Historical Review and Assessment of Clinical ... - CiteSeerX
12
ANNALS OF CLINICAL AND LABORATORY SCIENCE, Vol. 15, No. I Copyright © 1985, Institute for Clinical Science, Inc. Historical Review and Assessment of Clinical Hemoglobinometry in the United States* F. WILLIAM SUNDERMAN, M.D., P h .D. Institute for Clinical Science, Hahnemann University, Philadelphia, PA 19103 ABSTRACT An historical review of clinical hemoglobinometry has been presented. Investigators who have made important contributions to our knowledge of hemoglobin have been cited. A questionnaire was distributed to 750 clinical laboratories in the United States to ascertain (a) the type of instrumentation used routinely to mea- sure hemoglobin; (b) the methods that are now being used for clinical hemoglobinometry; (c) reference material that is used for daily quality control; and (d) the methods used for primary standardization. The results of the 263 responses to the questionnaire are reported. It is noteworthy that at the present time, 78 percent of the responding laboratories use the same instrumentation system. An assessment has been made of the precision of hemoglobin measure- ments undertaken in clinical laboratories in the United States over the past four decades. The data indicate that hemoglobin measurements dur- ing the past four years have become significantly more precise. There is probably no single factor responsible for this timely improvement; how- ever, it may be inferred that the shift from manual to automated meth- odology in recent years is an important contributing factor. tacular substance became capable of holding oxygen so loosely that it could be instantly released to meet the needs of animal tissues. In addition, this same component became capable of furnishing alkali to combine with the carbonic acid that was liberated by the tissues so that when the circulating fluid reached the lungs, the surplus carbonic acid was free to escape immediately into the atmo- sphere. That phenomenal substance was hemoglobin, a name given to it by Hoppe-Seyler in 1862.16 This year marks the 300th anniversary 1 0091-7370/85/0100-0001 $01.80 © Institute for Clinical Science, Inc. Historical Commentary In some millenial epoch in the evolu- tionary development of animal life on our planet, a phenomenal substance evolved in the circulating fluid of animals that enabled this fluid to extract from the atmosphere a hundred times more oxy- gen than could be absorbed by simple aqueous solutions. Moreover, this spec- * Presented as an invited lecture at the meeting of the American Society of Clinical Pathologists, New Orleans, LA, October 30, 1984.
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Historical Review and Assessment of Clinical ... - CiteSeerX

ANNALS O F CLINICA L A N D LABORATORY SC IE N C E, Vol. 15, No. I Copyright © 1985, Institute for Clinical Science, Inc.
Historical R eview and Assessm ent o f Clinical H em oglobinom etry in the U nited States*
F. W ILLIAM SUNDERMAN, M .D ., Ph .D.
Institute fo r Clinical Science, Hahnemann University, Philadelphia, PA 19103
ABSTRACT
An historical review of clinical hemoglobinometry has been presented. Investigators who have made im portant contributions to our knowledge of hemoglobin have been cited.
A questionnaire was distributed to 750 clinical laboratories in the United States to ascertain (a) the type of instrum entation used routinely to measure hemoglobin; (b) the m ethods that are now being used for clinical hemoglobinometry; (c) reference material that is used for daily quality control; and (d) the m ethods used for prim ary standardization. The results of the 263 responses to the questionnaire are reported. It is noteworthy that at the present time, 78 percent of the responding laboratories use the same instrum entation system.
An assessment has been m ade of the precision of hemoglobin m easurem ents undertaken in clinical laboratories in the U nited States over the past four decades. The data indicate that hemoglobin m easurem ents du ring the past four years have becom e significantly more precise. There is probably no single factor responsible for this timely improvement; however, it may be inferred that the shift from manual to autom ated m ethodology in recent years is an im portant contributing factor.
tacu lar substance becam e capab le of holding oxygen so loosely that it could be instantly released to m eet the needs of anim al tissues. In add ition , th is sam e com ponent becam e capable of furnishing alkali to combine with the carbonic acid that was liberated by the tissues so that when the circulating fluid reached the lungs, the surplus carbonic acid was free to escape im m edia te ly in to th e a tm osphere. That phenom enal substance washem oglobin , a nam e given to it by Hoppe-Seyler in 1862.16
This year marks the 300th anniversary1
0091-7370/85/0100-0001 $01.80 © Institute for Clinical Science, Inc.
Historical Commentary
In some millenial epoch in the evolutionary developm ent of animal life on our planet, a phenom enal substance evolved in the circulating flu id of anim als that en ab led th is f lu id to ex trac t from th e atm osphere a hundred times more oxygen than could be absorbed by simple aqueous solutions. Moreover, this spec-
* Presented as an invited lecture at the m eeting of the American Society of Clinical Pathologists, New Orleans, LA, October 30, 1984.
2 SUNDERMAN
F i g u r e 1 . Robert Boyle, 1 6 2 7 - 1 6 9 1 .
of the introduction of chemical m easurements in the study of blood and the 30th anniversary of the first workshop in Clinical Pathology, which was appropriately devoted to the topic of hemoglobinome- try. The enthusiastic response from the participants of the first workshop in our country helped to inaugurate a new era of continuing education into all branches of medicine.
Early H istory
The study of blood chemistry actually began in 1684 when Robert Boyle published a treatise entitled Memoirs fo r the Natural History o f Humane Blood.5 Robert Boyle (figure 1), British physicist and chem ist who was bo rn in Ire lan d , became an Oxford University professor, was the author of the gas law that bears his nam e, and a scho lar w ho m ight appropriately bear the title of “first clinical scientist” . In his studies, Boyle considered the possibility that blood served as a respiratory function and speculated upon the role played by the red blood p igm ent in the carriage of resp ira to ry gases. B oyle’s tre a tise o v e rtu rn ed the
abstract Aristotelian m etaphysical concepts that were predom inant in his day and heralded the m odern era by which the acquisition of knowledge is obtained from experimental observations.
The introduction of the experimental m ethod for the acquisition of knowledge in the 17th century was a vision seen only by a few farsighted thinkers. N evertheless, it becam e, w ith all its im p erfec tions, the guiding light for the furtherance of science and medicine for the past 300 years.
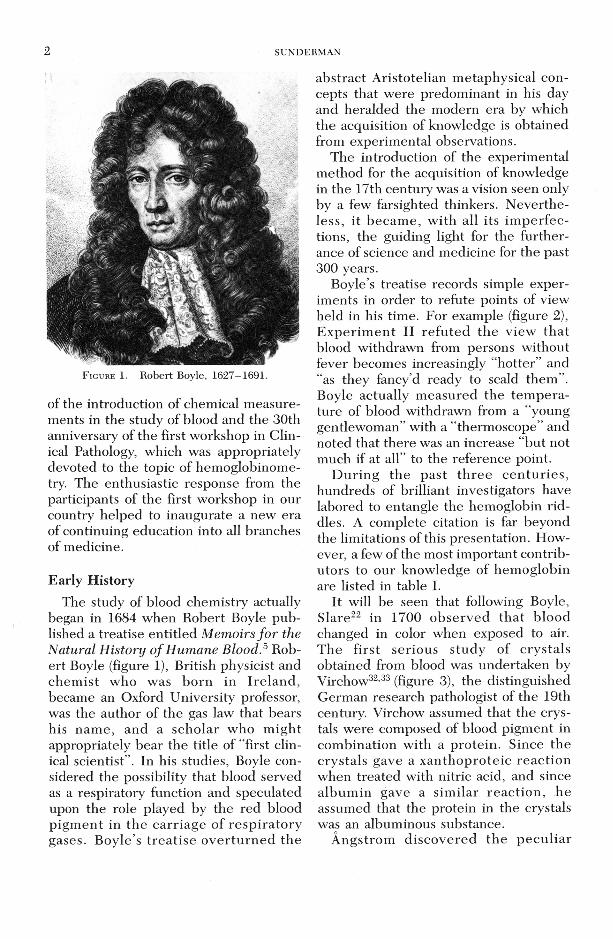
Boyle’s treatise records simple experiments in order to refute points of view held in his time. For example (figure 2), E x p erim en t II re fu ted the view that blood withdrawn from persons without fever becomes increasingly “hotter” and “as they fancy’d ready to scald them ”. Boyle actually m easured the tem p era ture of blood withdrawn from a “young gentlewom an” with a “therm oscope” and noted that there was an increase “but not much if at all” to the reference point.
D u rin g the past th re e c e n tu rie s , hundreds of brilliant investigators have labored to entangle the hemoglobin riddles. A complete citation is far beyond the limitations of this presentation. However, a few of the most im portant contributors to our knowledge of hem oglobin are listed in table I.
It will be seen that following Boyle, S lare22 in 1700 observed th a t blood changed in color when exposed to air. T he first serious study of crysta ls obtained from blood was undertaken by Virchow32,33 (figure 3), the distinguished German research pathologist of the 19th century. Virchow assumed that the crystals were composed of blood pigm ent in com bination with a protein . Since the crystals gave a xan thop ro te ic reac tion when treated with nitric acid, and since a lbum in gave a sim ilar reac tio n , he assumed that the protein in the crystals was an albuminous substance.
A ngstrom d iscovered th e p e c u lia r
CLINICAL HEMOGLOBINOMETRY 3
To the IV. (Primary) Title O F T H E
fftfto ry ofHumane Blood,
Experiment I
HAving for fome rcafons, that need pot here be men*
non a, been induc'd to enquire of more than one perfon, that has us’d to let many men Blood, whether they did not obferve, that fome perfons found a manifeil and confiderable change in the heat of the Blood, as it came to iiTue out firft or laft i I was aniwered Affirmatively ;ind told that feveral perfons that had no Fcaver faid, that after their Blood had run out a while, they found it come lenfibly hotter than before; and iotne of them complain'd, chat ir came with a degree of Heat that was troublefom, and as they fancy’d, ready to icaid them.
To the fame Title
O F T H E
Hipor/ o f Nm atie Blood.
tpejxriment II.
T Got« Chirurgeon to put a feal’d 1 Wcather-glafs, adjufied by the
’Standard of Grefham Colled ge, into 'the Porringer wherein he was going to bleed a young Gentlewoman, that, « th e Blood ran out of the open
it might- fall upon the Ball of xhe Inflrument; in which the Liquor was made by thewarrmh to afcend a good way, but not much ( if at. all ) nearer than about an Inch to the fmaller upper Ball of the Ther* moftope.
F i g u r e 2. Copy of two pages from Boyle’s Memoirs fo r the Natural H istory o f Humane Blood.
spectra l cha rac te ris tic s of b lood and hem oglobin in 1855. H em oglobin was first iso la ted in c ry sta lline form by Hoppe-Seyler16 in 1862.
I t appears tha t the first quantitative m easurem ents of hemoglobin w ere made by Sir William Gowers10 (figure 4), the em inent Victorian neurologist and energetic, inventive genius who, in addition to his contributions to the furtherance of neurology, becam e in te re s te d in art, music, and the construction of in stru m ents useful for the practice of m edicine. G ow ers’ in s tru m e n ts in c lu d ed a hem oglobinom eter,13 a hemocytometer, a candle ophthalmoscope, a magnifying otoscope, and a gauge for m easu ring sugar in urine. Gowers’ hemoglobinom-
eter consisted of a small stand that held two glass tubes of equal bore. O ne tube contained a colored standard composed of a mixture of glycerine, gelatine, carm ine, and picro-carm ine. D ilutions of b lood w ere m ade in the o th e r tu b e , w hich was ca lib ra ted , u n til th e color m atched that of the standard. Gowers’ h em o g lo b in o m e try re m a in e d for a quarter of a century the accepted m ethod for estimating the concentration of hem oglobin. His m ethod was supplanted by procedures proposed by Sahli21 and by H aldane.14
M olecular W eightH iifn e r17 was the first sc ien tis t to
investiga te th e m olecular w eigh t of
4 SUNDERMAN
TA BLE I
I m p o r ta n t C o n t r i b u t o r s t o O ur K n o w led g e o f H e m o g lo b in
Name Date C o n t r ib u t io n s
B o y le 1684
S l a r e 21 1700V irc h o w 3 2 ' 33 1847
Angstrom2
16.H o p p e - S e y le r 1862
G o w e rs13 1878
H U Ener17 1887
F i r s t c o n s i d e r e d t h a t b lo o d s e r v e d a r e s p i r a t o r y f u n c t i o n
S t u d ie d e f f e c t s o f a i r u p o n b lo o d " H a e m a to id in c r y s t a l s " ; P r o t e i n
s t u d i e s o n r e d b l o o d c e l l s D is c o v e r e d t h e s p e c t r u m o f
h e m o g lo b in C r y s t a l l i z e d h e m o g lo b in ; S p e c tru m s
o f OxyHb + M etH b; Named "H em o g lo b in "
E a r l i e s t c l i n i c a l m e th o d f o r e s t i m a t i o n o f h e m o g lo b in
Q u a n t i t a t i v e s p e c t r o p h o to m e t r y ;M o le c u la r w e i g h t ; c o n c e n t r a t i o n
Fe
B a r c r o f t &H i l l 3
A d a i r 1
31F a h r a e u s
K u n k e l & W a l l e n iu s 18
B r a u n i t z e r 6
H a l d a n e s 1899 S u g g e s te d C>2 c a p a c i t y b e a d o p te d a s S m ith m e a s u re o f h e m o g lo b in ; K jF e iC N jg
m e th o d ; P e rm a n e n t c a r b o x y - h e m o g lo b in s t a n d a r d
) M o le c u la r w e i g h t ; P h y s i c a lc o n s t a n t s ; r e s p i r a t o r y p h y s io l o g y
i F o u n d m o le c u la r w e i g h t o f h e m o g lo b in t o b e a p p r o x i m a t e ly 6 7 ,5 0 0 ; H em o g lo b in m o le c u le c o n t a i n s f o u r a to m s o f Fe a n d i s t h u s f o u r t im e s H ü f n e r 's v a lu e
S v e d b e rg & 1926 C o n f irm e d A d a i r ’ s v a l u e f o rm o le c u la r w e i g h t ; M am m alian h e m o g lo b in h a s m o le c u la r w e ig h t o f a p p r o x i m a t e ly 6 4 ,5 0 0
1 927 S y n t h e s i z e d h e m in i d e n t i c a l w i th t h a t o b t a i n e d f ro m h e m o g lo b in
1 955 S e p a r a t e d h e m o g lo b in v a r i a n t s b y e l e c t r o p h o r e s i s
1 961 E s t a b l i s h e d am in o a c i d s e q u e n c e s i n p o l y p e p t i d e c h a in s
1970 S p a t i a l r e l a t i o n s h i p s i n v e s t i g a t e d b y X - ra y d i f f r a c t i o n
hemoglobin. He found that 100 grams of ox hemoglobin contained 0.34 grams of iron which is 0.34/56 = 0.00607 gramatom of iron. Thus, if each molecule of hem oglobin con ta ined only one ironatom , th e m olecu lar w eigh t w ould be100/0.00607 or approximately 16,500.
Barcroft and Hill3 also determ ined them olecular w eigh t of hem oglob in . In1910, they estim ated that the least possible molecular weight of the compoundin a dialyzed solution was 16,669. Respira to ry physiology owes m uch o f itsknowledge to the research contributionsof Barcroft and his collaborators.
Thirty-eight years after H iifner’s studies, Adair1 found by direct osmotic pressure m easurem ents tha t the m olecular
w eigh t of hem oglob in was 67 ,500 ,— approximately four times Hüfner s value. His findings portended to hemoglobin’s quarternary structure. Adair’s value was confirmed by Svedberg and Fahraeus31 th ro u g h th e ir d e te rm in a tio n s of sed im entation rates in the ultracentrifuge.
Composition
The task of identifying the principal constituents of hemoglobin (native glo- bin, p ro toporphyrin , and ferrous iron) engaged the minds of some of the most b rillian t chem ists o f th is cen tu ry , and especially that of Hans Fischer. In 1927, F ischer12 achieved a scientific trium ph by synthesizing hem in, which was identical with that p repared from hemoglobin.
Although reports had appeared in the lite ra tu re suggesting tha t whole blood contained m ore than one type of hem oglobin , it rem a in e d for K unkel and W allenius18 in 1955 to separate four variant hem oglobins by starch gel e lectro pho resis and to op en an e n tire ly new area in the field of hematology.
The study of the amino acid sequence of adult hem oglobin was e laborated in 1961 by a group of workers in Munich under the leadersh ip of B raunitzer7 at the Max Planck In stitu te . Based upon their studies of the chemical structures of the alpha and beta chains and of heme, the molecular weight of hum an hemoglobin was calculated to be 64,458.® During the same period, the spatial relationships in the hemoglobin molecule were investigated by Perutz20 of Cambridge University using X-ray d iffraction p ro cedures.
In the history of hem oglobinom etry, the invesitga to rs lis ted in tab le I p ro vided contributions that served as a basis for th e fu rth e ran ce of m ost of the research in this im portant area of clinical science.
CLINICAL HEMOGLOBINOMETRY 5
F ig u r e 3. Rudolf Virchow, 1821-1902.
The Q uantitative M easurem ent of Hemoglobin
The q u a n tita tiv e m ea su rem e n t of hemoglobin has m aintained a prom inent place in clin ical m ed ic in e ev er since Gowers13 introduced the first m ethod for estim ating hem oglobin in blood. O ver the past century, countless hemoglobin m easurem ents have been made in hosp itals, clinics, and phy sic ian s’ offices. Scores of m ethods have been devised, and co n c en tra te d efforts have been directed toward securing uniformity and accuracy of results.
Inaccuracies in hemoglobinom etry in the U nited States becam e conspicuous during World War II, when reviews were m ade of blood analyses on w orkers in defense plants. At the end of the war, local and national organizations u n d e rtook a num ber of surveys to assess the accuracy of m easurem ents made in clinical laboratories.
The first survey was m ade in 1946 by the C om m ittee on Laboratories of the Pennsylvania Medical Society.4 This was perform ed by the d istribu tion of carefully prepared solutions to the directors of hospital laboratories, with the request
that analyses be made on two solutions and the results re tu rned anonymously. The mean result of 53 analyses for the first solution was 9.9 grams per dl, with a standard deviation of ±1.4; that of the second solution was 15.1 grams per dl, with a standard deviation of ±1 .1 . This survey was follow ed by a n u m b er of na tional su rveys, which revea led d is crepanc ies of th e sam e and of even greater magnitude.
N ational, s ta te , and local pathology societies becam e actively engaged in devising m ethods to correct faulty analyses in clin ical labora to ries. At the request of the Virginia Pathology Society, a m onth ly P roficiency Testing Service was started in 194924,25 by which laboratory directors might determ ine the accuracy of analyses performed under their direction. The service included the distrib u tio n of carefu lly p rep a red oxyhemoglobin solutions, in addition to other analytes routinely m easured in clinical laboratories.
In 1950, the American Society of Clinical Pathologists and the C ollege of American Pathologists organized a hem oglobin symposium as the main feature of
F i g u r e 4. Sir William Gowers, 1845-1915.
6 SUNDERMAN
th a t y e a r’s jo in t annual m eeting . The studies and rev iew s p re p a re d by the au thors for th is sym posium led to the publication in 1953 of the first com prehensive m onograph of clinical hemoglo- binometry.28,29
The first workshop in clinical hemoglo- b inom etry was h e ld on S ep tem b e r 7, 1954 under the auspices of the American Society of Clinical Pathologists and the U.S. Naval Medical School in Bethesda (figure 5). Elaborate preparations were made for this workshop with the production of a 60 m inute audiovisual film, the publication of a workshop m anual,2' and the acquisition of sufficient in strum entation to enable 120 participants to make iron analyses on b lood , spectroscop ic m easu rem en ts of hem oglob in d e riv a tives, e le c tro p h o re tic separa tions of hemoglobins, calibration of pipets, etc. I t is g ratify ing th a t th e en th u siastic response from the participants and the success of this initial workshop served as a stimulus for the establishm ent through jo in t efforts of th e F irs t In te rn a tio n a l Workshop at Royal Army Medical College in Millbank, London on July 9, 1957 (figure 6) and th e F irs t P u e rto Rican Workshop in Rio Piedras on Novem ber 18, 1957. These first workshops helped to inaugu ra te a new era of con tinu ing education into all branches of medicine. Today, th ere are literally thousands of w orkshops and sem inars u n d e rtak en each year by specialty organizations and institutions of higher learning throughout the world.
In 1955, under the sponsorship of the N ational R esearch C ouncil and the N ational A cadem y of Science (NAS- NRC),9 a plan was proposed for the centralization of standards in hemoglobinom- etry in this country. An “ad hoc” panel was established that supplied and distributed an NAS-NRC certified solution of cyanmethemoglobin. The criteria for this cyanm ethem oglobin standard was p u b lished in 1958.8 The standardization was
based upon th e m easu rem en t of the ex tinction coefficien t o f a so lu tion of cyanm ethem oglob in . The NAS-NRC standards programs was later turned over to the College of American Pathologists.
Rapid advances in clinical hemoglobi- nom etry were made in the score of years after World War II. A summarization of these advances was published as a monograph in 1964.30
In 1963, the European Society of H aem atology es tab lish ed a s tandard iz ing com m ittee which, in 1964, became the In ternational C om m ittee for Standards in H aem atology (ICSH). The C om m itte e ’s reco m m en d a tio n s for s ta n d a rd ization of cyanmethem oglobin were accepted at the International Congress of H aem atology he ld in Stockholm and p u b lish ed in 1967.11 A bout the sam e tim e, the N ational In s titu te of Public Health in Holland began distributing an international cyanmethemoglobin reference solution (referred to as haemiglo- bincyanide [HiCH]) through the World Health Organization.
In our country, an organization known as the National Com m ittee for Clinical L aborato ry S tandards (NCCLS) was founded in 1966 to “promote the developm en t and vo lun tary use of national standards and guidelines that are needed for im proved operation of clinical laboratories”. This organization (NCCLS) has rem ained active and has been responsible through its Com m ittee on Hem atology to publish from tim e to tim e reference p ro ced u res for the q u an tita tiv e determ ination of hemoglobin in blood.19
This b r ie f rev iew has a tte m p te d to epitomize some of the highlights in the h isto ry of clin ical hem oglob inom etry over the years.
Current Status of Clinical Hemoglobinometry
A questionnaire to ascertain the status of hem oglob inom etry in the U n ited
CLINICAL HEMOGLOBINOMETRY 7
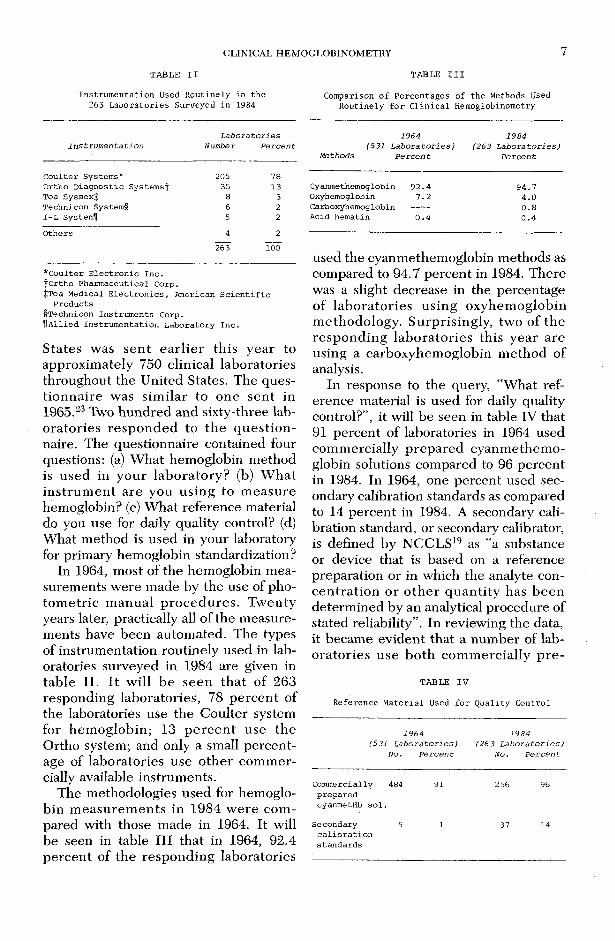
TA BL E I I T A BL E I I I
I n s t r u m e n t a t i o n U s e d R o u t i n e l y i n t h e C o m p a r i s o n o f P e r c e n t a g e s o f t h e M e th o d s U se d2 6 3 L a b o r a t o r i e s S u r v e y e d i n 1 9 8 4 R o u t i n e l y f o r C l i n i c a l H e m o g lo b in o m e t r y
L a b o r a t o r i e s 1 9 6 4 1 9 8 4I n s t r u m e n t a t i o n N u m b er P e r c e n t (5 3 1 L a b o r a t o r i e s ) ( 2 6 3 L a b o r a t o r i e s )
_______________________________________________________________ M e th o d s P e r c e n t P e r c e n t
C o u l t e r S y s te m s * 20 5 7 8O r t h o D i a g n o s t i c S y s t e m s ^ 35 1 3T o a S y s m e x J 8 3T e c h n ic o n S y s te m § 6 2I - L S y s te m f l 5 2
O t h e r s 4 2
263" 1 0 0
* C o u l t e r E l e c t r o n i c I n c . f O r t h o P h a r m a c e u t i c a l C o r p .$ T o a M e d ic a l E l e c t r o n i c s , A m e r ic a n S c i e n t i f i c
P r o d u c t s § T e c h n ic o n I n s t r u m e n t s C o r p .^ A l l i e d I n s t r u m e n t a t i o n L a b o r a t o r y I n c .
States was sen t e a rlie r th is year to approxim ately 750 clinical laboratories throughout the United States. The questio n n a ire was sim ilar to one sen t in 1965.23 Two hundred and sixty-three laborato ries re sp o n d ed to th e q u e s tio n naire. The questionnaire contained four questions: (a) W hat hemoglobin m ethod is u sed in your labo ra to ry? (b) W hat in s tru m e n t are you using to m easu re hemoglobin? (c) W hat reference material do you use for daily quality control? (d) W hat m ethod is used in your laboratory for prim ary hemoglobin standardization?
In 1964, most of the hemoglobin m easurem ents w ere m ade by the use of photom etric m anual p ro ced u res . Tw enty years later, practically all of the m easurements have been autom ated. The types of instrum entation routinely used in laboratories surveyed in 1984 are given in tab le II. I t w ill b e seen th a t of 263 responding laboratories, 78 pe rcen t of the laboratories use the C oulter system for hem oglobin ; 13 p e rc e n t use the Ortho system; and only a small percentage of laboratories use o ther com m ercially available instrum ents.
The methodologies used for hemoglobin m easu rem en ts in 1984 w ere com pared with those m ade in 1964. It will be seen in table III that in 1964, 92.4 percen t of the responding laboratories
C y a n m e th e m o g lo b in 9 2 . 4 9 4 . 7O x y h e m o g lo b in 7 . 2 4 . 0C a r b o x y h e m o g lo b in -------- 0 . 8A c id h e m a t i n 0 . 4 0 . 4
used the cyanmethem oglobin m ethods as compared to 94.7 percent in 1984. There was a slight decrease in the percentage of labo ra to ries using oxyhem oglobin m ethodology. Surprisingly , two of the resp o n d in g labo ra to ries th is year are using a carboxyhem oglobin m ethod of analysis.
In response to the query, “W hat reference material is used for daily quality control?’’, it will be seen in table IV that 91 percent of laboratories in 1964 used com m ercially p repared cyanm ethem oglobin solutions compared to 96 percent in 1984. In 1964, one percent used secondary calibration standards as compared to 14 percent in 1984. A secondary calibration standard, or secondary calibrator, is defined by NCCLS19 as “a substance or device that is based on a reference preparation or in which the analyte concen tra tio n o r o th e r q u an tity has b een determ ined by an analytical procedure of stated reliability” . In reviewing the data, it becam e evident that a num ber of labo rato ries use b o th com m ercially p re-
TA BLE I V
R e f e r e n c e M a t e r i a l U sed f o r Q u a l i t y C o n t r o l
1 9 6 4 1 9 8 4(5 3 1 L a b o r a t o r i e s ) (2 6 3 L a b o r a t o r i e s )
N o. P e r c e n t N o . P e r c e n t
C o m m e r c ia l ly 4 8 4 9 1 2 5 6 96p r e p a r e d c y a n m e tH b s o l .
S e c o n d a r y 5 1 37 14c a l i b r a t i o n s t a n d a r d s
00
Fig
ur
e 5
. T
he t
opic
for
the
fir
st w
orks
hop
was
Clin
ical
Hem
oglo
bino
met
ry.
SUNDERMAN
FIR
ST
IN
TE
RN
AT
ION
AL
WO
RK
-SH
OP
RO
YA
L A
RM
Y M
ED
ICA
L C
OL
LE
GE
M
XL
LB
AK
K,
LO
ND
ON
Ju
ly 9
, 19
57
F.
Wil
liam
Sus
ider
inan
, M
.D.,
Dir
ecto
r
Fig
ur
e 6
. T
he t
opic
for
the
fir
st i
nter
natio
nal w
orks
hop
was
Hem
oglo
bin
Stan
dard
izat
ion.
CDCLINICAL HEMOGLOBINOMETRY
10 SUNDERMAN
T A B L E V
C o m p a r i s o n o f P e r c e n t a g e s o f C l i n i c a l L a b o r a t o r i e s U s in g P r i m a r y H e m o g lo b in S t a n d a r d i z a t i o n s
1 9 6 4 1 9 8 4( 5 3 1 L a b o r a t o r i e s ) (2 6 3 L a b o r a t o r i e s )
N o . P e r c e n t N o . P e r c e n t
I r o n a n a l y s e s 12 2 . 3 8 3 . 0O x y g e n c a p a c i t y 2 0 . 4 1 0 . 4E x t i n c t i o n
c o e f f i c i e n t -- 16 6 . 1N one 51 7 9 7 . 4 2 3 8 9 0 . 5
pared standards and secondary calibration standards for daily reference.
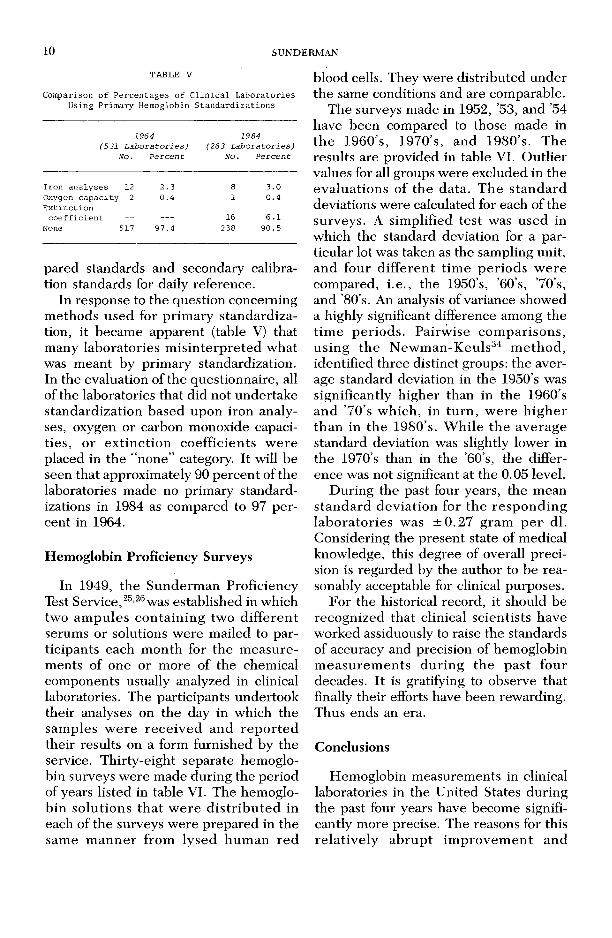
In response to the question concerning m ethods used for prim ary standardization, it becam e apparent (table V) that many laboratories m isin te rp re ted what was m eant by prim ary standardization. In the evaluation of the questionnaire, all of the laboratories that did not undertake standardization based upon iron analyses, oxygen or carbon monoxide capacities, or ex tinc tion coefficients w ere placed in the “none” category. It will be seen that approximately 90 percent of the laboratories made no prim ary standardizations in 1984 as compared to 97 p e rcent in 1964.
Hemoglobin Proficiency Surveys
In 1949, the Sunderm an Proficiency Test Service,25,26 was established in which two am pules con ta in ing two d iffe ren t serums or solutions w ere mailed to participants each m onth for the m easu rem ents of one or m ore of the chemical components usually analyzed in clinical laboratories. The participants undertook their analyses on the day in which the sam ples w ere rece iv ed and re p o rte d their results on a form furnished by the service. Thirty-eight separate hemoglobin surveys w ere made during the period of years listed in table VI. The hemoglob in so lu tions th a t w ere d is tr ib u te d in each of the surveys w ere prepared in the sam e m an n er from lysed hum an red
blood cells. They were d istributed under the same conditions and are comparable.
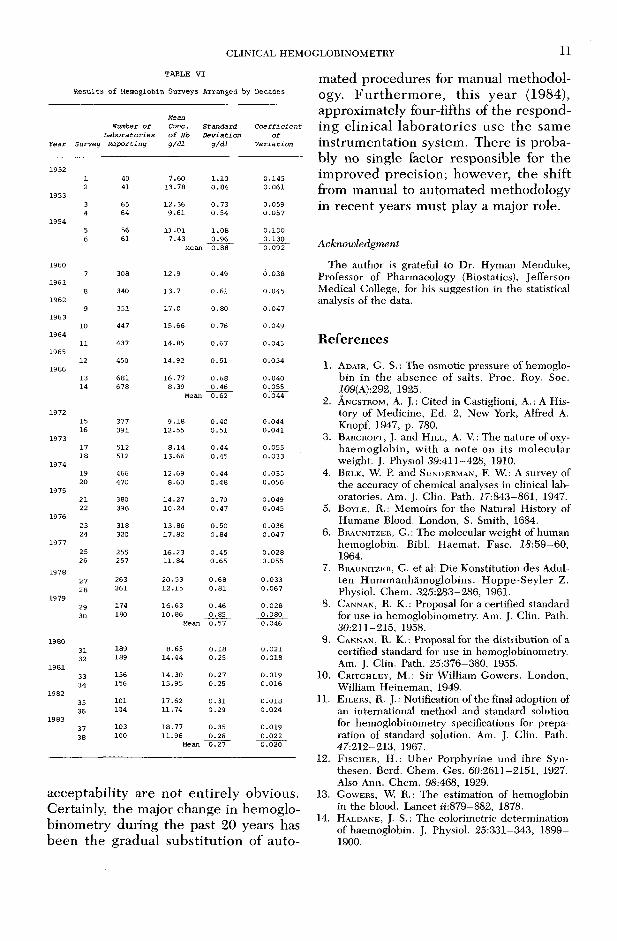
The surveys made in 1952, ’53, and ’54 have been compared to those made in th e 1960’s, 1970’s, and 1980’s. The results are provided in table VI. O utlier values for all groups were excluded in the evaluations of th e data. T he s tan d ard deviations were calculated for each of the surveys. A sim plified test was used in which the standard deviation for a particular lot was taken as the sampling unit, and four d iffe ren t tim e periods w ere compared, i.e ., the 1950’s, ’60’s, ’70’s, and ’80 s. An analysis of variance showed a highly significant difference among the tim e periods. Pairw ise com parisons, u sing th e N ew m an-K euls34 m ethod , identified three distinct groups: the average standard deviation in the 1950’s was significantly h igher than in the 1960’s and ’70’s w hich, in tu rn , w ere h ig h er th an in the 1980’s. W hile th e average standard deviation was slightly lower in the 1970’s than in the ’60 s, the difference was not significant at the 0.05 level.
During the past four years, the mean s tan d ard dev ia tion for th e resp o n d in g labo ra to ries was ± 0 .2 7 gram p e r dl. Considering the present state of medical knowledge, this degree of overall precision is regarded by the author to be reasonably acceptable for clinical purposes.
For the historical record, it should be recognized that clinical scientists have worked assiduously to raise the standards of accuracy and precision of hemoglobin m easu rem en ts du ring th e past four decades. It is gratifying to observe that finally their efforts have been rewarding. Thus ends an era.
Conclusions
Hemoglobin m easurem ents in clinical laboratories in the United States during the past four years have becom e significantly m ore precise. The reasons for this re la tive ly ab ru p t im provem en t and
CLINICAL HEMOGLOBINOMETRY 11
TABLE V I
R e s u l ts o f H em oglobin S u rv ey s A rran g ed by D ecades
Year S u rv e y
Number of
Laboratories
Reporting
Mean
Cone,
o f Hb
g/d i
Standard
Deviation
g/d l
Coefficient
of
Variation
19521 40 7 .6 0 1 .1 0 0 .1 4 52 41 1 3 .7 8 0 .8 4 0 .0 6 1
19533 65 1 2 .3 6 0 .7 3 0 .0 5 94 64 9 .6 1 0 .5 4 0 .0 5 7
19545 56 1 1 .0 1 1 .0 8 0 .1 0 06 61 7 .4 3
Mean0 .9 6
. 0 .8 80 .1 3 00 .0 9 2
19607 308 1 2 .9 0 .4 9 0 .0 3 8
196 18 340 1 3 .7 0 .6 1 0 .0 4 5
19629 351 1 7 .0 0 .8 0 0 .0 4 7
1 96310 447 1 5 .6 6 0 .7 6 0 .0 4 9
196411 437 1 4 .8 5 0 .6 7 0 .0 4 5
196512 450 1 4 .9 2 0 .5 1 0 .0 3 4
196613 681 1 6 .7 7 0 .6 8 0 .0 4 014 6 78 8 .3 9
Mean0 .4 60 .6 2
0 .0 5 50 .0 4 4
197215 377 9 .1 8 0 .4 0 0 .0 4 416 391 1 2 .5 5 0 .5 1 0 .0 4 1
1 97317 512 8 .1 4 0 .4 4 0 .0 5 518 512 1 3 .6 6 0 .4 5 0 .0 3 3
1 97419 466 1 2 .6 9 0 .4 4 0 .0 3 520 470 8 .6 0 0 .4 8 0 .0 5 6
197521 380 1 4 .2 7 0 .7 0 0 .0 4 922 396 1 0 .2 4 0 .4 7 0 .0 4 5
1 97623 318 1 3 .8 6 0 .5 0 0 .0 3 624 320 1 7 .8 2 0 .8 4 0 .0 4 7
197 725 255 1 6 .2 3 0 .4 5 0 .0 2 826 257 1 1 .8 4 0 .6 5 0 .0 5 5
1 97827 263 2 0 .5 3 0 .6 8 0 .0 3 328 261 1 2 .1 5 0 .8 1 0 .0 6 7
1 97929 174 1 6 .6 3 0 .4 6 0 .0 2 830 180 1 0 .8 6
Mean0 .8 50 .5 7
0 .0 8 00 .0 4 6
198031 189 8 .6 5 0 .1 8 0 .0 2 132 189 1 4 .4 4 0 .2 5 0 .0 1 8
198133 156 1 4 .3 0 0 .2 7 0 .0 1 934 156 1 5 .9 5 0 .2 5 0 .0 1 6
198235 101 1 7 .6 2 0 .3 1 0 .0 1 836 104 1 1 .7 4 0 .2 9 0 .0 2 4
198337 103 1 8 .7 7 0 .3 5 0 .0 1 938 100 1 1 .9 6
Mean0 .2 60 .2 7
0 .0 2 20 .0 2 0
acceptability are not en tire ly obvious. Certainly, the major change in hemoglo- binom etry during the past 20 years has been the gradual substitu tion of au to
m ated procedures for manual m ethodology. F u rth e rm o re , th is year (1984), approximately four-fifths of the responding clin ical labo ra to ries use the sam e instrum entation system. There is probably no single factor responsible for the im proved precision; however, the shift from manual to autom ated methodology in recent years must play a major role.
A cknowledgment
The author is grateful to Dr. Hyman Menduke, Professor of Pharmacology (Biostatics), Jefferson Medical College, for his suggestion in the statistical analysis of the data.
References
1. A d a i r , G. S. : The osmotic pressure of hem oglobin in the absence o f salts. Proc. Roy. Soc. i09(A):292, 1925.
2. A n g s t r o m , A . J.: Cited in Castiglioni, A . : A History of Medicine, Ed. 2, New York, Alfred A . Knopf, 1947, p. 780.
3. B a r c r o f t , J. and H i l l , A. V.: The nature of oxy- haem oglob in , w ith a note on its m olecular weight. J. Physiol 39:411-428, 1910.
4. B e l k , W. P. and S u n d e r m a n , F. W.: A survey of the accuracy of chemical analyses in clinical laboratories. Am. J. Clin. Path. J7:843-861, 1947.
5 . B o y l e , R . : Memoirs for the Natural History of Humane Blood. London, S. Smith, 1684.
6. B r a u n i t z e r , G.: The molecular weight o f human hem oglobin. Bibl. Haemat. Fasc. 18:5 9 -6 0 ,1964.
7. B r a u n i t z e r , G. et al: D ie Konstitution des Adulten H um m anhäm oglobins. H oppe-Seyler Z. Physiol. Chem. 325:283-286, 1961.
8. C a n n a n , R. K.: Proposal for a certified standard for use in hemoglobinometry. Am. J. Clin. Path. 30:211-215, 1958.
9. C a n n a n , R. K. -. Proposal for the distribution of a certified standard for use in hemoglobinometry. Am. J. Clin. Path. 25:376-380, 1955.
10. C r i t c h l e y , M.: Sir W illiam Gowers. London, William Heineman, 1949.
11. E i l e r s , R. J.: Notification of the final adoption of an international method and standard solution for hemoglobinometry specifications for preparation of standard solution. Am. J. Clin. Path. 47:212-213, 1967.
12. F i s c h e r , H.: Uber Porphyrine und ihre Synthesen. Berd. Chem. Ges. 60:2611—2151, 1927. Also Ann. Chem. 98:468, 1929.
13. G o w e r s , W. R.: The estimation of hemoglobin in the blood. Lancet it:879-882, 1878.
14. H a l d a n e , J. S.: The colorimetric determination of haemoglobin. J. Physiol. 25:331-343, 1899- 1900.
12 SUNDERMAN
15. H a l d a n e , J. and S m i t h , J. L .: The mass and oxygen capacity o f the blood in man. J. Physiol. 25:331-343, 1899-1900.
16. H o p p e - S e y l e r , F.: Ueber das Verhalten des Blut- farbstorres im Spectrum des Sonnenlichtes. Arch. path. Anat. u. Physiol. 23:446-449, 1862.
17. H ü f n e r , G.: Beitrag zur Lehre vom Blutfarbstoffe. Beitr. f. Physiol. Carl Ludwig z.s. 70 Geburst. (etc.) 74—81, 1887.
18. K u n k e l , H. C. and W a l l e n i u s , G.: New hem oglobins in normal adult blood. Science 122:288,1955.
19. National C om m ittee for Clinical Laboratory Standards: Reference Procedure for the Quantitative Determination of Hemoglobin in Blood. Vol. 4, No. 3, 1984, pp. 5 4 -7 8 . 771 East Lancaster Avenue, Villanova, PA 19085.
20. P e r u t z , M. F.: Stereochemistry o f cooperative effects in hemoglobin. Nature 228:726, 1970.
21. Sahli, H. L.: Lehrbuch d e Klinischen U ntersuchungsm ethoden. Ed. I. Leipzig: D euticke, 1894.
22. S l a r e , F.: Some affects of the air upon blood, explained by an experiment of the change of colour in a clear liquor, upon the admission of air. Philosphical Trans., London ii:235-240, 1700.
23. S u n d e r m a n , F. W .: Status o f clinical hem oglo- binom etry in the U nited States. Am. J. Clin. Path. 4 3 :9 -15 , 1965.
24. S u n d e r m a n , F. W .: The origin of proficiency testing for clinical laboratories in the United States. Proceedings of the Second National Conference on Proficiency Testing. Bethesda, 1975, pp. 6 -7 .
25. S u n d e r m a n , F. W .: Twenty-five years o f profi
ciency testing for clinical laboratories. Ann. Clin. Lab. Sci. 2:420-424, 1972.
26. S u n d e r m a n , F . W., C o p e l a n d , B. E ., M a c F a t e , R. P., M a r t e n s , V. E ., N a u m a n n , H. N . , and S t e v e n s o n , G. F.: Hemoglobin standardizations. A commentary on procedures to insure reliable hemoglobinometry. Am. J. C l i n . Path. 25:489- 493, 1955.
27. S u n d e r m a n , F . W., C o p e l a n d , B. E ., M a c F a t e , R. P., M a r t e n s , V. E ., N a u m a n n , H. N . , and S t e v e n s o n , G. F . : Manual of Workshop in Clinical Hemoglobinometry of American Society of Clinical Pathologists. Am. J. Clin. Path. 25:695- 713, 1955.
28. S u n d e r m a n , F . W ., M a c F a t e , R. P., M a c - F a d y e n , D. A., S t e v e n s o n , G. F . , and C o p e l a n d , B. E.: Symposium on clinical hem oglobinometry. Am. J. Clin. Path. 23:519-598, 1953.
29. S u n d e r m a n , F. W ., M a c F a t e , R. P., M a c - F a d y e n , D. A., S t e v e n s o n , G. F . , and C o p e l a n d , B. E.: Clinical Hemoglobinometry. Baltimore, Williams and Wilkins, 1953.
30. S u n d e r m a n , F. W., and S u n d e r m a n , F. W., Jr.: Hemoglobin: Its Precursors & Metabolites. Philadelphia, J. B. Lippincott Co., 1964.
31. S v e d b e r c , T. and F a h r a e u s , R .: A new method for the determination of the molecular weight of the proteins. J. Am. Chem. Soc. 48:430, 1926.
32. V i r c h o w , R.: D ie pathologischen Pigm ente. Arch. f. path. Anat. u. Physiol, u. f. klin. Med. J:379-404, 1847.
33. V i r c h o w , R .: D ie pathologischen Pigmente. II. Chemischephatsachen. Arch. f. path. Anat. u. Physiol, u. f. klin. Med. 7:409-486, 1847.
34. W i n e r , B. J.: Statistical Principles in Experimental Design. New York, McGraw-Hill, 1962, pp. 77 -85 .