
Postural Sway in Older Patients with Sagittal Imbalance and ...
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
Physiotherapy Research InternationalPhysiother. Res. Int. (2009)Published online in Wiley InterScience(www.interscience.wiley.com) DOI: 10.1002/pri.434
Hip subluxation and dislocation in cerebral palsy – a prospective study on the effectiveness of postural management programmes
TERESA E POUNTNEY, Chailey Heritage Clinical Services, North Chailey, East Sussex BN8 4JN, UK
ANNE MANDY, University of Brighton, Mithras House, Lewes Road, Brighton BN2 4AT, UK
ELIZABETH GREEN, Chailey Heritage Clinical Services, North Chailey, East Sussex, BN8 4JN, UK
PAUL R GARD, Pharmacology and Therapeutics Division, University of Brighton, Mithras House, Lewes Road, Brighton BN2 4AT, UK
ABSTRACT Background and Purpose. Hip subluxation and dislocation are common sequelae in children with bilateral cerebral palsy and are currently managed by surgical interventions. This study aimed to investigate the effectiveness of early postural manage-ment programmes on hip subluxation and dislocation at fi ve years, and the need for treat-ment in children with bilateral cerebral palsy, and to compare these fi ndings with a historical control group. Methods. A prospective cohort study followed 39 children who commenced using postural management equipment under 18 months of age. Levels of ability, type and amount of equipment use and treatments were recorded every three months. At 30 and 60 months, the hips were X-rayed and the hip migration percentage was measured. The results were compared with the historical control group. Results. Children who used equipment at recommended and moderate levels had signifi cantly less chance of both hips being subluxed than those using equipment at minimal levels (two-tailed Fisher’s exact c2 p = 0.024). The frequency of children with hip problems was signifi cantly less in the intervention group in comparison to the historical control group at fi ve years (c2 = 11.53, df = 2, p = 0.006). The frequency of children receiving bilateral or unilateral treat-ments, i.e. surgery, use of a hip and spinal orthosis and/or botulinum toxin injections, in the intervention group was signifi cantly less compared to the historical control group (two-tailed Fisher’s exact p = 0.001). Conclusion. The early provision of postural management equipment has a role to play in reducing the number of hip problems and therefore the need for treatment of hip subluxation/dislocation in cerebral palsy at fi ve years of age. Copyright © 2009 John Wiley & Sons, Ltd.

Pountney et al.
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
Key words: cerebral palsy, hip dislocation, postural management programmes
(Reimers, 1980; Turker and Lee, 2000). A review of the literature on adductor releases for hip subluxation and their effectiveness in reducing pain, improving personal care, increasing range of motion, improving sitting or preventing pelvic obliquity was limited because of poorly designed studies (Stott et al., 2004). This review identifi ed particu-lar diffi culties related to the heterogeneity of the participants and the variability in surgi-cal interventions. Further studies are needed to determine which surgical approaches are most effective.
A prevention programme involving 206 children with cerebral palsy reported that at fi ve years, none had developed hip disloca-tion (Hagglund et al., 2005). However, this heterogeneous group of children with cere-bral palsy, of whom only a proportion was non-ambulant, had an extensive programme of surgery including soft tissue or bony surgery, selective dorsal rhizotomies and intrathecal baclofen. The outcomes of surgi-cal intervention are not always successful in controlling further progression to disloca-tion in the long term (Miller and Bagg, 1992; Young et al., 2001; Pountney et al., 2002). Adolescents and adults have reported pain at surgical sites, which persists over many years (Schwartz et al., 1999; Hodgkinson et al., 2001).
Other less invasive approaches to the management of hip subluxation have become popular over the past 10 years, particularly the use of postural management equipment. This approach offers a planned programme of activities and interventions to control an individual’s posture and function. Postural management equipment offers positioning in lying, sitting and standing to encourage
BACKGROUND
Hip subluxation and dislocation are common sequelae in children with bilateral cerebral palsy and have a debilitating effect on func-tion, pain, ability to sit and personal care (Cooperman et al., 1987; Cornell, 1995). High rates of subluxation and dislocation were reported in children not walking independently (Scrutton and Baird, 1997; Scrutton et al., 2001; Morton et al., 2006; Soo et al., 2006). A population study moni-toring hip development in children with cere-bral palsy found that at fi ve years of age, 54% of children not walking independently had one or both hips subluxed or had treatment for their hips (Scrutton and Baird, 1997; Scrutton et al., 2001). Scrutton and Baird described children as having a hip problem if they had either surgery or botulinum toxin A injection to the muscles surrounding the hips or a hip and spinal orthosis (HASO) and/or a migration percentage of >32% by fi ve years of age. Of children not walking at fi ve years, 38.1% had both hips affected and 15.8% had unilateral problems. Soo et al. (2006) reported that at Gross Motor Function Classifi cation System (GMFCS) Levels IV and V, rates of hip displacement were 69% and 90%, respectively (Palisano et al., 1997). These fi gures indicate that there are high rates of subluxation and dislocation, which continue to increase into adolescence impact-ing on functional ability, pain and a need to address the prevention of hip subluxation (Miller and Bagg, 1992).
To date, hip subluxation and dislocation have been largely treated by surgical inter-ventions, which include preventative soft tissue and reconstructive bony surgery

Effectiveness of postural management programmes
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
active movement, maintain muscle length, control/prevent deformity and increase function (Gericke, 2006). Chailey Heritage Clinical Services has developed a range of postural management equipment to support children in postures which simulate a higher functional ability (Pountney et al., 2004). Some evidence to support this approach in controlling hip migration in the form of cohort studies is available (Hankinson and Morton, 2002; Pountney et al., 2002). A ret-rospective study of 60 children found that children with cerebral palsy using postural management equipment in lying, sitting and standing before hip subluxation occurred were signifi cantly more likely to maintain hip integrity than children who did not use the full range of equipment or used it after hip subluxation had occurred (Pountney et al., 2002). The use of a sleep system with children positioned in supine and a hip abduction of 20° bilaterally found a signifi -cant decrease in hip migration percentage over one year (Hankinson and Morton, 2002).
The evidence for different approaches to the management of hip subluxation/disloca-tion is not conclusive with only limited robust evidence for the use of surgical inter-ventions and postural management equip-ment to control hip dislocation. Further research is required to determine the most effective approaches to prevent and manage hip subluxation. In this study, the focus will be on the effectiveness of early provision postural management equipment to prevent hip subluxation and dislocation.
METHODS
This a prospective longitudinal cohort design study following the progress of children with cerebral palsy up to fi ve years of age compared with a subset of a historical control
group of children with cerebral palsy. The historical control group was created from a population study in the South East of England monitoring hip development using serial X-ray measurements from age 18 to 60 months. A subset of this study (n = 202) who were not walking at fi ve years will be used to determine the effect of the therapeutic inter-vention, postural management equipment, for comparison in this study (Scrutton and Baird, 1997; Scrutton et al., 2001). The control group was drawn from the same geographic population, and therefore other aspects of the children’s treatment were likely to be similar, improving the validity of the study. The researcher has been allowed access to the raw data on the subset of children not walking independently from Scrutton and Baird’s study from their 2001 paper to compare fi ndings with the inter-vention group using postural management programmes.
Ethical approval was given by the East Sussex, Brighton and Hove Local Research Ethics Committee. The conditions have been adhered to and an informed consent for par-ticipation and publication has been obtained from the parents of all children taking part in the study.
Participants
Children were recruited from child develop-ment centres and acute hospital trusts in the South Thames Health Region of England.
Inclusion criteria (prospective)
Children with a diagnosis of bilateral cere-bral palsy who were aged 18 months or less (18 months was chosen as, at this stage, dif-ferences in hip development become statisti-cally apparent [Scrutton et al., 2001] and allowed time for postural management
Pountney et al.
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
equipment to be effective); no other condi-tion likely to affect their musculoskeletal development at referral to the study; and children not walking independently by fi ve years of age.
Inclusion criteria (historical)
The subset of the historical control group not walking independently at fi ve years of age.
Hip migration percentage
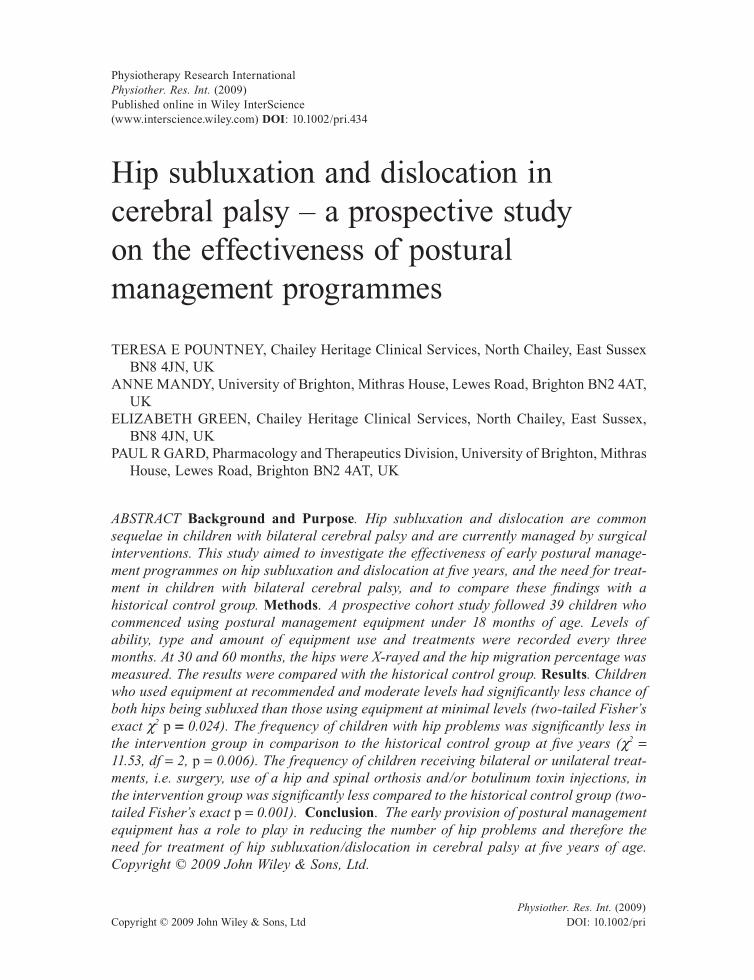
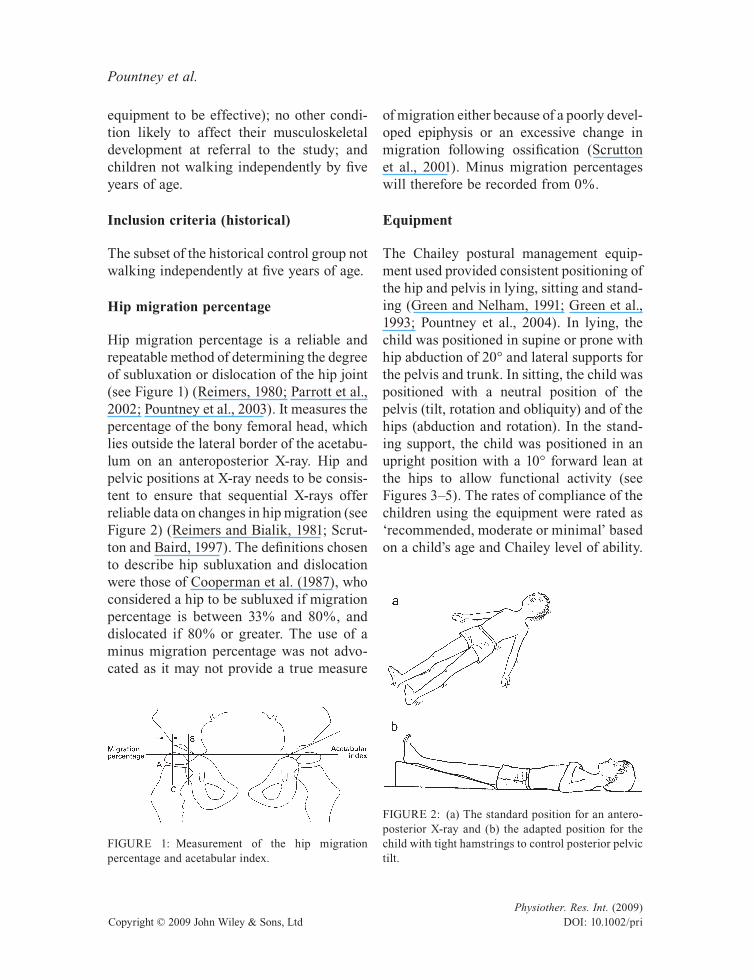
Hip migration percentage is a reliable and repeatable method of determining the degree of subluxation or dislocation of the hip joint (see Figure 1) (Reimers, 1980; Parrott et al., 2002; Pountney et al., 2003). It measures the percentage of the bony femoral head, which lies outside the lateral border of the acetabu-lum on an anteroposterior X-ray. Hip and pelvic positions at X-ray needs to be consis-tent to ensure that sequential X-rays offer reliable data on changes in hip migration (see Figure 2) (Reimers and Bialik, 1981; Scrut-ton and Baird, 1997). The defi nitions chosen to describe hip subluxation and dislocation were those of Cooperman et al. (1987), who considered a hip to be subluxed if migration percentage is between 33% and 80%, and dislocated if 80% or greater. The use of a minus migration percentage was not advo-cated as it may not provide a true measure
of migration either because of a poorly devel-oped epiphysis or an excessive change in migration following ossifi cation (Scrutton et al., 2001). Minus migration percentages will therefore be recorded from 0%.
Equipment
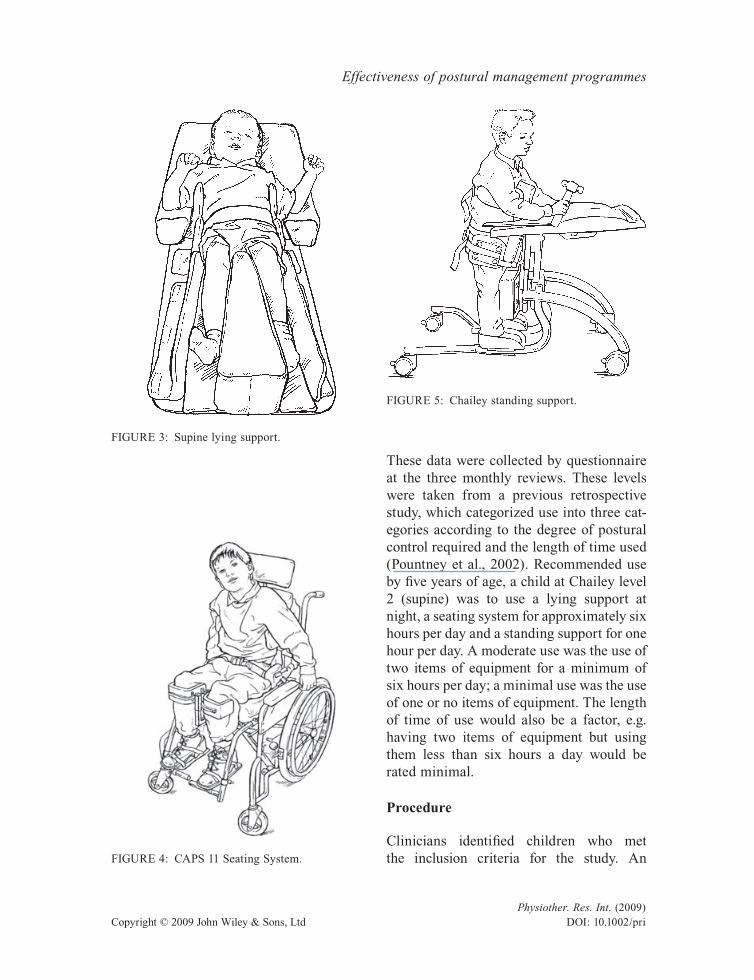
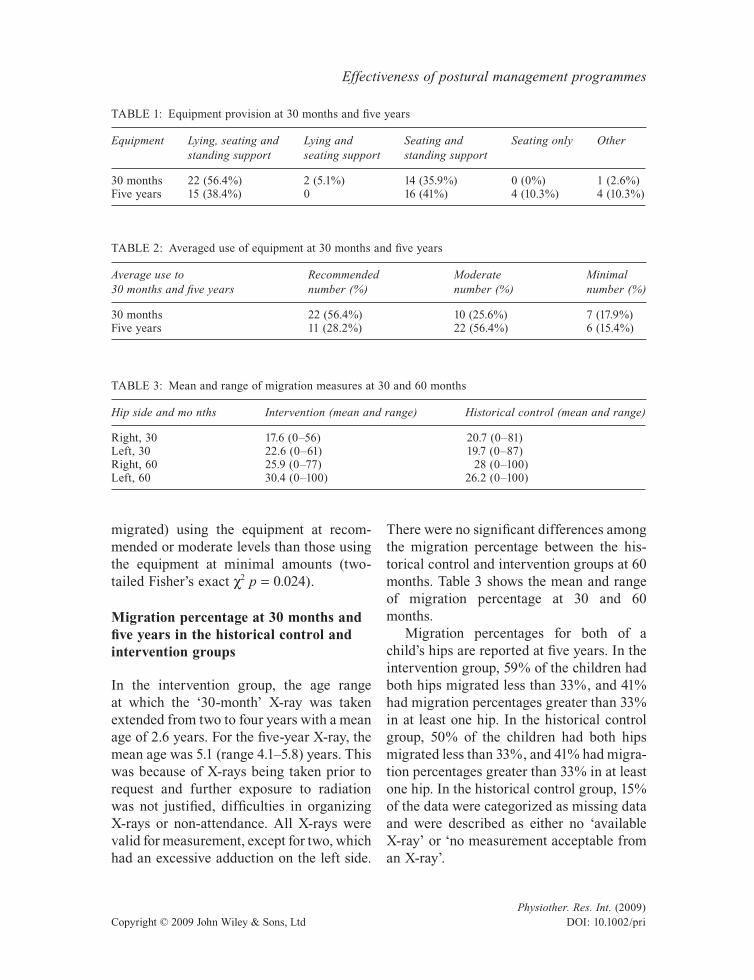
The Chailey postural management equip-ment used provided consistent positioning of the hip and pelvis in lying, sitting and stand-ing (Green and Nelham, 1991; Green et al., 1993; Pountney et al., 2004). In lying, the child was positioned in supine or prone with hip abduction of 20° and lateral supports for the pelvis and trunk. In sitting, the child was positioned with a neutral position of the pelvis (tilt, rotation and obliquity) and of the hips (abduction and rotation). In the stand-ing support, the child was positioned in an upright position with a 10° forward lean at the hips to allow functional activity (see Figures 3–5). The rates of compliance of the children using the equipment were rated as ‘recommended, moderate or minimal’ based on a child’s age and Chailey level of ability.
FIGURE 1: Measurement of the hip migration percentage and acetabular index.
FIGURE 2: (a) The standard position for an antero-posterior X-ray and (b) the adapted position for the child with tight hamstrings to control posterior pelvic tilt.
Effectiveness of postural management programmes
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
These data were collected by questionnaire at the three monthly reviews. These levels were taken from a previous retrospective study, which categorized use into three cat-egories according to the degree of postural control required and the length of time used (Pountney et al., 2002). Recommended use by fi ve years of age, a child at Chailey level 2 (supine) was to use a lying support at night, a seating system for approximately six hours per day and a standing support for one hour per day. A moderate use was the use of two items of equipment for a minimum of six hours per day; a minimal use was the use of one or no items of equipment. The length of time of use would also be a factor, e.g. having two items of equipment but using them less than six hours a day would be rated minimal.
Procedure
Clinicians identifi ed children who met the inclusion criteria for the study. An
FIGURE 3: Supine lying support.
FIGURE 4: CAPS 11 Seating System.
FIGURE 5: Chailey standing support.

Pountney et al.
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
information sheet was sent to the clinician for the parents to read and discuss together, and an informed consent was obtained by the researcher. The initial assessment included relevant past and present medical history, medications, current equipment, Chailey levels of ability, current treatments and issues affecting equipment provision, e.g. sleep patterns and refl ux. The child’s postural management requirements were discussed with the parents and local thera-pist, and were prescribed and fi tted accord-ing to each child’s clinical need.
The children were reviewed on a three monthly basis: the Chailey levels of ability were recorded, the equipment was adjusted and updated, and a questionnaire was com-pleted by the researcher or the parents detail-ing which equipment the child used and the amount of time spent in the equipment in the previous three months. Other relevant infor-mation relating to a child’s physical develop-ment was recorded. At fi ve years of age, each child was classifi ed on the GMFCS (Palisano et al., 1997).
At 30 months and fi ve years of age, the child’s paediatrician was approached to request a hip and pelvic X-ray. Information regarding positioning for the X-ray was sent to the radiography departments. X-rays were obtained and measured, and hip status was categorized as both hips safe, i.e. under 33%, one or both hips subluxed.
RESULTS
Fifty-two children were recruited to the study from health authorities in East and West Sussex, Kent, Surrey and London. Thirteen children withdrew from the study: seven died (a refl ection of the severity of their impairment and age), one for social reasons, one had developmental dysplasia of the hips, one had the diagnosis changed to
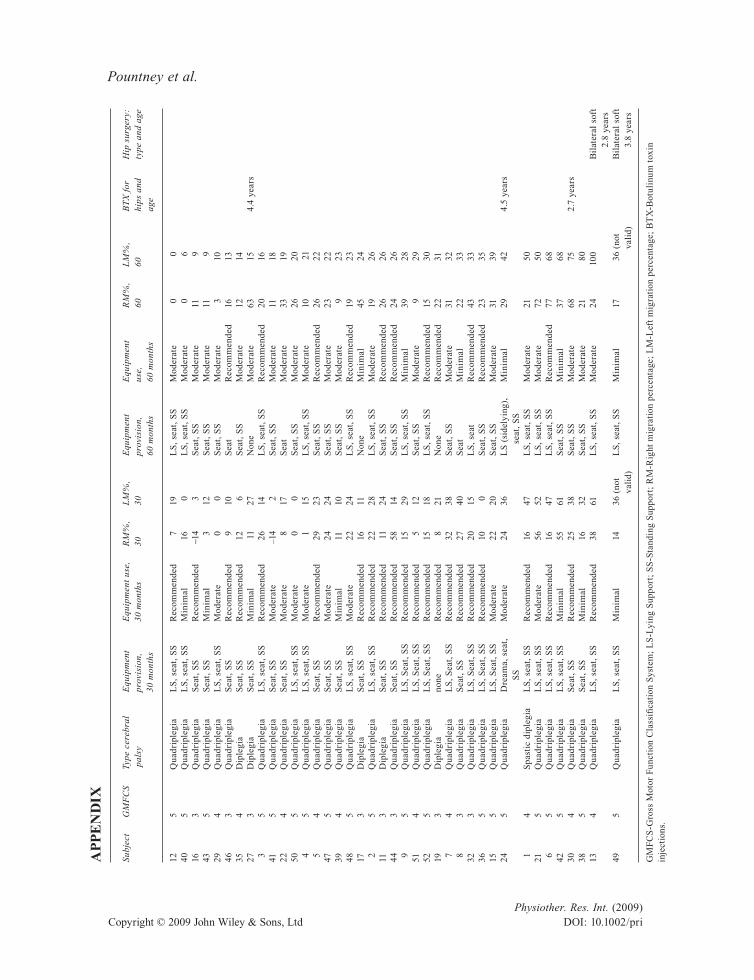
hemiplegia, two had on going ill health, and one child walked by age fi ve. Thirty-nine children were therefore included in this anal-ysis, 23 boys and 16 girls. Appendix 1 shows the characteristics of the sample: GMFCS, distribution of cerebral palsy, equipment provision, treatments and percentage hip migration. No data on the GMFCS in the historical control group were available as they were not in use at this time; however, all children were not walking at fi ve years and therefore would have been classifi ed at levels III–V.
Chailey levels of ability
The Chailey level of abilities in supine at 30 months ranged from levels 2 to 6, with 17 children (43.6%) at level 2 (unable to main-tain symmetry in supine) and 9 children (23.1%) at level 6 (able to roll and use hands in midline). By 60 months of age, 21 chil-dren (55.3%) were at level 2 in lying, and a further 2 (28.9%) had reached level 6.
Postural management equipment provision and use in the intervention group
The range of postural management equip-ment provided at 30 months and fi ve years of age included combinations of lying, stand-ing and seating supports, and is shown in Table 1.
Data on the use of equipment were col-lected from the questionnaires completed at each review point. The level of use at 30 and 60 months was averaged and categorized as ‘recommended, moderate or minimal use’ (see Table 2).
A Fisher’s exact test was used to compare the use of equipment and hip status. At fi ve years, there was a higher frequency of chil-dren with both hips not subluxed (<33%
Effectiveness of postural management programmes
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
migrated) using the equipment at recom-mended or moderate levels than those using the equipment at minimal amounts (two-tailed Fisher’s exact χ2 p = 0.024).
Migration percentage at 30 months and fi ve years in the historical control and intervention groups
In the intervention group, the age range at which the ‘30-month’ X-ray was taken extended from two to four years with a mean age of 2.6 years. For the fi ve-year X-ray, the mean age was 5.1 (range 4.1–5.8) years. This was because of X-rays being taken prior to request and further exposure to radiation was not justifi ed, diffi culties in organizing X-rays or non-attendance. All X-rays were valid for measurement, except for two, which had an excessive adduction on the left side.
There were no signifi cant differences among the migration percentage between the his-torical control and intervention groups at 60 months. Table 3 shows the mean and range of migration percentage at 30 and 60 months.
Migration percentages for both of a child’s hips are reported at fi ve years. In the intervention group, 59% of the children had both hips migrated less than 33%, and 41% had migration percentages greater than 33% in at least one hip. In the historical control group, 50% of the children had both hips migrated less than 33%, and 41% had migra-tion percentages greater than 33% in at least one hip. In the historical control group, 15% of the data were categorized as missing data and were described as either no ‘available X-ray’ or ‘no measurement acceptable from an X-ray’.
TABLE 1: Equipment provision at 30 months and fi ve years
Equipment Lying, seating andstanding support
Lying andseating support
Seating andstanding support
Seating only Other
30 months 22 (56.4%) 2 (5.1%) 14 (35.9%) 0 (0%) 1 (2.6%)Five years 15 (38.4%) 0 16 (41%) 4 (10.3%) 4 (10.3%)
TABLE 2: Averaged use of equipment at 30 months and fi ve years
Average use to 30 months and fi ve years
Recommendednumber (%)
Moderatenumber (%)
Minimalnumber (%)
30 months 22 (56.4%) 10 (25.6%) 7 (17.9%)Five years 11 (28.2%) 22 (56.4%) 6 (15.4%)
TABLE 3: Mean and range of migration measures at 30 and 60 months
Hip side and mo nths Intervention (mean and range) Historical control (mean and range)
Right, 30 17.6 (0–56) 20.7 (0–81)Left, 30 22.6 (0–61) 19.7 (0–87)Right, 60 25.9 (0–77) 28 (0–100)Left, 60 30.4 (0–100) 26.2 (0–100)

Pountney et al.
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
Comparison of hip problems at fi ve years between the control and intervention groups
At fi ve years of age, the intervention group was compared with a subset (n = 202) of the historical control group of children not walking at fi ve years defi ned as follows:
• had hip surgery and/or botulinum toxin A injection for the hips;
• had been prescribed a HASO by an orthopaedic surgeon; and/or
• having a hip migration percentage >32% (Scrutton and Baird, 1997; Scrutton et al., 2001).
Table 4 shows the comparison between the subset of the historical control group not walking at fi ve years (Scrutton et al., 2001) and the intervention group. In the historical control group of children who were not walking independently at fi ve years, 38.5% had a bilateral hip problem and 15.5% had a unilateral problem. In the intervention group, 10.3% had a bilateral problem and 25.6% had a unilateral problem. Although unilat-eral problems were greater in the interven-tion group, overall there was an 18.2% reduction in hip problems. There was a sig-nifi cant difference between the observed and expected frequencies of children in the historical control and intervention groups
with hip problems. Children in the interven-tion group were signifi cantly less likely to have hip problems (χ2 = 11.53, df = 2, p = 0.006).
Treatment for hip problems
Table 5 shows the frequency of children having bilateral and unilateral treatments, i.e. surgery, use of a HASO and/or botuli-num toxin injections, in both the historical control and intervention groups. Signifi -cantly less children in the intervention group received bilateral or unilateral treatment, and signifi cantly more had no treatment (two-tailed Fisher’s exact p = 0.001).
Table 6 shows the frequency and type of treatments of children in the historical control and intervention groups. Surgical treatment was reduced from 46% in the control group to 5.1% in the intervention group. No children in the intervention group used a HASO but three children received botulinum toxin injections into the muscles surrounding the hip. There was a signifi cant difference between the observed and expected frequency of children in the historical control and intervention groups having surgical interventions. Children in the intervention group were signifi cantly less likely to have a hip surgery (χ2 = 11.5322.91, df = 1, p ≤ 0.001).
TABLE 4: Frequency of bilateral and unilateral problems in the historical control and intervention groups
Group Historicalcontrol
Intervention
Bilateral problem 77 (38.1%) 4 (10.3%)Unilateral problem 32 (15.8%) 10 (25.6%)No problem 93 (46.1%) 25 (64.1%)Total 202 (100%) 39 (100%)
TABLE 5: Treatment for bilateral and unilateral problems
Treatment Control Intervention
Bilateral problem 65 (32.2%) 5 (13%)Unilateral 37 (18.3%) 0 (0%)No treatment 98 (48.5%) 34 (87%)Missing cases 2 (1%) 0 (0%)Total 202 (100%) 39 (100%)

Effectiveness of postural management programmes
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
DISCUSSION
These fi ndings indicate that children using postural management equipment up to the age of fi ve years at recommended or moder-ate levels had a signifi cantly greater chance of both hips being less than 33% migrated at fi ve years. Equipment use involves an ongoing commitment by families, carers, teachers and clinicians, and the length of the study, over fi ve years, meant that the use of equipment at times was somewhat variable because of illness and social/family situa-tions. Moderate use appears to be suffi cient to show a difference in outcomes; however, this has not been precisely quantifi ed.
The historical group had a substantial number of missing data on migration per-centage either because of a lack of X-ray or an unacceptable measurement. This number is likely to include hips, which could not be measured because of hip and pelvic posi-tions and may have had a confounding effect on the comparison between the historical control group and the intervention group.
The lying support was the least used item of equipment, with the majority of children using the seating and standing supports, which offer a more functional and inclusive position for activity. Many children with cerebral palsy have sleep problems including
the risk of refl ux and respiratory problems (Khan and Underhill, 2006). This may have impacted on the families’ reluctance to inter-fere with a child’s sleep routine, which might cause an increased risk of night-time distur-bance. The use of a lying support dropped between 30 and 60 months with nine fewer children using the support and is comparable with clinical practice.
Recent work by Soo et al. (2006), which found children at levels IV and V on the GMFCS, had hip subluxation rates of 69% and 90%, respectively, at a mean age of 11.7 years. Rates of displacement in the interven-tion group at levels IV and V were 10% and 23% at fi ve years, and this cohort will be followed to see if these levels are sustained over time in this cohort.
Treatment, particularly surgery, in the intervention group was reduced compared with that of the historical control group without an increase in hip migration per-centage. Over the period of the study, there have been changes in orthopaedic practice away from early soft tissue hip surgery; however, the large reduction is unlikely to be entirely due to change in practice. The fi ndings on use and migration percentage suggest that postural management equip-ment is a factor in this reduction. These fi ndings contrast with the fi ndings of the
TABLE 6: Comparison of treatment for hip problems in the control and intervention groups
Treatment Control group (number of children)
Intervention group(number of children)
Surgery 93 (46%) 2 (5.1%)Hip orthosis 48 (23.7%0 0 (0%)Botulinum toxin injections 0 (0%) 6 (15.4%)No treatment but >32% 55 (27.2%) 22 (56.4%)No treatment 6 (3%) 9 (23.1%)Total 202 (100%) 39 (100%)
Pountney et al.
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
Hagglund et al. (2005) study where surgery was the main intervention for hip dysplasia under fi ve years.
The reduction in bilateral hip problems may refl ect the position that the children adopted in the equipment, i.e. controlling a child’s hip and pelvis in neutral tilt, obliquity and rotation, and the hips in neutral ab/adduction and rotation. Applying forces to reduce asymmetry, the hip and pelvic posi-tions may lead to improved hip outcomes and have a protective effect for spinal cur-vature, but comparative studies are needed to determine this.
This study has focused on its role in the management of hip subluxation and suggests that the use of postural management equip-ment can play a role in the management of deformity besides the accepted role of improved postural control for functional activities (Pountney and Green, 2006).
Further research is required in the man-agement of hip dislocation in children with cerebral palsy, both for early intervention and in terms of long-term outcomes. Migra-tion percentage alone may not indicate a need for treatment but should be set in the context of a child’s pain and function or the postural effect on the spine. The views of children and their families on these inter-ventions need to be sought as different inter-ventions can affect the quality of life. Combinations of different approaches, such as postural management equipment, botuli-num toxin injections and surgery, may achieve long-term successful outcomes but requires collaborative working to maximize outcomes.
Limitations of the study included the use of a historical control group, which intro-duced, particularly, changes in surgical practice; the size of the cohort; and con-founding variables, which could not be controlled within the family setting.
This study suggests that the use of pos-tural management equipment in hip man-agement could reduce levels of subluxation and consequent surgery if introduced early and if used at recommended and moderate amounts. Recommendations would be in line with a consensus statement on the use of postural management programmes, which includes provision of postural management equipment at the earliest stages particularly in children at levels IV and V on the GFMCS (Gericke, 2006).
CONCLUSION
The early provision of postural management equipment has a role to play in reducing the levels of hip problems and therefore the need for treatment for hip subluxation/dislocation in children with cerebral palsy at fi ve years. However, there is a continuing risk of hip subluxation into adolescence, and infl uences affecting the long-term outcomes of inter-ventions need to be determined.
ACKNOWLEDGEMENTS
This study was funded by the Action Medical Research, the Märit and Hans Rausing Charitable Foundation, Rosetrees Trust, and other trusts and foundations who wish to remain anonymous.
The authors thank David Scrutton for his support and generosity in sharing his original data.
REFERENCES
Cooperman DR, Bartucci E, Dietrick E, Millar EA. Hip dislocation in spastic cerebral palsy: long term consequences. Journal of Pediatric Ortho-paedics 1987; 7: 268–276.
Cornell MS. The hip in cerebral palsy. Developmental Medicine and Child Neurology 1995; 37: 3–18.
Gericke T. Postural management for children with cerebral palsy: consensus statement. Develop-mental Medicine and Child Neurology 2006; 48: 244.
Green EM, Nelham RL. Development of sitting ability, assessment of children with a motor

Effectiveness of postural management programmes
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
handicap and prescription of appropriate seating systems. Prosthetics and Orthotics International 1991; 15: 203–216.
Green EM, Mulcahy CM, Pountney TE, Ablett B. The Chailey standing support for children and young adults with motor impairment: a developmental approach. British Journal of Occupational Therapy 1993; 56: 13–18.
Hagglund G, Andersson S, Duppe H, Lauge-Pedersen H, Nordmark E, Westbom L. Prevention of severe contractors might replace multilevel surgery in cerebral palsy: results of a population-based health care programme and new techniques to reduce spasticity. Journal of Pediatric Orthopae-dics part B 2005; 14: 269–273.
Hankinson J, Morton RE. Use of a lying hip abduc-tion system in children with bilateral cerebral palsy: a pilot study. Developmental Medicine and Child Neurology 2002; 44: 177–180.
Hodgkinson I, Jindrich ML, Duhaut P, Vadot JP, Metton G, Berard C. Hip pain in 234 non-ambulatory adolescents and young adults with cerebral palsy: a cross-sectional multicentre study. Developmental Medicine and Child Neurology 2001; 43: 806–808.
Khan Y, Underhill J. Identifi cation of sleep problems by questionnaire in children with severe cerebral palsy. Developmental Medicine and Child Neu-rology 2006 (Suppl); 48: 23.
Miller F, Bagg MR. Age and migration percentage as risk factors for progression in spastic hip disease. Developmental Medicine and Child Neurology 1992; 37: 449–455.
Morton JF, Brownlee MG, MacFadyen AK. The effects of progressive resistance training for chil-dren with cerebral palsy. Clinical Rehabilitation 2005; 19(3): 283–289.
Palisano R, Rosenbaum P, Walter S, Russell D, Wood E, Galuppi B. Development and reliability of a system to classify Gross Motor Function in children with cerebral palsy. Developmental Medicine and Child Neurology 1997; 39: 214–223.
Parrott J, Boyd RN, Dobson F, Lancaster A, Love S, Oates J, Wolfe R, Nattrass GR, Graham HK. Hip displacement in spastic cerebral palsy: repeatabil-ity of radiologic measurement. Journal of Pediat-ric Orthopaedics 2002; 22: 660–667.
Pountney TE, Green EM. Hip dislocation in cerebral palsy. British Medical Journal 2006; 332: 772–775.
Pountney TE, Mandy A, Green EM, Gard P. Man-agement of hip dislocation with postural
management. Child: Care, Health and Develop-ment 2002; 28: 179–185.
Pountney TE, Mandy A, Gard P. Repeatability and limits of agreement in measurement of hip migra-tion percentage in children with bilateral cerebral palsy. Physiotherapy 2003; 89: 276–281.
Pountney TE, Mulcahy CM, Clarke S., Green EM. Chailey Approach to Postural Management. Chailey Heritage Clinical Services, 2004.
Reimers J. The stability of the hip in children. A radiological study of the results of muscle surgery in cerebral palsy. Acta Orthopaedica Scandi-navica 1980 (Suppl); 184: 1–100.
Reimers J, Bialik V. Infl uence of femoral rotation on the radiological coverage of the femoral head in children. Pediatric Radiology 1981; 10: 215–218.
Schwartz L, Engel JM, Jensen MP. Pain in persons with cerebral palsy. Archives of Medical Reha-bilitation 1999; 80: 1243–1246.
Scrutton D, Baird G. Surveillance measures of the hips of children with bilateral cerebral palsy. Archives of Disease in Childhood 1997; 56: 381–384.
Scrutton D, Baird G, Smeeton N. Hip dysplasia in bilateral cerebral palsy: incidence and natural history in children aged 18 months to 5 years. Development Medicine and Child Neurology 2001; 43: 586–600.
Soo B, Howard JJ, Boyd RN, Reid SM, Lanigan A, Wolfe R, Riddihough D, Graham HK. Hip dis-placement in cerebral palsy. The Journal of Bone and Joint Surgery 2006; 88: 121–129.
Stott NS, Piedrahita L, AACPDM. Effects of surgical adductor releases for hip subluxation in cerebral palsy: an AACPDM evidence report. Develop-mental Medicine and Child Neurology 2004; 46: 628–645.
Turker RJ, Lee R. Adductor tenotomies in children with quadriplegic cerebral palsy: longer term follow-up. Journal of Pediatric Orthopaedics 2000; 20: 370–374.
Young NL, Wright JG, Lam TP, Rajaratnam K. Wind-swept deformity in spastic quadriplegic cerebral palsy. Pediatric Physical Therapy 1998; 10: 94–100.
Address correspondence to: Teresa E. Pountney, Chailey Heritage Clinical Services, North Chailey, East Sussex BN8 4JN, UK (E-mail: [email protected]).
(Submitted April 2008; accepted October 2008)
Pountney et al.
Physiother. Res. Int. (2009)Copyright © 2009 John Wiley & Sons, Ltd DOI: 10.1002/pri
AP
PE
ND
IX
Subj
ect
GM
FC
STy
pe c
ereb
ral
pal
syE
quip
men
tpr
ovis
ion,
30 m
onth
s
Equ
ipm
ent
use,
30 m
onth
sR
M%
,30
LM
%,
30E
quip
men
tpr
ovis
ion,
60 m
onth
s
Equ
ipm
ent
use,
60 m
onth
s
RM
%,
60L
M%
,60
BT
X f
orhi
ps a
ndag
e
Hip
sur
gery
:ty
pe a
nd a
ge
125
Qua
drip
legi
aL
S,
seat
, S
SR
ecom
men
ded
719
LS
, se
at,
SS
Mod
erat
e 0
040
5Q
uadr
iple
gia
LS
, se
at,
SS
Min
imal
16 0
LS
, se
at,
SS
Mod
erat
e 0
616
3Q
uadr
iple
gia
Sea
t, S
SR
ecom
men
ded
−14
3S
eat,
SS
Mod
erat
e11
943
5Q
uadr
iple
gia
Sea
t, S
SM
inim
al 3
12S
eat,
SS
Mod
erat
e11
929
4Q
uadr
iple
gia
LS
, se
at,
SS
Mod
erat
e 0
0S
eat,
SS
Mod
erat
e 3
1046
3Q
uadr
iple
gia
Sea
t, S
SR
ecom
men
ded
910
Sea
tR
ecom
men
ded
1613
354
Dip
legi
aS
eat,
SS
Rec
omm
ende
d12
6S
eat,
SS
Mod
erat
e12
1427
3D
iple
gia
Sea
t, S
SM
inim
al 1
127
Non
eM
oder
ate
6315
4.4
year
s 3
5Q
uadr
iple
gia
LS
, se
at,
SS
Rec
omm
ende
d26
14L
S,
seat
, S
SR
ecom
men
ded
2016
415
Qua
drip
legi
aS
eat,
SS
Mod
erat
e –
14 2
Sea
t, S
SM
oder
ate
1118
224
Qua
drip
legi
aS
eat,
SS
Mod
erat
e 8
17S
eat
Mod
erat
e33
1950
5Q
uadr
iple
gia
LS
, se
at,
SS
Mod
erat
e 0
0S
eat,
SS
Mod
erat
e26
20 4
5Q
uadr
iple
gia
LS
, se
at,
SS
Mod
erat
e 1
15L
S,
seat
, S
SM
oder
ate
10 2
1 5
4Q
uadr
iple
gia
Sea
t, S
SR
ecom
men
ded
2923
Sea
t, S
SR
ecom
men
ded
2622
475
Qua
drip
legi
aS
eat,
SS
Mod
erat
e24
24S
eat,
SS
Mod
erat
e23
2239
4Q
uadr
iple
gia
Sea
t, S
SM
inim
al11
10S
eat,
SS
Mod
erat
e 9
2348
5Q
uadr
iple
gia
LS
, se
at,
SS
Mod
erat
e22
24L
S,
seat
, S
SR
ecom
men
ded
1923
173
Dip
legi
aS
eat,
SS
Rec
omm
ende
d16
11N
one
Min
imal
4524
25
Qua
drip
legi
aL
S,
seat
, S
SR
ecom
men
ded
2228
LS
, se
at,
SS
Mod
erat
e19
2611
3D
iple
gia
Sea
t, S
SR
ecom
men
ded
11
24S
eat,
SS
Rec
omm
ende
d26
2644
3Q
uadr
iple
gia
Sea
t, S
SR
ecom
men
ded
5814
Sea
t, S
SR
ecom
men
ded
2426
95
Qua
drip
legi
aL
S,
Sea
t, S
SR
ecom
men
ded
1529
LS
, se
at,
SS
Min
imal
3928
514
Qua
drip
legi
aL
S,
Sea
t, S
SR
ecom
men
ded
512
Sea
t, S
SM
oder
ate
929
525
Qua
drip
legi
aL
S,
Sea
t, S
SR
ecom
men
ded
1518
LS
, se
at,
SS
Rec
omm
ende
d15
3019
3D
iple
gia
none
Rec
omm
ende
d 8
21N
one
Rec
omm
ende
d22
31 7
4Q
uadr
iple
gia
LS
, S
eat,
SS
Rec
omm
ende
d32
38S
eat,
SS
Mod
erat
e31
32 8
3Q
uadr
iple
gia
Sea
t, S
SR
ecom
men
ded
2740
Sea
tM
inim
al22
3332
3Q
uadr
iple
gia
LS
, S
eat,
SS
Rec
omm
ende
d20
15L
S,
seat
Rec
omm
ende
d43
3336
5Q
uadr
iple
gia
LS
, S
eat,
SS
Rec
omm
ende
d10
0S
eat,
SS
Rec
omm
ende
d23
3515
5Q
uadr
iple
gia
LS
, S
eat,
SS
Mod
erat
e22
20S
eat,
SS
Mod
erat
e31
3924
5Q
uadr
iple
gia
Dre
ama,
sea
t,S
SM
oder
ate
2436
LS
(si
dely
ing)
,se
at,
SS
Min
imal
2942
4.5
year
s
14
Spa
stic
dip
legi
aL
S,
seat
, S
SR
ecom
men
ded
1647
LS
, se
at,
SS
Mod
erat
e21
5021
5Q
uadr
iple
gia
LS
, se
at,
SS
Mod
erat
e56
52L
S,
seat
, S
SM
oder
ate
7250
65
Qua
drip
legi
aL
S,
seat
, S
SR
ecom
men
ded
1647
LS
, se
at,
SS
Rec
omm
ende
d77
6842
5Q
uadr
iple
gia
LS
, se
at,
SS
Min
imal
5561
Sea
t, S
SM
inim
al37
6830
4Q
uadr
iple
gia
Sea
t, S
SR
ecom
men
ded
2538
Sea
t, S
SM
oder
ate
6875
2.7
year
s38
5Q
uadr
iple
gia
Sea
t, S
SM
inim
al16
32S
eat,
SS
Mod
erat
e21
8013
4Q
uadr
iple
gia
LS
, se
at,
SS
Rec
omm
ende
d38
61L
S,
seat
, S
SM
oder
ate
24 1
00B
ilat
eral
sof
t 2.
8 ye
ars
495
Qua
drip
legi
aL
S,
seat
, S
SM
inim
al14
36 (
not
vali
d)L
S,
seat
, S
SM
inim
al17
36 (
not
vali
d)B
ilat
eral
sof
t 3.
8 ye
ars
GM
FC
S-G
ross
Mot
or F
unct
ion
Cla
ssifi
cat
ion
Sys
tem
; L
S-L
ying
Sup
port
; S
S-S
tand
ing
Sup
port
; R
M-R
ight
mig
rati
on p
erce
ntag
e; L
M-L
eft
mig
rati
on p
erce
ntag
e; B
TX
-Bot
ulin
um t
oxin
in
ject
ions
.
Copyright © 2022 FDOKUMEN




















