High degree of multi-drug resistance and hetero-resistance in pulmonary TB patients from Punjab...
8
MOLECULAR ASPECTS High degree of multi-drug resistance and hetero-resistance in pulmonary TB patients from Punjab state of India Parveen Kumar a , Veena Balooni a , Brijesh Kumar Sharma a , Virender Kapil a , K.S. Sachdeva b , Sarman Singh a, * a Division of Clinical Microbiology and Molecular Medicine, All India Institute of Medical Sciences, New Delhi 110 029, India b Central TB Division, Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India, New Delhi, India article info Article history: Received 11 June 2013 Received in revised form 3 October 2013 Accepted 14 October 2013 Keywords: MTBDRplus Line Probe Assay Mycobacterium tuberculosis Isoniazid Rifampicin summary Line Probe Assays (LPAs) have been recommended for rapid screening of MDR-TB. Aims of this study were (1) to compare the performance of LPA with standard Bactec MGIT 960 system and (2) to ascertain the pattern of genetic mutations in the resistance isolates. In phase I, a total of 141 Mycobacterium tuberculosis isolates from our routine laboratory were tested by LPA and Bactec MGIT 960 for DST. In phase II, 578 sputum specimens of suspected DR-TB patients were received from the Punjab state of India. Of them 438 specimens or their cultures were subjected to LPA. The presence of mutant bands with their corresponding wild type band was identified as “hetero-resistance”. In phase I, LPA showed high concordance with 96.4% positive agreement and 97.6% negative agreement with Bactec MGIT 960-DST. In phase II, 12 (2.7%) specimens were detected as invalid by LPA. Of the remaining 426 specimens, 184 (43.1%) had resistance to RIFand 142 (33.3%) to INH while 103 (24.1%) specimens showed resistance to both INH and RIF (MDR-TB) by LPA. Of the 142 INH resistant,113 (79.5%) showed mutations in katG and 29 (20.4%) in inhA. A high rate of hetero-resistance pattern was observed in rpoB gene (28.8%) and katG gene (9.8%). The most frequent mutation was S531L (81.1%) in rpoB region and S315T1 (100%) in katG gene. Ó 2013 Elsevier Ltd. All rights reserved. 1. Introduction Multi-drug resistant tuberculosis (MDR-TB) is considered when the causative agent Mycobacterium tuberculosis (M. tuberculosis) becomes resistant to at-least two first line anti-tubercular drugs e the isoniazid (INH) and rifampicin (RIF). India has an estimated 63,000 cases of notified MDR-TB, the highest in South-East Asia Region [1]. Though MDR-TB is seen in untreated cases also, the rate of MDR-TB in treated cases is very high [2]. The Global Plan to Stop TB 2011e2015 targets that all patients who have been previously treated for TB should be tested for MDR-TB using rapid tests by 2015 [3]. Drug susceptibility testing (DST) is conventionally performed using solid medium and is based on visible appearance of growth on the medium containing anti-tubercular drugs but these methods take longer time and are cumbersome. During this period patients may be inappropriately treated, drug-resistant strains may continue to spread and amplifying the resistance [4]. Given the number of people at risk the detection of drug susceptibility pattern of the pathogen must be rapid, inexpensive and easy to perform. Though in the last 10 years liquid culture based DST has reduced this time, still it is in weeks. Since resistance in M. tuberculosis is conferred by genetic mutation, molecular tech- niques (i.e. sequencing based) are preferred [5]. However, these techniques are cumbersome and costly for routine use. In the last 10 years two molecular methods have been endorsed by World Health Organization (WHO), in addition to the liquid culture based DST for rapid diagnosis and DST. These are Bactec MGIT 960 (Mycobacterium Growth Indicator Tube 960) liquid culture system [6], Line Probe Assay (LPA) [7] and Xpert MTB/RIF [8]. Government of India in its revised national TB control programme (RNTCP) has rolled out Bactec MGIT 960 and GenoType MTBDRplus in its na- tional programme while Xpert MTB/RIF is yet to be taken up by the national programme. Currently, two commercial LPA have been developed: INNO- LiPA Rif TB (LiPA) by Innogenetics, Zwijndrecht, Belgium and Ge- noType MTBDRplus by Hain Life Science GmbH, Nehren, Germany. The LiPA test can simultaneously detect M. tuberculosis and the presence of a mutation in the rpoB gene, which confers resistance to * Corresponding author. Tel.: þ91 11 2658 8484; fax: þ91 11 2658 8663, þ91 11 2658 8641. E-mail address: [email protected] (S. Singh). Contents lists available at ScienceDirect Tuberculosis journal homepage: http://intl.elsevierhealth.com/journals/tube 1472-9792/$ e see front matter Ó 2013 Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.tube.2013.10.001 Tuberculosis xxx (2013) 1e8 Please cite this article in press as: Kumar P, et al., High degree of multi-drug resistance and hetero-resistance in pulmonary TB patients from Punjab state of India, Tuberculosis (2013), http://dx.doi.org/10.1016/j.tube.2013.10.001
Transcript of High degree of multi-drug resistance and hetero-resistance in pulmonary TB patients from Punjab...

lable at ScienceDirect
Tuberculosis xxx (2013) 1e8
Contents lists avai
Tuberculosis
journal homepage: http : / / int l .e lsevierhealth.com/journals / tube
MOLECULAR ASPECTS
High degree of multi-drug resistance and hetero-resistance inpulmonary TB patients from Punjab state of India
Parveen Kumar a, Veena Balooni a, Brijesh Kumar Sharma a, Virender Kapil a,K.S. Sachdeva b, Sarman Singh a,*
aDivision of Clinical Microbiology and Molecular Medicine, All India Institute of Medical Sciences, New Delhi 110 029, IndiabCentral TB Division, Directorate General of Health Services, Ministry of Health and Family Welfare, Government of India, New Delhi, India
a r t i c l e i n f o
Article history:Received 11 June 2013Received in revised form3 October 2013Accepted 14 October 2013
Keywords:MTBDRplusLine Probe AssayMycobacterium tuberculosisIsoniazidRifampicin
* Corresponding author. Tel.: þ91 11 2658 8484; fa2658 8641.
E-mail address: [email protected] (S. Sing
1472-9792/$ e see front matter � 2013 Elsevier Ltd.http://dx.doi.org/10.1016/j.tube.2013.10.001
Please cite this article in press as: Kumar P,Punjab state of India, Tuberculosis (2013), h
s u m m a r y
Line Probe Assays (LPAs) have been recommended for rapid screening of MDR-TB. Aims of this studywere (1) to compare the performance of LPA with standard Bactec MGIT 960 system and (2) to ascertainthe pattern of genetic mutations in the resistance isolates. In phase I, a total of 141 Mycobacteriumtuberculosis isolates from our routine laboratory were tested by LPA and Bactec MGIT 960 for DST. Inphase II, 578 sputum specimens of suspected DR-TB patients were received from the Punjab state ofIndia. Of them 438 specimens or their cultures were subjected to LPA. The presence of mutant bands withtheir corresponding wild type band was identified as “hetero-resistance”. In phase I, LPA showed highconcordance with 96.4% positive agreement and 97.6% negative agreement with Bactec MGIT 960-DST. Inphase II, 12 (2.7%) specimens were detected as invalid by LPA. Of the remaining 426 specimens, 184(43.1%) had resistance to RIF and 142 (33.3%) to INH while 103 (24.1%) specimens showed resistance toboth INH and RIF (MDR-TB) by LPA. Of the 142 INH resistant, 113 (79.5%) showed mutations in katG and29 (20.4%) in inhA. A high rate of hetero-resistance pattern was observed in rpoB gene (28.8%) and katGgene (9.8%). The most frequent mutation was S531L (81.1%) in rpoB region and S315T1 (100%) in katGgene.
� 2013 Elsevier Ltd. All rights reserved.
1. Introduction
Multi-drug resistant tuberculosis (MDR-TB) is considered whenthe causative agent Mycobacterium tuberculosis (M. tuberculosis)becomes resistant to at-least two first line anti-tubercular drugs ethe isoniazid (INH) and rifampicin (RIF). India has an estimated63,000 cases of notified MDR-TB, the highest in South-East AsiaRegion [1]. Though MDR-TB is seen in untreated cases also, the rateof MDR-TB in treated cases is very high [2]. The Global Plan to StopTB 2011e2015 targets that all patients who have been previouslytreated for TB should be tested for MDR-TB using rapid tests by2015 [3].
Drug susceptibility testing (DST) is conventionally performedusing solid medium and is based on visible appearance of growthon the medium containing anti-tubercular drugs but thesemethods take longer time and are cumbersome. During this periodpatients may be inappropriately treated, drug-resistant strains may
x: þ91 11 2658 8663, þ91 11
h).
All rights reserved.
et al., High degree of multi-dttp://dx.doi.org/10.1016/j.tub
continue to spread and amplifying the resistance [4]. Given thenumber of people at risk the detection of drug susceptibilitypattern of the pathogen must be rapid, inexpensive and easy toperform. Though in the last 10 years liquid culture based DST hasreduced this time, still it is in weeks. Since resistance inM. tuberculosis is conferred by genetic mutation, molecular tech-niques (i.e. sequencing based) are preferred [5]. However, thesetechniques are cumbersome and costly for routine use. In the last10 years two molecular methods have been endorsed by WorldHealth Organization (WHO), in addition to the liquid culture basedDST for rapid diagnosis and DST. These are Bactec MGIT 960(Mycobacterium Growth Indicator Tube 960) liquid culture system[6], Line Probe Assay (LPA) [7] and Xpert MTB/RIF [8]. Governmentof India in its revised national TB control programme (RNTCP) hasrolled out Bactec MGIT 960 and GenoType MTBDRplus in its na-tional programme while Xpert MTB/RIF is yet to be taken up by thenational programme.
Currently, two commercial LPA have been developed: INNO-LiPA Rif TB (LiPA) by Innogenetics, Zwijndrecht, Belgium and Ge-noType MTBDRplus by Hain Life Science GmbH, Nehren, Germany.The LiPA test can simultaneously detect M. tuberculosis and thepresence of amutation in the rpoB gene, which confers resistance to
rug resistance and hetero-resistance in pulmonary TB patients frome.2013.10.001

P. Kumar et al. / Tuberculosis xxx (2013) 1e82
RIF [9]. Several studies had reported the sensitivity of 95% orgreater, and nearly 100% specificity for RIF resistance [10]. It hasbeen seen that more than 95% of RIF resistant isolates harbor amutations within the 81-bp hot spot region of the rpoB gene [11].The GenoType MTBDRplus assay (referred here after as LPA) has anadditional advantage over the LiPA because it can detect mutationsin rpoB gene as well as mutations in katG gene and inhA gene [12].Moreover, LPA is able to detect hetero-resistance, which is definedas the co-existence of the susceptible and resistant bacteria in thesame specimen/culture [13,14]. Hetero-resistance is a preliminarystage towards full resistance which is difficult to detect usingconventional DST methods. Nevertheless, liquid culture based DSTremains the most reliable and standard method.
However, very few studies have been carried out in India, thattoo on a very few number of patients to evaluate the performanceof LPA vis-à-vis Bactec MGIT 960 liquid culture for DST [15].Moreover, to best of our knowledgewe have not found even a singlepublication from Punjab state of India related to the prevalence ofvarious genotypes of M. tuberculosis and their drug susceptibilitypattern. Hence, the present study was aimed (I) to compare theperformance of LPA and Bactec MGIT 960-DST on a significantlylarger sample size of mycobacterial isolates made from variousclinical samples obtained from the patients belonging to Delhi re-gion and (II) applying LPA directly on sputum samples from sus-pected MDR patients of a study naïve north-western region(Punjab) of India. The study also deciphers the pattern of mutationin M. tuberculosis obtained from these two different pools ofpatients.
2. Materials and methods
2.1. Study settings
The study was carried out in two phases, after certification oflaboratory by Government of India. In phase I, standardization of LPAin our local settings was done. For this, we tested 141M. tuberculosisisolateswith known resistance patterns by BactecMGIT 960first lineDST. The isolates were obtained from clinical specimens of patientsfrom Delhi region of India. These specimens were submitted to ourTB reference laboratory for culture and DST. All study participantsgave informed consent, as a standard routinediagnostic procedure ofthe laboratory. All Bactec MGIT 960-DST results were blinded to themicrobiologists performed the LPA. Inphase II, the prospective studywas carried out directly on clinical specimens for rapid screening ofMDR cases under the programmatic management of drug resistantTB (PMDT), plan B of RNTCP, India.
2.2. Specimens
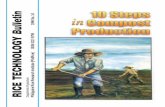
A total of 578 sputum specimens of suspected drug resistant-TB(DR-TB) patients from designated microscopy centers (DMCs) ofeight districts (Amritsar, SAS Nagar, Ludhiana, Sangrur, Patiala,Gurdaspur, Jalandhar and Rupnagar) of Punjab state were sent toour TB Laboratory for LPA testing. The specimens were transportedfrom the DMCs to the laboratory in the cold chain within 72 h ofcollection as per the guidelines of PMDT [16]. Only smear positivespecimens (1þ to 3þ) or Bactec MGIT 960 positive cultures wereused for LPA testing as per the manufacturer’s protocol (HAINLifescience, MTBDRplusV2_0212_304A-02-02.pdf) [17]. Thedetailed algorithm of the study protocol is shown in Figure 1.
2.3. Processing of specimens
The sputum specimens were processed using the modifiedPetroff’smethod [18]. In brief, about 3e4ml of specimenwasmixed
Please cite this article in press as: Kumar P, et al., High degree of multi-dPunjab state of India, Tuberculosis (2013), http://dx.doi.org/10.1016/j.tub
with an equal volume of 0.5% NALC-4% NaOHmixture in 50ml ridgecapped round bottom processing tube. The mixture was vortexedand incubated at 37�C for 10 min. Then mixture was neutralizedwith phosphate buffer (pH 6.8) up to a total volume of 50 ml andcentrifuged at 10,000 rpm for 10 min. The pellet was re-suspendedin 2 ml of the phosphate buffer and smears were prepared forZeihleNeelsen staining. The smears were graded for acid fast bacilli(AFB) positivity as per WHO standard guidelines routinely adoptedin all TB laboratories, as 1þ, 2þ or 3þ. If the entire smear exami-nation (100 oil fields) demonstrated 1e9 AFB, the specimen wasconsidered scantyþ and subjected to Bactec MGIT 960 culture and,if culture flashed positive it was subjected to LPA.
2.4. Bactec MGIT 960 culture and DST
After processing, 500 ml of the decontaminated specimens wereinoculated in Bactec MGIT 960 culture tubes containing 800 mlmixture of oleic acid, albumin, dextrose and catalase (OADC) andpolymyxin B, amphotericin B, nalidixic acid, trimethoprim, azlo-cillin (PANTA) supplement as per the manufacturer’s instructions(Becton Dickinson Diagnostic Instrument Systems, Sparks, MD,USA). The left over sediments of the decontaminated specimenswere stored at �20�C. All the manipulation of the specimens wasperformed under the Class II-B biosafety cabinet in a BSL-2B labo-ratory. In phase I, mycobacterial isolates obtained in Bactec MGIT960 culture, were identified as M. tuberculosis by in-house devel-oped multiplex PCR assay [18] before subjecting them to 4 first line(streptomycin, isoniazid, rifampicin and ethambutol) SIRE DST byBactec MGIT 960 system and the results were continuously moni-tored by BD Epi-centre� software V 5.75A [19].
2.5. GenoType MTBDRplus (LPA) testing
The LPA was performed according to the manufacturer’s pro-tocol (MTBDRplusV2_0212_304A-02-02.pdf) [17]. The test is basedon the DNA hybridization on strip technology and has three steps:DNA extraction, multiplex polymerase chain reaction (PCR)amplification, and reverse hybridization. All the three steps of LPAtesting were performed as per the WHO recommendations [7]. Inbrief: DNA extraction was performed in the BSL-2 laboratory,master mix preparation in a second room with UV chamber, andPCR amplification and hybridization were performed in anotherroom. Five hundred microliter of decontaminated specimen and1 ml of Bactec MGIT 960 culture was used for the DNA extractionusing the GenoLyse kit (GenoLyse_1011_51610-08-02.pdf) [20].Amplification of the targets was performed by adding 35 ml of PNMmix, 10 ml of reaction buffer and 5 ml of template DNA in each re-action mix except the negative control. PCR reaction was run in anMTC-100 thermal cycler (MJ Research, USA) at the amplifyingconditions of initial denaturation at 95 �C for 15 min and 10 cyclesof 95�C for 30 s, 58�C for 2 min and additional 30 cycles of dena-turation at 95�C for 25 s, annealing at 53�C for 40 s, elongation at70�C for 40 s; and a final extension at 70�C for 8 min. Afteramplification, the hybridization was carefully performed in theTwinCubator as per the manufacturer’s instructions. Briefly, 20 ml ofbiotin labeled amplicon with 1 ml of hybridization buffer was hy-bridized on the strip. After the washing with stringent buffer,streptavidin-alkaline-phosphatase conjugate was added to thestrip’s membrane. An alkaline phosphatase mediated staining re-action was allowed to occur and the strips were allowed to air dryfor the interpretation of the results. During the evaluation of LPA onmycobacterial isolates and clinical samples, the Bactec MGIT 960-DST results were blinded to the person who carried out LPA (PK &VB). For quality control, M. tuberculosis H37Rv (TMC-102) was runas positive control and sterile molecular grade water was used as a
rug resistance and hetero-resistance in pulmonary TB patients frome.2013.10.001

Study Settings
Phase I Phase II
Routine Laboratory isolates of M. tuberculosis from Delhi, India (n=141)
MDR(n=58)
Bactec MGIT 960DST
RIFR
(n=6)SEN
(n=65)INHR
(n=12)
54 MDR2 RIFR
2 INHR
6 RIFR 65 SEN9 INHR
3 INHS
Suspected DR -TB sputum samplesfrom Punjab, India (n=578)
AFB +ve(n=455)
MTBDRplus438 (403+35)
MGIT culturen=155
AFB -ve(n=123)
3+ve(n=131)
2+ve(n=100)
Sc. +ve(n=52)
1+ve(n=172)
Culture +ve(n=35)
Culture -ve(n=140)
MDRn=103 (24.1%)
RIFR
n=81 (19.0%)SEN
n=203 (47.6%)INHR
n=39 (9.1%)
Gene region/ Mutated codon
n=76 (73%) [rpoB]n= 93 (90.3%) [katG]
Hetero-resistance n=27 (26.2%) [rpoB]n=10 (9.3%) [katG]
Gene region/Mutated codon
n=55 (67%)
Hetero-resistance n=26 (32%)
Gene region/Mutated codonn=35 (89.7%)
Hetero-resistance n=4 (10.2%)
MTBDRplus
INVALIDn=12 (2.7%)
MTBDRplus results 426
Figure 1. Study design and major observations. In phase I, 141 M. tuberculosis isolates with known Bactec MGIT 960-DST patterns were tested by GenoType MTBDRplus assay (LPA).In phase II, the prospective study was carried out directly on sputum specimens for rapid screening of MDR cases under the PMDT (plan B) of RNTCP, India, which shows a higherprevalence of hetero-resistance pattern in the Punjab state of India.
P. Kumar et al. / Tuberculosis xxx (2013) 1e8 3
negative control in each run. For the external quality control, pro-ficiency panels with blinded codes were sent to the NationalReference Laboratory (NRL), National JALMA Institute of Leprosyand other Mycobacterial Diseases, Agra. The panels passed theproficiency testing and laboratory accredited as IntermediateReference Laboratory (IRL) for the LPA testing by RNTCP, India. Alltests and procedures at our laboratory undergo random externalquality assessment (EQA) with NRLs and Supra National ReferenceLaboratories of India.
2.6. Interpretation of results
The results were interpreted according to manufacturer’s in-structions [17]. Briefly, the banding pattern comprising only wildtype (WT) bands without mutant bands on the strip was inter-preted as sensitive. A strain was interpreted resistant if it showed:absence of one or more WT bands, presence of any mutant bandwith or without the presence of complementary WT band. Anisolate that revealed hybridization to mutant as well as to thecorresponding (WT) probe was considered heterogeneous popu-lation of bacteria or a mixed infection of a sensitive and a resistantstrain. If the (WT) 8 band was faint as compared to the amplifica-tion control and no corresponding mutant band was seen, in thatcase also the strain was considered sensitive.
2.7. DNA sequencing
The verification of hetero-resistance was done by thesequencing of rpoB and katG gene. Amplicons of 543 bp rpoB generegion and 455 bp of katG 315 promoter regions were targeted forsequencing using the primers rpoB-f (CTTGCACGAGGGTCAGACCA),rpoB-r (ATCTCGTCGCTAACCACGCC), katG-f (AACGACGTCGAAA-CAGCGGC) and katG-r (GCGAACTCGTCGGCCAATTC) as describedpreviously [21]. The PCR mixture consisted of 1X PCR Buffer II,
Please cite this article in press as: Kumar P, et al., High degree of multi-dPunjab state of India, Tuberculosis (2013), http://dx.doi.org/10.1016/j.tub
0.2 mM concentrations of each deoxynucleotide triphosphate(dNTP), 5 pmol of each primer, and 1 U of AmpliTaq Gold poly-merase (Applied Biosystems) and 5 ml of DNA template. The PCRreaction was first activated by incubation at 95�C for 15 min. Thereaction mixture was then subjected to 35 cycles of amplification:denaturation at 95�C for 30 s, annealing at 60�C for 30 s, andelongation at 72�C for 30 s and followed by a final extension step for7 min at 72�C. PCR products were purified with QIAquick PCR pu-rification kits (Qiagen) and sequencing of the PCR products wasdone commercially (Applied Biosystems, US) to avoid bias. Thesequencing results were analyzed by using BioEdit software version7.1.9 and sequence alignment was done by using clustal Wat EMBL-EBI website. The analysis of the rpoB and katG sequencing resultswere compared with the M. tuberculosis H37Rv (NC_000962).
2.8. Statistical analysis
The results of LPA were analyzed and compared with BactecMGIT 960-DST as gold standard. The data were statically analyzedto calculate the sensitivity, specificity, positive agreement andnegative agreement. All the LPA and Bactec MGIT 960-DST datawere maintained and analyzed on MS Excel 7.0. Sequence analysiswork was done by above mentioned bioinformatics tools.
3. Results
3.1. Performance of GenoType MTBDRplus (LPA) on M. tuberculosiscultures
A total of 141 clinical isolates of M. tuberculosis obtained fromBactec MGIT 960 were tested for first line anti-TB DST. Out of these,58 isolates were MDR, 6 RIF mono-resistant, 12 INHmono-resistantand 65 isolates were susceptible to these drugs (Tables 1 and 2).Considering the phenotypic DST method as the gold standard, the
rug resistance and hetero-resistance in pulmonary TB patients frome.2013.10.001

P. Kumar et al. / Tuberculosis xxx (2013) 1e84
LPA had sensitivity of 93.1% (54/58) with positive agreementof 96.4% for MDR-TB and sensitivity of 96.8% (62/64) for RIF resis-tance with positive agreement of 98.4%. For INH resistance thesensitivity of LPA was 92.8% (65/70) with positive agreement of96.2%. All susceptible isolates were also susceptible in LPA (97.3%sensitivity and 98.6% positive agreement). The specificity fordetecting RIF, INH or multi-drug resistant isolates was 100%(Tables 1 and 2). The negative agreement for the MDR detectionwas 97.6%.
The frequencies of mutations found in MDR and mono-resistantisolates are shown in Table 3. As mentioned above among the 64phenotypically RIF resistant isolates, 62 isolates also showedresistance banding pattern in LPA. The most prevalent mutations inrpoB gene identified were: S531L in 33.8% (21/62) isolates, 526e529 in 25% (16/62) isolates, H526D in 17.7% (11/62), H526Y, 530e533, 516e519 of each in 3.2% (2/62) isolates and D516V in 1.6% (1/62) isolates (Table 3). The mixed pattern was seen in 14.5% (9/62)isolates, where the most frequent mutation was S531L (77%, 7/9).
Among 70 phenotypically INH resistant culture isolates, 65 werealso found to be INH resistant by LPA. Of these 87.6% (57) showedmutations in katG gene and 12.3% (8) showed mutations in inhAgene. The most frequent katG gene mutation was S315T1, in 84.6%(55/65 isolates), whereas inhA gene mutation at position C15T wasseen in 7.7% (5/65 isolates), �15/116 in 4.6% and mutation at codon315 was observed at low frequency (3%) (Table 3).
3.2. Performance of GenoType MTBDRplus (LPA) on sputumspecimens
In phase II, a total of 578 sputum specimens of suspected DR-TBpatients from Punjab state of India were processed in our labora-tory under the PMDT (plan B) of RNTCP as shown in the flow chart(Figure 1). The Punjab state is located in the north-western regionof the country and adjoins the Punjab province of Pakistan. Of the578 sputa from MDR-TB suspected cases, 78.7% (455/578) weredetected as smear AFB positive and 21.2% (123/578) smear negative.Among 455 smear positives, 131 (28.8%) specimens were AFB 3þ;100 (22%) AFB 2þ; 172 (37.8%) AFB 1þ; and 52 (11.4%) scantyþ. LPAwas performed on 403 smear positive specimens and 35 (out of 52scanty positive samples) Bactec MGIT 960 culture positive samples,as shown in the flow chart (Figure 1).
Of the 438 specimens (breakup as given in above paragraph), 12(2.7%) specimens did not show TUB band, and were considered asinvalid test for evaluation. Hence, remaining 426 were furtheranalyzed for DST and gene mutation patterns. Of the 426, 203(47.6%) were sensitive to both INH and RIF.
A total of 103 (24.1%) specimens showed resistance to both INHand RIF and classified as MDR-TB. Interestingly, RIF mono-resistance was seen in 81 of 426 (19%), unlike routine isolateswhere the rate of RIF mono-resistance was only 5.6% (8 of 141).However, 39 (9.1%) specimens were detected as INH mono-resistant by LPA.
Table 1Performance of Line Probe Assay (MTBDRplus) and Bactec MGIT 960 in the drugsusceptibility testing against primary anti-tubercular drugs on Delhi samples.
MTBDRplus Bactec MGIT 960
MDR RIF mono-resistant
INH mono-resistant
Pan-sensitive
Total
MDR 54 e e e 54RIF mono-resistant 2 6 e e 8INH mono-resistant 2 e 9 e 11Pan-sensitive 0 e 3 65 68Total 58 6 12 65 141
Please cite this article in press as: Kumar P, et al., High degree of multi-dPunjab state of India, Tuberculosis (2013), http://dx.doi.org/10.1016/j.tub
The most prevalent mutation in RIF resistant specimens wasabsence of wild type band (WT8) 530e533 in 30.9% (57/184)specimens. The frequency of this mutation was more in RIF mono-resistant (43.2%) as compared to MDR (21%). Forty two (22.8%)specimens showed the corresponding S531L mutation (31% in MDRand 12.3% in RIF mono-resistant). The mutation detected at thecodon 513e519 was seen in 4.3%; H526Y in 2.7% and 510e513 in2.1% specimens, whereas other mutations were observed at lowlevel (<2%). In our study a high (28.8%, 53 of 184) prevalence ofhetero-resistance (mix pattern) was observed in the Punjab spec-imens. The most frequent mutation was S531L (81.1%) followed byH526Y (16.9%) and D516V (7.5%). However, 3 unidentified combi-nations of mutations were also observed. These combinations weremissing wild type bands WT1, and WT3, WT1 and WT8, WT7 andWT8 (Table 4).
One hundred forty two (33.3%) specimens showed resistant toINH. Of these, 79.5% (113/142) revealed mutations in katG gene and20.4% (29/142) in inhA gene. The two mutations in katG gene:S315T1 (42.2%) and 315 (26%) were most prevalent Fourteen pa-tients harbored hetero-resistant M. tuberculosis (9.8%) that showedS315T1 (100%) mutation bands only.
When comparing the mutations in two regions, the prevalenceof S531L mutation was higher in Delhi (33.3%) than Punjab region(22.8%). However, this mutation was more frequent is RIF mono-resistant isolates from Delhi (50%) compared to the Punjab region(12.3%). The loss of WT bands was responsible for the RIF resistance29.6% in Delhi and 45.1% in Punjab region. However, prevalence of.mutation bands was 53.1% in Delhi samples and 27.1% in Punjabsamples which were RIF resistant. The loss of WT bands wasobserved more frequently in INH resistance cases in Punjab. Apartfrom these differences, a higher prevalence of hetero-resistance inrpoB gene (28.8%) was observed in the Punjab region. Moreover,hetero-resistance in katG gene was observed in 9.8%, while no suchpattern was observed in Delhi region (Tables 3 and 4).
3.3. Confirmation of hetero-resistance by sequencing
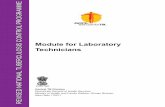
The co-existence ofWTandmutated sequences in rpoB and katGgene region was confirmed by sequencing results considering it asgold standard. In sequencing results the two peaks: one WT andanother mutant base at the resistance associated codons wereobserved which confirmed the hetero-resistance (Figure 2). Out of62 RIF and 14 INH hetero-resistant strains detected by LPA, 38 and 9strains were sequenced for the confirmation of hetero-resistantpattern at specific codon in rpoB and katG gene region, respec-tively (Table 5). The rpoB, sequencing showed mutant base (TTG)with another peak of corresponding WT base (TCG) and wild typecodon (TCG) with double peak of mutant base (TTG) at 531 codon(Figure 2a and b). Hetero-resistance detected at codon 526 and 516showed double signals of WT and mutant base at their corre-sponding codons (Table 5). One specimens found harboring dualmutations in LPA (mutation 2A and 2B) also showed mixture ofboth mutations (TAC, GAC) with WT base (CAC) (Figure 2d). In katGhetero-resistant samples, the peaks of mutation (ACC) were mixedwith WT (AGC) at the 315 codon. Thus, occurrence of mixture ofpeaks of WT and mutation base in same sample at specific codonconfirmed the hetero-resistant (Table 5, Figure 2).
4. Discussion
Diagnosis of MDR-TB by conventional DST is time consumingand cumbersome. Recently, molecular methods for DST have beendeveloped which overcome these limitations. The most valuablemolecular methods are LPA and Xpert MTB/RIF. WHO recommendsthe implementation of LPA and Xpert MTB/RIF for initial diagnosis
rug resistance and hetero-resistance in pulmonary TB patients frome.2013.10.001

Table 2Concordance between Line Probe Assay (MTBDRplus) and Bactec MGIT 960 based drug susceptibility test results in Delhi samples.
MTBDRplus Bactec MGIT 960
INH RIF INH þ RIF Sensitive
Resistant (70) Sensitive (71) Resistant (64) Sensitive (77) MDR (58) Non-MDR (83) Resistant (76) Sensitive (65)
Resistance 65 (92.8%) 0 62 (96.8%) 0 54 (93.1%) 0 74 (97.3%) 0Sensitive 5 (7.1%) 71 (100%) 2 (3.2%) 77 (100%) 4 (6.9%) 83 (100%) 2 (2.7%) 65 (100%)Total 141 141 141 141
Table 4Pattern of gene mutations in sputum samples obtained from suspected MDR-TBpatients of Punjab.
Gene Mutationpattern
Gene region/Mutatedcodon
MDR isolates(103)
RIF mono-resistant (81)
INH mono-resistant(39)
rpoB DWT2 510e513 3 (2.9%) 1 (1.2%) e
DWT3 513e517 1 (0.9%) 1 (1.2%) e
DWT7 526e529 1 (0.9%) 1 (1.2%) e
DWT8 530e533 22 (21.3%) 35 (43.2%) e
DWT1, 3 e 1 (0.9%) 1 (1.2%) e
DWT1, 8 e 1 (0.9%) e e
DWT2, 3 510e517 2 (1.9%) e e
DWT3, 4 513e519 5 (4.8%) 3 (3.7%) e
DWT4, 5 516e522 1 (0.9%) 1 (1.2%) e
DWT5, 6 518e525 e 1 (1.2%) e
DWT7, 8 e 1 (0.9%) e e
MUT1 D516Vmixed 1 (0.9%) 1 (1.2%) e
MUT2A H526Ymixed e 4 (3.8%) e
P. Kumar et al. / Tuberculosis xxx (2013) 1e8 5
and DST in patients suspected of MDR-TB. The LPA is widely andglobally used on clinical samples and isolates [5,22e24]. The per-formance of LPA on M. tuberculosis cultures is reported to correlatevery well with DST performed by Bactec MGIT 960. In previousstudies, the sensitivity of the LPA for the detection of RIF resistanceis reported to vary from 95% to 99% [15,24,25]. Its performance inour settings showed high sensitivity (96.8%) and specificity (100%)for detecting RIF resistance, but somewhat lower (92.8%) sensitivityfor INH resistance, most probably due to multiple mutationsinvolved in INH resistance. Moreover, the assay showed 93.1%sensitivity and 100% specificity for MDR isolates. In our study, onlyin 4 phenotypically MDR isolates, there was discordance betweenBactec MGIT 960-DST and LPA-DST. In these 4 cases Bactec MGIT960 showed MDR but mutation analysis by LPA showed that 2isolates had mutations in rpoB gene and 2 in katG and these wereclassified as RIF and INHmono-resistant, respectively, by LPA. Thus,overall positive agreement for RIF (also considered as surrogate ofMDR) was 96.4% as reported by others [26e28]. Phenotypic INHmono-resistant was also missed in 3 isolates and were detected assensitive by LPA. This indicates that in these isolates other muta-tions imparted the resistance which are not targeted by LPA [29].The high rate of RIF resistance detection can be explained by thewell-known fact that RIF resistance is highly associated with mu-tations in the 81 base pair region of the rpoB gene [23,25] and thatmutations outside this location are rare [30e32].
In RIF resistant isolates the S531L mutation was the mostprevalent (33.8%). Though not many studies are available forcomparison but our findings are in concordance with three previ-ous studies published from India [15,33,34]. In these studies thismutation has been reported ranging from 15% to 41%. While, fromother high burden countries the frequency of this mutation hasbeen reported upto 75% [25,26,35]. In INH resistant isolates S315T1mutation in katG region was the most (84.6%) common. In otherstudies also it has reported in the range of 50e95% [11,35e37].
On the basis of its high accuracy, in phase II the LPA was per-formed directly on sputum specimens from suspected MDR-TBpatients, under plan B of PMDT. Our results showed that 97.3%
Table 3Pattern of gene mutations in clinical isolates obtained from routinely screenedpulmonary TB patients of Delhi region.
Gene Mutationpattern
Gene region/Mutated codon
MDR isolates(54)
RIF mono-resistant (8)
INH mono-resistant (11)
rpoB DWT3, 4 513e519 1 (1.9%) e e
DWT7 526e529 15 (29.4%) 1 (16.5%) e
DWT8 530e533 2 (3.8%) e e
DWT7, MUT2A H526Y 2 (1.9%) e e
DWT7, MUT2B H526D 9 (16.6%) 2 (33.3%) e
MUT2A H526Ymixed 2 (3.8%) e e
MUT3 S531Lmixed 5 (9.8%) 2 (16.5%) e
DWT8, MUT3 S531L 17 (33.3%) 4 (50%) e
katG DWT 315 2 (3.7%) e e
DWT, MUT1 S315T1 46 (85.1%) e 9 (83.3%)inhA DWT1 �15/116 2 (3.7%) e 1 (8.3%)
DWT, MUT1 C15T 4 (7.4%) e 1 (8.3%)
Please cite this article in press as: Kumar P, et al., High degree of multi-dPunjab state of India, Tuberculosis (2013), http://dx.doi.org/10.1016/j.tub
test results were valid if the LPA was run on smear positive speci-mens. Several authors have reported 98.6%e100% (47/47) validityof test results with smear positive samples [23,38]. This differencecould be because the number of sample size in these studies wasvery small, while our study included very large sample size. In ourstudy, the distributions of mutations identified both in rpoB andkatG genes were evidently different from other studies [26,39]. Wefound S531L rpoB gene mutation in 30.9% RIF resistant specimens,which is a lower frequency of mutations as reported (46e79%) byothers [26,39]. But the loss of WT bands observed was much higherthan reported by Tolani et al. (2012) [34]. In INH resistant speci-mens, significantly higher prevalence of mutations in katG gene(79.5%) was seen as compared in inhA gene (20.4%). This observa-tion is in agreement with other reports where in katG gene muta-tions is reported in 46%e90% specimens as compared to the inhAgene mutations (20%e42%) [37,40,41].
Our significant finding was high rate of hetero-resistancepattern observed in these samples; which was 28.8% in rpoB
MUT3 S531Lmixed 22 (21.3%) 19 (23.4%) e
MUT1 & 2A D516Vmixed,H526Ymixed
1 (0.9%) 1 (1.2%) e
MUT3 & 2A S531Lmixed,H526Ymixed
e 1 (1.2%) e
MUT2A, 2B H526Ymixed,H526D
1 (0.9%) e e
MUT2A, DWT7 H526Y 4 (3.8%) 1 (1.2%) e
MUT2B, DWT7 H526D 1 (0.9%) e e
MUT3, DWT 7 526e529,531Lmixed
1 (0.9%) e e
MUT3, DWT8 S531L 32 (31%) 10 (12.3%) e
MUT2A, DWT1 H526Ymixed 1 (0.9%) e e
MUT3, DWT8,3,4
S531L,513e519
1 (0.9%) e e
katG DWT 315 26 (25%) e 11 (28.2%)DWT, MUT1 S315T1 44 (42.7%) e 16 (41%)MUT1 S315T1 mixed 10 (9.7%) e 4 (9.8%)DWT, MUT2 S315T2 2 (1.9%) e e
inhA DWT1 �15/116 11 (10.6%) e 2 (5.1%)DWT1, MUT1 C15T 10 (9.7%) e 6 (15.3%)
rug resistance and hetero-resistance in pulmonary TB patients frome.2013.10.001

Figure 2. Confirmation of hetero-resistance by sequencing of rpoB and katG gene showing dual peaks of wild-type (WT) sequence (TCG) and mutant base (TTG) at codon 531 ofrpoB. (c) Dual peaks of wild-type (WT) sequence (CAC) and mutant base (TAC) at codon 526 of rpoB. (d) Mixed peaks of wild-type (WT) sequence (CAC) with dual mutation (TAC/GAC) at codon 526 of rpoB. (e) Dual peaks of wild-type (WT) sequence (AGC) with mutant base (ACC) at codon 315 of katG.
P. Kumar et al. / Tuberculosis xxx (2013) 1e86
region and 9.8% in katG region. The sequencing analysis of rpoB andkatG gene regions confirmed the hetero-resistance. There are onlyvery few publications on hetero-resistance from whole world andonly one from India [34]. The Uzbekistan [13] study reported only20% hetero-resistance, while study published from Pakistan [14]showed 4% hetero-resistance. The highest hetero-resistance wasreported by Tolani et al. [34] from India only. This lone studypublished by Tolani et al. from Mumbai (South west India) showed34% hetero-resistance. It is noteworthy that fromMumbai only highrates of XDR and TDR-TB have been reported [42]. The differencebetween hetero-resistance rates in samples from Punjab and theMumbai is veryminimal and it may be scary to think that in comingdays Punjab may also face similar fate of high XDR and TDR-TB. Thestudy area (Punjab state of India) is least explored for drug resis-tance using such large studies and this is probably the first study ofits kind. In recent years Punjab state of India has become a newfound center for drug use and more than 20% young adults areengaged in drug abuse; both snuffing and intravenous (personalcommunication). Since there are no similar studies, it is difficult toprovide any better explanation. However, it is interesting that studyfrom Pakistan which is demographically adjoining area to Punjab
Please cite this article in press as: Kumar P, et al., High degree of multi-dPunjab state of India, Tuberculosis (2013), http://dx.doi.org/10.1016/j.tub
did not show high rate of hetero-resistance. The most plausiblereason for that could be uncertainty of sampling sites and verysmall sample size. [14] However, in the Mumbai study D516Vmutation was the most frequent while in our study commonestmutationwas S531L and D516V was seen only in 7.5% specimens. Itcould be because they studied the specimen collected from the fourDOTS centres which are located in the urban area of Mumbai, whileour samples came from the 8 different rural districts of Punjabstate. This could be a differential factor in two areas.
The development of hetero-resistance can occur in two ways:the co-existence of two sub-populations (sensitive and resistant) ofsame M. tuberculosis strain or two separate strains of sensitive andresistant M. tuberculosis occurring simultaneously in the samesample. Similarly, Hofmann-Thiel et al. [13] reported that in 71%cases of hetero-resistance was due to the presence of mix pop-ulations of different genotypes of M. tuberculosis. However, singlestrain of Beijing genotype was responsible for hetero-resistance in29% cases [13]. This finding signifies that high rate of hetero-resistance complicates the treatment and control strategies. Therate of hetero-resistance is related to the level of prevalence of DR-TB in particular regions [43]. Thus, in present study high rate of
rug resistance and hetero-resistance in pulmonary TB patients frome.2013.10.001

Table 5Hetero-resistance detection by LPA and sequencing.
Hetero-resistant by LPA Sequencing
LPA pattern (n) Hetero-resistant codon Codon pattern n
MUT3 (48) S531L mixed TCG þ TTG mixed 29/29MUT2A (6) H526Ymixed CAC þ TAC mixed 5/5MUT1 (2) D516Vmixed GAC þ GTC mixed 1/1MUT3 & 2A (1) S531Lmixed, H526Ymixed TCG þ TTG mixed
CAC þ TAC mixed1/1
MUT2A, 2B (1) H526Ymixed, H526Dmixed CAC þ TAC mixedCAC þ GAC mixed
1/1
MUT1 & 2A (2) D516Vmixed, H526Ymixed nd e
MUT3, DWT7 (1) 526e529, 531Lmixed TCG þ TTG mixed 1/1MUT2A, DWT1 (1) H526Ymixed nd e
MUT1 (14) S315T1 mixed AGC þ ACC mixed 9/9
nd e not done.
P. Kumar et al. / Tuberculosis xxx (2013) 1e8 7
rpoB hetero-resistance may be due to the higher prevalence of RIFresistance than INH. Also, the evolution of resistance is due to se-lective pressure of inadequate therapy. In our study majority ofpatients were either relapse cases on category-II treatment or oncategory-I treatment for more than 2 months. These strains notonly cause recrudescence in the same patient but get transmittedmore successfully to the others. We know that after Cat-I treatmentmany patients show initial clinical improvement but later on theirclinical condition worsens. Hetero-resistance explains such phe-nomenon very well where sensitive populations initially more innumber and major cause of illness get eradicated but later on theresistant population arise either from a different parent cell or fromthe resistant sister cells multiplying in un-competitive mannerleading to aggravation of the clinical condition. Not only thesestrains cause renewed disease in the same patient but get trans-mitted more successfully to the others [13].
In this study, mutations in the coding region 530e533(WT8þS531L) in rpoB gene and the S315T mutation of the katGgene were observed most frequently in the drug resistance strains.However, S531L mutation was higher in the specimens of MDRcases (31%) compared to the RIF mono-resistant cases (12.3%). Asmentioned above that�95% of RIF resistant strains carry mutationswithin 81-bp region of the rpoB gene [11], very few of these mu-tations have been tested for their phenotypic characters. Our re-sults show that S531L, H526D and D516V gene mutations wereresponsible for developing the high level of acquired resistance[44,45]. Earlier also these mutations have been associated withhigh levels of RIF resistance with MIC value of �100 mg/ml [46,32].However, mutations in codons 511, 516, 518 and 522 can result in alower resistance to RIF [32,44,47].
Molecular DST by LPA and Xpert-MTB/RIF have been globallyevaluated and reported the sensitivity of 95% or greater and nearly100% specificity with phenotypic DST. Moreover, unlike Xpert-MTB/RIF, LPA able to detect hetero-resistance at very low level of mixpopulation (1:100) [13]. This may not be identified by phenotypicDST as low amount of resistance bacteria. Molecular DST can bedirectly apply on the clinical specimens and low number of mix-tures of resistant and sensitive bacilli present in specimens can bedetect by the molecular methods. This may not be identified byphenotypic DST as low amount of resistant bacteria are oftenovergrown by majority population giving “sensitive” phenotypicDST results [43,34]. However, Folkvardsen et al. (2012) reportedphenotypic DST is more sensitive than LPA and sequencing indetecting the 1% INH resistant M. tuberculosis [48].
In the comparative analysis, we found a significant difference inthe prevalence of mutations between Delhi vs. Punjab regions ofIndia (Tables 3 and 4). The prevalence of S531Lmutationwas higherin Delhi than Punjab region. However, high rate of hetero-resistance was observed in samples obtained from Punjab region.
Please cite this article in press as: Kumar P, et al., High degree of multi-dPunjab state of India, Tuberculosis (2013), http://dx.doi.org/10.1016/j.tub
Earlier studies have also shown that the nature and frequency ofmutations in clinical specimens vary considerably according to thegeographical location [49] but very little information is available onspecific mutational patterns from India. Also, Nation-wide andState-wide representative data on prevalence of mutations in DR-TB are lacking. Therefore, we emphasize that efforts should befocused towards continued surveillance for DR-TB cases.
The performance of the LPA in our setting showed high agree-ment with BactecMGIT 960-DSTwhichwas similar to that reportedpreviously, with high sensitivity and specificity for detection ofdrug resistance [27,36,39]. We found that the LPAwas able to detect24.1% MDR-TB in clinically suspected cases of MDR-TB from Punjabstate. This was on expected lines as Jain et al. [50] have also re-ported that in treated cases the rate of MDR-TB is 19.8% while intreatment naïve cases MDR is <5% and the rate of mono-drugresistance (27.3%) was also high [2]. We also found high fre-quency of mutations in MDR-TB suspected cases: S531L, 530e533,H526Y and D516V for RIF resistance, S315T1 and 315 in katG geneand C15T and �15/116 inhA gene for INH resistance. A high rate ofhetero-resistance pattern was observed in rpoB gene (28.8%) andkatG gene (9.8%). We found that apart from the ability of rapiddetection of MDR isolates, LPA plays a significant role in thedetection of mono-resistance. Its significance was noteworthy indetecting the combination of mutations and occurrence of hetero-resistance found in DR isolates that cannot be identified by BactecMGIT 960-DST. Moreover, the test has a short turnaround time. Inconclusion, the LPA assay has been validated as a rapid and reliablefirst-line diagnostic test for direct as well as indirect DST. Theoverall performance of LPA showed very high agreement withconventional liquid culture based DST. Thus, it is very useful tool forthe management of TB.
Acknowledgments
The authors would like to thank all district TB officers (DTOs)and staff of the Designated Microscopy Centers (DMCs) of Punjab,to recruit the TB patients and sending samples to us.We thank FIND(Foundation for Innovative New Diagnostics) for providingMTBDRplus test kits and consumables for carrying out this studyunder the PMDT plan B of RNTCP. We also wish to thank BiomeriuxIndia for providing TwinCubators free of cost to us. The authors alsothankMr. Manitosh for the help in sequence analysis andMr. VinodKumar for his technical assistance.
Ethical approval
Not required.
Funding
None.
Competing interests
None declared.
References
[1] World Health Organization. Tuberculosis in the South-East Asia Region: theregional report. Geneva: WHO; 2012. SEA/TB/338. Retrieved from: http://whothailand.healthrepository.org/handle/123456789/1430.
[2] Revised National Tuberculosis Control Programme. Response to challenges ofdrug resistant TB in India January 2012 (Update 2012). Retrieved from: http://www.tbcindia.nic.in/pdfs/RNTCP%20Response%20DR%20TB%20in%20India%20-%20Jan%202012%20update.pdf; 2012.
[3] Stop TB Partnership. The global plan to stop TB 2011e2015: transforming thefight towards elimination of tuberculosis. Geneva, Switzerland: WHO Press;
rug resistance and hetero-resistance in pulmonary TB patients frome.2013.10.001

P. Kumar et al. / Tuberculosis xxx (2013) 1e88
2010. Retrieved from: http://www.stoptb.org/assets/documents/global/plan/TB_Global Plan ToStopTB2011-2015.pdf.
[4] Singh P, Katoch VM. Multi-drug resistant tuberculosis: current statusand emerging tools for its management in India. J Commun Dis 2006;38:216e29.
[5] Makinen J, Marttila HJ, Marjamäki M, Viljanen MK, Soini H. Comparison of twocommercially available DNA line probe assays for detection of multidrug-resistant Mycobacterium tuberculosis. J Clin Microbiol 2006;44:350e2.
[6] World Health Organization. Use of liquid TB culture and drug susceptibilitytesting (DST) in low and medium-income settings. Geneva: World HealthOrganization; 2007.
[7] World Health Organization. Policy statement. Molecular line probe assay forrapid screening of patients at risk of multidrug-resistant (MDR) TB. Geneva.Retrieved from: http://www.who.int/tb/features_archive/policy_statement.pdf; 2008.
[8] World Health Organization. Policy statement: automated real-time nucleic acidamplification technology for rapid and simultaneous detection of tuberculosisand rifampicin resistance: Xpert MTB/RIF system. Retrieved from: http://www.who.int/tb/features_archive/xpert_rapid_tb_test/en/index.html; 2011.
[9] Rossau R, Traore H, De Beenhouwer H, Mijs W, Jannes G, De Rijk P, Portaels F.Evaluation of the INNO-LiPA Rif TB assay, a reverse hybridization assay for thesimultaneous detection of Mycobacterium tuberculosis complex and its resis-tance to rifampin. Antimicrob Agents Chemother 1997;41:2093e8.
[10] Morgan M, Kalantri S, Flores L, Pai M. A commercial line probe assay for therapid detection of rifampicin resistance in Mycobacterium tuberculosis: asystematic review and meta-analysis. BMC Infect Dis 2005;5:62.
[11] Telenti A, Honore N, Bernasconi C, March J, Ortega A, Heym B, Takiff HE,Cole ST. Genotypic assessment of isoniazid and rifampin resistance in Myco-bacterium tuberculosis: a blind study at reference laboratory level. J ClinMicrobiol 1997;35:719e23.
[12] Hain Lifescience GmbH. GenoType MTBDRplus, version 1.0 [product insert].http://www.hain-lifescience.com/pdf/304xx_pbl.pdf; 2007. Nehren, Germany.
[13] Hofmann-Thiel S, van Ingen J, Feldmann K, Turaev L, Uzakova GT,Murmusaeva G, Soolingen D, Hoffmann H. Mechanisms of hetero resistance toisoniazid and rifampin of Mycobacterium tuberculosis in Tashkent, Uzbekistan.Eur Respir J 2009;33:368e74.
[14] Farooqi JQ, Khan E, Alam SJM, Ali A, Hasan Z, Hasan R. Line probe assay fordetection of rifampicin and isoniazid resistant tuberculosis in Pakistan. J PakMed Assoc 2012;62:767e72.
[15] Singhal R, Arora J, Lal P, Bhalla M, Myneedu VP, Behera D. Comparison of lineprobe assay with liquid culture for rapid detection of multidrug resistance inMycobacterium tuberculosis. Indian J Med Res 2012;136:1044e7.
[16] Revised National Tuberculosis Control Programme. Guidelines on program-matic management of drug resistant TB (PMDT) in India, May 2012. Retrievedfrom: http://www.tbcindia.nic.in/pdfs/Guidelines%20for%20PMDT%20in%20India%20-%20May%202012.pdf; 2012.
[17] Hain Lifescience GmbH, Nehren, Germany. GenoType MTBDRplus, version 2.0[product insert] http://www.hain-lifescience.de/en/instructions-for-use.html.
[18] Gopinath K, Singh S. Multiplex PCR assay for simultaneous detection anddifferentiation of Mycobacterium tuberculosis, Mycobacterium avium com-plexes and other mycobacterial species directly from clinical specimens. J AppMicrobiol 2009;107:425e35.
[19] Becton and Dickinson, USA. BACTEC MGIT-960 SIRE kit for the anti-mycobacterial susceptibility testing of Mycobacterium tuberculosis. Retrievedfrom: http://www.bd.com/ds/technicalCenter/clsi/clsi-960sire.pdf.
[20] Hain Lifescience GmbH, Nehren, Germany. GenoLyse [product insert]. http://www.hain-lifescience.de/en/instructions-for-use.html.
[21] Campbell PJ, Morlock GP, Sikes RD, Dalton TL, Metchock B, Starks AM,Hooks DP, Cowan LS, Plikaytis BB, Posey JE. Molecular detection of mutationsassociated with first- and second-line drug resistance compared with con-ventional drug susceptibility testing of Mycobacterium tuberculosis. Anti-microb Agents Chemother 2011;55:2032e41.
[22] Cavusoglu C, Turhan A, Akinci P, Soyler I. Evaluation of the GenoType MTBDRassay for rapid detection of rifampin and isoniazid resistance in Mycobacte-rium tuberculosis isolates. J Clin Microbiol 2006;44:2338e42.
[23] Hillemann D, Weizenegger M, Kubica T, Richter E, Niemann S. Use of thegenotype MTBDR assay for rapid detection of rifampin and isoniazid resis-tance in Mycobacterium tuberculosis complex isolates. J Clin Microbiol2005;43:3699e703.
[24] Miotto P, Piana F, Cirillo DM, Migliori GB. Genotype MTBDRplus: a further steptoward rapid identification of drug-resistantMycobacterium tuberculosis. J ClinMicrobiol 2008;46:393e4.
[25] Huyen MNT, Tiemersma EW, Lan NTN, Cobelens FGJ, Dung NH, Dinh NS,Buu TN, Kremer K, Hang PT, Caws M, O’Brien R, Soolingen DV. Validation ofthe GenoType� MTBDRplus assay for diagnosis of multidrug resistant tuber-culosis in South Vietnam. BMC Infect Dis 2010;10:149.
[26] Barnard M, Albert H, Coetzee G, O’Brien R, Bosman ME. Rapid molecularscreening for multidrug-resistant tuberculosis in a high-volume public healthlaboratory in South Africa. Am J Respir Crit Care Med 2008;177:787e92.
[27] Ling D, Zwerling A, Pai M. GenoType MTBDR assays for the diagnosis ofmultidrug-resistant tuberculosis: a meta-analysis. Eur Respir J 2008;32:1165e74.
[28] Albert H, Bwanga F, Mukkada S, Nyesiga N, Ademun P, Lukyamuzi G, Haile M,Hoffner S, Joloba M, O’Brien R. Rapid screening of MDR-TB using molecularLine Probe Assay is feasible in Uganda. BMC Infect Dis 2010;10:41.
Please cite this article in press as: Kumar P, et al., High degree of multi-dPunjab state of India, Tuberculosis (2013), http://dx.doi.org/10.1016/j.tub
[29] Feuerriegel S, Oberhauser B, George AG, Dafae F, Richter E, Rüsch-Gerdes S,Niemann S. Sequence analysis for detection of first-line drug resistance inMycobacterium tuberculosis strains from a high-incidence setting. BMCMicrobiol 2012;12:90.
[30] Heep MB, Brandstatter U, Rieger N, Lehn E, Richter S, Rusch-Gerdes,Niemann S. Frequency of rpoB mutations inside and outside the cluster I re-gion in rifampin-resistant clinical Mycobacterium tuberculosis isolates. J ClinMicrobiol 2001;39:107e10.
[31] Ozkutuk N, Gazi H, Surucuoglu S, Gunduz A, Ozbakkaloglu B. Characterizationof rpoB mutations by Line Probe Assay in rifampicin resistant Mycobacteriumtuberculosis clinical isolates from the Aegean region in Turkey. Jpn J Infect Dis2007;60:211e3.
[32] Bahrmand AR, Leonid PT, Hadizadeh TA, Yari S, Edward AG. High-levelrifampin resistance correlates with multiple mutations in the rpoB gene ofpulmonary tuberculosis isolates from the Afghanistan border of Iran. J ClinMicrobiol 2009;9:2744e50.
[33] Siddiqi N, Shamim M, Hussain S, Choudhary RK, Ahmed N, Prachee,Banerjee S, Savithri GR, Alam M, Pathak N, Amin A, Hanief M, Katoch VM,Sharma SK, Hasnain SE. Molecular characterization of multidrug-resistantisolates of Mycobacterium tuberculosis from patients in North India. Anti-microb Agents Chemother 2002;46:443e50.
[34] Tolani MP, D’souza TB, Mistry NF. Drug resistance mutations and hetero-resistance detected using the GenoType MTBDRplus assay and their implica-tion for treatment outcomes in patients from Mumbai, India. BMC Infect Dis2012;12:9.
[35] Rienthong D, Rienthong S, Boonin C, Woraswad S, Kasetjaroen Y. Rapiddetection for early appearance of rifampin and isoniazid resistance in Myco-bacterium tuberculosis. Siriraj Med J 2009;61:49e55.
[36] Nestani T, Kempker RK, Kalandadze I, Kurbatova E, Leonard ML,Apsindzelashvili R, Bablishvili N, Kipiani M, Blumberg HM. Use of a moleculardiagnostic test in AFB smear positive tuberculosis suspects greatly reduces timeto detection of multidrug resistant tuberculosis. PLoS One 2012;7:e31563.
[37] Mokrousov I, Narvskaya O, Otten T, Limenschenko E, Steklova L,Vyshnevskiy B. High prevalence of katG Ser315Thr substitution amongisoniazid-resistant Mycobacterium tuberculosis isolates from NorthwesternRussia, 1996e2001. Antimicrob Agents Chem 2002;46:1417e24.
[38] Miotto P, Piana F, Penati V, Canducci F, Migliori GB, Cirillo DM. Use of geno-type MTBDR assay for molecular detection of rifampin and isoniazid resis-tance in Mycobacterium tuberculosis clinical strains isolated in Italy. J ClinMicrobiol 2006;44:2485e91.
[39] Lacoma A, Sierra GN, Prat C, Ruiz-Manzano J, Haba L, Roses S, Maldonado J,Domínguez J. GenoType MTBDRplus assay for molecular detection of rifampinand isoniazid resistance in Mycobacterium tuberculosis strains and clinicalsamples. J Clin Microbiol 2008;46:3660e7.
[40] Kiepiela P, Bishop KS, Smith AN, Roux L, York DF. Genomic mutations in thekatG, inhA and aphC genes are useful for the prediction of isoniazid resistancein Mycobacterium tuberculosis isolates from Kwa-Zulu Natal, South Africa.Tuber Lung Dis 2000;80:47e56.
[41] Baker LV, Brown TJ, Maxwell O, Gibson AL, Fang Z, Yates MD, Drobniewski FA.Molecular analysis of isoniazid-resistant Mycobacterium tuberculosis isolatesfrom England and Wales reveals the phylogenetic significance of the ahpC-46A polymorphism. Antimicrob Agents Chem 2005;49:1455e64.
[42] Udwadia ZF, Amale RA, Ajbani KK, Rodrigues C. Totally drug-resistant tuber-culosis in India. Clin Infect Dis 2012;15:579e81.
[43] Nikolayevskyy V, Balabanova Y, Simak T, Malomanova N, Fedorin I,Drobniewski F. Performance of the Genotype� MTBDRPlus assay in thediagnosis of tuberculosis and drug resistance in Samara, Russian Federation.BMC Clin Pathol 2009;9:2.
[44] Williams DL, Spring L, Collins L, Miller LP, Heifets LB, Gangadharam PR,Gillis TP. Contribution of rpoB mutations to development of rifamycin cross-resistance in Mycobacterium tuberculosis. Antimicrob Agents Chemother1998;42:1853e7.
[45] Zaczek A, Brzostek A, Augustynowicz-Kopec E, Zwolska Z, Dziadek J. Geneticevaluation of relationship between mutations in rpoB and resistance ofMycobacterium tuberculosis to rifampin. BMC Microbiol 2009;9:10.
[46] Bobadilla-del-Valle M, Ponce-de-Leon A, Arenas-Huertero C, Vargas-Alarcon G, Kato-Maeda M, Small PM, Couary P, Ruiz-Palacios GM, Sifuentes-Osornio J. rpoB gene mutations in rifampin-resistant Mycobacterium tuber-culosis identified by polymerase chain reaction single-stranded conforma-tional polymorphism. Emerg Infect Dis 2001;7:1010e3.
[47] Bodmer T, Zurcher G, Imboden P, Telenti A. Mutation position and type ofsubstitution in the beta-subunit of the RNA polymerase influence in vitroactivity of rifampin-resistant Mycobacterium tuberculosis. J Antimicrob Che-mother 1995;35:345e8.
[48] Folkvardsen DB, Svensson E, Thomsen V, Rasmussen EM, Bang D, Werngren J,Hoffner S, Hillemann D, Rigoutsd L. Can molecular methods detect 1% isoni-azid resistance in Mycobacterium tuberculosis? J Clin Microbiol 2013;51:1596e9.
[49] Cavusoglu C, Hilmioglu S, Guneri S, Bilgic A. Characterization of rpoB muta-tions in rifampin-resistant clinical isolates of Mycobacterium tuberculosis fromTurkey by DNA sequencing and Line Probe Assay. J Clin Microbiol 2002;40:4435e8.
[50] Jain A, Mondal R, Prasad R, Singh K, Ahuja RC. Prevalence of multidrugresistant Mycobacterium tuberculosis in Lucknow, Uttar Pradesh. Indian J MedRes 2008;128:300e6.
rug resistance and hetero-resistance in pulmonary TB patients frome.2013.10.001