H.E.L.P. - Shop ICRC
794
H.E.L.P. Cours de santé publique pour la gestion Public Health Course in the Management of Humanitarian Aid Translated from the French by Martha Grenzeback International Committee of the Red Cross 19, avenue de la Paix 1202 Geneva, Switzerland T +41 22 734 60 01 F +41 22 733 20 57 E-mail: @icrc.org www.icrc.org © ICRC, October 2001 Original: French
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of H.E.L.P. - Shop ICRC

H.E.L.P.Cours de santé publique
pour la gestion Public Health Coursein the Managementof Humanitarian Aid
Translated from the French by
Martha Grenzeback
International Committee of the Red Cross19, avenue de la Paix1202 Geneva, SwitzerlandT +41 22 734 60 01 F +41 22 733 20 57E-mail: @icrc.org www.icrc.org© ICRC, October 2001
Original: French

iii
H.E.L.P.: Health Emergencies in Large Populations
ISBN 2-88145-116-0ª International Committee of the Red Cross
Geneva, 2001

TABLE OF CONTENTS
Preface V
Introduction VII
Module 1: Planning 1
Module 2: Food and Nutrition 47
Module 3: Environment 131
Module 4: Communicable Diseases 217
Module 5: Medical and Surgical Care 283
Module 6: The Health Care System 345
Module 7: Epidemiology 359
Module 8: From Emergencies to Development 435
Module 9: Protecting the Victimsof Armed Conflict 459
Module 10: Recapitulation and Conclusion 513
Module 11: Alphaland/Betaland 603
Module 12: Organization of the Course 759
Bibliography 775
iii

Preface
The HELP course was created by the International Committee of the Red Cross in
1986. At the time, it was designed to give health care professionals the skills they
needed to provide effective assistance to victims, particularly large populations, in
situations of armed conflict. This objective remains more relevant than ever.
Humanitarian interventions have become more complex and the constraints involved
in carrying them out are increasingly difficult to overcome. Training humanitarian
personnel thus continues to be a priority.
In situations of armed conflict, assistance is, of course, an important aspect of
humanitarian interventions. However, it is essential that assistance be linked to the
protection of victims and the re-establishment of their self-sufficiency. By establishing
these links, the HELP course gives participants a vision of a humanitarian strategy that
covers all the needs of victims while fully respecting their dignity.
From the outset the ICRC has offered the HELP course to professionals of all the
agencies involved in humanitarian crises, particularly those of the National Red Cross
and Red Crescent Societies. Thus, the ICRC has sought not only to share its
experiences, but also to establish a basis for more effective coordination in the field
among agents who have learned the same principles of action.
In the light of the interest in humanitarian problems shown by the universities, the
ICRC has consistently striven to promote the HELP course in academic circles,
particularly in schools of public health. Currently around 10 universities are directly
collaborating in the administration and teaching of the course. Several of them have
already incorporated the content of the course into their own curricula. In this way the
HELP course is helping to formalize instruction in humanitarian aid at the academic
level.
This manual describes in detail all the objectives of the HELP course. It will be
updated periodically by a group of experts comprising both health care professionals
and academic administrators.
I am proud of the excellent work already done by the ICRC team in this context, and
hope that the HELP course will continue to reflect the needs of victims, thereby
contributing to the appropriate training of health care personnel.
Jakob Kellenberger
President, International Committee of the Red Cross
Geneva, Switzerland
v

INTRODUCTION

ix
INTRODUCTION
The first HELP (Health Emergencies in Large Populations) course, lasting threeweeks, was held in Geneva in 1986 as a joint initiative of the InternationalCommittee of the Red Cross, the University of Geneva, and the World HealthOrganization. The purpose of the course is to give personnel involved inmass aidoperations the public-health tools that will enable them to plan coherent andappropriate relief actions. The course emphasizes the decision-making processmore than the actual technical aspects.
Since 1986, three strategic orientations have been established. The first has beento decentralize the course and offer it in areas close to relief operations in LatinAmerica, Asia, Eastern Europe, and Africa. The second has been to adopt asystematic policy of seeking collaboration with schools of public health incountries where the course is offered so that eventually these schools will be ableto take over the organization of the HELP course and integrate its content intheir standard curricula. This policy has also helped sensitize academic circles tohumanitarian problems in general. The third strategy has been to offer thecourse to people with solid experience in humanitarian operations but noprofessional training in the health field. This step hasmade it possible to broadenthe discourse on humanitarian aid and to give these ‘‘non-professionals’’ theknowledge they need for a better understanding of health operations, therebyfostering a stronger interdisciplinary approach in the field.
Since the ICRC is the main coordinator of the course, the needs of victims insituations of armed conflict are the primary focus. However, the tools developedin the course are applicable in other emergency situations as well. The subjectmatter has been divided into the following modules:
. general management principles
. food and nutrition
. water and environmental sanitation
. the control of communicable diseases
. the management of war-wounded victims
. the organization of health care facilities
. the application of epidemiology to emergency situations
. links between emergencies and development
HELP/SOS: INTRODUCTIONviii

. the role of international humanitarian law in the field of health
. recapitulation and conclusion.
GENERAL MANAGEMENT PRINCIPLES
The variety and complexity of emergency situations call for a rational approachto health problems. During the course, general management principles will beapplied with respect to:
. identification of health problems
. identification of constraints in situations of armed conflict
. establishment of priorities
. determination of objectives and strategies
. implementation of the measures required to achieve those objectives
. evaluation of results in terms of both cost-effectiveness and the impact on thehealth status of the target population
FOOD AND NUTRITION
This sphere often presents major problems in emergency situations. An overallview of the food system is imperative.
An assessment of needs and constraints, a well-designed programme, theimplementation of that programme, and a suitable monitoring system are allnecessary elements in any strategy to re-establish access to food resources.
The course will emphasize the following:
. assessment of food needs, data collection, anthropometry, identification ofvulnerable groups
. organizational methods, and implementation and monitoring of foodprogrammes
. organization of food distributions and management of nutrition rehabilita-tion centres
WATER AND ENVIRONMENTAL SANITATION
Environmental management is an absolute priority in emergency situations,which present increased risks attributable to precarious hygiene conditions,particularly in cases of overcrowding.
INTRODUCTION ix

xi
The course covers:
. methods for assessing environmental problems (water, shelter, energy, etc.)
. techniques for re-establishing access to clean water
. measures for providing victims with satisfactory housing
. the control of communicable-disease vectors.
The course will emphasize the ways that environmental sanitation measuresaffect health.
CONTROL OF COMMUNICABLE DISEASES
Controlling communicable diseases can be a major problem in emergencysituations, particularly when a population is living crowded together inprecarious hygiene conditions.
The course covers the following:
. strategies for controlling major communicable diseases (diarrhoeal diseases,cholera, tuberculosis, measles, intestinal parasites, etc.)
. development of programmes including, if possible, environmental sanitation,health education, community participation, and preventive and therapeuticmedical care, in the context of the constraints imposed by a disaster situation.
MANAGEMENT OF WAR-WOUNDED VICTIMS
The care of war wounds comprises several stages: first-aid measures, care beforeadmission to a hospital, evacuation, surgical treatment, and rehabilitation.
This module will examine:
. the importance of each stage, pointing out the impact that good-quality firstaid can have on reducing mortality among patients with war injuries
. the general principles of war surgery
. the connection with the issue of arms control.
ORGANIZATION OF HEALTH CARE FACILITIES
Disasters often generate a high demand for medical assistance that completelyoverwhelms existing facilities. TheHELP course covers the general organizationof health facilities in emergency situations, examining various types of action:
HELP/SOS: INTRODUCTIONx

. establishment of new medical facilities (hospitals, dispensaries, mobile units,etc.)
. standardization of treatment regimens and selection of essential drugscorresponding to identified needs.
Emphasis is laid on the role of primary health care in emergency situations.
EPIDEMIOLOGY AS APPLIED TO EMERGENCY SITUATIONS
Epidemiology is particularly important in emergency situations. Initially, itplays an essential role in the identification of health problems and the analysis ofpossible solutions. During the humanitarian operation, epidemiologicalmonitoring offers the possibility of modifying the original strategy as needed.
These basic epidemiological tools will be studied in the course:
. selection of health indicators
. sampling techniques
. data-collecting methods
. data analysis.
A special session will be arranged for study of the EPIINFO computer program,which allows computerized management of the data collected.
LINKS BETWEEN EMERGENCIES AND DEVELOPMENT
Emergency situations must be analysed from the overall perspective ofdevelopment. To that end, the course seeks:
. to identify points of human, social, economic, and ecological vulnerability
. to implement measures designed to prevent new disasters, or at least to limittheir effects in humanitarian terms.
THE ROLE OF INTERNATIONAL HUMANITARIAN LAWIN THE FIELD OF HEALTH
In a situation of armed conflict, populations must be protected.
The course will discuss the following points:
. basic principles of international humanitarian law: the Geneva Conventionsand their Additional Protocols
INTRODUCTION xi

xiii
. identifying groups at risk: displaced populations, hostage populations, ethnicand religious minorities isolated in a hostile environment
. making national or local authorities responsible for the protection of victims’access to essential services
. protecting populations living in particularly dangerous regions
. establishing the neutrality of certain zones or buildings in order to provide aidto victims under reasonably safe conditions
. the rights and duties of health care personnel.
RECAPITULATION AND CONCLUSION
This last module addresses general issues of humanitarian relief, such as:
. the impact of aid on the evolution of conflicts
. the role of health care personnel, particularly with respect to armaments andtheir effects on health
. evaluating the impact of humanitarian aid
. coordination between the various humanitarian agencies, and their relationswith political agencies.
This module will help participants to orient humanitarian aid within a globalcontext that includes the political environment.
Thematerial covered in this course was published by the ICRC inWar andPublicHealth in 1996. The teaching method is based on problem-solving. To that end,course planners have developed a simulation exercise presenting most of thehealth problems that may confront a population in a situation of armed conflict.Course participants are given the knowledge they need to analyse problemscorrectly and to propose context-appropriate solutions. Accordingly, eachmodule is divided into educational objectives falling into three categories. Eachobjective includes:
. a description
. identification of the category to which the objective belongs, namely:
. ‘‘framework’’—objective defining the framework and limits of themodule;
. ‘‘tool’’—objective giving participants the knowledge they need to operatewithin the previously defined framework;
HELP/SOS: INTRODUCTIONxii

. ‘‘practice’’—objective giving participants the opportunity to put theirnew knowledge into practice.
. formulation of the objective as it is presented to participants
. the teaching method used for the objective
. the anticipated length of the learning session
. references for purposes of recapitulation
. a link to the next objectives.
At the end of each module, the instructors will describe actual cases from theirown experience and analyse them together with the course participants.
Participants have access to a number of reference works to help them solveproblems. Where possible, links will be established with Internet databases.
The course material constitutes a set of inter-related educational objectives. Thismanual offers insight into the logic underlying the selection of educationalobjectives and their sequence.
Participants will evaluate the course after each module using several criteria: towhat degree the material presented meets their expectations, the quality of theeducationalmedia used, and the instructors’motivation and credibility. Anothermore general evaluation is carried out at the end of the course to rate the choice ofmodules, their sequence, and the relative emphasis they are given.
The participants’ achievements are evaluated in several ways:
. a multiple-choice test is used to determine what they have learned
. to evaluate their ability to make correct decisions in a given context, they areasked to write a summary report on the simulation, analysing the problemsand proposing solutions
. their behaviour is evaluated on the basis of their participation in discussionsand their ability to work as part of a team in their respective work groups.
This manual is designed to help the instructors of the HELP course understandthe philosophy, educational goals, and teaching method of the course. We hopeit will help them make sense of the complex assemblage of elements thatconstitutes a relief operation, and integrate their contributions harmoniously. Itwill also provide a basis of discussion for a working group charged with the taskof regularly updating the objectives of the course to reflect new public-healthdevelopments in emergency situations.
INTRODUCTION xiii

PLANNING
MODULE
1

3
LIST OF OBJECTIVES
. Outline a planning procedure to be applied throughout the course
. Describe the basic principles of an initial assessment
. Develop a method for setting priorities
. Break a general objective down into specific ones
. Develop a method of allocating responsibility for concrete tasks that permits aprecise identification of the resources that must be mobilized
. Define the concept of strategy, which is essential for directing an operation
. Define the concepts of evaluation and monitoring.
HELP/SOS: PLANNING2

DESCRIPTION OF THEPLANNING CYCLE
1. DESCRIPTION
Although many parameters cannot be controlled in emergency situations,especially during armed conflicts, every relief operation should follow as strict aplan as possible. This will give the actions undertaken a logical framework.
The planning sequence is as follows:
. definition of problems
. establishment of priorities
. determination of objectives
. development of a strategy
. mobilization of resources
. monitoring and evaluation of results.
These stages contain three steps:
. the process of initial assessment, which leads to the selection of the problemsthat should take priority;
. programme design—including the establishment of objectives, the develop-ment of a strategy, and the mobilization of resources;
. the evaluation of results.
The planning procedure proposed in this course does not claim to be morerigorous than others, but it has the advantage of being both simple and well-suited to health problems.
2. CATEGORY
Framework: outlining a planning procedure to be applied throughout the course.
3. FORMULATION
Describe with words, sentences or diagrams what the word ‘‘planning’’ means toyou.
PLANNING 3

5
4. TEACHING METHOD
Question assigned to each work group, which will present its answer to the fullassembly of participants.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Outline of the planning process, showing the sequence of theplanning stages in linear form to facilitate an understanding of theirlogical progression
. Box 2: Planning outline: cyclic presentation of programmes, underliningthe link between the evaluation and monitoring stage and theprogramme’s objectives
. Box 3: Planning outline: simplified version.
HELP/SOS: PLANNING4

PROBLEMS
PRIORITIES
OBJECTIVES
ACTIVITY PLANNING
MOBILIZATION OF RESOURCES
Logicalplanning
sequence in emergency
situations
Ass
essm
ent
Monitoring
Population’s state of health Local
services
Initial
Tactical
Normative
Str
ateg
y
Box 1
OUTLINE OF THEPLANNING PROCESS
PLANNING 55

7
INITIALASSESSMENT
EVALUATION/SUPERVISION
STRATEGY
IDENTIFICATION OF PROBLEMS
ESTABLISHMENT OF PRIORITIES
FORMULATION OF OBJECTIVES
MOBILIZATION OF RESOURCES
Programmes
Box 2
PLANNING OUTLINE
HELP/SOS: PLANNING66
INITIAL ASSESSMENT
PLAN OFACTION
EVALUATION/ MONITORING
Box 3
PLANNING OUTLINESIMPLIFIED VERSION
PLANNING 77
9
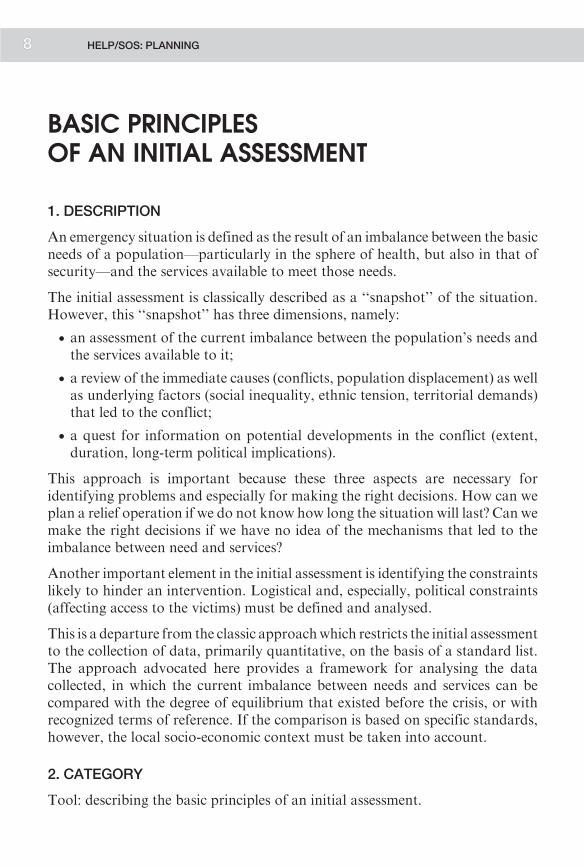
BASIC PRINCIPLESOF AN INITIAL ASSESSMENT
1. DESCRIPTION
An emergency situation is defined as the result of an imbalance between the basicneeds of a population—particularly in the sphere of health, but also in that ofsecurity—and the services available to meet those needs.
The initial assessment is classically described as a ‘‘snapshot’’ of the situation.However, this ‘‘snapshot’’ has three dimensions, namely:
. an assessment of the current imbalance between the population’s needs andthe services available to it;
. a review of the immediate causes (conflicts, population displacement) as wellas underlying factors (social inequality, ethnic tension, territorial demands)that led to the conflict;
. a quest for information on potential developments in the conflict (extent,duration, long-term political implications).
This approach is important because these three aspects are necessary foridentifying problems and especially for making the right decisions. How can weplan a relief operation if we do not know how long the situation will last? Can wemake the right decisions if we have no idea of the mechanisms that led to theimbalance between need and services?
Another important element in the initial assessment is identifying the constraintslikely to hinder an intervention. Logistical and, especially, political constraints(affecting access to the victims) must be defined and analysed.
This is a departure from the classic approachwhich restricts the initial assessmentto the collection of data, primarily quantitative, on the basis of a standard list.The approach advocated here provides a framework for analysing the datacollected, in which the current imbalance between needs and services can becompared with the degree of equilibrium that existed before the crisis, or withrecognized terms of reference. If the comparison is based on specific standards,however, the local socio-economic context must be taken into account.
2. CATEGORY
Tool: describing the basic principles of an initial assessment.
HELP/SOS: PLANNING8

3. FORMULATION
Plan an initial assessment in a given situation.
4. TEACHING METHOD
Assignment presented towork groups, whowill use theDelta exercise as the basisfor their response in the plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Concept of imbalance between victims’ needs and available services
. Box 2: Imbalance during a crisis: Defines the main components of an initialassessment, and introduces the notion of problems that result froman imbalance between needs and services. It also shows howdifferent factors contribute to the problems identified. The way inwhich these problems are likely to develop is the fourth componentof the initial evaluation
. Box 3: Examples of health problems related to an imbalance between needsand services
. Box 4: Influence of different sectors on the needs/services imbalance.
LINK WITH NEXT OBJECTIVES
This objective has helped the course participants to understand the definition ofan imbalance between health problems (malnutrition, tuberculosis, war injuries)and the inability of local services to cope with them. The next step will be to setpriorities.
PLANNING 9

11
ESSENTIALSERVICES
VICTIMS’NEEDS
Increase in needs associated with:
• Increased population
• Increased morbidity due to sanitary conditions
Emergence of new needs, such as treatment of war injuries
Deterioration in effectiveness of services:
• Insufficient means
• Abandonment of facilities by personnel for security reasons
• Disrupted organization
Destruction of medical facilities
Box 1
CONCEPT OF IMBALANCE BETWEENVICTIMS’ NEEDS
AND AVAILABLE SERVICES
HELP/SOS: PLANNING110

CAUSES DEVELOPMENT
ESSENTIALSERVICES
VICTIMS’NEEDS
The immediate causes are easy to identify: war, drought, etc.
The underlying causes are underdevelopment, ethnic tension, discrimination, etc.
The development of the situation depends on the political will to resolve an armed conflict, willingness to tackle the underlying causes of the crisis, the possibilities of mediation by the United Nations, response from the international community, etc.
Box 2
IMBALANCE DURING A CRISIS
PLANNING 111

13
ESSENTIALSERVICES
VICTIMS’NEEDS
Types of problems that may arise:
• Injured people going untreated
• Injured people without access to existing health facilities
• Injured people receiving inadequate care
• Population without access to safe water
Box 3
EXAMPLES OF HEALTH PROBLEMSRELATED TO AN IMBALANCE BETWEEN
NEEDS AND SERVICES
HELP/SOS: PLANNING112
ECONOMIC SECTOR
PO
LITI
CA
L S
EC
TOR
SO
CIO
-CU
LTU
RA
L S
EC
TOR
ECOLOGICAL ENVIRONMENT
ESSENTIALSERVICES
VICTIMS’NEEDS
Box 4
INFLUENCE OF DIFFERENTSECTORS ON THE
NEEDS/SERVICES IMBALANCE
PLANNING 113

15
SETTING PRIORITIES
1. DESCRIPTION
Setting priorities is a two-step procedure.
. The first step is to develop a simple method for establishing priorities on thebasis of:
. the magnitude of the health problems encountered, as expressed by thenumber of people affected, morbidity, mortality, and the impact onpublic health.
. the feasibility of intervention—meaning that a technical solution suitablefor the problems identified actually exists, and that there are noconstraints that might prevent the implementation of that solution.
. The second step is to examine the feasibility of applying this method to armedconflicts, since in such situations many parameters cannot be analysed (thenumber of people affected, for example, or the potential development ofconstraints impeding a technical solution that initially seemed appropriate).
Despite these restrictions with respect to armed conflicts, this method has theadvantage of presenting health problems in terms of their magnitude and thefeasibility of resolving them. Nevertheless, a health problem that seems to haveno immediately applicable solution due to objective constraints should notnecessarily be excluded. If technical action is impossible, then such measures asnegotiations with the authorities to gain access to victims, for example, become apriority. In other cases, seeking alternative technical solutions might be anobjective.
2. CATEGORY
Tool: developing a method of setting priorities.
3. FORMULATION
Identify the criteria that should be taken into account in establishing prioritieswith respect to health problems.
4. TEACHING METHOD
Assignment presented to work groups, followed by summary in plenary session.
HELP/SOS: PLANNING14

5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
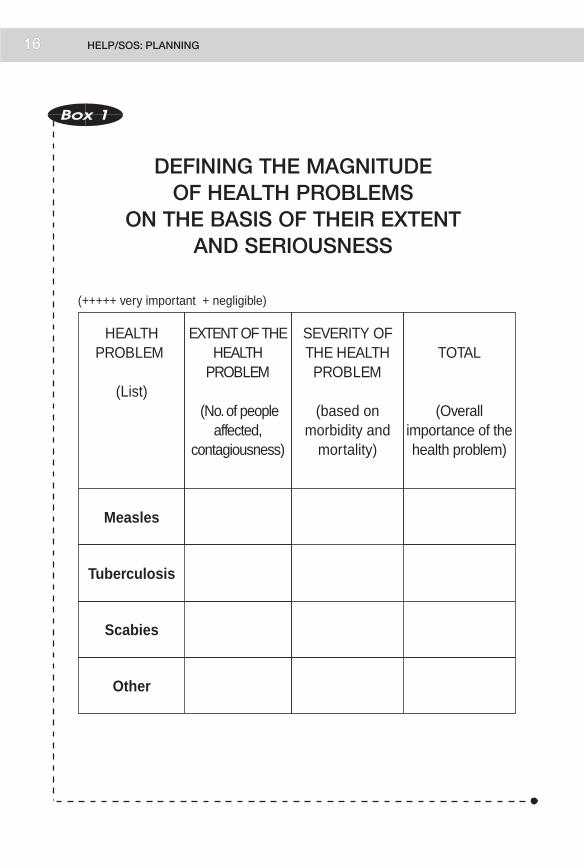
. Box 1: Defining the magnitude of health problems on the basis of theirextent and seriousness
. Box 2: Potential constraints in conflict situations that may limit the numberand effectiveness of solutions to health problems
. Box 3: Setting priorities: the magnitude of health problems as defined inBox 1 is balanced against potential constraints (Box 2) to determinethe feasibility of taking action.
LINK WITH NEXT OBJECTIVES
The next topic is the determination of objectives.
PLANNING 15
17
(+++++ very important + negligible)
EXTENT OF THE HEALTH
PROBLEM
(No. of people affected,
contagiousness)
Measles
Tuberculosis
Scabies
HEALTH PROBLEM
(List)
TOTAL
(Overall importance of the health problem)
Other
SEVERITY OF THE HEALTH PROBLEM
(based on morbidity and
mortality)
Box 1
DEFINING THE MAGNITUDEOF HEALTH PROBLEMS
ON THE BASIS OF THEIR EXTENTAND SERIOUSNESS
HELP/SOS: PLANNING116

Box 2
POTENTIAL CONSTRAINTSIN CONFLICT SITUATIONS
1. POLITICAL CONSTRAINTS
. Insecurity
. Structural breakdown of the parties to the conflict
. Mobility of victims
. Disinformation
2. LOGISTICAL CONSTRAINTS
. Shipping delays
. Administrative formalities
. Storage problems
. Communication problems
3. TECHNICAL CONSTRAINTS
. Unfeasibility of usual technical solutions in anemergency situation
. Deterioration of local health services
PLANNING 17

19
Technical feasibility of possible solutions
TotalType of problem
Magnitude of problem
Constraint Action tobe taken
Box 3
SETTING PRIORITIES
ANALYSIS OF PRIORITIES ACCORDINGTO THREE CRITERIA:
1. The magnitude of the health problems, asdefined in Box 1
2. Constraints
3. The feasibility of an effective technical solutiongiven the constraints of the emergencysituation
HELP/SOS: PLANNING18

DEFINING OBJECTIVESAND ACTIVITIES
1. DESCRIPTION
The first step is to distinguish between ‘‘objective’’ and ‘‘goal.’’ A goal is a generaldeclaration of what we seek to accomplish—for example, ‘‘to improve health.’’Definition of objectives is the first step in constructing a programme of action. Itnormally comprises four elements:
. statement of the health problem
. determination of the target group
. quantification of expected results
. time limit for achieving these results.
It may reasonably be wondered if such precision in defining an objective iscompatible with the imponderables involved in a situation of armed conflict.Although stating problems is simple enough, it is much more difficult todetermine the target population (owing to population movements) and toquantify results (using what base of reference?).
Nonetheless, every health programme must begin with the formulation ofobjectives, even if adjustments must be made as the situation develops. Whenobjectives cannot be established, the question arises as to whether the institutionof a health programme is in fact realistic. At that point it may be wise toreconsider the priority of the health problem and the feasibility of resolving it—afactor that was probably overestimated at the outset.
Objectives are set at several levels:
. general objectives defining the overall intent of an operation—for example,to reduce the rate of malnutrition from 20% to 5% in a given populationgroup over a period of three months. This objective does not specify themeans by which the desired result is to be achieved
. intermediate objectives, which help define the strategy to be used. Forexample, efforts might be directed towards influencing the incidence ofdiarrhoeal diseases, health education, or access to food
. specific, or operational, objectives, which specify the type of action to betaken. This is themost concrete level, where relief administrators decide what
PLANNING 19

21
they will actually do in practical terms. For example, they may choose toreduce the incidence of diarrhoeal diseases by improving the water supply,installing latrines, etc.
Breaking down an objective into increasingly specific, concrete elements bringsthe focus around to practical activities such as diggingwells and building latrines.An activity can be defined as a product resulting from the pooling of human,material, and financial resources. This seems obvious, and activities could beproposed directly on the basis of a general objective. However, the intellectualexercise of breaking down a general objective into more specific elements hasseveral advantages:
. it is an opportunity to review all possible means of intervention, whereas byfixing on a certain type of activity at the outset, planners risk choosing thosethat are most familiar but not necessarily the most appropriate in a givensituation
. all the activities selected can be linked to a health objective, therebymaintaining unity in a health programme that generally encompasses severalfields of activity
. it permits a later reconstruction of the process by which the activitiesinstituted were initially selected. This factor is important in emergencysituations involving a high personnel turnover.
In conclusion, the instructor must stress the usefulness of breaking the generalobjective down into progressively simpler and more concrete elements, even insituations of armed conflict where uncertainty about how the situation is likely todevelop may make this procedure seem to be a purely academic exercise withoutany practical impact.
2. CATEGORY
Tool: breaking a general objective down into specific objectives.
3. FORMULATION
Define an objective, and break a general objective down into specific objectives.
4. TEACHING METHOD
Assignment presented to work groups, who will be called upon to take a generalobjective in the Delta exercise as an example.
HELP/SOS: PLANNING20

5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Characteristics of an objective
. Box 2: General, intermediate, and specific objectives
. Box 3: Characteristics of a specific objective
. Box 4: Breaking down a general objective into specific objectives andactivities
LINK WITH NEXT OBJECTIVES
Next comes the concept of tasks.
Box 1
CHARACTERISTICS OF AN OBJECTIVE
AN OBJECTIVE SHOULD INCORPORATE:
1. Statement of the health problem
2. Definition of the population targeted by the interventionprogramme
3. Statement of the results expected from that intervention
4. Estimated length of time necessary to achieve theexpected result
PLANNING 21

Delineating specific objectives leads to the definition of concrete activities that must be carried out in order to achieve those objectives.
Box 2
GENERAL, INTERMEDIATE,AND SPECIFIC OBJECTIVES
. GENERAL:‘‘Improve health,’’ etc.
. INTERMEDIATE:‘‘Reduce the incidence of diarrhoeal diseases,’’ etc.
. SPECIFIC:‘‘Improve water supply,’’ etc.
Box 3
CHARACTERISTICSOF A SPECIFIC OBJECTIVE
S SPECIFIC, SIMPLE
M MEASURABLE
A ACCURATE
R REALISTIC
T TIME-BOUND(achieved within a certain period)
HELP/SOS: PLANNING22 23

IV. TASKS
I. GENERAL OBJECTIVE
II. SPECIFIC OBJECTIVE
III. ACTIVITIES
• Provide food assistance for a displaced population
• Immediately restore access to food by food distributions to the population
• Plan food distributions• Carry out the food distributions• Evaluate the results of the food distributions
• Ascertain the eating habits of the population• Calculate a food ration• Plan the purchase of food resources• Plan the storage of food resources
Box 4
BREAKING DOWNA GENERAL OBJECTIVE INTO
SPECIFIC OBJECTIVESAND ACTIVITIES
PLANNING 223

25
DEFINING TASKS
1. DESCRIPTION
The activities selected to achieve a health objective must in turn be broken downinto tasks. For example, planning the storage of food resources will involve suchtasks as choosing storage sites, measuring the capacity of the storage areas to beused, assessing the structure of the buildings, etc.
In short, defining a task provides a concrete view of what must be done.
In emergency situations as well as normal situations, activities are usually brokendown into tasks empirically. However, a formal definition of tasks offers severaladvantages. For one thing, it prevents the repetition of identical tasks at differentlevels of intervention. It also forces the relief administrator to proceed logically.A storage site cannot be selected if the frequency of food distributions has notbeen decided. The definition of tasks also makes it possible to give one personclear responsibility for performing a specific task.
The connection between defining tasks and mobilizing resources is obvious. Inthe previous example, the relief administrator knows exactly what sort of storagespace is required. Similarly, once a food ration has been calculated, it is clearwhat kinds of foods must be mobilized.
If, in this last example, a specific food ration has been calculated for, respectively,food distributions, nutrition rehabilitation programmes, and food programmesfor hospital patients, the administrator knows exactly what kind and quantitiesof food resources will be needed.
2. CATEGORY
Tool: planning the precise allocation of responsibilities for concrete tasks,thereby permitting an exact calculation of the resources needed.
3. FORMULATION
Break down an activity of your choice into tasks.
4. TEACHING METHOD
Assignment presented to work groups, followed by a plenary session.
HELP/SOS: PLANNING24
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Breaking down an activity into tasks
. Box 2: Relations between tasks and resources needed.
LINK WITH NEXT OBJECTIVES
The next objective concerns the concept of strategy. This concept can be appliedfirst to the mobilization of resources and subsequently to activities andobjectives.
PLANNING 25

27
Box 1
BREAKING AN ACTIVITY DOWNINTO TASKS
ACTIVITY
. Determine the rate of malnutrition in a child population
TASKS
. Measure the children
. Weigh the children
. Talk to the mothers
. Other tasks
Box 2
RELATIONSHIP BETWEEN TASKSAND RESOURCES NEEDED
TASKS
. Measure the children
RESOURCES NEEDED
. Personnel to measure the children
. Measuring instruments
. Notebook and writing implements to record the results
. Other
HELP/SOS: PLANNING26

THE CONCEPT OF STRATEGY
1. DESCRIPTION
The concept of strategy has three applications:
. as applied to general objectives, strategy means delimiting the mainorientations of an action by choosing fields of intervention according torelative priorities and the mandates of the agencies operating in a conflictsituation
. as applied to activities, strategy consists in determining the activities that willbe included in the programme and the order in which they will be performed
. as applied to resources, strategy involves choosing the resources that will beuseful and deciding on the order in which they will be mobilized.
In situations of armed conflict, determining strategies is an essential step, sincechanging circumstances dictate frequent adjustments—not so much on the levelof general orientations, which remain constant, as on the level of choosingactivities and mobilizing resources. The determination of a strategy—and thechanges that must be made as an intervention progresses—is thus crucial formonitoring and understanding the development of an intervention. Thecomplicated task of constructing a strategy amid the constraints of theemergency situation should not obscure the fact that this strategy is not an endin itself, but a means of achieving an objective.
2. CATEGORY
Tool: employing the concept of strategy as an essential element in managing anoperation.
3. FORMULATION
Plan a strategy in a given context.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 40 minutes
. 20 minutes for work in groups
PLANNING 27

29
. 20 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Normative and tactical strategies
LINK WITH NEXT OBJECTIVES
The idea that it is important tomonitor the development of a strategy provides anintroduction to the concepts of evaluation and epidemiological surveillance.
IDENTIFICATION OF PROBLEMS
OBJECTIVES
EVALUATIONAND
SUPERVISION
IDENTIFICATION AND SELECTION OF ACTIVITIES TO BE CARRIED OUT
DECISION TO TAKE ACTIONBASED ON:
STR
ATEG
IES
• institutional mandate• urgency of problems• constraints that must be overcome
normative
tacticalConsider all possibilitiesand choose the most appropriate
MOBILIZATION OF RESOURCES
IN ORDER TO IMPLEMENTSELECTED ACTIVITIES
Box 1
NORMATIVE AND TACTICAL STRATEGIES
HELP/SOS: PLANNING228

EVALUATION ANDEPIDEMIOLOGICAL SURVEILLANCE
1. DESCRIPTION
Emergency operations are ‘‘under-evaluated’’ in the sense that their impact on thevictims is not evaluated. The concept of evaluation can be examined in two ways:
. by type of evaluation:
. Onemethod of evaluation is to take successive ‘‘snapshots’’ of a situation,in order to compare them with each other as well as with the first‘‘snapshot’’ taken at the time of the initial assessment. This will showwhether the operation’s objectives have been achieved.
. The secondmethod is tomonitor the situation systematically bymeans ofregularly collected indicators. This form of surveillance is particularlywell suited to monitoring the development of health problems and thefunctioning of relief programmes—for example, regular monitoring ofthe malnutrition rate, the number of hospitalizations, market prices, etc.
These two forms of evaluation are complementary
. in terms of the planning cycle. At each point of this cycle, the followingquestions must be asked:
. Mobilization of resources:
. Were resources appropriate in quality and quantity?
. Did the resources arrive on time?
. Activities:
. What was the volume of activity—for example, number of medicalconsultations, number of surgical procedures, number of food rationsdistributed?
. Were the activities suited to the established objectives?
. Objectives:
. Were they achieved?
. Problems:
. Are the health problems identified in the initial assessment still top priority?
. Has the nature of the problems changed?
PLANNING 29

31
To answer these questions, not only must an epidemiological system be set up tocollect data, but problems, priorities, objectives, and strategy must all have beendefined at the outset to provide some basis for judging the results obtained.
Three additional points should be mentioned with respect to the essential linkbetween evaluation and planning. That link is clear in the context of a logicalplanning framework.
. There is a connection between surveillance indicators and the definition ofobjectives. The defining of objectives implies that there are health problemsto be resolved. Those problems are the basis for identifying indicators thatwill reflect the impact of programmes. Specific objectives often includeconcepts such as malnutrition rates and the incidence of diarrhoeal diseases,which are in fact indicators that can be used in a surveillance system.
. Evaluation must be associated with a decision-making process. The ultimategoal of an evaluation is to provide a basis for taking decisions.
. Should a programme be modified?
. Should an activity or programme be terminated?
. Should a strategy be modified?
. Amonitoring and evaluation systemmust be planned at the same time as theintervention programmes:
. If a food distribution is planned, how is its impact going to be measured?
. If an immunization programme is going to be implemented, how are itsimpact and coverage going to be measured?
Finally, the instructor must emphasize the increasing pressure from donorsnowadays to see the results of humanitarian operations expressed in terms oftheir impact on the victims, rather than solely in financial terms.
It is often argued that the institution of a monitoring system constitutes adiversion of human resources that could be better used for other activities. Theinstructormust stress that if an operation is not up to standard or is part of a poorstrategy and there is no way of analysing this situation, the victims will suffer. Amonitoring system can never be considered a poor use of resources.
2. CATEGORY
Tool: defining the concepts of evaluation and monitoring.
HELP/SOS: PLANNING30

3. FORMULATION
Describe the concepts of evaluation and epidemiological surveillance in anemergency situation, and offer arguments to support the construction of amonitoring system at the outset of a humanitarian operation.
4. TEACHING METHOD
Assignment presented to work groups, followed by a plenary session.
5. DURATION
Total duration: 50 minutes
20 minutes for work in groups
30 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: The concepts of evaluation and monitoring
. Box 2: Epidemiological programmes
. Box 3: Roles of monitoring and evaluation
. Box 4: Evaluation and the planning cycle
. Box 5: Logical framework
LINK WITH NEXT OBJECTIVES
Monitoring and evaluation are the last stage of the planning process. At thispoint the instructor will ask the participants if they would like clarification of anyof the points studied in this module. The instructor must emphasize thatparticipants will be expected to apply this planning procedure in the course of thefollowing modules. Accordingly, it is important that everyone understand theprinciple and the terminology.
PLANNING 31

33
Routine surveillance of certain indicators as a means of monitoring both the situation
and programme functioning
Early-warning system to anticipate worsening problems and potential disaster
Regular evaluation of programme impact and developments in the overall situation.
Initialassessment of the situation
Conflict
Time
Environment
Population
Box 1
THE CONCEPT OF EVALUATIONAND SURVEILLANCE
HELP/SOS: PLANNING332

Box 2
EPIDEMIOLOGICAL PROGRAMMES
. Early-warning system
. Initial assessment
. Surveillance
. Ad hoc evaluation
. Investigation of an epidemic
Box 3
ROLES OF MONITORINGAND EVALUATION
1. Regular collection of data to provide an objective basis for:
. defining trends
. detecting epidemics
. reorienting programmes
. terminating programmes
2. Overall evaluation of a situation for comparison with theinitial situation
PLANNING 33

35
INITIALASSESSMENT
OF THESITUATION
• Evaluation of impact (mortality, security)
• Evaluation of resources (quantity, quality)
• Evaluation of the choice of priorities
• Evaluation of programme results (coverage, solving problems, etc.)
• Evaluation of services provided (quantity and quality)
• Evaluationof choiceof activities
CHOICE OFPRIORITIES
DETERMINATIONOF OBJECTIVES
CHOICE OFACTIVITIES
EVALUATION
MOBILIZATIONOF
RESOURCES
Box 4
EVALUATION AND THE PLANNING CYCLE
HELP/SOS: PLANNING334

Planning
Situation
General objectives
Strategic orientations
Specificobjectives
Activities
Resources
Indicators Possible levels of analysis(appropriate-ness,effect-iveness, efficiency, impact,coherence, etc.)
Sources of data for evaluation indicators
Evaluation methods
Contextual interpretation (constraints hindering the action)
Box 5
LOGICAL FRAMEWORK
PLANNING 335
37
PROTECTION AND ASSISTANCE FORA POPULATION SUFFERING FROM THECONSEQUENCES OF INTERNAL UNREST:THE EXAMPLE OF SAKILI/ABSHA—DELTA
INTRODUCTION
Delta ranks third in area on the African continent, with an estimated populationof 57.8 million distributed among 200 tribes.
In April 1990, the government in power began a process of political change thathas not yet ended. Although the combined effects of the economic crisis and theinstability of the central authorities have not yet brought the country to a state ofgeneralized violence, there have been many signs of a weakening of security(looting in the capital and elsewhere, clashes between different communities).
The situation in Absha (a province in the southwest of the country), particularlythe clashes between communities, has attracted the attention of the internationalcommunity. The year 1992 saw many developments in conflicts between theSaika, who have been immigrating into Absha since colonial times in order toexploit the mining resources of the region, and the populations of Takanganeseorigin, who now wish to benefit from the rich local resources themselves. Theinternal disturbances in the Absha region have left a large number of peoplehomeless. Around 65,000 people, mostly of Saika origin, who have lived inAbsha for generations, have become targets of Takanganese violence, andultimately have had to flee their homes. Although many would have liked toreturn home, most of them realized they had no alternative but to head for theSaika region, about five days away by train.
In January the first disturbances began in Merugonu, resulting in three deathsand dozens wounded. Some 500 people sought refuge in the train station, hopingto be able to leave the region by train, but about 10 days later they agreed toreturn home.
From January to September 1992, sporadic clashes led many people to move tothe area around the train station and the premises of the mining company. Someinjuries were recorded.
HELP/SOS: PLANNING36

On 14 and 15 September, serious incidents in Sakili resulted in the deaths of 24people and the injury of 70 more, the destruction and looting of hundreds ofhomes, and congregations of people around the military camps as well as thetrain station. Most of the victims were of Saika origin, although someTakanganese were also affected by the violence.
Given the deterioration of the situation, the international community hasdecided to send in a team to assess the situation.
YOU ARE A MEMBEROF AN INTERNATIONAL MEDICAL TEAM GIVENTHE TASK OF ASSESSING THE SITUATION.
THE FIRST OBJECTIVEOF THIS EXERCISE IS TO PREPARE
YOUR ASSESSMENT BY DRAWING UP:
. A list of the main data you would liketo assemble
. A list of sources you will consult to findthese data
PLANNING 37

39
THE SITUATION OF THE VICTIMS IN SAKILI1. DESCRIPTION OF THE SITUATION
1.1 BASIC STATISTICS
1.1.1 Classification of the victims
The victims can be divided into four categories:
. Saikans living around the train stations (in the customs building, in tents, orin the station): 30,000
. Saikans living in more or less adequate accommodation (schools, miningcompany premises [Minex Co.]): 5,469
. Saikans who have taken shelter with relatives in town: 23,299
. Takanganese whose homes were destroyed during the clashes: around 3,000.
1.1.2 Mortality rate
The deaths were recorded by Saikans. The very precise figures reported at theoutset made us doubt their reliability. However, having checked them againststatistics furnished by the churches, we can assume that they are relativelyaccurate.
The following table shows the variations in the mortality rate for 10,000 peopleper day:
SAKILI:
Mortality rate for 10,000 people per day
Week August 1992 September 1992
1 1: 1.2 1.4
2 1.1 1.7
3 1 2.1
4 1.2 1.6
HELP/SOS: PLANNING38

Most of the deaths occurred among children under the age of five, as indicated inthe table above.
This is the mortality rate for all that part of the affected population that isoriginally from Saika and living in Sakili. The deaths were due primarily to anepidemic of measles at the end of August and an epidemic of diarrhoea inSeptember.
1.2 FOOD AND NUTRITIONAL DATA
1.2.1 The nutritional situation
An overall nutritional assessment showed a malnutrition rate of 20% amongchildren under the age of five years (i.e., under 80% of standard weight-for-height), with 2% suffering from acute malnutrition (under 70% of standardweight-for-height, and/or symptoms of kwashiorkor).
Among children under age five whose families live around the train station, themalnutrition rate is 30% (8% of those acutely malnourished).
1.2.2 The food situation
We can distinguish between two population groups.
1.2.2.1 The group living at the station
Analysis of the food and financial resources of this group shows that:
. their financial resources are limited, deriving from:
Week
Total deaths
Age < 1 year
Age 1 - 5 year(s)
Over 5 years
1 2 3 4 5 6 7 8
200 100 97 62 58 60 95 95
100 32 35 28 31 40 47 51
62 30 32 22 19 14 23 18
38 38 30 12 8 6 25 26
PLANNING 39

41
. sale of furniture and personal belongings
. wages, for the employees of Minex Co. and Absha Railways Company(ARC): 800 families out of a total of 7000.
. their food resources are also limited:
. a small local market has been created by the Saikans since the events inAugust
. around 10%of the families in this groupwork forMinexCo. As a generalrule, this company provides its employees with food, but this rationcovers at best only 20-30%of their basic food needs. Local agencies makelimited or sporadic food distributions amounting to 1 kg per family
. it is unsafe to go to rural areas to obtain food.
1.2.2.2 The other groups
The other groups are made up primarily of families connected with the miningcompany (Minex Co.) or the ARC. They live in better sanitary conditions, andsome people receive wages and food aid from their companies. Others are helpedby their families, with whom they are staying. These groups have some access tofood and financial resources, but for a limited period of time and in insufficientquantities to cover their needs.
1.3 THE ENVIRONMENT
The situation of the people living around the station is comparable to that ofpeople in a camp for displaced persons, where the following elements must betaken into account:
. Shelter:
Shelters made out of local materials (wood, sacks, plastic sheeting).
. Camp layout:
The shelters are numerous and close together (overcrowding), and problems willarise during the rainy season.
The access roads to the camp are in good condition, but there are no real meansof transport inside the camp. The camp measures about 400 by 300 metres.
. Water:
Themain source of water is themunicipal water system (the source of the water isa river five kilometres away from town). There are five taps in the station itself. In
HELP/SOS: PLANNING40

the camp, there are two privately owned hand-pumped wells that can be used bythe displaced population.
Quality:
According to the authorities, the water is chlorinated by the water-treatmentplant. However, the supply of chorine regularly runs out. The quality of thewell water has not been evaluated.
Quantity:
According to the authorities, the quantity of water distributed in the campby the municipal water system is some 90 cubic metres per day.
. Human Waste:
50 latrines have been dug.
1.4 MORBIDITY
The distribution of diseases follows a typical pattern, with a high percentage ofdiarrhoeal diseases (30%), fever caused by malaria (20%), skin infections (8%),and acute respiratory infections (12%). Many cases of tuberculosis have beendiagnosed, and several cases of measles have recently been recorded.
1.5 DISPENSARY ACTIVITIES
The health authorities opened a dispensary in the camp on 10 September (most ofthe morbidity data were collected there).
The medical staff consists of one doctor, two nurses, and four health workers, allof Saika origin. They see patients every day from 7:00 a.m. to 5:00 p.m. Patientswith serious medical problems cannot be evacuated to the hospital at night; infact, owing to the unsafe conditions in town at night, people do not dare go there.On average, 210 new cases arrive at the dispensary every day.
1.6 PUBLIC HEALTH ACTIVITIES
Public health education programmes have been set up, focusing in particular onwaste disposal and water usage.
The Red Cross has introduced a home visit programme, referring medical casesto the dispensary, and Saikan volunteers are setting up an aid programme forelderly people.
PLANNING 41

43
1.7 HOSPITALS
Those people requiring hospitalization are for the most part children sufferingfrom malnutrition, fever, and diarrhoeal diseases.
At the hospital, a special ward has been set aside for displaced persons, in order tokeep them separate from patients of Takanganese origin. This ward has acapacity of 36 beds. The rate of admission is 20 patients per week.
ON THE BASIS OF THIS DATA,COURSE PARTICIPANTS WILL BE ASKED TO:
. Identify health problems
. Set priorities
. Establish general and specific objectives
. Break down a specific objective into activities and anactivity into tasks
HELP/SOS: PLANNING42

2. FACTORS FOR ANALYSING POTENTIALDEVELOPMENTS IN THE SITUATION
2.1 TRANSPORTATION FROM SAKILI TO TUMWE
Since there is only one train a month from Bashiku to Tumwe, people areessentially trapped in the station and its environs. When the train arrives eachmonth at the Sakili station, it is already carrying passengers from Bashiku.Nonetheless, a few hundred people usuallymanage to get on tomake the five-daytrip to Tumwe.
2.2 SITUATION AT WIZEKOL
In the third week of September, disturbances broke out inWizekol, leading 3,000Saikans to congregate at the train station there.
2.3 SITUATION AT TUMWE
The estimated number of arrivals from January to August 1992, was 8,000.Mostof the people displaced from the province of Absha remained in the camp nearthe city of Tumwe before moving on to their final destination by their ownmeans.
POPULATION IN THE TUMWE CAMPS
Estimated number of people presentin the Tumwe camp per week,
from mid-August to the end of September 1992
Week August 1992 September 1992
1 --- 3,000
2 --- 2,700
3 2,400 3,250
4 2,600 3,500
PLANNING 43

45
. Housing:
During the first few months, group shelters were provided for the displacedpopulation. As the camp population increased, however, plastic sheeting wasdistributed for making tents.
. Food situation:
Food distributions have been regularly organized. The food consists primarily ofwhite flour. Since the malnutrition rate is high (more than 12% in children),supplementary rations are also provided for those children with a weight-for-height ratio of less than 70% and 75%.
. Morbidity:
An epidemic of severe diarrhoea broke out in August 1992. It probablyoriginated in Wizekol, where the same pathology was observed and caused thedeaths of a number of adults and children. During the rainy season (August-September), malaria was the main cause of mortality. The mortality rate in theTumwe camp is even higher than in Sakili.
2.4 POLITICAL SITUATION IN THE COUNTRY
The political situation in the country is far from stable. There is a generaltendency towards anarchy.
2.5 INTERNATIONAL CONTEXT
The international community is concerned about this situation but does not see itas a priority for two reasons:
. the international political context is very tense and other serious armedconflicts are drawing public attention
. a similarly tense situation developed in Delta in previous years, giving rise tohumanitarian operations that failed to solve the problem.
USING THESE FACTS, THE PARTICIPANTSWILL BE CALLED UPON
TO PLAN THEIR LONG-TERM STRATEGIES.
HELP/SOS: PLANNING44

Saika
Absha
Delta
Tumwe
Distance 100 km
Wikezol
Sakili
Merugonu
Bashiku
Box 1
PLANNING 445

Sakili
Sakilitrain station
camp
train station
Minex
Region mostly populated by Saikans
Region populatedmostly by Takanganese
Box 2
HELP/SOS: PLANNING46

FOOD AND NUTRITION
MODULE
2

49
LIST OF OBJECTIVES
. Draw a diagram of the food supply chain
. Know how to identify disruptions in agricultural production and fooddistribution
. Know how to recognize disruptions in access to food resources.
. Understand the importance of rapid assessment procedures as a tool forunderstanding rural populations’ reactions to upheavals in the agro-food andsocial systems during emergency situations
. Analyse a family’s food consumption
. Know how to identify and measure malnutrition, and be in possession ofenough basic facts to plan a strategy. This objective will allow participants tomake use of the skills learned earlier as practice for later use in the field
. Establish a framework in which to study skills useful for planning a fooddistribution
. Know the criteria for developing a suitable food ration
. Plan food distribution and nutritional rehabilitation programmes for a givenpopulation
. Be able to name the essential elements required for a population census
. Know what information is necessary to determine the strategy best suited toreducing malnutrition in a population
. Know what information is necessary to plan a surveillance system for a fooddistribution
. Acquire the essential facts for an understanding of the logistical requirementsassociated with food distributions
. Master a strategic tool for defining the obligatory interaction betweennutritional rehabilitation programmes and programmes designed to restoreaccess to food resources for a vulnerable population
. Study the general principles of organizing a nutritional rehabilitation centre.
HELP/SOS: FOOD AND NUTRITION48

DESCRIPTIONOF THE FOOD SUPPLY CHAIN
1. DESCRIPTION
Generally speaking, there are several links in a food supply chain: production ofagricultural resources, transformation into food products, distribution on themarket, family access to food resources, distribution of food within the family,and biological utilization of the food. Theway this chain functionswill determinethe nutritional status of the population and, more specifically, of children; andnutritional status will in turn determine health status.
Armed conflict affects all or part of this food supply chain. Strategies forhumanitarian action in this context must therefore take all the links of the foodsupply chain into consideration. Thus, an effort must be made to break thecommon habit of basing emergency food strategies exclusively on themeasurement of malnutrition rates. If the field of nutrition is expanded toencompass the concept of the food supply chain, it becomes feasible to planstrategies that incorporate the different links of this chain to one extent oranother, since the further up the chain action is taken, the greater thepreventive effect will be.
The food supply chain is not an isolated concept. For example, since biologicalutilization of food is linked to the incidence of communicable diseases, the foodsupply chain is closely connected with programmes for controlling communic-able diseases.
2. CATEGORY
Framework: Diagramming a food supply chain.
3. FORMULATION
Describe a food supply chain with respect to a population type of your choice:rural, urban, semi-nomadic, etc.
4. TEACHING METHOD
Assignment presented to work groups, who will be asked to write their results ona transparency for presentation and discussion in the plenary session.
FOOD AND NUTRITION 49

51
5. DURATION
Total duration: 35 minutes
. 15 minutes for work in groups
. 20 minutes for plenary session.
6. RECAPITULATION
. Box 1: Food supply chainSimple linear version of the food supply chain, without offshoots tothe other systems that influence it—for example, the control ofcommunicable diseases, which affects both biological utilization offood and food production
. Box 2: Food supply chain and macroeconomicsDefinition of production, economic channels, and availability offood resources
. Box 3: Effects of humanitarian aid on the food supply chain
. Box 4: Accessibility of food resources
. Box 5: Definition of food consumption, including feeding of children
. Box 6: Definition of biological utilization of food
. Box 7: Nutritional status and health status
. Box 8: Nutritional status as an indicator for an underlying disturbance; thisdisturbance may be limited to one link of the food supply chain, andmay require responses not directly related to food, such as measuresaffecting biological utilization and control of communicablediseases
. Box 9: Food supply chain and systems
LINK WITH NEXT OBJECTIVES
Beginning with this general outline of the food supply chain, we will study themain tools needed to evaluate its successive links and to plan appropriate actionat each level.
HELP/SOS: FOOD AND NUTRITION50

Production
Availability
Accessibility
Consumption
Economic Channels
Nutritional Status
Health Status
Biological Utilization
Box 1
THE FOOD SUPPLY CHAIN
FOOD AND NUTRITION 551

53
Box 2
FOOD SUPPLY CHAINAND MACROECONOMICS
AGRICULTURAL PRODUCTION:
. Agronomic analysis
. Climate analysis
. Analysis of agricultural practices
. Analysis of the agrarian system
. Analysis of imports
ECONOMIC CHANNELS:
. Analysis of communicationsystems
. Analysis of market prices
. Analysis of food stocks
AVAILABILITY OF FOOD RESOURCES:
. Availability of food resources in the immediateenvironment (quantity and quality)
HELP/SOS: FOOD AND NUTRITION52

biologicalutilization
of food
foodconsumption
nutritionalstatus
availability offood resources
agriculturalproduction
economicchannels
health status
Population’s potential access to food resourcesRequirements:
• Food resources must be available• The population must have the ability to obtain them (purchasing power, barter)• Security conditions must be satisfactory
Foodresources
Population’sfood
needs
accessibil i ty
Box 3
ACCESSIBILITY OF FOOD RESOURCES
FOOD AND NUTRITION 553

55
Box 4
DEFINITION OF FOOD CONSUMPTION
STUDY OF FOOD CONSUMPTION WITHIN THE FAMILY
. Types and quantities of food resources
. Mode of preparation
. Number of meals
. Distribution of food within the family
STUDY OF INFANT FEEDING
. Breast-feeding
. Weaning
. Feeding of young children
Box 5
DEFINITION OF BIOLOGICAL UTILIZATIONOF FOOD
FOOD ABSORPTION MAY BE HINDERED BY:
. Diarrhoeal diseases
. Intestinal parasites
LINKS WITH THE OTHER COMPONENTSOF THE HEALTH SYSTEM:
. Environmental sanitation
. Control of communicable diseases
HELP/SOS: FOOD AND NUTRITION54

Box 6
NUTRITIONALSTATUS/HEALTH STATUS
1. Nutritional status can be objectively measured.
2. The mortality rate is closely and exponentially correlatedwith the malnutrition rate.
3. The risk of infections is closely associated with themalnutrition rate.
4. Malnutrition may be a belated sign of a disruption in thefood supply chain, but it may also be related to infections.
FOOD AND NUTRITION 55

57
PRODUCTION
ECONOMICCHANNELS
AVAILABILITY
ACCESSIBILITY
CONSUMPTION
BIOLOGICALUTILIZATION
NUTRITIONALSTATUS
HEALTH STATUS
The measure of nutritional status reflects disruptions in the food supply chain
12
Box 7
NUTRITIONAL STATUS: INDICATOROF AN UNDERLYING PROBLEM
HELP/SOS: FOOD AND NUTRITION556

biologicalutilization
of food
foodconsumption
nutritionalstatus
availabilityof food
resources
agriculturalproduction
economicchannels
health status
Foodresources
Population’sfood
needs
accessibil i ty
Macroeconomicsystem
• Production• Imports• Stocks• Transport
• Diseases• Malnutrition
Social system• Social organization
• Food habits
Microeconomicsystem
• Family purchasing power
Healthsystem
Box 8
FOOD SUPPLY CHAIN AND SYSTEMS
FOOD AND NUTRITION 557

59
DISRUPTION OF AGRICULTURALPRODUCTION AND FOOD DISTRIBUTION
1. DESCRIPTION
This objective is not designed to provide participants with the skills needed toinstitute agricultural-production programmes, but to help them realize thatarmed conflicts can disrupt agricultural production, a problem that cansometimes be corrected by simple measures. This section will also discussdisruptions in the process by which agricultural products are made into foodproducts.
The present objective is twofold:
1. To identify basic indicators for assessing disruptions in the production andprocessing of agricultural goods following an armed conflict:
. access to farmland
. access to agricultural inputs: seeds, fertiliser, fuel, tools, etc.
. availability of manpower
. destruction of factories
. lack of spare parts and fuel for factories.
2. To note the importance of the compensation mechanisms that help offset adeficit in agricultural production and facilitate the transition to a survivaleconomy.
The problems linked to the distribution of agricultural and food productsthrough the economic system can be studied in the same way. For example,situations of armed conflict disrupt means of communication and cause supplyshortages, thereby leading to price increases.
2. CATEGORY
Tool: the ability to identify disruptions of agricultural production and fooddistribution.
3. FORMULATION
Identify the indicators that can be used to assess disruptions of agriculturalproduction and food distribution.
HELP/SOS: FOOD AND NUTRITION58

4. TEACHING METHOD
Discussion in plenary session of:
. disruptions in agricultural production
. disruptions in the distribution of food products.
5. DURATION
Total duration: 25 minutes.
6. RECAPITULATION
. Box 1: Breakdown of the food supply chain
. Box 2: Factors disrupting agricultural production during an armed conflict
. Box 3: Factors disrupting the distribution of food resources during anarmed conflict
LINK WITH NEXT OBJECTIVE
Disruptions in the production, processing, and distribution of agro-foodcommodities have an impact on the most vulnerable socio-economic groups’access to food resources.
FOOD AND NUTRITION 59

61
PRODUCTION
ECONOMICCHANNELS
AVAILABILITY
ACCESSIBILITY
FOODCONSUMPTION
BIOLOGICALUTILIZATION
NUTRITIONALSTATUS
HEALTH STATUS
• Armed conflict• Drought• Floods • Earthquakes
Box 1
BREAKDOWN OF THE FOOD SUPPLY CHAIN
HELP/SOS: FOOD AND NUTRITION660

AGRICULTURALPRODUCTION
Destructionof crops
Restricted access to agricultural areas
Restrictedaccess to
agriculturalinputs
Lack of fuel
Shortage of spare parts for agricultural equipment
Lack of manpower(due to military
recruiting)
Box 2
FACTORS DISRUPTINGAGRICULTURAL PRODUCTIONDURING AN ARMED CONFLICT
FOOD AND NUTRITION 661

63
ECONOMICCHANNELS
FOR THEDISTRIBUTION OF
FOODRESOURCES
Disruption ofimportmechanisms
Changes in the type of foodresources available
Insecurity
Militaryrequisition of
means of transport
Restriction ofthe circulation of food resources to avoid supporting the adversary
Stockpiling of food resources
to increase prices
Destructionof com-
municationlines
Box 3
FACTORS DISRUPTING THE DISTRIBUTIONOF FOOD RESOURCES DURING
AN ARMED CONFLICT
HELP/SOS: FOOD AND NUTRITION662

IDENTIFYING DISRUPTIONSOF ACCESSTO FOOD RESOURCES
1. DESCRIPTION
The disruptions in food production and distribution alreadymentioned will haverepercussions on the most vulnerable groups’ access to food resources. Thisperspective offers a different approach than the usual classification of vulnerablegroups—children, pregnant and nursing women, and the sick. Here, a group’svulnerability is defined as a function not only of physiological characteristics, butalso economic, ethnic, and political criteria.
Market price increases deny the poorest individuals access to food resources,obliging them to sell their cattle or their jewellery, or to migrate to morefavourable regions. Access to food resources may also be affected by ethnicorigin or political affiliation.
To pinpoint the factors impeding access to food resources, indicators—usuallyunquantifiable—will have to be sought through talks with the people affected. Inthis endeavour, it is essential to be a good listener and to be familiar with thesociocultural and political environment.
Restrictions on access to the usual food sources trigger compensationmechanisms—the population seeks out foods that it does not normally consume,obtained from sources used only in emergency situations when the usual sourcesare insufficient or exhausted. A population’s ability tomodify its strategy of foodaccess will depend on its way of life and degree of preparation for the risk ofinterrupted access to the usual food resources. A rural population, for example,may be less vulnerable than an urban population, whose compensationmechanisms are more limited.
The most common procedure for assessing access to food resources is byqualitative evaluation methods based on interviews with the victims of thesesituations.
2. CATEGORY
Tool: the ability to recognize disruptions in access to food resources.
FOOD AND NUTRITION 63

65
3. FORMULATION
Identify indicators permitting assessment of a given population’s access to foodresources.
4. TEACHING METHOD
Assignment presented to work groups, followed by a plenary session.
5. DURATION
Total duration: 25 minutes
. 10 minutes for work in groups
. 15 minutes for plenary session.
6. SYNTHESIS
. Box 1: Factors disrupting access to food resources
LINK WITH NEXT OBJECTIVES
The next objective covers the concept of rapid assessment procedures.
HELP/SOS: FOOD AND NUTRITION64

ACCESS TOFOOD
RESOURCES
Inability toadapt to thenew parametersof economic circulation
Disruptions in the social and familystructure (orphans, single-parentfamilies, etc.)
Diminishedincome
Increasedfood
prices
Restricted accessto food resources
on grounds of ethnic,social, or political
affiliation
Disruptions in availability offood resources
SEARCH FOR COMPENSATION MECHANISMS TO GAIN ACCESS
TO OTHER SOURCES OR FORMS OF FOOD
Box 1
FACTORS DISRUPTING ACCESSTO FOOD RESOURCES
FOOD AND NUTRITION 665

67
RAPID ASSESSMENT PROCEDURES
1. DESCRIPTION
Rapid assessment procedures are methods of qualitative evaluation. They areparticularly useful when social, anthropological, or microeconomic informationis sought. Such procedures obviate the need for systematic sampling of an entirepopulation, because they survey specific focus groups selected for their ability tofurnish the desired information. These focus groups may be people with a specialstatus in the population—village leaders, health care personnel, women’sassociations, etc.
The advantage of these procedures is that they provide a quick way of gatheringinformation from a small number of people without any need for enormoussurveys covering large numbers of people. Rapid assessment procedures arebased on informal meetings with the focus groups, interviews with keyrespondents of a community, or questionnaires distributed to those respondents.Obviously this method presents certain risks, particularly since the natural biasinherent in the ‘‘selection’’ of focus groups or respondents means that the resultsmay not reflect the true situation of all the people affected by a given situation.Data collected by means of rapid assessment procedures may have to beconfirmed by more direct methods.
Rapid assessment procedures are very useful for gathering information on agiven population’s agro-food system. They provide a view of the microeconomicand social mechanisms of such systems, as well as an understanding of thepopulation’s responses to changes caused by war.
2. CATEGORY
Tool: An appreciation of the importance of rapid assessment procedures forunderstanding a population’s reactions to upheavals in the agro-food and socialsystems during an emergency situation.
3. FORMULATION
Define rapid assessment procedures.
4. TEACHING METHOD
Question-and-answer session involving all participants.
HELP/SOS: FOOD AND NUTRITION66

5. DURATION
Total duration: 30 minutes.
6. RECAPITULATION
. Box 1: Rapid assessment procedures: principles
LINK WITH NEXT OBJECTIVES
Rapid assessment procedures are just as applicable to other spheres as they are tofood and nutrition. They are also useful for gathering data on security problemsin war situations.
Box 1
RAPID ASSESSMENT PROCEDURES
PRINCIPLES
. Method of qualitative evaluation
. Interviews
. Focus groups
. Risk of bias in selection of interviewees
. Confirmation of data by comparing different sourcesof information
FOOD AND NUTRITION 67
69
DISRUPTIONS IN FOOD CONSUMPTIONWITHIN THE FAMILY UNIT
1. DESCRIPTION
The consumption of foodwithin the family is affected not only by the disruptionspreviously mentioned, but also by factors intrinsic to the family unit. The familyunit must be understood in the broad sense, since in many societies it comprisesthe extended family or even the clan.
Food consumption can be assessed in many ways, including direct observation,an oral enquiry concerning foods eaten in the preceding 24 hours or the precedingweek, and surveys based on systematic records of meal content made within thehousehold. Other indirect methods are based on analysis of food waste.
The choice of the food consumed depends on cultural habits and the foodresources available. Nutritional value will depend on the nature of the food andthe method of preparation used, particularly the cooking method.
In emergency situations, consumption is influenced by access to both foodresources and the energy sources needed to prepare them.
Individual food consumption depends on the level of education (particularlywith respect to the feeding of children) and the nature of the social relationshipsbetween the members of a single family. In some cases, for example, a certainfamily hierarchy determines each individual’s access to food. This factor isradically altered in situations of armed conflict, which challenge customarysocial relationships.
All these factors help shape patterns of food consumption that are specific notonly to a given population, but also to the particular circumstances in which thatpopulation is living.
Analysis of food consumption also involves technical considerations. Basically,once the type and quantities of food consumed by each member of a householdhave been estimated, it remains to be determined whether this consumption isadequate to maintain a satisfactory nutritional status. To assess this factor, twotools are required:
. a knowledge of the nutritional values of the main foods, and the ability toread a table providing this type of information
HELP/SOS: FOOD AND NUTRITION68

. a knowledge of individual nutritional requirements according to thefollowing parameters: age, gender, activities, physiological condition(pregnancy, lactation, growth).
2. CATEGORY
Tool: Analysing a family’s food consumption.
3. FORMULATION
What data will you look for in order to analyse a family’s food consumption?
4. TEACHING METHOD
Assignment presented to work groups, who will be asked to write the results oftheir work on transparencies.
5. DURATION
Total duration: 40 minutes
. 20 minutes for work in groups
. 20 minutes for summary in the plenary session.
6. RECAPITULATION
. Box 1: Factors disrupting family food consumption
. Box 2: Assessment of family food consumption
. Box 3: Protein and calorie content of common foods
. Box 4: Energy requirements according to age and physiological parameters
LINK WITH NEXT OBJECTIVES
An adequate food consumption level does not necessarily imply a satisfactorynutritional status. Factors such as illness may impede food absorption.
FOOD AND NUTRITION 69
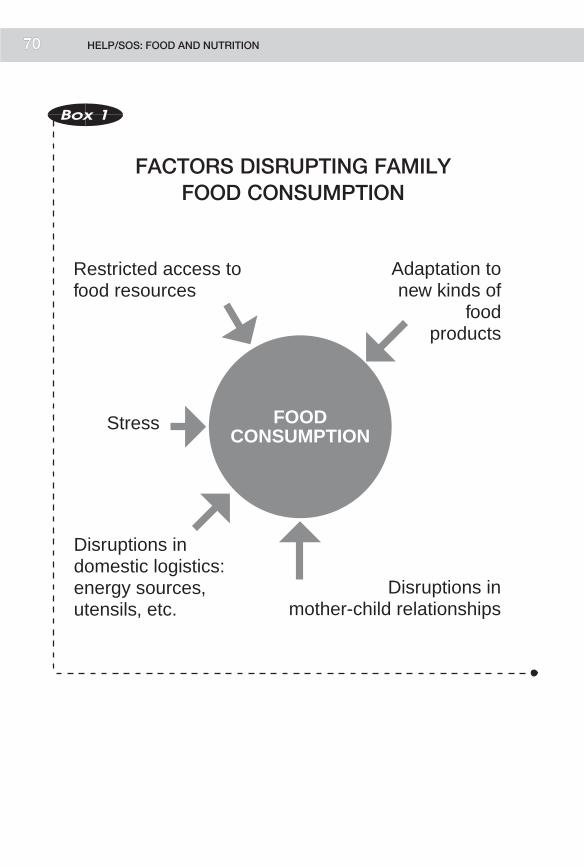
71
FOODCONSUMPTION
Disruptions indomestic logistics: energy sources, utensils, etc.
Stress
Restricted access tofood resources
Adaptation to new kinds of
foodproducts
Disruptions inmother-child relationships
Box 1
FACTORS DISRUPTING FAMILYFOOD CONSUMPTION
HELP/SOS: FOOD AND NUTRITION770

Familyunit
Foodresources
Observation
• Description of the family unit: number, age, etc.
• Types of food resources
• Source of food resources
• Strategy at the family level
• Food preparation
• Number of meals
• Distribution of food to different members of the family
• Assessment of the degree to which the food consumed meets the specific nutritional requirements of each member of the household
Box 2
ASSESSMENT OF FAMILYFOOD CONSUMPTION
FOOD AND NUTRITION 771
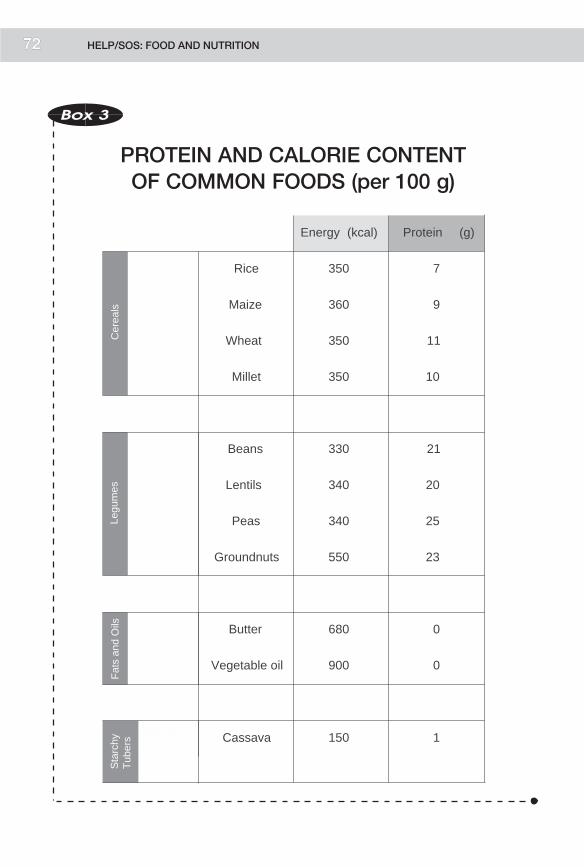
73
Energy (kcal) Protein (g)
Rice 350 7
Maize 360 9
Wheat 350 11
Millet 350 10
Beans 330 21
Lentils 340 20
Peas 340 25
Groundnuts 550 23
Butter 680 0
Vegetable oil 900 0
FRUITSFARINEUX Cassava 150 1
Cer
eals
Legu
mes
Fat
s an
d O
ilsS
tarc
hyT
uber
sBox 3
PROTEIN AND CALORIE CONTENTOF COMMON FOODS (per 100 g)
HELP/SOS: FOOD AND NUTRITION772

Box 4
ENERGY REQUIREMENTS
1. SIMPLIFIED FORMULA
. Children 100 kcal/kg/day
. Adults 30-40 kcal/kg/day
2. BY AGE
kcal/kg/day
. 0-1 year 820
. 1-3 year(s) 1,360
. 4-6 years 1,830
. 7-9 years 2,190
. 10-14 years 2,600
ADULT MALE
Moderately active 3,000
ADULT FEMALE
Moderately active 2,200
. Pregnant + 350
. Lactating + 750
Adapted from C. de Ville de Goyet, J. Seaman, and U. Geijer,The Management of Nutritional Emergencies in Large Populations (WHO, 1978)
FOOD AND NUTRITION 73

75
STUDY OF MALNUTRITION
1. DESCRIPTION
This objective is designed to give course participants a grounding in:
. types of malnutrition
. methods of measuring a population’s nutritional status
. causes of malnutrition
. possible strategies for the nutritional rehabilitation of malnourishedindividuals.
In defining malnutrition, the instructor must discuss the different types ofmalnutrition: marasmus, kwashiorkor, and stunted growth. The concepts ofacute and chronic malnutrition must be clarified, together with the parametersthat may induce one form or another. In addition, the instructor must definevitamin deficiencies, particularly those most common in emergency situations:A, B1, and C deficiencies.
The methods of assessing a population’s nutritional status are exclusivelyanthropometric. The instructor should explain why children are the groupchosen for anthropometric measurement. Next, participants will study thedifferent measurement systems and the advantages and disadvantages of each.Emergency operations generally focus on acute malnutrition. The instructor willexplain the criteria for classifying acute malnutrition as moderate or severe.
An analysis of the causes of malnutrition is useful for determining what types ofaction are most appropriate. The problem may lie in access to food, but it mayalso be the result of public health problems such as a measles epidemic or anunhealthy environment.
Nutritional rehabilitation involves treating the causes. For moderate forms ofmalnutrition, a supplementary dry ration may be added to the basic food ration.For severe forms, it may be preferable to establish a nutritional rehabilitationcentre which, depending on need and local constraints, may be open daily oraround the clock. In any case, the instructor must stress that a nutritionalrehabilitation programme ismeaningless unless the family unit has access to foodresources (either of its own or provided through food distributions) to cover itsbasic nutritional needs after the nutritional rehabilitation programme has ended.
HELP/SOS: FOOD AND NUTRITION74

2. CATEGORY
Tool: ability to diagnose and measure malnutrition and the basic skills to plan astrategy.
3. FORMULATION
Define the various forms of malnutrition and the methods used to measure it inemergency situations.
What strategies can be used in emergency situations to reduce the malnutritionrate?
4. TEACHING METHOD
Assignment presented to work groups, who will be asked to write the results oftheir work on transparencies.
5. DURATION
Total duration: 60 minutes
. 30 minutes for work in groups
. 30 minutes for summary in the plenary session.
6. RECAPITULATION
. Box 1: Types of malnutrition (the instructor should give precise definitionsof these various forms of malnutrition)
. Box 2: Anthropometric methods for assessing nutritional status
. Box 3: Criteria for choosing a method of anthropometric assessment inemergency situations
. Box 4: Presentation of anthropometric assessment results (percentage andZ-score)
. Box 5: Cut-off points for body mass index (BMI)
. Box 6: Classification of malnutrition based on arm circumference
. Box 7: Classification of malnutrition based on ratio of weight to height
. Box 8: Classification of malnutrition based on QUAC-stick measurements
. Box 9: Some effects of war, drought, and volcanic eruptions on the foodsupply chain
. Box 10: Indicators and methods for evaluating a food supply chain. (It shouldbe em-phasized that anthropometric indicators are only one type of anumber of indicators for assessing a particular food and nutritionsituation.)
FOOD AND NUTRITION 75

77
LINK WITH NEXT OBJECTIVES
At this stage course participants possess most of the skills they need to identifyfood and nutrition problems within a population and to formulate bothoperational objectives and a strategy for achieving them.
Box 1
TYPES OF MALNUTRITION
PROTEIN-ENERGYMALNUTRITION
. Marasmus
. Kwashiorkor
. Stunted growth
. Acute malnutrition
. Chronic malnutrition
VITAMIN DEFICIENCIES
. A
. B1
. C
TRACE ELEMENTS
. Iron (anaemia)
Box 2
ASSESSMENT OF NUTRITIONAL STATUS
ANTHROPOMETRIC METHODS
. Weight/height
. Arm circumference
. Arm circumference/height (QUAC stick)
. Height/age
. Weight/age
. Body mass index(BMI)
HELP/SOS: FOOD AND NUTRITION76

Box 3
CRITERIA FOR CHOOSINGAN ANTHROPOMETRIC ASSESSMENTMETHOD IN EMERGENCY SITUATIONS
. Relevance to what needs to bemeasured: acutemalnutrition
. Reliability of the method:Arm circumference (AC)/height +++Weight/age? +
. Simplicity: AC/height
. Speed
. Acceptability to the population
. Population groups:BMI method is applicable to adults
Box 4
PRESENTATION OF ANTHROPOMETRICASSESSMENT RESULTS
" Z-SCORE:
Anthropometric data expressed in terms of the numberof standard deviations from the reference value (mean)
" PERCENTAGE:
Actual weight as a percentage of standard weightfor a given height
FOOD AND NUTRITION 77

79
25 – 20.1
MEN
«A»: Normal Nutritional Status 23.8 – 18.5
20 – 16«B»: Moderate Malnutrition 18.4 – 16
< 16«C»: Severe Malnutrition < 16
WOMEN
Box 5
CUT-OFF POINTSFOR BMI
at risk formalnutrition
CHILD’S NUTRITIONAL STATUS
< 135 mm
moderatemalnutrition
< 125 mm
severe malnutritionwith high risk of
mortality< 110 mm
ARMCIRCUMFERENCE
Box 6
CLASSIFICATION BASEDON ARM CIRCUMFERENCE
HELP/SOS: FOOD AND NUTRITION78

severemalnutrition kwashiorkor
moderate malnutrition
OEDEMAPRESENT
OEDEMAABSENT
≥ 70 % -
< 80 %severe
malnutrition marasmus-kwashiorkor
severemalnutrition marasmus
< 70 %
severemalnutrition kwashiorkor
normal≥ - 2 SD
severemalnutrition kwashiorkor
moderate malnutrition< - 2 SD
severemalnutrition marasmus-kwashiorkor
severemalnutrition marasmus
< - 3 SD
%
WEIGHT/HEIGHT
Box 7
CLASSIFICATION BASED ON WEIGHTFOR HEIGHT
Box 8
CLASSIFICATION BASEDON QUAC-STICK MEASUREMENTS
A: SATISFACTORY NUTRITIONAL STATUS 5 85%
B: MODERATE MALNUTRITION < 85% AND 575%
C: SEVERE MALNUTRITION < 75%
FOOD AND NUTRITION 79

81
DOMESTIC TRANSPORTSERVICES
ACCESSIBILITY OFFOOD RESOURCES
(Population’s ability to gain accessto food resources)
• Communications• Transport facilities• Storage
• Economic access - Purchasing power - Food prices• Access and political factors (blockades)• Access and social factors (discrimination)
DISTRIBUTION ANDCONSUMPTION OF FOOD
RESOURCESWITHIN THE FAMILY
• Redistribution of food resources according to social norms favouring the survival of the more or the less vulnerable groups
• Consumption of uncustomary foods (compensation mechanisms)
NATURAL RESOURCES
PRODUCTION
AVAILABILITY OF FOODRESOURCE
• Surfaces covered by lava• Mined areas• Current rainfall compared with the norm
• Crop assessment• Assessment through interviews with peasants• Reduction of arable land (mines, security risks)
• Balance between food resources and population (number)• Wholesale prices
IMPORTS• Import documentation• Chambers of commerce• Ministries of agriculture
BIOLOGICAL UTILIZATIONOF FOODS
• Normal activities• Trace element deficiencies• Diseases that impair food absorption (diarrhoeal diseases, intestinal parasites, etc.)
NUTRITIONAL STATUS• Acute malnutrition• Chronic malnutrition
Box 9
SOME EFFECTS OF WAR, DROUGHT,AND VOLCANICERUPTIONS
HELP/SOS: FOOD AND NUTRITION880

• methods
• peasant interviews• satellite images
• evaluation of market prices• Rapid Appraisal Assessment (RAA)
Prices of basic food products,income, migration
• assessment within the household - 24-hour diet history
- observation throughout an entire day
• market assessment - sale of humanitarian relief rations
Household food consumption
• assessment of morbidity at the family level, through health centres
Prevalence of diarrhoeal diseases, measles, and parasitic infections
• weight/height• AC/height• mortality
Malnutrition
• peasant interviews (household food stocks)• interviews with authorities
Ministry of Agriculture/Port authorities/WFP/FAO
Quantities of food available
Examples of Indicators
Agricultural production
Box 10
INDICATORS AND METHODSFOR ASSESSING A FOOD SUPPLY CHAIN
FOOD AND NUTRITION 81

83
DEFINITION OF AN AGRO-FOOD POLICYFOR DIFFERENT POPULATION GROUPS
1. DESCRIPTION
Course participantsmust define an agro-food and nutritional programme for thevarious population groups suffering the effects of the conflict situation describedin the Alphaland-Betaland simulation. For this purpose they will use theplanning procedure studied earlier. This means they must:
. identify the problems involved in access to food resources for eachpopulation group
. define the priorities and constraints of potential interventions
. establish objectives and strategies for each population group.
2. CATEGORY
Practice: This objective gives participants an opportunity to use the skills alreadytaught, as they will need to do later on in the field.
3. FORMULATION
In theAlphaland-Betaland simulation, youmust identify all the population groupswith problems involving the main links of the food supply chain as defined in thefirst objective of this module. These problems may be related to agriculturalproduction, food distribution and storage, access to food—in short, malnutritionproblems. You should not limit yourselves to problems that already exist, but takea longer view and anticipate problems likely to ensue from the conflict situation.
Second, you must decide which population groups will take priority, accordingto the seriousness and urgency of their problems as well as the feasibility ofpossible interventions. You must therefore study the foreseeable constraints.
Finally, you must define an operating strategy, listing the specific programmesyou plan to set up.
4. TEACHING METHOD
The participants will work on the assignment in their work groups. However, thesession will be divided into two parts:
HELP/SOS: FOOD AND NUTRITION82

1. First, the work groups will be asked to draw up a list of the problems of eachpopulation group affected by the conflict, and present it in a plenary session.
2. Using this preliminary material, each work group will be randomly assigned adifferent population group. Each group will then establish objectives andstrategies for the population assigned to it.
Note: Obviously specific action to be taken for the benefit of one populationgroup will affect the other groups. Participants must be urged to coordinate theirstrategies. For example, food distributions are known to attract populationgroups. Consequently, this might interfere with agricultural rehabilitationprogrammes designed to keep people in their homes.
5. DURATION
Total duration: 180 minutes
. identification of most urgent problems: 90 minutes
. 60 minutes for work in groups
. 30 minutes for a plenary session
. objectives and intervention strategies: 90 minutes
. 60 minutes for work in groups
. 30 minutes for summary in the plenary session.
6. RECAPITULATION
. Box 1: Two programmes to study in detail
. Box 2: Map of the province of Gamma
. Box 3: Map of the province of Chi
. Box 4: Map of the Epsilon district
. Box 5: Map of the Awalei camp
On the blackboard summarize the objectives and strategies recommended by thework groups.
LINK WITH NEXT OBJECTIVES
In the course of this section, the course participants have summed up a complexsituation and defined types of intervention. Now they will focus on the study oftwo kinds of programmes:
FOOD AND NUTRITION 83

85
. food distributions
. nutritional rehabilitation programmes.
These programmes have been selected because health care personnel are oftenfaced with the task of planning them.
Box 1
TWO PROGRAMMESTO STUDY IN DETAIL
. FOOD DISTRIBUTION
. NUTRITIONAL REHABILITATION
HELP/SOS: FOOD AND NUTRITION84

Betaland
GammaProvince
Alphaland
border
Karam
district
Epsilondistrict
WabiRiver
GowiRiver
TanaRiver
BowiRiver
BeloRiver
Gamma
district
Brew
district
Box 2
FOOD AND NUTRITION 85

87
Alphaland
ChiProvince
Sigmadistrict
Maquerdistrict
Lirumidistrict
Chi
Chidistrict
Chidistrict
Betaland
Box 3
HELP/SOS: FOOD AND NUTRITION86

border
Epsilon district
Sigmadistrict
BetalandGammaProvince
AlphalandChiProvince
Bowi River
Box 4
FOOD AND NUTRITION 87

89
Awaleicamp
BowiRiver
ATP
dispensary
governmentaldispensary
spring
well
Zotew
e
swamps
Box 5
HELP/SOS: FOOD AND NUTRITION88

PRINCIPLES OF PLANNINGA FOOD DISTRIBUTION
1. DESCRIPTION
We have seen that the decision to carry out food distributions is a complexprocess, whichmust take into consideration the conflict situation’s impact on theentire food supply chain. The criteria for such a decision relate not only tonutritional status, but also to local agricultural potential, the possibility ofguaranteeing access to local food resources by alternate means, potentialdevelopments in the current situation, and the possibility of enforcinginternational humanitarian law to protect the means of production if they areinaccessible for security reasons. By taking these factors into consideration, thedecision-maker can avoid two major pitfalls:
. waiting until malnutrition rates are very high before deciding to organizefood distributions. The preventive approach is preferable; the decision tointervene should be dictated by restrictions on access to the usual foodresources
. distributing food at the wrong time and in the wrong place, a step likely tointerfere with local crops, thereby much reducing their market value anddestabilizing the local economy.
Once the decision to organize food distributions has been made, care must betaken not to create dependency or reduce the beneficiaries’ motivation to resumetheir normal activities. This is especially true for rural populations, althoughurban populations who depend onwages for their livelihood experience the sameproblem.
The steps of organizing a food distribution, in logical order, can be defined asfollows:
. determine sociocultural food habits. In general, this information will alreadyhave been obtained during the investigation of household food consumption
. compose a food ration
. enumerate beneficiaries
. select foods and determine the number of beneficiaries so that the quantity offood that must be shipped in can be determined
. decide on a distribution strategy
FOOD AND NUTRITION 89

91
. transport and store food preparatory to its distribution to beneficiaries
. set up a site for distributing food
. organize a food distribution
. set up a programme to monitor food distribution
. plan alternatives to food distributions.
2. CATEGORY
Framework: establishing a framework for the study of the skills required to plana food distribution.
3. FORMULATION
Define a conceptual framework that will help to determine the skills required toplan a food distribution.
4. TEACHING METHOD
Discussion in plenary session involving all participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: A food distribution’s place in the food supply chain (it must beemphasized that food distributions are only a temporary, palliativemeasure).
. Box 2: Factors to consider before instituting a food distribution.
. Box 3: Practical principles for planning a food distribution.
. Box 4: Planning the logistics of a food distribution.
LINK WITH NEXT OBJECTIVES
In the next objectives, the main steps of planning a food distribution will bestudied.
HELP/SOS: FOOD AND NUTRITION90
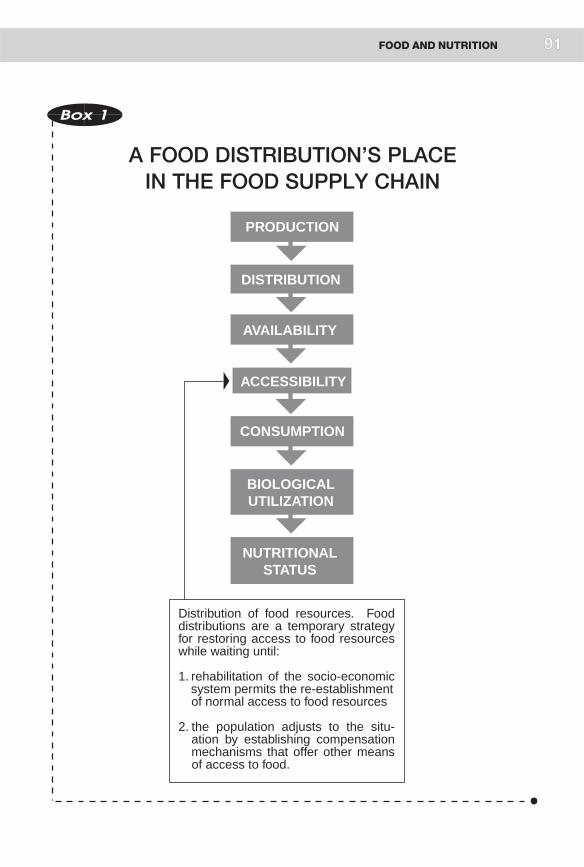
PRODUCTION
DISTRIBUTION
AVAILABILITY
ACCESSIBILITY
CONSUMPTION
BIOLOGICALUTILIZATION
NUTRITIONALSTATUS
Distribution of food resources. Food distributions are a temporary strategy for restoring access to food resources while waiting until:
1. rehabilitation of the socio-economic sssystem permits the re-establishment
of normal access to food resources
2. the population adjusts to the situ- aaation by establishing compensation aamechanisms that offer other means aaof access to food.
Box 1
A FOOD DISTRIBUTION’S PLACEIN THE FOOD SUPPLY CHAIN
FOOD AND NUTRITION 991

93
Box 2
FACTORS TO CONSIDERBEFORE INSTITUTINGA FOOD DISTRIBUTION
1. Study a variety of indicators reflecting the statusof the food supply chain; do not rely solely on themalnutrition rate.
2. Assess in advance potential economic, social,and political repercussions, and plan measuresto minimize them.
HELP/SOS: FOOD AND NUTRITION92
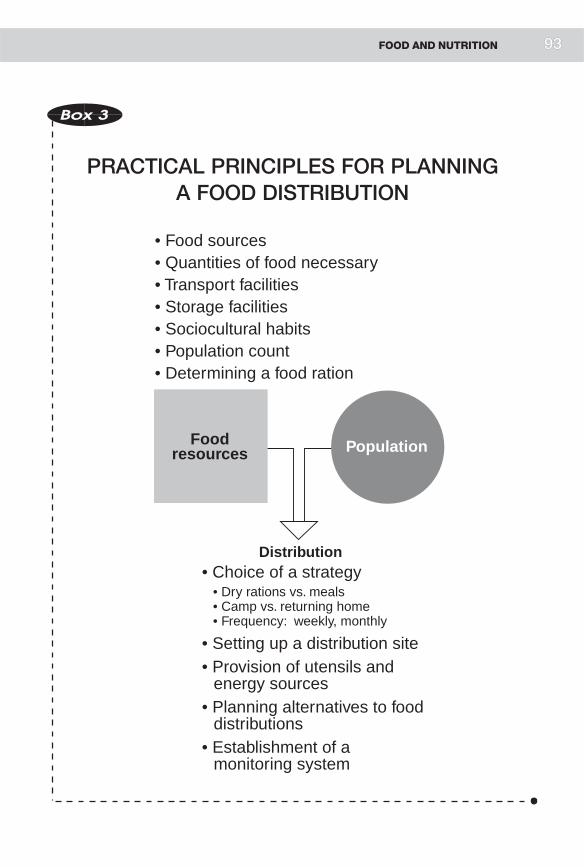
• Choice of a strategy • Dry rations vs. meals • Camp vs. returning home • Frequency: weekly, monthly
• Setting up a distribution site • Provision of utensils and energy sources
• Planning alternatives to food distributions
• Establishment of a monitoring system
• Food sources• Quantities of food necessary• Transport facilities• Storage facilities• Sociocultural habits• Population count• Determining a food ration
PopulationFoodresources
Distribution
Box 3
PRACTICAL PRINCIPLES FOR PLANNINGA FOOD DISTRIBUTION
FOOD AND NUTRITION 993

95
Determine sociocultural habits
Calculate a food ration
Count the population
Identify available foodsources
Identify transport andstorage facilities
Choose a strategy
Select a distribution site
Utensils, energy
DistributionPlan alternativesto a food distribution
Plan a monitoringsystem
Box 4
PLANNING THE LOGISTICSOF A FOOD DISTRIBUTION
HELP/SOS: FOOD AND NUTRITION994

COMPOSING A FOOD RATION
1. DESCRIPTION
Several factors must be considered in composing a food ration. The main ones are:
. sociocultural habits. The purpose of a food distribution is not to modify apopulation’s eating habits
. the logistical imperatives of emergency situations. It is unrealistic to try todistribute fresh food in situations where preserving and distributing the foodpresent insurmountable problems
. economic factors. The distributed food has a certain economic value on thelocal market. Beneficiaries are likely to resell some of it in order to purchaseother goods. Moreover, consideration must be given to the potentialinfluence of food distributions on the price of local foodstuffs, themechanisms of trade, and the management of local food stocks
. political factors: The distribution of food attracts the interest of armedgroups and political forces in the area. Care must be taken to keep food aidproducts from arousing the rapacious impulses of those with the power toappropriate them through looting, imposing an embargo, etc.
. the nutritional value of the foods chosen. The foods distributed must coverthe energy and protein needs of the various groups of beneficiaries
. the individual needs of moderately malnourished people and pregnant andlactating women, whose supplementary needs must be included in the basicration.
All these factors must be taken into account in the planning of a food ration. It istrue that from a strictly nutritional perspective, the most important aspects arethe food’s nutritional value and cultural acceptability. However, logistical,economic, and political factors play an important part in the organization andimplementation of food distributions.
2. CATEGORY
Tool: knowledge of the factors involved in composing an appropriate food ration.
3. FORMULATION
Identify the factors involved in composing a food ration for emergencydistributions.
FOOD AND NUTRITION 95

97
4. TEACHING METHOD
Assignment presented to work groups, followed by a discussion in plenarysession.
5. DURATION
Total duration: 40 minutes
. 20 minutes for work in groups
. 20 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: General factors to consider in designing a food ration
. Box 2: Nutritional factors to consider in designing a food ration
. Box 3: Sociocultural, economic, and political factors
LINK WITH NEXT OBJECTIVES
Designing a food ration involves selecting foods that are easy to distribute so thatbeneficiaries will have an optimal chance of obtaining access to them. The nextobjective will explain how to quantify the food resources needed to cover a givenpopulation’s food needs.
HELP/SOS: FOOD AND NUTRITION96

Nutritionalfactors
Politicalfactors
Socioculturaland
environmentalfactors
Economicfactors
Foodration
Box 1
FACTORS TO CONSIDER IN DESIGNINGA FOOD RATION
FOOD AND NUTRITION 997

99
Nutritionalvalue of food
Nutritionalneeds
BASIC PRINCIPLE
Choice offoods
conditionedby usual
constraintsof a food
distribution
Averagefamily
nutritionalrequirements
Factors to consider inan emergency situation
•Age• Sex• Activities• Physiological status
• Calories• Protein• Vitamins• Trace elements
Box 2
NUTRITIONAL FACTORS TO CONSIDERIN DESIGNING A FOOD RATION
HELP/SOS: FOOD AND NUTRITION998

Box 3
SOCIOCULTURAL, ECONOMIC,AND POLITICAL
FACTORS
SOCIOCULTURAL FACTORS:
. Food habits
. Mode of food preparation
ECONOMIC FACTORS:
Value of distributed food on the local market
POLITICAL FACTORS:
Risk of armed groups being attracted by the fooddistributions:
. depending on types of food
. depending on mode of distribution
} dry rations
} meals
FOOD AND NUTRITION 99

101
CONDUCTING A POPULATION CENSUS
1. DESCRIPTION
The selection of foods and the calculation of the food ration determine what willbe given to a beneficiary. Counting the number of beneficiaries of the distributionconstitutes the second stage in planning the total quantities of food resources thatwill be needed.
Carrying out a population census in an emergency situation is a delicate task forseveral reasons:
. in some cases it is difficult to find conflict victims who are actually sufferingfrom lack of food if they are scattered among a population whose way of lifehas not been affected by the conflict
. the population may be on the move, fleeing or displaced as a result of aprecarious security situation
. there may be no access to potential victims in conflict zones
. food distributions may attract population groups unaffected by theemergency situation but who hope to benefit from the aid all the same
. the number of beneficiaries may be inflated owing to multiple registration ofthe same people or families, or to exaggerated reports of the number ofpeople per family if registration is based on the statement of the head of thefamily.
Certain rules must be followed:
. carry out the census all at one time to avoid the problem of populationmovements in the interim; this means assembling all beneficiaries in the sameplace at the same time
. provide each family with a registration card showing exact name, address,and number of family members
. seek assistance from local authorities who are known to be familiar with thepopulations involved and to have influence over them.
2. CATEGORY
Tool: possession of the essential knowledge for conducting a populationcensus.
HELP/SOS: FOOD AND NUTRITION100

3. FORMULATION
What are the pitfalls to avoid and the rules to follow in conducting a populationcensus?
4. TEACHING METHOD
Assignment presented to work groups, followed by summary in plenary session.
5. DURATION
Total duration: 40 minutes
. 20 minutes for work in groups
. 20 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Difficulties involved in conducting population censuses duringemergency situations
. Box 2: Some rules to observe in taking a census
LINK WITH NEXT OBJECTIVES
At this stage, we have decidedwhat to distribute and have drawn up a list of thosewho are to receive it. The next stage is to select a food distribution strategy.
FOOD AND NUTRITION 101

103
Box 1
TAKING A CENSUS
DIFFICULTIES IN EMERGENCY SITUATIONS
1. Identification of population groups whoare particularly vulnerable to lack of accessto food resources
2. Population instability
3. Attraction exerted by food distributions
Box 2
CENSUS
SOME RULES TO OBSERVE
1. Carry out the census all at one time
2. Register beneficiaries
3. Seek assistance from local authorities
HELP/SOS: FOOD AND NUTRITION102

PRINCIPAL STRATEGIESFOR REHABILITATING A POPULATIONGROUP’S NUTRITIONAL STATUS
1. DESCRIPTION
The title of this section requires an explanation. The focus here is not on methodsfor the nutritional rehabilitation of individuals, but strategies for reducingmalnutrition rates within a population group. Before discussing nutritionalrehabilitation programmes per se, two points should be made.
First, the causes of malnutrition must be identified:
. lack of food
. unhealthy environment
. sociocultural factors
. political factors (stress, insecurity)
. morbidity (diarrhoeal diseases, measles, etc.).
In conflict situations, a number of contributing factors are usually intertwined,and the reduction of malnutrition requires a multidisciplinary approach.
Second, when the main cause of malnutrition is lack of food, it must be specifiedthat the essential programme for reducing malnutrition focuses on giving thepopulation groups in question access to basic food resources. Specific nutritionalrehabilitation programmes can then be introduced.
Nutritional rehabilitationprogrammesarebasedoneitherof twopossible strategies:
Malnourished individuals will be provided with food either in the form ofdry rations distributed as part of a system of food distributions, or in theform of meals served to beneficiaries at feeding centres.
Both strategies have their advantages and disadvantages. One advantage of dryrations is that they do not conflict with families’ traditional eating habits, and canbe integrated in the basic relief ration. Accordingly, the implementation of thisprogramme does not involve any significant extra work. Nor does it interferewith family life, in contrast to supplemental feeding in a feeding centre, whichrequires the malnourished child to go to the centre every day or remain there(depending on the kind of centre), usually accompanied by his or her mother. As
FOOD AND NUTRITION 103

105
a result, family life, especially the daily chores and the care of the other children,is badly disrupted. Theoretically, the overall needs of the malnourished can becovered by dry rations, whereas the coverage provided by specialized centres isoften limited. However, when the supplementary food ration for malnourishedbeneficiaries is integrated in the basic ration, there is a risk that it will not beconsumed by the person it is intended for, but by the entire family. This approachobviously requires strict surveillance of malnourished individuals within thepopulation, and is used for cases of moderate malnutrition where the weight-for-height (WFH) is over 80% (Z-score of -2).
In an emergency situation, dry rations are the strategy of choice for rehabilitatingcases ofmoderatemalnutrition.Moreover, given the additional nutritional needsof certain population groups—pregnant and lactating women (quantitativeneeds) and young children (qualitative needs), increasing the basic emergencyration can be considered as a way of meeting the needs not only of malnourishedindividuals, but also of the groups typically classified as ‘‘vulnerable.’’ Thisstrategy has its limitations, however, since it can cover only the needs of themoderately malnourished. Accordingly, in situations involving large numbers ofseverely malnourished people (<80%ofWFH), the establishment of specializedcentres must be considered.
Such centres fall into two categories:
. nutritional rehabilitation centres (supplementary feeding centres) open dailyfor the treatment of people with aWFH of between 80% and 70% (<-2 to -3Z-score). In these centres beneficiaries are fed two to four meals a day, butreturn home at night
. 24-hour nutritional rehabilitation centres (therapeutic feeding centres) forpeople with a WFH of less than 70% of the reference (Z-score of -3) or whopresent oedema (kwashiorkor). In these centres, beneficiaries are given six toeight meals in every 24-hour period.
Malnutrition criteria are not the only aspects of planning a nutritionalrehabilitation programme. Course participants should also understand that suchfactors as security and the total number of people suffering from malnutrition areessential considerations in the development of a nutritional strategy. If there is avery large number, say several hundred, of children with a Z-score of less than -3, itmay prove impossible to set up enough therapeutic feeding centres toaccommodate them all. In such a case it would be wiser to invest in facilitiesthat require fewer staff but permit coverage of all malnourished children.
In the course of this learning objective the Z-score will be mentioned, but notactually studied, since it will be examined in detail in the module on
HELP/SOS: FOOD AND NUTRITION104

epidemiology. Here the instructor will merely point out the connection betweenthe Z-score and the QUAC stick and WFH ratio.
Finally, stress should be laid on the role of basic care in the management ofmalnutrition—particularly immunizations andmedical care, the details of whichwill be studied in later objectives.
2. CATEGORY
Tool: basic information to determine the most appropriate strategy for reducingmalnutrition within a population.
3. FORMULATION
What are the advantages and disadvantages of the following two approaches toreducing malnutrition?
. distribution of specific foods to population groups
. provision of meals in specialized centres for the malnourished.
4. TEACHING METHOD
Assignment presented to work groups, followed by discussion in plenary session.
5. DURATION:
Total duration: 30 minutes
. 10 minutes for work in groups
. 20 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Should themalnourished be given food to take home, or should theybe fed in specialized centres?
. Box 2: Criteria for deciding between strategies
. Box 3: Types of nutritional rehabilitation centres (NRC)
LINK WITH NEXT OBJECTIVES
In this section, course participants have learned to define a specific strategy for agiven situation. The next objective will give them the tools for understanding thebasics of nutritional rehabilitation on the individual level.
FOOD AND NUTRITION 105

107
Malnourished
MealsFood
Admission of malnourished to centres where they are fed prepared meals—"on-the-spot"feeding
Distribution of supplementary food in the form of dry rations (included in the general ration)—"take-home" distributions
Box 1
SHOULD THE MALNOURISHED BE GIVENFOOD TO TAKE HOME, OR SHOULD
THEY BE FED IN SPECIALIZED CENTRES?
HELP/SOS: FOOD AND NUTRITION1106

Criteria forchoosing
strategies
• Seriousness of the malnutrition
• Extent of the malnutrition (number of people affected)
• Logistics of creating a facility
• Social disruptions created by an NRC
• Anticipated impact of each strategy
Box 2
DECISION CRITERIA
FOOD AND NUTRITION 1107

109
Distributionof meals duringthe day
No residential infrastructure
Distribution of meals over a period of up to24 hours
Need for residential infrastructure.
NUMBER OFMEALS
2
3
4
5
6
8
Box 3
TYPES OF NUTRITIONALREHABILITATION CENTRES
HELP/SOS: FOOD AND NUTRITION108

PLANNING A MONITORING SYSTEMFOR FOOD DISTRIBUTIONS
1. DESCRIPTION
Food distributions play a part in the food supply chain by artificially restoringaccess to food resources for certain population groups. A monitoring systemmust be able to provide answers to the following questions:
. Are the beneficiaries receiving their food rations?
. Are the rations they receive appropriate to their nutritional needs?
. Has the malnutrition rate been reduced to the target limit set in the initialobjectives?
. Are the distributed foodstuffs found in significant quantities in the localmarket?
. Are the food distributions having an impact on local market prices?
. Has agricultural production been resumed?
. Are the usual food distribution channels open?
The indicators that will be monitored in order to provide the answers to thesequestions should not be limited to anthropometric (malnutrition rates) andlogistical (number of rations distributed in relation to the number ofbeneficiaries) indicators, but should also include market prices and changes inlocal resources. This last point is particularly important, since it will be the basisfor decisions concerning the management of the programme—namely,modifications of the food ration (for example, a reduction to half-rations ifbeneficiaries regain independent access to a certain quantity of food), orrestrictions on the rations or refinements of the registration system if largequantities of food distributed by humanitarian agencies turns up on the market.Finally, this information will influence the decision as to whether fooddistributions can be safely terminated, by providing assurance that beneficiarieshave a reliable alternative: successful agricultural rehabilitation programmescoexisting with the food distributions, or the institution of other mechanisms tore-establish access to food.
Course participants must grasp the importance of establishing a surveillancesystem to evaluate the programme’s impact on beneficiaries—including thedetrimental effects it may have, such as attraction of other population groups,
FOOD AND NUTRITION 109

collapse of the prices of local products as a result of the surplus created by foodrelief, etc.
2. CATEGORY
Tool: The basics for planning a surveillance system for a food distribution.
3. FORMULATION
List the indicators that can be used to monitor a food distribution programme.
4. TEACHING METHOD
Assignment presented to work groups followed by summary in plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Indicators associated with different links of the food supply chain
. Box 2: Ask participants to remember the indicators learned for thesurveillance of food distributions, since they will be used again inthe module on epidemiology
LINK WITH NEXT OBJECTIVES
The results of this objective will be reviewed in the lesson on epidemiology andintegrated with the material on indicators presented in other modules:environment, communicable diseases, and health services.
HELP/SOS: FOOD AND NUTRITION110 111

PRODUCTION
DISTRIBUTION
AVAILABILITY OFFOOD RESOURCES
ACCESSIBILITY
CONSUMPTION
BIOLOGICALUTILIZATION
NUTRITIONALSTATUS
Changes in type of agricultural production
Price of foodstuffs on the local
market
Morbidity
Presence of food relief products
within the household
Anthropometric indicators
Presence ofhumanitarian reliefproducts for sale on
the local market
Box 1
INDICATORS FOR MONITORINGA FOOD DISTRIBUTION
FOOD AND NUTRITION 1111

113
Box 2
The institution of surveillancesystems will be studied in the uniton epidemiology.
Remember the indicators learned inconnection with the food supplychain.
HELP/SOS: FOOD AND NUTRITION112

LOGISTICAL IMPLICATIONSOF TRANSPORT, STORAGE,AND DISTRIBUTION OF FOODSTUFFS
1. DESCRIPTION
Dry foods are used for food distributions (cereals, legumes, oil) because of theirnutritional value and ease of handling. Course participants should know theaverage weight of a food ration for one month (16 to 18 kilos) and the volumerepresented by one tonne of food (2 m3).
The choice of a location for storage facilities depends on several factors:
. proximity to sources of food supplies
. security
. proximity to distribution points.
With respect to storage, course participants should know:
. the main principles of warehouse architecture: necessary surface, height,ventilation, construction materials, resistance to bad weather, precautionsagainst theft, etc.
. the rules for the actual storage of foodstuffs
. the rules for maintaining supplies in good condition—particularly theprecautions that must be taken to protect them from insects and vermin.
With respect to transport, participants should know the capacity of the primarymeans of transport: trucks and airplanes.
If possible, food aid should be distributed close to where the beneficiaries areliving. This will spare them long, arduous journeys, since they usually have nomeans of transportation. Moreover, this strategy ensures that populationsremain close to their means of production, thereby favouring a resumption ofnormal activities (rehabilitation). Distributions far away from the beneficiaries’place of residence, in contrast, are apt to lead to the establishment of camps at thedistribution point, making rehabilitation more difficult.
Foodstuffs can be distributed in different ways. The foodstuffs making up thebasic ration may be distributed in bulk to heads of families on the basis of the
FOOD AND NUTRITION 113

115
number of people in the household. Beneficiaries may also receive family parcelscontaining the components of the food ration.
Once the strategy has been decided, the distribution site must:
. remain accessible to transport at all times
. offer safe conditions for both the beneficiaries and the humanitarian agents
. be large enough to accommodate a substantial number of beneficiaries—anumber that may increase as the conflict situation develops further.
The lay-out of the site should take into account the need for a water supplyduring the distribution, and facilities for first aid, in case they are needed.Nevertheless, fixed installations must be avoided at all costs since this wouldencourage beneficiaries to form permanent camps on the site.
2. CATEGORY
Tool: a basic understanding of the logistic requirements of food distributions.
3. FORMULATION
Knowledge of the main logistic rules to follow in carrying out a well-organizedfood distribution.
4. TEACHING METHOD
Information given directly to participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Logistic factors (choice of food items, ration, transport, storage)
. Box 2: Strategy for a food distribution
. Box 3: Organization of a food distribution site
LINK WITH NEXT OBJECTIVES
The next objective will establish the link between food distribution programmesand nutritional rehabilitation programmes.
HELP/SOS: FOOD AND NUTRITION114

Box 1
LOGISTIC FACTORS
CHOICE OF FOODSTUFFS:
cereals
legumesoil
EXAMPLE OF DAILY FOOD RATION PER PERSON:
cereals = 400 glegumes = 100 g ¤ 550 goil = 50 g
TRANSPORT:
TYPE LIMITATION
boat (time)airplane (cost)truck (distance)
STORAGE:
1 tonne = 2 m3
FOOD AND NUTRITION 115

117
BeneficiariesFoodstuffs
Deliver the foodas close to
the beneficiaries’homes as possible
Have the beneficiariescome to central
distribution points
BeneficiariesFoodstuffs
Box 2
STRATEGY FOR AFOOD DISTRIBUTION
HELP/SOS: FOOD AND NUTRITION1116

Logistical planning:• Adequate food stocks• Storage facilities• Transport
Populationsurvey
Distribution of cereals
Distributionof legumes
Distributionof oil
Registration
WaterFirst aid
Stock ofcereals
Stock oflegumes
Stock ofoil
Beneficiaries
Entrance
Exit
Box 3
ORGANIZATION OF AFOOD DISTRIBUTION SITE
FOOD AND NUTRITION 1117
119
LINK BETWEEN FOOD DISTRIBUTIONSAND NUTRITIONAL REHABILITATIONPROGRAMMES
1. DESCRIPTION
Nutritional rehabilitation programmes must be linked with programmesdesigned to restore access to food resources, including food distributions. It islogical to assist the malnourished, but illogical to do so only to return them to asystem inwhich, once again, they have no access to food resources. The two typesof programme are complementary, although in emergency situations prioritymust be given to programmes that provide access to food resources for allpopulations identified as vulnerable.
2. CATEGORY
Tool: strategy to define the complementary link between nutritional rehabilita-tion programmes and programmes designed to restore access to food resourcesfor a vulnerable population.
3. FORMULATION
What is the connection between nutritional rehabilitation programmes and fooddistributions?
4. TEACHING METHOD
Assignment presented in plenary session.
5. DURATION
Total duration: 15 minutes.
6. RECAPITULATION
. Box 1: Complementary relationship between the distribution of foodrations and a nutritional rehabilitation programme
. Box 2: Complementary relationship between the two types of programme,shown for a normal population distribution
LINK WITH NEXT OBJECTIVES
The next objectives cover nutritional rehabilitation.
HELP/SOS: FOOD AND NUTRITION118
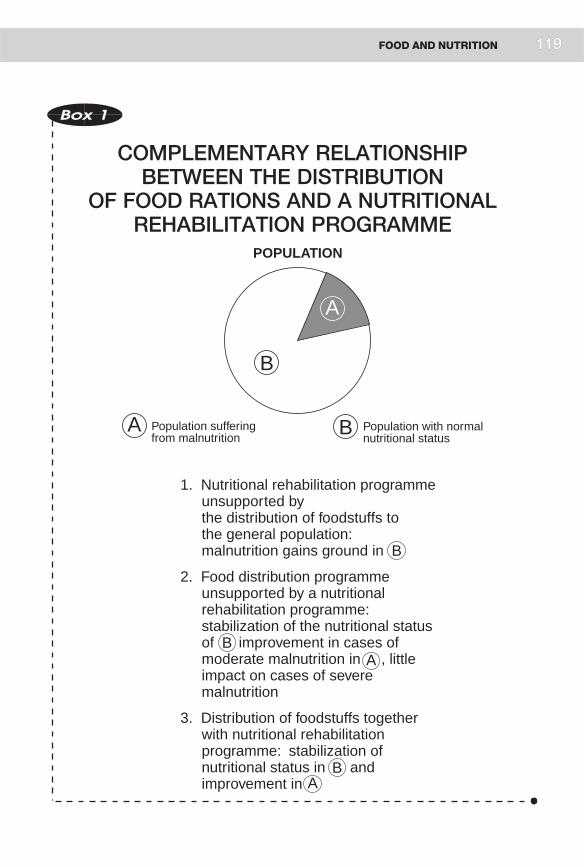
1. Nutritional rehabilitation programme unsupported bythe distribution of foodstuffs tothe general population: malnutrition gains ground in
2. Food distribution programme unsupported by a nutritional rehabilitation programme: stabilization of the nutritional status of improvement in cases of moderate malnutrition in , little impact on cases of severe malnutrition
3. Distribution of foodstuffs together with nutritional rehabilitation programme: stabilization of nutritional status in and improvement in
Population sufferingfrom malnutrition
Population with normalnutritional status
POPULATION
B
A
B
B
B
B
A
A
A
Box 1
COMPLEMENTARY RELATIONSHIPBETWEEN THE DISTRIBUTION
OF FOOD RATIONS AND A NUTRITIONALREHABILITATION PROGRAMME
FOOD AND NUTRITION 1119

121
Impact of nutritional rehabilitation: improvement of the nutritional status of subjects < -2 Z-score
-2 Z-score average
Impact of food distributions to the general population: increases the average nutritional status of the entire population
-2 Z-score average
Box 2
COMPLEMENTARY RELATIONSHIPBETWEEN FOOD DISTRIBUTIONS
AND NUTRITIONAL REHABILITATION SHOWNFOR A NORMAL POPULATION DISTRIBUTION
HELP/SOS: FOOD AND NUTRITION1120

PRINCIPLES OF ORGANIZINGA NUTRITIONAL REHABILITATION CENTRE
1. DESCRIPTION
Children are admitted to nutritional rehabilitation centres according toanthropometric criteria.However, childrenwhose nutritional status is borderlinebut who show associated risk factors such as medical or social problems(orphans, unaccompanied children, etc.) are also eligible for admission to suchcentres.
Any plan for a nutritional rehabilitation centre must make provision for fourkinds of activity:
. Feeding: the feeding of severely malnourished children must follow strictrules. During the first days, the child should not be given more than 100 kcaland 3 g of protein per kilo of bodyweight per day.Gradually this allowance isincreased until it reaches 200 kcal and 5 g of protein per kilo of body weightper day. At this stage severely malnourished children may gain 10 to 20 g perkilo of bodyweight per day, andmoderatelymalnourished onesmay gain 5 to10 g. The number of meals the child receives per day depends on the severityof the malnutrition and the degree of nutritional recovery; the feeding regimeis gradually modified until it approximates a normal diet by the end of thechild’s stay in the centre. We will not detail here how to make high-energymilk (milk, sugar, and oil), recipes for which can be found in the nutritionalmanuals available to course participants. Course graduates can consult suchmanuals once they are actually in the position of having to plan a nutritionalrehabilitation programme.
. Prevention:
. immunization against measles is imperative for all children (a measlesepidemic in a nutritional rehabilitation centre would be a real disaster)
. systematic administration of vitaminA to all children. The recommendeddose is 200,000 IU for children over the age of six months, and 50,000 IUfor children under six months
. administration of mebendazole to all children over a year old
. measures against hypothermia (blankets, instructions to mothers)
. supply of potable water
FOOD AND NUTRITION 121

123
. sanitation: clean buildings, proper food handling and storage, personalhygiene.
. Medical care:
. treatment of common medical problems: diarrhoeal diseases, fevers,anaemia, respiratory infections, skin infections
. supply of essential drugs.
. Epidemiological surveillance:
. childrenwill be individuallymonitored from the time they are admitted tothe centre until the time they leave. Records should be made of WFH,associated medical problems, social situation, compliance (in the case ofday care centres), the child’s progress towards nutritional recovery
. on the general level, different variables will be monitored: the number ofadmissions to the centre, the number of deaths, the average length of stay,the number of children present each day, the number of children who failto complete the nutritional rehabilitation programme.
Course participants will not be asked to design a nutritional rehabilitation centre.The architecture of health facilities, as exemplified by dispensaries, will bestudied in the module on medical and surgical care.
2. CATEGORY
Tool: grasp of the general principles of organizing a nutritional rehabilitationcentre.
3. FORMULATION
List the activities essential to the functioning of a nutritional rehabilitationcentre: definition of admission criteria, preparation of food recipes, organizationof meals, epidemiological monitoring.
4. TEACHING METHOD
Assignment presented to work groups followed by summary in plenary session.
5. DURATION
Total duration: 60 minutes
. 30 minutes for work in groups
. 30 minutes for summary in plenary session.
HELP/SOS: FOOD AND NUTRITION122

6. RECAPITULATION
. Box 1: Activities in a nutritional rehabilitation centre
. Box 2: Nutritional needs of the malnourished
. Box 3: Foods used for nutritional rehabilitation
. Box 4: Meals in a nutritional rehabilitation centre
. Box 5: Public health activities in a nutritional rehabilitation centre
. Box 6: Medical activities in a nutritional rehabilitation centre
. Box 7: Epidemiological activities: individual monitoring
. Box 8: Epidemiological activities: programme monitoring
LINK WITH NEXT OBJECTIVES
In the course of the next objective, participants will be asked to make practicaldecisions concerning the organization of a food and a nutritional aidprogramme, obliging them to apply the tools already studied.
Box 1
ACTIVITIES IN A NUTRITIONALREHABILITATION CENTRE
. NUTRITIONAL ACTIVITIES
. PUBLIC HEALTH ACTIVITIES
. MEDICAL ACTIVITIES
. EPIDEMIOLOGICAL ACTIVITIES
FOOD AND NUTRITION 123

125
Box 2
NUTRITIONAL NEEDS OF THE MALNOURISHED
FIRST WEEK:100 kcal + 3 g protein per kgof body weight per day
SUBSEQUENTLY:200 kcal + 5 g protein
per kg of body weightper day
THEN:Feed on demand whenappetite returns
Box 3
FOODS USED FORNUTRITIONAL REHABILITATION
1. HIGH-ENERGY MILK (HEM)
Powdered milk 80 g } 1,000 kcal
Oil 60 g } = and
Sugar 50 g } 30 g protein
Enough water for a total volume of 1 litre
100 ml = 100 kcal + 3 g protein
2. CEREAL BLENDS prepared from:
CSM (corn-soy-milk)
WSM (wheat-soy-milk)
Powdered milk, oil, sugar
100 ml = 100-150 kcal + 4 g protein
3. NORMAL DIET
* Mother’s milk is essential throughout the process of nutritional rehabilitation.
HELP/SOS: FOOD AND NUTRITION124

Box 4
MEALS IN A NUTRITIONALREHABILITION CENTRE
WEEK
1. HEM . 6-8 meals per day according to degreeof malnutrition
. meals during the night for severecases of malnutrition
2. HEM } 6 meals per day, alternating
CEREAL BLENDS } feedings of HEM and cereal blends
3. } CEREAL BLENDS} HEM
4. } MEALS based} on family feeding
5. } FAMILY MEALS
Criteria for discharge: <Weight gain > 85%Return to normal diet
Box 5
PUBLIC HEALTH ACTIVITIES INA NUTRITIONAL REHABILITATION CENTRE
. Vitamin A: Prophylactic dose of200,000 IU (every 3 months)
. Mebendazole: 200 mg in onedose (children over 1 year old)
. Immunizations against measlesand other diseases included in the
Expanded Programme ofImmunization (EPI) if there isany doubt as to child’s immunestatus
. Health education for child’scaregiver (mother)
FOOD AND NUTRITION 125

127
Box 6
MEDICAL ACTIVITIESIN A NUTRITIONAL
REHABILITATION CENTRE
. Treatment of vitamin deficiencies:A: 200,000 IU (days 1, 2, 7)E: 200 mg injected intramuscularlyfor the first three days, followed by250 mg orally per day
. Treatment of anaemia:Folic acid: 5 mg per day. Wait 2weeks before administering iron
. Dehydration/diarrhoea:oral rehydration salts (ORS)
. Infections: antibiotic treatment forpulmonary infections, forexample
. Intestinal parasites: systematicadministration of 200 mg ofmebendazole
. Hypothermia: mother, blankets
. Skin problems (scabies,infections): topical treatment
Box 7
EPIDEMIOLOGICAL MEASURES:INDIVIDUAL MONITORING
BEFORE:
. Selection (WFH and clinicalexamination)
. Registration (name, WFH,clinical examination, date, etc.)
DURING:
. Weight monitoring
. Clinical and therapeuticmonitoring
. Monitoring of feedingregimen: number ofmeals
AFTER:
. Monitoring within the family
HELP/SOS: FOOD AND NUTRITION126

Box 8
EPIDEMIOLOGICAL ACTIVITIES:PROGRAMME MONITORING
MONITORING OF NUTRITIONALACTIVITIES
. Number of admissions
. Number of children present
. Number of ‘‘defaulters’’
. Number of deaths
. Number of people sent to the hospital
. Number of discharges
MONITORING OF PUBLIC HEALTHACTIVITIES
. Vaccinations, health education sessions
MONITORING OF MEDICALACTITIVIES
. Morbidity distribution
FOOD AND NUTRITION 127

129
PLANNING A FOODAND NUTRITIONAL STRATEGYFOR A GIVEN POPULATION
1. DESCRIPTION
The course participants will apply previously studied tools in the framework ofthe simulation exercise.
2. CATEGORY
Practice: planning food distribution and nutritional rehabilitation programmesfor a given population.
3. FORMULATION
In the framework of the Alphaland-Betaland simulation, plan a food andnutritional aid programme for the population of the refugee camp. All aspects ofthe programme must be covered:
Food distributions:
. determine the number of beneficiaries
. define a food ration
. plan a logistical chain of operations
. organize a distribution site
. plan the organization of the distributions
. plan a surveillance system for the food distributions.
Nutritional rehabilitation:
. choose a strategy
. identify and select beneficiaries
. set up any facilities that may be needed
. arrange for epidemiological surveillance of this aspect of the programme.
HELP/SOS: FOOD AND NUTRITION128

4. TEACHING METHOD
Assignment presented to work groups, followed by summary in plenary sessionof the plans prepared by each group.
5. DURATION
Total duration: 120 minutes
. 60 minutes for work in groups
. 60 minutes for summary in plenary session.
6. RECAPITULATION
The instructor should already have studied and planned the food and nutritionalrehabilitation programmes for the Alphaland-Betaland simulation, and willcomment on the reports presented by the different groups during the plenarysession.
Box 1
In summing up this module, the instructorwill present a few concrete cases tounderline the principles that have beentaught in the course. The exampleschosen should demonstrate assessmentof food access problems, present blue-prints for action at various levels of thefood supply chain, and, finally, indicatethe results of such action. Ideally theinstructor should use examples of situa-tions in which he or she was involved.
FOOD AND NUTRITION 129

PRODUCTION OFAGRICULTURAL
RESOURCES
DISTRIBUTION OFFOOD RESOURCESIN THE ECONOMIC
SYSTEM
AVAILABILITY OFFOOD
RESOURCES
ACCESSIBILITY OF FOOD RESOURCES
FAMILYCONSUMPTION
BIOLOGICALUTILIZATION
NUTRITIONALSTATUS
Restoration of agricultural production
Short-term activities(artificial)
Rehabilitation of distribution routes
Re-establishment of income
Distribution of food resources
(humanitarian aid)
Nutritional rehabilitation
Necessityof linking
the two in order to form an
(artificial) food
supplychain
Medium-term
activities
Box 2
EFFECTS OF HUMANITARIAN AIDON THE FOOD SUPPLY CHAIN
HELP/SOS: FOOD AND NUTRITION1130

ENVIRONMENT
MODULE
3

133
LIST OF OBJECTIVES
. Identify the interactions between a population and its environment, and theways in which conflict situations disrupt them
. Know the criteria for choosing a site for a displaced-persons camp
. Know the classification of the diseases in which water plays an important rolein transmission
. Know the recommended quantity and quality of water required by apopulation in an emergency situation
. Identify the components of a water supply system
. Identify the various types of water sources
. Know how to calculate the quantity of rain water that can be collected in agiven spot
. Acquire five tools for understanding how a well functions
. Identify the advantages and disadvantages of surface water as a water source
. Know how a natural spring functions
. Know the factors involved in selecting a water source during a conflict situation
. Know what factors will make water storage necessary, and the various storagemethods possible
. Formulate a request for a pump
. Know the various water-treatment methods
. Know the characteristics of a water-distribution system
. Plan a water supply system
. Define the context for the study of human-waste disposal
. Acquire a simple means of classifying the various methods of human-wastestorage and disposal
. Describe the functioning of the main types of dry-pit latrine
. Know the principal communicable disease vectors and the methods forcontrolling them
. Know the methods of garbage disposal
. Know the impact of housing on health
. Plan the installation of adequate shelter and a system to control human wasteand garbage.
HELP/SOS: ENVIRONMENT132

DEFINITION OF THE CONCEPTOF INTERACTION BETWEEN A POPULATIONAND ITS ENVIRONMENT
1. DESCRIPTION
The relationship between population and environment can be schematized as adiagram showing, on one hand, the elements originating in the environment whichare necessary to maintain a population’s life and health (water, food, energy, rawmaterials for work, materials for building shelter), and, on the other, the waste apopulationdischarges into the environment (in the formofhumanexcreta,garbage,and liquid waste). Between these two poles a vicious circle may be created—forexample, human waste contaminates the water, leading to a proliferation ofcommunicable disease vectors, etc. The interactions between these parametersdepend on geological and climatic conditions, as well as the level of development.
Emergency situations engender major disruptions of the normal equilibriumbetween a population and its environment. Overcrowding, for example—characteristic of situations involving displaced populations—in a hostileenvironment breeds health catastrophes, and risks triggering a process in whichincreasing contamination of the environment spirals out of control, with aconsequent increase in morbidity.
At this level, course participants must clearly establish the link betweenenvironment and health: improving the water supply helps reduce the incidenceof diarrhoeal diseases and the rate of malnutrition, and controlling human wastereduces the incidence of ankylostomiasis (hookworm disease), for example. Theimpact of sanitation measures on morbidity will be studied in detail in thesections specifically dealing with water, waste, and vectors.
2. CATEGORY
Framework: identifying the interactions between a population and its environ-ment, and disruptions of these interactions by conflict situations.
3. FORMULATION
Show graphically or describe in words the interactions that normally existbetween a population and its environment, as well as the disruptions in theserelations that may be caused by conflict situations.
ENVIRONMENT 133

135
4. TEACHING METHOD
Assignment presented to work groups and summary in plenary session.
5. DURATION
Total duration: 60 minutes
. 30 minutes for work in groups
. 30 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Concept of interaction between a population and its environment
. Box 2: Ways that infectious diseases are transmitted
. Box 3: Factors detrimental to the relationship between a population and itsenvironment during a crisis
LINK WITH NEXT OBJECTIVES
This objective introduces the general topics of the module on environment,namely choosing a site for a displaced-persons camp, water, human waste,garbage, vectors, energy supply, and shelter.
HELP/SOS: ENVIRONMENT134

ENVIRONMENT
POPULATION
INTERACTION• human waste• garbage• waste water
• water• energy• materials/ shelter• vectors
This interaction depends on numerous factors, including climate, geographical and ecological characteristics, development level, education, etc.
OUT IN
Box 1
CONCEPT OF INTERACTIONBETWEEN A POPULATIONAND ITS ENVIRONMENT
ENVIRONMENT 1135

137
ENVIRONMENT
POPULATION
Direct Contact
Contamination of:• Water• Food• Soil• Insects• Insects Food
Box 2
WAYS THAT INFECTIOUS DISEASESARE TRANSMITTED
HELP/SOS: ENVIRONMENT1136
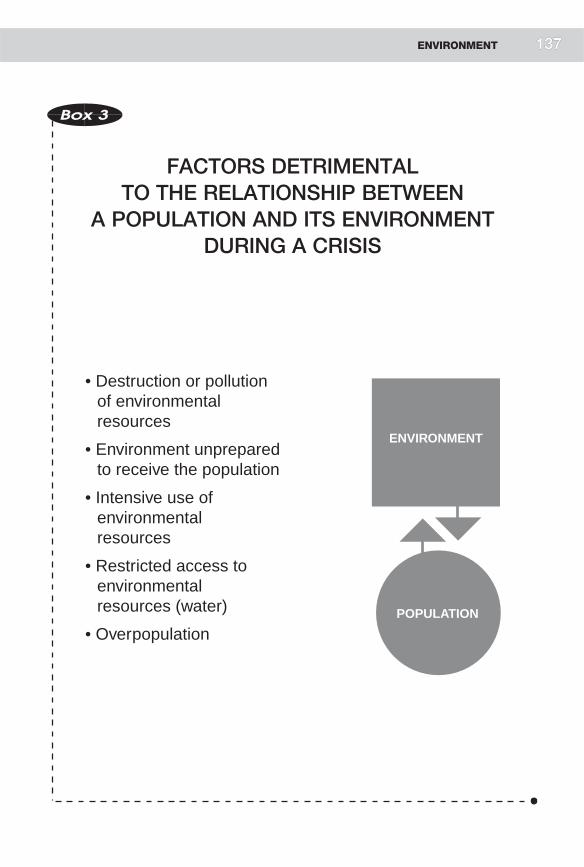
• Destruction or pollutionof environmentalresources
• Environment unpreparedto receive the population
• Intensive use ofenvironmentalresources
• Restricted access toenvironmentalresources (water)
• Overpopulation
ENVIRONMENT
POPULATION
Box 3
FACTORS DETRIMENTALTO THE RELATIONSHIP BETWEEN
A POPULATION AND ITS ENVIRONMENTDURING A CRISIS
ENVIRONMENT 1137

139
CHOOSING A SITE FOR ADISPLACED-PERSONS CAMP
1. DESCRIPTION
Humanitarian organizations are rarely in a position to choose the spot where afleeing population will be accommodated. The decision is usually a political one,made by the government of the host country.When a choice is possible, it shouldmeet specific criteria, including:
. the safety of the population
. access to water
. communication routes
. enough space to prevent overcrowding
. absence of existing or potential environmental dangers (flooding, unhealthyconditions)
. potential for developing agricultural activity, cottage industries, etc.
In negotiating with the authorities over a site, relief administrators must counterthe political arguments of the host country’s government with argumentsconcerning the impact that an unsuitable site will have on the health of displacedpersons. Course participants must understand the importance of having a goodgrasp of the technical arguments for choosing a particular site so that they canplay their role skillfully in negotiations with the political authorities.
2. CATEGORY
Tool: knowledge of the criteria for choosing a site for a displaced-persons camp.
3. FORMULATION
List in order of importance the criteria to consider when choosing a camp site fordisplaced persons.
4. TEACHING METHOD
Assignment presented to work groups and summary in plenary session.
HELP/SOS: ENVIRONMENT138

5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Criteria to consider in choosing a site for a displaced-persons camp
LINK WITH NEXT OBJECTIVES
Access to water is an essential factor in selecting a site for a refugee camp. Waterwill be the topic of the next objectives.
Box 1
CRITERIA TOCONSIDER IN CHOOSINGA SITEFOR A DISPLACED-PERSONS CAMP
. Access to water
. Security
. Access to food resources
. Communication routes
. Absence of natural dangers (flooding)
. Salubriousness
. Possibility of natural drainage
. Agreement with the local population
ENVIRONMENT 139

141
CLASSIFICATION OF THE MAINWATERBORNE DISEASES
1. DESCRIPTION
Many diseases can be transmitted by water, notably:
. diseases transmitted by the ingestion of germs present in thewater: diarrhoealdiseases, cholera, typhoid, amebiasis, etc.
. diseases caused by inadequate personal hygiene associatedwith lack of water:scabies, skin infections, trachoma, etc.
. diseases transmitted by an intermediate host that lives in water: schistoso-miasis, etc.
. diseases carried by water-dependent vectors: malaria, yellow fever, denguefever, etc.
This classification gives participants an overall view of the main communicablediseases directly affected by water supply programmes.
2. CATEGORY
Tool: familiarity with the classification of waterborne diseases.
3. FORMULATION
Classify communicable diseases by their relation to water rather than by thepathogens that cause them.
4. TEACHING METHOD
Discussion involving all participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Classification of communicable diseases by their relation to water
HELP/SOS: ENVIRONMENT140

LINK WITH NEXT OBJECTIVES
To reduce the transmission of these diseases, a satisfactory water supply isneeded. What does ‘‘satisfactory’’ mean?
Box 1
CLASSIFICATIONOF COMMUNICABLE DISEASESBY THEIR RELATION TO WATER
. Ingestion of polluted water:
. cholera
. amoebiasis
. inadequate personal hygiene due to lack of water:
. scabies
. trachoma
. presence in the water of an intermediate host carrying thepathogenic agent:
. schistosomiasis
. development of vectors of communicable disease in water:
. malaria
. yellow fever
. combination of the causes above:
. amoebiasis: polluted water and inadequatepersonal hygiene
ENVIRONMENT 141

WATER SUPPLY STANDARDS
1. DESCRIPTION
The importance of water in maintaining life and preventing disease is wellestablished. Recommended standards already exist for the quantity and qualityof water that should be available to disaster victims, and these recommendationscan be used as references for any water supply system set up in emergencysituations.
Water quantity:
Life is not possible without water. An inadequate supply of water will increasemorbidity—of diarrhoeal diseases, for example, since transmission of pathogenicagents will rise as a result of deficient hygiene caused by lack of water. Similarly,the incidence of trachoma will increase. The normal water requirement tomaintain health is 20 litres per person per day, although under certaincircumstances, when constraints are insurmountable, this limit can be loweredto 5 litres. Nevertheless, the goal should remain 20 litres and every effort must bemade to remove the constraints. For nutritional rehabilitation centres therecommended water requirement is 20-30 litres of water per child, while forhospitals it is 100-200 litres per patient.
Water quality:
The key factor in terms of public health is the microbiological quality of thewater, meaning the absence of pathogens. Water’s microbiological quality ismeasured by the presence of Escherichia coli (E. coli), which is an indicator offaecal contamination. The rule of thumb in emergency situations is that if thenumber of E. coli colonies exceeds 10 after a 24-hour culture period (at 42o), thewater should be treated before it is consumed.
Chemical pollution is also a factor to consider, especially in Eastern Europeancountries where this kind of pollution is very common in industrial areas; andconflicts cause populations to migrate precisely towards urban areas. Chemicalpollution is technically difficult to remedy. In emergency situations, it may benecessary to supply water from uncontaminated sources or to move populationsto unpolluted areas.
The waywater looks and smells must also be considered, since consumersmay bedisinclined to accept turbid, malodorous water.
HELP/SOS: ENVIRONMENT142 143

Course participants should remember this principle:
Quantity is more important than quality. A large quantity of reasonably cleanwater (0-10 E. coli) is preferable to a small quantity of perfectly clean water(0 E. coli).
2. CATEGORY
Tool: familiarity with the recommended standards of quality and quantity for thewater available to a population in emergency situations.
3. FORMULATION
What are acceptable standards for the water supplied to a population in anemergency situation?
4. TEACHING METHOD
Question presented to all groups, and summary of the participants’ spontaneousanswers.
5. DURATION
Total duration: 15 minutes.
6. RECAPITULATION
. Box 1: Water supply recommendations (simplified version)
. Box 2: Water supply recommendations (full version)
LINK WITH NEXT OBJECTIVES
The preceding objectives concerned the importance of water for public health(disease prevention) and recommended measures to ensure that in unstablesituations the water supply will achieve its purpose: the maintenance of goodhealth. The next objectives will address the technical aspects of implementing aneffective water supply system.
ENVIRONMENT 143

145
Box 1
WATER SUPPLYRECOMMENDATIONS
(SIMPLIFIED VERSION)
Give priority to quantitywhile respecting quality
QUANTITY:
. 15-20 litres per person per day
QUALITY:
. 0-10 E. coli/100 ml
. Follow recommendations concerningtoxic substances
Q > q
HELP/SOS: ENVIRONMENT144

Box 2
WATER SUPPLY RECOMMENDATIONS
(FULL VERSION)
QUANTITY:
. 20 litres per person per day
QUALITY:
. Physical characteristics:
. appearance
. smell
. taste
. Microbiological characteristics:
. 0-10 E. coli/100 ml
. Chemical characteristics:
. arsenic < 0.05/mg/l
. fluoride < 1.5 mg/l
. cyanides < 0.1 mg/l
. mercury < 0.001 mg/l
. lead < 0.05 mg/l
ENVIRONMENT 145

147
COMPONENTS OF A WATER SUPPLY SYSTEM
1. DESCRIPTION
The purpose of this section is to define the various components of a water supplysystem:
. water sources
. water storage
. water distribution
. water use
. human consumption
. other kinds of use
. disposal of waste water and unused water.
At this stage, course participants will be asked to identify these components.Emphasis must be laid on the fact that the health impact of the water supplysystem will depend on the performance of each component. Clean water may bedistributed (in accordance with the recommendations defined above), but it willhave no impact on health if the population continues to use its usual watersources, which may be polluted.
2. CATEGORY
Framework: components of a water supply system.
3. FORMULATION
Describe what a water supply system means to you.
4. TEACHING METHOD
Assignment presented to work groups.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
HELP/SOS: ENVIRONMENT146

6. RECAPITULATION
. Box 1: Components of a water supply system
. Box 2: Components of a water supply system and their relation toengineering
LINK WITH NEXT OBJECTIVES
This objective will be followed by an examination of each component of a watersupply system and the technical tools required to put it in place.
SOURCES
STORAGE
DISTRIBUTION
USE
DISPOSAL
Box 1
COMPONENTSOF A WATER SUPPLY SYSTEM
ENVIRONMENT 1147

149
SOURCES
STORAGE
DISTRIBUTION
USE
DISPOSAL
TypesEquipment
Choosing a source
TypesSedimentationFlocculation
FiltrationChemical treatment
TypeAccess (distance betweenwater-carrying network and
population)Flow
Consumption by humansConsumption by animals
Agricultural useConsumption by hospitals
Drainage of rain waterDisposal of waste water
Box 2
THE COMPONENTSOF A WATER SUPPLY SYSTEM
AND THEIR RELATION TO ENGINEERING
HELP/SOS: ENVIRONMENT1148

THE MAIN SOURCES OF WATER
1. DESCRIPTION
There are four main sources of water:
. rainwater: the quantity of available water varies according to climate andseason (unreliable over time), but the quality is satisfactory withouttreatment. This source of supply can therefore be considered as an adjunctto a permanent system.
. surface water (rivers, lakes): the quantity of water available is usually large,but as a rule the water is polluted.
. spring water: the flow varies considerably depending on the spring. Thequality is satisfactory if the water is protected from faecal contamination atthe point where it emerges.
. groundwater: the water is safe and available in variable quantities dependingon geology and climate. Extracting the ground water involves sinking a welland constructing an infrastructure for it. The quality of the water thusobtained is satisfactory, as long as the water table itself has not beencontaminated (chemical pollution).
2. CATEGORY
Tool: knowledge of the different types of water sources.
3. FORMULATION
List the various sources of water, noting in each case the quantity and quality ofwater that can be obtained without technical intervention.
4. TEACHING METHOD
Assignment presented to all participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Water sources
. Box 2: Assessment of a water supply point
. Box 3: Assessment of a water supply point (continued)
ENVIRONMENT 149

151
. Box 4: Criteria for selecting a water source
LINK WITH NEXT OBJECTIVES
The development of water sources poses specific technical problems, some simpleand some complex. The next sections will examine water source engineering,which comprises essentially:
. methods of collecting rain water
. developing and protecting natural springs
. sinking wells
. pumping well water or surface water.
Rainwater
Wells
Naturalsprings
Surfacewater
Ground water
Box 1
WATER SOURCES
HELP/SOS: ENVIRONMENT1150

Box 2
ASSESSMENT OF A WATER SUPPLY POINT
(ICRC Assessment Form)
I. Site
City, villageLocalityProvince
II. Type of supply point
a) Spring:
. approximate flow
. development
. protection
b) Well:
. dug by hand/bored with a hand drill/mechanically drilled
. year of construction
. depth
. present level of water (from the ground)
Ask users these questions:
. maximum level observed / when?
. minimum level observed / when?
. amount of water pumped each day
. protection (cover, stone slab, etc.)
. type of soil (clay, sand, humus, gravel, etc.)
. nature of the aquifer (layer containing water)
ENVIRONMENT 151

153
Box 3
(ICRC Assessment Form-continued)
c) Surface:
. description (stream, river, lake, etc.)
. in use all year? (dry season)
. estimated volume of water extracted each day
III. Equipment
a) Pump: manual or motorized
. type
. brand
. year of installation
. maximum possible flow
. if immersed, depth of the well
b) Tank:
. volume
. distance from water supply point
. difference in altitude between water supply point and tank
c) Pipes:
. material
. diameter
. condition
IV. Use
. number of people served
. length of waiting time
. quality of the water: smell/ taste/ colour
V. Remarks
HELP/SOS: ENVIRONMENT152

Box 4
CRITERIA FOR SELECTINGA WATER SOURCE
QUANTITY OF WATER:
. immediate capacity
. reliability over time (dry season)
QUALITY OF WATER:
. current quality
. risk of pollution
TECHNOLOGY REQUIRED:
. type of technology required
. to develop it
. to maintain it
. acceptability to local consumers
ACCESSIBILITY:
. geographical
. social
. financial (Is a fee charged?)
. safe access in conflict zones
ENVIRONMENT 153
COLLECTING RAINWATER
1. DESCRIPTION
Rainwater is easily collected from hard roofs (sheet metal, tiles, etc.); such roofsneed simply be fitted with gutters that channel the water into cisterns. Althoughquantities can be predicted by multiplying the surface of roofs thus equipped bythe usual rainfall in the region, they will always be uncertain owing to climaticirregularities.
2. CATEGORY
Tool: calculating the quantity of rainwater that can be collected in a givenlocation.
3. FORMULATION
Know the parameters for calculating rainwater volume.
4. TEACHING METHOD
Assignment presented to all participants in plenary session.
5. DURATION
Total duration: 10 minutes
. 10 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Rainwater collection and criteria for calculating rainwater volume
LINK WITH NEXT OBJECTIVES
Given the unreliability of this method of water supply, other water sources willhave to be sought as well.
HELP/SOS: ENVIRONMENT154 155

1) Rainfall
2) Surface
3) Collection
4) Storage
Rainfall x surface = volume of available water
Storage = volume of accessible water
Irregular supply depending on climatic conditions
Box 1
RAINWATER COLLECTIONAND PARAMETERS FOR CALCULATING
RAINWATER VOLUME
ENVIRONMENT 1155

157
NATURAL SPRINGS
1. DESCRIPTION
Natural springs are springs in which the water comes spontaneously out of theground, usually as a result of gravity. To eliminate the disadvantages common toall surface water, the spring must be protected at its origin (the eye of the spring).The aim must be to improve the filtration of the water through the geologicallayers of earth. The natural filtration process can be reinforced by theinterposition of layers of sand and gravel between the eye of the spring and thebeginning of the distribution system. The area uphill from the spring must befenced off to prevent faecal contamination by animals.
2. CATEGORY
Tool: an understanding of the way a natural spring functions.
3. FORMULATION
Learn how a natural spring works.
4. TEACHING METHOD
Lecture and debate.
5. DURATION
Total duration: 30 minutes.
6. RECAPITULATION
. Box 1: How a spring functions (1)
. Box 2: How a spring functions (2)
. Box 3: Springs—advantages and disadvantages
. Box 4: Main steps in exploiting a natural spring
LINK WITH NEXT OBJECTIVES
The principle of natural filtration through geological layers applies to wells,which will be studied in the next objective.
HELP/SOS: ENVIRONMENT156

Ground water
Storage
Protection of the areauphill from the spring
Collection box
Runoff ofunused water
inout
Box 1
NATURAL SPRINGS:
HOW THEY WORK (1)
Collection box
Regulation reservoir
in
in
out
out
Box 2
NATURAL SPRINGS:
HOW THEY WORK (2)
ENVIRONMENT 157

159
Box 3
NATURAL SPRINGS
ADVANTAGES:
1. Development is simple andinexpensive
2. Maintenance is simple
DISADVANTAGES:
Yield is generally limited.
Box 4
MAIN STEPS IN EXPLOITINGA NATURAL SPRING
. Locate the eye of the spring (the point where thewater emerges)
. Develop a filtration system (natural or engineered)
. Protect the area around the spring from possiblecontamination
. Set up a water-distribution system
. Develop a drainage system for runoff
. Set up a maintenance and monitoring system
HELP/SOS: ENVIRONMENT158

WELLS
1. DESCRIPTION
This objective is divided into six parts:
. Defining a framework of all the tools necessary for understanding how a wellworks and evaluating it. The topics that should be remembered are: theprinciple of filtering water through the walls of a well, methods of drilling,types of pumps, ways of protecting a well, and the indicators required forevaluating the operation of a well.
. The principle of filtering water through the walls of a well:
Ground water passes through geological strata before collecting in the well.This filtration through the soil gives the water a satisfactory bacteriologicalquality without any need for treatment.
. Boring the well:
A distinction is made between wells that are dug manually and those that arebored by mechanical means (mechanical diggers); the diameter of manuallydug wells is relatively wide (1-2 metres), and the depth may vary from a fewmetres to several dozen metres. Tube wells, strictly speaking, are wells of asmaller diameter (20-30 cm). They may be deeper than 100 metres.Constructing such a well may involve relatively simple equipment (drills)or very sophisticated equipment (truck-mounted drilling rigs). The type ofwell chosenwill depend on the nature of the soil, the level of the groundwater,local experience in well construction, and the availability of equipment.
. Protecting a well:
Once the well has been dug, the water that collects in it must be considered assurface water. Covering the well and protecting the area around it areessential to avoid contamination from water infiltrating from the surface(rainwater, water spilled in the process of using the well) and carrying with itpolluting elements (such as faecal material). Accordingly, the well headshould be covered by a concrete slab and surrounded by an apron measuring1-2 metres in diameter, covering the soil around the well.
Protecting a well also means situating it far enough away from the latrines toavoid contamination from them. The distance required will depend on thegeological nature of the soil, but a minimum of 30 metres is recommended.
ENVIRONMENT 159

161
. Pumps:
Once the well is covered (for protection), a pump will be needed to draw outthe water. A pump may be hand operated or motorized, and in each of thesetwo categories, a distinction is made between suction pumps and cylinderforce pumps.
. Handpumps versus motorized pumps:
The choice between these two kinds of pumps depends on various factors:
. The desired flow: the yield of a hand pump is limited to 700-900 litres ofwater per hour
. Local habits
. Ease of maintenance: motorized pumps require fuel for the generator andregular maintenance.
. Suction pumps versus cylinder force pumps:
The distinction between these two kinds of pumps lies in the location of thepiston in the pump. In suction pumps, the piston is in the part of the pumpsituated outside the well; it ‘‘sucks’’ the water out. In cylinder force pumps,the piston is located in the immersed part of the pump, and pushes the waterout of the well.
The choice between these two kinds of pumps will depend on the water levelin the well. If the water level is more than seven metres below the part of thepump that is outside the well, a suction pump cannot be used (owing to lawsof physics). This limit must take into account the change in water level causedby pumping. Cylinder force pumps can be used under all circumstances,whatever the water level. Submersible pumps are a particular type of cylinderpump, in which the entire pump is submerged in water. These are electricpumps, usually powered by a generator adjoining the well. There is a trend,however, towards using solar energy to power such pumps; the technology isreliable and eliminates the need for fuel which, in conflict situations, may bestolen and used for military purposes.
The maintenance of cylinder force pumps is more complicated, since theymust be removed from the well for that purpose.
. Evaluating the functioning of a well:
Two kinds of data are necessary for evaluating a well:
. descriptive: type of pump, type of generator, condition of protectiveapron, depth of water level, depth of well
HELP/SOS: ENVIRONMENT160

. dynamic: refill capacity, or the time it takes the well to regain its originalwater level after being pumped partly dry. This test measures the well’spotential yield and seasonal variations in the water level (evaluation ofyield over the whole year).
Course participants should be familiar with the assessment check list.
2. CATEGORY
Tools: five tools for understanding how a well functions.
3. FORMULATION
This objective will focus on five tools necessary for understanding and evaluatinga well’s operation:
. principle of filtering water through the walls of a well
. main methods of drilling
. protecting a well
. main categories of pumps
. evaluating the operation of a well.
4. TEACHING METHOD
Discussion and presentation of technical transparencies to all groups.
5. DURATION
Total duration: 40 minutes.
6. RECAPITULATION
. Box 1: General framework: theoretical diagram of a well
. Box 2: Well-digging methods
. Box 3: Natural filtration and forced filtration
. Box 4: Protection of a well (cross-section)
. Box 5: Protection of a well (aerial view)
. Box 6: Pumps—principles of operation
. Box 7: Pumps—mechanisms of operation
. Box 8: Evaluating a well
ENVIRONMENT 161

163
LINK WITH NEXT OBJECTIVES
The next objective will cover the parameters to consider in choosing the rightpump.
4 Pump
3 Protection
1 Bore-hole
Water
2 Ground water
Box 1
WELLS
THEORETICAL DIAGRAM
HELP/SOS: ENVIRONMENT1162

MotorizedManualMEANS
Drilling
Digging
ME
TH
OD
S
4
31
1
2 Mechanical
drillingBoring withan auger
Mechanical diggerHand-digging
1. The most common method—easy to use.
2. The surface and depth of the well are limited.
3. Speed is the only advantage thismethod has over technique .
Mechanical drilling allows deep digging, andconsequently a sufficient volume of availablewater and a better guarantee of water quality. However, it requires motorized equipment.
1
2
3
4
Box 2
WELL-DIGGING METHODS
ENVIRONMENT 1163

165
water ground water
water
water
well walls
ground water
Box 3
NATURAL FILTRATIONAND FORCED FILTRATION
HELP/SOS: ENVIRONMENT1164

water
danger of contamination(well water is in fact surface water)
protection of the well head protection of area around the well
ground water
ground water
Box 4
PROTECTION OF A WELL
(CROSS-SECTION)
ENVIRONMENT 1165
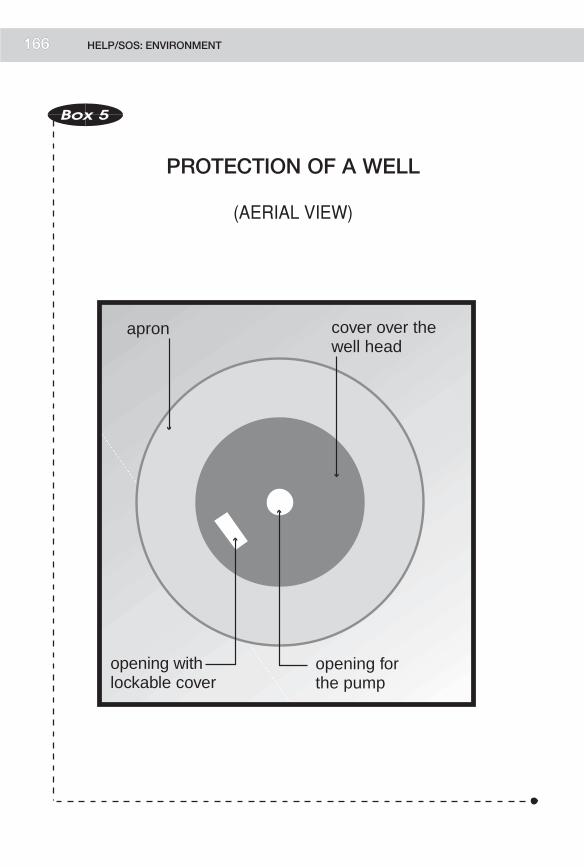
167
apron cover over thewell head
opening forthe pump
opening withlockable cover
Box 5
PROTECTION OF A WELL
(AERIAL VIEW)
HELP/SOS: ENVIRONMENT1166

Principle works if the distance between the level of the well head and the level of water in the well is less than 7 metres.
piston
piston
water
1 2Pulls thewater up
Pushes thewater up
1
Box 6
PUMPS
PRINCIPLES OF OPERATION
ENVIRONMENT 1167

169
Box 7
PUMPS
MECHANISMS OF OPERATION:HAND-OPERATED VS. MOTORIZED
CHARACTERISTICSOF HAND-OPERATED PUMPS
. Inexpensive
. Easy to repair
. Low maintenance costs
. Not dependent on external energysources
CHARACTERISTICSOF MOTORIZED PUMPS
. Greater yields, for large populations
. None of the advantages of hand-operatedpumps
HELP/SOS: ENVIRONMENT168

• Topographical data
• Specifications of the well (depth, year of construction)
• Information on water variables
• Population statistics (number)
• Pump specifications (type, capacities)
• Water storage specifications
storage
distribution
population
generator
pump
Box 8
EVALUATING A WELL
ENVIRONMENT 1169

171
CHOOSING A PUMP
1. DESCRIPTION
Choosing a pump depends on several factors:
. the height to which the water must be ‘‘hoisted,’’ including the distancebetween the water level and the ground level, and the distance between theground level and the place where the water will be stored. This calculationmust also take into account energy losses associated with the system itself(loss of energy in pipes) and differences in the water level caused by pumpingsessions and seasonal changes.
. the desired daily yield (the selection of the water source in itself reflects acorrelation between the desired yield and the possible yield). The pump mustbe able to supply that yield.
. the pumps normally used in the area (avoid installing unfamiliar equipment ifpossible).
. the diameter of the well.
Tables exist to facilitate the selection of a pump on the basis of these parameters.The role of the health care personnel in the fieldmust be emphasized; they shouldbe able to provide all this information to the engineers, who will then choose theright pump for the situation.
2. CATEGORY
Tool: formulating a request for a pump.
3. FORMULATION
Write a fax to an engineer requesting a pump for a well presenting certainparameters.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
HELP/SOS: ENVIRONMENT170

6. RECAPITULATION
. Box 1: Criteria for choosing a pump
. Box 2: Choosing a pump (power)
LINK WITH NEXT OBJECTIVES
This objective sums up the technical aspects of a well. Both well water and springwater are essentially subterranean water that flows to the surface. The nextobjective will address the problems involved in using surface water.
motorizedhand-operated
Mechanism of operation
push
pull
Prin
cipl
e of
oper
atio
n
CHOICE BASED ON:
• Yield
• Distance between water level and ground level (7 metres)
• Depth of the well: if the well is deeper than 50-60 metres, hand pumps cannot be used
• Regular access to energy sources (in conflict situations, access to energy sources often poses a problem)
• Cost
• Equipment customarily used in the region
Box 1
CRITERIA FOR CHOOSING A PUMP
ENVIRONMENT 1171

173
Yield in m3/hour
(*) Parameters:
• Height between the point where the water enters the pump and the level where the water will be stored
• Losses (distance, friction)
Par
amet
ers
(*)
100 m3
110 metres
example 110 metres
100 m3( )
Box 2
CHOOSING A PUMP
(POWER)
HELP/SOS: ENVIRONMENT1172

SURFACE WATER
1. DESCRIPTION
Since, in principle, surface water must be assumed to be bacterially polluted,provision must be made for storing and treating it. Surface water generally hasthe advantage of being available in large quantities (rivers, lakes), althoughseasonal variations may occur. Moreover, it is immediately accessible. As a wayof minimizing organic pollution without need for treatment, the water can becaptured in the geological stratum underlying the river, a procedure that willinvolve digging a cavity underneath the river bed. This cavity will collect waterthat has been filtered through the surrounding layer of earth. In emergencysituations, however, the best option is to pump the water directly from the riverand then to treat it.
The pumps used are the same kinds used for wells. The type of pump chosen willdepend on the difference in altitude between the water surface and the storagecontainer.
2. CATEGORY
Tool: knowledge of the advantages and disadvantages of using surface water as awater source.
3. FORMULATION
List the advantages and disadvantages of using surface water as a source of watersupply.
4. TEACHING METHOD
Discussion, followed by a debate.
5. DURATION
Total duration: 15 minutes.
6. RECAPITULATION
. Box 1: Surface water
ENVIRONMENT 173

175
LINK WITH NEXT OBJECTIVES
Now that the various types of water source have been reviewed, the next objectivewill cover the criteria for choosing among these different sources.
storagefor
treatment
Surface water must be considered polluted by definition
Water can be sought underthe riverbed
collectionbox
water
Box 1
SURFACE WATER
HELP/SOS: ENVIRONMENT1174

SELECTING A WATER SOURCE
1. DESCRIPTION
This objective requires the use of several tools studied previously. Basically, thechoice of a water source will depend on the following criteria:
. technical criteria:
. estimated volume and reliability of yield. The potential yield of the sourceshould correspond to the volume desired for the population, based on therecommendation of 20 litres per person per day.
. estimated time, difficulty, and cost of work required to develop thesource.
. integration of the source with the other components of the water supplysystem—need for storage with or without treatment of the water;distribution network (size, gravity flow); consumption (cultural accept-ability of the source).
. political criteria:
. safe access to the source (conflict zone or not).
. reliable access over time (negotiations with the parties to the conflict).
All these factors will affect the selection of a water source. It is crucial that courseparticipants understand that technical criteria are only one aspect of choosing awater source. Safe access and the source’s integration in the overall water supplysystem are also important. At this point an initial reference could be made to therules of international humanitarian law concerning the protection of indis-pensable objects.
2. CATEGORY
Tool: knowledge of the factors involved in selecting a water source in a conflictsituation.
3. FORMULATION
Describe the factors involved in selecting a water source in a conflict situation.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
ENVIRONMENT 175

177
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Criteria for selecting a water source
. Box 2: Choosing a water source on the basis of the technological inputrequired to exploit it
LINK WITH NEXT OBJECTIVES
This objective provides an opportunity to ascertain whether course participantshave assimilated the technical skills to decide whether or not pumping and/ortreating water is necessary, depending on the nature of the source. It also servesas an introduction to the next objectives, concerning water storage andtreatment.
Box 1
CRITERIA FOR SELECTINGA WATER SOURCE
. VOLUME OF WATER AVAILABLE
. REGULARITY OF THE SOURCE (SEASON)
. WORK NEEDED TO DEVELOP THE SOURCE:
SURFACE WATER = pumping, storage, and treatment
WELL = pumping, possibly storage, no treatment
NATURAL SPRING =no pumping, possibly storage, no treatment
HELP/SOS: ENVIRONMENT176

Pumping system needed
Water treatment
needed
NoneNaturalspring
Protectedwells with
hand-operatedpumps
Surfacewater with
gravity
Surfacewater
withoutgravity
Protectedwells withmotorized,
solar-poweredpumps
None Simple Sophisticated
Simple
Sophisticated
Box 2
CHOOSING A WATER SOURCEON THE BASIS
OF THE TECHNOLOGICAL INPUTREQUIRED TO EXPLOIT IT
ENVIRONMENT 1177

179
WATER STORAGE
1. DESCRIPTION
The origin of the water will determine whether it is potable or not. If the water isfrom a protected source, such as a well, for example, and the demands on it areheavy (several hundred or thousand people), a certain quantity of water will haveto be stored as a reserve to keep the distribution network supplied, so that a pumpwill not have to operate 24 hours a day. For low-yield natural springs which cansupply the needs of only a very limited number of people, a storage systemmay benecessary to build up water reserves.
The second reason for setting up a storage system is the necessity of treating thewater—for example, when the water source is a river. Water treatment will bestudied in the next section.
Possible storage units include:
. concrete tanks, which take a long time to build and require specificconstruction expertise
. ready-to-assemble steel tanks (OXFAMkit), which offer several advantages:they can be transported as kits, are easy to set up, come in various sizes, andare quickly available. In emergency situations, they are the method of choicefor storing water where no local solution exists
. collapsible tanks (bladders), which do not require any special installationsother than a supporting platform to protect them from the roughness of theground. However, they are less resilient than the other options.
The storage units are supplied from the water source by a distribution system.This system may be static (pipe system) or mobile (tanker trucks). Having watertrucked in is a last resort, since it is expensive. Although the tanker is itself astorage unit, static tanks must be set up so that tankers can quickly unload theirwater, thereby increasing the number of trips possible from source to storagepoint. In emergency situations, collapsible tanks (bladders) are often used as aquickly available temporary solution, to be replaced subsequently by steel orother hard tanks. Note that collapsible tanks can be mounted on the beds ofordinary trucks to make tankers.
HELP/SOS: ENVIRONMENT178

2. CATEGORY
Tool: knowledge of the factors necessitating water storage facilities, and of thevarious water storage systems.
3. FORMULATION
What are the criteria for deciding whether or not to store water for purposes ofconsumption?
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: The principle of water storage
LINK WITH NEXT OBJECTIVES
One of the reasons for storing water is to treat it, which is the subject of the nextobjective.
ENVIRONMENT 179

181
• Well• Natural spring• Rainwater
WATERSOURCES
STORAGE
Storage in order to regulate distribution
Storage in order to treat the water and regulate
distribution
• River• Lake
TYPES OF STORAGE:
• Metal tanks • Concrete tanks • Collapsible (rubber) tanks • OXFAM kits • Tanker trucks for transport (mobile storage)
STORAGE:First stage in water treatment • Means of treatment (schistosomiasis) • Ease of treatment (sedimentation)
Box 1
WATER STORAGE
HELP/SOS: ENVIRONMENT1180

WATER TREATMENT
1. DESCRIPTION
Water quality can be raised to the reference level already mentioned by severalmethods, often used in combination:
. water storage is a measure that in itself tends to reduce the transmission ofcertain communicable diseases (e.g. schistosomiasis), as well as the quantityof organic material, making subsequent chemical treatment more effective
. slow sand filtration is a reliable and inexpensive means of providing goodquality water without chemical treatment. This method can be used on thehousehold level or on a very large scale, as in the provision of safe water for arefugee camp. The principle is simple. Non-potable water (for example,surface water) is forced through a layer of sand two metres thick, so thatparticles are filtered out by the sand grains and a layer of bacteria (theSchmutzdecke), which is created in the top centimetres of the sand layer,destroys the micro-organisms in the water.
. chemical treatments:
. coagulation and flocculation procedures use products such as aluminiumsalts to agglomerate organic particles, producing precipitate. Not onlydoes the water become clearer, but this technique increases theeffectiveness of chemical treatment with chlorine at a later stage
. disinfectant treatment usually involves the use of chlorine products(bleach, calcium hypochlorite, etc.). The principle is simple. An adequateconcentration of free chlorine must be maintained in the water for 30minutes to kill bacteria. The rate of free chlorine must be 0.5 mg. per litreof water (0.5 parts per million, or ppm). In the water, chlorine combineswith organic particles and is thereby neutralized, hence the importance ofreducing organic matter by sedimentation, flocculation, or filtration.Residual free chlorine is measured with the same instruments used to testthe water in swimming pools. These instruments operate on the basis ofcolorimetry
These procedures are themost frequently used in emergency situations. Owing tothe increasing number of conflicts in developed urban areas, however, reliefworkers may face the problem of having to rehabilitate water treatment stations,which use very sophisticated techniques. This process will be not be describedhere, however.
ENVIRONMENT 181

183
Boiling water to make it potable is not practical in emergency situations, whenenergy sources are often in short supply.
2. CATEGORY
Tools: familiarity with the various water treatment methods.
3. FORMULATION
Examine the ways the different water treatment methods work.
4. TEACHING METHOD
Presentation (debate).
5. DURATION
Total duration: 40 minutes.
6. RECAPITULATION
. Box 1: Methods of improving water quality
. Box 2: Slow sand filtration
. Box 3: Flocculation and sedimentation
. Box 4: How chlorine works
. Box 5: Bactericidal effect of chlorine
LINK WITH NEXT OBJECTIVES
At this stage the course participants have all the information they need to obtainadequate quantities of clean water. The next step is to distribute it.
HELP/SOS: ENVIRONMENT182

Box 1
METHODS FOR IMPROVING WATER QUALITY
STORAGE AND SEDIMENTATION:
. Reduction of schistosomiasis
. Sedimentation of organic matter
SLOW SAND FILTRATION:
. Physical effect of filtration
. Bacteriological effect on pathogens
CHEMICAL TREATMENT:
. Flocculation with aluminium salts
. Disinfection with free chlorine
BOILING:
. Action against pathogens
ULTRAVIOLET RADIATION:
. Action against pathogens
ENVIRONMENT 183
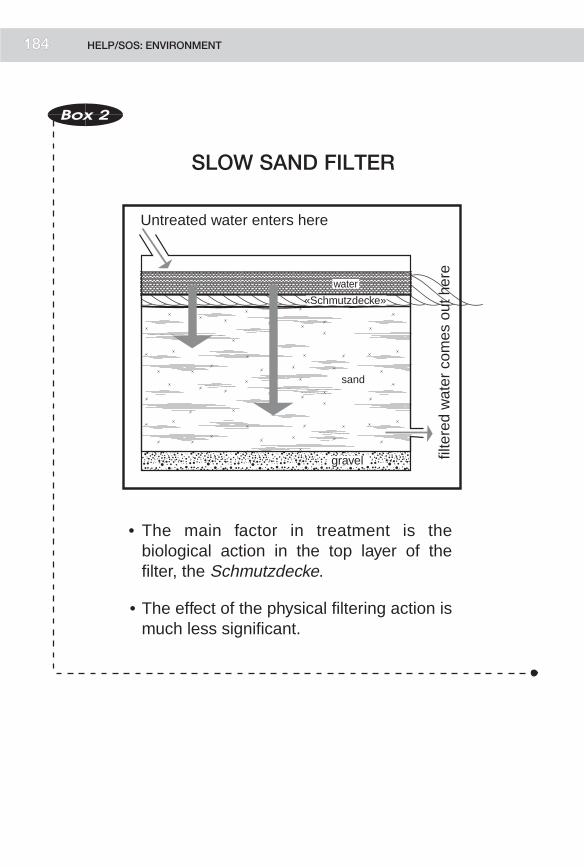
185
water
«Schmutzdecke»
sand
gravel
• The main factor in treatment is the biological action in the top layer of the filter, the Schmutzdecke.
• The effect of the physical filtering action is much less significant.
Untreated water enters here
filte
red
wat
er c
omes
out
her
e
Box 2
SLOW SAND FILTER
HELP/SOS: ENVIRONMENT1184

aluminium salts
sedi
men
t is
drai
ned
off h
ere
sedimentation
• Flocculation does not kill bacteria, but reduces the amount of organic matter, thereby increasing the effectiveness of subsequent chlorine treatment.
aluminium salt+
organicparticles
=flocculation
Box 3
FLOCCULATIONAND SEDIMENTATION
ENVIRONMENT 1185

187
pathogen chlorine organic matter
The combination of chlorine with organic matter releases free chlorine,
which has a bactericidal effect.
Chlorine combines withorganic matter.
CL-
CL-CL-
CL-
CL-
CL- CL-CL- CL-CL-
CL-CL-
CL-CL-
Box 4
HOW CHLORINE WORKS
COMBINATION OF CHLORINEWITH ORGANIC MATTER
HELP/SOS: ENVIRONMENT1186

Time
Concentrationof CL-
Theoretical curve where there is no combination with organic matter
Demand forchlorine
Real curve
Box 5
FREE CHLORINE
BACTERICIDAL EFFECT WITH:0.5 MG/LITRE OF FREE CHLORINE
ENVIRONMENT 1187

189
WATER DISTRIBUTION SYSTEMAND FACTORS INFLUENCINGWATER CONSUMPTION
1. DESCRIPTION
Clean water is now available in adequate quantities. The next step is to make iteasily accessible to the population. This concept is important for two reasons:
. In general, water consumption depends directly on ease of access.Accordingly, access is an important factor to consider if water programmesare to have a favourable impact on health.
. Access to water can become very difficult in conflict situations, particularly ifwater sources are at a distance (trips to fetch watermay be risky) or located indangerous areas (containing land mines, for example).
In some situations no distribution system may be necessary, if the populationconsists of a limited number of people living close to their water sources. In suchcases water can be obtained directly from the well or spring.
However, if the water source is remote and/or the population is large, theinstallation of a water-distribution system must be envisaged. Priority should begiven to gravity-fed systems, meaning that the storage units (tanks) are put at ahigher altitude than the homes of the people who require the water supply.Greater height may be achieved naturally (hills) or artificially (water towers). Inboth cases a pumping system will be required. From the water tanks adistribution system must be set up; the number and arrangement of its brancheswill depend on the dispersion and social organization of the population, as well asthe funds available. In displaced-persons camps, the distribution system must besufficiently ramified to prevent long waiting lines at water distribution points.Increasingly, conflicts affect urban populations whose water supply depends oncomplex systems. The destruction of these systems creates specific technicalproblems with respect to the rehabilitation of pumping stations and watertreatment facilities, as well as distribution systems.
Water consumption depends on several factors:
. the distance between the distribution point and the user’s home
. sociocultural habits
. security.
HELP/SOS: ENVIRONMENT188

Obviously, all these factorsmust be taken into account when a water distributionsystem is planned. The distribution network should offer convenient access towater, but it should not encourage a level of consumption that exceeds thecapacity of the water source.
Course participants must realize that a water programme’s impact on health willdepend on the quality of all the components in the water supply system.Consequently, we cannot simply repair one of those components withoutconsidering the others.
Another factor to consider is that supplying clean water for households does notguarantee that the water is clean when it is consumed. Water stored in the homemay be contaminated by hands soiled with faecal matter. Minimal quantities offaecal matter containing shigella organisms, for example, are enough to makewater unsafe. At every stage of the water supply system, personal hygiene andhealth education are also important factors.
2. CATEGORY
Tool: familiarity with the characteristics of a water distribution system.
3. FORMULATION
List the main characteristics of a water-distribution system and the factors thatinfluence water consumption.
4. TEACHING METHOD
Assignment presented to work groups and summary in plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Diagram of a water distribution network
. Box 2: Importance of hygiene when water is used or consumed
LINK WITH NEXT OBJECTIVES
Course participants have all the essential tools for planning a water supply system.
ENVIRONMENT 189

191
• 1 tap for 40-50 families• Water consumption increases if the distance between the home and the water supply point is decreased• The security factor must be considered
Tank
Water main
TapsRack
Box 1
DIAGRAM OF A WATER-DISTRIBUTIONNETWORK
HELP/SOS: ENVIRONMENT1190

SOURCE
STORAGE
DISTRIBUTION
DISPOSAL OFWASTE WATER
USE/CONSUMPTION
HEALTHEDUCATION
Box 2
IMPORTANCE OF PERSONAL HYGIENEWHEN WATER IS USED
OR CONSUMED
ENVIRONMENT 1191

193
PLANNING A WATER SUPPLY SYSTEMFOR A GIVEN POPULATION
1. DESCRIPTION
With the skills already learned, course participants can plan a water supplysystem for a refugee population that has just arrived in a new environment. Theymust:
. analyse water-related problems, using information on morbidity, socio-cultural habits, etc.
. analyse local water supply potential
. set objectives based on the quantity and quality of water to be supplied
. plan short- and long-term strategies.
. selection of water sources
. treatment method (if necessary)
. storage system
. distribution system
. set up a system to evaluate the operation of the water supply network andimpact on health (choose health indicators).
2. CATEGORY
Practice: planning a water supply system.
3. FORMULATION
Plan a water supply system for the Awalei camp in the simulation exercise. Youmust proceed through all the planning stages: analysing existing water problems,setting objectives, choosing strategies, planning the resources needed to carry outthe measures decided on, and, finally, establishing a monitoring system.
4. TEACHING METHOD
Groupwork based on theAlphaland-Betaland simulation exercise, followed by aplenary session at which all the groups will present the results of their work. Theinstructor should summarize the strategy that he or she recommends in thisspecific case.
HELP/SOS: ENVIRONMENT192
5. DURATION
Total duration: 90 minutes
. 60 minutes for work in groups
. 30 minutes for summary in plenary session.
6. RECAPITULATION
The recapitulation of the material in this case will be based on the instructor’sanalysis of the situation. The instructor will have studied and interpreted thewater supply problems and examined possible strategies for supplying water inthe simulation exercise.
LINK WITH NEXT OBJECTIVES
The institution of a water supply system must take into account environmentalsanitation measures, such as waste disposal, in order to avoid such problems ascontamination of the water supply.
ENVIRONMENT 193
195
HEALTH AND FAECAL RISK
1. DESCRIPTION
In emergency situations involving large numbers of people, overcrowdingsubstantially increases the risk of faecal contamination of people, water, and,more generally, the environment.
The problem can be outlined as follows:
. A single person produces an estimated 50-200 g of faecal matter per day ingross weight, which represents a total volume of 0.06 m3 per year. Faecalmatter may contain numerous pathogenic agents, such as the poliomyelitisand hepatitis viruses, cholera vibrios, salmonella, shigella, amoebae, hook-worm eggs, etc. Children’s stools are more pathogenic than those of adults.
. Pathogenic agents are transmitted in various ways: by direct contact betweena person and faecal matter, by contamination of water or food which is thenconsumed by the population, or through the intermediary of infected vectorsthat come into contact with people. Risk of infection is high when twoconditions are met: overcrowding and an absence of measures to prevent thedispersal of faecal matter in the environment. Faecal risk depends on theconjunction of these two conditions, although it is also affected by otherfactors, such as the sociocultural customs of the population in question.
This module will examine the technical measures that can be taken to minimizefaecal risk. First the main methods of storing faecal matter will be studied,followed by the criteria to be applied in choosing the right method for a specificemergency situation. Finally, measures for evaluating the effectiveness of thechosen method will be identified. Social aspects and health education methodswill be studied in greater depth in the module on communicable diseases.
2. CATEGORY
Framework: defining the framework for studying the disposal of human waste.
3. FORMULATION
What are themain diseases that can be transmitted by faecalmatter, andwhat arethe main modes of transmission?
Define the concept of faecal risk.
HELP/SOS: ENVIRONMENT194

4. TEACHING METHOD
Assignment presented to work groups, followed by summary in plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: The ‘‘chain’’ of human waste
. Box 2: Faecal risk: factors in production and transmission
LINK WITH NEXT OBJECTIVES
This objective defines the general context for studying methods of human wastedisposal and the way they reduce faecal risk. The next objectives will focus on thedifferent steps defined in that context.
PRODUCTION
STORAGE
DISPOSAL
USE
Box 1
CHAIN OF HUMAN WASTE
ENVIRONMENT 195

197
PRODUCTION
TRANSMISSION BY:
POPULATION
• 150-200 g gross weight per day
• Stools may contain numerouspathogens • salmonella (106/g)
• vibrio (106/g) • virus (poliomyelitis 106/g) • amoeba (104/g) • others
• Children’s stools are more contaminating than those of adults
• Direct contact • Contaminated water• Contaminated food • Faecal matter• Flies
Box 2
FAECAL RISK
HELP/SOS: ENVIRONMENT1196

WASTE STORAGE AND DISPOSAL METHODS
1. DESCRIPTION
The purpose of this section is to give participants a simple way to determinequickly the options available for storing and disposing waste. These options canbe classified according to two criteria:
. whether waste is stored where it is produced (i.e., where defecation takesplace) or elsewhere
. whether waste is stored under dry or wet conditions.
Methods of storage at the site of production under dry conditions include theestablishment of defecation areas and the various types of dry-pit latrines.
Methods of storage at the site of production under wet conditions include septictanks and water-dependent latrines.
The method of storage away from the site of production under wet conditions ismains drainage.
The last technique is transfer by bucket. Defecation takes place in the home, andthe faecal matter is collected and transported to a central location in a bucket,usually under dry conditions.
The instructor should briefly describe the technical aspects of the variousoptions. He or she should not go too deeply into construction techniques, butrather show the operating principles and technical limitations of each method.
The focus should be on dry-system latrines, which are the only feasible wastedisposal method in the vast majority of emergency situations.
2. CATEGORY
Tool: acquiring a simple means of classifying the various methods of wastestorage and disposal.
3. FORMULATION
What are the main methods available for human waste storage and disposal?
4. TEACHING METHOD
Assignment presented to work groups and discussion in plenary session,followed by a technical explanation of the principles underlying each method.
5. DURATION
Total duration: 60 minutes
ENVIRONMENT 197

199
. 10 minutes for work in groups
. 15 minutes for summary in plenary session
. 35 minutes for technical explanation.
6. RECAPITULATION
. Box 1: Outline of various human waste storage and disposal methods
. Box 2: Factors influencing the choice of a human waste disposal method
LINK WITH NEXT OBJECTIVES
The next objective will address the construction and operation of dry-pit latrines.
away from theproduction site
at theproduction site
STORAGE
wet
dry
STO
RA
GE
/DIS
PO
SA
LIN
EN
VIR
ON
ME
NT:
sewerseptic tank
bucketdry-pitlatrine
In emergency situations, latrinesare the best option:
• No use of water ( , )• No handling of human waste ( )• Unsophisticated ( )
1
2
3
4
4
3
1 2
Box 1
HUMAN WASTE STORAGEAND DISPOSAL METHODS
HELP/SOS: ENVIRONMENT1198

Choice of atechnicalmeasure
suited to theenvironment
Culturalacceptability
to thepopulation
+
Box 2
FACTORS INFLUENCINGTHE CHOICE OF A HUMAN WASTE
DISPOSAL METHOD
ENVIRONMENT 199

201
LATRINES
1. DESCRIPTION
The aim of this section is to describe a classic dry-pit latrine and explain how itoperates: dimensions, structure, and the distance that must be maintained fromwater sources in order to avoid contamination. This will be followed by a reviewof the principal types of dry-pit latrines: simple latrines, double-pit compostinglatrines, and ventilated latrines (to avoid creating breeding grounds for flies).
The cultural aspect must be addressed in discussions of measures facilitating useof latrines, particularly when the desired waste disposal plan is not customary forthe population concerned.
2. CATEGORY
Tool: description of the way the main types of dry-pit latrines work.
3. FORMULATION
Describe the parameters that must be respected in building a dry-pit latrine.
4. TEACHING METHOD
Discussion by the whole group.
5. DURATION
Total duration: 30 minutes.
6. RECAPITULATION
. Box 1: Latrines: how they work
. Box 2: VIP latrines
. Box 3: Examples of more sophisticated latrines
LINK WITH NEXT OBJECTIVES
The problem of flies associated with the construction of latrines can serve as anintroduction to the next objective, which concerns the collection and disposal ofgarbage. Garbage, too, may pose a serious problem by fostering the proliferationof communicable disease-carrying vectors.
HELP/SOS: ENVIRONMENT200

cover
opening
extra height
pit 1-3metres deep
humanwaste
structure
floor
roof
Box 1
LATRINES:
HOW THEY WORK
ENVIRONMENT 2201

203
waste
fly screen
pipe
fliestrapped bythe screen
fliesattracted bythe lightflies
Box 2
LATRINES
VIP LATRINE
HELP/SOS: ENVIRONMENT2202

reinforcedpit lining
This type of latrine is essential if the ground water is likely to be contaminated by human waste.
DOUBLE-PIT LATRINE
The two compartments are used alternately. When one side is full, it is sealed off for 6 months to a year. At the end of that time, the compartment is emptied and the waste can be used as fertilizer. During that time the other compartment is used.
Box 3
LATRINES:
TWO EXAMPLES
OF MORE
SOPHISTICATED LATRINES
ENVIRONMENT 2203

205
COMMUNICABLE DISEASE VECTORS
1. DESCRIPTION
The first step here is to make a list of commonly found communicable diseasevectors. Although the composition of the list does not change in an emergencysituation, the problemof vectors increases as a result of the unsanitary conditionstypical of such situations.
The second step will be to address possible ways of controlling communicable-disease vectors:
. reduction at the source
. reduction of transmission
. reduction of the vector population.
These methods can be classified as follows:
. physical methods: drainage, mosquito nets, traps
. chemical methods: larvicides, insecticides, rodenticides, etc.
2. CATEGORY
Tools: familiarity with the main communicable disease vectors and the methodsfor controlling them.
3. FORMULATION
List the main communicable disease vectors and the methods for controllingthem.
4. TEACHING METHOD
Assignment presented to all participants.
5. DURATION
Total duration: 30 minutes.
6. RECAPITULATION
. Box 1: The main communicable disease vectors
. Box 2: Anopheles and malaria
HELP/SOS: ENVIRONMENT204
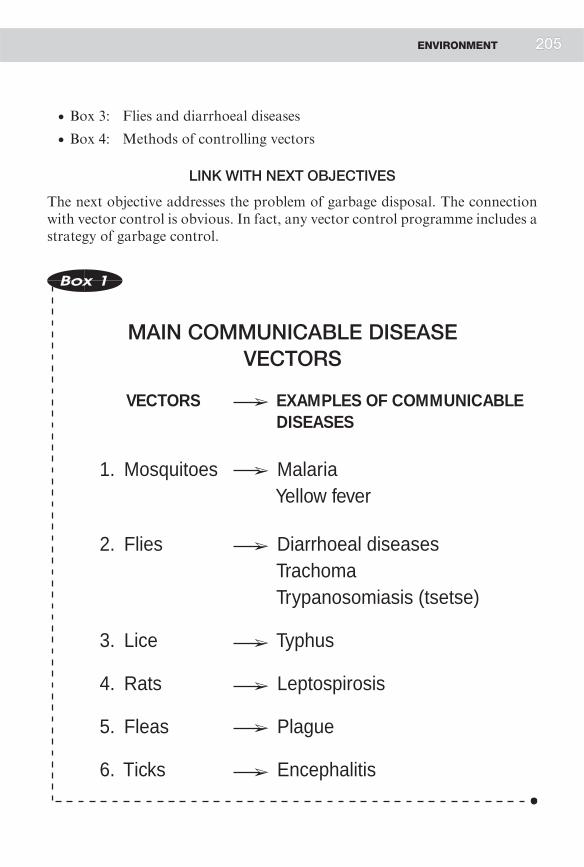
. Box 3: Flies and diarrhoeal diseases
. Box 4: Methods of controlling vectors
LINK WITH NEXT OBJECTIVES
The next objective addresses the problem of garbage disposal. The connectionwith vector control is obvious. In fact, any vector control programme includes astrategy of garbage control.
VECTORS EXAMPLES OF COMMUNICABLE DISEASES
1. Mosquitoes Malaria Yellow fever
2. Flies Diarrhoeal diseases Trachoma Trypanosomiasis (tsetse)
3. Lice Typhus
4. Rats Leptospirosis
5. Fleas Plague
6. Ticks Encephalitis
Box 1
MAIN COMMUNICABLE DISEASEVECTORS
ENVIRONMENT 2205

207
Box 2
ANOPHELES (MOSQUITOES) AND MALARIA
DEVELOPMENT OF THE ANOPHELES MOSQUITO:
Source ———‚ stagnant water
Factors favouring vector proliferation:
. Rainy season
. Poor drainage
CONTAMINATION OF ANOPHELES:
Biting an infected person
TRANSMISSION OF THE DISEASE:
Bite by an anopheles carrying the parasite
Box 3
FLIES AND DIARRHOEAL DISEASES
1. FACTORS FAVOURINGTHE DEVELOPMENT OF FLIES:
. Poor hygiene
. Poor sanitation
2. CONTAMINATION OF FLIES BY CONTACTWITH HUMAN WASTE
3. TRANSMISSION OF DIARRHOEAL DISEASESTHROUGH CONTAMINATION OF FOODBY PATHOGEN-CARRYING FLIES
HELP/SOS: ENVIRONMENT206
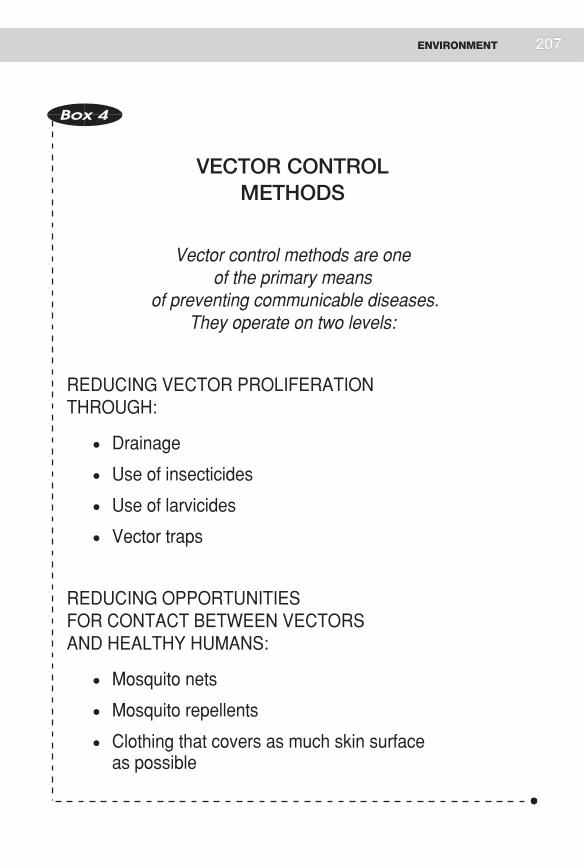
Box 4
VECTOR CONTROLMETHODS
Vector control methods are oneof the primary means
of preventing communicable diseases.They operate on two levels:
REDUCING VECTOR PROLIFERATIONTHROUGH:
. Drainage
. Use of insecticides
. Use of larvicides
. Vector traps
REDUCING OPPORTUNITIESFOR CONTACT BETWEEN VECTORSAND HEALTHY HUMANS:
. Mosquito nets
. Mosquito repellents
. Clothing that covers as much skin surfaceas possible
ENVIRONMENT 207

209
GARBAGE DISPOSALMETHODS
1. DESCRIPTION
Solid waste (garbage) constitutes a public health problem because it maycontribute to an increase in communicable disease vectors if not correctlymanaged.
We have already studied the principal vectors of communicable diseases. Solidwaste offers a breeding ground for flies, mosquitoes, and rats in particular. Aspecific problem that should be mentioned is the proliferation of anopheles inaccumulations of water in old tins or other containers.
Technically, there are two ways of disposing of garbage:
. incineration: burning whatever garbage can be burned
. burial: burying anything that cannot be burned.
Spraying insecticides directly on garbage is not feasible in the medium term.
2. CATEGORY
Tool: knowledge of garbage disposal methods.
3. FORMULATION
List the main communicable disease vectors that proliferate in garbage, andpropose garbage disposal methods.
4. TEACHING METHOD
Assignment presented to all participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Garbage control methods
HELP/SOS: ENVIRONMENT208

LINK WITH NEXT OBJECTIVES
The organization of sanitation services to dispose of human waste and garbage isclosely linked to the organization of shelter—specifically, the distance to watersupply points, latrines, and garbage pits or collection bins. The next objectivefocuses on the problem of shelter in the short and medium terms, giving dueconsideration to sanitation parameters.
Box 1
GARBAGE CONTROL METHODS
. INCINERATION
. BURIAL
ENVIRONMENT 209

211
THE CONNECTION BETWEEN HOUSINGAND HEALTH
1. DESCRIPTION
The role of housing will be addressed on two levels: the shelter itself and thesurrounding sanitary services. The impact of housing on health is oftenunderestimated, yet shelter plays a major role in more than one respect:
. Nutrition. Cold increases energy needs—under certain circumstances bymore than a third
. Transmission of communicable diseases. In collective shelters where severalhundred people are crowded together, the risk of epidemics of such diseasesas scabies, tuberculosis, and measles is evident
. Shelter also plays an essential social role, helping to reconstitute a favourablesocial atmosphere for people still suffering from the shock of a hasty move.
At the beginning of an action to assist a displaced population, relief workers willdistribute sheets of plastic for temporary shelter until less precarious facilities canbe set up: tents, or shelters built with local materials. A definitive solution is notsuggested until later, when the political situation has been stabilized. Certainstandards should be mentioned, such as the minimum surface area required perperson in a camp—30 square metres.
An important aspect of shelter is energy sources. Energy is needed for cooking,heating, and possibly lighting public areas. In emergency situations, wood is themost immediately useable energy source. However, if deforestation problems areto be avoided, it is at best a temporary measure for which an alternative must befound quickly: electricity, purchase of charcoal, solar energy. The instructorshould provide a few examples of simple measures for saving energy, such asenergy-saving stoves.
Latrine construction, the organization of water supply points, the establishmentof garbage collection points, and housing arrangements must all be part of anoverall plan that establishes such parameters as number of people per latrine,number of people per water supply point, etc.
2. CATEGORY
Tool: knowledge of housing’s impact on health.
HELP/SOS: ENVIRONMENT210

3. FORMULATION
Describe the health benefits you expect from salubrious housing.
4. TEACHING METHOD
Assignment presented to all participants.
5. DURATION
Total duration: 30 minutes.
6. RECAPITULATION
. Box 1: Housing and health: risks associated with inadequate shelter
. Box 2: Possible housing solutions
. Box 3: Choosing energy sources
. Box 4: Energy-saving stoves
LINK WITH NEXT OBJECTIVES
Course participants are now ready for the next objective, for which they will haveto put into practice the tools they have acquired for managing human waste andgarbage and for organizing shelter.
ENVIRONMENT 211

213
AMENITIES
RISKS
Rain
Heat
Cold
Overcrowding
• Buildings adapted tothe climate and tosocial customs
• Adequate energysources
• Blankets
• Family housing
Box 1
HOUSING AND HEALTH:
RISKS ASSOCIATEDWITH INADEQUATE SHELTER
HELP/SOS: ENVIRONMENT2212

Box 2
POSSIBLE HOUSINGSOLUTIONS
SHELTER OPTIONS:
. Emergency shelter (plastic sheeting)
. Temporary shelter
. tents
. shelters constructed with local materials
. Permanent housing in the context of a reintegrationor rehabilitation programme
FACTORS TO CONSIDERIN SELECTING HOUSING OPTIONS:
. Need for an immediate solution
. Climate
. Cost
. Social customs
. Probable development of the situation
ENVIRONMENT 213

215
Box 3
CHOOSING ENERGY SOURCES
ENERGY SOURCES
. Wood
. Charcoal
. Kerosene
. Gas
. Electricity
. Solar energy
SELECTION CRITERIA
. Availability
. Custom
. Cost
. Risks
opening fire heat smoke
Box 4
ENERGY-SAVING STOVE
HELP/SOS: ENVIRONMENT214

PLANNING A SYSTEMFOR HUMAN WASTE AND GARBAGEDISPOSAL IN A GIVEN SITUATION
1. DESCRIPTION
This objective will give course participants the opportunity to plan a humanwaste and garbage disposal system and to identify adequate housing solutions forthe short and medium term.
2. CATEGORY
Practice: planning adequate housing and a system for managing human wasteand garbage.
3. FORMULATION
Using the data corresponding to the Awalei camp in the Alphaland-Betalandsimulation, plan adequate shelter and a system for managing human waste andgarbage.
4. TEACHING METHOD
Assignment presented to each work group.
5. DURATION
Total duration: 60 minutes
. 30 minutes for work in groups
. 30 minutes for summary in plenary session.
6. RECAPITULATION
The synthesis will be based on the instructor’s analysis of the situation.
LINK WITH NEXT OBJECTIVES
In general, sanitation measures focusing on the environment are integrated inprogrammes to control communicable diseases. They will be mentioned again in
ENVIRONMENT 215

the introduction to the next module (on communicable diseases), under theheading ‘‘primary prevention.’’
Box 1
The instructor should present
concrete examples of action
involving water supply and
environmental hygiene.
HELP/SOS: ENVIRONMENT216

COMMUNICABLE DISEASES
MODULE
4

219
LIST OF OBJECTIVES
. Outline the natural cycle of communicable diseases
. Define the areas where treatment and primary, secondary, and tertiarypreventive measures are carried out
. List the main communicable diseases commonly found in emergencysituations, as well as the factors that increase their prevalence and severity
. Know the main principles of an expanded programme of immunization (EPI)
. Know the limitations of chemoprophylaxis and mass treatment in the controlof certain communicable diseases in emergency situations
. Know the advantages of short treatments in emergency situations
. Recognize the importance and the limitations of health education in emergencysituations and know the steps involved in implementing a health educationprogramme
. Know the essential rules for drawing up a questionnaire to assess childmortality within a population
. Know the essential clinical and therapeutic aspects of meningococcal meningitis
. Know the essential clinical and therapeutic aspects of tuberculosis
. Know the essential clinical and therapeutic aspects of diarrhoeal diseases andcholera
. Know the essential clinical and therapeutic aspects of malaria
. Know the essential clinical and therapeutic aspects of shigellosis
. Know the essential clinical and therapeutic aspects of measles
. Know the essential clinical and therapeutic aspects of hookworm disease(ankylostomiasis)
. Know the essential clinical and therapeutic aspects of yellow fever, diphtheria,scabies, and trachoma
. Use the planning tools already studied to establish priorities among the maincommunicable diseases
. Plan a programme for controlling measles in a given situation
. Plan a programme for controlling malaria in a given situation
. Plan a programme for controlling tuberculosis in a given situation
. Plan a programme for controlling diarrhoeal diseases in a given situation
. Plan a programme for controlling meningococcal meningitis in a given situation
. Plan a programme for controlling hookworm disease in a given situation.
HELP/SOS: COMMUNICABLE DISEASES218

THE NATURAL CYCLEOF COMMUNICABLE DISEASES
1. DESCRIPTION
Since the concept of the natural cycle of communicable diseases is basic to thisentire module, course participants must assimilate it properly. This cycle can bedefined as a successionof events ensuing froman encounter between ahumanbeingand a microbial agent (viral, bacterial, or parasitic). Depending on theaggressiveness of the pathogen and the susceptibility of the human being, theresulting reactions may range from biological manifestations to benign, moderate,or severe clinical symptoms. The last stage may consist in recovery, sequelae, thecontinued presence of the pathogenic agent in the cured individual, or even death.The disease may leave the individual with complete or partial immunity.
2. CATEGORY
Framework: outlining the natural cycle of communicable diseases.
3. FORMULATION
Make a diagram of the natural cycle of communicable diseases.
4. TEACHING METHOD
Work in groups.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Cycle of communicable diseases
LINK WITH NEXT OBJECTIVES
This diagram provides a basis for identifying the main levels of prevention.
COMMUNICABLE DISEASES 219

221
Healthy carriers
Cure
Responses to attack by pathogenic agents
• Individual responses:- biological infection- minimal clinical symptoms- severe clinical symptoms
• Collective responses: - epidemic
Relapses
Death
Population• Factors affecting
vulnerability:- lack of immunity- overcrowding
Pathogenic agents(viruses, bacteria, parasites)
• Transmission(humans,vectors,water, etc.)
Sequelae
Box 1
CYCLE OF COMMUNICABLEDISEASES
HELP/SOS: COMMUNICABLE DISEASES2220

LEVELS OF PREVENTION IN THECONTROL OF COMMUNICABLE DISEASES
1. DESCRIPTION
Beginning with the natural cycle of communicable diseases described in theprevious objective, participants will explore the concept of levels of prevention.Hygienic and environmental measures, for example, are intended to reduce theenvironment’s potential for harm: less human waste means fewer germs; morewater means reduced transmission of germs, etc. These measures clearly pertainto the level of primary prevention, namely preventing disease. On the same level,immunization programmes also prevent disease, by modifying the individual’simmune status.
The instructor might take the example of simple cases of diarrhoeal diseases toexplain that early management of such cases prevents the development of moresevere forms of the disease; this constitutes secondary prevention. The concept oftreatment can be considered separately or included in the topic of secondaryprevention, since it prevents serious forms of the disease and death.
Finally, tertiary prevention consists in managing the sequelae of communicablediseases—for example, paralysis after an attack of polio, or malnutrition after acase of the measles.
The spheres corresponding to these levels of interventionwill be sketched directlyon the natural cycle of communicable diseases.
2. CATEGORY
Framework: defining the spheres corresponding to treatment and primary,secondary, and tertiary prevention.
3. FORMULATION
Starting with the natural cycle of communicable diseases, identify the main levelsof prevention—primary, secondary and tertiary prevention (including treat-ment) — and provide examples for each of these levels.
4. TEACHING METHOD
Work in groups, followed by plenary session.
COMMUNICABLE DISEASES 221

223
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Levels of prevention in the control of communicable diseases.
LINK WITH NEXT OBJECTIVES
Once the context of themodule has been defined, the next stage will be to identifythe main communicable diseases found in emergency situations.
Healthy carriers
Cure
Responses to attack by pathogens
• Individual responses:• biological infection• moderate clinical symptoms• major clinical symptoms
• Collective responses: • epidemic
Relapses
Sequelae
Population
Transmissionof pathogen
PRIMARY PREVENTION
TERTIARY PREVENTION
SECONDARYPREVENTION/
TREATMENT
Box 1
LEVELS OF PREVENTION IN THE CONTROLOF COMMUNICABLE DISEASES
HELP/SOS: COMMUNICABLE DISEASES2222

MAIN COMMUNICABLE DISEASESIN EMERGENCY SITUATIONSAND ASSOCIATED RISK FACTORS
1. DESCRIPTION
The thought of an emergency situation often conjures up visions of communi-cable diseases; the media cannot mention a war or an earthquake withoutevoking the risk of epidemics. Certainly large population movements areaccompanied by a rapid and substantial increase in cases of measles, diarrhoealdiseases, pulmonary infections, etc., if the appropriate measures are not quicklytaken.
The reasons for this increase in communicable diseases are obvious:
. a displaced population comes into contact with new pathogens
. the risk of transmission increases with overcrowding
. inadequate hygiene leads to an increase in the number of disease vectors
. a high malnutrition rate fosters an increase in communicable diseases
. basic care and prevention measures may deteriorate or cease altogether (e.g.,interruption of immunization campaigns as a result of war)
. water sources may be contaminated
. the proportion of children is usually higher in a displaced population.
Mortality associated with communicable diseases also increases as a result of thedeterioration of the medical services that would normally take care of seriouscases of these diseases.
Themain diseases found in both displaced populations and overcrowded prisonsare the following:
. measles
. diarrhoeal diseases (including cholera and dysentery)
. acute respiratory infections (pneumonia)
. malaria
. meningococcal meningitis
. tuberculosis
COMMUNICABLE DISEASES 223

225
. intestinal parasites
. skin infections (scabies)
. AIDS.
2. CATEGORY
Tool: listing the main communicable diseases found in emergency situations, aswell as the factors that help increase their prevalence and severity.
3. FORMULATION
List the main communicable diseases found in emergency situations, and thefactors that help increase their prevalence and severity.
4. TEACHING METHOD
Work in groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: The main communicable diseases in emergency situations
. Box 2: Factors contributing to increased incidence of communicablediseases in emergency situations
LINK WITH NEXT OBJECTIVES
By matching the main levels of prevention (primary, secondary, and tertiary)with the major communicable diseases present in emergency situations, we candraw up a list of the principal tools required to establish control programmes:
. expanded programme of immunization
. chemoprophylaxis and mass treatments
. short treatments
. health education
HELP/SOS: COMMUNICABLE DISEASES224
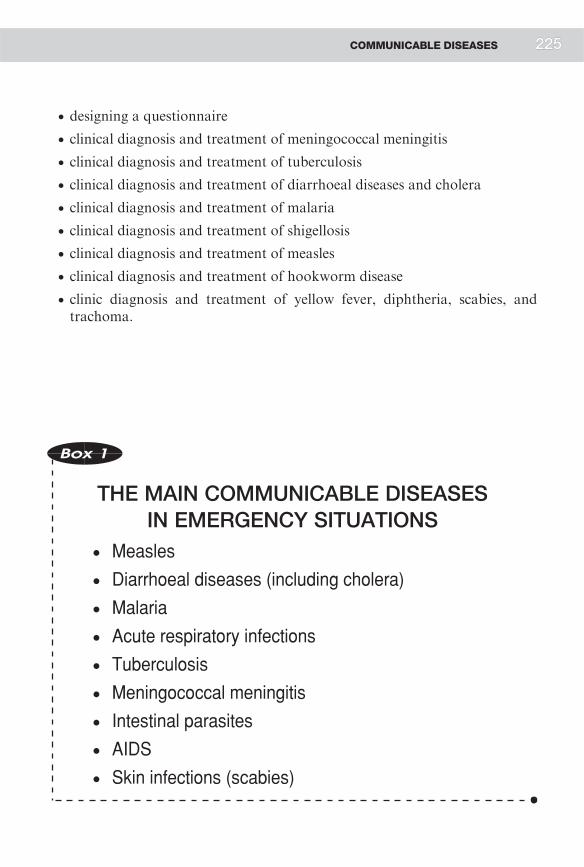
. designing a questionnaire
. clinical diagnosis and treatment of meningococcal meningitis
. clinical diagnosis and treatment of tuberculosis
. clinical diagnosis and treatment of diarrhoeal diseases and cholera
. clinical diagnosis and treatment of malaria
. clinical diagnosis and treatment of shigellosis
. clinical diagnosis and treatment of measles
. clinical diagnosis and treatment of hookworm disease
. clinic diagnosis and treatment of yellow fever, diphtheria, scabies, andtrachoma.
Box 1
THE MAIN COMMUNICABLE DISEASESIN EMERGENCY SITUATIONS
. Measles
. Diarrhoeal diseases (including cholera)
. Malaria
. Acute respiratory infections
. Tuberculosis
. Meningococcal meningitis
. Intestinal parasites
. AIDS
. Skin infections (scabies)
COMMUNICABLE DISEASES 225

227
Box 2
FACTORS CONTRIBUTINGTO INCREASED INCIDENCE
OF COMMUNICABLE DISEASESIN EMERGENCY SITUATIONS
. Presence of pathogenic agents new to a displacedpopulation or a host population
. Exhaustion
. No immunity
. Overcrowding
. Large proportion of children
. No environmental sanitation measures
. Increased number of vectors
. No personal hygiene
. Insufficient water
. Unsafe water
. High malnutrition rate
. No preventive health measures(e.g. immunization)
. Deterioration or lack of basic health services
. Breakdown of the family structure
HELP/SOS: COMMUNICABLE DISEASES226

EXPANDED PROGRAMMEOF IMMUNIZATION (EPI)
1. DESCRIPTION
In the practical exercise, course participants will have to make decisionsconcerning the institution and practical organization of an immunizationprogramme. In this objective, the important aspects of organizing an EPI will becovered:
. diseases covered by the EPI
. vaccine characteristics (types, storage requirements, etc.). The Schwarzantigen should be emphasized as the recommended measles vaccine
. the principle of ascertainingwhether an immunization programmewas in forcebefore the crisis. Formal proof of adequate immunization coverage (meaningmore than 95% of the vulnerable sectors in a refugee camp) is necessary
. determination of targeted age groups. Given the specific conditions ofemergency situations, the instructor should emphasize in particular the needto vaccinate children aged 6 months to 12 years against measles, noting thatthe use of the Schwarz vaccine will necessitate a second injection for childrenbetween the ages of 6-9 months. The magnitude of the risk factors affectingdisplaced and refugee populations justifies expanding the age groups eligiblefor the various types of immunization
. organizing an EPI involving several different vaccines (measles, polio,tetanus, diphtheria, whooping cough) is not much more work thanorganizing an immunization campaign for only one vaccine (logically, thetop-priority measles vaccine). In either case, however, immunization againstmeasles is absolutely essential
. educating the population is a key factor in the success of an immunizationcampaign
. the concept of a cold chain must be thoroughly understood. The instructorwill review the main types of equipment used (refrigerators, freezers or coldboxes, etc.), and will explain the use of cold-chain monitor cards, which, keptwith the stored vaccines, change colourwhen storage temperature exceeds themaximum
. evaluation of the effectiveness of an immunization campaign. Emphasisshould be laid on the concepts of coverage and vaccine efficacy
COMMUNICABLE DISEASES 227

229
. establishing a surveillance system to monitor the effectiveness of animmunization campaign is essential. This effectiveness is determined on thebasis of the cases seen by the dispensaries, being measured by the proportionof cases occurring in immunized patients. The concept of the serologiceffectiveness (rate of seroconversion) of each vaccine should be mentioned
. importance of linking any mass immunization campaign with a routine EPI.
All this information is essential for planning an immunization campaign.
2. CATEGORY
Tool: familiarity with the main elements of an expanded programme ofimmunization.
3. FORMULATION
Explain the importance of the main aspects of an expanded programme ofimmunization.
4. TEACHING METHOD
Question-and-answer session involving all participants.
5. DURATION
Total duration: 30 minutes.
6. RECAPITULATION
. Box 1: Communicable diseases covered by the EPI
. Box 2: Characteristics of the principal vaccines
. Box 3: EPI immunization schedule
. Box 4: Age groups for measles immunization
. Box 5: Formula for calculating vaccine efficacy
. Box 6: Illustration of changes in the proportion of cases which occur inimmunized children at different levels
. Box 7: The cold chain
LINK WITH NEXT OBJECTIVES
The practical organization of an immunization campaign will be discussed in alater objective (practice).
HELP/SOS: COMMUNICABLE DISEASES228

Box 1
COMMUNICABLE DISEASES COVEREDBY THE EXPANDED
PROGRAMME OF IMMUNIZATION (EPI)
1. . Measles
. Poliomyelitis
. Tetanus
. Diphtheria
. Pertussis
2. . Tuberculosis (countries withhigh incidence)
. Hepatitis B (1997 EPI)
. Yellow fever (countries wherethe disease is endemic)
COMMUNICABLE DISEASES 229

231
Vaccines
BCG
Diptheria
Tetanus
Pertussis
Poliomyelitis
Measles
Yellow fever
Nature of vaccine
AttenuatedM. bovis
Toxoid
Toxoid
Killed whole-cell pertussis
bacterium
Attenuated live viruses
Attenuated live viruses
Attenuated live viruses
Form
Freeze-dried
Fluid
Fluid
Fluid
Fluid
Freeze-dried
Freeze-dried
No. of doses
and route
1 I/D
3 I/M
3 I/M
3 I/M
4 oral
1 S/C
1 S/C
Heatstability
Medium in dried form,
low in reconstituted
form
High
High
Medium
Low
Medium in dried form,
low in reconstituted
form
Medium in dried form,
low in reconstituted
form
Efficacy
0-80% TB lung
75-86%meningitisand millary
TB
> 87%
> 95%
Around 80%
>90%industrialized
countries;
72-98% inhot climates
>90% at 12 months of
age;85% at 9
months of age
9>92%seroconver-
sion to vaccine
Duration of immunity
after primary series
Unknown
5 years
5 years
Unknown
Lifelong if boosted by wild virus
Lifelong if boosted by wild virus
10 years (booster)
Disease
Tuberculosis
Diptheria
Tetanus
Pertussis
Poliomyelitis
Measles
Yellow fever
Source: Immunization Policy, WHO/EPI/GEN/95.3 (1995)
HBsAgHepatitis BHepatitis B Fluid 3 I/M High 75-95% >10 years
Box 2
CHARACTERISTICSOF THE PRINCIPAL VACCINES
HELP/SOS: COMMUNICABLE DISEASES230

Box 3
EPI IMMUNIZATIONSCHEDULE
AGE VACCINES HEPATITIS B
Scheme A Scheme B
Birth BCG, OPV 0 HB 1
6 weeks DPT 1, OPV 1 HB 2 HB 1
10 weeks DPT 2, OPV 2 HB 2
14 weeks DPT 3, OPV 3 HB 3 HB 3
9 months Measles
Yellow fever*
Source: Immunization Policy,WHO/EPI/GEN/95.03 (1995)
* In countries where yellowfever poses a risk
COMMUNICABLE DISEASES 231

233
AGE 0 6 9 12 24 36 48 60 72
I. If no previous immunization, immunize all children between 9 months and 12 years: one injection
II. Give children between the ages of 6 months and 9 months two injections: one at 6 months and the other at 9 months2nd inj.
1st inj.
months
12 years
Box 4
AGE GROUPS FORMEASLES IMMUNIZATION
Box 5
FORMULA FOR CALCULATINGVACCINE EFFICACY
PCV =PPV - (PPV x VE)
1 - (PPV x VE)
PCV = Proportion of Cases Vaccinated
PPV = Proportion of Population Vaccinated
VE = Vaccine Efficacy
HELP/SOS: COMMUNICABLE DISEASES232

Total number of children
Number of unvaccinated children
Assumptions:
Measles incidence among unimmunized children: 50% per year
Measles incidence among immunized children: 5% per year (vaccine efficacy=90%)
40% 80%
60,000 20,000100,000 100,000
Number of measles cases in unvaccinated children 30,000 10,000
Total number of cases 32,000 14,000
Proportion of total cases which are in vaccinated children
6.7% 4.0%
Number of vaccinated children 40,000 80,000
Coverage
Source: Immunization Policy,WHO/EPI/GEN/95.03 (1995)
Number of measles cases in vaccinated children 2,000 4,000
Box 6
ILLUSTRATION OF CHANGESIN THE PROPORTION OF CASES
WHICH OCCUR IN IMMUNIZED CHILDRENAT DIFFERENT LEVELS,
FOR A HYPOTHETICAL POPULATIONOF 100,000 CHILDREN
COMMUNICABLE DISEASES 2233

235
Box 7
THE COLD CHAIN
REFRIGERATION REQUIREMENTS PER VOLUME:
For one child, EPI vaccines in their packaging represent30 ml, requiring:
36 ml in a cold box60 ml in a refrigerator120 ml in a cold room
TRANSPORT CHARACTERISTICS:
. Volume to transport
. Time required for transport
. Expected duration of immunization campaign
CHOOSING THE EQUIPMENT COMBINATIONFOR THE COLD CHAIN:
. Cold room
. Type of refrigerators (electric, gas, oil)
. Cold boxes
TEMPERATURE MONITORING
HELP/SOS: COMMUNICABLE DISEASES234

COLLECTIVE CHEMOPROPHYLAXISAND MASS TREATMENTS
1. DESCRIPTION
Chemoprophylaxis consists in administeringmedicines to healthy subjects in orderto protect them from certain diseases. Chemoprophylaxis may be indicated for anumber of diseases—malaria, cerebrospinal meningococcal meningitis, bilharzia-sis—and its effectiveness should be discussedwith respect to each specific situation.For example, in areas of resistance to common antimalarials, chemoprophylaxisposes seriousproblems, owing to thedangerof inducing resistance tonewdrugs andthe logistical problems of organizing such campaigns. The instructor shouldemphasize the practical difficulties and cost of organizing this sort of programme.
If chemoprophylaxis is difficult to implement under normal conditions, its use iseven more problematic in emergency situations. The only cases where chemopro-phylaxis can be considered would be formalaria and for certain population groups(pregnant women in the second and third trimesters, children between the ages ofthree months and five years) in very specific situations, and if a common, locallyeffective antimalarial is available. In the case of cerebrospinal meningitis,chemoprophylaxis may be considered for patients’ close contacts. Nevertheless,chemoprophylaxis is rarely appropriate in emergency situations and should not bepractised in the management of cholera epidemics.
Mass treatments consist in the systematic treatment of subjects who are or arepresumed to be infected with a disease, as well as healthy carriers of the disease.Since in practice it is difficult to distinguish between healthy carriers anduninfected subjects without systematic testing, such treatment would have toinclude all the people in a community. This is difficult to do in an emergency. Incertain communities where intestinal parasites are very prevalent, masstreatment of the population may be indicated in the period before sanitationmeasures begin to have an impact.
Generally speaking, both chemoprophylaxis and mass treatments are largelyinappropriate in any strategy to control communicable diseases in emergencysituations, given their uncertain efficacy, difficult implementation, and high cost,as well as the problem presented by the instability of the population.
2. CATEGORY
Tool: familiarity with the limitations of chemoprophylaxis and mass treatmentsin the control of certain communicable diseases in emergency situations.
COMMUNICABLE DISEASES 235

237
3. FORMULATION
Define the terms ‘‘chemoprophylaxis’’ and ‘‘mass treatment,’’ and indicate thelimitations of these measures in a general strategy for controlling communicablediseases in an emergency situation.
4. TEACHING METHOD
Work in groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Factors limiting the feasibility of collective chemoprophylaxis andmass treatments
LINK WITH NEXT OBJECTIVES
The material learned in this objective will be applied to the study ofcommunicable-disease control in the context of the simulation exercise.
Box 1
FACTORS LIMITING THE FEASIBILITYOF COLLECTIVE CHEMOPROPHYLAXIS
AND MASS TREATMENTS
. Risk of inducing resistance to the drugs used
. Difficult implementation when chemoprophylaxis mustbe repeated regularly (malaria)
. Effectiveness of mass treatment limited to medium termif it is not accompanied by sanitation measures(hookworm disease)
. Population instability
HELP/SOS: COMMUNICABLE DISEASES236

THE RESPECTIVE ADVANTAGESOF SHORT AND LONGTREATMENTS
1. DESCRIPTION
Short treatments should not be considered as treatments ‘‘on the cheap.’’ It hasbeen proven that short treatments for tuberculosis, for example, are much moreeffective than long ones. In any case, analysis of the results for individualpatients does not necessarily indicate a conclusive difference in effectiveness.The short treatment of meningococcal meningitis, which is based on a singleintramuscular injection of chloramphenicol, is effective, but so is the classictreatment, which consists in the intravenous administration of antibiotics over aperiod of several days. The problem is best approached from the perspective ofpublic health, with due consideration of the risks of patient non-compliance,which are higher in long courses of treatment. Also significant is the fact thatshort treatments reduce the workload of the health services—not a negligiblefactor during an epidemic or the acute phase of a conflict crisis. The relativecosts of the two therapeutic approaches should be briefly mentioned, and thecost analysis should take into account not only the cost of the drugs themselves,but also the considerations just mentioned. Short treatments for tuberculosismake patients’ sputum negative in two to three weeks, thereby checking thespread of the disease more quickly. Reduction of the burden on the healthservices must also be figured into the costs of medical care using shorttreatments. Reducing work disability is less important in situations involvingdisplaced populations.
The main diseases posing an alternative between short and long treatments are:
. tuberculosis
. meningococcal meningitis
. amoebiasis
. bilharziasis.
2. CATEGORY
Tool: familiarity with the advantages of short courses of treatment in emergencysituations.
COMMUNICABLE DISEASES 237

239
3. FORMULATION
List the advantages of short courses of treatment in emergency situations.
4. TEACHING METHOD
Assignment presented to entire group.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Advantages of short-course treatment in emergency situations.
LINK WITH NEXT OBJECTIVES
This objective raises the problem of patient compliance. Health education is oneof the factors that helps improve compliance.
Population
Box 1
ADVANTAGES OF SHORT-COURSETREATMENT IN EMERGENCY SITUATIONS
. Overcrowding
. Large number of patients
. Instability
Despite these unfavourable conditions, treatments should beoriented towards an optimal balance between:
. Therapeutic effectiveness
. Patient compliance
. The cost of treatment perpatient cured
. Health services’ workload
. Minimization of negative ef-fects (for example, inductionof resistance to antibiotics)
HELP/SOS: COMMUNICABLE DISEASES238

PLANNING A HEALTHEDUCATION PROGRAMME
1. DESCRIPTION
Health education is not, of course, relevant to communicable diseases alone.However, such diseases are a convenient vehicle for approaching this subject.The purpose of health education is to encourage behaviour that is conducive tohealth. In normal situations, attempts will be made to convince populations orgroups to modify their behaviour in light of one or more health problems.Emergency situations are more complex since the seriousness of the problemsinvolved necessitates rapid changes in behaviour, often in a new environment.This may also be a good argument for encouraging new behaviours.
A health education programme includes the following stages:
. let the community identify what it perceives to be its health problems
. together with the community, examine its usual response to these problems,by observing, conducting interviews, and studying documents
. define a health education programme:
. set priorities and objectives together with the community
. help the community choose the solution best suited to its health problems,taking into account both the desired impact and any local constraints(cost, social perception of behaviour modifications)
. identify and seek the resources needed to implement themeasures decidedupon
. evaluate the results obtained.
The training of community health workers should be oriented towards thecommunity’s basic problems and focused on apprenticeship rather than theory.Instruction should be based primarily on practice in the tasks that futurecommunity healthworkers will have to carry out in the course of their dailywork.
2. CATEGORY
Tool: recognizing the importance and the limitations of health education inemergency situations, and familiarity with the steps involved in implementing ahealth education programme.
COMMUNICABLE DISEASES 239

241
3. FORMULATION
Define health education and identify the steps involved in implementing a healtheducation programme. Outline the importance and limitations of healtheducation in emergency situations.
4. TEACHING METHOD
Question-and-answer session involving all participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Developing a health education programme
LINK WITH NEXT OBJECTIVES
This tool will be applied in the simulation exercise, in the context of latrine use.
Box 1
DEVELOPING A HEALTHEDUCATION PROGRAMME
. Identification of health problems by the community
. Study of behaviours adopted to cope with theseproblems: Should they be modified?
. Determination of the objectives of a health educationprogramme
. Identification of practical measures, acceptable to thecommunity, to modify these behaviours
. Implementation of the measures
. Evaluation of results
HELP/SOS: COMMUNICABLE DISEASES240

DRAWING UP A QUESTIONNAIRETO IDENTIFY THE MAIN CAUSESOF CHILD MORTALITY
1. DESCRIPTION
Child mortality can be studied from data collected in dispensaries and hospitals,but these sources may not include deaths occurring at home. In emergencysituations, administrative sources of information, such as death registers, arerarely accessible. For this reason, direct surveys within the community are alsonecessary.
Verbal autopsies are based on questions asked of mothers concerning the causesand number of deaths among their own children during a certain period.
The questionnaire must:
. take local dialect into account, particularly in the definition of termsdescribing diseases
. define the period under investigation in terms of important eventsremembered by the respondents, since not everyone has the same conceptof time
. not be overly structured. It is useless to ask for too many details concerningthe circumstances of a death; they will be difficult to interpret, owing tomultiple interpretations of the questions.
This questionnaire can be given to focus groups, in accordance with rapid-assessment procedures—as long as due consideration is given to the limitationsof this technique as a means of gaining a representative view of an entirepopulation. If time and resources permit, a survey of a correctly sampled sectorof the population is preferable. The course participants should be told thatsampling techniques will not be covered until later on, in the epidemiologymodule.
2. CATEGORY
Tool: familiarity with the essential rules for devising a questionnaire to assesschild mortality within a population.
COMMUNICABLE DISEASES 241

243
3. FORMULATION
Define the essential rules for drawing up a questionnaire to assess child mortalitywithin a population.
4. TEACHING METHOD
Question-and-answer session involving all participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Considerations in drawing up a questionnaire
LINK WITH NEXT OBJECTIVES
This tool will be applied in the simulation exercise to study child mortality in theAwalei camp.
Box 1
CONSIDERATIONS IN DRAWING UPA QUESTIONNAIRE
. Local idioms
. Duration of the period of investigation
. Structure of the questions
. Selection of respondents
HELP/SOS: COMMUNICABLE DISEASES242

ESSENTIAL CLINICALAND THERAPEUTIC ASPECTSOF MENINGOCOCCAL MENINGITIS
1. DESCRIPTION
This objective is designed to give participants the clinical and therapeuticknowledge essential for understanding the overall organization of a programmeto control meningococcal meningitis.
Clinical aspects
Meningococcal meningitis is caused by the Neisseria meningitidis bacterium,which is a gram-negative diplococcus comprising various serogroups—A, B, C.The classic clinical symptoms are:
. fever
. stiff neck
. headache
. vomiting.
In children the clinical symptoms are less obvious, and stiff neck is not necessarilypresent. Serious cases may be characterized by purpura fulminans, coma, orconvulsions.
Diagnosis is based on the results of an examination of the cerebrospinal fluid(lumbar puncture), which reveals the presence of meningococcus. Once thediagnosis has been confirmed for the first cases of an epidemic, thebacteriological tests need not be repeated for every patient presenting theclinical signs of meningitis. The disease can be diagnosed on the basis of theclinical symptoms alone.
Therapeutic aspects
In emergency situations, the recommended treatment for meningococcalmeningitis is an intramuscular injection of an oily suspension of chloramphenicolfollowed by a second injection 48 hours later.
2. CATEGORY
Tool: familiarity with the essential clinical and therapeutic aspects ofmeningococcal meningitis.
COMMUNICABLE DISEASES 243

245
3. FORMULATION
Present the essential clinical and therapeutic aspects of managing cases ofmeningococcal meningitis.
4. TEACHING METHOD
Question-and-answer session in plenary session.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Meningococcal meningitis
LINK WITH NEXT OBJECTIVES
The material learned in this objective will be used in the simulation exercise.
HELP/SOS: COMMUNICABLE DISEASES244

Box 1
MENINGOCOCCAL MENINGITIS
1. Infectious agent:Gram-negative diplococcus:Neisseria meningitidis. Several serogroups: A, B, C.
2. Cycle:Reservoir: manThe disease is spread directly from person to personby respiratory droplets.The incubation period averages 3-4 days.
3. Clinical signs:fevervomitingheadachestiff neckcomplications: . sepsis
. purpura
. intravascular coagulation
4. Diagnosis:. blood culture. analysis of CSF
5. Control measures:Treatment: antibioticsPrimary prevention: immunization of groups at riskSecondary prevention: tracing patients’ contactsProphylactic antibiotic treatment of patients’ contacts
6. Epidemiology:Universal diseaseLarge-scale epidemics are common in the sub-Saharan African countries(the ‘‘meningitis belt’’). Children and young adults living in groups are athighest risk.
COMMUNICABLE DISEASES 245

247
ESSENTIAL CLINICAL ANDTHERAPEUTIC ASPECTSOF TUBERCULOSIS
1. DESCRIPTION
This objective is designed to give participants the clinical and therapeuticknowledge essential for understanding the overall organization of a programmeto control tuberculosis.
Tuberculosis may have pulmonary and extrapulmonary manifestations (bone,renal, splenic, peritoneal, meningeal, etc.). The instructor will describe first themode of transmission, and then the transition from tubercular infection totubercular disease. Study will be limited to the clinical profile and treatmentoptions for pulmonary tuberculosis, since that is the most common andcontagious form of the disease.
Clinical aspects
Pulmonary tuberculosis (the disease) is manifested by the following clinicalsymptoms:
. cough that continues for at least three weeks
. haemoptysis (bloody sputum) may be present
. weight loss
. low-grade fever (38o C)
. sweating
. fatigue.
Where several of these clinical signs are in evidence, a sputum analysis isindicated to detect the mycobacteria responsible for tuberculosis (Mycobacter-ium tuberculosis). This is performed by direct microscopic examination afterZiehl-Neelsen staining. The goal is to detect patients with positive sputum, notonly in order to treat them, but also to decrease the risk of mycobacterialtransmission to the people around them (the primary prevention aspect oftreatment). People infected with pulmonary tuberculosis can be divided into fourcategories:
. category I: new cases with positive sputum
HELP/SOS: COMMUNICABLE DISEASES246

. category II: relapses or treatment failures in patients previously treated butagain presenting positive sputum
. category III: patients with infected organ tissue but negative sputum
. category IV: chronic cases—patients with positive sputum who have alreadybeen treated for tuberculosis. Most of these cases involve multi-drug-resistant forms of the disease.
Therapeutic aspects
The main drugs used in treating tuberculosis are:
. isoniazid (H)
. rifampicin (R)
. ethambutol (E)
. streptomycin (S)
. pyrazinamide (Z).
Three points are important for an understanding of treatment regimens:
. short-course therapy (6-8 months) is now recommended instead of longtreatments (15-18 months) because of its greater effectiveness. Shortantituberculous regimens comprise two stages:
. an intensive initial stage of 2 months
. a consolidating stage of 4-6 months
. institution of the DOT (Directly Observed Therapy) strategy is imperative
. the treatment regimen will depend on the category of the patient:
category I: H2R2Z2E2orS2 + H4R4
category II: H3R3Z3E3S3 + H5R5E5
category III: H2R2Z2 + H2-6R2-6
category IV: treatment is not very effective, except with second-line drugs.
Finally, mention should be made of the high incidence of tuberculosis in patientsinfected with HIV.
2. CATEGORY
Tool: familiarity with the essential clinical and therapeutic aspects oftuberculosis.
COMMUNICABLE DISEASES 247

249
3. FORMULATION
Present the essential clinical and therapeutic aspects of managing a campaignagainst tuberculosis.
4. TEACHING METHOD
Question-and-answer session involving all participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Tuberculosis
LINK WITH NEXT OBJECTIVES
The information learned in this objective will be used in the simulation exercise.
HELP/SOS: COMMUNICABLE DISEASES248

Box 1
TUBERCULOSIS1. Infectious agent:
Acid-fast bacillus: Mycobacterium tuberculosis
2. Cycle:Reservoir: manAirborne transmission. The risk of transmission depends mainlyon the concentration of mycobacteria.The risk of developing the disease is very low in personswith healthy immune systems.
3. Clinical signs:Pulmonary tuberculosis.Onset is progressive: . malaise
. low-grade fever
. night sweats
. weight loss
. coughOnce the disease has developed, haemoptysis may be observed.
4. Diagnosis:Examination of sputum to detect mycobacteria (active TB)Lung X-ray (unfeasible in emergency situations)
5. Control measures:Treatment: 6-9 months, with 4 antibiotics for 2 months followedby 2 antibiotics for 4-7 months. Drug resistances are increasingly common.DOT (Directly Observed Therapy)Primary prevention: vaccination with BCG for children underone year old offers protection against tuberculous meningitisand acute miliary tuberculosisChemoprophylaxis: for infected persons who have not developed thediseaseThe treatment of patients with positive sputum reduces transmission.Such treatment can therefore be considered as a primary preventionmeasure for the communitySecondary prevention: early diagnosis and treatment of cases.
6. Epidemiology:Universal disease. Predisposing factors:
. poverty
. overcrowding
. immunodeficiencies (e.g., HIV infection)
COMMUNICABLE DISEASES 249

251
ESSENTIAL CLINICAL AND THERAPEUTICASPECTS OF DIARRHOEAL DISEASESAND CHOLERA
1. DESCRIPTION
Diarrhoeal diseases are among the most common causes of mortality amongchildren. Cholera is one particular example of a diarrhoeal disease.
Clinical aspects
Several questions must be asked of a patient or the mother of a child presentingdiarrhoeal stools:
. nature of the stools:watery, containingblood andmucus (indicating dysentery)
. number of stools per day
. duration of each diarrhoeal episode.
The health practitioner performing the clinical examination should look first forsigns of dehydration:
. apathy
. skin folds
. sunken eyes
. dry tongue.
Therapeutic aspects
The most essential therapeutic measure is to prevent or treat dehydration. It is infact dehydration that is apt to cause death.
In cases of simple diarrhoea (without signs of dehydration), themother should beasked to increase the child’s liquid intake (possibly through a solution of oralrehydration salts—ORS) while continuing to feed or breast feed the child.
In cases presenting signs of dehydration, rehydration with ORS is imperative.This treatment must be maintained throughout the diarrhoeal episode.
Cases of acute diarrhoea accompanied by severe dehydration will requireintravenous rehydration with Ringer’s lactate. If the child’s condition permits it,oral rehydration should be continued.
HELP/SOS: COMMUNICABLE DISEASES250

Certain cases of diarrhoeal disease with specific etiologies, such as shigellosis,amebiasis, giardiasis, and cholera, require appropriate antibiotic treatment inaddition to rehydration.
Cholera
Cholera is a specific diarrhoeal disease caused by the bacterium Vibrio cholerae(serotype 01 and its classic biotypes, El Tor, and the new 0139). The diarrhoeaassociated with cholera is watery and profuse, and quickly leads to severedehydration, acidosis, and potassium depletion. It is accompanied by oftenuncontrollable vomiting.
Treatment consists primarily in rehydration with ORS. If the patient does not oris unable (being comatose, for example) to drink adequate amounts, rehydrationmust be performed intravenously using Ringer’s lactate solution. Infusions of 8-12 litres of Ringer’s lactate per day may be necessary.
Antibiotic treatmentwill help reduce the volumeof the stools and the length of timeduring which vibrio bacteria are excreted. The recommended antibiotic isdoxycycline. Sulfonamides are no longer effective and therefore shouldnot beused.
The principles involved in controlling a cholera epidemic will be addressed in themodule on epidemiology.
2. CATEGORY
Tool: familiarity with the essential clinical and therapeutic aspects of diarrhoealdiseases and cholera.
3. FORMULATION
Present the essential clinical and therapeutic aspects of managing cases ofdiarrhoeal diseases and cholera.
4. TEACHING METHOD
Question-and-answer session involving all participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Cholera
LINK WITH NEXT OBJECTIVES
The material learned in this objective will be used in the simulation exercise.
COMMUNICABLE DISEASES 251

253
1. Infectious agent: Vibrio cholerae • Three serotypes of the 01 group
(Ogawa, Inaba, Hikojima) divided into two biotypes (classic and El Tor)• New serotype in India: 0139
2. Cycle:
3. Physiopathology: The toxin secreted by the vibrio acts on the intestinal mucus membrane and induces hypersecretion resulting in diarrhoea (rice-water stools) and vomiting.
4. Clinical signs: • profuse, uncontrollable diarrhoea similar in appearance to rice water • vomiting • dehydration • acidosis • shock Note: Many infected people remain asymptomatic.
5. Diagnosis: • detection of vibrios in the stools
6. Control measures: Treatment: • rehydration
• antibiotics
Primary prevention: • personal hygiene• clean water• proper disposal of liquid waste• food hygiene• proper disposal of patient stools
Note: no effective vaccine
Secondary prevention: early diagnosis and treatment of cases
reservoir(man) stools and vomit
contamination• water• food (seafood)• clothing
transmission to man• consumption of contaminated water• contact with soiled clothing
Box 1
CHOLERA
HELP/SOS: COMMUNICABLE DISEASES2252

ESSENTIAL CLINICALAND THERAPEUTIC ASPECTS OF MALARIA
1. DESCRIPTION
This objective is designed to give participants the clinical and therapeuticknowledge essential for understanding the overall organization of a programmeto control malaria. The approach to this topic will be based on the natural cycleof communicable diseases:
. transmission by means of the anopheles mosquito: point out the connectionwith the vector-control measures studied in the previous module
. the concept of immunity: emphasize the temporary nature of immunity oncetransmission is discontinued
. the main clinical symptoms: fever, chills, etc.
. the difficulty of making a precise diagnosis without a laboratory—thesensitivity and specificity of clinical symptoms form the basis for diagnosis
. seriousness of certain clinical pictures, due to the strain of the parasite(cerebral malaria caused by plasmodium falciparum), due to age (malaria inchildren), due to physiological condition (malaria in pregnant women), ordue to complications (anaemia, renal insufficiency, pulmonary oedema,blackwater fever, etc.)
. laboratory tests: blood smears—thick and thin blood films
. the treatment for malaria with emphasis on:
. the main antimalarials: chloroquine, quinine, mefloquine, antifolates,schizontocides (combinations of sulfonamides and pyrimethamine,antibiotics, quinghaosu), gametocytocides
. the problem of resistance to antimalarials: types of resistance (R1, R2,R3) and the development of the problem of drug resistance in the world
. recommended treatments for different areas of resistance
. the limitations of prophylaxis in emergency situations
. environmental measures (vector control) and individual protectionmeasures (mosquito nets, mosquito repellents)
. mention the development of a vaccine and the results of the first tests inthe field.
COMMUNICABLE DISEASES 253

255
2. CATEGORY
Tool: familiarity with the essential clinical and therapeutic aspects of malaria.
3. FORMULATION
Present the essential clinical and therapeutic aspects of managing cases ofmalaria.
4. TEACHING METHOD
Question-and-answer session involving all participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Malaria
LINK WITH NEXT OBJECTIVES
The material learned in this objective will be used in the simulation exercise.
HELP/SOS: COMMUNICABLE DISEASES254

Gametocytes developinto sporozoites insidethe mosquito
Infected female anophelesinjects sporozoites along withits saliva when it bites ahuman being
1/2 hour to pass from theblood to the liver, wherethe sporozoite developsinto a schizont
Rupture of liver cell,releasing merozoites
Passage through the red bloodcells, where the merozoitesturn into trophozoites
Rupture of red blood cellsRelease of merozoitesand gametocytes
Red blood cell
Liver cell
Trophozoite
Bloodvessel
Infection of female anopheleswhen it bites a malaria patient
Liver
Schizonts
3. Physiopathology: The fever is caused by the release of malarial pigment into the blood when the schizonts rupture. Plasmodium falciparum, when parasitemia is high, causes microcirculation problems (brain, kidneys).
4. Clinical signs: 4.1 Plamodium falciparum: •1-2 weeks incubation • high fever • chills, sweating pernicious attacks: cerebral malaria—febrile coma 4.2 Plasmodium vivax •10-20 days incubation • fever • headache, body aches
5. Diagnosis: Detection of the parasite in the blood (blood smears—thin and thick film)
6. Control measures: Treatment: antimalarials (chloroquine, quinine, mefloquine, qinghaosu)
Primary prevention: mosquito nets, repellents, mosquito control
1. Infectious agent:Four types of parasite in man:
• Plasmodium falciparum • Plasmodium malaria • Plasmodium vivax • Plasmodium ovale
2. Cycle:
Box 1
MALARIA
COMMUNICABLE DISEASES 2255
257
ESSENTIAL CLINICALAND THERAPEUTIC ASPECTSOF SHIGELLOSIS
1. DESCRIPTION
Shigellosis is caused by a gram-negative bacillus (Shigella). These bacilli invadethe intestinal lining, where they cause micro-abscesses, bleeding, and destructionto the intestinal mucosa. The reservoir is man. The disease is transmitted throughdirect contact with infected people and through contaminated food and water.An important point to remember is that a small number of bacilli is enough tocause the disease and lead to major epidemics.
Shigellosis is characterized by diarrhoeal stools containing mucus, pus, andblood, accompanied by fever and abdominal pain. The mortality rate is high inchildren under the age of one year.
Treatment involves:
. the usual treatment for diarrhoeal diseases: rehydration
. antibiotic treatment. Tests should be made to determine the degree ofantibiotic resistance in the area in question so that themost effective drug canbe selected: nalidixic acid, ciprofloxacin, etc.
Prevention consists in environmental sanitation measures: correct disposal ofhuman waste, a clean water supply, and health education.
2. CATEGORY
Tool: familiarity with the essential clinical and therapeutic aspects of shigellosis.
3. FORMULATION
Present essential clinical and therapeutic aspects of shigellosis.
4. TEACHING METHOD
Question-and-answer session involving all participants.
5. DURATION
Total duration: 10 minutes.
HELP/SOS: COMMUNICABLE DISEASES256

6. RECAPITULATION
. Box 1: Shigellosis
LINK WITH NEXT OBJECTIVES
The material learned in this objective will be used in the simulation exercise.
Box 1
SHIGELLOSIS
(Bacterial Dysentery)
1. Infectious agent:Shigella organisms: gram-negative bacilli, comprising four subgroups
2. Cycle:Reservoir: manTransmission is by direct contact with infected people or consumptionof contaminated food or water
3. Physiopathology:Invasion of the intestinal mucosa leading to the formationof micro-abscesses, haemorrhaging, and destruction of intestinal cells
4. Clinical signs:Diarrhoea with fever and abdominal pain
5. Diagnosis:Stool culture: resistance to antibiotics
6. Control measures:Treatment: . rehydration
. antibiotics
Primary prevention: . hygiene measures(water, food, personal hygiene)
COMMUNICABLE DISEASES 257

259
ESSENTIAL CLINICALAND THERAPEUTIC ASPECTS OF MEASLES
1. DESCRIPTION
This objective is designed to give participants the clinical and therapeuticknowledge essential for understanding the overall organization of a programmeto control measles. The approach to this topic will be based on the natural cycleof communicable diseases:
. airborne transmission: effect of overcrowding
. immunity: concept of susceptible groups—mainly children between the agesof 6 months and 5 years, but under certain circumstances the susceptiblerange may be extended to age 14. It is important to point out that sincematernal antibodies are present in breastfed infants between the ages of 6-9months, a second injection of the vaccine will be necessary after the childpasses the age of 9 months
. clinical signs: fever, morbilliform rash, cough, red eyes, Koplik’s spots
. measles treatment:
. routine care: hydration, proper feeding, fever reduction, good hygiene
. prevention of infectious complications, e.g., pulmonary and ear, nose,and throat infections
. therapeutic doses of vitamin A (200,000 IU)
. notification of the epidemiological centre concerning cases of measlesrecorded among the population and in health facilities, and their immuniza-tion status, in order to facilitate evaluation of the efficacy of a previousimmunization programme.
2. CATEGORY
Tool: familiarity with the essential clinical and therapeutic aspects of measles.
3. FORMULATION
Present the essential clinical and therapeutic aspects of managing cases of measles.
4. TEACHING METHOD
Question-and-answer session involving all participants.
HELP/SOS: COMMUNICABLE DISEASES258

5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Measles
LINK WITH NEXT OBJECTIVES
The material learned in this objective will be used in the simulation exercise.
Box 1
MEASLES
1. Infectious agent:Measles virus
2. Cycle:Reservoir: manThe disease is transmitted directly from person to person by meansof Pflugge dropletsThe incubation period is 10 days
3. Clinical signs:Fever, enanthema, cough, rhinitis, conjunctivitis, Koplik’s spotsSpreading maculopapular rashComplications: . ear infections
. pneumonia
. encephalitis
. malnutrition
. vitamin A deficiency
4. Diagnosis:Clinical diagnosis
5. Control measuresTreatment: . symptomatic
. vitamin A
. antibiotic prophylaxisPrimary prevention: . vaccination
COMMUNICABLE DISEASES 259

261
ESSENTIAL CLINICALAND THERAPEUTIC ASPECTSOF ANKYLOSTOMIASIS
1. DESCRIPTION
This objective is designed to give participants the clinical and therapeuticknowledge essential for understanding the overall organization of a programmeto control intestinal parasites, using hookworm infestation (ankylostomiasis) asa representative example.
There are two kinds of hookworm: Ancylostoma duodenale and Necatoramericanus. They feed on blood, attaching themselves to the intestinal mucosaand ‘‘pumping’’ blood out of the intestinal villi. The amount of blood lost by thehost depends on the type of hookworm (A. duodenale is 10 times morehaematophagic than N. americanus) and the extent of the infestation.
Clinical aspects
Digestive symptoms are present during the initial phase of the primaryinfestation, taking the form of epigastric pain, nausea, vomiting, and diarrhoea.
Anaemia is caused by intestinal blood loss and may be severe.
Therapeutic aspects
The recommended treatment is albendazole. A single dose of 400 mg cures 80%of all cases. Three doses of 200 mg for three consecutive days cures all cases. Adaily dose of 100 mg of mebendazone for three days is also very effective.
Anaemia is treated with ferrous sulfate.
2. CATEGORY
Tool: familiarity with the essential clinical and therapeutic aspects of hookwormdisease.
3. FORMULATION
Present the essential clinical and therapeutic aspects of managing cases ofhookworm disease.
HELP/SOS: COMMUNICABLE DISEASES260

4. TEACHING METHOD
Question-and-answer session involving all participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Hookworm disease
LINK WITH NEXT OBJECTIVES
The material learned in this objective will be used in the simulation exercise.
COMMUNICABLE DISEASES 261

263
1. Infectious agent: Nematodes • Necator americanus
• Ancylostoma duodenale2. Cycle:
3. Physiopathology: Lesions of the intestinal mucosa
4. Clinical signs: • pulmonary symptoms (cough, infiltrates) • microhaemorrhages anaemia • growth retardation and failure to gain weight (chronic infection)
5. Diagnosis: • detection of eggs in the stools
6. Control measures: Treatment: albendazole
Primary prevention:• latrines• wearing shoes
Secondary prevention:• early diagnosis and treatment• mass treatment
Tertiary prevention: treat anaemia
eggs
stools
maturationin the soil (1 week)
larvaeenter
human hostthrough the skinor are swallowed
through thelymphatics
through thebloodstream
nematodesin the digestive
tract
lungsbronchialtubestrachea
( )
Box 1
HOOKWORM DISEASE
HELP/SOS: COMMUNICABLE DISEASES2262

ESSENTIAL CLINICAL AND THERAPEUTICASPECTS OF YELLOW FEVER, DIPHTHERIA,SCABIES, AND TRACHOMA
1. DESCRIPTION
The purpose here is to give participants some idea of the clinical and therapeuticaspects of other communicable diseases, although these diseases will not be usedto illustrate control programmes in the simulation exercise.
2. CATEGORY
Tool: familiarity with the essential clinical and therapeutic aspects of yellowfever, diphtheria, scabies, and trachoma.
3. FORMULATION
Present essential clinical and therapeutic aspects of yellow fever, diphtheria,scabies, and trachoma.
4. TEACHING METHOD
Question-and-answer session involving all participants.
5. DURATION
Total duration: 10 minutes.
6. RECAPITULATION
. Box 1: Yellow fever
. Box 2: Diphtheria
. Box 3: Scabies
. Box 4: Trachoma
LINK WITH NEXT OBJECTIVES
The material presented here will be useful for discussions of the concrete examplesof controlprogrammescitedby the instructorson thebasisof theirownexperiences.
COMMUNICABLE DISEASES 263

265
Box 1
YELLOW FEVER1. Infectious agent:
Yellow fever virus
2. Cycle:Reservoir: primates. The disease is transmitted by mosquitoes(Aedes aegypti)
3. Clinical signs:Fever, headache, muscular pains, albuminuria, renal insufficiency,jaundice, haemorrhage
4. Diagnosis:Serologic diagnosis
5. Control measures:Treatment: . symptomaticPrimary prevention: . immunization (10 years)
. mosquito control
Box 2
DIPHTHERIA
1. Infectious agent:Gram-positive aerobic bacillus:Corynebacterium diphteriae
2. Cycle:Reservoir: manThe disease is transmitted bydirect contact with infectedpatients or carriers.The incubation period is 2-5 days
3. Clinical signs:Pharyngeal and laryngealdiphtheria, formation of whitishmembranes in the pharynxand larynx
C. diphtheriae endocarditisToxic complications(myocarditis)
4. Diagnosis:Detection of C. diphtheriaecultured on special media
5. Control measures:Treatment: antibiotics, antitoxinPrimary prevention:immunizationSecondary prevention: patientquarantine
HELP/SOS: COMMUNICABLE DISEASES264

Box 3
SCABIES
1. Infectious agent:Mite: Sarcoptes scabiei
2. Cycle:Reservoir: manTransmission: by direct contact orfrom infested bedding
3. Clinical signs:Skin disease (papules,intradermic burrows) affecting thefinger-webs, the genitals, andflexor surfacesComplications: superimposedbacterial infections
4. Diagnosis: clinical
5. Control measures:Treatment: anti-mite lotionPrimary prevention: personalhygiene (water)Secondary prevention: earlytracing of contacts
6. Epidemiology:Universal disease, affectingall ages
Box 4
TRACHOMA
1. Infectious agent:Chlamydia trachomatis
2. Cycle:Reservoir: manTransmission: by direct contact(person to person) and throughthe intermediary of flies
3. Clinical signs:Follicular conjunctivitisRepeated infections cause scar-ring lesions of the cornea
4. Diagnosis: clinical
5. Control measures:Treatment: antibioticsPrimary prevention: personalhygiene (water is very important)
6. EpidemiologyCommon in Africa and the MiddleEast
COMMUNICABLE DISEASES 265

267
SETTING PRIORITIES AMONG THE PROBLEMSPERTAINING TOCOMMUNICABLE DISEASESIN A GIVEN SITUATION
1. DESCRIPTION
Using the data from the simulation exercise, participants will be expected toidentify the main problems deriving from communicable diseases and to setpriorities. They will have to apply the planning skills studied in the first module,first determining the magnitude of the problems (mortality, morbidity, number ofcases, etc.), and then ascertaining the feasibility of instituting an effectiveprogramme to deal with them.
The main communicable diseases encountered in the simulation are:
. diarrhoeal diseases (including a few cases of cholera)
. measles
. tuberculosis
. meningococcal meningitis (two cases)
. intestinal parasites
. scabies
. respiratory infections
. malaria
. AIDS.
The course participants have received enough information on communicablediseases and possible modes of intervention to be able to grasp this practicalobjective.
2. CATEGORY
Practice: using assimilated planning skills to set priorities among the maincommunicable diseases.
3. FORMULATION
Set priorities among the main communicable diseases by determining both themagnitudeof each (mortality,morbidity, numberof cases, etc.) and thepossibilitiesfor action in the framework of the Alphaland-Betaland simulation.
HELP/SOS: COMMUNICABLE DISEASES266

4. TEACHING METHOD
Assignment presented to work groups, followed by a plenary session duringwhich each group presents its results on transparencies.
5. DURATION
Total duration: 60 minutes
30 minutes for work in groups
30 minutes for summary in plenary session.
6. RECAPITULATION
The instructormust prepare the assignment in advance in order to compare his orher own priorities with those of the participants.
. Box 1: The six diseases to be used for the rest of the exercise
LINK WITH NEXT OBJECTIVES
The six communicable diseases for which the participants will be asked to plan anintervention programme do not necessarily reflect any particular order ofpriorities. These diseases were chosen to provide participants with a fairly widerange of decision-making opportunities.
Box 1
SIX COMMUNICABLE DISEASES FORWHICH CONTROL PROGRAMMES WILL BEDEVISED IN THE SIMULATION EXERCISE:
. Measles
. Malaria
. Tuberculosis
. Diarrhoeal diseases
. Meningococcal meningitis
. Hookworm disease
COMMUNICABLE DISEASES 267

269
PLANNING A PROGRAMMEFOR THE CONTROL OF MEASLESIN A GIVEN SITUATION
1. DESCRIPTION
Any plan for a programme to control measles must take into account thetechnical limitations of each measure, logistical constraints, the cultural context,and political constraints, particularly difficulties in gaining access to apopulation under certain circumstances. The development of the programmeshould follow the planning outline explained in Module 1:
. objectives
. strategy
. necessary resources
. method of evaluating the impact achieved.
With respect to strategy, the participants, working in groups, must refer to thenatural cycle of communicable diseases and determine the measures that thegroup wants to take at each level: primary and secondary prevention, treatment,and tertiary prevention.
The primary prevention measure is obvious: immunization. However, the groupmust take a number of decisions:
. what age groups should be immunized?
. what type of vaccine should be used?
. what general strategy should be followed? Mass immunization for measlesalone, or integration of measles immunization in an expanded programme ofimmunization (EPI) including several diseases?
The objective established for the measles immunization programme shouldclearly express the desired rate of coverage. The practical strategymust review allthe activities chosen:
. informing the community
. training the staff who will carry out the programme
. managing the cold chain
HELP/SOS: COMMUNICABLE DISEASES268

. setting up an evaluation system focusing on the detection of measles casesappearing after the immunization campaign
. following up the mass campaign with a routine EPI to immunize childrenreaching the age for immunization, or new arrivals in the case of displacedpopulations.
The work group should underline the importance of immediate, systematicimmunization of all children admitted to nutritional rehabilitation centres.
The programme should also make provision for measles cases presenting athealth facilities:
. prevention of infectious bacterial complications (selection of an antibiotic)
. therapeutic dose of vitamin A
. basic health care and proper feeding and hydration.
Such a programme comprises a combination of measures. Rather than merelyproviding a list of the measures it plans to take, the group must also explain whyit chose these particular measures and rejected other possibilities.
Insofar as time permits, the group should also quantify the resources needed toimplement the programme it is proposing. To that end, it must clearly specify theuse it plans to make of local resources (personnel and vaccines).
2. CATEGORY
Practice: planning a measles control programme for a given situation.
3. FORMULATION
Plan a measles control programme for the Awalei camp.
4. TEACHING METHOD
Each work group must plan control programmes for two diseases. Althougheach groupwill be asked to present its results for only one disease, its work on thesecond disease will have prepared it to discuss the results of the group presentingthe programme for that disease.
5. DURATION
Total duration: 120 minutes
. 60 minutes for work in groups
. 60 minutes for presentations in plenary session.
COMMUNICABLE DISEASES 269

271
6. RECAPITULATION
The instructor will have prepared a measles control programme to compare withthose of the students. He or she will ask the other groups, particularly the groupthat studied measles as its second disease, to comment on the programme ofaction submitted by the presenting group. The instructor will then offercomments and share any relevant personal experiences.
LINK WITH NEXT OBJECTIVES
In this programme, the group mentions the necessity of treating patients in adispensary and of hospitalizing severe cases. This subject will arise again in thesection on planning a patient care system in health facilities (in the module onmedical and surgical care).
HELP/SOS: COMMUNICABLE DISEASES270

PLANNING A PROGRAMMEFOR THE CONTROL OF MALARIAIN A GIVEN SITUATION
1. DESCRIPTION
Any plan for a programme to control malaria must take into account thetechnical limitations of each measure, logistical constraints, the cultural context,and political constraints, particularly difficulties in gaining access to apopulation under certain circumstances. The development of the programmeshould follow the planning outline explained in Module 1:
. objectives
. strategy
. necessary resources
. method of evaluating the impact achieved.
With respect to strategy, the participants, working in groups, must refer to thenatural cycle of communicable diseases and determine the measures that thegroup wants to take at each level: primary and secondary prevention, treatment,and tertiary prevention.
Primary prevention in this casemeans environmental sanitationmeasures: vectorcontrol, drainage, mosquito nets, and repellents.
Secondary prevention and treatment involve the institution of an effective systemfor early detection and treatment of cases of malaria. To this end, participantsmust decide how such a systemwill be organized: for example, whowill screen forcases, who will treat them, and what treatment regimen will be used. The groupmust also decide on a policy concerning themanagement of serious cases, thoughwithout going into the details of treatment regimens.
Rather than merely providing a list of the measures it plans to take, the groupmust also explain why it chose these particular measures and rejected otherpossibilities, such as mass chemoprophylaxis.
Insofar as time permits, the group should also quantify the resources needed toimplement the programme it is proposing.
2. CATEGORY
Practice: planning a malaria control programme for a given situation.
COMMUNICABLE DISEASES 271

273
3. FORMULATION
Plan a malaria control programme for the Awalei camp as a simulation exercise.
4. TEACHING METHOD
Each work group must plan control programmes for two diseases. Althougheach groupwill be asked to present its results for only one disease, its work on thesecond disease will have prepared it to discuss the results of the group presentingthe programme for that disease.
5. DURATION
Total duration: 120 minutes
. 60 minutes for work in groups
. 60 minutes for presentations in plenary session.
6. RECAPITULATION
The instructor will have prepared a malaria control programme to compare withthose of the students. He or she will ask the other groups, particularly the groupthat studied malaria as its second disease, to comment on the programme ofaction submitted by the presenting group. The instructor will then offercomments and share any relevant personal experiences.
LINK WITH NEXT OBJECTIVES
In this programme, the group mentions the necessity of treating patients in adispensary and of hospitalizing severe cases. This subject will arise again in thesection on planning a patient care system in health facilities (in the module onmedical and surgical care).
HELP/SOS: COMMUNICABLE DISEASES272

PLANNING A PROGRAMMEFOR THE CONTROL OF TUBERCULOSISIN A GIVEN SITUATION
1. DESCRIPTION
Any plan for a programme to control tuberculosis must take into account thetechnical limitations of each measure, logistical constraints, the cultural context,and political constraints, particularly difficulties in gaining access to apopulation under certain circumstances. The development of the programmeshould follow the planning outline explained in Module 1:
. objectives
. strategy
. necessary resources
. method of evaluating the impact achieved.
With respect to strategy, the participants, working in groups, must refer to thenatural cycle of communicable diseases and determine the measures that thegroup wants to take at each level: primary and secondary prevention, treatment,and tertiary prevention.
Immunization with BCG is not an effective measure, since it prevents only theserious forms of tuberculosis (miliary tuberculosis and tuberculous meningitis),and tuberculosis in children under the age of one year. Prevention ofovercrowding will decrease transmission of tubercle bacilli from TB patients tothe rest of the population.
The priority is to identify and treat patients presenting positive sputum. Such aprogramme involves the following steps:
. identify patients showing clinical signs of tuberculosis. A choice must bemade between two possibilities: active screening (health care personnel go outand try to screen for the disease within the community) and passive screening(health care personnel diagnose those patients that show up of their ownaccord at a health care facility). The second strategy is recommended.However, once a patient has been definitively diagnosed with the disease,health care personnel must screen the members of the patient’s immediatecircle.
COMMUNICABLE DISEASES 273

275
. establish bacteriological proof of tuberculosis by detecting tubercle bacilli inpatient sputum
. treat patients according to the categories defined byWHO (new case, relapse,treatment failure, chronic case)
. follow up patients after treatment in order to catch relapses.
Before designing this kind of programme, the group must define the inevitableconstraints on efforts to control tuberculosis. First of all, the quality of thelaboratory must be ascertained, since the selection of programme beneficiarieswill depend exclusively on laboratory results. Radiology is an inappropriatemeans of determiningwhat patients should be admitted to the programme. Theremust be some assurance that the patients will be able to continue their treatmentfor the required period (6-8 months), since patient compliance is the main factorin ensuring a cure. The instructor should comment on the absolute necessity ofapplying the DOT (Directly Observed Therapy) strategy. In unstable situations(such as war), this factor is difficult to appreciate. Finally, programmeadministrators must make sure that the resources needed to run the programwill be available. It would be a professional blunder to have to stop treatment forlack of means. Course participants will have to take all these factors intoconsideration when deciding whether or not to institute a programme to treattuberculosis.
Rather than merely providing a list of the measures it plans to take, the groupmust also explain why it chose these particular measures and rejected otherpossibilities.
Insofar as time permits, the group should also quantify the resources needed toimplement the programme it is proposing.
2. CATEGORY
Practice: planning a tuberculosis control programme for a given situation.
3. FORMULATION
Justify the advisability or inadvisability of implementing a campaign againsttuberculosis. If the argument is in favour, plan a tuberculosis control programme.
4. TEACHING METHOD
Each work group must plan control programmes for two diseases. Althougheach groupwill be asked to present its results for only one disease, its work on the
HELP/SOS: COMMUNICABLE DISEASES274

second disease will have prepared it to discuss the results of the group presentingthe programme for that disease.
5. DURATION
Total duration: 120 minutes
. 60 minutes for work in groups
. 60 minutes for presentations in plenary session.
6. RECAPITULATION
The instructor will have prepared a tuberculosis control programme to comparewith those of the students. He or she will ask the other groups, particularly thegroup that studied tuberculosis as its second disease, to comment on theprogramme of action submitted by the presenting group. The instructor will thenoffer comments and share any relevant personal experiences.
LINK WITH NEXT OBJECTIVES
In this programme, the group mentions the necessity of treating patients in ahospital facility, particularly during the intensive phase of the treatment. Thissubject will arise again in the section on planning a patient care system in healthfacilities (in the module on medical and surgical care).
COMMUNICABLE DISEASES 275

277
PLANNING A PROGRAMMEFOR THE CONTROL OF DIARRHOEALDISEASES IN A GIVEN SITUATION
1. DESCRIPTION
Any plan for a programme to control diarrhoeal diseases must take into accountthe technical limitations of each measure, logistical constraints, the culturalcontext, and political constraints, particularly difficulties in gaining access to apopulation under certain circumstances. The development of the programmeshould follow the planning outline explained in Module 1:
. objectives
. strategy
. necessary resources
. method of evaluating the impact achieved.
With respect to strategy, the participants, working in groups, must refer to thenatural cycle of communicable diseases and determine the measures that thegroup wants to take at each level: primary and secondary prevention, treatment,and tertiary prevention.
Primary prevention in this case means environmental sanitation measures:ensuring an adequate supply of clean water, appropriate management of humanwaste, health education.
Secondary prevention should include the early treatment of cases of diarrhoealdisease in order to prevent the development of dehydration. The group mustdecide on a strategy for ensuring access to rehydration solution: distribution ofORSpackets to all families, distribution of the ingredients forORS solution to allfamilies, or restriction ofORS to health care facilities, to be handed out on a case-by-case basis.
Treatment regimens for severe cases must be established (selection of theantibiotics to be used against specific pathogens such as shigella, and a plan forinfusions in cases of severe dehydration necessitating intravenous rehydration).
Rather thanmerely providing a list of themeasures it plans to take, the groupmustalso explain why it chose these particular measures and rejected other possibilities.
HELP/SOS: COMMUNICABLE DISEASES276

Insofar as time permits, the group should also quantify the resources needed toimplement the programme it is proposing.
2. CATEGORY
Practice: planning a programme for the control of diarrhoeal diseases in a givensituation.
3. FORMULATION
Plan a programme for the control of diarrhoeal diseases.
4. TEACHING METHOD
Each work group must plan control programmes for two diseases. Althougheach groupwill be asked to present its results for only one disease, its work on thesecond disease will have prepared it to discuss the results of the group presentingthe programme for that disease.
5. DURATION
Total duration: 120 minutes
. 60 minutes for work in groups
. 60 minutes for presentations in plenary session.
6. RECAPITULATION
The instructor will have prepared a diarrhoeal disease-control programme tocompare with those of the students. He or she will ask the other groups,particularly the group that studied diarrhoeal diseases as its second focus, tocomment on the programme of action submitted by the presenting group. Theinstructor will then offer comments and share any relevant personal experiences.
LINK WITH NEXT OBJECTIVES
In this programme, the group mentions the necessity of treating patients in adispensary and of hospitalizing severe cases. This subject will arise again in thesection on planning a patient care system in health facilities (in the module onmedical and surgical care).
COMMUNICABLE DISEASES 277

279
PLANNING A PROGRAMMEFOR THE CONTROL OF MENINGOCOCCALMENINGITIS IN A GIVEN SITUATION
1. DESCRIPTION
Any plan for a programme to control meningococcal meningitis must take intoaccount the technical limitations of each measure, logistical constraints, thecultural context, and political constraints, particularly difficulties in gainingaccess to a population under certain circumstances. The development of theprogramme should follow the planning outline explained in Module 1:
. objectives
. strategy
. necessary resources
. method of evaluating the impact achieved.
With respect to strategy, the participants, working in groups, must refer to thenatural cycle of communicable diseases and determine the measures that thegroup wants to take at each level: primary and secondary prevention, treatment,and tertiary prevention.
The relevant measures of prevention are:
. immunization. In non-epidemic periods, routine immunization againstmeningococcalmeningitis is not recommended, owing to the limited durationof the immunity it affords to young children. Nonetheless, in areas at highrisk for an epidemic of meningococcal meningitis, an immunizationcampaign before the beginning of the usual epidemic season might be apossibility worth considering. The decision to immunize at the beginning ofan epidemic is justifiable as long as immunization can be carried outquickly—which means, for example, that vaccines and a trained health careteam are available. The immunization campaign must be organized right atthe beginning of the epidemic in order to be effective. Accordingly, thecommunicable disease surveillance system must be of a high calibre, able todetect and provide bacteriological confirmation of the disease from the firstcases. Criteria can be set for initiating an immunization campaign, based onthe increase in cases over two consecutive weeks. The rule of thumb is that a
HELP/SOS: COMMUNICABLE DISEASES278

doubling of the number of cases is grounds for immunizing people betweenthe ages of 1 and 25 years.
. mass chemoprophylaxis is out of the question.
Treatment: In emergency situations where resources of personnel and space arelimited, the treatment for meningococcal meningitis consists in a singleintramuscular injection of an oily solution of chloramphenicol. This injectionmay be repeated 48 hours later.
Rather than merely providing a list of the measures it plans to take, the groupmust also explain why it chose these particular measures and rejected otherpossibilities—for example, mass chemoprophylaxis.
Insofar as time permits, the group should also quantify the resources needed toimplement the programme it is proposing.
2. CATEGORY
Practice: planning a programme for the control of meningococcal meningitis in agiven situation.
3. FORMULATION
Plan a programme for the control of meningococcal meningitis.
4. TEACHING METHOD
Each work group must plan control programmes for two diseases. Althougheach groupwill be asked to present its results for only one disease, its work on thesecond disease will have prepared it to discuss the results of the group presentingthe programme for that disease.
5. DURATION
Total duration: 120 minutes
. 60 minutes for work in groups
. 60 minutes for presentations in plenary session.
6. RECAPITULATION
The instructor will have prepared a programme for the control of meningococcalmeningitis to compare with those of the students. He or she will ask the othergroups, particularly the group that studied meningitis as its second disease, to
COMMUNICABLE DISEASES 279

281
comment on the programme of action submitted by the presenting group. Theinstructor will then offer comments and share any relevant personal experiences.
LINK WITH NEXT OBJECTIVES
In this programme, the group mentions the necessity of treating patients in adispensary and of hospitalizing severe cases. This subject will arise again in thesection on planning a patient care system in health facilities (in the module onmedical and surgical care).
HELP/SOS: COMMUNICABLE DISEASES280

PLANNING A PROGRAMMEFOR THE CONTROL OF HOOKWORMDISEASE IN A GIVEN SITUATION
1. DESCRIPTION
Any plan for a programme to control hookworm disease must take into accountthe technical limitations of each measure, logistical constraints, the culturalcontext, and political constraints, particularly difficulties in gaining access to apopulation under certain circumstances. The development of the programmeshould follow the planning outline explained in Module 1:
. objectives
. strategy
. necessary resources
. method of evaluating the impact achieved.
With respect to strategy, the participants, working in groups, must refer to thenatural cycle of communicable diseases and determine the measures that thegroup wants to take at each level: primary and secondary prevention, treatment,and tertiary prevention.
Primary prevention is based on environmental sanitation measures, particularlythe proper disposal of human waste.
The treatment of hookworm in dispensaries is simple: a single dose ofalbendazole or mebendazole. However, it is difficult to make a precise diagnosison the basis of clinical symptoms. In regions where the disease is endemic, thepresence of anaemia is grounds for systematic treatment against hookworm.Mass treatment should be considered only in specific communities, as a stopgapuntil environmental sanitationmeasures take effect (suchmeasures are known tohave a delayed impact).
Rather than merely providing a list of the measures it plans to take, the groupmust also explain why it chose these particular measures and rejected otherpossibilities—for example, mass treatment.
Insofar as time permits, the group should also quantify the resources needed toimplement the programme it is proposing.
COMMUNICABLE DISEASES 281

2. CATEGORY
Practice: planning a programme for the control of hookworm disease in a givensituation.
3. FORMULATION
Plan a programme for the control of hookworm disease.
4. TEACHING METHOD
Each work group must plan control programmes for two diseases. Althougheach groupwill be asked to present its results for only one disease, its work on thesecond disease will have prepared it to discuss the results of the group presentingthe programme for that disease.
5. DURATION
Total duration: 120 minutes
. 60 minutes for work in groups
. 60 minutes for presentations in plenary session.
6. RECAPITULATION
The instructor will have prepared a programme for the control of hookwormdisease to comparewith those of the students. He or she will ask the other groups,particularly the group that studied hookworm disease as its second disease, tocomment on the programme of action submitted by the presenting group. Theinstructor will then offer comments and share any relevant personal experiences.
LINK WITH NEXT OBJECTIVES
In this programme, the group mentions the necessity of treating patients in adispensary and of hospitalizing severe cases. This subject will arise again in thesection on planning a patient care system in health facilities (in the module onmedical and surgical care).
HELP/SOS: COMMUNICABLE DISEASES282

MEDICAL AND SURGICAL CARE
MODULE
5

285
LIST OF OBJECTIVES
. Define the concept of levels of medical and surgical care, and identify thegeneral criteria essential to the proper functioning of a therapeutic care system
. Identify the levels at which a health care facility can be evaluated, using theconceptual outline of a health care facility
. Calculate the number of medical consultations, hospitalizations, and hospitalbeds for a given population
. Identify the steps of a medical consultation and the connection withstandardized procedures
. Construct algorithms to help community health workers (CHWs) makediagnoses
. Know one method of evaluating the performance of health care personnel
. Know two methods of assessing the quantities of drugs necessary for a healthcare facility
. Formulate criteria for deciding whether to build a health care facilityindependent of the local facilities
. Define the architectural design of a dispensary based on an analysis of theactivities and tasks to be carried out there
. Define the stages involved in providing care to the war-wounded
. Identify the main features of a first-aid programme
. Know the general principles of surgical triage
. Identify the basic principles for evaluating an existing surgical facility todetermine whether it is adequate to assume responsibility for the care of warcasualties
. Know the basic rules of war surgery
. Understand the importance of postoperative care and rehabilitation in theoverall process of caring for wounded patients
. Plan a programme for the care of war casualties in a given situation
. Define the causes of the psychosocial problems experienced by the victims ofarmed conflict, and strategies to cope with them.
HELP/SOS: MEDICAL AND SURGICAL CARE284

IDENTIFICATION OF DIFFERENT LEVELSOF MEDICAL AND SURGICAL CARE
1. DESCRIPTION
People tend to associate medical and surgical care with health care facilities, eventhough such care is also provided outside such facilities—in the home, forexample, or on the battlefield. Primary health care strategy encompasses manyactivities, including the assumption of responsibility for basic medical care by thecommunity itself. Current research on first aid provided to thewar-injured showshow important it is to their survival.
Thus, three essential levels of medical and surgical care can be distinguished:
. primary level: care is provided by the community, community healthworkers, first-aid workers, and combatants (first aid)
. secondary level: care is provided by health professionals in dispensaries andhealth centres. At this level, care consists essentially of ambulatory services,as well as occasional hospital care for cases that, although uncomplicated,require a few days of medical observation
. third level: care is provided in hospitals by health professionals whose skillsmay be highly specialized.
Intermediary levels could be defined as well, but for emergency situations thisclassification is adequate for an understanding of how these different care levelsshould be integrated.
A few basic principles apply to all care levels:
. decentralization. Many kinds of medical and surgical care can be providedperipherally by the community, first-aid workers, and community healthworkers, who must be trained for the purpose
. professionalism. The higher the level of care, the greater the need forpersonnel with the training to cope with increasingly complex cases
. tasks. At each level, the tasks to be performed must be defined clearly.
. medical and surgical problems. The tasks defined must, of course,correspond to themedical and surgical problems prevalent in the population.In displaced populations, themainmedical problems are either not specific toany particular region (diarrhoeal diseases, pulmonary infections, measles,
MEDICAL AND SURGICAL CARE 285

287
skin infections) or specific to certain areas (malaria, bilharziasis). To thesemust be added the psychological problems engendered by the stress suchpopulations undergo in situations of armed conflict, including displacements(whether forced or voluntary) and inhuman treatment (rape, torture, etc.).Such situations give rise to real psychological wounds that must be treated bytrained professionals
. application of skills. This factor is not defined by the complexity of the cases ahealth professional is able to handle, but rather by the match between thework to be done and the capacities of the person charged with performing it.Responsibility must be assigned according to this principle. Complex casesshould be handled by personnel trained to manage them. Conversely, havinga doctor treat scabies when community healthworkers are available to do it issenseless and indicates a poor allocation of skills
. integration between the levels. A correct definition of the areas ofresponsibility corresponding to the different levels reduces the risk of thesecondary or tertiary levels being completely swamped as a result of theunderlying level’s failure to perform the tasks allocated to it. Such a definitionnecessitates a standardization of the tasks that each level is called upon toperform, as well as standardized procedures for transferring cases from onelevel to another. When the number of sick or wounded patients is high, thesetransfer procedures must follow the rules of triage in order to provide accessto care to the largest possible number of patients, given the limited capacitiesof the health facilities
. the care chain. Whether for war-wounded or other patients, the concept ofthe care chain is the same. The rule is to begin with primary care or first aidand transfer the patient to higher care levels as his or her condition dictates
. accessibility. In armed conflict situations, access to care centres is oftencomplicated by insecurity, discrimination against certain political, ethnic, orreligious groups, or cost, since victims may be completely destitute.
2. CATEGORY
Framework: defining the concept of levels of medical and surgical care andidentifying the general criteria essential to the proper functioning of a therapeuticcare system.
3. FORMULATION
Define levels of medical and surgical care and identify the general criteriaessential to the proper functioning of a therapeutic care system.
HELP/SOS: MEDICAL AND SURGICAL CARE286

4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 40 minutes
. 20 minutes for work in groups
. 20 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Structures
. Box 2: Tasks
. Box 3: Skills
. Box 4: Decentralization of skills
. Box 5: Factors disrupting the equilibrium of the system
LINK WITH NEXT OBJECTIVES
This objective provides the context for identifying the tools needed for planningmedical and surgical care services. The primary level of care will be studied in thecontext of primary health care, which will be covered in the module on healthcare systems.
MEDICAL AND SURGICAL CARE 287

289
TERTIARYLEVEL
• Hospitals
SECONDARYLEVEL
• Health centres• Dispensaries
PRIMARY LEVEL• Primary health care centres
• Family
PATIENTS
Box 1
MEDICAL AND SURGICALCARE LEVELS
(STRUCTURES)
HELP/SOS: MEDICAL AND SURGICAL CARE2288

TERTIARYLEVEL
• Care ofhospitalized patients
SECONDARY LEVEL• Ambulatory care not covered
at the primary levelPneumonia, trauma, cardiovascular diseases, etc.
PRIMARY LEVEL• First aid
• Routine care: fever, diarrhoea, scabies, etc.
MALADESPATIENTS
Box 2
MEDICAL AND SURGICALCARE LEVELS
(TASKS)
MEDICAL AND SURGICAL CARE 2289

291
TERTIARYLEVEL• Care of
hospitalized patients
SECONDARY LEVEL• Ambulatory care
PRIMARY LEVEL• Routine care
PRO
FESS
IONA
LISM
PATIENTS
Box 3
MEDICAL AND SURGICALCARE LEVELS
(SKILLS)
HELP/SOS: MEDICAL AND SURGICAL CARE2290
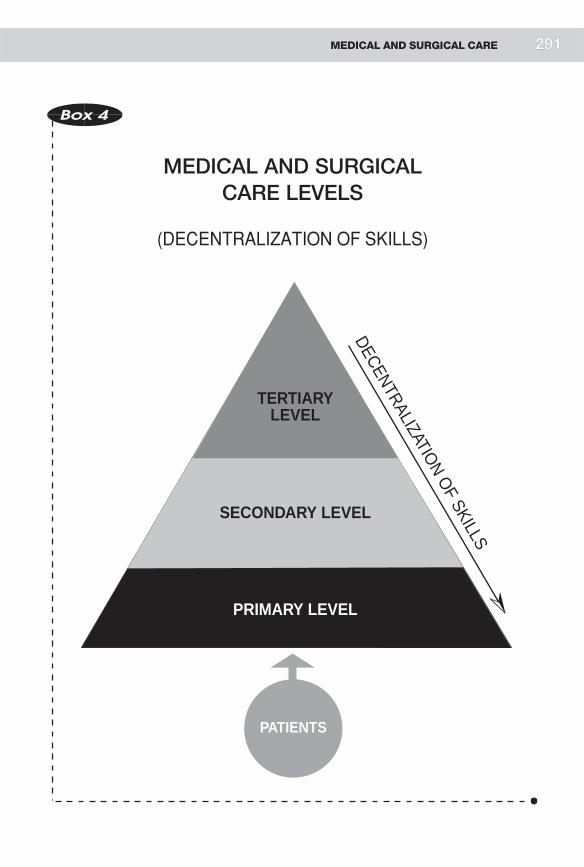
TERTIARYLEVEL
SECONDARY LEVEL
PRIMARY LEVEL
DECENTRALIZATION O
F SKILLS
MALADESPATIENTS
Box 4
MEDICAL AND SURGICALCARE LEVELS
(DECENTRALIZATION OF SKILLS)
MEDICAL AND SURGICAL CARE 2291

293
TERTIARYLEVEL
SECONDARY LEVEL
PRIMARY LEVEL
Factors disrupting the equilibrium of the system in emergency situations:
• Large number of patients (at the outset) • Lack of health care personnel • Destruction or deterioration of health care facilities • Inaccessibility of care
PRO
FESS
IONA
LISM
DECENTRALIZATION O
F SKILLS
PATIENTS
Box 5
FACTORS DISRUPTING THE EQUILIBRIUMOF THE SYSTEM
HELP/SOS: MEDICAL AND SURGICAL CARE2292

HEALTH CARE FACILITIES
1. DESCRIPTION
A health care facility can be defined by the following seven parameters:
. the patients receiving care there
. the health care personnel who work in it
. permanent medical equipment available
. drugs and other renewable supplies
. the sanitary infrastructure (water, electricity, kitchen, bathroom facilities,etc.)
. the buildings
. the administration of the facility.
These parameters can be applied to both primary health care centres andhospitals. Obviously they vary considerably depending on the case. They willprovide the basis for understanding the principles of assessing health facilities. Inmany emergency situations, humanitarian personnel need to assess existinghealth facilities in order to determine how much support will be needed to copewith the emergency. Two levels of assessment are essential.
. Quantitative assessment involves assessing each of the seven parametersseparately:
. the number of patients admitted, classified by age and type of ailment
. the number of care providers
. the nature and quantity of medicines available
. the condition of the medical equipment
. the number and condition of the buildings
. the condition of the sanitary infrastructure
. administrative factors: salaries, statistics.
. Qualitative evaluation involves examining the seven parameters in relation toeach other, in order to gauge the quality of the care provided:
. Are the buildings large enough to accommodate all the patientscomfortably?
MEDICAL AND SURGICAL CARE 293
295
. Are the health care personnel competent enough to handle the medicalproblems brought to the facility (an important point, for example, in thecase of war wounds treated by surgeons with little experience in this typeof work)?
. Does the health care personnel follow the diagnosis and treatmentprotocols recommended by the health ministry, WHO, or the ICRC?
. Are drugs of adequate quality available in sufficient quantity to meetpatients’ needs?
. Are the medical personnel able to operate the medical equipmentavailable (X-ray and laboratory equipment, etc., and to make proper useof the results?
. Will the sanitary infrastructure accommodate an increase in the numberof patients?
. Does the administrative system include patient registration? Are thesalaries of the health care personnel paid regularly? Are medical statisticsavailable?
The quantitative assessment is relatively easy. It consists, no more and no less, incounting what is available. Certain aspects of the qualitative assessment, incontrast, are very subjective. A way of getting around this difficulty is to analysethe performance of the health care personnel compared with standardprocedures used as references. For a global assessment of the quality of care,certain general indicators may be chosen, such as the mortality rate followinglaparotomies in surgical units, or a combination of factors—such as the presenceof electricity 24 hours a day, strict anaesthetic protocols, and continuedpostoperative care and supervision—that indicate a priori that the surgicalfacility’s impact on the mortality rate will be favourable.
Many manuals provide lists of data to collect. The emphasis should be onanalysing this information to gain as objective a view as possible of the quality ofcare provided by a given health care facility.
2. CATEGORY
Tool: identifying the levels at which a health care facility can be evaluated, usingthe conceptual outline of a health care facility.
3. FORMULATION
What is a health care facility, and what is the procedure for evaluating it?
HELP/SOS: MEDICAL AND SURGICAL CARE294

4. TEACHING METHOD
Assignment presented to work groups, followed by discussion in plenary session.
5. DURATION
Total duration: 50 minutes
. 30 minutes for work in groups
. 20 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Diagram of a health care facility
. Box 2: Chain of medical care
. Box 3: Tools for assessing and planning health care facilities
LINK WITH NEXT OBJECTIVES
The next two objectives deal with specific tools for evaluating the performance ofhealth care personnel, on one hand, and analysing a population’s drugrequirements, on the other.
MEDICAL AND SURGICAL CARE 295

297
Patients
Population
ADMINISTRATION
HEALTH CARE PERSONNEL
SANITARY INFRASTRUCTURE
DRUGS AND OTHER RENEWABLE
SUPPLIESPERMANENT MEDI-
CAL EQUIPMENT
Bui
ldin
gs
Bui
ldin
gs
Box 1
DIAGRAM OF AHEALTH CARE FACILITY
HELP/SOS: MEDICAL AND SURGICAL CARE2296

Hospital
HEALTH CARE PROFESSIONALS
SANITARY INFRA-STRUCTURE
• water • hygiene
DRUGS AND OTHER RENEW-ABLE SUPPLIES
PERMANENT MEDI-CAL EQUIPMENT
Administration
Administration
Bui
ldin
gsB
uild
ings Dispensary
HEALTH CARE PROFESSIONALS
SANITARY INFRA-STRUCTURE
• water • hygiene
DRUGS AND OTHER RENEW-ABLE SUPPLIES
PERMANENT MEDI-CAL EQUIPMENT
PRIMARY LEVEL• family• primary health care facility
Population
Patients
Patients
Patients
Box 2
CHAIN OF MEDICAL CARE
MEDICAL AND SURGICAL CARE 2297

299
Patients
Population
ADMINISTRATION
HEALTH CARE PERSONNEL
SANITARY INFRASTRUCTURE
DRUGS AND OTHER RENEWABLE
SUPPLIESPERMANENT MEDI-
CAL EQUIPMENT
Bui
ldin
gs
Bui
ldin
gs
1. Number of patients likely to use the facility (population, situation)2. Interaction between patient and health care personnel (e.g., medical consultation)3. Concept of standardization4. Standardized medical examination: algorithm5. Essential drugs6. Analysis of the performance of health care personnel7. Architecture8. Medical administration
Box 3
WHAT TOOLS ARE NEEDEDTO PLAN AND ASSESS
A HEALTH CARE FACILITY?
HELP/SOS: MEDICAL AND SURGICAL CARE2298

ESTIMATING THE NUMBEROF POTENTIAL PATIENTSIN A DISPLACED POPULATION THAT HASJUST ARRIVED IN A GIVEN LOCATION
1. DESCRIPTION
The quantitative approach to medical problems in emergency situations isessential for planning the resources that will be needed to cope with theemergency. However, quantification is made difficult by such factors as:
. population mobility and fluctuations in population count (displacedpopulations)
. preventive measures, which by definition reduce the number of patients and,by the same token, the work load of the health care facilities
. the stress engendered by the situation (insecurity and uncertainty regardingthe future), which gives rise to psychosomatic problems.
Despite these complicating factors, some basis of calculation must be used toplan health care facilities (number of facilities, drug supplies, number of healthcare personnel). Three estimates in particular are important. One of them is thenumber of out-patient medical consultations for a displaced population. As aninitial estimate, we should figure that in normal situations the average number ofannual consultations per person is two. This average takes into accountvariations determined by a population’s relative geographical proximity tohealth care centres, and variations based on age and sex. The number ofconsultations for a displaced population can be expected to double compared tonormal situations, for several reasons:
. easy access to health care facilities. In general, dispensaries are built indisplaced-person camps
. the amount of free time available to the population. Displaced persons areunemployed, although some time is occupied by activities necessary forsurvival: fetching water, waiting in line for food distributions, etc.
. the high prevalence of serious medical problems that is common in displacedpopulations, since such populations may have had no access to care formonths before reaching the camp, or have suffered from deterioratingpreventive care services.
MEDICAL AND SURGICAL CARE 299

301
Thus, for a population of 50,000 people, a need for some 500 consultations perday can be anticipated, corresponding to 1% of the population. Similarly, it canbe estimated that for every 1,000 people, 40 will have to be hospitalized withinthe year. This figure is based on the average rate of hospitalization indeveloping countries. Although clearly in emergency situations a large numberof patients will require hospitalization, limited resources mean that only themost severe cases are actually hospitalized. This calculation is thereforeacceptable. For a population of 50,000 people, this represents a total of aboutfive patients per day who will need to be hospitalized, or 1% of the patients whoseek medical help.
On the basis of these estimates, we can calculate the number of beds required. Thefirst step is to estimate an average length of hospitalization—for example, sevendays. On the basis of these two figures (number of patients requiringhospitalization and average length of hospitalization), it is possible to estimatethe number of patients who will require hospitalization—let us say 50, allowingan extra reserve for seasonal variations, epidemics, etc. One bed is required forevery 1,000 people.
The instructor must explain these calculations.
2. CATEGORY
Tool: calculating the number of medical consultations, hospitalizations, andhospital beds required for a given population.
3. FORMULATION
Estimate the number of medical consultations, the number of patients requiringhospitalization, and the number of hospital beds necessary for a displacedpopulation of 50,000 people.
4. TEACHING METHOD
Assignment presented in plenary session.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Quantifying the number of patients
HELP/SOS: MEDICAL AND SURGICAL CARE300

LINK WITH NEXT OBJECTIVES
The number of patients who will need to seek assistance from a health carefacility has been defined. The next objective will help course participants to planthe general organization of a health care facility.
Box 1
NUMBER OF POTENTIAL PATIENTS WHOWILL REQUIRE ACCESS
TO A HEALTH CARE FACILITY
1% of the population require out-patient care
1% of patients seeking out-patient carerequire hospitalization
1/1000 the number of beds required forhospitalization is 1 per 1,000 people(excepting epidemics)
MEDICAL AND SURGICAL CARE 301

THE COMPONENTS OF A MEDICALCONSULTATION AND THE CONCEPTOF STANDARDIZATION
1. DESCRIPTION
Amedical consultation can be broken down into a series of successive steps thatcall upon health care personnel to demonstrate a combination of technical skills,interpersonal relation skills, and intellectual abilities:
. reception of the patient by the health care giver
. patient history
. clinical examination
. diagnosis or diagnostic orientation
. decision about what to do (treatment, no treatment, transfer, further tests)
. conduct of treatment
. compliance with treatment
. patient follow-up.
All these steps can be broken down further into precise tasks. For example, afterthe patient has explained why he or she is seeking medical advice, the health carepersonnel must ask a number of questions concerning the complaint. The clinicalexamination must follow a strict order. Once the diagnosis has been made, thereshould be a standard policy to follow, based primarily on treatment regimens,from which, in turn, standard lists of drugs are derived.
This leads into the idea of standardizing all the steps in a medical consultation, aconcept essential to the proper functioning of any care unit. In emergencysituations, rapid turnover in health care staff is not unusual, and each new teammay introduce its own way of caring for patients. This means, for example, theintroduction of new drugs. ‘‘Standardized’’ management should not precludehumane relations between health care personnel and patients. Moreover,standardization permits effective coordination between health care facilitiesworking at the same care level, thus preventing competition between dispensariesof different organizations which might otherwise risk foundering in an excess ofmedical care.
HELP/SOS: MEDICAL AND SURGICAL CARE302 303

2. CATEGORY
Tool: identifying the steps of a medical consultation and their connection withstandardized procedures.
3. FORMULATION
Identify the steps of a medical consultation and derive standardized proceduresfrom them.
4. TEACHING METHOD
Assignment presented to work groups followed by plenary session.
5. DURATION
Total duration: 40 minutes
. 20 minutes for work in groups
. 20 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Concept of medical consultation
. Box 2: Concept of standardization
LINK WITH NEXT OBJECTIVES
The next objective develops a method for evaluating the work of health carepersonnel. The standardization of tasks provides reference points for this type ofevaluation.
MEDICAL AND SURGICAL CARE 303

305
ADMINISTRATION
Registration
Patient
Reception
Record
Follow-up
Patient historyObservance
Treatment
Examination
Options
Building
Decision (diagnosis)
HEALTH CARE PERSONNEL
SANITARY INFRASTRUCTURE
DRUGS AND OTHER RENEWABLE
SUPPLIESPERMANENT
MEDICAL SUPPLIES
No treatment
Transfer
Box 1
CONCEPT OF MEDICALCONSULTATION
Box 2
CONCEPT OF STANDARDIZATION
EXAMPLE:
. Standardization of the clini-cal examination (algorithm)
. Essential drugs
. Treatment regimens
. Standardization of referralsfrom one level of care toanother
. Standardization applies to allsteps of a medical consultation
HELP/SOS: MEDICAL AND SURGICAL CARE3304

CONSTRUCTING AN ALGORITHM
1. DESCRIPTION
The activities of community health workers are oriented mainly towardsprevention: immunization, water and environmental sanitation, nutrition, etc.Therapeutic activities do form a part of their tasks, but only to a very limitedextent.
Diagnostic protocols are a particularly important tool for CHWs working in thefield of therapeutic care. Medical manuals usually start with the disease and goon to describe its symptoms. Here the procedure is the opposite: starting with asymptom, we look for the most probable pathology; the progressive addition ofsymptoms will generate a list of successive diagnoses. It is best to begin with thesymptoms most representative of the top-priority ailments.
The instructor should emphasize that algorithms permit a standardizeddiagnostic approach.
2. CATEGORY
Tool: constructing algorithms that will assist CHWs to make diagnoses.
3. FORMULATION
Construct an algorithm based on two symptoms of your choice.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 50 minutes
. 20 minutes for work in groups
. 30 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Principle for constructing an algorithm
MEDICAL AND SURGICAL CARE 305

307
LINK WITH NEXT OBJECTIVES
Algorithms constitute references that health care personnel must apply in thepursuit of their activities. These references are an important element forevaluating the performance of health care personnel.
An algorithm is constructed on the basis of symptoms. A symptom is chosen, to which further symptoms or clinical signs are added progressively. At each stage the most plausible diagnosis is selected.
SYMPTOMS :
DISEASES:Fever Oedema Tachypnea
Skin rash Jaundice
Measles
Hepatitis
Kwashiorkor
Pneumonia
Malaria
Fever
Morbilliform rash Measles
Tachypnea Pneumonia
Fever alone, in a regionof endemic malaria during
the rainy season
+
+
Malaria
Box 1
PRINCIPLE OF CONSTRUCTINGAN ALGORITHM
HELP/SOS: MEDICAL AND SURGICAL CARE3306

EVALUATING THE PERFORMANCEOF HEALTH CARE PERSONNEL
1. DESCRIPTION
The purpose of this sort of evaluation is not to make value judgements about thequality of the work done by health care personnel, but to identify professionaldeficiencies in order to remedy them. Standardized diagnostic and treatmentprocedures serve as objective references for determining to what degree the tasksperformed by the health care personnel correspond to established standards.This also provides the basis for performance profiles for health care personnel,and identifies the spheres in which training is needed.
This method is effective for evaluating simple clinical and therapeutic tasks forwhich a standard can be defined. Such an evaluation assesses the quality of servicesprovided (output), not the actual impact of those services on health (outcome).
2. CATEGORY
Tool: knowledge of a method for evaluating the performance of health carepersonnel.
3. FORMULATION
Explain how to apply a method for evaluating the performance of health carepersonnel.
4. TEACHING METHOD
Question-and-answer session involving all participants.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Analysing the performance of health care personnel conductingmedical consultations
LINK WITH NEXT OBJECTIVES
The material learned here will be used to evaluate the quality of the servicesprovided by the two dispensaries in the Awalei camp.
MEDICAL AND SURGICAL CARE 307

309
ASSESSING THE DRUG REQUIREMENTSOF A HEALTH CARE FACILITY
1. DESCRIPTION
Humanitarian agencies, asked to provide drugs for health care facilities, oftenface the problem of assessing the drug requirements of those facilities. There aretwo ways of quantifying the requirements of any given facility:
. requirements based on consumption, as estimated by the administrators ofthe health care facility. The standard of reference is the facility’s normal drugconsumption level
. requirements based on morbidity rate and standard treatments, whichinvolves analysing current medical problems and the standard responses tothem. The point of reference in this case is a standardized consumption levelbased on the ailments requiring treatment.
The second method is the most commonly used in emergency situations, sinceprevious local consumption levels have no meaning where new facilities havebeen installed to cope with the emergency, and are irrelevant in mass influxes ofdisplaced people.
These methods are designed solely to assess the quantities of drugs necessary in agiven situation; they cannot be used to evaluate the use made of the drugs (aqualitative assessment that comes under the heading of performance evaluation).
2. CATEGORY
Tool: knowledge of two ways to assess the quantities of drugs necessary for ahealth care facility.
3. FORMULATION
Howwould you assess the quantities of drugs necessary for a health care facility?
4. TEACHING METHOD
Assignment presented to entire group.
5. DURATION
Total duration: 20 minutes.
HELP/SOS: MEDICAL AND SURGICAL CARE308
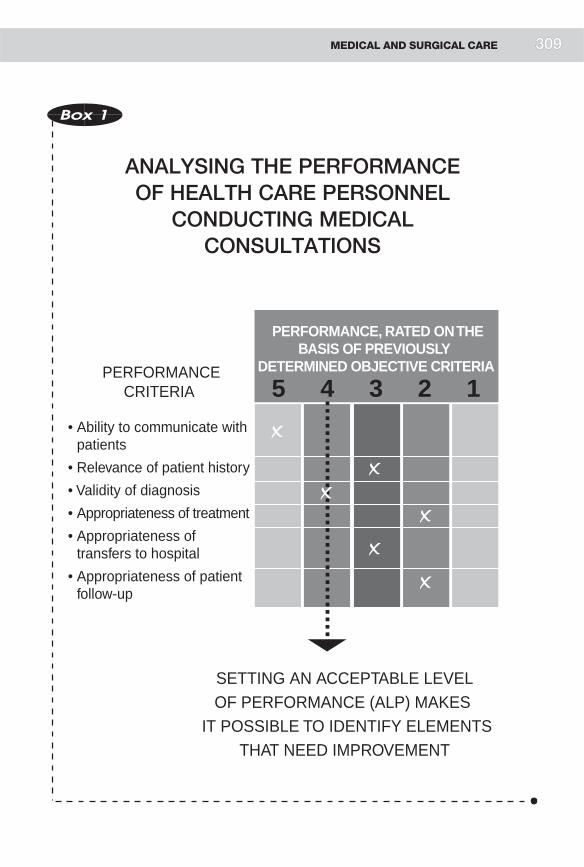
PERFORMANCE, RATED ON THE BASIS OF PREVIOUSLY
DETERMINED OBJECTIVE CRITERIA PERFORMANCECRITERIA
• Ability to communicate with patients
• Relevance of patient history
• Validity of diagnosis
• Appropriateness of treatment
• Appropriateness of transfers to hospital
• Appropriateness of patient follow-up
5 4 3 2 1
✗
✗
✗
✗
✗
✗
SETTING AN ACCEPTABLE LEVELOF PERFORMANCE (ALP) MAKES
IT POSSIBLE TO IDENTIFY ELEMENTSTHAT NEED IMPROVEMENT
Box 1
ANALYSING THE PERFORMANCEOF HEALTH CARE PERSONNEL
CONDUCTING MEDICALCONSULTATIONS
MEDICAL AND SURGICAL CARE 3309
311
6. RECAPITULATION
. Box 1: Methods for estimating the drug needs of a health care facility
. Box 2: Estimation of drug needs based on morbidity and standardtreatments
LINK WITH NEXT OBJECTIVES
This tool must be combined with two other tools: treatment regimens, in order toestablish the quantities of drugs needed to treat different ailments, and theformula for estimating the number of patients in a given population. These twotools have already been discussed.
These objectives are relevant to existing health care facilities. In emergencysituations, however, another problem often arises: should new facilities bebuilt?
Box 1
METHODS FOR ESTIMATING THE DRUGNEEDS OF A HEALTH CARE FACILITY
METHOD BASED ON CONSUMPTION
Reference: usual consumption levelin the health care facility in question
METHOD BASED ON MORBIDITYAND STANDARD TREATMENTS
Reference: standardized consumption
HELP/SOS: MEDICAL AND SURGICAL CARE310

Box 2
ESTIMATION OF DRUG NEEDSBASED ON MORBIDITY
AND STANDARD TREATMENTS
EXAMPLE FOR 10,000 PEOPLE:
MORBIDITY:
Children Adults
No. of malaria cases – –
No. of cases of diarrhoeal disease – –
No. of cases of respiratory infection – –
No. of cases of skin infections – –
STANDARD TREATMENTS:
Respiratory infections: No. of penicillin tablets for a complete course oftreatment
Malaria: No. of chloroquine tablets (or other medication) for acomplete course of treatment
Morbidity 6 Standard Treatments
=
Estimated Drug Requirements
MEDICAL AND SURGICAL CARE 311

313
CRITERIA FOR DECIDING WHETHERTO BUILD A HEALTH CARE FACILITYFOR A DISPLACED POPULATION
1. DESCRIPTION
Two situations may arise with respect to the medical problems of a displacedpopulation:
. There is already a local health care facility accessible to the displacedpopulation. In this case, an assessment of the facility’s quantitative andqualitative capacities will indicate the extent to which it will be able to absorbthe extra workload engendered by the arrival of the refugees.Ways to remedythe facility’s quantitative and/or qualitative deficit must be considered:training health care personnel, providing drugs, adding new personnel. Thisstrategy must take several factors into account:
. the risk of providing a level of care that is too sophisticated for the localsocio-economic context
. the risk of making the facility totally dependent on international aid andinducing the authorities in charge of the facility to relinquish theirresponsibility
. the risk of diverting too many local resources to the displaced populationat the expense of the local population
. the advantage that international aid affords to a ‘‘chronically’’inadequate local health care facility; in this respect, the aid contributesto a development process
. the advantage to the local personnel, who reap the benefit of outsideexpertise in coping with the situation and are thus better prepared forfuture emergencies.
. There is a local health care facility, but the high demand for services leadsrelief administrators to consider building an autonomous facility. Thisstrategy must take several factors into account:
. possible competition between the two health care facilities, especiallysince the new facility, built with international assistance, will probablyhave more resources than the local facility. The local population may beattracted to the new facility
. the greater effectiveness of an autonomous facility, if needs are high.
HELP/SOS: MEDICAL AND SURGICAL CARE312

. the possibility of installing an autonomous facility while supporting thelocal facility at the same time. This, however, creates the risk ofdependence on international aid
. the possibility that the local population will feel that the health careresources intended for it are being appropriated by the displacedpopulation.
. There is no local facility, leaving no choice but to build new facilities. In thiscase, efforts must be made to:
. scatter the facilities through the camp
. standardize diagnostic and therapeutic procedures to eliminate competi-tion between different facilities
. invest in personnel recruited from among the displaced population
. avoid diverting health care personnel from the local health care system(by offering higher salaries), since this is likely to reduce the capacities oflocal facilities in the region.
2. CATEGORY
Tool: formulating the criteria for deciding whether to build a new health carefacility independent of existing local facilities.
3. FORMULATION
List arguments for or against the construction of a health care facilityindependent of existing local facilities.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 40 minutes
. 20 minutes for work in groups
. 20 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Flow chart for deciding whether to build a dispensary for a displacedpopulation
. Box 2: Support versus replacement
MEDICAL AND SURGICAL CARE 313
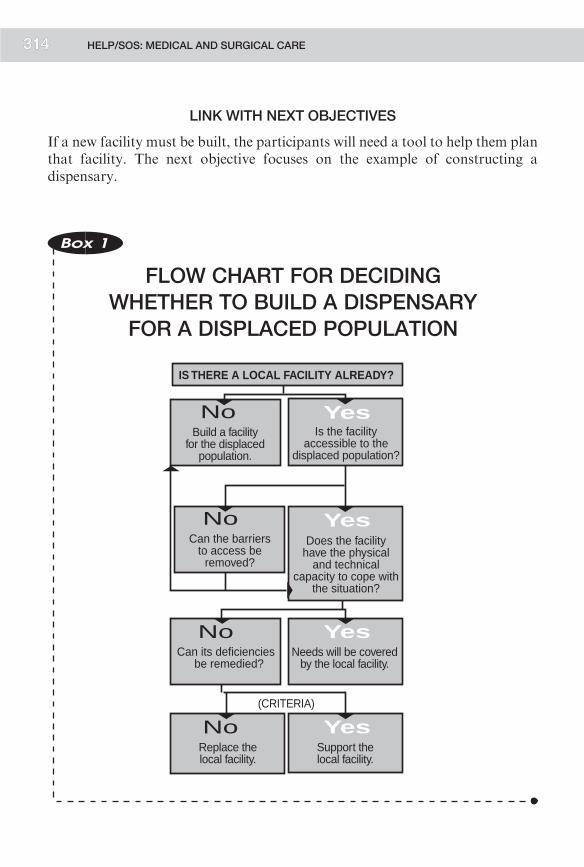
315
LINK WITH NEXT OBJECTIVES
If a new facility must be built, the participants will need a tool to help them planthat facility. The next objective focuses on the example of constructing adispensary.
IS THERE A LOCAL FACILITY ALREADY?
Is the facilityaccessible to the
displaced population?
Yes
Does the facilityhave the physical
and technicalcapacity to cope with
the situation?
Yes
Needs will be coveredby the local facility.
Yes
Build a facilityfor the displaced
population.
No
Can its deficiencies be remedied?
No
Can the barriersto access be
removed?
No
Support thelocal facility.
YesReplace thelocal facility.
No(CRITERIA)
Box 1
FLOW CHART FOR DECIDINGWHETHER TO BUILD A DISPENSARYFOR A DISPLACED POPULATION
HELP/SOS: MEDICAL AND SURGICAL CARE3314

Box 2
SUPPORT VERSUSREPLACEMENT
CRITERIA TO CONSIDERWHEN CHOOSING A STRATEGY
. Attitude of the local authorities
. Attitude of the local population
. Short-term effectiveness
. Long-term impact
. Control over the managementof the facility
. Financial implications
. Level of expertise required
. Risk of competition
. Control over the management of the local facility(corruption)
MEDICAL AND SURGICAL CARE 315

317
ARCHITECTURAL DESIGNOF A DISPENSARY
1. DESCRIPTION
Although health care personnel are not responsible for the construction of healthcare facilities, they should be involved in their architectural design. A health carefacility should be planned around the tasks that will be carried out in it. Thisdovetails with the concept of standardized diagnostic and therapeutic proceduresalready discussed. Thus, for a dispensary a list should be made of the activitiesthat are to be carried out in it:
. reception of patients (area for waiting, registration, initial triage, etc.)
. examination of patients (single consultation room, separate consultationrooms for adults and children or for women and men)
. testing (laboratory or other)
. observation of serious cases (a room for day hospitalization)
. distribution of drugs (distribution point)
. external care (bandaging room)
. flow of patients in the dispensary
. storage of drugs and medical supplies
. sanitary infrastructure (water supply, toilets, incinerator, etc.)
. administration.
The precise tasks corresponding to each general activity must be defined. Forexample, the steps involved in a medical examination are as follows:
. the patient must be able to lie down on an examination table (examinationtable)
. the health care personnel must be able to move around the examination table(space around the table)
. the health care personnel must be able to reach their basic examinationequipment (cupboard or shelf within arm’s reach of the examination table)
. the health care personnel must be able to wash their hands (washstand in theconsultation room)
HELP/SOS: MEDICAL AND SURGICAL CARE316

. the health care personnel must be able to sit at a table to write down theirrecommendations, and the patient must be able to sit facing the health careprovider (a table and two chairs).
This procedure also makes it easy to determine what equipment the health carepersonnel will need, as well as the space required to work comfortably (oneexamining table measuring 190 cm x 60 cm, one table measuring 90 cm x 90 cm,etc.).
2. CATEGORY
Tool: designing a dispensary by analysing the activities and tasks to be carriedout in it.
3. FORMULATION
What elements do you think are important in the design of a dispensary?
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Activities in a dispensary
. Box 2: Space required to perform the tasks involved in a clinicalexamination
LINK WITH NEXT OBJECTIVES
The participants have all the tools necessary to plan a therapeutic care system in agiven situation (simulation).
MEDICAL AND SURGICAL CARE 317

319
Decisions
Registration
Clinicalexamination
Keepingpatientsunder
observation(ORS)
Transfer
• X-rays• Lab
Injections
BandagingPatient history
ReceptionTreatment
IN OUT
Distribution ofdrugs
Diagnostictests
Box 1
ACTIVITIESIN A DISPENSARY
HELP/SOS: MEDICAL AND SURGICAL CARE3318

The patient sits down
The health care profes-sional must be able to write
The patient must be ableto lie down and the health care professional must have access to both sides of the examination table
Access to medical supplies
The health care professional must be able to wash hands
Reception
Patient history
Clinicalexamination
Chair
TableChair
Examinationtable
Cupboard
Washstand (basin)
30 x 30
100 x 60 30 x 30
200 x 40
100 x 30
40 x 30
80 x 80
150 x 110 80 x 80
300 x 140
150 x 30
90 x 30
TASKS
ORGANIZAT
ION
SUPPLIES
DIMENSIO
NS
SPACE
(cm
)
(cm)
Box 2
SPACE REQUIRED TO PERFORMTHE TASKS INVOLVED
IN A CLINICAL EXAMINATION
MEDICAL AND SURGICAL CARE 3319

321
CONCEPT OF CARE LEVELSAS APPLIED TO WAR-WOUNDED
1. DESCRIPTION
The concept of health care levels as defined previously can also be applied to themanagement of war injuries.
. Primary level: the first contact between the injured person and a person ableto provide first aid (a combatant, a first-aid worker, a health careprofessional, etc.).
. Secondary level: the first health care facility to which the injured person istaken (first-aid post, dispensary, health centre, advance medical post, etc.),where the patient’s condition will be stabilized if this was not done at theprimary level. It is here that a decision will be made to keep the patient underobservation, send him home, or evacuate him to a surgical unit. The facilitiesat this level do not have the skills or the necessary organization to performsurgery.
. Tertiary level: the surgical facility with the capacity and competence to carryout the surgical procedures called for by the condition of the patient.
. An evacuation system permits the transfer of wounded from one level toanother as their condition warrants.
. Every possible combination of these three levels may arise.
. The wounded may move from the primary level to the tertiary level by beingevacuated by helicopter directly from the place they were injured to a surgicalunit (tertiary level).
. In other cases, the wounded may not receive any first aid before they areevacuated to secondary level care centres, where they are given basic care.
. Yet another possibility is that the wounded are evacuated to a hospital to beoperated on, but the hospital does not have the necessary capabilities to carryout the appropriate surgical intervention.
The purpose of this objective is for participants to identify the levels of care. Theinstructor must stress the importance of continuity between the different levels(care chain).
HELP/SOS: MEDICAL AND SURGICAL CARE320

Another important part of this objective is to highlight the impact of health careon the rate of survival. It is estimated that 60-65% of war-wounded will survivewithout treatment. First aid and surgery increase the survival rate by 5-15%.
2. CATEGORY
Framework: defining the stages in the provision of care to war casualties.
3. FORMULATION
Define the main stages in the provision of care to war casualties and identifythose stages you think most important for their survival.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 40 minutes
. 20 minutes for work in groups
. 20 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Levels of care for war-wounded
. Box 2: Survival rate
. Box 3: Quality of survival
LINK WITH NEXT OBJECTIVES
The instructor should introduce the tools that will be discussed in the nextobjectives:
. impact of first aid on the survival curve
. concept of triage
. management of care for wounded in surgical units
. rules of war surgery.
MEDICAL AND SURGICAL CARE 321
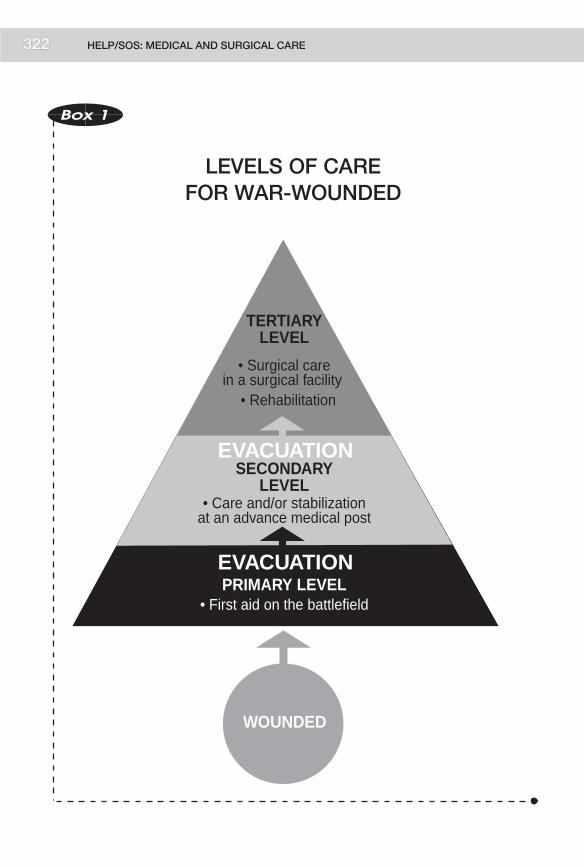
323
TERTIARYLEVEL
• Surgical carein a surgical facility
• Rehabilitation
SECONDARYLEVEL
• Care and/or stabilizationat an advance medical post
PRIMARY LEVEL• First aid on the battlefield
EVACUATION
EVACUATION
WOUNDED
Box 1
LEVELS OF CAREFOR WAR-WOUNDED
HELP/SOS: MEDICAL AND SURGICAL CARE3322

Box 2
SURVIVAL RATE
(WAR CASUALTIES)
. 60-65% of war casualtiessurvive without operations
. First aid and surgicalintervention increasethe rate of survivalby 5-15%
. It is difficult to establish therespective impacts on thesurvival rate of first aid andsurgical intervention
. First aid is an option even ifthere is no subsequentsurgical care
. The success of a first-aidprogramme depends ongood preparation beforethe conflict
. 3% of war casualtiesbenefit from emergencysurgical intervention
Source: Surgical unit, ICRC
Box 3
QUALITY OF SURVIVAL
(WAR CASUALTIES)
. Appropriate first aid to prevent, for example,a bone infection (osteomyelitis)
. Quality of surgical care:
. War surgery expertise
. Adequate facilities
. Quality and follow-up of rehabilitation
MEDICAL AND SURGICAL CARE 323

325
CHARACTERISTICSOF A FIRST-AID PROGRAMME
1. DESCRIPTION
First aid may be provided at both the primary and secondary levels of the healthcare chain.
Several factors are important in this respect:
. Since first aid is generally provided near the conflict zone, security for boththe casualties and the first-aid workers is an essential issue.
. The protective role of the Red Cross emblem and the neutrality andimpartiality of first-aid workers should be mentioned at this point, althoughthey will be studied in greater detail in the module on internationalhumanitarian law.
. An emergency preparation plan is a key factor in the success of any first-aidprogramme: supplies must be ready, means of transport available, etc.
. Life-saving technical measures can be performed at the primary and/orsecondary levels as permitted by the skills of the medical personnel and thephysical means available:
. putting the patient in a correct position
. applying a pressure bandage
. immobilizing a fracture
. ensuring that airways are not blocked
. initiating intravenous drip
. giving antibiotics.
. Evacuation to a first-aid centre for the administration of more sophisticatedtreatment, if such treatment was not possible where the injured person waspicked up. The first-aid centre will carry out surgical triage of the wounded.
2. CATEGORY
Tool: identifying the main features of a first-aid programme.
3. FORMULATION
What are the characteristics of a first-aid programme in situations of armedconflict?
HELP/SOS: MEDICAL AND SURGICAL CARE324

4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: First aid
LINK WITH NEXT OBJECTIVES
Transfers from one level of health care to another follow precise rules—the rulesof surgical triage.
Box 1
FIRST AID
. SECURITY
. Aid givers
. Wounded
. SHELTER
. TREATMENT
. Respiration
. Control of bleeding
. Bandaging
. Stabilization of fractures
. Intravenous drip
. Antibiotics
. Pain relief
. Tetanus prophylaxis
. EVACUATION
MEDICAL AND SURGICAL CARE 325

327
SURGICAL TRIAGE
1. DESCRIPTION
In emergency situations, the workload entailed by the number of wounded andthe severity of their wounds exceeds the capacity of the surgical facilities. Surgicaltriage is the process of sorting the wounded into categories preparatory toevacuating them to a higher level of care, taking into account their condition andthe surgical facilities’ capacity to accommodate and treat them. In manysituations this procedure must be undertaken in order to evacuate first thosecasualites whose condition requires urgent and rapid attention and whosechances of survival are good. Cases which are stable and can wait will beevacuated later, after the urgent cases have been treated. People with minorinjuries should not be sent to a surgical facility—at least not initially—in ordernot to overburden facilities that are already under pressure. Similarly, hopelesscases should not be evacuated first.
These points should be remembered:
. Surgical triage should be carried out by an experienced individual with theauthority to enforce his or her decisions
. Surgical triage is a continuous process that must take account of changes inthe condition of the wounded (a patient’s condition may deteriorate rapidlyfrom ‘‘not urgent’’ to ‘‘urgent’’)
. The teams doing the triage should already know the rules
. Many of the situations in which the ICRCoperates involvemajor evacuationdelays due to unsafe conditions and logistic constraints, giving rise to anatural ‘‘triage’’: seriously wounded patients die before they can be taken toan aid post
. Both the physical and technical capacities of the surgical facilities must beassessed before any wounded are sent there
. The assessment of surgical facilities is a continuous process that mustcontinue throughout the crisis, since capacity will change with the arrival ofthe wounded
. A system of communication between first-aid posts and referral facilities isessential. The surgical facilities must be aware of changes in the numbers andcondition of the wounded at the first-aid posts, and the first-aid postsmust beaware of the current capacities of the surgical facilities, so that appropriateadjustments can be made in the evacuation process.
HELP/SOS: MEDICAL AND SURGICAL CARE326

This course will not address the clinical details of surgical triage. It is a specializedskill, and few course participants will ever have the opportunity to practice it.They should, however, understand its purpose and general principles.
2. CATEGORY
Tool: knowledge of the general principles of surgical triage.
3. FORMULATION
Define surgical triage.
4. TEACHING METHOD
After presenting the question to the entire group, the instructor will expand onthe general principles of triage from the definition provided, stressing theevaluation of surgical facility capacity and competence.
5. DURATION
Total duration: 60 minutes.
6. RECAPITULATION
. Box 1: Concept of surgical triage
. Box 2: Organization of surgical triage
. Box 3: Categories
. Box 4: Parameters of response
LINK WITH NEXT OBJECTIVES
The need to assess a surgical facility’s skill level and capacities has beenmentioned. That will be the next objective.
MEDICAL AND SURGICAL CARE 327

329
LEVEL III
LEVEL II
LEVEL I
• Optimal use of resources for the benefit of the greatest numberof wounded
• Continuous process permitting constant establishment of priorities for access to care and transfer between differenthealth care levels
TRIA
GE
Box 1
SURGICAL TRIAGE
(CONCEPT)
HELP/SOS: MEDICAL AND SURGICAL CARE3328

Box 2
SURGICAL TRIAGE
(ORGANIZATION)
PREPARATION FORFUTURE EMERGENCIES:
. Establishment of procedures:
. categories
. clear allocationof responsibilities
. Drills
PERFORMANCE DURINGTHE EMERGENCY:
. Strict observance of rules andprocedures
DISCUSSION AFTERTHE EMERGENCY:
. Analysis of triage
. Conclusions to be drawn
Box 3
SURGICAL TRIAGE
(CATEGORIES)
. PRIORITY FOR SURGERY
. NO SURGERY
. CAN WAIT FOR SURGERY
MEDICAL AND SURGICAL CARE 329

331
Box 4
RESPONSE PARAMETERS
1. ASSESSMENT OF THE SITUATION
. Description of the situation
. Security
. Number of wounded and type of injuries
2. CRISIS MANAGEMENT
. Hierarchy
. Allocation of responsibilities
3. COLLECTION OF VICTIMS
. Seek and rescue operations
. Triage
. Evacuation to advance medical post
. Advance medical post. set-up and infrastructure. continued triage. stabilization
. Hospitalization. capacity. skills
4. REGULATION
. Monitor availability of medical facilities
. Monitor availability of transport
. Follow evacuation priorities
5. POST-CRISIS MANAGEMENT
. Post-Traumatic Stress Disorder (PTSD)
. Analysis of emergency response
HELP/SOS: MEDICAL AND SURGICAL CARE330

EVALUATION OF A SURGICAL FACILITY
1. DESCRIPTION
The general outline already introduced to define a health care facility also appliesto surgical units. The instructor should seek to develop the following points:
. access to surgical facilities during armed conflicts: security, impartiality,attitude of authorities
. quantitative analysis of the surgical facility (capacities):
. number of health care personnel, sanitary infrastructure, medical andsurgical equipment, drugs, bandaging supplies, etc.
. qualitative analysis:
. abilities of surgical personnel (the skills required to carryout a laparotomycompetently, motivated personnel, an understanding of the professionalcode of ethics).
The concept of indicators should be discussed: presence of electricity, mortalityrate after laparotomies, post-operative care with continuous supervision.
This objective should give health care personnel the tools to gauge an existingsurgical facility’s capacity to provide the right care for war injuries. This, in turn,will allow them to decide to what extent the facility can be helped to:
. cope with a quantitative deficit—for example, lack of personnel or lack ofsupplies
. cope with a qualitative deficit—for example, ignorance of the rules of warsurgery or no organizational framework for the management of war injuries.
2. CATEGORY
Tool: identifying the basic principles for assessing an existing surgical facility, inorder to determine to what extent it will be able to assume the charge of war-wounded.
3. FORMULATION
What would you assess first in an existing surgical facility that is likely to receivewar casualties?
4. TEACHING METHOD
Assignment presented to entire group.
MEDICAL AND SURGICAL CARE 331

333
5. DURATION
Total duration: 30 minutes.
6. RECAPITULATION
. Box 1: Assessment of a surgical facility: quantitative aspect
. Box 2: Assessment of a surgical facility: quality of care
. Box 3: Eight basic criteria for assessing a surgical facility
LINK WITH NEXT OBJECTIVES
Assessing a surgical facility includes evaluating the personnel’s knowledge of therules of war surgery—the topic of the next objective.
ADMINISTRATION• organization?
PERSONNEL• number?
RENEWABLE SUPPLIES• quantities?
PERMANENTEQUIPMENT
• kinds?• condition?
SANITARYINFRASTRUCTURE
• water?• toilets?• electricity?• buildings? WOUNDED
• number?• type of injuries?
WOUNDED• access tohealth carefacilities?
Box 1
ASSESSMENT OF A SURGICAL FACILITY
(QUANTITATIVE ASPECT)
HELP/SOS: MEDICAL AND SURGICAL CARE3332

REHABILITATION• quality of care
POST-OPERATIVECARE
• quality of care
RECEPTION
NOACTION
TRIAGE
DIAGNOSTIC
ADDITIONAL TESTS,X-RAYS, LAB, ETC.
• reliability• quality
IN OUT
• quality of choices
• reliabilityanaesthesia
surgery
support (blood)
DECISIONS• quality of the decision
SURGICALOPERATION
• analysis of performance
Box 2
ASSESSMENTOF A SURGICAL FACILITY
(QUALITY OF CARE)
MEDICAL AND SURGICAL CARE 3333

335
Box 3
ASSESSINGA SURGICAL FACILITY
8 BASIC CRITERIA
1. Is there an admission book or regular procedure for admitting and
registering patients?
2. Is there a person in charge of the admissions or the hospital whocontrols a systemwhereby the patients are assessed and then go
to a ward or operating theatre?
3. Is there an accurate operation book?
4. Is there a comprehensible and working system by which patients
get intravenous fluids or drugs?
5. Is the hospital secure (far enough from fighting, etc.)?
6. Is laparotomy performed safely with full, relaxed anaesthesia
(including endotracheal intubation) by a trained anaesthetist andis the patient supervised for 24 hours in a lighted roomwhere he or
she receives intravenous fluids?
7. Can five ormore laparotomies be performed in 24 hours under thesame conditions as described in 6?
8. Are patients walking on crutches? (not: do patients have crutchesby their beds?)
If these criteria are not met, the facility does not have the ability or
capacity to treat war injuries requiring surgical intervention.
Source: Adapted from Robin Coupland, Surgical Unit, ICRC.
HELP/SOS: MEDICAL AND SURGICAL CARE334

THE RULESOF WAR SURGERY
1. DESCRIPTION
The following rules will allow health care personnel assessing a surgical facility todetermine whether the principles of war surgery are being applied—for example:
. wounds are excised and all dead tissue is removed
. wounds are left open
. the policy of delayed primary closure is followed
. antibiotics are systematically administered to all wounded.
This learning objective is not intended to give participants specific surgical skills,but to make them more sensitive to these few rules. Ascertaining whether theprinciples of war surgery are being applied is an important aspect of assessing asurgical facility.
2. CATEGORY
Tool: knowledge of the essential rules of war surgery.
3. FORMULATION
Give some examples of essential rules of war surgery.
4. TEACHING METHOD
Explanatory lecture.
5. DURATION
Total duration: 15 minutes.
6. RECAPITULATION
. Box 1: Essential rules of war surgery
MEDICAL AND SURGICAL CARE 335

337
LINK WITH NEXT OBJECTIVES
Surgical care is not limited to actual surgical operations. To guarantee the bestpossible chances of survival and functional recovery, surgerymust be followed byproper post-operative care and appropriate physiotherapy.
Box 1
ESSENTIAL RULESOF WAR SURGERY
. Excise wounds
. Leave wounds open
. Delay primary closure
. Administer antibiotics
. Do not change dressings too often
Source: Surgical Unit, ICRC
HELP/SOS: MEDICAL AND SURGICAL CARE336

POST-OPERATIVE CAREAND REHABILITATION
1. DESCRIPTION
Stress must be laid on the importance of post-operative care for the survival ofwounded patients. Correctly performed operations are pointless if the patientdies afterwards for lack of proper care. Thus, the concept of the health care chainis not restricted to the operating theatre, but continues with post-operative care,including physiotherapy.
Physiotherapy is essential for recovering functional capacity as completely aspossible. Physiotherapy is also important for patients who must be fitted withprostheses.War injuries to the limbsmay result in amputations. The rehabilitationof amputees with prostheses will help their reintegration into socio-economic life.
That reintegration marks the end of the process of caring for the wounded. Theinstructor should stress that the chain of health care, like any other chain, is onlyas strong as its weakest link.
2. CATEGORY
Tool: understanding the importance of post-operative care and rehabilitation inthe overall process of caring for the wounded.
3. FORMULATION
What are the main advantages to be expected from post-operative care?
4. TEACHING METHOD
Assignment presented to entire group.
5. DURATION
Total duration: 20 minutes
6. RECAPITULATION
. Box 1: Post-operative care
. Box 2: Rehabilitation
MEDICAL AND SURGICAL CARE 337

339
LINK WITH NEXT OBJECTIVES
Upon completing this objective, the participants will have the tools they need toplan a programme for the care of war casualties in a given situation.
Box 1
POST-OPERATIVE CARE
. Intensive care throughout the 24 hours following theoperation
< SURVIVAL
. Care throughout the period of hospitalization(antibiotics, feeding, etc.)
< QUALITY OF SURVIVAL
Box 2
REHABILITATION
. Orthopaedic rehabilitation:
< QUALITY OF LIFE
. Socio-economic rehabilitation:
< QUALITY OF LIFE
HELP/SOS: MEDICAL AND SURGICAL CARE338

PLANNING A PROGRAMME FOR THE CAREOFWARCASUALTIES IN AGIVEN SITUATION
1. DESCRIPTION
The instructor will assign the participants an exercise allowing them to put intopractice the tools they have been taught. This exercise should pose the necessityof instituting first aid, and then proceeding to triage. Finally, the participantsshould find themselves in a situation where they have to decide whether or not toinvolve an existing local surgical facility in the care of the wounded. Their choiceat this point will be whether to reinforce the existing facility or to set up anindependent facility.
The case study can be taken from the Alphaland-Betaland simulation or it can becreated specially for this combination of objectives. Another possibility is to usethe ‘‘Lokichokio’’ case. The instructor will take the opportunity of the summarypresented in the plenary session to review any tools that have not been fullyassimilated
2. CATEGORY
Practice: planning a programme to provide care for war-wounded patients in agiven situation.
3. FORMULATION
Plan a programme to provide care for war-wounded patients in the framework ofthe Alphaland-Betaland simulation.
4. TEACHING METHOD
Assignment presented to work groups, followed by full assembly.
5. DURATION
Total duration: 90 minutes
. 30 minutes for work in groups
. 60 minutes for summary in plenary session.
LINK WITH FOLLOWING TOPICS
War situations cause not only physical injuries, but also psychological ones. Thatis the subject of the next exercise.
MEDICAL AND SURGICAL CARE 339

341
PSYCHOSOCIAL PROBLEMS
1. DESCRIPTION
The purpose of this objective is to introduce some idea of the psychosocialproblems suffered by victims of armed conflict. The clinical aspects that pertainto some of these problems will not be discussed.
The humanitarian organizations’ tendency has been to give priority to victims’physiological needs (humanitarian assistance) and security needs (protection).The victims who come under the ICRC’s mandate are particularly vulnerable topsychological problems caused by the trauma towhich they have been exposed asdirect victims or witnesses. This dimension of the impact of war is beginning toreceive serious attention. Within any population, certain groups are particularlyvulnerable. Children, for example, require stable, secure conditions for properdevelopment—conditions that are often disrupted in wartime.
Considerationmust be given not only to psychological effects on individuals, butalso to the effects on the individual’s integration in a society traumatized by thewar.
This learning objective can be broken down into two parts:
Impact on the Individual
Factors that may cause psychological disturbances in the individual are:
. the impossibility of meeting one’s own physiological needs (food, water,medical care), the break-up of the family unit, insecurity, danger, torture, thedeath of family and friends, participation in slaughter, sexual violence,imprisonment, interruption of work, the experience of discrimination, etc.
Psychological problems are expressed in varying degrees: state of shock,traumatism, psychiatric illness. In children, these problems may manifestthemselves by a loss of cultural identity, learning difficulties, introversion,indifference to human suffering, and other symptoms.
Psychological problems must be treated in the context of local socioculturalcustom. The best strategy is to sensitize health care personnel to such problems sothey can spot them, and to train local personnel to deal with them.Care should betaken not to over-medicalize psychological assistance. It should be rememberedthat there are three levels of care:
HELP/SOS: MEDICAL AND SURGICAL CARE340

. mental illness calls for psychiatric care
. the maintenance of mental health requires psychological support
. psychological development depends on education.
One possible strategy for fostering mental health is to include it in a system ofprimary health care.
Impact on Society
Individuals’ integration in society is disrupted by the radical changes that warmakes in that society. For example, the collapse of the economic system leads to afight for survival, loss of jobs, an upheaval in social positions (emergence of anew social class), the abandonment of schools (ending the integration of childreninto society by means of education), and the impossibility of conducting culturaland religious activities. All these factors militate against the social integration ofindividuals.
There are many possible courses of action. Generally speaking, society must berestored to its normal functions: promotion of economic activity, maintenance ofeducational activity, development of social programmes, etc.
Refugee and displaced populations have very substantial social problemsbecause the social organization of a camp is artificial.
In conclusion, psychosocial problems derive from disturbances in the individualpsyche and interference with the normal factors of social integration. Earlyrecognition of such problems and the institution of remedialmeasures will permitthe re-establishment of a certain social stability.
2. CATEGORY
Framework: defining the causes of psychosocial problems in victims of armedconflict and the strategies to cope with them.
3. FORMULATION
What are the causes of the psychosocial problems suffered by victims of armedconflict? What strategies can be used to combat them?
4. TEACHING METHOD
Assignment presented to work groups and discussed in a plenary session.
MEDICAL AND SURGICAL CARE 341

343
5. DURATION
Total duration: 60 minutes
. 30 minutes for work in groups
. 30 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Psychological impact on the individual
. Box 2: Disruption of social integration
. Box 3: Care levels
LINK WITH NEXT OBJECTIVES
End of the module on medical and surgical care.
-----------" INDIVIDUAL
Box 1
PSYCHOLOGICAL IMPACTON THE INDIVIDUAL
. Insecurity
. Danger
. Break-up of the family unit
. Torture
. Death of friends and relatives
. Violence
. Sexual aggression
. Imprisonment
. Discrimination
. Others
HELP/SOS: MEDICAL AND SURGICAL CARE342

-----------"
INDIVIDUAL
INDIVIDUAL INDIVIDUALSocialrelations
INDIVIDUAL
Box 2
DISRUPTIONOF SOCIAL INTEGRATION
IMPACT ON SOCIAL RELATIONS
. Struggle for survival
. Promotion of ethnic hatred
. Upheaval of social classes
. Loss of social integration due to closure of schools
. Withdrawal caused by insecurity, loss of employment
. Other
MEDICAL AND SURGICAL CARE 343

Box 3
CARE LEVELS
Mental illness Psychiatry(care according to localcultural environment)<
Mental health Psychological support(incorporated into primaryhealth care)<
Developmentof intellectualcapacities
< Education
HELP/SOS: MEDICAL AND SURGICAL CARE344

THE HEALTH CARE SYSTEM
MODULE
6

347
LIST OF OBJECTIVES
. Define the concept of a health care system in an emergency situation
. Design a health care system for a given situation.
HELP/SOS: THE HEALTH CARE SYSTEM346

CONCEPT OF THE HEALTH CARE SYSTEMIN AN EMERGENCY SITUATION
1. DESCRIPTION
This objective constitutes a turning point in the course. Up until now, thelearning objectives have been linked to specific modules: food and nutrition,environmental sanitation, control of communicable diseases, and medical andsurgical care. From now on, however, objectives will pertain to all the modulesalready studied, the context being the health care system in emergency situations.
The health care system in such situations can be depicted in two ways:
. A simplified version in which the modules are arranged as a pyramid
. the base is constituted by food, water, and environmental health
. the middle contains preventive health care measures: immunization andcontrol of communicable diseases
. the top level consists of therapeutic activities.
This model shows clearly that without solid bases, a population’s state of healthis going to deteriorate, and that the basic requirements of life (water and food),preventive measures, and therapeutic measures must all work together.
. A more elaborate version in which the general frameworks defined in thedifferent modules are lined up in parallel columns, so that the food supplychain,withall its links, is next to thewater supplychain,which in turn isnext tothe waste disposal chain, followed by the steps for controlling communicablediseases and the chain of medical and surgical care with its various levels.Listing the emergency activities corresponding to each of the links of thesechains provides an overviewof either an artificially created health care systemor the support provided for one or more of the components of an existinghealth care system—for example, provision of drugs for surgical facilitiestogether with a water supply programme and aid to food production, etc.
The instructor must stress the interactions between all these components: watersupply affects nutritional status, health education affects the control ofcommunicable diseases, etc. Finally, the instructor should mention some of themajor integrative functions of a health care system—functions that determine itsorientation and organization: epidemiology, planning, personnel training, legal
THE HEALTH CARE SYSTEM 347

349
protection (international humanitarian law), and fostering community respon-sibility.
2. CATEGORY
Framework: defining the concept of a health care system in emergency situations.
3. FORMULATION
Define the concept of a health care system in emergency situations.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for plenary session.
6. RECAPITULATION
. Box 1: Vicious circle of medical care unsupported by preventive measures
. Box 2: Health care pyramid on a weak foundation
. Box 3: Health care pyramid
. Box 4: Health care system
. Box 5: Health care system in emergency situations (organization)
. Box 6: Concept of primary health care (PHC)
. Box 7: Primary health care: essential elements
. Box 8: Are PHC criteria applicable to health care operations in emergencysituations?
. Box 9: PHC in various kinds of situations
. Box 10: How a health care system works: examples of integrative functions
LINK WITH NEXT OBJECTIVES
The next objective will focus on the construction of a health care system based onthe strategy of primary health care.
HELP/SOS: THE HEALTH CARE SYSTEM348

MEDICALCARE
• Diarrhoeal diseases• Measles• Scabies• Pulmonary infections• Malnutrition• Malaria
• Polluted water• Flies• No immunizations• Mosquitoes• Precarious shelter • No food resources
Return to anenvironmentcharacterized by:
Reoccurence ofmedical
problems
Box 1
VICIOUS CIRCLEOF MEDICAL CARE UNSUPPORTED
BY PREVENTIVE MEASURES
THE HEALTH CARE SYSTEM 3349

351
WATER ANDENVIRONMENTALSANITATION
FOODAND
NUTRITION
PUBLIC HEALTH
MEDICALCARE
Box 2
HEALTH CARE PYRAMIDON A WEAK FOUNDATION
FOODAND
NUTRITION
MEDICALCARE
PUBLIC HEALTH
WATER ANDENVIRONMENTALSANITATION
• Immunization
• Health education
Box 3
HEALTH CARE PYRAMID
HELP/SOS: THE HEALTH CARE SYSTEM350

HEALTH CARE SYSTEM
Foodsupply
Battle againstcommunicable diseases
Nutritionalrehabilitation
Immunization
Control of epidemics
Sanitation
Medical care
Shelter
Battle against vectors
Psychological support
Water supply
POPULATION’SHEALTH
Box 4
HEALTH CARE SYSTEM
THE HEALTH CARE SYSTEM 3351

353
WaterSupply
Sources
Storage
Distribution
Water consumption
Water use
Disposal of liquid waste
Environ-mental
Sanitation
Human waste management
Garbagemanagement
Energysources
Shelter
Vectorcontrol
Control of Communica-ble Diseases
Primary prevention
(immunization)
Secondary prevention
Tertiary prevention
Treatment of communicable
diseases
Control of epidemics
Medical-Surgical
Care
Primarylevel
medical care
Secondary level
medical care
Tertiarylevel
medical care
Transfer between
levels
Management of War
Injuries
First aid
Secondary level care
Evacuationand transport
Tertiary level surgical
care
Psycho-logical
Support
Psycho-social support for individualsand families
Psycho-social support
at the community
level
Psycho-social support
at the institutional
level
Food andNutrition
Agricultural production
Economicsystem
Foodavailability
Accessibilityof food
resources
Food consumption
Biologicalutilization of
food
Nutritional status
POPULATION’S HEALTH
Box 5
HEALTH CARE SYSTEMIN EMERGENCY SITUATIONS
(ORGANIZATION)
HELP/SOS: THE HEALTH CARE SYSTEM3352

Box 6
CONCEPT OF PRIMARY HEALTH CARE (PHC)
PHC CORRESPONDS TO AHEALTH CARE SYSTEM BASED ON:
. Acceptability to thecommunity
. Specific, recognizedbases
. Accessibility to the entirecommunity
. Community participation
. Coverage of costs
. Coordination with allthe elements of thehealth care system
. Integration in economicand social development
Box 7
PRIMARY HEALTH CARE:ESSENTIAL ELEMENTS
. Health education
. Promotion of good nutrition
. Clean water supply
. Environmental sanitation
. Mother and child welfare,including birth control
. Immunization (EPI)
. Prevention and control oflocal endemic diseases
. Treatment of commonmedical problems
. Supply of essential drugs
THE HEALTH CARE SYSTEM 353

355
Box 8
ARE PHC CRITERIA APPLICABLETO HEALTH CARE OPERATIONSIN EMERGENCY SITUATIONS?
. Accessibility
. Acceptability
. Coordination of activities
. Sustainability
. Balance between preventive and therapeutic measures
. Decisions and responsibilities
. Cost
. Coverage of costs
. Community participation
. Integration in the general health care system
. Integration in economic and social development
HELP/SOS: THE HEALTH CARE SYSTEM354

Refugee Populations
yes
?
dependson agencies
involved
no
yes
• agencies • State authorities
?
+++
no
yes
no
DisplacedPopulations
yes
?
dependson agencies
involved
?
yes
• agencies • local authorities
?
+++
no
yes
?
ResidentPopulations
(Armed Conflict)
?
?
depends onagenciesinvolved
yes ?
yes
• agencies • community • local authorities
yes
+++
no/yes(after conflict)
yes
yes
ResidentPopulations
(Natural Disaster)
yes
?
depends on agenciesinvolved
yes
yes
• agencies • community • local authorities
yes
+++
no/yes(after disaster)
yes
yes
Criteria
Accessibility
Acceptability
Coordinationof activities
Sustainability
Balance between preventive and
therapeuticmeasures
Decisions, responsibilities
Community participation
Costs
Costs covered
Integration in health care
system
Integration in socio-economic
development
NormalSituations
depends on decentralization
yes, if community participates
yes
yes, if costs are covered
yes
• community • authoritie
yes
according to communityresources
yes
yes
yes
Box 9
PHC IN VARIOUS KINDSOF SITUATIONS
THE HEALTH CARE SYSTEM 355

357
LEGAL PROTECTION (INTERNATIONALHUMANITARIAN LAW)
PERSONNELTRAINING
DELEGATION OFRESPONSIBILITY
TO THE COMMUNITY
SURVEILLANCE/EVALUATION(EPIDEMIOLOGY)
PLANNING
WaterSupply
Sources
Storage
Distribution
Water consumption
Water use
Disposal of liquid waste
Environ-mental
Sanitation
Human waste management
Garbagemanagement
Energysources
Shelter
Vectorcontrol
Control of Communica-ble Diseases
Primary prevention
(immunization)
Secondary prevention
Tertiary prevention
Treatment of communicable
diseases
Control of epidemics
Medical-Surgical
Care
Primarylevel
medical care
Secondary level
medical care
Tertiarylevel
medical care
Transfer between
levels
Management of War
Injuries
First aid
Secondary level care
Evacuationand transport
Tertiary level surgical
care
Psycho-logical
Support
Psycho-social support for individualsand families
Psycho-social support
at the community
level
Psycho-social support
at the institutional
level
Food andNutrition
Agricultural production
Economicsystem
Foodavailability
Accessibilityof food
resources
Food consumption
Biologicalutilization of
food
Nutritional status
POPULATION’S HEALTH
Box 10
HOW A HEALTH CARE SYSTEM WORKS
EXAMPLES OF INTEGRATIVE FUNCTIONS
HELP/SOS: THE HEALTH CARE SYSTEM3356

DESIGNING A HEALTH CARE SYSTEMFOR A GIVEN SITUATION
1. DESCRIPTION
Using the table defined in the previous objective, the instructor will ask thecourse participants to design a health care system for the Awalei camp in theAlphaland-Betaland simulation. The participants must write down the activitiesthey have planned for each component of the health care system, the object beingto obtain a global view of the activities in this camp.
The participants will refer to the transparencies they created in their work groupswhile working on the various modules.
2. CATEGORY
Practice: designing a health care system for a given situation.
3. FORMULATION
Write down in the table defined earlier all the activities you have planned for thepopulation of the Awalei camp in the Alphaland-Betaland simulation.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 50 minutes
. 30 minutes for work in groups
. 20 minutes for summary in plenary session.
6. RECAPITULATION
Tables will be presented by the participants following their group work.
LINK WITH NEXT OBJECTIVES
The synoptic chart showing the various activities undertaken tomaintain health inthe simulation exercise is a springboard to the next module, which focuses onepidemiology.
THE HEALTH CARE SYSTEM 357

The purpose of epidemiology is to assess health problems, their extent, theirdistribution, and their determinants. It may also provide a basis for decisionsconcerning the best strategy for tackling health problems. Another purpose is todescribe trends in health problems, and to evaluate the way services work. Inaddition, it facilitates the adoption of any remedial measures that may be neededto improve programme functioning.
The health care systemmodel, by providing a global view of health care activitiesand the interactions between them, will serve as a matrix for the study ofepidemiology—notably in the choice of indicators and sources of information.
HELP/SOS: THE HEALTH CARE SYSTEM358

EPIDEMIOLOGY
MODULE
7

361
LIST OF OBJECTIVES
. Identify epidemiology’s role in emergency situations
. Identify the basic epidemiological tools needed to institute a surveillancesystem
. Define the concept of indicators, and know the attributes of an indicator andthe attributes of tests measuring these indicators
. Identify possible sources of epidemiological data and list the criteria forselecting a source
. Apply the concepts of sensitivity, specificity, and positive predictive value totwo examples
. Define the concepts of cross-sectional studies, case control studies, and cohortstudies
. Design a questionnaire with the EPIINFO programme and create a data file
. Use EPIINFO to calculate frequencies and create tables and graphs
. Define and calculate an arithmetic mean, themean deviation, the variance, andthe standard deviation
. Express rates and define relative risk and attributable risk
. Know the various sampling methods
. Calculate the size of a sample using the formulas and EPIINFO
. Know how to do cluster sampling
. Know the statistical principles underlying the concepts of the Chi-square testand Student’s T-test
. Know the basic principles involved in making a decision subsequent to anepidemiological study in an emergency situation
. Design an epidemiological surveillance system for the Awalei camp in theAlphaland-Betaland simulation
. Identify the main steps in investigating an epidemic
. Plan measures for controlling a cholera epidemic.
HELP/SOS: EPIDEMIOLOGY360

THE ROLE OF EPIDEMIOLOGYIN EMERGENCY SITUATIONS
1. DESCRIPTION
The role of epidemiology will be defined in terms of the epidemiologicalprogrammes that are relevant in emergency situations:
. the initial assessment of a new situation: ‘‘snapshot’’ of the situation at theoutset
. epidemiological surveillance: regular monitoring of activities being carriedout in a given situation
. ad hoc evaluation: ‘‘snapshots’’ of the situation for comparison with theinitial ‘‘snapshot’’
. early warning system: institution of a surveillance system to detect impendingemergencies, so that preventive measures can be taken or preparations made
. investigation of an epidemic in an emergency situation.
Since participants have made initial assessments throughout the simulationexercise, the instructor need only review briefly the basic principles of suchassessments as studied in the planning module.
Early warning systems are developed in order to predict and/or prevent slowlydeveloping natural disasters (such as droughts). They are less successful indetecting signs of emergency in armed conflict situations. Usually, humanitarianagencies do not gain access to victims until the latter are already in dire straits,although if the situation had been monitored, preventive measures could havebeen taken.
Epidemiological surveillance has been mentioned during group work on thesimulation, but not discussed in depth. Such surveillance is one of the weakpoints of humanitarian action in situations of armed conflict, owing in part to thedifficulty of collecting data regularly, as well as health care personnel’s failure tounderstand the importance of epidemiological surveillance of health interven-tions. One area in which epidemiological surveillance is satisfactory is in refugeeand camps for displaced persons, owing to their relative stability and the easyaccess to data that they afford.
EPIDEMIOLOGY 361

363
Investigating epidemics is also an important part of epidemiology. Epidemicsoften arise during emergency situations.
Thus, epidemiology is a vast field. At the outset the goal will be to teachparticipants the basic tools essential for applying epidemiology in these variousways. Subsequently, these tools will be put to use in epidemiological surveillanceand the investigation of an epidemic.
2. CATEGORY
Framework: identifying epidemiology’s role in emergency situations.
3. FORMULATION
Define epidemiology’s potential roles in emergency situations.
4. TEACHING METHOD
Assignment presented to work groups, followed by a plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Epidemiological programmes
. Box 2: The epidemiological process
. Box 3: Types of epidemiology
. Box 4: Descriptive epidemiology
LINK WITH NEXT OBJECTIVES
The next objective concerns the selection of epidemiological tools.
HELP/SOS: EPIDEMIOLOGY362

Early warning system to anticipateworsening problems and potential disaster
Regular assessment of programme impact and developments in the general situation
Initialassessmentof thesituation
Routine surveillance of a certain number of indicators.
Conflict
TIME
Environment
Population
Box 1
EPIDEMIOLOGICAL PROGRAMMES
EPIDEMIOLOGY 3363

365
INDICATORS
SOURCES OF INDICATORS
MEASUREMENT OF INDICATORS
FORMULATION OF RESULTS
STATISTICAL ANALYSISOF RESULTS
INTERPRETATION OF RESULTS
Box 2
THE EPIDEMIOLOGICALPROCESS
HELP/SOS: EPIDEMIOLOGY3364

DESCRIPTIVEEPIDEMIOLOGY
STATISTICALANALYSIS
ANALYTICALEPIDEMIOLOGY
INDICATORS
SOURCES OFINDICATORS
MEASUREMENTOF INDICATORS
FORMULATIONOF RESULTS
STATISTICALANALYSIS OF
RESULTS
INTERPRETATIONOF RESULTS
Box 3
TYPES OF EPIDEMIOLOGY
EPIDEMIOLOGY 3365

367
• Frequency• Distribution according to:
PlaceTime
Persons
Box 4
DESCRIPTIVE EPIDEMIOLOGY:HEALTH PROBLEMS
HELP/SOS: EPIDEMIOLOGY3366

EPIDEMIOLOGICAL TOOLS
1. DESCRIPTION
The instructor will use a surveillance system as a frame of reference for definingepidemiological tools. This frame will incorporate the following:
. selection of indicators
. collection of indicators
. statistical analysis of indicators
. interpretation of indicators
. making decisions on the basis of that interpretation.
The tools corresponding to these different steps are the following:
. choosing indicators
. definition of an indicator
. prevalence and incidence
. attributes of an indicator
. attributes of a test to measure an indicator (cost, reliability, acceptability,sensitivity and specificity)
. collecting indicators
. choice of a data source
. sampling methods
. determining the size of a sample
. formulating the data
. rates
. frequency
. distribution by persons, in time, and in space
. relative risk
. tabulation
. graphic presentation
. statistical analysis of data
. indices of central tendency
EPIDEMIOLOGY 367

369
. indices of dispersion (variance, standard deviation)
. Chi-square test
. T-test
. interpreting results
. variables
. indicators and operational objectives
. case control.
This is an ambitious study programme; if the participants do not know muchabout epidemiology, the instructor should concentrate on the topics of choosingindicators, selecting data sources, and processing data, and dispense with thesection corresponding to statistical analysis.
The first step is essential. If the indicators selected are not relevant, or the sources ofinformation unreliable, the statistical processing of the data will lead to falseinterpretations. In contrast, if the indicators are appropriate and collected properlybut the health care personnel in the field are not able to perform the statisticalanalysis required, they can send their data to specialists who will do it for them.
2. CATEGORY
Framework: identifying the basic epidemiological tools needed to institute asurveillance system.
3. FORMULATION
Define the tools you need to set up a surveillance system.
4. TEACHING METHOD
Assignment presented to entire group.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: The tools required in the epidemiological process
LINK WITH NEXT OBJECTIVES
The first tool to be studied is indicators.
HELP/SOS: EPIDEMIOLOGY368

1. Definition of an indicator2. Selection of an indicator, attributes of an indicator
1. Choice of a source of indicators2. Sampling methods3. Calculating the size of a sample
1. Attributes of a test to measure an indicator
2. Principles for planning a survey
1. Calculating a rate2. Calculating a frequency3. Distribution by persons in time and
in space
1. Indices of central tendency2. Indices of dispersion3. Chi-square test4. T-test
1. Concept of variables2. The connection between the
definition of an indicator and the definition of an objective
3. Making decisions
INDICATORS
TOOLS
SOURCES OFINDICATORS
MEASUREMENTOF INDICATORS
FORMULATIONOF RESULTS
STATISTICALANALYSIS
OF RESULTS
INTERPRETATIONOF RESULTS
Box 1
TOOLS REQUIREDIN THE EPIDEMIOLOGICAL PROCESS
EPIDEMIOLOGY 3369

371
INDICATORS
1. DESCRIPTION
Indicators describe a situation, and their repeatedmeasurement over time revealschanges and tendencies in that situation. Theymust therefore bemeasurable, andcapable of being measured more than once.
Types of indicators:
. Indicators of impact. Such indicators may describe a state of health in terms ofmortality, morbidity, or nutritional status. They are impact indicators becausethey provide information about the impact of a measure on the population’sstate of health. Of course, such indicators provide only a partial picture, sinceusually they arequantitative indicators; to obtain awider viewof apopulation’shealth we would, for example, have tomeasure the index of psychological well-being. Moreover, the changes measured by the indicators cannot be directlyattributed to the effects of theaction taken.Analysis of thedata furnishedby theindicators must take into account many variables that influence health.
. Indicators of services. These are indicators that measure the quantity ofservices furnished—for example, the number of food rations distributed, thenumber of medical consultations performed, the number of patientshospitalized. This sort of measurement says nothing of the quality of theservices—are the patients well taken care of? Are the food rations distributedfairly? Measuring the performance of health care personnel in a dispensaryprovides an indicator of service quality, as does measuring the satisfaction ofthe beneficiaries of a food distribution.
. Indicators of resources supplied. This would include, for example, overallquantities of food distributed, the quantity of drugs provided to a dispensary,the number of health care personnel working in a hospital. These indicatorsprovide no information on the quality of services, nor on their impact on thevictims’ state of health.
The instructor will emphasize the health care personnel’s role in the selection ofindicators at all levels, and the importance of indicators reflecting quality ofservice and impact on health—with the reserve that these factors are oftendifficult to analyse, since numerous variables affect one’s the state of health.
Morbidity indicators may measure the number of cases of a disease at a givenmoment or during a certain period (prevalence), or measure the number of newcases appearing during these same time frames (incidence).
HELP/SOS: EPIDEMIOLOGY370

Variables:
Let us suppose that we aremeasuring the rate of malnutrition over a period of sixmonths. Repeated measurements show that the malnutrition rate drops from15% to 5% in the course of the six months. Can this result be attributed to thefood distributions that took place during these same six months? Not unless wehave additional information on, for example:
. the quality of the food distributions
. the quantities of food resources distributed
. the mortality rate—which might show that the drop in the malnutrition rateis in fact due to a high death rate
. the total number of the population: the drop in the malnutrition rate may bedue to the departure of masses of people, leaving behind only those who arehealthy.
Thus, each indicatormust be considered in conjunctionwith variables that roundout the analysis. In practice, these variables must be identified and measured atthe same time as the indicator itself.
An indicator must have the following attributes:
. relevance. The indicator does in fact measure what we are trying tomeasure—for example, in an emergency situation we want to measure therate of acute malnutrition rather than the rate of chronic malnutrition.
. precise definition. If not precisely defined, data gathered from differentsources will not be comparable, and any subsequent comprehensive analysisof these data will be impossible (or possible but false!).
. measurable: An indicator must be measurable—that is, a test is available tomeasure it accurately.
. sensitive: An indicator must be sensitive to changes in the thing that is beingmeasured.
Attributes of a test to measure an indicator:
. representativeness: Concordance between what is sought and what the testactually measures.
. validity: Validity is measured by two properties: sensitivity and specificity.
. applicability: Possibility of performing the test in emergency situationsdespite constraints of time and access and acceptability to the population.
EPIDEMIOLOGY 371

373
. standardization: The test should be simple enough so that it can be performedin exactly the same way by anyone called upon to perform it.
Indicator and operational objectives:
The instructor must remind the participants that operational objectives include astatement of the problem, quantification of the results sought, the length of timeneeded to achieve these results, and the population group or services for whichthese objectives have been established. The indicatormust cover these data—thatis, it must be chosen to reflect the health problem identified at the time theobjective was determined, be applied to the same population group, and bemeasured in the time frame determined.
2. CATEGORY
Tool: defining the concept of an indicator, and knowing the attributes of both anindicator and the tests that measure indicators.
3. FORMULATION
Define the concept of indicator.
List the attributes of an indicator.
List the attributes of a test to measure an indicator.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 60 minutes
. 20 minutes for work in groups
. 40 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Indicators
. Box 2: Attributes of indicators
. Box 3: Attributes of tests to measure indicators
LINK WITH NEXT OBJECTIVES
The participants have acquired a general understanding of indicators. The nextobjective addresses the sensitivity, specificity, and predictive value of a test.
HELP/SOS: EPIDEMIOLOGY372

Box 1
INDICATORS
. Types of indicators:
. Input indicators (resources)
. Output indicators (services)
. Outcome indicators (problems)
. Impact indicators (health status)
. Complexity increases with the level:
INPUT ? IMPACT
+ +++
. Indicators and determination of objectives
. Indicators and variables
. Attributes of an indicator
Box 2
ATTRIBUTESOF AN INDICATOR
. RELEVANT
. PRECISELY DEFINED
. MEASURABLE
. SENSITIVE
EPIDEMIOLOGY 373

375
Box 3
ATTRIBUTES OF A TESTOR DATA COLLECTING METHODIN EMERGENCY SITUATIONS
GENERAL ATTRIBUTES:
. Representativeness
. Validity
. Reliability
ATTRIBUTES MORE SPECIFIC TO EMERGENCIES:
. Applicability
. Rapidity
. Simplicity
. Reproducibility
. Acceptability
. To the population
. To the authorities
HELP/SOS: EPIDEMIOLOGY374

DATA SOURCES
1. DESCRIPTION
Once we have defined the indicators we want to use, we must determine where,how, and at what rate they can be efficiently collected. In situations of armedconflict, not all sources of information are accessible, and sometimes it isnecessary to resort to indirect and less reliable sources. This poses the risk ofhaving to make decisions based on mediocre data.
Sources of data:
. the victims. Nutritional status is measured directly within the population.Measuring the nutritional status of children visiting health facilities wouldcreate a bias, since greater numbers of malnourished children are brought infor medical advice
. health facilities. Hospitals and health care centres can provide data onmorbidity and the specific causes of mortality
. the local market. Information can be gleaned in the market concerning theprices of foodstuffs, which is one indicator for monitoring food distributions
. administration. Governmental bodies, where functioning, can provide dataon mortality, population censuses, etc.
The choice of data sources is based on:
. the relevance of the data source to the indicator to be measured
. continuity of access. In situations of armed conflict, access to informationsources is often difficult, irregular, and even dangerous
. reliability, which depends on how motivated health care personnel or otherpeople are to collect data according to defined standards and frequency. Thatmotivation, in turn, depends on an understanding of the link between datacollection and decisions. Sources providing information should receivefeedback, as this is essential for maintaining their motivation. Another pointto stress is that data should be reliable over time (consistency).
2. CATEGORY
Tool: identifying data sources and listing the criteria for selecting a source ofinformation.
EPIDEMIOLOGY 375

377
3. FORMULATION
What are the main data sources and what characteristics should be looked for ina data source?
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Data sources
LINK WITH NEXT OBJECTIVES
Indicators must be tested if they are to provide the necessary data. Thecharacteristics to be looked for in such tests are the focus of the next objective.
Box 1
DATA SOURCES
SOURCES:
. Population
. Health careservices
. Local market
. Administrative bodies
SELECTION CRITERIA:
. Relevance of thesource to the indicatorsought
. Accessibility
. Reliability
HELP/SOS: EPIDEMIOLOGY376

SENSITIVITY, SPECIFICITY, AND POSITIVEPREDICTIVE VALUE OF A TEST
1. DESCRIPTION
The object here is to explain the concepts of a test’s sensitivity, specificity, andpositive predictive value (PPV).
A test’s sensitivity is defined as the proportion of positive cases that are identifiedby the test (ratio between the number of positive cases detected by the test and theactual number of positive cases).
The specificity of a test is defined as the proportion of negative cases that areidentified by the test (ratio between the number of negative cases detected by thetest and the actual number of negative cases).
The positive predictive value of a test is the probability that an individualdeclared positive by a test actually has the disease.
2. CATEGORY
Tool: applying the concepts of sensitivity, specificity, and PPV to two examples.
3. FORMULATION
Define the sensitivity, specificity, and PPV of the tests in the two followingexamples.
4. TEACHING METHOD
Assignment presented to each participant, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for plenary session.
6. RECAPITULATION
. Box 1: The principles of test sensitivity and specificity
. Box 2: Sensitivity, specificity, and positive predictive value: definitions
EPIDEMIOLOGY 377

379
. Box 3: Calculating sensitivity, specificity, and positive predictive value
. Box 4: Application of sensitivity, specificity, and PPV to meningitis
. Box 5: Application of sensitivity, specificity, and PPV to malaria
. Box 6: Application of sensitivity, specificity, and PPV to bacillary dysentery
LINK WITH NEXT OBJECTIVES
There are different ways of conducting epidemiological studies. The nextobjective describes them briefly.
+
+
+
–
–
–
Healthy subjects Subjects withthe disease
What is the capacity of the test to distinguish subjects withthe disease (sensitivity) from healthy subjects (specificity)?
+
Results: correct false false correctTest
Box 1
THE PRINCIPLES OF TEST SENSITIVITYAND SPECIFICITY
HELP/SOS: EPIDEMIOLOGY3378

Actual status➀ of the population tested:
Test②detecting the disease
yesDisease
+
no
Sensitivity Specificity
–
total number of true positives Sensitivity =
number of true positivesdetected by the test
total number of true negatives Specificity =
number of true negativesdetected by the test
number of positive tests PPV =
number of true positivesdetected by the test
➀ The actual status of the population can be determined by more precise tests.
② The sensitivity, specificity, and PPV of most of the tests used in emergency situations are known.
PPVtrue
positivesfalse
positives
falsenegatives
truenegatives
Box 2
SENSITIVITY, SPECIFICITY,AND POSTIVE PREDICTIVE VALUE
(DEFINITIONS)
EPIDEMIOLOGY 3379

381
Disease
Test68 18
++
–
–Calculate: Sensitivity
SpecificityPPV
12 202
Box 3
CALCULATING SENSITIVITY, SPECIFICITY,AND POSITIVE PREDICTIVE VALUE
MENINGITIS Bacteriological confirmation
Clinicaldefinition
Fever +headache + stiff neck
45 30
5 20
++
–
–
+ cloudy CSF+–
40 2
10 48
+ –
Box 4
MENINGITIS: APPLICATIONOF SENSITIVITY, SPECIFICITY, AND PPV
HELP/SOS: EPIDEMIOLOGY380

MALARIA Laboratory confirmation
Clinical definition
Fever >38.5°Headache
Fever >38.5°HeadacheNo respiratory infection +
+–
90 80
10 70
+ –
+–
80 30
20 120
+ –
Box 5
MALARIA: APPLICATIONOF SENSITIVITY, SPECIFICITY, AND PPV
BACILLARY DYSENTERY
Identification of thebacillus in patient’s stools
Clinical definitionDiarrhoea with bloody stools and fever
Diarrhoea with blood actually seen in the stools, and fever
+–
80 50
20 50
+ –
+–
70 2
30 98
+ –
Box 6
BACILLARY DYSENTERY: APPLICATIONOF SENSITIVITY, SPECIFICITY, AND PPV
EPIDEMIOLOGY 381

383
CROSS-SECTIONAL STUDIES,CASE CONTROL STUDIES,AND COHORT STUDIES
1. DESCRIPTION
Epidemiological studies can be carried out in various ways:
. cross-sectional studies
. case control studies
. cohort studies.
. Cross-sectional studies are the type most often used in emergency situations.They provide a veritable snapshot of the situation at a given moment. Thefirst study corresponds to the initial assessment of an emergency situation.Subsequent cross-sectional studies are basically ad hoc assessments designedto monitor developments in the situation. The advantages of cross-sectionalstudies are as follows:
. they provide information quickly, capturing the situation at a givenmoment
. they are simple to carry out (if access to the population is guaranteed)
. they quickly provide a view of current health problems and theirdistribution.
. Case control studies are used to compare two population groups, onedisplaying a specific characteristic (for example, malnutrition), and the otherwithout that characteristic. A retrospective study of the two groups is carriedout in order to determine the factors that gave rise to the characteristic inquestion. This method is employed, for example, in areas of low-gradeconflict to evaluate the causes of the conflict’s impact on certain villages,when some villages have been directly affected by the conflict and others havenot. Gaining access to all the information requiredmay be difficult, however,owing to population movements, deaths, the disappearance of localadministrative bodies such as health services, etc.
. Cohort studies are prospective studies that examine the relation between ahealth problem and a presumed cause of that problem. In practice, theyfollow subjects exposed to a risk factor over a certain period of time in order
HELP/SOS: EPIDEMIOLOGY382

to determine whether those subjects will develop the health problem that isthought to be associated with the risk factor. This method is rarely used inemergency situations to establish links between health problems and possiblecauses. Cohorts of sick people or malnourished children are monitored inorder to determine a measure’s impact on their condition, but this practicedoes not constitute a cohort study; it is, rather, part of themonitoring processof a surveillance programme. The main advantage of cohort studies is thatthey can confirm a connection between a health problem and a potentialcause (within the statistical limitations of the sampling technique used).However, they require time to produce results, and during that time subjectsin the study may disappear from the cohort. This is a major problem inemergency situations.
2. CATEGORY
Tool: defining the concepts of cross-sectional studies, case control studies, andcohort studies.
3. FORMULATION
Define cross-sectional studies, case control studies, and cohort studies.
4. TEACHING METHOD
Assignment presented to entire group.
5. DURATION
Total duration: 15 minutes.
6. RECAPITULATION
. Box 1: Cross-sectional studies, case control studies, and cohort studies
LINK WITH NEXT OBJECTIVES
These studies require the use of questionnaires to obtain exact information onpeople’s health status, capacity of local services, etc. The purpose of the nextsection is to show how to create a questionnaire with the help of a computer.
EPIDEMIOLOGY 383

385
TIME
Initial assessment=
Cross-sectional study
Case control studies=
Retrospective studies
Cohort studies=
Prospective studies
Evaluation of results =
Cross-sectional studies
Box 1
CROSS-SECTIONAL STUDIESCASE CONTROL STUDIES
HELP/SOS: EPIDEMIOLOGY3384

DESIGNING A FORM USING EPIINFOAND CREATING FILES
1. DESCRIPTION
Forms for collecting quantitative data are easy to design, and can be put directlyon a computer.Where questions aremeant to elicit qualitative data, however, theway they are formulated is very important.
Possible problems include:
. tendentious questions that influence responses
. questions about security that respondents are not eager to answer
. questions using vocabulary, expressions, or syntax that are incomprehensibleto the intended respondents.
Crude mortality in the Awalei camp will be used as an example. Thequestionnaire should elicit the following information:
. name
. age
. sex
. place of origin
. length of stay in the camp
. cause of death
. family size.
Once the questionnaire has been created, participants will enter the data gatheredin the Awalei camp.
2. CATEGORY
Tool: designing a questionnaire using EPIINFO and creating a data file.
3. FORMULATION
Design a questionnaire using EPIINFO and enter the data relating to mortalityin the Awalei camp.
EPIDEMIOLOGY 385

387
4. TEACHING METHOD
Practical work assigned to the participants.
5. DURATION
Total duration: 30 minutes.
6. RECAPITULATION
. Box 1: Creating a questionnaire with EPIINFO
. Box 2: Entering data in a questionnaire
LINK WITH NEXT OBJECTIVES
Once the data have been collected, participants must put them ‘‘in order’’ intables and graphs. This will be covered by the next objective. (Assignmentsinvolving EPIINFO may all be grouped together.)
Box 1
CREATING A QUESTIONNAIREWITH EPIINFO
. Name <letters>
. Age <figures>
. Sex <upper-case letter: M or F>
. Place of origin <upper-case letters>
. Date of arrival <date>
. Causes of death <letters>
. Length of stay <figures>
HELP/SOS: EPIDEMIOLOGY386

Box 2
ENTERING DATAIN A QUESTIONNAIRE
Name Age SexPlace Date Causes
of origin of arrival of death
6 months
3 years
7 months
62 years
EPIDEMIOLOGY 387
389
FREQUENCIES, TABLES, GRAPHS,AND CHARTS WITH EPIINFO
1. DESCRIPTION
There are three main parameters of data distribution: time, space, and persons.EPIINFO will classify data by age, sex, place, and date. The participants will beasked to use the EPIINFO ANALYSIS function to calculate frequencies and tomake tables and graphs using the parameters obtained with the questionnaire.
2. CATEGORY
Tool: using EPIINFO to calculate frequencies and to make tables and graphs.
3. FORMULATION
Calculate frequencies and make graphs using the parameters from thequestionnaire previously created with EPIINFO.
4. TEACHING METHOD
Practical work assigned to participants.
5. DURATION
Total duration: 30 minutes.
6. RECAPITULATION
. Box 1: Frequencies, tables, and graphs using EPIINFO
LINK WITH NEXT OBJECTIVES
Formating data in this waymakes for quick visualization. However, interpretingthe data requires statistical analysis, followed by causal analysis. The nextobjectives deal with the statistical analysis of data. (All the practical assignmentsusing EPIINFO may be grouped together.)
HELP/SOS: EPIDEMIOLOGY388

Box 1
FREQUENCIES, TABLES,AND GRAPHS USING EPIINFO
. Calculate frequency by gender
. Calculate frequencies by age
. Calculate the average length of stay
. List names in alphabetical order
EPIDEMIOLOGY 389

391
NORMAL DISTRIBUTIONOF DATA (GAUSSIAN CURVE)
1. DESCRIPTION
To represent the distribution of a variable, plot the values of the variable on theX-axis of a graph, and their corresponding frequencies on the Y-axis. Normaldistributions have specific properties:
. they are defined by their arithmetic mean, a measure of central tendency
. they are symmetrical, their values differing from the arithmetic mean by thevalue of the standard deviation
. 68%of the values will lie between+1 and -1 standard deviations of themean,and 96% will lie between +2 and -2 standard deviations.
Measures of central tendency:
. the arithmetic mean, or average: the sum of all the values divided by thenumber of values
. the median: the value that is physically at the centre of the set of all the values
. the mode: the value that occurs most frequently in a set of values.
The arithmetic mean is the most frequently used measure of central tendency.
Measures of dispersion:
. the mean deviation: the sum of the individual deviations (regardless ofnegative or positive signs) divided by the number of observations
. the variance: the sum of the squares of individual deviations divided by thenumber of observations
. the standard deviation: the square root of the variance.
These indices are used to express variations of a value found in a givenpopulation.
2. CATEGORY
Tool: defining and calculating an arithmetic mean, the mean deviation, thevariance, and the standard deviation.
HELP/SOS: EPIDEMIOLOGY390

3. FORMULATION
Define the arithmetic mean, the mean deviation, the variance, and the standarddeviation.
Calculate these parameters for a set of values.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Normal distribution of data
. Box 2: Calculating the arithmetic mean, the median, the mode, the meandeviation, the variance, and the standard deviation
LINK WITH NEXT OBJECTIVES
This tool will also be used to define the basic principle underlying the statisticalinterpretation of results obtained by sampling.
EPIDEMIOLOGY 391

393
Arithmetic mean(measure of
central tendency)
-2 SD -1 SD X +1 SD +2 SD
68% of the population
measure of dispersion
96% of the population
(SD = a standard deviation)
Box 1
NORMAL DISTRIBUTION OF DATA
(GAUSSIAN CURVE)
HELP/SOS: EPIDEMIOLOGY3392

Box 2
MEASURES OF CENTRAL TENDENCY
Weight of five-year-old male children
21.8
20.3
20.1
20.1
19.9
19.7
19.2
18.7
18.7
18.7
18.1
17.9
17.3
16.5
15.2
14.1
Calculate:
. the arithmetic mean
. the median
. the mode
. the mean deviation
. the variance
. the standard deviation
EPIDEMIOLOGY 393

395
RATE, RELATIVE RISK, ATTRIBUTABLE RISK
1. DESCRIPTION
In order to compare a certain variable in two different populations, the datamustbe expressed in the form of a rate. A rate is characterized by a numerator—thenumber of cases observed in each population—and a denominator—the totalnumber of subjects at risk in each population.Rates are expressed in percentages,per-thousands, and per-hundred thousands, depending on current norms. Theincidence of tuberculosis, for example, is usually expressed as the number of newcases of tuberculosis per year per 100,000 people. In emergency situations, thecrude mortality rate is expressed as the number of deaths per day per 10,000people. The expression of rates using standard denominators for a given variablepermits quick comparison of data from two populations.
Relative risk is defined as the ratio between the value of a variable in peopleexposed to a certain factor and the value of that same variable in peoplewho havenot been exposed to the factor.
Attributable risk is defined as the value of the variable in people exposed to acertain factor minus the value of the variable in people who are not exposed tothat factor.
2. CATEGORY
Tool: expressing rates and defining relative risk and attributable risk.
3. FORMULATION
Define the morbidity rate and the mortality rate.
Calculate relative risk in a given example.
Calculate attributable risk in a given example.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
HELP/SOS: EPIDEMIOLOGY394

. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Examples of rates
. Box 2: Odds ratio
. Box 3: Relative risk and attributable risk
. Box 4: Incidence and prevalence: definitions
. Box 5: Calculating incidence and prevalence
. Box 6: Relation between the prevalence, incidence, and duration of adisease
LINK WITH NEXT OBJECTIVES
Data are not usually collected for an entire population, but for a sample thereof.The next objectives concern samplingmethods and the way the size of a sample isdetermined.
Box 1
EXAMPLES OF RATES
MORTALITY RATE:
. Crude mortality ratee.g., 2/10,000/day
. Mortality rate by agee.g., mortality amongchildren < 5 years
infant mortality rate(child < 1 year)
These rates are usuallyexpressed per 1,000
. Mortality rate by causeof deathe.g., pneumonia
MORBIDITY RATE:
. Incidence rate
. Prevalence rate
EPIDEMIOLOGY 395

397
BACILLARY DYSENTERY
odds ratio =
MALNOURISHED
50 102
46 409
+
+
–
–
a b
c d
bc
(odds ratio = 4.3)
ad
Box 2
ODDS RATIO
ESTIMATION OF RELATIVE RISK
HELP/SOS: EPIDEMIOLOGY3396

EXAMPLE: period from 1 March 1997 to 1 June 1997
SwampNo. of malaria
cases212
No. of malariacases
3181 Km
RELATIVE RISK =
Incidence inpopulation exposed
to the risk
Incidence inpopulation not exposed
to the risk
ATTRIBUTABLE RISK =
Incidence inpopulation exposed
to the risk — incidence inpopulation not exposed
to the risk
VILLAGE A2,632
people
VILLAGE B8,534
people
Box 3
RELATIVE RISKAND ATTRIBUTABLE RISK
EPIDEMIOLOGY 3397

399
Box 4
PREVALENCE AND INCIDENCE
PREVALENCE:
number of people in a populationwho have the disease in questionat a given time
INCIDENCE:
number of new cases of the diseasein question during a given period.
HELP/SOS: EPIDEMIOLOGY398

period 1 period 2
Incidence: number ofnew cases
Prevalence:number of cases
Onset of the disease End of the disease
Duration of the disease
Box 5
INCIDENCE AND PREVALENCE DURINGA GIVEN SPAN OF TIME
EPIDEMIOLOGY 3399

401
Box 6
RELATION BETWEEN THE PREVALENCE,INCIDENCE, AND DURATION
OF A DISEASE
P = I x D
EXERCISES:
. In a hospital, 12 new cases of mine injuries are admittedeach month. They remain hospitalized for 6 weeks onaverage.
How many beds are occupied by the injured?
. 200 patients are currently being treated in a programmeto combat tuberculosis. Their course of treatment lasts9 months.
How many new cases are admitted to theprogramme each year?
. A nutritional rehabilitation centre serves 800 children.Each week, 65 new cases are admitted.
What is the average length of stay in the centre?
Source: E. Brenner, Help.
HELP/SOS: EPIDEMIOLOGY400

SAMPLING METHODS
1. DESCRIPTION
Collecting data on an entire population would require an excessive investment intime, labour, and money. Instead, the usual practice is to study a representativesample of the population.
Several methods are possible:
. simple random sampling. The individuals for the sample are selected atrandom; each individual has the same chance of being chosen.
. stratified random sampling. The population to be studied is divided intogroups according to such characteristics as geographical location, socialmilieu, etc., and simple random sampling is carried out in each group.
. systematic sampling. Subjects are chosen according to a set interval (everyfifth individual, for example); each individual does not have the same chanceof being chosen.
. cluster sampling. A cluster of individuals is selected at random, and eachindividual in the group is examined.
. Each of these methods requires a sampling frame: a list of all the individuals,a list of all the houses (random and systematic sampling), or a cumulative listof populations (cluster sampling).
The choice between these methods will depend on:
. the degree of precision required. Simple random sampling is morerepresentative than cluster sampling.
. the geographical distribution of the population. For a population dispersedamong many villages, cluster sampling is more appropriate; in a camp,systematic sampling is preferable.
. cost. Cluster sampling is less expensive than simple random sampling.
. access to the population.
2. CATEGORY
Tool: knowledge of the various sampling methods.
3. FORMULATION
List the various sampling methods and their relative advantages.
EPIDEMIOLOGY 401

403
4. TEACHING METHOD
Assignment presented to the whole group.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Sampling methods
LINK WITH NEXT OBJECTIVES
The next objective will focus on determining the size of a sample.
Box 1
SAMPLING METHODS
. Simple random sampling
. Stratified random sampling
. Systematic sampling
. Cluster sampling
HELP/SOS: EPIDEMIOLOGY402

CALCULATING THE SIZE OF A SAMPLE
1. DESCRIPTION
Calculating the size of a sample is based on complex concepts. Three basicprinciples should be mentioned at the outset:
. the mean obtained for a series of samples of the same size within a singlepopulation is identical to the true mean (i.e., the average that would havebeen obtained by measuring all the individuals of one population)
. the curve of themeans obtained by this series of same size samples is a normaldistribution curve
. the standard deviation in a distribution of the means obtained for this seriesof same-size samples is called the standard error.
As mentioned, 96% of the values for a variable are situated between +2 standarddeviations and -2 standard deviations. By analogy, it can be said that 96% of samesize samples taken within a single population will be found to lie between +2standard errors and -2 standard errors. Conversely, any sample taken in a givenpopulationhasa96%chanceof fallingbetween+2standarderrors and -2 standarderrors (the usual convention is to assume a 95% chance that the value found by asamplewill fall between+1.96 and -1.96 standard errors). This percentage, 95%, isthe degree of probability that the value found in the sample will fall between+1.96standard errors. If we wanted that probability to be 99%, we would have to take+2.58 standarderrorsasour limits.This spread isknownas the confidence interval.Of course, if only one sample is to be taken, we do not know what the limits of theconfidence interval are. This is why, in calculating the size of a sample, we mustdetermine the size of that interval; the greater the interval, the less precision in oursample, and vice versa. For greater precision—precision meaning that the valuefound by the sample does not differ too much from the true mean—the size of thesample must be increased. A compromise must be sought between the degree ofprecision and the size of the sample. Finally, the last parameter to be considered isthe estimated value of the factor sought,which, for an infinite population,would bethe proportion of the population possessing that factor, and, for a mean, theestimated standard deviation.
This gives the following formulas:
For an infinite population: size of sample = Z2 x pq/D2, where:
. Z = 1.96 (level of confidence is 95%)
EPIDEMIOLOGY 403

405
. p = the value of the proportion
. q = 1-p
. D = degree of precision
For means: size of sample = Z2 x SD/D2, where:
. Z = 1.96 (level of confidence is 95%);
. SD = estimated standard deviation
. D = level of precision sought.
Thus, the size of the sample is determined by the level of confidence and thedesired confidence interval.
Once a result has been obtained, we can refine the calculation of the confidenceinterval by turning this reasoning around, so that for a mean we would calculate:
. standard error = standard deviation / square root of the size of the sample
. confidence interval for a confidence level of 95% = the mean found +1.96standard errors.
These explanations of how to determine the size of a sample are very simple. Theinstructor should not embark on any sophisticated statistical arguments; thepurpose of this objective is simply to illuminate the basic statistical principles ofsampling. Finally, the instructor should show the participants how to useEPIINFO to calculate the size of a sample.
2. CATEGORY
Tool: calculating the size of a sample using first the formulas provided and thenEPIINFO.
3. FORMULATION
Calculate the size of a sample for given values using first the statistical formulasprovided and then EPIINFO.
4. TEACHING METHOD
Explanation of the formula for calculating the size of a sample.
Work in groups to calculate the size of several samples according to given valuesfor the precision and proportion sought.
This EPIINFO practice can be combined with other assignments using EPIINFO.
HELP/SOS: EPIDEMIOLOGY404

5. DURATION
Total duration: 60 minutes
. 30 minutes for work in groups
. 30 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Calculating the size of a sample: basic concepts
. Box 2: Estimating the value of the factor to be measured in order tocalculate the size of a sample
. Box 3: Basic principles for calculating the size of a sample
. Box 4: Formula for calculating the size of a sample to find a proportion bysimple random sampling
LINK WITH NEXT OBJECTIVES
These formulas are used to calculate simple random samples. Themethod used tocalculate sample size in cluster sampling will be studied in the next objective.
Box 1
CALCULATING THE SIZEOF A SAMPLE
BASIC CONCEPTS:
. Level of confidence (related to standard error)
. Confidence interval
. Degree of precision
. Estimated value of the factor to be measured
EPIDEMIOLOGY 405

407
Box 2
ESTIMATING THE VALUEOF THE FACTOR TO BE MEASUREDIN ORDER TO CALCULATE THE SIZE
OF A SAMPLE
p = value of the factorq = 1-p
p q pxq
0.1 0.9 0.09
0.2 0.8 0.16
0.3 0.7 0.21
0.4 0.6 0.24
0.5 0.5 0.25
0.6 0.4 0.24
0.7 0.3 0.21
0.8 0.2 0.16
0.9 0.1 0.09
When in doubt, use 50%,which gives the largest sample size.
HELP/SOS: EPIDEMIOLOGY406

The mean of the values found in repeated samples from the same population is equal to the true mean.
The values found in successive samples follow a normal distribution curve and deviate from the true mean by the standard error.
95% of the values found in successive samples from the same population fall between +1.96 and -1.96 standard errors.
-2 -1 +1 +2
standard error standard errormean
standard error standard errormean
-1.96 +1.96
95%of thevalues
Box 3
BASIC PRINCIPLESFOR CALCULATING THE SIZE
OF A SAMPLE
EPIDEMIOLOGY 4407

409
Estimated prevalence sought (when in doubt, use 50%, which will make the sample as large as possible)
Tolerable margin of error(degree of precision sought)
Size of the sample
q = 1 – p
Z = 1.96 for a 95% level of confidence
N = Z2 pqD2
Box 4
FORMULA FOR CALCULATINGTHE SIZE OF A SAMPLETO FIND A PROPORTION
BY SIMPLE RANDOM SAMPLING
HELP/SOS: EPIDEMIOLOGY4408

CLUSTER SAMPLING
1. DESCRIPTION
Cluster sampling involves the following steps:
. determine the sizeof the samplebyusing the same formulaas for simple randomsampling,N=Z2xpq/D2,multiplying the resultobtainedby2 (this is necessarybecause cluster sampling is not as precise as simple random sampling)
. determine the number of clusters—at least 30, though more can be used
. determine the size of each cluster by dividing the size of the sample by thenumber of clusters
. situate the clusters:
. prepare a sampling frame—namely, a list of the places concerned and theirrespective populations—and make a cumulative list of those populations
. determine a sampling interval by dividing the total population by thenumber of clusters
. choose a random number that is smaller than the sampling interval
. apply this random number to the list of cumulative population totals tofind the first cluster
. add the sampling interval to that random number to find the secondcluster, and continue to add the sampling interval to find successiveclusters until the end of the list has been reached.
Cluster sampling is commonly used todetermine immunization coverage. It can alsobe used to measure malnutrition in dispersed populations. Its main disadvantage isthat a list of populations is required in order to constitute a sampling frame.
2. CATEGORY
Tool: technique of conducting cluster sampling.
3. FORMULATION
Use cluster sampling in a given situation.
4. TEACHING METHOD
Assignment presented to work groups, following an explanation of themethodology.
EPIDEMIOLOGY 409

411
5. DURATION
Total duration: 40 minutes
. 15 minutes for work in groups
. 25 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Preparing for cluster sampling
. Box 2: Geographical determination of clusters
. Box 3: Cluster sampling: situate the clusters
LINK WITH NEXT OBJECTIVES
The results obtained by sampling are an estimation of the true values that wouldbe obtained if the entire populationweremeasured.Whenwe compare the resultsof two samples from two different populations, we are in fact comparing twoestimates, which cannot be affirmed with any certainty to be either the same ordifferent. Statistical tests can be used to calculate the risk of error. These tests willbe briefly discussed in the next objectives.
Box 1
PREPARING FOR CLUSTER SAMPLING
1. Determine the size of the
sample by using the sameformula as for random
sampling:
N = (Z2 x pq)/D2
REMEMBER, the result must
be multiplied by 2!
2. Determine the number of
clusters. There should be atleast 30.
3. Determine the size of each
cluster by dividing the total sizeof the sample by the number of
clusters.
4. Determine the geographicallocation of each cluster.
HELP/SOS: EPIDEMIOLOGY410

Sampling frame List of populations Cumulative sum ofpopulations
Localities
Pop. 1
Pop. 2
Pop. 3
Pop. 4
Pop. 5, etc.
Pop. 1
Pop. 1+2
Pop. 1+2+3
Pop. 1+2+3+4
Pop. 1+2+etc.
• Draw a random number (only condition:the number must be smaller than thesampling interval)
• Add the sampling interval to the random number to obtain the location of the second cluster. Add the sampling interval again and again until the number of the total population is attained.
• Identify the population con-taining this random number
Randomnumber
• Total pop./no. of clusters =
Total population
Selection of thefirst cluster
Samplinginterval
Box 2
GEOGRAPHICAL DETERMINATIONOF CLUSTERS
EPIDEMIOLOGY 4411

413
Box 3
CLUSTER SAMPLING
SITUATE THE CLUSTERS
Places Number of Inhabitants
Place 1: 562Place 2: 1,066Place 3: 973Place 4: 5,272Place 5: 197Place 6: 428Place 7: 912Place 8: 1,088Place 9: 3,227Place 10: 56Place 11: 512Place 12: 493Place 13: 182Place 14: 217Place 15: 342Place 16: 228Place 17: 128Place 18: 4,235Place 19: 3,520Place 20: 636Place 21: 488Place 22: 152Place 23: 1,037Place 24: 137Place 25: 112
HELP/SOS: EPIDEMIOLOGY412

STATISTICAL TESTS
1. DESCRIPTION
The results obtained by sampling are an estimation of the true values that would beobtained if the entire population were measured. When we compare the results oftwo samples from twodifferent populations,we are in fact comparing two estimates,which cannot be affirmed with any certainty to be either the same or different.
Statistical tests can be used to calculate the risk of error. The basic principlesunderlying these tests are as follows:
. the null hypothesis is the assumption that two populations are identical. Theobject of a statistical test is to prove this hypothesis true or false. If it is true,this means there is no difference between the populations, or that the minordifferences observed were engendered by the sampling process. If it is false,this means that there is in fact a difference between the two populations.
. type I and type II errors. Rejecting the null hypothesis when it is in fact true isa type I error; accepting the null hypothesis when it is false is a type II error.Statistical tests are intended tomeasure the probability of making one type oferror or the other. In practice, such tests measure primarily the probability ofmaking a type I error.
. the p-value represents the level of risk we are willing to accept of making atype I error. In general a risk level of less than 5% (p=0.05) is consideredacceptable. That is, in order to reject the null hypothesis, there must be achance of less than 5 out of 100 that the difference observed is due to thesampling procedure. If the p-value is greater than 0.05, we cannot say the nullhypothesis is true without making a type II error. Type II errors depend onthe size of the sample, the significance level (probability of a type I error), andthe magnitude of the difference in the factor being sought in the twopopulations. The power of a test (i.e., probability of not committing a type IIerror) is defined by the value 1-b.
. the Chi-square test measures the differences between the values observed andthe theoretical values that would have been obtained if the populationsmeasured were identical. It is carried out as follows:
. calculate the difference between the value observed and the theoreticalvalue for each population group: (O-T)2/T
. adding together the differences found for each population groupproduces the Chi square
EPIDEMIOLOGY 413

415
. refer to Chi-square tables to determine the probability of a type I error,based on the Chi-squared value and the table’s degree of freedom(number of columns -1) x (number of rows - 1)
. if the probability is less than 0.05, the differences between the populationsare significant.
. Student’s T-test compares twomeans obtained by sampling two populations,by establishing the ratio between the difference between the two means andthe standard error of the difference. We calculate the latter by taking thesquare root of the sum of the squares of the standard deviations and dividingit by the size of the sample.
Participants should do exercises using EPIINFO.
Study of the statistical aspects of epidemiology should be limited to the essentialconcepts. The instructor must remind students that the goal is to set up asurveillance system, in which the first steps, selecting indicators and sources ofinformation, will take priority for personnel in the field. It is always possible laterto have a statistician perform a statistical analysis of the data—but not to ask thestatistician to collect a second batch of data because those provided the first timearound were neither relevant nor reliable.
2. CATEGORY
Tool: knowledge of the statistical principles of the Chi-square test and Student’sT-test.
3. FORMULATION
Explain the statistical principles of the Chi-square test and Student’s T-test.
4. TEACHING METHOD
Explanation of basic principles, followed by application exercises for the twotests.
5. DURATION
Total duration: 40 minutes.
6. RECAPITULATION
. Box 1: Statistical tests (concepts)
. Box 2: Chi-square
HELP/SOS: EPIDEMIOLOGY414

LINK WITH NEXT OBJECTIVES
Statistical analysis can show, for example, that the differences found in themalnutrition rates for two populations are statistically significant. However,analysis should not stop there. The reason for the difference must be discoveredbefore operational decisions can be taken. The link between interpreting resultsand the decision-making process will be studied in the next objective.
Box 1
STATISTICAL TESTS(CONCEPTS)
. Null hypothesis
. Type I and typeII errors
. P-value
. Chi square
. Student’s T-test
87*(58)**
115(140)
202
5,805
6,0074,2421,765
4,127(4,072)
1,678(1,694)
* values observed** values expected
Village A
Malaria
No malaria
Village B
Box 2
CHI-SQUARE
EPIDEMIOLOGY 415

417
INTERPRETATION OF RESULTSAND THE DECISION-MAKING PROCESS
1. DESCRIPTION
Before any data can be interpreted, the reliability of the study—themethod used,the reliability of the data sources, the value of the statistical analysis—must beverified. The interpretation of the data is based on a range of considerations:
. the establishment of connections between a health problem and its possiblecauses.
. Seeking the causes of a health problem is not axiomatic in the initialassessment; as we have seen, initial assessments are cross-sectional studiesthat provide a snapshot of a situation at a given moment. This is why it isimportant in the course of the initial assessment to ask questions aboutthe factors that led to the current situation. Of course rigorousretrospective studies cannot be undertaken, since they would take toomuch time, but at least essential information should be gathered tosupport decisions concerning the appropriateness and modalities of anaction. A multisectoral analysis of data provides further insights intocauses. Thus, a malnutrition rate will not be analysed exclusively in termsof access to food resources, but also in connection with the prevalence ofcontagious diseases (measles, diarrhoea); the rate of diarrhoeal diseaseswill be analysed in relation to water supply, etc.
. The instructor should emphasize the importance of drawing onanalogous situations that may be of assistance in making the rightdecisions. This underlines the need to preserve and make available the‘‘memory of humanitarian action.’’
. It is easier to match up a health problem with its causes in the context of asurveillance programme. However, cohort studies are rarely undertaken toestablish a formal association between a health problem and a risk factor.
. predictions of future developments. This is probably one of the most difficultthings to do in emergency situations. Decisions about taking measures andthe form such action should take must make allowance for possible changesin the situation. Thus, the malnutrition rate must be examined as a functionof potential harvests. Food distributions are not advisable if we know thatcrops are about to be harvested. The main stumbling block in taking a
HELP/SOS: EPIDEMIOLOGY416

decision is the development of the political situation. The duration of aconflict is impossible to foresee.
. obstacles to action. Analysing potential constraints is an important part ofdeciding how to act. Unsafe conditions sometimes necessitate recourse tomajor logistic resources (aeroplanes). Difficulties in gaining access to victimsalso make specific strategies necessary.
. feedback. People who have provided information should be informed of thedecisions taken on the basis of that information.
2. CATEGORY
Tool: knowledge of the basic principles involved in making decisions after anepidemiological study in an emergency situation.
3. FORMULATION
Identify the basic principles involved in making decisions after an epidemiolo-gical study in an emergency situation.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Interpretation of results: malnutrition rate
. Box 2: Implications of the choice of indicator in interpreting results:example of mortality rate
. Box 3: Decisions
. Box 4: Importance of reliable data
. Box 5: An epidemiological approach to situations of armed conflictimproves decision quality
. Box 6: Initial assessment: three-dimensional snapshot of the situation
EPIDEMIOLOGY 417

419
LINK WITH NEXT OBJECTIVES
This is the last objective dealing with epidemiological tools. The next objectiveswill cover the practical use of these tools in epidemiological programmes.
Mortality rate
Census
Specific morbidity rates
Access to food resources
Social environment
Political environment
Availability of food resources
Interpretation of the MALNUTRITION RATE
DECISION:• ACTION?• WHAT KIND OF ACTION?
Box 1
INTERPRETATION OF RESULTS
MALNUTRITION RATE
HELP/SOS: EPIDEMIOLOGY4418

• Rate of immunization coverage
• Water supply
• Access to food
• Monitoring the political situation
• Systematic census
Causes of death:• measles• meningitis• diarrhoea• malaria• malnutrition
Causes of variations in total number of children ≤ 1 year:• displacement• influx of refugees• more accurate count
Rate of infant mortality
Interpretationof results
Number of deaths among children≤ 1 year
Number of children aged ≤ 1 year
=
DE
CIS
ION
S
Box 2
IMPLICATIONS OF THE CHOICEOF INDICATOR IN INTERPRETING RESULTS
EXAMPLE OF MORTALITY RATE
Initiate a programme
Modify a programme
Terminate a programme
Do nothing
DECISIONS
FEEDBACK sources of information
EVERY ASSESSMENT MUST BE
FOLLOWED BY A DECISION
Box 3
DECISIONS
EPIDEMIOLOGY 419

421
In conflict situations, the reliability of data collected is uncertain because of:• the disorganization of the main sources of information (hospitals, displaced populations)• the deterioration of local administration systems• occasionally systematic disinformation.
The decisions that must be taken are often risky decisions concerning the possibility of implementing programmes, and are therefore also risky in terms of the desired results.
DATA OFDUBIOUSRELIABILITY
DECISIONS OFDUBIOUSRELIABILITY
Box 4
IMPORTANCE OF RELIABLE DATA
Box 5
AN EPIDEMIOLOGICAL APPROACHTO SITUATIONS OF ARMED CONFLICT
IMPROVES DECISION QUALITY
1. A quantitative and qualitativeapproach to health problems,permitting the establishment ofclear priorities.
2. An analytical approach to healthproblems, which permitsidentification of their causesand thereby facilitates theimplementation of a preventiveapproach.
3. A constant analysis of healthproblems, which makes it pos-sible to monitor their develop-ment and to measure the effectsof humanitarian action.
4. A systematic epidemiologicalapproach to armed conflictsituations, establishing a basisfor comparative analysis andconclusions of a general nature.
HELP/SOS: EPIDEMIOLOGY420

VICTIMS
Environment:• political• geographical • health• economic
• victims’ health status• capacity of local services
Potential developmentof the situation towards:
Causes of thevictims’ situation:
DECISION:IS OUTSIDE ACTION NECESSARY?
Current situation:
• stabilization• aggravation
• immediate causes• remote causes
Box 6
INITIAL ASSESSMENT:THREE-DIMENSIONAL SNAPSHOT
OF THE SITUATION
EPIDEMIOLOGY 4421

423
SETTING UP AN EPIDEMIOLOGICALSURVEILLANCE SYSTEMIN A GIVEN SITUATION
1. DESCRIPTION
A surveillance system involves routine collection of data in order to evaluatetrends. Several factors must be considered:
. choosing indicators on the basis of their relevance to the operation’sobjectives. These objectives may concern health problems or the functioningof health services. The coordinator of the course should insist from the outsetthat each work group keep its transparencies, particularly the ones listing theobjectives for each module established during the simulation exercise. Thiswill be a source for choosing indicators. For each indicator, participants willneed to identify the variables that will subsequently be used to interpret it.The overall outline of the activities planned in the simulation will assist in thisidentification. Finally, participants can also refer to standard lists found inbooks.
. selecting sources for collecting indicators. The participants must identifythese sources and analyse their reliability and relevance to the indicatorsought.
. establishing data collection methods. The method may involve distributingforms to health facilities to collect data on morbidity, or carrying outrepeated anthropometric surveys among the population. Participants mustdesign questionnaires and protocols for such surveys (when should variablesbe measured, what size should the sample be, what anthropometricmeasurement should be used, what age bracket examined, etc.).
. centralization of data. Who collects the questionnaires, and where are theysent? Who coordinates the data from repeated assessments? Who organizesthe data, in what form, for what purpose, and for whom?
. statistical analysis. Who does it?
. data interpretation. Who does it?
. decision-making. Who will be given the data for decision-making purposes?
. feedback. How will the decisions taken be communicated to the people whoinitially furnished the information?
HELP/SOS: EPIDEMIOLOGY422

Participantsmust define a structure permitting the flow of data from its source tothe decision-makers and back to those who furnished information. They mustalso provide practical details concerning the way this structure works for eachstage.
2. CATEGORY
Practice: designing an epidemiological surveillance system for the Awalei campin the Alphaland-Betaland simulation.
3. FORMULATION
Construct an epidemiological surveillance system for the Awalei camp in theAlphaland-Betaland simulation. You will need the list of objectives you havemade for the various modules studied so far, which will help you choose theindicators for your surveillance system. Do not forget to identify the variablesthat will allow you to interpret the variations in the indicators you have chosen.You must define a structure that will permit the flow of information from itssources to the decision-makers. At each stage, describe the resources youwill use:questionnaires, personnel, computer equipment.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 120 minutes
. 60 minutes for work in groups
. 60 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Epidemiological surveillance
. Box 2: Choosing indicators for epidemiological surveillance
LINK WITH NEXT OBJECTIVES
A surveillance system is also designed to detect epidemics. The issues involved incoping with an epidemic will be studied in the next objectives.
EPIDEMIOLOGY 423

425
Routine surveillance of a certain number of indicators as a way of monitoring the
situation and programmes
Planning an epidemiological surveillance system involves:
• Choosing indicators • Selecting indicator sources • Establishing methods for
collecting indicators • Formulating results • Analysing results • Distributing results • Making decisions based on results
TIME
Box 1
EPIDEMIOLOGICAL SURVEILLANCE
HELP/SOS: EPIDEMIOLOGY4424

Box 2
CHOOSING INDICATORSFOR EPIDEMIOLOGICAL SURVEILLANCE
Three kinds of factors must be considered in the choiceof indicators:
1. Technical factors
. Indicator relevance: What is being measured?Programme functioning, health status, etc.
. Reliability of information sources
. Possibility of systematic data collection
2. Coordination
. Link with the indicators specified at the timeof the initial assessment
. Link with operational objectives
. Standardization of indicators collected by differentpeople or groups involved in the humanitarianoperation
3. Political factors
. Are the information sources at liberty to furnish thenecessary data?
. Is regular access guaranteed?
EPIDEMIOLOGY 425

427
STRATEGY FOR COPINGWITH AN EPIDEMIC
1. DESCRIPTION
An epidemic is defined as an abnormal increase in the number of cases of adisease in a given region. The alarm signal may be spontaneous testimony fromthe population itself, a warning from the health services, or rumours of indefiniteorigin.Whatever the source, at that signal three kinds of action will be necessary:
. Epidemiological action.
. Confirm the rumours and establish a diagnosis. A few fever-relateddeaths are not enough to decide that meningitis was the cause, nor are thedeaths of adults as a result of diarrhoea sufficient to conclude that cholerahas struck. Certainly these symptoms will give the diagnostic process adirection, but any diagnosis must be confirmed by both an examinationof the suspected cases and microbiological analysis—of cerebrospinalfluid, to detect meningococci, or the stools, to detect vibrios, etc.
. Once a diagnosis has beenmade, confirm that an actual epidemic is underway—that is, establish that the number of cases is greater than usual. Thiswill require the implementation of an active screening system.
. Note the characteristics of the people with the disease (distribution of thedisease by population sector).
. Establish an epidemiological incidence curve, noting all the cases on ahistogram by days or weeks (to show distribution over time).
. Pinpoint all the cases on a map (distribution in space).
. Identify the source of the epidemic. This can be done with the help ofpreviously collected data that show a first group of cases in a specificplace (for example, cases of cholera associated with a particular watersupply point or foodmarket). If a cross-sectional study is not adequate, itmay be necessary to carry out a case control study to determine the sourceof the epidemic.
. Track the spread of the epidemic by noting cases on a map as they aredetected.
. Set up a reporting system.
. Therapeutic action. After a diagnosis has been made, it is necessary to:
. decidewhat treatment is appropriate. Itmay be necessary to perform testsof antibiotic resistance, for example, in shigellosis epidemics. One
HELP/SOS: EPIDEMIOLOGY426

epidemic may involve several hundred cases, so an effective treatmentshould be found quickly.
. determine a treatment regimen on the basis of previous tests of potentialdrug resistances, and define a standard clinical picture; every casepresenting this picture will be treated. When cases are very numerous, it isoften impossible to performmicrobiological tests for each one individually.
. supply material resources (drugs, infusions, etc.) to health facilities.
. ensure that the treatment regimens are applied by the health services.
. seek out cases and provide early treatment (this reduces mortalityconsiderably), and make sure that health services are accessible to allsectors of the population.
. set up a reporting system in the health facilities.
. therapeutic action is important not only for the patients who receive care,but also for the rest of the population, who, seeing that those sufferingfrom the disease are looked after, will be more willing to accept thepreventive measures proposed to control the epidemic.
. Preventive action.
. environmental sanitation measures (cholera).
. immunization (meningococcal meningitis).
. health education (cholera).
2. CATEGORY
Tool: identifying the main stages of investigating an epidemic.
3. FORMULATION
Describe the main stages of investigating an epidemic.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 40 minutes
. 20 minutes for work in groups
. 20 minutes for summary in plenary session.
EPIDEMIOLOGY 427

429
6. RECAPITULATION
. Box 1: Managing an epidemic
. Box 2: Investigating an epidemic: identifying the disease
. Box 3: Investigating an epidemic: defining a ‘‘typical’’ case
. Box 4: Defining a ‘‘typical’’ case: sensitivity and specificity
. Box 5: Investigating an epidemic: confirming the epidemic
. Box 6: Investigation of an epidemic: surveillance system
LINK WITH NEXT OBJECTIVES
The tools necessary to implement therapeutic and preventive action have alreadybeen amply studied in the module on communicable diseases and the module onmedical care (treatment protocols). The next objective will focus on theepidemiological aspect, using a cholera epidemic as an example.
Box 1
MANAGING AN EPIDEMIC
. Confirm the rumours: identify the disease involved(laboratory)
. Define a ‘‘typical’’ case (clinical symptoms)
. Confirm the epidemic
. Set up a surveillance system
. Decide on control measures and implement them:
. treatment
. preventive measures
. Maintain open dilogue with the political authoritiesand the media
HELP/SOS: EPIDEMIOLOGY428

Box 2
INVESTIGATING AN EPIDEMIC
IDENTIFYING THE DISEASE
Clinical diagnosis
+
Laboratory confirmation
Box 3
INVESTIGATING AN EPIDEMIC:
DEFINING A ‘‘TYPICAL’’ CASE
1. Establish with certainty theexistence of cases of commu-nicable diseases, for example,meningitis, cholera, andmeasles.
Rumours should not be a basisfor instituting a whole set ofemergencymeasures, and bacteriologicalconfirmation should beobtained for diseases suchas meningitis and cholera.
2. Establish the link between dulydocumented cases and thebeginning of an epidemic.There may be a number ofsporadic cases but no confir-mation of an epidemic.
3. Once the cases have beendocumented and their epi-demic character confirmed,subsequent cases will be diag-nosed and treated solely on thebasis of clinical criteria.
EPIDEMIOLOGY 429

431
Clinical criterion defining a case of cholera as profuse watery diarrhoea
Sensitivity 94%Specificity 40%
confirming the diagnosis
70 30
5 20
+
+
–
–
BACTERIOLOGICAL TEST
CLINICAL TEST
Box 4
DEFINING A ‘‘TYPICAL’’ CASE:SENSITIVITY AND SPECIFICITY
RATE OF ATTACK: Proportion of the population developing the disease during a given period of time
No. of cases
Time(Weeks)
50 -
40 -
30 -
20 -
10 -
1 2 3 4 5 6 7
- - - - - - -
EPIDEMIC CURVE
Box 5
INVESTIGATING AN EPIDEMIC:CONFIRMING THE EPIDEMIC
HELP/SOS: EPIDEMIOLOGY430

Box 6
INVESTIGATIONOF AN EPIDEMIC
SURVEILLANCE SYSTEM
. Record details of all cases: age, sex, onsetof disease, place where the disease has beennoted, etc.
. Monitor treatment and progress of thedisease:
. duration
. mortality
. Formulate data:
. tables
. graphs
. maps
. Interpret the data
. Publications
EPIDEMIOLOGY 431

433
CONTROLLING A CHOLERA EPIDEMIC
1. DESCRIPTION
The purpose of this objective is to:
. prove there actually is a cholera epidemic
. confirm the cases (examination of stools to confirm presence of vibrios)
. confirm the epidemic
. identify the source of the epidemic (case-control study)
. propose treatment regimens
. propose preventive measures
. environmental sanitation
. health education
. state the arguments against immunization and population quarantine
. set up a surveillance system.
2. CATEGORY
Practice: planning measures to control a cholera epidemic.
3. FORMULATION
Plan measures for controlling cholera, using the Alphaland-Betaland simulationas an example.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 60 minutes
. 30 minutes for work in groups
. 30 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Investigating an epidemic
HELP/SOS: EPIDEMIOLOGY432

LINK WITH NEXT OBJECTIVES
The module on epidemiology has provided an opportunity to review severalaspects of a health care system. Monitoring indicators have been selected in allthe modules studied thus far. This objective ends the module on epidemiology.
EPIDEMIOLOGICAL ASPECT
• Confirm the case or cases• Confirm the epidemic• Identify the source of the epidemic• Establish criteria for diagnosing
cases• Monitor the development of the
epidemic
THERAPEUTIC ASPECT
• Define an effective standard treatment• Treat cases• Follow up cases
PREVENTIVE ASPECT
• Identify measures to prevent transmission of the disease• Implement those measures
RUMOURSCASES
Box 1
INVESTIGATING AN EPIDEMIC
EPIDEMIOLOGY 4433

FROM EMERGENCIESTO DEVELOPMENT
MODULE
8

437
LIST OF OBJECTIVES
. Define a conceptual outline of development
. Define the various kinds of vulnerability
. Identify the main types of capacities within a community that can be used as aspringboard for development
. Show that in drought conditions malnutrition is the result of a complexinteraction involving vulnerability on different levels
. Identify both specifically emergency-oriented measures and measures thatpermit progress towards self-sufficiency in the medium term
. Describe the transition from an emergency situation to development after anatural disaster
. Identify emergency and development activities undertaken as an armed conflictwinds down.
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT436
THE CONCEPT OF DEVELOPMENT
1. DESCRIPTION
It is probably presumptuous to try to define what development is. The instructorshould prepare a conceptual outline of development that will provide a basis forvarious interpretations.
The instructor might begin with the idea that every society changes with time andaccording to modifications of its environment. This is the result of constantinteractions between the political, economic, social, and cultural systems thatmake up society. Changes may be rapid or imperceptible. The economic sector isoften considered a key element, since without economic growth, no developmentis possible.However, if the resources generated by economic growth are not fairlydistributed, social divisions increase between the wealthy and the most destitute.A balance must be found between ultra-liberalism and systematic planning. Thesocial sectormust rely on the economy if it is to develop. Free access to health careandeducationdoesnotmean that these servicesdonothaveacost.Abalancemustbe foundbetween the shareof the economic sector’s income that is redistributed inthe social sector, and the share that is reinvested in the economic sector. Theecological sectorhas a strong influenceon thedevelopmentof the economic sectorand, in some respects, on the social sector. The political sector may range fromdictatorship to themost complete anarchy.Democracy constitutes a compromisebetween these two extremes.
A society’s level of development is the result of the interactions between its ownsystems, within which all the members of the society have their proper place.However, another dimension must be added to these interactions between thesystems of a society. The economic sectors of different countries are linkedthrough international trade, just as the explosion of the communication mediahas influenced the cultural sectors. There is also a trend towards democratizationin the political sectors. Thus, development within a society is not only theconsequence of the balance between the society’s own systems; it also depends onthat society’s interactions with international systems (globalization). Thedevelopment process is a dynamic concept that is constantly changing.Development can thus be defined as a certain population’s opportunity to selectthe economic, social, cultural, and political options that suit it and that respectthe rights of every individual. Development is based on respect for human rights,meaning that for a given population there should be a reasonable equilibriumbetween collective rights and individual rights.
FROM EMERGENCIES TO DEVELOPMENT 437

439
An equilibrium is impermanent by definition, and development can beconsidered as a house of cards that will be shaken, damaged, or destroyed bythe aggressions of wars and natural disasters. Earthquakes and floods will havean impact on the economic system in particular. War has the lamentabledistinction of attacking virtually all systems, injuring or destroying the economicsector, social structures, the social fabric, and the political system. War is theantithesis of development.
War, like natural disasters, strikes at the most vulnerable people and the mostfragile elements of social systems first. This idea can be translated into a simpleformula stating that aggressions of all kinds (wars or natural phenomena) willfocus on vulnerable points and exercise an impact on populations, systems, andthe interactions between these systems. The impact may be minimal orcatastrophic.
On the basis of this formula, different possible types of action can be defined:
. prevention of ecological phenomena (drought)
. prediction of earthquakes and volcanic eruptions
. reduction of vulnerability (minimization of impact)
. preparation of a disaster response
. rehabilitation
. reconstruction.
The link between humanitarian action and development depends on the strategyfollowed for rehabilitation and reconstruction. In fact, the possibilities fordevelopment—that is, for making systems better suited to withstand harmfulphenomena and more in tune with the demands of the population—will be moreeasily accepted and effective if they are based on existing capabilities.
In conclusion, the instructor must emphasize the fact that the goal is not to give aprecise definition of ‘‘development,’’ but to come up with a conceptualframework in which each individual can find his or her own definition. Thisoutline will provide the basis for a simple formula integrating forms ofvulnerability and the impact of harmful phenomena on society, as well assuggesting possible types of action.
This module will use the example of natural disasters for a general study of thelink with development. However, the tools developed in this module, particularlythe definition of various kinds of vulnerability and their implications, areperfectly applicable to situations of armed conflict.
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT438

2. CATEGORY
Framework: defining a conceptual outline of development.
3. FORMULATION
What does the word ‘‘development’’ mean to you?
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for plenary session.
6. RECAPITULATION
. Box 1: Development: (concept 1)
. Box 2: Development: (concept 2)
LINK WITH NEXT OBJECTIVES
Using this outline, participants will have to define and identify the different kindsof vulnerability at which natural disasters will strike.
FROM EMERGENCIES TO DEVELOPMENT 439

441
Political institutions
Economic sector Socio-cultural sector
Populations
DICTATORSHIP ANARCHY
PLANNEDECONOMY
ULTRA-LIBERALISM
NATIONALIZEDPRIVATIZED
Box 1
DEVELOPMENT
(CONCEPT 1)
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT4440

Political institutions
Economic sector Sociocultural sector
Populations
International environment
Ecological and geographicenvironment
Box 2
DEVELOPMENT
(CONCEPT 2)
FROM EMERGENCIES TO DEVELOPMENT 4441

443
VULNERABILITY
1. DESCRIPTION
Vulnerability is part of the overall conceptual outline of development:
. Population groups such as children and the elderly are traditionally consideredas vulnerable groups.We shouldalso includebroader social sectors that quicklybecome destitute in times of crisis—groups that have no financial or foodreserves tohelp themcopewithacrisis thatdeprives themof theirusualmeansofsubsistence. In such a crisis, the social fabric is rewoven or destroyed.
. Economic systems are more or less vulnerable to natural disasters. Systemsbased on a rural economy depend on climatic conditions, types ofproduction, and the national and international environment to guaranteepeasants the resources they need for subsistence. Urban economic systemsare more sophisticated and therefore more vulnerable to such misfortunes asa breakdown of communication lines, a deteriorating economic system, etc.
. Social systems are vulnerable in crises. Not only may social infrastructures(hospitals, schools, etc.) be destroyed by earthquakes, floods, volcaniceruptions, etc., but social programmes are sometimes halted during crises forlack of financial means or human resources.
. Political systems themselves are sometimes challenged—for example, afterepisodes of famine following drought.
. The ecological environment is also vulnerable; erosion and deforestation areoften the beginning of a deficit in agricultural production.
A crisis will attack populations and systems at all their vulnerable points,eventually triggering a disaster.
2. CATEGORY
Tool: defining the different kinds of vulnerability.
3. FORMULATION
Using the conceptual outline of development already defined, explain thedifferent kinds of vulnerability and provide examples.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT442

5. DURATION
Total duration: 30 minutes
. 15 minutes for group work
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Examples of vulnerability.
LINK WITH NEXT OBJECTIVES
The next section will show how these different kinds of vulnerability interact,resulting in a human disaster that requires humanitarian action.
FROM EMERGENCIES TO DEVELOPMENT 443

445
INTERNATIONAL ENVIRONMENT
ECOLOGICALENVIRONMENT
POLITICAL INSTITUTIONS
ECONOMIC SECTOR
SOCIOCULTURALSECTOR
POPULATION
• Economic recession• Globalization
• Skewed distribution of political power
• Subjugation of judicial power
• Vulnerable groups: the elderly, pregnant women, the unemployed, etc.
• Urban/rural populations• Overpopulation• Monoculture• Mechanized agriculture
• Dysfunction• Non-earthquake-proof
building• Corruption• Drought, pollution
Box 1
EXAMPLESOF VULNERABILITY
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT4444

THE INTERACTION BETWEENDIFFERENT KINDSOF VULNERABILITY
1. DESCRIPTION
The aforementioned assaults on vulnerability occur in a logical series. Theinstructor will use the example of drought to show how such a series of disastersmay occur:
. ecological disaster: lack of rain and no retention of water (erosion,deforestation)
. agricultural disaster: drop in agricultural production
. food disaster: reduced availability of food resources
. social disaster: restricted access to food resources for the most vulnerablesocial groups, and migration of these groups to urban centres
. individual disaster: physical harm to individuals, especially those mostvulnerable (children) who are victims of malnutrition.
This approach links the various kinds of vulnerability, and effectively shows thedanger of taking measures only to deal with the ultimate consequences of adisaster, in this case malnutrition, without taking into account that disaster’sunderlying causes.
The link between humanitarian operations and development activities should bepointed out in this context, notably the connection between handling theconsequences of a disaster and concurrently planning activities that will reducevulnerability. The prevention of recurrent episodes of malnutrition will involveaction in the ecological, economic, and social systems.
Humanitarian disasters spotlight vulnerable areas, permitting the identificationof those spheres in which development efforts must be made to prevent futuredisasters.
2. CATEGORY
Tool: showing that malnutrition is the result of a chain reaction in which droughtworks against vulnerability at various levels.
FROM EMERGENCIES TO DEVELOPMENT 445

447
3. FORMULATION
Taking the example of a drought, show how it can lead to a nutritional disaster,describing the interaction of the various kinds of assaults against vulnerability atdifferent levels.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Spiral of disasters
LINK WITH NEXT OBJECTIVES
The areas of vulnerability revealed during a crisis allows us to pinpoint systemicweaknesses. In reducing those weaknesses, the essential focus must be on localcapabilities.
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT446

Ecological disaster
Agricultural disaster
Food disaster
Social disaster
Nutritional disaster
Human disaster
Box 1
SPIRAL OF DISASTERS
FROM EMERGENCIES TO DEVELOPMENT 447

449
THE CONCEPT OF CAPACITY
1. DESCRIPTION
Reducing vulnerability in order to prevent new crises is a step towardsdevelopment. This step involves creating the conditions for a new equilibriumbetween the systems and populations concerned. Development activities mustfocus on the development of people, and should be planned and implemented bythe population itself. To this end, development should be based on the capacitiesalready existing within a community. These capacities may be:
. at the social level—strong social structure, high level of professional training(for example, in the health field)
. at the economic level—efficient economic infrastructure (communications,industrial network, etc.), diversified agriculture
. at the political level—structured political system able to define and upholdsocial and economic policies by democratic means
. at the ecological level—high natural resource potential
. at the cultural level—strong sense of identification with the cultural milieu,translating into shared views on development models.
By relying on local capacities and maintaining a sustained presence, reliefagencies will be able to effect a transition from emergency and rehabilitationactivities to activities that form part of a development process.
2. CATEGORY
Tool: identifying the main kinds of capacities within a community that couldprovide the basis for initiating a development process.
3. FORMULATION
Identify the main kinds of capacities based on the conceptual outline ofdevelopment.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT448

5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Capacities
. Box 2: Breaking the chain of vulnerability by building on local capacities
. Box 3: Modification and reinforcement of capacities: progress towardsdevelopment
LINK WITH NEXT OBJECTIVES
Reducing vulnerability by building on local capacities is the basis for anydevelopment process. In emergency situations, however, relief agencies oftensettle for implementing measures with immediate effects but no long-termimpact.
FROM EMERGENCIES TO DEVELOPMENT 449

451
INTERNATIONAL ENVIRONMENT
POLITICAL INSTITUTIONS
ECONOMIC SECTOR
SOCIOCULTURAL SECTOR
POPULATIONS
• Solidarity• Awareness of the universality
of certain problems
• Structured state• Ability to effect change
• Level of education• Professional training
• Communication network• Diversified economy• Import-export balance
• Strong social structure• Media support
Box 1
CAPACITIES
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT4450
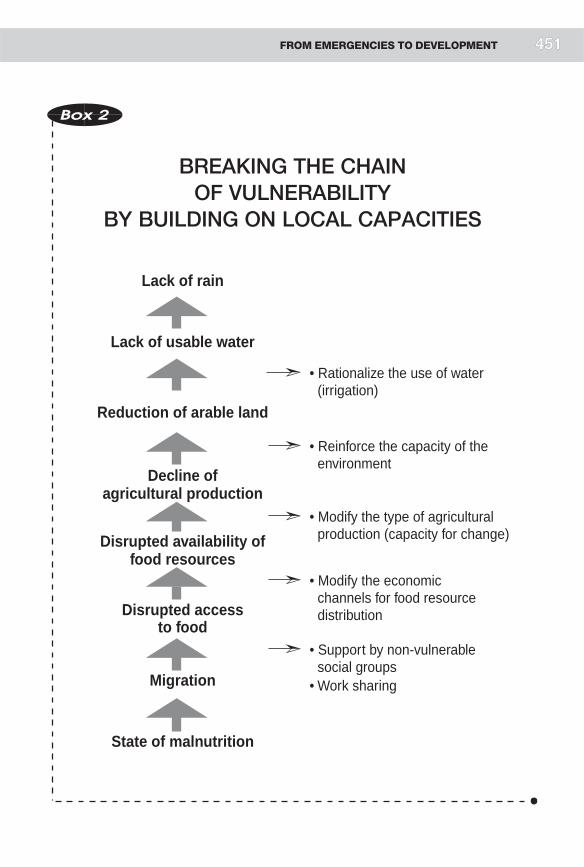
Lack of rain
Lack of usable water
Reduction of arable land
Decline ofagricultural production
Disrupted availability offood resources
Disrupted accessto food
Migration
State of malnutrition
• Rationalize the use of water (irrigation)
• Reinforce the capacity of the environment
• Modify the type of agricultural production (capacity for change)
• Modify the economicchannels for food resource distribution
• Support by non-vulnerable social groups
• Work sharing
Box 2
BREAKING THE CHAINOF VULNERABILITY
BY BUILDING ON LOCAL CAPACITIES
FROM EMERGENCIES TO DEVELOPMENT 4451

453
Political institutions
Economic sector Sociocultural sector
Populations
The reinforcement of capacities creates a new dynamic, with a new equilibrium.
Box 3
MODIFICATION AND REINFORCEMENTOF CAPACITIES:
PROGRESS TOWARDS DEVELOPMENT
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT4452

TRANSITION FROM ANEMERGENCY-ENGENDERED ARTIFICIALHEALTH CARE SYSTEM TO ASELF-SUFFICIENT HEALTH CARE SYSTEM
1. DESCRIPTION
During crises, it is easy to create a totally artificial health care system. Fooddistributions take the place of local production, the admission of physiologicallyvulnerable people to supplementary feeding centres takes responsibility awayfrom the family, mass immunization campaigns as needed take the place of anexpanded programme of immunization, temporary shelter (tents) takes the placeof permanent homes, essential drugs are widely distributed, medical services arefree, local personnel is recruited at high cost from local facilities nearby, andhospital care is provided by aid workers from abroad.
The development of this type of health care system into one which can stand onits own will be easier if from the outset relief agencies consider possiblealternatives to replace these specifically emergency-oriented measures—forexample, rehabilitation of agricultural activity, support for local compensatorymechanisms, development of income-generating activities, training of localpersonnel, and establishment of self-managed pharmacies. This assumes that thehumanitarian agencies have identified local capacities and are willing to furnishadequate support long enough to guarantee the transition towards localmanagement of the health care system.
2. CATEGORY
Tool: identifying both the measures specifically oriented towards resolving theemergency and those permitting a transition to self-sufficiency in themedium term.
3. FORMULATION
Using the conceptual outline of a health care system, identify both emergency-oriented measures and measures permitting a transition to self-sufficiency in themedium term.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
FROM EMERGENCIES TO DEVELOPMENT 453

455
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Health care system—development
LINK WITH NEXT OBJECTIVES
These tools will permit the participants to plan the transition from emergencymeasures to development activities in two practical examples.
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT454

Box 1
HEALTH CARE SYSTEM
DEVELOPMENT
Foodand
Nutrition
WaterSupply
Environ-mental
Sanitation
Control ofCommunicable
Diseases
Medical-SurgicalCare
Managementof WarInjuries
Psycho-logicalSupport
Agricultural
production
Sources Human-
waste
management
Primary
prevention
(immunization)
Primary-
level
medicalcare
First aid Psychosocial
support for
individualsand families
Economic
system
Storage Garbage
management
Secondary
prevention
Secondary
level medicalcare
Secondary
level care
Foodavailability
Distribution Energysources
Tertiaryprevention
Tertiarylevel
medical care
Evacuation andtransport
Psychosocialsupport at the
community
level
Accessibility
of food
resources
Water
consumption
Shelter Treatment of
communicable
diseases
Food
consumption
Water use Vector
control
Control of
epidemics
Transfer
between
levels
Tertiary
level
surgical care
Psychosocial
support at the
institutionallevel
Biologicalutilization
of food
Disposalof liquid
waste
Nutritionalstatus
POPULATION’S HEALTH
Using the above table, fill in examples of specific measures:
. for emergencies
. for long-term development
FROM EMERGENCIES TO DEVELOPMENT 455

457
FROM EMERGENCY TO DEVELOPMENTAFTER A NATURAL DISASTER
1. DESCRIPTION
The course participants will apply the tools they have acquired to two kinds ofnatural disaster: drought and volcanic eruption.
2. CATEGORY
Practice: planning the transition from emergency measures to developmentactivities after a volcanic eruption or a drought.
3. FORMULATION
Plan the transition from emergencymeasures to development activities, using theexample of a volcanic eruption or a drought.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session. Each groupmay choose one of the two practical exercises in the simulation.
5. DURATION
Total duration: 60 minutes
. 30 minutes for work in groups
. 30 minutes for summary in plenary session.
LINK WITH NEXT OBJECTIVES
The next objective is to study the transition from emergency to development insituations of armed conflict.
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT456

THE EMERGENCY DEVELOPMENTCONTINUUM AND SITUATIONSOF ARMED CONFLICT
1. DESCRIPTION
We have seen that the transition from emergency measures to developmentactivities, designed to reduce the areas of vulnerability identified during the crisis,is based on the use of local capacities. Unfortunately, however, in war situationsthe destruction of local capacities is often part of military strategy. Such strategymay include:
. destruction of agricultural potential through the use of land mines
. destruction of health care facilities
. population displacement
. threats to health care personnel, forcing them to leave the health carefacilities.
Thus, war destroys local capacities, which make the ‘‘continuum’’ harder toimplement. Human resources have fled, facilities have been destroyed, socialservices (notably education) no longer function, etc.
International humanitarian law is designed to protect the victims of armedconflict. Through the limits it imposes on the means of warfare, it also helpsprotect capacities more directly oriented towards rehabilitation, reconstruction,and development.
The identificationduringconflictsofbothcapacitiesandvulnerablepointsprovidesthe basis for a strategy oriented along three already defined axes:
. transfer of responsibility to the competent authorities
. support for local capacities
. replacement of local capacities.
The first two orientations eventually lead to a process of development.
2. CATEGORY
Framework: emergency and development activities in the wake of armed conflicts.
FROM EMERGENCIES TO DEVELOPMENT 457

3. FORMULATION
What are the constraints limiting a simultaneous approach to resolving theemergency and fostering development in situations of armed conflict?
4. TEACHING METHOD
Assignment presented to entire group.
5. DURATION
Total duration: 15 minutes.
LINK WITH NEXT OBJECTIVES
This objective has introduced the idea of continuity in emergency operations.This is the final aspect of the management of humanitarian action. The nextmodule will place it in the practical context of armed conflict.
HELP/SOS: FROM EMERGENCIES TO DEVELOPMENT458
PROTECTING THE VICTIMSOF ARMED CONFLICT
MODULE
9

461
LIST OF OBJECTIVES
. Define the concept of international humanitarian law
. Know the legal bases of international humanitarian law (the law of Geneva)
. Define the context for the application of international humanitarian law in thehealth sphere
. Introduce participants to the rules of international humanitarian lawconcerning the protection of health care systems and victims of armed conflict,as laid down in the Geneva Conventions
. Introduce participants to the rules of international humanitarian lawconcerning the protection of health care systems and victims of armed conflict,as laid down in the two Additional Protocols
. Know the components of the International Movement of the Red Cross andthe Red Crescent
. Understand the ICRC’s approach to obtaining access to victims of armedconflict
. Define what the emblem of the Red Cross and the Red Crescent represents
. Examine the approach taken by the ICRC on behalf of persons detained inarmed conflict
. Know the basic rules concerning protection of the wounded
. Know the basic principles concerning protection of refugees and displacedpeople
. Be familiar with the basic documents of human rights law
. Know the essential differences between international humanitarian law andhuman rights law
. Know some basic rules of the law of The Hague.
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT460

ARMED CONFLICT AND INTERNATIONALHUMANITARIAN LAW
1. DESCRIPTION
Armed conflicts do not occur unexpectedly. Beyond the immediate factors thattrigger them, analysis reveals other, deeper causes, such as territorial demands,socio-economic inequality, economic interests, the defence of political ideolo-gies, burgeoning nationalism, the struggles of ethnicminorities, racism, and armsproliferation. Dealing with these deeper causes is essentially a political matter,involving the promotion of development and human rights at the same time. Theresolution of armed conflicts is also a political affair, requiring the implementa-tion of diplomatic, economic, and military measures.
The instructor should mention the right to make war (jus ad bellum), andcomment on Chapter VII of the Unitied Nations Charter, as well as the role ofthe Security Council.
Alongwith efforts to achieve the political resolution of conflicts and to treat theircauses, steps must be taken tominimize the consequences of armed conflicts. Thedesire to limit the effects of war does not imply acceptance of the principle of war;it reflects, rather, a pragmatic approach based on the realization that despiteefforts to keep the peace, war exists.
International humanitarian law is a body of rules designed to limit the violence ofconflicts and protect the victims of those conflicts. It seeks to resolve thehumanitarian problems that arise duringwar (jus in bello). The effectiveness of itsapplication depends on the possibility of obtaining direct access to victims. Tothis end, strict neutrality is imperative; without that, the parties to conflicts willnot willingly allow humanitarian organizations access to victims. Accordingly,humanitarian organizations cannot take a stand in any conflict. Impartialitytowards victims is another essential principle of humanitarian relief. Finally,political non-alignment is a crucial condition in defining the priorities of anyhumanitarian action.
Course participants often have trouble understanding these two ideas:
. humanitarian action addresses the consequences of conflict
. the purpose of international humanitarian law is to limit the effects of war.
PROTECTING THE VICTIMS OF ARMED CONFLICT 461
463
Students tend to think international humanitarian law should play a role in theresolution of conflicts. Certainly, humanitarian action, by maintaining a marginof humanity in a conflict, may contribute to the restoration of peace; but its mainpurpose is to protect the victims of armed conflict. The instructor should explainat this point that the law of armed conflict has two branches:
. the law of war (law of The Hague), which comprises rules limiting the meansof conducting hostilities
. international humanitarian law (law of Geneva), which comprises rulesguaranteeing the protection of victims of armed conflict, as well as ruleslimiting the means of conducting hostilities.
2. CATEGORY
Framework: defining the concept of international humanitarian law.
3. FORMULATION
Define the concept of international humanitarian law.
4. TEACHING METHOD
Assignment presented to the entire class.
5. DURATION
Total duration: 15 minutes.
6. RECAPITULATION
. Box 1: Development of armed conflict in perspective
. Box 2: United Nations terminology
. Box 3: United Nations Charter: Chapter VII
. Box 4: Causes of armed conflict
. Box 5: Indications of impending armed conflict
. Box 6: Regional distribution of locations with at least one major armedconflict, 1989-98
. Box 7: Consequences of armed conflict (1)
. Box 8: Consequences of armed conflict (2)
. Box 9: Definition of international humanitarian law (1)
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT462

. Box 10: Definition of international humanitarian law (2)
. Box 11: Two lines of action for international humanitarian law
LINK WITH NEXT OBJECTIVES
The next objective will address the law of Geneva.
Peace
Crisis
Conflict
Peace
Reconstruction
Resolution
Box 1
DEVELOPMENT OF ARMED CONFLICTIN PERSPECTIVE
PROTECTING THE VICTIMS OF ARMED CONFLICT 4463

465
Box 2
UNITED NATIONS TERMINOLOGY
1. PEACE-MAKING
Process aimed at reconciling hostile parties, primarily by the
diplomatic means laid down in Chapter VI of the United Nations
Charter (peaceful resolution of conflicts).
2. PEACE-KEEPING
Involves establishing a neutral United Nations presence among
the belligerents or the parties to a conflict, with their consent, by
deploying UNpeace-keeping forces, military troops, police forces,
observers, or UN civilian personnel. Three principles are
essential: the consent of the parties, impartiality, and prohibition of
the use of force except in cases of self-defence.
3. PEACE ENFORCEMENT
Collective coercive action initiated by the Security Council under
the provisions of Chapter VII in order to end a threat to
international peace and security, a breach of the peace, or an act
of aggression. Means of military and non-military coercion include
economic sanctions (embargo), blockades, demonstrations of
force, and armed operations.
4. PEACE-BUILDING
A series of actions carried out in order to define and create the
conditions and support the structures necessary for consolidating
peace after a conflict. Its aims are to prevent a renewal of
hostilities and to eliminate any structural causes giving rise to
conflicts (economic and social factors).
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT464

Box 3
UNITED NATIONS CHARTER:CHAPTER VII
ARTICLE 39The Security Council shall determine the existence of any threat tothe peace, breach of the peace, or act of aggression and shall makerecommendations, or decide what measures shall be taken inaccordance with Articles 41 and 42, to maintain or restoreinternational peace and security.
ARTICLE 40In order to prevent an aggravation of the situation, the SecurityCouncil may, before making the recommendations or deciding uponthe measures provided for in Article 39, call upon the partiesconcerned to comply with such provisional measures as it deemsnecessary or desirable. Such provisional measures shall be withoutprejudice to the rights, claims, or position of the parties concerned.The Security Council shall duly take account of failure to comply withsuch provisional measures.
ARTICLE 41The Security Council may decide what measures not involving theuse of armed force are to be employed to give effect to its decisions,and it may call upon theMembers of the United Nations to apply suchmeasures. These may include complete or partial interruption ofeconomic relations and of rail, sea, air, postal, telegraphic, radio, andother means of communication, and the severance of diplomaticrelations.
ARTICLE 42Should the Security Council consider that measures provided for inArticle 41 would be inadequate or have proved to be inadequate, itmay take such action by air, sea, or land forces asmay be necessaryto maintain or restore international peace and security. Such actionmay include demonstrations, blockade, and other operations by air,sea, or land forces of Members of the United Nations.
PROTECTING THE VICTIMS OF ARMED CONFLICT 465

467
Box 4
CAUSES OF ARMED CONFLICT
IMMEDIATE CAUSES
. Socio-economicinequalities
. Territorial claims
. Collapse of statestructures
. Ethnic conflicts
. Tribal conflicts
. Political antagonism
. Human rights violations
. Other factors
LONG-TERM CAUSES
. Deterioration of the globalenvironment
. Competition for rawmaterials
. Competition for access towater
. Dissemination of a vio-lence-based culture
. Expansion of the arms trade
. Other factors
Box 5
INDICATIONS OF IMPENDINGARMED CONFLICT
. Proliferation of arms in thecountry
. Declaration of a state ofemergency
. Suppression of civil rights
. Freedom of assembly
. Freedom of the press
. Propaganda fomentingviolence and hatred(role of the media)
. Population migration
. Arbitrary arrests
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT466

Box 6
REGIONAL DISTRIBUTIONOF LOCATIONS WITH AT LEASTONE MAJOR ARMED CONFLICT,
1989-98
(AT LEAST 1000 BATTLE-RELATED DEATHS)
Region 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998
Africa 9 10 10 7 7 6 6 5 8 11
Asia 11 10 8 11 9 9 9 10 9 8
Central and
South 5 5 4 3 3 3 3 3 2 2
America
Europe 2 1 2 4 5 4 3 2 1 1
Middle East 5 5 5 4 4 5 4 4 4 4
Total 32 31 29 29 28 27 25 24 24 26
Source: Uppsala Conflict Data Project.
PROTECTING THE VICTIMS OF ARMED CONFLICT 467

469
• economic• health
Consequences ofarmed conflict for
combatants• prisoners • wounded
Consequences ofarmed conflict for
systems and civilianpopulations
Civilianpopulations
Systems
Box 7
CONSEQUENCES OF ARMED CONFLICT(1)
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT4468

Box 8
CONSEQUENCES OF ARMED CONFLICT(2)
CONSEQUENCES FOR VICTIMS
. Population displacement
. Injuries
. Harassment
. Famine
. Disappearances
. Summary trials
. Imprisonment
. Separation of families
. Ethnic cleansing
. Genocide
CONSEQUENCES FOR SYSTEMS
. Destruction of crops
. Destruction of hospitals
. Suppression of judiciary structures
. Deterioration of social structures
. Destruction of housing
PROTECTING THE VICTIMS OF ARMED CONFLICT 469

471
Box 9
DEFINITION OF INTERNATIONALHUMANITARIAN LAW (1)
International humanitarian law, also known as the law of armed conflictor the law of war, comprises the rules which, in times of armed conflict,seek to protect persons who are not or are no longer taking part in thehostilities, and to restrict the methods and means of warfare employed.
Source: ICRC, International Humanitarian Law: Answers to Your Questions
Box 10
DEFINITION OF INTERNATIONALHUMANITARIAN LAW (2)
International humanitarian law (IHL)has two separate branches:
. the law of Geneva, or humanitarian law proper, which isdesigned to safeguard military personnel who are not or nolonger taking part in the fighting and persons not activelyinvolved in hostilities, particularly civilians
. the law of The Hague or the law of war, which establishes therights and obligations of belligerents in the conduct of militaryoperations, and limits the means of harming the enemy.
Those two branches of IHL are not completely separate,however, because the effect of some rules of the law of TheHague is to protect victims of conflicts, while the effect of somerules of the law of Geneva is to limit the action that thebelligerents can take during hostilities. With the adoption of theAdditional Protocols of 1977, which combine both branches ofIHL, that distinction is now ofmerely historical and didactic value.
Source: ICRC, International Humanitarian Law: Answers to Your Questions
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT470

Party to theconflict
Party to the
conflict
Civilianpopulations
Prisoners
Detainees
Wounded
Protection and assistance for victims (1)
Limit the means of making war (2)
Box 11
TWO LINES OF ACTIONFOR INTERNATIONAL HUMANITARIAN LAW
PROTECTING THE VICTIMS OF ARMED CONFLICT 4471

473
THE LAW OF GENEVA
1. DESCRIPTION
The law of Geneva, or humanitarian law proper, is constituted by the fourGeneva Conventions of 1949 and their twoAdditional Protocols of 1977. Its roleis to protect the victims of armed conflict.
To explain the specific characteristics of each of the Conventions, the instructormay use a timeline as a frame of reference:
. the battle of Solferino, after which the wounded were left uncared for, led tothe original Geneva Convention of 1864 for the Amelioration of theCondition of the Wounded in Armies in the Field
. the battle of Lissa and the fate of shipwrecked combatants led to the SecondGeneva Convention (1899) for the Amelioration of the Condition ofWounded, Sick and Shipwrecked Members of Armed Forces at Sea
. World War I, and the many prisoners of war it generated, led to the ThirdGeneva Convention (1929) Relative to the Treatment of Prisoners of War
. World War II, with the many civilian victims it claimed, led to the FourthGeneva Convention (1949) Relative to the Protection of Civilian Persons inTime of War
. the need for better protection for victims of international armed conflict,particularly civilian populations, led to the adoption in 1977 of Protocol Iadditional to the Geneva Conventions
. the proliferation of non-international armed conflict claiming many victimsled to the adoption in 1977 of Protocol II additional to the GenevaConventions.
The instructor should mention the following points:
. international humanitarian law is one of the most developed branches ofpublic international law
. international humanitarian law includes some 600 articles for the protectionof the victims of armed conflict, and as many rules limiting the means of war
. international humanitarian law makes a distinction between internationalarmed conflicts, which are covered by the four Geneva Conventions andAdditional Protocol I, and non-international armed conflicts, which are
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT472

covered by Article 3 common to the Geneva Conventions and AdditionalProtocol II.
2. CATEGORY
Tool: knowledge of the legal bases of international humanitarian law (the law ofGeneva).
3. FORMULATION
What are the main categories of victims of armed conflict?
4. TEACHING METHOD
Assignment presented to the entire group.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: International humanitarian law: history
. Box 2: The Geneva Convention and their Additional Protocols: fields ofapplication
LINK WITH NEXT OBJECTIVES
The next objective addresses the application of international humanitarian law inthe health field.
PROTECTING THE VICTIMS OF ARMED CONFLICT 473

475
Box 1
INTERNATIONAL HUMANITARIAN LAW:HISTORY
. Battle of Solferino 1859
. First Geneva Convention 1864
. Battle of Lissa 1866
. Second Geneva
Convention 1899
. World War I 1914-1918
. Third Geneva
Convention 1929
. World War II 1939-1945
. Fourth Geneva
Convention 1949
. Revision of the
four Geneva
Conventions 1949
. The two Protocols
additional to the Geneva
Conventions 1977
Facts often precede laws.
Box 2
THE GENEVA CONVENTIONSAND THEIR ADDITIONAL PROTOCOLS:
FIELDS OF APPLICATION
INTERNATIONAL ARMED CONFLICTS
. Geneva Conventions
. Additional Protocol I
NON-INTERNATIONAL ARMED CONFLICTS
. Article 3 of the Geneva Conventions
. Additional Protocol II
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT474

THE APPLICATION OF INTERNATIONALHUMANITARIAN LAW IN THE HEALTH FIELD
1. DESCRIPTION
The purpose here is to define the framework for applying the rules ofinternational humanitarian law in the health sphere. The instructor shouldstrive in particular to incorporate the international humanitarian law moduleinto the general context of the course, and, to that end, may use the outline of thehealth care system as described previously as a frame of reference. Two aspects ofthe rules of international humanitarian law will be studied:
. the general protection of victims
. the protection of the health care system.
The general protection of victims involves, for example, protecting their lives,physical and mental integrity, human dignity, family integrity, freedom ofmovement, and right to a fair and regular trial. It consists in protecting peopleagainst disappearances, arbitrary arrest, torture, inhuman and degradingtreatment, harassment, forcible displacement, separation of families, forcibleenlistment of children in the armed forces, etc.
Protection of the health care system consists in protecting objects indispensableto survival, health care services (hospitals, public health services), and medicalpersonnel.
These two aspects are related. If the health care system is not protected, victimssoon suffer—for example, detainees languishing in an unsanitary environment.Another example is populations who are obliged to flee their homes becauseaccess to essentials such as water and food is barred to them.
2. CATEGORY
Framework: defining the context for applying international humanitarian law inthe health sphere.
3. FORMULATION
Define your conception of protecting the victims of armed conflicts, withparticular reference to the health field.
PROTECTING THE VICTIMS OF ARMED CONFLICT 475

477
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Application of international humanitarian law in the field of health:concept of protection
. Box 2: Protection of victims and health care systems in armed conflict
LINK WITH NEXT OBJECTIVES
The next objective will address the general protection of victims of armed conflictand the protection of health care systems based on the rules of the GenevaConventions.
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT476

Partyto the conflict
Partyto the
conflictVictims
Healthcare
system
Box 1
APPLICATION OF INTERNATIONALHUMANITARIAN LAW
IN THE FIELD OF HEALTH
CONCEPT OF PROTECTION
PROTECTING THE VICTIMS OF ARMED CONFLICT 4477

479
Box 2
PROTECTION OF VICTIMSAND HEALTH CARE SYSTEMS
IN ARMED CONFLICT
PROTECTION OF THE HEALTH CARE SYSTEM:EXAMPLES OF RULES
C. III, Art. 26 Feeding of POWs
C. III, Arts. 29-32 Hygiene and medical attention for POWs
C. IV, Art. 23 Consignments of food, medical supplies, and clothingfor civilian populations
C. IV, Art. 18 Protection of hospitals
P. I, Art. 71 Protection of personnel participating in relief actions
P. I, Art. 54 Protection of objects indispensable to the survival ofthe civilian population
P. I, Art. 55 Protection of the natural environment
P. II, Art. 11 Protection of medical units and transport
P. II, Art. 10 General protection of medical duties
P. II, Art. 14 Protection of objects indispensable to the survival ofthe civilian population
P. II, Art. 15 Protection of works and installations containingdangerous forces
PROTECTION OF VICTIMS: EXAMPLES OF RULESArt. 3 common to the four Geneva Conventions
P. II, Art. 13 Protection of the civilian population
P. II, Art. 7 Protection and care of the wounded, sick, andshipwrecked
P. I, Art. 51 Protection of the civilian population
P. II, Art. 4 Fundamental guarantees
P. II, Art. 5 Persons deprived of their liberty
Note: C = Convention, P = Protocol
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT478

BASIC RULES FOR THE PROTECTIONOF VICTIMS OF ARMED CONFLICTAND THEIR HEALTH CARE SYSTEMS:THE GENEVA CONVENTIONS
1. DESCRIPTION
First, the instructor will present examples of rules from the Geneva Conventionsto protect the victims of armed conflicts:
. wounded:
Article 3 common to the four Geneva Conventions
Article 7 (C I): non-renunciation of rights
Article 13 (C I): definition of protected persons
Article 15 (C I): search for casualties and their evacuation
. shipwrecked:
Article 3 common to the four Geneva Conventions
Article 7 (C II): non-renunciation of rights
Article 13 (C II): definition of protected persons
Article 18 (C II): search for casualties after an engagement
. prisoners of war:
Article 3 common to the four Geneva Conventions
Article 4 (C III): definition of prisoners of war
Article 7 (C III): non-renunciation of rights
Articles 12, 13, 14, 15, 16 (C III): general protection of prisoners of war
Article 18 (C III): property of prisoners
Article 20 (C III): conditions relating to the evacuation of prisoners
. civilian populations:
Article 3 common to the four Geneva Conventions
Article 4 (C IV): definition of protected persons
Article 8 (C IV): non-renunciation of rights
PROTECTING THE VICTIMS OF ARMED CONFLICT 479

481
The instructor will then use the same approach to identify the essential rules inthe Geneva Conventions for the protection of health care systems. The healthcare system must be considered in the broad sense, namely, in terms of food,sanitation, public health, and medical care.
. wounded:
Articles 19, 20, 21, 22, 23 (C I): protection ofmedical units and establishments
Article 24 (C I): protection of permanent medical personnel
. shipwrecked:
Article 22 (C II): protection of hospital ships
Article 23 (C II): protection of medical establishments ashore
Article 36 (C II): protection of the personnel of hospital ships
. prisoners:
Article 25 (C III): definition of housing conditions
Article 26 (C III): definition of food conditions
Article 29 (C III): hygiene measures
Article 30 (C III): medical attention
Article 33 (C III): rights and privileges of retained medical and religiouspersonnel
. civilian populations:
Article 18 (C IV): protection of hospitals
Article 20 (C IV): protection of hospital personnel
Article 55 (C IV): provision of supplies for the population in occupiedterritories
Article 91 (C IV): medical attention for internees
Many other examples might be used. It must be remembered that the aim is togive participants some awareness of the existence of international humanitarianlaw and the ways it is applied, not to make them experts in this field. Theinstructor should stress commonArticle 3, which sums up the general protectionafforded to victims of armed conflict.
2. CATEGORY
Tool: knowledge of the rules of international humanitarian law concerning theprotection of victims of armed conflicts and the health care systems on which
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT480
they depend, with particular reference to the rules laid down in the GenevaConventions.
3. FORMULATION
We are going to identify a number of rules of international humanitarian lawenunciated in the Geneva Conventions that guarantee the protection of victimsof armed conflicts and the health care systems on which they depend. In the nextsection we will do the same thing again, this time focusing on the rules ofinternational humanitarian law contained in the two Protocols additional to theGeneva Conventions.
4. TEACHING METHOD
Lecture.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Basic rules for the protection of victims of armed conflict, takenfrom the Geneva Conventions (the wounded)
. Box 2: Basic rules for the protection of health care systems, taken from theGeneva Conventions (health care systems for wounded)
. Box 3: Basic rules for the protection of health care systems, taken from theGeneva Conventions (health care systems for civilian populations)
. Box 4: Common Article 3: a miniature convention
LINK WITH NEXT OBJECTIVES
The next objective will use the same approach for the rules of the two Protocolsadditional to the Geneva Conventions.
PROTECTING THE VICTIMS OF ARMED CONFLICT 481

483
Box 1
BASIC RULES FOR THE PROTECTIONOF VICTIMS OF ARMED CONFLICT, TAKEN
FROM THE GENEVA CONVENTIONS
THE WOUNDED(examples of rules)
. Art. 3
. Art. 7 (C I) non-renunciation of rights
. Art. 13 (C I) definition of protected persons
. Art. 15 (C I) search for casualties and theirevacuation
PRISONERS OF WAR(examples of rules)
. Art. 3
. Art. 7 (C II) non-renunciation of rights
. Art. 13 (C II) definition of protected persons
. Art. 18 (C II) conditions relating to theevacuation of prisoners
CIVILIAN POPULATIONS
. Art. 3
. Art. 4 (C IV) definition of protected persons
. Art. 8 (C IV) non-renunciation of rights
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT482

Box 2
BASIC RULES FOR THE PROTECTIONOF HEALTH CARE SYSTEMS,
TAKEN FROM THEGENEVA CONVENTIONS
HEALTH CARE SYSTEMSFOR WOUNDED
. Art. 19 (C 1) protection of medical unitsand establishments
. Art. 24 (C I) protection of permanent medicalpersonnel
HEALTH CARE SYSTEMSFOR PRISONERS
. Art. 25 (C III) definition of housingconditions
. Art. 26 (C III) definition of food conditions
. Art. 29 (C III) hygiene measures
. Art. 30 (C III) medical attention
PROTECTING THE VICTIMS OF ARMED CONFLICT 483

485
Box 3
BASIC RULES FOR THE PROTECTION
OF HEALTH CARE SYSTEMS,
TAKEN FROM THE
GENEVA CONVENTIONS
HEALTH CARE SYSTEMS
FOR CIVILIAN POPULATIONS
. Art. 18 (C IV) protection of hospitals
. Art. 20 (C IV) protection of hospital
personnel
. Art. 55 (C IV) provision of supplies for the
population in occupied
territories
. Art. 91 (C IV) medical attention for
internees
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT484

Box 4
COMMON ARTICLE 3:A MINIATURE CONVENTION
In the case of armed conflict not of an international character occurring inthe territory of one of the High Contracting Parties, each Party to the conflictshall be bound to apply, as a minimum, the following provisions:
1. Persons taking no active part in the hostilities, including members ofarmed forces who have laid down their arms and those placed hors decombat by sickness, wounds, detention, or any other cause, shall in allcircumstances be treated humanely, without any adverse distinctionfounded on race, colour, religion or faith, sex, birth or wealth, or any othersimilar criteria.
To this end, the following acts are and shall remain prohibited at any timeand in any place whatsoever with respect to the above-mentioned persons:
a) violence to life and person, in particularmurder of all kinds,mutilation,cruel treatment and torture;
b) taking of hostages;
c) outrages upon personal dignity, in particular, humiliating anddegrading treatment;
d) the passing of sentences and the carrying out of executions withoutprevious judgement pronounced by a regularly constituted courtaffording all the judicial guarantees which are recognized asindispensable by civilized peoples.
2. The wounded and sick shall be collected and cared for.
An impartial humanitarian body, such as the International Committee of theRed Cross, may offer its services to the Parties to the conflict.
The Parties to the conflict should further endeavour to bring into force, bymeans of special agreements, all or part of the other provisions of thepresent Convention.
The application of the preceding provisions shall not affect the legal statusof the Parties to the conflict.
PROTECTING THE VICTIMS OF ARMED CONFLICT 485

487
BASIC RULES FOR THE PROTECTIONOF CIVILIAN POPULATIONSAND THEIR HEALTH CARE SYSTEMS:ADDITIONAL PROTOCOLS I AND II OF 1977
1. DESCRIPTION
This topic will be approached in the same way as the previous one, withparticipants being asked to look for the rules protecting victims and their healthcare systems in the two Additional Protocols. Since the course deals mainly withcivilian populations, study can be limited to this category of victims. Participantswill be expected to take the Geneva Convention articles identified in the previoussection and add to them others that they themselves select from the AdditionalProtocols—for example:
Protocol I:
Article 50: definition of civilians and civilian population
Article 51: protection of the civilian population
Article 54: protection of objects indispensable to the survival of the civilianpopulation
Article 55: protection of the natural environment.
Protocol II:
Article 4: fundamental guarantees
Article 13: protection of the civilian population
Article 14: protection of objects indispensable to the survival of the civilianpopulation
Article 17: prohibition of forced movement of civilians
Article 18: right to assistance.
At the end of this objective, participants should have a chart representing thevictims and the health care system, and featuring the principle articles ofinternational humanitarian law that guarantee the protection of the victims andthe various components of the health care system.
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT486

2. CATEGORY
Tool: knowledge of the main rules of international humanitarian law containedin the two Additional Protocols which guarantee the protection of civilianpopulations and health care systems.
3. FORMULATION
Using the outline of a health care system as a basis, identify the main rules ofinternational humanitarian law in the twoAdditional Protocols which guaranteethe protection of victims and their health care systems.
4. TEACHING METHOD
Assignment presented to work groups. Each groupwill have to identify andwritedown in the corresponding blank on the chart of the health care system thearticles it thinks would best provide protection.
5. DURATION
Total duration: 60 minutes
. 30 minutes for work in groups
. 30 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Basic rules for the protection of civilian populations and their healthcare systems: Additional Protocol I
. Box 2: Basic rules for the protection of civilian populations and their healthcare systems: Additional Protocol II
LINK WITH NEXT OBJECTIVES
There are rules to protect victims and their health care systems. In practice, it isnecessary to enforce these rules. The next objectives will cover modes of applyingthe rules of international humanitarian law.
PROTECTING THE VICTIMS OF ARMED CONFLICT 487

489
Box 1
BASIC RULES FOR THE PROTECTIONOF CIVILIAN POPULATIONS AND THEIR
HEALTH CARE SYSTEMS:ADDITIONAL PROTOCOL I
. Art. 50 definition of civilians and civilianpopulation
. Art. 51 protection of the civilian population
. Art. 54 protection of objects indispensable tothe survival of the civilian population
. Art. 55 protection of the natural environment
Box 2
BASIC RULES FOR THE PROTECTIONOF CIVILIAN POPULATIONS AND THEIR
HEALTH CARE SYSTEMS:ADDITIONAL PROTOCOL II
. Art. 4 fundamental guarantees
. Art. 13 protection of the civilian population
. Art. 14 protection of objects indispensable tothe survival of the civilian population
. Art. 17 prohibition of forced movement ofcivilians
. Art. 18 right to assistance
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT488

THE INTERNATIONAL RED CROSSAND RED CRESCENT MOVEMENT
1. DESCRIPTION
‘‘The International Committee of the Red Cross (ICRC) and the InternationalFederation of Red Cross and Red Crescent Societies form, together with theNational RedCross andRedCrescent Societies, the InternationalRedCross andRed Crescent Movement. These institutions meet in principle every four years,with representatives of the States party to the Geneva Conventions, at anInternational Conference of the Red Cross and Red Crescent.
The ICRC: The ICRC, an independent humanitarian institution, is the foundingbody of the Movement. Acting as a neutral intermediary in the event of armedconflict or disturbances, it seeks on its own initiative, or on the basis of theGeneva Conventions and the Protocols additional thereto, to protect and assistvictims of international or non-international armed conflict and those affectedby internal disturbances or tension.
The National Societies: In its own country, every National Society serves as anauxiliary to the public authorities in humanitarian matters. Its primary task is toback up army medical services in time of conflict. To do that, it has to prepareitself in peacetime. Furthermore, each National Society may carry out specificactivities in accordance with the Fundamental Principles (collection of blood,training of first-aid workers and nurses, running of dispensaries or hospitals, andproviding aid to the disabled, young people, the elderly, etc.).
The Federation: The International Federation of Red Cross and Red CrescentSocieties provides support for the humanitarian activities carried out by theNational Societies in behalf of vulnerable groups. By coordinating internationalrelief operations in disaster situations and encouraging development aid, itendeavours to prevent and alleviate human suffering.’’
Source: ICRC, Answers to Your Questions.
The instructor will emphasize the ICRC’s role within the International RedCross and Red Crescent Movement, particularly its responsibility for recogniz-ing new National Societies. Mention should also be made of the Statutes of theMovement, which specify the responsibilities of the different components of theMovement. The instructor will conclude with a brief summary of the Seville
PROTECTING THE VICTIMS OF ARMED CONFLICT 489

491
Agreement, which defines the respective roles of the ICRC, the Federation, andthe National Societies.
2. CATEGORY
Tool: familiarity with the components of the International Red Cross and RedCrescent Movement.
3. FORMULATION
What are the components of the International Red Cross and Red CrescentMovement?
4. TEACHING METHOD
Lecture.
5. DURATION
Total duration: 15 minutes.
6. RECAPITULATION
. Box 1: The International Conference of the Red Cross and Red Crescent
. Box 2: Fundamental principles of the International Red Cross and RedCrescent Movement
LINK WITH NEXT OBJECTIVES
This objective situates the ICRC within the International Red Cross and RedCrescentMovement, thus facilitating an understanding of its protective action insituations of armed conflict. That action will be the subject of the next objectives.
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT490

INTERNATIONAL
COMMITTEE
OF THE
RED CROSS
INTERNATIONALCONFERENCE
OF THERED CROSS
ANDRED CRESCENT
INTERNATIONAL
FEDERATION
OF RED CROSS
AND RED
CRESCENT
SOCIETIES
NATIONAL
RED CROSS
AND RED
CRESCENT
SOCIETIES
STATES
PARTY
TO THE
GENEVACONVENTIONS
Box 1
THE INTERNATIONAL CONFERENCEOF THE RED CROSS AND RED CRESCENT
Box 2
FUNDAMENTAL PRINCIPLESOF THE INTERNATIONAL RED CROSSAND RED CRESCENT MOVEMENT
. HUMANITY
. IMPARTIALITY
. NEUTRALITY
. INDEPENDENCE
. VOLUNTARYSERVICE
. UNITY
. UNIVERSALITY
PROTECTING THE VICTIMS OF ARMED CONFLICT 491
493
THE ICRC AND ACCESS TO THE VICTIMSOF ARMED CONFLICT
1. DESCRIPTION
The participants have seen that the rules of international humanitarian lawguarantee a general protection for the victims of armed conflicts. Moreparticularly, they have studied the rules applicable to the health field.
The States Parties undertake to respect and to ensure respect for the GenevaConventions (common Article 1). In practice, it is necessary to ascertain thatthese rules are indeed being respected by the parties to a conflict. Direct access tovictims is therefore essential. To obtain that access, the ICRC gives first priorityto negotiations with the parties to the conflict; its goal is to persuade them to giveICRC representatives unfettered access to victims in order to assess theirsituation and, if necessary, take appropriate measures on their behalf. The ICRCbases this activity on the right of initiative accorded it by the GenevaConventions, and on Protocol I (Art. 81, para. 1). In situations of non-international armed conflicts, the ICRC may offer its services under theprovisions of Article 3 common to the four Geneva Conventions.
The Geneva Conventions and their additional Protocols constitute theconventional basis for ICRC action. In situations where the violence does notreach the intensity of an armed conflict, the ICRC bases its action on the Statutesof the Movement, which grant it a right of humanitarian initiative. This is thestatutory basis for its action.
Negotiations are the strategy of choice for the ICRC. They are easier to conductif the parties have recognized international humanitarian law and its modes ofapplication before the outbreak of the conflict. The instructor should mentionhere the importance of disseminating international humanitarian law in times ofpeace, before a conflict arises. This educational effort is carried out not only inthe armed forces, but also among school children and students. Dissemination ofinternational humanitarian law among young people can be considered as adevelopment activity, the purpose being not only to prevent potential violence inconflicts, but also to help reduce violence generally.
Negotiations will be more likely to succeed if the parties to the conflict arealready familiar with the strategy employed by humanitarian agencies.Transparency concerning such agencies’ modus operandi in conflict situationsis essential. For example, the parties to the conflict know that the ICRC hasalways been discreet aboutwhat it sees in such situations, and this gives the ICRCbetter chances of gaining access to the victims.However, this policy should not beseen as an endorsement of the parties to the conflict, covering all their
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT492

infringements of international humanitarian law. In the event of seriousviolations, the ICRC reserves the right to appeal to international opinion.
The strategies used by humanitarian agencies will be reviewed in the session oncoordination; the purpose of the present section is primarily to illustrate theimportance of international humanitarian law as a basis for ICRC action.
2. CATEGORY
Tool: knowledge about the ICRC and the issue of access to victims of armedconflict
3. FORMULATION
What are the possible strategies for gaining access to victims of armed conflict?
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Access to victims of armed conflict
LINK WITH NEXT OBJECTIVES
Now that access has been negotiated, the next objective will focus on the RedCross emblem, in particular its protective role.
Box 1
ACCESS TO VICTIMS
OF ARMED CONFLICT
. CONVENTIONAL BASIS
. STATUTORY BASIS
. NEGOTIATIONS
. DISSEMINATION
PROTECTING THE VICTIMS OF ARMED CONFLICT 493

495
THE EMBLEMS OF THE RED CROSSAND THE RED CRESCENT
1. DESCRIPTION
The emblem of the Red Cross was adopted by the International Conference of1863 as the distinctive sign of societies bringing relief to wounded soldiers. In1876, theOttomanEmpire decided to use the red crescent instead of the red cross.
Two ideas are important to note with respect to the use of the emblem:
. protective use. This is the emblem’s essential significance. In times of conflict,the emblem is the visible manifestation of the protection accorded by theGeneva Conventions. It indicates to the combatants that the following areprotected by the Geneva Conventions and their Additional Protocols:
. people (National Society volunteers, medical personnel, ICRC delegates,etc.)
. medical units (hospitals, first-aid posts, etc.)
. means of transport.
In order tomaintain this protective function, it is essential that the emblem not beemployed for improper purposes (usurpation), let alone perfidious ones such as,for example, to protect vehicles used to transportmunitions or combatants. Suchabuses are considered war crimes.
When used for protective purposes, the emblem is usually large in dimension.
. indicative use. In times of peace, the emblem indicates that the person orobject bearing it has a connection with the International Red Cross and RedCrescent Movement. When used for such purposes, the emblem is small indimension.
2. CATEGORY
Tool: knowledge of the two fundamental roles of the Red Cross emblem.
3. FORMULATION
What does the Red Cross emblem represent to you?
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT494

4. TEACHING METHOD
Assignment presented to the entire group.
5. DURATION
Total duration: 15 minutes.
6. RECAPITULATION
. Box 1: Uses of the emblem
. Box 2: Uses in times of armed conflict
. Box 3: Misuse of the emblem
LINK WITH NEXT OBJECTIVES
The next objectives will cover some essential points concerning the protection ofcertain categories of victims.
Box 1
USES OF THE EMBLEM
PROTECTIVE USE OF THE EMBLEM
Protection accorded by the GenevaConventions
INDICATIVE USE OF THE EMBLEM
In both wartime and peacetime, shows that a person orobject is associated with the International RedCross andRed Crescent Movement.
PROTECTING THE VICTIMS OF ARMED CONFLICT 495

497
Box 2
USES IN TIMES OF ARMED CONFLICT
In times of armed conflict, the protective emblemmay be usedonly by:
. The medical services ofthe armed forces
. National Red Cross andRed Crescent Societies(under certain conditions)
. Civilian hospitals andother medical units
. Other voluntary reliefsocieties (undercertain conditions)
The ICRC is entitled to use the emblem at all times forboth protective and indicative purposes.
Box 3
MISUSE OF THE EMBLEM
. IMITATION
. USURPATION
. PERFIDY
. Misuse of the emblem as a protective device in time of warjeopardizes the entire protective system established byinternational humanitarian law.
. Misuse of the emblem as an indicative device undermines itssignificance in the eyes of the public and thus diminishes itsprotective power in wartime.
Source: ICRC, International Humanitarian Law: Answers to Your Questions
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT496

PROTECTION OF DETAINEESIN THE CONTEXT OF ARMED CONFLICT:THE ICRC’S APPROACH
1. DESCRIPTION
Detainees are at particular risk of suffering mistreatment or torture, disappear-ing, or not receiving the food they need. Their protection depends on the ICRC’shaving access to them in order to register them. This registration must not beconsidered as an administrative measure, but rather as a means of protection.Once detainees are registered, the ICRC can, in the course of subsequent visits,request to see the individuals it has recorded, thereby reducing the risk that theywill disappear. This supposes that the ICRC has negotiated with the authoritiesfor permission to make repeated visits, to see all the detainees, and to see all theplaces of detention. The ICRC also negotiates for the right to see detainees alone,without witnesses, so that the detainees will feel free to tell ICRC representativesabout their problems, whether allegations of mistreatment and torture, healthconcerns, or family troubles.
The ICRC sets four imperative conditions for its visits. Its delegates must beallowed to:
. visit all the detainees
. visit all places where detainees are held
. repeat visits to detainees
. interview detainees without witnesses.
Aid to detainees is based on the same general principles defined previously:
. evaluation of health problems and of the penitentiary system’s capacity tocope with them
. definition of a strategy of action—encouraging authorities to takeresponsibility, recommendations, support for the health care system,replacement of the health care system.
The ICRC’s mandate is to protect and assist persons detained for politicalreasons. To that end, the ICRC always seeks to obtain direct access to suchpersons by negotiating visiting conditions with the authorities. To increase itschances of success in these negotiations, the ICRC does not inquire into thereasons for which the persons in question have been detained; but this does notmean that the ICRC accepts the principle of detention for political reasons.
PROTECTING THE VICTIMS OF ARMED CONFLICT 497

499
During its visits to political prisoners, the ICRC comes into contact with criminallaw offenders as well. When these offenders are in particularly precarioussituations, the ICRC may consider their problems and propose an approachcovering ‘‘all detainees.’’ Emphasis should be laid on the limits of this approach,since the ICRC cannot be responsible for the penitentiary services of an entirecountry.
The instructor will give a few practical examples.
2. CATEGORY
Tool: familiarity with the ICRC’s approach to assisting detainees in the contextof armed conflicts.
3. FORMULATION
What are the rules followed by the ICRC to ensure the protection of detainees inthe context of armed conflicts?
4. TEACHING METHOD
Lecture.
5. DURATION
Total duration: 10 minutes.
6. RECAPITULATION
. Box 1: ICRC strategy for protecting political detainees
LINK WITH NEXT OBJECTIVES
The second example of protection for the victims of armed conflict will be theprotection of the wounded.
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT498

Box 1
ICRC STRATEGY FOR PROTECTINGPOLITICAL DETAINEES
. Political detainees
. Conditions for visits
. Visit all detainees
. Visit all places of detention
. Repeat visits to detainees
. Interviews without witnesses
. Strategy
. Transfer of responsibility to authorities
. Support for health care system
. Replacement of health care system
. ‘‘All detainees’’ approach
. Humanitarian necessity
. Limits
PROTECTING THE VICTIMS OF ARMED CONFLICT 499

501
PROTECTION OF WAR-WOUNDED
1. DESCRIPTION
The strictly surgical aspect of assisting war-wounded has already been discussedin the medical and surgical module. Protection of the wounded is a conceptinvolving the entire health care chain. The importance of first aid for the survivalrate of war-wounded has already been mentioned. Consequently, woundedpeople must be reached as soon as possible. In practice, health care personnelmust obtain from the authorities assurances allowing them to extend theirservices to the wounded. During evacuations of wounded to health care centres,the protection of the injured person must be guaranteed. Accordingly, the ICRChas rules concerning such evacuation:
. to promote respect for the wounded, particularly those in the hands of theenemy (dissemination of international humanitarian law)
. to protect the evacuation of wounded to health care centres—principle linkedto respect for the rules governing transportation of the wounded:
. ambulances and vehicles are marked with the Red Cross emblem
. no arms are permitted in ambulances (wounded and accompanyingsoldiers must lay aside their weapons)
. to protect health care facilities
. to protect the wounded in health care facilities, especially when woundedmembers of various ethnic or political groups are all hospitalized in the samefacility.
All wounded must be guaranteed access to hospitals according to need, not race,religion, or political opinions. Their protectionmust be ensured during their stayin the hospital, particularly where the care-providing facility is under theresponsibility of the adverse party to that of the wounded.
2. CATEGORY
Tool: knowledge of the basic rules for protecting the wounded.
3. FORMULATION
You are in charge of care for the wounded in an armed conflict: what measureswould you take to ensure their protection?
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT500
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Protection of war-wounded
LINK WITH NEXT OBJECTIVES
The next category of victims of armed conflict requiring protection is refugeepopulations.
Box 1
PROTECTIONOF WAR-WOUNDED
. DISSEMINATION OF INTERNATIONALHUMANITARIAN LAW
. RULES FOR TRANSPORTING WOUNDED
. PROTECTION OF HEALTH CARE FACILITIES
. PROTECTION OF WOUNDED IN HEALTH CAREFACILITIES
PROTECTING THE VICTIMS OF ARMED CONFLICT 501

503
INTERNATIONAL HUMANITARIAN LAWAND POPULATION DISPLACEMENT
1. DESCRIPTION
. Preventing displacement
Population displacement is usually accompanied by a major increase in themortality rate, particularly among children, as well as immense physical andpsychological suffering. Respect for the rules of international humanitarian law,which guarantee respect for persons not participating in the conflict, is anoutstandingmeans of preventing such displacement. Keeping individuals in theirusual area of residence is possible only if their protection is guaranteed—hencethe importance of negotiations with all the parties to the conflict, so that respectfor civilian populations will be taken into account in military strategies.
. Refugees
Several categories of refugee must be distinguished:
. Refugees as defined by the 1951 Convention on Refugees and the Protocol of1967, namely refugees who fear personal persecution on account of their race,political opinions, or religion. The High Commissioner for Refugees (HCR)has primary responsibility for these refugees. The principle of ‘‘non-refoule-ment’’ should be stressed (prohibition of expelling refugees to territories wherethey might be endangered).
. Persons living outside their own country owing to an armed conflict or asituation of internal violence—that is, refugees who have fled because of thesituation, not because they are personally objects of persecution. In thesesituations the ICRC and the HCR have complementary mandates. TheICRC has a direct mandate when the host State is at war with these refugees’State of origin, and also when the refugees face major security risks.
. Individual cases—for example, during an international armed conflict,nationals of a State who, in fleeing the fighting, enter the territory of theadverse State. Contrary to the 1951 United Nations Convention Relating tothe Status of Refugees or the Organization of African Unity Convention of1969, international humanitarian law does not base the protection of refugeeson a legal definition. However, it contains general rules applying torefugees—for example, the rules concerning the conduct of hostilities, andthe FourthGenevaConvention’s provisions concerning refugees from enemycountries. The principle of ‘‘non-refoulement’’ is recognized in the FourthConvention (Art. 45, para. 4).
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT502

. Displaced persons
Persons displaced inside their own country as direct victims of an armed conflictor internal violence are the main focus of the ICRC’s mandate. In all suchsituations, international humanitarian law is applicable.
The protection of displaced persons is covered by numerous rules stipulated inthe Geneva Conventions and their Additional Protocols. The instructor shouldgive some examples of applicable rules: commonArticle 3, Article 14 of ProtocolII on the protection of objects indispensable to the survival of the civilianpopulation, Article 17 of Protocol II on the prohibition of forced movement ofcivilians. These rules are designed not only to protect people when they aredisplaced, but also, and especially, to prevent displacement by guaranteeing theirprotection in their place of origin.
2. CATEGORY
Tool: knowledge of the basic principles concerning the protection of refugees anddisplaced persons.
3. FORMULATION
What are the rules of international humanitarian law for ensuring the protectionof displaced persons and refugees?
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Protection of refugees and displaced persons
. Box 2: International law on refugees
LINK WITH NEXT OBJECTIVES
The next objectives will focus on other legal instruments for protecting people.
PROTECTING THE VICTIMS OF ARMED CONFLICT 503

505
Box 1
PROTECTION OF REFUGEESAND DISPLACED PERSONS
. Prevention ofdisplacement
. Refugees:
. 1951 United NationsConvention
. Rules of internationalhumanitarian law
. Displaced persons
. Rules of internationalhumanitarian law
Examples:
Common Article 3
Art. 14, Protocol II
Art. 17, Protocol II
. Role of rules of internationalhumanitarian law in prevent-ing displacement
Box 2
INTERNATIONAL LAW ON REFUGEES
. 1951 UN ConventionRelating to the Statusof Refugees
. 1967 Protocol Relatingto the Status ofRefugees
. Convention of theOrganization of AfricanUnity (OAU)
. 1984 CartagenaDeclaration onRefugees
. Resolutions adoptedby the UN GeneralAssembly
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT504

HUMAN RIGHTS LAW
1. DESCRIPTION
A brief overview of documents concerning human rights law will be sufficient.The instructor may mention:
General documents:
. Universal Declaration of Human Rights (1789)
. United Nations Charter (1949)
. International Covenant on Civil and Political Rights (1966)
. International Covenant on Economic, Social and Cultural Rights (1966)
. Proclamation of Teheran (1968)
Documents concerning specific groups of people:
. United Nations Convention Relating to the Status of Refugees (1951)
. Declaration of the Rights of the Child (1959)
Documents concerning specific subjects:
. Universal Declaration on the Eradication of Hunger and Malnutrition(1974)
. Declaration on the Protection of All Persons from Being Subjected to Tortureand Other Cruel, Inhuman or Degrading Treatment or Punishment (1975)
. Principles of Medical Ethics relevant to the Role of Health Personnel,particularly Physicians, in the Protection of Prisoners and Detainees againstTorture and Other Cruel, Inhuman or Degrading Treatment or Punishment(1982)
. Basic Principles on the Independence of the Judiciary (1985)
Documents produced by regional bodies:
. American Declaration of the Rights and Duties of Man (1948)
. European Convention on Human Rights (1950)
. African Charter on Human and Peoples’ Rights (1981).
2. CATEGORY
Tool: knowledge of the basic documents of human rights law.
PROTECTING THE VICTIMS OF ARMED CONFLICT 505

507
3. FORMULATION
Name the main documents concerning human rights law.
4. TEACHING METHOD
Assignment presented to work groups followed by plenary session.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Documents concerning human rights law
LINK WITH NEXT OBJECTIVES
The essential rules of international humanitarian law and human rights law havebeen studied. The next objective consists in analysing the differences betweenthese two kinds of law.
Box 1
DOCUMENTS CONCERNINGHUMAN RIGHTS LAW
. GENERAL DOCUMENTS
. DOCUMENTS CONCERNING SPECIFIC GROUPSOF PEOPLE
. DOCUMENTS CONCERNING SPECIFIC SUBJECTS
. DOCUMENTS PRODUCED BY REGIONAL BODIES
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT506

INTERNATIONAL HUMANITARIAN LAWAND HUMAN RIGHTS LAW
1. DESCRIPTION
International humanitarian law and human rights law have the same purpose,which is to guarantee the respect due to human beings without discrimination.They differ on several points, specifically:
. International humanitarian law is applicable only in situations of armedconflict, while human rights law is applicable at all times.
. International humanitarian law protects fundamental rights of the victims ofarmed conflicts, whereas human rights law protects a whole body of rightsranging from fundamental rights—the hard core of human rights—to muchmore general rights, such as, for example, the right to development. As a result,the protection of fundamental rights accorded by human rights law loses force.
. The rules of international humanitarian law are very detailed, and lay downthe duties of the parties to the conflict very strictly. This precision is not foundin the law of human rights.
. Derogations are possible in human rights law, except for the rights includedin the ‘‘hard core’’ of human rights. They are not possible in internationalhumanitarian law. What is more, a victim cannot renounce his or herrights—a provision designed to prevent victims from renouncing their rightsunder duress.
The instructor must emphasize the power of international humanitarian law,which focuses on the protection of fundamental rights in situations of armedconflict according to specific rules.
2. CATEGORY
Tool: knowledge of the essential differences between international humanitarianlaw and human rights law.
3. FORMULATION
What are the essential differences between international humanitarian law andhuman rights law?
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
PROTECTING THE VICTIMS OF ARMED CONFLICT 507

509
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: International humanitarian law and human rights law
. Box 2: Other legal instruments for the protection of individuals
LINK WITH NEXT OBJECTIVES
The role of international humanitarian law in protecting the victims of armedconflict includes the establishment of rules concerning the conduct of hostilities.
Box 1
INTERNATIONAL HUMANITARIAN LAWAND HUMAN RIGHTS LAW
. INTERNATIONAL HUMANITARIAN LAW ANDHUMAN RIGHTS LAW: FIELDS OF APPLICATION
. INTERNATIONAL HUMANITARIAN LAW ANDHUMAN RIGHTS LAW: PROTECTED RIGHTS
. PRECISION OF INTERNATIONAL HUMANITARIAN LAW
. DEROGATIONS OF HUMAN RIGHTS LAW
Box 2
OTHER LEGAL INSTRUMENTSFOR THE PROTECTION OF INDIVIDUALS
. NATIONAL RIGHTS
. REGIONAL CONVEN-TIONS AND CHARTERS
. CUSTOMARY LAW
. STATUTORY RULES OFTHE INTERNATIONALRED CROSS AND REDCRESCENT MOVEMENT
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT508

LAW OF THE HAGUE
1. DESCRIPTION
The law of The Hague contains provisions limiting the means of conductinghostilities. Some examples:
. Declaration of St. Petersburg of 1868 to the Effect of Prohibiting the Use ofCertain Projectiles in Wartime
. Geneva Protocol of 17 June 1925 for the Prohibition of the Use in War ofAsphyxiating, Poisonous or other Gases and of Bacteriological Methods ofWarfare
. Convention of 10 December 1976 on the Prohibition of Military or AnyOther Hostile Use of Environmental Modification Techniques
. Convention on Prohibitions or Restrictions on the Use of CertainConventional Weapons Which May Be Deemed to Be Excessively Injuriousor to Have Indiscriminate Effects (1980).
The aim is not to give participants an exhaustive list of the rules of the law of TheHague, but to make them aware that not all means of warfare are permissible.
2. CATEGORY
Tool: knowledge of some essential rules of the law of The Hague.
3. FORMULATION
What rules would you like to have at your disposal to limit the effects of warfare?
4. TEACHING METHOD
Assignment presented to the entire group in plenary session.
5. DURATION
Total duration: 20 minutes.
6. RECAPITULATION
. Box 1: Examples of rules of the law of The Hague
PROTECTING THE VICTIMS OF ARMED CONFLICT 509

511
. Box 2: Timeline of international humanitarian law
. Box 3: The development of international humanitarian law
LINK WITH NEXT OBJECTIVES
All these legal elements help define a context for the specific responsibilities ofhealth care personnel. This point will be addressed in the final recapitulation, inthe objective entitled ‘‘Roles andResponsibilities ofHealth Care Professionals inAssisting and Protecting the Victims of Armed Conflicts.’’
Box 1
EXAMPLES OF RULESOF THE LAW OF THE HAGUE
. DECLARATION OF ST. PETERSBURG
. GENEVA PROTOCOL OF 17 JUNE 1925
. CONVENTION OF 1976 ON THE PROHIBITIONOF ENVIRONMENTAL MODIFICATIONTECHNIQUES
. 1980 CONVENTION ON PROHIBITIONS ORRESTRICTIONS ON THE USE OF CERTAINCONVENTIONAL WEAPONS
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT510

Box 2
TIMELINE OF INTERNATIONALHUMANITARIAN LAW
1864 Geneva Convention for the Amelioration of the Condition of the Wounded in Armies inthe Field
1868 Declaration of St. Petersburg to the Effect of Prohibiting theUse of Certain Projectiles inWartime
1899 Conventions of The Hague respecting the Laws and Customs of War on Land and theAdaptation to Maritime Warfare of the Principles of the Geneva Convention of 1864
1906 Revision and expansion of the Geneva Convention of 1864
1907 Revision of The Hague Conventions of 1899 and adoption of new conventions
1925 Geneva Protocol for the Prohibition of the Use in War of Asphyxiating, Poisonous orother Gases and of Bacteriological Methods of Warfare
1929 Two Geneva Conventions:. revision and expansion of the Geneva Convention of 1906. Geneva Convention relative to the Treatment of Prisoners of War (new)
1949 Four Geneva Conventions:
I Amelioration of the Condition of the Wounded and Sick in Armed Forces inthe Field
II Amelioration of the Condition of Wounded, Sick and Shipwrecked Membersof Armed Forces at Sea
III Treatment of Prisoners of War
IV Protection of Civilian Persons in Time of War (new)
1954 The Hague Convention for the Protection of Cultural Property in the Event of ArmedConflict
1972 Convention on the Prohibition of the Development, Production and Stockpiling ofBacteriological (Biological) and Toxin Weapons and on their Destruction
1977 Two Protocols Additional to the four Geneva Conventions of 1949, reinforcing theprotection of victims of international (Protocol I) and non-international (Protocol II)armed conflicts
1980 Convention on Prohibitions or Restrictions on the Use of Certain ConventionalWeaponsWhichMay BeDeemed to be Excessively Injurious or to Have IndiscriminateEffects. This Convention includes:
. Protocol I on Non-Detectable Fragments
. Protocol II on Prohibitions or Restrictions on the Use of Mines, Booby-Trapsand Other Devices
. Protocol III on Prohibitions or Restrictions on the Use of Incendiary Weapons
1993 Convention on the Prohibition of the Development, Production, Stockpiling and Use ofChemical Weapons and on Their Destruction
1995 Protocol on Blinding Laser Weapons (Protocol IV to the 1980 Convention) (new)
1996 Revised Protocol on Prohibitions or Restrictions on theUse ofMines, Booby-Traps andOther Devices (Protocol II [revised] of the Convention of 1980)
1997 Convention on the Prohibition of the Use, Stockpiling, Production and Transfer of Anti-Personnel Mines and on Their Destruction
PROTECTING THE VICTIMS OF ARMED CONFLICT 511

Box 3
THE DEVELOPMENTOF INTERNATIONAL HUMANITARIAN LAW
. Health concerns have formed the basis for thedevelopment of certain aspects of internationalhumanitarian law, in particular:
. the Protocol on Blinding Laser Weapons adopted bythe Conference of Vienna in October, 1995
. the Convention on the Prohibition of the Use,Stockpiling, Production and Transfer of Anti-PersonnelMines and on Their Destruction, signed in Ottawa inDecember, 1997
HELP/SOS: PROTECTING THE VICTIMS OF ARMED CONFLICT512

RECAPITULATION AND CONCLUSION
MODULE
10

LIST OF OBJECTIVES
. Define the general context of humanitarian action
. Identify factors in humanitarian relief that influence conflicts, and use them towork out a strategy of choice for delivering humanitarian relief
. Identify the various levels of evaluating humanitarian action
. Identify the ethical questions that should be asked at each stage of planning ahealth programme
. Define the roles and responsibilities of health care professionals in situations ofarmed conflict
. Know how to coordinate humanitarian operations.
HELP/SOS: RECAPITULATION AND CONCLUSION514 515

CONSTRUCTIONOF A GENERAL FRAMEWORK
1. DESCRIPTION
The purpose of this objective is to construct a general framework for orientinghumanitarian action in its political context. To this end, the instructor shouldbegin with the evolutionary cycle of conflicts:
. stable situation
. crisis factors
. crisis
. armed conflict
. resolution of the conflict
. reconstruction
. stable situation.
Two levels should be distinguished here:
. humanitarian management of the consequences of armed conflict
. political management of armed conflict.
Humanitarian action is concerned primarily with the humanitarian conse-quences of armed conflicts. It should be remembered that a goal of humanitarianaction is to cover the needs of victims impartially. This means humanitarianworkers must have access to the victims. One way of obtaining that access is tonegotiate with the parties to the conflict (this is the ICRC’s strategy). Duringsuch negotiations, the ICRC relies in particular on the rules of internationalhumanitarian law and the principles of humanity, impartiality, and neutrality.Neutrality is defined in relation to the parties to the conflict, while impartialityconcerns the victims.
Humanitarian action involves two essential aspects: assistance to and protectionof victims. Although it deals with the humanitarian consequences of armedconflicts, it must also try to minimize those consequences by taking a preventiveapproach, thereby reducing the conflict’s impact on the victims. In this respect,emergency action is akin to development projects designed to reduce causes ofinstability that might lead to crises and conflicts. This sort of prevention must be
RECAPITULATION AND CONCLUSION 515

517
clearly distinguished from prevention of the conflicts themselves, which is amatter of political management.
The political management of conflicts includes political measures to resolveconflicts, such as coercive diplomacy and the deployment of military forces toimpose peace. To keep a situation from developing from crisis into conflict,preventive diplomacy and peace-keeping forces have an essential role. Thesepolitical actions tackle the consequences and immediate political causes ofconflicts. However, the deeper causes of conflicts must also be taken intoaccount: underdevelopment, social inequality, interethnic tension, intolerance,territorial disputes, etc. At this more general level, all the activities linked todevelopment must be considered: economic development, education, democra-tization, promotion of human rights, etc.
Many agencies take a hand in all this. Some of them have an exclusivelyhumanitarian mandate (ICRC), while others play a political role (States). TheUnitedNationshasbothapolitical role (SecurityCouncil) andahumanitarianrole,through the intermediary of its specialized agencies (UNHCR, WHO, UNICEF).
This panorama of activities involved in the political and humanitarianmanagement of armed conflicts, together with the agencies that participate inthem, provides a general frame of reference that will help us address such generalsubjects as:
. the impact of aid on the development of conflicts
. the evaluation of measures
. the role and responsibility of health care professionals
. ethics and health care
. the coordination of humanitarian agencies.
2. CATEGORY
Framework: defining a general context for humanitarian action.
3. FORMULATION
Define a framework integrating both the humanitarian and the politicalmanagement of situations of armed conflict.
4. TEACHING METHOD
Assignment presented to work groups, followed by plenary session.
HELP/SOS: RECAPITULATION AND CONCLUSION516

5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: The development of an armed conflict
. Box 2: Humanitarian consequences of armed conflict
. Box 3: Responses to humanitarian problems
. Box 4: Humanitarian operations
. Box 5: Addressing the conduct of hostilities
. Box 6: Causes of armed conflict
. Box 7: Addressing the causes of armed conflict
. Box 8: The pieces of the puzzle
. Box 9: Levels of response
. Box 10: The protagonists in humanitarian situations
. Box 11: Political and humanitarian agencies
. Box 12: Implications of political factors in humanitarian operations
LINK WITH NEXT OBJECTIVES
The next objective addresses the first general subject: the impact of aid on thedevelopment of conflicts.
RECAPITULATION AND CONCLUSION 517

519
Peace
Crisis
Conflict
Peace
Reconstruction
Resolution
Box 1
THE DEVELOPMENTOF AN ARMED CONFLICT
HELP/SOS: RECAPITULATION AND CONCLUSION5518
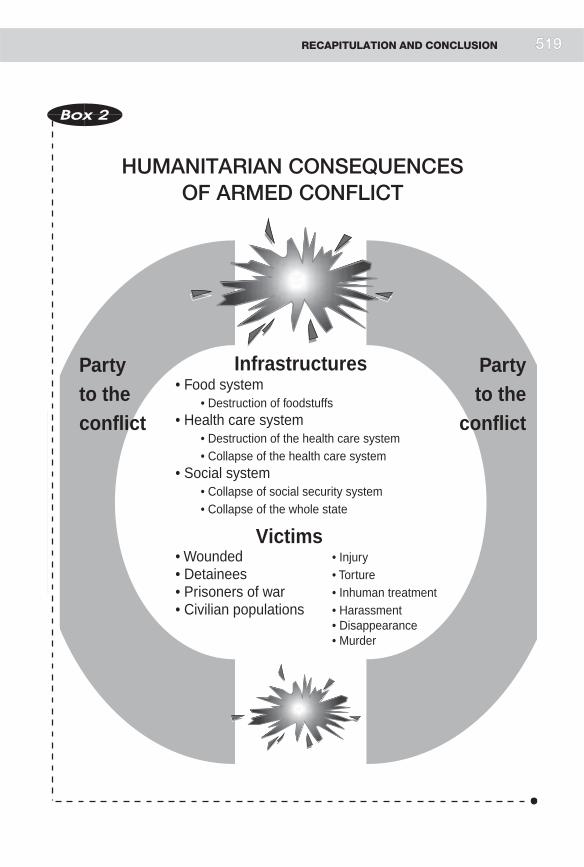
Partyto the conflict
Partyto the
conflict
Infrastructures
Victims
• Food system• Destruction of foodstuffs
• Health care system • Destruction of the health care system• Collapse of the health care system
• Social system• Collapse of social security system• Collapse of the whole state
• Wounded • Injury• Detainees • Torture• Prisoners of war • Inhuman treatment• Civilian populations • Harassment
• Disappearance • Murder
Box 2
HUMANITARIAN CONSEQUENCESOF ARMED CONFLICT
RECAPITULATION AND CONCLUSION 5519

521
Partyto the conflict
Partyto the
conflict
Negotiationswith the partiesto the conflict
Relations withthe media
Relations withother agencies
Dissemination of IHL
Link withdevelopment activities Emergency
Emergency Civilianpopulations
WoundedWounded Detainees
Victims
Protection of the victims
Wars
Box 3
RESPONSESTO HUMANITARIAN PROBLEMS
HELP/SOS: RECAPITULATION AND CONCLUSION5520

Partyto the conflict
Partyto the
conflictVictims
Victim protectionand assistance
Box 4
HUMANITARIAN OPERATIONS
RECAPITULATION AND CONCLUSION 5521

523
Health care systemSupplies
Civilianpopulations
Wounded
Victims
Infrastructures
Wounded
Partyto the conflict
Party to the conflict
Conduct ofhostilities
Detainees
Detainees
War victim protectionand assistance
Box 5
ADDRESSING THE CONDUCTOF HOSTILITIES
HELP/SOS: RECAPITULATION AND CONCLUSION5522

Peace
Crisis
Conflict Wars
Peace
Reconstruction
Resolution
Factors leading to destabilization
• Socio-economic inequalities• Arms trade: small- and large-calibre
weapons • Discrimination• Cult of violence• Territorial disputes• Human rights violations• Deterioration of the environment• Overuse of resources • Competition for resources,
water and electricity• Collapse of governmental
mechanisms
Box 6
CAUSESOF ARMED CONFLICT
RECAPITULATION AND CONCLUSION 5523

525
Peace
Crisis
Conflict Wars
Peace
Reconstruction
Resolution
Military interventionto enforce peace
Militaryintervention
to maintain peace
Preventivediplomacy
Coercivediplomacy
Rehabilitation
Justice
Promotion ofhuman rights
Democratization
Education
Economicdevelopment
Socialdevelopment Cultural
development
Box 7
ADDRESSING THE CAUSESOF ARMED CONFLICT
HELP/SOS: RECAPITULATION AND CONCLUSION5524

Partyto the
conflict
Partyto theconflict
Peace Peace
Enforcement of peace
Peace-keeping
Preventivediplomacy
Coercivediplomacy
Rehabilitation
Justice
Promotion ofhuman rights
Democratization
Education
Economicdevelopment
Socialdevelopment Cultural
development
Negotiationswith the partiesto the conflict
Relations withthe media
Relations withother agencies
Dissemination of IHL
Link with developmentactivities
Emergency
Emergency Civilianpopulations
Wounded
DetaineesVictims
Protection of victims
Wars
Wounded
Box 8
THE PIECES OF THE PUZZLE
RECAPITULATION AND CONCLUSION 5525

527
Partyto the
conflict
Partyto the conflict
Peace
Responses to fundamental causes
Responses to immediate causes
Response to the crisis
Humanitarian response
Peace
Negotiationswith the partiesto the conflict
Relations withthe media
Relations withother agencies
Dissemination of IHL
Link with developmentactivities Emergency
Emergency Civilianpopulations
Wounded
DetaineesVictims
Protection of victims
Wars
Wounded
Level I Level I
Level II Level IV
Level IV
DevelopmentPromotion ofhuman rights EducationDisarmament
DevelopmentPromotion ofhuman rights
EducationDisarmament
Preventive diplomacyPeace-keeping
JusticeRehabilitation
Reconstruction
Coercive diplomacyApplication ofpeace plan
Protection of victimsEmergency reliefEmergency rehabilitation
Level III
Stable situation
Destabilization
Stabilization
Return to stable situation
Box 9
LEVELSOF RESPONSE
HELP/SOS: RECAPITULATION AND CONCLUSION5526

Partyto the
conflict
Partyto theconflict
Peace Peace
Application of peace plan
Peace-keeping
Preventivediplomacy
Coercivediplomacy
Rehabilitation
Justice
Promotion ofhuman rights
DemocratizationEducation
Economicdevelopment
Socialdevelopment Cultural
development
Relations withthe media
Relations withother agencies
Dissemination of IHL
Link with developmentactivities
Emergency
Emergency Civilianpopulations
Wounded
DetaineesVictims
Protection of victims
Wars
Wounded
MEDIA NGOs
UNHCR
RED CROSSICRC
UNICEF
STATESUN
Negotiationswith the partiesto the conflict
Box 10
THE PROTAGONISTSIN HUMANITARIAN SITUATIONS
RECAPITULATION AND CONCLUSION 5527

529
Partyto the
conflict
Partyto theconflict
Peace Peace
Promotion ofhuman rights
Democratization
Education
Economicdevelopment
Socialdevelopment Cultural
development
Diffusion du DIH
Emergency Civilianpopulations
WoundedWounded
Victimes
Protection des victimes
Guerres
Humanitarianagencies
Politicalactivities
Peace-keeping
Preventivediplomacy
Coercivediplomacy
Rehabilitation
Justice
Application of peace plan
Link withdevelopment activities
Emergency
Negotiationswith the partiesto the conflict
Relations withother agenciesRelations with
the media
Box 11
POLITICALAND HUMANITARIAN AGENCIES
HELP/SOS: RECAPITULATION AND CONCLUSION5528

Partyto the
conflict
Partyto theconflict
Peace Peace
Application plan de paix
Promotion ofhuman rights
Democratization
Education
Economicdevelopment
Socialdevelopment Cultural
development
Diffusion du DIH
Urgence
Blessés
Victimes
Protection des victimes
Guerres
Humanitarianagencies
Politicalactivities
Peace-keeping
Preventivediplomacy
Coercivediplomacy
Rehabilitation
Justice
Detainees
Emergency
Link withdevelopment activities
Civilianpopulations
Negotiationswith the partiesto the conflict
Relations withother agencies
Relations withthe media
Box 12
IMPLICATIONS OF POLITICAL FACTORSIN HUMANITARIAN OPERATIONS
Risks of this strategy?
RECAPITULATION AND CONCLUSION 5529
531
IMPACT OF AID ON THE DEVELOPMENTOF CONFLICTS
1. DESCRIPTION
The role of humanitarian aid, particularly with regard to health, has been clearlyestablished in the preceding objective. Initially, course participants will analysethe negative effects of poorly planned humanitarian aid: taking responsibilityaway from the victims, attraction of populations not targeted by the operation,artificial changes in ways of life, etc.
The influence of humanitarian aid on the development of conflicts can beanalysed from two perspectives:
. influence on the level of violence of the conflict. Humanitarian aid mayincrease the level of violence (harassment of victims receiving aid, attacks onhumanitarian convoys, etc.), but it may also help reduce the level of violence.The humanitarian agencies that deliver aid are able to identify protectionneeds and to reduce violations of international humanitarian law. Theinstructor should emphasize the complementary nature of aid and protectionfor victims of armed conflict.
. influence on the duration of armed conflict. It is clear that poorly monitoredaid, part of which is diverted by the parties to the conflict, may prolong theconflict. In certain situations, on the other hand, aid may foster a resumptionof dialogue between the parties to the conflict, thereby helping to curtail theconflict.
The instructor will analyse various possible ways of looking at humanitarian aid,and ask participants to justify their choice of strategy. Possible strategic optionsare:
. to cease all forms of assistance
. to provide aid only if international humanitarian law is respected
. to distribute aid equally between the parties to the conflict
. to use military means to protect and/or deliver humanitarian aid
. to improve the strategy already being followed by humanitarian agencies,based on an analysis of the victims’ needs.
HELP/SOS: RECAPITULATION AND CONCLUSION530

The instructor will discuss the ICRC’s approach, which is based on an analysis ofvictims’ needs, non-discrimination, linkage between assistance and protection,direct access to the victims, support for compensatory mechanisms, andrestoration of self-sufficiency.
2. CATEGORY
Tool: knowledge of the factors in humanitarian aid that influence thedevelopment of conflicts, and the use of that knowledge to identify the righthumanitarian aid strategy.
3. FORMULATION
Identify the factors in humanitarian aid that influence the development ofconflict and use those factors to propose the right strategy for humanitarian aid.
4. TEACHING METHOD
Assignment presented to work groups.
5. DURATION
Total duration: 60 minutes
. 30 minutes for work in groups
. 30 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Effects of humanitarian aid
. Box 2: Influence of humanitarian aid on the development of armedconflicts
. Box 3: Influence of humanitarian aid on the duration of armed conflicts
. Box 4: Influence of humanitarian aid on the violence of conflicts
. Box 5: Humanitarian aid strategies
. Box 6: ICRC humanitarian aid strategy
LINK WITH NEXT OBJECTIVES
The influence of humanitarian aid on the development of conflicts under-lines—as if that were necessary—the importance of evaluating the impact ofhumanitarian action.
RECAPITULATION AND CONCLUSION 531

533
Box 1
EFFECTSOF HUMANITARIAN AID
POSITIVE EFFECTS
. Saves lives
. Relieves suffering
. Contributes to the protection of victims
. Rehabilitates local systems
NEGATIVE EFFECTS
. Takes responsibility away from the victims
. Alters behaviours and habits
. Attracts victims
. Helps support political systems
. Contributes to the war effort
HELP/SOS: RECAPITULATION AND CONCLUSION532

Peace
Crisis
Conflict
Peace
Reconstruction
Resolution
Level of violence
Duration
Box 2
INFLUENCE OF HUMANITARIANAID ON THE DEVELOPMENT
OF ARMED CONFLICTS
RECAPITULATION AND CONCLUSION 5533

535
Box 3
INFLUENCE OF HUMANITARIANAID ON THE DURATIONOF ARMED CONFLICTS
INCREASES THE DURATION OF CONFLICTS BY:
. maintaining an ‘‘acceptable’’ level of violence
. delaying political solutions to conflicts
DECREASES THE DURATION OF CONFLICTS BY:
. favouring a renewal of dialogue between the parties tothe conflict
Box 4
INFLUENCE OF HUMANITARIAN AIDON THE VIOLENCE OF ARMED CONFLICTS
INCREASES THE LEVELOF VIOLENCE BECAUSE:
. aid is used to buy arms
. aid recipients are har-assed by armed groups
. assisted populationsbecome hostages ofarmed groups seekingto extort more aid
DECREASES THE LEVELOF VIOLENCE BECAUSE:
. the presence of reliefworkers helps protectvictims
. indirect violence linkedto lack of food, water,and health care isreduced
HELP/SOS: RECAPITULATION AND CONCLUSION534

Box 5
HUMANITARIAN AID STRATEGIES
. No aid
. Aid conditional on re-spect for internationalhumanitarian law
. Aid distributed equallybetween the parties tothe conflict
. Protection of humani-tarian aid by militarymeans
. Improvement of theconventional strategybased on Red Crossprinciples
Box 6
ICRC HUMANITARIANAID STRATEGY
. Principles:
. Impartiality
. Neutrality
. Independence
. Link between assis-tance and protection
. Direct access tovictims
. Support for compen-satory mechanisms
. Restoration ofself-sufficiency
RECAPITULATION AND CONCLUSION 535

537
EVALUATION OF HUMANITARIAN ACTION
1. DESCRIPTION
The purpose of this section is to show the necessity of evaluating humanitarianaction, and to provide a tool for defining various kinds of evaluation.
The aims of evaluating humanitarian action are to:
. promote crucial management of ongoing action
. draw conclusions from completed action
. provide practical responses to specific problems for which no satisfactorysolution has as yet been devised
. contribute to the development of staff training.
Tools for defining the various kinds of evaluation
First, the instructor will review the stages of the planning process:
. initial assessment
. definition of problems
. determination of objectives
. planning of activities
. mobilization of resources
. evaluation of results.
For the stages involving resources, activities, and objectives, participants will beasked to provide examples of indicators, the instructor having already reviewedthe criteria for judging their quality (SMART).
Next, the instructor will describe the evaluation criteria:
. description of activities
. compliance with procedures
. effectiveness
. efficiency
. coherence
. relevance
. sustainability
. impact.
HELP/SOS: RECAPITULATION AND CONCLUSION536

The third step will be to combine planning and evaluation in a single diagram (seeTable 4). Participants will be asked to plot evaluation examples on this graph. Theexamplesmay be drawn from their own experience or from the simulation exercise.
Using this graph, the instructor will stimulate discussion on potential resistanceto evaluations deriving from fear of undermining the operation, constraintsgenerated by armed conflict, lack of resources, lack of expertise, etc.
Finally, it should be stressed that:
. provision for evaluating results must be made at the same time that theactions themselves are being planned
. evaluations are essential for improving policies relating to humanitarianaction
. evaluations permit improvement of ongoing operations.
2. CATEGORY
Tool: ability to correlate the various criteria for the evaluation of results with theplanning process.
3. FORMULATION
Identify the purposes of evaluating humanitarian concepts, and, on the basis ofyour own experiences (or the simulation exercise), give examples of evaluations.
4. TEACHING METHOD
Assignmentpresented toworkgroups.The instructorwillmatch the examplesgivenwith the appropriate stages of the planning process, and define the evaluationcriteria of these examples, thereby reconstructing the recapitulation depicted inTable 4.
5. DURATION
Total duration: 60 minutes
. 20 minutes for work in groups
. 40 minutes for summary in plenary session.
6. RECAPITULATION. Box 1: The role of evaluations of humanitarian action
. Box 2: Planning process
. Box 3: Evaluation criteria
. Box 4: Integration of planning stages and evaluation criteria
. Box 5: Logical framework: planning and evaluation tool
RECAPITULATION AND CONCLUSION 537

539
LINK WITH NEXT OBJECTIVES
The evaluation of results permits an improved definition of policies for dealingwith humanitarian crises, as well as the formulation of recommendationsconcerning ethics to which all involved parties should adhere when conductinghumanitarian operations. This is the next topic.
TIME
Causes
Conflict
ICRC takes action
Warningsystem
Monitoring
End of humanitarian action
Initialassessment
Interimevaluations
of humanitarian action
Finalevaluation
of humanitarian action
Box 1
THE ROLE OF EVALUATIONSOF HUMANITARIAN ACTION
HELP/SOS: RECAPITULATION AND CONCLUSION5538
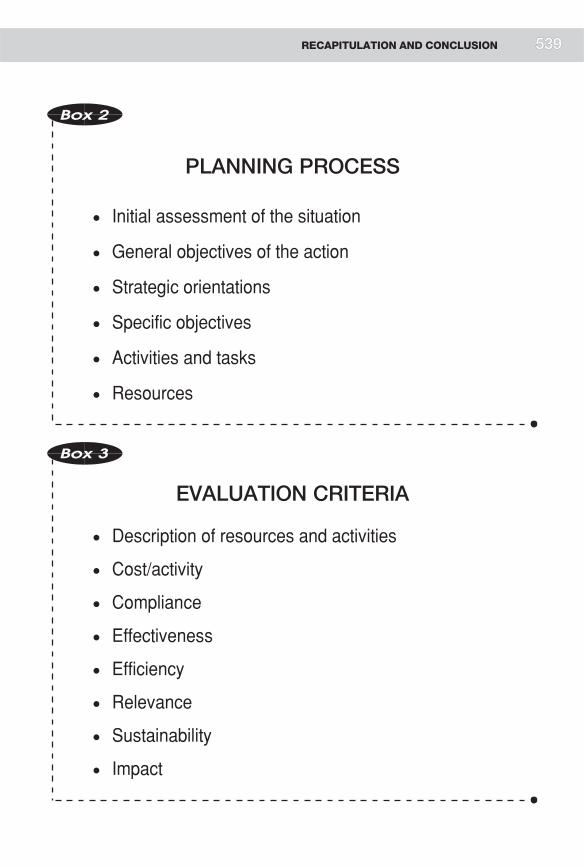
Box 2
PLANNING PROCESS
. Initial assessment of the situation
. General objectives of the action
. Strategic orientations
. Specific objectives
. Activities and tasks
. Resources
Box 3
EVALUATION CRITERIA
. Description of resources and activities
. Cost/activity
. Compliance
. Effectiveness
. Efficiency
. Relevance
. Sustainability
. Impact
RECAPITULATION AND CONCLUSION 539

541
Situations
Generalobjectives
Strategicorientations
Specificobjectives
Activities
Resources
Effecti
vene
ss
Efficien
cy
Impa
ct
Releva
nce
Compli
ance
Cost/a
ctivit
y
Types of evaluation
Planning stages
ICRCdocuments• Sitrep• Annual activity report
=Description of resourcesmobilized and activities
Angola:Evaluation of the quality of medicalconsultations =Study of compliancewith specific standards
Somalia:Evaluation of a disseminationprogramme
=Study ofcompliance
Mozambique:Evaluation of immunizationprogrammeimplemented by ICRC
=Study of immunizationcoverage
Azerbaijan:Evaluation of TB programme• % of patients cured• Application of DOT• Study of drug resistance
=• Study of effectiveness• Study of compliance
Delegation of plans,evaluation of a strategicorientation:• Study of relevance• Study of coherence
ICRC• Sitrep• Activity reports Angola
SomaliaAzerbaijan
AzerbaijanMozambique
Delegation ofprojects
Where do the evaluation examples described at the beginning of thissection fit in relation to planning stage and type of evaluation?
Descri
ption
of
reso
urce
s and
activ
ities
Box 4 INTEGRATION OF PLANNING STAGESAND EVALUATION CRITERIA
HELP/SOS: RECAPITULATION AND CONCLUSION5540

Planning
Situation
Generalobjectives
Strategicorientations
Specificobjectives
Activities
Resources
Indicators Possible evalu-ation criteria(relevance,effectiveness, efficiency, impact,coherence,etc.)
Data sources for evaluation indicators
Evaluationmethods
Contextualinterpretation(constraints on the implemen-tation of the humanitarianaction)
Box 5
LOGICAL FRAMEWORK
PLANNING AND EVALUATION TOOL
RECAPITULATION AND CONCLUSION 5541

543
ETHICS AND HEALTH CARE ACTION
1. DESCRIPTION
Humanitarian action implemented in the context of armed conflict may involvenumerous pitfalls:
. losing control of the aid and assisting the combatants instead of the victims
. paying for access to the victims, by helping the combatants so that they willallow the humanitarian aid to pass
. making the victims completely dependent on humanitarian aid, withoutplanning sustainable solutions
. contributing to the destruction of economic and social systems by assistingvictims
. introducing inappropriate technologies in an unsuitable context
. creating tensions between resident and displaced populations
. dissociating assistance and protection—helping victims while turning a blindeye to serious violations of international humanitarian law.
During a humanitarian action, the people involved do not always have a clearperception of the boundaries of humanitarian ethics. Certainly they rememberthe main principles, but often have trouble defining their practical applications.To give participants some guidance, the instructor will review the planningoutline, and ask them to identify the ethical problems that may arise at eachplanning stage.
The initial assessment—The purpose of an initial assessment is to determinewhether the local services are adequate to meet the basic needs of the population.Interpretation of the results of this assessment will give rise to questions withregard to the following points:
a) the needs of the victims. Interpretation of this concept depends not only on aprofessional analysis of health problems, but also on the cultural backgroundof the victims. Something that is essential in one society is not necessarily so inanother. Similarly, humanitarian action takes place in a variety of socio-economic contexts. In less developed countries, the idea of essential needscoincides with that of vital needs. In contrast, in developed countries wherevital needs are covered, victims will speak of needs that to an outsider appearnon-essential, but that are essential to them. Should the relief administrator
HELP/SOS: RECAPITULATION AND CONCLUSION542

address such needs, at the risk of creating programmes with doublestandards?
b) local services. Although it is possible to determine whether the quantity ofservices is sufficient in a given situation, determining whether the quality isappropriate is much trickier. The services provided can be compared torecognized standards of reference, but those standards must be interpreted inthe light of the local habits and socio-economic level. What is acceptable inone environment may not be in another. In practical terms, at what pointshould services be considered inappropriate in a given context, prompting theimplementation of measures to improve or replace them?
Determination of objectives—An objective involves four elements:
a) a health problem. Participants have already studied the questions that mustbe asked in order to define the priority of a particular health problem relativeto others.
b) quantification of the expected results—what level is desired?
. a return to the usual situation, with the risk of stabilizing victims at aninadequate standard of living
. a superior level, with the risk of creating dependence on foreign aid.
c) a target group:
. Who should decide which population groups take priority: agencies, thevictims themselves, donors?
. What should be done if a target group cannot be precisely identified becauseit is mixed in with armed groups who should not benefit from humanitarianaid?
d) a time limit:
. Should the length of time allocated to a humanitarian action be determinedon the basis of specific problems that must be resolved, or should theduration of the action also take into account the time required to establishlinks with development programmes?
Determination of strategies:
. Is a programme chosen according to the needs of the victims, or according toits media visibility?
. Do the victims participate in choosing the programme?
RECAPITULATION AND CONCLUSION 543

Mobilization of resources:
. Are the resources mobilized appropriate? (That is, drugs have not passedtheir expiration date, health care personnel are trained and have soundprofessional experience, etc.)
. Should local personnel be offered higher wages than the local average, inorder to attract people who know the sociocultural milieu well—even thoughthis poses the risk of draining off personnel who are indispensable for theproper functioning of the local services?
Epidemiological surveillance:
. Have means been provided for evaluating humanitarian action?
. Are decisions appropriate in light of epidemiological surveillance results?
2. CATEGORY
Framework: identifying the ethical questions that must be asked at the variousplanning stages of a health care programme.
3. FORMULATION
Identify the ethical questions that must be asked at the various planning stages ofa health care programme.
4. TEACHING METHOD
Each work group will be assigned to study one stage of the planning process; allparticipants will then meet and put the stages together.
5. DURATION
Total duration: 60 minutes
. 20 minutes for work in groups
. 40 minutes for summary in plenary session, during which all the work on thedifferent stages of the planning process will be combined.
6. RECAPITULATION
. Box 1: Ethics and planning: initial assessment
. Box 2: Ethics and planning: determination of objectives
. Box 3: Ethics and planning: determination of strategies
HELP/SOS: RECAPITULATION AND CONCLUSION544 545

LINK WITH NEXT OBJECTIVES
Now that the technical, legal, and ethical aspects of humanitarian action havebeen discussed, the next step is to define the roles and responsibilities of healthcare personnel in armed conflict.
Box 1
ETHICS AND PLANNING
INITIAL ASSESSMENT
. Interpretation of the concept of victims’ needs
. Interpretation of the quality of local services:which standards?
. Should an assessment be made if we know there willbe no follow-up?
RECAPITULATION AND CONCLUSION 545

547
Box 2
ETHICSAND PLANNING
DETERMINATION OF OBJECTIVES
. Aim for the reestablishment of the situation existingprior to the conflict, or aim higher?
. What are the criteria for deciding which populationgroup takes priority?
Box 3
ETHICS AND PLANNING
DETERMINATION OF STRATEGIES
. Course of action whena group of victims isunder the control of anarmed group
. Course of action whenthe institution of a pro-gramme (e.g., againsttuberculosis) requirescertain conditions thatare not present
. Are activities chosenaccording to the vic-tims’ needs or accord-ing to their visibility?
. To what extent do thevictims participate indecision-making?
. Provide direct aid orpush the authorities totake responsibility?
HELP/SOS: RECAPITULATION AND CONCLUSION546

ROLES AND RESPONSIBILITIESOF HEALTH CARE PROFESSIONALSIN ASSISTING AND PROTECTINGTHE VICTIMS OF ARMED CONFLICT
1. DESCRIPTION
At the outset, emphasis must be laid on the close connections between assistanceand protection activities. The ICRC takes a global approach to the victims ofconflicts, in which provision for physiological needs by guaranteeing access tofood, water, and health care is combinedwith respect for human dignity, physicalintegrity, the family unit, etc.
ICRC strategy, based on direct access to victims, gives delegates the opportunityto identify the aid and protection needs of those victims.
In this respect, health care personnel have a privileged position conferred by theirregular contact with the population and the professional skills they offer. Thisposition gives them special responsibilities, not only to perform their professionalduties properly according toacceptednorms, but also to identify anddealwith theprotection problems of the victims for whom they are responsible.
The fact that they witness violations of international humanitarian law giveshealth care personnel responsibilities not only towards the victims, but alsotowards the outside world. However, the instructor should note the power andthe limitations of testimony to the media, to governments, and, more generally,to civil society. It is not always easy to reconcile personal ethics, medical ethics,and the institutional strategies of the organizations in which the health carepersonnel work. By basing its strategy on access to victims, the ICRC givespriority to negotiations with the parties to the conflict, which limits its possibilityof bearingwitness to the outsideworld—although this possibility is not excluded,when massive and repeated violations of humanitarian law are committed.
Protection-orientedmeasures also concern the health care system. The instructorshould review the rules of law that protect hospitals, health care personnel,objects essential for survival, etc.
Health care personnel also have a responsibility to work for the development andapplication of international humanitarian law. One example that can be cited is
RECAPITULATION AND CONCLUSION 547

that of mines, in which the surgical issue eventually led to the treaty prohibitinganti-personnel mines. Another example is the prohibition of laser weapons.
Health care professionals have a duty to influence their organizations to respectethical considerations.
2. CATEGORY
Tool: familiarity with the role and responsibilities of health care personnel insituations of armed conflict.
3. FORMULATION
Define the role and responsibilities of health care personnel in situations ofarmed conflict.
4. TEACHING METHOD
Assignment presented to work groups.
5. DURATION
Total duration: 30 minutes
. 15 minutes for work in groups
. 15 minutes for summary in plenary session.
6. RECAPITULATION
. Box 1: Primary role of health care professonals: to provide care
. Box 2: Definition of health (WHO)
. Box 3: Roles of health care professionals
. Box 4: Consequences of armed conflict for people and populations
. Box 5: Definition of health in situations of armed conflict (ICRC)
. Box 6: Health care professionals’ role in protection
. Box 7: Health care professionals and international humanitarian law
. Box 8: Ethical problem of health care professionals confronted withviolations of international humanitarian law: what attitude to take?
. Box 9: Health care professionals and the conduct of hostilities
. Box 10: Anti-personnel mines: from conception to effects
. Box 11: Strategy for a total ban of anti-personnel mines
HELP/SOS: RECAPITULATION AND CONCLUSION548 549

. Box 12: Prohibition of anti-personnel mines
. Box 13: Blinding laser weapons
LINK WITH NEXT OBJECTIVES
Health care professionals have an obvious role in the provision of assistance andprotection to victimsof armed conflict. Theywork in humanitarianorganizationsthat have their own mandates and strategies for providing humanitarianassistance. The last objective of this module will address the problem ofcoordinating humanitarian actions.
Box 1
PRIMARY ROLE OF HEALTH CAREPROFESSIONALS: TO PROVIDE CARE
RECAPITULATION AND CONCLUSION 549

551
Box 2
DEFINITION OF HEALTH
(WHO)
Box 3
ROLES OF HEALTH CAREPROFESSIONALS
1. Care for the sick and wounded
2. Prevent disease
3. Maintain health
Health is a state of complete physical,
mental, and social well-being
and not merely the absence
of disease or infirmity.
HELP/SOS: RECAPITULATION AND CONCLUSION550

Box 4
CONSEQUENCES OF ARMED CONFLICTFOR PEOPLE AND POPULATIONS
. Murder
. Torture
. Mistreatment
. Rape
. Voluntary enlistment
. Hostage-taking
. Arbitrary detention
. Loss of judicial guar-antees
. Harassment
. Reprisals
. Indiscriminate attacks
. Mass exodus
. Deprivation of themeans for survival
. Break-up of families
. Internment
. Ethnic cleansing
. Deportation
. Genocide
Box 5
DEFINITION OF HEALTH IN SITUATIONSOF ARMED CONFLICT
(ICRC)
In situations of armed conflict, security is an essentialelement in improving and maintaining health.
Security means that the essential needs of the victimsare covered on a sustainable basis and that theirfundamental rights are respected.
RECAPITULATION AND CONCLUSION 551

553
Box 6
HEALTH CARE PROFESSIONALS’ROLE IN PROTECTION
1. Care for sick and wounded
2. Prevent disease
3. Maintain health
4. Protect victims
Box 7
HEALTH CARE PROFESSIONALSAND INTERNATIONALHUMANITARIAN LAW
Health care professionals must incorporate the rules of
international humanitarian law in their strategy of action
on behalf of the victims of armed conflict, in order to
ensure the protection of both the victims themselves
and the objects indispensable to their survival.
HELP/SOS: RECAPITULATION AND CONCLUSION552

Torture
Harassment Murder
Hostage-taking
Forceddisplacement
Ethniccleansing
Arbitrarydetention
Indiscriminateattacks
Rape
Inhumantreatment
Deportation Genocide
Box 8
ETHICAL PROBLEM OF HEALTH CAREPROFESSIONALS CONFRONTED
WITH VIOLATIONS OF INTERNATIONALHUMANITARIAN LAW:
WHAT ATTITUDE TO TAKE?
. Discuss and negotiate the end of the violations with thosedirectly and hierarchically responsible for them.
. Denounce those responsible for violations of internationalhumanitarian law
RECAPITULATION AND CONCLUSION 553

555
Emergency
Civilianpopulations
Wounded
Victims
Wounded
Party to the conflict
Party to the conflict
Conduct ofhostilities
Protection and assistanceof war victims
Health care systemSuppliesInfrastructures
Detainees
Detainees
Box 9
HEALTH CARE PROFESSIONALSAND THE CONDUCT OF HOSTILITIES
HELP/SOS: RECAPITULATION AND CONCLUSION5554

Research/conception
Production
Marketing/storage
Use
Public health Individual
Effects observedon health
Box 10
ANTI-PERSONNEL MINES:FROM CONCEPTION TO EFFECTS
RECAPITULATION AND CONCLUSION 5555

557
Political level
Epidemiological level
Legal level
Surgical level
Box 11
STRATEGY FOR A TOTAL BANOF ANTI-PERSONNEL MINES
HELP/SOS: RECAPITULATION AND CONCLUSION5556

Box 12
PROHIBITIONOF ANTI-PERSONNEL MINES
. International Strategy Conference Towards A GlobalBan On Anti-Personnel Mines, Ottawa(October, 1996)
. International Conference of Brussels(June, 1997)
. Diplomatic Conference on Landmines,Oslo (September, 1997)
Adoption of the Convention on the Prohibition of theUse, Stockpiling, Production and Transfer ofAnti-Personnel Mines and on Their Destruction(Ottawa Treaty)
Art. 1, para. 1:
‘‘Each State Party undertakes never under any circumstances
a) To use anti-personnel mines;
b) To develop, produce, otherwise acquire, stockpile, retain ortransfer to anyone, directly or indirectly, anti-personnel mines;
c) To assist, encourage or induce, in any way, anyone to engage inany activity prohibited to a State Party under this Convention.’’
. Ottawa Conference (December, 1997)Ottawa treaty open for signature.121 States have signed.
RECAPITULATION AND CONCLUSION 557

559
Box 13
BLINDING LASER WEAPONS
Problem:
The use of such weapons causes permanentblindness.
In September, 1995, in Vienna, the ReviewConference of the States Party to the 1980Convention on Prohibitions or Restriction on theUse of Certain Conventional Weapons adopteda Protocol on Blinding Laser Weapons(Protocol IV).
‘‘Article 1:
It is prohibited to employ laser weapons specificallydesigned, as their sole combat function or as one oftheir combat functions, to cause permanent blind-ness to unenhanced vision, that is to the naked eyeor to the eye with corrective eyesight devices. TheHigh Contracting Parties shall not transfer suchweapons to any State or non-State entity.’’
(Adopted on 13 October 1995)
HELP/SOS: RECAPITULATION AND CONCLUSION558

COORDINATING HUMANITARIAN ACTION
1. DESCRIPTION
The coordination of humanitarian action is a recurring problem for which nosatisfactory solution has been found. Nonetheless, the instructor should not turnthis educational objective into an unstructured forum with no real content.
The rule is to go from the simplest to the most complex. Initially, the instructorshould analyse the problem of coordination within the context of health careactions, thereafter expanding the subject to include all humanitarian activities,and finally raising the issue of the interface between humanitarian action and theresolution of armed conflict.
At each of these levels, three questions must be asked:
. What do we want to coordinate?
. Are the protagonists willing to be involved in a process of coordination?
. What are the means for ensuring some form of coordination?
1.1. Coordination in the health sphere
What should be coordinated?
This question leads to the definition of a humanitarian action intended to protectand assist victims of armed conflicts.
Course participants must, then, be called upon to reconstruct a humanitarianaction from basic elements. For example, in the health sphere, these elementscorrespond to a whole range of activities, such as nutritional rehabilitation, drugdistributions, support for a hospital, an immunization campaign, developmentof a water source, etc.
We return to the general outline of a health care system to help us identify what
should be coordinated.
The first aspect is coordination between activities deriving from the sameprogramme (vertical coordination). A useful example is the food supplychain; without coordination, food distributions may compromise efforts torehabilitate agricultural production. Another example is nutritional rehabi-litation,whichmust be coordinatedwithmeasures to guarantee family accessto food resources.
The second aspect is coordination between vertical programmes designed tohave an impact on health (horizontal coordination). Participants should be
RECAPITULATION AND CONCLUSION 559

561
reminded of the relationship between water supply programmes andenvironmental and sanitation programmes on one hand, and programmesfor the control of communicable diseases on the other.
Since these two aspects of coordination have been explained in the moduleon health care systems; they need not be reviewed in detail.
Who should be coordinated?
Numerous agents are involved in health care activities in armed conflict,including the health ministries of the countries in question, national non-governmental organizations, international non-governmental organizations,UN humanitarian organizations, and the ICRC.
As a general rule, everyone recognizes the need for coordination, but no onewants to be coordinated.What happens in the field is probablymore the result ofdialogue and collaboration than any structured coordination effort based on aparticular vision of the health care system.
In setting objectives, each agency tends to define and conduct its activitiesindependently. Before actually embarking on an action, however, the mainagencies confer to some extent concerning their intentions in a given situation.Although this informal mechanism does not prevent all the deplorableduplications of effort, it does reduce their number.
In the framework of health care and relief activities, there is a certaincollaboration between agencies in the form of exchanges of material resources,loans of logistical means, and provision of services—for example, if the ICRCruns short of food supplies, it might borrow from the WFP.
What means are available for purposes of coordination?
In the health sphere, planning and epidemiology are two tools that provideconcrete bases for coordination. One example is the definition of clear objectives,which reveals exactlywhat each agency intends to do in a given situation.Anotherexample is epidemiological surveillance, whichmakes it easier to pinpoint gaps inthe supply of health services and to offer agencies solutions for filling them.
Agents in the field organize meetings for the exchange of health information.Such meetings provide opportunities for everyone to find out what activities arebeing planned or implemented by the various health care agencies.
Another point to mention is the coordinating work that takes place inpreparation for future crises—work that focuses on the standardization ofequipment, operational policies, and training. For example, engineers meetperiodically to standardize the medical equipment used in humanitarian actions,
HELP/SOS: RECAPITULATION AND CONCLUSION560

in order to facilitate equipment loans and exchanges later on. Similarly, in thetraining field, certain basic terms of reference are taught to all health carepersonnel in the courses given by the various humanitarian agencies.
The idea of coordination is thus acknowledged and accepted, in principle if not in
practice, by all the agents involved in health care activities. The allocation of tasks is
often determined by the mandate or recognized expertise of a particular agency.
However, the coordination apparatuses that are instituted on the national level
rarely have any way of enforcing decisions—hence the spectacle of agencies that
propose actions without having the means to carry them out, or propose actions that
do not fit into an overall plan.
1.2. Coordination of activities linked to humanitarian problems of all kinds
What should be coordinated?
Mention has already been made of the problem of protecting victims of armedconflict, and the health implications of the application of internationalhumanitarian law, which prevents forced displacement of populations, offersprotection for hospitals, etc.
This link between assistance activities and protection activities was discussed atlength in the preceding objective with respect to the responsibilities of health careprofessionals, whose concern must be to preserve both the health and the dignityof the victims for whom they are responsible. The vital interrelation betweenassistance and protection must form part of the strategies of every humanitarianagency. We saw that one of the responsibilities of health care professionals is toinfluence institutional policies in this respect.
However, within a humanitarian agency coordination between assistanceactivities and protection activities is not always easy, and sometimes poses ethicaldilemmas for health care professionals. Relief operations must, after all, haveaccess to the victims. But when health care activities take place in a context wherethe rules of international humanitarian law are repeatedly and seriously violatedwithout any prospect of an end, the continuation of relief activitiesmay be viewedas an endorsement of those perpetuating the violations. Evenmore serious, if theaid isnotmonitoredandsomeof it isdiverted, it providesactual support forarmedgroups who deliberately violate international humanitarian law.
To deal with this situation, agencies have developed various policies. The ICRC’sdoctrine concerning the denunciation of massive violations of internationalhumanitarian law could be mentioned here.
The overall approach to the problems of victims may pose coordinationdifficulties within each agency; one can imagine the problems involved in trying
RECAPITULATION AND CONCLUSION 561

563
to coordinate several humanitarian agencies with different mandates andstrategies. The ICRC and Amnesty International could be cited as an example:The ICRC gives priority to negotiation, whereas Amnesty International’sstrategy is to denounce violations publicly.
The linkagebetween activities defined as emergencymeasures and those consideredasdevelopmentactivities is anotherdimension that shouldbeanalysedaspartof theoverall approach to the problems of victims of armed conflict. Direct aid to thevictims tends to encourage dependence, thereby compromising programmesdesigned to develop local capacities. Emergency activities, particularly those aimedat rehabilitating national systems, must be planned with some thought to theirpotential for becoming self-sufficient in the medium term.
Who should be coordinated?
The number of humanitarian agencies involved in a given context is often large.This factor is compounded by differences in mandate, objectives, strategies, andavailable resources.
At this point the instructor should mention a number of humanitarian agencieswith a general approach (victims of armed conflict, overall needs, assistance andprotection, long and short term) such as the ICRC, and agencies with a morespecific focus, such as Medecins sans Frontieres (MSF) for health, the UNHighCommissioner for Refugees (UNHCR) for refugees and displaced persons,WFPfor food, Amnesty International for detainees, UNICEF for children, etc.
What means are available for purposes of coordination?
In the field, humanitarian agencies have their own mechanisms of coordina-tion—basicallymeetings at which humanitarian agents exchange information ontheir activities and future plans. Such mechanisms carry little weight in thedecisions made by the various agencies, however, for various reasons:
. no agency has a formal mandate to ensure coordination
. certain agencies are unable to act within a framework defined by criteriaother than their own
. agencies want to remain independent in both their operations and their fund-raising efforts
. agencies that are openly in conflict are difficult to coordinate.
Beyond this limited coordination in the field of operations, mechanisms ofcoordination can be found within certain blocs of humanitarian agencies. Theresponsibilities of the various components of the Red Cross and Red CrescentMovement were defined in the Seville Agreement of December, 1997. UNHCRcoordinates actions to benefit refugees with the governments of the host
HELP/SOS: RECAPITULATION AND CONCLUSION562

countries, and has concluded a framework agreement (Partnership in Action, orPARinAC) with the NGOs to define respective responsibilities in jointoperations. The UN’s humanitarian interests are coordinated by the UN Officefor the Coordination of Humanitarian Affairs (OCHA), which is responsible forpolicies on humanitarian issues, mobilization of UN political organs, andcoordination of humanitarian activities. On the international level, the Inter-Agency Standing Committee (IASC), incorporating seven UN bodies and guestorganizations (ICRC, Federation of Red Cross and Red Crescent Societies,Interaction, and the International Council of VoluntaryAgencies [ICVA]),meetstwice a year to develop common humanitarian policies, exchange information onthe different members’ respective operations, and resolve disputes. It is a forumfor dialogue more than an actual mechanism for coordinating humanitarianaction, however, since it has no power to enforce decisions, nor to launch jointfundraising appeals in order to distribute the funds afterwards among thedifferent humanitarian agencies.
The Code of Conduct for the International Red Cross and Red CrescentMovement and NGOs is a document establishing humanitarian agencies’consent to the application of fundamental humanitarian principles. In thisaspect, it permits greater cohesion among humanitarian agencies.
Any real coordination among humanitarian agencies is practically impossible toachieve as long as mandates and strategies differ. Moreover, the principle itself isnot in fact a desirable goal, since some humanitarian agencies are notindependent of political agencies. Ultimately, interagency coordination wouldpresent the risk that humanitarian objectives would be subordinated to politicalobjectives involved in the resolution of armed conflict. This brings us to the nextpoint.
1.3 Relations between humanitarian agencies and other interested parties
What should be coordinated?
At this stage, some remarks should be made about the general context in whichan armed conflict develops, and the principal types of relief action should belinked to the phases of development. The instructor might describe:
. development activities, which work to resolve the underlying causes of thearmed conflict (promotion of human rights, reduction of socio-economicinequalities, access to education, etc.)
. activities designed to prevent crises from developing into situations of armedconflict (preventive diplomacy, installation of UN observers, deployment ofpeace-keeping forces, arms embargo, etc.) and activities that, during periodsof crisis, seek to minimize the humanitarian consequences of a potential
RECAPITULATION AND CONCLUSION 563

565
conflict (dissemination of the principles of international humanitarian law,alerts to humanitarian agencies, etc.)
. activities during the conflict, some aiming to resolve it (coercive diplomacy,forces to restore peace, etc.) and others seeking to limit its humanitarianconsequences (victim assistance and protection)
. activities during the post-conflict phase to promote rehabilitation andeconomic, social, and judicial reconstruction
. and finally we come back to development activities.
All these activities can be analysed from two perspectives:
. emergency versus development activities
. humanitarian versus political activities.
Although it is difficult to achieve any real coordination between activities sodiverse, measures can be taken to prevent them from interfering with each other.For example, measures specifically related to an emergency must be preventedfrom adversely effecting development projects (food aid should not endangeragricultural development programmes), while humanitarian activities must notcontribute to an increase in violence or compromise a possible political solution(through the diversion of humanitarian aid, for example).
A similar problem is political activities that contribute to an increase ofhumanitarian problems, such as the application of economic sanctions thatworsen the situation of the most vulnerable population sectors.
The positive impact that humanitarian measures may have on political activityshould also be analysed. The resolution of humanitarian problems helps reducehatred and violence, thereby contributing to the restoration of a lasting peace. Inuncontrolled situations dominated by insecurity and violations of internationalhumanitarian law, the following question might be asked:
At what point should humanitarian organizations recognize their impotenceand ask political agencies to act in order to restore a modicum of security?
This question leads to others:
. What criteria would be used to define a situation as unmanageable forhumanitarian organizations?
. Who would have the responsibility for deciding that a situation had becomeunmanageable for humanitarian organizations: humanitarian agencies,political agencies, or both?
Basically, all agencies share a desire to restore peace, and know that both politicaland humanitarian activities can contribute to this end. Mixing the two kinds of
HELP/SOS: RECAPITULATION AND CONCLUSION564

activities, however, may endanger the fundamental principles of humanitarianaction: impartiality, neutrality, and independence.
Who should be coordinated?
Still referring to the basic outline of an evolving conflict, the instructor will askparticipants to link the activities that have been identified at each level with theresponsibilities of the agencies involved (based on their mandates).
Next, two issues will be studied:
. spheres where the responsibilities of different agencies overlap
. possible links between different entities (humanitarian agencies, donors,UNHCR, NGOs, UN, States, OSCE, NATO, etc.).
Depending on the case, such links may reinforce the activities of the differentbodies—in the following fields of endeavour, for example:
. making the public aware of the causes of humanitarian problems(humanitarian agencies and the media)
. financial coverage of humanitarian operations (humanitarian agencies anddonors)
. diplomatic and humanitarian action (humanitarian agencies and States).
However, they may also be detrimental:
. armed escorts for humanitarian agencies, leading to loss of neutrality(humanitarian agencies and military forces)
. use of the media to obtain greater publicity for the humanitarian agencies asorganizations (humanitarian organizations and media)
. subordination of humanitarian objectives to political ones (humanitarianagencies and donor States).
Ideally, political and humanitarian agencies should act exclusively within theirown respective spheres of responsibility, while fitting their activities into acoherent whole. The encroachment of humanitarian agencies on the politicaldomain or of political agencies on the humanitarian domain is usually the resultof operational constraints:
. lack of access to victims, leading humanitarian agencies to take politicalpositions
. media pressure on political agencies to act, leading them to take action in thehumanitarian field if political measures are not possible
. financial pressure exercised by donors on humanitarian agencies for targetedaction that does not necessarily correspond to the victims’ real needs, butrather to political agents’ need for visibility.
RECAPITULATION AND CONCLUSION 565
567
Somehow the following paradoxmust be resolved: conceptually, the two types ofaction are interdependent, but in practice, their implementation must bedissociated. This dissociation is important during the conflict stage, when theprinciple of neutrality is essential for humanitarian agencies. This is whycentralized coordination, involving the determination of objectives by a singlebody, is not necessarily desirable. At most, we might aspire to a space fordialogue, and in certain cases mutual consultation.
The fact that both political (Security Council) and humanitarian (UNHCR,UNICEF, WHO) agencies coexist within the UN should permit the UN tomanage all its activities according to a coherent, overall plan. However, thissituation also implies the risk that humanitarian objectives will be integratedwithbroader, political objectives.
What means are available to effect a minimum of mutual consultation?
In the field, a dialogue between all involved parties is essential to achieve the aimof reciprocal notification about planned or current operations.
Opportunities for a more general dialogue between humanitarian agencies andpolitical agencies also exist. In the ICRC, the aim of humanitarian diplomacy isto provide coherence to the organization’s relations with UN bodies, the NGOs,and political bodies. The Conference of the Red Cross and Red CrescentMovement, which brings together the components of the Red Cross and RedCrescent Movement and the States, is an example of a systematic encounterbetween humanitarian and political agents.
In addition, issue-oriented meetings take place regularly between political andhumanitarian bodies—for example, the Wolfsberg meetings organized by theICRC.
2. CATEGORY
Summary: coordinating humanitarian action.
3. FORMULATION
This objective is divided into three parts. For each part participants will be askedthree questions.
. Coordination in the health field:
. What should be coordinated?
. Who should be coordinated?
. What means are available for purposes of coordination?
HELP/SOS: RECAPITULATION AND CONCLUSION566

. Coordination of all the activities linked to humanitarian problems:
. What should be coordinated?
. Who should be coordinated?
. What means are available for purposes of coordination?
. Relations between humanitarian agencies and the other agents involved inarmed conflicts:
. What should be coordinated?
. Who should be coordinated?
. What means are available to ensure a minimum of mutual consultation?
4. TEACHING METHOD
Assignment presented to work groups, with a plenary session after each group ofquestions.
5. DURATION
Total duration: 180 minutes
. 30 minutes (per group of questions) for work in groups
. 30 minutes (per group of questions) for summary in plenary session.
6. RECAPITULATION. Box 1: Coordination (health care activities as a starting point)
. Box 2: Types of relationships between agencies
. Box 3: Outline of a health care system
. Box 4: Outline of a health care system, including agencies
. Box 5: Coordination of health care activities
. Box 6: Factors limiting effective coordination in the health field
. Box 7: What canbe done to improve the coordinationof heath care activities?
. Box 8: Assistance and protection: coordination
. Box 9: Assistance and protection: agents
. Box 10: Relations between agents: the example of the ICRC
. Box 11: Factors limiting the coordination of humanitarian aid
. Box 12: What can be done to improve the coordination of humanitarian aid?
. Box 13: Humanitarian activities and conflict-resolving activities
. Box 14: Humanitarian agencies and political agencies
RECAPITULATION AND CONCLUSION 567

569
. Box 15: Relationships between agencies in the general context of armedconflict: the example of the ICRC
. Box 16: Factors limiting coordination between humanitarian and politicalaction
. Box 17: What can be done to improve the interface between humanitarianand political action?
. Box 18: Political and humanitarian spheres
. Box 19: Interference of one kind of agency in the domain of the other
. Box 20: The actors are different
. Box 21: NATO
. Box 22: UN
. Box 23: UN General Assembly
. Box 24: UN Security Council
. Box 25: Security Council interventions during the Gulf War
. Box 26: ECOSOC
. Box 27: UNICEF
. Box 28: MDM
. Box 29: MSF
. Box 30: OXFAM
. Box 31: UNDP
. Box 32: World Bank
. Box 33: Commission on Human Rights
. Box 34: ICRC
. Box 35: International Federation of Red Cross and Red Crescent Societies
. Box 36: National Red Cross and Red Crescent Societies
. Box 37: OCHA
. Box 38: IASC
. Box 39: UNHCR
. Box 40: WHO
. Box 41: OSCE
HELP/SOS: RECAPITULATION AND CONCLUSION568

Box 1
COORDINATION(Health Care Activities as a Starting Point)
1. Coordination ofhealth care activities
. What?
. Who?
. How?
2. Coordination ofhumanitarian aid:
. What?
. Who?
. How?
3. Coordinationof all war-linkedactivities:
. What?
. Who?
. How?
Box 2
TYPES OF RELATIONSHIPSBETWEEN AGENCIES
. Concentration
. Confusion
. Consultation
. Conferring
. Coordination
. Cooperation
. Contribution
. Coercion
. Competition
. Confrontation
. Conflict
RECAPITULATION AND CONCLUSION 569

571
Watersupply
Sources
Storage
Distribution
Water consumption
Water use
Disposal of liquid waste
Environ-mental
sanitation
Human waste management
Garbagemanagement
Energysources
Shelter
Vectorcontrol
Control of communica-ble diseases
Primary prevention
(immunization)
Secondary prevention
Tertiary prevention
Treatment of communicable
diseases
Control of epidemics
Medical-surgical
care
Primarylevel
medical care
Secondary level
medical care
Tertiarylevel
medical care
Transfer between
levels
Management of war
injuries
First aid
Secondary level care
Evacuationand transport
Tertiary level surgical
care
Psycho-logical
support
Psycho-social support for individualsand families
Psycho-social support
at the community
level
Psycho-social support
at the institutional
level
Food andnutrition
Agricultural production
Economicsystem
Foodavailability
Accessibilityof food
resources
Food consumption
Biologicalutilization of
food
Nutritional status
POPULATION’S HEALTH
Box 3
OUTLINE OF AHEALTH CARE SYSTEM
HELP/SOS: RECAPITULATION AND CONCLUSION5570

Control of communica-ble diseases
Primaryprevention
(immunization)
Secondaryprevention
Tertiary prevention
Treatment of communicable
diseases
Control of epidemics
ICRC
OXFAM
NationalRC and RCSocieties
NationalNGOs
UNHCR
CARE
WFP
UNICEF
WHO
Others
Healthministries
MSF SCF
Fed. ofRC and RCSocieties
Watersupply
Sources
Storage
Distribution
Water consumption
Water use
Disposal of liquid waste
Environ-mental
sanitation
Human waste management
Garbagemanagement
Energysources
Shelter
Vectorcontrol
Medical-surgical
Care
Primarylevel
medical care
Secondarylevel
medical care
Tertiarylevel
medical care
Transfer between
levels
Managementof war
injuries
First aid
Secondarylevel care
Evacuationand transport
Tertiary level surgical
care
Psycho-logicalsupport
Psycho-social support for individualsand families
Psycho-social support
at the community
level
Psycho-social support
at the institutional
level
Food andnutrition
Agriculturalproduction
Economicsystem
Foodavailability
Accessibilityof food
resources
Foodconsumption
Biologicalutilization of
food
Nutritionalstatus
POPULATION’S HEALTH
Box 4
OUTLINE OF A HEALTH CARESYSTEM, INCLUDING AGENCIES
RECAPITULATION AND CONCLUSION 5571
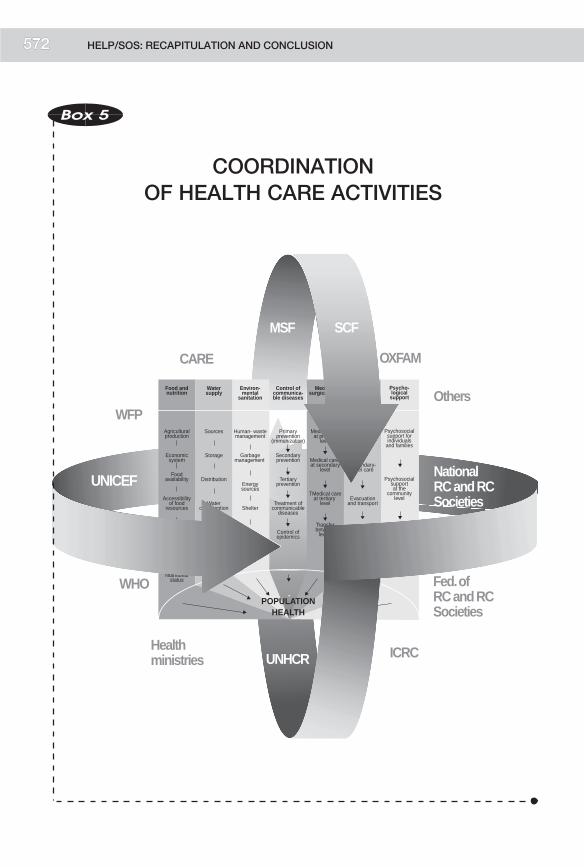
573
UNICEF
ICRC
OXFAM
NationalRC and RCSocieties
NationalNGOs
UNHCR
CARE
WFP
WHO
Others
Healthministries
MSF
Fed. ofRC and RCSocieties
Environ-mental
sanitation
Human- waste management
Garbagemanagement
Energysources
Shelter
Vectorcontrol
Control of communica-ble diseases
Primary prevention
(immunization)
Secondary prevention
Tertiary prevention
Treatment of communicable
diseases
Control of epidemics
Management of War
Injuries
First aid
Secondary-level care
Evacuationand transport
Tertiary-level surgical
care
Food andnutrition
Agricultural production
Economicsystem
Foodavailability
Accessibilityof food
resources
Food consumption
Biologicalutilization of
food
Nutritional status
POPULATIONHEALTH
SCF
Watersupply
Sources
Storage
Distribution
Water consumption
Water use
Disposal of liquid waste
Psycho-logical
support
Psychosocialsupport for individuals
and families
Psychosocialsupportat the
community level
Psychosocialsupport at the
institutionallevel
Medical-surgical Care
Medical care at primary
level
Medical care at secondary
level
TMedical care at tertiary
level
Transfer between
levels
SCF
Box 5
COORDINATIONOF HEALTH CARE ACTIVITIES
HELP/SOS: RECAPITULATION AND CONCLUSION5572

Box 6
FACTORS LIMITING EFFECTIVECOORDINATION IN THE HEALTH FIELD
. Sector-based approach
. Competition betweenagencies
. Selective planning
. Lack of standardization(health policies,equipment)
. Priority given to highly‘‘visible’’ activities
. Focus on short-termimpact
. Lack of credibility ofagencies that do not havethe necessary capacities
Box 7
WHAT CAN BE DONETO IMPROVE THE COORDINATIONOF HEALTH CARE ACTIVITIES?
FROM THE SIMPLEST TO THE MOST DIFFICULT:
. Development of tools foranalysing common pro-blems and strategies
. Multidisciplinary evaluation
. Better communicationbetween headquartersand the field
. Joint evaluation by severalagencies
. Joint fundraising
. Mandate given to oneorganization
RECAPITULATION AND CONCLUSION 573

575
Party
to the
conflict
Party
to the
conflictVictims
Healthcare
system
Box 8
ASSISTANCE AND PROTECTION:
COORDINATION
HELP/SOS: RECAPITULATION AND CONCLUSION5574

Partyto the conflict
Partyto the
conflictVictims
Health-care
system
OXFAM
ECHO
UN HumanRights
Commission
Nat. RC andRC Soc.
NGOs
UNHCR
CARE
WFP
UNICEF
WHO
Healthministries
MSF
Human rightsorganizations
MediaAmnesty
InternationalSCF
PHR
Fed. RC and RC Soc.
ICRC
Box 9
ASSISTANCE AND PROTECTION:
AGENTS
RECAPITULATION AND CONCLUSION 5575

577
Partyto the conflict
Partyto the
conflictVictims
Healthcare
system
ICRC
OXFAM
ECHO
UN HumanRights
Commission
Nat. RC andRC Soc.
NGOs
UNHCR
CARE
WFP
UNICEF
WHO
Healthministries
MSF
Human rightsorganizations
MediaAmnesty
InternationalSCF
PHR
Fed. RC andRC Soc.
Box 10
RELATIONS BETWEEN AGENTS:
THE EXAMPLE OF THE ICRC
HELP/SOS: RECAPITULATION AND CONCLUSION5576

Box 11
FACTORS LIMITINGTHE COORDINATION
OF HUMANITARIAN AID
. The donor is also a humanitarianagency
. Selective view of needs
. Different strategies (discreet negotiations vs.public denunciation)
. Conflict between the strategies of assistanceand protection
. Difficulty for one agency to coordinatewith agencies that have strategies conflictingwith its own
. Competition for financial resources
. Competition for media attention
RECAPITULATION AND CONCLUSION 577
579
Box 12
WHAT CAN BE DONETO IMPROVE THE COORDINATION
OF HUMANITARIAN AID?
POSSIBILITIES
. Promote better understanding of the strengths andweaknesses of the various strategies
. Establish cooperation agreements between differentagencies, for example:
. Seville Agreement: the Red Cross and Red Crescent Movement
. PARinAC: Agreement between UNHCR and the NGOs
. Set upmechanisms of coordinationwithin each group ofagencies, for example:
. OCHA
. ICVA
. Set up mechanisms of coordination between groups ofagencies, for example:
. IASC
. True coordination would require:
. Joint evaluations
. A shared programme
. Joint fund-raising appeals
Is this realistic?Is this desirable?
HELP/SOS: RECAPITULATION AND CONCLUSION578

Peace
Crisis
Conflict
Peace
Reconstruction
Resolution
Resolution of the political crisis
Resolution of the humanitarian crisis
Box 13
HUMANITARIAN ACTIVITIESAND CONFLICT-RESOLVING ACTIVITIES
RECAPITULATION AND CONCLUSION 5579

581
OXFAMECHO
UN Commissionon Human Rights
Nat. RC and RCSocieties
NGOs
UNHCR
CARE
WFP
UNICEF
WHO
Healthministries
MSF
SecurityCouncil
MilitaryPersonnel
UN Forces
ICRC
World Bank
NATO
UN GeneralAssembly
States
DevelopmentAgencies
Human rightsorganizations
Media
AmnestyInternational
SCF
PHR
Fed. RC and RCSocieties
Box 14
HUMANITARIAN AGENCIESAND POLITICAL AGENCIES
HELP/SOS: RECAPITULATION AND CONCLUSION5580

Military forcesUN (political organ:
Security Council, GeneralAssembly, Economicand Social Council
UN (peacekeepingforces, peaceenforcementinterventions)
Media
Parties to theconflict
Developmentagents
Governmental organizations.
NGOs
CICRICRC
States
Specializedagencies of theUN, UNHCR,
WHO
Intergovernmentalagencies
Box 15
RELATIONSHIPS BETWEEN AGENCIESIN THE GENERAL CONTEXT
OF ARMED CONFLICT
THE EXAMPLE OF THE ICRC
RECAPITULATION AND CONCLUSION 5581

583
Box 16
FACTORS LIMITING COORDINATIONBETWEEN HUMANITARIANAND POLITICAL ACTION
. Independence of humani-tarian agencies
. Humanitarian strategybased on strict neutrality
. Limitations on choice ofmeans (embargo, militarymeans)
. Insecurity limitinghumanitarian action
. Humanitarian objectivesas a substitute for politicalobjectives
. Impact of humanitarianaction on conflict develop-ment
Box 17
WHAT CAN BE DONE TO IMPROVE THEINTERFACE BETWEEN HUMANITARIAN
AND POLITICAL ACTION?
. Better understanding of mandates
. Promotion of diplomacy
. Participation in forums including both humanitarian andpolitical agencies (e.g., Wolfsberg)
. International Conference of the Red Cross and RedCrescent Movement
HELP/SOS: RECAPITULATION AND CONCLUSION582

Party
to the
conflict
Party
to the
conflict
Peace Peace
Application plan de paix
Promotion ofhuman rights
Democratization
Education
Economicdevelopment
Socialdevelopment Cultural
development
Diffusion du DIH
Urgence
Victimes
Protection des victimes
Guerres
Humanitarianactivities
Politicalactivities
Peace-keeping
Preventivediplomacy
Coercivediplomacy
Rehabilitation
Justice
Detainees
EmergencyLink with
developmentactivities
Civilianpopulations
Negotiationswith the partiesto the conflict
Relations withother agencies
Relations withthe media
Wounded
Box 18
POLITICALAND HUMANITARIAN SPHERES
RECAPITULATION AND CONCLUSION 5583

585
Party
to the
conflict
Party
to the
conflict
Peace Peace
Promotion ofhuman rights
Democratization
Education
Economicdevelopment
Socialdevelopment
Culturaldevelopment
Diffusion du DIH
Victimes
Protection des victimes
Guerres
Humanitarianagencies
Politicalactivities
Peace-keeping
Preventivediplomacy
Coercivediplomacy
Rehabilitation
Justice
Application of peace plan
Link withdevelopment
activitiesEmergency
Negotiationswith the partiesto the conflict
Relations withother agenciesRelations with
the media
EmergencyCivilian
populations
Wounded Wounded
Box 19
INTERFERENCE OF ONE KINDOF AGENCY
IN THE DOMAIN OF THE OTHER
HELP/SOS: RECAPITULATION AND CONCLUSION5584

Coordination: The actors are different
Partyto the conflict
Partyto the
conflictVictims
Healthcare
system
Means Means
Strategies Strategies
Objectives Objectives
Priorities Priorities
Mandate Mandate
Box 20
THE ACTORS ARE DIFFERENT
RECAPITULATION AND CONCLUSION 5585

587
Box 21
NATO
NORTH ATLANTIC TREATY ORGANIZATION
History: The North Atlantic Treaty was signed in 1949.
Mission: The Treaty creates a political and military defence alliance
to prevent aggression against its members.
Structure: A civilian administration comprising 16 members under theauthority of the North Atlantic Council.
A military administration under the authority of the Military
Committee supervises the various commands.
The Euro-Atlantic Partnership Council is a framework fordialogue and cooperation with the countries of Central and
Eastern Europe.
The aim of Partnership for Peace is to promote dialogue
and cooperation with non-member States (Switzerland,Sweden).
Action: . Evaluation of military needs
. Coordination of arms control policies
. Establishment of cooperative ties with Central andEastern European partners
. Mobilization in the framework ofmissions tomaintain and
re-establish peace
. Fact-finding in conflict situations
HELP/SOS: RECAPITULATION AND CONCLUSION586
Box 22
UN
UNITED NATIONS ORGANIZATION
History: The idea of creating an international organization wasexpressed in the Moscow Declaration (30 October 1943),which recognized:
‘‘the necessity of establishing at the earliest practicable datea general international organization, based on the principleof the sovereign equality of all peace-loving states, andopen to membership by all such states, large and small, forthe maintenance of international peace and security.’’
The United Nations Charter was signed at the Conferenceof San Francisco on 26 June 1945.
Mission: ‘‘We the peoples of the United Nations, determined. to save succeeding generations from the scourge of war,which twice in our lifetime has brought untold sorrow tomankind, and
. to reaffirm faith in fundamental human rights, in thedignity and worth of the human person, in the equal rightsof men and women and of nations large and small, and
. to establish conditions under which justice and respectfor the obligations arising from treaties and other sourcesof international law can be maintained, and
. to promote social progress and better standards of life inlarger freedom [...].’’
Preamble of the Charter of the United Nations
Objectives: . To maintain international peace and security. To develop friendly relations among nations based onrespect for the principle of equality between peoples
. To develop international cooperation in the economic,social, intellectual, and humanitarian spheres
. To promote respect for human rights and fundamentalfreedoms.
RECAPITULATION AND CONCLUSION 587

589
Box 23
UN
GENERAL ASSEMBLY
. Is composed of all the Member States.
. Meets in sessions (regular, special, emergencyspecial).
. Functions in the following frameworks:
. plenary session
. committees (7)
(1) Disarmament and International Security Committee
. specific political issues
(2) Economic and Financial Committee
(3) Social, Humanitarian and Cultural Committee
(4) Special Political and Decolonization Committee
(5) Administrative and Budgetary Committee
(6) Legal Committee
. Passes resolutions (decisions,recommendations).
HELP/SOS: RECAPITULATION AND CONCLUSION588

Box 24
UN
SECURITY COUNCIL
The Security Council is composed of 15 members:
. 5 permanent members
. 10 non-permanent members
The presidency rotates monthly among the MemberStates according to alphabetical order.
The permanent members may exercise their right of veto.
The Security Council’s objective is to maintaininternational peace and security:
. Investigation of disputes (Art. 34).
. Recommendations concerning the resolution of disputes (Arts. 36and 38).
. Arms regulation (Art. 26).
. Recommendations in cases of threats to peace (Art. 39).
. Call for economic sanctions and other measures not involving theuse of armed force (Art. 41).
. Call for armed intervention (Art. 42).
RECAPITULATION AND CONCLUSION 589

591
Box 25
SECURITY COUNCIL INTERVENTIONS
DURING THE GULF WAR
2 August 1990 Resolution 660 condemns the invasion and calls
for the immediate withdrawal of Iraqi troops.
6 August 1990 Resolution 661 imposes mandatory economicsanctions and creates a sanctions committee.
25 August 1990 Resolution 665 institutes a naval blockade.
25 September 1990 Resolution 670 institutes an aerial blockade.
20 November 1990 Resolution 678 authorizes recourse to any means
necessary to restore peace.
16 January 1991 The Security Council authorizes an armed inter-
vention by Kuwait’s allies, marking the beginningof Operation Desert Storm.
26 February 1991 Iraq requests a cease-fire.
3 April 1991 Resolution 687 establishes the conditions for acease-fire.
HELP/SOS: RECAPITULATION AND CONCLUSION590

Box 26
ECOSOC
ECONOMIC AND SOCIAL COUNCIL
Structure: ECOSOC is composed of 54 members elected according
to geographical quotas.
ECOSOC holds one session a year.
Decisions are taken by majority vote by the members
present.
Action: . Promotion of economic and social
development
. Promotion of international cooperation in the
economic, social, cultural, and education
spheres
. Promotion of respect for human rights and fundamental
freedoms
RECAPITULATION AND CONCLUSION 591

593
Box 27
UNICEF
UNITED NATIONS CHILDREN’S FUND
History: The UN General Assembly established UNICEF byResolution 57 (1946) as a temporary body to provide aid to
children in countries at war.
With Resolution 802 (1953), the UN General Assemblymade this body permanent and expanded its mandate.
Mission: To aid countries, particularly developing countries, to
provide permanent health services for children.
In 1996 the UNICEF Executive Board expanded theorganization’s mandate to include, in particular, promotion
of children’s rights.
Structure: The Executive Board has 36 members. It meets several
times a year. The members of the Executive Board arerecruited according to geographical quotas.
Action: . Promotion of children’s rights
. Mobilization of material resources for aid to developingcountries
. Response to the protection needs of children in
emergency situations
HELP/SOS: RECAPITULATION AND CONCLUSION592

Box 28
MDM
MEDECINS DU MONDE
(Doctors of the World)
History: Organization founded in 1980.
Mission: The fundamental principles on which the action of MDM is
based can be summed up by the motto:
‘‘Heal, bear witness, stand up for human rights.’’
Structure: International secretariat based in Paris.
The structures of the national sections are
autonomous.
Action: MDM sections are concentrated mainly in the sphere
of health. MDMacts in both emergency situations and long-
term operations, such as rehabilitation and health-relateddevelopment.
MDM acts on behalf of vulnerable populations, in both
developed and developing countries.
MDM takes a public stand on human rights violations.
RECAPITULATION AND CONCLUSION 593

595
Box 29
MSF
MEDECINS SANS FRONTIERES(Doctors without Borders)
History: Organization founded in 1971 in Paris.
Mission MSF’s action is based on a charter that defines the contextand form of its activities:
‘‘neutrality and impartiality in the name of universal medicalethics and the right to humanitarian assistance.’’
Structure: MSF comprises several sections, each directed by apresident and a general manager. The International Councilmeets every three months.
Action: MSFacts in emergency situations (natural disasters, epidemics,armed conflict). It deals primarily in health matters.MSF also develops rehabilitation programmes.
MSF is very active in the field of human rights, and takes apublic stand when human rights are violated.
Box 30
OXFAM
History: OXFAM began in 1942 as the Oxford Committee for
Famine Relief.
Mission: Its philosophy of action has developed from emergency
action to long-term programmes, and emphasizes buildinglocal capacities.
Strategy: OXFAMworks closely with government authorities in order
to build local capacities. This approach goes hand in handwith advocacy.
Action: OXFAM works in emergency situations, focusing in
particular on water and sanitation programmes.
HELP/SOS: RECAPITULATION AND CONCLUSION594

Box 31
UNDP
UNITED NATIONS DEVELOPMENT PROGRAMME
History: UNDP was created in 1966 by UN General Assembly
Resolution 2029.
Mission: To assist countries in their efforts to achieve sustainable
human development.
Structure: UNDP is under the authority of the UN Economic and
Social Council.
Its Executive Board defines general policy and approvesrequests for assistance.
It is constituted by 36 members selected according to
geographical quotas.
UNDP collaborates with the World Bank, ILO, WHO,
FAO, etc.
Action: . Assists countries to strengthen their
capacities.
. Implements development programmes for theeradication of poverty, the creation of employment,
and the protection and rehabilitation of the
environment.
RECAPITULATION AND CONCLUSION 595

597
Box 32
WORLD BANK
The World Bank comprises:
. International Bank for Reconstruction and
Development
. International Development Association
. International Finance Corporation
. Multilateral Investment Guarantee Agency
History: It was created following the Bretton Woods Conference in1944, and began operations in 1946.
Mission: To promote financial exchanges at the international leveland to help finance the rebuilding of countries devastated
during World War II.
Structure: The Board of Governors includes a governor for each
member State. It meets once a year with the Board of theIMF, and comprises 22 administrators.
In 1977 the World Bank created a unit designed to act in
post-conflict situations.
Action: . Provides loans for production projects
. Finances economic reforms(structural adjustment)
HELP/SOS: RECAPITULATION AND CONCLUSION596

Box 33
COMMISSION ON HUMAN RIGHTS
History: The Commission on Human Rights was established in
1946 by Resolutions 5 and 9 of the UN Economic andSocial Council.
Mission: To protect and promote human rights.
Structure: The Commission has 48 members (originally 18) who areelected by the Economic and Social Council for three years
according to geographical quotas.
The Commission has created a certain number ofsubsidiary bodies, such as the Sub-Commission on
Prevention of Discrimination and Protection of Minorities.
Action: . Establishment of standards:
Recommendations, reports on human rights, women’s
status, freedom of information, the protection of mino-
rities, the prevention of discrimination, etc.
. Monitoring procedures:
‘‘1503 procedure’’ for examining individual communica-
tions (complaints).
Analyses of a situation or problem by a special
rapporteur.
RECAPITULATION AND CONCLUSION 597

599
Box 34
ICRC*
INTERNATIONAL COMMITTEE OF THE RED CROSS
History: . 1859: Solferino
. 1863: International Committee for Relief to WoundedSoldiers
. 1864: First Geneva Convention
. 1880: International Committee of the Red Cross
Mission: To protect and assist victims of war.
Structures: Committee composed of 25 members meeting in anAssembly that decides general policy. The ICRC is headed
by a board of four directors.
Action: . Protects and assists victims of war
. Promotes, develops, and monitors the application of
international humanitarian law
. Maintains and disseminates the fundamental principlesof the Red Cross and Red Crescent Movement
. Recognizes new National Societies
* The ICRC’s role has already been described in Module 9,‘‘Protecting the Victims of Armed Conflict’’.
HELP/SOS: RECAPITULATION AND CONCLUSION598

Box 35INTERNATIONAL FEDERATON OF
RED CROSS AND RED CRESCENT SOCIETIES
History: The League of Red Cross Societies was created following an
international conference in 1919.
It became the Federation in 1991.
Mission: To encourage and support the humanitarian action of themember Societies.
Structure: General Assembly meeting every two years, in which each
Society has one vote. It elects the President for a term of four
years.
The permanent Secretariat of the Federation is based in
Geneva.
Action: . Develops National Societies. Provides assistance in situations of natural disasters andepidemics, and supports refugees outside countries inarmed conflict.
Box 36
NATIONAL RED CROSSAND RED CRESCENT SOCIETIES
History: Originally created to assist military medical services inproviding care for wounded or sick soldiers. Today theyengage in many activities.
Mission: To assist and protect vulnerable people.
Structure: There is only one National Society in each country. It isdirected by a president and a secretary-general.
Action: . Aid to vulnerable people (children, the elderly, thehandicapped, etc.)
. Training (first-aid workers, nurses, etc.)
. Creation of health care centres (hospitals, dispensaries)
. Disaster relief
RECAPITULATION AND CONCLUSION 599

601
Box 37
OCHA
OFFICE FOR THE COORDINATION
OF HUMANITARIAN AFFAIRS
History: Created in 1997 to replace the Department ofHumanitarian Affairs.
Mission: To coordinate humanitarian affairs within
the UN.
Structure: Directed by the Under-Secretary-General forHumanitarian Affairs.
Two offices: New York and Geneva.
Action: . Develops policies to address all humanitarian
problems
. Mobilizes political organs (Security Council) on
behalf of humanitarian causes
. Coordinates emergency humanitarian action through
consultations in the Inter-Agency Standing Commit-tee (IASC)
HELP/SOS: RECAPITULATION AND CONCLUSION600

Box 38
IASCINTER-AGENCY STANDING COMMITTEE
History: Created in 1992 (General Assembly Resolution 46/182).
Mission: To coordinate humanitarian aid.
Structure: Composition:. Seven UN bodies: OCHA, UNHCR, UNICEF,WFP, UNDP,
WHO, and FAO. Guest organizations: ICRC, Federation, Interaction, Inter-
national Council of Voluntary Agencies (ICVA). Meetings: twice yearly
Action: . Develops common humanitarian policies. Allocates responsibilities among UN agencies. Promotes the principles of humanitarian action outside IASC. Identifies gaps in mandates and operational capacities. Resolves disputes between agencies
Box 39
UNHCR
UNITED NATIONS HIGH COMMISSIONER FOR REFUGEES
History: The United Nations General Assembly appointed a High
Commissioner for Refugees in 1949. The statutes of theOffice of the High Commissioner for Refugees were
adopted in 1951.
Mission: To give international protection to refugees, assist themmaterially, and find a lasting solution to their problems.
Structure: The Executive Committee holds its annual session in
Geneva in October. It has 53 members.
Action: Protects and assists refugees and displaced persons in the
world.
RECAPITULATION AND CONCLUSION 601

Box 40
WHOWORLD HEALTH ORGANIZATION
History: Founded in 1948.
Mission: To enable all people to attain the highest possible level ofhealth.
Structure: TheWorld Health Assembly is held each year in May at thePalaisdesNations inGeneva. It elects theDirector-General.
The Executive Board, composed of 32 members, meetstwice a year in Geneva.
Action: . Assists governments with their health policies. Proposes international conventions in the health sphere. Monitors the trends in health and disease in the world. Promotes emergency standards. Promotes scientific cooperation in the health field
Box 41
OSCEORGANIZATION FOR SECURITY AND COOPERATION IN EUROPE
History: Created in 1970 as the Conference on Security and Co-operation in Europe (CSCE), it became the OSCE in 1994.
Mission: To provide a forum for East-West dialogue and negotiation.
Structure: The OSCE has a membership of 55 States.The Summit of heads of State or government meets everytwo years.The OSCE Ministerial Council is composed of ministers offoreign affairs and is the central decision-making body.The Permanent Council is based in Vienna. It is made up ofthe heads of the State member delegations, and meetsweekly.
Action: . Resolutions calling for respect for international humanitar-ian law in situations of armed conflict
. Activities in the spheres of arms control, preventive diplomacy,
human rights, election monitoring, economic security, etc.
HELP/SOS: RECAPITULATION AND CONCLUSION602

ALPHALAND/BETALAND
MODULE
11

605
CONTENTS
. What’s been happeningBackground to the conflict in Alphaland and Betaland’s response
. Information about BetalandBetaland: BackgroundBetaland: Food, nutrition, and agricultureBetaland: Demographic, economic, and social data
Transportation and communicationBetaland: Health systems and programmes
Health surveillance dataHospital information from Gamma province
Betaland: Water and sanitation
. The refugees in Awalei campAwalei Camp health servicesAwalei Camp food and nutritionAwalei Camp environmental healthAwalei Camp—General refugee issues
. MapsRegional and local maps
Information on different aspects of theemergency in Alphaland-Betaland isgrouped according to general topics. Thereis considerable overlap between sections.Although this information may seemscattered and incomplete, in field situationsemergency programmes must often bedesigned on the basis of even scantierinformation.
HELP/SOS: ALPHALAND/BETALAND604

ALPHALAND/BETALAND
INTRODUCTION
Alphaland has a sorry history of ethnic tensions. The Kuloros from the easternpart of the country have traditionally held key positions in the NationalDemocratic Party, which has controlled the Alphaland government for manyyears. There is increasing belief among the Zowaran minority that externaldevelopmentaid forAlphalandhasbeenpreferentially channelled towardKulorohomelands. During the last two years a drought has swept the north-east of thecountry, which is home to most of the Zowarans. During this time Zowaransbelieved little actionwas taken by the national government tomitigate the hungerand suffering brought about by crop failure and the forced sale of livestock.
An opposition group, the ZowaranDemocratic Union (ZDU), was formed threeyears ago (1996) to protest themarginalization of the north-east. In early 1999, asresentment among the Zowarans increased, rioting broke out in the town of Khi.Two weeks later the town was seized by an armed faction of the ZDU, theZowaran Liberation Movement (ZLM). Shortly afterward, the insurgents weredriven out by the Alphaland army. The ZLM then moved its operations to theSigma area, where it took the town of Trit. In early November 1999, taking theoffensive, they seized the town of Bhao, according to a ZLM spokespersonspeaking on the BBC from Stockholm. The intense fighting has driven unknownnumbers of Alphaland civilians across the border into Betaland. The Alphalandgovernment has sought to play down ZLM territorial claims, insisting that it willsoon re-establish control over its territory and that civilians will be able to returnhome safely.
On the Betaland side of the border, civilianswere overwhelming resources as theysettled in Gamma province. Unable to cope with their needs, the Betalandgovernment has requested international assistance. At the same time theBetaland government is attempting to mediate between the two parties to theAlphaland conflict.
The arrival of the Zowaran refugees in Betaland has complicated the internalpolitics of the country.Members of the Zowaran ethnic group are found on bothsides of the Alphaland/Betaland border. There have been calls for anindependent Zowaraland in the past. At the present time Betaland has movedfrom military rule to an essentially one-party state controlled by the NationalCouncil of the Revolution (NCR).
ALPHALAND/BETALAND 605

607
Although the president and many of his ministers are Zowarans, the real powerin Betaland rests with the military, who traditionally come from other ethnicgroups in Betaland. Although the president reportedly would like to take a moresupportive stance toward the Alphaland refugees, the government fears thatdoing so would give the Alphaland army a pretext for operations against ZLMsympathizers who have fled intoBetaland, and incur the risk ofAlphaland armedsupport for nascent Zowaran discontent in Betaland. In a recent CNN interview,a political scientist indicated that it could lead to a major escalation of hostilities,as old territorial claims and past injustices (real and imagined) were resurrected.
Meanwhile, in Gamma province in Betaland, most of the refugees have settled inan area of Gamma district near the village of Awalei, about 22 km from Khron,the nearest town, and 34 km from the border with Alphaland. This area wasselected for people arriving from Alphaland who did not have family memberswith whom they could settle in the Epsilon area. Some sources put the self-settledpopulation in Epsilon district at 20,000, while other officials give a much higherfigure. Manymore refugees seem to have settled in Awalei in the Gamma districtof Gamma province, although they have not been enumerated. At the presenttime, according to the recently formed Provincial Office of RefugeeAffairs, up to3,000 refugees a day are entering the area.
Refugees are living in huts they have made from grass, branches, and bananaleaves. Fuel for cooking is a problem. While most refugees have settled in theAwalei area, some are living near the village of Zowete. Water is being obtainedfrom the Bowi River, but there are problems with this water source. Sanitationprovisions for the refugees are reported to be poor. So far relations with the localcommunity are not a major problem, but there are indications that trouble maybe on the way. Although the refugees brought some food supplies with them,these have been exhausted. The community and various Betaland organizationshave been trying to help out, but this is clearly not enough. Although no surveyshave been completed, it appears that malnutrition may be a significant problem.How different this is from the chronic nutrition problems in Gamma province isalso unknown.
Health problems in the province include many common endemic and epidemiccommunicable diseases, such as P. falciparum malaria, cholera, measles,tuberculosis, AIDS, meningitis, diarrhoea, respiratory infections, and skindiseases. The trauma already caused by the disruption of the community has nowbeen increased by an influx of war casualties.
Obstetrical complications are common, and although thematernalmortality rateis unknown, it is thought to be quite high.
HELP/SOS: ALPHALAND/BETALAND606

Health services in Gamma province include a provincial hospital in the city ofGamma and smaller hospitals in Brew, Khron, and Takri. The hospital inKhronis the closest and so far seems the most affected by the refugee influx andincreased demand for services. There are health centres and medical postsscattered around the three districts of Gamma province. Community healthworkers (CHWs) are being trained, but in insufficient numbers. Severalorganizations are starting to provide limited health services for refugees.Already a major shortage of drugs and supplies is looming.
Transport into the area is by road, rail, and air. All of these means areproblematic at various times and in various ways. Roads around Khron aresubject to flooding, and access to some areas may be cut off for several days.
YOUR JOB
Your first duty will be to serve as part of the team that will assess urgent needs.Later your role will change and you will have to implement measures and makedecisions concerning the organization of assistance.What aid is needed, how canit best be provided using resources already present in Betaland or among therefugees themselves, and what must be brought in from outside?
TheAlphaland-Betaland simulation containsmuch of the information needed tomake decisions and set priorities for humanitarian aid. It is presented as bits andpieces of information that have been gathered from many sources but have beenarranged by topic in the following pages. Some information is in obvious conflict,and key facts are often missing. As in many real-life situations, there is neverenough information on hand to take decisions with the absolute confidence thatyou havemade the right choices. At first informationwill seemdisconnected, andin many cases extraneous. As you move through the simulation, the pieces willbegin to come together, and the picture of a refugee population with its manyneeds and a local population beset by drought and famine will emerge.
Emergencies are complex, and many factors affect the way populations cope.Failure to consider these can result in serious misjudgements about the types ofassistance to be provided and the manner in which programmes are to beimplemented.
ALPHALAND/BETALAND 607

609
ALPHALAND: BACKGROUND INFORMATION
No. 1001 Date: 13/12/99 Alphaland
Source: Geneva, journalist’s report (AFP)
AFP--NEW DISPATCH CONCERNING THE GENERAL SITUATIONON THE BORDER BETWEEN ALPHALAND AND BETALAND
As a result of the fighting in the northern part of Alphaland, many civilians areconcentrated near the border between Alphaland and Betaland. According toBetaland sources, civilians have crossed the border and are gathering onBetaland territory.
In the past, several factors have contributed to the development of tensionsbetween the different ethnic groups in Alphaland. First, the key positions in thegovernment have traditionally been held by the members of the Kuloro ethnicgroup from the eastern part of the country. They have been accused ofchannelling the country’s resources towards the development of their own area oforigin, instead of considering the development needs of the country as a whole.Second, during the last two years a drought has swept the north-east of thecountry, where the Zowaran ethnic group lives. The government have beenaccused of ignoring the drought and not taking any measures to alleviate thesuffering of the population.
An opposition group called the ZLM (Zowaran Liberation Movement) wascreated in the province ofKhi in 1997.Until recently, it was exclusively a politicalgroup, vocal in its criticisms of government attitudes.
Beginning in 1999, as the government increasingly ignored the affectedpopulation, resentment grew, sparking rioting in the town of Khi early inNovember of that year. Two weeks later the ZLM took control of the town. Atthe beginning of December the ZLM rebels were pushed back by thegovernmental armed forces and fled to the Sigma area, concentrating aroundthe town of Trit, which they controlled. Intense fighting is now raging around thetown of Bhao. According to some sources Bhao is now under the control of theZLM, although the Alphaland government has issued a statement saying that itsown armed forces control the town.
From Lambda, the capital of Alphaland, the Alphaland government has issuedthis statement: ‘‘The governmental armed forces control most of Khi province,
HELP/SOS: ALPHALAND/BETALAND608

and soon the situation will return to normal. Before long the population who fledto Betaland will be able to return to Alphaland safely. The Government ofAlphaland will not tolerate any intervention by the Betaland government inAlphaland’s internal affairs, and any support to the ZLMwill be seen as an act ofaggression against Alphaland.’’
No. 1002 Date: 14/12/99 Alphaland
Source: Geneva, UN Statistical Yearbook, 1998
THE GEOGRAPHY OF ALPHALAND
East: Coastal area (Lambda, the capital city, is located on the coast).
South: Mountainous terrain, the highest point being 3,000 metres (10,000 feet)above sea level.
In the centre: A plateau with an altitude of 1,000-1,500 metres above sea level.
West and north-west: A desert known as the Danikal.
North: A mountainous region located between the coast on the east and theDanikal on the west.
The total size of the country is 900,000 square kilometres.
No. 1003 Date: 14/12/99 Alphaland
Source: Geneva, UN Statistical Yearbook, 1998
THE POLITICAL SITUATION IN ALPHALAND*
The political power in Alphaland is in the hands of the NDP (NationalDemocratic Party) whose members are mainly from the Kuloro and Kaniankaethnic groups. From 1992 to 1996, following a period of rapid economicdevelopment, the NDP controlled the entire country. The per capita GNP rosefrom US$ 500 in 1992 to $840 in 1996. In the last general election (1995), onlyNPD candidates were allowed to run for office. In 1996, an opposition group,ZDU (Zowaran Democratic Union), was organized in the north and east of thecountry. The ZDU was tolerated by the NDP government, though it has neverbeen officially recognized.
* Written before 1 January 1996.
ALPHALAND/BETALAND 609

611
No. 1004 Date: 14/12/99 Alphaland
Source: Geneva, UN Statistical Yearbook, 1998
ETHNIC GROUPS IN ALPHALAND
Ethnic groups in Alphaland are classified here by geographical location and bythe proportion they constitute of the country’s population:
. Kuloro: coastal area (52%)
. Dokole: the mountains in the south (10%)
. Nisonke: south-east (3.5%)
. Kanianka: central plateau (29%)
. Gonlani: north-west and west; they are nomads living mainly in the Danikaldesert (1.5%)
. Zowara: north (4%).
No. 1005 Date: 14/12/99 Alphaland
Source: Geneva, UN Statistical Yearbook, 1998
POPULATION STATISTICS --- ALPHALAND
The total population ofAlphaland in 1998was 21,800,000 inhabitants (estimatedfrom the 1995 census). The age distribution was as follows:
. 0-4 years: 18%
. 5-14 years: 26%
. 15-64 years: 53%
. over 65: 3%
. Urban population: 15%
. Rural population: 85%.
The past several years have seen increased migration from rural areas to urbanareas, where growth and new employment have been concentrated.
. Population density: 22 per km2
. Average annual rate of urban population increase: 7%
. Life expectancy at birth: males: 44.3 years; females: 47.5 years
. Infant mortality rate (<1 year): 102 per 1,000 live births
HELP/SOS: ALPHALAND/BETALAND610

. Child mortality rate (<5 years): 212 per 1,000
. Crude mortality rate: 23 per 1,000 population
. Birth rate: 51 per 1,000 population.
No. 1006 Date: 14/12/99 Alphaland
Source: Geneva, UN Statistical Yearbook, 1998
THE HEALTH SYSTEM --- ALPHALAND
The country’s main health problems are tuberculosis, diarrhoeal diseases, acuterespiratory infections, malaria and measles. Health care facilities (hospitals,health centres and clinics) are concentrated in the towns, and in the coastal areaswhere half of the population is living. According to 1995 figures, the country has:
. 50 hospitals (7,200 beds)
. 1,200 health centres
. 2,300 rural health posts.
Health care personnel:
. 450 doctors
. 2,900 nurses
. 7,700 health care aides.
Physicians aremainly to be found in towns, while the health care aides include thecommunity health care workers who have been trained in the period since 1990.
The health care system spans the public and private sectors. In the public healthcare system, of which 55% is constituted by in-patient facilities and 48% byambulatory facilities, health care is free. The private sector includes bothfacilities run by doctors themselves and facilities run by missions or non-profitorganizations. The fees charged vary accordingly. Some facilities are operated byindustrial concerns for the benefit of their employees and dependents.
No. 1007 Date: 14/12/99 Alphaland
Source: Washington DC, World Bank World Development Report, 1998
ALPHALAND’S MAIN RESOURCES
Agriculture is the country’s main economic resource; 85% of the population isemployed in subsistence farming. The main crops are sorghum, millet, maize,
ALPHALAND/BETALAND 611

613
beans, and various fruits (mangos, papayas, citrus fruits, bananas). Most of theagricultural sector, however, is concentrated in the coastal area and on thecentral plateau. The south and south-east are forested. The north is a savannaarea where cattle and goats are the most important food resource, althoughpeasants cultivate a little millet and sorghum. In the north-west, the nomads livealmost exclusively on cattle.
During the last 10 years, a large number of wells have been dug in the north,leading to an increased number of cattle and stimulating an expansion ofveterinarian services. Attracted by permanent sources of water, the nomads havebegun to settle more permanently around the bore-holes, although health andtrading infrastructures are still inadequate. The high concentration of livestockin some areas has led to deterioration of the grazing land. This is especiallyobvious in the semi-arid area near the Danikal desert, where nomads drive theirherds during the dry season.
For the past four years, the country has drawn most of its resources from thecoastal region. An agricultural development programme has been implementedand the production of coffee, tea, and vegetables has more than doubled duringthis period. Fishing activities have increased as well, and a canning factory wasbuilt at Lambda, the capital, permitting the export of a large part of the country’sproduction.
No. 1008 Date: 14/12/99 Alphaland
Source: Geneva, UN Statistical Yearbook, 1998
RELIGION IN ALPHALAND
Islam is the official religion of the country, and 85%of the population isMuslim.In the south, the Dokole maintain their own animist tradition. A few smallgroups of Christians can be found in the large towns.
No. 1009 Date: 14/12/99 Alphaland
Source: The Times Atlas of the World, 1998
THE CLIMATE IN ALPHALAND
Alphaland’s climate has two main seasons: a wet season lasting from October toMarch, and adry season lasting fromApril to September.Rainfall is considerableon the coast (1,500 mm), whereas the semi-desert areas have a precipitation rateranging from 500 mm to 700 mm (average from 1986 to 1997). Over the last two
HELP/SOS: ALPHALAND/BETALAND612

years, rainfall in the semi-desert regions has been less than average, leading to asevere drop in agricultural production. In the Danikal rain is rare.
No. 1010 Date: 14/12/99 Alphaland
Source: Washington DC, The World Bank, 1998
ALPHALAND’S NATIONAL BUDGET
The local currency is theAlpha, which in 1996was devalued to 3 perUS dollar. In1996 the total government budget was 27 billion Alphas. The government givespriority to the Ministries of Defence, Industry, Agriculture and Trade, while theMinistry of Health receives less than 2% of the national budget. Despitegovernmental willingness to reorient the health system towards a focus onprimary health care, few financial resources have been earmarked for such care.
No. 1011 Date: 14/12/99 Alphaland
Source: Geneva, UN Statistical Yearbook, 1998
COMMUNICATION LINKS IN ALPHALAND
. Railway lines: Lambda-Khi and Lambda-Noma andKeso (one-metre-gaugetrack)
. Roads: Hard-surfaced roads between Lambda-Noma and Keso, andLambda-Khi. The network of non-hard-surfaced roads is quite good andcovers most of the country.
. Airports: The international airport is at Lambda, with regional airports atKhi and Noma.
No. 1012 Date: 15/12/99 Alphaland
Source: Geneva, representative of Alphaland diplomatic mission in Geneva
PRESS INTERVIEW GIVEN BY A REPRESENTATIVEOF THE ALPHALAND DIPLOMATIC MISSION
During a press interview, a representative of theAlphaland diplomaticmission inGeneva acknowledged the existence of security problems in the north of thecountry, but stated that the Government of Alphaland had taken steps to bringthe situation under control. Although he understood the role of thehumanitarian agencies, he felt there was no reason for them to become involved
ALPHALAND/BETALAND 613

615
in the situation. He was not in a position to issue visas to enter the country;humanitarian agencies would have to apply in writing to theMinister of InternalAffairs for permission to enter the country, and any visas issued did not includethe right to travel in the northern parts of the country. The ICRC asked therepresentative to forward to his government its formal request for an Alphalandvisa.
HELP/SOS: ALPHALAND/BETALAND614

THE PRESENT SITUATION IN ALPHALAND
No. 1013 Date: 15/12/99 Alphaland/Betaland
Source: Geneva, Reuters Oce
INFORMATION PROVIDED BY REUTERS IN GENEVA
The Reuters office in Geneva confirms the statement of the government ofBetaland that several thousand Alphaland refugees are arriving daily in theBetaland province of Gamma. Fighting is reportedly continuing around thestrategically located town of Bhao, which is evidently still under the control ofgovernment troops. Furthermore, reliable reports indicate that the town of Tritwas taken by the guerrilla group during the night of 12-13 December 1999,although the Alphaland government denies this.
No. 1014 Date: 15/12/99 Alphaland/Betaland
Source: London, BBC report by Jane Standley in Betaland
INFORMATION FROM BBC EVENING NEWS REPORT
The town of Khi is still controlled by governmental forces, which are beingreinforced by air. Severe fighting has raged in and around the town of Bhao forthe past twoweeks. Refugees arriving fromBhao report that the hospital in Bhaois overflowing with wounded, perhaps as many as 300 having been admitted.
No. 1015 Date: 15/01/99 Alphaland
Source: Sako, representative of the ZLM
THE SITUATION IN SAKO
Authorizationby themilitaryauthoritiesof theBetalandarmed forceshasmade itpossible to cross the border intoAlphaland and to visit Sako andTrit. In Sako thesituation is as follows.First of all, Sako is aZLMmilitary camp.NumerousarmedZLMsoldiers are walking around.A few trucks carrying guerrilla troops can alsobe seen. Near the town (500 metres away) is a small transit camp for civiliansheading for Betaland. At the time of the survey, the number of civilians in thetransit camp was estimated at 300. Usually civilians stay in Sako for only two orthree days before heading on toBetaland, although someof themhave been in the
ALPHALAND/BETALAND 615

617
Sako transit camp for several weeks, hoping that the situation might calm downenough so that they could return home.The situation in and aroundSako is quiet;in fact, there is no fighting there, since the area is tightly controlled by the ZLM.
According to the military commander in Sako, the town of Bhao is completelysurrounded by the ZLM and is about to fall under its control. Civiliansmentioned hearing rumours that a new ZLMoffensive was being planned for thepurpose of seizing control of the Alphaland provincial capital of Khi. All theroads around the town of Khi are occupied by the ZLM, except the road betweenKhi and Lambda which remains under the control of the government forces. It isthought that after Bhao falls the ZLM may press forward towards the coast inorder to gain access to the sea on the east.
No. 1016 Date: 15/01/99 Alphaland
Source: Sako, a nurse in the ZLM Forces
THE HEALTH STATUS OF THE PEOPLE IN SAKO
A ZLM military nurse provides care for the military and civilian populations inSako. He gives first aid to wounded soldiers before evacuation. Most of the mildcases are sent to Trit, where the health centre is operating normally, while theserious cases are evacuated to the hospitals of Betaland (mainly Khron).
He also treats civilian patients arriving at the health centre, the most commoncomplaints being diarrhoea, malnutrition, skin infections, and respiratorydiseases. Last week a number of children showed signs of measles, but they werein good general health, and hewas not concerned about them. Themain causes ofdeath seem to be diarrhoeal diseases (two weeks ago two adults died as a result ofsevere diarrhoea) and malnutrition.
The civilians have little food with them, and the ZLM does not have food todistribute. The nurse asks assessment teams of humanitarian agencies to give theZLM food so that the movement can in turn provide food for civilians.
No. 1017 Date: 16/01/99 Alphaland
Source: Merer, representative of the ZLM
THE SITUATION IN MERER --- ALPHALAND
Merer is a small village located between Sako andTrit. Before the conflict it was avillage of 2,500 inhabitants; now, according to the ZLM’s information, only a
HELP/SOS: ALPHALAND/BETALAND616

few hundred people are left in the village. Most of the inhabitants have fled westor north towards Betaland. Most of the houses have been abandoned. Thedispensary, the school, and other public buildings have been looted.
No. 1018 Date: 16/01/99 Alphaland
Source: Sirale, representative of the ZLM
THE SITUATION IN SIRALE
Sirale was a small village of 850 inhabitants. Today, almost all the civilianinhabitants have fled, and only a few ZLM soldiers are left in the village.
No. 1019 Date: 18/01/99 Alphaland
Source: Trit, representative of the ZLM
THE SITUATION IN TRIT
Trit was a city of 15,000 inhabitants before the conflict. Now it is estimated thatonly 6,000-7,000 people remain in the city, which has suffered badly from theconflict. Many houses have been destroyed, and the walls are scarred by bulletsand mortars. ZLM fighters are present in the town, living in private houses thathave been abandoned by civilians.
Trit has a strategic importance, since the town controls the road between Bhaoand Khi. If government forces want to go to Bhao they have to go through Trit;the road through Danote is far more difficult, and the government armed forcesdo not have the resources for an airlift into Bhao.Nonetheless, ZLM representatives do not think that government forces willattack Trit, because the ZLM controls the road to Khi.
No. 1020 Date: 18/01/99 Alphaland
Source: Trit, doctor at the Trit hospital
THE HEALTH CARE SITUATION IN TRIT
Before the conflict, the Trit hospital consisted of four buildings, with a capacityof 80 beds, and provided services to a population of 35,000 people. The hospitalhas suffered badly in the present conflict. One building has been destroyed andthe others have been looted. Activities are now concentrated in two buildings,which have been temporarily repaired. Two doctors from the ZLM are working
ALPHALAND/BETALAND 617

619
in the hospital, one treating military personnel (he has had some surgicalexperience) while the other takes care of the civilian population (formerly he wasan internist in the main university hospital in the capital city).
On the day of a BBC visit, there were 23 wounded in the Trit hospital, most ofthem suffering from lesions in the extremities caused by bullet and mine injuries.Since no beds were available, they were lying on mats on the floor. Most of thedressings were dirty, and the doctor was not performing operations, since he hadneither surgical equipment nor anaesthetic drugs. Some patients were receivingantibiotics (penicillin) through intravenous drips.
Some of the wounded had been evacuated fromSako, while others came directly toTrit.The serious caseshavebeen transferred toSako,whence theywere supposed tobe sent on to Betaland. Last week, however, some of the wounded who had beentransferred to Sako for evacuation to Betaland were returned to Trit.
Around 30 civilians are hospitalized in the second building, including 18 childrenwith such diseases as measles, diarrhoea with dehydration, and pulmonaryinfections. One child with measles has a severe eye infection. Two adults and onechild have superficial war injuries. The patients are lying on the floor, since thehospital beds have been stolen.
The doctors complain of the lack of equipment and drugs. Moreover, they haveno food for the patients. Water is drawn from a small river nearby; the bore-holein the hospital compound can not be used, since the pump was damaged duringthe fighting.
The doctors feel that with the necessary equipment and supplies they couldhandle most of the cases admitted to Trit hospital.
No. 1021 Date: 18/01/99 Alphaland
Source: Trit, representative of the local population
INFORMATION ON THE LOCAL POPULATION OF TRIT
Most of the civilian population of Trit have fled. Those who remain in the towntry to survive as best they can. The ZLM lets civilians circulate freely, and accessto surrounding fields is safe, although a few mines were laid during the fightingsome weeks ago. The cattle still remaining (about 200) are kept in the fields closeto the town.
Commercial activity has dwindled to virtually nothing. Both civilians andmilitary personnel have little purchasing power, stocks of merchandise are
HELP/SOS: ALPHALAND/BETALAND618

almost non-existent, and new supplies cannot be obtained from Khi. Themunicipal administration has been supplanted by a ZLM administration, whosemain concern is dealing with the influx of displaced people arriving from Khi.There are reportedly 3,000 displaced people in Trit. Although most of them areon their way north towards the border with Betaland, some remain in Trit inhopes that the situation will calm down and they will be able to return to theirvillages.
Relations between the military and the civilian population are good. Theadministration has asked the assessment team for emergency aid for Trit.
No. 1022 Date: 18/01/99 Alphaland
Source: Trit, representative of the local population
ASSESSMENT OF THE NUTRITIONAL SITUATION IN TRIT
Anthropometric measurements were taken from two samples of children, onefrom the displaced population and one from the resident population.
GROUP I
(RESIDENT)
GROUP II
(DISPLACED)
SAMPLE SIZE 123 98
Over 90% WFH 56% 43%
80%-90% WFH 32% 32%
Below 80% WFH 10% 20%
Kwashiorkor: 2% 5%
Vitamin A deficiency 1% 3%
WFH = Weight-for-height
No. 1023 Date: 14/12/99 Alphaland
Source: Geneva, representative of WHO diarrhoeal diseases dept., Geneva
CHOLERA IS NOW ENDEMIC IN THE NORTHERN PARTSOF ALPHALAND
Cholera has been endemic in Alphaland for many years, especially in thenorthern part of the country. The last serious outbreak occurred five years ago,when 600 people became sick, and about 70 died.
ALPHALAND/BETALAND 619

621
N
S
W E
Betaland
Alphaland
plain
semi-desertareaDanikal
desert
Takri
Kappa Lum
Srzo
Gamma
Khi
Anil
Lambda
KesoNoma plain
mountainousarea
mountainousarea
Border
Tana River
100 Km
Communications:
Roads
Railways
Harbours Airports
Box 1
HELP/SOS: ALPHALAND/BETALAND6620

N
S
W E
Betaland
Alphaland
Takri
Kappa Lum
Srzo
Gamma
Khi
Anil
Lambda
KesoNoma
Border
Tana River
Bazim
Podbe
Barganxa
GonlaniZowara
NisonkeKanianka
Kuloro
Nyanka
100 Km
Box 2
GEOGRAPHICAL LOCATIONOF ETHNIC GROUPS
ALPHALAND/BETALAND 6621

623
N
S
W E
Betaland
Alphaland
plain
semi-desertregionDanikal
desert
Takri
Kappa Lum
Srzo
Gamma
Khi
Anil
Lambda
KesoNoma plain
Mountainousarea
Mountainousarea
Border
Tana River
100 Km
Box 3
TOPOGRAPHY
HELP/SOS: ALPHALAND/BETALAND6622

BETALAND – BACKGROUNDINFORMATION
No. 1024 Date: 14/12/99 Betaland
Source: Washington DC, State Department country profile: Betaland, 1997
THE POLITICAL SITUATION
Since decolonization, the country’s government has been based on a constitutionstipulating that all parties be part of the political life of the country. From 1968-1995, Betaland has been governed by a succession of civilian governments, witheconomic and social stability providing the basis for a political consensus. In1995, the economy began to show some signs of weakness, reflecting partly theslowing international economy, and partly increasing social inequalities inBetaland.
In 1993, the army seized political power, with the stated goal of reducing socialinequalities in the country. It ruled the country from 1993 to 1996 under a state ofemergency, having suspended constitutional guarantees and outlawed theexisting political parties for those three years. From 1996 on the only authorizedpolitical party was the NCR (National Council of the Revolution), which hadbeen created by the military.
In 1996, elections were organized under pressure from various donor countries,although only the NCRwas allowed to enter candidates. Following the electionsa civilian government was sworn in, but it was in fact controlled by the military.
Beginning in 1996, the government took steps to liberalize the economy. TheInternationalMonetary Fund and theWorld Bank have encouraged Betaland toimplement structural changes.
The President of the Republic is a Zowaran, and most of the ministers are fromthe same tribe. Caught between its own poor economic performance and thestrict military control, the government has only limited options in settingnational priorities. So far the ZLMhas been the only political party that has beentolerated apart from the official party.
The situation in Alphaland has been a source of concern to the Betalandgovernment. In the past, the southern part of the country (the Danikal and
ALPHALAND/BETALAND 623

625
Epsilon regions) was more or less autonomous, and it took a long time to imposecentral administration on this area. Current events in the north of Alphalandhave prompted concern that southern Betaland may begin agitating for greatautonomy. The Zowaran people live on both sides of the border, and, since theoutbreak of conflict in Alphaland, there has been increasing pressure for thecreation of an autonomous territory that would include the Zowarans of bothAlphaland and Betaland. Should this demand be declared, it is likely that thearmed forces would reassume full control of the country. Informed sources saythe President of the Republic would like to assist refugees from Alphaland, butfears that the conflict may spread into Betaland, with potential involvement ofthe Alphaland armed forces on Betaland soil. Such a situation would probablylead to the collapse of the government, a new military coup, and war.
HELP/SOS: ALPHALAND/BETALAND624

DESCRIPTION OF THE PRESENT POLITICAL SITUATION
No. 1025 Date: 14/12/99 Betaland
Source: Paris, dispatch from an AFP reporter
INITIAL PICTURE OF THE GENERAL SITUATIONON THE ALPHALAND-BETALAND BORDER (AFP reporter)
This morning the Betaland Minister of the Interior issued the followingstatement: ‘‘Hundred of thousands of refugees have fled Alphaland, seekingrefuge in Betaland. The Government of Betaland urgently seeks the support ofthe international community in providing assistance for these victims of war. TheGovernment also offers its services to both parties in order to mediate a politicalresolution to the conflict.’’
No. 1026 Date: 15/12/99 Betaland
Source: Geneva, UNHCR representative in Geneva
UNHCR ACTIVITIES IN BETALAND
The UNHCR has closely followed the events in Betaland. Thus far, it has notbeen approached by the Betaland government to intervene on behalf of therefugees from Alphaland. The UNHCR has no permanent representative ineither country, but it has asked its representative in Zomaland, a neighbouringcountry, to go to Betaland in order to discuss protection for the refugees with thegovernment authorities.
No. 1027 Date: 14/12/99 Betaland
Source: Geneva, representative from the Betaland diplomatic mission
PRESS RELEASE FROM THE DIPLOMATIC MISSIONOF BETALAND IN GENEVA
The Secretary of the Permanent Diplomatic Mission of Betaland in Genevaconfirms his government’s statement concerning the situation on the borderbetween Alphaland and Betaland. He has no more information to add, otherthan that the situation is very tense and that new refugees are arriving daily inBetaland. He says that his government stands ready to help the civilian
ALPHALAND/BETALAND 625

627
population fleeing into Betaland. He confirms that the government of Alphalandhas issued a warning against any intervention by the Betaland government, andthis morning recalled its ambassador in Kappa. He emphasizes that humanitar-ian agencies wishing to assist the refugees in Betaland are welcome, provided thatstandard immigration regulations are respected.
No. 1028 Date: 14/12/99 Betaland
Source: The Times Atlas of the World, 1998
THE GEOGRAPHY OF BETALAND
The country is divided into four parts:
1. North and central areas: Plateau with an altitude of 1,000-1,500 metres abovesea level, ending abruptly at the desert
2. East: Coastal area
3. South: Semi-desert region separated from the coast by a range of mountains
4. Southwest: Desert region (the Danikal).
The total area of the country is 792,000 square kilometres.
The central area is mainly savanna. The coastal area is a narrow strip of fertileland with heavy rainfall, and is intensively farmed. This area, particularly theTanaRiverDelta, providesmost of the agricultural produce for domestic use andfor export. In the north there are extensive forests.
No. 1029 Date: 14/12/99 Betaland
Source: Washington DC, State Department country profile: Betaland, 1997
BETALAND --- ETHNICITY
. The Barganxa live on the central plateau and in the semi-desert region, andaccount for 16% of the population.
. The Podbe live mainly on the central plateau, and account for 22% of thepopulation.
. The Bazim live in the north, and represent only 7% of the population.
. TheNyanka live along the coast and are the largest tribe, representing 48%ofthe population.
HELP/SOS: ALPHALAND/BETALAND626

. The Gonlanis are nomads living in the Danikal, and represent 2% of thepopulation.
. TheZowarans live in the semi-desert region in the south, and account for 5%of the population.
No. 1030 Date: 14/12/99 Betaland
Source: Rome: World Food Programme, State of the World’s Agriculture, 1998
AGRICULTURE IN BETALAND
1. On the plateau, farming and livestock grazing are the main agriculturalactivities. Subsistence farming is the rule, and large commercial farms are few.The main crops are maize, beans, millet, sweet potatoes and vegetables. Someareas produce palm oil. Cattle providemeat andmilk and are used for work inthe fields. Coffee is a more recent crop which was introduced mainly forexport. Substantial private coffee plantations have been established south ofFen.
2. On the coastal plain, farmers traditionally maintain a subsistence agriculturaleconomy based on shifting cultivation. Subsistence crops are maize, cassava,yams, coconuts, bananas, and palm oil, but these crops are now also beingproduced in large quantities to meet the growing demands of the towns.During the past few years, large areas of land have been taken over by thegovernment for commercial production for export, mainly bananas and,more recently, sugar cane. Peasants have been organized into cooperatives. Amajor sugar factory has been opened in Szro as a joint venture with amultinational corporation. The delta areas are planted with rice, most ofwhich is exported.
3. The semi-desert area is sparsely populated. The population is stable, living insmall villages, and supports itself by subsistence farming. The main crops aremillet, chickpeas, sesame, and groundnuts. In addition, villagers keep a fewcattle, goats and sheep.
4. In the Danikal, grazing cattle is the main activity. There is some agriculturalproduction around the towns and villages. Traditionally, good relations haveprevailed between the Zowarans and the nomadic Gonlanis; the latter wouldtake their cattle to the Zowaran villages during the dry season, when theeastern pastures were exhausted. The Zowarans, who live between the desertand the coast, play an important role as traders. Brew has always been animportant market place (for the coast and for Alphaland).
ALPHALAND/BETALAND 627

629
No. 1031 Date: 14/12/99 Betaland
Source: Geneva, Times Atlas of the World, 1997
THE CLIMATE IN BETALAND
Betaland has two seasons: a rainy season from November to April, and a dryseason from May to October.
The Danikal has a precipitation rate of less than 200 mm per year, with anaverage temperature of 36 degrees Centigrade.
0
5
10
15
20
25
0
50
100
150
200
250
300mmGRADE CELSIUS
AVERAGE TEMP
RAIN IN mm
J F M A M J J A S O N D
22 22 22 20 18 16 16 17 21 23 23 23
266 243 213 55 5 0 0 0 5 30 149 270
PLATEAU AREA
HELP/SOS: ALPHALAND/BETALAND6628

0
5
10
15
20
25
30
0
50
100
150
200
250
300
mmGRADE CELSIUS
AVERAGE TEMP
RAIN IN mm
J F M A M J J A S O N D
27 27 26 25 22 21 20 21 22 26 26 26
276 248 200 106 56 33 30 27 20 132 134 233
COASTAL AREA
–
0
5
10
15
20
25
30
35
0
50
100
150
200
250
mmGRADE CELSIUS
AVERAGE TEMP
RAIN IN mm
J F M A M J J A S O N D
28 26 27 27 25 22 21 23 27 30 31 31
124 236 109 5 0 0 0 0 0 3 27 38
–
SEMI-DESERT AREA
ALPHALAND/BETALAND 6629

No. 1032 Date: 14/12/99 Betaland
Source: Geneva, UN Statistical Yearbook, 1998
BETALAND POPULATION STATISTICS
Total population: 11,200,000, estimated on the basis of the 1992 national census
Main population centres:
. Kappa (the capital): 450,000
. Szro: 210,000
. Lum: 65,000
. Gamma: 122,000
. Takri: 25,000
The urban population has increased dramatically during the last 10 years.
Distribution of urban and rural population: 10% urban, 90% rural.
Migration fromrural areas towards the townshas intensifiedduring the last 10years,as a result of poor economic conditions and lack of development in rural areas.
Geographical distribution of the population:
COASTAL
AREAPLATEAU
SEMI-DESERT
AREADANIKAL
Population 5,600,000 4,700,000 650,000 250,000
Area 150,000 km2 286,000 km2 156,000 km2 200,000 km2
Density 37 per km2 16.4 per km2 4 per km2 1 per km2
Overall population density: 14 per km2
Breakdown of population by age:
. 0 to 4: 20%
. 5 to 14: 27%
. 15 to 64: 50%
. >64: 3%
HELP/SOS: ALPHALAND/BETALAND630 631

Life expectancy at birth: men: 49 years; women: 52 years
Infant mortality rate: 110 (per 1000 live births )
Child mortality rate (<5 yrs): 160 (per 1000 )
Annual population growth rate: 2.6%
Population doubling time: 27 years
No. 1033 Date: 14/12/99 Betaland
Source: London, The Economist, ‘‘Emerging Market Indicators: Betaland: 1998’’
BETALAND’S ECONOMY
In 1998, the gross national product was estimated at $2.4 billion. For severalyears the GNP has been falling as a result of the economic recession in thecountry and regionally.
GNP 1998 1998 1999 (est.)
($bn) 2.85 2.74 2.40
This represents an average of US$ 214 per capita in 1998, down from $269 in1997.
No. 1034 Date: 14/12/99 Betaland
Source: Washington, State Department country profile: Betaland, 1997
INDUSTRY IN BETALAND
The construction of the railway from Kappa to Szro made the development ofcommercial agriculture possible. Themain crops are cotton and coffee, creating acash economy for many areas. Cotton produced in the villages is bought by localgins and mills, of which the two major ones are located in Kappa and Fen. Theysupply local needs, while producing a substantial surplus for export. Coastalfishing, though generally on a small and primitive scale, is anothermajor activity.A fishing project has been set up in Lum, where a factory is now producingcanned and dried fish, the goal being to increase exports. Many small fishingsettlements have fish-drying facilities.
ALPHALAND/BETALAND 631

633
No. 1035 Date: 14/12/99 Betaland
Source: London: The Economist, ‘‘Emerging Market Indicators: Betaland: 1998’’
BETALAND’S ECONOMY
Although the trend has been to promote the development of private investment,the State is still present in the economy, mainly in industry. It also continues tosubsidize heavily staple foods produced for local consumption, particularly thoseproduced for urban areas.
No. 1036 Date: 14/12/99 Betaland
Source: New York: UNDP Annual Report on Development Programmes, 1997
DEVELOPMENT POLICY IN BETALAND
For the past decade the Betaland government has stressed the development ofrural cooperatives, and improvement of rural agricultural production. While itrealizes that the results of these efforts have been considerable, this approachhas clearly not achieved all its aims. Beginning in 1992, a new approach wasdeveloped to encourage the development of large-scale commercial agriculturalprojects, often as joint ventures between Betaland companies and internationalinvestors. Large areas of land have been opened up as a result of this initiative,which has also caused agricultural workers to migrate. There has been increasingconcern over this policy’s destructive effects on households in rural communities,and workers are encouraged to settle with their families in the new agriculturalareas.
No. 1037 Date: 14/12/99 Betaland
Source: Geneva, UN Statistical Yearbook, 1998
RELIGIONS IN BETALAND
Amajority of the population, perhaps as many as 70%-80%, identify themselvesas Muslims. Many people have also incorporated aspects of Islam into theirindigenous religious practices. The branch of Islam that predominates is theMakelite school of the Sunni sect. Most of the rest of the population practicetraditional animism (in the north of the country), while 5%-10% are Christians(in the south).
HELP/SOS: ALPHALAND/BETALAND632

No. 1038 Date: 14/12/99 Betaland
Source: Washington DC, State Department country profile: Betaland, 1997
COMMUNICATION MEDIA IN BETALAND
. Railways: The railway from Kappa to Szro is 600 km long. The extension toGamma has not yet been completed. A passenger train runs between the twotowns twice a week. The duration of the trip is 15 hours. Freight trains rundaily, and are the main means of transporting food from the coast to thecapital, wood from the forests located in the north, and minerals to Szro forexport. From Szro, trains transport most imported items, either in containersor in standard freight cars.
. Air-routes:Kappa has an international airport with several flights every dayto Europe and to the principal cities of neighbouring countries. The towns ofSzro, Gamma, and Takri each have an airport with an asphalt or concreterunway. There are a number of small unpaved airstrips throughout thecountry.
. Roads: The road network between the main towns is good, with hard-surfaced roads between Kappa and Szro, Szro and Gamma, Gamma andTakri, and Szro and Lum. Most of the roads linking the small towns andvillages are unpaved, and are generally impassable during the rainy season.
No. 1039 Date: 14/12/99 Betaland
Source: Geneva, UN Statistical Yearbook, 1998
BETALAND: GENERAL HEALTH INFORMATION
The main health problems in the country are malaria, diarrhoeal diseases,measles, acute respiratory infections, malnutrition, tuberculosis, and schistoso-miasis (bilharziasis). HIV/AIDS is an emerging problem. In some cases it istransmitted through poor blood supply and injection practices, but mostly it isacquired through heterosexual transmission.
The health system is divided into public and private sectors. The public sectorservices are free in principle, although through a cost-sharing scheme introducedin 1998 patients pay part of the cost of drugs and laboratory tests. In urban areasthere are many private clinics run by individual doctors on a fee-for-servicesbasis. In both cities and rural areas, particularly the latter, there are hospitals runby missionary organizations which generally charge modest fees.
ALPHALAND/BETALAND 633

635
Of the 300 medical doctors in Betaland, 250 are based in urban areas. Thedistribution of nursing personnel (1,400 nurses) is similar since the mainhospitals, which employ the majority of the nurses, are in urban areas. Medicalaides provide many of the therapeutic services in the country, and their trainingemphasizes management of rural health centres. They number about 300, buthave tended to remain in urban health centres, replacing doctors going intoprivate practice.
In the early 1980s, the Ministry of Health launched a major programme to trainprimary health care workers (PHCWs), in line with the WHO Health for Allstrategy. Most of the 2,000 PHCWs trained to date have remained in rural areas.They are supervised by the district medical officer, or the district primary healthcare supervisor.
Of the Betaland government budget, an average of 4.5% is allocated to theMinistry of Health.
No. 1040 Date: 14/12/99 Betaland
Source: Geneva, WHO malaria control programme
MALARIA IN BETALAND
A 30-day in vivo malaria study to determine levels of resistance to chloroquinewas carried out in the Szro area* in 1997. One group, presenting with positiveblood films for Plasmodium falciparum but without clinical signs of malaria, wastreated with chloroquine (25 mg per kg of body weight) for three days. Of thesecases, 75% proved sensitive to chloroquine, 12% showed R1 resistance, 8%showed R2 resistance, and 5% had R3 resistance.
A second group with blood smears testing positive for P. falciparum andshowing clinical signs of malaria was also treated with chloroquine (25 mg perkg of body weight) for three days. Of this group, 45% were sensitive tochloroquine, 30% showed R1 resistance, 15% had R2 resistance, and 10% hadR3 resistance.
In the past two years individual reports of emerging resistance to Fansidar (SP–sulfadoxine and pyrimethamine) have become increasingly common, though nostudies have yet been done. Mefloquine has now become widely available, butthere have been no reports to date of resistance.
* Bulletin of the WHO 78 (1997): 234-246.
HELP/SOS: ALPHALAND/BETALAND634

N
S
W E
Alphaland
plain
Takri
Kappa Lum
Srzo
Gamma
KhiAnil
Lambda
KesoNoma plain
Mountainousarea
Mountainousarea
Border
Tana River
100 Km
Communications:
Roads
Railways
Harbours Airports
KhronZotewe
AwaleiBugda
BaidoBrew
Karam Burlo
Golra
SakoTrit Bhao
Betaland
Box 4
GEOGRAPHICAL PLAN ON THEEVALUATION OF GAMMA, KHRON, AWALEI,
BREW, TAKRI, SAKO AND TRIT
ALPHALAND/BETALAND 6635

637
N
S
W E
Betaland
Alphaland
plain
semi-desertregionDanikal
desert
Takri
Lum
Srzo
Gamma
Khi
Anil
Lambda
KesoNoma plain
Mountainousarea
Mountainousarea
Border
Tana River
100 Km
Communications:
Roads
Railways
Harbours Airports
Kappa
You are here
Box 5
INFORMATION FROM KAPPA
HELP/SOS: ALPHALAND/BETALAND6636

No. 1041 Date: 14/12/99 Betaland
Source: Geneva, WHO, division of strengthening of health services
HEALTH SYSTEMS IN BETALAND
Betaland has health problems similar to those of other countries in the region.The government is a signatory of the Alma-Ata Declaration, and theMinistry ofHealth has been implementing a strategy to reorient its health services accordingto the principles of primary health care in collaboration with technical advisorsfrom WHO.
Immunization programmes have been reinforced, and full immunizationcoverage rates (12-23 months) have increased to 50% in urban areas, but remainlow (20-30%) in rural areas. National immunization rates for 1997-1998 areestimated to be 38% for measles, 46% for polio, and 51% for DPT3.
Urban Rural
Access to safe water 60% 12%
Access to latrines 50% 17%
The major causes of death in children are diarrhoea, acute respiratory infection,malaria, and measles. Wasting (weight for age) is present in 23% of children andstunting (weight for height) in 47%.The infantmortality rate in 1996was estimatedat 154, and childhood mortality at 232.* Among adults (based on hospital data),AIDS, tuberculosis, various cancers, pregnancy-related problems and vehicleaccidents are the leading causes of death. AIDS prevalence is estimated at 22%(based on antenatal clinic surveys) in urban areas, and 9% in rural areas.
* UNICEF: State of the World’s Children, 1998
No. 1042 Date: 14/12/99 Betaland
Source: Geneva, UNICEF representative
WATER PROJECTS IN BETALAND
UNICEFhas started an important water programme in the area south ofKappa.It is aimed at providing safe water to 50,000 people living mainly in rural areas.UNICEF has a representative in Betaland, and is sponsoring a variety ofprogrammes.
ALPHALAND/BETALAND 637

639
INFORMATION FROM KAPPA
No. 1043 Date: 16/12/99 Betaland
Source: Kappa, permanent secretary, Ministry of the Interior
INTERVIEW GIVEN BY THE PERMANENT SECRETARY,BETALAND MINISTRY OF THE INTERIOR
Q: What is the situation on the border?
A: We are very concerned about the situation on the Alphaland border. Wefear that a guerrilla type of war may spread all over this region, and theauthorities of Lambda continue to falsely accuse us of harbouring armed groupson our territory. This tense situation, coupled with inflammatory statementsfrom Alphaland, increases the risk of conflict between the armed forces of thetwo countries.
Q: Do you think that this situation can continue long?
A: It is difficult to say, but you know the political situation has been tense forquite a long time in Sigma district, and I don’t see how it can be resolved quickly.However, our government is prepared to help in any negotiation process leadingto a just and acceptable solution for all parties.
Q: How many refugees are crossing the border daily?
A: According to the latest information we have, about 10,000 refugees werearriving per day during the first week of December, but the number of newarrivals has decreased since then.
Q: How many people live in Sigma district?
A: Around 1.5 million.
Q: What will your government’s position be if the influx continues?
A: So far our government’s policy has been to accept all refugees, but if theirnumber continues to increase as rapidly as it has recently, wemay have to changeour policy.
Q: In what way?
A: We will patrol the entire border and limit refugees to a few restricted areas.
Q: Do the press and the humanitarian agencies need special permits to gainaccess to the border area?
HELP/SOS: ALPHALAND/BETALAND638

A: They do for access to the border itself. My office will issue humanitarianagencies a travel permit for the border area. It is best, however, to contact themilitary authorities at Gamma for final authorization.
(The Secretary suggests travelling to Gamma by air, and there contacting thegovernor of the province, who will provide the relief team with a vehicle.Furthermore, the Ministry of the Interior will send one of its representatives toGamma with the team.)
No. 1044 Date: 17/12/99 Betaland
Source: Kappa, UNHCR representative
MEETING WITH THE UNHCR REPRESENTATIVE IN KAPPA
The UNHCR representative is based in a neighbouring country, where there arelong-standing refugee problems. He made his first visit to Betaland in July 1999as the first groups of refugees arrived in the country, but for the most part theywere taken care of by relatives living in Epsilon, and there was deemed to be littleneed for outside assistance. At that time he appointed a local representative tofollow the situation.
The UNHCR representative arrived in Kappa four days ago after receivinginformation that a large number of refugees from Alphaland had entered thecountry. He had contacted the various government ministries involved in thesituation. Two days ago he spent a day in the region of Awalei visiting sites wherethe new groups of refugees are concentrated. At present he estimates there areabout 40,000 refugees in the camp and approximately 20,000 self-settled inEpsilon.
He believes them to be in a precarious situation, especially those in the camp.UNHCR has taken steps to provide assistance to the refugees. Actions to betaken include:
. Refugees are to be registered by UNHCR.
. UNHCR has asked the government to aid the refugees. It has been agreedthat a governmental medical team would begin to work in the camp, foodwould be distributed by the government, and, in addition, self-settledrefugees scattered around Epsilon would be given access to medicalservices.
ALPHALAND/BETALAND 639

641
No. 1045 Date: 18/12/99 Betaland
Source: Kappa, permanent secretary, Ministry of Defence
INFORMATION PROVIDED BY THE MINISTRY OF DEFENCE
The Permanent Secretary of the Ministry of Defence said his Ministry wasfollowing the situation closely because of the potential risk of conflict betweenthe two countries. The Permanent Secretary recalled that the government ofAlphaland had issued a statement saying that any intervention by Betalandwould be seen as an act of aggression against Alphaland. The government ofBetaland does not want to provide any support to the ZLM, but is ready torender assistance to the civilian population of Alphaland. It is hoped that suchaid will not be seen as intervention in Alphaland’s internal affairs. For themoment the border is open to the civilian population fromAlphaland, but not tomembers of the ZLM. However, if the influx of refugees continues to increaserapidly, the government might choose to close the border in order to avoidsecurity problems in Epsilon district. The Ministry of Defence is not opposed tofacilitating humanitarian agencies’ access to the border area.
No. 1046 Date: 18/12/99 Betaland
Source: Kappa, deputy secretary, Ministry of the Interior
GOVERNMENTAL REGULATIONS CONCERNING ACCESSTO REFUGEE AREAS
Access to the province is restricted for all non-citizens. It is necessary to secure aspecial permit to visit Gamma province. In Gamma, another authorization mustbe obtained from the Ministry of Defence for access to Epsilon district. Theborder is strictly controlled by the army, and access to Alphaland by land isprohibited.
No. 1047 Date: 23/12/99 Betaland
Source: Kappa, ICRC delegate
ICRC MANDATE: VISIT TO THE MINISTRY OF HEALTH IN KAPPA
The ICRC informs the Permanent Secretary of the Ministry of Health that, incollaboration with the Betaland Red Crescent Society (BRCS), the ICRC wouldlike to assess the situation inGammaprovince. The ICRC is especially concerned
HELP/SOS: ALPHALAND/BETALAND640

about war-wounded, prisoners, and the civilian population. The ICRC haspermission from the Ministry of the Interior to enter the province and go toKhron, where the problems seem to be particularly acute.
No. 1048 Date: 16/12/99 Betaland
Source: Kappa, ICRC delegate
ROLE OF THE ICRC
During a visit to the provincial health office inGamma, the delegate informed theauthorities that the ICRC has a mandate to ensure that the war-wounded haveaccess to medical care. He noted that UNHCR’s responsibility is protection andassistance for refugees, but that the ICRC assists all victims of war, including theaffected civilian population.
No. 1049 Date: 17/12/99 Betaland
Source: Kappa, representative of the Ministry of Agriculture
DEVELOPMENT POLICY: AGRICULTURE IN BETALAND
1. Government development policy
The country was unprepared for self-rule immediately after independence, and ittook several years for clear long-term development policies to emerge. It wasrecognized that development offered the only hope of escaping growingindebtedness and dependence on foreign countries. The following objectiveswere accordingly selected from the options available:
1. Develop the coastal plain through agricultural programmes to produce cashcrops and through an expansion of timber operations.
2. Promote peanut production in the Zowaran area. This would bring moneyinto the region, stimulating further development.
A few years later, when the nomads began asking for development assistance intheir desert and semi-desert areas, the government, acknowledging that thecontinual migration in search of new pastures was creating problems, undertooka well-drilling programme to support cattle ranches on marginal land. The aim,partially realized, was to limit nomadic movement to smaller regions and toincrease the meat supply for urban areas.
ALPHALAND/BETALAND 641

643
2. Development on the coastal plain
Development on the coastal plain has been a priority, and the area northwardsfrom Szro has seen the most development initiatives. Activities here focused onthe harvest of mature hardwood and the promotion of cash crops such asbananas, sugar cane, cotton, and palm oil. This meant extending the railwaynorthwards along the coast, a project that provides seasonal employment,mainly for Zowaran and Gonlani workers. The new railway-line constructionand timber harvesting are being carried out by a consortium headed by the UK-based Lonrho. Financial support for crop-processing factories and cash-cropdevelopment is provided by other multinationals in the consortium. However,the Betaland government is responsible for marketing, through a marketingboard, and its loan guarantees depend on world market prices. Most of thecountry’s development resources are allocated to the coastal plain.
3. Development on the plateau
During colonial times, great hopes were placed on the anticipated income frommineral resources on the plateau. These hopes motivated the construction of arailwayand the establishmentof the townofKappaasone stationon the line. It soonbecame evident, however, that themineral resources were of a lower grade than hadbeen expected, and Kappa became in fact the end of the line. Since it was a colonialadministrative centre, industries developed around the town. When independencecame, Kappa was the appropriate place for the seat of the new government.
Since then, Kappa has increased greatly in size. Themajority of people migratingto the city are Zowarans andGonlanis who joined the informal sector when timeswere hard at home. To keep this migration in check, the government heavilysubsidizes cereal prices in Kappa, thereby stimulating a very substantial blackmarket, as well as mass speculation in areas affected by the drought where thegovernment cannot control cereal prices.
Most of the attempts to develop the plateau have failed; only along the railwayfrom Kappa to Szro have cash crops of coffee and cotton proved successful.
4. Development in Zowaraland
Ten years of exceptionally good climatic conditions with above-average rainfallled the population, with the help of the government and foreign investors, tointensify peanut cultivation onmarginal land. This trendwas further encouragedby high prices in the world commodity markets. At the same time, good pastureland on the edge of the desert became even scarcer than before. The government
HELP/SOS: ALPHALAND/BETALAND642

saw an opportunity here to develop a network of wells in the region and to createpilot cattle ranches in an effort to settle the nomads.
In Epsilon district, the government has embarked on the development of smallirrigated plots for the cultivation of cereals with a higher protein yield, as away oftackling protein malnutrition in the country. Seeds for the new high-proteincereals have already been distributed on a pilot basis in some places in Epsilonand on the plateau.
No. 1050 Date: 16/12/99 Betaland
Source: Kappa, director of the Department of Nutrition, Ministry of Health
NUTRITIONAL POLICY IN BETALAND
1. Nutritional surveillance at the national level
Betaland’s nutritional surveillance system is based on anthropometric measure-ments taken in the health care centres. Community health workers gather data,mainly anthropometric measurements, which they categorize using the Gomezclassification system. This programme is new and has taken a long time to set up.Data has not been collected for long enough yet to permit a longitudinal study,and the Department of Health Statistics has no facilities to analyze the existingdata. However, a pilot study was completed for the year 1997.
According to theDepartment ofNutrition, the overall national nutritional statusaccording to the Gomez classification and using NCHS reference standards is:20% at Grade 0 (normal nutrition); 62.5% at Grade I (mild malnutrition); 15%at Grade II (moderate malnutrition); and 2.5% at Grade III (severemalnutrition). Kwashiorkor is generally considered to be most common alongthe coast and in the Zowaran tribe. Anemia is very common, but its actualprevalence is difficult to gauge, since there is no standardized way for healthworkers to assess it in the absence of laboratory facilities. According to a surveytaken among the Zowaran tribe in 1996, the prevalence of vitamin A deficiencyamong children under six years of age is 5%. Bitot’s spots were used as thecriterion for diagnosis.
2. Feeding programme for malnourished children
. Children below 6 years with Grade II and III malnutrition are treated free ofcharge.
. Children with Grade III malnutrition are admitted to the nearest hospital forin-patient treatment.
ALPHALAND/BETALAND 643

645
. Children with Grade II malnutrition receive one ration of milk six days aweek. The milk is made from 50g of milk powder in 250 ml of water.However, the supply is not quite adequate to cover the whole country.
. Malnutrition is detected by the maternal and child health (MCH) clinicsystem. No statistics are available concerning the current extent ofprogramme coverage.
3. Programme for nutritional education and weaning products
Public healthworkers are responsible for educatingmothers about how to feed theirchildren. The government has designated a food factory to produce a weaningmixture based on cereals enriched with soy flour and dried skim milk (DSM), andfortified with vitamins and minerals. This product, called Nutrifort, is tasty andinexpensive, and it is the focusof amajormarketing campaign throughoutBetaland.Therehavebeen someproblemsbecause theproduct is newandunfamiliar.Mothersshould be encouraged to buy this product rather than imported brands of babyformula and other products which are inferior and more expensive. A nutritionaleducation training programme is provided for public health workers to give them agood knowledge of available foods and the means of preventing malnutrition.
4. Programme in collaboration with the Ministry of Agriculture
To improve the general nutritional status of the population, the Ministry ofAgriculture, in collaboration with international organizations, has developed, ina small irrigated zone near the Tana river on the outskirts of Epsilon, a variety ofbulgur wheat with improved protein content and better yield. The objectives ofthis programme are to eradicate kwashiorkor in Epsilon and to help the Zowarantribe achieve self-sufficiency in agricultural production within 10 years. Someseeds from the improved variety have been distributed free in the Epsilon areaand on the plateau. In theDanikal region, a number of ranches have been createdto help the nomads settle down, and to supply the large cities with meat.
No. 1051 Date: 18/12/99 Betaland
Source: Kappa, representative of the Betaland National Institute of Nutrition (NIN)
FOOD HABITS OF THE LOCAL POPULATION IN BETALAND
The population’s food preferences vary according to ethnic group.
. The staple foods for subsistence farmers are millet and sorghum. Other foodsinclude peanuts, beans, and peas, as well as a variety of fruits and other
HELP/SOS: ALPHALAND/BETALAND644

vegetables in season. Rice and wheat are eaten on a limited scale. Meat issometimes consumed. Along the coast, dried or smoked fish is widelyconsumed.
. The nomads live essentially on milk supplemented with cereals (sorghum),especially during the dry season. Meat is not eaten regularly—perhaps onceor twice a month. Sugar, rice, dates, tea, coffee and butter are obtained bybarter. The food gap for subsistence farmers comes during the wet season,when they are waiting for the new crops, and for nomads during the dryseason, when milk production declines.
No. 1052 Date: 21/12/99 Betaland
Source: Kappa, NIN representative
INFORMATION PROVIDED BY THE NIN REPRESENTATIVE IN KAPPA
The extent of protein-energy malnutrition in Betaland
Malnutrition is an endemic problem in Betaland. It is estimated that half of thepopulation does not have an adequate calorie intake. The main causes are: lackof food in the markets in some areas, low production levels, high prices, lowincome for the majority of the population, food habits, poor nutritionaleducation at the family level (weaning), and the high cost of seeds andfertilizer.
Food storage facilities at the family level are poor. It is estimated that in ruralareas 25%-30% of food is lost due to faulty storage.
Studies carried out in health centres show that 65% of children under the age offive years are malnourished; of those, 25% are severely malnourished (below70% of standard weight-for-age). Studies made in the population at large showthat 10%-20% of children, depending on region, are malnourished (below 80%of standard weight-for-height).
A programme to rehabilitate severely malnourished children has been set up inhealth centres. The centres distribute pappa (an enriched food made locally) tofamilies withmalnourished children. However, this programme covers only 20%of Kappa.
In emergency situations related to drought conditions, nutritional rehabilitationcentres are set up with the assistance of NGOs.
The high rate of child mortality is partly related to the high level of malnutritionin the country.
ALPHALAND/BETALAND 645

647
Other nutritional problems:
Vitamin A deficiency:
In 1993, a study carried out in the desert regions (Danikal and western Epsilon)showed that the prevalence of clinical vitamin A deficiency (Bitot’s spots) was2.5%. Another study showed that 40% of the children in rural areas had avitamin A blood level of less than 100 mcg/l.
A prevention programme based on the distribution of capsules containing200,000 IUof vitaminA through health centres was planned, but so far only 10%of the target population has been covered.
Anaemia:
Anaemia is amajor concern in pregnant women. It is estimated that 20%have anHgb level of less than 9g/dl.
No. 1053 Date: 18/12/99 Betaland
Source: Kappa, representative of the Ministry of Social Affairs
HOUSING PREFERENCES IN BETALAND
The most common housing for subsistence farmers in rural areas is a circularcone-roofed tukul, built fromwooden poles, maize stalks, mudmixed with straw,and grass thatch or corrugated iron sheets. The usual rural settlement patternconsists of scattered homesteads surrounded by cultivated fields. Nomads live incollapsible, portable huts made of acacia branches bent into a dome-shapedframework and covered with grass mats. Urban housing is varied, althoughmostof the houses are built of kiln-fired bricks or cement blocks and roofed withcorrugated iron.
No. 1054 Date: 27/12/99 Betaland
Source: Kappa, representative of the Ministry of Works and Supplies
THE AVAILABILITY OF BUILDING MATERIALS
Most commonly used building materials are available in the country. There is acement plant in Szro, but its output is insufficient for the country’s needs, so somecement must be imported from surrounding countries. Building stone and sandare available throughout the country.Wood is abundant in the north, but a largeproportion of it is exported. Wood is expensive in the south. Corrugated metal
HELP/SOS: ALPHALAND/BETALAND646

sheets are imported, and are almost always available in several thicknesses.Plywood and block board are made in Szro. Artisans are available throughoutthe country and their skills are graded by the technical training they haveundergone.
No. 1055 Date: 17/12/99 Betaland
Source: Kappa, permanent secretary, Ministry of Transport
TRANSPORTATION IN BETALAND
The permanent secretary says that communications betweenKappa andGammaare very good. Although it takes 24 hours to reach Gamma by road, by air it isonly two hours. At the present time there are only two flights per week. Fuel isrestricted in the country, all of it being imported through Szro harbour. Fuelration permits are issued by theMinistry of the Interior. The current cost of fuel is2 Betas per litre.
1. Communication System
. Postal service is generally good, although internal delivery is often slow.
. Telephone connections exist between most cities and towns. Majorpopulation centres now have Ericsson direct-dial digital systems.
. Fax machines are available in most post offices.
. E-mail service is available only in Kappa. Messages are downloaded toKappa from London only two or three times a week.
2. Transport System
Railway
The State of Betaland is the official owner of the railway system, except for thenew line from Szro to the north, which is run by the development consortium.Line repair and maintenance are good, but train maintenance and replacementare generally poor. Freight trains run daily each way between Kappa and Szroand between Szro and Gamma.
Carrying capacity
The network is overloaded and transportation delays are rather long (1-2 months),but faster service is sometimes available for a price. The train linking the capitalcity with the harbour has a maximum capacity of 50 freight cars, each with a
ALPHALAND/BETALAND 647

649
capacity of 40 tonnes. The train from Szro to Gamma usually has 20-30 freightcars, each with a 40 tonnes capacity. The cost of transportation is 400 Betas per100 km of tonne.
Road transport
There are two main transport companies, one in Kappa and the other one inSzro. The total number of lorries of the two companies combined is about 80.Road transport is handicapped by two main problems: Breakdowns are veryfrequent, with spare parts extremely difficult to find, and there is often a lack offuel. When there is a national fuel shortage, road transport is only possible if anextra fee is paid—meaning that it is available only to people able to pay thisunofficial levy. The transport companies also have to serve the personal interestsof their protectors. The cost is quite variable and depends on the demand, theperson who wishes to ship goods, and the places where the goods have to bedelivered. As an indication, costs can vary from 100 Betas/tonne/100 km to350 Betas/tonne/100 km—or more, when fuel is scarce.
Air transport
The national airline transports mainly passengers with two Boeing 737s and twoVickers Viscount propjets. The total volume of domestic air freight is negligible.There are regular international flights to Kappa by Air France, British Airways,KLM, and Air Maybe, all of which carry cargo. Cargo planes, mainly DC-3s,D-6s and C-130s, are available in the region.
No. 1056 Date: 27/12/99 Betaland
Source: Kappa, information officer, civil aviation authority
KAPPA AIRPORT
The Kappa airport is the country’s main airport, and handles most of theinternational air traffic.
Runway characteristics:elevation: 1041 metres
average temperature (C): 21 degrees
slope: 1.09%
length: 3000 metres
aircraft: all types, including DC10, B747, AB340-400, C5A,
Antonov 124
HELP/SOS: ALPHALAND/BETALAND648

fuel octane: 100/JA1
surface: tarmac and concrete
alternate aerodromes: Lambda (Alphaland), Bonauro (Basamland)
aids: ILS, DME, VOR, NDB, LSA -(07), LVA, LR, LTX, LB,
LO, MD, MC, MT, MTD, MS, MTX, MO, L4, L5, L9.
Updated information on this airport can be found in the latest editions ofWeeklyInternational Notams, International Flight Manual, and ICAO’s Air NavigationPlan for the region.
No. 1057 Date: 27/12/99 Betaland
Source: Kappa, information officer, civil aviation authority
AIR TRAFFIC
Air traffic is dense between the provincial capitals and the capital city of thecountry. There are two commercial flights every week between Kappa andGamma (AirBeta), and three flights weekly between Kappa and Takri. It ispossible to rent small aircraft in Kappa from BetaLuk Air Transport (motto:BetaLuk Next Time).
No. 1058 Date: 27/12/99 Betaland
Source: Kappa, information officer, Betaland ports authority
THE PORT OF SZRO
The port of Szro has the following characteristics:
depth at the entrance: 11-16.5 m pallets: 10,000
wharves: 5 storage for
containers: 40,000 m2depth alongside wharf: 8 m
fuel: availablemaximum safe draft
alongside wharf: 10 m potable water: available
mobile cranes: 35 MT, 55 MT minor repairs: limited facilities
container crane: 1 (max. 12 MT) towage: compulsory
forklifts: 24 pilotage: compulsory
ALPHALAND/BETALAND 649

651
No. 1059 Date: 27/12/99 Betaland
Source: Kappa, information officer, Betaland ports authority
THE PORT OF GAMMA
The port of Gamma has the following characteristics:
depth at entrance: 7.62 m
depth at wharf side: 3.66 m
max. draft: 3.3 m
max. ship length 167.5 m
loading and unloading by ship’s gear
minor repairs: available
towage: compulsory
pilotage: compulsory
No. 1060 Date: 27/12/99 Betaland
Source: Kappa, information officer, Betaland ports authority
THE PORT OF LUM
The port of Lum has the following characteristics:
1 wharf 73 m long and 4.3 m wide
minor repairs: unavailable
towage: unavailable
pilotage: compulsory
NB: The approach can be dangerous in north and north-west winds.
No. 1061 Date: 27/12/99 Betaland
Source: Kappa, information officer, Betaland ports authority
PORT FACILITIES
The Betaland ports authority authorizes the use of the country’s ports for thedelivery of humanitarian assistance. However, it is emphasized that humanitar-ian supplies are subject to the usual customs procedures, and that portwarehousing capacity is strictly limited.
HELP/SOS: ALPHALAND/BETALAND650

No. 1062 Date: 27/12/99 Betaland
Source: Kappa, representative of the Ministry of Communications
INFORMATION ON TELEPHONE AND RADIO COMMUNICATIONS
According to the International Telecommunications Union (1997), the countryhas had television broadcasting capabilities since 1984, but there is only onechannel, controlled by the government (Antenna Betaland).
Both radio stations are government controlled.
Telephone
The Posts andTelecommunications Corporation (Bethatel)maintains 30,000 linesto subscribers in various parts of the country. There are five automatic exchangesin Kappa and one in Gamma, all with digital switching. There are 70 manualexchanges in various towns. International calls can be directly dialed fromKappa and Szro; calls from other places require the assistance of theinternational operator. Cellular phones are available in Kappa, but there is noreception outside the capital.
Fax
Fax service is widely available in the commercial centres. Where there aretelephone services, every post office has a fax service.
Telex
Telex facilities, though less widely used than in the past, have 800 subscribers.
Several commercial companies have recently begun offering e-mail services inKappa and Szro.
Radio communications
TheBRCShas a short-wave radio system that connects the capital, Kappa, to themajor cities in the provinces, although transmissions are often interrupted.Authorization to establish a radio system must be obtained from the Ministriesof Communications and the Interior. Use of radio transmitters in sensitive areasnear the border is restricted by the Betaland army.
ALPHALAND/BETALAND 651

653
No. 1063 Date: 27/12/99 Betaland
Source: Kappa, representative of the Ministry of Transport
ROAD BETWEEN KHRON AND AWALEI
During the rainy season, the road between Khron and Awalei is cut off by highwater from the Bowi River, although only for three to four days at a time.
No. 1064 Date: 27/12/99 Betaland
Source: Kappa, representative of the Ministry of Transport
WATERWAYS IN BETALAND
The main river is the Tana River, which is navigable between Puri and Gammathe whole year, although only for shallow draft vessels (1-2m).
No. 1065 Date: 16/12/99 Betaland
Source: Kappa, director-general, Betaland Ministry of Health
HEALTH INFORMATION PROVIDED BY THE DIRECTOR-GENERAL,BETALAND MINISTRY OF HEALTH
Themain issues of health policy in Betaland can be summarized as follows.Up to1992, the government health policy focused on the provision of curative andemergency care. The aim was to create one central referral hospital in eachprovince (provincial hospital) and at least one hospital in each district.Government plans also called for the establishment of dispensaries staffed bydoctors and nurses in every village with more than 5,000 inhabitants. Althoughprivate medical practice was allowed, private doctors were few, and locatedmainly in thecapital.Publichealthprogrammeswereorganizedasdisease-specificschemes aimed at controlling endemic diseases such as tuberculosis, leprosy,schistosomiasis, and malaria on a national basis. Each programme had its ownbudget and administrative support, and its own health workers. The universityhospital in Kappa was in charge of training new doctors and nurses for thecountry.Medical assistants and nursing aides were trained at the provincial level.
Thispolicy failed toproduce theanticipated improvement inhealth statusbecauseof insufficient funding and because it did not increase access to health facilities.
From1992on, full support was given to the primary health care programme,whichrelied on village health workers. They were recruited from among the villagers by
HELP/SOS: ALPHALAND/BETALAND652

the traditional political and health authorities, with the consent of the localpopulation, and underwent a two-month training programme. Their responsi-bilities were to promote improved sanitation, good nutrition, and healthy homedeliveries for babies, aswell as todiagnose and treat commondiseases.Theywere tobepaidby the community inwhateverwaywasmost appropriate—this oftenmeantthat villagers cultivated the agricultural land of the village health workers.
Nevertheless, this programme never really succeeded. Most of the village healthworkers were ignored by other health workers. The programme as a whole wasnever very well organized or planned. In some villages, the village health workerbecame the ‘‘doctor’’, often selling drugs and treatments, while in others he or shewas ignored by the other villagers, who did not provide the support the healthworker needed. The village health worker programme is still underway but hasnot yet been fully implemented. The state budget for the next five years will covertraining for 3,000 village health workers, but this training is the responsibility ofthe individual provinces. Furthermore, no satisfactory agreement has beenreached yet on how to pay them—that is, whether they will be full-timeemployees of the health system, or be paid in kind by villagers.
No. 1066 Date: 16/12/99 Betaland
Source: Kappa, director-general, Betaland Ministry of Health
THE BETALAND HEALTH SYSTEM STRUCTURE
HEALTH SYSTEM ORGANIZATION
Ministry of Health (Kappa)
Provincial Health Office
The provincial health office (headed by a provincial health officer) comprises thefollowing departments:
. Public health department, in charge of public health programmes, EPI,primary health care, TB/leprosy control, etc.
. Health services department, in charge of the hospitals and health centres
. Training department, overseeing health assistant, nursing aide, and PHCworker training
. Pharmacy and medical supplies department
. Administrative services department, with sections for personnel, informationsystems, equipment, and financing for provincial and district services.
ALPHALAND/BETALAND 653

655
District Health Office
The health services in a district are managed by two persons, a district healthofficer (DHO) for public health services (including health centres anddispensaries) and a medical superintendent, in charge of the district hospital.The DHO and his or her staff are responsible for supervising the medicalassistants and nursing aides, and the village health workers in the dispensariesand first aid posts. The DHO is also responsible for the mobile teams that takecare of the EPI, malaria, and tuberculosis. Most health centres are run by nursesor medical assistants and the dispensaries by medical assistants or nursing aides.They offer out-patients and in-patients (in the case of health centres) bothpreventive and curative health care. PHC workers are supposed to be supervisedby the health worker in charge of the nearest health facility, but generally no suchsupervision takes place.
No. 1067 Date: 16/12/99 Betaland
Source: Kappa, director-general, Ministry of Health
INFORMATION ON HEALTH EDUCATION PROGRAMMES IN BETALAND
Doctors: Six years post-secondary school and one year as a staff doctor in theKappa or Szro hospital. Doctors do not work below the hospital level, except forthe small but increasing number in private practice in the main cities.
Enrolled nurses/midwives: Three years. Mostly oriented toward hospital-basedcurative care, including one year of midwifery.
Registered nurses/midwives: A special public health training course was startedtwo years ago. The University of Betaland in Kappa started a four-yearprogramme leading to aBachelor of Science degree in nursing (BSN) in 1989, anda Master of Science in nursing (MSN) in 1992.
Primary health care workers: Sixweeks: two-week theoretical course, usually heldin the provincial capital, followed by four weeks of practical work (in a healthcentre). A national reference manual has been written, based on the WHO text,The Primary Health Centre.
Medical assistants:Three years of post-secondary school in one of six schools runby government or mission hospitals. Medical assistants are qualified to diagnoseand treat common illnesses in clinics and dispensaries, and to implementimmunization programmes without direct medical supervision. They are alsoable to provide in-patient care for uncomplicated illnesses.
HELP/SOS: ALPHALAND/BETALAND654

No. 1068 Date: 16/12/99 Betaland
Source: Kappa, director-general, Ministry of Health
THE COST OF HEALTH SERVICES
General health budget:
1. National health budget: 4.5% of the Betaland government’s annual budget.
2. There is no national health insurance system, although some private systemsexist in the commercial sector. In the wake of recent health sector reforms,hospitalizations, out-patient services, and prescribed medicines require someco-payment, which is set by each facility according to local policy.
3. Some doctors and nurses work on a private basis after regular hours. Somefull-time private practices exist, particularly in Kappa.
4. Most drugs, including antibiotics, can be bought in pharmacies, as well as theopen market. Some recent problems with bogus drugs have come to theattention of the Ministry of Health.
Cost of treatment:
Diarrhoeal diseases: The cost of one packet of oral rehydration salts (ORS) is$US 0.40, whereas the cost of one hospitalization for intravenous rehydrationmay reach $US 15.00.
Malaria: The cost of one course of chloroquine treatment for acute malaria is$0.40, and one course of mefloquine is $6.70.
Measles:The cost of immunizing one child is $1.25 (all costs), whereas the cost ofhospitalizing a child with measles complications may reach $15.00.
Tuberculosis: The cost of curing a case of TB is estimated at $145.
Cost of drugs (Obscure Pharmaceutical Company):
Chloroquine: $15 (1,000-tablet tin)
Mebendazole: $4.50 (1,000-tablet tin)
Fansidar: $45 (1,000-tablet tin)
Albendazole: $18.00 (250 tablets)
Pyrantel pamoate: $7.50 (1,000-tablet tin)
Co-trimoxazole: $14 (500 tablets)
Quinine: $12 (100 vials)
ALPHALAND/BETALAND 655

657
Chloramphenicol: $7.50 (500-tablet tin)
Amoxicillin: $37 (500-tablet tin)
No. 1069 Date: 16/12/99 Betaland
Source: Kappa, director-general, Ministry of Health
ORGANIZATION OF DRUG DISTRIBUTION WITHIN THE HEALTH SYSTEM
. Drug distribution structure: National central pharmacy— provincial centralpharmacy— provincial hospital — district hospital — health care centres —dispensaries — health posts.
. Each year the main office of the Ministry of Health in Kappa determines thequantities of drugs and medical equipment that will be sent to the provincialhealth department. Each province is responsible for dispatching supplies tothe hospitals and the main health care centres. Drugs are allocated to thevillage health posts by the health care centre under the supervision of thedistrict health office. Very often, the health posts do not receive the drugs thatthey need. In some places, the population has organized a revolving drugfund (Bamako Initiative) to pay for the most basic drugs.
. ORS, aspirin, and penicillin are formulated locally in Kappa.
. There are a few private pharmacies in the big towns.
. The purchase of medicines in the local market by humanitarian agencies hasto be approved, for fear of creating shortages. At present agencies areencouraged to import their medical supplies directly while observing nationalessential drug policies.
No. 1070 Date: 16/12/99 Betaland
Source: Kappa, director of the malaria control programme, Ministry of Health
MALARIA CONTROL PROGRAMME IN BETALAND
The National Malaria Control Programme (NMCP) was created in the early1960s. At that time it was thought that malaria could eventually be eradicated bymeans of various control methods (vector control and chemoprophylaxis).Decades later, however, it was necessary to review the original strategy, giventhat mosquitoes, especially the predominant species Anopheles gambiae andA. funestus, were resistant to the widely used DDT. It also became obvious thatPlasmodium falciparum was increasingly resistant to chloroquine, the standardfirst-line treatment. The programme is structured as follows:
HELP/SOS: ALPHALAND/BETALAND656

Head of NMCP (Kappa)
|
Provincial directors of NMCP
|
District NMCP officers
|
District hospitals health centres and dispensaries PHC workers
vector control programme
No. 1071 Date: 16/12/99 Betaland
Source: Kappa, director of the malaria control programme, Ministry of Health
MALARIA CONTROL STRATEGY
Two objectives have been set for the national control programme:
1. reduction of malaria-related mortality
2. reduction of malaria transmission.
To reducemortality, theministry is promoting improved casemanagement at thehealth facility level. Although there is pressure from WHO and otherinternational agencies to encourage effective home treatment of malaria,particularly in children, with drugs available through grocery shops, this ideahas been resisted by the Betaland Medical Association. In the past three yearspromotion of insecticide-treated bednets has begun, but this campaign currentlycovers only a small part of the country and is entirely donor-funded. One of thestandard methods of malaria control in Betaland has been to spray houseinteriors with insecticide–originally DDT, and now pyrethroids. In theoryresistance to insecticides is monitored regularly. Communities are encouraged toclear brush from around dwellings and to fill in areas where rainwater collects, toeliminate mosquito breeding grounds.
No. 1072 Date: 16/12/99 Betaland
Source: Kappa, director of the malaria control programme, Ministry of Health
MALARIA TREATMENT IN BETALAND
Malaria: treatment policy
Although resistance to chloroquine has been noted in some places (Szro), therecommended treatment remains as follows:
ALPHALAND/BETALAND 657

659
. Chloroquine: 600 mg base, followed six hours later by 300 mg, then 300 mgdaily for three days.
. If there is no response to chloroquine, acutemalaria (P. falciparum) should betreated with sulphadoxine and pyrimethamine (Fansidare or SP)—threetablets stat.
. Cerebral malaria or complicated malaria should be treated with intravenousquinine.
. Mefloquine is only available at the provincial hospitals, and from privatepharmacies in major cities.
No. 1073 Betaland
Source: Kappa, director of the HIV control programme, Ministry of Health
BETALAND NATIONAL HIV PROGRAMME
The Betaland HIV programme has emphasized behaviour modification—through the promotion of safe health practices and the social marketing ofcondoms—as well as cooperation with international organizations and scientificorganizations researching AIDS and HIV. A major part of the HIV programmehas focused on the development of a national primary and secondary schoolcurriculum dealing with self-esteem, negotiating skills, and human sexuality,including HIV, AIDS, and other sexually transmitted infections (STI). Parts ofthis curriculumhave been instituted, but other parts have been ignored in schoolswhere the teaching staff felt uncomfortable with the material. The director saysthat awareness of HIV/AIDS and STI issues has increased dramatically inBetaland, but evidence of behavioural change is less clear. A number of NGOshave recently initiated AIDS control programmes in Betaland. One of the firstmeasures was to distribute condoms among lorry drivers travelling betweenGamma and Kappa.
All Betaland hospitals have access to HIV diagnostic kits using dried blood spottests, and some of the larger hospitals have ELISA equipment. The directoradmits that supply logistics have at times been less than ideal, with reagents andkits sitting in central medical stores until they are out of date while individualhealth facilities go without these supplies altogether. It is the policy of theMinistry of Health that no reusable syringes or needles be used in Betaland, butthe director acknowledges that most facilities are obliged to boil or sterilize theirdisposable syringes for reuse.
Condoms are now socially marketed in most of the larger cities of Betaland.
HELP/SOS: ALPHALAND/BETALAND658

No. 1074 Date: 16/12/99 Betaland
Source: Kappa, director of the AIDS control programme, Ministry of Health
HIV PREVALENCE IN BETALAND
With help from WHO, a national map of HIV prevalence estimates has beencompleted. These data are largely based on seroprevalence studies fromantenatal clinics. In the major cities, Kappa and Gamma, seroprevalence hasbeen increasing by about 3% a year for the past three years, and is now estimatedto be 18%. In Takri the figure is 15%, and for the coastal towns of Srzo and Lumthe percentages are 19% and 22%, respectively. In small towns along theprincipal highways seroprevalence is consistently above 15%. In areas awayfrom the main roads, figures drop, and in remote regions accessible only by dirtroads, prevalence is 1%-2%. Overall, it is estimated that 11% of Betaland’spopulation is infected. Residents of Betaland commonly believe that the diseaseis principally a disease of migrants, mostly from Alphaland, and that thoseBetalanders who contract the disease most certainly did so from contact with amigrant.
Figures for secondary and referral hospitals show that about 40% of patients inthe medicine wards and about 5% of children in the paediatric wards are HIV-positive. The figures for rural and first referral hospitals are somewhat lower,depending on location. In all tuberculosis wards sampled, HIV prevalence wasover 50%.
No. 1075 Date: 16/12/99 Betaland
Source: Kappa, director of the programme for control of diarrhoeal disease (CDD),Ministry of Health
DIARRHOEAL DISEASE CONTROL PROGRAMME IN BETALAND
In Betaland, diarrhoeal diseases are a major cause of death among preschool agedchildren. In 1992, the Ministry of Health mapped out a plan of action aimed atreducing mortality and morbidity among children. Two points were emphasized:
. the need for extensive use of oral rehydration therapy (ORT)
. the need to make safe water more widely available, especially in rural areas.
It was decided to implement the following measures:
. Large quantities of oral rehydration salts would be made available throughthe maternal and child health programme.
ALPHALAND/BETALAND 659

. The training of village health workers would stress the importance of oralrehydration therapy.
. The Ministry of Health would provide support to the National Safe WaterProject.
No. 1076 Date: 16/12/99 Betaland
Source: Kappa, director of tuberculosis control programme, Ministry of Health
TUBERCULOSIS CONTROL PROGRAMME IN BETALAND
Before 1990 the NTBP programme worked through the provincial and districthealth systems in an advisory and training capacity. In spite of these educationalefforts there were, in practice, no standard criteria for diagnosis, and treatmentregimens were not standardized either. BCG immunization was not a routinepart of the EPI.
In Gamma province, tuberculosis cases were diagnosed by medical assistants andnursing personnel, and treated by doctors.Usually patients were treated on an out-patient basis, although severe cases could be hospitalized for amonth or two in theTB ward (50 beds at the Gamma hospital, and 15 beds at the Brew health centre).Out-patients were asked to return to the dispensary where the treatment wasinitiated every two months for a follow-up, at which time they were given theirdrug allocation for the next two months. Not surprisingly, the treatmentcompletion rate was low, below 40% in many areas. At that time the treatmentmost commonly prescribed was streptomycin, isoniazid (INH), and thiacetazone.
Since 1990 the national policy has been to refer suspected TB patients to districtor provincial hospitals. Once diagnosed, patients are hospitalized for twomonthsand receive intensive treatment with four drugs: INH, rifampicin, pyrazinamideand ethambutol. At the end of twomonths they are discharged but continue on aregimen of INHand rifampicin under the direction of their local health centre foranother six months. This approach has greatly improved the treatmentcompletion rate, and reduced the number of relapses. However, hospitalsuperintendents have complained about the large amount of resources requiredto treat TB patients.
In 1998 DOTS (directly observed treatment, short course) was started in severalprovinces. Although it is now a national policy, it is not yet used nationwide.Considerable training is still required, especially at the health centre level. TheWHO office in Betaland is encouraging the NTBP programme managers toconsider using community monitors as treatment observers so that TB patients
HELP/SOS: ALPHALAND/BETALAND660 661

do not have to go to the health centre every day for treatment monitoring.However, this approach has not been tried in Betaland yet.
Drugs are supplied by the NTBP programme through the central medical stores.The director admits that there are frequent stock-outs of TBdrugs at the provincialand district levels. The most recent treatment completion rate for the country as awhole is 45%, and he does not have specific figures for Epsilon district.
Although aTB information system exists, the register is apparently not always upto date, and the national office does not regularly receive information fromabout25% of the facilities that treat tuberculosis.
No. 1077 Date: 16/12/99 Betaland
Source: Kappa, permanent secretary, Betaland Ministry of Health
INFORMATION PROVIDED BY THE PERMANENT SECRETARY, MINISTRYOF HEALTH, ON THE SITUATION PREVAILING ON THE BORDER
Q: Sir, how many refugees have arrived on the border?
A: Many, many—most of them settle near Khron.
Q: How far from Khron?
A: About five miles.
Q: What is their health situation?
A: Very bad. They are malnourished, many are sick, and the town hospitalseems to be overcrowded with patients.
Q: What are the most common medical problems among the refugees?
A: Malaria, tuberculosis, bilharziasis, diarrhoeal diseases, pneumonia, andvarious parasitic infections are common.
Q: Are there wounded?
A: Yes, they, too, have been hospitalized at Gamma.
Q: What medical services are available in Gamma?
A: Gamma is the capital of a province comprising three districts: Gamma,Epsilon and Takri. The provincial hospital is in Gamma, and there are healthcentres and dispensaries in other towns and villages.
Q: What is the population of Gamma province?
A: The estimate is roughly 800,000, but most of the population lives along thecoast.
ALPHALAND/BETALAND 661

663
Q: What is the refugees’ food situation?
A: The refugees have very little food with them. They can buy some in themarket in Gamma, but it is not enough for everyone.
Q: Have there been any disease outbreaks among the refugee population?
A: I have been told that there are many cases of measles and meningitis. This isalso a danger for our population. I have asked the health officer for Gammaprovince to take all necessary measures to prevent these problems from spreading.
Q: Howare relations between the residents ofGammaprovince and the refugees?
A: The Alphaland refugees are of Zowaran origin and our people in this areaare from the same tribe. Actually, people living in the Sigma area of Alphalandoften travel to Epsilon district for trading purposes, and residents of Epsilonregularly cross into the Sigma area.
No. 1078 Date: 17/12/99 Betaland
Source: Kappa, director of tuberculosis control programme, Ministry of Health
COST OF TB DRUGS FROM CENTRAL MEDICAL STORES
Isoniazid tablets 100 mg 12.5 Betas for 1,000
tablets 300 mg 23 Betas for 1,000
Rifampicin tablets 150 mg 30 Betas for 100
tablets 300 mg 50 Betas for 100
Pyranizamide tablets 500 mg 190 Betas for 1,000
Ethambutol tablets 100 mg 45 Betas for 1,000
tablets 400 mg 125 Betas for 1,000
No. 1079 Date: 17/12/99 Betaland
Source: Kappa, director of Expanded Programme of Immunization (EPI),
Ministry of Health
EPI IN BETALAND
In 1989, the government decided to implement a nationwide EPI. Theprogramme was launched at the beginning of 1991. The immunization scheduleis as follows:
. BCG: one dose at birth
. DPT: three doses at four-week intervals, beginning at the age of threemonths
HELP/SOS: ALPHALAND/BETALAND662

. Polio: three doses at four-week intervals, beginning at the age of threemonths
. Measles: one dose at the age of nine months
. Tetanus: for women of childbearing age or pregnant women, two doses atfour-week intervals, and one dose during each subsequent pregnancy.
The objectives of the national EPI are to reduce the incidence of measles,neonatal tetanus, and poliomyelitis by half within four years.
No. 1080 Date: 17/12/99 Betaland
Source: Kappa, director of EPI, Ministry of Health
AVAILABILITY OF VACCINES IN BETALAND
Vaccines are imported through UNICEF and then stored at the centralpharmacy in Kappa. Usually, the cold chain works effectively from the countryof origin to Kappa airport, the Central Medical Stores, the provincial airports,the provincial medical stores, and finally the EPI teams.
Though the vaccine supply in Gamma is sufficient for the usual EPI activities inthe province there are frequent gaps in vaccine distribution to the various EPIteams.Moreover, equipment maintenance (refrigerator repairs, adequate supplyof cold boxes) is difficult and time-consuming. Vaccinations are performed in thehealth centres; sometimes, in remote areas, mass campaigns are organized withmobile teams sent from the provincial health office. Transportation is often aproblem, since programme vehicles are frequently used for other purposes andare therefore unavailable for EPI services when required. Fuel and maintenanceare also a growing problem.
No. 1081 Date: 17/12/99 Betaland
Source: Kappa, director of EPI, Ministry of Health
MASS IMMUNIZATION CAMPAIGN
Starting in 1997, a National Immunization Days (NIDs) mass immunizationcampaign was organized in the country for DPT, polio (using oral polio vaccine)and measles. Following the initiation of this campaign, the estimatedimmunization coverage for measles increased from 35% to 55%, and the figurefor full immunization coverage (in ages 12-24 months) increased from 35% to65%. However, the campaign has not been followed by any improvement inroutine EPI services. Furthermore, provincial and district health offices are
ALPHALAND/BETALAND 663
665
complaining about the great demand thatNIDs place on their own infrastructureand resources, for which they receive little additional support from the Ministryof Health.
No. 1082 Date: 17/12/99 Betaland
Source: Kappa, representative from Assistance in Precarious Time (APT)
INFORMATION PROVIDED BY APT REPRESENTATIVE
This organization has been present in the country for one year. Its role is to coverthe medical needs of the population migrating from rural areas to the areaaround Kappa, where the migrants are concentrated in informal settlements.APT runs two health centres and provides support in the form of personnel andequipment to several others. The organization has six expatriates working inBetaland, three doctors and three nurses.
No. 1083 Date: 17/12/99 Betaland
Source: Kappa, representative of the Episcopal Council (a coordinating body
of the Christian churches in Betaland)
ROLE OF THE EPISCOPAL COUNCIL (EC)
The EC has representatives all over the country, and is a coordinating body forthe various development efforts of the Christian churches in Betaland. Althoughthe EC is not oriented towards emergency situations, it has sent 200 kg of drugsand 5,000 blankets to its office in Gamma for distribution to the refugees. Anappeal for aid toBetaland is currently beingmounted by the dioceses of Salisburyand Winchester in England.
No. 1084 Date: 17/12/99 Betaland
Source: Kappa, representative of National Charity Services (NCS)
THE ROLE OF THE NCS IN ASSISTING THE REFUGEES
This organization does social work on the outskirts of Kappa. Its representativefeels that the NCS should be providing assistance to the refugees, and is ready tooffer some relief assistance (food, drugs, etc.).
HELP/SOS: ALPHALAND/BETALAND664

No. 1085 Date: 17/12/99 Betaland
Source: Kappa, representative of the Ministry of Agriculture
WATER DEVELOPMENT POLICY
The Department of Water Resources Development has been attached to theMinistry of Agriculture since 1992. It has two functions: (1) to develop anirrigation network in agricultural areas; and (2) to improve rural populations’access to clean water.
No. 1086 Date: 21/12/99 Betaland
Source: Kappa, representative of the Water Development Project (WDP)
INFORMATION ON THE WDP IN BETALAND
TheWDP is a government-sponsoredorganization responsible for supplyingwaterto themajor towns of the country. Only 10%of the villages in Betaland have accessto protected sources ofwater. TheWDPhas a large amount of equipment providedby the government using funds from UNICEF.
No. 1087 Date: 21/12/99 Betaland
Source: Kappa, WDP representative
THE WATER SITUATION IN KHRON
The water supply system for the town of Khron derives its water from the BowiRiver, which is 1.5 km south of town. The water is pumped into a reservoir abovethe town. The pumping system has two components, one of them pumping fromthe river and the other pumping to the reservoir. The pumping system is locatedin the western part of the city.
No. 1088 Date: 21/12/99 Betaland
Source: Kappa, WDP representative
THE GUTIR WATER PROJECT
In cooperation with theMinistry of Health and in the framework of a local PHCproject, the WDP has completed the construction of a well in Gutir. The villageof Gutir was chosen for the following reasons:
ALPHALAND/BETALAND 665

667
. strong community involvement
. the geological features of the area
. the integration of the water project into the PHC programme
. the large number of people who will benefit from the project.
There are 1,326 inhabitants in the area (1997), and 500 of them live within800 metres of the well. The well is 15 metres deep, 2 metres wide, and has anaverage annual capacity of 20 cubic metres. The lining is of concrete and the wellhead is protected by a concrete apron. The pump is a handpump (IndianMarkII). The potential yield is 10 cubic metres per day, which is sufficient for thesurrounding population. In order to cover the needs of the entire populationliving in a radius of three kilometres, it will be necessary to install a motorizedpump connected to a reservoir which would be established on a hill north of thevillage. An evaluation of this proposal will be carried out in the near future aspart of the World Bank’s Second Rural Development Project. The village feelsthat a better solution, and one requiring less ‘‘free’’ labour from the village,would be to dig a new well 1.5 kilometres to the west.
No. 1089 Date: 21/12/99 Betaland
Source: Kappa, WDP representative
INFORMATION ON THE WATER SYSTEM IN BURLO
The project was commissioned and initiated in 1997. Its aim was to protect a springthat currently supplies water for 400 people. The WDP has provided the necessaryequipment (cement, pipes, tools), and the community has provided the manpower.Maintenance is carriedoutbymembersof thecommunityafter trainingby theWDP.
No. 1090 Date: 16/12/99 Betaland
Source: Kappa, director of the Department of Nutrition, Ministry of Health
NUTRITIONAL STATUS OF THE REFUGEE POPULATION
The Department of Nutrition has no precise figures concerning the nutritionalstatus of the refugees. The director has asked his counterpart in Gamma toenquire about the food situation of this population. So far, she has not receivedany information. From what she has heard from other sources, however, therefugees are in poor nutritional condition, and a large number of children aresuffering from malnutrition.
HELP/SOS: ALPHALAND/BETALAND666

No. 1091 Date: 23/12/99 Betaland
Source: Kappa, representative of the Ministry of Agriculture
FOOD STORAGE WAREHOUSES IN BETALAND
There are several warehouses in the country containing food stored foremergencies. Although this food is primarily for the local population, thegovernment is ready to loan food to the humanitarian agencies for a period ofthree months. The agencies must replenish the local warehouses with the sametype of food within three months.
The main warehouses in the country are:
LOCATION CAPACITY (MT) STOCKS DATE
KAPPA 5,000 3,245 07/10/97
KAPPA 2,500 1,276 23/02/97
SRZO 7,000 1,100 24/03/98
LUM 2,500 ? ?
GAMMA 6,000 1,345 12/07/97
Other warehouses belong to private organizations:
TAKRI 6,000 4,300 10/10/98
KHRON 200 40 21/12/98
No. 1092 Date: 17/12/99 Betaland
Source: Kappa, representative of the Department of Water Resources,
Ministry of Agriculture
WATER RESOURCES FOR THE REFUGEES
According to the Department of Water Resources Development, access to safewater should be no problem for the refugees. The population of the Awalei camphas access to the Bowi River, which can provide an adequate amount of water.The refugees who are living in the villages of Epsilon district have access to thesame sources of water that the local population uses.
ALPHALAND/BETALAND 667

669
No. 1093 Date: 03/01/99 Betaland
Source: Kappa, UNICEF representative
MATERIALS AVAILABLE FROM UNICEF
UNICEF is ready to provide the equipment to construct a water supply systemfor the refugee camp (pumps, pipes, water tanks, concrete, filtering andsedimentation equipment, etc.).
No. 1094 Date: 17/12/99 Betaland
Source: Kappa, permanent secretary, Ministry of Agriculture
REFUGEES’ IMPACT ON THE LOCAL AGRICULTURAL SYSTEM
Summary of a discussion with the permanent secretary of the Ministry ofAgriculture:
Q: The region where the refugees have settled is a drought-prone area. Don’tyou think that the influx of refugees will create a demand that will rapidly exceedthe area’s resources?
A: Wehavebeenquite concernedabout thedroughtover thepast twoyears, butthe problem is not new. During the last decade the Gonlanis living in theDanikaldistrict have increased their livestock. At the same time the Zowarans haveextended their fields westwards on marginal lands to cultivate groundnuts, onlandtraditionally sharedwith thenomads.Thiswaspossible in theyearsof regularandgood rainfall before thedrought.But thedroughthas created tensionbetweenthe two groups. Over the last two years the Gonlanis have lost their cattle as aresult of thedroughtandhavehad to findwork inEpsilonandon thecoastal plain.
Q: But adevelopment programmewas established forEpsilon district, was it not?
A: Yes, in fact there were two programmes, one for the development of grazinglands to the west of Brew, and one for agricultural development in the easternpart of Epsilon. These programmes were scheduled to be completed within fiveyears, but lack of financial resources have caused delays in implementation.
Q: Obviously, with the population increase caused by Alphaland refugees, thesituation will deteriorate further, and these projects might end up having alimited impact.
A: That is why we are trying to group the refugees in a camp near Gamma, butmany of them prefer to stay with their relatives in Epsilon.
HELP/SOS: ALPHALAND/BETALAND668

Q: Why Gamma? Is it far from where the refugees are crossing the border?
A: InGamma there is plenty of water, andwe think that it will be easier to assistthe refugees who sought refuge inKappa and Szro there.Wewill try to keep themfrom settling in Epsilon, where it is more difficult to bring in aid and they mayhave a greater impact on the fragile environment.
Q: Is it possible to route external aid through Szro?
A: Yes, it is quite possible, and some food that is locally produced between Szroand Gamma may be available.
Q: Youmentioned that there is plenty of water inGamma;what are its sources?
A: The water supply for the town is drawn from the Tana River. Even duringthe dry season there is enough water, and the refugee camp is situated very closeto the river.
Q: Does the government have food stocks thatmight be available for use by therefugees?
A: Yes, there are some in Szro. At present I cannot tell you how many tonnesmight be available. I know that some food has been sent to Gamma and has beendistributed by the government to the refugees in the Gamma camp.
No. 1095 Date: 18/12/99 Betaland
Source: Kappa, representative of the NGO ‘‘Survival’’
PLANS OF THE NGO ‘‘SURVIVAL’’
Survival is an NGO that specializes in responses to emergency situations. It is aninternational organization, with headquarters in Oslo and national branches in anumber of countries. A Survival representative based in Kappa is currentlyvisiting in Gamma. Survival wants to organize food distributions and set updispensaries for the refugees in Awalei Camp. This is only an assessment missionfor the Kappa-based representative, and no plans for action have been made.
No. 1096 Date: 18/12/99 Betaland
Source: Kappa, BRCS representative
INFORMATION PROVIDED BY THE BRCS REPRESENTATIVE
TheBetalandMinistry of the Interior has asked the BRCS to coordinate relief forthe refugees. The first convoy left Gamma two days ago for Awalei Camp with
ALPHALAND/BETALAND 669

671
2,500 blankets, 50 tents, and 15 tonnes of sorghum. The BRCS has alreadycontacted UNHCR and several NGOs for assistance.
No. 1097 Date: 18/12/99 Betaland
Source: Kappa, representative of the Ministry of Social Affairs
ROLE OF THE MINISTRY OF SOCIAL AFFAIRS IN ASSISTINGTHE REFUGEE POPULATION
The Ministry of Social Affairs seeks to address the basic needs of the mostvulnerable people: orphans, poor families in urban areas, etc. This ministry’smandate is restricted, so it cannot provide refugee assistance.
HELP/SOS: ALPHALAND/BETALAND670

N
S
W E
Betaland
Alphaland
plain
semi-desertregion
Danikaldesert
Takri
Lum
Srzo
Gamma
Khi
Anil
Lambda
KesoNoma plain
Mountainousarea
Mountainousarea
Border
Tana River
100 Km
Communications:
Roads
Railways
Harbours Airports
Kappa
You are here
Box 6
INFORMATION FROM GAMMA:CAPITAL OF GAMMA PROVINCE
ALPHALAND/BETALAND 6671

673
N S
WE
Gam
ma
Bre
w
Gut
irAl A
liKar
am
Bur
lo
Gol
ra
Gol
bi
El G
hei
Bug
da
Aw
alei
Zot
ewe
Opa
la
Pan
os
Maq
uer
Sanb
are
Nan
da
Min
ote
Sako
Khr
on
Toc
aye In
pala
Cub
ma
Lag
un
Mah
ad
Bai
do
Bor
der
Kar
amdi
stri
ct
Eps
ilon
dist
rict
Bre
wdi
stri
ct
Gam
ma
dist
rict
Gam
ma
prov
ince
10 K
m
Tan
a R
iver
Gow
i Riv
er
Wab
ie R
iver
Bel
e R
iver
Bow
i Riv
er
Alp
hala
nd
Bet
alan
dBox 7
GAMMA PROVINCE
HELP/SOS: ALPHALAND/BETALAND6672

INFORMATION FROM GAMMA
No. 1098 Date: 21/12/99 Betaland
Source: Gamma, governor of Gamma province
INFORMATION PROVIDED BY THE GOVERNOR OF GAMMA PROVINCE
Q: How many people normally live in Gamma province?
A: The town itself has 120,000, and the district 900,000. In Epsilon district thereare 100,000 people.
Q: Do you know how many people live in Sigma district?
A: Probably around 200,000.
Q: And in the Danikal desert?
A: It is only an estimate, but we think that there are about 500,000 nomadsliving in Alphaland and Betaland.
Q: Do you know how many refugees are arriving daily?
A: According to our reports an average of 1,000-2,000 people are crossing theborder daily.
Q: When did the first refugees arrive in Betaland?
A: The first group arrived in July 1999, and since then they have been comingregularly. In the beginning it was just an increase in the usual flow of people backand forth across the border, and people stayed with their relatives on theBetaland side. In the past month, however, we have been receiving people whohave no family to stay with because they are from an area far to the south ofSigma, and we have had to relocate these people to the Awalei camp .
Q: The camp was established one month ago?
A: Yes, and its population increased steadily for two or three weeks During thepast few weeks, the number of new arrivals has decreased. Only 50 to 100 wereadmitted to the camp each day this past week.
Q: Do all the others settle in Epsilon?
A: Yes, but last week apparently not many people crossed the border.
Q: Why not?
A: Maybe the fighting is intensifying inside Sigmaand civilians cannot get to theborder, or the situation has settled down and they prefer to stay in their villages.
ALPHALAND/BETALAND 673

675
Q: But the drought is very severe in Sigma, and the people may still want tocome even if the military situation calms down.
A: Nobody knows what will happen, so we had better prepare to receive quite alarge number of refugees.
Q: Doyou think that the presence of refugees will increase antagonismbetweenthe Zowaran and Gonlani ethnic groups?
A: There have been some difficulties recently due to drought and grazingproblems. The military has intensified its control over the whole district toprevent any outbreaks of violence.
No. 1099 Date: 19/12/99 Betaland
Source: Gamma, representative, provincial office for refugee affairs
INFORMATION PROVIDED BY THE PROVINCIAL OFFICEOF REFUGEE AFFAIRS
Summary of a discussion with the administrator for refugee settlements in Gammaprovince, appointed by the government in October:
Q: Can you give us an overview of the refugee situation in Gamma province?
A: Well, I just came back from a quick trip around the whole area. As a matterof fact there are two problems. The first problem is at the refugee camp nearKhron (Awalei). It was opened one and a half months ago for refugees arrivingfrom Sigma without relatives in Epsilon with whom they could stay. At that timethe rate of arrivals was quite high, up to 3,000 per day, and that waswhy the campwas created. A camp administrator was appointed, and a census is takenregularly. According to last week’s figures, there are 35,000 people in the camp.During the past week 3,500 new arrivals have been registered.
Q: What is the registration procedure?
A: For each new admission to the camp, we record the name of the head of thefamily, the number of familymembers, the age of eachmember, and the village oforigin.
Q: Is any medical screening carried out?
A: At the beginning we could not do any screening because we didn’t have thestaff. Screening began threeweeks agowhen theGammaprovincial health officersent a medical team to the refugee camp. They began to provide medicalassistance to the camp population and to screen the new arrivals.
Q: What are the main medical problems they have noted?
HELP/SOS: ALPHALAND/BETALAND674

A: I haven’t received their report yet, but I know that malnutrition, tuberculosis,diarrhoeal diseases, and chest infections are the most common complaints.
Q: Apart from Awalei camp, what is the second problem?
A: There is a large group of refugees in Epsilon district. It is difficult to gaugetheir number since they are scattered among the local population. I asked eachdistrict administrator to contact all chiefs and village headmen in their districts toask how many refugees were living in their villages. I can give you a copy of thesurvey findings.
Q: We have been told that the nomads who normally live in the Danikal beganto settle in the western part of Epsilon some years ago. Can you give us someinformation about this?
A: It is true that nomads settled around Brew and Karam, but it is difficult tosay how many there are.
Q: What is the government’s current position concerning the nomads?
A: We try to help them as much as we can, but opportunities in Epsilon arerather limited, and quite a number of them have migrated to Kappa and Szro.
Q: But the refugees cannot settle in Kappa and Szro. What are your plans forrefugees arriving in the future?
A: The flow of refugees is decreasing. I crossed over to Sako, which is a smallcamp located south of Khron on the Alphaland side, and discussed the issue witha representative of the ZLF group. He told me that they are trying to keep thepopulation inside Sigma province, but they need some form of aid, such as foodand medical care, to assist the displaced population in Sigma province.
Q: How many people are still living in Sigma?
A: I do not even have a rough estimate, but obviously if people remain on theAlphaland side of the border, it will ease the pressure on our resources.
No. 1100 Date: 24/01/99 Betaland
Source: Gamma, representative of the Ministry of Agriculture
DEVELOPMENT PROJECT IN KARAM --- HISTORY
Epsilon district has been stricken by a series of droughts. In 1988 and 1995,majordroughts in the district resulted in the migration of thousands of rural dwellerstowards large towns, where they hoped to find the food they needed to survive.Although food aid was chaotic, many people stayed on in town after the crisishad passed, hoping to find permanent work in factories.
ALPHALAND/BETALAND 675

677
To avoid such disasters in future, a plan for agricultural rehabilitation anddevelopment was drawn up for the district, and a pilot study was carried out nearKaram. The objectives of the plan were:
. to decrease migration towards the towns
. to reduce morbidity and mortality
. to increase food availability
. to increase family income
. to increase agricultural output
. to maintain an ecological equilibrium.
The population in the pilot area was 12,000, living on 400 square kilometres.
No. 1101 Date: 24/01/99 Betaland
Source: Gamma, representative of the Ministry of Agriculture
LAND AVAILABILITY
Each family receives 0.46 hectare of land for agriculture and 1 hectare forgrazing. The minimum for a subsistence living is 1.5 hectares of cultivable land,and 9 hectares of pasture land.
No. 1102 Date: 01/24/99 Betaland
Source: Gamma, representative of the Ministry of Agriculture
RESOURCES OF THE POPULATION IN THE PILOT PROJECT REGION
Most of the population supports itself by subsistence farming, with fewer than15% of the families making their livings from other economic activities. Thepopulation’s main resources are agriculture, livestock, food aid, and trade.
No. 1103 Date: 24/01/99 Betaland
Source: Gamma, representative of the Ministry of Agriculture
FUNCTION OF THE MARKET IN THE PILOT REGION
The market is important to the local economy. It is essential for the exchange ofproducts, and gives subsistence farmers access to cash. There are 12 majormarkets in the area, and no village ismore than 3-6 hours away fromone of them.
HELP/SOS: ALPHALAND/BETALAND676

The most common items sold are agricultural implements, animals, food(cereals), wood, cooking utensils, clothes and tools.
The main problems farmers face are high prices, remoteness of the market,insufficient demand for their products, and lack of cash. The traditionalmeans ofaccumulating wealth has been raising livestock, which can easily be sold innormal times. Now, however, the lack of fodder and the spread of disease amonglivestock have seriously disrupted the cattle markets. To solve this problem,people must diversify the means by which they accumulate wealth. To do this,however, the population must:
. develop exchange mechanisms
. obtain access to markets
. increase cash income
. diversify their sources of income.
No. 1104 Date: 24/01/99 Betaland
Source: Gamma, representative of the Ministry of Agriculture
AGRICULTURE-RELATED PROBLEMS IN THE PROJECT REGION
In 1999, there was a 34% reduction in land under cultivation, and a 73%reduction in food production. The causes were:
1. Lack of means: Oxen play an important role in agriculture. During droughtperiods it is difficult to feed them, and farmers are often forced to sell them atlow prices to buy food. This problem is further aggravated by the fact thatnomads come from remote areas of the Danikal to Epsilon in order to grazetheir cattle. As a result, relations between the two communities are ratherhostile.
2. Seeds: Famine results in seed stores being eaten, creating a shortage of seedsthe following year.
3. Insecticides, fertilizers: Pests take an especially heavy toll on crops, bothbefore harvest and after storage. Fertilizer prices are very high, and mostsubsistence farmers cannot afford them.
4. Water:Water is insufficient for irrigation because there are few dams to createrainwater storage capacity.
5. Land: The lack of arable land is obvious.
ALPHALAND/BETALAND 677

679
6. Food production: Yield per hectare is very low, the average being about736 kilos per hectare. Food yield may drop as low as 200 kilos perhectare in a drought period. Current agricultural development projectshave the goal of increasing food production by achieving the followingobjectives:
. to increase yield per hectare
. to improve farming techniques
. to increase the use of fertilizers
. to increase the use of pesticides
. to improve seed quality.
No. 1105 Date: 24/01/99 Betaland
Source: Gamma, representative of the Ministry of Agriculture
LIVESTOCK-BREEDING-RELATED PROBLEMSIN THE PROJECT REGION
Cattle is an important source of food and income for subsistence farmers. Cows,sheep, camels, and poultry suffered heavily from the drought and their numberswere considerably reduced. Donkeys are more resistant to drought, and the localpeople keep their donkeys even when they migrate to cities and towns.
Improved livestock breeding practices have not been promoted in this area. Theyield of meat, milk, and eggs is far less than it could be, considering the labourinvested. The destructive aspects of animal husbandry—over-grazing and soilerosion—are more visible than the productive ones. The grazing system is basedon a traditional social consensus concerning the use of land for pasturage, not onany scientific considerations.
Objectives of the animal husbandry project:
. to increase output of animal products
. to decrease the prevalence of animal diseases
. to improve cattle feeding practices
. to organize improved pasturage habits
. to improve pasture quality.
HELP/SOS: ALPHALAND/BETALAND678

No. 1106 Date: 24/01/99 Betaland
Source: Gamma, representative of the Ministry of Agriculture
WATER-RELATED PROBLEMS IN THE PROJECT REGION
A thorough survey of water resources has been carried out in the area. These arethe principal findings:
1. The main reasons for poor natural water storage are:
. soil erosion
. lack of vegetation related to:
– large number of cattle
– deforestation
– ignorance of resource management techniques.
2. The main reasons for the lack of man-made water-storage facilities are:
. lack of technical skills
. lack of material (pipes, cement, etc.).
The project’s objectives are:
. to develop water storage capacities by means of small dams
. to decrease soil erosion
. to increase reforestation, especially on the slopes of hills
. to develop additional means of water storage
. to develop local skills and capacity in the above areas.
No. 1107 Date: 24/01/99 Betaland
Source: Gamma, representative of the Ministry of Agriculture
HEALTH PROBLEMS IN THE AREA
Existing health problems derive from several factors:
1. Water quality:Astudy has shown that the following sources are used for waterfor human consumption:
. 54% from springs
. 25% from rivers
ALPHALAND/BETALAND 679

681
. 12% from ponds
. 9% from hand-dug wells.
Eighty-three percent of the people surveyed think that the water they use is safe.
2. Living conditions: Housing is of poor quality, and in most cases humans andanimals live in close proximity. Only 2% of the houses have latrines.
3. Health: Immunization coverage is very poor; fewer than 20%of children aged12-23months have had all three doses ofDPT. The level of health awareness islow among mothers. Both the wasting and stunting types of malnutrition areendemic.
Health-related objectives of the agricultural project are:
. to increase access to clean water
. to promote the construction and use of latrines
. to increase immunization coverage
. to reduce malnutrition
. to improve housing conditions.
No. 1108 Date: 03/01/99 Betaland
Source: Gamma, representative of the Ministry of the Interior
FOOD STOCKS IN BETALAND
The country has reserve food stocks for use in case of emergency. It is difficult toestimate the quantities that would be available for aid efforts. The authoritieshave indicated that the BRCS could utilize these stocks to feed refugees, providedthat it replenishes them within three months.
No. 1109 Date: 18/12/99 Betaland
Source: Gamma, Gamma provincial nutritionist, provincial health office
ASSESSMENT OF THE POPULATION’S NUTRITIONAL STATUSIN GAMMA PROVINCE
Epsilon district:
From the end of October to mid-November 1997, an assessment of nutritionalstatus was made in Epsilon district, the area where the refugees are settling.Among children under the age of six, the following findings were recorded:
HELP/SOS: ALPHALAND/BETALAND680

. 23% of the children were between 80%-90% of ideal weight-for-height(WFH)
. 12% were below 80% WFH
. The team also evaluated children from a community of nomads who were atthe market in Brew selling their cattle. In this sample:
. 42% of the children were between 80%-90% WFH
. 19% were below 80% WFH.
No. 1110 Date: 21/12/99 Betaland
Source: Gamma, representative of Gamma provincial administration
GAMMA PROVINCE POPULATION STATISTICS
The province has a total population of 830,000 inhabitants, distributed asfollows:
. Gamma district 500,000
. Epsilon district 205,000
. Danikal district 200,000
The principal towns are:
. Gamma 120,000
. Khron 12,000
. Brew 32,000
. Karam 12,800
. Takri 25,000
Epsilon district is divided into four administrative sectors:
. Golra 49,650
. Brew 64,500
. Khron 70,700
. Karam 39,500
No precise figures are currently available for the refugee population, but it isthought to total some 90,000.
ALPHALAND/BETALAND 681

683
No. 1111 Date: 17/12/99 Betaland
Source: Gamma, officer in charge, civil aviation authority, Gamma airport
GAMMA AIRPORT
Runway characteristics:
elevation: 345 metres
average temperature (C): 28 degrees
length: 1800 metres
aircraft: maximum B727
fuel available: none
aids: MD, MC, MT, L4, NDB, LR, LB, LO, L9,
visual flight rules
No. 1112 Date: 19/12/99 Betaland
Source: Gamma, representative of the EPI in Gamma
THE EPI IN GAMMA PROVINCE
Report from a meeting with the team leader of the EPI for Gamma province
In 1998, the EPI team had to cope with a number of logistical problems. The EPIvehicle broke down repeatedly and was often out of commission for severalweeks. In addition, owing to the difficulty of obtaining supplies of vaccine fromtheCentralMedical Stores inKappa, the teamwas unable to keep to the scheduleset out in the Annual Provincial Work Plan, although the UNICEF supply ofvaccine to Central Medical Stores is reportedly adequate for the country’s needs.The EPI team is ready to provide assistance to the refugees if the necessarysupport is available (petrol, vaccines, etc.). The provincial health director is alsoconvinced that the EPI team should immunize the refugees in order to minimizethe risk of outbreaks of disease in the local population.
HELP/SOS: ALPHALAND/BETALAND682

No. 1113 Date: 19/12/99 Betaland
Source: Gamma, representative of the EPI in Gamma
ACTIVITIES OF THE EPI IN GAMMA
MEASLES IMMUNIZATION
YearGamma
Town
Gamma
District
Epsilon
DistrictDanikal
1995 2,300 5,000 550 0
1996 2,500 5,500 780 0
1997 2,400 5,000 620 0
1998 2,100 4,500 520 0
Total 9,300 20,000 2,470 0
TUBERCULOSIS IMMUNIZATION (BCG)
YearGamma
Town
Gamma
District
Epsilon
DistrictDanikal
1995 2,100 3,250 420 0
1996 1,850 4,220 528 0
1997 1,720 2,850 615 0
1998 1,510 2,720 412 0
Total 7,180 13,040 1,975 0
POLIO IMMUNIZATION (OPV)
Gamma Town Gamma DistrictEpsilon
District
Danikal
Year
1st 2nd 3rd 1st 2nd 3rd 1st 2nd 3rd any
1995 2,900 1,870 1,240 5,480 3,230 2,430 730 230 70 0
1996 3,200 2,450 1,450 5,700 3,300 2,200 880 340 90 0
1997 2,800 1,950 1,520 5,200 3,200 1,900 690 320 70 0
1998 2,700 1,840 1,320 4,950 3,100 1,850 750 180 60 0
Total 11,700 8,100 5,530 19,480 12,830 8,380 3,050 1,070 290 0
ALPHALAND/BETALAND 683

685
No. 1114 Date: 19/12/99 Betaland
Source: Gamma, representative of the EPI in Gamma
EPI ACTIVITY IN GAMMA PROVINCE(WEEKS OF ACTIVITY IN EACH LOCATION)
LOCATION Jan Feb Mar Apr May June July Aug Sept Oct Nov Dec
Gamma
town-- xx -- xx xx xx xx xx xx xx xx --
Gamma
district
x x x x x -- x -- x x x --
Epsilon x x x -- x x x x -- -- x --
Danikal -- -- -- -- -- -- -- -- -- -- -- --
x = week of activity
No. 1115 Date: 21/12/99 Betaland
Source: Gamma, provincial health officer
THE HEALTH SITUATION IN GAMMA
Q: How many refugees have arrived so far in your province?
A: There are about 100,000 refugees, 60,000 of them concentrated nearGammain an area we allocated for them. The remaining 40,000 are scattered in Epsilondistrict, mainly around the town of Brew, where most are living with relatives.But we think many more refugees will soon be arriving.
Q: How many more do you anticipate?
A: It is difficult to say, but certainly several hundred thousand more.
Q: Is there fighting near the border?
A: Not according to our reports. Most of the fighting is taking place in theinterior of the Sigma region. Some wounded people arrived at the border and wemanaged to evacuate them to the hospital in Gamma.
Q: Civilians or military personnel?
A: Both.
Q: What are the main medical problems among the refugee population?
A: Well, several cases of meningitis have been reported, and two have beenhospitalized.
HELP/SOS: ALPHALAND/BETALAND684

Q: Was the diagnosis confirmed?
A: Both were meningococcal, and two of the cases were from the refugee campnear Gamma.
Q: What has been done to prevent an outbreak?
A: For themoment we have no vaccine formeningococcal meningitis available.I have asked theMinistry of Health in Kappa to provide us with 100,000 doses ofvaccine as an emergency allocation.
Q: Is the provincial EPI functioning well?
A: Yes, we are covering the whole province, with childhood immunizationsavailable from all health facilities and one mobile team. Our regular source ofsupply is Central Medical Stores in Kappa.
Q: What is the nutritional status of the refugees?
A: It seems not too bad. The refugees were short on food for quite a long time intheir own country, because of the drought. During the several weeks spenttravelling to the border they had very little access to food.
Q: What is the malnutrition rate?
A: I don’t know the exact figure. A nurse fromKhron has been sent to the campto take a survey.
Q: What other medical problems are you aware of?
A: Malaria is endemic in Gamma district.
Q: Which species?
A: Falciparum, and recent studies at Szro show a high level of drug resistance.I’ll give you copies of these studies if I can figure out what I did with them. Somany reports, so little time!
Q: What about the refugees’ water and sanitation situation?
A: There is plenty of water in the Bowi River, but we are concerned about thepoor sanitation in the camp. In Epsilon, refugees will soon have a major waterproblem because the region has been affected by the drought, and the refugeeshave brought their cattle with them.
Q: Are there enough medical staff to attend to the refugees?
A: No. We have a district medical team from Khron working in the camp, andan NGO has set up one dispensary in the camp. This is clearly not enough.
ALPHALAND/BETALAND 685

687
HEALTH FACILITIES IN GAMMA PROVINCE
No. of
Beds
Doctors Nurses HA VHW Equipment Nurses/
Midwives
Provincial
hospital, 1 A
500 10 50 80 0 X-ray, Lab 40N/10M
District
hospital, 3 B
100 2(F) 9 10 0 X-ray, Lab 7N/2M
Health
centres, 4 C
40 1(G) 19 19 0 4 basic labs 8N/4M
Dispensaries,
21 D
0 0 10 40 0
Health posts,
200 E
0 0 0 0 200
TOTAL 640 13 88 149 200 55N/16 M
A: Gamma town
B: District hospitals at Brew , Khron and Karam
C: One each in Epislon and Danikal (Khron and Karam), and two in Gamma district
(one in the north, one in the south)
D: 12 in Gamma district, 6 in Epsilon (V1, 2, 3, 4, 5, Golra), 3 in Danikal (V1, 2, Takri).
E: 100 in Gamma district, 30 in Epsilon, 70 in Danikal
F: Health centre in the north of Gamma district (one district hospital planned)
HA: Health assistants
VHW: Village health workers
Note: There is one missionary hospital in Takri with 2 doctors, 3 expatriate nurses,
20 local nurses trained at the hospital, 30 support personnel, 200 beds, one leprosy
ward, and one TB ward.
No. 1116 Date: 21/12/99 Betaland
Source: Gamma, provincial health officer for Gamma
HEALTH SERVICES IN GAMMA PROVINCE
Hospitals:
Gamma:The provincial hospital has 500 beds, with departments for medicine,surgery, paediatrics, and obstetrics and gynecology, as well as an
HELP/SOS: ALPHALAND/BETALAND686

infectious disease unit. There are 10 doctors, 50 nurses, and80 paramedical personnel. Radiology and laboratory facilities areavailable.
Brew: A 120-bed hospital offering basic medicine, surgery, pediatrics, andobstetrical services. The serious surgical cases are sent to the Gammahospital or to Takri. There are 3 doctors, 8 nurses, and 14 paramedicalpersonnel. Laboratory and radiology facilities are available.
Khron: A small hospital with 50 beds, staffed with 2 doctors, 5 nurses, and 12aides. There is a small laboratory and one X-ray machine that workswhen there is electricity.
Takri: The Takri mission hospital has 200 beds with 2 doctors, 1 surgeon, and20 nurses (5 of them expatriates). It provides service in medicine,surgery, paediatrics, obstetrics, and TB care, and has laboratory andX-ray facilities.
Health centres:
There are 21 health centres in the province, 12 in the district of Gamma,6 in the district of Epsilon, and 3 in the Danikal. Each of these healthcentres is headed by a nurse or medical assistant, with supervision by adoctor who is usually based in a nearby hospital.
Health posts:
One hundred small health posts, each headed by a PHCW, are scatteredthroughout the province, mostly in small villages.
No. 1117 Date: 21/12/99 Betaland
Source: Gamma, provincial director of the malaria control programme
THE MALARIA CONTROL PROGRAMME IN GAMMA PROVINCE
The malaria control programme is active in the province. In 1998, 195,000 pa-tients were treated for malaria by health facilities in the province. A total of38,000 blood smears were examined, 57% of which were positive (80%P. falciparum). Most laboratory tests are done in facilities in Gamma district.In the rest of the province, the laboratories are poorly equipped and often outof reagents. Treatment regimens have been standardized by the Ministry ofHealth.
ALPHALAND/BETALAND 687

689
No. 1118 Date: 21/12/99 Betaland
Source: Gamma, director, provincial vector control programme
THE VECTOR CONTROL COMPONENTOF THE MALARIA CONTROL PROGRAMME
Vector control programme: Findings of a 1997study in the north of Gamma
Resistance to: DDT Dieldrin Dichlorvos Tetramethrin
A. gambiae Yes Yes Yes Yes
A. funestus No Yes Yes Yes
A. pharenses Yes Yes Yes Yes
No further studies have been done to assess the geographic distribution ofresistance to insecticides, but the following policy has been established:
. in the coastal area spraying house interiors with dichlorvos is standard;
. in other parts of the country, where malaria is less prevalent, dieldrin is usedin the form of residual spray.
No. 1119 Date: 21/12/99 Betaland
Source: Gamma, director of the provincial diarrhoeal disease control programme
THE DIARRHOEAL DISEASE CONTROLPROGRAMME IN GAMMA PROVINCE
Activities of the Control of Diarrhoeal Disease (CDD) programme in GammaProvince during the period 1998-99:
1. Priority was given to the town ofGamma and its environs, mainly because it isa densely populated area.
. Mothers were taught to treat mild and severe cases of diarrhoea with ORS,and 150,000 packets of ORS were distributed in 1998 through dispensariesand by PHC workers within the framework of the maternal and child healthprogramme.
. The water supply for the town of Gamma was improved, and by the end of1998, 80% of the town’s population had access to piped water.
2. In other parts of the province, very little has been done to control diarrhoealdisease. The water resources department has carried out a few projects in
HELP/SOS: ALPHALAND/BETALAND688

Epsilon district, mainly digging and protecting wells. An ORT programmewas promoted by PHC workers, but has had little impact on the incidence ofdiarrhoeal diseases, partly because it was not well received by the public. Themothers were in fact taught how to prepare ORT solution using ordinary saltand sugar, but this way of treating diarrhoea goes against traditional beliefs.Further, studies carried out by the University of Betaland have shown thatwithin a few months after receiving instruction, mothers are not followingdirections, putting too much salt and not enough sugar in the solution. Therehas been some discussion about instituting a home-available fluidsprogramme, and a study group sponsored by the University of Betalandand the Ministry of Health is looking into this approach.
3. In 1998 and at the beginning of 1999, the activities of the water resourcesdevelopment department have decreased steadily, due to lack of financialsupport.Most of the budget allocated for this department has been devoted toan irrigation project in the north-east of Epsilon district, andmeasures relatedto water quality improvement and protection are a low priority.
No. 1120 Date: 18/12/99 Betaland
Source: Gamma, provincial manager, EPI
VACCINE AVAILABILITY IN GAMMA PROVINCE
The EPI in Gamma has the following vaccines in stock:
. measles: 23,000
. BCG: 5,000
. DPT: 12,000
. oral polio vaccine: 15,000
No. 1121 Date: 19/12/99 Betaland
Source: Gamma, representative of the EPI in Gamma province
MEASLES EPIDEMICS IN GAMMA
In 1999, ameasles epidemic occurred in the area of Lagun. Fifty-six children agedfrom one to three years were hospitalized at the Gamma hospital for measles-related complications. The Lagun area had apparently been well covered by theEPI, and this epidemic raised questions about vaccine efficacy. The immuniza-tion status of the 56 hospitalized children was assessed. Only 49 children had
ALPHALAND/BETALAND 689

691
been immunized, 28 of them during the mass campaign. Investigation revealedthat at the time of the mass campaign, the area had been flooded and the EPIvehicle was stopped on the road north-east of Lagun for four days. During thosedays the EPI team helped the local population to deal with the results of thefloods. The vaccine that spent four days in the vehicle was probably inadvertentlyused during the campaign, although the monitor card for this lot of vaccinescould not be found. Of the remaining 21 children, 12 had not been vaccinatedagainst measles, and 8 had probably been vaccinated at or before 9 months. Inone case, immunization status could not be determined.
No. 1122 Date: 21/12/99 Betaland
Source: Gamma, director of the provincial diarrhoeal disease programme
A CHOLERA OUTBREAK IN GAMMA PROVINCE
Cholera epidemic, 1998:
In November 1998, an outbreak of cholera occurred in Epsilon district. Thedistrict has been affected by sporadic cases of cholera over the years, but this wasthe first serious outbreak reported in five years. In this outbreak 335 clinical casesof cholera were confirmed by the Khron and Brew hospital laboratories. Isolatesfrom 123 patients were further investigated at the Gamma provincial hospital,and at the University Teaching Hospital in Kappa. Vibrio cholerae wasconfirmed in all 123 isolates, and all were of the El Tor biotype. Twenty of the335 patients with clinically diagnosed cholera died (6%). The number of deathsoccurring at home was estimated at 30%-50%.
No. 1123 Date: 21/12/99 Betaland
Source: Gamma, director of the Gamma tuberculosis control programme
THE TUBERCULOSIS CONTROL PROGRAMMEIN GAMMA PROVINCE
Before 1993, the tuberculosis control programmewas organized around amobileteam that screened individuals with a portable X-ray machine; suspected caseswere referred to the nearest hospital for further tests. This strategy has beenabandoned,mainly because of its high cost and ineffectiveness, but the equipmentis still available, and a team can be put together again whenever needed.
HELP/SOS: ALPHALAND/BETALAND690

The policy on TB control is as follows:
1. Screening for clinical signs of TB in the health centres.
2. Referring suspected cases to hospitals with X-ray and laboratory facilities.
3. Treating those cases presenting with AFB (acid-fast bacilli)-smear positivesputum or with lesions visible on X-ray. The treatment has been standardizedby the Ministry of Health.
4. Prevention: BCG for all children under one year of age.
No. 1124 Date: 21/12/99 Betaland
Source: Gamma, director of the Gamma tuberculosis control programme
ACTIVITIES OF THE TUBERCULOSIS CONTROL PROGRAMMEIN GAMMA PROVINCE
1. SPUTUM EXAMINATIONS
TOTAL POSITIVE NEGATIVE
1995 490 120 370
1996 665 175 490
1997 950 270 680
1998 975 740 235
2. X-RAY EXAMINATIONS FOR TUBERCULOSIS
TOTAL POSITIVE NEGATIVE
1995 789 234 555
1996 870 89 781
1997 679 76 603
1998 546 97 449
ALPHALAND/BETALAND 691
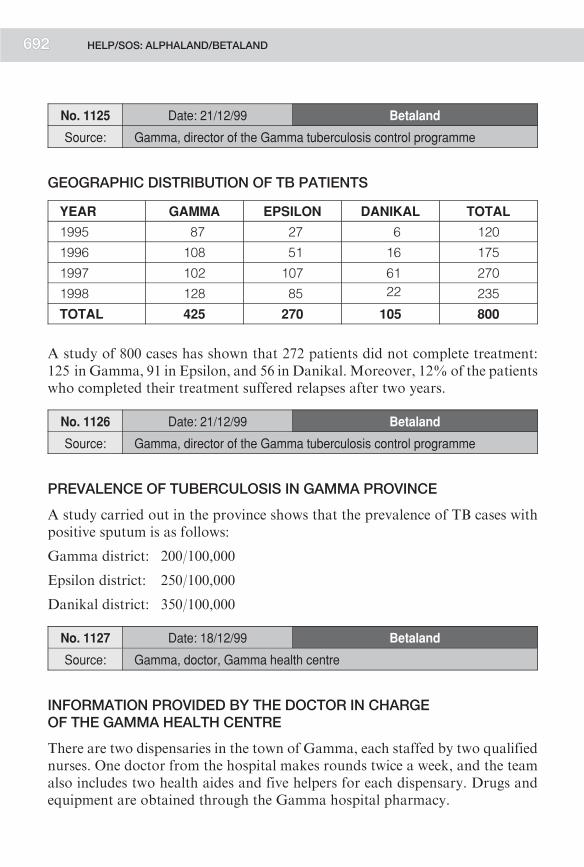
693
No. 1125 Date: 21/12/99 Betaland
Source: Gamma, director of the Gamma tuberculosis control programme
GEOGRAPHIC DISTRIBUTION OF TB PATIENTS
YEAR GAMMA EPSILON DANIKAL TOTAL
1995 87 27 6 120
1996 108 51 16 175
1997 102 107 61 270
1998 128 85 22 235
TOTAL 425 270 105 800
A study of 800 cases has shown that 272 patients did not complete treatment:125 in Gamma, 91 in Epsilon, and 56 in Danikal. Moreover, 12% of the patientswho completed their treatment suffered relapses after two years.
No. 1126 Date: 21/12/99 Betaland
Source: Gamma, director of the Gamma tuberculosis control programme
PREVALENCE OF TUBERCULOSIS IN GAMMA PROVINCE
A study carried out in the province shows that the prevalence of TB cases withpositive sputum is as follows:
Gamma district: 200/100,000
Epsilon district: 250/100,000
Danikal district: 350/100,000
No. 1127 Date: 18/12/99 Betaland
Source: Gamma, doctor, Gamma health centre
INFORMATION PROVIDED BY THE DOCTOR IN CHARGEOF THE GAMMA HEALTH CENTRE
There are two dispensaries in the town of Gamma, each staffed by two qualifiednurses. One doctor from the hospital makes rounds twice a week, and the teamalso includes two health aides and five helpers for each dispensary. Drugs andequipment are obtained through the Gamma hospital pharmacy.
HELP/SOS: ALPHALAND/BETALAND692

Activities in November 1999:
. number of new out-patient visits: 2,200
. principal diagnoses:malaria: 30%diarrhoea: 15%upper respiratory infections: 20%lower respiratory infections: 5%intestinal parasites: 8%skin infections: 3%otitis: 5%others: 14%suspected HIV: 12 patients.
Preventive health services are provided at each dispensary, includingmother andchild care, expanded programme of immunization, and family planning.
No. 1128 Date: 21/12/99 Betaland
Source: Gamma, director of the Gamma malaria control programme
RESULTS OF MALARIA TESTS IN GAMMA PROVINCE
Blood smears in the three districts:
GAMMA EPSILON DANIKAL
TOTAL NUMBER
OF SMEARS
34,000 3,000 1,000
POSITIVE SMEARS 24,437 1,728 28,700
P. FALCIPARUM+ 21,260 55,200 9,200
P. VIVAX+ 3,177 1,176 19,500
Hospital Information from Gamma province
No. 1129 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma provincial hospital
VISIT TO GAMMA HOSPITAL
Gamma provincial hospital is a 500-bed hospital with wards for paediatrics,medicine, surgery, obstetrics, and tuberculosis. The staff comprises 10 doctors,
ALPHALAND/BETALAND 693

695
50 qualified nurses, 80 medical and nursing assistants, and 120 service personnel(cleaners, cooks, etc.).
Supplies:Lists of drugs and equipment were provided (see annexed list). Demandhas increased since health facilities have begun to refer Alphaland refugees to thehospital, and essential drugs are often out of stock.
Food: Since the influx of new patients (refugees), the food supply has beeninadequate.
Water: The hospital receives its water from the municipal water supply system.There have been no breakdowns in supply recently, although sometimes thesupply is interrupted for several hours a day.
Electricity: Electricity is supplied by the city’s generating station. However, thehospital has its own generator in case of power failure.
No. 1130 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
ACTIVITIES OF GAMMA HOSPITAL
During the month of November the number of admissions increased:
. Medicine 412
. Paediatrics 621
. Surgery 132
. Obstetrics and gynecology 72
. Infectious diseases 34 (including 18 new TB cases)
. Total: 1,271
During the month of November the number of refugees admitted to the hospitalwas relatively low (67), but during the first two weeks of December 112 refugeesarrived in the hospital wards. The main causes of hospitalization were:
. Paediatrics: dehydration due to diarrhoea, pneumonia, measles, malaria.
. Internal medicine: malaria, schistosomiasis, tuberculosis, AIDS, cardiacfailure, respiratory disease, chronic diseases.
. Surgery: trauma including fractures, pancreatitis, stones in the urinary tract,hernia, prostatic hypertrophy, intestinal perforation due to typhoid fever.
HELP/SOS: ALPHALAND/BETALAND694

. Gynecology and obstetrics: fibroid uterus, ovarian cysts, cervical cancer,ruptured ectopic pregnancy, obstructed labour, and other complications oflabour and delivery.
With the arrival of the refugees, the surgical staff has been taking care of manywar-wounded. None of the surgical staff is experienced in this field. Moreover, asudden influx of wounded creates organizational problems within the hospital.Last week 23 wounded arrived at the hospital at the same time.
No. 1131 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
RADIOLOGY AT GAMMA HOSPITAL
The hospital has two functioning general purpose X-ray machines, and qualifiedpersonnel (one technician and two assistants) to operate them.Most of the usualtests can be performed. There is a chronic shortage of film and chemicals, but forthe moment supplies are adequate.
No. 1132 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
LABORATORY AT GAMMA HOSPITAL
The hospital laboratory is staffed with three qualified laboratory technicians andsix laboratory assistants. Most routine tests involving serology, biochemistry,parasitology, microbiology, and blood banking can be performed, includingHIV testing.
No. 1133 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
ACTIVITIES OF THE INTERNAL MEDICINE DEPARTMENT
There are two acute care wards with 65 beds each. Staff consists of 2 doctors,12 nurses, 14 medical and nursing assistants, and 15 support personnel. InNovember 1999, 412 new patients were admitted, 9 of them refugees.
ALPHALAND/BETALAND 695

697
Among the main causes of hospitalization in November were:
. uncomplicated malaria, 82
. cerebral malaria, 45 (9 deaths)
. pneumonia, 34 (3 deaths)
. AIDS, 30
. intestinal amoebiasis, 20
. asthma, 20 (1 death)
. dengue fever, 16
. fever of unknown origin, 14
. hepatitis (A or B) , 13 (1 death)
. typhoid fever, 12 (2 deaths)
. congestive heart failure, 5 (2 deaths)
. pleurisy, 5
. peptic ulcer, 4
. stomach cancer, 3 (1 death)
. hepatic amoebiasis, 3 (1 death)
. viral encephalitis, 3
. severe anaemia, 3 (1 death)
. pyelonephritis, 3
. snake bites, 3 (1 death)
. peripheral neuropathy (vitamin B deficiency), 2
. visceral leishmaniosis, 1 (from the north of the country)
. maduromycosis, 1
. pyomyositis, 1
. acute lymphangitis, 1
. S. haematobium infection, 1 (from the coastal region)
. sexually transmitted diseases, 9
. herpes zoster, 8.
Number of deaths: 22
HELP/SOS: ALPHALAND/BETALAND696

No. 1134 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
ACTIVITIES OF THE PAEDIATRICS DEPARTMENT
The paediatrics department has two wards totalling 140 beds. The staff includes3 doctors, 14 nurses, 16 medical and nursing assistants, and 20 supportpersonnel. The number of admissions in November 1999 was 621.
. *malaria, 189 (70 cerebral malaria; 30 deaths)
. malnutrition, 50 (5 deaths)
. *dehydration, 45 (13 deaths)
. pneumonia, 35 ( 3 deaths)
. *complicated measles, 30 (11 deaths)
. bronchitis, 24 (2 deaths)
. dysentery, 20
. *anemia, 19 (6 deaths)
. *fever of unknown origin, 17 (1 death)
. trypanosomiasis, 12
. pertussis, 5 (1 death)
. acute rheumatic fever, 3
. meningitis, 3 (1 death)
. tetanus neonatorum, 1 (1 death)
. TB lymphadenitis, 2
. acute poliomyelitis, 1.
In November, 22 refugee children were admitted to the paediatrics department,and during the first two weeks of December, 61 refugee children werehospitalized.
* The majority of children with these diagnoses were also moderately or severely malnourished.
ALPHALAND/BETALAND 697

699
No. 1135 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
ACTIVITIES OF THE OBSTETRICS AND GYNECOLOGY DEPARTMENT
The department has a staff of one obstetrician/gynaecologist, 10 midwives,14 medical or nursing assistants, and 5 support staff. The maternity ward has60 beds, and in November 1999 admitted 72 patients, for the following reasons:
. normal delivery, 42 (mean weight of infant at birth, 2.1 kg)
. spontaneous abortion, 9
. interpartum deaths, 6
. breech delivery, 3
. postpartum haemorrhage, 2
. pre-eclampsia, 2.
The gynecology ward has 15 beds and admitted 6 new patients in November 1999,for the following reasons:
. salpingitis, 3 (1 gonorrhea)
. carcinoma of the uterus, 2
. ruptured ectopic pregnancy, 5.
In November, two refugees were admitted to the obstetrics/gynecologydepartment, and in the first two weeks of December, 12 were admitted.
No. 1136 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
ACTIVITIES OF THE SURGICAL DEPARTMENT
The surgical ward has a capacity of 80 beds, and a staff of 3 surgeons, 7 nurses,18 medical or nursing assistants, and 10 support staff. The operating rooms andcentral sterile supply department have their own staff. The hospital has fouroperating rooms, two of them major and two of them minor. The hospital hasonly two abdominal surgical packs, three C-section packs, and four minorsurgical packs. At full capacity the operating room can accommodate up to120 major surgeries a month. For 1998 the average was 95 per month.
HELP/SOS: ALPHALAND/BETALAND698

Until September 1999 the department was able to cope with the situation. In thepast month, however, the number of surgical cases increased sharply, mainlywar-wounded arriving from Alphaland. Some of the wounded were brought tothe hospital by ambulance from the Khron health centre, but most of them werebrought by the army. During November 1999, 132 patients were admitted to thesurgical ward—90 Betaland civilians and 32 Alphaland war-wounded. Duringthe first two weeks of December 1999, the ward admitted 85 Betaland civiliansand 33 Alphaland war-wounded.
Since the refugees began fleeing Alphaland, a total of 65 patients with warinjuries have been admitted. This breaks down to 34 compound (open) limbfractures, 9 soft tissue infections, 6 thoracic injuries, 12 abdominal injuries, and4 head injuries. The number of patients regularly exceeds the number of availablebeds. The daily census in the 80 bed ward is often 105 or greater. Patients who donot require intensive surgical care have been transferred to the internal medicineward. The department is increasingly short of equipment, especially orthopaedicdevices, antibiotics, sutures, and anaesthetic drugs.
No. 1137 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
BLOOD BANK, GAMMA HOSPITAL
Donors to the hospital’s blood bank are recruited mainly from patients’ familiesand some volunteers (12% of the total). All blood is tested for malaria, syphilisand HIV. The hospital uses an average of 100 units of blood per month. In thepast two weeks, it has been increasingly difficult to find blood for patients,especially for the war-wounded, who generally arrive at the hospitalunaccompanied by family members.
No. 1138 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
ACTIVITIES OF THE INFECTIOUS DISEASE DEPARTMENT
The infectious disease department has two wards, TB and isolation, with a totalof 50 beds. Staff includes one doctor, three nurses, five medical or nursingassistants, and five support personnel.
. The TB department ward has 45 beds.
ALPHALAND/BETALAND 699

701
In November there were six admissions.
In the first two weeks of December there were eight admissions, four of themrefugees.
Data collected during the first half of 1999 indicate that 58% of patients withpulmonary TB were HIV positive, as were 76% of patients with extra-pulmonary TB.
. The isolation ward has five rooms.
InNovember there were five admissions: for rabies (1), shigella (2), and typhoid (2).
In December there were seven admissions: for meningitis (4), hepatitis (2), andshigella (1).
No. 1139 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
BED OCCUPANCY IN GAMMA HOSPITAL IN NOVEMBERAND DECEMBER
DEPARTMENT # OF BEDS NOVEMBER DECEMBER
Medicine 130 88% 92%
Surgery 80 85% 115%
Pediatrics 140 102% 128%
Ob/Gyn 60 75% 82%
Infectious diseases 50 84% 92%
No. 1140 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
SUPPLIES OF DRUGS AND EQUIPMENT IN GAMMA HOSPITAL
The medical supply system in Betaland is highly centralized. Each provincialhealth office sends a request every three months to Central Medical Stores inKappa, based on requests from district health officers who have determinedneeds in the various health facilities. Following this request from the province,Central Medical Stores dispatches a stock of drugs and equipment within 30-90 days. Frequently, however, the quantities received are less than those orderedby the provincial health office. From the provincial office, the drugs are
HELP/SOS: ALPHALAND/BETALAND700

distributed first to the various districts and then to the hospitals and healthcentres. The last shipment from Kappa was received three months ago. Thedemand for health services by the arriving refugees has contributed to a morerapid consumption ofmedical supplies than usual. In particularly short supply atboth Gamma hospital and the district hospitals are antibiotics, anaesthetics,bandages, X-ray films, and laboratory reagents.
No. 1141 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
DRUG SHORTAGES AT GAMMA HOSPITAL
During the past three months the hospital has had increasing problems with drugsupplies from Central Medical Supply. The days of stock-outs over the last threemonths are listed below.
No. 1142 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
AVAILABILITY OF VACCINES AND SERA
BCG vaccine injection
Diphtheria-pertussis-tetanus vaccine injection
Diphtheria-tetanus vaccine injection
Measles vaccine injection
Poliomyelitis live attenuated vaccine oral solution
Tetanus vaccine injection
Meningococcal vaccine injection
Rabies vaccine injection
Antirabies hyperimmune serum injection
Antivenin sera injection
There are not enough vaccines to cover the needs of the existing EPI. If avaccination campaign is to be organized for the refugees, it will be necessary toobtain additional supplies, perhaps from outside Betaland.
ALPHALAND/BETALAND 701

703
No. 1143 Date: 19/12/99 Betaland
Source: Gamma, medical director of Gamma hospital
DRUGS FOR TUBERCULOSIS AND LEPROSY
The following drugs will be available only for the specialized wards. If needed,they can be obtained solely on a special request basis.
Clofazimine capsule, 100 mg
Dapsone tablet, 50 mg, 100 mg
Prothionamide tablet, 125 mg
Ethambutol tablet,100-500 mg
Isoniazid tablet, 100-300 mg
Pyrazinamide tablet, 500 mg
Rifampicin tablet, 150-300 mg
Streptomycin vial for injection, 1 g
No. 1144 Date: 19/12/99 Betaland
Source: Gamma, representative of the provincial water development project
office (WDPO)
WATER AVAILABILITY IN GAMMA PROVINCE
In Gamma the water resources department is responsible for:
. Ensuring a safe water supply for the town ofGamma. This includes pumping,flocculation, sedimentation, and chlorination;
. Developing and improving the water supply in other towns and villages inGamma province;
. Developing irrigation programmes using water from the Tana river, as partof a Ministry of Agriculture project.
However, most of the water resources department’s efforts are devoted to thetown of Gamma itself and the irrigation programmes. Only 25%of the houses intown are directly connected to the water supply; the others rely on public standpipes. In the region of Awalei, water sources are plentiful, and the water table ishigh. The refugees have settled near the Bowi river, which provides sufficientwater in all seasons. TheWDPOhas special equipment for digging bore-holes, aswell as a good stock of handpumps donated by UNICEF.
HELP/SOS: ALPHALAND/BETALAND702
No. 1145 Date: 19/12/99 Betaland
Source: Gamma, representative of the Betaland Red Crescent Society
INFORMATION FROM A REPRESENTATIVEOF THE RED CRESCENT SOCIETY
The local branch of the BRCS is composed of twomembers employed full time atthe BRCS office—onewith an administrative background, the other a nurse with10 years’ experience—and 60 members working on a voluntary basis, all withfirst-aid training. So far, the only assistance it has provided to refugees has beento distribute 2,000 blankets and 20 tonnes of food. The local BRCS branch isready to give further assistance if the head office inKappa can provide additionalsupplies and funds.
ALPHALAND/BETALAND 703

705
N S
WE
Gam
ma
Bre
w
Gu
tirAl A
liKar
am
Bu
rlo
Gol
ra
Gol
bi
El G
hei
Bu
gda
Aw
alei
Zot
ewe
Op
ala
Pan
os
Maq
uer
San
bar
eN
and
a
Min
ote
Sak
o
Kh
ronT
ocay
e Inp
ala
Cu
bm
a
Lag
un
Mah
ad
Bai
do
bor
der
Kar
amd
istr
ict
Ep
silo
nd
istr
ict
Bre
wd
istr
ict
Gam
ma
dis
tric
t
Gam
ma
pro
vin
ce
10 K
m
Tan
a R
iver
Gow
i Riv
erW
abi R
iver
Bel
e R
iver
Bow
i Riv
er
Alp
hal
and
Bet
alan
d
You
are
her
e
Box 8
INFORMATION FROM KHRON
HELP/SOS: ALPHALAND/BETALAND7704

INFORMATION FROM KHRON
No. 1146 Date: 21/12/99 Betaland
Source: Khron, representative of the Ministry of Agriculture
SURVIVAL STRATEGY OF THE LOCAL POPULATION IN EPSILON
In times of famine people adopt a strategy allowing them to get through thedifficult period. Traditionally, the local population’s disaster strategy hasincluded the following emergency measures:
1. Migration in search of work outside Epsilon, mainly around the town ofGamma
2. Taking loans from wealthy families
3. Selling their livestock (sheep, goats, cows, chickens, donkeys).
However, the crisis is now so serious that people tend to adopt more drasticmeasures, including reduced food consumption and temporary migration of themost vulnerable families.
No. 1147 Date: 21/12/99 Betaland
Source: Khron, representative of the Ministry of Agriculture in Khron
SOCIAL CHANGES WITHIN FAMILIES IN TIMES OF AUSTERITY
During the nutritional survey in Epsilon district, important social changes werediscovered to be occurring. Elderly people are tending to abandon their homesand to move in with their married children. This practice increases the assetsavailable to the newly combined household.
At the same time, food allocation is becoming more and more of a problemwithin families. Children, pregnant women, and nursing mothers may receivemore or better food than other household members, or food may bepreferentially provided to income-generating members. The number ofmarriages, especially in rural areas, has decreased drastically during the last sixmonths, probably as a result of the difficult conditions currently prevailing.
When families have exhausted their normal food supplies, they tend to shifttowards ‘‘famine foods’’: edible plants, roots, berries, and wild vegetables and
ALPHALAND/BETALAND 705

707
fruits. Generally such foods are mixed with coarse grain, and served as the soledaily meal.
No. 1148 Date: 21/12/99 Betaland
Source: Khron, representative of the Ministry of Agriculture in Khron
INTER-FAMILY EXCHANGES IN TIMES OF AUSTERITY
The recent survey among selected rural families in Epsilon found that a numberof subsistence farmers were travelling to the north and west in search of relativeswho could help them and their families. Exchanges and other ‘‘deals’’ arefrequently made in Betaland during these times of austerity.
No. 1149 Date: 27/12/99 Betaland
Source: Khron, representative of the Public Power Corporation, Khron
ELECTRIC POWER IN THE TOWN OF KHRON
The town’s diesel-powered generating station was built 10 years ago and has acapacity of 5,000 KW. The grid supplies the town centre, the hospital, schools,the airport, the town council administration offices, and residences and shopsclose to the town centre. Fuel for the station must be trucked in by lorry.
No. 1150 Date: 21/12/99 Betaland
Source: Khron, district representative, Ministry of Works
INFORMATION PROVIDED BY THE DISTRICT REPRESENTATIVE,MINISTRY OF WORKS
Floods occur regularly in the province, especially around the town of Mahad onthe Bowi River. During the rainy season the road between Gamma and Khron isoften impassable for several days at a time.
The southern part of the town of Khron is sometimes affected by floods. In thisarea, the buildings are of poor quality and the last flood in 1996 severely damagedhouses. A rehabilitation planwas drawn up, but it was never implemented, due tolack of funding.
HELP/SOS: ALPHALAND/BETALAND706

No. 1151 Date: 27/12/99 Betaland
Source: Khron, officer in charge, civil aviation authority, Khron airport
KHRON AIRPORT
Runway characteristics:
elevation: 1329 metres
temperature: 24 degrees
length: 1300 metres
aircraft: maximum C-130
non-hard surface: —fuel available: none
No. 1152 Date: 27/12/99 Betaland
Source: Khron, officer in charge, civil aviation authority, Khron airport
RUNWAY IN KHRON
The Khron airport runway has a non-hard surface, and consequently landing isnot always possible during the rainy season.
No. 1153 Date: 23/12/99 Betaland
Source: Khron, doctor at Khron hospital
DRUGS USED BY PRIMARY HEALTH CARE WORKERS IN BETALAND
One of the tasks of the PHCW is to treat common medical problems such asdiarrhoea, respiratory infections, fever, and conjunctivitis. For this purpose theyare authorized to use the following drugs and supplies:
. aspirin, 300 mg
. co-trimoxazole tablets, 250 mg
. chloroquine tablets, 150 mg
. chloroquine syrup
. mebendazole tablets, 100 mg
. ferrous sulfate + folic acid, 60 + 25 mg
. aluminum hydroxide tablets
. tetracycline eye ointment
ALPHALAND/BETALAND 707

709
. gentian violet
. compresses
. cotton
. bandages.
No. 1154 Date: 24/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
MALARIA CONTROL PROGRAMME IN EPSILON DISTRICT
The malaria control programme is functioning poorly in the district. Thepromotion of insecticide-impregnated bednets has temporarily come to a halt forlack of bednets and insecticide. The doctor does not favour promoting thisapproach until adequate resources seem likely to be consistently available. Someantenatal clinics in the district are still striving to provide pregnant women withchloroquine chemoprophylaxis. The doctor doubts that many of those whoreceive tablets actually take them.
No. 1155 Date: 27/12/99 Betaland
Source: Khron, administrator of the Khron hospital
TRAINING PRIMARY HEALTH CARE WORKERS
Epsilon district was among the first districts to start training PHCWs. At presentthere are 20 health posts in the district staffed by PHCWs. The PHCW trainingcourse lasts threemonths, and at the endof that period the trainee shouldbe able to:
. weigh children
. give mothers nutritional advice
. identify malnourished individuals and refer them to the hospital
. give advice on proper water use
. help communities protect water sources
. help communities build latrines
. prepare communities for vaccination campaigns when the EPI team is sentout from Khron
. identify epidemics (meningitis, measles)
. treatdiarrhoea, respiratory infections,malaria, skin infections, conjunctivitis,and intestinal parasites.
HELP/SOS: ALPHALAND/BETALAND708

The director hopes that the community component of the Integrated Manage-ment of Childhood Illnesses (IMCI) will be available soon. This will be a veryhelpful tool, he thinks, to improve health at the community level.
No. 1156 Date: 21/12/99 Betaland
Source: Khron, doctor at Khron hospital
RATE OFMALNUTRITION IN THE UNDER-5 CLINIC AT KHRON HOSPITAL
Children brought in to the clinic between November 1998 and November 1999were weighed, giving the following results:
MONTH N0. CHILDREN
N0.
MALNOURISHED
(<80% WT/AGE)
NOVEMBER 552 147
DECEMBER 645 147
JANUARY 1102 256
FEBRUARY 879 212
MARCH 906 226
APRIL 752 194
MAY 763 276
JUNE 841 260
JULY 758 190
AUGUST 842 246
SEPTEMBER 705 154
OCTOBER 627 113
NOVEMBER 584 147
No. 1157 Date: 24/12/99 Betaland
Source: Khron, manager of the EPI for Khron
EPI EQUIPMENT AVAILABLE IN KHRON
One electric 285 L/10 CFT refrigerator is available, running on 110V/60HZ, witha 40-litre freezer component, UNICEF code 11 402 10 (1995). There aresix portable cold boxes of 4.35 litres each without ice packs and a 1.7-litre coldbox with ice packs. Twenty-five ice packs are on hand. There are also four large
ALPHALAND/BETALAND 709

711
cold boxes with a net vaccine capacity of 21 litres (UNICEF code 11 850 52).These canmaintain a temperature of below 10o C for 174 hours when the outsidetemperature is 32o C or less, or a safe temperature for 132 hours when the outsidetemperature is 43o C. Also available are 3,000 2-cc syringes and 4,000 needles.
No. 1158 Date: 27/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
TUBERCULOSIS IN KHRON HOSPITAL
Suspected cases of tuberculosis are referred to the hospital, where they undergo asputum test and a chest X-ray. Confirmed cases are treated according to thestandardMinistry of Health regimen, which includes twomonths in hospital andsix months of out-patient care. Currently 56 patients are receiving TB treatmentat the hospital, including 38 with pulmonary TB. Of these, 21 were diagnosedfrom positive sputum and 17 on the basis of X-ray findings. Of 18 patients withextra-pulmonary TB, 14 are HIV-positive.
Upon discharge, TB patients are referred back to the health centre from whichthey were sent. The doctor does not know how many of these actually completetheir treatment. Those patients living in Khron are followed up by the hospital,and the doctor doubts whethermore than half ever finish their treatment. He seesmany coming back for a second or third course of TB treatment. The hospital hasnot yet started a DOTS programme.
No. 1159 Date: 22/12/99 Betaland
Source: Khron, doctor at Khron hospital
CASES OF MENINGITIS IN KHRON HOSPITAL
Case ##1: Eight-year-old boy, 18 kg. Arrived at the hospital on 15 December,referred by the dispensary at Gamma refugee camp. He was living in a hut withhis parents, three brothers (two, five, and ten years old) and his aunt. They hadarrived at the camp from Sigma district at the end of September. Symptoms ofthe disease appeared on 8 November. In the morning he complained of aheadache. He had some fever. He received 100-mg tablets of chloroquine (threeon 12 November, two on 13 November) and took them. But he becameincreasingly worse and was accordingly referred to the hospital.
In the hospital: Temperature was 40oC; rigours and headache were present. Thepatient was vomiting, had a slightly enlarged spleen, a rigid neck, and Kerning’s
HELP/SOS: ALPHALAND/BETALAND710

sign. The malaria smear was positive, the cerebrospinal fluid turbid, and on thethird day the laboratory reported growth of Neisseria meningitidis, Group A.
The treatment prescribed was two grams of intravenous chloramphenicol dailyfor five days, then by mouth for five days. The patient was also given 360 mg ofquinine per day by intravenous drip for three days, then two tablets of Fansidar.He was discharged on the 11th day of hospitalization. According to the NationalReference Laboratory, type A is most prevalent but type C is present in Gammaprovince and probably in Khi province.
Case ##2 : Six-year-old girl, admitted to hospital on 18 December, referred by theGamma camp dispensary. She was living two huts away from case #1 with hermotherandher twobrothers.Theyarrived in thecampon20November fromSigmadistrict. The illness started on 10December. Before going to sleep she felt exhaustedand feverish. On the morning of the 11th, she was comatose and a rash developed.
On admission, a typical purpuric rash of meningococcemia was present. Malariasmears were negative. The cerebrospinal fluid was turbid, and the culture grewNeisseria meningitis. Treatment was started immediately, but the patient died onthe evening of admission.
No. 1160 Date: 21/12/99 Betaland
Source: Khron, doctor at Khron hospital
SHIGELLA IN KHRON HOSPITAL
During the past two months there has been an increase in the number of cases ofbloody diarrhoea noted in the district, although few of them were actuallyreferred to the hospital. It is the doctor’s understanding that a number of deathshave occurred in the villages.He noted that those cases coming to the hospital didnot seem to respond to treatment with co-trimoxazole and amoxicillin as readilyas in years past. Without a bacteriology department, the hospital is unable toassess drug sensitivities.
No. 1161 Date: 21/12/99 Betaland
Source: Khron, doctor at Khron hospital
SEXUALLY TRANSMITTED DISEASES IN KHRON
Sexually transmitted diseases have been a problem in Khron, particularly inrecent years, according to the doctor at Khron hospital. It seems to the doctor,
ALPHALAND/BETALAND 711

713
looking through the hospital records, that the proportion of patients in the out-patient register with a diagnosis of sexually transmitted infections (STIs) hasgreatly increased in the past two years. Part of this he thinks is due to theincreased number of lorries staying overnight on their way to cross the borderinto Alphaland. At first the most commonmanifestation was urethral discharge,but about a year ago an increase in ulcerative diseases such as chancroid andsyphilis began to be noted. He also says that probably most people with STIs donot come to the clinic but receive treatment in town—either self-treatment or, hebelieves, treatment from hospital staff members who are running STI clinics onthe side. He also suspects that the medicines used are stolen from the hospital,although they may be coming from other sources, since drugs are readilyavailable in the Khron markets.
He says that he is indeed worried about HIV. So far most of the new AIDS caseshe has seen are in persons with herpes zoster or extrapulmonary tuberculosis. Hewonders about some of the adult meningitis cases he saw over the last year whichdid not respond to antibiotics. He did not test those patients for HIV because, atthe time, testing kits were in short supply and he was reserving them for testingblood in obstetrical emergencies.
No. 1162 Date: 21/12/99 Betaland
Source: Khron, doctor at Khron hospital
HEALTH INFORMATION SYSTEM IN KHRON HOSPITAL
Khron hospital is responsible for collecting and integrating data from thehealth centres in Epsilon district and sending them on to the district medicalofficer (DMO). After she reviews them they are forwarded to the provincialmedical officer. The hospital has been doing this, since the DMO lacks thenecessary clerical staff. The doctor at Khron is concerned that the figures whichthey are now reporting on a monthly basis do not include all the healthinformation from the refugee camps. In the case of services that staff fromKhron hospital provide at the MoH health centre, records are not consistentlykept. The doctor has been including these figures with the hospital out-patientsdepartment data, since the drugs and services supplied are hospital resources.He thinks that the Betaland information system does not accurately reflect thedisorders the refugees may have. Further, data from other groups providingservices to refugees are not being included in the district information system. Hehas discussed this issue with them, but their response is that they are too busytaking care of the refugees’ many needs to bother with ‘‘filling out stupid forms’’for the district.
HELP/SOS: ALPHALAND/BETALAND712

No. 1163 Date: 21/12/99 Betaland
Source: Khron, doctor at Khron hospital
FOOD IN KHRON HOSPITAL
During a visit to the hospital, the assessment teamwas told by a patient that foodin the hospital was not available in sufficient quantities to feed patients threetimes daily, and that it was of very poor quality.
No. 1164 Date: 21/12/99 Betaland
Source: Khron, administrator of Khron hospital
ORGANIZATION OF THE OUT-PATIENTS DEPARTMENTOF KHRON HOSPITAL
Khron hospital has an out-patients department (OPD) serving the town’spopulation. It is attached to the hospital, so that patients who are referred to thehospital by district health centres also go through theOPDbefore being admittedto the hospital.
The OPD is divided into four sections:
1. Adult patients are seen by a qualified nurse (100 to 150 consultations per day).
2. TheMCH section is run by a paediatric nurse (70 to 80 children per day) and amidwife (20 to 25 mothers per day).
3. Dressings and injections are administered by an aide.
4. Medical consultations with the doctor total 30 to 40 cases per day. Most arereferred from other departments in the hospital or from health centres in thedistrict.
Drugs are supposed to be paid for on a cost-sharing basis, but in reality, due todrug shortages, most prescribed drugs are bought at the pharmacy in town.
No. 1165 Date: 23/12/99 Betaland
Source: Khron, doctor in charge at Khron hospital
REQUESTFORDRUGSFORWARDEDTOTHEPROVINCIALHEALTHOFFICE
The doctor in charge at Khron hospital has made a request to the provincialhealth office for a special allocation of drugs. The arrival of the refugees has
ALPHALAND/BETALAND 713

715
resulted in a rapid depletion of his usual allocation of drugs, and the hospital hasa critical shortage of:
. antibiotics (injections)
. infusions, particularly Ringer’s lactate
. chloroquine
. Fansidar
. quinine, injectable
. bandages.
In addition, since there are not enough beds to accommodate all the patientsadmitted, he has asked for 20 more. So far he has been able to cope with the newdemands because the Assistance to All (ATA) team has provided the followingdrugs:
. ampicillin injections, 1 gm 300
. ampicillin tablets, 250 mg 2000
. procaine penicillin, 1 mu 200
. gentamycin, 75 mg 100
. erythromycin, 250 mg 500
. mefloquine 500
. Ketamine vials. 50
No. 1166 Date: 23/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
DRUG REQUEST BY KHRON HOSPITAL TO THE AWALEI ATAHEALTH TEAM
Having had no response from the provincial health office concerning the requestfor drugs he sent some days ago, the doctor fromKhron hospital is submitting arequest in writing to the ATA team for the following drugs:
. metronidazole, 250 mg 20,000
. benzylpenicillin, 3 mu 2,000
. chloramphenicol, 1 g 1,000
. cloxacillin tablets, 500 mg 10,000
. sulfadiazine-pyrimethamine 5,000
HELP/SOS: ALPHALAND/BETALAND714

. diazepam injections, 10 mg 200
. dextran, 500 ml 100
. glucose 5% 100
. Ringer’s lactate 200
. isotonic saline 100
. lidocaine 1%, 50 ml 20
. quinine injections, 600 mg. 100
He feels that ATA should support the hospital since many refugees from thecamp are hospitalized in Khron.
No. 1167 Date: 23/12/99 Betaland
Source: Khron, EPI manager in Khron
AVAILABILITY OF VACCINES IN KHRON
The person in charge of the EPI in Epsilon district is based inKhron. She is readyto help the refugees and to implement an immunization campaign in the Awaleicamp. A team can be organized with health personnel from Khron hospital whohave previously worked in EPI campaigns. Unfortunately, the EPI does not havea functioning motor vehicle. The hospital’s only operative vehicle is used forpatient transport, since the hospital ambulance broke down months ago. TheEPI has a refrigerator in the hospital and one portable cold box. At the momentthe EPI has the following vaccines in stock:
. measles: 200 doses
. BCG: 80
. DPT: 300
. polio (OPV): 400
An order for meningitis vaccine has been placed with the provincial healthofficer, but the vaccine will not be received any time soon, since the provincialhealth officer must first obtain authorization from the Ministry of Health inKappa for non-standard vaccines.
ALPHALAND/BETALAND 715

717
No. 1168 Date: 23/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
FACILITIES AT KHRON HOSPITAL
The hospital of Khron is a 65-bed facility with five main buildings and othersubsidiary structures:
. a building housing the hospital’s administrative offices, the X-ray andlaboratory departments, the OPD, and a storeroom for drugs, supplies, andequipment
. a ward block housing the medicine ward and the surgical ward
. a ward block housing the paediatric ward and the maternity ward
. a small isolation unit for infectious diseases
. an operating theatre and a sterile supply department
. an annex to the first building containing kitchen and food storage facilities
. a garage and workshop
. a shed for the diesel-powered generator and the pump for the hospital’s watertower
. hospital staff are housed in the Betaland government housing area a shortdistance away.
The buildings are constructed of concrete, with corrugated iron roofs. Thebuilding housing the paediatric and maternity wards is in bad condition. Theroof was damaged three years ago by a storm, and has never been properlyrepaired. The structure was further damaged by last year’s heavy rains.
The annex to the first building is very small (3 x 4 metres); the kitchen floor iscovered with gravel, and the food storage area is not rodentproof. A fencesurrounds the hospital. The hospital is connected to Khron’s water system, butthere is a 5-m3 reservoir within the hospital compound, for use when themunicipal supply is cut off. Electricity is provided by the diesel-poweredgenerating plant that serves the town of Khron. The electrical supply isfrequently interrupted owing to mechanical problems at the generating plant.The hospital has a 40-KW generator, but this generator broke down six monthsago. A request for repair has been made to the Ministry of Works office inGamma, but the ministry’s mechanic does not think it can be repaired. Allbuildings have flush toilets, but most of them are not working. Patients and theirfamilies use pit latrines that are located at the far end of the hospital compound.
HELP/SOS: ALPHALAND/BETALAND716

No. 1169 Date: 23/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
SERVICES PROVIDED BY KHRON HOSPITAL
The hospital covers the needs of 70,000 persons who live within its catchmentarea. Only uncomplicated cases can be hospitalized at Khron; serious cases arereferred to Gamma, as are cases requiring special tests.
The number of admissions since November 1998 is:
1998 November
December
1999 January
February
March
April
May
June
July
August
September
October
November
December
258
194
222
194
172
175
212
206
215
201
210
187
337
335
145 refugees
229 refugees
No. 1170 Date: 23/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
PATIENTS REFERRED FROM KHRON TO GAMMA PROVINCIAL HOSPITAL
October 1999 (25 patients, age given in parenthesis):
. acute abdomen (49)
. heart failure (72)
. ectopic pregnancy (24)
. fever and convulsions (2)
ALPHALAND/BETALAND 717

719
. appendicitis (6)
. breast cancer (52)
. rheumatic fever (15)
. head injury (31)
. complicated delivery (29)
. respiratory distress (1)
. tests for stomach problem (45)
. uterine cancer (42)
. chronic headache (tests) (54)
. head injury (12)
. appendicitis (5)
. heart failure (67)
. psychiatric disorder (34)
. metrorrhagia (22)
. open fracture of the left leg (24)
. goitre (34)
. dysuria (56)
. fracture of femur (67)
. sterility (tests) (32)
. gastric ulcer (59)
. cataract (72).
November 1999:
Fifty-seven patients were referred to Gamma provincial hospital (more than thedouble the number in the previous month):
. surgical cases: 18 war-wounded, 12 others
. medical cases: 15
. paediatric cases: 12.
Many other patients had to be transported to Gamma hospital because theycould not be accommodated inKhron. In addition, several woundedwho arrivedin Khron on 5 December had to be evacuated to hospitals in Brew or Takribecause high water made the road between Khron and Gamma impassable.
HELP/SOS: ALPHALAND/BETALAND718

No. 1171 Date: 23/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
OPD ATTENDANCE AT KHRON HOSPITAL
Adults Children <5
1998 November
December
1999 January
February
March
April
May
June
July
August
September
October
November
2,532
2,678
2,234
2,456
2,678
2,387
2,217
2,291
1,876
765
1,657
1,874
2,987
1,186
975
1,047
1,289
1,345
1,276
1,123
1,086
876
721
865
987
1,456
During the first two weeks of December the number of consultations was 734 forchildren under 5, and 1,530 for patients over 5.
No. 1172 Date: 24/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
OCCUPANCY RATE FOR KHRON HOSPITAL (24 December 1999)
On 24 December the number of hospitalized patients was 112, distributed asfollows:
Medicine 21
Surgery 29
Paediatrics 42
OB/GYN 10——————————
TOTAL 102
The occupancy rate was 187%.
ALPHALAND/BETALAND 719

721
No. 1173 Date: 24/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
MAIN CAUSES OF HOSPITALIZATION IN KHRON HOSPITAL
In December 1999, the following patients were seen at Khron hospital. Somewere admitted for treatment, and others were referred directly to hospitals atGamma, Takri, and Brew.
War-woundedBullet injuries:
. upper limb: 6
. lower limb: 7
. abdomen: 4
. thorax: 3
. polytrauma: 5
Mine injuries:
. upper limb: 2
. lower limb: 11
. abdomen: 1
Shrapnel injuries:
. upper limb: 2
. lower limb: 3
. abdomen: 2
. thorax: 1
. polytrauma: 7
At present, there are 11 war-wounded in the hospital, all others having beenreferred to the following hospitals:
Gamma: 18 Brew: 7 Takri: 11
Some who had minimal injuries have been sent back to Awalei camp.
HELP/SOS: ALPHALAND/BETALAND720

Surgical cases (not war-related)
In December seven cases were admitted:
. two are still in hospital
. five were referred to Gamma hospital.
Medical cases
Many cases of cerebral malaria, acute respiratory infections, and severe anaemiawere hospitalized in December 1999. In all, 12 were admitted (two of them werereferred to Gamma hospital).
Paediatric cases
Malaria, meningitis, dehydration, and pneumonia are among the most frequentcauses of hospitalization. Twenty-six cases have been admitted (three referred toGamma). At present, the paediatric ward is the busiest department, with42 children in hospital.
OB/GYN
Nine patients were hospitalized in December. Three remain in hospital.
No. 1174 Date: 24/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
DEATHS IN KHRON HOSPITAL
During the first two weeks of December, 15 patients died in hospital. The causesof death were:
. meningitis (6 yrs) 1
. cerebral malaria 5
. pneumonia 3
. dehydration 4
. unknown causes 2
Eighty percent of the decedents were children.
ALPHALAND/BETALAND 721

723
No. 1175 Date: 24/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
KHRON HOSPITAL LABORATORY
The Khron hospital laboratory has basic equipment, and the technician canperform the following tests:
. blood smears for malaria
. blood cell counts
. blood typing and crossmatching
. hemoglobin/hematocrit
. urine tests
. stool examination (parasites)
. HIV
. blood glucose (glucose metre).
The spectrophotometre has been nonfunctioning for the past four months.
No. 1176 Date: 24/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
RADIOLOGY AT KHRON HOSPITAL
The radiology equipment is very basic. There is only one 30 mA machine whichcan take chest films, extremities, and abdominal flat plates. In addition, there is ashortage of X-ray film and sometimes chemicals. Multiple requests have beensent to the provincial health officer, without eliciting any response so far.
No. 1177 Date: 24/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
PROBLEMS RELATED TO THE PRESENCE OF WAR-WOUNDED
1. Transportation:
The main problem in evacuating wounded from the camp to Khron hospital andthence to Gamma, Brew or Takri hospitals has been the lack of transport. TheKhron hospital has only one ambulance, which is currently not in working order.Only oneEPI vehicle is available for transportingwounded and other patients. In
HELP/SOS: ALPHALAND/BETALAND722
general, the sick and wounded reach the hospital by their own efforts (trucks,cars, walking, etc.). The ATA health centre team is able to transport somepatients in its own vehicle.
2. Hospital capacity:
Khron hospital is overcrowded, and the occupancy rate is above 100% for alldepartments. The hospital is finding it difficult to admit more patients, and evenmembers of the local population are having trouble gaining access to hospital care.
3. Attitude of the government:
The government of Betaland is worried about the presence of many wounded inthe various hospitals in the province. As most of the wounded are related to theZLM forces in some way, it fears that the Alphaland government will considerprovision of medical care as direct support to the ZLM by the Betalandgovernment. On the other hand, it is under pressure from all humanitarianorganizations working in the area to maintain open access to governmenthospitals.
No. 1178 Date: 27/12/99 Betaland
Source: Khron, administrator of Khron hospital
STAFF AT THE KHRON HOSPITAL
The hospital’s professional staff includes one doctor, 4 medical assistants,18 nurses (one of them a public health nurse) 16 nursing aides, one labtechnician, and one X-ray technician.
No. 1179 Date: 23/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
HOSPITAL IN THE CAMP
The doctor at Khron hospital is worried about the increasing numbers ofrefugees being admitted to Khron hospital, and feels that a solution must befound immediately, because he believes that his staff and the hospital facilities areno longer able to cope with the situation. There are two solutions, as he sees it: toincrease the capacity of Khron hospital, or to build a field hospital in the campfor the refugees. He prefers the second option, because it would keep the refugee
ALPHALAND/BETALAND 723

725
patients separate from patients from the local communities, thereby avoidingpotential problems. He has discussed this with the district and provincial medicalofficers, but so far has received no definite response.
No. 1180 Date: 29/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
MALNOURISHED CHILDREN IN KHRON HOSPITAL
On 29 December 1999, there were 32 children hospitalized in Khron hospital,21 of them with severe malnutrition. The paediatric ward cannot accept morechildren, since the occupancy rate is already well over 200%. Moreover, thehospital is not equipped or staffed to care for such a large number ofmalnourished children.
No. 1181 Date: 21/12/99 Betaland
Source: Khron, representative of the water development project
WATER RESOURCES IN AWALEI
The Bowi river never goes dry, although the water level may drop by as much as20 cm during the dry season. The width of the river varies from 5-20 metres. Theamount of water available is sufficient for the consumption needs of both thelocal population and the refugees.
Near the village of Zotewe is a well that was dug 20 years ago by the inhabitantsof the village. In 1993, during a general assessment of local water resources,WDPtechnicians assessed this well. They estimated that the well had:
. a capacity of 21 cubic metres during the wet season
. a capacity of 11 cubic metres during the dry season
. a depth of 20 metres.
The level of the water in the well was recorded over the period of one year (1998):
Jan Feb Mar Apr May June July Aug Sept Oct Nov Dec
Water
level (m)
11.0 12.0 12.0 11.0 10.0 9.0 8.0 7.0 6.0 7.0 8.0 10.0
A bacteriological study of the well water at that time showed that the water wasalmost completely free of faecal coliforms. Since 1998, however, the water has
HELP/SOS: ALPHALAND/BETALAND724

not been tested. Generally in this area the water table is about 10 metres belowthe surface. The geological composition of the ground is such that diggingwells isnot very difficult. In places the rocky layer is rather superficial.
No. 1182 Date: 28/12/99 Betaland
Source: Khron, manager of the water plant in Khron
WATER PLANT IN KHRON
There is a shortage of chlorine for the water plant in Khron, preventing propertreatment of the town’s water.
No. 1183 Date: 24/12/99 Betaland
Source: Khron, doctor in charge, Khron hospital
HEALTH STAFF IN THE CAMP
Following a request from the health authorities in Khron, the provincial healthofficer has asked that one doctor, two nurses, and five aides be sent fromGammaprovincial hospital to theMoHhealth centre in theAwalei refugee camp, in orderto allow the Khron hospital staff to return to their duties.
No. 1184 Date: 23/12/99 Betaland
Source: Khron, doctor at Khron hospital
THE PRACTICE OF TRADITIONALMEDICINE IN THE CAMP
Traditional medicine is widely used in Epsilon by the local population. As bothcommunities belong to the same ethnic culture, it is almost certain thattraditional healers may be present in the camp, providing treatment.
No. 1185 Date: 21/12/99 Betaland
Source: Khron, representative, Betaland Council of Churches
THE STORAGE CAPACITYOF THE WAREHOUSE IN KHRON
The capacity of the warehouse that the Betaland Council of Churches (CoC)owns in Khron is 200 cubic metres (10 x 5 x 4). The CoC headquarters in Kappa
ALPHALAND/BETALAND 725

727
recently sent 80 tonnes of food, part of which has been distributed to the refugeesby the BRCS. The CoC intends to buy food in the north of the country and totransport it south. Distribution will be handled by the BRCS, since the CoC doesnot have the manpower to organize food distributions. It plans to deliver1,200 tonnes of food to the refugee-affected areas in the coming weeks.
No. 1186 Date: 03/01/99 Betaland
Source: Khron, manager of Khron food warehouse, Ministry of Agriculture
EVALUATION OF FOOD STOCKS IN THE KHRON WAREHOUSE
The following stocks were on hand as of 3 January 1999:
millet: 158.5 tonnes
groundnuts: 30.5 tonnes
oil: 11 tonnes.
HELP/SOS: ALPHALAND/BETALAND726

N S
WE
Gam
ma
Bre
w
Gu
tirAl A
liKar
am
Bu
rlo
Gol
ra
Gol
bi
El G
hei
Bu
gda
Aw
alei
Zot
ewe
Op
ala
Pan
os
Maq
uer
San
bar
eN
and
a
Min
ote
Sak
o
Kh
ronT
ocay
e Inp
ala
Cu
bm
a
Lag
un
Mah
ad
Bai
do
bor
der
Kar
amd
istr
ict
Ep
silo
nd
istr
ict
Bre
wd
istr
ict
Gam
ma
dis
tric
t
Gam
ma
pro
vin
ce
10 K
m
Tan
a R
iver
Gow
i Riv
erW
abi
Riv
er
Bel
e R
iver
Bow
i Riv
er
Alp
hal
and
Bet
alan
d
You
are
here
Box 9
INFORMATION FROM AWALEI
ALPHALAND/BETALAND 7727

729
Zot
ewe
IV
II
I
V
III
clin
ic (
G)
clin
ic(A
PT
)
wat
er s
ourc
e
Bow
i Riv
er
wel
l
Aw
alei
cam
p
swam
p
100
mN S
WE
Khr
on
Sako
Box 10
HELP/SOS: ALPHALAND/BETALAND7728

INFORMATION FROM AWALEI
No. 1187 Date: 21/12/99 Betaland
Source: Awalei, Provincial Refugee Affairs representative in Awalei camp
THE WATER TRUCK IN KHRON
The town of Khron has aWDPwater truck with a capacity of eight cubic metres.This truck could be used to distribute water to the refugees in the camp.
No. 1188 Date: 23/12/99 Betaland
Source: Awalei, traditional healers
TRADITIONAL HEALERS IN AWALEI CAMP
It has not been possible to talk with the traditional healers who are present in thecamp. It will take some time to establish enough trust. However, a nurse, himselfa refugee, explains that most of the treatments provided are for fever, cough,headache, abdominal pain, amenorrhoea, and psychological problems.
Common treatments are scarification, external use of ointments (oil, butter), andingestion of various mixtures of roots, herbs, and bark.
No. 1189 Date: 23/12/99 Betaland
Source: Awalei, interview with a group of refugee mothers, Awalei camp
A GROUP OF MOTHERS TALK ABOUT THE LOCAL TREATMENTOF DIARRHOEA
When a child is suffering from an episode of diarrhoea, the traditional treatmentconsists of ingesting spices. In addition, the child is not allowed to breast-feed ordrink cow’s milk until the diarrhoea stops. Among the 12 mothers who wereinterviewed, only one had heard of oral rehydration therapy.When the diarrhoeais associated with abdominal pains, the traditional healer performs scarificationat the location of the pain.
ALPHALAND/BETALAND 729

731
No. 1190 Date: 23/12/99 Betaland
Source: Awalei, assessment team
USE OF ORS IN THE MoH HEALTH CENTRE IN THE CAMP
Mothers are not given proper instruction on how to use oral rehydration salts for achild suffering from diarrhoea. When giving instructions, health workers do notmention the quantity and quality of water that should be mixed with the ORS.
No. 1191 Date: 23/12/99 Betaland
Source: Awalei, assessment team, Awalei camp
IMMUNIZATION IN AWALEI CAMP
So far, no immunization campaigns have been carried out in the camp. There isnot enough vaccine in Khron hospital, needles and syringes are in short supply,and the existing cold chain does not have the capacity for additional vaccinestorage.
No. 1192 Date: 23/12/99 Betaland
Source: Awalei, assessment team in Awalei camp
ORGANIZATION OF THE MoH HEALTH CENTRE IN AWALEI CAMP
The health centre is a large hut (10 x 5 metres) with a wooden frame and athatched roof. There are several rooms inside used for consultations, bandagingand injections, and treatment. The personnel, equipment and supplies areprovided by Khron hospital. The available medical equipment is very basic,consisting in a stethoscope, a blood pressure cuff, an otoscope, and, fordressings, one pair of forceps and one scissors set.
At the entrance to the clinic a guard allows patients to enter two or three at a time.Patients usually wait outside for several hours before they can enter. Usuallythere are 15 to 20 persons inside the health centre at any time. The medicalassistant works the whole day, seeing 200-250 patients a day. He asks eachpatient the purpose of the visit and, if necessary, performs a quick physicalexamination, but usually he makes his diagnosis on the basis of the symptomsdescribed to him. There are no standardized treatment regimens. A patient withbronchitis may receive penicillin, co-trimoxazole, or tetracycline. The drugsprescribed are written on a piece of paper which is handed to the aide in charge ofthe pharmacy. Each patient receives the full course of treatment at the initial visit.
HELP/SOS: ALPHALAND/BETALAND730
Each week a BRCS vehicle delivers a supply of drugs from Khron hospital. Thedrugs sent by the hospital are rather limited in amount and variety, and they donot meet the medical needs of many patients. The doctor from the ATA healthcentre helps by sharing some drugs from the ATA clinic.
The health centre does not have a record system. The nurse keeps a list of thediagnosis and age of each patient in a log book, but he has no time to keepindividual records. Drug and supply stockkeeping is poorly managed, and nopermanent records of stock movement are kept.
The water for the health centre is drawn directly from the river, and stored in a200-litre drum. The nurse has requested disinfectant tablets for the water, but sofar has not received any from the hospital.
There is no latrine and no electricity. Syringes and needles are boiled in apressure-cooker over a charcoal fire.
No. 1193 Date: 23/12/99 Betaland
Source: Awalei, Awalei camp assessment team
THE ATA HEALTH CENTRE IN THE CAMP --- GENERAL OBSERVATIONS
The health centre is a tent that is divided into three parts: a consultation room,containing an examination table, an ordinary table, and two chairs; a room forbandages and injections; and a room for dispensing medications. The basicmedical equipment needed for physical examinations (stethoscope, bloodpressure cuff, otoscope/ophthalmoscope, timer) is present, and there arefacilities for simple laboratory tests (microscope, centrifuge, reagents). However,this equipment is not in use at the moment because the lab technician has notarrived yet.
The health centre has a portable 25-KW generator which is used for lighting inthe evenings and to power a small portable electric sterilizer.
The water used in the health centre is drawn from the river and stored in fiveplastic 100-litre drums. It is treated with chlorine tablets before use.
A medical assistant posted at the entrance performs triage, working with atranslator. According to the presenting symptoms, the nurse will either prescribetreatment herself or send the patient to the doctor for further examination. Thedoctor also works with a translator. He examines each patient carefully, andmanages to see about 40 per day. There are no standardized regimens for thetreatment of specific diseases.
ALPHALAND/BETALAND 731

733
Between the morning and afternoon clinic sessions, the medical assistant appliesdressings and administers injections.
No. 1194 Date: 23/12/99 Betaland
Source: Awalei, medical assistant at the ATA health centre
CASE OF CLEFT PALATE BROUGHT TO THE ATA HEALTH CENTRE
The medical assistant at the ATA health centre is furious with the doctor ofKhron hospital, to whom she referred a three year old patient with a cleft palaterequesting that he be evacuated to the provincial hospital or to the UniversityTeaching Hospital in Kappa for surgery. Two weeks later the patient was sentback fromKhronwith a letter from the doctor saying that nothing could be donefor him at the moment. The ATA medical assistant says she will contact theBRCS directly or the Ministry of Health so that the patient can go to Kappa oreven abroad if necessary for the appropriate surgery.
No. 1195 Date: 24/12/99 Betaland
Source: Awalei, assessment team, Awalei camp
CHILDREN’S HYGIENE
Most of the children in the camp appear dirty and many of them seem to sufferfrom skin infections. Almost all appear to have taenia, some have scabies, and anumber have tropical ulcers. They play in pools of dirty rainwater which areheavily contaminated with human waste.
No. 1196 Date: 24/12/99 Betaland
Source: Awalei, medical assistant at the ATA health centre, Awalei camp
STUDY OF THE PREVALENCE OF INTESTINAL PARASITES
The medical assistant at the ATA health centre in the camp, aided by the Khronhospital laboratory, has studied the prevalence of intestinal parasites in thepatients who visit the ATA health centre. A total of 120 stool specimens wereexamined, and 60% tested positive for intestinal parasites:
. ankylostomes (hookworms): 57%
. ascaris: 20%
. trichuris: 13%
HELP/SOS: ALPHALAND/BETALAND732

. enterobius (pinworms): 1%
. giardia: 7%
. strongyloides (threadworms): 2%
Given these findings, he wants to organize a mass campaign of chemotherapy inthe camp, delivering a single dose of mebendazole (200 mg).
No. 1197 Date: 24/12/99 Betaland
Source: Awalei, medical assistant at the MoH health centre in the Awalei camp
HEALTH STATISTICS FROM THE MoH HEALTH CENTRE
A total of 1,600 patients have been seen at the MoH health centre in the camp.Those returning a second time for the same problem have not been countedseparately. The distribution of complaints was as follows:
. malaria: 480 (30%)
. fever: 200 (12.5%)
. diarrhoea: 152 (9.5%)
. bronchitis: 129 (8%)
. tuberculosis: 32 (2%)
. abdominal pain: 300 (19%)
. headache: 79 (5%)
. skin infections: 102 (6.4%)
. intestinal parasites: 80 (5%)
. urinary infections: 51 (3.2%)
. dental problems: 63 (4%)
. wounded: 43
. referred to the hospital: 56
No. 1198 Date: 24/12/99 Betaland
Source: Awalei, doctor at the ATA health centre
MALARIA PREVENTION IN THE CAMP
The only measure undertaken to prevent malaria in the camp has been thedistribution of chloroquine tablets to some pregnant women.
ALPHALAND/BETALAND 733

735
No. 1199 Date: 24/12/99 Betaland
Source: Awalei, medical assistant at the MoH health centre in Awalei camp
FOLLOW-UP OF MENINGITIS CASES
No follow-up action was taken following the identification of two cases ofmeningitis in the camp and their referral toKhron hospital. Themedical assistanthas no information on the type of organisms responsible, and is concerned thatother camp inhabitants may be carriers. He fears that the situation may be ripefor an outbreak of meningitis.
No. 1200 Date: 24/12/99 Betaland
Source: Awalei, MoH health centre in Awalei camp
THE MEDICAL ASSISTANT IN THE MoH HEALTH CENTREIS OVERWORKED
The medical assistant complains that he has too much work to do. He worksfrom 7 a.m. to 7 p.m. When he closes the health centre there are still patientswaiting to be seen. He has asked the doctor at Khron hospital to send additionalstaff for the health centre. He also complains that many patients use both healthcentres in the camp, going from one to the other for the same health problem.He thinks the treatment given in the ATA health centre is of higher quality,which makes patients attending the MoH health centre angry with the medicalstaff.
No. 1201 Date: 24/12/99 Betaland
Source: Awalei, medical assistant at the MoH health centre in Awalei camp
TUBERCULOSIS IN THE CAMP
Fourteen people with suspected tuberculosis have been sent to the hospital fortests. Of these 14 cases, three tested negative and were sent back to the camp. Thepublic health nurse from Khron has sent a note saying that eight patients havesputum testing positive for AFB, and he asked the camp medical assistant tocontact the families for follow-up. Unfortunately, the medical assistant does notknow where these families are living, and has no time to leave the health centreand go looking for them in the camp.
HELP/SOS: ALPHALAND/BETALAND734
No. 1202 Date: 27/12/99 Betaland
Source: Awalei, doctor at the ATA health centre, Awalei camp
TREATMENT OF TB PATIENTS IN THE ATA HEALTH CENTRE
The doctor at the ATA health centre has started to treat TB patients withstreptomycin (two months), isoniazid (eight months), rifampicin (two months),and pyrazinamide (eight months). He thinks that this course of treatment ispreferable to the regimen used by the Ministry of Health.
No. 1203 Date: 04/01/99 Betaland
Source: Awalei, assessment team
IMMUNIZATION STATUS OF THE CHILDREN IN AWALEI
According to a rough estimate made by the assessment team, about 15% ofchildren under the age of five years are fully immunized, and 25%have had someimmunizations. Few families have brought their children’s immunization recordswith them.
No. 1204 Date: 04/01/99 Betaland
Source: Awalei, assessment team, Awalei camp
HEALTH EDUCATION AMONG MOTHERS IN THE CAMP
According to estimates by the assessment team, only 20% of the mothers wereable to recall any of seven key messages about children’s health.
No. 1205 Date: 21/12/99 Betaland
Source: Awalei, representative of the Betaland Red Crescent Society
FOOD DISTRIBUTION IN THE CAMP BY THE BRCS
The BRCS arrived on the morning of 15 December 1999 with two lorriescontaining a total of 20 tonnes of food. The distribution was supposed to benefitthe new arrivals in Section II. As no census had been taken, the representatives ofthe refugee council were asked to identify new arrivals and to send them to thefood distribution area. The distribution started at 9 a.m. near the MoH healthcentre. Each family was entitled to 25 kilos of sorghum, 4 kilos of peas, and 1 kilo
ALPHALAND/BETALAND 735

737
ofmilk powder, regardless of the number of people in the family. The name of thehead of the family was recorded on a sheet of paper. Very rapidly, severalthousand refugees gathered around the distribution point, and the distributionended in chaos. So far, the BRCS has delivered 40 tonnes of food to the camp.
No. 1206 Date: 21/12/99 Betaland
Source: Awalei, nurse at the MoH health centre in Awalei
REFUGEE CHILDREN’S NUTRITIONAL STATUS
TheMoHhealth centre has been open for twomonths. During that period, 1,456children have been treated there. Of those, 20% were severely malnourished.Their nutritional status was evaluated on the basis of clinical criteria, since themedical assistant did not have the time or the equipment to take anthropometricmeasurements.
No. 1207 Date: 21/12/99 Betaland
Source: Awalei, doctor at the ATA health centre in Awalei camp
NUTRITIONAL STATUS OF THE CHILDREN AT AWALEI CAMP
The ATA health centre was opened two months ago. Since then, 428 childrenhave been weighed, and 36% showed severe malnutrition (below 80% of weight-for-height).
No. 1208 Date: 21/12/99 Betaland
Source: Awalei, food assessment team
REFUGEE FOOD STOCKS
It is thought that half of the refugee families have some food stocks with them.However, quantities are very small and will not cover basic nutritional needs forlong. In some huts, the team has found food that was distributed by the BRCS10 days ago.
HELP/SOS: ALPHALAND/BETALAND736

No. 1209 Date: 03/01/99 Betaland
Source: Awalei, nurse in charge of the nutritional rehabilitation centre
at Awalei camp
ORGANIZATION OF THE NUTRITIONAL REHABILITATIONCENTRE IN THE CAMP
A NGO called Food For All has set up a feeding centre in the camp. It wasopened on 28 November 1999, and is a structure with a wood frame and athatched roof. It measures 10 x 8 metres, and has a kitchen separate from themain building. The meals consist of biscuits and enriched milk supplementedwith vitamin A. Each meal provides an average of 300 kcal. The childrenattending the centre are usually referred by one of the two health centres in thecamp, although some of them are brought directly by theirmothers. Admission isbased on anthropometric measurements; only children with weight-for-heightvalues below 80% are admitted. Two meals per day are provided (morning andafternoon), and the mothers receive one meal in the morning. Upon admissioneach child receives a blanket and a bar of soap.
A nurse is responsible for the medical supervision of the centre. She providesbasic health care, and if necessary refers the children to one of the health centres.She has been asking the health centre staff to vaccinate the children in the feedingcentre, but nothing has been done so far.
No. 1210 Date: 03/01/99 Betaland
Source: Awalei, Betaland Red Crescent Society delegate in Khron
FOOD RATION DISTRIBUTED BY THE BRCS
The food ration that the BRCS has undertaken to deliver is as follows:
. 200 gm of millet/person/day
. 60 gm of peanuts/person/day
Unfortunately, distribution is irregular, and it has not yet been possible todistribute the quantities mentioned above, owing to the low level of food stocksin the Khron warehouse. For the moment the BRCS has on hand eight tonnes ofmillet and two tonnes of peanuts.
ALPHALAND/BETALAND 737

739
No. 1211 Date: 03/01/99 Betaland
Source: Awalei, person in charge of the nutritional rehabilitation centre,
Awalei camp
ACTIVITY OF THE FEEDING CENTRE IN THE CAMP
Admission figures are as follows for the first four weeks of operation:
Week 1: 58 Week 2: 116
Week 3: 127 Week 4: 142
On 3 January 1999, when the assessment team visited the centre, 367 childrenwere present.
No. 1212 Date: 21/12/99 Betaland
Source: Awalei, representative of provincial refugee affairs office
HOUSING IN THE CAMP
Shelters are small, 10-15 square metres, and made with local material (woodenpoles, grass matting, and a thatched roof). There is no water close at hand, andlatrine facilities are almost non-existent. Cooking is done outside the shelters onan open wood fire.Most families have no blankets and no cooking utensils. Fireshave broken out in the camp more than once, destroying many shelters, and onechild has been seriously burnt. She was sent to the hospital in Gamma where sheis awaiting a skin graft.
No. 1213 Date: 21/12/99 Betaland
Source: Awalei, Awalei refugee camp administrator
LACK OF SANITATION IN THE CAMP
The camp administrator explains: ‘‘It is not the habit of refugees to use latrines,nor to dispose properly of solid waste.’’ A representative of the Council ofRefugees explains: ‘‘We don’t want to dig latrines now, because there is a goodchance we will be returning to our homes in Alphaland soon.’’
HELP/SOS: ALPHALAND/BETALAND738

No. 1214 Date: 21/12/99 Betaland
Source: Awalei, ATA representative
QUALITY OF WATER IN THE CAMP
The ATA representative is worried about the quality of the water used in thecamp. At the ATA health centre, he sees a lot of diarrhoea cases. He thinks thatthe Bowi River is heavily polluted by the cattle that the refugees brought withthem. Tomorrow he has an appointment with the camp administrator to discussthe possibility of separating the animals from the population and keeping themout of the camp.
No. 1215 Date: 21/12/99 Betaland
Source: Awalei, interview of a refugee
INTERVIEW WITH A REFUGEE WHO HAS BEEN WORKINGIN WELL CONSTRUCTION
In the camp, there is a refugee who worked on building wells in Alphaland. Hewas employed in the WRMP (Water Resources and Management Programme)sponsored byUNICEF inAlphaland. He is ready to help build wells in the camp,if the necessary equipment can be obtained.He says thatmany refugees will workwith him, provided that they are paid with food.
No. 1216 Date: 27/12/99 Betaland
Source: Awalei, doctor at the ATA health centre
CAMP USE OF THE WELL BELONGING TO THE VILLAGE OF ZOTEWE
The doctor believes that the water of the Zotewe well could be used for the entirecamp if an electric pump were installed. It could then be channelled through anetwork that could be built quickly throughout the camp.
No. 1217 Date: 27/12/99 Betaland
Source: Awalei, assessment team, Awalei camp
PRESENCE OF WATER SOURCES NEAR THE CAMP
One kilometre north-east of the camp is a spring on the side of a small hill.Its yield is estimated at 12 litres per minute, and it is used by the villagers
ALPHALAND/BETALAND 739

741
who live nearby. The spring is not protected, and flows directly into theriver.
No. 1218 Date: 27/12/99 Betaland
Source: Awalei, assessment team
EVALUATION OF THE ZOTEWE WELL’S REFILL CAPACITY
A specialist has tested the Zotewe well’s refill capacity, and found yield to bearound 15 litres per minute.
No. 1219 Date: 23/12/99 Betaland
Source: Awalei, representative of Ministry of Works and Supplies in Khron
EVALUATION OF ROAD CONDITIONS BETWEEN KHRON AND AWALEI
The camp is connected to the main Khron-Awalei road by a small dirt side road.After heavy rains, lorries will have some difficulty in reaching the camp along theside road.Moreover, the mainKhron-Awalei road is frequently cut off at a placecalledWakiwherea small bridge is submergedby risingwatersduringheavy rains.
No. 1220 Date: 21/12/99 Betaland
Source: Awalei, administrator of the refugee camp, provincial refugee affairs office
LIVING CONDITIONS IN THE CAMP
The administrator has been appointed by the office of the provincial governor torepresent the Betaland government in the camp. He has been in the camp for twoweeks, and provided the following information.
Site:
The camp is near the road which leads from the border to Khron (22 kilometresfromKhron and 34 kilometres from the border). It is located on both sides of theBowiRiver, and is divided into five sectors. Sector IV is located near the village ofZowete. The closest village is Awalei with 750 inhabitants. The site was chosen bythe Betaland provincial authorities for several reasons:
. it is located near a water source (Bowi River)
. it is far enough from the border to prevent contact with the ZLMwhich couldbe misinterpreted by the Alphaland government
HELP/SOS: ALPHALAND/BETALAND740

. it is far enough from Khron to prevent many refugees from settling in thetown.
Census:
At the moment it is difficult to know exactly howmany refugees are in the camp.According to the administrator, there are about 80,000 people in the camp, but alist provided by some of the refugee leaders gives the figure of 123,890.
Water resources:
The Bowi River runs through the camp. At the present time of the year there isplenty of water. Many shelters have been constructed very close to the river’sedge. Some families draw water directly from the river, while others draw waterfrom small ponds near their shelters. Few households have water containers.
Topography:
The camp overlooks the Bowi River valley. Sector IV is on the right bank but theother four sectors are on the left bank. The surface areas of sectors I, II, III, andVare all about 800 x 300 metres, but sector IV measures about 100 x 100 metres.
Shelter:
The refugees are living in huts made of local materials: mats and poles for walls,with grass for the roof. Some tents have been sent by the Red Crescent Society.Wood for fuel is available from woodlands in the immediate vicinity, althoughthe local population is concerned about the refugees’ heavy use of firewood.
Food resources:
The refugees brought very little food with them, and most of it is gone now.Various agencies have distributed food on a number of occasions, but the rationwas inadequate (estimated at about 150 gm of cereals, 30 gm of beans, and 50 gmof milk powder per person per day). Only sections IV and II were assisted withfood. The refugees cannot afford to buy food in the local market inAwalei. Thereis almost no suitable land in the immediate surroundings for growing gardens.
Organization:
The sections correspondmore or less to the refugees’ place of origin. A council ofrefugees has been set up with representatives from each sector. They were electedinformally by the refugees themselves in each section. The council’s role is mainlyto discuss the practical organization of the camp with the local authorities and
ALPHALAND/BETALAND 741

743
representatives of the humanitarian agencies. Shelters are not organized in anyparticular order or according to any particular plan. Roads and market areashave not been planned for, since the sections grew spontaneously.
Health:
The refugees’ health status is poor. The children are malnourished, and manyrefugees complain of health problems such as diarrhoea, fever, skin infections,and cough. Two health centres have been set up in the camp, one operated by theMinistry of Health, using staff from Khron hospital, and one by ATA. Thesevere cases are evacuated to Khron hospital.
Sanitation:
The camp lacks sanitation. Human waste and solid waste are widely spread overthe camp, and in the surrounding grass and woods.
Animals:
Some families have brought their animals with them. Cows, donkeys (used totransport firewood), sheep, and goats are all present in the camp. It is estimatedthat there are about 200-300 cows, 20 donkeys, and several hundred sheep.
No. 1221 Date: 23/12/99 Betaland
Source: Awalei, representative of the refugees in Awalei camp
COMPLAINT FROM A GROUP OF REFUGEES
One of the most frequent complaints by the refugees is that they are not involvedin the decision-making process concerning the type of assistance theywill receive,and arrangements for their future. They would like to be responsible fororganizing and distributing relief assistance within the camp. For example, theybelieve they could organize food distributions in such a way as to avoid the chaosthat accompanied the BRCS food distribution.
No. 1222 Date: 23/12/99 Betaland
Source: Awalei, representative of villages surrounding Awalei camp
THE LOCAL POPULATION’S ATTITUDE TOWARD THE REFUGEES
The local population welcomes the refugees, and agrees with the governmentalpolicy. However, the families living around the camp are concerned about possible
HELP/SOS: ALPHALAND/BETALAND742

competitionwith therefugees for resources.Forexample, somerefugeeshavebegunto cultivate gardens around the camp without authorization from communityleaders. The local authorities inKhron have asked the refugees not to proceedwithgardens for the moment. Wood used for fuel is another concern of the localcommunities. Consumption is high and the price of firewood on the local markethas begun to rise. Thewell at Zowete can no longer cover the needs of both the localand refugee populations. In Khron, the waiting time for out-patient consultationshas doubled since the arrival of the refugees. The Awalei community leaders thinkthat sooner or later problems will arise between the two communities.
No. 1223 Date: 27/12/99 Betaland
Source: Awalei, headman, Awalei village
THE REFUGEES’S IMPACT ON THE VILLAGE OF AWALEI
The headmanofAwalei village is worried about the arrival of the refugees. Some ofthem have already started to cultivate lands that belong to the local population,and they go to theAwalei dispensary, so that the local population has to wait muchlonger than in the past. Their presence in the area is driving the prices ofcommodities in the local market higher every day. Drugs, blankets, and foodwhich were originally distributed to the refugees in the camp can now be found forsale in the market. The local population fears that new diseases may spread to thevillagers, since it is known thatmany refugees are sick. They especially worry aboutmeningitis and AIDS. The headman also mentions that the camp will mostprobably be flooded, since this area is prone to floods in the rainy season.
No. 1224 Date: 28/12/99 Betaland
Source: Awalei, a refugee in Awalei camp
IN-DEPTH INTERVIEWS WITH REFUGEES IN AWALEI CAMP
The assessment team has carried out a number of in-depth interviews withrefugees in a convenience sample. Typical of many stories is the followingaccount:
‘‘I arrived with my family in the camp 10 days ago (17 December 1998). I amoriginally fromTrit (60 kilometres fromAwalei). Following heavy fighting in thetown I ran away with my family. For a few days I stayed not too far from Trit,waiting to see if the situation would get any better. But, as the fighting was stillraging, I decided to seek refuge in Betaland.’’
ALPHALAND/BETALAND 743

745
He went on to say that on the way, he and his family stayed two days in Sako, andfollowing the advice of the ZLM he came to Awalei camp. He says that there weremany wounded in Trit, and that the city was repeatedly attacked by aircraft usingbombs and rockets. In addition, the town was being shelled by heavy artillery.
In Trit he had been employed in a health centre as a nurse. Although the city wasunder the control of the ZLM and despite a shortage of drugs and equipment, hewas still working.
No. 1225 Date: 28/12/99 Betaland
Source: Awalei, a refugee in Awalei camp
IN-DEPTH INTERVIEWWITHAREFUGEEFROMLOGIYE INAWALEI CAMP
The head of the family is a woman who arrived at the campwith her two childrenand her parents. Her husband stayed behind in their village, Logiye. Violentfighting occurred in and around Logiye two months ago. She decided to leaveand went directly to Khron. When Awalei camp was created, the Betalandauthorities sent her there from Khron. She has received a little food from theBRCS.As soon as possible her father will return toAlphaland, and depending onthe situation, the family will follow later. She is rather pessimistic that thesituation will improve in the near future.
No. 1226 Date: 28/12/99 Betaland
Source: Awalei, a refugee in Awalei camp
IN-DEPTH INTERVIEWWITHAREFUGEEFROMPAKERE INAWALEICAMP
The refugee interviewed comes from Pakere, near Sako, where he was a labourer.With his family he went through Sako, where he stayed for two days. The ZLMwanted to draft his son into its armed forces. He decided to leave Sako by night,and came to Betaland. He was among the first refugees to arrive in the camp,and considers himself lucky to have some work on a farm near the camp.
No. 1227 Date: 28/12/99 Betaland
Source: Awalei, a refugee
INTERVIEW WITH A REFUGEE FROM BHAO
The town of Bhao has been the centre of fierce fighting for the last three months.The town itself has always remained firmly under the control of governmental
HELP/SOS: ALPHALAND/BETALAND744

troops. There is a small runway located near the town (three kilometres east)which is also under government control, and it is used by military aircraft tobring in military supplies and reinforcements. The civilian population cannot getout of the city, and therefore has almost no access to its usual sources of foodsupplies. However, the soldiers allow some people to take their cattle to graze inareas immediately surrounding the town. In doing this, several people have beenkilled by crossfire outside the town.
When this refugee left one month ago, the market was empty, and there was acomplete lack of drugs in the hospital. The town’s water system had ceasedfunctioning, and people were drawing their water directly from the river, often atconsiderable personal risk. Slipping out of town at night, crossing the front lines,and reaching Betaland also involved substantial danger. Not many people areready to take such a risk.
No. 1228 Date: 28/12/99 Betaland
Source: Awalei, a refugee in Awalei camp
INTERVIEW WITH A REFUGEE FROM MAQUER
This family had been living on a farm 12 kilometres away from Maquer in theSigma district of Alphaland. Over the past several years climatic conditions havedeteriorated, and last year a severe drought occurred in the area north-west ofTrit. After the bad drought of 1995, a development programme had beendevised for the area, but it was poorly managed and failed to yield a reasonablelevel of agricultural production. This year there was no rain in October, andlittle in November, so almost certainly crops will fail again this year.Furthermore, it is increasingly difficult to travel around Sigma district lookingfor food. The towns of Khi, Trit and Lirumi are not easily accessible owing tothe fighting. For a combination of these various reasons, this refugee decided toleave Alphaland and seek refuge in Betaland. He says he intends to stay as longas the fighting continues, and may stay here permanently if the conflict drags on.
No. 1229 Date: 28/12/99 Betaland
Source: Awalei, refugees in Awalei camp
INTERVIEW WITH A GROUP OF REFUGEES IN THE CAMP
At the request of the provincial refugee authorities, the refugees have organized arefugee council in the camp to represent their interests to the camp authorities
ALPHALAND/BETALAND 745

747
and the various NGOs working in the camp. The refugee council has identifiedseveral problems in the camp:
Short term: A major problem is access to food and medical care. Most familieshave no food stocks, and a large part of the population is sick but has difficultygaining access to health services because of the long waits and congestion at theclinics. The refugee community wants a hospital to be built in the camp. At themoment there are adequate amounts of water, but the refugees are worried aboutthe dry season.
Long term: Although the refugees do not want to stay in Betaland, and hope toreturn home soon, they do want permission to start their own income-generatingactivities such as gardens, shops, restaurants, bicycle and radio repair, etc.
No. 1230 Date: 27/12/99 Betaland
Source: Awalei, assessment team, Awalei camp
CAMP CENSUS CARRIED OUT BY THE ASSESSMENT TEAM
The assessment team has taken a quick survey to estimate the population size. Asit was not possible to count the refugees individually, the team made an estimatebased on the number of huts and the average number of people living in each hut.From a small hill near the camp, it was possible to get an overview of the campand to count the huts; the average number of people per hut was then estimatedfrom a sample of 100 huts chosen at random.
The results are:
SECTION HUTSPERSONS
PER HUT
TOTAL
REFUGEES
I 2,200 6.04 13,000
II 1,600 5.77 9,000
III 1,280 6.23 8,000
IV 1,120 6.29 7,000
V 840 6.22 5,300
TOTAL: 7,040 42,300
HELP/SOS: ALPHALAND/BETALAND746
No. 1231 Date: 30/12/99 Betaland
Source: Awalei, interview with a refugee
AN ORPHAN
During the assessment a woman came to the teamwith an unaccompaniedminorof about 11 years of age. He was fromMubayio, and had lost his parents aroundDihun during the trip to Betaland. The woman says that she will take care of himfor the moment, but a solution must be found because she cannot keep him forlong; her resources are meagre and she has her own family to look after.
No. 1232 Date: 30/12/99 Betaland
Source: Awalei, a refugee in Awalei camp
A MISSING PERSON
A woman has asked the assessment team to make enquiries about her husband,who disappeared in Bhaowhen the family was crossing the front lines. They wereseparated when they were caught in a crossfire. She arrived at the camp threeweeks ago and has had no news from her husband.
No. 1233 Date: 30/12/99 Betaland
Source: Awalei, a refugee in Awalei camp
A REFUGEE ASKS FOR NEWS OF HIS SON, WHO HAS BEEN WOUNDED
A refugee asks the assessment team to help him find his son who was wounded inBhao, managed to cross the front lines, and arrived in Sako, whence he wasevacuated to Khron Hospital. The doctor in Khron told him that his son hadbeen transferred to Takri. He has no news of him for three weeks.
ALPHALAND/BETALAND 747

749
N
S
E
Betaland
Alphaland
plain
Takri
Kappa Lum
Srzo
Gamma
KhiAnil
Lambda
KesoNoma plain
mountainousarea
mountainousarea
Border
Tana River
100 Km
Communications:
Roads
Railways
Harbours Airports
KhronZotewe
AwaleiBugda
BaidoBrew
Karam Bulro
Golra
SakoTrit
Bhao
You are here
W
Box 11
INFORMATION FROM BAIDO,BREW, KARAM, TAKRI, BULRO AND GOLRA
HELP/SOS: ALPHALAND/BETALAND7748

No. 1234 Date: 08/01/99 Betaland
Source: Takri, district administrator, Epsilon
FOOD RESOURCES IN EPSILON DISTRICT
Food resources are rather limited in Epsilon district. Over the past three years, apersistent drought has dramatically reduced the district’s agricultural output.The population seems to be coping with the situation with increasing difficulty.Few families have any food stocks left. The local economy is showing the firstsigns of serious disruption by the drought. Cereal prices are steadily rising on thelocal market, whereas the price of livestock is lower than it usually is at this timeof the year. So far the rains have not reached normal levels, and it is feared thatonce more the crops will fail. Food production from the development projectscarried out on the central plateau and east of Karam cannot compensate for thefood deficit in the district resulting from the prolonged drought.
No. 1235 Date: 08/01/99 Betaland
Source: Takri, administrator of Epsilon district
AGRICULTURAL PRODUCTION IN EPSILON
Jan Feb Mar Apr May June July Aug Sept Oct Nov Dec
Millet G G G H S S
Sorghum S G G G H
Sesame G G H H S S S S S
Peas H H H H H H S S G G G
Peanuts G H H S S G G
S = SOWING G = GROWTH H = HARVEST
No. 1236 Date: 27/12/99 Betaland
Source: Takri, officer in charge, civil aviation authority, Takri airport
TAKRI AIRPORT
Runway characteristics:
elevation: 897 metres
mean temperature: 34 degrees
length: 1400 metres
ALPHALAND/BETALAND 749

751
aircraft: maximum C46 or C-130
fuel available: none
aids: MD, MC, MT, visual flight rules
No. 1237 Date: 08/01/99 Betaland
Source: Takri, doctor from the hospital at Takri
TAKRI HOSPITAL
Takri is the main town of the Danikal district, and has about 25,000 inhabitants.The whole district has an estimated population of 200,000. Officially there are norefugees in the district.
Health services:
The town has one hospital and two dispensaries.
Hospital facility:
Takri is a 200-bed mission hospital that offers curative services (medicine,surgery, paediatrics, obstetrics/gynecology). The technical support services arevery good. The laboratory can handle bacteriological and biochemical work,electrolytes, HIV testing using ELISA, and a full range of parasitological tests.The hospital also has a well-functioning blood bank. The radiology departmenthas three functioning X-ray machines, and there are three operating theatres.
Personnel:
. 3 doctors (one surgeon)
. 20 nurses
. 32 aides
. 5 technicians.
Activities:
To date the hospital has admitted 17 war-wounded (11 were referred by Khronhospital):
on 12/12/99: 8
on 12/15/99: 6
on 12/18/99: 3
HELP/SOS: ALPHALAND/BETALAND750

At present, the hospital is coping with the situation, and has the capacity toaccept more wounded. However, once ready for discharge, the wounded willhave to be transferred somehow toKhron or toAlphaland, and the hospital doesnot the necessary means of transport to do this.
No. 1238 Date: 03/01/99 Betaland
Source: Takri, manager of Takri food warehouse, Ministry of Agriculture
EVALUATION OF FOOD STOCKS IN THE TAKRI WAREHOUSE
Millet: 5,831 tonnes
Groundnuts: 104 tonnes
Oil: 65 tonnes
ALPHALAND/BETALAND 751

753
(OTHERS)
No. 1239 Date: 28/12/99 Betaland
Source: Bugda, nurse at the Bugda dispensary
ASSESSING THE IMPACT OF THE REFUGEE INFLUX FROM RECORDSOF THE BUGDA DISPENSARY
According to the nurse, the arrival of the refugees has had a minimal impact onhis dispensary. Most of the refugees in Epsilon are scattered through the district,living with relatives. He heard that a camp had been set up near Awalei. InBugda, there are only about a hundred refugees, as far as he knows. This is fewerthan 10% of all the people in the village of Bugda. So far he has observed noproblems between the two communities.
No 1240 Date: 04/01/99 Betaland
Source: Golra, nurse, Golra dispensary
GOLRA DISPENSARY
Golra is a small town of 5,000 inhabitants. The dispensary there serves apopulation of about 12,000. There are 500-600 refugees in the town and theimmediate environs. The dispensary is located in the centre of town, in a smallconcrete building divided into four rooms. One nurse is in charge of thedispensary, one aide is responsible for bandaging and injections, and anotheraide handles preventive services (MCH and public health activities in the town).An average of 45 patients are seen per day.
No. 1241 Date: 03/01/99 Betaland
Source: Burlo, health worker at the Burlo health post
BURLO HEALTH POST
Burlo isavillageof600 inhabitants (withanother1,200 in the surroundingarea). Itis oneof thepilot villages selected for thePHCWproject.Thehealthpost is a smallbuildingdivided in two.There is no runningwater, andnoelectricity.A latrinehasbeenbuilt nearby.OnePHCWworksat thepostpart time (half aday, three timesaweek). He sees about five patients per working day and makes rounds in thevillage, visiting water sources and discussing health issues with mothers.
HELP/SOS: ALPHALAND/BETALAND752

No. 1242 Date: 05/01/99 Betaland
Source: Karam, nurse, Karam dispensary
KARAM HEALTH CENTRE
The Karam health centre provides services for a population of 25,000 people. Itcomprises two buildings. One is the dispensary, which is divided into four rooms:one room for consultations, one room for bandaging and injections, a waitingroom, and a room for the MCH clinic. The second building is divided into twoparts, one for in-patients (10 beds), and one for administration and storage.Water comes from the municipal water system, which draws it from a deep welltwo kilometres away from town. The health centre has functioning flush toilets.Electric power is provided by a diesel-powered generating station in town. Thehealth centre does not have a standby generator. Syringes, needles, and surgicalinstruments are sterilized with an electric sterilizer.
No. 1243 Date: 04/01/99 Betaland
Source: Baido, medical assistant, Baido dispensary
BAIDO DISPENSARY
Baido has 6,000 inhabitants, 2,034 of them living in the town proper. There are230 refugees, most of whom live in town. The dispensary is a small buildingdivided into separate areas for consultations, bandaging and injections, waiting,and administrative work. Water is obtained from a well inside the compound.The staff consists of one nurse and two health aides.
On average, the nurse sees 30-40 persons a day. She also takes part in preventiveactivities: immunization, family planning, and occasional home visits, usuallywith one of the health aides.
No. 1244 Date: 05/01/99 Betaland
Source: Brew, doctor at Brew hospital
BREW HOSPITAL
Brew is a town of 15,000 inhabitants. The whole catchment area contains 35,000 in-habitants. There are an estimated 4,000-5,000 refugees in the area, many livingaround the town of Brew where jobs are easier to find.
ALPHALAND/BETALAND 753

755
Health facility: the 120-bed hospital is divided into five wards:
. medicine: 40 beds
. surgery: 30 beds
. paediatrics: 30 beds
. obstetrics/gynecology: 10 beds
. infectious diseases: 10 beds.
Services supporting the hospital include:
. water supply from the town mains
. electric power supplied from the municipal grid, with a standby generatorof 60KW
. sanitation: flush toilets (non-functioning)
. laboratory for basic testing
. radiology: two X-ray machines in working order.
Staff:
. 2 doctors (one surgeon)
. 18 nurses (one anaesthetist)
. 14 aides
. 3 technicians.
Activities:
The level of activity at the hospital has increased since the arrival of the refugees,but the hospital is coping with the situation. The surgical ward has been the mostaffected, since 15 war-wounded have been hospitalized since November (7 wereevacuated from Khron to Brew). During the last week the work load for thesurgical department has increased threefold. Drugs, equipment, and food for thehospital are in short supply, and additional supplies have been ordered fromGamma.
HELP/SOS: ALPHALAND/BETALAND754

No. 1245 Date: 03/01/99 Betaland
Source: Zotewe, headman, village of Zotewe
PEOPLE OF ZOTEWE VILLAGE
The village of Zotewe has 180 residents. The refugees’ arrival has brought manyproblems for the villagers. These include the refugees’ usurpation of their landsfor gardens, use and consequent contamination of their well, and purchase offood from their market, which has depleted available resources and driven upprices.
ALPHALAND/BETALAND 755

757
Min
ote
Nan
da
Ko
her
a
Maq
uer
San
bar
e
Imir
e
Sag
ere
Go
do
Sed
idad
le
Ro
der
Nu
taye
le
Led
id
Rey
et
Lir
um
iK
hi
Sir
iqu
eBab
uyi
o
Ko
sha
Deg
ore
Pro
tolo
Ro
linid
i
Bu
lo
Sak
oP
aker
e
Bh
ao
Dan
ote
Ria
nq
uin
Rid
i
Pal
ame
Hin
dar
So
lgat
eL
ore
r
Ker
ar
Pu
tse A
wle
f
Gu
aney
e
Tik
ayo
rie
Gu
erer
Kh
alim
u
N S
WE
Trit
Sig
ma
dis
tric
t
Kh
i dis
tric
t
Kh
alim
u d
istr
ict
Lir
um
i dis
tric
t
Maq
uer
dis
tric
t
10 K
m
Kh
i pro
vin
ce
Bet
alan
d
Alp
hal
and
Roy
e
You
are
here
Box 12
INFORMATION FROM ALPHALAND IN THEREGION OF SAKO, MERER AND TRIT
HELP/SOS: ALPHALAND/BETALAND7756

Min
ote
Nan
da
Koh
era
Maq
uer
San
bare
Imir
e
Sag
ere
God
o
Sed
idad
le
Rod
er
Nut
ayel
e
Ledi
d
Rey
et
Liru
mi
Khi
Sir
iqueB
abuy
io
Kos
ha
Deg
ore P
roto
lo
Rol
inid
i
Bul
o
Sak
oP
aker
e
Bha
o
Dan
ote
Ria
nqui
n
Rid
i
Pal
ame
Hin
dar
Sol
gate
Lore
r
Ker
ar
Put
se
Aw
lef
Gua
neye
Tika
yori
e
Gue
rer
Kha
limu
N S
WE
Trit
Sig
ma
dist
rict
Khi
dis
tric
t
Kha
limu
dist
rict
Liru
mi d
istr
ict
Maq
uer
dist
rict
10 K
m
Khi
pro
vinc
e
Bet
alan
d
Alp
hala
nd
Roy
e
Box 13
ALPHALAND/BETALAND 7757

N S
WE
Gam
ma
Bre
w
Gut
irAl A
liKar
am
Bur
lo
Gol
ra
Gol
bi
El G
hei
Bug
da
Aw
alei
Zot
ewe
Opa
la
Pan
os
Maq
uer
Sanb
are
Nan
da
Min
ote
Sako
Khr
on
Toc
aye In
pala
Cub
ma
Lag
un
Mah
ad
Bai
do
bord
er
Kar
amdi
stri
ct
Eps
ilon
dist
rict
Bre
wdi
stri
ct
Gam
ma
dist
rict
Gam
ma
prov
ince
10 K
m
Tan
a R
iver
Gow
i Riv
erW
abi R
iver
Bel
e R
iver
Bow
i Riv
er
Alp
hala
nd
Bet
alan
d
You
are
her
e
Box 14
INFORMATION ON THE DEVELOPMENTPROJECT IN KARAM
HELP/SOS: ALPHALAND/BETALAND7758
ORGANIZATION OF THE COURSE
MODULE
12

761
SELECTION OF PARTICIPANTS
1. TYPE OF APPLICANTS SOUGHT
Participants must be trained in the field of health (physicians, nursing staff,nutritionists, sanitary engineers, etc.). Also eligible for consideration areapplicants who, although having no specific training in the health field, do havea good knowledge of relief actions (agronomists, anthropologists, economists,jurists, etc.).
2. ADVERTISEMENT OF THE COURSE
The course should be advertised as widely as possible, by means of:
. a leaflet including:
. details concerning the place and dates of the course
. a summary of course content
. a summary of the methods used in the course
. a registration form to be sent to the ICRC (on the back).
This leaflet should be widely distributed through the network of the NationalRedCross andRedCrescent Societies, theUN system (especiallyWHO), and themajor voluntary agencies.
. a poster depicting the first page of the brochure
. an announcement on the ICRC Website.
3. REGISTRATION
Once the registration form has been received, a complete registration packet willbe sent to the applicant, requesting full details concerning his or her training,experience in the field, and motives for taking the course.
These registration packets will provide the basis for selecting the 25 applicantswho will participate in the course.
4. SELECTION CRITERIA
Selection is based on:
. academic training
HELP/SOS: ORGANIZATION OF THE COURSE760

. experience in emergency operations
. future responsibilities in the field of emergency relief
. association with areas and countries where humanitarian aid operations aretaking place.
Consideration will also be given to the balance between the countries representedin the course, particularly the balance between industrialized countries anddeveloping countries.
Once the participants have been chosen, each applicant will be informed, andthose accepted will be asked to confirm their participation. Some of those notaccepted will be put on a waiting list, to take the places of candidates who areultimately unable to participate.
ORGANIZATION OF THE COURSE 761

763
COURSE REGISTRATIONAPPLICATION FORM(Last page of the brochure)
REGISTRATION(Write in capital letters)
Last name: ________________________________________________________________
First name: ________________________________________________________________
Occupation: _______________________________________________________________
Institutional affiliation: ___________________________________________________
Address: ___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
___________________________________________________________________
Fax: ________________________________________________________________________
Nationality: ________________________________________________________________
Once this form has been received, a completeregistration packet, which will serve
as the basis for the selection of participants, will be sent.Registration forms should be sent to:
International Committee of the Red CrossH.E.L.P. 99 --- Geneva19, avenue de la PaixCH-1202 Geneva
Tel.: +41-22-730-2223Fax: +41-22-733-9674
E-mail: [email protected]
HELP/SOS: ORGANIZATION OF THE COURSE762
H.E.L.P. Course19, avenue de la Paix
CH-1202 Geneva
Tel.: +41-22-730-2689Fax:+41-22-733-2057

REGISTRATION PACKET(Page 1)
REGISTRATION H.E.L.P. 99 --- GENEVA(Write in capital letters)
Last name: ________________________ First name: ________________________
Birth date: _______ /_______ / _______day month year
Sex: M q F q
Nationality: ________________________________________________________________
Address: ___________________________________________________________________
___________________________________________________________________
Fax: ______________________________ Tel.: __________________________________
E-mail: _____________________________________________________________________
Employer’s address: _____________________________________________________
___________________________________________________________________
___________________________________________________________________
Sponsor/Registration fees will be paid by: ___________________________
______________________________________________________________________________
______________________________________________________________________________
Fluency in French:Excellent Good Satisfactory Poor
q q q q
PHOTO
ORGANIZATION OF THE COURSE 763
765
REGISTRATION PACKET(Page 2)
Academic record:
(List your diplomas in medical and health-related disciplines,as well as training courses taken, in chronological order.)
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Professional experience:
(Give a brief account of any professional experience relevant to thecurriculum of this course, beginning with the most recent.)
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Reasons for taking this course:
(Explain briefly what you expect to gain from this course and whatyou intend to do after completing it.)
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
HELP/SOS: ORGANIZATION OF THE COURSE764

REGISTRATION PACKET(Page 3)
Describe the field experience that best shows the kind of activity inwhich you have been involved.
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
This form must be supplemented by letters of reference from twopeople with whom you have worked. (These references may besent separately.)
Date: _______ /_______ / _______ Signature: _________________________
day month year
Participants will be selected two months before the beginning ofthe course. However, late applications will be considered as spaceallows.
Thank you for sending this packet to:
International Committee of the Red Cross19, avenue de la PaixCH-1202 GenevaFax: ++41 22 733 96 74E-mail: [email protected]
ORGANIZATION OF THE COURSE 765
H.E.L.P. Course19, avenue de la PaixCH-1202 GenevaFax: ++41 22 733 [email protected]

767
COURSE ADMINISTRATION
1. CENTRE
This course is best conducted in residence in order to facilitate group workoutside of ‘‘working hours’’.
2. LOCATION
The course should be held in premises large enough for five groups to workseparately. Equipment should be checked for proper functioning: video,computer, slide projector, etc.
3. EQUIPMENT
A list of standard equipment for the course is annexed, and can be adapted asneeded. One point should be noted in particular: Web access has proven useful,since it givesparticipants contactwith specialistsoutside thecourse centre, and thepossibilityofasking specificquestionsandreceivinganswers throughthe Internet.
Equipment should include an overhead projector, VCR, slide projector,computer, and printer.
4. INSTRUCTORS
The instructors’ role is to:
. help participants acquire the necessary skills for resolving health problems inemergency situations—for example:
. defining nutritional needs
. defining a food supply chain
. establishing the link between environment and health.
. help participants resolve the health problems presented in the simulation:
. analysing food strategy
. participating in the development of a water supply system
. commenting on programmes for the control of communicable diseases
. assessing the categorization of wounded.
. describe and discuss their own experiences and those of the participants.
HELP/SOS: ORGANIZATION OF THE COURSE766
Instructors must have in-depth knowledge and sound experience, but ‘‘primadonna’’ types who see the course as a forum in which to show off should beavoided.
A good instructor will be on hand to assist participants during group work andwill be capable, during plenary sessions, of accurately summarizing the materialand providing examples of similar problems experienced in the field—withoutlaunching into ex cathedra lectures.
5. WORK GROUPS
The 25 participants in the course will be divided into five groups of five peopleeach. Efforts should be made to achieve a homogeneous distribution of peopleamong the groups, based on:
. participant profile: there should not be one group of doctors, one group ofnurses, etc.
. participants’ national origin: nationalities should be mixed.
. institutional affiliation: there should not be an ICRC group, a UNHCRgroup, etc.
The group dynamic establishes itself fairly quickly, usually by the second day,when the participants have grasped the instructionmethod used, are beginning tomaster the simulation exercise, and are getting to know one other. Since theparticipants come from very diverse backgrounds, expression of all opinionsshould be encouraged. The work group must be able to reach conclusionsacceptable to all its members, but should be given the opportunity to air anydifferences or disputes during the plenary session.
Unless the groups are seriously dysfunctional, their composition should not bealtered during the course.
6. USE OF THE SIMULATION EXERCISE
Generally speaking, the simulation exercise involves a mixed population ofrefugees, displaced persons, and local residents presenting the usual medicalproblems encountered in disaster situations.
The data bank contains general information on the situation:
. a description of the political background
. economic and social conditions in the country
. a description of the country’s infrastructure
ORGANIZATION OF THE COURSE 767

769
. talks with national and local leaders
. maps.
The advantage of a single simulation is that it allows participants to work with asituation presenting all the complexity of real life, whereas short case historiesdealing with individual aspects of an emergency tend to restrict the possibilitiesfor interaction between all the different parameters involved in this kind ofsituation.
The instructors must study the simulation exercise before the course begins.Depending on the way the group work develops, they may wish to includeadditional information.
7. USE OF TIME
The course lasts three weeks. An attempt is made to give equal time to thedifferent modules, while maintaining enough flexibility to devote extra attention
!5
!5
!5
25
!5
!5
WORK GROUPS
The internal dynamic of each group and the interactionbetween the groups depend on a balanced distribution ofparticipants according to:
. Profession
. Experience
. Institutional affiliation
HELP/SOS: ORGANIZATION OF THE COURSE768

to subjects of special interest to the participants. A certain degree of schedulingmay be necessary if guest instructors are to take part, but within each module thetimetable should remain very flexible, with changes always possible.
When the course is organized on a residential basis, the participants should havethe option of working outside set hours. In general, the work groups meet tostudy the simulation exercise in detail and to prepare the report they will submitat the end of the course. This means that the classrooms must be availablepractically around the clock.
To break the monotony that may set in after a week and a half or so, effortsshould be made to offer activities outside the classroom. For example, it issometimes possible to organize such field trips as:
. a visit to the scene of a disaster (volcano in the Philippines)
. a visit to a camp for displaced persons.
POSSIBLE TIMETABLE
MONDAY TUESDAY WEDNESDAY THURSDAY
Week 1 19 April 20 April 21 April 22 April
Management Introduction Food and Water and
basics to the nutrition shelter
simulation
exercise
Food and
nutrition
Week 2 26 April 27 April 28 April 29 April
Communicable Communicable Health care Health care
diseases diseases services services
Week 3 3 May 4 May 5 May 6 May
Epidemiology Epidemiology Introduction Coordination
to international
Surveillance Surveillance humanitarian law Ethics
ORGANIZATION OF THE COURSE 769

771
8. REFERENCE MATERIAL
To help participants solve problems, a variety of referencematerials will be madeavailable.
. Dispatch of reference materials before the course:
Although logical, in practice this has not proved very effective. Most of theapplicants who are sent a series of documents to read before the coursebegins do not look at them. In their defence, it must be said that most ofthem have extensive professional commitments that do not leave themmuch time to prepare for the course.
. Materials on hand during the course:
A great deal of literature is available on health care in emergency situations.It can be classified as follows:
. basic textbook: War and Public Health (ICRC)
. reference materials:
. the most commonly used general manuals, such as:
? Assisting in Emergencies (UNICEF)
? Handbook for Emergencies (UNHCR)
. specialized manuals, such as:
? War Surgery (ICRC)
? Manual of Epidemiology for District Health Management(J.P. Vaughan and R.H. Morrow)
. professional journals: many journals regularly publish articles ofrelevance to this course, such as:
? Disasters
? The Lancet
? Bulletin of the World Health Organization
? Health Planning and Policy
. audiovisual materials:
Videos and slide presentations are increasingly popular. Some materialsof this kind will be available to participants for viewing during ‘‘offhours’’, while others can be used for the subject summaries presented atthe end of the plenary assemblies. Nevertheless, some effort should bemade to keep the course from turning into a film festival.
HELP/SOS: ORGANIZATION OF THE COURSE770

MATERIAL
. 25 name tags
. 25 folders
. 25 binders
. 30 note pads
. 30 pens
. 30 pencils with erasers
. 25 highlighters (fluorescentyellow)
. 5 rolls of scotch tape withdispensers
. 3 rolls of double-sided tape
. 5 calculators
. 5 pairs of scissors
. 5 rulers
. 2 staplers and extra staples
. 1 staple remover
. 2 paper punches, one large
. 2 pencil sharpeners
. 25 plastic sheet protectors
. 25 black markers
. 5 four-colour sets of markers forwhiteboards
. 1 box of large paper clips
. 1 bottle of liquid white-out
. 3 boxes of transparencies
. 3 sets of markers for theoverhead projector
. 10 boxes of diskettes(for EPIINFO)
. 1 French-English dictionary
. 1 telephone directory
. 1 list of ICRC internal telephonenumbers
. 1 roll of ICRC tape
. 1 box of rubber bands
. 25 ICRC plastic bags
. 1 ICRC stamp and red ink pad
ORGANIZATION OF THE COURSE 771

773
COURSE EVALUATION
1. COURSE EVALUATION BY PARTICIPANTS
The course must be evaluated to determine whether the content, teachingmethod, reference material, and instructors have met the participants’expectations.
At the end of each module, an evaluation form will be passed out to theparticipants so that they can evaluate and comment on that module. Thesebatches of formswill subsequently be analysedmodule bymodule, and at the endof the course, all the comments will be compiled to obtain an overall participantevaluation of the course.
A more detailed form will also be distributed at the end of the course to find outwhether:
. the overall length of the course is satisfactory
. the allocation of hours among the modules is appropriate
. the choice of a single simulation meets participants’ expectations
. the teaching staff is satisfactory (active participation, experience, etc.).
2. EVALUATION OF SKILLS LEARNED BY THE PARTICIPANTS
The participants’ achievements are evaluated in three ways:
. A test comprising 100 multiple-choice questions is administered at thebeginning and at the end of the course to determine what the participantshave learned.
. Each work group is asked to write a complete report on the simulation, inwhich the participants must:
. identify health problems
. establish priorities and objectives
. plan programmes, including an evaluation programme.
This report will demonstrate the participants’ ability to sum up an emergencysituation and propose ways of responding to it.
. Finally, the participants will be asked to write a dissertation on a missioncarried out after the course. This report should reflect the use of some of the
HELP/SOS: ORGANIZATION OF THE COURSE772

planning techniques taught by the course. If possible, arrangements may bemade with the cosponsoring university to recognize this work with theconferral of a diploma, if the dissertation meets the necessary standards. Thework will be evaluated according to the following criteria:
. It should be based on work carried out after the course.
. It should show the application of the skills taught in the course: planning andepidemiological methods.
. It should present results analytically.
. It should include elements of discussion.
. It should include a relevant bibliography.
ORGANIZATION OF THE COURSE 773

CONCLUSION
In developing the HELP/SOS course, we have tried to be as thorough as possiblewith respect to content, and as effective as possible with respect to teachingmethods.
Time will tell the true value of this instruction, after enough participants havehad the opportunity to test their knowledge in real field conditions. For thisreason, it is essential to maintain contact with graduates of the course, so thatthey can share their experiences for the enrichment of the course.
Another way of enhancing the course is to reinforce the links existing between theoperational agencies and the university sphere. The health problems that must bemanaged in emergency situations have increasingly complex interactions, andsometimes require carefully worked out technical solutions that the universitiescan help to identify.
The content of the course and the teaching method are systematically reviewedevery two years by a scientific council comprising the coordinators of the course(ICRC and academic bodies), field staff, and experts representing the ICRC,academic bodies and humanitarian agencies.
HELP/SOS: ORGANIZATION OF THE COURSE774

BIBLIOGRAPHY
PUBLIC HEALTH
BRAVEMAN P. A., TARIMO E., Screening in primary health care, WHO, Geneva, 1994.
FORBES Martin S., Refugee women, Zed Book Ltd., 1991.
GUILBERT J. J.,Educational handbook for health personnel,WHO,Geneva, revised and updated,1998.
KATZ F. M., SNOW R., Assessing health workers’ performances, WHO, Geneva, 1980.
MSF, Refugee health: An approach to emergency situations, 1997.
NOJI Eric, The public health consequences of disasters, Oxford University Press, 1997. ‘‘Publichealth impact of Rwanda refugee crisis: What happened in Goma, Zaire, in July 1994?’’, The
Lancet, 1995, 345: 339-344.
PALMERCelia, ‘‘Reproductive health for displaced populations in emergencies’’, RRNNetworkPaper, 1998.
PERRIN Pierre, War and public health, Handbook on war and public health, ICRC, 1996.
PROTHERO M. R., ‘‘Forced movements of population and health hazards in tropical Africa’’,International Journal of Epidemiology, 1994, 23: 657-664.
SIMMONDS S., VAUGHAN P., GUNN W., Refugee community health care, Oxford UniversityPress, 1986.
SUMMERFIELD Derek, ‘‘The impact of war and atrocity on civilian populations: Basic
principles for NGO interventions and a critique of psychosocial trauma projects’’, ODI, NetworkPaper, 1995.
TELFORD John, ‘‘Counting and identification of beneficiary populations in emergency
operations: Registration and its alternatives’’, RRN Good Practice Review, September 1997.
UNHCR, Reproductive health in refugee situations: An inter-agency field manual, Geneva, 1995.
UNICEF, Assisting in emergencies, 1986.
WHO, The community health worker: Working guide, Geneva, 1987.
Mental health of refugees, 1996.
PLANNING
CHALINDERAndrew, ‘‘Temporary human settlement planning for displaced populations’’,RRNGood Practice Review, No. 6, January 1998.
REINKE W. A., Health planning, qualitative aspects and quantitative techniques, John HopkinsUniversity School of Hygiene and Public Health, Baltimore, 1972.

777
FOOD & NUTRITION
BEGHIN I., CAP M., DUJARDIN B., A guide to nutritional assessment, WHO, Geneva 1988.
BOUDREAU Tanya, ‘‘The food economy approach: A framework for understanding rurallivelihoods’’, RRN Network Paper No. 26, May 1998.
CDC, ‘‘Famine-affected, refugee, and displaced populations: Recommendations for public health
issues’’, MMWR, 24 July 1992, Vol. 41, No. RR-13.
CEKAN J., ‘‘Seasonal coping strategies in central Mali: Five villages during the ‘Soudure’’’,Disasters, Vol. 16-1: 66-73.
CEKAN Jindra, MacNEIL Amy, LOEGERING Steve, ‘‘Monetisation: Linkage to food security’’,ODI Network Paper No. 17, November 1996.
DeMAYER E. M., Preventing and controlling iron deficiency anaemia through primary health care,
WHO, Geneva, 1989.
HARRISON G. A., Famine, Oxford University Press, 1988.
ILSI (International Life Sciences Institute), Nutrition Foundation, Washington, 1990.
JASPARS Susanne, YOUNG Helen, ‘‘General food distribution in emergencies from nutritionalneeds to political priorities’’, ODI, Good Practice Review, No. 3, 1996.
MACFARLANES.B. J., ‘‘Error in calculatingweight-for-height’’,Disasters,Vol. 19,No. 1; 37-49.
MESFIN W. M., Rural vulnerability to famine in Ethiopia: 1958-1977, Vikas, 1984.
MOUREY A., Food security in armed conflicts: The ICRC’s approach and experience,November 1996.
MSF, Nutrition guidelines, 1st Edition, 1995.
OXFAM, Practical guide to selective feeding programmes, 1984.
RAHMATO D., ‘‘Peasant survival strategies in Ethiopia’’, Disasters, Vol. 12-4: 326-344.
Household Food Economy Analysis, Kakuma Refugee Camp, Kenya, Save the Children Fund,UK: 1-4.
‘‘Assessments of mortality, morbidity and nutritional status in Somalia during the 1991-92famine’’, JAMA, 1994, 272: 371-376.
‘‘Acute malnutrition and high childhood mortality related to diarrhea: Lessons from the 1991
Kurdish refugee crisis’’, JAMA, 1993, 270: 587-590.
‘‘Is mid-upper-arm circumference a useful tool for screeening in emergency settings?’’, The Lancet,1995, 245: 631-633.
‘‘Access to basic food supplies’’, in UNICEF, Assisting in emergencies, pp. 163-176.
‘‘A case study of Somali refugees in Hartisheik camp, eastern Ethiopia: Health and nutrition
profile, July 1988-June 1990’’, Journal of Refugee Studies, 1992, 5: 313-326.
‘‘Famine-affected populations’’, MMWR RR-13, pp. 3-16, 44-50.
‘‘Factors associated with anemia in refugee children’’, J. Nutrition, 1997; 127: 2194-98.
‘‘The need for adult therapeutic care in emergency feeding programs’’, JAMA, 1993.
‘‘Impact of food delays on refugees’’, Field Exchange, 1997; 2: 10-11.
HELP/SOS: BIBLIOGRAPHY776

‘‘Supplementary feeding programme: Current guidelines’’, Field Exchange, 1997, 2: 10-11.
‘‘Treatment of severe child malnutrition in refugee camps’’, European Journal of Clinical Nutrition,1993, 47: 750-754.
REED B. A., HABICHT J. P., ‘‘Sales of food aid as sign of distress, not excess’’, The Lancet 1998,
351: 128-130.
REFUGEE POLICY GROUP, Mitigating micronutrient malnutrition in humanitarian crises,June 1995.
SEN Amartya, Poverty and famines. An essay on entitlement and deprivation, Clarendon PressOxford.
SHOHAM J., CLAY E., ‘‘The role of socio-economic data in food needs assessment and
monitoring’’, Disasters, Vol. 13-1: 44-72.
STEPHENSON R. S., ROMANOVSKY P. C., ‘‘Problems of beneficiary registration in foodemergency operations’’, Disasters, 1987 (11/03); 163-172.
SUERTENS C., DEDEURWAERDER M., ‘‘Food availability in the refugee camp of Kahindo,Goma, Zaire, November 1994’’, MSF-B Medical News, 1994, Vol. 3-5: 16-22.
WHO,Management of severe malnutrition: Amanual for physicians and other senior health workers,
Geneva, 1999.
YOUNGH., JASPAR S., ‘‘Nutrition, disease and death in times of famine’’,Disasters, 1995, 19-2:94-109.
‘‘Nutritional assessments, food security and famine’’, Disasters, 1995, 19-1: 26-36.
WATER AND SANITATION
CAIMCROSS S., FEACHEM R., Environmental health engineering in the tropics, Wiley, 1993.
CHALINDER A., ‘‘Water and sanitation in emergencies’’, ODI — RRN Good Practice Review,No. 1, June 1994.
DAVIS J., LAMBERT R., Engineering in emergencies — A practical guide for relief workers,IT Publications, 1995.
MICUTA W., Modern stoves for all, Bellerice Foundation, 1985.
MSF, Public health engineering in emergency situation, First Edition, 1994.
NEMBRINI P. G., CONTI R., ‘‘Water for Mogadishu: Water supply in a war-torn town’’, Bull.
Appl. Geol., 2/2 December. 1997, 151-165.
ROBERTS L., CHARTIER Y., MALENGA G., TOOLE M., ROLKA H., Keeping clean waterclean in a Malawi refugee camp: A randomized intervention trial, CDC Atlanta, 1995.
THOMSON M. C., ‘‘Disease prevention through vector control’’, OXFAM Practical HealthGuide No. 10, 1995.
UNHCR, Handbook on the use of disinfection in refugee situations, Geneva, 1997.
Vector and pest control in refugee situations, Geneva, April 1997.
Water manual for refugees’ situations, Geneva, 1992.
BIBLIOGRAPHY 777

779
COMMUNICABLE DISEASES
BISEG., CONINXR., ‘‘Epidemic typhus in a prison in Burundi’’,Transaction of the Royal Societyof Tropical Medicine and Hygiene, 1997, 91: 133-134.
BRES P., Public health action in emergencies caused by epidemics, WHO, Geneva, 1986.
CONINX R., DUPUY C., HERMANN C., CRUZ PIRES RIBEIRO G., MARGOT M.,
LUCIC K., ‘‘Vaccination of the civilian population in a country atwar: It can be done; it can also beevaluated. The ICRCexperience inMozambique’’, Journal of Tropical Pediatrics, 1998,Vol 00; 1-3.
ELIAS C. J., ALEXANDER B. H., SOKLY T., ‘‘Infectious disease control in a long-term refugeecamp: The role of epidemiologic surveillance and investigation’’, American Journal of PublicHealth, 1990, Vol. 80, No. 7, 824-828.
HAELTERMAN E., BOELAERTM., SUETENS C., BLOK L., HENKENSM., TOOLEM. J.,
‘‘Impact of a mass vaccination campaign against a meningitis epidemic in a refugee camp’’,
Tropical Medicine and International Health, 1996, Vol. 1, No. 3: 385-392.
HALLAM A., ‘‘Evaluating humanitarian assistance programmes in complex emergencies’’, RRN
Good Practice Review, No. 7, September 1998.
ICRC/WHO, Guidelines for the control of tuberculosis in prisons, Geneva, 1998.
KESSLER C., CONNOLLY M., LEVY M., CHAULET P., Tuberculosis control in refugees and
displaced persons, WHO/TB/1996, 209.
PAWLOWSKI Z. S., SCHAD G. A., STOTT G. J., Hookworm infection and anemia, WHO,
Geneva, 1991.
SIDDIQUE A. K., AKRAMK., ZAMAN K., MUTSUDDY P., EUSOF A., SACK R. B., ‘‘Vibrio
cholerae 0139: How great is the threat of a pandemic?’’, Tropical Medicine and InternationalHealth, 1996, Vol. 1, No. 3: 393-398.
VARAINE F., CAUGANT D. A., RIOU J. Y., KONDE K., SOGA G., NSHIMIRIMANA D.,
MUHIRWA G., OTT D., HØIBY E. A., FERMON F., MOREN A., ‘‘Meningitis outbreaks andvaccination strategy’’, Transactions of the Royal Society of Tropical Medicine and Hygiene, 1997,
91: 3-7.
VEEKEN H., RITMEIJER K., HAUSMAN B., ‘‘Priority during a meningitis epidemic:
Vaccination or treatment?’’, WHO Bulletin, 1998, Vol. 76: 135-141.
WHO, Guidelines for cholera control.
Guidelines for the management of drug-resistant tuberculosis, Geneva, 1997.
Guidelines for the management of drug-resistant tuberculosis, Geneva, 1998.
Immunization policy, WHO/EPI/GEN/95. 03, Rev. 1.
Malaria control among refugees and displaced populations.
Parasitic diseases in water resources development. The need for intersectoral negotiation, Geneva,1993.
The management of bloody diarrhoea in young children, WHO/CDD/1994. 49.
‘‘Why treatment centres failed to prevent cholera deaths among Rwandan refugees in Goma,Zaire’’, The Lancet, 1995, 345: 359-361.
HELP/SOS: BIBLIOGRAPHY778

Tuberculosis control in refugee situations, Geneva, 1997.
YODER P. S., HORNIK R. C., ‘‘Symptoms and perceived severity of illness as predictiveof treatment for diarrhea in six Asian and African sites’’, Soc. Sci. Med., 1996, Vol. 43, No. 4:
429-439.
MEDICAL AND SURGICAL CARE
AMELOOT L., ‘‘About the stress management’’, MSF-B Contact 55, 1998: 9-13.
BERCKMANS P., DAWANS V., SCHMETS G., VANDENBERGH D., AUTIER P.,
‘‘Inappropriate drug-donation practices in Bosnia and Herzegovina, 1992 to 1996’’, The NewEngland Journal of Medicine, 1997, Vol. 337, No. 25: 1842-1845.
BOWYER G.,W., ‘‘Afghan war-wounded: Application of the Red Cross wound classification’’,The Journal of Trauma, 1995, Vol. 38(1): 64-67.
BOWYERG.W., STEWARTM. P.M., RYAN J.M., ‘‘Gulf war wounds: Application of the RedCross wound classification’’, Injury, 1993, 24(9): 597-600.
BURKLE F. M., Disaster medicine, Medical Examination Publishing Co., Inc., 1984.
COUPLAND R. M., The Red Cross wound classification, ICRC, Geneva, 1991.
‘‘Hand grenade injuries among civilians’’, JAMA, 1993, 270: 24-626.
‘‘The effects of weapons: Surgical challenge andmedical dilemma’’, Journal of the Royal College ofSurgeons of Edinburgh, 1996, 41: 65-71.
Amputation for war wounds, ICRC, Geneva, 1992.
War wounds of limbs: Surgical management, Butterworth-Heinemann, Oxford, 1993.
‘‘Weapons intended to blind’’ (Editorial), The Lancet, 17 December 1994, Vol. 344: 1649-1650.
COUPLAND R. M., HOIKKA V., SJOEKLINT O. G., CUENOD P., CAUDERAY G. C.,
DOSWALD-BECK L., ‘‘Assessment of bullet disruption in armed conflicts’’, The Lancet,4 January 1992, 339: 35-37.
COUPLANDR.M., PARKERP. J., GRAYR. C., ‘‘Triage of war wounded: The experience of theInternational Committee of the Red Cross’’, Injury, 1992, 23(8): 507-510.
CRAIG G., ‘‘Treating the Afghan war-wounded’’, Journal of the Royal Society of Medicine, 1993,Vol. 86: 404-405.
ESSEX B. J., ‘‘Diagnostic pathways in clinical medicine’’, Medicine in the Tropics, ChurchillLivingstone, 1980.
HAYWARD-KARLSSON J., JEFFERY S., KERR A., SCHMIDTH.,Hospital for war-wounded
—A practical guide for setting up and running a surgical hospital in an area of armed conflict, ICRC,1998.
JEFFERY S. J., ‘‘Antipersonnel mines: Who are the victims?’’, J Accid Emerg Med; 1996, 13:343-346.
KLECZKOWSKI B.M., PIBOULEAUR.,Approaches to planning and design of health facilities indeveloping areas, Volume 1, Offset Publication No. 29, WHO, Geneva, 1976.
BIBLIOGRAPHY 779
781
Approaches to planning and design of health facilities in developing areas, Volume 2, Offset
Publication No. 37, WHO, Geneva, 1977.
Approaches to planning and design of health facilities in developing areas, Volume 3, Offset
Publication No. 45, WHO, Geneva, 1979.
Approaches to planning and design of health facilities in developing areas, Volume 4, OffsetPublication No. 72, WHO, Geneva, 1983.
Housing Research and Development Unit, University of Nairobi, Design for medical buildings —A manual for the planning and building of health care facilities under conditions of limited resources,Nairobi, 1988.
MSF, Clinical guidelines, diagnostic and treatment manual, 4th Ed., 1999.
PAINE L. H. W., SIEM TJAM F., Hospitals and the health care revolution, WHO, Geneva 1988.
ROWLEY D. I., War wounds with fractures: A guide to surgical management, ICRC, 1996.
WHO, District hospitals: Guidelines for development, Geneva, 1992.
Guidelines for the management of hospital outpatient services, Government of Kenya, Ministry ofHealth, 1982.
Guidelines for drug donations, revised, 1999.
The new emergency health kit.
The use of essential drugs, Geneva, 1998.
The hospital in rural and urban districts, Geneva, 1992.
THE HEALTH CARE SYSTEM
AMONOO-LARTSONR., EBRAHIMG. J., LOVELH. J., RANKENJ. P. ,District health care.Challenges for planning, organisation and evaluation in developing countries,MacMillan Press, 1984.
CRIEL B., MACQ J., BOSSYNS P., HONGORO C., ‘‘A coverage plan for health centres inMurewa district in Zimbabwe: An example of action research’’, Tropical Medicine and
International Health, 1996, Vol. 1, No. 5: 699-709.
GOYENSP., PORIGNOND., SORONGANEE.M., TONGLETR., HENNARTP., VISH. L.,
‘‘Humanitarian aid and health services in eastern Kivu, Zaire: Collaboration or competition?’’,Journal of Refugee Studies, 1996, Vol. 9, No. 3: 268-280.
WHO, Health system decentralization: Concepts, issues and country experience, Geneva, 1990.
The role of the hospital in the district: Delivering or supporting primary health care, Geneva, 1990.
EPIDEMIOLOGY
LWANGA S. K., CHO-YOOK TYE, Teaching health statistics, WHO, Geneva, 1986.
MITCHELL J., SLIM H., ‘‘Listening to rural people in Africa: The semi-structured interview inrapid rural appraisal’’, Disasters, Vol. 15, No. 1; 68-72.
MOREN A. et al., ‘‘Practical field epidemiology to investigate a cholera outbreak in a
Mozambican refugee camp in Malawi, 1988’’, Journal of Tropical Medicine and Hygiene, 1991,94: 1-7.
HELP/SOS: BIBLIOGRAPHY780

‘‘Infectious disease surveillance during emergency relief to Buthanese refugees in Nepal’’, JAMA,
1994; 272: 377-381.
‘‘Morbidity and mortality surveillance in Rwandan refugees–Burundi and Zaire, 1994’’,MMWR,1996; 45: 104.
‘‘Surveillance and control of meningococcal meningitis epidemics in refugee populations’’, WHOBulletin, 1990, 58: 587-596.
PAGE R., TIMMRECK T., Basic epidemiological methods and biostatistics: A practical handbook,
Ed. Jones and Bartlett, London, 1995.
WARDPatrick, RIMMERMartin, ‘‘Cibler les pauvres dans le nord de l’Irak: Le role desmethodesde recherche formelles et informelles dans les operations d’aide d’urgence’’, ODI, Dossier
Thematique No. 8, April 1995.
EMERGENCIES AND DEVELOPMENT
HENDRICKSONDylan, ‘‘Humanitarian action in protraced crises: The new relief agenda and itslimits’’, ODI, RRN Network Paper No. 25, April 1998.
ICRC, Beyond survival: Agricultural and veterinary rehabilitation.
MacNAIR Rebecca, ‘‘Room for improvement: The management and support of relief workers’’,ODI, RRN Network Paper No. 10, September 1995.
MACRAE Joanna, ‘‘Dilemmas of post-conflict transition: Lessons from the health sector’’, ODI,
RRN Network Paper No. 12, September 1995.
SHARP Kay, ‘‘Between relief and development: Targeting food aid for disaster prevention inEthiopia’’, ODI, RRN Network Paper No. 27, September 1998.
INTERNATIONAL HUMANITARIAN LAW
BACCINO-STRADA A., Manual on the rights and duties of medical personnel in armed conflicts,
ICRC, 1982.
BAUDET-SAULNIER F., Dictionnaire pratique du droit humanitaire, La Decouverte, 1998.
DUNANT Henry, A memory of Solferino, ICRC, 1986.
ICRC, Answers to your questions, Geneva, 1997.
Banning anti-personnel mines: The Ottawa treaty explained, ICRC, 1997.
Getting to know the ICRC, Geneva, 1997.
‘‘Internally displaced persons’’, Geneva Symposium, 23-25 October 1995.
‘‘International humanitarian law and protection’’, Report of the workshop, Geneva, 18-
29 November 1986.
‘‘Protection towards professional standards’’, Report of the workshop,Geneva, 17-19 March 1998.
Rules for behaviour in combat, ICRC, 1985.
Summary of the Geneva Conventions of 12 August 1949 and their Additional Protocols.
The Additional Protocols to the Geneva Conventions of 12 August 1949, 1977.
BIBLIOGRAPHY 781

783
The emblem.
The fundamental principles of the Red Cross and Red Crescent, Geneva, 1996.
The Geneva Conventions of 12 August 1949.
The SIrUS Project, Geneva, 1997.
VON FLUE C., LAVOYER J. P., ‘‘Comment les ONG peuvent-elles contribuer a promouvoir ledroit humanitaire international?’’, RRN/ODI Journal, 1997.
ARMED CONFLICTS
BAUWENS W., REYCHLER L., The art of conflict prevention, Brassey’s, 1994.
BOUTROS Boutros Ghali, An agenda for peace, United Nations, 1992.
DUFFIELD M., ‘‘War and famine in Africa’’, OXFAM Research Paper No. 5, 1991.
MACRAE J., ZWI A., FORSYTHE V., Post-conflict rehabilitation: Preliminary issue forconsideration by the health sector, London School of Hygiene and Tropical Medicine, Departmentof Public Health, 1996.
PERRIN Pierre, ‘‘Effects of conflicts and security crisis on humanitarian actions’’, Final report ofthe research project on a study on the health and prospective medical assistance for affected persons,
Tokyo, 1996.
‘‘Impact de l’assistance humanitaire sur l’evolution des conflit’’, Revue Internationale de la Croix-Rouge, No. 830, June 1998, pp. 343-358.
INTERNATIONAL RELATIONS
DEWITT D., HAGLUND D., KIRTON J., Building a new global order, Oxford University Press,1993.
COORDINATION
BENNETT J., NGO coordination at field level, ICVA, 1994.
ODI, ‘‘Recent changes in the international relief system’’, Briefing Paper, January 1993, 1-4.
VAN BRABANT Konenrad, ‘‘The coordination of humanitarian action: The case of Sri Lanka’’,
RRN Network Paper No. 23, December 1997.
ETHICS
FORSYTHED., ‘‘Choicemore ethical than legal: The International Committee of theRedCross’’,
Ethics & International Affairs, Vol. 7, 1993.
MACRAE J., ‘‘The origins of unease: Setting the context of current ethical debate’’, Background
paper for the Forum on Ethics and Humanitarian Aid, Dublin, 9 September 1996.
MINEAR L., WEISS T., Principes humanitaires et dilemmes lors des operations en zones de conflitsarmes, UNDP-DHA, 1994.
HELP/SOS: BIBLIOGRAPHY782

Humanitarian charter and minimum standards in disaster response, Sphere Project, International
Federation of Red Cross and Red Crescent Societies, Geneva, 1998.
Code of conduct for the International Red Cross and Red Crescent Movement and non-governmentalorganizations (NGOs) in disaster relief.
SLIM H., ‘‘Doing the right thing: Relief agencies, moral dilemmas and moral responsability inpolitical emergencies and war’’, Studies on emergencies and disaster relief, 1997.
GENERAL
CAHILLK.,A framework for survival: Health human rights and humanitarian assistance in conflictsand disasters, 1993.
‘‘Civilians in war’’, XXVIth International Conference of the Red Cross and Red Crescent, 1995.
CRAMER M., The true cost of conflict, Earthscan Publications, 1994.
‘‘Humanitarian aid to Somalia’’, Evaluation report, Netherlands Development Cooperation,
1994.
The international response to conflict and genocide: Lessons from the Rwanda experience, Joint
Evaluation of Emergency Assistance to Rwanda, March 1996.
ICRC, Landmines must be stopped!, Geneva, 1999 1998.
ICRC action on behalf of prisoners, Geneva, May 1998.
‘‘Humanitarian values and response to crisis’’, XXVIth International Conference of the Red Crossand Red Crescent, 1995.
ZOLBERG A. R., SUHRKE A., AGUAYO S., Escape from violence, conflict and the refugee crisisin the developing world, Oxford University Press, 1989.
BIBLIOGRAPHY 783

MISSION
The International Committee of the Red Cross (ICRC) is an
impartial, neutral and independent organization whose
exclusively humanitarian mission is to protect the lives and
dignity of victims of war and internal violence and to provide
them with assistance. It directs and coordinates the
international relief activities conducted by the Movement in
situations of conflict. It also endeavours to prevent suffering
by promoting and strengthening humanitarian law and
universal humanitarian principles. Established in 1863, the
ICRC is at the origin of the International Red Cross and Red
Crescent Movement.