Health Reforms in Rajasthan: An Empirical Study on Agencification
22
Health Reforms in Rajasthan: An Empirical Study on Agencification Avantika Singh* Abstract Agencification, or the carving out of independent agencies from the government, is a New Public Management approach for restructuring government through separation of the policy formulation and policy implementation functions. This research is devoted to an empirical investigation of agencification in the public health system of the State of Rajasthan in India. The objective of this research is to make a meaningful contribution to the understanding of the rationale for agencification, composition of agencies, autonomy and control of agencies, and service delivery by agencies. This research employs organisation theory perspectives such as interorganisational relations to explicate mechanisms for achieving functional integration and coordination between agencies and parent departments. Agencies studied in this research are legally independent bodies with not-for-profit status, which function within the policy framework provided by the parent ministry/department. However, there is no explicit performance contracting and accountability for results, and the idea of agencies is path dependent and linked to the reforms process. Because of resource dependence, agencies achieve functional integration with the parent ministry/department. Most of the agencies deliver services through a network of private providers and voluntary organisations, which establish coordination through the exchange of resources and information. Coordination is more formalised and dependent on Memorandums of Understanding (MoUs), contracts and paper-based reports than on trust, norms, reciprocity and informal communication. Introduction “Agencification”, or the disaggregation of the government through the carving out of independent “agencies” has gained currency among national governments undertaking reforms based on the New Public Management (NPM) 1 principles. Under agencification, the policy formulation function is retained by the parent ministry/department, while the policy implementation function is hived off to the agency, along with autonomy and accountability for the achievement of results. The agency either delivers public services directly or outsources the delivery of public services to providers from the private and voluntary sectors. Agencification is looked upon to “reinvent” government by making it more effective, efficient, accountable and performance-oriented. The central argument of this paper is that despite their legal independence and structural disaggregation, agencies are dependent for resources on the parent department, and that coordination is established in service delivery networks through exchange of resources and information, and that the actors in the
Transcript of Health Reforms in Rajasthan: An Empirical Study on Agencification
Health Reforms in Rajasthan: An Empirical Study on Agencification
Avantika Singh*
Abstract
Agencification, or the carving out of independent agencies from the government, is a New Public Management approach for restructuring government through separation of the policy formulation and policy implementation functions. This research is devoted to an empirical investigation of agencification in the public health system of the State of Rajasthan in India. The objective of this research is to make a meaningful contribution to the understanding of the rationale for agencification, composition of agencies, autonomy and control of agencies, and service delivery by agencies. This research employs organisation theory perspectives such as interorganisational relations to explicate mechanisms for achieving functional integration and coordination between agencies and parent departments.
Agencies studied in this research are legally independent bodies with not-for-profit status, which function within the policy framework provided by the parent ministry/department. However, there is no explicit performance contracting and accountability for results, and the idea of agencies is path dependent and linked to the reforms process. Because of resource dependence, agencies achieve functional integration with the parent ministry/department. Most of the agencies deliver services through a network of private providers and voluntary organisations, which establish coordination through the exchange of resources and information. Coordination is more formalised and dependent on Memorandums of Understanding (MoUs), contracts and paper-based reports than on trust, norms, reciprocity and informal communication.
Introduction
“Agencification”, or the disaggregation of the government through the carving out of independent “agencies” has gained currency among national governments undertaking reforms based on the New Public Management (NPM)1 principles. Under agencification, the policy formulation function is retained by the parent ministry/department, while the policy implementation function is hived off to the agency, along with autonomy and accountability for the achievement of results. The agency either delivers public services directly or outsources the delivery of public services to providers from the private and voluntary sectors. Agencification is looked upon to “reinvent” government by making it more effective, efficient, accountable and performance-oriented. The central argument of this paper is that despite their legal independence and structural disaggregation, agencies are dependent for resources on the parent department, and that coordination is established in service delivery networks through exchange of resources and information, and that the actors in the

62 - Avantika Singh
network are held together by formal mechanisms of coordination rather than by informal ones.
During the early 1990s, “health reforms” – changes in “health policy and institutional arrangements of the health sector” (WHO SEARO 1997) – were initiated in several states across India with a view to “improve the functioning and performance of the health sector and ultimately the health status of the people” (ibid.). Reform-related changes in policy and institutional arrangements include redefining the state in a steering role, and involving non-state actors in the delivery of public health services, and reforms in regulation, agencification and public-private partnerships (PPPs). This paper empirically investigates one such institutional reform, agencification, in the public health system of Rajasthan, a state in north-western India. The empirical analysis is done with respect to the rationale for agencification, autonomy and control of agencies, composition of agencies, mechanisms to achieve functional integration between agencies and their parent ministry/department, service delivery by agencies, and coordination among agencies, parent ministry/department, and service providers. Perspectives from organisation theory such as interorganisational relations and coordination have also been employed to explicate the rationale for agencification and the delivery of services through networks.
Section 2 provides a brief background on the performance of the public health system in India and Rajasthan. Section 3 presents a review of the existing literature on agencification, and examines the relevance of the literature on institutional analysis and interorganisational relations in the context of agencification. In section 4, findings of the empirical analysis of agencification in the public health system of Rajasthan are discussed. In the concluding section, I move from practice to theory by drawing lessons from the agencification process in Rajasthan. I discuss the similarities and points of departure between agencification in Rajasthan and Western formulations of agencification, and derive how the present analysis of agencification advances our understanding of NPM.
The Public Health System in India and Rajasthan
India spends 5.2% of its Gross Domestic Product (GDP) on health, of which 83% is private and 17% is public health expenditure2. Since, health is a State subject3 as specified by the Constitution of India, the State governments are responsible for provision of health care services in India. 15% of the total public health expenditure is contributed by the Union government, and 85% by all the State governments combined (Ministry of Health and Family Welfare, MoHFW 2005a). Traditionally, however, the Union Ministry of Health & Family Welfare (MoHFW), Government of India (GoI), has been carrying out the

Health Reforms in Rajasthan - 63
policy formulation role, and the State governments have been responsible for provision of health services. In Rajasthan, apart from policy guidance received from MoHFW, the ministry of health at the State level with assistance from the Secretariat (staffed by bureaucrats) formulates some policies, projects, and schemes. Policy implementation is the responsibility of the line department, known the Directorate of Medical & Health Services (DMHS), which is largely staffed by health professionals.
Located in the northwest of the country, Rajasthan is the largest state in India in terms of area. Rajasthan is one of the states in India with low performance on health and developmental indicators. The birth rate, total fertility rate (TFR), and infant mortality rate (IMR) in Rajasthan are higher than that for the entire country4. While the topography of Rajasthan (almost two-thirds of the State is either desert or hilly) compounds the problem of physical access to healthcare, a number of factors such as high proportion of marginalised groups, low female literacy and unfavourable sex ratio5, add to the complexity of social access to healthcare.
Agencification
What are Agencies?
Agencification involves transfer of activities hitherto done by the government to agencies (Pollitt and Talbot 2004), and may be referred to as “internal structural devolution” (Christensen and Lægreid 2004, 129). Existing departments may be either hived off into agencies, or agencies may be formed as “new” organisations. Agencification has been referred to as “boutiquing” of government (Schick 2002), and agencies have been described as an “administrative fashion accessory” (Pollitt et al. 2001, 286). Most literature on agencification has emerged in OECD countries and is written in a comparative perspective (Pollitt and Talbot 2004; Talbot et al. 2000). The terms “agencification” and “agencies” have come to mean different things to various national governments and scholars (see Allix and Van Thiel 2005; Aucoin 1995; Boston et al. 1996; Halligan 2004; Roberts 1997).
A large segment of the literature deals with “signposting the zoo” (Gill 2002), i.e., the terminology to describe “agencies” and the definitional aspects of agencies (Greve et al. 1999; Pollitt 2003; Thynne 2004; Van Thiel 2000). In order to understand what an “agency” exactly is, it is important to understand what is not an agency. An agency is not a division or directorate within a ministry or department. It is neither a corporate entity with commercial purpose. While Thynne (2004) classifies agencies on the basis of legal existence, Pollitt and Talbot (2004) emphasise structural separation from the core irrespective of legal
64 - Avantika Singh
independence. Thus, an agency is an entity with some measure of structural disaggregation from the parent ministry/department (Halligan 2004; Pollitt et al. 2001; Pollitt and Talbot 2004). Autonomy (Common et al. 1992; du Gay 2004; Thynne 2004; Pollitt and Talbot 2004; Verhoest et al. 2003) coupled with performance contracting and accountability for results (Christensen and Lægreid 2004; Pollitt et al. 2001; Roberts 1997) is regarded as a defining characteristic of agencies. However an agency is not a statutorily fully independent body free from ministerial instruction. Though the ultimate control of an agency lies with the parent ministry (du Gay 2004; Pollitt and Talbot 2004), the form of control shifts from ex ante to ex post (Verhoest et al. 2004). An agency performs public tasks such as service provision, regulation, adjudication and certification (Pollitt et al. 2001), and is therefore a public organisation (Pollitt and Talbot 2004).
The literature on agencification is rather euphoric, and there is an implicit assumption that agencification can improve the effectiveness of government, and that agencification principles are universally applied (OECD 1995). However, Pollitt et al. (2001) suggest that the behaviour of agencies is context-specific because of the different political systems.
Yesilkagit (2004) has examined the separation of functions through agencification from the point of view of the principal-agent problem and transaction costs. Being disaggregated from the ministerial hierarchy, agencies are supposed to be more autonomous, innovative, adaptable, responsive and efficient. In other words, agencies are expected to function in a more business-like fashion (Halligan 2004). In the case of public hospitals, it is expected that agencification can help overcome problems such as chronic under-funding, poor HR practices and a fragmented approach to policy implementation (Yeoh 2003). In the present day dynamic environment, with the reduced ability of the government to fund welfare through taxes (Pollitt and Bouckaert 2004), the bureaucratic structure no longer suffices for government to fulfil its emergent role (Osborne and Gaebler 1992), and the agency structure is considered more appropriate for service delivery and financing (Schick 2002). Though citizens’ expectations of the quality of public services are rising (Pollitt and Bouckaert 2004), they have lost faith in the government (Gill 2002; Nye et al. 1997). Common (1998), Dolowitz and Marsh (1998), and Gill (2002) suggest that agencification is thus, an opportunity for government to regain its legitimacy. La Guerre (1994) and Levitt (1991) have described the decision to agencify as the outcome of coercion, Christensen and Lægreid (2004) have described it as an “ideological import”, and Van Thiel (2000) has described it as ad hoc. Pollitt and Talbot (2004) propose the task specific path dependency (TSPD) model, according to which two sets of factors, namely path (nature of cultural and institutional norms in a particular jurisdiction) and task specificity (nature of the
Health Reforms in Rajasthan - 65
actual work to be done), influence the spread and application of agencies. Since agencies can be governed at arm’s length from the government, agencification is also expected to “depoliticise” government (Gill 2002). To sum up, there emerge varying perspectives on the rationale for agencification in the literature, and the question on rationale for agencification is not answered firmly.
Perspectives on Interorganisational Relations and Agencies
In some cases, agencies directly deliver services to citizens, while in others, they perform a planning, financing and coordinating role, and outsource the service delivery function to private providers (PPs) and voluntary organisations6 (VOs). Therefore, it is imperative to study the interorganisational relations and coordination among agencies and service providers (PPs and VOs). The study of interorganisational relations (IOR) has been particularly applied to the delivery of social services and human services (Goes and Park 1997; Hall 2002; Provan and Milward 1995). In the field of public management, interdependence and complexity in the nature of problems necessitate extensive collaboration between various types and levels of actors (Mason 1993), thereby making networks the preferred mode of governance in contrast to markets and hierarchies. Networks are formal and informal relationships (Jones et al. 1997) comprising relatively enduring resource transactions, flows, linkages (Oliver 1990), and information exchanges between two or more organisations such that that their individual autonomy remains intact (Kapucu 2005) while fulfilling mutually beneficial ends.
The political economy perspective of networks focuses not on the actors per se, but on the interorganisational linkages7 (Benson 1975; Milward and Provan 1998). Resource control is an important issue in IOR (Baker 1990; Ring and Van de Ven 1994; Schmidt and Kochan 1977; Ulrich and Barney 1984; Van de Ven and Walker 1984; Whetten 1981). Various types of resources have been described in the literature, viz., money, authority (Benson 1975), information, social support, facilities, personnel (Hall 2002) and even clients (Boje and Whetten 1981).
Several organisation theorists have described coordination in networks (Chisholm 1989; Jennings 1994; O’Toole 1997; Whetten 1981). In network organisations, coordination is increasingly maintained through organic, informal social systems (Eccles and Nohria 1992; Gerlach 1992), open-ended contracts, and social capital (Axelrod and Cohen 2000; Coleman 1990; Fukuyama 1995, 2001; Granovetter 1992; Ostrom 1991; Putnam 1993) rather than through formal contracts and authority.
Gaps in the Literature on Agencification

66 - Avantika Singh
Most literature on agencification has emerged with reference to OECD countries and is limited to the analysis of prominent agencies. Though perspectives from economics, management and governance have been employed to describe agencification, the agencification literature has not reached a stage of maturity as yet, and there is need for greater conceptual as well as empirical research in this area. The scholarship on the experience of developing countries with agencification is weak. There is an opportunity to employ organisation theory perspectives to understand the emergence of agencies, and the delivery of services by agencies through networks. A key aim of this paper is to make a modest contribution to the agencification literature in the context of the public health system in Rajasthan. This paper aims to empirically verify the existing literature on agencification, as well as apply organisation theory perspectives to explicate the rationale for agencification and coordination among agencies, parent ministry/department and service providers.
Agencification of the Public Health System in Rajasthan: An Empirical Analysis
Definitional Aspects of Agencies in the Public Health System of Rajasthan
Given that agencification is a relatively less researched area, an exploratory study was conducted in Rajasthan at State-level, and in one district. The findings from the empirical study on agencification in the public health system of Rajasthan reveal that National Health Programmes (NHPs) such as those for control of blindness, vector borne diseases, leprosy and Tuberculosis (TB), and promotion of Reproductive and Child Health (RCH), were earlier (before agencification) implemented by the Directorate of Medical and Health Services (DMHS) located in the State capital, Jaipur. In the district, the Chief Medical and Health Officer (CM&HO) was responsible for implementing these health programmes. With agencification, the implementation function with regard to these NHPs has been hived off from DMHS to separate agencies at State level as well as at district level8. On the other hand, the National AIDS Control Programme is implemented through new agencies created at national and State level. All the agencies created at State as well as district level for the implementation of NHPs are referred to as category A agencies for the purpose of this paper. Category B agencies refer to the agencies known as Rajasthan Medicare Relief Societies (RMRS) established to manage public hospitals9. With State governments hard-pressed for resources, there has been a need to look for alternative options of financing. Working on the assumption that if people paid for the services, the quality of services would improve, the idea of forming independent hospital boards was floated.

Health Reforms in Rajasthan - 67
In Rajasthan, both categories of agencies are neither ministerial departments nor corporate entities with for-profit motive. All of them are registered under the Rajasthan Societies Registration Act 1958, making them legally independent, structurally disaggregated bodies, with not-for-profit status. Both categories of agencies undertake public functions, i.e., category A agencies are responsible for implementation of NHPs, while category B agencies are responsible for management of public hospitals and making them financially sustainable.
Rationale for Agencification
Various rationales for agencification (in case of category A agencies) emerge from the empirical analysis, such as to divorce policy formulation from policy implementation, and to bring in a greater measure of autonomy and responsiveness in order to overcome “bureaupathologies” (Khandwalla 1999), viz., procedural and financial delays associated with government, excessive rule-boundedness, unutilised budgetary allocation, utilisation of funds for purposes other than those they were meant for, duplication of activities, and sub-optimal resource allocations and output. Donor-supported programmes are implemented through the agency mode because agencification helps donors circumvent the pitfalls of directly working with government departments, and is expected to fulfil their concerns for outcomes. The rationale for agencification through the creation of RMRS (category B agencies) was to decentralise management of health facilities, grant autonomy at local level, ensure financial sustainability of the health facility by generating, retaining and using resources at local level for improving availability and quality of services, and make available modern diagnostic and treatment facilities at affordable cost to the citizens.
Through the creation of agencies and development of service delivery networks, the government has expanded public participation in health care by involving VOs and PPs, such that the responsibility for achieving the health goals of the country is shared with other actors in society, and accountability towards the society is strengthened. Agencification has come to be established as a best practice and adopting it would help add legitimacy to the actions of the government. Moreover, agencification is also tied to international aid. For example, in Rajasthan agencies have been formed where specific disease control programmes are supported by the World Bank. National Rural Health Mission (NRHM), which is a seven-year long (2005-12) implementation programme for strengthening healthcare in rural areas of 18 (out of 28) States of India (MoHFW 2005a) is being implemented through agency structures both at State and district levels. Beginning in the early 1990s and continuing, the agency structure is increasingly being adopted for implementation of health programmes. Thus, agencification is linked to the reforms process and is path dependent.
68 - Avantika Singh
Composition of Agencies
As per the requirements of the Rajasthan Societies Registration Act 1958, each registered Society has to have a Governing Body and an Executive Committee. The Governing Body is responsible for strategic planning and performs a steering role, and the Executive Committee is entrusted with day-to-day management of the affairs of the society.
In the case of agencies in the public health system of Rajasthan, though the composition of the Governing Body varies from one agency to another, we can generalise it to some extent. The Health Secretary is the chairperson, and the State Programme Officer (RCH/AIDS/Blindness/Malaria/TB/Leprosy) is the Member Secretary of the category A agency at State level. The members of the Governing Body include officials from DMHS as well as other departments (Finance, Women and Child Development, Education, Social Welfare, etc.), eminent professionals, representatives from private sector, VOs and GoI. The category A agency at district level has the District Collector as the chairperson and the CM&HO as the Member Secretary. The members of the Governing Body include the Zila Pramukh10, officials from various departments at district level, representatives of VOs and PPs, eminent professionals, philanthropists and social workers. In case of category B agencies, the District Collector/ Sub-Divisional Magistrate (SDM)/ Project Director (PD)/ or any other official directed by Divisional Commissioner/ Health Secretary serves as the chairperson of the Governing Board. The CM&HO or Hospital Superintendent or any other health official serves as the Member Secretary of the agency. The members of the Governing Body include other health officials and medical specialists in the district, officials from other departments, Zila Pramukh, representatives from VOs and PPs, businessmen, social workers and philanthropists.
The members of the Executive Committee (of both categories of agencies) are mostly drawn from the Governing Body. The Chairperson and Member Secretary are common to Governing Body and Executive Committee. The Chairperson presides over meetings of Governing Body and Executive Committee. The Member Secretary is vested with all executive and financial powers, and is responsible for planning, implementation and monitoring of the agency’s activities.
Autonomy of Agencies
Because they are legally independent personalities, both categories of agencies in Rajasthan are financially independent from the parent ministry/department/ parent hospital. Each agency operates a separate bank account, and has separate financial rules and procedures. Moreover, these agencies have easier and faster

Health Reforms in Rajasthan - 69
billing and payment systems as compared to the government department. In the earlier case, payments had to be routed through the Treasury of the State government, making the process cumbersome and time-consuming. However, now payments are made through cheques and demand drafts, thus, improving the availability of funds for carrying out various interventions. Earlier, files would move up to the level of the Health Secretary for approval. Agency heads are now empowered to make certain decisions, which is expected to reduce the red tape in getting approvals. These agencies are less procedure-oriented and more flexible as they are not bound by the rules and procedures of the parent department. Though most officials are deputed from government departments to agencies, the agencies can hire professional as well as administrative staff on short-term contracts as required. They do not need to adhere to remuneration and other benefits as offered by the State government. They may pay higher salaries, but there may be no social security measures such as pension and gratuity.
The category B agency, i.e., RMRS raises its own resources and spends them at local level. Apart from the seed money given by the State government at start-up, RMRS does not receive any grants from the State government. Its sources of funds include user charges, grants (from other sources), donations, and income from sale of medicines. Prior to formation of RMRS, hospital income (if any) had to be deposited with the State Treasury. However, because of its independent legal status, RMRS can plough its income back into the hospital for various purposes such as maintenance, repairs and renovation of hospital premises, purchase of medical equipment, purchase of drugs, provision of free services to the poor and the disadvantaged, contracting out hospital support services, and other functions such as computerisation. By contracting out hospital support services such as cleaning, catering, laundry etc. and diagnostic services such as CT scanning, through a competitive bidding process RMRS has created competition in service delivery.
Control of Agencies
Despite their operational autonomy, both categories of agencies are not statutorily independent from ministerial instruction. The objectives and bye laws of the agency may be altered, or the agency dissolved with the consent of the Union/ State government, in accordance with the provisions of the Rajasthan Societies Registration Act 1958. The ultimate control of these agencies lies with the government as category A agencies at State level are headed by senior officials of the Secretariat/ DMHS, category A agencies at district level are headed by the District Collector and CM&HO, and category B agencies are headed by the District Collector and the the concerned hospital superintendent.

70 - Avantika Singh
The agencies operate as per policy guidelines received from the ministry/department, and certain (if not all) administrative law procedures. Category A agencies are primarily financed by donors such as the World Bank through the Union government. However, they are entitled to receive grants and donations from other sources as well. In contrast, category B agencies are financially less dependent on financing from the government as they have a number of sources of funds, particularly user charges.
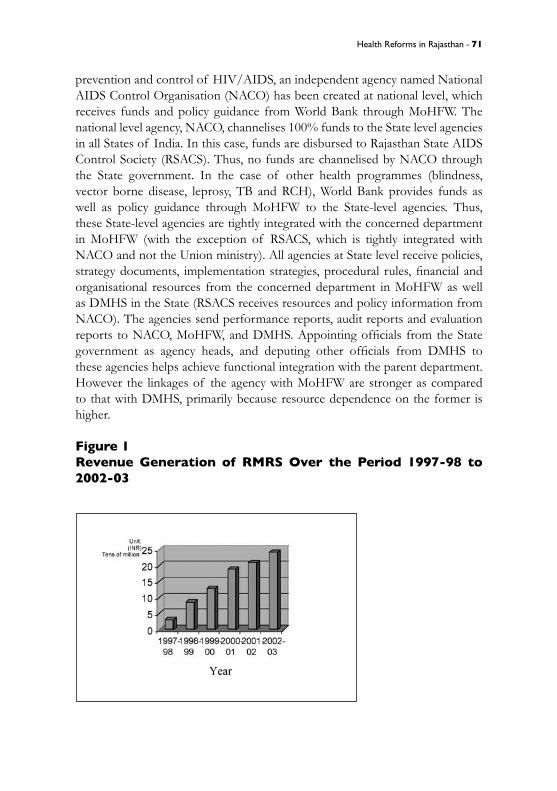
Control systems in both categories of agencies are ex post as the agencies are required to submit performance reports and audited financial statements to the parent ministry/department. However, there is no explicit performance contracting. Though these agencies have performance targets, such as number of cataract surgeries to be conducted or number of new TB patients to be identified, these are not however, linked to incentives or the continuance of funding. There is a condition on RMRS to spend 25% of its income on providing free services (including medicines, investigations and other hospital services) to patients possessing Medicare Relief Cards. These include patients from Below Poverty Line (BPL) families, widows, freedom fighters, orphans, senior citizens (over 70 years of age), prisoners and accident emergency cases. The areas of concern in the performance of RMRS include low utilisation of healthcare by BPL patients, and the inability of RMRS located in areas with larger proportion of poorer families to sustain themselves. However, there is no mechanism for cross-subsidising low-performing RMRS from high performing RMRSs because each RMRS is an independent body. The revenue generation of RMRS has increased from INR011 30.2 million in 1997-98 to INR 240.9 million in 2002-03, as depicted in figure 1. The cumulative number of BPL beneficiaries has increased from 0.36 million in 2001-02 to 1.06 million in 2003-04. However, the total number of BPL families identified through a survey and provided cards was 2,301,058 (Bhatnagar 2005).
Functional Integration of Agencies with Parent Ministry/Department
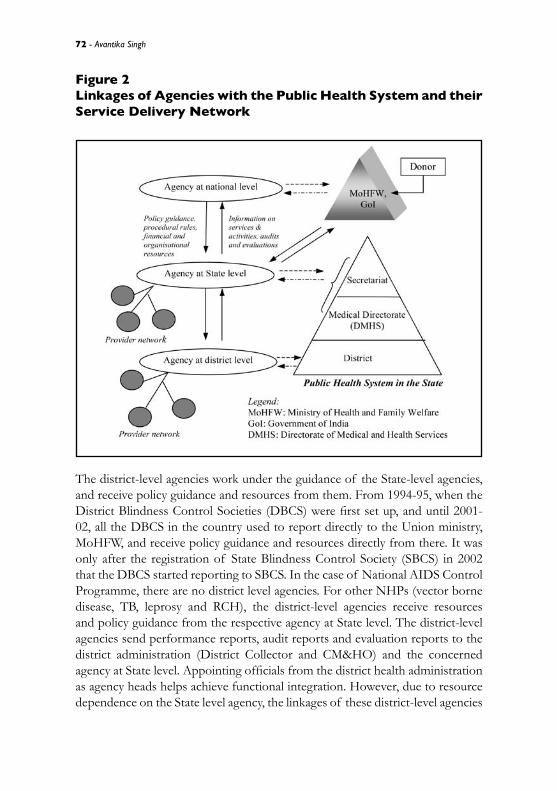
Applying the interorganisational relations perspective, dyadic linkages of the agencies with the parent ministry/department have been traced with respect to the exchange of resources, such as funds, supplies, equipment, human resources, and information. The flow of resources and information may be one-way or two-way, more frequent or less frequent, strong or weak, and hierarchical or horizontal. Interdependencies between the agency and the parent department necessitate coordination to achieve the common objective of performance. Figure 2 illustrates a generic representation of the linkages of category A agencies with the parent ministry/department and service providers. As illustrated in figure 2, donors provide assistance through the Union ministry, MoHFW. For
Health Reforms in Rajasthan - 71
prevention and control of HIV/AIDS, an independent agency named National AIDS Control Organisation (NACO) has been created at national level, which receives funds and policy guidance from World Bank through MoHFW. The national level agency, NACO, channelises 100% funds to the State level agencies in all States of India. In this case, funds are disbursed to Rajasthan State AIDS Control Society (RSACS). Thus, no funds are channelised by NACO through the State government. In the case of other health programmes (blindness, vector borne disease, leprosy, TB and RCH), World Bank provides funds as well as policy guidance through MoHFW to the State-level agencies. Thus, these State-level agencies are tightly integrated with the concerned department in MoHFW (with the exception of RSACS, which is tightly integrated with NACO and not the Union ministry). All agencies at State level receive policies, strategy documents, implementation strategies, procedural rules, financial and organisational resources from the concerned department in MoHFW as well as DMHS in the State (RSACS receives resources and policy information from NACO). The agencies send performance reports, audit reports and evaluation reports to NACO, MoHFW, and DMHS. Appointing officials from the State government as agency heads, and deputing other officials from DMHS to these agencies helps achieve functional integration with the parent department. However the linkages of the agency with MoHFW are stronger as compared to that with DMHS, primarily because resource dependence on the former is higher.
Figure 1Revenue Generation of RMRS Over the Period 1997-98 to 2002-03
72 - Avantika Singh
Figure 2Linkages of Agencies with the Public Health System and their Service Delivery Network
The district-level agencies work under the guidance of the State-level agencies, and receive policy guidance and resources from them. From 1994-95, when the District Blindness Control Societies (DBCS) were first set up, and until 2001-02, all the DBCS in the country used to report directly to the Union ministry, MoHFW, and receive policy guidance and resources directly from there. It was only after the registration of State Blindness Control Society (SBCS) in 2002 that the DBCS started reporting to SBCS. In the case of National AIDS Control Programme, there are no district level agencies. For other NHPs (vector borne disease, TB, leprosy and RCH), the district-level agencies receive resources and policy guidance from the respective agency at State level. The district-level agencies send performance reports, audit reports and evaluation reports to the district administration (District Collector and CM&HO) and the concerned agency at State level. Appointing officials from the district health administration as agency heads helps achieve functional integration. However, due to resource dependence on the State level agency, the linkages of these district-level agencies
Health Reforms in Rajasthan - 73
with the State-level agency are stronger as compared to that with the district administration.
The appointment of the District Collector as Chairperson and the concerned Hospital Superintendent as Member Secretary of category B agencies (RMRS) helps achieve functional integration with the local hospital/district health administration. Though RMRS has a considerable amount of autonomy with regard to the generation and utilisation of funds, it is dependent on the local hospital for other organisational resources. RMRS are required to work within the broader policy framework set by and as per directives issued by the State government/ hospital administration.
Service Delivery by Agencies
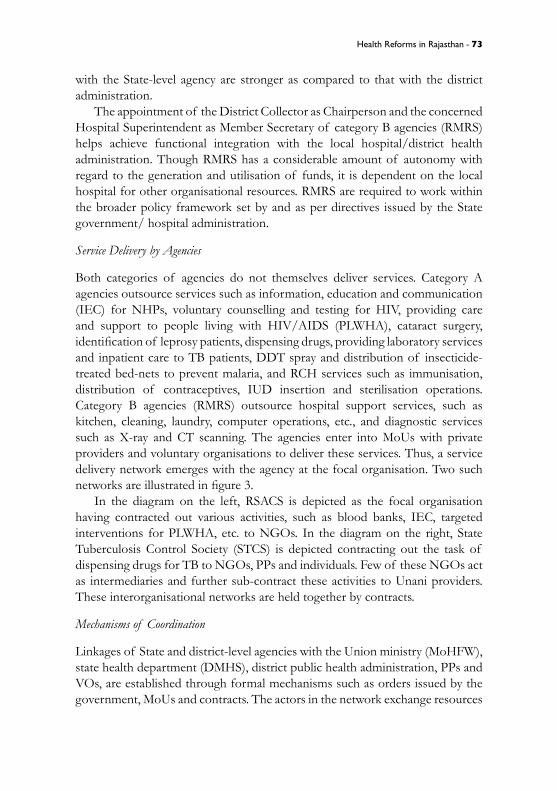
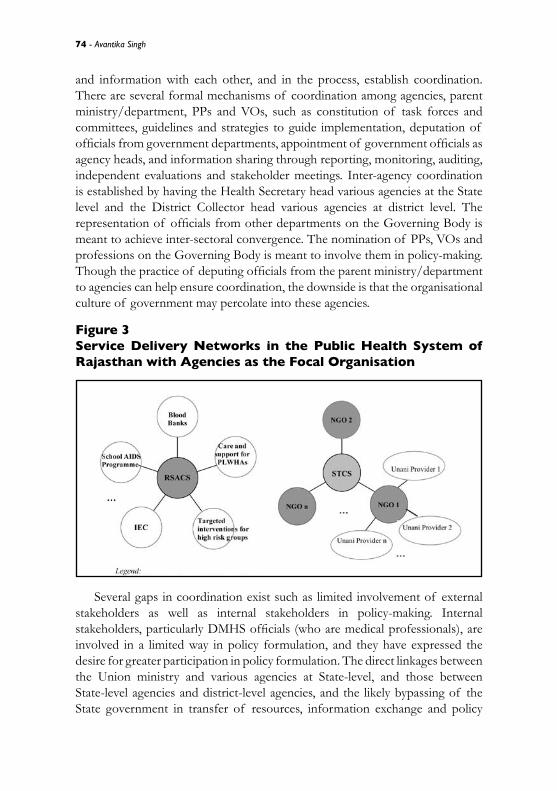
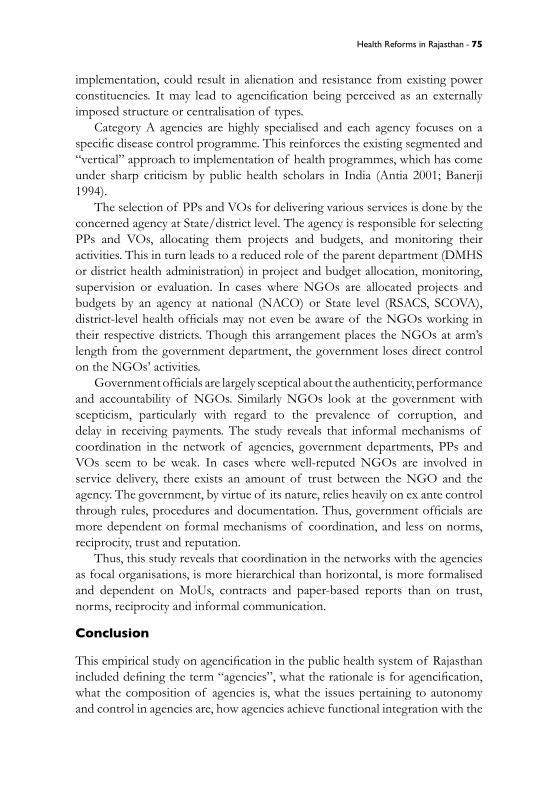
Both categories of agencies do not themselves deliver services. Category A agencies outsource services such as information, education and communication (IEC) for NHPs, voluntary counselling and testing for HIV, providing care and support to people living with HIV/AIDS (PLWHA), cataract surgery, identification of leprosy patients, dispensing drugs, providing laboratory services and inpatient care to TB patients, DDT spray and distribution of insecticide-treated bed-nets to prevent malaria, and RCH services such as immunisation, distribution of contraceptives, IUD insertion and sterilisation operations. Category B agencies (RMRS) outsource hospital support services, such as kitchen, cleaning, laundry, computer operations, etc., and diagnostic services such as X-ray and CT scanning. The agencies enter into MoUs with private providers and voluntary organisations to deliver these services. Thus, a service delivery network emerges with the agency at the focal organisation. Two such networks are illustrated in figure 3.
In the diagram on the left, RSACS is depicted as the focal organisation having contracted out various activities, such as blood banks, IEC, targeted interventions for PLWHA, etc. to NGOs. In the diagram on the right, State Tuberculosis Control Society (STCS) is depicted contracting out the task of dispensing drugs for TB to NGOs, PPs and individuals. Few of these NGOs act as intermediaries and further sub-contract these activities to Unani providers. These interorganisational networks are held together by contracts.
Mechanisms of Coordination
Linkages of State and district-level agencies with the Union ministry (MoHFW), state health department (DMHS), district public health administration, PPs and VOs, are established through formal mechanisms such as orders issued by the government, MoUs and contracts. The actors in the network exchange resources
74 - Avantika Singh
and information with each other, and in the process, establish coordination. There are several formal mechanisms of coordination among agencies, parent ministry/department, PPs and VOs, such as constitution of task forces and committees, guidelines and strategies to guide implementation, deputation of officials from government departments, appointment of government officials as agency heads, and information sharing through reporting, monitoring, auditing, independent evaluations and stakeholder meetings. Inter-agency coordination is established by having the Health Secretary head various agencies at the State level and the District Collector head various agencies at district level. The representation of officials from other departments on the Governing Body is meant to achieve inter-sectoral convergence. The nomination of PPs, VOs and professions on the Governing Body is meant to involve them in policy-making. Though the practice of deputing officials from the parent ministry/department to agencies can help ensure coordination, the downside is that the organisational culture of government may percolate into these agencies.
Figure 3Service Delivery Networks in the Public Health System of Rajasthan with Agencies as the Focal Organisation
Several gaps in coordination exist such as limited involvement of external stakeholders as well as internal stakeholders in policy-making. Internal stakeholders, particularly DMHS officials (who are medical professionals), are involved in a limited way in policy formulation, and they have expressed the desire for greater participation in policy formulation. The direct linkages between the Union ministry and various agencies at State-level, and those between State-level agencies and district-level agencies, and the likely bypassing of the State government in transfer of resources, information exchange and policy
Health Reforms in Rajasthan - 75
implementation, could result in alienation and resistance from existing power constituencies. It may lead to agencification being perceived as an externally imposed structure or centralisation of types.
Category A agencies are highly specialised and each agency focuses on a specific disease control programme. This reinforces the existing segmented and “vertical” approach to implementation of health programmes, which has come under sharp criticism by public health scholars in India (Antia 2001; Banerji 1994).
The selection of PPs and VOs for delivering various services is done by the concerned agency at State/district level. The agency is responsible for selecting PPs and VOs, allocating them projects and budgets, and monitoring their activities. This in turn leads to a reduced role of the parent department (DMHS or district health administration) in project and budget allocation, monitoring, supervision or evaluation. In cases where NGOs are allocated projects and budgets by an agency at national (NACO) or State level (RSACS, SCOVA), district-level health officials may not even be aware of the NGOs working in their respective districts. Though this arrangement places the NGOs at arm’s length from the government department, the government loses direct control on the NGOs’ activities.
Government officials are largely sceptical about the authenticity, performance and accountability of NGOs. Similarly NGOs look at the government with scepticism, particularly with regard to the prevalence of corruption, and delay in receiving payments. The study reveals that informal mechanisms of coordination in the network of agencies, government departments, PPs and VOs seem to be weak. In cases where well-reputed NGOs are involved in service delivery, there exists an amount of trust between the NGO and the agency. The government, by virtue of its nature, relies heavily on ex ante control through rules, procedures and documentation. Thus, government officials are more dependent on formal mechanisms of coordination, and less on norms, reciprocity, trust and reputation.
Thus, this study reveals that coordination in the networks with the agencies as focal organisations, is more hierarchical than horizontal, is more formalised and dependent on MoUs, contracts and paper-based reports than on trust, norms, reciprocity and informal communication.
Conclusion
This empirical study on agencification in the public health system of Rajasthan included defining the term “agencies”, what the rationale is for agencification, what the composition of agencies is, what the issues pertaining to autonomy and control in agencies are, how agencies achieve functional integration with the
76 - Avantika Singh
parent ministry/department, how the agencies deliver services, and how they establish coordination with parent ministry/department and service providers. The analysis reveals that the model of agencification adopted in Rajasthan is quite different from the “original” Western conceptualisation of agencification. The agencies studied in this research are registered as “Societies” under the Rajasthan Societies Registration Act 1958, making them legally independent, structurally disaggregated bodies with not-for-profit status. These agencies undertake public functions such as implementation of National Health Programmes and management of public hospitals. They are financially independent from the parent ministry/department/hospital. Though they have operational flexibility, they function within the broad policy framework and policy guidelines provided by the parent ministry/department. However, unlike the Western forms of agencies described in the literature, there is no explicit performance contracting and accountability for results in the case of agencies in the public health system of Rajasthan. Moreover, the idea of agencies in Rajasthan has not generated from “within” – it is path dependent and inextricably linked to the reforms process.
There are a number of ways in which agencies achieve functional integration with the parent ministry/department. The agencies are headed by government officials. Several officials are deputed from the ministry/department to the agencies. The functional integration of State-level agencies with the Union ministry, MoHFW, is stronger as compared to that with the State health department (DMHS) primarily because resource dependence on the former is higher. Similarly, due to greater resource dependence on the State-level agency, the linkages of district-level agencies with the State-level agency are stronger as compared to that with the district administration.
Most of the agencies enter into MoUs with private providers and voluntary organisations to deliver services. Thus, a service delivery network emerges with the agency as the focal organisation. The actors in the network exchange resources and information with each other, and in the process, establish coordination. Coordination is established through formal mechanisms such as MoUs, contracts, orders issued by the government, implementation guidelines and strategies, task forces, committees, stakeholder meetings, deputation of officials, reporting, monitoring, auditing and evaluation. However, several gaps in coordination exist, such as limited involvement of external and internal stakeholders in policy-making, and loss of direct control of the health department (DMHS or district health administration) over the selection of PPs and VOs, allocation of projects, transfer of budgets and policy guidelines, monitoring, supervision and evaluation. Coordination is more formalised and dependent on MoUs, contracts and paper-based reports than on trust, norms,

Health Reforms in Rajasthan - 77
reciprocity and informal communication. The underlying reasons could be the procedure-oriented nature of government work, and scepticism and lack of trust of government in NGOs and vice versa.
In the Western formulations of agencification based on the NPM, when government is unbundled through agencifying, agency heads are selected through lateral entry, are given autonomy and made accountable for achieving results, and rewards are linked to performance. However, in the case of Rajasthan, agencification has been “imported” only as an organisational structure, mostly at the behest of donors. Agency structures in this case serve as a channel for resource flow and implementation of health programmes.
For successful implementation of NPM in the public health system of Rajasthan, it is important for comprehensive and simultaneous implementation of NPM reforms. Agencification has to be accompanied by policy changes that bring about lateral entry, greater accountability, performance measurement, results orientation and incentive schemes in the public sector. For this to happen, political commitment needs to be high.
This research has made a modest attempt at analysing agencification from organisation theory perspectives. This research reveals the immense potential for applying “interorganisational relations” to the study of emerging service delivery networks as a result of disaggregation of government. Thus, this research suggests a way forward for building scholarship on New Public Management. Other issues pertaining to agencification that can be addressed through future research include how different from government is the organisational culture of agencies, how to address equity issues through public hospitals with autonomous boards (RMRS), and how to improve coordination through the development of social capital in networks with agencies as the focal organisation.
Acknowledgements
The author is grateful to Prof. M. Ramesh, Lee Kuan Yew School of Public Policy, National University of Singapore, Singapore, for his comments on earlier versions of this paper.
Notes
* Faculty Member, Department of Policy Studies, TERI University, India Habitat Centre, Lodhi Road, New Delhi 110003, India. Telephone): +91-9968381455, email): [email protected], [email protected]. The author was recipient of Sir Ratan Tata Trust (SRTT) Fellowship at Institute of Rural Management, Anand (IRMA), India. She acknowledges the financial support provided by SRTT, Mumbai, India for carrying out this research.1. New Public Management (NPM) originated in UK during the late 1970s under the leadership of Margaret Thatcher, and was soon embraced by New Zealand, Australia and other OECD countries. Its variants later spread to other countries including India. There are two strands under

78 - Avantika Singh
NPM, namely, managerialism and marketisation. NPM marks a departure from the Old Public Administration (Dunleavy and Hood 1994), and has been described as the “reinvention” of government through change in its role from “rowing” to “steering” (Osborne and Gaebler 1992) or the shift from “government” to “governance”. Contributors to NPM include Aucoin (1990), Barzelay (2001), Ferlie et al. (1996), Hood (1991), Kettl (1997), Kickert (1997), Minogue et al. (1998), Pollitt (1993), Pollitt and Bouckaert (2004) and Walsh (1995). 2. Public health expenditure as percentage of total expenditure on health in India is third lowest in the world. The only countries that spend less than India are Myanmar and Georgia (World Bank 2003).3. India has a federal polity, and the legislative powers are distributed between the Union and the States, as mandated by the Constitution of India. Public health and sanitation, hospitals and dispensaries are defined and enlisted in List - II (State List) of the Seventh Schedule of the Constitution. Population control and family planning, medical education and medical profession are defined and enlisted under the List - III (Concurrent List) of the Seventh Schedule of the Constitution. While only the State Legislatures can legislate on the subjects in the State list, both the Parliament and the State Legislatures can legislate on those in the Concurrent list, and the legislations made by the Parliament supersede those made by the State Legislatures (Ministry of Law and Justice).4. The birth rate in Rajasthan was 28.6 per 1000 as compared to 23.8 for all India during 2005 (Indiastat 2006), TFR was 3.7 per woman in Rajasthan as compared to 2.9 for all India during 2004 (Indiastat 2005 and 2006), and IMR was 68 infant deaths per 1000 live births in Rajasthan as compared to 58 for all India during 2005 (MoHFW 2005b). 5. According to the 2001 Census, Scheduled Castes and Scheduled Tribes together make up 29.8% of the population of the State as compared to 24.4% for all India, just 43.9% of the female population is literate in Rajasthan as compared to 53.7% in the whole of India, and the sex ratio is 922 females per 1000 males in Rajasthan as compared to 933 for the whole of India (Registrar General of India, RGI 2001). 6. In this paper, the term “voluntary organisations” has been employed as a broader term to include nongovernmental organisations (NGOs) as well as voluntary association such as Lions Club or Rotary Club. 7. Whetten (1981) has described four forms of interorganisational linkages, namely, dyadic linkage, organisation set, action set and network. Dyadic linkage refers to the mutually beneficial interactions between two otherwise independent organisations. Organisation set is the sum total of the interorganisational linkages established by a “focal organisation”. The linkages between other interacting organisations are ignored. Actions sets are clusters of organisations working together to accomplish a specific purpose. In contrast to the three forms mentioned above, a network consists of all the interorganisational linkages in a population. A network can be visualised as a system comprising of several inter-connected sub-systems. 8. The agencies at State level include Rajasthan State AIDS Control Society (RSACS), State Blindness Control Society (SBCS), State Leprosy Elimination Society (SLES), State Vector Borne Disease Control Society (formerly State Malaria Control Society) (SVBDCS), State Tuberculosis Control Society (STCS), and State Health and Family Welfare Society for Voluntary Sector (SHFWSVS/ SCOVA). The agencies at district level include District RCH Society (DRCHS), District Leprosy Elimination Society (DLES), District Tuberculosis Control Society (DTCS), and District Blindness Control Society (DBCS). 9. At the initiative of the then Health Secretary, RMRS were first created during 1995-96 at hospitals attached to medical colleges and district hospitals. RMRS were later created at all Community Health Centres in the State. In 2005, the State government took a decision to replicate these agencies at each public institution of curative care (including Primary Health Centres) in Rajasthan.10. Zila Pramukh is the chairperson of the Zila Parishad (District Council). The Panchayati Raj
Health Reforms in Rajasthan - 79
System of local self government comprises a three tier architecture of Gram Panchayats (village councils) in the villages, Panchayat Samitis (intermediate bodies) at sub-district level, and Zila Parishad at district level. All these bodies consist of democratically elected representatives. 11. 1 US$ = ~40 INR (Indian National Rupees).
References
Allix, M., and S. Van Thiel. 2005. ‘Mapping the field of quasi-autonomous organizations in France and Italy’. International Public Management Journal 8 (1): 39-55.
Antia, N. H. 2001. ‘Health for all through a decentralized people’s movement’. Health for the Millions 27 (4): 10-11.
Aucoin, P. 1990. ‘Administrative reform in public management: Paradigms, principles, paradoxes and pendulums’. Governance 3 (2): 115-137.
Axelrod, R., and M.D. Cohen. 2000. Harnessing complexity: Organizational implications of a scientific frontier. New York: The Free Press.
Baker, W.E. 1990. ‘Market networks and corporate behavior’. American Journal of Sociology 96 (3): 589-625.
Banerji, D. 1994. ‘A simplistic approach to health policy analysis: The World Bank team on the Indian health sector’. International Journal of Health Services 24 (1): 151-159.
Barzelay, M. 2001. The new public management: Improving research and policy dialogue. Berkeley, CA: University of California Press.
Benson, J.K. 1975. ‘The interorganizational network as a political economy’. Administrative Science Quarterly 20 (2): 229-249.
Bhatnagar, S. 2005. Health sector reforms in Rajasthan (Presentation shared by the author).Boje, D.M., and D.A. Whetten. 1981. ‘Effects of organizational strategies and contextual
constraints on centrality and attributions of influence in interorganizational networks’. Administrative Science Quarterly (26): 378-395.
Boston, J., J. Martin, J. Pallot, and P. Walsh. 1996. Public management: The New Zealand model. Oxford: Oxford University Press.
Chisholm, D. 1989. Coordination without hierarchy: Informal structures in multiorganizational systems. Berkeley, CA: University of California Press.
Christensen, T., and P. Lægreid. 2004. ‘Governmental autonomisation and control: The Norwegian way’. Public Administration and Development 24 (2): 129-135.
Coleman, J.C. 1988. ‘Social capital in the creation of human capital’. American Journal of Sociology 94 (Supplement): S95-S120.
Common, R. 1998. ‘Convergence and transfer: A review of the globalisation of new public management’. International Journal of Public Sector Management 11 (6): 440-450.
Common, R., N. Flynn, and E. Mellon. 1992. Managing public services: Competition and decentralisation. Oxford: Oxford University Press.
Dolowitz, D.P., and D. Marsh. 1998. ‘Policy transfer: A framework for comparative analysis’. In Beyond the new public management: Changing ideas and practices in governance, eds., M. Minogue, C. Polidano and D. Hulme. Northampton: Edward Elgar.
du Gay, P. 2004. ‘Against “Enterprise” but not against “enterprise” for that would make no sense’. Organization 11 (1): 37-57.
Dunleavy, P., and C. Hood. 1994. ‘From old public administration to new public management’. Public Money and Management 14 (3): 9-16.
Eccles, R.G., and N. Nohria. 1992. Beyond the hype: Rediscovering the essence of management. Boston, MA: Harvard Business School Press.
Ferlie, E., L. Asburner, L. Fitzgerald, and L. Pettigrew. 1996. The new public management in action. Oxford: Oxford University Press.

80 - Avantika Singh
Fukuyama, F. 1995. ‘Social capital and the global economy’. Foreign Affairs 74 (5): 89-103._______. 2001, ‘Social capital, civil society and development’. Third World Quarterly 22 (1): 7-20. Gerlach, M.L. 1992. ‘The Japanese corporate network: A blockmodel analysis’. Administrative
Science Quarterly 37 (1): 105-139. Gill, D. 2002. ‘Signposting the zoo – From agencification to a more principled choice of government
organisational forms’. OECD Journal on Budgeting 2 (1): 27-80.Goes, J.B., and S.H. Park 1997. ‘Interorganizational linkages and innovation: The case of hospital
services’. Academy of Management Journal 40 (3): 673-696. Granovetter M.S. 1992. ‘Problems of explanation in economic sociology’. In Networks and
organizations: Structure, form and action, eds., N. Nohria and R.G. Eccles, 25-56. Boston, MA: Harvard Business School Press.
Greve, C., M. Flinders, and S. Van Thiel. 1999. ‘Quangos – What’s in a name? Defining quangos from a comparative perspective’. Governance 12 (2): 129-146.
Hall, R. H. 2002. Organizations: Structures, processes and outcomes. 8th ed. New Delhi: Prentice Hall of India.
Halligan, J. 2004. ‘The quasi-autonomous agency in an ambiguous environment. The Centrelink case’. Public Administration and Development 24 (2): 147-156.
Hood, C. 1991. ‘A public management for all seasons?’ Public Administration 69 (1): 3-19.Indiastat. 2005/2006. ‘Selected state-wise total fertility rate in India (1988 to 2004)’. Rajya Sabha
Unstarred Question No. 4745, dated 06.05.2005; and Lok Sabha Unstarred Question No. 161, dated 22.11.2006. Available at http://www.indiastat.com/india/ShowDataSec.asp?secid=369063&ptid=17795, accessed 15 June 2007.
_______. 2006. ‘State-wise birth rates in India (2003 to 2005)’. Ministry of Health and Family Welfare, Govt. of India, and Rajya Sabha Unstarred Question No. 1258, dated 04.08.2006. Available at http)://www.indiastat.com/india/ShowDataSec.asp?secid=390929&ptid=17791, accessed 15 June 2007.
Jennings, E.T., Jr. 1994. ‘Building bridges in the intergovernmental arena: Coordinating employment and training programs in the American states’. Public Administration Review 54 (1): 52-60.
Jones, C., W.S. Hesterly, and S.P. Borgatti. 1997. ‘A general theory of network governance: Exchange conditions and social mechanisms’. Academy of Management Review 22 (4): 911-45.
Kapucu, N. 2005. ‘Interorganizational coordination in dynamic context: Networks in emergency response management’. Connections 26 (2): 33-48.
Khandwalla, P.N. 1999. Revitalizing the state: A menu of options. New Delhi: Sage. Kettl, D.F. 1997. ‘The global revolution in public management: Driving themes, missing links’.
Journal of Policy Analysis and Management 16 (3): 446-462. Kickert, W., ed. 1997. Public management and administrative reform in Western Europe.
Northampton, UK: Edward Elgar. La Guerre, J. 1994. Structural adjustment, public policy and administration in the Caribbean. St.
Augustine, Trinidad: School of Continuing Studies. Levitt, K.P. 1991. The origins and consequences of Jamaica’s debt crisis 1970-1990. Kingston:
Consortium Graduate School of Social Sciences. Mason, J.C. 1993. ‘Strategic alliances: Partnering for success’. Management Review 82 (5): 10-15. Milward, H.B., and K.G. Provan. 1998. ‘Principles for controlling agents: The political economy
of network structure’. Journal of Public Administration Research and Theory 8 (2): 203-221.
Minogue, M., C. Polidano, and D. Hulme, eds. 1998. Beyond the new public management: Changing ideas and practices in governance. Cheltenham: Edward Elgar.
MoHFW. 2005a. National rural health mission (2005-2012) – Mission document. New Delhi: MoHFW.
Health Reforms in Rajasthan - 81
_______. 2005b. ‘State-wise infant mortality rate by sex and residence in India (2005)’. Available at http://www.indiastat.com/india/ShowDataSec.asp?secid=409099&ptid=17794, accessed 15 June 2007.
Ministry of Law and Justice. ‘Seventh Schedule’. Constitution of India. Available at http://lawmin.nic.in/coi/SEVENTH-SCHEDULE.pdf, accessed 14 May 2007.
Nye, J.S., P.D. Zelikow, and D.C. King, eds. 1997. Why people don’t trust government. Cambridge, MA: Harvard University Press.
OECD. 1995. Governance in transition: Public management reforms in OECD countries. Paris: OECD.
Oliver, C. 1990. ‘Determinants of interorganizational relationships: Integration and future directions’. Academy of Management Review 15 (2): 241-265.
Osborne, D., and T. Gaebler. 1992. Reinventing government: How the entrepreneurial spirit is transforming the public sector. Reading, MA: Addison-Wesley.
Ostrom, E. 1991. ‘Rational choice theory and institutional analysis: Toward complementarity’. American Political Science Review 85 (1): 237-243.
O’Toole, L.J., Jr. 1997. ‘Treating networks seriously: Practical and research-based agendas in public administration’. Public Administration Review 57 (1): 45-52.
Pollitt, C. 1993. Managerialism and the public services. Cambridge: Blackwell. _______. 2003. ‘Agencies, apples and pears: Mapping the agency debate’. Paper for the 7th
International research symposium on public management, Hong Kong, 2-4 October. Pollitt, C., and C. Talbot. 2004. Unbundled government: A critical analysis of the global trend to
agencies, quangos and contractualisation. London: Routledge. Pollitt, C., and G. Bouckaert. 2004. Public management reform: A comparative analysis. 2nd ed.
Oxford: Oxford University Press. Pollitt, C., J. Birchall, and K. Putnam. 1998. Decentralising public service management. London:
Macmillan. Pollitt, C., K. Bathgate, J. Caulfield, A. Smullen, and C. Talbot. 2001. ‘Agency fever? Analysis of
an international policy fashion’. Journal of Comparative Policy Analysis: Research and Practice 3 (3): 271-290.
Provan, K.G., and H.B. Milward. 1995. ‘A preliminary theory of network effectiveness: A comparative study of four community mental health systems’. Administrative Science Quarterly 40 (1): 1-33.
Putnam, R.D. 1993. Making democracy work: Civic traditions in modern Italy. Princeton, NJ: Princeton University Press.
Registrar General of India. 2001. Primary census abstract: Census of India 2001. Available at http://www.censusindia.net/results/pca_main.html, accessed 26 January 2007.
Ring, P.S., and A.H. Van de Ven. 1994. ‘Developmental processes of corporative interorganizational relationships’. Academy of Management Review 19 (1): 90-118.
Roberts, A. 1997. ‘Performance-based organizations: Assessing the Gore plan’. Public Administration Review 57 (6): 465-478.
Schick, A. 2002. ‘Agencies in search of principles’. OECD Journal on Budgeting 2 (1): 7-26.Schmidt, S.M., and T.A. Kochan. 1977. ‘Interorganizational relationships: Patterns and motivations’.
Administrative Science Quarterly 22 (2): 220-234. Talbot, C., C. Pollitt, K. Bathgate, J. Caulfield, A. Reilly, and A. Smullen. 2000. ‘The idea of agency:
Researching the agencification of the (public service) world’. American Political Studies Association Conference. Washington DC, August.
Thynne, I. 2004. ‘State organisations as agencies: An identifiable and meaningful focus of research?’ Public Administration and Development 24 (2): 91-99.
Ulrich, D., and J.B. Barney. 1984. ‘Perspectives in organizations: Resource dependence, efficiency, and population’. Academy of Management Review 9 (3): 471-481.
Van de Ven, A.H., and G. Walker. 1984. ‘The dynamics of interorganizational coordination’. Administrative Science Quarterly 29 (4): 598-621.
82 - Avantika Singh
Van Thiel, S. 2000. ‘Quangocratization: Trends, causes and consequences’. Utrecht: Universiteit Utrecht.
Verhoest, K., B.G. Peters, G. Bouckaert, and B. Verschuere. 2003. ‘The study of organizational autonomy: A conceptual and methodological review’. Working paper. Catholic University of Leuven.
Verhoest, K., B. Verschuere, B.G. Peters, and G. Bouckaert. 2004. ‘Controlling autonomous public agencies as an indicator of new public management’. Management International 9 (1): 25-35.
Walsh, K. 1995. Public services and market mechanisms: Competition, contracting and the new public management. London: Macmillan Press.
Whetten, D.A. 1981. ‘Interorganizational relations: A review of the field’. The Journal of Higher Education 52 (1): 1-28.
WHO SEARO. 1997. Public private sector partnerships for health: Role of governments. New Delhi: WHO SEARO.
World Bank. 2003. World development indicators 2003. Washington, D.C.: World Bank.Yeoh, E.K. 2003. ‘Experiences in hospital sector reform, the performance of hospitals under
changing socio-economic conditions. WHO global study undertaken in collaboration with the International Hospital Federation’. World Hospitals and Health Services 39 (2): 2.
Yesilkagit, K. 2004. ‘The design of public agencies: Overcoming agency costs and commitment problems’. Public Administration and Development 24 (2): 119-127.