Health economic impact of risk group selection according to ASCO-recommended biomarkers uPA/PAI-1 in...
12
CLINICAL TRIAL Health economic impact of risk group selection according to ASCO-recommended biomarkers uPA/PAI-1 in node-negative primary breast cancer Volker R. Jacobs • Ronald E. Kates • Eva Kantelhardt • Martina Vetter • Rachel Wuerstlein • Thorsten Fischer • Manfred Schmitt • Fritz Jaenicke • Michael Untch • Christoph Thomssen • Nadia Harbeck Received: 6 February 2013 / Accepted: 20 March 2013 / Published online: 9 April 2013 Ó Springer Science+Business Media New York 2013 Abstract Invasion factors uPA/PAI-1 are guideline-rec- ommended (ASCO, AGO) biomarkers for decision support regarding adjuvant chemotherapy (CTX) in women with primary breast cancer. They define a high-risk group with strong benefit from adjuvant CTX and a low-risk group with uncertain benefit and excellent survival without CTX. In a target population (age [ 35/N0/G2/HR?/HER2-), administration of adjuvant CTX is not mandatory in Ger- many and other countries. Based on existing data, this economic model was developed to determine for the first time health economic impact of uPA/PAI-1 testing. Incremental cost-effectiveness ratio (ICER) resulting from uPA/PAI-1 testing was estimated for the target population by Markov modeling and sensitivity analysis. Survival data, CTX–uPA/PAI-1 interactions, and uPA/PAI-1 hazard ratios were derived from the Chemo N0 trial and other evidence. Incremental costs were computed from a payer’s perspective appropriate to the German setting. Incremental effectiveness in life years (ly) was estimated taking into account age-adjusted life expectancy, disease-free survival (with/without CTX), and 2 years post-relapse survival. Sensitivity analysis was performed by varying residual adjuvant CTX benefit in the low-risk group, denoted HR_CTX(LR), in range 0.8–0.99. All patients receive adjuvant endocrine therapy. Test is restricted to patients willing to forgo CTX if both markers are below specific cut-off values and to undergo CTX otherwise. For a typical 55-year-old patient, comparing to an ‘‘all-CTX’’ strategy without the test, ICER (all-CTX vs. test) [ €50,000 if HR_CTX(LR) [ 0.85, with savings of €18,500 per low- risk patient attributable to the test. The cost-effectiveness of forgoing CTX is very high as HR_CTX(LR) approaches one. Conversely, comparing to a ‘‘no-CTX’’ strategy (e.g., patients who initially refuse CTX) without the test, the test is very cost-effective at all ages in the target group if high- risk patients are willing to undergo CTX: ICER (test vs. no- CTX) \ €6,000 at age 55 and even better at younger ages, remaining \ €25,000 up to age 75. The main determinants Volker R. Jacobs and Ronald E. Kates contributed equally to this work. V. R. Jacobs (&) Á T. Fischer Frauenklinik (OB/GYN), Paracelsus Medical University (PMU), Mu ¨llner Hauptstr. 48, 5020 Salzburg, Austria e-mail: [email protected] R. E. Kates Á R. Wuerstlein Á N. Harbeck Breast Center, Frauenklinik Maistrasse, University of Munich (LMU), Munich, Germany E. Kantelhardt Á M. Vetter Á C. Thomssen Frauenklinik (OB/GYN), University Clinic of Halle/Saale, Halle (Saale), Germany R. Wuerstlein Á N. Harbeck Comprehensive Cancer Center (CCC), University of Munich (LMU), Munich, Germany M. Schmitt Frauenklinik (OB/GYN), Technical University Munich (TUM), Munich, Germany F. Jaenicke Frauenklinik (OB/GYN), University Clinic of Hamburg- Eppendorf, Hamburg, Germany M. Untch Frauenklinik (OB/GYN), Helios-Klinikum Berlin-Buch, Berlin, Germany N. Harbeck Breast Center, Frauenklinik Großhadern, University of Munich (LMU), Munich, Germany 123 Breast Cancer Res Treat (2013) 138:839–850 DOI 10.1007/s10549-013-2496-z
Transcript of Health economic impact of risk group selection according to ASCO-recommended biomarkers uPA/PAI-1 in...

CLINICAL TRIAL
Health economic impact of risk group selection accordingto ASCO-recommended biomarkers uPA/PAI-1 in node-negativeprimary breast cancer
Volker R. Jacobs • Ronald E. Kates • Eva Kantelhardt • Martina Vetter •
Rachel Wuerstlein • Thorsten Fischer • Manfred Schmitt • Fritz Jaenicke •
Michael Untch • Christoph Thomssen • Nadia Harbeck
Received: 6 February 2013 / Accepted: 20 March 2013 / Published online: 9 April 2013
� Springer Science+Business Media New York 2013
Abstract Invasion factors uPA/PAI-1 are guideline-rec-
ommended (ASCO, AGO) biomarkers for decision support
regarding adjuvant chemotherapy (CTX) in women with
primary breast cancer. They define a high-risk group with
strong benefit from adjuvant CTX and a low-risk group
with uncertain benefit and excellent survival without CTX.
In a target population (age [ 35/N0/G2/HR?/HER2-),
administration of adjuvant CTX is not mandatory in Ger-
many and other countries. Based on existing data, this
economic model was developed to determine for the first
time health economic impact of uPA/PAI-1 testing.
Incremental cost-effectiveness ratio (ICER) resulting from
uPA/PAI-1 testing was estimated for the target population
by Markov modeling and sensitivity analysis. Survival
data, CTX–uPA/PAI-1 interactions, and uPA/PAI-1 hazard
ratios were derived from the Chemo N0 trial and other
evidence. Incremental costs were computed from a payer’s
perspective appropriate to the German setting. Incremental
effectiveness in life years (ly) was estimated taking into
account age-adjusted life expectancy, disease-free survival
(with/without CTX), and 2 years post-relapse survival.
Sensitivity analysis was performed by varying residual
adjuvant CTX benefit in the low-risk group, denoted
HR_CTX(LR), in range 0.8–0.99. All patients receive
adjuvant endocrine therapy. Test is restricted to patients
willing to forgo CTX if both markers are below specific
cut-off values and to undergo CTX otherwise. For a typical
55-year-old patient, comparing to an ‘‘all-CTX’’ strategy
without the test, ICER (all-CTX vs. test) [ €50,000 if
HR_CTX(LR) [ 0.85, with savings of €18,500 per low-
risk patient attributable to the test. The cost-effectiveness
of forgoing CTX is very high as HR_CTX(LR) approaches
one. Conversely, comparing to a ‘‘no-CTX’’ strategy (e.g.,
patients who initially refuse CTX) without the test, the test
is very cost-effective at all ages in the target group if high-
risk patients are willing to undergo CTX: ICER (test vs. no-
CTX) \ €6,000 at age 55 and even better at younger ages,
remaining \ €25,000 up to age 75. The main determinantsVolker R. Jacobs and Ronald E. Kates contributed equally to this
work.
V. R. Jacobs (&) � T. Fischer
Frauenklinik (OB/GYN), Paracelsus Medical University (PMU),
Mullner Hauptstr. 48, 5020 Salzburg, Austria
e-mail: [email protected]
R. E. Kates � R. Wuerstlein � N. Harbeck
Breast Center, Frauenklinik Maistrasse, University of Munich
(LMU), Munich, Germany
E. Kantelhardt � M. Vetter � C. Thomssen
Frauenklinik (OB/GYN), University Clinic of Halle/Saale, Halle
(Saale), Germany
R. Wuerstlein � N. Harbeck
Comprehensive Cancer Center (CCC), University of Munich
(LMU), Munich, Germany
M. Schmitt
Frauenklinik (OB/GYN), Technical University Munich (TUM),
Munich, Germany
F. Jaenicke
Frauenklinik (OB/GYN), University Clinic of Hamburg-
Eppendorf, Hamburg, Germany
M. Untch
Frauenklinik (OB/GYN), Helios-Klinikum Berlin-Buch, Berlin,
Germany
N. Harbeck
Breast Center, Frauenklinik Großhadern, University of Munich
(LMU), Munich, Germany
123
Breast Cancer Res Treat (2013) 138:839–850
DOI 10.1007/s10549-013-2496-z

of cost utility are age and residual CTX benefit in low-uPA/
PAI-1 patients. The uPA/PAI-1 test is cost-effective in the
target group compared to either an ‘‘all-CTX’’ or a ‘‘no-
CTX’’ scenario. This model thus lends health economic
support to current guideline recommendations that
uPA/PAI-1 testing is beneficial for BC patients with no
lymph node involvement.
Keywords Economics � Biomarker � Cost model �Markov model � Cost-effectiveness analysis � Prevention of
chemotherapy � Costs
Background and objectives
In primary breast cancer, administration of an adjuvant
chemotherapy regimen is justified for those patients whose
expected survival benefit from the regimen outweighs
expected negative effects of the therapy. This premise
underlies essentially all adjuvant therapy guidelines. The
complexity of therapy decision support derives in large part
from the requirement of determining individual ‘‘expected
survival benefit,’’ which is heterogeneous even within
breast cancer sub-groups defined by conventional factors
such as lymph node involvement (N), tumor stage (pT),
age, and hormone receptor (HR±) status. According to
current guidelines in Germany, for example, patients with
age [ 35/N0/G2/HR?/HER2- are currently considered to
be at ‘‘intermediate’’ relapse risk and have an undetermined
indication for adjuvant chemotherapy based on these
established clinicopathological factors alone.
Without additional information, the optimal adjuvant
therapy decision for a patient within a heterogeneous sub-
group represents a compromise between benefits for some
and harm (or at best wasted resources) for others. In a
typical population of node-negative (N0), primary breast
cancer patients treated by chemotherapy, the mixture of
effects comprises considerable benefit (avoidance of
relapse) for a low percentage of patients, mild to moderate
harm (immediate and possibly long-term but nonlethal
side-effects of chemotherapy) for a much larger group, and
severe harm (e.g., cardiac insufficiency) in a small group.
Demands are increasing to verify health care resource
allotment for cost-effectiveness worldwide since health
care resources are limited even in high income countries
[1]. This is related to the use of adjuvant chemotherapy [2]
as well as CTX-related concomitant medication as G-CSF
[3] and anti-hormonal therapy [4]. Cost-effectiveness
computations for use of prognostic biomarkers for adjuvant
chemotherapy selection in breast cancer have a potentially
strong role to play in decision support, but there are also
substantial methodological challenges [5], particularly
regarding the applicability of prognostic studies.
Also new gene profiling tests support market access with
economic evaluations [6–8]. Requirements for publishing
economic evaluations have been defined to standardize and
assure quality and transparency of potential interests [9].
In most countries, including Germany, which has a cost-
related and disease-specific flat-rate reimbursement system,
therapy policies take not only the patient’s point of view,
but also a societal or payer point of view, i.e., including
costs into account. In order to objectify therapy decisions
from the perspective of these stakeholders, cost-effective-
ness ratios, e.g., Euros per quality adjusted life year,
abbreviated €/QALY, can be compared with a given will-
ingness to pay (WTP) threshold. This method can support
difficult health care policy choices by putting a common
quality metric on different disease contexts.
With the establishment and recommendation of novel
prognostic and especially predictive factors, we can utilize
evidence-based models to reveal some of the previously
hidden heterogeneity in survival and therapy benefits and
thus improve the level of therapy optimization from any
point of view in question. In clinical practice, of course,
there are costs associated with the determination of novel
factors. Therefore, the objective of health economics
modeling in this context is to quantify the cost-effective-
ness of a proposed test, by taking into account therapy
decisions based on the test and their consequences for the
entire subsequent course of events—including stochastic
variations within the population.
Tumor invasion factors uPA/PAI-1 have been guideline-
recommended by AGO Germany [10] since 2002 and
ASCO since 2007 [11]; quality-assured biomarkers for
decision support regarding adjuvant chemotherapy (CTX)
in primary breast cancer patients and considerable experi-
ence on the uPA/PAI-1 testing process in clinical practice
including realistic costs is now available. Despite the
strong evidence basis for uPA/PAI-1 [12–18], no cost-
effectiveness evaluation of the type discussed above has
been performed and published so far [19]. The present
model is intended as a first step to fill this gap by esti-
mating the financial benefit and cost-effectiveness for the
ideal and optimal application of uPA/PAI-1 testing in
defined target groups. The objective is accomplished here
by comparing the expected total net survival benefits and
costs of a therapy strategy utilizing the uPA/PAI-1 test
results to a base case, i.e., a therapy strategy not utilizing
the test. As explained in detail below, the estimation
methodology utilizes a Markov-state model of disease-free
and post-relapse survival with competing survival risks
typical for otherwise healthy women within a range of ages
in the target population. The resulting analysis will quan-
tify the cost-effectiveness of uPA/PAI-1 testing versus two
alternative scenarios (‘‘all-CTX’’ or a ‘‘no-CTX’’) by
computing the consequences of adjuvant therapy decisions
840 Breast Cancer Res Treat (2013) 138:839–850
123

based on the test for the subsequent course of events in
virtual populations.
Methods and health economic model
Formulation of cost-effectiveness as a virtual study
At the top level, cost-effectiveness of testing in a target
group is formulated here as a virtual study comparing the
consequences of two possible decisions trees: one with
uPA/PAI-1 testing and the other without it (testing case
versus base case). Quantitative testing of uPA and PAI-1 in
tumor tissue is performed with a standardized ELISA test.
Results of uPA and PAI-1 testing are defined by specific
cut-off levels with 3.0 ng/mg for uPA and 14.0 ng/mg for
PAI-1 in overall protein. A result of B cut-off level is
defined as low or negative and [ considered high or
positive. In the base case with no uPA/PAI-1 testing, the
decision for or against adjuvant chemotherapy can only be
affected by policy for the target group (and in principle by
other individual factors). In the testing case, the decision
recommendation will depend in addition on uPA/PAI-1
testing results, i.e., it will be the same as the usual policy
for one test outcome and will be different for the other.
Each computation described here can thus be thought of
as a two-armed virtual study performed on a virtual pop-
ulation drawn randomly from the target patient group and
assigned randomly to one of the two arms (testing or base
case).
The main figure of merit used here is denoted ‘‘incre-
mental cost-effectiveness ratio’’ (ICER), defined as the
ratio of incremental cost to incremental effectiveness.
These are computed as follows: For each virtual patient,
survival and costs are followed over time. ‘‘Incremental
effectiveness’’ in the present context involves the differ-
ence in survival distributions in the study arms for those
patients whose chemotherapy decision is changed by the
test. In principle it could also involve corresponding dif-
ferences in quality of life and possible severe harm (e.g.,
cardiac insufficiency) in a small group, but these differ-
ences are not included explicitly here.
Computation of incremental cost differences requires
inclusion of only those costs that could differ between the
virtual study arms; hence, primary surgery and endocrine
therapy costs are excluded from the analysis. Testing costs
for uPA/PAI-1 are obviously absent in the base case.
Chemotherapy costs—both direct and indirect—will differ
between the study arms for those patients whose chemo-
therapy decision is changed by the test. In addition, costs
due to treatment following relapse could also differ
between the study arms.
As mentioned earlier, from some perspectives, e.g., for
payers, it is customary to compare the ICER to a WTP
threshold, e.g., 50,000 Euro/ly. The cost-effectiveness of
the uPA/PAI-1 test in population subgroups can then be
objectified by asking whether the ICER is likely to exceed
this WTP or not in the subgroup. This particular compar-
ison is provided here only as a reference and not as a
recommendation.
Target population characteristics
The target population for the present analysis consists of
primary breast cancer patients staged as metastasis-free
(M0), node-negative (N0), pathological grade G2,
age [ 35 years, estrogen receptor and/or progesterone
receptor positive (HR?), and HER2 negative. In the target
population, it is assumed that all patients due to their HR?
status will receive adjuvant endocrine therapy appropriate
to their menopausal status (tamoxifen or aromatase inhib-
itors) according to current guidelines—i.e., for at least 5
years, unless they suffer relapse. The scenarios considered
here exclude the option of neo-adjuvant (rather than adju-
vant) chemotherapy in the tested (target) population, but
have no effect on this choice for the remaining population
if, e.g., node positive, G3, HR-, or HER2?, or age B35.
Markov states
The health economic computations utilize a Markov sur-
vival model with three possible states abbreviated as fol-
lows: relapse-free survival (RFS), post-relapse survival
(PRS), and death by any cause (D), the ‘‘absorbing state’’.
Markov models can be defined by their transitions and
transition rates. The possible transitions in the present
model are RFS ? PRS, RFS ? D, and PRS ? D. The
transition RFS ? D highlights the competing risks of
‘‘death due to breast cancer relapse’’ and ‘‘death from other
causes’’. This latter competing risk, which of course
depends on the age of the patient, is an important health
economic consideration, because it influences the potential
survival benefits of therapy.
Design of virtual studies
Two virtual study designs (scenarios) are considered, dif-
fering in the assumption of how patients would be treated
without the test. In each design, the health economic
impact of risk group selection by uPA and PAI-1 testing is
calculated by comparing the survival and cost sequences in
two hypothetical cohorts of virtual patients randomly
drawn from this population and eligible in principle for
Breast Cancer Res Treat (2013) 138:839–850 841
123
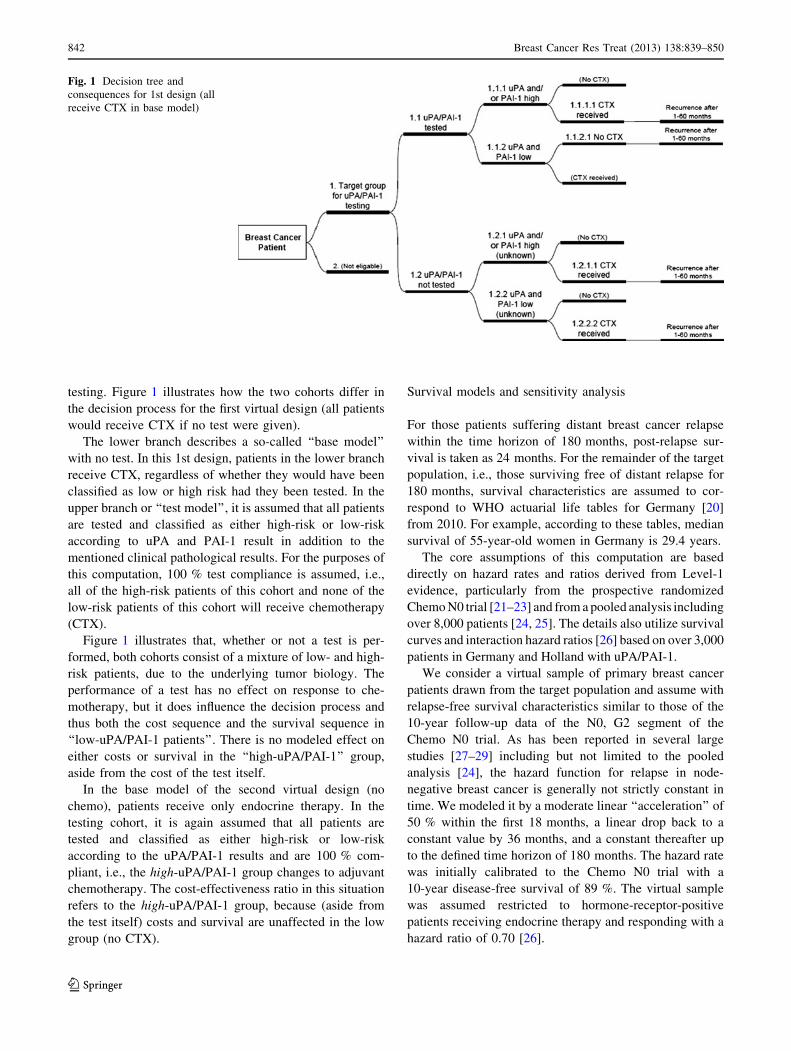
testing. Figure 1 illustrates how the two cohorts differ in
the decision process for the first virtual design (all patients
would receive CTX if no test were given).
The lower branch describes a so-called ‘‘base model’’
with no test. In this 1st design, patients in the lower branch
receive CTX, regardless of whether they would have been
classified as low or high risk had they been tested. In the
upper branch or ‘‘test model’’, it is assumed that all patients
are tested and classified as either high-risk or low-risk
according to uPA and PAI-1 result in addition to the
mentioned clinical pathological results. For the purposes of
this computation, 100 % test compliance is assumed, i.e.,
all of the high-risk patients of this cohort and none of the
low-risk patients of this cohort will receive chemotherapy
(CTX).
Figure 1 illustrates that, whether or not a test is per-
formed, both cohorts consist of a mixture of low- and high-
risk patients, due to the underlying tumor biology. The
performance of a test has no effect on response to che-
motherapy, but it does influence the decision process and
thus both the cost sequence and the survival sequence in
‘‘low-uPA/PAI-1 patients’’. There is no modeled effect on
either costs or survival in the ‘‘high-uPA/PAI-1’’ group,
aside from the cost of the test itself.
In the base model of the second virtual design (no
chemo), patients receive only endocrine therapy. In the
testing cohort, it is again assumed that all patients are
tested and classified as either high-risk or low-risk
according to the uPA/PAI-1 results and are 100 % com-
pliant, i.e., the high-uPA/PAI-1 group changes to adjuvant
chemotherapy. The cost-effectiveness ratio in this situation
refers to the high-uPA/PAI-1 group, because (aside from
the test itself) costs and survival are unaffected in the low
group (no CTX).
Survival models and sensitivity analysis
For those patients suffering distant breast cancer relapse
within the time horizon of 180 months, post-relapse sur-
vival is taken as 24 months. For the remainder of the target
population, i.e., those surviving free of distant relapse for
180 months, survival characteristics are assumed to cor-
respond to WHO actuarial life tables for Germany [20]
from 2010. For example, according to these tables, median
survival of 55-year-old women in Germany is 29.4 years.
The core assumptions of this computation are based
directly on hazard rates and ratios derived from Level-1
evidence, particularly from the prospective randomized
Chemo N0 trial [21–23] and from a pooled analysis including
over 8,000 patients [24, 25]. The details also utilize survival
curves and interaction hazard ratios [26] based on over 3,000
patients in Germany and Holland with uPA/PAI-1.
We consider a virtual sample of primary breast cancer
patients drawn from the target population and assume with
relapse-free survival characteristics similar to those of the
10-year follow-up data of the N0, G2 segment of the
Chemo N0 trial. As has been reported in several large
studies [27–29] including but not limited to the pooled
analysis [24], the hazard function for relapse in node-
negative breast cancer is generally not strictly constant in
time. We modeled it by a moderate linear ‘‘acceleration’’ of
50 % within the first 18 months, a linear drop back to a
constant value by 36 months, and a constant thereafter up
to the defined time horizon of 180 months. The hazard rate
was initially calibrated to the Chemo N0 trial with a
10-year disease-free survival of 89 %. The virtual sample
was assumed restricted to hormone-receptor-positive
patients receiving endocrine therapy and responding with a
hazard ratio of 0.70 [26].
Fig. 1 Decision tree and
consequences for 1st design (all
receive CTX in base model)
842 Breast Cancer Res Treat (2013) 138:839–850
123

It was further assumed that in the target population 60 %
will test with high uPA/PAI-1 status, the other 40 % low.
The assumed hazard ratio for patients in the target group
with high uPA/PAI-1 status compared to low uPA/PAI-1
status (no adjuvant chemotherapy) is HR_high-low = 2.5,
which represents a compromise between [26] and the
Chemo N0 trial and is consistent with the pooled analysis
[23]. Note that this hazard ratio is unaffected by adjuvant
endocrine therapy, which has no interaction with uPA/PAI-
1. The residual adjuvant CTX benefit in low uPA and PAI-
1 tested patients is uncertain, but is assumed to lie in the
range from HR_CTX(LR) = 0.8–0.99.
Cost and quality adjustment models
Costs for medication and uPA/PAI-1 testing
Costs of medication including febrile neutropenia (FN)
prophylaxis was calculated as provider’s costs in € of 2010
at an academic hospital chemotherapy unit in Germany.
Cost were taken from hospital charts and purchase
department and divided into direct and indirect costs. The
currency conversion rate is approx. €1.00 = US$ 1.30 in
March 2013.
Cost calculations
All cost calculations were performed according to official
prices or service costs charged in 2010 in the German
health care system. The calculations are based on CTX
standards of the Certified Breast Center of Martin-Luther-
University of Halle an der Saale, Germany, which are
Guideline-based and comparable to other German breast
centers and hospital settings.
Cost calculations were performed for (1) direct CTX
medication costs including the individual guideline-based
CTX regimen, (2) CTX-related concomitant medication for
prevention of, e.g., emesis, sickness, and CTX-related
toxicity as well as for (3) prophylaxis of febrile neutrope-
nia, a common side effect of CTX’s hematological toxicity.
Medication costs were taken from the official 2010 German
pharmaceutical price list (Rote Liste Service GmbH,
Frankfurt, Germany) [30].
Standard CTX regimen in the target group of breast
cancer as previously defined was applied with 6 cycles of
FEC 500/100/500 mg/m2 (q21) or 3 cycles of 5-Fluoro-
uracil, Epirubicin, and Cyclophosphamid FEC 500/100/
500 mg/m2 (q21) followed by 3 cycles of Docetaxel DOC
100 mg/m2 (q21). For this model the ratio of CTX was
defined with 70 % FEC and 30 % FEC ? DOC regimens.
The average standard patient was defined with a body
surface area (BSA) of 1.75 m2, and all costs were calcu-
lated accordingly.
CTX-related co-medication was calculated according to
CTX standard protocols and included for each FEC
500/100/500 cycle (aprepitant, ondansetron, dexamatha-
son, mesna, and furosemide) and for each DOC 100 cycle
(dexamethason, dimetindenmaleat, ranitidine) with the
prescription value of the smallest medication package
size.
FN prophylaxis was calculated at a hypothetical optimal
application rate of 100 % according to the EORTC
Guideline [31], which implies for CTX regimen FEC and
FEC-DOC an upfront G-CSF application of 100 % with
pegfilgastrim (Neulasta�) with a dose of one for each CTX
cycle (6 applications).
For CTX application of anthracycline, a port is guide-
line-recommended to avoid common CTX-related periph-
eral vascular toxicity and allow easy access for laboratory
and i.v. application. Therefore revenues for implantation
and explantation on an out-patient base according to Ger-
man ambulatory reimbursement in 2010 were included. To
prevent clotting of blood in this foreign body material,
repeated flushing with heparin is mandatory (n = 7; n = 1
before and n = 6 after each CTX cycle), for which the
service price is included. This price is taken from the
German Medical Fee Schedule (Gebuhrenordnung fur
Arzte (GOA) 2010) [32].
The following CTX-related diagnostics necessary for
each CTX application were estimated: Laboratory param-
eters like small and complete blood count to potentially
identify neutropenia, and other blood parameter and tumor
markers were estimated and defined with a flat rate of €40
per cycle. Cardiac ultrasound to identify potential cardiac
side effects of anthracycline CTX was performed after
every 3rd CTX cycle with anthracycline (29 for FEC
regimen; 19 for FEC-DOC regimen). The internal transfer
price of the hospital (= price between departments) of
€57.60 per cardiac ultrasound was used.
Additional direct and indirect medical and non-medical
costs as well as secondary and tertiary costs effects of CTX
for patients, health care and the entire social system were
not included. These include anything from i.v. fluids,
preparation of CTX, transportation costs, waste manage-
ment, out of pocket payments by patients, CTX-related
comorbidity to comortality, rehospitalization, wigs for
CTX-related alopecia, sickness benefits, earlier return to
work.
uPA/PAI-1 test costs
The costs for uPA/PAI-1 testing were analyzed in detail
and divided into direct and indirect costs. Costs were
estimated according to appropriate resource consumption
[33].
Breast Cancer Res Treat (2013) 138:839–850 843
123

Results
Cost calculations
For this model, the direct costs of the two standard CTX
regimen 69 FEC 500/100/500 and 39 FEC 500/100/500
followed by 39 DOC 100 including CTX, concomitant
medication, FN-prophylaxis and diagnostics like cardiac
ultrasound and laboratory parameter were calculated
according to actual provider costs in 2010 at €17,608.68
(Table 1) and €20,098.59 (Table 2), respectively. The
average direct costs of CTX at an estimated application
rate of 70 % for 69 FEC 500/100/500 and 30 % of 39
FEC 500/100/500 ? 39 DOC 100 were calculated as 0.79
€17,608.68 ? 0.39
€20,098.59 = €12,326.08 ? €6,029.58 = €18,356.38.
Estimated costs of i.v. port handling and care were
€1,040.26 (Table 3).
The estimated direct costs of uPA/PAI-1-testing were
€275.97; indirect costs including administration, han-
dling, and in-house or on-site transportation or mailing
were estimated as €110.00 for a total of €385.97
(Table 4). If samples need to be sent to an external
laboratory, additional transportation costs would occur,
depending on distance between hospital and laboratory,
single or consolidated shipment, and type of transporta-
tion used.
Incremental cost-effectiveness
Potential savings in direct, per-patient expected costs of
two leading CTX regimens (69 FEC or 39 FEC–39 DOC)
resulting from uPA/PAI-1 test were calculated from a
German health provider’s perspective. In this scenario,
adjuvant CTX costs are saved in 40 % of patients by
testing; including medications, prophylaxis, diagnostics,
additional supporting therapies and procedures, CTX costs
about €20,000 for both regimens considered (69 FEC
€19,366; 39 FEC ? 39 DOC €22,145; Fig. 2); relapse
medical costs were modeled at €40,000.
ICER of uPA/PAI-1 testing compared to ‘‘all-CTX’’-
scenario
In the first scenario, suppose that all patients of the target
group receive adjuvant CTX in the absence of the test, but
with the test, patients with low uPA and PAI-1-concen-
trations in the tumor tissue are spared adjuvant CTX.
Consider a patient with low uPA and PAI-1-concentra-
tions in the tumor within the target population of
35 \ age \ 75, N0, G2, HR?, HER2-: Survival curves
without CTX were estimated using Chemo N0 10-year dis-
ease-free survival of 89 % assuming endocrine therapy
benefit (hazard ratio HR = 0.7). Expected lost life years (ly)
due to relapse—with versus without test—were estimated
Table 1 Direct costs for 6
cycles of FEC 500/100/500 with
concomitant medication and
upfront FN prophylaxis
Comment Costs (€)
Diagnostics
Cardiac ultrasound After every 3rd CTX cycle 57.60
Laboratory parameter Blood count, tumor marker, etc. 40.00
Concomitant medication
Aprepitant 125 mg To prevent nausea and emesis 63.55
Ondansetron 8 mg To prevent nausea and emesis 160.14
Dexamethason 16 mg To prevent nausea and emesis 16.58
Uromitexan 400 mg To prevent urotoxicity 54.68
Uromitexan 400 mg To prevent urotoxicity 54.68
Lasix 20 mg To induce diuresis 16.95
Dexamethason To prevent nausea and emesis 34.68
CTX
5-Fluorouracil 875 mg Chemo 15.48
Epirubicin 175 mg Chemo 762.67
Cyclophosphamid 875 mg Chemo 132.64
FN prophylaxis
Pegfilgastrim Upfront for 6 cycles at each 1,563.53
Summary
3 CTX cycles with 1 cardiac ultrasound 8,804.34
Costs for 69 FEC with 2 cardiac ultrasounds 17,608.68
844 Breast Cancer Res Treat (2013) 138:839–850
123

from corresponding survival curves using age-adjusted life
expectancy minus 2 years post-relapse survival.
Figure 2 shows the ICER as a function of patient age
assuming CTX benefit (DFS) for low-uPA/PAI-1 patients
of HR_CTX(LR) = 0.90, corresponding to about the
midpoint of the uncertainty range. For example, at age 55,
median DFS benefit of CTX would be only about 0.25 ly (3
months) at an estimated net cost of €18,500 or about
ICER = €75,000/ly. The figure indicates that the test is
cost-effective at a €50,000 threshold above age 45, since
the ICER for CTX would otherwise exceed €50,000. Note
that in this virtual study, the cost-effectiveness does not
depend on the efficacy of chemotherapy in the high-uPA/
PAI-1 group.
Sensitivity analysis on residual adjuvant CTX benefit
in low-uPA/PAI-1 patients
Figure 3 shows the results of sensitivity analysis performed
by varying residual adjuvant CTX benefit in the low-uPA
and/orPAI-1 group in the range HR_CTX(LR) = 0.8–0.99
for age 55 years. If the test is not given, then the resulting
cost per ly of giving adjuvant CTX to all patients
(increasing curve) and the survival impact (decreasing
curve, right axis) depend on the assumed adjuvant CTX
benefit in low-risk patients. If the health care provider were
willing to pay €50,000 for 1 ly, then a HR of at most 0.85
would be required in the low-risk group. Very low CTX
benefit (HR approaching 1) is associated with astronomical
costs/ly.
The figure also shows estimated net savings (about
€18,500, lowest curve) in chemotherapy costs per low-risk
patient who does not receive adjuvant chemotherapy as a
result of her favorable uPA/PAI-1 test.
ICER of uPA/PAI-1 testing compared to ‘‘no-CTX’’-
scenario
We now consider a virtual subset of the target group as
defined above who would opt against the general chemo-
therapy recommendation but whose rejection of CTX
would be reversed by a high-uPA/PAI-1 test result (100 %
test compliance). In this scenario, CTX is unaffected in
low-uPA/PAI-1 patients.
Figure 4 shows the favorable ICER of uPA/PAI-1 test-
ing compared to a ‘‘no-CTX’’ scenario as defined above. In
this scenario, the test is very cost-effective at all ages
within the range considered: The ICER (test vs. no-CTX
strategy) remains below €6,000 at age 55 and is even more
favorable at younger ages, remaining below €25,000 up to
age 75. The median survival benefit per high-uPA/PAI-1
patient is substantial at all ages considered. Unlike the
Table 2 Direct costs of 3
cycles of FEC 500/100/500
followed by 3 cycles of DOC
100 with concomitant
medication and upfront FN
prophylaxis
FEC 500/100/500 Costs (€)
3 CTX cycles FEC with 1 cardiac ultrasound (see Table 1) 8,804.34
DOC 100
Diagnostics Comment Costs (€)
Laboratory parameter Blood count, tumor marker, etc. 40.00
Concomitant medication
Dexamethason i.v. Allergy prophylaxis 16.58
Fenistil Allergy prophylaxis 8.72
Ranitidin 50 mg Allergy prophylaxis 14.54
Dexamethason p.o. To prevent nausea and emesis 34.68
CTX
Docetaxel 175 mg Chemo 2,086.70
FN prophylaxis
Pegfilgastrim Upfront for 6 cycles at each 1,563.53
Summary
Costs for 3 cycles 11,294.25
Costs for 39 FEC ? 39 DOC 20,098.59
Table 3 Cost for venous port implantation and explantation and port
care
Service (including
port)
Comment Costs
(€)
Port implantation As out-patient, before CTX 496.01
Port explantation As out-patient, after CTX 487.97
Port irrigation n = 7 as out-patient, each at
€8.04
56.28
Summary 1,040.26
Breast Cancer Res Treat (2013) 138:839–850 845
123

0
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
200,000
0.80 0.82 0.84 0.86 0.88 0.90 0.92 0.94 0.96 0.98 1.00
hazard ratio of chemo in low-risk group
ICE
R
0.0
0.1
0.2
0.3
0.4
0.5
0.6
ly b
enef
itcost savings/patientdelta cost/ lydelta ly
Fig. 3 Sensitivity analysis with respect to uncertain CTX benefit for
low uPA/PAI-1 patients
Table 4 Direct and indirect
cost calculation for uPA/PAI-1-
testing
Direct costs for uPA/PAI-1 test Costs (€)
Preanalytics
Acceptance of specimen, weighing, visual assessment
Morcellation of tissue in dismembrator, lysis over night
Analytics
Centrifugation of lysis substrate
Determination of overall protein, BCA test 10.00
Aliquotation, dilution series, storage
FEMTELLE ELISA test for uPA/PAI-1 160.97
Quality management 20.00
Calculation of concentration in (a) ng/ml and (b) ng/mg
Of overall protein, technical validation of calculation
Biomedical validation of calculation
Postanalytics
Writing, print out and mailing of report, answering of queries, documentation (IT)
Labor time for technical assistant 40.00
Consumable supplies 45.00
Summary of direct costs for uPA/PAI-1 test 275.97
Indirect costs for uPA/PAI-1 test Costs
(€)
Administration
Writing of invoice, controlling of payment, purchase, etc. 10.00
Transportation
Specimen in LN from office/hospital/OR to pathology 15.00
Pathology
Acceptance of specimen, visual assessment, cutting of test specimen, control cut for HE-
section, report
25.00
Documentation, communication with physician and transport, dry ice for transportation 30.00
Transport
Dry ice transport over night to laboratory 30.00
Summary of indirect costs for uPA/PAI-1 test 110.00
Overall costs for uPA/PAI-1 test 385.97
-
20,000
40,000
60,000
80,000
100,000
120,000
140,000
160,000
180,000
200,000
35 40 45 50 55 60 65 70 75
age
ICE
R
0.0
0.1
0.2
0.3
0.4
0.5
0.6
ly b
enef
it
delta cost/ lydelta ly
Fig. 2 ICER for CTX (without the uPA/PAI-1 test) in the low-risk
group. Decrease of ly-benefit results from decreasing life expectancy
with age (dashed curve, right axis)
846 Breast Cancer Res Treat (2013) 138:839–850
123

other scenarios, the computation is independent of residual
adjuvant CTX benefit in the low-uPA/PAI-1 patients,
because they do not receive CTX in either case; the
strongest influence is the well-established strong benefit of
adjuvant CTX in high-uPA/PAI-1 patients.
Discussion
According to current guidelines in Germany and other
countries, ‘‘intermediate-risk’’ primary breast cancer
patients (M0/N0/G2/HR?/HER2-, age [ 35) have an
undetermined indication for adjuvant chemotherapy, based
on these factors alone. By refining risk and therapy
response assessment, the uPA/PAI-1 test can be used to
determine an adjuvant chemotherapy indication (negative
for low and up to cut-off uPA and PAI-1 values, otherwise
positive).
This model has examined the health economic conse-
quences, in particular the ICER, of applying the uPA/PAI-1
test for adjuvant chemotherapy determination in this target
group compared to (1) an ‘‘all-CTX’’ and (2) a ‘‘no-CTX’’
scenario. Cost-effectiveness was quantified taking com-
peting mortality risks into account and assuming 100 %
test compliance. Risks for harmful consequences and
quality of life losses associated with chemotherapy were
not included. Under these assumptions, cost utility depends
on patient age. The computations reveal a strong positive
case for uPA/PAI-1 testing within the collectives consid-
ered here.
In the first scenario (test vs. ‘‘all-CTX’’), assuming CTX
benefit in low-uPA/PAI-1 patients given by
HR_CTX(LR) = 0.90, the test was cost-effective at a
€50,000 threshold above age 45, since the ICER for CTX
would otherwise exceed €50,000. Note that in this virtual
study, the cost-effectiveness does not depend on the effi-
cacy of chemotherapy in the high-uPA/PAI-1 group.
However, the residual benefit of CTX in low-uPA/PAI-1
patients is an important uncertain parameter. For this
reason, sensitivity analysis was performed in the ‘‘all-
CTX’’ vs. test scenario by varying the residual CTX benefit
for low-uPA/PAI-1 patients within an uncertainty range.
For a typical 55-year-old, the ICER (all-CTX vs.
test) [ €50,000 if HR_CTX(LR) [ 0.85, with savings of
€18,500 per low-risk patient attributable to the test.
In clinical breast cancer practice, adjuvant therapy rec-
ommendations by physicians can include concomitant,
patient-specific health factors or subjective opinions that
may or may not be guided by systematic evidence. More-
over, the decision for chemotherapy in an individual breast
cancer patient may reflect her personal physiological,
emotional, or other subjective considerations. The conse-
quence is that in a sub-group (such as node-negative
patients over 35 years with HR-positive, HER2-negative,
G2 tumors) for whom chemotherapy is recommended but
survival benefits are heterogeneous, we will find patients
who opt against the chemotherapy recommendation in the
absence of a test but who would comply with a recom-
mendation to undergo CTX if the uPA/PAI-1 test indicates
high risk. Under these assumptions, the cost-effectiveness
of uPA/PAI-1 testing for these patients was strongly posi-
tive throughout a broad age range.
The cost-effectiveness of the uPA/PAI-1 test as com-
puted here compared to the all-CTX scenario would be
strengthened by inclusion of long-term survival risks
associated with chemotherapy such as cardiac toxicity and
leukemia. Cost-effectiveness in this scenario would be
further strengthened by if QALY rather than ly were used
as the figure of merit, the precise numbers depending of
course on assignment of quality of life differences to
treatment states.
The incremental costs were computed here from a
payer’s perspective appropriate to the German setting. If
our calculations are to be used as a rough guide to cost-
effectiveness in other settings, it is important to remember
that cost-effectiveness of any test regarding adjuvant che-
motherapy in primary breast cancer will generally depend
on specifics of the country and the health care system
involved. Important country-specific factors include the
following:
• Target group for which guidelines allow an option for
no adjuvant chemotherapy (here age [ 35/N0/G2/
HR?/HER2-).
• Accepted quality-of-life adjustment for chemotherapy.
• Competing survival risks (Life tables).
• Direct and indirect costs of chemotherapy.
• Willingness of the health care provider to pay.
Cost estimates for the present model—notably for che-
motherapy, concomitant medication and FN prophylaxis as
well as port use—were comprehensively defined in
‘‘Methods and health economic model’’ section. In
0
5,000
10,000
15,000
20,000
25,000
30,000
35 40 45 50 55 60 65 70 75
age at primary therapy
ICE
R
0.0
1.0
2.0
3.0
4.0
5.0
6.0
ly g
aine
d pe
r hi
gh-r
isk
delta cost/ lydelta ly
patie
nt d
ue to
test
Fig. 4 Favorable ICER of uPA/PAI-1 testing compared to ‘‘no-
CTX’’-scenario as a function of age
Breast Cancer Res Treat (2013) 138:839–850 847
123

practice, costs can vary both by health-care system and
even within a single country in time due to changes in CTX
regimens that reflect medical advances, incorporation of
trial results, changing medication prices, use of generics,
bonus concepts, etc. A strong cost driver is the decision for
upfront FN prophylaxis, whose costs can exceed those of
chemotherapy medication itself.
Costs excluded from this calculation cover multiple
secondary and tertiary effects of CTX. If included, these
often hidden costs could also exceed those of primary CTX
and related medication and if taken into account would
tend to strengthen the case for uPA/PAI-1 testing.
The true benefits and costs in practice will depend on
compliance by patients and physicians. In contrast to the
potential savings estimated here assuming 100 % test
compliance, one observes deviations from 100 % compli-
ance to both conventional guidelines and validated tests,
resulting in cases of undertreatment and overtreatment
despite clear indications.
As an additional limitation, in clinical practice, the
fraction of G2, HR?, HER2- patients for whom CTX
savings could be realized could be affected by
• existence of sufficient tissue for the assay,
• availability of logistics for test performance,
• additional clinico-pathological decision criteria.
Finally, note that the perspective (patient rather than
payer) could affect all computations.
In a recent publication, a Markov model was applied to
estimate and compare cost-effectiveness of adjuvant che-
motherapy for scenarios corresponding to 1st–3rd genera-
tion regimens compared to a no-therapy scenario in a UK-
setting [2]. Prognostic information was considered, but not
factors predictive of therapy response (in the sense of a
survival model interaction). Despite differences in costs,
WTP, inclusion of QoL losses in the model, and the greater
diversity of the target group considered [2], there is a
parallel to the present work in their conclusion that for an
ER-positive patient receiving endocrine therapy, ‘‘no che-
motherapy’’ becomes the optimal treatment strategy in
terms of cost-effectiveness for 10-year recurrence-free
survival exceeding about 82 % (for age [ 60) to about
86 % (age [ 40). This favorable level of RFS applies to a
rather low fraction of patients using only conventional
factors, but to a considerably higher percentage using the
prognostic information of uPA/PAI-1. The consequence is
thus to enlarge the group of patients who can be spared
chemotherapy.
In the case of the 70-gene test (MammaPrintTM), cost
utility compared to Adjuvant onlineTM or St. Gallen
guidelines was studied from a Dutch perspective [6]. There
were a few technical differences in survival simulation to
the method used here, particularly the model assumption
that patients classified as true low or false high risk had a
zero probability to experience a relapse and the use of
different data sources. Nonetheless, the conclusion of cost-
effectiveness of the test is similar and occurs for the same
reasons as in our comparison of uPA/PAI-1 testing with the
‘‘all-CTX’’ strategy. Moreover, the computations support
the hypothesis mentioned above that our conclusions would
be strengthened if QoL losses due to chemotherapy were
included. Similar conclusions were reached when including
the 21-gene assay (Oncotype DXTM) in the comparison [7,
8].
Cost-effectiveness computations for use of biomarkers
in adjuvant chemotherapy selection in breast cancer are
likely to play an increasingly important role with the
advent of new tests and the potentially complex structure of
tumor classification gene expression. It is entirely possible
that a fusion of different tests, such as the 21-gene assay
and uPA/PAI-1, could isolate an even lower-risk group
than either test alone and strengthen the case for omission
of chemotherapy. Cost-effectiveness computations, e.g.,
using Markov models, could also play a key role in
approval of tests that improve prediction of response to
specific chemotherapy regimens, particularly in the case of
an expensive, targeted therapy that is highly effective in a
specific group. Validated multivariate predictive models
(interaction of test result with therapy) have enormous
impact on these calculations. However, health economic
analysis poses rather specific requirements on the design
and quality of studies used to provide transition rates and
other data in Markov state models [5]. These include the
need for models reporting hazard ratios within a multi-
variate model, meta-analysis or pooled analysis, efforts to
correct for publication bias, etc. Small studies claiming a
putative marker to be prognostic in a univariate model are
seldom of use in these computations. Future biomarker
studies could profit from consideration of health economics
considerations during the design phase.
Conflict of interest All authors besides one declared no conflict of
interest.
Disclosures REK received consulting fees from American Diag-
nostica unrelated to this project.
References
1. Sullivan R, Peppercorn J, Sikora K, Zalcberg J, Meropol NJ,
Amir E, Khayat D, Boyle P, Autier P, Tannock IF, Fojo T,
Siderov J, Williamson S, Camporesi S, McVie JG, Purushotham
AD, Naredi P, Eggermont A, Brennan MF, Steinberg ML, De
Ridder M, McCloskey SA, Verellen D, Roberts T, Storme G,
Hicks RJ, Ell PJ, Hirsch BR, Carbone DP, Schulman KA,
Catchpole P, Taylor D, Geissler J, Brinker NG, Meltzer D, Kerr
848 Breast Cancer Res Treat (2013) 138:839–850
123

D, Aapro M (2011) Delivering affordable cancer care in high-
income countries. Lancet Oncol 12(10):933–980
2. Campbell HE, Epstein D, Bloomfield D, Griffin S, Manca A,
Yarnold J, Bliss J, Johnson L, Earl H, Poole C, Hiller L, Dunn J,
Hopwood P, Barrett-Lee P, Ellis P, Cameron D, Harris AL, Gray
AM, Sculpher MJ (2011) The cost-effectiveness of adjuvant
chemotherapy for early breast cancer: a comparison of no che-
motherapy and first, second, and third generation regimens for
patients with differing prognoses. Eur J Cancer 47(17):
2517–2530
3. Hershman DL, Wilde ET, Wright JD, Buono DL, Kalinsky K,
Malin JL, Neugut AI (2012) Uptake and economic impact of first-
cycle colony-stimulating factor use during adjuvant treatment of
breast cancer. J Clin Oncol 30(8):806–812
4. Lux MP, Hartmann M, Jackisch C, Raab G, Schneeweiss A,
Possinger K, Oyee J, Harbeck N (2009) Cost-utility analysis for
advanced breast cancer therapy in Germany: results of the ful-
vestrant sequencing model. Breast Cancer Res Treat 117(2):
305–317
5. Williams C, Brunskill S, Altman D, Briggs A, Campbell H,
Clarke M, Glanville J, Gray A, Harris A, Johnston K, Lodge M
(2006) Cost-effectiveness of using prognostic information to
select women with breast cancer for adjuvant systemic therapy.
Health Technology Assess 10(34):1–204
6. Retel VP, Joore MA, Knauer M, Linn SC, Hauptmann M, Harten
WH (2010) Cost-effectiveness of the 70-gene signature versus St.
Gallen guidelines and Adjuvant Online for early breast cancer.
Eur J Cancer 46(8):1382–1391
7. Retel VP, Joore MA, van Harten WH (2012) Head-to-head
comparison of the 70-gene signature versus the 21-gene assay:
cost-effectiveness and the effect of compliance. Breast Cancer
Res Treat 131(2):627–636
8. Yang M, Rajan S, Issa AM (2012) Cost effectiveness of gene
expression profiling for early stage breast cancer: a decision-
analytic model. Cancer 118(20):5163–5170
9. Lippman ME, Ethier S, Hayes DF (2009) Cost-effective analyses
in breast cancer research and treatment. Breast Cancer Res Treat
115(2):221–222
10. AGO Guidelines. www.ago-online.de/index.php?lang=de&site=
mamma_guide_topical&topic=mamma_guide
11. Harris L, Fritsche H, Mennel R, Norton L, Ravdin P, Taube S,
Somerfield MR, Hayes DF, Bast RC Jr (2007) American Society
of Clinical Oncology 2007 Update of Recommendations for the
Use of Tumor Markers in Breast Cancer. J Clin Oncol
25(33):5287–5312
12. Duffy MJ, Reilley D, O’Sullivan C, O’Higgins N, Fennelly JJ,
Andreasen P (1990) Urokinase-plasminogen activator, a new and
independent prognostic marker in breast cancer. Cancer Res
50(21):6827–6829
13. Janicke F, Schmitt M, Hafter R, Hollrieder A, Babic R, Ulm K,
Gossner W, Graeff H (1990) Urokinase-type plasminogen acti-
vator (uPA) antigen is a predictor of early relapse in breast
cancer. Fibrinolysis 4(2):69–78
14. Janicke F, Schmitt M, Graeff H (1991) Clinical relevance of the
urokinase-type and tissue type plasminogen activators and of
their type 1 inhibitor in breast cancer. Sem Thromb Hemostasis
17:303–312
15. Janicke F, Schmitt M, Pache L, Ulm K, Harbeck N, Hofler H,
Graeff H (1993) Urokinase (uPA) and its inhibitor PAI-1 are
strong, independent prognostic factors in node-negative breast
cancer. Breast Cancer Res Treat 24:195–208
16. Foekens JA, Schmitt M, van Putten WLJ, Peters HA, Kramer
MD, Janicke F, Klijn JG (1994) Plasminogen activator inhibitor-1
and prognosis in primary breast cancer. J Clin Oncol 12(8):
1648–1658
17. Stephens RW, Brunner N, Janicke F, Schmitt M (1998) The
urokinase plasminogen activator system as a target for prognostic
studies in breast cancer. Breast Cancer Res Treat 52(1–3):99–111
18. Harbeck N, Thomssen C (2011) A new look at node-negative
breast cancer. Oncologist 16(Suppl 1):51–60
19. Jacobs VR, Kates R, Kantelhardt EJ, Vetter M, Schmitt M, Jaenicke
F, Untch M, Thomssen C, Harbeck N (2010) Health economic
impact of risk group selection according to ASCO-recommended
biomarkers uPA/PAI-1 in node-negative primary breast cancer. 33rd
Annual San Antonio Breast Cancer Symposium, San Antonio, TX,
USA, December 7–12, 2010. Cancer Res 70(24 Suppl):196–197
20. World Health Organization (WHO). World Health Statistics
2010. WHO, Geneva, Switzerland 2010
21. Harbeck N, Schmitt M, Meisner C, Friedel C, Untch M, Schmid M,
Sweep CGJ, Lisboa BW, Lux MP, Beck T, Hasmuller S, Kiechle
M, Janicke F, Thomssen C, for the Chemo-N0 Study Group (2013)
Ten-year analysis of the prospective multicenter Chemo-N0 trial
validates ASCO-recommended biomarkers uPA and PAI-1 for
therapy decision making in node-negative breast cancer patients.
Eur J Cancer 2013 (in print). 10.1016/j.ejca.2013.01.007
22. Harbeck N, Schmitt M, Vetter M, Krol J, Paepke D, Uhlig M,
Paepke S, Janicke F, Geurts-Moespot A, von Minckwitz G,
Sweep F, Thomssen C (2008) Prospective biomarker trials
Chemo N0 and NNBC-3 Europe validate the clinical utility of
invasion markers uPA and PAI-1 in node-negative breast cancer.
Breast Care (Basel) 3(s2):11–15
23. Schmidt M, Victor A, Bratzel D, Boehm D, Cotarelo C, Lebrecht
A, Siggelkow W, Hengstler JG, Elsasser A, Gehrmann M, Lehr
HA, Koelbl H, von Minckwitz G, Harbeck N, Thomssen C (2009)
Long-term outcome prediction by clinicopathological risk clas-
sification algorithms in node-negative breast cancer—comparison
between Adjuvant!, St Gallen, and a novel risk algorithm used in
the prospective randomized Node-Negative-Breast Cancer-3
(NNBC-3) trial. Ann Oncol 20(2):258–264
24. Look MP, van Putten WL, Duffy MJ, Harbeck N, Christensen IJ,
Thomssen C, Kates R, Spyratos F, Ferno M, Eppenberger-Castori
S, Sweep CG, Ulm K, Peyrat JP, Martin PM, Magdelenat H,
Brunner N, Duggan C, Lisboa BW, Bendahl PO, Quillien V,
Daver A, Ricolleau G, Meijer-van Gelder M, Manders P, Fiets
WE, Blankenstein MA, Broet P, Romain S, Daxenbichler G,
Windbichler G, Cufer T, Borstnar S, Kueng W, Beex LV, Klijn
JG, O’Higgins N, Eppenberger U, Janicke F, Schmitt M, Foekens
JA (2002) Pooled analysis of prognostic impact of urokinase-type
plasminogen activator and its inhibitor PAI-1 in 8377 breast
cancer patients. J Natl Cancer Inst 94(2):116–128
25. Look M, van Putten W, Duffy M, Harbeck N, Christensen IJ,
Thomssen C, Kates R, Spyratos F, Ferno M, Eppenberger-Castori
S, Fred Sweep CG, Ulm K, Peyrat JP, Martin PM, Magdelenat H,
Brunner N, Duggan C, Lisboa BW, Bendahl PO, Quillien V,
Daver A, Ricolleau G, Meijer-van Gelder M, Manders P, Edward
Fiets W, Blankenstein M, Broet P, Romain S, Daxenbichler G,
Windbichler G, Cufer T, Borstnar S, Kueng W, Beex L, Klijn J,
O’Higgins N, Eppenberger U, Janicke F, Schmitt M, Foekens J
(2003) Pooled analysis of prognostic impact of uPA and PAI-1 in
breast cancer patients. Thromb Haemost 90(3):538–548
26. Harbeck N, Kates RE, Look MP, Meijer-Van Gelder ME, Klijn
JG, Kruger A, Kiechle M, Janicke F, Schmitt M, Foekens JA
(2002) Enhanced benefit from adjuvant chemotherapy in breast
cancer patients classified high-risk according to urokinase-type
plasminogen activator (uPA) and plasminogen activator inhibitor
type 1 (n = 3424). Cancer Res 62(16):4617–4622
27. Janicke F, Prechtl A, Thomssen C, Harbeck N, Meisner C, Untch
M, Sweep CG, Selbmann HK, Graeff H, Schmitt M, German N0
Study Group (2001) Randomized adjuvant chemotherapy trial in
high-risk, lymph node-negative breast cancer patients identified
Breast Cancer Res Treat (2013) 138:839–850 849
123

by urokinase-type plasminogen activator and plasminogen acti-
vator inhibitor type 1. J Natl Cancer Inst 93(12):913–920
28. Kim SJ, Shiba E, Kobayashi T, Yayoi E, Furukawa J, Takatsuka
Y, Shin E, Koyama H, Inaji H, Takai S (1998) Prognostic impact
of urokinase-type plasminogen activator (PA), PA inhibitor type-
1 and tissue-type PA antigen levels in node-negative breast
cancer: a prospective study on multicenter basis. Clin Cancer Res
4(1):177–182
29. Schmitt M, Harbeck N, Brunner N, Janicke F, Meisner C,
Muhlenweg B, Jansen H, Dorn J, Nitz U, Kantelhardt EJ,
Thomssen C (2011) Cancer therapy trials employing level-of-
evidence-1 disease forecast cancer biomarkers uPA and its
inhibitor PAI-1. Expert Rev Mol Diagn 11(6):617–634
30. Rote Liste (German pharmaceutical price list). www.rote-liste.de
31. Aapro MS, Bohlius J, Cameron DA, Dal Lago L, Donnelly JP,
Kearney N, Lyman GH, Pettengell R, Tjan-Heijnen VC,
Walewski J, Weber DC, Zielinski C, European Organisation for
Research and Treatment of Cancer (2011) 2010 update of EO-
RTC guidelines for the use of granulocyte-colony stimulating
factor to reduce the incidence of chemotherapy-induced febrile
neutropenia in adult patients with lymphoproliferative disorders
and solid tumours. Eur J Cancer 47(1):8–32
32. German Medical Fee Schedule (Gebuhrenordnung fur Arzte/
GOA). www.gesetze-im-internet.de/go__1982/
33. Hanseatische Krankenkasse (HKK) Erste Krankenkasse zahlt
Brustkrebs-Test [First health care fund reimburses breast cancer
test]. Press Release, November 10th 2010. www.hkk.de/top/
presse/pressearchiv/mitteilung_einzelansicht/?tx_ttnews%5Btt_-
news%5D=147&tx_ttnews%5BbackPid%5D=554%cHash=8963
6c6086
850 Breast Cancer Res Treat (2013) 138:839–850
123