Health behavior models in the age of mobile interventions: are our theories up to the task
27
Health behavior models in the age of mobile interventions: are our theories up to the task? William T Riley, PhD 1 , Daniel E Rivera, PhD 2 , Audie A Atienza, PhD 3 , Wendy Nilsen, PhD 4 , Susannah M Allison, PhD 5 , and Robin Mermelstein, PhD 6 1 National Heart, Lung, and Blood Institute, NIH, 6701 Rockledge Dr, Room 10224, MSC 7936, Bethesda, MD 20892-7936, USA 2 School for Engineering of Matter, Transport, and Energy, Ira A. Fulton School of Engineering, Arizona State University, Tempe, AZ 85287-6106, USA 3 National Institute of Health, National Cancer Institute, 6130 Executive Boulevard, EPN 4082, Bethesda, MD 20892-7335, USA 4 Office of Behavioral and Social Science Research, NIH, 31 Center Dr., Room B1C19, MSC 2027, Bethesda, MD 20892-2027, USA 5 National Institute of Mental Health, NIH, 6001 Executive Boulevard, Room 6226, MSC 9615, Bethesda, MD 20892-9615, USA 6 Department of Psychology and Public Health, Health Research and Policy Center, University of Illinois at Chicago, 850 West Jackson Boulevard, Suite 400, Chicago, IL 60607, USA Abstract Mobile technologies are being used to deliver health behavior interventions. The study aims to determine how health behavior theories are applied to mobile interventions. This is a review of the theoretical basis and interactivity of mobile health behavior interventions. Many of the mobile health behavior interventions reviewed were predominately one way (i.e., mostly data input or informational output), but some have leveraged mobile technologies to provide just-in-time, interactive, and adaptive interventions. Most smoking and weight loss studies reported a theoretical basis for the mobile intervention, but most of the adherence and disease management studies did not. Mobile health behavior intervention development could benefit from greater application of health behavior theories. Current theories, however, appear inadequate to inform mobile intervention development as these interventions become more interactive and adaptive. Dynamic feedback system theories of health behavior can be developed utilizing longitudinal data from mobile devices and control systems engineering models. Keywords Mobile phones; Handheld computers; Health behavior interventions; Smoking cessation; Weight management; Adherence; Chronic disease management; Health behavior theory; Dynamical systems; Control systems engineering The development, evaluation, and dissemination of computerized health behavior interventions have expanded rapidly in the last decade. Advances in Internet-based infrastructure and accessibility promoted the migration of computerized health behavior Correspondence to: W Riley, [email protected]. NIH Public Access Author Manuscript Transl Behav Med. Author manuscript; available in PMC 2011 July 25. Published in final edited form as: Transl Behav Med. 2011 March 1; 1(1): 53–71. doi:10.1007/s13142-011-0021-7. NIH-PA Author Manuscript NIH-PA Author Manuscript NIH-PA Author Manuscript
Transcript of Health behavior models in the age of mobile interventions: are our theories up to the task

Health behavior models in the age of mobile interventions: areour theories up to the task?
William T Riley, PhD1, Daniel E Rivera, PhD2, Audie A Atienza, PhD3, Wendy Nilsen, PhD4,Susannah M Allison, PhD5, and Robin Mermelstein, PhD6
1National Heart, Lung, and Blood Institute, NIH, 6701 Rockledge Dr, Room 10224, MSC 7936,Bethesda, MD 20892-7936, USA2School for Engineering of Matter, Transport, and Energy, Ira A. Fulton School of Engineering,Arizona State University, Tempe, AZ 85287-6106, USA3National Institute of Health, National Cancer Institute, 6130 Executive Boulevard, EPN 4082,Bethesda, MD 20892-7335, USA4Office of Behavioral and Social Science Research, NIH, 31 Center Dr., Room B1C19, MSC2027, Bethesda, MD 20892-2027, USA5National Institute of Mental Health, NIH, 6001 Executive Boulevard, Room 6226, MSC 9615,Bethesda, MD 20892-9615, USA6Department of Psychology and Public Health, Health Research and Policy Center, University ofIllinois at Chicago, 850 West Jackson Boulevard, Suite 400, Chicago, IL 60607, USA
AbstractMobile technologies are being used to deliver health behavior interventions. The study aims todetermine how health behavior theories are applied to mobile interventions. This is a review of thetheoretical basis and interactivity of mobile health behavior interventions. Many of the mobilehealth behavior interventions reviewed were predominately one way (i.e., mostly data input orinformational output), but some have leveraged mobile technologies to provide just-in-time,interactive, and adaptive interventions. Most smoking and weight loss studies reported atheoretical basis for the mobile intervention, but most of the adherence and disease managementstudies did not. Mobile health behavior intervention development could benefit from greaterapplication of health behavior theories. Current theories, however, appear inadequate to informmobile intervention development as these interventions become more interactive and adaptive.Dynamic feedback system theories of health behavior can be developed utilizing longitudinal datafrom mobile devices and control systems engineering models.
KeywordsMobile phones; Handheld computers; Health behavior interventions; Smoking cessation; Weightmanagement; Adherence; Chronic disease management; Health behavior theory; Dynamicalsystems; Control systems engineering
The development, evaluation, and dissemination of computerized health behaviorinterventions have expanded rapidly in the last decade. Advances in Internet-basedinfrastructure and accessibility promoted the migration of computerized health behavior
Correspondence to: W Riley, [email protected].
NIH Public AccessAuthor ManuscriptTransl Behav Med. Author manuscript; available in PMC 2011 July 25.
Published in final edited form as:Transl Behav Med. 2011 March 1; 1(1): 53–71. doi:10.1007/s13142-011-0021-7.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
interventions from prototype stand-alone software to robust, scalable, interactive, andtailored web-based programs. As a result, web-based health behavior interventions haveproliferated in recent years and appear to be an efficacious method for delivering healthbehavior interventions in a cost-effective manner [1–3].
The next evolution, or revolution, of computerized health interventions, mobile technologyand health (mHealth), appears to be underway. Mobile phones have achieved rapid and highpenetration. There are over 285 million wireless subscribers in the USA alone [4], and anestimated 67.6% of adults worldwide own cell phones [5]. Approximately 75% of US highschool students own a mobile phone [6]. In contrast to the initial Internet digital dividewhich limited the reach of computerized health behavior interventions for those in lowersocioeconomic groups, mobile phone use has been widely adopted across socioeconomicand demographic groups and appears greater among those populations most in need of theseinterventions [6, 7]. The penetration rates in developing countries, where wirelesstechnologies have leapfrogged the wired computer infrastructure, have producedconsiderable excitement in the global health community to reach and follow individuals whowere previously unreachable via traditional communication channels [8, 9].
Compared to Internet interventions delivered to desktop and laptop computers, mobileinterventions have the capacity to interact with the individual with much greater frequencyand in the context of the behavior. As sensing technologies integrated with the mobile phonevia Bluetooth or other data transmission process continue to develop, health behavior changeinterventions can be delivered based not only on self-reports and time/location parametersbut also on psychophysiological state, social context, activity level, and behavior patterns[10]. The availability of these rich, complex, and frequent data inputs provides the potentialto deliver health behavior interventions tailored not only to the person’s baselinecharacteristics but also to his/her frequently changing behaviors and environmental contexts[11].
To better leverage the potential of mobile technologies for health behavior interventions,health behavior theories and models need to be able to guide the development of complexinterventions that adapt rapidly over time in response to various inputs. Existing healthbehavior theories and models have served for many years as guides to interventiondevelopment and delivery, and these theories have been the basis not only for face-to-facecounseling interventions but also mass media and social marketing efforts. Models such asthe Health Belief Model [12], Theory of Planned Behavior [13], Social Cognitive Theory[14], the Transtheoretical Model [15], and Self-Determination Theory [16] have served asthe basis for many of the eHealth web and desktop/laptop computer interventions and haveinformed how interventions can be tailored to the individual’s baseline status.
As intervention developers take full advantage of mobile technologies, health behaviormodels will be required to guide not only tailored adjustments at intervention initiation butalso the dynamic process of frequent iterative intervention adjustments during the course ofintervention. The content and timing of a specific mobile phone intervention delivered viavoice, text, resident application, mobile web, or other modality can be driven by a range ofvariables including (a) the target behavior frequency, duration, or intensity; (b) the effect ofprior interventions on the target behavior; and (c) the current context of the individual (time,location, social environment, psychophysiological state, etc.). Such interventions requirehealth behavior models that have dynamic, regulatory system components to guide rapidintervention adaptation based on the individual’s current and past behavior and situationalcontext. Some have argued that current health behavior models are inadequate even for low-tech interventions [17], but the predominately linear and static nature of these models
Riley et al. Page 2
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

severely limits their ability to guide the dynamic, adaptive interventions possible via mobiletechnologies.
To evaluate the theoretical basis and adaptive nature of mobile interventions, the currentliterature on mobile technology health behavior interventions was reviewed. For this review,we define “mobile technology” as computer devices that are intended to be always on andcarried on the person throughout the day (i.e., during normal daily activities). Mobile phonesare the prototype device within this space, and most of the interventions reviewed usedmobile phone platforms, but precursors to current smart phones and text messaging systemssuch as personal digital assistants (PDAs) and two-way pagers also are consistent with thisdefinition. Excluded from this definition are devices that are portable (e.g., laptops,netbooks, iPads) but are not intended to be carried on the person throughout the day.Although technically mobile, we also excluded interventions that involved phone-basedcounseling, whether live or by interactive voice response (IVR), that could be deliveredsimilarly via landline (i.e., phone-based counseling via mobile phone). Prior to the adventand widespread use of multipurpose mobile devices, special purpose devices weredeveloped for the delivery of health behavior interventions [18, 19], but these pioneeringprototypes often lacked the portability, connectivity, input–output interface, and/orcomputing power of current multi-purpose devices and are not included in this review. Thisreview is also limited to the use of these mobile devices for delivering health behaviorinterventions, not assessments. There is a substantive literature on the use of mobile devicesfor health behavior assessment (e.g., ecological momentary assessment), and self-monitoringalone has been shown to be an effective health behavior intervention [20], but we excludedfrom this review mobile programs that involved assessment input only or that used mobiledevice output solely for the purpose of encouraging input (i.e., reinforcing recordingadherence).
For this review, a Medline search of “mobile phone,” “cell phone,” “text messaging,”“personal digital assistant,” “PDA,” “palmtop,” “handheld computer,” and “pager”published through June 2010 was conducted. Articles meeting the definition describedabove were selected, and additional articles were identified from references of these initiallyselected articles. A considerable number of these articles were proof-of-concept reports thatdescribed technical development, an ongoing study, or reported only usability/satisfactiondata. To insure review of fully functional mobile interventions, we narrowed the selectioncriteria to studies that reported some form of clinical outcome data, with or withoutrandomized controlled conditions. Nearly all of the articles identified meeting these criteriafell into one of four major health behavior areas: smoking, weight loss (including diet andexercise interventions), treatment adherence (i.e., adherence to medical recommendationsincluding both taking medication and attending appointments), and chronic diseasemanagement. Therefore, we limited this review to mobile health behavior interventions inthese four areas. Others have reviewed subsets of the research reviewed here for thepurposes of estimating effect sizes (e.g., [21, 22]). In contrast to meta-analytic reviews ofeffect size, the purpose of this review is to assess how theory has been employed in thedevelopment of mobile health behavior interventions and how the interactive and adaptivepotential of these interventions may require new dynamic systems theories of healthbehavior.
REVIEW OF MOBILE HEALTH BEHAVIOR INTERVENTIONSSmoking cessation
Seven studies were identified that used mobile technology to deliver smoking cessationinterventions. In Table 1 and subsequent tables of the other three areas reviewed, wesummarize for each study the basic study characteristics (e.g., sample, design), a brief
Riley et al. Page 3
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

description of the intervention, the theoretical basis of the intervention if reported, theinteractivity of the intervention, and the primary outcome. For interactivity, we specify if theintervention output was adjusted based on input provided by the user, if this adjustment wasmanual (e. g., healthcare professional reviewed data and determined intervention output) orautomatic (e.g., intervention output generated by computer algorithms), and if theadjustment occurred at intervention initiation (i.e., tailored or personalized based on initialassessment) or during the course of the intervention, or both. The concept of “just-in-time”of Intille et al. is used to characterize interventions that adjust based on data obtained duringthe course of the intervention [30]. As opposed to the term “real-time” which is commonlyis used in the mobile assessment literature to denote input occurring at the time of arecording prompt or the behavior being monitored, mobile interventions are often laggedover minutes, hours, or days as sufficient data are obtained to adapt the intervention, hencethe use of “just-in-time” to describe adaptations occurring during the course of theintervention.
As shown in Table 1, the seven studies identified are from three research groups whodeveloped and evaluated interventions delivered via mobile phone text messaging (aka shortmessaging service (SMS)). These interventions consisted primarily of text message outputalthough Whittaker et al. [26] also delivered mobile videos of role models and their quittingexperiences. All of the interventions were computer-tailored at treatment initiation. Theintervention developed by Riley and colleagues [23, 25] tailored both content and timing ofthe text messages to the times users indicated via an associated Internet site that urges andhigh-risk situations were likely to occur. All of these interventions also adjusted just-in-timevia text message requests from users for assistance which generated immediate return textmessages with tips and strategies to manage urges or withdrawal. The Brendryen [27, 28]and Riley interventions [23, 25] also adjusted the intervention based on smoking status (e.g.,different messages before vs. after quitting, resetting quit dates if relapse occurred).
With the exception of the Rodgers intervention [24, 29], these mobile smoking cessationinterventions provided a theoretical basis, citing Social Cognitive Theory, Self-RegulationTheory, the Transtheoretical Model, and cognitive–behavioral theory. These theoriesprimarily appear to have informed the content of the text messages which included skills tomanage urges and the facilitation of social support. The Transtheoretical Model was used toadapt the content of the text messages to the preparation, action, and maintenance stages ofthe quit process. In a separate report, Brendryen and colleagues [31] provided a detaileddescription of the intervention mapping process for the development of the Happy Endingintervention based on Self-Regulation Theory, Social Cognitive Theory, cognitive–behavioral therapy, motivational interviewing, and relapse prevention. In a stepwiseapproach, they performed a needs assessment and devised proximal change objectives basedon the self-observation, self-evaluation, and self-reaction processes of Self-RegulationTheory and the behavioral determinants posited by Social Cognitive Theory and relatedmodels. They generated theory-based methods and practical strategies to address thesechange objectives and developed the resulting intervention to deliver each of thesestrategies. This report provides a well-devised framework for the application of theory to amobile health behavior intervention.
Quit rates from the interventions evaluated in these studies range from 8% [29] to 53% [26]with a follow-up period ranging from 4 weeks to 12 months. A recent Cochrane review ofrandomized studies of mobile phone-based interventions for smoking cessation, whichincluded all of the randomized controlled trials (RCT) reviewed here, found a significantshort-term increase in self-reported quitting (relative risk= 2.18; 95% confidence interval1.80 to 2.65) but considerable heterogeneity and lack of sufficient evidence for long-term
Riley et al. Page 4
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

effects [32]. Although promising, the effects of mobile technologies for smoking cessationrequire more study, especially of the long-term effects of these interventions.
Weight loss, diet, and physical activityWe identified 12 studies reporting on mobile health behavior interventions for weight loss,diet, and/or physical activity. Four of these interventions were delivered via PDA, and eightwere delivered via mobile phone, predominately SMS. These interventions represent a rangeof interactivity from non-tailored weekly informational text messages [33] to real-time dietand exercise monitoring with multiple daily customized messages based on input [34]. Mostauto-adjusted the intervention based on computer algorithms, but the two interventionsencouraging walking in Chronic Obstructive Pulmonary Disease (COPD) patients weremanually adjusted by health professionals [35, 36]. The mobile weight loss programdeveloped by Bauer et al. [37] computer-generated text messages based on weekly inputfrom the overweight children in the study, but these messages were reviewed and modifiedby staff before sending. Diet, weight, and exercise data were provided via self-report for allinterventions except the Hurling et al. [38] study which used accelerometer data wirelesslytransmitted via Bluetooth to the mobile phone. Output from these interventions waspredominately text although tabular and graphic comparisons to targets/goals were providedby some interventions (e.g., [34, 39, 40]) and one intervention used a mobile phone programthat adjusted music tempo to encourage an appropriate walking pace [35].
Of the 12 studies summarized in Table 2, seven specified a theoretical basis for the mobileweight loss, diet, or physical activity intervention developed. Consistent with the moregeneral weight loss intervention literature, Social Cognitive Theory was the primarytheoretical basis for these interventions although the Theory of Planned Behavior was citedby one study [38]. In a well-controlled evaluation of a theoretically-based program, Haapalaand colleagues [40] randomly assigned overweight adults to control or a mobile phoneweight loss program. The intervention was based on Self-Efficacy Theory and a SystemsContingency Approach described by Hiltz [45] in which the amount, frequency, and type ofcomputer-mediated communication are hypothesized to influence learning effectiveness.These theories were combined in a contingency model of mobile phone weight loss thatcombines program factors (e.g., content), frequency of interaction with the program,exogenous variables, and changes in processes and outcomes. Text messages instructedusers in a staggered reduction of food intake and prompted daily weight reporting withimmediate tailored feedback. The program evaluated weight balance, calculated dailyenergy requirement, set daily weight goals and food consumption recommendations, andprovided feedback on the days remaining to the long-term weight target. Weight loss goalswere user defined, but typically averaged 2 kg/month. Weight was reported via mobilephone on average 4.4 times per week. Compared to controls, those in the mobile phoneintervention lost significantly more weight (4.5 vs. 1.1 kg) and had a greater reduction inwaist circumference (6.3 vs. 2.4 cm) after 1 year in the program.
As an example of interactivity in mobile weight management interventions, Patrick andcolleagues [43] reported on a 4-month, randomized trial of a mobile phone text messagingprogram for weight loss that, although not specified, appeared consistent with SocialCognitive Theory and that involved considerable interactivity. Text messages werepersonalized and varied not only in content but also in their interactive nature. Some textswere simple push reminders while others queried the user about their dietary behavior,obtained a reply, and then provided an intervention based on the reply. Although weight lossin the text messaging condition was modest over 4 months (2.88 kg), it was significantlygreater than in the print only condition.
Riley et al. Page 5
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

In a recently published study, Burke et al. [34] provided another example of interventioninteractivity via mobile device. They compared paper-based dietary and exercise monitoringto PDA-based monitoring and PDA-based monitoring plus daily feedback message in anRCT of 210 overweight and obese adults. The PDA monitoring program was based on theplatform developed by Beasley et al. [39], but the PDA monitoring plus feedback conditionadded daily messages of positive reinforcement and guidance for goal attainment tailored tothe input provided based on self-regulation theory. All three conditions also received 20group intervention sessions over a 6-month period. Compared to the monitoring onlyconditions which obtained a percent weight loss of 4.8 (PDA) and 4.6 (paper-based), thePDA plus daily feedback condition obtained a mean percent weight loss of 6.5.
Consistent with other reviews [46], these initial studies of mobile interventions for weightloss show modest but significant weight loss and related outcomes. Mobile interventions forweight loss, diet, and physical activity are poised to take advantage of a number of advancesin monitoring that could be leveraged to improve outcomes. Computerized dietarymonitoring has been used extensively in this field [47], and these self-monitoring procedureshave been adapted to mobile platforms. Recent research has begun to use cell phone camerasto assess dietary intake [48, 49] which may result in less underreporting of intake than fromself-monitoring. As mobile phones increasingly incorporate accelerometers, the potentialexists to use the automated data obtained from these accelerometers to monitor activitylevels and provide just-in-time interventions [50, 51]. These richer and potentially moreprecise measures of dietary intake and physical activity can provide the basis for robust andinteractive weight loss interventions delivered via mobile devices.
Treatment adherenceTen studies were identified that evaluated the use of mobile technology to improve treatmentadherence (Table 3). Of these, eight targeted medical appointment adherence and twoaddressed medication adherence, specifically HIV treatment adherence. All of theappointment adherence interventions were delivered via SMS while both of the medicationadherence interventions were delivered via two-way pager. Given the substantial use oftechnology for measuring medication adherence [52] and the availability of smart pillboxesfor improving adherence [53], it is surprising that only two studies have developed andevaluated a medication adherence intervention on a mobile platform, both using two-waypagers which have limited capabilities.
In 2003, Safren and colleagues [54] published the earliest evaluation of a mobile technologyidentified in this review. In HIV patients with poor adherence, they used a commercialsystem (Medimom) to enter patients’ drug regimens and transmit pager alerts to remindpatients to take their medications at the specified times. Based on electronic pill bottle data(MEMS), those randomly assigned to the pager reminder condition had significantimprovements in medication adherence compared to those in a medication monitoring onlycondition at 2 and 12 weeks. In a more recent study, Simoni and colleagues [55] developedand evaluated a similar pager dosing reminder program for HIV patients with additionaltexts providing education, adherence assessments, and entertainment. This intervention,however, failed to produce significant improvements in adherence over the 9-month trialrelative to usual care or peer support, possibly due to the mixed functions of the pagerprompt (i.e., prompt taking medications, provide education). Neither study provided atheoretical basis for the intervention provided. Both studies tailored the intervention atinitiation based on the medication regimen of each patient, but there were no adjustmentsmade during the course of the intervention.
Among the eight studies providing appointment reminders via mobile technologies, allprovided only a single, unadjusted output reminding the patient of their appointment, usually
Riley et al. Page 6
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
timed to within a few days of the scheduled appointment. The only two-way interaction wasin the Koshy et al. study [56] which provided the patient with the ability to text reply tocancel the appointment. None of the studies provided a theoretical basis for the interventionprovided.
Despite the simple nature of these appointment adherence interventions and their lack ofinteractivity and theoretical basis, most resulted in a significant increase in appointmentadherence. The only exception was Bos et al. [57], which had high appointment adherencerates to orthodontic visits across conditions. It is important to note, however, that only twostudies used randomized controls [58, 59]; the others used historical or nonrandomizedcontrols. Additionally, the three studies that compared SMS to traditional phone callreminders found no difference between these two modalities [57–59].
Disease managementIn addition to the treatment adherence research reviewed above, a number of treatmentadherence interventions are incorporated within a chronic disease management program.The use of mobile phones for disease management has been substantially reviewedelsewhere [46, 60–62], particularly in the area of diabetes management. Based on the criteriafor this review, we identified 20 studies: 16 in diabetes management, three in asthmamanagement, and one in hypertension management (Table 4). Across the 20 studies, onlyone [63] specified a theoretical basis for the intervention, using Social Cognitive Theory toprovide personalized SMS messages to support diabetes management in children with type 1diabetes. In part, this lack of theoretical basis may reflect the well-established practiceguidelines for managing type I and type 2 diabetes [64], but as the field extends theseinterventions beyond medication adjustments and integrates automated measures of physicalactivity, medication adherence, food intake, and other target variables into these systems[65], using health behavior theories to inform these interventions could improve outcomes.
The interventions developed and evaluated in these studies focused primarily on patientinput (e.g., blood glucose readings, insulin doses, carbohydrate intake, exercise, forcedexpiratory volume (FEV1), or blood pressure) which were reviewed by a health professionalto provide periodic regimen adjustments and treatment recommendations. Therefore, exceptfor the two PDA interventions that did not transfer data to a central server [66, 67], any just-in-time intervention adjustments were made manually. These manually adjustedinterventions are consistent with telemedicine models, but they have limited scalability dueto the provider burden required to review and deliver these interventions. Lanzola andcolleagues have proposed a multi-tier intervention model in which lower-tier diseasemanagement interventions are provided via automated treatment algorithms and higher tierinterventions involving the healthcare provider occur only if the lower-tier interventions areineffective [68].
Although advances in automating disease management intervention output are needed, thefield is leveraging advances in objective, real-time input. Data entry burden is a persistentproblem in disease management [69]. In one study of adolescents on intensified insulintherapy, one quarter failed to send at least 50% of their four daily blood glucose values [70].With the advent of Bluetooth-enabled glucometers, data entry burden is eliminated. Since2008, three of the studies reviewed used this or similar technology and found significantreductions in HbA1c [71–73]. Another study used Bluetooth-enabled blood pressure devicesto provide automated transmission for hypertension control in diabetes patients [74].
Although the automatic transmission of testing data eliminates data entry burden, it does noteliminate the responsibility of the patient to perform regular testing, and a number of thestudies used reminders via pager or mobile phone SMS to obtain blood glucose [72, 75, 76]
Riley et al. Page 7
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

or to take medications [77]. For example, Turner and colleagues provided blood glucosemeasurement reminders in an interactive manner with type 2 diabetes patients [72]. If noblood glucose data were automatically transmitted for 3 days, or if hypo- or hyper-glycemiapersisted, patients received additional reminders.
Outcomes from the mobile disease management studies were generally positive andstatistically significant. Among the 12 diabetes management studies with HbA1c as aprimary outcome, ten found significant reductions in HbA1c. This is consistent with a recentsystematic review of mobile phone use for diabetes self-management in which nine of tenstudies reviewed reported significant improvement in HbA1c [46]. All three mobile asthmamanagement interventions found significant improvements in the primary outcome. Forexample, in a small randomized controlled trial of no SMS vs. SMS daily reminders to takeasthma medication, Strandbygaard et al. [77] found that the percent adherence based onobjective inhaler dose counts decreased in the control condition (84.2% to 70.1%) butincreased in the intervention condition (77.9% to 81.5%) over the 12-week study period.Therefore, the ability of mobile disease management programs to assess patient statusfrequently and adjust treatment remotely appears to improve treatment outcomes and toserve as a basis for more comprehensive and automated mobile disease managementinterventions.
SUMMARY OF MOBILE HEALTH BEHAVIOR INTERVENTION FEATURESThe application of mobile technologies to health behavior interventions is a nascent butrapidly growing field that has only begun to leverage the full capabilities of mobile phonesand other mobile technologies. Most of the mobile interventions described in this reviewused text messaging (aka SMS) functionality of mobile phones. Text messages can bedelivered simply and inexpensively across mobile phone operating platforms and to a largepercentage of mobile phone users given the ubiquitous nature of this feature even on “lesssmart” mobile phones. As smart phone penetration rates increase and interoperabilitybetween operating platforms improves, however, additional features of mobile phones canbe used.
In addition to voice, text, and data inputs, researchers have begun to use video input viacamera features on these phones. Although video input has been primarily used fortelemedicine purposes [78, 79], health behavior researchers have begun to use cameras fordietary assessment [48]. Another significant set of input features are automated sensors,either resident on the smartphone (e.g., accelerometers and GPS) or connected viaBluetooth. Much of the mobile health behavior interventions to date have focused ontransmitting data from glucometers and spirometers, but an expanding variety of sensortechnologies can be used to assess physiological states, movement, location, and othervariables using mobile phones.
These early mobile health behavior interventions also have only begun to leverage theoutput functionality of these phones. As with input, most of the output delivery to date hasbeen via text messaging. A few studies have used other output functions such as audio (e.g.,[35]) or video (e.g. [26]), but device-resident or wireless Internet applications onsmartphones provide a rich array of possible data and display outputs (e.g., progress charts,animation, videos, games) that could be used to deliver health behavior interventions.
Most apparent from this review, however, is the limited use of the rapid two-way interactionof inputs and outputs that could be used to deliver just-in-time health behavior interventions.Disease management and weight loss mobile health interventions have relied predominatelyon input while adherence and smoking cessation mobile health interventions have relied
Riley et al. Page 8
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

predominately on output. Among applications relying on input, many employed a user-initiated or unprompted input procedure despite a considerable ecological momentaryassessment literature supporting the use of prompted inputs [80]. Following input, someapplications provided tailored intervention responses, but others failed to deliver even aconfirmation message, despite the potential importance of this feature for encouragingcontinued input. Of the applications that predominately pushed out intervention messages, afew encouraged confirmation of receipt or some other reply response (e.g., [43]), but mostdid not. None of the adherence interventions made just-in-time adjustments, but most ofthese interventions were single prompt appointment reminders with no longitudinal basis foradjustment, and none obtained the input necessary to make treatment adjustments. Most ofthe smoking and weight loss mobile interventions provided some form of “just-in-time”response based on a prior input, but the frequency or intensity of interactivity variedsubstantially among these interventions from requests for additional text message assistancecommon among the smoking interventions (e.g., [23, 27]) to regular interventionadjustments based on dietary and exercise inputs [34, 43]. The disease managementinterventions also typically provided just-in-time intervention adjustments, but most reliedon manual adjustments by a health care professional to do so. Although more complexintervention adjustments might be best reserved for health professional judgment, standardtreatment algorithms can be used to automate, with 100% treatment fidelity, many of thesetreatment adjustments, greatly improving scalability, and reducing professional time andcosts.
Given the lag between intervention development, evaluation, and eventual publication, thearticles reviewed, although published as recently as the June 2010, describe interventionsdeveloped a number of years ago. Therefore, the limited interactivity of the mobileinterventions reviewed may not reflect current status, and the National Institutes of Healthcurrently funds a number of ongoing projects that use more intensive interactivity and just-in-time interventions than described in this review [81]. To insure that the mobileinterventions reviewed were mature enough for actual use, we limited our review to studiesthat subjected these interventions to some form of clinical outcome assessment. As a result,we did not report on recent mobile intervention development from proof-of-concept (e.g.,[82]), usability/feasibility (e.g., [83]), or ongoing research reports (e.g., [84]) in which morerecently developed interventions are described. Given the recent interest in and rapidprogression of mHealth interventions, reports on more intensively interactive mobile healthbehavior interventions are likely to be published in the coming years.
THEORETICAL BASIS FOR MOBILE HEALTH BEHAVIOR INTERVENTIONSAND NEW DIRECTIONS
Our review of the studies of health behavior interventions delivered via mobile technologiesreveals a paucity of discussion regarding the health behavior theories or models that providethe basis of the intervention. Even among those studies that provided a theoretical basis,very few attempted to evaluate any of the theoretical components hypothesized to beaffected by the intervention. Studies in the smoking and weight loss areas tended to use atheoretical model for their intervention, drawing predominately from Social CognitiveTheory or its variants (e.g., self-efficacy). Among these studies are extensive and thoughtfulexamples of using theory to guide mobile intervention development (e.g., [31, 40]). Incontrast, most of the mobile interventions studied in the treatment adherence and diseasemanagement areas did not report a theoretical basis for intervention development, but thismay be the result of reliance on evidence based clinical guidelines (e.g., diabetesmanagement) or on the simplicity of the intervention delivered (e.g., appointmentreminders).
Riley et al. Page 9
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

A simple reminder intervention, however, is an excellent example for the necessity of theoryto guide intervention. Text messaging reminders to attend appointments, take medications,exercise, etc. appear relatively straightforward and are consistent with the “cue to action”component of many health behavior theories, but the history of health behavior theoriescautions us about assuming that behavior change is straightforward or that innovative modesof delivery alone are sufficient to produce behavior change. In the 1950s, mobileneighborhood tuberculosis screenings were innovative, but the added salience andconvenience did not substantially increase screenings. Researchers studying uptake of theseneighborhood screenings learned that the perceived threat (severity and susceptibility) oftuberculosis, the perceived benefit of being screened, and the perceived barriers to gettingscreened contributed to a person obtaining these screenings. These findings led to the HealthBelief Model [85] and the various health behavior theories and models that followed.Therefore, a greater reliance on health behavior theories to guide mobile technologyintervention development, even for apparently simple interventions, should result ininterventions that address more comprehensively the potential mechanisms of behaviorchange, resulting in more effective interventions.
While mobile technology applications of health behavior interventions should be guided byour current health behavior models, it is important to acknowledge that these current modelsappear inadequate to answer many of the intervention development questions likely to ariseas interventions better leverage the interactive capabilities of mobile technologies. Somehave argued that these theories are inadequate even for traditional interventions [17], butthey are particularly limited at informing just-in-time intervention adaptations. Dunton andAtienza have noted that the increasing availability of time-intensive information (i.e.,longitudinal data obtained at an intensive frequency) allows for the intra-individual tailoringof interventions but that current health behavior theories are based on delineating between,not within-person differences [86]. Boorsboom and colleagues have argued that between-person theories do not imply, test, or support causal accounts valid at the individual level[87]. As a result, these theories and models have been used with considerable success totailor health behavior interventions based on pre-intervention factors, but typically have notbeen used to adapt the intervention to the individual over the course of the intervention [88,89]. As these interventions become deliverable on mobile devices, the content ofinterventions can be adapted for each individual not only initially but also over time basedon his/her prior outcome data, prior responses to specific intervention outputs, currentenvironmental and/or social context, and a range of other variables that might influence theoptimal intervention based on the current state of the individual (i.e., ecological momentaryinterventions) [90].
In addition to adapting the content of the intervention over time, mobile technologyapplications of health behavior interventions also have the ability to adapt the timing of theinterventions based on these same data. For example, following a prompt to exercise, howlong should the program wait before prompting again and how should the timing andcontent of the follow-up prompt be tailored based on prior pattern of responses to prompts?In this review, only a few studies adjusted the timing of the interventions, usually during thetransition from behavior change to maintenance (e.g., [23, 40]), but these timing adjustmentswere set a priori across all participants and were not dynamically determined at theindividual level.
The development of time-intensive, interactive, and adaptive health behavior interventionsvia mobile technologies demands more intra-individual dynamic regulatory processes thanrepresented in our current health behavior theories. These theories do not preclude thepossibility that some conceptual components change over time, and some concepts such asreciprocal determinism in Social Cognitive Theory are explicitly dynamic in nature [14].
Riley et al. Page 10
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Moreover, a rich behavior change process–outcome literature describes dynamic interactionsin face-to-face behavioral interventions that could be applied to behavioral interventions viamobile technologies [91]. Adoption of dynamical system models for mobile health behaviorinterventions does not require that our current health behavior theories and models bediscarded, but the predominately static, linear nature of these theories appears to be a poorfit with the intra-individual dynamics of future mobile technology interventions.
Control systems engineering [92] may provide the dynamical system models needed totransform our current health behavior theories into the dynamic theories required for thetime-intensive, interactive, and adaptive health behavior interventions delivered via mobiletechnologies. Control systems engineering examines how to influence dynamical systems toachieve a desired outcome. These dynamical systems are multivariate, time-varyingprocesses, often nonlinear in nature, in which variables that can be manipulated (e.g., systeminput variables) lead to changes in outcomes of interest (e.g., system output variables)adjusting for exogenous effects (e.g., disturbance variables). Control engineering approacheshave been proposed for adaptive interventions to determine, for example, when and howmuch to change the frequency of family counseling to prevent the development of conductdisorder in children [93].
There are a number of practical advantages of using dynamical systems to inform adaptive,time-intensive interventions delivered via mobile technologies. Control systems engineeringprinciples and procedures are mature and provide a robust computational framework formodeling, simulation, and systematic decision making over time. These control systemprinciples and procedures fit well with the rich longitudinal data and real-time interventionadaptations potentially available via mobile technologies. Interventions based on theoriesenriched by control system models also provide engineers and health behavior researcherswith a common language for collaborating on new interventions delivered via mobiletechnologies [94].
Perhaps more importantly, these feedback control systems have the potential to reshapehealth behavior theories and improve our understanding of human behavior. Feedbackregulatory processes are core to neurobiology. Basic neuronal processes are time-intensive,adaptive interactions of excitatory and inhibitory synaptic processes that have been modeledat the single neuron level [95]. The communalities between brain circuitry and controlsystem engineering principles are so compelling that some brain processes are described viaengineering feedback systems (e.g., [96]). Since the brain appears to regulate itself and otherorgans using feedback control processes, it seems reasonable that the brain also regulateshuman behavior via similar feedback control processes. Optimal feedback control systemshave been applied to basic sensorimotor control [97] and to reinforcement learning models[98]. Therefore, the application of feedback control systems to current health behaviortheory concepts provides not only potential theoretical models that are amenable to the time-intensive, interactive nature of mobile health behavior interventions but also theoreticalmodels that are more consistent with the putative neurobiological and environmentalprocesses that regulate these behaviors.
One significant example of regulatory feedback for disease management processes is indiabetes where frequent adjustments to diet and insulin dose are determined based on bloodglucose levels. Control engineering approaches have been applied to the glucose–insulinclosed-loop system [99], and this application illustrates the potential of this approach toproduce the desired outcome in systems that possess measurement error, model uncertainty,noise, and lagged effects. This work could serve as a basis for developing mobiletechnologies for diabetes management that take advantage of advanced closed-loop controlsystem models to automate and better regulate blood glucose for insulin-dependent patients.
Riley et al. Page 11
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Detailed descriptions of applications of control systems engineering to other health behaviorinterventions such as substance use have been described elsewhere [93, 100], but to illustratethe application of control systems engineering to mobile health behavior interventions, weprovide a simple model for intervening on smoking urges depicted in Fig. 1 whichrepresents an individual’s smoking behavior in terms of a production–inventory model[101]. Using a fluid analogy, smoking urge is accumulated as an inventory that is built up byan “inflow” of negative emotional stimuli (e.g., sadness, irritation) and external stimuli (e.g.,presence of others smoking, drinking coffee) and depleted by an urge “outflow” resultingfrom smoking events and the salutary effects of positive affect and dosages of interventioncomponents such as medications and psychosocial interventions. In a control systemsconceptualization, smoking urge (y(t)) is the controlled variable, while smoking activityrepresents a manipulated variable (u1(t)) whose action serves to reduce the urge to smoke.Environmental stimuli and positive and negative affect represent external disturbancevariables (d1(t), d2(t)) whose changes build up or deplete the smoking urge inventory. Thedose of intervention components represents additional manipulated variables (u2(t)) that canbe selected adaptively by a set of decision rules or mathematical algorithms (referred to asthe intervention controller in Fig. 1) based on assessed participant response. A differentialequation drawn from the general principle of conservation of matter can be used to describethe relationship between these variables [102]
where Kd1, Kd2, Ku1, and Ku2 represent coefficients that quantify the rate of change in urgebased on changes in manipulated variables (intervention dosages, smoking activity) anddisturbance variables (negative and positive affect, environmental stimuli). The inherentdynamics of smoking behavior in Fig. 1 constitutes a closed-loop feedback system in whichincreases in smoking urge precipitate a decision to smoke (the relationship between urge andsmoking activity is denoted by the “urge controller” box in Fig. 1).
The potential of mobile technologies to generate the intensive longitudinal data setsreflecting the behavior of a smoker over time and observed in different settings and contextsis important for building a dynamical system model such as the individual smoking behaviormodel illustrated above. Mobile devices can collect information in real time about thecontrolled, manipulated, and disturbance variables, as represented by sensor locations in Fig.1. Model estimation techniques such as system identification [103] and functional dataanalysis [104] can be used to estimate the Kd1, Kd 2, Ku1, and Ku2 coefficients from thesedata. These modeling techniques also can be applied to reverse-engineer the functionalrelationship underlying the urge controller which reflects the actions of an individualsmoker. With a dynamical systems model, it becomes possible to apply control systemsengineering to develop algorithms that use real-time assessments and predicted responsesfrom the model to adaptively decide on the timing and dose of the intervention components.Mobile technology is an enabler to advanced control algorithms such as model predictivecontrol [105] that employ formal optimization methods to decide on current and future dosesof intervention components while satisfying clinical practice preferences and restrictions[100]. The use of these control technologies in a smoking cessation intervention as shown inFig. 1 parallels the closed-loop control system for diabetes management describedpreviously. The optimization process leads to specific intervention decisions (u2(t)) forproviding behavioral strategies and/or medication prompts to replace smoking as a means ofreducing smoking urge.
Riley et al. Page 12
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

In addition to being sensitive to threshold (or mean) levels of key variables, a control systemframework can adapt to and consider variability of key controlling or explanatory variables.Most theories of health behavior change to date have focused on mean levels of predictivevariables, but with the advent of newer data technologies, we can develop models that focuson lability or stability of key controlling factors. For many health behaviors, maintaining astable level or tighter range for some key variables may be as or more important thanincreasing or decreasing mean levels.
Novel dynamic health behavior theories and their application to health behaviorinterventions via mobile technologies will require empirical validation. Adaptive treatmentmethodologies has been applied to interventions that adjust over the course of weeks ormonths, not hours or days, but these methodologies can be applied to mobile technologyinterventions [106]. Other methodological considerations for adaptive interactivetechnologies applied to eHealth also may be appropriate to consider for mHealthinterventions [107, 108]. The opportunity via mobile devices to collect intensive context-and time-dependent (longitudinal) data and to systematically vary intervention componentsenables researchers to test not only these components but also the theoretical concepts anddynamic models that underlie them.
The application of mobile technologies to health behavior interventions is an exciting andrapidly growing field. The ability to provide frequent, time-intensive interventions in thecontext of the behavior holds considerable promise but also poses many challenges to ourcurrent health behavior theories and models. To meet these challenges, our current healthbehavior theories and models need to expand from elucidating between-person differencesto explaining within-person changes over time and to evolve to incorporate dynamicfeedback control systems to “close the loop.” Health behavior interventions delivered viamobile technologies offer not only the impetus to transform our current theories into moredynamic feedback control models but also the potential to provide the intensive longitudinaldata necessary to test and improve our theoretical intervention models. To date, only asubset of mobile health behavior interventions have been theory-based, but a theory-driveniterative model of mobile intervention development holds promise for improving not onlyour mobile health behavior interventions but also our theoretical and empiricalunderstanding of health behavior change.
References1. Webb TL, Joseph J, Yardley L, Michie S. Using the Internet to promote health behavior change: A
systematic review and meta-analysis of the impact of theoretical basis, use of behavior changetechniques, and mode of delivery on efficacy. Journal of Medical Internet Research. 2010; 12:e4.[PubMed: 20164043]
2. Tate DF, Finkelstein EA, Khavjou O, Gustafson A. Cost effectiveness of Internet interventions:Review and recommendations. Annals of Behavioral Medicine. 2009; 38:40–45. [PubMed:19834778]
3. Norman GJ, Zabinski MF, Adams MA, Rosenberg DE, Yaroch AL, Atienza AA. A review ofeHealth interventions for physical activity and dietary behavior change. American Journal ofPreventive Medicine. 2007; 33:336–345. [PubMed: 17888860]
4. CTIA. 2009. http://www.ctia.org/advocacy/research/index.cfm/AID/103235. International Communications Union. 2010.
http://www.itu.int/ITU-d/ict/publications/idi/2010/Material/MIS_2010_Summary_E.pdf6. Pew Internet &American Life Project. 2010.
http://www.pewInternet.org/~/media//Files/Reports/2010/PIP_Mobile_Access_2010.pdf7. Leena K, Tomi L, Arja R. Intensity of mobile phone use and health compromising behaviours: How
is information and communication technology connected to health-related lifestyle in adolescence?Journal of Adolescence. 2005; 28:35–47. [PubMed: 15683633]
Riley et al. Page 13
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

8. Kosaraju A, Barrigan CR, Poropatich RK, Casscells SW. Use of mobile phones as a tool for UnitedStates health diplomacy abroad. Telemed J E Health. 2010; 16:218–222. [PubMed: 20156128]
9. Kaplan WA. Can the ubiquitous power of mobile phones be used to improve health outcomes indeveloping countries? Global Healthcare. 2006; 2:9–22.
10. Pharow P, Blobel B, Ruotsalainen P, Petersen F, Hovsto A. Portable devices, sensors andnetworks: Wireless personalized eHealth services. Studies in Health Technology and Informatics.2009; 150:1012–1016. [PubMed: 19745466]
11. Patrick K, Griswold WG, Raab F, Intille SS. Health and the mobile phone. American Journal ofPreventive Medicine. 2008; 35:177–181. [PubMed: 18550322]
12. Becker, MH., editor. Health Education Monographs. Vol. 2. 1974. The health belief model andpersonal health behavior; p. 324-473.
13. Godin G, Kok G. The theory of planned behavior: A review of its applications to health-relatedbehaviors. American Journal of Health Promotion. 1996; 11:87–98. [PubMed: 10163601]
14. Bandura A. Social cognitive theory: An agentic perspective. Annual Review of Psychology. 2001;52:1–26.
15. Prochaska JO, Velicer WF. The transtheoretical model of health behavior change. AmericanJournal of Health Promotion. 1997; 12:38–48. [PubMed: 10170434]
16. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, socialdevelopment, and well-being. Amer Psychol. 2000; 55:68–78. [PubMed: 11392867]
17. Ogden J. Some problems with social cognition models: A pragmatic and conceptual analysis.Health Psychology. 2003; 22:424–428. [PubMed: 12940399]
18. Burnett KF, Taylor CB, Agras WS. Ambulatory computer-assisted therapy for obesity: A newfrontier for behavior therapy. J Cons Clin Psychol. 1985; 53:698–703.
19. Prue DM, Riley A, Orlandi MA, Jerome A. Development of a computer-assisted smokingcessation program: A preliminary report. J Adv Med. 1990; 3:131–139.
20. Brownell KD. Adherence to dietary regimens. 2: Components of effective interventions.Behavioral Medicine. 1995; 20:155–164. [PubMed: 7620227]
21. Fjeldsoe BS, Marshall AL, Miller YD. Behavior change interventions delivered by mobiletelephone short-message service. American Journal of Preventive Medicine. 2009; 36:165–173.[PubMed: 19135907]
22. Krishna S, Boren SA. Healthcare via cell phone: A systematic review. Telemed e-Health. 2009;15:231–240.
23. Obermayer JL, Riley WT, Asif O, Jean-Mary J. College smoking-cessation using cell phone textmessaging. J Amer Coll Health. 2004; 53:71–78. [PubMed: 15495883]
24. Rodgers A, Corbett T, Bramley D, et al. Do u smoke after txt? Results of a randomized trial ofsmoking cessation using mobile phone text messaging. Tobacco Control. 2005; 14:255–261.[PubMed: 16046689]
25. Riley WT, Obermayer J, Jean-Mary J. Internet and mobile phone text messaging intervention forcollege smokers. J Amer Coll Health. 2008; 57:245–248. [PubMed: 18809542]
26. Whittaker R, Maddison R, McRobbie H, et al. A multimedia mobile phone-based youth smokingcessation intervention: Findings from content development and piloting studies. Journal ofMedical Internet Research. 2008; 10:e49. [PubMed: 19033148]
27. Brendryen H, Kraft P. Happy Ending: A randomized controlled trial of a digital multi-mediasmoking cessation intervention. Addiction. 2008; 103:478–484. [PubMed: 18269367]
28. Brendryen H, Drozd F, Kraft P. A digital smoking cessation program delivered through Internetand cell phone without nicotine replacement (happy ending): Randomized controlled trial. Journalof Medical Internet Research. 2008; 10:e51. [PubMed: 19087949]
29. Free C, Whittaker R, Knight R, Abramsky T, Rodgers A, Roberts G. Txt2stop: A pilot randomizedcontrolled trial of mobile phone-based smoking cessation support. Tobacco Control. 2009; 18:88–91. [PubMed: 19318534]
30. Intille, SS.; Kukla, C.; Farzanfar, R.; Bakr, W. Just-in-time technology to encourage incremental,dietary behavior change. AMIA 2003 symposium proceedings; p. 874
Riley et al. Page 14
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
31. Brendryen H, Kraft P, Schaalma H. Looking inside the black box: Using intervention mapping todescribe the development of an automated smoking cessation intervention happy ending. TheJournal of Smoking Cessation. 2010; 5:29–56.
32. Whittaker R, Borland R, Bullen C, Lin RB, McRobbie H, Rodgers A. Mobile phone-basedinterventions for smoking cessation. Cochrane Database of Systematic Reviews. 2009;4:CD006611.
33. Joo N, Kim B. Mobile phone short message service messaging for behaviour modification in acommunity-based weight loss programme in Korea. Journal of Telemedicine and Telecare. 2007;13:416–420. [PubMed: 18078554]
34. Burke LE, Conroy MB, Sereika SM, et al. The effect of electronic self-monitoring on weight lossand dietary intake: A randomized behavioral weight loss trial. Obesity. 2011; 19:338–344.[PubMed: 20847736]
35. Liu WT, Wang CH, Lin HC, et al. Efficacy of a cell phone-based exercise programme for COPD.The European Respiratory Journal. 2008; 32:651–659. [PubMed: 18508824]
36. Nguyen HQ, Gill DP, Wolpin S, Steele BG, Benditt JO. Pilot study of a cell phone-based exercisepersistence intervention post-rehabilitation for COPD. Int J COPD. 2009; 4:301–313.
37. Bauer S, de Niet J, Timman R, Kordy H. Enhancement of care through self-monitoring andtailored feedback via text messaging and their use in the treatment of childhood overweight.Patient Education and Counseling. 2010; 79:315–319. [PubMed: 20418046]
38. Hurling R, Catt M, De Boni M, et al. Using Internet and mobile phone technology to deliver anautomated physical activity program: Randomized controlled trial. Journal of Medical InternetResearch. 2007; 9:e7. [PubMed: 17478409]
39. Beasley JM, Riley WT, Davis A, Singh J. Evaluation of a PDA-based dietary assessment andintervention program: A randomized controlled trial. Journal of the American College of Nutrition.2008; 27:280–286. [PubMed: 18689560]
40. Haapala I, Barengo NC, Biggs S, Surakka L, Manninen P. Weight loss by mobile phone: A 1-yeareffectiveness study. Public Health Nutrition. 2009; 12:2382–2391. [PubMed: 19323865]
41. Atienza AA, King AC, Oliveira BM, Ahn DK, Gardner CD. Using hand-held computertechnologies to improve dietary intake. American Journal of Preventive Medicine. 2008; 34:514–518. [PubMed: 18471588]
42. King AC, Ahn DK, Oliveira BM, Atienza AA, Castro CM, Gardner CD. Promoting physicalactivity through hand-held computer technology. American Journal of Preventive Medicine. 2008;34:138–142. [PubMed: 18201644]
43. Patrick K, Raab F, Adams MA, et al. A text message-based intervention for weight loss:Randomized controlled trial. Journal of Medical Internet Research. 2009; 11:e1. [PubMed:19141433]
44. Fjeldsoe BS, Miller YD, Marshall AL. MobileMums: A randomized controlled trial of an SMS-based physical activity intervention. Annals of Behavioral Medicine. 2010; 39:101–111. [PubMed:20174902]
45. Hiltz SR. Productivity enhancement from computer-mediated communication: A systemscontingency approach. Communications of the ACM. 1988; 31:1438–1454.
46. Krishna S, Boren SA. Diabetes self-management care via cell phone: A systematic review. JDiabetes Sci Technol. 2008; 2:509–517. [PubMed: 19885219]
47. Ngo J, Engelen A, Molag M, Roesle J, Garcia-Segovia P, Serra-Majem L. A review of the use ofinformation and communication technologies for dietary assessment. British J Nutr. 2009;101:S102–S112.
48. Boushey CJ, Kerr DA, Wright J, Lutes KD, Ebert DS, Delp EJ. Use of technology in children’sdietary assessment. Euro J Clin Nutr. 2009; 63:S50–S57.
49. Six BL, Schap TE, Zhu FM, Mariappan A, Bosch M, Delp EJ, et al. Evidence-based developmentof a mobile telephone food record. Journal of the American Dietetic Association. 2010; 110:74–79. [PubMed: 20102830]
50. Hynes M, Wang H, Kilmartin L. Off-the-shelf mobile handset environments for deployingaccelerometer based gait and activity analysis algorithms. Conf Proc IEEE Eng Med Biol Soc.2009; 2009:5187–5190. [PubMed: 19964383]
Riley et al. Page 15
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
51. Bexelius C, Lof M, Sandin S, Trolle Lagerros Y, Forsum E, Litton JE. Measure of physical activityusing cell phones: Validation using criterion measures. J Med Internet Res. 2010; 29:e2. [PubMed:20118036]
52. Farmer KC. Methods for measuring and monitoring medication regimen adherence in clinical trialsand clinical practice. Clinical Therapeutics. 1999; 21:1074–1090. [PubMed: 10440628]
53. Naditz A. Medication compliance—helping patients through technology: Modern “smart”pillboxes keep memory-short patients on their medical regimen. Telemed J E Health. 2008;14:875–880. [PubMed: 19062349]
54. Safren SA, Hendriksen ES, Desousa N, Boswell SL, Mayer KH. Use of an on-line pager system toincrease adherence to antiretroviral medications. AIDS Care. 2003; 15:787–793. [PubMed:14617500]
55. Simoni JM, Huh D, Frick PA, et al. Peer support and pager messaging to promote antiretroviralmodifying therapy in Seattle: A randomized controlled trial. Journal of Acquired ImmuneDeficiency Syndromes. 2009; 52:465–473. [PubMed: 19911481]
56. Koshy E, Car J, Majeed A. Effectiveness of mobile-phone short messaging service (SMS)reminders for ophthalmology outpatient appointments: Observational study. BMC Ophthalmology.2008; 8:9. [PubMed: 18513438]
57. Bos A, Hoogstraten J, Prahl-Andersen B. Failed appointments in an orthodontic clinic. BAm JOrthod Dentofacial Orthop. 2005; 127:355–357.
58. Leong KC, Leong KW, Mastura I, et al. The use of text messaging to improve attendance inprimary care: A randomized controlled trial. Family Practice. 2006; 23:699–705. [PubMed:16916871]
59. Chen ZW, Fang LZ, Chen LY, Dai HL. Comparison of an SMS text messaging and phonereminder to improve attendance at a health promotion center: A randomized controlled trial.Journal of Zhejiang University Science B. 2008; 9:34–38. [PubMed: 18196610]
60. Blake H. Mobile phone technology in chronic disease management. Nursing Standard. 2008;23:43–46. [PubMed: 19093357]
61. Russel-Minda E, Jutai J, Speechly M, Bradley K, Chudyk A, Petrella R. Health technologies formonitoring and managing diabetes: A systematic review. J Diabetes Sci Technol. 2009; 3:1460–1471. [PubMed: 20144402]
62. Skinner C, Finkelstein J. Using cell phones for chronic disease prevention and management. AMIAAnnual Symposium Proceedings. 2008; 6:1137. [PubMed: 18999018]
63. Franklin VL, Waller A, Pagliari C, Greene SA. A randomized controlled trial of Sweet Talk, a textmessaging system to support young people with diabetes. Diabetes Med. 2006; 23:1332–1338.
64. American Diabetes Association. Executive summary: Standards of medical care in diabetes—2009.Diabetes Care. 2009; 32:S6–S12. [PubMed: 19118288]
65. Hedtke PA. Can wireless technology enable new diabetes management tools. J Diabetes SciTechnol. 2008; 2:127–130. [PubMed: 19885187]
66. Ma Y, Olendzki BC, Chiriboga D, et al. PDA-assisted low glycemic index dietary intervention fortype 2 diabetes: A pilot study. Euro J Clin Nutr. 2006; 60:1235–1243.
67. Forjuoh SN, Reis MD, Couchman GR, Ory MG. Improving diabetes self-care with a PDA inambulatory care. Telemed Health. 2008; 14:273–279.
68. Lanzola G, Capozzi D, D’Annunzio G, Ferrari P, Bellazzi R, Larizza C. Going mobile with amulti-access service for the management of diabetes patients. J Diabetes Sci Technol. 2007;1:730–737. [PubMed: 19885142]
69. Arsand E, Tufano JT, Ralston JD, Hjortdahl P. Designing mobile dietary management supporttechnologies for people with diabetes. Journal of Telemedicine and Telecare. 2008; 14:329–332.[PubMed: 18852310]
70. Rami B, Popow C, Horn W, Waldhoer T, Schober E. Telemedical support to improve glycemiccontrol in adolescents with type 1 diabetes mellitus. European Journal of Pediatrics. 2006;165:701–705. [PubMed: 16670859]
71. Quinn CC, Clough SS, Minor JM, Lender D, Okafor MC, Gruber-Baldini A. WellDoc™ mobilediabetes management randomized controlled trial: Change in clinical and behavioral outcomes and
Riley et al. Page 16
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

patient and physician satisfaction. Diabetes Technology and Therapeutics. 2008; 10:160–168.[PubMed: 18473689]
72. Turner J, Larsen M, Tarassenko L, Neil A, Farmer A. Implementation of telehealth support forpatients with type 2 diabetes using insulin treatment: An exploratory study. Inform Prim Care.2009; 17:47–53. [PubMed: 19490773]
73. Cho JH, Lee HC, Lim DJ, Kwon HS, Yoon KH. Mobile communication using a mobile phone witha glucometer for glucose control in type 2 patients with diabetes: As effective as an Internet-basedglucose monitoring system. Journal of Telemedicine and Telecare. 2009; 15:77–82. [PubMed:19246607]
74. Logan AG, McIsaac WJ, Tisler A, et al. Mobile phone-based remote patient monitoring system formanagement of hypertension in diabetic patients. Amer J Hypertension. 2007; 20:942–948.
75. Leu MG, Norris TE, Hummel J, Isaac M, Brogan MW. A randomized controlled trial of anautomated wireless messaging system for diabetes. Diabetes Technology and Therapeutics. 2005;7:710–718. [PubMed: 16241873]
76. Hanauer DA, Wentzell K, Laffel N, Laffel LM. Computerized automated reminder diabetes system(CARDS): Email and SMS cell phone text messaging reminders to support diabetes management.Diabetes Technology and Therapeutics. 2009; 11:99–106. [PubMed: 19848576]
77. Strandbygaard U, Thomsen SF, Backer V. A daily SMS reminder increases adherence to asthmatreatment: A three-month follow-up study. Respiratory Medicine. 2010; 104:166–171. [PubMed:19854632]
78. Chung P, Yu T, Scheinfeld N. Using cellphones for teledermatology, a preliminary study.Dermatology Online Journal. 2007; 13:2. [PubMed: 18328196]
79. Tang FH, Law MY, Lee AC, Chan LW. A mobile phone integrated health care delivery system formedical images. Journal of Digital Imaging. 2004; 17:217–225. [PubMed: 15534754]
80. Shiffman S, Stone AA, Hufford MR. Ecological momentary assessment. Annual Review ofClinical Psychology. 2008; 4:1–32.
81. National Institutes of Health. [Accessed 29 Oct 2010] 2010. http://projectreporter.nih.gov(reporter_searchresults.cfm?&new=1&icde=5933670&loc=2&CFID=17945345&CFTOKEN=13189329)
82. Skevofilakas M, Mougiakakou SG, Zarkogianni K, et al. A communication and informationtechnology infrastructure for real-time monitoring and management of type 1 diabetes patients.Conf Proc IEEE Eng Med Biol Soc. 2007; 2007:3685–3686. [PubMed: 18002797]
83. Holtz B, Whitten P. Managing asthma with mobile phones: A feasibility study. Telemed J EHealth. 2009; 15:907–909. [PubMed: 19919198]
84. Ryan D, Pinnock H, Lee AJ, et al. The CYMPLA trial. Mobile phone-based structured interventionto achieve asthma control in patients with uncontrolled persistent asthma: A pragmatic randomizedcontrolled trial. Primary Care Respiratory Journal. 2009; 18:343–345.
85. Rosenstock IM. Historical origins of the Health Belief Model. Health Education Monographs.1974; 2:328–335.
86. Dunton, Atienza. The need for time-intensive information in healthful eating and physical activityresearch: A timely topic. JADA. 2009; 109(1):30–35.
87. Boorsboom D, Mellenbergh GJ, van Heerden J. The theoretical status of latent variables.Psychological Review. 2003; 110:202–219.
88. Neville LM, O’Hara B, Milat AJ. Computer-tailored dietary behaviour change interventions: Asystematic review. Health Education Research. 2009; 24:699–720. [PubMed: 19286893]
89. Lustria ML, Cortese J, Noar SM, Glueckauf RL. Computer-tailored health interventions deliveredover the Web: Review and analysis of key components. Patient Education and Counseling. 2009;74:156–173. [PubMed: 18947966]
90. Heron KE, Smyth JM. Ecological momentary interventions: Incorporating mobile technology intopsychosocial and health behaviour treatments. British Journal of Health Psychology. 2010; 15:1–39. [PubMed: 19646331]
91. Llewelyn S, Hardy G. Process research in understanding and applying psychological therapies. TheBritish Journal of Clinical Psychology. 2001; 40:1–21. [PubMed: 11317944]
Riley et al. Page 17
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

92. Åström, KJ.; Murray, RM. Feedback systems: An introduction for scientists and engineers. 2008.http://www.cds.caltech.edu/~murray/amwiki
93. Rivera DE, Pew MD, Collins LM. Using engineering control principles to inform the design ofadaptive interventions: A conceptual introduction. Drug and Alcohol Dependence. 2007; 88(suppl2):S31–S40. [PubMed: 17169503]
94. Navarro-Barrientos, JE.; Rivera, DE.; Collins, LM. A dynamical systems model for understandingbehavioral interventions for weight loss. In: Chai, SK.; Salerno, JJ.; Mabry, PL., editors. 2010international conference on social computing, behavioral modeling, and prediction (SBP 2010).Heidelberg: Springer; 2010. p. 170-179.
95. Deco G, Jirsa VK, Robinson PA, Breakspear M, Friston K. The dynamic brain: From spikingneurons to neural masses and cortical fields. PLoS Computational Biology. 2008; 4:e1000092.[PubMed: 18769680]
96. Saper CB, Chou TC, Scammell TE. The sleep switch: Hypothalamic control of sleep andwakefulness. Trends Neuroscience. 2001; 24:726–731.
97. Todorov E. Optimality principles in sensorimotor control. Nature Neuroscience. 2004; 7:907–915.98. Lewis FL, Vamvoudakis KG. Reinforcement learning for partially observable dynamic processes:
Adaptive dynamic programming using measured output data. IEEE Transactions on Systems,Man, and Cybernetics Part B, Cybernetics. 2010; 41:14–25.
99. Bequette BW. Glucose clamp algorithms and insulin time–action profiles. J Diabetes Sci Technol.2009; 3:1005–1013. [PubMed: 20144413]
100. Nandola, N.; Rivera, DE. A robust model predictive control formulation for hybrid systems withapplication to adaptive behavioral interventions. American Control Conference; Baltimore, MD.2010. p. 6286-6292.
101. Schwartz JD, Rivera DE. A process control approach to tactical inventory management inproduction-inventory systems. Int J Production Economics. 2010; 125:111–124.
102. Ogunnaike, BA.; Ray, WH. Process dynamics, modeling, and control. New York: OxfordUniversity Press; 1994.
103. Ljung, L. Prentice Hall information and system sciences series. New York: Prentice Hall; 1999.System identification: Theory for the user.
104. Ramsay, J.; Silverman, B. Functional data analysis. New York: Springer; 2005.105. Camacho, EF.; Bordons, C. Model predictive control. 2. New York: Springer; 2004.106. Collins LM, Murphy SA, Bierman KL. A conceptual framework for adaptive preventive
interventions. Prevention Science. 2004; 5:185–196. [PubMed: 15470938]107. O’Grady L, Witteman H, Bender JL, Urowitz S, Wiljer D, Jaded AR. Measuring the impact of a
moving target: Towards a dynamic framework for evaluating collaborative adaptive interactivetechnologies. Journal of Medical Internet Research. 2009; 11:e20. [PubMed: 19632973]
108. Resnicow K, Strecher V, Couper M, et al. Methodologic and design issues in patient-centered e-health research. American Journal of Preventive Medicine. 2010; 38:98–102. [PubMed:20117564]
109. Downer SR, Meara JG, Da Costa AC. Use of SMS text messaging to improve outpatientadherence. MJA. 2005; 183:366–368. [PubMed: 16201955]
110. Downer SR, Meara JG, Da Costa AC, Sethuraman K. SMS text messaging improves outpatientattendance. Australian Health Review. 2006; 30:389–396. [PubMed: 16879098]
111. Foley J, O’Neill M. Use of mobile short message service (SMS) as a reminder: The effect onpatient attendance. European Archives of Paediatric Dentistry. 2009; 10:15–18. [PubMed:19254521]
112. da Costa TM, Salomao PL, Martha AS, Pisa IT, Sigulem D. The impact of short message servicetext messages sent as appointment reminders to patients’ cell phones at outpatient clinics in SaoPaulo, Brazil. International Journal of Medical Informatics. 2010; 79:65–70. [PubMed:19783204]
113. Kwon HS, Cho JH, Kim HS, et al. Development of web-based diabetic patient managementsystem using short message service (SMS). Diabetes Research and Clinical Practice. 2004;66S:S133–S137. [PubMed: 15563964]
Riley et al. Page 18
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
114. Ostojic V, Cvoriscec B, Ostojic SB, Reznikoff D, Stipic-Markovic A, Tudjman Z. Improvingasthma control through telemedicine: A study of short-message service. Telemed J E Health.2005; 11:28–35. [PubMed: 15785218]
115. Kim HS, Yoo YS, Shim HS. Effects of an Internet-based intervention on plasma glucose levels inpatients with type 2 diabetes. Journal of Nursing Care Quality. 2005; 20:335–340. [PubMed:16177585]
116. Kim HS, Kim NC, Ahn SH. Impact of a nurse short message service intervention for patients withdiabetes. Journal of Nursing Care Quality. 2006; 21:266–271. [PubMed: 16816608]
117. Kim HS, Jeong HS. A nurse short message service by cellular phone in type-2 diabetic patientsfor six months. Journal of Clinical Nursing. 2007; 16:1082–1087. [PubMed: 17518883]
118. Benhamou PY, Melki V, Boizel R, et al. One-year efficacy and safety of Web-based follow-upusing cellular phone in type 1 diabetic patients under insulin pump therapy: The PumpNet study.Diabetes Metabol. 2007; 33:220–226.
119. Yoon KH, Kim HS. A short message service by cellular phone in type 2 diabetic patients for 12months. Diabetes Research and Clinical Practice. 2008; 79:256–261. [PubMed: 17988756]
120. Newton KH, Wiltshire EJ, Elley CR. Pedometers and text messaging to increase physical activity:Randomized controlled trial of adolescents with type 1 diabetes. Diabetes Care. 2009; 32:813–815. [PubMed: 19228863]
121. Prabhakaran L, Chee WY, Chua KC, Abisheganaden J, Wong WM. The use of text messaging toimprove asthma control: A pilot study using mobile phone short messaging service (SMS).Journal of Telemedicine and Telecare. 2010; 16:286–290. [PubMed: 20576744]
Riley et al. Page 19
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Implications
Practice
Mobile technologies are rapidly evolving as a method for delivering health behaviorinterventions that can be tailored to the individual throughout the intervention, but thecontent and timing of these interventions have not been consistently grounded in healthbehavior theories, so practitioners need to consider the theoretical and empirical basis ofmobile health behavior interventions.
Policy
Investment in the development of mobile health behavior interventions needs to bebalanced with investment in theoretically grounded content development and evaluationprocedures that are responsive to this rapidly evolving area.
Research
In addition to the responsive evaluation of mobile health behavior interventions,researchers need to utilize these applications to test and advance more dynamic healthbehavior theories, taking advantage of control systems engineering and other dynamicfeedback models to advance new theories that can be better applied to the intensiveadaptability possible from mobile health behavior interventions.
Riley et al. Page 20
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

Fig. 1.Illustration of control systems dynamical model for smoking urge
Riley et al. Page 21
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Riley et al. Page 22
Tabl
e 1
Smok
ing
cess
atio
n m
obile
inte
rven
tion
stud
ies
Ref
eren
ceSt
udy
char
acte
rist
ics
Inte
rven
tion
desc
ript
ion
The
oret
ical
bas
isIn
tera
ctiv
ityO
utco
me
Obe
rmay
er e
tal
. [23
]N
=46,
age
18–
25-y
ear s
mok
ers;
pre–
post
SMS
for m
anag
ing
urge
s tim
ed a
ndta
ilore
d to
like
ly h
igh-
risk
situ
atio
ns a
ndto
stag
e of
cha
nge;
add
ition
al m
essa
ges
prov
ided
by
text
requ
est
Self-
Reg
ulat
ion;
Tra
nsth
eore
tical
Mod
elO
utpu
t aut
o-ad
just
edin
itial
ly a
nd ju
st-in
-tim
e
Qui
t rat
e (b
io-v
alid
ated
)of
17%
at 6
wee
ks
Rod
gers
et a
l.[2
4]N
=1,7
05 a
dult
smok
ers;
RC
T of
SMS
mes
sage
s vs.
no tr
eatm
ent
SMS
with
mot
ivat
iona
l sup
port,
qui
tin
form
atio
n, a
nd d
istra
ctio
n (g
ener
alin
tere
st in
fo);
addi
tiona
l mes
sage
spr
ovid
ed b
y te
xt re
ques
t
Non
e re
porte
dO
utpu
t aut
o-ad
just
edin
itial
ly a
nd ju
st-in
-tim
e
Qui
t rat
e of
28%
for
inte
rven
tion
vs. 1
3% fo
rco
ntro
l at 6
wee
ks
Rile
y et
al.
[25]
N=3
1, a
ge 1
8–25
-yea
r sm
oker
s;pr
e–po
stSa
me
as O
berm
ayer
et a
l. [2
3]Se
lf-R
egul
atio
n; T
rans
theo
retic
al M
odel
Out
put a
uto-
adju
sted
initi
ally
and
just
-in-
time
Qui
t rat
e (b
io-v
alid
ated
)of
42%
at 6
wee
ks
Whi
ttake
r et a
l.[2
6]N
=17,
age
16–
45-y
ear s
mok
ers;
pre–
post
Vid
eos o
f rol
e m
odel
qui
tting
exp
erie
nces
inte
rspe
rsed
with
SM
S m
essa
ges
prov
idin
g qu
ittin
g as
sist
ance
Soci
al C
ogni
tive
Theo
ry; S
ocia
l Mar
ketin
gO
utpu
t aut
o-ad
just
edin
itial
ly a
nd ju
st-in
-tim
e
Qui
t rat
e of
53%
at 4
wee
ks
Bre
ndry
en a
ndK
raft
[27]
N=3
96 a
dult
smok
ers;
RC
T of
inte
rven
tion
vs. s
elf-
help
boo
klet
IVR
and
SM
S m
essa
ges a
s par
t of m
ulti-
chan
nel s
mok
ing
cess
atio
n in
terv
entio
nta
ilore
d to
smok
ing
stat
us; m
ost a
lso
rece
ived
NR
T
Self-
Reg
ulat
ion;
Soc
ial C
ogni
tive
Theo
ry;
Cog
nitiv
e–B
ehav
iora
l Mod
elO
utpu
t aut
o-ad
just
edin
itial
ly a
nd ju
st-in
-tim
e
Qui
t rat
e of
38%
for
inte
rven
tion
vs. 2
4% fo
rse
lf-he
lp b
ookl
et a
t 12
mon
ths
Bre
ndry
en e
t al.
[28]
N=2
90 a
dult
smok
ers;
RC
T of
inte
rven
tion
vs. s
elf-
help
boo
klet
Sam
e as
Bre
ndry
en a
nd K
raft
[27]
Self-
Reg
ulat
ion;
Soc
ial C
ogni
tive
Theo
ry;
Cog
nitiv
e–B
ehav
iora
lO
utpu
t aut
o-ad
just
edin
itial
ly a
nd ju
st-in
-tim
e
Qui
t rat
e of
20%
for
inte
rven
tion
vs. 1
0% fo
rse
lf-he
lp b
ookl
et a
t 12
mon
ths
Free
et a
l. [2
9]N
=200
adu
lt sm
oker
s; R
CT
ofin
terv
entio
n vs
. gen
eric
text
mes
sage
s
Sam
e as
Rod
gers
et a
l. w
ith S
MS
text
sad
apte
d fo
r UK
par
ticip
ants
Non
e re
porte
dO
utpu
t aut
o-ad
just
edin
itial
ly a
nd ju
st-in
-tim
e
Qui
t rat
e (b
io-v
alid
ated
)of
8%
for i
nter
vent
ion
vs.
6% fo
r con
trol a
t 6m
onth
s
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Riley et al. Page 23
Tabl
e 2
Wei
ght l
oss (
diet
, phy
sica
l act
ivity
) mob
ile in
terv
entio
n st
udie
s
Ref
eren
ceSt
udy
char
acte
rist
ics
Inte
rven
tion
desc
ript
ion
The
oret
ical
bas
isIn
tera
ctiv
ityO
utco
me
Joo
and
Kim
,[3
3]N
=927
adu
lt pu
blic
hea
lthce
nter
pat
ient
s; p
re–p
ost
Wee
kly
info
rmat
iona
l SM
S m
essa
ges r
egar
ding
diet
and
exe
rcis
eN
one
repo
rted
Out
put n
ot a
djus
ted
Wei
ght l
oss o
f 1.6
kg
at 1
2w
eeks
Hur
ling
et a
l.[3
8]N
=77
norm
al a
nd o
verw
eigh
tad
ults
; RC
T of
inte
rven
tion
vs.
exer
cise
adv
ice
alon
e
Web
-bas
ed p
rogr
am fo
r man
agin
g pe
rcei
ved
barr
iers
and
sche
dulin
g w
eekl
y ex
erci
se;
rem
inde
rs v
ia e
mai
l or S
MS
mes
sagi
ng;
acce
lero
met
er d
ata
obta
ined
and
tran
smitt
ed v
iam
obile
pho
ne fo
r rea
l-tim
e w
eb fe
edba
ck
Theo
ry o
f Pla
nned
Beh
avio
r; C
ompo
nent
s of
othe
r the
orie
s
Out
put a
uto-
adju
sted
initi
ally
Phys
ical
act
ivity
incr
ease
of 1
2 M
ET m
in fo
rin
terv
entio
n vs
. 4 M
ET m
info
r con
trol a
t 9 w
eeks
Atie
nza
et a
l.[4
1]N
=36
heal
thy
adul
ts; R
CT
ofin
terv
entio
n vs
. prin
t mat
eria
lsPD
A p
rogr
am a
sses
sing
veg
etab
le a
nd w
hole
grai
n in
take
and
pro
vidi
ng b
ehav
iora
l stra
tegi
esto
mot
ivat
e ch
ange
s to
diet
ary
inta
ke
Self-
Reg
ulat
ion
Theo
ry;
Soci
al C
ogni
tive
Theo
ryO
utpu
t man
ually
adj
uste
d in
itial
lySe
rvin
gs o
f veg
etab
les o
rgr
ain
fiber
per
1,0
00 k
cal o
f1
for i
nter
vent
ion
vs. 0
for
cont
rols
at 8
wee
ks
Kin
g et
al.
[42]
N=3
7, a
ge ≥
50 y
ears
unde
ract
ive
adul
ts; R
CT
ofin
terv
entio
n vs
. prin
t mat
eria
ls
PDA
pro
gram
ass
essi
ng p
hysi
cal a
ctiv
ities
,ve
geta
ble
and
who
le g
rain
inta
ke, a
ndpr
ovid
ing
beha
vior
al st
rate
gies
to m
otiv
ate
chan
ges t
o di
etar
y in
take
Self-
Reg
ulat
ion
Theo
ry;
Soci
al C
ogni
tive
Theo
ryO
utpu
t aut
o-ad
just
ed in
itial
ly a
ndju
st-in
-tim
eIn
crea
se o
f mod
erat
e+p
hysi
cal a
ctiv
ity o
f 178
min
/wee
k fo
r int
erve
ntio
nvs
. dec
reas
e of
80
min
/w
eek
for c
ontro
l at 8
wee
ks
Bea
sley
et a
l.[3
9]N
=174
ove
rwei
ght o
r obe
sead
ults
; RC
T of
inte
rven
tion
vs.
pape
r dia
ry
PDA
die
tary
self-
mon
itorin
g pr
ogra
m w
ithfe
edba
ck c
ompa
red
to p
erso
naliz
ed ta
rget
s for
very
low
fat d
iet r
ecom
men
datio
ns
Non
e re
porte
dO
utpu
t aut
o-ad
just
ed in
itial
ly a
ndju
st-in
-tim
eTo
tal f
at in
take
dec
reas
e of
31 g
/day
for i
nter
vent
ion
vs. 2
2 g/
day
for c
ontro
l at 3
wee
ks
Liu
et a
l. [3
5]N
=48
adul
t CO
PD p
atie
nts;
RC
T of
inte
rven
tion
vs. n
otre
atm
ent
Mus
ic te
mpo
del
iver
ed v
ia m
obile
pho
nepr
ogra
m a
djus
ted
base
d on
ISW
T to
enc
oura
gea
wak
ing
pace
at 8
0% m
ax e
ffor
t
Non
e re
porte
dO
utpu
t man
ually
adj
uste
d in
itial
lyan
d ju
st-in
-tim
eIS
WT
dist
ance
incr
ease
of
68.4
m fo
r int
erve
ntio
nfr
om b
asel
ine
to 1
2 w
eeks
Ngu
yen
et a
l.[3
6]N
=17
adul
t CO
PD p
atie
nts;
RC
T of
mob
ile c
oach
ed v
s.m
obile
mon
itorin
g al
one
Dai
ly lo
g vi
a SM
S of
exe
rcis
e an
d sy
mpt
oms;
Wee
kly
SMS
mes
sage
s rei
nfor
cing
logg
edex
erci
se b
y nu
rse
Non
e re
porte
dO
utpu
t man
ually
adj
uste
d ju
st-in
-tim
eIn
crem
enta
l cyc
le te
stch
ange
of +
1.3
W fo
rm
onito
ring
vs. −
5.5
W fo
rco
ache
d
Haa
pala
et a
l.[4
0]N
=125
ove
rwei
ght a
dults
; RC
Tof
inte
rven
tion
vs. n
o tre
atm
ent
Con
tinge
ncy
prog
ram
via
SM
S th
at in
stru
cted
user
s in
a st
agge
red
redu
ctio
n of
food
inta
keba
sed
on w
eigh
t, da
ily e
nerg
y re
quire
men
ts,
and
shor
t- an
d lo
ng-te
rm w
eigh
t goa
ls
Self-
Effic
acy
Theo
ry;
Syst
ems C
ontin
genc
yA
ppro
ach
Out
put a
uto-
adju
sted
initi
ally
and
just
-in-ti
me
Wei
ght l
oss o
f 4.5
kg
for
inte
rven
tion
vs. 1
.1 k
g fo
rco
ntro
l at 1
2 m
onth
s
Patri
ck e
t al.
[43]
N=6
5 ov
erw
eigh
t adu
lts; R
CT
of in
terv
entio
n vs
. prin
tin
form
atio
n
Tailo
red
SMS
mes
sage
s tha
t enc
oura
ged
goal
setti
ng, s
elf-
mon
itorin
g, a
nd a
ddre
ssed
bar
riers
to w
eigh
t los
s
Non
e re
porte
dO
utpu
t aut
o-ad
just
ed in
itial
ly a
ndju
st-in
-tim
eW
eigh
t los
s of 2
.9 k
g fo
rin
terv
entio
n vs
. 0.9
kg
for
prin
t inf
orm
atio
n at
4m
onth
s
Fjel
dsoe
et a
l.[4
4]N
=88
post
nata
l wom
en; R
CT
ofin
terv
entio
n vs
. ini
tial
beha
vior
al c
ouns
elin
g on
ly
Tailo
red
SMS
mes
sage
s enc
oura
ging
phy
sica
lac
tivity
sent
3–5
tim
es p
er w
eek
prov
ided
inco
njun
ctio
n w
ith tw
o be
havi
oral
cou
nsel
ing
sess
ions
; wee
kly
SMS
goal
che
ck w
ithre
spon
se
Soci
al C
ogni
tive
Theo
ryO
utpu
t aut
o-ad
just
ed in
itial
ly a
ndju
st-in
-tim
eW
alki
ng fo
r exe
rcis
edu
ratio
n in
crea
se o
f 6.7
min
for i
nter
vent
ion
vs. 0
.3m
in fo
r con
trol a
t 13
wee
ks
Bur
ke e
t al.
[34]
N=2
10 o
verw
eigh
t or o
bese
adul
ts; R
CT
of P
DA
+ ta
ilore
dIn
add
ition
to 2
0 gr
oup
sess
ions
ove
r 6 m
onth
s,PD
A p
rogr
am o
f sel
f-m
onito
ring
and
sum
mar
you
tput
of d
ieta
ry in
take
(sam
e di
etar
y
Self-
Reg
ulat
ion
Theo
ryO
utpu
t aut
o-ad
just
ed in
itial
ly a
ndju
st-in
-tim
eW
eigh
t los
s of 6
.5%
for
PDA
+ ta
ilore
d fe
edba
ck,
4.8%
for P
DA
alo
ne, a
nd
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Riley et al. Page 24
Ref
eren
ceSt
udy
char
acte
rist
ics
Inte
rven
tion
desc
ript
ion
The
oret
ical
bas
isIn
tera
ctiv
ityO
utco
me
feed
back
, PD
A m
onito
ring,
and
pape
r-ba
sed
mon
itorin
gm
onito
ring
prog
ram
as B
easl
ey e
t al.
[39]
) and
exer
cise
act
ivity
with
or w
ithou
t cus
tom
tailo
red
mul
tiple
dai
ly m
essa
ges b
ased
on
inpu
t
4.6%
for p
aper
-bas
eddi
etar
y m
onito
ring
at 6
mon
ths
Bau
er e
t al.
[37]
N=4
0 ov
erw
eigh
t chi
ldre
n; p
re–
post
Wee
kly
text
mes
sage
que
stio
ns o
n m
aint
aini
ngdi
et a
nd p
hysi
cal a
ctiv
ity fo
llow
ing
12-w
eek
grou
p in
terv
entio
n. F
eedb
ack
base
d on
resp
onse
s pro
vide
d re
info
rcem
ent,
prom
oted
soci
al su
ppor
t, re
min
ded
skill
s lea
rned
dur
ing
treat
men
t, an
d m
otiv
ated
par
ticip
ants
(rev
iew
edan
d m
odifi
ed b
y st
aff b
efor
e se
ndin
g)
Cog
nitiv
e–B
ehav
iora
lO
utpu
t (se
mi)
auto
-adj
uste
din
itial
ly a
nd ju
st-in
-tim
eB
MI s
tand
ard
devi
atio
nsc
ore
redu
ctio
n of
0.0
7fr
om e
nd o
f gro
upin
terv
entio
n to
12
mon
ths
ISW
T In
term
itten
t Shu
ttle
Wal
k Te
st
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Riley et al. Page 25
Tabl
e 3
Adh
eren
ce m
obile
inte
rven
tion
stud
ies
Ref
eren
ceSt
udy
char
acte
rist
ics
Inte
rven
tion
desc
ript
ion
The
oret
ical
bas
isIn
tera
ctiv
ityO
utco
me
Safr
en e
t al.
[54]
N=8
2 H
IV +
pat
ient
s; R
CT
of in
terv
entio
nvs
. mon
itorin
g on
lyTa
ilore
d do
se re
min
ders
via
two-
way
pag
er, a
long
with
oth
erre
min
ders
(e.g
., m
eals
,ap
poin
tmen
ts)
Non
e re
porte
dO
utpu
t man
ually
adju
sted
initi
ally
Dos
e ad
here
nce
of 6
4% fo
r int
erve
ntio
nvs
. 52%
for c
ontro
l at 1
2 w
eeks
Bos
et a
l. [5
7]N
=343
orth
odon
tic p
atie
nts;
non
rand
omiz
edco
mpa
rison
of t
ext m
essa
ge, p
hone
, mai
l, an
dno
rem
inde
r
SMS
appo
intm
ent r
emin
der
Non
e re
porte
dO
utpu
t not
adj
uste
dA
ppoi
ntm
ent a
ttend
ance
of 9
0.6%
for
mai
l, 90
.4%
for p
hone
, 82.
4% fo
r SM
S,an
d 83
.7%
for n
o re
min
der o
ver 3
wee
ks
Dow
ner e
t al.
[109
]N
=2,8
64 g
ener
al m
edic
al o
utpa
tient
s with
mob
ile p
hone
s; h
isto
ric c
ontro
l of
inte
rven
tion
vs. n
o re
min
der
SMS
appo
intm
ent r
emin
der
Non
e re
porte
dO
utpu
t not
adj
uste
dA
ppoi
ntm
ent a
dher
ence
of 8
5.8%
for
inte
rven
tion
vs. 7
6.6%
for c
ontro
l ove
r 1m
onth
Dow
ner e
t al.
[110
]N
=45,
110
gene
ral m
edic
al o
utpa
tient
s;hi
stor
ic c
ontro
l of i
nter
vent
ion
vs. n
ore
min
der
SMS
appo
intm
ent r
emin
der
Non
e re
porte
dO
utpu
t not
adj
uste
dA
ppoi
ntm
ent a
dher
ence
of 9
0.2%
for
inte
rven
tion
vs. 8
0.5%
for c
ontro
l ove
r 3m
onth
s
Leon
g et
al.
[58]
N=9
93 p
rimar
y ca
re o
utpa
tient
s; R
CT
ofSM
S, p
hone
or n
o re
min
der
SMS
appo
intm
ent r
emin
der
Non
e re
porte
dO
utpu
t not
adj
uste
dA
ppoi
ntm
ent a
dher
ence
of 5
9.6%
for
SMS,
59.
0% fo
r pho
ne, a
nd 4
8.1%
for
cont
rol o
ver 3
mon
ths
Kos
hy e
t al.
[56]
N=9
,512
oph
thal
mol
ogy
outp
atie
nts;
nonr
ando
miz
ed c
ompa
rison
of i
nter
vent
ion
vs. n
o re
min
der
SMS
appo
intm
ent r
emin
der w
ithab
ility
to te
xt re
ply
to c
ance
lap
poin
tmen
t
Non
e re
porte
dO
utpu
t not
adj
uste
dA
ppoi
ntm
ent a
dher
ence
of 8
8.8%
for S
MS
vs. 8
1.9%
for c
ontro
l ove
r 6 m
onth
s
Che
n et
al.
[59]
N=1
,859
pre
vent
ive
scre
enin
g pa
tient
s; R
CT
of S
MS,
pho
ne o
r no
rem
inde
rSM
S ap
poin
tmen
t rem
inde
rN
one
repo
rted
Out
put n
ot a
djus
ted
App
oint
men
t adh
eren
ce o
f 87.
5% fo
rSM
S, 8
8.3%
for p
hone
, and
80.
5% fo
rco
ntro
l ove
r 2 m
onth
s
Sim
oni e
t al.
[55]
N=2
24 H
IV +
pat
ient
s; R
CT
of p
ager
+ p
eer
supp
ort,
page
r onl
y, p
eer s
uppo
rt on
ly, o
rus
ual c
are
Tailo
red
dose
rem
inde
rs v
ia tw
o-w
ay p
ager
alo
ng w
ith e
duca
tiona
l,en
terta
inm
ent,
and
adhe
renc
eas
sess
men
t tex
ts
Non
e re
porte
dO
utpu
t man
ually
adju
sted
initi
ally
Dos
e ad
here
nce
of 5
0.1%
for p
ager
+ p
eer
supp
ort,
41.8
% fo
r pag
er, 4
7.0%
for p
eer
supp
ort a
nd 4
4.4%
for u
sual
car
e at
3m
onth
s
Fole
y et
al.
[111
]N
=276
ped
iatri
c de
ntal
pat
ient
s; h
isto
rical
cont
rol o
f int
erve
ntio
n vs
. no
rem
inde
rSM
S ap
poin
tmen
t rem
inde
rN
one
repo
rted
Out
put n
ot a
djus
ted
App
oint
men
t adh
eren
ce o
f 89.
6% fo
r SM
Svs
. 76.
1% fo
r con
trol o
ver 1
mon
th
Da
Cos
ta e
t al.
[112
]N
=7,8
90 g
ener
al o
utpa
tient
app
oint
men
ts;
nonr
ando
miz
ed c
ompa
rison
of i
nter
vent
ion
vs. n
o re
min
der
SMS
appo
intm
ent r
emin
der
Non
e re
porte
dO
utpu
t not
adj
uste
dA
ppoi
ntm
ent a
dher
ence
of 8
0.6%
for S
MS
vs. 7
4.4%
for c
ontro
l ove
r 11
mon
ths
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.

NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Riley et al. Page 26
Tabl
e 4
Dis
ease
man
agem
ent m
obile
inte
rven
tion
stud
ies
Ref
eren
ceSt
udy
char
acte
rist
ics
Inte
rven
tion
desc
ript
ion
The
oret
ical
bas
isIn
tera
ctiv
ityO
utco
me
Kw
on e
t al.
[113
]N
=185
adu
lt di
abet
es p
atie
nts;
pre–
post
Glu
cose
read
ings
reco
rded
via
SM
S,re
view
ed b
y pr
ovid
er w
ho se
ntre
com
men
datio
ns v
ia S
MS
Non
e re
porte
dO
utpu
t man
ually
adj
uste
d ju
st-in
-tim
eH
bA1c
dec
reas
ed 7
.5%
to7.
0% a
t 3 m
onth
s
Leu
et a
l. [7
5]N
=50
adul
t dia
bete
s pat
ient
s;R
CT
of p
ager
rem
inde
rs v
s.ro
utin
e ca
re
Two-
way
pag
er re
min
ders
for v
ario
usdi
abet
es se
lf-m
anag
emen
t act
iviti
es(c
usto
miz
ed)
Non
e re
porte
dO
utpu
t man
ually
adj
uste
d at
bas
elin
eH
bA1c
dec
reas
ed 8
.5%
to8.
2% fo
r int
erve
ntio
n vs
.8.
5% to
7.9
% fo
r con
trols
at
3 to
6 m
onth
s
Ost
ojic
et a
l. [1
14]
N=2
6 ad
ult a
sthm
a pa
tient
s; R
CT
of te
xt v
s. no
text
mes
sage
reco
rdin
g
Dai
ly S
MS
reco
rdin
g of
pea
k flo
wre
view
ed b
y pr
ovid
er w
ho se
nt w
eekl
ytre
atm
ent a
djus
tmen
t mes
sage
s via
text
Non
e re
porte
dO
utpu
t man
ually
adj
uste
d ju
st-in
-tim
eFE
V1
incr
ease
d fr
om77
.63%
to 8
1.25
% fo
rin
terv
entio
n vs
. 78.
88%
to78
.25%
for c
ontro
ls a
t 16
wee
ks
Kim
et a
l. [1
15]
N=4
2 ad
ult t
ype
2 di
abet
espa
tient
s; p
re–p
ost
SMS
mes
sage
s sen
t by
prov
ider
s bas
edon
revi
ew o
f dat
a pr
ovid
ed b
y pa
tient
via
Inte
rnet
Non
e re
porte
dO
utpu
t man
ually
adj
uste
d ju
st-in
-tim
eFa
stin
g pl
asm
a gl
ucos
ede
crea
sed
from
174
to 1
45.4
m/d
L at
12
wee
ks
Kim
et a
l. [1
16]
N=4
5 ad
ult t
ype
2 di
abet
espa
tient
s; p
re–p
ost
Sam
e as
Kim
et a
l. [1
16]
Non
e re
porte
dO
utpu
t man
ually
adj
uste
d ju
st-in
-tim
eH
bA1c
dec
reas
ed 8
.1%
to7.
0% a
t 12
wee
ks
Fran
klin
et a
l. [6
3]N
=92,
age
8–1
8-ye
ar ty
pe 1
diab
etes
pat
ient
s; R
CT
ofco
nven
tiona
l ins
ulin
ther
apy,
conv
entio
nal t
hera
py w
ith S
MS,
and
inte
nsiv
e th
erap
y w
ith S
MS
Pers
onal
ized
dai
ly S
MS
mes
sage
s to
supp
ort d
iabe
tes m
anag
emen
tSo
cial
Cog
nitiv
e Th
eory
Out
put a
uto-
adju
sted
at i
nitia
tion
HbA
1c d
ecre
ased
10.
0 to
9.2
for i
nten
sive
ther
apy
+SM
S; n
o ch
ange
in o
ther
grou
ps
Ram
i et a
l. [7
0]N
=36,
age
10–
19-y
ear t
ype
1di
abet
es p
atie
nts;
rand
omiz
edcr
osso
ver d
esig
n of
inte
rven
tion
vs. u
sual
car
e pa
per d
iary
reco
rdin
g
SMS
reco
rdin
g of
blo
od g
luco
se, i
nsul
indo
se, a
nd c
arbo
hydr
ate
inta
ke w
ithw
eekl
y fe
edba
ck (a
utom
ated
if O
K,
gene
rate
d by
dia
beto
logi
sts i
fad
just
men
ts n
eede
d)
Non
e re
porte
dO
utpu
t man
ually
adj
uste
d ju
st-in
-tim
eH
bA1c
cha
nge
of 9
.1%
to8.
9% (i
nter
vent
ion)
to 9
.2%
(con
trol);
and
8.9
% to
9.9
%(c
ontro
l) to
8.9
%(in
terv
entio
n) a
t 3 a
nd 6
mon
ths
Ma
et a
l. [6
6]N
=15
adul
t typ
e 2
diab
etes
patie
nts;
pre
–pos
tPD
A d
ieta
ry m
onito
ring
with
gly
cem
icin
dex
feed
back
use
d to
aug
men
t a si
x-co
ntac
t dia
bete
s man
agem
ent
inte
rven
tion
Non
e re
porte
dO
utpu
t aut
o-ad
just
ed ju
st-in
-tim
eH
bA1c
dec
reas
e fr
om 8
.0%
to 7
.5%
at 6
mon
ths
Kim
and
Jeon
g,[1
17]
N=5
1 ad
ult d
iabe
tes p
atie
nts;
pre
–po
stSa
me
as K
im e
t al.
[115
]N
one
repo
rted
Out
put m
anua
lly a
djus
ted
just
-in-ti
me
HbA
1c d
ecre
ased
from
8.1%
to 7
.0%
for
inte
rven
tion
and
7.6%
to7.
7% fo
r con
trol a
t 6 m
onth
s
Ben
ham
ou e
t al.
[118
]N
=30
adul
t typ
e 1
diab
etes
patie
nts;
rand
omiz
ed c
ross
over
of
SMS
feed
back
vs.
self-
mon
itorin
gon
ly
Prov
ider
s ack
now
ledg
ed re
ceip
t of
wee
kly
trans
mitt
ed g
luco
se lo
gs a
ndpr
ovid
ed re
com
men
datio
ns
Non
e re
porte
dO
utpu
t man
ually
adj
uste
d ju
st-in
-tim
eH
bA1c
cha
nge
of 8
.3%
to8.
2% fo
r int
erve
ntio
n an
d8.
2% to
8.3
% a
t 6 m
onth
s
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.
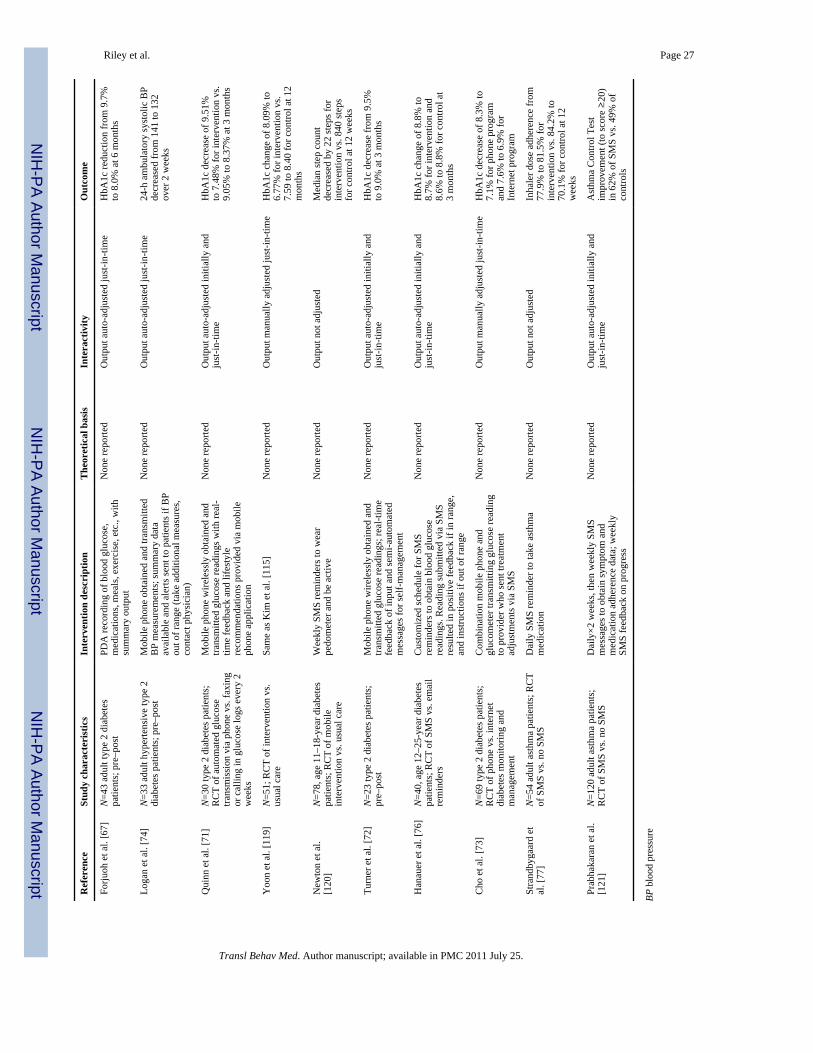
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
NIH
-PA Author Manuscript
Riley et al. Page 27
Ref
eren
ceSt
udy
char
acte
rist
ics
Inte
rven
tion
desc
ript
ion
The
oret
ical
bas
isIn
tera
ctiv
ityO
utco
me
Forju
oh e
t al.
[67]
N=4
3 ad
ult t
ype
2 di
abet
espa
tient
s; p
re–p
ost
PDA
reco
rdin
g of
blo
od g
luco
se,
med
icat
ions
, mea
ls, e
xerc
ise,
etc
., w
ithsu
mm
ary
outp
ut
Non
e re
porte
dO
utpu
t aut
o-ad
just
ed ju
st-in
-tim
eH
bA1c
redu
ctio
n fr
om 9
.7%
to 8
.0%
at 6
mon
ths
Loga
n et
al.
[74]
N=3
3 ad
ult h
yper
tens
ive
type
2di
abet
es p
atie
nts;
pre
–pos
tM
obile
pho
ne o
btai
ned
and
trans
mitt
edB
P m
easu
rem
ents
; sum
mar
y da
taav
aila
ble
and
aler
ts se
nt to
pat
ient
s if B
Pou
t of r
ange
(tak
e ad
ditio
nal m
easu
res,
cont
act p
hysi
cian
)
Non
e re
porte
dO
utpu
t aut
o-ad
just
ed ju
st-in
-tim
e24
-h a
mbu
lato
ry sy
stol
ic B
Pde
crea
sed
from
141
to 1
32ov
er 2
wee
ks
Qui
nn e
t al.
[71]
N=3
0 ty
pe 2
dia
bete
s pat
ient
s;R
CT
of a
utom
ated
glu
cose
trans
mis
sion
via
pho
ne v
s. fa
or c
allin
g in
glu
cose
logs
eve
ry 2
wee
ks
Mob
ile p
hone
wire
less
ly o
btai
ned
and
trans
mitt
ed g
luco
se re
adin
gs w
ith re
al-
time
feed
back
and
life
styl
ere
com
men
datio
ns p
rovi
ded
via
mob
ileph
one
appl
icat
ion
Non
e re
porte
dO
utpu
t aut
o-ad
just
ed in
itial
ly a
ndju
st-in
-tim
eH
bA1c
dec
reas
e of
9.5
1%to
7.4
8% fo
r int
erve
ntio
n vs
.9.
05%
to 8
.37%
at 3
mon
ths
Yoo
n et
al.
[119
]N
=51;
RC
T of
inte
rven
tion
vs.
usua
l car
eSa
me
as K
im e
t al.
[115
]N
one
repo
rted
Out
put m
anua
lly a
djus
ted
just
-in-ti
me
HbA
1c c
hang
e of
8.0
9% to
6.77
% fo
r int
erve
ntio
n vs
.7.
59 to
8.4
0 fo
r con
trol a
t 12
mon
ths
New
ton
et a
l.[1
20]
N=7
8, a
ge 1
1–18
-yea
r dia
bete
spa
tient
s; R
CT
of m
obile
inte
rven
tion
vs. u
sual
car
e
Wee
kly
SMS
rem
inde
rs to
wea
rpe
dom
eter
and
be
activ
eN
one
repo
rted
Out
put n
ot a
djus
ted
Med
ian
step
cou
ntde
crea
sed
by 2
2 st
eps f
orin
terv
entio
n vs
. 840
step
sfo
r con
trol a
t 12
wee
ks
Turn
er e
t al.
[72]
N=2
3 ty
pe 2
dia
bete
s pat
ient
s;pr
e–po
stM
obile
pho
ne w
irele
ssly
obt
aine
d an
dtra
nsm
itted
glu
cose
read
ings
; rea
l-tim
efe
edba
ck o
f inp
ut a
nd se
mi-a
utom
ated
mes
sage
s for
self-
man
agem
ent
Non
e re
porte
dO
utpu
t aut
o-ad
just
ed in
itial
ly a
ndju
st-in
-tim
eH
bA1c
dec
reas
e fr
om 9
.5%
to 9
.0%
at 3
mon
ths
Han
auer
et a
l. [7
6]N
=40,
age
12–
25-y
ear d
iabe
tes
patie
nts;
RC
T of
SM
S vs
. em
ail
rem
inde
rs
Cus
tom
ized
sche
dule
for S
MS
rem
inde
rs to
obt
ain
bloo
d gl
ucos
ere
adin
gs. R
eadi
ng su
bmitt
ed v
ia S
MS
resu
lted
in p
ositi
ve fe
edba
ck if
in ra
nge,
and
inst
ruct
ions
if o
ut o
f ran
ge
Non
e re
porte
dO
utpu
t aut
o-ad
just
ed in
itial
ly a
ndju
st-in
-tim
eH
bA1c
cha
nge
of 8
.8%
to8.
7% fo
r int
erve
ntio
n an
d8.
6% to
8.8
% fo
r con
trol a
t3
mon
ths
Cho
et a
l. [7
3]N
=69
type
2 d
iabe
tes p
atie
nts;
RC
T of
pho
ne v
s. in
tern
etdi
abet
es m
onito
ring
and
man
agem
ent
Com
bina
tion
mob
ile p
hone
and
gluc
omet
er tr
ansm
ittin
g gl
ucos
e re
adin
gto
pro
vide
r who
sent
trea
tmen
tad
just
men
ts v
ia S
MS
Non
e re
porte
dO
utpu
t man
ually
adj
uste
d ju
st-in
-tim
eH
bA1c
dec
reas
e of
8.3
% to
7.1%
for p
hone
pro
gram
and
7.6%
to 6
.9%
for
Inte
rnet
pro
gram
Stra
ndby
gaar
d et
al. [
77]
N=5
4 ad
ult a
sthm
a pa
tient
s; R
CT
of S
MS
vs. n
o SM
SD
aily
SM
S re
min
der t
o ta
ke a
sthm
am
edic
atio
nN
one
repo
rted
Out
put n
ot a
djus
ted
Inha
ler d
ose
adhe
renc
e fr
om77
.9%
to 8
1.5%
for
inte
rven
tion
vs. 8
4.2%
to70
.1%
for c
ontro
l at 1
2w
eeks
Prab
haka
ran
et a
l.[1
21]
N=1
20 a
dult
asth
ma
patie
nts;
RC
T of
SM
S vs
. no
SMS
Dai
ly×2
wee
ks, t
hen
wee
kly
SMS
mes
sage
s to
obta
in sy
mpt
om a
ndm
edic
atio
n ad
here
nce
data
; wee
kly
SMS
feed
back
on
prog
ress
Non
e re
porte
dO
utpu
t aut
o-ad
just
ed in
itial
ly a
ndju
st-in
-tim
eA
sthm
a C
ontro
l Tes
tim
prov
emen
t (to
scor
e ≥
20)
in 6
2% o
f SM
S vs
. 49%
of
cont
rols
BP b
lood
pre
ssur
e
Transl Behav Med. Author manuscript; available in PMC 2011 July 25.