Contraception and Beyond: The Health Benefits of Services Provided at Family Planning Centers
Upload
khangminh22Category
view
0download
0
HEALTH AND FAMILY WELFARE
SERVICES
ANNUAL REPORT
2021-22
(upto January)


INDEX
Sl.No. Subjects Page No.
CHAPTER - I 1-11
I HEALTH AND FAMILY WELFARE SERVICES SECRETARIAT
PART - 1
1 Organisation Chart 15-16
1.1 Functions of the Health Department 17
1.2 Important National & State Health Programmes 18-68
1.2.1 Universal Immunization Programme 18-19
1.2.2 National Leprosy Eradication Programme 20-25
1.2.3 National Tuberculosis Control Programme 25-29
1.2.4 National Programme For Control Of Blindness Visual Impairment 29-32
1.2.5 Karnataka State AIDS Prevention Society 32-39
1.2.6 National Vector Borne Diseases Control Programme (NVBDCP) 40-43
1.2.7 Communicable Diseases (CMD) 43-46
1.2.8 Child Health Programme 47-53
1.2.9 HMIS & RCH Portal 53-57
1.2.10 Mother Health 57-62
1.2.11 Emergency Management and Research Institute (EMRI) 62-66
1.2.12 Pre-Conception and Pre-natal Diagnostic Techniques Programmes (PC & PNDT) 67-68
1.3 School Health Programme 68-70
1.4 ASHA Programme 71
1.5 Health Services 72
1.6 National Urban Health Mission 72-76
1.7 National Programme for Prevention and Control of Fluorosis (NPPCF)
76-77
1.8 Citizen Friendly Facilities 77-78
1.9 Regulation of Private Medical Establishments 79
1.10 Health Education and Training 79
1.11 Mental Health Programme 79-86
1.12 Information, Education & Communication (IEC) programme 86-87
1.13 State Health Transport Organization 87
1.14 Integrated Disease Surveillance Project (IDSP) 87-93
1.15 Nutrition Programmes 93-96

1.16 National Iodine Deficiency, Disorder Control Programme (NIDDCP) 96-97
1.17 National Programme for Prevention and Control Of Deafness 98-99
1.18 Karnataka State Drug Logistics and Ware Housing Society 99-100
1.19 State Institute of Health & Family Welfare 100-101
1.20 Public Health Institute 101-103
1.21 Food Safety & Standards 104-107
1.22 Suvarna Arogya Suraksha Trust 107-111
1.23 Ayushman Bhart - Health and Wellness centre in Karnataka 111-116
1.24 Community Monitoring 117
1.25 Oral Health 118-121
1.26 Quality Assurance 122-125
1.27 Family Welfare 125-133
PART II
DRUG CONTROL DEPARTMENT
2.1 Introduction 136
2.2 Organization Setup 137-138
2.3 Enforcement Wing 137-140
2.4 Drugs testing Laboratory 141-143
2.5 Pharmacy Education 143-148
2.6 Finance 148-149
PART III
AYUSH DEPARTMENT
3.1 Organogram 151
3.2 Departmental Brief Note, Staff Position 152
3.3 Health Sector (Details Of Hospitals & Dispensaries) 152
3.4 Government Central Pharmacy & Drug Testing Laboratory) 153
3.5 Ayush Drugs Control 153
3.6 Statutory Boards 153
3.7 Ayush Medical Education 154
3.8 Herbal Gardens 154
3.9 Achievements of the year 2020-21 155
3.10 Proposed Plan for the year 2021-22 155
3.11 New Proposal for the year 2021-22 155-156

CHAPTER-I
Health and Family Welfare Secretariat

2

3
HEALTH AND FAMILY WELFARE DEPARTMENT
The Health and Family Welfare Department was constituted by DPAR. It has been operational since 1982. Department aim is to provide good health system to public. Role of the Health and Family Welfare Department:- Health and Family Welfare Department is providing good health system in the state to its people. It is the responsible for overall administration of Health and Family Welfare Services, AYUSH Department, Drugs Control Department, Health and Family Welfare Engineering division, Food Safety and Standards Department, National Health Mission, Karnataka State Aids Prevention Society, Suvarna Arogya Suraksha Trust, Karnataka State Medical Equipment Supplies Corporation, Karnataka Ayurveda and Unani Practitioners Board and Karnataka Homoeopathy Board. Health and Family Welfare Department implements the policies of State Government and Govt. of India. It is responsible for the administration and disciplinary matter of the Head of the Department under its purview, budgetary planning, monitoring and control and the supervision of implementation of schemes and serving as the link with the State Government the Legislature and its committees. The Hon’ble Health and Family Welfare and Medical Education Minister is the Head of the Health and Family Welfare Department. Administratively, the Department is headed by Principal Secretary to Government to supervise the overall policy and administration of the Department. The Principal Secretary is assisted by Private Secretary and Joint Secretary and Deputy Secretary. FUNCTIONS AND DUTIES. The Principal Secretary, Health & Family Welfare Department is assisted by the Joint Secretary and Deputy Secretaries in Administrative matters, releasing funds, Service matters. IFA assist in financial matters and Head of the Legal Cell assist in Legal matter. Services Section:
Service matter of all Government Medical Officers and Group A Officers of the Department of Health and Family Welfare and related court cases. C&R Section: Service matters / court cases of all Group-B, C and D cadres of the Health and Family Welfare Department. Enquiry Section: Joint enquiry of the cadre of Group-A Doctors and enquiry Cases of retired Group-A Doctors of Health & Family Welfare Department, Lokayukta cases, ACB Cases and Court Cases.

4
Health-1 Section:
Issues relating to the Engineering Unit of the Department of Health and Family Welfare.
Upgrading of Primary Health Center, Community Health Center, Taluk Hospital and
District Hospital (Bangalore and Kalaburagi Division)
RIDF /NABARD matters
Providing clinical facilities to medical nursing college /paramedical students (Bangalore
and Kalaburagi Division)
Constructions of MCH Hospital
Control of infections diseases.
Issues related to H1N1 and all other infections diseases.
Matter pertaining to persons affected by endosalphan.
Providing answers to questions of Karnataka Legislative assembly and Council.
Health-2 Section:
Upgradation of Primary Health Centre, Community Health Centre, Taluk Hospital and District Hospital (Mysore and Belagavi Division)
Matters relating to Arogya Kavacha-108 and Health Helplin-104 projects and Court Cases.
Issues relating to Karnataka State AIDS Prevention Society and Court Cases.
Providing clinical facilities to medical nursing college/paramedical students (Mysore and Belagavi Division)
Issues pertaining to Ayushman Bharath –Arogya Karnataka Project under Suvarna Arogya Suraksha Trust and Court cases.
Food Safety and Quality Authority matters and court cases.
Nomination for the Arogya Raksha Samithi (Taluk Hospital and District Hospital)
Mental Health programs.
Issues related to Tobacco Control
Sanctioning Mobile Medical units.
Providing answers to questions of Karnataka Legislative assembly and Council.

5
Family Welfare:
NHM and Family Welfare Programs.
Nomination for PC&PNDT Act Committees.
Issues pertaining to family welfare and training organizations.
Matters pertaining to Messrs HLL and KAPL.
Issues relating to the purchase of diagnostic laboratories / equipment and medicines.
Registration matters of hospitals relating to reimbursement of KPME Act, Medical
Bills.
Issues relating to Karnataka State Drug Logistic and Warehousing Society.
Issues pertaining to Indian Population Plan.
Other subject Excluding Sanjay Gandhi Trauma and Orthopedics.
Indian System of Medicine:
Matters pertaining to AYUSH Department and AYUSH College.
Issues pertaining to Karnataka Homeopathic Medical Board.
Matters pertaining to Karnataka Ayurveda and Unani Medical Board.
All matters pertaining to the Department of Drug Control and related to Pharmacy Colleges.
Receipt and Issue:
Receiving and forwarding acknowledgments relating to the Department of Health and Family Welfare.
Identifying and transmitting acknowledgment letters to the relevant branch and sending copies and other copies to other departments of the Ministry.
Service matters of all staff members of the Department of Health and Family Welfare.
Supply of stationery to these branches, Co-ordination:
1. All Co-ordination related to Health & Family Welfare Department.
2. Matters related to Karnataka Legislation.
3. Collecting general information from all the departments.
4. Annual reports of Heads of the Departments, Consolidation of information to the Governor’s speech and other reports.
5. Letter and Files Management System, Organising meetings related to Court cases and etc.

6
Head of Legal Cell: Giving instruction and advise in legal matters relating to Hon’ble Supreme Court, High Court and KAT pertaining to Health and Family Welfare Department. Authorisation to the Government Advocate to appear on behalf of the Government in legal matters. Internal Financial Advisor. Government appoints Internal Financial Advisor for a Department, in the inputs of the IFA in Secretariat decision making process to examine and advise on all issues having in impact on the Departments budget, having a financial implication of short, medium and long term nature, render advise on financial prudence, preparation of Department budget, tracking of audit report and Action taken report an items covered in the Government of Karnataka (Consultation with Financial Adviser) Rules and circular or orders issued from time to time, budget speech, MPIC matters etc. Details of Department Boards and Corporation coming under Administrative control on the Health and Family Welfare Department.
a) Health and Family Welfare Services . b) Department of AYUSH c) Drugs Control Department. d) Health and Family Welfare Engineering division. e) Food Safety and Standards Department f) National Health Mission g) Karnataka State Aids Prevention Society h) Suvarna Arogya Suraksha Trust i) Karnataka State Medical Equipment Supplies Corporation j) Karnataka Ayurveda and Unani Practitioners Board. k) Karnataka Homoeopathy Board. l) Karnataka State Medicine Plant Authority.
1. Health and Family Welfare Services:- The Origination, objective, functions and duties are Origination: The Commissioner is the Head of the Department of Health and Family Welfare Services, under whom the Administrative Affairs of the Karnataka Administrative Service, K.A.S. The Chief Administrative Officer of the senior hierarchy and the Chief Accounting Officers of the Karnataka State Accounting Department are in charge of managing the financial matters. Directors, Joint / Deputy Directors / Programme Officers are responsible for technical matters Objective: The Department of Health and Family Welfare aims to provide National and state health programs and radical health services to the public through its health care institutions.

7
2. Department of AYUSH Origination: The Commissioner is the Head of the Ayush Department, Joint Director (Medical Education) of the Department to perform the duties relating to the Ayush Medical Colleges. Serves in cooperation with 4 Deputy Directors and Administrators in each of the KAS senior ranks as Chief Administrators and Ayurveda, Unani, Homeopathy and Naturopathy & Yoga practices. Deputy Director of Government Central Pharmacy is working to prepare Ayurveda and Unani medicine. Objective: Establishment of AYUSH Colleges as per Government of India Guidelines / Instructions to promote Indian Ancient Medicine Practices to provide better health services to the public and to provide medical services. 3. Drugs Control Department Origination: The Drugs Controller is headed by the Drugs Controller Department. Additional Drugs Controller, Deputy Drugs Controller, Assistant Drugs Controller and Drugs inspectors are working as subordinate officer. Principal Scientific Officer head of the Drug Testing Laboratory, Chairman/Member Secretary are headed by Board of Examining Authority to conduct Pharmacy Course Examinations. Objective: To ensure the Quality of Drugs and Cosmetics manufactured and marketed in the State in the interest of public health by exercising strict control and vigilance on the Drugs marketed in the State, the department ensures safety of drugs and there availability on the controlled price to the consumers. 4. Food Safety and Standards Department Origination: The Commissioner is the Head of the Department of Food Safety and Quality Control, Administration of the Food Safety and Quality Control Department and other administrative matters. There are team officials and field level officers / food safety officers. Objective: The Food Safety and Standard Act has been implemented in the State of Karnataka since August 5, 2011 and is a comprehensive Food and Drug Act, with the objective of Providing quality and whole foods at all levels.

8
5. National Health Mission: Origination: For the implementation of the National Health Mission in the State, Mission Director (IAS) has been appointed and Administrative matters KAS rank officers works with the chief executives and accountants and other officers. Objective: The goal of the National Health Mission is to improve the health of the poor living in the state, especially in the hut and other disadvantaged communities, by rebuilding the public health system, actively participating and actively participating with urban local bodies, to improve the health of the state's people 6. Karnataka State Aids Prevention Society Origination: The project director is the head of Karnataka State AIDS Prevention Society. The organization is working in the state with the requirements set out in the guidelines of the National AIDS Prevention Organization to manage its functions Objective Sexually transmitted infections and genital tract infections can spread from one person to another. There are as many as 20 sexually transmitted infections and genital tract infections, including syphilis and gonorrhoea infections, along with testing and treatment information. People are delivered to the general public through clinics. What is still noteworthy is that the adequate treatment and prevention of sexually transmitted infections and genital tract infections aims to reduce the HIV infection rate by 40%. 7. Suvarna Arogya Suraksha Trust Origination Executive Director, Head of the Suvarna Arogya Suraksha Trust, the Government of Karnataka has long term active in its mission of providing health care to its residents. Objective: The Suvarna Arogya Suraksha Trust was established in 2009 with the specific objectives of implementing health plans. First, the Vajpayee Arogyashree Scheme has been providing cashless treatment to BPL families for three years since 2009. Then in 2014, the Rajiv Arogya Bhagya Scheme was introduced to provide APL families with tertiary stage diseases. Since the inception of the project, 250386 patients have been treated under these plans. Second-line treatments were administered by RSBY Scheme. Under this scheme, 62 lakh families were provided with insurance. The project was completed in 2016 to August 2018, and there have been 168377 beneficiaries receiving treatment facilities.

9
The Universal Health Care Plan, “Arogya Karnataka,” was launched on 02.03.2018 to bring together all social health plans to unveil the Vision Document 2025, which aims to improve efficiency, impact and provide universal, equal and sustainable health services as integrated Karnataka Public Health Policy 2017. Under this scheme Rs 2.00 lakh free treatment in the second stage, third stage and emergency treatments around 1516 methods of treatment under National Food Security Act -2013 are provided for the application of the eligibility criteria on the basis of the application. Upto 19 lakh APL families receive financial assistance upto 30% of the package rate. 8. Karnataka State Medical Supplies Corporation: Origination
The Managing Director is the head of the company, registered with the Karnataka State Medical Supplies Corporation under the Company Act, with all the required posts for procuring, storing and supplying drugs and chemicals to all medical and health institutions under the Health and Family Welfare Services.
Objective
The Department of Health and Family Welfare has allocated grants from the state government to purchase medicines and chemicals for state-run hospitals, teaching hospitals under medical education and district panchayat hospitals. The medicines will be supplied through the District Drug Stores in accordance with the demand of various hospitals under this grant.
9. Karnataka Ayurveda and Unani Practitioners Board. Origination: Under the Chairmanship of elected President Medical officer of the AYUSH Department is deployed as Registrar, administers the functions of Karnataka Ayurveda and Unani Physician Board. Objective: In addition to registering for the medical profession in Karnataka Ayurveda and Unani systems of medicine, also regulate the profession of physician. 10. Karnataka Homoeopathy Practitioners Board. Origination: Under the Chairmanship of elected President Medical officer of the AYUSH Department is deployed as Registrar, administers the functions of Karnataka Homeopathic Board. Objective:
In addition to registering for the medical profession in Karnataka Homeopathy Systems of medicine, also regulate the profession of physician.

10
V) THE ACTS, RULES, REGULATIONS INSTRCTIONS AND MANUAL S USED BY THE EMPLOYEES OF HEALTH AND FAMILY WELFARE DEPARTME NT IN DISCHARGING ITS FUNCTIONS .
a) Acts:- 1) Official secrets Act 2) ESMA Act 1968. 3) The Karnataka State Civil Service Rules (RPPP) Act, (1957/2018) 4) The Karnataka State Civil Service (Determination of Age) Act, 1974. 5) The Karnataka Lokayukta Act. 6) The Karnataka Administrative Tribunal Act. 7) KTPP Act. 8) KPME Act. 9) The Karnataka Epidemic Diseases Act 2020 and The Karnataka Epidemic Diseases
(Amendment) Act, 2020 10) The Karnataka State Civil Services Regulation (Transfer of Medical Officer and
other Staff) Act, 2011 11) The Karnataka Ayurveda and Unani Practitioner Act. 12) The Karnataka Homoeopathy Practitioners Act. 13) The Karnataka State compulsory Rural Service Act, 2015. 14) The Karnataka Compulsory Service Training by candidates completed Medical
Courses Act, 2012. 15) The Karnataka Good Samaritan and Medical Professional (Protection and
Regulation during Emergency situations) Act, 2018. 16) The Karnataka Educational Institutions (Prohibition of Capitation Fee) Act, 1984. 17) Central Council for Homoeopathy Act 18) Central Council for Indian Medicine Act
b) Rules
1) The Karnataka Civil Services (CCA) Rules 1957 2) The Karnataka Government Servant (Seniority) Rules 1957 3) The Karnataka Civil Services (General Recruitment Rules) 1977 4) The Karnataka Civil Services (Recruitment for the posts of stenographers/typists)
Rules 1983. 5) The Karnataka Civil Services (Conduct) Rules 1966 6) The Karnataka Civil Services (RPP and P) Rules 1978 7) The Karnataka Civil Services (Medical attendance) Rules1963 8) The Karnataka Civil Services (Typist and junior assistant/Second Division
Assistant Change of cadre) Rules 1985 9) The Karnataka Civil Services (Special recruitment of SC/ST candidates to Certain
Group A and B posts) Rules 1985 10) The Karnataka Civil Services (Performance Report) Rules 1994 11) The Karnataka Public Service Commission (Consultation) Regulation 12) The Karnataka KTPP Rules 2000 13) The Karnataka State Civil Services Regulations (Transfer of Medical Officer and
other Staff) Rules, 2011 14) The Karnataka Directorate of Health and Family Welfare Services (Recruitment of
Senior Medical Officers /Specialists, General Duty Medical Officers and Dental Health Officers) (Special) Rules, 2019

11
15) The Karnataka Ayurveda and Unani Practitioner Rules. 16) The Karnataka Homoeopathy Rules. 17) Karnataka State compulsory Rural Service Act 2015 18) The Karnataka State Human Immunodeficiency virus and Acquired Immune
Deficiency Syndrome (Ombudsman and Legal Proceedings) Rules, 2020. 19) The Karnataka Compulsory Service Training by candidates completed Medical
Courses (Counselling, Allotment and Certification) Rules, 2015. 20) The Selection of candidates for admission to Post Graduate degree courses in
Ayurveda, Yoga, Naturopathy, Unani, Sowa-Rigpa and Homoeopathy (Amendment) Rules, 2020.
21) The Karnataka Conduct of Entrance Test for selection and admission to Post Graduate Medical and Dental Degree and Diploma Courses Rules, 2006
22) Central Council for Homoeopathy Rules. 23) Central Council for Indian Medicine Rules.
c) Instruction, Manual and others.
i. Karnataka Government Secretariat Manual of Office procedure. ii. Karnataka of Contingent Expenditure Code
iii. Karnataka Financial Code iv. Karnataka Treasury Code v. Criminal Procedure Code
vi. Reservation for women vii. Reservation roster for Scheduled Castes, Scheduled Tribes and other Backward
Classes. viii. Department Promotion Committee. ix. The Executive orders, official memoranda, circulars and other general instructions
issued by Government from time to time

12

13
PART- I
HEALTH AND FAMILY WELFARE SERVICES
AROGYA SOUDHA,
MAGADI ROAD, BENGALURU

14

15
1. ORGANOGRAM – NHM :

16
2. ORGANOGRAM – H&FWS :

17
1.1. FUNCTIONS OF THE HEALTH DEPARTMENT:
The Department is headed by the Commissioner of Health & Family Welfare Services and the Director of Health & Family Welfare Services. The Commissioner is the administrative head and Director is the technical head. National Health Mission (NHM) is headed by a Mission Director (NHM). Karnataka State AIDS Prevention Society is headed by Project director.
These officers are assisted by Additional Directors, Joint Directors, Deputy Directors &
Demographer in implementing and monitoring health programmes. The Chief Administrative Officer and Chief Accounts Officers cum Financial Adviser assist in administrative and financial matters of this Department.
At the District level, District Health and Family Welfare Officer is the head of Public
Health Services. Implementation and monitoring of various National & State Health Programmes in all below 100 beds health care service institutions which are under Zilla Panchayat Sector are done by the District Health and Family Welfare Officer. He is assisted by
1. District Reproductive & Child Health Officer 2. District Programme Management Officer 3. District TB Officer 4. District Malaria Officer 5. District Family Welfare Officer 6. District Surveillance Officer 7. District Leprosy Officer (who also oversees Blindness Control Programme).
Above 100 beds healthcare services institutions are under state sector. The District Surgeons of District Hospitals are responsible for providing curative, emergency and preventive services including referral services. Presently 16 District Hospitals are under the control of Health & Family Welfare Department.
176 Taluk Health Officers are positioned at Taluk headquarter.They are the
implementing authorities of Public Health, National and State Health Programs in their respective Taluks. The Medical Officers of Health at Primary Health Centre Level are responsible for the implementation of various National and State Health Programs including Family Welfare Programme and Maternal and Child Health Services. To provide Primary Health Care throughout the State, a network of 8871 Sub Centres, 2359 Primary Health Centres, 207 Community Health Centres and 146 Taluk Hospitals have been provided.
The Department of Health and Family Welfare Services implements various National
and State Health programmes of Public Health importance to provide comprehensive Health Care Services to the people of the State through various Health and Medical Institutions. Health Care Services rendered are classified into Curative Services, Health Education and Training and School health services, nutritional services, laboratory services.
Health and Family Welfare department was responsible for implementation of Rural
Health component of Minimum Needs Programme, National Health Mission (NHM), National Leprosy Eradication Programme, Revised National Tuberculosis Control Programme, National Programme for Control of Blindness, National Vector Borne Disease Control Programme (NVBDCP), National Guinea Worm Eradication Programme, Prevention and control of Communicable Diseases like Diarrhoea, Kyasanur Forest Diseases, National Iodine Deficiency Disorder Control Programme and AIDS Prevention Programme.

18
1.2. IMPORTANT NATIONAL AND STATE HEALTH PROGRAMMES:
The Department of Health and Family Welfare Services implements various National
and State Health programs of Public Health importance and also provides comprehensive Health
Care Services to the people of the State through various Health and Medical Institutions.
Progress of implementation of Major Programmes is as follows:
1.2.1. UNIVERSAL IMMUNIZATION PROGRAMME:
Goals:
• Immunization of all children against 13 vaccine preventable diseases and all pregnant women with TD Vaccines.
• To maintain Polio free status
• To achieve Measles Elimination & Rubella Control by year 2023
Objectives:
• To prevent incidence and deaths due to vaccine preventable diseases by providing free vaccines to all eligible beneficiaries in the state.
• To maintain highly sensitive surveillance system for early identification and control of all Vaccine preventable diseases.
Achievements:
• Pulse Polio Programme was held on 31th January 2021 and achieved 102% coverage for children aged less than 5 years oral polio vaccine.
• Intensified Mission Indradhanush 3.0 was implemented in Bengaluru Urban, BBMP, Bellary, Bagalkote, Belagavi, Bidar, Chikkaballapur, Davangere, Gadag, Kalburgi, Koppal, Raichur, Vijayapura (February & March 21). 95% targeted pregnant women and 94% children were covered.
• Pneumococcal conjugate vaccine (PCV) vaccine has been introduced by Honourable Chief Minister, Government of Karnataka and Honourable Minister, Health and Family Welfare and Medical Education Department on 22.10.2021 under Routine Immunization Programme.

19
Achievement -2021-2022 (April to January 2022) as per H.M.I.S Report
Sl
No Vaccines
2021-22 (in Lakhs)
Target Achievement (April to Jan
2022) %
1 Hepatitis-B 934570 648494 69
2 OPV-0 719428 77
3 OPV-1 898730 96
4 OPV-2 850412 91
5 OPV-3 853512 91
6 BCG 860182 92
7 Penta-1 898820 96
8 Penta-2 854673 91
9 Penta-3 858381 92
10 Rota-1 864400 92
11 Rota-2 818421 88
12 Rota-3 827078 88
13 IPV-1 860395 92
14 IPV-2 821545 88
15 PCV-1
(Date : 22.10.2021 to 31.12.2021)
186914 125396
54
16 Measles & Rubella (MR)- 1st Dose 934570 834005 89
17 JE-1 (10 districts) 267168 267168 93
18 Fully Immunization
(9 to 11 month) 934570
844901 90
19 JE -2 (10 districts) 267168 241164 84
20 Measles & Rubella (MR)-
2nd Dose (16-24 months) 934570
768798 82
21 DPT-Booster 780707 84
22 OPV-Booster 780184 83
23 DPT-Booster -2 (5 years) 1121483
804750 72
24 Td – 10 years 758512 68
25 Td – 16 years 714992 64

20
1.2.2 NATIONAL LEPROSY ERADICATION PROGRAMME :
Introduction : National Leprosy Control Programme was started in 1955. Tremendous achievement was made
in the Programme with regard to accessibility and service delivery with the successful implementation of the Programme. The prevalence rate of leprosy dropped from 40/10000 population in the year 1986 to 0.21/10000 population in January 2022 - Karnataka.
Main objectives under National Leprosy Eradication Programme are:
Elimination of leprosy i.e. Leprosy prevalence of less than 1 case per 10000 population in all the Districts of the State.
Strengthening Disability Prevention & Medical Rehabilitation of persons affected by leprosy. Reduction in the level of stigma associated with leprosy.
At present 02 districts have prevalence rate 0.50 to 1 (Bidar, & Koppal) i.e. 10000 population. As
on January 2022 there are 1617 Leprosy cases under treatment.
Activities under National Leprosy Eradication Programme:
1. Case Detection and Management:
Active Case Detection and Regular Surveillance for Leprosy (ACD& RS) : This activity is planned to cover all the Taluks.
• In high endemic area twice in a year • in low endemic area once in a year, • Any village/ urban pocket within the low endemic blocks, If reporting even a
single child case among new cases – Twice in a year. • Training for all cadres for this activity through Virtual was done in the month of
August 2020.
Chikkaballapur, Bengaluru (Rural), Ramanagara, Mysore, Mandya, Chamarajanagara,
Bagalkote & Vijayapura District supervision of the programme was carried out by State level Officers:

21

22
2. ASHA’s involvement: New activity (ABSULS –Asha Based surveillance Leprosy suspects) as per Government of India
guidelines was rolled out in 2017-18. For the financial year 2021-22 A total of 22331 ASHAs were trained. Incentives were paid to
ASHAs for case detection (Rs.250/case) & after treatment completion i.e.Paucibacillary (PB) 6 months (PB Rs.400/case) & Multi Bacillary (MB) 12 months – (MB Rs.600/-case).
3. Training Programme: Virtual Training of Division wise Medical officers, Health workers and Staff Nurse as a newer
initiative Training of RBSK, RKSK and UHC is undertaken and completed.
For the financial year 2021-22 – 990 Medical Officers and 2415 Health workers have been sensitized. RBSK teams are being sensitized to pick up suspected Leprosy cases.
4. IEC Activities:
Special Drive to remove stigma surrounding leprosy and prevent discrimination was
planned in the form of
Sl. No. Media No. of districts
1. Mass Media(TV Radio Press) 30+ Bruhat Bengaluru
Mahanagara Palike (BBMP)
2. Outdoor Media (Hoardings Wall Paintings Banner Rally) 3. Rural Media (IPC Meeting School Health Quiz) 4. Advocacy meeting (Meeting with Zilla Parishad NGOs) 5. IEC Activities – State 1
Sparsh Leprosy Awareness Campaign 2021-22 (Anti Leprosy fortnight – 30th Jan 2022 to Feb 13th 2022):
As per the guidelines of the Government of India, the campaign was successfully carried out in Karnataka to reach the village level in collaboration with the Panchayat Raj Department.

23

24
Physical Target and Achievements for Eradication of Leprosy
from 2013-14 to 2021-22 New Cases Detected
PR Cases Cured Deformit
y Rate
Deformity Gr. II cases
Child cases Year
Target Achievement
% Target Achievement
%
2013-14 - 3461 - 0.45 - 3295 - 3.72 129 320
2014-15 - 3314 - 0.44 - 3260 - 4.41 146 287
2015-16 - 3065 - 0.40 - 3037 - 3.39 104 209
2016-17 - 2897 - 0.40 - 2710 - 3.52 102 166
2017-18 - 2892 - 0.38 - 2774 - 4.05 117 171
2018-19 - 2789 - 0.34 - 2869 - 2.94 82 147
2019-20 - 2724 - 0.33 - 2674 - 2.50 68 121
2020-21 - 1500 - 0.19 - 2323 - 2.60 39 69
2021-22 (till Jan 22)
- 1420 - 0.21 - 1262 - 2.89 41 59
4. Welfare measures for the Persons Affected by Leprosy:
1. 5% of Group ‘D’ Jobs are reserved for the Persons affected by Leprosy during recruitment. 2. 12 Reconstructive Surgery Operations done as on 31st Jan 2022 Rs.8000/- paid (As per
Guidelines) incentive for RCS undergone Persons Affected by Leprosy. 3. Micro Cellular Rubber Footwear provided to 3746 Persons Affected by Leprosy (PALs).
4. 1315 Self-care kits provided to foot ulcer cases.
5. 139 Lepra reaction cases treated with supportive drugs.
6. Splints, crutches and other needed appliances provided.
7. Prevention of Deformity (POD) camps conducted regularly in all the Taluk level hospital.
8. Medical facilities are being provided to the Persons Affected by Leprosy family member residing in 20 Leprosy colonies in the State.
25
9. Grant-in Aid is provided by State Govt. for the NGO hospitals providing treatment to the Persons Affected by Leprosy at the rate Rs.500/bed for adults and Rs.275/bed for children per month.
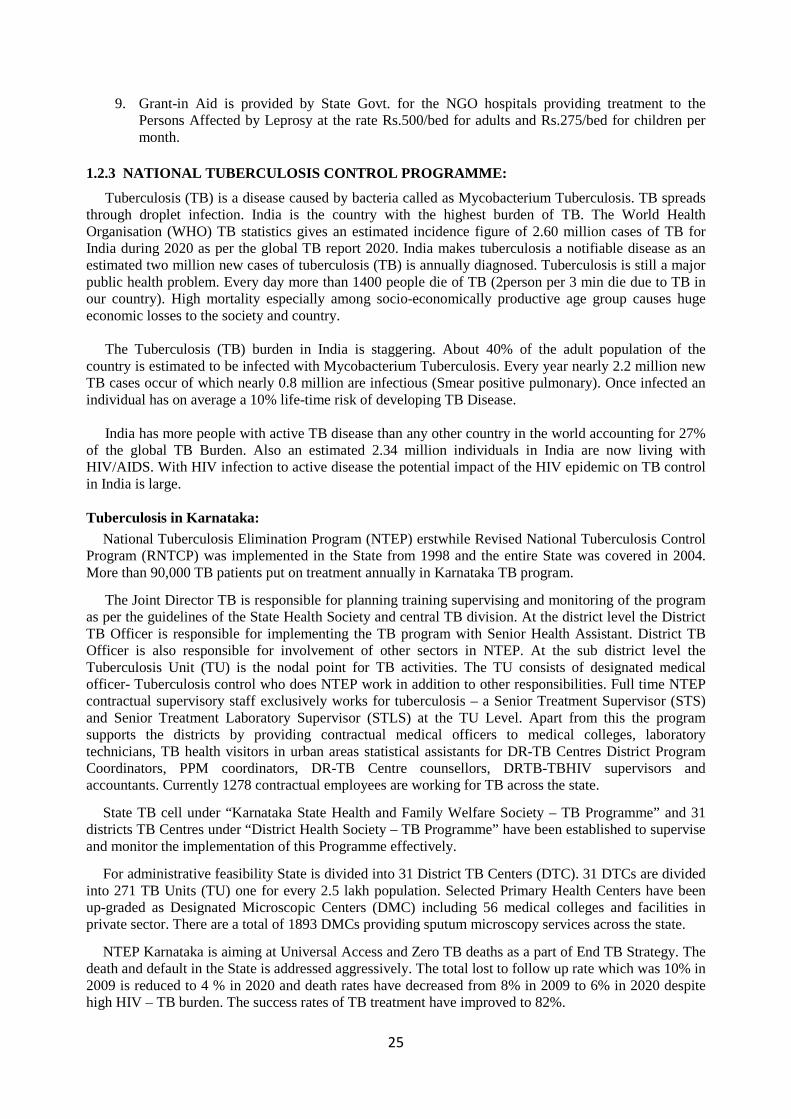
1.2.3 NATIONAL TUBERCULOSIS CONTROL PROGRAMME:
Tuberculosis (TB) is a disease caused by bacteria called as Mycobacterium Tuberculosis. TB spreads through droplet infection. India is the country with the highest burden of TB. The World Health Organisation (WHO) TB statistics gives an estimated incidence figure of 2.60 million cases of TB for India during 2020 as per the global TB report 2020. India makes tuberculosis a notifiable disease as an estimated two million new cases of tuberculosis (TB) is annually diagnosed. Tuberculosis is still a major public health problem. Every day more than 1400 people die of TB (2person per 3 min die due to TB in our country). High mortality especially among socio-economically productive age group causes huge economic losses to the society and country.
The Tuberculosis (TB) burden in India is staggering. About 40% of the adult population of the
country is estimated to be infected with Mycobacterium Tuberculosis. Every year nearly 2.2 million new TB cases occur of which nearly 0.8 million are infectious (Smear positive pulmonary). Once infected an individual has on average a 10% life-time risk of developing TB Disease.
India has more people with active TB disease than any other country in the world accounting for 27%
of the global TB Burden. Also an estimated 2.34 million individuals in India are now living with HIV/AIDS. With HIV infection to active disease the potential impact of the HIV epidemic on TB control in India is large. Tuberculosis in Karnataka:
National Tuberculosis Elimination Program (NTEP) erstwhile Revised National Tuberculosis Control Program (RNTCP) was implemented in the State from 1998 and the entire State was covered in 2004. More than 90,000 TB patients put on treatment annually in Karnataka TB program.
The Joint Director TB is responsible for planning training supervising and monitoring of the program as per the guidelines of the State Health Society and central TB division. At the district level the District TB Officer is responsible for implementing the TB program with Senior Health Assistant. District TB Officer is also responsible for involvement of other sectors in NTEP. At the sub district level the Tuberculosis Unit (TU) is the nodal point for TB activities. The TU consists of designated medical officer- Tuberculosis control who does NTEP work in addition to other responsibilities. Full time NTEP contractual supervisory staff exclusively works for tuberculosis – a Senior Treatment Supervisor (STS) and Senior Treatment Laboratory Supervisor (STLS) at the TU Level. Apart from this the program supports the districts by providing contractual medical officers to medical colleges, laboratory technicians, TB health visitors in urban areas statistical assistants for DR-TB Centres District Program Coordinators, PPM coordinators, DR-TB Centre counsellors, DRTB-TBHIV supervisors and accountants. Currently 1278 contractual employees are working for TB across the state.
State TB cell under “Karnataka State Health and Family Welfare Society – TB Programme” and 31 districts TB Centres under “District Health Society – TB Programme” have been established to supervise and monitor the implementation of this Programme effectively.
For administrative feasibility State is divided into 31 District TB Centers (DTC). 31 DTCs are divided into 271 TB Units (TU) one for every 2.5 lakh population. Selected Primary Health Centers have been up-graded as Designated Microscopic Centers (DMC) including 56 medical colleges and facilities in private sector. There are a total of 1893 DMCs providing sputum microscopy services across the state.
NTEP Karnataka is aiming at Universal Access and Zero TB deaths as a part of End TB Strategy. The death and default in the State is addressed aggressively. The total lost to follow up rate which was 10% in 2009 is reduced to 4 % in 2020 and death rates have decreased from 8% in 2009 to 6% in 2020 despite high HIV – TB burden. The success rates of TB treatment have improved to 82%.

26
TB Notification under Nikshay Registration:
Tuberculosis is a notifiable disease. All providers must notify TB patients including public and private providers through “NIKSHAY” which is a case based wed based application for TB patient’s registration. This software was launched in May 2012 and it is disseminated to all districts. There is a significant response from private providers. Around 30000 health facilities have been registered on NIKSHAY till date and out of which 2022 health facilities are notifying TB cases. A total of 20095 TB cases have been notified from private sector in 2020 and in this current year despite of Covid 19 pandemic 16879 cases have been notified so far from January 2021 to December 2021.
Paediatric TB:
Paediatric tuberculosis (i.e. TB among the population aged less than 14 years) has always been accorded high priority by NTEP. In our state screening of TB among SAM children is of high priority. To overcome the delay and to augment the diagnosis of paediatric TB 125NAAT machines are placed at district/sub district level. There are exclusive paediatric drugs with different weight bands which help in successful outcomes.
DR-TB (Drug Resistant TB):
Programmatic management of drug resistant TB aims at diagnosis treatment and follow-up of patients with drug resistant TB. For the diagnosis of DRTB three dedicated mycobacteriology laboratories are established one is Intermediate Reference laboratory at Bangalore and other is CDST laboratory at KIMS Hubballi and RIMS Raichur. These laboratories are certified by Government of India (CTD) to perform both genotypic and phenotypic tests. The diagnosis treatment and follow up of the patient is done free of cost. The cost of treating MDR patients is 2-6 lakh rupees which are provided free to the patients. Currently all TB patient samples are tested for MDR-TB and 3000 MDR patients are getting free treatment. The Xpert MTB/RIF is a cartridge-based automated diagnostic test that can identify Mycobacterium tuberculosis (MTB) DNA and resistance to rifampicin (RIF) by nucleic acid amplification technique (NAAT). The state has 65geneCBNAAT machines and 60 TruNAAT machines which are placed at the district/sub district level and at places where there is high HIV-TB burden thereby ensuring early quality diagnosis and management happens to these patients.
TB-HIV collaborative activities. – The NTEP Programme closely collaborates with AIDS control programme at state and district level for early diagnosis follow up and treatment of HIV infected TB patients.
TB- HIV collaborative services include:
1. PITC (provider initiated testing and counselling) for presumptive TB patients. 2. HIV testing for the all TB patients. 3. Providing CB NAAT testing for all the presumptive TB and presumptive MDR TB cases for
all the symptomatic HIV infected patients. 4. Linking all HIV infected TB patients to ART centres. 5. Providing ART to all HIV infected TB patients irrespective of their CD4 counts. 6. Providing daily FDC to all co-infected patients 7. Providing Co-trimaxozole preventive therapy (CPT) to all HIV infected TB patient
CBNAAT (Cartridge Based Nucleic Acid Amplification Test) and Trunat: The Xpert MTB/RIF is a cartridge-based automated diagnostic test that can identify Mycobacterium
tuberculosis (MTB) DNA and resistance to rifampicin (RIF) by nucleic acid amplification technique (NAAT). Results are obtained from unprocessed sputum samples in 90 minutes with minimal biohazard and very little technical training required.

27
The TB program in Karnataka recognizes the need of targeting special populations. TB control program in Karnataka has identified special populations and has planned target interventions. The target interventions include active surveillance in these populations’ and utilizing genotypic methods for the diagnosis TB and resistant TB.
The following innovations stand out in programme strengthening in Karnataka state are:
1. Political and administrative stewardship towards TB elimination 2. Joint TB HIV visits to districts involving officials from KSAPS and State TB Centre
for monitoring TB HIV collaborative activities. 3. All TB suspects testing for HIV. 4. Designing of formats for reporting HIV TB collaborative activities. 5. Micro planning (TU wise analysis) for identifying low performing TUs and planning
focused interventions. 6. Guiding tool for ACSM activities. 7. Social media activities-What Sapp group (NTEP family), Twitter and Facebook
(Tuberculosis in Karnataka) accounts for State TB Centre. 8. Involvement of field general health staff for pulmonary TB suspect referral. 9. Incentives for ASHAs for sputum sample transportation in difficult to reach areas in
some districts. 10. Utilization of ophthalmic camps organized by NGO (Muslim forum) for creating TB
awareness. 11. Focused DTOs review. 12. Drugs stock exercises done in all districts. 13. Involving 104 services for TB care. 14. Using ICT technology (99 DOTS) to monitor adherence of TB treatment in co-
infected patients who are on daily DOT. 15. Patient charter and patient forums. 16. Nutritional support through NGO’s in certain districts. 17. Enrolling MDR TB patients in Jan Dhan and PMSBY. 18. Adaptation of integrated patient centered care and district specific action plan aiming
towards TB elimination 19. Support research in medical college and use the result of the studies in program
intervention. 20. Kshaya Muktha Karnataka, a strategic document for guiding the districts for making
TB free released out in month of December 2020 During Covid19 Pandemic:
1. The state took up innovative case finding strategies to address this issue with a four pronged approach.
a) All presumptive TB patients to be identified by house to house visits by ASHAs and enrolled in Presumptive TB register. These patients to be further screened on chest X-ray and CBNAAT
b) All the ILI and SARI patients admitted in various hospitals of the state must be tested for TB by offering upfront CBNAAT.
c) All COVID negative patient details to be collected from RT PCR labs, patients traced back and tested for TB by offering upfront CBNAAT.
d) All persons who contacted APTAMITRA care line in Karnataka to be contacted, traced back and specimens collected and tested for TB by offering upfront CBNAAT

28
2. State supplied 2 months door step drugs to all the TB patients in order to prevent drug stock outs
at the patient’s end. 3. In the month of August from 10th August to 17th August a contact Tracing Drive 4. State has initiated Bidirectional Screening of TB patients for COVID symptoms and Covid
positive patients for TB symptoms from October 2020.
Month long Active TB Case Finding was conducted throughout the state between 1st December 2020 to 31st December 2020 in Karnataka by reaching an unreached population, 2800 TB patients were identified because of the activity.
For 7th National Summit on Good, Replicable Practices and
Innovations in Public Health Care Systems in India, Karnataka state poster has chosen under best practices on NTEP during Covid 19 times.
Pilots in Karnataka which have become National Policies are:
1. ATT-ART-CD4(HIV-TB) 2. PITC (provider initiated testing and counselling) for presumptive TB patients 3. TB-DM bi-directional screening 4. Human Resource for Health (aligning NTEP with NHM).
The Standards for Tuberculosis Care in India (STCI) is developed published and disseminated by the Central TB Division (CTD) Government of India in 2014. These standards apply to all health care providers in the country both public and private and establish a common yardstick for TB management. The Standards for TB Care is widely disseminated in the state through the medical college professional bodies and through NGOs and partner organizations.
The current strategy of TB is as envisaged in the sustainable development goals (SDG) and it is called “The END TB STRATEGY.”
The END TB STRATEGY has a Vision: “Tuberculosis free India–achieving universal access by provision of quality diagnosis and treatment
for all Tuberculosis patients in the community”.
Goal: To decrease the morbidity and mortality by early diagnosis and early treatment of all Tuberculosis
cases there by cutting the chain of transmission.
Objective: “Universal Access to TB Care”
FUNDING:
Government of India 60% and Government of Karnataka 40% funds for this programme. Funds are released to the district TB Societies from State Health Societies (NHM).
2021-22 Approved Budget as per ROP SOE 2021-22 (upto Jan)
12353.05 (in lakhs) 3785.64 (in lakhs)

29
PERFORMANCE OF NATIONAL TUBERCULOSIS ELIMINATION PR OGRAMME (NTEP) KARNATAKA:
(Source-Nikshay)
Year Population (in lakhs)
Annual Total TB Case Notification Rate.
Treatment Success rate
Public Private Total New Cases
Re-treatment cases
National average 114 11 125 87% 70%
2013 629 97 1 98 83% 57% 2014 635 97 3 100 83% 59% 2015 643 96 8 104 84% 64% 2016 650 92 9 101 84% 67% 2017 658 94 14 108 84% 68% 2018 668 102 22 124 85% 64% 2019 676 106 30 136 85% 68% 2020 704 69 24 93 84% 81%
2021 716 74 27 101 81% 74%
1.2.4 NATIONAL PROGRAMME FOR CONTROL OF BLINDNESS& VISUAL IMPAIRMENT: National Program for Control of Blindness was launched in 1976 with the goal to reduce the prevalence of blindness from 1.4% (1974) to 0.3% by the year 2020 by developing eye care infrastructure human resources, improving accessibility quality of eye care services. As per the survey of 2007, level of prevalence of blindness has come down to 1.0%. The present prevalence rate of blindness is 0.36 % as per National Survey 2015-19.The present prevalence rate of blindness is 1.61 in Karnataka as per National Rapid Assessment of Blindness Survey (2015-2019) carried out by NPCB&VI across 31 district of the State.
1. The Karnataka State Health and Family Welfare Society (Blindness Control Division) is working under National Health Mission (NHM) headed by Mission Director. The State Programme Officer will implement and monitor the programme through a network of Districts Programme Managers (Blindness Control Division) at Districts level as per the Guidelines of NPCB. Government of India releases the funds to the State Society for onward distribution of funds to all Districts Health &Family Welfare Society (Blindness Control Division) based on the Target assigned to each Districts.
2. Cataract is the major cause of Blindness. 99% of the Cataract surgeries are IOL inserted
surgeries. The patient affected with cataract are treated free of cost in Govt. hospitals and NGO hospitals who have MoU with NPCB. Cataract camps are being conducted on regular basis throughout the state in both the government and voluntary sector.
3. Diabetic Retinopathy, Glaucoma management, Laser Technique, Corneal Transplantation, Vitreo
Retinal Surgery, Treatment of Childhood Blindness etc., are also treated under NPCB in order to provide improved eye care services and control the incidence of blindness. The patient affected with any of the above eye diseases will also be treated free of cost in Govt. hospitals and NGO hospitals who have MoU with NPCB.
4. In order to detect refractive errors in school going children, the school teacher having their
proximity to the children is trained in primary eye screening. The identified children experiencing difficulties in reading are immediately referred to the Para medical Ophthalmic Officers (PMOOs) for eye screening. The children detected with refractive error are provided free spectacles.

30
5. 40 Eye Banks registered under Human Organs Transplantation Act are functioning in Karnataka
including 7 Functioning Government Eye Banks. As per the policy of Govt. of India under NPCB eye bank infrastructure is also improved to increase cornea collection and Keratoplasty. Incentives are also given to all the eye banks registered under HOTA for collecting eye balls in order to increase the cornea collection
6. Karnataka state initiated Diabetic Retinopathy project at Chikkaballapur district by Vittala Institute of ophthalmology.
7. To make our state corneal blindness black log eye collection centre to be opened in all District Hospitals.
8. 6 Districts are strengthened with mobile ophthalmic units to reach the underserved and reached & unreached in the year 2018-19 approved to procure 11 more mobile vans for DMOU (District Mobile Ophthalmic Unit). Tele ophthalmic unit – implemented at Tumkur District.
9. Retinopathy of Prematurity screening & treatment being done by NarayanaNethralaya.
Adherent leucoma, triple procedure post op 6/24
Cataract Eye Surgeries in Government Base Hospital

31
School Eye Screening
Free Spectacles distribution to School Eye
Cataract Surgeries Target & Achievements
Year Target Achievement
% 2013-14 3,54,560 3,62,481 102.23 2014-15 4,04,563 3,63,661 89.89 2015-16 4,04,563 3,74,971 92.69 2016-17 4,04,563 3,66,737 90.65 2017-18 4,04,563 3,83,497 94.79 2018-19 4,04,563 3,90,630 96.56 2019-20 4,04,563 3,61,711 89.41 2020-21 4,04,563 1,94,755 48.14 2021-22
(Up to Jan ) 4,31,744 2,80,884 65.06

32
Achievement of School Eye Screening Programme
Year No. of
Children Screened
No. of Children detected with
Refractive Error
No. Spectacles given to Children
2013-14 32,47,402 32,487 30,161
2014-15 29,05,004 47,003 37,786 2015-16 43,75,400
77,261
38,379
2016-17 41,55,367 1,00,426 45,553 2017-18 44,93,399 1,10,883 47,871 2018-19 46,39,151 2,31,958 56,487
2019-20 53,71,134 1,39,998 86,220
2020-21 16.16,707 66,011 67,166
2021-22 (Up to Jan)
43,23,429 80,845 34,207
Eye Balls Collection Target & Achievement
Year Target Achievement % 2013-14 5,600 3,499 62.48 2014-15 5,600 3,938 70.32 2015-16 5,600 3,572 63.79 2016-17 5,600 3,527 62.98 2017-18 5,600 5,914 105.61 2018-19 5,600 5,561 99.30 2019-20 5,600 5,427 96.91 2020-21 5,600 1,790 31.96
2021-22 (Up to Jan) 5,600 4,442 79.32
Financial Progress (Rs. in lakhs)
Year Budget Allocation Expenditure % 2017-18 3230.26 1998.54 62%
2018-19 3002.87 2676.58 89%
2019-20 3043.39 2825.82 93%
2020-21 3601.87 1518.81 42%
2021-22 3249.92 1172.19
(Provisional exp. up to Jan 2022)
36%
1.2.5 KARNATAKA STATE AIDS PREVENTION SOCIETY:
Karnataka State AIDS Prevention Society (KSAPS) was registered as a Society on 9th December 1997; it is an autonomous institution and the highest policy-making structure with respect to HIV/AIDS in Karnataka. The Governing council is headed by the Chief Minister and the Vice chairman is the Minister for Health and Family Welfare Services.
The Chairman of Executive Committee is Secretary to Government Health & Family Welfare Department. As per NACO, high prevalent states in India are Nagaland, Mizoram, Tripura, Manipur and Meghalaya. KSAPS is implementing National AIDS Control Programme (NACP IV). Karnataka has 30 Category “A” districts.

33
KSAPS is implementing NACP IV funded by National AIDS Control Organization (NACO), New Delhi:
Karnataka has been conducting HIV Sentinel Surveillance since 1998. Surveillance is carried out annually by testing for HIV at designated sentinel sites and now the annual frequency of HSS was shifted to biennial (once in two years). The prevalence among antenatal clinic (ANC) attendees as per HSS 2012-13 was 0.53%. This is close to the NFHS-3 estimate of 0.69% in 2006. HIV prevalence among ANC attendees indicates decline in adult HIV prevalence in the state from 1.5% in 2004 to 0.38% in 2016-17. In 2018-19 16th round of HIV Sentinel Surveillance has been conducted at ANC sites where HIV prevalence among ANC attendees is 0.22% and in 2016-17 HRG HSS of FSW is 3.33% MSM is 5.40% in Karnataka. Presently 17th round of HSS activity is going on in all NACO designated ANC/HRG sites.
Declining trend among ANC attendees-Karnataka
Karnataka State AIDS Prevention Society Programmes: 1. Targeted Intervention:
Response from Karnataka State AIDS Prevention Society (KSAPS) has been to saturate targeted interventions (TIs) in Karnataka under the thrust area of NACP -IV.
I. Core TI (FSW, MSM, TG& IDU):
This saturation currently covers around 84248 Female Sex Workers (FSWs) under targeted
interventions and 27107 Men who have sex with Men (MSM), 2282 transgender are covered under this programme. This programme is funded by NACO through KSAPS.
1 TI is implementing Injecting Drug User (IDU) programme of which is in Kolar covering 1097
IDUs. 2 Opioid Substitution Therapy (OST) centres 1 in Bangalore and 1 in Kolar covers intravenous drug user population.
1.5
1.3
1.1
0.86 0.89
0.69
0.53
0.36 0.38
0.22
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
2004 2005 2006 2007 2008 2010 2012 2014-15 2016-17 2018-19

34
II. Bridge TI (Migrant & Truckers):
8 TI projects in Karnataka covers 1,42,000 destination migrants. 4 truckers TIs cover a population of 80,000 long distance male truckers. The Truckers program is implemented at Trans-shipment locations.
Under this program, registration of HRGs for HIV prevention program takes place. Supply of
free condoms, STI drugs, needles and syringes for IDUs. Constant follow up of all registered HRGs for regular medical check-up for STI management (once in 3 months) and HIV testing (Once in 6 months). Linkages to ART and other care and support services for HIV positive HRGs. Mainstreaming through linkages to social welfare schemes of central and state government.
2. HIV Counselling & Testing Centres:
In Karnataka Total 473 Stand-alone ICTCs and 2896 FICTC centres are functioning.
• An integrated counselling and testing centre is a place where a person is counselled and tested and checked for HIV, Tuberculosis, ANC and postnatal follow up on his own free will or as advised by a medical provider.
• An ICTC shall be located in health facilities owned by the government, in the private/not for-profit sector, in public sector organizations/other government departments such as the Railways, Employees' State Insurance Department (ESID), etc. and in sectors where nongovernmental organizations (NGOs) have a presence.
ICTCs can be classified into two types:
Standalone Integrated Counselling and Testing Centres and Facility-integrated Counselling and Testing Centres Fixed-facility ICTCs are those that are located within an existing health-care facility/ hospital/centre. 1. “Stand-alone Integrated Counselling and Testing Centres”: SICTC having a full-time
counsellor and laboratory technician who undertake HIV counselling and testing. Such facilities
exist in medical colleges and district hospitals, and in some sub district hospitals.
2. “Facility- integrated Counselling and Testing Centres”: FICTC which does not have full-time
staff and provides HIV counselling and testing as a service along with other services. Existing staff
such as the auxiliary nurse midwife (ANM)/staff nurse/health visitor/laboratory technician
(LT)/pharmacist are expected to undertake HIV counselling and testing. Such ICTCs will usually be
established in facilities that do not have a very large client load and where it would be
uneconomical to establish a stand-alone ICTC
Such facilities are 24-hour PHCs as well as private sector/not-for-profit hospitals, private
laboratories, public sector organization-run hospitals or facilities, and in the NGO sector.

35
HIV Cases Tested and found Positive in ICTC
Year
General clients ANC
Target
Achievement
Target
Achievement
Tested Achieve
ment
% +ve Positivity
% Tested Achieve ment% +ve
Positivity
%
2013-14 1467137 1664848 113.48 29473 1.77 1292519 1178907 91.21 1445 0.12
2014-15 1540494 1906237 123.74 26509 1.39 1253456 1232862 98.36 1295 0.11
2015-16 1617519 1945282 120.26 21989 1.13 1287757 1280862 99.46 1034 0.08
2016-17 1698395 1940589 114.3 20004 1.03 1287757 1321668 103 856 0.06
2017-18 1973772 2220292 112.49 18862 0.85 1315595 1418176 74.09. 891 0.06
2018-19 2225423 2473845 111.16 18143 0.73 1315595 1423045 108.17 776 0.05
2019-20 2634744 2578245 97.85 15685 0.60 1381375 1447231 104.72 623 0.04
2020-21 2634744 1629561 61.85 9504 0.58 1209010 1209938 100.0 580 0.05
2021-22 (April to Jan)
2634744 1847397 70.11 8520 0.46 1209010 1062484 87.8 477 0.04
3. Care Support & Treatment:
During 2021-22, 70 ART Centers and 306 Link ART Centers have been functioning. The
cumulative number of HIV cases registered at ART Centers till January 2022 were 3,63,841 out of which 1,69,902 cases are alive and on ART.
Cumulative Status report on ART (till January- 2022)
Indicator Adult
TS/TG Child
Total Male Female Male Female
Pre ART-Registration 175954 168205 1005 10200 8477 363841
Ever Started on ART 142203 139077 794 7888 6479 296441
Alive on ART 69737 89548 471 5478 4668 169902
Reported on ART Death 53716 32899 180 1558 1155 89508
"Test-Treatment": The "test-treatment" outbreak began in the state from June 14, 2017, where HIV-infected individuals are free of anti-retroviral therapy at any stage of the infection and CD-4 number.
3. STI/RTI (SEXUALLY TRANSMITTED INFECTIONS/REPRODUCTI VE TRACT INFECTIONS):
Major route of transmission of HIV in Karnataka in unprotected sexual intercourse and HIV is
primarily considered to be a sexually transmitted infection. A person with STI/RTI is 2 to 9 times prone
to get HIV. HIV positive patients with STI are more likely to acquire HIV. Hence, control of STIs
contributes significantly to the reduction in HIV transmission. Up to 40% of HIV transmission can be
cut down by treating STI, hence STI control could be considered as the most cost effective programme.

36
There are 54 Designated STI/RTI Clinics (DSRCs) and 2 State Reference Centres (SRCs) in
Karnataka, The DSRCs are located in all District Hospitals and some Taluka Hospitals. SRC is located
in Bengaluru Urban District and Hubli, Dharwad District.
DSRC - Physical and Financial Achievement
Year Physical
Target Achievement
2018-19 413384 277184 (67%)
2019-20 420808 288971 (69%)
2020-21 428042 183400(42.8%)
2021-
22(April to
Jan22)
435485 193196(44.37%)
5. Information Education Communication, Youth and Mainstreaming. Under IEC, awareness will be created through various medias like mass media, folk media,
outdoor media, print media, Trainings, Through Red Ribbon clubs creating of awareness on prevention of HIV/AIDS, available Government services and schemes for PLHIV, Adolescent Health Education Programme, HIV and AIDS (Prevention and Control) Act 2017, creating awareness to youth, women and general population regarding Care and Support, reduction of Stigma and discrimination . The following IEC activities undertaken from April 2021 till Jan 2022:
Creating awareness on HIV/AIDS through following various medias:
• Communication agency has been hired for creating awareness on HIV/AIDS through various social media like Facebook, instagram, twitter, etc.
• Broadcast of Radio spots of 30 secs each on HIV and AIDS Act, 2017, helpline, blood donation through 3 private radio channels (Big FM, Radio City and Radio Mirchi)
• Broadcast of Radio spots of 30 secs each and 3 panel discussion on HIV and AIDS Act 2017, Blood Donation, Basics of HIV, Social protection schemes through All India Radio State hook, FM and Vivid Bharathi.
• Telecast of TV spots, panel discussion and laptop branding on HIV/AIDS through Doordarshan. • Interdepartmental meeting at district level with various departments, organisations,
institutions.
• World of work meeting to factories at district level implementation of IEC activities.

37
• Telecast of video bytes of KSAPS and services through Public music TV channel. • Organising International Youth Day on 12.8.2021 at district level. • Essay, poster writing and slogan writing competition on HIV/AIDS and Youth by NSS students of
High schools across the State. • Broadcast of audio spots at bus stations on HIV and AIDS Act, 2017, social protections scheme,
Blood donation across the State. • On eve of International Youth Day, Poster writing competition on HIV/AIDS in 5 districts. • Branding of BMTC, KSRTC, NEKSRTC and NEKSRTC buses across the State. • Broadcast of Radio spots of 30 secs each on blood donation and Youth through 3 private radio
channels (Big FM, Radio City and Radio Mirchi) on eve of International Youth Day. • Broadcast of Radio spots of 30 secs each on HIV and Youth, Blood Donation through All India
Radio (State hook, FM and Vivid Bharathi) on eve of International Youth Day. • Printing and supply of Kshema Newsletter to all districts. • Quiz competition for school/college students at district level. • On eve of National Voluntary Blood Donation Day, poster writing competition on Blood donation in
5 districts. • Digital wall painting on HIV and AID Act, 2017, Social Protection schemes, helpline a 10 districts. • Broadcast of Radio spots of 30 seconds each on blood donation through 3 private radio channels (Big
FM, Radio City and Radio Mirchi) on eve of National Voluntary Blood Donation Day. • Telecast of Video bytes through TV news channels. • Branding of bus shelters in Bangalore. • Broadcast of Radio spots of 30 seconds each on Blood Donation through All India Radio (State hook,
FM and Vivid Bharathi) on eve of National Voluntary Blood Donation Day. • Telecast of panel discussion on various services through Doordarshan. • Live interaction of college students with Hon’ble Minster for Health and Family Welfare,
Government of India on eve of India@75. • Telecast of spots in cinema theatres across the State. • 3 days State level folk workshop conducted from 9th to 11th Nov 2021 at Gadag district. • State level quiz competition for the college students. • State Level World AIDS Day was observed on 21.12.2021 at Belagavi districts. • Broadcast of Radio spots of 30 seconds each on Blood Donation through All India Radio (State hook,
FM and Vivid Bharathi) on eve of World AIDS Day. • Organizing Door to Door Campaign in 15 districts selecting 15 talukas. • Around 920 folk shows were performed covering all the districts. • Around 50962 members of various departments, institutions, organisation, agriculturists, etc were
sensitised on HIV/AIDS and services.

38
Government facilities available to HIV infected and affected persons
April 2021 to Jan 2022 Sl. No.
Name of the scheme To whom Benefit Concerned
Dept. Beneficiaries
1 Anna anthyodaya 35 Kgs Ration like Rice, dal
HIV infected and affected Family
Food & Civil Dept. 783
2 CABA (Children affected by AIDS)
Rs. 1000 HIV infected & affected children
Women & Child Dept. 946
3 Rajiv Gandhi Housing
free house HIV infected & affected family
Rajiv Gandhi Rural Development Corporation
20
4 Mythree Rs. 500/- per month pension
TS/TG Women & Child Dept. 33
5 TA for ART Travel reimbursement
local TA as per actuals Those who are under Second line ART treatment
Dept. Health & Family Welfare
7736
6 Free testing HIV people get free
Testing and Treatment HIV infected & affected family
Dept. Health & Family Welfare
13518
7 RTE Education ACT
free admission in private schools
HIV infected & affected Children
Dept. of Primary Education 9
8
Chetana Scheme 1. Loan of Rs. 50,000/- will be given to FSW. Out of Rs. 50,000/- only 25,000/-to be remitted at the low rate of interest and remaining Rs. 25,000/- is subsidy amount.
female sex worker Dept. of Women Development Corporation
405
9 Higher education and Scholarship
Under this scheme, Rs. 23,000/- Scholarship and free education.
HIV infected & affected Children under special category
Dept. of Higher Education 51
10
Dhana Shree yojana
1. Loan of Rs. 50,000/- will be given to PLHIV (only Women) . Out of Rs. 50,000/- only 25,000/-to be remitted at the low rate of interest and remaining Rs. 25,000/- is subsidy amount.
This scheme particularly HIV positive women only
Dept. of Women Development Corporation
459
11 Free legal services
free legal services PLHAs Karnataka State Legal Authority 110

39
6.Blood Safety: State Blood Council was established in Karnataka during 1996-97 to provide adequate and safe
blood and blood products at reasonable rates. At present there are 248 registered blood banks in Karnataka of which 66 are supported by NACO. Out of 248 blood banks, 43 are in Governments Sectors (State Govt. - 40, Central Govt.- 3), IRCS blood banks are - 8, Voluntary/Charitable blood banks-89 and 108 are in private sector (106 private Hospital Blood Banks & 2 are Private Stand Alone Blood Banks)
Blood Safety Indicators (2014-15 to 2021-22 up to January 2022)
Indicator 2014-15 2015-16 2016-17 2017-18 2018-19 2019-20 2020-21 2021-22
(till Jan 2022)
Total blood units collection 694151 754485 746716 787330 844419 877654 625062 578182
Blood units collected from VBD 408974 519260 539878 593108 657612 766860 536744 486942
7. Programme Component wise expenditure of KSAPS Budget
Sl. No. Programme
2021-22 (31.01.2022)( Rs. in Lakhs) Approved Budget for
2021-22
Total Grants received/available
for the year 2021-22 Expenditure
Expenditure Against Total amount for the
year (%)
1 Targeted Interventions 2671.47 2609.33 1908.58 73.14
1.1 Link Worker Scheme
155.09 191.71 144.19
75.21
2 Sexually Transmitted Infection / Reproductive Tract Infections Services
136.22 114.88 112.63
98.04
3 Blood Safety 548.54 548.55 210.90 38.45
4 Lab Services 214.33 176.13 96.38 54.72
5 ICTC/HI-TB/PPTCT 4517.23 4451.97 3370.75 75.71
6 Information, Education & Communication
386.64 323.76 224.44 69.32
7 ART/CCC 3575.00 4251.51 2019.04 47.49
8 Institutional Strengthening 1185.00 941.09 536.59 57.01
9 Strategic Information Management System
82.08 59.31 28.51 48.07
10 UNICEF 1030.50 984.52 0 0
11 State Fund
11a 2210-06-101-7-15-103 Grant in Aid Salary
450.00 225.00 49.82 22.14
11b 2210-06-101-7-15-100 Reimbursement of Travel cost to HIV patient
250.00 125.00 60.10 48.08
11c 2210-06-101-7-15-059 LWS programme
150.00 75.00 59.47 79.29
Total 15352.1 15077.76 8821.4 58.50

40
1.2.6 NATIONAL VECTOR BORNE DISEASES CONTROL PROGRAMME (NVBDCP):
State is implemented the activities for prevention and control of Vector Borne Diseases like Malaria, Filaria, Dengue, Chikungunya and Japanese Encephalitis as per the guidelines of GOI, Directorate of NVBDCP Delhi. Accordingly, in each of the Districts, Program implementation is being done though District Vector Borne Disease Control Officers, Taluka Health Officers and through Administrative Medical Officers CHC and PHC. Certain activities are managed at the State level such as drug procurement, information education and communication (IEC) and training.
Details of NVBDCP
Year Malaria cases/
deaths Dengue cases/
deaths Chikungunya
cases AES/JE cases
AES/JE deaths
2016 10607/0 6083/8 1528 406/ 11 0/0
2017 7381/0 17844/ 10 3511 332/ 23 0/ 0 2018 5289/0 4848/4 2951 380/35 0/5
2019 3499/ 0 18183/ 17 3994 388 /33 0/ 4 2020 1701/0 3823/5 1326 342/19 4/2 2021
(till December) 888/0 7359/0 2163 349/21 0/1
1. Malaria:
The State is heading towards Malaria Elimination and the State Framework of Malaria Elimination is launched on 12th May 2017 with the vision of eliminating Malaria from the State by 2025. The State is experiencing downward trend of Malaria incidence. During 2021, a decrease of 44 % in total Malaria cases is marked up to December as compared to same period of 2020. The State is under category-2 as per elimination criteria. During 2021, 78 % of the cases are from D.Kannada and 4 % is from Upper Krishna Project followed by Udupi with 3% and Raichur, Hassan, Belagavi & Yadagiri. Special inputs have been provided in terms of Human resource & Logistics to the Districts of Dakshina Kannada & Udupi for achieving the reduction in Malaria morbidity and heading towards goal of elimination.

41
District wise contribution of Malaria till December 2021
II. Dengue & Chikungunya
During 2021, till end of December 7359 confirmed Dengue cases are reported in
the State, showing an increase compared to same period of last year. Five deaths are confirmed from i.e. Ramanagar-02 and one death each from Belagavi, Chamarajanagara & Dakshina Kannada, Further, a total of 2163 Chikungunya confirmed cases have also been reported showing increase compared to same period of last year.
0
2000
4000
6000
8000
10000
12000
2016 2017 2018 2019 2020 2021 tillDEC
10607
7381
5289
3499
1701888
16931170 846 566 235 179
Malaria cases
Pf cases
Dakshina Kannada, 78%
UKP Project Area, 4%
Udupi, 3%
Raichuru, 1%
Hassan, 1%
Belgaum, 1%
Yadageri, 1% Others (24 dist.), 11%

42
District wise contribution of Dengue incidence till December 2021
District-wise contribution of Chikungunya incidence till December 2021
BBMP, 19%
Shivamogga, 7%
Kalaburagi, 6%
Udupi, 6%
Ballari, 6%
Koppal, 5%Vijayapura,
4%
Davanagere, 4%
Dakshina Kannada, 4%
Gadag, 4%
Haveri, 4%
Others, 31%
Shivamogga, 13%
Kalaburagi, 11%
Kolar, 9%
Vijayapura, 8%
Mandya, 7%Tumakuru,
7%
Yadageri, 7%
Chitradurga, 5%
Davanagere, 5%
Others, 28%

43
III. Acute Encephalitis syndrome/ Japanese Encephalitis (AES/ JE) : AES cases are being reported from most of the districts. During 2021 till December,
State has reported a total of 349 AES and 21 JE cases and one JE death from Vijayapura district.
These JE cases are reported from the Districts of Kolar, Vijayapura, Bagalkote, Dharwad,
Gadag, Uttar Kannada, Kalburgi, Yadgiri, Mysuru, Udupi, Chikkamagaluru & Dakshina
Kannada. 10 Sentinel Surveillance Laboratories have been established for diagnosis of JE.
Vaccination against JE is taken up in JE endemic districts of Bellary, Raichur, Kolar, Mandya,
Koppal, Bijapur, Dharwad, Chitradurga and Davangere and are now under Universal
Immunization Programme.
IV. Filariasis:
Filaria is endemic in 9 districts viz; Dakshina Kannada, Uttara Kannada, Udupi, Raichur,
Vijayapura, Bagalkot, Kalaburagi, Bidar & Yadgir. Three Districts vi. Dakshina Kannada, Udupi and
Uttara Kannada have qualified all three Transmission Assessment Survey. Out of Six Districts which are
observing MDA, three Districts such as Kalaburagi, Yadgir, Bidar are completely under Mass Drug
Administration (MDA) with Ivermectin, DEC & Albendazole and remaining three Districts such as,
Vijayapura, Bagalkot & Raichur are partly under MDA as 2 Evaluation Units each of these districts are
under Transmission Assessment Survey (TAS).
1.2.7 COMMUNICABLE DISEASES (CMD): The Communicable diseases (CMD) wing of this Directorate of Health &F.W.Services is Prevention and Control of Communicable Disease by regular monitoring, issuing appropriate guidelines & training. To Control the mortality and morbidity in community by taking necessary action like, water testing, chlorination and proper information and education. Main Objectives:
1. Issue of guidelines from time to time to District level programme officers regarding the control of communicable diseases.
2. Regular monitors of the diseases by issuing appropriate guidelines to the District Health Authorities
3. Investigation of outbreaks. 4. Supply of KFD vaccines to KFD affected districts their demands. 5. Implementations of instructions issued by Government of India and Government of
Karnataka, if any 6. To make necessary plan of action to improving Endosulfan victims health. 7. Necessary action for preventing and control of H1N1 infection.

44
Programmes monitoring :
a. Communicable Disease
1. Gastro Enteritis 2. Cholera 3. Typhoid 4. Viral Hepatitis
5. Kyasanur Forest Disease 6. Leptospirosis 7. Anthrax 8. Plague 9. H1N1 (Influenza-A)
b. Other Programmes
1. Handigodu Syndrome 2. Dog bite
3. Snake bite 4. Guinea Worm Eradication
Programme 5. Rehabilitation programme of
Endosulfan
Progress Achieved year wise 2015 to end of December-2021
2016 2017 2018 2019 2020 2021
Attacks Deat
hs
Attacks Deat
hs
Attacks Deat
hs
Attacks Deat
hs
Attacks Deat
hs
Attacks Dea
ths
Gastroenteritis 135125 9 152869 2 169936 0 218562 7 157852 0 135935 5
Cholera 84 1 2 0 19 3 5 0 18 0 4 0
Typhoid 57112 0 90607 90755 0 108298 0 54684 0 47137 0
Viral Hepatitis 5226 4 5957 4 5848 1 5194 0 3078 0 3917 0
KFD 32 1 46 3 22 0 445 15 287 5 23 0
Leptospirosis 503 2 475 2 568 3 896 0 544 0 906 1
H1N1 110 0 3260 15 1733 72 2030 96 458 3 13 0
Handigodu
Syndrome 495 Handigodu Syndrome cases are under treatment, No new cases are found since 2005
Dog Bites 258035 13 275639 7 313090 20 309105 13 275598 2 294880 6
Snake Bites 12182 55 10818 49 10244 62 11093 39 10551 20 11049 31
Plague Control Programme (2016 to end of December-2021)
Surveillance 2015 2016 2017 2018 2019 2020 2021
Rodent collection 1186 1226 407 40 No
Surveillance done
No Surveillance
done
No Surveillance
done Sera Collection & Examined
1055 1003 287 40
REP Survey in 24 23 60 6
( Rodent Sera samples have been analysis at NICD-Bangalore.)

45
Handigodu Syndrom - Handigodu Syndrome disease prevalent only in Shivamoggaand Chikkamagalore Districts. Cases under treatment:
1. Shimoga District 206 2. Chikkamagalore District 289
Total cases under treatment 495 (No further cases since 2005)
Kyasanur Forest Disease: -
Kyasanur Forest Disease (KFD) is reported from few districts
Sl. No.
Name of the District
2016 2017 2018 2019 2020 2021
Cas
es
Dea
ths
Cas
es
Dea
ths
Cas
es
Dea
ths
Cas
es
Dea
ths
Cas
es
Dea
ths
Cas
es
Dea
ths
1 Shimoga 14 41 39 2 18 0 343 12 185 4 15 0 2 U.Kannada 2 0 6 1 4 0 93 3 89 1 5 0 3 Belagavi 16 0 1 0 0 0 2 0 0 0 0 0 4 Chikkamagaluru 0 0 0 0 0 0 1 0 12 0 3 0 5 Kodagu 0 0 0 0 0 0 0 0 0 0 0 0 6 Mysore 0 0 0 0 0 0 3 0 0 0 0 0 7 Chamarajanagara 0 0 0 0 0 0 2 0 0 0 0 0 8 Hasana 0 0 0 0 0 0 1 0 1 0 0 0 9 Udupi 0 0 0 0 0 0 2 0 0 0 0 0
Total 32 41 46 3 22 0 445 15 287 5 23 0 H1N1 (Influenza-A):
Comparative Statement of H1N1 Samples Tested and Confirmed cases
Sl. No Particulars 2014 2015 2016 2017 2018 2019 2020 2021
1 Specimen Examined 2349 13168 3494 16835 10435 4600 4937 2032
2 H1N1 cases confirmed by lab test 303 3565 110 3260 1733 1198 458 13
4 Reported deaths 34 94 0 15 87 96 3 0

46
Communicable Diseases Control Programme: The Directorate has given the responsibilities to the CMD-Section to control and eradicate the
communicable diseases. They are,
1. Regular monitoring of the diseases by issuing appropriate guidelines to the District Health
Authorities.
2. Investigation of outbreaks/epidemics.
3. Monitoring the drinking water sources by analysing the water samples and issuing instructions
for chlorinating the unfit water sources.
4. Conducting workshops to sensitize the medical and paramedical staff about KFD.
5. Creating awareness about these diseases among the public.
6. Immunization of risk group population in KFD endemic district under KFD control programme
7. To strengthen the passive surveillance activities of communicable diseases.
8. To visit all the district and check the under reporting of communicable diseases from District
Hospitals, private Hospitals and peripheral health institutions.
9. All communicable diseases surveillance activities to be activated.
10. To involve all the local bodies for preventing the communicable diseases through the supply of
safe drinking water and maintain environmental sanitation.
Action plan for the year 2022-23:
1. Up gradation of Viral Diagnostic Laboratory at Shimoga.
2. To bring down incidence of KFD by maximum coverage of vaccination in endemic districts.
3. Strengthening of VDL Shimoga with fully function of RTPCR equipment for accurate & speedy
diagnosis of KFD cases by occupied the new building.
4. To prevent the death and reduce the epidemics due to cholera and Gastroenteritis.
5. Creating the awareness for preventing H1N1.
6. Providing medical and financial support to be Endosulfan victims for in priority their health
status.
The Communicable Diseases unit is entrusted with the task of not only controlling the
waterborne communicable diseases but also preventing these diseases in the form of epidemics and
minimizing the morbidity and mortality (Human suffering and deaths)

47
12.8 REPRODUCTIVE AND CHILD HEALTH PROGRAMMES :
The Child Health Programme comprehensively integrates interventions that improve child survival
and addresses factors contributing to Infant and Under 5 Mortality. Many initiatives have been taken up
to provide preventive, promotive, curative & rehabilitative health care services through evidence-based
interventions like Facility Based New born Care (SNCU, NBSU, NBCC), Home Based New born Care,
Janani Shishu Suraksha Karyakrama (JSSK), Child Death Review, Kangaroo Mother Care and Lactation
Clinic, Integrated Management of Neonatal & Childhood Illnesses (IMNCI), Intensified Diarrhoea
Control Fortnight (IDCF), Home Based Care of Young Child (HBYC), Social Awareness & Action to
Neutralise Pneumonia Successfully (SAANS), World Breastfeeding Week (WBW), National New born
Week (NNW).
Child Health Achievements:
• The Millennium Development Goal (MDG) for Under 5 Mortality Rate has already been
achieved in Karnataka.
• The current Under 5 Mortality Rate is 28 (SRS 2018), Under 5 Mortality Rate has been reduced
by 20 points since 2009.The current goal is to reduce Under 5 Mortality Rate from 28 to 25
according to Sustainable Development Goal (SDG) 2030.
• Infant Mortality Rate (IMR) in Karnataka is declining steadily. It is declined from 41 in 2009 to
21 as per Sample Registration System (SRS) 2019 (20 Points in reduction).
• Neonatal Mortality Rate (NMR) is 25 in 2009 to 16 as per SRS 2018, (9 Points in reduction).
Current goal is to reduce NMR from 16 to <12 according to Sustainable Development Goal
(SDG-3) 2030.
• The current Early Neonatal Mortality Rate is 12 as per SRS 2018.

48

49
1. Facility Based New Born Care (FBNC):
• New Born Care Corner (NBCC): 1070 NBCC are functioning at all delivery points. New-born care corners are established in labour rooms & Operation Theatres in all the 24X7 PHCs, CHCs, and Taluk Hospitals and District hospitals. NBCCs are provided with Radiant warmer, resuscitation bag and suction apparatus for immediate care of the new born baby. The staffs are trained in Navajatha Shishu Suraksha Karyakrama (NSSK) to provide care to new born including resuscitation of an asphyxiated baby. 1070 NBCCs are functional in Karnataka.
• New Born Stabilization Units (NBSU): 165 NBSUs are functional till date. NBSUs have been established in all First Referral Units (FRUs) and Taluk Hospitals, adjoining the labour room or OT and provided with radiant warmer, Phototherapy Units. Each NBSU is provided 2 Staff Nurses who are trained in Facility Based Integrated Management of Neonatal & Child hood Illnesses (F-IMNCI). Babies needing resuscitation, low birth weights or premature new-borns are given initial treatment, well stabilized at the NBSUs & then referred in appropriate way to the higher centres.
• Special New-born Care Unit (SNCU): 42 SNCUs are functioning at all district hospitals& Government medical college hospitals and some high performing Taluk hospitals. Special New born Care Units are units in a large hospital generally at district level with more than 3000 deliveries per year and meant to reduce the case fatality among sick new borns, either born within the hospital or outside including home delivery. It is a separate unit near the labour room with 12 or more beds, and managed by adequately trained paediatricians, medical officers, staff nurses and support staff to provide 24x7 services. It also acts as the teaching and training hub for imparting the skills of new born care.
In Karnataka, 42 SNCUs are functioning in all District Hospitals and District Level Hospitals. Among them, 14 SNCUs attached to Government Medical Colleges and 5 SNCUs attached to District hospitals have been upgraded to provide Neonatal intensive care. 42 SNCUs consists of 822 beds and approximate 70,000 admissions per year.

50
Eight more new Taluk Level SNCUs at Hospet Bellary, Humnabad Bidar, Jewargi Kalaburgi, Sira Tumkuru, Holenarsipura Hassan, KR Pete Mandya and Gokak Belagavi and Sir. C V Raman Nagar Hospital, Bangalore upgrading to SNCUs is under process. Functions of Special New-born Care Units (SNCU):
Care of low birth weight new-borns Breastfeeding support Managing all sick new-borns (except those requiring mechanical ventilations) Some units have CPAP and ventilation facilities also. Follow-up of all babies discharged from the SNCUs. Immunisation services Referral services
• Kangaroo Mother Care wards: Kangaroo Mother Care (KMC) ward are being established
in all the District Hospitals adjacent to SNCUs to strengthen the supportive care to the newborn. KMC wards are established in all hospitals with SNCUs and health care personals are trained in KMC at state level. Further community KMC will be rolled out in order to increase the survival of low birth weight babies.
• Lactation Clinics: Lactation clinics are established in district hospitals to increase the early initiation of breast feeding and exclusive breastfeeding rates. This will be established at all the delivery points and further existing lactation clinics will be upgraded to lactation management centres and mothers will be supported to store the expressed breast milk.
• Neonatal Transportation: Neonatal ambulances ensemble with intensive care will be provided for four divisions to transfer sick neonates. This will be rolled out to all other districts based on the experience of piloting.
2. Integrated Management of Neonatal & Childhood Illnesses (IMNCI): IMNCI was first initiated in Raichur in 2005 and expanded in a phased manner to all 31 districts including BBMP as on 2017-18.Integrated Management of Neonatal & Childhood Illnesses (IMNCI) programme is an innovative approach where the field level workers (ANMs & Anganwadi workers) are trained to

51
identify common diseases of early child hood (Pneumonia, Diarrhoea, Measles, Ear Infections, Malaria, Malnutrition, Anaemia) and manage or arrange prompt, timely referral. IMNCI was first initiated in Raichur in 2005 and expanded in a phased manner to include all 30 districts from about 2012.By 2011, with the establishment of FRUs and New Born Stabilization Units, the Facility based IMNCI concept was introduced in addition to the Community based component and Medical Officers and Staff Nurses of all Health facilities have been trained and are implementing the same. Supportive supervision of the programme has been under taken through the Community Medicine Department of the 10 Government Medical Colleges. This supervision was initiated from 2014 onwards.
3. Home Based Newborn Care (HBNC): ASHAs visit the neonates at least 6 times in the first 42 days after delivery. 41,565 ASHAs are trained to identify common neonatal illnesses & educate the mothers regarding Breast feeding & care of new born. In case of SNCU graduates and low birth weight babies, additional visits at 3rd, 6th, 9th & 12th month at the incentive of Rs. 50/- per each visit is carried out by ASHA. They are provided with a kit containing essential equipment & drugs to car for the new born. Knowledge of ASHAs is being reinforced through the SATCOM facility where the State Officials directly interacted with ASHAs and cleared their doubts. Similarly, Medical Officers and Staff Nurses of PHCs were also oriented regarding RMNCH+A strategies through SATCOM.
4. Janani Shishu Suraksha Karyakrama (JSSK): Janani Shishu Suraksha Karyakrama (JSSK) was introduced in early 2012 to reduce the out of pocket expenditure of the parents towards the treatment of sick new born. An amount of Rs. 200/- for Drugs and Consumables, Rs. 100/- for diagnostics and Rs.300/- for Referral Transport was allocated per sick new born as an indicative unit of calculation. The required amount may be spent with justification. In the year 2013-14, the facility was extended for any sick child below one year of age.
5. Child Death Review (CDR): Child and infant Death Review have been implemented in all Districts of Karnataka. State and District level Child Death Review committees have been formed and are meeting regularly. All reports being sent are being reviewed validated and feedback given to districts. Through all these efforts the State has reduced the Under 5 Mortality to 28 per 1000 live births and Infant Mortality Rate to 21 per 1000 live births as per SRS 2019. State level Reorientation and review of CDR was conducted for district & Taluk administrators for successful implementation of CDR and thereby take necessary actions to fill the gaps to reduce the Child deaths.
6. Intensified Diarrhoea Control fortnight (IDCF): IDCF programme has been observed throughout the state every year (May and June). All the grass root level of workers like ASHAs, Anganwadi workers and ANMs are involved in active participation and distribution of ORS and ZINC tablets. These health care workers visit the houses of under 5 children and give awareness to the parents regarding preparation of ORS solution, management of Diarrhoea at household, sanitation and hygiene, hand washing techniques.
7. National New born Week: New born week is being celebrated in Karnataka since 2016. This is a
programme launched by Government of India to highlight care of new borns and to emphasize the importance of improving new born care. It is celebrated every year in the second week of November. Multiple training programmes, awareness activities and IEC activities are carried out in the community and at health care facilities across the state.
8. Home Based Care Of Young Child (HBYC):
Newborn babies are followed up till 42 days under HBNC program, however infants from around 3 months of age and beyond face problems such as discontinuation of breast feeding delay in initiation or incomplete complementary feeding beyond six months, poor care seeking for sickness, etc. In addition, poor hygiene and sanitation (WASH), and child rearing practices in the home during this period may also lead to sub-optimal physical growth and development of the child. Thus to reduce

52
the adverse impact of these factors and to provide support for nutrition and early childhood development, the Home- Based Care of Young Child (HBYC) has been launched as part of the National Health Mission and POSHAN Abhiyaan under which additional 5 visits by ASHA during 3rd, 6th, 9th, 12th& 15th months of age. HBYC TOT Training in 19 POSHAN districts (including 2 aspiration districts) has been completed and the training of front line workers like ASHA, AF and ANM is being conducted at Raichur and Yadgiri districts.
9. Social Awareness and Action to Neutralise Pneumonia Successfully (SAANS):
Childhood Pneumonia is caused by a combination of risk factors related to the host i.e. the child and infecting organisms (microbes). Within the child, low birth weight, malnutrition, nonexclusive breastfeeding (during the first 6 months of life), indoor air pollution, lack of complete immunization, lack

53
of hygiene and many other socio economic factors lead to Pneumonia in children. Childhood Pneumonia continues to be the top most infectious killer among under-five children, contributing to 15 percent of under-five deaths in the country. Around 1.4 lakh children die due to Pneumonia annually in the country. TOT training at state level for rolling out of SAANS program was conducted during month of November 2020 and district level training are under progress.
Health Indicators:
Table: 12.37 Achievement of the Health & Family Welfare Services programme in Karnataka Sl No
Indicator 2011 2012 2013 2014 2015 2016 2017 2018 2019
1 Neonatal mortality rate (per 1000 live births)
24 23 22 20 19 18 18 16 -
2 Infant Mortality Rate (per 1000 Live births)
35 32 31 31 31 24 25 23 21
3 Under-Five Mortality Rate (per 1000 Live births)
40 37 37 37 35 29 28 28 -
* Data Source: Sample Registration System (SRS)
1.2.9 HMIS & RCH Portal HMIS (Health Management Information System):
The physical progress of Health Programmes in general and RCH programmes in Particular is captured through Health Management Information System (HMIS). The Data components of HMIS formats as per the guidelines of GOI is captured from around 12,500 health institutions on monthly basis in HMIS web portal. The Old HMIS application is developed by Vayam Technologies and the New HMIS portal is developed from NIC, HMIS Division, GoI, MOHFW.

54
Facility wise HMIS data is available from August 2010. HMIS is completely shifted from old HMIS portal to new HMIS portal from July 2020.
Data reporting period is 1stto 30th of previous month and the data has to be fed with in 5th of
preceding month. Different types of formats designed to capture information:
o Daily data entry (OPD, IPD, SARI, ILI, Fever Cases)- from PHC and above health facilities (Initiative in new HMIS portal).
o Monthly Format (Physical Performance of facilities) – from all the facilities. * Monthly Information System – (Physical Performance) from all the facilities. * Monthly format (Infrastructure Details) – From all the facilities. (HR details, Population,
Area covered, Building Status, Equipment’s, Drugs, vaccines availability, Contraceptives) from all the facilities.
*Stock format - ( IFA Tablets, Syringe) from all the facilities. Data reporting unit is PHC / CHC/ SDH /DH / SC all the units are provided with separate user
credentials: • Many type of reports are available in HMIS portal for monitoring the data reported by facilities
live report, dash board, analytical report etc.., • Based on the infrastructure availability and services being provided the performance of health
facilities are graded (Star Rating of Health facilities). • District / Taluk performance can be analysed based on composite index of 16 RMNCH+A
indicators.
HMIS portal screenshot with HMIS logo

55
State level workshop on HMIS and RCH portal RCH - REPRODUCTIVE AND CHILD HEALTH PORTAL
RCH (Reproductive and Child Health)portal is a centralized web based application for early identification and tracking of the individual beneficiary throughout the reproductive lifecycle.Application facilitates to ensure timely delivery of full component of antenatal, postnatal & delivery services and tracking of children for complete immunization services. RCH portal has been designed to meet the requirements of the RMNCH program by incorporating additional functionality and features of the MCTS.
RCH portal started in the State from October 2018 and around 75.64% of pregnant woman and
72.92% of Children registered in RCH portal during the year 2021-22.

56
RCH portal helps Beneficiaries in providing Information about desired services, Government Schemes & Benefits, advance information about the due services, Facilitate better interaction with Health Service Provider and Free consultation from Central Helpdesk (Toll Free No)
RCH portal helps Jr.HAF / ASHAs in auto generation of work-plan, better guidance from senior
supervisors, micro planning for Filed Visit, Payment of incentives to the Health Service Providers
RCH portal helps State, District and Taluk Officers in Planning, Decision making, analysis, better planning for Vaccination Supply &Management Group /Individual SMS’s to health workers and monitor the High risk cases and LBW cases closely.
The RCH portal will be linked with other department applications like for issuance of Birth certificate (Directorate of Economics and Statistics) and to capture services provided by ICDS W&CD department.
ANMOL (ANM ONLINE):
ANMOL Launched in the month of November 2019 in Karnataka state. ANMOL (ANM On
Line), a job aid tool for ANMs is providing a readily available information such as due list dashboard and guidance based on data entered etc.
ANMOL helps To ensure effective and timely delivery of quality healthcare services to all
potential beneficiaries including rural and unreached urban population. It establishes better communication of ANMs with beneficiaries and Doctors through remote assistance which will improve the quality of services and bring awareness among potential beneficiaries and unserved community through images, videos and educating them about Government initiatives on health, maintenance of good hygiene, basic health care & precautions.

57
ANMOL benefits: 1. Designed to Meet ANM Needs 2. Easy to understand UI (User Interface) 3. Counselling alerts for Anaemic, high risk, LBW beneficiaries etc. 4. Works offline without internet connectivity, syncs at availability 5. Save time with one click access to daily , weekly or customizable work plan 6. Digital e-Register a step towards paperless registers 7. Multilingual support (Localization) 8. Audio, Video counselling to support IEC activities 9. Ready reports in Dashboard for any meetings or self-review 10. Auto generate VHND due list with required logistics saving time and effort 11. Receive Notifications and updates from State / GoI
1.2.10 MOTHER HEALTH:
The Mother health programme involves providing qualitative maternity care which is equitable, affordable and accessible by all sections of the society. The following are the aims and objectives of the mother health programme.
• To promote safe pregnancy and child birth. • To reduce preventable causes of maternal death. • To reduce out of pocket expenditure for delivery services. • To promote institutional delivery. • To reduce caesarean section rate. • To provide comprehensive 24/7 MCH services at high delivery points • To provide basic MCH services at all delivery points.
In order to accomplish the above goals and objectives, the following schemes are implemented across the State 1. Janani Suraksha Yojane (JSY):
Janani Suraksha Yojane (JSY) is a centrally sponsored scheme under National Health Mission implemented in Karnataka since 2006. It is an important initiative of the Government to reduce maternal mortality and early neonatal mortality.
Sl No. Type of Delivery (Normal & LSCS) Monetary benefit per case
1. Institutional Deliveries (Urban) Rs. 600/-
2. Institutional Deliveries (Rural) Rs. 700/-
JSY Eligibility criteria: - Pregnant women belong to BPL/SC/ST.
Incentive is paid within 48hrs of delivery at the facility where delivery occurs through PFMS on to the bank account of the pregnant women of any age and Para belonging to BPL/SC/ST.
JSY Physical Expenditure for the last 5 years.
Year Target Achievement % of
Achievement 2017-18 425587 282731 66
2018-19 248949 325197 130 2019-20 350000 498557 142
2020-21 574469 481609 84 2021-22
(April-Jan) 631213 2,65,082 42
2. Janani Shishu Suraksha Karyakrama (JSSK)
JSSK is a centrally sponsored scheme under National Health Mission implemented in Karnataka since 2011.

58
Goals & Objectives of the JSSK scheme:
• To ensure zero expenditure to Pregnant Women by providing the following five entitlements in all public facilities at free of cost to all section of society (i.e. irrespective of the economic status).
free drugs and consumables free diagnostics free blood free diet and free transport services from home to health institutions and back to home.
Sl. No.
Year No. of beneficiaries
availed (JSSK)
Financial expenditure (Rs. in lakhs)
1. 2018-19 5,64,549 5699 2. 2019-20 5,12,126 5465 3. 2020-21 5,04,388 3348 4. 2021-22(till Jan) 4,58,827 1525
3. Pradhan Mantri Surakshit Matritva Abhiyan(PMSMA)
This is a centrally sponsored scheme under National Health Mission implemented in the state since
August 2016.PMSMA is conducted on 9th of every month at all Government facilities. In case, of 9th falling on a holiday, the PMSMA is conducted on the next working day.
Goals & Objectives of PMSMA:
• To promote quality antenatal checkups especially, for the High Risk pregnant women in 2nd& 3rd trimester.
� The Programme aims to reach out all pregnant women who are in the 2nd and 3rd Trimester of pregnancy.
� Provide antenatal checkups from the medical officers and specialists. � Provide necessary investigations on the same day at the same site.
Sl. No.
Data element 2016-17 2017-18 2018-19 2019-20 2020-21 2021-22
(April-Jan) (Number of Pregnant
Women )
1 Total number of pregnant women Received Antenatal care under PMSMA in the current month
420422 512163 490886 512559 516894 387670
2 Received Antenatal care under PMSMA in 2nd or 3rd trimester for 1st time
78566 154794 132580 162170 185418 139062
3 Total Number of high risk pregnancies identified
89044 131141 177011 130949 137825 103368
4 Total Number of Private Volunteers provided services monthly
98 96 97 102 99 98
435 Private Volunteers have been Registered from 2016-2022

59
4. LaQshya Programme:
LaQshya is a flagship program of NHM aimed at improving intrapartum and postpartum care processes thereby decreasing maternal mortality and neonatal mortality.
LaQshya is the targeted approach in improving the quality of maternal and new born care services and encompasses the following.
1) Up gradation of the labour room and maternity OT as per the LaQshya standards. 2) Providing the requisite number of Human resource to the facility as commensurate with delivery
load 3) Providing necessary equipment as a part of infrastructure up gradation. 4) Up scaling the knowledge, attitude and practices of the services providers i.e., obstetricians,
Medical officers, staff nurses and housekeeping staff. The program is being implemented in 124 facilities across the state from 1st April 2018. The
following is the district wise number of LaQshya facilities
LaQshya Facilities Certification Status in Karnataka as on 25-01-2022
Sl No.
Type of Facility
No. of Facilities Selected
National Certification
Achieved
State Certification
Achieved
1 MC 19 13 4
2 DH 19 11 6
3 SDH 72 23 13
4 CHC 14 7 3
Total 124 54 26
5. MCH Wings:
Mother and Child Health (MCH) Wings are established to provide exclusive and comprehensive obstetric and new born care to all pregnant women and new born child.
MCH Wings are established to bring down the maternal mortality ratio and infant mortality rate.
The present Maternal Mortality Ratio (MMR) which is an indicator of quality maternal care is 92 in Karnataka and Infant Mortality rate (IMR) is 21
MCH Wings bring in additional equipment and human resource commensurate with the delivery load. Services provided in MCH Wings:
1. 24 Hrs Normal delivery services.
2. 24 Hrs Caesarean delivery services.
3. 24 Hrs New Born Care services.
4. Blood Storage Unit.
5. Laboratory services.
6. Ultra Sonography Services for pregnant women.

60
Criteria for Establishment of MCH Wings.
1. Should cater to a population of at least 5Lakh. 2. Should be established in a First Referral Unit only.
3. The facility should have a Bed Occupancy Rate (BoR) of more than 70 for MCH beds.
4. The nearest MCH Wing should be more than 100Km.
The MCH Wings have been established from the following source of funds:
1. National Health Mission. 2. NABARD. 3. RIDF. 4. Smart City.
5. First Referral Unit (FRU):
First Referral Unit (FRU) is defined as “a facility providing full range of FRU services including
C-Sections along with facilities for handling other medical emergencies and accordingly a minimum strength of 4 medical officers who are either qualified or especially trained to work as surgeon, Obstetrician, Physician and Paediatrician) are required to be in position.
FRUs are the First Referral Units established to provide Comprehensive Obstetric and New Born
Care proposed by GoI for every 5 Lakh populations (3 Lakhs in hilly areas). Karnataka has established FRUs at all district head quarters and taluk head quarters hospitals. Further in Karnataka at CHCs where Obstetricians, Paediatricians and Anaesthesiologist are posted at are also considered as FRUs.
Critical determinant of First Referral Unit:- There are 10 functionality indicators for designating
a facility as FRU. (As per the guidelines Functionalization of FRU released by GoI). These are as follows.
1. 24- Hour delivery services including normal and assisted deliveries. 2. Emergency Obstetrics Care including surgical interventions like Caesarean Sections. 3. New Born Care. 4. Emergency Care for Sick Children. 5. Full range of family planning services including Laparoscopic services. 6. Safe Abortion Services. 7. Treatment of STI/RTI. 8. Blood Storage facility. 9. Essential Laboratory services. 10. Referral (transport) services. However, of the above the following 3 indicators are critical determinants for a facility to be declared
as a FRU 1. Availability of surgical interventions like Caesarean Sections. 2. New Born Care. 3. Blood Storage facility on 24 hrs basis.
FRUs are of 3 types, namely:
1. District FRUs including Medical College Hospitals, District Hospitals and equivalent hospitals such as KC General Hospital, Jayanagara General Hospital etc.
2. Sub District Hospital FRUs (SDH) stationed at taluka Head quarters. 3. Community Health Center FRUs (CHCs) placed at Hoblis

61
The following is the breakup of FRUs in the State
Sl. No. Type of FRUs
Total No. Of designated
FRUs
Functional FRUs
1 District Hospitals (DH)* 38 38 2 Sub District Hospitals (THs)** 147 140 3 Community Health Centers (CHCs) 104 73
TOTAL 289 251
Amongst 289 FRUs which are designated for the 251 facilities are functional for Caesarean section deliveries. Maternal Mortality Ratio (MMR):
The Office of the Registrar General of India has released a special bulletin in the month of July 2020 on the trends in the Maternal Mortality all over the country. The maternal death is defined as the death of any women during pregnancy, child birth and lactation beginning from the first month of pregnancy to 42 days following delivery, due to any cause directly or indirectly related to Obstetrics excluding suicides, homicides and accidents. The maternal deaths are expressed in terms of Maternal Mortality Ratio which means no of women succumbing to pregnancy and childbirth causes per every lakh of live births.
The bulletin is released to assess the progress made by each state in the field of maternal health so that least and acceptable mortality is achieved. The current bulletin pertains to the analysis of the maternal deaths over the time period 2016-18 throughout the country. The MMR of the country is 113 which mean that 113 women are losing lives to pregnancy and child birth causes for every lakh live births. The MMR of Karnataka is 92 which is above the national average. Percentage decline in MMR over the previous year report and State Ranking based on the decline is as below.
Measures undertaken by the state to achieve the decline in the MMR:
The Department of Health and Family welfare Services welcomes the Special Bulletin on MMR released by GoI, today. The MMR which determines the progress made by the Society in saving lives of pregnant women during pregnancy, childbirth and lactation is 92 in Karnataka. The State has shown reduction in the maternal deaths by 5 points and by 5 .2 percentage as compared to the previous report pertaining to the period 2015-17.
213
178
133
10897 92
0
50
100
150
200
250
2004-06 2007-09 2011-13 2014-16 2015-17 2016-18
Karnataka MMR Trend (Source SRS)

62
The State stands at 9th position in terms of ranking in MMR as compared to other states throughout the country. Karnataka is one of the 7 states to have achieved National Health policy Goal of MMR less than 100. The next aim of the state is to achieve the Sustainable Development Goal (SDG) of MMR of less than 70 which is to be achieved by 2030.
The department congratulates all the stake holders in the provision of quality Maternity Care in
achieving the reduction of Maternal Deaths. While admitting that the Department has miles to go in the achievement of SDG Goal of MMR less than 70, the Department has already started the implementation of Programmes aimed at achieving acceptable Maternal Mortality.
1. Prioritization of MCH services in all Govt. Hospitals considering the vulnerability of the pregnant women.
2. Functionalization of 84 % of First Referral Units which act as the point of care for all comprehensive Obstetric and New born care services
3. New Recruitment of MCH specialists ,staff nurses and Health Assistants over the last 3 years 4. Improved access to the Govt. hospitals for the MCH services. Functionalization of the MCH
wings enhancing the quality of maternity care. Implementation of LaQshya programme in 124 hospitals which is aimed at improving the quality of labour and operation theatre services thereby contributing to reduction of maternal deaths.
5. Improved access to nutrition services in the form of iron and calcium supplementation and regular de-worming programmes.
6. Capacity building of the Doctors and nurses in the care of the pregnant women through Dakshata and LaQshya.
7. Tracking and monitoring the High risk pregnant women. 8. Monthly monitoring of the maternal and child health by Chief Secretary, Karnataka state through
video conferencing. 9. Review of the maternal health programme by senior officers of the Department. 10. Review of the maternal deaths at the District level by Deputy Commissioners, CEOs and DHOs.
1.2.11 EMERGENCY MANAGEMENT AND RESEARCH INSTITUTE (EMRI):
Arogya Kavacha (108): “Arogya Kavacha” 108 Emergency service was started in the state of Karnataka on November 1,
2008, by the Karnataka Health and Family Welfare Department under a Private Public Partnership
through an MOU signed with GVK EMRI.
The Role and Mission of ‘108’ is to save lives by providing a comprehensive ‘Emergency
Response Service’ to those in Medical, Police or Fire emergencies, through a single integrated number -
108. We operate 24 x 7 and 365 days of the year with a fleet of 711 well equipped ambulances. The
ambulances are manned by a trained Emergency Medical Technician (EMT) and a trained driver (Pilot).
This service is available across the length and breadth of Karnataka i.e., all the 30 Districts.
Ambulances are stationed strategically in all Districts and Taluks across Karnataka so they can
reach the incident location within the shortest possible time anywhere in the state. The services are
operated through a centralized Emergency Response Centre located at Bangalore. At present there is one
ambulance for every 85000 populations with a total of 711 Ambulances throughout the state.

63
This service can be utilized by any individual who requires emergency help (Medical, Police, or
Fire) irrespective of his economic status, caste, creed, colour, ethnicity, gender, and/or literacy levels. The process of calling for an ambulance is simplified to such an extent that a call to the toll-free number ‘108’ with details of emergency, the number of people involved and the incident location supported with a landmark; would trigger an ambulance dispatch . This is an absolutely FREE SERVICE starting from the phone call till the point of reaching the hospital.
The medical emergencies can be availed for Accident and Trauma (Vehicular and non vehicular),
complaints related to Cardiac, Respiration, Diabetes, pregnancy, Stroke/Convulsions, Suicide attempts Poisoning cases, Assault/Violence, Animal Attacks, Neonatal, Building Collapse, Fire, Burns, hazardous material ingestion etc.,
From April 2021 to Jan 2022, 679782 Emergency calls are attended, 528071 emergencies cases
are attended and out of these 148804 pregnant women have utilized the services and 40118 lives are saved.
Janani SurakshaVahini:
Janani Suraksha Vahini Programme was initiated under NHM in 2009-10 to ensure 24/7 round the clock, free referral transport between the facilities for pregnant women and sick neonates/ infants. Out of the existing ambulances of the CHCs/ THs/ DHs one ambulance of each facility was designated as JSV Ambulance. At present there are 180 JSV Ambulances. Drivers are outsourced by District Health Societies from Manpower Agencies by calling tenders as per KTPP Act.

64
2 drivers (1 Regular and 2 Out sourced) are given to each vehicle to work in 8th hourly shifts. Total number of beneficiaries under JSV from April 2021 to Jan 2022 is 64478.
Nagu-Magu:
To provide Drop Back facility for post postnatal mothers and new born from Government Health Facilities to their residence, 200 drop back vehicles called as “Nagu-Magu” were inaugurated on 5th February 2014. The Nagu-Magu vehicles are deployed one each at the District Hospital and Taluka Level Hospitals. Drivers for Nagu-Magu Vehicle are outsourced by District Health Societies from Manpower Agencies by calling tenders as per KTPP Act.
Total number of beneficiaries under Nagu-Magu from April 2021 to January 2022 is
82414. Bike Ambulances: (First Response Unit):
The Bike Ambulances/ First Response unit (FRU) is inaugurated on 15th of April 2015 by Government of Karnataka. It is the “Platinum Ten Minutes” trauma care initiative aimed at reducing deaths due to road accidents. It is a unique initiative and is the first of its kind to be taken up by the State Government in our Country. The first aid and medical care during the “Platinum Ten Minutes” is paramount to save the life of an accident victim, hence the pioneering attempt to start motorbike ambulance service.

65
The motorbike ambulance service is another pilot and pioneering initiative to ensure first aid to the victims during the Golden Hour They are useful for negotiating the small streets and heavy traffic in the large urban areas where it would be difficult to move ambulances through crowds. The fleet of high-powered touring motorcycles are available when required to respond to various trauma/medical incidents. The Bike ambulances will be currently deployed in Bangalore (19 Nos), Mangalore (2 Nos), and one each to the corporation areas of Mysore, Kalburgi, Belagavi, Hubli-Dharwad, Davangere, Tumkur, Vijayapura, Shimoga and Kolar Districts where heavy traffic congestion and narrow streets would be easily overcome by the agile nature of the bikes. The programme will be implemented through GVK-EMRI who are already experience in providing such services through Arogya Kavacha-108. Riders are paramedics or EMTs who are recruited and trained on managing emergencies. Motorbike ambulance drivers would be fully trained in rendering first aid and would start resuscitation measures to save the victim.
Two-wheelers by virtue of their size could manoeuvre through narrow and busy roads and reach
accident spots with ease while they would be followed by a fully equipped four-wheel ambulance for shifting the victim to a nearest hospital for further treatment if necessary.
Bike ambulance is able to respond to a medical emergency much faster than an ambulance or a
car in heavy traffic which can increase survival rates for patients suffering cardiac arrest/ accident/ other emergencies.
From April 2020 to Jan 2021, 20791 emergencies are attended by the bike ambulances.
Arogya Sahayavani-104: The Government of Karnataka has started the Arogya Sahayavani-104 service with the moto of
reaching the unreached, to provide all the health care services available in the public sector.
Those patients residing in the remote rural villages, who cannot access the medical doctors in the
hospitals, can now contact with the doctors through Arogya Sahayavani-104. “104” is a toll free number
through which people can avail consultation for minor ailments, counseling services, information on
services available in public Health facilities, directory services (Eye bank, Blood Bank) and grievance
redressal (Services, Epidemics, Corruption, Hygiene, Drugs and Diagnostics, ASHA grievances, etc., )

66
Arogya Sahayavani-104 call centre is situated at IT Park Hubli and Sir. C V Raman Nagar
Hospital, with a capacity of 100 seater each. People (Citizens) from any part of the state can avail their
service by calling 104. From April 2021 to Nov- 2021, 44,74,704 calls are received at the call centre
out of which 37,24,791 calls are provided with the different services. At present around 10000 calls per
day on an average is being received at both the call centres.
Vatsalya Vani:
For the first time in India, A Three way call conferencing structure for Mother Child tracking
system called “VatsalyaVani” is launched in Karnataka by Hon’ble Chief Minister Shri. Siddaramaiah on
21st December 2015. This programme is implemented through Arogya Sahayavani-104.
Vatsalya Vani call centre will offer the below services throughout the state:
1. Monitor all pregnant woman and child through ANC/PNC advice.
2. Promote, protect and maintain the health of the mother and child through advice e.g. nutrition,
health & wellbeing.
3. Providing information of various government health programs and schemes and their
entitlements
4. Identify and track High Risk Pregnancies and low weight birth babies.
5. Motivate mothers for Institutional Delivery and family planning methods.
6. Arrange and monitor transfer to nearest delivery point through state ambulances.
7. Eliminate home deliveries.
8. Track Immunization status.
9. Prevent dropouts.
10. Ensure complete service delivery.

67
1.2.12 PRE-CONCEPTION AND PRE-NATAL DIAGNOSTIC TECH NIQUES PROGRAMMES (PC & PNDT) : Purpose:
Prevent Sex detection and selective abortion of female foeticide and increase the sex ratio of females. Objective of the act:
The Pre-conception and Pre-Natal Diagnostic Techniques (Prohibition of Sex-Selection) Act, 1994 to provide for the prohibition of sex selection, before or after conception, and for regulation of pre-natal diagnostic techniques for the purpose of detecting genetic abnormalities or metabolic disorders or sex-linked disorders and for the prevention of their misuse for sex determination leading to female foeticide and for matter connected therewith or incidental thereto.
Social discrimination against women and a preference to sons have promoted female foeticide in
various forms skewing the sex ratio of the country and also in our State towards male. Female foeticide began in early 1990s when ultrasound techniques gained widespread use in
India. Pre- Conception & Pre – Natal Diagnostic Techniques (PCPNDT) act was enacted by Parliament of India in 1994 with the intent to prohibit prenatal diagnostic techniques for determination of sex of the foetus leading to female foeticide.
Government of Karnataka is strictly enforcing PCPNDT act by taking action against all erring
who are conducted sex determination and abortion and by stepping up the awareness regarding the worth of girl child.0-6 Child Sex Ratio (CSR)is 946 in 2001 Census & 948 2011 Census. In the report of Civil Registration System 2018, the Sex ratio at Birth is increased to 957.
Indicators of Sex Ratio:
Sources Sex Ratio Sex ratio at Birth (SRS-2019) 940 Sex Ratio at Birth (Civil Registration of Birth 2019)
947
Sex Ratio at Birth (NFHS-5) 978 Child Sex Ratio (Census 2011) 948
Activities: 1. All statutory committees under the act are constituted at State & District level. Under the
Chairmanship of District Commissioner who is also District Appropriate Authority, the District Inspection & Monitoring Committee shall inspect all the scanning centres every quarterly.
2. A total of 5268 scanning centres are registered of which 4991 are private scanning centres and 277 are government scanning centres.
3. Till date a total of 89 cases have been registered for violating PC & PNDT act, of which 56 cases are penalized for violation 33 cases are pending for judgement.
4. BALIKA software is developed for effective reporting of F-forms through which all the registered scanning centres must report.
5. Under PC & PNDT rules, 2014 to empower the Untrained Registered Medical Practitioners who conduct the scanning are given Competency Based Test and Education in collaboration with Department of Medical Education. A total of 198 doctors have successfully cleared the exams and issued certificates.
6. All machine manufactures, Dealers, refurbishes are registered under PC&PNDT State Cell and also, they submitting quarterly sales report.

68
7. Division wise PC&PNDT awareness workshop conducted to District Health & Family Welfare officers, District Family Welfare officers, Taluk Health Officers, District Advisory Committee Members, District Inspection and Monitoring Committee Members and PCPNDT case workers.
8. To create awareness among public, effective IEC is publicised through radio and video jingles. 9. Further to reinforce and strengthen the objectives of the act, Government of Karnataka is
conducting Decoy operations to expose the suspects indulging in offence of determining sex and awarding remuneration of Rs.50000 on success of each sting operation.
1.3. SCHOOL HEALTH PROGRAMME :
Rashtriya Bal Swasthya Karyakram:
School Health Programme has subsumed under Rashtriya Bal Swasthya Karyakram (RBSK). This programme commenced from the year of 2013-14, under this programme 0 to 18 years children are screened for 38 health conditions broadly classified under 4’D’s. The screening is conducted by 02 dedicated RBSK Mobile Health Teams constituted in each Taluka consisting of 2 Medical Officers, 1 Staff Nurse and 1 Ophthalmic Assistant/ Pharmacist, the main aim of this programme is to conduct health screening so as to identify children with health conditions and to refer for appropriate timely treatment. Rashtriya Bal Swasthya Karyakram (RBSK) is implemented in the State in all Rural and Urban areas children studying in 1st to 12th standard in Government, Government Aided, Government Residential Schools / Colleges and in Anganawadi Canters. Children in 0-18 years age group are screened annually and children found positive for various heart related condition, Neuro problems, Cleft Lip Palate and others are referred to hospitals empaneled under Suvarna Arogya Suraksha Trust (SAST) for cash less treatment. As per the guidelines, the DHOs are implementing this programme successfully in all taluks. The activities of Rashtriya Bal Swasthya Karyakram (RBSK) are as follows:
1. Screening of 0 to 6 weeks children through delivery points and ASHA – HBNC visits. 2. Screening of 6 months to 6 years children at Aganwadi Centres. 3. Screening of 6 to 18 years children (1stto 12thstd.) at Schools and Colleges. 4. Health screening to identify children with 38 Health Conditions, broad classified under 4’D’s
(Defects at birth, Developmental delays, Diseases and Deficiencies) under the age group 0 to 18 years.
5. Children requiring further management are referred to the nearest health facility. 6. Health Education to Anganwadi workers, Teachers and Students as well as students regarding
Personal Hygiene, Environmental Sanitation, Safe drinking water and use of latrines are being taught regularly. This programme is being implemented in Co-ordination with Department of Health and Family
Welfare, Women and Child Development, Public Instruction and PU Board.
Progress report for the period of 2021-22 (Apr-21 to Jan-22): Sl. No. Beneficiaries Annual
Target Achievement %
1 Health Screening of 0-18 years children (Anganwadi Centres, Schools & Colleges)
1,45,48,039 1,08,69,883 74.71

69
Weekly Iron & Folic Acid Supplementation Program (WIFS) : Introduction:
Anemia not only in women and children but also it is more commonly seen in adolescents, with the main reason of poor nutritional food and now this is a routine health problem. There is an increase in prevalence of persons suffering from Iron deficiency Anemia, which is an as an alarming call for public health. More than 55% of adolescents are suffering from Anemia, the numbers are more in Girls than the Boys, the reason being the speedy growth and increased blood flow during the menstruation.
The girls aged between 10-19 years are more vulnerable for Anemia as this is the period of
getting mature and starting of menstruation, the development will be hampered due to lack of nutrition and mainly due to poor iron supplementation.
To address this the department of health & Family Welfare , initiated the National WIFS
program , where in weekly based Iron-Folic Acid supplementation tablets (Pink & Blue) will be distributed to children aged 5 to 19 years and Bi annual De-worming the children aged from 1-19 years , through administering the Tablet-Albendazole at School and Anganwadi centres.
Objective- To reduce the prevalence and severity of nutritional anaemia in children’s.
Target (Beneficiaries):
Students studying in 1st to 5th standard and 6th to 10th standard for all Government and Government Aided School Children. Strategies:
Weekly once IFA tablets (WIFS) :
- Each IFA – Pink tablet contains 45 mg of Iron with 400 mcg Folic Acid, it is given to children of 5 to 10 years age group weekly once for 52 weeks.
- Each IFA – Blue tablet contains 60 mg of Iron with 500 mcg Folic Acid, it is given to children of 11 to 19 years age group weekly once for 52 weeks.
Total No of beneficiaries: • IFA-Pink- 28,62,843 • IFA-Blue- 33,38,541
Biannual De-worming (Albendazole 400 mg), six months apart, for control of helminthes
infestation.
Information and counselling for improving dietary intake and for taking actions for prevention of intestinal worm infestation.
Albendazole tablets given to adolescents under National Deworming Day (NDD) Program – 2021-22:
Target Achievement %
WIFS-IFA (Pink) & (Blue) Tab. 62,01,384 51,38,667 82.86
NDD – Albendazole Tab. 2,03,17,943 1,64,96,630 81.19

70
“SHUCHI” Yojane:
There is a need to maintain good hygiene during menstruation in women and adolescent girls. It is observed that the adolescent girls remain absent to school due to infections occurred due to
unhygienic practices in menstrual management, also it keeps them away from their routine economic / family activities. On this ground to eradicate the myths and misconceptions on menstruation through various awareness generation programs on hygiene and utilizing sanitary napkin pads, it is observed the need to adopt the scheme adolescent girls towards improving their health and school attendance.
In general most of the women, due to lack of knowledge, non-priority and sometimes due to
financial problem, use old/ torn cloths available in home to manage menstruation. The same cloth may be reused by other family members with ought proper washing and drying it under the sunlight. This may lead to local skin infections and spreads within the family.
Keeping in mind the above issues, the Government of Karnataka has started the Shuchi-Yojane
in FY 2013-14, for distribution of free sanitary napkin pads to all Adolescents in the state. Monthly one unit of Sanitary napkin packet will be distributed freely to each adolescent. Objectives:
1. To bring awareness on menstruation in adolescent. 2. To educate adolescent girls on practice and benefits of sanitary pads. 3. To change the view on menstrual hygiene in community and Adolescents. 4. To promote the usage through free distribution of Sanitary napkins.
Beneficiaries:
1. Students from 6th to 12th class(10-18 years), registered in all Government, Aided and Residential schools
2. Adolescent girls in hostels from the Department of Social Welfare and Minority Welfare Department.
Current Status: • Procurement of Sanitary Napkin Pads for FY 2021-22, is under progress.

71
1.4 ASHA PROGRAMME:
1 Introduction:
Accredited Social Health Activist (ASHA), are working in a voluntary spirit. The primary
responsibility of the ASHA is to encourage the community for access the services in Public Health
system and also generate the awareness to community on various health schemes. It is launched under
National Health Mission in 2005.
1. Objectives:
To bring the considerable changes in Public health system and effective health service delivery to vulnerable and marginalised community in Rural and Urban area.
2. Goals : 1. Awareness about Nutrition related issues.
2. Reduce IMR & MMR through counselling, community level management, early detection
and referrals.
3. Community oriented services at the doorstep of people through creating awareness of health
program and schemes to people in community.
3. Implementation :
It is implemented through Health Sub center, Primary Health Center, Urban Primary
Health center and Community Health Center for providing the Information on health services.
Monitoring of this programme at Public Health institutions level, One ASHA Facilitator is
identified, in Taluk and District Level, ASHA Mentors have been recruited, These are working
under District RCH Officer and Taluk Health officer.
4. Physical and Financial Achievement:
Year Physical Finance (In Lakhs) Target Achievement Target Achievement
2019-20 42524 41752 20380 19813.00 2020-21 42524 41785 20412 16636.00 2021-22 4524 41542 21686.52 15983.98
5. Outcome of the programme:
1. Promotion of Institutional deliveries. 2. Reduction in MMR 3. Reduction IMR 4. Family Planning implementation and spacing.

72
1.5 HEALTH SERVICES: Urban Health Services:
The District Hospitals under Health & Family Welfare Department provide curative, referral, counselling and 24x7 emergency delivery services along with preventive, promotive and rehabilitative services. Other Major Hospitals and Teaching Hospitals provide Secondary level Services. The details of Hospitals are as follows:
Hospitals No. of Institutions No. of Beds
District Hospitals 16 6095
Other Hospitals under HFW 11 2218
Teaching & Autonomous Hospitals (including Medical Education) 36 18715
1.6 NATIONAL URBAN HEALTH MISSION:
Preamble:
1. National Urban Health Mission was launched on May 1 2013 as a sub-mission of the National Health Mission (NHM) to strengthen the primary health care system in cities & towns to provide essential primary health services to the entire urban population and Special focus on People living in listed unlisted slums and other low income neighbourhoods All other vulnerable population such as homeless rag-pickers street children rickshaw pullers and other temporary migrants.
2. It aims to improve the health status of the urban poor particularly the slum dwellers and other staged sections by facilitating equitable access to quality health care through a revamped public health system partnerships and with the active involvement of the urban local bodies.
3. Considered all districts and state headquarters and towns and cities with more than 50000
populations are incorporated and implemented in all 80 cities and towns of Karnataka as per the Government of India guidelines. Totally 365 Urban Primary Health Centres (UPHCs) out of which 205 UPHCs are in Non-Metro and 160 UPHCs (Including 27 Maternity Hospital) are in Metro city which comes under urban development department. All the 365 Urban Primary Health Centers (UPHC) 9 Urban Community Health Centres (UCHC)/Referral Hospital 8 Mobile Medical Units (MMUs) 34 Health KIOSKs and 2 Transit clinics are implemented in urban area with inter-sectoral coordination with urban development and Municipalities.
4. The NUHM activities are implemented in Metro city through BCH&FWS constituted
during 2014-15 but made more functional from 2016-17 onwards. The BBMP has 198 wards which includes the 135 wards of erstwhile BBM and 63 wards coming under Bengaluru District Health & Family Welfare Officer in so far as provision of health services are concerned. The NUHM implementations in all the 198 wards were brought functionally under the unified command of BCH & FWS headed by the Commissioner BBMP.

73
5. As a community activity special outreach camps will be conducted by Auxiliary Nurse
Midwives (ANM) to ensure health care delivery at the door-step. Community participation will be facilitated by the Mahila Arogya Samithi (MAS) which will act as a bridge between the communities and the nearest health facility.
6. The Urban ASHAs will play the role of provider of first contact care and also generate
community awareness with regards to various health issues sanitation and nutrition. Special care will be taken to ensure that MAS would be constituted by drawing representation of people from local population by ensuring adequate representations to the SC ST and other minorities.
Introduction:
1. National Urban Health Mission (NUHM) aims to improve the health status of the urban poor particularly the slum dwellers and other disadvantaged sections by facilitating equitable access to quality health care through a revamped public health system partnerships and with the active involvement of the urban local bodies.
2. The main focus of the NUHM will be urban poor population living in listed and unlisted slums all other vulnerable populations such as homeless rag-pickers street children rickshaw pullers construction brick lime kiln workers commercial sex workers and others.
3. NUHM will cover all the District headquarters and other cities/towns with a population of 50000 and above (as per census 2011) in a phased manner. Cities and towns with population below 50000 will be covered under NRHM.
4. As per 2011 census 236.25 lakh people reside in urban areas and the urban slum population is 38.61 lakhs in Karnataka state. The challenge is that the state has 38.67% of population living in urban areas as against the National Average of 31.57%.
5. Under NUHM the emphasis will be to improve existing public health delivery system with a thrust on making available adequate health human resources upgrading the existing health facilities in terms of infrastructure and equipment and also establishing new health facilities wherever necessary by providing specialist care as well as strengthening emergency response systems. This will enable the Health and Family Welfare Department or City Municipalities/Corporations to effectively provide adequate primary health care to the urban poor focus on promotive, preventive and curative aspects of both communicable and non-communicable diseases domestic violence on women and strengthen trauma care and emergency care to the urban poor.
6. The strategy will comprise of strengthening the existing primary health care centres establishing new primary health care centres wherever appropriately needed. Further special outreach camps will be conducted by ANMs and ASHAs to ensure health care delivery at the door-step. Community participation will be facilitated by the Mahila Arogya Samithis (MAS) which will act as a bridge between the communities and the nearest health facility. The ASHAs will play the role of provider of first contact care and also generate community awareness with regard to various health issues sanitation and nutrition.

74
7. It is generally felt that there is non-availability of reliable data on health status of people
living in urban areas. A comprehensive baseline survey and mapping is being undertaken to gain insight into the dynamics of health needs of existing listed and unlisted slum pockets urban poor concentration areas and other vulnerable population. This will help in assessing their health seeking behavior health indicators such as morbidity and mortality patterns ongoing health needs and existing provisions for health care and out of pocket expenses etc.
8. An amount of Rs 5081.05 Lakhs is provided during 2013-14 of which State share is Rs 1270.00 Lakhs and Central share is 3811.00 Lakhs. Sanction has been accorded by the Government for implementation Of National Urban Health Mission in 135 wards of BBMP 63 wards of Bangalore Urban Mysore Bagalkote Mangalore and Ullal of Dakshina Kannada. Total number of cities taken up for implementation of NUHM in 2014-15 were 25 of which 5 are part of 2013-14 and 18 are new cities. The amount approved was Rs. 86.24 Crores of which GOI share was Rs. 64.68 Crores and GOK share was Rs. 21.56.Crores.The 18 new cities are Belagavi, Bellary, Bidar, Vijayapura, Chikkaballapur, Davangere, Hubli-Dharwad, Gadag, Kolar ,Kalaburagi ,Sedum ,Gangavathi , Raichur, Udupi, Yadgir, Dandeli Puttur and Bantwal. In 2015-16 total budget approved is Rs. 104.21 Crores.
9. During the financial year 2016-17 54 cities /Towns have been added to the list with a total amount of Rs 131 crores with a Centre state sharing pattern of 60:40.
10. In the financial year 2017-18 2 cities have been added to the list 11. In the state of Karnataka for FY 2019-20 National Urban Health Mission is implemented in
79 cities.
12. In the financial year 2020-21 1 more city name shikaripura has been added to the list. 13. In the state of Karnataka for FY 2020-21 National Urban health Mission is implemented in
80 cities.
Demographic Glance (based on 2011 census)
1 Total Population (In lakhs) 610.95
2 Urban Population (In lakhs) 236.25
3 Urban Population as percentage of total population 38.67
4 Urban slum population (in lakhs) 32.91
5 Slum population as percentage of urban population 13.95
6 Number of Metro cities 1
7 Number of Million + cities (> 10 lakh population) 0
8 Number of cities with 1 to 10 lakh population 25
9 Number of towns with less than 1 lakh but more than 50000 population
53
10 Number of State HQs/Dist. HQs which have less than 50000 population but are covered under NUHM
1

75
Human Resource:
To improve existing public health delivery system with a thrust on making available
adequate health human resources upgrading the existing health facilities in terms of
infrastructure and equipment and also establishing new health facilities wherever necessary by
providing specialist care as well as strengthening emergency response systems.
Designation FY 2021-22
RoP Approved In position Vacant
ANM 1264 1081 183
LHV 43 28 15 Staff Nurse 595 554 41 Lab technician 316 311 05 Pharmacist 323 286 37 X-ray and Mammogram Technician 6 + 1 6+1 0 OT Assistant 8 8 0 Medical officer Full time 187 168 19 Medical officer Part time 338 185 53 Specialist 45 38 7 Lower Division Clerk / DEO cum Accountant
237 236 1
Group-D 307 307 0
Jr Health assistant (New position) 629 304 325
Infrastructure:
One urban primary health centre (UPHC) may be planned for every 50-60 thousand
population under NUHM. In case there is an existing Urban Family Welfare Centre Urban RCH
Centre Urban Health Centre Urban Health Post etc. the same may be upgraded and strengthened
as UPHC. Where none exists new UPHCs will have to be planned and the Dist. Health Society
will initiate the process of identification of location/ land. NUHM will provide both capital and
recurrent cost for up gradation and maintenance of the UPHCs as per the norms. The Dist.
Health Society can also hire premises for new UPHCs where land is not available.

76
Financial Progress from 1st April 2021 to 31st January, 2022(Provisional)
Physical Number
Total Budget
allocated Expenditure
(Rs in lakhs))
1.Medical Officers 525 2217.77 925
2.Paramedics: (ANM, SN, LT, Pharmacists, Male Health worker X-ray technician and OT assistant)
3185 5133.56 2742.28
3.Support Staff (LDC+ Group D) 544 642.29 478.02 4.Urban ASHAs 3329 798.96 693.95 5.MAS 4071 203.55 6.4
6.Untied Grants to UPHCs 365 296.50 204.63
7.Untied Grants to UCHC 9 45.00 32
1.7 NATIONAL PROGRAMME FOR PREVENTION AND CONTROL O F FLUOROSIS (NPPCF):
Fluorosis, a public health problem is caused by excess intake of fluoride through drinking water/food products/industrial emission over a long period. It results in major health disorders like dental fluorosis, skeletal fluorosis and non-skeletal fluorosis.
As a first step towards mitigation of Fluorosis in the State, all 19 endemic districts PHCs and Sub Centers have been stratified based on the incidence of fluorosis by consumption of water which is more than 1.5 PPM fluoride content. It has been categorized into strata wise accordingly. To achieve the set goals of mitigation of fluorosis in the state well before the year of 2030, the state has brought out a strategic frame work for micro level implementation of activities in villages as per the API classifications.
The programme aims to achieve the set objectives with the following activities.
Physical progress report of NPPCF Programme for the FY 2021-22 (up to Jan 2022)
Laboratory Activity
Total No. of Water samples test done for Fluorosis 9317 Total No. of Water samples found above 1.5 PPM 2856 Total No. of Urine samples test done for Fluorosis 13814 Total no. of Urine samples found above the limit (1.0 PPM) 9568 Survey Activity (Community and School Survey) Total persons Surveyed for Fluorosis 54888 Total school surveyed 865 No. of cases with suspected dental fluorosis 9495 No. of cases with suspected skeletal fluorosis 3812

77
IEC Activities No. of Digital Wall Painting 70 No. of Street Play 67 No. of Poster 19297 No. of Radio / Audio Jingle 761 No. of Flex / Hoarding 20 No. of Paper Advertisement 24 No. of Standees 273 Medical Management of Fluorosis No. of persons provided with vitamin-C and calcium supplementation 4397 No. of beneficiaries provided with mobility aids 969 Other Provisions for Medical Management 33
Financial progress report of NPPCF Programme for the FY 2021-22 (up to Jan-22)
Budget Approved (Rs. In Lakhs)
Expenditure (Rs. In Lakhs)
Percentage
318.61 155.32 48.75%
1.8 CITIZEN FRIENDLY FACILITIES: Citizen Help Desk:
It is a novel scheme implemented in District Hospitals and Major Hospitals. The objective of the Scheme is to guide and help the patients to get proper and timely need care. There are redactors in patients waiting time and the patient grievances are reduced at the local level. So far, 50 Citizen Help Desk is serving the patients round the clock in order to reach health services.
Dialysis Programme: Dialysis centres were functioning in 57 centres as on March 2017. The list of centres included
• 20 District Hospitals • 3 Major Hospitals • 34 Taluk Hospitals
In the Budget speech for FY 2017-18, Honourable Chief Minister announced setting up Dialysis centres at all Taluk Hospitals under PPP mode with fund support from NHM.
Accordingly, Under PPP mode, Out of 171 centres proposed, 167 centres have been established for providing dialysis services as on date.
Physical Progress:
2016-17 2017-18 2018-19 2019-20 2020-21 2021-22 Total Dialysis centers
57 119 163 167 167 167
No. of Dialysis machines
252 394 543 588 588 594
Total no. of Dialysis cycles
81,422 1,37,111 3,08,347 4,28,973 3,92,311 3,19,663

78
Telemedicine:
Telemedicine facility was started in association with ISRO since 2004. In the First phase they were started in District hospital Chamarajanagar, Mandya, Tumkur, Chitradurga, Shimoga, Karwara, Chikmagalur, Gadag and Taulk hospitals at Maddur, Sagara and Yadgir.Hub centers (Centres from whom expert advice is given) identified are - Jayadeva Institute of Cardiology , ST. John’s Medical college Hospital, Narayana Hrudayalaya, NIMHANS at Bangalore and JSS Hospital at Myosre.During 2008-09 in 2nd Phase Telemedicine centres were started at District hospitals- Kolar, Madikeri, Belgaum, Bellary, Dharwad, Davangere, Gulbarga, Udupi, Bijapura & GH Lingasagur, Raichur District. Hub centres at Bowring and Lady Curzon hospital, Indira Gandhi child health Institute, Institute of Nephro & Urology centre. ISRO was unable to continue V-SAT Connectivity due failure of V-Sat in September 2010. Later onward functioning through Broad band connectivity.department connectivity established to all the centres along with new centers, they are Wenlock Hospital Mangalore, District hospital Koppal, Haveri & General Hospital Hospete. New hub centres are Kidwai Institute of Oncology, Karnataka Diabetic centre and K.R. hospital, Mysore. 49,704 patients were given expert advice through telemedicine during 2015-16.
In 2013-14 through Keonics with the help of KSWAN connectivity from e-govrnance department connectivity established to all the centres along with new centers, they are Wenlock Hospital Mangalore, District hospital Koppal, Haveri & General Hospital Hospete. New hub centres are Kidwai Institute of Oncology, Karnataka Diabetic centre and K R hospital, Mysore.
Telemedicine at Taluk Hospitals :
1. Introduction
Rural population can avail the specialist opinion at door step through electronic devices is called as Telemedicine. Telemedicine Services implemented in all the districts. We have established 39 hub centres, General physician, Gynaecologist, Paediatrician and other Specialist working in shift basis. Total 3152 Health and wellness centres – HWCs are providing Teleconsultation services in the state.
2. Purpose :To provide quality health care services & provide specialist services.
3. Benefits :
a) Rural population can consult the specialist from home though android smart mobile n directly call doctor and can get specialist consultation or
b) Patient can visit nearer health & wellness centre / Primary health centre with the help of MLHP / health workers and upload the patient records to hub centre and consult specialist doctors opinion and get e-prescription.
c) MBBS Doctors those who are Primary health care centre / community health care centres if they required specialist opinion they can transfer all medical records to district hospital/ Government Medical college and consult the specialist opinion and get the e-prescription.
d) Specialist services are available timely to the patient without any cost 4. Target : We have given target of minimum 2 Tele consultation per day to health
workers/ MLHPs those patients who required specialist opinion they can consult
specialist through Telemedicine.

79
1.9 REGULATION OF PRIVATE MEDICAL ESTABLISHMENTS:
On 13-8-2007 Karnataka Private Medical Establishment Act got approval from Honourable Governor, Government of Karnataka. The Karnataka Private Medical Establishment Act, 2007 and Karnataka Private Medical Establishments Rules, 2009 are in force. This legislative aim to regulate, control and monitor Private Medical Establishments in Karnataka for providing quality care according to medical ethics by prescribing service quality.
Karnataka, Private Medical Establishments amendment 2017, got approval from Honourable Governor, Government of Karnataka on 04-01-2018, and 06-01-2018 the amendment was officially notified.
Registration and Grievance Redressal Authority:
There shall be a registration and grievance redressal authority in each district consisting of the following members nominated in such manner with such qualification as may be prescribed, namely:
1. The Deputy Commissioner of the district. – Chairman 2. District Health and Family Welfare Officer -- Member Secretary 3. District Ayush officer- Member 4. One member each from Indian medical association and one more association- Members 5. One woman representative when the authority is dealing with a grievance redressal- Member Where upto January 2022 applications for registration of Private medical establishments were
scrutinized and 29616 institutions are issued registration certificates.
1.10. HEALTH EDUCATION AND TRAINING: The Health Education and Training Section of this Directorate is organized below programmes mainly responsible for:
1. Arrangements of Medical team and Ambulances to VIP and VVIP’s. visiting to Karnataka. 2. Deputation of Departmental A& B group Officers and Officials different for Trainings at
Administration Training Institute Mysore. Fiscal Policy Institute, Kengeri, Bangalore. 3. Deputation of In-Service Doctor for 12 Months PGDPHM Course at Public Health Management
at Indian Institutes of Public Health, Leprosy Hospital, Magadi road, Bangalore. 4. Signature of part-iv confidential reports of Belgaum Division Doctors. 5. Celebration of State level Doctor’s day programme on July 1st Bengaluru at Directors Office. 6. Submission of Nomination received from elected bodies for Arogya Raksha Samithi to
Government. 7. Submission of Nomination received online, from Candidates to work Haj as Medical Personnel,
to Government. 8. Submission of list of Doctors who are eligible to issue Compulsory Health Certificates to
Amarnath Yathries , to Government 9. Submission of Nominations of Departmental of Staffs for various Awards like Sarvothama
Award and Florence Nightingale Award to Government. 1.11. MENTAL HEALTH PROGRAMME:
District Mental Health Programme (DMHP) is implemented in all the 30 districts and BBMP in Karnataka, Also taken up in 10 Taluka under Taluka Mental Health Program (TMHP).
Trainings have been taken up in all the 30 districts and BBMP:
Persons trained 2017-18 2018-19 2019-20 2020-21 2021-22
(Till January)
Medical Officers 1,673 1,616 1,481 1,702 1,321
Paramedical workers 9,375 4,734 2,862 3,788 3,571

80
RBSK/RKSK 658 490 804 988 548 AYUSH 873 475 655 854 578 Teachers (Schools, Colleges & Anganwadi)
9,379 7,590 8,553 16,180 12,098
Students (Schools & Colleges)
5,013 8,532
KSAPS, WCD & counselors
1,648 3030 1,550 1,936 2,778
Police/Prisons staff 1,473 6,671 6,902 6,236 6,749 Faith Healers/NGOs/ Elected representatives
1,380 818 2351 1,027 907
ASHA workers 23,775 21,816 24,316 18,294 18,373 VRW, MRW - 2,214 8,553 2,095 1,956 Agri, Horticulture staff 1,257 938 ANM , Health Assistants , Community Health Workers
6,426 4487
PLD Bank Staff 233 506 RNTCP , NCD , DDWO, NTCP , Panchayath Raj Officials & Volunteers
2,256 1,749
Total 50,234 47,240 58,027 68,285 65,091
Clinical Services of District Mental Health Programme
Clinical Service 2017-18 2018-19 2019-20 2020-21 2021-22
(Till January)
Outreach camps no. 1,711 884 1192 644 1167
Home visits no. 3,688 6067 5,426 2,495 1416
Outreach - patients reached 19,242 29,997 38,957 21,503 16208
Home visits - patients reached
6,269 5,642 5,061 6,468 1610
No of Beneficiaries
Counseling Centers 2017-18 2018-19 2019-20 2020-21 2021-22(Till
January) Counseling Service in
Colleges 17,433 28,118 48,779 7,349 10961
Counseling Service in workplaces
7,480 8,533 16,952 11,059 4881
Counseling Service in Urban slums
5,775 8,555 13,187 4,757 3298
Total 30,688 45,206 78,918 23,165 19140

81
No. of Consultations under DMHP Karnataka
DMHP Expenditure Percentage

82
IEC activities
Year Camps conducted
Patients catered.
Awareness Programmes Conducted
No. of participants
World schizophrenia Day Celebration 24th May 2019 174 3464 288 19802
World Mental Health Day 10th October 2016 459 56368 2017 155 2479 1461 47543 2018 301 7022 2440 71083 2019 224 4985 613 50751 2020 518 2021 667 20312
International Day Against Drug Abuse and Illicit Trafficking observation 26th June 2016 107 7267 2017 585 61426 2018 243 3857 618 79903 2019 172 2531 404 28833 2020 438 2021 629
Suicide Prevention Day 10th September 2016 459 56368 2017 155 2479 1461 47543 2018 301 7022 2440 71083 2019 286 3695 502 30007 2020 509 2021 1022 18312
Community Mental Health Day care center Programme (Manasadhara):
Community Mental Health Day care center Programme, funded by the state. One for each District.Day Care Centre/Rehabilitation centre for the recovered mentally ill persons by recognized NGO’s, are functional in 10 districts (Bangalore Rural, Udupi, Tumkur, Dharwad, Gadag, Mandya, Haveri, Mysore, Kolar and Belagavi). Efforts are continued to start these centres in all the districts.
Tele- counselling- Mental Health support during Covid-19 As on 14th February 2022, 27,24,780 telephonic consultation sessions have been made across the
state, services has been extended to 88,847 migrants, 8,736 doctors and 25,410 health workers also.
“Manochaitanya” : (Super Tuesday clinic) Programme is a unique initiative of Govt. of Karnataka. Under
this programme, on selected Tuesdays Psychiatrist from DMHP/DH/Medical college/Private, provide specialist Services to the mentally ill at the Taluka level hospitals.
In the year 2021-22 this programme is functional in all Taluks of the State and have catered to the needs of 2,56,332 (till Jan 2022) patients.

83
Progress Report of Karnataka State Mental Health Authority: Government of Karnataka has released funds for Karnataka State Mental Health Authority to implement provisions of the Mental Health Care Act 2017.
1. Mental Health Care Act 2017 is being implemented for providing care and treatment for mentally ill persons and to protect rights of persons with mental illness.
2. Government has established Karnataka State Mental Health Authority with Additional Chief Secretary / Principal Secretary to Government, Health and Family Welfare Department, as the Chairman of the Authority.
3. Commissioner, Health and Family Welfare Services, is appointed as the Chef Executive Officer.
4. The Official Members and Non Official Members are selected. 5. Mass media Programme in Radio to create awareness of general public and reduce the stigma
towards Mental illness. 6. Karnataka State Mental Health Rules has been approved by Government of India, will be
notified soon Karnataka INNOVATIONS in MENTAL Health
I. Artificial intelligence & Data analytics to enhance mental health care services n Karnataka
1. AI and Data Sciences, including computational techniques such as Machine Learning, Deep Learning, Natural Language Processing, image and video analysis, speech recognition, etc., have the potential to significantly improve delivery of mental health care. Significant research focus worldwide with promising outcomes, though at early stages
2. A project in Karnataka under NHM has been initiated to employ AI techniques to analyze data from the DMHP program and health services such as Arogyavani-104.
3. The goal is to identify temporal and geo-spatial patterns in treatment seeking across districts and talukas, correlations between awareness/training efforts as part of the DMHP program and outcomes in terms of increased patient visits for mental health treatment.
4. This can help to fine-tune policies and actions plan at program, district and taluk level towards improving the efficacy of the DMHP program. For example - identifying taluks and districts requiring support on their efforts, those requiring attention for increasing the efforts, optimizing utilization of funds, planning drug availability, etc.

84
Proposed approach for data analytics and visualization
e-Manas II. Karnataka Mental Healthcare Management System (KMHMS)
Since 2018-2019 more than 10 lakh persons are seeking mental healthcare consultation across
different public health institutions in Karnataka. To be compliant with the Mental Health Care Act, 2017
and Rules (2018), Karnataka Mental Healthcare Management Systems or e-Manas has been developed
as an online platform for comprehensive mental health services. Karnataka e-Manas is an initiative of
NHM GOK in collaboration with NIMHANS and IIIT-B. Probably first in the country.
The goals are to do away with manual registers with public authorities, health institutions and
functionaries, simplify data entry (only once at the time of service delivery),
This web solution brings all the stakeholders in mental health in Karnataka together: Karnataka
State Mental Health Authority, Karnataka State Mental Health Review Board, all public and private
Mental Health Care Establishments, Mental Health Professionals (psychiatrists, psychologists, social
workers, mental health nurses), persons with mental illness and their caregivers.
1. The software supports maintenance of a Karnataka state-wide registry of all facilities and all
persons providing mental health care.
2. The application for the registration of mental health establishment and procurement of
provisional certificate will be fully online.
3. Basic Medical Records (BMR) of the patient (both in-patient and out-patient records) would be
accessible to a treating professional anywhere across the state. Thus patients need not carry paper
copy of the document. Thus, this web-based platform aims to provide seamless care anywhere in
Karnataka.
4. The web platform also incorporates the processes related to patient’s Advance Directive (AD)
and Nominated Representative (NR).
5. Through the portal a patient / care-giver can raise their grievances online to be addressed by
respective District Mental Health Review Board.

85
6. The portal is linked with assurance schemes like Ayushman Bharat-Arogya Karnataka and is
being integrated with Arogya Sahayavani 104 and 108 ambulance services.
7. The software is scalable for deployment at national level.
8. The different modules under the e-Manas platform are
a. Registration of Mental Health Establishments (MHE)
b. Registration of Mental Health Professionals (MHP)
c. Out-Patient / In-Patient Module: Maintenance of outpatients and inpatients Basic Medical
Records of the person seeking mental health care across both public and private mental health
facilities and integrated with ABArK, 108 and 104 services
d. Enlisting Outpatient Clinics
e. Patient Portal/ Registering Grievances
f. Registering Advance Directive (AD) and Nominated Representative (NR)
g. Mental Health Authority Portal / MHA Dashboard / MHRB Dashboard.
III. KSHEMA- Karnataka State Holistic Empowering-programme for Mental Aliments • KSHEMA - An innovative community based rehabilitation program in Karnataka.
• People recovering from severe mental Disorders (SMD) require more than just medications - empowering them to achieve their life goals, which have been hit by mental illness should be part of their holistic treatment. Unfortunately, services beyond mere provision of medications are scanty and are confined to very few academic institutes and expensive private settings.
• Community-based rehabilitation (CBR) envisages use of available resources to provide such services in the place where persons with mental illness normally live. Both Mental Health Care Act and Rights of Persons with Disabilities Act mandate such services. However, there are no replicable models of CBR in the country.
• Karnataka has always pioneered the care of persons with mental illness. In a first, the state has recruited social workers at 10 Taluks. Each social worker would have to provide rehabilitation services for about 300 persons with SMDs. This is eminently doable.
• KSHEMA is a 3-year project that intends to implement and evaluate CBR in 10 taluks of Karnataka. It is a sustainable model, since we would be using the available resources. This project has potential to be a model, which other parts of the state and the country may emulate.
• Under this project, all patients with SMDs would be offered comprehensive rehabilitation addressing their needs in the domains of health, education, livelihood, social relationships and empowerment. Use of tele technology to train the grass root level staff and to monitor the progress of each individual with mental illness are in-built innovations in this project. Already about 700 beneficiaries are being offered services at different levels.
4. An e-initiative for Monitoring District Mental Health Program in Karnataka: Helps to track the objectives and goals of the program. Recognizing the need for good quality data which is regular, a web based Mental Health Program Management Information System (MHP-MIS) has been initiated across the 31 DMHPs in Karnataka since December 2016 and has been fully functional with effect from April 2017.

86
5. Care at Door-Step (CAD): Generally, about 30–50% of Severe Mentally ill patients seeking care, drop out after registering under DMHP.
It is critical that patients with severe mental illnesses do not miss treatment and take the treatment for the longer period of time; Studies have shown that the functioning, disability levels and symptoms improve consistently if treatment adherence is maintained. Till date, many registered cases have been brought back under the CADs treatment umbrella. The program is being expanded across the state.
6. Tele-mentoring: Adopting the technology, Tele-On Consultation Training (OCT) is being offered to PHC medical officers. The PHC medical officers, while seeing their general patient pool, are offered guidance and training to identify and treat psychiatric disorders.
Brief summary of KTM program till date
1.12 INFORMATION EDUCATION COMMUNICATION (IEC) :
IEC activities are being implemented to create awareness in the communities on various service facilities being provided at various levels under National Health programmes. Activities are planned for both at state and district sectors.
1. Printing & distribution of education materials like Posters, Folders, Flipbook, Handbills, wall
calendar, site-signage, sun-board & Printing & fixing of flex on existing hoardings at the District level & distribution to peripheral health institutions on National Health programme
2. Publicity done through bus branding on KSRTC / NWKRTC / NEKRTC / BMTC buses & display of health messages on bus shelters & bus tickets.
3. Health information disseminated through LED TVs in Railway bogies & Railway stations. Installation of Standees & display of health messages on various National Health Programmes & Schemes at Metro Stations.
4. Dissemination of Health & FW services messages through Social media like Facebook, Twitter, whatsapp, LinkedIn, etc
5. Panel discussion on various Health programme in Doordarshan by subject experts & Telecast of TV spots & scrolling messages in local city cable Network.
6. Broadcasting and conducting of interviews, Radio jingles and phone in programme in Akashvani & Private FM radio on various Health Programme.
7. Press advertisement was given on National Health Events / Days in State, Regional, District & taluka level newspapers.
1. Total of DMHP psychiatrist / TMHP psychiatrist enrolled for TOT training 36
2. No of DMHP psychiatrist / TMHP psychiatrist completed TOT training 28
3. Total number of TOT training hours 556 hours
4. Total number of PCD enrolled for Tele-OCT
i. Total number of doctors received at least one session of training: 435 ii. Total number of doctors received minimum of two sessions: 320 iii. Total number of doctors received three sessions : 208
435
5. Total number of KTM training hours 994 hours
6. Total number of CVC 27
7. Total number of patients catered 4449

87
8. Press conferences / Press meets by Hon’ble Health Minister & Hon’ble Principal Secretary on National Health Events.
9. Telecast of spots in selected cinema theatres. 10. Conducted major & mini exhibitions and tablo on special occasions like Dasara, Kannada
Rajyotsava & Jatras. 11. Conducted awareness on Health programmes and schemes in hilly and remote area villages,
thandas & hadi’s through different folk forms. 12. Essay competition, Speaking competition, Debate Competition & Quiz competition to school &
college students. 13. Sensitization programme for NGO’s, Stree Sakthi Members, Religious Leaders & Elected
Panchyat Members. 14. Created awareness among mothers department is conducting Mothers Meeting, Healthy baby
shows & Nutrition Food Demonstration Programmes. 15. Conducted VHND & VHNC meetings every month across the state. 16. 104 calls ringtone is adopted on corona virus awareness messages. 17. Panel boards are used in all Airports to create awareness with specific messages. 18. BBMP and other major city corporations are creating awareness through audio jingles in
garbage collection vans/autos in all localities. 19. LED vans are used to create awareness in rural areas and videos spots displayed to create
awareness.
1.13 STATE HEALTH TRANSPORT ORGANISATION :
State Health Transport Organization is working under Health and Family Welfare Department to implement all the National Health Programmes effectively. State Health Transport Organization is headed by the Chief Transport Officer at the State Level.
The Department has total fleet strength of 1760 vehicles. These vehicles are allotted in the health institutions like Primary Health Centres, Community Health Centres, Taluk Level General Hospitals, District hospitals and District Health and Family Welfare Offices.
Different types of vehicles including ambulances are being used to implement the National Programmes and Medical Emergency to shift patients to the higher level hospitals. After formation of Zilla Panchayat the vehicles working in the respective districts, are being maintained by the DHO’s under the administrative control of the corresponding Zilla Panchayat.
Fleet strength for the Year 2021-22 is as below as on January 2022
1 Vehicles allotted to the Programme implementing officers 805
2 Ambulance vehicles allotted for Emergency services 955
Total 1760
1.14. INTEGRATED DISEASE SURVEILLANCE PROJECT (IDSP):
The Integrated Disease Surveillance Project was launched in 2005 and became programme in the year 2012. The general objectives of the program aims at establishing a decentralized state based system of surveillance for communicable diseases so that timely and effective public health actions can be initiated in response to health challenges in the country at the state and national level.
To improve the efficiency of the existing surveillance activities of disease control programs and facilitate sharing of relevant information with health administration community and other stakeholders so as to detect disease trends over time and evaluate control strategies.

88
The Specific Objectives of Integrated Disease Surveillance Programme are:
1. To integrate and decentralize surveillance activities. 2. To establish systems for data collection reporting analysis and feedback using Information
Technology. 3. To strengthen laboratory support for disease surveillance and laboratory confirmation of
outbreak. 4. To develop human resources for disease surveillance and action; To involve all stakeholders
including private sector and communities in surveillance activities. Integrated Health Information Platform (IHIP) IHIP is near-real-time. Web-enabled electronic health information system intended to capture village-level case-based disease surveillance data under IDSP. WHO Country Office India has designed and developed Integrated Health Information Platform (IHIP) with IDSP. The IT Platform shall also enable greater collaboration with other existing disease surveillance program and sectors with support from WHOM in future. All types of surveillance standards data standards and IT standards are incorporated In IHIP. Along with the 6 other Sates IHIP was launched on 26th November 2018 Secretary Health MoHFW, GoI in the Karnataka State. The reporting for “S” “L” and “P” Forms under the IHIP is 42%, 81% and 75% respectively for the month of November, 2021. Existing System (IDSP):
1. Reporting: Weekly reporting of Syndromic (S) Presumptive (P) and Confirmed (L) cases of communicable diseases from Public and P & L reporting from Private health care facilities throughout the state.
2. Data Analysis and Feedback: Analysis of the weekly ‘S’ ‘P’ and ‘L’ reports at State and
Districts Surveillance unit as vigilance against identifying impending outbreaks . Weekly feedback by higher institutions to the peripheral reporting units/health staff to initiate proper containment measures.
3. Network of Laboratories: 20 District Public Health Laboratories at the district level are
strengthened by providing Laboratory Equipments, Reagents, kits, consumables, contingency and Manpower – Microbiologist, Laboratory Technician, Laboratory Assistant and Laboratory attendant for sentinel surveillance and lab confirmation of communicable diseases
4. Human Resource & Training: Recruitment of Epidemiologists Microbiologists Entomologist Data Managers and Data Entry Operators on contractual basis to support surveillance activities. Peripheral/Districts Health staff trained to identify and report various diseases defined in the S P and L formats.
5. Media scanning& Verification cell: Media Scanning and Verification cell is function in the
SSU and DSU by sending the media alerts to the Districts/Taluks by scanning print & electronic media and expect the districts to verify the incident and to send the report. These interns verify the Media Alert by the CSU GoI and SSU respectively.
6. IT strengthening: The video-conferencing facility is available at DSU & SSU and is used
regularly for the supervision monitoring and to discuss the issues pertaining to implementation of the programme.
7. Outbreak Response and Management: State and District Rapid response teams are identified
involving DSO DVBDCP officer RCH Officer Physician Pediatrician Epidemiologist

89
Microbiologist Entomologist Veterinary Doctors and Designated officers from Food Safety headed by District Surveillance Officer to investigate cause and contain the outbreaks. The teams are instructed to report outbreaks on daily basis with mandatory nil reports.
8. Water testing: All District Surveillance laboratories are carrying out bacteriological examination of water. H2S media for water quality monitoring and media stain are prepared here and distributed to the peripheral health centres. Training for the Lab Technicians of Bangalore Urban and Banglaore Rural Districts has been done and the water testing examination will be initiated soon.
Table 1 Financial Progress
Year Total Budget allocated Expenditure
2013-14 444.02 308.53 2014-15 550.72 374.60 2015-16 566.82 469.54 2016-17 528.10 501.59 2017-18 532.14 423.01 2018-19 317.21 237.76 2019-20 642.44 614.78 2020-21 275.15 223.71(prov) 2021-22 256.86 102.00(up to Jan-2022) (Prov)
Table 2: Physical Progress of IDSP reporting 2013-2021
Sl. No. Parameter 2013 2014 2015 2016 2017 2018
2019
2020
2021 2022
1 S Form 85% 92% 95% 96% 98% 95% 96% 62% 42% 44%
2 P form 90% 92% 94% 91% 97% 91% 95% 60% 81% 84%
3 L form 87% 92% 93% 88% 95% 90% 95% 60% 75% 75%
4 Warning Alerts 59 131 35 55 296 32 69 77 46% 5%
5 Media Alerts 187 53 41 236 197 55 83 33 73% 8%
6 Outbreaks Investigated 313 291 323 273 289 192 268 69 88% 1%
7 Laboratory Network 10 13 19 19 22 27 28 28 28% 28%

90
Year-wise outbreaks reported from 2013 to
2022 Karnataka
Year No. of
outbreaks No. lab
utilised No. lab
confirmed
2013 313 235 156
2014 291 265 198
2015 323 189 114
2016 273 227 147
2017 289 259 177
2018 192 168 121
2019 286 268 182
2020 69 58 46
2021 88 73 28
2022 1 1 1

91
Table 3: Physical Progress of DPHLs- (Up-to January 22)
Sl. No
Name of DPHL
Year wise Utilization of DPHL- Serology
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
( up
to
jan)
1 Chitradurga 157 243 516 1259 1604 3472 2059 4538 2100 3141 1044 2342 195
2 Udupi 321 246 149 1244 1491 2525 4055 5054 5405 5040 3959 7356 613
3 Bijapur
Approved in ROP 2013-14. Manpower appointment in 2016. Lab started
functioning from 2016.
274 1338 1375 2758 1453 5994 500
4 Yadgiri 475 1493 1894 4518 2051 4473 373
5 Chamarajanagar 378 4839 2010 2456 519 627 52
6 Koppal
Approved in ROP 2014-15. Manpower appointment in 2016. Lab started
functioning from 2016.
225 915 665 2509 1530 3225 269
7 Bagalkote 48 604 973 2657 822 918 77
8 Davanagere 34 1895 2041 2225 865 4293 358
9 Gadag ._ 905 1083 2647 2170 4800 400
10 Gulbarga 193 4061 7310 6640 1248 6184 515
11 Haveri 216 2147 3697 1691 242 2985 249
12 Tumkur
Approved in ROP 2017-18.
._ 4662 1282 2020 1161 3825 319
13 Kolar ._ 1901 358 1849 904 238 20
14 Dakshin Kannada ._ 1984 7855 6619 1988 5691 474
15 Bellary
Approved in ROP 2018-19. Renovation of the Lab and equipment procurement is in progress
22 433 2748 229
16 Dharwad 0 79 1483 124
17 Chickmagalur 2228 81 830 69
18 Chikkaballapura 2402 1256 1553 129
19 Ramanagar 1663 573 967 81
20 Mysore Approved in ROP 2019-20.Equipment procurement is in progress 6812 822 1754 146
NOTE : Serology tests includes Dengue IgM ELISA, Dengue NS1 ELISA, Chikungunya IgM ELISA, Leptospira ELISA, Heapatitis A & E, Widal, Weil Felix & Scrub Typhus .

92
Table 4: Physical Progress of DPHLs- Culture & Sensitivity (Up-to January.22)
Sl. No Name of DPHL
Year wise Utilization of DPHL- Culture & Sensitivit y(till Jan 22)
2010
2011
2012
2013
2014
2015
2016
2017
2018
2019
2020
2021
2022
1 Chitadurga 40 120 74 219 374 434 808 1292 2681 3092 1517 3338 278
2 Udupi 65 31 14 159 412 307 694 899 2283 3190 1939 2363 197
3 Bijapur
Approved in ROP 2013-14. Manpower appointment in 2016. Lab started
functioning from 2016.
392 765 2232 2271 1094 1510 126
4 Yadgiri .- 212 454 240 136 176 15
5 Chamarajanagar .- 232 574 1512 1803 2416 201
6 Bagalkote
Approved in ROP 2014-15. Manpower appointment in 2016. Lab started
functioning from 2016.
.- 73 1588 899 476 2298 192
7 Koppal 136 1430 732 2415 664 503 42
8 Davanagere .- 415 1294 2134 703 452 38
9 Gadag .- 52 145 698 444 757 63
10 Gulbarga .- 132 602 1066 1672 613 51
11 Haveri .- 750 2999 2768 1689 2292 191
12 Tumkur
Approved in ROP 2017-18.
.- 120 2601 3822 1803 3302 275
13 Kolar .- 233 853 1167 603 841 70
14 Dakshin Kannada .- 114 760 1280 938 615 51
15 Bellary
Approved in ROP 2018-19. Renovation of the Lab and equipment procurement is in progress
524 218 227 19
16 Dharwad 778 213 212 18
17 Chickmagalur 107 204 219 18
18 Chikkaballapura 0 19 353 29
19 Ramanagar 0 0 0 0
20 Mysore
Approved in ROP 2019-20.Equipment procurement is in progress 517 115 179
15
NOTE : Culture tests includes tests done for Typhoid Fever, Cholera & Other Enteropathogens, Diphtheria, other clinical samples, Water culture & OT swab cultures.

93
Table 5: IDSP Training status
1.15. NUTRITION PROGRAMMES:
1. Vitamin ‘A’ Administration Programme: This programme is implemented for pre-school children of 9 months to 5 years age. The children are administered Vitamin ‘A’ solution orally to prevent Night Blindness, formation of Bitot Spots and other Vitamin ‘A’ deficiencies leading to blindness. The Vitamin ‘A’ solution necessary for this programme is procured under NHM PIP by KSMSCL.
Two programmes are implemented under this viz.:
I. Measles Rubella Vitamin ‘A’ Programme: One ml of Vitamin ‘A’ solution containing 1 lakh IU is administered orally to the children of 9 months along with Measles Rubella Immunization. This is a routine monthly programme.
Sl.No Year Target Achievement %
1 2021-22 (Till January)
9,19,899 6,90,041 75
(ii) Vitamin ‘A’ supplementation programme : This programme is implemented biannually to the children of 11/2 to 5 years. 2ml. of Concentrated Vitamin ‘A’ solution containing 2 lakh IU is administered to the children orally, to improve immunity and reduce morbidity and mortality among pre-school children.
Designation
2014
-15
2015
-16
2016
-17
2017
-18
2018
-19
2019
-20
2020
-21
2021
-22
(Up
to
Jan)
Medical Officers 365 133 131 177 1063 920 120 6
Staff Nurse/ Pharmacists 29 114 53 51 425 315 240 2 Medical College Doctors & DPHL Microbiologists
- - 20 23 50&4 23&1 80 1
ASHA mentors 72 40 - - 0 140 300 3
Lab tech. - 20 119 135 19 189 20 0 Sensitization to multi-sector group involving School Teachers, Self help group members, AWW, High School Students, ASHA, Grama Panchayat members
567 203 616 489
200
1
One day sensitization for PRIs 40 5
Training on IHIP for new jointers 240 14
one training for Data Entry and Block Health Team
80 24 160 6
Training for private practioners 75 0 200 2
Total 466 307 890 589 2278 2077 1600 40

94
Sl.No Year Target Achievement %
1 2021-22 (March)
37,39,752 35,73,173 96
2 2021-22 (December)
Reports awaited
2. Mass Deworming Programme: This programme is implemented Bi-annually during February and August every year. Albendazole tablets are distributed to pre-school children. 1/2 tablet containing 200mg is given to children of 1 to 2 years. And 1 tablet containing 400mg is given to children of 2 to 5 years of age. National Deworming Day is implemented as per GOI Guidelines. These albendazole tablets are procured under NHM PIP by KSMSCL.
The progress is as follows:
Year Target Achievement % 2021-22 (April) 1,50,50,866 1,42,87,408 95 2021-22 (November) 50,26,312 42,22,646 84
FINANCIAL PROGRESS
Year Approved
(Rs. in lakhs) Expenditure (Rs. in lakhs)
(Vitamin A) 292.68 Supply under Process
Albendazole tablets 149.94 Supply under Process
Nutrition Rehabilitation Centres (NRCs) in Karnataka:
Nutrition Rehabilitation Centres refers to a unit for ‘inpatient, centre based’ care of children with severe malnutrition. Children with Severe Acute Malnutrition (SAM) are usually treated either in facility/hospital based care units without medical complications. The Medical officers visit A.W.Centres and conduct health check-up once in 3 months. The children diagnosed with Mal-Nutrition and other deficiencies are treated suitably. Severely malnourished children are referred to Paediatricians for treatment at Taluka Hospitals/ District Hospitals/ Nutrition Rehabilitation centres.
Under nutrition is associated with high rates of mortality and morbidity due to common childhood illness including diarrhoea, acute respiratory infections, malaria and measles. To prevent deaths due to severe acute malnutrition (SAM) specialized treatment and prevention interventions are required. In Karnataka there are 32 Nutrition Rehabilitation Centres. 20 are attached to District Hospitals and 12 are attached to Medical Colleges. Usually they are either 20 beds or 10 bed capacity. With a trained Medical Officer, Staff Nurses and Diet Counsellors at the Rehabilitation Centre.

95
Children and Mother/care taker will stay for a maximum of 14 days in the NRC. In addition to providing nutritious food to children, awareness is being created to Mothers /care takers on preparation of nutritious food. An amount of Rs.275/- to compensate the loss of wages, Rs. 125/- for food for parents, Rs.125/- for food and Rs. 125/- for drugs for SAM child is being provided. Taluka Nutrition Rehabilitation Centres (NRCs) :
As per the instructions of the Chief Secretary, Government of Karnataka 49 taluka NRCs were established in 25 districts during March 2019. The beneficiaries are provided with treatment along with food. The mother / guardian is paid wage compensation loss of Rs. 275/- per day for 14 days or as long as the child is admitted in the centre. The centre is managed with existing hospital staff. A total of 950 (from April to December 2021) admissions have been done in the Taluka NRCs, CHCs and PHCs, in addition to the admissions done District Level 32 NRCs detailed as below.
PHYSICAL PROGRESS of NRC is as follows.
Year Admissions
Discharged with target weight gain
Referred (Medical Transfer)
Children followed up
2021-2022 (till
January)
4,047 2,099 77 2,582
Financial Progress 2021-22
Nutrition Rehabilitation
Services (32 NRCs) (till
January)
Approved (Rs. in lakhs)
Expenditure (Rs. in lakhs)
Remarks
324.00 95.85 District NRCs are functioning as District Covid centres, during the pandemic the
admission in NRCs was low.
Anemia Mukt Bharath:
India is one of the countries with anemia as a serious public health concern today. Almost 50 percent of the pregnant women, 59 percent of children under five years of age, 54 percent of adolescent girls and 53 percent of non-pregnant non-locating women of our country are anemic.
Anemia impairs cognitive and motor development among children, increase their susceptibility to illness, and in adults reduces work capacity and productivity. In pregnancy, this contributes to high maternal and neonatal mortality and morbidity, obstetrical risks like impairment of fetal development and low birth weight, neural tube defect, Post Partum Hemorrhage, still birth, prematurity and maternal deaths.
Government of India has also made a commitment to Global World Health Assembly with target of 50% reduction of anemia among women of reproductive age by 2025 and the POSHAN Abhiyan (2018-2020), ambitious to reduce prevalence of anemia among children 6-59 months, adolescents and women of reproductive age 15-49 years by 3 percentage points per year.

96
IEC activities for Anemia Mukt Bharath Financial Progress 2021-22
Approved (Rs. in lakhs) (till
January)
Expenditure (Rs. in lakhs)
125.00 Activities under process
Achievements:
• With reference to W.P. 38157/2011in the Honble High Court Karnataka Bengaluru the Justice Rtd. Justice Venugopala Gowda Committee is conducting a virtual meeting to monitor and guide on the control and prevention of Malnutrition among children and Women the State.
• Further to complying to directions of the above committee a regular weekly Health Check Up camps is being conducted for children, adolescent and women jointly in coordination by Departments of H&FW, WCD, Education and RDPR.
• The HOD of Community Medicine, BMCRI has been nominated as Nodal Officer by the Department of Medical Education for this regular weekly Taluka Level Health Camps.
• While Deputy Director, Nutrition and RBSK have been identified as the Coordinating Officers by Department of Health and Family Welfare.
• The details of the above camp conducted till 08.12.2021, data source from google spread sheet https://docs.google.com/spreadsheets/d/1r-onHosAvo92FQw BTMktOstQskSjURY-hRnqWbBox4/edit?usp=sharing
• The above camp initially was scheduled to be held on Wednesday of every week, as a State proclaimed Wednesday as COVID Vaccination day through out the State. The above camp is now been rescheduled and is conducted every Friday across the State.
• In coordination guidance and handholding with the NRC- SCoE Maharashtra a virtual orientation has been conducted for the NRC staff and Pediatricians of NRCs at 8 Districts namely Haveri, Kolar, Shivamogga, Ballari, Mysore, Chikkaballapura, IGICH, Bengaluru and NRC SCoE Karnataka Vani Vilas, Bengaluru on the following three topics.
1. Treatment Protocols for children below 6 months at NRCs. 2. Effective breastfeeding techniques under the IYCF programme. 3. Structural Play therapy at NRCs.
1.16. NATIONAL IODINE DEFICIENCY DISORDER CONTROL P ROGRAMME (NIDDCP):
National Iodine Deficiency Disorders Control Programme (NIDDCP) is implemented in the State to create awareness about usage of Iodized salt in daily diet to prevent Iodine Deficiency Disorders (IDD) like Cretinism, Deafmutism, Dumbness, Physical and Mental Retardation, Goiter, etc.
Dakshina Kannada, Bellary, Uttara Kannada, Kodagu, Chikkamaglur, Bengaluru(U),
Bengaluru(R), Shivamogga are recognized to be Endemic Districts. During 2021-22, 270 Goitre cases reported and put on treatment as per the report sent from the districts.
Salt Testing Kits (STK) have been distributed to ASHA workers in 8 Endemic districts to test the
Iodine content in salt samples at community/household level and to promote the importance of consumption of Iodized Salt in daily diet and to prevent Iodine Deficiency Disorders. In all the Districts Salt Testing Kits for Demonstration Purpose of Iodine Content in Salt Samples by Health Workers in Sub Centres, Community Health Centres (CHC), Primary Health Centres (PHC), Taluka Hospitals, District Hospitals is provided. These programmes shall be continued during 2022-23 also.

97
Every year October 21st to 27th is observed as “Global IDD Day and week”. During 2021-22, on this occasion various activities were conducted as per the guidelines of Government of India. During this occasion at the State level a virtual meeting was conducted by Deputy Director (Nutrition) involving the District Surveillance Officers (DSO) prior to IDD Day and week in promoting awareness by the health workers at district/ Taluka level on the importance of Iodine and the various disorders caused by Iodine deficiency. The various topics such as GOI perspective on NIDDCP, Iodine Deficiency Disorders with particular reference to pregnant women and school going children (6-12 years age group), demonstration of Salt Samples for analysis of Iodine content using Salt Testing Kits (STK) were discussed. The importance of Iodine and Iodine Deficiency Disorders (IDD) publicity was done through All India Radio by Deputy Director, Nutrition. At district level newspaper publications on the importance of Iodine to prevent IDD were emphasized, demonstration of Salt Samples at the community Level ( by following the guidelines for Covid-19 prevention) to test the presence of Iodine content using STK by ASHA/Health personnel were done to create awareness about iodized salt in daily diet to prevent Iodine Deficiency Disorders.
PHYSICAL PROGRESS 2021-22
Particulars 2021-22 (Upto Jan)
Goitre Cases 270
Salt samples tested in 8 Endemic districts using Salt Testing kits (STK)
Year Total samples Above 15ppm Below 15ppm 0ppm
2021-22 (Upto January)
35,17,713 33,94,402 (96.49%) 1,12,747 (3.21%)
10,564 (0.30%)
Salt samples tested for Iodine content at State IDD Laboratory
Year Total Satisfactory (>15ppm)
Non-Satisfactory (<15ppm)
2021-22 (Upto January)
6442 6259 (97.16%) 183 (2.84%)
Urine samples tested for Iodine Excretion at State IDD Laboratory
Year Total Samples tested
Normal (>10µg/dl)
Mild (>5 to <10µg/dl)
2021-22 (Upto January)
3100 3100 (100%) -

98
1.17 NATIONAL PROGRAMME FOR PREVENTION AND CONTROL OF DEAFNESS (NPPCD):
As per WHO estimates in India, there are approximately 63 million people, who are suffering
from significant auditory impairment; this place the estimated prevalence at 6.3% in Indian population. As per NSSO survey, currently there are 291 persons per on lakh population who are suffering from severe to profound hearing loss (NSSO, 2001). Of these, a large percentage is children between the ages of 0 to 14 years. In Karnataka State, according to estimated population of 2018census, it is estimated that there are 20,839 children are suffering from hearing impairment in the age group of 0-6 years and most of these are from birth. Long term objective of NPPCD Programme: To prevent and control major causes of hearing impairment and deafness, so as to reduce the total disease burden by 25% of the existing burden.
Hearing Impairment / Deafness Statistics for the Year 2021-22 (up to Jan-22)
Number of cases
Examined with
0-5 years 6-15 years 16-50 years > 50 years Total No. of Cases M F Total M F Total M F Total M F Total
Deafness 560 542 1102 1980 1884 3864 6674 5602 12276 6120 4241 10361 27603
Mild Deafness
124 119 243 497 545 1042 1957 1678 3635 1425 1109 2534 7454
Moderate Deafness
109 124 233 546 500 1046 1822 1560 3382 2033 1262 3295 7956
Severe Deafness
135 138 273 424 438 862 1529 1282 2811 1780 1206 2986 6932
Profound Deafness
192 161 353 513 401 914 1366 1082 2448 882 664 1546 5261
ENT surgeries performed for the Year 2021-22 (up to Jan-22)
Name of the ENT
Surgery Male Female Total No. of Cases
Myringoplasty 90 86 176 Tympanoplasty 228 287 515 Myringotomy 81 62 143 Grommet insertion 25 19 44 Stapedectomy 53 27 80 Mastoidectomy 158 153 311
Total 635 634 1269
No. of patients referred for Rehabilitation Services and Fitted with Hearing Aids for the Year 2021-22 (upto Jan-22)
Referred for Up to 14 years 15-50 years > 50 years
Total No. of Cases
M F Total M F Total M F Total
No. of persons referred for rehabilitation
116 111 227 121 109 230 255 150 405 862
Number of hearing aids fitted
651 584 1235 1967 1707 3674 2292 1425 3717 8626

99
New Born Screening of hearing impairment for the Year 2021-22 (Up to Jan-22)
Newborn Withouthigh risk Newborn With high risk Total No. of Cases
Pass Refer Total
Pass Refer Total
Male Female Male Female Male Female Male Female 8987 8424 456 324 18191 3031 2471 1237 958 7697 25888
Financial Progress for the FY 2021-22 (Up to Jan-22)
Budget Approved (Rs. in lakhs)
Expenditure (up to Jan-2021)
(Rs. in lakhs) Percentage
815.19 176.63 21.67 1.18. KARNATAKA STATE DRUGS LOGISTIC WAREHOUSING SO CIETY : Introduction and Objectives:
Karnataka State Drug Logistics and Warehousing Society Bangalore was established with and objective to cater to the needs of Health Institutions coming under the Directorate of Health and Family Welfare Services as well as those Hospitals coming under the control of Directorate of Medical Education and such other programmes coming under Health and Family Welfare Services.
Objectives:
Karnataka State Drug Logistics and Warehousing Society Bangalore is headed by Additional director. He functions under the Administrative control of the Commissioner Health & Family Welfare services and the Director of Health & Family welfare Services. The requirement of Drugs Chemicals & other items of all State Sector Hospital Teaching Hospitals under the Directorate of Medical Education and the Hospitals/Institutions coming under ZP are procured and supplied in accordance with the budget allotted and the indent of individual Hospitals/Institutions through District Drugs Warehouses.
Action plan:
1. To ensure reach of quality and affordable health care services in a transparent and equitable manner to all by delivering essential drugs medical equipment’s and Lab consumables in a timely manner to public health care systems by efficient procurement, Storage and supply chain management.
2. In the State 27 District Warehouses are catering to the needs of hospitals. As per the indents of the Health Institutions, drugs are supplied to them through the troop Carriers. In the state 28 Troop Carriers are provided to the warehouses. Cold storage Room has been installed in all 27 Dist. Drug Warehouse.
3. Online Drug Inventory Management System, has been followed for Indenting of Drugs from various Health Institutions & Medical Educational Institutions. Drugs and Chemicals are also supplied to combat natural calamities and disaster managements as per the directions of the Government from time to time.
4. The Equipment’s and Furniture required for different health institutions are procured by calling tender by KSMSCL.

100
5. Essential Need Based Drugs are provided to 2889 Health Institutions in the State. Quality control Section regularly checks the quality of the drugs and supplies to all Health institutions.
6. During the Covid-19 Pandemic 1st and 2nd wave action was initiated for timely procurement and supply of drugs, equipment’s and Consumables to warehouses and Government health Institutions. Effective Management for keeping up sufficient buffer stock of covid-19 essential drugs as per GoI guidelines.
7. The overall quality of the service delivery improved by meeting the demand for proper procurement, supply and consumption of essential medicines, essential equipment, by providing proper supply chain system and Quality Control.
Budget Allocations: Budget released for KSDLWS, Bangalore for procurement of Equipments, Drugs and Chemicals and expenditure for the year 2021-22 (upto January-2022) is
as follows: Year Budget Released
(Rs. in Lakhs) Expenditure
(Rs. in Lakhs) 2021-22 (Jan 2022) 94189.96 46243.82
1.19. STATE INSTITUTE OF HEALTH AND FAMILY WELFARE:
Salient features of the SIHFW:
1. Works as the State Level Nodal Agency for the training under department of the Health and Family Welfare.
2. Works in formulating state training policy, planning, implementation and monitoring evaluation of the in-service training to Medical and paramedical personal in the department.
3. 19 District Training Centres, 4 Health & Family Welfare Training Centres are working under SIHFW, and helps in dissimilating the trainings to districts and sub district levels.
Training Programmes taken up during 2021-22
1. Maternal Health Trainings : SBA, SBA Refresher, RTI/STI, IMEP. 2. Child Health Trainings : IMNCI, F-IMNCI, NSSK, IYCF, FBNC. 3. Family Planning Trainings : Specialized Skill programme in IUCD insertion, MTP, Minilap and
Laparoscopic training. 4. PPIUCD training to newly recruited Medical officers & Staff Nurses. 5. ASHA’s Induction, ASHA’s Training in ASHA Module 6&7 and ASHA NIOS Training. 6. Induction training to newly recruited Medical Officers.
7. Training for Pharmacists.
Achievements for 2021-22 (Both Physical and Financial)
Details regarding achievements for the year 2020-21 upto January - 2021 (Both Physical and Financial) enclosed in the Annexure.

101
Other remarkable achievements for the year
a) 7th batch of CPHN Course for in service LHV’s/ANMs Started in March-2021. b) 5th Batch PGDHP & E Course for in service BHEO’s is running. c) The NBEMS (National Board of Examinations in Medical Sciences) New Delhi, has allotted 104
DNB seats in various specialties at 02 General Hospitals & 15 Taluk Hospital of Karnataka, 9 Specialties in DNB, 7 Specialties in Diploma, and 2 Specialties in DrNB (Super Specialities) have been sanctioned 130 DNB, 136 Diploma and 3 DrNB Seats, Till date 158 Students have received admission to the Govt. hospital and selection of the candidates for the year 2021-22 is ongoing by MCC, DGHS, Govt. of India and list will be available by the end March 2022.
Achievements for the year 2021-22 under (NHM)
Sl. No.
Details of the Training Batches No. of persons trained
Achievement
1 Maternal Health Trainings 13 68 A sum of Rs. 18.03 lakhs have been incurred as expenditure
out of Rs. 59.65 lakhs approved.
2 Child Health Trainings 19 364 3 Family planning Trainings 17 123 4 Other Trainings under NHM 22 593 5 ASHAs Training for Induction &
ASHA Module 6&7 31 851
6 ASHA NIOS Training 2 60
1.20. PUBLIC HEALTH INSTITUTE:
The Public Health Institute is one of the oldest health institution and main food and water laboratory in the State. The following sections are working in this institute.
1. Diagnostic Bacteriology Section. 2. Water Bacteriology Section. 3. Water Chemical Section
Chemical Examiners Section
1. Yellow Fever Vaccine Section. 2. Training Section. 3. Media Preparation Section. 4. Sentinel Lab under NVBDCP and L3 Laboratory under IDSP. 5. State Food Laboratory Section.
Diagnostic Bacteriology Section:
1. In the Diagnostic Bacteriology Section stool samples for detection of Vibrio Cholera Organisms, are being received and analyzed and the reports are being sent to the concerned Institutions.
2. Water samples for detection of V Cholera Organisms are being received and analyzed and the reports sent to the concerned Institutions.
3. Food samples are being received from private and government institutions for detection of pathogenic Organisms and analyzed.
4. Swabs are being received from operation theatres from the Government Institutions for detection of Clostridium Tetanus Organisms.

102
Water Bacteriology Section:
1. Water samples from both Government and Private Institutions for bacteriological examination are being received and analyzed.
2. The samples are analyzed for E. Coli Organisms and Coli Form Organisms which are the indicators for the facial contamination of the water.
Water Chemical Section:
1. In this section, water samples are received for analysis of dissolved solids, PH, alkalinity, turbidity, total hardness and others chemicals like Iron, Nitrates, Calcium, Chlorides, Sodium, Potassium, Fluorides, Sulphates for potable purposes.
Chemical Examiner Section:
Samples are received for analysis of the following 1. Lokayukta trap case Samples. 2. Excise Samples. 3. Narcotic Samples 4. Blood and Urine Samples for the estimation of Alcohol 5. Chemical analysis of Bleaching Powder.
Vaccine Section:
1. Yellow fever vaccination is being given to International travelers, who travel to African and South American Countries. This is the only center for Yellow Fever Vaccination in Karnataka State.
2. Menu vaxAcwy(Meningitis Vaccine) is provided to the Hajj Pilgrims (9120 doses given) in Karnataka State.
Training Section:
1. Training programmes are being conducted for both Junior and Senior Medical Laboratory technologists of Government Institutions from all over Karnataka in the Diagnostic bacteriology, water bacteriology, media preparation sections.
2. Students from Government and Private Institutions of Both Post graduate and under graduate Medical, Dental, BAMS, Microbiologist, Home Science & Para Medical are visiting for enhancement of Knowledge in the Laboratories.
Media Preparation Section:
1. Required media to culture Micro Organisms are prepared and distributed to various sections of this Institution.
Sentinel Lab under NVBDCP and L3 Laboratory under IDSP
1. The Blood samples received for detection of vector borne disease like Chickungunya, Dengue and Japanese encephalitis (J.E) are tested.
Food Laboratory
1. Suspected food samples are being tested and analyzed as per Food Safety and Standards Act, if
the samples are found adulterated, legal procedure will be initiated by the food safety officers as
per the provisions of the food safety and standards Act.

103
2. The State Food Laboratory is strengthened by way of supply of equipments and glassware’s by
the KHSDRP.
3. From 5th August, 2011, Prevention of food Adulteration act repealed and Food Safety and
Standards Act came into effect in the Karnataka State. This Act will consolidate various act and
orders relating to food, under this Act FSSAI has been established. FSSAI has been created for
laying down science based standards for articles of food and to regulate manufacture, storage,
distribution, sale and import to ensure availability safe and whole some food for human
consumption. The government of Karnataka has notified the authorities and laboratories as per
the requirement of food safety and standards Act for implementation.
Action Plan for 2021-22
1. Construction of New State food laboratory is completed with the assistance of KHSDRP and
purchase of equipments is also under progress.
2. Up gradation of the existing Divisional Labs are under process with the assistance of KHSDRP
and FSSAI, New Delhi as per FSSAI guidelines.
3. Divisional Food Lab, Belgaum, Gulbarga and Mysore will be strengthened by procuring the
required instrument with Central Assistance (FSSAI).
FSSA 2006 Report of Karnataka State during the year 2021-22
Month Registration Licensing Total
Samples Received
samples Analyzed
Unsafe/ Misbrand/
Adulterated April 7498 1998 350 350 0/4/1
May 4628 1424 120 120 0/6/3
June 4950 5641 315 315 0/2/2
July 10512 3570 320 320 2/3/1
August 11127 4347 315 315 2/4/2
September 10891 3086 310 310 4/2/12
October 9240 3229 300 300 3/9/15
November 8282 3215 350 350 4/2/12
December 10714 4251 310 310 2/8/10
January 10267 2521 330 330 2/1/5
February 10359 2276 315 315 1/2
March 0 0 0 0 0
TOTAL 98468 35558 3335 3335 20/43/64

104
1.21. Food Safety and Standards : Introduction :
Food Safety and Standards Act, 2006 came into force from August-5, 2011 in Karnataka State. Which consolidates various Acts & order Food Safety and Standards Act emphasizes on science based standards for articles of food and to regulate their manufacture, storage, distribution, sale and import to ensure availability of safe and wholesome food for human consumption. After the implementation of this Act, all other Food Related Acts have been repelled. In Karnataka State, the Commissioner, Health & Family Welfare Services, has been additionally designated as Food Safety Commissioner. 238 various posts have been re designated and 177 new posts have been created in the Government Order vide No: HFW 317 CGE 2011, dated: 23-08-2012 and for filling up of these posts Executive Orders have been issued. Cadre and recruitment rule has came into existence with effect from 05.01.2017, accordingly 158 Food Safety Officers posts will be filled through KEA (Karnataka Examination Authority). As per the Government of India notification arrangements is being made inducting sub divisional officer in the districted quarter will be placed on in charge arrangement to the post of designated officer as he is facilitated sufficient staff under his control and empowered to execute standing orders at his level which enables him to carry out duties of designated officer and effective enforcement of FSS Act and rules.
FSSA 2006 Report of Karnataka State during the year 2020-21
Month for the year
2020-21 Registration Licensing
Total Samples Received
samples Analyzed
Unsafe/ Misbrand/
Adulterated April 1333 767 03 46 01/01/06 May 1620 1895 90 66 02/03/05 June 4450 5201 155 134 02/02/04 July 3620 2721 110 114 02/02/02 August 4220 1700 287 171 02/00/02 September 5066 2128 722 783 17/26/22 October 3034 2063 347 258 03/09/18 November 2133 994 459 449 03/13/22 December 6016 980 621 568 11/6/33 January 8230 2516 193 420 2/6/15 February 5400 1900 700 700 02/03/05 March - - - - -
TOTAL 45122 22865 3687 3709 43/65/111
PUBLIC HEALTH INSTITUTE, SHESHIDRI ROAD, BANGALORE. PERFORMANCE
REPORT FOR THE YEAR OF 2021-22 PUBLIC HEALTH INSTITUTE, SHESHIDRI ROAD, BANGALORE.
Sl.NO.
SECTIONS OF PHI
Cumulative total no of samples analysed from
April-2021to – FEB-2022
I WATER BACTERIOLOGY
Bacteriological analysis of water for drinking
purpose,analysedBorewell/Tapwater/Others
290/419/1305
Number found fit for potable purpose. 365/285/786 Number found unfit for potable purpose 150/157/519

105
II DIAGNOSTIC BACTERIOLOGY
1
Bacteriological analysis of water for isolation of V,
Cholera No of samples received.
26
Number of sample analysed. 26 Number of samples positive for V. Cholera. 0
2 Bacteriological analysis of stool sample for isolation of
V. Cholera
01
Number of samples negative for V, Cholera 0 Number of samples positive for V. Cholera 01
3 Bacteriological analysis of food for Coli forms and other
specific pathogens,analysed
22
Number of samples found positive 01 Number of samples found negative 21
III Yellow Fever Vaccination and International Certificate
Give
1512
IV CHEMICAL EXAMINER’S LABORATORY
1 Liquor Samples -
Opening balance 0
Samples received 03
Samples Analyzed 03
Total 03
No samples found positive 0
Pending 0
2 ACB
Opening balance 0
Samples received 72
Samples Analyzed 72
Total 72
No samples found positive 72
Pending 0
V STATE FOOD LABORATORY
a No of food samples received under FSSA 3355
1 Opening balance ( under FSSA ) 0
2 Total samples 3355
3 No of food samples analyzed 3355
4 No of samples Found unfit for Analysis 0
5 No of samples Found unsafe 20
6 No. of samples misbranded/substandard 43/64
7 Closing balance 0
b No of food samples received under Non FSSA 8117
1 Opening balance during the year. ( under Non-FSSA ) 220
2 Total samples 8337
3 No of food samples analyzed during the year 7800
4 No of samples Found unfit for analysis 69
5 No of samples found unsafe 174
6 No. of samples found misbranded/ substandard. 60/58
7 Closing balance 537

106
VII TRAINING SECTION
Post Graduate Doctors
1 Post Graduate. MD trained/visited Microbiologist 32 2 Post Graduate MDS trained/visited Microbiologist 30 Under Graduate Doctors
3 Doctors MBBS trained/visited 10 4 Doctors B D S trained/visited 10 Students from other Institution
5 Post Graduates 00 6 Sanitary health inspector 10 7 Under Graduate 05 Nursing Student
8 B Sc Nursing 06 9 General Nursing ( LHV’S ) 12
10 Senior Lab Technicians 06 11 Junior Lab Technicians 10 12 Nodal Officers/DSO/A.O/DO’s 00
13 F.S.O 10 14 Excise sub inspectors 00
VIRAL SENTINAL SURVEILLANCE LAB 1 Chickangunya;- No. of samples received 566 No. of samples tested 566 No of Positives 124 No.of equivocal 04
2 Dengue:- No of samples received 656 No. of samples tested 656 No. of Positives 98 No.of equivocal 6
3 J E:
No. of samples received No. of samples tested No. of Positives No.of equivocal

107
Action Plan for 2021-22:
• Up gradation of the existing state Lab and Divisional Labs are under process with the
assistance of KHSDRP and FSSAI, New Delhi .
Allocation of Funds and Expenditure for the year 2021-2022 :
SL NO Head of Account Released
Lakhs
( Rs)
Expenditure
Lakhs (Rs)
1 2210-06-107-0-01 2100.84 1289.80
1.22. SUVARNA AROGYA SURAKSHA TRUST: “Ayushman Bharat-Arogya Karnataka” Scheme:
Government of Karnataka has been very proactive in the goal of providing health care to its
residents from a long time. Yeshasvini scheme the first such scheme was initiated in 2003. Later Suvarna Arogya Suraksha Trust was established in 2009 with the specific objectives of implementing health schemes. The first scheme was Vajpayee Arogyashree Scheme which provided cashless treatment for tertiary care to BPL families. In 2014 Rajiv Arogya Bhagya was introduced for APL families for tertiary care. About 250386 patients benefitted from VAS and RAB since their inceptions under VAS and RAB. RSBY Scheme provided secondary health care services to 62 lakh families in an insurance mode and about 168377 beneficiaries availed treatment under this scheme from the year 2016 till its closure on August 2018.
In line with the policy goals of the “Karnataka Integrated Public Health Policy 2017” which
envisages merging all social health insurance schemes into a single health assurance plan to improve efficiency and outreach and to achieve the goal of Universal, Equitable and Sustainable healthcare as envisaged in the Vision document-2025; all the existing schemes were merged and “Arogya Karnataka” a Universal Health care Scheme was launched on 2/3/2018, wherein cashless treatment upto Rs. 2.00 lakh for specified 1516 secondary, tertiary and emergency health care treatments was provided in an Assurance Mode based on eligibility criteria as per the National Food Security Act 2013. 19 lakh APL families are also covered for financial assistance upto 30% of the package rates.
Government of India has come out with its own scheme called Ayushman Bharat - National Health Protection Mission, on 25.9.2018, later renamed as Pradhan Mantri Jan Arogya Yojana (PMJAY), to provide health protection to over 10 Crore poor families identified based on the latest Socio-Economic Caste Census (SECC) data, (50 crore beneficiaries). Since both Arogya Karnataka and Ayushman Bharat have the same goal, scope and similar modalities for providing specified treatments to the poor and vulnerable sections of society, integrating both the schemes was imperative for smooth implementation especially at the field level. A single integrated scheme under a co-branded name as “Ayushman Bharat-Arogya Karnataka” is now being implemented in an Assurance Mode.
A MoU has been signed with National Health Agency, Government of India in order to implement this integrated scheme on 30/10/2018. The Government Order No. HFW 69 CGE 2018 dated 15.11.2018 was issued for implementation of integrated Ayushman Bharat-Arogya Karnataka scheme. This is the only scheme at present that covers beneficiaries of all the other hitherto existing schemes and is an Universal Health Coverage Scheme.

108
Entitlement and Eligibility for availing the scheme are as below;
i. Eligible Patient: A patient who is a resident of Karnataka State and belongs to “Eligible Household” as defined under the National Food Security Act, 2013; This category shall also include the beneficiaries listed in the SECC data and the enrolled members of the hitherto existing Rashtriya Swasthya Bhima Yojane.
ii. General Patient: A patient who is a resident of Karnataka State but does not come under the definition of “Eligible Household” as defined under the National Food Security Act, 2013, or does not produce the eligible household card.
Enrolment of patients:
One-time enrolment of patients, on an IT portal to be established by SAST as and when they approach any PHI for treatment for the first time or any other enrolment facility as designated from time to time
For single incident patient can get treatment under the scheme by producing his Aadhaar card and PDS card.
A patient approaching an empanelled private hospital in case of emergency without a referral from a PHI can be enrolled at a designated enrolment centre or a PHI after stabilization and discharge from hospital
AB-ArK Card:
Under the Ayushman Bharat- Arogya Karnataka scheme the enrolment card called AB-ArK Card and an unique AB-Ark ID is generated and provided to the patient at the enrolment centre on payment of a fee of Rs.10/-.
Enrolment cards are issued in Common service centres, B1, K1 and Seva Sindhu centers on a payment of Rs. 35/-.
Cost of treatment to be borne by the Government
For “Eligible Patients” the financial assistance up to Rs.5.00 lakh will be provided for specified simple secondary care, complex secondary health care, tertiary health care and emergency health care per annum, for a family. This will be on family floater basis meaning one or more persons of the family can use the full cover of Rs. 5.00 lakhs. One person can also use the entire Rs.5.00 lakh.
For “General Patient” the benefit limit is 30% of Government package rates, with overall annual limit of Rs.1.50 lakh per family, per year on co-payment basis.
Under integrated Ayushman Bharat-Arogya Karnataka scheme, the treatments provided for primary health care and benefit packages are as follows;
The scheme covers 1650 treatment packages. Primary treatments and 291 simple secondary procedures will be limited to PHIs only 254 complex secondary procedures, 900 tertiary procedures and 169 emergency procedures will
be performed in PHIs and empanelled Private hospitals. Complex secondary procedures and tertiary procedures require referral from PHIs. 36 Sub procedures. For 169 emergency procedures, patients can directly go to the empanelled hospitals of their
choice and avail treatment without referral.
Implementation Performance:
No. of hospitals empanelled Government 2907+ Private –562 = Total 3469. No. of Arkid Cards issued from April 2021 to January 2022: 9,97,866 (Total
Cards1,53,11,656)

109
During the current financial year (2021-22) from April 2021 till January 2022, total preauth approved for 8,98,722 cases amounting to Rs.1170.75/- crores. In the current financial year total claims of 7,58,167 amounting to Rs.1238.31/- crores has been paid to the network hospitals for treating AB-ArK beneficiaries.
(Expenditure is higher than grant releases, and most of the expenditure is borne by the central (GOI) share of grants and Opening Balance)
The total budget allocated for the year 2021-22 is Rs.977.85/- crores.
COVID-19:
The Government of Karnataka has proactively initiated various measures to combat ongoing COVID-19 pandemic. In the beginning treatment was carried out only in the Public Health Institutes later private hospitals, nursing homes and other licensed health facilities have been permitted for treatment and management of COVID 19 patients, to ensure that all who fall prey to the virus get the necessary treatment and nobody is deprived of institutional treatment. The Government issued vide its Notification No: HFW/228/ACS/2020 23-06-2020 to provide treatment in private hospitals.
108 ambulance facilities has been provided for the admission of Covid-19 infected, referred from
the public health authority. For effective management of the covid-19 infected patients admitted in public health institute and private empanelled hospitals on referral basis, injection Remedesevere has been supplied from the district ware house of Karnataka State Ware House and drug Logistics. For such treatment facility provided by SAST the treatment cost has been funded by the AB-ArK head of account.
During the current financial year 2021-22 till January 2022, Covid-19 treatment provided
through Suvarna Arogya Suraksha Trust and treatment cost borne under Ayushman Bharat Arogya Karnataka Scheme Head of Account, the details is as follows;
No. of hospitals empanelled 299 Government + 1058 Private = Total 1357. Total Preauth of 1,43,95 amounting to Rs.715.20/- crores has been approved as on 31st January
2022.
Jyothi Sanjeevini Scheme (JSS) :
This health assurance scheme is specifically for the benefit of all State Government Employees and their dependents without any cap on the financial limit and the treatment is totally cashless. The scheme was launched on 20-01-2015. The only expenditure to be borne by the beneficiary is:
1. If the beneficiary wishes to have a higher stent, prosthetics or implants other than those specified
under SAST benefit package. 2. If the beneficiary wishes to avail a higher ward other than the ward eligible for will have to be
borne by the beneficiary. Eligibility of general ward, semi-private and private wards depends on the basic pay drawn by the employee. During the current financial year (2021-22) from April 2021 till January 2022, a total of 1496
employees have availed benefit and an amount of Rs.1816.74 lakhs has been paid to the network hospitals for treating these beneficiaries.
The total budget allocated for the year 2021-22 is Rs.15.00/- crores.

110
Organ Transplant Scheme:
Government of Karnataka has implemented the ‘Organ Transplantation Scheme’ for poor/BPL patients of Karnataka, vide GO No. HFW 64 FPE 2018, Bengaluru, dated: 3-12-2018. Main features of the scheme are as under;
The scheme is applicable only for BPL recipients, receiving organs from live related donors and such transplants will be conducted in Government hospitals.
However in the event of the Government hospitals not having the capacity to perform such transplant then it may be referred to empanelled private hospitals.
In the event of cadaveric transplants (brain dead), the transplant can be conducted in government or private empanelled hospital as per the registration of the recipient and availability of the Organ in the retrieval centre.
The allotment policy of the Jeevasarthakathe society will be followed for preauthorization of the procedure other conditions like BPL/Poor recipient is also applicable. .
Eligibility:
Poor/BPL patients of Karnataka State identified by BPL card and Aadhar card are eligible under the scheme.
The beneficiary should visit Public Health Institutes (INU, SJICR, PMSSY, IGE) and after evaluation should register for Organ transplant after getting the approval from the authorization committee (Hospital level/District/ State level authorization).
Referral:
All public Health Institutes can evaluate the patients for Organ transplant and can refer to the hospitals of centre of excellence for further process of Human Organ transplant.
The center of excellence can evaluate the patient and direct the patient to register under the Jeevasarthakathe for cadaveric organ transplant.
In the event of the patient opting for live related organ transplant, he/she can be evaluated and can register for human organ transplant. If the centre of excellence has not having the capacity to conduct the organ transplant those shall refer to empanelled network hospitals
Treatment & Benefit packages:
The total cost of Kidney Transplant surgery is –Rs.3 lakhs per patient, per year The total cost of Heart Transplant surgery is –Rs.11 lakhs per patient, per year The total cost of Liver Transplant surgery is –Rs.12 lakhs per patient, per year Suvarna Arogya Suraksha Trust (SAST) is the nodal agency to implement the scheme. SAST will be
responsible for empanelment of private hospitals, pre-authorization and payments for transplants to hospitals as per the mechanism followed in the Ayushman Bharat-Arogya Karnataka Scheme. Enrollment of patients in SAST:
The enrolment of the patients shall be based on Aadhar and PDS Card and shall be done in the hospital conducting transplant. The hospital will obtain the authorization from the appropriate authorization committee and submit the same along with other required documents during preauthorization. Implementation Performance:
As on 31/01/2022, the achievement under Organ Transplant Scheme is as follows: • No. of hospitals empanelled Government : 3+ Private : 9 = Total : 12

111
• Total no. of beneficiaries availed treatment: Liver 03(Cadaveric 01+ live 02), Heart 02, Kidney:19 ( Cadaveric 10+ Live 09) Total – 24.
During the current financial year (2021-22) from April 2021 to January2022, total of 24 transplants approved amounting to Rs. 93.10/- lakhs and a total of 218 Immunosuppression cases amounting to Rs. 22.95/- lakhs have been approved.
1.23: AYUSHMAN BHARAT- HEALTH & WELLNESS CENTERS IN KARNA TAKA:
Preamble:
The goal of Universal Health Coverage (UHC) is to ensure that all people obtain the health
services they need: preventive, promotive, curative, rehabilitative and palliative without the risk
of financial hardship.
Objectives: • To reduce out of pocket expenditure
• To strengthen two way referral system and follow-up care
• To screen population for NCDs thereby identify, treat and reduce morbidity and mortality
• Thus help country in reaching goal three of sustainable development Goal (SDG) which aims to remove poverty
Achievements and Projected Goal in 2021-22:- • State Health department has recruited 2614 CHOs additionally under NHM through online
examinations in transparent way. • NHM has operationalized 6742 (93%). Health Centres as HWCs against the target of
7257The remaining HWCs will be made operationalized by end of March-2022 • Karnataka Stood 1st Rank in India for operationalization of AB-HWCs in FY-2020-21
Provision of wellness activities for Health Promotion in all 6742 HWCs • NCD- Camps and Community screening in all villages
For early identification of HTN, DM & 3 Common cancers (Breast, oral and cervical)

112

113
• Implementation of Yoga and Traditional therapies at HWCs
To address HTN & DM and other health issues in SC, PHC & UPHC and promotion of Health
• Ayushman Bharath- School Health ambassadors in all Schools
Identification of Developmental delays, Nutritional deficiency, mental health and counselling to all the students on personal hygiene • Strengthening screening for Mental Health care at all SC-HWCs, training on mental
health given to Community health officers and Frontline health workers
• Strengthening Tele-consultation services to community through e- Sanjeevini programme at all SCs, PHCs & UPHCs.
• Awareness on all Health activities and programmes as per health calendar through regular Health promotion sessions in Wellness area
• Formation of Jan Arogya samithi at all 2172 PHC and 4581 Sub centre level by involving the local Panchayat Raj Representatives and community.

114
81 Essential drugs and 14 Diagnostics at SC-HWCs: as per the government norms
Service delivery provided at AB-HWCs (source AB-HWC portal upto January
2022)
Services Number
Total Foot falls 6,04,69,105
Total availed for medicine 5,46,72,478
Total availed for diagnostic facilities 1,96,52,791
screened for HTN 89,88,275
On treatment among screened for HTN 11,66,080
screened for DM 77,40,347
On treatment among screened for DM 10,19,767
screened for Breast cancer 11,16,590
On treatment among screened for Breast cancer 9,553
screened for cervical cancer 9,02,491
On treatment among screened for cervical cancer 791
New programmes Implemented at HWCs:
• State has started Home-based palliative care at 4581 Sub Centre level HWCs to provide need based
support to the community and reduce Health care demand
• State has initiated awareness activities under Eat Right Movement in all 6742 HWCs to provide
awareness to community for having nutritious rich food aiming to reduce salt, sugar and Fat
consumption
• NHM has started Fit India Movement to improve the health status among the community and
Frontline Health care workers in all 6742 HWCs, more than 9000 sessions were conducted to assess
the health status of the community and staff

115
IEC Activities: Hoarding Creative:
Train External Branding:

116
Health and Wellness centre Hoarding:
Airport Panel Board:

117
1.24 Community Monitoring: Preamble
Under National Health Mission Untied funds are provided to the health Facilities to Improvement of health facility by taking up necessary civil works and patient friendly amenities. Under National Health Mission for every Financial Year every District Hospital, Taluk Hospital, CHC and PHC will be allotted untied fund of Rs.10.00 lakhs, Rs.5.00 lakhs, Rs.5.00 lakhs and Rs.1.75 lakhs respectively. Grants to health institutions are released in accordance with the health center's performance based on Number of In-Patients, Number of Out-Patients, Number of laboratory tests and Surgical interventions done at the facilities.
Goal: Effective and purposeful utilization of resources at the community level through community participation, monitoring and supportive supervision of Institutions. Objectives:
1. Implementation of Activities pertaining to the Institutions through community monitoring - by decentralized community participation.
2. Community monitoring through formation of ARS committees. Allocation and utilization of emergency funds (Untied Grants) for local needs for facility improvement and elevate health status of community.
Physical and Financial Achievement:
Sl.No
Health Facility
2020-21 2021-22 (till Jan) Physical Financial Physical Financial
target ach target ach target ach target ach
1 District Hospitals
35 35 350.0 233.79 35 35 350.0 88.89
2 SDH 147 147 735.0 594.01 147 147 735.0 168.37
3 CHCs 202 202 1010.0 803.57 203 203 1015.0 203.24
4 PHCs 2172 2172 3801.0 3026.86 2172 2172 3801.0 784.86
5 Sub Centres 9135 9135 1473.6 713.38 9135 9135 1473.6 122.68
6 VHSNC 26087 26087 2608.7 1602.63 26087 26087 2608.7 641.34
Outcome: Improvement in the utilization of untied fund by the community lead institution and Strengthening of Health system. There has been considerable improvement in community involvement and participation with supportive supervision

118
1.25 Oral Health: Introduction: National Oral Health Programme (NOHP) According to the World Health Organisation (WHO), Oral health is a state of being free from chronic mouth and facial pain, oral and throat cancer, oral sores, birth defects such as cleft lip and palate, periodontal (gum) disease, tooth decay and tooth loss, and other diseases and disorders that affect the oral cavity.
Oral health has been neglected over the years, especially in the underprivileged areas. Amongst many reasons, low level of awareness among the population and the care providers even, has led to continued neglect of dental care.
State has made progress in providing comprehensive oral health care through its exiting care
system. Danta Bhagya Oral Health Policy in Karnataka was announced during FY 2014-15. Under this policy Danta Bhagya Yojane was introduced with the main objective to provide free complete dentures/Partial Denture (artificial teeth set) for senior citizens to improve the quality of life. Aims & Objectives: National Oral Health Programme (NOHP)
To improve the determinants of oral health.
To reduce morbidity from oral diseases.
To integrate oral health promotion and preventive services with general health care system.
To encourage Promotion of Public Private Partnerships (PPP) model for achieving better oral health.
Danta Bhagya
Completely edentulous patients over the age of 45 years having BPL card will be given complete dentures free of cost and Patients with 3 or more missing teeth can get partial dentures having BPL card.
Apart from giving free complete dentures, this programme also focus on prevention of dental diseases and oro-mucosal lesions.
The programme is underway in 7 District Hospitals, 2 Government Dental Colleges and 43 Private Dental Colleges who are in MoU with Government of Karnataka.

119
Activities: National Oral Health Programme (NOHP) Dental Chair, Equipment
Updradation od Dental Units Source 2016-17 2017-18 2018-19 2019-20 2020-21 2021-22 NOHP Dental Chair 10 - 19 1 25 5
State
- 66 - 71 - - B Class Autoclave 179 Instruments Cabinets
374
Consumables Every year under NHM Dental units are provided with funds for procuring Dental Consumables DH-50000, TH-35000 and CHC- 25000.
Sl No Year Funds (in Lakhs) Total No of Facilities 1 2016-17 38 21 2 2017-18 0 - 3 2018-19 112.40 367 4 2019-20 112.40 367 5 2020-21 112.40 367
Dental Services Provided across Karnataka
Particulars 2019-20 2020-21 2021-22 OPD 758697 577745 638226 Restorative Treatments 113632 53926 74299 Oral Prophylaxis 43861 10461 16931 Root Canal Treatment 13629 4586 7605 Extractions 135949 76210 100821 Surgical Procedures 8652 4568 8410 Oral Cancer diagnosed 3061 2897 1575 Treated by only medications 313786 304106 315496

120
Danta Bhagya
Sl No Years Financial Expenditure Beneficiaries
1 2015-16 8.93 1606 2 2016-17 17.57 3293 3 2017-18 56.21 4802 4 2018-19 37.64 5537 5 2019-20 43.27 5907 6 2020-21 38.09 1517*
Total 22662
Training-interactive session and Training for Asha and Health Workers
Sl No Years Training 1 2020-21 31 2 2021-22 31
Dental Camps
Sl No Years Dental Camps 1 2019-20 225 2 2020-21 176 3 2021-22 100

121

122
1.26 Quality Assurance Programme: Preamble:
Quality Assurance division under National Health Mission is enable for maintenance of quality related aspects of all the public health care facilities in the state. Quality Assurance Programs under NHM, Government of Karnataka implementation started in 2015-16.Quality Assurance Programs are:
1. Kayakalpa 2. Swachh Swasth Sarvatra (SSS) 3. National Quality Assurance Program (NQAP) 4. Mera Aspataal (MA) 5. Biomedical Waste Management (BMWM) 6. Patient Safety 7. Infection Prevention & Control (IPC)
QA Goal Provision of Quality Health Care Services in Public Health Facilities (PHFs) in Karnataka
Objective of QA
Up gradation of all Public Health Facilities (PHFs) for NQAS Certification. All Public Health Facilities (PHFs) to qualify for Kayakalpa award. Integration of all Public Health Facilities (PHFs) for Mera Aspataal-Patient feedback system.
Kayakalpa:
Swachh Bharat Abhiyan (SBA) was launched by the Hon. Prime Minister on 2nd October 2014, focuses on promoting cleanliness in public spaces. In 2015-16, Government of Karnataka implemented Kayakalp program in public health facilities as a major mechanism of social protection to meet the health care needs of large segments of the population. Cleanliness and hygiene in hospitals are critical to preventing infections and also provide patients and visitors with a positive experience and encourages moulding behavior related to clean environment.
“Kayakalp”-an initiative for awards to public health facilities launched in May 2015.
“Kayakalp” award is to encourage public health facility in the country to work towards standards of excellence to help the facilities stay clean and hygienic.
Kayakalp Measure Public Health Facilities under following 7 Thematic Areas: 1. Facility Upkeep 2. Sanitation and Hygiene 3. Waste Management 4. Infection Control 5. Support Services 6. Hygiene Promotion 7. Beyond Hospital Boundary 8. Eco-Friendly Hospital (DH,TH,CHC)

123
Kayakalpa Award Status 2015-21
Kayakalpa 2015-16 2016-17 2017-18 2018-19 2019-20 2020-21 Total Award Facilities 03 103 290 479 611 900
Swachh Swasth Sarvatra (SSS):
Swachh Swasth Sarvatra joint initiative of Ministry of Health & Family Welfare and Ministry of Drinking Water & Sanitation launched on 29th December 2016 to achieve high levels of sanitation and hygiene in and around public health facilities.
SSS fund were approved to a total of 150 CHCs@10lakh per CHC from 2017-18 and 175 UPHCs@50,000/- from 2020-21 to implement SSS program and achieve Kayakalpa award.
As of now a total of – 44 CHCs and 22 UPHC won the ‘Swachha Rathna Award ’
National Quality Assurance Program (NQAP):
National Quality Assurance Program (NQAP) envisages to instill the culture of quality and Safety in our health systems. It includes development of standards and tools which are pro public health, flexible, evidence based, current as per professional knowledge, explicit, user friendly and have a uniform measurement system. Under the ambit of NQAP, National Quality Assurance Standards (NQAS).
NQAS has got accreditation from International Society for Quality in Healthcare (ISQua).
In Karnataka 2021-22, 438 Public Health Facilities is the target set by QI NHSRC for National Certification. Out of which 31 PHFs (DHs-08, 24*7PHCs-18 and UPHCs-05) are NQAS Certified. Remaining 408 will be subjected for NQAS SLA (Virtual)
NQAS Certification (National/State) Status
before 30.11.2021
NQAS National Certification
Total 31 Mera Aspataal (My Hospital)
Every health system should aspire to provide patient-centric care. This can be best done by empowering citizens to have their voice heard, involve them in making health care system more accountable and creating a system that acts on their feedback. Towards this end, the Ministry of Health and Family Welfare launched the Mera Aspataal application on 29th August 2016.
“Mera Aspataal” is a simple, intuitive, and multi-lingual application that captures patient feedback in a very short time on the services received from the health facilities. It works through multiple communication channels, including Short Message Service (SMS), Outbound Dialing (OBD), a mobile application, and a web portal.
The application allows feedback to be consolidated, analysed and disseminated on a frequently updated dashboard. Analysed data is used to improve quality of services in healthcare facilities. Thus the Mera Aspataal allows patients to connect with the healthcare providers and policymakers and to have their opinion heard and acted upon.

124
Integration :
Presently Total 322 (52 DH, 142 TH, 2 CHC, 2 MCH, 51 PHC and 73 UPHC) Health Care Facilities are integrated with Mera Aspataal Application. Presently 32TH under integration process. SQAU planned for remaining facilities integration process in a phased manner in the FY 2021-22.
BIOMEDICAL WASTE MANAGEMENT (BMWM)
Biomedical Waste is defined as any waste, which is generated during the diagnosis, treatment or immunization of human beings or animals, or in research activities pertaining thereto, or in the production or testing of biological.
Unsafe disposal of Biomedical Waste has huge impact on the Environment & Human Health. Hence, Ministry of Environment, Forest and Climate Change has notified BMW Rules on 28th March 2016 and its Amendments thereof. It is mandatory for all the hospitals under Department of Health and Family Welfare to adhere to BMW Rules 2016 and its amendments for safe & scientific disposal of Biomedical Waste.
OBJECTIVES BMWM UNIT: • To assist the Healthcare Facilities under the Department in implementation of the Biomedical
Waste Management Rules 2016 and its Amendments thereof. • To supervise, handhold and monitor the HCF’s to comply with the statutory requirements of
Biomedical Waste Management Rules 2016. • To plan the logistics and budget needed for BMW management in the State. • To provide guidelines in implementation of the rules. • To design and plan for periodic training to Healthcare Personnel of the Department. • To liaise and coordinate with the State Pollution Control Board.
BMWM Implementation:
• Formation of Biomedical Waste Management Committee & Infection Control Committee in each of the Hospital.
• Segregation of Biomedical Waste at the point of Generation in respective Color Coded Closed Bins (Yellow, Red, Blue & White) as per BMW Rules 2016.
• Training of all the staffs working in the hospital on BMW Management periodically and maintain records.
• Valid Authorisation and timely renewal from the prescribed control board for generating Biomedical Waste.
• Maintain Biomedical Waste Management Register in all wards and availability of the same in the Hospital Website.
• Minutes of the all the meetings related to BMW should be recorded and submitted along with Annual Report.
• Timely submission of Annual Report in the prescribed format to Pollution Control Board, etc.
• Facilities Valid MOU with Common Treatment Facilities (CTF)

125
Financial Utilization Status in FY 2021-22
Under QA a total of Rs.3052.01lakh including HR and Committed budget in 2021-22 For which financial utilization guidelines prepared and disseminated to district for proper utilization of provided fund.
In 2021-22 a total of Rs.176.35 Lakhs for approved to Quality Assurance NQAS Traversing Gaps.
For Kayakalp Assessment and Awards Approved Rs.935.60 Lakhs. For SSS Rs.115.29 Lakhs Committed amount of 2020-21 for 2021-22 and released to districts For Bio Medical Waste Manages Approved Rs.1041.84 For Patient Safety (Fire Audit) Approved Rs.83 Lakhs 2021-22 till December expenditure is Rs.735.50 lakhs, which is 24.10%.
1.27 Family Welfare Programme Introduction:
India is the first country that launched a National Family Planning Programme in 1952, emphasizing fertility regulation for reducing birth rates to the extent necessary to stabilize the population at a level consistent with the socio-economic development and environment protection. Dramatic growth has been driven largely by increasing numbers of people surviving to reproductive age, and has been accompanied by major changes in fertility rates, increasing urbanization and accelerating migration.
Objectives:
• Main objective of the programme is to empower the couple to enjoy the reproductive health, improve maternal and child health status.
• Overall reduction in the malnourishment among children and adolescents. • To sustain the TFR (Total Fertility Rate) achieved in the state. • To reduce the regional imbalances in the TFR focusing more on Northern Karnataka. • Ensure access to family planning services to eligible couples and reduce the unmet need by an
improved access to voluntary family planning services, supplies and information. • Improve the modern contraceptive usage and demand satisfied by modern contraceptives.
Goals:
• Ensure universal access to sexual and reproductive health-care services, including for family
planning, information, and education, to attain replacement level fertility: TFR < 1.8 (Karnataka
state has achieved)Expanding the basket of choices and scaling up the usage of current methods
available and roll out of newer contraceptives (Injectable Antara and Chaaya)
• Ensuring healthy birth spacing by enhancing the focus on spacing methods.
• Strengthening the sterilization services through quality service delivery and demand generation.
• Strengthening the supply chain of family planning commodities

126
Implementation:
Formulation of Statutory Bodies like (SQAC, DQAC, SFPIS Subcommittee and QACs at Family Planning Centres co-located at the delivery points). The Basket of choices for Sterilization Methods are provided to the target couples (Eligible Couples) increasing access to contraceptives through distribution of contraceptives at the doorstep of beneficiary through health care workers. An effective Model for Behaviour Changes Communication through Social networking & Convergence Inter/Intra Sectoral and Strategic Planning cycle has been adopted for promoting family planning methods. Updated the CAC software from 2.0.7 to 2.0.8
Activities done for implementation of the Family Planning Programme:
1. Integrated Training/ Orientation/ Review Meeting under Family Planning for LHV, ANM, Pharmacists.
2. Integrated Training/ Orientation/ Review Meeting under Family Planning for Medical Officers/GDMOs/ Gynaecologists
3. Integrated training on Post Abortion Family Planning for Medical officers and nursing officers. 4. Meeting-cum-Sensitization Training regarding Strengthening of Family Planning Services,
Implementation to streamline the co-ordination between the heath staff and delivery point and filed level to boost the family planning services (Post-partum, Post-abortion, IUCD and Sterilization).
5. Data entry operators training on upgraded CAC state monitoring system.
Physical and Financial Achievement:
Year Physical Finance Target Achievement Target Achievement
2018-19 1791012 986870 2682.05 1984.04 2019-20 1792044 977970 2776.43 2316.75 2020-21 1719093 776093 2730.04 1015.47 2021-22 1117321 649437 3145.32 582.52
- Schemes of the programme: 1. ESB Scheme (Ensure Birth Spacing ): Spacing of minimum 2 years before 1st Child (ESB-I),
Spacing of minimum 3 years between the two child (ESB-II), 2. Family Planning Indemnity Scheme: Claim benefit to the Failures, Deaths and , Complications
following Sterilizations. 3. HDC Scheme : Door step delivery of Family planning commodities through ASHA. Contraception methods -Permanent methods: 1) Female sterilization: a) Minilap / interval tubectomy b) Laparoscopic sterilization c) Post partal sterilization. 2) Male sterilization : No scalpel vasectomy.

127
Temporary methods / Spacing methods: 1) OCP: a) Mala- N tab.
b) Chhaya tab.
c) Emergency contraceptive pill.
2) CC/ Nirodh:
3) Injectables / inj. Antara
4) IUCD : Interval IUCD / PPIUCD / PAIUCD.
STRATEGIES ADOPTED
1. Strengthening spacing methods including condom usage, oral pills and IUCD
2. Emphasis on Postpartum family planning services more focus on Post-Partum Intra Uterine Contraceptive Device (PPIUCD)
3. Capacitating the health care providers with hands on trainings to provide services including PPIUCD
4. Strengthening quality of services with regular quality assurance measures including supportive supervision and monitoring.
5. Providing of spacing tools at the doorsteps through ASHAs and grass root health functionaries.
6. Appropriate IEC and also counseling services through RMNCH counselors and other health care providers.
7. Popularizing NSVs among men to encourage male participation and Gender equity.
Family Welfare:
The State offers an excellent family welfare programme operating through the existing health infrastructure. The main objective of the programme is to provide better health services in general and family planning services in particular to check the rapid growth of population. Table 1provides details of the State’s achievements in sterilization and IUD during the last seven years.
Though sterilization continues to be the main method of family planning the spacing between the
births of two children is also equally emphasized.

128
Table : Performance of Family Welfare Sterilization Programme:
Year Sterilization IUD Couples Target Achievement Target Achieve-
ment Protected
(%) Vasectomy
Tubectomy
Total
2012-13 484980 2857 330445 333302 311822 189981 66.42
2013-14 407102 1390 310025 311415 311883 159540 66.89
2014-15 449495 1006 321007 322013 303924 188756 63
2015-16 450997 1039 316922 317961 308356 181620 63
2016-17 454287 922 295520 296442 277007 181618 *** 51.3
2017-18 462141 917 306273 307190 *592008 214916 *** 51.3
2018-19 **406217 770 279996 280766 *505267 209353 *** 51.3
2019-20 **441371
787 295726 296513 **551908 233965
***51.3 2020-21
**468920 730
210688 211418 438366 217313 ****68.2
2021-22 up to
January **490516
624 173095 173791 237455 174333
****60.87
Note:- * No. of IUD & PPIUCD insertion ** 2021-22 ELA *** NFHS 4( 2015-16) and **** NFHS 5 (2019-20)
Sl. No. Indicators NFHS 4 survey NFHS 5 survey
1 MCPR 51.3 68.2 2 TFR 1.8 1.7 3 Female sterilization 48.6 57.2 4 Male sterilization 0.1 0 5 IUCD /PPIUCD 0.8 2.9 6 OCP 0.4 2.10 7 CC 1.3 4.1
8 Injectables 0 0.5

129

130
Photos/ Maps/ Chats/graph:

131
Any Special Achievement:
• Private Hospitals for Comprehensive Abortion Care (CAC) services (under the provision of MTP Act 1971)
• FPLMIS operationalization and functioning at all the facilities and indentation through SMS by ASHAs.
• Roll out of Inj. Antara at all the PHC facilities. Listing of all the CHAAYA beneficiaries by ASHA workers.
Outcome of the Programme:
• Total Sterilization 168821 done in FY 2021-22 (Female Sterilization (168821), Male sterilization (462))
• Contraceptive prevalence for modern methods is 68.2%

132
• Karnataka state has achieved Total Fertility Rate of 1.8 and has attained replacement level fertility
• Ensuring healthy birth spacing by enhancing the focus on spacing methods • Family Planning Logistics Management Information system has been
operationalized in 80% of the total facilities • Ensure access to family planning services to eligible couples and reduce the
unmet need by an improved access to contraceptives • Improve the modern contraceptive usage
CAC programme: Updated data entry, increased in number of women receiving the services.
Action Plan:
1. Focus on improving uptake of spacing methods in FY 2022-23 esp. newer contraceptives Chhaya & Inj Antara
2. Fixed Day Services for IUCD and Male sterilization (NSV) to be organized 3. Saturation of Antara roll out at all PHCs and Sub Center through orientation trainings 4. Strengthen sterilization services through quality service delivery and demand
generation and adequately trained manpower for female and Male sterilizations 5. Strengthen FP counselling services at facilities and community level 6. Comprehensive IEC & multimedia campaigns 7. Regular review and follow up of low performing districts, blocks (Taluks) and high
case load facilities. 8. Family Planning commodities distribution and family planning counselling during
Routine Immunization sessions and through Mobile Medical Units 9. Strengthen delivery of contraceptives at the doorstep of beneficiaries (2 months of
requirement) by ASHAs and through ANMs at Sub Centre 10. Conduct virtual trainings of the ROP approved batches 11. Strengthen FPLMIS operationalization and FP supply chain review at district and
Taluk level.

133

134
PART-II
DRUGS CONTROL DEPARTMENT

135

136
DRUGS CONTROL DEPARTMENT
2.1 Introduction:
The State Drugs Control Department is existing since 1956 as an independent department under the control of the Ministry of Health and Family Welfare. It is headed by the state Drugs Controller. The main objective of the Department is to implement the Drugs and Cosmetics Act, 1940 and Rules there under and to ensure the quality of the Drugs and Cosmetics manufactured and marketed in the State in the interest of the public health. By exercising strict control and vigilance on the drugs marketed in the State, the Department eradicates the menace of Spurious and substandard drugs, ensures safety of drugs and their availability on the controlled prices to the public.
Drugs Control Department, Palace Road, Bengaluru
The Department has three wings:
1. The Enforcement Wing 2. Drugs Testing Laboratory and 3. The Pharmacy Education.

137
Drugs Control Department discharges the statutory functions involved in the enforcement of the following enactments:
Drugs & Cosmetics Act, 1940 & rules thereunder Drugs (Prices Control) Order, 2013(an order issued under the Essential Commodities Act). Drugs & Magic Remedies (Objectionable Advertisement) Act,1954 & Rules, Narcotics Drugs & Psychotropic Substances Act, 1985in relation to manufactured drugs covered
under the Drugs & Cosmetics Act, 1940 & Rules thereunder.
During the financial year 2021-22 a total provision of Rs. 7041.80 granted under the State scheme.
The establishment and construction work of laboratory buildings of 2 Regional Drugs Testing Laboratories one at Hubli and the other at Bellary in North Karnataka, are completed through KHSDRP and have already started functioning in respective own buildings. The Department is taking initiatives to get the NABL accreditation in the National level for these two laboratories. Drug Testing Laboratory, Bangalore has already having NABL Accreditation. SAKALA:
The Department is providing 26 services under SAKALA Scheme to assure the accomplishment of services to the public within the specified time frame. From 01.04.2021 to 31.01.2022, a total of 14742 applications are disposed.
The licensing activity of the drugs sales establishments is fully computerized and the licensing
process is online while the computerization of process of licensing to drug manufacturing units is under progress. The Department has successfully adopted the LMS/FMS software under e-governance for its internal files and letters management.
The Department has also successfully implemented e-sampling program for the process of Drug
Testing and Analysis in the State Drugs Testing Laboratories as a part of e-governance. The information about the substandard drugs is being published through the Departmental web portal, as soon as it is declared as substandard quality. The information is reflected in the department portal and around 42,000 auto generated SMS alerts will reach the various stakeholders like, retailers, wholesalers, Doctors & enforcement officers to prevent the use of substandard drugs. The information is also published in the Newspapers time to time.
In order to encourage the Pharmacy Education in the State, Admissions through CET has been introduced for the B. Pharma Education.
In the financial year 2021-22 Rs. 500.00 lakhs has been allocated for the construction of sub office of Udupi District.
2.2 Organisation set up:
Drugs controller is the head of the Drugs Control Department. Drugs Controller is assisted by one Additional Drugs Controller. Drugs Control Department is organized into enforcement/administration division, Drugs Testing Laboratory and Pharmacy Education division organogram is as below,

138
Working strength of the Drugs Control department of categories Group-A, Group-B, Group-C and Group-D with respect to the sanctioned, filled up and remained vacant posts is as follows as on 31.01.2022.
Number of posts
Sanctioned Filled up Vacant
Group-A 116 97 19 Group-B 254 156 98
Group-C (Technical) 67 16 51
Group-C (Non-Technical) 238 148 90
Group-D 111 35 76
Grand Total 786 452 334
Note: 158 posts created by government vide G.O.No. HFW/383/PTD/2012 Dt. 06/01/2015 Group A- Principal-01, Professor-12, Assistant professor-20, Group B- Lecturers- 42, Gazetted Assistant-01, Group C- Superintendant-02, Junior Engineer-01, First Division Assistant-08, Computer operator-08, Librarian-02, Store keeper-02, Second Division Assistant-08, Typist-08, Lab Technicians(Drugs)-02, Lab. Technician-10, Group D- Lab. Supervisor-20, Attendor-08, Gardener-02, Animal Supervisor-01.
2.3 Enforcement Wing:
Enforcement wing consists of an Additional Drugs Controller assisted by 13 Deputy Drugs Controller, (8 DDC’s posts are Vacant) Deputy Drugs Controller are assisted by 60 Assistant Drugs Controllers (8 ADC’s posts are vacant) under Assistant Drugs Controllers 112 Drugs Inspectors are

139
provided. 01 System analyst post is sanctioned to technically support the enforcement wing.(91 Drugs Inspectors posts and 09 Assistant Drugs Controllers post are vacant as on 31.01.2022). Recruitment process by KPSC is under process. Enforcement wing is laterally assisted by State Intelligence Branch, 6 Drugs Inspectors are working under an Assistant Drugs Controllers at Bengaluru under the supervision of Additional Drugs Controller and 2 drugs Inspectors in each of the 8 regional Deputy Drugs Controller offices under the supervision of the regional Deputy Drugs Controller. Enforcement wing is technically assisted by a System Analyst. Circles office’s are headed by Assistant Drugs Controllers and are functioning under the jurisdiction of each regional offices of Deputy Drugs Controller.
Sl.No. DDC REGIONAL OFFICE ADC CIRCLES
01 Bengaluru Bangalore: Circle-1, Circle-2, Circle-3, Circle-4, Circle-5, Circle-6, and Bangalore Rural Circle
02 Mysore Mysore: Circle-1 & Circle-2, Chamarajanagara Circle, Kodagu Circle and Mandya Circle.
03 Hubballi Dharwad Circle, Karwara Circle, Haveri Circle, Gadag Cirlce.
04 Gulbarga Gulbarga Circle, Bidar circle and Bijapur circle
05 Bellary Bellary Circle, Koppal Circle, Raichur Circle and Yadgir Circle
06 Belgaum Belagavi Circle and Bagalkot Circle,
07 Davanagere Chitradurga Circle, Davangere Circle and Shimoga Circle
08 Mangalore Udupi Circle, Mangalore Circle, Hassan Circle and Chikkamangalur Circle
09 Tumkur Tumkur Circle, Chikkaballapur Circle, Kolar Circle and Ramanagara Circle
PERFORMANCE OF ENFORCEMENT WING:
PARTICULARS 2021-22 (31.01.2022) Number of manufacturers units in the state
a Drugs Manufacturing units 414 b Loan License Manufacturers 443 c Cosmetic Manufacturing units 77 d Cosmetic Loan License Manufacturing units 43 e Repacking Units 09 f Approved Laboratories 41 g Blood Banks 253 h Blood storage Centers 242 i Cord Blood Bank (Stem Cells) 05
Total Number of Sales premises in the State 45110 Blood Banks / Blood storage Centers 253/242
STATUTORY ACTION TAKEN Sales Suspension 1184

140
License Cancellations 786 Manufacturing License Cancellations 02 Stop Production 03 Product permission Cancellations 05 Blood Bank Stop Collection 02 Number of prosecution cases launched under Drugs and Cosmetic Act, 1940 and Drugs (Price Control) order 1995/2013& DMR
50
Number of cases convicted 07
PROSECUTIONS INSTITUTED: The following are the details pertaining to the prosecutions instituted under Drugs and Cosmetic
Act, 1940 and Rules 1945, Drugs (Price Control) Order, 2013. (An order issued under Essential Commodities Act. 1955) and Drugs and Magic Remedies (Objectionable advertisement) Act, 1954 and Rules thereunder, during the year 2021-22 (1st April 2021 to 31.01.2022).
Sl.No. Particulars
Legislation D&C Act
1940 D.P.C.O
1995/2013 D.M.R
01 Prosecutions pending at the beginning of the year(i.e. as on 01.04.2022)
602 37 03
02 Prosecutions launched (up to 31.01.2022) (During 2021-22)
50 - -
03 Total (as on 31.01.2022) 652 37 03
04
Prosecutions decided(as on 31.03.2022)
05
07
-
-
-
-
a. Cases ended in acquittal/discharged (as on 31.01.2022)
b. Cases ended in Convictions (as on 31.01.2022)
05 Prosecutions pending as on 31.01.2022 640 - -
Total Number of cases as on 31.01.2022
640 37 03

141
2.4 DRUGS TESTING LABORATORY WING:
Drugs Testing Laboratory division is headed by Principal Scientific officer and is assisted by 3 Chief Scientific Officer’s of 3 laboratories. 19 scientific officers are working as government analysts. Out of 113 junior scientific officers this year 31 Junior Scientific Officers(JSO) are recruited and are deputed for 3 months training. 02 JSO posts remained vacant as on 29.02.2020. Chief Scientific Officers are assisted by Gazetted Assistant.
Drugs Testing Laboratory is provided with Hi-tech equipment’s and trained technical personnel
and is equipped to analysis all types of drugs and cosmetic (except vaccines, sera, blood & blood products). There are three Drugs Testing Laboratories in Karnataka, one in Bangalore and one each as Regional Drugs Testing Laboratories in North Karnataka at Hubli and Bellary. 1. Drugs Testing Laboratory, Bangalore.
(a) Number of samples analyzed 2564 (b) Number of samples found to be Standard quality 2347 (c) Number of samples found to be Not of Standard quality 217

142
2.Regional Drugs Testing Laboratory, Hubballi
3. Regional Drugs Testing Laboratory, Bellary
(a) Number of samples analyzed 1107
(b) Number of samples found to be Standard quality 1068
(c) Number of samples not found to be Standard quality 39
(a) Number of
samples analyzed,
2564
(b) Number of
samples found to
be Standard
quality, 2347
(c) Number of
samples found to
be Not of
Standard quality,
217
(a) Number of
samples analysed,
1089(b) Number of
samples found to
be Standard
quality, 1053
(c) Number of
samples found to
be Not of Standard
quality, 36
(a) Number of samples analysed 1089 (b) Number of samples found to be Standard quality 1053 (c) Number of samples found to be Not of Standard quality 36

143
Total samples from all the three laboratories for the period 2021-22 Sl.No. DTL/RDTL Total No. of Samples analysed Standard quality Not of Standard Quality
1 Bangalore 2564 2347 217
2 Hubballi 1089 1053 36
3 Bellary 1107 1068 39
Total 4760 4468446844684468 292292292292
2.5 Pharmacy Education:
Administrative control and supervision of Pharmacy Education vests with Drugs Controller. There is one Government College of Pharmacy situated in Bangalore. Board of examination authority is functioning for managing the affairs for conducting examinations for Diploma Courses in Pharmacy.
Government College of Pharmacy, Bangalore
(a) Number of
samples
analysed, 1107(b) Number of
samples found
to be Standard
quality, 1068
(c) Number of
samples found to
be Not of Standard
quality 39

144
Pharmacy Education consists of two wings i.e. 1. Government College of Pharmacy at Bangalore. 2. Board of Examining authority at Bangalore (BEA)
Government college of Pharmacy, Bangalore started in the year 1964 under the administrative
control of this Department. The Pharmacy education imparted at Diploma, Degree and Post Graduate levels. The Government of India through AICTE is supporting with 100% assistance for the development of Post –graduate courses in Pharmacy. The following disciplines are established under the Post-graduate course
1. Pharmaceutics 2. Pharmacology 3. Pharmacognosy 4. Pharmaceutical Chemistry
Details of the candidates for final examinations for the period 2020-21
Name of the Course Duration Month
01.04.2020 to 31.03.2021
Appeared Passed
D Pharm (Diploma in Pharmacy) 2 years First Year 70 67
Final Year 61 52
B Pharm (Degree in Pharmacy) 4 years
First Year 56 40
Second year 52 34
Third year 51 47
Final Year 53 46
M Pharm (Master’s Degree in Pharmacy)
2 years First Year 30 30
Final Year 31 31
Board of Examination Authority, Bangalore:
The Board of Examining Authority is entrusted with the responsibility of enforcing education regulations stipulated by the Pharmacy Council of India at Diploma level in the State with respect to conduct of examinations at Diploma level for the students admitted in the Government and Private Pharmacy Colleges in the State. The Principal Government College of Pharmacy is functioning as ex-officio Chairman, and the Deputy Drugs Controller on deputation functioning as ex-officio Member Secretary of the Board. There are 304 Private Colleges imparting Diploma in Pharmacy Education and one Government College of Pharmacy in the State.
Details of the students appeared for D Pharm examinations conducted by Board of Examining Authority during the period 01.04.2021 to 31.03.2022.
Sl.No. Number of the Course
Duration Annual Exam
Month / Year
Appeared Passed
1. D Pharm (Diploma in Pharmacy)
2Years March 2021 First Year
22237 5814
October 2021 Final Year
21095 Results not yet decided

145
Achievements of Drugs Control Department for the year 2021-22
Under the Karnataka Guarantee of Services to citizens Act-2011. The Drugs Control Department is providing 26 services of which 5 services are related to grant and renewal of licenses for sale of Drugs. Grant of Licenses for the establishment of Medical Stores/Chemist & Druggists. 16 services are related to manufacturing of drugs & cosmetics which are included in the current year.
Sl. No. Service List Designated
Officer
Designated Officer time
limit
Competent Authority
Competent Authority
time limit to Dispose
Appellate Authority
Time limit to Dispose
1 Grant of License Assistant
Drugs Controller
30 Working days
Regional Deputy Drugs
Controller
15 Working days
Additional Drugs
Controller
15 Working
Days
2 Renewal of License Assistant
Drugs Controller
30 Working days
Regional Deputy Drugs
Controller
15 Working days
Additional Drugs
Controller
15 Working
Days
3 Registered Pharmacist
Change/Cancellation
Assistant Drugs
Controller
7Working days
Regional Deputy Drugs
Controller
15 Working days
Additional Drugs
Controller
15 Working
Days
4 Competent Person
Change/Cancellation
Assistant Drugs
Controller
7 Working days
Regional Deputy Drugs
Controller
15 Working days
Additional Drugs
Controller
15 Working
Days
5 Changing of Name Assistant
Drugs Controller
7 Working days
Regional Deputy Drugs
Controller
15 Working days
Additional Drugs
Controller
15 Working
Days
6 Grant of Fresh Drug
Manufacturing license
Drugs Controller
60 days Deputy
Secretary HFW
15 days Principal Secretary
HFW 15 days
7 Renewal of Drug Manufacturing
license
Drugs Controller
210 days Deputy
Secretary HFW
15 days Principal Secretary
HFW 15 days
8 Issue of WHO GMP
Certificate Drugs
Controller 7 days
Deputy Secretary
HFW 15 days
Principal Secretary
HFW 15 days
9 Issue of Free Sale
certificate Drugs
Controller 7 days
Deputy Secretary
HFW 15 days
Principal Secretary
HFW 15 days
10 Issue of Market
Standing Certificate Drugs
Controller 7 days
Deputy Secretary
HFW 15 days
Principal Secretary
HFW 15 days
11 Issue of GMP
Certificate as per Sch. ‘M’
Drugs Controller
7 days Deputy
Secretary HFW
15 days Principal Secretary
HFW 15 days
12 Issue of No Conviction Certificate
Deputy Drugs
Controller 7 days
Drugs Controller
15 days Principal Secretary
HFW 15 days
13 Issue of Production capacity certificate
Drugs Controller
7 days Deputy
Secretary HFW
15 days Principal Secretary
HFW 15 days
14 Issue of Licence
Validity Certificate.
Deputy Drugs
Controller 7 days
Drugs Controller
15 days Principal Secretary
HFW 15 days

146
15 Issue of Essentiality
Certificate Drugs
Controller 7 days
Deputy Secretary
HFW 15 days
Principal Secretary
HFW 15 days
16 Issue of Neutral Code Number
Deputy Drugs
Controller 7 days
Drugs Controller
15 days Principal Secretary
HFW 15 days
17 Issue of
Manufacturing and Marketing Certificate
Drugs Controller
7 days Deputy
Secretary HFW
15 days Principal Secretary
HFW 15 days
18 Issue of Quality and Capacity Certificate
Drugs Controller
7 days Deputy
Secretary HFW
15 days Principal Secretary
HFW 15 days
19 Issue of Performance
Certificate. Drugs
Controller 10 days
Deputy Secretary
HFW 15 days
Principal Secretary
HFW 15 days
20 Issue of Installation /
Registration / Products certificate
Drugs Controller
7 days Deputy
Secretary HFW
15 days Principal Secretary
HFW 15 days
21
Issue of Certificate of pharmaceutical
Products (COPP) For the recommended
products
Drugs Controller
20 days Deputy
Secretary HFW
15 days Principal Secretary
HFW 15 days
22 Issue of Good
Laboratory Practice Certificate
Drugs Controller
7 days Deputy
Secretary HFW
15 days Principal Secretary
HFW 15 days
23 Grant of License for Change in Premises
Assistant Drugs
Controller
30 Working days
Regional Deputy Drugs
Controller
15 Working days
Additional Drugs
Controller
15 Working
Days
24 Grant of License for
Change in Constitution
Assistant Drugs
Controller
30 Working days
Regional Deputy Drugs
Controller
15 Working days
Additional Drugs
Controller
15 Working
Days
25
Grant of License for Change in Premises
& change in Constitution
Assistant Drugs
Controller
30 Working days
Regional Deputy Drugs
Controller
15 Working days
Additional Drugs
Controller
15 Working
Days
26 Issue of No
conviction Certificate
Deputy Drugs
Controller 7 days
Drugs Controller
15 days Principal Secretary
HFW 15 days
Right to information Act, 2005: Under Right to Information Act, 2005 in Drugs Control
Department, Drugs Controller for the State of Karnataka is the public Authority, the Additional Drugs Controller is designated as first Appellate Authority, 41 officers are designated as public information officers in Head office, Regional Deputy Drugs Controller offices, all District Circle offices, Drugs Testing Laboratory Bangalore, Regional drugs testing Laboratories Hubballi and Bellary, Government College of Pharmacy.
Drugs Testing Laboratory Bangalore has received NABL accreditation.
Regional Drugs Testing Laboratories, at Hubballi and Bellary are under process of obtaining NABL accreditation.

147
The Department has implemented e-sampling system in laboratory. As soon as drug is declared as substandard quality, the information will be reflected in departmental portal and around 42,000 auto generated SMS alerts will reach the various stock holders like retailers, wholesalers, Doctors and Enforcement Officers to prevent the use of substandard drugs.
“Technical Cell” is established in the department for the speedy disposal of the application filed
by the manufacturers in order to boost the exports. In the Current year special inspection drive was conducted to detect/prevent misuse of drugs
falling under NDPS Act.
An awareness programme was conducted on the drug abuse on June 26 on the occasion of International Anti-Drugs Abuse Day in the department auditorium several students from various pharmacy colleges were invited and participated.
Under strengthening of the State Drugs Regulatory System in order to increase the analysis of
no. of samples scientific Equipments are yet to purchase through tender at an estimate cost of Rs.3.00 crores and installation of modular clean room at an estimate cost of Rs.5.00 crores
Department in association with NIC is monitoring the blood bank networking in the name of
Jeeva Esanjeevani at URL https://blood.kar.nic.in/for citizens to access the availability of blood and blood components
1030 product permissions are granted for exports on priority to the manufacturers in the year 2021-22 based on the NOC. 1901 Certificate of Pharmaceutical Products (COPP) is issued to the manufacturers for the registration of their products in various countries in the year 2021-22.
For the first time a consensual agreement was made between the Management of Private
Pharmacy Colleges and the Government for the government seats in the private colleges in order to encourage the pharmacy course and to ensure that the meritorious students get seats in the private colleges at government fixed fee. Accordingly in the academic year 2019-20, for D-Pharmacy, for B-Pharmacy, for M-Pharmacy and for Pharm-D are made available for poor and meritorious students.
Conducting of examinations for the D. Pharmacy course is by online transmission of question papers to various examination centers.
In order to provide quality education for D.Pharmacy students stringent norms are notified and new college applications are scrutinized in the high power committee meeting .
Construction of sub office at Mandya (estimate cost of Rs.209.00 lakhs) and Udupi (estimate cost of Rs.288.00 lakhs) is completed. Construction of sub office at Tumkur (estimate cost of Rs.270.00 lakhs) is under progress.
Product permissions granted to manufacture of drugs & cosmetics for sale during 2021-2022 are detailed below: Details Domestic Export Total Drugs 566 1030 1596 Cosmetics 168 02 170

148
Action taken during Covid-19:
Department has taken necessary steps to ensure the availability of quality essential drugs and hand sanitizer. Further, adequate surgical masks are also made available to citizens during pandemic period.
Officers of the department made Chemists and Druggists to upload the details of purchase of drugs for the symptoms of ILI and SARI in the Pharma Portal by citizens. These data was compiled and forwarded to Apthamithra web Portal to keep a tab/vigil on covid cases during pandemic period.
War room is created to address the issues pertaining to the Remdesivir injection and oxygen and was made functioning round the clock with helpline number - 8951755722. Officers of the Department were deputed at all Oxygen manufacturing units to monitor manufacture and supply on priority to the Covid patients in 2nd wave of Covid-19 situations.
State level Vigilance Squad is created in the department to monitor and prevent misuse, hoarding and black marteking of Remdesivir injection and oxygen during pandemic period and 11 cases were booked.
2.6 FINANCE:
Budget Allotment and Expenditure for the year 2021-22 (Rs. in lakhs)
Sl. No.
BUDGET HEAD Budget allotment for 2021-22
Expenditure for the year 2021-22
(upto January)
1 2210-06-104-0-01 Drugs Controller 2549.80 1850.64
2 2210-06-104-0-02 Drugs Testing Laboratory 1663.00 1147.28
3 2210-05-105-1-14 Govt. College of Pharmacy 1050.00 618.02
4 4210-03-105-02-03 Drugs Controller - Buildings 500.00 95.21
5 2210-06-104-0-15 Strengthening of State Drugs Regulatory System Scheme
800.00 2.99
6 4210-04-200-1-05 Construction of sub offices and other civil works (Strengthening of State Drugs Regulatory System)
479.00 192.69
Total 7041.80 3906.83
(55.48%)

149
REVENUE RECEIPTS FOR THE YEAR 2021-22 (Rs. in lakhs)
SL. NO. BUDGET HEAD 2021-22 Budget
Estimate
Revenue Receipts for the year 2021-22
(upto January 2022)
1.
0210-04-104-2-01 Drugs Controller 500.00 592.56
2.
0210-03-105-0-01 Government College of Pharmacy,
Bangalore 900.00 529.70
TOTAL
1400.00 1122.26

150
PART III
AYURVEDA, YOGA & NATURE CURE, UNANI, SIDDHA AND HOMEOPATHY (AYUSH
DEPARTMENT)

151
3.1. ORGANOGRAM:
z
Government of Karnataka
Principal Secretary
Health and Family Welfare
Chief
Administrative
Officer
Deputy Director-(Ayu)
Deputy Director-(Unani)
Deputy Director-(Hom)
Deputy Director (NC&
Yoga)
Administrative
Officer
Drug Inspector
Bangalore, Mysore,
Belgaum, Kalaburgi
District AYUSH Officers
Chief Planning &
Development
Officer
SENIOR MEDICAL OFFICER (AYUSH) and
MEDICAL OFFICER (AYUSH)
Asst. Drug
Controller
Joint Director
(M.E)
Deputy Director
(Pharmacy)
Prog. Officer:
Prog. Officer-CSS
Prog. Officer-NHM
Prog. Officer-IEC TRAINING
Principals Govt/
Aided /Un Aided
Ayush Medical Colleges
Planning Officer
Accounts
Officer
COMMISSIONER
Department of AYUSH
Drug Testing
Laboratrory
Deputy Drug
Controller

152
3.2 Departmental Brief Note, Staff Position of the Department:
The Department of AYUSH has the mandate of regulating AYUSH Education and drug
enforcement and is also responsible for health service delivery under the Ayush systems.
The Department is headed by Commissioner AYUSH, assisted by a Joint Director (Medical Education), one Chief Administrative Officer (KAS Senior Scale), Drug Licensing Authority, one each of Deputy Directors for Ayurveda, Unani, Homoeopathy and Nature Cure &Yoga, a Chief Planning and Development Officer, an Administrative Officer and an Accounts Officer. District AYUSH Officers are incharge of Dist. Hospitals, Taluk Hospitals and Dispensaries under the overall control of the respective Zilla Panchayats.
2021-22(Upto Jan) Budget details:
(Rs. In lakhs) State Sector ZP Sector
Budget Expenditure Budget Expenditure Non-plan 21401.19 13607.29 13060.69 9688.29
The Staff Position of the Department is as follows: Non-Teaching Teaching Total Sanctioned Filled Vacant Sanctioned Filled Vacant Sanctioned Filled Vacant
Group-A 1122 746 376 203 102 101 1325 848 477
Group-B 76 25 51 126 07 119 202 32 170
Group-C 1189 410 779 0 0 0 1189 410 779
Group-D 1592 439 1195 0 0 0 1592 397 1195
Total 3979 1578 2401 329 109 220 4308 1687 2621
3.3 HEALTH SECTOR:
At the district level, the department is represented by the District Ayush Officer (DAO), who is under the administrative control of the concerned Zilla Panchayat. The DAO is responsible for day to day functioning of the hospitals and dispensaries in the district, which are the main service delivery arms of the department.
The system wise break up is given here under dated 31.01.2022:
Sl.No.
Systems Government Hospitals No. of dispensaries
No. of Hospitals No. of Beds.
01 Ayurveda 115 1821 564 02 Unani 18 392 50 03 Homoeopathy 18 260 43 04 Nature Cure 05 46
05 05 Yoga 03 15 Total 159 2534 662

153
3.4 GOVERNMENT CENTRAL PHARMACY:
One Government Central Pharmacy at Bangalore is manufacturing Ayurveda and Unani
medicines, which are being supplied to all Government Ayurveda, Unani Hospitals and Dispensaries in the state.
DRUG TESTING LABORATORY:
Is functioning in Bangalore to ensure the quality of AYUSH Raw Drug samples and Medicines.
Statement showing the Details of Samples tested by Drug Testing Laboratory in the year 2021-22
01-04-2021 to 31-01-2022 Sl.No. Types of Drugs Tested Total
1 Legal Sample 128 2 Survey Sample 638 3 Ayurveda Medicines 01 4 Unani Medicines 03 5 Raw Drugs 31
Total 801 Total Number of Samples tested - 801
3.5 AYUSH DRUGS CONTROL:
Is responsible for regulating manufacture of ASU drugs by companies licensed in the state under
the provisions of the Drugs and Cosmetics Act, 1940 and the rules there under.
There is one Deputy Drug Controller (DDC), one Assistant Drug Controller and one Drug Inspector in the head quarter at Bangalore. The DDC is the ASU drug licensing authority. The Director / Commissioner Ayush is the drug controller for ASU drugs. ASU drug control units are also functioning at Mysore, Belagavi and Kalaburgi.
Details of Licensed manufacturing Units as on 31-01-2022 are as follows:-
3.6 STATUTORY BOARDS: There are two statutory boards namely the Karnataka Ayurveda and Unani Practitioner’s Board (KAUP) and the Karnataka Board of Homoeopathy Systems of medicine functioning under the department, responsible for registration of practitioners of the respective systems.
Sl. No Systems No. of
Manufacturing license holders. Loan
license No. of Sales
Whole sale Retail 1 Ayurveda 226 231 0 0 2 Unani 0 0 0 0
Total 226 231 0 0

154
Details of registered practitioners as on 31.01.2022
Sl.No Name of System No. of practitioners 01 Ayurveda 1213
02 Unani 32
03 Naturopathy & Yoga 63
04 Siddha 0
05 Homoeopathy 14973
TOTAL 16281
3.7 AYUSH MEDICAL EDUCATION: Department of Ayush regulates admissions to all Ayush colleges in the state.
The details of Medical Colleges under this department as follows in the state.
System Government Total No. of
Colleges Aided colleges Unaided Colleges No. Intake No. Intake No. Intake No. Intake Ayurveda 4 320 2 120 72 4045 78 5385 PG 0 86 0 0 0 820 0 906 Unani 1 60 0 0 04 240 05 300 PG 0 8 0 0 0 07 0 15 Homoeopathy
1 100 0 0 17 1290 18 1450
PG 0 28 0 0 0 101 0 129 Yoga & Nature Cure
1 60 0 0 10 540 11 600
PG 0 0 0 0 0 35 0 35 Total 7 662 2 120 103 7078 112 9020 Note: 2021-22 academic year admissions not yet completed
These AYUSH Medical colleges are affiliated to Rajiv Gandhi University of Health Sciences.
Selection of candidates for all these Medical colleges is through a Common Entrance Examination as decided by Government from time to time.
3.8 HERBAL GARDENS:
Herbal gardens are being maintained at Bangalore. Mysore and Bellary which are attached to the Ayurveda Medical Colleges. The Medicinal plants required for students demonstration and green herbs required for the hospitals are being grown in these herb gardens. Further “Dhanvantri Vana” has been established in 37 acres of land at Nagadevnahalli near Bangalore University campus for development of herbarium and about 500 varities of Herbs have been raised. Depending upon the basic facilities of the Dispensaries and Hospitals Herbal gardens are being developed across the state. The medicinal plants grown here are distributed to the public. BIO MEDICAL WASTAGE MANAGEMENT:
Under the guidelines of the Karnataka State Pollution Control Board and Hon’ble Lok Adalath, from 2011-12. AYUSH Department has adopted Bio-Medical wastage management of Government AYUSH Hospitals and Dispensaries in the state.

155
3.9 ACHIEVEMENTS OF THE YEAR 2021-22:
• Cabinet approval has been granted for the opening of the New AYUSH University in Shimoga City, which has been approved by the AYUSH University Act in both Houses.
• 50 bedded integrated AYUSH hospitals have been newly constructed and started in Gadag and Mangalore cities at the cost Rs.9.00 crores each.
• 7th International Day of Yoga is celebrated on 21-06-2021 with the slogan “Be with Yoga Be at Home”
• 176 AYUSH Health and Wellness centres have been developed under National Ayush Mission. 3.10 PROPOSED PLAN FOR THE YEAR 2022-23:
• It is proposed to construct a 50 bedded integrated AYUSH hospital at Yadagiri city at an estimated cost of Rs.13.00 crores.
• It is proposed to construct a 50 bedded integrated AYUSH hospital at Haveri city at an estimated cost of Rs.12.00 crores.
• Under National AYUSH Mission scheme, it is proposed to upgrade 84 AYUSH dispensaries to AYUSH Health and Wellness Centers.
3.11 2022-23 And Financial Achievements, Classification And Activities For 2021-22
Sl. No
Head of Account
Budget for 2021-22
Revised Budget for
2021-22
Expenditure Up to
Jan- 2022
Estimated Budget for
2022-23 1 2210-02-101-1-03
Ayush Directorate, Dist. Offices, Health IEC and Training Programmes
1618.60 1618.60 (+)262.70 (-) 500.00
1381.30
797.17 1703.00
2 2210-02-101-1-04 Land & Bldg for AYUSH
100.00 100.00 14.87 200.00
3 2210-02-101-2-04 Opening & Maintenance of Taluk & Dist. Hospitals
1019.00 1019.00 (+)6.58 1025.58
645.62 1578.20
4 2210-05-101-1-03 Opening & Maintenance of Government AYUSH Medical Colleges (Under Graduate and Post Graduate) and Teaching Hospitals
11667.00 11667.00 (+)1615.76
13282.76
8515.70 15107.00
5 2210-05-101-3-01 AYUSH- Drugs manufacturing institutions and Drug Testing Laboratories Govt. Central Pharmacy
393.00 393.00 (+)7.29 400.29
256.46 519.00
6 2210-05-101-6-00 AYUSH- Cultivation and Development of Medicinal plants and Karnataka State Medicinal Plants authority
146.00 146.00 95.82 442.00
7 2210-05-200-0-11 (State Share) AYUSH-National Ayush Mission-CSS
3055.00 3055.00 (+)9.97 3064.97
654.45 3242.00

156
8 2210-05-200-0-13 (Central Share) AYUSH- National Ayush Mission - CSS
0.00 1.00 0 2700.00
9 4210-03-101-1-01 AYUSH Buildings Major Works(Capital Out lay)
2000.00 2000.00 715.29 3000.00
19998.60
21401.19 13607.29 28491.20
* * * * *
Copyright © 2022 FDOKUMEN