
GROUP TRUST BOARD MEETING IN PUBLIC1 A G E N D A
135
GROUP TRUST BOARD MEETING IN PUBLIC 1 The next meeting of the group trust board will take place on Wednesday 25 July 2018 at 1.00pm in the Sir William Wells atrium, ground floor, Royal Free Hospital. Dominic Dodd Chairman A G E N D A ITEM LEAD PAPER ADMINISTRATIVE ITEMS 2018/94 Apologies for absence – M Basterfield, James Tugendhat, D Sloman, E McManus D Dodd 2018/95 Declaration of interests D Dodd 1. 2018/96 Minutes of meeting held on 27 June 2018 D Dodd 2. 2018/97 Matters arising report D Dodd 3. 2018/98 Record of items discussed at the Part II board meeting on 27 June 2018 D Dodd 4. QUALITY, PATIENT SAFETY AND EXPERIENCE 2018/99 #Pride video D Dodd Verbal 2018/100 End of lfe care Dr Jo Wilson PhD, consultant nurse palliative care and Dr Hannah Western, clinical service lead, palliative care C Streather Verbal 2018/101 Learning from deaths review – quarter 3 report C Streather 5. 2018/102 Director of infection prevention and control reports: • Annual report 2017/18 • Quarterly report D Sanders 6. 2018/103 Complaints annual report 2017/18 D Sanders 7. 2018/104 Patients’ voices A Raja 2018/105 Go see visits E Kearney 8. 2018/106 Workforce race equality standard update D Grantham 9. 2018/107 Gender pay review gap D Grantham 10. FINANCE AND PERFORMANCE 2018/108 Financial performance report C Clarke 11. 2018/109 Operational performance report P Ridley 12. GOVERNANCE AND REGULATION: REPORTS FROM BOARD COMMITTEES – DISCUSSION BY EXCEPTION ONLY 2018/110 Chair’s and chief executive’s report D Dodd / D Sloman 13. 1 In accordance with the Health & Social Care Act 2012, all Trust Board meetings must be held in public. All decisions which require the board’s collective approval can only be made at a Trust Board (or a Part II meeting held in closed session to discuss confidential matters).
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of GROUP TRUST BOARD MEETING IN PUBLIC1 A G E N D A

GROUP TRUST BOARD MEETING IN PUBLIC1
The next meeting of the group trust board will take place on Wednesday 25 July 2018 at 1.00pm in the Sir William Wells atrium, ground floor, Royal Free Hospital.
Dominic Dodd Chairman
A G E N D A
ITEM LEAD PAPER
ADMINISTRATIVE ITEMS
2018/94 Apologies for absence – M Basterfield, James Tugendhat, D Sloman, E McManus
D Dodd
2018/95 Declaration of interests D Dodd 1.
2018/96 Minutes of meeting held on 27 June 2018 D Dodd 2.
2018/97 Matters arising report D Dodd 3.
2018/98 Record of items discussed at the Part II board meeting on 27 June 2018
D Dodd 4.
QUALITY, PATIENT SAFETY AND EXPERIENCE
2018/99 #Pride video D Dodd Verbal
2018/100 End of lfe care
Dr Jo Wilson PhD, consultant nurse palliative care and Dr Hannah Western, clinical service lead, palliative care
C Streather Verbal
2018/101 Learning from deaths review – quarter 3 report C Streather 5.
2018/102 Director of infection prevention and control reports:
• Annual report 2017/18
• Quarterly report
D Sanders 6.
2018/103 Complaints annual report 2017/18 D Sanders 7.
2018/104 Patients’ voices A Raja
2018/105 Go see visits E Kearney 8.
2018/106 Workforce race equality standard update D Grantham 9.
2018/107 Gender pay review gap D Grantham 10.
FINANCE AND PERFORMANCE
2018/108 Financial performance report C Clarke 11.
2018/109 Operational performance report P Ridley 12.
GOVERNANCE AND REGULATION: REPORTS FROM BOARD COMMITTEES – DISCUSSION BY EXCEPTION ONLY
2018/110 Chair’s and chief executive’s report D Dodd /D Sloman
13.
1 In accordance with the Health & Social Care Act 2012, all Trust Board meetings must be held in public. All decisions which require the board’s collective approval can only be made at a Trust Board (or a Part II meeting held in closed session to discuss confidential matters).

2018/111 Quality improvement and leadership committee (25 June 2018) J Owen 14.
2018/112 Clinical standards and innovation committee (16 July 2018) A Schapira Verbal
2018/113 Group services and investment committee (5 July 2018) W Goldwag 15.
2018/114 Population health and pathways committee (3 July 2018) C Clarke 16.
OTHER BUSINESS
2018/115 Questions from the public D Dodd
2018/116 Any other business D Dodd
2018/117 Date of next meeting – 26 September 2018 D Dodd

Paper 1
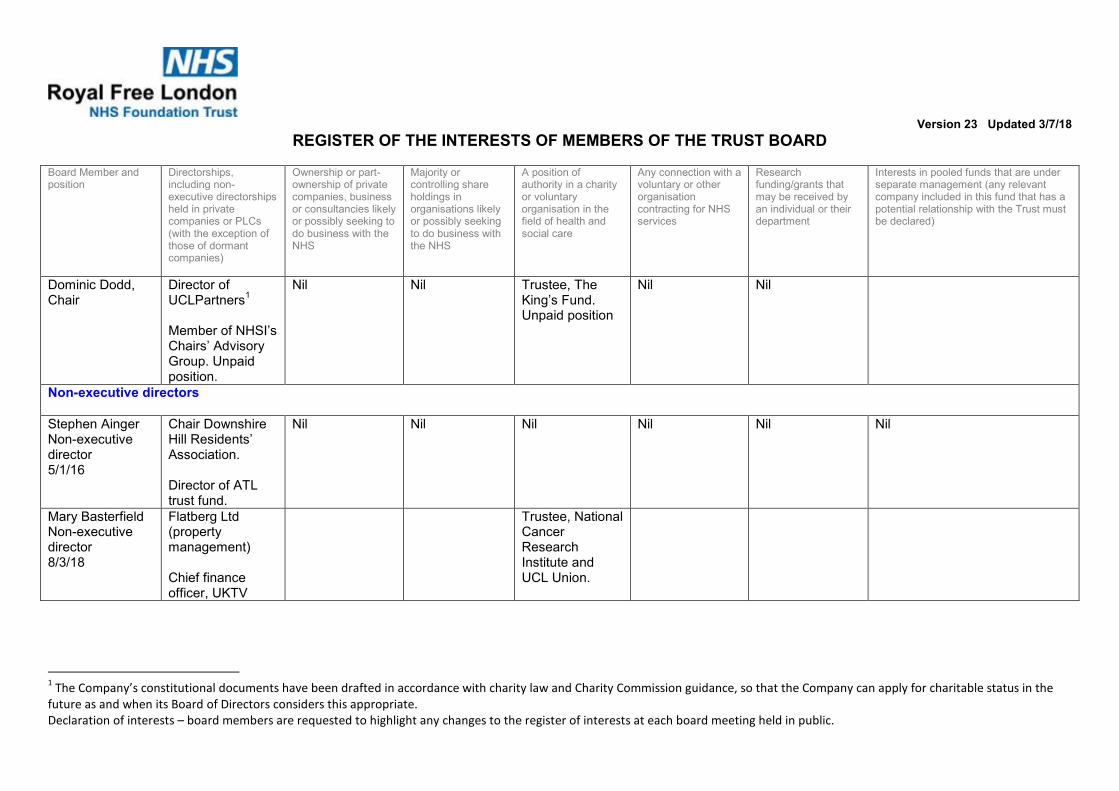
Register of interests – trust board 23 May 2018 1
REGISTER OF INTERESTS OF MEMBERS OF THE BOARD OF DIRECTORS
Executive summary
The trust constitution requires trust board members to declare interests which are relevant and material to the NHS board of which they are a member. The register of interests is presented at each board meeting.
The group chief executive, group chief finance officer and group director of capital and estates have amended their declarations. .
Action required
Board members are asked to provide an update if they have any changes in interests since the last meeting.
Board members are asked to declare any interests which are relevant to matters on the board agenda.
The board is asked to ratify the register, subject to any further changes made.
Public Patient and Carer involvement
The register will be made available to the public.
Report From Dominic Dodd, chairman Author(s) Alison Macdonald, board secretary Date 19 July 2018
Report to Date of meeting Attachment number
Trust Board 25 July 2018 Paper 1
Version 23 Updated 3/7/18
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
REGISTER OF THE INTERESTS OF MEMBERS OF THE TRUST BOARD
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
Dominic Dodd, Chair
Director of UCLPartners
1
Member of NHSI’s Chairs’ Advisory Group. Unpaid position.
Nil Nil Trustee, The King’s Fund. Unpaid position
Nil Nil
Non-executive directors
Stephen Ainger Non-executive director 5/1/16
Chair Downshire Hill Residents’ Association.
Director of ATL trust fund.
Nil Nil Nil Nil Nil Nil
Mary Basterfield Non-executive director 8/3/18
Flatberg Ltd (property management)
Chief finance officer, UKTV
Trustee, National Cancer Research Institute and UCL Union.
1 The Company’s constitutional documents have been drafted in accordance with charity law and Charity Commission guidance, so that the Company can apply for charitable status in the
future as and when its Board of Directors considers this appropriate.

Version 23 Updated 3/7/18
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
Wanda GoldwagNon-executive director
• Chair of the Office of Legal Complaints (OLC)
• Lay Member QC Appointments Panel
• Advisor SmedvigVenture Capital
Director, Goldwag Consultancy Ltd
Nil Nil Adopted sister is chief pharmacist of Barnet Enfield and Haringey Mental Health Trust
Nil I have a shareholding via Smedvig Capital in Antidote Technologies Ltd the clinical trial matching platform
Jenny Owen, Non-executive director
Nil Nil Nil Board member of Housing and Care 21
Vice chair of Alzheimer’s Society
Member of General Advisory Council King’s Fund
Housing 21 and Care 21
Alzheimer’s Society
Nil Nil

Version 23 Updated 3/7/18
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Akta Raja Non-executive director
• RFL Property Services Company Ltd
• Enhabit Ltd • Geneff Ltd • Thornriver
Management Ltd • Riverside Homes
Ltd • Ansor Ltd (not
currently trading)
Nil Nil Nil Nil Nil Nil
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
Professor Anthony Schapira Non-executive director
Upper Hampstead Walk Residents’ Association. AHV Schapira Ltd
Non-executive director, Ministry of Justice
Nil Nil Parkinson’s Disease Society Research Strategy Group
Nil Medical Research Council, Wellcome Trust, Parkinson’s Disease Society and other charitable sources of research funding
Nil

Version 23 Updated 3/7/18
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
James Tugendhat
Non-executive director
Director of BHFS One Ltd and BHFS Two Ltd
Nil Nil Nil Nil Nil Nil

Version 23 Updated 3/7/18
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Executive directors
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
Caroline Clarke Deputy group chief executive & chief finance officer
Director RFL Property Services Company
Nil Nil Director
Royal Free Charity (1/4/16)
Trustee, Overcoming MS
Trustee, Healthcare Finance Managers Association
Nil Nil
Deborah Sanders Group chief nurse
Nil Nil Nil Board member, The Royal Free Hospital Nurses’ Home of Rest Trust
Trustee, Royal Hospital for Neuro-disability
Nil Nil Nil
Kate Slemeck, RFH chief executive
Nil Nil Nil Chair of NHS Elect Advisory Committee Chair of NHS Providers COO Network
Husband works for Canon who provide the trust’s managed print service.
Nil Nil

Version 23 Updated 3/7/18
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Chris Streather
Group chief
medical officer
Nil Nil Nil Nil Unpaid advice to
ZPB on e-
rostering which
will contribute to
a report
commissioned
from them by
Allocate. It
involved two
meetings and
reviewing a
document and
Health Education
England (HEE)
also were
involved. The
trust has a
contract with
Allocate, but not
ZPB, for whom
this work was
done.
Nil Nil

Version 23 Updated 3/7/18
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
State when directorship commenced
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS State when interest acquired
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS State when interest acquired
A position of authority in a charity or voluntary organisation in the field of health and social care
State when position accepted
Any connection with a voluntary or other organisation contracting for NHS services
State when position accepted
Research funding/grants that may be received by an individual or their department
State when funding/grant commenced
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
State when interest acquired
David Sloman Group chief executive
Director, UCLPartners2
Nil Nil London Procurement Partnership board member.
Relative who works for Haringey CCG
Provider SROfor NCL STP and chair of digital programme board
Member of London health and social care strategic partnership board
Nil Nil
2 The Company’s constitutional documents have been drafted in accordance with charity law and Charity Commission guidance, so that the Company can apply for charitable status in the
future as and when its Board of Directors considers this appropriate.

Version 23 Updated 3/7/18
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Non-voting directors
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
David Grantham
Group director of
Workforce and
OD
Nil Nil Nil Board Member
and Treasurer
London
Healthcare
People
Management
Academy –
March 2013
Chair of NHS
Employers
Medical
Workforce
Forum – August
2010
Board Member Health Education North and East London (HENCEL) – July 2014 Board Member and Treasurer London Streamlining Programme(s) – March 2014
Nil Nil
Emma Kearney
Group director of
corporate affairs
and
communications
Director, EK
Consulting Ltd
Nil Nil Nil Nil Nil Nil
Andrew Panniker
Group director of
capital and
estates
Managing director RFL Property Services Company
Nil Nil Nil Director, Royal
Free Charity
Development Co
Nil Nil

Version 23 Updated 3/7/18
Declaration of interests – board members are requested to highlight any changes to the register of interests at each board meeting held in public.
Peter Ridley
Group director of
Planning
Nil Nil Nil Nil Nil Nil Nil
Board Member and position
Directorships, including non-executive directorships held in private companies or PLCs (with the exception of those of dormant companies)
Ownership or part-ownership of private companies, business or consultancies likely or possibly seeking to do business with the NHS
Majority or controlling share holdings in organisations likely or possibly seeking to do business with the NHS
A position of authority in a charity or voluntary organisation in the field of health and social care
Any connection with a voluntary or other organisation contracting for NHS services
Research funding/grants that may be received by an individual or their department
Interests in pooled funds that are under separate management (any relevant company included in this fund that has a potential relationship with the Trust must be declared)
Steve Shaw
Chief executive
BH
Nil
Glenn
Winteringham
Chief information
officer
Nil Nil Nil Nil Nil Nil Nil

Paper 2
1
MINUTES OF THE TRUST BOARD
HELD ON 27 JUNE 2018
Present
Mr D Dodd Mr S Ainger Ms M Basterfield Ms C Clarke Ms W Goldwag Ms J Owen Ms A Raja Prof A Schapira Ms D Sanders Ms K Slemeck Sir David Sloman Dr Chris Streather Mr J Tugendhat
Chairman Non-executive director Non-executive director Group chief finance officer and deputy group chief executive Non-executive director Non-executive director Non-executive director Non-executive director Group chief nurse Chief executive – Royal Free Hospital Group chief executive Group chief medical officer Non-executive director
Invited to attendMr D Grantham Ms E Kearney Ms V Manchanda Mr A Panniker Mr P Ridley Mr G Winteringham Mrs J Dewinter Ms A Macdonald
Group director of workforce and organisational development Group director of corporate affairs and communications Associate non-executive director Group director of capital and estates Group director of planning Group chief information officer Lead governor Board secretary (minutes)
Others in attendance
Rachael Brady Kam Kalirai Dr J Mountford Dr Kerrie Whitwell Ms M Buckley Ms H Swarbrick
CPG pathway manager Associate director – service improvement (for item 2018/79) Director of quality (for item 2018/79) ED consultant and CPG pathway lead (for item 2018/79) Head of safeguarding (for item 80) Director of midwifery (for item 2018/83)
2018/74 APOLOGIES FOR ABSENCE AND WELCOME Action
Ms E McManus Group chief transformation officer Dr S Shaw Chief executive – Barnet Hospital
The chairman welcomed those present to the meeting.
2018/75 DECLARATION OF INTERESTS
There were no further changes advised and the report on the register of interests was noted.
Paper 2
2
2018/76 MINUTES OF MEETING HELD ON 23 MAY 2018
The minutes were accepted as an accurate record of the meeting.
2018/77 MATTERS ARISING REPORT
The matters arising report was noted.
2018/78 RECORD OF ITEMS DISCUSSED AT PART II BOARD MEETING ON 23 MAY2018
The report was noted.
2018/79 ROYAL FREE EMERGENCY DEPARTMENT – CLINICAL PRACTICE GROUP IMPROVEMENT PROJECT – FOCUS ON PATIENT STREAMING
Dr Kerrie Whitwell, ED consultant and CPG pathway lead, Kam Kalirai, Associate Director –Service Improvement, Ms Rachael Brady, CPG pathway manager, and Dr James Mountford, director of quality, were in attendance for this item.
Dr Whitwell described the major changes in the Royal Free Emergency Department (ED) in recent years, notably the major expansion in the size of the department, with major building work going on at the same time as clinical services were being provided. The team had been keen to participate in the quality improvement (QI) and clinical practice group (CPG) work to tackle the performance issues the department was facing. There had been an increase in the number of breaches yet the overall number of attendances had not risen and there were more breaches occurring in the evenings. A number of workstreams had been put in place, notably streaming, rapid assessment and triage and ED processes. As a result more patients were being streamed more quickly, ambulance handover times had improved, ambulance patients were being seen by a doctor more quickly and the number of treatment unit breaches had reduced. The ED had achieved 95% of patients treated or discharged within four hours on 18 April and on several days seen and the team would be working to sustain these improvements going forward.
The chairman asked how this could be sustained. Dr Whitwell responded that it would be important to challenge people not following the new processes and also to ensure that they were in place 24/7. Mr Tugenhdat, non-executive director, asked about patient satisfaction. Dr Whitwell responded that a specific patient survey had not yet been undertaken but improved performance was clearly best from a patient safety perspective. The group director of workforce and OD asked whether this had resulted in a better training environment for junior doctors. Dr Whitwell responded that junior doctors were very closely supervised and the department received positive feedback from them. The changed processes had not really impacted on them directly.
Mr Ainger, non-executive director, asked if any lessons had been learned from the redevelopment. Dr Whitwell said that the design generally worked well but it had been necessary to move GPs out of the minors area into the ambulatory space.

Paper 2
3
Ms Godwag, non-executive director, asked about working with the community to reduce attendances. Dr Whitwell responded that this was not something that the hospital could directly influencing but was working with the clinical commissioning group (CCG) to get earmarked GP appointments to which patients could be redirected.
The group chief executive asked how it felt to participate in QI work. Dr Whitwell responded that the results were very satisfying but obtaining the data had been challenging.
The chairman thanked the team for attending and presenting their work which had improved the patient experience in the Royal Free ED.
2018/80 ANNUAL SAFEGUARDING REPORT
Ms H Swarbrick, head of safeguarding, was in attendance for this item. The group chief nurse noted that the report had been discussed at the relevant board and hospital committees. This was the first report since the establishment of the group structure, but safeguarding arrangements had remained largely as before with the head of safeguarding having overall responsibility with site based leads. The head of safeguarding met regularly with the hospital directors of nursing.
She noted that there had been a quality improvement (QI) project to support vulnerable families needing early intervention.
There had been a Care Quality Commission (CQC) inspection of looked after children in Barnet which had included a review of the Royal Free London safeguarding arrangements from which there was a very positive report, with some recommendations for further developments.
The group chief nurse noted that safeguarding training compliance was still not as high as it should be, but 88% of staff requiring level 3 (the highest) training were compliant.
The head of safeguarding then commented on the midwifery vulnerable women’s team which had been very highly regarded in the CQC report as it had delivered excellent outcomes and received positive feedback from users. She added that a review of the death of a patient at Barnet Hospital with learning disabilities had concluded that the appropriate reasonable adjustments had been put in place and the patient had received high quality care.
Ms Owen, non-executive director, congratulated the safeguarding team on the proactive work that was being done and asked if there was sufficient resource.
The head of safeguarding responded that the number of case reviews which the trust needed to contribute to was increasing, with 15 already this year. Contributing to the reviews required a lot of work and there were often extensive action plans that also needed trust input. However this was currently manageable.
The chairman expressed thanks on behalf of the board to the safeguarding team for the excellent work they were doing.

Paper 2
4
The board noted the report and agreed that it provided sufficient assurance that the trust was meeting its responsibilities in ensuring appropriate safeguarding arrangements were in place.
2018/81 PATIENTS’ VOICES
The group director of planning, read out a complaint made by the mother of a patient who contacted the trust to complain about the lack of treatment plan for her son, who had recently been diagnosed with bone marrow cancer and advised that he should be treated within two weeks or it could develop into a much more serious form of cancer. The patient (and his mother) were concerned that treatment had not yet commenced and were unclear about the treatment plan. The resolution was that the oncology consultant advised that the patient has a probable diagnosis of myelodysplastic syndrome (MDS a premalignant but potentially serious disease of bone marrow failure). He had been referred for MDS assessment and possible treatment at Barts. There was no need to treat his MDS in two weeks and, as explained in clinic, it was likely that he had had this condition for two years or more. The immediate treatment needed was ongoing intravenous iron. The first dose was provided at RFH but the hospital was liaising with the patient’s local hospital so he could receive this nearer to home. There patient had clearly not understood the information provided to him in clinic and/or there had been a misunderstanding between the patient and his mother. The patient’s consultant relayed all of the above to the patient in a phone call and the patient then updated his mother accordingly.
The compliment was from a cancer patient who asked the specialist nurse to thank the people who looked after him while he was having a trans-arterial embolization (TAE – treatment for liver cancer) He said the hospital had proved the papers wrong with all the bad press the NHS gets . He specifically referred to the consultant interventional radiologist who carried out the procedure and had one of the nurses in the interventional radiology area. He also said that the staff on 11 East were a credit to the NHS and he couldn’t thank them enough.
Ms Raja, on-executive director, would present the patients’ stories item next time.
Akta Raja
2018/82 GO SEE VISITS
Mr Ainger, non-executive director, reported back on his visit to therapies, accompanied by Ms Manchanda, to therapies. They had heard about the innovative work that was being done with patients, for example setting goals and the launch of social media channels for patients. However, they were trying to work out what the group structure meant for them in financial and business terms. Ms Manchanda echoed that the team were looking for external help to arrive at a more strategic vision of the service.
The group director of planning reported that his team were working with therapies on a demand and capacity plan.
Ms Basterfield, non-executive director, reported on her visit to the Starlight neonatal unit at Barnet Hospital where she had learnt about ‘orange hats’ (knitted hats for vulnerable babies needing more supervision) and the “what matters to you” campaign. She had been struck by how calm and controlled the unit was and the very cohesive team. The close links between the Royal Free

Paper 2
5
and Barnet units had also been discussed.
The board noted the report.
2018/83 PROGRESS AGAINST THE CLINICAL NEGLIGENCE SCHEME FOR TRUSTS (CNST) INCENTIVE SCHEME MATERNITY SAFETY ACTIONS
The director of midwifery was in attendance for this item.
The group chief nurse introduced this item explaining that this was the first year the Clinical Negligence Scheme for Trusts (CNST) scheme had run. The maternity element of the trust’s CNST contributions for 2018/2019 had been increased by 10% to create a maternity incentive fund. The scheme required the trust to self-certify (with board sign off) their progress against ten actions and discuss this with their commissioners before submitting a template board report to NHS Resolution by Friday 29 June 2018. She had reviewed the evidence on behalf of the board which showed compliance with the 10 standards and the evidence was available to view at the board meeting. This had been discussed at the Barnet and Royal Free Hospital clinical standards and patient safety committees and had also been approved by the clinical commissioning groups.
She noted that this was a self-certification but was subject to audit.
The group director of planning asked what the refund would be and how it would be used. The director of midwifery responded that this was £90k and would be credited to the division’s FIP. The division was also trying to achieve a midwife to birth ratio of 1:28 which was a cost pressure.
The board:
• Confirmed that it was satisfied that the evidence provided to demonstrate compliance with/achievement of the maternity safety actions met the required standards and that the self-certification was accurate.
• Noted that the content of this report had been shared with the commissioners of the trust’s maternity services
2018/84 FINANCIAL PERFORMANCE REPORT
The group chief finance officer presented this report, noting that the trust had submitted a deficit plan of £65.8m for the 2018/19 financial year. Currently the trust was trading in line with expectations and income budgets and plans were being re-profiled as North Central London clinical commissioning group (CCG) contracts had now been signed. She anticipated that private practice unit (PPU) income would recover and would therefore meet the plan in quarter 1 overall.
The 2018/19 financial plan included delivery of £45.4m financial improvement programme (FIP) savings. The trust had identified £40.9m of plans to deliver the £45.4m FIP target and delivered £4.0m of FIP year to date compared to a plan of £3.4m.
The trust’s cash balance of £39.5m was still artificially high due to the Parcel B land sale receipts being ring fenced for the Chase Farm capital development.
Paper 2
6
Focus continued on reducing debt with CCGs and NHS England (NHSE) who accounted for the majority of the aged debt in order to minimise loan drawdown and therefore interest charges.
The board noted the current financial position of the trust.
2018/85 OPERATIONAL PERFORMANCE REPORT
The group director of planning presented this report. He noted that the challenge continued to be to meet the cancer 62 day standard and the referral to treatment time (RTT) standard which in May was 84.7% compared with the 92% standard. However there had been some success in treating patients who had waited over 52 weeks, with the figure reducing from 41 patients in April to 23 in May.
The A&E performance was improving with overall performance in May 89.8% and 91.1% in June month to date.
The board noted the current operational performance of the trust.
2018/86 CHAIR’S AND CHIEF EXECUTIVE’S REPORT
The chairman reminded the board that the annual members’ meeting would be taking place on 18 July. He thanked all those involved in arranging the Oscars (staff achievement) awards notably the communications, facilities and estates teams, and congratulated the nominees and winners.
The group chief executive reported that the handover date of 12 July 2018 for Chase Farm Hospital (CFH) remained on track. He also highlighted that with the opening of the last area to be provided as part of the Royal Free Hospital Emergency Department redevelopment, this would no longer be a feature in his report.
Finally he highlighted that the trust had now completed all the Information Commissioner’s Office (ICO) undertakings and confirmation was awaited from the ICO that they were satisfied with the action taken by the trust.
The board noted the report.
2018/87 QUALITY IMPROVEMENT AND LEADERSHIP COMMITTEE
Ms Owen, chair of the committee, highlighted that the committee had discussed joy in work at its meeting earlier that week and had discussed how to deal with the transition of business to the new committee arrangements which would be discussed in the confidential board meeting later.
The board noted the report from the committee.
2018/88 CLINICAL STANDARDS AND INNOVATION COMMITTEE
Prof Schapira, chair of the committee noted that never events were a standing item at the meetings and the committee would continue to monitor them closely.
The board noted the report from the committee.

Paper 2
7
2018/89 GROUP SERVICES COMMITTEE
Ms Goldwag, chair of the committee, noted that the board had given delegated authority to the committee to approve the establishment of the RFL Property Services Ltd and the committee had had a number of detailed discussions about the legal and commercial aspects of this. The committee had now approved the establishment of the company which had now commenced trading.
The board noted the establishment of RFL Property Services Ltd and noted the report from the committee.
2018/90 AUDIT COMMITTEE
The board noted the report from the committee.
2018/91 QUESTIONS FROM THE PUBLIC
Noelle Skivington, Enfield Healthwatch, asked for more information about the property services company. The chief finance officer responded that the trust had established a wholly owned subsidiary company which would initially manage the assets and facilities at Chase Farm Hospital. The aim was to trade more efficiently and effectively than an in house department and use the skills developed in building Chase Farm Hospital more widely. The group chief executive added that this was completely the opposite of PFI as all profits from the company would be ploughed back into the trust.
Ms Skivington then asked for more information about RTT and ‘pop ons’. The group chief executive explained that expert advice had been commissioned to identify the data quality issues and address them once and for all. In the meantime the access team were managing waiting lists manually and on a patient by patient basis. The group chief medical officer added that clinical harm reviews had been carried out for all patients waiting more than 52 weeks and to date no moderate or serious harm had been identified.
2018/92 ANY OTHER BUSINESS
There was no other business.
2018/93 DATE OF NEXT MEETING
The next trust board meeting would be on 25 July 2018 at 1300 in the boardroom, 2nd floor, Royal Free Hospital.
Agreed as a correct record
Signature …………………………………..date 25 July 2018……………………………. Dominic Dodd, chairman

Paper 3
Matters arising – trust board 25 July 2018
Trust Board Matters arising report as at 25 July 2018
Actions completed since last meeting of the Trust Board
MinuteNo
Action Lead Complete Board date/agenda item
Outstanding
FROM TRUST BOARD HELD ON 25 APRIL 20182018/612018/62
Patients’ voicesLearning from deaths review
Presentation on end of life care – to be presented alongside next learning from deaths review
The group chief medical officer undertook to include the actual learning from deaths in future reports, which would be derived from the serious incidents investigation reports. He would also ensure that the time taken to conclude investigations was kept under review.
Group chief medical officer
On agenda
FROM TRUST BOARD HELD ON 21 MARCH 20182018/43 Gender pay gap
Ms Owen, non-executive director, said that she would like to see a very focused plan of three items with clear outcomes defined. The group chief executive commented that it was necessary to fully understand the data in order to arrive at an action plan, but an action plan would be brought back to the board in due course.
Group director of workforce and OD
To be scheduled for the July 2018 board meeting.

Paper 4
Confidential trust board meeting update – trust board July 2018
ITEMS DISCUSSED AT THE CONFIDENTIAL BOARD MEETING HELD ON 27 JUNE 2018
Executive summary
Decisions taken at a confidential trust board are reported where appropriate at the next trust board held in public. Those issues of note and decisions taken at the trust board’s confidential meeting held on 27 June 2018 are outlined below. The board discussed the trust’s financial position and performance report, although a detailed discussion also took place within the public part of the meeting. The following matters were also discussed at the meeting:
• Referral to treatment time (RTT) update – the trust is currently dealing with data quality issues which are impacting on management of waiting lists and ability to meet the waiting time standards. This is reported to the board every month in the public operational performance report.
• Operating plan update – the plan has been updated and resubmitted reflecting feedback from NHS Improvement. A summary of the plan will be published in due course.
• Financial strategy – the board received an update. A further update will be provided in the confidential July meeting and the draft strategy will be presented to the board in September.
• Partnership with West Hertfordshire Hospitals NHS Trust (WHHT)- the board confirmed its support to continue to work with WHHT with a view to WHHT becoming a clinical partner.
• Establishment of the Royal Free property services company – the board had delegated the detailed discussion and final decision to the group services and investment committee, which had approved the establishment of the company on 26 June 2018.
• Confidential chair and chief executive’s report – this report contained an update on never events (an update is included in the public chair and chief executive’s report) and property matters which remain confidential for commercial reasons.
• Board committees review – the board confirmed the cessation of the quality improvement and leadership committee and the population health committee and the creation of the people and population health committee, with a review to take place in six months’ time.
Action required
For the board to note.
Report From
D Dodd, chairman
Author(s)Date
A Macdonald, board secretary 16 July 2018
Report to Date of meeting Attachment number
Trust Board 25 July 2018 Paper 4

Paper 5
Page 1 of 6
Learning from deaths 2017/18: Q3
Executive summary
From April 2017, we have been developing our review process to meet the national learning from deaths (LfD) guidance. We have identified those patient deaths that meet the key criteria and we launched our learning from deaths (LfD) policy in September 2017.
Data are provided for all information gathered and validated to date, which includes Q1 and Q2 updates and Q3 data.
Q3 summary:
553 patient deaths 0 stillbirths (reporting delay) 31 patient deaths that meet the review criteria 22 patient deaths selected for random review 58 patient deaths listed for review 16 patient deaths still under review 42 patient deaths reviewed 2 patient deaths considered likely to be avoidable > 50% (Likert 1-3) 4 patients who died who had learning disabilities 0 LD patient deaths considered likely to be avoidable > 50% (Likert 1-3) 4 patient deaths reported as serious incidents
2 patient deaths were considered likely to be avoidable > 50% (Likert 1-3). These were both identified as incidents prior to the learning from deaths (LfD) process, and reported as serious incidents.
Action required/recommendation (to note, for information, to agree, to consider)• To note report • To agree the National submission on Learning from deaths (LfD).
Trust strategic priorities and business planning objectives supported by this paper Delete those that do not apply
Board assurance risk number(s) if you do not know risk number, please leave blank , or mark relevant cell with an X
1. Excellent outcomes – to be in the top 10% of our peers on outcomes
Yes
2. Excellent user experience – to be in the top 10% of relevant peers on patient, GP and staff experience
Yes
3. Excellent financial performance – to be in the top 10% of relevant peers on financial performance
Yes
4. Excellent compliance with our external duties – to Yes
Report to Date of meeting Attachment numberTrust Board 25 July 2018 Paper 5

Paper 5
Page 2 of 6
meet our external obligations effectively and efficiently
5. A strong organisation for the future – to strengthen the organisation for the future
yes
CQC Regulations supported by this paper Please delete those that do not applyRegulation 4 Requirements where the service provider is an individual or partnership Regulation 5 ⃰ Fit and proper persons: directors Regulation 6 Requirement where the service provider is a body other than a partnership Regulation 7 Requirements relating to registered managers Regulation 8 ⃰ General Regulation 9 Person-centred care Yes Regulation 10 Dignity and respect Yes Regulation 11 Need for consent Yes Regulation 12 Safe care and treatment Yes Regulation 13 Safeguarding service users from abuse and improper treatment Regulation 14 Meeting nutritional and hydration needs Regulation 15 Premises and equipment Yes Regulation 16 Receiving and acting on complaints Yes Regulation 17 Good governance Yes Regulation 18 Staffing Regulation 19 Fit and proper persons employed Regulation 20⃰ Duty of candour Yes Regulation 20A⃰ Requirement as to display of performance assessments Care Quality Commission (Registration) Regulations 2009 (Part 4)Regulation 12 Statement of purpose Regulation 13 Financial position Regulation 14 Notice of absence Regulation 15 Notice of changes Regulation 16 Notification of death of a service user Regulation 17 Notification of death or unauthorised absence of a service user who is detained or liable
to be detained under the Mental Health Act 1983 Regulation 18 Notification of other incidents Regulation 19 Fees Regulation 20⃰ Requirements relating to termination of pregnancies Regulation 22A⃰ Form of notifications to the Commission
Risks attached to this project/initiative and how these will be managed (assurance)• Failure to review all relevant deaths – triangulation of data sets from SIRP, stillbirths,
Dr Foster and complaints against all trust deaths • Increased numbers of avoidable deaths identified – provides opportunities for more
learning • Delay of at least 4 months to identify deaths 30 days post discharge from Dr Foster
could lead to family distress if incidents are identified – update bereavement literature to inform families
• There are no dedicated resources to manage or undertake the learning from deaths (LfD) process, so time delays will probably occur – this process will be fitted into current job roles.
Equality analysis Please choose one • No identified negative impact on equality and diversity • Positive evidence that proposal has considered equality and diversity • Any adverse impact on equality and diversity has been remedied or escalated
Report from Deborah Sanders, Group Chief Nurse Chris Streather, Group Chief Medical Officer
Author(s) Hester Wain, Deputy Director of Patient Safety and Risk Date 23/06/18

Paper 5
Page 3 of 6
Contents 1. Learning from deaths (LfD) Review Summary ................................................................ 3
2. Learning from deaths (LfD) Quarter 3 of 2017/18 data review ........................................ 3
1. Learning from deaths (LfD) Review Summary
Please note that because the learning from deaths (LfD) reviews are a continuing process, the data are dynamic, and there have been updates to the data since the last report.
Q1 Q2 Q3
Number of patient deaths 479 459 553
Number of stillbirths 9 4 0
Number of patient deaths that meet the review criteria 28 36 31
Number of patient deaths selected for random review 5 11 22
Number of patient deaths listed for review 33 48 58
Number of patient deaths still under review 3 13 16
Number of patient deaths reviewed 30 35 42
Number of patient deaths considered likely to be avoidable > 50% (Likert 1-3)
2 2 2
Number of patients who died who had learning disabilities 2 3 4
Number of LD patient deaths considered likely to be avoidable > 50% (Likert 1-3)
0 0 0
Number of patient deaths reported as serious incidents 4 2 4
2. Learning from deaths (LfD) Quarter 3 of 2017/18 data review
On average there are 156 deaths per month across RFL; 47% RFH: 53%BH. For Q3 we planned to review 10.5% of patient deaths. The planned reviews include those patient deaths that meet the key criteria and other patient deaths that have been selected at random, with a 50:50 location split RFH/BH and other.
There were two patient deaths considered likely to be avoidable identified. These were both identified as incidents prior to the learning from deaths (LfD) process, and reported as serious incidents.
Serious incident ID Site Likert Avoidability
2017/25733 BH 3. Probably avoidable, more than 50/50
2017/29464 BH 4. Possibly avoidable but not very likely, less than 50/50
2017/29762 RFH 3. Probably avoidable, more than 50/50
2017/29969 BH 5. Slight evidence of avoidability

Paper 5
Page 4 of 6

Paper 5
Page 5 of 6

Paper 5
Page 6 of 6

Paper 6.1
1
Report to Date Attachment numberTrust board 25 July 2018 Paper 6.1
Paper title:Director of infection prevention and control annual report, 2017/18
Executive summary In line with the revised Health and Social Care Act (2008) trusts are required to have appropriate management and clinical governance systems in place to deliver effective infection prevention and control. This document reports on the activity for the year 2017/18 to provide assurance that the IPC programme has been taken forward, that IPC activity has striven to assure compliance with the Health and Social Care Act detailed below.
Action requiredThe Board is asked to confirm that the report provides sufficient information to provide assurance of sustained compliance with the Hygiene Code.
Trust strategic aims and business planning objectives supported by this paper• Improving clinical effectiveness • Enhancing the patient experience • To be in the top 10% of hospitals in England for quality including reductions in HCAIs
CQC outcomes supported by this paperOutcome 8 Cleanliness and infection control QCQ Compliance (regulation 12 (2) h)
Risks attached to this project / initiative and how these will be managed (assurance)The revised Hygiene Code Risk matrix will be monitored at the Infection Control Committee. The risks associated with the Hygiene Code have been included in the Board Assurance Framework.
Equality impact assessment
• no adverse equality impact
Public, patient and carer involvementAll IPC reports available to public scrutiny and discussed at open Board meetings
Report from: Deborah Sanders Authors: Damien Mack, microbiology consultant, IPC doctor;
Anand Sivaramakrishnan, consultant microbiologist, IPC doctor; Dianne Irish, consultant virologist; Yvonne Carter, Head of IPC nursing
Date: July 2018

Paper 6.1
2
1.0 Introduction and Summary This report outlines activity and events related to infection control for 2017/18. As always,
healthcare associated infection (HCAI) continues to be an important issue for the trust and this
report will include some site specific information to better enable actions for improvement and
patient safety. The trust target remains ‘zero avoidable infections’. For reportable organisms,
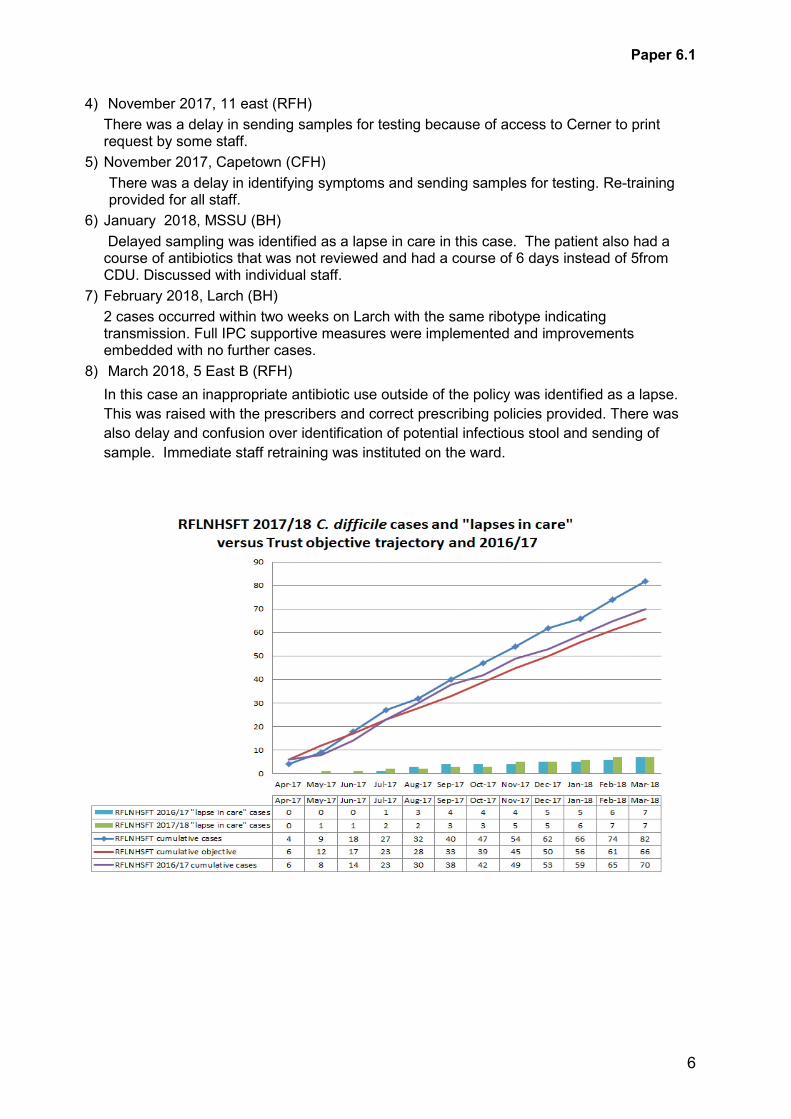
the threshold for the enlarged Trust C.diff, toxin positive, attributable infections was 66, with an
actual outcome of 82 cases. There were eight lapses in care which means actions were
identified that may have contributed to C.diff acquisition. Overall this is a reduction from 14
lapses in care cases in 2015/16, but seven in 2016/17.
There were three MRSA bacteraemias against a target of zero attributed to the Trust.
2.0 Description of infection control arrangements
The director of nursing is the director of infection prevention and control (DIPC) and chair of
the infection prevention and control committee (IPCC). The IPC team is headed by the DIPC,
who is a board member and activity is directed by the lead infection control doctor and
microbiologist and by the head of IPC nursing. In the group model the chief nurse will be the
DIPC and the IPCC will be a group committee.
The IPCC meets quarterly and has representation from across the trust. The consultant
microbiologists with special interest in antimicrobial prescribing are members of the IPCC and
the Drugs and Therapeutics Committee and act as a link between the two. Within the trust
committee structure the IPCC reports to the clinical standards and innovation committee and
directly through the DIPC to the Board. The IPCC is reported to by the decontamination
committee and the fortnightly divisional leads IPC group and Clostridium difficile action group.
The monthly divisional leads meeting are held to review ongoing infection control data,
infection control activity, activity to keep C.diff cases below threshold and current IPC issues.
The meetings are chaired by the hospital director of nursing and attended by the IPCT,
divisional infection control clinical leads, divisional nurse directors and operational managers
as well as allied healthcare professionals (AHPs). Monthly reports of infection control activity
within each clinical division are recorded as part of the divisional clinical governance grid.
3.0 Infection Control Team Staffing
Director of infection, prevention and control - D Sanders – director of nursing.
Royal Free Hospital Barnet and Chase Farm Hospitals Medical Staff Consultant microbiology 5 PA
(infection control lead) Consultant microbiology 5. PA Virologist 1. PA
Medical Staff Consultant microbiology 11 PA
Nursing Staff Head of IPC Nursing 1 wte Clinical Lead Nurse 2 wte Clinical Nurse Specialist 4.8 wte Clinical nurse specialist 1 wte - funded by renal services Senior practice educator 1 wte

Paper 6.1
3
IPC practice educators 3 wte Audit and surveillance nurse 1 wte Hand hygiene co-ordinator 1 wte Data administrator 1 wte Antibiotic pharmacist 0.5 wte at RF and 0.5 at BCFH
4.0 Healthcare associated Infections
4.1 MRSA acquisitions
New cases of MRSA are assessed as acquisitions if a positive screen or swab is identified
more than 48 hours after admission. Acquisitions of MRSA thought to have occurred within the
trust are on average five per month which is a steady, low rate. There have been sporadic
cases of MRSA acquisition, but no outbreaks.
Since the beginning of 2009, the trust commenced mandatory MRSA screening of elective
admissions following Department of Health requirements. This mandate has now been lifted,
but the trust screens high risk patients and is reducing screening in groups such as out-patient
and day cases
Screening admissions helps to reduce MRSA acquisition by earlier identification, and
management of colonised patients, as well as improving the accuracy with which the site of
acquisition can be attributed. The IPCC agree to maintain high screening schedule to ensure
patient safety.
4.2 MRSA and MSSA bacteraemia
There were three attributable MRSA bacteraemias within the trust, the threshold remains zero.
1) Tottenham Hale Kidney Dialysis Centre.
The patient had MRSA in their urinary stents and required a procedure to be performed at
which point the stents could have been removed. At the time of the procedure no urology
report was available and the procedure cancelled. This was escalated to SIRP panel, with
learning to ensure integration of IT systems and on-going review with the urology team.
2) 10 North
The patient had aspiration pneumonia, also with community strain MRSA. It was agreed
that this was a 3rd party case with CCG but was still assigned to the trust. A subsequent
appeal was unsuccessful.
3) The third case concerned a patient with advanced liver disease transferred from another
hospital. It was identified and reported to the ward that the patient was MRSA colonised
but no decolonisation was commenced for 5 days which could have led to migration of
MRSA to pleural drain and eventual bacteraemia. It is possible that this could have been
prevented if decolonisation had taken place and reduced the MRSA load.

Paper 6.1
4
MRSA and MSSA bacteraemia episodes at RFLNHSFT
MSSA bacteraemias have been reported as part of the national mandatory reporting scheme,
although no targets for reduction have been set.
The annual MRSA audit was carried out to check staff knowledge of the policy across all sites. The MRSA audit confirmed that the majority of staff are knowledgeable and competent in risk assessing, screening, isolation, treatment & post treatment screening of patients with MRSA. However gaps in knowledge were also identified, highlighting the need for education and training on the areas that need improvement. Recommendations included the IPC practice educators training the ward based clinical practice educators in the management of patients with MRSA as per policy, who can in turn educate their staff. The findings of the audit were disseminated at corporate level and cascaded down to ward level, raising awareness at ward meetings and huddles on all the issues and practices listed in the questionnaire.

Paper 6.1
5
There is regular surveillance, feedback and teaching to all the satellite units. Activity for
mandatory reporting and reduction of Gram negative bacteraemias was aimed at reducing
MSSA bacteraemias through improved practice. Recent RCA learning included:
• Improved recording of screens requested to address delay in acting on positive results.
• Delay in removing line with signs of infection has been escalated to SIRP.
4.3 Clostridium difficile
In April 2015, Monitor made an important change to the C.difficile infections target, in that only
lapses in care leading to such infections should be recorded. Lapses in care infections are
determined by the local clinical team applying a checklist based assessment developed by
Public Health England, with outcomes reviewed and agreed by local commissioners.
The threshold for the year was to record fewer than 66 cases where a lapse of care was an
underlying factor; over the period April 2017 to March 2018, the trust observed 82 confirmed
cases (70 cases in 2016/17). Following the assessment process of each case 8 of the 82
were deemed to be lapses in care.
1) May 2017, 12 west (RFH)
Antibiotic prescribing differed from standard trust policy with the reason not documented, nor the discussion with the microbiologists. Learning discussed with the prescribers
2) July 2017, 7 west,(RFH)
There were two cases within two weeks on the ward with the same ribotype indicating transmission. Full IPC supportive measures were implemented with improvements embedded and no further cases identified.
3) September 2017, Capetown (CFH)
The RCA identified extended Metronidazole administration for three weeks with no patient improvement. This was not reviewed or documented. Clinical staff reminded to discuss with Microbiology for extended prescribing.
Paper 6.1
6
4) November 2017, 11 east (RFH)
There was a delay in sending samples for testing because of access to Cerner to print request by some staff.
5) November 2017, Capetown (CFH)
There was a delay in identifying symptoms and sending samples for testing. Re-training provided for all staff.
6) January 2018, MSSU (BH)
Delayed sampling was identified as a lapse in care in this case. The patient also had a course of antibiotics that was not reviewed and had a course of 6 days instead of 5from CDU. Discussed with individual staff.
7) February 2018, Larch (BH)
2 cases occurred within two weeks on Larch with the same ribotype indicating transmission. Full IPC supportive measures were implemented and improvements embedded with no further cases.
8) March 2018, 5 East B (RFH)
In this case an inappropriate antibiotic use outside of the policy was identified as a lapse.
This was raised with the prescribers and correct prescribing policies provided. There was
also delay and confusion over identification of potential infectious stool and sending of
sample. Immediate staff retraining was instituted on the ward.

Paper 6.1
7
The learning from the lapses in care and the actions agreed are included into the trust
infection prevention action plan. Examples include:
• Refresh Deep Clean programme across all sites • Review of all cleaning audit reports at monthly Divisional Lead meetings • Arrange external expert review of C.diff reduction strategies and management plans • Reduce antibiotic usage • Improved antimicrobial stewardship – business case to GEC • IT integration: stool chart/algorithm, antibiotic stewardship, patient tracking and
isolation • Clinical audit programme • Clinical team engagement in RCA process • ‘Board to Ward’ support • Inclusion of antimicrobial stewardship in appraisal
The annual Clostridium difficile audit was carried out to assess staff knowledge of the policy
across all sites. The C. diff audit demonstrated a good level of basic knowledge about the
management of patients with diarrhoea and isolation and investigation procedures. The audit
found that there still remains a gap in knowledge on when to send a stool specimen and the
need to educate staff on the type five to seven as an assessment to trigger sending stool
specimen for C. diff testing. Recommendations included IPCN’s to work closely with the ward
manager and clinical practice educator to improve the areas for development identified in the
findings and orientation to the stool chart to be carried out to all new starters on the ward. The
harmonised Bristol stool chart that was introduced in the beginning of 2016 has a detailed
guidance on the management and accurate record of patients who develop diarrhoea. There
will be on-going training and education across the site to ensure everybody understands how
to utilise the stool chart. The IPCN will take the opportunity during the winter road show and
the clinical practice events to speak to staff and educate on C. diff.
4.4 Carbapenemase producing enterobacteriaceae (CPE) and other non-fermenting (NF) organisms.
The DH guidance, or ‘Toolkit’ for management of CPEs many recommendations are still being
embedded, such as isolation for the period of screening, which impacts isolation facilities in
Paper 6.1
8
general, particularly in renal dialysis services and the financial and time resources needed for
the screening, education, care and follow-up of patients (Appendix A)
All cases are investigated for possible source and screening is instituted to ensure that there
is no further transmission. There have been two single unit outbreak investigations as
detailed below and a larger scale outbreak at Barnet Hospital, which is now resolved.
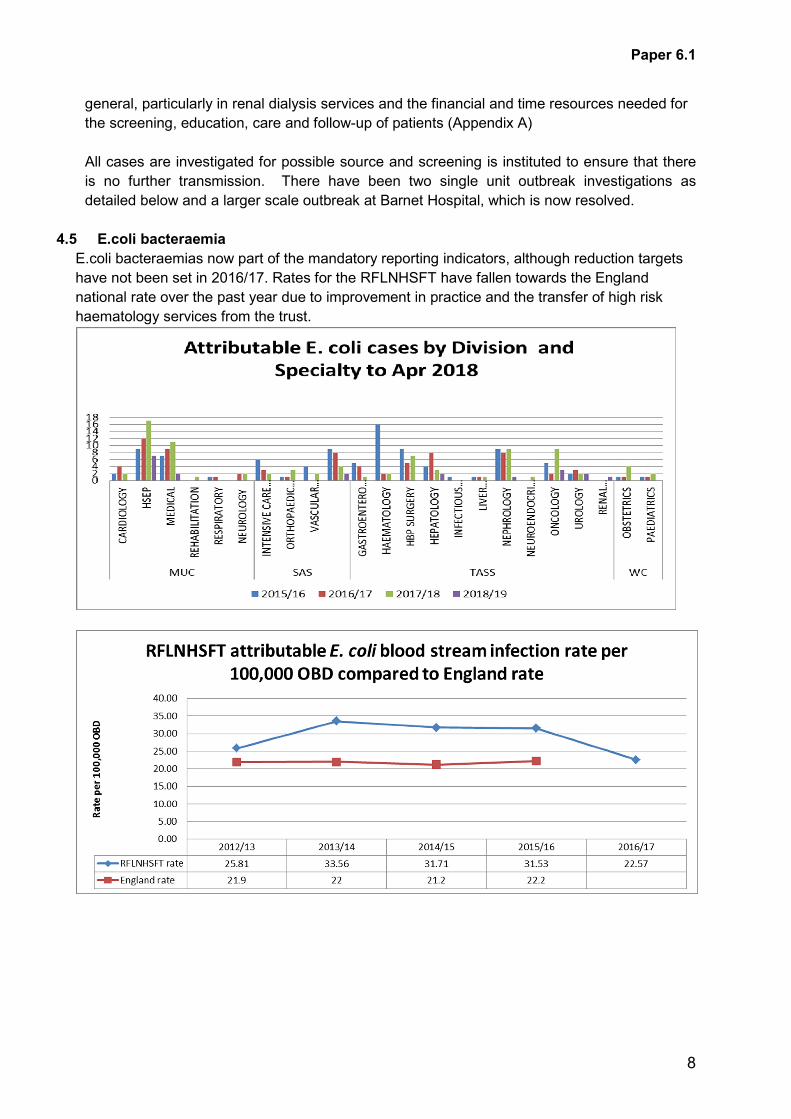
4.5 E.coli bacteraemia
E.coli bacteraemias now part of the mandatory reporting indicators, although reduction targets
have not been set in 2016/17. Rates for the RFLNHSFT have fallen towards the England
national rate over the past year due to improvement in practice and the transfer of high risk
haematology services from the trust.

Paper 6.1
9
5.0 Outbreaks and periods of increased incidence (PII).
C.difficile
There were been a total of six C.diff toxin positive cases acquired between 9 north and 9 west (RFH) from April to June 2017. Supportive measures were implemented and weekly meeting were held. Investigation identified the need to re-energise the deep cleaning programme, along with some practice and antimicrobial stewardship improvements. On the 1st of September 9 west ward discontinued supportive measures as there were no new cases. 9 north ward continued with special measures as a further two new cases were identified on 23rd and 24th August 2017. Following deep cleans, both wards demonstrated a significant reduction in cases.
7 west ward (RFH) also had a period of increased incidence of C.diff cases. The ward completed supportive IPC measures successfully and there were no new cases reported. IPCN will continue to C.diff teaching and monitor commode cleaning and hand hygiene compliances. Medical staff were supportive and engaging which helped improve the hand hygiene on the ward among medical staff. The ward has Electronic prescribing and therefore all antibiotics were reviewed and stopped on the stipulated date and the ward has been deep
Capetown ward at Chase Farm had an increase in patients identified with C. diff, although ‘typing’ indicated no direct transmission. The ward underwent a deep clean and hydrogen peroxide vapour (VHP) clean. Teaching has been undertaken for all staff relating to the early detection of C.diff through the better understanding of the Bristol Stool Chart.
Larch Ward at Barnet hospital had three cases of C diff toxin positive cases with the same ribotype. The ward underwent deep cleaning and HPV fogging and was placed on IPC supportive measures for four weeks. There have been no further cases.
Carbapenemase producing enterobacteriaceae – CPE
An outbreak of three cases in 12 west, Royal Free hospital was investigated in liaison with PHE.
This was related to three overseas patients with social interaction between patients and
families. A full supportive programme was instituted including interpreters, appropriate language
documents and information, with no further cases identified from weekly ward and admission
screening for a period of one month.
An outbreak in 10 east ward, Royal Free hospital, involved two patients having the same strain
of Klebsiella pneumoniae. The ward was placed on supportive measures for four weeks. No
further patients tested positive.
A more sensitive laboratory test was introduced at Barnet hospital to align with that at the Royal
Free hospital. Subsequent to this there was a Following the report of cases identified on more
sensitive laboratory testing at Barnet Hospital, an outbreak was declared. The outbreak
continued from January 2018 to June, but has now been de-escalated. An outbreak committee
was instituted with representation from Public Health England. A fortnightly CPE management
group has been established to manage preventative actions and respond in a timely manner to
any newly ientifed cases, whether from admission screen or sampling later in an in-patient stay.
Each sporadic case now identified is investigated, with ‘contacts’ screened and full IPC
measures instituted.

Paper 6.1
10
Tuberculosis
There were two incidences of TB exposure at Barnet hospital, one on ITU and the other on MSSU. The ITU patient was in isolation on Walnut but following negative smear tests, became unwell and was transferred to an open bay on ITU where another sputum test was found to be positive. Staff and patient follow-up was undertaken, with no reports on transmission. In MSSU, a patient was in an open bay and then transferred to the Royal Free Hospital, on transfer the patient was screened smear negative and culture positive. A full investigation was undertaken, with contact screening and no reports of transmission.
Chicken pox exposureIn August one case of chicken pox was confirmed on Mulberry ward at Barnet hospital. Eight patients were identified as being exposed. Blood samples were obtained from all 8 patients which indicated that they all had immunity. All exposed staff were referred to OH. There were been no reports of transmission.
Whooping coughThere was a confirmed pertussis in a seven week old infant admitted to a cubicle on Galaxy ward who was admitted for just under 13 hours. Two staff members had contact with the baby and both were referred to occupational health. There were no patient exposures and no reports of transmission.
Norovirus
10 north ward, Royal Free hospital was closed for admissions following a Norovirus outbreak
after the admission of a patient from a care home that was affected with Norovirus. There were
four confirmed patients and 22 further symptomatic patients, with seven staff affected. The ward
was closed to admissions for 10 days. All affected patients were isolated. The ward was deep
cleaned and VHP cleaned before opening to admissions.
7 west ward, Royal Free hospital, was closed to admissions following a Norovirus outbreak for
13 days. There were six confirmed cases of Norovirus. Eleven staff was also affected. The
ward was deep cleaned and VHP cleaned before re-opening.
Paper 6.1
11
Larch ward, Barnet hospital, was closed to admission for 8 days from 8th February due to a
norovirus outbreak. There were 7 symptomatic patients with 1 confirmed norovirus positive
patient. Three staff were affected. All symptomatic patients were isolated or discharged before
the ward was terminally cleaned, VHP fogged and reopened to admissions.
Influenza
CCU and Rowan ward, Barnet hospital, were closed due to an influenza outbreak. There were
eight confirmed cases of flu A among patients and 2 staff members had flu like symptoms. Both
areas were deep cleaned and VHP fogged before reopening.
Starlight neonatal unit, Barnet hospital, had bays closed intermittently due to an influenza A
outbreak from 05.02.18 to 20.02.18. Three babies were positive, two staff members and one
parent had flu like symptoms. All symptomatic babies were isolated and bays terminally cleaned
before reopening.
6.0 High consequence infectious diseases management.
The IPC team are joining with the infectious disease team in attending NHS England and HSE
planning meetings to discuss national policy, guidance and preparedness, particularly around
the use of protective clothing. Further NHS England and HSE working is planned for later this
summer.
7.0 Virology
Samples for Virology tests were performed in the virology department at the Royal Free
hospital until September last year, when molecular testing moved to the HSL laboratories.
From March 2018 serological tests on RFH samples have also been performed by HSL. All
positive virology results that require infection control interventions involving patients,
healthcare workers and in the community are telephoned out by Virology medical staff on an
urgent basis.
From April 2017 to March 2018, there were 2374 laboratory confirmed viral infections that
required IPC interventions, 91% (n=2155) were from patients with respiratory viral infections
(Figure 1).Of these, 1571 infections were identified on RFH site and 584 infections on the
BCF site. In addition, there were 34 chicken pox/shingles infections, two measles infections
and 109 norovirus infections recorded from the RFH site.

Paper 6.1
12
Figure 1: Virology IPC Activities from July 2014 to March 2018
Respiratory illness
From April 2017 to March 2018, there were 625 influenza infections identified at the Royal Free London NHS Foundation Trust of which 367 infections were influenza A and 258 were influenza B infections. These figures represent a 50% increase in influenza infections from the previous year 2016/17, of which 80% occurred between January and March 2018. This was mainly due to a significant increase in influenza B infections which started to rise from December 2017 and continued until late March 2018. The dominant strain of influenza B circulating during winter season 2017/2018 was the Yamagata strain (which was not present in the trivalent vaccine but was present in the quadrivalent vaccine). The dominant influenza A strain circulating was H3N2.
Table 1 Respiratory Infections for April 2017 – March 2018
RFH BarnetAdenovirus - 87 19Coronavirus 117 26Enterovirus/Rhinovirus 650 228Influenza A 260 107Influenza B 180 78Metapneumovirus 91 28Parainfluenza 98 34Parechovirus 5 4RSV 83 60Total 1571 584

Paper 6.1
13
Figure 2 Common Viral Respiratory Infections Recorded from July 2014 – March 2018
Rash illness There were 34 cases of varicella zoster infections and 2 cases of measles that were identified and managed by the virology medical staff.
Gastrointestinal infections
At the Royal Free hospital site, gastrointestinal infections identified other than norovirus
included 13 adenovirus infections,4 astrovirus infections, 6 sapovirus infections and 6
rotavirus infections
8.0 Surgical site infection surveillance (SSI)
Under the mandatory surveillance scheme one three-month module of orthopaedic surgical site infection surveillance per year is required. Regular meetings have been incorporated within the orthopaedic specialty group audit programme to feedback and discuss results of surveillance.
With low numbers the fluctuations that show reports out of ‘normal range’ have very narrow margins and are seen as trends to address more often than severe service issues.
The Surgical site infection (SSI) surveillance committee was restructured in September with the first meeting being held in October 2017. This is a multidisciplinary committee with a large group of members from all three trust sites, including orthopaedic surgeons, microbiologists, infection control nurses, SSI surveillance nurse, matron, ward and theatre nursing staff. The meetings are also been attended by the Chase Farm hospital medical director and SAS divisional director.

Paper 6.1
14
The committee agreed in its first meeting to continue mandatory reporting of surgical site infections in total hip and total knee replacements. Following the guidance from Public Health England (PHE) the data is currently collected, analysed and reported from CFH site alone, which is the main site of elective joint replacements. The data is being collected and analysed from the other two sites with the intention to submit data to PHE from all sites. This data is discussed at local SSI meetings and is not reported nationally. The spinal surgery surgical site infections has also been included in the surveillance program.
Public Health England Surgical Site Infection Surveillance Service has recently identified the Trust as an outlier for SSIs in Knee Replacements in the reported period of Oct – Dec 2017. The national rate of SSI after TKR is 0.8%, in comparison our reported rate is 1.1%. The Trust responded to PHE detailing the contributory factor and the measures being taken to reduce the risk.
The Trust has reported a total of three SSIs in the last four periods of data collection, one in each of the last three collection periods.
Root cause analysis are carried out on all patients who have developed an SSI in order to ascertain if there have been any lapses in care or if there are any ways in which risk of developing SSI could have been reduced. As a result of this, there have been changes to current practice, including the following: 1. Changes in theatre environment and process to reduce the number of unnecessary
interruptions. 2. Introduction of Chlorhexidine washcloths for patient use before attending for surgery. 3. Development of a protocol for the use of PICO dressings in high risk patients and patients
who go on to have wound complications following surgical procedure. The protocol will be part of the new digital solution in the Chase Farm Hospital building. It is envisaged this will further increase adherence to the protocol. This is also part of on-going work to develop Clinical Pathways to eliminate unwarranted variation across the Trust.
4. Robust monitoring of adherence to the Trust prophylactic antibiotic policy. Feedback from this has led to teaching from our microbiologists to prescribers around the reasons for the specifics in terms of drug choices and doses and risks of side effects and clearer guidelines are being developed.
5. The setting up of a cross-site SSI committee to promote best practice.
Further work includes: 1. Monitoring the use of Chlorhexidine washcloths to ascertain reliability in terms of usage. 2. Making the prophylactic antibiotic policy part of the new digital solution, reducing the
likelihood of deviation from the protocol and reducing the risk of error in prescribing. 3. The use of antimicrobial sutures. 4. The use of the ‘One Together Assessment Toolkit’ to assess infection prevention practice
across the surgical pathway.
Audits have been undertaken to look into the use of standardised antibiotics before elective joint surgery which have been presented in both orthopaedic and anaesthetic audit meetings. Improvements have been made to the protocol for use of pre-operative antibiotics.
9.0 Infection surveillance The list of surveillance and clinical audit topics is included as appendix 1. This formed the
basis of the surveillance and audit programme for 2017/18.
10.0 Invasive device management
10.1 Peripheral intravenous cannulae

Paper 6.1
15
A trust-wide audit of peripheral cannula management was conducted in 2017/18.
Findings:
Actions for improvement include training and re-training for staff and ensuring the use of a cannulation pack as without one, staff are observed to use insufficient equipment and training to use ‘single’ extensions, not doubles, unless specifically required.
10.2 Urinary catheter point prevalence survey – HOUDINI
A point prevalence survey was undertaken for all in-patients at the Royal Free Hospital, Barnet Hospital and Chase Farm Hospital. During the audit period, there were 932 inpatients included in the audit across the Trust. 205 patients had a urethral indwelling catheter, an increase of 4% compared to the previous year’s audit. Based on HOUDINI forms, nursing documentation, medical notes or asking the nurse, 197 (96%) of those urinary catheters had a clinical indication to remain in-situ. Out of 88 urine sample tested, 20 (or 10% of the total no of patients with urinary catheter) have a confirmed positive bacteriuria, but not a confirmed infection.
11.0 Quality Improvement (QI) programme. As part of the QI programme around reduction of Gram negative bacteraemias, a focus has been directed at reduction of catheter associated urinary tract infections, especially by the introduction of a ‘catheter passport’ to improve communication between healthcare settings and community and hospital staff by also involving patients in their care. (appendix 3)
12.0 Education Members of the IPCT continue to provide mandatory infection prevention and control training
for induction and annual updates for all relevant staff, particularly those who are unable to
access e-learning modules easily. In addition, ad hoc training is performed in clinical areas
depending on local needs. The MaST e-learning modules have been re-written and up-dated
in line with current best practice and policy.

Paper 6.1
16
13.0 Practice educators (PEs)
There are currently four practice educator posts. They continue ward based teaching and skill
competence assessments as part of their daily role.
14.0 Antibiotic stewardship The CQUIN outcomes are still awaited for 2017-18. The downward trend in antibiotic use
continues.
Antimicrobial stewardship rounds are ongoing across a vast majority of specialties at the
Royal Free hospital but coverage is not as intensive at Barnet hospital but additional
resources have been requested to improve this.
Teaching sessions for doctors, nurses and pharmacists are ongoing by various members of
the antibiotic stewardship and infection control teams. Antimicrobial stewardship training for
nursing staff has been reinvigorated by a programme led by the IPCC lead nurse.
There were several antibiotic shortages over the year, notably piperacillin/tazobactam and
clindamycin. Antibiotic policies were reviewed and amended in order to address these
shortages, which have now been alleviated.
This multicentre ‘ARK’ study aimed at empowering Junior Doctors to make definitive decisions
to review and stop empiric antibiotic treatment was launched at the Royal Free hospital earlier
this year. Feedback thus far has been excellent from both this and other centres.

Paper 6.1
17
15.0 Service validation The trust has declared compliance to the Care Quality Commission in relation to IPC aspects of the Health and Social Care Act (2008) Hygiene Code. The CQC has agreed unconditional compliance. The CQC report for the inspection in 2016 made recommendations for improvement in some aspects of hand hygiene and in continuing to keep doors closed in isolation rooms as well as individual recommendations by service. The IPC team has worked with each division to address shortfalls including:
- Implementation of enhanced IPC and hygiene measures when wards fall below practice or cleaning standards
- Additional hand hygiene training and validation audits of clinically based audits - Daily IPCT visits to wards to review practice and three times weekly visit to each isolation
room to review isolation measures and discuss care with patients. The Trust also collaborates with the CCG and CSU advisors in the PIRs and RCAs for infections to ensure open and transparent reporting, learning from the outcomes and sharing learning from other organisations.
16.0 Public and patient involvement PLACE audit programme continues including patient representatives, Matrons, IPCNs and Facilities staff to enhance patient inclusion in maintaining a clean environment. The IPC Nurses are always available to discuss face-to-face issues with patients, relatives and visitors when requested.

Paper 6.1
18
Appendix 1
Infection prevention and control (IPC) carbapenemase producing enterobacteriaceae (CPE) assurance analysis
Ref – (PHE acute trust toolkit for the early detection, management and control of CPE – 2013). https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/329227/Acute_trust_toolkit_for_the_early_detection.pdf
B.2 Hospital / trust checklist of actions to prevent and minimise spread of carbapenemase-producing Enterobacteriaceae Number of cases Trust engagement
Action Comment
Board to make it a high priority to minimise spread and to support all infection prevention and control (IP&C) measures
Paper presented to LEC on request Activity presented to GEC within DIPC quarterly report and approved/
AS/ DM /YC
Prepare a dedicated management plan including IP&C measures
Paper presented to LEC
Paper presented to CPPSC on request
AS/ DM /YC
Hospital-wide
Run awareness / training campaign for staff especially, but not exclusively, medical and nursing staff; maintain staff awareness of high-prevalence countries and UK problem areas
Training on-going by IPC practice educators and CNSs. Prioritise high risk areas and areas with higher numbers of identified cases
IPCT
On admission screen suspected cases eg previously positive cases OR history of hospitalisation abroad in last 12 months OR in a UK hospital with a known problem in last 12 months (if known)
Screening in place in high risk areas – BH - critical care, Spruce (HSE, stroke) Mulberry (immunocompromised) and Cedar (surgery). RFH – critical care, renal, hepatology, oncology and HSEP
Rolling out to further wards with targeted training for staff
All
IPCT
Implement isolation strategy at triage / admission for suspected or recent laboratory-confirmed patients
All confirmed and direct contacts ‘flagged’ on EPR to allow identification for screening, particularly on future admissions.
IPCT All
Hold regular management team meetings to review epidemiology and IP&C strategies, including root cause analyses where applicable
Meetings in progress. All
Implement communication strategy; report as a Serious Incident (SI) and inform PHE Centre if evidence of onward transmission
PHE informed of management meetings and transmission
All

Paper 6.1
19
Ensure that any transmission becomes a top trust priority, with leadership from board to ward
Outbreak meetings include Director of IPC and site executive team as well as staff from all relevant clinical and support services.
All
Laboratory
Optimise and review laboratory methods to detect producers (refer to Standard Operating Procedure)
Laboratory testing methods harmonised across all Trust sites to ensure effective detection of cases.
Micro-biology
Screen by plating rectal swabs (or faeces) and manipulated site swabs eg from skin breaks / catheter sites onto either a) proprietary chromogenic agars designed to be selective for carbapenemase-producing Enterobacteriaceae or onto b) MacConkey or CLED agar with meropenem or ertapenem discs. Examine for colonies on the selective plate or within the zone. Prior broth enrichment may be useful: use a rectal swab to inoculate 5 -10 ml broth containing a 10 μg ertapenem disc, then subculture as above
As above. Micro-biology
Infection prevention and control
It is recommended that Directors of IP&C ensure that the incident / problem is raised at Board level
Included in DIPC quarterly Board report. Raised at BEC
DIPC YC/ AS/ DM
Implement the Carbapenemase-producing Enterobacteriaceae Management Plan immediately, with strict adherence to standard precautions; affected patients should be isolated in a single room with en suite facilities or dedicated commode
Implemented. This is part of the harmonised Group policy
X3 daily review of isolation capacity and CPE requirements. Escalated at bed/site meetings.
All
Optimise care bundles and clinical practice for indwelling devices (review the need for the latter)
Part of clinical practice skills and competence assessments. Awaiting IT support to enable audit data entry for reporting at ward, divisional and Trust level.
All IT
Reinforce and optimise hand hygiene with soap and water or, on visibly clean hands only, an alcohol hand rub as an alternative
Daily reinforcement by IPC PEs, Senior staff and weekly audits
All
http://www.hpa.org.uk/ProductsServices/MicrobiologyPathology/UKStandardsForMicrobiologyInvestigations/TermsOfUseForSMIs/AccessToUKSMIs/SMIUKProtocols/smiP08LaboratoryDetectionandReportingofBacteria/

Paper 6.1
20
Minimise spread by effective routine and terminal cleaning including all hand-contact and sanitary areas (increase frequency if evidence of spread); review procedures for effective decontamination of equipment
Outbreak cleans in place for affected wards.
Hydrogen peroxide vapour decontamination (fogging) in place following terminal clean on discharge
Deep clean schedule in place
All Facilities and ward teams.
Designate cohort staffing depending on risk assessment, number of cases and feasibility
Part of risk assessment at ‘IPC supportive measures’ meetings and outbreak meetings.
All
Ensure effective incident tracking via a robust surveillance system, with an incident / outbreak management team, full epidemiological investigation, maintaining line list and epidemic curve
Tracking, bed moves and time-line of current cases and contacts in place.
Outbreak team
Prepare a readmission, discharge and transfer strategy for affected patients and contacts
In place – ‘Flagging’ of known cases and contacts GP/patient notification form in place for patients already discharged.
All
Plan and facilitate adequate communication to other healthcare providers (intra- and inter-regionally)
Case-by-case basis
Communication by PHE colleagues.
All PHE
Screening
Screen index case and case-contacts as per criteria; case find and isolate immediately; determine the extent of spread; convene an outbreak control team if spread suspected; electronically flag affected patient(s) record
In place All
Instigate weekly and discharge screening of all patient contacts (as identified) in affected units / wards for a period of 4 weeks after the last case was detected; cohort contacts if possible / feasible
In place in related wards
Outbreak team to determine further screening requirements
All
Screening of staff or household members for carriage is NOT routinely recommended as it is unlikely to provide additional benefit to control measures, whereas promotion of strict standard precautions will
Staff screening not in place. Strict source isolation measures in place for positive patients and direct patient contacts
All
B.3 Planning checklist for hospital / trust20 Infection Prevention & Control (IP&C) teams for the management of an outbreak, suspected outbreak or cluster of cases colonised or infected with carbapenemase-producing Enterobacteriaceae

Paper 6.1
21
1) Early communications √ Ensure senior managers, the board, and key senior clinical / ward staff are made aware of the case(s)
2) Instigation of immediate control measures √ Immediately refer to your dedicated plan for the management of carbapenemase-producing Enterobacteriaceae √ Refer to the PHE acute trust toolkit to ensure all early control measures to prevent spread have been instigated
3) Convene an incident / outbreak control team (OCT) – consisting of: √ Infection control leads – clinician and nurse √ Microbiologist √Infectious disease physician (if available / appropriate) √ Trust executive representation √ Clinical representation and senior nurse manager √ Estates / domestic service representation √ Communications department √ Pharmacy / medicines management team √ Senior representative from the local Public Health England (PHE) Centre
4) OCT review: √ Line list of cases – produce and maintain an epidemic curve (or running tally for repeat sporadic cases √ Microbiological investigations to date – diagnostic and screening, plus results √ Epidemiological investigations to date √ Current hypothesis(es) for incident / outbreak / cluster √ Control measures to date and effectiveness, include compliance / audit history √ Antimicrobial practices and compliance to policies √ Staff training and awareness
5) OCT produce incident / outbreak control plan including: √ Agreement on leadership, roles and responsibilities √ Frequency of meetings and reporting schedule (may change over time) √ Action plan for on-going investigations and control measures (include timelines) √ Plans for maintaining and reinforcing enhanced cleaning schedule (increased frequency and terminal cleaning for rooms of affected patients), if evidence of transmission √ Transfer and discharge arrangements for affected patients √ Additional expert advice required √ Consideration of external expert or peer support visit in ‘difficult to control’ outbreaks √Communications strategy including patients, relatives, the media and additional professionals / organisations as outlined in 6)

Paper 6.1
22
Appendix 2.
Infection Surveillance Programme 2017/18
Type of surveillance Performed by: Reported to: Frequency CompleteMandatory surveillance
MRSA bacteraemia Consultant microbiologist Clinical Lead IPC nurse
DH, PHE, NHS London IPCC Division Boards Divisional leads IPC group Wards/Matrons
MESS website Quarterly – Jan, Apr, July, Oct Monthly Fortnightly Weekly
√
MSSA bacteraemias Consultant microbiologist Clinical Lead IPC nurse
DH, PHE, NHS London IPCC Division Boards Divisional leads IPC group Wards/Matrons
MESS website Quarterly – Jan, Apr, July, Oct Monthly Fortnightly Weekly
√
E.coli bacteraemia- total numbers
Consultant microbiologist Clinical Lead IPC nurse
DH, PHE, NHS London IPCC Division Boards Divisional leads IPC group Wards/Matrons
MESS website Quarterly – Jan, Apr, July, Oct Monthly Fortnightly Weekly
√
Clostridium difficile in >2yrs Lapse in Care cases
Consultant microbiologist Clinical Lead IPC nurse
DH, PHE, NHS London IPCC Divisional leads IPC group Wards/Matrons
Quarterly returns Quarterly – Jan, Apr, July, Oct Fortnightly Weekly
√
Orthopaedic SSI-Total knee replacement -Total hip replacement - Hemiarthroplasty
Audit & surveillance nurse in Surgery, with IPC in-put.
DH, PHE IPCC Orthopaedic surgeons Wards/Matrons
Quarterly returns Quarterly – Jan, Apr, July, Oct Twice per year Weekly
√
Alert organism surveillance Completed
Alert organism surveillance
IPCT Clinical Lead IPC nurse
IPCC Wards/Matrons
Quarterly – Jan, Apr, July, Weekly
√
CPO point prevalence audit
IPCT IPCC Divisional leads IPC group Wards/Matrons
Annual √

Paper 6.1
23
MRSA acquisitions –(MRSA acquisitions – (colonisation and infection)
IPCT Clinical Lead IPC nurse Consultant microbiologist Clinical Lead IPC nurse
Data maintained on IPC database, √
Other Completed
RFH - High impact intervention audit reports
All Matrons indicators Monthly Will commence with Perfect Ward roll-out
By ward/ division report
Urinary catheter care audit.
IPCT IPCC Divisional leads IPC group Wards/Matrons
Annual √
MRSA screening of all admissions
Ward staff no-longer mandatory By ward/ division
Alert organism monthly list – changes, up-dates, new patients
IPCN’s On Freenet ‘Clinical applications’ All alerts appear automatically on patient records.
Daily up-date √
Cerner alert IPCN’s Cerner Daily up-date √Hand hygiene audit All Matrons indicators Monthly √
Antibiotic usage Pharmacy IPCT
Periodic √
Handgel usage Supplies IPCT
Periodic √

Paper 6.1
24
Appendix 3

Paper 6.2
1
Executive summary This is the trust report from the director of infection prevention and control for the Royal Free London NHS Foundation Trust.
In line with the revised Health and Social Care Act (2008) trusts are required to have appropriate management and clinical governance systems in place to deliver effective infection control. Included at appendix A are the ten compliance criteria from the Health and Social Care Act to assist the board in assessing the information provided.
In line with the Health and Social Care Act (2008, rev 2015) Code of Practice on the prevention and control of infections and related guidance, trusts are required to have appropriate management and clinical governance systems in place to deliver effective infection control. Within criterion 1 of the Code of Practice is a requirement that there is a programme of activity and planned development for IPC within the organisation to keep to a minimum the risk for infection and the general means by which it plans to control such risks.
Equality impact assessment• Positive impact which supports equity of service
Report to Date of meeting Attachment number
Trust board 25 July 2018 Paper 6.2
Director of infection prevention and control (DIPC) quarterly report
Action required The Board is asked to confirm that the report provides sufficient information to provide assurance of sustained compliance with the Hygiene Code.
Trust strategic priorities and business planning objectives supported by this paper
Board assurance risk number(s)
1 Improving clinical effectiveness R1 2 Enhancing the patient experience
CQC outcomes supported by this paperOutcome 8 Cleanliness and infection control QCQ Compliance (regulation 12 (2) h)
Risks attached to this project / initiative and how these will be managed (assurance)The revised Hygiene Code Risk matrix will be monitored at the Infection Control Committee. The risks associated with the Hygiene Code have been included in the Board Assurance Framework

Paper 6.2
2
Report From D Sanders, group chief nurse and director of infection prevention and control. Author(s) D Mack, Microbiology Consultant, IPC Doctor
Anand Sivaramakrishnan, Consultant Microbiologist, IPC Doctor Dianne Irish, Consultant Virologist Y Carter, Head of IPC Nursing IPC team
Date 13 July 2018

Paper 6.2
3
Introduction
The Health and Social Care Act (2008) Code of Practice on the prevention and control of infections and related guidance outlines the actions NHS Trusts in England must take to ensure a clean environment for the care of patients, in which the risk of infection is kept as low as possible. The 10 compliance criteria are attached at appendix A. The criteria have been revised for the 2015 edition, including a larger focus on antimicrobial stewardship
Monitoring Progress against the Health and Social Care Act, including internal audit. Hygiene code compliance will continue to be monitored through the Infection Prevention and Control Committee and through hospital unit divisional lead monthly meetings. The trust’s internal auditors annually assess trust arrangements and ensure robust evidence of compliance in all criteria. The most recent comprehensive CQC inspection identified no specific ‘infection prevention and control’ improvement recommendation, but the IPC team will support clinical divisions and services to make improvements in the infection prevention and control elements raised in the divisional and service reports.
1. Infection report
1.1 Meticillin-sensitive and Meticillin-resistant Staphylococcus aureus bacteraemia. (MRSA and MSSA)
Reduction of hospital acquired Staphylococcus aureus bacteraemias including those due to MRSA continue to be an important infection control priority for the trust. The MRSA target for 2018/19 is zero for all organisations.
From April 2018, post infection reviews are only required for CCGs with a rate of 1.6 or more community onset MRSA blood stream infections per 100,000 population and trusts with a hospital onset MRSA blood stream infection rate of 1.7 per 100,000 bed-days or more. Any CCG or trust with a rolling rate that breaches this threshold within year will also have to formally undertake and report post infection reviews. Royal Free London NHS FT is not on the list of trusts required to carry out reviews.
Since April 1st, there have been three cases of MRSA bacteraemia. The first case occurred in ITU South in Barnet hospital where a central venous catheter line remained in-situ for clinical reasons longer than routinely recommended, but with clinician and microbiology approval. This was attributed to the Trust with no lapses in care identified.
The second case was in Olive Ward at Barnet Hospital, but cultures taken on admission indicated that there had been acquisition prior to admission to Barnet Hospital and was not attributed to the Trust.
Case three occurred on 5 South at the Royal Free Hospital. The patient was found to be colonised with MRSA on the admission screen. The patient fell whilst using the commode 3/6/18 and sustained a fracture which was surgically fixed. Post operatively the patient developed a fever and an MRSA bacteraemia was detected which was attributed to the Trust. The post infection review indicated lessons for learning including pre-operative screening and timely MRSA decolonisation, the need for more robust documentation and staff training up-dates, particularly for agency and bank staff.
The learning from any lapses is shared at the divisional leads IPC meetings.
1.2 MRSA colonization trust acquisitions.
The trust MRSA colonization acquisition rate remains low across all sites, (an acquisition is defined as any patient not previously known to be MRSA positive but has been swabbed whilst in the RFLNHSFT after the first 48 hours of admission and found to be positive). Although the national requirement has reduced, the

Paper 6.2
4
Trust screening process remains inclusive of in-patient admissions as it is felt to be integral in reducing acquisition rates and contributes to safer patient care.
1.3 Clostridium difficile (C.diff)
The threshold for the trust for 2018/19 set by Public Health England (PHE) is 65 cases of acquired C.diff, a reduction of one from last year. Following revisions to its risk framework NHS Improvement, confirmed that for the purposes of its governance risk ratings of foundation trusts’ with effect from quarter one 2015/16 national performance against the C. difficile indicator will include only those infections that result from a lapse in care. Infections which result from a lapse in care are determined by the local clinical team applying a checklist based assessment developed by PHE with outcomes reviewed and agreed by local commissioners.
Since April 1st there have been 13 cases of attributable C.diff, 4 below threshold. There have been no lapses in care so far identified.
The deep clean and vapourised hydrogen peroxide (VHP) programme is now embedded and along with antibiotic stewardship improvements are key actions for the trust for the next year.
The actions which will be also be focused on for the next year include: • Continue Deep Clean programme across all sites • Review of all cleaning audit reports at monthly divisional lead meetings • External expert review of C.diff reduction strategies and management plans (Professor Mark Wilcox
- consultant microbiologist, head of research and development in microbiology at the Leeds Teaching Hospitals (LTHT), the lead on Clostridium difficile for Public Health England (PHE), medical advisor to national infection prevention & control lead (NHS Improvement, England)
• Reduce antibiotic usage • Improved antimicrobial stewardship – business case to GEC

Paper 6.2
5
• IT integration: stool chart/algorithm, antibiotic stewardship,patient tracking and isolation • Clinical audit programme – Perfect Ward roll-out • Clinical team engagement in RCA process • ‘Board to Ward’ support • Inclusion of antimicrobial stewardship in appraisal
There have been further reductions in piperacillin-tazobactam, carbapenam, and total antibiotic usage in 2017/18 and this remains a focus of antimicrobial stewardship activities.
Education continues and includes learning from the identified lapses in care. This program continues from details in previous DIPC reports.
1.4 E.coli bacteraemias.
From April 2017 a government initiative extended the surveillance of bacteraemias caused by Gram-negative organisms to include Klebsiella species and P. aeruginosa in addition to the existing E. coli collection with the intention of reducing such infections by 50% by 2021. The reporting of these cases will be driven through the hospital unit divisional leads group and the Infection Prevention and Control Committee. A report will be provided once cases are reviewed according to PHE guidance. The reduction in these infections is one of the stated aims in the Quality Account for 2018/19.
It is recognised that the trust rates are above the England average and further work is essential to reduce Gram negative bacteraemias. The quality improvement (QI) programme to achieve this is set out in Appendix B. The work already undertaken has been recognised as significant progress by Ruth May, NHSI executive director of nursing, deputy CNO and national director for infection, prevention and control as per previous report.

Paper 6.2
6
1.5 Carbapenemase producing enterobacteriaceae (CPE) and other non-fermenting (CP-NF) organisms.
There have been sporadic cases of CPE and CP-NF identified through admission screening at the Royal Free hospital with one identified transmission on 10 East Ward. Full IPC measures were instigated on the ward with no further cases.
Following the report of cases identified on more sensitive laboratory testing at Barnet Hospital, the outbreak has now been de-escalated. A fortnightly CPE management group is established to manage preventative actions and respond in a timely manner to any newly ientifed cases, whether from admission screen or sampling later in an in-patient stay. Each sporadic case now identified is investigated, with ‘contacts’ screened and full IPC measures instituted.

Paper 6.2
7
1.6 Influenza
The winter of 2017/18 identified more patients than previous years with both Flu A and Flu B as reported in the last quarterly report. Staff vaccination rate reached 72%. The programme to increase to 75% in preparation for winter 2018/19 has been implemented using a Quality Improvement methodology (QI):
1.7. Quality Improvement The IPC team is using a quality improvement initiative to identify drivers for improvement in all infection indicators. The overall aim has four elements, as detailed in the previous quarterly report.
1. Reduce Gram negative bacteraemias as per national (PHE) 50% reduction target by 2021. This is equal to 10% reduction per year.
2. Reduce C.diff to below threshold of 65 attributable cases form April 2018 to March 31st 2019
3. Zero MRSA BSIs by March 31st 2019
4. Undertake mandatory surgical site infection surveillance for 2018/19 and maintain orthopaedic SSIs within national parameters

Paper 6.2
8
2 Orthopaedic surgical site infection report The mandatory requirements from DH for surveillance is one category of orthopaedic surgery for one quarter within each financial year as a group requirement. The IPC surveillance nurse is currently on long-term leave however this requirement will be met.
The surgical site infection surveillance (SSIS) committee drives the SSI programme within orthopaedic surgery as a Group committee. RCA’s from all infections are reported to the orthopaedic specialty team and surgical Board and reported to the SSI committee for learning and dissemination of best practice.
Learning from the recent RCAs includes:
1. Changes in theatre environment and process to reduce the number of unnecessary interruptions. 2. Introduction of Chlorhexidine washcloths for patient use before attending for surgery. 3. Development of a protocol for the use of PICO dressings in high risk patients and patients who go
on to have wound complications following surgical procedure. The protocol will be part of the new digital solution in the Chase Farm Hospital building. It is envisaged this will further increase adherence to the protocol. This is also part of on-going work to develop Clinical Pathways to eliminate unwarranted variation across the Trust.
4. Robust monitoring of adherence to the Trust prophylactic antibiotic policy. Feedback from this has led to teaching from our microbiologists to prescribers around the reasons for the specifics in terms of drug choices and doses and risks of side effects and clearer guidelines are being developed.
5. The setting up of a cross-site SSI committee to promote best practice.
Further work includes:
1. Monitoring the use of Chlorhexidine washcloths to ascertain reliability in terms of usage. This will be followed up with actions as appropriate.
2. Making the prophylactic antibiotic policy part of the new digital solution, reducing the likelihood of deviation from the protocol and reducing the risk of error in prescribing.
3. Consideration of the use of antimicrobial sutures in various surgical specialties. 4. The use of the ‘One Together Assessment Toolkit’ to assess infection prevention practice across
the surgical pathway.
3. Viral infections 4.
410 laboratory-confirmed viral infections were identified by the virology laboratory at the Royal Free hospital (RFH) between April and June 2018, which required IPC interventions from the virology doctors at Royal Free hospital, (See Figure 1).
Figure 1: Virology IPC Activity from April 2018 – June 2018
85% of the infections were due to respiratory viruses (See Figure 2).
8% of the infections were gastrointestinal infections
6% of the infections were rash illnesses. There were 16 cases of varicella zoster virus infections and 6 cases of measles identified during this period at RFH site.
1 case of acute hepatitis E infection recorded
RFHApr May Jun Total
Respiratory 96 64 47 207Gastro/Other 17 23 15 55Total 113 87 62 262
BarnetApr May June Total
Respiratory 71 44 26 141Gastro/Other 1 3 3 7Total 72 47 29 148

Paper 6.2
9
Figure 2: Virology IPC Activity from October 2014 – June 2018
0102030405060708090
100110120130140150160170180190200210220230240250260270280290300310320330340350360
Oct-1
4
Nov
-14
Dec
-14
Ja
n-1
5
Feb
-15
Ma
r-15
Apr-1
5
Ma
y-1
5
Ju
n-1
5
Ju
l-15
Aug
-15
Sep
-15
Oct-1
5
Nov
-15
Dec
-15
Ja
n-1
6
Feb
-16
Ma
r-16
Apr-1
6
Ma
y-1
6
Ju
n-1
6
Ju
l-16
Aug
-16
Sep
-16
Oct-1
6
Nov
-16
Dec
-16
Ja
n-1
7
Feb
-17
Ma
r-17
Apr-1
7
Ma
y-1
7
Ju
n-1
7
Ju
l-17
Aug
-17
Sep
-17
Oct-1
7
Nov
-17
Dec
-17
Ja
n-1
8
Feb
-18
Ma
r-18
Apr-1
8
Ma
y-1
8
Ju
n-1
8
Resp Viruses Other Viruses
RFH
Respiratory illness Respiratory Infections - Apr-Jun 18 Gastro/Other Infections - Apr-Jun 18
Figure 3: Common Viral Respiratory Infections Recorded from October 2014 – June 2018
0
20
40
60
80
100
120
140
160
180
Oct-1
4
No
v-14
De
c-14
Jan-1
5
Feb
-15
Mar-1
5
Apr-1
5
May-1
5
Jun-1
5
Jul-1
5
Aug
-15
Sep
-15
Oct-1
5
No
v-15
De
c-15
Jan-1
6
Feb
-16
Mar-1
6
Apr-1
6
May-1
6
Jun-1
6
Jul-1
6
Aug
-16
Sep
-16
Oct-1
6
No
v-16
De
c-16
Jan-1
7
Feb
-17
Mar-1
7
Apr-1
7
May-1
7
Jun-1
7
Jul-1
7
Aug
-17
Sep
-17
Oct-1
7
No
v-17
De
c-17
Jan-1
8
Feb
-18
Mar-1
8
Apr-1
8
May-1
8
Jun-1
8
Influenza RSV Rhinovirus Parainfluenza Coronavirus Swine Flu H1N1RFH
RFH BarnetAdenovirus – NPS/BAL 10 11Coronavirus 11 5Enterovirus/Rhinovirus 107 75Influenza A 40 15Influenza B 6 0Parainfluenza 29 30Parechovirus 1 1RSV 3 4Total 207 141
RFH BarnetAdenovirus - FAE 2 1Astrovirus 1 0Hepatitis A 1 0Measles 6 0Norovirus 19 1Rotavirus 2 0Sapovirus 7 0VZV 16 5Total 54 7

Paper 6.2
10
Gastrointestinal illness During this quarter, there were 28 laboratory confirmed viral infections : 2 rotavirus infections, 7 sapovirus infections and 19 norovirus infections. Of the 19 norovirus infections, the majority were from patients with chronic norovirus infection There were no norovirus outbreaks.
Figure 4: Norovirus PCR Positive Stool Samples recorded from RFH : July 2014 June 2018
5. Serious Incidents, outbreaks related to HCAIs
In critical care south and Cedar ward at Barnet hospital there was a CPE outbreak as noted above. The outbreak was de-escalated as there were no new cases from either Cedar or critical care for 4 consecutive weeks. It was agreed that it would be beneficial to the Trust to widen the focus to all divisions rather than narrow focus on ITU and surgery, to provide governance assurance that pro-active preventative measures are in place and recognition of CPE incidents can be timely, with good feedback to all clinical teams. As a result CPE management meetings have been set up with a wider invitation circulation.
There have been two tuberculosis incident (PHE ref: 193701 and 193710). The first case is a patient admitted to ED at Barnet hospital on 16/04/2018 and transferred to the SAU on 17/04/2018 into an open bay. After 22 hours the patient was transferred to a side room on MSSU when it was confirmed that he was multi-drug resistant (MDR) TB positive. Contact tracing was done in A&E and SAU for both staff and patients who were exposed and letters will be sent out to all concerned.
The second case is a patient who was admitted to Barnet ED on 22/03/18 and was there for a total of four hours. He was transferred to the open bay on MSSU, then to Walnut before going into a side room there. Contact tracing is being done on MSSU and Walnut and letters sent out to all concerned.
On 18/06/18 a period of increased incidence was declared on the Starlight neonatal unit after there were three cases of MRSA acquisitions (colonisations) within a period of seven days from 04/06/2018 to 11/06/2018. All babies were isolated and the unit remained opened to admissions. Supportive measures were instituted which included enhanced cleaning, hand hygiene, environmental audits and teaching by the IPCT on hand hygiene and general IPC issues. Weekly meeting were held to review patients and outcomes of implemented measures. As at 10/07/2018 there no further positive cases.

Paper 6.2
11
6. IPC team activity
The quality improvement (QI) programme related to reducing urinary catheter associated infections has been a priority as part of the Gram negative bacteraemia reduction programme and to improve patient safety. The current focus is the catheter ‘passport’ which allows patients to participate in their own catheter management and share information across primary and secondary healthcare as a seamless care activity.
Further training and support with antibiotic stewardship for nurses is undertaken in all clinical areas to support prescribers and ensure nurses are clear on their role in antibiotic administration. Appendix B
The IPC team is supporting the Chase Farm new hospital build with site visits and IPC advice.
7. Hand hygiene
Hand hygiene is audited by staff within clinical areas and data entered on the ‘reporting portal’ as summarised below. Verification audits are undertaken by the IPCNs and individual training and feedback provided within the clinical area directly to the staff.
8. Serious Incidents. There have been No SIs this quarter relating to infection risks.
9. Antibiotic stewardship Surgical antibiotic prophylaxis at the Royal Free hospital and incidents related to teicoplanin.A case series of 8 patients from 2015 - 18 was presented at a recent audit meeting: four patients were under the vascular team and all had anaphylaxis with acute onset within 10 minutes of receiving teicoplanin. Seven patients had raised mast cell tryptase levels in samples taken shortly after the reaction and five patients were followed up in allergy clinic:(four had positive intra-dermal tests to teicoplanin and one test was not positive but all other causal agents were excluded.). Six patients had definite prior exposure to teicoplanin, five within the previous five months. This was discussed at the drugs and therapeutic committee and medical staff committee. It was noted that at RNOH the rate of IgE-mediated anaphylaxis to teicoplanin had been calculated at between 0.046% and 0.059% (equating to between 1:2088 and 1:1655). RNOH continue to use teicoplanin as surgical prophylaxis, but by 15-30 min intravenous infusion rather than slow bolus injection. It was agreed that the same precautions should be implemented at RFH, and any such incidents monitored closely.
Update 5th July 2018 - There has been one incident of anaphylaxis likely due to teicoplanin use as surgical prophylaxis in the last 5 months since infusions replaced bolus injections. This was discussed at the anitibiotic stewardship committee on 4/7/18 and it was agreed that, whereas teicoplanin remained the best drug from a microbiological perspective, it would be appropriate to review the prophylaxis policy to see if other agents could be used in some situations.
10. Validation The trust has declared compliance to the Care Quality Commission in relation to IPC aspects of the Health and Social Care Act (2008) Hygiene Code. The CQC has agreed unconditional compliance. The Trust also collaborates with the CCG CSU advisors in the PIRs and RCAs for infections to ensure open and transparent reporting, learning from the outcomes and sharing learning from other organisations.

Paper 6.2
12
Appendix A

Paper 6.2
13
Appendix B Antibiotic stewardship for nurses
Antibiotic prescription:
Check start and end date
Administer for documented duration only.
Administration past end date is a medication error
Best route for administration
Check with prescriber to switch from IV to oral administration at 48 hours.
Administration time
Administer antibiotics on time – missing doses contributes to the development of antibiotic resistance
Review prescription after 48 hours
Check if prescription should continue, change or stop
Think about your patient
• are there any signs of reaction?
• are blood levels needed and checked?
• has C.diff been identified – if so antibiotics need review.
Antibiotic records and patient transfers
Include records of infection, antibiotic prescriptions and administration in transfer notes
H H
Do you know why your patient is on antibiotics?
Has an infection been confirmed?
All antibiotic prescriptions should have a reason written in the patient notes
? Every time you administer an antibiotic, do you know:
• why?
• the usual dose?
• route of administration?
• common side effects?
Find more information in the BNF or Trust Microguide.
i-phone Android

Paper 7
Page 1 of 14
Annual complaints report
Executive summary
This report provides information on the complaints received in the trust between 1 April 2017
and 31 March 2018. It provides a summary of the complaints received, the areas concerned,
the main issues raised and trends identified, as well as the actions taken in response or
those planned for the future. It also looks at our performance against agreed targets and the
number of complainants who have come back dissatisfied following their initial response.
Action required/recommendation
For information and consideration.
Trust strategic priorities and business planning objectives
supported by this paper
Board assurance risk
number(s)
2. Excellent user experience – to be in the top 10% of relevant
peers on patient, GP and staff experience
4. Excellent compliance with our external duties – to meet our
external obligations effectively and efficiently
5. A strong organisation for the future – to strengthen the
organisation for the future
CQC Regulations supported by this paper
Regulation 9 Person-centred care
Regulation 10 Dignity and respect
Regulation 11 Need for consent
Regulation 12 Safe care and treatment
Regulation 13 Safeguarding service users from abuse and improper treatment
Regulation 14 Meeting nutritional and hydration needs
Regulation 15 Premises and equipment
Regulation 16 Receiving and acting on complaints
Regulation 17 Good governance
Regulation 18 Staffing
Regulation 20⃰ Duty of candour
Risks attached to this project/initiative and how these will be managed (assurance)
N/A
Equality analysis
No identified negative impact on equality and diversity
Report to Date of meeting Attachment number
Trust board 25 July 2018 Paper 7

Paper 7
Page 2 of 14
Report from: Deborah Sanders, group chief nurse
Author(s): Stephen Evans, head of complaints & PALS
Date: 13 July 2018

Paper 7
Page 3 of 14
Annual Complaints Report – 2017/18
Introduction
Feedback from patients, relatives and carers provides the trust with a vital source of insight
about people’s experiences of healthcare at the Royal Free London NHS Foundation Trust,
and how our services can be improved. The ultimate aim of the trust’s complaints process is
to listen and respond to the issues being raised and use the information received to improve
our services and, in turn, the experience of our patients.
This report provides information on the complaints received in the trust between 1 April 2017
and 31 March 2018. It provides a summary of the complaints received, the areas concerned,
the main issues raised and trends identified, and the actions taken in response or those
planned for the future. It also looks at our performance against agreed response targets and
the number of complainants who came back dissatisfied following receipt of their initial
response.
Background
The statutory instrument for complaints in the NHS is contained in the Local Authority Social
Services and National Health Service Complaints (England) Regulations 2009. The
legislation expects that each responsible body has arrangements for dealing with complaints
to ensure that:
1. complaints are dealt with efficiently;
2. complaints are properly investigated;
3. complainants are treated with respect and courtesy;
4. complainants receive, so far as is reasonably practical -
I. assistance to enable them to understand the procedure in relation to
complaints; or
II. advice on where they may obtain such assistance;
5. complainants receive a timely and appropriate response;
6. complainants are told the outcome of the investigation of their complaint; and
7. action is taken if necessary in light of the outcome of a complaint.
The Department of Health issued Listening, Responding, Improving: A guide to better
customer care in February 2009 to support organisations in responding to and learning from
complaints.
The Parliamentary Health Service Ombudsman (PHSO) Principles of Good Complaint
Handling has six principles:
1. getting it right
2. being customer focused
3. being open and accountable
4. acting fairly and proportionately
5. putting things right
6. seeking continuous improvement.

Paper 7
Page 4 of 14
Complaints received
There were 1,534 complaints received between 1 April 2017 and 31 March 2018. 765 of
those were complaints regarding Royal Free Hospital services, 591 were regarding Barnet
Hospital services and 178 were regarding Chase Farm Hospital services. This is very similar
to the combined total of 1,567 complaints received in 2016/17 – 853 of which were for Royal
Free Hospital services, 565 for Barnet Hospital services and 149 were Chase Farm Hospital
services.
The 1,534 complaints received are from 1,410,262 inpatient and outpatient episodes, which
equates to a complaint ratio of 0.1%, the same percentage as 2014/15, 2015/16 and
2016/17.
As of 13 July 2018, 1,489 of the complaints have been responded to. Of those, 132 have
been fully upheld, 668 have been partially upheld and 689 have not been upheld. There
have been 1,518 response target dates in this time period and we met 1,151 of them, which
equates to an overall response rate of 76%.
Q1 Q2 Q3 Q4 Overall
Deadlines met 313 of 411 324 of 441 298 of 377 216 of 289 1,151 of 1,518
Percentage 76% 73% 79% 76% 76%
Weekly meetings between the complaints managers and the corporate complaint leads on
the Royal Free Hospital site continue, and regular meetings between the complaints
managers and the corporate complaints lead for Barnet and Chase Farm take place
regularly. The corporate complaints teams are also assisting with the extending and
negotiating of deadlines where necessary.
However, disappointingly, the end of year position (76%) is the same as 2016/17. The
average response rate for Barnet hospital and Chase Farm hospital for 2017/18 was 67%
and the Royal Free Hospital average response rate was 85%.
In Q1 the newly appointed complaints manager for the medicine and urgent care (MUC)
division at Barnet and Chase Farm facilitated responses to a number of the historic
complaints but, working through the back-log methodically, whilst dealing with the new cases
coming through, impacted on performance (43%).
In Q2 the surgery and associated service (SAS) division at the Royal Free met 24 of 51
targets (47%) and the women’s, children’s and imaging (WC&I) division at Barnet met 20 of
40 targets (50%). The director of nursing for Barnet Hospital requested that action be taken
to improve performance. Consequently, weekly meetings are now taking place between the
divisional complaints managers and senior staff in the divisional governance management
teams to monitor complaint progress and help escalate matters when needed. The
performance for Barnet and Chase Farm in Q1 of 2018/19 has improved to 73%.
We appreciate that any missed target reflects poorly on the trust and potentially exacerbates
a complainant’s feelings of upset and frustration, and we are working hard to improve the
response rate in this regard. The trust’s default position is to respond to complaints in 35
working days and the average response time for those complaints closed in 2017/18 was 43
working days.

Paper 7
Page 5 of 14
Complaints re-opened following receipt of their first response
As demonstrated by the table below, the number of complainants who have re-opened their
complaint regarding services provided by the Royal Free Hospital, following receipt of their
first response letter, has fallen gradually since 2010/11 but would appear to have now
plateaued. Despite the increase in numbers received since the acquisition in 2014, there has
been a decrease in the number of re-opened complaints regarding services provided by
Barnet hospital and Chase Farm Hospital. This figure too would appear to have now
plateaued.
NB: the numbers for 2017/18 are accurate as of 13 July 2018 and may continue to change
over the next few months.
2010/11 2011/12 2012/13 2013/14 2014/15 2015/16 2016/17 2017/18
Royal Free Hospital
86 of 877
(10%)
75 of 797 (9%)
57 of 709 (8%)
50 of 653 (8%)
60 of 698 (8%)
37 of 785 (5%)
42 of 853 (5%)
43 of 765 (6%)
Barnet & Chase Farm
Hospitals
53 of 225
(24%)
59 of 207
(29%)
53 of 295
(18%)
31 of 337 (9%)
26 of 461 (6%)
41 of 671 (6%)
45 of 714 (6%)
41 of 769 (5%)
Top 10 Subjects (primary)
The table below is a breakdown of the complaints by primary subject, along with a
comparison of the primary subjects reported in last year’s annual report. The top 10 subjects
are very similar to 2016/17 but have changed order slightly.
2016/17 2017/18
Clinical treatment 391 Clinical treatment 394
Communications 335 Communications 297
Values & behaviours (attitude) 209 Values & behaviours (attitude) 218
Appointments 184 Appointments 215
Car parking 102 Car parking 96
Transport 75 Admission / discharge 60
Nursing or midwifery care 74 Transport 50
Admission / discharge 60 Nursing or midwifery care 50
Waiting times 28 Waiting times 37
Access to treatment / drugs 16 Administration 37
The top 10 subjects are predominantly the same and the top 5 are identical. Clinical
treatment and communication issues are again the most common primary subjects of the
complaints received. Attitude and appointment complaints continue to be a feature, as does
car parking issues across all sites.
Further analysis of the top 3 subjects
A more detailed analysis of the top three subjects i.e. complaints regarding clinical treatment,
communication and attitude will follow below, along with examples of actions taken and
changes implemented in response to those complaints. In addition, the same analysis will be
undertaken for the nursing care complaints received.

Paper 7
Page 6 of 14
Clinical treatment
There were 531 complaints received where clinical treatment was recorded as a subject of
the complaint – in 394 cases it was the primary or sole reason for the complaint. The 531
complaints were received from 1,410,262 inpatient and outpatient episodes, which equates
to a complaint ratio of 0.04% (2014/15 was 0.02%, 2015/16 was 0.04% and 2016/17 was
0.04%). There is no identifiable trend in terms of staff member.
Of the 531 complaints received, 23 have been fully upheld (38 are still under investigation).
Detailed explanations have been provided to each complainant along with apologies and
information regarding the action taken as a result. There has been escalation to the serious
incident process whenever appropriate and/or the involvement of human resources for
further investigation.
The table below breaks the clinical treatment complaints down by primary specialty and
primary sub-subject for the 10 most complained about specialties.
Delays with treatment taking place is again the common underlying theme for the complaints
received and the adult section of our emergency departments, along with orthopaedics and
obstetrics/maternity, are again the most common specialties to be referred to.
Example actions taken in response to the complaints are listed below:
Aw
are
ne
ss u
nd
er
anae
sth
eti
c
De
lay
or
failu
re t
o u
nd
ert
ake
sca
n/X
-ray
De
lay
or
failu
re in
act
ing
on
/ o
rde
rin
g te
st
resu
lts
De
lay
or
failu
re in
tre
atm
en
t fo
r in
fect
ion
De
lay
in in
du
ctio
n o
f la
bo
ur
De
lay
or
failu
re t
o m
on
ito
r w
ou
nd
De
lay
or
failu
re in
tre
atm
en
t o
r p
roce
du
re
De
lay
or
failu
re t
o d
iagn
ose
De
lay
or
failu
re t
o f
ollo
w u
p
De
lay
in o
bta
inin
g cl
inic
al a
ssis
tan
ce
Failu
re t
o f
ollo
w u
p o
n o
bse
rvat
ion
s /
reco
gnis
e
de
teri
ora
tin
g p
atie
nt
Inad
eq
uat
e p
ain
man
age
me
nt
Inap
pro
pri
ate
pro
ced
ure
or
tre
atm
en
t
Inju
ry s
ust
ain
ed
du
rin
g tr
eat
me
nt
or
op
era
tio
n
Mis
man
age
me
nt
of
lab
ou
r
Tota
lEmergency Dept - Adults
0 7 3 0 0 0 8 20 1 1 1 1 8 1 0 51
Orthopaedics & Trauma
0 1 0 1 0 1 11 3 2 0 0 0 5 2 0 26
Obstetrics & Maternity 0 1 2 2 1 0 1 1 1 0 0 1 1 1 13 25
Cardiology 1 0 1 0 0 1 7 2 1 0 2 0 2 2 0 19
Plastic Surgery 0 0 0 0 0 1 9 0 4 0 0 1 1 1 0 17
Urology 0 0 1 0 0 0 6 1 4 0 0 0 1 1 0 14
Paediatrics 0 1 1 0 0 0 2 2 2 0 0 0 4 0 0 12
Breast Surgery 0 0 0 1 0 0 4 4 0 0 0 1 1 0 0 11
Ophthalmology 0 0 0 0 0 0 4 0 0 0 0 0 4 3 0 11
Gynaecology 0 0 0 1 0 0 4 0 2 0 0 0 2 0 1 10
Total 1 10 8 5 1 3 56 33 17 1 3 4 29 11 14 196

Paper 7
Page 7 of 14
Whilst arrangements for review or follow up are suitable to be discussed via telephone,
certain conditions, such as wounds, cannot be assessed adequately via telephone
because they require a visual or physical examination. For such cases, foundation year 2
ED doctors should seek a local, senior emergency department opinion, rather than a
remote, junior surgical opinion. This will be reiterated during junior doctor induction and
teaching sessions and included in the ED handbook. The surgical teams, including
plastics, will also be advised that their junior staff should not give such opinions over the
telephone.
A complaint highlighted that some patients have not been receiving their cardiology test
results in a timely manner due to a breakdown in the registrar review process. A new
process has therefore been instigated within cardiology so that all results, requiring
review from a registrar, are distributed to the on-call cardiology registrar, who will do them
within the week that the test happens. An escalation process has also been instigated to
chase outstanding administration work via the educational supervisors.
The ED consultant has discussed this case with the doctor concerned and provided him
with education on the management of a clavicle injury and possible underlying chest
injuries. There will also be a teaching session on this case [anonymously] to ensure there
is learning for all the ED junior doctors.
Communication
There were 424 complaints received where communication was recorded as a subject of the
complaint – in 297 cases it was the primary or sole reason for the complaint.
The complaints related to a wide range of departments and specialties and there is no
obvious trend in terms of numbers received or the departments or staff member(s) involved.
The table below breaks the communication complaints down by specialty and the sub-
subject for the 10 most complained about specialties.
Bre
akd
ow
n in
co
mm
un
icat
ion
be
twe
en
sta
ff
Bre
akd
ow
n in
co
mm
un
icat
ion
re
ap
po
intm
en
ts
Co
mm
un
icat
ion
Fai
lure
be
twe
en
de
par
tme
nts
Co
mm
un
icat
ion
fai
lure
wit
hin
de
par
tme
nt
Co
mm
un
icat
ion
wit
h p
atie
nt
Co
mm
un
icat
ion
wit
h r
ela
tive
s/ca
rers
Co
mm
un
icat
ion
wit
h G
P
Co
nfl
icti
ng
info
rmat
ion
De
lay
in g
ivin
g in
form
atio
n/r
esu
lts
De
lay
in r
ep
ort
ing
resu
lts
Inad
eq
uat
e o
r in
suff
icie
nt
info
rmat
ion
pro
vid
ed
Inco
rre
ct E
ntr
y o
n M
ed
ical
Re
cord
s
Inco
rre
ct/i
nac
cura
te in
terp
reta
tio
n
Inco
rre
ct/N
o in
form
atio
n g
ive
n
Pat
ien
t N
ot
List
en
ed
to
Insu
ffic
ien
t in
form
atio
n p
rovi
de
d p
rio
r to
co
nse
nt
Tota
l
Emergency Dept - Adults
0 0 0 0 8 3 1 1 0 0 0 3 1 0 2 0 19
Urology 1 1 0 0 10 1 0 0 2 0 0 0 0 1 0 1 17
Obstetrics & Maternity
0 1 0 0 10 0 0 1 1 0 1 1 0 1 1 0 17

Paper 7
Page 8 of 14
Dermatology 0 1 0 0 7 0 0 3 2 0 2 0 0 0 0 0 15
Orthopaedics and Trauma
0 0 1 0 10 0 0 0 0 0 0 0 0 0 1 0 12
Gynaecology 0 0 0 0 5 2 1 0 1 0 1 0 0 2 0 0 12
Radiology 0 0 0 0 4 0 0 0 1 2 2 0 0 1 1 0 11
Cardiology 0 0 0 0 5 1 0 0 1 1 1 2 0 0 0 0 11
Plastic Surgery 0 1 1 1 5 2 0 0 0 0 0 0 0 0 0 0 10
Ophthalmology 0 0 0 0 7 1 0 0 0 0 0 1 0 0 0 0 9
Total 1 4 2 1 71 10 2 5 8 3 7 7 1 5 5 1 133
The specialties involved and numbers received are lower than last year’s report. The top ten
specialties and sub-subjects are very similar to last year’s report but elderly medicine, the
outpatient appointment centre and general surgery have been replaced by gynaecology,
radiology and plastic surgery. Communication with the patient is once again the key
underlying theme.
Example actions taken in response to the complaints are listed below:
The overseas visitors team will work with the senior nurses on 11 West ward to produce
a patient information leaflet about treatment for a high consequence infectious disease
and chargeable treatments.
The dermatology service at Barnet Hospital will be implementing a cryotherapy consent
form that has to be read and signed by patients prior to receiving this treatment.
Furthermore, following comments about the quality of the images available on the current
information leaflet for cryotherapy, the dermatology service has agreed to make colour,
laminated copies of the information leaflets available for each clinic room so that patients
can better visualise what to expect.
Corneal abrasion (scratch to the eye) will now be something that the ophthalmology staff
discuss more thoroughly with patients before going ahead with injections, and it will now
become part of the formal consent procedure.
The ophthalmology team have now employed another member of staff to support the
ophthalmology service at the Whittington Hospital site and prevent difficulties in patients
getting through to the clinic.
The urology service is in the process of arranging a new system that will link all the
administrative telephone lines in the service together and therefore enable the
management team to view the performance of the administrative team in answering calls
and voicemail messages. We hope that this will ensure that patients will not encounter
problems getting through to the department.
Values and behaviour – attitude
There were 307 complaints received where attitude was recorded as a subject of the
complaint – in 218 cases it was the primary or sole reason for the complaint.
The complaints related to a wide range of departments and specialties. 165 (54%) related to
Royal Free Hospital services and 142 (46%) related to Barnet and Chase Farm Hospital

Paper 7
Page 9 of 14
services, whereas in last year’s report the Royal Free Hospital services accounted for 65% of
the attitude complaints.
There is no obvious trend in terms of individuals involved but the adult emergency
departments and our obstetric services again received the most complaints in this regard.
The table below breaks the complaints down by specialty and the sub-subject for the 10 most
complained about specialties.
Att
itu
de
of
Nu
rsin
g
staf
f/M
idw
ive
s
Att
itu
de
of
Me
dic
al s
taff
Att
itu
de
of
Ad
min
&
Cle
rica
l sta
ff
Att
itu
de
of
oth
er
staf
f
Failu
re t
o a
ct in
a p
rofe
ssio
nal
man
ne
r
Ru
de
ne
ss
Tota
l
Emergency Dept - Adults 9 11 2 0 0 2 24
Obstetrics & Maternity 8 7 0 0 1 1 17
Radiology 0 7 1 2 1 3 14
Orthopaedics and Trauma 6 4 2 0 0 0 12
Dermatology 2 3 2 0 0 1 8
Gynaecology 1 2 4 0 0 2 9
Phlebotomy 1 1 2 2 0 1 7
Outpatient Appointment Centre 0 0 3 2 0 2 7
Respiratory Medicine 2 4 0 1 0 0 7
Rheumatology 2 3 1 0 0 0 6
Cardiology 1 3 1 0 0 1 6
Total 32 45 18 7 2 13 117
Example actions taken in response to the complaints are listed below:
The urology secretary concerned will be attending a professional telephone skills course.
The outpatient appointment centre has now introduced new software which allows us to
record all calls made to the department. The software records who called, when, and
how long the conversation lasted. This should help improve the standard of service
being provided and, with the greater degree of monitoring, will allow us to take further
action on any complaints about unsatisfactory call handling.
The switchboard operator in question has listened to the recordings that were made, in
the presence of her manager, and was shocked by how abrupt she was. This incident
has been recorded on her staff file and will be followed up during the course of her
ongoing appraisal and assessment.
The outpatient appointment centre manager has listened to the recording of the phone
call and agrees that the matter could have been handled much better by the member of
staff and that her tone was inappropriate at times. The member of staff has been spoken
to about this matter by her line manager and it has been placed on her record so that it
can be monitored and discussed during her upcoming appraisal.

Paper 7
Page 10 of 14
The doctor who discussed the ‘do not attempt resuscitation’ form with the patient is going
to have a debrief with their line manager and clinical lead in order to improve the way in
which they conduct such conversations in future.
Nursing and midwifery care
There were 94 complaints received where nursing/midwifery care was recorded as a subject
of the complaint – in 50 of those complaints it was the primary or sole reason for the
complaint being lodged.
The directors of nursing review and sign off all complaint responses, ensuring that
appropriate explanations and apologies have been provided in each case and action taken in
response to the points raised. The directors of nursing are also informed of any issues
raised regarding unsafe practice or potential serious incidents.
The table on pages 14 and 15 of this report breaks the nursing complaints down by the
primary location and primary sub-subject for the complaints received. The data highlights
that the concerns raised about nursing care are spread across a number of wards; 48 in
total. A patient’s care needs not being met and a lack of support for patients during their
admission were the most common underlying themes, although if you were to group together
the 5 different sub-subjects linked to nutrition and hydration this would also become a theme.
No area received a concerning number of complaints during the financial year (no ward had
more than 5 complaints recorded against them) and there was no identifiable trend in terms
of staff members involved.
Example actions taken in response to the complaints are listed below:
The maternity day unit at Barnet Hospital has set up a service improvement group, with a
named consultant taking the lead, looking at ways to improve the service to our women.
Matron for 9 North ward met with complainant to discuss the complaint and apologise in
person for what happened with the nurse. This was an agency member of staff who has
not worked on the ward since this incident and the bank team have been made aware so
that they don’t book this agency nurse anymore.
It took too long to commence a patient’s NG feed, partially because of difficulties in
ensuring that it was in the correct position and partially because staff did not carry out the
correct protocols. In light of our findings, we have advised the doctor to call the radiology
team when requesting x-rays to confirm the position of a NG tube and for Sister to remind
her staff to escalate any issues to senior staff, where necessary. Sister for 9 North ward
will also ask the clinical practice educator to perform an audit on NG feeding
documentation and to arrange for any necessary training arising from there.
The nurse from 8 East ward has acknowledged that, on reflection, the problems
encountered by a patient were caused by her lack of knowledge of what was required.
Consequently, the matter is now being taken forward in line with appropriate internal
processes.
The senior matron for renal and urology plans to have a 30 minute surgery every day on
10 South A ward where he is available to talk to families about concerns they might have.

Paper 7
Page 11 of 14
5 East B ward are setting up a daily clinic for relatives of patients to ask questions and
raise concerns about their loved ones treatment.
Examples of actions taken in response to other complaints received
In addition to apologies and explanations, the majority of our complaint responses will
include details of specific action(s) taken as a result of the complaint that has been received.
Some general examples of actions taken/changes implemented are listed below:
A review of the signage from the ground floor to the cashier’s office indicates that it is
insufficient. There will therefore be increased the signage from the main entrance along
the route to the cashier’s office.
It has been identified that there was an operational issue with the Dictate IT system,
which resulted in letters that were ready for printing and distribution to patients between
the 15 May 2017 and 9 June 2017, not being sent out until July 2017. We can confirm
that this issue has been rectified and the process amended to ensure this does not
happen again, including daily audits of the letters distribution. We have also had
assurances that all letters are now sent out on a daily basis from the Dictate IT system.
This matter is being taken very seriously and has been reported internally as a serious
incident in order to ensure that all patients affected are reviewed and followed up
appropriately.
The dermatology service is currently experiencing capacity issues and there has also
been an increase in the referrals received, which is impacting on the time patients wait to
receive their appointments/treatment. Consequently, the dermatology department is
currently undergoing restructuring and are in the process of recruiting more staff to help
with the flow of patients.
A reduced car parking rate over night was considered many years ago but a flat fee was
eventually decided upon because this keeps the administration costs down. When we
changed to ParkingEye the decision was made to keep a flat fee so as to keep changes
to a minimum during the transition from pay and display to automatic number plate
recognition controlled cameras. However, when the multi-storey car park closes, we will
be introducing a capped fee at 8 hours parking.
The diabetes clinic has recently taken on a pump nurse, who can undertake reviews by
telephone and email, which both increases convenience for patients and means that
clinic consultations by medical staff can take less time, thereby reducing delays.
Your complaint was discussed at the weekly urology operations meeting on 4 September
2017. Whilst those in attendance noted that the correct pathway was followed, it was felt
by all that the patient’s experience was not ideal and the clinical director for nephrology,
urology and transplantation has agreed that the urology management team would review
the pathway (for patients transferring across from Barnet Hospital) to see if there were
any improvements that could be made in this regard.

Paper 7
Page 12 of 14
The operations manager will ensure that the general surgery on-call contact details are
available on 5 North A ward, and has been working with the breast team, in conjunction
with the nursing teams working on DSU, to develop a 23 hour mastectomy pathway.
Due to the patient’s circumstances she is entitled to claim back her taxi fares to the
hospital. The fact that this was not widely known by staff is a failing, which stems from a
lack of clear guidance within the treasury team. Finance are therefore leading on a piece
of work to implement new processes and procedures which will be available to patients,
clinic and ward staff, and the cashiers office staff by the end of March 2018.
Complaints referred to the Parliamentary & Health Service Ombudsman (PHSO)
The PHSO continue to record any preliminary reviews of complaint files as investigations in
their annual figures, as opposed to only those cases that went on to be formally investigated.
The draft reports produced by the PHSO also continue to make recommendations for
financial payment in recognition of distress caused but the number of cases this has applied
to has decreased over the last 3 years.
Of the 1,534 complaints opened in this financial year, 5 have so far been escalated to the
PHSO by the complainant. 2 of those are complaints regarding services provided by Barnet
& Chase Farm Hospitals and 3 are regarding services provided by the Royal Free Hospital.
To date, 1 Barnet Hospital case has been closed and not upheld and the other 4 cases are
currently under investigation.
Summary
The primary subjects remain largely the same as the last financial year, with the most
common subjects being clinical treatment, communication, attitude, delays and appointment
issues. However, the actions outlined in this report demonstrate that trends are acted upon
and the complaints received in the trust are used to inform pieces of work aimed at improving
the patient experience. The responses provided invariably outline action(s) that have been
taken in response to the concerns raised or explain what is planned as a result of issues
identified during the investigation.
Policy and procedure and the way in which complaints are recorded and dealt with is
harmonised across trust sites. We have systems in place to systematically review the
complaints received and ensure that investigations are undertaken appropriately, in line with
legislation, and escalated within the trust as necessary. The data collected is used to inform
reports, is disseminated amongst divisional teams and taken to various committees to inform
ongoing work within the trust.

Paper 7
Page 13 of 14
Dis
char
ge A
rran
gem
en
ts (
inc
Lack
of
or
Po
or
Pla
nn
ing)
Acq
uir
ed
pre
ssu
re u
lce
r
Cal
l be
ll o
ut
of
reac
h
Cal
l Be
ll -
failu
re t
o r
esp
on
d
Car
e n
ee
ds
no
t ad
eq
uat
ely
me
t
Cat
he
ter
care
Can
nu
la m
anag
em
en
t
Can
nu
lale
ft in
situ
on
dis
char
ge
Co
nti
ne
nce
issu
es
Failu
re t
o p
rovi
de
ad
eq
uat
e c
are
Failu
re t
o c
om
ply
wit
h h
and
-hyg
ien
e r
eq
uir
em
en
ts
Failu
re t
o a
do
pt
infe
ctio
n c
on
tro
l me
asu
res
Failu
re t
o id
en
tify
fo
od
alle
rgy
Failu
re t
o m
on
ito
r o
bse
rvat
ion
s
Failu
re t
o m
on
ito
r p
ress
ure
ulc
er
Failu
re t
o p
rovi
de
ass
ista
nce
wit
h e
atin
g/d
rin
kin
g
Failu
re t
o p
rovi
de
fo
od
ap
pro
pri
ate
to
clin
ica
l co
nd
itio
n
Failu
re t
o p
rovi
de
flu
ids
Inad
eq
uat
e s
up
po
rt p
rovi
de
d
Lack
of
nu
trit
ion
an
d h
ydra
tio
n
Mo
vin
g an
d h
and
ling
issu
es
Pat
ien
t fe
lt n
egl
ect
ed
Slip
s tr
ips
and
fal
ls -
un
wit
ne
sse
d
Tota
l
Barnet Hospital
AAU 1 1
Beech 1 1 1 3
Cedar 1 1 1 1 1 5
Damson 1 1 1 3
Delivery Suite 1 1
Emergency Dept 1 1
EPU 1 1
Juniper 1 1
Larch 2 2
Mulberry 2 2
MDU 1 1
MSSU 1 1 1 3
Outpatients dept 1 1
Olive 1 1 2
Palm 1 1 2
Post-op care unit 1 1
Rowan 1 1
Spruce 1 3 1 5

Paper 7
Page 14 of 14
Victoria 2 1 1 4
Walnut 3 1 4
Willow 1 1 2
X-ray dept 1 1
Chase Farm Hospital
Adelaide 1 1
Capetown 1 1
Canterbury 1 1
Day surgery unit 1 1
Endoscopy 1 1
Wellington 2 2
UCC 1 1
Royal Free Hospital
Emergency Dept 1 1 1 3
ICU 4 West 1 1
Fracture clinic 1 1
PITU 1 1 2
3 North A 1 1
5 East B 1 1 1 3
5 South 1 1 1 3
5 West A 1 1
6 South 1 1
7 East A 1 1
8 East 1 1 2
8 North 1 1 2
8 West 1 1
9 North 1 3 1 5
9 West 1 1 1 1 4
10 South A 1 1 2
11 East 2 1 3
11 West 1 1
11 South 1 1 2
Total 1 2 2 1 27 3 3 2 1 11 1 1 1 2 1 3 5 2 11 2 3 2 6 94

Paper 8
1
GO SEE VISITS
Executive summary
The board agreed to a new approach to go see visits at its December 2017 meeting, building on the previous programme of go see visits designed to increase visibility and engagement between trust leaders and governors with staff.
Go see visits are open to all group directors, including site chief executives, non-executive directors and governors. They will take place monthly and ‘visit’ all areas of the trust, including corporate support services. Prior to the visits, a fact sheet will be provided giving some key information about the areas. This will include information on staffing and where appropriate, patient or client feedback. The current sheet is in the process of being reviewed. Visits are not designed to be inspections, but opportunities to listen to staff and where appropriate, meet patients.
While non-executives will continue to be paired with governors, executive directors will visit a separate set of areas.
Three key questions will be asked:
1. What is working? 2. What is not working? 3. What would you like to change?
This information will be fed back verbally at the following trust board meeting. Logistically this will mean there is feedback from more than one area. This will be dealt with by a list of areas visited being circulated in the papers and the chairman asking for any specific areas to be highlighted.
Since the last meeting the following visits have taken place. Work has now commenced on organising the next set of visits.
Area Director
Diabetes, Barnet Hospital Akta Raja and George Verghese Post operative observations Stephen Ainger Microbiology Jenny Owen and Judy Dewinter New Chase Farm Hospital Dominic Dodd and David Sloman
Action required
The board is asked to note the report.
Report to Date of meeting Attachment number
Trust Board 25 July 2018 Paper 8

Paper 8
2
Report From Emma Kearney, director of corporate affairs and communications
Author(s) Alison Macdonald, board secretary Date 16 July 2018
Page 1 of 1
Workforce Race Equality Standards (WRES): board actions update
Executive summary
This is a scheduled progress update on the trust board actions supporting progress against
the NHS Workforce Race Equality Standards (WRES). It highlights in particular the recent
recruitment changes to encourage improved recruitment of BME staff into senior roles. It is
too early to tell if this initiative will make a difference but once embedded at 8a and above it
is proposed that it is extended to other leadership levels.
The quarter 2 WRES figures will be ready at the end of July 2018.
Action required
For noting.
Trust strategic priorities and business planning objectives
supported by this paper
Board assurance risk
number(s)
4. Excellent compliance with our external duties – to meet our
external obligations effectively and efficiently
x
5. A strong organisation for the future – to strengthen the
organisation for the future
x
CQC Regulations supported by this paper
Regulation 17 Good governance
Risks attached to this project/initiative and how these will be managed (assurance)
Equality analysis
• No identified negative impact on equality and diversity – actions are aimed at a
positive impact
Report from Yemisi Oluyede, head of workforce health, equality and diversity
Author(s) Yemisi Oluyede, head of workforce health, equality and diversity; David
Grantham, group director of workforce and organisational development
Date 25 July 2018
Report to Date of meeting Attachment number
Group Trust Board 25 July 2018 Paper 9
Paper 9

Group Board WRES actions update: 25th July 2018
1
NHS WORKFORCE RACE EQUALITY STANDARD:BOARD ACTIONS
PROGRESS UPDATE
1. • Approved a new initiative whereby all
recruiting managers for posts in Bands 8a
and above are expected to email the
Group Chief Executive Officer (CEO) to
confirm reasons why they have not
appointed any shortlisted Black or Minority
Ethnic (BME) candidate(s) and what more
the candidate could do to develop their
skills or experience to be more likely to be
appointed in future
• This process was implemented for all 8a and above recruitment from 1st June
2018
• There has been a total of 18 Band 8a and above roles recruited into since
the 1st of June 2018 (to 16th July 2018)
• Out of the 18 recruiting panels, 4 were not recorded as having attended
recruitment and selection training, and one panel had less than 50% of
those on the panel trained. In total, 13 recruiting panels were fully trained
in recruitment and selection. Recruitment and selection training includes
unconscious bias
• In total, for the 18 roles, there were 58 applications, 31 BME and 27 white
• A total of 26 applicants were shortlisted, 12 BME and 14 white.
• A total of 15 candidates were successful in the interview process, 4 BME
and 11 white
• For the 8 unsuccessful BME candidates 4 recruiting managers have sent
details to the Group CEO to confirm reasons why they have not appointed
any of the shortlisted BME candidates
• The process of monitoring 8a and above recruitment activity, shortlisted
candidates, letters to the CEO and follow up is being conducted manually but
work is underway to embed this in TRAC, the Trust’s recruitment system
2. • Approved the implementation of
recruitment and selection as mandatory
training (MaST) for all recruiting
• The education and workforce development committee (EWDC) has approved
that the recruitment and selection is included in MaST for recruiting managers
• Enforcement will be managed through manager self-declaration on the TRAC
Paper 9

Group Board WRES actions update: 25th July 2018
2
managers recruitment system. Training delivered will be recorded on OLM against which
manager declarations that they have received training can be verified
• Adding recruitment and selection training to the MaST report is complicated
by the fact that identifying who may or may not be a recruiting
manager/individual is not straightforward. This is because individuals other
than budget holders may undertake this activity. Having managers declare
and a system of verification against training records will though provide
robust monitoring
3. • Agreed to 1) the re-launch of executive
support for diverse panels with a letter
signed by the CEO, group chief medical
officer, group chief nursing officer, and
group director of workforce and
organisational development to go out to all
recruiting managers with evidence of
progress with indicator 2) a similar letter to
go out to all BME staff on diverse panels
to reinforce support
• Completed
• Letter of support was sent to all trained BME recruiters on 1st June 2018
4. • Agreed that all new hospital executive
teams undergo unconscious bias and
mentor training in order to cascade
executive BME mentoring into hospital
units
• Completed
• All new hospital executive teams have undergone unconscious bias training.
They have also received mentoring training as part of the leadership
development. Their details and information on the scheme are available to
BME staff
5. • Agreed to BME staff listening sessions for
site chief executives to commence
• The chairman will be commencing the BME staff listening sessions for
hospitals from this month by holding a Royal Free Hospital session on
Tuesday 24th July 2018. This information has been placed in Freemail and in
Paper 9

Group Board WRES actions update: 25th July 2018
3
other communication channels
• Agreed to support the “no bystanders
campaign” as part of the LGBT campaign
for this year in addressing bullying and
harassment
• The “no bystanders campaign” for LGBT was launched in November 2017
with executive support. The initiative was well received by staff. Executives
also participated in the London Pride this year in support of the staff LGBT
network
• The campaign was extended to cover all bullying and harassment, not just of
LGBT staff, and has continued with monthly initiatives such as reporting on
routes for resolution, details of cases tackled etc in Freenet and Freepress
• The trust has launched its speaking up champions and recruiting more
champions to cover all sites to help address staff concerns about bullying and
harassment
• Trust executive champions have been identified providing robust governance
and leadership, regularly reviewing how many cases are reported and solved,
providing visible assurances of cases being dealt with
7. • Agreed to support staff disability networks
preparing for the new NHS standards
coming into place by April 2019
• Staff disability networks are planning to have hospital and site based events
in November 2018 to cover disability confidence, access to work and
remploy. The disability network was promoted at the recent health and
wellbeing events
8. • Agreed that best practice experience
should be explored against London Trusts
and national WRES guidance on those
WRES indicators where the Trust has not
made progress i.e. 6, 7 & 8.
• WRES indicator 6 (bullying and
harassment)
• Exploratory meetings are arranged with Imperial NHS Trust to gain further
understanding of how they have used QI methodology to improve WRES
overall
• The trust has attended and presented at the national WRES event (October
2017) and continues to engage with the national WRES team and London-
wide WRES work
Paper 9

Group Board WRES actions update: 25th July 2018
4
• WRES indicator 7 (career progression)
• WRES indicator 8 (discrimination)
9. • Supported communicating back to the
trust’s BME staff what they said during the
BME staff listening sessions held in 2016,
what the trust has done about what was
said, the current results from WRES
indicators, and to highlight areas of
improvement and further actions to be
taken on all indicators.
• The chairman, CEO and the CEO, Royal Free Hospital will be holding a BME
staff listening session at Royal Free Hospital on Tuesday 24th June
2018. The discussions with BME staff will cover what the trust has done so
far, improvements, gaps and future actions
• Dates for other hospitals and sites will be scheduled for September and
October 2018
10.• Continue existing Quality Improvement
(QI) work on WRES disciplinary cases
indicator (indicator 3)
• The trust is one of the 5 working with NHS England and NHS Improvement
on a WRES 3 project - a write up is in progress and publication awaited
• The Trust has commenced work with other London Trusts using the ‘just
culture’ approach to review disciplinary processes, managed by the
Employee Relations team
11.• New – improving non mandatory training
and development data for WRES to
support measuring access to non-
mandatory training (indicator 4)
• The EWDC is looking at how all areas conducting training for various staff
occupational groups can update the OLM system to ensure that the WRES
training data is more accurate
12.• New – reducing gaps in workforce WRES
indicators and engaging internal and
external stakeholders in assessing the
trust’s progress
• The Equality Delivery System (EDS2) for the trust due for a stakeholder
review and grading assessment. A survey is going out to all staff and
managers to help inform this and the trust’s performance on equality and
diversity
Paper 9

Group Board WRES actions update: 25th July 2018
5
Paper 9

Paper 10
1
Gender Pay Gap (GPG) and pay gap by other protected characteristics: Board update
Executive summaryThis paper informs the board of the further work the trust has undertaken and priorities for action to address the gender pay gap (GPG), and gaps appearing when pay data has been examined against other protected characteristics, including ethnicity.
The board has previously indicated its commitment to eliminating the gender pay gap, but also to ensuring equality across other protected characteristics, which would include pay. The analysis of pay against other protected characteristics therefore goes further than the statutory requirement for GPG reporting, which the trust complied with in March 2018. The trust’s GPG data can be accessed here. The trust’s median GPG was 13.32% compared with a median public sector average of 13.10% and median private sector average of 15.9%.
The key findings of the further work are that:
• The overall GPG is predominantly driven by consultant clinical excellence awards and incremental scale (which rewards long service and there are less female than male consultants with longer service, reflecting changes in the make-up of the profession over time).
• The overall pay gap between black and minority ethnic staff and white staff is 7.96%. This is predominantly driven by the proportions of BME/white staff and the bands they occupy, and the known under-representation of BME staff in senior roles at 8a and above.
• It has not been possible to meaningfully analyse data against other protected characteristics which is due to smaller cohorts or lack of reporting of those characteristics. There are also some limitations of the ability to analyse the data in excel.
Despite the limitations of the analysis possible it has been useful to inform a number of priorities to address the GPG and other gaps. These are:
• Reform of the local CEA arrangements (in the light of national changes) • Reinforcement of the guidelines and process for reviews of starting salaries – this can be
managed within the recruitment service and through scrutiny of decisions • Promoting flexible working and staff support – the trust is considering options for further
promoting and encouraging flexible working • Ensuring the trust’s talent management arrangements (options being considered by GEC
next month) takes account the need to improve the representation of women and BME staff in more senior roles as part of addressing pay gaps
Action required/recommendationTo note the further analysis of pay gaps and support the actions recommended above.
Report to Date of meeting Attachment number
Trust board 27 July 2018 Paper 10

Paper 10
2
Trust strategic priorities and business planning objectives supported by this paper
Board assurance risk number(s)
3. Excellent financial performance – to be in the top 10% of relevant peers on financial performance
4. Excellent compliance with our external duties – to meet our external obligations effectively and efficiently
5. A strong organisation for the future – to strengthen the organisation for the future
CQC Regulations supported by this paper Regulation 17 Good governance Regulation 18 Staffing Regulation 19 Fit and proper persons employed Care Quality Commission (Registration) Regulations 2009 (Part 4)Regulation 13 Financial position
Risks attached to this project/initiative and how these will be managed (assurance)The key risk for the trust is to take positive steps to close the gaps between the earnings of male and female and BME staff as identified in the report.
Equality analysis: The trust’s gender pay gap issues are incorporated within the equality action plan section of the Staff Experience, Retention Plan (SERP).
Report from
David Grantham, Director of Workforce and OD
Authors Yemisi Oluyede, Head of Workforce Health, Equality and Diversity & Sharon Churchley, Head of Workforce Information
Date 16 July 2018
Paper 10
3
Gender Pay Gap (GPG) and pay gap by other protected characteristics: Board update
1. Introduction
When it considered the Gender Pay Gap (GPG) report in March 2018 the board requested an update in July 2018. This paper summarises actions and analysis since then and makes some additional recommendations for addressing pay gaps.
2. Pay gap reporting and legislative requirements
The Equality Act 2010 (specific duties and public authorities) regulations 2017 required all public sector organisations that have 250 or more employees to publish and report their gender pay gap (GPG). The GPG is calculated as the average pay of all men in an organisation in comparison to the average pay of all women in the same organisation. Non-public companies and organisations have also been made subject to this requirement.
The objective of GPG reporting is to identify if there are disparities in hourly pay rates, gaps in existing bonus schemes and to better understand where there may be uneven distribution of men and women across pay grades within a workforce so that action can be taken to try to address this.
Gender pay is not equal pay. Equal pay relates to paying male and female employees in the same or similar jobs the same pay rate for work of equal value. The GPG is about the overall position on pay including access to overtime, bonuses and identifying and addressing the differential distribution of genders within a workforce.
The trust published its GPG data in March 2018.
In addition, under the Equality Act’s public sector equality duty (PSED) the trust has an obligation to pursue equality objectives. It has previously identified two priorities:
a. a representative and supported workforce b. inclusive leadership representative of the communities we serve
To support the first objective, and its wider equality duty, the trust has sought to examine differences in pay not only by gender but also by other protected characteristics, particularly ethnicity. The purpose is to inform actions that will promote equality.
3. Hourly rate GPG
The trust’s gender pay data shows female employees earn an hourly average pay of 17.68% less than men (table 1 below). This data is inclusive of all staff groups, including medical and dental.
Table 1: The overall pay gap based on the basic hourly rate for all employees is as follows:

Paper 10
4
Table 1 Male Female Pay Gap Mean hourly rate for all employees
£23.61 £19.44 17.68%
Median hourly rate for all employees
£20.31 £17.60 13.32%
As the board noted in March 2018, the gender pay gap is driven by a number of factors including the predominance of female staffing in the nursing and support staff professional group, the consultant workforce (through the impact of seniority and bonus payments) and the under-representation of women in very senior roles.
4. Bonus/additional payment GPG
Clinical excellence awards (CEAs) and distinction awards/discretionary points are the only bonus payments made, and paid only to medical staff. CEA awards are determined locally in the trust while national awards are determined nationally. There is a 22.13% mean pay gap overall for these bonus payment.
Table 2: The overall bonus payments for all employees are as follows:
Table 2 Male Female Pay Gap Mean bonus amount (per annum)
£13,834.46 £10,783.63 22.13%
Median bonus amount (per annum)
£11,934.00 £5,976.20 50.00%
The proportion of male and female consultants receiving bonus payments is outlined in Table 3:
Table 3 Employees Paid Bonus
Total relevant employees within a 12 month period
Percentage of employees receiving a bonus
Gender
Female 94 272 34.56% Male 178 390 45.64%
A greater proportion of male consultants are in receipt of awards than females. This will in part reflect that historically larger proportion of the consultant workforce was male and awards, when made, were for the duration of a consultant’s career. However, it is also known that women consultants have historically been less likely to apply for CEAs. There may also be an impact too from women consultants being more likely to have had career breaks (for maternity) or to have worked part-time. This may have meant they have had less opportunity to demonstrate that their work has been ‘over and above’ or, perhaps more likely, that decision makers have not recognised the context in which their applications have been made, perhaps undervaluing such applications against those working full-time.
The CEA scheme has now been reformed and future awards will be non-consolidated and for a maximum duration of 3 years. The trust also has the opportunity to review and refine the process for applications and their assessment, within certain parameters set out ion amendments to the consultant contract. This should begin the process of ensuring greater equity in future awards building on the trust’s work to operate a diverse decision making group (with BME and female representation) and objective scoring in previous years.

Paper 10
5
5. Proportion of male and female staff in each pay quartile
Female employees account for 74% of the total workforce and male employees 26%. When pay is divided into quartiles (1 being the lowest and 4 the highest) the evidence is that females are more likely to work in roles within the 2nd (Q2) and 3rd (Q3) quartiles and are underrepresented in the highest paid quartile.
1st quartile represents the lowest paid while the 4th is the highest.
Table 4: The proportion of male and female in each pay quartile:
Table 4 Female Male Female % Male% Quartile1 2019 748 72.97% 27.03% 2 2211 572 79.45% 20.55% 3 2097 621 77.15% 22.85% 4 1774 1070 62.38% 37.62%
Some of this reflects the structure of the workforce and dominance of women within the nursing profession (roles usually in Q2 and Q3). There is an issue about improving the proportion of women in the highest paid roles. Males are over-represented in Q4, partly reflecting the consultant grade and the seniority and CEAs paid to male consultants.
6. Pay gap against other protected characteristics
Further analysis has been conducted to see if there are pay gaps with possible significant trends against other protected characteristics taking into consideration age, length of service, pay bands, staff group and proportion of employees in each group. This has proved challenging as data is not always sufficient to allow meaningful analysis eg for disability where there is a much smaller proportion of the workforce with a declared disability. We have concentrated analysis where the data is available for cohorts of more than 10% of employees.
6a. Ethnicity
The overall average pay gap between BME and White staff is 7.96%. This has been determined by looking at the pay gaps between BME and White where the total at length of service, staff group, band and age is greater than 10%. The ‘other’ group is relatively small and made up if the staff who have not disclosed ethnicity (just 1.52% of total employees).
Please note that these figures do not include bank staff and analysis has only been possible based on the mean (average), rather than median pay. Nevertheless it gives an indication of the distribution of pay differences.
For BME and white staff, pay gaps based on length of service are outlined in table 5 below:
Table 5 % of Headcount Avg. Hourly Rate Difference Pay Gap %
Length of Service BME Other White BME Other White BME Other BME < 1 year 53.00% 1.58% 45.43% £17.10 £19.47 £19.53 £2.43 £0.06 12.46%
1 - 3 years 47.78% 2.20% 50.02% £19.12 £20.85 £20.00 £0.88 -£0.85 4.39%
3 - 5 years 44.27% 1.75% 53.98% £18.59 £17.83 £20.75 £2.16 £2.92 10.39%
5 - 10 years 49.70% 0.81% 49.49% £19.64 £15.16 £21.35 £1.72 £6.20 8.04%

Paper 10
6
> 10 years 47.21% 0.87% 51.92% £21.73 £20.58 £24.14 £2.41 £3.56 10.00%Grand Total 47.87% 1.52% 50.61% £19.70 £19.80 £21.41 £1.70 £1.61 7.96%
It shows that there is a pay gap issue at certain lengths of service (in < 1 year, 3 – 5 Years and > 10 years).
Further analysis of the data informing table 5 above broadly indicates that:
• BME consultants with less than 1 years’ service are paid a lower rate than white appointees, although numbers are small.
• When looking at any cohorts with 3 - 5 years’ service there is a need to consider that these employees may have been hired on a higher spine point at a lower band up to 5 years ago and this may have influenced how they have moved through the bands over the years.
• BME Band 7s in the Additional Professional Scientific and Technical staff group, are paid at lower spinal points than white – but this is based on relatively small numbers.
• BME Band 6s in the Admin and Clerical staff group, although there are more whites proportionally, more BMEs are on lower spinal points.
• BME Bands 7 and 8Bs > 10 years’ service the majority of these staff are female but those who are white are paid on higher spine points
• Consultants with > 10 years’ service demonstrate a 3% BME pay gap, but proportionally 37% female so gender pay is also an issue.
6b. Disability
Due to the low numbers of staff disclosure for disability i.e. only 1.05% of staff disclosed that they have a disability, it’s not possible to identify any pay gap.
6c. Sexual Orientation
Staff disclosing as non-heterosexual accounts for 1.99%, therefore, it’s not possible to identify any pay gap as the numbers are too small for any comparison to take place.
6.d Gender-re-assignment
This status is not captured nationally by ESR so there is no trust data at present against which any analysis could be conducted.
6e. Pregnancy or Maternity
These cannot be analysed as the pay of those staff on maternity leave will be skewed by statutory maternity pay or additional unpaid leave which may take them over their maternity leave entitlement and as such there are no inferences to be drawn.
7. Conclusion
Apart from gender, ethnicity is the other protected characteristic that has shown gender pay gaps when further analysed. All other protected characteristics do not have sufficient information to draw a similar inference.
Paper 10
7
The work analysing data needs to continue, especially in those areas that this further analysis has indicated there are potential issues. Nevertheless even on the basis of the work done, there are a number of actions to be pursued that will impact the position.
These include continuing activity already underway:
• Continuing to promote equal opportunities for career progression and ensuring fairness in processes and procedures (including the steps to improve BME and female staffing at senior levels)
• Promoting applicants from all backgrounds by using diverse interview panels and advertising posts and extending advertising channels
• Creating opportunities for all employees to progress, such as providing secondment and acting up opportunities and ensuring appraisals and personal development plans are undertaken.
• Challenge systems and mind-sets to ensure that they do not disadvantage women or other groups through provision of unconscious bias training and online testing.
• Appropriate senior role models mentoring and coaching staff • Presenting the findings of this and the GPG report to the new trust’s Women’s
network and the BME staff network to engage key stakeholders and seek further qualitative insights into addressing the causative/underlying factors that affect the pay gaps in the workplace.
Other steps informed by this analysis are:
• Reform of the local CEA arrangements (in the light of national changes) – a draft process is being developed with the Local Negotiating Committee and medical staff committees
• Reinforcement of the guidelines and process for reviews of starting salaries – this can be managed within the recruitment service and through scrutiny of decisions
• Promoting flexible working and staff support – the trust is considering options for further promoting and encouraging flexible working
• Ensuring the trust’s talent management arrangements (options being considered by GEC next month) takes account the need to improve the representation of women and BME staff in more senior roles as part of addressing pay gaps.
8. Recommendation
The Board is asked to note the further work and analysis (and that this is continuing) and to endorse and support the steps being taken to start addressing the pay gaps identified outline above.

Page 1 of 2
Finance report for M3 June
Executive summary
At end of quarter 1 (April to June 2018) the trust reported an actual deficit of £19.5m which is
an adverse variance of £22k.
The 2018/19 financial plan includes delivery of £45.4m financial improvement programme
(FIP) savings. The trust delivered £5.8m of FIP year to date compared to a plan of £5m. The
trust has identified £45.2m of plans and imminent schemes to deliver the £45.4m FIP target.
The cash balance on 30 June was £28.1m. This continues to be high due to the Parcel B
land sale receipts being ring fenced for Chase Farm capital redevelopment. The trust
anticipates that it will need to access working capital loans from September onwards. Focus
continues on reducing debt with clinical commissioning groups (CCGs) and NHS England
who account for the majority of the aged debt in order to minimize loan drawdown and
therefore interest charges.
Action required
For information
Trust strategic priorities and business planning objectives
supported by this paper
Board assurance risk
number(s)
1. Excellent outcomes – to be in the top 10% of our peers on
outcomes
2. Excellent user experience – to be in the top 10% of relevant
peers on patient, GP and staff experience
3. Excellent financial performance – to be in the top 10% of
relevant peers on financial performance
x
4. Excellent compliance with our external duties – to meet our
external obligations effectively and efficiently
5. A strong organisation for the future – to strengthen the
organisation for the future
CQC Regulations supported by this paper
Regulation 17 Good governance
Regulation 13 Financial position x
Risks attached to this project/initiative and how these will be managed (assurance)
Report to Date of meeting Attachment number
Trust Board 25 July 2018 Paper 11
Paper 11

Page 2 of 2
Equality analysis
• No identified negative impact on equality and diversity
Report from: Caroline Clarke, group chief finance officer
Author(s): Senior Finance Team
Date: 19th July 2018
Paper 11

The Royal Free London
Finance Report TB Part 1
1
Paper 11

Contents
2
Q1 Performance Slides 3 to 5
Paper 11

YTD Performance Q1 – Key Headlines
3
Performance against Plan
In Year Performance - FY18
Agency Spend Vs. Last year
Cash Flow forecast
• YTD performance against plan - £0.02m adverse
FIP Performance
• YTD FIP delivery of £5.8m - £0.8m above plan
Better Payment Performance Code Capital Expenditure
Agency spend for the month was £1.9m. Agency spend is £0.7m above target at end of Q1
YTD Forecast
Plan Actual Variance Plan Actual Variance
£m £m £m £m £m £m
23.2 25.1 -1.9 72.4 72.4 0.0
Number Value £'m Number Value £'m % Number % Value
NHS 1,030 £17.96 269 £9.95 26% 55%
Non NHS 49,401 £168.62 39,201 £122.90 79% 73%
Total 50,431 £186.58 39,470 £132.85 78% 71%
Total within 30 days
Paper 11

CFO Message
Delivered an actual
deficit of £19.5m at
end of Q1; £22k
worse than plan
1 At end of Q1, the Trust delivered an actual deficit of £19.5m. This was £22k worse than plan.
Key headlines at end of quarter 1 are
• Clinical income over performance of £1.1m. Clinical income over performance driven predominantly by high level of non-
elective activity
• Earlier than planned delivery of FIP
• Emerging risks at end of Q1 relate to unfunded costs relating to GDE
Delivered £5.8m of
FIP at end of Q1;
£0.8m better than
plan
2 The Trust delivered £5.8m of FIP at end of Q1. This was £0.8m better than plan. Earlier than planned delivery of FIP schemes
was the key driver for the FIP performance in Q1. The Trust has currently identified £45.2m of plan and imminent schemes
to deliver the £45.4m FIP target for the year. This includes £21.6m (48%) of non-recurrent schemes. The Trust is committed
to identifying £40m of recurrent FIP schemes by the end of this financial year.
The reliance on non-recurrent FIP will have an adverse impact on the underlying performance of the trust.
Cash position –
£28.1m at end of
May
3 The cash balance on the 30th of June was £28.1m
Cash at the end of June is better than plan by £5.9m due to slight slippage on capital asset spend. The forecast for the remainder of the year remains as per plan, however it is expected that the phasing of cash receipts will improve as negations with NCL continue on SLA cash payments.
The Trust is continuing to manage its cash position in the best interests of both patients and creditors.
Emerging Risks at
Q1
4 At end of Q1 there are some emerging risks that will impact on the delivery of FY19 plan. Some of the emerging risks are
• Above than planned expenditure relating to GDE • Income risks. These cannot be quantified as the quarter 1 reconciliation process has not taken place however contracts
are performing to a level above what is affordable to CCGs.• Slippage against FIP plans identified
4
Q1 Performance FY19Paper 11

Q1 OverviewQ1 Performance FY19
5
Plan Actual Variance Plan Actual Variance Plan Actual Variance
£ '000s £ '000s £ '000s £ '000s £ '000s £ '000s £ '000s £ '000s £ '000s
NHS Clinical Income 55,649 58,693 3,044 171,243 172,407 1,164 692,391 692,391
TEDD Income 16,475 13,971 (2,504) 49,424 46,108 (3,317) 197,697 197,697
Non NHS Clinical Income 2,730 2,258 (472) 7,375 6,612 (762) 33,774 33,774
Other Operating Income 11,119 8,219 (2,900) 27,236 25,643 (1,593) 104,622 104,622
Total Income 85,973 83,141 (2,832) 255,278 250,771 (4,507) 1,028,484 1,028,484
Pay (45,402) (44,824) 578 (135,023) (134,224) 799 (545,839) (545,839)
Other Pay (Apprentice Levy) (211) (186) 25 (594) (594) (2,301) (2,301)
Non-Pay Expenditure (Excl. TEDD) (26,119) (25,906) 213 (77,223) (77,191) 31 (297,604) (297,604)
TEDD Expenditure (15,859) (13,097) 2,761 (47,680) (44,254) 3,426 (190,763) (190,763)
Total Operating Expenditure (87,589) (84,013) 3,577 (260,520) (256,263) 4,257 (1,036,506) (1,036,506)
SLR (0) (0) 0 (0) 0 0 (0) (0)
EBITDA (1,616) (871) 745 (5,242) (5,493) (251) (8,022) (8,022) 0
Interest, Dividends & Depreciation (4,051) (3,954) 97 (14,237) (14,008) 229 (57,804) (57,804)
P/L Disposal of Fixed Assets
Investment In Joint Ventures
Surplus/Deficit (5,667) (4,826) 842 (19,479) (19,501) (22) (65,826) (65,826)
ForecastIn Month YTD
In-month variance driven predominantly due to plan
re-phasing
Paper 11

Page 1 of 1
Operational performance report
Action required/recommendation
The board is asked to review the current performance of RFL against the key cancer, A&E
and RTT operational performance standards
Trust strategic priorities and business planning objectives
supported by this paper
Board assurance risk
number(s)
1. Excellent outcomes – to be in the top 10% of our peers on
outcomes
X
2. Excellent user experience – to be in the top 10% of relevant
peers on patient, GP and staff experience
X
3. Excellent financial performance – to be in the top 10% of
relevant peers on financial performance
4. Excellent compliance with our external duties – to meet our
external obligations effectively and efficiently
X
5. A strong organisation for the future – to strengthen the
organisation for the future
CQC Regulations supported by this paper
Regulation 8 ⃰ General
Regulation 9 Person-centred care
Regulation 10 Dignity and respect
Regulation 12 Safe care and treatment
Regulation 17 Good governance
Regulation 18 Staffing
Regulation 20A⃰ Requirement as to display of performance assessments
Risks attached to this project/initiative and how these will be managed (assurance)
Failure to achieve and maintain compliance against Monitor risk assessment framework
standards and targets.
Equality analysis
• No identified negative impact on equality and diversity
Report from Peter Ridley
Director of planning
Authors Sally Dootson, chief executive (Barnet), Sarah Dobbing, chief executive
(RFH) Senita Robinson, performance lead
Date 17 July 2018
Report to Date of meeting Attachment number
Part 1 Trust board meeting 25 July 2018 Paper 12
Paper 12

Royal Free London –operational performance
July 2018
Paper 12

2
Operational performance summary report
Where we are Predictions Key Risks
Cancer – May 2018
• Performance in May was reported at 86.9%
• The majority of breaches were in the Lower GI, Lung HPB and Upper GI
• Un-validated June performance is 78.32%
• The backlog has increased again since May, now at 151 patients with 58 diagnosed over 62 days. This is driving continued high risk of non-compliance.
• We have seen high referrals in:• Skin• Bladder• Prostate
• Other than skin, these have driven the trust PTL and backlog above target
• Lower GI backlog has persistently increased and requires further pathway work to address
RTT –May 2018
• Performance in May 2018 was 82.6%, slight decrease on March and April
• 23 over 52 week waiters, compared to 35 in March and 41 in April
• Expect increase of >52 week waiters due to ‘pop-ons’ caused by validation of the outpatient waiting list. Current unvalidatedfigure is 66.
• The quality and availability of our data in this area is a priority for improvement, external consultants from MBI are currently reviewing the new PTL logic.
A&E –June 2018
• Overall performance in June is92.2%
• Above trajectory and 2017/18performance at this time.
• Further 15 AAU beds at RFH to be opened.
• AAU proposal in development at BH.
• Performance problems at other trusts, leading to redirections of ambulance and walk-in activity at RFH site.
• Staffing at BH site.
Paper 12

3
62 Day Cancer – Performance Summary
Current Period May: stable, above year, above trajectory and standard at both site and Trust level
Relative position May 2018: 2nd quartile in London
% cancer patients waiting < 62 days from GP referral to first treatment
Source: NHS England, July 2018
86.9%
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
Standard 2018/19 2017/18 Trajectory
Paper 12

4
In May, 5 out of 13 tumour sites accounted for 20% of the trust’s total breaches:
● Lower GI – 3 breaches (performance 57.9%)
● HPB – 0.7 breaches (performance 50%)
● Lung (RF and BCF) – 1.2 breaches (performance 63.64%)
● Upper GI – 0.6 breaches (performance 75%)
62 Day Cancer – Sources of Current Performance
February Performance by Tumour site Observations
Number of excess patient breaches*
* Actual breaches minus breaches that would have been incurred if the tumour site were exactly at 85% standard
-3
-2
-1
0
1
2
3
438% of total RFL breaches
Paper 12
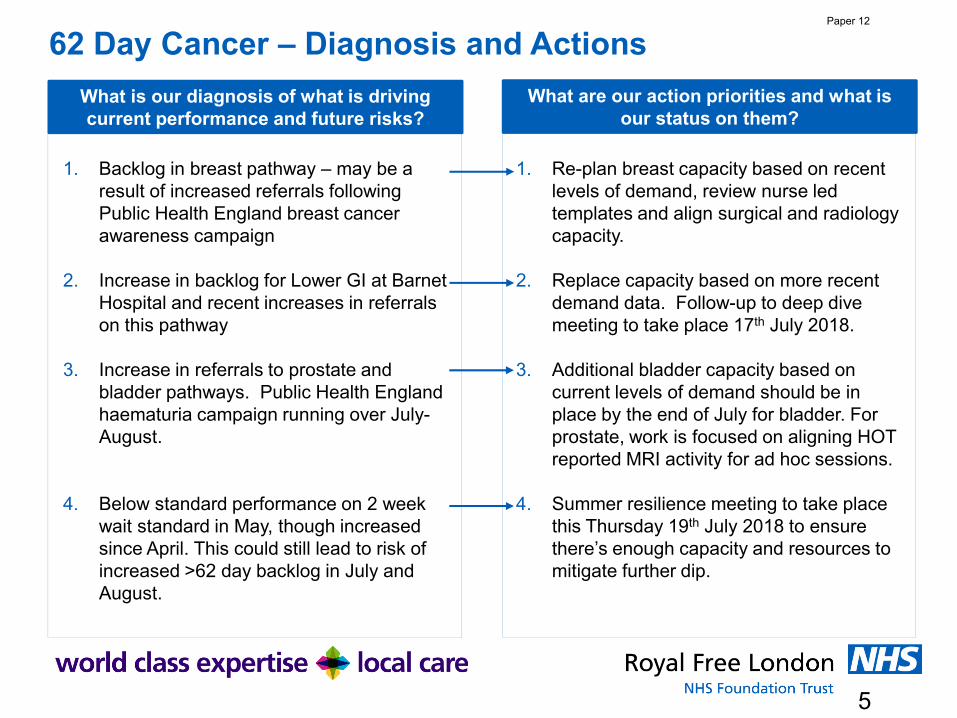
5
62 Day Cancer – Diagnosis and Actions
What is our diagnosis of what is driving current performance and future risks?
What are our action priorities and what is our status on them?
1. Backlog in breast pathway – may be a result of increased referrals following Public Health England breast cancer awareness campaign
2. Increase in backlog for Lower GI at Barnet Hospital and recent increases in referrals on this pathway
3. Increase in referrals to prostate and bladder pathways. Public Health England haematuria campaign running over July-August.
4. Below standard performance on 2 week wait standard in May, though increased since April. This could still lead to risk of increased >62 day backlog in July and August.
1. Re-plan breast capacity based on recent levels of demand, review nurse led templates and align surgical and radiology capacity.
2. Replace capacity based on more recent demand data. Follow-up to deep dive meeting to take place 17th July 2018.
3. Additional bladder capacity based on current levels of demand should be in place by the end of July for bladder. For prostate, work is focused on aligning HOT reported MRI activity for ad hoc sessions.
4. Summer resilience meeting to take place this Thursday 19th July 2018 to ensure there’s enough capacity and resources to mitigate further dip.
Paper 12

6
RTT – Performance Summary
Current Period May 2018: stable and below standard and trajectory
Relative position May 2018: 4th quartile in London
% patients waiting < 18 weeks from referral to treatment
Source: NHS England, June 2018
82.6%
70%
75%
80%
85%
90%
95%
100%
Standard Trajectory 2018/19 2017/18
Paper 12

7
RTT – Sources of Current PerformanceCurrent Period Performance by Specialty/Hospital Combination
* Actual breaches minus breaches if achieving 85% standard
Barnet Hospital Royal Free Hospital
Current Period > 52 week waiters
Introduction of new patient tracking list
August 2017May-18 = 23
Paper 12

8
RTT – Diagnosis and Actions
What is our diagnosis of what is driving current performance?
What are our action priorities and what is our status on them?
1. The Patient Tracking List (the waiting list) continues to suffer from unexpected ‘pop-on’ long-waiting patients.
2. The full suite of waiting list and performance reports is not yet available to operational and clinical teams to enable them to monitor their performance and act on early warnings.
3. Need for productivity improvements in outpatients and theatres.
4. Need for close oversight of new >52 week waiters.
1. Phase 3 logic is currently being reviewed by external consultants from MBI. They will complete this review within 3 weeks and we expect that work will need to be done to address problems they identify.
2. These reports will rely on construction of accurate waiting lists. Currently, the validation team are focusing on validating the outpatient waiting list and this is driving additional pop-ons to the PTL.
3. The outpatients productivity programme work has started and we are refreshing our theatres productivity programme. This will include a re-designed theatres productivity dashboard.
4. Weekly PTL reviews of >40 week waiters and regular escalation meetings for specialties of concern.
Paper 12

9
A&E – Performance Summary
Current Period June 2018: Improvement across both sites, above trajectory but below standard
Relative position June 2018: 2nd quartile in London
% patients waiting < 4 hours in A&E
Source: NHS England, July 2018
50%
55%
60%
65%
70%
75%
80%
85%
90%
95%
100%
Standard Trajectory 2018/19 2017/18
Paper 12

10
A&E – Barnet Sources of Current Performance
Current Period Performance
Performance against 4 hour standard
DTOC and MOs
Total DTOC and MO bed days DTOC by borough – June 2018
50%
60%
70%
80%
90%
100%
Standard Trajectory 2018/19 2017/18
June ED performance is above trajectory.DTOC lower but not consistently at target.The improvement plans continue to embed changes:• Ambulance handover• Ambulatory majors• ED workforce• Flow / length of stay
Paper 12
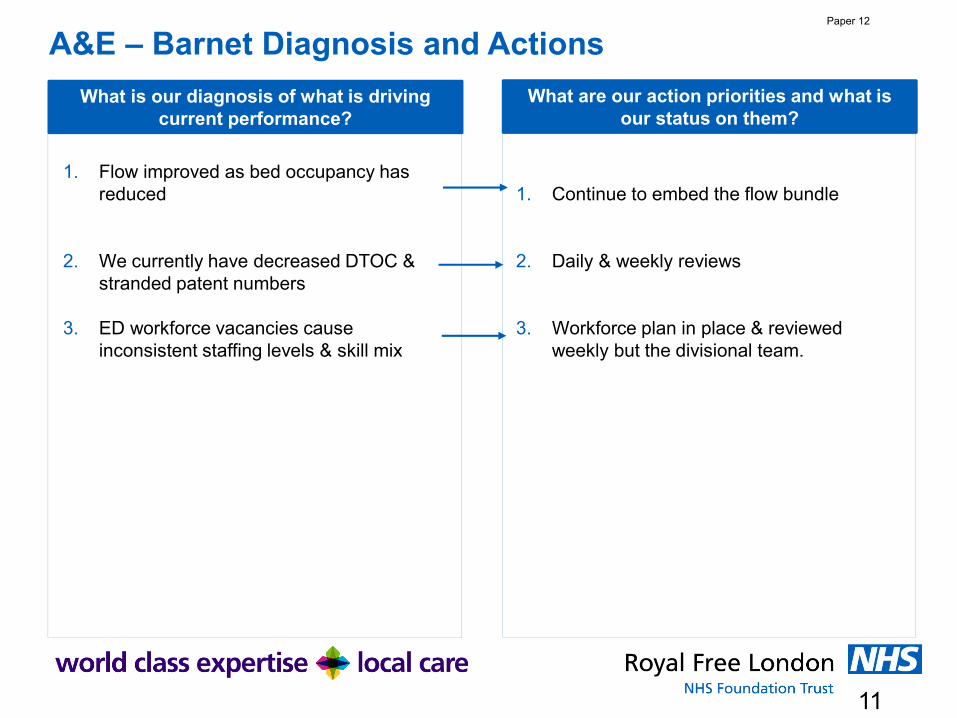
11
A&E – Barnet Diagnosis and Actions
What is our diagnosis of what is driving current performance?
What are our action priorities and what is our status on them?
1. Flow improved as bed occupancy has reduced
2. We currently have decreased DTOC & stranded patent numbers
3. ED workforce vacancies cause inconsistent staffing levels & skill mix
1. Continue to embed the flow bundle
2. Daily & weekly reviews
3. Workforce plan in place & reviewed weekly but the divisional team.
Paper 12

12
A&E – Royal Free Sources of Current Performance
Current Period Performance
Performance against 4 hour standard
DTOC and MOs
Total DTOC and MO bed days DTOC by borough – June 2018
50%
60%
70%
80%
90%
100%
Standard Trajectory 2018/19 2017/18
Similar to performance last year; slightly below trajectory and below standard
Current actions• Improved flow through the hospital
(high number of discharges)• Improved streaming and ambulance
handover times• Focus on improving ED escalation
processes to manage surges in demand
Paper 12

13
A&E – Royal Free Diagnosis and Actions
What is our diagnosis of what is driving current performance?
What are our action priorities and what is our status on them?
1. ED process delays. ED process delays contribute significantly to breaches
2. ED workforce capacity. We need to complete our middle grade and consultant establishments.
3. In-hospital flow. Current average length of stay for patients who stay at least 1 day is 6.6 days (down from 7.3 in May).
4. Out of hospital capacity. DTOCs have increased as we have improved our process for capturing information. The % of stranded patients has declined as we have focused on MDT reviews of these patients.
1. CPG work now focusing on improvement in: Streaming, the SitRep process and AAU. Initial nurse assessment time has improved with 90% of patients last week seen within 15 minutes.
2. Revised ED workforce plan has been developed, with support from ECIP.
3. The AAU is helping patient flow.
4. Improved focus on DTOCs and additional resource within the discharge team has led us to identify more patients who are delayed, and therefore an increase in DTOCs. Each division has a weekly stranded patient review.
Paper 12
Paper 13
1 X:\ Chair and CEO report 25 July 2018
CHAIRMAN’S AND CHIEF EXECUTIVE’S REPORT
Executive summary
This is a combined chairman’s and chief executive’s report containing items of interest / relevance to the board.
Action required
The board is asked to note the report.
Report From D Dodd, group chairman and D Sloman, group chief executive Author(s) Alison Macdonald, board secretary Date 16 July 2018
Report to Date of meeting Attachment number
Trust Board 25 July 2018 Paper 13
Paper 13
2 X:\ Chair and CEO report 25 July 2018
CHAIRMAN’S AND CHIEF EXECUTIVE’S REPORT
A TRUST DEVELOPMENTS
CHASE FARM HOSPITAL REDEVELOPMENT UPDATE
The official handover date of the new CFH from the builders IHP is Monday 23 July. Prior to this date the builders will complete the final preparations and testing of equipment in the new hospital. The trust remains on track to have completed the move by the middle of September. The key dates for moves are:
• 15 August – radiology fully open • 3 September: theatres open, ward and day surgery open • 10 September: Out-patients department, older persons assessment unit and
chemotherapy open • 13 September: urgent care centre opens
THE PEARS BUILDING
Work on the piling for the building, which will house the UCL Institute of Immunity and Transplantation, is well underway and the construction team's new accommodation is now in place and in use. It is hoped to use this for some of the meetings with stakeholders as it offers excellent views of the site.
A design company and two local schools have been chosen to work on a project to provide informative and attractive artwork on the extensive area of hoardings. It is hoped to have these in place in the autumn.
The construction working group, which includes local residents, representatives of the school and St Stephen's Church, Camden councillors and officers, meets next week and resumes monthly meetings in September. Current subjects under discussion include improving pedestrian access and the marshalling of traffic on the trust site.
On 28 June a "drop-in" in the Peter Samuel Hall provided information about the building and the research programme, as well as an opportunity to ask questions, and a similar facility was part of the annual members' meeting on 18 July.
B REGULATION
INFORMATON COMMISSIONER’S OFFICE (ICO) UNDERTAKINGS
The trust has now met all the requirements of the undertakings agreed with the Information Commissioner. The final stage of this was the publication of the report of the audit carried out by Linklaters LLP into the use of the Streams app (designed to deliver improved care to patients with acute kidney injury (AKI)), which took place on 12 June 2018.
The trust is awaiting confirmation from the Information Commissioner that she is satisfied that the requirements of the undertakings have been met.

Paper 13
3 X:\ Chair and CEO report 25 July 2018
C BOARD AND COUNCIL MATTERS
ROYAL FREE LONDON GROUP EXECUTIVE CHANGES
To ensure the Royal Free London group is in the best possible position to deliver a world class experience for patients and our staff, a review of the roles of its executive directors has been completed.
From September 2018, Caroline Clarke, group deputy chief executive, will formally take responsibility for group strategy and planning, partnerships and transactions, business development and population health. She will also represent the group on any of the subsidiary boards the Royal Free London wholly owns.
Peter Ridley will formally take the role of group chief finance and compliance officer focussing on financial recovery and stability, performance, corporate secretariat and compliance.
Emma Kearney will become group director of public affairs and communications and will lead on the trust’s relations with stakeholders, internal and external communications, patient information, management of the council of governors and Freedom of Information.
All other RFL group roles will remain the same.
D LOCAL NEWS AND DEVELOPMENTS
ADDRESSING RECENT NEVER EVENTS
Never events are defined by NHS Improvement as “serious incidents that are entirely preventable because guidance or safety recommendations providing strong systemic protective barriers are available at a national level, and should have been implemented by all healthcare providers”. There are fifteen types of incident which are determined nationally and which must be reported if they occur.
Unfortunately, we reported four never events in June 2018, and one in July 2018, making a total of 7 reported in 2018/19.
The trust take these incidents very seriously and is working closely with our commissioners, NHSI and NHSE including inviting commissioners to participate in the serious incident investigation panels, to provide an additional external perspective.
The trust is actively undertaking risk assessments against all never event criteria in all areas, to help identify any additional gaps in processes. Every never event is subject to a detailed investigation and root cause analysis and action plans are put in place which are monitored both within the trust and by commissioners and NHS Improvement.
The actions from all the never events have been combined in an assurance plan that includes themes for improvement and learning from other organisations. Each hospital is providing updates to the weekly Executive-led Safety Huddles, where robust challenge is made and teams are supported to gain solutions.

Paper 13
4 X:\ Chair and CEO report 25 July 2018
The clinical standards and innovation committee has oversight on behalf of the board and receives a regular updates on the status of never events, their investigation and action plans.
MINISTERIAL VISIT
Jackie Doyle-Price MP, junior minister for health and social care, visited the Royal Free Hospital to launch a campaign to increase the number of people signed up to the organ donation register from black, Asian and other non-white minority ethnic backgrounds. The minister spoke to surgeons and nurses on the transplant unit and to specialist organ donor nurses about some of the historic cultural and religious barriers to donation from non-white communities. Black, Asian and minority ethnic patients make up a third of the active kidney transplant waiting list. People from black and Asian communities are more likely to develop conditions such as high blood pressure, diabetes and certain forms of hepatitis than white people. This makes them more likely to need a transplant. Generally, these patients wait significantly longer for a kidney transplant than white patients if they are fortunate enough to receive an organ from a donor. Sadly, many will die waiting.
The Royal Free London is one of the leading transplant centres in the country and transplants more than 250 livers and kidneys every year. In 2017/18 the hospital transplanted 139 kidneys and 118 livers.
FAMILY AND FRIENDS TEST (FFT)
The NHS friends and family test (FFT) was introduced in 2013 to enable patients to feed back on their care and treatment to enable hospitals and other providers to improve services.
It asks patients whether they would recommend hospital wards, A&E departments, maternity services and out-patient clinics to their friends and family if they needed similar care or treatment. The June results are below.
Royal Free London combined data
% likely/extremely likely to recommend June 2018
(range: 0 – 100%)
Number of patient responses
In-patient 91% 1365
A&E 85% 4991

Paper 13
5 X:\ Chair and CEO report 25 July 2018
Barnet Hospital % likely/extremely likely to recommend June 2018
(range: 0 – 100%)
Number of patient responses
In-patient 89% 500
A&E 82% 2334
Antenatal care 89% 46
Labour and birth 100% 42
Postnatal hospital ward 100% 42
Postnatal community care 98% 96
Out-patients 89% 212
Chase Farm Hospital % likely/extremely likely to recommend June 2018
(range: 0 – 100%)
Number of patient responses
In-patient 96% 131
Out-patients 98% 201
Royal Free Hospital % likely/extremely likely to recommend – June 2018
(range: 0 – 100%)
Number of patient responses
In-patient 91% 734
A&E 88% 2657
Antenatal care 100% 20
Labour and birth 93% 40
Postnatal hospital ward 90% 40
Postnatal community care 98% 96
Out-patients 96% 248
*The postnatal community care question is only reported as a whole trust figure and not split by site.

Paper 13
6 X:\ Chair and CEO report 25 July 2018
ROYAL FREE LONDON WOMEN’S NETWORK
A women’s network is being launched on 25 July to offer a platform to encourage, motivate and mentor the women of the RFL.
As part of the launch, there will be speeches from Dame Ruth Carnall, former chief executive of NHS London, and Kate Slemeck, chief executive of the RFH and the meeting will also discuss how gender may have impacted on women’s career. Natalie Forrest, chief executive of CFH, will also attend the launch at CFH to get involved with the discussions and share her experiences.
A survey has been undertaken to find out what the women of the RFL want from the network, which showed a lot of interest in mentoring and career progression and women at various levels, from band 2 to executives have expressed an interest in the network.
COMMUNICATIONS BOARD REPORT: JUNE 2018
We welcomed Prime Minister Theresa May to the trust to launch the government’s new strategy for the NHS. Her speech was broadcast live from the Royal Free Hospital and her visit to our children’s ward was featured prominently across the national media and on social media.
Media coverage
Main positive story: The i newspaper published an in depth feature of the Royal Free Hospital’s partnership with DeepMind and the development of our Streams app. The story featured one of our patients and two RFL members of staff, along with representatives from DeepMind.
The table below shows the sentiment of press mentions in June:
June Royal Free Hospital
Barnet Hospital Chase Farm Hospital
Total
Positive 32 0 4 36Neutral 49 0 2 51Negative 44 0 2 46Total 125 0 8 133
Digital Communications
Total number of Facebook followers: 5862 (+ 216) Number of Posts: 36, reaching 139,398 people.
Total number of Twitter followers: 15814 (+292) Number of Tweets: 136, reaching 339,175 people.
Our top tweet was about Theresa May’s visit to the Royal Free Hospital. It featured a photo of the Prime Minister delivering her speech to senior leaders from the NHS, and RFL staff, in the atrium.

Paper 13
7 X:\ Chair and CEO report 25 July 2018
Internal communications
Oscars 2017/18: Last month, we held our annual outstanding staff celebration and rewards (Oscars) which recognise individuals, teams and services that made an exceptional difference to the care and wellbeing of our patients, their carers or staff during 2017/18. Almost 300 staff attended, as well as actress and presenter Michelle Collins who hosted the event. We promoted the winners on social media and in all of our internal communications channels.
What matters to you day: We took part in international ‘what matters to you?’ day on 6 June. The initiative encouraged us to ask our colleagues and patients “what matters to you?”, rather than “what’s the matter with you?” Staff held local events, funded by the Royal Free Charity, and we captured their feedback and covered the day on social media, on Freenet and in Freepress.
Trust objectives: We launched our new trust objectives for 2018/19 at the beginning of June. Our aim was to help staff understand that they represent the main priorities that will help us meet our group goals by 2021. We shared them with staff through articles in Freemail, on Freenet, in Freepress and screensavers.
E NATIONAL NEWS AND DEVELOPMENTS
NEW SECRETARY OF STATE FOR HEALTH AND SOCIAL CARE
The Rt Hon Jeremy Hunt MP, who recently became the longest serving health secretary, has been promoted to Foreign Secretary.
His replacement is the Rt Hon Matt Hancock MP who was previously Secretary of State for Digital, Culture, Media and Sport and prior to that Minister of State at the Department for Digital, Culture, Media and Sport, 2016-18. Before becoming an MP, he worked as an advisor for then Shadow Chancellor, George Osborne, later becoming his chief of staff.
Other members of the ministerial team are:
• Stephen Barclay MP, Minister of State for Health • Caroline Dinenage MP, Minister of State for Care • Lord O'Shaughnessy, Parliamentary Under-secretary of State (Lords) • Steve Brine MP, Parliamentary Under-secretary of State for Public Health and
Primary Care • Jackie Doyle-Price MP, Parliamentary Undersecretary of state for Mental Health and
Inequalities

Paper 14
Page 1 of 2 FINAL
Report from the quality improvement and leadership committee (QILC) meeting held
25 June 2018
Executive summary
To follow is a report outlining the key items discussed and actions taken at the QILC meeting held on 25 June 2018.
Signature initiative – Joy in Work The committee discussed implementing a quality improvement (QI) ‘’signature initiative’’ focussing on ‘’Joy in Work’’ (JiW). This aim of the initiative was to help improve staff wellbeing and experience across the trust, whilst meeting the trust’s objective of embedding continuous QI into its day-to-day work. All considered the following topics would be good areas of focus within the JiW initiative; bullying and harassment, improving staff members sense of ‘belonging’, and ensuring staff were supported and respected by management. However, it was agreed that further analysis should take place on staff’s views as to what issues mattered to them.
The committee also agreed the six principles that underpinned the design of the signature initiative programme but requested the inclusion of an additional principle around ‘’being bold’’ and for patient engagement to be made explicit. It also suggested a number of amendments to the membership of the JiW steering group and in terms of governance, agreed that the group should report into the group executive committee (GEC) and in turn to the trust board.
Transitional and future arrangements for QILC business In light of the trust board’s proposal to disband the QILC, the chair agreed to redistribute the committee’s responsibilities to a number of the other group board committees as follows:
• QI, cancer action plan and end of life care would transfer to the clinical standards and innovation committee.
• Leadership (other staff), patient and staff engagement, equalities, dementia action plan, Friends and Family Test scores would transfer to the new people and population health committee.
• Leadership (top leaders) would transfer to the remuneration committee. • CQC business would transfer to GEC. • PALs and complaints would continue to report into the hospital patient and staff
experience and workforce committees with an annual report to the trust board.
The final QILC would take place on 23 July 2017. A report on bringing the committee to a close, i.e. its work thus far, progress against its goals etc. would be provided and would form the purpose of the meeting. A copy of the closure report is attached at Annex A.
Report to Date of meeting Attachment number
Trust Board 25 July 2018 Paper 14

Paper 14
Page 2 of 2 FINAL
Action required
The trust board is asked to:
• note the report from the QILC meeting on 25 June 2018; and
• note the QILC closure report setting out the role of the QILC, its work thus far,
progress against its goals and areas of future focus within the new reporting
structure.
Trust strategic priorities and business planning objectives supported by this paper
2. Excellent user experience – to be in the top 10% of relevant peers on patient, GP and
staff experience
4. Excellent compliance with our external duties – to meet our external obligations
effectively and efficiently
CQC Regulations supported by this paper
Regulation 9 Person-centred care Regulation 13 Safeguarding service users from abuse and improper treatment Regulation 16 Receiving and acting on complaints Regulation 18 Staffing
Risks attached to this project/initiative and how these will be managed (assurance)Any risks would be outlined in the report.
Equality analysisNo identified negative impact on equality and diversity
Report from Jenny Owen, non-executive director and chair of the QILC
Author(s) Veronica Jackson, committee administrator
Date 18 July 2018

Paper 14 - Annex A
FINAL
Quality improvement and leadership committee (QILC) closure report
Background The QILC was established in July 2017 following the establishment of the RFL group. It has ensured that group strategic priorities were advanced through seeking and securing assurance on quality improvement (QI), leadership and patient and staff experience.
The committee has met eight times over the year. Meetings were originally held bi-monthly. From March 2018 the committee moved to monthly meetings, alternating between a full two-hour and a one-hour agenda to focus on progressing a number of QILC’s goals, or to take forward any pressing agenda items.
The meetings were chaired by Jenny Owen, non-executive director (NED). There has been full representation at the meetings from NEDs, group and hospital executives, senior colleagues from the trust’s workforce and organisational development, quality improvement and patient experience departments, the Royal Free Charity and governors. There were two occasions when the QILC only became quorate later on in proceedings; this was due to members having sent apologies for the first part of the meetings.
Decision to disband the QILC and the population health and pathways committee (PHPC) In June 2018, the trust board agreed to disband the QILC and redistribute its responsibilities to a number of the other board subcommittees. In addition, the current population health and pathways committee was disbanded and a new people and population health committee (PPHC) established with new terms of reference and membership. The focus of the PPHC would move from being externally focussed to a large proportion of its work being internally focussed on staff and patient experience / engagement, two key areas of QILC focus. There are synergies between the public health agenda and the wellbeing and support of staff (who are also part of the population). The last QILC meeting would take place on 23 July 2018.
Group goals and board assurance framework (BAF) The following goals were allocated to the committee in July 2017.

Paper 14 - Annex A
FINAL
The committee has regularly reviewed its goals. Throughout the year, it has submitted two goal change requests to the trust board which were approved:
i. Proposal to amend the two group goals relating to leadership merging them into one goal with a proposed alternative measure. The revised goal was ‘Top 10% for leadership’ and the leading indicator was ‘recognition and value of staff by managers and the organisation (KF5 – staff survey)’.
ii. Request to transfer the goal, Top 10% for workforce efficiency (55% of clinical income) to the group executive committee (GEC).
The committee has regularly reviewed its associated BAF risks, particularly in terms of risk scoring and timescales and actions. In line with ii) above, it agreed that the risk G-026 (reliance on high levels of agency staff) should be re-allocated to the GEC given staffing more widely was the responsibility of that committee with staffing levels aligned to the Financial Improvement Plans which, again, were also reviewed by that committee.
Work of the committee to date The remainder of the report sets out the role of the QILC, its work thus far, progress against its goals and areas of future focus within the new reporting structure. All meeting agendas have been organised around QILC’s goals.
• Goal: All sites self-assessed as Care Quality Commission (CQC) outstanding
CQC assurance The committee discussed how it would take assurance that its goal would be achieved and as such the chair specifically requested a report on the framework for CQC assurance within the group structure. It noted that this was aligned with the CQC quarterly self-assessment undertaken by services across the trust and the CQC’s new inspection approach. The committee considered it would be helpful to look at other trust’s that had been rated as outstanding by the CQC and the evidence behind that so that the trust could have greater confidence in its self-assessment scores, especially where staff had rated these as outstanding. The committee considered that the trust’s CQC self-assessment process was robust but might need to be accelerated in view of the impending Well Led review.
CQC quarterly self-assessments The committee has received the trust CQC quarterly self-assessment reports. This included the first iteration of the report completed under the group operating structure with management and coordination of the self-assessment having been devolved to the divisions and under new teams. It noted the challenges for staff in self-assessing themselves, e.g. as a result of greater staff reflection on Never Events and the difficulties in self-assessing a service as ‘good’ or ‘outstanding’ as staff tended to take a cautious approach when self-assessing themselves.
Other reports The committee has received and discussed the following CQC-related reports with particular focus on areas for improvement:
- Camden and Islington psychiatric service CQC report. - CQC national inpatient survey. - Children and young people’s inpatient and day case survey.
Well Led review 2018 The committee has also held discussions in respect of the trust’s preparations for its externally facilitated Well Led review, noting the agreed specific areas of focus which included patient and staff engagement (including bullying and harassment (B&H) and freedom to speak up).

Paper 14 - Annex A
FINAL
• Goal: Top 10% versus peers – staff recommend the trust as a place to work (FFT>90%)
Staff experience and retention The committee has received regular progress updates in respect of staff experience and retention plan. In the latter part of the year, the report was reformatted to focus more specifically on progress made against the workforce efficiency and staff satisfaction goals and included a summary of work on staff retention. The chair considered the presentation and layout of the new report was helpful. However, she wished to see the inclusion of targets by year as this would provide a clear visual for
managing progress and slippage. The committee noted that part of the hospital site’s patient and staff experience committees would now centre on workforce issues, and as such would become the patient and staff experience and workforce committees (PSE&WCs).
Updates have covered:
- The challenge in defining a suitable set of metrics against the goal. - The aspiration to increase the goal baseline from 61% to 80% by 2020/21. - Staff retention, including improving retention within nursing and midwifery and ICU Barnet
Hospital and Royal Free Hospital, and exit interviews. - Friends and Family Test (FFT), noting that the quarter 4 staff FFT was extended to
include key questions on B&H and discrimination and that the local executive committees (LECs) were analysing the data and undertaking thematic reviews.
- Associated BAF risks. - Staff Oscars.
National staff survey 2017 The committee received the results from the national staff survey 2017. It was pleased to see that response rates had increased but noted that there was disparity across sites / groups in terms of the numbers responding and that action was underway to determine the reasons for this. Given the challenging national context, it was pleased to see that the trust had maintained a good position in terms of patent and staff engagement. Discussions focussed on improving non-clinical staff engagement particularly in terms of how they could benefit from the trust’s work on clinical practice groups (CPGs) and quality improvement (QI) and its leadership programmes.
Guardian of safe working reports – Barnet Hospital, Royal Free Hospital and GPs The committee has also received the guardian of safe working reports for quarters 1 – 3 2017-18. The chair requested that any comments from the LECs be included in the reports.
• Goal: Top 10% for workforce efficiency (55% of clinical income)
Workforce efficiency The committee held discussions on where workforce efficiency should best sit in the new reporting structure. It noted that it was relatively easy to measure the trust’s clinical income position but the challenge lay on how the committee could get a handle on that, how it could be reduced, and what were the right measures to steer progress in the right direction. It also noted that there were a number of fora where this information was already being reviewed, e.g. GEC, the workforce and planning committee, and the group services and investment committee which focussed on group clinical and non-clinical support services specifically.
At its March meeting, the committee agreed to request the board transfer the goal to the GEC which was subsequently approved.

Paper 14 - Annex A
FINAL
• Goal: Patients would want to be treated at RFL (FFT>90%) • Goal: Match leader on staff and patient engagement
Patient involvement Throughout the course of its business, the committee has regularly discussed patient involvement, improving the patient experience and the patient experience collaboration. It decided to focus one of its one hour meetings on the issue of patient involvement in April 2018. A detailed discussion was held on how to find and recruit patients to participate in key trust projects and areas of work, such as CPGs, board committees and other formal structures, and QI projects, and how staff could be supported with that undertaking. The committee noted that there were a number of the trust’s existing groups that could offer a useful pool of patients to liaise with, e.g. patient governors, membership and volunteer base, plus the availability of tools, guidance and training, both of which provided a sense that patient involvement at a trust level could be achievable. At its May meeting, a follow up report was discussed and the committee approved a four tier approach (by the nature of activity required) to patient involvement but suggested that this work be rolled out in stages, e.g. Tier 1 (the most high level) undertaken first. There was recognition that the patient involvement initiative needed to be meaningful and not simply a tick box exercise.
The committee has received a number of other progress updates that have demonstrated the trust’s commitment to put the patient, carer and its staff at the heart of all it does in delivering excellent experiences. These reports comprise detail from the quarterly reports that were presented to the clinical review group and which formed part of the quality assurance process for commissioners.
Friends and Family Test (FFT) scores The committee has received quarterly updates in respect of the FFT scores for inpatient, A&E, outpatients and maternity. The reports have also captured a number of comments on the trust’s services which were made on public sites such as NHS Choices. The committee noted the challenge in achieving the target (>90%) given that the FFT data was captured from a number of different metrics, plus there was the risk that only those people that had a disappointing experience would respond to the FFT survey. In addition, there was also currently no benchmarking available due to the varying data collection methods. At the end of 2017, the FFT scores were then reviewed by the local PSE&WCs.
Dementia The committee has received updates in regards to the key achievements against the pathways (patients and carers, staff and the organisation) within the dementia strategy, noting the large amount of work undertaken and successes thus far, e.g. high take up of John’s Campaign which was a good example of how the learning and embedding of improved patient and staff experience was happening across the organisation; pride at the success of the work on the CAPER Anchor; and the dementia-friendly refurbishment of ward 10 North which included a flagship day room facility. The committee received a presentation on the Say Delirium pathway, a project for identifying and managing patients with dementia and delirium on ward 8 West. The later QILC meetings have also focussed on the findings from the national audit of dementia care in general hospitals, with specific focus paid to the action plan in place to address those areas requiring improvement before the re-audit of the trust in Spring 2018.
Cancer The committee has received updates in regards to the cancer patient experience and cancer projects. It has received the findings the national cancer patient experience surveys, noting the positive feedback received and those areas were less favourable reviews were given. The committee noted that a number of detailed improvement actions were underway, such as discussions with the informatics team on improving the collation of data in relation to the completion of treatment summaries. The lead cancer nurse would call on the clinical standards and innovation committee (in the new reporting structure) should help be needed to steer the improvement work along.

Paper 14 - Annex A
FINAL
PALs and complaints report The committee has routinely received a report outlining the number and nature of complaints and PALS cases the trust received each quarter, plus an annual report. In light of the new group governance structure, the committee noted that the site-based patient and staff experience and workforce committees (PSE&WC) were reviewing the reports but agreed that a board committee should also have oversight of the reports as one of the recommendations arising from the Francis Report was that boards needed to be sighted on this information. The report was updated to include a section on complaints via the council of governor’s inbox. The committee was pleased to note that action had been taken to address the issue of outstanding responses to Barnet Hospital complaints.
Quality accounts The committee has reviewed various reports in respect of the trust’s quality accounts 2017-18; the development timetable, draft versions of the final quality accounts and updates on the 2018-19 patient experience priorities. On the latter, it suggested minor amendments to the wording around ‘improving our involvement with stakeholder’s so that it referred to ‘patients and carers’ specifically, and in terms of ‘improving infection prevention and control’ requested that MRSA be replaced with E-coli.
• Goal: Promote equality and diversity
Workforce Race Equality Standards (WRES) The chair requested that the reports on the trust’s compliance with the WRES become a standing item on the QILC agenda. The committee noted that the trust’s protocol in respect of its WRES responsibilities was able to demonstrate that positive steps had been made since its implementation two years ago but work was in chain to improve equality and diversity further. Particular areas of focus were:
- Reducing the likelihood of black and ethnic minority (BME) staff entering formal disciplinary within transplant and specialist services division to 1.0. The committee noted that a large amount of work had been done to improve the position and more was in chain to improve that further. The chair considered that this was an area of importance in terms of the trust’s values and therefore the data on this should be spread across the group to enable greater awareness and future learning.
- Progress against the WRES indicators: diverse interview panels introduced, unconscious bias training being undertaken, the assurance process for determining why BME candidates were unsuccessful in being appointed into Band 8a roles, BME listening sessions, and WRES data.
- Understanding how the trust could recognise if there was an issue with unconscious bias and if so, how would it monitor the solution, and also how could recruitment managers be supported on overcoming any unconscious bias they may hold.
Workforce Disability Equality Standards (WDES) The committee received updates in respect of the WDES. The WDES metrics were in the process of being finalised by NHS England with a proposed publication date of autumn 2018 but there would be further consultation with trusts before then as to what they may be. The committee noted that there was an issue around staff disclosing that they had a disability, and there was disparity in the figures with more staff having reported themselves as having a disability in the 2016 staff survey compared to the numbers on ESR. The QILC delegated the final say on which logo should be used to represent the trust’s staff disability forum to staff.
In the latter part of the year, the WRES / WDES report was reformatted to focus more specifically on progress made against the equality goals.
Gender pay gap The committee received the report which was fulfilling a statutory duty under Equality Act 2010 regulations which required all public sector organisations with 250 or more employees to calculate and publish details of their gender pay gap. It noted that, overall, the trust’s position was better than

Paper 14 - Annex A
FINAL
that seen in the private sector but there were areas that required improvement. Furthermore, more sophisticated analysis of the data would be undertaken, with a clear and focussed action plan, and communications in place.
Annual equality monitoring report 2017 The committee reviewed and approved the annual equality information monitoring report on behalf of the board for publication on the trust’s website by the end of March 2018.
Equality Delivery System 2 (EDS2) progress update The committee chose not to endorse the new approach proposed to simply the process of the ED2 grading event. It considered the new process was challenging for two reasons; firstly, the time commitment on staff having to attend five separate grading events and secondly, the difficulty in ensuring there was consistency in the grading as one group could grade the trust differently from the others.
• Goal: Top 10% for leadership • Goal: Directors developed, appointed to other Trusts
The committee has received regular updates on the development of the trust’s leadership curricula against the leadership framework and on the proposals around talent succession planning for the group. In the latter part of the year, the report was reformatted to focus more specifically on progress made against the leadership goals. Discussions have centred on ensuring that there was the resource available to respond to the demand in participation, clarity on the specifics of the committee’s goals in respect of excellent leadership and how performance against that would be measured, and identifying business critical roles. At its May meeting, the committee heard from two members of staff on their experience of having participated in the Step up to Lead programme and the Licence to Lead programme.
As noted above, the two group goals relating to leadership were merged into one goal, ‘Top 10% for leadership’.
• Goal: Quality improvement (QI) embedded as our method of transformation
QI progress The committee has received regular updates in respect of the trust’s QI initiative, including reviewing the QI risk register. In the latter part of the year, the report was reformatted to focus more specifically on progress made against the QI goal. The committee noted that, overall, QI was being successfully integrated across the trust but work was needed to ensure that impetus was not lost and that the Institute for Healthcare Improvement’s (IHI’s) Improvement Science in Action work was aligned with the site’s daily priorities.
Presentations A QI presentation opened each committee meeting and provided the opportunity to ensure front line staff’s voice was present in the committee’s work and to give members chance to hear first-hand from staff what it is like doing QI work at the trust. The presentation topics have been:
a) What Matters To You – Children’s ward coffee morning for parents and families
b) #Endpjparalysis campaign – ward 10 North
c) Barnet Hospital ED discharge summary QI project
d) WRES – reducing the likelihood of BME staff entering formal disciplinary process to 1.0
e) Theatres – Chase Farm Hospital
f) ICU nurse retention QI project
g) QI in Royal Free Hospital anaesthesia and theatres

Paper 14 - Annex A
FINAL
Joy in work The chair requested its one hour QILC in June focus on the QI ‘’signature initiative’’ - ‘Joy in Work (JiW). Discussions centered on those challenging topics that JiW could address such as bullying and harassment, improving staff members sense of ‘belonging’, and ensuring staff were supported and respected by management, but ultimately staff’s views would be sought on the issues they considered were important and could benefit from JiW. Subject to a minor amendment, the committee agreed the six principles that underpinned the design of the signature initiative programme.
• Reporting At its meeting in July 2017, the committee agreed that the chief executive and director of nursing at Chase Farm Hospital should be invited to attend future QILC meetings.
The committee has received detailed reports from each of the hospital’s PSE&WCs on action taken and decisions made since their inception under the new group governance structure. It was clear that there was a huge amount of work going on at a local level, and QILC was pleased to see that efforts had been made in improving patient and staff experience across all three hospital sites. It noted that the staff experience element of the meetings were well attended and were being well received by staff. The committee was also pleased to see that Barnet Hospital’s committee had a patient representative at the meeting which was adding a new, real dimension to the discussions. It was hoped that clarity around the trust’s patient participation and engagement processes would assist the Royal Free Hospital’s and Chase Farm Hospital’s PSE&WCs in recruiting patient representatives to sit on their meetings.
• Transfer of responsibilities At its meeting on 25 June 2018, and subsequent agreement at the trust board on 27 June 2018, QILC approved the transfer of its responsibilities as follows:
- QI would move to the clinical standards and innovation committee (CSIC) - ‘Top leaders’ (i.e. very senior managers / senior managers) would move to the
remuneration committee (RemCo) - ‘Other staff’ would move to the PPHC - Patient engagement would move to PPHC - Staff engagement would move to PPHC - Equalities (WRES and WDES) would move to PPHC - Dementia (action plan and national audit) would move to PPHC - Cancer (action plan and annual patient survey) would move to CISC - PALs and complaints would continue to go to the local PSE&WCs with an annual report
to the trust board - Friends and Family Test (FFT) scores would move to PPHC - CQC self-assessment would move to GEC - End of life care would move to CSIC
It also undertook a review of a number of the specific reports it currently received and agreed where they would sit in the new reporting structure as follows:
- CQC children and young people’s inpatient and day case survey report and the CQC national survey of adult inpatient report – PPHC
- JiW updates – GEC and then to the trust board - PLACE assessments - local PSE&WCs - Guardian of safe working reports – GEC and LECs. - Gender pay gap reports and follow up work – GEC and then to the trust board. - Reports PSE&WCs – PPHC
Report to the trust board Throughout its operation, QILC has provided the trust board with a written report from each of its meetings. On those occasions where it was not possible to provide a written report immediately after

Paper 14 - Annex A
FINAL
the meeting, the chair of the committee has provided a verbal update with a written report submitted to the next meeting for completeness. All reports have covered the key items discussed at the meetings, provided assurance to the board where necessary and highlighted any risks to the trust, plus outlined any actions agreed.
A copy of this closure report would go to the trust board on 25 July 2018, along with a verbal update from the final QILC meeting on 23 July 2018.

Paper 15
Page 1 of 2
Final
Report from group services and investment committee (GSIC) meeting held 5 July
2018
Executive summary
The GSIC met on 5 July 2018. The key agenda items are outlined below.
Royal Free London Property Services Company Limited The committee received a progress update on the setting up of RFL Property Services Limited.
Future subsidiaries The committee received a report on the timetable and process for setting up two further subsidiaries in respect of the trust’s decontamination services and pharmacy services. Business cases for both entities would be submitted to GSIC in September and October.
Adult assessment unit – Barnet Hospital The committee approved a business case for the development of adult assessment and ambulatory care at Barnet Hospital.
Health Services Laboratory (HSL) The committee received a paper outlining HSL’s potential business development opportunities in the acute local sector.
GSIC goals and Board Assurance Framework risks The committee undertook regular review of its group goals;
• efficiency leader on corporate services • CFH deficit eliminated • double contribution of private patients • being a digital exemplar • efficiency leader on middle office operations
The committee also reviewed its forward planner.
Action required
The board is asked to note the report.
Trust strategic priorities and business planning objectives supported by this paper
Board assurance risk number(s)
1. Excellent outcomes – to be in the top 10% of our peers on outcomes
x
Report to Date of meeting Attachment number
Trust Board 25 July 2018 Paper 15

Paper 15
Page 2 of 2
Final
2. Excellent user experience – to be in the top 10% of relevant peers on patient, GP and staff experience
x
3. Excellent financial performance – to be in the top 10% of relevant peers on financial performance
x
4. Excellent compliance with our external duties – to meet our external obligations effectively and efficiently
x
5. A strong organisation for the future – to strengthen the organisation for the future
x
CQC Regulations supported by this paperRegulation 15 Premises and equipment Regulation 17 Good governance Regulation 13 Financial position
Risks attached to this project/initiative and how these will be managed (assurance)
N/A
Equality analysis
No identified negative impact on equality and diversity
Report from Wanda Goldwag, non-executive director and chair of GSIC Author(s) Duncan Gordon-Smith, trust secretaryDate 13 July 2018
Paper 16
Page 1 of 2 FINAL
Report from the population health and pathways committee (PHPC)
Executive summary
The PHPC held met on 3 July 2018. The key items discussed and decisions taken are outlined below.
Hospital partnership developments The committee received updates in respect of its partnership developments with North Middlesex University Hospital (NMUH) and West Hertfordshire Hospital (West Herts). Discussions centred on the Case for Change with NMUH; the contribution of the Clinical Practice Groups to the partnerships; the West Herts’ model for its clinical partnership with the Group; the potential for Group subscription services; mutual sustainability versus the future platform for population health; and defining the Group’s growth strategy.
The committee also discussed partnership developments with the Royal National Orthopaedic Hospital (RNOH), with specific reference on identifying any dimensions to the partnership that could help the committee’s approach to integrated care. It was noted that MSK / orthopaedics and its links to pain management would be a helpful area for consideration. Given the general relevance of the MSK agenda to PHPC, it was agreed that the MSK team would be invited to attend a future meeting to discuss their work to date.
Royal free vanguard ‘health as a social movement’ programme
The committee received a report which detailed the health and wellbeing initiative, ‘Health as a social movement’ undertaken across the trust and the findings from the independent valuation. The programme focussed on facilities staff on lower pay bands at the Royal Free Hospital with the aim of working with those staff to co-produce a programme of activities to improve their health and wellbeing. The committee was pleased to hear that there had been some excellent outcomes seen as a result of this work; reduced sickness absence, staff felt valued and respected, and social events had enabled staff and managers to connect outside of the work setting. In light of the successes, the trust had been awarded further funding to see through the initiative for another three years and it was noted that the work around that would link into the trust’s quality improvement ‘Signature Initiative’ in respect of Joy in Work (JiW).
New people and population health committee
The committee discussed the recent board decision to disband the quality improvement and leadership committee (QILC) (and redistribute its responsibilities) and the PHPC, replacing them with a new people and population health committee. It noted that a large proportion of the work of the new PPHC would focus on ‘the person’ and that there were synergies between the public health agenda and the wellbeing and support of staff (who were also part of the population).
Report to Date of meeting Attachment number
Trust Board 25 July 2018 Paper 16

Paper 16
Page 2 of 2 FINAL
The committee agreed to subsume the following responsibilities from QILC;
• Patient and staff engagement • Equalities • Friends and Family Test scores • Leadership (in respect of ‘other staff’ (‘top leaders’ would go to the remuneration
committee)) • Dementia
It was noted that a review of the PPHC’s terms of reference, including membership, would be discussed at an upcoming trust board meeting.
Group goals
In light of the transfer of responsibilities from QILC, the new PPHC would now own nine goals in total.
The committee received a paper setting out options for developing a lead indicator and sub-indicators for the group goal, ‘Develop partnerships with non-hospital providers’. Discussion focussed on defining what the committee was looking to achieve from the goal in a broader sense, agreeing its leading indicators and how success against the goal would be measured.
It was agreed that a final view on the committee’s group goals and indicators would be taken at its meeting in September.
Action required
The committee is asked to note the report.
Trust strategic priorities and business planning objectives supported by this paper
Board assurance risk number(s)
1. Excellent outcomes – to be in the top 10% of our peers on outcomes
x
2. Excellent user experience – to be in the top 10% of relevant peers on patient, GP and staff experience
x
3. Excellent financial performance – to be in the top 10% of relevant peers on financial performance
x
4. Excellent compliance with our external duties – to meet our external obligations effectively and efficiently
x
5. A strong organisation for the future – to strengthen the organisation for the future
x
CQC Regulations supported by this paperRegulation 17 Good governance
Risks attached to this project/initiative and how these will be managed (assurance)Any risks would be outlined in the report.
Equality analysis• No identified negative impact on equality and diversity
Report from James Tugendhat, non-executive director and chair of the PHPC Author(s) Veronica Jackson, committee administratorDate 18 July 2018




















