Institutional Directors and Board Compensation: Spanish Evidence
Upload
khangminh22Category
view
0download
0
Board of Directors Meeting Part One
Thursday 25 November 2021 09:30am – Via MS Teams
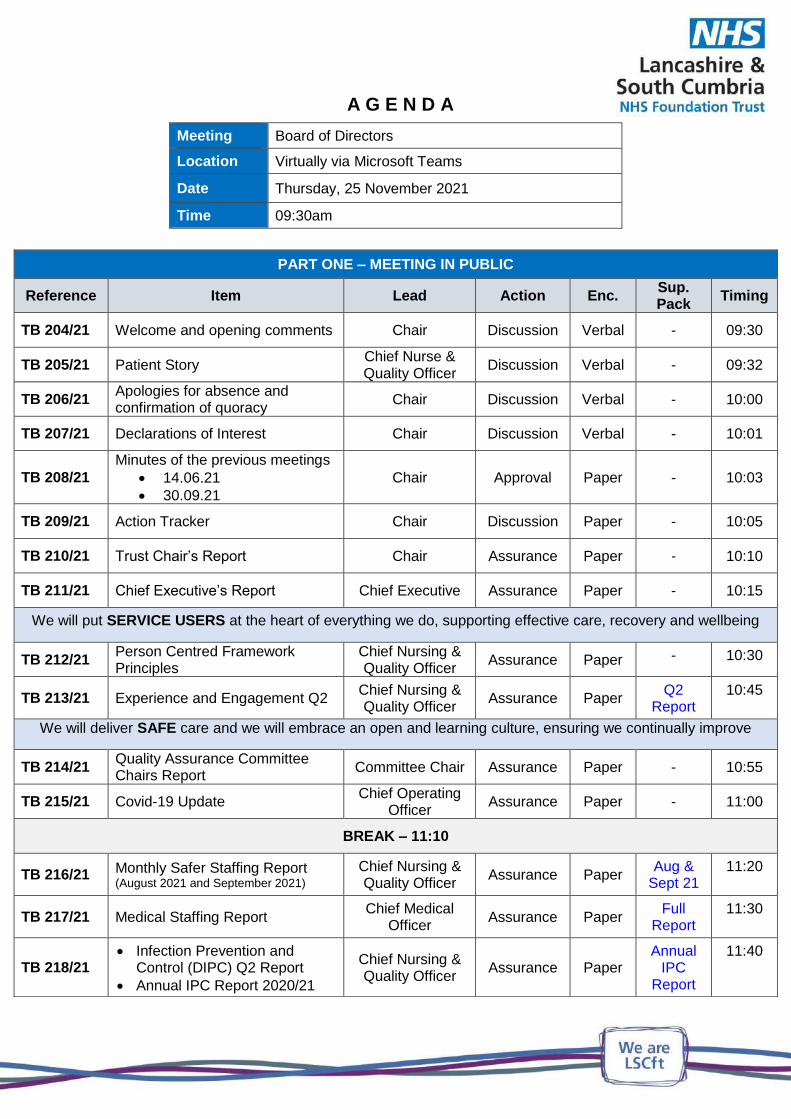
A G E N D A
Meeting Board of Directors
Location Virtually via Microsoft Teams
Date Thursday, 25 November 2021
Time 09:30am
PART ONE – MEETING IN PUBLIC
Reference Item Lead Action Enc. Sup. Pack
Timing
TB 204/21 Welcome and opening comments Chair Discussion Verbal - 09:30
TB 205/21 Patient Story Chief Nurse & Quality Officer
Discussion Verbal - 09:32
TB 206/21 Apologies for absence and confirmation of quoracy
Chair Discussion Verbal - 10:00
TB 207/21 Declarations of Interest Chair Discussion Verbal - 10:01
TB 208/21
Minutes of the previous meetings
14.06.21
30.09.21
Chair Approval Paper - 10:03
TB 209/21 Action Tracker Chair Discussion Paper - 10:05
TB 210/21 Trust Chair’s Report Chair Assurance Paper - 10:10
TB 211/21 Chief Executive’s Report Chief Executive Assurance Paper - 10:15
We will put SERVICE USERS at the heart of everything we do, supporting effective care, recovery and wellbeing
TB 212/21 Person Centred Framework Principles
Chief Nursing & Quality Officer
Assurance Paper - 10:30
TB 213/21 Experience and Engagement Q2 Chief Nursing & Quality Officer
Assurance Paper Q2
Report 10:45
We will deliver SAFE care and we will embrace an open and learning culture, ensuring we continually improve
TB 214/21 Quality Assurance Committee Chairs Report
Committee Chair Assurance Paper - 10:55
TB 215/21 Covid-19 Update Chief Operating
Officer Assurance Paper - 11:00
BREAK – 11:10
TB 216/21 Monthly Safer Staffing Report (August 2021 and September 2021)
Chief Nursing & Quality Officer
Assurance Paper Aug &
Sept 21 11:20
TB 217/21 Medical Staffing Report Chief Medical
Officer Assurance Paper
Full Report
11:30
TB 218/21 Infection Prevention and
Control (DIPC) Q2 Report
Annual IPC Report 2020/21
Chief Nursing & Quality Officer
Assurance Paper Annual
IPC Report
11:40

We will respond to people’s needs by striving for the highest STANDARDS of quality, proactively reducing health
inequalities
TB 219/21 Audit Committee Chair’s Report Committee Chair Assurance Paper - 11:55
TB 220/21 Trust Performance Report Director of
Information & Performance
Assurance Paper Full TPR Month 7
12:00
TB 221/21 Board Assurance Framework (BAF) Q2 21/22
Chief Improvement &
Compliance Officer
Assurance Paper BAF Q2 Report
12:10
TB 222/21
Information Governance and Caldicott Guardian Annual Report 2020/21
Chief Medical Officer
Assurance Paper IG&CG Report 20/21
12:20
TB 223/21
Emergency Preparedness, Resilience & Response (EPRR) Annual Core Standards Review
Chief Operating Officer
Approval Paper - 12:30
TB 224/21 CQC Update
Chief Improvement &
Compliance Officer
Assurance Paper CQC
Action Plan
12:40
TB 225/21 Appoint a Director to LSCFT Nominee No 1 Ltd
Chief Operating Officer
Approval Paper - 12:50
TB 226/21 Mental Health Improvement Plan Chief Operating
Officer Assurance Paper - 12:55
LUNCH – 13:10
We will employ and retain the best STAFF, as our culture will be inclusive and a supportive place to work
TB 227/21 People & Culture Committee Chairs Report
Committee Chair Assurance Paper - 13:30
TB 228/21 Annual Medical Appraisal and Revalidation Report 2020/21
Chief Medical Officer
Approval Paper AMARR
Full Report
13:35
We will provide SUSTAINABLE services that are delivered in an effective and efficient way, at the time people need it
TB 229/21 Finance & Resource Committee Chairs Report
Committee Chair Assurance Paper - 13:45
TB 230/21 Ward and Agency Spend Chief Operating
Officer Assurance Paper - 13:50
TB 231/21 Finance Report Chief Finance
Officer Assurance Paper - 14:00
We will value our partners by listening and collaborating effectively across the SYSTEM
TB 232/21 Provider Collaborative Committee Chairs Report
Committee Chair Assurance Paper - 14:10
TB 233/21 Transformation Progress Update Chief Integration
Officer Assurance Paper - 14:15
BREAK – 14:25
End of Part One Board of Directors Meeting
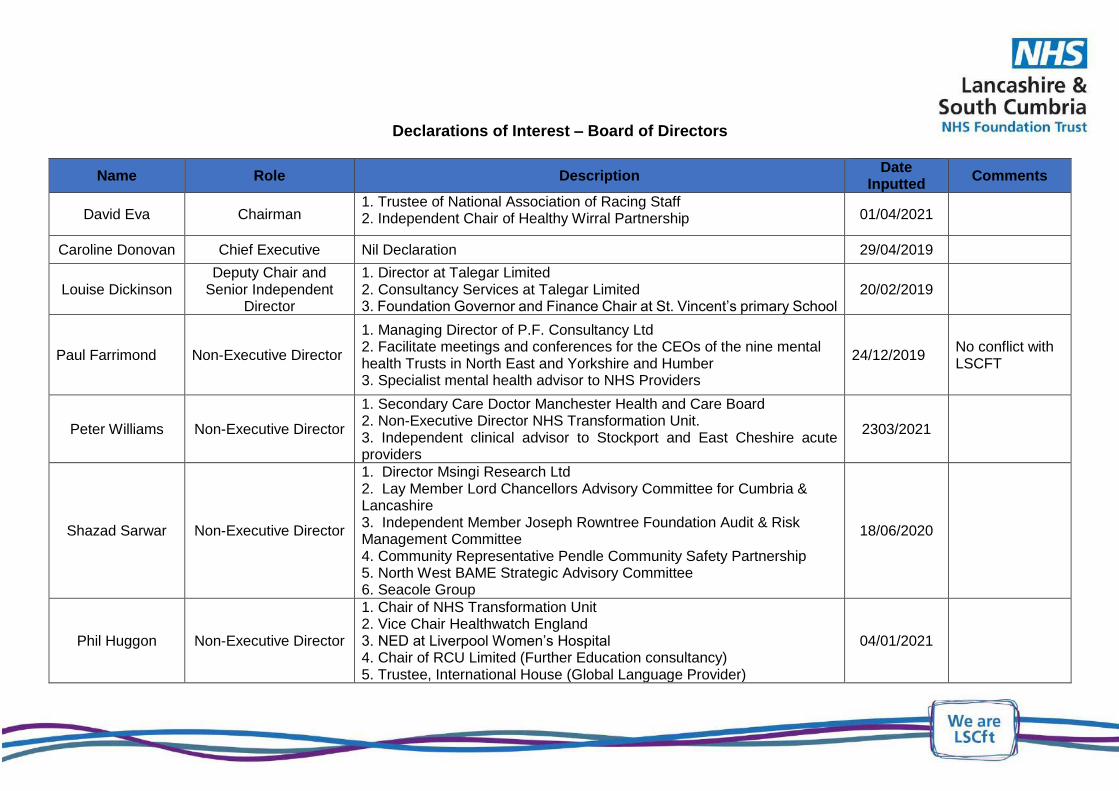
Declarations of Interest – Board of Directors
Name Role Description Date
Inputted Comments
David Eva Chairman 1. Trustee of National Association of Racing Staff2. Independent Chair of Healthy Wirral Partnership 01/04/2021
Caroline Donovan Chief Executive Nil Declaration 29/04/2019
Louise Dickinson Deputy Chair and
Senior Independent Director
1. Director at Talegar Limited2. Consultancy Services at Talegar Limited3. Foundation Governor and Finance Chair at St. Vincent’s primary School
20/02/2019
Paul Farrimond Non-Executive Director
1. Managing Director of P.F. Consultancy Ltd2. Facilitate meetings and conferences for the CEOs of the nine mentalhealth Trusts in North East and Yorkshire and Humber3. Specialist mental health advisor to NHS Providers
24/12/2019 No conflict with LSCFT
Peter Williams Non-Executive Director
1. Secondary Care Doctor Manchester Health and Care Board2. Non-Executive Director NHS Transformation Unit.3. Independent clinical advisor to Stockport and East Cheshire acuteproviders
2303/2021
Shazad Sarwar Non-Executive Director
1. Director Msingi Research Ltd2. Lay Member Lord Chancellors Advisory Committee for Cumbria &Lancashire3. Independent Member Joseph Rowntree Foundation Audit & RiskManagement Committee4. Community Representative Pendle Community Safety Partnership5. North West BAME Strategic Advisory Committee6. Seacole Group
18/06/2020
Phil Huggon Non-Executive Director
1. Chair of NHS Transformation Unit2. Vice Chair Healthwatch England3. NED at Liverpool Women’s Hospital4. Chair of RCU Limited (Further Education consultancy)5. Trustee, International House (Global Language Provider)
04/01/2021
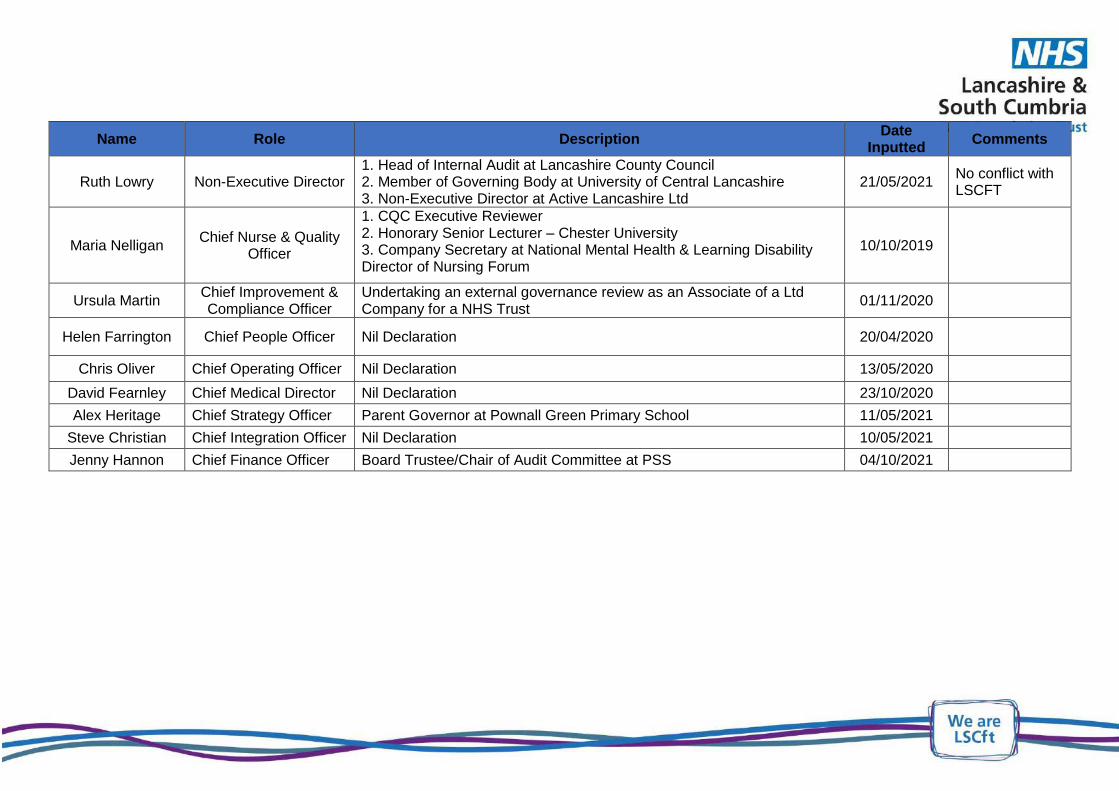
Name Role Description Date
Inputted Comments
Ruth Lowry Non-Executive Director 1. Head of Internal Audit at Lancashire County Council 2. Member of Governing Body at University of Central Lancashire 3. Non-Executive Director at Active Lancashire Ltd
21/05/2021 No conflict with LSCFT
Maria Nelligan Chief Nurse & Quality
Officer
1. CQC Executive Reviewer 2. Honorary Senior Lecturer – Chester University 3. Company Secretary at National Mental Health & Learning Disability Director of Nursing Forum
10/10/2019
Ursula Martin Chief Improvement & Compliance Officer
Undertaking an external governance review as an Associate of a Ltd Company for a NHS Trust
01/11/2020
Helen Farrington Chief People Officer Nil Declaration 20/04/2020
Chris Oliver Chief Operating Officer Nil Declaration 13/05/2020
David Fearnley Chief Medical Director Nil Declaration 23/10/2020
Alex Heritage Chief Strategy Officer Parent Governor at Pownall Green Primary School 11/05/2021
Steve Christian Chief Integration Officer Nil Declaration 10/05/2021
Jenny Hannon Chief Finance Officer Board Trustee/Chair of Audit Committee at PSS 04/10/2021

BOARD OF DIRECTORS
Minutes of the Part One Board of Directors meeting held on 14 June at 9.00am, virtually on MS Teams
PRESENT: David Eva (Chair) Caroline Donovan, Chief Executive Louise Dickinson, Non-Executive Director Paul Farrimond, Non-Executive Director Phil Huggon, Non-Executive Director Shazad Sarwar, Non-Executive Director Peter Williams, Non-Executive Director Steve Christian, Chief Integration Officer John Glover, Chief Digital Officer Alex Heritage, Chief Strategy Officer Ursula Martin, Chief Improvement & Compliance Officer Dominic McKenna, Acting Chief Finance Officer Maria Nelligan Chief Nursing & Quality Officer Chris Oliver, Chief Operating Officer
IN ATTENDANCE: Jo Sandham, Company Secretary Dianne Scambler, Deputy Company Secretary (minutes)
OBSERVERS: Ken Lowe, Public Governor
TB 115 21 WELCOME AND OPENING COMMENTS The Chair welcomed everyone to the meeting.
TB 116 21 APOLOGIES FOR ABSENCE AND CONFIRMATION OF QUORACY Apologies for absence were given by Helen Farrington, Chief People Officer and David Fearnley, Chief Medical Officer. Confirmation of quoracy was given.
TB 117 21 DECLARATIONS OF INTEREST No declarations of any interest were received.
TB 118 21 AUDIT COMMITTEE CHAIRS REPORT The Chair of Audit Committee presented a verbal report in respect of the Audit Committee meetings held on 11 June and immediately prior to the Trust Board meeting.
The Audit Chair advised the Board that KPMG had notified the Trust over the weekend, that they were experiencing IT issues that had resulted in the late circulation of the amended ISA 260 Report to the Audit Committee and that these issues may affect the signing of the audit opinion and its submission. In the event of any such delay, KPMG would write a detailed explanation to NHSE/I
The Audit Committee had now received a number of year-end documents, including the annual Head of Internal Audit Opinion, of which the Trust received substantial assurance, which was an improvement on last year’s opinion of moderate assurance.
The Committee also received a progress report of internal audit activity during 22 April to 7 June 2021 and approved the 2021/22 Internal Audit Plan, which was
CONFIRMED
25.11.21

caveated on the fact that the Plan may be subject to change following the outcome of the HSIS review commission by the Chief Finance Officer.
The Audit Committee received the draft External Auditors ISA 260 Opinion and flagged to the Board the issuing of an unqualified opinion on the financial statements which is the highest achievable standard. The Committee noted the work undertaken to ensure appropriate treatment of the ICS hosting arrangements in the Trust’s accounts, particularly in relation to deferred income, with £4.2m of the deferred ICS income balance now being disclosed as an unadjusted audit difference. It was highlighted to the Board that the external auditor had identified one risk around financial sustainability, absence in cost improvements programme (CIP) monitoring, which in their opinion highlighted a potential risk of a significant weakness in that the Trust does not have in place adequate arrangements to achieve financial sustainability in the medium term.
However, following the Audit Committee’s strenuous challenge against this view the wording within the opinion and annual report had been amended to better reflect the Trust’s position in relation to CIP monitoring, the Trust having halted CIP monitoring throughout the pandemic as directed by NHSE/I.
The Management Letter of Representation had also been amended to reflect the amended wording in preparation for signing by the Acting Chief Finance Officer.
The Chair of Audit Committee took the opportunity to formally thank the Chief Improvement and Compliance Officer, Company Secretary and members of the Finance team for their diligence throughout the year-end process.
The Audit Committee were recommending the Board of Directors to approve the Annual Report and Accounts for 2020/21.
TB 119 21 FINAL EXTERNAL AUDIT ISA 260 (OPINION) The Board of Directors considered the final external audit ISA 260 Report that gave the year-end position of the Trust. The Board of Directors discussed the work undertaken to ensure adequate assurance and the appropriate treatment of the ICS hosting arrangements in the Trust’s accounts, particularly in relation to deferred income, with £4.2m of the deferred ICS income balance now being disclosed as an unadjusted audit difference. This reflects a potential error in the accounting treatment because of insufficient audit evidence.
At the request of the Audit Committee, the wording within the Report had also been amended to better reflect the Trust’s position in relation to CIP monitoring during 2020/21 as part of its Value for Money review and opinion.
The Board of Directors noted the assurances provided within the report.
TB 120 21 EXTERNAL AUDIT REPORT ON THE ACCOUNTS The Board of Directors received the external auditor’s report for 2021/21 that was presented alongside the ISA 260. The report provided a summary of the findings and key issues arising from the auditors 2020/21 audit of the Trust’s financial statements.
The Auditors have issued an unqualified opinion on the Trust’s accounts. The key risks identified included valuation of land and buildings and the treatment of deferred income, none of which has led to any material misstatements. They also

concluded that the Trust has sufficient arrangements in place to achieve value for money, although there was a recommendation for the Trust to improve its financial governance around CIP in line with the commentary within the ISA 260 discussion.
It was confirmed that the Annual Governance Statement had been prepared in line with DHSC requirements, with no significant inconsistencies having been identified. It was reported that there is a new requirement, this year, for a shorter version of the External Auditors Report to be published on the Trust’s website, alongside the Trusts Annual Report and Accounts for 2021/22.
The Board of Directors noted the assurances provided within the report.
TB 121 21 MANAGEMENT LETTER OF REPRESENTATION ON THE FINANCIAL ACCOUNTS The management letter of representation on the accounts was presented as the standard NHS organisation letter that is required to be signed alongside the annual accounts. The wording had been amended in line with those comments made by the Audit Committee on the ISA 260 Opinion and Annual Audit Report.
The Board of Directors granted approval for the Acting Chief Finance Officer to sign the letter of representation.
TB 122 21 ANNUAL REPORT (INCLUDING ANNUAL GOVERNANCE STATEMENT) AND ACCOUNTS 2020/12 The Chief Improvement and Compliance Officer presented the item, noting that the Audit Committee had received the final Annual Report and Accounts for 2020/21 and recommended the Trust Board to approve the documents.
The Annual Report (including the Annual Governance Statement) and Accounts reflected the Head of Internal Audit Opinion, which concluded substantial assurance for the Trust overall, an improvement on the moderate assurance rating received for 2019/20.
There was recognition that the scope of work that had been curtailed due to the challenges and pressures that the Trust had faced during Covid-19 and was not as broad as expected. Due to the impact of the pandemic, there was limited coverage of quality areas highlighted in risk assessments and these would be taken forward as part of the 2021/22 risk assessment and planning process.
The Board noted that the Quality Account had not been included within the Annual Report in line with NHS Improvement/England guidance received noting the extended deadline for submission of the Quality Account. The Trust Board would be required to sign the Quality Account off towards the deadline.
The Board of Directors approved the Annual Report and Accounts for 2020/21. Electronic signatures would be added to the documents for final submission to NHS Improvement/England.
TB 123 21 ANY OTHER BUSINESS None.
TB 124 21 DATE AND TIME OF NEXT MEETING The next Trust Board meeting was scheduled to take place on 28 June 2021, 10.00am.
1
BOARD OF DIRECTORS
Minutes of the Part One Board of Directors meeting held in public, Virtually, via MS Teams, on 30 September 2021 at 9.30am.
PRESENT: Louise Dickinson, Deputy Chair in the Chair Caroline Donovan, Chief Executive Paul Farrimond, Non-Executive Director Ruth Lowry, Non-Executive Director Shazad Sarwar, Non-Executive Director Steve Christian, Chief Integration Officer Helen Farrington, Chief People Officer David Fearnley, Chief Medical Officer Alex Heritage, Chief Strategy Officer Ursula Martin, Chief Improvement & Compliance Officer Maria Nelligan Chief Nursing & Quality Officer Chris Oliver, Chief Operating Officer Dom McKenna, Acting Chief Finance Officer
IN ATTENDANCE: Andy Chittenden, Interim Company Secretary (minutes) Paul Jebb, Deputy Chief Nursing & Quality Officer (items 168-169) Phil Horner, Director of Information and Performance (items 168-183)
OBSERVERS: Jenny Hannon, Designate Chief Finance Officer (Items 168–182) Ken Lowe, Public Governor, Deputy Lead Governor, (Items 168-185) Alexa Traynor, Director of Communications Dianne Scrambler, Deputy Company Secretary
TB 168/21 WELCOME AND OPENING COMMENTS The Chair welcomed everyone to the meeting. Apologies were received from Chair David Eva.
TB 169/21 PATIENT STORY One of the Trust’s service users named Susan was introduced to the Board, together with Linda, one of the Trust’s staff working within the Preston Positive Lifestyle Team. Susan explained her story and patient experience over several years through her artwork, accompanied by her own vocal narrative.
As an adult Susan had experienced poor mental health, forcing her to leave both her job and home in London to return to the northwest. Her early experiences of accessing mental health services had included a lack of consistency between different teams and team members that she had been supported by; poor handovers and a sense that she was not always consulted about her support and care in the ways she would wish to be. There were numerous admissions to in- patient services during her journey.
As Susan spoke about her experiences, she revealed that it had been four years since her most recent admission and that the Positive Lifestyle Service had been a very significant factor in her recuperation and in particular how the encouragement for Susan to access her hobbies and those things she is good at such as art and fashion had been fundamental in rebuilding better mental health.
Board members asked a number of questions about Susan’s experience and the importance of non-medical interventions in supporting patients on their recovery.
CONFIRMED
25.11.21
2
The Board thanked Susan and the team for coming to the meeting and sharing their insights. The Chief Nursing Officer explained to the Board how such insights were being used to increase the degree to which person centred care planning was being promoted and developed. Susan, Paul Jebb and Linda left the meeting.
TB 170/21 APOLOGIES FOR ABSENCE AND CONFIRMATION OF QUORACY Apologies for absence were received from David Eva, Trust Chair. Confirmation of quoracy was given.
TB 171/21 DECLARATIONS OF INTEREST
There were no new declarations of any conflicts of interests.
TB 172/21 MINUTES OF THE PREVIOUS MEETING The minutes of the previous meeting held on 29 July 2021 were confirmed as a true and accurate record, subject to minor typographical amendments.
TB 173/21 ACTION TRACKER Board members noted the content of the action tracker that were due for September 2021 and where appropriate items were closed off or agreed for follow up outside of the meeting.
TB 174/21 TRUST CHAIR’S REPORT
The Chair highlighted the visit by the recently appointed Secretary of State for Health and Social, Sajid Javid at The Grange Community Centre in Blackpool, the forthcoming Governor Elections and the recent Annual Members Meeting. It was reported that feedback from the Secretary of State and his team on the Trust’s mental health urgent assessment centre at Blackpool Victoria Hospital had been very positive. The Board were also advised of the activity that had taken place by the Non-Executive Directors and the Use of the Common Seal for a number of contracts. The Board of Directors noted the report.
TB 175/21 CHIEF EXECUTIVE’S REPORT The Chief Executive introduced her report and drew the Board’s attention to the continued high demand on services and the Trust’s ongoing focus on the Covid pandemic. The Board was also updated on the refurbishment and opening of the Mental Health Urgent Assessment Centre (NHUAC) at Royal Preston Hospital. Development of the new rehabilitation service in Wesham were reported. The Trust has been recognised with two being shortlisted for HSJ Awards; Mental Health Innovation for Advice & Guidance and Staff Engagement for Inspiring Culture Change through Inclusive Engagement. The Trust’s Eco-therapy project ‘MySpace’ which was featured recently on ‘Granada Reports’ is a previous winner of an HSJ Award. The Board was pleased to hear of a continuing focus on staff wellbeing with approximately 750 staff have been involved with the engagement initiative ‘Listening into Action’ and the recent launch of a new Staff Network to support inclusivity. The publication of the Trust’s progress against the Workplace Race

3
Equality Standard had also shown progress against seven of the nine key indicators. The CEO welcomed the introduction of the Trust’s new Ward Accreditation Scheme with Duxbury Ward in Chorley being the first to be designated ‘Gold’. Ted Baker, the CQC’s Chief Inspector of Hospitals had participated in an online staff engagement in September, setting out in more detail The Board welcomed a wide range of positive developments. Management assurances were sought and provided [in relation to BAF Strategic Risk No 2 - failure to recruit, develop, retain a diverse and talented workforce, due to a national workforce shortage and reputational factors, which may impact upon the quality of care] on the incidence of and response to staff sickness levels; preparations for adequate resourcing to face winter pressures; partnership working across the region, including mutual aid; recruitment and retention of staff. Action: A paper to the November 2021 Board, responding to any perceived gap in control over BAF risk No 2, addressing staff resourcing and wellbeing, or if available earlier, the Board development session in October. HF The Board sought further assurance as to the pace and depth of transformational activity within the organisational structure and the roll out of enabling strategies into the localities. Action: Papers to the November 2021 Board updating the Board on transformation progress and in embedding Trust-wide enabling strategies into the Localities. AH & SC
The Board noted the content of the report.
TB 176/21 SERVICE USER & CARER CHAIR’S REPORT
The Chair of the Service User & Carer Council provided an update to the Board since its last meeting on 6 September 2021. The report provided assurances on key areas that included agreement to elect a new Chair and Vice Chair for the Council. Information was also provided in relation to Youth Voices, the Research and Development Strategy and the implementation of the Integrated Response Service (IRS). The Board noted the content of the Chair’s Report.
TB 177/21 QUALITY & ASSURANCE COMMITTEE CHAIR’S REPORT
The Chair of the Quality & Assurance Committee presented the report and highlighted approval of the Terms of Reference for three sub-committees which report into the Committee. Assurances had also been received and scrutinised in a number of areas that included Serious Incidents and Inquests; Reducing Restrictive Practices and Infection, Prevention and Control. The Board noted that the Committee had welcomed a comprehensive action plan following a deep dive of The Guild that had highlighted improvements made around ligature risks and staffing challenges.
4
The Committee welcomed the assurance provided by the response and action plan to the CQC inspection of The Harbour, in which actions are anticipated to be complete by April 2022. The Committee also reported to the Board the challenge to resource inquests and investigations of serious incidents. There were 54 reported as ‘open’ and under investigation currently at the time of the Committee’s meeting. Of these, 25% were reported as concluding later than planned, thereby potentially delaying the learning arising from those investigations. It was reported that the Committee would continue to focus on the improvement of Trust processes for investigations and to triangulate assurances received with the control over BAF Risk No 3 [Failure to learn and improve as an organisation underpinned by ineffective systems and a lack of an open and transparent culture may impact upon care] – currently scored at 15, for which the Lessons Learned Framework is a key control mechanism. This scrutiny would include being appraised of the changes to the National Safety Strategy effective April 2022. The Board was pleased to note the Committee’s focus on the Quality Dashboard which now included reporting on protected characteristics to improve insight into the Trust’s performance. Management assurances were sought and provided that the content of the follow on papers in the Board pack [Items 178-181 on Covid 19; Safer Staffing and Safeguarding] had been shared with and scrutinised by the Quality Assurance Committee
The Board noted the content of the report.
TB 178/21 COVID-19 UPDATE
The Chief Operating Officer presented the Covid-19 report. Across the months of July and August there had been three ward outbreaks, an outbreak being were there are two or more positive Covid cases on any one ward. There have, however been low incidences were individual patients have tested positive on admission to the Trust. All three outbreaks were contained within the ward in which Covid was detected and there was no ward to ward transmission. Staff absence due to Covid continues to be affecting the Trust’s services, with approximately 75 staff per day absent. –being substantially lower than the peak of 250 per days in 2020 but higher than the lowest figures since the pandemic began (the low point being less than 50 per day). The Board was updated on the latest positions re Public Health England Guidance on Isolation; Trust Covid 19 vaccination rates, asymptomatic testing; and worker vaccination status in the care home environment. Management assurances were sought and provided that the vaccine cold chain remains reliable; the supply of blood test tubes, which had been interrupted nationally, was no longer hampering timely pathology investigations; that specific plans were in place to encourage all those within the remaining 20% of unvaccinated staff to consider and accept appropriate vaccination. These plans included working with nursing staff group; care home workers; the faith sector; BAME staff groups; and that the Communications Team were integral to the plans.

5
The Board noted that the report triangulated with a recognised gap in control to mitigate BAF Risk 5 [Failure to respond to the increased demand for services as a result of Covid 19 pandemic, due to ineffective recovery planning and the availability of appropriate resources to meet demand which may impact on the quality and wellbeing of service users] – currently scored at 15. The Board was pleased to note that the Trust’s Infection, Prevention and Control (IPC) measures were working to reduce the incidence of patient to patient transmission. Action: The Covid 19 report at the November 2021 meeting to include greater detail of the work being undertaken to ensure that all remaining staff, including those with protected characteristics are fully engaged by the Trust in relation to the benefits of appropriate vaccination against Covid 19. CO. The Board noted the content of the report.
TB 179/21 MONTHLY SAFER STAFFING REPORT (JUNE and JULY 2021)
The Chief Nurse and Quality Officer introduced the monthly safer staffing report that informed the Board and public of staffing levels within in-patient units as part of its requirement of NHS England and the National Quality Board (NQB) reporting. The report also provided assurance that there is continued detailed internal oversight and scrutiny in place to ensure safer staffing levels are maintained which continue to be challenging to meet, due to competition for staff amongst providers and the pandemic. The incidence of ‘red flag’ triggers, principally due to a shift being worked with a single RN on duty continued during the summer with notable higher incidence at The Harbour and The Guild. Assurance was provided that night fill rates have been bolstered by block booking agency RNs to backfill gaps in the establishment and that a range of other mitigating actions have been tested and found effective. It was reported that 12 months previously, the Trust had had 157 vacancies across in patient wards but this had been reduced to 57 at the time of the report. It was reported that the Trust is also placing significant emphasis on filling all the vacancies for Healthcare Support Workers across the localities. They will be deployed quickly by reducing the period between advert and start date. The Board was pleased to note the assurance provided that the Trust’s recruitment activity is attracting applications and interest from talented candidates who have choice in selecting from amongst several employers. The Board noted that the report triangulated with BAF Risk 2 [Failure to recruit, develop and retain a diverse and talented workforce, due to a national workforce shortage and reputational factors, may impact on the quality of care] – currently scored at 16. The Board anticipated further information and assurance both in the following Item 182 Annual Safer Staffing Report as well as the November 2021 Board paper already actioned under the prior Item 175. The Board of Directors noted the content of the report, the increasing challenges in delivering safe staffing particularly in the current pandemic, the mitigations and action plans in place and were assured that safe staffing levels had been maintained during June and July with the support of rostered and non-rostered nursing and MDT staff.
6
TB 180/21 ANNUAL SAFER STAFFING REVIEW (Jan 2020 – July 2021) As with the immediately preceding Item 181 Safer Staffing Report (June and July 2021), the Board noted that Item 182 triangulated with BAF Risk 2 [Failure to recruit, develop and retain a diverse and talented workforce, due to a national workforce shortage and reputational factors, may impact on the quality of care] – currently scored at 16. The Chief Nursing and Quality Officer presented the report, drawing the Board’s attention to the findings of the Annual Safer Staffing Review (Acute and PICU wards) which covered 19 months including the first year of the pandemic. The report met the Trust’s compliance requirement under NQB guidance. In an environment characterised by the current national shortage of registered nurses and the increasing dependency / acuity of service users, it had been challenging for the Trust to maintain safe staffing levels during 2020 and into 2021. However, through dedication and commitment, Matrons, Ward Managers and their teams have maintained safer staffing levels at safer levels. Management assurances were sought and provided on a wide range of related aspects of the system of controls by which safer staffing levels are delivered. The Board noted that not all the posts which had been filled are fully funded and that they are funded in the short term from under-spending elsewhere in the establishment. All Adult and PICU wards have received a CQC Mental Health Act inspection within the past 2 years. There are opportunities emerging from these inspections including requirements for improvement in seclusion environments: patient involvement in care planning: maintaining contact with relatives during COVID pandemic. The Board of Directors noted the progress of safer staffing within the Trust; noted the level of temporary staffing required to support safer staffing and endorsed, by a show of hands, the range of ongoing responses to the 27 recommendations arising from the report and summarised therein at Section18 of that report.
TB 181/21 SAFEGUARDING ANNUAL REPORT
The Chief Nursing and Quality Officer presented the annual report that provided the Board with an overview of the Trust’s achievements, safeguarding developments and challenges that have taken place during the reporting period. These illustrate the breadth and depth of initiatives carried out in respect of Safeguarding from April 2020 to March 2021. The Board noted that the report triangulated with BAF Risk 4 [Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care, which may impact upon the quality of care and could incur regulatory action] – currently scored at 16. The report was presented in two parts, with part one detailing the achievements made throughout the year, demonstrating how LSCFT fulfils its legislative duties in relation to all aspects of safeguarding adults and children, and part two describing those achievements relating to the LSCFT Safeguarding Service and enhanced commissioned services the Trust is contracted to host for safeguarding children/adults and Looked after Children services.
7
Performance targets had been met and the safeguarding team strengthened. Management assurances were sought and provided that succession plans for safeguarding leadership are in place. The Board was pleased to note that a Consultant Social Worker had been recruited into the leadership team. The Board of Directors approved the Annual Report and agreed the Safeguarding priority actions for 2021/22.
TB 182/21 MENTAL HEALTH IMPROVEMENT PLAN
The Chief Operating Officer introduced the Mental Health Improvement Plan that provided assurance of significant and sustained improvement across the mental health crisis pathway. The report set out progress against key service metrics. The Board noted that the report triangulated with BAF Risk 5 [Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care, which may impact upon the quality of care and could incur regulatory action] – currently scored at 15. Despite higher demand on services (such as a 30% increase in demand from 2019 to 2021 experienced by the Home Treatment Team), performance had improved since the pre-pandemic period in some areas. The Trust continues to work to reduce the incidence of breaches of the A & E 12 hour target and the use of s136 place of safety detentions which remain greater than the Trust aims for but compare well compared to peer providers. The Trust continues to seek solutions to inappropriate out of area placements, though this remains a challenge with an average of almost 30 beds occupied daily in the independent sector provision of out of area placements. Length of stay has increased and the incidence of stranded stays in the acute setting has also increased under increased demand for access to services. The Board was pleased to hear that collaborative work with Blackpool Council has resulted in improved performance and better service quality for patients. Management assurances were sought and provided in relation to the improvements being consistent across different localities; that learning from success in one locality can be transferred into others; that service design is being planned based on anticipated need rather than raw population figures; that where improvements were being demonstrated in the short term, management had plans in place to embed the improvements and ensure that they became sustainable. The Board noted the content of the report, in particularly welcoming the improvements identified but recognising that much more remained to be achieved to fulfil the Trust’s ambition for mental health service provision.
TB 183/21 TRUST PERFORMANCE REPORT (July – Aug 2021)
The Director of Information and Performance introduced the Trust Performance Report, provided in a revised format with metrics now being grouped by CQC domain to bring better visibility to each domains and to facilitate performance monitoring. Management assurances were sought and provided that whilst some metrics within the report still required manual compilation and are therefore of lower data quality that a digitised system, further work is ongoing to digitise the collection of remaining data collection. The Board noted that the report triangulated with BAF Risk 4 [Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care, which may impact upon the quality of care and could incur regulatory action] – currently scored at 16.
8
Of the 160 indicators, exceptions were reported in for 132; of these, 33 relate to Quality; 73 relate to Operational Performance; and 26 relate to Workforce. The Board’s attention was drawn to performance in a number of areas including but not limited to rapid tranquilisation; dementia discharge; falls; stranded patients; eating disorder service and the incidence of RIDDOR incidents.a Management assurances were sought and provided that the waiting list for CAMHS is actively managed by locality; any that trends in RIDDOR incidents were being examined and that as yet, none were emerging. The review process has been iterated and strengthened. The Board was pleased to note three service area indicators showing notable trend improvement:
No reported incidents of Physical Violence with Harm reported.
The number of reported restraints continues to show improvement and exceeded (by being below) the target for the second month.
The number of Out of Area Bed Days fell in August to below maximum use threshold set by the Trust.
Six indicators have moved from requiring improvement to achieving target from July to August 2021, and four indicators have moved from achieving target to requiring improvement in the same period.
The Board of Directors noted the report; confirmed an aspiration to see the report developed to provide greater detail on locality performance, and intra-locality performance. The Board acknowledged that the Quality Assurance Committee includes locality performance within its purview. The report was noted.
TB 184/21 CQC UPDATE
The Chief Improvement & Compliance Officer introduced the paper that provided the Board with an update of the work being undertaken relating to CQC compliance across the Trust. The Board noted that the report triangulated with BAF Risk 4 [Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care, which may impact upon the quality of care and could incur regulatory action] – currently scored at 16. The report provided an update of the action plan developed to respond to the inspection of two core services (older adult impatient and adult impatient/psychiatrist intensive care) at The Harbour, Blackpool, in April 2021. Management assurances were sought and provided as to progress being made in three principal areas: CQC Inspection report and subsequent action plan for The Harbour which had been inspected by the CQC in April 2021; the update on five virtual visits by the CQC to review care for those detained under the Mental Health Act since April 2021; and noted the work being undertaken regarding the Trust’s compliance with the CQC Fundamental Standards of Care which would enhance the Trust’s readiness for any future CQC inspection.
9
The report also updated on the work that the Trust is undertaking with retained advisers the Good Governance Institute and Enable East to improvement against the CQC’s Fundamental Standards of Care and to support with organisational development, by implementing the Creative Capable Teams programme, which has been successfully implemented in Scarisbrick Inpatient Unit and in the inpatient wards in Dane, Garth, South Cumbria. Updates on the work undertaken will be shared with the Board at the October Board development event.
The Board was pleased to note that two non-executive directors had visited Dover Ward and had seen at first hand the initiatives being undertaken there, facilitated by Enable East engagement. Action: A paper to the November Board setting out the work undertaken and assurance arising from each Network Locality re self-assessment position against the Fundamental Standards of Care. UM The report was noted.
TB 185/21 LEARNING FROM EXPERIENCE REPORT (April 2021 – June 2021)
The Chief Improvement and Compliance Officer presented a report that provided assurance on the triangulation of governance mechanisms to ensure learning and improvement work will be more targeted and focused. The report contained quantitative and qualitative analysis, using information from the Datix system, and included incidents, complaints, claims, inquests and mortality information. A summary of key issues, identified in Quarter 4 was also provided along with recommendations in respect to findings that will be reported on in the next report. The Board noted that the report triangulated with BAF Risk No 3 [Failure to learn and improve as an organisation underpinned by ineffective systems and a lack of an open and transparent culture may impact upon care] – currently scored at 15. Management assurances were sought and provided as to the Trust’s performance in relation to incident reporting, compared to peer (the Trust reports similar but growing numbers of incidents); the reducing incidence of restraint being used; the reducing use of seclusion being used; the embedding of lessons learned across network localities thereby improving care and the patient experience. The Board noted that the NHS plans to introduce a new National Safety Strategy in 2022 which will drive further methodological change. In the interim period the Board anticipated the report style providing a greater insight into the data as it relates to people with protected characteristics. The Board noted the ongoing very considerable number of inquests (no = 180) which the Trust is supporting and sought assurances, that were provided, that colleagues were adequately supported in the preparation for and involvement in inquests. Action: An amendment to be made to the templates for Board and Committee papers to provide for consideration to be given by authors to what insights the report provides for people with protected characteristics. AC The Board of Directors noted the report and endorsed the following management actions already completed in Q1:
10
Learning from inquests is strengthened so that it is routinely captured and shared with teams – including having debriefs and tracking lessons learnt.
Launch of the Report to Improve Campaign by the end of Quarter 2 to support improved incident reporting and learning.
TB 186/21 PEOPLE & CULTURE COMMITTEE CHAIR’S REPORT
The Chair of the People & Culture Committee introduced the report that gave an overview of activity undertaken and assurances received at the previous meeting on 12 August 2021. The Board noted that the report triangulated with BAF Risk 2 [Failure to recruit, develop and retain a diverse and talented workforce, due to a national workforce shortage and reputational factors, may impact on the quality of care] – currently scored at 16. Assurances had been received in a number of areas that included, the Trust’s Attendance Management Policy, Appraisals process and compliance, progress made against the Quarter 1 BAF actions and the WRES 2021 results. The Committee had also escalated to the Board it’s recommendation that a Board development session consider vacancy rates, recruitment and retention, but noted that this theme had already been anticipated earlier in the meeting (Item 175) and a paper actioned for the November 2021 Board. The Board of Directors noted the report.
TB 187/21 WORKFORCE RACE EQUALITY STANDARD REPORT
WORKFORCE DISIBILITY EQUALITY STANDARD REPORT The Chief People Officer introduced two reports that gave an overview of the Workforce Race Equality Standard (WRES) and Workforce Disability Equality Standard (WDES) and which updated the Board on the positive progress made against action plans to strengthen the Trust’s performance against both of the standards during 2020/21, identifying further key priorities for 2021/22. The Board noted that the report triangulated with BAF Risk 2 [Failure to recruit, develop and retain a diverse and talented workforce, due to a national workforce shortage and reputational factors, may impact on the quality of care] – currently scored at 16. Management assurances were sought and provided as to the extent of the Trust’s ambition not only to achieve the standards but to surpass them and to do so at a local team and service level. Action: A further paper to the January 2022 Board on the performance of the Trust compared to peer Trust performance (both WRES and WDES) and to include the Trust’s performance and plans to widen participation in the workforce amongst people with learning disabilities and autism. HF The Board of Directors noted the two report, the actions, measures and targets implemented to support progress against the metrics, endorsed the two action plans for 2021/22 and approve the contents of both reports being shared with commissioners and NHS England.
TB 188/21 SPEAKING OUT SAFETY REPORT – QUARTER 1
The Chief Improvement and Compliance Officer presented a report on the speaking out safely system and process, an update on the Freedom to Speak Up
11
promotional and development work in Quarter 1, together with an analysis of the Dear Caroline concerns raised in the same period. The report also provided assurance of the ongoing work within LSCFT to ensure that staff are supported to speak up, challenges to speaking up are overcome, speaking up becomes everyday business, and we learn and develop from concerns that are raised. The Board noted that the report triangulated with BAF Risk No 3 [Failure to learn and improve as an organisation underpinned by ineffective systems and a lack of an open and transparent culture may impact upon care] – currently scored at 15. Management assurances were sought and provided that the wide range of approaches to solicit concerns from within the staff body are designed to be as inclusive as possible and take into account the intelligence available as to the methods by which staff have indicated that they wish to have available to raise concerns. Action: A report in November 2021 collating the data and themes arising from Speaking Out Safely developments with incidents of whistleblowing and if practicable to include insights into the incidence of sickness absence and incident reporting. UM The Board of Directors noted the report and confirmed their assurance of the process.
TB 189/21 FINANCE & RESOURCES COMMITTEE CHAIR’S REPORT The Chair of the Committee presented the Chair’s Report that gave an overview of activity transacted at its meeting on 22 September 2021. A number of items had been approved that included its Terms of Reference; the project initiation document for investments to be made at Whalley; the recommended appointment of a contractor and the Environmental Management Carbon Net Zero Policy. Management assurances were sought and provided in relation to action planning following the EPR audit by MIAA; the further development of the EPR and the capital programme. The Committee was pleased to note that NHSX had reported upon its review of the Trust’s cyber metrics arrangements; assessing the Trust as category blue (high performance / complete) across its review domains. The Committee Chair escalated to the Board the Committee’s view that the successful completion of the capital programme would be affected by the increasing costs of material costs and the high level demand for labour on improvement and construction projects. Resolution The Board resolved by a show of hands to ratify the terms of reference of the Finance and Resources Committee (which the Committee had approved as fit for purpose on 22 September 2021). The iterated ToR therefore came into effect on 30 September 2021.
The Board noted the content of the report.
TB 190/21 FINANCE REPORT
The Acting Chief Finance Officer presented the Finance Report that summarised the financial position of the Trust as at the end of August 2021, and appraised the Board of the drivers of the position.

12
The Board noted that the report triangulated with BAF Risk 7 [Failure to deliver the Trust’s annual financial plan for 21/22 caused by a lack of robust cost improvements which may impact the rust’s ability to deliver high quality care] – currently scored at 15. The Board noted that the Trust has a slight overspend at month 5, but expected to breakeven at both H1 and financial year outturns. There remains risk of the financial outturn, driven by ward staffing challenges, increased medic and agency spend, slippage on efficiencies and the requirement to make assumptions about funding in H2 as the guidance from NHSE/I remains outstanding (note: it was issued to the system immediately before the month end but was not available at the date on which the report had been written). The Board noted that high agency spend alone year to date continue to constrain the Trust’s self-assessment of its own Use of Resource performance indicator to a ‘3’ (ie worse) against a plan of ‘2’ and noted that further assurances would be sought at both Committee and Board level. The Board of Directors noted the Trust’s current financial position.
TB 191/21 PROVIDER COLLABORATIVE COMMITTEE CHAIR’S REPORT
The Chair of the Lead Provider Collaborative Committee introduced the report that gave an overview of activity undertaken at their last meeting on 17 September 2021. The Board noted that the work of the Committee and the report triangulated with BAF Risk 6 [Failure to actively collaborate across the system and undertake appropriate due diligence as part of the Lead Provider Collaborative due to a lack of capacity and capability within the organisation which may result in care being provided that is not based on local population needs and may provide poor patient experience] – currently scored at 15. The Committee had been updated on the financial position, risks and mitigations in a paper describing Go Live preparations for the transfer of the two NHSE specialist commissioning programmes transferring into the Lead Provider model, as well as the risks likely to still be unmitigated at that point. ‘Go Live’ decisions for CYP Tier 4 and Adult Secure Mental Illness service effective 1 October 2021 would be further discussed in a private Board meeting later the same day. A decision on the Go Live date for Adult Secure LD & A would be deferred until a greater level of assurance had been provided. The Board of Directors noted the report.
The meeting closed at 2pm.

Agenda Item Number: TB 210/21
TRUST CHAIRS REPORT
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: David Eva, Trust Chair
Prepared by: Umme Batan, Corporate Governance Officer
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will respond to peoples’ needs by striving for the highest STANDARDS of quality across all of our services
Aligned to Board Assurance Framework Risk
4.0 Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care may impact on quality of care and could incur regulatory action
Recommendation/Required Action
The Board of Directors is asked to note the content of
the Trust Chair’s Report.
1.0 NON-EXECUTIVE DIRECTOR ACTIVITY
In line with the organisations response to the Covid pandemic and in line with national
NHSE/I guidance, since April 2020, all essential meetings have been undertaken
virtually via Microsoft Teams. This has included the Trust’s Board of Director meetings.
As a result, all Board, Committee and Council of Governors meetings have been held
virtually via Microsoft Teams and this will continue until further notice. Public members
continue to have the opportunity to attend Part One of all Board of Director meetings.
Non-Executive Directors have continued to support Executive Directors and Governors
in attending weekly Director Engagement Visits. The visits from October – November
2021 took place in person.
Non-Executive Director Paul Farrimond visited the Orchard in October 2021 and was
shown around the service, followed by a meeting with the Bay locality leaders, Dr
Alison Napier, Medical Director and Richard Chillery, Director of Operations. Paul also
deputise for the Trust Chair at the Wesham Engagement & Recruitment Event and met
with the Fylde Coast locality leaders, rehab service managers and staff, HSIS lead
engagement officers, service users and members of the Wesham community.

Agenda Item Number: TB 210/21
Non-Executive Director Shazad Sarwar joined the North West Wellbeing Workshop for
Chairs, Chief Executives, Wellbeing Guardians and Staff Side Chairs event on behalf
of the Trust Chair.
The Trust Chair has continued to attend the fortnightly North West Providers/CCG
Chairs meeting virtually. These meetings are led by Amanda Doyle and the agenda
continues to be focussed mainly on Covid, plans to recover service delivery and the
progress on system (ICB) development. The Chair and Chief Executive of the ICB have
now been announced (David Flory and Kevin Lavery) and the Non-Executive roles are
out to advert (closing date November 21st).
The Chair continues to meet with the Chief Executive on weekly basis, the Deputy
Chair/Senior Independent Director monthly and has started to meet with the Executive
Directors on a bi-monthly basis as well as having bi-monthly meetings with the local
NHS FT Chairs.
The Chair has met with various council leaders/adult social care leads which has been
interesting and hopefully a start to building the relationships that can support work in
the localities.
The Chair joined the judging panel for the Time to Shine Awards and also presented
the Chairs Time to Shine Award during the virtual ceremony. The awards evening was
a great opportunity to thank the award winners and nominees for this amazing work
and to thank staff and volunteers for the way they have responded to the huge
challenges we have faced.
The Deputy Chair has attended various meetings on behalf of the Chair including the
Provider Collaborative Board, Central Lancashire ICP Chairs Forum, Special Adult
Social Care and Health Scrutiny Committee: Mental Health,
The Deputy Chair has also been leading on the Trust Chair Recruitment in consultation
with the Interim Company Secretary.
2.0 COUNCIL OF GOVERNORS
The Council of Governors met formally on 20 October 2021 and on 08 November 2021
for an update from the Chief Executive and Executive Directors. The meetings took
place via Microsoft Teams. The following items were considered during the formal
meeting in October:
Assurance from the CoG sub-committee Chairs report; Nomination
Remuneration Committee, Quality and Assurance Committee and Membership
Engagement Committee
The Council approved the recommendation form the Nomination Remuneration
Committee to re-appoint Non-Executive Director Shazad Sarwar for a second
term of three years office commencing 01 December 2021 to 30 November
2024.
The Council approved the extension of the current Lead Governor and Deputy
Lead Governor roles terms of office for a further three months till 31 March
2022 to retain continuity in the Trust Chair’s appointment process.
The Council approved the Membership and Engagement Strategy.
Agenda Item Number: TB 210/21
The Council approved the extension for the Governor Nominations till 05
November 2021.
The Council approved the appointment process for the Lead Governor.
The Council approved the External auditor’s provision update.
The following updates were provided by the Chief Executive and Executive Directors during
the meeting in November:
Update on the Trust including Covid-19 update from the Chief Executive
Update from the Chief Nurse & Quality Officer on the Service User & Carer
Enabling Strategy
Update from the Chief Integration Officer on the Provider Collaborative
approaches
3.0 GOVERNOR RESIGNATION
The Council of Governors received a resignation from Public Governor Brian Gumbley
(Central Lancashire Constituency) in October 2021, this vacancy was included in the
Governors Elections 2021.
The Council also received a resignation from Public Governor Val Richards (North
Lancs/South Cumbria Constituency) in November 2021. This has resulted in a vacancy
in North Lancs/South Cumbria. This vacancy will be included in the by-election 2021.
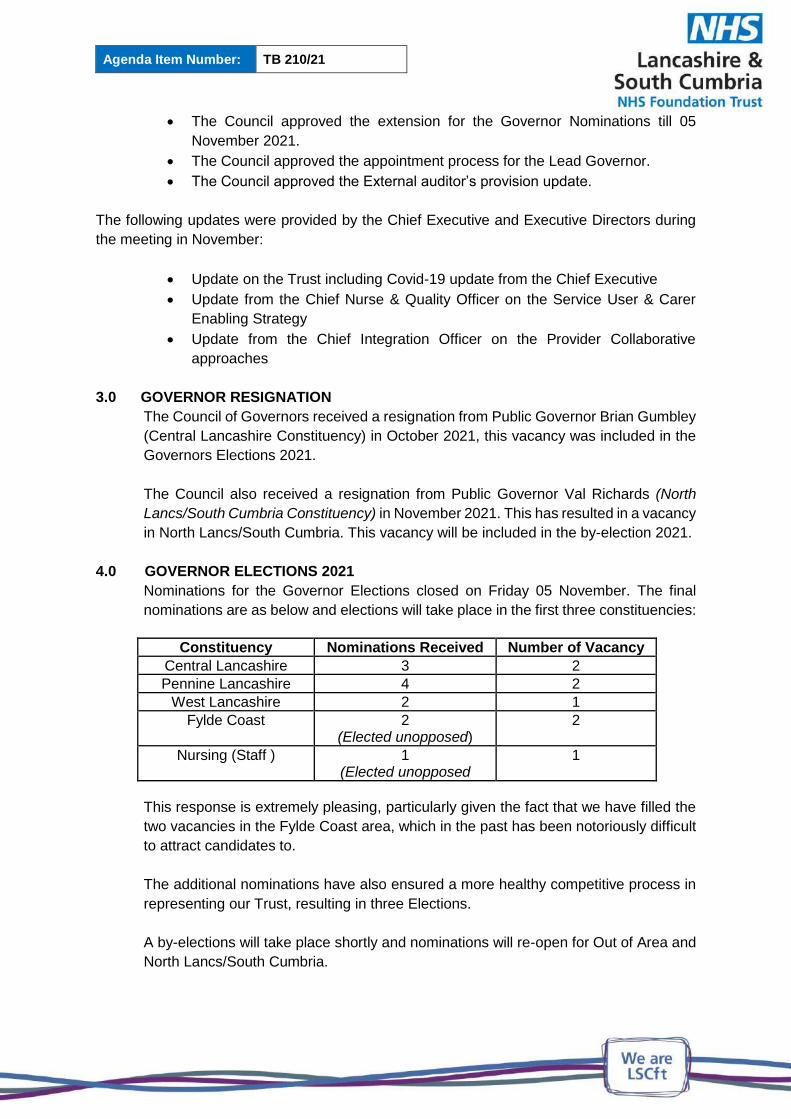
4.0 GOVERNOR ELECTIONS 2021
Nominations for the Governor Elections closed on Friday 05 November. The final
nominations are as below and elections will take place in the first three constituencies:
Constituency Nominations Received Number of Vacancy
Central Lancashire 3 2 Pennine Lancashire 4 2
West Lancashire 2 1 Fylde Coast 2
(Elected unopposed) 2
Nursing (Staff ) 1 (Elected unopposed
1
This response is extremely pleasing, particularly given the fact that we have filled the
two vacancies in the Fylde Coast area, which in the past has been notoriously difficult
to attract candidates to.
The additional nominations have also ensured a more healthy competitive process in
representing our Trust, resulting in three Elections.
A by-elections will take place shortly and nominations will re-open for Out of Area and
North Lancs/South Cumbria.

Agenda Item Number: TB 210/21
5.0 USE OF THE COMMON SEAL
The Board are advised that the Common Seal has been applied as below since the
July 2021 Board of Directors meeting:
Underlease at Barbara Castle Way Health Centre, Blackburn
Contract, Transfer and Legal Charge for sale of Ridge Lea Hospital, Lancaster
6.0 BOARD ACTION
The Board of Directors is asked to note the content of the Trust Chair’s Report.

Agenda Item Number: TB 211/21
CHIEF EXECUTIVE REPORT
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Caroline Donovan, Chief Executive
Prepared by: Alexa Traynor, Director of Communications and Engagement
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will respond to peoples’ needs by striving for the highest STANDARDS of quality across all of our services
Aligned to Board Assurance Framework Risk
4.0 Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care may impact on quality of care and could incur regulatory action
Recommendation/Required Action
Trust Board is requested to note the report.
Introduction
The Trust Strategy 2021 - 2026 was launched in September 2021.The vision and values
outlined in the Trust Strategy are supported by six strategic priorities, which outline key areas
of focus for our Trust. This report provides progress against the six priorities since the last
Board meeting.
1. We will put SERVICE USERS at the heart of all we do, supporting effective care,
recovery and wellbeing
1.1 Demand
Nationally pressure in the NHS is at the highest it’s ever been. Across Lancashire and South
Cumbria we are noting a significant increase across our urgent mental health pathway.
Demand across the Trust’s urgent care services in Q2 2021/22 show a 25% increase on the
level of demand in Q4 2020 (pre-Covid). The Trust continues to work in partnership with
Lancashire Constabulary and NWAS to mitigate the increase Paramedic and Police Calls
being received through the Mental Health Access line. The Access line has experienced a
29% increase in call volume between July and September 2021 compared to the same period
last year.
The Trust is preparing for winter making sure patient ‘flow’ through pathways is maximised,
avoiding attendances to hospital, supporting patients in the least restrictive environment and
safely discharging and supporting service users in communities when an admission cannot
be avoided.
A Winter Silver Command Room has been established which will provide direct management
of operational response to winter pressures, to ensure it is coordinated and integrated with
our partners and to strengthen our response to be as effective as possible.
The ICS has also established a seven day Gold Command room to support the flow across
the region and ensure timely escalation to regional and national bodies.
1.2 Winter Planning
Across all health & social care systems there are early triggers to suggest the NHS and social
care partners are going to face an extremely pressured winter. Nationally and regionally,
covid-19 cases are rising and placing additional pressures across the acute sectors as well as
the on-going impact on workforce.
To support system resilience, winter plans have been driven via the Place Based A&E Delivery
Boards; additional funding has been released to support increasing mental health demand.
Winter plans are being coordinated locally with ICS and regional leads and will ensure that
plans can be implemented at pace to allow for delivery within winter and ensure maximum
impact.
The key focus of the 2021/22 winter plan:
- The health and wellbeing of our workforce is a critical element to the plan and therefore
there will be a significant emphasis on a highly effective flu campaign
- Increasing our clinical and managerial workforce going into winter

- Increasing our weekend clinical offer to ensure 7 day timely access to assessment,
treatment and discharge
- Early decisions to increase the Mental Health Liaison Team will support winter
pressures
- Increasing our well-being support will feature within winter planning
- The Resilience Hub has launched a marketing campaign to promote on-going support
to teams across L&SC through winter
- Managing demand by signposting patients to alternative services where appropriate
- Timely and effective assessment, decision making and treatment.
- Maintaining flow throughout the in-patient units and the out of hospital system,
ensuring that patients who are medically fit for discharge do not stay in hospital
unnecessarily
The Trust is planning to run a “Perfect Week” in January 2022, this will increase clinical and
operational support across the organisation to support with patient flow. This is being led by
the transformation team and will include partnership working with local authority and primary
care colleagues.
1.3 Launch of street triage pilot in South Cumbria
A joint pilot with Cumbria Constabulary for Street Triage in Barrow launched in October, to
make sure that people who need mental health treatment receive it as quickly as possible.
The pilot involves our mental health nurses working alongside the police in Barrow to reduce
the number of detentions made under Section 136 of the Mental Health Act.
When police attend an incident out of hours, and believe that an individual involved has a
mental illness, learning disability or substance misuse problem, they can contact the street
triage team to carry out an immediate assessment.
This determines whether the person should be held under Section 136 of the Mental Health
Act and if not, whether any follow up is needed from mental health, social or substance misuse
services. It means those people who do need care and treatment receive the right services
quickly, and that those who don’t are not unnecessarily detained.
In its launch week, the team successfully helped to prevent five Section 136 suite admissions.
1.4 Covid-19 update
Across the North West, more than 10.2 million vaccines have been administered, which
includes over 5.1 million first doses. The North West case rate is now higher than the national
figure but is increasing less quickly.
Across Lancashire and South Cumbria, case rates have been rising with high pockets of
prevalence in the Ribble Valley, Blackpool and Central Lancashire.
We’re still responding to post Covid lockdown demand increases in both mental health and
community services. We are also starting to experience small outbreaks and increases in staff
Covid absence again.
It remains, and will continue to be, incredibly important to continue to follow the protective
measures learnt over the last year, and encourage our staff, patients, and communities to do
the same to minimise the risk of the rising infection rates
Our Covid vaccination campaign continues running centrally from Ribble House in addition to
a roving service to our sites. Across LSCft the vaccination rates are 82.61% for first dose,
79.43% second dose and 28.57% for the booster (3rd dose). Weekly testing remains in place
and available at all our clinical sites, however compliance is low. Our Flu vaccine uptake is
currently at 34.90%.
The recent Government announcement on the introduction of mandatory Covid-19 vaccination
for all frontline health and social care workers will mean staff need to provide evidence they
have been fully vaccinated against Covid-19 in order to be deployed.
The requirements will come into force in the spring, subject to the passage of the regulations
through Parliament. There will be a 12-week grace period between the regulations being made
and coming into force to allow those who have not yet been vaccinated to have both doses.
Enforcement would begin from 1 April, subject to Parliamentary approval.
1.5 New landmark strategy to improve the lives of autistic people
Improving the lives of autistic people is the focus of a new multi-million pound strategy
launched by the Government. Backed by nearly £75 million in the first year, it aims to speed
up diagnosis and improve support and care for autistic people. The funding includes £40
million through the NHS Long Term Plan to improve capacity in crisis services and support
children with complex needs in inpatient care.
Autistic people face multiple disadvantages throughout their lives, with too many struggling to
get support that is tailored to their needs at an early enough stage and facing stigma and
misunderstanding, often leaving them lonely or isolated. Through this new strategy, steps will
be taken to improve diagnosis, which is crucial to help people get the support they need and
improve society’s understanding of autism. The 5-year strategy was developed following
engagement with autistic people, their family and carers. It will support autistic children and
adults through better access to education, more help to get into work, preventing avoidable
admissions to healthcare settings, and training for prison staff to better support prisoners with
complex needs. The Trust will ensure this landmark national strategy is delivered locally to
improve the lives of people in Lancashire and South Cumbria with Autism.
1.6 Peer Facilitators
The Trust continues to develop its peer support service, to introduce peer facilitators across
the care pathways working in multi-disciplinary teams to bring a lived experience perspective
to colleagues, service user, carers and students.
The peer facilitators provide formalised peer support and practical assistance to help service
users regain control over their lives and their own unique recovery process to achieve a better
quality of life despite mental health difficulties.

The Trust has now recruited over 35 peer facilitators and 3 peer facilitator support worker
supervisors who will support the development, supervision and mentoring of our facilitators
across the Trust.
2. We will employ and retain the best STAFF because our work culture will be
inclusive and a supportive place to work
2.1 Lancashire Resilience Hub promotional campaign
The Lancashire and South Cumbria Resilience Hub was created in response to the pandemic
to help support public sector workers psychologically affected by Covid-19. The Resilience
Hub team is dedicated to supporting those who work in the emergency services, health and
social care, teachers, carers, local authority staff and volunteers as well as their immediate
family members too.
Since its launch at the start of the Covid-19 pandemic, the Resilience Hub has helped people
get back to doing the things they love most. This includes those who have worked on the
frontline of the pandemic, those who struggled with the transition of working from home and
the changing demand of their jobs and sadly, to those who have lost loved ones.
The Trust launched a new marketing campaign in September 2021 urging all public sector
workers in Lancashire and South Cumbria to ‘check in’ on how they’re feeling using the
Resilience Hub self-assessment tool.
During the first month since the marketing campaign the Resilience Hub has seen a
287% increase in referrals. More than 500 people completed the self-screening tool on the
new website and 120 of those went on to refer themselves to the Resilience Hub for the first
time.
2.2 LSCft Time to Shine Awards
The Trust hosted its inaugural ‘Time to Shine’ staff awards in November. This year’s
celebration was an inclusive virtual celebration with awards being sponsored by the Executive
Team and Non-Executive Directors. Almost 500 teams and colleagues from across the Trust
were nominated for the nine different Time to Shine awards in each network – with the winners
from the networks going forward for a chance to win one of 12 Trust wide awards. The winning
and highly commended entries on the night were:
Clinical Team of the Year
Winners:
District Nursing Teams in Central and West
Ribblemere Mother and Baby Unit
Non-Clinical Team of the Year
Winner:
Recovery College and HARRI Bus
Highly Commended:
Fylde: Admin Team - Complex Needs Nursing Services
Central and West: Medical Secretaries based at Charnley Fold
Outstanding Contribution to Service User and Carer Experience
Winner:
Recovery Riders
Highly Commended:
Corporate: Lesley Whittaker - Enhancing Experience Matron
Pennine: Lisa Harrison – Activities co-ordinator for Health And Wellbeing Team
Outstanding Contribution to Quality and Patient Safety
Winner:
Complex Packages of Care Team (CPoC)
Highly Commended:
Corporate: Infection Prevention Control Team
Central and West: Central and West PICU Teams – Lathom Ward and Avenham Ward
Outstanding Contribution to Service Improvement
Winner:
Blackburn with Darwen Pulmonary Rehabilitation Team
Highly Commended:
Fylde: Fylde Coast Rapid Intervention and Treatment Team (RITT)
Outstanding Contribution to Education and Research
Winner:
Dr Miranda Budd & the Primary Care TAPP Team
Highly Commended:
Corporate: The tissue Viability and the Research and Development Team
Specialist: Louise Hamer – Senior Nurse - Youth Endowment Fund
Outstanding Contribution to Partnership Working
Winner:
Frequent Attenders Team Lancaster and Morecambe
Highly Commended:
Pennine: Blackburn with Darwen Integrated Neighbourhood Team
Central and West: The Central Allocation Team for Care and Health (CATCH)
Outstanding Contribution to Inclusion and Inequalities
Winner:
Shorelands Older Adults Community Mental Health Team
Highly Commended:
Corporate: Equality, Diversity and Inclusion Team
Pennine: Covid Vaccination Team (Disability Team)
Outstanding Contribution to Valuing our Workforce
Winner:
Jo Harrison – Equality, Diversity and Inclusivity Team
Highly Commended:
Fylde: Michelle White - Blackpool Community Mental Health Team
Pennine: Dr Rachel Domone – Consultant Clinical Neuropsychologist
People Choice Award
Winner:
The Lancashire and South Cumbria Resilience Hub
Chief Executive’s Award
Winner:
Sam Tyrer - Prevention and Engagement Lead
Chair’s Award
Winner:
Lorraine Khalaf - Service Manager for the Mental Health Crisis Line and the Wellbeing
Helpline and Texting Service
2.3 Awards
The Trust’s Associate Director of Safeguarding, Bridgett Welch, recently received a
prestigious national NHS Safeguarding Award personally presented to her by Catherine
Randall, Associate Director of Safeguarding at NHSE/I.
Bridgett received the award for her outstanding leadership, personalised care, trauma
informed practice and making a difference to her patients, colleagues and the population.
The Byron Ward, at the Harbour, were also awarded a National safeguarding star award for
Person Centred Care. A great achievement that we will look to understand best practice from
and embed across our inpatient wards.
Paul Jebb, Associate Chief Nurse, Patient Experience, Engagement & Safeguarding, has also
been awarded The Patient Experience Professional of the year award.
2.4 HSJ awards

The Trust is proud to have been shortlisted for two HSJ Awards at this year’s ceremony which
took place on November 18th. The shortlisted entries were for:
Mental Health Innovation for Advice and Guidance
Staff Engagement for Inspiring Culture Change through Inclusive Engagement
Unfortunately, the Trust did not win an award this year, however, the shortlisted nominations
are the result of a lot of hard work and it’s incredibly positive that our commitment to
improvement and our work to generate a truly inclusive culture, that puts service users at the
heart of everything we do, has been recognised by the HSJ.
2.5 Medical Awards
A number of our Doctors have been shortlisted for this year’s Regional North West RCPsych
awards. The virtual awards ceremony is on the 25th November, the nominations include:
Dr Ben Cross – Foundation Year Doctor of the Year
Dr Shon Chattopadhyay – Core Trainee of the Year
Dr Will Davis – Higher Trainer of the Year
Dr Chris Linton – Trainer of the Year
Dr Marisa Wray – Trainer of the Year
2.6 Equality, Diversity and Inclusion Award
Max Oosman, An LSCft Community Mental Health Practitioner with 49 years’ experience
within the NHS, has won a top award from the Royal College of Nursing (RCN).
Max was named the RCN’s North West Veteran Award for Outstanding Contribution to
Equality, Diversity and Inclusion at a recent virtual celebration event.
The award is for individuals that have provided long service to the health and social care
community, overcome significant inclusivity barriers, and championed positive outcomes for
equality, diversity and inclusion.
2.7 Education
We continue to invest in developing our staff to ensure that we have a strong culture of
development and learning. It is a great achievement that, in addition to the current 15 Trainee
Advanced Clinical Practitioners (ACPs), a further 8 Trainee ACPs have recently commenced
their MSc in Advanced Clinical Practice. Furthermore, we have 23 Registered Nursing
Associates undertaking the pre-registration nurse degree apprenticeship to ‘top-up’ to
Registered Nurses.
3. We will delivery SAFE care and we will embrace an open and learning culture,
ensuring we continually improve
3.1 Liaison and Diversion win Positive Practice Award
The Lancashire and Cumbria Liaison and Diversion team have won an award as part of the
positive practice in mental health collaborative.
The Seni Lewis Award recognises partnership working between healthcare and the police.
The award is named after Olaseni Lewis, a young man who sadly died following a police
restraint in 2010.
“Seni's Law” was passed into British law in November 2018 and introduced changes to limit
the use of force on mental health patients.
The Liaison and Diversion team were nominated for the work they do to ensure people with
vulnerabilities have access to the best support at each point of the Criminal Justice Pathway.
3.2 Quality Improvement Fellowship
The Trust has appointed 8 staff to the role of Improvement Fellow, following recent interviews
as part of cohort 1. The staff appointed come from a range of professions and networks and
will take part in an induction day for the Fellows planned in December where they will meet
each other and start to connect with the Continuous Improvement and Patient Safety agendas,
both of which are key to their role.
The programme begins in January with Lancaster University modules in Improvement Science
commencing and the Advance Mindset diagnostic with Matthew Syed Consulting. This will
provide our Fellows with unique insights into where their developmental areas lie and their
focus can be on applying their learning to these areas to overall strengthen their improvement
approach and practise. There are 4 places remaining for cohort 1 and an interview process
has been established to ensure LSCFT take the full complement of staff onto the fellowship
programme this year.
3.3 National Apprenticeship Awards 2021
The Trust has also been successful in getting to the regional final category ‘Apprentice
Employer of the Year’. We are also delighted to have a number of apprentices who have been
selected to go through to the regional final of the National Apprenticeship awards this year.
Apprentice of the Year
Andrew Corns – Business administration apprentice
Abdulhai Dawood – Customer Care Apprentice
Rising Star
Abbie Greenwood
Kyle Lingham
3.4 Ward Accreditation
The Trust has developed a Ward Accreditation scheme for all Trust inpatient wards. The
internal visiting team consists of a peer network Director of Nursing, Head of Nursing and
Professional Practice, Expert by Experience and Peer Matron. All Adult inpatient wards will
receive an initial ward accreditation visit by the end of December 2021. So far there have been
2 gold awards (Duxbury and Worden) and 2 silver awards (Avenham and Ramsey). In early
2022, we will be scheduling visits to Children and Young People ward at the Cove and the
Trust’s Secure Mental Health Services at Guild Lodge.
3.5 Listening into Action
Work is progressing across the 10 wave 2 LiA programmes, which are as follows
1. Flexible Working
2. Admin &Clerical
3. Trusted Triage, Assessment and Transfer
4. Digital skills
5. Safer-Red to Green
6. Dual Diagnosis
7. Just Culture
8. Care Co-ordination
9. Person Centred Care
10. Recruitment
In addition this cohort sees the introduction of the Inspiring Change programme and the Trust
are an early adopter of this programme. The Inspiring Change programme consists of two
elements which focus on Staff Health and Wellbeing. Three Leadership behaviours and 5
Courageous Changes have been agreed within the Trust, following a staff engagement
exercise in July 2021. The leadership behaviours are practiced and embedded into day to
day working by 100 change leaders in the Trust, supported by 10 Change Navigators, who
are coached and supported to help take this forward. With regard to courageous changes for
staff health and wellbeing, work has commenced on flexible and agile working, health and
wellbeing facilities for staff and development of a campaign with some health and wellbeing
pledges and practices to be adopted across the Trust.
LiA groups Midway Check in took place on 15 November to hear an update of all LiA work and
progress to date. It was a successful event attended with over 120 staff and received very
positive feedback. The Pass it on event, which is the event at the end of the twenty week
improvement cycle, has been scheduled for 25 February 2022.
4. We will respond to people’s needs by striving for the highest STANDARDS of quality,
proactively reducing health inequalities
4.1 Lancashire and South Cumbria Health Equity Commission
Lancashire and South Cumbria is set to have its own Health Equity Commission (HEC),
chaired by international expert in health equity, Professor Sir Michael Marmot.
This follows an agreement by Health and Community Leaders to form a regional Lancashire
and Cumbria HEC to improve health inequalities and help transform the health and wellbeing
of people living in the region.
With Professor Sir Michael Marmot as the Chair, the HEC will consist of regional health,
community, business and public sector leaders and influencers, as well as independent
experts. The Commission will aim to provide local leaders, organisations and partnerships with
the support they need to make health inequalities and the ‘prevention agenda’ a joint priority
and provide a loud and clear voice in the region. The initial scope of the HEC is to influence
all partners to mobilise health and care to reduce health inequalities and its role in the
economy.
As part of the development of the HEC the Trust hosted a workshop, facilitated by the HEC,
to explore the relationship between mental health, learning disability and autism and health
inequalities to inform the new HEC strategic plan. The workshop was very well attended by
colleagues from local authority, criminal justice, Department of Work and Pensions and
representatives from the VCFSE sectors. The session provided a rich conversation
considering all aspects of mental health, learning disability and autism and health inequalities.
We look forward to furthering the development of this important work in the coming months as
the HEC establishes and we drive forward our approach to population health management.
In the same week, the Trust was pleased to welcome Sir Michael Marmot as guest speaker to
our November staff “Engage” session to hear about the how Sir Michael’s health inequalities
strategy directly links to the progressive work we are doing here at the Trust. This highly
engaging session as followed by a discussion on how our Trust Inequalities Strategy will
maximise our opportunities for integration, population health planning and provision of care
closer to home to deliver better, more equitable care for our service users.
4.2 Black History Month
Throughout October, our Race Equality Network held a number of events in recognition of
Black History Month. The Trust programme included external and internal experts addressing
topics such as equality, diversity and inclusion, health and wellbeing, and celebrating culture
and development.
The Trust continues to take positive and proactive action to address equality, diversity and
inclusion across our organisation, focusing on programmes of work to improve opportunities
for career progression, remove discrimination and build cultural competence, capability and
confidence across the Trust.
As such we are delighted to continue our work around equality and inclusion with the second
stage of the Yvonne Coghill review beginning shortly.
The review will see Yvonne working with service users, carers and communities to examine
health inequalities in relation to race and barriers to service access.
5. In order to support our local communities by excelling at everything we do together,
we will always collaborate with our SYSTEM partners
5.1 New Chief Executive Designate of the NHS Lancashire and South Cumbria
Integrated Care Board
Kevin Lavery has been appointed by NHS England and NHS Improvement as the new Chief
Executive of the Lancashire and South Cumbria Integrated Care Board.
He is an experienced CEO with public and private sector experience in the UK and overseas
and is currently a Director of Tuhura and Partners in New Zealand.
This appointment is a significant step in the development of the Integrated Care System in
Lancashire and South Cumbria to improve care for the people of Lancashire and South
Cumbria.
5.2 H2 Plan
The Trust has submitted a balanced financial plan for the second half of the year as part of
Lancashire and South Cumbria’s Integrated Care System’s wider plans.
5.3 Initial Response Service (IRS)
The IRS will start in Pennine Lancashire in January 2022. When IRS commences, we will
gradually start diverting referrals from our START team in Pennine Lancashire to a single team
based in The Mount in Accrington.
The new IRS team will triage each referral and make contact with the referrer to let them know
the outcome. The change will be made gradually to allow a smooth transition in to this new
way of accessing mental health services.
We are on track to go live with our IRS model for the Central Lancashire and West Lancashire
Service in February 2022 .This will be based at our Avondale Unit on the Royal Preston
Hospital Site.
5.4 Lead Provider Collaborative
LSCft is working as the Lead Provider for two Specialist Mental Health Lead Provider
Collaboratives (LPC) across Lancashire and South Cumbria; Children and Young People Tier
4 Mental Illness, Eating Disorder and Learning Disabilities Services (CYP), and Adult Low and
Medium Secure Specialist Services (AS).
The CYP service successfully transferred from NHSE/I with delegated commissioning
responsibility passed to LSCft on 1 October 2021 and adult secure services on 1 November.
The LPC Team would like to thank colleagues who have supported the Trust reach this
position, which now provides a significant opportunity for the Trust to commission, plan and
deliver services that can further improve the lives and outcomes of our local communities.
6. We will provide SUSTAINABLE services that are delivered in an effective and
efficient way, at the time people need it.
6.1 Community Mental Health Services Transformation
Mental health services that are available in the community to support people with severe
mental illness are improving. As part of the NHS Long Term Plan and learning from patients,
carers, staff and stakeholders and experiences through Covid, we have ambitious plans to
transform community mental health services for adults and older adults across Lancashire and
South Cumbria.
Within each ICP, monthly stakeholder partnership meetings have now been set up as delivery
vehicles for the transformation.
6.2 Expansion of our inpatient provision

The Trust has agreed with Mersey Care NHS Foundation Trust (MCFT) to lease of part of its
site at Whalley. This has been a centre for people with learning disabilities for many years, but
we plan to develop its function to provide adult mental health services, including a new
PICU. This will allow us to add much needed capacity to our estate, benefiting service users
across Lancashire and South Cumbria.
Work to refurbish the part of the site known as Woodview will begin in the next few weeks,
and is expected to be completed in about a year. Both Trusts are committed to continuing to
have service users, carers and the local community at the heart of all we do, to deliver the
highest quality of care and support.
As soon as we can, we will set out what this means for the rest of the site. Any wider plans
will subject to business cases and agreements by our two Trusts’ Boards, which will come no
earlier than February 2022.
The Trust is also continuing to at pace with the development of Wesham Rehabilitation Unit.
The Trust recently held a community engagement and recruitment event at Ribby Hall to
introduce the upcoming Wesham Rehabilitation Centre, which saw great attendance from the
local residents and applicants.
The event, which presented an opportunity for the people of Wesham to talk to clinical leads
and service managers, also saw all advertised roles appointed over the course of the day from
health care assistants, to registered mental health nurse, OT clinical specialist and deputy
team leaders.

Agenda Item Number: TB 212/21
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Maria Nelligan, Chief Nurse and Quality Officer (DIPC)
Prepared by:
Maria Nelligan, Chief Nurse and Quality Officer (DIPC)
Paul Jebb, Associate Chief Nurse, Patient Experience and Engagement
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will put SERVICE USERS at the heart of everything we do, supporting effective care, recovery and wellbeing.
Aligned to Board Assurance Framework Risk
4.0 Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care may impact on quality of care and could incur regulatory action
Recommendation/Required Action
Trust Board is requested to note the report For discussion/approval.
Version Control:
Version Report to Date Reported
V2 Maria Nelligan, Chief Nurse and Quality Officer
18/11/21
1. Introduction As part of the Trust drive to meet the strategic priority relating to ‘We will put SERVICE USERS at the heart of everything we do, supporting effective care, recovery and wellbeing’. Work was undertaken at the beginning of 2020 to co-design a person centred framework. Five sessions were held to engage with service users, carers and staff in the development of the framework, these focus groups were facilitated by Tommy Whitelaw a well know speaker and advocate of person centred care. Person centred relates to how we engage with each other, service users, carers and staff. Tommy also attended Trust Engage in February 2021 to capture wider views, which enabled a discussion with Teams around the concept of person centeredness including:
What matters to you?
Who maters to you?
PERSON CENTRED CARE FRAMEWORK
Agenda Item Number: TB 212/21
Following these groups, co-production work was undertake with the service user and carer council and different staff groups to develop the framework. The agree framework can be found in appendix 1. 2. Listening Into Action In autumn 2021 a LiA programme around person centred care was also launched. The LiA was led by Lesley Davison, and supported by a triumvirate of staff to enable the work to be taken forward. The work programmes for the LiA were;
Exploring and piloting Dialog as a tool to develop care plans in partnership with the patient
Development of a drama to provide education around person centeredness
Develop a campaign around understanding language and #DropTheJargon
Development and approval of a Person Centred Framework and development of an intranet site to share tools to support the delivery of person centred care.
The LiA will be reported on via the LiA reporting process after the 20 week cycle.
One Page Profiles The aim of a one-page profile is to give a brief overview about a person, outlining what others love about them, what they love doing, who they love being with, and how they like others to help them. You will see some of these out with in teams. One-page profiles are not designed to convey detail, but to give an enticing and positive flavour of personality, strengths and aspirations. A one-page profile provides information to use as a starting point for discussions about a person and their life. One-page profiles are a great person-centred involvement technique; their simplicity belies their potential for radically transforming negative views about people. The positivity shining out from an effective one-page profile serves to give the sense of a person being fully human. A one-page profile is one way of helping us to see beyond the person’s illness. We will be rolling these out across the Trust and encouraging staff and patients to complete them and display them on the room door, or for staff, in a communal area for others to read and know about the person. We are asking the Trust board to complete the one page profile (appendix 2) and share these across the organisation and on social media which will support the roll out across corporate and network teams. 3. Recommendations
The Board is asked to note the work completed in collaboration with service users and staff and approve the Person Centred Care Framework.

Agenda Item Number: TB 212/21
Appendix 1 Person Centred Framework
Agenda Item Number: TB 212/21

Agenda Item Number: TB 212/21
Appendix 2
Getting to know me PDF file
Getting to Know
Me- 1 page profile - blue.docx

Agenda Item Number: TB 213/21
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Maria Nelligan, Chief Nurse and Quality Officer (DIPC)
Prepared by: Paul Jebb, Associate Chief Nurse, Patient Experience and Engagement
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will respond to peoples’ needs by striving for the highest STANDARDS of quality across all of our services
Aligned to Board Assurance Framework Risk
1.0 Failure to engage effectively with service users and carers caused by a lack of meaningful service user and carer engagement and collaboration within the organisation, may impact on the Trust’s ability to provide high level quality care
Recommendation/Required Action
To update the Board of Directors on the work of the
Experience and Engagement Teams as well as the
Recovery College and Prevention Lead.
EXECUTIVE SUMMARY
To update the Board of Directors of the work undertaken by the Patient Experience and Engagement Team.
Introduction and background
This report has been developed to provide an overview to the Board of Directors of the work of the Experience and Engagement Team as well as the Service User and Carer Council, the Lancashire Recovery College and the Trust Prevention Lead.
Key Activities
Recruitment and Development of Trust and Network Service User and Carer Councils
Carer engagement and challenges relating to implementing Triangle of Care across community services
Success in the wider engagement of HARRI in communities
Continued growth of Recovery College access to carers, staff involvement and development of Minerva Centre hub
Continued development of FFT upgrade and text pilot
EXPERIENCE AND ENGAGEMENT REPORT Q2
(JULY - SEPTEMBER 2021)
EXPERIENCE AND ENGAGEMENT REPORT Q2
(JULY - SEPTEMBER 2021)
Agenda Item Number: TB 213/21
Local survey calendar and ongoing uploading to the new ENVOY database for FFT.
Escalation of risk
Growing partnership with Lancashire Volunteer Partnership (LVP) in relation to volunteer support and recruitment
Recruitment of Peer Facilitators and ongoing recruitment of Peer Supervisors.
Conclusion and Recommendations
The Board is asked to note the paper and the ongoing work to enhance experience and engagement across the Trust.
Agenda Item Number: TB 214/21
QUALITY AND ASSURANCE COMMITTEE CHAIRS REPORT
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Paul Farrimond, Committee Chair
Prepared by: Marion Fountain, Executive PA
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will respond to peoples’ needs by striving for the highest STANDARDS of quality across all of our services
Aligned to Board Assurance Framework Risk
3.0 Failure to learn and improve as an organisation underpinned by ineffective systems and a lack of an open and transparent culture, may impact on delivering safe care
Recommendation/Required Action
The Board of Directors are asked to note the
assurance and escalation provided within the Quality
and Assurance Committee chairs report.
1.0 INTRODUCTION
The Board of Directors are presented with the Chair’s Report of the Quality and
Assurance Committee held on 20th October 2021. The Chair’s report provides an
overview of assurance received and escalation to discussions held, as required.
2.0 RECOMMENDATION
The Board of Directors are asked to:
note the assurance and escalation provided within the Chair’s report.

Chair’s Report
MEETING: Quality and Assurance Committee DATE OF MEETING: 20/10/2021 CHAIR OF MEETING: Paul Farrimond
ITEMS APPROVED
There were no items for approval.
ASSURANCE RECEIVED
Deep Dive – Pennine The Committee welcomed the comprehensive deep dive in April 2021 highlighting the current position within the network and the improvements made since the triumvirate formed in April 2021. Recruitment is a challenge, however, the Home Treatment Team, which have carried a number of vacancies over the past 12 months currently now only have one vacancy and the IRS have 7 vacancies – they have recruited in excess of 50 staff. There remains recruitment challenges around medical staff in some specialities and agency locum consultants continue to be used. The Committee were advised of the completion of Sir Tom’s room at Pendleview, the new 24/7 Freephone Crisis line which was formed at the start of COVID, the Mental Health Wellbeing Line which is available from 7 until 11pm each night and weekends and supported by volunteers, the new street triage service which will be implemented from December 21 in collaboration with the Police and the Rapid Assessment Team, which will operate from 8 am until 8 pm, 7 days a week. The Committee also learned that the Oxygen team and COPD team won a joint HSJ award for their partnership working with East Lancashire Hospitals around COVID. The Committee were also made aware of the increasing demand on the services, particularly in relation to the assessment wards, the model of which is currently under review in the Trust. The numbers of unallocated cases for care co-ordinators are reducing and a weekly working group has been formed. Serious Incidents (SI) and Inquests Monthly Report The Committee were advised that there are currently 49 SIs open and under investigation with 25 being reported during August and September 2021. Incidents resulting in apparent/actual/suspected self-inflicted harm meeting SI criteria continue to account for the highest number of StEIS reported SI incidents – 15 out of 25. There have been no new homicide incidents reported and no Duty of Candour issues. The Committee heard that work is ongoing to improve both the quality and quantity of incident reporting. The team are currently identifying themes around incident reporting within each network to understand why some areas are higher reporters of incidents of harm than others. The Trust is undertaking a thematic analysis of the SIs to help plan for the introduction of the new national patient safety strategy from April 2022.

Chair’s Report
There continues to be a high volume of Inquests - there are currently 175 open cases, with 43 to be heard between October and December 2021. The staff continue to be supported. Quarter 1 Infection Prevention and Control (IPC) Report The Committee received the Quarter 1 Infection Prevention and Control report which highlighted that the flu annual campaign is ongoing together with the COVID booster. It was confirmed that the Trust are promoting LAMP testing. Annual Infection Prevention and Control Report The Committee were provided with an overview of the arrangements currently in place with reporting mechanisms, governance arrangements, Estates work and wider safety issues including the completed workplan for the team for the previous year and the scheduled workplan for this current year. In relation to the PLACE assessments, particularly in relation to the food, the Committee heard that work is ongoing in relation to improving these scores and additional investment of £125,000 has been allocated to catering. Experience and Engagement Report Quarter 1 2021 The Committee were informed of the wide range of work undertaken across the Trust. They were advised that the Trust’s Service Users’ and Carers’ Council has been established and there has been engaging activity across a whole range of different groups. The Committee heard that the Trust is part of the Health Education England’s Trailblazer programme as well as being part of the Observe and Act initiative, which is being developed by Shropshire Community Health Trust and NHSE. The purpose of this is to look at the total experience of a service from the service user/carer perspective, learn from it, share good practice and make improvements. The Committee also heard that there is a new Friends and Family provider – Envoy. Medicines Optimisation and Controlled Drugs Annual Reports The Committee received these two reports, hearing of the highlights over the previous year and the main challenges going forward. The highlights from the Medicines Optimisation Annual Report included the continuation of delivery of patient safety activity throughout COVID; 15 areas of the three year medicines optimisation strategy have made progress; successful vaccination of inpatients, homeless and travellers; funding approved for the introduction of clozapine one-stop clinics; rapid tranquilisation compliance has improved; the number of medication incidents has decreased as has the severe harm incidents with 3 occurring (this is the lowest reported within the past 4 years); 64 new or updated procedures were approved
Chair’s Report
and 15 new Patient Group Directions; an annual medication safety plan was approved and progressed; training resources were developed to deliver effective symptom control for the dying; engagement at ICS level to progress changes; implementation of the automated and remote fridge temperature monitoring; My Perfect Ward app purchased and also purchased AdIOS software to strengthen assurance around controlled drug prescribing. There was a discussion around the roll out of the electronic prescribing programme, and EPMA specifically, in relation to timescales and integration with the Mental Health Law auditing (T2/T3 monitoring and oversight). The Committee heard the main challenges going forward were maintaining and enhancing staff wellbeing, developing and sustaining a workforce to meet an increasing demand, impact on pressures felt in other professional designations eg nurses and medics, shared care and physical health monitoring. The Committee were informed that following the Never Event and the use of the wrong syringe for administering insulin, the Trust is moving away from using syringes and are using pen devices. In relation to the Controlled Drugs Annual Report, the Committee were advised that the Trust have a good reporting culture and the number of controlled drug instances was the lowest ever reported in the last 3 years. Of the 243 incidents recorded, zero met the NHSE/I criteria for catastrophic or severe category of harm, 26 were classed as moderate risk and 25 were high risk – this is the highest number of high risk incidents in the past 3 years. 18 of the 25 high risk incidents were administration errors – all required additional monitoring but there was no evidence of harm caused. The top 3 categories were suspected or actual illicit drug misuse, administration errors (this is the first time administration errors have been in the top 3 since the 2018/19 annual report) and record keeping. The Committee heard that e-learning training is above 80% compliance and some face to face training has resumed and the Controlled Drug Procedure has been updated. They also heard that guidelines are being improved within the organisation around opiates and community nursing teams working collaboratively providing training and supporting end of life medications.
ITEMS TO ESCALATE TO THE BOARD
ITEMS FOR ESCALATION MITIGATING ACTION
Oversight and assurance of ECT at the Committee – this was raised at the meeting as this is a potential gap in assurance monitoring.
To be addressed going forward with an assurance report being planned for a future meeting form the clinical lead in the Trust.

Chair’s Report
ITEMS TO ESCALATE TO THE BOARD
ITEMS FOR ESCALATION MITIGATING ACTION
Learning framework – further assurance required at Committee regarding how learning from Serious Incidents is being embedded in the Trust. Updated Terms of Reference The Committee was reminded that the request for two Non-Executive Directors to be present for quoracy was made when there were three Non-Executive Directors as members. There is now only two Non-Executive Directors. Health & Safety Sub Committee- discussion regarding door top alarm work being undertaken cross the Trust as part of the capital plan and the lead in time for work due to suppliers. SIRO/Caldicott Guardian Terms of Reference The Committee confirmed that amendments were required to these as the Chief Finance Officer will now be the Executive Director responsible for this Group.
A clinical audit and internal audit planned, which will be received by the Committee. The quoracy should be amended or another Non-Executive Director should join the membership of this Committee. Ongoing delivery of works and monitoring via Health & Safety Committee aligned to the risk priorities.
ITEMS RECEIVED FOR INFORMATION
The following reports were received for information: Update on Community Rehab Pathways for Community and Inpatients The Committee received this report following the NICHE review around the bed base and heard that 94 rehabilitation beds had been identified throughout the last year. They were informed of the Getting It Right First Time (GIRFT) review and the recommendations following this review. Quality Dashboard The Committee received an update on the Trust Performance report for the month of August 2021. The number of incidents continues to show a downward trend and a Just Culture campaign is planned around monitoring and reporting of all incidents. The incidents of harm continue to remain below the target of 3% and physical violence with harm remains at zero. There has been a positive impact from Reducing Restrictive Practice work and work continues on specific wards.

Chair’s Report
The Committee heard that there were two medication cases with harm – this is being investigation but there is no trend. There has been an increase in falls and 2 have occurred with harm. The Committee also heard that 7 RIDDOR incidents were reported – 4 of these relate to one ward. There has been a positive improvement in rapid tranquilisation. In relation to protected characteristics, the Committee were advised that work is progressing but some issues have been identified around data completeness – once these are rectified, these will be reported into this dashboard. Update on Verita Action Plan The Committee were advised of the work which had commenced on this Action Plan, which is discussed at the Mental Health Law Sub-Committee. An advert to recruit more Associate Hospital Managers is ongoing and plans to update their contract and handbook and work on their Training Needs Analyses and appraisal process is underway. Plan for Establishing New Clinical Pathways The Committee were informed that a new Clinical Strategy has been approved by the Board, a new Clinical Senate has been formed to provide greater clinical engagement, Clinical Pathway Lead roles are currently being advertised with interviews taking place at the end of November 2021, there is a system leadership approach to align the various aspects of clinical leadership with service delivery and development and revised Best Practice Groups have been established (11 or 12 currently) and are being reviewed – the Chair noted that Eating Disorders is not included and the Chief Medical Officer confirmed that this would be included. . Chair’s Reports from: Complaints Assurance Group Health and Safety Sub-Committee Safeguarding Sub-Committee Patient Safety and Effectiveness Sub-Committee Infection Prevention and Control Sub-Committee Patient Experience Sub-Committee Research and Development Sub-Committee The monthly safer staffing and annual safer staffing reports were included within the pack for information – these reports had already been presented to the Board of Directors on 30th September 2021.
Agenda Item Number: TB 215/21
COVID-19 UPDATE
Report provided for: Report to: Board of Directors
Information ☒ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Chris Oliver, Chief Operating Officer / Deputy CEO
Prepared by: Chris Oliver, Chief Operating Officer / Deputy CEO
Emma McGuigan, Deputy Chief Operating Officer
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will deliver SAFE care by embracing an open and learning culture, ensuring we continually improve
Aligned to Board Assurance Framework Risk
5.0 Failure to respond effectively following the Covid-19 pandemic, due to ineffective recovery planning and the availability of appropriate resources to meet demand which may impact on the quality and wellbeing of service users
Recommendation/Required Action
The Trust Board is asked to note the Covid-19 update
report
EXECUTIVE SUMMARY
This report provides the Board with an update of the current work programme underway by
the Trust in responding to the Covid-19 pandemic.
Introduction and background
The Trust has a duty of care to both its workforce and patients / service users as part of the
national response to the covid 19 pandemic. This paper will provide the Board of Directors
with an update on the current position regarding transmission within the Trust from a patient
and staff perspective, as well as updating on the vaccination role out and ongoing
asymptomatic testing programme.
Key Issues
Patient Transmission – There were no outbreaks across the wards in Lancashire and South
Cumbria throughout September and there was one ward outbreak in October. This is a great
achievement as throughout this period the incidence of covid transmission in the community
has been increasing. Across the contracted out of area bed base there have bene a
significantly higher number of outbreaks, which have contributed to reduced bed availability
overall. . It is very pleasing to see the Trust Infection Prevention and Control (IPC) measures

Agenda Item Number: TB 215/21
working to reduce the number of patient to patient transmission. On the sites which had wards
declared as an outbreak there have been no evidence of ward to ward transmission, further
evidencing teams adhering to the IPC guidance. The Trust continues to promote inpatient
testing across all our wards and retesting for our patients after any period of leave. Where
there are no covid outbreaks, we continue to support visiting across our inpatient units. This
is managed in a coordinated way to ensure we maintain the safety of our patients and staff
whilst also encouraging visiting to support with well-being and social support.
Staff Transmission – In the last Board report I updated that staff absence through June was
increasing and this continued into July with just over 100 staff being absent from work due to
covid. The level of absence as we moved into August reduced slightly to c. 75 staff and has
remained relatively static with 78 staff absent due to covid, with 40 of those staff currently
testing positive. Since August 2021 national guidance has enabled all non-household
contacts to return to work where the individual has been doubly vaccinated.
Trust Vaccination – The Trusts vaccination programme continues to be delivered with 80.36%
of staff vaccinated, and 71.36% of our BAME colleagues. The Trust continues to vaccinate
all inpatients (within Trust or private provider units) within the agreed JCVI cohorts and is
supporting the ICS with the wider vaccination of Health Inclusion Groups (HIG) this includes;
Homeless population
LD community & Inpatients
Private MH Inpatient providers
GRT Communities
The Trust has commenced the covid booster campaign in October 2021 and have been
running clinics at Ribble house as well attending the main staff sites to improve uptake.
Mandatory vaccine status for NHS staff
The Department of Health and Social Care have recently updated that the covid vaccine will
become mandatory in spring 2022. Further detailed guidance is expected throughout the
coming weeks. The Trust is currently reviewing the vaccine uptake across all our clinical
services and undertaking a detailed data cleanse.
We have been working with our E&I team and our inclusion council to raise awareness
regarding the benefits of the covid-19 vaccine. Our staff networks are supporting this. We are
planning additional Trust wide communication across winter to promote access to the vaccine.
At our monthly Engage sessions, the Chief Operating Officer/ Deputy Chief Executive discuss
with our staff teams about the importance and access to the covid vaccine and booster.
Asymptomatic Testing – The Trust has commenced the rollout of LAMP testing (loop mediated
isothermal amplification). LAMP testing will compliment LFT testing and has more benefits to
both staff and the Trust due to the fact that staff only have to test weekly with a small saliva
sample. Staff do not need to self-report any results as the reporting is via an electronic
dashboard and the access to drop off points for samples increases on a weekly basis across
the ICS. Over 1,000 staff have registered for the weekly LAMP testing. Our Chief Nurse and
Agenda Item Number: TB 215/21
Chief Medical Officer have supported the Trust-wide comms campaign to encourage our
clinical staff to register for LAMP testing. We have rolled out LAMP testing to all our inpatient
facilities and larger community teams and LAMP testing is available to all our staff. The
collection points have been increased to ensure availability and timely results. For corporate
staff and / or staff working from home Lateral Flow testing is available via the government
website. All staff continue to have access to supplies of Lateral Flow testing until they have
transitioned onto LAMP.
Vaccination status for care home - From the 11th November 2021 all staff that work in or who
are required to attend or visit a care home will be required to provide evidence that they have
received both doses of the COVID vaccination or that they are medically exempt from the
vaccination. The Trust have reviewed their community teams and the risk to service disruption
remains low. The Trust has completed a data cleanse of the information for our community
teams to provide assurance that services will be able to be maintained throughout the winter.
Escalation of risk
The impact on staffing with increasing community transmissions, self-isolation and contract
tracing remains our most significant challenge over the winter months.
Conclusion and Recommendations
The Board is asked to note the information provided within this report.
Agenda Item Number: TB 216/21
MONTHLY SAFER STAFFING REPORT AUGUST – SEPTEMBER 2021
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Maria Nelligan, Chief Nurse & Quality Officer (DIPC)
Prepared by:
Julie Anne Murray, Deputy Chief Nurse and Quality Officer
Shamine Hall, Nursing & Quality Matron (Safer Staffing)
Andrew Hodgson, Workforce Systems Performance Manager
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will deliver SAFE care by embracing an open and learning culture, ensuring we continually improve
Aligned to Board Assurance Framework Risk
2.0 Failure to recruit, develop and retain a diverse and talented workforce, due to a national workforce shortage and reputational factors, may impact on the quality of care
Recommendation/Required Action
The Board is asked to:
Receive the report;
Note the increasing challenges in delivery safer
staffing particularly in the current pandemic;
Note the mitigations and action plans in place;
Be assured that safe staffing levels have been
maintained during August- September 2021 with the
support of rostered and non-rostered nursing and
MDT staff.
VERSION CONTROL:
Version Report to Date Reported
V1 Executive Team 16 November 2021
V1.1 Trust Board 25 November 2021
EXECUTIVE SUMMARY
1. Introduction and background
The monthly reporting of safer staffing levels is a requirement of NHS England and the
National Quality Board (NQB) in order to inform the Trust Board and the public of staffing
levels within in-patient units. This report provides assurance that there is continued detailed
internal oversight and scrutiny in place to ensure safer staffing levels are maintained.

Agenda Item Number: TB 216/21
This report details the in-patient daily nurse staffing levels during the months of August and
September 2021 reporting of the planned and actual hours of Registered Nurses (RNs),
Registered Nursing Associates (RNAs) and Health Care Support Workers (HCSWs).
This report provides an update on LSCFT nurse staffing for August and September 2021.
During the reporting period it is evident that staffing challenges continue, which also reflects
the current national picture, exacerbated by the impact of the COVID-19 pandemic. Despite
these challenges, ward managers and clinical teams have maintained safer staffing levels
albeit with the Harbour going into Business Continuity to do so. All inpatient wards have had
a comprehensive safer staffing review; the recommendations and associated work plan are
overseen by the Safer Staffing Group.
2. Key Issues
Overall fill rates have reduced from 82% in July to an overall fill-rate of 77% in August and
78% in September; meeting SS requirements continued to be challenging during August and
September. The current COVID-19 pandemic has contributed to this with a number of RNs
and HCSWs self-isolating or shielding as per government advice.
There was an overall day fill-rate of 69% (August) and 73% (September) and 83% on nights
in August and 82% September 2021. For Registered Nurses (RNs) the fill-rate was 64% on
days in August and 64% on days in July and on nights the fill rates for RNs was 79% (August)
and 77% (September). This is a decrease on day and night fill rates for RNs. The day fill-rates
in August and September have been impacted by vacancies and sickness across the majority
of sites as demonstrated in appendix 1.
During August and September the number of incidences of 1 RN on duty increased from 305
in June and July to 1226 in August and September (675 and 551 incidences reported
respectively). This significant increase is due to strengthening reporting. Previously red flags
raised by WMs were used however it was identified that this did not capture all incidences.
Therefore, from August 2021, it was agreed that this data would be pulled directly from
Healthroster. As a comparison, had July’s data been taken directly from Healthroster the
incidences on 1 RN on duty would have been 707. For August and September, the 1226
incidences is approximately 17% and 14% respectively of shifts.
The majority of incidents of 1 RN on duty were at the Harbour (264) and the Guild (649); the
level of RN vacancies at both sites is the main contributory factor. Wards are supported by a
Duty Matron based at The Harbour the Guild have a supernumerary Senior Staff Nurse on-
site. Additionally, inpatient areas have a total of 66 RNs commencing from 2021 cohorts (59
NRNs, 6 experienced RNs and 1 RTP); of which the Guild have 24 RNs (23 NRNs)
commencing in September and Harbour have 12 (10 NRNs). On commencement with the
Trust the majority of these will be awaiting their NMC registration and therefore will not be
counted as RNs until this is received which is likely to be over the September/October period.
Mitigating actions include Ward Managers and Matrons supporting wards, altering skill-mix
and the use of Temporary Staffing. During August 500 WTE Bank and Agency shifts supported
the maintenance of Safer Staffing (98 WTE RN and 402 WTE HCSWs); in September this
Agenda Item Number: TB 216/21
increased to 470 (91 WTE RN and 379 WTE HCSWs). Furthermore, the Harbour implemented
Business Continuity due to staffing pressures in July 2021.
RN vacancies for in-patients increased by 1 from 157 to 158 during the bi-monthly period; this
is still reduction of 70 since August 2020. As stated above, the majority of the 59 NRNs are
awaiting their NMC registration and once this is received the RN vacancy figure will be
significantly reduced.
During August and September 14 RNs left the in-patient areas, 10 of whom remained in the
Trust moving to non-inpatient teams. Of the 4 who left 2 RNs remained on the bank. Is it of
note that 10 NRNs withdrew from starting.
Proactive recruitment continues and the Trust is being supported by NHSE/I to develop
recruitment of RNMHs internationally however due to the pandemic situation in India this was
paused until the end of June 2021 which has resulted in a delay. There have been 13 RNs,
recruited internationally, who have joined the Trust to date. Five of whom are yet to complete
their OSCE (and therefore not yet registered with NMC). Job offers have been made to a
further 77 RNMHs through international recruitment. Therefore the Trust has achieved 90
recruits towards the 125 target. Pastoral and clinical support has been funded by NHSE to
support the project.
3. Safer Staffing Risk
There remains continued challenges in maintaining safer staffing due to the national shortage
in Registered Nurses and the impact of the COVID pandemic. This risk is noted on the
corporate risk register and mitigations are in place both short and longer term. Alongside the
development of RNMHs through international recruitment, the Trust has a ‘grow your own’
model in place from Apprentice Health Care Assistants through to Registered Nursing
Associates (RNAs) and Registered Nurses (RNs). A programme of supporting and developing
Registered Nursing Associates (RNAs) to ‘top-up’ to RNLDs commenced in January 2021 and
a 2nd cohort commenced in September 2021. Additionally, further programmes to ‘top-up’
RNAs to RNMH and Adult RN have been implemented with a cohort of 12 RNMH and 5 Adult
RN commenced in September 2021. Additionally, the Trust has extending the nursing career
pathway with opportunities for advanced clinical practice and consultant levels posts. These
initiatives will support the recruitment and retention of RNs.
4. Conclusion and Recommendations
The Board is asked to:
Receive the report;
Note the increasing challenges in delivery safer staffing particularly in the current
pandemic;
Note the mitigations and action plans in place;
Be assured that safe staffing levels have been maintained during August and
September with the support of rostered and non-rostered nursing and MDT staff.
Agenda Item Number: TB 217/21
MEDICAL STAFFING REPORT
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: David Fearnley, Chief Medical Officer
Prepared by: Catherine Pollard, Business Manager, Medical Directorate
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will employ and retain the best STAFF, as our culture will be inclusive and a supportive place to work
Aligned to Board Assurance Framework Risk
2.0 Failure to recruit, develop and retain a diverse and talented workforce, due to a national workforce shortage and reputational factors, may impact on the quality of care
Recommendation/Required Action
The Board of Directors is asked to note the progress
on the plan and seek any further assurance.
EXECUTIVE SUMMARY Introduction and background A Medical Staffing paper was presented to the Board of Directors in May 2021, and indicated areas of future focus. Following further engagement with medical staff a 10 point plan is being developed and an update is presented in this report. Key Issues There is a gradual improvement in medical staffing recruitment, and the 10 point plan has been developed to continue and accelerate this improvement. A new task and finish group, chaired by the CMO has been established to review weekly medical staffing changes, monthly budget statements and support further engagement with the Local Negotiating Committee and the British Medical Association. The group will oversee delivery of the plan through to 2022/23 and will provide assurance that medical staffing is safe, effective and affordable. Escalation of risk The Board will be aware of the financial pressures arising from the use of agency locums, and this report provides a summary of the main actions that will be undertaken to address this financial risk whilst maintaining a safe and effective medical workforce. Conclusion and Recommendations The Board of Directors is asked to note the progress on the plan and seek any further assurance. The People and Culture Committee and Finance and Resource Committee will receive assurances on the plan to monitor its effectiveness.
Agenda Item Number: TB 218/21
DIRECTOR OF INFECTION PREVENTION AND CONTROL (DIPC)
QUARTER 2, JULY - SEPTEMBER 2021
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☒ Date of Meeting: 25/11/2021
Presented by: Maria Nelligan, Chief Nurse & Quality Officer (DIPC)
Prepared by: Amanda Miskell, Associate Chief Nurse (ACN), Infection Prevention and Safety, Deputy DIPC
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will deliver SAFE care by embracing an open and learning culture, ensuring we continually improve
Aligned to Board Assurance Framework Risk
4.0 Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care may impact on quality of care and could incur regulatory action
Recommendation/Required Action
To note decreased outbreaks due to Covid 19. To approve the updated Influenza BAF November 2021 (Appendix 1) To note the commencement of the annual influenza vaccination campaign To approve the Autumn/Winter plan summary, September 2021 (Appendix 2)
Version Control
Version Report to Date Reported
Version 1.0 Maria Nelligan 15.11.2021
Version 1.0 IPC Sub-Committee 15.11.2021
Agenda Item Number: TB 218/21
Director of Infection Prevention & Control (DIPC) Report Q2
1. Purpose of the Report The purpose of this report is to provide assurance to the Board in relation to the implementation of the Health and Social Care Act 2008 (revised 2015) also noted as mandatory in criterion 1, the Care Quality Commission standards, Regulation 12, Safe Care & Treatment and Regulation 15, Premises & Equipment. This is also in line with Winning Ways document (DH 2003).
2. Executive Summary
Q2 of 2021/2022 remains an unprecedented time in terms of IPC responses nationally. The pandemic continues with an impact on service provision overall, however resilience and prioritisation of safe care continue to keep staff and patients as safe as possible as guidance changes and restrictions are lifted. The epidemiology in relation to Covid 19 prevalence continues to be fluid in addition to other respiratory infections. The annual influenza campaign commenced at the end of September 2021 and will continue into Quarter 4 with a final national and regional submission of uptake on 28th February 2022. The seasonal influenza campaign will include more digital resources this year to aid efficiencies. The Immunisation & Vaccination group continues to drive this progress alongside the Covid 19 booster programme. This report includes an updated version of the Influenza assurance framework to be approved at Board v1 (Appendix 1). This report also includes the LSCft summary slides in response to the National Autumn Winter plan 2021 (Appendix 2).
3. HealthCare Associated Infections (HCAI’s) Non Covid There were no cases of blood stream infections associated with health provision in the community or hospital stay during Q2. There were no cases of preventable Clostridium Difficile Infection (CDI) associated with health provision in the community, antimicrobial prescribing or delivery via the Outpatients Parental Antimicrobial Treatment (OPAT) service, dentistry, and or hospital stay, including possible transmission. Excluding Covid 19, there have been no identified infections related to transmission or causation within the Trust. There was one confirmed case of Salmonella in August 2021 in a rehabilitation setting. Response was delivered the same day from IPC and involved a multi-disciplinary team response including the Environmental Officer and food standards agency. Root Cause analysis identified and concluded that this was related to the six types of pork scratchings products which were recalled from sale in August after being linked to a Salmonella outbreak. All had best before dates of 19 Feb 2022 and were found in the service user’s room. There was no transmission to any other which evidences excellent IPC practices and the patient made a full recovery. There has been learning from a Post Infection Review (PIR) of a potential line infection associated with the OPAT service in March 2021. Line associated infection was not a cause of death on the death certificate. All PIRs will now be tabled at the weekly Post Incident Group (previously for Pressure Ulcers only), with IPC membership, and a PIR completed for all incidents where learning can be extrapolated.

Agenda Item Number: TB 218/21
4. Outbreaks In July and August the Trust reported two outbreaks of Covid on In-patient wards. The first in July resulted in a ward becoming “Red” at The Guild on 21st July. This was the wards second Covid outbreak and on this occasion three patients and four staff tested positive. None of the nine contacts converted to positive. All made a good recovery and didn’t require an acute intervention or treatment. The ward was Red for 15 days and all patients stepped down at day 15. Following a deep clean the ward resumed normal business which has remained since. Root cause analysis does not indicate an index case or likely transmission. The community had sustained transmission of Covid 19 infection. One bed was closed for the duration. The staff were all reported as RIDDOR due to the close proximity and timescales with each of the RCAs. The second outbreak was in the Bay locality. The ward became “Red” on 9th August. This was the wards first outbreak of Covid and this resulted in four patients and one member of staff testing positive. None of the six contacts tested positive. The ward remained Red and then Amber for 18 days until all patients stepped down. Following a deep clean the ward resumed normal business which has remained since. Root cause analysis does not indicate an index case or likely transmission. The community had sustained transmission of Covid 19 infection. One bed was closed for the duration. The outbreaks were presented at and supported by the Outbreak Control Team (OCT) which reconvened once each outbreak was declared and IIMARCHs completed, which are approved by the DIPC and shared with Public Health England (North West). The IPC locality nurse supported the outbreak wards with daily visits and staff complete the daily Covid checklist to ensure compliance with IPC policies and procedures. The revised isolation care plan is also implemented where a patient is asked to isolate. On both these occasions the outbreaks were managed as “cohorts” due to the patient’s presentation, exposure and ability to isolate. No outbreaks were reported in September.
As with any Covid outbreak the IPC measures were robust in bringing both to a timely close. In terms of prevention the organisation encourages:
a) Screening for Covid 19 on admission and weekly remains a priority to rapidly identify and manage any asymptomatic carriers and locality IPCNs ensure and support colleagues in their responsibilities for admission, weekly and contact screening. Self-testing for patients is actively encouraged. b) Vaccination for inpatients continued in Q2 and access to the vaccination status for patients is available on Lancashire Person Record Exchange Service (LPRES). c) Daily summaries are competed and distributed to ensure that colleagues are sighted on all outbreaks and the location of any Covid positive patients. d) To maintain support and consistent IPC advice a member of the IPCT attends the bed meeting at least once a day. This commenced in February 2021 but will conclude as visibility of the IPC team and the daily summaries reach a wider audience.
e) The IPCT liaise closely with Health & Safety colleagues during any identification of a Covid 19 infection or outbreak. This ensures any staff testing positive have a RCA completed. During Q2 the majority, 90% and above have been related to social and household contacts, not work.
Epidemiology and prevalence is reported to Silver for consideration in Covid 19 activity impacting on the Trusts ability to provide services and respond safely. Outbreak activity in table 1 below.
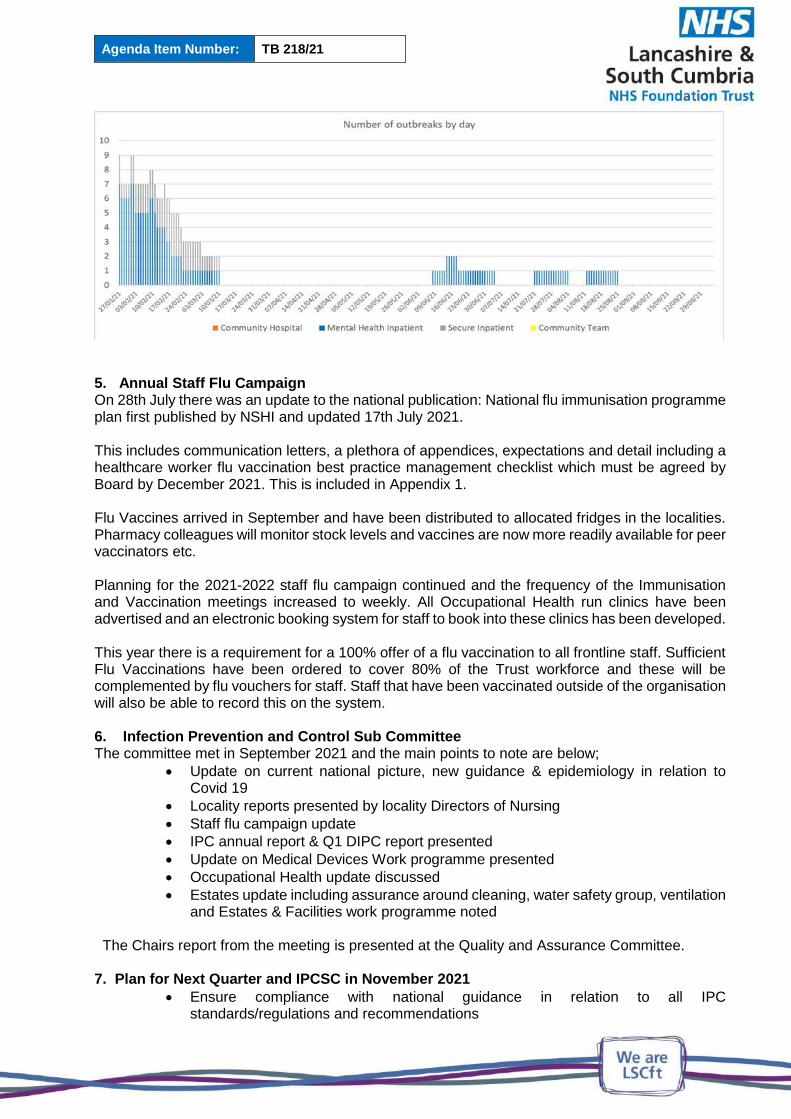
Agenda Item Number: TB 218/21
5. Annual Staff Flu Campaign On 28th July there was an update to the national publication: National flu immunisation programme plan first published by NSHI and updated 17th July 2021. This includes communication letters, a plethora of appendices, expectations and detail including a healthcare worker flu vaccination best practice management checklist which must be agreed by Board by December 2021. This is included in Appendix 1. Flu Vaccines arrived in September and have been distributed to allocated fridges in the localities. Pharmacy colleagues will monitor stock levels and vaccines are now more readily available for peer vaccinators etc. Planning for the 2021-2022 staff flu campaign continued and the frequency of the Immunisation and Vaccination meetings increased to weekly. All Occupational Health run clinics have been advertised and an electronic booking system for staff to book into these clinics has been developed. This year there is a requirement for a 100% offer of a flu vaccination to all frontline staff. Sufficient Flu Vaccinations have been ordered to cover 80% of the Trust workforce and these will be complemented by flu vouchers for staff. Staff that have been vaccinated outside of the organisation will also be able to record this on the system.
6. Infection Prevention and Control Sub Committee The committee met in September 2021 and the main points to note are below;
Update on current national picture, new guidance & epidemiology in relation to Covid 19
Locality reports presented by locality Directors of Nursing
Staff flu campaign update
IPC annual report & Q1 DIPC report presented
Update on Medical Devices Work programme presented
Occupational Health update discussed
Estates update including assurance around cleaning, water safety group, ventilation and Estates & Facilities work programme noted
The Chairs report from the meeting is presented at the Quality and Assurance Committee. 7. Plan for Next Quarter and IPCSC in November 2021
Ensure compliance with national guidance in relation to all IPC standards/regulations and recommendations

Agenda Item Number: TB 218/21
Continue to provide robust education, support and specialist advice to LSCFT staff.
Review IPC policies and SOPs including Dress Code Policy and involvement in national pilot
Monitor progress against annual Work programme at IPCSC
Update locality work plans for IPC
Develop a new Hand hygiene audit tool for link practitioners following revision
Ensure all IPC information resources are up to date on Sharepoint page
8. Recommendations
To note decreased outbreaks due to Covid 19
To approve the updated Influenza BAF November 2021 (Appendix 1)
To note the commencement of the annual influenza vaccination campaign
To approve the Autumn/Winter plan summary, September 2021

Agenda Item Number: TB 218/21
Appendix 1 – Healthcare worker flu vaccination best practice management checklist v1 - 03/08/2021
For public assurance via trust boards by December 2021.
A Committed Leadership Trust Self-Assessment
A1 Board record commitment to achieving the ambition of vaccinating all frontline healthcare workers
July 2021
A2 Trust has ordered and provided a quadrivalent (QIV) flu vaccine for healthcare workers
Spring 2021
A3 Board receive an evaluation of the flu programme 2020 to 2021, including data, successes, challenges and lessons learnt
February 2022
A4 Agree on a board champion for flu campaign DIPC
A5 All board members receive flu vaccination and publicise this Autumn 2021
A6 Flu team formed with representatives from all directorates, staff groups and trade union representatives
Via Silver
A7 Flu team to meet regularly from September 2021 Immunisation & Vaccination Group scheduled throughout the year Peer vaccinators support forum Part of regional & national meetings
B Communications Plan Trust Self-Assessment and approved at Board Autumn 2021
B1 Rationale for the flu vaccination programme and facts to be published – sponsored by senior clinical leaders and trades unions
From September 2021 Communication Plan Silver
B2 Drop in clinics and mobile vaccination schedule to be published electronically, on social media and on paper
August - November 2021
B3 Board and senior managers having their vaccinations to be publicised September - October 2021
B4 Flu vaccination programme and access to vaccination on induction programmes
From October 2021
B5 Programme to be publicised on screensavers, posters and social media From September 2021
B6 Weekly feedback on percentage uptake for directorates, teams and professional groups
Jabometer visuals on Sharepoint for all Localities Uptake shared with Silver and all Directors of Nursing
C Flexible Accessibility In place via clinics, peer vaccinators, events, Induction, training, IPCT, dial a jab and vouchers
Agenda Item Number: TB 218/21
C1 Peer vaccinators, ideally at least one in each clinical area to be identified, trained, released to vaccinate and empowered
Started September 2021
C2 Schedule for easy access drop in clinics agreed Started September 2021 and ongoing
C3 Schedule for 24 hour mobile vaccinations to be agreed Part of plan and Jabathons
D Incentives Amazon Vouchers monthly prize draw
D1 Board to agree on incentives and how to publicise this Via Communication plan
D2 Success to be celebrated weekly Jabometer visuals on Sharepoint for all Localities Uptake shared with Silver and all Directors of Nursing
Appendix 2 – Autumn Winter plan summary LSCft September 2021 in response to national publication
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1020982/COVID-19-response-
autumn-and-winter-plan-2021.pdf
Autumn Winter plan
summary slides v1.pptx
Autumn Winter Plan summary slides PDF
Agenda Item Number: TB 218/21
ANNUAL INFECTION PREVENTION & CONTROL (IPC) REPORT
2020/21
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☒ Date of Meeting: 25/11/2021
Presented by: Maria Nelligan, Chief Nurse & Quality Officer (DIPC)
Prepared by: Amanda Miskell, Associate Chief Nurse (ACN), Infection Prevention and Safety, Deputy DIPC
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will deliver SAFE care by embracing an open and learning culture, ensuring we continually improve
Aligned to Board Assurance Framework Risk
4.0 Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care may impact on quality of care and could incur regulatory action
Recommendation/Required Action
The Board to note the contents of this annual report.
The Board to note the finalised 2020/2021 Work
Programme for IPC and approve the new Work
Programme for 2021/2022
EXECUTIVE SUMMARY
The Annual Infection Prevention & Control Report will provide Board members with
assurance that its Infection Prevention & Control responsibilities and obligations are being
met under the Health & Social Care Act and Care Quality Commission regulations. This
report includes a summary of activity and outcomes in relation to the promotion and
management of Infection Prevention & Control within Lancashire and South Cumbria NHS
Foundation Trust for year 2020/2021. The report will also highlight Covid response,
Nosocomial incident data, Estates and Facilities IPC responses, in particular to cleanliness
and refurbishments, the assessment and safe use of Personal Protective Equipment,
reporting to Regional and National bodies for Vaccination, current key priorities and the work
programme for the year 2021/2022.
Introduction and background
During 2020 and at the start of the pandemic the Trust immediately took proactive steps to
protect patients, visitors and staff. Responding to the challenges of the pandemic has

Agenda Item Number: TB 218/21
facilitated the ongoing collaborative with other safety forums including estates and facilities,
staff side, health and safety, the senior leadership team and operational leads.
Key Issues
Covid 19 response – an increase in incidents relating nosocomial outbreaks, high
prevalence of Covid 19 infections with sustained transmission in the community
affecting patients and staff. Variants of concern and mutation and increased
transmissibility. Consistent changes to information and categorisation of SARS CoV 2
resulting in Covid 19 infection. The implementation of a mass vaccination programme.
Environmental Issues – New information regarding the impact of environments and
buildings and the management of Covid 19 within them. Enhanced cleaning regimes.
Use of cleaning materials and frequency of cleaning. PLACE programme and
outcomes. New refurbishments and management of Water Safety, Waste, Ventilation
and changing facilities.
Influenza Programme – The Trust vaccinated more staff in 2020-2021 compared to
2019-2020. However as a new electronic process was used (ESR) compared to a
manual arrangement the year before compliance with the national target appeared to
be lower. This was due to a significantly higher denominator for 2020-2021 and the
inability to remove all staff working from home and or shielding during the pandemic.
Escalation of risk
Buildings that are fit for purpose and ability to manage infection risks within them.
Estates and Facilities response to required works, including water safety.
Capability of Rio in relation to IPC physical health assessments including Covid 19 testing and
diagnostics.
Conclusion and Recommendations
The Infection Prevention & Control Service, including the Communicable Disease Control
function for the wider community will maintain a continuous review of the performance,
resources and arrangements for infection prevention control and safety within the
organisation to ensure that the highest standard of infection prevention and safety is
achieved for all localities and the wider populations.
The Trust Board is asked to note the Annual Report, including the infection prevention &
control work programme for 2021/2022 that will be monitored by the Infection Prevention &
Control Sub-Committee (IPCSC).

Agenda Item Number: TB 219/21
AUDIT COMMITTEE CHAIRS REPORT
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Ruth Lowry, Committee Chair
Prepared by: Dianne Scambler, Deputy Company Secretary
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will respond to peoples’ needs by striving for the highest STANDARDS of quality across all of our services
Aligned to Board Assurance Framework Risk
7.0 Failure to deliver the Trust’s annual financial plan caused by lack of robust cost improvements and an inability to attract appropriate investment to meet demand may impact on the Trust’s ability to deliver high quality care
Recommendation/Required Action
The Board of Directors are asked to:
note the assurance and escalation provided
within the chairs report
1.0 INTRODUCTION
The Board of Directors are presented with the Chairs Reports of the Audit Committee
held on 01 November 2021. The chairs report provides an overview of assurance
received and escalation to discussions held, as required.
2.0 RECOMMENDATION
The Board of Directors are asked to:
note the assurance and escalation provided within the chairs report

CHAIRS REPORT
MEETING: Audit Committee - Part I and Part II DATE OF MEETING: 01/11/2021 CHAIR OF MEETING: Ruth Lowry, Non-Executive Director
ITEMS APPROVED
Minutes of the previous meeting – The minutes of the meeting held on 22 July 2021 were confirmed as an accurate record, subject to amendment to include Rob Fenton’s (Senior Manager, KPMG) attendance. External audit provision The Committee agreed to recommend that the Council of Governors approves KPMG’s proposal to extend the current contract to 2023/24.
Internal Audit and Counter Fraud The Committee approved commencement of the proposed process for the appointment of Internal Audit and Counter Fraud Services, from 2022/23.
ASSURANCE RECEIVED
Risk Management Update Report The Committee discussed how the Corporate Risk Register was linked to the BAF, and asked that the Risk Register be shared with the Committee at the next meeting. We also discussed ways in which we could better gain assurance over the adequacy and effectiveness of the systems and processes for the management of the Trust’s strategic risks and the role of the Audit Committee, in conjunction with Board Committees. The deep dive process will be reviewed. We recognised specifically that good connectivity is necessary between the Audit and Quality Assurance Committees in relation to clinical risk. The Interim Company Secretary proposed an improved Committee process for monitoring progress against the strategic risks that could be adopted. This involves the relevant committees reviewing the relevant risk scores based upon the assurances they receive and escalating any changes through the Chair’s Report to the Board. This will be actioned.
CHAIRS REPORT
Associate Hospital Managers Review Update Although there have been delays in implementing some of the actions in the Improvement Plan whilst legal advice has been sought, the Committee was pleased to note the progress to date, and that most actions are expected to be complete by January 2022. The action plan had been presented to various stakeholder meetings including the Associate Hospital Managers Forum, where it had been extremely well received. Annual Cyber Security Assurance Report The annual audit is expected to be undertaken shortly, with re-certification expected. Despite the pandemic, good progress has been made in implementing the plan and the Trust has good evidence of its compliance against the standards. The Committee received additional assurance that the Trust is effectively raising the awareness of its staff to the risks arising around cyber security. NHSx Digital: Cyber Metrics Report The Committee were pleased to note that the Trust has achieved the highest level of performance against the management of high severity alerts, unsupported systems, secure backups and the Data Security and Protection Toolkit. Internal Audit; Quarter 2 Progress Report The Committee was informed of the internal audit activity taking place against the plan. Work under the 2020/21 Internal Audit Plan is now complete. The last two remaining reviews, Data Security and Protection Toolkit and EPR gateway review have both received substantial assurance. Work has now commenced on a number of reviews contained within the 2021/22 Internal Audit Plan The Committee was also advised that preliminary conversations had taken place to inform the 2022/23 Audit Plan. Internal Audit: Quarter 2 Follow Up Summary Report The Committee was informed that 21 recommendations had now been completed. Out of the 24 recommendations still outstanding, only two are address high risks, and three recommendations are not yet due. Additional detail has been requested on what recommendations are still outstanding and who the responsible officers are. This will allow the Committee to be better focus on what further assurances are required. Anti-Fraud: Quarterly Progress Report A fraud risk analysis is now to be undertaken in line with the Government Counter Fraud Profession’s fraud risk assessment methodology; and the Anti-Fraud Service has begun to update our existing fraud risk assessment toolkit.

CHAIRS REPORT
The Anti-Fraud Service had issued six Fraud Prevention Checks, alerting the Trust to potential frauds but their checks indicate that there have been no attempts against the Trust of the kinds described in the alerts. Anti-Fraud, Bribery and Corruption Policy and Recovery Plan The draft policy was presented to the Committee as part of the consultation process with key stakeholders. The Committee were supportive of the amended document.
Breaches and Waivers Report – Quarter 2 The Committee noted that there had been no breaches during the quarter and seven waivers which did not require any further investigation. One waiver however, which related to the supply of anti-ligature windows, was escalated to the Finance and Resources Committee. The Audit Committee asked for confirmation that the original procurement process had included the whole of the Trust’s estate, since it was foreseeable then that all the windows across the whole of the estate would have to be replaced with the same products. This query would be escalated to the Finance and Resources Committee for a full analysis of the expected work and cost across the Trust’s estate. Losses and Special Payments Report – Quarter 2 The Committee was informed that all the payments were within delegated limits and were made in accordance with Standing Financial Instructions. There were 12 losses and nine special payments during the period totalling £12,531.65. The Committee requested that additional detail to be included in subsequent reports that would allow any patterns or trends to be identified. Trust Improvement Towards ‘Well Led Preparedness’ The Committee was provided with an update on the support commissioned from the Good Governance Institute (GGI) to assist the organisation as it readiness itself for a future CQC visit. In addition we were informed that GGI will be undertaking a review of the Trust’s response to the COVID pandemic, in anticipation of the national review that will commence early in 2022. The Committee was informed of the interim findings into the Well-led review that outlined examples of good practice and areas for development against five priorities that have been identified by GGI – leadership, strategy, culture, risk management and workforce. The final report will be presented to Board at the end of November. Quality Account – Review of Process I have requested a review of the process by which the Quality Account was prepared in 2021, to be included in the review of the year-end reporting processes.

CHAIRS REPORT
External Auditor The Committee recommended that the Council of Governors approve the extension of the external audit contract with KPMG until completion of the audit for 2023/24.
ITEMS TO ESCALATE TO THE BOARD
ITEMS FOR ESCALATION MITIGATING ACTION
Risk Management Update
Further work being considered in line with risk management improvement work and outcome from well led review regarding risk management – specifically strengthening connectivity between the corporate risk register and BAF and reviewing the roles of the Committees and Audit Committee with regard to roles in monitoring and oversight of strategic risks.
ITEMS RECEIVED FOR INFORMATION
No items were received for information at this meeting.
Agenda Item Number: TB 220/21
TRUST PERFORMANCE REPORT (TPR) EXCEPTION SUMMARY –
MONTH 7
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☒ Decision ☐ Date of Meeting: Date: 25/11/2021
Presented by: Phil Horner, Director of Information & Performance
Prepared by: Anne Thompson, Head of Performance
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will respond to peoples’ needs by striving for the highest STANDARDS of quality across all of our services
Aligned to Board Assurance Framework Risk
4.0 Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care may impact on quality of care and could incur regulatory action
Recommendation/Required Action
The TPR is presented to provide assurance to Trust
Board of Directors for the Trust’s key performance
metrics.
A 201 indicators in total are reported, with notable
performance described.
Trust Board of Directors are requested to review and
discuss Trust performance for October 2021.
EXECUTIVE SUMMARY
1. Report Overview
The TPR is presented in a revised format following discussions with the Executive
Team
o Metrics are grouped by CQC domain in order to bring visibility to the domains
and drive improvement
Discharge LOS (Acute Pathway) (Metric 45 – IP4) has been recalculated to include
any direct discharges from PICU as well as Adult Acute Treatment wards, to align
with NHS Benchmarking calculations. As there are very few direct discharges from
PICU this has made little difference to overall performance
Three new Quality Indicators are included covering Serious Incident Investigations
and the numbers ongoing beyond the 60 working day deadline (metrics 4 – 6 QUA
46, QUA 47, QUA 48)
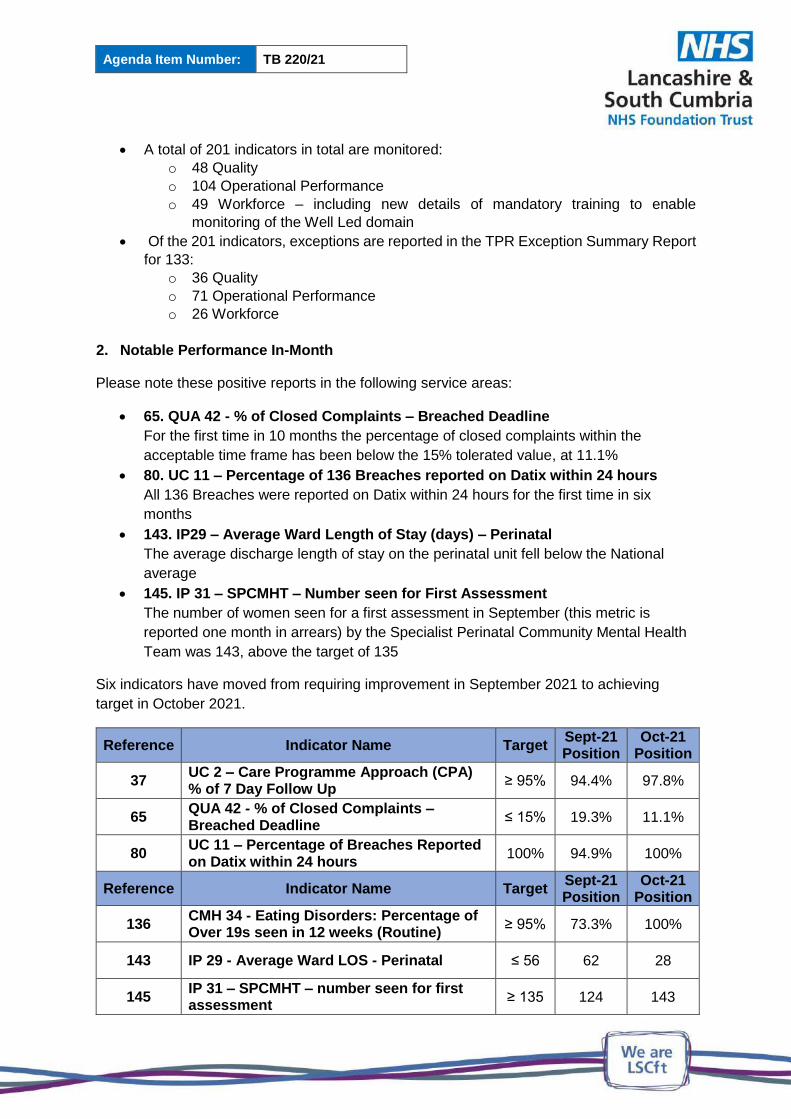
Agenda Item Number: TB 220/21
A total of 201 indicators in total are monitored:
o 48 Quality
o 104 Operational Performance
o 49 Workforce – including new details of mandatory training to enable
monitoring of the Well Led domain
Of the 201 indicators, exceptions are reported in the TPR Exception Summary Report
for 133:
o 36 Quality
o 71 Operational Performance
o 26 Workforce
2. Notable Performance In-Month
Please note these positive reports in the following service areas:
65. QUA 42 - % of Closed Complaints – Breached Deadline
For the first time in 10 months the percentage of closed complaints within the
acceptable time frame has been below the 15% tolerated value, at 11.1%
80. UC 11 – Percentage of 136 Breaches reported on Datix within 24 hours
All 136 Breaches were reported on Datix within 24 hours for the first time in six
months
143. IP29 – Average Ward Length of Stay (days) – Perinatal
The average discharge length of stay on the perinatal unit fell below the National
average
145. IP 31 – SPCMHT – Number seen for First Assessment
The number of women seen for a first assessment in September (this metric is
reported one month in arrears) by the Specialist Perinatal Community Mental Health
Team was 143, above the target of 135
Six indicators have moved from requiring improvement in September 2021 to achieving
target in October 2021.
Reference Indicator Name Target Sept-21 Position
Oct-21 Position
37 UC 2 – Care Programme Approach (CPA) % of 7 Day Follow Up
≥ 95% 94.4% 97.8%
65 QUA 42 - % of Closed Complaints – Breached Deadline
≤ 15% 19.3% 11.1%
80 UC 11 – Percentage of Breaches Reported on Datix within 24 hours
100% 94.9% 100%
Reference Indicator Name Target Sept-21 Position
Oct-21 Position
136 CMH 34 - Eating Disorders: Percentage of Over 19s seen in 12 weeks (Routine)
≥ 95% 73.3% 100%
143 IP 29 - Average Ward LOS - Perinatal ≤ 56 62 28
145 IP 31 – SPCMHT – number seen for first assessment
≥ 135 124 143
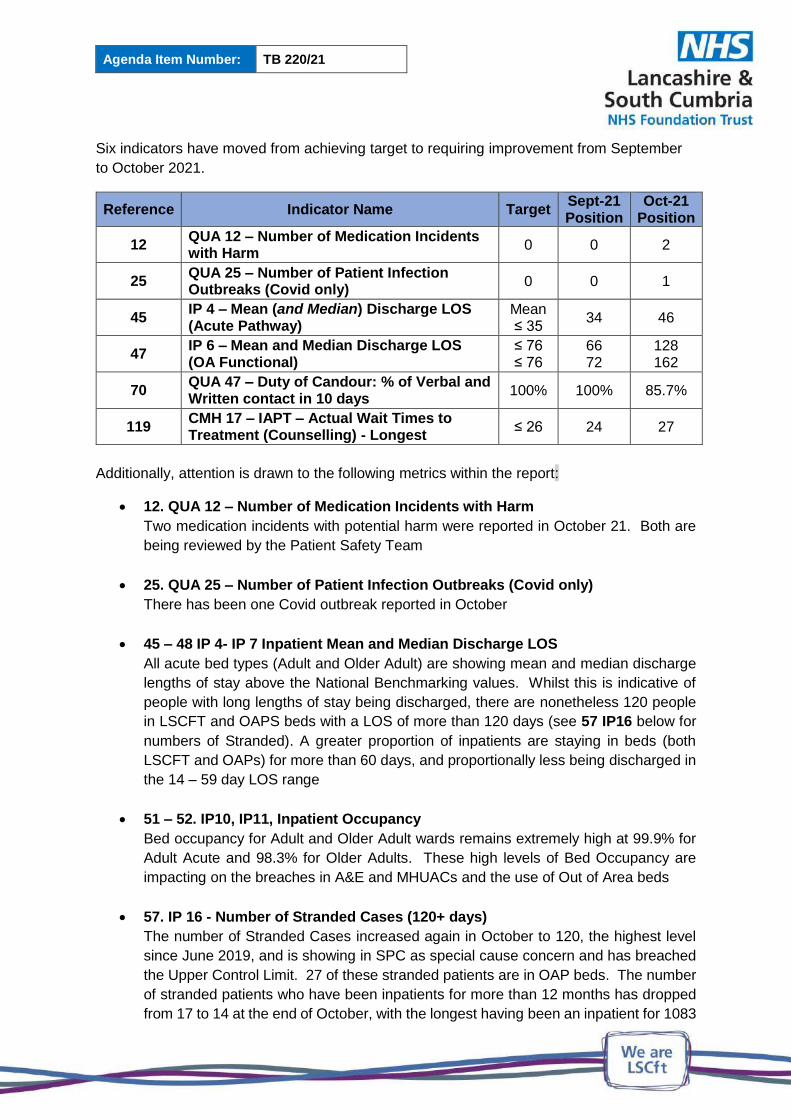
Agenda Item Number: TB 220/21
Six indicators have moved from achieving target to requiring improvement from September
to October 2021.
Reference Indicator Name Target Sept-21 Position
Oct-21 Position
12 QUA 12 – Number of Medication Incidents with Harm
0 0 2
25 QUA 25 – Number of Patient Infection Outbreaks (Covid only)
0 0 1
45 IP 4 – Mean (and Median) Discharge LOS (Acute Pathway)
Mean ≤ 35
34 46
47 IP 6 – Mean and Median Discharge LOS (OA Functional)
≤ 76 ≤ 76
66 72
128 162
70 QUA 47 – Duty of Candour: % of Verbal and Written contact in 10 days
100% 100% 85.7%
119 CMH 17 – IAPT – Actual Wait Times to Treatment (Counselling) - Longest
≤ 26 24 27
Additionally, attention is drawn to the following metrics within the report:
12. QUA 12 – Number of Medication Incidents with Harm
Two medication incidents with potential harm were reported in October 21. Both are
being reviewed by the Patient Safety Team
25. QUA 25 – Number of Patient Infection Outbreaks (Covid only)
There has been one Covid outbreak reported in October
45 – 48 IP 4- IP 7 Inpatient Mean and Median Discharge LOS
All acute bed types (Adult and Older Adult) are showing mean and median discharge
lengths of stay above the National Benchmarking values. Whilst this is indicative of
people with long lengths of stay being discharged, there are nonetheless 120 people
in LSCFT and OAPS beds with a LOS of more than 120 days (see 57 IP16 below for
numbers of Stranded). A greater proportion of inpatients are staying in beds (both
LSCFT and OAPs) for more than 60 days, and proportionally less being discharged in
the 14 – 59 day LOS range
51 – 52. IP10, IP11, Inpatient Occupancy
Bed occupancy for Adult and Older Adult wards remains extremely high at 99.9% for
Adult Acute and 98.3% for Older Adults. These high levels of Bed Occupancy are
impacting on the breaches in A&E and MHUACs and the use of Out of Area beds
57. IP 16 - Number of Stranded Cases (120+ days)
The number of Stranded Cases increased again in October to 120, the highest level
since June 2019, and is showing in SPC as special cause concern and has breached
the Upper Control Limit. 27 of these stranded patients are in OAP beds. The number
of stranded patients who have been inpatients for more than 12 months has dropped
from 17 to 14 at the end of October, with the longest having been an inpatient for 1083
Agenda Item Number: TB 220/21
days, currently in a PICU bed. In total, 10 of the 14 longest stays are at the Harbour
(3 in Older Adult wards, 3 in PICU and 4 in Acute wards); there is one in an acute OAP
bed and 2 in acute LSCFT beds in Central
70. QUA 47 – Duty of Candour: Percentage of Verbal and Written Contact in 10
days
Two of 14 incidents requiring Duty of Candour during October 2021 did not receive an
appropriate Duty of Candour letter within the 10 working day time frame although there
has been other contact during that time. This is being followed up with the clinical
teams
71 & 72. QUA 45 - Section 132 Compliance (%) – Rights attempted to be read
within 72 hours and UC 3 % Rights given to people detained under section
135/136
The QUA 44 indicator refers to people admitted under the Mental Health Act being
given their Section 132 Rights on the ward, and has consistently underperformed for
the past two years. The s132 protocol has been ratified and moves the reporting to 72
hours from July 21. There is a plan to relaunch the process including information about
how and where to capture S132 rights and where to access reporting and monitoring
information. Compliance has improved for the second month and is at the highest
(73.0%) since tracking began
74. UC 5 and 76 UC 7 – Number of Section 135 and Section 136 Place of Safety
Breaches (24 hours)
Although there were less detentions in October than in the previous two months, there
were more 24 hour breaches with compliance dropping to 72%. Lack of availability of
beds was the cause of the delays
88. UC 19 – Mental Health Number of 12 Hour Breaches
The number of 12 hour breeches in A&E rose again to 55, 4.9% of attendances
breaching, which is comparable to pre-pandemic levels. Demand in A&E and across
the Urgent Care Pathway was high in October and bed availability was the key reason
for these breaches. The longest stay in A&E was 75:47 hours
92 & 93. UC 23 & UC 24- Mental Health Urgent Assessment Centre performance
Diversions to MHUAC in October declined slightly to 116, however 22 people waited
longer than the 4hr target so 81.0% achieved the 4 hour target, there were 14 people
(12.1%) who were 12 hour breaches in MHUACs
102. IP 18 – Inappropriate Out of Area Placement (OAP) Occupied Bed Days
The impact of closure of 37 Trust beds for Covid and Estates reasons, in addition to an identified need for increased Trust bed capacity, is undoubtedly a factor in reliance on independent sector beds. However, reliance on unplanned OAPs in October was beyond the number of closed Trust beds. Stranded cases (mentioned above) are emerging as a key factor in driving up the Inappropriate OAP use
Agenda Item Number: TB 220/21
103. CMH 7 – Number of cases waiting for a care coordinator in Community
Mental Health Teams (CMHTs)
964 people were waiting for allocation of a care coordinator in CMHTs at the end of
October. Improvement has been made in Central Lancashire reducing the numbers
waiting by more than 100, due to new starters in the team and caseload management.
Development of the teams has been agreed and funding secured, but there remain
problems recruiting to the large number of vacancies. RAG rating and dynamic risk
assessments are in place for assessing and managing risk whilst people are waiting,
and support from Duty Workers is in place. In turn this is having a knock-on effect on
the Forensic CMHT caseload
114. CMH 12 – IAPT Prevalence – Cumulative Target
The Nationally set target is to achieve 25% Prevalence in Quarter 4, and it is an
incremental target, with each Quarter’s target higher than the previous quarter’s. The
total for the year is 43,330 people starting treatment, of whom we should have seen
24,800 by the end of October. Instead we had seen a total of 16,481, which is a
shortfall of 8,319 (33.5%). This position has deteriorated in month. In October 2,187
people entered treatment, against a monthly target of 3,653, a shortfall of 1,466. In
addition a further 1,200 would have to be seen every month for the rest of the financial
year to make up the short fall already accrued, which is more than double the numbers
currently being seen. There are a number of Trainees who are now able to provide
Triage Assessment appointments which will assist in reaching prevalence targets.
Work is ongoing with the ICS and commissioners to look at a Communication Strategy,
with new materials and newsletters, which is integral to meeting prevalence target
118. CMH 16 - IAPT Actual Wait Times to treatment (Cognitive Behavioural
Therapy) Longest waits
There were 25 people waiting more than 26 weeks for CBT at the end of October, an
increase of 7 from last month. The longest wait being 34 weeks, in The Bay locality,
where eleven of the long waits are located, with a further 11 in Central (max 29 weeks),
2 in Pennine Lancashire (max 28 weeks) and one waiting 29 weeks in Fylde
123 – 127. CMH 21 – CMH 25 - Children and Young People’s Mental Health Access
Targets
Some improvement is being achieved against Access and Waiting Times targets for
Children and Young Peoples Mental Health Services, but none have yet been met.
The service continues to struggle with increased demand and difficulty in recruiting to
establishment vacancies
128. CMH 26 – Children’s Community Referral to Treatment (RTT) (combined
CITNS)
Children’s services are provided in both Central and Pennine Lancashire. Increased
demand and an increase in complexity of referrals are compounded by problems

Agenda Item Number: TB 220/21
recruiting to vacancies to detrimentally impact on Referral to Treatment times.
Alternative ways of delivering the service are being investigated, including
implementing non clinical support posts to free up more clinical time, telephone triage
and the offer of self-guided support as a prerequisite to seeing a therapist in parts of
the service.
129 & 133. CMH 29 & CMH 33 – Eating Disorders Routine Referrals
The routine assessment target has improved in month with the service now having
benefit realisation of the sub-contract with Spring North whom have had CYP cases
allocated which is freeing some capacity to also begin working with adult cases, the
partnership is hopeful that this will be an improving picture month on month
137. CMH 35 – MAS Assessment % seen in 6 week
Trust Performance of the MAS ‘Seen in 6 weeks’ target (Referral to Assessment)
improved to 63.1% against a target of 70%. Only the Fylde Locality met the target
seeing 96.9% within the time frame. Trajectories are in place in the localities to recover
performance
148. CPH 3 - 92% of Community Dental Waits less than 18 weeks
Current dental activity levels are reduced due to the national BDA Covid requirement
to leave each clinic room fallow. The fallow period is reducing from 15 to 10 minutes
(still 30 minutes for Aerosol Generating Procedures) in November which will help
slightly. The service is experiencing increased referrals from General Dental
Practitioners working on their backlogs (created by 35 million lost dental appointments
due to Covid natioanlly). Recovery above 92% at current activity level would take
approximately 24 months, but changing national dental guidance re fallow times and
PPE management could reduce this period, a new CDO (Chief Dental Officer) SOP is
expected early 2022. The national CDO Covid guidance remains in place but the dental
management team will respond immediately to any changes as they occur, this will be
monitored through the monthly dental improvement and assurance group. Final
validation of the entire waits is now complete and will be continued on a six month
rolling basis
3. Conclusion and Recommendations
Trust Board are requested to review and discuss Trust performance for October 2021.
Link below for the TPR Exception Summary Report:
TPR Exception Summary Report for Month 7 October 2021

Agenda Item Number: TB 221/21
BOARD ASSURANCE FRAMEWORK AT Q2 2020-21
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Ursula Martin, Chief Improvement and Compliance
Officer
Prepared by:
Ursula Martin, Chief Improvement and Compliance
Officer
Andy Chittenden, Interim Company Secretary
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will employ and retain the best STAFF, as our culture will be inclusive and a supportive place to work
Aligned to Board Assurance Framework Risk
3.0 Failure to learn and improve as an organisation underpinned by ineffective systems and a lack of an open and transparent culture, may impact on delivering safe care
Recommendation/Required Action
During Q2 the Executive Team has continued to identify and put in place controls to mitigate the 8 identified risks of failure to achieve the 6 strategic objectives. Risk in some areas has increased in line with the intensity of demand and competition for staffing felt across the NHS region and system. This paper updates the Board as a whole on the work undertaken to mitigate risk; the assurance sought and scrutinised by the Board’s assurance committees together with slight adjustments to risk scoring.
Version Control
Version Report to Date Reported
1.0 Executive Team 16/11/21
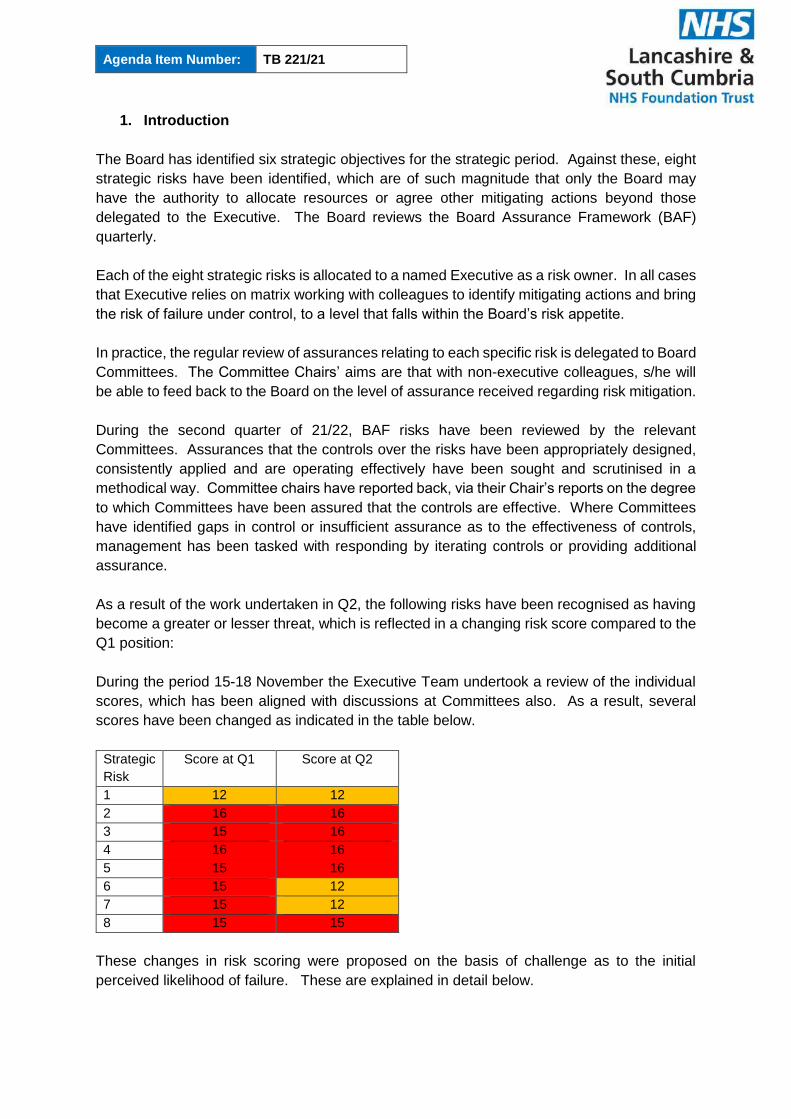
Agenda Item Number: TB 221/21
1. Introduction
The Board has identified six strategic objectives for the strategic period. Against these, eight
strategic risks have been identified, which are of such magnitude that only the Board may
have the authority to allocate resources or agree other mitigating actions beyond those
delegated to the Executive. The Board reviews the Board Assurance Framework (BAF)
quarterly.
Each of the eight strategic risks is allocated to a named Executive as a risk owner. In all cases
that Executive relies on matrix working with colleagues to identify mitigating actions and bring
the risk of failure under control, to a level that falls within the Board’s risk appetite.
In practice, the regular review of assurances relating to each specific risk is delegated to Board
Committees. The Committee Chairs’ aims are that with non-executive colleagues, s/he will
be able to feed back to the Board on the level of assurance received regarding risk mitigation.
During the second quarter of 21/22, BAF risks have been reviewed by the relevant
Committees. Assurances that the controls over the risks have been appropriately designed,
consistently applied and are operating effectively have been sought and scrutinised in a
methodical way. Committee chairs have reported back, via their Chair’s reports on the degree
to which Committees have been assured that the controls are effective. Where Committees
have identified gaps in control or insufficient assurance as to the effectiveness of controls,
management has been tasked with responding by iterating controls or providing additional
assurance.
As a result of the work undertaken in Q2, the following risks have been recognised as having
become a greater or lesser threat, which is reflected in a changing risk score compared to the
Q1 position:
During the period 15-18 November the Executive Team undertook a review of the individual
scores, which has been aligned with discussions at Committees also. As a result, several
scores have been changed as indicated in the table below.
Strategic
Risk
Score at Q1 Score at Q2
1 12 12
2 16 16
3 15 16
4 16 16
5 15 16
6 15 12
7 15 12
8 15 15
These changes in risk scoring were proposed on the basis of challenge as to the initial
perceived likelihood of failure. These are explained in detail below.
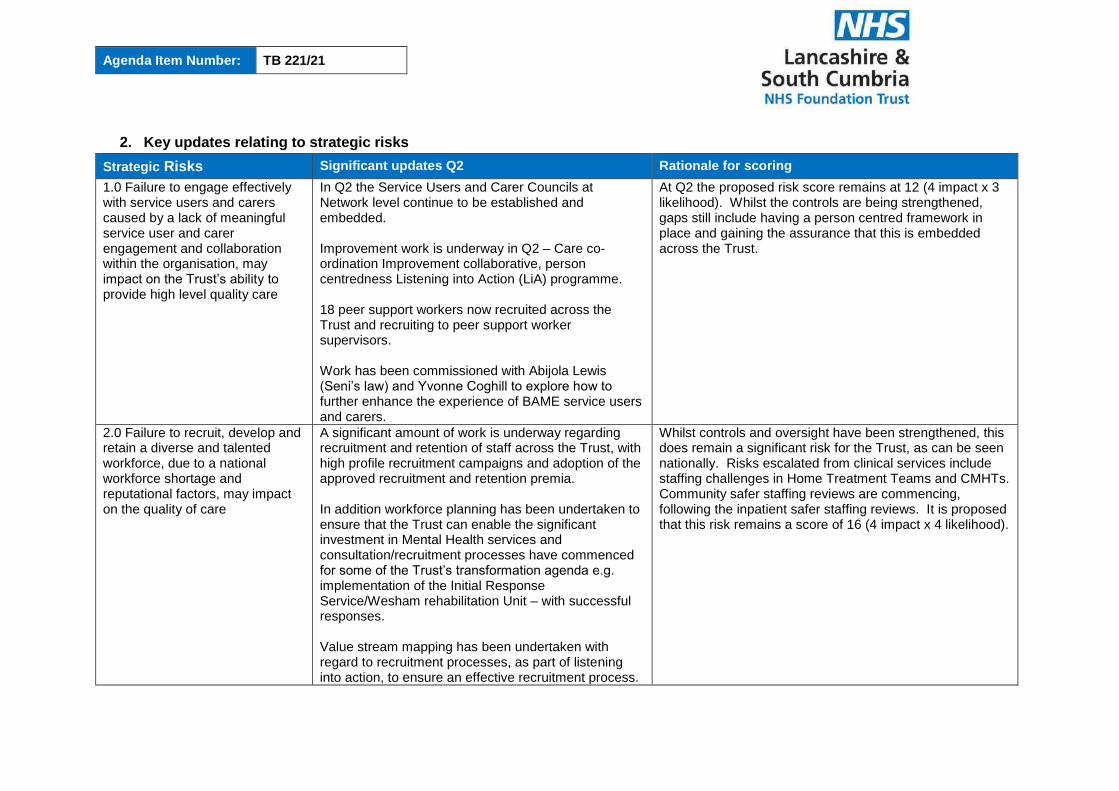
Agenda Item Number: TB 221/21
2. Key updates relating to strategic risks
Strategic Risks Significant updates Q2 Rationale for scoring
1.0 Failure to engage effectively with service users and carers caused by a lack of meaningful service user and carer engagement and collaboration within the organisation, may impact on the Trust’s ability to provide high level quality care
In Q2 the Service Users and Carer Councils at Network level continue to be established and embedded. Improvement work is underway in Q2 – Care co-ordination Improvement collaborative, person centredness Listening into Action (LiA) programme. 18 peer support workers now recruited across the Trust and recruiting to peer support worker supervisors. Work has been commissioned with Abijola Lewis (Seni’s law) and Yvonne Coghill to explore how to further enhance the experience of BAME service users and carers.
At Q2 the proposed risk score remains at 12 (4 impact x 3 likelihood). Whilst the controls are being strengthened, gaps still include having a person centred framework in place and gaining the assurance that this is embedded across the Trust.
2.0 Failure to recruit, develop and retain a diverse and talented workforce, due to a national workforce shortage and reputational factors, may impact on the quality of care
A significant amount of work is underway regarding recruitment and retention of staff across the Trust, with high profile recruitment campaigns and adoption of the approved recruitment and retention premia. In addition workforce planning has been undertaken to ensure that the Trust can enable the significant investment in Mental Health services and consultation/recruitment processes have commenced for some of the Trust’s transformation agenda e.g. implementation of the Initial Response Service/Wesham rehabilitation Unit – with successful responses. Value stream mapping has been undertaken with regard to recruitment processes, as part of listening into action, to ensure an effective recruitment process.
Whilst controls and oversight have been strengthened, this does remain a significant risk for the Trust, as can be seen nationally. Risks escalated from clinical services include staffing challenges in Home Treatment Teams and CMHTs. Community safer staffing reviews are commencing, following the inpatient safer staffing reviews. It is proposed that this risk remains a score of 16 (4 impact x 4 likelihood).

Agenda Item Number: TB 221/21
Strategic Risks Significant updates Q2 Rationale for scoring
In addition a review of the control framework for temporary staff has been undertaken.
3.0 Failure to learn and improve as an organisation underpinned by ineffective systems and a lack of an open and transparent culture, may impact on delivering safe care
The Trust continues to embed the Learning Framework across the Trust, with improved investigation, training and learning processes and opportunities. In Q2 the Trust has delivered 3 learning lessons sessions. Listening into Action Just Culture work continued across Q2, with the Trust piloting a revised incident investigation methodology and also trialling some reflective sessions following an incident for staff. Q2 saw the commencement of an internal audit, as part of the Trust’s internal audit programme regarding learning from serious incidents actions.
Gaps in control regarding this strategic risk include having the time and capacity to learn when things go wrong and also sharing learning from best practice. Learning and improvement forums will help with this going forward, as will visibility of safety and quality information, which has been enhanced at Trust, network and core service level. Ward and team information is in development with business intelligence team. The optimisation work being undertaken with the new DCIQ incident and risk management system will support this. Other gaps include not being able to systematically provide assurance regarding learning and shared learning from incidents, complaints, PALS etc., although this is evolving. With the gaps in control identified, it is proposed to amend the risk score from 15 (5 impact x 3 likelihood) to 16 (4 impact x 4 likelihood).
4.0 Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care may impact on quality of care and could incur regulatory action
The Trust recognises the improvement journey it has embarked upon and has a number of actions aligned to this strategic risk, which aligns to the Trust Quality Strategy and People, Improvement & Culture Strategy in particular. In Q2, the Trust has continued with its quality improvement work across the Trust including Reducing Restrictive Practice Improvement collaborative, Listening into Action and we have launched a Health & Social Care Needs improvement collaborative. Ward accreditation continues to be implemented across the Trust and community safety metrics have also been launched The Trust has also commenced recruitment of clinical leads across the Trust, whose role will be to review
Whilst controls and oversight have been strengthened, further work to be done relating to pathways and outcomes measures therefore it is proposed that the risk remains a score of 16 (4 impact x 4 likelihood).

Agenda Item Number: TB 221/21
Strategic Risks Significant updates Q2 Rationale for scoring
pathways and ensure unwanted variation Face to face director engagement visits have recommenced and executive team meetings are being held fortnightly at sites across the Trust to promote increased visibility and support staff.
5.0 Failure to respond to the increased demand for services as a result of the Covid-19 pandemic, due to ineffective recovery planning and the availability of appropriate resources to meet demand which may impact on the quality and wellbeing of service users
In Q2 transformation work continues to be a priority and recruitment has commenced for Initial Response Service and Wesham Rehabilitation. Street Triage implemented in South Cumbria and plans to implement in localities in Lancashire agreed.
In Q2 increased controls include a focus on Wellbeing with LiA work and a review of the psychological resilience hub having been commenced.
In addition commencement of roll out of booster injections for staff and continue support for staff to receive injections
The Trust is seeing increases in demand across all services, some more pronounced than others. Whilst transformation plans are in place regarding service provision to continue to meet the demand, gaps in control relate to workforce, access and waiting times for some services. A risk score of 15 is recommended following previous discussion at the Board of Directors. With the gaps in control identified, it is proposed to amend the risk score from 15 (3 likelihood x 5 impact) to 16 (4 likelihood x impact).
6.0 Failure to actively collaborate across the system and undertake appropriate due diligence as part of the development of the Lead Provider Collaborative due to a lack of capacity and capability within the organisation may result in care being provided that is not based on local population needs and poor patient experience
Specialist commissioning Lead Provider Collaborative LPC) live from 1st October 2021, with infrastructure, governance and oversight in place. System Transition Board and programmed activity in place for MH, LD&A to support the further delivery of the LSCFT LPC model.
Following engagement with the LPC Committee to which scrutiny of this risk is assigned, this risk is proposed to be re-scored at 12 (3 impact x 4 likelihood) from 15 (3 impact x 5 likelihood). The rationale is underpinned by specific focus on lead provider programmes. LSCFT has successfully transferred the NHSE specialist programmes and now agreed a “shadow form” arrangement with ICS on local MHLDA commissioning from 1st April 2021
7.0 Failure to deliver the Trust’s annual financial plan for 2021/22 caused by lack of robust cost improvements may impact on the
H2 plans under development in accordance with national timescales. Efficiency IP plans under development, further opportunities to be identified through ICS wide work and internal benchmarking.
The Trust has not failed in delivery of the financial plan (albeit Covid has been an extraordinary year) and discussions held during the planning round has ensured that the Trust has attracted the appropriate investment into our services going forward. However, the continued overspend and uncertainty for the second half of 2021/22 is
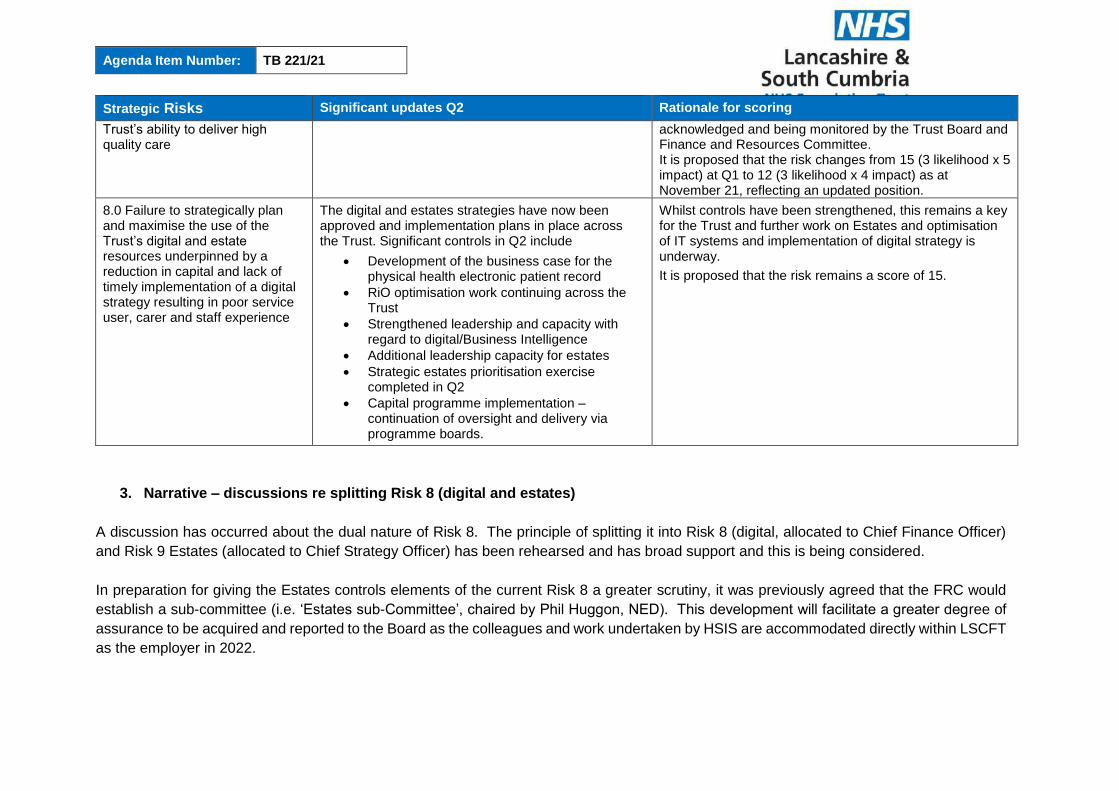
Agenda Item Number: TB 221/21
Strategic Risks Significant updates Q2 Rationale for scoring
Trust’s ability to deliver high quality care
acknowledged and being monitored by the Trust Board and Finance and Resources Committee. It is proposed that the risk changes from 15 (3 likelihood x 5 impact) at Q1 to 12 (3 likelihood x 4 impact) as at November 21, reflecting an updated position.
8.0 Failure to strategically plan and maximise the use of the Trust’s digital and estate resources underpinned by a reduction in capital and lack of timely implementation of a digital strategy resulting in poor service user, carer and staff experience
The digital and estates strategies have now been approved and implementation plans in place across the Trust. Significant controls in Q2 include
Development of the business case for the physical health electronic patient record
RiO optimisation work continuing across the Trust
Strengthened leadership and capacity with regard to digital/Business Intelligence
Additional leadership capacity for estates
Strategic estates prioritisation exercise completed in Q2
Capital programme implementation – continuation of oversight and delivery via programme boards.
Whilst controls have been strengthened, this remains a key for the Trust and further work on Estates and optimisation of IT systems and implementation of digital strategy is underway.
It is proposed that the risk remains a score of 15.
3. Narrative – discussions re splitting Risk 8 (digital and estates)
A discussion has occurred about the dual nature of Risk 8. The principle of splitting it into Risk 8 (digital, allocated to Chief Finance Officer)
and Risk 9 Estates (allocated to Chief Strategy Officer) has been rehearsed and has broad support and this is being considered.
In preparation for giving the Estates controls elements of the current Risk 8 a greater scrutiny, it was previously agreed that the FRC would
establish a sub-committee (i.e. ‘Estates sub-Committee’, chaired by Phil Huggon, NED). This development will facilitate a greater degree of
assurance to be acquired and reported to the Board as the colleagues and work undertaken by HSIS are accommodated directly within LSCFT
as the employer in 2022.
Agenda Item Number: TB 221/21
4. Risk Management Update
The Trust has undertaken significant work to date regarding risk management including
development of a Risk Management Strategy, development of a training programme relating
to Risk Management, significant review of risk registers across the Trust (to new network
structure) and development of a corporate risk register and further development of the Board
Assurance Framework. It is recognised that there is still further work to do as we progress
our improvement journey and move toward an integrated governance framework within the
Trust, where governance, performance and risk management systems are aligned.
In order to further support this, the Trust are working with the Good Governance Institute, as
they support well led preparations. In October the Board of Directors held the first workshop
looking at risk appetite across our strategic risks and described how this would be utilised
going forward as we begin to deliver our Trust Strategy and enabling strategies. Further work
is being undertaken relating to this and an update will be given to Board in Q3 version of this
report, as well as an update on the Well Led review being conducted by Good Governance
Institute relating to risk management.
5. Summary
Overall, the threats of failure to achieve the Trust’s strategic objectives has not reduced in the
quarter. Pressures across the NHS and the Lancashire and South Cumbria system remain
intense, with demand and workforce challenges being a major challenge for all service
providers, including the Trust.
The Board is invited to:
Scrutinise the assurance provided.
Provide management with constructive challenge as to the appropriate design,
consistent application and effective operation of controls over all BAF risks.
Request further sources of assurance if deemed appropriate.

Agenda Item Number: TB 222/21
ANNUAL INFORMATION GOVERNANCE AND CALDICOTT
GUARDIAN REPORT 2020/2021
Report provided for: Report to: Board of Directors
Information ☒ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by:
Dr David Fearnley, Chief Medical Officer and Caldicott Guardian
Jenny Hannon, Chief Finance Officer and Senior Information Risk Owner (SIRO)
Prepared by:
Dr Ayesha Rahim, Perinatal Psychiatrist, Deputy Chief Medical Officer,
Chief Clinical Information Officer, Deputy Caldicott Guardian
Michelle Brammah, Data Protection Officer
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will respond to peoples’ needs by striving for the highest STANDARDS of quality across all of our services
Aligned to Board Assurance Framework Risk
4.0 Failure to deliver the highest quality of care across all of our services caused by a lack of person centred care may impact on quality of care and could incur regulatory action
Recommendation/Required Action
The Board is asked to note the annual report and seek
any further assurance.
EXECUTIVE SUMMARY
Introduction and background
The annual Information Governance and Caldicott Guardian report for 2020 was deferred due
to the Covid-19 pandemic and this report is presented to cover the extended period including:
the work that has taken place during 2020/21
the common approach that has been shared to ensure that individual privacy is
balanced with clinical practice
objectives for 2021/2022.
Agenda Item Number: TB 222/21
Key Issues
The Caldicott Guardian (CG) report was previously written and presented on an annual basis
to the Trust Board and was separate to the Information Governance (IG) Assurance Update.
The IG Assurance report was a quarterly paper and part of a former Corporate Governance
and Assurance Sub Committee.
Given the close working relationship between the functions and the joint objectives for
2021/2022 these two reports have been merged to present a unified account, reinforcing the
importance and effectiveness of IG and the CG working together.
This report is to provide assurance in regard to the work both the IG function and the Caldicott
Guardian undertake to ensure that the Trust is compliant with a range of legislative
frameworks; specifically safeguarding the privacy and confidentiality of personal data (Staff
and patients) by providing appropriate advice and guidance to assure that operational
practices and processes conform to NHS and statutory standards.
The paper sets out the working interface primarily between the Caldicott Guardian (CG) and
the Data Protection Officer (DPO). It also demonstrates the working alliance with the Senior
Information Risk Officer (SIRO). The document provides insight into the fundamental
collaboration essential to sustain and improve quality of care to the patient and staff. It draws
together accountability for information risk which Data Protection law mandates and the
application of ethical and clinical oversight to support patients under our care.
Escalation of risk
Currently there are no risks to escalate. However, a new IG Risk Assurance Framework was
agreed for implementation at the August 2021 JSCG. The framework is a standardised suite
of risks applicable to all networks and corporate services with identified universal controls and
assurance measures. Networks and corporate areas will be expected to ascertain and record
local risks affiliated to the framework, employing IG incident reviews to inform the risk
assessments and local controls and assurance. All risks will be aligned with the Board
Assurance Risk Framework.
Conclusion and Recommendations
In summary, this paper is to offer assurance that the joint working between the IG and CG
functions has significantly strengthened and there is an agreed plan to further consolidate the
partnership. The future work will continue to support the delivery of safe, quality services to
patients whilst protecting the data protection rights of individuals.
Completion of the joint objectives for 2021/2022 will be monitored by the quarterly Joint SIRO
and Caldicott Guardian (JSCG) Sub-Committee and made a standing agenda item. A Chair’s
report will inform progress to both the Executive team and the Quality Committee.

Agenda Item Number: TB 223/21
EMERGENCY PREPAREDNESS, RESILIENCE & RESPONSE
(EPRR) ANNUAL CORE STANDARDS REVIEW
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Chris Oliver, Chief Operating Officer/Deputy CEO
Prepared by: Neil Furness, Head of EPRR
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will deliver SAFE care by embracing an open and learning culture, ensuring we continually improve
Aligned to Board Assurance Framework Risk
5.0 Failure to respond effectively following the Covid-19 pandemic, due to ineffective recovery planning and the availability of appropriate resources to meet demand which may impact on the quality and wellbeing of service users
Recommendation/Required Action
The Board is presented this paper in order to be
provided with assurance on the EPRR Assurance
Statement for submission into the regional assurance
process.
1.0 Introduction
1.1 Following a reduced submission in 2020/21 as a result of the national response to the Covid-19 pandemic, the annual Emergency Preparedness, Resilience & Response (EPRR) Assurance process has been increased to a pre-covid level of questions for the 2021/22 submission. 1.2 The assurance process comprises of a self-assessment against 37 questions from which an overall declaration is provided (full, partial or non-compliance).
1.3 A letter from the Steven Groves (National Director of EPRR) (ref PAR628, dated 22/07/2021), provides a reminder of the statutory requirement for formal assurance of EPRR readiness in our own organisation and the wider NHS; and a breakdown of what this will entail for 2021/22.
1.4 This report provides the EPRR Statement for assurance to the Board following approval at the Patient Safety and Effectiveness Sub Committee.
Agenda Item Number: TB 223/21
2.0 Assurance Breakdown 2.1 This year, there are eight area (domains) of EPRR that assurance is provided against. These are:
1. Governance 2. Duty to Risk Assess 3. Duty to Maintain Plans 4. Command and Control 5. Response 6. Warning and Informing 7. Cooperation 8. Business Continuity
3.0 2021/22 Declaration
3.1 The first assurance is an updated assurance position of any organisations that were rated partially or non-compliant in 2020/21. 3.2 Assurance Statement The declaration and submission LSCFT submitted for 2020/21 and an update on the 2019/20 submission of “FULL compliance”, which subsequently meant that there were no improvement actions generated. Appendix A provides details of the update.
4.0 Assurance Process Findings
4.1 The 2021/22 assurance process was undertaken with the support of the Emergency Preparedness & Resilience Group (EPRG) and was presented and agreed at the 14th September EPRG meeting. In addition, Chris Oliver, Chief Operating Officer & Deputy Chief Executive as well as fulfilling the role of Trust Accountable Emergency Officer (AEO) as part of the requirements from the NHS England EPRR Response Framework (2015) agreed the submission. Approval for the submission was obtained at the Patient Safety and Effectiveness Sub Committee on 4th November 2021.
Additionally, a requirement of the process was for the relevant CCGs to review our submission and to submit this to NHS England Lancashire & South Cumbria EPRR
team. This was undertaken with Greater Preston & Chorley, South Ribble CCGs as well as East Lancashire & Blackburn with Darwin CCGs who completed their review and submitted to NHS England on 19th October 2021.
At the 3rd November Local Health Resilience Partnership meeting, attended by Lancashire and Cumbria NHS trusts and CCG it was noted that LSCFT’s submission of Substantial is an outlier to other trust’s submission. However, NHS England are assured that we have the process in place in order to move to a fully compliant score during 2021 / 2022.
The assurance process has identified four of the 37 standards that have an “Amber”* rating. These are:
No. 6 Duty to Risk Assess – Risk Assessments
No.32 Response – Management of business continuity incidents

Agenda Item Number: TB 223/21
No.60 Chemical, Biological, Radiological & Nuclear (CBRN) – Equipment & Supplies
No.68 CBRN – Staff Training (decontamination)
* Not compliant with core standard. The organisation’s EPRR work programme demonstrates evidence of progress and an action plan to achieve full compliance within the next 12 months
A programme of work has been identified and endorsed by the EPRG who will receive updates on progress at each meeting. A copy of the work plan for each of the four amber standards is detailed at Appendix B.
4.2 Assurance Statement A copy of the Assurance statement is found at Appendix C.
5.0 Conclusion Whilst we continue to face challenging times due to our on-going covid-19 response and the onset of winter, emergency planning will continue to be a key area for the trust, with the support of the re-established Emergency Preparedness & Resilience Group (EPRG), to maintain and improve/enhance our resilience arrangements.
6.0 Recommendation The Board are receiving the Assurance Statement and supporting papers for assurance purposes.
Agenda Item Number: TB 223/21
Appendix B.
EPRR Assurance 2020 – Lancashire & South Cumbria Update
Name of Trust/CCG: Lancashire & South Cumbria NHS Foundation Trust
Compliance 2019
Progress made during
2020 on partially or
non-compliant areas
identified last year.
(Return N/A if fully or
substantially compliant)
N/A
The declaration and submission
LSCFT submitted for 2020/21 was a
“FULL compliance”, which
subsequently meant that there were no
improvement actions generated.
Therefore this criterion does not apply
to LSCFT and the trust does not have
an improved status to report on.
2021 Update
Not applicable as refers to 2019
compliance
Mid Term Covid
Review
Date of debrief /
Review Key Lessons
The Head of Emergency Planning has
been at the forefront of the response
from initial monitoring, Incident Room
activation, through to the current
position. This has enabled the capture
the Trust’s status and learning
opportunities from the response as it
has progressed, through hot debriefs
of staff, comprehensive logging and
ongoing monitoring. From this, a
comprehensive review and lessons
learned report (including an action plan
to address improvement opportunities)
has been compiled.
Please see appendix A for a copy of
the report
2021 Update
The trust continues to operate its
Covid-19 Silver Command. Lessons
learnt are being monitored via the
Emergency Preparedness &
Resilience Group. Additionally, the
trust has commissioned a piece of
work with the Good Governance
Institute (GGI) to review it’s working
practices and it’s command and control
during / as part of our on-going
response to the pandemic. To support
this, the trust has started to collate key
information such as timelines, key staff
information and details of where
NWICC updates were distributed to
and what action was taken.
Agenda Item Number: TB 223/21
Process for embedding
the learning from the
review
Include changes to
procedures and
communications
The action plan associated with the
systematic review and lessons
learned report will be a standing
agenda item on the Emergency
Preparedness and Resilience
Group EPRG), where it will be
monitored through to completion.
Subject to the nature of the action,
an implementation, training and
communication plan will be
deployed to ensure all necessary
staff are fully aware of and trained in
any changes to systems and
processes.
The process for embedding any
learning will form of the Emergency
Preparedness and Resilience
Group’s action plan.
Winter Plans
Areas from review that
have influenced Winter
planning
The Head of Emergency Planning
has already begun preparations for
the LSCFT Winter Plan 2020/21 by
undertaking a series of preparatory
actions:
Tasking each lead member of the Emergency Preparedness & Response Group (EPRG) to: o Review their Network’s or
Support Services’ winter plans from 2019/20 to ensure learning from previous years in incorporated into this year’s plan;
o Study existing organisational and system pressures (i.e. normal pressures and those exacerbated by the response to Covid-19), to identify issues and develop initiatives and solutions;
o Participate in the offer from Richard Freeman, (Head of Winter & UEC, NHS England & NHS Improvement - North West Region) of peer reviews;
o Develop Winter and Christmas/New Year rotas as early as possible to ensure and validate essential staff cover for critical services
Trust Winter Planning is being
actioned by the Deputy Chief
Operating Officer and will be
reported via the applicable sub-
committee.

Agenda Item Number: TB 223/21
throughout winter and the festive period
Liaising closely with the Senior Responsible Officer for the C&SR CCG/Greater Preston CCG’ Winter Planning Group
Linking in with the Senior Planning, Transformation & Delivery Officer within Blackburn with Darwen CCG and East Lancashire CCG to undertake joint working where appropriate.
Using the above to feed into, and ensure that appropriate arrangements to support LSCFT, are integrated into the ICS Winter Plan.
All of the above actions, together with the relevant learning from the systematic review and lessons learned report and action plan, will actively inform winter preparedness activities for LSCFT.

Agenda Item Number: TB 223/21
Appendix B – 2021/22 Work Plan
Organisation: Lancashire & South Cumbria NHS Foundation Trust
Plan owner: Neil Furness, Head of EPRR
Core
Standard
reference
Core Standard description Improvement required to achieve
compliance Action to deliver improvement Deadline
7 Duty to Risk Assess – Risk
Assessments
Currently, there are a limited number of
emergency planning risks recorded in
the trust. A plan is underway to review
what emergency planning risks are
applicable to the rust in conjunction with
local LRF risks. Once the risks have
been defined, they will be reviewed at
each Emergency Preparedness &
Resilience Group meeting as a standard
agenda item.
Task and Finish Group has been
established to determine the emergency
planning risks and these are to be
monitored at each Emergency
Preparedness & Resilience Group
meeting.
December 2021
32 Response – Management of
business continuity incidents
Due to the restructuring of the trust into
a locality model and the demands of
Covid a new initiative is underway to
The status of all business continuity
plans are a standard agenda item on the
quarterly Emergency Preparedness &
December 2021

Agenda Item Number: TB 223/21
Core
Standard
reference
Core Standard description Improvement required to achieve
compliance Action to deliver improvement Deadline
ensure all services, including corporate
areas, have an up to date Business
Continuity plan. These will be stored in
MS teams to allow greater access.
Progress on the works is being
monitored via the Emergency
Preparedness and Resilience group.
Resilience Group meeting. Initial update
provided at the 14/09 meeting with a full
update provided at the 07/12 meeting.
60 CBRN – Equipment & Supplies
List of required equipment and supplies
for a "Response Box" are explicitly listed
within the HAZMAT/CBRN Plan with
guidance for building managers to
develop their response boxes to include
all of the information and resources
needed.
However, not assured that this is in place
in LCFT locations. Need to ensure all
sites have a response box in place and
Task and Finish group to be established
to conduct a full review of the process
including which sites are applicable that
the relevant equipment and supplies are
in place including support from
Lancashire Police.
December 2021
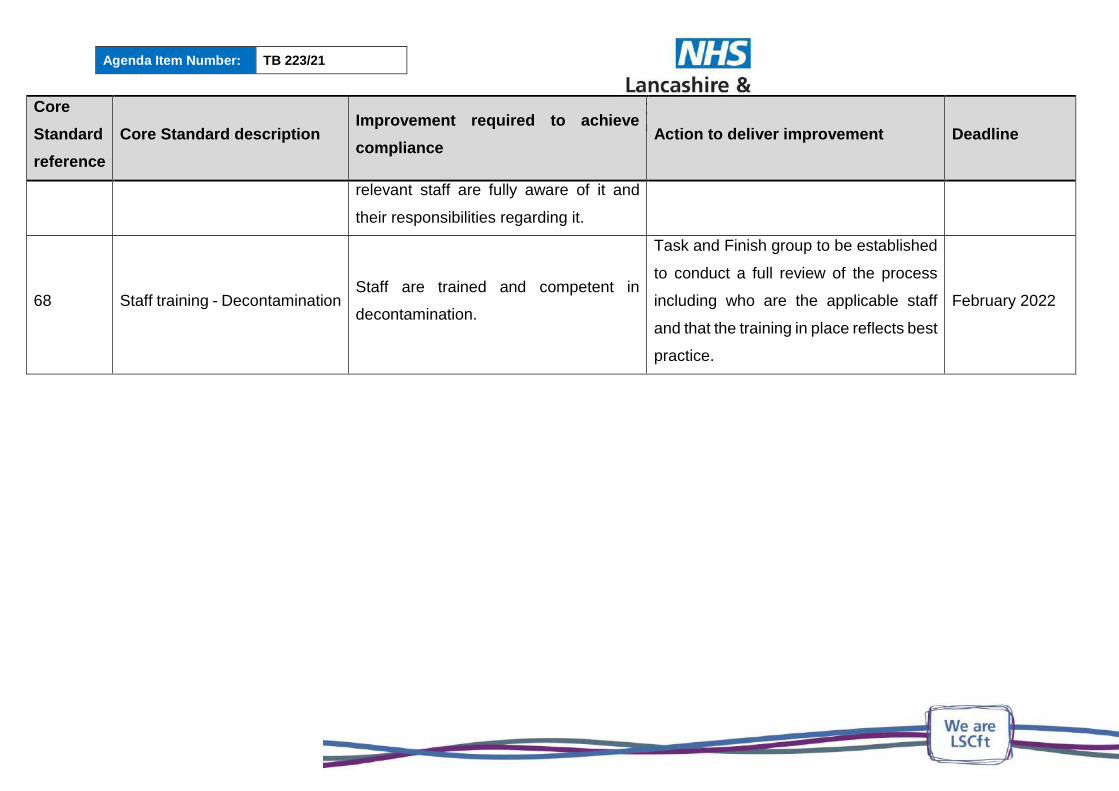
Agenda Item Number: TB 223/21
Core
Standard
reference
Core Standard description Improvement required to achieve
compliance Action to deliver improvement Deadline
relevant staff are fully aware of it and
their responsibilities regarding it.
68 Staff training - Decontamination Staff are trained and competent in
decontamination.
Task and Finish group to be established
to conduct a full review of the process
including who are the applicable staff
and that the training in place reflects best
practice.
February 2022
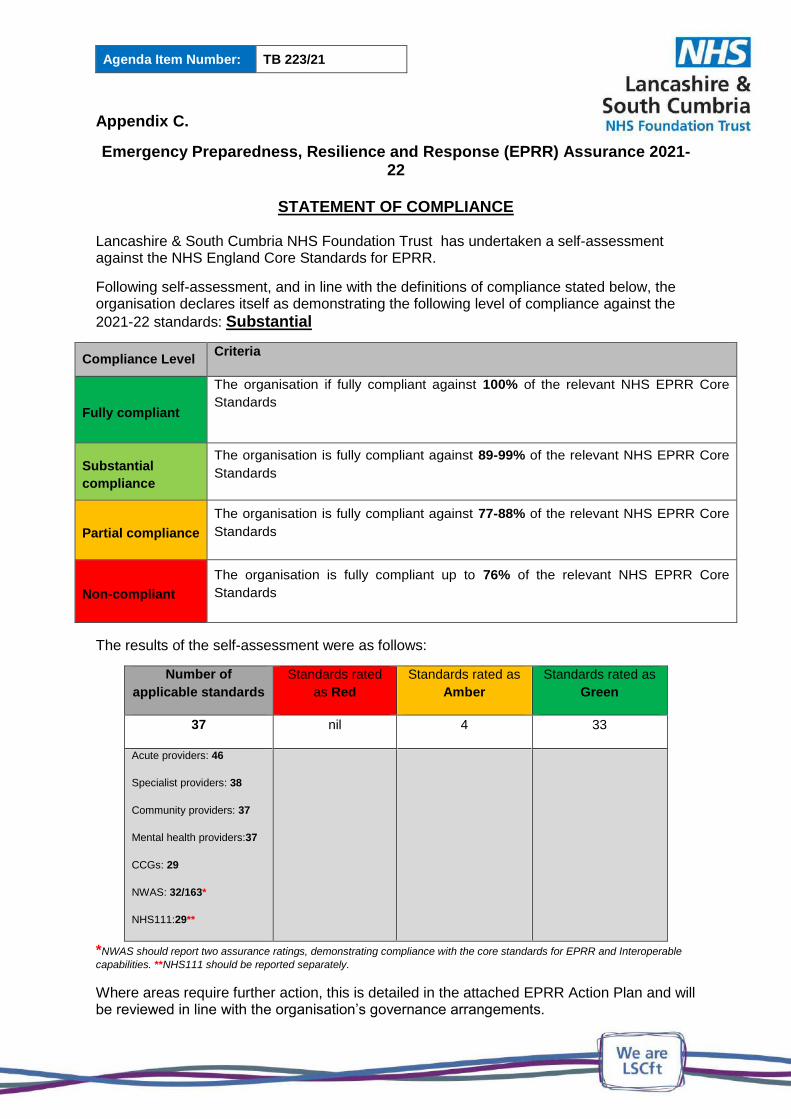
Agenda Item Number: TB 223/21
Appendix C.
Emergency Preparedness, Resilience and Response (EPRR) Assurance 2021-22
STATEMENT OF COMPLIANCE
Lancashire & South Cumbria NHS Foundation Trust has undertaken a self-assessment against the NHS England Core Standards for EPRR.
Following self-assessment, and in line with the definitions of compliance stated below, the organisation declares itself as demonstrating the following level of compliance against the
2021-22 standards: Substantial
Compliance Level Criteria
Fully compliant
The organisation if fully compliant against 100% of the relevant NHS EPRR Core
Standards
Substantial
compliance
The organisation is fully compliant against 89-99% of the relevant NHS EPRR Core
Standards
Partial compliance
The organisation is fully compliant against 77-88% of the relevant NHS EPRR Core
Standards
Non-compliant
The organisation is fully compliant up to 76% of the relevant NHS EPRR Core
Standards
The results of the self-assessment were as follows:
Number of
applicable standards
Standards rated
as Red
Standards rated as
Amber
Standards rated as
Green
37 nil 4 33
Acute providers: 46
Specialist providers: 38
Community providers: 37
Mental health providers:37
CCGs: 29
NWAS: 32/163*
NHS111:29**
*NWAS should report two assurance ratings, demonstrating compliance with the core standards for EPRR and Interoperable
capabilities. **NHS111 should be reported separately.
Where areas require further action, this is detailed in the attached EPRR Action Plan and will be reviewed in line with the organisation’s governance arrangements.
Agenda Item Number: TB 223/21
I confirm that the above level of compliance with the EPRR Core Standards has been or will be confirmed to the organisation’s board / governing body.
______________________________________________________________Chris Oliver Signed by the organisation’s Accountable Emergency Officer
27/11/2021 06/10/2021
Date of board / governing body meeting Date signed
Agenda Item Number: TB 224/21
CARE QUALITY COMMISSION (CQC) UPDATE
Report provided for: Report to: Board of Directors
Information ☒ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Ursula Martin, Chief Improvement & Compliance Officer
Prepared by: Stefan Verstraelen, Director of Governance
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will put SERVICE USERS at the heart of everything we do, supporting effective care, recovery and wellbeing.
Aligned to Board Assurance Framework Risk
1.0 Failure to engage effectively with service users and carers caused by a lack of meaningful service user and carer engagement and collaboration within the organisation, may impact on the Trust’s ability to provide high level quality care
Recommendation/Required Action
For members of the board to take note of the report
with assurance offered to the board on progress of the
CQC action plan following the April 2021 inspection to
the Harbour (Blackpool) inpatient unit. The board are
asked to note CQC preparedness and CQC State of
Care report
EXECUTIVE SUMMARY
The board are asked to receive this paper, giving an update on CQC preparedness.
Key issues within this report include:
- An update on The Harbour Visit action plan, with assurance offered that the action
plan is being progressed;
- An update on the CQC preparedness work and this is outlined for information;
- An update of the CQC’s recently published State of Care report and this is outlined
for information.
1. CQC ACTION PLAN
The CQC inspected The Harbour on an announced visit in April 2021 and visited two core
services (Adult wards for adults of working age and Psychiatric Intensive Care Units and wards

Agenda Item Number: TB 224/21
for older adults with mental health problems). Whilst the CQC found that the services were
safe and staff demonstrated high levels of care, with lots of good practice identified, there were
a number of recommendations made by the CQC.
Adult wards for adults of working age and Psychiatric Intensive Care Units core
service
- The trust must ensure that staffing levels and skill mix are appropriate to meet the
needs of patients (Regulation 9 (1) Person Centred Care - The care and treatment of
service users must be appropriate, meet their needs and reflect their preferences)
- The trust should ensure that ongoing recruitment plans are delivered and that the
recruitment trajectory is met
- The trust should ensure that supervision takes place in line with trust policy
- The trust should ensure that staff have access to regular team meetings
- The trust should ensure effective engagement with staff and increased visibility of
senior leaders post COVID-19
- The trust should ensure governance and performance monitoring systems are in place
to monitor delivery of ward activities and record the rationale for cancelled leave
Wards for older adults with mental health problems core service
- The trust must ensure that staffing levels and skill mix are appropriate to meet the
needs of patients (Regulation 9 (1) Person Centred Care - The care and treatment of
service users must be appropriate, meet their needs and reflect their preferences)
- The trust should ensure that ongoing recruitment plans are delivered and that the
recruitment trajectory is met
- The trust should ensure that staff have access to regular team meetings
- The trust should ensure that staff receive appropriate specialised training
- The trust should ensure effective engagement with staff and increased visibility of
senior leaders post COVID-19
- The trust should ensure governance and performance monitoring systems are in place
to monitor delivery of ward activities and record the rationale for cancelled leave
An updated action plan from this CQC inspection is appended as additional information for the
board to scrutinise. The action plan is overseen by the Improvement Management Group for
The Harbour, which meets weekly, chaired by the Chief Nursing and Quality Officer, and has
been received by Improvement Management Board, chaired by Chief Executive Officer and
Quality Assurance Committee. Assurance can be offered to the board on the actions being
taken to address the findings of the CQC, a lot of which were in train prior to the inspection.
2. CQC PREPAREDNESS
The trust continues to progress the improvement journey aligned to CQC preparedness under
the Excelling Together programme. There are a number of activities as part of this CQC
preparedness work.
Agenda Item Number: TB 224/21
Well led preparedness – following the AQUA review undertaken in 2019, the trust have
commissioned the Good Governance Institute (GGI) to work with the trust to ascertain the
improvement and progress made since the last well led review. The GGI are also supporting
the trust with implementing its risk management strategy, specifically with training on risk
management and in addition provision of training for staff relating to good governance,
complaints handling and family liaison officer training. We have also invited the GGI to review
our Covid response, in preparation for the Covid Enquiry. The GGI work continues to progress
with interviews with key internal and external stakeholders and observation and scrutiny of
meetings and documents across all eight Key Lines of Enquiry (KLoEs). This will be reported
to board early 2022.
Core service preparedness – as part of the preparedness for core services, the trust is
undertaking a number of programmes of work.
Improvement board - The Improvement Board chaired by the CEO continues its scrutiny of
the improvement work across the Trust. This has a number of reporting workstreams aligned
to CQC domains of Safe, Effective, Caring, Responsive and Well led, each led by an Executive
Director, with an overarching CQC Steering Group. The Improvement Board oversees areas
where there is challenging performance and improvement is required, sharing of practice and
the CQC preparedness programme. This includes a number of clinical practice improvement
workstreams e.g. therapeutic environments, Reducing Restrictive Practice, person
centeredness etc.
Self assessments – networks have been asked to self-assess against the core services
fundamental standards. This exercise was undertaken in June 2021 and again in September
2021. This self-assessment exercise has been supported by performance data, triangulated
quality and governance information, visits and inspections and staff collectively in teams
considering the CQC fundamental standards and identifying positive practice and areas for
improvement. The exercise will be completed again in January 2022 and will be presented to
the board as part of board development and assessing CQC preparedness.
Ward accreditation and time to shine mock inspections – the trust have implemented a
ward accreditation scheme, aligned to CQC fundamental standards. All inpatient wards will
receive a visit by end December 2021 and improvement and follow up visits will be planned
depending on the status of the ward; gold, silver, bronze, white. The board will receive an
update on the ward accreditation scheme early 2022. In addition to the ward accreditation
scheme, a number of time to shine mock CQC inspections are being undertaken across other
core services. This is to ensure that staff are familiar with a CQC inspection process and are
able to identify evidence required as part of the inspection process, but also talk positively
about the things they are proud of and help identify improvements. Over seventy teams have
received a visit thus far from a multi disciplinary inspection team, with more visits scheduled
up to March 2022. Reports from the time to shine visits are shared with the teams, with any
urgent issues escalated to network leadership and any improvement actions are monitored
via network governance meetings and report to CQC Steering Group and Improvement Board.
Agenda Item Number: TB 224/21
Previous inspection reviews – the trust developed an action plan following the 2019
inspection (South Cumbria actions were integrated following the merger of services in October
2019). The board received regular updates of this action plan and monitored delivery. There
were two internal audits of the actions in the action plan, which gave assurance of delivery.
Work is underway to review current performance against the recommendations given by the
CQC in 2019, specifically the Must Do and Should Do recommendations outlined within the
report. There are examples of where we had achieved compliance with the recommendations
at the time of delivering the action plan, Covid has had an impact e.g. delivery of face to face
training. The review of this is therefore key to understanding any risks of performance against
these recommendations ahead of a future inspection.
Staff engagement – there is a significant programme of staff engagement underway across
the trust with programmes such as Health & Wellbeing, Equality, Diversity and Inclusion,
leadership development and Listening into Action being examples of work currently underway.
The trust recognise that staff are our greatest asset and key to the delivery of the improvement
programme is a happy and motivated workforce.
Communication – there is a communication plan in place as part of the Excelling Together
improvement journey. This is to ensure that all staff across the organisation are aware of the
improvement work being undertaken and are able to articulate issues like the revised strategy
for the trust, values etc. A booklet will be circulated to all staff in December 2021 and we will
be holding workshops for staff in early 2022 to talk about the improvement journey, recognising
the work we have done to date, but also the work planned ahead as part of delivery of our
clinical strategy and enabling stratgies.
3. CQC STATE OF CARE REPORT
The Care Quality Commission (CQC) most recently (21 October 2021) published ‘The state
of health care and adult social care in England 2020/21’ report.
The Care Quality Commission (CQC) explains in the ‘The state of health care and adult social
care in England 2020/21’ report that there is recognition that COVID-19 will continue to cast a
long shadow over all aspects of everyday life, in particular the health and care system, and
the toll it has taken on the workforce, which now faces the challenges ahead, whilst already
exhausted and depleted. The CQC has concerns that this may have implications for the quality
of care and that COVID-19 has a damaging impact on people who use health and social care
services. There is acknowledgement that staff in health and social care services cannot work
any harder, and that they need support to work differently.
Although many of the underlying problems and issues pre-date COVID-19, such as access to
children and young people’s mental health services, concerns about closed cultures in
services for people with a learning disability or autistic people, and poorer experience and
outcomes around childbirth for black and minority ethic women, it has become clear that
COVID-19 has exacerbated inequalities and continues to do so. Significantly so, this means
that people who were less likely to receive good care before and during the pandemic, are in

Agenda Item Number: TB 224/21
many cases the same groups disproportionally impacted by COVID-19. For example, in
relation to community care for people with a learning disability, it is apparent that their physical
health, including how COVID-19 may present, was not always considered.
The CQC continues to explain that to help address the multiple challenges faced by the care
system, the government has now made a welcome £5.4 billion investment, which must be
used to enable new ways of working that recognise the interdependency of all care settings.
Increased funding and stability in social care is the key not only to unlocking improved access
and quality of care for the people who use it, but to easing pressure on the NHS by reducing
emergency attendances and delayed discharges. Close working between providers,
commissioners and all other parts of the health and care system is essential to safely manage
risk through the forthcoming winter. As waiting lists for investigation and treatment lengthen,
ensuring that they are managed well, fairly and safely will be increasingly crucial; closer
collaboration with primary care services and third sector organisations will be vital to this.
New models for urgent and emergency care are needed, to ensure people receive the care
they need where and when they need it, also to avoid them being inappropriately funnelled
into emergency departments. In the medium to longer term, integrated care systems must set
out plans for how social care and all parts of the health and care system work better together
to respond to the needs of their local community. Unsurprisingly, success will involve making
sure people get the right treatment in the right place at the right time, managing activity away
from acute services where possible, to where people can be better cared for.
To make this happen, more attention needs to be given to relationships and support outside
the formal healthcare system, as well as to training and recruitment across all sectors. Better,
more coordinated care for people happens when local services work well as a system; good
collaboration makes a difference in helping people to access care, even during the pandemic.
Every system needs to learn from examples of innovation, to ensure that their local population
receives the care it needs, with leaders focused on delivering a transformation in the way that
people access and experience care. The future must be focused on outcomes for all people
who need care, supported by transformational changes to workforce, funding, commissioning
and oversight.
Key Issues
The review by the CQC of the State of Care has highlighted four key issues, which are outlined
and detailed in the ‘The state of health care and adult social care in England 2020/21’ report.
The four key issues and associated key points have been summarised below:
1) People’s experiences of care
Many people have struggled to get the care they need, and there is also evidence that
some people have not sought care and treatment as a result of COVID-19.
Agenda Item Number: TB 224/21
Ongoing issues that people from some groups have faced in accessing and receiving
high-quality care. Over the last year, the pandemic has further exposed and
exacerbated these inequalities.
People with a learning disability have faced increased challenges as a result of the
pandemic.
The need for mental health care has increased, with children and young people
particularly badly affected.
The strain on carers has intensified. Carers UK estimated in June 2020 that an
additional 4.5 million people had become unpaid carers since the pandemic began.
Health and social care staff are exhausted and the workforce is depleted. People
across all professions, and carers and volunteers, have worked tirelessly to help those
who needed care. The negative impact of working under this sustained pressure,
including anxiety, stress and burnout, cannot be underestimated.
Despite the widespread disruption caused by the pandemic, surveys have shown that,
when people were able to access the care they needed, they were often positive about
that care.
2) Flexibility to respond to the pandemic
After the initial prioritisation of urgent care, there was a gradual push to bring systems
back in line with pre-pandemic levels. Of the NHS acute areas examined (cancer,
cardiovascular, A&E and mental health services), cancer services have achieved the
best response and recovery.
The NHS was able to expand its critical care capacity to respond to the needs of the
patient population at a time of crisis, although it put extra pressure on staff and other
types of care and treatment.
There are serious concerns about ambulance handover delays at hospitals, which puts
the safety of patients at risk
The ‘discharge to assess’ model for managing transfers of care has helped to support
services in both health and social care. It has been a good step towards helping people
after they leave hospital, although there needs to be greater consistency in how it is
implemented.
The vital role of adult social care was made clear during the pandemic, but urgent
action is needed to tackle staffing issues and the increased pressures and stresses
caused by staff shortages.
GP practices had to rapidly move to a more remote model of care in the pandemic –
this was welcomed by many people needing GP care, but it did not benefit everyone
and some struggled to get the appointments they wanted.
Access to NHS dental care was an issue since before COVID-19, and there are clear
signs that this has been compounded by the pandemic.
3) Ongoing quality concerns
Through reviews of high-risk mental health services, there are concerns that people
continue to be put at risk in a small number of services where there are warning signs
of closed cultures.
Agenda Item Number: TB 224/21
Improvements in maternity care are far too slow, with continuing issues around staff
not having the right skills or knowledge, poor working relationships, and not learning
from when things go wrong. Other concerns include a lack of engagement with local
women by maternity services and limited action taken by these services to improve
equitable access.
While services have largely maintained levels of Deprivation of Liberty Safeguards
during 2020/21, they need to have a continued focus on people subject to a deprivation
of liberty. There are ongoing concerns about delays in authorisations, which mean that
individuals are deprived of their liberty longer than necessary, or without the
appropriate legal authority and safeguards in place.
4) Challenges for systems
Collaborative working was varied among the local systems; cross-sector working was
helped by good communication, information sharing and shared values.
There was a lack of integration of adult social care providers into system-level planning
and decision-making.
Most systems had some understanding that inequalities in care existed in their areas
before the pandemic, as well as how they had worsened or changed due to the
pandemic. But tackling these inequalities was often not a main priority for them.
Workforce planning is a major priority and challenge for local systems and providers.
Recruitment and staff retention continue to be severe problems. In adult social care,
the situation is serious and deteriorating. There must be a sharp focus on developing
a clearly defined career pathway and training, supported by consistent investment that
will enable employers to attract and retain the right people.
The ‘The state of health care and adult social care in England 2020/21’ report holds no
surprises for the trust and all applicable issues described in the report had already been
identified and recognised by the trust, with work under way.
It is assuring to learn from the CQC that despite the widespread disruption caused by the
pandemic, surveys have shown that, when people were able to access the care they needed,
they were often positive about that care. Through their feedback received, it is apparent that
the vast majority of our service users and their carers have had a good experience from the
services we provide.
However, the trust also acknowledge that many challenges remain and those have been
appropriately identified on the Board Assurance Framework (BAF):
4. CONCLUSION
Members of the board are asked to consider the contents of this paper for information and
assurance.
Agenda Item Number: TB 225/21
APPOINT A NEW DIRECTOR OF NOMINEE NO 1 LTD
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☐
Discussion ☐ Decision ☒ Date of Meeting: 25/11/2021
Presented by: Chris Oliver, Chief Operating Officer and Deputy CEO
Prepared by: Andy Chittenden, Interim Company Secretary
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will employ and retain the best STAFF, as our culture will be inclusive and a supportive place to work
Aligned to Board Assurance Framework Risk
3.0 Failure to learn and improve as an organisation underpinned by ineffective systems and a lack of an open and transparent culture, may impact on delivering safe care
Recommendation/Required Action
The Board is invited to appoint Alex Heritage as a
Director of LSCFT Nominee No 1 Ltd with immediate
effect.
1. Introduction
LSCFT incorporated LSCFT Nominee No 1 Ltd on 18 January 2018. The company does not
trade but is a member of Healthcare Support & Infrastructure Services LLP (‘HSIS’) and
entitled to a 1% share of profits generated by HSIS.
LSCFT is the sole shareholder of LSCFT Ltd which is a company limited by shares.
Companies House returns re LSCFT Nominee No 1 Ltd are upto date, with the exception of
the director rotation following the resignation of the previous Chief Finance Officer.
2. Recommendation
The Board is invited to appoint Alex Heritage as a Director of LSCFT Nominee No 1 Ltd with
immediate effect.

Agenda Item Number: TB 226/21
MENTAL HEALTH IMPROVEMENT PLAN
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☒ Date of Meeting: 25/11/2021
Presented by: Chris Oliver, Chief Operating Officer / Deputy CEO
Prepared by: Phil Horner, Director of Information & Performance
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will respond to peoples’ needs by striving for the highest STANDARDS of quality across all of our services
Aligned to Board Assurance Framework Risk
3.0 Failure to learn and improve as an organisation underpinned by ineffective systems and a lack of an open and transparent culture, may impact on delivering safe care
Recommendation/Required Action
To provide an update for the Board on a range of key performance metrics linked to the urgent care mental health pathway. The Board is asked to receive this report as Assurance that there has been significant and sustained improvement across the adult mental health crisis pathway.
1.0 Introduction There is continued focus on the mental health urgent care pathway at a local, regional and
national level. The agreed data sets below monitor key measurables within the urgent care
pathway, both to identify current performance trends and to gauge the impact of supportive
actions intended to develop more efficient, effective and sustainable services that would
meet the needs of key stakeholders including service users, carers, the Trust and the wider
ICS system. While post-Covid demand pressures have resulted in deteriorations in
performance of some metrics compared to the Lockdown period, the data indicate areas of
improved performance compared to pre-Lockdown activity, even where demand is now at a
significantly higher level and for some key metrics demand is the highest levels ever recorded.
In addition there is a continued reduction in the number of beds in the system due to social
distancing measures and planned ward refurbishment.
Because of specific concerns regarding the Urgent Mental Health Care pathways in
Lancashire, there has been particular focus on these pathways in previous reports. South
Cumbria data has been further woven into this report to provide a more rounded view of Trust
performance.
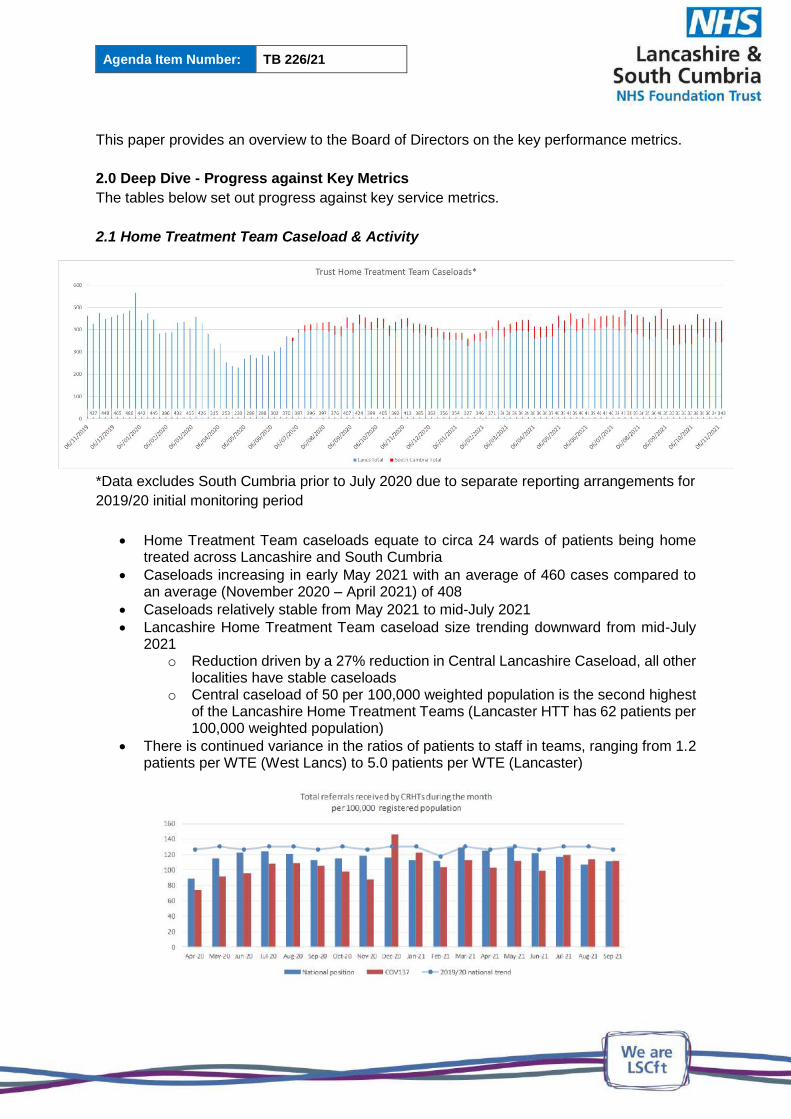
Agenda Item Number: TB 226/21
This paper provides an overview to the Board of Directors on the key performance metrics.
2.0 Deep Dive - Progress against Key Metrics
The tables below set out progress against key service metrics.
2.1 Home Treatment Team Caseload & Activity
*Data excludes South Cumbria prior to July 2020 due to separate reporting arrangements for
2019/20 initial monitoring period
Home Treatment Team caseloads equate to circa 24 wards of patients being home treated across Lancashire and South Cumbria
Caseloads increasing in early May 2021 with an average of 460 cases compared to an average (November 2020 – April 2021) of 408
Caseloads relatively stable from May 2021 to mid-July 2021
Lancashire Home Treatment Team caseload size trending downward from mid-July 2021
o Reduction driven by a 27% reduction in Central Lancashire Caseload, all other localities have stable caseloads
o Central caseload of 50 per 100,000 weighted population is the second highest of the Lancashire Home Treatment Teams (Lancaster HTT has 62 patients per 100,000 weighted population)
There is continued variance in the ratios of patients to staff in teams, ranging from 1.2 patients per WTE (West Lancs) to 5.0 patients per WTE (Lancaster)

Agenda Item Number: TB 226/21
NHS Benchmarking shows referrals to LSCFT Home Treatment Teams as having been lower than the Benchmark for much of the Covid period, but with higher than typical monthly referrals since July 2021
LSCFT Home Treatment Teams accept 99% of referrals, compared to a Benchmark of 93%, suggesting that more appropriate referrals are made to the teams
Home Treatment Team face-to-face activity levels overall fell steeply when Lockdown 1 commenced in March 2020, and the impact that social distancing, lockdown and other Covid-related measures have had is evident in the above graph
The reduction in face-to-face activity was balanced to a degree with increased telephone activity
Both face-to-face and overall activity increased as Lockdown eased
Home Treatment Team face-to-face contacts increased in March to their highest since October 2020 and have remained above the post-RiO mean since then

Agenda Item Number: TB 226/21
The rate of clinical contacts per 100,000 registered population in September was
Benchmarked as 14.3% below the national mean, and 6.6% below the national median
Home Treatment Team staffing in LSCFT is currently 22.8% below the Benchmarked mean rate per 100,000 registered population
2.2 Mental Health Liaison Activity
Full team activity presented (A&E and ward-based activity) and updated to include historic South Cumbria data
Lower activity in teams November 2020 – February 2021 accounted for by lower ward-based activity (i.e. activity has remained weighted towards A&E departments)
The increase in activity in March 2021 is therefore notable as this activity is predominantly with A&E departments
This pattern has continued, with a further increase in activity in May 2021, which was sustained into June
Face-to-face activity fell in July and August, in line with a decrease in attendances at A&E
However, activity again increased in September and October, being 27% higher than in the same period 2020, and 28% higher than the same period in pre-Covid 2019
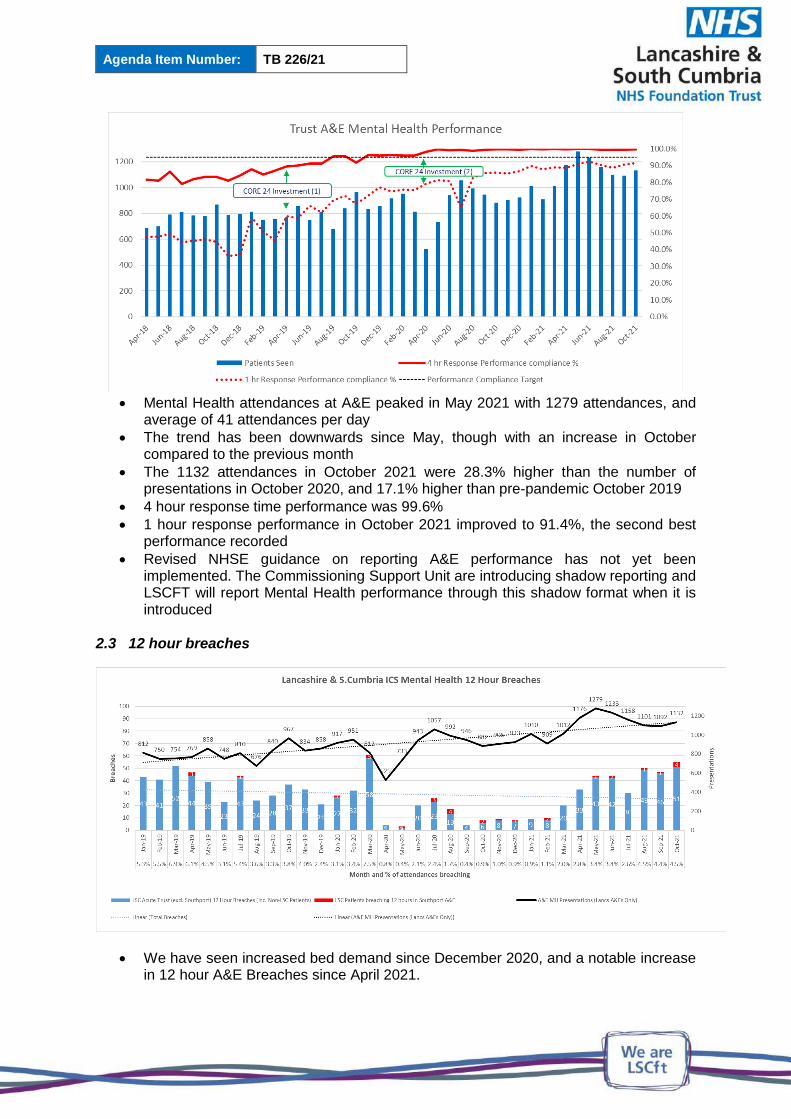
Agenda Item Number: TB 226/21
Mental Health attendances at A&E peaked in May 2021 with 1279 attendances, and
average of 41 attendances per day
The trend has been downwards since May, though with an increase in October compared to the previous month
The 1132 attendances in October 2021 were 28.3% higher than the number of presentations in October 2020, and 17.1% higher than pre-pandemic October 2019
4 hour response time performance was 99.6%
1 hour response performance in October 2021 improved to 91.4%, the second best performance recorded
Revised NHSE guidance on reporting A&E performance has not yet been implemented. The Commissioning Support Unit are introducing shadow reporting and LSCFT will report Mental Health performance through this shadow format when it is introduced
2.3 12 hour breaches
We have seen increased bed demand since December 2020, and a notable increase in 12 hour A&E Breaches since April 2021.
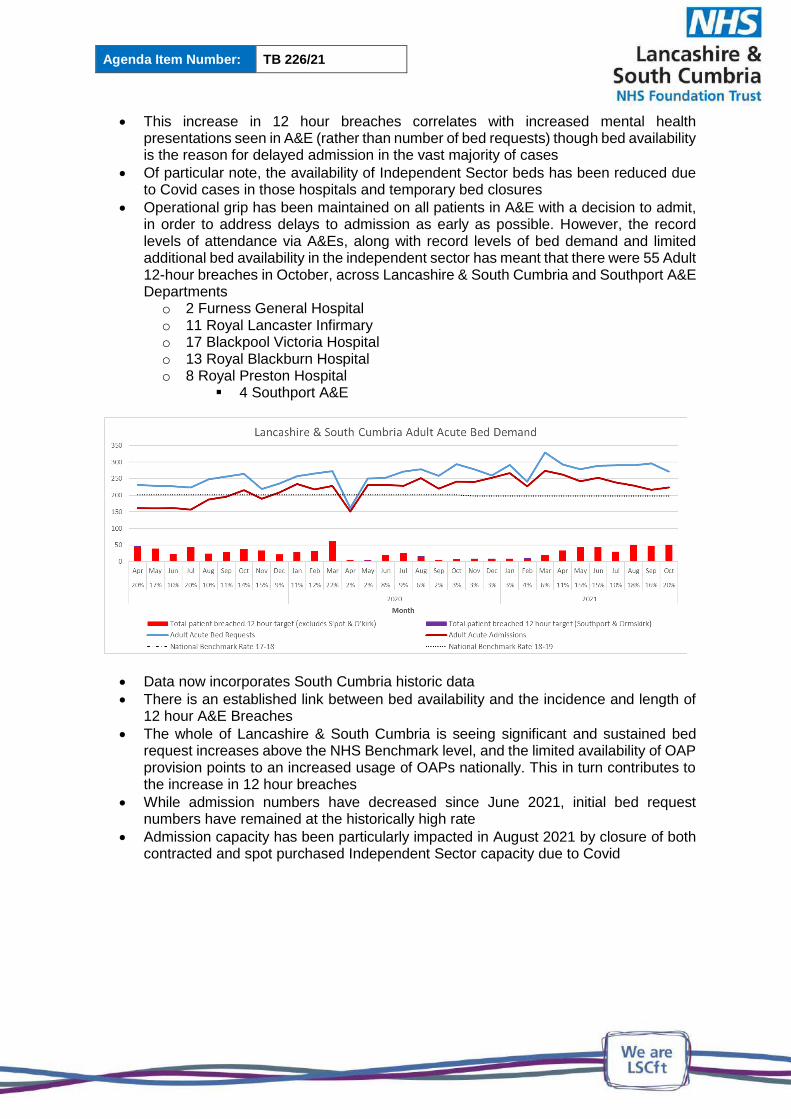
Agenda Item Number: TB 226/21
This increase in 12 hour breaches correlates with increased mental health presentations seen in A&E (rather than number of bed requests) though bed availability is the reason for delayed admission in the vast majority of cases
Of particular note, the availability of Independent Sector beds has been reduced due to Covid cases in those hospitals and temporary bed closures
Operational grip has been maintained on all patients in A&E with a decision to admit, in order to address delays to admission as early as possible. However, the record levels of attendance via A&Es, along with record levels of bed demand and limited additional bed availability in the independent sector has meant that there were 55 Adult 12-hour breaches in October, across Lancashire & South Cumbria and Southport A&E Departments
o 2 Furness General Hospital o 11 Royal Lancaster Infirmary o 17 Blackpool Victoria Hospital o 13 Royal Blackburn Hospital o 8 Royal Preston Hospital
4 Southport A&E
Data now incorporates South Cumbria historic data
There is an established link between bed availability and the incidence and length of 12 hour A&E Breaches
The whole of Lancashire & South Cumbria is seeing significant and sustained bed request increases above the NHS Benchmark level, and the limited availability of OAP provision points to an increased usage of OAPs nationally. This in turn contributes to the increase in 12 hour breaches
While admission numbers have decreased since June 2021, initial bed request numbers have remained at the historically high rate
Admission capacity has been particularly impacted in August 2021 by closure of both contracted and spot purchased Independent Sector capacity due to Covid
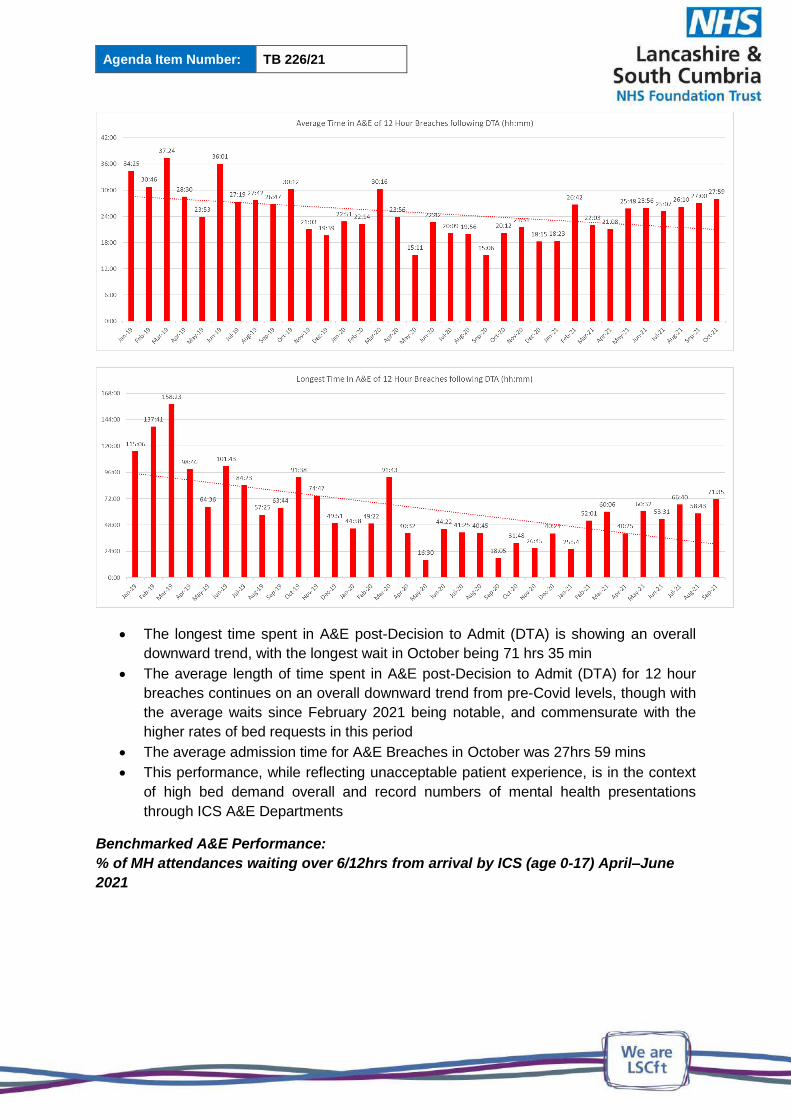
Agenda Item Number: TB 226/21
The longest time spent in A&E post-Decision to Admit (DTA) is showing an overall
downward trend, with the longest wait in October being 71 hrs 35 min
The average length of time spent in A&E post-Decision to Admit (DTA) for 12 hour
breaches continues on an overall downward trend from pre-Covid levels, though with
the average waits since February 2021 being notable, and commensurate with the
higher rates of bed requests in this period
The average admission time for A&E Breaches in October was 27hrs 59 mins
This performance, while reflecting unacceptable patient experience, is in the context
of high bed demand overall and record numbers of mental health presentations
through ICS A&E Departments
Benchmarked A&E Performance:
% of MH attendances waiting over 6/12hrs from arrival by ICS (age 0-17) April–June
2021

Agenda Item Number: TB 226/21
% of MH attendances waiting over 6/12hrs from arrival by ICS (age 18+) April–June
2021
The ultimate aim must be to eliminate any avoidable time spent in A&E, and the
above data and comparisons are presented for Benchmarking LSCFT performance against North West Region performance
The data reflect total time in A&E (not the contracted response times reported earlier in this paper) and also include time in A&E prior to referral to Mental Health Liaison Teams
Lancashire & South Cumbria responsiveness to children and young people under 18 is relatively positive, with 90.8% of presentations discharged from A&E within 6 hours of arrival, and 98.2% within 12 hours of arrival
Lancashire & South Cumbria responsiveness to people over the age of 18 is comparable to the other North West systems, with marginally smaller numbers of longer waits in A&E in Lancashire & South Cumbria: 72.3% of patients leaving A&E within 6 hours and 92.5% within 12 hours
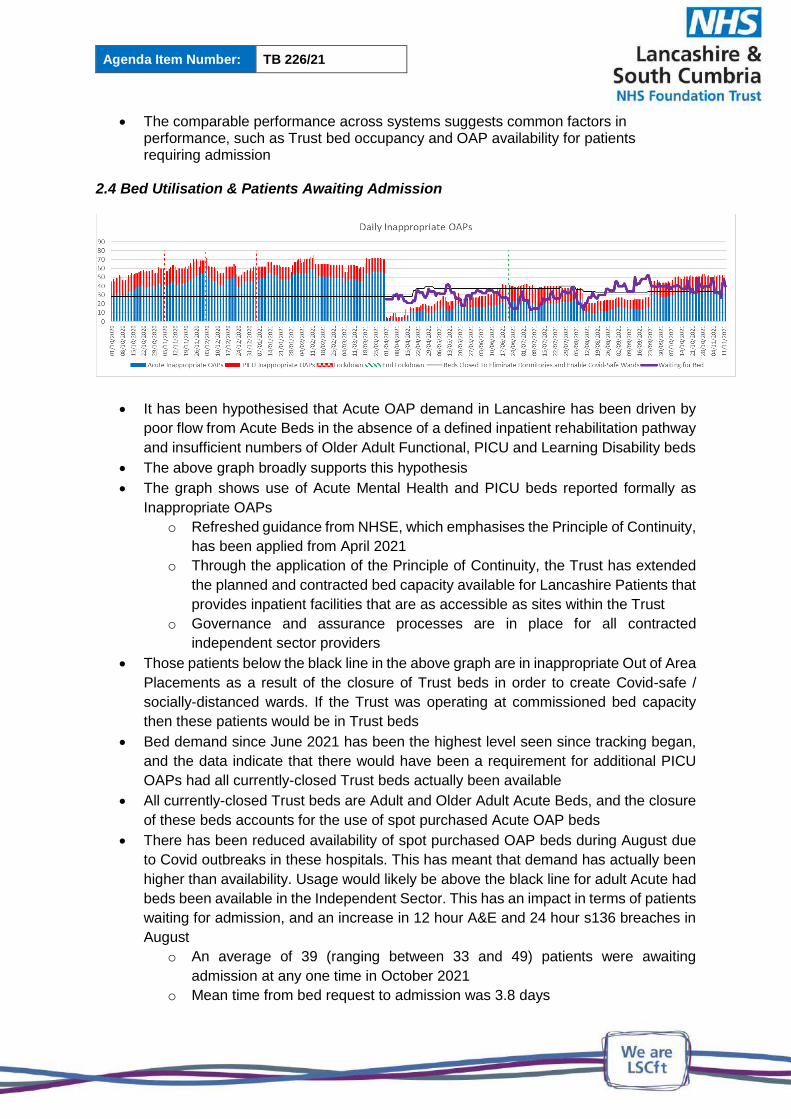
Agenda Item Number: TB 226/21
The comparable performance across systems suggests common factors in performance, such as Trust bed occupancy and OAP availability for patients requiring admission
2.4 Bed Utilisation & Patients Awaiting Admission
It has been hypothesised that Acute OAP demand in Lancashire has been driven by
poor flow from Acute Beds in the absence of a defined inpatient rehabilitation pathway
and insufficient numbers of Older Adult Functional, PICU and Learning Disability beds
The above graph broadly supports this hypothesis
The graph shows use of Acute Mental Health and PICU beds reported formally as
Inappropriate OAPs
o Refreshed guidance from NHSE, which emphasises the Principle of Continuity,
has been applied from April 2021
o Through the application of the Principle of Continuity, the Trust has extended
the planned and contracted bed capacity available for Lancashire Patients that
provides inpatient facilities that are as accessible as sites within the Trust
o Governance and assurance processes are in place for all contracted
independent sector providers
Those patients below the black line in the above graph are in inappropriate Out of Area
Placements as a result of the closure of Trust beds in order to create Covid-safe /
socially-distanced wards. If the Trust was operating at commissioned bed capacity
then these patients would be in Trust beds
Bed demand since June 2021 has been the highest level seen since tracking began,
and the data indicate that there would have been a requirement for additional PICU
OAPs had all currently-closed Trust beds actually been available
All currently-closed Trust beds are Adult and Older Adult Acute Beds, and the closure
of these beds accounts for the use of spot purchased Acute OAP beds
There has been reduced availability of spot purchased OAP beds during August due
to Covid outbreaks in these hospitals. This has meant that demand has actually been
higher than availability. Usage would likely be above the black line for adult Acute had
beds been available in the Independent Sector. This has an impact in terms of patients
waiting for admission, and an increase in 12 hour A&E and 24 hour s136 breaches in
August
o An average of 39 (ranging between 33 and 49) patients were awaiting
admission at any one time in October 2021
o Mean time from bed request to admission was 3.8 days
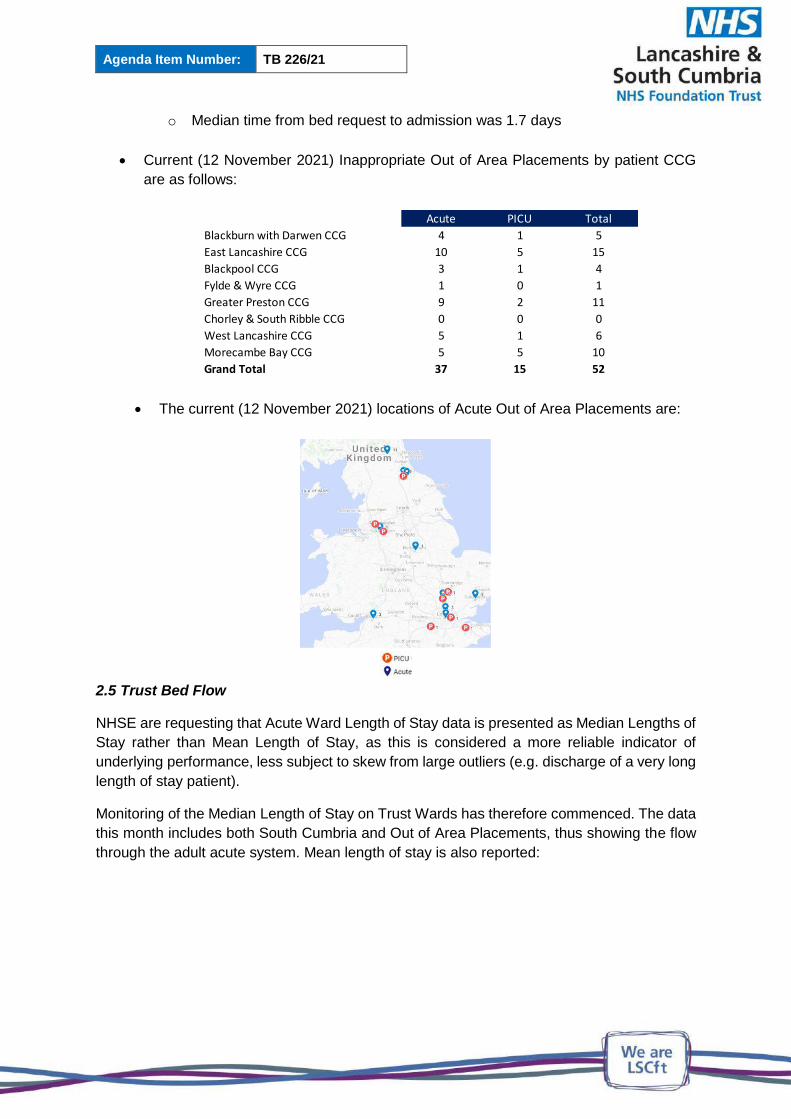
Agenda Item Number: TB 226/21
o Median time from bed request to admission was 1.7 days
Current (12 November 2021) Inappropriate Out of Area Placements by patient CCG
are as follows:
The current (12 November 2021) locations of Acute Out of Area Placements are:
2.5 Trust Bed Flow
NHSE are requesting that Acute Ward Length of Stay data is presented as Median Lengths of
Stay rather than Mean Length of Stay, as this is considered a more reliable indicator of
underlying performance, less subject to skew from large outliers (e.g. discharge of a very long
length of stay patient).
Monitoring of the Median Length of Stay on Trust Wards has therefore commenced. The data
this month includes both South Cumbria and Out of Area Placements, thus showing the flow
through the adult acute system. Mean length of stay is also reported:
Acute PICU Total
Blackburn with Darwen CCG 4 1 5
East Lancashire CCG 10 5 15
Blackpool CCG 3 1 4
Fylde & Wyre CCG 1 0 1
Greater Preston CCG 9 2 11
Chorley & South Ribble CCG 0 0 0
West Lancashire CCG 5 1 6
Morecambe Bay CCG 5 5 10
Grand Total 37 15 52

Agenda Item Number: TB 226/21
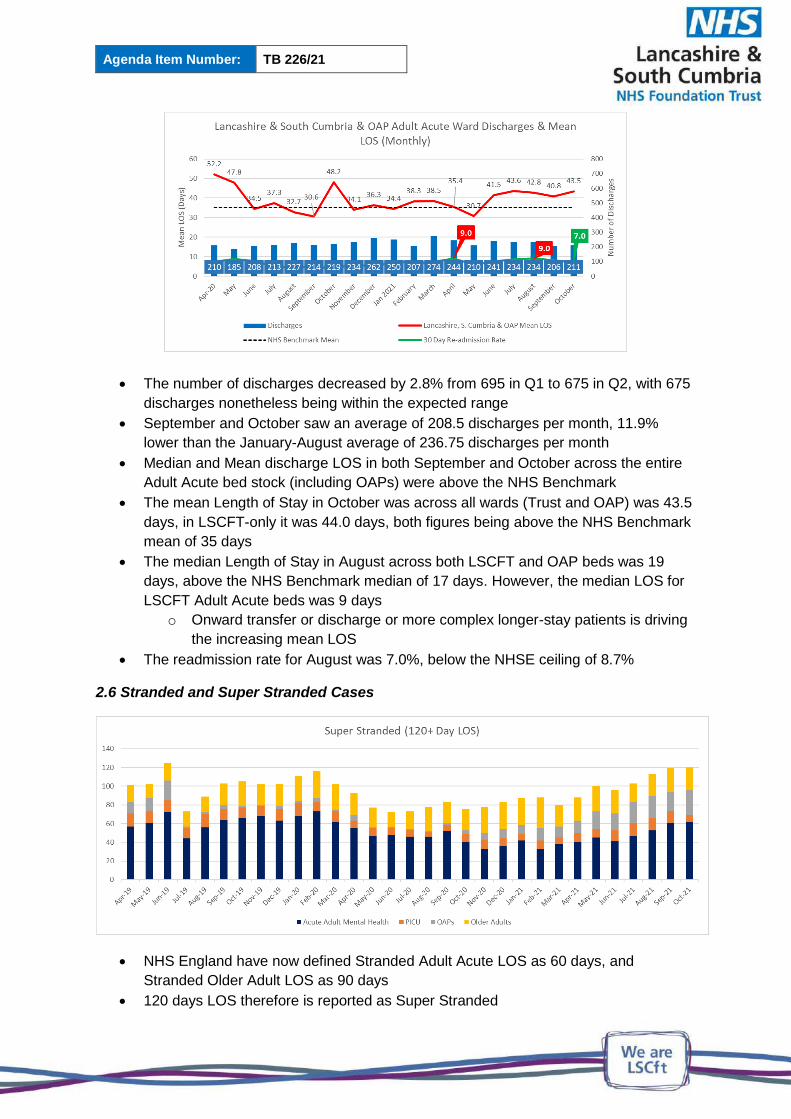
Agenda Item Number: TB 226/21
The number of discharges decreased by 2.8% from 695 in Q1 to 675 in Q2, with 675
discharges nonetheless being within the expected range
September and October saw an average of 208.5 discharges per month, 11.9%
lower than the January-August average of 236.75 discharges per month
Median and Mean discharge LOS in both September and October across the entire
Adult Acute bed stock (including OAPs) were above the NHS Benchmark
The mean Length of Stay in October was across all wards (Trust and OAP) was 43.5
days, in LSCFT-only it was 44.0 days, both figures being above the NHS Benchmark
mean of 35 days
The median Length of Stay in August across both LSCFT and OAP beds was 19
days, above the NHS Benchmark median of 17 days. However, the median LOS for
LSCFT Adult Acute beds was 9 days
o Onward transfer or discharge or more complex longer-stay patients is driving
the increasing mean LOS
The readmission rate for August was 7.0%, below the NHSE ceiling of 8.7%
2.6 Stranded and Super Stranded Cases
NHS England have now defined Stranded Adult Acute LOS as 60 days, and
Stranded Older Adult LOS as 90 days
120 days LOS therefore is reported as Super Stranded
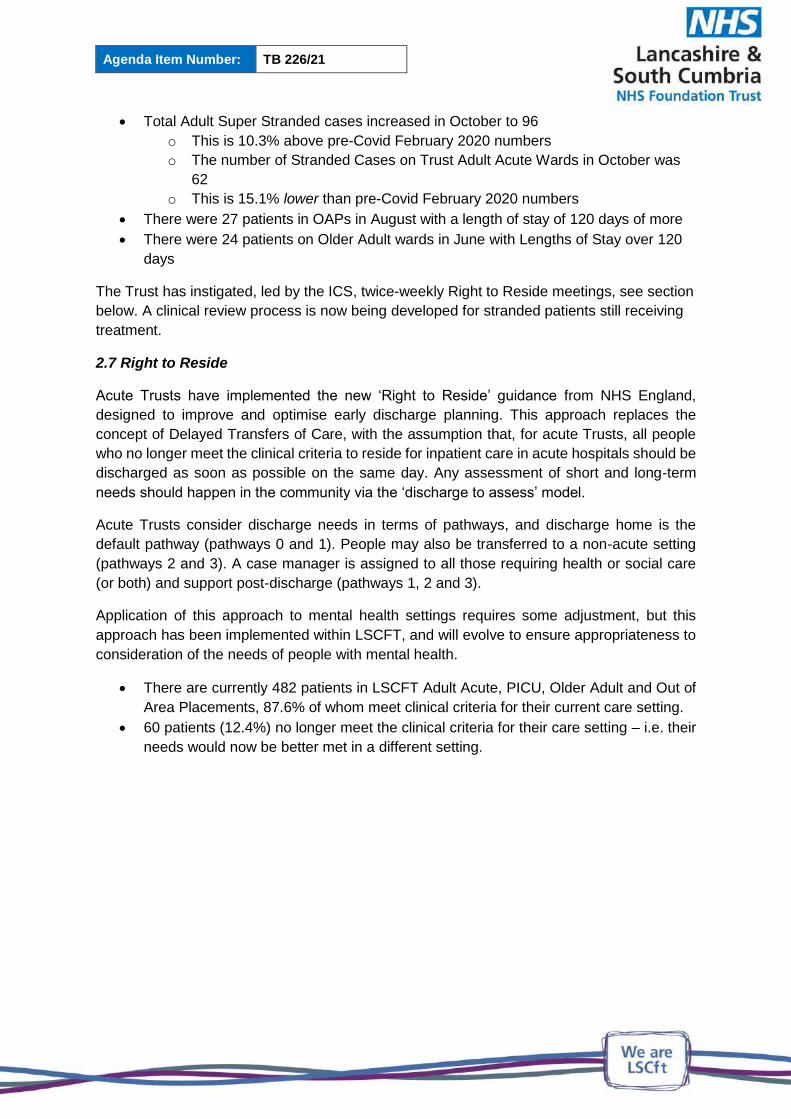
Agenda Item Number: TB 226/21
Total Adult Super Stranded cases increased in October to 96
o This is 10.3% above pre-Covid February 2020 numbers
o The number of Stranded Cases on Trust Adult Acute Wards in October was
62
o This is 15.1% lower than pre-Covid February 2020 numbers
There were 27 patients in OAPs in August with a length of stay of 120 days of more
There were 24 patients on Older Adult wards in June with Lengths of Stay over 120
days
The Trust has instigated, led by the ICS, twice-weekly Right to Reside meetings, see section
below. A clinical review process is now being developed for stranded patients still receiving
treatment.
2.7 Right to Reside
Acute Trusts have implemented the new ‘Right to Reside’ guidance from NHS England,
designed to improve and optimise early discharge planning. This approach replaces the
concept of Delayed Transfers of Care, with the assumption that, for acute Trusts, all people
who no longer meet the clinical criteria to reside for inpatient care in acute hospitals should be
discharged as soon as possible on the same day. Any assessment of short and long-term
needs should happen in the community via the ‘discharge to assess’ model.
Acute Trusts consider discharge needs in terms of pathways, and discharge home is the
default pathway (pathways 0 and 1). People may also be transferred to a non-acute setting
(pathways 2 and 3). A case manager is assigned to all those requiring health or social care
(or both) and support post-discharge (pathways 1, 2 and 3).
Application of this approach to mental health settings requires some adjustment, but this
approach has been implemented within LSCFT, and will evolve to ensure appropriateness to
consideration of the needs of people with mental health.
There are currently 482 patients in LSCFT Adult Acute, PICU, Older Adult and Out of
Area Placements, 87.6% of whom meet clinical criteria for their current care setting.
60 patients (12.4%) no longer meet the clinical criteria for their care setting – i.e. their
needs would now be better met in a different setting.

Agenda Item Number: TB 226/21
2.8 Access Line and 136 Usage
Lancashire Police calls to the Mental Health Access Line in September and October were at similar levels, and while not as high as the May peak, continue the trend for high call numbers from the police, with around 10 calls per day
There were 147 uses of s136 by Lancashire Police in October 2021, an average of 4.7 per day
o This is a reduction of 16.3% from September 2021 o The October daily rate was 12.9% higher than the 4.2 per day in February 2020
(pre-Covid)
Police report increased confidence in the Mental Health Access Line service, which coincides with more consistent staffing of the Access Line as staffing deficits reduce
2.9 s136 Usage and Breaches
There was a step-change increase in s136 detentions in March 2021, which has been sustained into August 2021
o Average number of daily detentions September 2020 – February 2021: 4.1 o Average number of daily detentions March – June 2021: 5.5 o Average number of daily detentions October 2021: 5.4 o October 2021 detention rate was 32.2% higher than Sept. 2020–Feb. 2021
Of 168 detentions in October 2021, there were 47 breaches of the 24 hour target
Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct
Police calls to MHAL 124 137 124 113 193 139 144 138 138 210 243 252 260 214 211 178 240 206 189 213 239 241 274 331 317 304 303 299 319
Total Number of Lancashire s136 Detentions 123 116 127 136 124 82 119 117 121 113 97 114 138 130 160 141 143 126 120 141 105 178 170 176 166 159 174 170 147
20202019 2021

Agenda Item Number: TB 226/21
o 28.0% of all detentions o 58.0% of all admissions via s136
13 (7.7%) of detentions were repeat detentions in-month, involving 12 people: o 11 people were detained twice o 1 person was detained three times
Detentions to locality Health Based Places of Safety varied in volume and number of breaches:
October breaches by locality were: o Central & West: 26% o Pennine: 21% o Fylde: 35% o Bay: 34%

Agenda Item Number: TB 226/21
Management monitoring and actions remain in place to minimise s136 breach numbers and Length of Stay though bed capacity pressures are impacting notably on s136 admission times
o For Trust Health Based Places of Safety, average length of stay has increased in the two months, with the average in October at 60hrs 51min)
o The longest LOS (146hrs 40mins) in October was the longest since August 2019
Length of Stay of breaches in Health Based Places of Safety is directly related to bed availability and is in the context of the current heightened levels of bed demand
Availability of PICU beds is a notable factor in longer breach times 2.10 Mental Health Crisis Line
The Mental Health Crisis Line was established in May 2020 to provide rapid access
to clinical services for people in mental health crisis
Abandoned calls had become a recognised issue within the service. Patient
preference (e.g. for particular call takers) is a known factor, and potential barriers to
some callers, such as automated welcome messages, have been removed
The service have acquired a new telephony system which enables improved activity
reporting and the service is now able to breakdown the times at which callers abandon
their call to the Crisis Line.
There were a total of 2177 calls in October, a reduction from May’s peak of 2268, but
a 29.7% increase compared to April 2021
o Of the calls in October:
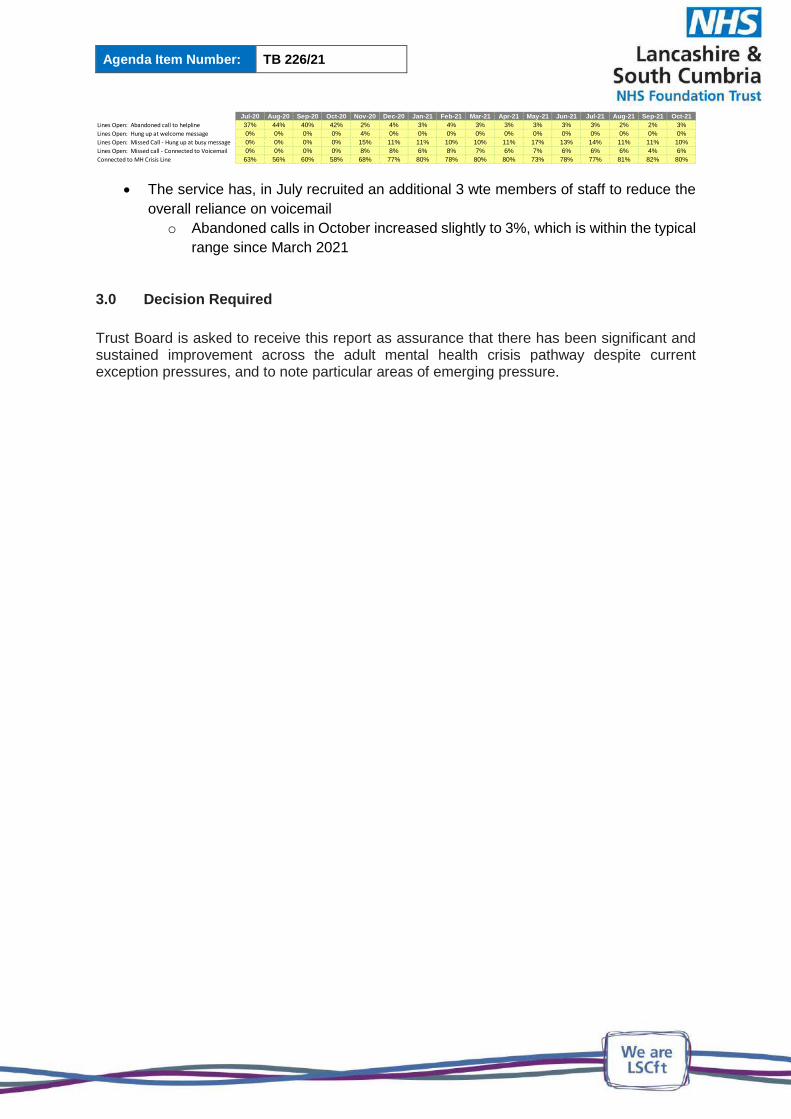
Agenda Item Number: TB 226/21
The service has, in July recruited an additional 3 wte members of staff to reduce the
overall reliance on voicemail
o Abandoned calls in October increased slightly to 3%, which is within the typical
range since March 2021
3.0 Decision Required
Trust Board is asked to receive this report as assurance that there has been significant and sustained improvement across the adult mental health crisis pathway despite current exception pressures, and to note particular areas of emerging pressure.
Jul-20 Aug-20 Sep-20 Oct-20 Nov-20 Dec-20 Jan-21 Feb-21 Mar-21 Apr-21 May-21 Jun-21 Jul-21 Aug-21 Sep-21 Oct-21
Lines Open: Abandoned call to helpline 37% 44% 40% 42% 2% 4% 3% 4% 3% 3% 3% 3% 3% 2% 2% 3%
Lines Open: Hung up at welcome message 0% 0% 0% 0% 4% 0% 0% 0% 0% 0% 0% 0% 0% 0% 0% 0%
Lines Open: Missed Call - Hung up at busy message 0% 0% 0% 0% 15% 11% 11% 10% 10% 11% 17% 13% 14% 11% 11% 10%
Lines Open: Missed call - Connected to Voicemail 0% 0% 0% 0% 8% 8% 6% 8% 7% 6% 7% 6% 6% 6% 4% 6%
Connected to MH Crisis Line 63% 56% 60% 58% 68% 77% 80% 78% 80% 80% 73% 78% 77% 81% 82% 80%

Agenda Item Number: TB 227/21
PEOPLE & CULTURE COMMITTEE CHAIRS REPORT
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Peter Williams, Committee Chair
Prepared by: Rebecca Walker, Executive PA
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will respond to peoples’ needs by striving for the highest STANDARDS of quality across all of our services
Aligned to Board Assurance Framework Risk
3.0 Failure to learn and improve as an organisation underpinned by ineffective systems and a lack of an open and transparent culture, may impact on delivering safe care
Recommendation/Required Action
The Board of Directors are asked to note the
assurance and escalation provided within the People
and Culture Committee chairs report.
1.0 INTRODUCTION
The Board of Directors are presented with the Chairs Report of the People & Culture
Committee held on 28th October 2021. The chairs report provides an overview of
assurance received and escalation to discussions held, as required.
2.0 RECOMMENDATION
The Board of Directors are asked to:
note the assurance and escalation provided within the chairs report

CHAIRS REPORT
MEETING: People & Culture Committee DATE OF MEETING: 28/10/2021 CHAIR OF MEETING: Peter Williams, Non-Executive Director
ITEMS APPROVED
None
ASSURANCE RECEIVED
Employer Relations Activity The Committee received an assurance report on the management of employee relations cases and confirmation that the average length of disciplinary investigations is below 12 weeks. The committee were informed of 46 live disciplinary cases, with 8 being bank workers. There are 13 live grievances and 7 employment tribunals. . The Committee was made aware of the disproportionate number of BME and male staff currently in a disciplinary process. The chair asked for disability to be included in the next report to provide a fuller picture. Communications and Engagement Delivery Plan Update: Assurance was received regarding the progress of the delivery plan and it was confirmed there is a subcommittee being established. The Chair acknowledged the positive work in relation to branding and the staff award virtual ceremony, taking place on 11 November 2021. National Staff Survey 2020 Action Plan: The committee was informed the national staff survey 2021 launched on the 4 October 2021 and results will be published by the survey coordination centre in February 2022. The committee received assurance on the improvement work completed against the five priorities identified following the 2020 staff survey results :
Staff Engagement
Equality Diversity and Inclusion
Safety Culture
Health and Wellbeing
Quality of Appraisals

CHAIRS REPORT
The Committee also received an overview of the results of the pilot Quarterly Staff Survey QSS) which now replaces the Staff Friends and Family Test (SFFT) and was carried out in Q2. The response rate was 19%. The results showed improvements in staff experience relating to appraisal, values and behaviours and a maintained position in relation to inclusion. However, the results indicate a deteriorating position in relation to staff engagement and health and wellbeing. The Committee was made aware that the QSS results could be indicative of the results the Trust may expect in the 2021 national staff survey. Workforce and Resource Plan: The Deputy Chief People Officer presented the resourcing improvement plan and provided assurance that Step One (Workforce Plan) and Step Two (Workforce Resourcing tool) of the four step plan have been completed and that the Executive Team had approved additional investment to support recruitment activity at a Network level to support the implementation of Steps 3 (Recruitment Optimisation and Live Data) & 4 (Training and Consistency). The ‘request to recruit’ improvement plan is being piloted in Fylde Coast and is aimed at reducing the process by 9 days (from 15 days to 6) in line with the recommendations delivered as part of the LiA improvement programme. There was a discussion around the current workforce establishment, over recruiting above budgeted establishment and how we balance new recruits with growing our own. It was noted that further workforce transformation is still required. Completion of all 4 steps in the improvement is required to provide greater assurance against our workforce supply challenges and progress against these plans will be presented at the next Committee meeting.
ESCALATION
MITIGATING ACTION
It was highlighted that BME and Male staff were disproportionately represented in relation to the disciplinary cases. In relation to the response of the latest quarterly staff survey there was only a 19% response and the results indicated poorer staff experience as compared to that reported in the 2020 national staff survey for staff engagement and health and wellbeing.
The Chief People Officer agreed to carry out a deep dive and report back to the next committee. There are action plans in place in the localities to mitigate and a comprehensive communications plan to support increasing the national staff survey response rate and share with staff the actions taken to respond to the feedback received in 2020. .

CHAIRS REPORT
ITEMS RECEIVED FOR INFORMATION
W&E Chairs Report: A brief update on hybrid working was reported and it was noted that a task and finish group is developing the framework and implementation plan. The chair asked for clarification on this work at the next meeting. The health and wellbeing website is now live and receiving positive feedback. In September the Trust acknowledge Pride and in October Black History Month where there were a broad range of talks, awareness raising and socials were planned and successfully delivered. The first BAME Medics network meeting took place in September with support from the Chief Medical officer. There has been recognition externally for:
Pav Akhtar received High commended in Equality & Inclusion Influencer of the Year at the Employers Network for Equality & Inclusion
Max Osman won the RCN North West Veteran Award for Outstanding Contribution to Equality, Diversity & Inclusion
Shortlisted for a HSJ Award for Staff Engagement Workforce Performance Report: The committee was presented with the latest performance against workforce KPIs. Of note is the increase of use of temporary staffing and more recently as a consequence of workforce growth requirements. The Committee received assurance of the plans to mitigate against this under the workforce and resourcing planning item. Sickness absence was reported at 8.2% in September which is an increase on the previous month however expected as the start of seasonal sickness. COVID absence stable at 1.1%. The committee were informed of the continue challenge of face to face training and attendance reported as 44%, there is work between Quality Academy and the localities to improve attendance. Workforce Policies The Committee noted the following ratified policies:
Appraisal Policy (New Policy)
Substance Misuse & Problem Gambling Policy
Flexible Working Policy To add all policies had been approved at Joint Negotiating Consultation Committee, JNCC in October 2021.
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☐
Discussion ☐ Decision ☒ Date of Meeting: 25/11/2021
Presented by: Dr David Fearnley, Chief Medical Officer
Prepared by: Angela Maclennan, Professional Standards, Appraisal & Revalidation Lead
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will employ and retain the best STAFF, as our culture will be inclusive and a supportive place to work
Aligned to Board Assurance Framework Risk
3.0 Failure to learn and improve as an organisation underpinned by ineffective systems and a lack of an open and transparent culture, may impact on delivering safe care
Recommendation/Required Action
The Board is asked to approve the report and agree the statement of compliance for submission to the Higher Level Responsible Officer at NHS England & Improvement.
EXECUTIVE SUMMARY
Doctors who hold a licence to practice are required to revalidate every five years. As a
Designated Body, the Trust is required to comply with the Responsible Office Regulations and
ensure that those doctors with whom it has a prescribed connection are engaged in the annual
appraisal process. This report summarises appraisal and revalidation activity during 2020/21,
and includes the statement of compliance for review and agreement by the Board. This will
then be submitted to NHSE&I.
Key Issues
Due to the pandemic, medical appraisal was optional for doctors during 2020/21. The report
details the number of doctors who did choose to have an appraisal, and the continuing high
quality of those appraisals which were completed.
Revalidation dates were also amended by the GMC as a result of the pandemic, with doctors
being given additional time to ensure they were ‘revalidation ready’. However a number of
revalidation recommendations were made by the Responsible Officer during the year.
The ‘Appraisal 2020’ model was introduced by NHS England in September 2020, with a focus
on support and wellbeing and less emphasis on documentation and written evidence. This
Agenda Item Number: TB 228/21
ANNUAL MEDICAL APPRAISAL & REVALIDATION REPORT 20/21
approach has continued during the 2021/22 appraisal year and the benefits of this will be
embedded going forward.
Concerns about doctors continued to be reviewed by the Trust’s Professional Standards
Monitoring Group and the report includes a summary of the concerns considered and actions
taken during the year.
Annual reporting to NHSE&I is optional for the 2020/21 appraisal year, but the Trust has
chosen to complete an annual report and the Board is asked to approve the Statement of
Compliance for submission to the Higher Level Responsible Officer.
Agenda Item Number: TB 229/21
FIANANCE AND RESOURCE COMMITTE CHAIRS REPORT
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Shazad Sarwar, Committee Chair
Prepared by: Vicki Waddington, Executive PA
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will provide SUSTAINABLE services that deliver real value
Aligned to Board Assurance Framework Risk
7.0 Failure to deliver the Trust’s annual financial plan caused by lack of robust cost improvements and an inability to attract appropriate investment to meet demand may impact on the Trust’s ability to deliver high quality care
Recommendation/Required Action
The Board of Directors are asked to note the
assurance and escalation provided within the Quality
and Assurance Committee chairs report.
1.0 INTRODUCTION
The Board of Directors are presented with the Chairs Report of the Finance and
Resource Committee on 18 October 2021 2021. The chairs report provides an overview
of assurance received and escalation to discussions held, as required.
2.0 RECOMMENDATION
The Board of Directors are asked to:
note the assurance and escalation provided within the chairs report

CHAIRS REPORT
MEETING:
Finance and Resource Committee
DATE OF MEETING: 18/10/2021
CHAIR OF MEETING:
Shazad Sarwar, Non-Executive Director
ITEMS APPROVED
Data Quality Policy The data quality policy was approved.
ASSURANCE RECEIVED
Financial Position The H1 plan outlined a breakeven position and remains in line with previous month’s reports and funding for H2 remains unconfirmed. Risks remain as previous months which include and were noted as ward spend, medical spend and efficiency plans. The 2022/23 planning guidance is not expected until December 2021, as part of the H2 planning cycle the Trust will produce an indication of the run rate for next year. Cash Flow It was expected that the Trust will remain at a breakeven position and a £15.5m cash balance is predicted for the end of the year. 2022/23 planning has been initiated at network level and the capital planning has commenced to allow for conversations to start to take place with the system. Ward and Agency Spend Next Steps Services have been requested to review and deliver an action plan which included trajectories for improvement in relation to overspends. Wards have identified a £670k saving over the next 6 months which if continued would equate to £1.9m during 2022/23. In addition, medics have identified £131k over a 6 month period, the run rate would be impacted by £800k with an annual saving of £2.1m. The impact on the finance against the trajectories will continue to be monitored on a monthly basis. Delivery of Investment Schemes Revised 21/22 Plan An in year recurrent pressure was highlighted. The Executive Team have agreed to progress with the mitigation which will be balanced against schemes which have not yet started.

CHAIRS REPORT
Anti-Ligature Phasing plan The proposal is to develop a multi-year plan for the roll out of the programme, services have been prioritised and it has been identified the focus in year would be on Ribble ward and the Orchard. Risk was noted while the prioritisation of the wards in year and the development of the 4 year implementation plan take place. Capital Planning Chairs Report Dashboards will be developed for any programme over £1m and the risk, themes and trends were noted. HSIS Chairs Report The HSIS Board meeting held in September 2021 was the last HSIS Board meeting, this will be replaced by an Estates and Facilities sub-committee which will report to the Finance & Resource Committee. The Hard FM contract is going out to market with the ambition to have a new supplier by 01 April 2022.
ITEMS TO ESCALATE TO THE BOARD
ITEMS FOR ESCALATION MITIGATING ACTION
Wards and Agency Spend Paper This will be presented in part 1 of the Board in November 2021 Medical Spend Yearly Comparison It was asked the medical spend yearly comparison, ward and agency spend and the finance report be shared with Board members ahead of the November 2021 meeting.
ITEMS RECEIVED FOR INFORMATION
What Good Looks Like in a Digital Setting The framework consists of 7 success measures, once the framework is available, the Trust will undertake the assessment which will then be shared via the Digital sub-committee and the Finance & Resource Committee.

Agenda Item Number: TB 230/21
WARD AND AGENCY SPEND
Report provided for: Report to: Board of Directors
Information ☒ Assurance ☐
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Chris Oliver, Chief Operating Officer
Prepared by: Dominic McKenna, Director of Operational Finance
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will provide SUSTAINABLE services that deliver real value
Aligned to Board Assurance Framework Risk
7.0 Failure to deliver the Trust’s annual financial plan caused by lack of robust cost improvements and an inability to attract appropriate investment to meet demand may impact on the Trust’s ability to deliver high quality care
Recommendation/Required Action
To inform the Board of the actions subsequent to report
on ward and agency spend and the revised spending
trajectories of the services.
1.0 Introduction This paper is prepared subsequent to the previous work presented on ward and medical
agency spend. As part of the response, services were challenged to review expenditure and
deliver revised trajectories for expenditure until the end of the financial year which could be
reported on a monthly basis to the Committee.
2.0 Process For the previous work, expenditure for both wards and medics in the early part of the financial
year was used to extrapolate an outturn position for the whole financial year. Services were
asked to validate this, establish meaningful actions that would impact and produce a trajectory
against which they could be measured on a monthly basis.
For the identified wards the estimated initial overspends were:
Pennine £1,185,548
Fylde Coast £1,633,268
Central & West £1,089,500
Total £3,908,316

Agenda Item Number: TB 230/21
For Medical staffing, the values were:
The Bay £423,672
Central & West £759,442
Pennine £475,740
Specialist £1,996,030
Total £3,767,858
Fylde’s financial position with regard to medical spend was not material so there not asked to participate in this work. 3.0 Revised Trajectories Each service reviewed the positions and identified actions which would impact. For some services (e.g. Specialist medics) the assumptions on spend had been impacted so the forecast didn’t hold as a starting point. Each response was accompanied by actions, action owners and timescales which could be monitored. For wards, the trajectories are summarised in financial terms as:
Pennine £959,034 +£226,514
Fylde Coast £1,280,331 +£352,937
Central & West £999,317 +£90,183
Total £3,238,863 +£669,633
Over the six period, if achieved this would improve the positions by £670k, with a monthly improvement for March of £160k, which if continued into 2022/23 would see an annual improvement of £1.9m. For medical spend, the trajectories are summarised in financial terms as:
The Bay £423,672 +£167,743
Central & West £759,442 +£188,277
Pennine £475,740 +£53,224
Specialist £1,996,030 -£278,297
Total £3,767,858 +£130,947
Over the six period, if achieved this would improve the positions by £131k. Most areas are seeing improvement but Specialist have recently taken on additional posts since the original forecasts were made. Further work continues in the service to identify recovery actions. The combined trajectories, if achieved, would see a run rate improvement of £800k by the end of the year, with an annual impact of over £2.1m if sustained.

Agenda Item Number: TB 230/21
4.0 Summary Clinical services have been presented with a challenge and have reviewed expenditure and cost drivers. They have developed action plans with key timescales which should see £800k of in year savings and £2.1m of recurrent savings if maintained. The trajectories will be reviewed and reported to the Committee on a monthly basis. Further work continues to identify further opportunities in most areas, but particularly in Specialist services.
Appendix A – Summary of Ward Positions
Original Forecast
October November December January February March
Treatment Blackburn Hyndburn -£292,175 -£333,915 -£375,654 -£417,393 -£459,133 -£500,872
Treatment Blackburn Darwen -£115,393 -£131,877 -£148,362 -£164,847 -£181,331 -£197,816
PICU Blackburn Calder -£284,002 -£324,573 -£365,145 -£405,717 -£446,288 -£486,860 -£1,185,548
Treatment Harbour Shakespeare -£196,110 -£224,125 -£252,141 -£280,157 -£308,172 -£336,188
Treatment Harbour Stevenson -£54,257 -£62,008 -£69,759 -£77,510 -£85,261 -£93,012
Treatment Harbour Churchill -£104,601 -£119,544 -£134,487 -£149,430 -£164,373 -£179,316
Treatment Harbour Orwell -£91,782 -£104,893 -£118,005 -£131,117 -£144,228 -£157,340
PICU Harbour Byron -£283,150 -£323,600 -£364,050 -£404,500 -£444,950 -£485,400
PICU Harbour Keats -£222,840 -£254,675 -£286,509 -£318,343 -£350,178 -£382,012 -£1,633,268
Treatment Chorley Duxbury -£146,008 -£166,867 -£187,725 -£208,583 -£229,442 -£250,300
Treatment Chorley Worden -£253,230 -£289,405 -£325,581 -£361,757 -£397,932 -£434,108
PICU Chorley Avenham -£150,726 -£172,259 -£193,791 -£215,323 -£236,856 -£258,388
Treatment Ormskirk Scaribsrick -£34,183 -£39,067 -£43,950 -£48,833 -£53,717 -£58,600
PICU Ormskirk Lathom -£51,394 -£58,736 -£66,078 -£73,420 -£80,762 -£88,104 -£1,089,500
Total -£2,279,851 -£2,605,544 -£2,931,237 -£3,256,930 -£3,582,623 -£3,908,316 -£3,908,316
Revised Forecast
October November December January February March
Treatment Blackburn Hyndburn -£273,322 -£300,530 -£322,737 -£346,244 -£355,452 -£364,659
Treatment Blackburn Darwen -£105,466 -£114,984 -£124,502 -£144,015 -£149,965 -£155,916
PICU Blackburn Calder -£301,550 -£337,889 -£369,227 -£401,783 -£420,121 -£438,460 -£959,034
Treatment Harbour Shakespeare -£225,729 -£245,845 -£268,105 -£291,738 -£315,372 -£339,005
Treatment Harbour Stevenson -£65,563 -£64,623 -£63,907 -£63,192 -£62,476 -£61,761
Treatment Harbour Churchill -£54,430 -£50,869 -£47,307 -£43,745 -£40,183 -£36,622
Treatment Harbour Orwell -£76,087 -£76,130 -£76,172 -£76,214 -£76,257 -£76,299
PICU Harbour Byron -£225,599 -£244,799 -£266,625 -£292,221 -£317,817 -£343,413
PICU Harbour Keats -£316,999 -£338,245 -£359,492 -£380,739 -£401,986 -£423,232 -£1,280,331
Treatment Chorley Duxbury -£118,441 -£134,642 -£150,844 -£166,045 -£180,246 -£194,448
Treatment Chorley Worden -£249,981 -£285,394 -£320,808 -£354,221 -£386,634 -£419,048
PICU Chorley Avenham -£206,680 -£235,496 -£261,407 -£283,318 -£305,229 -£327,141
Treatment Ormskirk Scaribsrick -£83,482 -£94,193 -£104,903 -£111,613 -£118,323 -£125,034
PICU Ormskirk Lathom £27,137 £32,580 £38,023 £47,467 £56,910 £66,353 -£999,317
Total -£2,276,195 -£2,491,058 -£2,698,013 -£2,907,622 -£3,073,152 -£3,238,683 -£3,238,683
Variance
October November December January February March
Treatment Blackburn Hyndburn £18,853 £33,385 £52,917 £71,149 £103,681 £136,213
Treatment Blackburn Darwen £9,927 £16,893 £23,860 £20,831 £31,366 £41,900
PICU Blackburn Calder -£17,549 -£13,315 -£4,082 £3,934 £26,167 £48,400 £226,514
Treatment Harbour Shakespeare -£29,620 -£21,719 -£15,964 -£11,582 -£7,199 -£2,817
Treatment Harbour Stevenson -£11,306 -£2,615 £5,852 £14,318 £22,785 £31,251
Treatment Harbour Churchill £50,171 £68,675 £87,180 £105,685 £124,190 £142,694
Treatment Harbour Orwell £15,694 £28,764 £41,833 £54,902 £67,972 £81,041
PICU Harbour Byron £57,551 £78,801 £97,425 £112,279 £127,133 £141,987
PICU Harbour Keats -£94,158 -£83,571 -£72,983 -£62,396 -£51,808 -£41,220 £352,937
Treatment Chorley Duxbury £27,567 £32,224 £36,881 £42,538 £49,195 £55,852
Treatment Chorley Worden £3,248 £4,011 £4,773 £7,536 £11,298 £15,060
PICU Chorley Avenham -£55,954 -£63,237 -£67,616 -£67,995 -£68,374 -£68,753
Treatment Ormskirk Scaribsrick -£49,299 -£55,126 -£60,953 -£62,780 -£64,607 -£66,434
PICU Ormskirk Lathom £78,531 £91,316 £104,101 £120,887 £137,672 £154,457 £90,183
Total £3,656 £114,486 £233,224 £349,308 £509,471 £669,633 £669,633
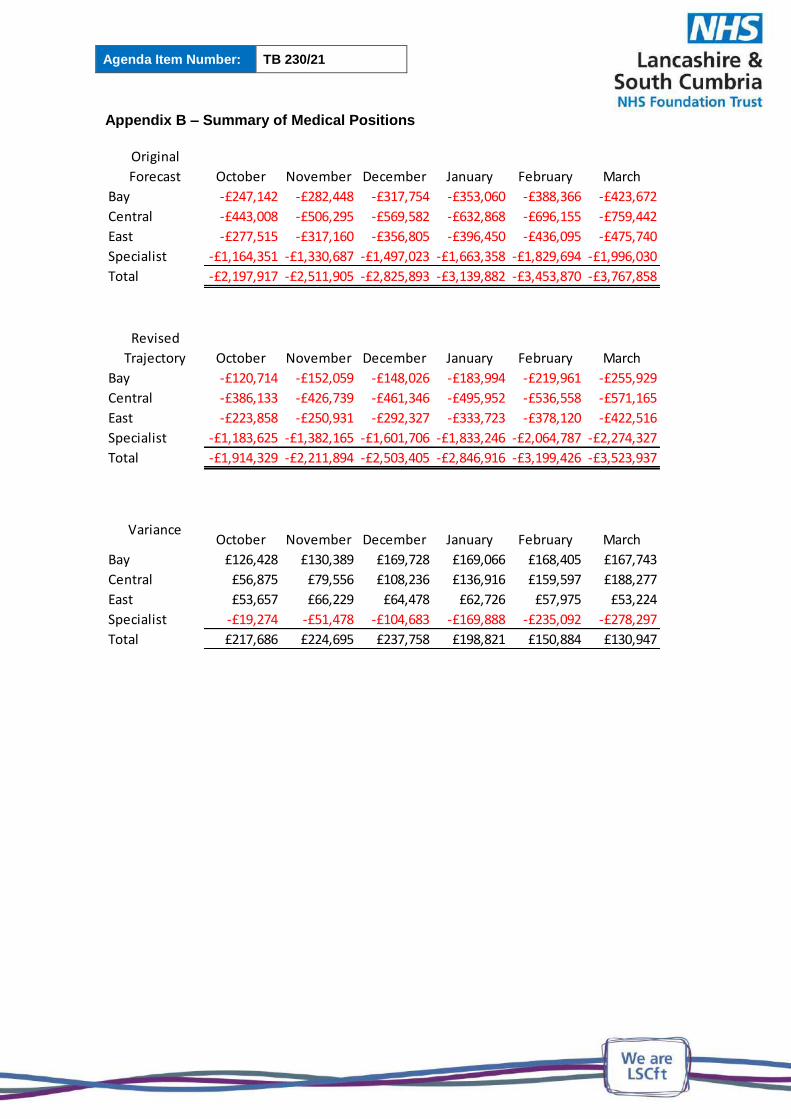
Agenda Item Number: TB 230/21
Appendix B – Summary of Medical Positions
Original
Forecast October November December January February March
Bay -£247,142 -£282,448 -£317,754 -£353,060 -£388,366 -£423,672
Central -£443,008 -£506,295 -£569,582 -£632,868 -£696,155 -£759,442
East -£277,515 -£317,160 -£356,805 -£396,450 -£436,095 -£475,740
Specialist -£1,164,351 -£1,330,687 -£1,497,023 -£1,663,358 -£1,829,694 -£1,996,030
Total -£2,197,917 -£2,511,905 -£2,825,893 -£3,139,882 -£3,453,870 -£3,767,858
Revised
Trajectory October November December January February March
Bay -£120,714 -£152,059 -£148,026 -£183,994 -£219,961 -£255,929
Central -£386,133 -£426,739 -£461,346 -£495,952 -£536,558 -£571,165
East -£223,858 -£250,931 -£292,327 -£333,723 -£378,120 -£422,516
Specialist -£1,183,625 -£1,382,165 -£1,601,706 -£1,833,246 -£2,064,787 -£2,274,327
Total -£1,914,329 -£2,211,894 -£2,503,405 -£2,846,916 -£3,199,426 -£3,523,937
VarianceOctober November December January February March
Bay £126,428 £130,389 £169,728 £169,066 £168,405 £167,743
Central £56,875 £79,556 £108,236 £136,916 £159,597 £188,277
East £53,657 £66,229 £64,478 £62,726 £57,975 £53,224
Specialist -£19,274 -£51,478 -£104,683 -£169,888 -£235,092 -£278,297
Total £217,686 £224,695 £237,758 £198,821 £150,884 £130,947
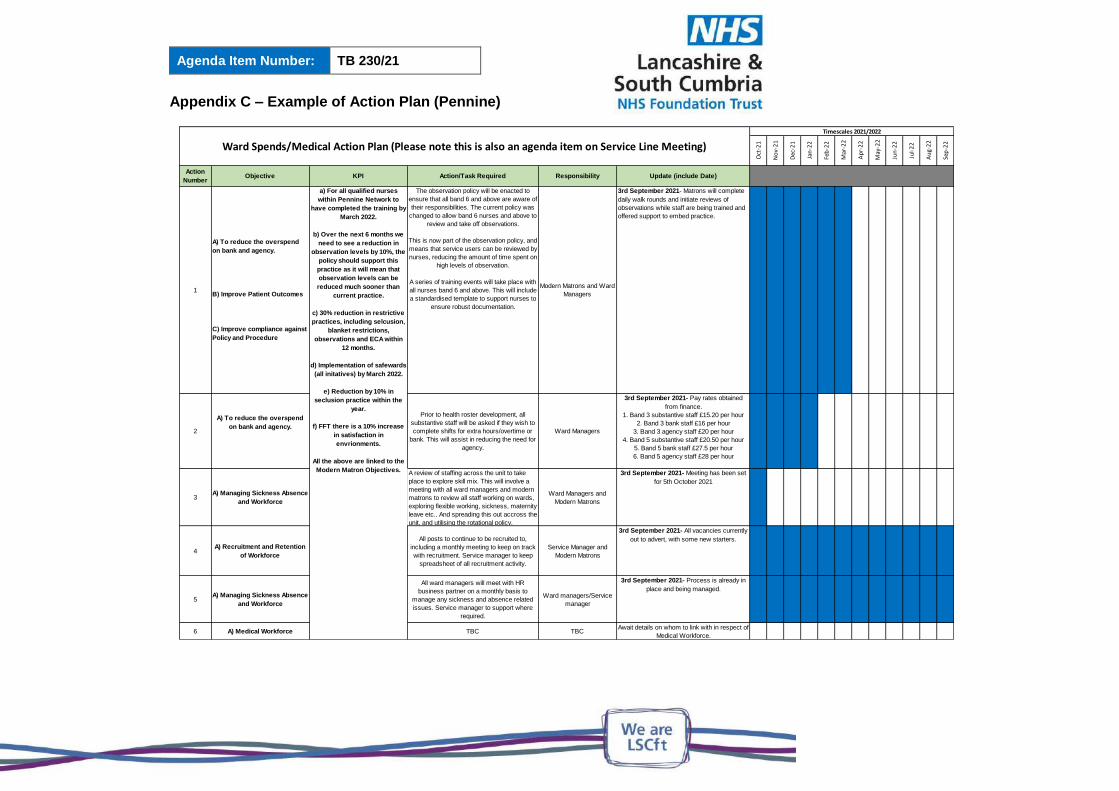
Agenda Item Number: TB 230/21
Appendix C – Example of Action Plan (Pennine)
Oct
-21
No
v-2
1
Dec
-21
Jan
-22
Feb
-22
Mar
-22
Ap
r-2
2
May
-22
Jun
-22
Jul-
22
Au
g-2
2
Sep
-22
Action
NumberObjective KPI Action/Task Required Responsibility Update (include Date)
1
A) To reduce the overspend
on bank and agency.
B) Improve Patient Outcomes
C) Improve compliance against
Policy and Procedure
The observation policy will be enacted to
ensure that all band 6 and above are aware of
their responsibilities. The current policy was
changed to allow band 6 nurses and above to
review and take off observations.
This is now part of the observation policy, and
means that service users can be reviewed by
nurses, reducing the amount of time spent on
high levels of observation.
A series of training events will take place with
all nurses band 6 and above. This will include
a standardised template to support nurses to
ensure robust documentation.
Modern Matrons and Ward
Managers
3rd September 2021- Matrons will complete
daily walk rounds and initiate reviews of
observations while staff are being trained and
offered support to embed practice.
2
A) To reduce the overspend
on bank and agency.
Prior to health roster development, all
substantive staff will be asked if they wish to
complete shifts for extra hours/overtime or
bank. This will assist in reducing the need for
agency.
Ward Managers
3rd September 2021- Pay rates obtained
from finance.
1. Band 3 substantive staff £15.20 per hour
2. Band 3 bank staff £16 per hour
3. Band 3 agency staff £20 per hour
4. Band 5 substantive staff £20.50 per hour
5. Band 5 bank staff £27.5 per hour
6. Band 5 agency staff £28 per hour
3A) Managing Sickness Absence
and Workforce
A review of staffing across the unit to take
place to explore skill mix. This will involve a
meeting with all ward managers and modern
matrons to review all staff working on wards,
exploring flexible working, sickness, maternity
leave etc.. And spreading this out accross the
unit, and utilising the rotational policy.
Ward Managers and
Modern Matrons
3rd September 2021- Meeting has been set
for 5th October 2021
4A) Recruitment and Retention
of Workforce
All posts to continue to be recruited to,
including a monthly meeting to keep on track
with recruitment. Service manager to keep
spreadsheet of all recruitment activity.
Service Manager and
Modern Matrons
3rd September 2021- All vacancies currently
out to advert, with some new starters.
5A) Managing Sickness Absence
and Workforce
All ward managers will meet with HR
business partner on a monthly basis to
manage any sickness and absence related
issues. Service manager to support where
required.
Ward managers/Service
manager
3rd September 2021- Process is already in
place and being managed.
6 A) Medical Workforce TBC TBCAwait details on whom to link with in respect of
Medical Workforce.
Ward Spends/Medical Action Plan (Please note this is also an agenda item on Service Line Meeting)
Timescales 2021/2022
a) For all qualified nurses
within Pennine Network to
have completed the training by
March 2022.
b) Over the next 6 months we
need to see a reduction in
observation levels by 10%, the
policy should support this
practice as it will mean that
observation levels can be
reduced much sooner than
current practice.
c) 30% reduction in restrictive
practices, including selcusion,
blanket restrictions,
observations and ECA within
12 months.
d) Implementation of safewards
(all initatives) by March 2022.
e) Reduction by 10% in
seclusion practice within the
year.
f) FFT there is a 10% increase
in satisfaction in
envrionments.
All the above are linked to the
Modern Matron Objectives.

Agenda Item Number: TB 231/21
FINANCE REPORT MONTH 7
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Jenny Hannon, Chief Finance Officer
Prepared by: Dominic McKenna, Director of Operational Finance
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will provide SUSTAINABLE services that deliver real value
Aligned to Board Assurance Framework Risk
7.0 Failure to deliver the Trust’s annual financial plan caused by lack of robust cost improvements and an inability to attract appropriate investment to meet demand may impact on the Trust’s ability to deliver high quality care
Recommendation/Required Action
The members of the Board are asked to note the
Trust’s current financial position.
EXECUTIVE SUMMARY The paper summarises the financial position of the Trust as at the end of October 2021, and apprises the Board of the drivers of the position.
KEY ISSUES The Trust has a slight overspend at month 7, due to underfunding of national pay awards, but expects to achieve a breakeven at and financial year outturns. Financial positions are presented prior to the agreement of the Trust’s H2 plan.
ESCALATION OF RISK There remains risk the financial outturn driven by ward staffing, agency spend, slippage on efficiencies and the financial strain the partners in the system find themselves exposed to..
CONCLUSION AND RECOMMENDATIONS The Board are asked to review note the Trust’s financial position
TRUST SUMMARY AT MONTH 7
Actual Plan Var Forecast Plan VarINCOME AND EXPENDITUREOperational surplus / (deficit) -£1,398 £0 -£1,398 -£2,194 £0.0 -£2,194CIPs (against Trust Plan) £2,930 £3,550 -£620 £8,640 £10,878 -£2,238Cash and Liquidity (£000) £57,075 £25,971 £31,104 £14,805 £19,468 -£4,663Capex (£000) £9,870 £18,132 £8,262 £27,653 £22,929 -£4,724Use of Resources 3 2 3 2Agency (£000) £8,266 £4,060 -£4,206 £13,827 £6,960 -£6,867OAPs (£000) £3,497 £2,073 -£1,424 £4,942 £2,482 -£2,460
Note Agency target represents the base ceiling given to the Trust and is taken from 2020-21
YTD Out-Turn
For H2, the plan had not been agreed at the time of forming the financial position for month 7 and therefore contains a number of assumptions which are altered by the subsequent agreement of the plan, most pertinent of which is confirmation of an actual breakeven after ICS funding. This position is driven by a number of items:
KeyMajor ConcernsMinor concerns, within toleranceIn line with planNHSI RatingNo evident concernsMinor concern, potentially requiring scrutinyMajor concern, requiring scrutinySignificant Risk, action required
The Trusts position to month 7 is consistent with the previous month, except for the overspends driven by the pay award. The planning is anchored to the prior years run rate.
As with previous years, the Trust is experiencing pressures in inpatient areas. These are expected to amount to £1.1m in Secure and£4.4m in other ward areas. Wards are significantly overspending against budget, and this has increased by about £1.4m from the previous year. Efficiencies are £3.5m behind target for the year plus we are seeing an overspend against the Covid income, and ashortfall on other income. Finally, we have seen a large run rate increase in medic costs, mainly due to filling vacancies with agency at a cost premium.
These overspends have been modelled to be mitigated to some degree by an assumption that in non-inpatient areas a shortage of particular skilled workers will lead to a slippage in recruitment. Additionally, we expect the new developments to attract a number of workers already employed by the Trust into new roles creating vacancies. There is still a residual gap, which is deemed mitigated in the main by an assumption that the amber efficiency schemes are delivered which attracts c£0.9m. Finally, we are assuming the same level of top up and Covid funding in H2 as H1. This is by no means certain given the reduction in the ICS envelope however it is in line with the amounts being paid to us..
This position assumes no underspend against the MHIS.
Position AnalysisRun Rate Changes
Wards -1.4 Subcontracted Beds / OAPs -0.6 Efficiency Improvement -3.5 Non Contract Income -0.5 Noncontract Income -1.5 Increase in Medics Costs -0.5 Pay Award Costs -2.2
Unmitigated Deficit -10.2
Overspend Mitigated by:Slippage on recruitment assumptions 2.6Amber EIP Schemes 0.9M7-12 Top Up 4.5
Mitigations 8.0
Mitigated Position -2.2
TRUST SUMMARY CONTINUED AT MONTH 7Clinical and managerial focus remains on addressing the impact of Covid 19 and the dispensing the vaccine, as well as restoration of services and the increased demand, however key financial metrics continue to be monitored. Agency costs exceeds the control total by c99% (£4.2m ytd). The drivers for this are being reviewed by clinical services, with particular focus on ward staffing and medical agency expenditure.
Overall on core infrastructure schemes capital expenditure is broadly in line with the plan, but the change to spend phasing on the Wesham and MH Dormitory schemes that was identified earlier in the year has shifted significant expenditure toward the end of the year. Spend on these schemes has now accelerated, and though not without risk we are confident the majority of these can be concluded in 2021/22 with slippage of c£500k into 2022/23. The Trust received additional resource envelope cover with the ICS for spend on the Hurstwood (c£3.1m) and precommitments (c£2.6m - primarily Wesham) which although not included in plan figures have been incorporated into the Trusts working plans and forecasts. With the plans in place this gave the Trust sufficient headroom to manage the programme within its resource envelope. A number of potential pressures to forecast have been identified, which after mitigations have resulted in a gap of c£0.8m. If the Trust continues with the current planned schemes approved including the mitigations, re-prioritisation is likely to be required in order to remain within the funding envelope. Even if this can be managed there will remain a risk of potential overspends due to the limited flexibility in the plan and funding.
The Trust continues to benefit from the significant increases to planned cash levels as a result of year end working capital, and underlying cash remains healthy.
Whilst not reflected in these financial positions, the Trust has now submitted a plan for H2, which assumes a breakeven for the planning period.
With the deterioration of the I&E position the metrics show a decline from M06, arising from the unfunded pay award leaving only liquidity on plan. However the overall metric remains unchanged as that had been constrained by an agency rating of 4. If the I and E position remains as forecast the metrics will remain likely remain unchanged leaving the trust with an overall outturn metric of 3. Should the I and E position improve the overall metric will still likely be constrained by the forecast agency rating of 4. Agency forecasts remain at 4 and this continues to constrain overall forecast performance to a 3. It should be noted that the agency target is taken from pre-Covid 2020-21 plans. Note also that the Single Operating Framework published in late June indicates that Use of Resources Ratings will be revised but that new metric calculations and their weightings have not yet been published. The figures presented use the historic UOR calculations and are based on extrapolated figures, they are not currently reportable or collected centrally and are included for indicative purposes only.
INCOME AND EXPENDITURE
Actual Plan Variance Actual Plan Variance£'m £'m £'m £'m £'m £'m
Income 266.3 249.6 16.7 463.2 428.1 35.2
Pay (184.6) (177.5) (7.1) (320.8) (302.7) (18.1)Non Pay (72.9) (61.9) (11.0) (127.0) (107.9) (19.1)Total Costs (257.5) (239.4) (18.1) (447.8) (410.6) (37.2)
EBITDA 8.8 10.2 (1.4) 15.4 17.5 (2.1)
Capital Charges (9.3) (9.1) (0.1) (15.8) (15.6) (0.1)Financing (1.0) (1.1) 0.1 (1.8) (1.8) (0.0)
Operational surplus / (deficit) (1.4) (0.0) (1.4) (2.2) (0.0) (2.2)
Year To Date (Current) Annual
We have sought to extrapolate the financial projections for the whole year to provide an early warning of any issues that may compromise delivery of a financial breakeven. Although not formalised, the Trust is receiving income for Covid and Top up, so has recognised this in the position in line with NHSE guidance. There has so far been no resolution to the shortfall on pay inflation at this point so that causes a £2.2m adverse variance against an assumed breakeven requirement.

INCOME AND EXPENDITURE BY LOCALITY FULL YEAR
AnnualBudget Actual Variance Budget Actual Variance£'000 £'000 £'000 £'000 £'000 £'000
Healthcare Income 215,784 216,078 294 369,250 372,597 3,347
CENTRAL & WESTIncome 3,009 3,339 330 5,081 5,331 251Expenditure 42,909 45,374 -2,465 73,770 77,961 -4,191
-39,900 -42,035 -2,136 -68,689 -72,630 -3,941PENNINEIncome 1,122 2,117 994 1,979 3,397 1,418Expenditure 36,056 36,620 -564 62,714 63,971 -1,257
-34,934 -34,503 430 -60,735 -60,574 161FYLDE COASTIncome 351 465 113 650 829 179Expenditure 24,850 26,158 -1,308 43,025 46,113 -3,088
-24,498 -25,693 -1,194 -42,375 -45,283 -2,909THE BAYIncome 702 926 223 1,239 1,516 277Expenditure 20,817 19,994 822 36,240 35,075 1,166
-20,114 -19,069 1,046 -35,002 -33,559 1,443SPECIALISTIncome 3,696 4,037 341 5,775 7,168 1,393Expenditure 41,023 40,443 579 70,829 71,748 -919
-37,326 -36,406 920 -65,053 -64,580 474OTHER
-48,771 -49,220 -449 -79,781 -80,199 -418CCE
Capital Charges 10,241 10,550 -309 17,616 17,967 -352
-59,011 -59,770 -758 -97,396 -98,167 -770TOTAL
0 -1,398 -1,398 0 -2,195 -2,195
This summary measures performance against internal budgets, which also supposes a breakeven against a plan of breakeven to the end of month 7.
Most clinical areas are performing near expectations. Central and West services are experiencing pressures on wards and are also experiencing cost pressures from the use of agency and locums in coveringmedical vacancies.
The outturn position sees a continuation of the pressure on wards, particularly in Central and West, but with further pressures emerging at Specialist Services, particularly with regard to recruitment assumptions in Perinatal and The Bay.
Capital Charges are expected to remain in line with budget.
The overall shortfall is a recognition that the system has not yet determined a solution for the shortfall in pay award funding which is expected to amount to £2.2m for the year.

CASH AND LIQUIDITY
CASH AND LIQUIDITY
Actual Plan Variance£57.1m £26.0m £31.1m
Forecast Plan Variance£'m £'m £'m
£14.8m £19.5m -£4.7m
BETTER PAYMENTS PRACTICE CODEBPPC NHS Volume BPPC Non NHS Volume
92% 94%
BPPC NHS Value BPPC Non NHS Value
96% 96%
Year To Date (Current)
Annual
The Trust continues to benefit from the significant increases to planned cash levels as a result of year end working capital, and underlying cash remains healthy.
£0
£20
£40
£60
£80
1 2 3 4 5 6 7 8 9 10 11 12
Cash Forecast
Strategic Headroom Operating Headroom Minimum Threshold Actual/Forecast Plan
£m
£0
£5
£10
M01 M02 M03 M04 M05 M06 M07 M08 M09 M10 M11 M12
NHS Debt
1-30 31-90 90+
£m
£0
£5
M01 M02 M03 M04 M05 M06 M07 M08 M09 M10 M11 M12
Non NHS
1-30 31-90 90+
£m
Where possible the Trust is supporting suppliers by paying all invoices within 7 days and where problems exist facilitating payments on account to support said suppliers.

CAPITAL
Current PositionOverall on core infrastructure schemes capital expenditure is broadly in line with the plan, but the change to spend phasing on the Wesham and MH Dormitory schemes that was identified earlier in the year has shifted significant expenditure toward the end of the year. Spend on these schemes has now accelerated, and though not without risk we are confident the majority of these can be concluded in 2021/22 with slippage of c£500k into 2022/23.Forecast PositionThe Trust received additional resource envelope cover with the ICS for spend on the Hurstwood (c£3.1m) and precommitments (c£2.6m - primarily Wesham) which although not included in plan figures have been incorporated into the Trusts working plans and forecasts. With the plans in place this gave the Trust sufficient headroom to manage the programme within its resource envelope. A number of potential pressures to forecast have been identified, which after mitigations have resulted in a gap of c£0.8m. If the Trust continues with the current planned schemes approved including the mitigations, re-prioritisation is likely to be required in order to remain within the funding envelope. Even if this can be managed there will remain a risk of potential overspends due to the limited flexibility in the plan and funding.
£0
£5,000
£10,000
£15,000
£20,000
£25,000
£30,000
APR MAY JUN JUL AUG SEP OCT NOV DEC JAN FEB MAR
CAPEX
CUM SPEND (Total) CUM FORECAST (Total) CUM PLAN (Total)
£000

STAFFING
0
200
400
600
800
1,000
1,200
1,400
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Agency Spend by Type
Medical and Dental Nursing, midwifery and health visiting staff
Scientific, therapeutic and technical staff Health care assistants and other support staff
Managers and infrastructure support Other
Agency Ceiling
12,000
14,000
16,000
18,000
20,000
22,000
24,000
26,000
28,000
30,000
32,000
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar
Staffing Spend by Category
Substantive Bank Agency Plan Total
Staffing Spend
• The Trust continues to overspend in ward areas with a heavy reliance on agency, but more so bank staff. Nursing are reviewing ward staffing levels. Secure Services have revised establishments to better reflect need however the financial gap will be left with the service pending discussions with commissioners and service reviews.
• Temporary staffing has accounted for 12.4% of pay costs to the end of August. Agency now constitutes 4.5% of Trust spend.
• Overall staffing has been impacted by developments and to a lesser extent by Covid. Costs have increased due to pay award, but also recruitment to vacancies.
Agency Spend
• Agency expenditure continues to be dominated by medical and dental expenditure. We have seen an increase in agency use this year over last. This has become particularly pronounced in medical and ward spend. The causes are being reviewed alongside appropriate remedial actions. This month has seen an increase of medical spend with particular rises in Specialist Services.
• Although not reported this year, the previous Agency Ceiling was £7.0m, but is not flexed for Covid costs.
• Overall expenditure is expected at current rates to exceed the agency ceiling by c£6.9m for the year, 99%.

COVID BRIDGE TO MONTH 7
The Trust was provided with £9.3m to address Covid matters for the first 6 months of the year and overspent by c£0.2m against it.The Trust s seeking £9.9m for H2, and although not yet confirmed is being paid in line with that.The main area of expenditure is in relation to the increase in OAPs activity due to increased presentations, but also in relation to the OAPS consequential to the number of beds that have had to be stood down as dormitories carry increased Covid.The Trust expects to spend in line with the £9.9m for H2, however there is significant risk if this is not the case and figures have not yet been circulated to trust level.The Trust is incurring, and recovering costs, for the Vaccine centre for the financial year
Covid Scheme Costs 2021-22 H1 Actual H2 PlanM7
ActualM8-12
ForecastH2
Forecast£000's £000's £000's £000's £000's
OAPs - Increased demand 5,388 6,026 982 5,067 6,049OAPS - Dormitory Closures 2,951 2,977 512 2,481 2,993Extended Service Hours 177 0 0 0 0Agency COVID-19 Absence 23 24 0 20 20Bank COVID-19 Absence 565 360 22 300 322PPE Locally Procured 70 120 43 100 143Covid Booking System 21 12 4 10 14Decontamination & Waste 48 48 5 40 45IPC additional workforce at MH sites 22 120 18 100 118Increase in contingency beds in Pennine 46 54 8 45 53Covid Ward Catering Costs 32 32 5 27 32Other 2 3 0 3Total 9,657 9,892 1,602 8,290 9,892
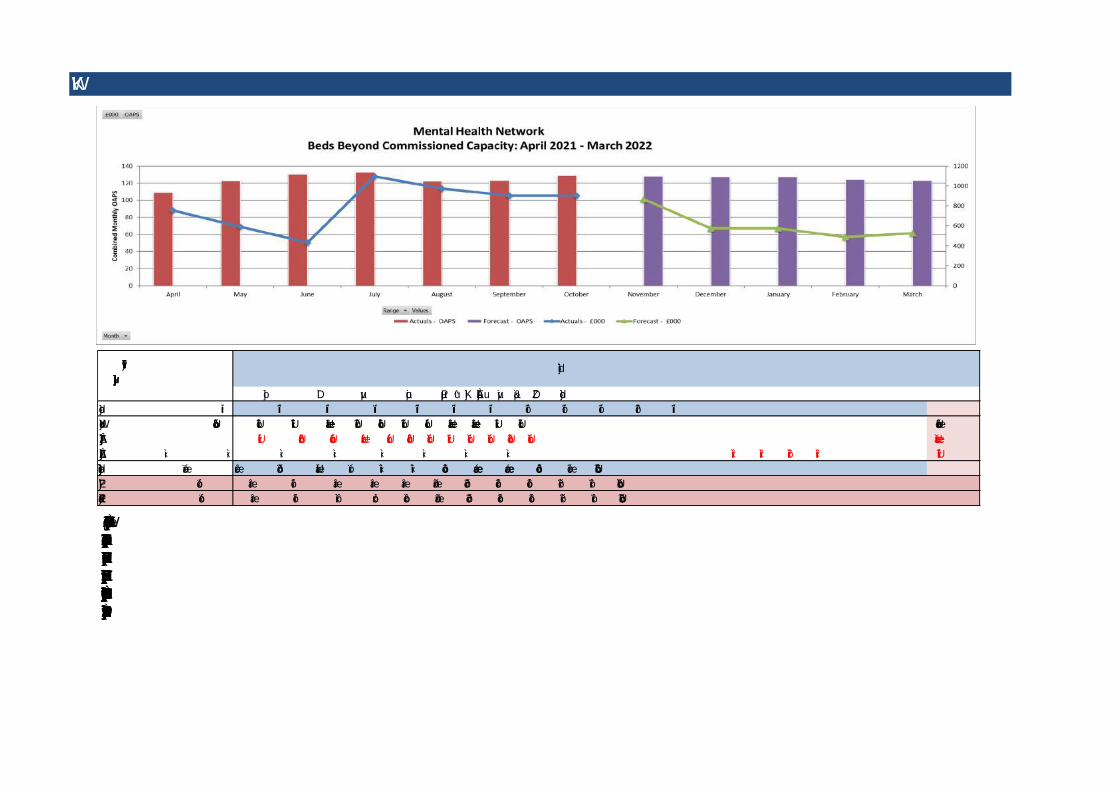
OAPs
The Trust has spent £14.9m on OAPs at month 7. £9.2m of this is Covid related and therefore reimbursed. Of the remaining £5.7m, the CCGs are liable for the amount for the comparable period under the current arrangement, so pay £2.2m. The Trust therefore pays £3.4m. The outturn of £4.9m spend for the Trust is £2.4m more than budgeted, but is in line with last year's expenditure.The closure of beds for dormitory work has impacted on capacity. Whilst there is no certainty for H2 yet, an assumption has been made that indemnification for Covid costs will continue, however should this arrangement not continue, the position could be compromised. Additionally, any delays in reopening could lead to pressure on funding with underspend on MHIS having to be considered.
21/22 Beds beyond Commissioned Capacity
April May June July August September October November December January February March TotalTotal Beds 109 122 131 133 122 123 129 128 127 127 124 123Total OAPs £1,764 £2,038 £2,212 £2,355 £2,142 £2,086 £2,272 £2,197 £2,255 £2,255 £2,013 £2,207 £25,798Covid Recovery Costs -£1,011 -£1,449 -£1,777 -£1,259 -£1,169 -£1,184 -£1,370 -£1,329 -£1,370 -£1,370 -£1,246 -£1,370 -£15,905Wesham Recovery Costs £0 £0 £0 £0 £0 £0 £0 £0 -£310 -£310 -£280 -£310 -£1,212Total Cost (£'000s) £753 £589 £434 £1,095 £973 £902 £902 £868 £575 £575 £487 £527 £8,682Charge to CCGs £377 £295 £217 £295 £295 £295 £451 £434 £287 £287 £243 £263 £3,740Charge to LCFT £377 £295 £217 £800 £679 £607 £451 £434 £287 £287 £243 £263 £4,942
Trajectory
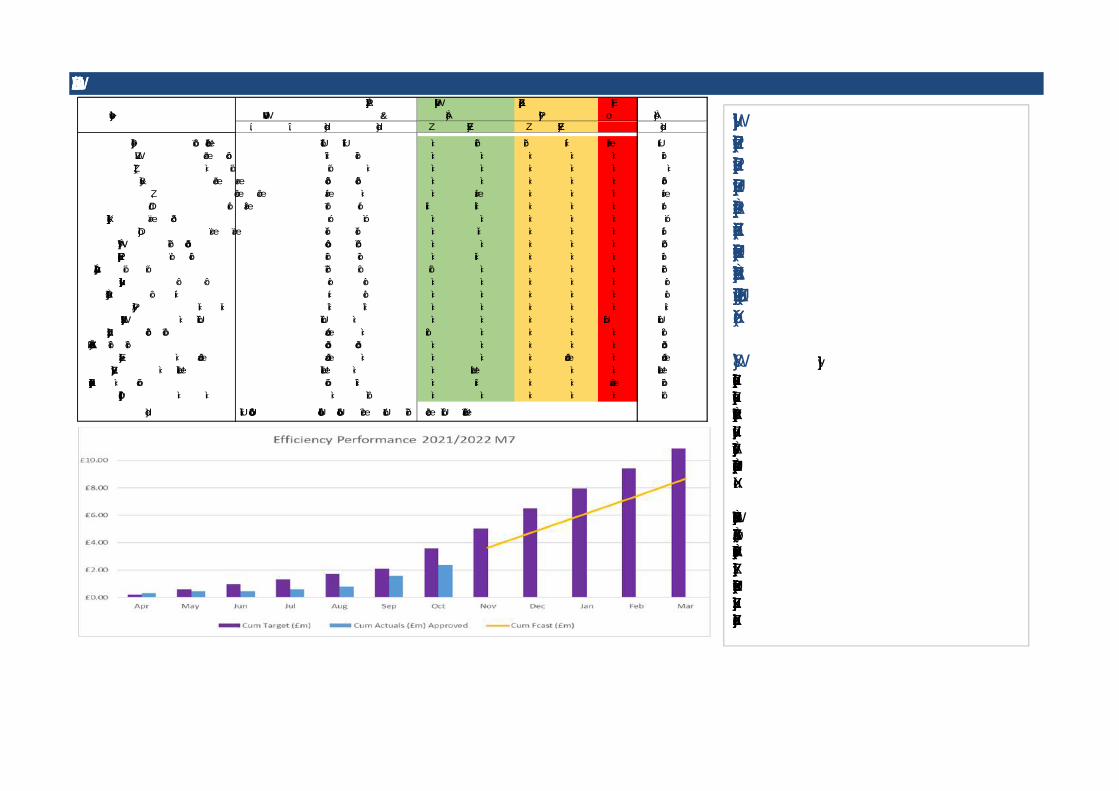
EFFICIENCY IMPROVEMENT PROGRAMME
Current PositionDue to the lateness of the planning guidance and establishment of the financial gap, there has been some delays in developing the efficiency plans for the year. The Trust set an annual target of £10.9m. At month 7, the Trust has delivered £2.9m against a plan to this point of £3.6m, a shortfall of £0.7m.
Forecast PositionThe position for the full financial year is as yet undetermined due to the lack of settlement in respect of financial planning in H2. However the Trust has made certain assumptions around expectations and has derived an additional H2 challenge of £8.8m, giving a full year target of £10.9m.
Plans are being delivered which amount to £3.9m. A further £3.9m of schemes have also been developed and are pending QIA sign off. £7.8m is therefore considered certain.Of the £0.8m of amber schemes, a workingassumption has been made that either these or compensatory schemes will be. A scheme to
Locality/DepartmentNo
Clear DeliveryH1 H2 Total Total Rec Non Rec Rec Non Rec Total
Locality 1% £883 £1,354 £2,237 £1,321 £0 £141 £240 £111 £125 £1,939Pharmacy £54 £78 £132 £108 £0 £0 £0 £0 £0 £108Chief Exec £0 £71 £71 £0 £0 £0 £0 £0 £0 £0
Finance £54 £95 £148 £148 £0 £0 £0 £0 £0 £148HR £58 £58 £115 £0 £0 £115 £0 £0 £0 £115IMT £169 £215 £383 £17 £120 £200 £0 £0 £0 £337
Director of Operations £35 £44 £79 £70 £0 £0 £0 £0 £0 £70Medical £53 £53 £107 £107 £0 £10 £0 £0 £0 £117
Property Services £240 £447 £687 £480 £0 £0 £0 £0 £0 £480Nursing & Quality £63 £118 £181 £26 £0 £100 £0 £0 £0 £126
Improvement & Compliance £71 £71 £142 £61 £81 £0 £0 £0 £0 £142Communications £8 £8 £16 £16 £0 £0 £0 £0 £0 £16
Strategic Development £8 £11 £19 £16 £0 £0 £0 £0 £0 £16Integration £10 £10 £20 £20 £0 £0 £0 £0 £0 £20
OAPS Reduction £0 £1,600 £1,600 £0 £0 £0 £0 £0 £1,600 £1,600Secure B&A Reduction £148 £627 £775 £0 £361 £0 £0 £0 £0 £361
New Developments Overheads £238 £238 £476 £476 £0 £0 £0 £0 £0 £476NCA Lost Income £0 £475 £475 £0 £0 £0 £0 £475 £0 £475
Non Recurrent Gains £0 £2,500 £2,500 £0 £0 £2,500 £0 £0 £0 £2,500Further Secure Transformation £0 £717 £717 £210 £0 £313 £0 £0 £85 £608
S136 Efficiencies £0 £0 £0 £800 £0 £0 £0 £0 £0 £800
Total £2,090 £8,788 £10,878 £3,876 £562 £3,379 £240 £586 £1,810 £10,453
Planned TargetAchieving
FYEPlan Awaiting
ApprovalRequires Further
Scoping
USE OF RESOURCES
FINANCE AND USE OF RESOURCES RATING
Plan Actual Plan Actual 1 2 3 4 Weighting
Capital service cover rating 2 3 2 3 2.5 1.75 1.25 <1.25 20%
Liquidity rating 1 1 1 1 0 -7 -14 <-14 20%
I&E margin rating 2 3 2 3 1.00% 0.00% -1.00% <=-1% 20%
I&E margin: distance from financial plan 1 2 1 2 0.00% -1.00% -2.00% <=-2% 20%
Agency rating 3 4 3 4 0.00% 25.00% 50.00% >=50% 20%
Overall 2 3 2 3 100%
Year to Date Annual
Note that the Single Operating Framework was published in late June and Use of Resources Ratings will be revised. The new metric calculations and their weightings have not yet been published. The figures presented use the historic calculations and are based on extrapolated figures, they not currently reportable or collected centrally and are included for indicative purposes only. Note also that the agency target has been taken from 2020-21:
- With the deterioration of the I&E position the metrics show a decline from M06, leaving only liquidity on plan. However the overall metric remains unchanged as that had been constrained by an agency rating of 4. - If the I&E position remains as forecast the metrics will remain likely remain unchanged leaving the trust with an overall outturn metric of 3. Should the I&E position improve the overall metric will still likely be constrained by the forecast agency rating of 4.
Note Adjustments for allowances have not yet been formally confirmed and are therefore currently excluded.
BALANCE SHEET
Actual Plan Variance Actual Plan Variance£'m £'m £'m £'m £'m £'m
Non Current Assets 234.0 242.4 -8.4 247.4 242.9 4.6
Stock 0.0 0.1 -0.1 0.1 0.1 0.0
Trade Debtors 25.8 22.6 3.2 24.4 22.6 1.8
Other Current Assets 0.5 0.0 0.5 0.0 0.0 0.0
Cash 57.1 26.0 31.1 14.8 19.5 -4.7
Current Liabilities -75.0 -37.9 -37.1 -36.4 -32.4 -4.0
Working Capital 8.4 10.8 -2.4 2.9 9.8 -6.9
Non Current Liabilities -44.1 -44.0 0.0 -42.7 -42.7 0.0
198.3 209.2 -10.8 207.6 209.9 -2.3
Taxpayers Equity
PDC 128.8 136.1 -7.4 136.8 136.9 -0.1
I&E Reserve 6.3 9.8 -3.5 8.3 10.5 -2.2
Other Reserves 63.3 63.2 0.1 62.5 62.5 0.0
198.3 209.2 -10.8 207.6 209.9 -2.3
AnnualYear To Date (Current)
Key changes relate to capital changes (and corresponding changes to funding) and cash (and corresponding changes in I&E/Working Capital)- see respective sections.
Agenda Item Number: TB 232/21
PROVIDER COLLABORATIVE COMMITTEE CHAIRS REPORT
Report provided for: Report to: Board of Directors
Information ☐ Assurance ☒
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Phil Huggon, Committee Chair
Prepared by: Vicki Waddington, Executive PA
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will value our partners by listening and collaborating effectively across the SYSTEM
Aligned to Board Assurance Framework Risk
6.0 Failure to actively collaborate through the ICS, ICPs and wider partners due to a lack of capacity and capability within the organisation may result in fragmented services and reputational damage
Recommendation/Required Action
The Board of Directors are asked to note the
assurance and escalation provided within Provider
Collaborative Committee chairs report.
1.0 INTRODUCTION
The Board of Directors are presented with the Chairs Report of the Provider
Collaborative Committee on 15 November 2021. The chairs report provides an overview
of assurance received and escalation to discussions held, as required.
2.0 RECOMMENDATION
The Board of Directors are asked to:
note the assurance and escalation provided within the chairs report

CHAIRS REPORT
MEETING: Provider Collaborative Committee DATE OF MEETING: 15/11/2021
CHAIR OF MEETING:
Phil Huggon – Non-Executive Director
ITEMS APPROVED
No items were approved at the committee.
ASSURANCE RECEIVED
Go Live Commissioning Programmes for Specialist Commissioning Services (Children, Young People Tier 4 and Adult Secure) The Committee received a comprehensive report on the go live for Children, Young People Tier 4 and Adult Secure. Progress is being made and contracts have been created and are awaiting sign off. The Trust has received good engagement across the north west and colleagues in non-clinical and clinical roles are working closely to move the project forwards. There are still a couple of gaps in recruitment but these are being addressed and we are in the process of filling the posts. In relation to all financials there is work being completed on this and will be brought back to a future meeting to discuss and approve. The creation of balance score cards and a road map was agreed to be completed and brought to the next meeting for discussion. Development of the ICS MHLD&A Provide Collaborative Arrangements Assurance was received that we are on with the development of the ICS for MHLD&A and it was confirmed that all trust will have a lead provider model in place. It was confirmed that following a system wide reform on legislation in relation to the ICS we are now looking at the architecture of the plan and how the service will be delivered. Risk Register and Programme Plan The committee received an update on the risk register and the programme plan and it was confirmed that a number of positions have been filled by interim posts. A paper is being produced and will be present to Executive’s which will show the sustainable model and how we firm up being a
CHAIRS REPORT
lead provider. It was agreed that the Board Assurance Framework will be included on the agenda at future meetings, so that the risk levels can be reviewed. The committee confirmed that the risk level is still the same as we still pose the same amount of risk.
ITEMS TO ESCALATE TO THE BOARD
ITEMS FOR ESCALATION MITIGATING ACTION
The financial risk was assessed and assurance will be provided through a business case and partnership agreements and will be outlined in details
The Committee requested sight of any financial papers prior to their consideration by the Finance and Resource Committee
ITEMS RECEIVED FOR INFORMATION
Balance Score Cards and a Road map will be created
There are a lot of unknowns for the next couple of months on what we can expect the structure to look like but this was confirmed that from March 2022 we will have shadow forms of the structure.
Agenda Item Number: TB 233/21
TRANSFORMATION PROGRESS UPDATE
Report provided for: Report to: Board of Directors
Information ☒ Assurance ☐
Discussion ☐ Decision ☐ Date of Meeting: 25/11/2021
Presented by: Steve Christian, Chief Integration Officer
Prepared by: Louise Giles, Deputy Director of Transformation
Freedom of Information Act Exemption
No Exemption Not Applicable
Link to Strategic Priorities We will provide SUSTAINABLE services that deliver real value
Aligned to Board Assurance Framework Risk
6.0 Failure to actively collaborate through the ICS, ICPs and wider partners due to a lack of capacity and capability within the organisation may result in fragmented services and reputational damage
Recommendation/Required Action
The Board of Directors are asked to:
Note the report and progress
Note the significant engagement across
stakeholders and partners
Note the key risks and mitigating actions
across all programmes
1.0 Introduction This paper is to update the Trust Board on the progress of the three system wide transformation programmes which are:
• Community Mental Health Transformation • Initial Response Service ( IRS ) • Children and Young Peoples Mental Health and Emotional Wellbeing
2.0 Community Mental Health Transformation This programme is overseeing the single biggest investment in mental health services that we have seen in recent times; Lancashire and South Cumbria will receive £11.6m in NHS transformation funding. The aim is to develop a new model of care that is set out in the NHSE Community Mental Health Framework. The NHSE Community Mental Health Framework sets out a model of care that enhances community based support for people living with moderate to severe mental illness and complex needs. The funding provides local NHS organisations the opportunity to focus on population health and reduce inequalities. Lancashire and South Cumbria NHS Foundation

Agenda Item Number: TB 233/21
Trust (LSCFT) aims to deliver on this transformation programme through the strengthening of local partnerships with local authority-funded services and the Voluntary, Community, Social, Faith and Enterprise (VCFSE) sector. Nationally there have been early implementer sites of the model and a new 4 week waiting time target is being piloted with the ambition that people moderately to severely affected by mental illness can expect to receive the right treatment at the right time within 4 weeks from 2023/24. The following principles are fundamental to the new community models:
• Removing the idea of thresholds and multiple assessments – if someone is unwell and in need of support, they should receive it, as they would in acute care. If that service turns out to not be quite right then the system should be flexible enough to offer other options and step up and step down care as
• A ‘no wrong door’ policy, or even a ‘no door’ policy • People should be able to tell their story and experience just once • A focus on specific, tailored and inclusive support needed for underrepresented groups
– including the black, Asian and minority ethnic (BAME) population and people from lesbian, gay, bisexual, transgender, questioning and intersex (LGBTQI) communities.
• Personalised health and social care support – including entitlements under the Care Act and personal health budgets.
• Joint commissioning of services for people and communities There are some key elements of the model that are nationally mandated that include
• Implementing a core community mental health service model • Physical Health Checks in SMI • Individual Placement Support • Early Intervention Psychosis • Mental Health Rehabilitation • Eating Disorders • Complex Emotional Needs associated with diagnosis of PD • Expand the clinical and non-clinical workforce • Address Health Inequalities
The access into the community model will be at a neighbourhood level within Primary Care Networks (PCNs); which are groups of GP practices that specifically focus on the needs of local populations. The plan is to create Community Hubs with aligned services and teams wrapped around a number of PCNs with close connections to a local network of community groups and VCFSE organisations. The intention is that people will be able to access a multidisciplinary team (MDT) comprising:
• Mental health practitioners/consultants/support workers • Social care staff • VCFSE staff • Primary care staff • Substance misuse providers • Housing/finance/employment support • Peer support workers

Agenda Item Number: TB 233/21
The programme will introduce a new trusted assessment and formulation model that is strengths based, and goal/solutions focussed. Assessment and formulation (with input from the full MDT) will be delivered by both statutory staff, voluntary sector staff and peer workers trained to the same standard. Where appropriate, the same staff will coproduce a personalised care and support plan and provide a range of short-term clinical, social and community interventions designed to promote recovery and reduce risk of crisis. 2.1 Progress to date The progress for this programme;
• Governance structure in place with task and finish groups for the following
o Personality Disorder (PD) o Community Rehabilitation o VCFSE o Physical Health Checks o DIALOG+
• Significant stakeholder engagement taken place with the establishment of locality
delivery groups aligned to Place Based Partnership (formerly known as ICPs) • Marketplace engagement events held with VCFSE organisations in each locality • Project team recruited • Procurement commenced for the VCFSE sector offer • Community Hubs identified and we are commencing mobilisation to have one
operational in Jan / Feb 2022 • Recruitment to the PD SCM practitioner community roles commenced (11 recruited ) • Primary Care MH Practitioner (50% funded by ARRS) roles recruitment commenced
(14 recruited) with an SLA drafted • Alignment of LSCFT staff to PCNs and developing community hubs • Roll out of DIALOG+ commencing in Pennine and plans within all localities • Recruitment commenced for community rehab core team • Team/team events with stakeholders and clinical teams with early implementer sites
2.3 Next Steps Our plans for the next 12 months include:
• Expand the number of community mental health hubs • PDSA cycles to test and learn from the model • Expanding and or establish investment into commissioning local voluntary
organisations, including smaller/micro VCFSE organisations, grassroots, local community/faith and user-led organisations, to provide outreach services for people with SMI experiencing inequalities;
• Recruitment peer support / lived experience roles from minority groups with protected characteristics, including ensuring these roles receive appropriate support, supervision and remuneration
• Continue to draw on innovative workforce configurations and expand MDT approaches across clinical and non-clinical roles, including new roles e.g. peer support workers; MH pharmacists, Mental Health and Wellbeing Practitioners and Mental Health Practitioners in Primary Care.
Agenda Item Number: TB 233/21
• Build a more psychologically informed workforce and support staff to take up and then apply relevant local, regional and national CPD opportunities.
• Working towards the workforce reflecting and able to work with the diversity of local communities;
• Developing Integrated or other partnership approaches to workforce planning with local authorities and the VCFSE that result in integrated service deliver
• State of readiness monitoring against the five key principles moving away from CPA • Expansion and implementation of a service for physical health checks • Ongoing recruitment to all roles
2.4 Key Risks There are a number of key risks that include
Risk Identified Mitigating Actions
Recruitment of required posts has historically been a recognised difficulty within the trust, with posts not being filled, or being vacated shortly after they have been filled.
There will be a dedicated workforce group who will be
responsible for a system wide recruitment strategy.
Analysis will be completed to inform development of
an appropriate, skilled workforce. Comms will support
with the targeted recruitment strategy.
CMHT currently have a high number of unallocated cases which could significantly impact the delivery of the 4 week wait target.
Bipolar network, PD network, trauma service and clinical treatment team have reviewed caseloads and are working with CMHT to confirm who can be solely in the specialist service caseload as they have no need for CMHT input. There is no requirement for people to be care coordinated by CMHT to access these services. Service managers are identifying gaps in services where people are referred to CMHT when the service is not appropriate- will use this information to commission services in localities.
3.0 Initial Response Service (IRS)
We are implementing a new Initial Response Service (IRS) in each locality to support people in crisis as part of the community model. The aim of the service is to provide a responsive single point of access for urgent and routine requests for help, including signposting to relevant services. The intention is that by April 2022 each Locality / ICP will have the IRS service in place. 3.1 The Model for Access Through stakeholder engagement workshops which included staff, partners, service users and carers, the groups co-produced and articulated how a single access point (IRS) across Lancashire and South Lancashire would help people receive a quick and efficient response for help, reduce clinician administration burden and improve service user outcomes.
The development of a 24/7 Service provides one number across each Lancashire & South Cumbria locality for all age and the service will allow people to self-refer or be referred by a carer as well as by a professional. The service will provide urgent and routine mental health
Agenda Item Number: TB 233/21
support, advice and a single triage based on trusted assessment, through which people can access the mental health pathway for urgent or routine care, signposting and/or further support if needed. Emergency Services will also have direct access to the line.
The aim of the service is to provide a responsive single point of access for urgent and routine requests for help, including signposting to relevant services within and outside of LSCFT. A crucial part of the design is to enable this service to work alongside the Home Treatment Team (HTT) and therefore share skills and experience, promote positive learning and development for all staff within their roles. This would also offer flexibility to staff and the service. In addition, staff will all have interchangeable roles across the IRS and HTT.
Key design elements for IRS include:
A 24/7 single free phone number that signposts/ connects people to the right place first
time, every time
Enable self-referral or referral by a carer / professional
Quick and efficient responses to requests for help
Trusted Triage – patients will tell their story once
Provide advice, support, triage and routing to appropriate mental health services and
signposting to other local services as appropriate
Patients are directly booked into routine services via a trusted assessment through a
centralised booking system for the locality
Patients will be able to contact the IRS direct to book and reschedule appointments without
having to go direct to teams
Receive warm transfers from NHS111, North West Ambulance Service (NWAS) and Police
No requirement for any separate lines which includes current Crisis Line, Volunteer and
Access Line once rolled out across each locality
IRS will work closely with Patient Advice and Liaison Service (PALS) service to resolve
any disputes and low level concerns
A Street Triage Service will be integrated into the model to support the reduction in 136
detentions and A&E attendances for those in crisis conveyed by the Police or Ambulance
Service.
3.2 Progress to date
• Recruitment has commenced across all localities supported by a significant recruitment
campaign
• Significant engagement with stakeholders across all localities
• Pathways agreed with booked assessment slots across teams
• Street Triage pilot Tuesday – Friday 3pm – 1am commenced in Barrow in October with a
significant reduction in 136 detentions
• All age model agreed
• Go live plans agreed for a soft launch in Pennine commencing 12th January 2022, Central
and West Lancashire planned end of Jan / Feb 2022 dependant on estates handover
• The IRS estate which is the Mount in Accrington has been handed over
• 4 week training programme in progress for all new staff in place
• Street Triage in Pennine as a soft launch will commence on the 1st Dec 2021
• Volunteer Coordinator model agreed
• Patient Communications agreed

Agenda Item Number: TB 233/21
• Working with the deaf community to ensure access to the IRS.
3.3 Key risks A number of key risks across all localities have been identified for IRS including:
Risk Identified Mitigating Actions
Fylde Coast – Accommodation yet to be identified
Options appraisal and funding requirements to be agreed
CMHT - Currently have a high number of unallocated cases, this in turn impacts on the ability to undertake planned appointments booked from the IRS
Interim solution agreed that IRS Routine Care team will undertake the first appointment. This will reduce immediate pressure on CMHT and enable the service to work on current demand and unallocated cases
START Waiting lists/Caseloads - Team currently holds an existing caseload. This will impact on capacity
Team currently working through the trajectories and plan to clear the backlog, utilisation of bank staff will also support this process.
Recruitment to vacancies (new roles) identified will impact on the safe delivery of an effective and safe IRS Service.
Recruitment options via agency, bank and HEE to be considered to support transition and soft launch of IRS. Opportunity to have a rolling programme of recruitment and share resources in the early implementation / go live of the programme with other localities.
4.0 Children and Young People Mental Health and Emotional Wellbeing Transformation 4.1 Programme Overview
In Lancashire and South Cumbria, work has continued to build upon a strong platform of
leadership and collaboration to establish good governance that will enable the ICS to deliver
on improving outcomes and care for local Children and Young People, reducing pressures on
services and making best use of financial resources.
The ICS partners have worked with Niche Health and Social Care Consulting who have
undertaken an ICS wide review of current and future capacity of mental health and wellbeing
services for children and young people and completed a robust statistical modelling exercise.
The output has been translated into a sustainable financial model across the ICS.
The Strategic Commissioning Committee approved a system wide plan to progress a large-
scale transformation programme within an agreed financial envelope of £10.7 million over a 3
year period .The establishment of a Transformation team has been endorsed by the system.
The Children and Young People’s Emotional Wellbeing and Mental Health (CYPEWMH)
Transformation Plan for Lancashire (2015-2020) was first published in January 2016. The
document set out the initial iteration of a five-year plan for Lancashire, to support local
implementation of the national ambition and principles as set out in ‘Future in Mind –
promoting, protecting and improving our children and young people’s mental health and
wellbeing’ (2015) The plan’s aim was to improve the resilience, emotional wellbeing and
mental health of children and young people, especially those who are at increased risk due to

Agenda Item Number: TB 233/21
their vulnerability, making it easier for them and their families to access help and support when
they need it whilst improving the standard of mental health services across Lancashire and
now, South Cumbria.
4.2 Programme Collaboration
The transformation programme proposes to draw upon these local ambitions along with the key deliverables required within the NHS long term plan (2019) to create a programme of delivery to enact the vision for our Children and Young People to enable them to live their lives to their full potential. The ICS has a proven history of working with CYP, families and carers to co-produce new service models. Children and young people with lived experience of emotional health and wellbeing needs, along with their parents and carers, were recruited to undertake a four-month phase of co-production design of the C&YP THRIVE Redesign model.
It is important to us to ensure that the communities of Lancashire & South Cumbria are
equitably represented through our partners. The significant impact that the expertise and
impact our VSCFE partnerships can bring to the getting advice and the getting help quadrants
of Thrive cannot be underestimated therefore an additional £1.9 million investment has been
ring fenced to support these developing partnerships and pathways.
4.3 Programme Objectives
To deliver and embed the ICS transformation programme that ensures the deliverables for Children and Young People, addresses local need and delivers and embeds the THRIVE redesign model
To address health inequalities, particularly through disadvantaged groups and whereby there are multiple complexities
To deliver the best possible long term health outcomes for our children and young people
To build and maintain relationships within our system partnerships
To raise the profile of emotional wellbeing and mental health in children and young people across our footprint To provide local parity on care delivery models, commissioned delivery models and outcomes, pathway
To reduce unwarranted variation in the accessibility to mental health and wellbeing interventions
To enhance the “getting advise and getting help” quadrants of Thrive through the investment in our partnerships with VSCFE
4.4 Programme Priorities
To understand any variation in delivery models and outcomes, through a comprehensive
review of service delivery models in order to promote consistency and parity of service
delivery
To increase access to mental health and wellbeing provision for all children and young
people
To reduce waiting times to mental health and wellbeing interventions for all children and
young people through the achievement of a 4 week referral to treatment target
To enhance the lived experience and peer support collaboration across the ICS.

Agenda Item Number: TB 233/21
To Build and expand upon an intensive community support model, reducing the need for
hospital based stay
To reduce transitional gaps by enhancing the C&YP delivery model to flexibly meet the
needs up to 25 where required
4.5 Progress to Date
Programme team established through a collaborative approach with partners
The priorities for years 1 and 2 transaction of investment agreed based upon the engagement with the collaborative Thrive redesign
Recruitment commenced for the delivery of intensive community support teams
Recruitment commenced for the delivery of a risk support model
Workshops to support go live of the all age IRS completed for Pennine
Workshops completed to scope pathway interdependencies
MHST coverage plan completed with allocation agreed for next 3 years
Scoping of commissioning gaps and interdependencies commenced
Scoping of quality outcomes commenced 4.6 Key Risks
Risk Identified Mitigating Actions
Capacity to mobilise Thrive model at pace
Introduction of dedicated Transformation Team led by the Associate Director for clinical transformation for CYP from LSCFT in conjunction with all providers and commissioners
Recruitment of practitioners with required skill set across the ICS area
Recruitment planning already mobilised with agreements across providers to work collaboratively to increase workforce across ICS and attract talent into the area
Service provision is delivered across three Trusts, risk of fragmentation in delivery
Agreed LSCFT as the host for MH CYP transformation, collaborative approach to redesign and ongoing transformation programme
5.0 Decision Required The Trust Board are asked to
• Note the report and progress • Note the significant engagement across stakeholders and partners • Note the key risks and mitigating actions across all programmes
Copyright © 2022 FDOKUMEN