Governing Bodies meetings in common – Public
148
Governing Bodies meetings in common – Public Date: 13 April 2017, Time: 10.30–12.00 Venue: Olympic Room, Aylesbury Vale District Council, the Gateway, Gatehouse Road, Aylesbury, HP19 8FF Chair – Dr Graham Jackson No Agenda Item Action Lead PDF Page No. Welcome 1. Introductions Dr Graham Jackson, Chair Verbal 2. Apologies Dr Graham Jackson, Chair Verbal 3. Declaration of Interests in items for items on this meeting’s agenda/Formal Review of Registers of Conflicts of Interest and Hospitality/Gifts/sponsorship. Locations of public registers: Aylesbury Vale CCG: https://www.aylesburyvaleccg.nhs. uk/about-us/conflict-of-interest-pol/ Chiltern CCG: https://www.chilternccg.nhs.uk/publ ic/about-us/how-we-make- decisions/registers-of-interests/ For Noting & Mitigating Actions Dr Graham Jackson, Chair 3 4. Questions from the public Dr Graham Jackson, Chair Verbal/ Websites 5. Review and Approval of Minutes of previous meeting: • Meeting minutes – 09/03/2017 • Action Log and Matters Arising For Approval Dr Graham Jackson, Chair 6 23 Leadership Reports 6. Accountable Officer’s Report For Assurance Lou Patten, Accountable Officer Verbal Assurance and Governance 7. Finance Report (Month 11) For Assurance Robert Majilton Interim Chief Finance Officer 24 Page 1 of 148 Page 1 of 148
-
Upload
khangminh22 -
Category
Documents
-
view
6 -
download
0
Transcript of Governing Bodies meetings in common – Public

Governing Bodies meetings in common – Public Date: 13 April 2017, Time: 10.30–12.00
Venue: Olympic Room, Aylesbury Vale District Council, the Gateway, Gatehouse Road, Aylesbury, HP19 8FF
Chair – Dr Graham Jackson
No Agenda Item Action Lead PDF Page No.
Welcome
1. Introductions Dr Graham Jackson, Chair
Verbal
2. Apologies Dr Graham Jackson, Chair
Verbal
3. Declaration of Interests in items for items on this meeting’s agenda/Formal Review of Registers of Conflicts of Interest and Hospitality/Gifts/sponsorship. Locations of public registers: Aylesbury Vale CCG: https://www.aylesburyvaleccg.nhs.uk/about-us/conflict-of-interest-pol/ Chiltern CCG: https://www.chilternccg.nhs.uk/public/about-us/how-we-make-decisions/registers-of-interests/
For Noting & Mitigating Actions
Dr Graham Jackson, Chair
3
4. Questions from the public Dr Graham Jackson, Chair
Verbal/ Websites
5. Review and Approval of Minutes of previous meeting:
• Meeting minutes –09/03/2017
• Action Log and MattersArising
For Approval Dr Graham Jackson, Chair
6 23
Leadership Reports
6. Accountable Officer’s Report For Assurance Lou Patten, Accountable Officer
Verbal
Assurance and Governance
7. Finance Report (Month 11) For Assurance Robert Majilton Interim Chief Finance Officer
24
Page 1 of 148
Page 1 of 148

8. Quality and Performance Report (Month 11)
For Assurance Debbie Richards Deputy Accountable Officer and Interim Chief Finance Officer
68
9. Five Year Forward View Delivery Plan Update
For Information Dr Graham Jackson, Chair
Verbal
10. Amendments to terms of reference for Audit Committees meetings in common.
For Ratification Robert Majilton Deputy Accountable Officer and Interim Chief Finance Officer
101
11. Amendments to terms of reference for the joint Quality and Performance Committee
For Ratification Debbie Richards Director of Commissioning and Delivery
104
Decisions
12. CCGs Budget Setting 2017/18 For Decision Robert Majilton, Deputy Accountable Officer and Interim Chief Finance Officer
For Information
13. Approved Minutes from sub-committees, sub-groups or steering groups: a) Executive Committee –
23/02/2017b) Audit Committee – 01/02/2017
For Information Dr Graham Jackson, Chair
14. Date and Time of the next public meeting: 8 June 2017, 10:00am – 12:00pm; TBC, The Gatehouse, Aylesbury Vale District Council
Page 2 of 148
Page 2 of 148
129139
114

MEETING: Governing Bodies meetings in common AGENDA ITEM: 3
DATE: 13 April 2017
TITLE: Declaration of Interests in items for items on this meeting’s agenda/Formal Review of Registers of Conflicts of Interest and Hospitality/Gifts/sponsorship.
AUTHOR: Russell Carpenter, Corporate Governance Lead
LEAD DIRECTOR: Robert Majilton, Deputy Accountable Officer
Reason for presenting this paper: For Action For Approval For Decision For Assurance For Information
Summary of Purpose and Scope of Report: The Governing Bodies are asked to: • NOTE formal circulation of registers of declarations of interest and hospitality, gifts and
sponsorship.• NOTE link to registers published on external websites included on the agenda.• NOTE systems for declaration and thus formal opportunity in public to declare any
changes to published records.
This paper provides a summary and assurance on the CCGs compliance with statutory guidance on conflicts of interest and hospitality, gifts and sponsorship. This follows new guidance published by NHS England in June 2016 which strengthens requirements in declaring and recording interests for CCG members and employees.
Systems for declaration The guidance requires CCGs to have systems in place to satisfy themselves on a six-monthly basis that their register of interests is accurate and up-to-date. Accordingly this paper directly signposts members to online publication of registers of declarations of conflicts of interest (and hospitality, gifts and sponsorship), in addition to being made available for review (paper copies) at every meeting.
Members are reminded that declarations of interest should be made as soon as reasonably practicable and by law within 28 days after the interest arises (this could include an interest an individual is pursuing). Therefore the meeting in public provides an opportunity to declare any new or changed interests, with signed forms completed post declaration.
Page 3 of 148
Page 3 of 148

Signposting to registers
Aylesbury Vale CCG Chiltern CCG Registers of declarations of conflicts of interest
https://www.aylesburyvaleccg.nhs.uk/about-us/conflict-of-interest-pol/
https://www.chilternccg.nhs.uk/public/about-us/how-we-make-decisions/registers-of-interests/
Registers of declarations of gifts, hospitality and sponsorship
https://www.aylesburyvaleccg.nhs.uk/wp-content/uploads/2016/06/2016-10-Aylesbury-Vale-and-Chiltern-CCGs-Hospitality-and-Gifts-Register-FEBRUARY-2017.pdf
https://www.chilternccg.nhs.uk/public/about-us/how-we-make-decisions/strategies-and-policies/hospitality-and-gifts/
Note: Registers are updated on websites only after any change to entries or new declarations received. In relation to conflicts of interest, this applies whenever there is a change to entries for any of the CCG committees included and not just governing bodies.
Assurance in respect of national guidance A further consultation by NHS England across the NHS as a whole was completed with guidance published February 2017 to come into effect from June 2017. There are no new requirements separate to those already covered by local policy and implemented through application of NHS England’s existing guidance for CCGs. An annual CCGs self-assessment and Quarter 4 self-assessment have been completed and submitted to NHS England, having been approved by conflicts of interest guardians through Audit Committees on 29 March 2017. This also documents compliance with requirements on declarations of hospitality, gifts and sponsorship.
Conflicts of Interest: None arising in respect of this paper as it does not relate to commissioning decisions.
Strategic aims supported by this paper (please tick) Better Health in Bucks – to commission high quality services that are safe, accessible to all and achieve good patient outcomes for all
Better Care for Bucks – to commission personalised, high value integrated care in the right place at the right time
Better Care for Bucks – to ensure local people and stakeholders have a greater influence on the services we commission
Sustainability within Bucks – to contribute to the delivery of a financially sustainable health and care economy that achieves value for money and encourages innovation
Leadership across Bucks – to promote equity as an employer and as clinical commissioners
Governance requirements: (Please tick each box as is relevant to the paper)
Governance Element Y N N/A Comments/Summary Patient & Public Involvement
This paper describes implementation of national statutory guidance
Equality This paper describes implementation of national statutory guidance
Quality This paper describes implementation of national
Page 4 of 148
Page 4 of 148

statutory guidance Financial This paper describes implementation of national
statutory guidance Risks Failure to follow policy could bring the CCGs’
reputation into disrepute. Some challenge in evidencing decision making to ensure completeness of procurement decisions register.
Statutory/Legal The consequences of failing to manage conflicts of interest properly could have significant implications both legal and reputational
Prior consideration by Committees etc.
None
Membership Involvement
No members have had particular contribution to the policy, but are involved in implementation through standing declarations.
Supporting Papers:
1. Aylesbury Vale and Chiltern CCGs register of declarations of conflicts of interest – GoverningBodies meetings in common.
2. Aylesbury Vale and Chiltern CCGs register of hospitality, gifts and sponsorship.
Page 5 of 148
Page 5 of 148

AYLESBURY VALE AND CHILTERN CLINICAL COMMISSIONING GROUPS GOVERNING BODIES (meetings in common in public)
9th March 2017 Council Chamber, Chiltern District Council, King George V House King George V
Road, Amersham HP6 5AW
Governing Bodies Members Present: Dr Raj Bajwa - GP Chair (Chiltern CCG)
GP Clinical Chair – Chiltern CCG RB
Louise Patten Accountable Officer LP Graham Jackson GP Clinical Chair (Aylesbury Vale CCG) GJ Dr Karen West Clinical Commissioning Director Integrated
Care KW
Robert Majilton Deputy Accountable Officer and Director of Sustainability and Transformation
RM
Dr Rebecca Mallard-Smith Clinical Commissioning Director Unplanned Community
RMS
Tony Dixon Lay Member (Deputy Lay Chair, Chiltern CCG) TD Robert Parkes Lay Member (Deputy Lay Chair, Aylesbury
Vale CCG) RP
Graham Smith Lay Member (Chair of Primary Care Commissioning Committee)
GS
Dr Robin Woolfson Secondary Care Specialist Doctor RW Ross Carroll (RC) Lay Member RC
Others present (non-voting) Debbie Richards Director of Commissioning and Delivery (co-
opted member) DR
Kate Holmes Deputy Chief Finance Officer KH Nicola Lester Director of Transformation NL Louise Smith Associate Director Commissioning and Locality
Delivery – Item 13 LS
Leigh Franklin Executive Assistant and Office Manager (minute taker)
LF
Karen Kilshaw Personal Assistant (Visuals) KK
1&2 Welcome & Apologies Lead The Chair Dr Raj Bajwa (RB) welcomed the Governing Bodies members and members of the public.
Apologies Crystal Oldman – Registered Nurse Colin Seaton – Lay Member (Patient and Public Engagement)
3. Declarations of Interest in items on this meeting’s agenda Dr Raj Bajwa reminded the Governing Bodies members of their obligation to declare any Conflict of interest they may have on any agenda items at Governing Bodies meetings in common. Declarations previously made by members of the Governing Bodies are listed in the CCG’s Register of Interests published on the CCG websites and available for review at the meeting.
Page 6 of 148
Page 6 of 148

Declarations of interest from today’s meeting
ITEM CONFLICTS OF INTEREST AND ACTION 8. Process forApproval of AnnualAccounts andAnnual Report forthe year 2016-17
As this a process decision, all voting members can participate in decision to delegate authority to approve the Draft accounts and annual report to the Audit Committees. RB to remain as chair.
11. Primary Caredelegatedcommissioning –Chiltern CCG
This paper is for information and to note that the delegation agreement has been signed. No other conflicts of interest action is required as there is no commissioning decision requested. RB to remain as chair.
12. Scheme ofReservation andDelegation(Primary CareCommissioningCommittee, Qualityand PerformanceCommittee)
Member GPs are not conflicted as there is no financial benefit, and can therefore take part as voting members in the decision to delegate. As this is a process decision, member GPs will not be required to leave the room. No other conflicts of interest action is required as there is no commissioning decision requested. However, for the avoidance of doubt, the chair of the meeting will change to TD as Lay Member and Deputy Chair for Chiltern CCG (agreed in advance).
13. Primary CareImprovementScheme (followingrecommendationfrom Primary CareCommissioningCommittee)
The Primary Care Improvement Scheme has a conflict of interest for the CCG clinicians as it relates to primary care development and an associated payment scheme. Although the paper has been owned by the management team it has involved development with the clinicians due to the clinical content and this has been considered essential. Clinicians have not however been involved in the discussions and conclusions reached regarding financing. The paper was previously discussed at the Primary Care Committee (2nd March 17) and is for sign off including financial commitment. The conflicted Clinicians will leave the room at the governing bodies meetings in common and will refrain from participation in the final decision to approve the financial commitment for the scheme. Given the above, TD will remain as chair of the meeting. Conflict of Interest was noted from RB/GJ/KW/RMS.
14. GeneralPractice ResilienceProgramme(followingrecommendationfrom Primary CareCommissioningCommittee)
Conflict of interest arises if a member of the Governing Bodies from a member practice has or will in the future be selected for support using the Vulnerable Practice Scheme or General Practice Resilience Programme funding. However, it should be noted that no practice will directly receive funding from either of these routes. NHS England guidance on the use of funding for non-clinical training stipulates that funding must be used to support training on either care navigation or workflow optimisation within primary care. Member GPs are not conflicted as there is no financial benefit. As this is a process decision, they can take part as voting members in delegating to the Primary Care Operational Group the mechanics of programme investment (of which member GPs are not voting members). However, for
Page 7 of 148
Page 7 of 148

Quorum requirement Main meeting
Items 8, 11
Item 12, 13
Item 14
Chair from either group (or deputy lay Chair)
RB RB TD TD
Accountable Officer or Chief Finance Officer
LP LP RM LP
3 clinicians (1 of which must be a registered nurse or specialist hospital doctor and one must be a GP). Where GPs are conflicted in the decision, the meeting will be quorate with 3 clinicians and no GP.
RW GJ KW DR
RW GJ KW DR
RW LP DR
RW GJ KW RB
Two lay members RP TD GS RC
RP TD GS RC
RP RC
RP RC
the avoidance of doubt and transparency, the chair of the meeting will remain as TD. Conflict of Interest was noted from RB/GJ/KW/RMS.
4. Questions from the public RB noted that no questions had been submitted in advance of the meeting. No questions were raised from the floor.
5. Minutes of the meeting held on 12th January 2017, Action Log and Matters Arising 3.1 Minutes – 12 January. The minutes were approved unchanged.
3.2 Action Log – It was noted that all actions have been updated within the action log. In relation to an action on management of non-elective admissions, the CSU is looking at top 5 presentations in terms of value: Pneumonia, UTIs, Falls, Acute Kidney Infection (AKI) and Sepsis. Further update to GB as part of Urgent Care clinical director’s presentation in June 2017.
3.3 Matters arising – None were raised.
Leadership Reports 6. Accountable Officers Update
Presented by Lou Patten (LP). There are no conflicts of interest relating to this paper. LP informed Governing Bodies of local and national developments in the context of NHS Aylesbury Vale and NHS Chiltern CCGs. LP discussed the following:
Buckinghamshire System Transformation Work continues at pace with our local system transformation programme. We are currently developing a new role for our General Practice Nurse Leaders as we recognise they have a key role in this transformation. At the time of writing we are about to consult on the new proposals.
Sustainability & Transformation Plans (STP) LP attended a special Health and Social Care Select Committee (HASC) meeting to update on the STP and our local NHS plans supported by Dr
Page 8 of 148
Page 8 of 148

Graham Jackson and Neil Dardis, Chief Executive of Buckinghamshire Healthcare Trust. This was well attended with some challenging questions. It can be viewed here: https://buckscc.public-i.tv/core/portal/webcast_interactive/271795 Organisational Development - Merger NHSE met to understand whether they could facilitate merger of our two organisations for April 2017, given the tight timescale and the amount of work required, outside of our control, they have recommended that we wait until April 2018. We will continue to seek organisational change during the coming year.
Referrals Audit - update Further to the Governing Bodies recent decision (based on a recommendation by the Executive Committee), a clinical audit of referrals into secondary care during the period January-April 2017 is being set up across our providers. A report on this will come back to the Governing Bodies in June.
RC asked what issues and challenges had been raised by the HASC on the STP presentation. LP advised that there is a growing understanding that there are no proposed significant changes around restructuring in Buckinghamshire and the plans focus around our local plan for patients. There was challenge around the funding and gaps in working at scale through the STP, and how this may affect members of the public and the overall approach to health management.
TD commented that at a recent national audit chairs forum, the members had discussed guidance for audit committee chairs in STP areas on how they may best achieve assurance on delivery. As there is currently no specific guidance from NHS England, audit committee chairs in the STP area expected to meet to discuss how they might achieve their needs for assurance.
LP further advised that the STP will look at further refresh of finances, with a proposal to take that work to a future audit committee with a discussion at the end of April. GJ reiterated that the joint presentation as a collective system at the HASC was a positive step forward, and was well received with good debate between Health commissioners and social care colleagues.
KW asked that as we would now have to wait until April 2018 for merger could we clarify that we would continue with proposals to combine some of our working practices. LP confirmed that we would continue to ensure we used this next year to transition and continue with the significant work achieved so far. RB reiterated that we would look to continue to stream line the two organisations. RP suggested a master plan of next 12 months looking at milestones to achieve merger that could be shared with members of the public.
Assurance and Governance 7. Finance Report (Month 10)
Presented by Kate Holmes (KH). The purpose of this report is to Assure the Governing Bodies of the financial performance of the federated CCGs, in both summary federated view and by individual CCG to the end of January 2017. The supporting paper related to Month 10 (January) but there was also additional briefing on Month 11 February.
KH provided highlights as follows: (1) Financial Performance: To the end of January 2017 (10 months) the
Page 9 of 148
Page 9 of 148

total position is an under spend of £4,140k. The CCG’s reduced the forecast outturn by £1m; from achieving the 1% planned surplus of £5,967k down to £4,967k. Furthermore the CCG’s have reported a net, risk assessed, opportunity of £0.3m to NHSE.
(2) The forecast position deteriorated by c£2m in relation to two high costcritical care episodes at Guys & St Thomas Hospital in London. We arecontinuing to work to ensure that we aware of these episodes earlier inthe future. There is also further deterioration in the Frimley position andreducing Prescribing underspend.
(3) The CCGs continues to refresh its financial recovery plan, previouslypresented to NHSE and internal Committees, to ensure expenditureremains within planned levels through further expenditure controls andreviewing forecasts to identify mitigating opportunities. This will continueto be iterated to ensure that the CCG maximises it opportunities todeliver against its targets.
(4) Across Buckinghamshire CCGs there is a year to date under spend of£4,140k (AVCCG £1,616k and Chiltern CCG £2,524k) against abudgeted under spend of £4,973k. The position has been achieved bythe utilisation of Non-Recurrent mitigations of £10,994k andContingency of £3,128k released into the position to cover thecrystallisation of some of the risks and the additional in month pressure.
(5) KH also advised that the QIPP: actual delivery year to date being£11,298k against an equivalent plan of £13,785k (82% achievement),before mitigations. The year to date QIPP performance is consideredbelow target and is rated amber. Forecast achievement is also belowtarget at 83%, before mitigations, and also rated amber.
(6) To hold the CCG position QIPP is required to deliver an additional£2,000k above ytd run rate; mitigations identified through the summerand autumn balance sheet and forecast reviews enable us to cover thisstretch.
(7) Buckinghamshire CCGs have instigated a deep dive into the QIPPschemes to gain assurance in the robustness and deliverability of theschemes, look for in year mitigation and to build up a pipeline ofschemes that can be used to replace underperforming schemes or usedfor future years.
(8) KH also bought the Governing Bodies attention to a material error in thereport, unfortunately the wrong SLAM figures had been attached, allother figures and reporting were correct.
RW asked what proportion of the provider payments are in dispute. KH reported that all providers are paid on a monthly contractual basis, so cash flow is not affected, but we do have a system of data challenges with our Providers. KH advised that the whole CCG had been working hard to ensure correct levels of challenge have been taking place.
The QIPP clinics have been held regularly to support us in reducing spend, and the Verto project management system is now embedded into the organisation to help ensure good control of all projects in place.
DR further replied that alongside the data challenges with Providers, we also have an amount of activity coded by providers with high levels of un-coded activity. DR advised that they have formally written to the Provider to express concern at the level of un-coded activity, and have requested a recovery plan. This does add risk to our forecast, but we are working to mitigate this.
Page 10 of 148
Page 10 of 148

RM added that, in terms of the scale of financial recovery, a number of large elements have been landed, although the financial position remains susceptible to further movement. We are dependent on end of year reporting to determine our final position which has not yet completed. Whereas in previous years we would have agreed our close out position at the end of year with our providers, this is not the case for any provider this year, with a number of financial settlements still to be reached.
TD queried whether, in terms of the end of the year close, we are anticipating any further demands for payment from providers for activity we are not currently sighted on. KH responded that we have worked closely with providers and feel that our forecast outcome is robust as it can be, although recognising that we still have an overall net risk.
RM also advised that part of our financial recovery plan was to become an early adopter of the national QIPP support programme. We have been accepted on this and from next week there will be some external support to add further value to the process.
TD also asked about Continuing Healthcare (CHC) and the possibilities of large scale overspend, with a request for a report to the audit committees on any overspends anticipated. RM replied that there is a CHC recovery plan with specific issues and that it would be beneficial to take to the Audit Committee and to carry out a deep dive.
RC asked about the iMSK new service to develop Musculoskeletal project and to understand the slippage in the new project and the possible financial implications. RM acknowledged that there is slippage, but that had been mitigated against for this financial year but there would be a risk into next year if this continued. Work is being undertaken and the Programme Board will be considering the final business case to be bought to Governing Bodies at a future date.
The Governing Bodies noted the Financial Report for Month 10
8. Process for Approval of Annual Accounts and Annual Report for the year 2016-17 The Governing Bodies were asked to agree delegated authority to approve the Draft accounts and annual report to the Audit committee at their meeting on the 16 May 2017 and for final approval of any changes post Audit Committee to the Chairs, Chairs of the Audit Committee, Chief Officer and Chief Finance Officer on behalf of the Governing Bodies.
Under the CCG’s Scheme of Reservation & Delegation approval of the annual report and accounts is delegated to the audit committee. Under the audit committee terms of reference the audit committee will review the annual report and financial statements before submission to the Governing Bodies.
The National Annual Reporting guidance requires Governing Bodies to approve the final Annual Report and Accounts. This paper clarifies the process for approval of the annual accounts and report to be submitted by 12.00 on the 31 May 2017.
Page 11 of 148
Page 11 of 148

Due to the deadline for the submission of the draft accounts and annual report to the Department of Health (31 May 2017) and its proximity to the date by which the preparation and audit of these documents will be completed, it is proposed that the Governing Bodies agree to delegate authority to approve the final accounts and annual report to the Audit Committee at their meeting on the 16 May 2017.
Given the tight timetable for auditing the accounts there may be a requirement for adjustments post review by the Audit Committee. It is proposed that any such changes be approved by the Chairs, Chairs of the Audit Committee, Chief Officer and Chief Finance Officer on behalf of the Governing Bodies taking advice from the Auditors and other members of the Audit Committee. Such approval may be made virtually.
There are specific Certificates and Statements which are required to be signed by the Chief Officer (as Accountable Officer) and Chief Finance Officer. The Annual Report and Accounts are then published on the CCG website and presented to an Annual General Meeting to take place in September 2017.
Key dates 1. The draft annual report and accounts, the ISFE consistency
statement & supporting data collection templates and Head of InternalAudit Opinion to be submitted by Wednesday 26 April 2017
2. The Full Audited and signed Annual Report & accounts,approved by the Governing Bodies, ISFE consistency statement &supporting data collection templates and External audit completionreport to be submitted by Wednesday 31 May 2017
3. The annual report and accounts in full on the public website byFriday 9 June 2017.
4. A public meeting will be held by 30th September 2017 at whichthe annual report and account are presented.
RP asked that the minutes clarify that there will be two sets of accounts one for Aylesbury Vale CCG and one for Chiltern CCG.
The Governing Bodies approved the recommendations as requested.
9. Governing Bodies Assurance Framework (GBAF)
Presented by Robert Majilton (RM). The Governing Bodies were asked to note that the previous iteration of the Governing Bodies Assurance Framework was circulated to the Executive Committee on 23 February 2017. The Executive Committee discussed the revised approach to risk and will undertake a deep dive review of the Corporate Risk Register every quarter; the same timescale for which the Governing Bodies review the GBAF.
RM advised the following changes : 1. Risk 1 (The CCG fails to align its priorities and plans with the
Buckinghamshire health and care system) has increased to 12 (from 9),this reflects the risk around delivery of the iMSK transformation programmeescalated from the Executive Committee at their meeting on the 23February and that delivering changes in this pathway are currently delayed.
2. Risk 12 (internal capacity and capability) has increased to 12 (from 6),
Page 12 of 148
Page 12 of 148
related to departures of substantive Chief Finance Officer and Director of Nursing and Quality.
Against a maximum risk score of 350 (14 risks, each of which has a maximum score of 25), we have assessed our current level at 162 (46%) against a target of 86 (24.5%). Of the 14 identified principle risks, 4 are now extreme (15+) – Risks 9, 10, 11 and 13.
The following extreme measures are:- 1. Poor management of the QIPP programme, cost pressures and in-year
changes to CCG allocations may create an increased requirement for QIPPor reductions in spending plans (Risk 9)
2. Over-performance at providers; increased demand in the system may leadto capacity shortages/be unaffordable - and therefore CCG targets may notbe met (Risk 10)
3. The wider health and care system’s financial challenges may adverselyaffect the CCGs’ performance (Risk 11)
4. Performance issues across the system will adversely affect patients'treatment times (18 weeks etc.) and ultimately the delivery of patientservices and planned priorities (Risk 13).
All others are moderate or minor.
RW also asked about Risk 1 and the iMSK project and what the level of concern related to. RM said that the delay in this specific project but also the risk to transformational programmes and the approach and to ensure learning from this project within the health and social care system as a whole.
RC asked specifically about Risk 12 and addressing of vacant senior positions and the recruitment gap. RM advised that the CCGs are looking to recruit an interim Chief Finance Officer and until that point RM will be covering the position with the help of the two existing Deputies. He also advised that it has been decided to not replace the Director of Nursing and Quality position, the other Directors in the organisation having taken on added responsibilities to absorb that work.
LP added that with the growing importance of the STP, we would seek a more strategic approach with some shared resources and also as we move into the Accountable Care Organisation (ACO) we will be looking at some new ways of nurse leadership, for example Crystal Oldman is looking at how we deliver nursing in the future.
RW replied that this was re-assuring as he was concerned at the loss of professional leadership for nursing; as so much of the future plans are transformational and development of the workforce and would be concerned that by sourcing this from outside of the CCG would not allow enough strength and purpose.
LP advised that there is good clinical accountability for nursing in the organisation, with clear lines of accountability all the way through to the Governing Bodies. We also separately have nursing leadership around our work in community and primary care services; it is this that Crystal will be focusing on That piece of work will be presented to the Governing Bodies for assurance.
Page 13 of 148
Page 13 of 148

10. Quality and Performance Report (Month 10)
Presented by Debbie Richards (DR). DR noted the purpose of this report is to provide assurance and highlight quality and performance exceptions, together with actions to address the issues and risks identified.
DR reported on the Cancer targets; two of the eight national targets were not met in December; the 31 day (94%) target for standard treatment was narrowly missed in Aylesbury Vale by one patient. The 62 day standard target was missed by 16 patients and below the 85% standard target. We work closely with the Provider to understand the reasons why and to ensure there has been no resultant harm to patients.
We now have support from the national intensive support team (IST), an improvement team which helps providers and commissioners to work better together in managing patient pathways.
DR also reported on the RTT (Referral to Treatment within 18 weeks) the incomplete target was not met in December with performance at 90.3%, with both CCGs missing the 92% target. Buckinghamshire Healthcare NHS Trust has initiated a RTT recovery plan which is monitored each week, with an expectation to return to compliance with standard by the end of March 2017. Contributory factors include non- elective pressures such as the use of the day bed unit for escalation beds.
DR updated on the A&E performance – Buckinghamshire Healthcare NHS Trust delivered a performance of 86.9% for all types in January, against the 4 hour standard of 95%. This is a 7.1% adverse variance to plan of 94%. Total attendances in the month were 11,328 a reduction from the previous month of 470 patients.
Performance has started to improve and in February reached over 90%. We are now at Operational Pressure Escalation Level (OPEL) 1 having spent a lot of the last few months in an out of OPEL 3. NHSE have congratulated the whole system on the efforts made. A lot of work with is also taking place with Wexham Park/North Frimley and we are attending their A&E delivery board. We are also working to reduce the numbers of South bucks patients waiting for discharge who are medically fit but experienced delays on discharge to community placements.
DR has also been asked by the Regional Chair assurance and delivery at NHSE to co-host an improvement workshop with North West London on A&E Delivery so that we can share our learning and work. DR report that the Ambulance response time targets were not met in December SCAS continue to report on their Remedial Action Plan at regional level and their local action for Bucks at a more local level. The CCGs continue to work very closely with SCAS. Work continues with Buckinghamshire Healthcare NHS Trust to address the handover delays that have a direct impact on SCAS performance. DR finally reported that there were three MRSA cases provisional assigned in December.
RW queried delayed transfer of care (DTOC) and the difficulties for Providers with the process of moving people out of secondary care and current delays. DR advised that we are currently focussing on DTOC in Buckinghamshire
Page 14 of 148
Page 14 of 148
Healthcare NHS Trust and Frimley /Wexham Park, and noted that the HASC (Health and Social Care Committee) had recently led a review on DTOC and will be publishing their findings in two weeks’ time. This review will be circulated to the A&E Delivery Board.
We do currently have a low level of DTOC but are running higher than this time last year and are seeing a deteriorating trend. To mitigate this problem we are holding anonymised weekly calls, where Associate Directors will review pathways and escalate any blocks and escalate to DR any significant issues.
The reasons for DTOC are well understood and tend to be social care placement in the community, some domiciliary care or Continuing Healthcare or social care that my need complex packages of care that cannot be met by the independent sector. There can also be system shortage in Elderly Mental Illness (EMI) capacity in nursing homes and small groups of self-funders where families need to find places.
TD asked about the Buckinghamshire Healthcare NHS Trust CQC report on safety between Stoke and Wycombe, what the specific issues that were identified, and if the Governing Bodies could do anything to contribute to improving these issues. DR responded that this report was fully published in September 2016 and the quality improvement plan was fully reviewed and reported through the Quality and Performance Committee meeting. Although the headline report cited the Trust requirements improvement, 21 of 35 indicators were rated as good.
RM acknowledged discussion held by the Quality and Performance Committee, noting that it is important to recognise that this wasn’t a full review or full re-inspection report, and did not reflect progress made since it was published. RB asked to clarity whether CQC was expected to re-visit. DR replied that they are monitoring the plan and can opt to re-inspect at any time.
RC asked whether the social care funding announced in the government budget (£2bn extra funding over the next three years) would be ring fenced. DR advised that her understanding was that it might not be. LP said that we will ensure the Governing Bodies had clarification.
11. Primary Care delegated commissioning – Chiltern CCG
Presented by Graham Smith (GS), chair of the primary care commissioning committee (PCCC). GS advised the Governing Bodies that Chiltern CCG had requested delegated responsibilities for the commissioning of primary medical services from 1st April 2017.
This gives CCGs more control over general practice and is part of a wider strategy to support the development of place-based commissioning and a key enabler for the development of new care models. In preparation for full delegation of primary care responsibilities, the CCG has taken the following steps:
Page 15 of 148
Page 15 of 148

• It carried out a full consultation with member practices between July andSeptember 2016, culminating in a vote for delegation by 33 out of 34Chiltern Practices in October 2016.
• The Governing Bodies noted progress and approved the CCG’sproposal to make an application to NHS England in October 2016.
• Application agreed by Deputy Chair of the CCG and Lay Chair of theAudit Committee.
• Application signed by CCG’s Accountable Officer and submitted to NHSEngland Regional Team in November 2016.
• Application approved by NHS England in January 2017 and draftDelegation Agreement issued.
• Delegation Agreement signed by CCG’s Accountable Officer andsubmitted to NHS England by 1st March 2017.
RMS asked if there were plans for a level of communication to practices to explain CCG responsibility and NHS England responsibility (and in respect of commissioning versus contracting function). It was agreed that this would be helpful (and working with LMC to ensure communication is seamless). LP will ensure this is undertaken.
GJ noted that the GMS contract is not something we will be interfering with or changing at CCG level. The commissioning function coming together across Bucks allows us to manage bigger pieces of work and therefore a single primary care function makes sense. We can't assume practices understand what this function is.
LP
For Decision 12. Scheme of Reservation and Delegation (Primary Care Commissioning
Committee, Quality and Performance Committee) As this agenda item relates to primary care, RB asked TD (Deputy Chair – Chiltern) to take over as chair as was agreed prior to the meeting. However RB remained in the room.
This item was presented by Lou Patten (LP). The Governing Bodies through meetings in common were asked to: (1) REVIEW, APPROVE and RATIFY attached draft operational schemes of
reservation and delegation for Quality and Performance and Primary CareCommissioning Committee.
(2) NOTE that this request is based on a recommendation from the AuditCommittee as an assurance that the committee have reviewed a draft andconcluded delegations as appropriate, subject to amendments described.
Whereas the draft presented to the Audit Committee limited a £50k threshold for a specific number of decisions (.e.g. premises improvement grants and capital developments), it was discussed and recommended by the Audit Committees meetings in common that approval is limited to £50k for all decisions listed and delegated – to include direct awards/primary care improvement schemes. Any decision above the threshold would need to be escalated to the Governing Bodies with a recommendation from the Primary Care Commissioning Committee. This will also apply irrespective of the number of contracts or awards underneath. This allows for delegation so that the Governing Bodies are not stifled, but also recognising that some decisions may need to be escalated.
Page 16 of 148
Page 16 of 148

Decision: The Governing Bodies ratified the proposed limits recommended: (1) Approval is limited to £50k for all decisions listed and delegated to the
primary care commissioning committee.(2) Draft was amended to read that PCCC can “Advise on or approve
matters relating to primary care contracting within agreed levels,specifically in relation to commissioning Quality Outcomes Framework(QOF - subject to allowances within NHS England's legal framework).
In addition however, LP asked that with the approval of delegated commissioning to Chiltern CCG, the limits would need to be further reviewed. LP therefore recommended that that Governing Bodies accept the above decision, with the with the Primary Care Commissioning Committee to review when holding the first meeting post delegated commissioning coming into effect, with a further review by the Audit Committee before an additional recommendation to the Governing Bodies to approve and ratify.
TD queried the timescale for further Audit Committee review. LP replied that the first primary care commissioning committee meeting post delegation and therefore including both CCGs would take place in June, and therefore at the earliest it will be July 2017. This was acknowledged and agreed.
13. Primary Care Improvement Scheme (following recommendation from Primary Care Commissioning Committee) TD remained as chair of the meeting (Deputy Chair – Chiltern)
The Primary Care Improvement Scheme has a conflict of interest for the CCG clinicians as it relates to primary care development and an associated payment scheme. Although the paper has been owned by the management team it has involved development with the clinicians due to the clinical content and this has been considered essential. Clinicians have not however been involved in the discussions and conclusions reached regarding financing. The paper has previously been discussed at Primary Care Committee (2nd March 17) and is coming to Governing Bodies for sign off including financial commitment.
The interests of all clinicians in the organisation are recorded on the CCGs register of interests. The Conflict of Interest was specifically noted from RB/GJ/KW/RMS.
For the avoidance of doubt, member GPs in the room felt that they should not take part in the discussion leading to the commissioning decision that they would also refrain from participating in. GJ also emphasised that clinician discussion has taken place the previous week in public at the Primary Care Commissioning Committee but had not included financial elements. RB/GJ/KW/RMS left the room. TD advised that the Governing Bodies remained quorate, with LP taking on the clinical nurse role.
LS joined the meeting, and advised the Governing Bodies that the purpose of the supporting paper was to provide the Governing Bodies with details of the primary care development scheme. Whilst it is acknowledged that there may be further refinement to the clinical expectations as a result of on-going engagement, the overarching principles and financial envelope of the scheme stand firm and are not expected to change.
The paper suggests that a development model is progressed, designed to
Page 17 of 148
Page 17 of 148

enable primary care to transition to new models of care in line with the 5 year forward view whilst maintaining clinical quality of services. This model is built on the following 1. Foundation - A robust and reactive infrastructure from which to deliver, toinclude clustering of general practice and standardisation of practice2. Delivery - structured, evidenced based delivery vehicles which havedemonstrated improved clinical outcomes in those areas that are considered apriority to Buckinghamshire because of the health needs of the local population3. Outcomes – Improved population based outcomes
This model will be supported by a multiyear development scheme which builds on these three areas. The core principles behind the scheme are:
• Encompasses the Quality and Outcomes Framework (QOF) and thecurrent Quality Improvement Schemes (QIS)
• Reduces inappropriate workload, that does not add clinical value• Is built on evidence based care• Is responsive to the population health needs of localities and adds value
to patient care• Does not disadvantage practices that take up the proposed scheme• Aligns to national, STP and CCG strategies
It is proposed that practices will receive a one off payment which will support achievement of the foundation stage. This will be considered a gateway because without the fundamentals within the foundation stage practices will not be able to deliver the services in the ‘Care Delivery’ stage and work at scale as part of a new model of care. It is also proposed that the Care Delivery stage may involve changes to the Quality Outcome Framework (QOF) expectations for 17/18. Finally as part of the ‘care delivery alternative’ it is proposed that alternative evidenced based outcomes are delivered. This stage will require further work up by the CCG but proposed outcomes would apply to any provider and or a MCP/PACs.
The total budget requested is £1.5m. This will cover the practice support to transition to this way of working as well as the infrastructure within the CCG to provide support, training and technical solutions such as templates and protocols. The Governing Bodies were asked to approve the principles, direction and financial envelope available to the scheme. LP advised that the aim is to try and influence the Practices to work with us and this is a real opportunity to work together to gain improvements.
RM clarified the investment that this is a quality improvement scheme that both CCGs have supported in the past and it uses non-recurrent funding on schemes that could move into recurrent funding, these could be multi-year outcomes. TD asked whether the additional £200k could be accommodated in next year’s budget plans. RM said that this has been accounted for and can be accommodated going forward.
RW said that this was a great model and looked to reduce variations in care and very important, although didn’t entirely understand the funding parts but recognised that this was to ensure delivery.
RC asked if there was a danger that if practices don’t have partial payment they may be discouraged rather than encouraged to do the work. LS advised that this was recognised and that some have practices have further to go than
Page 18 of 148
Page 18 of 148

others, it will be challenging going forward but we will have clear markers and having carried out something similar before we hope to encourage most practices into new ways of working and want to encourage them to work differently and make the scheme attractive.
RM said that it is recognised that some Practices may find the scheme more difficult but would encourage clustering of practices and need to ensure support to the practices.
Decision: The Governing Bodies approved the principles, direction and financial envelope available to the scheme.
14. General Practice Resilience Programme (following recommendation from Primary Care Commissioning Committee) The Chairmanship of the meeting remained with TD (Deputy Chair – Chiltern). However member GPs RB/GJ/KW/RMS returned to the room for discussion but did not form part of decision.
GS updated the Governing Bodies on three elements of funded support on offer from NHS England and the steps taken by the CCGs to identify how the funding should be utilised within primary care. The three elements are Vulnerable Practice Scheme (VPS), funding to provide training for receptionists and clerical staff and the General Practice Resilience Programme (GPRP).
In July 2016, CCGs were allocated £35,000 non-recurrent funding each, specifically for practices identified as vulnerable. Work has been ongoing throughout the year to identify, support and work with practices that fit the original criteria as set out by NHS England in the scheme guidance.
So that this funding could be accessed in a consistent, transparent manner, the CCGs drew up a policy based on the NHS England guidance. The aim of the scheme was to assess and treat the causes of vulnerability, securing practice improvement and build longer term resilience rather than deliver short term quick fixes. The types of support included:
• Diagnostic services so improvements can be identified and understood• Specialist advice and guidance e.g. HR, management, finance, IT• Coaching, supervision or mentorship• Practice management capacity and support.
The Primary Care Operational Group has reviewed spend against the Vulnerable Practice Scheme on a monthly basis and funding has now been fully committed. NHS England is committed to investing £40m in the General Practice Resilience Programme (GPRP) until 2018/19. The funds available to NHS Aylesbury Vale and NHS Chiltern CCGs based on capitation share as follows:
Aylesbury Vale CCG Allocation £’s
Chiltern CCG Allocation £’s
Buckinghamshire CCGs Total £’s
2016/17 44,000 70,000 114,000 2017/18 22,000 35,000 57,000 2018/19 22,000 35,000 57,000
Page 19 of 148
Page 19 of 148

NHS England has identified the following menu of support for which the GPRP funding should be used at a local level to address specific issues:
• Diagnostic services to quickly identify areas for improvement support• Coaching / supervision / mentorship as appropriate to identify needs• Practice management capacity support• Rapid intervention and management support for practices at risk of
closure• Coordinated support to help practices struggling with workforce issues• Change management and improvement support to individual practices
or groups of practices.
LP noted we should ensure that they include Locality working and ensure that the General Practice nurses are included as a fundamental part of our transformation. In terms of management turnaround team support package a good idea to ensure rapid turnaround, there is still support available from NHS England and we should be sure to work with that capacity as well. RM said that this was not a huge amount of money within our new commissioning responsibilities and should be used through the Primary Care Commissioning Committee.
Decision: Governing Bodies:- • Noted the update from the Primary Care Commissioning Committee to
Governing Bodies on schemes related to building primary careresilience.
• Noted the use of Vulnerable Practice Scheme funding, previouslyapproved by the Primary Care Commissioning Committee.
• Were assured that plans to spend primary care resilience funding in2016/17 are in line with CCG-approved policies, stated commissioningintentions and have been subject to our financial policies.
• Noted that this funding does not form part of our discretionary spend (asthe funding is ring-fenced for specific uses) and that final approval willbe in line with our Scheme of Delegation. Given the CCG is in financialrecovery, this will be two of the Chief Officer, Deputy Chief Officer orChief Finance Officer to give final approval.
For Information 15. Approved Minutes from sub-committees, sub-groups or steering groups:
Approved Minutes from sub-committees, sub-groups or steering groups:
a) Executive Committee – 22/12/2016b) Executive Committee – 26/01/2017c) Primary Care Commissioning Committee – 02/12/2016d) Quality and Performance Committee – 26/01/2017e) Health and Wellbeing Board – 15 December 2016
Date of next meeting (in public): Thursday 13 April 2017, 10:30am – 12:30pm; Jubilee Room, The Gatehouse, Aylesbury Vale District Council
Page 20 of 148
Page 20 of 148

Acronyms
A&E Accident and Emergency KLOE Key Lines of Enquiry ACHT Adult Community Health Team LMC Local Medical Committee ACO Accountable Care Organisation LPF Lead Provider Framework AF Atrial Fibrillation M Million AGM Annual General Meeting MAGs Multi Agency Groups AQP Any Qualified Provider MCA Mental Capacity Act AT Area Team MCP Multi-speciality Community
Provider AVCCG Aylesbury Vale Clinical
Commissioning Group MK Milton Keynes University
Hospital Foundation Trust BAF Board Assurance Framework MCP Multispecialty Community
Provider BCC Buckinghamshire County
Council MusIC Musculoskeletal Integrated
Care BCF Better Care Fund NHSE NHS England BAF Board Assurance Framework NHSi NHS Improvement BHT Buckinghamshire Healthcare
Trust NOAC New Oral Anticoagulants
BAME Black and Minority Ethnic OCCG Oxfordshire Clinical Commissioning Group
BPPC Better Payment Practice Code OOH Out of Hours CCCG Chiltern Clinical
Commissioning Group OUH Oxfordshire University
Hospitals NHS Foundation Trust
CDIF Clostridium Difficile OPEL Operational Pressures Escalation Level
CFO Chief Finance Officer PACS Primary & Acute Care Systems
CHC Continuing Health Care PAS Patient Administration System
CIP Cost Improvement Programme PB Programme Board COI Conflict of Interest PBR Payment by Results COPD Chronic Obstructive Pulmonary
Disease PIRLS Psychiatric In Reach Liaison
Service CPA Care Programme Approach PLCV Procedures of Limited
Clinical Value CQC Care Quality Commission PMS Personal Medical Services CQRM Contract Quality Review
Meeting POD Point of Delivery
CQUIN Commissioning Quality & Innovation
POG Programme Oversight Group
SCWCSU South Central and West Commissioning Support Unit
PPE Patient & Public Engagement
CSIB Children’s Services Improvement Board
QIPP Quality, Innovation, Productivity & Prevention
CSP Care & Support Planning QIS Quality Improvement Scheme
CSR Comprehensive Spending Review
QOF Quality & Outcome Framework
CSU Commissioning Support Unit RAG Red, Amber, Green
Page 21 of 148
Page 21 of 148

K Thousand RBH Royal Berkshire Hospital DES Directly Enhanced Service RCA Root Cause Analysis DGH District General Hospital REACT Rapid Enhanced Assessment
Clinical Team DOLS Deprivation Of Liberty
Safeguards RRL Revenue Resource Limit
DST Decision Support Tool (CHC) RTT Referral to Treatment EDS Equality Delivery System SCAS South Central Ambulance
Service EOL End of Life SCN Strategic Clinical Network F&F Friends and Family SLA Service Level Agreement FHFT Frimley Health Foundation
Trust SLAM Service Level Agreement
Monitoring FOT Forecast Outturn STP Sustainability &
Transformation Plan FPH Frimley Park Hospitals NHS
Foundation Trust SUS Secondary Uses Service
GB Governing Bodies TOR Terms of Reference GMS General Medical Services TV Thames Valley HASU Hyper Acute Stroke Unit TVN Tissue Viability Nurse HETV Health Education Thames
Valley UECN Urgent Emergency Care
Network HWBB Health & Wellbeing Board YTD Year to Date ICS Inhaled Corticosteroids ICU Intensive Care Unit IFR Individual Funding Request IG Information Governance
Page 22 of 148
Page 22 of 148

ACTION LOG
MEETING: Item 05.
DATE: 13/04/2017
TITLE: Action Log
Previous
Meeting
Date (or
Date
raised
/added)
Action
Number /ID
Minutes
ReferenceAction Description
Responsibility
/OwnerTarget date
Completed
dateStatus Progress Details/Comments
09/03/2017 1 AO Report RP suggested a master plan of next 12 months looking at
milestones to achieve merger that could be shared with
members of the public.
RM 08/06/2017 Open In progress
09/03/2017 2 Quality and
Performance
Report (Month
10)
RC asked whether the social care funding announced in
the government budget (£2bn extra funding over the next
three years) would be ring fenced. DR advised that her
understanding was that it might not be. LP said that we will
ensure the Governing Body had clarification.
DR 08/06/2017 Open In progress
09/03/2017 3 Primary Care
delegated
commissioning –
Chiltern CCG
RMS asked if there were plans for a level of
communication to practices to explain CCG responsibility
and NHS England responsibility (and in respect of
commissioning versus contracting function). It was agreed
that this would be helpful (and working with LMC to ensure
communication is seamless). LP will ensure this is
undertaken.
LP 08/06/2017 Open In progress
Governing Body (in public)
Page 23 of 148
Page 23 of 148
FINANCIAL PERFORMANCE TO FEBRUARY 2017
MONTH 11 2016/17
Executive Summary This report covers the overall financial position, as at the end of month 11, of the Buckinghamshire CCGs and supported by detailed summaries for each individual CCG. This report includes the application of the agreed risk share across the CCGs.
At the end of February 2017 (M11), the CCGs’ total position is as follows:
• The forecast position has remained under pressure as a result of further additional activity in the acute sector, mainly atBuckinghamshire Healthcare Trust. This has been offset with a combination of lower activity and successful challenges for LondonProviders, and decrease in activity in Non-Contracted Activity. Prescribing continues to deteriorate together with Continuing Healthcare;the forecast for the latter includes a very high cost client, and the M11 element of the previously identified QIPP stretch. On the basis ofadditional assumed non recurrent allocations from NHS England, the CCGs have increased their forecast outturn surplus by £1m toreinstate the 1% budgeted surplus of £5,967k, albeit this was done in conjunction with flagging a potential net risk of £0.5m to NHSE.
• The CCGs continue to refresh their financial recovery plan which has been presented to NHSE, and internal committees, to ensure thatthe CCGs maximises its opportunities to deliver against its targets.
• There is a year to date surplus of £5,470k (AVCCG £2,125k and Chiltern CCG £3,345k) against a budgeted surplus of £5,470k. Thisincludes the historic surplus.
• The position has been achieved by the utilisation of Non-Recurrent mitigations of £13,478k and Contingency of £3,128k released into theposition to cover the crystallisation of some of the risks and the additional in month pressure.
• QIPP achievement across the CCGs totals 79% of target year to date (98% after mitigation) being an achievement of £15,658k(including £3,096k mitigation) versus a target of £15,904k. QIPP forecast achievement across the CCGs totals 98% of the target (100%after mitigation) being a forecast achievement of £18,021k (including £3,096k mitigation) versus a target of £18,336k.
• The forecast includes identified mitigations to cover the additional £1m of QIPP above YTD run rate in Month12. The reported forecastexcludes the 1% headroom held in reserve as required by the NHS England business rules for 2016/17.
Page 24 of 148
Page 24 of 148

Key Issues and Actions in Financial Position:
Actions for: Issue: Key Drivers: Financial Impact YTD: Action: Owner: Timeline: Further Detail:
CSU
Increased overspend visible across Continuing Health Care (CHC) and Funded Nursing Care (FNC)
Understand the key drivers behind the deteriorating position visible.
Current overspend (£6.8m)
CSU finance team to undertake a deep dive of expenditure in this area and link with CHC financial recovery team set up by the CCG and Arden Gem CCG. Create clear forecast risk assessments
CSU finance, CCG and Arden Gem CSU On-going
Limited availability of information for QIPP monitoring
Provider data and analysis Unknown
CSU to link with information analysts to ensure data required for monitoring is available and push back to providers where this is limited
Finance & Information Analytics
On-going implemented Sep '16
CCG
Implementation of vacancy control procedures
To control spend within Running Costs limits
Unknown
Control process in place with all posts being numbered and any proposed recruitment changes now reviewed by Senior Management Team on a weekly basis. Applies to agency staffing also.
CCG and CSU HR On-going implemented Sep '16
Implementation of discretionary spend procedures
Control all discretionary spend
Unknown Control process in place with anticipated spend being approved by the AO and CFO and scrutinised at SMT CCG
On-going Implemented Jan ‘17
Review and implement standard forecast risk assessment process across all portfolios
Improve risk management and understanding
Unknown Review best practice and implement a standard approach to risk assessment against forecast CCG with CSU Mar ‘17
Review of current QIPP status
Ensure full understanding of QIPP delivery/mitigation
Current joint QIPP programme of £5.6m ytd
Monthly QIPP clinics to be instigated to review current project status against target ; agreeing corrective actions and linking these to the QIPP monitoring process; Daily progress escalation calls have now been initiated and will be maintained.
CCG & CSU Financial Planning
On-going - Clinics from Sep 16; Escalation call Jan 17
Continue review of reserves, budget lines etc to identify areas of mitigation
CCG spend on NR element Unknown Continual review of budgets, transactions to identify slippage to
be used for mitigations. CCG and CSU Finance
On-going implemented Oct '16
Page 25 of 148
Page 25 of 148

Finance Dashboard
Indicator Target MeasureTarget Value £,000's
Actual Value £,000's
Target % Actual %Rating this
month% Distance
from Target Explanation of target measure
Financial Position in month Planned monthly surplus 14 14 100% 100% √ 0.00% Achievement of Plan target
Financial Position in month Planned historic c/fw d 483 483 100% 100% √ 0.00% Achievement of Plan target
Financial Position in month Total planned position 497 497 100% 100% √ 0.00% Achievement of Plan target
Financial Position year to date Planned YTD Surplus 156 156 100% 100% √ 0.00% Achievement of Plan target
Financial Position year to date Planned historic c/fw d 5,313 5,315 100% 100% √ 0.04% Achievement of Plan target
Financial Position year to date Total planned position 5,468 5,470 100% 100% √ 0.04% Achievement of Plan target
Financial position forecast outturn Planned Annual Surplus 5,967 5,967 100% 100% √ 0.00% Achievement of Plan target
QIPP year to date Total planned position 15,904 12,563 100% 79% X -21.01% Achievement of Plan target (excludes Mitigation)
QIPP forecast outturn Total planned position 18,336 14,437 100% 79% X -21.26% Achievement of Plan target (excludes Mitigation)
Creditors - Better Payment Practice Code %age Creditors paid in 30 days 11,150 10,680 95% 96% √ 0.78% Target number of Non NHS invoices paid in 30 days
On Plan √Take Note !Action Required X
-(ive) £ = negative performance (overspend against budget)
(this convention applies to all but the specif ic QIPP tables)
Key Note:
+ive £ = positive performance (underspend against budget),
Page 26 of 148
Page 26 of 148

Financial Performance:
To Date: Annual Plan YTD Plan YTD Actual
Previous Month
Variance £,000's £,000's £,000's £,000's % £,000's
Commissioning:Planned and Unscheduled Care 390,118 357,740 365,358 (7,618) (2.13%) (4,244)Prescribing 68,074 62,401 59,790 2,610 4.18% 2,491Joint & Continuing Care 108,377 98,696 103,927 (5,231) (5.30%) (5,177)PRC Delegated Co-Commissioning 25,893 23,035 22,983 52 0.22% 6Primary Care IT 1,378 1,263 1,106 157 12.46% 208Other / Reserves 14,518 5,807 (3,985) 9,793 168.63% 5,571Commissioning Sub Total 608,357 548,943 549,179 (236) (0.04%) (1,145)Running Costs 11,628 10,644 10,407 237 2.23% 259Quality Premium 0 0 0 0 0.00% 53Planned Surplus 172 158 0 158 100.00% 1432016/17 CCG Position 620,157 559,744 559,586 158 0.03% (689)C/Fwd 2015-16 Surplus 5,795 5,312 0 5,312 100.00% 4,829
625,952 565,056 559,586 5,470 0.97% 4,140
Variance to YTD Plan
Key Points
• As at the end of February 2017, the CCGs are reporting a year to date surplus of £5,470k, in line with the planned combined target surplus of £5,967k. The CCG has restored the target surplus to £5,967k from that reported in M10 of £4,967k, an improvement of £1,000k, due to additional mitigation identified in the financial recovery plan being confirmed. The majority of this was confirmation of funding for previously incurred costs for GP Access Fund and funding from NHSE in recognition of vascular charging issue, this is non-recurrent whilst the recurrent charging flows are resolved for 2017/18.
• The reported variance across planned and unscheduled care has worsened in month, with increased acute pressures mainly in Buckinghamshire Healthcare Trust but partly mitigated by a reduction for London Providers as a result of lower activity and successful challenges.
• The prescribing forecast for each CCG has now been adjusted to be fully in line with the current PPD forecasts for the year end and released at 100% into the position. There has, again, been a slight upward pressure in this month.
• The pressure on Joint and Continuing Care continues. The drivers for the pressure still exist, namely increased costs relating to the impact of the nationally agreed FNC price increase, increase in activity and cost due to the complexity of packages required.
• Delegated Primary Care Medical Co-commissioning relates to AV CCG and is showing a small surplus ytd based on information from NHS England. The forecast position of delivering a year-end underspend of £300k has not changed.
Page 27 of 148
Page 27 of 148

• The year to date position on Running Costs of £237k relates to, firstly, the previously planned QIPP requirement for Chiltern which remains on course toachieve the target of £200k at year end, and no longer required prior year accruals released into the position. Following guidance issued from NHSEngland, the Quality Premium allocation has been moved into programme.
• Each CCG is required to hold a 0.5% Contingency reserve. To hold the year to date position each CCG has needed to utilise 11/12th of this.• As per NHSE requirements the position does not include any release of the 1% Non-Recurrent Headroom.
QIPP Overview and Forecast Performance
The QIPP for the CCGs is as follows:
Best case is £18,336k of which £1,300k was unidentified in plan and £1,421k of schemes which are now requested to close as these will not deliver in 16/17.
There is a QIPP reserve set aside of £1,934k and other mitigation actions on the schemes is only £1,650k.
Therefore the likely case is:
£kChiltern CCG 10,071 Aylesbury Vale CCG 8,265 Best Case 18,336 less:Unidentified (2,721)Schemes not achieving (1,178)
Likely Case 14,437 Mitigation Identifed (3,899)
• The year to date QIPP performance is considered belowtarget and rated amber due to the unallocated QIPPschemes yet to be identified.
• QIPP actual savings to date of £12,563k against a plan of£15,904k (79% achievement). When combined withmitigation schemes a year to date saving of £15,658k isachieved (98% achievement).
• QIPP forecast achievement for the year is £14,437k for theyear (79% achievement) and after mitigation added is£18,021k (98% achievement).
• Bucks CCGs QIPP report shows that more than 50% of theschemes are forecasting to showing an underachievement at
Page 28 of 148
Page 28 of 148

the end of the year; however some of this effect has been offset with the remaining over performing schemes.
Forecasts, Risks and Mitigation
Combined CCGs Worst Most Likely Best£,000's £,000's £,000's
Planned and Unscheduled Care (7,741) (6,021) (6,021)Prescribing 2,707 2,857 3,017Joint & Continuing Care (5,543) (5,343) (4,909)Delegated Co Commissioning 300 300 306Running Costs / Quality Premium 384 384 434Other 4,721 4,721 5,571Reserves 3,275 3,275 3,275Total Forecast before C/fwd Surplus (1,896) 174 1,674C/fwd Surplus 15-16 5,793 5,793 5,793Total Forecast 3,897 5,967 7,467
Reserves * Worst Most Likely Best£'000 £'000 £'000
Headroom 0 0 0Contingency 3,128 3,128 3,128Mitigations/Other Impact 147 147 147Total Reserves 3,275 3,275 3,275
The change between the Worst and Most Likely positions:
Planned and Unscheduled Care relates to:
1. Non elective activity increasing above the levels already inthe most likely forecast over the winter period
2. A reduction in the RTT (Referral to Treat- waiting times)position for elective surgery that would impact theIndependent sector as acute hospitals look for capacity
Joint & Continuing Health Care
1. Increase activity and cost of packages with the impact ofWinter above that in the Most Likely forecast
Key Points
• Assessed risks are calculated to be circa £2,070k currentlymainly relating to activity pressures, continued growth inactivity across CHC and the prescribing forecastdeteriorating with winter activity. Note this is offset in thesub total “Total Forecast before C/fwd Surplus” by the in- year surplus for the CCGs of £174k.
• Assessed mitigations are calculated to be circa £1,570kbeing mitigations identified in the recovery plan.
• The CCG continues to explore avenues to give furthermitigations as at M11 the CCG has reported a net, riskassessed, risk to NHSE of £500k. These further mitigationsrequired are largely centred on the vascular activityidentified as specialist at Frimley, previously brought tocommittee’s attention.
Page 29 of 148
Page 29 of 148

• The CCGs plan contains a budget of £5,602k held for headroom reserve. According to the NHSE Business rules this has not been factored into the position at month 11.
• The CCG has developed a Financial Recovery Plan, which will continue to be iterated, that has been shared with NHSE to identify further mitigating opportunities in forecasts and budget slippage. As part of the plan a discretionary spend
control process has been adopted. Criteria against which to assess spend release requests have been developed.
Mitigations
The total mitigations utilised to hold the forecasted position is £16,606k has been released into the position and is represented by:
Use of 0.5% Contingency £ 3,128k Budget/Project slippage £ 830k Balance sheet releases £12,648k The Budget/Project slippage is the result of deep dives into the management accounts establishing if the budgets are required and if relating to projects will they be fully spent in year. This has been part of the financial recovery and will be constantly reviewed. This slippage relates to the following areas: Budget/Project Slippage Carers budget £232k New models of care Projects £150k Over 75 Projects £250k Enablement budget £198k Total £830k The Balance Sheet releases are a result of work reconciling the accruals from previous years against invoices paid relating to those accruals and establishing if the accrual is required or not. Again this is part of the financial recovery work that finance has undertaken.
Page 30 of 148
Page 30 of 148

Changes to Plan – Buckinghamshire CCGs Planned and
Unscheduled Care Prescribing
Joint & Continuing
Care
PRC Delegated Co-
CommissioningOther /
Reserves Running Costs Surplus Capital TotalRevenueM10 Revenue Plan Total 389,433 68,074 108,220 25,893 15,346 11,618 5,967 624,551 M11 Revenue allocations 684 - - - 707 10 - 1,401 M11 Revenue Plan Total 390,117 68,074 108,220 25,893 16,053 11,628 5,967 625,952
Capital
M10 Capital Plan Total 677 677 M11 Capital allocations - - M11 Capital Plan Total - - - - - - - 677 677
Key Points
In Month 11 the Chiltern CCG received a total allocation of £710k, out of which £628k was for GP Access Fund share of uncommitted funds and £82k is for Capital Grant for Primary care.
Aylesbury Vale CCG`s M11 increase in funding was £691k, out of which £387k was for GP Access Fund share of uncommitted funds, £300k for RTT funding and £4k was for LD Transformational care programme.
In M12 the CCG’s are anticipating an allocation of £700k from NHSE as part of the Financial Recovery Plan.
Page 31 of 148
Page 31 of 148
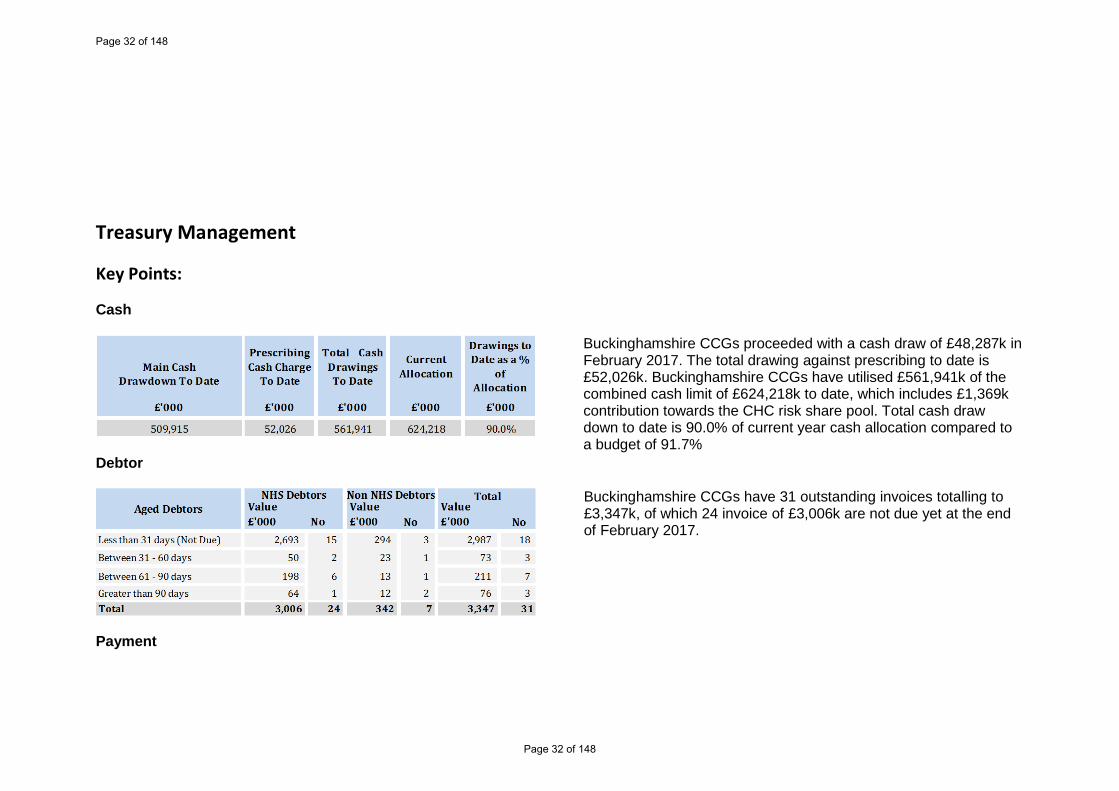
Treasury Management
Key Points:
Cash
Buckinghamshire CCGs proceeded with a cash draw of £48,287k in February 2017. The total drawing against prescribing to date is £52,026k. Buckinghamshire CCGs have utilised £561,941k of the combined cash limit of £624,218k to date, which includes £1,369k contribution towards the CHC risk share pool. Total cash draw down to date is 90.0% of current year cash allocation compared to a budget of 91.7%
Debtor
Buckinghamshire CCGs have 31 outstanding invoices totalling to £3,347k, of which 24 invoice of £3,006k are not due yet at the end of February 2017.
Payment
Page 32 of 148
Page 32 of 148

Value of invoice (YTD) £'000
Number (YTD)
Value of invoices
(YTD) £'000Number (YTD)
Value of invoice
(YTD) £'000Number (YTD)
Total invoices paid 341,843 4982 104,453 11150 446,296 16,132Total invoices paid within 30 days 340,172 4775 99,579 10680 439,751 15,455% Paid within 30 days 100% 96% 95% 96% 99% 96%
TotalNHS Invoices Non NHS Invoices
Better Payment Practice Code - payment within 30 days (cumulative YTD)
The Better Payment Practice Code, introduced by Treasury, requires the CCG to aim to pay all valid invoices by the due date or within 30 days of receipt of a valid invoice, whichever is the later. Buckinghamshire CCGs have achieved above target of 95% on NHS and non NHS invoices by number and volume YTD.
Capital
To date, the CCG’s have received capital allocations for £677k to cover the following activities:
Capital Schemes
Aylesbury Vale CCGBudget Actual Variance£000's £000's £000's
Hardware replacement programme 20 20 0Additional Hardware for increase in staff 20 3 17Improving Wi-fi technologies 20 0 20
Total 60 23 37
Chiltern CCGBudget Actual Variance£000's £000's £000's
Hardware replacement programme 17 0 17Intergration and Interopability 600 0 600Total 617 0 617
Key Points:
• Whilst there has been minimal spend the forecast remains breakeven against budget.
• Plans have been developed and implemented to spend the additional allocation of £677k during February and March on projects covering Interoperability and New ways of Working.
Page 33 of 148
Page 33 of 148

Buckinghamshire CCGs Financial Performance
The following pages show the Month 11 financial performance by individual CCG. Aylesbury Vale CCG on the left and Chiltern CCG on the right unless otherwise specified. It should be noted that the 1% headroom reserve held by each CCG has not been released into either the YTD position or within the full year forecast, in line with NHSE requirements.
Aylesbury Vale to date: Annual Plan YTD Plan YTD Actual
Previous Month
Variance £,000's £,000's £,000's £,000's % £,000's
CommissioningPlanned and Unscheduled Care 149,369 136,946 141,703 (4,757) (3.47%) (2,711)Prescribing 26,645 24,425 23,835 589 2.41% 603Joint & Continuing Care 44,094 40,179 42,212 (2,033) (5.06%) (1,488)Delegated Co-Commissioning 25,893 23,035 22,983 52 0.22% 6Primary Care IT 526 482 397 85 17.63% 104Other / Reserves 5,832 2,683 (3,327) 6,010 224.02% 3,170Commissioning sub-total 252,359 227,750 227,803 (54) (0.02%) (316)Running Costs 4,441 4,063 4,009 54 1.32% (0)Quality Premium Admin 0 0 0 0 0.00% 0Planned Surplus 86 79 0 79 100.00% 72Planned/Actual Spend Sub Total 256,886 231,891 231,813 79 0.03% (245)C/Fwd 2015-16 Surplus 2,233 2,047 0 2,047 100.00% 1,861Total CCG 259,119 233,938 231,813 2,125 0.91% 1,616
Variance to YTD Plan
Key Points
• The position at month 11 shows a surplus of £2,125k and a forecast surplus of £2,319k, which is in line with the original surplus agreed with NHS England. Included in this position is further release of mitigations identified in the recovery plan and previously been shown as a mitigating factor in the forecast outturn.
• The pressures in the Planned and Unscheduled Care and Joint and Continuing Care are narrated below.
• Running costs are at breakeven to plan after applying the risk share to the CSU contract.
• The position includes the release of eleven twelfths of the 0.5% contingency reserve
Chiltern to date: Annual Plan YTD Plan YTD Actual
Previous Month
Variance £,000's £,000's £,000's £,000's % £,000's
CommissioningPlanned and Unscheduled Care 240,749 220,794 223,656 (2,861) (1.30%) (1,532)Prescribing 41,429 37,976 35,955 2,021 5.32% 1,888Joint & Continuing Care 64,283 58,517 61,715 (3,198) (5.46%) (3,689)Delegated Co-Commissioning 0 0 0 0 0.00% 0Primary Care IT 852 781 709 72 9.27% 104Other / Reserves 8,686 3,125 (658) 3,783 121.07% 2,401Commissioning sub-total 355,998 321,193 321,376 (183) (0.06%) (828)Running Costs 7,187 6,581 6,398 183 2.79% 259Quality Premium Admin 0 0 0 0 0.00% 53Planned Surplus 86 79 0 79 100.00% 72Planned/Actual Spend Sub Total 363,271 327,853 327,773 80 0.02% (445)C/Fwd 2015-16 Surplus 3,562 3,265 3,265 100.00% 2,968Total CCG 366,833 331,118 327,773 3,345 1.01% 2,524
Variance to YTD Plan
Key Points
• The position at month 11 shows a surplus of £3,345k and a forecast surplus of £3,648k, which is in line with the original surplus agreed with NHS England. Included in this position is further release of mitigations identified in the recovery plan and previously been shown as a mitigating factor in the forecast outturn.
• The pressures in the Planned and Unscheduled Care and Joint and Continuing Care are narrated below.
• Running costs reflect an underspend relating to the QIPP target that is forecast to be delivered.
Page 34 of 148
Page 34 of 148

• The position includes the release of eleven twelfths of the 0.5% contingency reserve.
Page 35 of 148
Page 35 of 148

QIPP Overview and Forecast Performance - Combined CCG
Month 11 Forecast PositionYear to
Date Budget
Year to Date
Actual
Year to Date
Variance
Achieved Year to
Date
Impact Rating
Annual Budget
Forecast Actual
Forecast Variance
Forecast Achievement
Risk Rating
Name £000 £000 £000 % £000 £000 £000 %Running Costs - additional allocation (183) (183) 0 100% (200) (200) 0 100%FYE 15/16 schemes (80) (80) 0 100% (88) (88) 0 100%EOL Project (1,568) 0 (1,568) 0% (1,764) (196) (1,568) 11%Airedale (133) (81) (53) 60% (159) (108) (51) 68%CHC Procurement (DR) (571) (862) 291 151% (623) (968) 345 155%Over 75's (420) 0 (421) 0% (500) (79) (421) 16%HF Admission avoidance (SK) (318) (288) (30) 91% (451) (421) (30) 93%Falls (187) 0 (187) 0% (206) 0 (206) 0%Diabetes (60) (61) 0 101% (67) (68) 0 101%Reduce prescribing growth (1,199) (3,807) 2,608 318% (1,304) (4,150) 2,846 318%Respiratory (384) (256) (129) 0% (587) (306) (281) 52%Live Well (409) 0 (409) 0% (458) 0 (458) 0%PLCV (1,138) (1,988) 850 175% (1,250) (2,100) 850 168%Home Oxygen (183) (58) (125) 32% (213) (65) (148) 31%Direct Access Radiology (80) (80) (0) 100% (96) (95) (0) 100%Follow ups (SK) (763) (783) 20 103% (850) (870) 20 102%Data Challenges (650) (578) (72) 89% (731) (659) (72) 90%Daycase to O/Patient Procedures (41) (21) (20) 51% (45) (25) (20) 56%C2C challenge on protocols (SK) (594) (352) (242) 59% (645) (403) (242) 62%Dermatology - Monmouth (SK) (275) (275) 0 100% (300) (300) 0 100%Enhanced Services (366) (366) 0 100% (400) (400) 0 100%North Locality outpatient project (70) (70) (0) 100% (84) (84) (0) 100%Procedures out of acute and into community (SK) (44) (28) (16) 64% (50) (34) (16) 68%Genito Urinary (202) (115) (88) 0% (309) (221) (88) 72%Community Urology (SK) (44) (36) (8) 82% (50) (42) (8) 84%Right Care - Elective ( Circulation/Nutrition/GUM) (174) (174) 0 100% (190) (190) 0 100%Referral Management (291) (295) 4 101% (350) (350) 0 100%PTS - reduction in activity (428) (428) 0 100% (471) (471) 0 100%London Repatriation (SK) (59) (7) (52) 12% (67) (15) (52) 22%Resilience (92) (93) 0 100% (110) (110) 0 100%Move to Non Bed Based Services (714) 0 (714) 0% (818) (52) (766) 6%OUH - Discharge Co-ordinator (66) (0) (66) 0% (80) (14) (66) 18%Reduction in NEL admissions (177) 0 (177) 0% (194) (9) (186) 4%Demand Management in A&E (ST) - reduction in attendances (143) (13) (130) 9% (156) (20) (136) 13%Reduction of patients admitted with no procedure carried out (1,188) (1,188) 0 100% (1,300) (1,300) 0 100%DLS central appointment system (166) 1 (166) 0% (200) (17) (183) 8%D2A (229) 0 (229) 0% (250) (10) (240) 4%
Total Identified Savings (13,692) (12,563) (1,129) 92% (15,615) (14,437) (1,177) 92%Unidentified QIPP (2,212) 0 (2,212) 0% (2,721) 0 (2,721) 0%Total Gross QIPP Programme (15,904) (12,563) (3,341) 79% (18,336) (14,437) (3,897) 79%
Mitigation : QIPP Reserve (1,445) 1,445 (1,934) 1,934Project slippage (1,650) 1,650 (1,650) 1,650Contingency Reserves ( balance after FNC) 0 0 0 0Prescribing underspend 0 (0) 0 (0)
Gross QIPP Programme (incl mitigation) (15,904) (15,658) (246) 98% (18,336) (18,021) (313) 98%
Page 36 of 148
Page 36 of 148

Key Points:
• The majority of QIPP scheme progress will be reported separately through individual Programme Boards. • The table above shows the actual achievement to date of £12,563k (79%). When combined with mitigation schemes at year to date
saving of £15,658k is achieved (98% achievement). • Forecast achievement for the year is £14,437k for the year (79% achievement) and after mitigation added £18,021 (98%
achievement). • All schemes have been reviewed this month and potential achievement aligned to actual data received. • Targets relating to schemes that were not deemed able to deliver at all in year and recommended to be closed through the QIPP
clinics have been added to the unidentified QIPP balance currently with managers tasked to find alternative mitigation schemes to compensate. These schemes are detailed below :
QIPP Schemes requested to close 16/17 £k
Federation 240MSK 702Community 100IVF 193FY effect of the Advice and Guidance 186Total to tfr to unidentified QIPP balance 1421
• Although there are still a number of schemes that are still underperforming but the mitigation factor this month was due to the over achievement on the performing schemes as well as ; AVCCG QIPP reserve; Project slippage and prescribing underspend per reported position.
• For schemes such as Contract challenges and C2C challenges technical challenges only have been assumed to date with estimates relating to hard close Q1 and Q2.
• The year to date target and position reflects 64% of the overall QIPP target due to phasing meaning that some of the schemes are planned to commence part way through the year with other schemes that are currently underway are planned to increase in their saving delivery over the course of the year.
April May June July August Sept. Oct. Nov. Dec. Jan. Feb. March Total
£k £k £k £k £k £k £k £k £k £k £k £k £kCombined QIPP Target Profile by Month (965) (976) (1,031) (1,340) (1,343) (1,343) (1,555) (1,555) (1,558) (2,119) (2,120) (2,431) (18,336)
Page 37 of 148
Page 37 of 148

Page 38 of 148
Page 38 of 148

Forecasts, Risks
AVCCG Worst Most Likely Best£,000's £,000's £,000's
Planned and Unscheduled Care (4,094) (3,570) (3,570)Prescribing 588 645 705Joint & Continuing Care (2,231) (2,155) (1,990)Delegated Co Commissioning 300 300 306Running Costs / Quality Premium 60 60 60Other 3,516 3,516 3,949Reserves 1,292 1,292 1,292Total Forecast before C/fwd Surplus (570) 87 752C/fwd Surplus 15-16 2,232 2,232 2,232Total Forecast 1,662 2,319 2,984
Reserves * Worst Most Likely Best£'000 £'000 £'000
HeadroomContingency 1,292 1,292 1,292Risk Share Estimate 2,191Mitigations/Other Impact (2,191)Total Reserves 1,292 1,292 1,292
Key Points
• The first table shows the potential range of risks and opportunities for the financial year ending 31/3/17. The current range is from a £2,984k favourable variance (the “best case”) to £1,662k favourable (the “worst case”) with a most likely forecast of the required £2,319k surplus, after applying the risk share with Chiltern CCG.
• The forecasts are based on month 10 activity information which contains a level of challenge and therefore there is some uncertainty and risk within the system.
• The reserves being utilised within the forecast outturn are the surplus budget and all of the contingency reserve.
• The assessed risks are calculated at c£657k and covers: The pressures from increasing activity in the acute sector. Increasing activity and cost due to complexities of care
packages in Adult Continuing Healthcare. Prescribing activity increasing.
Chiltern CCG Worst Most Likely Best£,000's £,000's £,000's
Planned and Unscheduled Care (3,647) (2,451) (2,451)Prescribing 2,120 2,213 2,312Joint & Continuing Care (3,311) (3,187) (2,918)Delegated Co Commissioning 0 0 0Running Costs / Quality Premium 324 324 374Other 1,205 1,205 1,622Reserves 1,983 1,983 1,983Total Forecast before C/fwd Surplus (1,327) 87 922C/fwd Surplus 15-16 3,561 3,561 3,561Total Forecast 2,234 3,648 4,483
Reserves * Worst Most Likely Best£'000 £'000 £'000
HeadroomContingency 1,836 1,836 1,836Risk Share Estimate (2,191)Mitigations/Other Impact 2,643 452 452Total Reserves 2,288 2,288 2,288
Key Points
• The first table shows the potential range of risks and opportunities for this financial year. The current range is from a £4,483k favourable variance (the “best case”) to a £2,234k favourable variance (the “worst case”) with a most likely forecast of the required £3,648k surplus, after applying the risk share with Aylesbury Vale CCG.
• Activity data relating to month 10, where available, has been extrapolated and assessed to give the forecast out-turn position, should be treated with some caution.
• The reserves being utilised within the forecast outturn are the surplus budget and all of the contingency reserve.
• Assessed risks are calculated to be circa £1,414k currently mainly relating to activity pressures; potential QIPP under delivery and growth re CHC and national living wage etc. not managed to be contained within planned uplifts together with the potential prescribing activity increasing.
Page 39 of 148
Page 39 of 148

Page 40 of 148
Page 40 of 148

Commissioning
Planned and Unplanned Care Summary
Summary of position
Aylesbury Vale
Annual Plan
YTD Plan
YTD Actual
Previous month
variance to plan
£'000 £'000 £'000 £'000 % £'000Acute Commissioning 621 318 2,968 (2,650) (833.8%) (2,094)Planned Care 66,326 60,799 62,796 (1,997) (3.3%) (1,437)Urgent Care 44,261 40,572 41,659 (1,087) (2.7%) (172)Intermediate Care 1,629 1,494 1,488 5 0.3 % 2 Non-Contracted Activity 2,941 2,696 2,865 (170) (6.3%) (178)Exceptions and Prior Approvals 312 286 143 143 49.9 % 137Ambulance Services 6,684 6,127 6,189 (62) (1.0%) (68)Patient Transport 1,316 1,206 1,148 58 4.8 % 56Community Services 20,173 18,768 18,647 121 0.6 % 143NHS 111 769 705 659 46 6.6 % 40Local Enhanced Services 1,364 1,250 1,067 183 14.7 % 167Out of Hours 1,895 1,737 1,735 2 0.1 % 40Winter Resilience 1,077 987 337 650 65.9 % 655
Total Planned and Unscheduled Care 149,369 136,946 141,703 (4,757) (3.5%) (2,711)
YTD variance to plan
Month 11 Feb 2017
Summary of position
Chiltern
Annual Plan
YTD Plan
YTD Actual
Previous month
variance to plan
£'000 £'000 £'000 £'000 % £'000Acute Commissioning 11,690 10,824 15,307 (4,483) (41.4%) (2,989)Planned Care 128,589 117,873 118,598 (725) (0.6%) (565)Urgent Care 47,216 43,281 41,988 1,294 3.0 % 1,472Intermediate Care 2,592 2,376 2,423 (47) (2.0%) (51)Non-Contracted Activity 4,143 3,798 3,673 125 3.3 % 44Exceptions and Prior Approvals 451 414 165 249 60.2 % 237Ambulance Services 10,477 9,604 9,867 (263) (2.7%) (290)Patient Transport 2,338 2,143 1,756 387 18.0 % 392Community Services 24,862 22,790 22,356 434 1.9 % 386NHS 111 1,154 1,058 932 126 11.9 % 136Local Enhanced Services 1,458 1,337 1,337 (0) (0.0%) (0)Out of Hours 3,156 2,893 2,851 42 1.5 % (304)Winter Resilience 2,622 2,403 2,403 (0) (0.0%) (0)
Total Planned and Unscheduled Care 240,749 220,794 223,656 (2,861) (1.3%) (1,532)
YTD variance to plan
Month 11 Feb 2017
Key Points • For Planned and Unscheduled care, there are adverse variances of £4,757k in Aylesbury Vale and £2,861k in Chiltern against year to date plan for
month 11. Acute activity is based on M10 SLAM. There is a separate analysis of all the headline variances in Acute by provider in the following pages.
• The reported pressures relate to BHT- Non–Elective activity for general surgery and critical care bed days, Milton Keynes FT – Day case electives in T&O, Gynae and Cardiology, Frimley – Non-Elective activity for vascular, immunology through a rise in septicaemia, digestive procedures and excess bed days OUH- Non-Electives in clinical haematology, transplant surgery. These reported pressures have been offset by a reduction in activity and successful challenges (high cost patients at Guy’s and Bart’s) along with a reduction in Non-Contracted Activity.
• The majority of the independent sector is still showing underspends against contracts due to a decrease in activity except for BMI Bucks where an increase in activity due to seasonal catch up has deteriorated to an overspend position.
• Ambulance services continue to over perform, including hospital delays.
• Other areas are generally on budget.
Page 41 of 148
Page 41 of 148

Prescribing
Summary of position
Aylesbury Vale
Annual Plan YTD Plan YTD Actual Previous month
variance to plan
£'000 £'000 £'000 £'000 % £'000Prescribing 26,645 24,425 23,834 591 2.4 % 604High Cost Drugs 1 (1) 0
Total Prescribing 26,645 24,425 23,834 591 2.4 % 604
Month 11 Feb 2017YTD variance to plan
Summary of position
Chiltern
Annual Plan YTD Plan YTD Actual Previous month
variance to plan
£'000 £'000 £'000 £'000 % £'000Prescribing 41,087 37,663 35,646 2,017 5.4 % 1,888Medicines Management - Clinical 341 313 309 3 1.1 % ()
Total Prescribing 41,429 37,976 35,955 2,021 5.3 % 1,888
Month 11 Feb 2017YTD variance to plan
Key Points
• The prescribing calculation is now based on 9 months actual data from April to December. As previously outlined, the PPD basis has been adopted fully in line with previous years practice.
• As the entire forecast was in the position at month 9, there was perceived a risk that there could be a potential adverse movement on Prescribing which was included in the assumptions of a worst case scenario for the CCGs. This would be offset by mitigating actions. £150k of that risk assumption remains, and that is in line with the movement across the two CCGs in this month.
• The benefit from the Category M Price reduction included in line with revised NHSE reporting guidance is assumed in the forecast.
Page 42 of 148
Page 42 of 148

Mental Health, Joint & Continuing Care
Summary of position
Aylesbury ValeAnnual
PlanYTD Plan
YTD Actual
Previous month
£'000 £'000 £'000 £'000 % £'000Mental Health - Contracts 16,490 15,116 15,116 (0) (0.0%) (0)Mental Health - NCA 421 386 386 (0) (0.0%) (0)Mental Health - Other 2,311 2,118 2,326 (208) (9.8%) 226IAPT 54 50 48 2 4.7 % 2CAMHS 2,105 1,648 1,648 (0) (0.0%) (0)Mental Health - Advocacy 279 256 0 256 100.0 % 233Learning Difficulties 2,010 1,839 1,763 76 4.1 % (3)Mental Health Sub Total 23,670 21,412 21,286 126 0.6 % 457
CHC Adult Fully Funded 11,773 10,837 14,782 (3,945) (36.4%) (3,477)CHC Adult Joint Funded 812 744 547 197 26.5 % 179Funded Nursing Care 3,855 3,534 2,675 859 24.3 % 803CHC Children 637 584 577 7 1.2 % 29CHC Assessment & Support 607 556 833 (277) (49.8%) (267)Continuing Healthcare Sub Total 17,684 16,255 19,414 (3,159) (19.4%) (2,733)
Commissioning - Non Acute 1,698 1,556 1,446 110 7.1 % (49)Reablement 217 199 0 199 100.0 % 181End Of Life 494 452 388 64 14.3 % 59Carers 332 304 (322) 626 205.8 % 599Other Sub Total 2,740 2,512 1,512 1,000 39.8 % 789
Total MH, Joint & Continuing Care 44,094 40,179 42,212 (2,033) (5.1%) (1,488)
Month 11 Feb 2017
YTD variance to plan
Summary of position
ChilternAnnual
PlanYTD Plan
YTD Actual
Previous month
£'000 £'000 £'000 £'000 % £'000Mental Health - Contracts 21,911 20,085 20,086 (0) (0.0%) (0)Mental Health - NCA 763 699 701 (2) (0.3%) (0)Mental Health - Other 3,344 3,065 3,282 (217) (7.1%) (193)IAPT 611 538 537 0 0.1 % (0)CAMHS 3,306 2,577 2,582 (5) (0.2%) 4Mental Health - Advocacy 28 26 26 (0) (0.0%) (0)Learning Difficulties 3,113 2,851 2,767 84 3.0 % (7)Mental Health Sub Total 33,076 29,842 29,981 (140) (0.5%) (197)
CHC Adult Fully Funded 22,576 20,764 22,228 (1,464) (7.1%) (2,246)CHC Adult Joint Funded 1,115 1,022 874 148 14.5 % 135Funded Nursing Care 2,703 2,478 4,277 (1,799) (72.6%) (1,600)CHC Children 965 885 923 (38) (4.3%) 2CHC Assessment & Support 968 888 1,240 (352) (39.7%) (312)Continuing Healthcare Sub Total 28,328 26,036 29,542 (3,505) (13.5%) (4,022)
Commissioning - Non Acute 1,936 1,774 2,449 (674) (38.0%) (638)Reablement 110 101 0 101 100.0 % 92End Of Life 718 658 597 61 9.3 % 56Carers 115 105 (1,002) 1,107 1053.0 % 1,098Other Sub Total 2,879 2,639 2,043 595 22.6 % 607
Total MH, Joint & Continuing Care 64,283 58,517 61,567 (3,050) (5.2%) (3,611)
Month 11 Feb 2017
YTD variance to plan
Key Points
• In CHC, there is continued pressure from increases in activity and the cost of packages due to the complexity of packages required.This month, the forecast includes a significant provision for a highly complex package.
• The forecast has risen on the Commissioning non acute now includes the actual charges for continence and equipment that have beenidentified as risks previously. There has been an improvement in the year end forecast since last month of £48k.
• The nil balances on carers and reablement spend reflects the release of unutilised accruals (spend on these areas is included in theBetter Care Fund payments). A similar position exists for Mental Health – Advocacy in Aylesbury Vale.
• The adverse variance for CHC Assessment & Support relates to payments made to Arden and GEM CSU for the risk share agreement.• Mental Health other forecasts, which covers S117 arrangements, remain as per previous months at £240k adverse for Aylesbury and
£254k adverse for Chiltern.
Page 43 of 148
Page 43 of 148

PRC Delegated Co-Commissioning – Aylesbury Vale CCG only
Aylesbury Vale CCG Month 11 Year to Date Full YearGP Services 16/17 Plan Actual Variance Plan Actual Variance Plan FOT Variance Prior yr
£k £k £k £k £k £k £k £k £k £k
GP Contract payment 1,356 1,292 65 14,920 14,987 (67) 16,277 0 16,277 0 QOF payments 194 193 1 2,134 2,132 2 2,328 0 2,328 0 GP Seniority and Locums 35 21 14 385 384 0 420 0 420 0 GP Drug payments 146 141 5 1,611 1,605 6 1,758 0 1,758 0 GP Premises 247 291 (44) 2,712 2,676 37 2,959 0 2,959 0 GP Enhanced Services 106 104 2 1,168 1,093 75 1,275 0 1,275 0 GP Other Items 3 0 3 30 26 5 33 0 33 0 CCG Prescribing 0 (0) 0 0 (0) 0 0 0 0 0 Collaborative Fees 5 5 (0) 55 55 (0) 60 0 60 0 GP Premises other 2 2 0 19 25 (5) 21 0 21 0 GP General Reserves 0 0 0 0 0 0 762 25,593 (24,830) 0
Total 2,094 2,049 45 23,035 22,983 52 25,893 25,593 300 0
Key Points:
Overall the YTD position is a favourable variance of £52k against plan.
• GP Contracts £67k adverse partly due to unbudgeted MPIG a proportion of which is prior year and chargeable to NHS England andpartly due to up front set up cost payments for a new APMS contract.
• GP Premises £37k favourable due to outstanding rent reviews that the CSU have been commissioned to clear by 31st March 2017.
• GP Drugs £6k favourable due to seasonal variation.
• GP Enhanced Services £74k favourable due to Extended Hours slippage as not all practices have signed up.
• The actual FOT is £300k below plan. This has been achieved by a review and release of funds held in reserve, rather than a reductionin the planned expenditure by individual category.
Page 44 of 148
Page 44 of 148

Running Costs
Summary of position
Aylesbury Vale
Annual Plan
YTD Plan YTD Actual
Previous month
variance to plan
£'000 £'000 £'000 £'000 % £'000Administration & Business Support 2,544 2,325 2,419 (94) (4.1%) (113)Admin Projects 7 (7) 0.0 % (7)CEO/ Board Office 831 761 613 149 19.6 % 127Chair And Non Execs 34 31 26 6 18.3 % 5Clinical Governance 316 290 210 80 27.6 % 73Finance 87 80 80 (1) (0.7%) (0)Operations Management 628 576 656 (81) (14.1%) (85)
Total Running Costs 4,441 4,063 4,010 53 1.3 % (0)Quality Premium Admin 0 0 0 0 0.0 % 0Total Admin 4,441 4,063 4,010 53 1.3 % (0)
Month 11 Feb 2017YTD variance to
plan
Key Points
• The year to date running costs are reported as a £53kunderspend, after allowing for the risk share on both the CSUcontract and across the CCGs. This is based on a forecastunderspend of £60k at year end. This is the result of mitigatingactions following the inception of the one team management ofBuckinghamshire CCGs.
• NHS England has redefined the allocation for Quality Premium asProgramme and this has been moved accordingly.
Summary of position
ChilternAnnual
PlanYTD Plan
YTD Actual
Previous month variance to plan
£'000 £'000 £'000 £'000 % £'000Administration & Business Support 3,975 3,637 3,816 (179) (4.9%) 13CEO/ Board Office 594 544 536 8 1.5 % 20Chair And Non Execs 622 570 547 24 4.1 % 30Clinical Governance 210 192 293 (101) (52.4%) (93)Commissioning 224 205 283 (78) (37.8%) (81)Emergency Planning 4 3 2 1 29.0 % 1Finance 270 247 191 57 22.9 % 76General Reserve - Admin 200 183 (69) 252 0.0 % 167Medicines Management 137 125 174 (48) (38.4%) (32)Operations Management 926 849 600 249 29.3 % 69Performance 0 0 20 (20) 0.0 % (16)Primary Care Support 0 0 (5) 5 0.0 % 92Strategy & Development 26 24 10 14 59.1 % 13
Total Running Costs 7,187 6,581 6,398 183 2.8 % 259Quality Premium Admin 0 0 0 0 0.0 % 53
Total Admin 7,187 6,581 6,398 183 2.8 % 312
Month 11 Feb 2017YTD variance to
plan
Key Points
• The CCG has reviewed specific project spend and continues toaccrue, in anticipation of spend against identified projects.
• As before, the reported position reflects any favorable variancesagainst pay budgets where some vacancies exist withappropriate accruals in for non-pay budgets e.g. Rental costs etc.The forecast includes £25k of Q4 vacancy savings.
• There is a £200k QIPP target associated with efficiencies as aresult of the one team management approach ofBuckinghamshire CCGs and the current ytd favorable variance ison track to achieve the required target.
• The Chiltern Quality Premium for Chiltern is phased into M12,and will offset QIS 16/17 expenditure of £500k to be incurred inProgramme, alongside carried forward QIS 15/16 funding. Therevised NHS England guidance has seen this been re-categorised as Programme and moved accordingly. There is aresidual prior year balance of £91k which has been released intothe position.
Page 45 of 148
Page 45 of 148

Summary Headline variances acute provision – Aylesbury Vale CCG
The year to date position on main NHS contracts is £3.2m which is driven by Milton Keynes £1.1m and Buckinghamshire Hospitals £1.8m.
The position on Milton Keynes is up on M10 by £126k this is mainly Non Elective (NEL) and Day cases. The treatments functions for Day cases are Trauma & Orthopaedics (T&O), Cardiology, Gynae and Gastro and within NEL it is T&O, Respiratory, A&E and Cardiology
Buckinghamshire Hospitals is performing over plan significantly in critical care; some spells could be identified as specialist activity but will not be known until the end of spell in M12, and emergency activity. Planned care is performing over plan in gastro, urology and general medicine. Provision has been included in the forecast outturn for expected winter pressure on emergencies in the final month of the year. There continues to be a high level of U codes which remedial action is being sought from the trust.
Oxford University is also spending over plan year to date by £181k and Luton and Dunstable by £122k. Independents collectively are under by £231k mainly from Ramsay Horton which is £205k of this. This is due to referrals not coming through as expected in plan.
Summary Headline variances Acute provision – Chiltern CCG
The year to date position on main NHS contracts is £1.6m overspent against plan, predominantly driven by a year to date overspend of £2.03m at Frimley and Wexham Park hospitals. The year-to-date position has deteriorated by a further £467k from Month 10. This is due to the Outpatients missing data now being recorded in the YTD position, though this is adjusted out for FOT and remains a risk if the CCG does not win the challenge.. There are also increasing volumes of non-elective spells specifically in the vascular chapter and immunology (septicaemia). Vascular cases are being challenged as part of misattribution of specialist activity.
Buckinghamshire Hospitals is contributing a £488k underspend at month 11. This is largely due to significant underspends totalling c£1.4m in first outpatient, diagnostics and electives followed by higher than anticipated underperformance against the excluded drugs budget. Whilst emergency cases are over-performing, critical care is underperforming resulting in a net underspend of £547k before below the line adjustments. Consideration has been given within the forecast outturn for winter pressures and the expected performance for elective care. There continues to be a high level of U codes which remedial action is being sought from the trust.
Other providers account for the balance but overall are within tolerances with nothing significant to report.
Independent sector providers are observing continued reductions in activity YTD although a marginally improved M10. This is led by BMI Bucks £578k and Circle £197k.
The Care UK AQN has been closed and recommendations provided to the planned care board as a result of increasing forecast outturn.
Page 46 of 148
Page 46 of 148

Contract Update (Month 10 SLAM) Buckinghamshire Healthcare Trust - Aylesbury Vale CCG
Aylesbury
Point of Delivery (POD) Annual PlanCumulative
Plan Cumulative
Actual Cumulative
Variance
Cum. Variance
% Annual Plan Cumulative Plan Cumulative ActuaCumulative VariaCum. Variance %
Electives (DC and IP) 15,738 12,974 14,776 -1,802 -13.89% £17,185,979 £14,334,358 £15,020,559 -£686,202 -4.79%Maternity 4,352 3,649 2,760 889 24.35% £4,280,139 £3,588,281 £3,588,281 £0 0.00%Outpat Procedures 19,077 15,729 17,690 -1,961 -12.47% £2,582,653 £2,126,847 £2,398,604 -£271,757 -12.78%Outpatients - FA 46,555 38,386 36,698 1,688 4.40% £6,722,933 £5,542,990 £5,108,372 £434,618 7.84%Outpatients - FU 65,911 54,343 53,204 1,139 2.10% £5,803,214 £4,784,691 £4,608,409 £176,282 3.68%Outpatients - Unbundled Radiology 32,284 26,617 29,007 -2,390 -8.98% £2,259,928 £1,863,288 £2,093,589 -£230,302 -12.36%Direct Access - Radiology 24,161 20,135 19,573 562 2.79% £926,570 £772,142 £731,529 £40,613 5.26%Direct Access - Pathology 0 0 0 0 0.00% £2,407,776 £2,006,480 £2,103,833 -£97,353 -4.85%PbR Drug Exclusions 0 0 0 0 0.00% £3,919,185 £3,265,988 £2,571,041 £694,947 21.28%PbR Device Exclusions 0 0 0 0 0.00% £129,787 £108,156 £92,814 £15,341 14.18%Dabigatran Patients 0 0 0 0 0.00% £106,139 £88,449 £78,649 £9,800 11.08%Aids & Appliances 0 0 0 0 0.00% £140,564 £117,136 £97,767 £19,370 16.54%AQP Audiology 3,832 3,160 2,563 597 18.89% £558,310 £460,321 £558,029 -£97,708 -21.23%Rehab 1,185 993 1,219 -226 -22.73% £294,649 £247,021 £301,934 -£54,913 -22.23%Other (Paediatric Diabetes) 141 117 0 117 100.00% £182,004 £151,670 £0 £151,670 100.00%Other (Digital Hearing Aids) 0 0 0 0 0.00% £105,780 £88,150 £38,119 £50,031 56.76%Other (Cardiology DA) 765 637 550 87 13.67% £74,624 £62,186 £53,680 £8,506 13.68%Other (Best Practice Tariff) 0 0 0 0 0.00% £476,972 £397,477 £397,477 £0 0.00%Non face to Face 3,706 3,056 2,546 510 16.68% £101,798 £83,932 £67,749 £16,183 19.28%Block (Excl PTS) 0 0 0 0 0.00% £1,378,895 £1,149,079 £1,149,079 £0 0.00%CQUIN 0 0 0 0 0.00% £2,395,584 £1,996,320 £1,996,320 £0 0.00%NEL/Emergency admissions 14,857 12,442 12,348 94 0.76% £26,260,355 £22,015,531 £23,302,079 -£1,286,548 -5.84%Emergency excess bed days 5,683 4,763 4,054 709 14.89% £1,311,480 £1,099,486 £1,003,038 £96,448 8.77%Emergency Readmissions 0 0 0 0 0.00% -£562,370 -£471,466 -£433,021 -£38,445 8.15%MRET - Financial Adjustments 0 0 0 0 0.00% -£768,076 -£643,921 -£803,970 £160,049 -24.86%FINANCIAL ADJUSTMENT/QIPP -111 -93 0 -93 100.00% -£89,908 -£299,693 £0 -£299,693 100.00%FINANCIAL ADJUSTMENT 0 0 0.00% -£654,724 -£320,833 -£320,833 £0 0.00%CSRU( Cardiology/Stroke Assesment) 531 445 1,189 -744 -166.95% £371,518 £311,464 £454,344 -£142,880 -45.87%A&E 40,446 33,908 35,549 -1,641 -4.84% £5,048,262 £4,232,242 £4,471,365 -£239,124 -5.65%Critical Care Bed Days 1,837 1,540 1,912 -372 -24.14% £2,280,499 £1,911,870 £2,506,133 -£594,263 -31.08%Block (Crit Care Outreach) 0 0 0 0 0.00% £43,184 £35,986 £35,986 £0 0.00%Community Block 0 0 0 0 0.00% £16,332,214 £13,610,178 £13,610,178 £0 0.00%Patient Transport (Block) 0 0 0 0 0.00% £661,992 £551,660 £551,660 £0 0.00%Sub Total 280,950 232,804 235,638 -2,834 -1.22% £102,267,910 £85,267,464 £87,432,795 -£2,165,330 -2.54%Contract Challenges - Agreed 0 0 0 0 0.00% £0 £0 -£33,785 £33,785 NOT IN SLAMPotential for Non delivery of CQUIN Targets 0 0 0 0 0.00% £0 £0 -£39,926 £39,926 NOT IN SLAMAdjustments as per Q1 Hard close plus est Q2 LESS u Cod 0 0 0 0 0.00% £0 £0 -£276,746 £276,746 NOT IN SLAMMRET over performance as per risk share agreement - 50 0 0 0 0 0.00% £0 £0 £337,621 -£337,621 NOT IN SLAMFinancial Summary Risk Share (hardcoded in final adj) ta 0 0 0 0 0.00% £0 £0 -£606,204 £606,204 NOT IN SLAMAmber PLCV 15% agreement as per Q1 hardclose 0 0 0 0 0.00% £0 £0 -£69,404 £69,404 NOT IN SLAMGRAND TOTAL 280,950 164,909 166,031 -1,122 -0.68% £102,267,910 £85,267,464 £86,744,351 -£1,476,887 -1.73%
ACTIVITY FINANCE
Over/under plan 10%Over/under plan 3.00%Over/under plan <3.0%
Key
Page 47 of 148
Page 47 of 148
Key Points (by PoD):
• Overall Elective inpatient (EL IP) is performing in excess of plan by £686k and 1,802 spells, the main Specialties affected are Gastro884 cases £459k, Urology 217 cases £158k, General Medicine 343 cases £409k. Specialties that are performing under plan are T&O172 cases £236k, General Surgery 10 cases £53k, and Vascular Surgery 0 cases over £195k down.
• Overall Outpatients is performing under plan by £339k and 867 appointments (appts) , within this Outpatients (OP) firsts are under by£434k and 1,688 appts this being Plastics 725 appts £95k, T&O 423 appts £81k, Ophthalmology 669 appts £69k, Urology 469 appts£61k & Paeds £142k. OP Follow ups are under £176k and 1,139 appts within this is T&O 514 appts £45k, Ophthalmology 1,020 appts£83k & Paeds 122 cases £53k. Outpatient procedures is over by £271k and 1,961 cases this being Ophthalmology 992 cases £140k, &Plastics 726 & £95k in the main.
• Payment by Results (PbR) Drug Exclusions, the trust have indicated the plan is incorrectly profiled - to be discussed and amended ifjustified, trust allude to catch up which has yet to be shared.
• Other (Paediatric Diabetes) - Costs are being charged to IP and OP Paeds TFC as YOC had plan.• Overall NEL is £1,286k over, Due to abnormal high levels of Uncoded activity (U codes) in M10 which the trust has said will be resolved
at M11, the analysis is a TFC level only - General Medicine is over by 599 Spells and £1,411K, General Surgery is over by £150k and164spells under UZ credit plan raised with trust, T&O £272k and 92 Spells. Underperforming areas are Cardiology £39k and 179spells, Midwife Episodes £123k and 63 spells & plastics £278k and 377 spells & Gynae £150k, 156 spells.
• No QIPP benefit assumed until sight of schemes and profile.• FINANCIAL ADJUSTMENT – there is performance under plan as the Trust has assumed they will hit control target, this was adjusted at
month 3.• AE is over by £239k, 1,641 attendances, M1-M10 average run rate was 3,555 and in Month 10 is under this at 3496 , mainly HRGs
over YTD are VB011/7 25% & 3 Z around 50% of variance. VB03Z is Scans.• Critical Care - In month 2 an extra £70k was incurred for bed days with 4 organs monitored. M6 and M7 have been higher mainly
around 5 organs and 2 organs supported and M8 3 organs spell belonged to NHSE £300K adjusted out in M9 for freeze & M10 wassimilar run rate to M9 219 days, overall over by £594k due to 2, 4 & 5 Organs supported.
• MRET over performance as per risk share agreement - Elective POD has 50% put into plan less CQUIN as agreed.• 15% agreement on Amber PLCV.
Page 48 of 148
Page 48 of 148

Contract Update (Month 10 SLAM) Buckinghamshire Healthcare NHS Trust - Chiltern CCG
Chiltern
Point of Delivery (POD) Annual PlanCumulative
Plan Cumulative
Actual Cumulative
Variance
Cum. Variance
% Annual Plan Cumulative Plan Cumulative Actual Cumulative VarianceCum. Variance
%Electives (DC and IP) 21,257 17,540 18,099 -559 -3.19% £23,083,369 £19,165,637 £18,779,433 £386,204 2.02%Maternity 5,302 4,445 3,372 1,073 24.13% £5,214,654 £4,371,738 £4,371,738 £0 0.00%Outpat Procedures 23,301 19,211 23,033 -3,822 -19.90% £3,570,428 £2,646,281 £3,210,339 -£564,058 -21.32%Outpatients - FA 61,820 50,977 48,862 2,115 4.15% £9,122,994 £7,521,815 £6,781,777 £740,038 9.84%Outpatients - FU 93,575 77,152 78,309 -1,157 -1.50% £8,303,161 £6,845,871 £6,854,127 -£8,256 -0.12%Outpatients - Unbundled Radiology 45,603 37,599 38,383 -784 -2.08% £3,167,194 £2,611,319 £2,728,705 -£117,386 -4.50%Direct Access - Radiology 37,300 31,083 22,534 8,549 27.50% £1,341,518 £1,117,932 £857,582 £260,350 23.29%Direct Access - Pathology 0 0 0 0 0.00% £2,976,340 £2,480,283 £2,473,913 £6,370 0.26%PbR Drug Exclusions 0 0 0 0 0.00% £5,672,853 £4,727,378 £3,709,153 £1,018,224 21.54%PbR Device Exclusions 0 0 0 0 0.00% £88,776 £73,980 £100,923 -£26,943 -36.42%Dabigatran Patients 0 0 0 0 0.00% £139,256 £116,047 £138,090 -£22,043 -19.00%Aids & Appliances 0 0 0 0 0.00% £193,206 £161,005 £156,415 £4,590 2.85%AQP Audiology 4,326 3,567 3,080 487 13.64% £775,238 £639,176 £758,561 -£119,385 -18.68%Rehab 3,044 2,552 2,294 258 10.11% £757,100 £634,719 £570,541 £64,179 10.11%Other (Paediatric Diabetes) 234 195 0 195 100.00% £311,730 £259,775 £0 £259,775 100.00%Other (Digital Hearing Aids) 0 0 0 0 0.00% £193,583 £161,319 £85,330 £75,989 47.10%Other (Cardiology DA) 588 490 326 164 33.42% £57,342 £47,785 £31,818 £15,967 33.41%Other (Best Practice Tariff) 0 0 0 0 0.00% £554,518 £462,099 £462,099 £0 0.00%Non face to Face 4,267 3,518 3,582 -64 -1.81% £115,281 £95,048 £95,317 -£269 -0.28%Block (Excl PTS) 0 0 0 0 0.00% £1,790,321 £1,491,936 £1,491,934 £2 0.00%CQUIN 0 0 0 0 0.00% £2,912,717 £2,427,264 £2,427,264 £0 0.00%NEL/Emergency admissions 17,679 14,815 14,146 669 4.52% £31,554,591 £26,453,985 £27,183,348 -£729,363 -2.76%Emergency excess bed days 7,598 6,369 6,859 -490 -7.69% £1,771,624 £1,485,252 £1,656,647 -£171,395 -11.54%Emergency Readmissions 0 0 0 0 0.00% -£707,773 -£593,366 -£468,231 -£125,135 21.09%MRET - Financial Adjustments 0 0 0 0 0.00% -£778,923 -£653,015 -£595,171 -£57,844 8.86%FINANCIAL ADJUSTMENT/QIPP -86 -72 0 -72 100.00% -£667,184 -£555,989 £0 -£555,989 100.00%FINANCIAL ADJUSTMENT 0 0 0 0 0.00% -£1,197,003 -£700,000 -£700,000 £0 0.00%CSRU( Cardiology/Stroke Assesment) 1,598 1,339 3,217 -1,878 -140.19% £1,114,469 £934,322 £1,250,064 -£315,742 -33.79%A&E 25,122 21,061 23,306 -2,245 -10.66% £3,289,854 £2,758,069 £3,057,333 -£299,263 -10.85%Critical Care Bed Days 2,417 2,027 1,625 402 19.82% £3,162,474 £2,651,279 £2,103,801 £547,478 20.65%Block (Crit Care Outreach) 0 0 0 0 0.00% £56,657 £47,214 £47,214 £0 0.00%Community Block 0 0 0 0 0.00% £16,374,119 £13,645,099 £13,645,099 £0 0.00%Patient Transport (Block) 0 0 0 0 0.00% £868,545 £723,787 £651,410 £72,377 10.00%Sub Total 354,945 293,868 291,027 2,841 0.97% £125,183,028 £104,255,044 £103,916,572 £338,472 0.32%Contract Challenges - Agreed 0 0 0 0 0.00% £0 £0 -£24,563 £24,563 NOT IN SLAMPotential for Non delivery of CQUIN Targets 0 0 0 0 0.00% £0 £0 -£29,839 £29,839 NOT IN SLAMAdjustments as per Q1 Hard close plus est Q2 LESS u Codes W 0 0 0 0 0.00% £0 £0 -£206,500 £206,500 NOT IN SLAMMRET over performance as per risk share agreement - 50 % 0 0 0 0 0.00% £0 £0 £183,041 -£183,041 NOT IN SLAMFinancial Summary Risk Share (hardcoded in final adj) taper 0 0 0 0 0.00% £0 £0 £0 £0 NOT IN SLAMAmber PLCV 15% agreement as per Q1 hardclose 0 0 0 0 0.00% £0 £0 -£113,236 £113,236 NOT IN SLAMGRAND TOTAL 354,945 293,868 291,027 2,841 0.97% £125,183,028 £104,255,044 £103,725,475 £529,569 0.51%
ACTIVITY FINANCE
Page 49 of 148
Page 49 of 148

Key Points (by PoD):
• Overall EL IP is underperforming, the main underperforming Specialties are T&O down 264 cases and £482k, Dermatology down 220cases and £314k, General Surgery down 61 cases and £136k, Plastics down 14 and £94k, Vascular 71 cases down and £216k, Thereare a few Specialties up Gastro 660 cases £355k, General Medicine 134 cases £191k & Gynae 17 cases and £82k. There is also 50 %added in here less CQUIN to the plan from the MRET agreement over Risk share.
• Overall Outpatients are £167k underperforming , OP firsts are down by £740k and 2,115 apps this is mainly due to T&O 728 appts and£136k, Ophthalmology 1,046 appts £104k, Paediatrics 288 appts & £437k. OP Follow ups are over by 1,157 appts and £8k the mainvariances are Haematology as previously reported over 5,118 appts and £696k this is offset by Paediatrics 1,172 appts and £225k,Ophthalmology 1,870 appts £142k, Geriatric Medicine 232 appts £28K & Endocrinology 947 appts £104k. Outpatient Procedures areover by 3,822 cases and £564k, this is due to Ophthalmology 1,641 cases £220k, ENT 863 cases £118k, Urology 269 cases £72k,Plastics 635 cases £83k.
• Underperformance accounted for by RA28Z plain film XRAY & Ultrasound less than 20 minutes.• PbR Drug Exclusions The trust have indicated the plan is incorrectly profiled - to be discussed and amended if justified, trust allude to
catch up which has yet to be shared.• Other (Paediatric Diabetes) - Costs are being charged to IP and OP Paeds TFC as YOC had plan.• Overall NEL is £729k over, Due to abnormal high levels of U codes in M10 which the trust has said will be resolved at M11, the analysis
is a TFC level only - General Medicine is over by 298 Spells and £1,097K, Obstetrics is over by £165k and 7 spells under showingadverse case mix mainly normal delivery with CC and Caesarean Section with CC, T&O £251k and 76 Spells, Paediatrics £395k and202 spells, underspends are Cardiology £453k and 309 spells, Midwife Episode £386k and 174 spells & plastics £289k and 400 spells.XBDs are over by £171k and 490 bed days, TFCs are - Geriatric Medicine £135k - 1,004 bed day, Stroke Med 153 bed dyas , £28k &Thoracic Medicine £148k and 650 bed days over.
• No QIPP benefit assumed until sight of schemes and profile.• AE is over by £299k, 2,245 attendances, M1-M10 average run rate was 2,331 and in Month 10 is 2316 , mainly HRGs over YTD are
VB09 15 % &7/3 Z around 30% each over.• Critical Care -1 patient cost £214k in Months 1&2 due to 5 organs supported, months 3-5 stayed same level with next three months
dropping slightly, 7 cases slight increase in M9, M10 has seen a huge increase in 2 organs supported up 70 days over normal run rate,5 organs supported overall YTD is largest area of underspend £200k, 3 organs over by £743k.
• MRET over performance as per risk share agreement - 50 % into elective - Elective POD has 50% put into plan less CQUIN as agreed.• 15% agreement on Amber PLCV credit for CCGs.
Page 50 of 148
Page 50 of 148

Contract Update (Month 10 SLAM) Oxfordshire University Hospital NHS Foundation Trust - Aylesbury Vale CCG
OUH - Aylesbury
Point of Delivery (POD) Annual Plan Cumulative Plan Cumulative Actual Cumulative
Variance Cum. Variance % Annual Plan Cumulative Plan Cumulative Actual Cumulative VarianceCum. Variance %A&E Attendances 2,569 2,154 2,093 61 2.83% £339,390 £284,530 £288,771 -£4,242 -1.49%CQUIN 0 0 0 0 0.00% £0 £0 £0 £0 0.00%Direct Access - Pathology/Radiology 64,885 53,871 51,239 2,632 4.89% £219,222 £181,963 £176,290 £5,673 3.12%Elective Spells 2,576 2,138 2,431 -293 -13.68% £2,940,616 £2,440,828 £2,435,995 £4,832 0.20%First Outpatient Attendances 5,959 4,946 4,609 337 6.82% £921,440 £764,816 £704,019 £60,798 7.95%Follow Up Outpatient Attendances 10,879 9,030 10,086 -1,056 -11.69% £1,113,660 £924,300 £1,036,308 -£112,008 -12.12%ITU Bed Days 388 326 347 -21 -6.44% £348,383 £292,069 £326,643 -£34,574 -11.84%Maternity Pathway 288 241 178 63 26.28% £334,302 £280,263 £203,040 £77,224 27.55%Non Elective Spells 1,452 1,218 1,576 -358 -29.40% £2,670,907 £2,238,987 £2,392,513 -£153,526 -6.86%Other Items 1,538 1,277 1,652 -375 -29.38% £286,780 £238,998 £194,985 £44,014 18.42%Block Items 0 0 0 0 0.00% £63,137 £52,614 £52,614 £0 0.00%Outpatient Procedures 1,675 1,391 1,505 -114 -8.23% £307,226 £255,009 £309,261 -£54,251 -21.27%PbR Device/Product Exclusions 447 371 388 -17 -4.57% £268,166 £222,589 £214,537 £8,051 3.62%PbR Drug Exclusions 82 69 62 7 9.51% £674,608 £565,659 £608,935 -£43,276 -7.65%Unbundled Radiology 2,749 2,282 2,218 64 2.81% £298,458 £247,732 £258,174 -£10,442 -4.22%Sub Total 95,487 79,314 78,384 930 1.17% £10,786,295 £8,990,357 £9,202,086 -£211,728 -2.36%
ACTIVITY FINANCE
Key Points (by PoD):
• At Month 10, the Contract is £212k (2%) over plan. This represents an increase of £2k from the Month 9 position.• Non-Electives; Outpatient Follow Ups & Procedures account the majority of total over performance year to date.• These over-performing areas are off-set by underperformance within Outpatient First Attendances & the Maternity
pathway.• Maternity pathway costs continue to underperform as a result of the current changes within this service, although the month on month
figures are now pretty steady. .
Page 51 of 148
Page 51 of 148

Contract Update (Month 10 SLAM) Oxfordshire University Hospital Foundation Trust - Chiltern CCG
OUH - Chiltern
Point of Delivery (POD) Annual Plan Cumulative Plan Cumulative Actual Cumulative
Variance Cum. Variance % Annual Plan Cumulative Plan Cumulative Actual Cumulative Variance Cum. Variance %A&E Attendances 1,354 1,135 1,094 41 3.61% £174,379 £146,191 £151,052 -£4,860 -3.32%CQUIN 0 0 0 0 0.00% £0 0.00%Direct Access - Pathology/Radiology 729 606 545 61 10.04% £44,057 £36,569 £26,114 £10,454 28.59%Elective Spells 2,096 1,741 1,788 -47 -2.72% £2,328,202 £1,932,731 £1,742,300 £190,431 9.85%First Outpatient Attendances 4,135 3,432 3,259 173 5.04% £687,214 £570,399 £524,440 £45,959 8.06%Follow Up Outpatient Attendances 8,923 7,406 7,739 -333 -4.50% £1,011,812 £839,763 £922,344 -£82,580 -9.83%ITU Bed Days 235 197 263 -66 -33.67% £243,788 £204,382 £272,766 -£68,384 -33.46%Maternity Pathway 220 184 140 44 23.90% £325,872 £273,197 £211,493 £61,704 22.59%Non Elective Spells 1,433 1,202 1,148 54 4.49% £1,874,430 £1,571,651 £1,732,294 -£160,643 -10.22%Other Items 1,614 1,339 1,577 -238 -17.80% £272,251 £226,859 £181,704 £45,156 19.90%Block items 0 0 0 0 0.00% £12,428 £10,357 £10,357 £0 0.00%Outpatient Procedures 1,054 875 910 -35 -4.03% £194,655 £161,571 £165,486 -£3,915 -2.42%PbR Device/Product Exclusions 425 353 305 48 13.48% £255,675 £212,220 £214,642 -£2,422 -1.14%PbR Drug Exclusions 12 10 25 -15 -148.50% £462,030 £387,444 £437,831 -£50,387 -13.01%Unbundled Radiology 1,662 1,380 1,460 -80 -5.83% £188,345 £156,334 £175,189 -£18,856 -12.06%Sub Total 23,892 19,858 20,253 -395 -1.99% £8,075,138 £6,729,669 £6,768,012 -£38,344 -0.57%
ACTIVITY FINANCE
Key Points (by PoD):
• At Month 10 the contract is £38k (1%) over plan a £14k increase on the Month 9 position.• Non-Elective performance has reduced by £6k, £161k over spent against plan.• Electives performance is £190k under, £16k worse than last month.• Outpatient Follow-Up attendances performance over plan has increased in month by £11k.• Maternity pathway costs continue to perform under plan as a result of the current changes within this service, although the month on
month figures are now pretty steady.
Page 52 of 148
Page 52 of 148

Contract Update (Month 10 SLAM) Milton Keynes Healthcare Foundation Trust - Aylesbury Vale CCG Only
MK - Aylesbury
Point of Delivery (POD) Cumulative Plan Cumulative Actual Cumulative
Variance Cum. Variance % Cumulative Plan Cumulative Actual Cumulative VarianceCum. Variance %Accident and Emergency 4,105 4,318 213 5.20% £566,553 £593,352 £26,800 4.73%Best Practice Tariff 46 97 51 111.11% £21,706 £44,123 £22,417 0.00%Critical Care 70 106 36 51.35% £86,944 £100,245 £13,301 15.30%Drugs and Devices 0 33 33 0.00% £123,504 £125,217 £1,713 1.39%Electives 897 1,065 168 18.67% £915,630 £1,151,359 £235,729 25.74%Emergencies 2,162 2,716 554 25.63% £2,673,250 £3,136,719 £463,469 17.34%Financial Adjustments 0 0 0 0.00% -£94,920 -£62,025 £32,895 -34.66%Imaging 1,457 1,597 140 9.59% £135,398 £150,131 £14,733 10.88%Maternity Pathway 54 114 60 111.14% £85,533 £111,254 £25,720 30.07%Non-Tariff 0 0 0 0.00% £72,713 £74,739 £2,026 2.79%Other Non-Electives 79 168 89 113.22% £168,846 £180,143 £11,298 6.69%Outpatients 10,737 12,357 1,620 15.09% £1,225,181 £1,414,555 £189,375 15.46%Pathology 58 63 6 9.57% £902 £918 £16 1.73%CQUIN 0 0 0 0.00% £146,443 £172,388 £25,944 17.72%Sub Total 19,665 22,634 2,969 15.10% £6,127,683 £7,193,118 £1,065,435 17.39%
ACTIVITY FINANCE
Key Points (by PoD):
• A&E overall over by £27k and 213 cases, mainly due to VB08Z Emergency Medicine, Category 2 Investigation with Category 1Treatment, higher cost HRG being over by 1677 cases costing £22k, various up and downs throughout the rest of the HRGs.
• Critical Care is over by £13k, £41k on cost 1 organ significantly over plan 48 Bed days though 2&3 Organs supported both significantlydown, which could demonstrate less sick patients; XC04Z 3 Organ Support is under by £28k and 20 Bed days.
• Drugs & Devices is under by £2k mainly due to Cytokine modulators being £19k under, Stents over by £3k, Subfoveal choroidalneovascularisation over by £7k.
• Electives over by £236k, 168 cases. This being mainly T&O also over in Gynae/Cardiology, however Obstetrics is down by no actualssuggests switch with Gynae.
Page 53 of 148
Page 53 of 148

• NEL over by £463K YTD, of which £180k relates to XBDs overspend YTD, for NEL spells this is up due to mainly T&O, Respiratory,Cardiology and A&E, XBDs is up in general Medicine, case mix in NEL spells.
• Outpatients Overall is Over by £189k, 1,620 Cases - OPPROC is over by £63k – 377 Cases, mainly due to Specified Skin Examinationsand Investigations £25k, 168 Cases, OP Firsts is over by £80k – 519 cases due to T&O, Dermatology, General Medicine & Cardiology,OPFUPs are over by £50k – 415 cases due to Ophthalmology, T&O and Respiratory, other OP pods down by £4k.
• OPPROC is over by £53k – 326 Cases, mainly due to Specified Skin Examinations and Investigations £24k, 160 Cases, OP Firsts isover by £67k – 438 cases due to T&O, Dermatology, General Medicine & Cardiology ,OPFUPs are over by £31k – 331 cases due toOphthalmology, T&O and Respiratory, other OP pods down by £3k
Page 54 of 148
Page 54 of 148

Contract Update (Month 10 SLAM) Frimley Health Foundation Trust - Chiltern CCG Only
Frimley - Chiltern Source CubePoint of Delivery (POD) Cumulative Plan Cumulative Actual Cumulative Variance Cum. Variance % Cumulative Plan Cumulative Actual Cumulative Variance Cum. Variance %A&E 22,277 23,883 1,606 7.21% £3,215,469 £3,433,383 £217,914 6.78%CRITICAL CARE 1,740 2,915 1,175 67.52% £1,780,254 £2,105,165 £324,911 18.25%DAY CASE 3,127 3,373 246 7.87% £2,476,111 £2,692,818 £216,707 8.75%ELECTIVE INPATIENT 979 955 -24 -2.49% £2,937,439 £2,807,273 -£130,166 -4.43%EXCESS BED DAYS EL 246 257 11 4.37% £60,146 £63,678 £3,532 5.87%REGULAR DAY ATTENDARS 897 821 -76 -8.42% £409,058 £389,249 -£19,809 -4.84%EXCESS BED DAYS NEL 3,363 5,282 1,919 57.07% £797,088 £1,250,277 £453,189 56.86%NON-ELECTIVE INPATIENTS 8,320 9,438 1,118 13.44% £16,498,761 £17,909,116 £1,410,355 8.55%NON-ELECTIVE NON EMERGENCY 2,269 2,241 -28 -1.23% £3,216,822 £3,139,787 -£77,034 -2.39%OTHER 2,080 1,656 -424 -20.40% £267,329 £210,246 -£57,083 -21.35%OTHER 9,140 10,481 1,341 14.68% £910,415 £922,049 £11,635 1.28%OUTPATIENT FIRST 10,134 11,060 926 9.14% £1,744,358 £1,872,276 £127,918 7.33%OUTPATIENT FOLLOW UP 20,290 20,733 443 2.18% £2,133,547 £2,032,968 -£100,579 -4.71%OUTPATIENT PROCEDURES 3,391 4,111 720 21.25% £689,454 £838,792 £149,339 21.66%RADIOLOGY 95 194 99 104.27% £28,443 £44,042 £15,599 54.84%DRUGS AND DEVICES 0 0 0 0.00% £776,387 £798,628 £22,242 2.86%OTHER VARIANCES / ADJUSTMENTS 5,293 4,707 -587 -11.08% -£203,129 -£675,116 -£471,987 232.36%CQUIN 0 0 0 0.00% £920,877 £460,438 -£460,438 -50.00%Sub Total 88,348 97,400 8,466 9.58% £37,164,694 £39,711,121 £1,636,243 4.40%
ACTIVITY FINANCE
Key Points (by PoD):
• NEL/NELST/NELSD/PAEDLOS are collectively 1410k / 8.5% over plan (1097k / 7.4% at M9). Collectively M8 remains the activity peak at1066 with M9-10 slightly below. The average per month in 1516 was 852.
• Key subchapters performing over plan are largely unchanged: QZ - vascular, WA - immunology (mostly due to septicaemia). DZ -respiratory (a growth area M9&10). DZ11A - pneumonia maj CC 101k over plan of 86k in M10 alone
• M10 alone saw 300k over plan for the combined PODs; 210k in DZ respiratory, 55k in QZ vascular and 46k in FZ digestive. NEL PODalone follows the same key subchapters and is 253k over plan; each POD is individually over plan in M10 alone
Page 55 of 148
Page 55 of 148

• Vascular is being challenged as part of the misattribution process, although there is likely to be a resource implication so there has been noadjustment in likely case.
• However to note that QZ15 HRGs (Therapeutic Endovascular Procedures ) are considerably above plan, and are also linked to a significantlevel of CCU activity, which is being challenged, and pursued with NHSE (awaiting reply).
• NELXBD is over plan by 435k / 56.3% /1851 days (55.3% at M9). After increasing month on month M6-8, M9 activity dropped back to M5levels, which then increased again, within trend, for m10. Average M9 1516 to M6 1617 is 456 days per month. M10 alone is 31k overplan. 31k due to 127 days, 31k HA94Zin M10. M8 was the peak at 91k over plan. £40k due to WA03V septicaemia major CC (176 days,plan 2 days), 19k AA26A muscular, balance, cranial 83 days.
• A&E is 218k /6.8% (6.7% at M9) / 1614 attendances over plan. M10 activity is at similar levels to M9.• CCU is 285k / 16.3% over plan at M10 (16.1% M9). The position swung in M6, and has continued at the new high level at M7 and M9 with
a slight drop in M8. There have been 365 bed days in M9. 213 was the previous high before M6-8 peak. The price however has declinedin each of M7-9 and does not show the same trend as activity; case mix analysis has identified a significant proportion of CCU activity islinked to QZ15 HRGs, and therefore forms part of the Vascular challenge.
• DC & EL are 87k over plan jointly; the plan includes 2% growth in this area. DC are 217k over and EL are 130k under. DC is in line withthe peak of M8 & M5-6. EL is the lowest month in 1617. DC: In M10 alone DC is over by 21k; 8k in urology, 8k in paeds. (consistent withlast month) YTD urology and plastics are the highest specialties performing over plan. EL: In M10 alone, 88k under plan, 5k over in genmedicine. YTD EL is under plan by 48k, but over in cardiology by 53k. T&O is under plan by 94k.
• OPFA/FUP/OPPROCS/NLFUP collectively over plan by £171k (which is a movement from the under plan position by £136k at M9). Trusthave added the M1-6 missing data to SLAM at M10, commissioners did not agree this and this has therefore been raised as a challenge.
Page 56 of 148
Page 56 of 148

Treasury Management - Aylesbury Vale CCG
Statement of Financial Position Statement of Financial Position as at:
As at 31 Mar 16
As at 31 Jan 17 Movement
As at 28 Feb 17
28 February 2017 £'000 £'000 £'000 £'000
Non Current Assets 1,077 903 (18) 885
Total Non Current Assets 1,077 903 (18) 885
NHS Receivables - Revenue 537 (316) 2,821 2,505
NHS Prepayments and Accrued Income 564 857 (352) 505
Non-NHS Receivables - Revenue - 14 - 14
Non-NHS Prepayments and Accrued Income 115 2,224 (2,078) 146
Other Receivables 86 3 6 9
Total Trade and Other 1,302 2,782 397 3,179
Cash 47 1,902 (2,702) (800)
Total Current Assets 1,349 4,684 (2,305) 2,379
NHS Payables - Revenue (1,511) (3,947) 2,040 (1,907)
NHS Accruals and Deferred Income (3,522) (4,048) (1,600) (5,648)
Non-NHS payables - Revenue (418) (1,901) 1,496 (405)
Non-NHS payables - Capital (154) (58) 58 -
Non-NHS Accruals and Deferred Income (8,753) (11,065) 763 (10,302)
Other Payables (91) (433) 130 (303)
Provisions (156) (156) - (156)
Total Current Liabilities (14,605) (21,608) 2,887 (18,721)
Total non Current Liabilities (139) (26) - (26)
Total Assets Employed (12,318) (16,046) 564 (15,482)
General Fund (12,318) (16,046) 563 (15,483)
Total Taxpayers Equity (12,318) (16,046) 563 (15,483)
Page 57 of 148
Page 57 of 148

Key Points:
• Current trade and other receivables have increased by £397k to£3,179k from the previous month.
• The ledger balance of cash at 28th February appears to beoverdrawn by £800k, but the actual cash balance at bank was£301k at the end of February. This was caused by the timingdifference between payment journals hitting the ledger and cashleaving the bank account at month end;
• Total current liabilities at 28th February are £18,721k, adecrease of £2,887k from the previous month.
• Total taxpayer equity deployed to February 2017 has decreased£563k to £15,483k from the previous month;
Receivables
Value £'000 No
Value £'000 No
Value £'000 No
Less than 31 days (Not Due) 2,429 10 - - 2,429 10Between 31 - 60 days 34 1 - - 34 1
Between 61 - 90 days 18 3 13 1 31 4Greater than 90 days - - 1 1 1 1
Total 2,481 14 14 2 2,495 16
TotalAged Debtors
NHS Debtors Non NHS Debtors
Key Points:
• The overall value of aged debtors has increased from £88kin M10 to £2,495k in M11 of which £2,481k is not due yet;
• There is £1k aged debtors over 90 days in M11;• £1k has been provided as bad debt at the end of last
financial year.
Cash
£'000 £'000 £'000 £'000 £'000
211,018 18,630 229,648 256,064 89.7%
Prescribing Cash Charge
To Date
Total Cash Drawings To Date
Current Allocation
Drawings to Date as a %
of Allocation
Main CashDrawdown To Date
Key Points:
Page 58 of 148
Page 58 of 148

• The CCG processed a cash draw down of £19,623k inFebruary.
• The total drawing against prescribing to date is £18,630k.• Total cash draw down to date is £229,648k which includes
£539k CHC Risk Pool contribution.
• Total cash draw down to date is 89.7% of current year cashallocation compared to a budget of 91.7%.
Cash forecast v actual
Cash Receipts £'000
Cash Expenditure
£'000Cash Receipts
£'000
Cash Expenditures
£'000
Cash Receipts
£'000
Cash Expenditure
s £'000
Net cash expenditures /
receipts %
September 20,180 19,507 20,186 19,201 -6 306 1.5%
October 18,870 18,874 18,917 18,613 -47 261 1.4%
November 17,548 18,814 17,673 17,146 -125 1,668 9.4%
December 18,462 18,618 18,828 20,820 -366 -2,202 -11.7%
January 19,889 19,797 19,932 18,041 -43 1,756 8.8%
February 19,829 21,450 19,626 21,231 203 219 1.1%
Month
Forecast Actuals Variance
Payables Not Due Overdue Overdue Overdue Overdue Total
1-30 days 31-60 days 61-90 days 90+ days£'000 £'000 £'000 £'000 £'000 £'000
At 31 October 773 350 456 94 526 2,199At 30 November 2,239 455 247 440 442 3,823At 31 December 1,492 359 364 181 730 3,126At 31 January 2,593 2,477 152 359 876 6,457At 28 February 1,123 376 32 52 639 2,222
Aged Creditors - volume Nos Nos Nos Nos Nos Total Nos
At 31 October 162 101 41 42 184 530At 30 November 203 99 65 32 193 592At 31 December 166 122 69 48 219 624At 31 January 201 90 66 50 213 620At 28 February 159 94 46 44 217 560
Aged Creditors - value
Page 59 of 148
Page 59 of 148

Key Points: • Creditors (unpaid invoices on the system) decreased £4,235k from £6,457k at the end of January to £2,222k at the end of February of
which £1,123k is not yet due for payment. The decrease is mainly in overdue categories.• The total number of invoices outstanding has decreased from 620 in January to 560 in February of which 159 are not yet due for
payment.• Total value of creditors overdue has decreased from £3,864k at the end of January to £1,099k at the end of February. The largest 90+
days overdue ones are £199k to Oxford Health NHS Foundation Trust, and £188k to Buckinghamshire County Council.• Note: Creditors balances have been adjusted for invoices relating to future months.
BPPC
Value of invoice (YTD) £'000
Number (YTD)
Value of invoices
(YTD) £'000Number (YTD)
Value of invoice
(YTD) £'000Number (YTD)
Total invoices paid 158,856 2255 22,897 2269 181,753 4,524Total invoices paid within 30 days 157,838 2156 21,101 2155 178,939 4,311% Paid within 30 days 99% 96% 92% 95% 98% 95%
TotalNHS Invoices Non NHS Invoices
Better Payment Practice Code - payment within 30 days (cumulative YTD)
* 95% or more Green - 75% to 95% Amber - Less than 75% Red
The above table gives the percentage of invoices paid within a 30 day period for the year to date to 28th February.
The Better Payment Practice Code requires the CCG to aim to pay all valid invoices by the due date or within 30 days of receipt of a valid invoice, whichever is the later.
BPPC continued:
Key Points: • YTD NHS invoices paid continue to maintain at a high level of 99% in value and 96% in terms of number of invoices.• YTD Non NHS invoices at 92% by value and 95% by number.
The graph shows BPPC performance over the last twelve months:
Page 60 of 148
Page 60 of 148

Note: Monthly payment performance has achieved above 95% target with NHS by value and number and Non NHS by number.
Treasury Management – Chiltern CCG
Statement of Financial Position
Note:
The drop in BPPC non-NHS invoice value to 63% is mainly due to one BCC invoice for £924k which was on hold as there was an element of £124k to be charged to Milton Keynes and was waiting for a confirmation if this is chargeable. If this invoice is excluded then the revised achievement will be 90%
Page 61 of 148
Page 61 of 148

Statement of Financial Position(Balance Sheet) as at:
As at 31 Mar 16
As at 31 Jan 17 Movement
As at 28 Feb 17
28 February 2017 £'000 £'000 £'000 £'000
Non Current Assets 693 629 1 630
Total Non Current Assets 693 629 1 630
NHS Receivables - Revenue 978 1,635 (1,058) 577
NHS Prepayments and Accrued Income 1,131 1,603 34 1,637
Non-NHS Receivables - Revenue 1,132 99 247 346
Non-NHS Prepayments and Accrued Income 619 964 (724) 240
Other Receivables (330) (6) 5 (1)
Total Trade and Other 3,530 4,295 (1,496) 2,799
Cash 341 (1,548) 535 (1,013)
Total Current Assets 3,871 2,747 (961) 1,786
NHS Payables - Revenue (5,953) 8,983 (3,239) 5,744
NHS Accruals and Deferred Income (5,685) (17,738) (738) (18,476)
Non-NHS payables - Revenue (2,600) (4,233) (3,055) (7,288)
Non-NHS payables - Capital (310) (136) - (136)
Non-NHS Accruals and Deferred Income (16,660) (15,315) 10,844 (4,471)
Other Payables (1,099) (1,069) 55 (1,014)
Provisions (249) (249) - (249)
Total Current Liabilities (32,556) (29,757) 3,867 (25,890)
Total non Current Liabilities (41) (41) - (41)
Total Assets Employed (28,033) (26,422) 2,907 (23,515)
General Fund (28,033) (26,422) 2,907 (23,515)
Total Taxpayers Equity (28,033) (26,422) 2,907 (23,515)
Key Points:
• Total current trade and other receivables have decreased by£1,496k to £2,799k;
• The ledger balance of cash at 28th February appearsoverdrawn of £1,013k, but the actual cash balance at bank was£330k at the end of February. This was caused by the timingdifference between payment journals hitting the ledger and cashleaving the bank account at month end;
• Total current liabilities for February stand at £25,890k, adecrease of £3,867k on previous month;
• Total taxpayer equity deployed to February 2017 has decreased£2,907k to £23,515k;
Page 62 of 148
Page 62 of 148

Receivables
Value £'000 No
Value £'000 No
Value £'000 No
Less than 31 days (Not Due) 264 5 294 3 559 8
Between 31 - 60 days 16 1 23 1 38 2
Between 61 - 90 days 180 3 - - 180 3Greater than 90 days 64 1 11 1 75 2Total 524 10 328 5 853 15
Non NHS Debtors TotalNHS DebtorsAged Debtors
Key Points:
• The overall aged debtors have decreased to £853k in M11,of which £524k is not due yet.
• Over 31 days debtors have decreased to £260k, of which£64k is owed by Oxfordshire CCG. Agreement has beenreached with OCCG for settlement of this old debt and hasbeen cleared in M12.
Cash
Main Cash Drawdown To Date
£'000 £'000 £'000 £'000 £'000
298,897 33,396 332,293 368,154 90.3%
Prescribing Cash Charge
To Date
Total Cash Drawings To Date
Current Allocation
Drawings to Date as a %
of Allocation
Key Points:
• The CCG processed a cash draw down £28,664k inFebruary.
• The total drawing against prescribing to date is £33,396k.• Total cash draw down to date is £332,293k which includes
£830k CHC Risk Pool contribution • The percentage of total cash drawings charged against the
CCG overall allocation to date of £368,154 is 90.3%compared with a budget of 91.7%.
Cash forecast v actual
Page 63 of 148
Page 63 of 148

Cash Receipts £'000
Cash Expenditure
£'000Cash Receipts
£'000
Cash Expenditures
£'000
Cash Receipts
£'000
Cash Expenditur
es £'000
Net cash expenditures / receipts %
October 32,806 32,603 32,470 28,604 336 3,999 12.3%
November 29,761 29,765 28,382 27,775 1,379 1,990 7.0%
December 19,905 27,344 21,989 26,370 -2,084 974 4.4%
January 32,413 32,101 32,193 31,971 220 130 0.4%
February 31,078 31,234 32,163 32,138 -1,085 -904 -2.8%
Month
Forecast Actuals Variance
Page 64 of 148
Page 64 of 148

Payable Not Due Overdue Overdue Overdue Overdue Total
1-30 days 31-60 days 61-90 days 90+ days£'000 £'000 £'000 £'000 £'000 £'000
At 31 October 5,157 1,450 540 714 2,490 10,351
At 30 November 4,169 1,882 974 537 2,567 10,129
At 31 December 4,533 2,334 510 638 2,521 10,536
At 31 January 5,078 2,049 930 884 2,686 11,627
At 28 February 7,342 1,561 763 612 3,576 13,854
Aged Creditors - volume Nos Nos Nos Nos Nos Total Nos
At 31 October 568 346 125 177 490 1,706
At 30 November 645 282 214 109 645 1,895
At 31 December 533 432 194 186 691 2,036
At 31 January 531 281 240 169 766 1,987
At 28 February 524 237 194 137 952 2,044
Aged Creditors - valueNote: Creditors’ balances have been manually adjusted for invoices relating to future months.
Key Points: • Creditors as at 28th February stand at £13,854k, an
increase of £2,27k from previous month. • £7,342k of current creditors are not yet due for payment.• There is an increase of £890k in 90+ day’s overdue
creditors. The largest are £1,232k to Henley HealthcareLtd, £283k to Buckinghamshire County Council, £189k toFremantle Trust (The), and £149k to BuckinghamshireHealthcare NHS Trust.
BPPC
Value of invoice (YTD) £'000
Number (YTD)
Value of invoices
(YTD) £'000Number (YTD)
Value of invoice (YTD) £'000
Number (YTD)
Total invoices paid 182,988 2,727 81,556 8,881 264,544 11,608
Total invoices paid within 30 days 182,334 2,619 78,478 8,525 260,812 11,144
% Paid within 30 days 100% 96% 96% 96% 99% 96%
TotalNHS Invoices Non NHS Invoices
Better Payment Practice Code - payment within 30 days (cumulative YTD)
* 95% or more Green - 75% to 95% Amber - Less than 75% Red
The above table gives the percentage of invoices paid within a 30 day period for year to date at 28th February compared to the DoH target of 95%.
Key Points:
• Overall payments have maintained at a high level withvalue of invoices at 99% and number of invoices at 96%.
• Non NHS invoices have performed above target at 96% forvalue of invoices and above target at 96% for number ofinvoices.
• NHS invoices are above target at 100% for value ofinvoices and above target at 96% for number of invoices.
Page 65 of 148
Page 65 of 148

The graph below shows BPPC performance over the last twelve months.
Note: • Payment performance has achieved 95% DoH target in February.
Page 66 of 148
Page 66 of 148

Abbreviations and acronyms used: 2016/17 Financial Year from 1 April 2016 – 31 March 2017 k Thousand
A&E Accident and Emergency m Million
APMS Alternative Provider Medical Services MSK Musculo-Skeletal
AT Area Team MPIG Minimum Practice Income Guarantee
BPPC Better Payment Practice Code- target (currently 95% of invoices to be paid within 30 days of receipt of invoice or goods/service. NHSE NHS England
AVCCG Aylesbury Vale CCG PBR Payment By Results – payment system (based on Healthcare Resource Groups) used mainly in acute contracts
Break-even Position where actual costs are same as planned i.e. not in deficit or surplus (loss or profit) OUH Oxford University Hospitals NHS Foundation Trust
Budget A sum of money allocated for a specific purpose POD Point of Delivery – area of acute care activity of similar type (e.g. Inpatient or Outpatient)
CCG Clinical Commissioning Group PPD Prescription Pricing Department (central body that provides GP prescribing data)
CAMH Child & Adolescent Mental Health Services QIPP Quality, Innovation, Prevention and Productivity – plans and associated savings / changes in financial costs
CCGs Aylesbury Vale and Chiltern Clinical Commissioning Groups Reserves Monies set aside for a specific purpose e.g. Contingency reserves for unforeseen spend in year.
CHC Continuing Health Care RTT Referral to Treatment is the definition by which patients waiting to be treated are measured
CQUIN Commissioning Quality & Innovation Revenue Resource Limit (RRL) Total funding allocated for the year set by the Department of Health
CSU Commissioning Support Unit RBH Royal Berkshire Hospital
Deficit Financial variance where overall net costs are more than planned SCAS South Central Ambulance Service
Excess Bed Days Term used in acute contracts to describe days chargeable under PBR in excess of the standard tariff (for example a tariff might set 5 days as standard stay and days above this are charged to the CCG)
SLAM Service Level Agreement Monitoring – i.e. contract monitoring information
FPH Frimley Park Hospitals NHS Foundation Trust. STP Sustainability and Transformation Plan (now Local NHS Plan)
FOT Forecast Outturn (from 1/4/16 to 31/3/17) Surplus Financial variance where overall net costs are less than planned
FNC Funded Nursing Care Variance (Adverse) Difference against plan (overspend) GP General Practice or General Practitioner Variance (Favourable) Difference against plan (underspend)
HWPH Heatherwood & Wexham Park Hospitals NHS Foundation Trust now part of Frimley Park Hospitals FT YTD Year-to-date (from 1 April to the end of the
reported month)
HR Human Resource department (part of CSU)
Page 67 of 148
Page 67 of 148

MEETING: Governing Bodies meetings in common AGENDA ITEM: 8
DATE: 13th April 2017
TITLE: Quality and Performance Report – March 2017
AUTHORS: Adam Hooley and Lisa Beaumont
LEAD DIRECTOR:
Debbie Richards
Reason for presenting this paper: For Action For Approval For Decision For Assurance For Information
Summary of Purpose and Scope of Report:
The purpose of this report is to highlight quality and performance exceptions, and provide assurance on the actions being taken to address the issues and risks identified.
The following exceptions should be noted:-
• Cancer performance• RTT performance• A & E 4 hour wait• Ambulance response times• MRSA bacteraemia• C.Difficile
Conflicts of Interest: No conflict of interest identified.
Strategic aims supported by this paper (please tick) Better Health in Bucks – to commission high quality services that are safe, accessible to all and achieve good patient outcomes for all
Better Care for Bucks – to commission personalised, high value integrated care in the right place at the right time Better Care for Bucks – to ensure local people and stakeholders have a greater influence on the services we commission Sustainability within Bucks – to contribute to the delivery of a financially sustainable health and care economy that achieves value for money and encourages innovation Leadership across Bucks – to promote equity as an employer and as clinical commissioners
Page 68 of 148
Page 68 of 148

Governance requirements: (Please tick each box as is relevant to the paper)
Governance Element
Y N N/A Comments/Summary
Patient & Public Involvement
Equality Quality This report covers the three domains of quality (patient
safety, clinical effectiveness/patient experience) Financial Risks Risks are captured in a Quality and performance risk
register that is part of the overall risk reporting and are reviewed by the Quality and Performance Committee.
Statutory/Legal Delivery of constitutional standards for performance and quality
Prior consideration Committees /Forums/Groups
Reviewed at Executive Committee on 23rd March 2017 and circulated as part of papers to members of the Q&P Committee for the virtual meeting on 29th March 2017.
Membership Involvement
Supporting Papers:
As enclosed
Page 69 of 148
Page 69 of 148

QUALITY AND PERFORMANCE REPORT
AYLESBURY VALE CCG CHILTERN CCG
March 2017
Authors: Lisa Beaumont Adam Hooley
Paul Smith Rob Hicks
Page 70 of 148
Page 70 of 148

Page 71 of 148
Page 71 of 148
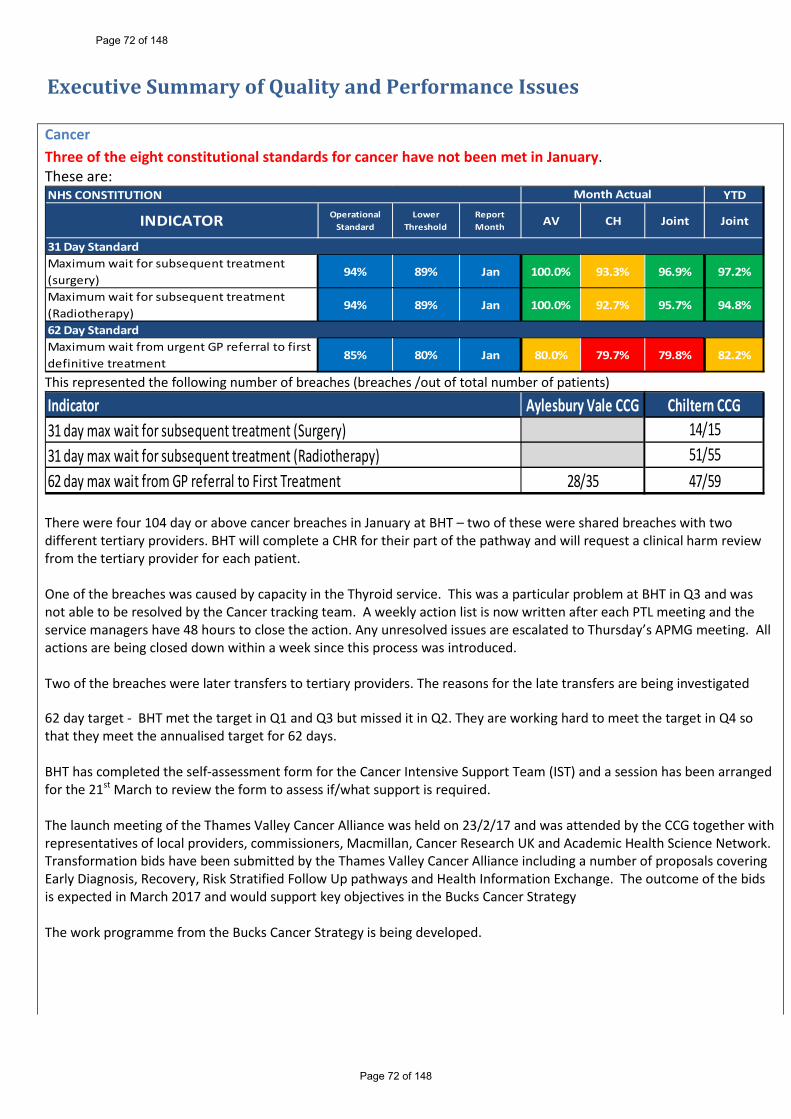
Executive Summary of Quality and Performance Issues Cancer Three of the eight constitutional standards for cancer have not been met in January. These are:
YTD
INDICATOR Operational Standard
Lower Threshold
Report Month AV CH Joint Joint
31 Day StandardMaximum wait for subsequent treatment (surgery)
94% 89% Jan 100.0% 93.3% 96.9% 97.2%
Maximum wait for subsequent treatment (Radiotherapy)
94% 89% Jan 100.0% 92.7% 95.7% 94.8%
62 Day StandardMaximum wait from urgent GP referral to first definitive treatment
85% 80% Jan 80.0% 79.7% 79.8% 82.2%
NHS CONSTITUTION Month Actual
This represented the following number of breaches (breaches /out of total number of patients)
31 day max wait for subsequent treatment (Surgery)Indicator
62 day max wait from GP referral to First Treatment
Aylesbury Vale CCG Chiltern CCG14/15
47/5928/3531 day max wait for subsequent treatment (Radiotherapy) 51/55
There were four 104 day or above cancer breaches in January at BHT – two of these were shared breaches with two different tertiary providers. BHT will complete a CHR for their part of the pathway and will request a clinical harm review from the tertiary provider for each patient. One of the breaches was caused by capacity in the Thyroid service. This was a particular problem at BHT in Q3 and was not able to be resolved by the Cancer tracking team. A weekly action list is now written after each PTL meeting and the service managers have 48 hours to close the action. Any unresolved issues are escalated to Thursday’s APMG meeting. All actions are being closed down within a week since this process was introduced. Two of the breaches were later transfers to tertiary providers. The reasons for the late transfers are being investigated 62 day target - BHT met the target in Q1 and Q3 but missed it in Q2. They are working hard to meet the target in Q4 so that they meet the annualised target for 62 days. BHT has completed the self-assessment form for the Cancer Intensive Support Team (IST) and a session has been arranged for the 21st March to review the form to assess if/what support is required. The launch meeting of the Thames Valley Cancer Alliance was held on 23/2/17 and was attended by the CCG together with representatives of local providers, commissioners, Macmillan, Cancer Research UK and Academic Health Science Network. Transformation bids have been submitted by the Thames Valley Cancer Alliance including a number of proposals covering Early Diagnosis, Recovery, Risk Stratified Follow Up pathways and Health Information Exchange. The outcome of the bids is expected in March 2017 and would support key objectives in the Bucks Cancer Strategy The work programme from the Bucks Cancer Strategy is being developed.
Page 72 of 148
Page 72 of 148

RTT Incomplete
YTD
INDICATOR Operational Standard
Lower Threshold
Report Month AV CH Joint Joint
Patients on incomplete non-emergency pathways (yet to start treatment) should have been waiting no more than 18 weeks from referral
92% 87% Jan 90.9% 91.1% 91.0% 91.7%
Patients waiting more than 52 weeks (Incomplete)
0 10 Jan 2 0 2 17
NHS CONSTITUTION Month Actual
Referral to Treatment waiting times for non-urgent consultant led treatment
The RTT Incomplete target was not met on a Bucks CCG’s basis in January (latest UNIFY data) with performance at 91.0%, with both CCGs missing the 92% target.
The BHT RTT recovery plan has yielded improvements and continues to receive focussed attention at the weekly BHT APMG. Weekend theatre lists for cataracts at BHT (in addition to the outsourcing at BMI) should further improve the situation in March.
Despite this improvement, the original trajectory showing achievement of the constitutional standard by the end of March is not being achieved. This performance was examined with BHT and it was agreed that the CCGs and BHT would amend their Operational Plan trajectory with NHSE/NHSI to show April as non-compliant. NHSE have informally notified the CCGs that there will be a further opportunity to amend trajectories on the 30th March. Should performance have improved it may be possible to change this to compliance in April.
A&E
A&E 4hr Wait YTD
INDICATOR Operational Standard
Lower Threshold
Report Month AV CH Joint Joint
Buckinghamshire Healthcare NHS Trust Feb 88.8% 90.3%Milton Keynes NHS Foundation Trust Jan 86.2% 92.3%Oxford University Hospital Jan 84.8% 86.3%Frimley Health Jan 84.7% 91.6%NHS England Jan 85.1% 89.6%
NHS CONSTITUTION Month Actual
A&E 4 Hour wait
95% 90%
The A&E 4hr wait target was not met at BHT and is not being met YTD by any local provider.
The Trust delivered a performance of 88.8% for all types in February, against the 4 hour standard of 95%. Total attendances in the month were 10,495, remaining the same as the previous month (10,500 for January). Average attendance per day for type 1 was 220, with 5 days over 240 attendances, and peaking at 267 on 6th February. 52% of all attendances this month were categorised as majors patients (reduction of 2% from January), a reduction, however, admission rate increased to 29.41% (up from 28% in January) demonstrating a further rise in acuity of major patients. On 7 days this month, the conversion rate to admission increased over 30%, and peaked at 36% in the middle of the month. The average number of admissions per day for February was 64, an increase of 3 per day from January. In line with the ambulances conveyances in the previous month, ambulance arrivals averaged at 60 per day in February.
Page 73 of 148
Page 73 of 148

A&E Longest Wait Audit BHT undertakes a monthly audit on the 10 longest waits in A&E and submits it to the Quality Team for review. The review of February’s audit showed the following:
• All patients reviewed had intentional rounding• Longest length of stay was 26 hours > down from 29 hours in January• 1 delay was a patient awaiting mental health assessment > this has improved from previous months where several
patients’ length of stay was extended due to this• Following discharge, none of the patients audited have re-attended A&E.• The longest time in hospital is 17 days – this patient remained on a medical ward throughout their stay
Ambulance Response Times YTD
INDICATOR Operational Standard
Lower Threshold
Report Month AV CH Joint Joint
Category A calls - emergency response arriving within 8 minutes (Red 1)
Jan 64.6% 60.4% 61.8% 64.3%
Category A calls - emergency response arriving within 8 minutes (Red 2)
Jan 66.3% 62.6% 64.0% 64.7%
Category A - ambulance arriving at the scene within 19 minutes
95% 90% Jan 89.5% 91.5% 90.8% 91.6%
75% 70%
NHS CONSTITUTION Month Actual
Category A ambulance calls
The Ambulance response time targets were not met in January.
At regional level SCAS continue to report on their Remedial Action Plan (RAP) at the contract review meetings (CRM). There is also a local action plan for the Buckinghamshire area at a more local level. The CCG’s Urgent Care team continue to develop and forge relationships to better understand the issues that SCAS are experiencing in the county, the resulting effect on response times and patients. The CCG Quality and Performance Committee has noted the long standing sub-standard performance and have invited SCAS to present at the March meeting on their plans to bring performance back into line, what quality issues this performance causes and how they are mitigating any such issues.
MRSA Bacteraemia At a Joint CCG level there was one MRSA case reported in February which was provisionally assigned to AV CCG. The Post Infection review (PIR) is still in progress.
C.DifficileThere were three cases over trajectory in February for the combined CCGs with Chiltern CCG four cases over target for the month. Quality and Performance Committee Update A Committee was held on 22nd February 2017. Alongside the standard agenda items, an update was received on the relaunch of the GP Clinical Concerns process, which has been live since the beginning of February, and will be reported on quarterly. Terms of Reference are currently being reviewed to reflect change in Director Portfolios. All known quality and performance risks are now on Verto.
Page 74 of 148
Page 74 of 148

Performance Commentary Cancer Three of the eight constitutional standards for cancer have not been met in January. These are:
YTD
INDICATOR Operational Standard
Lower Threshold
Report Month AV CH Joint Joint
31 Day StandardMaximum wait for subsequent treatment (surgery)
94% 89% Jan 100.0% 93.3% 96.9% 97.2%
Maximum wait for subsequent treatment (Radiotherapy)
94% 89% Jan 100.0% 92.7% 95.7% 94.8%
62 Day StandardMaximum wait from urgent GP referral to first definitive treatment
85% 80% Jan 80.0% 79.7% 79.8% 82.2%
NHS CONSTITUTION Month Actual
This represented the following number of breaches (/out of total number of patients)
31 day max wait for subsequent treatment (Surgery)Indicator
62 day max wait from GP referral to First Treatment
Aylesbury Vale CCG Chiltern CCG14/15
47/5928/3531 day max wait for subsequent treatment (Radiotherapy) 51/55
BHT met the 62 day target in Q1 and Q3 but missed it in Q2. They are working hard to meet the target in Q4 so that they meet the annualised target for 62 days. BHT has completed the self-assessment form for the IST and a session has been arranged for the 21st March to review the form to assess if/what support is required. The launch meeting of the Thames Valley Cancer Alliance was held on 23/2/17 and was attended by the CCG together with representatives of local providers, commissioners, Macmillan, Cancer Research UK and Academic Health Science Network. Transformation bids have been submitted by the Thames Valley Cancer Alliance including a number of proposals covering Early Diagnosis, Recovery, Risk Stratified Follow Up pathways and Health Information Exchange. The outcome of the bids is expected in March 2017 and would support key objectives in the Bucks Cancer Strategy The work programme from the Bucks Cancer Strategy is being developed.
Cancer - 104 Day Waiters There were four 104 day or above cancer breaches in January at BHT – two of these were shared breaches with two different tertiary providers. BHT will complete a CHR for their part of the pathway and will request a clinical harm review from the tertiary provider for each patient. One of the breaches was caused by capacity in the Thyroid service. This was a particular problem at BHT in Q3 and was not able to be resolved by the Cancer tracking team. A weekly action list is now written after each PTL meeting and the service managers have 48 hours to close the action. Any unresolved issues are escalated to Thursday’s APMG meeting. All actions are being closed down within a week since this process was introduced.
Page 75 of 148
Page 75 of 148

31 Day Subsequent Treatment – Surgery
The 31 Day Standard subsequent treatment where that treatment is ‘surgery’ target (94%) was met on a Bucks CCG’s basis in January with performance at 96.9%.
However, Chiltern CCG missed the target with performance at 93.3% this equates to 14 out of 15 patients being seen within the required standard. The one patient not seen within standard waited 38 days, the breach occurred at University College London Hospitals and was reported as ‘Capacity’.
The provider is required to inform commissioners for the reason for each breach and where this is not due to patient choice or related to the patient’s condition, the provider is required to undertake and submit a more detailed review. On completion these reports are submitted to the planned care and quality leads to inform improvement actions. This is the case for all cancer standards
31 Day Subsequent Treatment - Radiotherapy The 31 Day Standard subsequent treatment where that treatment is ‘Radiotherapy’ target (94%) was met on a Bucks CCG’s basis in January with performance at 95.7%.
However, Chiltern CCG missed the target with performance at 92.7% this equates to 51 out of 55 patients being seen within the required standard. Of the four patients not seen within standard two were ‘patient choice’, one was ‘capacity’ and one ‘unable to contact patient’. The breaches occurred at Oxford University Hospital (1); East & North Hertfordshire (2) and Royal Berkshire Hospital (1).
Page 76 of 148
Page 76 of 148

62 Day Standard Urgent GP Referral to First Treatment
The 62 Day Standard Referral to First Treatment target (85%) was not met on a Bucks CCG’s basis in January with performance at 79.8%. Year to Date the target is being missed with performance at 82.2%
Chiltern CCG missed the target with performance at 79.7% equating to 47 out of 59 patients having been seen within the required standard. Year to Date the CCG are below standard with performance at 82.7%.
Aylesbury Vale CCG missed the target with performance at 80.0% equating to 28 out of 35 patients being seen within the required standard. Year to Date the CCG are below standard with performance at 81.5%.
The days waiting (Joint CCG) for the 19 breaches are shown below.
Page 77 of 148
Page 77 of 148

Referral to Treatment (RTT) RTT Incomplete
YTD
INDICATOR Operational Standard
Lower Threshold
Report Month AV CH Joint Joint
Patients on incomplete non-emergency pathways (yet to start treatment) should have been waiting no more than 18 weeks from referral
92% 87% Jan 90.9% 91.1% 91.0% 91.7%
Patients waiting more than 52 weeks (Incomplete)
0 10 Jan 2 0 2 17
NHS CONSTITUTION Month Actual
Referral to Treatment waiting times for non-urgent consultant led treatment
The RTT Incomplete target was not met on a Bucks CCG’s basis in January (latest UNIFY data) with performance at 90.9%, with both CCGs missing the 92% target.
The BHT RTT recovery plan has yielded improvements and continues to receive focussed attention at the weekly BHT APMG. Weekend theatre lists for cataracts at BHT (in addition to the outsourcing at BMI) should further improve the situation in March.
Despite this improvement, the original trajectory showing achievement of the constitutional standard by the end of March is not being achieved. This performance was examined with BHT and it was agreed that the CCGs and BHT would amend their Operational Plan trajectory with NHSE/NHSI to show April as non-compliant. NHSE have informally notified the CCGs that there will be a further opportunity to amend trajectories on the 30th March. Should performance have improved it may be possible to change this to compliance in April.
The detailed position and actions for the major specialties:-
Page 78 of 148
Page 78 of 148

RTT: Over 52 week waiters
Aylesbury Vale CCG Incomplete Pathway: There were two breaches in January, one occurred at BHT (General Surgery) and one at Milton Keynes University Hospital (T&O). The patient at Milton Keynes University Hospital was subsequently treated in February, and the BHT patient has a treatment date of 16 March 2017.
Page 79 of 148
Page 79 of 148

A&E – Four Hour Waits The National target is 95%, the most recent A&E Performance-: • BHT - Performance in February was below standard at 88.8% (January 86.9%).• OUH – Performance in January was below standard at 84.8%.• FH – Performance in January was below standard at 84.7%.• MK- Performance in January was below standard at 86.2%NHS England performance in December was 85.1%.
Please note: A&E Data for BHT is more recent than for other Providers as the Trust submits data on a weekly basis to the CCGs.
Buckinghamshire Hospital Trust - BHT
The Trust delivered a performance of 88.8% for all types in February, against the 4 hour standard of 95%. The 88.8% all type performance was a 5.5% adverse variance to plan (94.3%) however; this was a 1.9% increase on January performance. February’s improved performance has also positively impacted on year to date performance which is now 90.3%.Total attendances in the month were 10,495, remaining the same as the previous month (10,500 for January). Average attendances per day for type 1 were 220, with 5 days over 240 attendances, and peaking at 267 on 6th February. 52% of all attendances this month were categorised as majors patients (a reduction of 2% from January), however, the admission rate increased to 29.41% (up from 28% in January) demonstrating a further rise in acuity of major patients. On 7 days during the month of February, the conversion rate to admission increased over 30%, and peaked at 36% in the middle of the month. The average number of admissions per day for February was 64, an increase of 3 per day from January. In line with the ambulances conveyances in the previous month, ambulance arrivals averaged at 60 per day in February.
The delayed transfers of Care (DTOCs) in February averaged at 17 throughout the month, peaking at 21. In the community, Adult Community healthcare teams (ACHT) consistently had 13-15% of capacity restricted by transfer of care waits. The consistently high acuity resulted in ITU having limited capacity throughout the month, and the number of medical outliers increasing.
The demand for both medical and surgical admissions this month resulted in the Trust utilising escalation beds throughout the month for patients expected to be discharged within 48 hours. St Josephs was utilised for medical patients and as discharge lounge, whilst SAU and the Day Surgery Unit were also utilised to accommodate non-complex patients. On one occasion this month (3rd February), the Trust declared an OPEL level 4 status. Command and control was put in place, alongside a number of system wide actions including representation on site from the Continuing healthcare (CHC) team, and also system calls with Hertfordshire to expedite discharges to these providers. Medical,
Page 80 of 148
Page 80 of 148

Nursing, Therapy and Operational support was also increased and allocated to support at both the front door and on the wards. During the month of February BHT through their three work streams (Flow from the Wards, Care Closer to Home and the Emergency Access Performance Management Group) have delivered the following actions which form the basis of their trajectory to achieve overall A & E improvement performance:
• Wards 8 and 9 were given support to accelerate their application of the SAFER, discharge planning and multi-agency daily discharge meeting
• Data now being collected and assessed on Expected Discharge dates (EDD), transport, discharges under 12 hours and Length of Stay (LoS). The data for EDD’s have had a positive impact on pre-planned discharges and reducing on the day booking for Non-emergency transport services with the average for February being 30%, a significant increase from the January performance of 16.4%
Further actions that BHT are working to include:
• Exploring expanded roles for ED clinicians working in the Ambulatory Emergency Care (AEC) unit and testing the
ability to run co-located surgical ambulatory care service. • Progress the Community transformation actions to establish the Rehabilitation, Re-ablement and Intermediate
Care team support from community hospitals • A frailty service review is being undertaken as part of the integrated model including Mudas, A&E streaming and
the community hospital reconfiguration. The CCG also continues to work with cross county partners and continue to ensure that there are levels of support in place (particularly to our East Berkshire Frimley system colleagues) to effectively encourage and support the safe and appropriate repatriation of patients across neighbouring counties. The system wide A & E delivery board discussed the importance of assuring plans are in place for the Easter period and an Easter readiness plan will be discussed at March A & E delivery board meeting before sign off in April. Oxford University Hospitals NHS Foundation Trust – OUH
The Trust has produced an urgent care action plan to address poor A&E performance and a corresponding improvement trajectory. This will be led by Oxfordshire CCG as the lead commissioner with Buckinghamshire involved as an associate.
SCAS Ambulance Response Times The Ambulance response time targets were not met in January. SCAS continue to report on their Remedial Action Plan (RAP) at regional level at the contract review meetings (CRM) and a local action plan for the Bucks area at a more local level. The CCG Quality and Performance Committee has noted the long standing sub-standard performance and have invited SCAS to present at the March meeting on their plans to bring performance back into line, what quality issues this performance causes and how they are mitigating any such issues. The CCG (and Urgent Care team in particular) continue to develop and forge these relationships to better understand the issues that SCAS are experiencing in the county and the effect on response times and on patients. SCAS actions:
• Continue to work to achieve on the agreed actions with the local action plan which is tracked at regular CCG hosted meetings and through their RAP which has identified a number of actions they are working to including:
• Greater operational onsite support has been agreed with Operational leads to provide additional hours and resource for onsite responses
• The standby points for Aylesbury and North of the county are currently being re-configured with aim to reduce length of response by up to 3% and ensure that the stand by points are more strategically positioned to meet the
Page 81 of 148
Page 81 of 148

demand in that area • Continue to work with CCGs and OOHs providers to improve GP call backs and to implement trusted assessor
(Specifically Paramedics) so crews can refer and leave without speaking to a GP• Individual outlier performance reviews for on scene and clear up delays• Implement one way taxi option transport for low acuity patients after crew assessment• Work continues with Buckinghamshire Healthcare Trust (BHT) to address the handover delays that have a direct
impact on SCAS performance and crews being able to leave the hospital to pick up other jobs in the community(see also CCG actions) and there have been improvements noted in this area.
CCG and System actions: • Commissioners continue to meet with colleagues from SCAS to work through the local action plan for Bucks
which aims to address the key issues which have been a challenge locally. It should be noted that whilst overdemand has increased from the previous year performance has remained relatively static and not deterioratedas is the case with other ambulance providers nationally
• SCAS continue to work towards achieving their agreed trajectory’s for each of the areas within the Thames Valleyregion including Buckinghamshire and to support the improvements through the action plan.
• Data has been gathered which highlights practices who have a low threshold for accepting patients following GPtriage and the CCG will be working closely with those practices and SCAS to help understand the reasons forthis, as quite often this will result in a hospital attendance and possible admission
• The CGG hosted a meeting between SCAS and BHT to agree a process to improve the current hand over delaysthat are being reported at Stoke Mandeville Hospital. The Emergency Care Improvement Programme (ECIP) teamwere also present to support the meeting and help deliver the rapid improvement guidelines (RIG). The findingsconcluded that although many of the processes, escalations points and culture within the A & E (in relation toworking relationship with SCAS) have significantly progressed there remains spatial and infrastructurechallenges.
Additional support is being provided by NHSE as and when required and the CCG has also been liaising with ECIP to agree support levels to address hand over delays.
Category A8 Minute Response Time – RED 1 (Target 75%): The target was not met in January for both Aylesbury Vale and Chiltern CCG’s with a Joint CCG performance of 61.8%. At Thames Valley level the target was not met in January. Performance at Thames Valley level has fallen from 75.5% in April to 73.9% in January. YTD performance is below target at 72.5%.
Page 82 of 148
Page 82 of 148

Category A8 Minute Response Time – RED 2 (Target 75%): The target was not met in January for both Aylesbury Vale and Chiltern CCG’s with a Joint CCG performance of 64.0%. At Thames Valley level the target was not met in January. Performance has fallen from 76.2% in April to 73.1% in January. YTD performance is below target at 73.4%.
Category A19 Minute Transportation Time (Target 95%):
The target was not met in January for both Aylesbury Vale and Chiltern CCG’s with a Joint CCG performance of 90.8%. At Thames Valley level the target was missed in January with performance at 94.2%, YTD performance remains just below target at 94.4%.
Page 83 of 148
Page 83 of 148

Page 84 of 148
Page 84 of 148

AV CCG Red 1 Long Waits
Chiltern CCG Red 1 Long Waits
These charts show the length of wait for those patients for whom the target is not met. There were no waits over 30 minutes.
Page 85 of 148
Page 85 of 148

Dementia Diagnosis Rate Dementia is a national and local priority, with Chiltern CCG currently ranked in the lowest quartile of CCGs for dementia diagnosis (difference between expected and actual diagnosis rates).
The Dementia Diagnosis Rate in Chiltern CCG improved in February with performance at 62.4%, (January 61.6%), against the national target of 66.7%.
The Clinical Director for Mental Health continues to proactively lead Chiltern CCG’s recovery plan to realise a significant increase in its overall diagnostic performance. Changing some GPs’ perceptions as to "why diagnose" is a challenge and this is reflected within the significant variance in individual practices performance i.e. those practices performing under 40% compared to those practices performing over 80%. The Clinical Chair and Clinical Director have been attending public engagement events to support the raising awareness of dementia and the importance of an early diagnosis.
Key new initiatives include:
• Locality managers are raising dementia and diagnostic rates at every Locality Meeting and offering support inimplementing the various tool kits if need be. Practice level dashboards are being provided at every practice visitand individual practice issues discussed. I.e. if the practice has no care homes, help is provided to develop anindividual practice level improvement plan.
Mental Health Care Programme Approach
The Quarterly Measure for Care Programme Approach (CPA) is: The proportion of people under adult mental illness specialities on CPA who were followed up within 7 days of discharge from psychiatric inpatient care during the period.
The CPA target (95%) was met on a Bucks CCG’s basis in Quarter 3 with performance at 95.9%. However YTD Chiltern CCG is missing the target with performance at 93.9%.
Page 86 of 148
Page 86 of 148

2016/17
CCG AV CCG C CCGBucks CCG's AV CCG C CCG
Bucks CCG's AV CCG C CCG
Bucks CCG's AV CCG C CCG
Bucks CCG's
Number on CPA 28 55 83 38 62 100 30 40 70 95 153 248
Number Followed-Up within 7 days
27 51 78 38 66 104 31 42 73 97 163 260
Performance (standard 95%)
96.4% 92.7% 94.0% 100.0% 93.9% 96.2% 96.8% 95.2% 95.9% 97.9% 93.9% 95.4%
Q1 Q2 Q3 YTD
Q3 figures are provis ional and may be subject to change, i f this occurs the table wi l l be updated in next month's report.
Risk Assessment (Adult)
All patients on a Care Programme Approach (CPA) to have a documented risk assessment (target 100%). At a joint CCG level the target was not met in February with performance at 93%. Year to Date, both Aylesbury Vale and Chiltern CCG’s are falling short of the target with performance at 98.2% and 98.6% respectively.
Apr-16 May-16 Jun-16 Jul-16 Aug-16 Sep-16 Oct-16 Nov-16 Dec-16 Jan-17 Feb-17 YTD
bumerator 20 20 20 20 20 20 19 20 20 20 17 216Denominator 20 20 20 20 20 20 20 20 20 20 20 220Percentage 100% 100% 100% 100% 100% 100% 95% 100% 100% 100% 85% 98.2%bumerator 20 19 19 19 20 20 20 20 20 20 20 217Denominator 20 20 20 20 20 20 20 20 20 20 20 220Percentage 100% 95% 95% 95% 100% 100% 100% 100% 100% 100% 100% 98.6%bumerator 40 39 39 39 40 40 39 40 40 40 37 433Denominator 40 40 40 40 40 40 40 40 40 40 40 440Percentage 100% 98% 98% 98% 100% 100% 98% 100% 100% 100% 93% 98.4%
2016-17Documented Risk
Assessment
Adult C CCG
Bucks CCG's
Adult AV CCG
Crisis Contingency Plan - Monthly (Adult)
All patients on a Care Programme Approach (CPA) have a crisis contingency plan (target 95%). At a joint CCG level the target was not met in February with performance at 93%. Aylesbury Vale CCG missed the target with performance at 94%. Chiltern CCG missed the target with performance at 93%. Year to Date both Aylesbury Vale and Chiltern CCG are missing the target.
Page 87 of 148
Page 87 of 148

Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb YTDbumerator 302 302 307 310 314 315 321 328 330 330 338 3497Denominator 334 345 337 340 338 339 338 354 359 368 361 3813Percentage 90% 88% 91% 91% 93% 93% 95% 93% 92% 90% 94% 92%bumerator 546 553 550 542 558 603 624 645 656 638 614 6529Denominator 609 615 611 602 622 603 664 679 696 670 658 7029Percentage 90% 90% 90% 90% 90% 100% 94% 95% 94% 95% 93% 93%bumerator 848 855 857 852 872 918 945 973 986 968 952 10026Denominator 943 960 948 942 960 942 1002 1033 1055 1038 1019 10842Percentage 90% 89% 90% 90% 91% 97% 94% 94% 93% 93% 93% 92%
Adult MH AV CCG
Adult MH C CCG
Bucks CCG's
2016-17Crisis Contingency Plan
Transforming care for People with Learning Disabilities
The Transforming Care Programme aims to improve services for people with learning disabilities and/or autism (including those without a learning disability), who display behaviour that challenges, including those with a mental health conditions. Monthly reporting to NHSE is through the Health and Social Care Information Centre (HSCIC) and is used to monitor inpatient flow of this cohort. Inpatients that are included in the monitoring/reporting meet the definition above and are adults and children. All children are admitted to inpatient facilities by Specialist Commissioners (who also fund these placements). All other inpatient admissions are by agreement with the CCGs commissioners and funding is by the Buckinghamshire CCGs.
Specialist Learning Disability inpatient beds are at the Dove Ward, Kingfisher Court, Kingsley Green Radlett (HPFT) – block contract of 4 beds Mental Health inpatient beds are at Whiteleaf Centre, Bierton Rd, Aylesbury (OHFT) – individuals with mental health conditions who do not have a learning disability, but do have a diagnosis of Autism/Asperger’s
Additionally, the CCGs may fund inpatient beds within the private sector out of the area; if local contracted beds are not clinically appropriate
In December 2016 a further 8 individuals (CCG and Spec Comm funded) were identified by NHSE as Buckinghamshire patients who meet the criteria of the Transforming Care reporting – those with no diagnosis of a learning disability.
Transforming Care - current inpatients as at 1st March 2017. Current inpatient AV CCG C CCG Joint CCG Acute mental Health 1 1 2 Specialist Out of Area 2 2 4 Specialist Learning Disability 0 3 3
Total 3 6 9
Page 88 of 148
Page 88 of 148
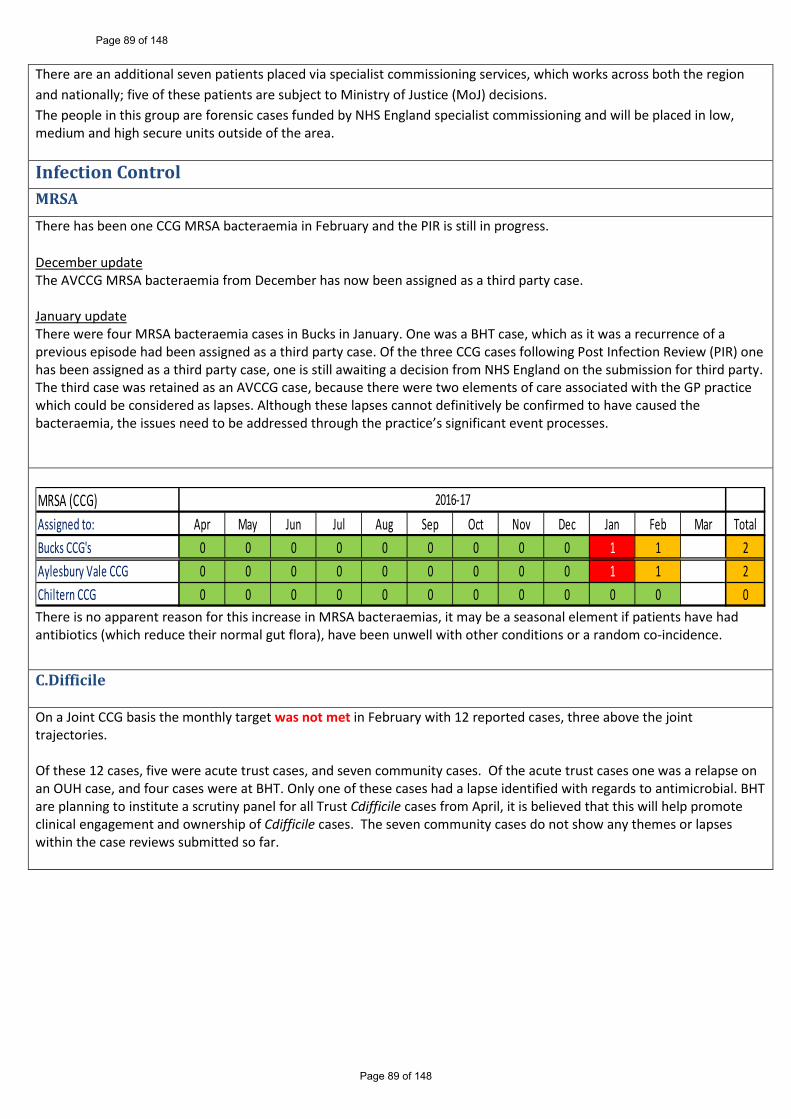
There are an additional seven patients placed via specialist commissioning services, which works across both the region and nationally; five of these patients are subject to Ministry of Justice (MoJ) decisions. The people in this group are forensic cases funded by NHS England specialist commissioning and will be placed in low, medium and high secure units outside of the area.
Infection Control MRSA There has been one CCG MRSA bacteraemia in February and the PIR is still in progress.
December update The AVCCG MRSA bacteraemia from December has now been assigned as a third party case.
January update There were four MRSA bacteraemia cases in Bucks in January. One was a BHT case, which as it was a recurrence of a previous episode had been assigned as a third party case. Of the three CCG cases following Post Infection Review (PIR) one has been assigned as a third party case, one is still awaiting a decision from NHS England on the submission for third party. The third case was retained as an AVCCG case, because there were two elements of care associated with the GP practice which could be considered as lapses. Although these lapses cannot definitively be confirmed to have caused the bacteraemia, the issues need to be addressed through the practice’s significant event processes.
Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Total0 0 0 0 0 0 0 0 0 1 1 20 0 0 0 0 0 0 0 0 1 1 20 0 0 0 0 0 0 0 0 0 0 0
2016-17MRSA (CCG)Assigned to:Bucks CCG's Aylesbury Vale CCGChiltern CCGThere is no apparent reason for this increase in MRSA bacteraemias, it may be a seasonal element if patients have had antibiotics (which reduce their normal gut flora), have been unwell with other conditions or a random co-incidence.
C.Difficile
On a Joint CCG basis the monthly target was not met in February with 12 reported cases, three above the joint trajectories.
Of these 12 cases, five were acute trust cases, and seven community cases. Of the acute trust cases one was a relapse on an OUH case, and four cases were at BHT. Only one of these cases had a lapse identified with regards to antimicrobial. BHT are planning to institute a scrutiny panel for all Trust Cdifficile cases from April, it is believed that this will help promote clinical engagement and ownership of Cdifficile cases. The seven community cases do not show any themes or lapses within the case reviews submitted so far.
Page 89 of 148
Page 89 of 148
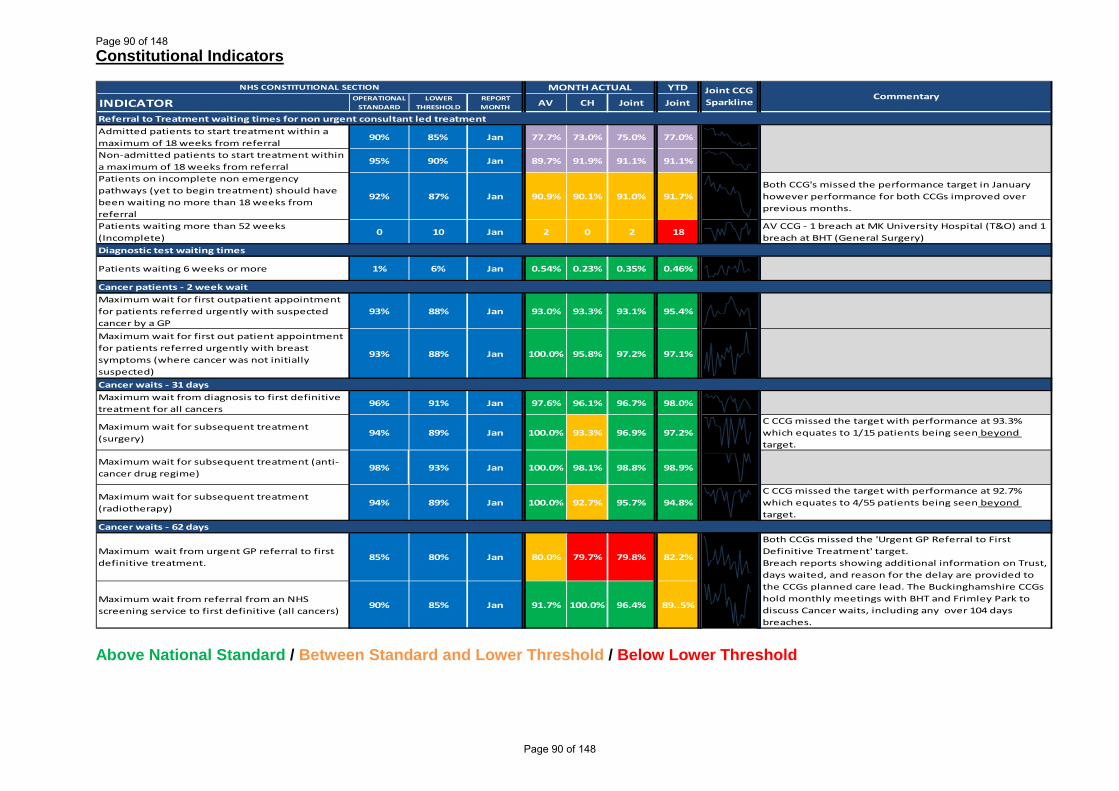
Constitutional Indicators
INDICATOR OPERATIONAL STANDARD
LOWER THRESHOLD
REPORT MONTH AV CH Joint Joint
Admitted patients to start treatment within a maximum of 18 weeks from referral
90% 85% Jan 77.7% 73.0% 75.0% 77.0%
Non-admitted patients to start treatment within a maximum of 18 weeks from referral
95% 90% Jan 89.7% 91.9% 91.1% 91.1%
Patients on incomplete non emergency pathways (yet to begin treatment) should have been waiting no more than 18 weeks from referral
92% 87% Jan 90.9% 90.1% 91.0% 91.7%Both CCG's missed the performance target in January however performance for both CCGs improved over previous months.
Patients waiting more than 52 weeks (Incomplete)
0 10 Jan 2 0 2 18AV CCG - 1 breach at MK University Hospital (T&O) and 1 breach at BHT (General Surgery)
Patients waiting 6 weeks or more 1% 6% Jan 0.54% 0.23% 0.35% 0.46%
Maximum wait for first outpatient appointment for patients referred urgently with suspected cancer by a GP
93% 88% Jan 93.0% 93.3% 93.1% 95.4%
Maximum wait for first out patient appointment for patients referred urgently with breast symptoms (where cancer was not initially suspected)
93% 88% Jan 100.0% 95.8% 97.2% 97.1%
Maximum wait from diagnosis to first definitive treatment for all cancers
96% 91% Jan 97.6% 96.1% 96.7% 98.0%
Maximum wait for subsequent treatment (surgery)
94% 89% Jan 100.0% 93.3% 96.9% 97.2%C CCG missed the target with performance at 93.3% which equates to 1/15 patients being seen beyond target.
Maximum wait for subsequent treatment (anti-cancer drug regime)
98% 93% Jan 100.0% 98.1% 98.8% 98.9%
Maximum wait for subsequent treatment (radiotherapy)
94% 89% Jan 100.0% 92.7% 95.7% 94.8%C CCG missed the target with performance at 92.7% which equates to 4/55 patients being seen beyond target.
Maximum wait from urgent GP referral to first definitive treatment.
85% 80% Jan 80.0% 79.7% 79.8% 82.2%
Maximum wait from referral from an NHS screening service to first definitive (all cancers)
90% 85% Jan 91.7% 100.0% 96.4% 89..5%
Cancer waits - 62 days
Referral to Treatment waiting times for non urgent consultant led treatment
Cancer patients - 2 week wait
Cancer waits - 31 days
Both CCGs missed the 'Urgent GP Referral to First Definitive Treatment' target.Breach reports showing additional information on Trust, days waited, and reason for the delay are provided to the CCGs planned care lead. The Buckinghamshire CCGs hold monthly meetings with BHT and Frimley Park to discuss Cancer waits, including any over 104 days breaches.
Diagnostic test waiting times
NHS CONSTITUTIONAL SECTION MONTH ACTUAL YTD Joint CCG Sparkline
Commentary
Above National Standard / Between Standard and Lower Threshold / Below Lower Threshold
Page 90 of 148
Page 90 of 148

INDICATOR OPERATIONAL STANDARD
LOWER THRESHOLD
REPORT MONTH AV CH Joint Joint
For guide to full commentary please see reference page.
Care Programme Approach (CPA): The proportion of people under adult mental illness specialities on CPA followed up within 7 days of discharge from psychiatric inpatient care during the period
95% 90%Q3
2016/1796.8% 95.2% 95.9% 95.4%
Care Programme Approach (CPA): The proportion of people under adult mental illness specialities on CPA followed up within 7 days of discharge from psychiatric inpatient care during the period (Monthly) (Adult)
Feb 92% 88% 89% 93%Both CCG's failed to achieve the 95% target. AV CCG - 11 out of 12 were followed-up within 7 days. C CCG - 22 out of 25 were followed-up within 7 days.
Care Programme Approach (CPA): The proportion of people under adult mental illness specialities on CPA followed up within 7 days of discharge from psychiatric inpatient care during the period (Monthly) (Older Adult)
Feb 100% 100% 100% 100%
All patients on CPA have a documented risk assessment (Adult)
85% 100% 93% 98%In the first eleven months of this year 433 out of 440 patients have had a documented risk assessment.
All patients on CPA have a documented risk assessment (Older Adult)
100% 100% 100% 100%
Patients on CPA have a crisis contingency plan (Adult)
94% 93% 93% 92%In February 952 out of 1019 Adult patients on CPA had a crisis contingency plan.
Patients on CPA have a crisis contingency plan (Older Adult)
97% 95% 96% 98%
The proportion of people that enter treatment against the level of need in the general population (the level of prevalence addressed or ‘captured’ by referral routes)
16% by quarter 4
Feb 17% 16% 16% 18%
The proportion of people who complete treatment who are moving to recovery.
50.0% Feb 63% 61% 62% 60%
People that wait 6 weeks or less from referral to entering a course of IAPT treatment against the number of people who finish a course of treatment in the reporting period"
50% Feb 99% 100% 100% 98%
People that wait 18 weeks or less from referral to entering a course of IAPT treatment against the number of people who finish a course of treatment in the reporting period"
75% Feb 100% 100% 100% 100%
Transforming Care (Patients placed via Specialist Commissioning Services)
Feb 7 7
Mental Health - Improving Access to Psychological Therapy (IAPT)
Learning Disabilities
YTD
Mental Health
Sparkline CommentaryMONTH ACTUAL
Feb
95%
NHS CONSTITUTIONAL SECTION
90%
100% Feb
95%
Above National Standard / Between Standard and Lower Threshold / Below Lower Threshold
Page 91 of 148
Page 91 of 148

INDICATOR OPERATIONAL STANDARD
LOWER THRESHOLD
REPORT MONTH AV CH Joint Joint
For guide to full commentary please see reference page.
Dementia Diagnosis rate 66.7% Feb 69.9% 62.4% 65.1% 65.1%Chiltern have a recovery trajectory, and performance has been showing a steady improvement.
NHS England Jan 85.1% 89.6%
Buckinghamshire Healthcare NHS Trust Feb 88.8% 90.3%
The CCG has worked with BHT to produce a recovery against trajectory and actions. The A&E performance will be monitored through the newly established A&E delivery board which identifies the 4 hour target as the priority and will focus soley on Urgent & Emergency Care. The CCG will work closely with the Trust and through the A&E delivery board aim to ensure improved performance against trajectory.
Milton Keynes NHS Foundation Trust Jan 86.2% 92.3%
Oxford University Hospital Jan 84.8% 86.3%The Trust has produced an urgent care action plan and a corresponding improvement trajectory.
Frimley Health Jan 84.7% 91.6%
Category A calls - emergency response arriving within 8 minutes (Red 1)
Jan 64.6% 60.4% 61.8% 64.3%
Category A calls - emergency response arriving within 8 minutes (Red 2)
Jan 66.3% 62.6% 64.0% 64.7%
Category A - ambulance arriving at the scene within 19 minutes
95% 90% Jan 89.5% 91.5% 90.8% 94.2%
Breaches of Mixed Sex Accommodation 0 10 Jan 0 0 0 3
Incidence of healthcare associated infection MRSA
Feb 1 0 1 2 A Post Infection Review (PIR) is in progress. .
Incidence of healthcare associated infection C. Difficile
Feb 3 9 12 94 Chiltern CCG was 4 cases over monthly target.
Category A ambulance calls
YTD
Dementia Diagnosis
95%
Sparkline Commentary
Outcomes - Safety
Yearly Target Joint 110
Yearly Target - 0
NHS CONSTITUTIONAL SECTION
Mixed Sex Accommodation
75% 70%
90%
All three targets were missed at CCG level and at Thames Valley level. SCAS continue to report on their Remedial Action Plan (RAP) at regional level at the contract review meetings, and a local action plan for the Bucks area at a more local level.
A&E 4hr Wait
MONTH ACTUAL
Spark lines – most spark lines show 12 months of data Above National Standard / Between Standard and Lower Threshold / Below Lower Threshold
Page 92 of 148
Page 92 of 148

Quality Commentary Safeguarding Serious Case Review The serious case review (SCR) for Baby M which was completed by the Buckinghamshire Safeguarding Children Board (BSCB) in May 2016 is finally going to be published on the BSCB website on Friday 17th March; publication was delayed due to the on-going criminal proceedings. The SCR relates to a 16 week old baby who suffered serious injuries in November/December 2014 and subsequently father received a custodial sentence for causing a child unnecessary harm, and the mother a suspended custodial sentence and a community order for neglect. Learning for health in this case centred around poor planning in the pre-birth period and improving the understanding of thresholds for intervention. Significant work has been undertaken to improve the understanding of thresholds across the partnership and there is now increasing evidence from internal and external audit that this has improved.
Stroke East Berkshire Stroke Pathway Update The East Berkshire Interim Stroke Service has now been operational for 2 months.
Wycombe Hospital There have been no reported incidents or issues since the mobile scanner was installed towards the end of January 2017. The mobile scanner will be returned as soon as the new scanner is operational. The timeline for the new scanner to be in situ and operational is still on track for the 1st June 2017. During February Northwick Park Hospital indicated they could only accept stroke patients within the 4 hour thrombolysis window; Wycombe agreed to accept those patients outside of the 4 hour window.
The implementation of the new stroke service is progressing well and the Trust is still on target to have the additional HASU unit capacity on stream on the 1st May 2017.
Wexham Park Hospital During February, WPH continued to be challenged in admitting rehabilitation patients in a timely way which resulted in some transfer delays to other providers. The WPH team has committed to focus on streamlining their internal clinical review and discharge processes to improve patient flow. The rehabilitation service is now fully operational 7 days a week, and it is expected that access to weekend rehabilitation and therapy input to patients will also contribute to overall patient flow. New admissions criteria and protocols have been agreed as it was acknowledged that some HASU providers had not been including the necessary assessments and paperwork when discharging patients to WPH.
The current contract to provide support services and 6 months reviews to all stroke survivors across Slough will be ending on the 31st March 2017. The East Berkshire CCG’s and the Local Authorities are in the process of reviewing all the service specifications and re-procuring these services across East Berkshire. In order to deliver an equitable service across East Berkshire both health and social have agreed to work together to ensure that there is a collaborative approach to commissioning a single service that will be in place from 1st October 2017. In the interim we will work with the Stroke Association to ensure an equitable interim service for all stroke survivors.
Monitoring All providers reported that the stroke activity has been lower than anticipated. Activity figures for January and February 2017 are shown in the table below. The operational implementation meetings are still continuing on a fortnightly basis.
Page 93 of 148
Page 93 of 148

Stroke Activity
Provider Normal and Agreed AdditionalActivity (Per Month)
Provider Activity January 17
Provider Activity February 17
Under/Over - YTD
Activity Variance Activity Variance BHT 28 28 0 27 -1 -1
ASPH 9 4 -5 4 -5 -10RBH 10 9 -1 4 -5 -4FPFT 21 17 -4 6 -15 -19Total 67 58 -9 39 -26 -34
MKUFT Stroke Service Due to the bed pressures faced by the Trust in February, there was often not a ring-fenced bed for stroke available leading to the performance taking a downward trend despite appropriate measures taken to meet the increased demand for beds - this included medical patients having to be moved off the stroke unit to create a bed, which is time consuming and often difficult considering that all medical beds were full. MK CCG has confirmed that outlying patients who are awaiting a bed on the stroke unit have commenced the stroke pathway and the stroke consultants visit them on the outlying wards.
Overall the Trust SSNAP performance has improved from ‘D’ to ‘C’.
In terms of stoke performance measures detailed in the quality schedule targets relating to spending 90% of time on the stroke unit, admission to the stroke unit within 4 hours of arrival in A&E and transferring patients for HASU to MKUFT ASU have not been met in February. The Trust has cited demand for medical admissions as the main reason for this underachievement. Two beds are ring-fenced in the stroke unit; however the ring-fencing is broken at the time of an 11 hour trolley wait. The volume of A&E activity and number of medical outliers impacted on the achievement of all 3 of these targets.
The Trust has appointed a ‘stroke champion’ in A&E to support the functions of the Stroke Advanced nurse practitioner. Linked to this the Trust is working towards stroke patients having a CT scan within one hour of admission. CT scan capacity is in place delivered through a responsive team. The Trust is working on requesting scans at the time of diagnosis.
Physiotherapy services are running 7 days per week and OT services 6 days per week. Challenges remain in relation to SALT services. Although the trust has reviewed the contract with the SALT service provider, they have been unable to recruit into either a substantive of locum post.
TIA services continue to cause concern. High risk patients are reviewed at Northampton at weekends, however some patients prefer to wait until Monday to attend MKUH. It was agreed at CQRM that the reasons for low risk TIA patients not attending scanning appointments would be explored.
MK CCG continues to monitor the Trust against an improvement action plan, which the Trust is reviewing to include trajectories and timescales. An action relating to cardiac monitoring and the use of telemetry has not been implemented as yet.
Source: MK CCG
Continuing Healthcare Reviews Arden and Gem continuing healthcare team are conducting a review of Seeley’s house week
Page 94 of 148
Page 94 of 148

commencing 20th March 2017. A member of the CCG quality team is participating in the review. All families involved in accessing Seeley’s house are being regularly communicated with by the Continuing Healthcare Team, day services have been provided where access has not been available to this respite service. Oxford Health NHS Foundation Trust A detailed review of the Quarter 2 and Quarter 3 submission for CQUIN have been completed for Oxford Health NHS Foundation Trust, the Trust has until the 27th March 2017 to submit a response to the Buckinghamshire CCGs. At the February 2017 contract meeting the Head of Quality raised a number of quality queries with the Trust related to performance standards, and to ascertain if any quality issues were present as a result of the performance achieved. The Buckinghamshire CCGs received re assurance that there were no issues in terms of quality of care for the related patients identified in the performance breaches. Feedback had been provided prior to the contracting meeting by the Head of Quality to enable the trust to conduct a review of the patients affected.
Page 95 of 148
Page 95 of 148

INDICATOR PROVIDER
FREQ
UEN
CY
THRESHOLDCURRENT PERIOD
CURRENT VALUE
TREND
STROKE
BHT M 80% Jan-17 94%
OUHFT M 85% Jan-17 84%
MKUFT M 85% Jan-17 84%
BHT M 95% Jan-17 80%
OUHFT M 85% Jan-17 82%
MKUFT M 90% Jan-17 69%
FHFT M 72% Jan-17 63%
Thrombolysis Stroke - (Door to Needle) <60 Minutes
BHT M 80% Jan-17 83%
SERIOUS INCIDENTS
BHT M - Feb-17 3OHFT M - Feb-17 0FPH M - Feb-17 2
HWPH M - Feb-17 0OUHFT M - Feb-17 7SCAS M - Feb-17 0
BHT M 0 Feb-17 0
OHFT M 0 Feb-17 0
FPH M 0 Feb-17 0
HWPH M 0 Feb-17 0
OUHFT M 0 Feb-17 0
All SIs logged
All Never Events Logged
SERIOUS INCIDENTS
COMMENT
% pts spent >90% of time SU 41/49 patients spent 90% on SU
11/13 Patients spent 90% on SUThe CCG has reviewed MKFT's Stroke Action plan but is requesting further assurance from MKCCG around when stroke targets will start to recover
STROKE
% pts admitted to SU <4hrs
Although the target was not met, patients were started on the Stroke Pathway regardless of the ward
40/49 were admitted within 4hoursPatients were started on Stroke Pathway regardless of the ward
9/13 Patients admitted within 4 hours - all patients were started on Stroke Pathway regardless of the ward
See Stroke Section of this report for further narrative
22%72% 63% 56% 72%
53% 58% 25%63% 69%
82% 92% 84% 85% 70% 63% 83% 68% 82% 80%
70% 72% 78% 71% 80% 83% 77%92% 89%
82%
60%88%
71% 60% 68% 70% 74% 82% 72% 63%
94% 94% 91%100%
88% 91% 93% 91% 90% 94%
90% 87% 89% 95% 96% 98% 96% 100% 96% 84%
44%89% 95% 89% 95% 84% 92% 75% 89% 84%
0
10
20
BHT OHFT FPFT HWPFT OUH
0
2
4
BHT OHFT FPFT HWPFT OUH
100%73% 75% 64%
100%71% 88% 56% 91% 83%
Quality Dashboard Page 96 of 148
Page 96 of 148

INDICATOR PROVIDER
FREQ
UEN
CY
THRESHOLDCURRENT PERIOD
CURRENT VALUE
TREND
BHT M - Feb-17 0OHFT M - Feb-17 0FPH M - Feb-17 1
HWPH M - Feb-17 0OUHFT M - Feb-17 1
MATERNITY
BHT M 26.5% Jan-17 28.7%
MKUFT M 26% Jan-17 30.8%
HWPH M 26% Jan-17 29.1%
BHT M - Jan-17 20.0%
MKUFT M - Jan-17 17.3%
BHT M - Jan-17 10.2%
MKUFT M - Jan-17 13.5%
SAFETY THERMOMETER
BHT M - Feb-17 97.5%
MKUFT M - Feb-17 99.1%
FHFT M - Feb-17 97.5%
OUHFT M - Feb-17 97.2%
BHT M - Feb-17 1.1%
MKUFT M - Feb-17 0.7%
FHFT M - Feb-17 1.0%
OUHFT M - Feb-17 0.2%
This has changed from 'harm free' to 'New Harm Free' as New Harm Free is a more accurate representation of how likely harm is to
occur to any given patient receiving treatment at a provider
C-Section Rate - Elective
C-Section Rate - Emergency
Slips/trips/falls
MATERNITY
SAFETY THERMOMETER
COMMENT
C-Section Rate - Combined
New Pressure Ulcers -
% of patients with NEW Pressure Ulcers
NEW Harm Free Care-
% of patients with no harm
0
10
BHT OHFT FPFT HWPFT OUH
32.5% 29.1%33.8%
25.7% 27.9% 26.2% 27.0% 27.3% 27.6% 28.7%
26.7% 25.5% 31.6% 26.7% 26.3% 30.3% 28.9% 32.4% 32.9% 29.1%
27.3%32.7%30.4%30.9%28.9%27.0%29.4%29.2%25.8%30.8%
18.9%21.7%18.7%21.3%17.9%17.3%19.9%18.8%13.5%17.3%
0.98%
0.97%
BHT OUH FHFT (HWP) MKFT
97.84% 97.84%
BHT OUH
FHFT (HWP) MKFT
National Average
20.0% 16.7%23.0%
8.6% 11.2% 9.3% 10.5% 11.8% 9% 10%
8.4% 11.0% 11.7% 9.6% 11.0% 9.7% 9.5% 10.4% 8.9%13.5%
12.5% 12.4% 10.8% 17.1% 16.7% 16.8% 16.5% 15.5% 18% 20%
Page 97 of 148
Page 97 of 148

INDICATOR PROVIDER
FREQ
UEN
CY
THRESHOLDCURRENT PERIOD
CURRENT VALUE
TREND
WORKFORCE
BHT MiA 3.5% Dec-16 3.1%
OHFT MiA 3.5% Dec-16 4.9%
BHT M - Jan-17 11.8%
TRAINING
Statutory Training BHT Q 85% Jan-17 81%
COMPLAINTS
BHT M - Jan-17 40
OUHFT M - Jan-17 81
COMMENT
Vacancy Rate
Sickness(This figure is reported month in
arrears)
COMPLAINTS
WORKFORCE
April deep dive for OHFT to focus on Workforce matters.
Total Number of Complaints Received
TRAINING
47 44 42 49 47 50 33 51 37 40
109 77 108 101 97 90 82116
67 81
86% 86% 86% 85% 86% 85% 85% 84% 84%
4.3% 4.1% 3.7% 3.9% 4.1% 3.4% 3.8% 4.3%4.9%
3.2% 3.0% 3.0% 3.2% 3.1% 3.6% 4.0% 3.9%3.1%
11.2% 11.1% 11.2% 11.4% 11.2% 11.7% 11.3% 10.9% 11.3% 11.8%
Page 98 of 148
Page 98 of 148

INDICATOR PROVIDER
FREQ
UEN
CY THRESHOLDCURRENT PERIOD
CURRENT VALUE
TREND
BHT M - Jan-17 94%
FPFT M - Jan-17 97%
OUHFT M - Jan-17 97%
MKUFT M - Jan-17 97%
National Average M - Jan-17 95%
BHT M - Jan-17 26%
FPFT M - Jan-17 25%
OUHFT M - Jan-17 19%
MKUFT M - Jan-17 17%
National Average M - Jan-17 23%
BHT M - Jan-17 78%
FPFT M - Jan-17 91%
OUHFT M - Jan-17 91%
MKUFT M - Jan-17 88%
National Average M - Jan-17 95%
BHT M - Jan-17 10%
FPFT M - Jan-17 20%
OUHFT M - Jan-17 22%
MKUFT M - Jan-17 10%
National Average M - Jan-17 12%
Friends and Family TestIn Patients
% Recommended
Friends and Family TestIn Patients
% Response Rate
Friends and Family TestA&E
% Response Rate
Friends and Family TestA&E
% Recommended
COMMENT
96%
95%
BHT FPFTOUHFT MKGFTNational Average
94%95%
BHT FPFTOUHFT MKGFTNational Average
24%23%
BHT FPFTOUHFT MKGFTNational Average
17%12%
BHT FPFTOUHFT MKGFTNational Average
Page 99 of 148
Page 99 of 148

Page 100 of 148
Page 100 of 148

MEETING: Governing Bodies meetings in common AGENDA ITEM: 10
DATE: 13 April 2017
TITLE: Amendments to terms of reference for audit committees
AUTHOR: Russell Carpenter, Corporate Governance Lead
LEAD DIRECTOR: Robert Majilton, Deputy Chief Officer
Reason for presenting this paper: For Action For Approval For Decision For Assurance For Information For Ratification
Summary of Purpose and Scope of Report:
The Governing Bodies meetings in common are asked to: 1. RATIFY approved amendments to terms of reference as are described.
Terms of Reference for both Audit Committees were approved in July 2016 following CCG federation; these are mirrored to allow each Audit Committee to meet separately should there be a necessity, but in all other respects Audit Committees meetings are held as meetings in common. It had however become necessary to propose and agree an amendment, to reflect changes in personnel, and allow the Audit Committees to continue to function. This amendment is outlined below.
Previous terms of reference (approved 27.07.16)
Proposed amendment
The Committee consists of not less than four members, one of which must be the designated Chair (the lay member from the Governing Body).
The other three members comprises: • Practice Member(s)/ Practice Member
Representative(s) – Up to two practicemember representatives appointed fromthe Group’s membership.
• Remaining Lay Members – Up to TwoLay Members (s) who will not bemembers of the Governing Bodyappointed to serve on the AuditCommittee.
A quorum shall be at least two members
The Committee consists of not less than three members, one of which must be the designated Chair (the lay member from the Governing Body).
The other members comprise: • Practice Member(s)/ Practice Member
Representative(s) – a representativeappointed from the membership of eitherCCG in the federation.
• Remaining Lay Member – who need notbe a member of the Governing Bodyappointed to serve on the AuditCommittee.
A quorum shall be two members
Page 101 of 148
Page 101 of 148

Points of discussion and approval by the Audit Committees meetings in common on 29 March 2017 (which were quorate to approve the amendment):
1. Benchmarking against other CCGs indicated a general pattern of quorum of twomembers. This shall remain the same.
2. Remaining lay member who “need” not rather than “will” not be a member of theGoverning Body appointed to serve on the Audit Committee . This aims to offer someflexibility should our lay member not appointed to the Governing Body be unavailablefor a meeting, and will allow the other deputy lay chair who is not the chair for ameeting (as they each alternate the role) to count to quorum.
All other proposed amendments described above were approved.
Conflicts of Interest: As Governing Bodies are rubber stamping what committees have already approved as their own amendments to tors, there are no material conflicts of interest which are relevant and therefore no action is required.
Strategic aims supported by this paper (please tick) Better Health in Bucks – to commission high quality services that are safe, accessible to all and achieve good patient outcomes for all
Better Care for Bucks – to commission personalised, high value integrated care in the right place at the right time
Better Care for Bucks – to ensure local people and stakeholders have a greater influence on the services we commission
Sustainability within Bucks – to contribute to the delivery of a financially sustainable health and care economy that achieves value for money and encourages innovation
Leadership across Bucks – to promote equity as an employer and as clinical commissioners
Governance requirements: (Please tick each box as is relevant to the paper)
Governance Element Y N N/A Comments/Summary Patient & Public Involvement
Equality Quality Financial Risks Statutory/Legal Both CCGs are required by statute to have in
place fully functioning Audit Committees which, for purposes of practicality, hold their meetings in common
Prior consideration Committees /Forums/Groups
None
Membership Involvement
Supporting Papers: None
Page 102 of 148
Page 102 of 148

Page 103 of 148
Page 103 of 148

MEETING: Governing Bodies meetings in common AGENDA ITEM: 11
DATE: 13 April 2017
TITLE: Quality and Performance Committee Terms of Reference – for ratification
AUTHOR: Lisa Beaumont, Associate Director of Nursing and Quality
LEAD DIRECTOR: Debbie Richards, Director of Commissioning and Delivery
Reason for presenting this paper: For Action For Approval For Decision For Assurance For Information For Ratification
Summary of Purpose and Scope of Report:
The Quality and Performance Committee would like to make the Governing Bodies meetings in common aware of some amendments to the Committee’s Terms of Reference, following the resignation of Secondary Care Nurse (and Chair) Sheran Oke, and following changes to the Executive Director’s portfolios.
Membership • The Committee does not now have a Secondary Care / Governing Body Nurse. Lisa
Beaumont agreed to cover this role in the interim.• The Committee does not have lay member representation, other than Health Watch,
who are non-voting, and who are unable to become voting members (in order topreserve their independence).
Chair • Karen West has agreed to become the new Chair, and Debbie Richards will be the
Deputy Chair.
Voting Members
• One lay member (vacancy)• One Clinical Commissioning Director (Chair)• Director of Commissioning and Delivery (Deputy Chair)• Secondary Care Specialist Doctor• Associate Director of Nursing and Quality
Quoracy Quoracy was agreed as any three of the membership described above to include at least one clinician from the CCGs, and the Committee Chair or Deputy Chair. This has proved a
Page 104 of 148
Page 104 of 148

challenge In March, when due to lack of quoracy a virtual meeting had to be held. The committee will endeavour to recruit a new lay member.
The Governing Bodies are asked to ratify RATIFY the changes to the Terms of Reference as outlined above and note the lay member vacancy, which is being addressed as part of a wider review of governance arrangements aligned to plans for merger by 1 April 2018.
Conflicts of Interest: As Governing Bodies are rubber stamping what committees have already approved as their own amendments to tors, there are no material conflicts of interest which are relevant and therefore no action is required.
Strategic aims supported by this paper (please tick) Better Health in Bucks – to commission high quality services that are safe, accessible to all and achieve good patient outcomes for all
Better Care for Bucks – to commission personalised, high value integrated care in the right place at the right time Better Care for Bucks – to ensure local people and stakeholders have a greater influence on the services we commission Sustainability within Bucks – to contribute to the delivery of a financially sustainable health and care economy that achieves value for money and encourages innovation Leadership across Bucks – to promote equity as an employer and as clinical commissioners
Governance requirements: (Please tick each box as is relevant to the paper)
Governance Element Y N N/A Comments/Summary Patient & Public Involvement
Equality Quality This report covers the three domains of quality
(patient safety, clinical effectiveness/patient experience).
Financial Risks Statutory/Legal Delivery of constitutional standards for
performance and quality. Prior consideration Committees /Forums/Groups
The Terms of Reference (ToR) were discussed and amendments agreed at the Quality and Performance Committee on 22 February 2017. A revised ToR was circulated to the virtual Committee on 29 March 2017.
Membership Involvement
Supporting Papers:
Quality and Performance Committee Terms of Reference, V3, 23 March 2017
Page 105 of 148
Page 105 of 148

Quality and Performance Committee
Terms of Reference V3 – March 2017
Purpose of the Quality and Performance Committee
Introduction The Quality and Performance Committee (referred to as the Committee) is established in line with NHS Chiltern and NHS Aylesbury Vale Clinical Commissioning Group’s Constitutions. It is a joint committee across Aylesbury Vale and Chiltern CCGs and, as of 1 July 2016, supersedes a joint Commissioning for Quality Committee which previously served the needs of both CCGs.
Objectives and constitutional requirements The Committee is accountable to the CCG’s Governing Body (meeting in common), and provides assurance on the quality and performance of services commissioned and promotes a culture of continuous improvement and innovation with respect to safety of services, clinical effectiveness, outcomes and patient experience. This includes a responsibility to promote research and the use of research and monitor reports made to the National Reporting and Learning System. The Committee makes recommendations on areas such as access, reducing inequalities, equality and diversity issues, and service improvements needed, and is responsible for advising on new developments for implementation such as NICE. The Governing Body approves and keeps under review the terms of reference for the quality and performance committee, which includes information on the membership of the quality and performance committee and is available upon request.
For the purposes of this document, quality is defined as the domains of patient safety, clinical effectiveness and patient experience.
Statutory framework The Committee is accountable for the monitoring and overseeing a robust organisation wide system of Board assurance that supports the work of the Audit Committee. The role of the Committee is to oversee the quality, performance and integrated governance arrangements on the effective discharge of the CCG’s function with particular focus on quality and performance. This includes oversight and monitoring of: • The quality of commissioned services including patient experience and safety• The effectiveness of commissioned services• Performance against service delivery indicators
Aim/objectives The Committee will: • Provide the Governing Body’s (meeting in common) with assurance that the
quality and performance of all commissioned services is systematically monitored.• Provide assurance that risks are identified, escalated and appropriately managed.• Support collaborative working and decision making that improves health and
social care outcomes in Buckinghamshire.• Support effective partnerships working between health, local authority and wider
Page 106 of 148
Page 106 of 148
partnership organisations in Buckinghamshire. • Ensure consistency in implementation of relevant policies in an evidence-based,
cost effective and safe manner, and support wider CCG commissioning intentions.
Specific duties and responsibilities
The Quality and Performance Committee will also: 1. Assure the Governing Body’s meeting in common of appropriate
arrangements, for both the CCG and providers of the quality of commissionedservices, in respect of safeguarding, infection control, incident management,complaints, workforce data, staff surveys, reporting of quality accounts, orany other area of quality. This will be undertaken through a series of reportsfrom providers, the Commissioning Support Unit (CSU) and from theBuckinghamshire CCGs.
2. Assure the Governing Body’s meeting in common of appropriatearrangements for both the CCG and providers of the performance ofcommissioned services against the constitutional standards e.g. Strokeservices, cancer waiting times and A & E performance etc.
3. Receive assurance on performance and quality risks, including clinical risks,ensuring risks are reviewed and appropriate action is taken to mitigate and /or close.
4. Receive assurance of the quality of clinical portfolios from portfolio holders toensure that all commissioned services are operating together in such a way asto deliver maximum benefit and a good patient experience and compliancewith NICE Quality Standards.
5. Receive assurance on QIPPS through Quality Impact Assessments (QIAs), toassess any impact on quality and performance, in order to provide challengewhere necessary.
6. Ensure that there is a continuing structured process for leadership,accountability and working arrangements for quality and performance withinthe CCGs, whilst also assuring the Governing Bodies the statutory EqualityDuty has been met.
The Committee, under the Governing Body Scheme of delegation has the delegated responsibilities for assuring the following:
• Contract performance• Clinical risk management• Quality, clinical effectiveness and health improvement• Patient safety and experience• Equality and diversity• Serious Incidents (SIs), complaints and PALS• Infection Control• Safeguarding
The Committee also has the delegated responsibility for the • Approval and ratification of policies relating to quality and patient safety• Ratify the ToR for reporting groups into the committee and approve their
work programmes
See Appendix 1 for reference: Extract from the Scheme of delegation
Accountability and reporting arrangements
The Committee is formally accountable to the CCG Governing Body’s (meeting in common) as one of its committees.
Page 107 of 148
Page 107 of 148

Whereas previously each CCG’s representative reported to their own Governing Body, this committee represents both CCGs will report and provide assurance as one body, on quality and performance through to the Governing Body (meeting in common). This will enable sharing of good practice and learning and thus help ensure quality and safety for all of the population for which the CCG’s commission services. It will also enable sufficient mechanisms are in place to support the delivery of Care Quality Commission (CQC) Essential Standards outcomes.
The Committee is accountable for monitoring and overseeing a robust organisational wide system of assurance that supports the work of the Audit Committee. It is the formal mechanism by which Aylesbury Vale CCG and Chiltern CCG discharge their responsibilities for quality assurance and contract monitoring in relation to the services they commission.
The Committee will assume responsibility for risk management relevant to its area of business through the review and critical appraisal of identified risks (perceived or actual) and/or serious concerns at each meeting, and report to the Governing Body on all such risks and the effectiveness of their means of control (through the Governing Body Assurance Framework).
The Committee may delegate certain of its responsibilities to sub-groups as required but will remain accountable for delivery as if these sub-groups were the Quality and Performance Committee.
The Committee gives delegated authority to the Quality and Performance Operational Group (QPOG), to provide assurance for the Governing Body (meeting in common) and escalation to the Executive Committee, in the alternative months when the Committee does not meet.
The Committee, via the monthly Quality and Performance Operational Group, will produce a monthly Quality and Performance Report to provide assurance for the Governing Body’s (in common), and will also produce an Annual Assurance Report on The Committee’s effectiveness for the Governing Body (in common).
The Governing Body will ratify the Committee’s terms of reference and forward business plan.
The Committee will receive and review minutes and reports from sub groups as appropriate.
The Committee will escalate any exceptions to the Governing Body or Executive Committee as appropriate for decision making or review.
Decision making and delegated authority
The Committee has delegated authority to take decisions in accordance with standing orders and schemes of delegation.
The Committee will work on the basis that decisions will be made by consensus wherever possible. Where this is not possible, a vote will be taken with a simple majority carrying the motion with the chair having a second, casting vote in the event of a tie. Only standing members of the Committee will be eligible to vote and each member shall have one vote. If an individual has a conflict of interest for a particular agenda item, they must abstain from voting on that item.
Page 108 of 148
Page 108 of 148

Where the committee need to discuss issues in relation to primary care, a confidential Part 2 of the meeting should be arranged, and any practicing GP’s on the committee will be excused from this confidential part of the meeting.
Membership and Quoracy
Membership The Chair of the Committee shall be a voting member and a Member of the Governing Body (in common). In the absence of the Committee Chair and / or appointed deputy, the remaining members present shall elect another member to chair the meeting. Only members have the right to vote. Note: CCG Clinical Chairs are not formal voting members but will have a standing invitation to attend the Committee.
Members (voting) • One lay member (vacancy)• One Clinical Commissioning Director (Chair)• Director of Commissioning and Delivery (Deputy Chair)• Secondary Care Specialist Doctor• Associate Director of Nursing and Quality
In attendance only (non-voting) • Associate Director of Performance• Head of Quality• Health Watch representative• Safeguarding Lead – for quarterly updates• IPC Lead Nurse - for quarterly updates• Other officers as and when by invitation
Others CCG staff will be required to attend meetings if requested. In addition the NHS England (Thames Valley) Quality Team will be invited to attend as they wish.
Quorum The Committee will be quorate to make decisions as delegated if the following mix of members are all present:
• Any three of the membership described above to include at least one clinicianfrom the CCGs, and the Committee Chair or Deputy Chair.
If quorum has not been reached, then the meeting may proceed if those attending agree, but any record of the meeting should be clearly indicated as notes rather than formal minutes, and no decisions may be taken by the non-quorate meeting. If a decision does need to be made before the date of the next meeting, the matter should be escalated preferably to the Executive Committee, but if required, the Governing Body (in common).
If a member is conflicted on a particular item of business they will not count towards the quorum for that item of business. If this course of action causes the decision to be non-quorate, the matter may be escalated preferably to the Executive Committee, but if required, the Governing Body.
Deputies will not generally be allowed but permission can be sought from the Chair.
The Committee may call additional experts to attend meetings on case-by-case basis to inform discussions.
Page 109 of 148
Page 109 of 148

Chair/deputy of a meeting
The named Chair of the Committee shall preside. In the absence of the Chair, another voting member will act in this role.
The group will be chaired by a Clinical Commissioning Director. In the absence of the Chair the Committee will be chaired by the Director of Commissioning and Delivery.
Member conduct Members of the Committee have a collective responsibility for its operation. They will participate in discussion, review evidence and provide objective expert input to the best of their knowledge and ability. However, this is with the exception of the GP leads in any discussion regarding primary care performance or quality issues. They will endeavour to reach a collective view prior to making any decision where authority to do so is delegated.
Attendance will be monitored and reported to the Committee quarterly with full disclosure in the CCGs Annual Reports.
Conflicts of interest There must be transparency and clear accountability of the Committee. The Chair will ask at the beginning of each meeting, as a standing item, whether any member has conflict of interest to declare about any items being discussed at the meeting in accordance with the CCGs’ conflict of interest policy. If a member has a direct or indirect connection with an issue on the agenda which may impact on their ability to be objective they must declare an interest to the Chair. A decision will then be taken by the Chair as to whether it is appropriate or not for this member to remain involved. All declarations of interest and decisions on participation shall be reported in the minutes.
A register of interests will be completed by all Committee members and updated at least annually, and will be available on the CCG website for public scrutiny.
Confidentiality To allow this Committee to operate effectively, members need to be able to openly discuss commercial and operational issues and requirements. Members accordingly agree to hold all information obtained in the course of meetings in the strictest of confidence and agree not to disclose any information discussed without first seeking authorisation to do so from the Chair.
Meeting arrangements
Each year, the Quality and Performance Committee will develop a forward plan of planned business aligned to the CCGs’ business cycle and share this with the Executive Committee.
The Committee will normally meet every alternate month for 2 ½ hours on the second or third Wednesday of the month. Exceptions to this arrangement will be considered in August and December. A minimum of 6 meetings to take place annually. The Quality and Performance Operational Group (QPOG) will meet monthly, and in the month when the Committee does not meet the QPOG will provide assurance to the Executive Committee, via the Quality and Performance Report (produced monthly). If the meeting is not quorum and too many apologies make a meeting unviable, a virtual meeting may be held, at the Chair’s discretion.
The administrative support to the meeting will be provided by the Quality Support Assistant, within the Quality Team. The following arrangements will be in place to
Page 110 of 148
Page 110 of 148

ensure the smooth organisation of each meeting: • Agenda items will be accepted up to 2 weeks in advance of the meeting.• Apologies should be sent in advance to determine quoracy.• Papers will be circulated a minimum of 4 days in advance of the meeting.• Members should review and update the action log 2 weeks in advance of the
meeting.• The agenda and associated papers will be circulated five working days ahead of
the meeting. This is the responsibility of the Associate Director of Quality andSafeguarding.
• The venue for the meeting will alternate between Chiltern CCG and AylesburyVale CCG. Arrangements to dial-in to the meeting will be made where possibleand practical, especially if required to ensure quoracy.
Where appropriate, excerpts of papers/minutes only will be sent to others who have attended meetings according to the confidentiality of information.
Agreed minutes of the Committee meetings will be sent to the Governing Body (in common) for information, and topics for the key issues report agreed at the meeting (prior to the issue of accepted minutes) released to the Executive Committee as soon as possible after the meeting for urgent or significant matters.
Guiding Principles The Committee will abide by the guiding principles below to discharge their duty effectively and diligently:
• The patient comes first – not the needs of any organisation or professionalgroup;
• Quality is everybody’s business – from the ward to the board; from thesupervisory bodies to the Regulators, from the commissioners to primary careclinicians and managers;
• If we have concerns, we speak out and raise questions without hesitation;• We listen in a systematic way to what our patients and our staff tell us about
the quality of care;• If concerns are raised we listen and ‘go and look’;• We share our hard and soft intelligence on quality with others and actively
look at the hard and soft intelligence on quality of others ;If we are not sure what to decide or do, then we seek advice from others.
Document Control Version control and review date Signatures (approval and review) Date of approval (by who/which committee)
These terms of reference will be reviewed annually.
Version (author and date)
Review date (by group/committee)
Reason for amendments
Signature (chair) and date to confirm acceptance and adoption
V 1.0 Lisa Beaumont
21/9/2016 Draft 1
V2.0 Lisa Beaumont
16/11/2016 Amendments required following review by Corporate Governance
Page 111 of 148
Page 111 of 148

Lead and Committee. V3.0 Lisa Beaumont
22/2/17 Amendments required following resignation of lay chair.
Appendix 1 For reference: Extract from the Scheme of Reservation and Delegation.
Page 112 of 148
Page 112 of 148

Appendix 1
No Policy Area Decision Comments QP
Q1 REGULATION AND CONTROL
Review then approve and ratify policies, procedures and other documents for the management of patient safety risk and quality, as otherwise described within the Development and Approval Policy for Formal CCG Documents
Y
Q2 REGULATION AND CONTROL
Ratify the Terms of Reference and annual work plans for all sub-groups that have accountability to the committee
Y
Q3 REGULATION AND CONTROL
Approve the Terms of Reference and annual work plans for the committee Y
Q4 QUALITY AND SAFETY Review closure of early warning alerts; reported through effective early warning systems which draw on a range of quality indicators and other sources of information to identify gaps in assurance about providers
Y
Q5 QUALITY AND SAFETY Ratify proposals for ensuring quality and developing clinical governance in services provided by the Group’s providers having regard to any guidance issued by the NHS England
Y
Q6 PARTNERSHIP WORKING
Agree the CCGs arrangements for contributing to and working with agencies responsible for Safeguarding and Infection, Prevention and Control
Y
Page 113 of 148
Page 113 of 148

MEETING: Governing Bodies meetings in common AGENDA ITEM: 12
DATE: Thursday 13th April 2017
TITLE: CCGs Budget Setting 2017/18
AUTHOR: Kate Holmes, Deputy Chief Finance Officer
LEAD DIRECTOR: Robert Majilton, Deputy Chief Officer
Reason for presenting this paper: For Action For Approval For Decision For Assurance For Information For Ratification
Summary of Purpose and Scope of Report:
Governing Bodies meetings in common are asked to: 1. NOTE the approval by Executive Team, at the meeting on 23/3/17, of the detailed
Programme and Running Cost budgets of the CCGs for 2017-18 outlined in this paper.
The purpose of the report is to provide an update briefing from the Chief Finance Officer on the detailed budgets for both NHS Aylesbury Vale CCG and NHS Chiltern CCG for the financial year 2017-18 following the approval of the Financial Plans at the Executive Meeting on 23rd February 2017.
In October the Executive Team reviewed an initial baseline allocation and associated financial plan based on planning assumptions through NHSE guidance which aligned with STP requirements and further updates were reviewed by Executive Team in December and February.
The agreed initial summary plans were submitted on 1st November, a further full draft plans submitted on 24th November; final versions of the plans submitted on 23rd December 2016, alongside the CCGs operational plans and contract signature with providers, and a further subsequently required submission was made on 24th February 2017.
The paper outlines the detail of the programme budgets and running cost budgets funded within this plan for the financial year 2017-18. Executive Team recognised that whilst approval was given for the start budgets of the CCGs for 2017-18 there may be a need to revise budgets in year (and especially during Q1) due to the following factors:
2. The CCGs operational plans have not yet fully been approved or rated green nationally byNHSE due to the level of QIPP within the plan and triangulation with activity.
3. The continued process for further identification of plans to cover the unidentified QIPP andoutcome of work by Deloittes’ as part of an NHS England support programme.
4. Any changes as result of in year moves due to system priorities (i.e. movement in detailed
Page 114 of 148
Page 114 of 148

budgets due to MSK, impact 111 etc and resubmission of STP. 5. Any in year change in national policy e.g. 5YFV delivery plan due end of March 2017.
Conflicts of Interest: None
Strategic aims supported by this paper (please tick) Better Health in Bucks – to commission high quality services that are safe, accessible to all and achieve good patient outcomes for all
Better Care for Bucks – to commission personalised, high value integrated care in the right place at the right time
Better Care for Bucks – to ensure local people and stakeholders have a greater influence on the services we commission Sustainability within Bucks – to contribute to the delivery of a financially sustainable health and care economy that achieves value for money and encourages innovation
Leadership across Bucks – to promote equity as an employer and as clinical commissioners This paper supports the delivery of the CCG’s statutory duties to remain within its allocated funding and to achieve a 1% target surplus by keeping the Executive updated on the current financial performance throughout the financial year.
Governance requirements: (Please tick each box as is relevant to the paper)
Governance Element Y N N/A Comments Equality Analysis Privacy Impact Assessment
Quality Impact Assessment (QIA)
Prior consideration Committees/ Forums
This financial performance position update has also reported through Executive Team and Audit Committee
Patient & Public Involvement (PPI)
There has been no direct PPI, however, lay members sit on Executive Team, Governing Body and Audit committee at which these are reviewed. Additionally Governing Body papers are available for public inspection both at the meeting and through the CCG website.
Membership Involvement
There has been no direct membership involvement, however, members representatives in the form of Clinical and portfolio leads sit on Executive Team and Governing Body at which these are reviewed. Papers are also available for review on the member’s website.
Risks Financial Consequences
Financial Approval
Supporting Papers:
Page 115 of 148
Page 115 of 148

CCGs detailed budget setting 2017-18
Page 116 of 148
Page 116 of 148

AYLESBURY VALE & CHILTERN CCGS
2017/18 BUDGET SETTING
Introduction
The 2017-19 financial plans for each CCG were reported to Executive team in October, December and most recently in February in alignment with corresponding required submission dates.
The detailed budgets for the financial year 2017-18 outlined in the paper should be read in conjunction with the papers referred to above to ensure Executive remain aware of the allocation received, the approach taken, links to the wider health economy Sustainability and Transformation Plan (STP) and the risks and opportunities pertaining to these budgets.
2017-19 Financial Framework
The CCGs operational financial plans are required to support and reconcile to the operational plans and demonstrate:
• How they will be delivering the nine must-dos;
• How they support the delivery of the local STP, including clear and crediblemilestones and deliverables;
• How they intend to reconcile finance with activity and workforce;
• Robust, stretching and deliverable activity plans which are directly derived from theirSTP;
• How local independent sector capacity is factored into capacity planning and localproviders engaged throughout;
• The planned contribution to nationally savings;
• How risks have been jointly identified and mitigated through an agreed contingencyplan;
• The impact of new care models, including where appropriate how contracts with SCproviders will be adjusted to reflect MCPs or PACS during 2017-19.
Page 117 of 148
Page 117 of 148

Business rules for 2017/18 – 2018/19 are largely consistent with 2016/17 with some key changes:
• Aim for in-year break even for each CCG, with expectations set for the minimumlevel of improvement in deficit CCGs.
• CCGs to plan for 0.5% contingency.• A central risk reserve is to be held in both 2017/18 ( total set at c£830m) and
2018/19 created by both commissioners and providers to help create this:• NHSE will contribute £200m, funded from drawdown• CCGs to ensure 1% of their allocation is planned to be spent Non-
Recurrently, but only half of this, equivalent to £360m nationally has to beuncommitted at the start of the year, with the other half being available forimmediate investment
• 0.5% of local CCG CQUIN scheme will also be held within the risk reservecontributing £270m nationally.
• From 2017/18 onwards, specialised commissioning will be required to build a similarreserve up to 1%, starting with 0.3%.
• Expectation is that both the commissioner sector and provider sector to be infinancial balance in both 2017/18 and 2018/19.
The financial plans for each CCG are compliant with all the required business rules as detailed above.
Baseline
The start point for the 2017-18 allocation is based on the assumptions outlined above, and aligned with those in the STP submission, updated for known recurrent adjustments. This was detailed in the previous reports to Executive Committee.
Baselines have then been adjusted by NHSE in respect of Specialist Services Identification Rules (IR) changes c£5.2m and impact of changes in HRG4+ tariff resulting in a c£1.6m reduction in allocation.
It should be noted that there are some additional non recurrent allocations remaining centrally examples of interest are those relating to GP Practice Resilience Programme, Vulnerable Practice Pilots and GP Development. These will be allocated in year and are assumed committed.
Other central sources of income assumed have been estimated at circa £5m across Bucks and have been shown within opportunities in the financial plans; these relate to centrally held funding associated with national Forward View. £1.1m confirmed income relating to IAPT schemes have been assumed within the main body of the financial plan.
It should be noted that funds associated with delegated primary care co-commissioning have only been included within the AVCCG plan; although the Chiltern CCG application has been sent to NHSE it has not yet been formally approved and as such funds for Chiltern CCG Primary Care Services remain in NHSE local area team plans.
Page 118 of 148
Page 118 of 148

The revenue resource limits assumed for each CCG is detailed in the table below:
Revenue Resource Limit
£'000 sign
AVCCG 2017/18
CCCG 2017/18
Programme Baseline Allocation +ve 230,512 361,776 Recurrent Changes In-Year +ve/(-ve) 8 (319)Primary Care Co-Commissioning +ve/(-ve) 26,455 - Running Cost Allocation +ve 4,453 7,172 Total Notified Allocation 261,428 368,629
Non Recurrent AllocationsOther Non Recurrent allocations +ve/(-ve) 1,748 1,786 In-Year drawdown/(drawup) (465) (770)Non Recurrent Requirement (-ve) (2,570) (3,615)Non Recurrent Return +ve 2,570 3,615 Marginal Rate Non Elective Collection +ve 1,107 2,246Marginal Rate Non Elective Return (-ve) (1,107) (2,246)Total Non Recurrent Allocation 1,283 1,016
Total In-Year Allocation 262,711 369,645
Estimated registered population +ve 211,862 341,672 Final per capita allocation +ve 1,088 1,059 Final per capita growth 1.31% 1.61%Final closing DfT -4.50% -4.30%
Other non-recurrent allocaton 2017/18 2017/18Quality PremiumCEOVWinter FundingGP AccessVanguard FundingCapital GrantsAdditional MHOtherPublic HealthIM&T / Dispensing doctors(16/17) - - IR Changes 2,481 2,681 HRG4 changes (733) (895)NHS PSOther Inter Org Non-Rec TransfersTotal 1,748 1,786
Page 119 of 148
Page 119 of 148

CCGs Agreed Financial Plans 2017/18
On 23rd February 2017 Executive Team agreed the CCGs allocations and requirements against it as identified in the paper presented.
After review and debate Executive Team agreed the high level budget for 2017-18 outlined above and associated QIPP requirements.
The resulting resource and application of funds for 2017-18 is reflected in the table below.
A detailed summary of the CCGs Programme Budgets is shown in Appendix A and the CCGs Running Costs Budgets in Appendix C.
It should be noted that at the current time only AVCCG has delegated Primary Care co-commissioned budgets and this is reflected in the current plans at initially transferred levels plus growth and additionally STP primary care growth assumptions then applied.
CCCG has permission for delegated Primary Care co-commissioned budgets with effect from 1/4/2017 and an Inter Authority Transfer (IAT) will be made from NHSE to the CCG in year to reflect the delegated responsibility change.
Headroom is budgeted at the full 100% in the CCGs plans, however, as referred to earlier only 50% may be planned to be utilised in year by the CCGs and the remaining 50% to be held back into a central national reserve.
Page 120 of 148
Page 120 of 148

Planned and Unscheduled Care
The above table details the budgets envelopes for our main providers of Planned and Unscheduled Care net of current QIPP expectations.
Joint and Continuing Care
Other includes the CCGs contribution to the BCF that is paid across to Buckinghamshire County Council to administer as part of the s75 agreement.
Page 121 of 148
Page 121 of 148

Medicines Management
The general Prescribing budget is shown above alongside the funding for the Medicines Management team.
Delegated Primary Care Co-Commissioning & Primary Care Budgets
At the current time only AVCCG has delegated Primary Care co-commissioned budgets and this is reflected in the current plans at initially transferred levels plus growth and additionally STP primary care growth assumptions then applied. For the first time the CCG will have to deliver a 1% surplus on these funds.
CCCG member practices have voted to move to delegated co-commissioning moving forward and the CCCG application has now been approved by NHSE.
A table detailing the proposed budget for delegated primary care co-commissioning services is shown below:
AVCCG CCCGPrimary Care Co-Commissioning £'000 £'000General Practice - GMS 12,823 26,061 General Practice - PMS 2,709 - Other List-Based Services (APMS incl.) 1,178 934 Premises cost reimbursements 2,752 4,806 Primary Care NHS Property Services Costs - GP - 128 Other premises costs 21 38 Enhanced services 1,275 2,009 QOF 2,328 3,770 Other - GP Services 3,369 2,587
Sub-total - Primary Care Co-Commissioning 26,455 40,333 *
* Delegated Budget for CCCG is outside of the current CCG Financial Plan as is held by NHSE currently. Figures included in the table above are for reference and are those expected to be transferred to the CCG in year.
Page 122 of 148
Page 122 of 148

Reserves & National Requirements
Reserves and ring fenced funding have been allocated as shown in the source and application table above as per national requirements.
No reward funding, relating to the 2016-17 CCG Quality Premium Scheme, is shown in the budget as the final achievement is not yet known however, this will be available to the CCG upon achievement in accordance with the scheme regulations.
It should be noted, as outlined above in the report, that only 50% of Headroom funds can be planned to be utilised by the CCG with the remaining 50% ring fenced into a central national reserve.
Running Costs
The running cost allowance, assumed in 2017/18 is virtually flat compared to those seen in 2016/17 and there has been no further reduction assumed. Plans have been developed that remain slightly within these expected running cost allowances.
The total CCGs running cost allocations totalled £7,059k, however, as agreed by the Executive team there has been a £300k QIPP applied to the running costs budget to support the CCGs position.
Page 123 of 148
Page 123 of 148

QIPP
The total agreed QIPP requirement for 2017-18 is currently £22,440k.
QIPP plans to support this requirement continue to be developed, tested and agreed with provider colleagues as appropriate.
Details of the schemes are constantly being reviewed etc. currently to ensure they are viable and will deliver the required savings
The detailed summary of schemes is shown in Appendix B
Risks & Opportunities
Risks Opportunities
- The planned surplus for 16-17 is notachieved and carried forward.
- release of unallocated 50% Headroomfrom NHSE.
- That schemes to support the QIPPtarget can be fully identified anddelivery achieved.
- 2016/17QIPP Scemes releaseadditional savings into 2017/18 (FYE).
- The PbR assumptions are changedduring the pbr consultation and causepressures to resource.
- Additional under spend on Prescribingbudgets per current PPA forecast.
- Cost increase and growth will begreater than STP assumptions.
- Further central allocations from NHSE linked to Forward View.
- Budgets for Prescribing not agreed tobe based on 16-17 out-turn.
- HRG4+ challenge to centre issuccessful.
- Investments cannot be met fromQIPP schemes.
- Potential to re-prioritise someinvestment funds.
- Planned underspend seen againstRunning Costs in previous years willnot be available to support QIPP in17/18 going forward.
- Return of some service fromSpecialised Commissioning are notfully funded and cause pressures tobaseline budgets.
There remain a significant number of risks to the financial position as outlined above which will require careful management within year; these have been outlined in our financial plan submission to NHSE
A number of opportunities/ mitigations have been identified but once again these will require careful management to ensure optimisation of these and minimisation of any further risks.
Page 124 of 148
Page 124 of 148

Key Agreements required from CCG Executive Team
Executive Team should be aware that whilst approval is being sought here for the start budgets of the CCGs for 2017-18 there may be a need to revise budgets in year (and especially during Q1) due to the following factors:
1. The CCGs operational plans have not yet fully been approved or rated greennationally by NHSE due to the level of QIPP within the plan and triangulation withactivity.
2. The continued process for further identification of plans to cover the unidentifiedQIPP and outcome of Deloittes’ work.
3. Any changes as result of in year moves due to system priorities (i.e. movement indetailed budgets due to MSK, impact 111 etc. and resubmission of STP.
4. Any in year change in national policy e.g. 5YFV delivery plan due end of March2017.
The Executive Team is asked to:
APPROVE the detailed Programme and Running Cost budgets of the CCGs for 2017-18 outlined in this paper.
Page 125 of 148
Page 125 of 148

Appendix A – Detailed CCGs Budgets 2017-18
2017/18 AVCCG CCCG TOTAL
Income and Expenditure
Total - 2017/18 Plan
Total - 2017/18 Plan
Total - 2017/18 Plan
Acute servicesAcute contracts -NHS (includes Ambulance services) 123,455 189,577 313,032Acute contracts - Other providers (non-nhs, incl. VS) 3,932 7,428 11,360Acute - Other (4,713) 8,267 3,554Acute - Exclusions / cost per case 104 450 554Acute - NCAs 3,668 5,085 8,753Acute - Pass-through payments - - -
Sub-total - Acute services 126,446 210,807 337,253
Mental Health services MH contracts - NHS 18,568 23,849 42,417MH contracts - Other providers (non-nhs, incl. VS) 2,167 3,436 5,603MH - Other (35) 2,706 2,671MH - Exclusions / cost per case - - -MH - NCAs 430 770 1,200MH - Pass-through payments - - -
Sub-total - MH services 21,130 30,761 51,891
Community Health ServicesCH Contracts - NHS 17,310 17,935 35,245CH Contracts - Other providers (non-nhs, incl. VS) 1,722 2,867 4,589CH - Other - - -CH - Exclusions / cost per case 3 498 501CH - NCAs - - -CH - Pass-through payments 3,499 - 3,499
Sub-total - Community services 22,534 21,300 43,834
Continuing Care servicesContinuing Care Services (All Care Groups) 16,911 27,416 44,327Local Authority / Joint Services 5,863 13,274 19,137Free Nursing Care 2,808 4,611 7,419
Sub-total - Continuing Care Services 25,582 45,301 70,883
Primary Care servicesPrescribing 27,225 39,927 67,152Community Base Services 990 1,337 2,327Out of Hours 1,760 3,243 5,003Practice Transformation Support 419 679 1,098PC - Other - - -
Sub-total - Primary Care services 30,394 45,186 75,580
Primary Care Co-CommissioningGeneral Practice - GMS 12,823 12,823General Practice - PMS 2,709 2,709Other List-Based Services (APMS incl.) 1,178 1,178Premises cost reimbursements 2,752 2,752Primary Care NHS Property Services Costs - GP - -Other premises costs 21 21Enhanced services 1,275 1,275QOF 2,328 2,328Other - GP Services 3,369 3,369Delegated Contingency 0 0
Sub-total - Primary Care Co-Commissioning 26,455 - 26,455
Other Programme servicesGP IT Costs 540 870 1,410NHS Property Services re-charge (excluding running cost) - 41 41Voluntary Sector Grants / Services - 171 171Social Care 19 733 752Other CCG reserves - 311 311Other Programme Services 2,774 3,524 6,2981% Non Recurrent - uncommitted funds (0.5%) 1,153 1,807 2,960Sub-total - Other Programme services 4,486 7,457 11,943
Total - Commissioning services 257,027 360,812 617,838
Running CostsCCG Pay costs 1,910 2,839 4,749CSU Re-charge 2,000 2,896 4,896NHS Property Services re-charge / CHP Charges 105 245 350Running Costs - Other Non-pay 342 988 1,330
Sub-total - Running costs 4,357 6,968 11,325
Contingency 1,327 1,865 3,192
Total Application of Funds 262,711 369,645 632,355
Page 126 of 148
Page 126 of 148

Appendix B – CCGs Federated QIPP Schemes - working version
QIPP from STP
Scheme workstream Assumed split 17/18 18/19 17/18 18/19 Contractaction/reduction
impact£k £k
BOB wideSpec Comm 0 0 n/a n/a
Mental Health OBC Integrated capn 68:32 208 432 removed from baseline contract
Prevention capn 68:32 - - n/a n/aNHS 111 procurement Urgent capn 68:32 1,208 - 7,550 - A&E attendances
Acute Services - good practice variation Planned contract 56:44 450 450 281 281
Daycases / Electives/ Regular day attenders/ Outpatients
Workforce - - n/a n/aDigital road map - - n/a n/a
- - - -
Bucks wide - -
CAMHs investment adj Integrated capn 68:32 208 - removed from budget in plan
MH Task force investment adj Integrated capn 68:32 835 - removed from budget in plan
Bed day reduction (+15LOS) Integrated contract 56:44 875 875 3,340 3,340 XS bed daysCommunity Hubs Planned contract 56:44 - -
STP wide acute collaboration Planned contract 56:44 - 600 - 400 Electivesmaternity investment reduction Planned contract 56:44 335 417
111/OOH service tender pressure Urgent capn 68:32 500- - add to budget in plan if still required
Urgent Care ( 2% reduction in NEL) Urgent contract 56:44 360 380 90 95 NELs
BCBV - NEL admissions (CCG Based) Urgent contract 56:44 - 1,176 - 294 NELsCommissioner QIPP - -
Out of hospital - residential care Integrated capn 68:32 100 100 remove from budget & set baseline
CHC Savings vs growth Integrated capn 68:32 1,000 1,000 remove from budget & set baseline
Right Care Opportunities Planned contract 56:44 - 2,000 - - Out patient & Electives
Primary Care BAU CI opportunities Planned contract 56:44 1,000 1,000
review - removed from Enhanced Services budget in plan?
Use of independent sector & WLI Planned contract 56:44 500 500 2,500 2,500 Out patients/diagnostics
BCBV - surgical thresholds Planned contract 56:44 - 400 - 267 Electives
Commissioning corporate efficiencies capn 68:32 300 300 CSUremoved from budget in plan
Total 6,879 9,630 CCG QIPP
FYE 16/17 schemes : - -
AiredaleIntegrated Care 141 - 35 - NEL
Over 75s Urgent Care 37 - 9 - NELGPAC (formerly DLS) & paramedic schemes Urgent Care 150 - 938 - A&E attendancesHeart Failure Lounge Planned Care 250 - 63 - NEL
MSK Planned Care 404 - 269 - Elective
EOLIntegrated Care 1,212 - 303 - NEL
- - New Pipeline : - - SCAS A&E avoidance/ GP triage Urgent Care 417 - 2,605 - A&E attendances
Airedale - pilot rollout Urgent Care 300 - 75 - NEL
Spinal Urgent Care 200 - 317 - BHT Spinal xs Bed daysTransitional Care Urgent Care 500 - 1,908 - xs bed daysMaximise us Community Beds baseline Urgent Care 150 - 573 - xs bed daysShort Stay Admissions Urgent Care 370 - 493 - NEL short stay
Cancer Planned Care 240 60 - NEL
Falls Planned Care 140 - 35 - NEL
COPD Planned Care 125 - 31 - NEL
Heart Failure Planned Care 766 - 192 - NEL
Community Integrated Hubs Planned Care - - - - outpatients
Ophthalmology Planned Care 100 - 67 - Electives
Dermatology Planned Care 30 - 150 - outpatients
Community Headache Planned Care 30 - 188 - A&E attendances / Diagnositics
Gynae Planned Care 144 - 96 - ElectivePrevention Planned Care - -
Follow ups Planned Care 705 - 7,053 - follow up
OPD to block Planned Care 317 - 1,585 - outpatients
LTC Planned Care 199 - 995 - outpatients
Referrals Planned Care 1,352 - 901 - Elective
Stoma - link with Cancer Planned Care 50 - - -
remove from baseline budget for Stomacare.
Hypertension Planned Care 143 - 36 - NEL
NEL Planned Care 153 - 38 - NEL
Urology Planned Care 55 - 37 - Elective
General Surgery Planned Care 105 - 70 - Elective
Contract Management Planned Care 368 - 245 - Elective
BAU service monitoring BAU -Contracts - - - - AllPrescribing Prescribing 500 - 333 - All
- - Unallocated 5,908 -
Total 22,440 9,630
Savings Activity
Page 127 of 148
Page 127 of 148

Appendix C – CCGs Federated Running Costs Budget
Committee/Team
Governing Bodies £391,727
Executive £839,832
Finance £433,343
Clinical Governance £590,641
Sustainability and Transformation £645,963
Commissioning and Locality £1,255,771
Integrated Commissioning £95,750
Medicines Management £501,598
Corporate Affairs £427,460
Strategy and Development £26,108
Non-Pay £6,416,758
TOTAL £11,625,000
Page 128 of 148
Page 128 of 148

Executive Committee Meeting : Minutes Thursday 26th January 2017 – 1:45pm – 4.30pm
Chair: Robert Majilton Present:
Robert Majilton RM Chair - Deputy Chief Officer Executive Committee Member Debbie Richards DR Director of Commissioning and Delivery Executive Committee Member Philip Murray PM Chief Finance Officer Executive Committee Member Dr Toby Gilham TG Clinical Director - Central Executive Committee Member Nicola Lester NL Director of Corporate Affairs Executive Committee Member Dr Conan Hassim CH Clinical Director -Southern Executive Committee Member Dr Dal Sahota DS Clinical Director – Urgent Care Executive Committee Member Dr Sian Roberts SR Clinical Director – Mental Health Executive Committee Member Dr Malcolm Jones MJ Clinical Director – Locality Lead Executive Committee Member
Other Attendees
Lisa Beaumont LB Associate Director of Quality & Safeguarding Dr Karen West KW Clinical Director – Integrated Care Dr Juliet Sutton JS Clinical Director - Children Dr Raj Bajwa RB Chair Chiltern CCG – Non Voting Dr Graham Jackson GJ Chair Aylesbury CCG – Non Voting Dr Charles Todd CT Clinical Director – Central Locality Dr Stuart Logan SL Clinical Director – Diabetes, CSP & Prevention Dr Peter Newman PN Clinical Director –Wooburn Green Locality –
Joined from Item 7 Dr Rebecca Mallard Smith
RMS Clinical Director – Joined from Item 7
Dr Roger Dickson RD Clinical Director – North Locality – Joined from Item 7
Dr Raj Thakkar RT Clinical Director – Planned Care – Joined from Item 8
Neil Flint NF Head of Commissioning for Planned Care- Item 8
Catherine Richards CR Transformation Manager – Planned Care - Item 8
Minute Taker
Leigh Franklin LF Executive Assistant Office Manager
Page 129 of 148
Page 129 of 148

No Agenda Item Discussion 1. Welcome &
Apologies Apologies received: Lou Patten
Dr Rashmi Sawhney Lisa Maclean
2. Declarations of Interest
RM reminded committee members of their obligation to declare any interest they may have on any issues arising at committee meetings which might conflict with the business of Aylesbury Vale or Chiltern CCGs, the standing declarations were as noted in the Declarations of interest register.
Declarations of interest from today’s meeting Agenda Item 12 – 24/7 Urgent Primary Care discussion all GPs that are Members of FedBucks Agenda Item 11 - Community Hubs discussion – KW and MJ declared an interest
The Chair agreed for all GPs to remain in the discussion as the Executive required the appropriate Clinical knowledge but will not contribute to the decision made.
3. Minutes of 22nd December 2017
The minutes were reviewed and approved with some minor changes.
4. Actions Log – 22nd December 2017
The Action log was reviewed with the following updates:-
EC/20 – New process instead of the MAD button for Practices - LB advised that the process has been updated since the circulation of the paper. LB apologised for the delay in setting up this new system, mainly due the correct resourcing in place to ensure monitoring. The re-launch will be 1st February directing Practices to use the member’s website, replacing the MAD button; the second part of the launch will be the ability to use the DXS system from mid-February.
The Process is quite self-explanatory. The team will be looking at trends and holding providers to account
Page 130 of 148
Page 130 of 148

on a quarterly basis. The system cannot hold PID patient Identifiable data.
There will be comms to launch in the GP bulletin at the end of January in both AV and Chiltern this will be a pilot with review in 6 months’ time, there will be a link to Quality team who will work closely with the Localities hoping to ensure we reinstate the confidence of using the system with the Practices.
PM raised the concern managing the IG risk, some of the contact points on the pathway were not nhs.net, and therefore will not be secure; they will all need generic nhs.net email addresses. LB will review and ensure contact email addresses that are sign posted are nhs.net.
The launch will be County wide. SR asked that they ensure the communication goes to the Locality meeting to allow membership involvement in the pathway. LB will discuss with the Locality teams.
EC/23 - RM updated on the Local Digital Roadmap and Estates Technology Transformation Funding The LDR has had minor changes to the documents circulated to Executive Committee, with a more detailed technical document and more accessible language for publication these are now all submitted to NHSE.
ETTF – awaiting confirmation of release of 1st phase of funding, have also asked for additional £300k from slippage and awaiting response to that. Have received capital support for interoperability.
DLS is now in liquidation and we have been in discussion with the liquidator. It was decided by SMT that it would be safer to close down the website and app, although relatively low usage due to clinical risk it was safer to close down.
5. AO Report RM updated the Executive Committee
The Month 9 position put the CCGs into Financial recovery, further information and discussion at agenda item 6.
Operational Plan – positive feedback has been received so far from NHSE, particularly the clinical stories. We now await further feedback before the final version can be submitted.
Briefings with Stakeholders A STP event was held last week attended by multiple stakeholders. RB reported that concern was expressed at the meeting that the Primary Care agenda in not currently reflected in STP discussion and many of the plans don’t include Primary Care. It was agreed at the meeting that a representative would put themselves forward to co-ordinate.
There will be a standard slide set available for any meetings with Councillor members to ensure we are
Page 131 of 148
Page 131 of 148
presenting a consistent message.
RM advised that this was PM’s last meeting and to thanked him for all his hard work.
6. Finance Report – Month 9
PM reported on the Financial Performance: To the end of November (9 months) the total position is an under spend of £4,475k against an equivalent budgeted surplus.
• The forecast position deteriorated by c£3m in relation to increasing activity at Frimley Health FT,CHC, Continence products, which together with the required QiPP stretch has resulted in the CCG’snot being able to mitigate further identified risks. For M9 the CCG’s have reported a net risk of£3.3m to NHSE which if not mitigated will result in us missing our financial targets.
• The CCGs have developed a financial recovery plan which has been presented to NHSE to ensureexpenditure remains within planned levels through further expenditure controls and reviewingforecasts to identify mitigating opportunities.
• The position has been achieved by the utilisation of Non-Recurrent mitigations of £8,724k andContingency of £3,128k released into the position to cover the crystallisation of some of the risksand the additional in month pressure.
• Buckinghamshire CCGs remain on target currently to achieve their 1% planned surplus requirementthough will need to mitigate the £3.3m risk to that position relating to further pressures across thecommissioning portfolio especially across Joint and Continuing Care through increased activity andcost of packages, Acute contracts mainly Non elective admissions and Prescribing activity.
• The reserves being utilised within the forecast outturn are those that have no specific criteria for use;the 0.5% contingency reserve and the surplus budget. The amount utilised year to date is not inexcess of the 9/12 level.
• In conjunction with NHSE guidance the 1% Headroom reserve remains uncommitted in the CCGposition.
SR queried the use of the delegated monies for members being used to help fill the gaps. PM advised that this money was the reported underspend that could not be carried forward for use into next year and was not assigned to any project. RM reiterated that it was important to understand the correct message to members. RB said that it would be sensible to advise members at the February PLT sessions.
PM also advised that that the ledger balance of cash appears overdrawn but the actual cash balance at the bank was not physically overdrawn. This was caused by timing difference between payment journals hitting the ledger and cash leaving the bank account.
QIPP: Actual delivery year to date being £10,252k against an equivalent plan of £11,666k (88% achievement), before mitigations
Page 132 of 148
Page 132 of 148

• The year to date QIPP performance is considered below target and is rated amber. Forecastachievement is also below target at 87%, before mitigations, and also rated amber.
• To hold the CCG position QIPP is required to deliver an additional £2,980k above ytd run rate;mitigations identified through the summer and autumn balance sheet and forecast reviews enable usto cover this stretch.
• Buckinghamshire CCGs have instigated a deep dive into the QIPP schemes to gain assurance inthe robustness and deliverability of the schemes, look for in year mitigation and to build up a pipelineof schemes that can be used to replace underperforming schemes or used for future years.
The Executive Committee noted the report
7. Financial Recovery Plan
PM advised that as reported, the financial position that emerged at the end of December put the CCGs ability to deliver its planned surplus under considerable pressure.
Following a large in month expenditure increase, c£3m, the CCG found itself in the position that it had very limited identified opportunity with which to manage further risk should it crystallise; this further risk was estimated at £4.1m with £800k of potential mitigation available.
As a result the CCG developed a formal Financial Recovery Plan that builds upon the work undertaken during the autumn when we had initiated an internal recovery approach.
The CCG has adopted a two strand approach of reviewing forecasts to ensure that our risk assessments are robust and in parallel develop mitigation plans to reduce expenditure, or maximise income, in the final quarter of the financial year.
PM talked the Executive Committee through the Financial recovery plan shared with NHS England. The Executive looked in detail at the possible opportunities available for recovery. PM will circulate the final recovery plan information sent to NHSE and would ask for any further help in recognising areas of potential savings.
DR asked that the teams ensure that they are putting all projects onto the Verto system, there have been workshop sessions and 1:1s to ensure all are familiar with the system, this will be the most productive way to ensure we all understand the projects that are on-going.
8. Quality & Performance Report
DR and RM updated the Executive Committee on the Quality and Performance report
Cancer Cancer performance is monitored at the monthly Cancer Assurance group (which reports to the Planned Care Programme Board) with input from performance, quality, contracts and clinical leadership. An SDIP has
Page 133 of 148
Page 133 of 148

been proposed to BHT, to be varied into the new contract (FY17/19) that aims to encourage the provider to review specialties and develop action plans that are pro-active and sustainably improve performance.
NHSE have also afforded the opportunity for national Intensive Support Team (IST) to support BHT and this is currently being progressed. They are currently working with OUH where there are significant pressures at both specialty and diagnostics level, affecting regional commissioning partners as the OUH is a prominent tertiary and specialist centre.
The cancer team are now looking at how to expand engagement across other providers (Frimley and OUH – as those with high levels of activity). Links have already been established with the Thames Valley Strategic Clinical Network and we plan to strengthen this relationship by inviting them and the newly formed Thames Valley Cancer Alliance to the Cancer Assurance Group meetings on a quarterly basis.
There were four 104 day cancer breaches in October at BHT. Clinical Harm Reviews (CHRs) have been completed for each patient and conclude that there was no harm caused by the extended wait for treatment.
There were three 104 day cancer breaches in November at BHT – theses were shared breaches with three different tertiary providers. BHT will complete a CHR for their part of the pathway and will request a clinical harm review from the tertiary provider for each patient.
RTT The RTT Incomplete target was not met on a Bucks CCG’s basis in November with performance at 90.6%, with both CCGs missing the 92% target.
For both CCG’s performance, at BHT and OUH is the major contributor to the failure to meet the 92% target.
The Senior Management team have taken the following actions: .
• A recovery plan has been received from BHT, reviewed and shared with NHSE. The plan wasjudged as requiring considerable additional work in order to provide the required level of assurance.The CCGs will work alongside BHT to decide the appropriate level of detail/ assurance requiredgoing forward.
• The expected recovery trajectory is for Paediatrics to be compliant by the beginning of February andoverall trust compliance by the end of March.
• A review of the weekly activity received from BHT. The latest activity report from BHT shows thebacklog has not reduced as much as planned in Ophthalmology, T&O, Paediatrics and GeneralSurgery.
The CCGs have bid for additional RTT funding (£200k) from NHSE and proceeded to implement these actions on the basis that the funding will be received but this may be a risk.
Page 134 of 148
Page 134 of 148

Ambulance Response times The Ambulance response time targets were not met in November.
SCAS actions: • Continue to work to achieve on the agreed actions with the local action plan which is tracked at
regular CCG hosted meetings
• A demand practitioner has been deployed to manage frequent callers and appropriately examine asappropriate
• Work with Buckinghamshire Healthcare Trust (BHT) to address the handover delays that have adirect impact on SCAS performance and crews being able to leave the hospital to pick up other jobsin the community
• SCAS are currently reviewing the resource for the additional stand points for Aylesbury and Chiltern.An additional stand point would mean that SCAS crew could reach a job quicker than they currentlydo with a more flexible approach to meeting job demand. A decision on this resource will be madewithin the next few weeks.
CCGs actions: • Commissioners meet with colleagues from SCAS to work through the local action plan for Bucks
which aims to address the key issues which have been a challenge locally. These meetings takeplace 6 weekly with the next one scheduled for February 23rd.
• SCAS continue to work towards achieving their agreed trajectories for each of the areas within theThames Valley region including Buckinghamshire and to support the improvements through theaction plan.
• Primary care team continue to work with SCAS on the paramedic pilots these have been wellreceived and are a good example of multidisciplinary working across different organisations.
• The CCGs have organised a meeting between SCAS and BHT to agree a process to improve thecurrent hand over delays that are being reported at Stoke Mandeville Hospital. The Emergency CareImprovement Programme (ECIP) team have also been invited to support the meeting and helpdeliver the rapid improvement guidelines (RIG).
• The Quality and Performance Committee will be inviting SCAS to the committee meeting on 22March 2017 to talk through their Bucks Improvement Plan to address performance issues, and theirRemedial Action Plan to address the quality issues raised in the performance notice issued to the
Page 135 of 148
Page 135 of 148

Trust on 20th January 2017.
CH expressed concerns about the on-going SCAS performance and Stoke. RM reported that SCAS have been asked to attend the next Quality & Performance meeting in March to give and update on their recovery plan.
On stroke LB reported that East Berkshire are working closely with providers. The interim dispersal pathway is working well, with 7 extra beds open. The scanner wasn’t working last weekend but BHT has recognised that the age of the scanners is a system wide issue, and BHT have plans for replacements. Their refurbishment plans are on track for the end of April. There will be an investigation into the two patients that were affected at the weekend from the broken scanner to ensure they came to no harm.
A&E
The A&E 4hr wait target was not met and has not been met YTD by any local provider.
Buckinghamshire Healthcare Trust (BHT) delivered a performance of 87.6% for all types in December 2016 against the 4 hour national standard of 95%. This is a 7.5% adverse variance to plan of 95.1%. The percentage of breaches for admitted patients related to 68.7%, or 993 breaches. In line with NHSE and NHSI winter planning requirements, BHT delivered a planned 85% occupancy rate in the run-up to the Christmas period and also took the following actions:- • Escalation beds were utilised to meet medical demand.• St Joseph’s Ward was utilised as both a discharge lounge and a general medical ward.• Paediatric demand also resulted in the escalation for external bed and cubicle cover.
DR advised that A&E has been high profile with the media. During January it has continued to be a challenge for BHT with the first week of January even more challenging that December declaring OPEL 4 Black, they have also experienced a second period of OPEL 4 but have recovered more quickly.
DR also advised that there are a number of Bucks medically fit patients remaining in Frimley compared to Berkshire patients, this is an on-going issue and the team continue to work through the challenges.
RD do we monitor the pressure on primary care during that period whilst these issues are happening. This was also raised recently at A&E Delivery Board and although it is difficult to measure it is certainly worth following up.
The Quality and Performance Report was noted by the Executive Committee.
9. Buckinghamshire Cancer Strategy 2016-21
Raj Thakkar (RT), Catherine Richards (CR) and Neil Flint (NF) joined the meeting.
Page 136 of 148
Page 136 of 148

The Bucks Cancer Strategy has been developed by the Cancer Strategy Group to provide an overview of the strategic direction that NHS Aylesbury Vale and NHS Chiltern Clinical Commissioning Groups wish to take to improve cancer care for our patients. The strategy closely aligns with the key priorities for cancer and has been developed as part of the CCGs Operational Plan 2017/18 - 2018/19.
The strategy has been approved by both the Bucks Cancer Strategy Group and the Planned Care Programme Board.
RT advised that this is the plan, how to deliver that plan is the next step. NF said that the detail of works will be circulated and discussed at the Cancer Strategy working group and presented back to the Executive. Clinicians will be invited to be involved in the plan.
CR advised that the newly established cancer alliance has put in transformation funding bids for a whole variety of initiatives to help improving data and IT across the Thames Valley area. The Cancer Alliance have realised the importance of IT and data movement. Feedback is expected by the end of March.
RT thanked CR for all her work
The Executive Committee agreed that the Cancer Strategy can be submitted to NHS England and attached to the CCG Operational Plan.
10. Community Hubs Pilots in Thame and Marlow
David Williams (DW), Natalie Fox (NF) and Syed Hasan (SH) joined the Executive Committee meeting from Buckinghamshire Healthcare Trust.
DW took the Executive Committee through the progress made on the Community Hub proposals; having worked together on a model for developing services in the community linking with Primary Care and the CCGs alongside recent public engagement events.
The Executive discussed in detail and made challenge on the presentation requesting further clarity and narrative from BHT. Further discussions will take place outside of the Executive Committee meeting with a report back on a regular basis on progress made.
11. 24/7 Urgent Primary Care: Using the historic OOHs contract as an opportunity for transformation
RMS advised the Executive Committee that she will be holding a 24/7 primary care workshop with members on 15th February to encourage everyone to be innovation as a locality or individually and look to transfer primary care over the next two years. RMS said that by September we should have a plan to be shaped over the next couple of years to ensure improved access to planned and urgent care and would like to open it up to the Executive to get their thoughts and opinions.
The Executive discussed and fed back ideas and thoughts. It was agreed that we must ensure we work with the members and gain a collective view. It was also important to work with Fedbucks as they will be part of the vision. It was agreed that there were a number of messages/communications that we needed to ensure the members were aware of. The Programme Board will design a strategy for the member engagement.
Page 137 of 148
Page 137 of 148

NL advised that she had forwarded some information on MCPs and PACs models that were worth reading they described the vanguard models.
Meeting Closed
Page 138 of 148
Page 138 of 148

AYLESBURY VALE AND CHILTERN CLINICAL COMMISSIONING GROUPS AUDIT COMMITTEE 30 November 2016
Nightingale Room, The Gateway, Gatehouse Road, Aylesbury
Voting Members Present Robert Parkes (RP), Audit Committee Chair, Aylesbury Vale CCG (chair) Tony Dixon (TD), Audit Committee Chair, Chiltern CCG Graham Hurst (GH), Lay Member, Chiltern & Aylesbury Vale CCGs Anita West (AW), Practice Managers Representative
Others present (non-voting) Philip Murray (PM), Chief Finance Officer, Chiltern & Aylesbury Vale CCGs Alan Cadman (ACa), Deputy Chief Finance Officer, Chiltern & Aylesbury Vale CCG David Guest (DG), Ernst and Young (External Auditors) Liz Wright (LW), RSM Tenon (Internal Auditors) Gareth Robins (GR), Counter Fraud Manager, TIAA Russell Carpenter (RCa) – Corporate Governance Lead (Minute taker)
Welcome 1. Introductions and apologiesThe Chair welcomed members and invitees to the meeting in common of the two CCGs’Audit Committees.
The following apologies were noted: • Kate Holmes (KH), Deputy Chief Finance Officer, Chiltern & Aylesbury Vale CCG• Maria Grindley (MG), Ernst and Young (External Auditors)
The meeting was noted as quorate to conduct its business. Members noted that Lesley Munro-Faure, previously a practice manager’s representative for Aylesbury Vale, had taken a role with FedBucks and therefore had resigned from CCG business.
2. Declaration of interests in items on this meeting’s agenda
RCa reminded committee members of their obligation to declare any interest they may have on any matters pertaining to the agenda.
Declarations of interest from sub committees: None declared that are not already in standing declarations. Declarations of interest from today’s meeting: RP noted that all members present were conflicted in respect of agenda item 12 (staff code of business conduct) as its contents would apply to them as individuals who are CCG employees, from CCG member practices or otherwise with one or more positions of authority. However it was agreed by members that they were still acting within their decision making authority to approve the Code on behalf of the Governing Body (and therefore to remain present for the item).
RCa noted that a register of declarations of members was also available for review; to embed a principle of the conflicts of interest policy in ensuring members interests are
Page 139 of 148
Page 139 of 148

accurately recorded. Chairs of other meetings are also asked to cross reference this with agenda planning to ensure conflicts are identified, mitigated, and reported on cover sheets so any required action by the meeting chair is clear. GH noted that he would need to update his record. Action 1 – RC to circulate a declaration form to GH after the meeting to update his entry. 3. Minutes of the last meeting. TD commented that the minutes could be more specific on what actions the committee is taking, and if a report is being noted the minute should state that, or otherwise be clear if further action is required. PM suggested the detail on the finance report conclude by reading “The committee closed this item by noting the contents of the report and the current financial situation” TD noted that a sentence referring to whether the Commissioning Support Unit had a procurement register was incomplete. RC replied that this is in progress and, when complete, would be published on the CCGs’ websites. It details procurement decisions following federation on 1 July and also includes single tender waivers above threshold of £50k. Action 2 – Procurement Decisions Register requires a quality assurance approval by committee to confirm what is publishable given commercial in confidence constraints. The minutes were also corrected to specify that the Deputy CFOs are now shared posts and not aligned separately to each of the CCGs. It was also agreed to ensure that an appropriate action log is put in place. 4. Matters Arising, not otherwise on the Agenda None 5. Financial Position PM introduced this item (Month 7). Debt Write-off • Following review of the aged debt and discussion at Governing Body an invoice raised
to Buckinghamshire County Council in 2014 has been written off. • During 2013 and 2014 Buckinghamshire County Council was not engaging in the joint
care arrangements to the satisfaction of the CCG and was putting claims on the CCG for cases which they deemed to be healthcare responsibility. Furthermore there was no acceptable level of engagement by the Council to arrive at satisfactory outcomes.
• In an attempt to stimulate engagement the CCG issued invoice 7027300082 dated 18/10/14 for £329,766.95 relating to the expected cost that the CCG had incurred for children and young people that needed to be shared or realigned to the sharing agreement with Buckinghamshire County Council.
• At the end of 14/15 the CCG was aware that the debt would be at risk of being collectable so generate a Provision for Doubtful Debts to cover this item. This provision
Page 140 of 148
Page 140 of 148

is still in the balance sheet and will be released into the Income and expenditure account to offset the write off.
• The CCG now feels that the Council is now engaged at the expected level to move agendas forward and become further integrated in the care for patients of Buckinghamshire. The time is right to cancel this debt.
• This was discussed at the Governing Body meeting 10th November 2016 and the action agreed to write back the debt, reported back to the Audit Committee.
• RP noted that this had been subject to formal provision/set aside, which has now been released.
Financial Performance: To the end of November (7 months) the total position is an under spend of £3,481k against an equivalent budgeted surplus. PM noted that this same report had also been discussed by the Executive Committee last week. • PM emphasised that the underlying position remains on track, although with future
QIPP delivery required to achieve its ambitions in order to sustain this (circa £4m in the remaining six months of the financial year).
• Buckinghamshire CCGs have instigated a deep dive into the QIPP schemes to gain assurance in the robustness and deliverability of the schemes, look for in year mitigation and to build up a pipeline of schemes that can be used to replace underperforming schemes or used for future years.
• To maintain the forecast position the CCG’s have utilised £9,126k of non-recurrent mitigations covering the use of contingency, noted below, the use of budget and project slippage and release of balance sheet accruals not required.
• Risks to achievement remain, with pressure expected to continue into the next financial year.
• RP emphasised that the CCGs are in a difficult position and that achieving the planned year-end position is by no means guaranteed.
• PM noted that there remains a QIPP opportunity, particularly in relation to continuing healthcare, where accruals are based on numbers of patients on the broad care management database used by the CSU. Some patients, particularly those in receipt of fast track end of life packages of care, may already have passed away, which can therefore result in over-accrual.
• In conjunction with NHSE guidance the 1% Headroom reserve remains uncommitted in the CCG position. However it is anticipated that, at Month 9, permission will be given to release this into the underlying position. Any CCG that finds that it still cannot achieve balance having done this will be in instant financial recovery.
• TD drew attention to planned QIPP savings in prescribing and a best case scenario of £3,678m, querying how realistic this estimate was now.
• AC confirmed that Prescribing forecast continues to be based on activity paid compared to plan, adjusted for further pressures later in the year. The CCG forecast underspend remains lower than forecasts from the PPA due to the volatile nature of the PPA forecasts at this time of year, although the figures are close to each other.
• PM added that many CCG CFO’s are seeing PPA forecasts further below their budgets, but with scepticism as to whether the position will hold. Hence the prudent position to retain a higher prescribing forecast at this stage of the financial year.
• TD added that London audit chairs had discussed that CCGs may be able to release part (0.5%) of the headroom, although this is speculation and not yet confirmed. PM and TD acknowledged that if this were to happen, its benefit may actually be limited.
Page 141 of 148
Page 141 of 148

• PM added that the CHC position is not expected to get materially worse, unless there were to be a run on high cost cases.
• There may also be a pressure to invest further in acute contracts given challenges with RTT (Referral to Treatment) and other constitutional targets such as cancer, which may then be the prompt for headroom release.
• Unplanned care was also noted as difficult to forecast, along with ongoing challenges and variance across providers in conversation rates from A&E attendance to full admission.
• TD queried the relationship between social care services in Berkshire and Buckinghamshire. PM replied that support would be based on residential address rather than registered practice and thus acute discharge should be liaising with the respective local authority team.
• It was acknowledged that Slough and Royal Borough of Windsor and Maidenhead may well have a more robust presence in Wexham A&E than Buckinghamshire. CHC and Local Authority are both routinely challenged to ensure Wexham patients are not treated any differently.
• TD queried the position of financial allocations. PM replied that these are already set for 2016-17 and 2017-18, with minor adjustments for:
o A change in identification rules (a mechanism by which healthcare activities can be identified as specialist and therefore for direct commissioning by NHS England).
o HRG (Healthcare Resource Group) 4+ - these are updated codes through which acute trusts charge for activity under payment by results (PBR), which is believed to save £1.5m across the two CCGs and therefore this has been removed from the allocation.
• Allocations are unlikely to materially change were the two CCGs to formally merge (which we are some distance away from); although there could be an additional challenge to make further savings.
• In summary, QIPP remains a challenge (for which there has recently been an audit) though the bigger opportunities are in planned care. As the position is activity driven, PM emphasised the need to ensure GP colleagues support the CCG in referring appropriately.
• The committee noted the accompanying report.
6. Internal Audit LW noted a final report for Aylesbury Vale on localities governance with reasonable assurance, with recommendation on governance arrangements, but to revisit in six months when governance around STPs is clearer. TD queried when the audit took place, which LW confirmed was late September/early October. LW introduced the progress report, with no audits in progress that will affect head of internal audit opinion with a draft annual report to the March meeting. LW noted RCa attended a GBAF workshop last week and use of three line of defence model. LW noted that RSM could also provide a Governing Body workshop on this. PM queried whether RSM had experienced other federations and whether the CCGs were in the position internal auditors would expect. LW replied that there are few CCGs who have gone through the process, but the CCGs are further along than expected compared
Page 142 of 148
Page 142 of 148

to other organisations with reasonable assurance obtained through audits undertaken to date. It was acknowledged that the plan will reduce upon entry to 2017/18 where audits are only undertaken once, although whilst remaining two separate statutory bodies then separate head of internal audit opinions may still be required. It was also acknowledged that there is the added complication of Sustainable Transformation Plans. Sustainable Transformation Plans TD highlighted that lay audit chairs have been encouraged to carefully scrutinise these for assurance on the risks, to which PM added it would need some time to ensure appropriate assurance. RP emphasised that the role of audit is about challenge of the process and not business detail. LW added that discussion is in progress region wide in respect of joint audit committees given a need for mutual assurance, but a concern is the transparency in decision making – where the responsibility of CCGs ends and responsibility of STPs (which have no statutory authority) begins. Following a short debate, it was agreed to further discuss and identify impact on the CCGs operating plan through a special meeting in January. Action 3 (RCa) Meeting to further discuss and identify impact on the CCGs operating plan of STP. 7. External Audit DG attended for MG and introduced this item. There were no particular concerns to report, though working is ongoing with CSU and CCG staff to work up an audit plan for 2017/18 with an annual report anticipated at the meeting of the committee in March 2017. PM noted that last year the Better Care Fund (BCF) was high profile in external audit, and this year STP and Primary Care given delegated commissioning arrangements. PM queried whether any other high profile issues were anticipated. SG confirmed there were no other issues anticipated. 8. Counter Fraud GR introduced this item and noted two referrals since the last meeting being investigated.
(1) Patients eligible for Full Nursing Care (FNC) on located on the relevant first floor in a nursing home based on needs for which the CCG is paying a higher rate cumulative circa £100,000 now be recovered. There had been some delay in transfer from the ground floor. Investigation is underway to determine whether this, known for some months by the management, constituted intent to de-fraud or an oversight.
(2) Discrepancies on payments made from a Personal Health Budget (PHB) not in line with agreed care plan. GR noted that experience from other CCG clients indicates that this is a civil rather than criminal matter. The recipient had indicated willing to re-pay and money concluded to have been inappropriately spent.
9. Single Tender Waivers amounts ACa introduced the STW, noting that 3 waivers were presented
(1) Maximum Group; telephony support for call centre that is part of Digital Life Sciences project in primary care. This is the most capable provider with technical expertise.
Page 143 of 148
Page 143 of 148

(2) Hunter Healthcare – two waivers relating to external consultants, one working on the Lead Provider Framework for the Commissioning Support Unit re-procurement and the other an interim deputy of contracts now substantively filled.
For the latter two interim roles, original contracts were both extended above original purchase orders, resulting in waivers to allow for the difference which takes costs above tender threshold and allow subsequent invoices to be paid. £ It was noted that there was an error in figures presented to committee in respect of the interim deputy director of contracts - £74314.80 shown on the single tender waiver log whereas £74614.80 shown on the waiver documentation. Minutes to clarify accurate figure – this should read as £76614.80. These single tender waivers presented were noted. 10. Integrated Risk Management Framework The Audit Committee were asked to:
(1) REVIEW, APPROVE AND RATIFY the revised integrated risk management framework.
(2) NOTE that the Senior Management Team (SMT) has been asked to agree a process decision in relation to risk escalation from project level to corporate risk level as is described in the draft framework/supporting flowchart guidance.
The CCGs’ Integrated Risk Management Framework has been reviewed and updated, aligned both to federation and the introduction of a new project management software system, Verto (as of November 2016). Both CCGs previous frameworks have been combined and condensed. This includes a risk module to replace the 4Risk software system for risk currently in use. It has also taken into account previous internal audit findings and recommendations. Specific amendments include the CCGs appetite for risk aligned to strategic aims/goals, and a flowchart/guidance to break down steps required in identifying, reporting, monitoring and escalating risks. Members were asked to note that this is in development, with an opportunity to comment on a draft before it is finalised. A supporting table, available to members to review on request, documents the CCGs committees and the format, content and frequency of risk registers and reports each is anticipated to receive. Members were also assured on how recommendations from previous audit reports have been incorporated. Audit Committee approved the revised Integrated Risk Management Framework following federation, subject to minor amendments:
(1) Emphasise that it corporately owned by the Chief Finance Officer but management responsibility is with Nicola Lester as Director of Corporate Affairs.
(2) Clarification as to reference to having a ‘high’ appetite for reputational and innovation / service delivery risks and what this means. Although there is appetite for new technology to innovate, it is less true to say that high risk would be acceptable in relation to service delivery given the current financial position. (Post meeting note – this point has been removed from the framework to avoid ambiguity)
11. Conflict Of Interest Implementation plan
Page 144 of 148
Page 144 of 148

RC introduced this item. New guidance was published by NHS England in June 2016 which strengthens requirements in declaring and recording interests for CCG members and employees. Committee was reminded that, at its last meeting, it had agreed that conflicts of interest remain a standing item. Therefore this would be the opportunity to keep Conflicts of Interest Guardians well briefed on conflicts of interest matters and issues arising. An update on the CCG’s compliance action plan was provided. RC noted challenges in embedding governance around use and management or registers, and accurate articulation of conflicts of interest through cover sheets used by authors to prompt necessary actions. Committee was also informed of a further consultation was undertaken in October 2016 in respect of conflicts of interest, gifts, hospitality and sponsorship across the NHS as a whole, with an indication of possible implications for the CCGs provided in the accompanying paper. CCGs await final guidance to be published in Spring 2017. PM referred specifically to an action which read: It is imperative that CCGs ensure complete transparency in their decision-making processes through robust record-keeping. If any conflicts of interest are declared or otherwise arise in a meeting, they must be accurately recorded in minutes. PM suggested that this should also include minute taking courses. RC replied that most administrative staff had already been trained in this, and effective use of the cover sheet by authors would further assist minute takers. It was agreed to amend the action to reflect that additional training would be provided as appropriate. 12. Code of Conduct RCa introduced this item, noting that this and Conflicts of Interest policy were the remaining incomplete parts of the constitutions agreed to support federation of the CCGs. The Audit Committee was asked to:
• REVIEW, COMMENT on and APPROVE revised local CCG Code of Conduct for recommendation to the Governing Body that it can be RATIFIED
It is mandatory for the CCG (in line with all other Government Bodies) to adopt a Code of Conduct for its employees. This document has been reviewed and updated to align with Federation of the CCGs and therefore to ensure both adopt a consistent approach. Both Audit Committee chairs were provided the opportunity to comment in advance of this paper circulating to the committee. Following feedback that subsequent sanctions for non-compliance with the Code were unclear, the document has been strengthened to re-inforce other CCG policies that come into effect in ensuring the Code is appropriately enforced. TD queried whether this was likely to require further changes to the Code once formal guidance resulting from the consultation is published. Members were assured that this was unlikely; the Code already cross references to the CCGs conflict of interest policy (and
Page 145 of 148
Page 145 of 148

others) with these to be further updated if required. 13. Policy Approvals Members were asked to discuss arrangements for approving and ratifying policies going forward, as in Chiltern this had previously been through Executive Committee. LW reflected that, in other CCGs, Audit has approved risk management and conflicts of interest and little else – with Finance Committee looking at operational detail. RCa added that a policy on governance for policy and other document approval and ratification was in development. TD commented that Audit’s role is to be assured that appropriate policies are in place and are reviewed as necessary. Action 4 (RCa) PM noted that SMT and Executive would review this, Executive approve this and commend it to Governing Body for ratification. 01:40 14. Quality/Performance Assurance PM introduced the item and noted that it was to prompt a discussion as to how the committee is best assured on provider quality, given no member has this formally as part of their role and that there are other committees which also address it. TD reflected an example of previous concern with care homes heard by the Quality Committee of which he was also a member, with the Director of Nursing asked to attend to further Audit to explain rectification actions. This was agreed a useful example to explain Audit Committees involvement, which may be prompted by the Governing Body asking it to further discuss a particular issue. In response to query on what is documented in the terms of reference, RCa replied that they state: “The Committee may also request specific reports from individual functions within the Group as they may be appropriate to the overall arrangements. Its work dovetails with that of the Quality and Performance Committee which the group has established to seek assurance that robust clinical quality is in place”. LW noted that in other organisations it is the GBAF used for this purpose where a gap in assurance is perceived and request a deep dive into a particular area. This can ensure a robust process rather than looking into specific clinical quality issues. RP queried what the next step would be if Audit felt there were to be a problem, which LW replied would be to escalate to the Governing Body. LW suggested that the Audit Committee was unusual as it did not receive the corporate risk register or the GBAF. PM replied that it had been receiving the corporate risk register, although not since the CCGs had federated. LW’s recommendation entailed review of GBAF for assurance on controls and assurances with deep dive into areas where these were not felt to be sufficient. RP also suggested that the committee have a clear work plan of its routine reports, including risk registers. TD commented on having previously seen red rated risks with insufficient assurance that they were being appropriately and effectively managed. RCa replied that the risk escalation process would assist this in ensuring oversight of extreme risks at corporate level. TD
Page 146 of 148
Page 146 of 148

replied that this may mean that some risks (where they do meet threshold for escalation) the committee wouldn’t be sighted on. A compromise agreed was to ensure the committee also undertook a periodic review of some project level risks. RP noted that this needed to be further scoped and was an action for PM. 15. Primary Care Delegated Commissioning This item was noted as related to Chiltern only and that it was quorate to:
1. Receive FOR ASSURANCE a copy of Chiltern CCG’s application for delegated commissioning of primary care (delegated commissioning application process and checklist for 2017/18).
2. NOTE that terms of reference for Aylesbury Vale’s primary care commissioning committee (PCCC) will be updated to reflect from April 1 2017 the meeting will be held in common with Chiltern CCG, with an equivalent set to be agreed for Chiltern CCG with the equivalent inclusion.
TD noted that the Governing Body had reviewed and made approved a proposal to apply for delegated commissioning, and if approved by NHS England assume responsibilities for the commissioning of primary medical services from 1st April 2017. Aylesbury Vale CCG had assumed this responsibility on 1 April 2016. The application was signed by both Tony Dixon and Lou Patten as CCGs’ Accountable Officer. TD also noted that there were risks, PM adding that moving forward this relates to increased responsibilities with challenged resources internally and few additional resources. CCGs will also be required to deliver an extra 1% surplus through this area of funding. Nationally overall sustainability in primary care is a further future challenge. These risks were noted. There was discussion on reference in the paper to delegated commissioning “Giving CCGs more control over general practice is part of a wider strategy to support the development of place-based commissioning and a key enabler of the development of new care models” And “More control of workforce and processes supporting primary care commissioning” appearing in the list of opportunities. AW raised concern in terms of how this could/would be interpreted by primary care, with an overall conclusion that “oversight” may be a better choice of word given a need to be sensitive with the phrasing. It was acknowledged that the wording was likely taken straight from some form of NHS England documentation. It was also noted that the governing body member GPs hadn’t taken part in the discussion and decision in respect of the application because of conflicts and may therefore not have noticed this choice of language – having been in receipt of a paper with similar content as that circulated to Audit. Members asked for the minutes of Audit to reflect this point, although existing published papers and minutes will remain as they were. RCa will inform Helen Delaitre (as author of the paper on delegated commissioning) of this feedback. 16. Missing phone Committee received a report on a missing IPhone as all losses are required to be reported
Page 147 of 148
Page 147 of 148

to the Audit Committee and be included in losses register that forms part of statutory accounts. This will cost £230 to replace, for which the staff member concerned will be making a contribution. The loss was noted, along with assurance that appropriate security risk mitigations taken.
17. Key Issues (for escalation to the Governing Body)
• Audit Committee approved a revised Integrated Risk Management Frameworkfollowing federation, subject to minor amendments including a need to emphasisethat it corporately owned by the Chief Finance Officer but managementresponsibility is with Nicola Lester as Director of Corporate Affairs.
• Audit Committee discussed a proposed process for policy approvals, and agreedthat the Executive Committee in December would approve and ratify a formal policydescribing how CCG policies and other documents are developed followed byapproval and ratification by committees such as Audit and the Governing Body.
• A difficult financial position with ongoing QIPP challenge, with achievement ofplanned year-end position on track but by no means guaranteed.
18. Any Other Business
No other business raised
The meeting closed at 12:05pm. The next meeting was noted as taking place on 1 February 2017 in the large meeting room at Chiltern CCG.
Page 148 of 148
Page 148 of 148