Cost-Effective Suppression and Eradication of Invasive Predators
Upload
khangminh22Category
view
2download
0
Global Polio Eradication InitiativeStrategic P lan
2004–2008
WHOPartners in the Global Polio Eradication Initiative

WHO Library Cataloguing-in-Publication Data
Global Polio Eradication Initiative.
Global Polio Eradication Initiative : strategic plan 2004-2008.
1.Poliomyelitis – prevention and control
2.Poliovirus vaccine
Oral – supply and distribution
3.Immunization programs – organization and administration
4.Strategic planning I.Title.
ISBN 92 4 159117 X
(NLM classification: WC 556)
© World Health Organization 2003
All rights reserved. Publications of the World Health Organization can be obtained from Marketing
and Dissemination, World Health Organization, 20 Avenue Appia,
1211 Geneva 27, Switzerland (tel: +41 22 791 2476; fax: +41 22 791 4857;
email: [email protected]). Requests for permission to reproduce or translate
WHO publications – whether for sale or for noncommercial distribution – should be addressed
to Publications, at the above address
(fax: +41 22 791 4806; email: [email protected]).
The designations employed and the presentation of the material in this publication do not imply
the expression of any opinion whatsoever on the part of the World Health Organization concerning
the legal status of any country, territory, city or area or of its authorities, or concerning the
delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines
for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they
are endorsed or recommended by the World Health Organization in preference to others of a
similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary
products are distinguished by initial capital letters.
The World Health Organization does not warrant that the information contained in this publication
is complete and correct and shall not be liable for any damages incurred as a result of its use.
Printed in Switzerland
Global Polio Eradication InitiativeStrategic Plan
2004–2008

2
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
Abbreviations and acronyms 3
1 Executive summary 4
2 Background 6
3 Goal 8
4 Objectives and milestones 94.1 Objective 1: Interrupt poliovirus transmission 94.2 Objective 2: Achieve certification of global polio eradication 174.3 Objective 3: Develop products for the Global OPV Cessation Phase 224.4 Objective 4: Mainstream the Global Polio Eradication Initiative 27
5 Cross-cutting challenges 325.1 Political commitment and engagement 325.2 External financing 325.3 High-quality polio vaccines 335.4 Conflict-affected countries and areas 335.5 Public information and social mobilization 335.6 Biocontainment 34
6 Roles of partner agencies 356.1 Governments 356.2 Spearheading partners 356.3 Donor and technical partners 366.4 International humanitarian organizations and NGOs 376.5 Vaccine manufacturers 38
7 2009 & Beyond – the Global OPV Cessation Phase 39
C o n t e n t s

3
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
A b b r e v i a t i o n s a n d
A c r o n y m s
AFP acute flaccid paralysisAFR WHO African RegionAMR WHO Region of the AmericasARVs anti-retroviral drugsCCM Country coordination mechanismCDC US Centers for Disease Control and Prevention (USA)CIDA Canadian International Development AgencycVDPV circulating vaccine-derived poliovirusDFID Department for International Development (United Kingdom)EC European CommissionEMR WHO Eastern Mediterranean RegionGAVI Global Alliance for Vaccines and ImmunizationGCC Global Commission for the Certification of the Eradication of PoliomyelitisGOARN Global Outbreak Alert and Reponse NetworkkfW Kreditanstalt für Wiederaufbau (Germany)ICCs interagency coordinating committeesIDS integrated disease surveillanceiNIDs intensified national immunization daysIPV inactivated poliovirus vaccineiSNIDs intensified subnational immunization daysITD intratypic differentiationITN insecticide treated netJICA Japan International Coorporation AgencyMDGs millennium development goalsmOPV monovalent oral polio vaccineNCCs national certification committeesNGOs nongovernmental organizationsNIDs national immunization daysOPV oral polio vaccineRCCs regional certification commissionsRED Reach Every DistrictSIAs supplementary immunization activities (e.g. NIDs, SNIDs, mop-ups)SEAR WHO South-East Asia RegionSNIDs subnational immunization daysTAGs technical advisory groupsTCG global Technical Consultative Group for Poliomyelitis EradicationUN United NationsUNF United Nations FoundationUNICEF United Nations Children’s FundUSAID United States Agency for International DevelopmentVAPP vaccine-associated paralytic poliomyelitisVDPVs vaccine-derived poliovirusesVPDs vaccine-preventable diseasesWHA World Health AssemblyWHO World Health OrganizationWPR WHO Western Pacific Region

4
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
E x e c u t i v eS u m m a r y
1BY end-2003, poliomyelitis had been
eliminated from all but 6 countries1 in theworld as a result of the Global Polio EradicationInitiative, the largest international public healtheffort to date. Nearly 5 million children arewalking who would otherwise have beenparalyzed by polio and 1.25 million childhooddeaths have been averted by distributing VitaminA during the polio immunization campaigns.
Once polio has been eradicated, the world will reap substantial financial, as well ashumanitarian, dividends due to foregone poliotreatment and rehabilitation costs. Depending onnational decisions on the future use of poliovaccines, these savings could exceed US$ 1 billionper year.
The Global Polio Eradication InitiativeStrategic Plan 2004-20082 outlines activitiesrequired to interrupt poliovirus transmission(2004-2005), achieve global certification andmainstream the Global Polio Eradication Initiative(2006-2008), and prepares for the Global OPVCessation Phase (2009 & beyond). This Plan reflectsthe major tactical revisions that were introduced in2003 to interrupt the final chains of poliotransmission, the revised timeframe for certificationof eradication, and the decision to stopimmunization with oral polio vaccine (OPV)globally as soon as possible after global certification.
Of the 4 objectives outlined in the Plan, theover-riding objective is the rapid interruption ofpolio transmission in the 6 remaining endemiccountries. Eliminating these reservoirs during2004-2005 is now an urgent international publichealth issue because the cessation of massimmunization campaigns in most polio-freecountries has left the world increasingly vulnerableto importations of this disease. Objective 1 of thePlan details the supplementary immunization,routine immunization, and surveillance activitiesneeded to finish the job of eradication and protectthe investment made in polio-free areas. Particular
attention is given to ‘intensifying’ supplementaryimmunization activities to improve quality andreach every child. The Plan highlights the 3countries linked to over 95% of cases in 2003:Nigeria, India and Pakistan. It recognizes, however,that with the reduction in polio transmission inIndia and Pakistan in late 2003, the risks to globaleradication are increasingly concentrated inNigeria. The postponement of eradication activitiesin key areas of that country in 2003 led to a markedincrease in the number of polio-paralyzed Nigerianchildren and the re-infection of at least 5neighbouring countries. The narrow window ofopportunity that now exists to eradicate polio canonly be exploited if the leaders of the endemic areasensure that every child is immunized duringintensified supplementary immunization activitiesin 2004 (SIAs).
Objectives 2 and 3 of the Plan outline activitiesfor certifying the world polio-free and preparing forthe Global OPV Cessation Phase that will follow.With the certification process and criteria havingbeen validated in three WHO regions, Objective 2focuses on improving surveillance quality(especially in the 19 countries yet to achievecertification-standard), reversing declines insurveillance sensitivity in the regions that have beencertified, and completing Phase II of the GlobalAction Plan for the Laboratory Containment of WildPolioviruses. Objective 3 outlines the implications ofthe 2003 decision to stop OPV after globalcertification. Although trivalent OPV will continueto be the vaccine of choice for routineimmunization through 2008, the plan outlines thework required to develop the specific productsneeded to facilitate the safe cessation of OPV. Theseproducts include: a 3rd edition of the Global ActionPlan for the Laboratory Containment of WildPolioviruses (specifying the longterm requirementsfor wild poliovirus, vaccine-derived poliovirusesand Sabin-strains), monovalent OPV (mOPV)stockpiles, IPV produced from Sabin strains (S-IPV), and appropriate IPV-containingcombination vaccines. The plan also discusses the
1 Countries with ongoing indigenous wild polioviruses in 2003, in order of intensity of transmission, were: Nigeria, India, Pakistan, Niger,Afghanistan and Egypt.
2 This plan replaces and updates the Global Polio Eradication Strategic Plan 2001-2005. WHO Document No. WHO/Polio/00.05.

5
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
development of mechanisms to ensure thatcountries which desire or need these productshave access to them by 2008.
The fourth and final objective of the planaddresses the work required to integrate and/ortransition the substantial human resources,physical infrastructure and institutionalarrangements that were established for polioeradication into other disease control, surveillanceand response programmes. This objective alsodetails the programme of work to ‘mainstream’those polio eradication activities that must becontinued indefinitely (i.e. surveillance,stockpiles, containment) into existing national,WHO and UNICEF structures and mechanismsfor managing other serious pathogens which aresubject to high biosafety levels.
The greatest risks to achieving the annualmilestones of this plan are ongoing wild
poliovirus transmission in any of the 6 remainingendemic countries and an increased frequency ofpolio outbreaks due to circulating vaccine-derived polioviruses (cVDPVs). Implementingthe full activities outlined in the Plan requirescontinued technical support from a strong polio eradication partnership, financing for theshortfall of US$ 150 million to interruptpoliovirus transmission, and identification offunding for the US$ 380 million budget toachieve global certification and mainstream theGlobal Polio Eradication Initiative.
The Global Polio Eradication InitiativeEstimated External Financial ResourceRequirements 2004–2008 outlines the resourcesrequired to implement the Global PolioEradication Initiative Strategic Plan 2004–20083
and the financial implications of the major risksto the annual milestones of the Plan. ❐
3 WHO/UNICEF Global Polio Eradication Initiative Estimated External Financial Resource Requirements 2004-2008.

In 1988 the World Health Assembly (WHA),the annual meeting of the ministers of health of
all Member States of the World HealthOrganization, voted to launch a global initiativeto eradicate polio. As a result of the Global PolioEradication Initiative, the largest internationalpublic health effort to date, by late-2003 polio hadbeen eliminated from all but 6 countries and fewerthan 1000 children had been paralysed by thedisease that year. More notably, nearly five millionchildren were walking who would otherwise havebeen paralysed by polio and 1.25 millionchildhood deaths had been averted by distributingvitamin A during the polio immunizationcampaigns.
The international decision to pursueeradication of this devastating disease was basedon sound evidence from the WHO Region of theAmericas (AMR) as to the technical feasibility ofsuch a goal, and on the political and societalsupport best exemplified by the commitment of
the service organization Rotary International toraise financial resources and advocate for polioeradication. In the 15 years since the decision toeradicate polio, an extensive network of nationalgovernments, international agencies, privatecorporations, foundations, bilateral donors,humanitarian organizations, nongovernmentalorganizations (NGOs) and development bankshave formed a “global polio partnership”,spearheaded by the World Health Organization(WHO), Rotary International, the US Centers forDisease Control and Prevention (CDC) and theUnited Nations Children’s Fund (UNICEF).
Between 1988 and the mid-1990s, there was alimited reduction in the number of endemiccountries as the partnership was developed,broader political commitment secured and furtherevidence of the operational feasibility of the AMRstrategies established, particularly in the WesternPacific Region (WPR). From the mid-1990s, itwas possible to rapidly scale-up eradication
6
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
B a c k g r o u n d2
GLOBAL OPVCESSATION PHASE
Figure 1: Key targets to interrupt poliovirus transmission (2004-2005), achieve global certification and mainstream the Global Polio Eradication Initiative (2006-2008), and during theGlobal OPV Cessation Phase (2009 & beyond)
� CERTIFY GLOBAL ERADICATION
� TRANSMISSION TO LONG-TERM POLIO IMMUNIZATION POLICY
� COMPLETE PHASE II OF LABORATORY CONTAINMENT
� STOP POLIOVIRUSTRANSMISSION
� ACHIEVE CERTIFICATION-
STANDARD SURVEILLANCE IN
ALL COUNTRIES
� FINISH SUPPLEMENTARY
IMMUNIZATION
2004 2005 2006 2007 2008 2009& beyond
2004 2005 2006 2007 2008 2009& beyond
2004–2008 & BEYOND
� MAINSTREAMING OF POLIO ERADICATION LONG-TERM ACTIVITIES AND HUMAN RESOURCES

activities so that by the end of the decade over 575 million children were regularly being reachedwith oral polio vaccine (OPV) through the effortsof an estimated 20 million volunteers in every low-and middle- income country in the world. Today,the technical feasibility of polio eradication hasbeen demonstrated through the elimination of thedisease from 210 countries, territories, areas, andlarge geographic areas of the six remainingendemic countries. By late 2003, the remainingchains of wild poliovirus transmission,concentrated primarily in just five states or provinces of Nigeria (1), India (2) and Pakistan (2), were the result of missing substantial numbers of children during both routine andsupplementary polio immunization activitiesduring the preceeding years.
Since the Global Polio Eradication Initiativewas launched, the work of the global poliopartnership, including national governments, has
been guided by a series of multi-year strategicplans, the last of which was published in 20004.The Global Polio Eradication Initiative StrategicPlan 2004–2008 replaces and updates the 2000Plan. This Plan outlines the key activities requiredto interrupt poliovirus transmission (2004–2005),achieve global certification and mainstream theGlobal Polio Eradication Initiative (2006–2008)and prepares for the subsequent Global OPVCessation Phase (2009 & beyond) (Figure 1). Theplan reflects the major tactical revisions of strategywhich were introduced in 2003 to interrupt wildpoliovirus transmission worldwide, the revisedtimeframe for the certification of polio eradicationglobally, and the substantial increase in theknowledge base for development of policies for theperiod after global certification of polioeradication. This Strategic Plan serves as the basisfor the annual work planning of individual partneragencies and national programmes. ❐
7
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
4 Global Polio Eradication Strategic Plan 2001–2005 (WHO/Polio/00.05).

8
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
T HE goal of the Global Polio EradicationInitiative is to ensure that poliovirus
transmission is interrupted globally throughcoordinated national and international action, that the full humanitarian and economic benefits
of eradication are realized, and that the lessons andinfrastructure from its implementation areutilized in the strengthening of health systemsand control of other important diseases. ❐
G o a l3

9
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
S t r a t e g i c A p p r o a c h :
Interruption of wild poliovirus transmission hasbeen pursued using a combination of routine andsupplementary immunization activities (SIAs),guided by high quality surveillance (see also section 4.2).
High routine coverage with at least threedoses of oral poliovirus vaccine (OPV3) has beenthe foundation of the Global Polio EradicationInitiative. However, global OPV3 coverage wasonly 67% in 1988 and never reaching more than80% in subsequent years. More importantly, evenwith good OPV3 coverage polio has persisted inmany developing countries due to a combinationof factors. For example, the level of seroconversionto OPV3 is often substantially lower indeveloping, tropical climates compared withtemperate climates due to host (e.g. concomitantinfections, malnutrition), programmatic (e.g. coldchain failures) and environmental factors,requiring substantially more doses to seroconvertan individual. Furthermore, sub-optimalsanitation, high population density and tropicalclimates combine to facilitate the transmission ofany enterovirus in these areas, including
polioviruses. In such settings, wild poliovirus cancontinue to circulate even in highly immunizedpopulations, requiring synchronized campaignswith OPV to interrupt transmission.
Consequently, in endemic countries nationalimmunization days (NIDs) during the lowtransmission season for polioviruses have beenconducted to interrupt the major chains oftransmission by rapidly increasing systemic andintestinal immunity among all children aged lessthan five years. All endemic countries hadintroduced NIDs by the end of 1999. Whereepidemiologically appropriate, NIDs have beencoordinated across national borders.5 House-to-house mop-up campaigns, targeting at least onemillion children, were added to NIDs to interruptthe final chains of transmission. In 1999 theWHA called for the acceleration of activities,urging endemic countries to increase the numberof NID rounds conducted each year, to addsubnational immunization days (SNIDs) inparticularly high-risk areas, and to introduce ahouse-to-house vaccine delivery strategy for NIDsand SNIDs.6 In April 2003, as a result of anincreasing geographic restriction of poliovirustransmission and increasingly limited resources,
4 . 1 O b j e c t i v e 1 :
I n t e r r u p t P o l i o v i r u s T r a n s m i s s i o n
O b j e c t i v e s a n dM i l e s t o n e s
4
By late 2003, wild poliovirus was endemic in only six countries. Of the three countries which accounted for 95% ofcases globally, two (India and Pakistan) were at the lowest levels of wild poliovirus transmission ever, again
reaffirming the biologic and technical feasibility of polio eradication. With the reduction of cases in these countries andimprovement of quality of activities, the risks to global eradication are increasingly concentrated in Nigeria, where casesincreased markedly in 2003, with subsequent re-infection of a number of neighbouring countries. Consequently, in 2003the number of countries suffering polio cases due to importations was the highest ever recorded. In 2003 alone, respondingto importations cost over US$ 20 million in emergency mop-up activities. Rapidly eradicating the final polio reservoirsin 2004 has now become an urgent international public health issue. With the cessation of mass campaigns in most polio-free countries, the world is increasingly vulnerable to polio and the consequences of importations are increasingly grave.The narrow window of opportunity which now exists to eradicate polio can only be exploited if the leaders of endemicareas, particularly in five key states/provinces worldwide, ensure that every child is immunized during intensified massimmunization activities in 2004.
5 Examples are: Operation MECACAR, west and central Africa synchronized NID operations and synchronization of activities between China andthe SAARC countries.
6 Fifty-second World Health Assembly. Poliomyelitis eradication. World Health Organization, Geneva, 1999 (resolution WHA52.22).
the global Technical Consultative Group forPoliomyelitis Eradication (TCG) advisedconcentrating advocacy, financing and humanresources on the remaining endemic areas toincrease both the number and quality of SIAs. Torapidly stop the final chains of transmission inreservoir areas, from 2004 a series of intensifiedmass immunization campaigns, overseen by thehighest levels of government, will target the verylimited number of states or provinces which nowthreaten the global eradication goal.
S i t u a t i o n A n a l y s i s :
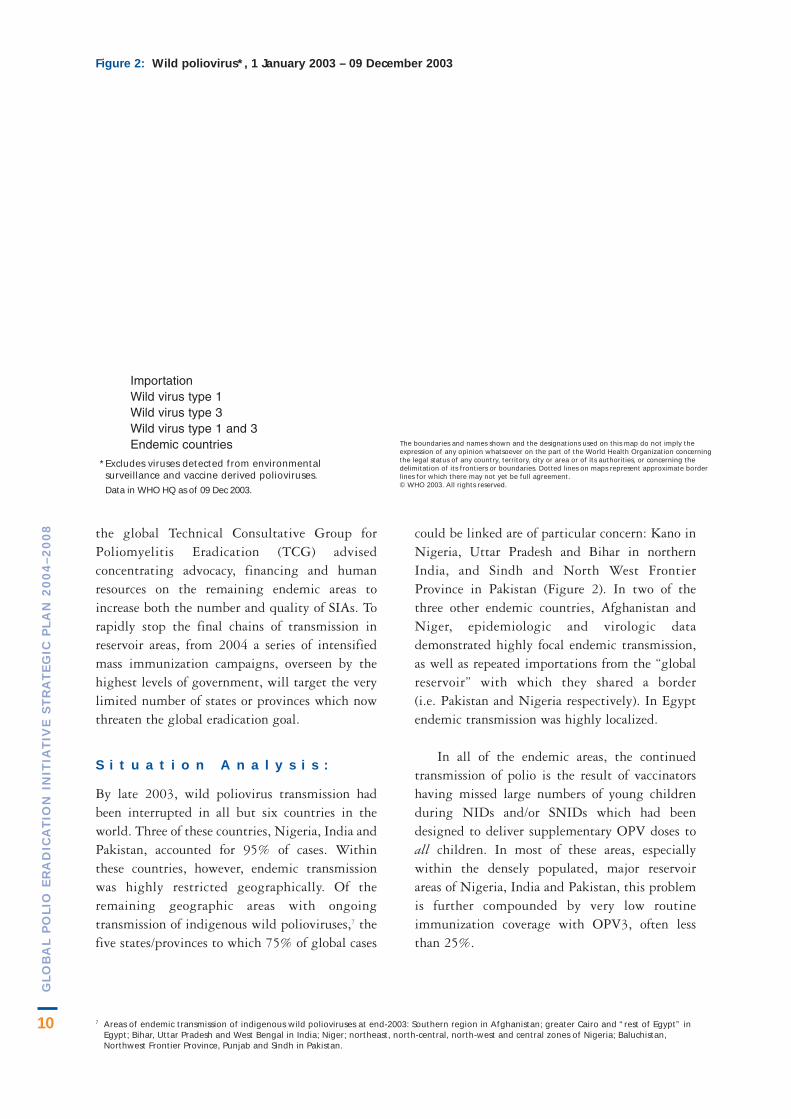
By late 2003, wild poliovirus transmission hadbeen interrupted in all but six countries in theworld. Three of these countries, Nigeria, India andPakistan, accounted for 95% of cases. Withinthese countries, however, endemic transmissionwas highly restricted geographically. Of theremaining geographic areas with ongoingtransmission of indigenous wild polioviruses,7 thefive states/provinces to which 75% of global cases
could be linked are of particular concern: Kano inNigeria, Uttar Pradesh and Bihar in northernIndia, and Sindh and North West FrontierProvince in Pakistan (Figure 2). In two of thethree other endemic countries, Afghanistan andNiger, epidemiologic and virologic datademonstrated highly focal endemic transmission,as well as repeated importations from the “globalreservoir” with which they shared a border (i.e. Pakistan and Nigeria respectively). In Egyptendemic transmission was highly localized.
In all of the endemic areas, the continuedtransmission of polio is the result of vaccinatorshaving missed large numbers of young childrenduring NIDs and/or SNIDs which had beendesigned to deliver supplementary OPV doses toall children. In most of these areas, especiallywithin the densely populated, major reservoirareas of Nigeria, India and Pakistan, this problemis further compounded by very low routineimmunization coverage with OPV3, often less than 25%.
Figure 2: Wild poliovirus*, 1 January 2003 – 09 December 2003
7 Areas of endemic transmission of indigenous wild polioviruses at end-2003: Southern region in Afghanistan; greater Cairo and “rest of Egypt” inEgypt; Bihar, Uttar Pradesh and West Bengal in India; Niger; northeast, north-central, north-west and central zones of Nigeria; Baluchistan,Northwest Frontier Province, Punjab and Sindh in Pakistan.
10
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
The boundaries and names shown and the designations used on this map do not imply theexpression of any opinion whatsoever on the part of the World Health Organization concerningthe legal status of any country, territory, city or area or of its authorities, or concerning thedelimitation of its frontiers or boundaries. Dotted lines on maps represent approximate borderlines for which there may not yet be full agreement.© WHO 2003. All rights reserved.
*Excludes viruses detected from environmentalsurveillance and vaccine derived polioviruses.
Data in WHO HQ as of 09 Dec 2003.
ImportationWild virus type 1Wild virus type 3Wild virus type 1 and 3Endemic countries
11
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
Although endemic polio transmission is nowgeographically restricted, wild poliovirusimportations have continued to paralyse childrenin polio-free areas. Between 1999 and mid-2003,a total of 12 such importations were detected withover 70 children paralysed in Africa, Asia, Europe,and the Western Pacific. In the first nine monthsof 2003 alone, virus from the northern Nigeriareservoir reinfected Burkina Faso, Chad, Ghana,Togo and part of Niger, as well as polio-free stateswithin Nigeria such as Lagos, requiring an inter-national immunization response. To date, all suchpolio outbreaks have eventually been controlledthrough large-scale OPV mop-up operations,though sometimes as late as six months after theindex case had been detected. In addition to therisk of importations, during 2000–2002 a total of28 polio cases in the Dominican Republic, Haiti,Madagascar and the Philippines, confirmed thereal, though rare, risk of polio outbreaks due tocirculating vaccine-derived polioviruses(cVDPVs). Although these cVDPV outbreakswere readily stopped with OPV mop-upoperations, the capacity to detect and respond to
such events must be in place until well after theuse of OPV in routine immunization has stopped.
E x p e c t e d R e s u l t s :
1. Intensified mass immunization activities inendemic areas (iSNIDs or iNIDs8): The highestpriority for the Global Polio Eradication Initiativeis the interruption of wild poliovirus transmissionin the remaining endemic countries of Nigeria,India, Pakistan, Niger, Egypt and Afghanistan.Among the remaining geographic areas withendemic transmission of indigenous wildpoliovirus,9 particular attention is required in thefive key reservoir states/provinces of Kano(Nigeria), Uttar Pradesh and Bihar (India) andSindh and North West Frontier Province(Pakistan). To stop transmission in all infectedareas as rapidly as possible, intensified activitiesare planned to repeatedly vaccinate the largecohorts of susceptible young children that rapidlyaccumulate in these areas due to large populations,high birth rates and very low routineimmunization coverage. Reaching over 90% of
8 iSNIDs: intensified subnational immunization days; iNIDs: intensified national immunization days.9 See footnote 7.
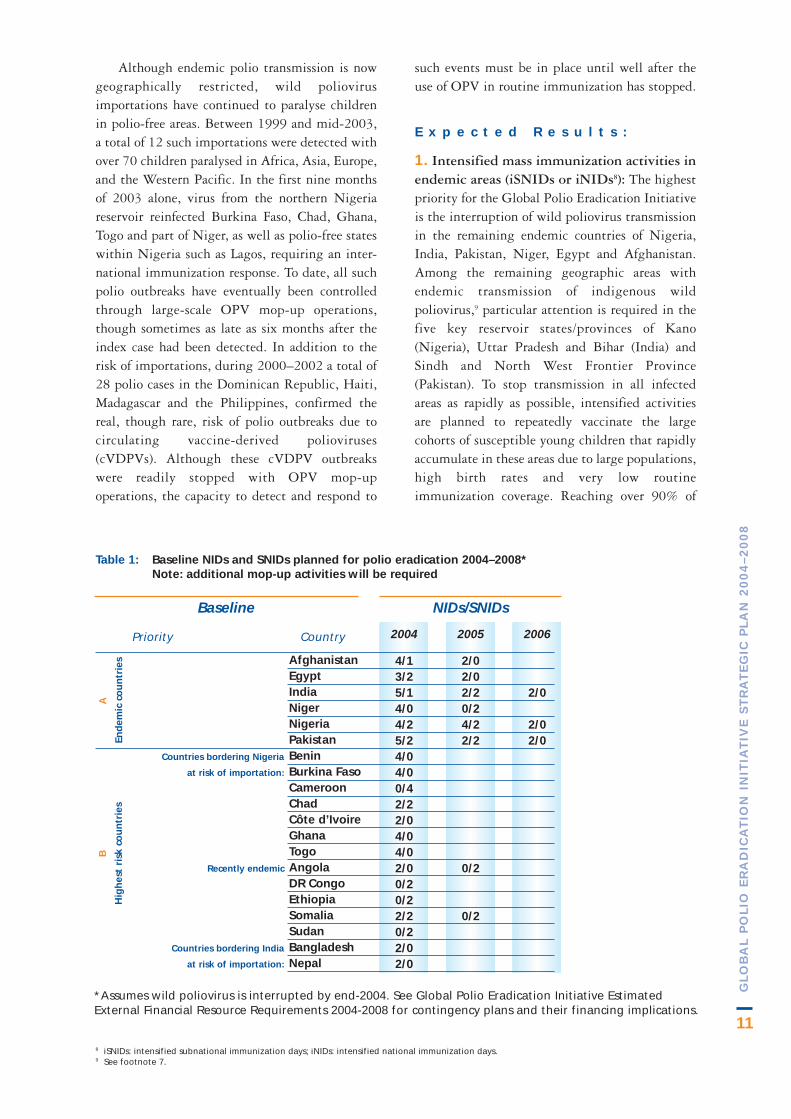
*Assumes wild poliovirus is interrupted by end-2004. See Global Polio Eradication Initiative EstimatedExternal Financial Resource Requirements 2004-2008 for contingency plans and their financing implications.
NIDs/SNIDsBaseline
Priority Country 2004
4/13/25/14/04/25/24/04/00/42/22/04/04/02/00/20/22/20/22/02/0
2006
2/0
2/02/0
2005
2/02/02/20/24/22/2
0/2
0/2
AfghanistanEgyptIndiaNigerNigeriaPakistanBeninBurkina FasoCameroonChadCôte d’IvoireGhanaTogoAngolaDR CongoEthiopiaSomaliaSudanBangladeshNepal
Countries bordering Nigeria
at risk of importation:
:
Recently endemic
Countries bordering India
at risk of importation:
Table 1: Baseline NIDs and SNIDs planned for polio eradication 2004–2008*Note: additional mop-up activities will be required
B
Hig
hes
t ri
sk c
ou
ntr
ies
A
End
emic
co
un
trie
s

12
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
children during intensified polio activities willrequire:
■ direct oversight by the highest political andhealth authorities in the country to ensureaccountability;
■ “mapping” of local political, religious,traditional and community leaders to ensurestate/province, district and community leveladvocacy efforts generate enhanced supportfrom influential opinion leaders;
■ detailed microplanning at the local level toensure that every household is identified,mapped and visited by an immunizationteam;
■ full engagement of local women’s groupsand other influential NGOs to ensuresufficient female vaccinators with access toall homes and communities;
■ enhanced communications strategies andactivities, based on epidemiologic andprogramme data;
■ sufficient financing and, where appropriate,innovative funding mechanisms, includingdirect financing to peripheral levelgovernment and nongovernmentalinstitutions, to ensure timely availability offunds at the point of operations;
■ additional technical assistance from poliopartners to ensure sufficient national andinternational expertise is available forstate/province and district planning andmonitoring.
iSNIDs or iNIDs will be conducted onemonth apart in series of 3–4 rounds, in allremaining endemic states or provinces, until 12months after the last indigenous case (Table 1).The effectiveness of these intensified activities will be highly dependent on the presence ofquality acute flaccid paralysis (AFP) surveillance,including very rapid processing of diagnosticspecimens and genetic characterization of isolatedviruses, to guide these activities.
2. Emergency response mop-ups to wildpoliovirus importations and/or cVDPVs: Thesecond priority will be to ensure that all polio-freecountries and areas treat the detection of animported wild poliovirus and/or cVDPV as apublic health emergency, with standard operatingprocedures to mount a rapid and massive mop-upresponse within four weeks of confirmation of sucha virus from a clinical case. To enhance nationalcapacity to initiate such a response, standardoperating procedures will be developed in eachcountry, as outlined in the requirements of theglobal and regional certification commissions. Atthe regional level, the polio partnership will targetits 2004 technical assistance to the rapidpreparation of these procedures in countries whichform epidemiologic blocks with the remainingreservoir areas (e.g. west and central Africa). Atthe global level, international requirements for thereporting of circulating polioviruses will berevised to enhance timeliness of their reporting.Adequate reserves of financial and vaccineresources are planned to facilitate emergency mop-up responses. By 2007 the management of theresponse to such events will be fully integratedwith existing WHO and UNICEF emergencyresponse mechanisms for other importantpathogens (e.g. yellow fever, meningitis).
3. Supplementary immunization in highest-risk polio-free areas: The third priority of theGlobal Polio Eradication Initiative will be toprevent the re-establishment of wild poliovirustransmission in polio-free areas, especially withinthe endemic countries themselves. Consequently,in addition to the iSNIDs at least two rounds ofiNIDs will continue to be conducted in each of theendemic countries for two years after the last caseis detected. Two rounds of NIDs or SNIDs willalso be conducted in the limited number of polio-free countries which are at particularly high risk ofre-establishing endemic transmission of importedwild poliovirus due to their proximity to anendemic area, large population size and/orsuboptimal OPV3 coverage. As of mid-2003, thesix large countries in which the re-establishmentof wild poliovirus transmission would beparticularly damaging were Angola, Bangladesh,the Democratic Republic of the Congo, Ethiopia,Nepal and the Sudan. As a result of the intensepolio transmission in northern Nigeria in 2003,and its repeated spread into bordering countries,NIDs or SNIDs are now also required in Benin,

13
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
Burkina Faso, Cameroon, Chad, Côte d’IvoireGhana and Togo. The NIDs or SNIDs in thesecountries will continue to be planned until the lastcase has been detected in the relevant reservoirareas. Specific countries and areas requiringadditional SIAs will be regularly reviewed andupdated, depending on routine immunizationcoverage, surveillance sensitivity, risk ofimportations and other factors. Table 1 outlinesthe proposed schedule of SIAs for these countries.
4. Enhanced routine immunization coverageagainst polio: The fourth priority will be tosupport the work of WHO and UNICEF,especially within the Global Alliance for Vaccinesand Immunization (GAVI), to improve routineimmunization coverage. In polio-free areasenhanced routine immunization coverage will becentral to limiting the spread of importationsand/or the emergence of cVDPVs. In endemicareas improvements in routine OPV coverage willenhance the impact of iNIDs, iSNIDs and
mop-ups. The importance of ensuring a “birthdose” of OPV will be reinforced. The Global PolioEradication Initiative will continue to identify forGAVI those areas at highest risk of importationsand/or cVDPVs for its international and nationaladvocacy work. Polio-funded staff will continue towork on routine immunization strengthening,giving particular emphasis to transferring poliolessons and experience to the effort to “ReachEvery District” (RED) in the areas at highest riskof importations. Special attention will be given tomicroplanning, logistics, social mobilization, andmonitoring and evaluation in the areas with lowOPV3 coverage (Table 2).
5. High quality surveillance and laboratories(see also objective 2): To interrupt endemicchains of wild poliovirus transmission,importations and/or cVDPVs, high quality SIAsmust be guided by excellent surveillance globallyfor circulating polioviruses. The highestsurveillance priority of the Global Polio
Table 2: Priority countries for improving OPV3 coverage to GAVI target*; WHO/UNICEF estimates for 2002 (based on data available as of October 2003)
CountryOPV3
% coverage
4842425448404041544557445043555057555946504040565339312525
AfghanistanAngolaBurkina FasoCambodiaCameroonCentral African RepublicChadCongoCôte d'IvoireDemocratic Republic of the CongoEthiopiaGuineaGuinea-BissauHaitiLao People's Democratic RepublicLiberiaMaliMozambiqueNauruPapua New GuineaSierra LeoneSomaliaSudanTimor-LesteVanuatuEquatorial GuineaGabonNigerNigeria
40–60%
<40%
CoverageCountryOPV3
% coverage
7279697962737074786179797778726378706068737663787377697974
BeninBoliviaBurundiChinaDjiboutiDominican RepublicIndiaIndonesiaLesothoMadagascarMalawiMicronesia (Federated States of )MyanmarNamibiaNepalPakistanParaguayPhilippinesSenegalSolomon IslandsSurinameSwazilandTogoTurkeyUgandaVenezuelaYemenZambiaZimbabwe
60–80%
Coverage
* GAVI target: by 2010 or sooner, all countries will have routine immunization coverage at 90% nationally with at least 80% coverage in everydistrict.
14
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
5
100%
30%
80%
85%
2 0 0 4
1*
100%
40%
90%
90%
2 0 0 5
0
100%
50%
100%
100%
2 0 0 6
0
NA
60%
100%
100%
2 0 0 7
0
NA
70%
100%
100%
2 0 0 8I n d i c a t o r s
Number of endemic countries
Percentage of planned SIAs
implemented in highest risk
polio-free areas (Table 1)
Percentage of countries
achieving GAVI targets for
DTP3/OPV3**
Percentage of emergency
mop-ups begun within four
weeks of case confirmation
Percentage of non-certified
countries with certification-
standard surveillance
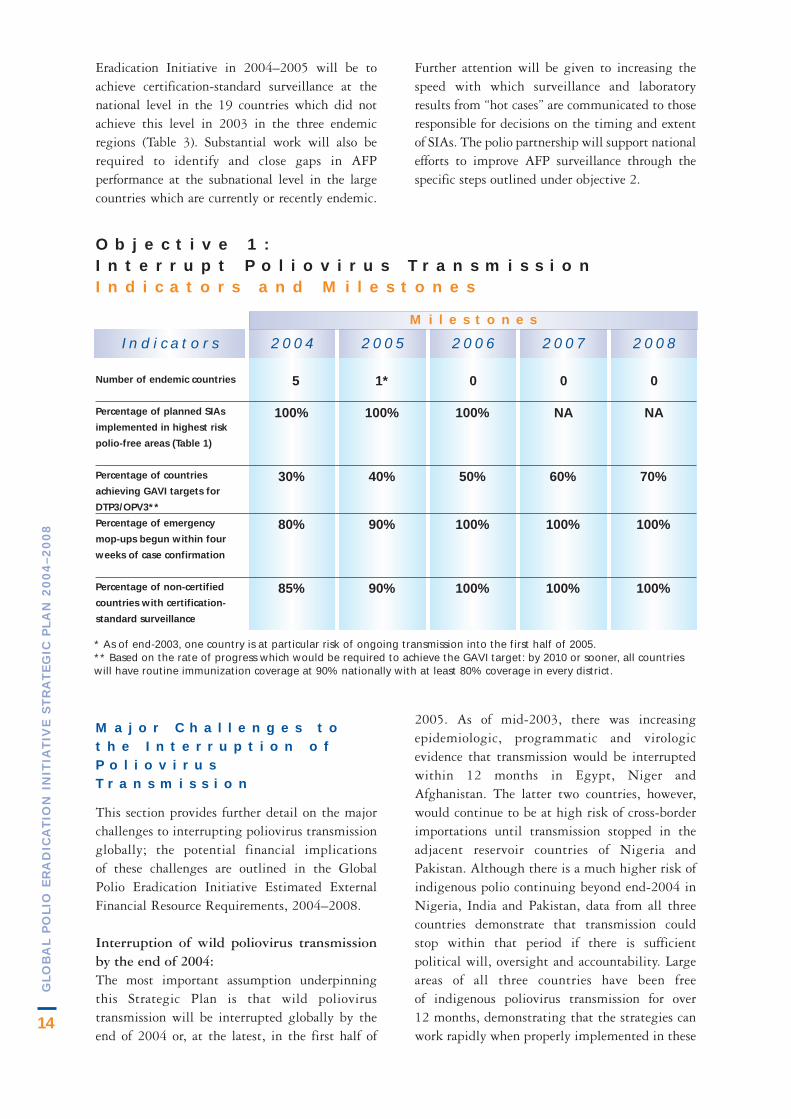
O b j e c t i v e 1 : I n t e r r u p t P o l i o v i r u s T r a n s m i s s i o nI n d i c a t o r s a n d M i l e s t o n e s
* As of end-2003, one country is at particular risk of ongoing transmission into the first half of 2005.** Based on the rate of progress which would be required to achieve the GAVI target: by 2010 or sooner, all countrieswill have routine immunization coverage at 90% nationally with at least 80% coverage in every district.
M a j o r C h a l l e n g e s t o t h e I n t e r r u p t i o n o fP o l i o v i r u sT r a n s m i s s i o n
This section provides further detail on the majorchallenges to interrupting poliovirus transmissionglobally; the potential financial implications of these challenges are outlined in the Global Polio Eradication Initiative Estimated ExternalFinancial Resource Requirements, 2004–2008.
Interruption of wild poliovirus transmissionby the end of 2004:The most important assumption underpinningthis Strategic Plan is that wild poliovirustransmission will be interrupted globally by theend of 2004 or, at the latest, in the first half of
2005. As of mid-2003, there was increasingepidemiologic, programmatic and virologicevidence that transmission would be interruptedwithin 12 months in Egypt, Niger andAfghanistan. The latter two countries, however,would continue to be at high risk of cross-borderimportations until transmission stopped in theadjacent reservoir countries of Nigeria andPakistan. Although there is a much higher risk ofindigenous polio continuing beyond end-2004 inNigeria, India and Pakistan, data from all threecountries demonstrate that transmission couldstop within that period if there is sufficientpolitical will, oversight and accountability. Largeareas of all three countries have been free of indigenous poliovirus transmission for over 12 months, demonstrating that the strategies canwork rapidly when properly implemented in these
M i l e s t o n e s
Eradication Initiative in 2004–2005 will be toachieve certification-standard surveillance at thenational level in the 19 countries which did notachieve this level in 2003 in the three endemicregions (Table 3). Substantial work will also berequired to identify and close gaps in AFPperformance at the subnational level in the largecountries which are currently or recently endemic.
Further attention will be given to increasing thespeed with which surveillance and laboratoryresults from “hot cases” are communicated to thoseresponsible for decisions on the timing and extentof SIAs. The polio partnership will support nationalefforts to improve AFP surveillance through thespecific steps outlined under objective 2.

15
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
countries. However, successfully building on thisclose political oversight will require the continueddevelopment of appropriate local responses tospecific challenges as they arise, such as the anti-OPV campaign in northern Nigeria in 2003, thelimited access to conservative tribal groups inparts of Pakistan and the persistent polioimmunity gap among underserved populations inIndia. In those limited endemic areas which arestill affected by conflict or insecurity, strategyimplementation will continue to depend onestablishing, at least temporarily, a safe workingenvironment.
In India the marked increase in the number (6) and quality of annual NID/SNIDrounds following the 2002 outbreak hassubstantially reduced the immunity gap10 inchildren from underserved communities (from42% in 2002 to just 13% in 2003) and, in 2003,was associated with the lowest mid-year levels oftransmission ever. With continued attention toreaching very young children and underservedpopulations in late 2003, particularly in thenorthern states of Bihar, Uttar Pradesh and WestBengal, transmission could be interrupted in2004. Of particular concern is western UttarPradesh, the only area in India where transmissionhas never been interrupted and where substantialnumbers of children are still missed during SIAs.Major challenges to achieving the necessary levelof SIA quality include ensuring programmecontinuity given the ongoing changes amongsenior health and political authorities in thecountry, heightening district level accountabilityfor the performance of immunization teams, andexpanding the ongoing efforts to reach all childrenin underserved populations. This work in endemicareas will need to be matched by faster, larger,high-quality mop-up responses to importationsinto polio-free areas, such as occurred in WestBengal in 2002 and Andhra Pradesh andKarnataka in 2003.
In Pakistan, a sufficient number ofNIDs/SNIDs have been planned to interrupttransmission by the end of 2004. However,ongoing gaps in SIA quality, particularly indistricts of northern Sindh and the North WestFrontier Province (NWFP), could leave asubstantial number of children unimmunized andcompromise the impact of these activities. The
mid-2003 decision of the President of Pakistan topersonally monitor progress should substantiallyimprove accountability in these areas. Because ofthe gaps in the formal health services in thesegeographic areas, further improvements in SIAquality require enhanced engagement of the localpolitical leadership to mobilize the non-healthtransportation, human and communicationsresources necessary to reach every child. Ofparticular importance will be fully implementingthe policy of having at least one woman (e.g. thelocal Lady Health Worker) on every vaccinationteam to ensure all communities and householdscan be visited to search for highest risk,unimmunized, very young children duringiSNIDs. The Federally Administered Tribal Areas(FATA) will require special attention to build thenecessary oversight and accountability by localpolitical and community leaders.
As of mid-2003, the greatest risk to the end-2004 global target was Nigeria, due to theintensity of transmission in the northern statesand the spread to recently polio-free areas bothwithin and outside the country. This exacerbationof transmission was caused by a combination ofsubstantial, ongoing gaps in SIA quality and thecancellation of key immunization activities inlate-2003. Of particular concern at mid-2003were data demonstrating that the polio immunitygap among children in some northern states,particularly Kano, was still >50%. Rapidlyclosing this immunity gap will require: (1) enhancing the microplanning, socialmobilization, logistics and vaccination teamsupervision during SIAs, (2) addressing ongoingcommunity concerns as to the safety of OPVfollowing widespread rumours and comments tothat affect, and (3) ensuring state and district levelauthorities are fully engaged in these activities. Tofacilitate this work, the polio partners haveenhanced their technical assistance to the keystates in coordination with federal authorities andprovided extensive background materials toaddress concerns over vaccine safety.
Frequency of circulating vaccine-derivedpoliovirus (cVDPV) outbreaks:The second major assumption underpinning thisplan is that cVDPVs will continue to be rareevents requiring only intermittent OPV mop-upcampaigns to stop transmission rather than
10 Immunity gap: percentage of children (non-polio AFP cases) receiving < 4 doses of OPV.

16
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
extensive, preventive SIAs to limit theiremergence. This assumption is based on theavailable data, primarily from the global AFPsurveillance and polio laboratory network, whichhas detected an average of only one cVDPVoutbreak each year in the period 1999–2002, witha total of 28 cases. During the period 1999 to June 2003, the laboratory network screened over11 000 polioviruses worldwide, 7000 of whichwere Sabin-related, usually isolated as acoincidental finding during the investigation ofAFP cases (29 were from the 3 cVDPV outbreaks,3 were from iVDPVs and 12 were “other” VDPVsof ambiguous origin).
Although cVDPVs appear to be rare events,the 3 recent episodes in Hispaniola, Madagascarand the Philippines have occurred undercircumstances which could become more prevalentin the period 2004–2008 and thus lead toadditional outbreaks. For example, common to allof these episodes was the absence of indigenouswild poliovirus, low routine OPV3 coverage and the cessation of supplementary OPV
immunization activities. With the revised tacticalapproach in 2003 to interrupt wild poliovirustransmission, an increasing number of countrieswith low OPV3 coverage will stop polio SIAs in2004–2005. It is anticipated that this decline inSIAs coverage will be in part compensated by anincrease in routine OPV3 as GAVI enhances itsefforts to increase coverage as laid out in itsStrategic Framework for that period. Furtheremphasis will be placed on the inclusion of thebirth dose of OPV, particularly in low coverageareas. In addition, there will be a heightening ofsurveillance and closer scrutiny of the VDPVswhich are detected through AFP and othersurveillance activities, to better understand therisk factors for, and frequency of cVDPVs.
Consequently, although the incidence ofcVDPV events could increase as a result of thereduction in SIAs globally, it is anticipated thatthey will continue to be rare. However, the globalTCG will by 2005 revisit its recommendations onthe need for additional SIAs to prevent theemergence of cVDPVs. ❐

17
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
4 . 2 O b j e c t i v e 2 :
A c h i e v e C e r t i f i c a t i o n o f G l o b a l
P o l i o E r a d i c a t i o n
S t r a t e g i c A p p r o a c h :
In 1997, the Global Commission for theCertification of the Eradication of Poliomyelitis(GCC) finalized the criteria for certifying whetherthe goal of polio eradication is achieved. Insummary, certification of the interruption of wildpoliovirus transmission is conducted on a regionalbasis. Each of the 6 Regional CertificationCommissions (RCCs) could consider certificationonly when all countries in that area had submittedthe appropriate documentation demonstrating theabsence of wild poliovirus transmission for at leastthree consecutive years in the presence of excellentsurveillance. The GCC further stated that forendemic and recently endemic countries, thenotification and investigation of AFP cases wouldbe the accepted standard for the purposes ofcertification. AFP surveillance would be of“certification standard” if three performancecriteria were achieved. First, the system shoulddetect at least one case of non-polio AFP for every100 000 population aged less than 15 years.Second, two adequate diagnostic specimens12
should be collected from at least 80% of AFPcases. Third, all specimens should be processed ata WHO-accredited laboratory.
For certification of global polio eradication, theGCC established the further criteria that allfacilities holding wild poliovirus infectious and
potentially infectious materials must haveimplemented appropriate biocontainmentmeasures. The process of laboratory containmentwas developed through international consultation.A draft action plan was widely distributed forcomment in 1998 prior to publication as theGlobal Action Plan for Laboratory Containment ofWild Polioviruses (WHO/V&B/99.32) in 1999,with a second edition in 2003.13 The plan outlinesphased activities to minimize the risk ofreintroduction of wild polioviruses fromdiagnostic and research laboratories to thecommunity. Phase I requires all countries toconduct a national search for laboratories and tocreate an inventory of those identified as holdingwild poliovirus or potentially infectious materials.RCCs have included phase I activities as acomponent of the regional certificationrequirements. Phase II requires that laboratorieslisted on national inventories destroy wildpoliovirus materials or maintain them underappropriate biosafety conditions. Formanufacturers of IPV produced from wildpolioviruses, specific guidelines defining biosafetyrequirements following the interruption oftransmission of wild polioviruses were developedand finalized in 2003 through a collaborativeprocess with national regulatory authorities andbiosafety professionals. Global certification willrequire the implementation of these requirementsin all countries where IPV production continues.
THE process for certification of the global eradication of poliomyelitis has been validated through the experience of thethree WHO regions that had been certified polio-free by end-2003. The global certification process is threatened,
however, by ongoing gaps in surveillance quality in the three remaining endemic regions, declining surveillance sensitivitywithin the three regions that have already been certified, and incomplete implementation of the Global Action Plan forthe Laboratory Containment of Wild Polioviruses (GAP II). In addition to interruption of wild poliovirus transmissionworldwide, achieving global certification by 2008 requires rapidly addressing persistent surveillance gaps in 19 countries of Africa, the Eastern Mediterranean and South-East Asia.11 Countries in regions which have already beencertified must maintain certification-standard surveillance and high immunity levels against poliovirus. All countriesmust have established national plans of action for rapidly responding to wild poliovirus importations and cVDPVs andhave completed Phase II containment activities. Vaccine manufacturers producing inactivated poliovirus vaccine (IPV)from wild poliovirus strains must have implemented enhanced biosafety procedures.
11 Of these 19 countries, 7 had a population of less than 1 million people and were unlikely to sustain undetected wild poliovirus transmission.12 Adequate diagnostic specimens: Two stool specimens collected at least 24 hours apart, within 14 days of onset of paralysis and received in good
condition at the laboratory.13 WHO Global Action Plan for Laboratory Containment of Wild Polioviruses. Second edition. World Health Organization, Geneva, 2003
(WHO/V&B/03.11).

18
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
S i t u a t i o n A n a l y s i s :
As required by the GCC, RCCs have beenestablished to oversee the process of reviewingnational surveillance and containmentdocumentation in each of the six WHO regions.National certification committees (NCCs) havebeen established in all countries to collate andverify the necessary information.14 As of mid-2003,three of the six WHO regions had been certifiedpolio-free. These regions included the 46 countries of the Americas in 1994, the 34 countries of the Western Pacific in 2000 and 51 countries of Europe in 2002. Although thethree remaining “endemic” regions have achieved“certification-standard” surveillance at theregional level, 19 of the 82 countries in thoseregions had yet to achieve this standard at thenational level during 2003 (10 in Africa, 7 in theEastern Mediterranean, 2 in South-East Asia)(Table 3). Within a number of other countries thequality of surveillance was not uniform and did not
meet the certification criteria for high qualitysubnational data. Figure 3 summarizes the statusof national AFP surveillance indicators in endemicand certified regions. Figure 4 illustrates theworldwide network of 145 virology laboratorieswhich forms the backbone of global AFPsurveillance,15 arranged in a hierarchical structureof national (123), regional (15) and globalspecialized (7) facilities. High quality performanceis assured through annual proficiency testing, aformal accreditation programme, and ongoingevaluation using standard indicators. In 2002,99% of the network laboratories were accreditedby WHO; 100% of specimens were tested in aWHO-accredited laboratory by referring samplesfrom countries where facilities were not accredited.
In mid-1999, the WHA urged all MemberStates “to begin the process leading to thelaboratory containment of wild poliovirus”.16 As ofmid-2003, 148 (68%) countries and territorieshad begun or completed their listing of
14 For the very limited number of geographic areas without a recognized national health authority (e.g. Somalia), the GCC has requested thatWHO and UNICEF assume responsibility for coordinating the collection, verification and submission of the documentation required forcertification.
15 The number and distribution of network laboratories are: 8 in the Americas, 16 in Africa, 12 in the Eastern Mediterranean, 48 in Europe, 17 inSouth-East Asia and 43 in the Western Pacific.
16 Fifty-second World Health Assembly. Poliomyelitis eradication. World Health Organization, Geneva, 1999 (resolution WHA52.22).
CountryAFP cases
reported (2003*)
28148131110659312811121885531
Non-polio AFP rate
0.402.701.302.007.300.601.301.601.701.700.590.700.480.432.373.090.471.240.73
AFP cases withadequate
specimens (%)
89717767739071710
790
1000
10072786067
100
Algeria
Botswana
Cameroon
Cape Verde*
Equatorial Guinea*
Liberia
Madagascar
Mozambique
Sao Tome and Principe*
Sierra Leone
Bahrain*
Cyprus*
Djibouti*
Kuwait
Lebanon
Somalia
West Bank and Gaza
Bhutan
Maldives*
Table 3: Countries not achieving one or more of the AFP Performance Indicators required for certification-standard surveillance in 2003 (data available as of 4 November 2003)
Region
Comoros, Mauritius, Reunion, Saint Helena, Seychelles and Timor-Leste did not report AFP cases in 2003 due to small populations.Data in HQ as of 4 November 2003.Red indicates targets not achieved.Green indicates targets achieved during 2002.*Total population <1 million, unlikely to have sustained, undetected indigenous transmission of wild polioviruses.Population Data source: United Nations Population Division, Department of Economic and Social Affairs, World PopulationProspects the 2002 revision.
AFR
EMR
SEAR

19
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
biomedical laboratories as part of the Phase Icontainment activities. This number includedseveral large industrialized countries such asAustralia, Canada, Germany and the United Statesof America. Worldwide, over 100 000 laboratorieshad been identified for surveying and 80 countries(37%) had finalized an inventory of laboratoriesstoring wild poliovirus materials. For IPVproduction facilities using wild poliovirus at thesesites, consensus has been reached on the need forBSL-3/polio level containment in all existingfacilities, with implementation and verificationactivities planned for completion in 2007–2008.
E x p e c t e d R e s u l t s :
1. “Certification-standard” surveillance: a) Polio-endemic regions: The highest prioritywill be to achieve and sustain certification-standard surveillance at the national level in the19 countries of the endemic regions which didnot achieve this level in 2002. Substantial workwill also be required to identify and close gaps inAFP performance at the subnational level in thelarge countries which are currently or recentlyendemic (Table 3). The polio partnership willsupport national efforts to improve AFPsurveillance through targeted technical assistanceat the national and subnational levels and, wherenecessary and appropriate, external financing ofequipment and operating costs. Attention will begiven to improving the speed of surveillance andvirologic data analysis and feedback at thecountry and regional levels, especially to meet theperformance indicators for emergency responsemop-ups in all regions. Joint national/international AFP surveillance reviews willcontinue to guide improvements.
b) Regions certified as polio-free: Assisted byRCCs and National Certification Committees(NCCs), countries in certified regions shouldsustain polio-free status by maintainingcertification-quality surveillance, achieving thehighest possible immunity levels against wildpoliovirus, and developing plans of action forrapidly reacting to importations of wild poliovirus.Priority will be given to identifying high-riskcountries or areas where AFP surveillancesensitivity has markedly declined and/or fromwhere enhanced AFP or supplementarysurveillance data may be required for the purposesof global certification. From 2005-2006,
partnership resources will increasingly be targetedto address those areas. At the same time, increasedattention will be given to integrating AFPreporting into appropriate national surveillancemechanisms, if this intergration has not alreadybeen done, or expanding the AFP surveillancecapacity to detect and investigate other diseases ofpublic health importance (see section 4.4).
2. Global access to a WHO-accreditedlaboratory: The priority in this area of work willbe to reduce the time required for intratypicdifferentiation (ITD) results to be available fromendemic areas; ITD capacity will be established inall countries with major poliovirus reservoirs. Forall other areas the priority will be to sustain,through global certification and OPV cessation,the international capacity that now exists toprocess all specimens from AFP cases in WHO-accredited laboratories. Consequently, emphasiswill be given to maintaining rather thanexpanding the existing laboratory network, withtargeted support to the small number of networklaboratories which have yet to achieveaccreditation. Special advocacy will be required,particularly from 2006 onward, to ensure that thenational public health institutions which housethe global polio laboratory network, but have amuch broader mandate, continue to designatesufficient human resources, facilities andequipment to polio eradication work. During thissame period, it is anticipated that the work of thepolio laboratory network will actually increase, as itaccommodates demands for supplementaryvirologic data in advance of global certification.These data requirements (e.g. targetedenvironmental surveillance) will be defined withthe GCC during the period 2004–2005.
3. Containment of wild polioviruses andVDPVs: The priority in this area will be thefurther dissemination and national levelimplementation of the activities outlined in thesecond edition of the Global Action Plan forLaboratory Containment of Wild Polioviruses (2003).Particular attention will be given to completingthe laboratory survey and inventory activities inall polio-free countries and preparing forimplementation of phase II laboratorycontainment activities prior to globalcertification. From the end of 2005, the date bywhich wild poliovirus transmission should havebeen interrupted for at least one year, phase II

20
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8Figure 3: AFP Performance Indicators 1 January 2003 – 25 November 2003
Figure 4: Global laboratory network for polio eradication, 2002
The boundaries and names shown and the designations used on this map do not implythe expression of any opinion whatsoever on the part of the World Health Organizationconcerning the legal status of any country, territory, city or area or of its authorities, orconcerning the delimitation of its frontiers or boundaries. Dotted lines on maps repre-sent approximate border lines for which there may not yet be full agreement.© WHO 2003. All rights reserved. Data in WHO HQ as of 25 November 2003.
Adequate stool collection rate
Non-polio AFP rate
< 60% 60%-80%
80% No AFP Surveillance
< 0.5 0.5 -1
1 No AFP Surveillance
The designations employed and the presentation of material on this map do not imply the expression of any opinion whatsoever on the part of the Secretariat of the World Health Organization concerning the legal status of any country,territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
Global Specialised Reference LaboratoryRegional Reference LaboratoryNational/Sub-national Laboratory

21
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
containment activities will be initiated in allcountries, with particular emphasis on largeindustrialized countries which contain the largeststocks of wild poliovirus.
BSL-3/polio containment will be completed infacilities producing IPV from wild poliovirus,followed by the necessary validation activities andlicensure by national regulatory authorities.During this period the GCC, in consultation withappropriate biosafety and other expert bodies, willestablish the national, regional and global levelprocedures needed for reviewing and verifying thecontainment documentation submitted by eachcountry as part of the certification process.Particular attention will also be given to verifyingthe thoroughness of national laboratory surveys toidentify potentially polio-infected materials, such as specimen collections from places andperiods when wild poliovirus was endemic. Theprocess for developing long-term containmentrequirements for wild and attenuated poliovirusstrains is outlined in section 4.3.
4. Completion of the certification processes:The priority in this area will be to support thework of RCCs in the three remaining endemicregions as they complete the process of trainingNCCs and then collect, review and decide onnational documentation through an intensiveseries of consultations. Particular attention will begiven to supporting the work of the RCC forAfrica, given the large number of countries forwhich it is responsible. At the global level, by theend of 2005 the GCC will seek to have finalized anumber of issues related to its operations,particularly (a) the additional data that will berequired for global certification from the threeregions which had been certified polio-free byend-2002, (b) the extent and role of environmentalsurveillance as a supplementary strategy prior toglobal certification, and (c) the mechanisms/procedures for reviewing and verifyingdocumentation on containment of laboratorystocks and IPV production. WHO and partnerswill continue to support the work of thecommissions by convening or facilitating thenecessary meetings, expert consultations, fieldvisits and other activities of these bodies. ❐
85%
100%
50%(phase I)
NA
60%(regional
certification)
2 0 0 4
90%
100%
75%(phase I)
NA
70%(regional
certification)
2 0 0 5
100%
100%
100%(phase I)
NA
85%(regional
certification)
2 0 0 6
100%
100%
100%(phase II)
60%
100%(regional
certification)
2 0 0 7
100%
100%
100% (phase II+)
100%
100%(global
certification)
2 0 0 8I n d i c a t o r s
Percentage of non-certified
countries with certification-
standard surveillance
Percentage of AFP specimens
processed in a WHO-
accredited laboratory
Percentage of countries
completing each laboratory
biocontainment phase
Percentage of manufacturers
producing wild-type IPV
under BSL-3/polio
Percentage of countries
submitting “final”
certification documentation
O b j e c t i v e 2 : A c h i e v e C e r t i f i c a t i o n o f G l o b a l P o l i oE r a d i c a t i o nI n d i c a t o r s a n d M i l e s t o n e s
M i l e s t o n e s

22
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
S t r a t e g i c A p p r o a c h :
The broad policy objective for the Global OPVCessation Phase is to minimize the risks of paralyticpoliomyelitis for current and future generations atthe lowest possible cost. The cessation of routineimmunization against smallpox following theeradication of that pathogen in 1977 established anexpectation that immunization against polio canalso stop after the interruption of wild poliovirustransmission and the containment of laboratorystocks and vaccine production facilities. Thesmallpox experience has offered important insightsinto the range of issues that arise in thedevelopment of such policy. However, the issue issubstantially more complex for polio due to avariety of reasons, including differences in thecharacteristics of the vaccines used and in thegeopolitics of the era in which each eradicationcampaign has been conducted.
Consequently, the focus of this area of work hasbeen to first define and quantify the risks ofparalytic poliomyelitis following globalcertification, due to either the continued use of theOPV or the continued handling of wild poliovirusesor potentially infectious materials. An agenda ofresearch and programme work was established toinform this risk framework and to study potential
strategies for their mitigation. Particular attentionwas given to defining the financial costs, economicimplications, technical and regulatory feasibility,and operational practicality of each potentialstrategy. Recognizing the implications of thisevolving work for polio eradication stakeholders, aswell as the international health community, aconsultative process was initiated to betterunderstand these influences. A communicationsprogramme of work was established to ensure thewide dissemination of relevant scientific andprogrammatic data on both the risks followingcertification and their management as additionalinformation became available.
In April 2003, the global TCG stated thatstopping OPV would require new policies in fourinterrelated areas: (1) routine immunization, (2) detection and notification of circulatingpolioviruses as public health emergencies, (3) polio vaccine stockpiles and outbreak responsemechanisms, and (4) long-term biocontainment ofall poliovirus strains.
S i t u a t i o n A n a l y s i s :
In 1998, a WHO-convened expert consultation onthe scientific basis for stopping polioimmunization concluded that given the rare but
4 . 3 O b j e c t i v e 3 :
D e v e l o p P r o d u c t s f o r t h e G l o b a l
O P V C e s s a t i o n P h a s e
SINCE 2000, polio outbreaks caused by vaccine-derived polioviruses (VDPVs) have conclusively demonstrated thatthe continued use of the OPV for routine immunization could compromise the goal of eradicating all paralytic disease
due to circulating polioviruses. To minimize the long-term risks associated with OPV, the world must stop the routine useof this vaccine as soon as possible after global certification, while surveillance sensitivity and population immunity arehigh. Although trivalent OPV will continue to be the vaccine of choice for routine immunization for the Global PolioEradication Initiative up to 2009, stopping OPV requires the development of a range of other products during the period2004–2008. A third edition of the Global Action Plan for the Laboratory Containment of Wild Polioviruses will beneeded by 2006, specifying the biosafety requirements for wild polioviruses, VDPVs and Sabin-strains in the GlobalOPV Cessation Phase of the programme (i.e. 2009 & beyond). Monovalent OPV (mOPV) will need to be licensed andstockpiled to complement or even replace the current “rolling stockpile” of trivalent OPV. The manufacture of IPV fromSabin strains (S-IPV) will be encouraged, as will the production and licensing of appropriate IPV-containingcombination vaccines for those middle- or low-income countries which might choose to introduce such a vaccine. Becauseof the long-term risks of wild poliovirus re-introduction, the ongoing need for an OPV stockpile, and the probable futureproduction of S-IPV, OPV production capacity will be needed indefinitely. During this period, every country must planfor the cessation of OPV use and decide whether or not to introduce IPV; countries deciding to introduce IPV must makeprovision for its procurement. Recognizing the challenges to developing and introducing new products, this work will beclosely coordinated with GAVI.

23
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
predictable risk of vaccine-associated paralyticpoliomyelitis (VAPP), the use of OPV for routineimmunization should eventually stop once wildpoliovirus transmission was interrupted, wildpoliovirus stocks were properly contained andthere was assurance that VDPV circulation wouldnot persist. Following the confirmation in 2000that VDPVs could indeed persist, circulate andcause polio outbreaks, subsequent consultationsidentified three potential options for stoppingroutine OPV immunization: coordinated cessationof OPV globally (possibly following immunizationcampaigns in low coverage areas), phasedreplacement of OPV with IPV for routineimmunization (for at least an interim period), andthe development and introduction of a new poliovaccine for routine immunization. In the same yearan expert review of new vaccines for the GlobalOPV Cessation Phase outlined substantial manu-facturing challenges and regulatory hurdles tointroducing a new poliovirus vaccine. Since thenthe polio research agenda has focused on thefeasibility and effectiveness of the first two options.
In 2001, the global TCG established an ad hocCommittee for Poliomyelitis Research to provideadditional oversight of the ongoing research forpost-certification policy development. By late-2002this research had progressed to the point where theglobal TCG could endorse a framework of the risksof paralytic poliomyelitis after global interruptionof wild poliovirus transmission. The frameworkclassifies these risks into two categories: those dueto the continued use of OPV and those due to futureimproper handling of wild polioviruses. Thespecific risks within both categories were defined,with working estimates of the frequency andpotential burden of disease associated with each(Table 4). From 2001, a briefing kit on thepotential risks, and post-certification policy ingeneral, has been widely disseminated amongnational health authorities, polio partners, otherstakeholders and interested bodies. These materialswere updated in 2003 as additional information onrisks following certification became available andthe processes for policy development were furtherclarified. In 2003, WHO also published a positionpaper on the introduction of IPV into OPV-usingcountries to assist the growing number of countries,particularly in polio-free regions, which wereconsidering or implementing a change to IPV forroutine immunization, primarily due to nationalassessments that the risk of VAPP was increasinglyunacceptable.
Among the key developments in the area ofpublic consultation was a 2002 meeting at which awide range of policy-makers from diversebackgrounds reaffirmed the internationalexpectation, particularly among low- and middle-income countries, that routine polio immunizationwould eventually stop. Of equal importance was theSeptember 2003 international consultation onvaccine-derived polioviruses which concluded thatVDPVs posed a real risk to the global goal ofeliminating paralytic poliomyelitis due tocirculating polioviruses. That meeting furtherconcluded that this risk would continue as long asOPV continued to be used, particularly in areas oflow routine immunization coverage.
In 2003, the Global Polio Eradication Initiativewas operating with a rolling stockpile of 50 milliondoses of trivalent OPV for responding to wildpoliovirus outbreaks and cVDPVs, with a plannedexpansion to 75 million doses for the period2006–2008 (as outlined below, prior to the cessationof routine OPV immunization a significantly largerstockpile of mOPV will be required). By late-2003,as a result of the above-mentioned scientificresearch, programme work and consultations, theGlobal Polio Eradication Initiative was workingtoward the cessation of routine immunization withOPV as soon as possible after global certification.This goal required enhancing the work to licensemOPV for the vaccine stockpile, as mOPV wouldallow a type-specific response to cVDPVs orcontainment failures and thus limit the number ofserotypes reintroduced to human populations. Theimplications of OPV cessation also led to anexpanded programme of work to mainstream the
Risk category
Risks of polioparalysis fromcontinued use oforal polio vaccine
Risks of paralysisfrom mishandlingof wild poliovirus
Risk
VAPP(vaccine-associated paralytic polio)
cVDPV(circulating vaccine-derived polio)
iVDPV(immuno-deficient excretors of
vaccine-derived polio)
Inadvertent release from a laboratory
Inadvertent release from an IPVmanufacturing site
Intentional release
Frequency
1 in 2.4 million dosesof OPV administered
One episode per year in 1999–2002(Haiti, Madagascar, the Philippines)
19 cases since 1963with 2 continuing to excrete; no secondary cases
None to date
One known eventin early 1990s
None to date
Estimated globalannual burden**
250–500 casesper year
Approx. 10 casesper year (total of29 cases in threeyears)
<1 case per year
No cases
* Study and data collection is ongoing for all categories ** Under current polio immunization policies
Table 4: Risks of paralytic poliomyelitis followingglobal certification*

24
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
polio vaccine stockpile and response activitieswithin WHO and UNICEF and to evaluate furtherthe potential large-scale production of IPV fromattenuated (e.g. Sabin) poliovirus strains. Finally, asWHO-coordinated research had indicated that morepotent poliovirus antiviral compounds could bedeveloped, the Global Polio Eradication Initiativecontinued to explore the potential role suchproducts might have in enhancing flexibility inoutbreak response scenarios.
E x p e c t e d R e s u l t s :
1. Strategy for cessation of routineimmunization with OPV: The priorities in thisarea of work will be to (a) refine existing estimatesof the frequency and risk associated with each typeof VDPV which could emerge with OPV-cessation,including the geographic areas or demographicgroups at highest risk (especially for cVDPV), (b) establish standard strategies and operatingprocedures for responding to circulating poliovirusafter OPV cessation, (c) develop local strategies toreduce specific VDPV risks (i.e. iVDPVs,17 VDPVsin orphanages), (d) evaluate seroconversion rates,operational feasibility, costs and productioncapacity of IPV, alone and in combination, for low-and middle-income settings, (e) maintain thecapacity to restart large-scale OPV-use if required,and (f) define the most cost-effective strategy forthe coordinated cessation of OPV. Becauseminimizing the risk of VDPV emergence andspread at the time of OPV cessation requires highsurveillance sensitivity and population immunity,these priorities must be sufficiently addressed by2006 to allow implementation to begin.18 Such atimeframe is needed to ensure that those countrieswhich will want to switch to IPV on an interim orlong-term basis are able to secure the necessaryvaccine and financing. To facilitate decisions onpost-OPV vaccination policies, from 2004onwards, there will be extensive consultation,particularly with OPV-using countries, on the risksassociated with OPV cessation. Further materialswill be developed to assist countries in decidingwhether or not to introduce IPV and if so how (e.g.guidelines, policy directives). Standard protocolswill be implemented to study some of theseexperiences. Additional work will be conducted toensure sufficient IPV capacity. Given the risksassociated with IPV production using wild
polioviruses, the development of IPV productsbased on attenuated (e.g. Sabin) strains ofpoliovirus will be encouraged.
2. Detection and notification of circulatingpolioviruses: With the elimination of wildpoliovirus transmission globally, the detection ofany circulating poliovirus must be treated as aninternational public health emergency to ensure itis contained with a rapid response. Consequently,routine AFP reporting and investigation will needto be supplemented by additional measures tofacilitate the rapid detection and immediatenotification of such events to national andinternational health authorities. AFP reportingwill also need to be aligned with other WHOactivities aimed at identifying events ofinternational public health importance. Enhancedsurveillance will be particularly important todetect potential cVDPVs, during andimmediately after OPV cessation. Within one yearof the last case of wild poliovirus, the reporting ofany circulating poliovirus will be incorporatedinto existing mechanisms for dealing with eventsof international public health importance, such asthe WHO International Health Regulations andthe Global Outbreak Alert and Response Network(GOARN). The ongoing polio research agendawill continue to explore new diagnostics, tools andstrategies for surveillance following globalcertification, including the potential role oftargeted environmental sampling.
3. Polio vaccine stockpiles and theirmanagement: By the end of 2003 theinternational rolling stockpile of trivalent OPVfor responding to wild poliovirus importationsand/or cVDPVs consisted of 50 million doses oftrivalent OPV. This stockpile will grow to 75 million doses as supplementary immunizationcampaigns are phased out in the period2006–2008. Both the number of doses and rangeof polio vaccines in this stockpile will expand inadvance of the cessation of OPV for routineimmunization. The number of doses required forthe stockpile over time will be calculated using acombination of national immunization policy andcoverage data and modelling of the possible spreadof reintroduced wild poliovirus after OPVimmunization has stopped. As noted above,mOPV will be required to ensure a type-specific
17 iVDPVs = individuals with primary immunodeficiency syndromes who are long-term excretors of vaccine-derived polioviruses (i.e. > 6–12 months).18 The experience from polio-free regions demonstrates that both surveillance sensitivity and polio immunization coverage begin to decline soon
after certification (the latter due primarily to the cessation of supplementary OPV immunization activities).

25
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
response to cVDPVs or containment failures. IPVstocks may be required for country(ies) which havechosen to forego routine immunization againstpolio but are considered at risk of due to a cVDPVor containment failure in another country. OPVstocks and production capacity will need to bemaintained in case routine immunization againstpolio must be reinstituted globally. The prioritiesin this area of work are the licensure of mOPV,finalization of the target number of stockpile dosesfor each vaccine during OPV cessation (and howthese will change over time relative to populationimmunity), long-term containment requirementsfor IPV and OPV production, and thedevelopment of sustainable operating proceduresto govern the maintenance and use of thestockpiles. The Global Polio Eradication Initiativewill also continue its work to support thedevelopment of candidate poliovirus antivirals andpublic health strategies for their use which mightenhance the flexibility of outbreak responseoptions.
4. Long-term containment of poliovirusstocks: Following global certification,containment issues become more complex as thebiosafety requirements for the handling of allpoliovirus strains are increased. Wild and vaccine-derived polioviruses in particular will need to behandled similar to other serious pathogens which
are under strict containment. In the period2004–2005 a third edition of the Global ActionPlan for the Laboratory Containment of WildPolioviruses (GAP III) will be developed to dealwith containment in the Global OPV CessationPhase. The development of this plan will be usedto establish international consensus on thetimeframe and mechanisms for ensuring that thecontainment requirements for laboratory stocks ofwild poliovirus and VDPVs are appropriate to therisks. The plan will also be used to define theadditional requirements, in advance of OPVcessation, needed to protect against silent infectionof production staff in sites which manufacture IPV.In contrast to GAP II, GAP III will also be used toestablish consensus on the relevant biosafety levelsfor handling Sabin and Sabin-derived poliovirusstrains during the Global OPV Cessation Phase.Requirements will be developed for laboratoriesand vaccine production sites, including thosewhich produce IPV from well-characterizedattenuated strains. During the period from 2006onward, tools and capacity will be developed forensuring that containment requirements aremaintained in the long term in all laboratories andvaccine production facilities that hold polioviruses.The longterm monitoring of containmentimplementation will be aligned with the processesalready in place for other pathogens which aresubject to high biosafety levels. ❐

26
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
Guidelines and
consultations on
“post-OPV”
options
Define strategies
to rapidly detect
circulating
viruses
Align
management
with other
stockpiles (yellow
fever, meningitis,
smallpox)
Research and
consult on
requirements for
Global OPV
Cessation Phase
2 0 0 4
Introduce local
strategies to
reduce VDPV risk
Assess feasibility
of incorporation
into IHR/GOARN*
Define mOPV, IPV
and trivalent OPV
stockpile sizes for
post-OPV era
Publication of
third edition of
Global Action
Plan (GAP III)
2 0 0 5
Consolidate OPV
cessation
strategy and
national IPV
decisions
Incorporate polio
surveillance into
IHR and GOARN
Licensure of at
least two mOPV
suppliers
Fully align with
security
processes for
similar pathogens
2 0 0 6
Introduce
protocols for
cVDPV response
in post-OPV era
Begin
environment
sampling
(if/where
appropriate)
Establish
contracts for
mOPV stockpile
Licensure of at
least one IPV
product from
Sabin strains
2 0 0 7
Finalize
introduction of
long-term
immunization
policies
Finalize
additional tools
for surveillance
(if applicable)
Begin assembly
of mOPV
stockpile
Begin
implementation
and verification
of GAP III
2 0 0 8I n d i c a t o r s
Cessation of OPV for routine
immunization
Detection and immediate
notification of circulating
polioviruses
Polio vaccine stockpiles and
emergency response
`
Long-term containment of
poliovirus stocks
* IHR = International Health Regulations; GOARN = Global Outbreak and Alert Response Network.
O b j e c t i v e 3 : D e v e l o p P r o d u c t s f o r t h e G l o b a l O P VC e s s a t i o n P h a s eI n d i c a t o r s a n d M i l e s t o n e s
M i l e s t o n e s

27
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
4 . 4 O b j e c t i v e 4 :
M a i n s t r e a m t h e G l o b a l P o l i o
E r a d i c a t i o n I n i t i a t i v e
S t r a t e g i c A p p r o a c h :
Polio eradication has relied heavily on three majoractivities: supplementary immunizationcampaigns, active surveillance with laboratoryinvestigation of cases, and heightened partnershipcoordination. Throughout the course of theGlobal Polio Eradication Initiative, substantialeffort has been made to use these activities, aswell as the resources of the Global PolioEradication Initiative, to improve the delivery ofother health services, where appropriate andfeasible.
In the area of SIAs (e.g. NIDs), the emphasishas been on (a) adding other interventions whichwere epidemiologically appropriate, operationallyfeasible and could be continued through routineimmunization contacts, (b) improving routineimmunization services by refurbishing thephysical infrastructure (e.g. cold chain), updatinghealth worker training, building data analysiscapacity and reinstituting supervisory systems,and (c) increasing community demand for, andawareness of, other health services, particularlyroutine immunization, through massive socialmobilization efforts. The range of interventionsthat could be added to polio campaigns, however,was often limited by the recruitment of largenumbers of community helpers with minimumtraining in health service delivery. Consequently,the greatest attention was given to vitamin A
supplements, which did not require extensivetraining or an injection and the delivery of whichhad already been linked to routine immunizationcontacts. In the area of surveillance, two generalapproaches have been taken to developing thecapacity needed for polio eradication in a waywhich strengthened surveillance in general. Inplaces with strong disease detection andnotification, AFP reporting was integrated, ifpossible, into that system. In places without suchcapacity, AFP surveillance was established as aframework for a national integrated diseasesurveillance system. In the area of partnershipcoordination, management and support, thespecific mechanisms which were developed, suchas interagency coordinating committees (ICCs),technical advisory groups (TAGs) and theAdvisory Group on Communication forImmunization and Polio Eradication, included intheir mandates the strengthening of routineimmunization.
To implement the polio eradication activities,the polio partnership invested heavily in humanresources, physical infrastructure, andinstitutional arrangements. Mainstreaming thisinvestment into national immunization andsurveillance systems will be critical to ensuringthat the experience, lessons and capacitydeveloped through polio eradication continue to benefit these areas, especially the “UnitedNations General Assembly Special Session/World
THE Global Polio Eradication Initiative has supported the delivery of other health services, particularly since the mid-1990s, through such activities as vitamin A supplementation, integrated disease surveillance, refurbishment of
routine immunization services, and, most recently, country-level implementation of the activities of the Global Alliancefor Vaccines and Immunization (e.g. new vaccine introduction; immunization services strengthening). During the period2004-2008, the polio partnership will accelerate the ‘mainstreaming’ of the Global Polio Eradication Initiative tooptimize these broader benefits and to institutionalize the longterm functions of the polio programme. First, the ongoingwork to transition or integrate the substantial polio-funded human resources, physical infrastructure and institutionalarrangements into other disease control, surveillance and response activities will be enhanced to sustain the broader benefitsof the international investment in polio eradication. This work will also minimize the risks that the conclusion of theGlobal Polio Eradication Initiative might pose for other programmes which rely on its infrastructure. Secondly, thelongterm work of polio eradication, particularly in the areas of containment, surveillance, stockpiles and response, willbe fully incorporated into existing, sustainable, national, WHO and UNICEF mechanisms and structures that havebeen established for other important pathogens (NOTE: the relevant milestones for mainstreaming these longterm functionsare included under Objective 3).

28
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
Fit for Children” and GAVI goals of increasingroutine immunization coverage19 and the globalmeasles mortality reduction targets.20 Linkageshave also been pursued to transfer the polioexperience to the scaling-up of other importantinterventions, particularly those contributing tomillennium development goals (MDGs).
As outlined under Objective 3, in the late1990s the Global Polio Eradication Initiativebegan working to ensure that longterm polio-related activities could eventually be incorporatedinto existing mechanisms that deal with otherserious pathogens. For example, since 1997-1998the WHO Biosafety Advisory Group (BAG) thatprovides guidance on general internationalbiosafety policy as well as specific expertise inareas such as smallpox, has assisted thedevelopment of the global action plans forlaboratory containment of wild polioviruses. In2002, the Global Polio Eradication Initiativebegan discussing the incorporation of polio intothe International Health Regulations (IHR), andsince 2003 the Global Outbreak Alert andResponse Network (GOARN) has been formallyinvolved in the tracking of, and response to, poliooutbreaks.
The longterm maintenance of polio diagnosticlaboratory capacity will be particularly important,but also challenging, due to the increasing rarityof the disease and decreasing relevance to nationalhealth priorities. Consequently, opportunities arebeing explored to sustain this national capacity bybetter intergrating its basic functions with that foreither pathogens, while maintaining sufficientinternational specialized centers for poliovirus.
S i t u a t i o n A n a l y s i s :
By mid-2003, the Global Polio EradicationInitiative had made a substantial impact on thecapacity to address other health priorities in manycountries. In all WHO regions, technicaloversight bodies for polio eradication, known astechnical consultative/advisory groups (TCGs/TAGs),21 were being used to address the broaderimmunization agenda. Polio-initiated, country-level ICCs became the cornerstone of GAVI’sprocess for providing support and are the model
for the Country Coordination Mechanism (CCM)used by the Global Fund to Fight AIDS,Tuberculosis, and Malaria (GFATM). As early as2001, 91% of the international polio-fundedpersonnel and 100% of the national personnelwere already spending an average of 44% and 22%of their time, respectively, on other immunizationand health issues in the countries in which theyworked.22 During the five-year period 1996–2000,the polio eradication partnership invested anestimated 20% (i.e. US$ 200 million) of itsbudget on equipment for routine immunizationand surveillance. In Africa alone, as much as 30%of the routine cold chain was replaced with poliofunding.
Since 1998, the inclusion of vitamin Asupplements in NIDs has averted an estimated1.25 million childhood deaths and strengthenedthe links between immunization contacts andmicronutrient supplementation. NIDs have alsofacilitated the piloting of campaign approaches forthe delivery of other interventions such asinsecticide treated nets (ITNs) for malariaprevention. The surveillance capacity developedfor polio has been extensively used to detect andrespond to diseases such as measles, neonataltetanus, meningitis, cholera and yellow fever. Inthe WHO African Region (AFR), the AFPnetwork has been used as the framework for“integrated disease surveillance” (IDS). By 1998,86% of AFR countries had included measles andneonatal tetanus and 60% cholera and meningitis.In the Americas, surveillance for polio and measleshas been closely integrated since 1994. Since2001, WHO and UNICEF have begunsystematically training polio-funded staff in keycountries to assist with the implementation of theRED strategy to boost routine coverage.
Because of the increasing reliance of otherinternational health programmes, particularly thepolio-funded human resources, the Global PolioEradication Initiative began in 1999-2000 a seriesof discussions on the longterm role that theseresources might play in the work of GAVI and othercommunicable disease surveillance and controlinitiatives. Recognizing that the potential utility ofthe polio-funded human resources network wentbeyond immunization, in 2003 the Global Polio
19 By 2010, routine immunization coverage of children under one year of age at 90% nationally, with at least 80% coverage in every district orequivalent unit.
20 Reduce measles deaths by 50% by end-2005, compared to 1995 levels.21 TCGs/TAGs: these annual or semi-annual meetings bring together expert advisers, researchers, field staff, national programme managers and
partner agencies to assist strategy development, guide policy and set operational priorities.22 WHO Polio Staff Survey 2001.

29
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
Eradication Initiative also started discussing thepossibility of sharing activities and costs with otherimportant health programmes such as the GOARNand the WHO and UNAIDS ‘3 x 5 Initiative’.From late 2003 the programme began workingwith the WHO Country Focus department toestablish a set of pilot countries for evaluating thefeasibility of expanding the work of this network inline with country-defined communicable diseasepriorities for WHO technical assistance, with aparticular emphasis on the control of vaccine-preventable diseases.
Despite the increasing work to share costswith other programmes, by the end of 2003, manynon-polio activities had become even more highlydependent on the polio eradication activities,funding and/or infrastructure. To minimize therisks inherent in this dependence, these activities,particularly those which are closely intertwinedwith polio campaigns (e.g. GAVI, vitamin Asupplementation), must be “mainstreamed” intoroutine programmes within countries, WHO andUNICEF.
E x p e c t e d R e s u l t s :
1. Transition polio “campaign” elements toroutine immunization programmes: Theoverriding goal of this area of work will be toensure full functional integration of the routineimmunization and polio eradication infra-structures at the country level (e.g. humanresources, equipment, institutional arrangements,vitamin A delivery). Such integration will helpensure that the strategic approaches and processesestablished for polio eradication bring districtlevel microplanning, social mobilization and “datafor decision-making” capacity for routineimmunization to the levels achieved for poliocampaigns. The work to develop country-specificplans for this integration will continue, withparticular attention to the 15 large and/orconflict-affected countries where almost 85% ofthe polio human resources have been deployed.This work will be closely coordinated with theGAVI Strategic Framework 2004–2005, as thepriority countries outlined in that frameworkclosely align with those where the polioinfrastructure is most extensive. As the country-specific planning advances, tools will be developedto facilitate the additional training needs for thisbroader programme of work. At the global level,
the polio communication tools will be expandedand updated (i.e. websites, newsletters, mediareleases, progress reports) to promote and facilitatethe active engagement of all key stakeholders inthis transition to broader immunization goals.
2. Expand or integrate AFP surveillance withother diseases of public health importance:This work will be pursued on a country-by-country basis through two approaches. AFPsurveillance will be integrated into routine diseasesurveillance systems in those countries withexisting structures and capacity, with the firstpriority being countries with the strongestsystems and which have been certified as polio-free. In those countries without such capacity, theAFP surveillance system will be further expandedto facilitate the detection, investigation andresponse to vaccine-preventable diseases (VPDs)and other diseases of public health importance(especially epidemic-prone diseases). By the end of2004, those countries requiring substantial long-term support to maintain surveillance capacitywill be identified. Planning will continue for theinstitutionalization of this external support intoan integrated surveillance capacity that ismaintained following global certification. Allsuch countries will, by the end of 2005, have thetraining materials and other tools needed toexpand the AFP system to include the reportingand investigation of additional diseases.Opportunities will be identified to expand theskills of polio-funded staff and facilitate theirreintegration, if appropriate, into nationalprogrammes.
3. ‘Mainstream’ Polio-Funded HumanResources: Between 2004 and 2006, the targetdate for stopping polio SIAs in all countries, theprogramme will complete the ongoing process oftransitioning to other funding sources those poliopositions which primarily provide technicalassistance for immunization activities and/or socialmobilization. Particular priority will be given toworking with funding streams which supportroutine immunization strengthening, accelerateddisease control (e.g. measles mortality reduction)and/or introduction of new vaccines. Where suchtechnical assistance is not needed, positions will be made redundant and opportunities sought with other programmes and organizations. By2006, the programme will also have refined thehuman resources capacity, particularly for field

30
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
surveillance and laboratory diagnosis, that will berequired through global certification and OPVcessation. In addition, from 2004 the programmewill begin evaluating what proportion of the timeof these polio-funded personnel at national, stateand district levels could be made available fortasks related to the surveillance and control ofother vaccine-preventable and communicablediseases. Where it is found feasible, the GlobalPolio Eradication Initiative will work with otherprogrammes to provide additional training,establish supervisory structures and share costs.Priority for this work will be given to the 15 countries which house 85% of the polio-fundedtechnical assistance, and begin with those whichwere polio-free by end-2002. The final phase ofthis ‘mainstreaming’ of the polio-funded humanresources will take place from 2008 through 2010,during which all longterm polio functions will befully incorporated into sustainable structuresdealing with multiple diseases or pathogens.
4. Mainstream the major institutionalarrangements for polio eradication: Thepriority in this area of work will be to ensure thecontinued use of polio-initiated InteragencyCoordinating Committees (ICCs) and, ifappropriate, TAGs, for routine immunization
activities. While the functions of these groups hadbeen expanded in virtually all countries andregions by the end of 2003, in many areas thefinancial and human resources required to conveneand support these groups were still being providedexclusively by the Global Polio EradicationInitiative. By the end of 2006, as SIAs areconcluded in almost all countries, thecontinuation of these institutional arrangementswill require that they are also fully supported byroutine immunization personnel and fundingstreams, potentially through GAVI itself.
5. Support the scaling-up of other healthinterventions: The focus of this work will be onidentifying and supporting those areas whereapplication of the experience and lessons frompolio eradication could facilitate the MDGs,especially Target 5, the reduction of under-fivemortality by two-thirds from 1990 levels by 2015.Particular attention will be given to ensuringexperiences in the areas of human resources,financing and administration and management aretransferred to the international efforts tosustainably reduce measles mortality andmorbidity, and to expand the coverage of healthinterventions such as vitamin A, ITNs and antiretroviral drugs (ARVs). ❐
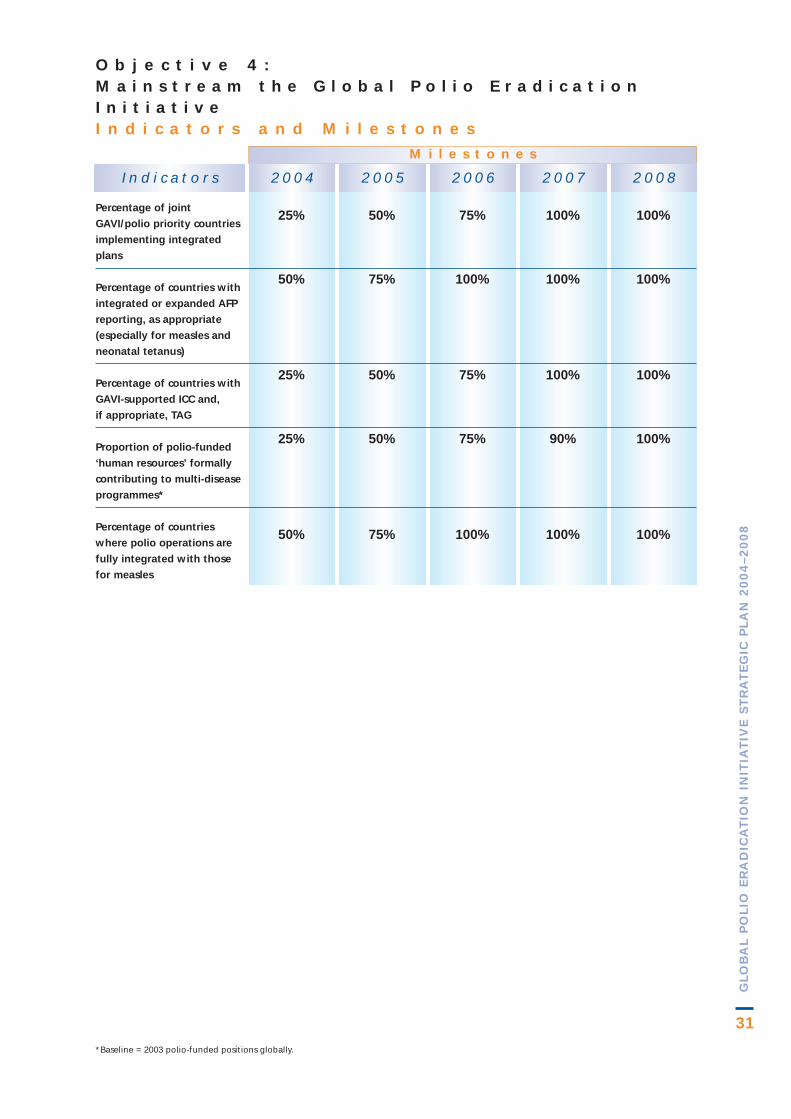
31
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
*Baseline = 2003 polio-funded positions globally.
25%
50%
25%
25%
50%
2 0 0 4
50%
75%
50%
50%
75%
2 0 0 5
75%
100%
75%
75%
100%
2 0 0 6
100%
100%
100%
90%
100%
2 0 0 7
100%
100%
100%
100%
100%
2 0 0 8I n d i c a t o r s
O b j e c t i v e 4 : M a i n s t r e a m t h e G l o b a l P o l i o E r a d i c a t i o nI n i t i a t i v e I n d i c a t o r s a n d M i l e s t o n e s
M i l e s t o n e s
Percentage of joint
GAVI/polio priority countries
implementing integrated
plans
Percentage of countries with
integrated or expanded AFP
reporting, as appropriate
(especially for measles and
neonatal tetanus)
Percentage of countries with
GAVI-supported ICC and,
if appropriate, TAG
Proportion of polio-funded
‘human resources’ formally
contributing to multi-disease
programmes*
Percentage of countries
where polio operations are
fully integrated with those
for measles

32
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
IN addition to 2 specific challenges outlined forstopping poliovirus transmission, there are 6
major challenges that cut across all of the fourobjectives outlined in this Strategic Plan. Thefollowing sections outline each of these challengesand the planned actions of the polio partnership tomitigate their possible detrimental effects.
5 . 1P o l i t i c a l C o m m i t m e n ta n d E n g a g e m e n t
First and foremost, continued high-level politicalsupport for, and engagement in, the global polioeradication effort is essential. In the remainingendemic countries such engagement is needed atnational and subnational levels to ensure high-quality implementation of the strategies (seesection 4.1). In polio-free countries endorsement isneeded to improve routine immunizationcoverage, sustain high-quality surveillance,achieve containment of poliovirus stocks, andensure the full documentation necessary forcertification. In those countries which also provideoverseas development assistance, continuedsupport of the political leadership will be criticalto ensure sufficient external financing for adisappearing disease.
To facilitate this continued politicalengagement, the polio partnership will continueto develop and implement country-by-countryadvocacy plans. Regional and global politicalforums will be exploited to maintain the visibilityof the Global Polio Eradication Initiative in thiscritical period.
5 . 2E x t e r n a l F i n a n c i n g
The second major cross-cutting challenge will be to close the 2004–2005 funding gap of
US$ 150 million to interrupt poliovirustransmission, and the US$ 380 million to achieveglobal certification and mainstream the GlobalPolio Eradication Initiative. The centralimportance of sufficient funding to the ultimatesuccess of the Global Polio Eradication Initiativebecame acutely evident in early 2003 when, forthe first time since 1999, it was necessary to cancelor postpone eradication activities due to a lack offinancing. This financing shortfall rapidlycompromised the quality of polio surveillance,especially in Africa, reduced the speed and qualityof emergency outbreak responses, and hinderedthe implementation of activities in key reservoirareas. Continued financing gaps wouldsubstantially impact all of the major milestonesoutlined in this plan.
To address this funding gap, the interagencyPolio Advocacy Group (PAG)23 will continue itsresource mobilization efforts. Special attentionwill be given to finalizing the commitment of G8members (particularly France, Germany andItaly), to closing the funding gap for eradicationactivities in Africa and identifying new partners,including those interested in mainstreaming thepolio infrastructure as outlined above. Attentionwill also be given to assisting Member States ofthe Organization of Islamic Conference (OIC) tooperationalize their 2003 summit resolution tofund polio activities. The heightened profile of polio eradication activities within the UNagencies, and the identification of polioeradication as a global public good for health, willsupport efforts to expand the polio partnershipand encourage other Organisation for EconomicCo-orperation and Development/ DevelopmentAssistance Committee (OECD/ DAC) countries toparticipate in this historic Initiative. The poliopartnership will put a particular emphasis onsecuring multiyear financial commitmentsthrough 2008.
C r o s s - C u t t i n gC h a l l e n g e s
5
23 PAG is an interagency group of external relations, resource mobilization and communications experts from WHO, UNICEF, UN Foundation andRotary International that coordinates the international advocacy and resource mobilization activities across the polio eradication partnership.

33
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
24 MOSS compliance refers to the “minimum operating security standards” required of UN agencies working in insecure or potentiallyinsecure areas.
5 . 3H i g h - Q u a l i t y P o l i oV a c c i n e s
A reliable supply of high-quality polio vaccineswill be needed for all of the major objectives of thisplan. Stopping the final chains of poliovirustransmission will require an estimated 2.5 billiondoses of WHO-prequalified OPV for SIAs duringthe period 2004-2005. Additional OPV will berequired for SIAs in high-risk countries as well asroutine immunization activities; given theincreasing work of the global community toimprove routine immunization through effortssuch as GAVI, the OPV requirements for routineimmunization could increase during this period.As plans for a vaccine stockpile are developed,arrangements will need to be made to ensurecontinued production capacity for stockpile OPVthrough the Global OPV Cessation Phase as wellas the continued availability of specific reagentsand procedures critical for its production andquality control. In addition to OPV, it isanticipated that there will be an increasingdemand for IPV, in a variety of formulations,regardless as to the long-term policy decisions forfuture polio immunization. The need to ensure theimplementation of appropriate containmentmeasures in large-scale IPV production facilitiesglobally will require close collaborative effortsbetween manufacturers, their governmentaloversight authorities, and international biosafetyand biosecurity functions.
To ensure adequate supply of high-qualitypolio vaccines, UNICEF and WHO, inconsultation with national governments, willcontinue to refine their long-term demandforecasting work for both OPV and IPV. WHOwill develop the criteria and process for pre-qualification of IPV containing vaccines. Thiswork will be shared regularly with OPV and IPVmanufacturers through annual meetings, as well asad hoc consultations as requested. The poliovaccine and immunization research and policyagendas will continue to inform this area of work.
5 . 4C o n f l i c t - A f f e c t e dC o u n t r i e s a n d A r e a s
Although the polio eradication strategies havebeen successfully implemented in all conflict-affected countries, these areas will continue to posespecial challenges for all aspects of the eradicationprogramme. In addition to the need to stop poliotransmission in Afghanistan, substantial work isneeded to improve and maintain populationimmunity in a much larger number of thesecountries. Special arrangements will be needed forsome of these countries and areas to verify andsubmit the necessary documentation forcertification. Such areas may also have particularinterests which must be represented indeliberations on future polio immunization policy.
Recognizing the special needs of conflict-affected areas, the polio partnership will continueto devote a substantial proportion of its technicalassistance to these areas, particularly through thedeployment of long-term human resources.Ongoing work with NGO networks will besustained and expanded. The close collaborationthat has been established with the UN securityapparatus in many of these areas will alsocontinue, including the deployment of a limitednumber of polio-funded security officers andfurther investment in MOSS compliance.24
5 . 5P u b l i c I n f o r m a t i o na n d S o c i a lM o b i l i z a t i o n
Throughout the Global Polio EradicationInitiative, the informing and engagement of thepublic sector has been central to activities rangingfrom strategy implementation in endemic areas toresource mobilization in donor countries. In donorcountries, a high profile and awareness of theGlobal Polio Eradication Initiative is needed tofacilitate resource allocation decisions throughglobal certification. In all countries, thedevelopment of long-term polio policies,particularly for routine immunization, willgenerate new demands in this area of work.

34
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
Social mobilization efforts must be enhancedin the remaining endemic areas to fully engage thepolio-affected populations, as well as to addressrumours which may have undermined publicconfidence in the programme. The appropriateselection and training of vaccinators, the inclusionof women and underserved groups at all levels, theneed for strong interpersonal communicationskills at the service delivery level, and thedevelopment of appropriate Information,Education and Communication (IEC) messagesand materials, remain key to the successfulvaccination of every child.
The Global Polio Eradication Initiative willcontinue to place a strong emphasis on publicinformation, social mobilization andcommunications during the period 2004-2008.The technical capacity which has been establishedin this area at the global, regional, national andsubnational levels will require additional inputsand leadership to enhance support to governmentefforts. The inter-agency mechanisms forcoordinating communications and socialmobilization inputs (e.g. the Advisory Group onCommunication for Immunisation and PolioEradication, the Advisory Group onCommunication for Immunisation (Africa), andNational Social Mobilisation Committees) willcontinue. New materials will be developed andwidely disseminated to support this work.
5 . 6B i o c o n t a i n m e n t
Timely completion of the containment activitiesoutlined in the Global Action Plan for the LaboratoryContainment of Wild Polioviruses, second edition (GAPII), is particularly important to the 2004–2008overall timeline for polio eradication. GAP IIrequires that by the end of 2004 all countries willhave completed a nationwide survey oflaboratories, established an inventory of allfacilities holding wild polioviruses or potentiallyinfectious materials, and implemented BSL-2/polio level safety measures. One year afterthe last wild poliovirus has been detected (e.g.from end-2005), all countries must begin eitherdestroying retained materials, or increasing thelevel of biocontainment to BSL-3/polio. While theprogress to date in implementing the GAP IIdemonstrates that this timeline is feasible,achieving these milestones requires acceleratingcontainment in a number of large industrializedcountries and initiating activities in many recentlyendemic countries. The timely introduction,validation and verification of BSL-3/poliocontainment measures at existing IPV productionand quality control facilities using wildpolioviruses, represents a particular challenge tomanufacturers and national oversight authorities.The expected results for containment, outlinedunder objectives 2 and 3 of this Strategic Plan,highlight the activities that will be undertaken toaddress these challenges. ❐

35
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
6 . 1G o v e r n m e n t s
National governments of polio-endemic, recently-endemic and polio-free countries are the ownersand beneficiaries of the Global Polio EradicationInitiative, undertaking the full range of polioeradication activities outlined in this StrategicPlan. National resources contributed towards theimplementation of polio eradication activitiesinclude both financial expenditures and in-kindcommitments, such as the time that is contributedby volunteers, health workers and others in theimplementation of NIDs. Substantial resources arealso expended by governments at national,state/province, district and local community levelsto pay for petrol, social mobilization, training andother costs. It has been estimated that polioendemic countries will have contributed volunteertime worth at least US$ 2.35 billion for polioeradication activities between 1988 and 2005.25
Governments of polio-endemic and recentlyendemic countries also conduct advocacy withdonor governments and at various multilateralforums.
6 . 2S p e a r h e a d i n gP a r t n e r s
World Health Organization (WHO): Throughits headquarters, regional and country offices,WHO provides the overall technical directionand strategic planning for the management andcoordination of the Global Polio EradicationInitiative. WHO is responsible for ensuring thatall components of the Global Polio EradicationInitiative Strategic Plan are well implemented,and has a key role in monitoring and evaluatingall aspects of the Plan. WHO also coordinatesoperational/basic scientific research, providesoperational support to ministries of health, andthe training/deployment of human resources.WHO is the lead technical agency for supportingAFP surveillance systems, the global polio
laboratory network, resource mobilization, donorcoordination, advocacy and public information.
Rotary International: Through its PolioPlusprogram, established in 1985, RotaryInternational was, with the Pan American HealthOrganization, the first to have the vision of apolio-free world and continues to play a centralrole in global efforts to eradicate polio. Rotary isthe world’s first service organization, with a globalnetwork of 1.2 million members in more than 160 countries. More than one million Rotarymembers have volunteered their time and personalresources to contribute to the immunization ofnearly two billion children in 122 countries. Inaddition, Rotary mobilizes millions of fellowvolunteers to assist during NIDs. Rotary alsoprovides urgently needed funds. To date, the organization has committed more than US$ 500 million to polio eradication. Rotary'sPolio Eradication Advocacy Task Force, with theassistance of the PolioPlus National AdvocacyAdvisors, has played a major role in highlightingpolio eradication in international forums and ininfluencing decisions by donor governments tocontribute over US$ 1.5 billion to the globaleradication effort. That amount, combined withdirect funds from Rotary, has accounted for morethan half the amount required for the entire globalinitiative. In June 2003, Rotary concluded asecond membership fundraising drive, whichexceeded its goal to raise an additional US$ 80 million for polio eradication.
US Centers for Disease Control and Prevention(CDC): The most important contribution of theAtlanta-based CDC continues to be deployment ofits epidemiologists, public health experts, andscientists to WHO, UNICEF and endemiccountries. In addition, a number of internationaland national staff in WHO and UNICEFheadquarters and in the regional and countryoffices of both organizations are funded by CDCgrants. CDC also provides funding for theprocurement of OPV required for mass
R o l e s o f P a r t n e rA g e n c i e s
6
25 Global Public Goods for Health: Health economic and public health perspectives, pg.41, Smith, R., et al, eds, Oxford University Press, 2003.

36
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
immunization campaigns, and a wide range oftechnical expertise and laboratory support. Thisincludes staff support for disease surveillance atglobal, regional and national levels and outbreakinvestigation, especially in areas within orbordering polio-free zones. CDC works as the“viral detective” of the four partners, using itsstate-of-the-art virological surveillance expertise toidentify the strain of poliovirus involved andpinpoint its geographical origin. CDC alsoprovides assistance in the development andmonitoring of the 145 members of the global poliolaboratory network, including funding short-termand long-term technical support in key countries.Finally, CDC conducts research which willfacilitate development of long-term immunizationand surveillance policies.
United Nations Children’s Fund (UNICEF):UNICEF is the lead partner in the procurement and distribution of polio vaccines for routine andsupplementary immunizations and with WHO, the strengthening of routine immunizationcomponents of the Strategic Plan. With WHO,UNICEF is the lead partner in the implementationof intensified NIDs, SNIDs and mop-up campaignsat country level. UNICEF provides technicalassistance to national coordinators to develop actionplans and secure logistics to access hard-to-reachplaces, including in countries affected by conflict.UNICEF also participates in the global process bywhich eradication policies and plans of action aredeveloped; develops materials for training andpublic information; strengthens social mobilizationefforts through its network of communicationsofficers; and provides cold chain support. UNICEFis also an active partner in resource mobilization,advocacy and public information.
6 . 3D o n o r a n d T e c h n i c a lP a r t n e r s
Agencies for international developmentcooperation: These agencies play a central role inthe Global Polio Eradication Initiative throughthe provision of multilateral and bilateral support.They also undertake high-level advocacy withendemic countries and among their peers, provideaccess to technical expertise within theircountries, and give significant technical inputthrough participation in global, regional and
country-level ICCs and technical oversight bodies.International development agencies havecontributed to the Global Polio EradicationInitiative’s resource mobilization strategy andhave assisted the development of long-term plansby making commitments through to globalcertification. Some of the long-standing partnersinclude Canada (CIDA), Germany (kfW), Japan(JICA), the United Kingdom (DFID) and theUnited States of America (CDC and USAID).These donors have contributed or committed US$ 1.76 billion to the Global Polio EradicationInitiative, or 59% of all the funds received orprojected, between 1985 and 2005. Partners suchas Australia, Denmark, Luxembourg, theNetherlands and Norway have made significantcontributions and are some of the leadingsupporters, especially on a per capita basis. TheGlobal Polio Eradication Initiative is alsowelcoming new donor partners such as Ireland,New Zealand and the Russian Federation. Inaddition to focusing on development agencies inOECD countries, the Global Polio EradicationInitiative is looking to expand its relationshipwith key Arab and Asian nations.
Foundations (see also ‘Rotary International’under Spearheading Partners): Foundationsprovide financial support, advocacy and assistancein partnership development. The United NationsFoundation (UNF) has provided substantialassistance through direct financial support,strengthening of the Global Polio EradicationInitiative’s fundraising capacity, leveraging fundsthrough matching grants and introducing otherpartners to the Global Polio Eradication Initiative.The UNF also works closely with thespearheading partners in global polio advocacyactivities and resource mobilization efforts. Afterthe Rotary Foundation, the Bill and MelindaGates Foundation has been the largest donorfoundation to the Global Polio EradicationInitiative having committed US$ 75 million. TheBill and Melinda Gates Foundation has also playedan important advocacy and promotion role forpolio eradication. The Rotary Foundation, the Billand Melinda Gates Foundation and UNF have alsosupported the Global Polio Eradication Initiativeby collaborating with the World Bank toimplement a loan buy-down mechanism whichwill buy polio vaccine for Nigeria and Pakistan.

37
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
Development Banks and MultilateralAgencies: Institutions like the World Bank andthe Inter-American Development Bank haveprovided access to country-level financing throughthe provision of “soft loans”. The World Bank hasalso collaborated with the Bill and Melinda GatesFoundation, Rotary International and UNF toimplement a funding mechanism to assist theprocurement of polio vaccines for Nigeria andPakistan. The European Commission (EC) hassupported the Global Polio Eradication Initiativein countries such as India and Nigeria.Intergovernmental bodies such as the G8, theAfrican Union and the Organization of the IslamicConference (OIC) have strongly supported theGlobal Polio Eradication Initiative by providing ahigh profile for polio eradication in their summitsand pledging both financial and political support.
Corporations: Corporations and members of theprivate sector have provided monetary and in-kindcontributions to the Global Polio EradicationInitiative. Most often their contributions are for aspecific area or purpose which requires targetedfunding. Aventis Pasteur is the Global PolioEradication Initiative’s longest standing corporatepartner having donated 120 million doses of OPVover a 10-year period. This vaccine has beenearmarked for campaigns in specific Africancountries which are emerging from conflict. Otherkey corporate supporters include Wyeth, whichfunds the African Regional Polio LaboratoryNetwork; the International Federation ofPharmaceutical Manufacturers Associations(IFPMA), which coordinated a 100 million dosevaccine donation from Aventis Pasteur,GlaxoSmithKline (GSK) and Chiron; DeBeers,which provided funding for polio campaigns inAngola; and British Airways, which funded animportant mop-up campaign in western Zambia.Private sector fundraising campaigns organized byRotary International and UNF, and by the variousUNICEF national committees, have alsogenerated significant support for the Global PolioEradication Initiative.
6 . 4I n t e r n a t i o n a lH u m a n i t a r i a nO r g a n i z a t i o n s a n dN G O s
International humanitarian organizations:Organizations such as the International Federationof Red Cross and Red Crescent Societies (IFRC)assist the Global Polio Eradication Initiative byconducting advocacy at international and nationallevels, and contributing financial, operational andtechnical support in selected priority countries.The Red Cross/Red Crescent societies contributeto the implementation of mass immunization andsurveillance activities in the field, with emphasison deploying networks of community-basedvolunteers for social mobilization. TheInternational Committee of the Red Cross (ICRC)assists in facilitating access in areas of conflict andrefugee populations.
Nongovernmental organizations: NGOs play akey role in the implementation of country-levelactivities. The NGO umbrella-organizationCORE through the efforts of its many memberssuch as ADRA, CRS, CARE, Plan International,Save the Children, and World Vision, assists thepolio eradication effort by building partnershipsbetween the government and the communitiesthey serve, supporting supplementalimmunization campaigns, assisting with AFPsurveillance, and monitoring the immunizationstatus of children. NGOs help train volunteers andhealth workers, transport vaccines and equipment,monitor the quality of the cold chain, and assistwith communication and social mobilizationactivities. NGOs also play an important advocacyrole, particularly at the national and subnationallevels. Some NGOs, such as the Albert B. SabinVaccine Institute which formally joined theGlobal Polio Eradication Initiative in 2003, playboth an international advocacy and technicaladvisory role. NGOs such as Médecin SansFrontières and Save the Children have beenimportant in reaching children in conflict-affectedcountries such as Angola, the Democratic Republicof the Congo and Somalia.

38
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
6 . 5V a c c i n eM a n u f a c t u r e r s
The vaccine industry plays a critical role insupporting routine and supplementary polioeradication activities by making availablesufficient quantities of assured quality poliovaccine. The manufacturers make sure thatsufficient quantities of vaccine are available in atimely manner by ensuring that the productionand investment plans for capacity increases are
initiated at the right times. To guarantee timelyavailability and a minimum of vaccine wastage,the vaccine industry also works in closecollaboration with UNICEF and WHO whichincludes sharing short- and long-term demandschedules and production plans. In addition, thevaccine industry provides technical inputs andinitiates research in response to productrequirements after certification as suggested anddefined by the new Strategic Plan. Furthermore,the industry has provided contributions in-kindon a number of occasions.

39
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
The experience of the smallpox eradicationinitiative, combined with the risks associated
with continued use of OPV, demonstrate the needto plan for a combination of longterm and time-limited polio eradication activities followingcertification of global polio eradication (target date2008). The ongoing development of the productsand policies needed for this phase of the GlobalPolio Eradication Initiative precludes a detailedassessment of the financial resources required atthat time; however, it is possible to anticipate themajor activities that will be required.
The longterm activities are those needed tominimize and manage the risks of re-introductionand re-establishment of wild polioviruses. Forexample, prior to the cessation of OPV, andindefinitely thereafter, all polioviruses will need tobe subject to longterm containment26.Independent verification of appropriate storageand handling of wild and vaccine-derivedpoliovirus strains will be needed, particularly formanufacturing sites that amplify wild poliovirusesto produce IPV. Stockpiles of monovalent OPV,and possibly other formulations, will need to be inplace and maintained in the longterm.Internationally-agreed mechanisms will berequired to govern the use of these stockpiles, withspecial attention to ensuring priority for thosecountries that decide to forego the use of IPV forroutine immunization. Because of their longtermnature, these activities will be incorporated intoexisting national, WHO and UNICEF structuresand mechanisms for managing the identification,response and containment of high prioritypathogens.
In addition to these longterm activities, anumber of time-limited actions will be needed tomanage the short-term risk of circulating vaccine-derived polioviruses (cVDPVs) that will beassociated with the cessation of OPV. Foremostamong these activities will be the heightening and
sustaining of AFP surveillance for at least twoyears after the cessation of OPV. Particularcapacity will be needed in those areas at highestrisk for the emergence of a cVPDV (i.e. those withvery low routine immunization coverage) and inthose countries which decide not to introduce IPV.Should the ongoing evaluation of supplementarysurveillance strategies (e.g. environmentalsampling) demonstrate the capacity tosignificantly enhance the detection of circulatingpolioviruses, these methods will have had to beintroduced at least 1 year in advance of OPVcessation. Finally, if there is evidence that boostingpopulation immunity substantially reduces therisk of cVDPV emergence, in some areas thecessation of OPV may need to be preceded bypulse immunization with OPV.
The use of IPV in routine immunizationprogrammes represents a special issue. Somecountries have indicated their desire to forego itsuse completely, some are considering a time-limited approach in which it would be used as partof a 3-5 year transition strategy during thecessation of OPV, and others have stated theirintention to continue longterm IPV use for routineimmunization. Although some countries mayforego the use of IPV, those which do decide to useit for a time-limited period or in the longterm,will need to have introduced that vaccine by 2008and made provision for its procurement for thenecessary period. Given the inter-relatedness ofdecisions on IPV introduction, the use ofcombination vaccines and longterm nationalpolicy for other antigens (e.g. pertussis componentof DTP), key stakeholders in the provision of suchvaccines for routine immunization, such as GAVI,will need to be centrally involved in this process.
The resource implications of the Global OPVCessation Phase will be developed as part of thework to establish appropriate products and policiesfor this period, outlined in Objective 3 of the
26 To be developed for the 3rd Edition of the Global Action Plan for Laboratory Containment of Wild Polioviruses.
2 0 0 9 & B e y o n d –t h e G l o b a l O P VC e s s a t i o n P h a s e
7
40
GL
OB
AL
PO
LIO
ER
AD
ICA
TIO
N I
NIT
IAT
IVE
ST
RA
TE
GIC
PL
AN
20
04
–2
00
8
Global Polio Eradication Initiative Strategic Plan2004-2008. The financing requirements will bedriven by internationally-agreed decisions during2005-2007 on the actual process for stoppingOPV, the size and composition of vaccinestockpiles, and the future role of other polio
vaccines. Given the longterm nature of many ofthe activities of the Global OPV Cessation Phase,the required resources will need to be raised andchannelled through the sustainable structures andmechanisms into which these activities will havebeen incorporated. ❐


The spearheading partners of the Global Polio Eradication Initiative are:
World Health OrganizationGlobal Polio Eradication Initiative
20, avenue AppiaCH-1211 Geneva 27
SwitzerlandTelephone (41 22) 791 2111
Fax (41 22) 791 4193Email: [email protected]
Website: www.polioeradication.org
WHO
ISBN 92 4 159117 X
Copyright © 2022 FDOKUMEN