
Generalized anxiety disorder prevalence and comorbidity with depression in coronary heart disease: a...
17
http://hpq.sagepub.com/ Journal of Health Psychology http://hpq.sagepub.com/content/18/12/1601 The online version of this article can be found at: DOI: 10.1177/1359105312467390 2013 18: 1601 originally published online 8 January 2013 J Health Psychol Phillip J Tully and Suzanne M Cosh coronary heart disease: A meta-analysis Generalized anxiety disorder prevalence and comorbidity with depression in Published by: http://www.sagepublications.com can be found at: Journal of Health Psychology Additional services and information for http://hpq.sagepub.com/cgi/alerts Email Alerts: http://hpq.sagepub.com/subscriptions Subscriptions: http://www.sagepub.com/journalsReprints.nav Reprints: http://www.sagepub.com/journalsPermissions.nav Permissions: http://hpq.sagepub.com/content/18/12/1601.refs.html Citations: What is This? - Jan 8, 2013 OnlineFirst Version of Record - Nov 20, 2013 Version of Record >> at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013 hpq.sagepub.com Downloaded from at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013 hpq.sagepub.com Downloaded from
Transcript of Generalized anxiety disorder prevalence and comorbidity with depression in coronary heart disease: a...

http://hpq.sagepub.com/Journal of Health Psychology
http://hpq.sagepub.com/content/18/12/1601The online version of this article can be found at:
DOI: 10.1177/1359105312467390
2013 18: 1601 originally published online 8 January 2013J Health PsycholPhillip J Tully and Suzanne M Cosh
coronary heart disease: A meta-analysisGeneralized anxiety disorder prevalence and comorbidity with depression in
Published by:
http://www.sagepublications.com
can be found at:Journal of Health PsychologyAdditional services and information for
http://hpq.sagepub.com/cgi/alertsEmail Alerts:
http://hpq.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
http://hpq.sagepub.com/content/18/12/1601.refs.htmlCitations:
What is This?
- Jan 8, 2013OnlineFirst Version of Record
- Nov 20, 2013Version of Record >>
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

Journal of Health Psychology18(12) 1601 –1616© The Author(s) 2012Reprints and permissions: sagepub.co.uk/journalsPermissions.navDOI: 10.1177/1359105312467390hpq.sagepub.com
Introduction
Major depressive disorder (MDD) is the most commonly researched internalizing/emotional disorder in coronary heart disease (CHD) patients. Previous meta-analyses indicate that MDD and depression symptoms confer greater CHD morbidity risk (Barth et al., 2004; Nicholson et al., 2006), culminating in the American Heart Association advocating routine depression screening among these patients (Lichtman et al., 2008). However, the fact that depression screen-ing and intervention have only translated to a modest impact on cardiovascular outcomes (Baumeister et al., 2011; Pizzi et al., 2011)
suggests that what is understood about the MDD–CHD link is in the nascent stages and incomplete. Recent findings also indicate that
Generalized anxiety disorder prevalence and comorbidity with depression in coronary heart disease: A meta-analysis
Phillip J Tully1,2,3 and Suzanne M Cosh1
AbstractGeneralized anxiety disorder prevalence and comorbidity with depression in coronary heart disease patients remain unquantified. Systematic searching of Medline, Embase, SCOPUS and PsycINFO databases revealed 1025 unique citations. Aggregate generalized anxiety disorder prevalence (12 studies, N = 3485) was 10.94 per cent (95% confidence interval: 7.8–13.99) and 13.52 per cent (95% confidence interval: 8.39–18.66) employing Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition criteria (random effects). Lifetime generalized anxiety disorder prevalence was 25.80 per cent (95% confidence interval: 20.84–30.77). In seven studies, modest correlation was evident between generalized anxiety disorder and depression, Fisher’s Z = .30 (95% confidence interval: .19–.42), suggesting that each psychiatric disorder is best conceptualized as contributing unique variance to coronary heart disease prognosis.
Keywordscomorbidity, coronary heart disease, depression, generalized anxiety disorder, meta-analysis
1The University of Adelaide, Australia2 School of Psychology, The University of Adelaide, Australia
3Cardiac Surgery Research and Perfusion, Department of Medicine, Flinders Medical Centre, Australia
Corresponding author:Phillip J Tully, Cardiac Surgery Research and Perfusion, Cardiac and Thoracic Surgical Unit, Flinders Medical Centre, Bedford Park, SA 5042, Australia. Email: [email protected]
467390 HPQ181210.1177/1359105312467390Journal of Health PsychologyTully and Cosh2012
Article
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

1602 Journal of Health Psychology 18(12)
other emotional constructs such as anxiety and negative affect, in particular, increase CHD risk, raising the possibility that MDD is not a discrete psychiatric risk factor for CHD (Frasure-Smith and Lesperance, 2008; Martens et al., 2010; Phillips et al., 2009; Scherrer et al., 2010; Tully et al., 2011). In fact, the extent to which the recent CHD prognostic findings reflect unique depression variance, independent from anxiety and negative affect, remains largely unchallenged. Quantifying the degree of comor-bidity between MDD and anxiety disorders in CHD can help inform whether these disorders contribute independent variance to cardiovascu-lar prognosis or, alternatively, whether the co-occurrence of disorders largely reflects common variance (e.g. negative affect, shared diagnostic symptoms and artificial diagnostic splitting). Although the extent of overlap between psycho-social constructs in CHD has long been high-lighted as crucial to define (Kubzansky et al., 2006; Kubzansky and Kawachi, 2000; Smith, 2010); Suls and Bunde, 2005; Tully et al., 2008), we are not aware of a previous study to pool such data together and thereby quantify the associa-tion between depression and anxiety in CHD patients.
Among all psychiatric disorders, generalized anxiety disorder (GAD) is the most commonly comorbid disorder with MDD, both concur-rently and across the lifespan, among individu-als primarily free from CHD (Krueger, 1999; Sherbourne et al., 1996; Watson, 2009). In fact, in primary care settings over half of unipolar MDD, cases are comorbid with GAD (Sherbourne et al., 1996), so much so that scholars have long debated whether these even form separate diag-nostic and clinical disorders (Mennin et al., 2008). Explanations for high comorbidity between GAD and MDD include shared diag-nostic criteria (i.e. fatigability, restlessness/psychomotor agitation, concentration and sleep difficulties) (American Psychiatric Association, 2000), common genetic factors and common diathesis (Mineka et al., 1998) and related cog-nitive processes such as rumination and worry (Brosschot et al., 2006; Soo et al., 2009). For
these reasons, GAD would serve as a suitable diagnostic exemplar to determine the extent to which depression shares variance with anxiety among CHD patients.
The dilemmas imposed by the overlap between depression and GAD are exemplified further in recent aetiological and prognostic studies. Recent research generally supports that MDD is associated with CHD, though largely contrasting results have been reported for GAD. For example, a recent epidemiological survey of 43,093 US civilians showed that the largest psy-chiatric association with physician diagnosed cardiovascular disease was attributable to GAD, as opposed to any other affect or mood disorder (adjusted odds ratio (OR): 1.83; 95% confidence interval (CI): 1.39–2.39) (Goodwin et al., 2009). Some studies have suggested that GAD is asso-ciated with cardiovascular outcome independent of MDD (Frasure-Smith and Lesperance, 2008; Martens et al., 2010; Phillips et al., 2009; Tully et al., 2011) and another dataset reported reduced cardiovascular risk attributable to GAD (Parker et al., 2011), raising the possibility that these psychiatric disorders are highly collinear in CHD. Given that the degree of interrelation between GAD and MDD in CHD patients and the overall prevalence of GAD are not known, a critical gap is evident with respect to interpreta-tion of the extant literature, particularly aetio-logical and prognostic studies.
Only by identifying the prevalence of GAD and the comorbidity rates between GAD and MDD will the extent of potential confounding variance in the MDD–CHD association be known. If comorbidity between GAD and MDD is small, then both GAD and MDD might best be conceptualized as discrete psychiatric risk factors in CHD. This, in turn, could feasibly redirect psychosocial research and interven-tions towards treatments tailored towards the phenotypic processes and biobehavioural mechanisms that confer CHD risk, beyond sim-ply depression. Conversely, if high comorbidity rates were evident, research and intervention efforts may facilitate a shift away from disor-der-specific treatments towards transdiagnostic
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

Tully and Cosh 1603
approaches targeting common and modifiable vulnerability risk factors for depression and anx-iety in CHD (Barlow et al., 2011; Dozois et al., 2009). Therefore, the purpose of this systematic review was to quantify the prevalence of GAD in CHD and comorbidity with MDD with two study aims:
1. What is the prevalence of GAD in popu-lations with verified CHD?
2. What are the current comorbidity rates between depression disorders and GAD in populations with verified CHD?
Methods
Literature search
Using standardized criteria (Stroup et al., 2000), one systematic search of the Medline, Embase, SCOPUS and PsycINFO electronic databases was performed for English language studies or unpublished doctoral dissertations, reporting the prevalence of GAD in CHD or comorbidity rates with depression published between January 1975 and May 2011. Free text searches without language restrictions included the term GAD in combination with CHD, cardiovascular disease, heart disease, ischaemic heart disease, myocar-dial infarction (MI), cardiac death, coronary artery bypass graft (CABG), percutaneous coro-nary intervention, angioplasty and heart failure. These cardiac search terms were then combined with ‘anxiety’ and several common structured diagnostic interview tools: Anxiety Disorder Interview Schedule (ADIS), Composite International Diagnostic Interview (CIDI), Diagnostic Interview Schedule (DIS), MINI International Neuropsychiatric Interview (MINI) and Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised (DSM-III-R) (SCID).
Selection criteria
Eligibility criteria were established before the literature search. Editorial, letter, case report,
conference abstract or qualitative reviews were excluded. Studies with post-stroke, cerebrovas-cular accident populations, heart transplant and mitral valve prolapse populations were also excluded, unless CHD patients were reported separately. Only studies with more than 50 patients were included to provide reliable prev-alence and comorbidity estimates and sufficient power for studies. Studies were eligible for inclusion if the sample showed physician veri-fied or documented CHD (e.g. positive stress test, coronary atherosclerosis, MI and coronary revascularization procedure) or end-stage heart failure. Studies employing only self-report CHD diagnosis/symptoms were ineligible.
Diagnosis of GAD and MDD (current and life-time) was derived from either structured inter-view or self-report with the Diagnostic and Statistical Manual of Mental Disorders (American Psychiatric Association, 1987, 2000, 2010) and International Classification of Diseases-10 (ICD-10; World Health Organization, 2007) criteria, or documented with relevant codes corroborated by a physician in medical records. Non-current International Classification of Disease codes for ‘anxiety states’ and ‘anxiety neurosis’ were not searched for and were excluded.
Data extraction
The two authors independently reviewed arti-cles for eligibility. In the case of title/abstract disagreements, the study was subjected to full-text review. Additional studies were identified by inspection of the reference section of arti-cles selected for full-text review. Disagreements were resolved by discussion. The quality of studies was not rated because there are no agreed upon measures of study quality, and the use of subjective rating scales may lead to bias (Petitti, 1994). Standardized data were extracted for each study including authors and citation, sample size, CHD sample characteristics, coun-try, age (mean (M), standard deviation (SD)) and percentage female sex, GAD criteria, current and lifetime GAD prevalence, GAD and MDD
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

1604 Journal of Health Psychology 18(12)
comorbidity rates. Like other meta-analyses (Hackett et al., 2005), articles were judged to be from the same cohort if there was evidence of overlapping study dates, recruitment sites and similar study sample characteristics and grant funding numbers. In the case of multiple reports for the same sample, the study with the most comprehensive data and largest sample was retained.
Search results
Figure 1 displays the flow chart for exclusion and selection of studies. Table 1 describes the characteristics of the included studies reporting GAD prevalence and CHD outcomes in CHD. From 1025 unique citations, 934 were excluded by title/abstract (Kappa agreement = .91). Among 91 subjected to full-text review, in
Full Text Review(n = 91)
+ 15 identified by manualsearching
Title/Abstract Exclusion(n = 934)
Non-CHD (n = 728)GAD not reported (n = 120)Review (n = 31)Paediatric (n = 7)Case report/letter (19)Stroke (n = 15)Non-English (n = 13)Animal (n = 1)
Primary Literature Search
(n = 1,025)
Full Text Exclusion(n = 94)
Not CHD / mixed (n = 27)None / insufficient GAD
prevalence (n = 41)Self-report CHD (n = 5)
Case-report/review (n = 7)< 50 patients (n = 3)
Duplicate sample (n = 11)
Met Inclusion Criteria Aim 1(n = 12)
Met Inclusion Criteria Aim 2
Reported proportion of GADpatients with MDD
(n = 3)
Met Inclusion Criteria Aim 2
Reported proportion ofMDD patients with GAD
(n = 4)
Figure 1. Flow chart of selected studies.CHD: coronary heart disease; GAD: generalized anxiety disorder; MDD: major depressive disorder.
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

Tully and Cosh 1605Ta
ble
1. O
verv
iew
of s
tudi
es r
epor
ting
GA
D p
reva
lenc
e am
ong
CH
D p
opul
atio
ns.
Stud
yC
ount
rySa
mpl
eA
ge, M
(S
D)
Fem
ale
%
(N)
GA
D c
rite
ria
Life
time
GA
DG
AD
/de
pres
sion
cr
iteri
a
Com
orbi
d de
pres
sion
am
ong
GA
Da (
%)
Com
orbi
d G
AD
am
ong
depr
essi
onb
(%)
Z (
SE)
r
Mar
tens
et
al.
(201
0)U
SA10
15 C
HD
NR
18.0
(18
3)D
IS, D
SM-II
I–
DIS
, DSM
-IIIc
80.1
9–
.52
(.03)
.48
Fras
ure-
Smith
et
al.
(200
8)
CA
N80
4 C
AD
60.0
(10
.6)
19.3
(15
5)SC
ID, D
SM-IV
–SC
ID, D
SM-IV
25.5
8d–
.17
(.02)
.17
Park
er e
t al
. (2
011)
AU
S43
6 po
st-
AC
S65
.7 (
12.2
)29
.7 (
145)
CID
I, D
SM-IV
YC
IDI,
DSM
-IV38
.6e
–.3
9 (.0
2).3
7
Sher
bour
ne
et a
l. (1
996)
USA
245
MI,
HF
61.1
(1.
0)40
.0 (
98)
DIS
, DSM
-III
YD
IS, D
SM-II
I–
––
–
Tul
ly e
t al
. (2
011)
AU
S15
8 pr
e-C
ABG
64.7
(10
.6)
20.9
(33
)M
INI,
DSM
-IV–
––f
––
–
Tod
aro
et a
l. (2
007)
USA
150
CH
D
reha
bilit
atio
n60
.6 (
12.3
)32
.0 (
48)
AD
IS, D
SM-IV
Y–
––
––
Val
kam
o et
al.
(200
3)FI
N14
4 an
giog
raph
y >
50%
NR
42.3
(36
)SC
ID, D
SM-II
I-R–
––
––
–
Fedo
roff
et a
l. (1
991)
USA
129
MI
56 (
16)
NR
PSE,
DSM
-IIIg
–PS
E, D
SM-II
Ig23
.08
–.0
3 (.0
6).0
3
Bank
ier
et a
l. (2
008)
USA
120
stab
le
CH
DN
R30
.8 (
37)
SCID
, DSM
-IV–
SCID
, DSM
-IV–
18.3
3.1
8 (.0
3)h
.18
Bank
ier
et a
l. (2
004)
USA
100
stab
le
CH
D67
.1 (
13.6
)31
(31
)SC
ID, D
SM-IV
–SC
ID, D
SM-IV
–45
.16
.34
(.06)
.33
(Con
tinue
d)
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

1606 Journal of Health Psychology 18(12)
Stud
yC
ount
rySa
mpl
eA
ge, M
(S
D)
Fem
ale
%
(N)
GA
D c
rite
ria
Life
time
GA
DG
AD
/de
pres
sion
cr
iteri
a
Com
orbi
d de
pres
sion
am
ong
GA
Da (
%)
Com
orbi
d G
AD
am
ong
depr
essi
onb
(%)
Z (
SE)
r
Haw
orth
et
al.
(200
5)U
K98
HF
67.0
(11
.0)
(17)
SCID
, DSM
-IV–
SCID
, DSM
-IVi
–9
.45
(.02)
.42
Birk
et-S
mith
et
al.
(200
9)D
EN86
CH
DM
edia
n 68
37 (
43)
PRIM
E-M
D,
DSM
-III-R
––
––
––
AC
S: a
cute
cor
onar
y sy
ndro
me;
AD
IS: a
nxie
ty d
isor
der
inte
rvie
w s
ched
ule;
AU
S: A
ustr
alia
; CA
BG: c
oron
ary
arte
ry b
ypas
s gr
aft
surg
ery;
CA
D: c
oron
ary
arte
ry d
isea
se;
CA
N: C
anad
a; C
HD
: cor
onar
y he
art
dise
ase;
CID
I: C
ompo
site
Inte
rnat
iona
l Dia
gnos
tic In
terv
iew
; DEN
: Den
mar
k; D
IS: D
iagn
ostic
Inte
rvie
w S
ched
ule;
FIN
: Fin
land
; HF:
he
art
failu
re; M
I: m
yoca
rdia
l inf
arct
ion;
MIN
I: M
INI I
nter
natio
nal N
euro
psyc
hiat
ric
Inte
rvie
w; N
L: N
ethe
rlan
ds; N
R: n
ot r
epor
ted;
PR
IME-
MD
: Pri
mar
y C
are
Eval
uatio
n of
M
enta
l Dis
orde
rs; P
SE: P
rese
nt S
tate
Exa
m; S
CID
: Str
uctu
red
Clin
ical
Inte
rvie
w fo
r D
SM-II
I-R; U
K: U
nite
d K
ingd
om; U
SA: U
nite
d St
ates
of A
mer
ica;
GA
D: g
ener
aliz
ed a
nxi-
ety
diso
rder
; M: m
ean;
SD
: sta
ndar
d de
viat
ion;
SE:
sta
ndar
d er
ror;
DSM
-III:
Dia
gnos
tic a
nd S
tatis
tical
Man
ual o
f Men
tal D
isord
ers,
Third
Edi
tion;
DSM
-III-R
: Dia
gnos
tic a
nd S
tatis
tical
M
anua
l of M
enta
l Diso
rder
s, Th
ird E
ditio
n, R
evis
ed; D
SM-IV
: Dia
gnos
tic a
nd S
tatis
tical
Man
ual o
f Men
tal D
isord
ers,
Four
th E
ditio
n; M
DD
: maj
or d
epre
ssiv
e di
sord
er.
a Num
ber
of G
AD
cas
es is
the
den
omin
ator
; num
ber
of d
epre
ssio
n ca
ses
is t
he n
umer
ator
.b N
umbe
r of
dep
ress
ion
case
s is
the
den
omin
ator
; num
ber
of G
AD
cas
es is
the
num
erat
or.
c Mar
tens
et
al. (
2010
) re
port
ed u
sing
DIS
to
dete
rmin
e G
AD
and
MD
D w
ith D
SM-IV
cri
teri
a, h
owev
er, r
efer
red
to t
he D
SM-II
I ver
sion
. The
aut
hors
rep
orte
d 12
-mon
th
GA
D r
ates
.d F
rasu
re-S
mith
and
Les
pera
nce
(200
8) a
lso
repo
rted
com
orbi
dity
for
17 o
ut o
f 43
GA
D p
atie
nts
with
pas
t hi
stor
y of
dep
ress
ion
indi
catin
g a
com
orbi
dity
rat
e of
39.
53 (
95%
C
I 25.
99-5
4.44
) e P
arke
r et
al.
(201
1) r
epor
ted
lifet
ime
GA
D c
omor
bid
with
dep
ress
ion/
dyst
hym
ia. A
CID
I + r
esea
rch
assi
stan
t pr
eval
ence
was
als
o re
port
ed fo
r cu
rren
t (1
5.5%
) an
d lif
etim
e G
AD
(28
.6%
).f T
ully
et
al. (
2008
) de
pres
sion
com
orbi
dity
cou
ld n
ot b
e ca
lcul
ated
bec
ause
onl
y hi
erar
chic
al e
xclu
sion
rul
es w
ere
repo
rted
.g F
edor
off e
t al
.’s (
1991
) di
agno
stic
cri
teri
a ar
e co
nsis
tent
with
DSM
-III G
AD
and
MD
D c
rite
ria.
h Ban
kier
et
al. (
2008
) re
port
ed 1
1 ou
t of
30
GA
D c
ases
in m
ixed
MD
D/a
nxie
ty g
roup
and
4/3
0 G
AD
cas
es in
anx
iety
-onl
y gr
oup.
The
fina
l rep
orte
d sa
mpl
e w
as r
estr
icte
d to
eith
er d
epre
ssio
n on
ly (
n =
30)
, no
psyc
hiat
ric
diso
rder
(n
= 3
0), m
ixed
dep
ress
ion–
anxi
ety
(n =
30)
and
anx
iety
onl
y (n
= 3
0) fr
om w
hich
the
2 ×
2 c
ontin
genc
y ta
ble
for
com
orbi
d G
AD
am
ong
MD
D w
as c
alcu
late
d.i H
awor
th e
t al
. (20
05)
repo
rted
dep
ress
ion
diso
rder
s (2
2 ou
t of
98,
tot
al 2
5%)
as m
ajor
dep
ress
ion
(14.
8%),
dyst
hym
ia (
2.3)
, min
or d
epre
ssio
n (2
.3),
brie
f dep
ress
ion
diso
r-de
r (3
.4)
and
adju
stm
ent
diso
rder
with
dep
ress
ion
(1.1
).
Tabl
e 1.
(C
ontin
ued)
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

Tully and Cosh 1607
addition to 15 identified by manual searching, a further 94 were excluded. A total of 12 studies were retained that reported GAD prevalence and seven of these also reported comorbidity with MDD.
Additional data from personal communication
The lead authors of some studies were con-tacted if required using the provided contact e-mail address. No response was received from the authors of one study (Bankier et al., 2008) who reported GAD prevalence results of 120 patients from a total recruited sample of 143. The GAD prevalence and MDD comorbidity rate were thus derived from the reported cohort of 120. A broad ‘all anxiety disorder’ category was reported in some studies. As the original GAD prevalence data in well-defined CHD groups could not be provided, these studies were excluded.
Statistical analyses
The Mix 1.7 software was employed for data analyses (Bax et al., 2006b); a software descrip-tion was reported by Bax et al. (2006a, 2007). The summation of current and lifetime preva-lence estimates was reported as the proportion of GAD patients within the total CHD sample. Aim 2 data were reported by describing the comorbidity between GAD and MDD (propor-tion of GAD patients with depression) and the comorbidity between MDD and GAD (propor-tion of depressed patients with GAD). Aim 1 and Aim 2 prevalence data were reported as proportions with 95 per cent CI calculated via the Wilson score method without continuity correction (Newcombe, 1998). To report GAD and MDD comorbidity rates, the r value was calculated (Rutledge and Loh, 2004), and then a standardized conversion to Fisher’s Z with standard error was applied (Field, 2001). Correlation effect sizes can be interpreted according to Cohen’s criteria (Cohen, 1992):
small < .10, medium = .10 to <.30, large = .30 to .50. Heterogeneity statistics were evaluated; I2 > 50 per cent in fixed-effects analyses repre-sents considerable heterogeneity, while in ran-dom effects models, when τ2 approaches zero, there is no homogeneity (Tak et al., 2010). When Aim 1 and 2 data were pooled together with a fixed-effects model, the inverse variance approach was selected. In the random effects models for Aim 1–Aim 2 data, the DerSimonian–Laird method (1986) was employed to provide a more conservative estimate of effect size (Tak et al., 2010). To evaluate the presence of publi-cation bias, the fail-safe N was reported, along with Begg and Mazumdar’s (1994) and Egger et al.’s (1997) tests.
Results
GAD prevalence in CHD
There were 12 studies (total N = 3485) reporting GAD prevalence among populations with docu-mented CHD. The Heart and Soul study recruited the largest sample, reporting GAD prevalence among 1015 stable CHD patients (Martens et al., 2010). A Canadian study recruited 804 stable coronary artery disease (CAD) patients (Frasure-Smith and Lesperance, 2008). An Australian study performed structured interviews 4 days after acute coronary syndrome among 436 patients (Parker et al., 2011). A primary care sample reported GAD prevalence rates for 245 patients with MI or heart failure (Sherbourne et al., 1996). Others reported prevalence among CHD patients attending cardiac rehabilitation (Todaro et al., 2007), an outpatient cardiology clinic (Bankier et al., 2008) and coronary angi-ography >50 per cent stenosis (Valkamo et al., 2003). The only CABG surgery study performed structured interview before surgery (Tully et al., 2011). Another report compared MI patients with stroke and spinal cord lesions, reporting MI patients separately (Fedoroff et al., 1991). The smallest studies were among 100 CHD patients (Bankier et al., 2004), 98 heart failure patients
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

1608 Journal of Health Psychology 18(12)
with left ventricular systolic dysfunction (Haworth et al., 2005) and 86 CHD outpatients (Birket-Smith et al., 2009).
When pooling the GAD prevalence data together, there was evidence of heterogeneity (I2 = 89.17%). When a random effect model was specified, the pooled GAD prevalence was 10.94 per cent (95% CI: 7.8–13.99; z = 7.01, p < .0001; τ2 = .0024), data shown in Figure 2. The fail-safe N statistic indicated that an additional 1051 missing studies would be required to bring the p value from .00 to .05. Neither Begg and Mazumdar’s nor Eggar’s test supported the evi-dence of publication bias. A sensitivity analysis was performed excluding the studies adopting DSM-III-R or earlier criteria. Again, there was evidence of heterogeneity (I2 = 90.09%), and a random effects model from seven prevalence studies supported a 2 per cent higher prevalence and 13.52 per cent pooled prevalence (95% CI: 8.39–18.66; z = 5.16, p < .0001; τ2 = .004). There was no evidence of publication bias from Begg and Mazumdar’s and Eggar’s test. The fail-safe N statistic indicated that an additional 394 miss-ing studies would be required to bring the p value from .00 to .05.
Lifetime GAD prevalence
Three studies reported lifetime GAD in CHD, and the combined N was 884 patients (Parker et al., 2011; Sherbourne et al., 1996; Todaro et al., 2007). Due to heterogeneity (I2 = 60.89%), a random effects model was specified and showed that the pooled lifetime GAD prevalence was 25.80 per cent (95% CI: 20.84%–30.77%; z = 20.67, p < .001; z = 10.19, p < .0001; τ2 = .0012). There was no evidence of publication bias from Begg and Mazumdar’s or Eggar’s test, and the fail-safe N statistic indicated that an additional 216 missing studies would be required to bring the p value from .00 to .05.
Pooled comorbidity results for depression and GAD in CHD
There were seven studies where the comorbidity between MDD and GAD could be calculated
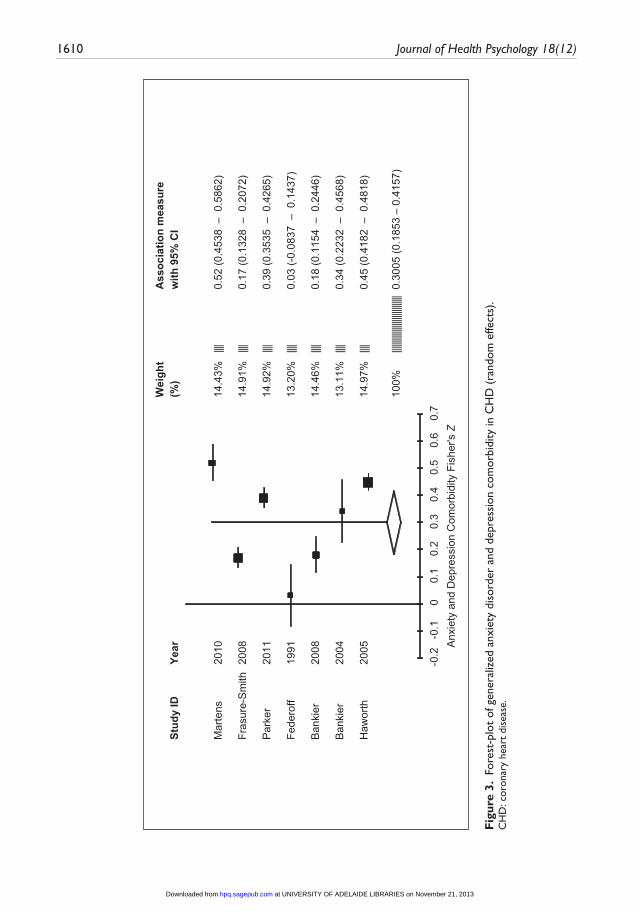
(N = 2702). One study provided comorbidity rates among a subsample of patients, but not the total recruited sample (Bankier et al., 2008). As there was evidence of heterogeneity (I2 = 97.20%), comorbidity data were pooled together in a random effects model, and this model sug-gested a modest association between MDD and GAD, Fisher’s Z = .30, 95 per cent CI: .19–.42; z = 5.11, p < .001; τ2 = .0228), data shown in Figure 3. There was no evidence of publication bias. The fail-safe N indicated that an additional 1861 missing studies were required to bring the p value from .00 to .05.
Proportion of GAD patients with comorbid depression in CHD
In moderator analyses, only studies reporting the proportion of MDD cases among GAD patients were included (combined N = 2384). As there was evidence of heterogeneity (I2 = 97.77%), comorbidity data were pooled together in a random effects model, which sug-gested a modest association, Fisher’s Z = .28 (95% CI: .10–.46; z = 3.19, p = .0015, τ2 = .0301). There was no evidence of publication bias. The two studies with stable CHD (Frasure-Smith and Lesperance, 2008; Martens et al., 2010) provided a higher comorbidity associa-tion in random effects model (Fisher’s Z = .34, 95% CI: .01–.69; z = 1.97, p = .05, τ2 = .0605) than the acute coronary syndrome studies (Fedoroff et al., 1991; Parker et al., 2011) (Fisher’s Z = .21, 95% CI: −.14 to .58; z = 1.19, p = .23, τ2 = .0629).
Proportion of depressed patients with comorbid GAD in CHD
The proportion of GAD cases among MDD patients could be determined in three studies (Bankier et al., 2004, 2008; Haworth et al., 2005). Comorbidity rates ranged between 18.33 per cent and 61.54 per cent. A random effects model was specified (I2 = 96.35%), and this test showed modest comorbidity between MDD and GAD (Z = .32, 95% CI: .13–.52; z = 3.2985,
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

Tully and Cosh 1609
Wei
ght
(%)
Ass
ocia
tion
mea
sure
with
95%
CI
Stud
y ID
Year
Mar
tens
2010
9.95
%|
0.10
44 (0
.085
6 –
0.1
232)
Fras
ure-
Sm
ith20
0810
.07%
||||
0.05
35 (0
.037
9 –
0.0
69)
Par
ker
2011
9.14
%|
0.16
06 (0
.126
1 –
0.1
95)
She
rbou
rne
1996
8.60
%|
0.13
47 (0
.091
9 –
0.1
774)
Tully
2011
8.31
%|
0.10
13 (0
.054
2 –
0.1
483)
Val
kim
o 20
039.
75%
|0.
0208
(0.0
00 –
0.0
442)
Toda
ro20
077.
23%
|0.
1867
(0.1
243
– 0
.249
)
Fedo
roff
1991
7.96
%|
0.10
08 (0
.048
8 –
0.1
527)
Ban
kier
2008
7.45
%|
0.12
5 (0
.065
8 –
0.1
842)
Ban
kier
2004
5.83
%|
0.24
(0.1
563
– 0
.323
7)
Haw
orth
2005
7.22
%|
0.11
22 (0
.049
7 –
0.1
747)
Birk
et-S
mith
2009
8.48
%|
0.04
65 (0
.002
– 0
.091
)
100%
0.10
94 (0
.078
8 –
0.13
99)
00.
10.
20.
30.
4
GA
D P
ropo
rtion
(95%
CI)
||||||
||||||
||||
Fig
ure
2. F
ores
t pl
ot o
f gen
eral
ized
anx
iety
dis
orde
r pr
eval
ence
in C
HD
(ra
ndom
effe
cts)
.C
HD
: cor
onar
y he
art
dise
ase;
GA
D: g
ener
aliz
ed a
nxie
ty d
isor
der;
CI:
conf
iden
ce in
terv
al.
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from
1610 Journal of Health Psychology 18(12)
Wei
ght
Ass
ocia
tion
mea
sure
Stud
y ID
Year
(%)
with
95%
CI
Mar
tens
2010
14.4
3%||||
0.52
(0.4
538
– 0
.586
2)
Fras
ure-
Sm
ith20
0814
.91%
||||0.
17 (0
.132
8 –
0.2
072)
Par
ker
2011
14.9
2%||||
0.39
(0.3
535
– 0
.426
5)
Fede
roff
1991
13.2
0%||||
0.03
(-0.
0837
– 0
.143
7)
Ban
kier
20
0814
.46%
||||0.
18 (0
.115
4 –
0.2
446)
Ban
kier
20
0413
.11%
||||0.
34 (0
.223
2 –
0.4
568)
Haw
orth
2005
14.9
7%||||
0.45
(0.4
182
– 0
.481
8)
100%
||||||||
||||||||
||||||||
|||||
0.30
05 (0
.185
3 –
0.41
57)
-0.2
-0.1
00.
10.
20.
30.
40.
50.
60.
7A
nxie
ty a
nd D
epre
ssio
n C
omor
bidi
ty F
ishe
r's Z
Fig
ure
3. F
ores
t-pl
ot o
f gen
eral
ized
anx
iety
dis
orde
r an
d de
pres
sion
com
orbi
dity
in C
HD
(ra
ndom
effe
cts)
.C
HD
: cor
onar
y he
art
dise
ase.
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

Tully and Cosh 1611
p < .0001). There was no evidence of publica-tion bias from Begg and Mazumdar’s and Eggar’s test. The fail-safe N indicated that an additional 391 missing studies were required to bring the p value from .00 to .05.
Discussion
This systematic review was the first to quan-tify the degree of overlap between categorical depression and anxiety disorders in CHD patients with meta-analysis techniques. The results suggested approximately 11 per cent–14 per cent GAD prevalence in CHD samples, dependent on the diagnostic criteria employed to determine psychiatric disorder status. This finding approximates previous MDD preva-lence estimates of 15 per cent in CHD samples (Thombs et al., 2008). The pooled lifetime GAD prevalence was 26 per cent. Generally speaking, the pooled comorbidity data showed correla-tions in the small to modest range (Cohen, 1992) between MDD and GAD and, thus, each psychiatric disorder is best conceptualized as sharing small to moderate variance in CHD populations.
The low comorbidity rates in CHD patients reported here noticeably contrast with those reported in clinical psychiatric samples. Evidence from three national epidemiological surveys in the Netherlands, United States and Australia (total N = 29,014) showed that GAD shared more variance with the mood disorders (r = .65) than with the other anxiety disorders (range r = .42–.58) in weighted analyses (Watson, 2009). A possible explanation for the discrepancy in comorbidity rates includes that the phenomenology of MDD in cardiovascular patients is discrepant from non-cardiovascular MDD, as previous authors have questioned (Carney and Freedland, 2012). For example, results from the Sequenced Alternatives to Relieve Depression showed that patients with CHD reported more symptoms of sympathetic nervous arousal (Fraguas et al., 2007). However, contrasting results have been reported as to whether a particular cardiovascular depression
subtype might be associated with CHD morbid-ity (Carney and Freedland, 2012; Hoen et al., 2010; Tully et al., 2011).
Indeed, it is also plausible that the phenome-nology of GAD is dissimilar among CHD patients. That said, Hoehn-Saric et al. (2004) reported that GAD patients without documented CHD scored significantly higher on cardiovas-cular and respiratory anxiety symptoms than other psychiatric patients and suggested that such symptoms were markers for somatic focussed worry in GAD. Challenging that ill-ness worry and fear would be significantly ele-vated in CHD patients, Marker et al. (2008) reported that persons without documented ath-erosclerosis scored significantly higher on a measure of heart focussed worry/fear than per-sons with heart disease. Similarly, a Swedish sample of 767 chronic stable angina patients found evidence for lower worries about the future among persons with MI history than those without MI history (25% vs 37%, p < .01) (Billing et al., 2000). Comparably, lower wor-ries were also found for persons with a heart failure diagnosis than persons without heart fail-ure (26% vs 36%, p < .01) (Billing et al., 2000).
As the pooled correlation between MDD and GAD was modest, these findings have implica-tions for interpretation of previous prognostic studies that have inferred heightened CHD mor-bidity risk to MDD and/or GAD. At the very least, findings here do not suggest that studies reporting prognostic CHD risk are merely con-founded by a large degree of shared variance between MDD and GAD. With respect to prog-nostic studies examining MDD and GAD con-currently, the Heart and Soul study showed that GAD increased the risk for subsequent major cardiovascular events between 61 per cent and 74 per cent, while MDD impacted the strength of this association by less than 5 per cent, cor-roborating independence of these psychiatric disorders (Martens et al., 2010). Also, Frasure-Smith and Lesperance (2008) showed that both MDD and GAD were associated with a twofold increased risk for major adverse cardiovascular outcome. However, the authors also noted that a
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

1612 Journal of Health Psychology 18(12)
diagnosis of either MDD or GAD conferred the greatest cardiovascular morbidity event risk, despite the small correlation between psychiat-ric disorders in the sample (Fisher’s Z = 17, p = .04). As such, it is not known whether MDD and GAD work through similar or discrepant biobe-havioural mechanisms to portend greater CHD morbidity risk. Curiously, despite low comor-bidity rates in CHD, both MDD and GAD have been associated with reduced vagal control and autonomic nervous system activity (Brosschot et al., 2006). Additionally, previous research links both MDD and GAD to CHD risk factors such as smoking, alcohol use, lower exercise and lower medication adherence (Barger and Sydeman, 2005; Grant et al., 2004; Martens et al., 2010; Wiltink et al., 2011).
Collectively, a sparse number of studies met the inclusion criteria, suggesting that further GAD research is required in CHD to clarify these preliminary findings. Dugas et al. (2010) highlighted the low rate of publications and concluded that GAD research continues to lag behind the other anxiety disorders. In CHD, previous research and intervention efforts appear to have consolidated depression as the predominant psychosocial factor (Denollet, 2008), whereas GAD research is seemingly in the nascent stages. For example, few of the CHD studies reported here investigated prog-nostic cardiovascular outcomes (Frasure-Smith and Lesperance, 2008; Martens et al., 2010; Parker et al., 2011) or receiver operating char-acteristic evaluations of self-report measures to identify GAD (Frasure-Smith and Lesperance, 2008; Haworth et al., 2005; Tully and Penninx, 2012). As other systematic reviews have shown, GAD is a chronic and disabling condition that deleteriously impacts upon quality of life (Bereza et al., 2009), with significant unmet needs (Sherbourne et al., 1996) and associated financial costs in primary care (Hoffman et al., 2008). Thus, given the relatively modest comor-bidity rates between GAD and MDD, the rec-ommendation for further GAD research in CHD cannot be understated. The predominance of CHD research concerning non-specific
self-reported anxiogenic constructs such as trait and state anxiety may hamper efforts to exam-ine specific disorders such as GAD. It was the case here that studies were excluded because various anxiety disorders were collapsed together into an ‘any anxiety disorder category’ that is not clinically informative in cardiac set-tings (Tully and Baker, 2012). In fact, such research practices neglect the heterogeneous presentation of anxiety disorders and the phe-notypic variance that makes each disorder rela-tively unique (Watson, 2009).
This study is presented with several strengths including the systematic data retrieval and meta-analyses techniques to provide a novel quanti-fication of the degree of overlap between depression and anxiety disorders that confer CHD risk. Studies prone to bias with samples fewer than 50 and those adopting self-reports of CHD were excluded. A large proportion of total variance was explained by heterogeneity in the studies, and one potential explanation was the types of CHD patients recruited. For example, only one study was identified among CABG surgery (Tully et al., 2011), one among cardiac rehabilitation attendees (Todaro et al., 2007) and two studies after acute coronary syndrome (Fedoroff et al., 1991; Parker et al., 2011). Other potential sources of heterogeneity include the type of diagnostic criteria to determine GAD, gender ratio and age of patients. A limita-tion concerns the categorical classification of depression and anxiety when these negative emotional constructs are known to reflect a con-tinuum, and critically appraised as potentially reflecting a single disorder (Mennin et al., 2008). Further research might investigate the overlap between MDD and GAD with continu-ous self-report measures that match diagnostic criteria (e.g. patient health questionnaire (PHQ)-9 and GAD-7) (Kroenke et al., 2010), and could pool together r values using a similar methodology to that outlined here.
In conclusion, these data approximate 11 per cent–14 per cent current and 26 per cent life-time GAD prevalence in CHD. The pooled data showed small to modest correlations between
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from
Tully and Cosh 1613
MDD and GAD and, thus, each psychiatric dis-order is best conceptualized as sharing moder-ate amount of variance in CHD populations. These findings support that GAD and MDD each contribute unique variance to CHD prog-nosis and may assist interpretations of the extant literature.
FundingThis research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
ReferencesAmerican Psychiatric Association (1987) Diagnostic
and Statistical Manual of Mental Disorders, Third Edition, Revised. DSM-III-R. Washington, DC: American Psychiatric Association.
American Psychiatric Association (2000) Diag-nostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision: DSM-IV-TR. Washington, DC: American Psy-chiatric Association.
American Psychiatric Association (2010) 300.02 Generalized anxiety disorder. Available at: http://www.dsm5.org/ProposedRevisions/Pages/proposedrevision.aspx?rid=167# (accessed 8 August 2010).
Bankier B, Barajas J, Martinez-Rumayor A, et al. (2008) Association between C-reactive pro-tein and generalized anxiety disorder in stable coronary heart disease patients. European Heart Journal 29(18): 2212–2217.
Bankier B, Januzzi JL and Littman AB (2004) The high prevalence of multiple psychiatric disorders in stable outpatients with coronary heart disease. Psychosomatic Medicine 66(5): 645–650.
Barger SD and Sydeman SJ (2005) Does generalized anxiety disorder predict coronary heart disease risk factors independently of major depressive disorder? Journal of Affective Disorders 88(1): 87–91.
Barlow DH, Farchione TJ, Fairholme CP, et al. (2011) The Unified Protocol for Transdiagnos-tic Treatment of Emotional Disorders: Therapist Guide. New York: Oxford University Press.
Barth J, Schumacher M and Herrmann-Lingen C (2004) Depression as a risk factor for mortality in patients with coronary heart disease: A meta-analysis. Psychosomatic Medicine 66(6): 802–813.
Baumeister H, Hutter N and Bengel J (2011) Psy-chological and pharmacological interventions for depression in patients with coronary artery dis-ease. Cochrane Database of Systematic Reviews 9: CD008012.
Bax L, Yu LM, Ikeda N, et al. (2006a) Development and validation of MIX: Comprehensive free software for meta-analysis of causal research data. BMC Medical Research Methodology 6: 50.
Bax L, Yu LM, Ikeda N, et al. (2006b) MIX: Com-prehensive free software for meta-analysis of causal research data. (Version 1.7).
Bax L, Yu LM, Ikeda N, et al. (2007) A system-atic comparison of software dedicated to meta-analysis of causal studies. BMC Medical Research Methodology 7: 40.
Begg CB and Mazumdar M (1994) Operating char-acteristics of a rank correlation test for publica-tion bias. Biometrics 50: 1088–1101.
Bereza BG, Machado M and Einarson TR (2009) Systematic review and quality assessment of economic evaluations and quality-of-life studies related to generalized anxiety disorder. Clinical Therapeutics 31(6): 1279–1308.
Billing E, Eriksson SV, Hjemdahl P, et al. (2000) Psychosocial variables in relation to various risk factors in patients with stable angina pectoris. Journal of Internal Medicine 247(2): 240–248.
Birket-Smith M, Hansen BH, Hanash JA, et al. (2009) Mental disorders and general well-being in cardiology outpatients – 6-year survival. Jour-nal of Psychosomatic Research 67(1): 5–10.
Brosschot JF, Gerin W and Thayer JF (2006) The perseverative cognition hypothesis: A review of worry, prolonged stress-related physiological activation, and health. Journal of Psychosomatic Research 60(2): 113–124.
Carney R and Freedland K (2012) Is there a high-risk subtype of depression in patients with coronary heart disease? Current Psychiatry Reports 14(1): 1–7.
Cohen J (1992) Power primer. Psychological Bulletin 112(1): 155–159.
Denollet J (2008) Depression, anxiety, and trait negative affect as predictors of cardiac events: Ten years after. Psychosomatic Medicine 70(8): 949–951.
DerSimonian, R., & Laird, N. (1986). Meta-analysis in clinical trials Controlled Clinical Trials 7(3), 177–188.
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from
1614 Journal of Health Psychology 18(12)
Dozois DJ, Seeds PM and Collins KA (2009) Transdiagnostic approaches to the prevention of depression and anxiety. Journal of Cognitive Psychotherapy 23(1): 44–59.
Dugas MJ, Anderson KG, Deschenes SS, et al. (2010) Generalized anxiety disorder publica-tions: Where do we stand a decade later? Journal of Anxiety Disorders 24(7): 780–784.
Egger M, Davey SG, Schneider M, et al. (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315: 629–634.
Fedoroff JP, Lipsey JR, Starkstein SE, et al. (1991) Phenomenological comparisons of major depres-sion following stroke, myocardial infarction or spinal cord lesions. Journal of Affective Disor-ders 22(1–2): 83–89.
Field AP (2001) Meta-analysis of correlation coef-ficients. Psychological Methods 6: 161–180.
Fraguas R Jr, Iosifescu DV, Alpert J, et al. (2007) Major depressive disorder and comorbid cardiac disease: Is there a depressive subtype with greater cardiovascular morbidity? Results from the STAR*D study. Psychosomatics 48(5): 418–425.
Frasure-Smith N and Lesperance F (2008) Depres-sion and anxiety as predictors of 2-year cardiac events in patients with stable coronary artery disease. Archives of General Psychiatry 65(1): 62–71.
Goodwin RD, Davidson KW and Keyes K (2009) Mental disorders and cardiovascular disease among adults in the United States. Journal of Psychiatric Research 43(3): 239–246.
Grant BF, Stinson FS, Dawson DA, et al. (2004) Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders: Results from the national epidemio-logic survey on alcohol and related conditions. Archives of General Psychiatry 61(8): 807–816.
Hackett ML, Yapa C, Parag V, et al. (2005) Fre-quency of depression after stroke: A system-atic review of observational studies. Stroke 36: 1330–1340.
Haworth JE, Moniz-Cook E, Clark AL, et al. (2005) Prevalence and predictors of anxiety and depres-sion in a sample of chronic heart failure patients with left ventricular systolic dysfunction. Euro-pean Journal of Heart Failure 7(5): 803–808.
Hoehn-Saric R, McLeod DR, Funderburk F, et al. (2004) Somatic symptoms and physiologic responses in generalized anxiety disorder and panic disorder: An ambulatory monitor study. Archives of General Psychiatry 61(9): 913–921.
Hoen PW, Conradi HJ, Denollet J, et al. (2010) Interview-based ratings of somatic and cognitive symptoms of depression and their impact on car-diovascular prognosis. Psychotherapy and Psy-chosomatics 79(5): 319–320.
Hoffman DL, Dukes EM and Wittchen HU (2008) Human and economic burden of generalized anxiety disorder. Depression and Anxiety 25(1): 72–90.
Kroenke K, Spitzer RL, Williams JB, et al. (2010) The Patient Health Questionnaire Somatic, Anxi-ety, and Depressive Symptom Scales: A system-atic review. General Hospital Psychiatry 32(4): 345–359.
Krueger RF (1999) The structure of common men-tal disorders. Archives of General Psychiatry 56(10): 921–926.
Kubzansky LD and Kawachi I (2000) Going to the heart of the matter: Do negative emotions cause coronary heart disease? Journal of Psychoso-matic Research 48(4–5): 323–337.
Kubzansky LD, Cole SR, Kawachi I, et al. (2006) Shared and unique contributions of anger, anxi-ety, and depression to coronary heart disease: A prospective study in the normative aging study. Annals of Behavioral Medicine 31(1): 21–29.
Lichtman JH, Bigger JT Jr, Blumenthal JA, et al. (2008) Depression and coronary heart disease: Recommendations for screening, referral, and treatment: A science advisory from the Ameri-can Heart Association Prevention Committee of the Council on Cardiovascular Nursing, Council on Clinical Cardiology, Council on Epidemiol-ogy and Prevention, and Interdisciplinary Coun-cil on Quality of Care and Outcomes Research: Endorsed by the American Psychiatric Associa-tion. Circulation 118(17): 1768–1775.
Marker CD, Carmin CN and Ownby RL (2008) Car-diac anxiety in people with and without coronary atherosclerosis. Depression and Anxiety 25(10): 824–831.
Martens EJ, De Jonge P, Na B, et al. (2010) Scared to death? Generalized anxiety disorder and cardiovascular events in patients with stable coronary heart disease: The Heart and Soul Study. Archives of General Psychiatry 67(7): 750–758.
Mennin DS, Heimberg RG, Fresco DM, et al. (2008) Is generalized anxiety disorder an anxiety or mood disorder? Considering multiple factors as we ponder the fate of GAD. Depression and Anxiety 25(4): 289–299.
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

Tully and Cosh 1615
Mineka S, Watson D and Clark LA (1998) Comor-bidity of anxiety and unipolar mood disorders. Annual Review of Psychology 49(1): 377–412.
Newcombe RG (1998) Two-sided confidence intervals for the single proportion: Comparison of seven methods. Statistics in Medicine 17: 857–872.
Nicholson A, Kuper H and Hemingway H (2006) Depression as an aetiologic and prognostic fac-tor in coronary heart disease: A meta-analysis of 6362 events among 146 538 participants in 54 observational studies. European Heart Journal 27(23): 2763–2774.
Parker G, Hyett M, Hadzi-Pavlovic D, et al. (2011) GAD is good? Generalized anxiety disorder pre-dicts a superior five-year outcome following an acute coronary syndrome. Psychiatry Research 188(3): 383–389.
Petitti DB (1994) Of babies and bathwater. American Journal of Epidemiology 140(9): 779–782.
Phillips AC, Batty GD, Gale CR, et al. (2009) Gener-alized anxiety disorder, major depressive disorder, and their comorbidity as predictors of all-cause and cardiovascular mortality: The Vietnam experience study. Psychosomatic Medicine 71(4): 395–403.
Pizzi C, Rutjes AW, Costa GM, et al. (2011) Meta-analysis of selective serotonin reuptake inhibi-tors in patients with depression and coronary heart disease. The American Journal of Cardiol-ogy 107(7): 972–979.
Rutledge T and Loh C (2004) Effect sizes and sta-tistical testing in the determination of clinical significance in behavioral medicine research. Annals of Behavioral Medicine 27(2): 138–145.
Scherrer JF, Chrusciel T, Zeringue A, et al. (2010) Anxiety disorders increase risk for incident myo-cardial infarction in depressed and nondepressed Veterans Administration patients. American Heart Journal 159(5): 772–779.
Sherbourne CD, Jackson CA, Meredith LS, et al. (1996) Prevalence of comorbid anxiety disorders in primary care outpatients. Archives of Family Medicine 5(1): 27–34. discussion 35.
Sherbourne CD, Wells KB, Meredith LS, et al. (1996) Comorbid anxiety disorder and the func-tioning and well-being of chronically ill patients of general medical providers. Archives of Gen-eral Psychiatry 53(10): 889–895.
Smith TW (2010) Conceptualization, measurement, and analysis of negative affective risk factors. In. A. Steptoe (Ed.), Handbook of Behavioral Medicine: Methods and Applications (pp. 155-168). New York: Springer.
Soo H, Burney S and Basten C (2009) The role of rumination in affective distress in people with a chronic physical illness. Journal of Health Psy-chology 14(7): 956–966.
Stroup DF, Berlin JA, Morton SC, et al. (2000) Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 283: 2008–2012.
Suls J and Bunde J (2005) Anger, anxiety, and depression as risk factors for cardiovascular disease: The problems and implications of over-lapping affective dispositions. Psychological Bulletin 131(2): 260–300.
Tak LM, Meijer A, Manoharan A, et al. (2010) More than the sum of its parts: Meta-analysis and its potential to discover sources of heterogeneity in psychosomatic medicine. Psychosomatic Medi-cine 72(3): 253–265.
Thombs BD, de Jonge P, Coyne JC, Whooley MA, Frasure-Smith N, Mitchell AJ, Zuidersma M, Eze-Nilam C, Lima BB, Smith CG, Soderlund K, Ziegelstein RC (2008) Depression screening and patient outcomes in cardiovascular care: a sys-tematic review. Journal of the American Medical Association 300(18): 2161–2171.
Todaro JF, Shen BJ, Raffa SD, et al. (2007) Preva-lence of anxiety disorders in men and women with established coronary heart disease. Journal of Cardiopulmonary Rehabilitation and Preven-tion 27(2): 86–91.
Tully PJ and Baker RA (2012) Depression and anxi-ety and morbidity outcomes after coronary artery bypass graft surgery patients: A practical and contemporary review. Journal of Geriatric Car-diology 9: 197–208.
Tully PJ and Penninx BW (2012) Depression and anxiety among coronary heart disease patients: Can affect dimensions and theory inform diag-nostic disorder based screening? Journal of Clin-ical Psychology 68(4): 448–461.
Tully PJ, Baker RA, Turnbull D, et al. (2008) The role of depression and anxiety symptoms and hospital readmissions after cardiac sur-gery. Journal of Behavioral Medicine 31(4): 281–290.
Tully PJ, Pedersen SS, Winefield HR, et al. (2011) Cardiac morbidity risk and depression and anxiety: A disorder, symptom and trait analysis among cardiac surgery patients. Psychology, Health and Medicine 16(3): 333–345.
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from

1616 Journal of Health Psychology 18(12)
Tully PJ, Winefield HR, Baker RA, et al. (2011) Con-firmatory factor analysis of the Beck Depression Inventory-II and the association with cardiac morbidity and mortality after coronary revascu-larization. Journal of Health Psychology 16(4): 584–595.
Valkamo M, Koivumaa-Honkanen HT, Hintikka J, et al. (2003) Life satisfaction in patients with chest pain subsequently diagnosed as coronary heart disease – Connection through depressive symptoms? Quality of Life Research 12(8): 1099–1105.
Watson D (2009) Differentiating the mood and anx-iety disorders: A quadripartite model. Annual Review of Clinical Psychology 5: 221–247.
Wiltink J, Beutel ME, Till Y, et al. (2011) Prevalence of distress, comorbid conditions and well being in the general population. Journal of Affective Disorders 130(3): 429–437.
World Health Organization (2007) International statistical classification of diseases and related health problems 10th revision version for 2007. Available at: http://www.who.int/classifications/apps/icd/icd10online/
at UNIVERSITY OF ADELAIDE LIBRARIES on November 21, 2013hpq.sagepub.comDownloaded from




















