Gender role and child health care utilization in Nepal
10
Health Policy 74 (2005) 100–109 Gender role and child health care utilization in Nepal Subhash Pokhrel a,∗ , Rachel Snow b , Hengjin Dong c , Budi Hidayat a , Steffen Flessa a , Rainer Sauerborn a a Department of Tropical Hygiene and Public Health, University of Heidelberg, INF 324, D-69120 Heidelberg, Germany b Michigan Centre on the Demography of Aging, 426 Thompson St., P.O. Box 1248, Ann Arbor, MI 48106, USA c Health Economics Research Group, Brunel University, Uxbridge, Middlesex UB8 3PH, UK Abstract Objective: To study the gender role in child health care utilization in Nepal. Methods: We analysed 8112 individual observations of age ≤15 years from 2847 households in 274 communities, obtained from the 1996 Nepal Living Standard Survey. Four steps of a health seeking action, namely illness reporting, choosing an external care, choosing a specific health care provider, and spending money to treat the sick child, were examined using discrete/continuous choice models. Results: There was no statistically significant difference between boys and girls by demographic, socio-economic and geo- graphical status in the sample. However, gender was associated with all four utilization decision steps. While the net effect of being a boy was modest in illness reporting (p < 0.10), it appeared stronger in the choice of external care, in the choice of public provider and in the choice of expenditure with the private provider (p < 0.05). Conclusion: Gender role not only affects illness reporting but also affects the decision to choose a health care provider and how much to spend on the sick child, i.e. it affects the entire steps of a health seeking action. © 2004 Elsevier Ireland Ltd. All rights reserved. Keywords: Child health; Utilization; Gender bias; Nepal 1. Introduction Gender refers to “women’s and men’s roles and re- sponsibilities that are socially determined” [1]. Gen- der differences in health, therefore, are caused by so- ciety’s response to secondary sex characteristics that distinguish males from females. Because a child ap- ∗ Corresponding author. E-mail address: [email protected] (S. Pokhrel). pears to be male, society provides opportunities and constraints that affect his health [2]. Several studies, in particular, those reported from South Asia, speak much on gender bias in health and health care [3–8]. While economic opportunities and threats are related to such a difference by some [3], cultural attributes have been given more importance in influencing the health care decisions by others [4,8]. A common ground, how- ever, is the recognition of the existence of strong son- preference in South Asian societies including Nepal, for both economic and non-economic reasons [3,9–11]. 0168-8510/$ – see front matter © 2004 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.healthpol.2004.12.013
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Gender role and child health care utilization in Nepal

Health Policy 74 (2005) 100–109
Gender role and child health care utilization in Nepal
Subhash Pokhrela,∗, Rachel Snowb, Hengjin Dongc,Budi Hidayata, Steffen Flessaa, Rainer Sauerborna
a Department of Tropical Hygiene and Public Health, University of Heidelberg, INF 324, D-69120 Heidelberg, Germanyb Michigan Centre on the Demography of Aging, 426 Thompson St., P.O. Box 1248, Ann Arbor, MI 48106, USA
c Health Economics Research Group, Brunel University, Uxbridge, Middlesex UB8 3PH, UK
Abstract
Objective: To study the gender role in child health care utilization in Nepal.Methods:We analysed 8112 individual observations of age≤15 years from 2847 households in 274 communities, obtained fromthe 1996 Nepal Living Standard Survey. Four steps of a health seeking action, namely illness reporting, choosing an external care,choosing a specific health care provider, and spending money to treat the sick child, were examined using discrete/continuouschoice models.Results: There was no statistically significant difference between boys and girls by demographic, socio-economic and geo-graphical status in the sample. However, gender was associated with all four utilization decision steps. While the net effect ofbeing a boy was modest in illness reporting (p< 0.10), it appeared stronger in the choice of external care, in the choice of publicprovider and in the choice of expenditure with the private provider (p< 0.05).Conclusion:Gender role not only affects illness reporting but also affects the decision to choose a health care provider and howm©
K
1
sdcd
(
ands,eak
ed toealth-
son-pal,
0
uch to spend on the sick child, i.e. it affects the entire steps of a health seeking action.2004 Elsevier Ireland Ltd. All rights reserved.
eywords:Child health; Utilization; Gender bias; Nepal
. Introduction
Gender refers to “women’s and men’s roles and re-ponsibilities that are socially determined”[1]. Gen-er differences in health, therefore, are caused by so-iety’s response to secondary sex characteristics thatistinguish males from females. Because a child ap-
∗ Corresponding author.E-mail address:[email protected]
S. Pokhrel).
pears to be male, society provides opportunitiesconstraints that affect his health[2]. Several studiein particular, those reported from South Asia, spmuch on gender bias in health and health care[3–8].While economic opportunities and threats are relatsuch a difference by some[3], cultural attributes havbeen given more importance in influencing the hecare decisions by others[4,8]. A common ground, however, is the recognition of the existence of strongpreference in South Asian societies including Nefor both economic and non-economic reasons[3,9–11].
168-8510/$ – see front matter © 2004 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.healthpol.2004.12.013

S. Pokhrel et al. / Health Policy 74 (2005) 100–109 101
In Nepal, child mortality is still high and differs sub-stantially between boys and girls. The 1–4-year-old fe-male child deaths per 100 male child deaths in 1970,1985 and 1996 were, respectively, 108.7, 128.2 and124.2, showing that the situation for girls relative toboys increasingly deteriorated during the 1970s andvery little progress could be achieved afterwards[12].A recent study has opened up a new argument that dif-ferential child mortality in Nepal may be due to thedifferential access to health care arising primarily fromillness perception, not necessarily from the decisionsto seek care or spend money on the sick children[13].
The current 5-year plan as well as the long-termhealth plan of His Majesty’s Government of Nepal hastargeted at reducing the child mortality rates furtherby embarking upon several “first-priority” preventiveand curative care interventions for childhood diseases,such as expanded program on immunization, diarrhoeaand acute respiratory tract infection control, nutrition,mother and child welfare, etc.[14]. In order to im-plement these programs more effectively than in thepast, policy makers and program managers need to un-derstand how different factors, including gender, mayaffect the household decisions with regard to the use ofchild health care. The purpose of this paper is, there-fore, to establish the extent to which gender role affectschild health care utilization in Nepal.
2. Methodology
2
asw n-t ac-c %o 30.N blicp lthp tral,r ers,7 ed att yi De-s pal’sh s, isc or
quality of care[14,15]. The current health care spend-ing level in Nepal is about 5% of its gross nationalproduct (GNP), of which 74% is accounted for out-of-pocket payment[16]. The infant and under-five childmortality rates have declined steadily in the past decadebut they are still one of the highest in the world and arecharacterized by substantial gender differentials[12].The focus of child health services has been on the ex-panded program on immunization, nutrition, controlof diarrhoeal and acute respiratory infections, and pro-grams that address leading causes of mortality and mor-bidity [14].
2.2. Sample design
We analysed the data obtained from the Nepal Liv-ing Standards Survey (NLSS) which was administeredby Nepal’s Central Bureau of Statistics (CBS), togetherwith the World Bank, in 1996. This survey included anationally representative sample of 3338 households(18,855 individuals) in 275 communities. A two-stagestratified sampling procedure was used: first selectingwards (the primary sampling units (PSU)) from the fourstrata (mountains, urban-hills, rural-hills and theTerai,the plains in the southern part) with probability pro-portional to sample size, and then choosing a fixednumber of households from each selected PSU withequal probability. The details of the survey design aredescribed elsewhere[17]. We analyzed 8112 individ-ual observations (4162 males and 3950 females) from2 erva-t uredb
2
phica d toh : (a)w suf-f (b)w ivent ndp tiona erec f thec ed.N
.1. Setting
Nepal is situated at the foot-hills of the Himalayith two-thirds of its land covered by hills and mou
ains, the extremely difficult terrain with regard toessibility. It has a population of over 23 million, 80f which is rural. The per capita income is US$ 2epal’s health care system relies heavily on the purovision of service delivery. The Ministry of Hearovides care through 79 hospitals located at cenegional and district levels, 178 primary health cent05 health posts and 3132 sub-health posts locat
he community level[14]. Since the new health policn 1991, private provision has expanded rapidly.pite the increase in number of service outlets, Neealth care infrastructure, especially in rural areaharacterized by a low level of utilization and po
847 households in 274 communities. These obsions include all children aged 15 years or less capty the survey.
.3. Survey instrument
NLSS surveyed on various economic, demogrand health-related behaviours. Questions relateealth, which we chose for our analysis, includedhether each household member was perceived to
er from an illness or injury in the past month,hether the individuals used health care services g
his illness/injury, and (c) if so, the type of place aractitioner that was consulted, and the consultand travel costs for the first two visits. If tests warried out and drugs were given as the result oonsultation during the visit, they were also includo costs for drug items were recorded separately.

102 S. Pokhrel et al. / Health Policy 74 (2005) 100–109
2.4. Statistical methods
The analytical framework employed in this paper isbased on the four-step construct of household decision-making process described by Pokhrel and Sauerborn[13]. It assumes that the child health care decisionsfollow a pathway that involves four steps in a hierarchy.The steps are: (a) whether or not a child is reportedill, (b) whether the sick child is offered an externalcare given illness, (c) to which provider the child wastaken to, and (d) depending upon what type of providerchosen, how much is spent for the treatment of the sickchild.
In order to translate this framework into a multivari-ate analysis, the four steps were considered sequentialdecision steps in which each decision is governed bydifferent stochastic processes[18–20]. This gave riseto a four-part model in which the decisions to report anillness, to choose an external care (versus no care), tochoose a type of provider (from a choice set comprisingof public, private, pharmacy, and traditional healers),and to choose the level of expenditure to treat the child,were modelled separately.
The first two steps (reporting an illness and choos-ing an external care) were modelled with logit spec-ifications [21]. The model goodness-of-fit for theseequations was assessed by Hosmer–Lemeshow test[22,23]. The third step [choosing one provider fromthe choice set{no or informal care, public providers,private providers}] was specified as a multinomiall edt rna-t ansT sti-m pen-d atep nu-m lersw rg-i ion-m tra-d ayd allyh less,m wasd y be-c bser-
vations pertaining to traditional healers and pharmacychoices.
Since people self-select providers, a correctionmight be needed in the OLS estimates of the expen-diture. A method derived by Lee[25] and applied in arecent study in Zambia[26] was applied. The selectionterms were found insignificant in both equations, andhence, the final model did not include selection terms.The details of the methods and results of these selec-tion models are given in[27]. All regression diagnosticsfollowing OLS were carried out.
2.5. Independent variables
Gender was measured by a dummy variable(0 = girls, 1 = boys). Other variables that were in-cluded as the independent variable are: income, ageof the child, mother’s socio-economic status (her edu-cation and employment as well as whether she headsthe household), household composition (number ofadults), location variables (mountain, hills or Terai), ru-ral/urban status, types of illness reported, and the timeto reach the nearest public clinic (proxy for health ser-vice availability). Because information on the severityof illness was not available, it was not included in themodel. Sanitation variables such as having piped waterwas also included as independent variables. Includingtypes of illness together with age of the child and san-itation variables helped us separate the gender’s neteffect from biological needs. Income was proxied byt
3
andf antt fer-e cio-e
am-p na feredf hes eret n top romR 256
ogit (MNL). Two specification tests were employo test the independence of the irrelevant alteives (IIA) assumption of the model, viz. Hausmpecification test and Small–Hsiao IIA test[21,24].he final step (the level of expenditure) was eated by ordinary least squares (OLS). The exiture decisions were modelled for users of privroviders and public providers separately. Forerical significance, pharmacy and traditional heaere included in the private provisions. This me
ng could affect our results because the decisaking dynamics behind seeking treatment fromitional healers and from other private providers miffer significantly, and these differences potentiave an important gender dimension. Nevertheerging these categories into private provisioneemed as the most appropriate analytical strategause the survey recorded a small number of o
otal annual expenditures per capita[26,28,29].
. Results
Table 1presents the characteristics of the maleemale children included in the sample. It is importo note that there was no statistically significant difnce between boys and girls by demographic, soconomic and geographical characteristics.
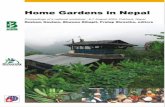
The four-step decision-making process in our sle is depicted inFig. 1. About 10% of the childreged 15 years or less were reported to have suf
rom an acute illness or injury 1 month prior to turvey date. Over two-thirds of the sick children waken to an external help. Of these, 56% were takeublic providers. The health expenditure ranged fs. 115 (US$ 2.05) with traditional healers to Rs.

S. Pokhrel et al. / Health Policy 74 (2005) 100–109 103
Table 1The characteristics of the sampled population (n= 8112a)
Characteristics Sex of the child
Male Female p-Value
Mean age of the child (years) 7.2 7.2 0.91Mean age of the mother (years) 33.3 33.4 0.56Mothers who attended school (%) 11.5 12.1 0.42Mothers who were not in self- or
wage-employment (%)22.3 22.3 0.64
Mothers heading the household (%) 8.0 7.4 0.39Mean income per capita (Rs.) 6187 6065 0.22Living in rural areas (%) 93.9 94.0 0.79Mean time taken to reach the nearest
health facility (min)80.7 82.9 0.55
a Male children = 4162; female children = 3950.
(US$ 4.57) with the private providers in 1995/1996value.
3.1. Decision to report an illness
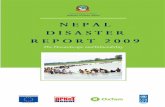
A boy had a 15% more chance to have been re-ported ill than a girl (the second column ofTable 2).The predicted probabilities of illness reporting were
higher for boys regardless of income (Fig. 2). Con-sistent with the results from the descriptive analysis[13], these predictions also show the non-linear rela-tionship between illness reporting and income-lowerfor the poorer who cannot afford to be ill, rising withwealth, and then falling again as health and wealth areassociated.
3.2. Decision to seek external care given illness
Compared to girls, boys were associated with a 42%more likelihood of seeking external care given illness,holing constant all other variables including the typeof illness reported (the fourth column ofTable 2). Thiseffect was strong (p< 0.05).
3.3. Decision to choose a health care provider
The last four columns ofTable 2report the relativerisk ratio (RRR) given by the multinomial logit model.The results show that, compared with no or informalcare, being a boy predicted the probability of using thepublic provider by 43% more than being a girl. Thiseffect was strong (p< 0.05). Gender had no effect in the
decisio
Fig. 1. Child health care utilization ns in Nepal (data source: NLSS 1996).
104 S. Pokhrel et al. / Health Policy 74 (2005) 100–109
Table 2Estimated odds ratio in logit models for child health care utilization decisions
Variable Report ill Seek care Choose provider
OR |Z| stat OR |Z| stat Public vs. no/informal Private vs. no/informal
RRR |Z| stat RRR |Z| stat
Male child 1.15 (1.81)* 1.42 (2.11)** 1.43 (2.17)** 1.07 (0.33)Age 1–5 years 0.75 (2.17)** 0.99 (0.04) 1.11 (0.28)Age 6–15 years 0.26 (9.89)*** 1.14 (0.45) 0.66 (1.10)Mother heads the household 1.51 (3.02)***
Mother’s schooling (years) 0.99 (0.23) 1.05 (1.31)Mother in wage-employment 0.70 (1.40) 1.03 (0.08)Income quartile 2a 0.99 (0.10)Income quartile 3a 1.18 (1.24)Income quartile 4 (highest)a 1.27 (1.67)*
Natural log of income 2.50b (4.65)*** 1.78c (3.68)*** 2.63c (4.66)***
Number of adults in the household: 3–5 0.69 (3.83)*** 0.88 (0.73) 1.14 (0.55)Number of adults in the household: >5 0.63 (3.06)*** 1.27 (0.87) 1.24 (0.60)Piped water source 0.80 (2.20)**
Mountain region 0.46 (2.44)** 0.93 (0.25) 0.03 (3.36)***
Hill region 0.51 (3.13)*** 0.97 (0.14) 0.22 (5.72)***
Rural area 1.14 (0.37) 1.67 (1.73)* 0.47 (2.31)**
Public clinic 1 hour away 0.54 (2.77)*** 0.57 (2.93)*** 0.92 (0.30)
Reported illness (ref: diarrhoea)Respiratory problems 0.50 (1.30) 0.67 (0.92) 1.59 (0.77)Fever 0.57 (2.14)** 0.48 (3.19)*** 1.59 (1.34)Skin diseases 2.90 (1.38) 0.91 (0.17) 3.94 (1.96)**
Injury 0.72 (0.77) 0.49 (1.70)* 1.50 (0.66)Others 0.57 (1.96)* 0.46 (3.09)*** 1.21 (0.50)
Log likelihood −2452.65 −426.85 −730.68Chi-square (d.f.) 247.43 (10)* 64.40 (11)* 189.69 (34)*
Model fit d e f
Observations 8112g 788h 788h
OR, odds ratio; RRR, relative risk ratio.a Income quartile 1 (lowest) to 4 (highest), quartile 1 being the reference group.b Income elasticity at mean = 0.30.c Income elasticities at mean estimated at 0.21 (public) and 0.60 (private).d Hosmer–Lemeshow Chi-square (8) = 5.3 (p= 0.73).e Hosmer–Lemeshow Chi-square (8) = 4.02 (p= 0.85).f Small–Hsiao tests of IIA assumption: Chi-square (18) = 24.048; prob > Chi-square = 0.15 (omitting public); Chi-square (18) = 16.04;
prob > Chi-square = 0.59 (omitting private). Hausman test of IIA assumption: Chi-square (18) = 7.796; prob > Chi-square = 0.982 (omitting pub-lic); did not meet asymptotic assumptions of the test (omitting private).
g Male children = 4162; female children = 3950.h Male children = 432; female children = 356.* Significant at 10%.
** Significant at 5%.*** Significant at 1%.

S. Pokhrel et al. / Health Policy 74 (2005) 100–109 105
Fig. 2. Predicted probability and actual frequency of illness reporting by the gender of the child and income quartile.
choice of private provider compared to no or informalcare.
3.4. Health expenditure decisions
Table 3 reports the estimated coefficients in themodels of health expenditure with public and privateproviders. Both models fit the data, and OLS assump-tions are held (the last four rows report the results ofthe regression diagnostics). Being a male child wasnot significantly associated with the health expenditurewith public providers. However, its effect was signifi-cant with the private provider. Households would spendmore money with private providers if the child was aboy, after holding all other variables including the typeof illness constant.
4. Discussion
The gender role within the household is importantto the extent it influences the propensity to seek healthcare. Although there is already an overwhelming liter-ature on gender bias in the allocation of health care andfood within households in South Asian societies[3–6],we contribute to the literature in at least three ways.Firstly, we examine gender’s effect in four outcomemeasures – illness reporting, choice of care, choice
of provider, and health expenditure – in a frameworkthat allows us to scrutinize how gender role changes ashouseholds make health care decisions in a sequentialnature. Secondly, we document gender’s effect on thedemand for child health care in a small and poor SouthAsian country that has extremely difficult terrain withregard to accessibility. Thirdly, we attempt to make thedistinction between ‘gender’ and ‘sex’ explicit by sepa-rating the biological effects from social discriminationin our multivariate analysis. We believe that once thetype of illness (biological effects) is controlled for, theremaining effect of sex on health care choices reflectthe gender effect.
The results show that gender bias exists in the illnessreporting, and it gets larger in the subsequent decisions.This indicates that the underlying household dynamicsof health care choice are different for boys and girls[13]. One possible explanation for this bias is the ex-istence of strong son-preference in Nepal[9–11]. Ifhealth care is considered as an investment, poor house-holds may not wish to invest in girls who will leave thefamily after marriage[3] and hence they deem girls’need for care less often than they would do so if thechild was a boy. As the size of the gap in predicted prob-ability of illness reporting remained the same acrossall income groups, we share with Das Gupta[4] thatdiscrimination against female children may not be mo-tivated primarily by economic hardship.

106 S. Pokhrel et al. / Health Policy 74 (2005) 100–109
Table 3Estimated coefficients in OLS for child health care expenditure decisions
Variable Health expenditure decisions
Public provider Private provider
Coefficient |t| stat Coefficient |t| stat
Male child 0.07 (0.53) 0.32 (2.06)**
Age of the child −0.01 (0.72) −0.01 (0.09)Mother heads household −0.13 (0.54) 0.40 (1.24)Mother’s schooling (years) −0.03 (1.21) −0.00 (0.02)Natural log of income 0.49 (3.89)*** 0.23 (1.57)Number of adults in the family −0.14 (3.34)*** 0.02 (0.44)Mountain region 0.04 (0.20) −0.10 (0.10)Hill region −0.08 (0.53) −0.28 (1.29)Rural area −0.07 (0.30) −0.27 (1.21)
Reported illness (ref: diarrhoea)Respiratory problems 0.23 (0.67) 0.80 (1.81)*
Fever 0.16 (0.89) 0.06 (0.25)Skin diseases −0.79 (2.05)** 0.48 (1.07)Injury 0.66 (1.85)* 1.13 (2.54)**
Others −0.09 (0.47) −0.04 (0.14)Constant 1.098 (0.91) 3.056 (2.17)**
Observations 280a 145b
R2 0.15 0.16Ramsey RESET test F(3, 262) = 0.51;p= 0.67 F(3, 127) = 2.17;p= 0.09Cook–Weisberg test Chi-square (1) = 4.33;p= 0.03c Chi-square (1) = 1.02;p= 0.31Normality of residuals µ = 0.0003;σ2 = 1.005 µ =−0.0003;σ2 = 1.008
S=−0.04;K= 3.23 S=−0.07;K= 2.67
µ, Mean;σ2, variance;S, skewness;K, kurtosis.a Male children = 165; female children = 115.b Male children = 77; female children = 68.c Following this test, White’s correction applied to get robust standard errors.* Significant at 10%.
** Significant at 5%.*** Significant at 1%.
We add on to the health care utilization literaturethe finding that gender not only counts in one measureof child health care utilization in Nepal, it counts in alldecision steps of one health seeking action. This under-scores once again the need for capturing the entire stepsof a health seeking action in the quantitative analysis[13]. Apart from influencing the decisions to report anillness and subsequently to seek care, gender was as-sociated with the choice of public providers, comparedto choice of no or informal care. But it did not influ-ence the choice of private providers compared to no orinformal care. Interestingly, it was found that the ex-penditure decisions at private providers go in favour ofboys. Such a finding is also reported from Kerala stateof India in which it was found that gender was not asso-
ciated with the decision to seek care but it influenced theselection of allopathic compared to alternative medicalsystems[6].
Studies elsewhere, particularly in Africa, find amixed effect of gender on health care use[30–32]. Ear-lier studies conducted in Burkina Faso in West Africa,for example, found no gender bias in the allocationof household resources in health care[30] or expen-ditures between boys and girls[31]. A more recentstudy that examined out-of-pocket health expenditurein the same country, however, found that males wereallocated considerably higher out-of-pocket expendi-ture on health than females while seeking treatmentin the health facility[32]. While discussing why theirfindings differed from the earlier studies, the authors

S. Pokhrel et al. / Health Policy 74 (2005) 100–109 107
point to different methodological approaches used toanswer the same question. Therefore, we recommendfuture studies similar to that of ours in these settingstoo.
As our study and many others described above werebased on revealed preference construct in which we ob-served households making health care choice and wereconcerned with the outcome and not the process bywhich these choices were evolved[27], we are unableto explain fully why people have son-preference withregard to health care utilization. Future research shouldseek the answer from the stated-preference paradigm,e.g. using a conjoint analysis in which all attributes ofa given choice should be analysed[33].
One caveat of our analysis is the assumption thathousehold members, in particular the parents, makeutilization decisions for their children[13]. If this isso, household members’ characteristics, such as house-hold head’s or father’s age, sex, occupation, and edu-cation might be important predictors of these decisions[34]. We were aware of these hypotheses and testedthem by estimating models that included the above-mentioned variables. We could not find any signifi-cant relationship between the characteristics of house-hold members (head, father) and child health carechoice. We suspect that the very little variation ofthese variables in our data may not have allowed usto detect this relationship. Once again, we share withRyan[33] that a conjoint analysis of heath care choicecould be a better alternative method to explore thisr
5
rityi e oft clearu beeno
per-c welli ralp s dis-c par-i e tol iesh role
in increasing health care utilization[35]. Although in-vesting in education is a continuous and long run un-dertaking coming outside health sector, there are twoadvantages of mothers’ education that can be relatedto child health care use. Mothers’ education, on onehand, may increase the likelihood of reducing her re-source constraints by increased income; it, on the otherhand, helps her better perceive illness of her childrenregardless of their gender as higher education and in-come may link her to certain social institutions thatfoster health care utilization[36].
Second, given gender’s broader social and culturalroots and its effect, particularly in illness perception, in-creasing service outlets and removing financial barriersthrough supply side subsidy may not work[8,37,38]. Ithas been argued elsewhere that demand side subsidiesthat enable the poorest households to purchase healthinsurance could help lower this gap[27], potentiallybecause the household decisions then do not becomea trade-off between who (a boy or a girl) should betreated.
6. Conclusion
The main contribution of this paper is the findingthat gender role not only affects illness reporting butalso affects the decision to choose a health care providerand how much to spend on the sick child, i.e. it affectsthe entire steps of a health seeking action. While thee etiesc reu digmi oc-c ptiono or-e haseh r gapi
A
s ofT n-t ankf ex-p hors.
elationship.
. Policy implications
Offering specific policy to reduce gender dispan child health care use in Nepal is beyond the scophis paper because any such discussion requires anderstanding of why the findings presented havebserved. However, two general points are made:
First, health policies should address altering theeption of girls’ illnesses. This may need strategiesnformed by additional research from socio-cultuerspectives and/or stated-preference techniqueussed above. While we could not attribute the disty in health care choice to mother’s education duittle variation observed for this variable, other studave found women’s education to play a positive
xistence of son-preference in South Asian sociould be linked to this differential child health case, more research from a stated-preference para
s needed to explore why this difference actuallyurs. Health polices that address altering the percef girls’ illnesses and potentially providing the post households with demand side subsidies to purcealth insurance are needed to reduce the gende
n child health care utilization.
cknowledgements
This study was carried out under the auspiceropical Medicine Heidelberg (TMH). We thank Ce
ral Bureau of Statistics (Nepal) and the World Bor providing us with the NLSS I dataset. The viewsressed and errors in the paper are that of the aut

108 S. Pokhrel et al. / Health Policy 74 (2005) 100–109
References
[1] WHO. Gender and health: technical paper. Geneva: WorldHealth Organization; 1998.
[2] Snow R. Reorienting public health: exploring differentials in hipfracture. In: Sen G, George A, Ostlin P, editors. Engenderinginternational health: the challenge of equity. The MIT Press;2002.
[3] Chen L, Huq E, D’Souza S. Sex bias in family allocation ofhealth care in Bangladesh. Population and Development Review1981;7:55–70.
[4] Das Gupta M. Selective discrimination against female childrenin rural Punjab, India. Population and Development Review1987;13:77–110.
[5] Pandey A, Sengupta PG, Mondal SK, Gupta DN, Manna B,Ghosh S, et al. Gender differences in healthcare seeking duringcommon illnesses in a rural community of West Bengal, In-dia. Journal of Health, Population and Nutrition 2002;20:306–11.
[6] Pillai RK, Williams SV, Glick HA, Polsky D, Berlin JA,Lowe RA. Factors affecting decisions to seek treatment forsick children in Kerala, India. Social Science and Medicine2003;57:783–90.
[7] Borooah VK. Gender bias among children in India in their dietand immunization against disease. Social Science and Medicine2004;58:1719–31.
[8] Basu AM. Cultural influences on health care use: two regionalgroups in India. Studies in Family Planning 1990;21:275–86.
[9] Niraula BB, Morgan SP. Son and daughter preferences in Be-nighat, Nepal: implications for fertility transition. Social Biol-ogy 1995;42:256–73.
[10] Leone T, Matthews Z, Dalla Zuanna G, Leone T, MatthewsZ, Dalla Zuanna G. Impact and determinants of sex pref-erence in Nepal. International Family Planning Perspectives
[ ugh-69–
[ lhi:
[ childealth
[ /59of
[ s inolicy
[ use-care71–
[ tan-tion.
[18] Manning WG, Newhouse JP, Duan N, Keeler E, Leibowitz A,Marquis S. Health insurance and the demand for medical care:evidence from a randomized experiment. American EconomicReview 1987;77:251–77.
[19] Pohlmeier W, Ulrich V. An econometric model of the two-partdecision making in the demand for health care. Journal of Hu-man Resources 1995;30:339–61.
[20] Liu TC, Chen CS. An analysis of private health insurance pur-chasing decisions with national health insurance in Taiwan. So-cial Science and Medicine 2002;55:755–74.
[21] Greene W. Econometric analysis. 3rd ed. New Jersey: PrenticeHall International Inc.; 1997.
[22] Hosmer DW, Lemeshow S. Applied logistic regression. 2nd ed.New York: John Wiley & Sons Inc.; 2000.
[23] Ha NT, Berman P, Larsen U. Household utilization and expen-diture on private and public health services in Vietnam. HealthPolicy and Planning 2002;17:61–70.
[24] StataCorp. Stata statistical software: release 7.0. College Sta-tion, TX: Stata Corporation; 2001.
[25] Lee L. Generalized econometric models with selectivity. Econo-metrica 1983;51:507.
[26] Hjortsberg C. Why do the sick not utilise health care? The caseof Zambia. Health Economics 2003;12:755–70.
[27] Pokhrel S, 2004. Role of price, income and gender onthe demand for child health care in Nepal: exploring afour-step construct on household decision making. Doc-toral Dissertation. University of Heidelberg Medical School,submitted.
[28] Deaton A. The analysis of household surveys—a microeco-nomic approach to development policy. Baltimore: Johns Hop-kins University Press; 1998.
[29] Rous JJ, Hotchkiss DR. Estimation of the determinants ofhousehold health care expenditures in Nepal with controls forendogenous illness and provider choice. Health Economics2003;12:431–51.
[ ndercare31–
[ f re-gateddies
[ ningkinaIn-
[ pa-appli-ine
[ R.kina
[ ctureAsia
2003;29:69–75.11] Karki Y. Sex preference and the value of sons and da
ters in Nepal. Studies in Family Planning 1988;19:178.
12] WHO. Women of South-East Asia: a health profile. New DeSouth East Asia Regional Office; 2000.
13] Pokhrel S, Sauerborn R. Household decision making onhealth care in developing countries: the case of Nepal. HPolicy and Planning 2004;19:218–33.
14] MOH. Annual report: Department of Health Services 2058(2002/03). Kathmandu: Ministry of Health, DepartmentHealth Services; 2003.
15] Acharya LB, Cleland J. Maternal and child health servicerural Nepal: does access or quality matter more? Health Pand Planning 2000;15:223–9.
16] Hotchkiss DR, Rous JJ, Karmacharya K, Sangraula P. Hohold health expenditures in Nepal: implications for healthfinancing reform. Health Policy and Planning 1998;13:383.
17] Prennushi G. Central Bureau of Statistics. Nepal living sdards survey I (1995/96). Survey design and implementaWashington, DC: World Bank; 1996.
30] Sauerborn R, Berman P, Nougtara A. Age bias, but no gebias, in the intra-household resource allocation for healthin rural Burkina Faso. Health Transition Review 1996;6:145.
31] Haddad L, Reardon T. Gender bias in the allocation osources within the household in Burkina Faso: a disaggreoutlay equivalent analysis. Journal of Development Stu1993;29:260–76.
32] Mugisha F, Kouyate B, Gbangou A, Sauerborn R. Examiout-of-pocket expenditure on health care in Nouna, BurFaso: implications for health policy. Tropical Medicine andternational Health 2002;7:187–96.
33] Ryan M. Using conjoint analysis to take account oftient preferences and go beyond health outcomes: ancation to in vitro fertilization. Social Science and Medic1999;48:535–46.
34] Dong H, Kouyate B, Cairns J, Mugisha F, SauerbornWillingness-to-pay for community-based insurance in BurFaso. Health Economics 2003;12:849–62.
35] Matsumura M, Gubhaju B. Women’s status, household struand the utilization of maternal health services in Nepal.Pacific Population Journal 2001;16:23–44.

S. Pokhrel et al. / Health Policy 74 (2005) 100–109 109
[36] McKinalay J. Some approaches and problems in the study ofthe use of services: an overview. Journal of Health and SocialBehaviour 1972;13:115–52.
[37] Magadi MA, Madise NJ, Rodrigues RN. Frequency and timingof antenatal care in Kenya: explaining the variations between
women of different communities. Social Science and Medicine2000;51:551–61.
[38] Obermeyer CM. Culture, maternal health care, and women’sstatus: a comparison of Morocco and Tunisia. Studies in FamilyPlanning 1993;24:354–65.