GENDER-RELATED THERAPIST ATTRIBUTIONS IN COUPLES THERAPY: A PRELIMINARY MULTIPLE CASE STUDY...
12
Journal of Marital and Family Therapy 1997, Vol. 23, NO. 3,335-346 GENDER-RELATED THERAPIST ATTRIBUTIONS IN COUPLES THERAPY A PRELIMINARY MULTIPLE CASE STUDY INVESTIGATION Sally D. Stabb Deborah L. Cox Texas Woman’s University Jerry L. Harber Private Practice, Memphis, TN Differential treatment by gender has been an ongoing area of concern and uncer- tainty both in society at large and in clinical research. In this investigation, thera- pist attributions over the course of therapy for three different couples were coded and analyzed to detennine if cause forpositive and negative events was assigned diflerentially to females and males. Additionally, the stability and globality di- mensions of the therapist’s attributions about the couples were examined for ste- reotypical gender-related patterns. Results indicate no gender differences in lo- cus of causal attributions but some gender-relatedpatterns in stability and globality dimensions. Implications for both couples therapy and gender bias in couples research are discussed. The question of therapist gender bias continues to generate controversy, research, and contradictory results. In spite of (or perhaps due to) conflicting findings, most agree that the topic is important and should be further investigated. Writers on women’s psychology consistently note females’ tendency to take the lion’s share of responsibility for emotional well-being in their relationships (Goodrich, 1991). Gilligan (1982) found women to possess a morality of responsibility toward others over self; women were more concerned with obligation and self-sacrifice than equity. Kaplan (1986) suggested that women assume responsibility for situations in which negative feel- ings may be aroused in their partners. In other words, when their partners experience some discomfort or anger, women tend to believe that they caused or should alleviate the aversive stimulus. Bradbury and Fincham (1990) reviewed studies of women’s depression and marital satisfaction, finding that women’s attributions for events in their relationships distinguished Sally D. Stabb, PhD, is an Associate Professor of Counseling Psychology, Department of Psychology and Philosophy, Texas Woman’s University, Denton, TX 76204. Deborah L. Cox, PhD, CCCC Counseling Center, Central Park Campus, 2200 West University Dr., McKinney, Tx 75069. Jerry L. Harber, DMin, 4646PoplarAve.. Suite 425, Memphis,TN 38117. Correspondence should be addressed to the first author at the Department of Psychology and Philosophy, Texas Woman’s University, Denton, TX 76204. Phone: (817) 898-2149 or -2303; Email: F-STABB @venus.twu.edu. July 1997 JOURNAL OF MARITAL AND FAMILY THERAPY 335
-
Upload
memphisseminary -
Category
Documents
-
view
0 -
download
0
Transcript of GENDER-RELATED THERAPIST ATTRIBUTIONS IN COUPLES THERAPY: A PRELIMINARY MULTIPLE CASE STUDY...

Journal of Marital and Family Therapy 1997, Vol. 23, NO. 3,335-346
GENDER-RELATED THERAPIST ATTRIBUTIONS IN COUPLES THERAPY
A PRELIMINARY MULTIPLE CASE STUDY INVESTIGATION
Sally D. Stabb Deborah L. Cox Texas Woman’s University
Jerry L. Harber Private Practice, Memphis, TN
Differential treatment by gender has been an ongoing area of concern and uncer- tainty both in society at large and in clinical research. In this investigation, thera- pist attributions over the course of therapy for three different couples were coded and analyzed to detennine if cause forpositive and negative events was assigned diflerentially to females and males. Additionally, the stability and globality di- mensions of the therapist’s attributions about the couples were examined for ste- reotypical gender-related patterns. Results indicate no gender differences in lo- cus of causal attributions but some gender-relatedpatterns in stability and globality dimensions. Implications for both couples therapy and gender bias in couples research are discussed.
The question of therapist gender bias continues to generate controversy, research, and contradictory results. In spite of (or perhaps due to) conflicting findings, most agree that the topic is important and should be further investigated.
Writers on women’s psychology consistently note females’ tendency to take the lion’s share of responsibility for emotional well-being in their relationships (Goodrich, 1991). Gilligan (1982) found women to possess a morality of responsibility toward others over self; women were more concerned with obligation and self-sacrifice than equity. Kaplan (1986) suggested that women assume responsibility for situations in which negative feel- ings may be aroused in their partners. In other words, when their partners experience some discomfort or anger, women tend to believe that they caused or should alleviate the aversive stimulus. Bradbury and Fincham (1990) reviewed studies of women’s depression and marital satisfaction, finding that women’s attributions for events in their relationships distinguished
Sally D. Stabb, PhD, is an Associate Professor of Counseling Psychology, Department of Psychology and Philosophy, Texas Woman’s University, Denton, TX 76204.
Deborah L. Cox, PhD, CCCC Counseling Center, Central Park Campus, 2200 West University Dr., McKinney, Tx 75069.
Jerry L. Harber, DMin, 4646PoplarAve.. Suite 425, Memphis,TN 38117. Correspondence should be addressed to the first author at the Department of Psychology and Philosophy, Texas Woman’s University, Denton, TX 76204. Phone: (817) 898-2149 or -2303; Email: F-STABB @venus.twu.edu.
July 1997 JOURNAL OF MARITAL AND FAMILY THERAPY 335
between those who were happily married and those who were distressed. The responsibility ethic becomes especially important as it relates to clinical and thera-
peutic issues. Clinicians may inadvertantly convey restrictive notions about women’s roles in relationships in therapeutic settings with women and couples (Hare-Mustin, 1983). In fact, early naturalistic studies revealed therapists’ differential treatment of males and fe- males (Stein, DelGaudio, & Ansley, 1976). Women receive more prescriptions for psycho- tropic medications and are seen for more therapy sessions than are men. Hare-Mustin (1983) suggests that the pathological labels often assigned to women by mental health prac- titioners actually reflect conditions of society in which females experience prolonged pow- erlessness and inequality. Hence, clinicians may perpetuate societal assumptions about women’s responsibility in relationships by continuing to hold traditional causal views of problems in women’s lives.
Additionally, Fitzgerald and Nutt (1986) and the most recent revision of the APA Ethi- cal Principles ofPsychoZogists (1992) strongly emphasize the ethical responsibility of thera- pists for competent, informed, nondiscriminatory, and respectful treatmenthesearctheory along gender lines. How gender bias may be reflected specifically through clinician attri- butions in couples therapy is the focus of this investigation.
The bulk of research to date on therapist gender bias has been conducted in an indi- vidual therapy setting. Although results do not always confirm gender bias, a substantial number of studies indicate that stereotyping, diagnostic and treatment biases, sexism, and sexual abuse of women in therapy are prevalent issues (see Nutt, 1992, and Nelson, 1993, for reviews). Feminist critique of family therapy includes concerns regarding the struc- turalhierarchical placement of males in dominant roles in the family, mother-blaming, as- sumptions about sharing power and responsibility embedded in the systemic concepts of circularity and complementarity, and assumptions about therapist neutrality (Nutt, 1992). Recently, family therapy has also received scrutiny for its biased treament of men, for ex- ample, by reinforcing the socialized limitations of male roles (Brooks, 1991; Deinhart & Avis, 1994).
Within the individual and family literature, the importance of exploring gender bias in marital therapy per se has certainly been mentioned (e.g., Weiner & Boss, 1985), but very little empirical research on gender bias in marital therapy seems to exist. In one such study, no evidence of gender bias was found, although, therapist gender (rather than client gender) was linked to differential clinical judgments of couples (Zygmond & Denton, 1988). How- ever, in their excellent review of gender-linked factors in communication that might affect marital therapy, O’Donohue and Crouch (1996) found no studies of therapists’ communica- tion behaviors. They note, “Another important question concerns the extent to which thera- pists are aware of their own gender-related communication expectations and patterns and the effects that these may have on clients” (O’Donohue &Crouch, 1996, p. 98). Nonclinical dyads and couples in counseling have been studied, but it is striking that therapist behavior remains largely unexamined.
There has been some research on therapist attributions as an indicator of gender bias in individual therapy. Deaux’s seminal work contributes a solid overview of the issues and research (1976). She points out that sex can be viewed as an object, subject, or task charac- teristic. Most relevant to the current discussion is sex as an object characteristic; that is, when observers (therapists) “have expectancies for the behavior of an individual male or female which derive from the stereotyped assumptions made of men and women as groups . . . and the resultant attributions differ to the extent that the stereotyped expectancies differ”
336 JOURNAL OF MARITAL AND FAMILY THERAPY July 1997
(Deaux, 1976, p. 336). In a later review Lopez (1989) notes that therapists have been shown to make differential gender attributions in a number of areas, including (a) ascription of more internality to women’s presenting problems and more situational triggers for men’s presenting problems, (b) problem formulation of hypothetical clients, (c) diagnosis and treatment recommendations, and (d) degree of seventy of problem. Lopez concludes that “clinicians’ causal ascriptions may be important in understanding patient variable biases in clinical judgment” (1989, p. 195). Fisher (1989), while finding no difference between male and female therapists’ causal explanations of male and female patients’ presenting prob- lems at intake, did find differences after five to six sessions in cross-sex pairings. Male therapists perceived female clients to be more responsible for difficulties in the therapeutic relationship, and the causes ascribed to them were seen as longer lasting and unlikely to change. This study was also noteworthy in its use of attributional coding from verbatim transcripts of individual therapy.
There have also been numerous studies of the attributions that couples themselves make in marital therapy (e.g., Bradbury & Fincham, 1990). Except for those which have devel- oped coding systems which allow for the identification and later analysis of attributions from transcripts of actual therapy sessions (Bradbury & Fincham, 1988; Stratton et al., 1986), these studies are less relevant to the current investigation. An expansion of such coding systems was used in the present study and will be discussed in the Methods section.
A number of methodological and conceptual problems also plague the research in thls area (Barak & Fisher, 1989; Lopez, 1989). These problems include conceptualizatiorddefinition, operationalizing concepts, unrepresentative samples, inappropriate measures, overuse of ana- logue studies, and covert political, social, or value agendas that lead to selective review and interpretation of data. In a related critique, systemic marital and family researchers note that although systemic conceptualizations of marital relationships and marital therapy are wide- spread, systemic assessment instruments or research designs are noticeably lacking (Jacobson, 1991; Liddle, 1991; Moon, Dillon, & Sprenkle, 1990). Concurrently, growing openness to the use of qualitative methods in psychological research reflects recognition of their appropriate- ness for many types of research questions (Hoshmand, 1989; Jacob, 1987; Lincoln & Guba, 1985; Patton, 1990; Polkinghorne, 1991; Sprenkle, 1994).
Most importantly, we could find no studies that specifically analyzed therapist attribu- tions in couples counseling. With this fact and the previously discussed gender bias issues in mind, as well as recent calls for less analogue research (Barak & Fisher, 1989) and more qualitative/process work (Hoshmand, 1989; Jacobson, 1991; Moon et al., 1990; Polkinghorne, 1991; Sprenkle, 1994), this investigation set out to make a preliminary inquiry into thera- pist causal attributions for positive and negative events in the course of three actual cases of couples therapy. A mixed qualitative/quantitative methodology was chosen for a number of reasons. First, case studies allow for an in-depth examination of process. Second, qualita- tive methods are recommended in the early stages of research, when one is investigating an area previously unexamined (Patton, 1990; Polkinghorne, 199 1). Third, content analysis via coding systems is a well-established qualitative methodology (Hoshmand, 1989; Jacob, 1987; Miles & Huberman, 1994). Coding in marital and family process research has re- cently gained substantial support and a sophisticated conceptual base (Alexander, Newell, Robbins, & Turner, 1995). Such coding systems also lend themselves to some degree of quantification for more traditional analysis. The combination of qualitative and quantita- tive methods--called triangulation-often enhances the overall quality of inquiry. In this case, the combined methodology involves qualitative data (verbatim transcripts of natu-
July 1997 JOURNAL OF MARITAL AND FAMILY THERAPY 337
rally occwing events-couples therapy) and both qualitative data analysis (content coding) and quantitative data analysis (statistical analysis of frequencies). Patton (1990) notes that although it is possible to move from qualitative data to quantitative analysis, the reverse process is rarely achievable.
In this investigation it was hypothesized that if the therapist were gender fair, there should not be a significant discrepancy between the causality assigned to the husband or the wife for either positive or negative events in the relationship. Alternately, the therapist might make predominantly systemic or relationship attributions for both positive and nega- tive events, thereby placing causality neither internally to either partner nor externally, but rather in their interaction as a dyad. In addition, evidence for stereotypical attributions toward men and women were examined in regard to the dimensions of stability and globality for negative and positive events. Often, attributions for negative events are seen as more stable and internal for women than for men; attributions for positive events are seen as less stable and less internal for women than for men (Deaux, 1976; Lopez, 1989). If such pat- terns were consistently displayed by a therapist in giving explanations or interpretations to a couple, that therapist might be considered to be showing gender bias.
METHOD
Participants The therapist in this study was a 50-year-old, married, white male. He is a marriage
and family therapist, a member of the American Association for Marriage and Family Thera- pists with 20 years experience and an eclectic orientation (cognitive-behavioral and human- istic). Although only one therapist was involved in the investigation, it should be noted that he closely fits the demographic profile of the typical marriage and family therapist recently found in a national, random sample of AAMFT members (Stabb, Mecca, & Myers, 1995). The thee therapy couples involved were all white, middle-class persons with an age range of 3 0 4 1 years. They had been married from 3 to15 years and attended between 6 and 9 sessions of therapy.
Coding System Therapist attributions were determined by using an expansion of the marital attribution
coding system developed by Stratton, Munton, Hanks, Heard, and Davidson (1988). This system was developed to identify and categorize attributions from the context of actual marital therapy transcripts. The modifications to the system involved expansions to include therapist attributions and to elaborate on the attributional dimension of locus of causality to include the couple as a systedunit. These changes allowed coding of statements in which the therapist was giving causal explanations to the couple together or to one or the other spouse about events in their relationship. Thus, attributions that the therapist made could be internal to either partner, external to either partner, or about the couple as a system. These couple attributions were designated relationship attributions in the coding scheme. Attribu- tions were also coded for stability and globality. Positive, negative, and neutral situations were coded as well. The complete coding system is too long and detailed for presentation here; see Table 1 for definitions and typical examples of the categories. Details of the coding system are available from the first author.
Five graduate student coders were trained on random sections of marital transcripts until reliability at acceptable levels (Siege1 & Castellan, 1988) was obtained. Reliability
338 JOURNAL OF MARITAL AND FAMILY THERAPY July 1997
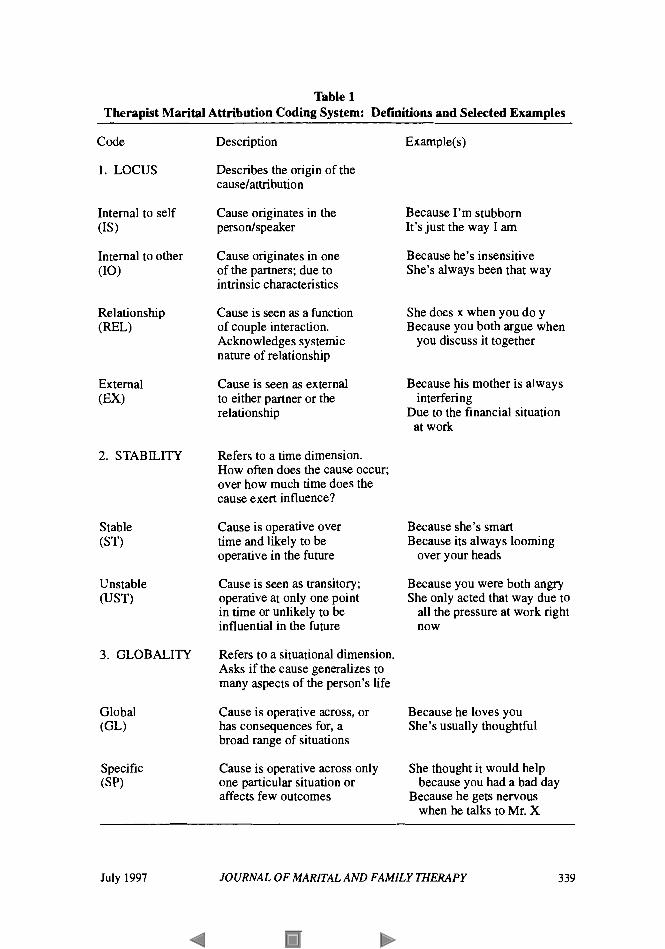
Table 1 Therapist Marital Attribution Coding System: Definitions and Selected Examples
Code
1. LOCUS
Internal to self (1s)
Internal to other (10)
Relationship (WL)
2. STABILITY
3. GLOBALITY
Description
Describes the origin of the causelattribution
Cause originates in the persodspeaker
Cause originates in one of the partners; due to intrinsic characteristics
Cause is seen as a function of couple interaction. Acknowledges systemic nature of relationship
Cause is seen as external to either partner or the relationship
Refers to a time dimension. How often does the cause occur; over how much time does the cause exert influence?
Cause is operative over time and likely to be operative in the future
Cause is seen as transitory; operative at only one point in time or unlikely to be influential in the future
Refers to a situational dimension. Asks if the cause generalizes to many aspects of the person’s life
Cause is operative across, or has consequences for, a broad range of situations
Cause is operative across only one particular situation or affects few outcomes
Example(s)
Because I’m stubborn It’s just the way I am
Because he’s insensitive She’s always been that way
She does x when you do y Because you both argue when
you discuss it together
Because his mother is always
Due to the financial situation interfering
at work
Because she’s smart Because its always looming
over your heads
Because you were both angry She only acted that way due to
all the pressure at work right now
Because he loves you She’s usually thoughtful
She thought it would help because you had a bad day
Because he gets nervous when he talks to Mr. X
July 1997 JOURNAL OF MARITAL AND FAMILY THERAPY 339
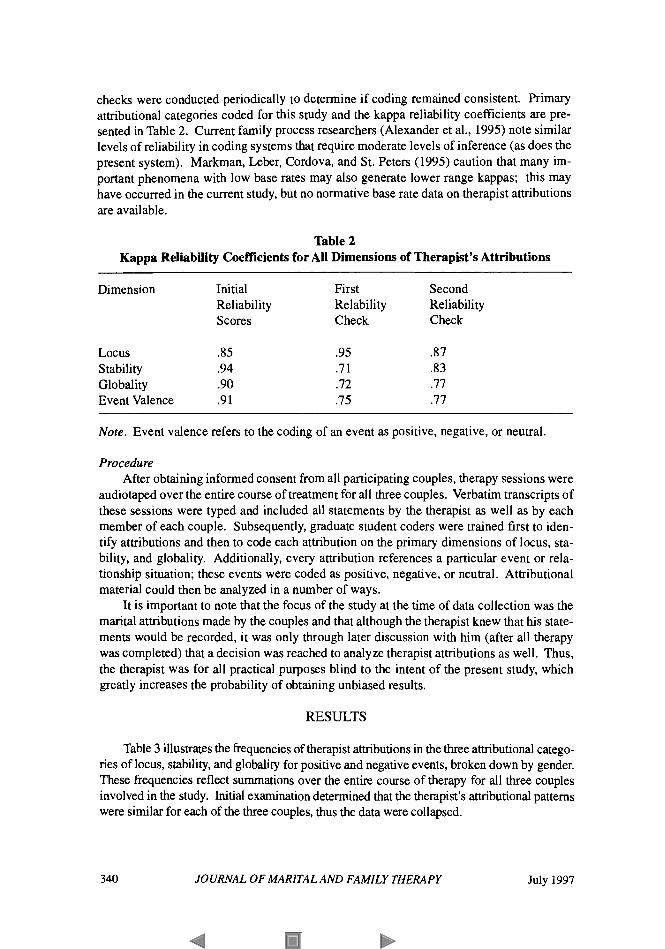
checks were conducted periodically to determine if coding remained consistent. Primary attributional categories coded for this study and the kappa reliability coefficients are pre- sented in Table 2. Current family process researchers (Alexander et al., 1995) note similar levels of reliability in coding systems that require moderate levels of inference (as does the present system). Markman, Leber, Cordova, and St. Peters (1995) caution that many im- portant phenomena with low base rates may also generate lower range kappas; this may have occurred in the current study, but no normative base rate data on therapist attributions are available.
Table 2 Kappa Reliability Coefficients for All Dimensions of Therapist’s Attributions
Dimension Initial First Second Reliability Relability Reliability Scores Check Check
Locus .85 .95 .87 Stability .94 .7 1 .83
Event Valence .91 .75 .77 Globality .90 .72 .77
Note. Event valence refers to the coding of an event as positive, negative, or neutral.
Procedure After obtaining informed consent from all participating couples, therapy sessions were
audiotaped over the entire course of treatment for all three couples. Verbatim transcripts of these sessions were typed and included all statements by the therapist as well as by each member of each couple. Subsequently, graduate student coders were trained first to iden- tify attributions and then to code each attribution on the primary dimensions of locus, sta- bility, and globality. Additionally, every attribution references a particular event or rela- tionship situation; these events were coded as positive, negative, or neutral. Attributional material could then be analyzed in a number of ways.
It is important to note that the focus of the study at the time of data collection was the marital attributions made by the couples and that although the therapist knew that his state- ments would be recorded, it was only through later discussion with him (after all therapy was completed) that a decision was reached to analyze therapist attributions as well. Thus, the therapist was for all practical purposes blind to the intent of the present study, which greatly increases the probability of obtaining unbiased results.
RESULTS
Table 3 illustrates the frequencies of therapist attributions in the three attributional catego- ries of locus, stability, and globality for positive and negative events, broken down by gender. These frequencies reflect summations over the entire course of therapy for all three couples involved in the study. Initial examination determined that the therapist’s attributional patterns were similar for each of the three couples, thus the data were collapsed.
340 JOURNAL OF MARITAL AND FAMILY THERAPY July 1997
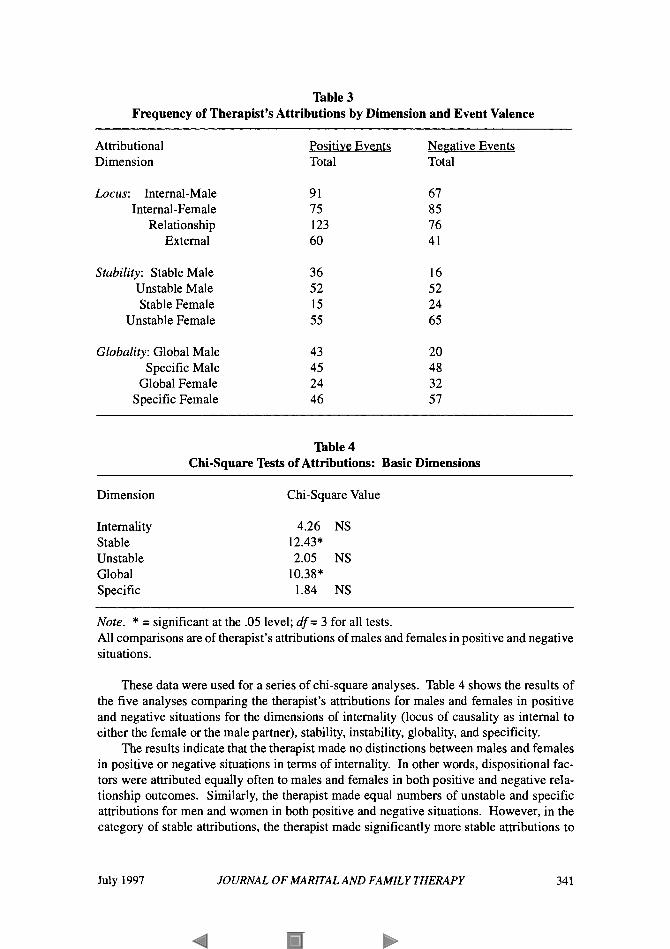
Table 3 Frequency of Therapist’s Attributions by Dimension and Event Valence
Attributional Dimension
Locus: Internal-Male Internal-Female
Relationship External
Stability: Stable Male Unstable Male Stable Female
Unstable Female
Globality: Global Male Specific Male
Global Female Specific Female
Positive Events Total
91 75 123 60
36 52 15 55
43 45 24 46
Negative Events Total
67 85 76 41
16 52 24 65
20 48 32 57
Table 4 Chi-square Tests of Attributions: Basic Dimensions
Dimension
Internality Stable Unstable Global Specific
Chi-square Value
4.26 NS
2.05 NS
1.84 NS
12.43*
10.38*
Note. * = significant at the .05 level; df= 3 for all tests. All comparisons are of therapist’s attributions of males and females in positive and negative situations.
These data were used for a series of chi-square analyses. Table 4 shows the results of the five analyses comparing the therapist’s attributions for males and females in positive and negative situations for the dimensions of internality (locus of causality as internal to either the female or the male partner), stability, instability, globality, and specificity.
The results indicate that the therapist made no distinctions between males and females in positive or negative situations in terms of internality. In other words, dispositional fac- tors were attributed equally often to males and females in both positive and negative rela- tionship outcomes. Similarly, the therapist made equal numbers of unstable and specific attributions for men and women in both positive and negative situations. However, in the category of stable attributions, the therapist made significantly more stable attributions to
July 1997 JOURNAL OF MARITAL AND FAMILY THERAPY 341
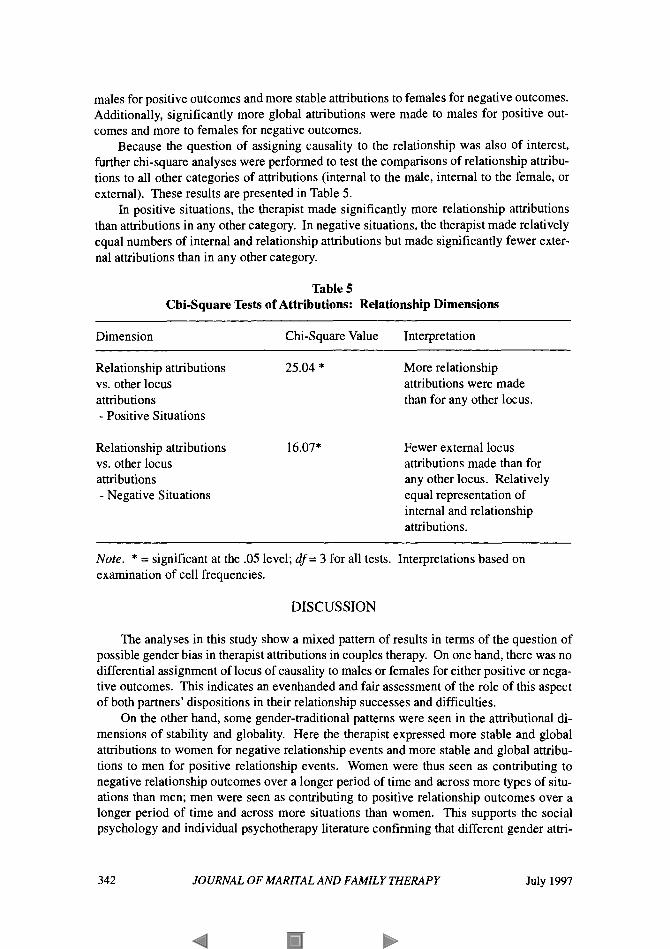
males for positive outcomes and more stable attributions to females for negative outcomes. Additionally, significantly more global attributions were made to males for positive out- comes and more to females for negative outcomes.
Because the question of assigning causality to the relationship was also of interest, further chi-square analyses were performed to test the comparisons of relationship attribu- tions to all other categories of attributions (internal to the male, internal to the female, or external). These results are presented in Table 5.
In positive situations, the therapist made significantly more relationship attributions than attributions in any other category. In negative situations, the therapist made relatively equal numbers of internal and relationship attributions but made significantly fewer exter- nal attributions than in any other category.
Table 5 Chi-square Tests of Attributions: Relationship Dimensions
Dimension Chi-square Value Interpretation ~~~~~~~~
Relationship attributions 25.04 * vs. other locus attributions - Positive Situations
Relationship attributions 16.07* vs. other locus attributions - Negative Situations
More relationship attributions were made than for any other locus.
Fewer external locus attributions made than for any other locus. Relatively equal representation of internal and relationship attributions.
Note. * = significant at the .05 level; df= 3 for all tests. Interpretations based on examination of cell frequencies.
DISCUSSION
The analyses in this study show a mixed pattern of results in terms of the question of possible gender bias in therapist attributions in couples therapy. On one hand, there was no differential assignment of locus of causality to males or females for either positive or nega- tive outcomes. This indicates an evenhanded and fair assessment of the role of this aspect of both partners’ dispositions in their relationship successes and difficulties.
On the other hand, some gender-traditional patterns were seen in the attributional di- mensions of stability and globality. Here the therapist expressed more stable and global attributions to women for negative relationship events and more stable and global attribu- tions to men for positive relationship events. Women were thus seen as contributing to negative relationship outcomes over a longer period of time and across more types of situ- ations than men; men were seen as contributing to positive relationship outcomes over a longer period of time and across more situations than women. This supports the social psychology and individual psychotherapy literature confirming that different gender attri-
342 JOURNAL OF MARITAL AND FAMILY THERAPY July 1997
butions exist and that they may underlie biases in clinical judgments (Deaux, 1976; Lopez, 1989). In particular, the results support similar findings by Fisher (1989), who found that male therapists made more stable attributions for negative events for female clients in indi- vidual therapy.
These findings reflect Hare-Mustin’s (1983) concerns regarding women and traditional psychotherapy. If more stable and global attributions are assigned for negative situations to women than to men in couples therapy, the potential for pathologizing women increases. Additionally, Fitzgerald and Nutt (1 986) encourage practitioners to increase awareness of all forms of oppression and how they interact with sexism. Although therapist attributions for relationship events reflect a more subtle form of sexism, they nonetheless bring poten- tial negative influence into the therapeutic situation. Therapists and counselors bear re- sponsibility for educating themselves on issues pertaining to women and for continually evaluating their own biases and values with regard to sex-role issues as they impact clients.
A completely new aspect of this research is the examination of therapist relationship attributions-assigning cause for good and bad events in the relationship to the couple as a unit. This systemic notion has been incorporated in the study of couples’ own attributions about their relationships (Bradbury & Fincham, 1990), but this is the first investigation of the therapist’s use of these attributions. Areview of Tables 3 and 5 shows that this therapist made significantly more relationship attributions for positive situations than for any other single locus category. This therapist modeled systemic, cooperative strategies and took a supportive and encouraging attitude toward his clients, a “look at the good things you have done together and can do in the future together” approach. Relationship attributions for negative events were not significantly higher than internal attributions for either partner alone but were more prevalent than seeing the cause of negative events as external to either partner or to the relationship. (External attributions were made significantly less often than all others in negative situations.)
This initial analysis of therapist relationship attributions makes a valuable contribution by operationalizing an aspect of systemic thinking in couples research and by addressing the congruence (or lack thereof) of systemic theory, research, and practice (Jacobson, 1991; Liddle, 1991; Moon et al., 1990). Although counting attributions is admittedly a linear process, at the content level, a relationship attribution is clearly a systemic concept. These attributions were frequently made, and the fact that they can be reliably identified is thus potentially useful.
In addition to the research implications discussed above, therapeutic and training ap- plications emerge as well. For example, initial work by Leslie and Clossick (1996) indi- cates that entry-level marriage and family therapists who have had training in gender issues from a feminist perspective show less sexism in clinical interventions than those without such training. Another possibility would be that therapists could monitor their gender- based attributional patterns through a coding system (perhaps a modified version of the one used here). Additionally, using different types of attributions-especially relationship attri- butions-with couples might be consciously incorporated into therapy, as has successfully been done in re-attribution therapy for individuals (Brehm & Smith, 1986). In a related vein, it would be interesting to compare marital therapies which emphasize re-attribution techniques and those which do not, especially in light of recent reviews which challenge the efficacy of more generic cognitive components in marital therapy (Alexander, Holtzworth- Munroe, & Jameson, 1994).
July 1997 JOURNAL OF MARITAL AND FAMILY THERAPY 343

Finally, it is important to keep in mind, as Bar& and Fisher (1989) note, that “gender diferences in psychotherapy may occur but are not by themselves indicative of gender bias” and that a therapist’s “gender-dependent behavior may represent an optimal approach to the client’s individual needs and expectations . . .” (p. 378). In fact, there may be times when one member of a couple may realistically be judged to be more causally central to marital dysfunc- tion. This very important point was not directly assessed in the present investigation. Also, in some forms of systemic couples work, the therapist might strategically destabilize entrenched patterns by consciously pressuring one member of the couple, and such a technique might be reflected in attributional material but not indicate gender bias.
If gender bias were present, it could be manifest in any number of ways that were not studied in the current investigation, such as turn-taking allocations, nonverbal expressions, or paralinguistic communication features. For example, we did examine therapist interrup- tions, which were distributed equally across wives and husbands. However, such raw fre- quency counts may not distinguish differential treatment of women and men; these microprocedures are perhaps better studied in a more in-depth qualitative analysis.
Data on each member of the three couples indicate that both men and women reported either no significant change in marital satisfaction or increased marital satisfaction at the end of therapy and at 18-month follow-up (as assessed by the Dyadic Adjustment Scale; Spanier, 1976). However, it is unknown how these actual outcomes as perceived by the couples were affected (if at all) by the gender-traditional stability and globality attributions of the therapist. Therapeutic change, or lack thereof, could certainly have been due to any number of the myriad factors operative in couples counseling.
It should be reiterated that no questions about gender biadfairness were asked of the couples. It is still possible that a more refined assessment, targeted to gender issues, would have picked up such effects. It would be interesting to know if clients were able to perceive these gender-traditional patterns in their therapist’s responses, and if so, what effect this perception had. The link between therapist attributions and the consequent effects on cli- ents is thus yet to be established. As a number of authorities note (Fisher, 1989; Goodrich, 1991; Kaplan, 1986; Nelson, 1993; Nutt, 1992; O’Donohue & Crouch, 1996), gender-tradi- tional patterns of attribution and communication may be so culturally ingrained in our so- cial interactions that clients and therapists alike might have difficulty identifying or chal- lenging them.
As with all research, this investigation had limitations, particularly the small and there- fore biased samples of both therapist and clients. The differences obtained here might be due to somethmg idiosyncratic about this therapist, about the situations these couples brought to therapy, and so forth. For example, different results, such as those noted by Fisher (1989), might be obtained with a female therapist. However, the study also makes a unique contri- bution by using a mixed qualitativelquantitative case study approach in a real setting to study therapist attributions in marital counseling. This study has generated many questions regarding both clinical application and future research directions. Although the focus here was on gender bias, it is hoped that the methods and ideas presented will be expanded upon by others with a variety of interests.
REFERENCES
Alexander, J. F., Holtzworth-Munroe, A,, & Jameson, P. B. (1994). The process and outcome of marital and family therapy: Research review and evaluation. In A. E. Bergin & S. L. Garfield
344 JOURNAL OF MARITAL AND FAMILY THERAPY July 1997
(Eds.). Handbook of psychotherapy and behavior change (4th ed.) (pp. 595-630). New York: John Wiley.
Alexander, J. F., Newell, R. M., Robbins, M. S., & Turner, C. W. (1995). Observational coding in family therapy process research. Journal of Family Psychology, 9,355-365.
American Psychological Association. (1992). Ethical principles of psychologists and code of con- duct. American Psychologist, 47, 1597-1611.
Barak, A., & Fisher, W. (1989). Counselor and therapist gender bias? More questions than answers. Professional Psychology: Research and Practice, 20,377-383.
Bradbury, T. N., & Fincham, F. D. (1988). Assessing spontaneous attributions in marital interaction: Methodological and conceptual considerations. Journal of Social and Clinical Psychology, 7,
Bradbury, T. N., & Fincham, F. D. (1990). Attributions in marriage: Review and critique. Psycho- logical Bulletin, 107, 3-33.
Brehm, S. S., & Smith, T. W. (1986). Social psychological approaches to psychotherapy and behav- ior change. In S. L. Garfield & A. E. Bergin (Eds.), Handbook ofpsychotherapy and behavior change (pp. 69-115). New York: John Wiley.
Brooks, G. R. (1991). Traditional men in marital and family therapy. In M. Bograd (Ed.), Feminist approaches for men in family therapy (pp. 51-74). New York: Haworth.
Deaux, K. (1976). Sex: Aperspective on the attributional process. In J. H. Harvey, W. J. Ickes, & R. E Kidd (Eds.), New directions in attribution research (Vol. 1, pp. 335-352). Hillsdale, NJ: Erlbaum.
Dienhart, A., & Avis, J. M. (1994). Working with men in family therapy: An exploratory study. Journal of Marital and Family Therapy, 20,397-417.
Fisher, E. H. (1989). Gender bias in therapy? An analysis of patient and therapist causal explana- tions. Psychotherapy, 26,389-401.
Fitzgerald, L. F., & Nutt, R. L. (1986). The Division 17 principles concerning the counseling/psycho- therapy of women: Rationale and implementation. The Counseling Psychologist, 14, 18O-216.
Gilligan, C. (1982). In a diyerent voice. Cambridge, MA: Harvard University Press. Goodrich, T. J. (Ed.). (1991). Women andpower: Perspectives forfamily therapy. New York: W. W.
Hare-Mustin, R. T. (1983). An appraisal of the relationship between women and psychotherapy.
Hoshmand, L. S. T. (1989). Alternate research paradigms: A review and teaching proposal. The
Jacob, E. (1987). Qualitative research traditions: Areview. Review of Educational Research, 57,1-50. Jacobson, N. S. (1991). Toward enhancing the efficacy of marital therapy and marital therapy re-
Kaplan, A. (1986). The “self-in-relation”: Implications for depression in women. Psychotherapy,
Leslie, L. A., & Clossick, M. L. (1996). Sexism in family therapy: Does training in gender make a
Liddle, H. A. (1991). Empirical values and the culture of family therapy. Journal of Marital and
Lincoln, Y. S . , & Guba, E. G. (1985). Naturalistic inquiry. Beverly Hills, CA: Sage. Lopez, S. R. (1989). Patient variable biases in clinical judgment: Conceptual overview and method-
ological considerations. Psychological Bulletin, 106, 184-203. Markman, H. J., Leber, B. D., Cordova, A. D., & St. Peters, M. (1995). Behavioral observation and
family psychology-strange bedfellows or happy marriage?: Comment on Alexander et al. (1995). Journal of Family Psychology, 9,371-379.
Miles, M. B., & Huberman, A. M. (1994). Qualitative data analysis. Thousand Oaks, CA: Sage. Moon, S. M., Dillon, D. R., & Sprenkle, D. H. (1990). Family therapy and qualitative research.
Nelson, M. L. (1993). A current perspective on gender differences: Implications for research in
Nutt, R. L. (1992). Feminist family therapy: A review of the literature. Topics in Family Psychologi-
122-1 30.
Norton.
American Psychologist, 38,593-601.
Counseling Psychologist, 17,3-101.
search. Journal of Family Psychology, 4,373-393.
23,234-242.
difference? Journal of Marital and Family Therapy, 22,253-269.
Family Therapy, 17,327-348.
Journal of Marital and Family Therapy, 16,357-373.
counseling. Journal of Counseling Psychology, 40,200-209.
cal Counseling, 1, 13-23.
July 1997 JOURNAL OF MARITAL AND FAMILY THERAPY 345
O’Donohue, W., & Crouch, J. L. (1996). Marital therapy and gender-linked factors in communica-
Patton, M. Q. (1990). Qualitative evaluation and research methods. Newbury Park, CA: Sage. Polkinghome, D. E. (1991). Two conflicting calls for methodological reform. The Counseling Psy-
chologist, 19, 103-1 14. Siegel, S., & Castellan, N. J. (1988). Nonparametric statistics for the behavioral sciences. New
York: McGraw-Hill. Spanier, G. B. (1976). Measuring dyadic adjustment: New scales for assessing the quality of mar-
riage and similar dyads. Journal of Marriage and the Family, 38,15-28. Sprenkle, D. H. (1994). The role of qualitative research and a few suggestions for aspiring authors
[Editorial]. Journal of Marital and Family Therapy, 20,227-229. Stabb, S. D., Mecca, S. J., & Myers, D. (1995). Marriage and family therapists’responses to conf-
dentiality issues with infidelitous couples. Manuscript submitted for publication. Stein, L. S., Del Gaudio, A. C., & Ansley, M. Y. (1976). A comparison of female and male neurotic
depressives. Journal of Clinical Psychology, 23, 19-21. Stratton, P., Heard, D., Hanks, H. G. I., Munton, A. G., Brewin, C. R., & Davidson, C. (1986).
Coding causal beliefs in natural discourse. British Journal of Social Psychology, 25,299-313. Stratton, P., Munton, A. G., Hanks, H. G. I., Heard, D., & Davidson, C. (1988). Leeds attributional
coding system. Leeds, U K : Leeds Family Therapy and Research Centre, Psychology Depart- ment, Leeds University.
Weiner, J. P., & Boss, P. (1985). Exploring gender bias against women: Ethics for marriage and family therapy. Counseling and Values, 30,9-23.
Zygmond, M. J., & Denton, W. (1988). Gender bias in marital therapy: A multidimensional scaling analysis. The American Journal of Family Therapy, 16,262-272.
tion. Journal of Marital and Family Therapy, 22,87-101.
346 JOURNAL OF MARITAL AND FAMILY THERAPY July 1997