Gender, Individualism-Collectivism orientation, and program orientation influences on nutrition...
91
GENDER, INDIVIDUALISM-COLLECTIVISM ORIENTATION, AND PROGRAM ORIENTATION INFLUENCES ON NUTRITION AMONG HISPANIC PREADOLESCENTS APPROVED BY SUPERVISING COMMITTEE: ________________________________________ Stella Lopez, Ph.D., Chair ________________________________________ Raymond Garza, Ph.D. ________________________________________ Ann Eisenberg, Ph.D. Accepted: _________________________________________ Dean, Graduate School
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Gender, Individualism-Collectivism orientation, and program orientation influences on nutrition...
GENDER, INDIVIDUALISM-COLLECTIVISM ORIENTATION, AND PROGRAM
ORIENTATION INFLUENCES ON NUTRITION AMONG HISPANIC
PREADOLESCENTS
APPROVED BY SUPERVISING COMMITTEE:
________________________________________
Stella Lopez, Ph.D., Chair
________________________________________
Raymond Garza, Ph.D.
________________________________________
Ann Eisenberg, Ph.D.
Accepted: _________________________________________
Dean, Graduate School

DEDICATION
This thesis is dedicated to my friends and family. Thank you so much for your constant support
and inspiration.

GENDER, INDIVIDUALISM-COLLECTIVISM ORIENTATION, AND PROGRAM
ORIENTATION INFLUENCES ON NUTRITION AMONG HISPANIC
PREADOLESCENTS
by
SARA GARCIA, B.A.
THESIS
Presented to the Graduate Faculty of
The University of Texas at San Antonio
in Partial Fulfillment
of the Requirements
for the Degree of
MASTER OF SCIENCE IN PSYCHOLOGY
THE UNIVERSITY OF TEXAS AT SAN ANTONIO
College of Liberal and Fine Arts
Department of Psychology
May 2014

iii
ACKNOWLEDGEMENTS
I would like to thank Dr. Stella Lopez for her guidance and constant encouragement. I
would not be where I am today if it were not for the opportunity and support provided to me by
her. I would also like to thank Dr. Garza for encouraging me to keep pursuing my goals, and
keep looking ahead to what is next. Thank you to Dr. Ann Eisenberg for her tremendous
feedback and support during the writing process. Finally, a special thanks to all the faculty and
staff in the department for always providing help and guidance when I needed it.
May 2014

iv
GENDER, INDIVIDUALISM-COLLECTIVISM ORIENTATION, AND PROGRAM
ORIENTATION INFLUENCES ON NUTRITION AMONG HISPANIC
PREADOLESCENTS
Sara Garcia, M.S. The University of Texas at San Antonio, 2014
Supervising Professor: Stella Lopez, Ph.D.
The present study examined the influence of gender and the individualism-collectivism
characteristic on Hispanic youth’s attitudes and behaviors about nutrition using a collectivist,
individualist, and standard intervention program. The standard, collectivist, and individualist
curricula were implemented in this pretest-posttest design. The Health Perception scale, Eating
and Exercise questionnaire, Health Behavior Questionnaire, and interview responses were used
to assess attitudes and behaviors. Data were collected from 146 Hispanic 6th
graders. The results
indicated that females reported better perceived health and eating habits than males overall.
Females who went through a collectivist intervention reported more control over food choices
and remembered more information about healthy behavior than males and females in the other
intervention conditions. In addition, males who went through the individualist intervention
reported higher associations of health with well-being. These findings suggest that programs that
incorporate the cultural dimension that is compatible with participants’ cultural orientation along
with gender could help improve attitudes and behaviors about nutrition.
v
TABLE OF CONTENTS
Acknowledgements ........................................................................................................................ iii
Abstract .......................................................................................................................................... iv
List of Tables ................................................................................................................................ vi
List of Figures ............................................................................................................................... vii
Chapter One: Introduction ...............................................................................................................1
Chapter Two: Method ....................................................................................................................10
Chapter Three: Results ...................................................................................................................18
Chapter Four: Discussion ...............................................................................................................27
Appendices.....................................................................................................................................36
References ......................................................................................................................................73
Vita

vi
LIST OF TABLES
Table 1 Inter-rater reliability analysis for Interviews .........................................................18
Table 2 Differences in Gender and Gender-IC Orientation ................................................19
Table 3 Descriptive Statistics for Program Orientation ......................................................19

vii
LIST OF FIGURES
Figure 1 Main Effect of Gender for HPS Scale ....................................................................20
Figure 2 Main Effect of Gender for EEQ Scale Scores .......................................................20
Figure 3 Main Effect of Gender for Question One Should not-Type Response ..................21
Figure 4 Main Effect of Gender for Question One Undefined Response ............................21
Figure 5 Main Effect of Gender for Question Four Behavior Change Responses ...............22
Figure 6 Interaction between IC orientation and Gender .....................................................23
Figure 7 Interaction Between Gender and Curricula Condition for Question One. .............26
1
CHAPTER ONE: INTRODUCTION
According to U.S. census data collected in 2010, the Hispanic population in the United
States accounts for more than half of the total population growth and is considered the nation’s
largest ethnic or racial minority (U.S. Census, 2012). This continuing growth among the
Hispanic population is accompanied by substantial health concerns (Boyles, 2011; CDC, 2012;
OMH, 2013). Recent data suggests Hispanic children are especially at risk of health problems
such as obesity and diabetes (CDC, 2012). Researchers have tried to address these health
concerns through programs designed specifically for children to adopt healthy attitudes and
behaviors about nutrition. However, developing these programs has been a challenge. One
important challenge has been to make an intervention program relevant to the Hispanic
population. The variable of culture has been proposed as an important aspect to incorporate into
intervention programs for this particular group. Previous research has found that Hispanic
children born outside of the United States have lower obesity rates compared to U.S.-born
Hispanic children. In fact, young Hispanic women are 40% more likely to be obese than Non-
Hispanic women (Singh & Yu, 2012; Schwartz, Des Rosiers, Huang, Unger, Zamboanga,
Knight, & Szapocznik, 2013; CDC, 2012). These findings suggest that a culturally focused
program on nutrition should be considered.
Culture and Nutrition
Previous research has reported that, regardless of race or ethnicity, only a small fraction
of children consume fruits and vegetables, drink three or more glasses of milk a day, have
breakfast daily, participate in physical activity, and know the foods in the food pyramid guide
(Lorson, Melgar-Quinonez, & Taylor, 2009; Pearson Biddle, & Gorely, 2008; Zapata, Bryant,
McDermott, & Helfelfinger, 2008; Shmeer, 2011; Ogden, Carroll, Kit, & Flegal, 2012).In one

2
study, Piernas and Popkin (2011), measured trends in portion sizes of energy dense foods for
U.S. children and adolescents from 1977-2006. Parents of African-American and Hispanic
children reported serving and consuming larger portions of calorie dense foods than did Non-
Hispanic White children. In addition, U.S.-born Hispanic children are more likely to be obese
than non-U.S.-born Hispanic children (Popkin & Udry, 1998; Gordon-Larson, Harris, Ward, &
Popkin, 2003; Singh, & Yu, 2012). Similarly, U.S.-born Spanish speakers are more likely to
develop higher BMIs than non-U.S.- born English-speakers (Guendelman, Fernandez, Thornton,
& Brinis, 2011).
Other cultural factors, such as the method of cooking preparation, traditional foods,
family support, acculturation, and economic deprivation, have also been examined with regards
to nutrition (Gans, et al., 1999; Taveras, et al., 2007; Schmeer, 2012). Using data from the 2012
National Survey of Children’s Health, researchers found that the association of living in a low
socioeconomic status community and being obese was stronger for Hispanic than non-Hispanic
children. Furthermore, Hispanic children who had less access to preventative health care due to
low socioeconomic status were 22% more likely to be overweight compared to African-
American or White children facing the same conditions (Lutfiyya, Garcia, Dankwa, Young, &
Lipsky, 2008).
Nutrition Programs
The Academy of Nutrition and Dietetics identified pre-adolescence and adolescence as
critical periods for obesity prevention. In order to see long-term changes in nutrition-related
attitudes, the Academy recommended that children should be exposed to nutrition programs
early because younger children are more amenable to changing their behaviors about nutrition
than older children who are becoming young adults. Similarly, the Academy found that school

3
and community environments are important settings to initiate primary interventions for young
adolescents (Hoelscher, Kirk, Ritchie, & Cunningham-Sabo, 2013).
These findings have guided efforts to design and implement programs for nutrition-
related changes (Sing & Yu, 2012; Schmeer, 2012; Lutfiyya, et al., 2008; Black, et al., 2012;
Hanni, Ahn, & Winkleby, 2013). For example, Somerville, Kessler, Wallace, and Burns-
Whitmore (2012) implemented a garden-based nutrition education program to increase the fruit
and vegetable intake of Hispanic youth. The program engaged children in activities, such as
preparing healthy snacks, in order to promote healthy eating among Hispanic children.
Another program utilized Internet-delivered nutrition interventions, developed for the
purpose of weight management and fat reduction. The intervention was catered to students and
was carried out by school teachers. The program consisted of eight modules, in which each
module provided information about healthy lifestyle choices and prompted students to answer
questions about their nutrition-related preferences. Based on student responses, the program
offered tailored feedback for each student on how to change unhealthy behaviors (Ezendam,
Noordegraaf, Kroeze, Brug, & Oenema, 2012).
In addition, there are several school-based intervention programs that promote daily and
healthy breakfast choices (Eilat-Adar, Koren-Morag, Siman-Tov, Livne, & Altmen, 2011),
include mandatory nutrition classes (Prelip, Kinsler, Thai, Erasquin, & Slusser 2012), encourage
dietary and physical activity change (Gortmaker, Lee, Mozaffarian, Sobol, Nelson, Roth, &
Wiecha, 2012), use peer modeling (Nixon, Moore, Douthwaite, Gibson, Vogele, Kreichauf,
Wildgruber, Manios, & Summerbell, 2012), and involve parent-focused programs (Van
Lippevelde et al., 2012; Hendrie et al., 2012; Campbell et al., 2013).These programs, however,
generally focus on the “what” –related (factual) information that children must learn. These

4
knowledge-based programs are informative, but are not designed to inspire long-term changes
that result in consistently healthy eating habits (McBean & Miller, 1999; Rosas et al., 2011;
Thomas, 2006; Zapata et al., 2008). Other programs focus on factors such as refusal skills or
self-efficacy and have been reported to influence children and adolescents in much the same way
as factually based nutrition programs (Nixon et al., 2012; Cerin, et al., 2009; McClain, Chappuis,
Nguyen-Rodriguez, Yaroch, & Spruijt-Metz, 2009; Peters, et al., 2009; Thomas, 2006). In order
to enact long-term behavior changes regarding nutrition, the literature suggests a need for
culturally targeted nutrition intervention programs (Barrera, Castro, Strycker, & Toobert, 2013;
Lindberg, Vega-Lopez, Kauffman, Calderon, & Cervantez, 2012).
Culturally Sensitive Nutrition Programs
Designing and implementing programs about nutrition for Hispanic youth should
incorporate specific cultural aspects that are relevant to the Hispanic population, such as
collectivism, acculturation, and language (Elder, et al., 2009; Oyserman & Lee, 2008; Sussner, et
al., 2008). Culture has the capability of influencing cognitions and self-concept, and programs
aimed at altering behaviors about nutrition should accommodate the participants’ culture in order
to maximize the programs’ effectiveness.
The relevance of cultural factors in behaviors about nutrition was reported in a study by
Liu, Chu, Frongillo, & Probst (2012). In this study, the researchers reported that second- and
third- generation Mexican-American adolescents consumed fewer fruits and vegetables and more
sweetened beverages as well as high fat foods in comparison to first-generation adolescents. The
researchers also found that second- and third- generation children who still spoke Spanish in the
home, but considered themselves acculturated into American culture, had a greater risk of
developing a high BMI, compared to children who did not consider themselves to be as

5
acculturated. These findings suggest that acculturation and language affect children’s behaviors
regarding nutrition and should be considered in efforts to influence Hispanic children’s attitudes
about nutrition.
Individualist-Collectivist Based Interventions
Two cultural variables that are prominent in the cross-cultural literature are individualism
and collectivism (IC; Triandis, 1995), which have been proposed as an important facet of culture.
Individualist cultures tend to value attitudes, beliefs, and behaviors that benefit the self, whereas
collectivist cultures tend to value attitudes, beliefs, and behaviors that reflect and support the
family, community, and the collective unit in general. In the U.S., the Hispanic population tends
to identify as collectivist, as opposed to Anglo-Americans, who tend to identify as individualist.
These basic cultural concepts have promising implications for effective intervention and
prevention programs for Hispanic youth. Programs can be oriented in a collectivist or
individualist way in order to make them more relevant to the target population, and bring about
long term change for the behaviors being targeted (Lopez, Garza, & Gonzalez-Blanks, 2012).
Specifically, a collectivist oriented nutrition program would contain knowledge-based
information and would be designed to inform the students how individual decisions to eat in a
healthy or unhealthy manner affects one’s group and how one’s collective unit (i.e., family and
peers) would affect one’s nutrition-related behaviors. An individualist oriented nutrition
program would contain knowledge-based information and would be designed to inform how
decisions to eat healthy or unhealthy foods fosters or impedes their achievement of their own
goals (Lopez et al., 2012).
A recent study examined the role of program orientation (individualist versus
collectivist), the participants’ IC characteristic, acculturation level, and their influence on

6
Hispanic youth’s attitudes towards smoking (Lopez et al., 2012). The collectivist condition
contained school-based materials but emphasized the interdependence between the individual
and family and peers. The individualist condition on the other hand, emphasized the individual’s
independence. Lopez et al. (2012) reported that Hispanic sixth graders who were exposed to the
collectivist-oriented intervention program about smoking reported more desirable and accurate
perceptions and communication about smoking compared to those in the individualist-focused
program. The findings strongly support the role of specific aspects of culture in effective anti-
smoking programs for Hispanic youth. Recognizing the theoretical and practical importance of
culture’s influence on individual behavior, the present study examined the influence of IC in
enhancing healthy attitudes and behaviors in nutrition among Hispanic youth.
Gender and IC Orientation
When IC orientation is assessed, gender is an important factor to consider. A previous
study of self-construal involving five countries found that women in the United States score
higher for collectivism on average than men did (Kashima, Kim, Gelfand, Yamaguchi, Choi, &
Yuki, 1995). In addition, women are more likely to express a collectivist ideology and resolve
dilemmas using strategies that reflect themes of social responsibility (Lykes, 1985). Similar
results were found in a study assessing competitive and cooperative behaviors among 3-12 year
old children. The results showed that girls favored cooperative rather than competitive
interactions with others, a characteristic that is associated with collectivism. In contrast, boys
favored more competitive interactions (Knight & Chao, 1989). Similarly, in a meta-analysis,
Marcus and Le (2013) found individuals with a collectivist orientation showed higher levels of
cooperation than those with an individualist orientation.
The tendency for women to be more collectivist than men are is especially true within

7
minority groups. In a study of gender differences in measures of cultural orientation as a function
of race/ethnicity, African-American and Hispanic women were found to be more collectivist, on
average, than African-American and Hispanic men (Gaines, Marelich, Bledsoe, Steers, &
Henderson, 1997). This result suggests that culture and gender can influence IC orientation, and
may in part, contribute to the ways men and women respond to collectivist or individualist
oriented interventions in regards to nutrition. Furthermore, women may be more likely to benefit
from a collectivist-oriented intervention, since they view themselves as being interdependent and
emotionally related to others (Green, Deshamps, & Paez, 2005; Kashima et al., 1995).
Surprisingly, few studies have examined the possible association between IC orientation and
gender in regards to nutrition interventions.
The possible association between gender and cultural aspects warrants careful
consideration in the development of programs about nutrition for Hispanic youth. Culturally
targeted and sensitive interventions should incorporate an individual’s collectivist or
individualist tendencies and examine their influence on eating habits.
The Current Study
Lopez, Gonzalez-Blanks, Garza, & Garcia (in review, 2014) examined the role of cultural
dimensions of IC in the development of healthy attitudes and behavior regarding nutrition among
Hispanic youth who varied in acculturation. The aim of the research was to examine how an
intervention program oriented towards a collectivist or an individualist perspective in attitudes
towards nutrition aided in the adoption of healthy attitudes about nutrition. In addition, the study
examined the influence of collectivism and individualism in the adoption of healthy attitudes and
behavior regarding nutrition. Overall, the study examined intervention program orientation
(individualist, collectivist, control or standard), the characteristic of individualism-collectivism,

8
and acculturation level, and their influence on Hispanic youth’s attitudes and behaviors about
nutrition.
The design of the previous study included three interventions. The standard curriculum
was modeled on the school district’s curriculum and contained knowledge-based facts about
nutrition and refusal skills. An individualist condition consisted of information contained in the
school-based materials along with information regarding how students’ decisions to eat in an
unhealthy manner impede one’s achievement of a goal. A collectivist condition also contained
school-based materials but with the addition of informing the students that individual decisions
to be nutritious and healthy affect one’s collective unit (e.g. family and peers), who would then
affect one’s behaviors. Sixth graders’ eating behavior and attitudes about nutrition were assessed
before and after the intervention program. In addition, their degree of individualism and
collectivism was also assessed.
The study found that individuals who were characteristically collectivist in orientation
reported healthier attitudes and behaviors in nutrition than those who were characteristically
individualist. It also found that collectivist individuals benefited more from a collectivist-
oriented intervention program than an individualist or standard-focused intervention program.
The present research aimed to expand on Lopez et al.’s (2013) results by examining the role of
gender and its combined influence with IC orientation on attitudes and behaviors about nutrition
among Hispanic children. In addition, the present study sought to investigate gender differences
that exist as a function of the IC-focused nutrition intervention programs. The present study
examined gender differences using the same dependent variables as Lopez et al. (2014). These
two sets of dependent variables were: (1) scores on health behavior questionnaires assessed at the
post-test phase, and (2) the participant’s responses to interview questions.

9
Hypotheses
The present study was designed to test gender differences in IC orientation and curricula
on program outcome. The following hypotheses were tested:
(1). It was expected that there would be gender differences on the dimension of
individualism-and collectivism. Specifically, girls were predicted to be more collectivist than
boys, but not less individualist than boys are.
(2). It was predicted that there would be a main effect for gender on several outcome
variables. Specifically, girls were expected to score higher on the nutrition behavior
questionnaires and to remember more nutrition information during post-test interviews than boys
would.
(3). It was also expected that there would be a gender by individualism-collectivism
orientation interaction effect such that, girls who identify as collectivist would report more
healthy eating habits and would remember more nutrition information in the post-test interviews
than girls who identify as individualist. However, boys who were collectivist were not expected
to differ significantly from boys who were individualist.
(4). A gender by curricula interaction effect was also predicted. Specifically, girls who
participate in the collectivist program were expected to score higher on the nutrition behavior
questionnaire and remember more nutrition information during post-test interviews than boys in
either condition.
The main effects and interactions of program and individualist-collectivist orientation on
each of the three main dependent variables were not assessed in the proposed research because
these results were already analyzed and reported by Lopez et al. (2014).

10
CHAPTER 2: METHOD
Participants
Participants were 6th
grade students recruited from San Antonio Independent School
District (SAISD) academies, which integrate specialized coursework in different fields. There
were three academies randomly assigned to receive the control (n=48), individualist (n=53), and
collectivist (n=45) curriculum. There were a total of 146 participants. The children were from
predominantly Mexican-American neighborhoods located in San Antonio’s inner city. There
were 88% Hispanic students in the control, 68% in the individualist, and 71% in the collectivist
condition. All participants were between 10 to 13 years of age (M = 11.4 years).
Materials
Child Demographics. Each student completed a demographics questionnaire that
included items about the students’ age, gender, grade level, and race.
Health Perception Scale (HPS). Students completed the 4-item HPS (Garcia-Maas,
1999; Gillis, 1994; Lawton, Moss, Fulcorner, & Cleban, 1982) which assessed the extent to
which an individual perceives him or herself as healthy (e.g., “How would you rate your overall
health at the present time?”). Responses were reported on a 3 or 4-point Likert scale. Higher
scores indicated a healthier self-perception (See Appendix C).
Lafrey health conception scale(LHCS). The 26-item LHCS (Laffrey, 1986) is a self-
report measure assessing individuals’ conception or definition of health. The LHCS consists of
four subscales measuring an individual’s conception of health with respect to clinical health
(e.g., “free of symptoms”), functional health (e.g., “able to do what I have to do”), adaptive
health (e.g., “cope with stressful events”), and eudemonistic health (e.g., “realize full potential”).

11
Total scale and subscales could range from 1(Strongly Disagree) to 6 (Strongly Agree). (See
Appendix F).
Eating and Exercise Questionnaire (EEQ). The 7-item EEQ (Brener, Kann, Kinchen,
Sundberg, & Ross, 2002; Centers for Disease Control and Prevention, 2002; Zullig, Pun, Patton,
& Ubbes, 2006) assessed frequency of eating healthy foods and exercising (e.g., “During the past
7 days, how many times did you eat fruit?”, “In an average week when you are in school, on how
many days do you go to P.E. class?”). Responses were reported on a 7-point Likert scale ranging
from “none” to “4 or more times per day.” Higher scores meant a high frequency of healthy
eating. The 5-item exercise subscale was responded to using an 8-point Likert scale ranging
from “0 days” to “7 days.” Higher scores meant a high frequency of exercise. The TV viewing
subscale is a single item that assessed the number of hours of TV watching on a school day, and
the scores ranged from “0 hours” to “7 hours” (See Appendix D).
Health Behavior Questionnaire (HBQ). The HBQ (Parcel et al., 1995) assessed both
eating and exercise behaviors. It has eight subscales (See Appendix E).
The 13-item dietary intention subscale assessed dietary intention using a dichotomous
response option (e.g., “Which would you put in your hamburger? Ketchup or tomatoes?”). The
students were presented with pairs of food items (one healthy and the other unhealthy) and were
asked which they would choose if they had to pick just one. Higher scores signified healthy
nutritious intent.
The 14-item usual food choice subscale also used a dichotomous response option. The
students were presented with pairs of food items and were asked which they eat most often.
Higher scores reflected high frequency of usual (nutritious) food choice.

12
The 14-item dietary knowledge subscale similarly presented a dichotomous response.
The students were presented with pairs of food items and were asked which was better for one’s
health. Higher scores represented knowledge of nutritious food.
The 9-item home eating behaviors subscale had a dichotomous response option and
assessed whether the students had control over food choices. Higher scores indicated healthy
eating at home.
The 18-item social support for physical activity was measured using a dichotomous
response option. Higher scores pointed to more social support for physical activity.
The 21-item social support for healthy eating also had a dichotomous response option.
The items assessed whether parents, teachers, or friends were supportive of healthy eating.
Higher scores denoted a high social support for healthy eating.
The 15-item self-efficacy for healthy eating measured the certainty students have in
eating some of the foods presented. Respondents could choose “Not Sure,” “A Little Sure,” or
“Very Sure.” Higher scores identified those with high self-efficacy for healthy eating (Parcel, et
al., 1995).
The 5 item self-efficacy for participating in physical activity subscale assessed the
certainty students were about being physically active. Responses were on a 3-point Likert scale
of “Not Sure,” “A Little Sure,” or “Very Sure.” Higher scores showed high exercise self-
efficacy.
Child Individualism-Collectivism Scale (CIC). The 22-item CIC scale (Soh & Leong,
2002) assessed the extent to which an individual was collectivist or individualist (e.g.,
collectivism: “Family members should stick together no matter what”; individualism: “I’d rather
depend on myself than others”) on a 10-point scale ranging from 1 (“Not true at all”) to 10

13
(“Very true”). IC orientation was determined by performing mean splits on IC scale scores (See
Appendix B).
Intervention Program
The curricula were designed to enhance and supplement the current school-based
curricula. LifeSkills (Botvin, 2006) and the Texas Health and Wellness book (Meeks & Heit,
2006) were used to create the three curricula based on the concepts of (1) individualism, (2)
collectivism, and (3) standard information (See Appendix G).
Collectivist Curriculum. In addition to knowledge-based information, the collectivist
curriculum was designed to inform the students how individual decisions to eat in a healthy or
unhealthy manner affects one’s group and how one’s collective unit (i.e., family and peers)
would affect one’s nutrition-related behaviors. It included aspects of health (e.g. “These foods
will also help increase your energy so you are able to participate in activities with friends and
family.”), cosmetic (e.g. “If you have a healthy weight, you will look your best and could gain
more friends”), and athletics (“You also won’t have as much fun playing the sports with your
friends if you eat unhealthy foods.”) that would be affected by nutrition.
Individualist Curriculum. In addition to knowledge-based information, the individualist
curriculum was designed to inform students how decisions to eat healthy or unhealthy foods
foster or impede their achievement of their own goals and how they affect their health (e.g. “By
eating healthy foods, you will have many more options to enjoy activities that are important to
you.”), cosmetic (e.g. “By eating healthily, you will be able to be the person who you want to
be.”), and athletics (e.g. “You would rather want to stand out in an athletic crowd by presenting
yourself as healthy and a person who takes care of their body by eating healthy.”).

14
Control Curriculum. The control curriculum was modeled closely on the curriculum
currently used in the SAISD. It contained knowledge-based facts about nutrition (e.g. “Choosing
to stay away from foods that are high in salt, fat, and increasing the amount of fruits and
vegetables can dramatically increase health status.”). There were no collectivist or individualist
themes in the control curriculum.
Procedure
The UTSA Institutional Review Board, the SAISD superintendent and the parent
committee granted approval for the study.
Participant Recruitment. Consent for participant recruitment was obtained from the
principals, teachers or coaches, and parents. Parental consent forms were distributed. Students
were instructed to return the signed parental consent forms. Students who returned signed parent
consent forms were asked to sign a child assent form as well. Students who did not return a
parent consent form were not included in the study. The intervention programs took place in the
students’ physical education or health classes.
Pretest Administration
The first day of the study consisted of the administration of the pretest to all 9 schools
within the same school-week. The pretest consisted of all the questionnaires described above.
All surveys were completed in English. No one requested a Spanish version of the
questionnaires.
Intervention Phase
A week later, a nutrition curriculum was administered to each academy. Based on
random assignment, three academies received the control curriculum, three academies received

15
the individualist curriculum, and three academies received the collectivist curriculum. The
procedures for each condition are outlined below.
Collectivist Condition. Students in the collectivist condition were instructed to gather
into groups. The groups were decided based upon the students’ peer groups to ensure a
collectivist nature of instruction. The groups varied from 4 students to 6 students, with a total of
13 groups across the 3 academies. After the groups were formed, the students were asked to
collaborate with their own group to formulate reasons regarding the importance of eating
healthy. The students wrote their reasons and then shared their responses with the class.
After the discussion of the students’ reasons to eat healthy foods, an experimenter
presented knowledge-based nutrition information and then discussed collectivist reasons that
revolved around a collectivist theme: how individuals’ decisions to maintain a healthy or
unhealthy nutrition lifestyle affects one’s group and how one’s collective unit would affect one’s
set of behaviors. For example, they discussed how poor nutrition can impact the students’
performance in sports and how peers will be less likely to select a player who is unhealthy. This
action could result in fewer opportunities to be involved with one’s group.
Individualist Condition. Students gathered in a classroom for the curriculum. In
addition to knowledge-based information, the curriculum was individualist in content. For
example, the students discussed how eating nutritious food can impact their own performance in
sports (e.g., “By eating fruits and vegetables, you will enjoy participating in activities that are
important to you.”) and how eating healthy enhances an individual’s ability and desire to become
a great athlete.
16
Control Condition. Students were presented the standard curriculum (e.g., “Eating fruits
and vegetables will give you the necessary nutrients.”). No deviations from this curriculum were
made, and no individualist and collectivist themes were introduced.
The three curricula were each 40 minutes long. A week later, the student assembled
again. A recap of the original content was first presented. Then students engaged in a drawing-
poster activity with regards to their curriculum program.
Posttest Phase
Four months later, posttest questionnaires were administered. The posttest session was
administered to all nine schools during the same school week. The questionnaires included the
HPS, HBQ, and EEQ. Afterwards, each student participated in a short, one-on-one, five-
question interview with the researcher that assessed his or her evaluation of the curriculum. The
questions were as follows: (1) “What did you think the lessons and posters were about?” (2) “Did
you learn anything from the lessons?” (3) “Were the lessons useful for you?” (4) “What did you
like about the lessons?” and (5) “What did you not like about the lessons?” They were then
thanked and allowed to return to their class. In summary, the present research used data from the
health behaviors questionnaire assessed at the post-test phase and participants’ responses to the
interview questions.
Interviews
Interview rater’s recruitment. Experimenters transcribed all the interviews.
Undergraduate and graduate research assistants from the University of Texas at San Antonio
(UTSA) read the transcriptions and identified the most common themes within the responses. A
different set of UTSA undergraduate research assistants served as interview raters. There was a
total of 8 raters. They were given all transcriptions and copies of the rating scale. The

17
following instructions were given in the smoking study. A similar set of instructions were
provided in the nutrition study.
Thank you for agreeing to participate in the rating of 6th
grader interviews. You are asked
to read every interview and rate each of the child’s responses according to the following
notes: Please place a tally mark next to every topic/theme (e.g. HEALTH
FACTS/REFERENCE TO TOPIC/SHOULD, etc) that fits the child’s response to each
question. Please note that child responses may fit more than one theme/topic. For example,
“Smoking makes your lungs black and you shouldn’t do it.” This response contains at least a
HEALTH FACT “makes your lungs black,” and a SHOULD NOT “you shouldn’t do it,”
(*note this example can fit other statements not mentioned depending on your own personal
criteria). Some of the responses may also include multiple references to one statement;
therefore multiple tally marks will be necessary. For example “Smoking makes your teeth
yellow and causes cancer.” This response contains at least two HEALTH FACTS, therefore
two tally marks in the blank for HEALTH FACTS are necessary. (*note this example can fit
other statements not mentioned depending on your own personal criteria). If you have any
questions feel free to contact the experimenters.
Interview rating scale. The scale is made up of the overall questions that were asked of the
students. The most prominent themes were specified for each question. Raters would have to
tally the number of times the students’ responses fit with each theme. Examples of themes that
were identified included health facts, reference to topic (i.e., nutrition and smoking), collectivist
oriented responses, individualist oriented responses, should, should not, behavior change, etc.
Table 1: Inter-rater reliability analysis for Interviews Scale or Subscale Chronbach’s Alpha
Nutrition Interview Rating Scale .896

18
CHAPTER 3: RESULTS
Strategy for Analysis
Questionnaire and interview responses from the study conducted by Lopez et al. (2014)
were analyzed. To test the first hypothesis, gender differences in IC orientation were analyzed
using an independent samples t-test. For the remaining hypotheses, a 2 (gender) X 2 (IC
orientation) X 3 (Intervention Curricula) MANOVA was conducted in order to analyze a
possible gender main effect and interaction effects with IC orientation and curriculum on
questionnaire and interview responses.
The independent variables used in the analysis were child gender (male, female),
participant individualist-collectivist (IC) orientation (individualist and collectivist) and program
orientation condition (individualist, collectivist, control). The data were analyzed using 2 x 2 x 3
fully crossed MANOVA and an independent samples t-test. The dependent measures were
participant responses to the HPS, EEQ, HBQ, and Laffrey HCS scales and subscales. Participant
IC orientation was determined by performing mean splits on IC scale scores which ranged from -
10 to +10. The number of male and female individualists and collectivists can be seen in Table 2.
In addition, the number of males and females in the collectivist, individualist, and control
intervention programs are presented in Table 3.
Surprisingly, the independent samples t-test analysis revealed no significant gender
differences on the dimension of individualism and collectivism. Thus, the first hypothesis which
stated there would be gender differences in IC-orientation was not supported.

19
Table 2: Differences in Gender and Gender-IC Orientation
Student Gender IC characteristic N
Male Individualist 41
Collectivist 34
Female Individualist 27
Collectivist 25
Table 3: Descriptive Statistics for Program Orientation
Program Orientation Student Gender N
Control Male 29
Female 15
Individualist Male 26
Female 20
Collectivist Male 21
Female 17
Total 128
Main effect of Gender
Support for the second hypothesis, which predicted that there would be main effects of
gender on several outcome variables, was found. The child gender (male, female) X program
orientation (collectivist, individualist, and control) MANOVAS on the questionnaire data
revealed significant main effects of gender for the HPS scale (F(1,141)= 4.08, p< .05), and EEQ
scale (F(1,141)= 5.11, p< .03). Females reported better perceived health on the HPS scale than
males did (Mfemales= 2.66, SD= .39; Mmales= 2.52, SD= .42). This main effect can be seen in
Figure 1. As seen in Figure 2, females also reported better eating habits than males did according
to the Eating and Exercising Habits scale (Mfemales= 3.18, SD= .097; Mmales= 2.89, SD=.08).

20
Figure 1: Main Effect of Gender for HPS Scale.
Figure 2: Main Effect of Gender for EEQ Scale Scores.
For the interview responses, a significant main effect of gender was found for question
one “What do you think the lessons were about?” for should-not oriented responses (F(1, 126)=
4.27, p< .05). As seen in figure 3, males reported more should-not type behavior responses (e.g.
“You should not eat un-healthy because it is bad for you”) than females did (Mmales= .09, SD=
.18; Mfemales= .03, SD= .09). In addition, a significant main effect of gender was found for
question one for the “other” undefined oriented responses (F(1, 126)= 5.67, p< .02). Females
responded with more undefined type responses (e.g. “Teaching me about how to grow up
healthy”) than males (Mfemales= .11, SD= .33; Mmales= .01, SD= .08) (See Figure 4).

21
Figure 3: Main Effect of Gender for Question One Should not-Type Response.
Figure 4: Main Effect of Gender for Question One Undefined Response
Additionally, a significant main effect of gender was present for question four “What did
you like about the lessons?” for behavior change-oriented responses (F(1, 125)= 5.95, p< .02).
Females reported liking the behavior changes they saw in themselves (e.g., now I don’t add too
much salt to my food”) after the program more than males did (Mfemales= .03, SD= .01; Mmales=
.000, SD= .007). This main effect can be seen in figure 5. Again, these results support the second
hypothesis.

22
Figure 5: Main Effect of Gender for Question Four Behavior Change Responses.
Gender and IC orientation
Partial support for the third hypothesis, which predicted a gender by IC-orientation
interaction effect on the questionnaire and interview responses, was found. The child gender
(male, female) X IC orientation (collectivist and individualist) MANOVAS for the questionnaire
data revealed a significant interaction of IC and gender on social support for physical activity
(F(1,107) = 5.20, p < .03). As seen in Figure 6, females who were high in collectivism reported
having more social support for physical activity than female individualist and male collectivists
and individualists. Post hoc comparisons using the Tukey HSD test indicated that the mean
scores for female collectivists (Mfemale.collectivism= 1.88, SD= .09) was significantly different than
the scores for female individualists (Mfemale.individualism= 1.75, SD= .19). However male
collectivists Mmale.collectivism= 1.83, SD= .11) did not differ significantly from male individualists
(Mmale.individualism= 1.82, SD= .14) or females of both IC orientations.

23
Figure 6: Interaction between IC orientation and Gender.
For the interview data, in response to question one (“What did you think the lessons were
about”), there was a significant interaction between gender and IC orientation (F(1,109) = 4.91,
p< .03). Not surprisingly, males who identified as being individualist gave more individualist-
oriented responses (“It doesn’t matter what others are doing, don’t eat unhealthy.”) than male
collectivists, female individualists, and female collectivists (Mmale.individualism= .16, SD= .29;
Mmale.collectivism= .03, SD= .10; Mfemale.individualism= .03, SD= .10; Mfemale.collectivism= .07, SD= .18).
However post-hoc comparisons using the Tukey HSD test revealed no significant differences
between groups.
Furthermore, there was a significant interaction between gender and IC orientation in
response to question three (“Were the lessons useful for you?”), for gain response (F(1,105)=
4.14, p< .05) and gain response with a topic reference (F(1,105)= 5.02, p< .03). Female
collectivists reported “yes” to gaining information more than female individualists and males of
both IC orientations on average (Mfemale.collectivism=.46, SD= .66; Mf.individualism=.13, SD= .36;
Mmale.individualism= .36, SD= .64; Mmale.collectivism= .24, SD=.49). In addition, when pressed for more
detail on what they gained, females who identified as collectivists made more topic references on
average (e.g. “information on nutrition”) than female individualists and males of both IC
24
orientations (Mfemale.collectivism= .41, SD= .59; Mfemale.individualism= .10, SD= .30; Mmale.collectivism= .17,
SD= .37; Mmale.individualism= .29, SD= .58). Post-hoc comparisons using the Tukey HSD test found
no significant differences between male and female individualists and collectivists in their
responses to question three. These results partially support the third hypothesis predicting gender
by IC-orientation interaction effects on the questionnaire and interview responses. Female
collectivists were predicted to report healthier attitudes and recall more nutrition information
during interviews than female individualists and males of both IC-orientations. However, post-
hoc tests only showed significant differences between female collectivists and female
individualists on one of the questionnaire subscales, and no significant differences between
males and females of both IC-orientations for interview responses.
Gender and Program Orientation
Partial support for the fourth hypothesis predicting a gender by curricula interaction
effect on interview and questionnaire responses was also found. A significant interaction for
program orientation and child gender were evidenced in the HBS control of food subscale
(F(2,119)= 3.84, p< .03). On average, females who went through the collectivist curriculum
reported having more control over food choices at home than males and females in the
individualist, and control curriculum conditions (Mfemale.collectivist= 1.71, SD= .1922; Mmale.collectivist=
1.61, SD= .19; Mfemale.individualist= 1.63, SD= .24; Mmale.individualist= 1.60, SD= .21). However post-
hoc comparisons using the Tukey HSD test found no significant differences between females and
males in any of the curricula conditions.
There was also a significant interaction for child gender and program orientation
condition in the HCS function subscale (F(2, 135)= 4.35, p< .02), and eudaimonistic subscale
(F(2, 135)= 3.80, p< .03). Males in the individualist condition reported higher associations of

25
health with functionality than males and females in the collectivist and individualist conditions
on average (Mmale.individulist= 5.34, SD= .74; Mfemale.individualist= 4.59, SD= 1.12; Mmale.collectivist= 5.08,
SD= .97; Mfemlae.collectivist= 4.83, SD= 1.04). Males in the individualist condition also reported
higher associations of health with well-being than females and males in the individualists and
collectivist conditions on average (Mmale.individualist= 5.11, SD= .79; Mfemale.individualist= 4.34, SD=
1.12; Mmale.collectivist= 5.06, SD= .87; Mfemale.collectivist= 4.61, SD= 1.12). Contrary to expectation,
post-hoc comparisons using the Tukey HSD tests found no significant differences between
groups for both the HCS function and eudaimonistic subscales.
In regards to the interview data, a significant interaction was found between gender and
curricula condition for question one (“What do you think the lessons were about?”)on the topic
reference (F(2, 122)= 3.81, p< .03), collectivist theme(F(2, 122)= 3.09, p< .05), and should-
statement oriented responses (F(2,122)= 4.71, p< .01). However, post-hoc comparisons using the
Tukey HSD test found no significant differences between groups for topic references or
collectivist-oriented responses, but did find significant differences between groups for should-
oriented responses.
For should-oriented responses the Tukey HSD test revealed significant differences
between males in the collectivist curricula condition and males in the control curricula condition.
The mean response of males in the collectivist condition (Mmale.collectivist= .29, SD= .34) was
significantly different than males in the control condition (Mmales.control = .01, SD= .06) such that
males in the collectivist condition provided more should oriented behavior responses (e.g. “You
should do sports instead of eating junk food”) than males in the control condition did. However
the females in the collectivist, individualist, and control conditions did not differ significantly
from each other or from males in each of the curricula conditions (Mfemale.collectivist= .08, SD= .19;
26
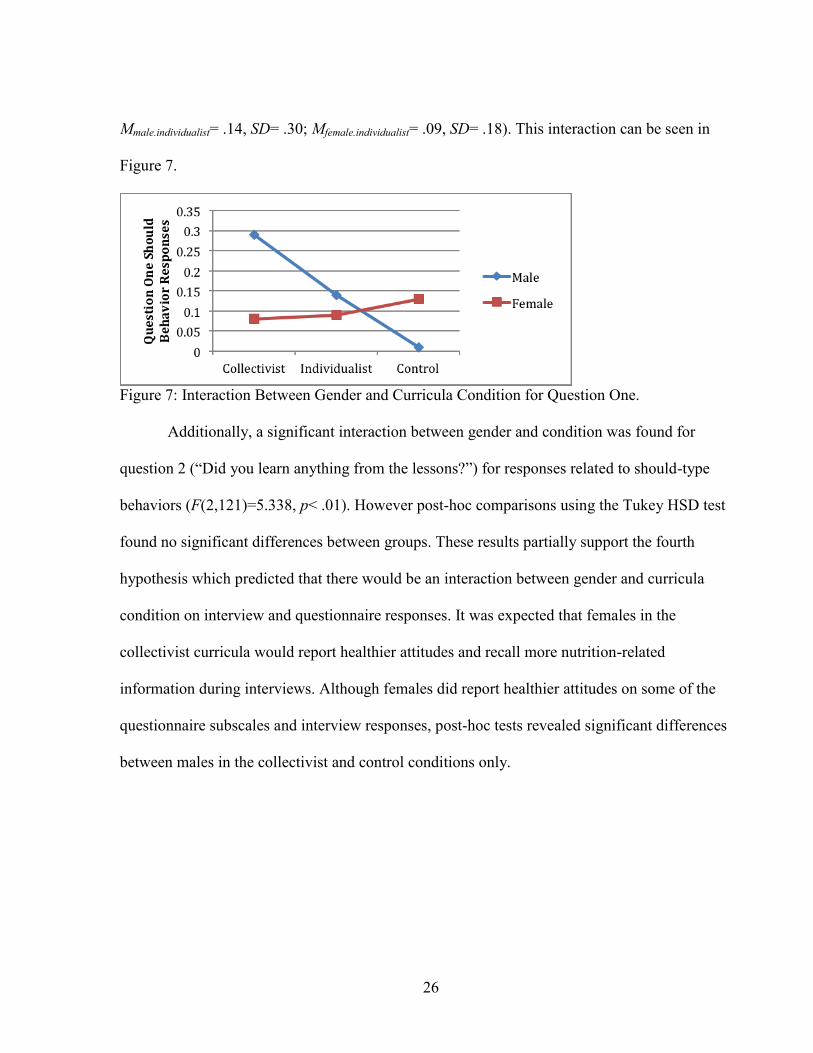
Mmale.individualist= .14, SD= .30; Mfemale.individualist= .09, SD= .18). This interaction can be seen in
Figure 7.
Figure 7: Interaction Between Gender and Curricula Condition for Question One.
Additionally, a significant interaction between gender and condition was found for
question 2 (“Did you learn anything from the lessons?”) for responses related to should-type
behaviors (F(2,121)=5.338, p< .01). However post-hoc comparisons using the Tukey HSD test
found no significant differences between groups. These results partially support the fourth
hypothesis which predicted that there would be an interaction between gender and curricula
condition on interview and questionnaire responses. It was expected that females in the
collectivist curricula would report healthier attitudes and recall more nutrition-related
information during interviews. Although females did report healthier attitudes on some of the
questionnaire subscales and interview responses, post-hoc tests revealed significant differences
between males in the collectivist and control conditions only.

27
CHAPTER FOUR: DISCUSSION
The purpose of the present study was to expand on the results found by Lopez et al. (in
review, 2014) by investigating gender differences that may exist as a function of IC-focused
nutrition intervention programs along with gender differences in IC-orientation. The results in
the present study both support and expand on the findings from Lopez et al. (in review, 2014),
and provide support for the idea that both culture and gender should be taken into consideration
when designing and implementing programs about nutrition for Hispanic youth. Participants’ IC
orientation and gender along with program orientation all have a significant role in the
effectiveness of the nutrition intervention programs. In general, both gender on its own and the
interactions between gender, program orientation, and IC orientation influenced participants’
health perceptions and attitudes.
Surprisingly, the first hypothesis was not supported by the data. There were no gender
differences in IC orientation; in other words, females in this sample of Hispanic middle school
students were not more collectivist than males. The lack of gender differences in IC orientation
could be attributed to various factors. First, sample size could have been an issue. There were
more males in the sample than females, and females of both IC orientations did not exceed 30
participants, which could have made it difficult to detect any true gender differences in IC
orientation. Second, the sample consisted of only Hispanic youth; thus, the participants all shared
a common ethnic background, which could account, in part, for the lack of variability among IC
orientations. Future research should incorporate a larger and more ethnically diverse sample in
order to test for gender differences in IC orientation.
In regards to the second hypothesis, as expected, females reported having better eating
habits and healthier perceptions of themselves overall than males. This finding supports the

28
second hypothesis which predicted that females would report better eating habits and health
behaviors overall. Previous research investigating gender differences in health and diet related
behaviors also found that females place a higher value on nutrition and eating healthy than males
do (Bothmer & Fridlund, 2005; Courtenay, McCreary, & Merighi, 2002; Wardle, Hasse, Steptoe,
Nillapun, Jonwutiwes, & Bellisle, 2004). This is not surprising considering the amount of social
and societal pressures females face to be thin and healthy from a very early age (Stephen &
Perrera, 2014; Mischner, Schie, & Engels, 2013; Dakanalis, Clerici, Caslini, Favagrossa,
Prunas…Zinetti, 2013). Females also begin to care about their appearance and weight at an
earlier age than males do. The sample in this study consisted of sixth graders, and, at this age,
boys may not yet place much emphasis on health or health related behaviors, which could
account, in part, for the gender differences in health perceptions and attitudes (Shriver, Harrist,
Paige, Hubbs-Tait, Moulton, & Topham, 2013).
Males and females also differed in the way they responded to the interview questions. In
response to a question concerning what the students thought the lessons were about, males were
more likely to respond with should-not oriented responses. For example, in response to the
question, males made statements such as “you should not eat unhealthy because it is bad for
you.” In contrast, females were more likely to respond with undefined responses (e.g. “Teaching
me about how to grow up healthy”). These findings suggest that both males and females were
able to recall the central ideas of the curriculum; however, they attuned to the information in
differing ways. Females focused on the global, overarching effects, while males focused on
specific behaviors and their immediate relation to health. In short, both males and females were
able to recall nutrition-related information during the post-test interviews, but did so in differing
ways. The difference in the way they remembered information partially supports the second

29
hypothesis that females would remember more nutrition information during interviews than
males would. Females did remember the global themes more than males did; however, males
were able to remember specific behavior-related information.
In addition, when responding to the question regarding what the students liked about the
lessons, females reported liking behavior changes they saw in themselves after the program more
than males did. This finding is in line with the previous results of Lopez et al.’s (2014) study as
well as with research suggesting that females place a greater emphasis on nutrition and health
related behaviors beginning at an early age (Bothmer & Fridlund, 2005; Courtenay et al. 2002;
Stephen and Perrera, 2014).
Surprisingly, there was only one significant difference present between the female
collectivist and female individualist groups for the questionnaire responses. Although the
MANOVA including gender and IC orientation revealed significant interactions between gender
and IC orientation on one of the HBS subscales and interview responses, post-hoc tests only
revealed significant differences between groups for the support for physical activity sub-scale.
Female collectivists reported higher social support for physical activity than female
individualists. Therefore, the third hypothesis stating that female collectivists would report better
health attitudes and recall more information was only partially supported. This result was
unanticipated and warrants further investigation. Only 25 female collectivists could be included
in the final sample and thus the small sample size could account in part, for the lack of
significant differences between males and females of both IC-orientations on the interview
responses and other questionnaire responses.
The fourth hypothesis was partially supported as well. Specifically, the curriculum that
presented knowledge-based information within a collectivist framework was effective for both

30
females and males in aiding in the retention of the nutrition-related information in comparison to
the individualist and control conditions. Females who went through the collectivist nutrition
intervention program reported better eating habits along with a more positive perception of
themselves as healthy than males and females in any of the other curriculum conditions.
However, even though post-hoc analysis revealed no significant differences between the
curricula groups on the questionnaire data, there are clear differences within the results that
warrant further investigation.
Although post-hoc analysis revealed no significant differences between groups on the
questionnaire data, the post-hoc analysis revealed significant differences between males in the
collectivist and control conditions for “should”-oriented responses to interview question one
“What do you think the lessons were about?” Males who went through the collectivist
curriculum provided more “should” statement responses (e.g. “You should eat healthy because it
is good for you”) than males in the control curriculum. This was not the predicted interaction, but
it provides some evidence for the collectivist curricula doing better at helping the students to
retain information on what they should do to stay healthy than the control curricula. This
difference between males in the collectivist and control curriculum partially supports the fourth
hypothesis in the sense that there were differences between students in the control and
collectivist curriculum. However, the significant difference was between males and not females,
which was not the predicted result. Future research could be done to investigate the gender X
curriculum interaction effects further, along with why students remembered the nutrition
information in a “should-oriented” way.
In addition, females who went through the collectivist curriculum reported having more
control over their food choices at home than males and females in the individualist or control
31
curriculum. Perhaps for females, a collectivist oriented program presents information in a way
that is more salient and relevant to the collective and social nature of their interactions regarding
health and body image.
Although the post-hoc analysis revealed no significant differences, males who went
through the individualist curriculum reported higher associations of health with being able to
fulfill daily responsibilities and maintain good bodily function on average. In addition, males in
the individualist curriculum reported higher associations of health with well-being and happiness
than males and females in each of the other curricula conditions. This finding could be explained
by the idea that males are encouraged to engage in physical activity more than females are and,
thus, associate health more with physical well-being and physical strength (Calasanti, King,
Pietila, & Ojala, 2013). The more one engages in physical activity, the higher his or her body-
esteem may be and the more likely he or she may be to associate nutrition and health with
wellness (Williams & Cash, 2001).
Overall, the results in the present study expand on the results reported by Lopez et al.
(2014). Both gender and culture should be considered key factors when using programs about
nutrition to bring about necessary health-related changes among Hispanic youth. In general, the
results support the idea that Hispanic males and females could benefit more from a collectivist-
oriented nutrition intervention program. However, males seemed to benefit from the
individualist-oriented curricula as well. In the survey and questionnaire responses, males who
went through the individualist curriculum showed a strong tendency to relate nutrition to
physical and emotional well-being. In contrast, in response to the interviews, males who went
through the individualist or collectivist curriculum displayed almost equal retention of the facts
and concepts from the program. Since the sample for this study only included Hispanics, the
32
differences in males’ behavior could be partially attributed to males being more collectivist than
individualist within the sample.
Future Research
This study provides an example of a simple and easy culturally relevant curriculum that
other researchers can expand upon and implement. Future work in this area can examine the
cross-cultural benefits of culturally-oriented intervention programs for other minority and non-
minority groups. In addition, future research can also sample from various levels of SES and
attempt to incorporate culturally relevant messages into other programs aimed at altering
attitudes and behaviors.
More work is needed to examine if Hispanic males could benefit more from an
individualist rather than a collectivist-oriented program. The results presented in this study were
fairly inconclusive in regards to males, so future research should examine the relevance of
gender for culturally oriented curricula for males more critically. Future research could also
investigate why Hispanic males as well as those in a collectivist curriculum remembered “should
not” behaviors better than other information. Future research investigating which aspects of the
curriculum students most attended to could help to inform teachers not only how characteristics
of students can affect the way they view information, but how that information can be presented
to best suit the student’s needs.
The present study examined only sixth graders. Yet previous research has found that pre-
adolescence is a critical period for obesity prevention and that, in order to see long-term changes
in nutrition-related behaviors and attitudes, children should be exposed to nutrition programs
early (Hoelscher et al., 2013). Future research should use a younger sample, perhaps from third

33
or fourth grade, in order to assess more long-term changes in nutrition related attitudes and
behaviors and the impact of the program on participants’ future health related attitudes.
Limitations
Surprisingly, the results from the interview data were fairly inconclusive. Since the
gender of the interviewer was not taken into account when the interviews were conducted, it is
possible that the gender of the interviewer could possibly have impacted the ways in which the
students responded to the questions. The male and female students may have provided different
responses or given different examples of the information they remembered depending on
whether the interviewer was male or female. Thus future studies should consider the gender of
the interviewer and its impact on students’ responses.
Another limitation of the study is that the sample size for the study was small, with a total
of 146 participants, and only 25 female collectivists in the analysis in contrast to the larger group
of 41 male individualists. This lack of equality between groups could have affected the results
and made it difficult to detect significant differences between groups in the post-hoc analysis.
Furthermore, the questionnaire and survey responses assessed in the present study were
administered to the participants in one post-test phase four months after the initial nutrition
curriculum was presented. Including a second post-test phase six to eight months after the initial
curriculum was presented would allow us to more reliably assess changes in behaviors and
attitudes regarding nutrition as a function of the intervention program.
Implications
Despite these limitations, it is clear that for this sample of Hispanic youth, a culturally-
oriented nutrition intervention program worked better than presenting the information in a purely
fact-based way. At the practical level, to be most effective, programs should integrate

34
participant characteristics, such as participant IC and gender. On another practical note, it would
be relatively inexpensive to incorporate this program into existing nutrition programs in schools.
These cultural concepts can be easily integrated into health-related school programs or classes.
Lesson plans can be revised to add the IC perspective as a program orientation. Coaches or
instructors can also be made aware of the relevance of these variables along with how gender and
culture can influence the students’ perceptions of the information.
At the theoretical level, the results presented here encourage and support further
examinations of underlying cultural dimensions as a means of increasing the effectiveness of
intervention programs. The content of culturally relevant programs needs to go beyond a
superficial integration of cultural differences in the promotion of healthy attitudes and behavior.
The research presented here promotes the relevance of collectivism, individualism, and gender in
the development and maintenance of healthy attitudes and behaviors about nutrition. It is
important to teach youth about healthy nutrition and to do so in a way they can easily identify
with. The cultural framework in which this information is communicated is more salient, more
relevant, and more motivational than a standard-focused program. It is clear that in order to
promote healthy attitudes and behaviors among individuals from diverse backgrounds, programs
should present information in a culturally relevant way, while also appealing to participant
characteristics such as gender.
The nutrition intervention program presented in this study can also be used in a global
context to address the growing obesity problem not only in the U.S. but internationally as well.
The Organization for Economic Co-operation and Development recently issued a report stating
that the obesity rates in Mexico are rapidly increasing, especially among children (OECD, 2011).
As a group, Hispanics generally tend to identify as collectivist, so a collectivist-oriented nutrition

35
intervention program could be useful in places such as Mexico in encouraging individuals to
adopt healthier attitudes and behaviors. If the nutrition intervention is provided to students during
early childhood, then they may engage in healthier behaviors as they get older, which could
prevent future health problems.
In conclusion, it is clear that culturally-oriented nutrition intervention programs work
better to bring about healthier attitudes and behaviors among Hispanic preadolescents. More
work is needed to investigate how culturally-oriented nutrition intervention programs could work
cross-culturally and among younger children. The results presented in this study indicate clear
gender differences in nutrition-related attitudes and adds to the existing knowledge that culture is
an important variable to consider when administering information to youth. The limitations of
this study limited the ability to detect clear differences among males and females in both IC-
orientation and curricula effectiveness. However, there was evidence to suggest that there are
interactions between gender and IC-orientation and gender and type of curricula, so future
research is needed to investigate these possible interactions.
Overall, the results from the current study and the results from Lopez et al. (in review,
2014) indicate that programs aimed at altering behaviors and attitudes about nutrition should
present the information in a way that meaningfully relates to factors such as culture and gender.
Furthermore, in order to address the rising issues of obesity on both the local and global level,
the present study represents the need to investigate gender differences regarding nutrition-related
attitudes more critically.

36
APPENDIX A
Interview Rating Scale_Nutrition Interview ID:______________ Interviewer ID: ____________ Rater ID:______________ What did you think the lessons and the posters were about? _______Health Facts (e.g. “It makes your lungs black/fat/makes you look older.”) _______Reference to topic (i.e. smoking, alcohol, nutrition) _______Collectivist Oriented Response (e.g. “About respecting your family and staying healthy.”) _______Individualist Oriented Response (e.g. “It doesn’t matter what others are doing, don’t smoke.”). _______Should (e.g. “You should do sports instead of smoking, drinking, or eat junk food.”) _______Should not (e.g. “You should not smoke or drink or eat unhealthy because its harmful.”) _______Behavior Change (e.g., now I don’t add too much salt to my food”) _______I don't know _______Other (e.g. “Teaching me about how to grow up and stay out of jail.”) Did you learn anything from the lessons? _______Yes _______No _______Health Facts _______Reference to topic (i.e. smoking, alcohol, nutrition) _______Should (e.g. “You should do sports instead of smoking, drinking, or eat junk food.”) _______Should not (e.g. “You should not smoke or drink or eat unhealthy because its harmful.”) _______Collectivist Oriented Response _______Individualist Oriented Response _______Behavior Change _______I don't know _______Other Were the lessons useful for you? _______Yes _______No _______Gained information _______Health Fact _______Reference to topic (i.e. smoking, alcohol, nutrition) _______Should _______Should not _______Behavior Change _______Collectivist Oriented Response _______Individualist Oriented Response _______I don't know _______Other What did you like about the lessons? _______Liked everything _______Liked nothing _______Gained information _______Health Fact _______Reference to topic (i.e. smoking, alcohol, nutrition) _______Should _______Should not _______Materials (e.g. “I liked the glitter and stencils a lot.”) _______Procedures (e.g. “I enjoyed working in a group with my friends.”)
37
_______Should (e.g. “You should do sports instead of smoking, drinking, or eat junk food.”) _______Should not (e.g. “You should not smoke or drink or eat unhealthy because its harmful.”) _______Collectivist Oriented Response _______Individualist Oriented Response _______Behavior Change _______I don't know _______Other What did you not like about the lessons? _______Liked everything _______Liked nothing _______Materials _______Procedures _______Should (e.g. “You should do sports instead of smoking, drinking, or eat junk food.”) _______Should not (e.g. “You should not smoke or drink or eat unhealthy because its harmful.”) _______Collectivist Oriented Response _______Individualist Oriented Response _______Behavior Change _______I don't know _______Other

38
APPENDIX B
Individualism/Collectivism Scale
How true are the following statements of you? Fill in the blank with a number from 0 to 10 to
show whether the statement is true for you, with 0 being “not true” and 10 being “very true” for
you.
0 1 2 3 4 5 6 7 8 9 10
Not true Somewhat true Very
at all true
_____ 1. I’d rather depend on myself than others.
_____ 2. If another student does really well in school, I would feel proud.
_____ 3. Doing badly in school will disappoint my parents very much.
_____ 4. Winning is everything.
_____ 5. Doing poorly in school will hurt my chances for a good job in the future.
_____ 6. I rely on myself most of the time; I rarely rely on others.
_____ 7. My parents expect me to get mostly A’s in school.
_____ 8. It is important that I do better than others.
_____ 9.1 do my homework because it bothers me when I don’t complete it.
_____ 10. The well-being of other students is important to me.
_____ 11. I often do “my own thing.”
_____ 12. If I don’t do well in school I won’t get the job I want in the future.
_____ 13. It’s important to me that I respect decisions made by my group.
_____ 14. My personal identity is very important to me.
_____ 15. To me , fun is spending time with others.
_____ 16. Family members should stick together, no matter what.
_____ 17. I feel good when I work with others.
_____ 18. Competition is the law of nature.
_____ 19. Parents and children must stay together as much as possible.
_____ 20. I don’t think I can get a good job if I do badly in school.
_____ 21. When another person does better than I do, I get tense.
_____ 22. It’s my duty to take care of my family, even if I have to sacrifice what I want.

39
APPENDIX C
Health Perception Scale
Please answer the following questions by placing and “X” next to the answer that you think best
describes your health.
1. How would you rate your overall health at the present time?
_______excellent
_______good
_______fair
_______poor
2. Is your health now better, about the same, or not as good as it was three years ago?
_______better
_______same
_______not as good
3. Do your health problems stand in the way of your doing the things you want to do?
_______not at all
_______a little
_______a great deal
4. Would you say that your health is better, about the same, or not as good as most people
your age?
_______better
_______same
_______not as good

40
APPENDIX D
Eating and Exercise Questionnaire
These questions have been adapted from the YRBS, a national youth behavior survey
administered by the CDC.
Eating
1. During the past 7 days, how many times did you drink 100% fruit juice, such as orange,
apple, or grape juice? (Do not count punch, Kool-Aid, sports drinks, or other fruit-
flavored drinks)
a. none
b. 1-3 times
c. 4-6 times
d. 1 time per day
e. 2 times per day
f. 3 times per day
g. 4 or more times per day
2. During the past 7 days, how many times did you eat fruit? (Do not count fruit juice)
a. none
b. 1-3 times
c. 4-6 times
d. 1 time per day
e. 2 times per day
f. 3 times per day
g. 4 or more times per day
3. During the past 7 days, how many times did you eat green salad?
a. none
b. 1-3 times
c. 4-6 times
d. 1 time per day
e. 2 times per day
f. 3 times per day
g. 4 or more times per day
4. During the past 7 days, how many times did you eat potatoes? (Do not count French fries,
fried potatoes, or potato chips)
a. none
b. 1-3 times
c. 4-6 times
d. 1 time per day
e. 2 times per day
f. 3 times per day

41
g. 4 or more times per day
5. During the past 7 days, how many times did you eat carrots?
a. none
b. 1-3 times
c. 4-6 times
d. 1 time per day
e. 2 times per day
f. 3 times per day
g. 4 or more times per day
6. During the past 7 days, how many times did you eat other vegetables? (Do not count
green salad, potatoes or carrots)
a. none
b. 1-3 times
c. 4-6 times
d. 1 time per day
e. 2 times per day
f. 3 times per day
g. 4 or more times per day
7. During the past 7 days, how many glasses of milk did you drink? (Include the milk you
drank in a glass or a cup or from a carton or with ceral)
a. none
b. 1-3 times
c. 4-6 times
d. 1 time per day
e. 2 times per day
f. 3 times per day
g. 4 or more times per day
Exercise
1. On how many of the past 7 days did you exercise at least 20 minutes that made you sweat
and breathe hard, such as a basketball, soccer, running, swimming laps, fast bicycling,
fast dancing, or similar exercise?
a. 0 days
b. 1 day
c. 2 days
d. 3 days
e. 4 days
f. 5 days
g. 6 days
h. 7 days

42
2. On how many of the past 7 days did you participate in physical activity for at least 30
minutes that did not make you sweat or breathe hard, such as fast walking, slow
bicycling, skating, pushing a lawn mower, or mopping floors?
a. 0 days
b. 1 day
c. 2 days
d. 3 days
e. 4 days
f. 5 days
g. 6 days
h. 7 days
3. On how many of the past 7 days did you exercise to strengthen or tone your muscles,
such as push-ups or sit-ups?
a. 0 days
b. 1 day
c. 2 days
d. 3 days
e. 4 days
f. 5 days
g. 6 days
h. 7 days
4. On the average school day, how many hours do you watch TV?
a. None
b. Less than 1hour per day
c. 1 hour per day
d. 2 hours per day
e. 3 hours per day
f. 4 hours per day
g. 5 or more hours per day
5. In an average week when you are in school, on how many days do you go to P.E. class?
a. 0 days
b. 1 day
c. 2 days
d. 3 days
e. 4 days
f. 5 days
g. 6 days
h. 7 days
6. During the average P.E class, how many minutes do you spend actually exercising or
playing sports?

43
a. I do not take P.E.
b. Less than 10 minutes
c. 10-20 minutes
d. 21-30 minutes
e. 31-40 minutes
f. 41-50 minutes
g. 51-60 minutes
h. more than 60 minutes

44
APPENDIX E
HEALTH BEHAVIOR QUESTIONNAIRE WHAT WOULD YOU DO?
1. If you were at the movies, which one would you pick?
popcorn with salt or butter popcorn without salt and butter
2. Which one would you pick to fix with dinner?
fresh or frozen vegetables canned vegetables
3. If you were going to eat your lunch, which would you do?
eat the food without adding salt shake salt on the food before eating
4. Which would you put on your hamburger?
INSTRUCTIONS: Circle one of the two foods that you would pick if you had to
choose just one.
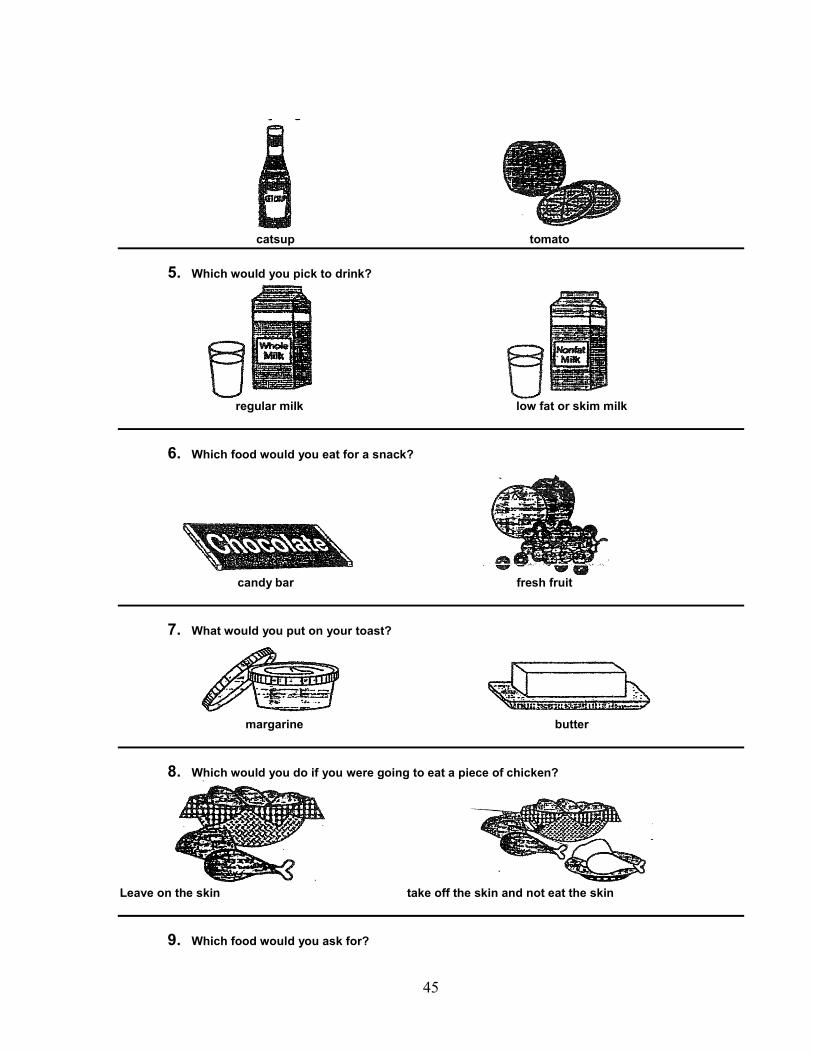
45
catsup tomato
5. Which would you pick to drink?
regular milk low fat or skim milk
6. Which food would you eat for a snack?
candy bar fresh fruit
7. What would you put on your toast?
margarine butter
8. Which would you do if you were going to eat a piece of chicken?
Leave on the skin take off the skin and not eat the skin
9. Which food would you ask for?
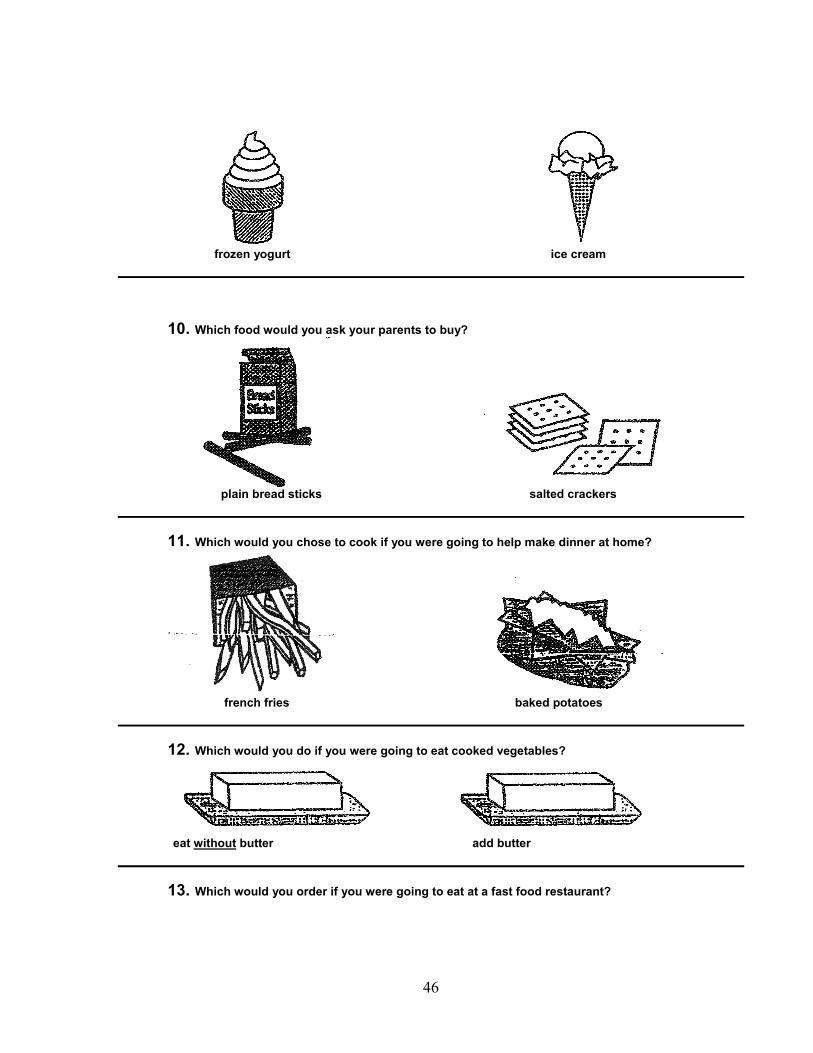
46
frozen yogurt ice cream
10. Which food would you ask your parents to buy?
plain bread sticks salted crackers
11. Which would you chose to cook if you were going to help make dinner at home?
french fries baked potatoes
12. Which would you do if you were going to eat cooked vegetables?
eat without butter add butter
13. Which would you order if you were going to eat at a fast food restaurant?
47
a regular hamburger a salad from the salad bar
WHAT FOODS DO YOU EAT MOST OF THE TIME?
1.
cookies an apple
2.
hot dog chicken
3.
INSTRUCTIONS: Circle one of the two foods that you
eat most often.
48
buttered popcorn unbuttered popcorn
4.
bran muffin with margarine french toast with butter and syrup
5.
chocolate cake an orange
6.
ice cream fresh fruit popsicle
7.
INSTRUCTIONS: Circle one of the two foods that
you eat most often.

49
sweet roll whole wheat roll
8.
turkey bologna
9.
regular milk lowfat or skim milk
10.
no salt salt
11.
frozen yogurt ice cream
12.
INSTRUCTIONS: Circle one of the two foods that
you eat most often.

50
french toast whole wheat toast
13.
margarine butter
14.
regular hamburger lean hamburger
WHICH FOOD IS BETTER FOR YOUR HEALTH?
1.
whole wheat bread white bread
2.
broiled beef broiled fish
INSTRUCTIONS: Circle one of the two foods that you think is
better for your health.

51
3.
cold cereal eggs and bacon
4.
beef beans
5.
chicken regular hamburger
6.
regular milk lowfat or skim milk
7.
INSTRUCTIONS: Circle one of the two foods that you think is
better for your health.

52
peanut butter bologna
8.
frozen yogurt ice cream
9.
green salad french fries
10.
raisins candy bar
11.
butter margarine
12.
INSTRUCTIONS: Circle one of the two foods that you think is
better for your health.

53
frozen corn canned corn
13.
french fries baked potato
14.
regular peanut butter freshly ground peanut butter
THINGS YOU DO MOST OF THE TIME
1. Do you choose or fix your own 1. YES 2. NO breakfast? 2. Do you choose or fix your own 1. YES 2. NO
INSTRUCTIONS: The questions in this section ask about what you do most of the time. Please answer by circling either YES or NO
for each question.

54
lunch on school days? 3. Do you choose foods at the 1. YES 2. NO grocery store? 4. Do you choose what you want to 1. YES 2. NO eat from the dinner table? 5. Do you choose or fix your own snacks? 1. YES 2. NO 6. Do you eat fresh fruit at home? 1. YES 2. NO 7. Do you eat ice cream at home? 1. YES 2. NO 8. Do you eat chips at home? 1. YES 2. NO 9. Do you put salt on your food 1. YES 2. NO at the dinner table?
PHYSICAL ACTIVITY
Note: Being physically active means doing exercises like running, jogging, walking fast, bike riding, swimming, dancing, skating, or any other activity that makes you breathe faster and your heart beat faster. 1. One or both of my parents are 1. YES 2. NO physically active. They do exercises like running, jogging, walking fast, bike riding, swimming, dancing, or skating. 2. One or both of my parents do 1. YES 2. NO exercises with me like running, jogging, walking fast, bike riding, swimming, dancing, or skating. 3. Most of my friends are physically 1. YES 2. NO active. 4. Most of my parents are physically 1. YES 2. NO active.
INSTRUCTIONS: The questions in this section ask about physical activity. Please answer by circling either YES or NO for each
question.

55
5. Most of my friends want me to be 1. YES 2. NO physically active when we play. 6. My friends and I have fun when we’re 1. YES 2. NO physically active playing together. 7. One or both of my parents want me to 1. YES 2. NO stay inside when I want to be physically active outside. 8. One or both of my parents will not let me 1. YES 2. NO do physical activities when I want to. 9. One or both of my parents like to watch 1. YES 2. NO me when I am being physically active. 10. When I am physically active, one or both 1. YES 2. NO of my parents smile and cheer for me. 11. Most of my classroom teachers criticize 1. YES 2. NO people who exercise. 12. When I am physically active at recess, 1. YES 2. NO most of my classroom teachers tell me to stop. 13. When I am physically active in PE 1. YES 2. NO class, my PE teacher tells me I am doing a good job. 14. Most of my friends tease me a lot 1. YES 2. NO when I am physically active. 15. When doing sports, most of my 1. YES 2. NO classmates choose me last for their team. 16. When I am physically active, most of my 1. YES 2. NO friends make fun of me. 17. When doing sports most of my 1. YES 2. NO classmates want me on their team. 18. When I am physically active, most of my 1. YES 2. NO friends tell me I am a good player

56
WHAT DO OTHER PEOPLE WANT YOU TO EAT?
1. Who wants you to eat popcorn without salt and butter on it? a. Your parents 1. YES 2. NO b. Your teachers 1. YES 2. NO c. Your friends 1. YES 2. NO 2. Who wants you to eat lots of fruits and vegetables? a. Your parents 1. YES 2. NO b. Your teachers 1. YES 2. NO c. Your friends 1. YES 2. NO 3. Who wants you to eat food without putting salt on it from the salt shaker? a. Your parents 1. YES 2. NO b. Your teachers 1. YES 2. NO c. Your friends 1. YES 2. NO 4. Who wants you to drink skim or low milk instead of whole milk? a. Your parents 1. YES 2. NO b. Your teachers 1. YES 2. NO c. Your friends 1. YES 2. NO 5. Who wants you to eat margarine instead of butter? a. Your parents 1. YES 2. NO b. Your teachers 1. YES 2. NO c. Your friends 1. YES 2. NO 6. Who wants you to eat the chicken meat without the skin? a. Your parents 1. YES 2. NO b. Your teachers 1. YES 2. NO
INSTRUCTIONS: The questions in this section ask about what other people want you to eat. Please answer by circling either YES or
NO for each question.

57
c. Your friends 1. YES 2. NO 7. Who wants you to eat a salad from the salad bar instead of eating a hamburger? a. Your parents 1. YES 2. NO b. Your teachers 1. YES 2. NO c. Your friends 1. YES 2. NO
HOW SURE ARE YOU?
1. How sure are you that you 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE can eat food without adding salt from a shaker? 2. How sure are you that you 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE can eat fresh or frozen vegetables instead of canned vegetables? 3. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE ask your parents for popcorn without salt and butter? 4. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE ask for lettuce and tomato instead of pickles on your hamburger? 5. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE drink low fat white milk instead of regular white milk? 6. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE eat cereal instead of a doughnut? 7. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE eat fresh fruit instead of a candy bar? 8. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE eat toast with margarine instead of real butter? 9. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE take the skin off of the chicken (and not eat the skin)?
INSTRUCTIONS: The questions in this section ask how sure you are about being able to eat some of the foods below. Please answer by circling either Not Sure,
A Little Sure, or Very Sure for each question.

58
10. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE ask for frozen yogurt instead of ice cream? 11. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE ask your parents to buy bread sticks instead of salted crackers? 12. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE eat a baked potato instead of french fries? 13. How sure are you that you 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE can drink fruit juice instead of a soft drink (soda pop)? 14. How sure are you that you 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE can eat cooked vegetables without adding real butter to them? 15. How sure are you that you 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE can eat a salad from the salad bar at a fast food restaurant instead of ordering a hamburger and fries?
PHYSICAL ACTIVITY
1. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE
choose to jog during recess? 2. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE be physically active 3-5 times a week? 3. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE exercise and keep moving for most of the time in physical education class? 4. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE improve your physical fitness by running or biking 3-5 times a week? 5. How sure are you that you can 1. NOT SURE 2. A LITTLE SURE 3. VERY SURE keep up a steady pace without stopping for 15-20 minutes when you are physically active?
INSTRUCTIONS: The questions in this section ask how sure you are about being physically active. Please answer by circling either Not Sure, A Little Sure, or
Very Sure for each question.

59
APPENDIX F
Laffrey Health Conception Scale
Instructions. Below are 28 statements to describe the meaning that “healthy” or “being healthy”
has for different people. Depending on your personal definition of health, you may agree or
disagree with the statements. Besides each statement is a scale which ranges from strongly
disagree (1) to strongly agree (6). For each item, please circle the number that best represents the
extent to which you agree or disagree with these statements. The more strongly you disagree
with a statement; the lower will be the number you circle. The more strongly you agree with a
statement, then the higher the number you circle. Please make sure your answer every item and
that you circle only one number per item. This is a measure of how you define health. There are
no right or wrong answers.
Health or “being healthy” means:
Strongly
Disagree
Moderately
Disagree
Slightly
Disagree
Slightly
Agree
Moderately
Agree
Strongly
Agree
1. Feeling
great- on top of
the world.
1 2 3 4 5 6
2. Being able
to adjust to
changes in my
surroundings.
1 2 3 4 5 6
3. Fulfilling my
daily
responsibilities.
1 2 3 4 5 6
4. Being able
to do those
things I have to
do.
1 2 3 4 5 6
5. Not
requiring a
doctor’s
services.
1 2 3 4 5 6
6. Creatively
living life to
the fullest.
1 2 3 4 5 6
7. Adjusting to
life’s changes. 1 2 3 4 5 6
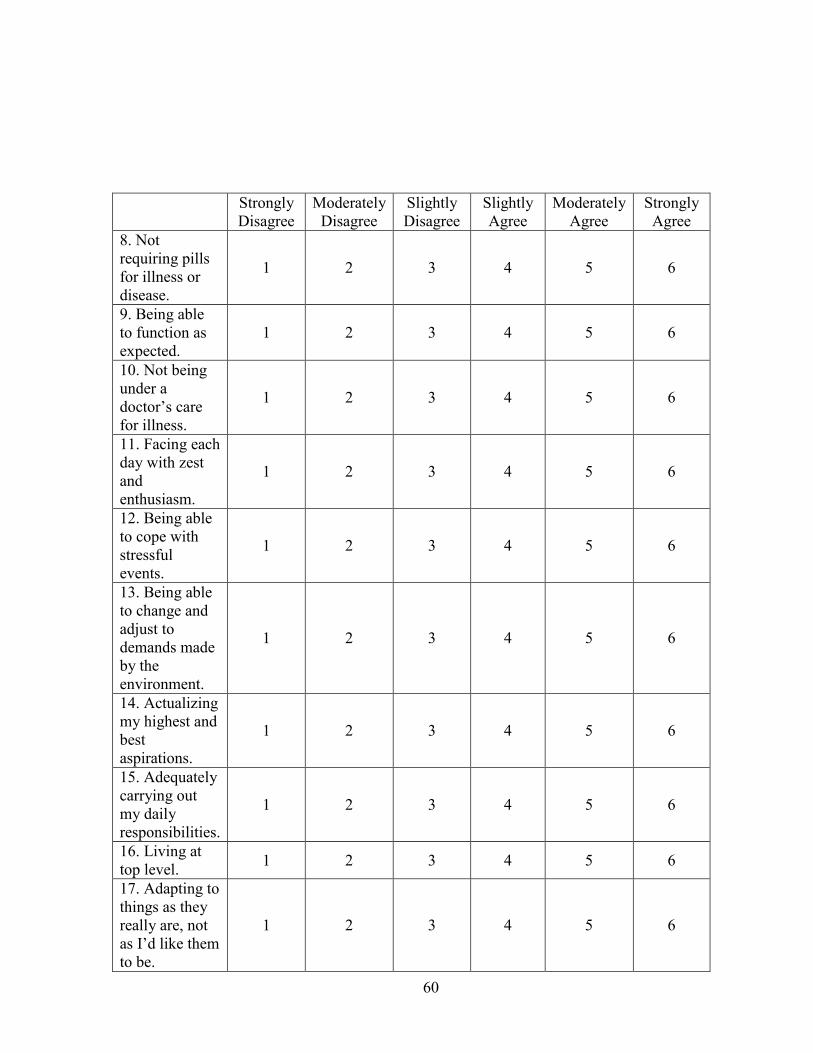
60
Strongly
Disagree
Moderately
Disagree
Slightly
Disagree
Slightly
Agree
Moderately
Agree
Strongly
Agree
8. Not
requiring pills
for illness or
disease.
1 2 3 4 5 6
9. Being able
to function as
expected.
1 2 3 4 5 6
10. Not being
under a
doctor’s care
for illness.
1 2 3 4 5 6
11. Facing each
day with zest
and
enthusiasm.
1 2 3 4 5 6
12. Being able
to cope with
stressful
events.
1 2 3 4 5 6
13. Being able
to change and
adjust to
demands made
by the
environment.
1 2 3 4 5 6
14. Actualizing
my highest and
best
aspirations.
1 2 3 4 5 6
15. Adequately
carrying out
my daily
responsibilities.
1 2 3 4 5 6
16. Living at
top level. 1 2 3 4 5 6
17. Adapting to
things as they
really are, not
as I’d like them
to be.
1 2 3 4 5 6
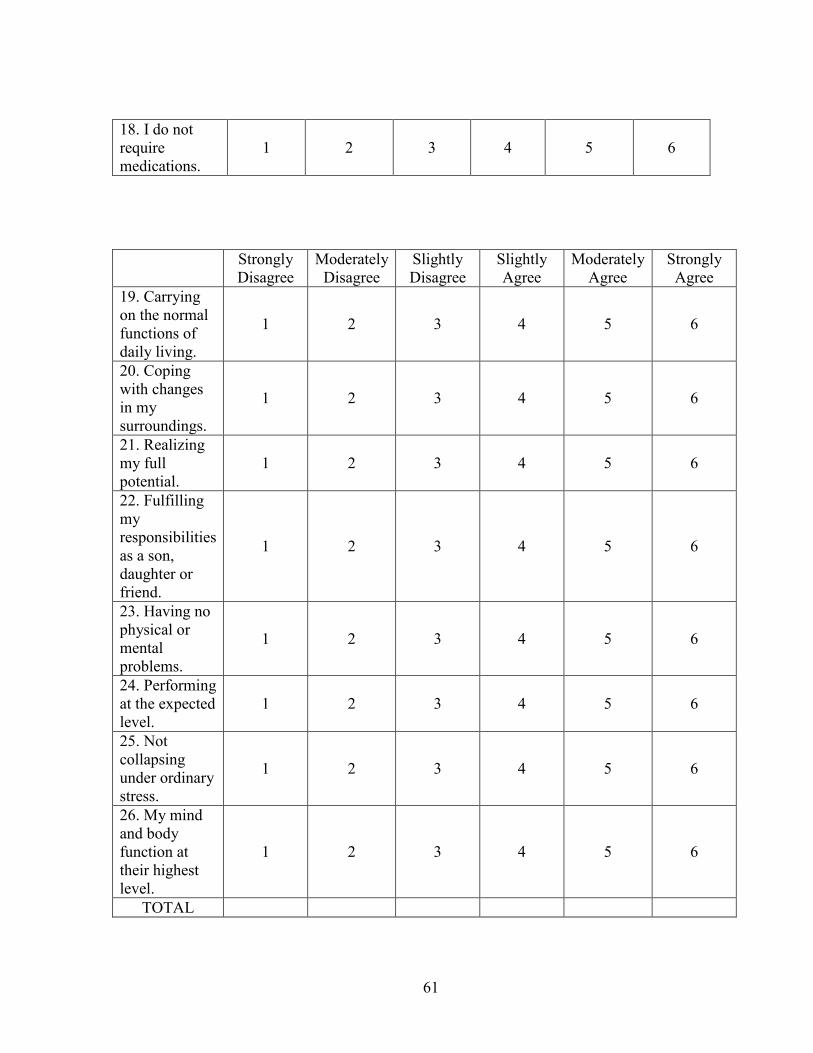
61
18. I do not
require
medications.
1 2 3 4 5 6
Strongly
Disagree
Moderately
Disagree
Slightly
Disagree
Slightly
Agree
Moderately
Agree
Strongly
Agree
19. Carrying
on the normal
functions of
daily living.
1 2 3 4 5 6
20. Coping
with changes
in my
surroundings.
1 2 3 4 5 6
21. Realizing
my full
potential.
1 2 3 4 5 6
22. Fulfilling
my
responsibilities
as a son,
daughter or
friend.
1 2 3 4 5 6
23. Having no
physical or
mental
problems.
1 2 3 4 5 6
24. Performing
at the expected
level.
1 2 3 4 5 6
25. Not
collapsing
under ordinary
stress.
1 2 3 4 5 6
26. My mind
and body
function at
their highest
level.
1 2 3 4 5 6
TOTAL

62
APPENDIX G
Curriculum for Nutrition (Collectivistic Style)
-Health
-Cosmetics
-Athletics
*****Immediately instruct students to form groups with their friends, where each group
contains four to five students. Assign numbers to each group of students and keep a record of
the members in each group.
My name is _______ and this is _________. We are here from the University of Texas at
San Antonio today to talk to you about health-related behaviors and decisions that you will be
making throughout your life. You are making many decisions, and these will stick with you, so
if you make healthy choices you are more than likely to make good decisions throughout your
life. We want you to make the best decisions!
Sometimes we have to make difficult decisions that are not only best for you, but also
best for everyone around us, including your friends and family members. Look at the friends
in your group and think of your family. Your decisions also affect your friends and family. (IF
COACHES HAVE REVIEWED NUTRITION): Your teachers/coaches have already spoken to
you about eating healthy and good nutrition. We are here to add to some of the information they
have already talked about.
*****For the poster themes: Instruct students to talk to each other in their groups and
create reasons why it is important to eat healthy. For each group, record three to four reasons
that they said. This will be used later for the poster activity.
These are all great reasons why you should eat healthy. Now we will go into more detail
about the risks of not eating healthy, including how it affects yourself as well as the people
around you, like your family and friends.
HEALTH
The word “diet” does not necessarily mean a plan for losing weight. It also means
“regular eating” or the food that a person typically takes in each day. The nutrients in food you
eat determine how healthful your diet is, and the healthier a person eats, the better they feel. The
six types of nutrients include proteins, fats, carbohydrates, vitamins, minerals, and water. All of
these nutrients are important for the body to function properly, but many people do not get the
proper nutrients in the meals they eat. This can lead to many health problems.
Point#1:
This is why it is important for you to choose the correct balance of nutrients. It is not
only important for yourself, but also for your friends. If your friends are in good physical
condition from eating healthy, you will be able to spend more time with them, and not have to
worry about them getting sick. If you eat the right nutrients, you also will be healthy and your
friends will want to spend more time with you to do things together.

63
Point#2: Not only do friends and family eat healthy and do things together, friends and family
members are also a good source of support, and you too provide a great deal of support to your
family and friends. If your parents and other family members were unhealthy due to their diet,
they would not be able to help you and provide for you as they do now. When you grow older,
you will also want to contribute to and help out your family, but its hard when you have poor
health because you chose to eat unhealthily. For example, if you are unhealthy, you could not
help around the house because you wouldn’t have energy!
Point#3:
Choosing a healthy diet can provide a positive influence to others around you, like your
family and friends, and you may also notice your friends deciding to eat a healthy diet. So you
and your friends can influence each other in a positive way, and be able to participate in more
activities together. Following the food pyramid is a great way to decide on what foods to eat. Choosing a
variety of grains, especially whole grains, will make sure your body has the essential fiber to
help prevent illnesses.
Point#4:
Fruits and vegetables are also extremely important foods that are rich in vitamins and
help prevent heart disease and some cancers.
Conversation with kids:
What are some of your favorite fruits? Vegetables?
What is your father’s, mother’s, friend’s favorite fruits? Vegetables?
Do you like it too?
[if not] Why don’t you try it if your friend/family member like it?
Point#5:
These foods will also help increase your energy so you are able to participate in
activities with friends and family. You do not want to feel left out of certain activities only
because you are not healthy enough. Eating a healthy diet can help you be more willing to spend
time and have fun with your friends and family.
Conversation with kids:
What are some activities/things you like to do with your friends?
What do they like to do?
You need lots of energy for these activities, which can be obtained from the right food!
You will have many more options to enjoy activities with your friends if you do not have to
worry about your health. All of your friends want you to be able to participate in sports and
activities with them, so it is important for you to be aware of the foods that you are eating.
Choosing a diet that does not contain high amounts of saturated fat, such as meat and dairy
products, will also reduce your risk for heart disease and certain cancers. Meat products like
beef usually contain more saturated fat than other meats such as chicken. Dairy products like
milk, cheese, and yogurt also contain high amounts of saturated fat, if you don’t choose the low

64
fat products. Choosing low fattening foods will also help increase energy levels. Salt is also a
concern because consuming high levels of sodium can increase the risk for high blood pressure,
heart disease, kidney disease, stroke, and diabetes. Choosing to stay away from foods that are
high in salt, fat, and increasing the amount of fruits and vegetables can dramatically increase
your healthy status. You will not have to worry about seeing the doctor every week, or every
month for conditions such as heart disease and diabetes.
SHOW AND EXPLAIN THE FAT MANIPULATIVE.
Point#6:
Some of your family members may be relying on you when you grow older for some
help and support. How are you going to provide them with that help if you yourself have poor
health due to your eating habits? Having diseases especially heart disease, diabetes and cancers
will severely limit your options with friends and family. It is possible that you will not be
physically able to see the people you like or love the most.
Also, treating diseases and cancers is extremely expensive. Even if you were physically able
to spend time with friends and family members, you may not have the extra money to spend on
activities with friends or family due to all the medical expenses.
Point#7:
Remember that you have options when eating. Even when you eat out, you can make
good decisions. Be sure you don’t add the extra fat, sugar, and salt to your portions and ask
family members or friends to not put too much salt on their food, or not to eat too much. If the
portions are too large, ask to share with a friend, or take the leftover portions home for lunch
the next day or for a snack later on. Also remember that fried foods are extremely high in fat,
and broiled foods contain much less fat. Even if fried foods taste great, remember not to eat too
much of it.
Every time you eat, you are getting calories from the food, and is the energy that your
body uses. Since breakfast refuels your body after a night of not eating, it is important to eat
more whole grains, fruits, and vegetables. Protein is also good for breakfast, like peanut butter,
yogurt, and low-fat milk and cheese. Healthy snacking throughout the day can keep you
energized and include foods like fruits and vegetables such as carrot and celery sticks. Grains,
pasta, low-fat crackers, and popcorn without a lot of salt and butter are also great snacks.
Conversations with kids:
What kind of snacks, healthy ones, do/can you and your family eat together?
What are some more healthy snacks you can eat as a family?
Point#8:
You also want your friends to be proud of you and your actions. Eating unhealthy and
gaining an unhealthy amount of weight means that you are not taking care of yourself. Your
friends may eventually choose not to associate with you because of the bad choices that you
make for yourself. It is also great to represent your friends and your family in a positive light,
choosing to eat healthy and take care of your body. You are a reflection of your friends,
family, and culture, and they will be proud of you and your actions if you decide to make the
right decision when it comes to nutrition.

65
Reading food labels is extremely useful in order to decide which foods to eat. The daily
value is the amount of nutrient that a person needs each day. The food label lists the Percent
Daily Value, the percentage of the recommended daily amount of the nutrient that is found in a
serving of the food. Inspect the food carefully so you don’t eat food that looks, feels, or smells
bad.
Point#9:
This will also prevent any foodborne illness from eating contaminated food. Your
friends and family will be impressed with how much you know about choosing the right foods. And your friends and family will be looking to you for guidance on healthy eating!
COSMETIC
Point#10:
Eating healthy foods is important so that you maintain a healthful weight. Healthy
weights vary from individual to individual depending upon body heights and body types. A
person’s weight is one of the first things that people notice, and you don’t want friends and
family or other people to judge you in a bad way if you don’thave a healthy weight. So it’s
important to maintain a healthy weight to have and keep the respect of your friends and family
members. If you have a healthy weight, you will look your best and could gain more friends
from the positive self-esteem that you gain from the healthy weight.
Point#11:
You will also look much more appealing to other people if you remain healthy. In
order to lose unwanted or excess weight, a person must increase the number of calories used by
physical activity, and do not lose the weight quickly. Continue to eat the correct amount of
servings from the Food Guide Pyramid, and choose lower-calorie foods, with small serving sizes.
Being underweight is also not considered healthy. In order for a person to gain necessary
weight, they should follow the Dietary Guidelines and increase the number of serving from the
food groups in the Food Guide Pyramid, as well as eat healthful snacks, but not before meals.
Eating healthy and maintaining a good weight for your particular body type will help you
present yourself to your friends in the best possible way. You will gain more respect from
friends because you will have a higher self-esteem due to your healthy weight, and your
friends and family will be proud of your accomplishments.
Your skin, eyes, and nails will also be much more attractive. Eating healthy means that
you are giving your body good nutrients that it needs, and can helpclear up facial blemishes.
You will look and feel much better, and be able to present yourself to your friends, family and
others in a positive light.
ATHLETIC
Medical doctors or physicians often use body composition, the proportion of fat tissue to
lean tissue in the body, to determine if a person’s weight is healthy. All people have some fat. A
female teen with a healthful body composition may have about 15 percent of body fat, and a
male teen with 10 percent. Obesity is the term for having too much body fat. Other ways of
determining if a person’s weight is unhealthy is by using the Body Mass Index. It measures

66
mass compared to height. Even if you are at a desirable weight, you still need to keep healthful
eating habits.
Having too much body fat from eating unhealthy foods, or by eating too large of portions,
will limit a person’s athletic ability or will hurt hi/her ability to engage in exercise or sports. Do
you ever see overweight athletes? No!
Point#12:
An overweight person will have difficulty in participating in many of the sports and activities as
his or her friends. Overweight people have a hard time keeping up with others that have a
healthful weight. People who do not eat healthy food will be much more tired and sick due to
lack of exercise. You also won’t have as much fun playing the sports as your friends. You’d be
out of breath too soon; you won’t be able to run and will need to catch up with your friends. That
isn’t fun! On the other hand, being healthy and having a healthy weight means you are eating the
right foods. And if you are, then you have the energy to play sports with the team or with your
friends.
Curriculum for Nutrition (Control Style)
-Health
-Cosmetics
-Athletics
*****Students will be instructed to sit at their desks, or on the floor. The students will
not be in any group formation.
My name is _______ and this is _________. We are here from the University of Texas at
San Antonio today to talk to you about behaviors and decisions that you will be making
throughout your life. You are making many decisions, and these will stick with you, so if you
make healthy choices you are more than likely to make good decisions throughout your life. We
want you to make the best decisions!
Your teachers/coaches have already spoken to you about eating healthy and good
nutrition. We are here to add to some of the information they have already talked about.
These are all great reasons why you should eat healthy. Now we will go into more detail
about the risks of not eating healthy, including how it affects yourself as well as the people
around you.
Health
The word “diet” does not necessarily mean a plan for losing weight. It also means the
food that a person typically takes in each day. Nutrients in the food determine how healthful

67
your diet is, and the healthier a person eats, the better they feel. The six types of nutrients
include proteins, fats, carbohydrates, vitamins, minerals, and water. All of these nutrients are
important for the body to function properly, but many people do not get the proper nutrients in
the meals they eat. This can lead to many health problems. This is why it is important to choose
the correct balance of nutrients.
Point#1:
In order to achieve goals in life, whether it be an athlete, doctor, or teacher, it is
extremely important to remember to eat healthy.
Following the food pyramid is a great way to decide on what foods to eat. Choosing a
variety of grains, especially whole grains, will make sure the body has the essential fiber to help
prevent colon cancer. Fruits and vegetables are also extremely important foods that are rich in
vitamins and help prevent heart disease and some cancers.
Point#2:
These foods will also help increase your energy.
Point#3:
Choosing a diet that does not contain high amounts of saturated fat, such as meat and
dairy products, will also reduce the risk for heart disease and certain cancers.
Point#4:
Choosing low fattening foods will also help increase energy levels. Salt is also a concern
because consuming high levels of sodium can increase the risk for high blood pressure, heart
disease, kidney disease, and stroke.
Point#5:
Choosing to stay away from foods that are high in salt, fat, and increasing the amount of
fruits and vegetables can dramatically increase health status. You would rather be doing the
activities that you enjoy rather than worrying about your health. Having diseases and cancers
will be extremely limiting.
Point#6:
Remember that you have options when eating. Even when you eat out, you can make
good decisions. Be sure you don’t add the extra fat, sugar, and salt to your portions, and if the
portions are too large, ask to share with a friend, or take the leftover portions home. Also
remember that fried foods are extremely high in fat, and broiled foods contain much less fat.
Point#7:
Every time you eat, you are getting calories from the food, and is the energy that your
body uses. Since breakfast refuels your body after a night of not eating, it is important to eat
more whole grains, fruits, and vegetables. Protein is also good for breakfast, like peanut butter,
yogurt, and low-fat milk and cheese. Healthy snacking throughout the day can keep you

68
energized and include foods like fruits and vegetables such as carrot and celery sticks. Grains,
pasta, low-fat crackers, and popcorn without a lot of salt and butter are also great snacks.
Eating healthy foods such as these will help your body stay healthy and lean. Being
overweight can increase the risks of heart disease, diabetes, and some cancers. In addition, being
overweight limits your activity with your friends.
Point#8:
Eating unhealthy and gaining an unhealthy amount of weight means that you are not
taking care of yourself. You are not giving yourself many options when you decide to eat
unhealthily.
Reading food labels is extremely useful in order to decide which foods to eat. The daily
value is the amount of nutrient that a person needs each day. The food label lists the Percent
Daily Value, the percentage of the recommended daily amount of the nutrient that is found in a
serving of the food. Inspect the food carefully so you don’t eat food that looks, feels, or smells
bad. This will also prevent any foodborne illness from eating contaminated food.
Cosmetic
Point#9:
Eating healthy foods is important so that you maintain a healthful weight- the weight that
is desirable for a person. Healthy weights vary from individual to individual depending upon
body heights and body types. Eating healthy will promote a higher self-esteem. You will have
more energy, and the body works best when it’s at a desirable weight.
Point#10:
You can also prevent many injuries if you eat healthy and maintain a healthy weight.
You will not have to worry about your balance as much, so the risk of falling is much less.
Serious injuries could be avoided, so you will not have to worry about having a permanent
injury, casts, or braces. In order to lose weight a person must increase the number of calories
used by physical activity, and do not lose the weight quickly. Continue to eat the correct amount
of servings from the Food Guide Pyramid, and choose lower-calorie foods, with small serving
sizes.
Being underweight is also not considered healthy. In order for a person to gain weight,
they should follow the Dietary Guidelines and increase the number of serving from the food
groups in the Food Guide Pyramid, as well as eat healthful snacks, but not before meals.
Point#11:
Your skin, eyes, and nails will also be much more attractive. Eating healthy means that
you are giving your body good nutrients that it needs, and can clear up facial blemishes. You
will look and feel much better.
Athletic
Medical doctors and physicians often use body composition, the proportion of fat tissue
to lean tissue in the body, to determine if a person’s weight is healthy. All people have some fat.
A female teen with a healthful body composition may have about 15 percent of body fat, and a
male teen with 10 percents. Obesity is the term for having too much body fat. Other ways of
69
determining if a person’s weight is unhealthy is by using the Body Mass Index. It measures
mass compared to height. Even if you are at a desirable weight, you still need to keep healthful
eating habits.
Point#12:
Having too much body fat from eating unhealthy foods, or by eating too large of portions,
will limit a person’s athletic ability. Do you ever see overweight athletes? No! People who do
not eat healthy food will be much more tired and sick due to the lack of exercise they typically
get.
Curriculum for Nutrition (Individualistic Style)
-Health
-Cosmetics
-Athletics
*****Students will be instructed to sit at their desks, or on the floor. The students will
not be in any group formation.
My name is_______ and this is ________. We are here from the University of Texas at
San Antonio today to talk to you about health-related behaviors and decisions that you will be
making throughout your life. You are making many decisions, and these will stick with you, so if
you make healthy choices you are more than likely to make good decisions throughout your life.
We want you to make the best decisions!
Sometimes you have to make difficult decisions that are best for you.
*****For the poster themes: Ask the students individually why they think it is important
to eat healthy. Record their responses for later poster themes.
These are great reasons why you should eat healthy. Now we will go into more detail
about the risks of not eating healthy, including how it greatly affects you.
HEALTH
The word “diet” does not necessarily mean a plan for losing weight. It also means the
food that a person typically takes in each day. The nutrients in food you eat determine how
healthful your diet is, and the healthier your are the better you feel.
The six types of nutrients include proteins, fats, carbohydrates, vitamins, minerals, and water. All
of these nutrients are important for the body to function properly, but many people do not get the
proper nutrients in the meals they eat. This can lead to many health problems such as diabetes
and heart disease. This is why it is important for you to choose the correct balance of nutrients
like the ones in fruits and vegetables.
Point #1:
In order to achieve your goals in life, whether you choose to be an athlete, doctor, or
teacher, it is extremely important to remember to eat healthy. You will not be able to achieve
your goals if you are unhealthy and constantly concerned with medical treatment because you
are unhealthy.

70
Following the food pyramid is a great way for you to decide on what foods to eat.
Choosing a variety of grains, especially whore grains, will make sure your body has the essential
fiber to prevent illnesses. Fruits and vegetables are also extremely important foods that are rich
in vitamins and help prevent heart disease and some cancers.
Conversation with kids:
What are some of your favorite fruits and vegetables?
Point #2:
These foods will also help increase your energy so you are able to participate in several
activities.
Conversation with kids:
What are some activities/things you like to do?
Point#3: Whatever the activity, you’ll need energy! Energy comes from good and
healthy food!
Choosing a diet that does not contain high amounts of saturated fat, such as meat and
dairy products, will also reduce your risk for heart disease, diabetes, and certain cancers.
Point #4:
Choosing low fattening foods will help increase your energy levels. Salt is also a
concern because consuming high levels of sodium can increase the risk for high blood
pressure, heart disease, kidney disease, stroke, and diabetes. You want to be the best possible
healthy person you can be.
Point #5:
Choosing to stay away from foods that are high in salt, fat, and increase the amount of
fruits and vegetables can dramatically increase your healthy status. You will not have to worry
about seeing the doctor every week, or every month. You will have many more options to enjoy
activities that are important to you, and those things that you like to do.
SHOW AND EXPLAIN THE FAT MANIPULATIVE.
Point#6:
You will also feel great about yourself. You don’t want to be spending your time going
to the doctor because of your weigh, or due to unhealthy eating habits. You would rather be
doing the activities that you enjoy rather than worrying about your health. Having heart
disease, diabetes, and cancers will be extremely limiting, and you won’t be able to become the
person that you want to be in life.
Point#7:

71
Remember that you have options when eating. Even when you eat out, you can make
good decisions. Be sure you don’t add the extra fat, sugar, and salt to you portions, and if the
portions are too large, as to share with a friend, or take the leftover portions home. Also
remember that fried foods are extremely high in fat, and broiled foods contain much less fat.
Even if fried foods taste great, remember not to eat too much of them.
Point#8:
Every time you eat, you are getting calories from the food, and is the energy that your
body uses. Since breakfast refuels your body after a night of not eating, it is important to eat
more whole grains, fruits, and vegetables. Protein is also good for breakfast, like peanut butter,
yogurt, and low-fat milk and cheese. Healthy snaking throughout the day can keep you
energized and include foods like fruits and vegetables such as carrot and celery sticks. Grains,
pasta, low-fat crackers, and popcorn without a lot of salt and butter are also great snacks.
Conversations with kids:
What kind of healthy snacks do you eat?
What are other snacks you can try?
What kinds of snacks do you think are healthy?
Would you enjoy eating these snacks?
Eating healthy foods such as these will help your body stay healthy and lean.
Point#9:
Eating unhealthy and gaining an unhealthy amount of weight means that you are not
taking care of yourself. You are not giving yourself many options when you decide to eat
unhealthily. It is important to give people a good impression of yourself. You will be the person
that comes to their mind first if you leave a positive impression. Remember that you are a
reflection of all the positive things that you are doing for your body.
Reading food labels is extremely useful in order to decide which foods to eat. The daily
value is the amount of nutrient that a person needs each day. The food label lists the Percent
Daily Value, the percentage of the recommended daily amount of the nutrient that is found in a
serving of the food. Inspect the food carefully so you don’t eat food that looks, feels, or smells
bad. This will also prevent any foodborne illness from eating contaminated food.
COSMETIC
Point#9:
Eating healthy foods is important so that you maintain a healthful weight. Healthy
weights vary from individual to individual depending upon body heights and body types. Eating
healthy will promote a higher self-esteem.
CRITICAL POINT:
You will respect yourself much more and also gain respect from other people. You will
be able to be the person who you want to be. You will have more energy, and your body works
best when you are at a desirable weight.
Point#10:

72
You can also prevent many injuries if you eat healthy and maintain a healthy weight.
You will not have to worry about your balance as much, so the risk of falling is much less.
Serious injuries could be avoided, so you will not have to worry about having a permanent
injury, casts, or braces. You will be able to worry less about how you appear if you are not
injured, and you will be able to do the things you like to do most. You can heal faster too. In
order to lose weight a person must increase the number of calories used by physical activity, and
do not lose the weight quickly. Continue to eat the correct amount of servings from the Food
Guide Pyramid, and choose lower-calorie foods, with small serving sizes.
Being underweight is also not considered healthy. In order for a person to gain weight,
they should follow the Dietary Guidelines and increase the number of serving from the food
groups in the Food Guide Pyramid, as well as eat healthful snacks, but not before meals.
Point#11:
Eating healthy and maintaining a good weight for your particular body type will help you
present yourself to your friends in the best possible way. You will have a higher self-esteem,
and you will be proud of your self..
Point#12:
Your skin, eyes, and nails will also be much more attractive. Eating healthy means that
you are giving your body good nutrients that it needs, and can help clear up facial blemishes.
You will look and feel much better and you will be able to present yourself in a positive light.
ATHLETIC
Medical doctors or physicians often use body composition, the proportion of fat tissue to
lean tissue in the body, to determine if a person’s weight is healthy. All people have some fat. A
female teen with a healthful body composition may have about 15 percent of body fat, and a
male teen with 10 percents. Obesity is the term for having too much body fat. Other ways of
determining if a person’s weight is unhealthy is by using the Body Mass Index. It measures
mass compared to height. Even if you are at a desirable weight, you still need to keep healthful
eating habits.
Point#13:
Having too much body fat from eating unhealthy foods, or by eating too large of portions,
will limit a person’s athletic ability, or will hurt his/her ability to engage in exercise or sports.
Do you ever see overweight athletes? No! An overweight person will not be able to be the great
athlete that he or she wants to. You would rather want to stand out in an athletic crowd by
presenting yourself as healthy and a person who takes care of their body by eating healthy. People who do not eat healthy food will be much more tired and sick due to the lack of exercise.
You will be too tired and sick to play to the best of your ability. You’d be out of breath too soon
or you won’t be able to run. All of this is not fun! On the other hand, being healthy and having a
healthy weight means you are eating the right foods. And if you are, then you have the energy to
play sports.
73
REFERENCES
Barrera, M., Castro, F., Strycker, L. A., & Toobert, J. D. (2013). Cultural adaptations of
behavioral health interventions: A progress report. Journal of Consulting and Clinical
Psychology, 81.2, 196-205.
Black , M. M., Quigg, M. A., Cook, J., Casey, H. P., Cutts, B. D., Chilton, M., … Frank, A. D.
(2012). Wic participants and attenuation of stress-related child health risks of household
food insecurity and caregiver depressive symptoms. Arch Pediatr Adolesc Med, 166, 444-
451.
Botvin, G.J. (Eds.). (2006). Lifeskills Training. Princeton, NJ: Princeton Health Press.
Bothmer, K. M., Fridlund, B. (2005). Gender differences in health habits and in motivation for
a healthy lifestyle among Swedish university students. Nursing and Health Sciences,
7, 107-118.
Boyles, S. (2011). One hundred sixty four Million Obese Adults by 2030: Half of American
Adults will be obese if trends continue. Retrieved from:
http://www.webmd.com/diet/news/20110825/report-164-million-obese-adults-by-2030.
Brener, N. D., Kann, L., McManus, T., Kinchen, S., Sundberg, E., & Ross, J. (2002). Reliability
of the 1999 youth risk behavior survey questionnaire. Journal of Adolescent Health, 31,
336-342.
Campbell, K., Lioret, S., McNaughton, S., Crawford, A. D., Salmon, J., Ball, K., & Hesketh, D.
K. (2013). A parent-focused intervention to reduce infant besity. Journal of the American
Academy of Pediatrics, 131, 652-660.
Calasanti, T., Pietela, I., Ojala, H., & King, N. (2013). Men, bodily control, and health behaviors:
The importance of age. Health Psychology, 32, 15-23.

74
Centers for Disease Control and Prevention (2002). Youth Risk Behavior Surveillance- United
States, 2011. Morbidity and Mortality Weekly Report, 51, 1-64.
Cerin, E., Barnett, A., & Baranowski, T. (2009). Testing theories of dietary behavior change in
youth using the mediating variable model with intervention programs. Journal of
Nutrition Education and Behavior, 41, 309-318.
Courtenay, H. W., McCreary, R. D., & Merighi, R. J. (2002). Gender and ethnic differences in
health beliefs and behaviors. Journal of Health Psychology, 3, 219-231.
Dakanalis, A., Clerici, M., Caslini, M., Favagrossa L., Prunas, A., Volpato, C., Riva, G., &
Zanetti, M. A. (2013). Internilization of sociocultural standards of beauty and disordered
eating behaviours: The role of body surveillance , shame and social anxiety. Journal of
Psychopathology, 1-5.
Eilat-Adar, S., Koren-Morag, N., Siman-Tov, M., Livine, I., & Altmen, H. (2011). School-based
intervention to promote eating daily and healthy breakfast: A survey and a case-control
study. European Journal of Clinical Nutrition, 65, 203-209. doi:10.1038/enj.2010.247
Elder, J.P., Ayala, G. X., Parra-Medina, D., & Talavera, G. A. (2009). Health communication in
the latino community: Issues and approaches. Annual Review of Public Health, 30, 227-
251.
Ezendam, N. M., Noordegraaf, V. S., Kroeze, W., Brug, J., & Oenema, A. (2012). Process
evaluation of fataintphat, a computer-tailored intervention to prevent excessive weight
gain among dutch adolescents. Health promotion international, 28, 26-36. doi:
doi:10.1093/heapro/das021.
Gaines, O. S., Marelich, D. W., Bledsoe, L. K., Steers, N. W., Henderson, M., Granrose, S. C.,
… Farris, R. K. (2013). Links between race/ethnicity and cultural values as mediated by

75
racial/ethnic identity and moderated by gender. Journal of Personality and Social
Psychology, 72, 1460-1476.
Gans, K. M., Lovell, H. J., Fortunet, R., McMahon, C., Carton-Lopez, S., & Lasater, T. M.
(1999). Implications of qualitative research of nutrition education geared to selected
hispanic audiences. Journal of Nutrition Education and Behavior, 31, 331-338.
Garcia-Maas, L. D., (1999). Intergenerational analysis of dietary practices and health perceptions
of Hispanic women and their adult daughters. Journal of Transcultural Nursing, 10, 213-
219.
Gillis, A. (1994). Determinants of health-promoting lifestyles in adolescent females. Canadian
Journal of Nursing Research, 26, 13-28.
Gordon-Larson, P., Harris, K. M., Ward, D. S., & Popkin, B. M. (2003). Acculturation and
overweight-related behaviors among hispanic immigrants to the U.S.: The national
longitudinal study of adolescent health. . Social Science & Medicine , 57, 2023-2034.
Gortmaker, L. S., Lee, M. R., Mozaffarian, S. R., Sobol, R. A., Nelson, F. T., Roth, A. B., &
Wiecha, L. J. (2012). Effect of an after-school intervention on increases in children's
physical activity. Journal of the American College of Sports Medicine, 450-457.
Green, G. E., Deschamps, J., & Paez, D. (2005). Variation of individualism and collectivism
within and between 20 countries. Journal of Cross-Cultural Psychology , 36, 321-339.
Guendelman, S., Fernandez, A., Thornton, D., & Brindis, C. (2011). Birthplace, language use,
and body size among Mexican American women and men: Findings from the national
health and nutrition examination survey (NHANES) 2001-2006. Journal of Health Care
for the Poor Underserved, 22, 590-605.

76
Hanni, K. D., Ahn, D. A., & Winkleby, M. A. (2013). Signal detection analysis of factors
associated with diabetes among semirural mexican american adults. Hispanic Journal of
Behavioral Sciences, 35, 260-277.
Hendrie, A. G., Brindal, E., Corsini, N., Gardner, C., Baird, D., & Golley, K. R. (2012).
Combined home and school obesity prevention interventions for children: What behavior
change strategies and intervention characteristics are associated with effectiveness?.
Health Education & Behavior, 39, 159-171.
Hoelscher, M. D., Kirk, S., Ritchie, L., & Cunningham-Sabo, L. (2013). Position of the academy
of nutrition and dietetics: Interventions for the prevention and treatment of pediatric
overweight and obesity. Journal of the Academy of Nutrition and Dietetics, 113, 1376-
1394.
Kashima, Y., Kim, U., Gelfand, M., Yamaguchi, S., Choi, S., & Yuki, M. (1995). Culture,
gender, and self: a perspective from individualism-collectivism research. Journal of
Personality and Social Psychology , 69, 925-937.
Knight, P. G., & Chao, C. (1989). Gender differences in the cooperative, competitive, and
individualistic social values of children . Motivation and Emotion, 13, 125-140.
Laffrey, C. S. (1986) Development of a health conception scale. Research in Nursing and
Health, 9, 107-113.
Lawton, M. P., Moss, M., Fulcomer, M., & Kleban, M. H., (1982). A research and service
oriented multilevel assessment instrument. Journal of Gerontology, 37, 91-99.
Leopold, C., & Leutner, D. (2012). Science text comprehension: Drawing main idea selection,
and summarizing as learning strategies. Learning and Instruction, 22, 16-26.

77
Lindberg, M. N., Stevens, V. J., Vega-Lopez, S., Kauffman, L. T., Calderon, R. M., &
Cervantez, A. M. (2012). A weight-loss intervention program designed for mexican
american women: cultural adaptations and results. Journal of Immigrant Minority Health,
14, 1030-1039.
Liu, J., Chu, H. Y., Frongillo, A. E., & Probst, C. J. (2012). Generation and acculturation status
are associated with dietary intakeand body weight in mexican american adolescents. The
Journal of Nutrition , 142, 298-305.
Lopez, S.G., Garza, R.T., & Gonzalez-Banks, A. (2012). Preventing smoking among Hispanic
preadolescents: Program orientation, participant individualism-collectivism, and
acculturation. Hispanic Journal of Behavioral Sciences, 34, 323-339.
Lopez, S.G., Gonzalez-Blanks, A., Garza, R.T., & Garcia, S. (2014). “Mejorando nuestra salud
comiendo saludable”: Cultual influences in promoting healthy nutrition among hispanic
preadolescents. Hispanic Journal of Behavioral Sciences. In review.
Lorson, B. A., Melgar-Quinonez, H. R., & Taylor, C. A. (2009). Correlates of fruit and vegetable
intakes in us children. Journal of the American Diet Association, 109, 474-478. doi:
10.1016/j.jada.2008.11.022
Lutifya, N. M., Garcia, R., Dankwa, M. C., Young, T., & Lipsky, S. M. (2008). Overweight and
obese prevalence rats in african american and hispanic children: An analysis of data from
the 2003-2004 national survey of children's health. JABFM, 21, 191-199.
Lykes, M. B. (1985). Gender and individualistic vs. collectivistic basis for notions about the self.
Journal of Personality, 53, 356-383.
Marcus, J., & Le, H. (2013). Interactive effects of levels of individualism-collectivism on
cooperation: A meta-analysis. Journal of Organizational Behavior , 34, 813-834.

78
McBean, L. D., & Miller, G. D. (1999). Enhancing the nutrition of America’s youth. Journal of
the American College of Nutrition, 18, 563-571.
McClain, A. D., Chappuis, C., Nguyen-Rodriguez, S. T., Yaroch, A. L., & Spruijt-Metz, D.
(2009). Psychosocial correlates of eating behavior in children and adolescents: A review.
International Journal of Behavioral Nutrition and Physical Activity, 6, 54-74.
Meeks, L., & Heit, P. (2006). Health and Wellness Texas. New York: Macmillan McGraw-Hill.
Mendelson, K., White, R. D., & Mendelson, J. R. (1996). Self-esteem and body esteem: Effects
of gender, age, and weight. Journal of Applied Developmental Psychology, 17, 321-346.
Mischner, H.S. I., Schie, T. H., & Engels, R. (2013). Breaking the circle: Challenging Western
sociocultural norms for appearance influences in young women’s attention to appearance-
related media. Body Image, 10, 316-325.
Mitchell, M. L. (2006). Thinking critically about children's drawings as a visual research
method. Visual Anthropology Review, 22, 60-73.
Nixon, C. A., Moore, H. J., Douthwaite, W., Gibson, E. L., Vogele, C., Kreichauf, S.,
Wildgruber, A., .. Summerbell, C. D. (2012). Identifying effective behavioral models and
behavior change strategies underpinning pre-school-based obesity prevention
interventions aimed at 4-6 year olds: A systematic review. International Association for
the Study of Obesity, 13, 106-117.
Ogden, L. C., Carroll, D. M., Kit, K. K., & Flegal, M. K. (2012). Prevalence of obesity and
trends in body mass index among us children and adolescents, 1999-2010. JAMA, 307,
483-490.
Orji, R., Vassileva, J., & Mandryk, L. R. (2013). Modeling gender differences in healthy eating
determinants for persuasive intervention design. Persuasive, 161-173.

79
Oyserman, D., & Lee, S. W. (2008). Does culture influence what and how we think? Effects of
priming individualism and collectivism. Psychology Bulletin, 134, 311-342.
Parcel, G.S., Edmundson, C. L., Theim, K.R., Epstein, L. H., Wilfey, D.E. (1995). Measurement
of self-efficacy for diet related behaviors among elementary school children. Journal of
School Health, 65, 23-27.
Pearson, N., Biddle, S. J., & Gorely, T. (2008). Family correlates of breakfast consumption
among children and adolescents: A systematic review. Appetite, 52, 1-7. doi:
10.1016/j.appet.2008.08.006
Pelander, T., Lehtonen, K., & Leino-Kilpi, H. (2007). Children in the hospital: Elements of
quality in drawings. Journal of Pediatric Nursing, 22, 333-341.
Peters, L. W., Wiefferink, C. H., Hoekstra, F., Buijs, G. J., Dam, G. T., & Paulussen, T. G.
(2009). A review of similarities between domain-specific determinants of four health
behaviors among adolescents. Health Education Research, 24, 198-223.
Piernas, C., & Popkin, M. B. (2011). Increased portion sizes from energy dense foods affect total
energy intake at eating occasions in us children and adolescents: Patterns and trends by
age group and sociodemographic characteristics, 1977-2006. The American Journal of
Clinical Nutrition, 94, 1324-1332.
Popkin, B. M., & Udry, J. R. (1998). Adolescent obesity increases significantly in second and
third generation u.s. immigrants: The national longitudinal study of adolescent health.
Journal of Nutrition , 128, 701-706.
Prelip, M., Kinsler, J., Thai, C., Erausquin, T. J., & Slusser, W. (2012). Evaluation of school-
based multicomponent nutrition education program to improve young children's fruit and
vegetable consumption. Journal of Nutrition Education and Behavior, 44, 310-318.

80
Rosas, L. G., Guendelman, S., Harley, K., Fernald, L.C., Neufeld, L., Mejia, F., & Eskenazi, B.
(2011). Factors associated with overweight and obesity among children of Mexican
descent: Results of binational study. Journal of Immigrant Minority Health, 13, 169-180.
doi:10.1007/s10903-010-9332-x
Schwartz, J. S., Rosiers, D. S., Unger, B. J., Zamboanga, L. B., & Knight, P. G. (2013).
Developmental trajectories of acculturation in hispanic adolescents: Associations with
family functioning and adolescent risk behavior. Child Development , 00, 1-18.
Schmeer, K. U.S. Department of Health and Human Services, (2011). Early childhood economic
disadvantage and the health of hispanic children (WP-11-01). Bowling Green State
University : National Center for Family & Marriage Research.
Shriver, H. L., Harrist, W. A., Paige, M., Hubbs-Tait, L., Moulton, M., & Topham, G. (2013).
Differences in body esteem by weight status, gender, and physical activity among young
elementary school-aged children. Body Image, 10, 78-84.
Singh, S. K., & Yu, S. M. (2012). The impact of ethnic-immigrant status and obesity-realted risk
factors on behavioral problems among u.s. children and adolescents. Scientifica , 2012, 1-
14.
Soh, S., & Leong, F. T. L.(2002). Validity of vertical and horizontal individualism and
collectivism in singapore: Relationships with values and interests. Journal of Cross-
Cultural Psychology, 33, 3-15.
Somerville, M., Kessler, A. L., Wallace, P. S., & Burns-Whitmore, B. (2013). The effect of a
garden-based nutrition education program on the consumption of fruits and vegetables by
hispanic children. California Journal of Health Promotion, 10, 20-25.

81
Stephen, D. I., & Perrera, A. T. (2014). Judging the difference between attractiveness and health:
Does exposure to model images influence the judgment made by men and women? PLOS
one, 9, 1-7.
Sussner, K. M., Lindsay, A. C., Greaney, M. L., & Peterson K. E. (2008). The influence of
immigrant status and acculturation on the development of overweight in Latino families:
A qualitative study. Journal of Immigrant Minority Health, 10, 497-505.
Taveras, E. M., Sobol, A. M., Hannon, C., Finkelstein, D., Wiecha, J., & Gortmaker, S.L. (2007).
Youth’s perceptions of overweight-related prevention counseling at a primary care visit.
Obesity, 15, 831-836. doi:10.1038/oby.2007.594.
Thomas, H. (2006). Obesity prevention programs for children and youth: Why are their results so
modest? Health Education Research, 21, 783-795. doi:10.1093/her/cy1143
Triandis, H.C. (1995). Individualism and collectivism. Boulder, CO: Westview Press.
U.S. Department of Health and Human Services, Center for Disease Control. (2012). Health,
united states, 2012. Retrieved from website: http://www.cdc.gov/nchs/data/hus/hus12.pdf
U.S. Department of Health and Human Services, Office of Minority Health. (2013). Obesity and
hispanic americans. Retrieved from website:
http://minorityhealth.hhs.gov/templates/content.aspx?ID=6459
Van Lippevelde, W., Verloigne, M., Bourdeaudhuij, I., Brug, J., Bjelland, M., Lien, N., & Maes,
L. (2012). Does parental involvement make a difference in school-based. International
Journal of Public Health , doi: 10.1007/s00038-012-0335-3
Wardle, J., Hasse, M. A., Steptoe, A., Nillapun, M., Jonwutiwes, K., & Bellisle, F. (2004).
Gender differences in food choice: The contribution of health beliefs and dieting.
Annual Behavioral Medicine,27, 107-116.

82
Williams, A. P., & Cash, F. T. (2001). Effects of a circuit weight training program on the body
image of college students. John Wiley and Sons Inc.
Zapata, L. B., Bryant, C. A., McDermott, R.J., & Hefelfinger, J.A. (2008). Dietary and physical
activity behaviors of middle schools youth: The youth physical activity and nutrition
survey. Journal of School Health, 78, 9-18.
Zullig, K. J., Pun, S., Patton, J. M., & Ubbes, V. A. (2006). Reliability of the 2005 middle school
youth risk behavior survey. Journal of Adolescent Health, 39, 856-860.

VITA
Sara Garcia is from San Antonio, TX. She studied psychology and earned a Bachelor’s
degree from Boston University and Master’s degree in Psychology from The University of Texas
at San Antonio. Her future plans include earning a Ph.D. in Educational Policy, Organization,
and Leadership from the University of Illinois at Urbana-Champaign.