Galapagos PowerPoint Template (Confidential)
47
Novel targets, better treatments Investor presentation | May 2018
-
Upload
khangminh22 -
Category
Documents
-
view
5 -
download
0
Transcript of Galapagos PowerPoint Template (Confidential)
Novel targets, better treatments
Investor presentation | May 2018
2
Disclaimer
This presentation contains forward-looking statements, including (without limitation) statements concerning the progress of our clinicalpipeline, the slides captioned “GLPG: strong investment case” “GLPG: data rich 2018” “Advancing our innovation to market” “Strong R&D”“Establishing commercial footprint” “Building the filgotinib franchise” “Inflammation market ~$65 B by 2027” “Ambition with filgotinib”“FINCH Ph3 design for RA” “DIVERSITY & SELECTION in IBD” “Filgotinib in psoriatic arthritis” “Filgotinib in ankylosing spondylitis” “$1.9Bmarket with large unmet needs” “IPF: $5B market by 2025” “Building an IPF franchise” “Ph3 program ISABELA 1&2” “CF approach totriple combo” “PELICAN” “FALCON” “’1972 for osteoarthritis” “MOR106 for atopic dermatitis” ”IGUANA Ph2 program” “2018 late-stageclinical newsflow,” statements regarding the development of the triple combination therapy CF program, statements regarding theexpected timing, design and readouts of ongoing and planned clinical trials (i) with filgotinib in RA, IBD, and other potential indications (ii)in the CF program, (iii) with GLPG1690, GLPG1205, and GLPG3499 in IPF, (iv) with GLPG1972 in OA, (v) with MOR106 in atopic dermatitis,and expectations regarding the commercial potential of our product candidates. When used in this presentation, the words “anticipate,”“believe,” “can,” “could,” “estimate,” “expect,” “intend,” “is designed to,” “may,” “might,” “will,” “plan,” “potential,” “possible,” “predict,”“objective,” “should,” and similar expressions are intended to identify forward-looking statements.
Forward-looking statements involve known and unknown risks, uncertainties and other factors which might cause the actual results,financial condition, performance or achievements of Galapagos, or industry results, to be materially different from any future results,financial conditions, performance or achievements expressed or implied by such forward-looking statements. Among the factors that mayresult in differences are the inherent uncertainties associated with competitive developments, clinical trial and product developmentactivities, regulatory approval requirements (including that data from the company's development programs may not support registrationor further development of its compounds due to safety, efficacy or other reasons), reliance on third parties (including Galapagos’collaboration partners AbbVie, Gilead, Servier and MorphoSys) and estimating the commercial potential of its product candidates. Afurther list and description of these risks, uncertainties and other risks can be found in Galapagos’ Securities and Exchange Commission(“SEC”) filing and reports, including Galapagos’ most recent Form 20-F filing for the year ended December 31, 2017. Given theseuncertainties, you are advised not to place any undue reliance on such forward-looking statements.
All statements contained herein speak only as of the release date of this document. Galapagos expressly disclaims any obligation to updateany statement in this document to reflect any change or future development with respect thereto, any future results, or any change inevents, conditions and/or circumstances on which any such statement is based, unless specifically required by law or regulation.
Under no circumstances may any copy of this presentation, if obtained, be retained, copied or transmitted.
3
GLPG: strong investment case
Late stage data from filgotinib
2018-2019
Building commercial infrastructure
Proven platform for innovation, deep pipeline
Candidates for $80+B inflammation & fibrosis
markets
Strong cash positionfor growth with
~$1.3 B
4
GLPG: data rich 2018
• Best-in-class JAK
• Topline results in 3 indications (RA, PsA, AS)
• Building commercial organization with Gilead
• ISABELA Ph3 program with ‘1690
• Franchise of 3 proprietary novel assets
• Individual components validated in patients
• Topline 1st triple in patients Q3 ‘18
• 19 Ph2 trials in ‘18
• Additional novel drugs into clinic
Filgotinib
IPF
CF
Expanding pipeline
5
Advancing our innovation to market
2020-2022
• Potential for multiple product launches
• New pipeline opportunities
2018-2019
• Pivotal trials
• Expansion of late stage pipeline
• Commercial preparations
2016-2017
• GILD partnership
• 2nd and 3rd PoC on novel targets
6
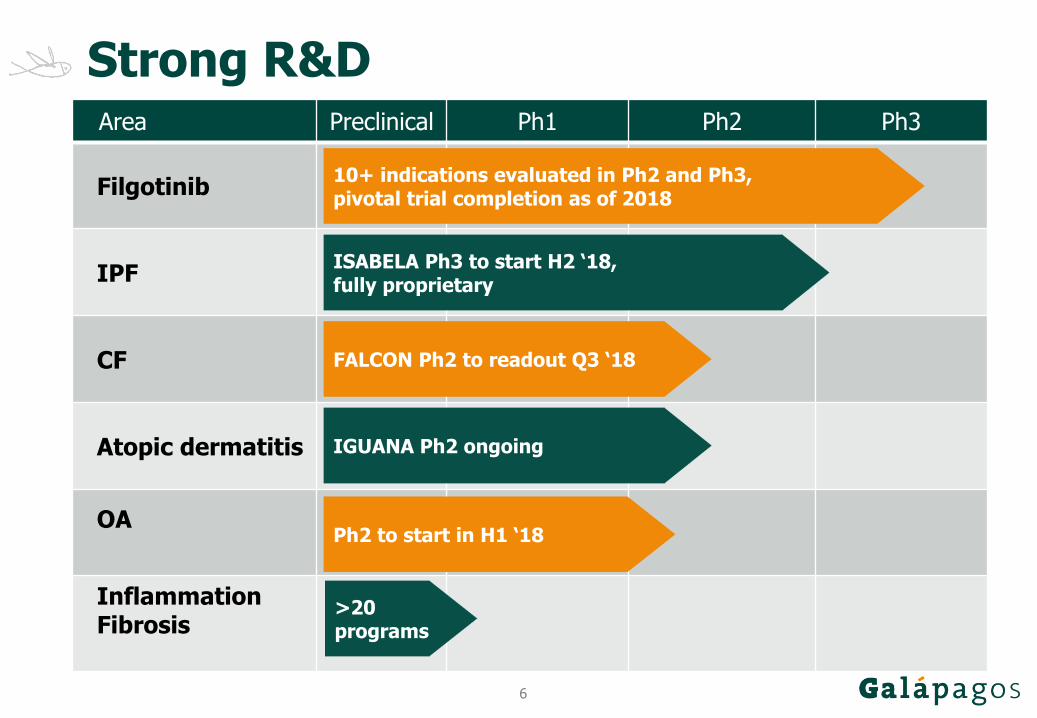
Strong R&DArea Preclinical Ph1 Ph2 Ph3
Filgotinib
IPF
CF
Atopic dermatitis
OA
Inflammation Fibrosis
FALCON Ph2 to readout Q3 ‘18
ISABELA Ph3 to start H2 ‘18,fully proprietary
10+ indications evaluated in Ph2 and Ph3,pivotal trial completion as of 2018
IGUANA Ph2 ongoing
>20 programs
Ph2 to start in H1 ‘18
7
Unique target discovery engine
NOVEL TARGETS
disease-modifying
multiple disease areas
first-in-class candidates
SMART DEVELOPMENT
rapid, multiple PoCs
swift moves to pivotal development
3 PROOFS OF CONCEPT
filgotinib (JAK1)
‘1690 (autotaxin)
MOR106 (IL17-C)
7
8
PartnershipsGilead: filgotinib
$750M upfront$1.35B in milestone paymentsprofit-split, co-promote in 8 EU countries20-30% royalties
AbbVie: CF
$600M milestonesprofit-split and co-promotion in BeneluxChina/Korea rights15-20% royalties
Servier: ‘1972
$290M milestonessingle digit % royaltiesUS rights
MorphoSys: MOR106
50/50 cost/benefit
9
Establishing commercial footprint
Further pipeline
expansion
‘1690 in IPF
global launch
Filgotinib
EU co-promotion
• Experience in launch and international operations
• Established global presence
• Partnerships as opportunity
• Orphan, shape the market
• Expand beyond EU
• Compact medical and patient community
• Rheumatology and IBD advanced markets
• First organizations in EU
• Leverage Gilead partnership
10
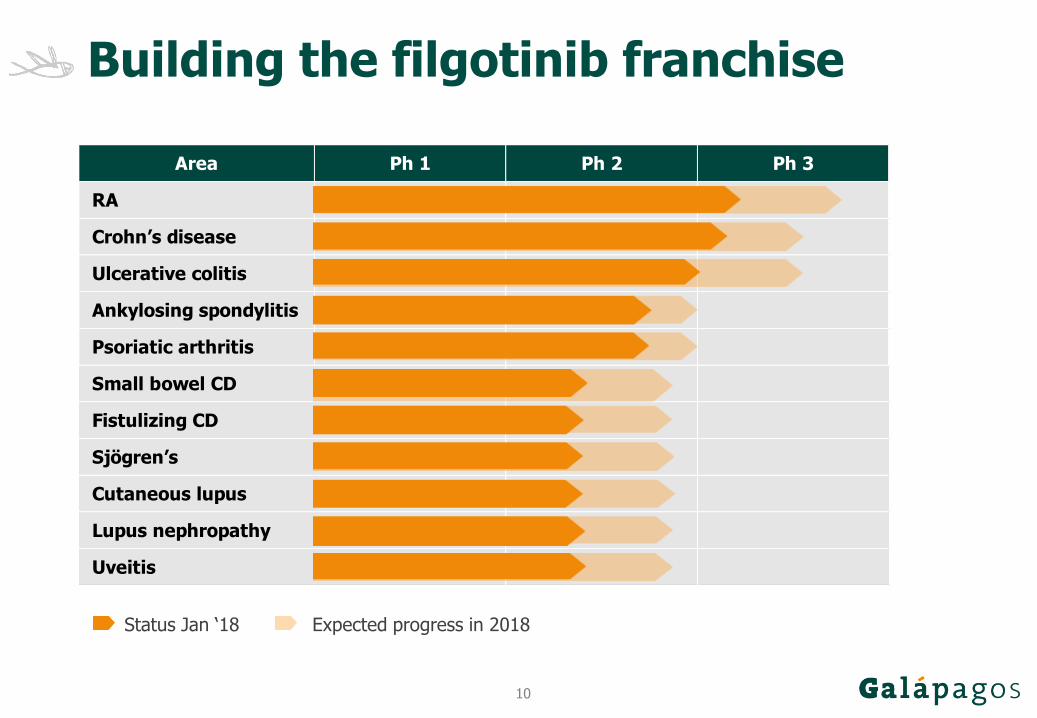
Building the filgotinib franchise
Status Jan ‘18 Expected progress in 2018
Area Ph 1 Ph 2 Ph 3
RA
Crohn’s disease
Ulcerative colitis
Ankylosing spondylitis
Psoriatic arthritis
Small bowel CD
Fistulizing CD
Sjögren’s
Cutaneous lupus
Lupus nephropathy
Uveitis
11
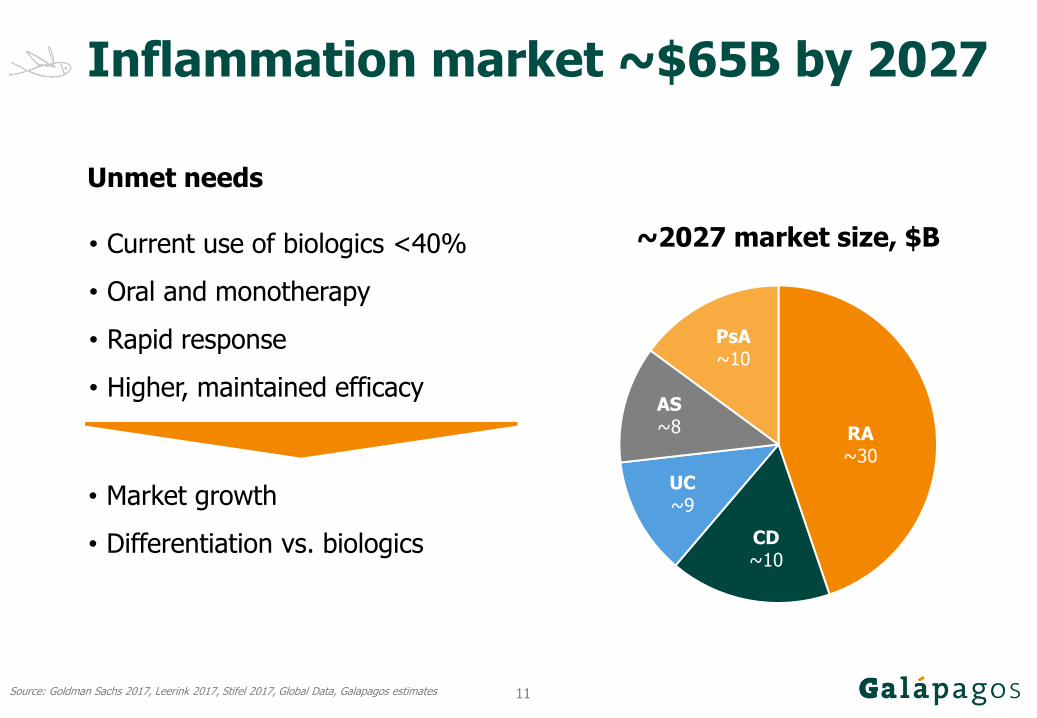
Inflammation market ~$65B by 2027
Source: Goldman Sachs 2017, Leerink 2017, Stifel 2017, Global Data, Galapagos estimates
• Current use of biologics <40%
• Oral and monotherapy
• Rapid response
• Higher, maintained efficacy
Unmet needs
RA~30
CD~10
UC~9
AS~8
PsA~10
~2027 market size, $B
• Market growth
• Differentiation vs. biologics
12
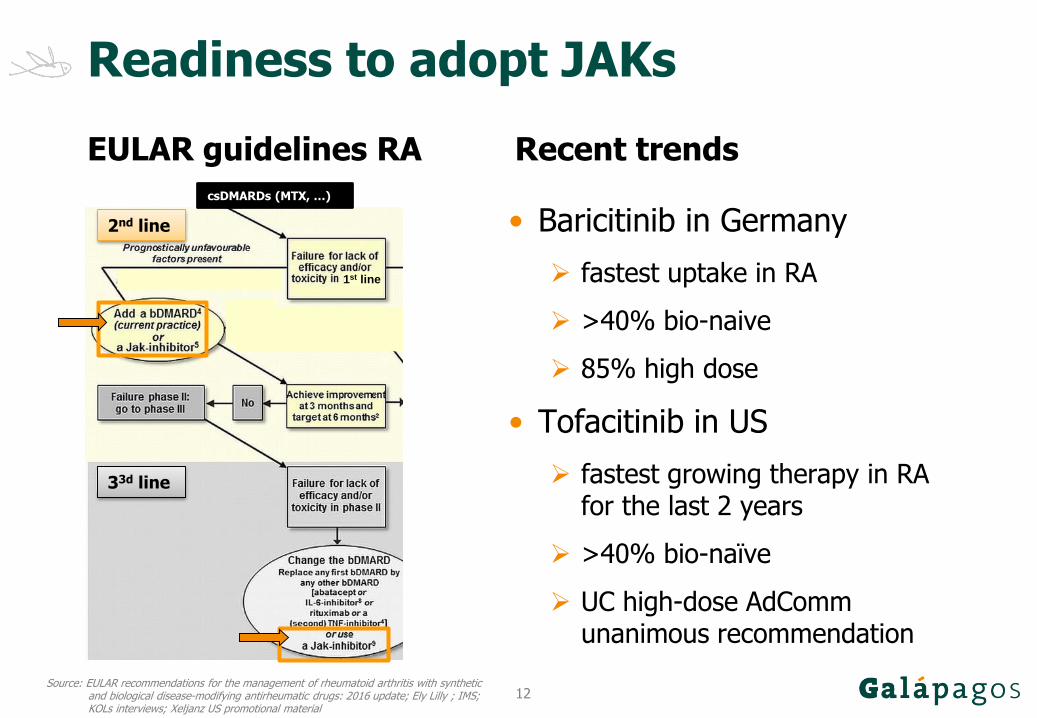
Readiness to adopt JAKs
• Baricitinib in Germany
fastest uptake in RA
>40% bio-naive
85% high dose
• Tofacitinib in US
fastest growing therapy in RA for the last 2 years
>40% bio-naïve
UC high-dose AdCommunanimous recommendation
2nd line
33d line
1st line
csDMARDs (MTX, …)
Source: EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2016 update; Ely Lilly ; IMS; KOLs interviews; Xeljanz US promotional material
EULAR guidelines RA Recent trends
13
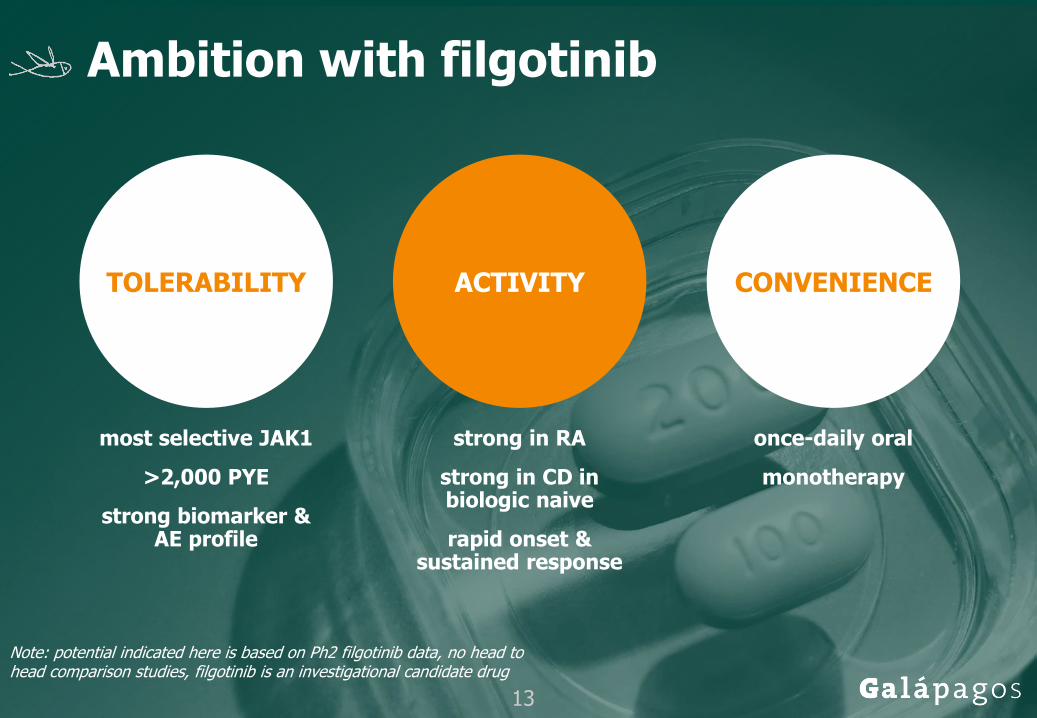
Ambition with filgotinib
most selective JAK1
>2,000 PYE
strong biomarker & AE profile
TOLERABILITY ACTIVITY CONVENIENCE
strong in RA
strong in CD in biologic naive
rapid onset & sustained response
once-daily oral
monotherapy
Note: potential indicated here is based on Ph2 filgotinib data, no head to head comparison studies, filgotinib is an investigational candidate drug
13
14
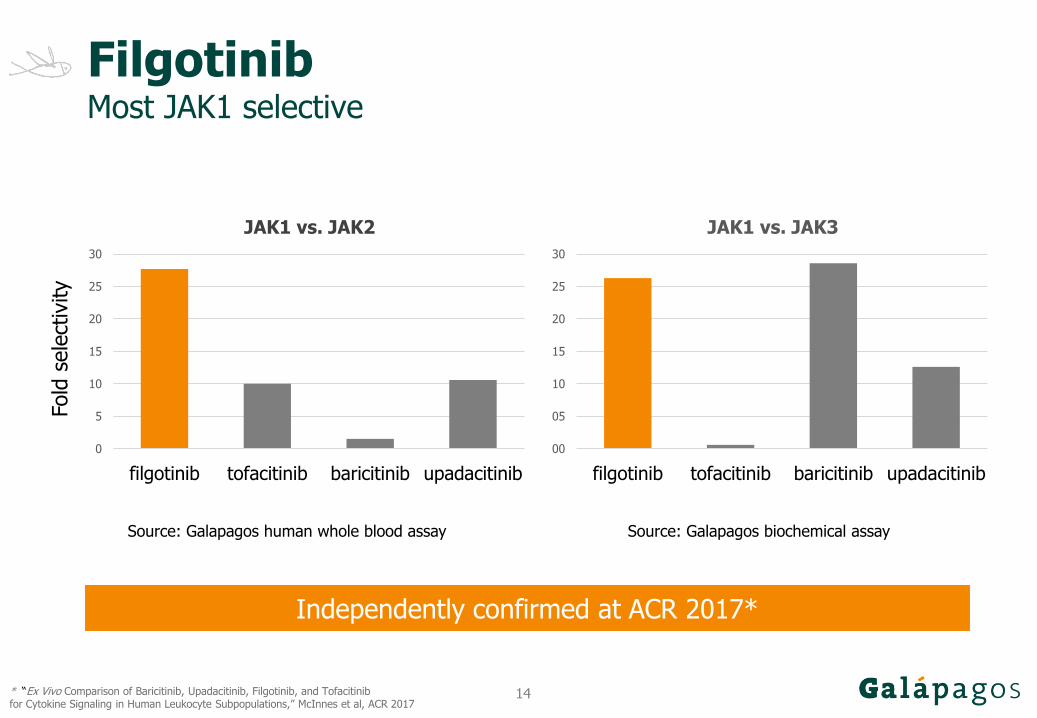
FilgotinibMost JAK1 selective
Independently confirmed at ACR 2017*
Source: Galapagos human whole blood assay
Fold
sele
ctiv
ity
0
5
10
15
20
25
30
filgotinib tofacitinib baricitinib upadacitinib
JAK1 vs. JAK2
00
05
10
15
20
25
30
filgotinib tofacitinib baricitinib upadacitinib
JAK1 vs. JAK3
Source: Galapagos biochemical assay
* “Ex Vivo Comparison of Baricitinib, Upadacitinib, Filgotinib, and Tofacitinibfor Cytokine Signaling in Human Leukocyte Subpopulations,” McInnes et al, ACR 2017
15
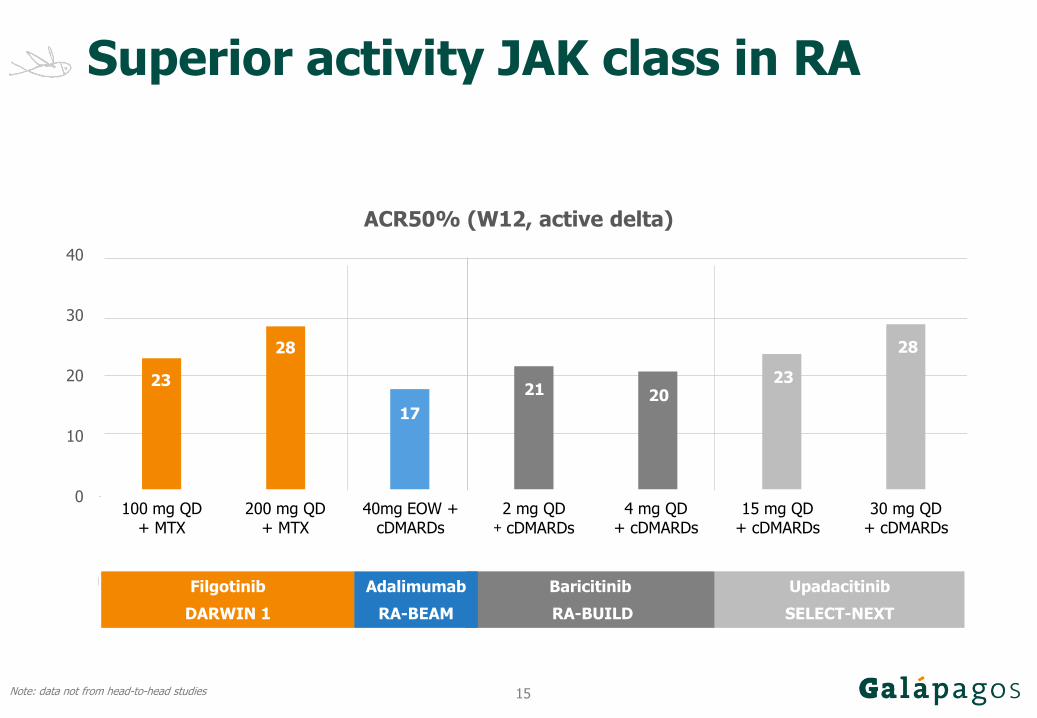
Superior activity JAK class in RA
23
28
17
21 2023
28
0
10
20
30
40
50
100 mg Q.D. + MTX(DARWIN-1, 2016, W12)
200 mg Q.D. + MTX(DARWIN-1, 2016, W12)
Adalimumab 40mg EOW(RA-BEAM, 2017, W12)
2 mg Q.D. + cDMARDS(RA-BUILD, 2017, W12)
4 mg Q.D. + cDMARDS(RA-BUILD, 2017, W12)
15 mg Q.D. + cDMARDs(SELECT NEXT, 2017,
W12)
30 mg Q.D. + cDMARDs(SELECT NEXT, 2017,
W12)
Filgotinib Baricitinib Upadacitinib
MTX IR (cDMARD IR)
ACR50% (W12)placebo active active delta
100 mg QD+ MTX
200 mg QD+ MTX
40mg EOW + cDMARDs
2 mg QD+ cDMARDs
4 mg QD+ cDMARDs
15 mg QD+ cDMARDs
30 mg QD+ cDMARDs
Filgotinib
DARWIN 1
Baricitinib
RA-BUILD
Upadacitinib
SELECT-NEXT
Adalimumab
RA-BEAM
ACR50% (W12, active delta)
Note: data not from head-to-head studies
16
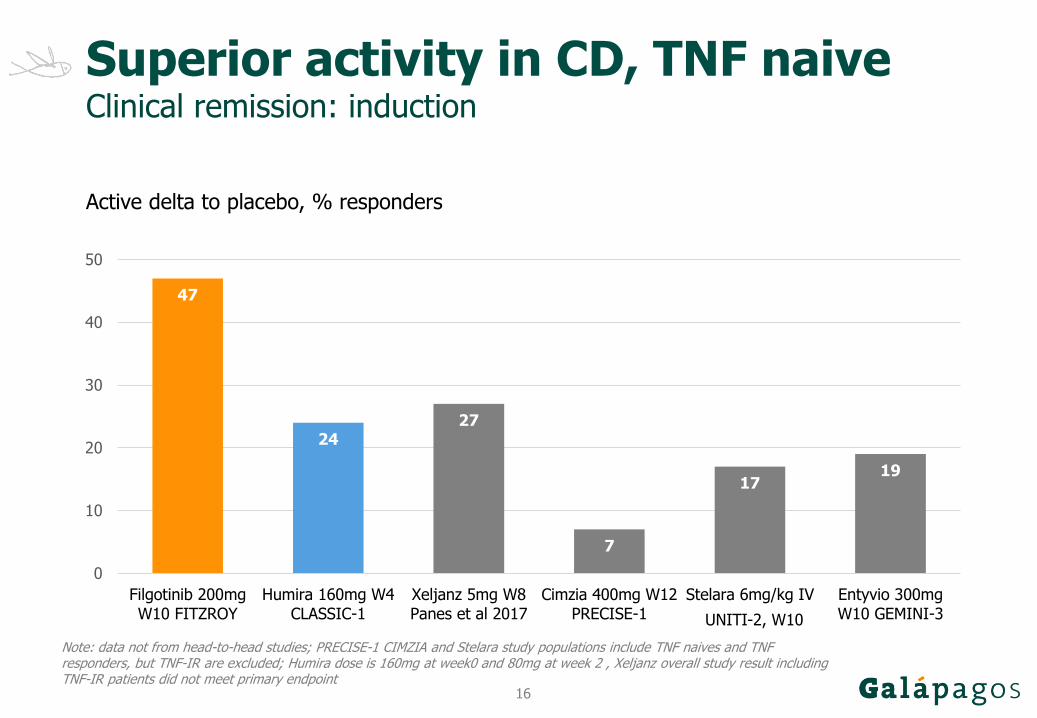
Superior activity in CD, TNF naiveClinical remission: induction
Active delta to placebo, % responders
Note: data not from head-to-head studies; PRECISE-1 CIMZIA and Stelara study populations include TNF naives and TNF responders, but TNF-IR are excluded; Humira dose is 160mg at week0 and 80mg at week 2 , Xeljanz overall study result including TNF-IR patients did not meet primary endpoint
47
27
47
2427
7
1719
0
10
20
30
40
50
Filgotinib 200mgW10 FITZROY
Humira 160mg W4CLASSIC-1
Xeljanz 5mg W8Panes et al 2017
Cimzia 400mg W12PRECISE-1
Stelara 6mg/kg IVW10
Entyvio 300mgW10 GEMINI-3UNITI-2, W10
17
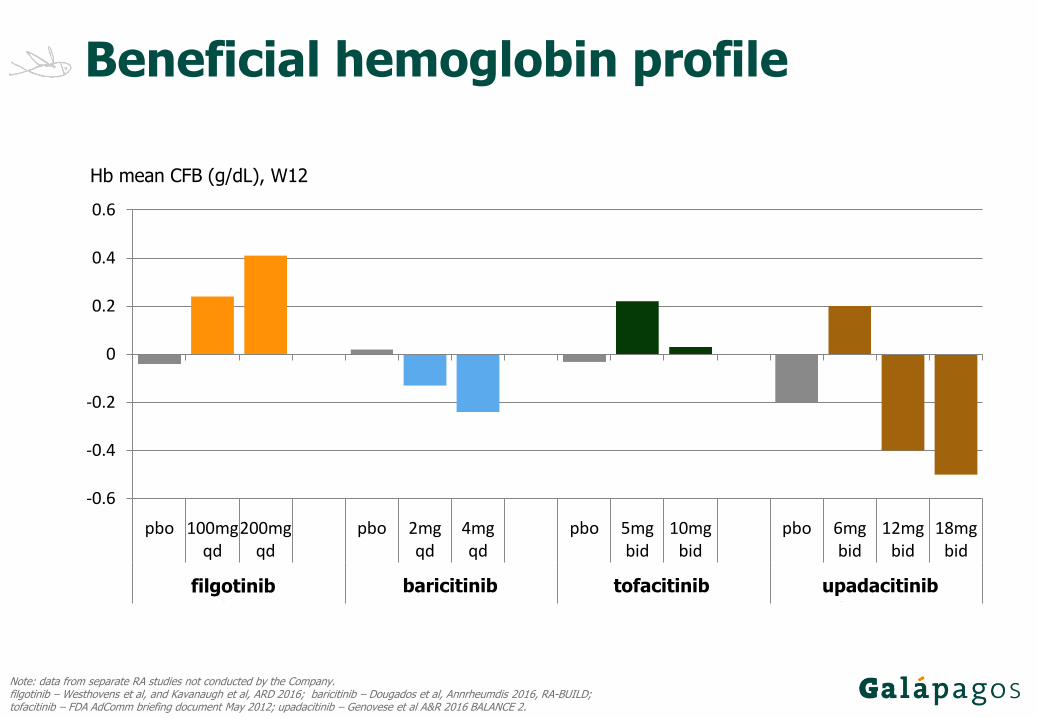
Beneficial hemoglobin profile
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
pbo 100mgqd
200mgqd
pbo 2mgqd
4mgqd
pbo 5mgbid
10mgbid
pbo 6mgbid
12mgbid
18mgbid
filgotinib baricitinib tofacitinib upadacitinib
Hb mean CFB (g/dL), W12
Note: data from separate RA studies not conducted by the Company.filgotinib – Westhovens et al, and Kavanaugh et al, ARD 2016; baricitinib – Dougados et al, Annrheumdis 2016, RA-BUILD; tofacitinib – FDA AdComm briefing document May 2012; upadacitinib – Genovese et al A&R 2016 BALANCE 2.
filgotinib baricitinib tofacitinib upadacitinib
18
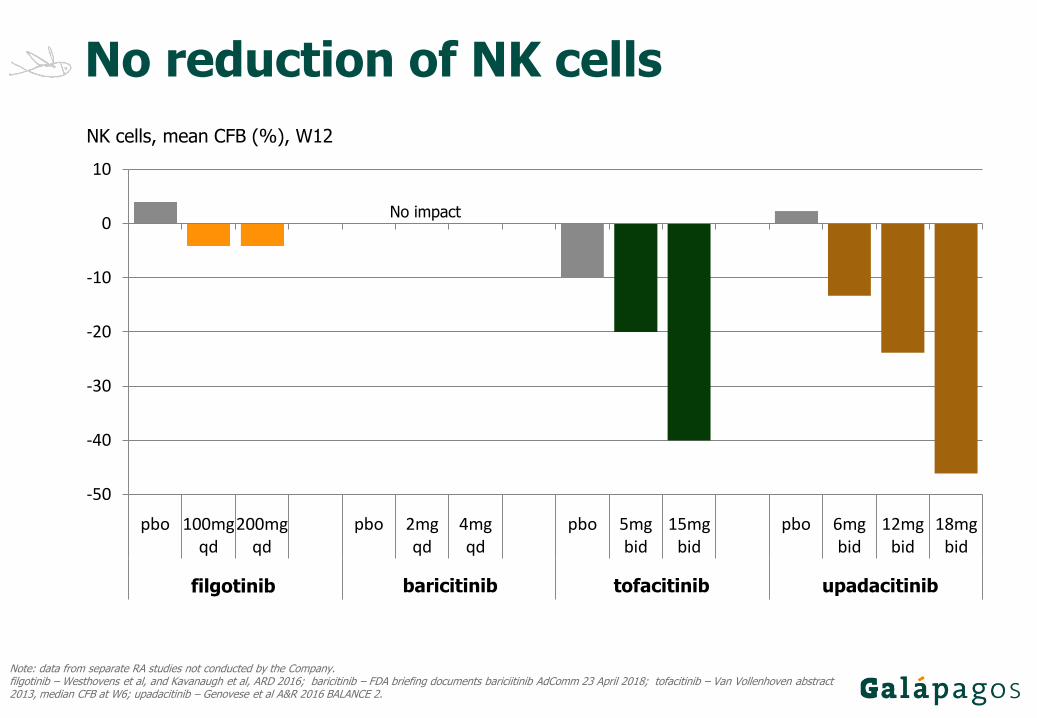
Note: data from separate RA studies not conducted by the Company.filgotinib – Westhovens et al, and Kavanaugh et al, ARD 2016; baricitinib – FDA briefing documents bariciitinib AdComm 23 April 2018; tofacitinib – Van Vollenhoven abstract 2013, median CFB at W6; upadacitinib – Genovese et al A&R 2016 BALANCE 2.
No reduction of NK cells
NK cells, mean CFB (%), W12
-50
-40
-30
-20
-10
0
10
pbo 100mgqd
200mgqd
pbo 2mgqd
4mgqd
pbo 5mgbid
15mgbid
pbo 6mgbid
12mgbid
18mgbid
filgotinib baricitinib* tofacitinib** upadacitinib
No impact
filgotinib baricitinib tofacitinib upadacitinib
19
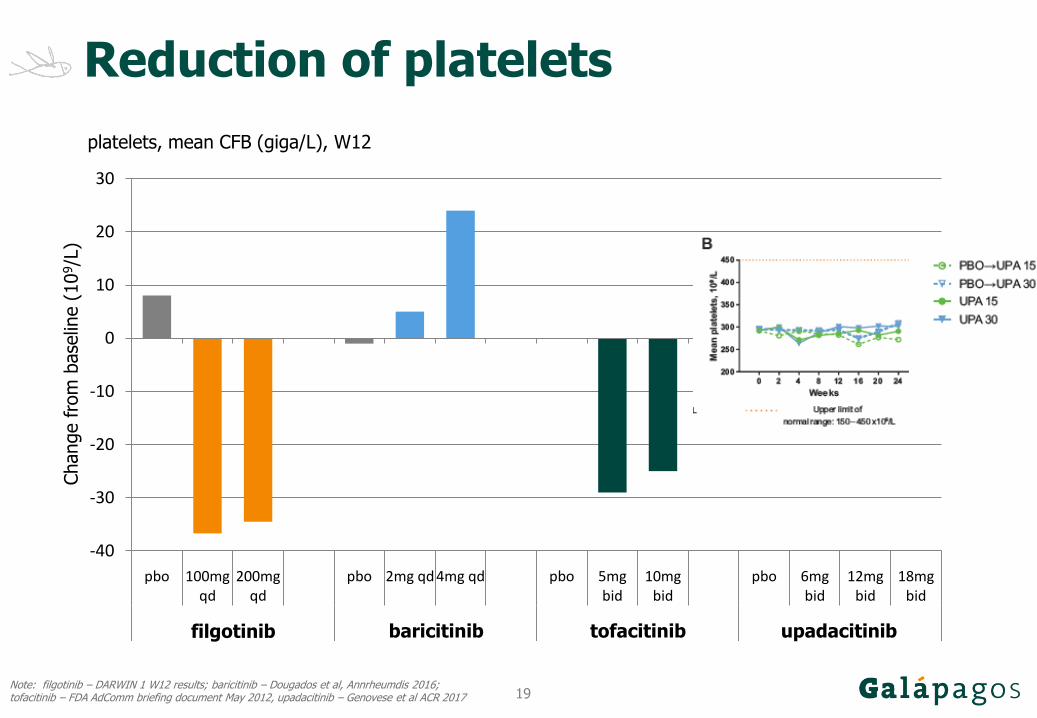
Reduction of platelets
-40
-30
-20
-10
0
10
20
30
pbo 100mgqd
200mgqd
pbo 2mg qd 4mg qd pbo 5mgbid
10mgbid
pbo 6mgbid
12mgbid
18mgbid
filgotinib baricitinib tofacitinib upadacitinib
Change fro
m b
ase
line (
10
9/L
)
Note: filgotinib – DARWIN 1 W12 results; baricitinib – Dougados et al, Annrheumdis 2016;tofacitinib – FDA AdComm briefing document May 2012, upadacitinib – Genovese et al ACR 2017
platelets, mean CFB (giga/L), W12
filgotinib baricitinib tofacitinib upadacitinib
20
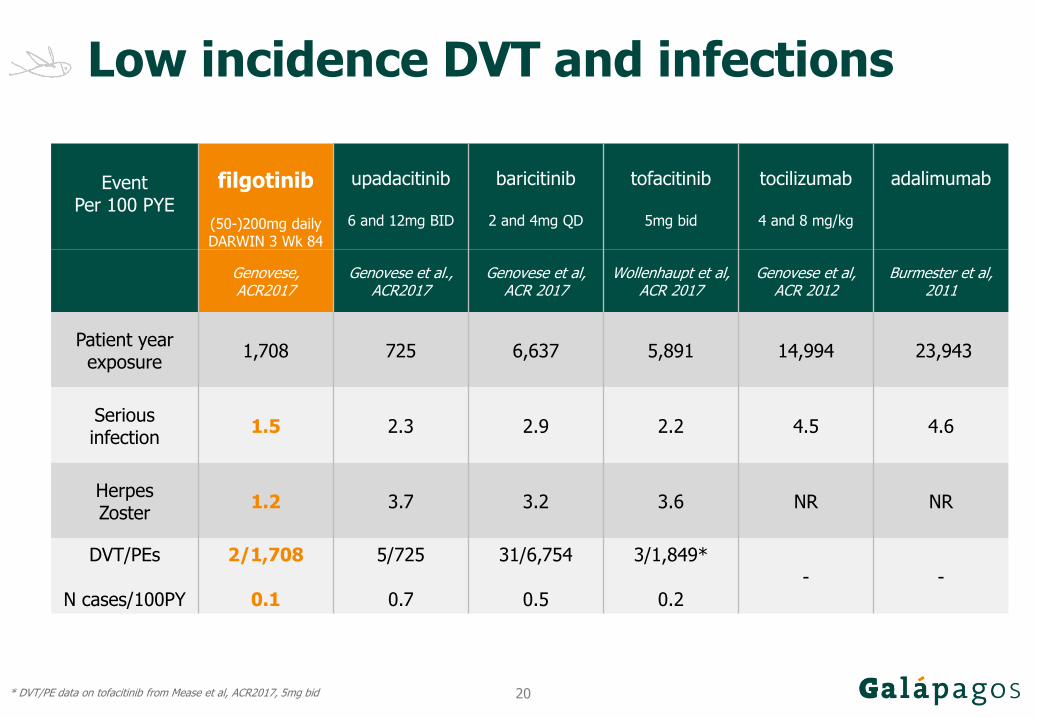
Low incidence DVT and infections
EventPer 100 PYE
filgotinib
(50-)200mg dailyDARWIN 3 Wk 84
upadacitinib
6 and 12mg BID
baricitinib
2 and 4mg QD
tofacitinib
5mg bid
tocilizumab
4 and 8 mg/kg
adalimumab
Genovese, ACR2017
Genovese et al., ACR2017
Genovese et al,ACR 2017
Wollenhaupt et al, ACR 2017
Genovese et al, ACR 2012
Burmester et al, 2011
Patient year exposure
1,708 725 6,637 5,891 14,994 23,943
Serious infection
1.5 2.3 2.9 2.2 4.5 4.6
Herpes Zoster
1.2 3.7 3.2 3.6 NR NR
DVT/PEs
N cases/100PY
2/1,708
0.1
5/725
0.7
31/6,754
0.5
3/1,849*
0.2- -
* DVT/PE data on tofacitinib from Mease et al, ACR2017, 5mg bid
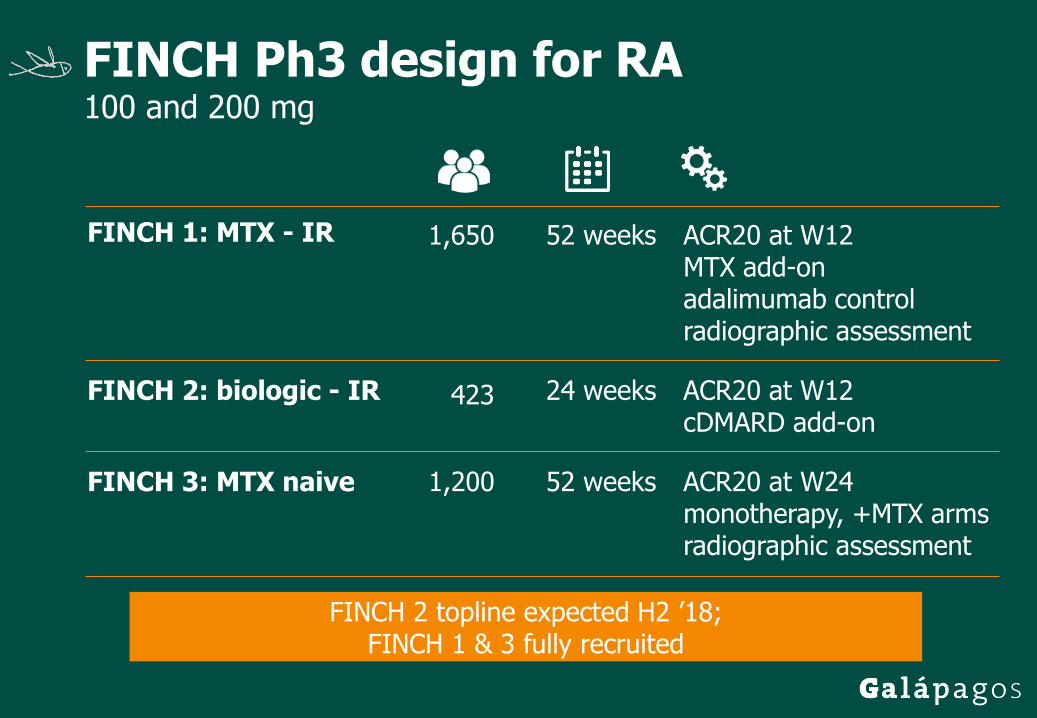
FINCH Ph3 design for RA100 and 200 mg
FINCH 1: MTX - IR ACR20 at W12MTX add-onadalimumab controlradiographic assessment
1,650 52 weeks
FINCH 2: biologic - IR 423 24 weeks ACR20 at W12cDMARD add-on
FINCH 3: MTX naive 1,200 52 weeks ACR20 at W24monotherapy, +MTX armsradiographic assessment
FINCH 2 topline expected H2 ’18; FINCH 1 & 3 fully recruited

DIVERSITY & SELECTION in IBD100 and 200 mg
DIVERSITY 1 PRO2, endoscopic response Induction & maintenance
Crohn’s Ph31,320 pts
58 weeks
DIVERSITY 2 Long term extension study
SELECTION 1 Mayo score components Induction & maintenance
UC Ph2/31,300 pts
58 weeks
SELECTION 2 Long term extension study
Interim decision SELECTION expected H1 ’18; recruitment completion DIVERSITY expected H2 ’19
23
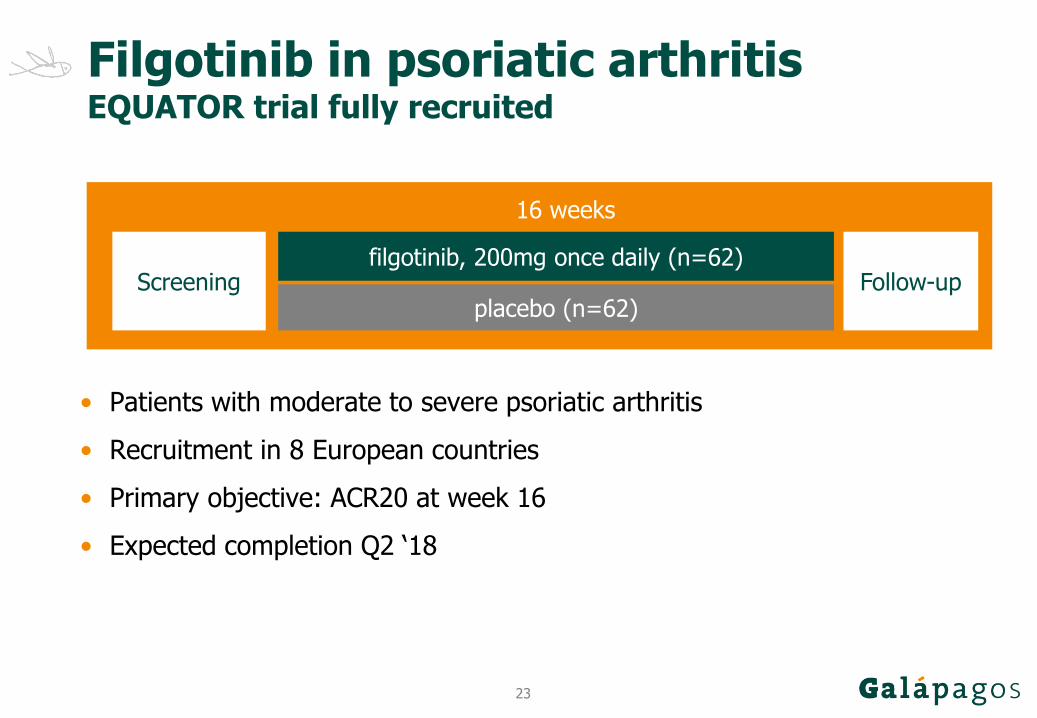
Filgotinib in psoriatic arthritisEQUATOR trial fully recruited
filgotinib, 200mg once daily (n=62)Screening
16 weeks
Follow-up
• Patients with moderate to severe psoriatic arthritis
• Recruitment in 8 European countries
• Primary objective: ACR20 at week 16
• Expected completion Q2 ‘18
placebo (n=62)
24
Filgotinib in ankylosing spondylitisTORTUGA trial fully recruited
filgotinib, 200mg once daily (n=50)Screening
12 weeks
Follow-up
• Patients with moderate to severe ankylosing spondylitis
• Recruitment in 8 European countries
• Primary objective: ASDAS at week 12
• Expected completion H2 ’18
placebo (n=50)
25
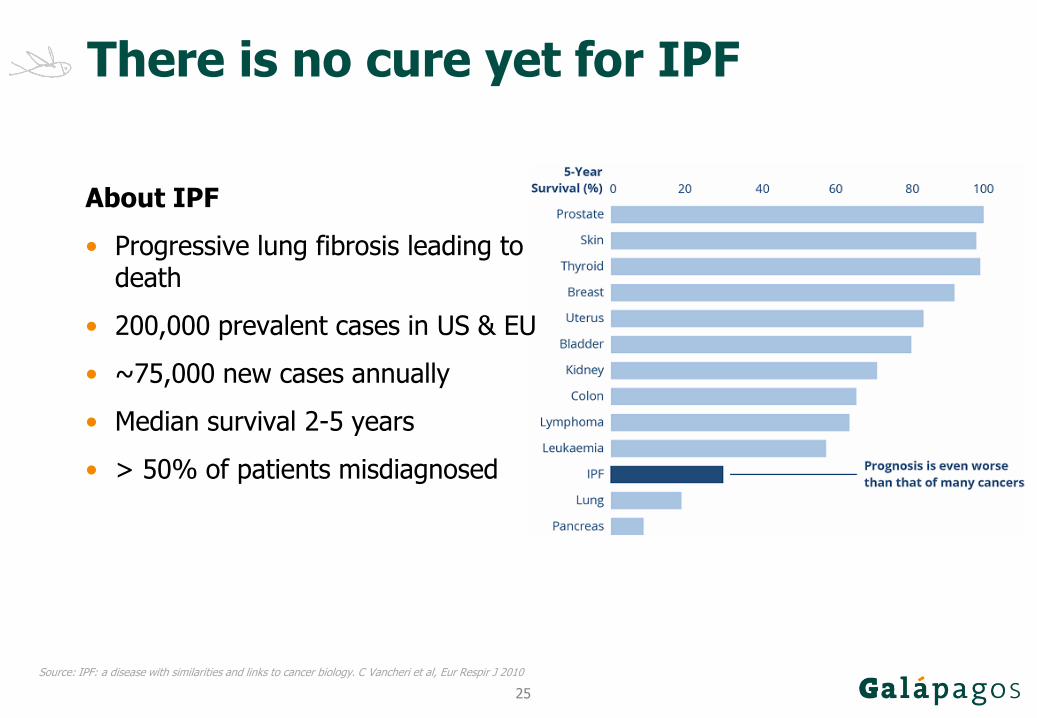
There is no cure yet for IPF
About IPF
• Progressive lung fibrosis leading to death
• 200,000 prevalent cases in US & EU
• ~75,000 new cases annually
• Median survival 2-5 years
• > 50% of patients misdiagnosed
Source: IPF: a disease with similarities and links to cancer biology. C Vancheri et al, Eur Respir J 2010
26
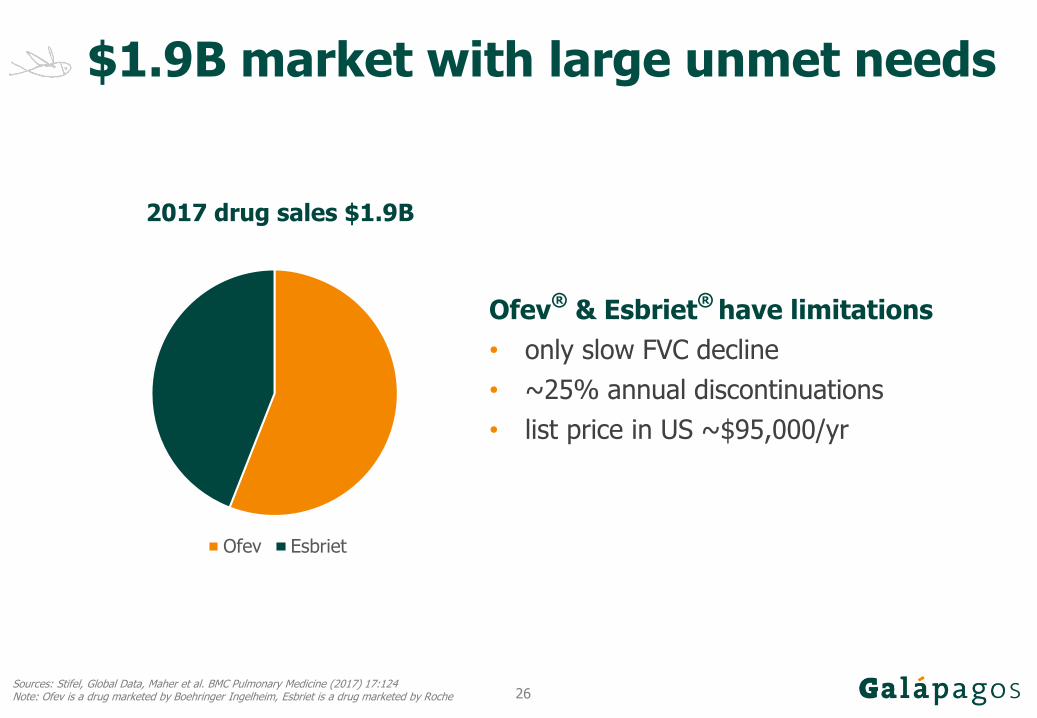
$1.9B market with large unmet needs
Sources: Stifel, Global Data, Maher et al. BMC Pulmonary Medicine (2017) 17:124Note: Ofev is a drug marketed by Boehringer Ingelheim, Esbriet is a drug marketed by Roche
2017 drug sales $1.9B
Ofev®
& Esbriet®
have limitations
• only slow FVC decline
• ~25% annual discontinuations
• list price in US ~$95,000/yr
Ofev Esbriet

27
IPF: $5B market by 2025
Sources: Stifel, Global Data, Galapagos assessment
Current unmet needs
• lengthy diagnosis
• low treatment rate and duration
• low survival
Improve treatment
• more diagnosed patients treated
• patients longer on treatment
• awareness and education
Improve outcomes
• shorten diagnosis time
• improve efficacy
• combination therapies
• long term treatment compliance
Galapagos aspiration
28
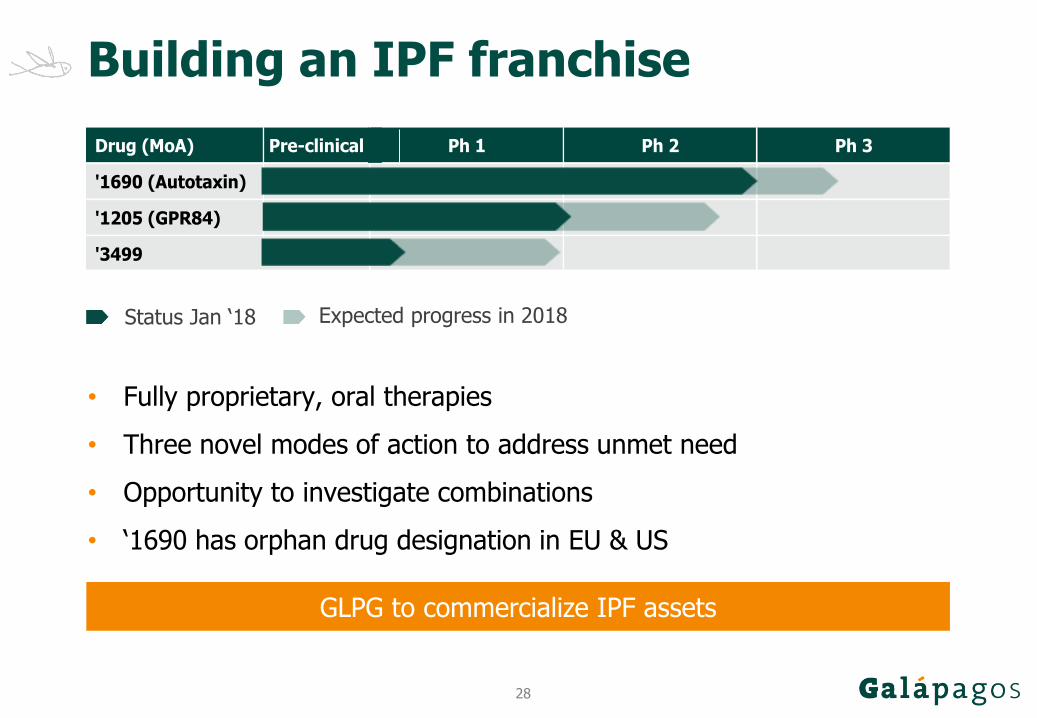
Building an IPF franchise
• Fully proprietary, oral therapies
• Three novel modes of action to address unmet need
• Opportunity to investigate combinations
• ‘1690 has orphan drug designation in EU & US
GLPG to commercialize IPF assets
Status Jan ‘18 Expected progress in 2018
Other Pipeline Assets
Area Drug (MoA) Pre-clinical Ph 1 Ph 2 Ph 3
'1690 (Autotaxin)
'1205 (GPR84)
'3499
IPF

29
Positive ‘1690 data in patients
FVC stabilization over 12-week period
Flora
‘1690 600mg QDPlacebo
Placebo‘1690
BSLN=6N=17
*= p<0.05
4N=3N=16
8N=4N=15
12N=4N=13
FUN=4N=15
30
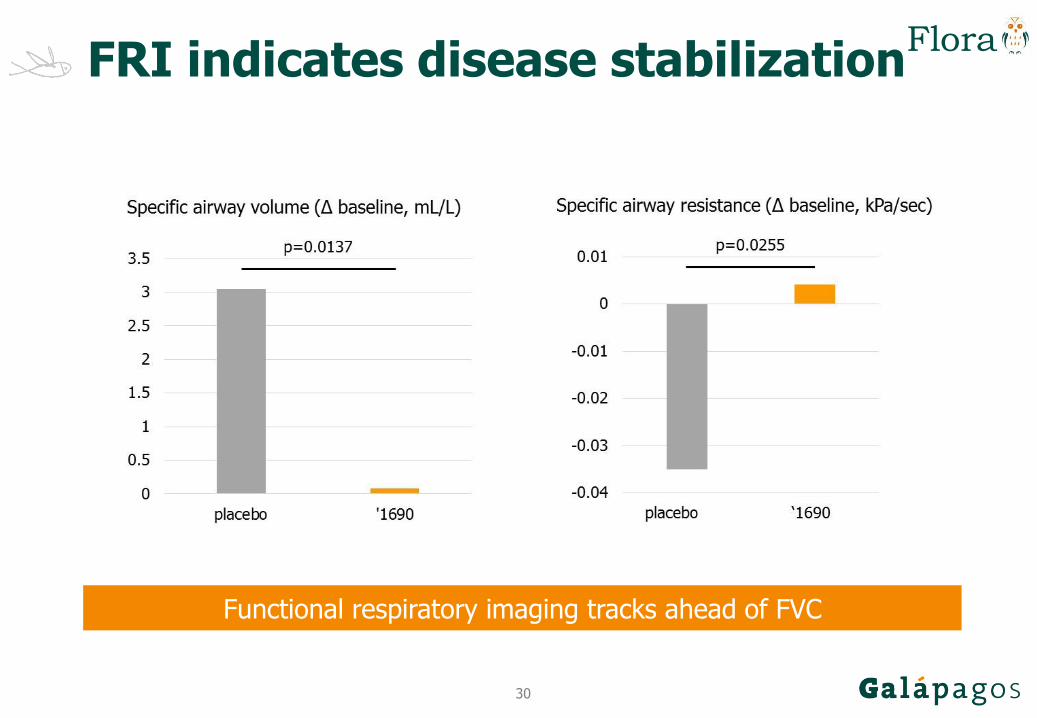
Functional respiratory imaging tracks ahead of FVC
FRI indicates disease stabilization
Flora
31
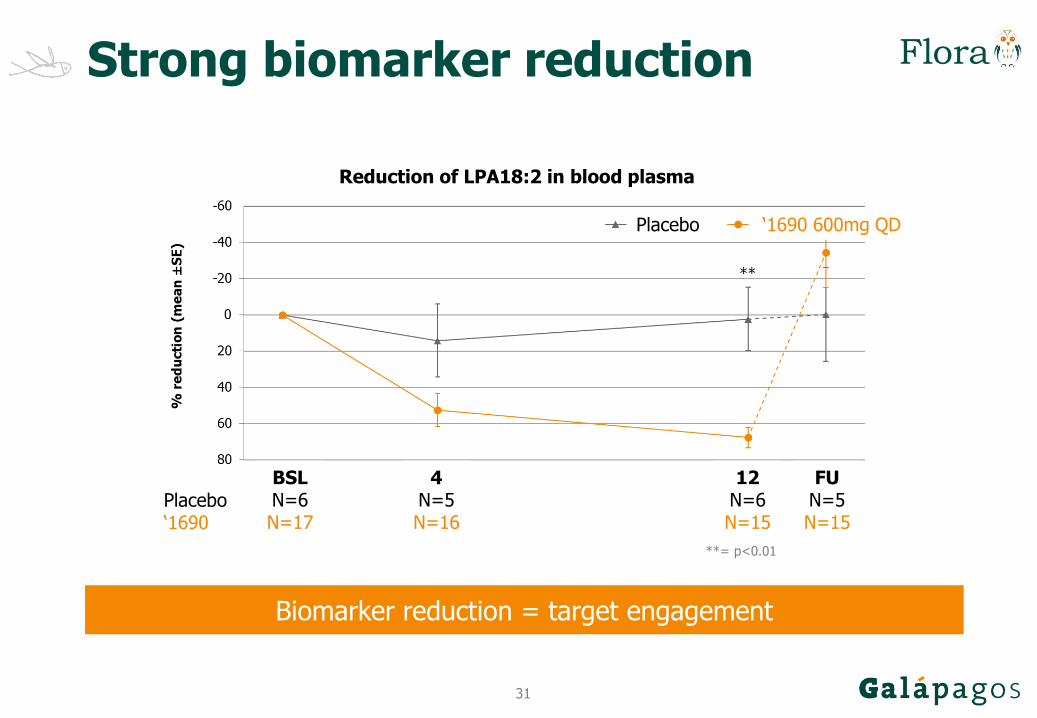
Strong biomarker reduction
Flora
Reduction of LPA18:2 in blood plasma
Biomarker reduction = target engagement
‘1690 600mg QDPlacebo
Placebo‘1690
BSLN=6N=17
**= p<0.01
4N=5N=16
12N=6N=15
FUN=5N=15
32
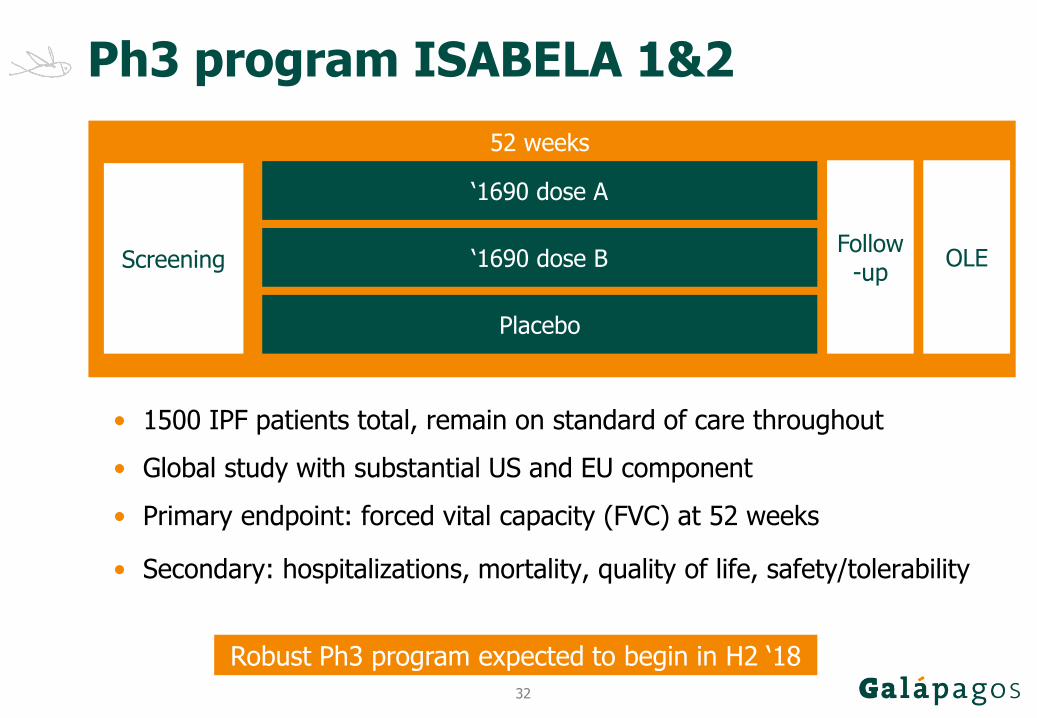
Ph3 program ISABELA 1&2
Topline Part 1 expected Q3 ‘18‘1690 dose B
Placebo
52 weeks
ScreeningFollow
-up
‘1690 dose A
OLE
• 1500 IPF patients total, remain on standard of care throughout
• Global study with substantial US and EU component
• Primary endpoint: forced vital capacity (FVC) at 52 weeks
• Secondary: hospitalizations, mortality, quality of life, safety/tolerability
Robust Ph3 program expected to begin in H2 ‘18
33
Ashcroft score (median)
PBS + veh
icle
BLM +
veh
icle
BLM +
Ninte Q
D, 60m
pk
BLM+G12
3999
9-5
1
2
3
4
5
Sco
re (
media
n)
DiseasedHealthyOfev
60mg/kgqd
‘349910mg/kg
bid
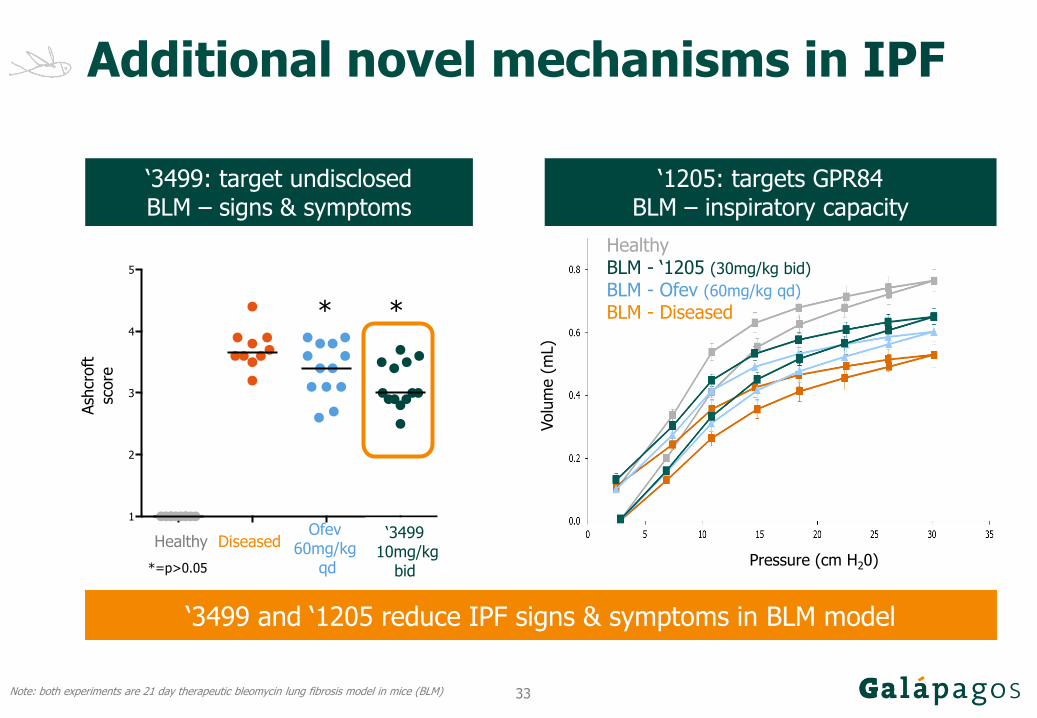
Additional novel mechanisms in IPF
‘3499 and ‘1205 reduce IPF signs & symptoms in BLM model
‘3499: target undisclosedBLM – signs & symptoms
‘1205: targets GPR84BLM – inspiratory capacity
Pressure (cm H20)
HealthyBLM - ‘1205 (30mg/kg bid)
BLM - Ofev (60mg/kg qd)
BLM - Diseased
Note: both experiments are 21 day therapeutic bleomycin lung fibrosis model in mice (BLM)
Volu
me (
mL)
Ash
croft
sc
ore
* *
*=p>0.05

34
• >130 patients, 10 countries, >60 sites in studies to date
• Interim results of 1st triple therapy in patients (FALCON) expected Q3 ‘18
• 2nd triple therapy completed dosing in healthy volunteers
2005 - today 2018 -
Validate triple combo in patients
Discover novel correctors & potentiators
Validate individual components in patients:
Potentiator: SAPHIRA
C1: ALBATROSS, FLAMINGO
C2: PELICAN
CF approach to triple combo
Comprehensive clinical network
Multiple triples in patient studies
Triple studies in US & Europe
35
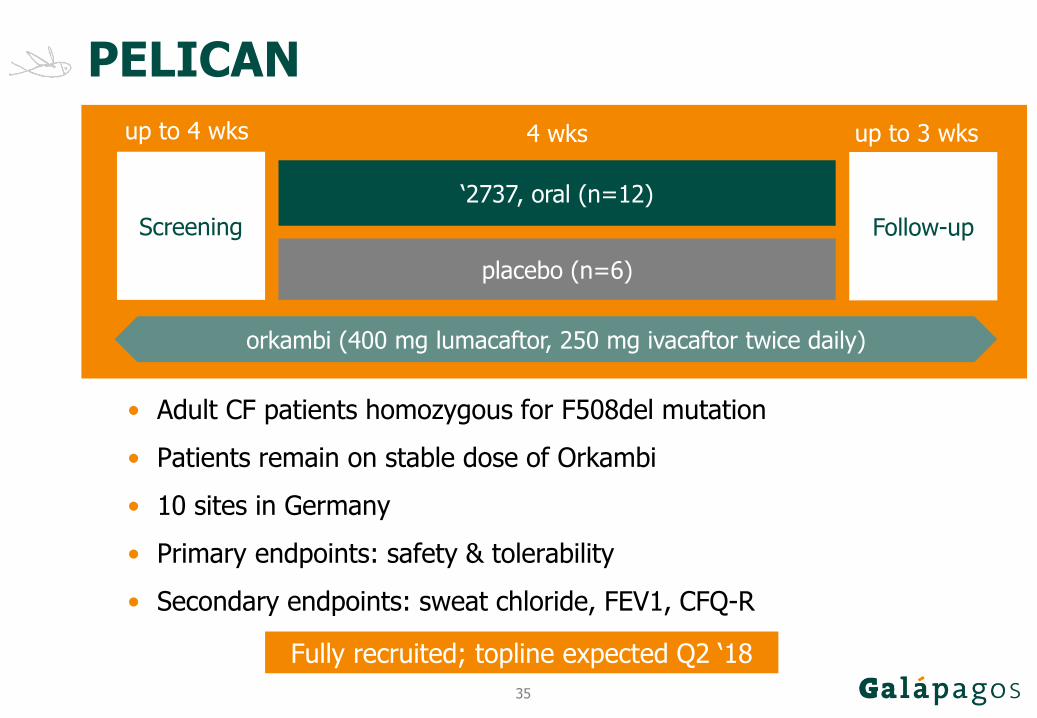
PELICAN
• Adult CF patients homozygous for F508del mutation
• Patients remain on stable dose of Orkambi
• 10 sites in Germany
• Primary endpoints: safety & tolerability
• Secondary endpoints: sweat chloride, FEV1, CFQ-R
Screening
4 wks up to 3 wks
Follow-up
‘2737, oral (n=12)
placebo (n=6)
up to 4 wks
orkambi (400 mg lumacaftor, 250 mg ivacaftor twice daily)
Fully recruited; topline expected Q2 ‘18
36
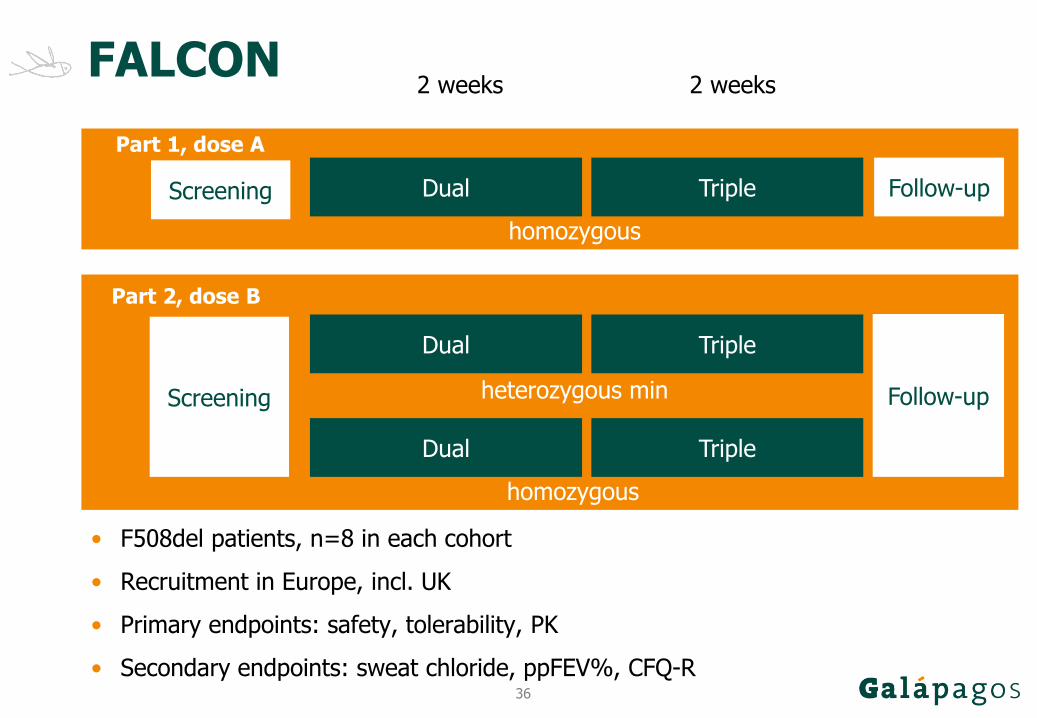
FALCON
• F508del patients, n=8 in each cohort
• Recruitment in Europe, incl. UK
• Primary endpoints: safety, tolerability, PK
• Secondary endpoints: sweat chloride, ppFEV%, CFQ-R
Screening
2 weeks
Follow-upDual
Topline Part 1 expected Q3 ‘18
Triple
2 weeks
Part 1, dose A
homozygous
Dual Triple
Part 2, dose B
Dual Triple
heterozygous min
homozygous
Screening Follow-up
37
‘1972 for osteoarthritis
Targets ADAMTS-5Inhibits cartilage breakdown biomarker in healthy volunteers
Phase 1: clear target engagement, favorable safety & PK
GLPG Ph1b 30-patient study in US: positive dataPh2 start in H1 ‘18
OA: breakdown of joint cartilage118 M patients in US, Europe & JapanNo disease-modifying drugs approved today
38
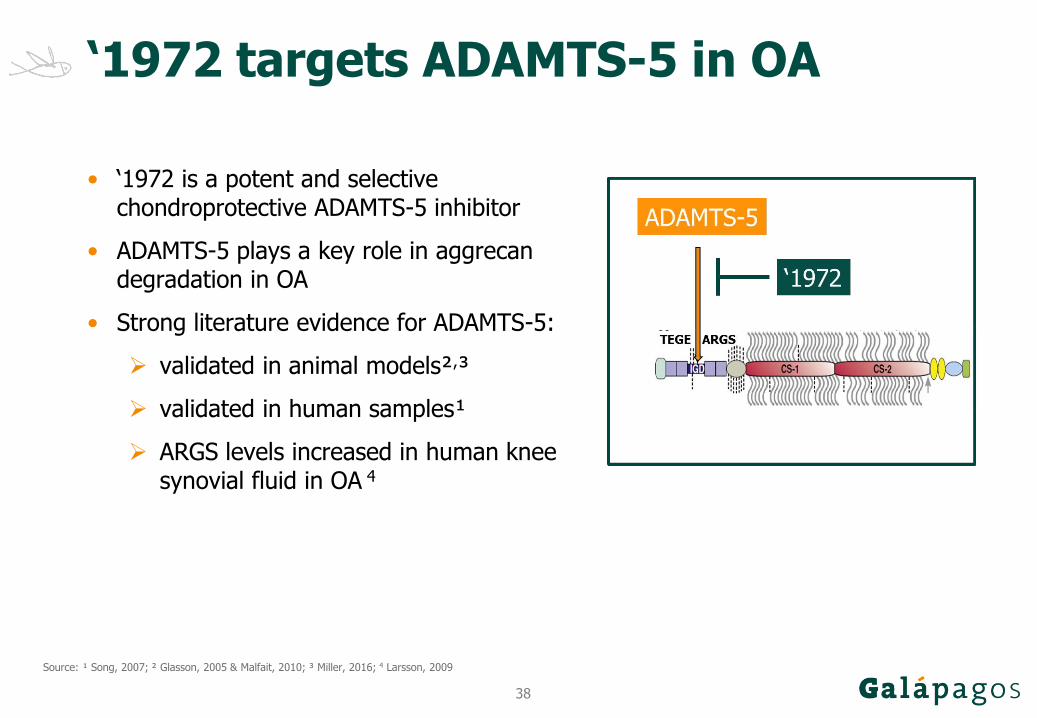
‘1972 targets ADAMTS-5 in OA
• ‘1972 is a potent and selective chondroprotective ADAMTS-5 inhibitor
• ADAMTS-5 plays a key role in aggrecandegradation in OA
• Strong literature evidence for ADAMTS-5:
validated in animal models²,³
validated in human samples¹
ARGS levels increased in human knee synovial fluid in OA 4
Source: ¹ Song, 2007; ² Glasson, 2005 & Malfait, 2010; ³ Miller, 2016; 4 Larsson, 2009
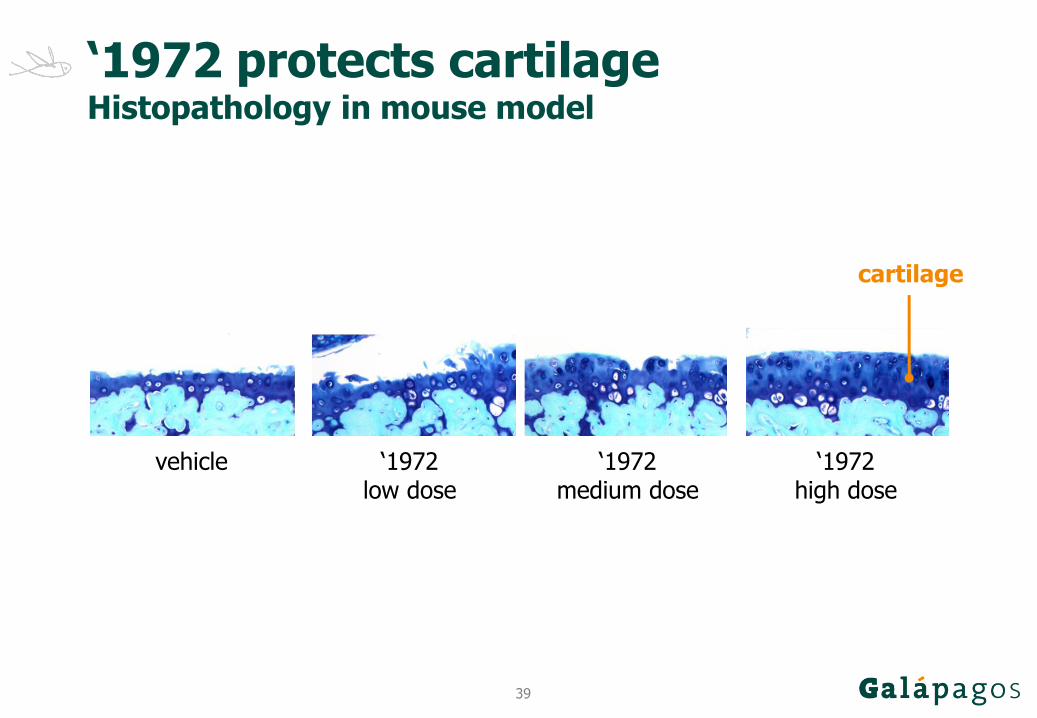
39
‘1972 low dose
‘1972 medium dose
‘1972 high dose
vehicle
‘1972 protects cartilageHistopathology in mouse model
cartilage
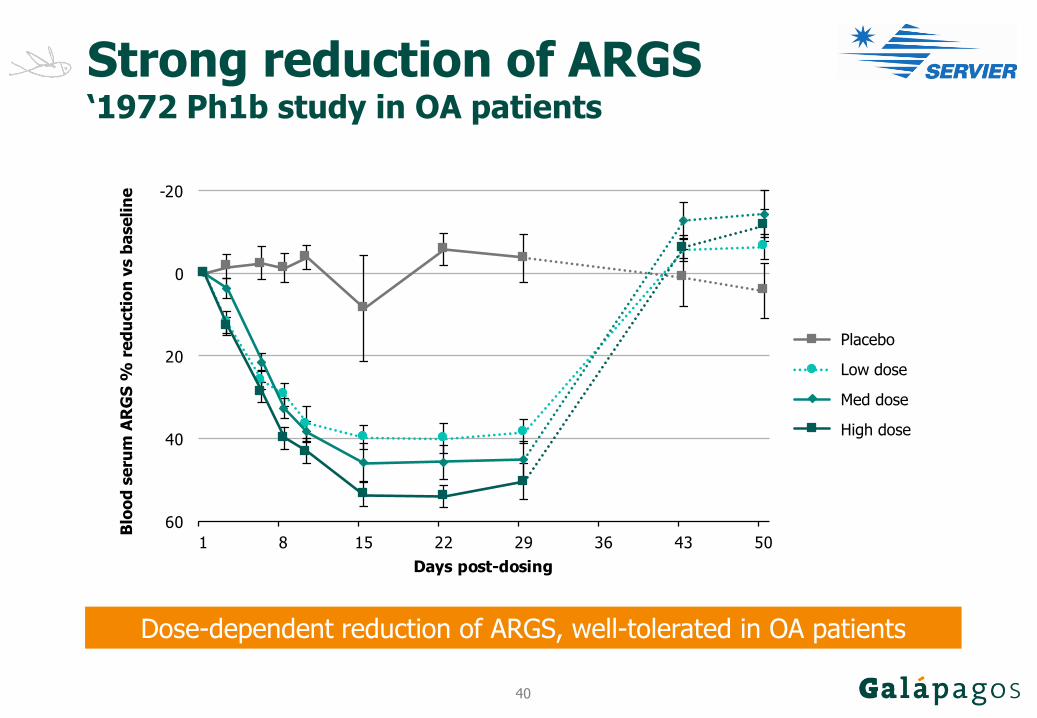
40
Strong reduction of ARGS‘1972 Ph1b study in OA patients
Dose-dependent reduction of ARGS, well-tolerated in OA patients
-20
0
20
40
60
1 8 15 22 29 36 43 50
AR
GS
% r
ed
ucti
on
vs b
aseli
ne
Days post-dosing
placebo
‘1972 dose 1
‘1972 dose 2
‘1972 dose 3
Blo
od
se
rum
AR
GS
% r
ed
ucti
on
vs b
ase
lin
e
Low dose
Med dose
High dose
Placebo
41
MOR106 for atopic dermatitis
AtopicD: disease causing very dry skin, severe itching 35M patients in US, Europe & Japan
First-in-class human MAbNovel MOA: IL-17C target discovered by Galapagos
Ph1 (SAD): favorable safety & PK in healthy volunteers Ph1b (MAD): 83% patients at EASI50 within 4 weeks at highest dose
Ph2 IGUANA study started in Q2 ‘18

42
Dual mode of action
• IL-17C target of MOR106
• Dual action described
• Local amplifier of inflammation
• First-in-class
IL-17A
Source: Haines & Cua, Immunity 2011

43
MOR106 Ph1bEASI, % change from baseline, pooled data, median
-100
-90
-80
-70
-60
-50
-40
-30
-20
-10
0
0 2 4 6 8 10 12 14
% c
hange f
rom
base
line
Weeks after start of treatment
Placebo
MOR106
Infusion
Source: Thaci et al, AAD 2018
44
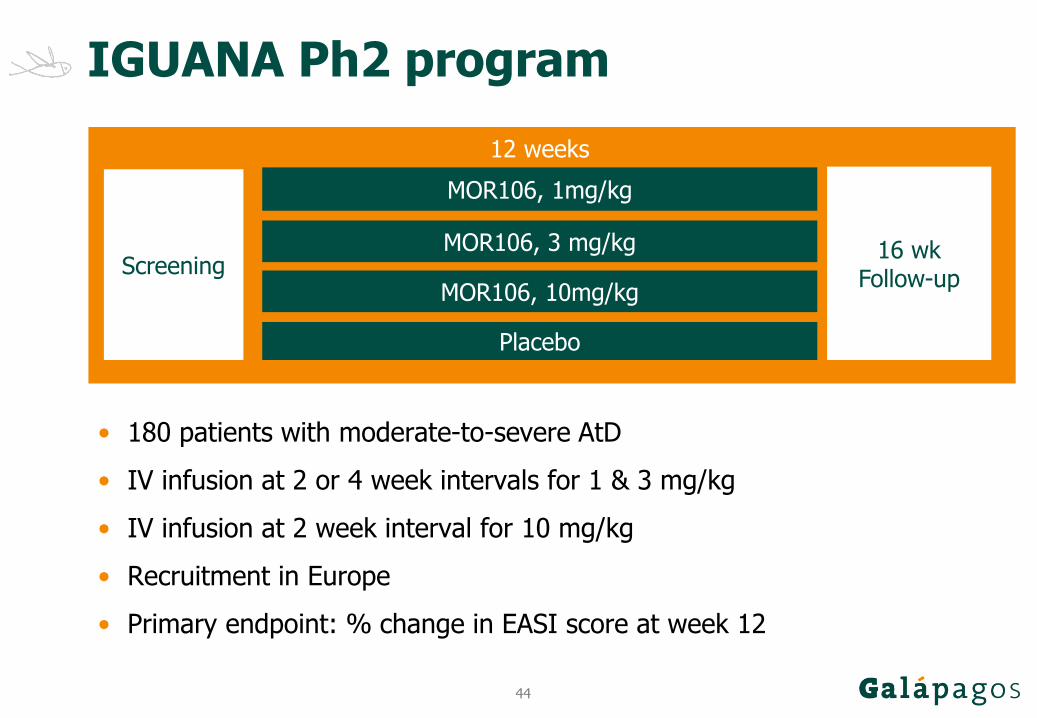
IGUANA Ph2 program
Topline Part 1 expected Q3 ‘18
MOR106, 3 mg/kg
Placebo
12 weeks
Screening16 wk
Follow-up
MOR106, 1mg/kg
• 180 patients with moderate-to-severe AtD
• IV infusion at 2 or 4 week intervals for 1 & 3 mg/kg
• IV infusion at 2 week interval for 10 mg/kg
• Recruitment in Europe
• Primary endpoint: % change in EASI score at week 12
MOR106, 10mg/kg
45
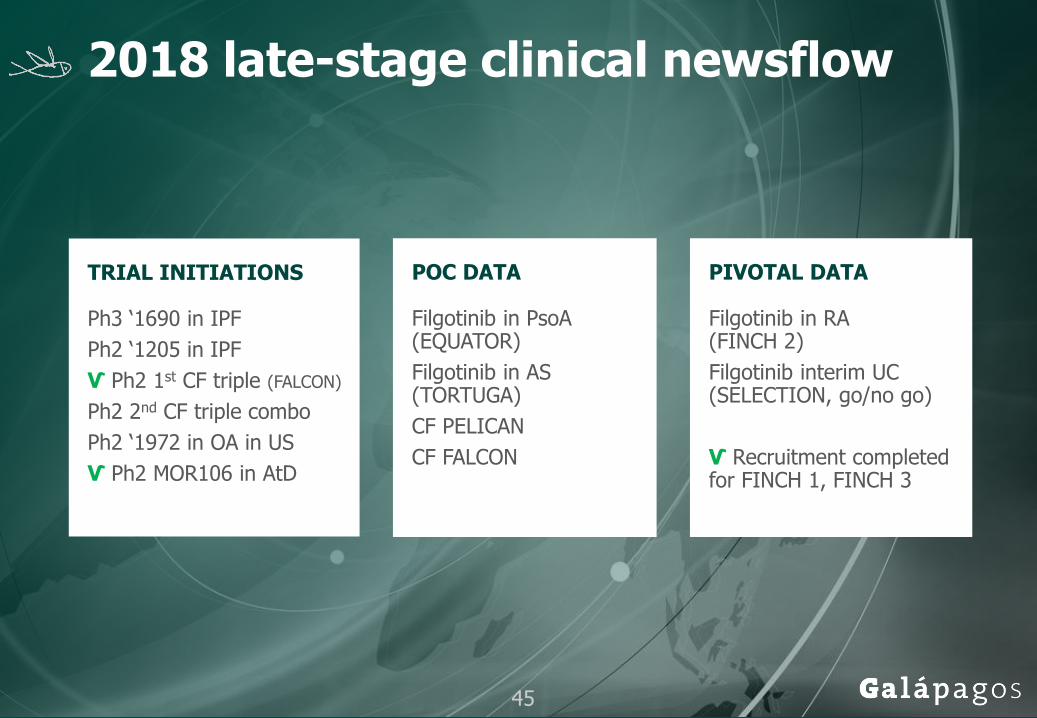
2018 late-stage clinical newsflow
TRIAL INITIATIONS
Ph3 ‘1690 in IPF
Ph2 ‘1205 in IPF
Ѵ Ph2 1st CF triple (FALCON)
Ph2 2nd CF triple combo
Ph2 ‘1972 in OA in US
Ѵ Ph2 MOR106 in AtD
POC DATA
Filgotinib in PsoA(EQUATOR)
Filgotinib in AS (TORTUGA)
CF PELICAN
CF FALCON
PIVOTAL DATA
Filgotinib in RA (FINCH 2)
Filgotinib interim UC (SELECTION, go/no go)
Ѵ Recruitment completed for FINCH 1, FINCH 3
45

glpg.com
47
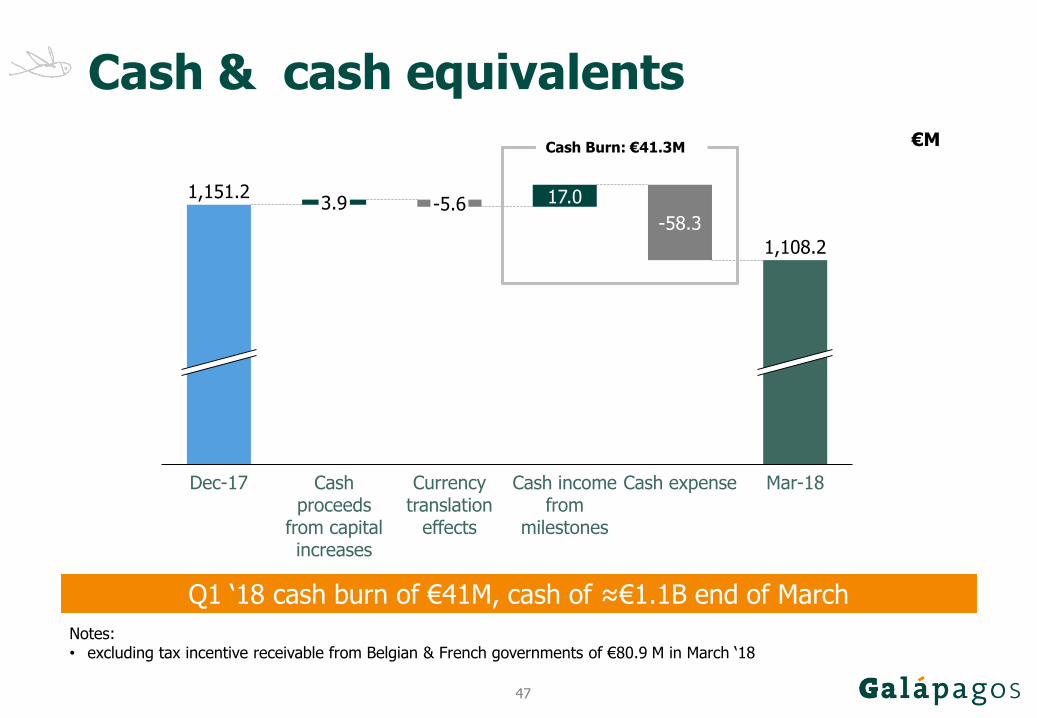
Cash & cash equivalents
17.03.91,151.2
Dec-17 Cash proceeds
from capital increases
-5.6
Currency translation
effects
Cash income from
milestones
-58.3
Cash expense Mar-18
1,108.2
€M
Notes:• excluding tax incentive receivable from Belgian & French governments of €80.9 M in March ‘18
Cash Burn: €41.3M
Q1 ‘18 cash burn of €41M, cash of ≈€1.1B end of March