GABAergic dysfunction in schizophrenia: new treatment strategies on the horizon
15
Psychopharmacology (2005) 180: 191–205 DOI 10.1007/s00213-005-2212-8 REVIEW Alessandro Guidotti . James Auta . John M. Davis . Erbo Dong . Dennis R. Grayson . Marin Veldic . Xianquan Zhang . Erminio Costa GABAergic dysfunction in schizophrenia: new treatment strategies on the horizon Received: 8 September 2004 / Accepted: 11 February 2005 / Published online: 28 April 2005 # Springer-Verlag 2005 Abstract Rationale: Cortical γ-aminobutyric acid (GABA) ergic neurons contribute to the orchestration of pyramidal neuron population firing as follows: (1) by releasing GABA on GABA A and GABA B receptors, (2) by releasing reelin in the proximity of integrin receptors located on cortical pyramidal neuron dendritic spines, and (3) through reelin contributing to the regulation of dendritic spine plasticity by modulating dendritic resident mRNA translation. In schizophrenia (SZ) and bipolar (BP) postmortem brains, the downregulation of mRNAs encoding glutamic acid de- carboxylase 67 (GAD 67 ) and reelin decreases the cognate proteins coexpressed in prefrontal cortex (PFC) GABA ergic neurons. This finding has been replicated in several laboratories. Such downregulation suggests that the neuro- pil hypoplasticity found in the PFC of SZ and BP disorder patients may depend on a downregulation of GABAergic function, which is associated with a decrease in reelin secre- tion from GABAergic neuron axon terminals on dendrites, somata, or axon initial segments of pyramidal neurons. Indirectly, this GABAergic neuron downregulation may play a key role in the expression of positive and negative symptoms of SZ and BP disorders. Objectives: The above described GABAergic dysfunction may be addressed by pharmacological interventions to treat SZ and BP disorders using specific benzodiazepines (BZs), which are devoid of intrinsic activity at GABA A receptors including α 1 subunits but that act as full positive allosteric modulators of GABA action at GABA A receptors containing α 2 , α 3 , or α 5 subunits. These drugs are expected to enhance GABA ergic signal transduction without eliciting sedation, amne- sia, and tolerance or dependence liabilities. Results and conclusions: BZs, such as diazepam, although they are efficient in equilibrating GABA A receptor signal transduc- tion in a manner beneficial in the treatment of positive and negative symptoms of SZ, may not be ideal drugs, because by mediating a full positive allosteric modulation of GABA A receptors containing the α 1 subunit, they con- tribute to sedation and to the development of tolerance after even a brief period of treatment. In contrast, other BZ- binding site ligands, such as 6-(2bromophenyl)-8-fluoro- 4H-imidazo [1,5-a][1,4] benzodiazepine-3-carboxamide (imidazenil), which fail to allosterically and positively mod- ulate the action of GABA at GABA A receptors with α 1 subunits but that selectively allosterically modulate corti- cal GABA A receptors containing α 5 subunits, contribute to the anxiolytic, antipanic, and anticonvulsant actions of these ligands without producing sedation, amnesia, or tol- erance. Strong support for the use of imidazenil in psycho- sis emerges from experiments with reeler mice or with methionine-treated mice, which express a pronounced reelin and GAD 67 downregulation that is also operative in SZ and BP disorders. In mice that model SZ symptoms, imidazenil increases signal transduction at GABA A receptors contain- ing α 5 subunits and contributes to the reduction of be- havioral deficits without producing sedation or tolerance liability. Hence, we suggest that imidazenil may be consid- ered a prototype for a new generation of positive allosteric modulators of GABA A receptors, which, either alone or in combination with neuroleptics, should be evaluated in GABAergic dysfunction operative in the treatment of SZ and BP disorders with psychosis. Keywords GABA A receptors . Imidazenil . Diazepam . Psychoses . Schizophrenia . Bipolar disorder . Reelin . GABA-mimetics . Benzodiazepines . Glutamic acid decarboxylase This work is dedicated to Professor Joseph A. Flaherty on the occasion of his promotion to Dean of the UIC College of Medicine. A. Guidotti . J. Auta . J. M. Davis . E. Dong . D. R. Grayson . M. Veldic . X. Zhang . E. Costa (*) Psychiatric Institute, Department of Psychiatry, University of Illinois at Chicago, 1601 Taylor St, Chicago, IL, 60612, USA e-mail: [email protected] Tel.: +1-312-4134593 Fax: +1-312-4134569
Transcript of GABAergic dysfunction in schizophrenia: new treatment strategies on the horizon

Psychopharmacology (2005) 180: 191–205DOI 10.1007/s00213-005-2212-8
REVIEW
Alessandro Guidotti . James Auta . John M. Davis .Erbo Dong . Dennis R. Grayson . Marin Veldic .Xianquan Zhang . Erminio Costa
GABAergic dysfunction in schizophrenia: new treatment strategieson the horizon
Received: 8 September 2004 / Accepted: 11 February 2005 / Published online: 28 April 2005# Springer-Verlag 2005
Abstract Rationale: Cortical γ-aminobutyric acid (GABA)ergic neurons contribute to the orchestration of pyramidalneuron population firing as follows: (1) by releasing GABAon GABAA and GABAB receptors, (2) by releasing reelinin the proximity of integrin receptors located on corticalpyramidal neuron dendritic spines, and (3) through reelincontributing to the regulation of dendritic spine plasticityby modulating dendritic resident mRNA translation. Inschizophrenia (SZ) and bipolar (BP) postmortem brains,the downregulation of mRNAs encoding glutamic acid de-carboxylase 67 (GAD67) and reelin decreases the cognateproteins coexpressed in prefrontal cortex (PFC) GABAergic neurons. This finding has been replicated in severallaboratories. Such downregulation suggests that the neuro-pil hypoplasticity found in the PFC of SZ and BP disorderpatients may depend on a downregulation of GABAergicfunction, which is associated with a decrease in reelin secre-tion from GABAergic neuron axon terminals on dendrites,somata, or axon initial segments of pyramidal neurons.Indirectly, this GABAergic neuron downregulation mayplay a key role in the expression of positive and negativesymptoms of SZ and BP disorders. Objectives: The abovedescribed GABAergic dysfunction may be addressed bypharmacological interventions to treat SZ and BP disordersusing specific benzodiazepines (BZs), which are devoidof intrinsic activity at GABAA receptors including α1
subunits but that act as full positive allosteric modulatorsof GABA action at GABAA receptors containing α2, α3,or α5 subunits. These drugs are expected to enhance GABAergic signal transduction without eliciting sedation, amne-sia, and tolerance or dependence liabilities. Results andconclusions: BZs, such as diazepam, although they areefficient in equilibrating GABAA receptor signal transduc-tion in a manner beneficial in the treatment of positiveand negative symptoms of SZ, may not be ideal drugs,because by mediating a full positive allosteric modulationof GABAA receptors containing the α1 subunit, they con-tribute to sedation and to the development of toleranceafter even a brief period of treatment. In contrast, other BZ-binding site ligands, such as 6-(2bromophenyl)-8-fluoro-4H-imidazo [1,5-a][1,4] benzodiazepine-3-carboxamide(imidazenil), which fail to allosterically and positively mod-ulate the action of GABA at GABAA receptors with α1
subunits but that selectively allosterically modulate corti-cal GABAA receptors containing α5 subunits, contributeto the anxiolytic, antipanic, and anticonvulsant actions ofthese ligands without producing sedation, amnesia, or tol-erance. Strong support for the use of imidazenil in psycho-sis emerges from experiments with reeler mice or withmethionine-treated mice, which express a pronounced reelinand GAD67 downregulation that is also operative in SZ andBP disorders. In mice that model SZ symptoms, imidazenilincreases signal transduction at GABAA receptors contain-ing α5 subunits and contributes to the reduction of be-havioral deficits without producing sedation or toleranceliability. Hence, we suggest that imidazenil may be consid-ered a prototype for a new generation of positive allostericmodulators of GABAA receptors, which, either alone or incombination with neuroleptics, should be evaluated inGABAergic dysfunction operative in the treatment of SZand BP disorders with psychosis.
Keywords GABAA receptors . Imidazenil . Diazepam .Psychoses . Schizophrenia . Bipolar disorder . Reelin .GABA-mimetics . Benzodiazepines . Glutamic aciddecarboxylase
This work is dedicated to Professor Joseph A. Flaherty on theoccasion of his promotion to Dean of the UIC College of Medicine.
A. Guidotti . J. Auta . J. M. Davis . E. Dong . D. R. Grayson .M. Veldic . X. Zhang . E. Costa (*)Psychiatric Institute, Department of Psychiatry,University of Illinois at Chicago,1601 Taylor St,Chicago, IL, 60612, USAe-mail: [email protected].: +1-312-4134593Fax: +1-312-4134569

Introduction
By regulating pyramidal neuron firing rates, γ-aminobu-tyric acid (GABA)ergic interneurons play an important rolein modulating the cortical signal transduction operative ininformation processing (Mountcastle 1998; McBain andFisahn 2001; Crick and Koch 2003). As an example, byreleasing GABA, prefrontal cortex (PFC) fast-spiking in-terneurons modulate the intermittent firing mode of pyra-midal neurons operative in circuits attending perceptions,emotions, learning, and memory (Sawaguchi et al. 1989;Rao et al. 1999, 2000; Benes and Berretta 2001; Sawaguchiand Iba 2001; Carter et al. 1999). A deficit or an excess ofGABA released from inhibitory interneuron axon terminalson GABAA or GABAB receptor subtypes located on den-dritic shafts, somata, or initial axon segments of pyrami-dal neurons influence their rhythmic excitability and theirfunctional output. Often, these changes are facilitatedor re-pressed by drugs or environmental stimuli that contributeto sensory perception distortions and cognitive function im-pairments. In extreme cases, lasting changes in GABAergictone bring about seizures, sedation, or even induce deep-sleep activity (Benes and Berretta 2001; Costa et al. 2001a;Hensch and Stryker 2004; Fagiolini et al. 2004). CorticalGABAergic interneurons (particularly in layers I to III), inaddition to GABA, coexpress and release reelin at synapses(Costa et al. 2001b; Rodriguez et al. 2002).
Reelin is an extracellular matrix (ECM) protein criticalfor brain function (for review, see Rice and Curran 2001)that regulates synaptic plasticity as it relates to long-termpotentiation (LTP) (Weeber et al. 2002) and protein syn-thesis in neuronal dendrites and their spines. This mecha-nism likely involves reelin binding to integrin receptors andthe activation of spine-resident mRNA translation (Donget al. 2003).
Dysfunction of cortical GABAergic neurotransmission inSZ and BP disorders
In physiological conditions, GABA and reelin modulatevarious aspects of cortical activities including cortical cir-cuitry plasticity (Jones 1993; Benes 2000; Selemon andGoldman-Rakic 1999; Costa et al. 2001b; Weeber et al.2002; Niu et al. 2004; Hensch and Stryker 2004), synchro-nous intermittent firing of cortical pyramidal neuron pop-ulation assemblies (Mountcastle 1998; Jones 2000;McBainand Fisahn 2001), and cortical information processes(Sawaguchi et al. 1989; Rao et al. 1999, 2000; Sawaguchiand Iba 2001, Carter et al. 1999; Crick and Koch 2003).
Thus, it is not surprising that the extent of glutamicacid decarboxylase 67 (GAD67) and reelin downregula-tion in PFC GABAergic neurons of schizophrenia (SZ)or bipolar (BP) disorder patients (Akbarian et al. 1995b;Impagnatiello et al. 1998; Fatemi et al. 2000; Guidotti et al.2000; Volk et al. 2000; Benes and Berretta 2001; Eastwoodand Harrison 2003; Knable et al. 2004;Woo et al. 2004) has
been associated with (1) the pyramidal neuron hypoplas-ticity, (2) the reduction of dendritic spine density (Selemonand Goldman-Rakic 1999; Rosoklija et al. 2000; Glantzand Lewis 2001; Black et al. 2004), (3) an alteration ofhigh speed synchronous cortical neuron population firing(Spencer et al. 2004), and (4) a working memory deficit andsymptoms of SZ (Perlstein et al. 2001; Spencer et al. 2004).Interestingly, PFC GABAergic downregulation is consis-tently associated with psychosis but has not been detected inmajor depression without psychosis (Guidotti et al. 2000).Thus, an important component underlying psychotic think-ing appears to be a deficit in the cortical GABAergic or-chestration of pyramidal neuron intermittent populationfiring.
To fully appreciate the importance that a primary corticalGABAergic transmission defect may have on SZ and BPdisorder morbidity, one may have to reach a better un-derstanding of the GABAergic neuron subtypes that aredefective in psychoses. This includes the need to identifythe location of the defective GABAergic axon terminalcontacts presynaptically and to identify the compensatorychanges in GABAA receptor subtypes expressed at den-drites, somata, or initial axon segments of glutamatergicpyramidal neurons postsynaptically (Table 1).
Table 1 Dysfunction of cortical GABAergic transmitter system inchronic psychosis
(1) The presynaptic component: a primary defect of corticalGABAergic interneurons?
↓GAD67 Benes et al. 1992; Akbarian et al. 1995a,b;Guidotti et al. 2000; Volk et al. 2000;Woo et al. 2004; Veldic et al. 2005
↓Reelin Fatemi et al. 2000; Guidotti et al. 2000;Eastwood and Harrison 2003; Veldic et al.2004; Abdolmaleky et al. 2005
↓GAT-1 Woo et al. 1998↓Parvalbumin Lewis et al. 2004↓NR2A Woo et al. 2004(2) The postsynaptic component: compensatory alterations inpyramidal neurons?(a) GABAA receptor upregulation↑3H muscimolbinding
Hanada et al. 1987; Benes et al. 1992,1996a,b; Dean et al. 2001
↑GABAA α1,α2,α5
mRNAsImpagnatiello et al. 1998;Lewis et al. 2004
↑GABAA α1,α2,α5
proteinsIshikawa et al. 2004; Lewis et al. 2004
(b) Neuropil hypoplasticity↓Dendritic spines Glantz and Lewis, 2001; Rosoklija
et al. 2000
GAD Glutamic acid decarboxylase, GAT1 GABA membranetransporter 1, NR2AN-methyl-D-aspartate receptor subunit 2A
192

The presynaptic component as a primary defect ofcortical GABAergic neurons in SZ and BP disorders
Heterogeneity of cortical GABAergic neurons
In primate neocortices, the density and morphology ofGABAergic inhibitory interneurons varies in different lay-ers [from 20 to 30% in the deep cortical layers to about 90%in layer I (Rodriguez et al. 2002)]. Every GABAergic neu-ron releases GABA but not every GABAergic neuron syn-thesizes, stores, or releases reelin (Rodriguez et al. 2002).Similar heterogeneity should be considered for the GABAergic neuronal proteins parvalbumin (PV) and calretinin(CR), which are coexpressed but not secreted with GABA.
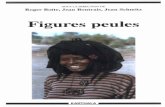
Double bouquet, basket, and chandelier cells are themost abundant cortical GABAergic interneuron subtypes(Fig. 1). Each of these subtypes establishes synapses withup to 200–250 different pyramidal neurons (Peters 1984;DeFilipe and Farinas 1992).
Because the firing frequency of the cortical GABAergicinterneurons is consistently the highest among the firingfrequencies of the other cortical neurons, these interneur-ons play a pivotal role in orchestrating the intermittentsynchronous population-firing pattern of pyramidal neu-rons (Peters 1984; DeFilipe and Farinas 1992; Jones 1993;Mountcastle 1998). This intermittent synchronous neuro-nal activity appears to be very important for cortical so-matosensory information processing. Furthermore, in theneocortex, this activity has been frequently associated withsensory representations (Mountcastle 1998; Carter et al.1999; McBain and Fisahn 2001; Crick and Koch 2003).
GABAergic neuron axon terminals synapse on differentreceptorial fields of pyramidal neurons (i.e., cell bodies,dendrites, and dendritic spine necks, or axon hillocks) (Fig. 1),providing a tailor-made control over the functional regula-tion of excitatory principal neurons (DeFilipe and Farinas1992). For example, basket cells in layers II, III, V, and VI,which innervate pyramidal cell somata and proximal den-drites (Fig. 1) (Halasy et al. 1996), modulate pyramidal cellfiring rates. In contrast, chandelier interneurons that syn-apse on the axon initial segment of pyramidal neurons in themiddle cortical layers (Fig. 1) can block action potentialgeneration at axon hillocks (Mountcastle 1998). Interneu-rons that innervate shafts of dendrite branches (i.e., doublebouquet in layers II and III or horizontal cells in layer I)influence the amplitude of glutamate-mediated dendriticvoltage-gated currents at restricted sites distal from thepyramidal neuron somata modulating local dendritic Ca2+-dependent action potentials (Miles et al. 1996).
Two isoforms of glutamic acid decarboxylase
In GABAergic neurons, the synthesis of GABA from glu-tamate depends on the expression of twomolecular forms ofglutamic acid decarboxylase (GAD), which are the rate-limiting enzymes in GABAbiosynthesis. These two distinctGAD isoforms have been termed GAD67 and GAD65 be-cause of their difference in molecular size (Soghomonianand Martin 1998). GAD67 and GAD65 differ in their struc-ture to allow for differences in their regulatory mechanisms.GAD67 expresses high-affinity binding for the cofactorpyridoxal phosphate and because of the saturation of thishigh-affinity binding site by tissue cofactor levels, the up-regulation of GAD67 activity is independent from the co-factor, but depends on the rate of new GAD67 mRNAtranslation (Soghomonian and Martin 1998). In contrast,GAD65 fails to express a high-affinity binding site for thecofactor and responds to GABAergic neuron depolarizationwith an upregulation of the enzyme affinity for the cofac-tor. Thus, GAD67 is physiologically regulated by a changein enzyme biosynthesis that is much faster than that ofGAD65.
While it is hypothesized that every GABAergic neuronexpresses both molecular forms of GAD, this hypothesishas not yet been thoroughly investigated. The necessity forthis type of scrutiny is becoming critically important toreaching a better understanding of the details of GABAfunction. This, in turn, is operative in the regulation of thestrength of excitatory glutamatergic afferents impinging onthe postsynaptic densities expressed in the head of corticalpyramidal neuron dendritic spines.
GABA and reelin: searching for a functional rolefor their neuronal coexistence
Neurochemical properties and emerging principles ofneuronal function (McBain and Fisahn 2001) indicate thatGABAergic interneurons play a far more complex role in
GABAergic Neurons B: large basket DB: Double Bouquet Ch: chandelier Ng: neurogliaform SB: small basket α2
α1
α1 α5
α5
NPS
α1
SZPGABAergic Tone Downregulation
α2
α1
α5
α5
Normal GABAergic Tone
α1α1
Fig. 1 Outline of principal cortical neuronal circuits in SZP (left)and NPS (right) (from Jones 1993, modified). Open circle NormalGABAergic interneurons. Filled triangle Layer V pyramidal glu-tamatergic neurons receiving normal GABAergic innervation. Filledcircle Downregulated GABAergic interneurons. Filled triangle witha filled circle Layer V pyramidal neurons receiving deficient GABAergic innervation. α GABAA receptor subunits. Note: The increasein α5 and α2 subunit expression in somata, dendrites, and axon hill-ocks of pyramidal neurons of SZP is indicated by a larger α symbol
193

cortical function than simply providing pyramidal neuronswith a rhythmic firing inhibition. Neurochemically, GABAergic interneurons have been classified by the expression ofspecific functionally important proteins. For example, se-lective interneurons express GABA associated with eitherreelin (Costa et al. 2001b) or two calcium-binding proteins(PV, CR) (Lewis et al. 2004). Reelin is constitutively re-leased from GABAergic interneurons into the ECM andplays a role in the regulation of extrasomatic protein syn-thesis (Dong et al. 2003). In contrast, PV and CR are notreleased extracellularly and their functional role in GABAergic transmission at the molecular level is not preciselyknown. Because PV and CR are calcium-binding proteins,they likely contribute to intracellular Ca2+ homeostasis andprobably modulate the activity of transcription factors incooperation with RNA polymerase II.
Although in humans, different levels of reelin are ex-pressed in different GABAergic neurons (higher in hori-zontal and bitufted cells and lower in basket and chandeliercells) (Guidotti et al. 2000), studies in primates suggest thatthe majority of GABAergic neurons in layers I, II, and IIIof PFC express reelin; however, only 30–50% of GABAergicneurons in layers V and VI express this protein (Rodriguezet al. 2002). Reelin, once released into the ECM, interactswith specific receptors including various integrin receptorsubtypes expressed in postsynaptic densities of pyramidalneuron dendrites. Reelin also contributes to the regulationof dendritic protein synthesis attendant to spine and neu-ropil plasticity (Dong et al. 2003). When recombinantreelin is applied to rat hippocampal slices, it enhances theinduction of LTP (Weeber et al. 2002); however, whenapplied to dissociated neuronal cultures of heterozygousreeler mouse hippocampus characterized by dendritic hy-poplasticity, it normalizes the expression of dendritic ar-borization (Niu et al. 2004).
When recombinant reelin is applied to cortical synapto-neurosome preparations, it modulates extrasomatic mRNAtranslation including that of the activity-regulated cytoskel-etal (Arc) protein. This modulation can be blocked byspecific integrin receptor antagonists (Dong et al. 2003),reinforcing the view that integrins are targets for a reelin-mediated signal transduction cascade. The dendritic syn-thesis of Arc and of other cytoskeletal proteins occurring inthe proximity of dendritic spine postsynaptic densitiesmodulates spine morphology and presumably the long-termplasticity operative in LTP as it relates to learning, memory,and cognitive function (Weeber et al. 2002). This plastici-ty is disrupted when the translation of dendritic residentmRNAs encoding Arc and for other regulatory proteins isreduced (Dong et al. 2003). Reelin–integrin receptor inter-actions may activate cytosolic tyrosine kinases that inducephosphorylation-mediated adapter protein functions (i.e.,DAB1) (Rice and Curran 2001). These include the ac-tivation of various polymerases that polyadenylate den-drite-resident mRNAs, thereby regulating their translation(Stewart and Schuman 2003). One may speculate that thevarious cortical GABAergic interneuron subtypes are likelyto orchestrate the release pattern of GABA and/or trophic
neuromodulators (i.e., reelin) that affect dendritic spineplasticity and indirectly influence learning and memory.
Is a selective population of GABAergic neurons alteredin SZ and BP disorders?
Several neuropathological studies of postmortem humanbrain have reported alterations of cortical GABAergic neu-rons in patients with SZ and BP disorders. These changesinclude a decrease in: (1) GAD67, (2) reelin, (3) GABAmembrane transporter 1 (GAT1), and (4) PV (Table 1).
To clarify the role of these neurochemical changes, whichmay influence the expression of psychotic symptoms in SZand BP patients by downregulating the level or rate ofGABA or reelin secretion, one can assess: (1) the number ofGABAergic neurons present in different cortical areas thatalso express reelin, (2) the cortical interneuron subtypes thatexpress the specific changes of GAD67 or GAD65, and (3)the type of GABAergic neurons that express either a down-regulation of reelin expression or a decrease in GAT1 in SZand BP patients. It is pertinent to state that the decreasedexpression of reelin, GAD67, GAT1, or PV in SZ and in BPpatients is unrelated to postmortem interval, dose, or dura-tion of antipsychotic medication. Even those psychiatricpatients who have never received antipsychotic treatmentexpress a downregulation of GAD67 and reelin (proteinsand mRNAs). Since protracted haloperidol treatment of rats(Impagnatiello et al. 1998) or of monkeys (Volk et al. 2000,2001) failed to change reelin, GAD67, andGAT1 expressionin the PFC, one could infer that antipsychotic medicationsper se fail to change reelin, GAD67, andGAT1 expression inSZ and BP patients.
Downregulation of proteins and mRNA in SZ and BPdisorders: is this a promoter dysfunction or a reductionin neuronal number?
Although several reports suggest that the number of non-pyramidal neurons is decreased in the telencephalon of SZand BP patients (for review, see Benes 2000), one may notethat this decrease has been strictly localized in cortical layerII. Hence, this decrease may not account for the 30–50%decrease in GAD67 or reelin expression estimated withquantitative RT-PCR in different cortical areas of SZ andBP disorder patients (Impagnatiello et al. 1998; Guidottiet al. 2000). The selective decrease in the number of non-pyramidal neurons in layers II of SZP would not explainthe large (30–50%) decrease in GAT1 expression in chan-delier cell axon terminal cartridges that has been estimatedin middle cortical layers of SZ brains by immunohisto-chemistry (Lewis et al. 2004). In addition, a lack of a con-comitant decrease in GAD65 expression has been reportedin the PFC of any given patient who also shows a decreasein GAD67 and reelin (Guidotti et al. 2000). Thus, we(Guidotti et al. 2000) and others (Lewis et al. 2004; Wooet al. 2004) have inferred that the decreases in GAD67 andreelin and the decreases in GAT-1 and PV expression ob-
194

served in SZ or BP patients are unrelated to neuronal lossand very likely represent a promoter-related downregula-tion of gene expression in selective GABAergic interneurons.
Immunohistochemical and in situ hybridization studieshave reported that a GAD67 deficit is particularly evident inthe middle cortical layers where it is probably selectivelyrestricted to chandelier cells (Lewis et al. 2004). However,there is also evidence that the decrease in GAD67 and reelinexpression is not restricted to cortical chandelier cellsbecause this decrease is also found in other GABAergicneurons in layers I, II and IV in SZ (Akbarian et al. 1995b;Woo et al. 2004; Veldic et al. 2004, 2005) and layer II in BP(Woo et al. 2004). Moreover, this decrease is also general-ized to different brain areas including the hippocampus(Impagnatiello et al. 1998; Heckers et al. 2002) and there-fore likely represents a systemic defect of gene expressionin various subtypes of GABAergic neurons.
The hypothesis that selective GABAergic neurons aredysfunctional and express a downregulation of specificgenes is strongly supported by a selective increase in DNA-methyltransferase-1 (DNMT1) expression in GABAergicneurons of layers I, II, and IV. This increase, determined byunbiased three-dimensional counts, was found in patientswith SZ and BP disorders with psychosis, but not in patientswith BP disorder without psychosis (Veldic et al. 2004, 2005).
In our laboratory, we have begun to study the DNAmethylation (D.R. Grayson, unpublished data) associatedwith the overexpression of DNMT1 in GABAergic neurons(Veldic et al. 2005). In future studies, it will be important toestablish the mechanisms that elicit this increased expres-sion of DNMT1 in GABAergic neurons of SZ patients. Infact, in the treatment of SZ, the reversal of the DNMT1overexpression elicited by the association of valproate withantipsychotics (Veldic et al. 2005) justifies the success thatthe coadministration of antipsychotics and valproate hasgained during the last few years (Wassef et al. 2003).
Postsynaptic component: GABAA
receptor upregulation
The influence of GABA released from presynaptic axonterminals onto synapses located at dendritic spine, somata,or axon initial segment of pyramidal neurons is determinedby the particular type of postsynaptic GABA receptor atwhich GABA binds (Table 1; Fig. 1). Three types of GABAreceptors have been identified. GABAA and GABAC recep-tors are ionotropic, whereas the GABAB receptor is meta-botropic and coupled to a GTP-binding protein.
Several studies have reported alterations of GABAA re-ceptors in SZ (Hanada et al. 1987; Benes et al. 1992;Impagnatiello et al. 1998; Lewis et al. 2004; Ishikawa et al.2004). In contrast, there are only few studies indicating thatthe GABAB receptor is downregulated in the hippocampusor in the entorinal and temporal cortices in SZ (for review,see Wassef et al. 2003). Although these studies suggest aputative GABAB receptor involvement in the pathophys-iology of SZ, clinical studies investigating the beneficialeffects of GABAB receptor agonists in the treatment of SZ
have been largely negative (Lees et al. 1977; Skausig andKorsgaard 1977). To the best of our knowledge, there are nostudies published on a modification of GABAC receptorexpression in brains of SZ or BP disorder patients.
We now summarize information concerning changes inGABAA receptor subtype expression in SZ as a backgroundto address the hypothesis that selective positive allostericmodulators specific to certain GABAA receptor subtypesmay deserve consideration as prospective therapies for anew pharmacological intervention for psychotic disorders.
GABAA receptor
GABAA receptors are heteropentameric structures thatinclude various subtypes composed of different combina-tions of α, β, and γ subunits (Barnard 2001). It is believedthat GABAA receptors express two GABA-binding sites
Fig. 2 Immunostaining depicting the distribution of GABAA re-ceptor α1 and α5 subunits in a BA9 (layer III) section of a NPS. A.GABAA α1 receptor subunit immunostaining. Notice intense stainingin somata of pyramidal neurons and small interneurons (polyclonalantibody 1:1,000, Upstate Lake Placid, NY). B. GABAA α5 receptorsubunit immunostaining. Notice intense staining in somata and apicaldendrites of pyramidal neurons (polyclonal antibody 1:1,000, NovusBiological, Littleton, CO). C. Typical example (large magnification)of GABAA α5 receptor subunit immunoreactivity in a pyramidalneuron and its apical dendrite. In this photomicrograph, for clarity theapical dendrite surrounding was eliminated. (For immunolabelingmethod details, see Rodriguez et al. 2002; Veldic et al. 2004). GABAAα1 andα5 receptor subunit antibody specificity was tested byWesternblot analyses of human PFC extracts. After 10% SDS/PAGE andblotting, a major band of immunoreactivity with the expected mo-lecular weight was detected with each antibody
195

(located on β subunits) on which this transmitter can bind.In addition, these receptors express a complementary pock-et at the interface between the α and γ subunits, wherebenzodiazepines bind and trigger the allosteric modulatoryaction for GABA (Costa and Guidotti 1996; Barnard 2001).So far, a large number of molecular forms (6α, 4β, and 3γ)of GABAA receptor subunits have been identified. There-fore, it is highly probable that neurons of the brain expressa considerable heterogeneity of GABAA receptor subtypes(Sieghart 1995; Costa and Guidotti 1996; Barnard 2001).Moreover, each of these subtypes possesses a distinct af-finity for GABA and for different BZs.
In the mammalian brain, GABAA receptor α subunitshave a very specialized regional cellular and subcellulardistribution (Fritschy and Möhler 1995). For example, inthe cortex, the most abundant GABAA receptor subunit isthe α1 subunit that is abundant in cell bodies and proximaldendrites of pyramidal neurons and in cell bodies ofGABAergic interneurons (Figs. 1, 2a). Cortical α5 subunitsare less abundantly expressed than the α1 subunits, but theyare concentrated in pyramidal neuron somata (layers III, V,and VI) and in their apical dendrites (Figs. 1, 2b; Akbarianet al. 1995a). Furthermore, α2 subunits in the cortex arelocalized in the somata and also very consistently in the
1.0
0.8
0.6
0.4
0.2
3 4 5 61
2 3 4 5 610
2 3 4 5 6100
2 3
1.0
0.8
0.6
0.4
0.2
4 6 81
2 4 6 810
2 4 6 8100
2
1.0
0.8
0.6
0.4
0.2
Cur
rent
s (I
/Imax
)
3 4 5 61
2 3 4 5 610
2 3 4 5 6100
2 3
D VDiazepam(200nM)
(5nM)IV Imidazenil
Zolpidem(300nM) (300nM)
GABA(µM) GABA(µM)
Z V
α1 1.0
0.8
0.6
0.4
0.2
0.03 4 5 6
12 3 4 5 6
102 3 4 5 6
1002 3
1.0
0.8
0.6
0.4
0.2
0.04 6 8
12 4 6 8
102 4 6 8
1002
1.0
0.8
0.6
0.4
0.2
0.0
Cur
rent
s (I
/Imax
)
4 6 81
2 4 6 810
2 4 6 8100
2
Diazepam(200nM)
Imidazenil(5nM)
Zolpidem
VZ
VI
V
D
α5
Fig. 3 Diazepam (D), imidazenil (I), and zolpidem (Z) activities onhuman α1 and α5 recombinant GABAA receptors. Cl− current in-tensity elicited by various concentrations of GABA in HEK 293 cellstransfected with human α1 (α1,β2,γ2) or α5 (α5,β2,γ2) GABAAreceptors was studied with the patch-clamp technique (whole cellconfiguration) as described by Costa et al. (2002a). The GABAEC50(μM) was 16±1.8 for the recombinant α1 GABAA receptors and 6.9±
1.2 for the recombinant α5 GABA receptors. The concentrations ofdiazepam (D), zolpidem (Z), and imidazenil (I) used in the ex-periments were twice the concentrations required to elicit maximalpotentiation of Cl− current intensities in recombinant α1 GABAAreceptors for diazepam and zolpidem, and maximal potentiation inrecombinant α5 GABAA receptors for imidazenil. V Vehicle. Eachvalue is the mean±SE of three experiments
196

axon initial segments of pyramidal neurons (Nusser et al.1996; Fritschy et al. 1998; Nyiri et al. 2001; Cruz et al.2003) (Fig. 1). In the hippocampus, α1 subunits are pri-marily expressed in GABAergic interneurons, whereas α5
subunits are localized at cell bodies and apical dendrites ofpyramidal neurons (Fritschy and Mohler 1995).
The various molecular forms of α subunits confer to theGABAA receptors a large range of GABA affinity oscil-lations that may span two- to threefold in magnitude fromα1 to α5 (Fig. 3; Costa and Guidotti 1996) and up to tenfoldfrom α1- to α2-containing GABAA receptors (Levitan et al.1988). Moreover, the susceptibility of GABAA receptorsexpressing different α subunits to the action of positiveallosteric modulators, such as the endogenous neurosteroids(Lambert et al. 2003) or exogenously administered BZligands (Fig. 3), varies dramatically. For example, maximalallosteric modulatory doses of diazepam and zolpidemshifted by more than twofold the action of GABA EC50 onα1-containing GABAA receptors, whereas diazepam isweaker and zolpidem is ineffective on the action of GABAEC50 at α5-containing GABAA receptors. In contrast, im-idazenil is more effective on α5 than on α1-containing re-ceptors. In addition, the sensitivity of GABAA receptorsto the action of positive allosteric modulators is not staticbut can change dynamically through various posttransla-tional modifications of receptor subunits (phosphorylationof subunits?) and thereby contribute to synaptic plasticity(Lambert et al. 2003).
Relationship between the strength of GABAergictransmission and GABAA receptor expression
Several lines of evidence suggest that GABAA receptordensity and subunit composition may change in relationto the strength of GABAergic transmission. For exam-ple, in the substantia nigra (SN), a 60–80% decrease inGABA content elicited by a lesion of the striato-nigralGABAergic pathway results in a local increase in the num-ber of high-affinity GABAA recognition sites by abouttwofold (Guidotti et al. 1979). Nyiri et al. (2001) reported aninput-dependent synaptic targeting of GABAA receptorscontaining α2 subunits in synapses innervated by basketcell axon terminals expressed in the hippocampal pyrami-dal neurons of rats. Impagnatiello et al. (1996) and Longoneet al. (1996) found that protracted upregulation of GABAA
receptor function induced in rats by a 2-week treatment withdiazepam (a full positive allosteric modulator of the actionof GABA at GABAA receptors) (up to 20 mg/kg/day)resulted in a large cortical and hippocampal decrease (40–50%) in the expression of mRNA and proteins encoding theGABAA receptor α1 and γ2 (short and long variants) sub-units and a 30% increase in themRNA and protein encodingthe GABAA receptor α5 subunit (for review, see Costa et al.2001a). On the other hand, protracted treatment with a fullnegative allosteric modulator (FG7142) of the action ofGABA at GABAA receptors resulted in an increased cor-tical expression in α1 subunits (Primus and Gallager 1992).
GABAA receptor upregulation in SZ and BP disorders
Studies in postmortem brains from patients diagnosed withSZ and BP disorders suggest that the primary defect ofGAD67 expression in cortical GABAergic neurons resultsin a decrease in GABA synthesis and presumably in acorresponding decline in synaptic GABA levels. If thiswere the case, one would anticipate compensatory upregu-lation of receptors and relevant changes in GABAA receptorsubunit composition expressed by pyramidal neurons atpostsynaptic sites. This hypothesis is at least indirectlysubstantiated in studies of postmortem SZ and BP disor-der brains in which the PFC shows an increase of specificGABAA receptor α subunits (Table 1).
That is, Benes et al. (1992) reported an upregulation of3H-muscimol binding to high-affinity GABAA recognitionsites expressed in superficial layers of the anterior cingulatecortex in the postmortem brain of SZ patients. An up-regulation of GABAA receptors—as detected by ligandbinding—was reported in the caudate nucleus, geniculategyrus, PFC layers II and III, dentate gyrus, and CA3 andCA4 areas of the hippocampus of SZP (Hanada et al. 1987;Benes et al. 1996a,b; Dean et al. 1999). In BA9 of BPdisorder patients with psychosis, an increased density of3H-flunitrazepam binding without changes in the density of3H-muscimol binding has been reported (Dean et al. 2001).This latter result suggests that in BP disorder patients withpsychosis, a defect of GABAergic transmission may resultin an upregulation of specific GABAA receptor subtypes(Table 1).
In the PFC of SZP, GABAergic chandelier cells thatinnervate the initial axon segment of pyramidal corticalneurons show a decreased expression in GAD67mRNA, PVimmunoreactivity, and GAT1 in presynaptic axon terminals(Lewis et al. 2004). In these brains, the initial segment ofpyramidal neuron axons postsynaptically coexpress a sig-nificant increase (up to 100%) in α2-containing GABAA
receptors (Lewis et al. 2004) (Table 1).In the PFC of SZP and matched nonpsychiatric subjects
(NPS), we studied the relationship between the downregu-lation of reelin mRNA and GAD67 protein expression andthe density of mRNAs encoding α1 and α5 GABAA recep-tor subunits. We detected a small (30–35%) increase in α1
mRNA while the increase in the mRNA encoding the α5
Table 2 In PFC of SZP, the increase of GABAA receptor α1 and α5mRNA subunits is paralleled by a decrease of reelin mRNA andGAD67 protein
a
Subjects α1 GABAA α5 GABAA Reelin GAD67/β-actin
mRNA (amol/μg RNA) OD ratio
NPS (n=7) 150±9.7 100±2.7 400±41 2.0±0.25SZP (n=7) 220±23* 210±11** 296±25* 0.55±0.08**
Each value is the mean±SEaMeasured in the temporal cortex of the same patients*p<0.05 when SZP are compared with NPS (Student’s t test)**p<0.01 when SZP are compared with NPS (Student’s t test)From Impagnatiello et al. 1998 (modified)
197

receptor subunits was about 100% (Table 2) (Impagnatielloet al. 1998). This GABAA receptor α5 subunit mRNA up-regulation appears to occur in SZP brains regardless of thedose of neuroleptics or of the duration of the exposure.
In the PFC of SZP, the increase in α1 and α5 subunitmRNA expression appears to correlate with an increasedtranslation in α1 and α5 subunit proteins. For example, in arecent immunohistochemical study, Ishikawa et al. (2004)reported that GABAA α1 subunit immunoreactivity wasincreased by ∼30% in the BA9 neuropil and pyramidalneuron somata of SZP.
In BA9 of a small group of SZP (n=5) and NPS (n=5)(Harvard Tissue Resource Center, Belmont, MA; Veldic etal. 2005) matched for age, gender, PMI, and cause of death—using the immunohistochemical technique described byVeldic; et al. (2004, 2005)—we confirmed the data ofIshikawa et al. (2004) showing that in SZP, the intensity ofGABAA α1 immunolabeling is slightly increased in pyra-midal neurons but not in the somata of GABAergic inter-neurons. However, in the same subjects, the optical densityof GABAA receptor α5 subunit immunolabeling in pyra-midal neuron somata was ∼twofold higher in SZ than inNPS. [Relative optical density calculated on a 256 Gy scale(Scion Image for Windows, Scion Corporation) was 15±3.2SEM inNPS and 37±3.6 in SZP (p<0.002) (Veldic, personalcommunication)].
Although confirmation of the data on the expression ofGABAA α1, α2, α3 receptor subunits are needed, the datathis far on GABAA receptor binding increase and on theupregulation of specific GABAA receptor subunit mRNAorprotein (α2 and α5) suggests that specific GABAA receptorsubtypes are upregulated in dendrites, cell bodies, or initialaxon segments of pyramidal neurons of SZ and BP disorderpatients (Fig. 1).
Since GABAA α5- and α2-containing receptors exhibitan affinity for GABA that is three- to tenfold, respectively,higher than the affinity of GABA for the α1-containingGABAA receptors (Costa and Guidotti 1996; Levitan et al.1988), it can be inferred that in SZ and BP disorders, pyra-midal neurons express GABAA receptors enriched with thetype of α subunits that confer higher affinity for GABA.This selective GABAA receptor upregulation could allevi-ate the disruption in synchronization and oscillatory firingactivity that is altered as a consequence of the deficit ofGABAergic transmission in SZP and probably in BPdisorder.
Pharmacological implications of selective GABAAreceptor subtype upregulation in the treatment of SZand BP disorders
Significance of GABAA receptor subunitchanges in SZ
The overwhelming evidence of a cortical and hippocam-pal GABAergic transmitter presynaptic defect and of apostsynaptic overexpression of α5- and α2-containingGABAA receptors in pyramidal neurons of SZ and BP dis-
orders suggest that to improve the efficacy of availabletreatments, future efforts should be directed at developingdrugs that can normalize the functional deficit of GABAergic neurotransmission.
It is highly likely that many atypical antipsychotic drugsactually acting at 5HT2A or dopamine receptors located onGABAergic interneurons in the cortex or in other brainregions, altering the firing rate of GABAergic neurons,may modulate GABAergic neurotransmission (Willins et al.1997; Williams et al. 2002; Jakab and Goldman-Rakic2000; Carlsson et al. 2001). However, it is clear that thepresently available treatments for SZ and BP disorders arenot directly targeted to the treatment of the molecular ab-normalities generated by the GABAergic dysfunction op-erative in SZ and BP morbidity.
Two principal strategies should be considered to correctthe primary GABAergic neuron defects: (1) targeting ab-normalities in nuclear epigenetic mechanisms (for recentreview, see Costa et al. 2004), and (2) enhancing the defec-tive GABAergic transmission with drugs acting as direct orindirect GABAA receptor agonists or as selective positiveallosteric modulators of GABA action at pertinent GABAA
receptor subtypes.Because selective cortical GABAA receptor subtypes are
upregulated in SZ, it can be inferred that direct or indirectGABA-mimetic drugs might make an appropriate con-tribution to a symptomatic therapy in SZ by increasingGABAergic tone at downregulated GABAergic synapses.Hence, theoretically, GABAergic synaptic transmissioncould be considered an important target in the developmentof new drugs that can ameliorate the symptomatology ofSZ and BP patients (Costa et al. 2002b, 2003, 2004; Wassefet al. 2003; Lewis et al. 2004).
Elaborating on these concepts, one might expect that (1)GABAA receptor agonists or drugs that increase GABAlevels at the synaptic cleft, or (2) positive allosteric mod-ulators of GABA action at selective GABAA receptor sub-types may ameliorate SZ psychotic symptoms, either whenadministered alone or in combination with antipsychotics ordrugs that correct the synaptic hypoplasticity generated bythe deficits of reelin and GAD67.
GABAA receptor agonists
Direct GABA-mimetic drugs, such as muscimol or 4,5,6,7-tetrahydroisoxazolo [5,4c]pyridin-3(2H)-one (THIP), orindirect GABA-mimetic drugs that increase GABA levelseither by blocking GABA reuptake in neurons [1-[2-bis(trifluoromethyl)-phenyl]methoxy]ethyl]-1,2,5,6-tetrahy-dro-3-pyridine-carboxylic acid (CI-966) (Giusti et al. 1990)or by inhibiting GABA metabolism (γ-acetylenic GABA,γ-vinyl GABA), have been employed as monotherapy or asadjuncts of antipsychotic medications to stimulate GABAA
receptor function. As summarized in Table 3, clinical ev-idence suggests that with the use of these drugs, their seda-tive side effects become a problem that cannot be overcame.Direct GABA-mimetics not only fail to improve psychoticsymptoms but also elicit confusion and further exacerbate
198

the existing thought disorders when used in high doses.These unwanted effects are presumably the consequenceof the disruption of phasic GABAergic synaptic activity,which are due to the indiscriminate and protracted actionof these drugs on a large number of different GABAA re-ceptor subtypes expressed throughout the brain. Hence, theuse of direct or of certain indirect GABAergic drugs for thetreatment of SZ is not tenable.
Full positive allosteric modulators of GABA action atGABAA receptors
Benzodiazepines (BZs) act as indirect GABAA receptoragonists by positively and allosterically facilitating the ac-tion of presynaptically released GABA (Costa and Guidotti1996). Unlike direct or indirect GABA receptor agonists,BZs do not disrupt the physiological oscillatory activity ofsynaptic transmission. BZs that act as full positive allostericmodulators amplifying the action of GABA at GABAA
receptors (i.e., chlordiaxepozide, diazepam) have been stud-ied extensively in double-blind trials as treatment for SZeither alone or as adjunctive drugs to be used with neuro-leptics. As reviewed by both Wolkowitz and Pickar (1991)and Carpenter et al. (1999), the consensus is that SZmonotherapy with BZs for a short time reduces positive andnegative symptoms in about one third to one half of thepatients studied. Moreover, BZs are potentially most usefulas adjuncts to neuroleptics in the initial treatment of SZ(Wolkowitz and Pickar 1991; Carpenter et al. 1999).
Although BZs appear to be potentially useful in thetreatment of SZ morbidity, several side effects limit theiracute or protracted use as follows. (1) BZs acting in-discriminately as full positive allosteric modulators at ev-ery GABAA receptor subtype in every brain structurecause amnesia and profound sedation, probably related totheir high affinity and intrinsic activity for α1-containing
GABAA receptors (Crestani et al. 2001;Möhler et al. 2001).(2) These BZs possess high dependence liability (Costa andGuidotti 1996; Costa et al. 2001a) and thus have limitedprotracted use. Finally, (3) The beneficial effects developrapidly, but unfortunately, in some patients, the beneficialeffects also regress rapidly (Wolkowitz and Pickar 1991).This regression in efficacy experienced by these patients ismost likely due to tolerance that results from the continualactivation of α1-containing GABAA receptors.
As shown in Fig. 4, protracted rat treatment with dia-zepam—a full positive allosteric modulator of the action ofGABA at GABAA receptors—induces tolerance to itspharmacological actions. Tolerance to the anticonvulsantactions of diazepam is presumably mediated by the maxi-mal amplification of GABA-gated Cl− current intensity oc-curring indiscriminately in every GABAA receptor subtype.This maximal amplification of the action of GABA atevery GABAA receptor subtype triggers an adaptive changein GABAA receptor subunit expression, decreasing α1 andγ2 subunits and increasing α5 subunits (Costa and Guidotti1996). The α5-containing GABAA receptors are known tobe less responsive to the maximizing action of commer-cially available BZs on GABA-gated Cl− current intensity.Hence, the doses of BZs must be increased to maintain thebeneficial actions obtained during the initial treatmentperiod. When the BZs that maximize GABA-gated Cl−
current intensity are indiscriminately withdrawn at the timein which tolerance to the drug is already operative, signs ofexcitatory activities are observed. These responses may inpart be due to the inadequacy of the function of the ab-normal GABAA receptor subunit assembly triggered by theprotracted synaptic facilitation of GABAergic signal trans-duction. Also, the expression of AMPA-preferring gluta-matergic receptor subunits in dendritic spine postsynapticdensities of the pyramidal neurons of different corticalareas may be upregulated and thus may complicate matters(Izzo et al. 2001).
Table 3 Schizophrenia is a GABAergic dysfunction that requires aGABAergic pharmacological intervention
Antipsychoticactivity
Unwanted sideeffects
Drugs acting at GABAA receptorsDirect agonists Muscimol Absent Psychosis, sedation
THIP Absent SedationFull positiveallostericmodulators
Diazepam Some Sedation, amnesia,tolerance,dependence
Partial positiveallostericmodulators
Bretazenil Some Short acting,sedation
Drugs acting at GABAB receptorsDirect agonist Baclofen Exacerbation –Drugs acting at GABAA and GABAB receptorsGABA transam.inhibitors
γ VinylGABA
Absent Confusion,disorientation
Long-term VEH Long-term DZ Long-term IMI
VEHb DZb IMIb VEHb DZb IMIb VEHb DZb IMIb0
1
2
3
4
5
Bic
ucul
line
thr
esho
ldch
ange
s (µ
mol
/kg)
0
1
2
3
4
5
0
1
2
3
4
5
*
(14 days)a (14 days)a (14 days)a
* ** *
Fig. 4 Imidazenil-induced inhibition of diazepam anticonvulsanttolerance. a Rats treated for 14 days with vehicle or with increasingdoses of diazepam, or with imidazenil (for dose schedule and detailsof the experiment, see Impagnatiello et al. 1996) were drug free for24 h before bicuculline test. b Acute challenge treatment with VEH(Vehicle), DZ [Diazepam (17.6 μmol/kg)], or IMI [imidazenil (2.5μmol/kg)] was carried out 30 min before bicuculline test. *p<0.05compared with respective vehicle-treated rats. (ANOVA followed byDunnett’s multiple range test). Each value is the mean±SE of sixanimals
199

At least theoretically, these limitations could be over-come with partial positive allosteric modulators of GABAaction at GABAA receptors expressing α1 subunits. Bre-tazenil (Table 3), a partial positive allosteric modulator ofthe action of GABA at several GABAA receptors, is vir-tually devoid of sedative action, tolerance, and dependenceliabilities when administered for short time periods torodents (Auta et al. 1994) or humans (Busto et al. 1994). Ithas been reported that this drug produces antipsychoticactivity of the magnitude seen with traditional neurolepticsin month-long open trials (Delini-Stula et al. 1992). How-ever, the bretazenil t-1/2 is short lasting due to its rapidmetabolism, and in rodents, prolonged administration ofhigh doses of this drug elicits sedation and amnesia, pre-sumably due to the formation of bretazenil metabolites thatmay be endowed with full agonist activity. For this reasonand because of its short half-life, bretazenil has never beenstudied in humans with randomized double-blind protocols.
BZ sites at GABAA receptors: a new model of receptorpharmacology
Today, new therapeutic opportunities arise due to increasinginsights into the diversity involved in signal transduction atGABAA receptors (Costa et al. 2001a, 2002a; Crestani et al.2001Möhler et al. 2001). TheGABAA receptors responsiveto BZs are characterized by the expression of α1, α2, α3, orα5 subunit combinations with β,γ subunits to form variousheteropentameric structures. Moreover, this BZ respon-siveness is facilitated by the contiguity of an α with a γsubunit.
The maximal amplification of GABA-gated channels bycommercially approved full positive allosteric modulatorsBZs, such as diazepam acting at α1 GABAA receptor sub-types, in addition to their anxiolytic, antiepileptic, andmuscle relaxant actions, is also the cause of undesirable sideeffects such as sedation, amnesia, tolerance, and depen-dence (Costa and Guidotti 1996; Costa et al. 2001a,b,2002a).
Recent studies (Crestani et al. 2001; Möhler et al. 2001)have established that the sedative and amnestic actions ofBZs are related to an amplification of GABA action atreceptors where an α1 GABAA receptor subunit is contig-uous to a γ2 subunit. In addition, tolerance liability is alsoassociated with α1-containing GABAA receptor subtypes.In contrast, their anxiolytic, anticonvulsant, and antipsy-chotic actions are presumably facilitated by similar actionsat GABAA receptors containing α2, α3, or α5 subunits.
Thus, opportunities for the molecular design of a newgeneration of ligands for BZ-binding sites that are partialagonists at certain GABAA receptor subtypes and that actspecifically at selective GABAA receptor subtypes may beemerging. These new drugs may impart reduced toleranceand dependence liabilities and could be designed to actselectively on certain GABAA receptor subtypes (e.g., α2-,α3-, and α5-expressing GABAA receptors) that may beoperative in the control of the psychotic symptoms of SZPwithout eliciting either sedation or amnesia.
Imidazenil, a selective BZ-binding site ligand devoid ofsedation, tolerance, and dependence liabilities
A BZ recognition site ligand that is devoid of intrinsicaction at α1-containing GABAA receptor subtypes butallosterically and maximally increases GABA action atα5 GABAA receptors is BZ 6-(2bromophenyl)-8-fluoro-4H-imidazo [1,5-a][1,4] benzodiazepine-3-carboxamide(imidazenil).
Imidazenil, unlike diazepam or zolpidem, fails to changeGABA-mediated activity at GABAA receptors includingα1
subunits, but selectively modulates the in vitro action ofGABA at recombinant GABAA receptors including α5
subunits through an allosteric positive action (Fig. 3; Costaet al. 2002a).
Because of this pharmacological profile, imidazenil isdevoid of the side effects related to the stimulation of α1-containing GABAA receptors, such as sedation and amne-sia, and probably because of its lack of action on α1
subunits, imidazenil is virtually devoid of tolerance anddependence liabilities.
We have published extensively on the unique behavioralprofile of imidazenil in rodents (Giusti et al. 1993; Autaet al. 1995; Costa and Guidotti 1996; Impagnatiello et al.1996; Costa et al. 2001b, 2002a,b; Auta et al. 2004) andprimates (Auta et al. 1995, 2000; Thompson et al. 1995;Costa et al. 2001b). We developed imidazenil in collabo-ration with Hoffman LaRoche. It is our opinion that thiscompound has an interesting profile as defined in the abovementioned publications and which justifies its testing in themaintenance treatment of SZ.
In Table 4, we compared the pharmacological actions ofdiazepam (a classic commercially available BZ ligand withfull BZ agonist profile at most GABAA receptor subtypesexpressed in the human brain) with that of imidazenil inrats. An important aspect of the pharmacological profile ofimidazenil that distinguishes this drug from diazepam andother commercially available BZs is its ability to elicitpotent anticonvulsant (anti-PTZ and bicuculline seizures)and anxiolytic (anti-proconflict or conflict) actions at dosesthat are several orders of magnitude lower than thoseeliciting sedation (reduction of motor activity, thiopentalpotentiation, ethanol potentiation).
Imidazenil has been reported to have a high affinity(subnanomolar KD) for BZ-binding sites and a low clear-ance rate in vivo (in rats, the t-1/2 is 90 min; in nonhumanprimates, the t-1/2 lasts longer than 6 h) (Costa and Guidotti1996). Moreover, imidazenil is virtually devoid of sedativeand amnestic action in monkeys. In monkeys, imidazenilfails per se to induce an amnestic response and actuallyblocks the cognition impairing action of alprazolam a fullallosteric modulator of GABA action at various GABAA
receptor subtypes (Fig. 5; see Auta et al. 1995; Thompson etal. 1995). Moreover, imidazenil, unlike diazepam, also failsto induce tolerance to its anticonvulsant (rats) or anti-amnestic actions (monkeys) when administered protract-edly in doses that fully occupy its recognition site onGABAA receptors (Giusti et al. 1993; Auta et al. 2000;Costa et al. 2001a). In future studies, it will be important to
200

investigate the mechanisms whereby imidazenil inhibitsbicuculline-induced convulsions in rats that are tolerant tothe antibicuculline action of diazepam (Fig. 4).
Hypothesis on the usefulness of imidazenil in thetreatment of SZ
The remarkably unique features of the pharmacologicalprofile of imidazenil (compared with diazepam or alprazo-lam) warrant the investigation of this drug as a prospectiveagent to treat psychotic symptoms in SZ and BP patientswith mania.
Our interest in the study of imidazenil is justified by theincreasing consideration given to the role of GABAergicinhibition in control of the thalamo-cortical afferent andreentrant cortico-thalamic pathways, as well as afferent sep-tal hippocampus and reentrant hippocampal–septal gluta-matergic pathways (Mountcastle 1998). These two pathwayshave an important GABAergic component that participatesin the regulation of sensory gating and memory acquisitionand perhaps in the consolidation of these functions. Thesecognitive functions are altered in SZ and BP patients with
mania (Lewis and Lieberman 2000). Since the expression ofGAD67 is decreased in the PFC and other brain areas ofSZ and BP patients with mania (Impagnatiello et al. 1998;Guidotti et al. 2000; Lewis et al. 2004; Woo et al. 2004),one might reason that if imidazenil were used in thetreatment of SZ, it could increase cortical GABAergic tone,thereby correcting the symptoms associated with the spe-cific cortical GABAergic downregulation typical of SZ.
Imidazenil’s action on the mousemethionine model of SZ
To investigate the hypothesis that imidazenil may correctthe behavioral consequences of the GABAergic transmis-sion deficit operative in SZ, we studied the effects ofimidazenil on the behavioral abnormalities induced in miceby protracted treatment with methionine (Tremolizzo et al.2002; Tremolizzo et al. 2005 ). These mice exhibit frontalcortex and hippocampal expression deficits of GAD67 andreelin mRNAs and proteins similar to those reported inpostmortem SZ and BP brains. These deficits are associatedwith prepulse inhibition of startle (PPI) and social interac-tion deficits, two characteristic behavioral markers asso-ciated with SZ (Tremolizzo et al. 2002; Tremolizzo et al.2005). We refer to these deficits collectively as the “syn-drome elicited by methionine”. It is important to keep inmind that methionine administration was shown to precip-itate psychotic episodes in SZP during a remission phase(Wyatt et al. 1971). These doses of methionine are devoid ofactions in normal individuals.
As shown in Fig. 6, imidazenil reduces the loss of PPIinhibition in mice receiving protracted methionine treat-ment (Tremolizzo et al. 2005). Moreover (Table 5), imid-azenil normalizes the social interaction deficits induced byprotracted methionine treatment (Tremolizzo et al. 2005).
A P
A P
A P
A P
A=Acquisition ; P=Performance
Vehicle
IMD+ALP
IMD 0.5 µmol/kg
ALP 1 µmol/kg
a
5min
Fig. 5 Imidazenil (IMD) antagonism of alprazolam (ALP)-inducedacquisition deficit in monkeys. Cumulative records from a Patasmonkey showing the pattern of response under a multiple schedulewith acquisition (A) and performance (P) components. Each recordrepresents a complete session (60 reinforcements) except for alpra-zolam (ALP) alone, which shows the first two A and P componentsrespectively during a 2-h session. Ordinate (a) represents 100 correctresponses (from Thompson et al. 1995). Note: The acquisitiondisruptive effect of ALP and the reversal of this effect with IMDpretreatment
Table 4 Comparison of the pharmacological profiles of imidazeniland diazepam in rats
Behavioral tests Imidazenil DiazepamED50 μmol/kg i.v
(1) Proconflict(antagonism)
0.060 2.0
(2) PTZ seizure(antagonism)
0.095 5.0
(3) Bicucullineseizures (antagonism)
0.95 8.l0
(4) Conflict (antagonism) 2.5 4.0(5) Motor activity (reduction) >60 4.0(6) Ataxia >60 4.0(7) ThiopentalLRR (potentiation)
>60 2.5
(8) Ethanol(potentiation)
>60 2.5
Structures
Behavioral tests predicting side effects (6, 7, 8) or clinically usefulmuscle relaxant, sedative (5), anxiolytic (4), anticonvulsant (2, 3),and antipanic activity (1). For details, see Giusti et al. 1993;Thompson et al. 1995LRR Loss of righting reflex, PTZ pentylenetetrazol
201

At these doses, imidazenil fails to change locomotor activ-ity of untreated mice.
These results suggest that a partial and selective agonistof the BZ recognition sites associated with GABAA re-ceptors expressingα2–α5 subunits, such as imidazenil, mayinhibit the onset of the syndrome elicited by methionine,which in many ways models behavioral symptoms of SZsuch as impaired PPI and social interaction deficits. More-over, the effect of imidazenil on PPI was studied on het-erozygous reeler mice that exhibit a 50% downregulation ofreelin expression and replicate the dendritic spine andGABAergic deficit described in SZ postmortem brain. Thisgenetic mouse model reveals a postpubertal PPI deficitthat is corrected by imidazenil but not by alprazolam (Costaet al. 2002b). With this background, imidazenil should betested in psychiatric patients. If it turns out to be effica-cious, further evidence will be provided that psychoticsymptoms can be ameliorated by stabilizing GABAergictone with a BZ that is devoid of sedative and amnestic
action and that fails to cause tolerance and dependenceliabilities.
Conclusions
Accumulating evidence reviewed in this paper suggests thata dysfunction of cortical GABAergic transmission resultingin a disturbance of cortical inhibitory activity and leading todesynchronization of modal or supramodal cortical asso-ciative functions might be at the root of SZ and BP disor-der morbidity. The altered GABAergic transmission in SZand BP disorders probably includes both a presynaptic anda postsynaptic component. For example, in cortical GABAergic neurons, several studies have consistently report-ed a defect of presynaptic GAD67, GAT1, PV, and reelinexpression (Table 1).
It is possible that in the PFC of SZP, the decrease inGAD67, with the resulting decrease in GABA synthesis andthe corresponding decline in the synaptic levels of GABA,may be responsible for the postsynaptic compensatory up-regulation of GABAA α2, α5 receptor density on dendrit-ic spines, somata, or initial axon hillocks of pyramidalneurons.
Evidence that in treatment for SZ, the most abundantlyupregulated GABAA receptors are those containing α2
and α5 subunits is of particular interest. The importanceof these findings for the treatment of SZ and BP disordersrests on the evidence that the susceptibility of GABAA
receptors to the action of positive allosteric modulatorsacting at BZ recognition sites depends on the type of αsubunit present in the heteropentameric structure of theGABAA receptors. For example, it is suggested that on thepyramidal neuron somata, GABAA receptors containing α1
subunits are highly expressed at synapses made by PV-positive basket cells (Nyiri et al. 2001). These receptorsmediate the sedative and amnestic effects of diazepam andother clinically used BZs. In contrast, GABAA receptorscontaining α5 subunits expressed with α2 subunits may behighly expressed at synapses formed by PV-negative basketcells on pyramidal cell bodies in the cortex and hippocam-pus. Furthermore, synapses established by chandelier axonterminals on axon initial segments of pyramidal neuronsshow a high density of GABAA receptors expressing α2
subunits (Nyiri et al. 2001; Lewis et al. 2004). GABAA
receptors containing α5 and/or α2 subunits mediate theanxiolytic and anticonvulsant actions of BZs.
In line with the rationale that a GABAergic transmissiondeficit in the brain of SZP may be corrected with the ad-ministration of drugs acting as positive allosteric modu-lators of GABA action at GABAA receptors, clinicallyavailable BZs, such as diazepam, or the experimentallynovel BZs, such as bretazenil, have been used in clinicaltrials in the treatment of SZ morbidity.
The consensus is that diazepam and bretazenil exertbeneficial antipsychotic effects comparable to those ofneuroleptics, but with the advantage of a rapid onset ofaction. However, the short half-life of bretazenil and thesedative and amnesic actions and the tolerance and depen-
Prepulse/Startle delay (msec)
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.1
0.2
0.3
0.4
0.5
0.6
0.7
70 140100 280 420
PP
figI
Rat
io
VEH
MET
A
070 100 140 280 420
MET+IMD
IMD
B
Fig. 6 Imidazenil reverses the decrease of prepulse inhibition ofstartle (PPI) elicited by protracted methionine treatment in mice. A.Mice receiving 5.2 mmol/kg s.c. of methionine (MET) twice a dayfor 15 days show acceleration of PPI decline elicited by increasingthe delay in the prepulse/startle interval (for details, see Tremolizzoet al. 2005) as compared to vehicle (VEH)-treated mice (p<0.01;repeated-measure ANOVA). Mice were without methionine for 16 hbefore testing. B. Imidazenil (IMD), 3 μmol/kg, 1 h before test at-tenuates the effect of methionine (no significant differences betweenmethionine + imidazenil and vehicle, repeated-measure ANOVA).Data from Tremolizzo et al. 2005 (modified)
Table 5 Imidazenil antagonizes the methioninea (MET)-inducedshortening of social interaction in mice
Protracted treatment Challenge
VEH Imidazenilb
(Social interaction/s/10 min)
VEH 215±6 260±20MET 110±11* 200±15
Each value is the mean±SE of six pairs of miceaMET 5.2 mmol/kg s.c. twice a day for 15 daysbImidazenil 3.3 mmol/kg s.c. 2 h before test*p<0.01 when protracted MET-treated mice are compared with theother groupsFrom Tremolizzo et al. 2005 (modified)
202

dence liabilities of diazepam, due to the maximal ampli-fication of GABA action at GABAA receptor subtypesexpressing α1 subunits, pose strong limitations for the pro-tracted use of these BZs in the treatment of SZ.
In contrast, imidazenil acts as a selective positive al-losteric modulator of GABA action at GABAA receptorsubtypes containing α5 subunits and is virtually devoidof intrinsic activity at GABAA receptors expressing α1
subunits.Imidazenil is capable of potent anticonvulsant, anti-
panic, and anxiolytic actions, but it is incapable of in-ducing sedation and amnesia in rodents and in primates.Moreover, imidazenil, unlike diazepam, fails to induceanticonvulsant tolerance even when administered in largepharmacological doses for protracted time periods to ro-dents and primates (Costa et al. 2001a; Auta et al. 2000).
These preliminary data suggest that imidazenil is an idealselective positive allosteric modulator of GABA action atGABAA receptors and may correct the GABAergic trans-mission deficits present in the brain of SZ or BP patients.
Since imidazenil reduces the auditory gating deficit andthe social interaction deficit associated with the GAD67
and reelin decrease in mouse models of SZ and does sowithout producing sedation or tolerance, the data supportthe concept that imidazenil should be clinically investigatedto evaluate its ability to correct SZ symptoms related toGABAergic transmission dysfunction and possibly to ame-liorate positive and negative symptoms in SZ and BP dis-order patients.
Acknowledgements This work is supported by RO1MH62188 toA.G., RO1MH62090 to E.C., and RO1MH6262A to D.R.G.
References
Abdolmaleky HM, Cheng KH, Russo A, Smith CL, Faraone SV,Wilcox M et al (2005) Hypermethylation of the reelin (RELN)promoter in the brain of schizophrenia patients: a preliminaryreport. Am J Med Genet B Neuropsychiatr Genet 134:60–66
Akbarian S, HuntsmanMM, Kim JJ, Tafazzoli A, Potkin SG, BunneyWE Jr, Jones EG (1995a) GABAA receptor subunit gene expres-sion in human prefrontal cortex: comparison of schizophrenicsand controls. Cereb Cortex 6:550–560
Akbarian S, Kim JJ, Potkin G, Hagman JO, Tafazzoli A, Bunney WEJr, Jones EG (1995b) Gene expression for glutamic acid decar-boxylase is reduced without loss of neurons in prefrontal cortexof schizophrenics. Arch Gen Psychiatry 552:258–266
Auta J, Giusti P, Guidotti A, Costa E (1994) Imidazenil, a partialpositive allosteric modulator of GABAA receptors, exhibits lowtolerance and dependence liabilities in the rat. J Pharmacol ExpTher 270:1262–1269
Auta J, Fraust WB, Lambert P, Guidotti A, Costa E, MoerschbaecherJM (1995) Comparison of the effects of full and partial allostericmodulators of GABAA receptors on complex behavioral pro-cesses in monkeys. Behav Pharmacol 6:323–332
Auta J, Guidotti A, Costa E (2000) Imidazenil prevention ofalprazolam-induced acquisition in Patas monkeys is devoid oftolerance. Proc Natl Acad Sci U S A 97:2314–2319
Auta J, Costa E, Davis J, Guidotti A (2004) Imidazenil: a potent andsafe protective agent against diisopropyl fluorophosphate toxic-ity. Neuropharmacology 46:397–403
Barnard EA (2001) The molecular architecture of GABAA receptors.In: Möhler H (ed) Handbook of experimental pharmacology, vol150. Springer, Berlin Heidelberg New York, pp 79–99
Benes FM (2000) Emerging principles of altered neural circuitry inschizophrenia. Brain Res Brain Res Rev 31:251–269
Benes FM, Berretta S (2001) GABAergic interneurons: implicationsfor understanding schizophrenia and bipolar disorder. Neuro-psychopharmacology 25:1–27
Benes FM, Vincent SL, Alsterberg G, Bird ED, SanGiovanni JP(1992) Increased GABAA receptor binding in superficial layersof cingulate cortex in schizophrenics. J Neurosci 12:924–929
Benes FM, Khan Y, Vincent SL, Wickramasinghe R (1996a) Dif-ferences in the subregional and cellular distribution of GABAAreceptor binding in the hippocampal formation of schizophrenicbrain. Synapse 22:338–349
Benes FM, Vincent SL, Marie A, Khan Y (1996b) Upregulation ofGABAA receptor binding on neurons of the prefrontal cortex inschizophrenic subjects. Neuroscience 75:1021–1031
Black JE, Kodish IM, Grossman AW, Klintsova AY, Orlovskaya D,Vostrikov V, Uranova N, Greenough WT (2004) Pathology oflayer V pyramidal neurons in the prefrontal cortex of patientswith schizophrenia. Am J Psychiatry 161:742–744
Busto U, Kaplan HL, Zawertailo L, Sellers EM (1994) Pharmacologiceffects and abuse liability of bretazenil, diazepam, and alprazo-lam in humans. Clin Pharmacol Ther 55:451–463
CarlssonA,Waters N, Holm-Waters S, Tedroff J, NilssonM, CarlssonML (2001) Interactions between monoamines, glutamate, andGABA in schizophrenia: new evidence. Annu Rev PharmacolToxicol 41:237–260
Carpenter WT Jr, Buchanan RW, Kirkpatric B, Breier AF (1999)Diazepam treatment of early signs of exacerbation in schizo-phrenia. Am J Psychiatry 156:299–303
Carter CS, Botvinick MM, Cohen JD (1999) The contribution of theanterior cingulate cortex to executive processes in cognition. RevNeurosci 10:49–57
Costa E, Guidotti A (1996) Benzodiazepines on trial: a researchstrategy for their rehabilitation. TIPS 17:192–200
Costa E, Auta J, Guidotti A (2001a) Tolerance and dependence toligands of the benzodiazepine recognition sites expressed byGABAA receptors. In: Möhler E (ed) Handbook of experi-mental pharmacology, vol 150. Pharmacology of GABA andglycine neurotransmission. Springer, Berlin Heidelberg NewYork, pp 227–250
Costa E, Davis J, Grayson DR, Guidotti A, Pappas GD, Pesold C(2001b) Dendritic spine hypoplasticity and downregulation ofreelin and GABAergic tone in schizophrenia vulnerability.Neurobiol Dis 8:723–742
Costa E, Auta J, Grayson DR, Matsumoto K, Pappas DG, Zhang X,Guidotti A (2002a) GABAA receptors and benzodiazepines: arole for dendritic resident subunit mRNAs. Neuropharmacology43:925–937
Costa E, Davis J, Pesold C, Tueting P, Guidotti A (2002b) Theheterozygote reeler mouse as a model for the development of anew generation of antipsychotics. Curr Opin Pharmacol 2:56–62
Costa E, Grayson DR, Mitchell CP, Tremolizzo L, Veldic M, GuidottiA (2003) GABAergic cortical neuron chromatin as a putativetarget to treat schizophrenia vulnerability. Crit Rev Neurobiol15:121–142
Costa E, Davis JM, Dong E, Grayson DR, Guidotti A, Tremolizzo L,Veldic M (2004) A GABAergic cortical deficit dominatesschizophrenia pathophysiology. Crit Rev Neurobiol 16:1–24
Crestani F, Löw K, Deist R, Mandelli M, Möhler H, Rudolph U(2001) Molecular targets for the myorelaxant action of diaz-epam. Mol Pharmacol 59:442–445
Crick FH, Koch C (2003) A framework for consciousness. NatNeurosci 6:119–126
Cruz DA, Eggan SM, Lewis DA (2003) Postnatal development ofpre- and post-synaptic GABAmarkers at chandelier cell inputs topyramidal neurons in monkey prefrontal cortex. J Comp Neurol465:385–400
203

Dean B, Hussain T, Hayes W, Scarr E, Kitsoulis S, Hill C, Opeskin K(1999) Changes in serotonin2A and GABA (A) receptors inschizophrenia: studies on the human dorsolateral prefrontalcortex. J Neurochem 72:1593–1599
Dean B, Pavey G,McLeodM, Opeskin K, Keks N, Copolov D (2001)A change in the density of [(3)H]flumazenil, but not [(3)H]muscimol binding, in Brodmann’s Area 9 from subjects withbipolar disorder. J Affect Disord 66:147–158
DeFilipe J, Farinas I (1992) The pyramidal neuron of the cerebralcortex: morphological and chemical characteristics of the syn-aptic inputs. Prog Neurobiol 39:563–607
Delini-Stula A, Berdah-Tordjman D, Neumann N (1992) Partialbenzodiazepine antagonists in schizophrenia: expectations andpresent clinical findings. Clin Neuropharmacol 15:405A–406A
Dong E, Caruncho H, LiuWS, Smalheiser NR, Grayson DR, Costa E,Guidotti A (2003) The reelin–integrin interaction regulates ArcmRNA translation in synaptoneurosomes. Proc Natl Acad Sci US A 100:5479–5484
Eastwood SL, Harrison PJ (2003) Interstitial white matter neuronsexpress less reelin and are abnormally distributed in schizophre-nia: towards an integration of molecular and morphologic as-pects of the neurodevelopmental hypothesis. Mol Psychiatry8:821–831
Fagiolini M, Fritschy JM, Low K, Mohler H, Rudolph U, Hensch TK(2004) Specific GABAA circuits for visual cortical plasticity.Science 303:1681–1683
Fatemi SH, Earle JA, McMenomy T (2000) Reduction in reelinimmunoreactivity in hippocampus of subjects with schizophre-nia, bipolar disorder and major depression. Mol Psychiatry5:654–663
Fritschy JM, Möhler H (1995) GABAA-receptor heterogeneity in theadult rat brain: differential regional and cellular distribution ofseven major subunits. J Comp Neurol 359:154–194
Fritschy JM, Weinman O, Wenzel A, Benke D (1998) Synapse-specific localization of NMDA and GABA (A) receptor subunitsrevealed by antigen-retrieval immunohistochemistry. J CompNeurol 390:194–210
Giusti P, Guidotti A, Danysz W, Auta J, Costa E (1990) Neurophar-macological evidence for an interaction between the GABAuptake inhibitor CI-966 and anxiolytic benzodiazepines. DrugDev Rev 21:217–225
Giusti P, Ducic I, Puia G, Arban R, Walser A, Guidotti A, Costa E(1993) Imidazenil: a new partial positive allosteric modulator ofγ-aminobutyric acid (GABA) action at GABAA receptors. JPharmacol Exp Ther 266:1018–1028
Glantz LA, Lewis DA (2001) Dendritic spine density in schizophre-nia and depression. Arch Gen Psychiatry 58:203
Guidotti A, Gale K, Suria A, Toffano G (1979) Biochemical evidencefor two classes of GABA receptors in rat brain. Brain Res172:566–571
Guidotti A, Auta J, Davis JM, Dwivedi Y, Gerevini VD,Impagnatiello F, Pandey G, Pesold C, Sharma R, Uzunov DP,Costa E (2000) Decrease in reelin and glutamic acid decarbox-ylase67 (GAD67) expression in schizophrenia and bipolardisorder: a postmortem brain study. Arch Gen Psychiatry 57:1061–1069
Halasy K, Buhl EH, Lorinczi Z, Tamas G, Somogyi P (1996) Synaptictarget selectivity and input of GABAergic basket and bistratifiedinterneurons in the CA1 area of the rat hippocampus. Hippo-campus 6:306–329
Hanada S, Mita T, Nishino N (1987) [3H] muscimol binding sitesincreased in autopsied brains of chronic schizophrenics. Life Sci40:259–266
Heckers S, Stone D, Walsh J, Shick J, Koul P, Benes FM (2002)Differential hippocampal expression of glutamic acid decarbox-ylase 65 and 67 messenger RNA in bipolar disorder andschizophrenia. Arch Gen Psychiatry 59:521–529
Hensch TK, Stryker MP (2004) Columnar architecture sculpted byGABA circuits in developing cat visual cortex. Science 303:1619–1621
Impagnatiello F, Pesold C, Longone P, Caruncho HJ, Fritschy JM,Costa E, Guidotti A (1996) Modifications of γ aminobutyricacidA receptor subunit expression in rat neocortex during tol-erance to diazepam. Mol Pharmacol 49:822–831
Impagnatiello F, Guidotti A, Pesold C, Dwivedi Y, Caruncho H, PisuM, Uzunov D, Smalheiser N, Davis J, Pandey G, Pappas G,Tueting P, Sharma R, Costa E (1998) A decrease of reelinexpression as a putative vulnerability factor in schizophrenia.Proc Natl Acad Sci U S A 95:15718–15723
Ishikawa M, Mizukami K, Iwakiri M, Hidaka S, Asada T (2004)Immunohistochemical and immunoblot study of GABA(A)alpha1 and beta2/3 subunits in the prefrontal cortex of subjectswith schizophrenia and bipolar disorder. Neurosci Res 50:77–84
Izzo E, Auta J, Impagnatiello F, Pesold C, Guidotti A, Costa E (2001)Glutamic acid decarboxylase and glutamate receptor changesduring tolerance and dependence to benzodiazepines. Proc NatlAcad Sci U S A 98:3483–3488
Jakab RL, Goldman-Rakic PS (2000) Segregation of serotonin 5-HT2A and 5-HT3 receptors in inhibitory circuits of the primatecerebral cortex. J Comp Neurol 417(3):337–348
Jones EG (1993) GABAergic neurons and their role in corticalplasticity in primates. Cereb Cortex 3:361–372
Jones EW (2000) Microcolumns in the cerebral cortex. Proc NatlAcad Sci U S A 97:5019–5021
Knable MB, Barci BM,Webster MJ, Woodruff JM, Torrey EF (2004)Molecular abnormalities in the hippocampus in severe psychi-atric illness: postmortem findings from the Stanley Neuropa-thology Consortium. Mol Psychiatry 9:609–620
Lambert JJ, Belelli D, Peden DR, Vardy AW, Peters JA (2003)Neurosteroid modulation of GABAA receptors. Prog Neurobiol71:67–80
Lees AJ, Clarke CR, Harrison MJ (1977) Hallucinations afterwithdrawal of baclofen. Lancet 16:858
Levitan FS, Schofield PR, Burt DR, Rhee LM, Wisden W, Kohler M,Fujita N, Rodriguez HF, Stephenson A, Darlinson MG, BarnardEA, Seeburg PH (1988) Structural and functional basis forGABAA receptor heterogeneity. Nature 335:76–79
Lewis DA, Lieberman JA (2000) Catching up on schizophrenia:natural history and neurobiology. Neuron 28:325–334
Lewis DA, Volk DW, Hashimoto T (2004) Selective alterations inprefrontal cortical GABA neurotransmission in schizophrenia: anovel target for the treatment of working memory dysfunction.Psychopharmacology 174:143–150
Longone P, Impagnatiello F, Guidotti A, Costa E (1996) Reversiblemodifications of GABAA receptor subunit mRNA expressionduring tolerance to diazepam-induced cognition dysfunction.Neuropharmacology 35:1465–1473
McBain CJ, Fisahn A (2001) Interneurons unbound. Nat RevNeurosci 2:11–23
Miles R, Toth K, Gulyas AI, Hajos N, Freund GF (1996) Differencesbetween somatic and dendritic inhibition in the hippocampus.Neuron 16:815–823
Möhler H, Crestani F, Rudolph U (2001) GABA(A)-receptorsubtypes: a new pharmacology. Curr Opin Pharmacol 1:22–25
Mountcastle VB (1998) Perceptual Neuroscience. The cerebralcortex. Harvard University Press, Cambridge, MA
Niu S, Renfro A, Quattrocchi CC, SheldonM, D’Arcangelo G (2004)Reelin promotes hippocampal dendrite development through theVLDLR/ApoER2-Dab1 pathway. Neuron 41:71–84
Nusser Z, Sieghart W, Benke D, Fritschy JH, Somogyi P (1996)Differential synaptic localization of two major gamma-amino-butyric acid type A receptor alpha subunits on hippocampalpyramidal cells. Proc Natl Acad Sci U S A 93:11939–11944
Nyiri G, Freund TF, Somogyi P (2001) Input-dependent synaptictargeting of alpha (2)-subunit-containing GABA (A) receptors insynapses of hippocampal pyramidal cells of the rat. Eur JNeurosci 13:428–442
Perlstein WM, Carter CS, Noll DC (2001) Relation of prefrontalcortex dysfunction to working memory and symptoms inschizophrenics. Am J Psychiatry 158:1105–1113
Peters A (1984) Chandelier cells. In: Jones EG, Peters A (eds)Cerebral cortex, vol 1. Plenum Press, NY, pp 361–380
204

Primus RJ, Gallager DW (1992) GABA receptor subunit mRNAlevels are differentially influenced by chronic FG7142 anddiazepam exposure. Eur J Pharmacol 226:21–28
Rao SG, Williams GV, Goldman-Rakic PS (1999) Isodirectionaltuning of adjacent interneurons and pyramidal cells duringworking memory: evidence for microcolumnar organization inPFC. J Neurophysiol 81:1903–1916
Rao SG, Williams GV, Goldman-Rakic PS (2000) Destruction andcreation of spatial tuning by disinhibition: GABAA blockade ofprefrontal cortical neurons engaged by working memory. JNeurosci 20:485–494
Rice DS, Curran T (2001) Role of the reelin signaling pathway incentral nervous system development. Annu Rev Neurosci 24:1005–1039
RodriguezMA, Caruncho HJ, Costa E, Pesold C, LiuWS, Guidotti A(2002) In Patas monkey GAD67 and reelin mRNA coexpressionvaries in a manner dependent of layer and cortical area. J CompNeurol 451:279–288
Rosoklija G, Toomayan G, Ellis S, Keilp J, Mann JJ, Latov N, HaysAP, Andrew AJ (2000) Structural abnormalities of subiculardendrites in subjects with schizophrenia and mood disorders:preliminary findings. Arch Gen Psychiatry 57:349–356
Sawaguchi T, Iba M (2001) Prefrontal cortical representation ofvisuospatial working memory in monkeys examined by localinactivation with muscimol. J Neurophysiol 86:2041–2053
Sawaguchi T, Matsumura M, Kubota K (1989) Delayed responsedeficits produced by local injection of bicuculline into thedorsolateral prefrontal cortex in Japanese macaque monkeys.Exp Brain Res 75:457–469
Selemon LD, Goldman-Rakic PS (1999) The reduced neuropilhypothesis: a circuit based model of schizophrenia. Biol Psy-chiatry 45:17–25
Sieghart W (1995) Structure and pharmacology of γ-aminobutyricacidA receptor subtypes. Pharm Rev 47:181–234
Skausig OB, Korsgaard S (1977) Hallucinations and baclofen. Lancet1:158
Soghomonian JJ, Martin DL (1998) Two isoforms of glutamatedecarboxylase: why? Trends Pharmacol Sci 19:500–505
Spencer KM, Nestor PG, Perlmutter R, Niznikiewicz MA, KlumpMC, Frumin M, Shenton ME, McCarley RW (2004) Neuralsynchrony indexes disordered perception and cognition inschizophrenia. Proc Natl Acad Sci 101:17288–17293
Stewart O, Schuman EM (2003) Compartmentalized synthesis anddegradation of proteins in neurons. Neuron 9:347–359
Thompson DM, Guidotti A, Costa E (1995) Imidazenil, a newanxiolytic and anticonvulsant drug, attenuates a benzodiazepine-induced cognition deficit in monkeys. J Pharmacol Exp Ther273:1307–1312
Tremolizzo L, Carboni G, Ruzicka WB, Mitchell CP, Sugaya I,Tueting P, Sharma R, Grayson DR, Costa E, Guidotti A (2002)An epigenetic mouse model for molecular and behavioralneuropathologies related to schizophrenia vulnerability. ProcNatl Acad Sci U S A 99:17095–17100
Tremolizzo L, Doueiri MS, Dong E, Grayson DR, Pinna G, Tueting P,Rodriguez-Menendez V, Costa E, Guidotti A (2005) Valproatecorrects a methionine-induced schizophrenia neuropathology inmouse. Biol Psychiatry 57:500–509
Veldic M, Caruncho H, Liu WS, Davis J, Satta R, Grayson DR,Guidotti A, Costa E (2004) DNAmethyltransferase-1 (DNMT1)is selectively overexpressed in telencephalic cortical GABAergicinterneurons of schizophrenia brains. Proc Natl Acad Sci U S A101:348–353
Veldic M, Guidotti A, Maloku E, Davis JM, Costa E (2005) Inpsychosis, cortical interneurons overexpress DNA-methyltrans-ferase 1. Proc Natl Acad Sci U S A 102:2152–2157
Volk DW, Austin MC, Pierri JN, Sampson AR, Lewis DA (2000)Decreased glutamic acid decarboxylase67 messenger RNAexpression in a subset of prefrontal cortical gamma-aminobu-tyric acid neurons in subjects with schizophrenia. Arch GenPsychiatry 57:237–245
Volk D, Austin M, Pierri J, Sampson A, Lewis D (2001) GABAtransporter-1 mRNA in the prefrontal cortex in schizophrenia:decreased expression in a subset of neurons. Am J Psychiatry158:256–265
Wassef A, Baker J, Kochan LD (2003) GABA and schizophrenia: areview of basic science and clinical studies. J Clin Psychophar-macol 23:601–640
Weeber EJ, Beffert U, Jones C, Christian JM, Forster E, Sweatt JD,Herz J (2002) Reelin and ApoE receptors cooperate to enhancehippocampal synaptic plasticity and learning. J Biol Chem277:39944–39952
Williams GV, Rao SG, Goldman-Rakic PS (2002) The physiologicalrole of 5-HT2A receptors in working memory. J Neurosci 1(22):2843–2854
Willins DL, Deutch AY, Roth BL (1997) Serotonin 5-HT2A receptorsare expressed on pyramidal cells and interneurons in the ratcortex. Synapse 27(1):79–82
Wolkowitz DM, Pickar D (1991) Benzodiazepines in the treatment ofschizophrenia: a review and reappraisal. Am J Psychiatry 148:714–726
Woo TU, Whitehead RE, Melchitzky DS, Lewis DA (1998) Asubclass of prefrontal γ-aminobutyric acid axon terminals areselectively altered in schizophrenia. Proc Natl Acad Sci U S A95:5341–5346
Woo TU, Walsh JP, Benes FM (2004) Density of glutamic aciddecarboxylase 67 messenger RNA-containing neurons thatexpress the N-methyl-D-aspartate receptor subunit NR2A in theanterior cingulate cortex in schizophrenia and bipolar disorder.Arch Gen Psychiatry 61:649–657
Wyatt RJ, Benedict A, Davis J (1971) Biochemical and sleep stud-ies of schizophrenia: a review of the literature 1960–1970.Schizophr Bull 4:10–44
205