
Future e-Health, QoS Provision and Cybersecurity Challenges
9
Journal of the Institute of Industrial Applications Engineers Vol.2, No.3, pp.113–121, (2014.7.25) DOI: 10.12792/JIIAE.2.113 ISSN:2187-8811 Paper Future e-Health, QoS Provision and Cybersecurity Challenges Eduard Babulak * Member, Ming Jin † Non-member Yoon Sang Kim ‡ Non-member (Received February 18, 2013, revised April 15, 2013) Abstract: In this paper, the authors discuss the importance of provision of Quality of Service (QoS) and Cybersecurity in the field of medical care and Electronic Healthcare Management. The main motivation to present our paper is to discuss the use of data communications, Internet, cloud and Smart Ubiquitous Computational Devices (SUCDs) in medical field while presenting possible scenarios related to ubiquitous access to Patient’s Electronic Health Record (PEHR) and remote control of Medical Surgical Robots via Internet and SUCDs. The message of the paper is to stress the importance of quality of service provision and cyber security in the field of telemedicine today and tomorrow. The SUCDs controlling, PEHR and surgical robots are quite new applications in medical practice and little is know about the possible scenarios that may be triggered by cyber security. The control data and PEHR are transmitted via data communications networks and Internet. As such, the quality of service provision and proper cyber security solutions are essential to patient’s safety and security Keywords: e-health, telerobotics, quality of service, cybersecurity, smart ubiquitous computing devices. 1. Introduction The world today is driven by the information exchange pro- viding support for the national and global cooperation. The supporting telecommunications infrastructures are becom- ing more complex providing the platform for the user driven real-time applications over the large geographical distances. The essential decisions made concerning the state welfare, health care systems, education, business, national security and defense, depend on Cybersecurity and QoS provision of telecommunications and data networks. Figure 2, illustrates the e-Health system in South Korea. The communication network infrastructure connects multi- ple departments and offices geographically located at vari- ous institutions and centers. Medical doctors with patients, access their medical records via Internet and MCNIs daily while utilizing the SUCDs. The MCNI(s) supporting the EHR in hospitals are very complex and essential part of e-Health Management Sys- tems worldwide. The medical doctors and staff expect se- cure and reliable services with best QoS provision regard- less of complexity of medical information flow(s) as an in- tegrated part of daily operation in hospital today. For legal purposes, the patient’s private data, such as medical record, insurance policies, etc. that may be transmitted via Inter- * Department of Computer Science and Engineering, Sungkyunkwan University, Suwon, Gyenggi, Korea. ([email protected]) † Department of Computer Science and Engineering, Korea Tech, Cheonan, South Korea. ([email protected]) ‡ Department of Computer Science and Engineering, Korea Tech, Cheonan, South Korea. ([email protected]) Figure 1: The patient record consultation with iPad [F1]. Figure 2: The e-Health in South Korea. net and ICT networks must be safe and secure against any unauthorized or illegal use. Published by IIAE. 2014 113
Transcript of Future e-Health, QoS Provision and Cybersecurity Challenges

Journal of the Institute of Industrial Applications Engineers Vol.2, No.3, pp.113–121, (2014.7.25)DOI: 10.12792/JIIAE.2.113 ISSN:2187-8811
Paper
Future e-Health, QoS Provision and Cybersecurity Challenges
Eduard Babulak∗ Member, Ming Jin† Non-memberYoon Sang Kim‡ Non-member
(Received February 18, 2013, revised April 15, 2013)
Abstract:In this paper, the authors discuss the importance of provision of Quality of Service (QoS) and Cybersecurity inthe field of medical care and Electronic Healthcare Management. The main motivation to present our paper is todiscuss the use of data communications, Internet, cloud and Smart Ubiquitous Computational Devices (SUCDs)in medical field while presenting possible scenarios related to ubiquitous access to Patient’s Electronic HealthRecord (PEHR) and remote control of Medical Surgical Robots via Internet and SUCDs. The message of thepaper is to stress the importance of quality of service provision and cyber security in the field of telemedicinetoday and tomorrow. The SUCDs controlling, PEHR and surgical robots are quite new applications in medicalpractice and little is know about the possible scenarios that may be triggered by cyber security. The controldata and PEHR are transmitted via data communications networks and Internet. As such, the quality of serviceprovision and proper cyber security solutions are essential to patient’s safety and security
Keywords: e-health, telerobotics, quality of service, cybersecurity, smart ubiquitous computing devices.
1. IntroductionThe world today is driven by the information exchange pro-viding support for the national and global cooperation. Thesupporting telecommunications infrastructures are becom-ing more complex providing the platform for the user drivenreal-time applications over the large geographical distances.The essential decisions made concerning the state welfare,health care systems, education, business, national securityand defense, depend on Cybersecurity and QoS provisionof telecommunications and data networks.
Figure 2, illustrates the e-Health system in South Korea.The communication network infrastructure connects multi-ple departments and offices geographically located at vari-ous institutions and centers. Medical doctors with patients,access their medical records via Internet and MCNIs dailywhile utilizing the SUCDs.
The MCNI(s) supporting the EHR in hospitals are verycomplex and essential part of e-Health Management Sys-tems worldwide. The medical doctors and staff expect se-cure and reliable services with best QoS provision regard-less of complexity of medical information flow(s) as an in-tegrated part of daily operation in hospital today. For legalpurposes, the patient’s private data, such as medical record,insurance policies, etc. that may be transmitted via Inter-
∗ Department of Computer Science and Engineering,Sungkyunkwan University, Suwon, Gyenggi, Korea.([email protected])† Department of Computer Science and Engineering,
Korea Tech, Cheonan, South Korea.([email protected])‡ Department of Computer Science and Engineering,
Korea Tech, Cheonan, South Korea.([email protected])
Figure 1: The patient record consultation with iPad [F1].
Figure 2: The e-Health in South Korea.
net and ICT networks must be safe and secure against anyunauthorized or illegal use.
Published by IIAE. 2014 113

114 E. Babulak, M. Jin and Y.-S. Kim
Figure 3: Telesurgery experiment with Raven system[F2]
Technology used in hospitals and medical field todayhave become essential part of research for hospital manage-ment and provision of services such as medical care diag-nosis and administration of medication. In medical practicetoday use of SUCDs and ICT and future health care tech-nology facilitates application for electronic health records.
The internet technology and electronics health recordhave become driving force in 21st century health care sys-tem. There are significant challenges healthcare provisionin South Korea and elsewhere such as quality, safety, ef-ficiency and medical care accessibility to remote locationsoutside large cities areas.
In this paper, the authors discuss the importance of QoSprovision and Cybersecurity challenges in future healthcommunication infrastructures. The paper presents the useof ICT and SUCDs in modern hospitals and medical infras-tructures, while addressing the importance of QoS and Cy-bersecurity provision in future hospitals, medical case andnational e-health management. The paper is structured asfollows. In section one, the authors introduce the use of ITand SUCDs in medical field. Section two presents the teler-obotic surgery scenario and work conducted in BioRoboticsLab at the University of Washington in Seattle. Sectionthree discuss the application of telemedicine, EHR andSUCDs and Health Care Economy. Section four discussesthe Cybersecurity challenges in the field of e-Health andtelemedicine. The section five discusses the importance ofQoS provision in future health communication infrastruc-tures. The final Section six presents conclusion and furtherresearch directions.
2. TELEROBOTIC SURGERY SCENARIO
As one of the leading institution in the field of medicalrobotics, the University of Washington is leading researchin surgical telerobotics. The telesurgery also known asremote surgery, enables a medical doctors to perform thesurgery on a patient remotely via Internet video-conferencesoftware[1].
A teleoperated surgical robotic system allows surgicalprocedures to be conducted across long distances while uti-lizing wired and wireless communication subject to properQoS provision that may affect the reliability and safety ofthe patient undergoing telesurgery.
Figure 3 shows one example of telesurgery with an openarchitecture portable surgical robotic system (Raven) devel-
Figure 4: System architecture of Raven II
oped in University of Washington. The system was devel-oped for both open and minimally invasive surgery. It hasbeen the subject of an intensive telesurgical experimentalprotocol aimed at exploring the boundaries of the systemand surgeon performance during a series of field tests undersynthetic fixed time delay. One standard task of the Fun-damentals of Laparoscopic Surgery (FLS) training kit wasused for the experimental protocol. Network characteriza-tion indicated a typical time delay in the range of 16-172msin field experiments.[2]
Figure 4 shows another telesurgery robotic system calledRaven-II - an advanced version of Raven. The system is aplatform for collaborative research on advances in surgicalrobotics. There are seven universities conducting researchesutilizing this platform. It has two 3-DOF (Degree in Free-dom) spherical positioning mechanisms capable of attach-ing interchangeable four DOF instruments. Its software isbased on open standards such as Linux and ROS (RobotOperating System) to facilitate software development. It isproven that the mechanism is robust enough for repeated ex-periments and animal surgery experiments, however, it isn’tdesigned to sufficient safety standards for human use.[3]
The surgical Telerobot(s) have become very valuabletechnology in the field of medical surgery, while enablingremote surgery on a patient in the environments with ex-treme conditions such as, battlefield or remote areas not ac-cessible to medical doctors. Development of surgical Tele-robotics is one of the key research areas in surgical medicalfield.
Currently, the surgical Telerobots are still in a developingstage and are becoming more computerized in conjunctionwith the mechatronics and automated technologies. The re-
IIAE Journal, Vol.2, No.3, 2014

Future e-Health, QoS Provision and Cybersecurity Challenges 115
mote surgery with Telerobot is controlled via microproces-sor communicating with control center via computer net-work and Internet Cloud. Given the critical data transmis-sion and real time control messaging over communicationnetwork, it is important to make sure that there are no mal-functions caused by poor QoS provision such as networkconnection breakdown or network malfunction. In order toprovide best QoS, security and safety, communication in-frastructure and Internet technology it is essential to buildproper network and communication devices with softwareand hardware security.
Typical network problems, such as increased communi-cation latency or connection failures must be controlled andmanaged by proper network management software such asHP Open View (HPOW: http://support.openview.hp.com),Packetter (PCT: http://www.packeteer.com/ ), etc. To createan infrastructure required for the surgical telerobotics, it iscritical to build a medical communication network infras-tructure that provide reliable services, proper QoS provi-sion. To improve the QoS provision for the surgical teler-obotics[4], researchers of BioRobotics Laboratory at Uni-versity of Washington proposed a design of a portable low-cost surgical master station for teleoperated surgical robots.
The QoS of proposed system was enhanced within fol-lowing aspects:
• low xost, aff-the-shelf hardware, interoperability plat-form for multiple surgical robots;
• Use of Internet connection;
• Data collection for experimental surgical telerobotics;
2.1 Telerobotics example at UW Lab The proposedsystem consist of off-the-shelf hardware, such as low-costhardware (i.e, laptop, omni haptic devices and USB (Uni-versal Serial Bus) foot pedal). The kinematic mapping be-tween the HID (Haptic Interface Devices) and the remotesurgical robot in this system is entirely in Cartesian spaceand the motion commands are position increments, ratherthan absolute position under the purpose of enhancing theconvenience of use of the proposed system.
Figure 5 illustrates the hardware configuration of pro-posed system. We can see the surgeon’s Graphical UserInterface (GUI) is appeared in laptop screen. The GUI al-lows the surgeon to execute high-level commands such asconfiguring the movement rate of surgical robot arm or se-lecting a remote IP of surgical Telerobot from a drop-downbox. It is also protected with the password based authenti-cation. The surgical video is appeared in the LCD monitorbehind the two omni haptic devices.
With this configuration, motions of HIDs in variousdirection causes corresponding movement in the surgicalfield. The reference frame for position increments is a right-handed frame, which is the X-axis pointing right, Y-axispointing up and Z-axis pointing out.
The Internet protocols and specific network communica-tion algorithms, create communication and control of theproposed telerobotics system. The communication system
Figure 5: System setup of proposed system in [4 and F4]
and implementation of surgical telerobotics at UW provesto be practical and cost-effective.
2.2 Interoperable Telesurgical Protocol (ITP) exampleat UW Lab Second example from University of Wash-ington[5], is a preliminary protocol for interoperability usedfor multiple robots performing telesurgery at various loca-tions. The objective of the protocol is to develop a commu-nication platform providing support for the multiple surg-eries across various interconnected heterogeneous surgicaltelerobotic master and slave systems. The secondary aim ofthe research work at UW is to compare two master stationdesigns side-by-side while improving their performance.The proposed protocol provides a platform for interconnect-ing multiple teleoperators and telesurgical systems.
The system testing and performance analysis of the pro-posed interoperability protocol were conducted betweenKagawa-Kawashima Group at the Tokyo Institute of Tech-nology and the BioRobotics Lab at the University of Wash-ington. The results showed the significant QoS improve-ment of telesurgery system[5]
2.3 Surgical Telerobotics with Information Securityexample at UW Lab Provision of proper QoS fortelesurgical system must be build side-by-side with properhardware and software security to prevent any possible at-tacks or intrusion on remote surgery and surgeons interac-tion. Any attack could cause problems such as fault move-ment of surgical robot arm during the surgery which couldlead to severe injuries or even life risks.
System performance, reliability, availability, simplicityas well as serviceability are essential in conjunction withproper security and QoS. The surgical telerobotics experi-ment at University of Washington promotes further researchin area of security and QoS. As shown in Fig. 6, any possi-ble security threats and attacks against mobile surgical teler-obotics systems could cost human lives.
Discussion in paper[6] addresses examples of malicioussignal jamming, intrusions via communication network thathave significant impact on the remote surgery and surgicaltelerobotics systems. These could be classified in five cate-gories:
i) attacks against the wireless communication,
IIAE Journal, Vol.2, No.3, 2014

116 E. Babulak, M. Jin and Y.-S. Kim
Figure 6: Cyber attack against medical system could lead tosevere accident threatening human life
ii attacks targeting surgeon-manipulator interaction,
iii attacks on the surgeon-side software (e.g., attacks ex-ploiting development (engineering) interfaces),
iv attacks on the manipulator-side software (e.g., attacks onthe programmable logical controllers (PLC)),
v physical attacks,
The analysis of the first category were, remote attacks tar-geting surgeon-manipulator interaction, such as Eves drop-ping, Jamming and Message modification (i.e., False datainjection). Typical examples in second category are simplereplay, delay attack, message dropping, combined delay anddrop attack, message modification and spoofing attack.
The authors discus new solution with mitigation strate-gies, while analyzing impact on system’s performance, se-curity and safety and suggesting further research directionsin developing telerobotics surgery systems with proper QoSprovision, communication security and human safety.
3. APPLICATION OF TELEMEDICINE, HER,SUCDs AND HEALTH CARE ECONOMY
The increased use of telemedicine services, HER system(s)and SUCDs in the healthcare contribute to more cost effec-tive e-Health Management and reduction in hospital read-missions. In 2012, the American Telemedicine Associationestimates that more than 10 million Americans directly ben-efited from telemedicine services[7].
Readmission to hospital is common, costly and maycauses overcrowding at emergency department of hospi-tals[8]. Until recently, In Ontario, Canada, over one-thirdof patients discharged from hospital are readmitted within90 days. It was estimated that these readmissions cost over$700 million per year[9].
Focused care after discharge can improve post-dischargeoutcomes[10]. Recent advances in SUDCs, mobile video,cloud access enabling multi-point, live video-supportedpost-discharge programs in conjunction with HER andtelemedicine (i.e., such as patient-care consultations or postdischarge meetings) contribute to significant reduction ofhospital readmissions.
3.1 Telepsychiaty Example In the South CarolinaDepartment of Mental Health (SCDMH), the use of video
Figure 7: Illegal cyber activity.
telepsychiatry solution utilizing Internet, SUCDs, cloudcomputing and video collaborative tools contributed tothe patient adherence to psychiatric treatment by nearly200%, reduced readmission, while saving $21.7 mil-lion. The telepsychiatry program, named Polycom R©RealPresence R© Platform[11], is powered by Polycom,Inc., a leading company in open standards-based unifiedcommunications solutions for voice and video. The Poly-com system creates direct connection between medical doc-tors and patients via high definition video conference whileeliminating the distance. It enables the doctors to observefurther non-verbal cues such as lack of eye contact, abnor-mal movement, or enlarged pupils, which can be even moreimportant than the cues observed with pure verbal interac-tion[12].
3.2 Remote Cardiac Monitoring Example Cur-rently, more than one million Americans receive remotecardiac monitoring to prevent readmissions for heart fail-ure(s), which often occur within 30 days of discharge andcost Medicare $6 billion annually. The Indianapolis-basedSt. Vincent Health successfully conducted a pilot programthat enables the nurses to consults the patients with the heartfailure and chronic obstructive pulmonary disease via re-mote video conference. The results showed that the read-missions was reduced by an astonishing 75 percent. In ad-dition, a Department of Veterans Affairs national home tele-health program demonstrated a 25 percent reduction in thenumber of days of bed care and a 19 percent reduction inhospital admissions[7]. Modern hospitals and medical cen-ters all over the world are exploring ways of utilizing moreeffectively the EHR, SUCDs, and telemedicine systems viamedical communication infrastructures, cloud computingand Internet.
4. CYBERSECURITY CHALLENGES
4.1 What is Cybersecurity Cybersecurity is thebody of technologies, processes and practices designed toprotect networks, computers, programs and data from at-tack, damage or unauthorized access.[13]∼[17] In short, wecan say that Cybersecurity is a security technique to pro-
IIAE Journal, Vol.2, No.3, 2014

Future e-Health, QoS Provision and Cybersecurity Challenges 117
Figure 8: Cyber-attacks around the world. [F5]
tect our networks for Cybersecurity attacks. Cybersecuritycomes from the combination of these two root words; cyberand security. Cyber means internet, networking and digitalcommunication. It’s all about technologies that we are hav-ing nowadays. Security is the degree of resistance to harmor protection from harm. The Fig. 7 illustrates example ofcybercrime motivated by money or cyber-terror.
Comparing with the traditional security concept in phys-ical world, Cybersecurity is more complex because the in-truders use Internet to attack a PC or even patient’s med-ical record remotely. In particular the mobile security isneeded because mobile technology is proliferating in to-day’s medical and corporate environments. While thereare significant opportunities to leverage these devices to in-crease the effectiveness of mobile workers, there are alsosignificant concerns about the privacy of sensitive corporatedata stored on the devices that IT must handle. McAfee’sGary Davis predicts that the next hacker target will be mo-bile devices. “Smartphone’s and tablets are at even greaterrisk than PCs”, Davis says, since they have fewer securityfeatures and often allow access to an individual’s entire net-work. Just in the last quarter, there was a 76 percent increasein malware on Android devices alone[18].
Some attacks occur at the national level. Due to its mas-sive scale and significant influence it is considered as a cy-berwar or cyber warfare. In contrast with the fact that tra-ditional war between organizations or nations in physicalworld is uncommon today, cyber wars are everywhere andhave never stop. Past month, the North Korea conducteda series of cyber-attacks on South Korea and United Statesgovernment websites[19].
Figure 8 illustrates cases of cyber-attacks world-wide, captured and visualized in real time by HoneynetProject[21]. The red dots on the world map represent cyber-attackers and the yellow dots represent the targets. Theseattacks were conducted systematically on worldwide scaleacross multiple countries and continents.
The Honeynet Project official website stated that theseevents are just small portion of cyber-attacks conducted allover the world in the past few years.
As a result, several Cybersecurity standards have beencreated including, the ISO/IEC 27001, IEC NERC 1300 andRFC 2196 published by IETF.
In the field of e-Health the cyber-attacks may compro-mise patient’s safety or even put human lives in danger. Inaddition to cyber-attacks it is important to consider the er-
rors cause by personnel. One way in which systems mayfail, is through the incorrect action of the system’s oper-ators[21]. No matter how great the cyber-attack defensemechanism or algorithm of the security system is, the sys-tem can be easily exposed to security threats if the securitysystem operator or administrator operates the system incor-rectly. In order to prevent any system errors or malfunction,it is essential to implement proper Cybersecurity mecha-nisms and policies[22]. The inappropriate design of userinterface may also misguide the operator/user and increasethe possibility of fault operation or security breach. Otherhuman errors and real world computer related crimes thatmay compromise human safety and system security may in-clude:
• Revealing the system password voluntary or underthreat;
• Physically stealing or destroying security devices.
In addition to human factors in Cybersecurity, natural dis-asters such as fires, earthquakes, floods and hurricanes canput the e-Health system(s) in great danger. Natural disas-ter(s) may compromise or destroy the Cybersecurity sys-tems and devices, as well as cause damage triggered bywidespread power outage. Without electricity, the MC-NIs, HER, Cybersecurity systems, banks, etc., are nonop-erational. From the above, we can see that Cybersecurity isextremely important and complex.
4.2 Importance of Cybersecurity With the increas-ing degree of ubiquitous connectivity to support critical op-erations in national e-Health system, state defense, banking,telecommunication, transportation, electric power grid con-trol, etc., the provision of proper Cybersecurity is essentialto any country all over the world[23].
The cyber-attacks may be motivated by political conflict,social tension, economics, religious belief, and any formof extremism[24] [25]. The cyber-attacks can occur at any-time, anywhere targeting any SCUBs or e-Health system. InTaiwan, a child at age of only 14 successfully hacked sev-eral learning website of his school, making them unavail-able for normal services[25]. Cyber-attacks could cause fa-tal disaster.
Nowadays, most of the nation’s critical infrastructuressuch as power grid are operated by cyber systems, whichmeans security incident in these cyber systems will affectthe physical critical infrastructures and cause a devastatingcrisis in our real world. Recent findings indicate the grow-ing threat of physical and cyber-based attacks in numbersand sophistication on electric grids and other critical infras-tructure systems[26].
From above, we can see that cyber-attacks are every-where and can be conducted at any time for any purposeby any person or organization from anywhere, and can leadto a severe consequence. Thus, Cybersecurity is extremelyimportant for safety of human world.
IT Management[19] pointed out key threats to comput-ers and security and divided them into 4 categories: Errors
IIAE Journal, Vol.2, No.3, 2014

118 E. Babulak, M. Jin and Y.-S. Kim
Table 1: Threats to Cybersecurity. [T1]
ThreatCategory Types of Threats
Errors andaccidents
· Human errors· Procedural errors· Software errors· Electromechanical problems· “Dirty data” problems
Naturalhazards -
Computercrimes
· Theft of hardware· Theft of software· Theft of online music and movies· Theft of time and services· Theft of information· Internet-related fraud· Taking over your PC: zombies,
botnets, and blackmail· Crimes of malice: crashing entire· systems
Computercriminals
· Individuals or small groups· Employees· Outside partners and suppliers· Corporate spies· Foreign intelligence services· Organized crime· Terrorists
and accidents, Natural hazards, Computer crimes as well asComputer criminals. The details is shown in Table. 1.
4.3 Human Safety and Security in Hospitals Orig-inally, one of the purposes of adopting ICT to hospital andmedical system is to increase the human safety by keep itfrom human errors. Humans tend to act on their percep-tions, and are emotional thus their performance is usuallyaffected by their emotions. Therefore, human errors are in-evitable and fault in hospital and medical operation usuallyresult in critical danger in human safety. By assess, de-tect and control with ICT, human errors can be dramaticallyeliminated and increased safety can be assured.
However, as the hospital and medical infrastructure re-lies on ICT more and more heavily, human safety can bethreatened by illegal access and attack in telemedicine sys-tem. Breach in Cybersecurity of hospital and medical in-frastructure can lead to fault operation of critical medicalfacilities related with radioactivity cure, or paralysis of en-tire medical system. Not like in common living residence,even power outage caused by cyber-attack in hospital cancause disaster that threatens patients’ life. Thus, Cyberse-curity in hospital and medical infrastructure should be givenenough attention.
4.4 Electronic Health Record and CybersecurityAs adopting the ICT in hospitals, almost all kinds of in-formation in hospital are recorded in digital format todayfor effective storing, sharing, searching and etc. An elec-tronic health record (EHR) is an evolving concept definedas a systematic collection of electronic health informationabout individual patients or populations[27]. EHRs may
include a range of data, including demographics, medicalhistory, medication and allergies, immunization status, lab-oratory test results, radiology images, vital signs, personalstats like age and weight, and billing information[28]. Thepatient data is private and sensitive, and should be protectedfrom illegal access.
Typical EHR system must be safe from any possible com-puter crime, improper identification access. While the infor-mation technology crime is becoming more sophisticatedand frequent, so have the people charged with preventingit and disciplining its outlaws. It includes enforcing laws,computer emergency response team and tools for fightingfraudulent & unauthorized online uses. Identification & Ac-cess: There are three ways a computer system can verifythat someone have legitimate right of access. The securitysystem in EHR could authenticate users’ identity by deter-mining (1) what you have, (2) what you know, or (3) whoyou are. Credit cards, debit cards, and cash-machine cardsall have magnetic strips or built-in computer chips that iden-tify users to the machine.
The computer room used to access information of EHRmay kept locked, requiring a key or may be guarded by se-curity officers, who may need to see an authorized signa-ture or badge (what you have). And the computers couldbe locked with password (what you know). Some securitys are using biometrics, the science of measuring individualbody characteristics (who you are). Protection of Software& Data: Procedures such as making backup disks, protect-ing against viruses can help security in EHR. Security pro-cedures for protection of software & data in EHR includecontrol of access (Access to online files is restricted to thosewho have a legitimate right to access), audit controls (fortracking which programs and servers were used, which filesopened, and so on to creates an audit trail) and people con-trols (people are the greatest threat to a computer system,security precautions begin with the screening of job appli-cants)
5. IMPORTANCE OF QOS PROVISION IN FU-TURE HEALTH COMMUNICATION INFRAS-TRUCTURE
The QoS is one of the most elusive, confounding, and con-fusing topics in data networking today[29]. While researchpapers on QoS hardly ever questioning raison d’etre it isfrequently the topic of heated debates. Why there are somany publications and even workshops on a topic which isquestioned vehemently while at the same time has so littleimpact on current products or services[30] The term ser-vice quality may have a different meaning to different peo-ple[31]. This is perhaps more accurately called QoS, as op-posed to service quality, which could be taken to mean theentirety of outcome and experience[32].
The great majority of users are not interested in the en-gineering of telecommunications networks or its QoS spec-ifications; instead they expect fast, reliable, and easy ac-cess to online resources, applications and Internet (i.e., on-line databases, banking services, e-commerce, e-mails, webservers, etc.)[33].
IIAE Journal, Vol.2, No.3, 2014
Future e-Health, QoS Provision and Cybersecurity Challenges 119
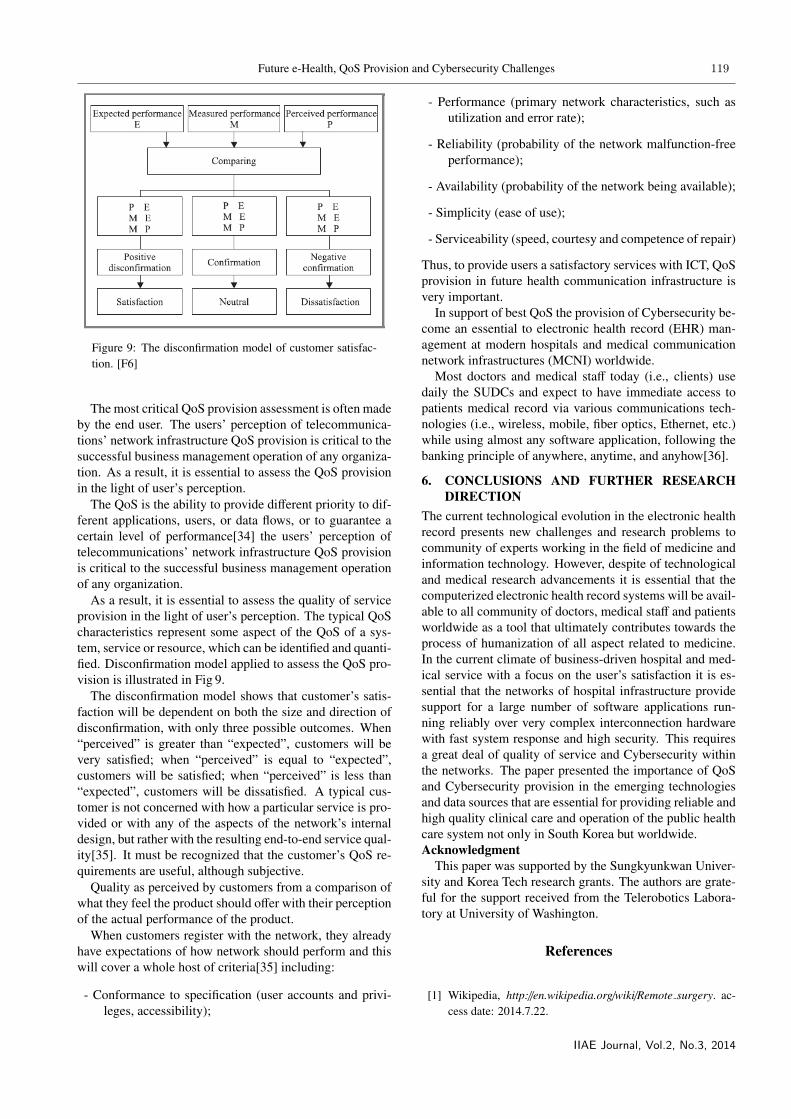
Figure 9: The disconfirmation model of customer satisfac-tion. [F6]
The most critical QoS provision assessment is often madeby the end user. The users’ perception of telecommunica-tions’ network infrastructure QoS provision is critical to thesuccessful business management operation of any organiza-tion. As a result, it is essential to assess the QoS provisionin the light of user’s perception.
The QoS is the ability to provide different priority to dif-ferent applications, users, or data flows, or to guarantee acertain level of performance[34] the users’ perception oftelecommunications’ network infrastructure QoS provisionis critical to the successful business management operationof any organization.
As a result, it is essential to assess the quality of serviceprovision in the light of user’s perception. The typical QoScharacteristics represent some aspect of the QoS of a sys-tem, service or resource, which can be identified and quanti-fied. Disconfirmation model applied to assess the QoS pro-vision is illustrated in Fig 9.
The disconfirmation model shows that customer’s satis-faction will be dependent on both the size and direction ofdisconfirmation, with only three possible outcomes. When“perceived” is greater than “expected”, customers will bevery satisfied; when “perceived” is equal to “expected”,customers will be satisfied; when “perceived” is less than“expected”, customers will be dissatisfied. A typical cus-tomer is not concerned with how a particular service is pro-vided or with any of the aspects of the network’s internaldesign, but rather with the resulting end-to-end service qual-ity[35]. It must be recognized that the customer’s QoS re-quirements are useful, although subjective.
Quality as perceived by customers from a comparison ofwhat they feel the product should offer with their perceptionof the actual performance of the product.
When customers register with the network, they alreadyhave expectations of how network should perform and thiswill cover a whole host of criteria[35] including:
- Conformance to specification (user accounts and privi-leges, accessibility);
- Performance (primary network characteristics, such asutilization and error rate);
- Reliability (probability of the network malfunction-freeperformance);
- Availability (probability of the network being available);
- Simplicity (ease of use);
- Serviceability (speed, courtesy and competence of repair)
Thus, to provide users a satisfactory services with ICT, QoSprovision in future health communication infrastructure isvery important.
In support of best QoS the provision of Cybersecurity be-come an essential to electronic health record (EHR) man-agement at modern hospitals and medical communicationnetwork infrastructures (MCNI) worldwide.
Most doctors and medical staff today (i.e., clients) usedaily the SUDCs and expect to have immediate access topatients medical record via various communications tech-nologies (i.e., wireless, mobile, fiber optics, Ethernet, etc.)while using almost any software application, following thebanking principle of anywhere, anytime, and anyhow[36].
6. CONCLUSIONS AND FURTHER RESEARCHDIRECTION
The current technological evolution in the electronic healthrecord presents new challenges and research problems tocommunity of experts working in the field of medicine andinformation technology. However, despite of technologicaland medical research advancements it is essential that thecomputerized electronic health record systems will be avail-able to all community of doctors, medical staff and patientsworldwide as a tool that ultimately contributes towards theprocess of humanization of all aspect related to medicine.In the current climate of business-driven hospital and med-ical service with a focus on the user’s satisfaction it is es-sential that the networks of hospital infrastructure providesupport for a large number of software applications run-ning reliably over very complex interconnection hardwarewith fast system response and high security. This requiresa great deal of quality of service and Cybersecurity withinthe networks. The paper presented the importance of QoSand Cybersecurity provision in the emerging technologiesand data sources that are essential for providing reliable andhigh quality clinical care and operation of the public healthcare system not only in South Korea but worldwide.Acknowledgment
This paper was supported by the Sungkyunkwan Univer-sity and Korea Tech research grants. The authors are grate-ful for the support received from the Telerobotics Labora-tory at University of Washington.
References
[1] Wikipedia, http://en.wikipedia.org/wiki/Remote surgery. ac-cess date: 2014.7.22.
IIAE Journal, Vol.2, No.3, 2014

120 E. Babulak, M. Jin and Y.-S. Kim
[2] M.J. Lum, J. Rosen, H. King, D.C. Friedman, T.S. Lend-vay, A.S. Wright, et al., “Teleoperation in Surgical RoboticsNetwork Latency Effects on Surgical Performance”, ConfProc IEEE Eng Med Biol Soc, pp.6860-6863, 2009.DOI:10.1109/IEMBS.2009.5333120.
[3] B. Hannaford, J. Rosen, D.W. Friedman, H. King, P. Roan,L. Cheng, et al., “Raven-II: An Open Platform for SurgicalRobotics Research”, IEEE Trans Biomed Eng Vol.60 No.4,pp.954-959, 2013. DOI:10.1109/TBME.2012.2228858.
[4] G. Sankaranarayanan, H. King, S.Y. Ko, M.J.H Lum, D.C.W.Friedman, J. Rosen and B. Hannaford, “Portable surgerymaster station for mobile robotic telesurgery”, Proceedingsof the 1st international conference on Robot communicationand coordination, pp.15-17, 2007.
[5] H.H. King, K. Tadano, R. Donlin, D. Friedman, M.J.HLum, V. Asch, et al., “Preliminary protocol for interop-erable telesurgery”, International Conference on AdvancedRobotics Advanced Robotics, pp.1-6, 2009.
[6] T. Bonaci, H.J. Chizeck, “Surgical Telerobotics Meets Infor-mation Security”, 21st Usenix Security Symposium, 2012.
[7] G. Slabodkin, “Problem of hospital readmissions, benefitsof telemedicine hit home [Internet]. Fierce Mobile Health-care”, http://www.fiercemobilehealthcare.com/story/problem-hospital-readmissions-benefits-telemedicine-hit-home.access date: 2013.02.01
[8] CADTH, “Canadian Agency for Drugs and Technologiesin Health”, http://www.cadth.ca/products/environmental-scanning/environmental-scans/environmental-scan-27.access date: 2014.7.22.
[9] CARP, http://www.carp.ca/advocacy/advarticle-display.cfm?documentID=6061. access date: 2014.7.22.
[10] C.W. Van, I.A. Dhalla, C. Bell, E. Etchells, I.G. Stiell, K.Zarnke, et al., “Derivation and Validation of an index to pre-dict early death or unplanned readmission after dischargefrom hospital to the community”, CMAJ , Vol.182, No.6,pp.551-557, 2010.
[11] Polycom, http://www.polycom.com/products-services/realpresence-platform.html. access date: 2014.7.22
[12] Polycom, http://www.polycom.com/company/news/press-releases/2012/201209100.html. access date: 2013.6.11.
[13] L. Wilbanks, “Cybersecurity: Welcome to My World”, ITProfessional, Vol.9, No.2, pp.61-64, 2007.
[14] L. Hoffman, “Exploring a national cybersecurity exercisefor universities”, Security & Privacy, Vol.3, No.5, pp.27-33,2005. DOI:10.1109/MSP.2005.120.
[15] W. Chou, “Cybersecurity Costs: Balancing Blanket Securitywith Real-World Practicality”, IT Professional, Vol.9, No.2,pp.16-20, 2007.
[16] S. Ghemouti-Helie, “A National Strategy for an Ef-fective Cybersecurity Approach and Culture”, ProcInt Conf Availab Reliab Secur, pp.370-373, 2010.DOI:10.1109/ARES.2010.119.
[17] J.D. Howard and T.A. Longstaff, “A common language forcomputer security incidents”, Technical report, Sandia Na-tional Laboratories, 1998.
[18] Dimensional Research, “The Impact of Mobile De-vices on Information Security: A Survey of ITProfessionals [Internet] Dimensional Research”,http://www.checkpoint.com/downloads/products/check-point-mobile-security-survey-report.pdf. access date:2014.7.22.
[19] “IT Management”, WILEY, 2011.
[20] HoneyMap [Internet] “Honeynet Project”,http://map.honeynet.org, access date: 2014.7.22.
[21] M.G. Lee, “Securing the human to protect the sys-tem: Human factors in Cybersecurity”, incorporat-ing the Cyber Security Conference, pp.1-5, 2012.DOI:10.1049/cp.2012.1519.
[22] A. Beautement, M.A. Sasse and M. Wonham, “The compli-ance budget: managing security behavior in organizations”,Proceedings of 2008 Workshop on New Security Paradigms,pp.47-58, 2008. DOI:10.1145/1595676.1595684.
[23] N. Ye, Y. Zhang and C.M. Borror, “Robustness ofthe Markov-chain model for cyber-attack detec-tion”, Reliability Vol.53, No.1, pp.116-123, 2004.DOI:10.1109/TR.2004.823851.
[24] R. Gandhi, A. Sharma, W. Mahoney, W. Sousan, Z. Qium-ing and P. Laplante, “Dimensions of Cyber-Attacks: Cul-tural, Social”, Economic, and Political, Technology andSociety Magazine, Vol.30, No.1, pp.28-38, 2011. DOI:10.1109/MTS.2011.940293.
[25] SINA, http://tech.sina.com.cn/it/2012-07-04/09317346411.shtml
[26] C.W. Ten, G. Manimaran and C.C. Liu, “Cybersecu-rity for Critical Infrastructures, Attack and Defense Mod-eling”, Systems, Man and Cybernetics, Part A: Sys-tems and Humans, Vol.40, No.4, pp.853-865, 2010.DOI:10.1109/TSMCA.2010.2048028.
[27] T.D. Gunter and N.P. Terry, “The Emergence of Na-tional Electronic Health Record Architectures in the UnitedStates and Australia”Models, Costs, and Questions, Jour-nal of Medical Internet Research, Vol.7, No.1, 2005.DOI:10.2196/jmir.7.1.e3 .
[28] Wikipedia, http://en.wikipedia.org/wiki/Electronic health re-cord#cite note-1. access date: 2014.7.22.
[29] P. Ferguson and G. Huston, “Quality of Service”, Wiley,1998.
[30] M. Ott, “What is wrong with QoS research?”, NEC InternalReport, C&C Research Laboratories, 1998.
[31] E. Babulak, “Trader’s quality of service specifications andeffects on system performance for video-on-demand”, Inter-national Conference of Multimedia and Expo, pp.837-842,2000. DOI:10.1109/ICME.2000.871490.
[32] R. Johnston and G. Clark, “Service Operations Manage-ment”, Financial Times, Prentice Hall, 2001.
IIAE Journal, Vol.2, No.3, 2014

Future e-Health, QoS Provision and Cybersecurity Challenges 121
[33] E. Babulak and R.A. Carrasco, “The university networkmodel for the quality of service provision analysis”, Inter-national Journal of Mathematics, Vol.2, No.7, pp.651-661,2002.
[34] Wikipedia, http://en.wikipedia.org/wiki/Quality of service.access date: 2014.7.22.
[35] D.J. Wright, “Assessment of alternative transport optionsfor video distribution and retrieval over ATM in residen-tial broadband”, IEEE Communication Magazine, Vol.35,No.12, pp.78-87, 1997. DOI:10.1109/35.642836.
[36] E. Babulak and R.A. Carrasco, “The IT quality of serviceprovision analysis in light of user’s perception and expecta-tions”, International Symposium of CSNDSP, 2002.
FIGURE SOURCES(F1) Collaborative Video Solution in Healthcare, Center
for Digital Government, May 2013 issue, Canada.
(F2) B. Hannaford, D.C. Friedman, H. King, M. Lum,J. Rosen, G. Sankaranarayanan, 2009, Evaluation ofRAVEN surgical Telerobot during the NASA ExtremeEnvironment Mission Operations (NEEMO) 12 Mis-sion, Technical Report, Deptment of Electrical Engi-neering, University of Washington.
(F3) B. Hannaford, J. Rosen, D.W. Friedman, H. King, P.Roan, L. Cheng, et al., Raven-II: An Open Platform forSurgical Robotics Research, IEEE Trans Biomed Eng60 (4) (2013) 954-959.
(F4) G. Sankaranarayanan, H. King, S.Y. Ko, M.J.H Lum,D.C.W. Friedman, J. Rosen, B. Hannaford, Portablesurgery master station for mobile robotic telesurgery,in: Proceedings of the 1st international conference onRobot communication and coordination, Greece, Oct.15-17, IEEE, 2007.
(F5) Honeynet Project. http://map.honeynet.org (Visitedon 11 Jun. 2013)
(F6) E. Babulak, Methodology to measure the quality ofservice in healthcare information and telecommunica-tions infrastructures, Journal of Telecommunicationsand Information Technology (2005) pp.133-138.
TABLE SOURCES(T1) IT manegement, WILEY, 2011.
ACRONYMS LISTISO: International Organization for StandardizationIEC: International Electrotechnical CommissionNERC: North American Electric Reliability CorporationRFC: Request for CommentsIETF: Internet Engineering Task Force
IIAE Journal, Vol.2, No.3, 2014




















