full-text.pdf - Cjasn
19
Article Secular Trends in the Cost of Immunosuppressants after Solid Organ Transplantation in the United States Margaret E. Helmuth, 1 Qian Liu, 1 Marc N. Turenne, 1 Jeong M. Park, 2 Murewa Oguntimein, 3 Sarah K. Dutcher, 3 Rajesh Balkrishnan, 4 Pratima Sharma, 5 Jarcy Zee, 1 Alan B. Leichtman, 1 and Abigail R. Smith 1 Abstract Background and objectives Immunosuppressive medications are critical for maintenance of graft function in transplant recipients but can represent a substantial financial burden to patients and their insurance carriers. Design, setting, participants, & measurements To determine whether availability of generic immunosuppressive medications starting in 2009 may have alleviated some of that burden, we used Medicare Part D prescription drug events between 2008 and 2013 to estimate the average annualized per-patient payments made by patients and Medicare in a large national sample of kidney, liver, and heart transplant recipients. Repeated measures linear regression was used to determine changes in payments over the study period. Results Medicare Part D payments for two commonly used immunosuppressive medications, tacrolimus and mycophenolic acid (including mycophenolate mofetil and mycophenolate sodium), decreased overall by 48%–67% across organs and drugs from 2008 to 2013, reflecting decreasing payments for brand and generic tacrolimus (21%–54%), and generic mycophenolate (72%–74%). Low-income subsidy payments, which are additional payments made under Medicare Part D, also decreased during the study period. Out-of-pocket payments by patients who did not receive the low-income subsidy decreased by more than those who did receive the low-income subsidy (63%–79% versus 24%–44%). Conclusions The decline in payments by Medicare Part D and by transplant recipients for tacrolimus and mycophenolate between 2008 and 2013 suggests that the introduction of generic immunosuppressants during this period has resulted in substantial cost savings to Medicare and to patients, largely reflecting the transition from brand to generic products. Clin J Am Soc Nephrol 14: 421–430, 2019. doi: https://doi.org/10.2215/CJN.10590918 Introduction Solid organ transplantation is a life-saving and cost- effective (1,2) treatment for patients with end-stage organ failure. In order to maintain a functioning graft, however, transplant recipients must remain on immunosuppressive medications for the rest of their lives. In 2000, the yearly average cost of standard maintenance immunosuppressive medication regi- mens for kidney transplant recipients was estimated to be between $10,000 and $14,000 (3). Since then, generic versions of some commonly prescribed im- munosuppressive medications, including tacrolimus, mycophenolate mofetil, and mycophenolate sodium, have become available (4). The fi rst generic versions of mycophenolate mofetil and tacrolimus were approved by the US Food and Drug Adminis- tration (FDA) in 2008 and 2009, respectively (5,6). Use of generic versions of these immunosuppressive med- ications increased rapidly after their initial market entry; by 2013, 80%–90% of prescriptions covered under Medicare Part D for tacrolimus or mycophenolate mofetil were dispensed as generics (7). A generic version of mycophenolate sodium, frequently prescribed as an alternative to mycophenolate mofetil, was approved in 2012. Generic substitution for brand-name products is thought to reduce pharmaceutic expenditures while delivering comparable therapeutic benefit (8). Medicare pays for 60%, 30%, and 39% of kidney, liver, and heart transplants, respectively (9). Medicare also covers immunosuppressive medications for eli- gible kidney transplant recipients for 3 years after transplant via Part B. Payment beyond that time and for all other organs requires that patients qualify for Medicare coverage on the basis of age or disability. Transplant recipients with other sources of coverage may have their immunosuppressive medications cov- ered by Medicare Part D when they become eligible. Coverage for immunosuppressive medications for the duration of transplant function has been recom- mended; however, such a policy has gained little traction in the United States (3,10). Generic immunosuppressive medications have the potential to reduce costs for transplant recipients, resulting in a wide range of social and economic benefits for patients and the United States health care system. Despite the expected benefits of more 1 Arbor Research Collaborative for Health, Ann Arbor, Michigan; 2 College of Pharmacy, University of Michigan, Ann Arbor, Michigan; 3 Center for Drug Evaluation and Research, US Food and Drug Administration, Washington, DC; and 4 Public Health Sciences, School of Medicine, University of Virginia, Charlottesville, Virginia 5 Department of Internal Medicine, University of Michigan, Ann Arbor, Michigan Correspondence: Margaret E. Helmuth, Arbor Research Collaborative for Health, 340 E. Huron Street, Suite 300, Ann Arbor, MI 48104. Email: margaret. helmuth@ arborresearch.org www.cjasn.org Vol 14 March, 2019 Copyright © 2019 by the American Society of Nephrology 421
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of full-text.pdf - Cjasn
Article
Secular Trends in the Cost of Immunosuppressants afterSolid Organ Transplantation in the United States
Margaret E. Helmuth,1 Qian Liu,1 Marc N. Turenne,1 Jeong M. Park,2 Murewa Oguntimein,3 Sarah K. Dutcher,3
Rajesh Balkrishnan,4 Pratima Sharma,5 Jarcy Zee,1 Alan B. Leichtman,1 and Abigail R. Smith1
AbstractBackground and objectives Immunosuppressive medications are critical for maintenance of graft function intransplant recipients but can represent a substantial financial burden to patients and their insurance carriers.
Design, setting, participants, & measurements To determine whether availability of generic immunosuppressivemedications starting in 2009mayhave alleviated some of that burden,weusedMedicare PartDprescription drugevents between 2008 and 2013 to estimate the average annualized per-patient payments made by patients andMedicare in a large national sample of kidney, liver, and heart transplant recipients. Repeated measures linearregression was used to determine changes in payments over the study period.
Results Medicare Part D payments for two commonly used immunosuppressive medications, tacrolimusand mycophenolic acid (including mycophenolate mofetil and mycophenolate sodium), decreased overall by48%–67% across organs and drugs from 2008 to 2013, reflecting decreasing payments for brand and generictacrolimus (21%–54%), and generic mycophenolate (72%–74%). Low-income subsidy payments, which areadditional payments made under Medicare Part D, also decreased during the study period. Out-of-pocketpayments by patients who did not receive the low-income subsidy decreased by more than those whodid receive the low-income subsidy (63%–79% versus 24%–44%).
Conclusions The decline in payments by Medicare Part D and by transplant recipients for tacrolimus andmycophenolate between2008 and2013 suggests that the introduction of generic immunosuppressants during thisperiod has resulted in substantial cost savings to Medicare and to patients, largely reflecting the transition frombrand to generic products.
Clin J Am Soc Nephrol 14: 421–430, 2019. doi: https://doi.org/10.2215/CJN.10590918
IntroductionSolid organ transplantation is a life-saving and cost-effective (1,2) treatment for patients with end-stageorgan failure. In order to maintain a functioninggraft, however, transplant recipients must remain onimmunosuppressive medications for the rest of theirlives. In 2000, the yearly average cost of standardmaintenance immunosuppressive medication regi-mens for kidney transplant recipients was estimatedto be between $10,000 and $14,000 (3). Since then,generic versions of some commonly prescribed im-munosuppressive medications, including tacrolimus,mycophenolate mofetil, and mycophenolate sodium,have become available (4). The first genericversions of mycophenolate mofetil and tacrolimuswere approved by the US Food and Drug Adminis-tration (FDA) in 2008 and 2009, respectively (5,6). Useof generic versions of these immunosuppressive med-ications increased rapidly after their initial marketentry; by 2013, 80%–90% of prescriptions covered underMedicare Part D for tacrolimus or mycophenolatemofetil were dispensed as generics (7). A generic versionof mycophenolate sodium, frequently prescribed as an
alternative to mycophenolate mofetil, was approvedin 2012. Generic substitution for brand-name productsis thought to reduce pharmaceutic expenditures whiledelivering comparable therapeutic benefit (8).Medicare pays for 60%, 30%, and 39% of kidney,
liver, and heart transplants, respectively (9). Medicarealso covers immunosuppressive medications for eli-gible kidney transplant recipients for 3 years aftertransplant via Part B. Payment beyond that time andfor all other organs requires that patients qualify forMedicare coverage on the basis of age or disability.Transplant recipients with other sources of coveragemay have their immunosuppressive medications cov-ered by Medicare Part D when they become eligible.Coverage for immunosuppressive medications forthe duration of transplant function has been recom-mended; however, such a policy has gained littletraction in the United States (3,10).Generic immunosuppressive medications have the
potential to reduce costs for transplant recipients,resulting in a wide range of social and economicbenefits for patients and the United States healthcare system. Despite the expected benefits of more
1Arbor ResearchCollaborative forHealth, Ann Arbor,Michigan; 2College ofPharmacy, Universityof Michigan, AnnArbor, Michigan;3Center for DrugEvaluation andResearch,US Food andDrug Administration,Washington, DC; and4Public HealthSciences, School ofMedicine, Universityof Virginia,Charlottesville,Virginia 5Departmentof Internal Medicine,University ofMichigan, Ann Arbor,Michigan
Correspondence:Margaret E. Helmuth,Arbor ResearchCollaborative forHealth, 340 E. HuronStreet, Suite 300, AnnArbor, MI 48104.Email: [email protected]
www.cjasn.org Vol 14 March, 2019 Copyright © 2019 by the American Society of Nephrology 421

affordable immunosuppressive medications, little infor-mation is available regarding the actual financial effect ofsubstitution with generic immunosuppressive medications(11). The objective of our study was to assess potential costsavings from substitution with generic immunosuppres-sive medications for organ transplant recipients and theMedicare Part D program. We examined the trajectoriesof per-patient payments for brand-name and generictacrolimus and mycophenolate mofetil and brand-namemycophenolate sodium in a large national sample over a6-year period, during which generic versions of these drugswere first introduced.
Materials and MethodsData and Study SampleThis study used data from the Scientific Registry of
Transplant Recipients (SRTR). The SRTR includes dataon all donors, wait-listed candidates, and transplantrecipients in the United States, submitted by members ofthe Organ Procurement and Transplantation Network(OPTN). The Health Resources and Services Adminis-tration (HRSA), US Department of Health and HumanServices, provides oversight to OPTN and SRTR con-tractor activities.SRTR data were used to identify all United States
kidney, liver, and heart recipients transplanted between1987 and 2013. The SRTR data set was linked to MedicarePart D prescription drug event data to identify immu-nosuppressive medication prescriptions filled between2008 and 2013 for transplant recipients whose immuno-suppressive medications were covered through a Part Dplan. This study period reflects years shortly beforeand after generic versions of the most common immu-nosuppressive medications became available. The linkeddata set was used to estimate transplant recipients’ out-of-pocket payments, Medicare Part D prescription drugplan payments, and Medicare Part D low-income sub-sidy payments for generic and brand-name oral immu-nosuppressive medications dispensed after heart, liver,or kidney transplantation.Patients were eligible for analysis if they received a
single-organ transplant and maintained graft function forat least 30 days after transplantation; had graft function onJanuary 1, 2008 for those transplanted before 2008; andhad at least one post-transplant Part D prescription drugevent during the study period for tacrolimus, mycophe-nolate mofetil, or mycophenolate sodium. Patients withrepeat transplants were allowed to contribute multipletransplants to the analysis if the above criteria were met foreach transplant. Prescription drug events for immunosup-pressive medications reported between graft failure andrepeat transplantation were excluded from analysis. Thisstudy was deemed exempt from Institutional ReviewBoard review.
Statistical AnalysesWe calculated the average annualized amount paid by
transplant recipients, Medicare Part D plans, and the Medi-care Part D low-income subsidy program for brand-name andgeneric tacrolimus and mycophenolate mofetil and brand-name mycophenolate sodium. The FDA approved generic
mycophenolate sodium in August of 2012 (not observed inour data; only brand-name mycophenolate sodium data arepresented in these analyses). An overall average annualizedper-patient payment amount that included brand-name andgeneric products was calculated to show overall paymenttrends during the study period. Because mycophenolatesodium is often used as a substitute for mycophenolate mofetil,and we only observed brand-name mycophenolate sodiumuse, the overall average per-patient payment amounts formycophenolate mofetil and mycophenolate sodium werecombined into one estimate for any mycophenolic acidproduct.Per-patient payment amounts were annualized to a full
calendar year to account for patients with partial years ofprescription drug data, i.e., patients transplanted or en-rolled/dis-enrolled from Medicare Part D during a givenyear, or patients with periods of missing prescription drugevents. Annualized per-patient payment amounts werecalculated as the total amount paid during the year,divided by the proportion of days with immunosuppres-sive medication prescription coverage during that year.Average annualized per-patient payment amounts werecalculated by averaging all patients’ annualized per-patientpayment amounts, across each year, weighted by theproportion of days each patient had immunosuppressivemedication prescription coverage. The proportion of dayswith immunosuppressive medication prescription cover-age was calculated using the total number of days’ supplyreported for each recipient’s prescription drug events foreach specific immunosuppressive medication in a year,divided by the number of days in that year. Many trans-plant recipients had multiple prescriptions for the sameimmunosuppressive medication, with overlapping daysof supply covering the same period of time. Medicare PartD prescription drug event data do not include informa-tion on dose prescribed; in these cases, days with over-lapping immunosuppressive medication prescriptionsof the same medication were only counted once. Theaverage annualized per-patient payment amount thusrepresents an estimate of the amount that would be paidby a patient, by a Part D plan, or in the form of a low-income subsidy, if the patient had been transplanted,enrolled in Medicare, and filled immunosuppressivemedication prescriptions covered by Part D for an entireyear.Overall, brand-name, and generic average annualized
per-patient payment amounts were calculated separatelyfor each organ and immunosuppressive medication foreach year from 2008 to 2013. Patient and low-incomesubsidy payment amounts were reported separately bypatient low-income subsidy status. All payment amountswere adjusted for price inflation using the Consumer PriceIndex for All Urban Consumers from the US Bureau ofLabor Statistics, and are expressed in 2013 dollars (12).To determine whether the change in overall average
annualized per-patient payments from the start (year2008) to the end (year 2013) of our study period wasstatistically significant, we used repeated measures linearregression with annualized payments as the outcome andcalendar year as a categorical variable and reportedP values from pairwise comparisons between years the2008 and 2013. Regression was done separately by organ
422 Clinical Journal of the American Society of Nephrology
Table 1. Descriptive statistics for transplant recipients with tacrolimus or mycophenolic acid prescription drug events throughMedicare Part D during 2008–2013, by organ type
Variable Kidney Liver Heart
Number of transplant recipients 27,625 15,882 6851Number of transplants 27,736 15,958 6874Yr of transplant1987–1990 223 (1%) 216 (1%) 124 (2%)1991–1995 1007 (4%) 1003 (6%) 539 (8%)1996–2000 4146 (15%) 2637 (17%) 1341 (20%)2001–2005 8560 (31%) 4643 (29%) 1949 (28%)2006–2010 10,963 (40%) 5753 (36%) 2266 (33%)2011–2013 2726 (10%) 1630 (10%) 632 (9%)
Male 15,787 (57%) 9638 (61%) 4980 (73%)Racea
White 14,382 (52%) 11,409 (72%) 4954 (72%)Black 6869 (25%) 1345 (9%) 1150 (17%)Hispanic/Latino 4417 (16%) 2308 (15%) 551 (8%)Asian/Other 1956 (7%) 815 (5%) 196 (3%)
Age at transplant, yrMedian (IQR) 52 (39–61) 54 (48–60) 54 (45–60),18 1023 (4%) 145 (1%) 107 (2%)18–34 3979 (14%) 824 (5%) 712 (10%)35–49 7002 (25%) 3861 (24%) 1577 (23%)50–64 11,762 (43%) 9779 (62%) 3919 (57%)65+ 3859 (14%) 1273 (8%) 536 (8%)
Age at first Medicare Part D claim during 2008–2013, yrMedian (IQR) 58 (45–66) 60 (53–65) 62 (50–66),18 557 (2%) 3 (0.0%) 5 (0.1%)18–34 2891 (11%) 647 (4%) 597 (9%)35–49 5620 (20%) 1894 (12%) 989 (14%)50–64 9618 (35%) 7992 (50%) 2630 (38%)65+ 8939 (32%) 5346 (34%) 2630 (38%)
BMIa
,18.5 1071 (4%) 372 (3%) 263 (4%)18.5–24.9 8519 (35%) 4375 (30%) 2429 (37%)25.0–29.9 7773 (32%) 5182 (35%) 2400 (37%)$30 6870 (28%) 4810 (33%) 1404 (22%)
Donor typea
Donation after circulatory death 1410 (5%) 474 (3%)Donation after brain death 15,446 (57%) 14,186 (93%)Living related donation 6933 (26%) 382 (3%)Living unrelated donation 3319 (12%) 140 (1%)
Previous transplant of the same organ type 3010 (11%) 884 (6%) 145 (2%)Number of human leukocyte antigen mismatches: 1–6 versus 0a 23,865 (88%)Recipient diagnosis (kidney)a
Diabetes 6168 (23%)Hypertension 6140 (22%)GN 6943 (25%)Cystic kidney disease 2410 (9%)Other 5728 (21%)
Recipient diagnosis (liver)b
Acute hepatic necrosis 933 (6%)Cholestatic liver disease/cirrhosis 2011 (13%)Noncholestatic cirrhosis 7933 (50%)Hepatitis C 6408 (40%)Malignant neoplasm 2812 (18%)Metabolic disease 584 (4%)Other liver disease 2307 (15%)
Recipient diagnosis (heart)a
Coronary artery disease 2925 (43%)Cardiomyopathy 3416 (50%)Congenital/valvular/other 501 (7%)
Ventricular assist device (heart)a 1746 (38%)
Data displayed as n (%) unless otherwise noted. IQR, interquartile range; BMI, body mass index.aMissing for at most 5% of patients, except BMImissing for 7% and 12% of Medicare Part D liver and kidney patients, respectively, andventricular assist device missing for 33% of Medicare Part D heart patients.bDiagnoses for liver transplant recipients are on the basis of primary and secondarydiagnoses andare notmutually exclusive. Each liverrecipient can have one or two diagnoses; therefore, percentages will not sum to 100%.
Clin J Am Soc Nephrol 14: 421–430, March, 2019 Immunosuppressant Cost after Solid Organ Transplantation, Helmuth et al. 423
type and immunosuppressive medication. All analyseswere conducted using SAS version 9.4 (SAS Institute,Inc., Cary, NC).
ResultsThere were 27,625 kidney, 15,882 liver, and 6851 heart
transplant recipients enrolled in Part D who were eligible forthis study, accounting for 8%, 14%, and 12% of all kidney,
liver, and heart transplant recipients since 1987, respectively. Inall three cohorts, recipients were predominantly male, white,and aged 50–64 years (Table 1). Among kidney transplantrecipients, 38% had living donor transplants, compared withonly 3% of liver recipients. Previous transplants of the sameorgan typewere reported for 11%, 6%, and 2% of kidney, liver,and heart transplant recipients, respectively. Compared withthe SRTR transplant population not included in our Medicare
Tacrolimus
$10,000
$8000
$6000
$4000
$2000
$10,000
$8000
$6000
$4000
$2000
Ave
rage
Ann
ualiz
ed M
edic
are
Par
t D P
aym
ents
$10,000
$8000
$6000
$4000
$2000
$0
2008 2009 2010 2011 2012 2013 2008Year
2009 2010 2011 2012 2013
$0
$0
Mycophenolic Acid
Kid
ney
Live
rH
eart
OverallBrand Tacrolimus or Mycophenolate Mofetil
Generic Tacrolimus or Mycophenolate Mofetil
Brand Mycophenolate Sodium
BA
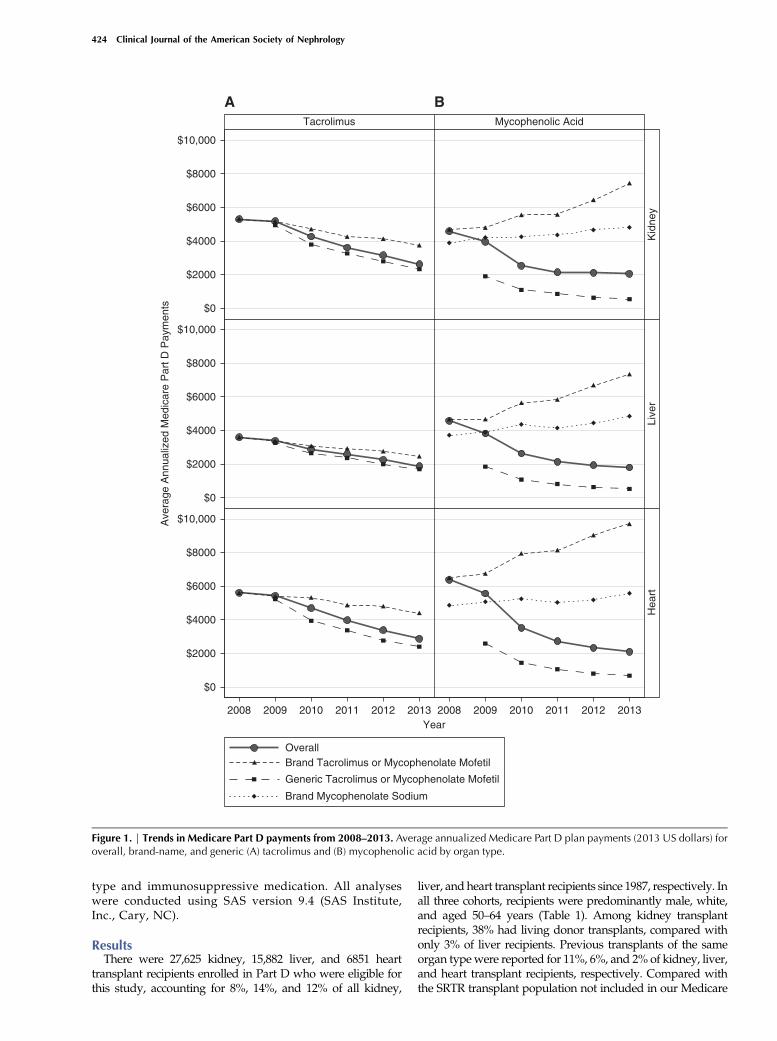
Figure 1. | Trends in Medicare Part D payments from 2008–2013. Average annualized Medicare Part D plan payments (2013 US dollars) foroverall, brand-name, and generic (A) tacrolimus and (B) mycophenolic acid by organ type.
424 Clinical Journal of the American Society of Nephrology
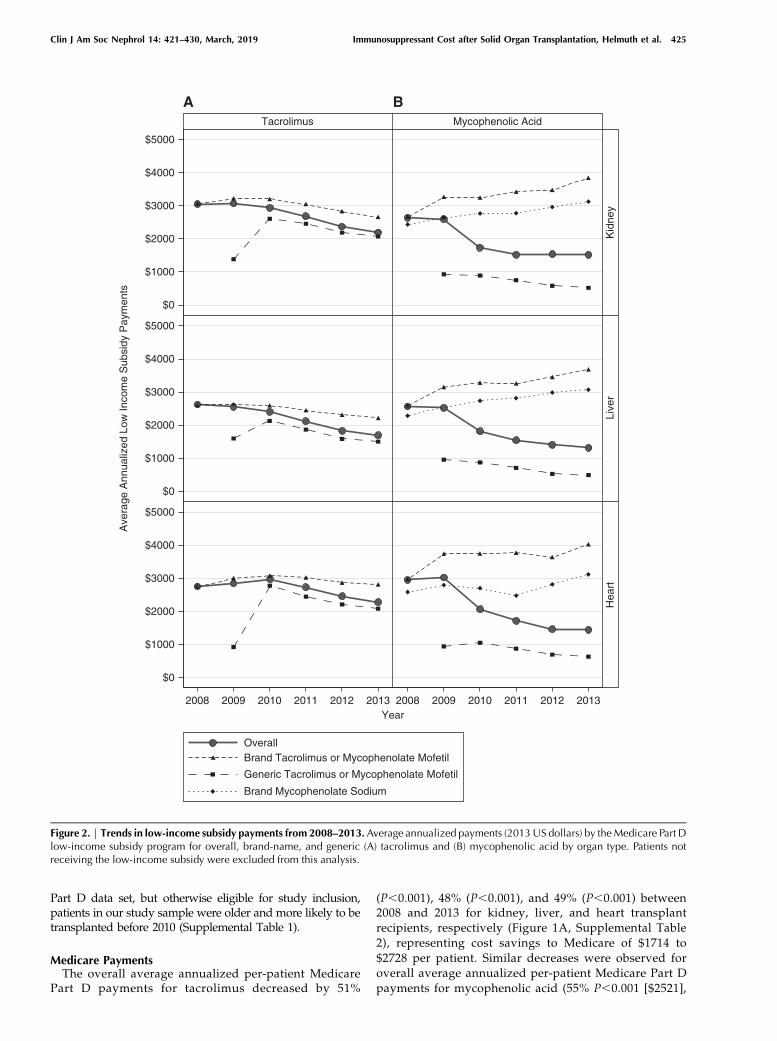
Part D data set, but otherwise eligible for study inclusion,patients in our study sample were older and more likely to betransplanted before 2010 (Supplemental Table 1).
Medicare PaymentsThe overall average annualized per-patient Medicare
Part D payments for tacrolimus decreased by 51%
(P,0.001), 48% (P,0.001), and 49% (P,0.001) between2008 and 2013 for kidney, liver, and heart transplantrecipients, respectively (Figure 1A, Supplemental Table2), representing cost savings to Medicare of $1714 to$2728 per patient. Similar decreases were observed foroverall average annualized per-patient Medicare Part Dpayments for mycophenolic acid (55% P,0.001 [$2521],
Tacrolimus
$5000
$4000
$3000
$2000
$1000
$5000
$4000
$3000
$2000
$1000
Ave
rage
Ann
ualiz
ed L
ow In
com
e S
ubsi
dy P
aym
ents
$5000
$4000
$3000
$2000
$1000
$0
$0
$0
Mycophenolic Acid
Kid
ney
Live
rH
eart
2008 2009 2010 2011 2012 2013 2008Year
2009 2010 2011 2012 2013
OverallBrand Tacrolimus or Mycophenolate Mofetil
Generic Tacrolimus or Mycophenolate Mofetil
Brand Mycophenolate Sodium
BA
Figure 2. | Trends in low-income subsidy payments from 2008–2013.Average annualized payments (2013US dollars) by theMedicare Part Dlow-income subsidy program for overall, brand-name, and generic (A) tacrolimus and (B) mycophenolic acid by organ type. Patients notreceiving the low-income subsidy were excluded from this analysis.
Clin J Am Soc Nephrol 14: 421–430, March, 2019 Immunosuppressant Cost after Solid Organ Transplantation, Helmuth et al. 425
61% P,0.001 [$2771], and 67% P,0.001 [$4262] for kidney,liver, and heart recipients, respectively; Figure 1B). Thedecline in overall average per-patient payments largelyreflects a shift toward increased generic use. Declines in theaverage overall per-patient Medicare Part D payments wereobserved for brand-name (29%, 32%, and 21% for kidney,liver, and heart recipients between 2008 and 2013,
respectively) and generic tacrolimus (53%, 48%, and 54%for kidney, liver, and heart recipients between 2009and 2013, respectively). Unlike for tacrolimus, overallper-patient payment amounts for Medicare Part D benefi-ciaries for brand-name mycophenolate mofetil and brand-name mycophenolate sodium increased over time for allorgans. From 2008 to 2013, average overall brand-name
Tacrolimus
$2500
$2000
$1500
$1000
$500
$2500
$2000
$1500
$1000
$500
Ave
rage
Ann
ualiz
ed P
atie
nt P
aym
ents
$2500
$2000
$1500
$1000
$500
$0
2008 2009 2010 2011 2012 2013 2008Year
2009 2010 2011 2012 2013
$0
$0
Mycophenolic Acid
Kid
ney
Live
rH
eart
OverallBrand Tacrolimus or Mycophenolate Mofetil
Generic Tacrolimus or Mycophenolate Mofetil
Brand Mycophenolate Sodium
BA
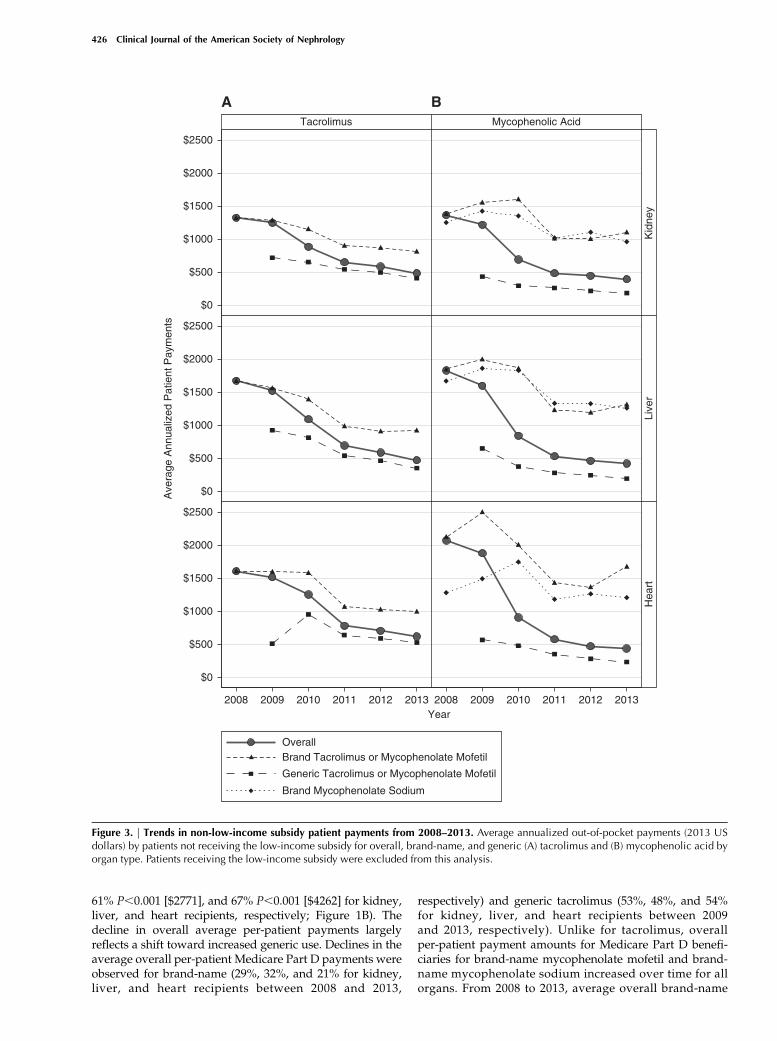
Figure 3. | Trends in non-low-income subsidy patient payments from 2008–2013. Average annualized out-of-pocket payments (2013 USdollars) by patients not receiving the low-income subsidy for overall, brand-name, and generic (A) tacrolimus and (B) mycophenolic acid byorgan type. Patients receiving the low-income subsidy were excluded from this analysis.
426 Clinical Journal of the American Society of Nephrology
mycophenolate mofetil per-patient payments for Part Dbeneficiaries increased by 59%, 57%, and 49% for kidney,liver, and heart recipients, respectively; average overallbrand-name mycophenolate sodium per-patient paymentsincreased by 23%, 30%, and 15%, respectively. By contrast,average overall per-patient payments for Medicare Part Dbeneficiaries for generic mycophenolate mofetil decreasedby 72%, 72%, and 74% between 2009 and 2013 for kidney,liver, and heart recipients, respectively.
Overall, per-patient Part D low-income subsidy paymentamounts for tacrolimus and mycophenolic acid decreasedbetween 2008 and 2013. Per-patient Part D low-incomesubsidy payment amounts for brand-name tacrolimus andgeneric mycophenolate mofetil also decreased between2008 and 2013; the brand-name mycophenolate mofetil andbrand-name mycophenolate sodium Part D low-incomesubsidy payments increased during this time period.Payment amounts for generic tacrolimus increased from
Tacrolimus
$60
$40
$20
$60
$40
$20
Ave
rage
Ann
ualiz
ed P
atie
nt P
aym
ents
$60
$40
$20
2008 2009 2010 2011 2012 2013 2008Year
2009 2010 2011 2012 2013
Mycophenolic Acid
Kid
ney
Live
rH
eart
OverallBrand Tacrolimus or Mycophenolate Mofetil
Generic Tacrolimus or Mycophenolate Mofetil
Brand Mycophenolate Sodium
BA
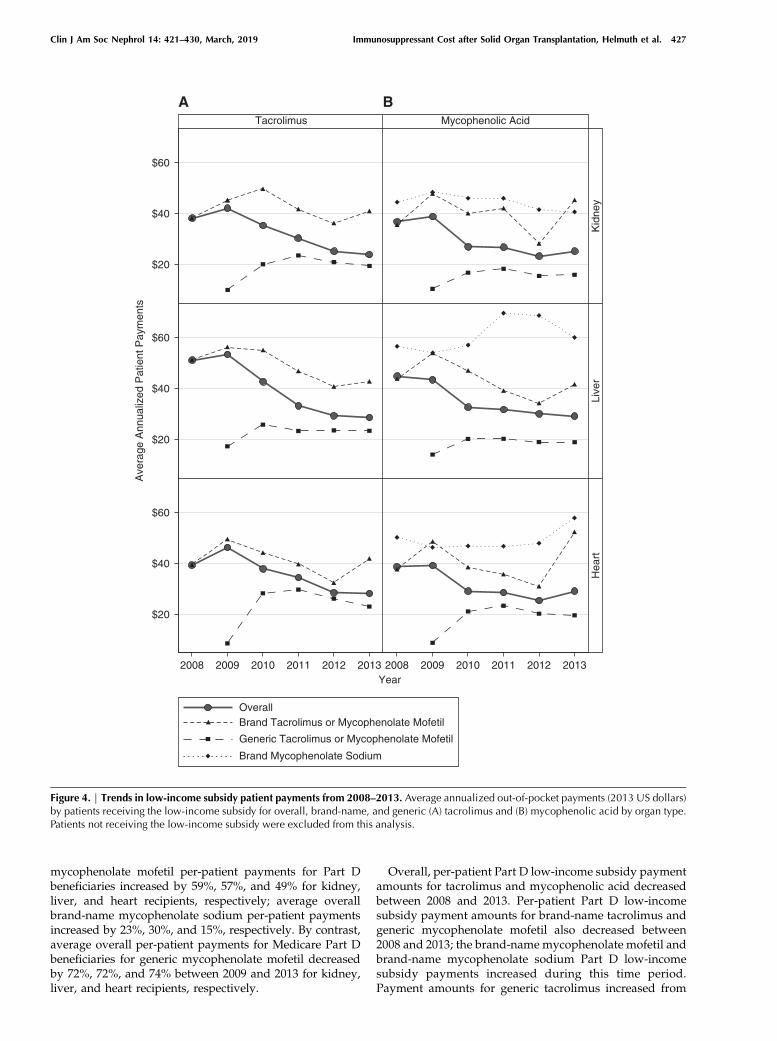
Figure 4. | Trends in low-income subsidy patient payments from 2008–2013. Average annualized out-of-pocket payments (2013 US dollars)by patients receiving the low-income subsidy for overall, brand-name, and generic (A) tacrolimus and (B) mycophenolic acid by organ type.Patients not receiving the low-income subsidy were excluded from this analysis.
Clin J Am Soc Nephrol 14: 421–430, March, 2019 Immunosuppressant Cost after Solid Organ Transplantation, Helmuth et al. 427

2009 to 2010, likely due to the low proportion of dayscovered in the first year of its introduction (average 16%),then decreased from 2010 to 2013 (Figure 2, SupplementalTable 3).
Patient PaymentsThe proportion of patients not receiving the low-income
subsidy ranged from 37% to 58%, 45% to 58%, and 46% to63% for kidney, liver, and heart patients, across drugs andyears. The overall average annualized out-of-pocket pay-ments for tacrolimus by transplant recipients with Part Dwho did not receive the low-income subsidy decreased by63% ($921, P,0.001), 72% ($1,323, P,0.001), and 61%($1,086, P,0.001) between 2008 and 2013 for kidney, liver,and heart transplant recipients, respectively (Figure 3A,Supplemental Table 4). As with the trend in averageoverall Medicare Part D per-patient payment amountsfor tacrolimus, patient out-of-pocket payments for tacroli-mus decreased over the study period for brand-name andgeneric immunosuppressive medications. The percentagedecreases in patient payments for all organs were greaterthan those observed for Part D payments. Annualizedaverages for generic tacrolimus for 2009 represent a rela-tively low proportion of days covered (average 16%), giventhat generic tacrolimus was not approved until Augustof 2009. Although overall annualized out-of-pocket per-patient payments for tacrolimus for patients receiving thelow-income subsidy were low (ranging from $24 to $53 peryear across organs and across years) compared with thosenot receiving the low-income subsidy, they also decreasedduring the study period, by 37% (P,0.001), 44% (P,0.001),and 28% (P=0.01) for kidney, liver, and heart recipients,respectively (Figure 4A, Supplemental Table 5).The average annualized out-of-pocket payments by
patients with mycophenolic acid prescriptions decreasedfrom 2008 to 2013 for all organs (Figure 3B). Unliketacrolimus, which showed a steady decline over the studyperiod, the overall out-of-pocket payment amounts forpatients not receiving the low-income subsidy decreasedmore rapidly between 2008 and 2010, then more slowlybetween 2011 and 2013, with overall decreases of 71%($1,065, P,0.001), 77% ($1,555, P,0.001), and 79% ($1,801,P,0.001) for kidney, liver, and heart recipients, respec-tively. Per-patient payments for generic mycophenolatemofetil decreased 58%, 71%, and 59% for kidney, liver, andheart transplant recipients, respectively, between 2009 and2013. Between 2008 and 2013, per-patient payments forbrand-name mycophenolate mofetil decreased by 20%,29%, and 21%; brand-name per-patient payments formycophenolate sodium decreased by 23%, 25%, and 6%.Although patients receiving the low-income subsidy maderelatively low out-of-pocket payments for mycophenolicacid (ranging from $23 to $45 per year), their payments alsodecreased by 31% (P,0.001), 35% (P,0.001), and 24%(P=0.06) between 2008 and 2013 for kidney, liver, and heartrecipients, respectively (Figure 4B).
DiscussionOverall, annual payments by patients for tacrolimus and
mycophenolic acid decreased from 2008 to 2013 for kidney,liver, and heart transplant recipients, and for the Medicare
Part D program. These trends are largely explained bysubstitution of generic immunosuppressive medicationsafter the introduction of generic products in 2008 and 2009.Across organs, the percentage of prescription drug eventsfor generic tacrolimus increased from 10% to 11% in 2009 to76% to 80% in 2013; generic mycophenolate mofetil in-creased from 28% to 30% of prescription drug events in2009 to 68% to 77% in 2013 (7). This led to a substantialreduction in the overall financial burden of immunosup-pressive medications to organ transplant recipients andMedicare Part D. The cost savings to Medicare result fromdecreases in per-patient Part D plan payments and per-patient Part D low-income subsidy program payments.This is the first study to document the cost savings to
organ transplant recipients and the Medicare program in alarge national sample after the introduction of genericimmunosuppressive medications. As this study shows, thedecrease in costs over time was often substantial. Fortransplant recipients not receiving the low-income subsidy,we observed declines in average out-of-pocket payments of$1000 to $1750 per patient per year between 2008 and 2013,depending on the organ type and drug. For the Medicareprogram, we observed savings of $1500 to $4500 perpatient per year in Part D plan payments between 2008and 2013, and additional savings to Medicare of $400 to$1500 per low-income subsidy recipient per year over thesame time period. This documentation of cost-savings isrelevant to ongoing policy discussions regarding theextension of Medicare coverage of immunosuppressantsbeyond 36 months post-transplant for kidney transplantrecipients not eligible for Medicare on the basis of age or adisability; it could inform evaluations of the cost effective-ness of such a reform.Ensuring that transplant recipients have consistent ac-
cess to affordable immunosuppressive medications iscritical to the medical and financial wellbeing of patients.Nonadherence with immunosuppressive medications isassociated with higher graft loss rates (13–15). In a surveyof United States kidney transplant programs investigatingcost-related medication nonadherence, .94% of programsdescribed the level of difficulty their patients encounterwhen paying for their immunosuppressive medications asserious or worse; 83% of programs reported being con-tacted by patients with concerns about the high cost ofmedications (16). Other studies have found higher non-adherence rates among individuals with lower socioeco-nomic status (17–19). Furthermore, return to dialysis afterkidney graft failure has high medical, economic, and societalcosts related to dialysis and repeat transplantation, compe-tition for scarce deceased donor organs, higher patientmortality, and reduced quality of life while on dialysis.Annual expenses for payers associated with graft failure andsubsequent return to dialysis and/or retransplantation areestimated to be between $70,000 and $106,000 comparedwith approximately $16,000 for patients with a functioninggraft (20).The overall reductions in per-patient payments by
beneficiaries and the Medicare Part D program supportthe hypothesis that the introduction of generic drugproducts provides economic (i.e., reduced costs to patientsand payers) benefits to organ transplant recipients, whichmay subsequently result in health benefits (i.e., increased
428 Clinical Journal of the American Society of Nephrology

access to medications and improved outcomes). Reductionsin the out-of-pocket burden of transplant recipients couldreduce the prevalence of cost-related medication nonad-herence and the associated risks and costs of graft failure.The possibility of longer and more widespread immuno-suppressive medication coverage for kidney transplantrecipients, such as Medicare coverage for the life of thetransplant (21), may be more palatable given reductions inpayments for the Medicare program.This study also highlights the large difference in out-of-
pocket payments between transplant recipients who didand did not qualify for the low-income subsidy. Given thissubstantial difference, we speculate that transplant recip-ients who do not meet the income eligibility requirementsfor the full or partial low-income subsidy, but are close tothe income cutoffs, may experience financial strain relatedto the yearly overall out-of-pocket payments for immuno-suppressive medications (range $436 to $2279 per year)and that this strain could result in a higher risk ofmedication nonadherence compared with those that receivethe low-income subsidy. Data to support this hypothesis areneeded.In assessing potential cost savings of generic substitu-
tion, we documented changes over time in paymentsspecific to brand and generic medications. In contrast topayments for generic and brand tacrolimus, which de-clined over the study period, Medicare Part D paymentsfor brand mycophenolic acid actually increased over timefor the remaining subset of transplant recipients continu-ing to use these brand-name products. This finding maybe explained by increases in brand prices after genericmarket entry, made possible by a subset of brand-loyalpatients (22,23).One limitation of this study is that it is restricted to
Medicare transplant recipients who obtained immunosup-pressive medications through Part D. Although MedicarePart B pays for immunosuppressive medications for trans-plant recipients covered by Medicare Part A at the time oftransplant (60%, 30%, and 39% of kidney, liver, and hearttransplant recipients, respectively) (9), these analyses can-not be performed using Part B claims because they do notinclude National Drug Codes required to distinguishbetween generic and brand medications. Our cost analysisdoes not include 36 months of coverage by Part B providedto kidney transplant recipients whose transplants arecovered by Medicare; immunosuppressant costs may differbetween Part B and Medicare Part D plans. Our annual-ization method assumes no medication nonadherence ordose adjustments over the year, which may not be valid;however, our results can still be interpreted as the paymentamount, assuming that the reported regimen was in placefor the full year, which has value for counseling potentialrecipients. Finally, this analysis is limited to post-trans-plant immunosuppressant costs and does not includeother transplant costs, i.e., pretransplant and transplanthospitalization costs, which have been reported elsewhereas ranging from $414,800 to $1,382,400 for the organsstudied (24).This study provides a description of trends in payments
for two immunosuppressive medications, tacrolimus andmycophenolic acid (including mycophenolate mofetil andmycophenolate sodium), since the introduction of generic
versions of these drugs. Reductions in overall per-patient payments by the Medicare Part D program andtransplant recipients during 2009–2013 supports thehypothesis that the introduction of generic versions ofthese drugs has resulted in substantial cost savings forpatients and payers. The cost effect of generic substitu-tion may be amplified by increased competition in theimmunosuppressive medication market (25). In addi-tion, we observed large differences in average yearlyout-of-pocket payments for immunosuppressive medi-cations between Part D beneficiaries who do and do notqualify for the low-income subsidy. Further research isneeded to assess whether there is a potential causal linkbetween recipient immunosuppressive medication pay-ments, adherence, and graft outcomes.
Acknowledgments
Heather VanDoren, senior medical editor with Arbor ResearchCollaborative for Health, provided editorial assistance on thismanuscript.Funding for this researchwasmadepossiblebytheFoodandDrug
Administration through grant 1U01FD005274-01. Views expressedinwrittenmaterials or publications andbyspeakers andmoderatorsdo not necessarily reflect the official policies of the Food and DrugAdministration or the Department of Health and Human Services;nor does any mention of trade names, commercial practices, or or-ganization imply endorsement by the United States government.The data reported here have been supplied by the HennepinHealthcare Research Institute (HHRI) as the contractor for the Sci-entific Registry of Transplant Recipients (SRTR). The interpretationand reportingof thesedata are the responsibility of the author(s) andin no way should be seen as an official policy of or interpretation bythe SRTRor theUnitedStates government. Thedata that support thefindings of this study are available from the Centers for Medicare &Medicaid Services (CMS) and from HHRI as the contractor for theSRTR.Restrictionsapply to theavailabilityof thesedata,whichwereused under license for this study. Data are available from cms.organd SRTR.org with the permission of CMS and HHRI.
DisclosuresA.B.L. reports grants from the US Food andDrug Administration
during the conduct of the study; other from Watermark ResearchPartners, Inc., Indianapolis, IN, outside the submittedwork.M.E.H.,M.N.T., J.M.P., R.B., P.S., J.Z., A.B.L., and A.R.S. report grants fromthe US Food and Drug Administration during the conduct of thestudy. The remaining authors have nothing to disclose.
Supplemental MaterialThis article contains the followingsupplementalmaterial online at
http://cjasn.asnjournals.org/lookup/suppl/doi:10.2215/CJN.10590918/-/DCSupplemental.Supplemental Material Title and Authors.Supplemental Table 1. Demographics for transplant recipients
with and without tacrolimus or mycophenolate Part D prescriptiondrug events during 2008 to 2013, by organ type.Supplemental Table 2. Average (SEM) annualized Medicare Part
D plan payments (2013 US dollars).Supplemental Table 3. Average (SEM) annualized Medicare Part
D low-income subsidy payments (2013 US dollars).Supplemental Table 4. Average (SEM) annualized out-of-pocket
payments by patients not receiving the low-income subsidy (2013US dollars).
Clin J Am Soc Nephrol 14: 421–430, March, 2019 Immunosuppressant Cost after Solid Organ Transplantation, Helmuth et al. 429

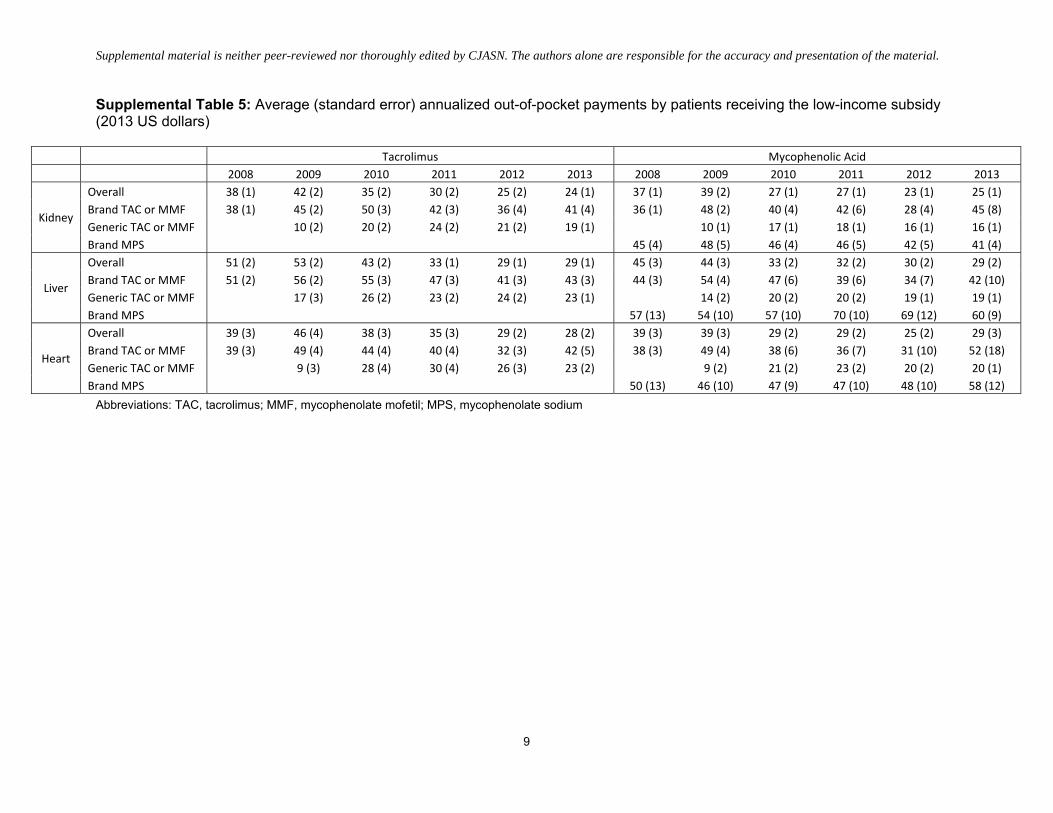
Supplemental Table 5. Average (SEM) annualized out-of-pocketpaymentsbypatientsreceivingthelow-incomesubsidy(2013USdollars).
References1. Loubeau PR, Loubeau JM, Jantzen R: The economics of kidney
transplantation versus hemodialysis. Prog Transplant 11:291–297, 2001
2. Laupacis A, Keown P, Pus N, Krueger H, Ferguson B, Wong C,Muirhead N: A study of the quality of life and cost-utility of renaltransplantation. Kidney Int 50: 235–242, 1996
3. Kasiske BL, Cohen D, Lucey MR, Neylan JF; American Society ofTransplantation: Payment for immunosuppression after organtransplantation. JAMA 283: 2445–2450, 2000
4. El Hajj S, Kim M, Phillips K, Gabardi S: Generic immunosup-pression in transplantation: Current evidence and controversialissues. Expert Rev Clin Immunol 11: 659–672, 2015
5. FDA approval of tacrolimus, 2009. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2009/065461s000ltr.pdf. Accessed November 20, 2018
6. FDA approval of mycophenolate mofetil, 2008. Available at:https://www.accessdata.fda.gov/drugsatfda_docs/appletter/2008/065413s000ltr.pdf. Accessed November 20, 2018
7. Liu Q, Smith AR, Park JM, Oguntimein M, Dutcher S, Bello G,HelmuthM,TurenneM,BalkrishnanR,FavaM,BeilCA,SaullesA,Goel S, Sharma P, Leichtman A, Zee J: The adoption of genericimmunosuppressant medications in kidney, liver, and hearttransplantation among recipients in Colorado or nationally withMedicare part D. Am J Transplant 18: 1764–1773, 2018
8. PhillipsCJ: Ahealth economicperspectiveon generic therapeuticsubstitution. Eur J Hosp Pharm Sci Pract 20: 290–292, 2013
9. Organ Procurement and Transplantation Network (OPTN) andScientific Registry of Transplant Recipients: (SRTR). OPTN/SRTR2016 Annual Data Report, Rockville, MD, Department of Healthand Human Services, Health Resources and Services Adminis-tration, 2018
10. Yen EF, Hardinger K, Brennan DC, Woodward RS, Desai NM,Crippin JS, Gage BF, SchnitzlerMA: Cost-effectiveness of extendingMedicare coverage of immunosuppressive medications to the lifeof a kidney transplant. Am J Transplant 4: 1703–1708, 2004
11. McDevitt-Potter LM,SadakaB, TichyEM,RogersCC,Gabardi S:Amulticenter experience with generic tacrolimus conversion.Transplantation 92: 653–657, 2011
12. USBureauof Labor Statistics,USDepartment of Labor:Consumerprice index—all urban consumers. Series ID: CUUR0000SA0,Washington, DC, US Bureau of Labor Statistics, 2014. Availableat: http://data.bls.gov/timeseries/CUUR0000SA0. Accessed July17, 2017
13. Schweizer RT, Rovelli M, Palmeri D, Vossler E, Hull D, Bartus S:Noncompliance in organ transplant recipients. Transplantation49: 374–377, 1990
14. De Geest S, Borgermans L, Gemoets H, Abraham I, Vlaminck H,Evers G, Vanrenterghem Y: Incidence, determinants, and con-sequences of subclinical noncompliance with immunosuppres-sive therapy in renal transplant recipients. Transplantation 59:340–347, 1995
15. Pinsky BW, Takemoto SK, Lentine KL, Burroughs TE, SchnitzlerMA, Salvalaggio PR: Transplant outcomes and economic costsassociated with patient noncompliance to immunosuppression.Am J Transplant 9: 2597–2606, 2009
16. Evans RW, Applegate WH, Briscoe DM, Cohen DJ, Rorick CC,Murphy BT, Madsen JC: Cost-related immunosuppressive medi-cation nonadherence among kidney transplant recipients. Clin JAm Soc Nephrol 5: 2323–2328, 2010
17. Frazier PA, Davis-Ali SH, Dahl KE: Correlates of noncomplianceamong renal transplant recipients. Clin Transplant 8: 550–557,1994
18. Gordon EJ, Prohaska TR, Sehgal AR: The financial impact ofimmunosuppressant expenses on new kidney transplant recipi-ents. Clin Transplant 22: 738–748, 2008
19. Rovelli M, Palmeri D, Vossler E, Bartus S, Hull D, Schweizer R:Noncompliance in organ transplant recipients. Transplant Proc21: 833–834, 1989
20. James A, Mannon RB: The cost of transplant immunosuppressanttherapy: Is this sustainable?CurrTransplantRep2:113–121,2015
21. HR 6139. Comprehensive immunosuppressive drug coverage forkidney transplant patients act of 2016. Available at: https://www.congress.gov/bill/114th-congress/house-bill/6139. AccessedNovember 20, 2018
22. Grabowski HG, Vernon JM: Brand loyalty, entry, and pricecompetition in pharmaceuticals after the 1984 drug act. J LawEcon 35: 331–350, 1992
23. Frank RG, Salkever DS: Generic entry and the pricing of phar-maceuticals. J Econ Manage Strategy 6: 75–90, 1997
24. Milliman research report. 2017 US organ and tissue transplantcost estimates and discussion. Available at: http://us.milliman.com/uploadedFiles/insight/2017/2017-Transplant-Report.pdf.Accessed November 20, 2018
25. Dave CV, Hartzema A, Kesselheim AS: Prices of generic drugsassociated with numbers of manufacturers. N Engl J Med 377:2597–2598, 2017
Received: September 4, 2018 Accepted: January 16, 2019
Published online ahead of print. Publication date available at www.cjasn.org.
See related Patient Voice, “Cost of Immunosuppressive Drugs andthe Patient with a Kidney Transplant,” and editorial, “Are GenericImmunosuppressive Drugs the Solution for Providing LifelongMedication Coverage to Transplant Recipients?,” on pages 317–318and 327–329, respectively.
430 Clinical Journal of the American Society of Nephrology
Supplemental material is neither peer-reviewed nor thoroughly edited by CJASN. The authors alone are responsible for the accuracy and presentation of the material.
1
Table of Contents
Supplemental Material Title and Authors ...................................................................................................................................................................... 2
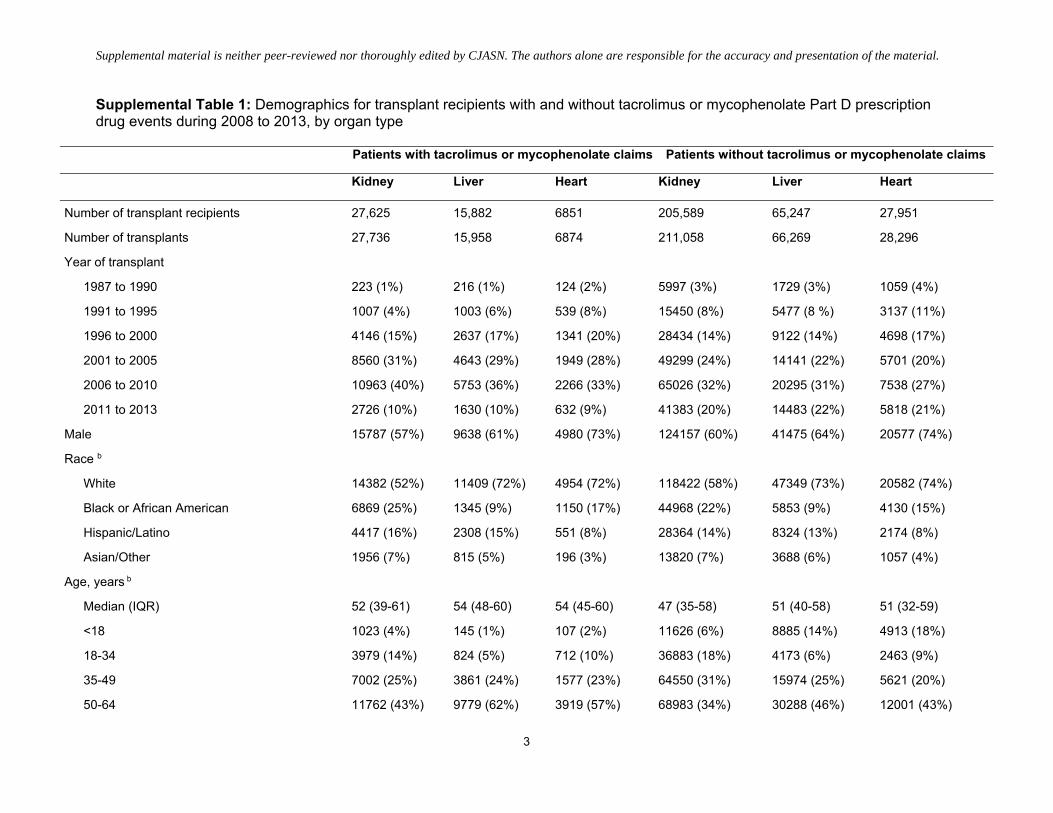
Supplemental Table 1: Demographics for transplant recipients with and without tacrolimus or mycophenolate Part D prescription drug events during 2008 to 2013, by organ type .............................................................................................................................................................................. 3
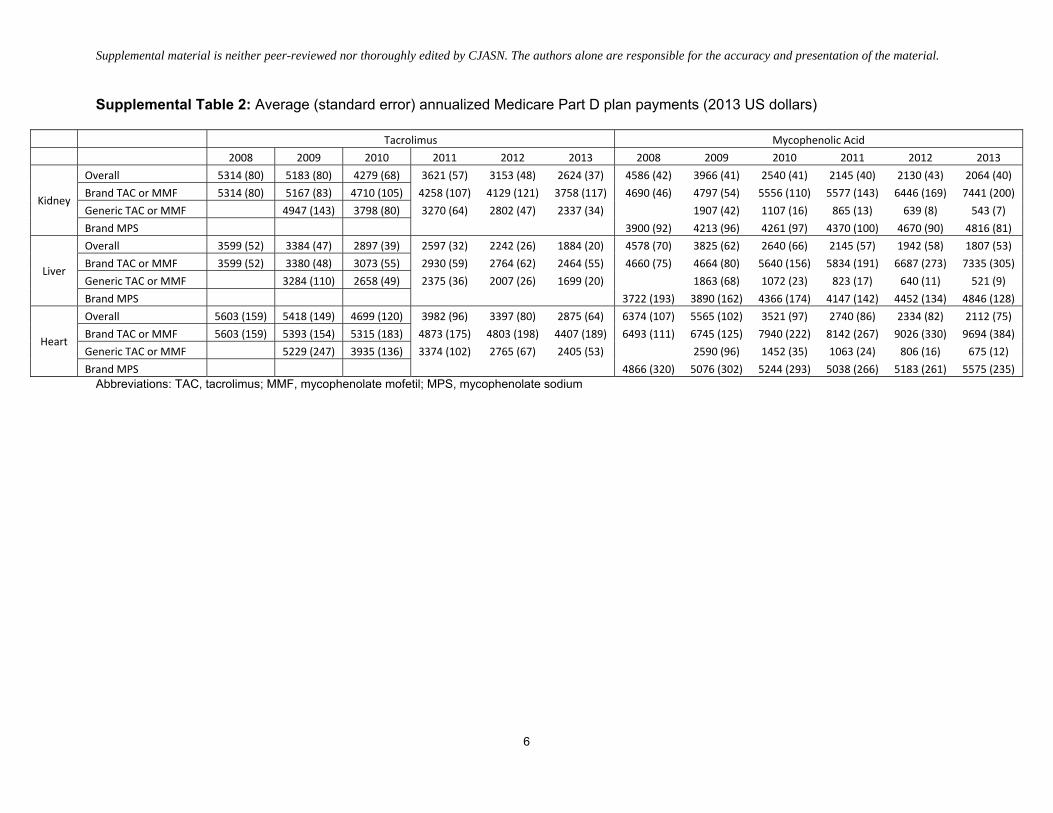
Supplemental Table 2: Average (standard error) annualized Medicare Part D plan payments (2013 US dollars) ....................................................... 6
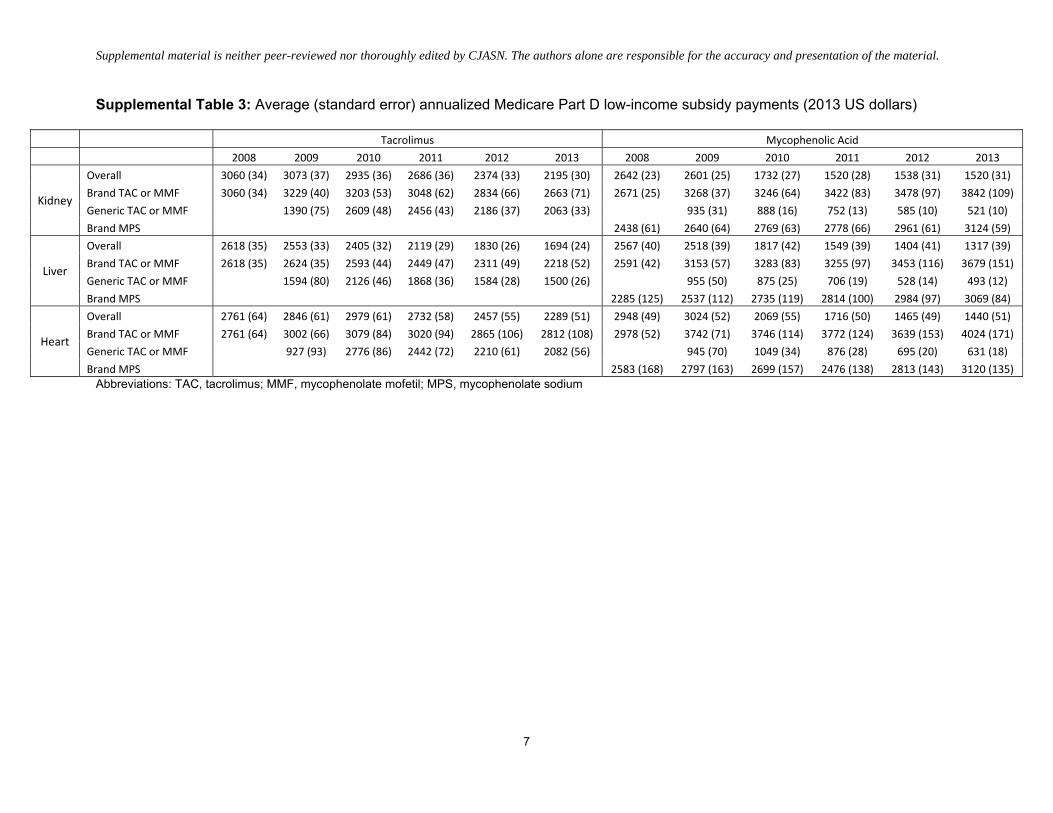
Supplemental Table 3: Average (standard error) annualized Medicare Part D low‐income subsidy payments (2013 US dollars) .............................. 7
Supplemental Table 4: Average (standard error) annualized out‐of‐pocket payments by patients not receiving the low‐income subsidy (2013 US dollars) ........................................................................................................................................................................................................................... 8
Supplemental Table 5: Average (standard error) annualized out‐of‐pocket payments by patients receiving the low‐income subsidy (2013 US dollars) ........................................................................................................................................................................................................................... 9
Supplemental material is neither peer-reviewed nor thoroughly edited by CJASN. The authors alone are responsible for the accuracy and presentation of the material.
2
Supplemental Material Title and Authors
Secular Trends in the Cost of Immunosuppressants after Solid Organ Transplantation in the United States
Margaret E. Helmuth, MA; Qian Liu, MPH; Marc N. Turenne, PhD; Jeong M. Park, PharmD; Murewa Oguntimein, PhD; Sarah K. Dutcher, PhD; Rajesh Balkrishnan, PhD; Pratima Sharma, MD, MBBS, MS; Jarcy Zee, PhD; Alan B. Leichtman, MD; Abigail R. Smith, PhD, MS
Supplemental material is neither peer-reviewed nor thoroughly edited by CJASN. The authors alone are responsible for the accuracy and presentation of the material.
3
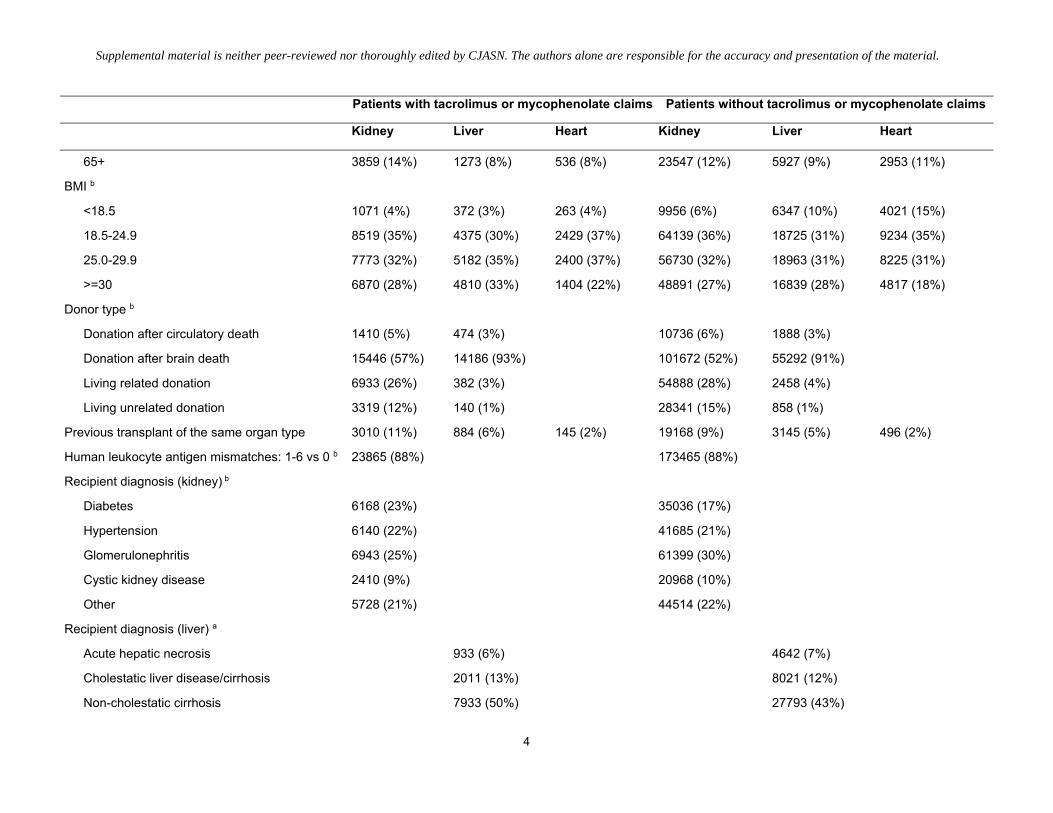
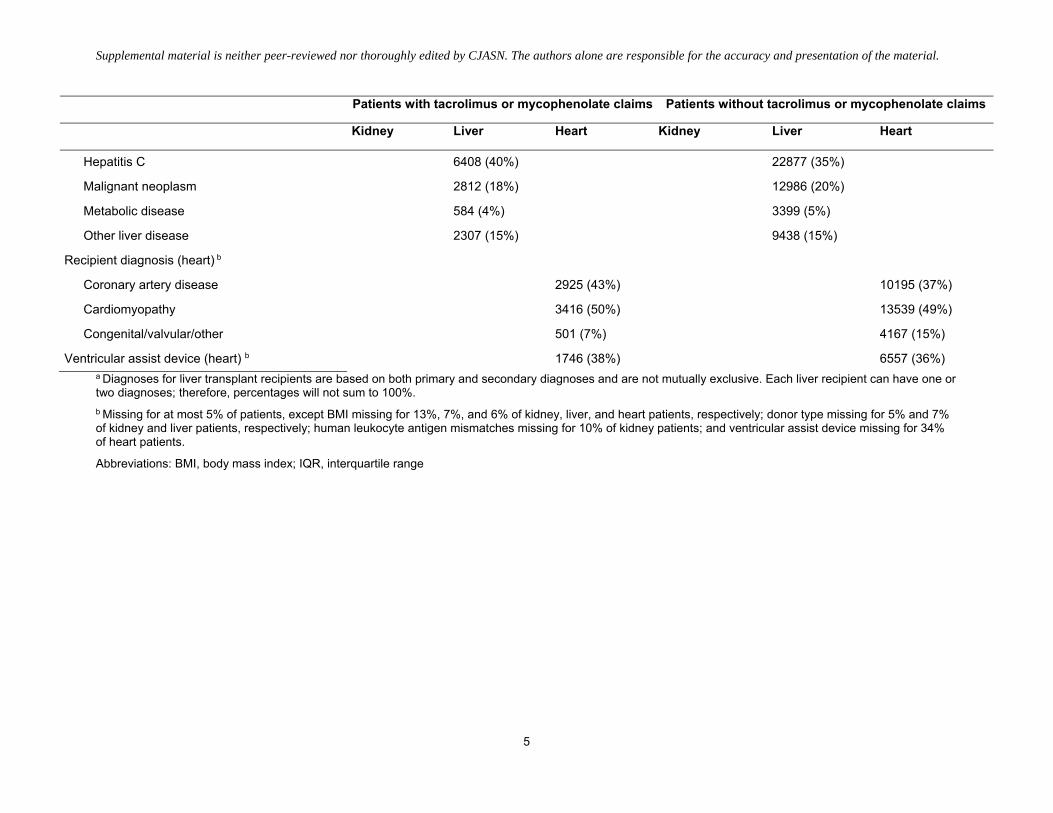
Supplemental Table 1: Demographics for transplant recipients with and without tacrolimus or mycophenolate Part D prescription drug events during 2008 to 2013, by organ type
Patients with tacrolimus or mycophenolate claims Patients without tacrolimus or mycophenolate claims
Kidney Liver Heart Kidney Liver Heart
Number of transplant recipients 27,625 15,882 6851 205,589 65,247 27,951
Number of transplants 27,736 15,958 6874 211,058 66,269 28,296
Year of transplant
1987 to 1990 223 (1%) 216 (1%) 124 (2%) 5997 (3%) 1729 (3%) 1059 (4%)
1991 to 1995 1007 (4%) 1003 (6%) 539 (8%) 15450 (8%) 5477 (8 %) 3137 (11%)
1996 to 2000 4146 (15%) 2637 (17%) 1341 (20%) 28434 (14%) 9122 (14%) 4698 (17%)
2001 to 2005 8560 (31%) 4643 (29%) 1949 (28%) 49299 (24%) 14141 (22%) 5701 (20%)
2006 to 2010 10963 (40%) 5753 (36%) 2266 (33%) 65026 (32%) 20295 (31%) 7538 (27%)
2011 to 2013 2726 (10%) 1630 (10%) 632 (9%) 41383 (20%) 14483 (22%) 5818 (21%)
Male 15787 (57%) 9638 (61%) 4980 (73%) 124157 (60%) 41475 (64%) 20577 (74%)
Race b
White 14382 (52%) 11409 (72%) 4954 (72%) 118422 (58%) 47349 (73%) 20582 (74%)
Black or African American 6869 (25%) 1345 (9%) 1150 (17%) 44968 (22%) 5853 (9%) 4130 (15%)
Hispanic/Latino 4417 (16%) 2308 (15%) 551 (8%) 28364 (14%) 8324 (13%) 2174 (8%)
Asian/Other 1956 (7%) 815 (5%) 196 (3%) 13820 (7%) 3688 (6%) 1057 (4%)
Age, years b
Median (IQR) 52 (39-61) 54 (48-60) 54 (45-60) 47 (35-58) 51 (40-58) 51 (32-59)
<18 1023 (4%) 145 (1%) 107 (2%) 11626 (6%) 8885 (14%) 4913 (18%)
18-34 3979 (14%) 824 (5%) 712 (10%) 36883 (18%) 4173 (6%) 2463 (9%)
35-49 7002 (25%) 3861 (24%) 1577 (23%) 64550 (31%) 15974 (25%) 5621 (20%)
50-64 11762 (43%) 9779 (62%) 3919 (57%) 68983 (34%) 30288 (46%) 12001 (43%)
Supplemental material is neither peer-reviewed nor thoroughly edited by CJASN. The authors alone are responsible for the accuracy and presentation of the material.
4
Patients with tacrolimus or mycophenolate claims Patients without tacrolimus or mycophenolate claims
Kidney Liver Heart Kidney Liver Heart
65+ 3859 (14%) 1273 (8%) 536 (8%) 23547 (12%) 5927 (9%) 2953 (11%)
BMI b
<18.5 1071 (4%) 372 (3%) 263 (4%) 9956 (6%) 6347 (10%) 4021 (15%)
18.5-24.9 8519 (35%) 4375 (30%) 2429 (37%) 64139 (36%) 18725 (31%) 9234 (35%)
25.0-29.9 7773 (32%) 5182 (35%) 2400 (37%) 56730 (32%) 18963 (31%) 8225 (31%)
>=30 6870 (28%) 4810 (33%) 1404 (22%) 48891 (27%) 16839 (28%) 4817 (18%)
Donor type b
Donation after circulatory death 1410 (5%) 474 (3%) 10736 (6%) 1888 (3%)
Donation after brain death 15446 (57%) 14186 (93%) 101672 (52%) 55292 (91%)
Living related donation 6933 (26%) 382 (3%) 54888 (28%) 2458 (4%)
Living unrelated donation 3319 (12%) 140 (1%) 28341 (15%) 858 (1%)
Previous transplant of the same organ type 3010 (11%) 884 (6%) 145 (2%) 19168 (9%) 3145 (5%) 496 (2%)
Human leukocyte antigen mismatches: 1-6 vs 0 b 23865 (88%) 173465 (88%)
Recipient diagnosis (kidney) b
Diabetes 6168 (23%) 35036 (17%)
Hypertension 6140 (22%) 41685 (21%)
Glomerulonephritis 6943 (25%) 61399 (30%)
Cystic kidney disease 2410 (9%) 20968 (10%)
Other 5728 (21%) 44514 (22%)
Recipient diagnosis (liver) a
Acute hepatic necrosis 933 (6%) 4642 (7%)
Cholestatic liver disease/cirrhosis 2011 (13%) 8021 (12%)
Non-cholestatic cirrhosis 7933 (50%) 27793 (43%)
Supplemental material is neither peer-reviewed nor thoroughly edited by CJASN. The authors alone are responsible for the accuracy and presentation of the material.
5
Patients with tacrolimus or mycophenolate claims Patients without tacrolimus or mycophenolate claims
Kidney Liver Heart Kidney Liver Heart
Hepatitis C 6408 (40%) 22877 (35%)
Malignant neoplasm 2812 (18%) 12986 (20%)
Metabolic disease 584 (4%) 3399 (5%)
Other liver disease 2307 (15%) 9438 (15%)
Recipient diagnosis (heart) b
Coronary artery disease 2925 (43%) 10195 (37%)
Cardiomyopathy 3416 (50%) 13539 (49%)
Congenital/valvular/other 501 (7%) 4167 (15%)
Ventricular assist device (heart) b 1746 (38%) 6557 (36%) a Diagnoses for liver transplant recipients are based on both primary and secondary diagnoses and are not mutually exclusive. Each liver recipient can have one or two diagnoses; therefore, percentages will not sum to 100%. b Missing for at most 5% of patients, except BMI missing for 13%, 7%, and 6% of kidney, liver, and heart patients, respectively; donor type missing for 5% and 7% of kidney and liver patients, respectively; human leukocyte antigen mismatches missing for 10% of kidney patients; and ventricular assist device missing for 34% of heart patients.
Abbreviations: BMI, body mass index; IQR, interquartile range
Supplemental material is neither peer-reviewed nor thoroughly edited by CJASN. The authors alone are responsible for the accuracy and presentation of the material.
6
Supplemental Table 2: Average (standard error) annualized Medicare Part D plan payments (2013 US dollars)
Tacrolimus Mycophenolic Acid 2008 2009 2010 2011 2012 2013 2008 2009 2010 2011 2012 2013
Kidney
Overall 5314 (80) 5183 (80) 4279 (68) 3621 (57) 3153 (48) 2624 (37) 4586 (42) 3966 (41) 2540 (41) 2145 (40) 2130 (43) 2064 (40) Brand TAC or MMF 5314 (80) 5167 (83) 4710 (105) 4258 (107) 4129 (121) 3758 (117) 4690 (46) 4797 (54) 5556 (110) 5577 (143) 6446 (169) 7441 (200) Generic TAC or MMF 4947 (143) 3798 (80) 3270 (64) 2802 (47) 2337 (34) 1907 (42) 1107 (16) 865 (13) 639 (8) 543 (7) Brand MPS 3900 (92) 4213 (96) 4261 (97) 4370 (100) 4670 (90) 4816 (81)
Liver
Overall 3599 (52) 3384 (47) 2897 (39) 2597 (32) 2242 (26) 1884 (20) 4578 (70) 3825 (62) 2640 (66) 2145 (57) 1942 (58) 1807 (53) Brand TAC or MMF 3599 (52) 3380 (48) 3073 (55) 2930 (59) 2764 (62) 2464 (55) 4660 (75) 4664 (80) 5640 (156) 5834 (191) 6687 (273) 7335 (305) Generic TAC or MMF 3284 (110) 2658 (49) 2375 (36) 2007 (26) 1699 (20) 1863 (68) 1072 (23) 823 (17) 640 (11) 521 (9) Brand MPS 3722 (193) 3890 (162) 4366 (174) 4147 (142) 4452 (134) 4846 (128)
Heart
Overall 5603 (159) 5418 (149) 4699 (120) 3982 (96) 3397 (80) 2875 (64) 6374 (107) 5565 (102) 3521 (97) 2740 (86) 2334 (82) 2112 (75) Brand TAC or MMF 5603 (159) 5393 (154) 5315 (183) 4873 (175) 4803 (198) 4407 (189) 6493 (111) 6745 (125) 7940 (222) 8142 (267) 9026 (330) 9694 (384) Generic TAC or MMF 5229 (247) 3935 (136) 3374 (102) 2765 (67) 2405 (53) 2590 (96) 1452 (35) 1063 (24) 806 (16) 675 (12) Brand MPS 4866 (320) 5076 (302) 5244 (293) 5038 (266) 5183 (261) 5575 (235)
Abbreviations: TAC, tacrolimus; MMF, mycophenolate mofetil; MPS, mycophenolate sodium
Supplemental material is neither peer-reviewed nor thoroughly edited by CJASN. The authors alone are responsible for the accuracy and presentation of the material.
7
Supplemental Table 3: Average (standard error) annualized Medicare Part D low-income subsidy payments (2013 US dollars)
Tacrolimus Mycophenolic Acid 2008 2009 2010 2011 2012 2013 2008 2009 2010 2011 2012 2013
Kidney
Overall 3060 (34) 3073 (37) 2935 (36) 2686 (36) 2374 (33) 2195 (30) 2642 (23) 2601 (25) 1732 (27) 1520 (28) 1538 (31) 1520 (31) Brand TAC or MMF 3060 (34) 3229 (40) 3203 (53) 3048 (62) 2834 (66) 2663 (71) 2671 (25) 3268 (37) 3246 (64) 3422 (83) 3478 (97) 3842 (109) Generic TAC or MMF 1390 (75) 2609 (48) 2456 (43) 2186 (37) 2063 (33) 935 (31) 888 (16) 752 (13) 585 (10) 521 (10) Brand MPS 2438 (61) 2640 (64) 2769 (63) 2778 (66) 2961 (61) 3124 (59)
Liver
Overall 2618 (35) 2553 (33) 2405 (32) 2119 (29) 1830 (26) 1694 (24) 2567 (40) 2518 (39) 1817 (42) 1549 (39) 1404 (41) 1317 (39) Brand TAC or MMF 2618 (35) 2624 (35) 2593 (44) 2449 (47) 2311 (49) 2218 (52) 2591 (42) 3153 (57) 3283 (83) 3255 (97) 3453 (116) 3679 (151) Generic TAC or MMF 1594 (80) 2126 (46) 1868 (36) 1584 (28) 1500 (26) 955 (50) 875 (25) 706 (19) 528 (14) 493 (12) Brand MPS 2285 (125) 2537 (112) 2735 (119) 2814 (100) 2984 (97) 3069 (84)
Heart
Overall 2761 (64) 2846 (61) 2979 (61) 2732 (58) 2457 (55) 2289 (51) 2948 (49) 3024 (52) 2069 (55) 1716 (50) 1465 (49) 1440 (51) Brand TAC or MMF 2761 (64) 3002 (66) 3079 (84) 3020 (94) 2865 (106) 2812 (108) 2978 (52) 3742 (71) 3746 (114) 3772 (124) 3639 (153) 4024 (171) Generic TAC or MMF 927 (93) 2776 (86) 2442 (72) 2210 (61) 2082 (56) 945 (70) 1049 (34) 876 (28) 695 (20) 631 (18) Brand MPS 2583 (168) 2797 (163) 2699 (157) 2476 (138) 2813 (143) 3120 (135)
Abbreviations: TAC, tacrolimus; MMF, mycophenolate mofetil; MPS, mycophenolate sodium

Supplemental material is neither peer-reviewed nor thoroughly edited by CJASN. The authors alone are responsible for the accuracy and presentation of the material.
8
Supplemental Table 4: Average (standard error) annualized out-of-pocket payments by patients not receiving the low-income subsidy (2013 US dollars)
Tacrolimus Mycophenolic Acid 2008 2009 2010 2011 2012 2013 2008 2009 2010 2011 2012 2013
Kidney
Overall 1458 (43) 1368 (43) 970 (34) 716 (25) 643 (19) 536 (14) 1500 (36) 1339 (36) 760 (27) 535 (15) 488 (14) 436 (11) Brand TAC or MMF 1458 (43) 1419 (45) 1271 (57) 994 (36) 961 (36) 897 (33) 1520 (39) 1713 (54) 1768 (96) 1114 (62) 1105 (67) 1217 (73) Generic TAC or MMF 790 (90) 717 (38) 594 (31) 544 (22) 452 (15) 476 (28) 324 (14) 286 (10) 237 (7) 200 (5) Brand MPS 1377 (86) 1566 (111) 1487 (90) 1121 (49) 1214 (49) 1056 (38)
Liver
Overall 1841 (40) 1671 (36) 1201 (31) 761 (19) 644 (14) 518 (10) 2013 (61) 1761 (54) 924 (42) 586 (22) 505 (18) 459 (16) Brand TAC or MMF 1841 (40) 1723 (38) 1535 (45) 1088 (27) 1001 (24) 1017 (25) 2032 (65) 2203 (76) 2052 (126) 1355 (75) 1313 (89) 1447 (100) Generic TAC or MMF 1017 (77) 890 (39) 592 (23) 510 (16) 384 (10) 713 (60) 408 (21) 306 (13) 267 (9) 210 (6) Brand MPS 1836 (186) 2048 (156) 2011 (159) 1466 (81) 1458 (72) 1384 (62)
Heart
Overall 1768 (71) 1667 (63) 1378 (59) 858 (35) 773 (29) 682 (24) 2278 (61) 2071 (67) 997 (43) 636 (24) 518 (20) 477 (18) Brand TAC or MMF 1768 (71) 1762 (68) 1745 (94) 1178 (55) 1131 (52) 1097 (50) 2343 (64) 2754 (93) 2210 (130) 1578 (88) 1505 (98) 1846 (118) Generic TAC or MMF 560 (80) 1043 (69) 704 (43) 647 (33) 579 (26) 622 (54) 526 (27) 386 (18) 307 (12) 256 (9) Brand MPS 1408 (171) 1642 (194) 1920 (188) 1299 (92) 1390 (91) 1327 (82)
Abbreviations: TAC, tacrolimus; MMF, mycophenolate mofetil; MPS, mycophenolate sodium
Supplemental material is neither peer-reviewed nor thoroughly edited by CJASN. The authors alone are responsible for the accuracy and presentation of the material.
9
Supplemental Table 5: Average (standard error) annualized out-of-pocket payments by patients receiving the low-income subsidy (2013 US dollars)
Tacrolimus Mycophenolic Acid 2008 2009 2010 2011 2012 2013 2008 2009 2010 2011 2012 2013
Kidney
Overall 38 (1) 42 (2) 35 (2) 30 (2) 25 (2) 24 (1) 37 (1) 39 (2) 27 (1) 27 (1) 23 (1) 25 (1) Brand TAC or MMF 38 (1) 45 (2) 50 (3) 42 (3) 36 (4) 41 (4) 36 (1) 48 (2) 40 (4) 42 (6) 28 (4) 45 (8) Generic TAC or MMF 10 (2) 20 (2) 24 (2) 21 (2) 19 (1) 10 (1) 17 (1) 18 (1) 16 (1) 16 (1) Brand MPS 45 (4) 48 (5) 46 (4) 46 (5) 42 (5) 41 (4)
Liver
Overall 51 (2) 53 (2) 43 (2) 33 (1) 29 (1) 29 (1) 45 (3) 44 (3) 33 (2) 32 (2) 30 (2) 29 (2) Brand TAC or MMF 51 (2) 56 (2) 55 (3) 47 (3) 41 (3) 43 (3) 44 (3) 54 (4) 47 (6) 39 (6) 34 (7) 42 (10) Generic TAC or MMF 17 (3) 26 (2) 23 (2) 24 (2) 23 (1) 14 (2) 20 (2) 20 (2) 19 (1) 19 (1) Brand MPS 57 (13) 54 (10) 57 (10) 70 (10) 69 (12) 60 (9)
Heart
Overall 39 (3) 46 (4) 38 (3) 35 (3) 29 (2) 28 (2) 39 (3) 39 (3) 29 (2) 29 (2) 25 (2) 29 (3) Brand TAC or MMF 39 (3) 49 (4) 44 (4) 40 (4) 32 (3) 42 (5) 38 (3) 49 (4) 38 (6) 36 (7) 31 (10) 52 (18) Generic TAC or MMF 9 (3) 28 (4) 30 (4) 26 (3) 23 (2) 9 (2) 21 (2) 23 (2) 20 (2) 20 (1) Brand MPS 50 (13) 46 (10) 47 (9) 47 (10) 48 (10) 58 (12)
Abbreviations: TAC, tacrolimus; MMF, mycophenolate mofetil; MPS, mycophenolate sodium