Journal of Eastern Mediterranean Archaeology and Heritage Studies 1.1 Front Matter
Upload
khangminh22Category
view
0download
0
There’s More To EPOGEN#{174}(Epoetin alfa)
Than Epoetin Affa.
ER�EN(EPOETIN ALFA)
RECOMBINANT
Programs available exclusively for dialysis patients and prosiders.
© 1994 Amgen Inc.
When you specify EPOGEN#{174}(Epoetinalfa), you get more than a product You alsoget a comprehensive support system. That’simportant, because the depth and quality of
professional support is a significant elementin long-term clinical success.
EPOGEN#{174}support encompasses theAmgen Reimbursement Hotline, the AmgenSAFETY NET#{174}Program, Professional Services,Professional Education Programs, and Clinical
Support Services. Your Amgen ProfessionalSales Representative can tell you more aboutthe ways these programs can satisfy your needs.
There simply is no comparable source of
professional support. That’s not surprising,because EPOGEN#{174}is a lot more than just adrug. It’s away of life.
For more information, please call1-800-77-AMGEN.
NORVASC#{174}© 1995, Pfizer Inc (ainIodIp1ne besylate) � �Lab. #{149}NHO #{149}Pratt#{149}Hoeng
INFeD not bevalid in patents on chronic renal dialysis who are also receMn� iron dextran complex.‘IRON DEXTRANINJECTION, USP) Although there are significant variations in body build and weight distribution among males and females, the accompanying
table andiormula representa convenientmeanstorestimating thetotal iron required. Thistotal iron requirement reflectstheWARNING � amount of iron neededto restore hemoglobin concentration to normal or near normal levels plus an additional allowance to
ThE PMENTERAL USEOFCOMPLEXESOFIRONAND CARBOHYDRATESHASRESULTEDIN ANAPHYLAC11C.TYPERE- provide adequate replenishment 01iron stores in most individuals with moderately or severely reduced levels of hemoglobin. ItACTIONS. DEATHSASSOCIATEDWITH SUCHADMINISTRATIONHAVEBEENREPORTED.ThEREFORE.INFeOSHOULD shOuldbe remembered that iron deficiency anemiawill not appear until essentially all iron stores have been depleted. Therapy,BEUSEDONLYIN ThOSE PATIENTSIN WHOM ThE INDICATiONSHAVt BEENCLEARLYESTABLISHEDAND LABORA� thOS,should aim at not only replenishment of hemoglobin iron but iron stores as well.TORYINVESTIGATiONSCONARM ANIRON DEFICIENTSTATENOTAMENAILETO ORALIRONTHERAPY. Factorscontributing to the formula are shown below.
DESCRIPTiON:INFeD(iron dextran injection, USP) is a dark brown, slightly viscous oterile liquid complex otfernc hydroxide mg blood iron = mL blood o g hemoglobin x mg ironand deotran for intravenous or intramuscular use. lb body weight lb bodyweight mL blood g hemoglobinEachmL contains the equivalent of 50 mg of elemental iron (as an iron deotrancompleo), approximately 0.9% sodium chIn- a) Blood volume 65 mLlkg of body weightride, in water for injection. Sodium hydroxide and/or hydrochloric acid may have been used to adjust pH. The pIt of the solutionis between 5 2 and 6 5 b( Normal hemoglobin (males and females)The iron dextran compleo has an averageapparent molecular wieght of 165.000. 0#{174}�15 kg (33 Ibs) 14.8 g/dlTherapeutic Class: fematinic 15 kg (33 Ibs) or less 12.0 g/dICUNICAJ.PHARMACOLOGY:General: After intramuscular injection, iron deotran is absorbed from the injection sde into the c) Iron content of hemoglobin 0.34%capillaries and the lymphatic system. Circulating iron dextran is removed from the plasma by cells ofthe reticuloendothelial d) Hemoglobin deficitsystem, which split the complex into its components of Iron and dextran. The iron is immediately bound to the available proteinmoieties to form tnemosiderinor fernitin, the physiological forms of iron, or to a lesser extenttotransfernin. This iron which is e) Weiohtsuf$ect to physiological control replenishes hemoglobin and depleted iron stores. � onthe above factors, individuals with normal hemoglobin levels will haveapproximately 33 mg of blood iron per kilo-Dextran, a pofyglucose, is either metabolizedorexcreted. Negligible amounts ofiron are lost viathe urinary or alimentary path- gram ofbOd� weght(15 mg/lb).ways after admrnistration of iron deotran. Note: The table and accomparyingformula are applicablefor dosagedeterminations only in patients with iron deficiency ane-The major portion of intramuscular injections of iron deotran is absorbed within 72 hours: most ofthe remaining iron is ab- mm: they are not to be used for dosagedeterminations in patients requinng Iron replacementfnr blood loss.sorbed over the ensuing 3 to 4 weeks. TOTAL INFsD REQUIREMENTFORHEMOGLOBINRESTORATIONAND IRON STORESREPLACEMENTVanous studies involving intravennusfyadministered 59Foiron dextran to iron deficient subjects, some of whom had coexistingdiseases, have yielded haft-Ide values ranging from 5 hours to more than 20 hours. The 5-hour value was determined for#{176}9Feiron deotran from a studythat used laboratoty methods to separate the circulating 50Feiron deotran from the transferrin-boundt9Fe.The 20-hour value reflects a half-life determined by measuring total � both circulating and bound. It should be under-stood that these baIt-Idevalues do not representclearance of iron from the body. Iron is not easily eliminated from the bodyand accumulation ofiron can betosic.INDICAT1ONSANDUSAGE:Intravenous or intramuscular injections of iron dextrar are indicated fortreatment of patients withdocumented iron deficiency in whom oral administration is unsatisfactory or impossible.CI�N_TRA1� product. Allanemias notassociated with iron deficiency.
PAflENTLEANSOD-�-
V WEIGHTlb
5 1110 2215 3320 4425 5530 6635 7740 8845 9950 11055 12160 13265 14370 15475 16580 17685 18790 19895 209
100 220105 231110 242115 253120 264
Milliliter Requirement of INFeDBasedOnObserved Hemoplobin of
WARNINDS: See BOXEDWARNINU.A risk ofcarcinogenesis may attend the intramuscular injection ofiron-carbohydrate complexes. Such complexes have beenfound underesperimental condItions to produce sarcoma when large doses or small doses injected repeatedly at the same sItewere given to rats, mice, and rabbits, and possibly in hamsters.The long latent period between the inection of a potential carcinogen und the appearuncoof a tumor makes It impossible tomeasure accurately the risk in man. T1herehave,however, beer several reports in the literature describing tumsrs at the injec-tion site in humans who had previously received intramuscular injections ofiron-carbohydrafe complexes.Large intravenous doses, such us used wIth total dose infusions (TOt), have been associatedwIth an increased incidence ofadverse effects. Theadverse effects frequently are delayed (1-2 days) reactions typified by one or mom ofthe following romp-toms: arthralgia. backache,chills, dizziness, moderateto highfever, headache,malaise,mvalgia, nausea,and vomiting. Theonset is usually 24-48 boors afteradministration and symptoms generally subside within 1-4 days. Thesesymptoms havealsobeen reported following intramuscular injection and generally subside within 3-7 days. Theetiology ofthese reuctions is notknown. The potentiul for a delayedreaction most be considered when estimating the risk/benefit sf treatment.The maximum daily dose should not exceed2 ml undiluted iron deotran.This preparation should be used with extreme care in patients with serious impairment of liver function.It should not be used dunng the acute phase of infectious kidney disease.Adverse reactions experienced following administration oflNFeb may exacerbatecardiovascular complications in patients withpre-eoisbn�cardiovascukir disease.PRECAUTI NS: General: Unwarranted therapy with purenferal iron will causeexcessstorage of iron with the consequent pos-sibility of exogenous hemosiderosis. Such iron overload is particularly apt to occur in patients with hemoglobinopathies andother refractory anemias that might beerroneously diagnosed us iron deficiency anemias.INFeDshould be used with caution in individuals with histories of significant allergies and/or asthma. �TabIe values were calcuiated based on a normal adult hemoglobin of 14.8 g/dl forweignts greaterthan 15 kg (33 (ha)and aAnaphytaxisand other hypersensitivIty reactions have been reported after uneventful test doses as well as therapeutic doses of hemoglobin of 12.0 gIdI forweights less than orequal to 15 kg (33 Ibs).iron deotran Injection. Therefore, administration of subsequent test doses during therapy should beconsidered. (See DOSAGE Thetotal amount of INFeDin mL required to treatthe anemiaand replenish Iron stores may be approximated as follows:AND ADMINISTRATION:Administration.) Adultsand6h!Idrn over lSkg(33!hs):See DosageTable.Alternatively the total dose may be calculated:Epinephrine should be immediately available in the event of acute hypersensitivity reactions (Usual adult dose: 0.5 mL of a Dose (ml) = 0.0442 (Desired Hb - Observed Hb) s LBW + (0.26 x LBW)1:1000 solution, by subcutaneous or intramuscular injection.) Nete: Patients using beta-blocking agents may not respond ado- � on Desired Hb=thetarget Hb in g/di$��t�it�rheumatoId arthritis may havean acuteexacerbationofpant pain andswetliog following theadmimstration of INFeD. � = Lean body weight in kg. A patient’slean bodyweight(oractual body weight It less than lean body weight) should
e inephrine. Isoproterenol or similar beta-agonist agents may be required in these patients. OS�V� Hb = the patient’s current hemoglobin in g/dl.Reports in the literature from countnes outside the UnIted States (in particular, New Zealand)have suggested thatthe use of be utilized when determining dosage.intramuscular iron deotrar in neonateshas beenassociated with an increased incidenceof gram-negative sepsis, pnmanilydue for males: LBW = 50 kg + 2.3 kg foreach inch of patient’s height over5 feetto E. Ccli. Forfemales: LBW = 45.5 kg + 2.3 kg foreach inch of patient’s height over 5 feetlnlermatfon ForPitlento: Patients should be advised olthe potential adverse reactions associated with the use of INFeD. To calculatea patient’s weightin kg when Ibsare known: patient’sweight in pounds �weight in kilogramsDru�/LabonatoryTest lntsrsctlons: Large doses of iron destrar (5 mL or more) have been reported to give a brown color to 22serum from a blood sample drawn 4 hours after administration. �,lldnen 5 - l5kg(11 -33Ibs): SeeDosa9eTableThe drag may causefalsely elevatedvalues of serum bilirubin and falsely decreasedvalues of serum calcium. INFeDshould not normally he given in the first four manths of life. (SeePRECAUTIONS:Pediatric Use.)Serum iron determinations (especially by colorimetric assays) may not be meaningful for 3 weeks following the administration Altemativolythe total dose may becalculatedof iron dextran. Dose )mL) = 0.0442 (Desired Hb - ObservedHb) s W + (0.26 s W)Serum ferritin peaks appronimatefy 7 to 9 daysafter an intravenous dose of INFeDand slowly returns to baselineafter about 3 � on tesire� Hb = the target Hb in g/dl (Normal Hbfor Children 15 kg or less is 12 g/dl)weeks. W=Weight in kg.Examination ofthe bone marrowfor iron stores may not be meaningful for prolonged periods following iron dextrun therapy To calculatea patient’s weight in kg when Ibsare known patient’sweight in pounds � weight in kilogramsbecause residual iron deotran may remain in the reticuloendothelial cells.Bonescans involving 99m Tc-diphosphonate have been reported to show a dense, crescentic ureaof activity in the buttocks, 2.2following the coetourofthe iliac crest, 1 fo6 daysafter intramusculurinjections of iron dextran. II. IronReplacementlorBloodLoss:Some individuals sustain blood tosseson an intermittentor repetitive basis. Such bloodBonescans with 99m Tc-Iabeledbone seeking agents, in the presenceof high serum ferritin levelsorfollowing iron deotran losses may occur periodically in patients with hemorrhagicdiatheses (familial telangiectasia: hemophilia: gastrointestinalinfusions, have been reported to show reduction of bony uptake, marked renal activity, and excessive blood pool and soft fit- bleeding) and on a repetitive basis from procedures such as renal hemodiatysis.sue accumulation. Iron therapy in these patients should be directed toward replacement of the equivalent amount of iron represented in the bloodCarclnogenesfa, Mutageneafa, lmpatrmeet Of Feedllly See WARNINGS. loss. The table and formula described under I. IronOeflclenqAneneiaare notapplicableforsimple iron replacement values.Pne�Rancy: PregnancyCategoiyC:(ror deotran has been shnwnto beteratogenic and embryocidalin mice, rats, rabbits, dogs, Quantitativeestimates nfthe individuars periodic bloodtossand hematocritduringtfne bleeding episode provide aconvenientand monkeys when given in doses ofabout 3times the maximum human dose. method forthe calculation ofthe required iron dose.No consistent adverse fetal effects were observed in mice, rats, rabbits, dogs and monkeys at doses of 50 mg iron/hg or less. The formula shown below is based on the approximation that 1 mL of normocytic, normochromic red cells contains I mg ofFetaland maternal toxicity has been reported in monkeys at a total intravenous dose of 9Omg iron/kQover a 14 day penod. elemental iron:Similar effects were observed in mice and rats on administration of a single dose of 125 mg iron/kg. vetal abnormalities in rats Replacement iron (in mg( Blood loss (in mL) s hematocritand dogs were observed at doses of 250 mg iron/hg and higher. The animals used In these tests were not iron deficient There Example: BlOOdloss of 500 mLwith 20% hematocritare no adequateand well-controlled studies in pregnant women. INFeDshould be used dunng pregnancy only ffthe potential Replacement Iron = 500 s 020 = 100mgbenefit justifies the potential riskto the fetus. INFeDdose = 100 mg � 2 mLPlacental Transfer Various animal studies and studies in pregnant humans havedemonstrated inconclusive results withrespect to the placental transfer of iron deotranas iron dextran. It appearsthat some iron does reachthe fetus, but the form in Admtntstratlon: The total amount of INFeDrequired forthe treatment of iron deficiency anemiaor iron replacement for bloodwhich if crosses the placenta is not clear. loss is determined from the table orappropriate formula. See DosageNetting Methent: Caution should be esercised when INFeDis administered to a nursing woman. Traces of unmetabolized iron � � PRIORTO RECEIVINGTHEIR F)RSTINFeD�HERAPEUTIC DOSE,AU. PATIENTSSHOULDBEGIVENdextran are excreted in human milk. AN INTRAVENOUSTESTDOSEOF0.5 mL 15cc PRECAUTIONS:Generat)THE TESTDOSESHOULDBEADMINISTEREDAlAPediatrIc tine: Not recommended for use in infants under 4 months of age. (See DOSAGEAND ADMINISTRATION.( GRADUAL�m OVERAT LEAST3OSECOI�DS.Aithoogh anaphytactic reactions known to occurfotlowing INFeDadministra-ADVERSEREACTIONS:Senses/Fatal: Anaphylaclic reactions have been reported with the use ofiron dextran in�ethon: on tion are usually evidentwithin afew minutes, or sooner, It is recommended thata period ofan hour orlonger elapse before theoccasions these reactions have beenfatal. Such reactions, which occur most often within the first several minotes ofadmin- mmainder of the initial therapeutic dose is given.istration, have beengenerally characterized by sudden onset of respiratory difficulty and/or cardiovascular collapse. (See booed Individual doses of 2 mL or less may be given on a daily basis until the calculated total amount required has been reached.WARNINGand PRECAUTIONS:General,pertaining to immediate availability of epinephrine.) INFeDis given undiluted at a slow�radual rats notto exceed50 mg (1 mL’ per minute.Cardiovascular Chest pain, chest tightness, shock, fiypotension, hypertension, tachycardia, flushing, arrhythmias. (Flushing 2. IntramuscularlnJectlon. PRIO TO RECEIVINGTHEIR FIRSTINFeDTI1ERAPEUTICDOSE,ALL PATIENTSSHOULDBEand hypotension may occur from too rapid injections by the intravenous route.) GIVEN� INTRAMUSCULARTESTDOSEOF0.5 mL (See PRECAUTIONS:General.)The test dose should be administered inDennatologlc: Urticaria, pruntus, porpura, rash. the same recommendedtest site and bythe sametechnique as described in the last paragraph ofthis section. Although ana-GastroIntestInal: Abdominal pain, nausea,vomiting, diarrhea. phylactic reactions knownto occurfollowing INFeDadminIstration are usually evident within afew minutes orsooner, It is rec-Hemalologlc/lymphatic: Leucocytosis, lympliadenopathy. ommended that at leastan hour or longerelapse beforethe remainder ofthe initial therapeutic dose is given.Musculoshelelal/soft tlsswe: Arthralgsa,arthnhs (may represent reactivation in patients with quiescent rheumatoid arthntis - � no adverse reactions are observed, INFeDcan be given according to thefollowing schedule until the calculatedtotal amountSeePRECAUTIONS:General),myulgia: backache:stenle abscess, atrophylfibrosis (intramuscular injection site): brown skin required has been macbed.Eachday’s dose should ordinarily not exceed0.5 ml (25 mg of iron) for infants under 5 kg (11 Ibs):and/or underlying tissue discoloration (staining), soreness or pain at or near intramuscularinjection sites: cellulitis: swelling: i.o mL (50 mg nfiron) for children under 10 kg (22 (ha): aed 2.0 mL (100 mg of iron) forntherpatients.inflammation: local phlebitis at or near intravenous inlechon site. INFeDshould be injected only into the muscle mass ofthe upper outer quadrant of the buttock - never into the arm orotherNeirologic: Convulsions, seizures, syncope, headache,weakness,unresponsiveness, paresthesia, febrile episodes, chills, exposedareas-and should be injected deeply, wttha2-inch or3-inch l9or20gauge needle. lfthe patientis standing he/shedizziness, disonentation, numbness. should be bearing his/herweight on the leg opposite the injection site, or if in bed, he/she should be in the lateral position withR��lrslory Respiratory arrest, dyspnea, brnnchospasm. injection site uppermost. To avoid injection or leakageinto the subcutaneous tissue, a Z-tracktechnique (displacement of the
olc, Hemafuria skin laterally priorto injection) is recommended.Delayedreactions: Arthralgiu, backache,chills, dizziness, fever, headache,malaise, myulgia, nausea, vomiting. (SeeWARN- NOTE:Do not mix INFeDwith other medications oraddto parenteral nutrition solutionsfor intravenous infusion.INGS.) Parenteral dreg products should be inspected visually for particulate matterand discoloration priorto administration, when-MIscellaneous: Febnleepisodes, sweating, shivering, chills, malaise, altered taste. everttse solution aed container permIt.OVERDOSAGE:Overdosagewith iron deotran is unlikelyto be associated with any acute mandestations. Dosagesof iron deo- HOW siwFtwo: INFeD (Iron Destran Injection, USP)containing 50 mg of elemental iron per mL is available in 2 ml singlefran in excess of the requirements for restoration of hemoglobin and replenishment of iron stores may leadto hemosiderosis. dose amberviats (for intramuscularor intravenous use) in cartons of 10 (NDC0364-3012-47).Periodic monitoring of serum ferritin levelsmay be helpful in recogniziog a deleterious progressive accumulation of iron re- �ore at controlled room temperature 15’ - 30’ C (59’ - 86 F).suIting from impaired uptake of iron from the reticuloeedothellal system in concurrent medical conditions such as chronic � Federal law prehiblts dIspensing without prescnlptloe.renal failore, Hodgkin’s disease and rheumatoid arthritis. The LD� of iron deotran is not less than 500 mg/kg in the mouse.DOSAGE AND ADMINISTRATION:Oral iron should be discontinued priorto administration of INFeD. Literature revised: July1995Doug.: ProductNo.: 1001-02 695310010364�E1I. Iran Owhc.loncyAnmla: Periodic hematologic determination (hemoglobin and hematocrit) is a simple and uccurate tech-nique for monitoring hematological response, and should be used as a guide in therapy. It should be recognized that iron slur-age m� lag behind the appearanceof normal blood morphology. Serum iron, total iron binding capacity (TIBC)and percentsaturation oftransferrin are other important tests for detecting and monitoring the iron deficient state. SCHEIN PfIARMACEU’flCAL, INC.Afteradministration of iron dextran complex, evidenceof a therapeutic response can beseen in a few days as ar increase in the Florham Park, NJ 07932 USA �reticulocyte count.Although serumferritin is usually a good guideto body iron stores, the correlation ofbody iron stores and seromferritin may P H A 1 M A C F U S I C A
IF1O
)g/dl)
1�162023273135394347515559636670747882869094
(g/dl)
151822262933374144485255596366707477818588
(g/dl)
1�1721242831353842454952555962666973768083
(g/dl)
131619232629323639424549525558626568717578
(g/d()
1�1518212427303336394245485154576063677073
(g/dl)
1�1417202225283134363942454850535659626467
(g/dl)
101315182123262831343639414446495254575962
10(g/dl)
1�14171921242628313335384042454750525457
Anewera in
cyclosporinetherapy
starts here.
©1996 Sandoz Pharmaceuticals Corporation
w w
to those when
dosage of the
same cyclosporine blood trough concentrations.
Intrasubject variability of the area under the
concentration-versus-time curve (%CV) in renal
transplant recipients was 9% to 21 % for Neoral and
19% to 26% for Sandimmune#{174} (cyclosporine). Today,
the Neoral combination of microemulsion technology
and comparable safety* offers an important option
for providing cyclosporine to your transplant
recipients.
*The principal adverse reactions of cyclosporine therapy are renal dysfunction,
tremor, hirsutism, hypertension, and gum hyperplasia.
Innovation Through Microemulsion
NEORAE �
cyclosixhneqapsulesa1ndJxo�Isolutionformic�emuIsion�
WARNINGOnly physicians experienced in immunosuppressive therapyand management of organ transplant patients should pre-
scribe Neoral#{174}. Patients receiving the drug should be man-aged in facilities equipped and staffed with adequatelaboratory and supportive medical resources. The physician
responsible for maintenance therapy should have complete
information requisite for the follow-up of the patient.
Neoral#{174}may be administered with other immunosuppressive
agents. Increased susceptibility to infection and the possibledevelopment of lymphoma and other neoplasms may resultfrom the degree of immunosuppression.
Neoral#{174} Soft Gelatin Capsules (cyclosporine capsules for
microemulsion) and Neoral#{174}Oral Solution (cyclosporine oral
solution for microemulsion) have increased bioavailabilityin comparison to Sandimmune#{174} Soft Gelatin Capsules (cy-
closporine capsules, USP) and Sandimmune#{174} Oral Solution(cyclosporine oral solution, USP). Neoral#{174}and Sandimmune#{174}
are not bioequivalent and cannot be used interchangeablywithout physician supervision. It is recommended that cy-
closporine blood concentrations be monitored in patients tak-ing Neoral#{174}and that dose adjustments be made in order to
avoid toxicity due to high concentrations and possible organrejection due to low concentrations. For a given trough con-
centration, cyclosporine exposure will be greater with Neoral#{174}than with Sandimmune#{174}. If a patient who is receiving excep-
tionally high doses of Sandimmune#{174} is converted to Neoral#{174},particular caution should be exercised. Comparison of blood
concentrations in the published literature with blood concen-trations obtained using current assays must be done with de-
tailed knowledge of the assay methods employed. (See BloodConcentration Monitoring under DOSAGE AND ADMINIS-TRATION.)
#{149}For de novo transplant recipients, start withthe same Neoral dosage you would use withSandimmune
I For maintenance patients, conversion to Neoralis generally safe and well tolerated
- Start with a simple 1:1 dosage conversionto Neoral (see boxed warning)
- Adjust the Neoral dosage to attainpreconversion blood trough concentrations
*ln controlled studies, the nature, severity, and incidence of the adverse
events that were observed in transplant recipients treated with Neoralwere comparable with those of patients who received Sandimmune inthose same studies when the dosage of the two drugs was adjusted toachieve the same cyclosporine blood trough concentrations. Theprincipal adverse reactions of cyclosporine therapy are renal dysfunc-tion, tremor, hirsutism, hypertension, and gum hyperplasia.
Reference1. Mueller EA, Kovarik JM, van Bree JB, et al. Pharmacokinetics andtolerability of a microemulsion formulation of cyclosporine in renalallograft recipients-a concentration-controlled comparison with thecommercial formulation. Transplantation. 1994;57:1178-1182.
� SANDOZSANDOZ PHMAt� CORPORAflON
EAST HAN�ER. NEWJERSEY 07936
Please see brief summary of prescribing informationon the following page.
NEO-0695-O1 Printed in U.S.A. 4/96
I Neoral and Sandimmune are not bioequivalentand cannot be used interchangeably withoutphysician supervision
I Available in 25-mgand 100-mg softgelatin capsulesand oral solution(100 mg/mL)
Innovation Through Microemulsion
NEORAE �
c�dospo�necapsulesand J(�o�lsolu�onformic�emulsion� ‘
WARNING: Only physicians experienced in immunosuppressive therapy and management of organtransplant patients should prescribe Neoral�. Patients receiving the drug should be managed infacilities equipped and staffed with adequate laboratory and supportive medical resources. Thephysician responsible for maintenance therapy should have complete information requisite for thefollow-up of the patient.Neoral#{174}may be administered with other immunosuppressive agents. Increased susceptibility to in-fection and the possible development oflymphoma and other neoplasms may result from the degreeof immunosuppression.
Neoral#{174}Soft Gelatin Capsules (cyclosporine capsules for microemulsion) and Neoral#{174}Oral Solution(cyclosporine oral solution for microemulsion)have increased bioavailability in comparison toSandimmune#{174}Soft Gelatin Capsules (cydosporine capsules. USP) and Sandimmune#{174}Oral Solution(cyclosporine oral solution, USP). Neorale and Sandimmune#{174}are not bioequivalent and cannot beused interchangeably without physician supervision. It is recommended that cyclosporine bloodconcentrations be monitored in patients taking Neoral� and that dose adjustments be made in orderto avoid toxicity due to high concentrations and possible organ rejection due to low concentrations.For a given trough concentration, cyclosporine exposure will be greater with Neoral#{174}than withSandimmune#{174}. If a patient who is receiving exceptionally high doses ofSandimmune#{174}is convertedto Neorale, particular caution should be exercised. Comparison of blood concentrations in the pub-lished literature with blood concentrations obtained using current assays must be done with detailedknowledge of the assay methods employed.
NEORAL#{174} SoftGelatinCapsules(cyclosporine capsulesfor microemulsion)
NEORAL#{174}OJ�IISolution(cyclosporine oral solutionfor microemulsion)cautioss Federal law prohibits dispensing without prescription.BRIEF SUMMARY: Please see package insert for full prescribing information
INDICATIONS AND USAGE Neorale is indicaeed for the prophylaxis of organ rejection in kidney,liver. and beare allogeneic transplants. Neoral#{174}has been used in combination with azathioprine andcorticosteroids.c0NTRAINDIcATI0Ns: Neorultm is coneraindicated in patients with a hypersensitivity to cyclosporineor to any of the ingredients ofthe formulation.
WARNINGS: (Set’ boxed WARNINGS)Cyclosporine. the active ingredient of Neoral#{174},can cause nephrotoxicity and hepatoeoxicity when used inhigh doses.It is not unusual for serum creatinine and BUN levels to be elevaeed during cyclosporine therapy. Theseelevations in renal transplant patients do not necessarily indicate rejection, and each patient must be fullyevaluaeed before dosage adjustment is initiated.Based on the historical Sandimmune� experience with oral solution. nephrotoxicity associated withcyclosporine had been noted in 25% ofcases of renal transplantation, 38% ofcases ofcardiac transplan-Cation, and 37% ofcases of liver transplantation. Mild nephroeoxiciey was generally noted 2-3 monthsafter renal transplant and consisted of an arrese in the fall ofthe pie-operative elevations of BUN andcreatinine at a range of 35-45 mg/dl and 2.0-25 mg/dl respectively. These elevations were often respon.sive to cyclosporine dosage reduction.
More overt nephrotoxicity was seen early after transplantation and was characterized by a rapidly risingBUN and creatinine. Since these events are similar to renal rejection episodes, care must be taken todifferentiate between them. This form ofnephrotoxicity is usually responsive to cyclosporine dosagereduction.Although specific diagnostic criteria which reliably differentiate renal graft rejection from drug toxicityhave not been found. a number of parameters have been significantly associated with one or the other. Itshould be noted however, that up to 20% of patients may have simultaneous nephrotoxicity and rejection.
A form ofa cydosporine-associated nephropathy is characterized by serial deterioration in renal functionand morphologic changes in the kidneys. From 5% to 15% oftransplant recipients who have receivedcyclosporine will fail to show a reduction in rising serum creatinine despite a decrease or discontinuationof cyclosporine therapy. Renal biopsies from these patients will demonstrate one or several ofthe tot-lowing alterations: tubular vacuohzation, tubular microcalcifications, peritubutar capillary congestion,arteriolopathy. and a striped form ofinterstitial fibrosis with tubular atrophy. Though none of these mor-phologic changes is entirely specific. a diagnosis ofcyclosporine-associated structural nephrotoxicityrequires evidence ofthese findings.
When considering the development ofcyclosporine-assodated nephropathy, it is noteworthy that severalauthors have reported an association between the appearance ofinterstitial fibrosis and higher cumulativedoses or persistently high circulating trough levels ofcydosporine. This is particularly true during thefirst 6 posttransplant months when the dosage tends to be highest and when, in kidney recipients. theorgan appears to be most vulnerable to the toxic effects ofcycbosporine. Among other contributing factorsto the development of interstitial fibrosis in these patients are prolonged perfusion time, warm ischemiatime, as welt as episodes ofacute toxidt� and acute and chronic rejection. The reversibility of interstitialfibrosis and its correlation to renal function have not yet been determined. Reversibility of arteriolopathyhas been reported after stopping cyclosporine or lowering the dosage.
Impaired renal function at any time requires close monitoring. and frequent dosage adjustment may beindicated.In the event of severe and unremitting rejection, when rescue therapy with pulse steroids and monoctonalantibodies fail to reverse the rejection episode, it may be preferable to switch to alternative inununosup’pressive therapy rather than increase the Neoral#{174}dose to excessive levels.Occasionally patients have developed a syndrome of thrombocytopenia and microangiopathic hemolyticanemia which may result in graft failure. The vasculopathy can occur in the absence ofrejection and isaccompanied by avid platelet consumption within the graft as demonstrated by Indium 151 labeledplatelet studies. Neither the pathogenesis nor the management of this syndrome is clear. Though resolu-tion has occurred after reduction or discontinuation ofcycbosporine and I) administration of streptokinaseand heparin or 2) plasmapheresis, this appears to depend upon early detection with Indium Ill labeledplatelet scans. (Set- ADVERSE REACTIONS)
Si#{216}ficant hyperkalemia (sometimes associated with hyperchloremic metabolic acidosis) and hyper-uncemia have been seen occasionally in individual patients.Hepatotoxicity associated with cycbosporine use had been noted in 4% of cases of renal transplantation.7% ofcases ofcardiac transplantation. and 4% ofcases of liver transplantation. This was usually notedduring the first month of therapy when high doses of c�rcbosporine were used and consisted of elevationsofhepatic enzymes and bilirubin. The chemistry elevations usually decreased with a reduction in dosage.As in patients receiving other imununosuppressants. those patients receiving cyclosporine are at increasedrisk for development of lymphomas and other malignancies. particularly those ofthe skin. The increasedrisk appears related to the intensity and duration ofimmunosuppression rather than to the use of specificagents. Because of the danger ofoversuppression ofthe immune system resulting in increased risk ofinfection or malignancy, a treatment regimen containing multiple imnnunosuppressants should be usedwith caution.There have been reports ofconvulsions in adult and pediatric patients receiving cyclosporine, particularlyin combination with high dose methylprednisolone.
Care should be taken in using cydosporine with nephrotoxic drugs. (See PRECAUTIONS)
Because Neoralw is not bioequivalent to Sandimmune#{174}.conversion from Neoral#{174}to Sandimmune#{174} using a1:5 ratio (mg/kg/day) may result in lower cydosporine blood concentrations. Conversion from Neoral#{174}toSandimmune� should be made with increased monitoring to avoid the potential of underdosing.
pREcAuTIoNs: General: Cyclosporine is the active ingredient of Neoral#{174},Hypertension is a commonside effect ofcyclosporine therapy. (See ADVERSE REACTIONS) Mild or moderate hypertension isencountered more frequently than severe hypertension and the incidence decreases over time. Anti-hypertensive therapy may be required. Control ofblood pressure can be accomplished with any of thecommon antihypertensive agents. However, since cyclosporine may cause hyperkalemia, potassium-sparing diuretics should notbe used. Calcium antagonists can be effective agents in treating cyclosporine-associated hypertension. However, care should be taken since interference with cydosporine metabolismmay require a dosage adjustment. (See Drug Inferacf ions)
During treatment with cydosponne. vaccination may be less effective; and the use oflive attenuatedvaccines should be avoided.Infonnation for Patienhe Patients should be advised that any change of cyclosporine formulationshould be made cautiously and only under physician supervision because It may result in the needfor a change In dosage.Patients should be informed of the necessity of repeated laboratory tests while they are receiving thedrug. Patients should be advised of the potential risks during pregnancy and informed of the increasedrisk of neoplasia.Patients should be given careful dosage instructions. Neoral#{174}Oral Solution (cyclosporine oral solution formicroemutsion) should be diluted, preferably with orange or applejuice that is at room temperature.Grapefruit and grapefruitjuice affect metabolism ofcyclosporine and should be avoided. The combinationof Neoral#{174}Oral Solution (cyclosporine oral solution for microemulsion) with milk can be unpalatable.
Patients should be advised to take Neorale � a consistent schedule with regard to time ofday andrelation to meals.
Laboratory Tests: Renal and liver functions should be assessed repeatedly by measurement of BUN,serum creatinine, serum bilirubin, and liver enzymes.
Drug Interactions: All of the individual drugs cited below are well substantiated to interact withcydosporine.Design Thaf May Potentiate Renal Dysfunction
Antibiotics Antjfungals Gastrointestinal Agents
gentamicin amphotericin B cimetidinetobransycin ketoconazole ranitidinevancomycm � Anti-inflam;nators Drugs Imrnunosuppressirvstnmethopnm with sulfamethoxazole
. . azapropazonAnt:neoplasfzcs dic(ofenacmelphalan
Careful monitoring of renal function should be practiced when Neoral#{174}is used with nephrotoxic drugs.
Drugs ThafAlter Cyclosporine Levels: Cydosporine is extensively metabolized. Cyclosporine concentra-tions may be influenced by drugs that affect microsomal enzymes, particularly cytochrome P-450 Ill-A.Substances that inhibit this enzyme could decrease metabolism and increase cydosporine concentrations.Substances that are inducers of cytochrome P450 activity could increase metabolism and decreasecyclosporine concentrations. Monitoring ofcirculating cyclosporine concentrations and appropriateNeoral#{174}dosage adjustment are essential when these drugs are used concomitantly.Drugs That Ltic�aac Cyclosporine Concentrations
Calcium Channel Antjfungals Antibiotics Glucocorticoids Other Drugs
Blockers fluconazole clarithromycin methylprednisolone allopurinoldultiazem itraconazole erythromycin bromocriptinenicardipine ketoconazole danazolverapamil metoclopramide
Drugs That Q.tacgsc Cyclosporine Concentrations
Antibiotics Anticonsulsants Other Drugs
nafcillin carbamazepine octreotiderifampin phenobarbttal ticlopidine
phenytoin
Rifabutin is known to increase the metabolism of other drugs metabolized by the cytochrome P.450 sys-tem. The interaction between rifabutin and cyclosporine has not been studied. Care should be exercisedwhen these two drugs are administered concomitantly.
Other Drug lnteractions: Reduced dearance of prednisolone, digoxin, and lovastatin has been observedwhen these drugs are administered with cyclosporine. In addition, a decrease in the apparent volume ofdistribution ofdigoxin has been reported after cyclosporine administration. Severe digitalis toxicity hasbeen seen within days ofstarting cyclosporine in several patients taking digoxin. Cyclosporine shouldnot be used with potassium-sparing diuretics because hyperkalemia can occur. During treatment withcyclosporine, vaccination may be less effective. The use oflive vaccines should be avoided. Myositis hasoccurred with concomitant lovastatin, frequent gingival hyperplasia with nifedipine. and convulsionswith high dose methylprednisolone. Further information on drugs that have been reported to interactwith cyclosporine is available from Sandoz Pharmaceuticals Corporation.
Carcinogenesis, Mutugenesis, and Impairment of Fertility: Cyclosporine gave no evidence of mutagenicor teratogenic effects in appropriate test systems. Only at dose levels toxic to dams, were adverse effectsseen in reproduction studies in rats. (See Pregnancy)
Carcinogenicity studies were carried out in male and female rats and mice. In the 78-week mouse study,evidence ofa statistically significant trend was found for Iymphocytic Iymphomas in females, and theincidence ofhepatocellular carcinomas in mid-dose males significantly exceeded the control value. In the24-month rat study. pancreatic islet cell adenomas significantly exceeded the control rate in the low doselevel. Doses used in the mouse and rat studies were 0.01 to 0.16 times the clinical maintenance dose. Thehepatocellular carcinomas and pancreatic islet cell adenomas were not dose related.
No impairment in fertility was demonstrated in studies in male and female rats.
Cydosporine has not been found to be mutagenic/genotoxic in the Ames Test, the V79-HGPRT Test, themicronucleus test in mice and Chinese hamsters, the chromosome-aberration tests in Chinese hamsterbone-marrow, the mouse dominant lethal assay. and the DNA-repair test in sperm from treated mice.A recent study analyzing sister chromatid exchange (SCE) induction by cyclosporine using humanlymphocytes in vitro gave indication ofa positive effect (i.e.. induction ofSCE), at high concentrationsin this system.An increased incidence of malignancy is a recognized complication of immunosuppression in recipientsoforgan transplants. The most common forms ofneoplasms are non-Hodgkin’s lymphoma and carci-nomas of the skin. The risk of malignancies in cyclosporine recipients is hipher than in the normal, healthypopulation but similar to that in patients receiving other immunosuppressive therapies. Reduction or dis-continuance of immunosuppression may cause the lesions to regress.
Pregnancy: Pregnancy Category C. Cyclosporine has been shown to be embryo- and fetotoxic in rats andrabbits following oral administration at maternally toxic doses. Fetal toxicity was noted in rats at 0.8 andrabbits at 5.4 times the human maintenance dose of6.O mg/kg. where dose corrections are based on bodysurface area. Cyclosporine was embryo- and fetotoxic as indicated by increased pre. and postnatal mor-tality and reduced fetal weight together with related skeletal retardations.There are no adequate and well’controlled studies in pregnant women. Neoral5 should be used duringpregnancy only if the potential benefit justifies the potential risk to the fetus.
The following data represent the reported outcomes ofll6 pregnancies in women receiving cyclosporineduring pregnancy, 90% ofwhom were transplant patients, and most ofwhom received cyclosporinethroughout the entire gestational period. The only consistent patterns of abnormality were prematurebirth (gestational period of28 to 36 weeks) and low birth weight for gestational age. Sixteen fetal lossesoccurred. Most of the pregnancies (85 of 100) were complicated by disorders, including pre-eclampsia.eclampsia, prematurelabor, abruptio placentae, oligohydramnios, Rh incompatibility and fetoplacentaldysfunction. Preterm delivery occurred in 47%. Seven malformations were reported in 5 viable infantsand in 2 cases offetal loss. Twenty-eight percent of the infants were small for gestationat age. Neonatalcomplications occurred in 27%. Therefore, the risks and benefits of using Neoral#{174}during pregnancyshould be carefully weighed.
Nursing Mothers: Since cyclosporine is excreted in human milk, nursingshould be avoided.
Pediatric Use: Although no adequate and well controlled studies have been completed in children, pa.tients as young as one year ofage have received Neoral#{174}with no unusual adverse effects.
ADVERSE REACTIONS: The principal adverse reactions ofcyclosporine therapy are renal dysfunction,tremor, hirsutism, hypertension, and gum hyperplasia. Hypertension. which is usually mild to moderate,may occur in approximately 50% ofpatients following renal transplantation and in most cardiac trans-plant patients.
Glomerular capillary thrombosis has been found in patients treated with cyclosporine and may progressto graft failure. The pathologic changes resemble those seen in the hemolytic.uremic syndrome and includethrombosis ofthe renal microvasculature, with platelet-fibrin thrombi occluding glomerular capillariesand afferent arterioles, microangiopathic hemotytic anemia, thrombocytopenia, and decreased renalfunction. Similar findings have been observed when other immunosuppressives have been employedposttransplantation. Hypomagnesemia has been reported in some, but not all, patients exhibiting convul-sions while on cyclosporine therapy. Although magnesium-depletion studies in normal subjects sugpestthat hypomagnesemia is associated with neurologic disorders, multiple factors, including hypertension,high dose methylprednisolone, hypocholesterolemia, and nephrotoxicity associated with high plasmaconcentrations ofcyclosporine appear to be related to the neurological manifestations of cyctosporinetoxicity.
In controlled studies, the nature, severity and incidence of the adverse events that were observed in493 transplanted patients treated with Neoralw were comparable with those observed in 208 transplantedpatients who received Sandimmune� in these same studies when the dosage of the two drugs was ad-justed to achieve the same cyclosporine blood trough concentrations.The following reactions occurred in 2% or less ofSandimmune#{174}-treated patients: allergic reactions,anemia, anorexia, confusion. conjunctivitis, edema, fever, brittle fingernails. gastritis, hearing loss,hiccups, hyperglycemia, muscle pain. peptic ulcer, thsombocyto�enia, tinnitus. The following reactionsoccurred rarely: anxiety, chest pain, constipation. depression, hair breaking, hematuria, joint pain,lethargy, mouth sores, myocardial infarction, night sweats, pancreatitis. pruritus. swallowing difficulty,tingling. upper CI bleeding. visual disturbance, weakness, weight loss.Increased susceptibility to infection and the possible development oflymphoma and other neoplasmsmay result from the degree of inxmunosuppression.
Sandoz Pharmaceuticals Corporation, East Hanover, New Jersey 07936 SEPTEMBER 1995 38371902
THERE’ S A POWERFUL ATTRACTIONBETWEEN QUALITY AND CLINICAL RESULTS.
INTRODUCING DEXFERRUM#{174} (IRoN DEXTRAN INJECTION, USP)n
THE NEW CHOICE IN THE INTRAVENOUS TREATMENT OF IRON DEFICIENCY ANEMIA.
Introducing a high quality, highly consistent,
and clinically tested intravenous iron from a leader
in quality parenterals.
The safety and efficacy of new DEXFERRUM
have been established with ESRD patients on
Epoetin alfa in controlled, multi-center trials.
American Regent Laboratories, known for
quality parenterals throughout the U.S., supports
the dialysis community with services such as a
reimbursement hotline and a patient assistance
program. Our clinical support specialists are
dedicated to helping you achieve optimum
patient outcomes.
Now you can prescribe injectable iron with a
new measure of confidence. Because with new
DEXFERRUM, the connection between quality
care and clinical results is virtually inseparable.
The parenteral use of iron-carbohydrate
complexes has resulted in anaphylactic-type
reactions and death. Therefore, DEXFERRUM
should not be administered to patients amenable
to oral iron therapy.
AME RICANREGENTA#{241}�LABORATORIES, INC. One Luitpold Drive, Shirley, New York 11967
Phone: (800) 645-1706, Fax: (516) 924-1731http://www.luitpold.com.
DEXFERRUM Reimbursement Hotline: (800) 282-77l2#{174}In Washington, D.C., metropolitan area: (202) 942.2453. ISS 3/96
New DEXFERRUM#{174}(RoN DEXTRAN INJECTION, usP)
The quality choice.Please see brief summary of the prescribing information on the following page.
WARNINGTHE PARENTERAL USE OF COMPL.EXES OF IRON AND CARBOHYDRATES HASRESULTED IN ANAPHYLACflC-1YPE REACTIONS. DEATHS ASSOCIATED WITHSUCH ADMINISTRATION HAVE BEEN REPORTED. THEREFORE, DEXFERRUM’SHOULD BE USED ONLY IN THOSE PATIENTS IN WHOM THE INDICATIONS HAVEBEEN CLEARLY ESTABUSHED AND LABORATORY INVEST1GA11ONS CONFIRM ANIRON DEFICIENT STATE NOT AMENABLE TO ORAL IRON ThERAPY.
DEXFERRUM#{174}(IRON DEXTRAN INJECTION, USP)
DESCRIPTION: DEXFERRUM (IRON DEXTRAN INJECTiON, USP) is a dark brown, slightlyvcacous s�de liq� comp�x of ferric oxyhydroxide and a bw mdecukr w�ght dextran
deeivative for intravenous use. Each ml contains: 50 mg elemental ran as an iron dextrancomp�x. Sodium chbride may has#{174}been added for ton�. Water for injection q.s. pH adjustedto 5.2 - 6.5 with hydrachbric acid and, ifnecessary, sodium hydroxkle. Ste�, nanpyragenic.
Therapeutic Class: Hematinic.
INDICATIONS AND USAGES DexFerrum is indicated for treatment of patients with docu’mented iron defkiency in whom oral administration is unsatisfactocy or impossible.
CONTRAINDICAT1ONS: Hypersensitivity to the product. ,6J1anemias not associated withiron deliciency.
WARNINGS: See BOXED WARNING.
A nsk d carcinogenesis may attend the inframusct�ar injection of iran-carbohydrate com#{231}�exes.Such camp�xes have been found under expenmental canditians to praduce sarcama whenurge doses or small doses injected repeatedly at the same site were g’r�en to rats, mice, andrabbits, and possibly in hamsters.
The bag latent period between the injection ofa potential carcinogen and the appearance ofa tumor makes it impossible to measure accurately the risk in man. There have, however,been several reports in the literature describing tumors at the injection site in humans whohod previously received intramuscular injections of iron’carbohydrate complexes.
Large intravenous doses, such as used with total dose infusions (TDO, have been associated
withan increased inddence ofadverse effects. The adverse effects frequently are deleyed(1‘2 days) reactions typilied by one or more ofthe �bwing symptoms: arthralgia, backache,chills, dizziness, moderate to high fever, headache, malaise, myalgia, nausea, and vomiting.The onset is usually 24-48 hours after administration and symptoms generally subside within
3.4 days. The etiolegy of these reactions is not known. The potential far a dekiyed reactionmust be considered when estimating the risk/beneit of treatment.
The maximum daily dose should not exceed 2 ml undiluted iron dextran.
This preparation should be used with extreme care in patients with serious impairment of liverfunction.
It should not be used during the acute phase of infectious kidney disease.
Adverse reactions experienced fc�bwing administration ofDexFerrum may exacerbate cardio-
vascular complications in patients �th pee-existing cardkwascuksr disease.
PRECAUTIONS: General: Unwarranted therapy withparenteral iron will cause excessstorage of iron with the consequent possibility ofexogenous hemasiderosis. Such iron overloadis particulorly aptto occur in patients withhemoglobinopathies and other refractory anemiasthat might be erroneously diagnosed as iron deficiency anemias.
DexFerrum should be used with caution in individuals with histories of significant allergiesand/or asthma.
Anaph�4axis and other hypersensiti� reactions have been reported after uneventful test dosesas wefi as therapeutic doses of iron dextran injection. Therefore, administration of subsequenttest doses dunng therapy shauk� be considered. lSee DOSAGE AND ADMINISTRAflON:Administration.l
Epinephrine should be immediately available in the eventofacute hypersensitivity reactions.
lUsual adult dose: 0.5 ml of a 1:1000 solution, by subcutaneous or intramuscular injection.lNote: Patients using beta-blocking agents may not respond adequately to epinephrine.Isoproterenol or similar beta-agonist agents may be required in these patients.
Patients with rheumatoid arthritis may have an acute exacerbation of joint pain and swellingfollowing the administration of DexFerrum.
Information For Pathnts: Patients should be advised ofthe potential adverse reactionsassociated with the use of DexFerrum.
D�ug/Laboratoiy Test Interadions Large doses of iran dextran 15ml or morel have beenreported b give a browii calar to serum from a blood sample drawn 4 hours after administration.
The drug may cause falsely elevated values of serum bilirubin and falsely decreased values of
serum calcium.
Serum iron determinations lespeaally by cdo�metrk assaysl may not be meaningful for 3 weeksfoHa*�ng the administration of iron dextran.
Serum ferritin peaks approximately 7 to 9 days after an intravenous dose of DexFerrum andslowly returns to baseline after about 3 weeks.
Examination ofthe bone marrow for iron stores may not be meaningful for prolonged per�dsfdb#ing iron dextran therapy because residual iron dextran may remain in the reticuben-dothelial cells.
Bone scans with99m Tc’bbeled bone seeleng agents, in the presence of h�hsenim fernitin levelsor following iron dextran infusions, have been reported to show reduction of bony uptake,marked renal activity, and excessive blood pod and soh tissue accumubtion.
Carcinogenuis, Mutagenesis, Impairment Of Fertililyt See WARNINGS.
Pregnancy: Teratogenic Effects, Pregnancy Category C: Iron desdran has been shown to beteratogenic and embryocidal in mice, rats, rabbits, dogs, and monkeys when given in dosesofabout 3 times the maximum human dose.
No consistentadverse fetol effects were observed in mice, rats, rabbits, dogs and monkeys atdoses of 50 rag iron/kg or less. Fetal and maternal toxicity has been reported in monkeys at atotal intravenous dose of 90 mg iron/kg over a 14 day penod. Similar effects were observedin mice and rats on administration of a single dose of 125 mg iron/kg. Fetal abnormalitiesin rats and dogs were observed at doses of 250 mg iron/kg and higher. The animals used inthese tests were not iron dek�nt. There are no adequate and weWcontrdled studies in pregnantwoman. DexFerrum shauki be used during pregnancy only ifthe potential bene�t justifies the
potential �sk to the fehis.
Placental Transfer Various animal studies and studies in pregnant humans have demon’
stroted incondus’ive results with respect to the plocental transfer of iron dextran as iron dextran.Itappears that some iron does reach the felus, but the form in which itcrosses the pkicenta is
not dear.
Nursing Mothersi Caution shodd be exercised when Dexferrum is administered to a nur�ngwoman. Traces of unmetabdized iron dextran are excreted in human milk.
Pediatric Use: Not recommended for use in infants under 4 months of age (See DOSAGEAND ADMINISTRA11ON).
ADVERSE REACflONS.� Severe/Fatak Anaphykidk reactions have been reported withtheuse of iron dextran injection; on occa�ons these reactions hose been fotol. Such reactions, whichoccur most often within the lirst severd minuses ofodministrotion, haee been gene�ly character’ized by sudden onsetof respiratory difficulty and/or carc&isoscubr cdkipse. (See boxedWARNING and PRECAUT1ONS: General, pertaining to immediate avaibbility of epinephrine.)
Cardiovascular Chestpain, chesttightness, shock, hypotension, hypertension, tachycardia,Bushing, arrhythmias. IFlushing and hypotension may occur from too rapid injections by theintravenous route.)
Dermatologk: Urticaria, pruritus7purpura, rash.
Gastrointestinal: Abdominal pain, nausea, vomiting, diarrhea.
Hematologk/Iymphatic: Leucacytosis, lymphodenopathy.
Musculosk.letoI/soft tissue: Arthralgia, arthatis (may represent reactivation in patientswith quiescent rheumatoid arthritis - See PRECAuTIONS: General), myalgia; backache;sterile abscess; brown skin and/or underlying tissue discoloration (staining); cdlulitis; swelling;inAammation; local phlebitis at or near intravenous injection site.
Neurologic: Convulsions, seizures, syncope, headache, weakness, unresponsiveness,paresthesia, febrile episodes, chills, dizziness, disorientation, numbness.
Respiratory’� Respiratory arrest, dyspnea, bronchospasm.
Urologk: Hematuria.
D.lay.d reactions: Arthralgia, backache, chills, dizziness, fever, headache, malaise,myalgia, nausea, vomiting (See WARNINGS).
Miscellaneous: Febrile episodes, sweating, shivering, chills, malaise, altered taste.
DOSAGE AND ADMINISTRAflON: Oral iron shodd be discontinued p#{241}orto administrationof DexFerrum. Dexferrum should not be administered intramuscularly.
Administration: Intravenous Injectionl PRIOR TO RECEMNG THEIR FIRST DEXFERRUMTHERAPEU11C DOSE, AU PA11ENTSSHOULD BE GIVEN AN INTRAVENOUS TEST DOSE OF0.5 mL (See PRECAIThONS: General.) THE TEST DOSE SHOULD BE ADMINISTERED AT AGRADUAL RATE OVER AT LEAST 5 MNUTES.
See full prescribing information for instructions on administration and dosage.
NOTE: Do not mix DexFerrum with other medications or add to porenteral nutrition solutionsfor intravenous infusion.
Parenteral drug products should be inspected visually for particulate matter and discolorationprior to administration, whenever the solution and container permit.
HOW SUPPUED DexFerrum#{174}(Iron Dextran Injection, USP) containing 50 rag of elementaliron per ml, is available in 2 ml single dose vials (for intravenous use) in cartons of 10 (NDC051 7-0234’lO).
Store at controlled roam temperature 15 ‘ 30C )59� ‘ 86SF).
CAU11ON: Federal law prohibits dispensing without presc,iption.
See produd package insert for full prescribing information.
tNO234Rev. 3/96
AMERICANREGENTA6’LABORATORIES, INC. One Luitpold Drive, Shirley, New York 11967
Phone: (800) 645-1706, Fax: (516) 924-1731http://www.luitpold.com.
DEXFERRUM Reimbursement Hotline: (800) 282-77l2#{174}51n Washington, D.C., metropolitan area: (202) 942-2453.

To: Collections Development Librarian
CalcijexCalcitriol Injection
BRIEF SUMMARY 1 mcg and 2 mcg/mLINDICAT1ONSAND USAGECalci�ex#{174}Icalcilnol ingectionl is indicated in the management ot hypocalcemia in patients undergoing chronicrenal dialysis. It has been shown to signiticanlty reduce elevated parathyroid hormone levels. Reduction of PINhas been shown to result in an improvement in renal osteodystrophy.CONTRAJNDICATIONSCalcijex#{174}Icalcalriol inlectionl should not be given to patients with hypercalcemia or evidence of vitamin 0toxicity.WARNINGSSince calcitriol is the most potent metabolite of vitamin D available, vitamin 0 and its derivatives should bewithheld during treatment
A non-aluminum phosphate-binding compound should be used to control serum phosphorus levels in patientsundergoing dialysis.
Overdosage of any form ofvitamin 0 is dangerous Isee also OVERDOSAGE). Progressive hypercalcemia due tooverdosage of vitamin 0 and Its metabolites may be so severe as to require emergency attention. Chronichypercalcemia can lead to generalized vascular calcification, nephrocalcunosis and other soft-tissuecalcification. The serum calcium times phosphate ICa s P1 product should not be allowed to exceed 70.Radiographic evaluation of suspect anatomical regions may be useful in the early detection ofthis condition.PRECAUTiONS:1. Geeeral
Excessive dosage of Calcites#{174}Icalcitriol inlectionl induces hypercalcemia and in some instanceshypercalciuria, therefore, early in treatment during dosage adjustment. serum calcium and phosphorusshould be determined at least twice weekfy. Should hypercafcemia develop, the drug should bediscontinued immediately.
Calcijes should be given cautiously to patients on digitalis. because hypercafcemia in such patients mayprecipitate cardiac arrhythmias.
2. tefenaitise for Ibe PedeetThe patient and his or her parents should be informed about adherence to instructions about diet andcalcium supplementation and avoidance of the use of unapproved nonprescription drugs, includingmagnesium’containing antacids. Patients should also be carefully informed about the symptoms ofhypercalcemia Isee ADVERSE REACTIONS).
3. Eseontief Laborelety TeatsSerum calcium, phosphorus, magnesium and alkaline phosphatase and 24’hour urinary calcium andphosphorus should be determined periodically. During the initial phase of the medication, serum calciumand phosphorus should be determined more frequentfy)twice weekly).
4. �wea�eaMagnesium.containing antacid and Calcifex should not be used concomitantfy, because such use may feedto the devefopinent of hypermagnesemia.
5. Carcieogee.sis. Metageessis. Impairment Sf FvtilifyLong’term studies in animals have not been performed to evaluate the carcinogenic potential of Calci,ex)calcitriof inlection). There was no evidence of mutagenicity as studied by the Ames Method. No significanteftects of calcitriof on fertility were reported using oral Cafcitriol.
6. Us. is Pregeescy: Pregnancy Category C:Calcitriol given orally has been reported to be teratogenic in rabbits when gwen in doses 4 and 15 times thedose recommended for human use
AU 15 fetuses in 3 litters at these doses showed external and skeletal abnormahties. However, none of theother 23 liners )l56fetuses) showed significant abnormalities compared with controls.
Teratology studies in rats showed no evidence of teratogenic potential. There are no adequate and well-controlled studies in pregnantwomen. Calci�es should be used during pregnancy only if the potential benefittustifies the potential risk to the fetus.
1. Nunsie� Melkersft is not known whether this drug is excreted in human milk. Because many drugs are excreted in humanmilk and because of the potential for serious adverse reactions in nursing intants from calcitriol, a decisionshould be made whether to discontinue nursing or to discontinue the drug, taking into account theimportance ofthe drug to the mother.
8. Pediatric UseSafely and efficacy of Calciles in children have not been established.
AD VERSE REACTiONSAdverse effects of Calcijex#{174})calcitriol injection) are, in general, similar to those encountered with encessivevitamin 0 intake. The early and late signs and symptoms of vitamin D intoxication associated with hypercalcemiainclude:1. tidy
Weakness, headache, somnolence, nausea, vomiting. dry mouth, constipation, muscle pain, bone pain andmetallic taste.
2. LatePolyuria, polydipsia, anorexia, weight loss, nocturia, conjunctivitis Icalcific), pancreatitis, photophobia,rhinorrhea, pruritus, hyperthermia, decreased libido, elevated BUN, albuminuria, hypercholesterotemia,elevated SOOT and SGPT, ectopic calcification, hypertension, cardiac arrhyshmias and, rarely, overtpsychosis.
Occasional mild pain on injection has been ob�ereed.OVF.RDOSAGEAdministration of Calcipex#{174}Icalcitriol inlection) to patients in excess of their requirements can cause
hypercalcemia, hypercatciuria and hyperphosphatemia. High intake ot calcium and phosphate concomitantwith Catcipesmay lead to similar abnormalities.
I. Trse�eet St Hypercakieda aid Overdosage is Petleets ee H..edlalysiaGeneral treatment of hypercafcemia Igreater than 1 mgldl above the upper limit of normal range) consists ofimmediate discontinuation of Calcites therapy, institution of a low calcium diet and withdrawal of calciumsupplements. Serum calcium levels should be determined daily until normocalcemia ensues. Hypercalcemiausually resolves in two to seven days. When serum calcium levels have returned to within normal limits,Calcifex therapy may be reinstituted at a dose 0.5 mcg less than prior therapy. Serum calcium levels shouldbe obtained atleast twice weekly after alt dosage changes.
Persistent or markedly elevated serum calcium levels may be corrected by dialysis against a calcium4reediatysate.
2. Treelaeet ofAccideefal Overdose,. at Calcitniel lejectiosThe treatment of acute accidental overdosage of Calcijes should consist of general supportive measures.Serial serum electrolyte determinations lespecialty calcium), rate of urinary calcium excretion andassessment of electrocardiographic abnormalities due to hypercalcemia should be obtained. Suchmonitoring is critical in patients receiving digitalis. Discontinuation of supplemental calcium and low calciumdiet are also indicated in accidental overdosage. Due to the relatively short duration ofthe pharmacologicalaction of calcitriol, further measures are probably unnecessary. Should, however, persistent and markedlyelevated serum calcium levels occur, there are a variety of therapeutic alternatives which may beconsidered, depending on the patients’ underlying condition. These include the use of drugs such asphosphates and corticosteroids as well as measures to induce an appropriate forced diuresis. The use ofperitoneal dialysis against a calcium-tree dialysate has also been reported.
IIOWSUPPUEDCalcites#{174}Icalcitriol infection) is supplied in 1ml ampufs containing1 mcg lUst No. 1200) and 2 mcg lUst No. 1210).Proteat kern I�kt
Store at controlled roomlemperature 15 to 30C 1W to WF).
Caution.Federal)USA)law prohibits dispensing without prescription.See complete Professional Use Information before prescribing.©Abbott 1906 06-4630’R5-Rev. Oct. 1990a Abbott Renal Core
Abbott Park, IL 60064-35001.800-457.9472
- II II II Name of Library I
Name of institution
I II Street address II City, State, Zip II II From II Your name II I
Street address
I City. State, Zip II My coLLeagues and I would Like to have access to �ASN and request that II our library subscribe to it. II II Signature Date II Reasons why JASN would be a valuable addition to our collection on this II subject. Check the appropriate box(es): II E News about scientific 1� Reference/citation for II advances research0 Reports on major fl Track trends in the specialty
I professional meetings U Continuing medical II � Information on licensing educationand certification fl OtherI � Student assignments II 3ournal of the American Society of NephroLogy II ISSN 1046-6673 I Published monthly I
� I Institutional rate $329/yr. / Add $65/yr. for postage outside the U.S. II ��38�6423 Toll-Free � W1Ih�IflS & Wilkins II Fax: 1-410-528-8596 �‘ A WAVERLY COMPANY I
� I Write: Williams & Wilkins, P.O. Box 23291, Baltimore, MD 21203-9990 I: ASNIJB6
- - - - - - - - - - - - - - - - -
In 1975, Bayer AG introduced Adalat#{174} (nifedipine) In the
in Europe. We’ve since made the Adalat brand available in United States,. . the one to
several formulations around the world, and nifedipme presc,.ii� j�
has been in clinical use for over twenty years.
Backed by a worldwide clinical database ofOnce-A-Day
tens of thousands of patients and hundreds
of clinical studies, the Adalat brand today
provides therapy for millions of
patients* around the globe. #{149}� #{149}#{149} #{149} E X T E N D E D
nITeaIPIneRELEAs E
lull I I TABLETS
3Omg,6Omg & 90mg
Providing a World of Confidencefor Hypertension Control
Frequency and type of side effects, eg, peripheral edema, headache, flushing/heat sensation,dizziness and fatigue/asthenia, are typical of dihydropyridine calcium channel blockers.Please see briefsummary ofPrescribing Information on foiowingpage. aData on file, Bayer Corporation, Pharmaceutical Division.
IRIEFSUMMARYCONSULTPACKAGEINSERT FOR FULL PRESCRIBING
INFORMATiONFor Oral Us.
PZ50002515 6/95IPSICATION AND USAGIf: ADAIATCCisIidkaiodfor the tr.ahnetd ofhypenlen-slot ffmayhas.dalomerItcombItaflunwithotharantthypeI1ensiveogent�COIITRAiIMICATJOII& tineehypenumtiMtytonifmhpina�WARNiNGS: Ixcesulwe Nypiteuslee: Athouphrn moat�ihenh din hypotnasiveeffectofaife�ineis mOdastandweltnlnrated, occasisedpeitentshave had excessivenod poorly tohiraled hypotennia� Thesereapameskane mealy occurredduring mitiultitration or at the thin of sebsequetti� dotagead)usimsd,and may be moreNsely’mpatItnN�cancnITitaIdbefo’bledcaItSeverehveolansiennod/or ‘mcreaSSdBaidVOhIIIwrsqairementshave beanreported in- abe received lumedialo rekese ca�s together with a beto-binchingagentmid who enderuent coronaryortoty bypasssurgery asia huh dosefeniantil anesthe-at ilie Itlaredion with hiph donefenteuf appearsto be Jim to the canshinalionofalke.idabe$e-bhckar,botthepassMlythatNmpyewewNhoifed�lsidsne,with low dates of ‘e other surgiod procederas,or with other norcolic intel’asaicscannotbendedoet. nndehans.traotadpmiontowhmasergecyuting high doneFnet� anesthesiais canfeewlaindthe physicianshouldha aware oftheseposantitdproblems and, if the patient’s cae�Nioe permits, sufficient time (at host 36 ken)shMhdIoeedhoaihd�lwtehwmhededofthebadypdortowrgey.hcveeaed Aegis .4/er Myscerdiel hfancfieer lately, patients,ponlissilanfythosemite ha,. severeohemative coronary artoty disease,have devekpedwSl dons.mooted increasedfrequency duration mWer severity ofaagma or anile myacardlal�eifamkenpanslenlingnde�iIteoratlh tlneofdosagn increase.Themechanismofdmeffedisnatesh#{225}ldietkte4leckx Wkbdoew#{233}Wltenilscoelineina a bela’blucker I is kapotlaidto lapse‘dxdane,if nansible rather thin, steppingeltrapify before beaianlm oifed�ine� Patientsma�ed6draenkomhteldedomm�eedhdrawOtheewNh’maiased-‘ probablyrel�lto’meaanedteeaitivllyteed,thahmIie& hdIlatinnofailed�lseVa�atwinatpnuedflisowirnnnceandoeaaasmanhashenrnpedsdtoinenaae�_h. H� Mires landy, patsnh(anealy adelereceiv� a kee-bhdon)bnve�heartfeilmaoftarh�agoihe�ne. Patientswithflghixmksoeno’
may be of risk forsuch an event, asthe aelsading often ofnifst�ine unuidbe exported to beof less benefit to these patients, owing totheirfixedlapedancetoBawacrossflwxnkvelve.PRECAUDON& Geanrel - N�eo.ealeen lecasse aflwlplwdncrnases per�hnrel vas.adm enhance carefid nanilnrmgof idandprasairs define the inliel �iikeatise mel�abeadyth� mntlntiism’thatma knownto lewarblandpruasam(SeeWAIfNINGS).
Pedylerel Idse.ex Mild in mndnrafs peripheral edema occurs‘ona dnne.dnpendnefmonnsewithADAtATC(llwplarnbaarblrartedrasnl npcmsimnlnfr8%at90mg�2%at6Omgandl9%at90mg&�y.1hledmaaisahctdksdphnaommnn thneahttnhmsaciaiedwithvana�alan ofdepeednatieiarinhswtdsinal bloodvnsn�s talent thinto loft ventriculardysfunctimienanneralnad IbM misatla� With patientsadios. taper-tension is cen#{231}flcatsdby cnngnnlfiewart fedora,earnshouldhe itdiento diBarantlaindmperkihereledneahomdweffothof’mcraasieghffvenerlcnbwdysfundinth(eraellae for Petleets: ADAIATCC is tat extended release lablot and should beswolowed whole and falcon tat an en9ify sinmack is shiM not be administeredwithfoot OOnOfcIIew,dividnorcronhtablnf�L#{226}eniteryTester tore usua11ytransient hut occasionallyniandicantelevationsofoiayiamwchasidktdlnn �ianphaiaan, � LOll, SGOT,eel � beensaint ThemladeesIt� to aledmleetherapyisnacarketin mastcasesbet probablein sante.Thesebthar*ry abeurmalties have rarely hen assedatodwith dinicel sympssn� however,chnhntonltwith arwithoet �enthce hasbeen reponiat Asanalincrease(<S%)m meanalioliw pbosphnemewasmind in IsItItntsVOOI.dwiIhADALaTCC Thiswasan Isolatedfoidlagtaellnralyrwnalledinvebieswltlth faNmitsui. the normal reap. be ‘instancesofelhrjc hepoilte lines bane reportedwith iledipiw freaitnnnt. In coetralndstudies,
did eat adverselyeffect serumwin acid, phirme, cliahalnralor poaossiunitNlfwll� hiwoiher calciemchannelblockers,decreasesplatelet aanmeeatisnis vitro.Limitedclinicalstudies have demonstrated a moderatebut statistically significantdecrease in �nt aggregationand increase in bleedingtime in someaitedipsee-� This is thaeeld to be a fteicfineci ibdillion of(alcieln frantped acrossthe�menthrant �cNnIcel significancehirthesefindings hashendemanstratetPositivedirect Csontbs’test with enwithout hemslytk annasiahas been raporlod but a
M�Lkede�rke mol poti�hy of thisAlthaughalei�tinnhasbennmedndelyinpaiinatswithmaeldysftaatianmid Ian hutrn� to exert a benefidaleffectincarteincasesrarereversibleehivetiamIt Bill andworn aaalinliw havehen reportedin pafeatswIlt prw.esintlagchronicrend ‘oaufflciency.1lwmbnlannh�tookdlpkethnrapyismicadainmmoaicaseskitprababhinsasw.Dew, hfeneclleees lefa.atkeaergkhhddng agents:(SeeWARNINGS).
Bayer �JPharmaceutIcalDivIsIon
Bayer CorporationPharmaceutical Division400 Morgan LaneWest Haven, CT 06516 USAMade n U S A and Germany
Once-A-Day
© 1996, Bayer Corporation X09136 M-14630
I#{174}#{149} U #{149} EXTENDE
nifedipineTA B L E TRELEAS
D
SE
3Omg,6Omg & 90mg
ADALATCCwasws$tofsraled alien atMinisierad ‘it combinationwitha his bisdier I, Thefallowingadverse eventshave bess reperted rarely si patients �ven nilet�pine It187 hy�emive �is in a phcebo�oolmlhd dmkal kid. However there have other formuIttions: eliergenk hepatitIs afopecta anemia, arthritis with ANA (+),been accasionalr�t�m reports suggesting that the combinationof nilsi�pine and depression,w�i)weesh�a, sxfollafIte�nnaiith, lever, ginhyperplini, gp�ece-bets-a#{233}e� bloddnt� drugsmaykcrease the hkekhoodrAcoi�estive hearifailer., med� hukapeern, mind cheeps, musclecrea�t, neivewness, paraneal syn&ons,severeh�en�orexacerbolisnaf� ItpOIiSnholthcOrIBO,SSndiWi�SeSSt purpura, Mines� sleep iksfurbancss syisope, lasts peivenien, throm�ocyiepenki,D�c Sincethere lIars been‘salted repoitsof palietiseith elevatedi�goxIt hvelt� IrDIISiSIdb�ndneaattfIepI#{232}phaIin ,tremora,dwticari�tI� there ti a pats�ie ‘eiseractiet hiween t�goxIt and ADALaTC� I ti remnrmended� a�usa� aid �scuniIwig ADAIATCC � � © 1995 � � SW PeloledIt USA
CaemorloAnlitoagulonfc Therehave beenrare repertsof ‘mcreased�alhroeiIt fleain �tieets taking coumorin anticoagelants to whomnifedipinewas administered.
the rslafiuitshipto nifedipine therapy is uncarlitQulrildine: Therelava beenrare reports of on interaction befesen qainidinsandififet�tine(olthe#{224}creasad�hndefquinidine).Odinr�ththepsakplaanohnddnflet�ieeundtheAU(mpyItcreaseItthepea-enceofcInelldiI� Ian�Ike�eunomIerneni#{231}ndieat’maeuneiliiseffsctof clue-tihie may be meMd by Is knoen ItMIUOBO(hI#{216}kCpIsdWOmeP’450, tie utzy,m� If nilediple there-pyisluIluadIto�flisflcerreIWIyrsaMapclnsl#{243}e,cmiisseMnllunisadvisetCir#{224}e�.eak, Melureeds, �#{225}.eet ad FerfMt� Ilhfedipine� adminis.mmd only to rats ferteoyearstinlwtn notsitown to becardoogenit Whengiven toraft�tomalini nifedi�cainadredmadfeddityatodateappuedeatofy3Otlnes*amuninemrecommendedfeiman�ne.Innunmatap�stedierwe�i�Preg..c�� PregnaecyCategoryC In rodents,rabbitsmid monkeys,tifedipine mshen shownto have a variety of embryotoxic placentotoxk and fetofosk effects,liduding stunted fefuses� mice and robbils( di�nd anomalies rots and r�blts),rth�foindiies(nice) deftpahte(mica),untdiplaceeiosmel chorine-k4(molcheys), mnlryonkmidhoiddeatbi(mts, lucamudrtdihlls), preg-nencylratsimleralaolndinnihvapedm),neddgcreasadimanondsurvivd rofs notevaluolod motherspedes). Onemp�garnmjm� basis,wee of the dosesassocintedwith these various effects are ti� than the maximum recommendedkenton dose
someare keen, hut alien slIM an order of mognitodeof ‘tThe digilid anelnldies seen Ii nife4ne.exponed rabbit pups era sirthingly similar tothee seen ‘in pyps expysed to phenytoin, and these are ‘in turn sitnflarto the phe-hinged defornitins that are the mast common malonantlini seen ni moron childrenwith at utoroexposureto phenytoin.Thornma eoadequ* mid wolconlulId studiosin ersintuweemut ADALATCCshnrddhnoeddeflthepotidhemdi�usathmthnpot.niinirishtothefeto�Nerolej M.fhens Nifsdi� isexcrn$edm IKImtMm&ThSrOfOr., a decisiunshouldhe made to disconilno. nursingor to discontinue the don� taking ‘into account theInpenianceof the drug tothe mother.ADVERSE IXPERIEIKES: The incidenceof adverse events donnatreotmeofwithAOALATCC to doses to 90 mgdnflywsrederivedfromonilkenler �xebe-coniroledcheicrdtrnds’m370 hvoenisntivs� Aoenslul50 n�m,cedeflyme osadconconwfatiffylt lll7ofthe3lbpolientsonADAtATCCweIiMoftfw 126 pollenlsnoAl adverseeventsreportedduring ADALATCC therapywsin tithufasel ‘ ofthnincausdrnitiiionsh�loinnikoiion,�moti cemmonadverseneed reportedwith ADALAT#{174}CCwasperipherulmienso.Thismadomheedondfhfrequencywas 18% oeADAtATCC3Un�dnfly, 22%on�LaTCC6doflyaed2P%unADAiATCC9On�deilyverss1Q%unplecebe.
Other continueadverseeventsreportedin the drove placsbo’conirnllodtrials iclede:lisodadin (19%, verses 13% placeboincidence);AushinaJlteatsinsaiinn(4%, venus0% placebo‘eicideeca);Dizziness(4%, venus 2% placebohicidence);Fatigee/asthenin(4%, verses 4% placebo incidence); Nausea (i%, venus 1%placehoincidence);Coedipalion(1%,vorsusO%plncahinddnnco).Where the frequencya) adverseeventswith ADALATCC and placebo issimilar, canedreheienshipcaanothesotdihshetThe felowl�g adverseevents ware reported with an incidenceof 3%or hiss rn doilydoses to 90 n#{231}Sidy en a Whele/Systeeda chest porn, leg porn Centred Nerwees Systems
oresthesin, vertiao Der.etel.elc: rash Genfr.l.testl.el: constipationleg cramps Reap1ret.r�� apistoxis, rhinith Uregeeit#{233}mipo’
teens,urinary frequencyOtheraduerseeventsrepontedwithaninddenceofhssthan 1.O%wsrr ______________lady en e Whele/Syoteufic taleNts, chilk fetid edeum,audi pam, pelvis pain,
. Curdisseocaler. atred fthdllaflon, bra�ycardla, canttmcarrest,extrasysook,�Nmiun, po�teinm, �th, postund hypatension,tethycank� caloneow no�‘estates Ceefrd Nerveen Systems onxinfy, confusiat� decreased�ido, deprensiat�hypertonia insomnia somnolence D.r.ef.leelc: prenites, sweatingGenfrekeeogingebdsinintd pa.� dienhea, drymsuth, &eeeosia esonhawi� Bate-lance, gastrointestinal hemorrhage, vomiting Heauet.Ioglc lymphoJenopathyMefekNc: gout, weight loss Msscwlosk.letel: arthralgia, arthritis, myolg’mRenpfraterysdyspoen,inoonsedcauphrehe,phth Spsdwi S.en.� abner-mid name, mnbly� co�is, ilpiopin, tinaiho UrS,SUNII/IIprSdmstIVec�nyndca� no�, keed�

Their iron therapy shouldn’t be �
Recommend SLOW FE#{174}for 60% fewer GI side effects.”2On average, your dialysis patients spend roughly 500 tough hoursdialyzing each year. So why should they spend 1 extra minute withGI upset? Consider SLOW FE. It’s been clinically proven to reduceGI side effects compared to other leading iron supplements-includ-ing a rate of constipation almost 69% less than Feosol#{174}*and 61% lessthan immediate-release ferrous sulfate.2 That’s because SLOW FEdelivers iron directly to the duodenum and jejunum, which increases
absorption and reduces the incidence of side effects. SLOW FE also
restores hemoglobin levels 2 1/2 times faster than Feosol.3
Also available: SLOW FE#{174}Slow Release Iron + Folic Acid.
References: 1. Brock C, Curry H. Comparative incidence of side effects of a wax-matrix and a sustainedrelease iron preparation. Gun Thec 1985;7:492’496. 2. Brock C,Curry H, Hanna C, et al. Adverse effects of iron supplementation: a comparative trial of a wax�matrix iron preparation and conventional ferrous sulfate tablets. Clln Therl985;7:568’573. 3. Daniels EH Jr, Ente G, Freed N, et al. Hemoglobin response to two modifiedrelease iron formulations in patients with iron deficiency anemia: an evalua-tor-blind trial. Today’s Therapeutic Trends. I 989;7: I 1� I 9.
Feosol is a registered trademark of SmithKline Consumer Healthcare, LP. 0 1996, Ciba Self-Medication, Inc. � 0 0
THE AMERICAN SOCIETY OF NEPHROWGY
andTHE NATIONAL INSTITUTE OF DIABETES AND DIGESTIVE AND KIDNEY DISEASES
Announce the 1996 Advances in Basic Science Conference:
Renal Developmental Biology#{149}:.++
November 6-9, 1996(Immediatelyfollowing the ASNAnnual Meeting.)
Hyatt RegencyNew Orleans, Louisiana
TOPICS WILL INCLUDE: CONFERENCE CO-CHAIRS:
Developmental Regulators Ellis D. Avner, M.D.Epithelial Development Richard P. Woychik, Ph.D.Vascular-Interstitial DevelopmentMethodologies of Developmental BiologyThe Cell Cycle, Apoptosis, and Signalling in Development
SPEAKERS WILL INCLUDE:
Dale Abrahamson, University of Alabama
Thomas Daniel, Vanderbilt UniversityGregory Dressier, Howard Hughes Medical Institute
Eric Neilson, University of PennsyivaniaFrank Rauscher III, The Wistar Institute
Plus twenty-five other distinguished scientists
For meeting registration and hotel reservation information contact:
American Society of Nephrology
1200 19th Street, N.W., Suite 300
Washington, DC, 20036-2422
Phone: 202/857-1190
Fax: 202/223-4579
The Official American Society ofNephrology Board Review Course...
...will
take place August 24-30, 1996 in San Francisco.
The American Society ofNephrology (ASN) Board Review
Course will be a week-long, in-depthreview of nephrology and hypertension fea-turing nationally renowned teachers. Thecourse is designed as an intensive preparationfor the Nephrology Board Examination to be
held in November 1996 and will also serve asan outstanding review for anyone in need of a
timely update. The course will feature a van-etyofformats includinglectures,interactive
workshops, computer-assisted prog rams andsmall-group, question-and-answer sessions. It willprepare participants for the upcoming boardexamination by blending relevant physiology and
pathophysiology with clinical discussions.The site for this user-friendly course will be the
Palace Hotel. Registration is as follows: ASNmembers - $735; ASN associate members -
$660; nonmembens - $840; nonmemberfellows - $700. “Early bind” reduced rates arealso available until April 15, 1996. To makeyour reservation or obtain an informationbrochure, call ASN national headquartersat 202/857-1 190. If you need to get in
� shape for the fall exam, leave yourMedical Education gym card at home and join us
in San Francisco.
American Society of Nephrology
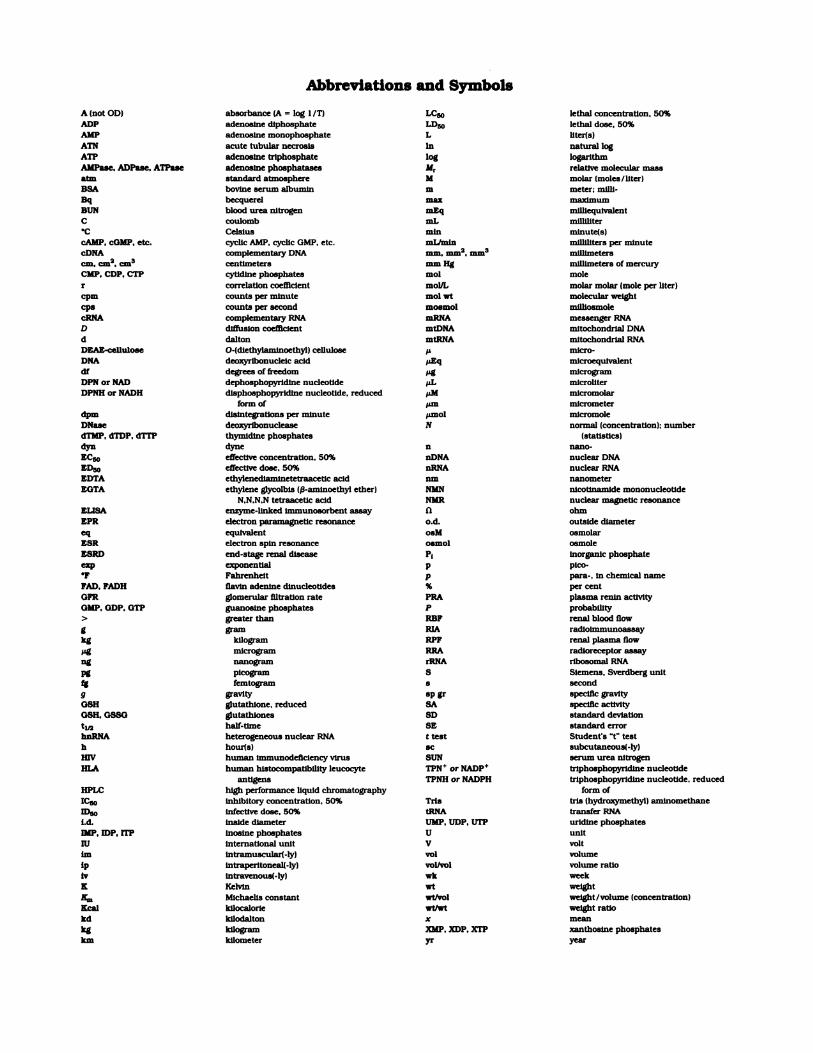
Abbreviations and Symbols
A (not OD) absorbance (A = log 1 IT) LC� lethal concentration, 50%
ADP adenosine diphosphate LD� lethal dose, 50%AMP adenoslne monophosphate L liter(s)
ATN acute tubular necrosis hi natural log
ATP adenosine triphosphate log logarithm
AMPase, ADPase. ATPase adenosine phosphatases M� relative molecular massatm standard atmosphere M molar (moles ItiterlBSA bovine serum albumin m meter; mUll.
Bq becquerel max maximumBUN blood urea nitrogen mEq mithequivalent
C coulomb mL milliliter
.C Celsius mm nnlnute(s(cAMP, cOMP, etc. cyclic AMP. cyclic GMP. etc. mLImin milliliters per minutecDNA complementary DNA mm. �2, �3 millimeterscm. cm2. cm3 centimeters mm Hg millimeters of mercuryCMP. CDP, en’ cytidine phosphates mol mole
r correlation coefficient molJL molar molar (mole per liter)
cpm counts per minute mol wt molecular weig�it
cpa counts per second mosmol milliosmole
cRNA complementary RNA mRNA messenger RNAD diffusion coefficient mtDNA mitochondrial DNA
d dalton mtRNA mitochondrial RNA
DEAE-cellulose O’(dlethylanimoethyll cellulose � micro-DNA deoxyribonucleic acid �.tEq nilcroequlvalent
dI degrees of freedom �ig microgram
DPN or NAD dephosphopyridine nucleotide �.L microliterDPNH or NADH disphosphopyridine nucleotide. reduced �sM micromolar
form of �LIfl micrometerdpm disintegratlons per minute �mol micromole
DNase deoxyribonuclease N normal (concentration); number
dTMP. dTDP, d� thymidine phosphates (statistics)
dyn dyne n nano.EC� effective concentration. 50% nDNA nuclear DNA
ED� effective dose, 50% nRNA nuclear RNA
EDTA ethylenedlamlnetetraacetlc acid nm nanometer
EGTA ethylene glycotbis (p-aminoethyl etherl NMN nicotinamide mononucteotideN,N,N.N tetraacetlc acid NMR nuclear magnetic resonance
ELISA enzyme-linked Immunosorbent assay 0 ohm
EPR electron paramagnetic resonance o.d. outside diameter
eq equivalent osM osmolarESR electron spin resonance osmol osmole
ESRD end-stage renal disease P5 inorganic phosphateexp exponential p pico.
F Fahrenheit p para.. In chemical name
FAD, FADH flavin adenine dinucleotides % per centGFR glomerular ifitration rate PRA plasma renin activity
GMP. GDP. GTP guanosine phosphates P probability> greater than RBF renal blood flowg gram RIA radiolmmunoassay
kg kilogram RPF renal plasma flow
Mg microgram RRA radioreceptor assayng nanogram rRNA ribosomal RNA
pg picogram S Siemens. Sverdberg unit
fg femtogram S secondg gravity sp gr specific gravity
GSH glutathione. reduced SA specific activity
GSH. GSSG glutathiones SD standard deviationti/a half.time SE standard error
hnRNA heterogeneous nuclear RNA t test Student’s “t” test
h hour(s) inc subcutaneous(.tyl
HIV human Immunodeficiency virus SUN serum urea nitrogen
lILA human hlstocompatibillty leucocyte TPN� or NADP� triphosphopyrldlne nucleotide
antigens TPNH or NADPH triphosphopyridine nucleotide, reduced
HPLC high performance liquid chromatography form of
IC� inhibitory concentration. 50% Tris ti’is Ihydroxymethyll aminomethane
ID50 infective dose. 50% tRNA transfer RNAl.d. inside diameter UMP. UDP, UTP uridine phosphates
IMP. IDP. tip Inosine phosphates U unit
lu international unit V volt
inn intramuscular(-ty) vol volume
ip intraperitoneall.ly) vol/vol volume ratiolv tntravenous(.lyl win weekK Kelvin wt weight
Km Michaells constant wi/vol weight/volume (concentration)
Kcal kilocalorie wt/wt weight ratiokd kilodalton x mean
kg kilogram XMP, XDP. XTP xanthosine phosphates
km kilometer yr year
THE AMERICAN SOCIETY OF NEPHROLOGYpresents
MOLECUlAR BIOLOGYFOR CLINICAL NEPHROLOGISTS
...
This two-day course is designed to bring practicing nephrologists up-to-speed on the fundamentals
of DNA/RNA structure, gene organization and other key definitions, terms and techniques that
constitute the ‘jargon of molecular biology.”
November 1-2, 1996(Immediately Preceding the ASN Annual Meeting)
New Orleans Marriott
New Orleans, Louisiana
Lectures and small group workshops will provide a concise, but complete, introduction to the
methods and applications ofrecombinant DNA technology. The course will help you to understand
and draw relationships between molecular biology, genetics and clinical medicine. N� prior
knowledge will be assumed.
LECTURES AND WORKSHOP TOPICS WILL INCLUDE:Basic Molecular Biology
Genetic Cloning and Engineering
Genes and Human Diseases
Gene Therapy
Course Directors: Steven Hebert, MD. and Robert Narins, MD.
Course Faculty
Joseph Bonventre, Boston, MA Peter Igarashi, New Haven, CT
Thomas Coffman, Durham, NC Richard Lifton, New Haven, CT
Leon Fine, London, England Philip Marsden, Toronto, Canada
Stephen Gluck, St. Louis, MO Orson Moe, Houston, TX
William Guggino, Baltimore, MD Alan Yu, Boston, MA
Steven Hebert, Boston, MA
Co-Sponsored by the National Kidney Foundation
Register Early...Attendance will be limited.
For meeting registration and hotel reservation information contact:American Society of Nephrology1200 19th Street, N.W., Suite 300
Washington, DC 20036-2422
Phone: 202/857-1 190; Fax: 202/223-4579; E-mail [email protected]
INSTRUCTIONS TO AUTHORS
Send manuscripts to the Editor:
Jared J. Grantham, M.D.JASN
University of Kansas Medical Center3901 RaInbow Blvd.
Kansas City, Kansas 66160-7361
T he Journal of the American Society ofNephrology willpublish original manuscriptsJudged by peers to be of
high quality and relevant to the broad field of Nephrology.Nephrology is an alliance of scientists and physicians whoseek to understand the functions of the kidneys and themeans to improve the medical care of individuals withrenal disease. The strength and vitality of the disciplineradiate, historically, from the dynamic interaction betweenthe basic and the clinical sciences. The Journal strives tonurture this relationship by providing the means for com-municating to nephrologists and others in related special-ities critical information of broad significance in the field.Subjects appropriate for the Journal include, but are notrestricted to:
. clinical nephrology. renal and epithelial physiology. biochemistry. pathology and immunology
. cellular and molecular biology
. renal pathophysiology
. body fluidI electrolyte and acid-base metabolism. hypertension. dialysis. renal transplantation
General Information
Manuscripts are of four types: Concise Reports, Com-prehensive Studies, Comments and Letters to the Edi-tor.
Concise Reports should contain in not more than 2500words (including abstract, figures, tables and references)important new observations of sufficient interest to ne-phrologists to warrant rapid publication. ComprehensiveStudies are traditional full length papers that addressresearch questions with exhaustive experimental designand methodology. Comments are brief reports limited tofewer than 1000 words (including introductory paragraphdescribing the origins and chief conclusions, one figure ortable, and fewer than 15 references) that are preliminary,negative or confirmatory. Highly innovative technical ad-vances will be considered. Letters to the Editor should beconfined to brief scientific commentary about articles pub-lished in JASN or to topics of general interest to nephrolo-gists. Reviews of basic and clinical topics ofinterest to thereadership will be solicited by the editors.
In the cover letter, designate one author as correspon-dent. All coauthors should have contributed in substantialways to the study and manuscript preparation.
Include in the cover letter a statement explaining whythe research is especially important. It is at this stage thatclaims of new or novel findings (“This is the first . . .“)
should be mentioned, not within the text of the paper. Thejournal office may solicit editorials to accompany articlesthat are especially newsworthy or controversial.
Include in the cover letter the names, addresses, tele-phone and areas of expertise of at least five individuals(peers) who may serve, at the discretion of the editors, asreviewers of the manuscript.
American Renal Training Centers
This series is to serve as a forum for concise yet compre-hensive updates on a subject of current interest in clinicalnephrology, centered around a patient presentation. Thearticles are to be authored by fellows in training under theguidance of a senior faculty member. The manuscriptsshould include:
. A brief focused patient presentation. If pertinenta radiologic or histologic figure can complementit.
. Background-not to exceed one paragraph.. Review of clinical and pathologic presentation of
the entity.. An overview of the etiology and the pathogenetic
mechanism of the disease.S Review of therapeutic approaches.S A summary-conclusion paragraph that contains
a “take home message”, and if at all possible,reverts back to the patient.
. No more than three tables or figures that confer acritical message or summarize information fromvarious sources.
. References should not exceed 20.
. The overall length of the communication shouldnot exceed 15 double-spaced typewritten pages.
Copyright Transfer: Include one of the two followingstatements on copyright interests signed by all authors.
“In consideration of the American Society of Nephrolo-gy’s taking action in reviewing and editing this submis-sion, the author(s) undersigned hereby transfer(s), as-sign(s) or otherwise convey(s) all copyright ownership tothe ASN in the event this work is published by the ASN.
Federal Government: ‘�I was an employee of the UnitedStates Federal Government when this work was investi-gated and prepared for publication: therefore, it is notprotected by the Copyright Act and there is no copyright ofwhich the ownership can be transferred.”
These signatures, that must accompany the cover letter,indicate that each author approved the final version of themanuscript and is prepared to take public responsibilityfor the work.
It is the policy of the Journal to expedite the reviewprocess. Authors will receive within 10 days of receipt atthe editorial office, acknowledgment that their manuscripthas been forwarded to an associate editor and reviewingeditors. Manuscripts that are judged by a panel of screen-ing editors to fall outside the range of interest of thereadership or that fall to satisfy technical requirementswill be promptly returned to the authors without furtherreview. In order to reduce postage expense, manuscriptssent to outside reviewers as privileged communicationswill be destroyed and not returned to the authors. Glossyprints and photographs from rejected manuscripts will bereturned to authors. Authors who have not received formalnotification of manuscript review status 2 1 days followingacknowledged receipt at the editorial office are encouragedto contact the editorial office for a status report.
Manuscript Preparation
. Submit an original manuscript and three photocopies,typed double-spaced in letter-quality print on one sideonly of standard (8’/2 X 1 1 inch) white bond paper.. Manuscripts submitted as Concise Reports and Com-prehensive Studies should be organized as follows: titlepage, abstract, introduction, methods, results , discussion,acknowledgments, tables, legends to figures, and refer-ences. Comments should contain: title page; introductoryparagraph; methods, results and discussion; acknowl-edgements; table or figure legend; and references. A brief
Disclaimer-The statements and opinions contained in the articles of JASN JOURNAL OF THE AMERICAN SOCIETY OFNEPHROLOGY are solely those of the individual authors and contributors and not of the American Society of Nephrologyor Wffliams & Wilkins. The appearance ofadvertisements In the Journal is not a warranty, endorsement or approval of theproducts or services advertised or of their effectiveness, quality or safety. The American Society of Nephrology and thePublisher disclaim responsibility for any injury to persons or property resulting from any ideas or products referred to inthe articles or advertisements.
description of methods may be included in the table orfigure legends. Letters to the Editor will be edited andshortened in consultation with the author.. On the title page type the full names, highest academicdegrees and affiliations of all the authors. The title shouldnot exceed 100 characters and spaces. Include an abbre-viated title of not more than 40 characters and spaces.. Abstract: State the problem considered, methods, re-sults, and conclusions in less than 250 words. List 5 indexterms not included in the title.. Use of Systeme International d’Unites (SI) for measure-ments is preferred throughout the manuscript. Factors forconverting frequently used components can be found inJAMA (1989:262:200-202).. Use generic names of drugs.. Do not use abbreviations in the title or abstract. Defineunusual abbreviations on the first use in the body of themanuscript. A list of accepted abbreviations can be foundIn the July and January issues of JASN.. Text footnotes should be typed on a separate page.. Foreign contributors, whose language is not English,should obtain help from colleagues who are proficient inscientific English.. It is assumed that all clinical investigation described inthe manuscript was conducted in accordance with theguidelines proposed in the Declaration of Helsinki. Docu-ment in the manuscript that informed consent was ob-tamed.
S � is assumed that all animal experimentation describedin the manuscript was conducted in accord with the NIHGuide for the Care and Use of Laboratory Animals, and themanuscript should contain a statement to that effect.. Tables: Double-space on separate sheets of standard-sized white bond paper. Title all tables and number inorder of appearance in the text. Footnotes may includemethods in Concise Reports and Comments. Use super-script letters to indicate footnotes typed at the bottom ofthe table.. Figures: Include clear photocopies of the figures with theoriginal and each copy of the manuscript as well as threesets of 5 x 7 inch glossy photographs for all line drawings,clearly labeled on the back. Graphs must be of professionalquality: computer-generated graphs should be of laserquality. High contrast prints for roentgenographic photo-graphs and electron micrographs are essential; halftonesmay be custom printed on special paper from engravingsapproved by the author and at the author’s expense.Photomicrographs should be sized to fit one column (8 cm)or two columns ( 1 7 cm); the maximum plate size is 1 7 x 22cm. Legends should state degree of magnification or scalebars should be used on the photograph and specified inthe length.. References: Cite in numerical order, only one referenceto a number. Citation of unpublished observations orpersonal communications (include separately permissionto quote from appropriate individual) should be placed inthe text in parentheses.
Journal articles, abstracts and books: List all authorswhen six or fewer; when seven or more, list only the firstthree and add et at. Journal names should be abbreviatedaccording to the BIOSIS list of serials.. Examples:1 . Abramson RG, King VF, Reif MC, Leal-Pinto E, Baruch
SB: Urate uptake in membrane vesicles of rat renalcortex: Effect of copper. Am J Physiol 1982;242:F 158-Fl 70.
2. Couser WG. �3lomerular diseases. In: Stein J. ed. Inter-nal Medicine. 2nd ed. Boston: Little Brown: 1987:834-86 1 .
. Manuscripts by Electronic Diskettes-Preparation ofDisks:Authors are encouraged to submit electronic diskettes oftheJlnal version of their manuscripts along with the typedREVISED manuscript. Diskettes produced on IBM or IBM-compatible computers are preferred, but those producedon most Apple/Macintosh or Wang computers can also beconverted. The following word processing programs arepreferred: XyWrite III Plus; Word Perfect 4.2, 5.0, or 5.1(IBM or Macintosh); Microsoft Word (IBM or Macintosh);Word for Windows; Wang 015 (WPS); and Wordstar (IBM).Among other word processing systems that we can convertare CPT 8000; MacWrite 2.2 or 4.5; MacWrite II; DisplayWrite 3 or 4; Multimate; PC Write; Volkswriter; and WriteNow. Authors preparing diskettes on Macintosh comput-ers should not use the Fast Save option. Files in ASCII canalso be used, but are not preferred. Identify the diskette byproviding journal name, manuscript number, senior au-thor’s name, manuscript title, name of computer file, typeof hardware, operating system and version number, andsoftware program and version number.
The journal does not assume responsibility for errors inconversion of customized software, newly released soft-ware, and special characters. Mathematics and tabularmaterial will be processed in the traditional manner.
. Manuscript checklist1 . Include the original typed manuscript and three photo-
copies.2. Send three sets ofglossy print figures: each manuscript
set should contain photocopies of figures.3. Include in cover letter: a) copyright transfer statement.
b) list of five candidates for peer review.4. Include all authors’ personal signatures.5. Designate a corresponding author and provide a tele-
phone number and address.
S Please read, correct, and return the original set of proofswith the manuscript and figure copy. Be sure that allEditor’s or printer’s queries are answered. Only minorcorrections are permitted. Authors will be charged forexcessive changes. Excess page charges will be assessedon articles and concise reports that exceed four pages inlength ($60.00 per printed page). Invited reviews, editori-als, and special articles will be exempt. The enclosed printsof your illustrations should be reviewed carefully and anycorrections noted on the figure proof. Return the cor-rected proof and manuscript within 48 hrs. to:
Journal Editing, Williams & Wilkins, 35 1 W. CamdenStreet, Baltimore, MD 21201-2436.Reprints: Authors of articles published in JASN will
receive reprint order forms with page proof. Reprint orderblanks must be returned within 10 days ofreceipt to avoidlate charges. Orders received late will be charged anadditional fee of 25%. Send Reprint Order blanks to:Journal Editing, Williams & Wilkins, 35 1 W. CamdenStreet, Baltimore, MD 21201-2436.
THE AMERICAN Socii�av OF NEPHROLOGY1200 19th Street, N.W., Suite 300, Washington, D.C. 20036-2412 #{149}202/857-1190
Application for Active and Corresponding Membership
LAST N�Ma Fmrr N�ai� MioDi..t lNm.&L(s)
PREFERRED MuUNG ADDRESS
CITY STATE/PROVINCE ZIP/POSTAL CODE Couwrit�
Busir’ass ADDRESS (IF NO’� uSrED ABOVE)
Cm� STATE/PROVINCE ZIP/POSTAL CODE Cour.rrsy
Busmass TELEPHONE BusiNEss F,�x E-w�n. ADDRESS
Date of Birth_________________ Sex__________________ Country of Citizenship
if you reside in the U.S., but are not a U.S. citizen, please provide visa status_____________________________
(Individuals residing in the U.S. with temporary visa status will applyfor corresponding membership.)
Academic Appointment: _______________ Full Time ______________ Part Time ______________ None
Primary Professional Interest (e.g., Adult Nephrology, Pediatric Nephrology, Pathology, Urology, Physiology, etc.)
Primary Institutional Affiliation (e.g., Medical School-Faculty/Clinical Dept., Medical School-Faculty/Research Dept., Hospital-
� Staff/Clinical Staff Private Practice, Armed Forces or Other Federal Services, etc.)
Present Hospital/University Appointments (titles and departmental affiliations)
Please indicate the amount of time spent on the following. Your total should amount to 100%.
Clinical________ Research_________ Teaching__________ Administration__________ Other_________
Professional Education and Training (To qualifyfor active and corresponding membership you must have an M.D., Ph.D. or
equivalent, such as D.O., D. VM., FR. C.P., M.B.B.S., Pharm.D., etc.)
Institutional Name/Address Degree Dates
For office use only:
IT� nate ent�r�i-I (“}�pj�fr�j�. Ch�i’fr name
Training in Nephrology (Give inclusive datesfor residences, fellowships, other relevant postgraduate education.)
Institution Name and Address Position Preceptor(s) Inclusive Dates
List your five most significant publications.
Describe your clinical experiences as a specialist and consultant in kidney disease and related conditions that wouldprovide basis for qualification of membership.
List other societies to which you belong..
Provide names and addresses of three persons from whom letters of reference may be requested if needed.
Please return your completed application with the first year’s dues (see below) payable to the ASN in U.S. funds.
_________$125-AcrivE MEMBERSHIP for residents of North or Central America_________$140-CoRREsroNDmiG MEMBERSHIP for those who meet the qualifications for Active Membership, but are
not residents of North or Central America. Corresponding Members will receive all Society mailings and
member discounts, but do not have the right to vote or hold office.
If you would like to pay by Visa or MasterCard, please list the cardholder’s name, number and expiration date below:
� Visa � MasterCard
CARDHOLDER’S NAME (PLEASE PRINT OR TYPE) SIGNATURE
CARD NUMBER EXPIRATION DATE
Copyright © 2022 FDOKUMEN