Formal and informal care for people with dementia: variations in costs over time
12
PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [King's College London] On: 18 January 2011 Access details: Access Details: [subscription number 931926339] Publisher Routledge Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37- 41 Mortimer Street, London W1T 3JH, UK Aging & Mental Health Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713404778 Formal and informal care for people with dementia: Factors associated with service receipt J. Schneider a ; A. Hallam b ; J. Murray b ; B. Foley b ; L. Atkin b ; S. Banerjee b ; M. K. Islam c ; A. Mann b a Centre for Applied Social Studies, University of Durham, b Institute of Psychiatry, King's College, University of London, c Department of Economics, Jahangirnagar University, Bangladesh Online publication date: 09 June 2010 To cite this Article Schneider, J. , Hallam, A. , Murray, J. , Foley, B. , Atkin, L. , Banerjee, S. , Islam, M. K. and Mann, A.(2002) 'Formal and informal care for people with dementia: Factors associated with service receipt', Aging & Mental Health, 6: 3, 255 — 265 To link to this Article: DOI: 10.1080/13607860220142486 URL: http://dx.doi.org/10.1080/13607860220142486 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of Formal and informal care for people with dementia: variations in costs over time

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [King's College London]On: 18 January 2011Access details: Access Details: [subscription number 931926339]Publisher RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Aging & Mental HealthPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713404778
Formal and informal care for people with dementia: Factors associatedwith service receiptJ. Schneidera; A. Hallamb; J. Murrayb; B. Foleyb; L. Atkinb; S. Banerjeeb; M. K. Islamc; A. Mannb
a Centre for Applied Social Studies, University of Durham, b Institute of Psychiatry, King's College,University of London, c Department of Economics, Jahangirnagar University, Bangladesh
Online publication date: 09 June 2010
To cite this Article Schneider, J. , Hallam, A. , Murray, J. , Foley, B. , Atkin, L. , Banerjee, S. , Islam, M. K. and Mann,A.(2002) 'Formal and informal care for people with dementia: Factors associated with service receipt', Aging & MentalHealth, 6: 3, 255 — 265To link to this Article: DOI: 10.1080/13607860220142486URL: http://dx.doi.org/10.1080/13607860220142486
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

Aging & Mental Health 2002; 6(3): 255–265
ISSN 1360–7863 print/ISSN 1364–6915 online/02/030255–11 © Taylor & Francis LtdDOI: 10.1080/1360786022014248 6
ORIGINAL ARTICLE
Formal and informal care for people with dementia: factors associated with service receipt
J. SCHNEIDER,1 A. HALLAM,2 J. MURRAY,2 B. FOLEY,2 L. ATKIN,2 S. BANERJEE,2
M. K. ISLAM3 & A. MANN2
1Centre for Applied Social Studies, University of Durham, 2Institute of Psychiatry, King’s College, University of London & 3Department of Economics, Jahangirnagar University, Bangladesh
AbstractDetails of service receipt by 132 people diagnosed with dementia and their carers were collected in South London(boroughs of Lewisham, Camberwell, Southwark and Croydon), a geographical area served by several health and socialcare providers. The data collected included the Caregiver Activity Survey, which details the informal care given. This paperreports the formal and informal services received by the people with dementia at entry to the study. The amount of timespent on specific caring tasks by all informal carers of people with dementia averaged seven hours per week, but wassignificantly higher for co-resident carers, even when controlling for the level of dependency of the person cared-for. Theodds ratios of receipt of formal services are given, according to where people were living: in the community or residentialcare, with co-resident carers or alone.
Introduction
The needs of people with dementia place a growingdemand on health and welfare resources. Moderateto severe dementia is estimated to affect 6% ofpeople aged over 65, doubling in prevalence withevery five years increase in age (Jorm et al., 1987).The age-specific prevalence of all forms of dementia,including mild disorders, has been estimated torange from 1.4% in people aged 60–64, to 32.2%in people aged 90–94 (Hoffman et al., 1991).Increasing longevity means that, over the next 30years, the number of people aged 80 or more in theUK is expected to double (Ageing Population Panel,2000). Therefore the needs for care for people withdementia are expected to escalate (Winblad et al.,1999). This increase will inevitably affect informalcarers as well as other services.
In the UK, it is estimated that over half ofpeople with moderate to severe dementia live withco-resident carers, over one third live in residentialor nursing homes, and the rest live alone(Schneider et al., 1992). The numbers of elderlypeople receiving taxpayer-subsidised local authorityhome care services are projected to increase by48% between 1996 and 2031 (Pickard et al., 2000).On the basis of current funding system, total
expenditure on long-term care is projected todouble to about £24 billion by 2031 (Wittenberget al., 1998, Fig. 5). Two thirds of these costsof long-term (residential and nursing) care fallto the taxpayer through state funding. Therefore,enabling people with dementia to continue to livein domestic settings is widely regarded as a cost-effective strategy from the perspective of thetaxpayer/state, while it can also be justified becauseit responds to the preference of most people toend their days in familiar surroundings (RoyalCommission on Long-Term Care, 1999).
Dementia is a high risk factor for admission tolong-term care. Philp et al., (1997) estimate thatover two years, dementia increases the risk ofadmission to a residential or nursing home by afactor of eight. In the UK, the care of people withdementia is shared by the National Health Service,the national system of social services departments(SSD) run by local authorities, voluntary organisa-tions, families and neighbours. We know fromprevious research that the role of the informal careris often crucial in transitions from domestic toresidential care (Philp et al., 1997) and in carers’overall willingness to continue in that role (McKeeet al., 1999). We also know a great deal about thephysical and psychological impact of care-giving on
Correspondence to: Justine Schneider, Centre for Applied Social Studies, 15 Old Elvet, Durham, DH1 3HL, UK.Tel: 0191 374 7243. E-mail: [email protected]
Received for publication 2nd July 2001. Accepted 6th January 2002.
Downloaded By: [King's College London] At: 10:24 18 January 2011

256 J. Schneider et al.
carers of people with dementia (Levin et al., 1990;Donaldson et al., 1997; Schneider et al., 1999;Murray et al., 1999). Quantitative information isalso available about how formal and informalsupports are combined. The Lund 80+ study(McCamish-Svensson et al., 1999) does not reportdetail about the types of support provided. More-over, this Swedish study presents formal andinformal care as mutually exclusive, while, in theUK at least, the two are more likely to be mutuallydependent, whether carers are seen as resources inthemselves, as co-workers with formal services or asco-clients with the cared-for person (Twigg, 1989).Livingston et al., (1997) looked at the costs ofcommunity care for a representative sample ofpeople aged over 65, but did not attempt to esti-mate informal inputs. Here, we illustrate the variedand complex combinations of services used bypeople with dementia in one geographical area.
An unusual aspect of this study is that wemeasure the inputs of informal carers as well asthose of formal health and social care services.While the contribution of informal carers is widelyrecognised, it is important also to specify the natureof that input and measure it as far as possible inorder to recognise fully the interplay between it andformal services. Therefore we explore the configu-rations of formal and informal care received bypeople living in their own homes, as well as inresidential or nursing care homes.
Key policy initiatives in Britain that reflect thepriority given to people with dementia and theircarers include a raft of policy and legislationpertaining to carers. The Royal Commission onLong-Term Care was appointed in 1997 to examinethe options for a sustainable system of funding,both for people living in their own homes and inother settings. The members were asked to recom-mend how the cost of such care should be sharedbetween public funds and individuals. In keepingwith the approach of the Royal Commission, thisstudy distinguishes between the different elementsof care.
The Carers (Recognition and Services) Act 1995gave local authority social services departments aresponsibility to assess the needs of carers of allpeople with disabilities and their ability to continuecaring. A review of its implementation (Social Serv-ices Inspectorate, 1998) found wide variations andrecommended, among several other developments,‘checking that support and services for carers areavailable fairly across the SSD’ (p. 16). Thisconcern with equity of service delivery is one thatextends into all care settings, and it can also beaddressed with reference to the present study.
A subsequent government initiative, Caring aboutCarers: A National Strategy for Carers (http://www.doh.gov.uk.carers.htm), aimed to meetcarers’ needs for: information, support in the caringwork they do, and care for their own personal
needs. This has been backed up by £750m centralfunding for prevention and rehabilitation and£140m for respite care, as well as by the Carersand Disabled Children Act. While little impact ofthe carers’ strategy would have been felt during thecourse of the study, it is taken here to illustrate theimportance of our findings for service assessmentor benchmarking, with a view to future develop-ments for the support of older people withdementia and their carers. The aims of this studywere to answer the following questions:
� What services do people use?� What factors are associated with service receipt?� What services do informal carers provide?� How do the answers to these questions vary
according to living arrangements or otherfactors?
Methods
We selected people with moderate to severedementia who were receiving support from a familymember or friend who could be seen as the ‘carer’.The criterion for being a carer was spending fourhours or more per week with the individual withdementia. The sample consisted of all those patientson secondary care caseloads who had carers. Thus,the people with dementia had all been diagnosedformally and were known to specialist services. Aproportion of these people were already living inresidential or nursing homes but nevertheless hadcarers by our definition at the start of the study.Carers and the people with dementia were inter-viewed in their homes by two researchers (BF andLA), using a range of instruments to measure healthstatus of both parties and carer ‘burden’. Initial face-to-face interviews with both carer and the personwith dementia were followed by telephone inter-views after about seven months (Time 2), andTime 3 face-to-face interviews after an average of16 months. Here, we focus on the services receivedat Time 1, and how these appear to be affected bylevels of disability and place of residence. Althoughthis was a longitudinal study, we consider thatservice receipt is best judged at entry to the study,since the effect of the study itself on service use orreporting rates is likely to be minimal, whereas atlater dates the research itself may have promptedpeople to access services.
Informal care was measured using the CaregiverActivity Survey (Davis et al., 1997). This asks thecarer about how much time has been spent in thepast week on a range of tasks. For the purpose ofthis analysis, the data were classified into threeprincipal forms of caring:
� General tasks, such as communicating with theperson with dementia, paperwork, householdchores, shopping, cooking and eating meals;
Downloaded By: [King's College London] At: 10:24 18 January 2011
Formal and informal care for people with dementia 257
� Specific tasks, such as bathing, dressing,grooming, taking to the lavatory, or providingtransport for the person with dementia, and
� Supervision, during which time the carer mightdo something, which was not directly part ofthe care function, such as reading, entertainingvisitors or watching television.
Some carers reported that they spent more hoursthan there are in one day in caring activities. Inseveral cases, it was necessary to adjust these esti-mates to more plausible amounts. Where the meantotal number of hours caring was reported to exceed24, the number of hours of supervision was adjusteddownwards, on the assumption that active caringtasks took precedence over supervision. The distinc-tion between ‘general’ and ‘specific’ tasks was drawnto facilitate costing (costs are not reported here).General tasks had no cost for co-resident carers, andsupervision was costed at a lower rate.
Carers were also asked to complete the GeneralHealth Questionnaire (Goldberg, 1972), an instru-ment normally used in its shorter form to detectrecent stress, but which, in the 28-item version usedhere, also allows for measurement of chronic psycho-logical symptoms (Goodchild & Duncan-Jones,1985; Brodaty & Luscombe, 1998).
Services received were measured using the ClientService Receipt Inventory (CSRI, Beecham, 1995)and taking the carer as the informant about servicesto the person with dementia. The CSRI has beenused in a wide range of studies of mental healthcare. The inventory is completed for each studyparticipant and is designed to measure exhaustivelythe services used by that individual during the lastthree months, as well as their accommodation andmedication.
The person with dementia was interviewed witha number of measures, including the Global Dete-rioration Scale (Reisberg et al., 1982), a ‘staging’scale that allows the interviewer to rate the severityof cognitive impairment on a seven-point scalefrom ‘none’ to ‘very severe’. The Global PhysicalHealth Rating from the Older Americans Researchan Service Centre, (OARS; Duke University, 1978)rates a person’s current physical functioning on asix point scale, ranging from ‘excellent health’ to‘totally impaired’. The rater is given descriptiveanchor points on which to base their judgement.
Results
Sample
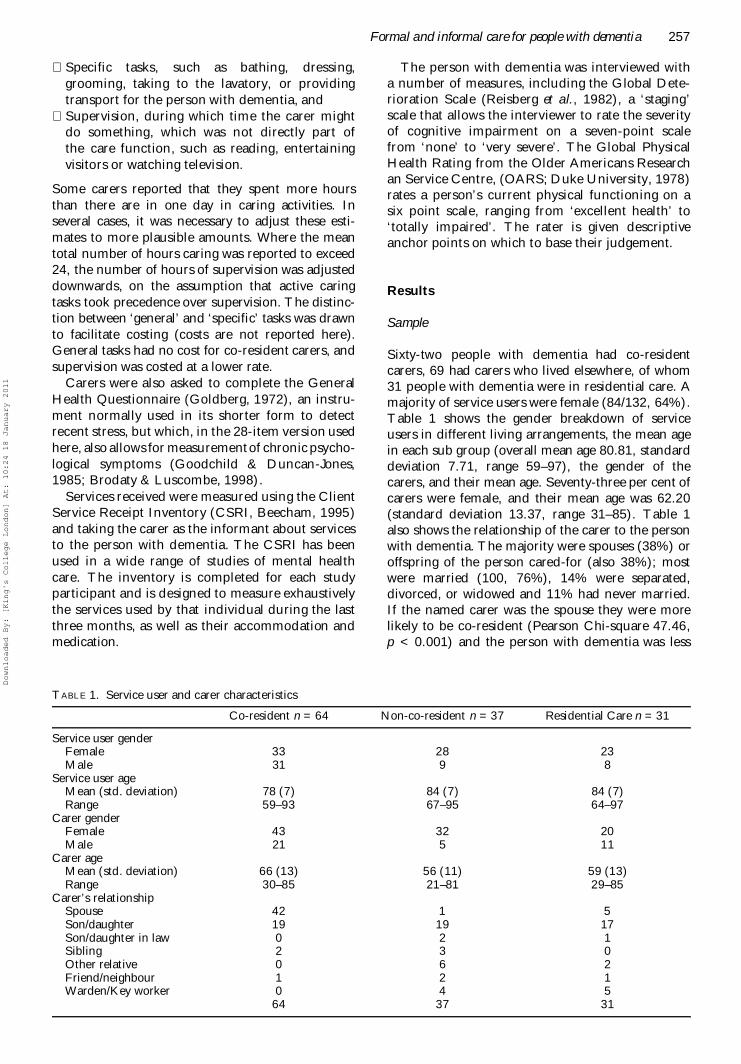
Sixty-two people with dementia had co-residentcarers, 69 had carers who lived elsewhere, of whom31 people with dementia were in residential care. Amajority of service users were female (84/132, 64%).Table 1 shows the gender breakdown of serviceusers in different living arrangements, the mean agein each sub group (overall mean age 80.81, standarddeviation 7.71, range 59–97), the gender of thecarers, and their mean age. Seventy-three per cent ofcarers were female, and their mean age was 62.20(standard deviation 13.37, range 31–85). Table 1also shows the relationship of the carer to the personwith dementia. The majority were spouses (38%) oroffspring of the person cared-for (also 38%); mostwere married (100, 76%), 14% were separated,divorced, or widowed and 11% had never married.If the named carer was the spouse they were morelikely to be co-resident (Pearson Chi-square 47.46,p < 0.001) and the person with dementia was less
TABLE 1. Service user and carer characteristics
Co-resident n = 64 Non-co-resident n = 37 Residential Care n = 31
Service user genderFemale 33 28 23Male 31 9 8
Service user ageMean (std. deviation) 78 (7) 84 (7) 84 (7)Range 59–93 67–95 64–97
Carer genderFemale 43 32 20Male 21 5 11
Carer ageMean (std. deviation) 66 (13) 56 (11) 59 (13)Range 30–85 21–81 29–85
Carer’s relationshipSpouse 42 1 5Son/daughter 19 19 17Son/daughter in law 0 2 1Sibling 2 3 0Other relative 0 6 2Friend/neighbour 1 2 1Warden/Key worker 0 4 5
64 37 31
Downloaded By: [King's College London] At: 10:24 18 January 2011

258 J. Schneider et al.
likely to be in residential care (Pearson Chi-square13.25, p < 0.001). Wives were no more likely thanhusbands to care for their spouse.
Most of the carers (121, 92%) and people withdementia (123, 93%) described their ethnic groupas ‘white’, and there were no sizeable groups fromany particular ethnic minority. Five people withdementia had been born in Ireland and four inJamaica. This is probably fairly representative ofthe older ethnic population in that part of London,although the younger population would have ahigher proportion of black residents and wouldinclude people from South Asia. Few (3%) of thepeople with dementia had been educated beyondsecondary school, but 12% of carers had tertiary orfurther education.
Nineteen of the people with dementia (14%)lived in residential homes, and 12 (9%) in nursinghomes. Clearly, being resident in non-domesticsettings, including nursing homes and residentialhomes, is likely to affect the services that peoplereceive. For instance, nursing homes have qualifiednurses on the staff who may deliver care that acommunity nurse might give to an individual livingin their own home. Because of the small numbers inresidential and nursing homes, meaningful compar-isons between these two settings cannot be made.Instead we restrict our analyses to comparingdomestic and non-domestic settings. Thirteen(10%) lived in sheltered housing, which implies thata person is supervised by a resident warden, but stilldepends on community-based health and socialcare services. For this reason, sheltered housing istaken here to be a ‘domestic’ setting. Amongst theother people living in domestic settings, 53 (40%)were in owner-occupied housing, and 35 (27%) inrented accommodation.
Variations in the sample
Table 2 summarizes the differences in the sampleaccording to where and with whom people lived;
residential (or nursing home) compared to domesticaccommodation, and, for those in domestic housing,whether the carer was co-resident or not. Carers’ages did not differ significantly between domesticand residential settings, but non-co-resident carerswere significantly younger than co-resident carers(many of whom were spouses). While third partieswere helping for more hours per week in domesticsettings than in residential ones, this did not differsignificantly between people with dementia livingwith their carers and those living apart from them.On every other demographic variable there weresystematic differences in the sample, which arediscussed below.
The services used
The total sample living in the community and thenumbers using each of the services measured areshown in Table 3, column 1. Apart from informalcare, which was an inclusion criterion for this study,the most commonly used services were GPs,community psychiatric nurses (CPNs), day centresrun by social services, and home care provided bysocial services ‘home help’. Certain services havebeen excluded from the table because each was usedby only one person in the sample: geriatric specialist,optician, health visitor, dietician, welfare benefitsofficer and ‘other’ hospital ward. Nobody recalledthe person with dementia visiting a dentist in thepreceding three months, only two people saw a phys-iotherapist (1.5%), three saw a psychologist (2.3%),and four saw an occupational therapist (3%).
In interpreting the comparisons made below, it isimportant to bear in mind that there may be somesubstitution, for example between inpatient care ondifferent types of ward. For this reason, the aggre-gate use of hospital care is presented. In general,the higher the level of aggregation of variables, themore reliable the service use estimates. Aggregateservice use levels are shown at the bottom ofTables 3 and 4.
TABLE 2. Variable means for people in domestic settings compared to people in non-domestic living arrangements
Residential vs. Domestic
Residentialcare n = 3
Mean
Domesticsettings n = 101
MeanT
statisticLevel of
significance (p)
95% Confidence Interval of the
mean difference
Age (person with dementia) 83.67 79.91 -2.37 0.019 -6.90, -0.62Physical health (PWD)1 16.32 9.44 4.34 < 0.001 3.78, 9.99Cognitive impairment2 5.10 4.18 3.37 0.001 0.38, 1.46Carer’s age 60.00 62.89 1.05 0.296 -2.56, 8.33Hours per week others care 3.37 7.81 2.58 0.014 0.96, 7.91Co-resident vs. Non-co residentAge (PWD) 77.58 83.72 4.16 0.000 -9.08, -3.22Physical health (PWD)1 10.69 7.39 2.23 0.028 0.36, 6.24Cognitive impairment2 4.42 3.72 2.49 0.015 0.14, 1.26Carer’s age 66.79 56.35 -4.06 0.000 -15.54, -5.34Hours per week others care 10.16 5.00 1.63 0.111 -1.26, 11.59
1 OARS; 2Global Deterioration Scale
Downloaded By: [King's College London] At: 10:24 18 January 2011

Formal and informal care for people with dementia 259
Factors associated with service receipt
The number of individual formal services receivedwas calculated. This variable shows an approxi-mately normal distribution, with a mode of six,median of seven and mean number of servicesreceived of 6.6 (standard deviation 2.5, range 0–14).The number of services received differed accordingto where people were living. People in residentialcare received fewer services than those in domesticaccommodation (mean 3.9 vs. 7.3, p < 0.001, 95%CI 2.5, 4.2). For those in domestic accommodationpeople with a co-resident carer received more serv-ices (mean 7.8 vs. 6.4, p = 0.01, 95% CI 0.3, 2.3).
Variations by living arrangements
Having seen that the number of services receivedvaried by living arrangements, we looked at the
types of services received. People with co-residentcarers were compared to those whose carer was notco-resident (Table 3) and people living in residentialcare were compared to those living in domesticsettings, including sheltered housing (Table 4).Table 3 shows that people without a co-residentcarer were less likely to see a psychiatrist, a GP or tobe taking medication. Similarly, they were less likelyto have ‘specific’ caring tasks performed by informalcarers (measured by the Care-giving ActivitySurvey). Not surprisingly, they were less likely toreceive respite from a home sitting service.However, they were more likely to receive two formsof social care: home help and meals ‘on wheels’,both services that are designed to enable people tocope at home. In terms of ‘aggregate’ services, there-fore, they were less likely to be treated in hospital asoutpatients, and less likely to receive primary healthcare. This is not surprising in view of their overalllower level of impairment. They received marginally
TABLE 3. Differences in service receipt by carer’s residence
ServiceTotal
n = 101Co- resident
n = 62Non-co-resident
n = 24Fisher’s
exact test
pInformal care
Informal carers other than main carer 94 60 34 0.705Inpatient services
Assessment/rehabilitation ward 5 4 1 0.650Medical ward 8 6 2 0.707Inpatient ward 30 23 7 0.113
Outpatient servicesOutpatient appointments 17 14 3 0.099Day hospital 8 6 2 0.707A&E or casualty 11 8 3 0.742NHS day care 3 3 0 0.297
Community health servicesPsychiatrist 35 31 4 0.000Psychologist 3 2 1 1.000Community psychiatric nurse 44 29 15 0.681
Primary careGP 49 39 10 0.002Nursing 19 15 4 0.186Occupational Therapist 4 4 0 0.294Physiotherapist 2 2 0 0.531Chiropodist 12 7 5 0.755Medication 76 53 23 0.031
Social CareRespite care 16 12 4 0.400LA SSD day care 43 30 13 0.299Voluntary organisation day care 1 1 0 1.000Social worker 11 5 6 0.204Home help 41 15 26 0.000Crossroads sitting service 10 10 0 0.012Meals on wheels 16 1 15 0.000
Informal careGeneral tasks 92 61 31 0.071Specific tasks 64 53 11 0.000Supervision 36 33 7 0.001
Aggregate servicesHospital 30 22 8 0.113Outpatient 34 27 7 0.028Community health care 99 64 35 0.132Social care 76 44 32 0.057Primary care 85 58 27 0.025All health and social care services 99 64 35 0.132
Downloaded By: [King's College London] At: 10:24 18 January 2011

260 J. Schneider et al.
more social care than people with co-resident carers(p = 0.057). This may be taken to suggest that somesocial services are targeted at people living alone. Ofcourse, co-resident carers who are elderly and disa-bled might qualify for such support in their ownright.
As noted above in relation to Table 2,people living in residential care were less likely tohave the informal support of a third party apartfrom their main carer (Table 4). They were lesslikely to receive inpatient hospital care or outpa-tient appointments, and community psychiatricnurses and psychiatrists had less frequent contactwith people in residential care. They were lesslikely to attend day care funded by the localauthority, or outpatient appointments. The lowerlevel of hospital, outpatient and community mentalhealth care is a finding that we discuss furtherbelow.
Stress experienced by informal carers
GHQ ‘caseness’ was positively associated with beinga co-resident carer (Fisher’s exact test, one-sided p =0.03). Longitudinal data analysis of the datacollected for this study will cast light on any causallinks between formal services and carers’ well-being.
Services provided by informal carers
Table 5 gives the hours per week devoted to general,specific, and supervisory tasks according to thecarer’s living arrangements. Taking each element ofinformal care (general, specific and supervision)people in domestic settings received more thanthose in residential settings (all p < 0.001). Whenpeople with dementia with co-resident carers werecompared to those with carers living elsewhere, the
TABLE 4. Total service receipt and differences by domestic or non-domestic accommodation
ServiceTotal132
% of TotalSample
Domestic101
Non-domestic 31
Fisher’sexact test
Informal care n % n n pInformal carers other than main carer 110 83% 94 16 0.000
Inpatient servicesAssessment/rehabilitation ward 5 4% 5 0 0.591Medical ward 10 8% 8 2 1.000Inpatient ward 32 24% 30 2 0.008
Outpatient servicesOutpatient appointments 17 13% 17 0 0.012Day hospital 8 6% 8 0 0.197A&E or casualty 12 9% 11 1 0.293NHS day care 3 2% 3 0 1.000
Community health servicesPsychiatrist 37 28% 35 2 0.002Psychologist 3 2% 3 0 1.000Community psychiatric nurse 47 36% 44 3 0.000
Primary careGP 59 45% 49 10 0.148Nursing 20 15% 19 1 0.043Occupational Therapist 4 3% 4 0 0.572Physiotherapist 2 1% 2 0 1.000Chiropodist 16 12% 12 4 1.000Medication 101 76 25 0.633
Social careRespite care 16 12% 16 0 0.023LA SSD day care 44 33% 43 1 0.000Voluntary organization day care 2 1% 1 1 0.416Social worker 12 9% 11 1 0.293Home help 41 31% 41 0 0.000Crossroads sitting service 10 8% 10 0 0.116Meals on wheels 16 12% 16 0 0.023
Informal careGeneral tasks 103 78% 92 11 0.000Specific tasks 68 52% 64 4 0.000Supervision 43 33% 36 7 0.196
Aggregate servicesHospital 32 24% 30 2 0.008Outpatient 35 27% 34 1 0.000Community health care 63 48% 59 4 0.000Social care 78 59% 76 2 0.000Primary care 111 84% 85 26 1.000All health and social care services 127 96% 98 28 0.084
Downloaded By: [King's College London] At: 10:24 18 January 2011

Formal and informal care for people with dementia 261
former group were found to receive significantlymore inputs (p = 0.012 for general tasks, p = 0.002for specific tasks, and p < 0.001 for supervision).
The amount of informal care depends on factorsother than co-residency. Regression analysissuggests that, controlling for co-residency and forthe person with dementia being in residential care,cognitive impairment measured by the GlobalDeterioration Scale was significantly associatedwith the number of hours of informal care provided(p < 0.001). The person with dementia’s physicalfunctioning (OARS) was also associated (p =0.004) with informal care given but in this equationthe coefficient is negative, indicating that the morefrail the person the less informal care hours theyreceived. This may because more mobile peoplewith dementia require greater supervision. TheGDS and OARS did not appear to be correlated(Kendall’s tau p = 0.243). The regression model,incorporating these and other variables pertainingto the carer and the cared-for person, as well asservice inputs and residency factors, explained atleast 41% of the variation in informal care hours
(Table 6). This table shows that, in addition towhere people were living, the level of dementia andphysical health both predicted the hours ofinformal care given to this group of people withdementia.
Having identified demographic factors that influ-ence informal care hours, we can summarise theinteractions between formal and informal care.Logistic regression analysis was used, with eachformal service tested as the dependent variable.Cognitive functioning (GDS), physical health(OARS), co-residency, and residential care wereentered into the model to control for these factors.When inserted in the logistic model as dependentvariables, the receipt of 13 services could bepredicted using logistic regression with a criterionof model adequacy of p = 0.01. The odds ratios forthe key significant variables are shown in Table 7.Several key findings emerge:
� Non-domestic care has a negative associationwith receipt of community psychiatric nursingcare, even controlling for dependency measures.
TABLE 5. Informal care hours per week by living arrangements
Domestic accommodation
Mean hours per week (standard deviation)
All 132 Co-residentcarer 64
Non-co-residentcarer 37
Residentialcare 31
General care tasks 18.68 (25.31) 28.52 (28.88) 14.57 (21.54) 3.55 (5.99)Specific care tasks 7.30 (14.16) 12.45 (18.26) 4.25 (7.25) 0.51 (1.44)Supervision 17.74 (38.83) 33.55 (50.45) 5.49 (14.28) 0.23 (1.26)TOTAL: excluding travelling time 43.72 (57.22) 74.53 (65.22) 24.30 (32.63) 4.29 (7.54)
TABLE 6. Linear regression on hours of informal care at Time 1
Independent variables Standardized coefficients t Significance
Constant 0.335 0.739Global deterioration scale 0.389 5.018 0.000OARS -0.212 -2.920 0.004Co-resident carer 0.292 3.278 0.001Residential care -0.343 -3.683 0.000
Adjusted R2 0.41; SE 43.36; F 20.68; p < 0.001; Dependent variable: total hours of informal care at Time 1
TABLE 7. Odds ratios and 95% confidence intervals derived from logistic regression models, taking service receipt asdependent variable
Likelihood of receiving: Co-resident carer Residential careGlobal deterioration
scale OARS
Respite care (hospital ornursing home)
2.17* 1.04, 4.51
Outpatient care 2.93* 1.05, 8.19Psychiatric appointment 4.16* 1.21, 14.23CPN appointment 0.12* 0.02, 0.64GP appointment 3.61* 1.33, 9.77 0.58* 0.36, 0.94Home help 0.07** 0.02, 0.24Meals on wheels 0.02** 0.003, 0.227Other informal carer 0.04** 0.005, 0.28 2.00* 1.11, 3.60Any community healthservices
2.65* 1.02, 6.86 0.81* 0.04, 0.83
Any social services 0.02*** 0.003, 0.12
* p < 0.05; ** p < 0.01; *** p < 0.001
Downloaded By: [King's College London] At: 10:24 18 January 2011

262 J. Schneider et al.
A consequent effect is lower use of communityhealth services by people in residential care.
� Use of social services was also significantly lowerfor people in non-domestic settings, and theywere less likely to have support from people otherthan the named carer.
� All other things being equal, the presence of aco-resident carer increases the probability of aperson with dementia receiving some services:outpatient care, psychiatrist appointments, andGP care. This could be because the co-residentcarer facilitates attendance. It can also beexplained by nursing care being provided insome non-domestic settings.
� A co-resident carer is associated with a lowerprobability that the person with dementia willreceive home help or meals on wheels.
� Seeing a GP was less likely for more disabledpeople as measured by OARS scores.
� People whose cognitive impairment as measuredby the GDS was greater were twice as likely toreceive support from other informal carers inaddition to the main carer interviewed.
� People whose cognitive impairment was greaterwere more likely to receive respite care.
Discussion
The sample, made up of individuals in southLondon and their carers, needs to be seen as a popu-lation in contact with secondary services. Despitethis element of selectivity, they may be held to betypical of the clients with dementia who, by virtue ofbeing ‘known to’ health and social care services, arethe people who mostly use these services. Of course,while the configuration of formal and informal serv-ices received by this sample may be illustrative ofthose received in other British urban settings bypeople with dementia, it tells us little about peoplewith dementia and their carers who are not incontact with services, nor about the situation ofpeople in other countries or service contexts.
When the sample characteristics were comparedaccording to where people live (Table 2), we foundsystematic differences in most variables, with theexception of the carer’s age. The only variable onwhich the groups do not appear to differ is in thenumber of hours care received from third parties.These analyses highlight a continuum of disabilityaccording to which the highest mean levels ofimpairment were found in non-domestic settings,and, within domestic settings, higher levels ofimpairment affected the individuals with co-residentcarers.
As is usually found in studies of service use,of those people interviewed, one half or fewerused the formal services about which they wereasked (Schneider et al., 1992; McNamee et al.,1999; Moriarty & Webb, 2000). It should be
acknowledged that service receipt data are alwayssubject to difficulties in recall. We must there-fore ask whether these difficulties are likely to berandomly distributed in our study sample. Theinformants of service use were carers who sawthe individual with dementia for at least fourhours per week, but one might assume that thelonger a carer spent with the person withdementia, the more services they would recall.We tested this by looking at the correlationbetween informal care hours and the number ofservices reported to have been used tested this.The results show a high correlation between thetwo variables (r = 0.441; p < 0.001) whereas theGlobal Deterioration Scale score did not appearto correlate either with number of services norwith informal care hours. By contrast, McNameeet al., (1999), using a different case-mix of olderpeople and a data collection method that reliedprimarily on documents, found that people livingalone used more services than others, particularlyinpatient care. This suggests that in our studythe informants for people living alone may haveunder-reported service use more than co-residentinformants. At the same time, the sample usedby McNamee et al., included a large proportionof physically frail older people whose hospitaluse may have affected this result. Overall, weconsider that it is safe to assume that servicesare more likely to be under-reported than over-reported, so that the estimates presented heremay be read as minimum estimates of accessingservices.
What services do people use?
Of course, service use is largely supply-led, and thesefindings cannot be extrapolated to other servicecontexts in other countries, for example. The serv-ices most frequently in contact with this sample ofpeople living in domestic settings were communitymental health services, general practitioner, localauthority day care, and home helps (Table 3).Perhaps partly due to under-reporting, some servicesappear to have been received by few people diag-nosed with dementia. Contact with professionalsallied to medicine was low overall. We found thatpeople in residential care appear to have reliedmostly on the home to provide formal services.However, since we did not disaggregate serviceinputs like nursing care, day care, and occupationaltherapy from board and lodging for residentialdwellers, few inferences can be made about unmetneeds. It should be noted, that people in residentialsettings were less likely than others to receivespecialist psychiatric services, but these would notnormally be provided ‘in-house’, even in nursinghomes as compared to residential homes.
Downloaded By: [King's College London] At: 10:24 18 January 2011

Formal and informal care for people with dementia 263
What factors are associated with service receipt?
These findings demonstrate some surprising andsome less surprising bilateral associations betweenwhere people were living and service receipt. In viewof the facilities normally provided in non-domesticsettings, it is not surprising to find that residentswere less likely to receive respite care, attend localday care, receive home help or meals on wheels. Thesame applies to the finding that people in residentialhomes were less likely to receive informal care forgeneral or specific tasks, but not supervision, onvisits. In short, people in residential care were lesslikely to receive all the ‘aggregate’ services exceptprimary care and all health and social care servicestaken together (which includes primary care).
In addition, we explored the relationship betweencognitive functioning, poor physical health, andnumber of services service received. The associa-tions between severity of mental impairments andreceipt of respite care imply effective targeting ofthis provision by the service providers at peoplewith higher levels of need. The presence of a co-resident carer has been shown to influence servicereceipt, even controlling for level of impairment.Multivariate analyses confirm that three factors (co-residency, being in non-domestic care, and thedependency of the person with dementia) arethe key predictors not only of the formal servicesprovided, but also of the amount of informal careprovided for people with dementia. These findingsare fairly robust, because our sample spans threelocal authority areas, so the people studied were notsubject to a single service allocation policy. Theysuggest that these three variables should beincluded in future analyses of care allocation.
What do informal carers provide?
This study focused on carers for people withdementia who are known to services, and found thatcarers supply general help with household chores tomost people, as well as performing specific personalcare tasks and providing supervision to many peoplewhom they care for. The hours that carers spent inthese activities represent a large proportion of theirtime. For instance, co-resident carers were occupiedfor an average of 75 hours per week, of which41 hours were spent on general and specific caringduties. This may be compared to a standard workingweek of 35–40 hours. Non-co-resident carers spenton average 24 hours, of which 19 hours, the equiva-lent of about three working days per week, was spenton caring activities excluding supervision. Thesefindings confirm the huge investment of labourmade by informal carers (Henwood, 1998; Warner& Wexler, 1998) and in particular the burden oncarers of people with dementia (Moriarty & Webb,2000). These rates of informal inputs apply only to
carers for people with dementia who are in contactwith secondary services. Thus, they are likely to beat the more severe end of the dementia spectrum.They could not be extrapolated to the whole popula-tion of carers for people with dementia, includingthose less severely affected.
What can be done to help carer stress?
The Resource Implications Study (Bamford et al.,1998) found that co-resident carers were more likelyto believe that their health had been affected and tohave a high GHQ than non-co-resident carers. Ourcross-sectional data support this, with co-residentcarers having a higher GHQ than non-co-residentcarers. This implies that some carers might benefitfrom formal interventions designed to support them,but this hypothesis remains to be tested.
How do the answers to these questions vary according toliving arrangements or other factors?
For people in residential or nursing care, theextremely low use of health services reported shouldlead us to ask whether there is a risk of neglect ofhealth needs as a result of being in non-domesticcare. For instance, we know from the NationalSurvey of NHS Patients that in the Health Authorityarea Lambeth, Southwark and Lewisham (whichoverlaps with our study districts) in the past threemonths, 63% of respondents aged 18+ had seentheir GP (1998, UK Data Archive). Older peoplemay be expected to attend even more frequently, yetin the study we report here we found that only10 out of 31 people in residential care (32%) hadseen a GP in same period, although 61% of peoplewith co-resident carers had done so (39 out of 64).Considering that this study comprised very elderlypeople with dementia whose frailty might be anobstacle to the expression of health needs, thisfinding suggests that people in non-domestic caremay be missing out on primary health care.
In the UK, nursing homes, but not residentialhomes, are required to have qualified nursing staff.Of our sample in non-domestic care, 12 were innursing homes and 19 in residential homes. Wecannot therefore assume that physical health needsare being met ‘in house’ in all non-domesticsettings. At the same time, the fact of being in acaring setting, residential or nursing, may preventor ameliorate some health needs. Further, detailedcomparisons would be required to explore thisissue. Evidence of differences between people indifferent settings could be a matter for concern inthe light of findings that poor physical health care isassociated with depression in residents of homesand hence detrimental to their quality of life (Mannet al., 2001), and that nursing staff were no better
Downloaded By: [King's College London] At: 10:24 18 January 2011

264 J. Schneider et al.
than other care staff at recognising depression inresidents (Bagley et al., 2000).
Questions remain about how far a residential ornursing home might exercise control over access toprimary care for patients with dementia, and howwell the non-domestic setting itself responds tosuch needs. In summary, the findings presentedhere raise some questions of equity. Formal healthcare and social services are generally provided atthe discretion of professionals, but usually onlyafter a request has been made, either by the personwith dementia or by their carer. To the extentthat dementia impairs an individual’s ability torecognize or to articulate their needs, the disorderitself can be a barrier to service receipt, over andabove other barriers, including lack of resources,problems of access and cultural insensitivity.
Conclusion
The data analysed for this study supply evidence ofthe delivery of ‘normal’ (non-experimental) healthand social care provision to people with diagnoseddementia who have carers in South London. Whileother research has established that people withdementia use more services than people without(e.g. Cullen et al., 1993), we have demonstratedsystematic differences in service receipt betweendifferent sub-groups of people with dementia. More-over, we have quantified the inputs of informalcarers in supporting people with dementia, not justin the community but also in long-term care.
Acknowledgements
The authors wish to acknowledge the helpful sugges-tions made about the structure and content of thispaper by the journal’s referees. This work wasundertaken by staff of the Health Services ResearchCentre at the Institute of Psychiatry, Kings College,University of London, who received funding fromthe Department of Health. The views expressed inthe publication are those of the authors and notnecessarily those of the Department of Health.
References
AGEING POPULATION PANEL (2000). The age shift: aconsultation document. London: Department of Tradeand Industry.
BAGLEY H., CORDINGLEY L., BURNS A., MOZLEY C.G.,SUTCLIFFE C., CHALLIS D. & HUXLEY P. (2000).Recognition of depression by staff in nursing and resi-dential homes. Journal of Clinical Nursing, 9, 445–450.
BAMFORD, C., GREGSON, B., FARROW, G., BUCK, D.,DOWSWELL, T., MCNAMEE, P. & BOND, J. (1998).Mental and physical frailty in older people: the costsand benefits of informal care. Resource Implications
Study of Medical Research Council Cognitive Func-tioning and Ageing Study. Ageing and Society, 18,317-354.
BEECHAM, J. (1995). Collecting and estimating costs. InM.R.J. KNAPP (Ed.), The economic evaluation of mentalhealth care. Aldershot: Arena.
BRODATY, H. & LUSCOME, G. (1998) Psychologicalmorbidity in carers is associated with depression inpatients with dementia. Alzheimer Disease and AssociatedDisorders, 12, 62–70.
CULLEN, M., BLIZARD, R., LIVINGSTON, G. & MANN, A.(1993). The Gospel Oak project 1987–1990. HealthTrends, 25, 142–146.
DAVIS, K., MARIN, D., KANE, R., PATRICK, D., PESKIND,E., RASKIND, M. & PUDER, K. (1997). The CaregiverActivity Survey (CAS): development and validation of anew measure for caregivers of persons with Alzheimer’sDisease. International Journal of Geriatric Psychiatry, 12,978–988.
DONALDSON, C., TARRIER, N. & BURNS, A. (1997). Theimpact of the symptoms of dementia on caregivers.British Journal of Psychiatry, 170, 62–68.
DUKE UNIVERSITY, CENTRE FOR THE STUDY OF AGING
AND HUMAN DEVELOPMENT. (1978). MultidimensionalFunctional Assessment: The OARS Methodology. DukeUniversity, Durham, North Carolina.
GOLDBERG, D. (1972). The detection of psychiatric illness byquestionnaire: a technique for the identification and assess-ment of non-psychotic psychiatric illness. London: OxfordUniversity Press.
GOODCHILD, M.E. & DUNCAN JONES, P. (1985).Chronicity and the General Health Questionnaire.British Journal of Psychiatry, 146, 55–61.
HENWOOD, M. (1998). Ignored and invisible? Carers’experiences of the NHS. London: Carers NationalAssociation.
HOFFMAN, A., ROCCA, W., BRAYNE, C. et al. (1991).The prevalence of dementia in Europe: a collaborativestudy of 1980–1991 findings. International Journal ofEpidemiology, 20, 76–748.
JORM, A.F., KORTEN, A.E. & HENDERSON, A.S. (1987).The prevalence of dementia: a quantitative integrationof the literature. Acta Psychiatrica Scandinavica, 76,465–479.
LEVIN, E., SINCLAIR, I. & GORBACH, P. (1990). Families,services, and confusion in old age. Aldershot: Avebury.
LIVINGSTON, G., MANELA, M. & KATONA, C. (1997).Cost of community care for older people, British Journalof Psychiatry, 171, 56–59.
MANN, A.H., SCHNEIDER, J., MOZLEY, C.G., LEVIN, E.,BLIZARD, R., NETTEN, A., KHARICHA, K. EGELSTAFF,R., ABBEY, A. & TODD, C. (2001). Depression andthe response of residential homes to physical healthneeds. International Journal of Geriatric Psychiatry. 15,1105-1112.
MCCAMISH-SVENSSON, C., SAMUELSSON, G., HAGBERG,B., SVENSSON, T. & DEHLIN, O. (1999). Informal andformal support from a multi-disciplinary perspective: aSwedish follow-up between 80 and 82 years of age.Health and Social Care in the Community, 7, 163–176.
MCKEE, K., WHITTICK, J., GILHOOLY, M., BALLINGER,B., GORDON, D., MUTCH, W. & PHILP, I. (1999). Thewillingness to continue caring in family supporters ofolder people. Health and Social Care in the Community, 7,100–108.
MCNAMEE, P., GREGSON, B., BUCK, D., BAMFORD, C.,BOND, J. & WRIGHT, K. (1999). Costs of formal care forfrail older people in England: the resource implicationsstudy of the MRC cognitive function and ageing study.Social Science and Medicine, 48, 331–341.
Downloaded By: [King's College London] At: 10:24 18 January 2011

Formal and informal care for people with dementia 265
MORIARTY, J. & WEBB, S. (2000). Part of their lives:community care for older people with dementia. Bristol:Policy Press.
MURRAY, J. (1995) Carers of confused and elderly people.In J. MURRAY (Ed.), Prevention of anxiety and depressionin vulnerable groups. London: Gaskell.
MURRAY, J., SCHNEIDER, J., BANERJEE, S. & MANN, A.(1999) Eurocare: a cross-national study of co-residentspouse carers for people with Alzheimer’s disease II. Aqualitative analysis of the experience of care-giving.International Journal of Geriatric Psychiatry, 14, 662–667.
PHILP, I., MCKEE, K.J., ARMSTRONG, G.K., BALLINGER,B.R., GILHOOLY, M.L.M., GORDON, D.S., MUTCH, W.J.& WHITTICK, J.E. (1997). Institutionalisation amongstpeople with dementia supported by family carers in aScottish city. Aging & Mental Health, 1, 339 -345.
PICKARD, L., WITTENBERG, R., COMAS, A., DAVIES, B. &DARTON, R. (2000). Relying on informal care into thenext century? Informal care for elderly people inEngland to 2031. Ageing and Society, 20, 745–772.
REISBERG, B., FERRIS, S., DE LEAN, M., CROOK., T.(1982) The Global Deterioration Scale (GDS) forassessment of primary degenerative dementia. AmericanJournal of Psychiatry, 139, 1136–1139.
ROYAL COMMISSION ON LONG-TERM CARE. (1999).With respect to old age: executive summary. London:Department of Health.
SCHNEIDER, J., KAVANAGH, S., KNAPP, M., BEECHAM, J. &NETTEN, A. (1992). Elderly people with advanced
cognitive impairment in England: Resource use andcosts. Ageing and Society, 13, 27–50.
SCHNEIDER, J., MURRAY, J., BANERJEE, S. & MANN, A.(1999). Eurocare: a cross-national study of co-residentspouse carers for people with Alzheimer’s disease I.Factors associated with carer burden. InternationalJournal of Geriatric Psychiatry, 14, 651–661.
SOCIAL SERVICES INSPECTORATE . (1998). A matter ofchance for carers? Inspection of local authority support forcarers. CI (98) 19, London: Social Care Group,Department of Health.
TWIGG, J. (1989). Models of carers: how do social careagencies conceptualise their relationship with informalcarers? Journal of Social Policy 18, 53–66.
UK DATA ARCHIVE (1998). National Survey of NHSPatients: General Practice, 1998. University of Essex: UKData Archive.
WARNER, L. & WEXLER, S. (1998). Eight hours a day andtaken for granted? London: Princess Royal Trust forCarers.
WINBLAD B., WIMO A., MOBIUS H., FOX J. &FRATIGLIONI, L. (1999). Severe dementia: a commoncondition entailing high costs at individual and societallevels. International Journal of Geriatric Psychiatry, 14,911–914.
WITTENBERG, R. PICKARD, L., COMAS-HERRERA, A.,DAVIES, B. & DARTON, R. (1990). Demand for long-termcare: projections of long-term care finance for elderly people.Canterbury: PSSRU, University of Kent at Canterbury.
Downloaded By: [King's College London] At: 10:24 18 January 2011