Folder ID: 1774384 Dates - Pubdocs.worldbank.org.
90
THE WORLD BANK GROUP ARCHIVES PUBLIC DISCLOSURE AUTHORIZED Folder Title: Clausen Papers - Special Programme for Research and Training in Tropical Diseases - Correspondence 03 Folder ID: 1774384 Dates: 12/1/1984 - 12/31/1984 Series: Alphabetical [subject] files Subfonds: Records of President A. W. Clausen Fonds: Records of the Office of the President ISAD Reference Code: WB IBRD/IDA EXC-09-3957S Digitized: 3/1/2019 To cite materials from this archival folder, please follow the following format: [Descriptive name of item], [Folder Title], Folder ID [Folder ID], World Bank Group Archives, Washington, D.C., United States. The records in this folder were created or received by The World Bank in the course of its business. The records that were created by the staff of The World Bank are subject to the Bank’s copyright. Please refer to http://www.worldbank.org/terms-of-use-earchives for full copyright terms of use and disclaimers. THE WORLD BANK Washington, D.C. © International Bank for Reconstruction and Development / International Development Association or The World Bank 1818 H Street NW Washington DC 20433 Telephone: 202-473-1000 Internet: www.worldbank.org
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Folder ID: 1774384 Dates - Pubdocs.worldbank.org.
THE WORLD BANK GROUP ARCHIVES
PUBLIC DISCLOSURE AUTHORIZED
Folder Title: Clausen Papers - Special Programme for Research and Training in Tropical Diseases - Correspondence 03
Folder ID: 1774384
Dates: 12/1/1984 - 12/31/1984
Series: Alphabetical [subject] files
Subfonds: Records of President A. W. Clausen
Fonds: Records of the Office of the President
ISAD Reference Code: WB IBRD/IDA EXC-09-3957S
Digitized: 3/1/2019
To cite materials from this archival folder, please follow the following format: [Descriptive name of item], [Folder Title], Folder ID [Folder ID], World Bank Group Archives, Washington, D.C., United States. The records in this folder were created or received by The World Bank in the course of its business.
The records that were created by the staff of The World Bank are subject to the Bank’s copyright.
Please refer to http://www.worldbank.org/terms-of-use-earchives for full copyright terms of use and disclaimers.
THE WORLD BANK Washington, D.C. © International Bank for Reconstruction and Development / International Development Association or The World Bank 1818 H Street NW Washington DC 20433 Telephone: 202-473-1000 Internet: www.worldbank.org
Pr D~ .r or """ ~ h; .r Vct) ~ l'1 ' A i-v-of / CL.'t' (
1~~
DE.:CT .. A.SSIFIED W J:1G· Arc.hives
@
I IIII II Ill II Il l II Ill II Ill II Ill II Ill 1111111 11111111 1774384
A1995-285 Other#: 18 209478B Clausen Papers - Special Programme for Research and Training In Tropical Diseases -Correspondence 03
-.I
The World Health Organization 1211 Geneva 27
Sheikh Ballclan Ben Mohaaed Al Nahyan Deputy Priae Mini1ter of the United
Arab Emirates Switzerland
•••
•••
Abu Dhabi Onited Arab Eairatea
December 12, 1984
Dear Sir,
We take the liberty of 1oliciting your 1upport for a unique venture in international collaboration. ?bia venture in reaearch and deYelopaent ii an invest'aent in the future of aan1tind and will require year• of work and sustained financial 1upport. BoveTer, we are conTinced that the reaulta will have a profound iapact on the health and vell-beina of bmunity.
The Special Progr .... for leaearch and Trainina in Tropical Di1ea1e1 (TDI.) - co-sponaored by the United Nation• Development Progr .... , the World Bank and the World Health Organization - 1eaka to develop the .. u, to control 1ix 11ajor tropical di1ea1e1 which today afflict or threaten over one thousand million people living in developina countrie1. We attach for your information a booklet deacribing in more detail the work and achievements of the Special Programme.
In spite of the exploaive growth of knowledge in the biological science• over the paat 30 year,, little progress baa been made toward, the control of these diaeaaea. In fact the menace ia increasing.
Million• of children die fl'ea ularia before reaching their fifth birthdays, and millions of thoae who reach adulthood are incapacitated by one or aore tropical infectiona. They are sentenced to spend their live• on the treadaill of illness and poYerty with no hope of isprovina the lot of their faailiea or their c011111Unitiea.
cc: The Miniater of Health, Abu Dhabi The Miniater for foreipi Affairs, Abu Dhabi Bil Bighneaa Sheikh H&lldan Bin Raahid Al Maltto1111, Minister of Finance
and Indutry, Ministry of Finance and Induatry, Dubai Per.anent Kisaion of the United Arab Fairates to the Unitecl Nation•
Office and other Specialized Agencie1 at GeneYa
ENCLS: Aa stated
bee: UNDP (2) World Bank EMllO (2) Att: TDR EMS/HQ
Sheikh Baadan In Mobaaed Al Rahyan, Deputy PriM Miniater of the United Arab lairatea, Abu Dhabi
%
The deTaatatina blow, to the individual and the faaily, of an acute attack of aalaria at h~eat ti .. or of peraaaent loaa of •iaht by the aae of 2.5 troa river blindaeH (oncbocerctaaia) ia euy to underatand. However, the aocial and econoaic iapacta upon a cOIIIIUllity and a country when tropical diauaea atrfie don huactreda of tbouaanda of people, go tar beyond the individual or aroaa atatiatica. In fact, epideaica of aalaria, aleepina aickn••• and river blindn••• often drive aelf-sufficient C01111Unitiea into atatea of dependent poverty.
The deatructive syabioaia of diaeaae and poverty auat, and caa be replaced by the synerai•• of health and productivity. To brtaa th1a abovt, the tropical countriea require both the tool• for preventioa and treataent of the tropical di•••••• and the acientific and technical capal,ilitie• to assure their effective application. Theae are the goala of TDl.
Over the paat eix years, TDl baa challanaad and atiaulated reaurchera at institutions throughout the world to work together toward theae enda. Thouaanda of acientiata in univeraitiea, reaearch inatitutiona, aoverDllellt miniatriea and induatry have responded and are now worlting aa aaabera of TDR te ... - in fundaaental reaearch laboratoriea, in hoapital clinic• aad in villaae he<h centres - to build the new tool• and prepare thea for uae in the villages of the tropica. TDl has catalysed the linkina of reaearcb activities into an effective worldwide network and baa focuaed the nev methods and knowledge ol the biological science• upon the tropical diaeaaea.
The results have been remarkable and reaearch carried out both within and outaide the Special Programme baa brought about aignificant progreaa. Some new tools for diseaae control have already reached the ataae of actual application in the field, while other• are close to it. Exaaplea of major development• toward• the control of the diseases include:
o A biological agent, Bacillus thuringienaia R-14, to control the flies tbat spread river blindneH 1a beina used extenaively in Weat Africa and ia beina teated againat aalaria-carrying mosquitoa.
o A new drug, mefloquine, for the treatmen.t of aalaria infection• reaiatant to atandard therapy baa been reaiatered for uae.
o Vaccine• which aay treat and prevent leproay are in the early 1tagea of teating in aan. However, the teats vill take five to eight year• to coaplete becauae of the slow natural biatory of the dheaae.
o Simple kita to measure the senaitivity of aalaria paraaitea to druga to aaaure the correct choice of treataent are beina uae4 widely.
o A aimple teat to diagnoae sleeping sickneaa (AfricaR trypanoaoaiaaia) at the villa&• level, an4 thua perait early intervention, ia ready for videapread application.
...
Sheikh Baadan Beu Moh ... .d Al Bahyan, Deputy Priae Miniater of the Uaitecl Arab Eairat••• Abu Dhabi
Among significant acbie• .. •nta at earlier at•&•• of developaent are the follovtna:
0
0
0
0
0
Vaccine• againat aalaria are now a real poaaibility follovin& the identificatioa and production of the aubatance• in the paraaite responsible for 11811'• illlllune reaction• •&•inst th•••
A totally new family of coapoU!lda for the treataent of aalaria. baaed on a traditional Chin••• raedy called Qinghaoau, ha• been ayntheaised and teatin& baa beaun.
Drugs for the treataent of river blindne••• critical for the control of this diaeaae, are bein& ayntheaised and teated.
Natural biological agenta are being teated in the field, auch as Bacillua aphaericua, which will destroy the la~•• of diae.aetranaaitting insects and recycle theaaelvea and in thia way prolong their effectiveneaa.
Simple and effective diagnostic teat• - vital to all diseaae control progra ... • - are being developed for Chagas' diaeaae, schistoaomiasis, malaria and leprosy.
Scientiata and institutions in over 120 countriea participate in TDI and provide the vision, knowledge and facilities required for the work. So far, their progreaa baa been outstanding, while the Programme'• catalytic effect• have kept coata low. In short, we believe TDR. to be one of the moat coat-effective inveataenta in health and development and one which merits your support. However, bringing a new drug or vaccine froa the laboratory to the needy family in the village takea many yeara of work, and for thil TDR. requi,rea both adequate and suatained financial suppo~t.
TDR depend• entirely upc,u voluntary contributions. Froa 1975 until 31 Auguat 1984, 27 government• an4 11 other organizations, together with the three co-aponaorina agencie•• have contributed over ust 155 aillion to the Programme (aee attached table). However, available fund• have fallen abort of the ainiaua required (about USS 33 million per year) to keep the Programae moving ahead. Unlesa contribution• are increased and sustained, TDR. will have to abandon many promising initiatives toward• new and effective tools to control the diaeaaea. Malaria, sleeping aickneaa, river blindneaa and leproay will continue to spread and thwart any hope of self reliance for the people living in the tropic&.
We are convinced that the partnership of J10deru acience and the Special Programae can 10 far to break the cycle of disea1e and poverty. Scientist• froa both the public and private aectora are already doing their part and it ia now up to governaenta and agencie1 to provide TDa with the funda necessary to coaplete the work.
3
-Slaet ................... Al ... ,. ••
Da,-tJ Prtae IUaiaur of u. Vatt..t Ba• lllirat.u, -""• Dhal,1
We etaeeTel7 ••,. tlaat , .. will at•• ••rioua coaatd•ratiea te our r.,.••• for tu ftaaact•l part1c1peti• •f your C.O.enant ta the Sfffial Prop .... aacl loolt fonra'l'4 to b•riq frc,a :,oa at :,oar •rlteat cOlffateaee. W. allolwl N aratefd it yeo wo.t.4 aa4 ,ov reply to Dr Balfcln X.lllff, D1reetor-Geaera1 ol tile Vorl4 Bulth OrgaahaUoa.
lraiford !loT•• Adataiatrator, U.f.te4 hU•• Dnelo,...c Proaraae
Sluerel:,,
A. w. Claaea Prff14nt, ?ha Worlcl Baek
(Sgd .) H. \\J1h!cr
a. Mahler, M.D. Director-C..eral, World Bealtla Orantaatin
4
, .
The World Health Organization 1211 Geneva 27
Mr Muhaaed Az-Zaruq Rajab Secretary-General of the General
Secretariat of the General People'• Conare•• of the Socialist People'• Libyan Arab Jaaahiriya
Switzerland
•••
...
Tripoli Libyan Arab Jamahiriya
December 12, 1984
Dear Mr Secretary-General,
We take the liberty of aoliciting your support for a unique venture in international collaboration. Thia venture in reaearch and developaent 1• an investment in the future of mankind and will require year• of work and sustained financial support. However, we are convinced that the reault1 will have a profound impact on the health and well-being of hU11&nity.
The Special Programme for Reaearch and Training in Tropical Disease• (TDR) - co-sponsored by the United Nations Development Programme, the World Bank and the World Health Organization - aeeka to develop the aeans to control aix major tropical di•••••• which today afflict or threaten over one thousand million people living in developing countries. We attach for your information a booklet deacribing in more detail the work and achievement• of the Special PrograJJlle.
In spite of tbe explosive growth of knowledge in the bioloaical sciences over the pa1t 30 yeara, little progreaa ha• been aade tovarda the control of these dbeaaes. In fact the menace 1s increasing.
Millions of children die from aalaria before reaching their fifth birthday•, and million• of thoae who reach adulthood are incapacitated by one or more tropical infections. They are sentenced to apend their live• on the treadmill of illneaa and poverty with. no hope of iaproving the lot of their f .. iliea or their coaaunitiea.
cc: The Secretary of the Gener~l People's Comaittee for Health, Tripoli Hie Excellency ICae .. M. Sb~rlala, Secretary of the People's General
Committee for Treaaury, Tripoli The Director of the United Nation• and Internati~nal Organizations
Affair•, Secretariat of the General People'• Co11111ittee for Foreign Affair,, Tripoli
Permanent Miaaion of the Socialiat People's Libyan Arab Jaaahiriya to the United Nation• Office at Geneva and the International Organizations in SWitzerland
ENCLS: Aa stated
bee: UNDP (2) World Bank EMRO (2) Att: TDR EMS/HQ NW'R&PC, Libyan Arab Jamahiriya
Ill' MvUNCI M-ZanMI lajalt. S.Cntary-Gaeral 2 ot the Geaual Secretariat ef tbe Getaeral People'·• C.IIITff• of tile Soct.aliat P•o,1•'• Libya ua~ Jaau.irt,a. Tripoli
The devaat.atill& blow, to tbe iacli-widul ••• tu fntl7, of aa acate attack of aalaria at harnat ti• or of peraunt lou of aia)tt by ti..••• of 2.5 froa ri-.er bllacla••• (oachocerct:uta) ta eaaJ to uierataa4. aow..er, th• aoctal aad ecoaoeic tapacta apea a c.o111n111itJ ••• a co .. try wbe1l trepieal diauHa atrtke down llndreda of thoaaaa4a of people, 10 far b•yOIMI tile individual or ar••• atatiattca. Ia faet, epi4 .. tca of aalarta, •l••tiaa atckn••• and river bliaclae•• oft .. drift aelf-e•fficiat caaiatu .. tau state• of dependeat poYerty.
tbe deatnacti'Ye •yabioaia of dieeaH au po-.erty net, au caa k replaced by the ayaergiaa of bealtb aa4 prodaetiYity. To brl•& thia alNMlt, the tropical couacrle• reqvire bot• tM tool• tor prneati• au treataeat of the tropical 4iaea••• aa4 tbe aciattftc aM taclnaical capabillti•• te &Hare their effective appliuttoe. The•• are tlte pala of Tl>I.
O•er the paat aiz , .. ra, Tim. haa cllalleaa .. aa4 atbntlat.l r .... rdaera at 1D.9titutiona tbrougbo•t tlle wort• to worl toa•t••r , ...... t ........ . Tbo .. anda of acieatiate ia uaiYeratti••• r•••arc~ t .. ttt•ti ... , 10Teraaeat •1n1atr1•• and tnduatry have reapoa~ aa4 -are aOlf worltaa •• INIIIMtra •I TDR teaaa - in fuadaaeatal reaearcb lal>oratoriea, la !aoapital cltatca ... _ in •1llage health centre• - to 1'uU4 tbe new tool• ••• p.repare tllea fw ue in the •illaa .. of the tropic•. TDI. Ila• cata1, .. , t'- lteltaa el r...arek act1-.1U•• into n e.ffectha werldwi .. utworlt od ha• foe .... tbe -.. thoda and. knowledge of the l>ioloatcal adaacH apoa tlMI ttoptcal •t•••-·
Tbe reeulta ha•• 'beea reaartahl• aa4 r .. earch carrte4 .. c '9c• v1t~a and outaide the Special Proar .... baa bro•aht altollt ataatficaa& pr•ar .... S~• new toola for dbeue coatnl ha•• alreactJ r•chff the ataae of act .. 1 appUcattoa 111 the field, vhUa otllera are cloae &;o 1t. baaplea of Mjer deYelopeenta toward• the control of the cl.ta-ea••• tacladez
o A biolog.iul •a•t• lac:illu tberiyieuta B-14, to coatrel the fliea that •F••• rt••• l,lbdaaa ta beiaa ue4 ext ... 1-.el7 ta Weat Africa n4 1• betaa t .. te4 aaaiut •larta-arrytaa 1a0aquttoa.
o Ann d"-, ••floq111••• fot tlle trut ... t of ularta ialeecta. -reaiatant to ataaiar• turapy baa"" regiatere4 fer ....
o Yacciaea which uy t~eat alMl ,r••••t lepr••J are ta tM eerly •t•a•• of te•till& ta .... BoweTer 1 the teat• will take ft~ t• eight year• to c:oaplete becaue of· tl&e alow u.taral la.tator,, el the c1, .......
o Staple ktta to 1MUUe tba aeuttt•ttJ of •lai:la ,.rant .. t• · dr111• ta •••11n the conaet choice of trutaeat ue 1Mt1aa..., widely.
o A aiapl• teat to dtaaaoa• .1 .. ,1., eicka ... (Af'lteaa tr:,paa .... taeie) at t11e nllqe lnel, ad t .ltu. pel'll1t earl)' 111terveat101t. la re.M17 for .u .. ,r._ applicati•.
. -,
•••
Mr lhsheaed Aa-Z•Aill a..jaa., Secretarr'e'DaTal of tile Gneral S.Uetarlat of tile Caeral Peopl•'• Coaar• .. of tile Soclaluc Pffple'• Libyaa Ara, JaaahtrS1•, Tripelt
aoa.1 •ip1f1cut ac:hieY .... ts at earlier •t•a•• of dnelopaent are the follon .. ,
0
0
0
0
0
facciau aaaiJl•t aalad.a are nov a rul poaaUillty folloiiriq tile Ueattfic.atloa aa4 pro4actioa of the •ubetaac:H ta the paraeite reapon•iltle for 118a'1 imue reac:tiona agaiaat tha.
A totally a .. faailJ of coapound1 for the treataent of aalaria, baaed on a traditional Cbiae,e reaedy c.alled Q1aghaoau, ha• beea ayatheais~ and teatina baa begua.
Druga for the treableot of rher blindaeH, critical for the control of thi• diaeue, are beiq •111theaiaed and telte4.
Natural biological aaenta are ~ing teated in the field 1 such•• Bacillu aphaericu,, which will de•troy the lar'fae of cliaea•etranaaitting inaecta and recycle thea•el•e• and in thi• way proloq their effecUYeaa••••
Si•ple aad effecti'fe d.iapoatic teata - 'fital to all diaean control progra-N - are being de'feloped for Chas••' dh••••, echieto•oai&ai•, llalaria and lapro•y.
Sciea.tiet• aDAl inatitutioa• iu o••r 120 co1111tri .. participate 1n TDI and pro•ide the viaioa, knowledge and facilitiea required for the work. So far, their progreaa baa beea outetaading, while the Proar .... •a catalytic effecta ba'fe kept co•ta l01r. ID abort, we beline TJ>Jt to be one of the mo•t c09t-effect1ve iDTeet ... ta 1• health and dnelopaeot and one vbich aeriu your support. ao .. ver, brin&in& a new drug or vaccine froa tbe laboratory to the needy faaily ia tbe Tillage c.tea aany yeara of work, aad for thia TDK require• both adeq ... te and auatained financial aupport.
TDa depe•d• .. tirely upoa 'foluatary coatributiOGa. FrOII 1975 uatil 31 Aua-at 1984, 27 ,~ernaeaata and 11 other organization•, together vitb the three co-apouoriq aaeaci .. , ba-..e contri'butecl o'fer usj 1SS a1111oa to the l'rogr•- (•ee attached tal)le). Bowner, &'failable fUDda h••• fall- abort of tu ailli- r941uire4 (about vst 33 aillioa per year} to keep tbe Progra .. • aoYiD& ahead. Uale•• contribution• are tncreaaed and autaia.ecl, TDa vtll ha.a to aNIMloe IMlllJ proaiaia1 initiati••• towu4a aew and effecthe toou to COlltrol the diaea•••• Mauria 1 deeptna licknen, ri'fer bl1114•••• and leproa1 rill coatiDM to •~ea~ a11d thwart &DJ hope of aelf reliance for the people li'filll ia the trop1ee.
We are conY1aee4 that tbe parturelup of IIOdera ednce an4 the Special Proara ... can 10 far to break the cycle of diaeaae aad po.,erty. Scientiata froa both tbe peblic aad priYate ••ctora are already doiaa their part and it ta now up to go'fernMDta and •&end.ea to pro•ide TDR. witb the funda aeceaury to coaplete the wort •.
3
' .
Mr Kvbaaed A&-Zar1M( Rajab, Secretary-General of the General Secretariat of tbe General People'• Coqreaa of tbe Socialiat People'• Libya• Ara~ Jaaahiriya, Tripoli
We aincerely hope that you will give 1erioua conaideratioa to our requeat for the financial participation of your Gevernaeat in the Special Proar .... and look forward to heariug froa you at your earlieat couvaaince. We ahould be arateful 1f 70u would aend your reply to Dr Balfdan Mahler, Director-General of the World Health Organization.
__ Bradford Mone Adainiatra-tor ~ . United Jlationa Develop11ent Proara-•
Sincerely,
(Signed) A. W. Clausen A. w. Clauaen Preeident, The World Bank
tS\:lu .J H. 1v1al1leli
H. Mahler, K.D. Director-General. World Health Oraanization
4

•,
The World Health Oraanisatiou 1211 Genna 27
Mr Mu.hamluld Ho•ni Mubarak Preaident of the Arab Republic of Egypt Cairo Switzerland
•••
•••
Egypt
December 12, 1984
Dear Mr Pre•ident,
We take the liberty of soliciting your support for a unique venture in international collaboration. This venture in research and development 1• ·an inveataent in the future of mankind and will require yeara of work and euatainecl financial support. However, we are convinced that the reaulta will have a profound impact on the health and well-being of ht111anity.
The Special Progruaa for R.e•earch and Training in Tropical Diau••• (TDI) - co-•ponaored by the United Nation• Development Progra ... , the World Bank an, the World Health Organisation - ••eta to develop the aeaaa to control six major tropical diseaeea which today afflict or threaten over one thoueand milli011 people living in developing countrie•. We attach for your information a booklet describing in more detail the work and achieveaenta of the Special Progr .....
In apite of the explosive growth of knowledge in the bioloaical acienc .. over the paat 30 years, little prosr••• bas been made toward• the control of these diseaaes. In fact the menace is increasing.
Million• of children die from malaria before reaching their fifth birthdays, and millions of those who reach adulthood are incapacitated by one or more tropical infection•• Thay are sentenced to ape.nd their liv .. on the treadaill of illne•• and poverty with no hope of improving the lot of their faaili•• or their c01111U11iti•••
ccs The Mini•ter of Health, Ministry of Health, Cairo The Minister of Foreign Affair•• Ministry of Foreign Affair•• Cairo Hie Excellency Dr Moustafa Kamel El Said, Minister of Econ011y and
Foreign Trad•• Cairo Permanent Mission of the Arab Republic of Egypt to the United Nation•
Office and Specialized Agenciea at Geneva
ENCLS: A. stated
bee: Dr Aleya Ayoub, Under Secretary of State, Endemic Disease Control, Ministry of Health, Cairo
Dr Mohamed Saif, Director-General, Tropical Medicine institute, Cairo UNDP (2) World Bank EMRO (2) Att: TDR EMS/HQ WHO Liaison Of-ficer in Cairo
Ml' ~batmaci Be•n1 Mab.-1'.aka h"Ueot oft.he Arab lepubllc •f '117pt, tauo
2
Tb•· dnutatiq ltlow. to tliie 11141Y14Nl eDd tb faJly. of an acute attack of ular1• u banut u- or of ,.runet loa• of •1gbt by the •&• of 2S troa ri,,•r bllaa• .. (oach.N«c:iaaJ.•) te eu7 to u.lereuact. HOVft11r • tb• aeeial a ee•Ollic ta,-.u .,.. • c aaauaity aa4 • c••t-rJ ,._ tropical d1aeon ui:fb down lwedreda of thouaDda of peopl•• 10 ta~ herccd tbe ind.hJ.4ual or aroa• atatbtlce.. la fact. eptd•1ca of ularia, deepta1 •iellDBa au rt-.er blind'll .. • oftea drtwe ••lf-eoffictiellt coaauiU•• .lato atat .. of deJM111.ct.at po'ferc,.
Tb• de1truct1"T• 1y11bio•f• of dhe••• nd poverty auet. aad caa be rept.cei by tbe a,nergin of health aad pro4uctiY1ty. To .. &-"lq tlaia •N11t• the tropical c:011atr 1•• r-.ure ktb ue to.1• for prttati04I and treatuat of the tropical dta••••• and the aciec~tfic aD4 tee.b.ntc.al ca,a\111~1•• to •••ur• their eftectiY• application. Thea• are t~ goal• of TDl.
Oftr the pa•t ab y.ra, TDI. bN cballenaed and •tialatad ruur.clwn:e at 1Dst1tat1on• t hroughout. the -.orld to work toae&ber toward th••• •nd•• Tb04aand• of scienttau ill uei•ar-alUee, r .. urch Wtitutiou, go••r--t miniatTte• and :indoatry have reapondecf and are ao:w 1fClrkf•a u -~•r• of ma tua - in f'ftdmatal r .. eue!l lakl'atort••, h hoapital clinic• ud in •illaa• health caatrea - to build the IMlV tool• and prei-r• thea tor us. in tile ~tll•g~ of the tropice. T1JI ha• catalyaed the link.ina of researcb act1•1t1•• into an effectiYe wcrldvide network and b•• focaae4 the a•• 111etboda an.t bewledge of tha biolosical adncu vpoo the tropical 41auae••
'the reeulu have b•en ruerkable aad reae&rcb carriecl ou.t both vitiate and outeide the Special Progra ... ha• brou&bt alK>ut aigniftcant proaru•• S01N oe• tool• for diae••• contrel ba¥e already reached CM ataga of aet11&1 appUcaUoo 1A the field. while otbr• are cl-. to it. luapl•• of ujor developenta tovarda the cootrol of the dteea••• hlclude:
o A btoloaieal aaaa.t, &ae1llua thuriag1e11eia K•l4. to control the fl1•• tha~ •pread ri••r bli.Ddn••• 1• b•taa ua-4 ext•••i•el.r to West Alrlca aa4 la betn.a teeted a1ainet ealarla-canyin& 1a0e1•1tos •
o A new droa • .-efloq1itoe, for the traata.st of aalaria ta.fecttcme ~ffi•taAt t.o etaadard therapy ha• ben registerecl fo~ u•~
o Vaccine• vhtctl may treat and preYetlt lop~o.-y are Jn the early stage• ot teatiQg 1a aaa. novever, the te•t• will take fi.,. to e1 ht :,aare to coaplete becou•• of the elow utur-al bi•to1')' of tti. dtauae..
o Staple kita to •~•ure th• aer:e.iUTitJ' of' :elaria paraaitff to drug• to aaeue the correct choice of treatuat are be1111, .... Widely.
o A staple teat to d1atnc.c a1ea,1n1 a1okn••• (Afr!caa tT,.,.... .. tui•) at tu •tlla&• 1 ... e1. all4 thu pendt ..... 1, utervaattoo, 1• rqcfy tor viie•pr••• •nliut1oa.
•••
Mr~ Road MtaN••lt• Prut41etac of the Arab lepw'blic of Jupt, C.airo
Jeoaa ataatftcaat &dlle"#...at• at ••rl1er •t•a•• of de•elopaeat are the following:
o Vace.ie• again.at aaluu ue now a r u l P'l••ibUtty followtna the ldeatifiutioa ~114 pi-oduct1oo of t h. suba~auc .. in the paraa1tf! rupouibl• for ua'• 1111n11• reac.Uoa• apiaat tb••
o A tot.ally n• faatly of coopow-da for t he treatlll«Dt of salarta. b..aae4 on a traditional Cb-1ncae r -*dJ c.a lled ( io.ghaoau, baa bcea syatbe•is d and testing haa bat on.
o Drugs for the treatment of rivu blindnus , critical £or the cCtttrol of tbia dia .... , are beiaa ayathea1sad aa4 teated.
ktual b1olcg1ul agenta are bd.na te.atecl 1• the field, such •• !aeJ.11 .. eph.eericaa, lfhieh •ill destroy tb• lai,,ae of dtJ....trauaittiag inaacta au re~ycle tb•u•h•• and 1a th1a .,.,. p:rolona tNil' effecti••a•.
o S111ple aad efhcttff di•gao•tic teat• - wital to All diseaae coatrol proar01N.e - are be1n& d.n.t•ped tor Oaaiaa• dtuaae, s chiatoaoaJ.a.le, ••larla and l eprceJ.
Scleattau &ad iuUtnUou 1a nu 120 countr1•• p&rtidpate ta tl).I aad pl'OYide tbe Yhion, k~owled,. aad faciliti•• reqtalract for tbe work. SO tai-. their proar .. • "-* beea. 01ltataad1ng, while the rroar-... • • utalyttc effect• have k..ept eoeta low. la ehort, •• believe TDl to be one of the llMt coat-effecU.Ye 1.DYutaeau ta he-alth au dewelopaeat au one which aertu 7our au:ppor t. Roft'1er • br1agiiaa • new drua. or v-acd.ne froa the labor4tory to the aeedy f•U1 ia the. village take• mauy yffra of work. alMII f or thia ! DA require• bGtb ade41\l&te .nt4 austained f inancial aupport.
TDI deP41a:ta eoU.rely ~poa Tel-tary coattihutioua. Proa l97S uattl 31 Avgut 1984, 21 ao,wenlllnta net ll other organJzatiou, tog•tb.e'r • 1th the thr• co-apoaaoriaa a1nc1 .. , haft coatriktad ever us.t l.U a1llioa to tbe hogra ... (aee auac:b-4 table). Hove•er, available fu.Dda hn• falln abort of the a.lat- r-.utre.t Callout ust 33 aillioa ,-r yur-) to keep the Prcar ....... 1n• ahead. Uale&e coatT1but1oua are iccr .. lMMI aiul auata.lud• 'm& will ha•• c. aha4oa ua7 proaiaillc iaitJati•• towara uw and effe.ettwe tools to coauol th• diaN•••• tf".alarh, slffping •ic:ltneu • Tiffr blillflneu &1lCI leproey will coaU•- te aprea.d au thwart · aa, hope of aelf reliance for the people 11YiAI 1u the tropiea.
V. ar• coPtacff tllat tt:.e partaffSblp of aodena acteec• a1t.S tu Special hoar.... caa ao tar to hr••k. th• cycle of d1aoa•• na ~•ei-ty. Sdentt.ta frea hotb th« p)llc utl prhate Net«• are alru4J 4.oiq tllei...,.art u4 J t 1• uw vp to &ffHaMaU anfl aanct.a• to provld• Tl)I. witb. tb• f-aada aeceaaar7 to coaplet• tb• woc-lt.
EgypU•a Sutitvtioaa ad acie11Uat. are ~ruc.t,-uoa 1a th• work of tt>I. tbcy Ila.-. curted n~ 12 r .. .urcb an4 dnelopant p.t'ojftt• an ti..
3
ii . . . -
~ ttu--4 8"a1 Mubarak, Pree14nt of the Arab lepbltc of S,,,c, Caire
S~id hoar--. ue ••pportecl tbr•• traia1na. projecta io E.ay-pt at • total C!Nt of usj 341 000 to the PrOP" ..... £&)'pt hu alao taua a actiYe part 1D cha 11&Da£e98Ut ot ~he Special ~oar .... •• a me-aber of it• Joint c~~41utina Boar• in 1978 aucl 1979. od au.'b••flueatly aa aa off1cial obaerNr te the hard. lie aTe Ye.ry 1rateful to ,our Co.uu..nt, it• 1net1tut1ona en4 aciutbta for tbe1r 1aportaat participatioa. BOW'Yer 1 1a viev of the taaka to l:Hl ac.cccplubc& and the opportuoiti.es befor~ ua 1 ••
are aak1JI& 1oa to •upport TDI. finucially ••well•• tecl\nicallT ••4 h thi• "•Y to work ,r1 th ua at all level• o-f the rroar•- te traaafona cite opport .. ttlea of today iato tll.e aev drea• aod vaccine• of toaorrew.
We eincerely b$pe, that you will gi•• aeriou couatderation. to ou reqaut for the financial particfpat1oa of yoar eo.erDMat ill. tb• Special Prograaae and look forward to hear!n1 fro-. yoa at your earlieat cooveateDce. We abould be grateful if you vo~ld aend yo.r reply to Dr B•lfdaa Mahle1' 1 Oir•ctor-GeneTal of the ~orld Be•lth Oraaaiaatioa.
S1ue:erely,
(Signed) A. W. Clausen (Sgd.) H. Mahler
4
Bra1lfoTd Morse Adst:iniltra tol.', Uaite4 NaUcaa t!H•elopzent Prcgrai.c.e
A. \1 . Clausen f reaidnt1
The llorld tank
ll. Mahler. K.D. D1rector-<;eaeral. Worl4 Hultll Cr.aa.batioa
The World Health Oraaniaation 1211 Geneva 27
Mr K. u. Chernenko Chairman of the Pre•idium of the
Supreme Soviet of the Union of Soviet Sociali•t Republics
Moacov
Switzerland
•••
•••
Union of Soviet Socialist Republics
December 12, 1984
Dear Mr Chairman,
We take the liberty of 1oliciting your support for a unique venture in international collaboration. lbie venture in reeearch and development i1 an inveet~ent in the future of mankind and will require year• of work and sustained financial 1upport. However, we are convinced that the result• will have a profound impact on the health and well-being of humanity.
The Special Progra~.me for Research and Training in Tropical Diaeaaea (TDR) - co-sponsored by the United Nations Develoyment Prograllllle, the World Bank and the World Health Organization - - seeka to develop the means to control six major tropical diseaees which today afflict or threaten over one thousand million people living in developing countries. We attach for your information a booklet describing in more detail the work and achievementa of the Special Programme.
In spite of the explosive growth of knowledge in the bioloiical sciences over the past 30 years, little progreas haa been made toward• the control of these diseases. In fact the menace is increasing.
Millions of children die from malaria before reaching their fifth birthday, and millions of those who reach adulthood are incapacitated by one or more tropical infections. They are sentenced to spend their lives on the treadmill of illness and poverty with no hope of improving t he lot of their families or their conaunitiea.
cc: The Minister of Health of the Union of Soviet Socialist Republics. Moacow
The Permanent Representative of the Onion of Soviet Socialist Republics to the United Nations Office and other International Organization• at Geneva
ENCLS: Aa 1tated
bee: Profeaaor F. F. Soprunov, Director. Martsinoveky Inetitute of Medical Parasitology and Tropical Medicine, Moecow
Dr Lev s. Iarotski, Deputy Director, Martainovaky In1titute of Medical Paraaitoloay and Tropical Medicine, Moecow
UNDP World Bank !UI.O (2) Att: Dr B. Nisetic, RPD
Mr I. u. Chernenko, Chaina11 of tb• Preaidiua of the Supr ... Soviet of the Union of Soviet Socialiat lepublic•, Moacow
2
'lbe devaetatina blow, to the individual and the family, of an acute attack of malaria at ba~••t ti .. or of peraanent 101• of eight by the age of 25 froa river blindneaa (onchocerciaaia) ia eaey to understand. However, the 1ocial and econoaic impact, upon a c01111unity and a country when tropical disea••• 1trike down hundred, of thoueand1 of people, go far beyond the individual or gro11 atatiatic1. In fact, eptd .. ic1 of aalaria, 1leepina sickne•• and river blindne1a often drive eelf-aufficient c0111Runitiea into state• of dependent poverty.
The deatructive aymbio•i• of diaeaae and poverty muat, and can be replaced by the 1ynergi1a of health and productivity. To bring thi1 about, the tropical countrie1 require both the tool1 for prevention and treatment of the tropical di•••••• and the acientific and technical capabilitiea to assure their effective application. These are the goal• of TDR.
Over the paat aeven years, TDR ha, challenged and etiaulated researcher• at inatitutiona throughout the world to work together toward the•• enda. Thouaand• of scientist• in univeraitiea. research inatitution•• government ainiatriea and induatry have responded and are nov working as member• of TDR tea .. - in funda .. ntal reaearch laboratorie•, in hoapital clinics and in village health centre• - to build the new tool• and prepare thea for uae in the village• of the tropic•. TDR has catalysed the linking of research activitiee into an effective worldwide network and ha• focused the new method, and knowledge of the biological 1cience1 upon the tropical diaeasea.
The results have been remarkable and reeearch carried out both within and out1ide the Special Progra111me ha• brought about significant progre••· Some new tools for di••••• control have already reached the stage of actual application in the field. while other, are cloee to it. Example• of major development• toward• the control of the dieeaaea include:
o A bioloaical agent. Bacillua thurinaienaie H-14, to control the fliea that apread river blindneaa ia beina used extenaively in Weat Africa and ia beiua teated againat malaria-carryin& moaquitoe.
o A new drua, mefloquine, tor the treatment of malaria infection• reaiatant to standard therapy haa been registered for use.
o Vaccine• which may treat and prevent leproey are in the early stage• of teetina in man. However, the teats will take five to eight yeara to complete becauee of the slow natural history of the diaea1e.
o Simple kit• to mea1ure the senaitivity of malaria parasite• to drug, to aaaure the correct choice of treatment are being uaed widely.
o A simple teat to diagnoae sleeping sickne•• (African trypano1oaiaeia) at the village level. and thua perait early intervention, ia ready for widespread application.
•••
Mr X. t.T. Chernenko, Chairman of the Preaidiua of the Supreae Soviet of the Union of Soviet Socialiat Republic•, Moacaw
Aaona aignificant achiaveaenta at earlier 1tage1 of developaent are th• followtnas
o Vaccine• againat malaria are now a real poaaibility following the identification and productiou of the aubatancea in the parasite responsible for man'• immune reaction• again1t them.
o A totally new family of compound• for the treataent of malaria, baaed on a traditional Chine1e remedy called Qinghaoau, ha1 been syntheaised and testing baa begun.
o Drugs for the treatment of river blindne1a, critical for the control of this disease, are being ayntbeaised and teated.
o Natural biological agents are being tested in the field, auch aa Bacillus 1phaericu1, which will deatroy the larvae of diaeaaetranamitting insect• and recycle themaelvea and in thia way prolona their effectiveness.
o Simple and effective diagnostic teat• - vital to all diaea•• control programmes - are being developed for Cbaaa•' di•••••, 1chi1tososiasia, malaria and leprosy.
Scientists and inatitutiona in over 120 countries participate in TDa and pr<YYide the vision, knowledge and facilities required for the work. So far, their progress ha• beea outstanding, while the Progra11111e'1 catalytic effect• have kept coats low. In short, we believe TDR to be one of the moat coat-effective inveetmenta in health and development and one which merita your support. However, bringing a new drug or vaccine from the laboratory to the needy family in the village takes many years of work, and for this TDR require• both adequate and sustained financial support.
TDR depends entirely upon voluntary contributions. From 1974 until 31 August 1984, 27 governments and 11 other organization•, together with the three co-sponsoring agencies, have contributed over USS 1.55 million to the Progralllle (see attached table). However, available funds have fallen abort of the ainimua required (about USS 33 million per year) to keep the Prograllllle moving ahead. Unless contribution• are increased and au1taiued, TDR will have to abandon aany promiaing initiative• toward• new and effective tools to control the diaeaaea. Malaria, aleepin& 1ickne1a, river blindneas and leprosy will continue to spread and thwart any hope of 1elf reliance for the people living in the tropics.
We are convinced that the partnerabip of modern acience and the Special Programne can go far to break the cycle of disease and poverty. Scientists from both the public and private 1ectora are already doing their part and it is now up to governments and agencies to provide TDR with the funda neceeaary to complete the work.
Soviet institution• and scientists are participatina in the work of TDI. They ha•• carried out 20 reaearch and developaent project• and oue
a
Mr K. u. Chernenko, Chairman of the Presidium of the Supr ... Soviet of the Union of Soviet Socialiat Republic•, Moscow
training course, at a total cost of over USS 500 000 to the PrograllllD8. The USSR has also taken an active part in the management of the Special Programme as a member of its Joint Coordinating Board from 1978 - 1983 and subsequently as an official observer to the Board. We are very grateful to your Government, its institution• and scientists for their important participation. However, in view of the ta1ks to be accomplished and the opportunities before ua, we are asking you to support TDR finaccially as well ae technically and in this way to work with us at all levels of the Programme to tranefprm the opportunities of today into the new drugs and vaccines of tomorrow.
We sincerely hope that you will give serious consideration to our request for the financial participation of your Government in the Special Programme and look forward to hearing from you at your earliest convenience. We should be grateful if you would send your reply to Dr Halfdan l-lahler, Director-General of the World Health Organization.
Sincerely,
4
Bradford Morse Administrator, United Nations Development Programme
A. W. Clausen President, The World Bank
H. Mahler, M.D. Director-General, World Health Organization
Tpe World Health Organization 1211 Geneva 27 Switzerland
December 12, 1984
Your Royal Highness,
H.R.H. Prince Abdallah Ibo Abdel Aziz First Deputy Prime Minister
of the Kingdom of Saudi Arabia Riyad Saudi Arabia
We take the liberty of soliciting your support for a unique venture in international collaboration. This venture in research and development is an investment in the future of mankind and will require years of work and sustained financial support. However, we are convinced that the results will have a profound impact on the health and well-being of humanity.
The Special Programme for Research and Training in Tropical Diseases (TOR) - co-sponsored by the United Nations D~velopment Programme, the World Bank and the World Health Organization - seeks to develop the means to control six major tropical diseases which today afflict or threaten over one thousand million people living in developing countries. We attach for your information a booklet describing in more detail the work and achievements of the Special Programme.
In spite ·of the explosive growth of knowledge in the biological sciences over the past 30 years, little progress has been made towards the control of these diseases. In fact the menace is increasing.
Millions of children die from malaria before reaching their fifth birthdays, and millions of those who reach adulthood are incapacitated by one or more tropical infections. They are sentenced to spend their lives on the treadmill of illness and poverty with no hope of improving the lot of their families or their communities.
cc: The Minister for Foreign Affairs of Saudi Arabia, Ministry for Foreign Affairs, Riyad
The Minister of Public Health, Ministry of Public Health, Riyad His Excellency Sheikh Mohammed Abalkhail, Minister of Finance and
National Economy, Minister's Office, Riyad Permanent Mission of Saudi Arabia to the United Nations Office and
Specialized Agencies at Geneva
ENCLS: As stated
bee: UNDP (2) World Bank EMRO (2) Att: TDR EMS/HQ WR&PC, Saudi Arabia
B.R.R. Prince Abdalla~ Iba Abdel Aais. Fir•t Deputy Pr1 .. Miat•t•r of the lioadoa of Saudi Arabia. i1yad
2
The de•••tatiag blow. to the 1nd1•1dual aad th• faaily, of an acute attack of malaria at la.ar,eat ti .. or of per11aaent lo•• of eight by the•&• of 2S frott river blindn••• (oachocerciaaia) ta •••Y to uaderataad. Bowe••r• the •oc:lal and ecoaoaic iapacta upoa a coanaity aa4 a couotrJ whea tropical diau••• atrik• d,ovn buud.reda of thouaanda of people, ao far beyoad the indi•td .. 1 or aro•• atatiatica. Ia fact, epi4 .. tca of aalarta, al .. piD& stckne•• aad river blindu••• ofte11 drive aelf-eafficieat cOllllUDitiea into statea of dependent poverty.
The deatructive a)'llbioaia of di••••• and poverty aoat. aad caa be replaced by the aynergiae of health and produeti•ity. To brina thia about, the tropical ccuntrie• require both the tool• for pre•entieu 8114 treataeut of the tropical diaeases aud the 1dentiftc aad tectmic.l up,abilitiea to aHur• their effective application. These are the aoala of T»a.
O.er the past 1b. year,• Tnl ha• challen1ed an4 atiaulatacl reaearchere at in1titution• throughout the vorld to work toa-ther towar4 th .. e end,. Thouean4a of 1cienti1t1 in univeraitte,. reaearch iaatitvtio .. , aa.ernaeat sinietriea and industry have responded and are now vorkiaa •• aee'bera of TDR teaaa - in fundaaental reeearcb laboratoria•, in hoapital cliutca aa4 in villaae health centres - to build the new tool• alMI prepare thea for uae in the village• of the tropic.a. TDI baa catalysed the Ua.ki.ng of rHearch activitiea into an effect!Ye vorldwide network and bu focuaed tile Dff •ethod• and knowledge of the biological ad•nc•• upoa the tropical diauea.
'nle results hav• been remarkable and research carr1e4 out both vttbiD and outeide the Special Progra ... ha• brouaht aboat •lgaificaat proare••• Some new tool• for disease control ha-.e .1lread1 reached the •t•&• of actul application in the field• while others are cloae to it. Example• of aajor developcent• toward• the control of the di•••••• include:
o A biological agent. !a~illua thur1nalen•1- R-14• to control the flie• tbt aprud river blindn••• h being 11•e.d exte.aeively 1a We.et Africa and 18 being teated aaain•t .. urta-carrytq. moaquito•.
o A new drug. sefloqutne. for the treatMnt of ularia infe-cttoaa reaiatant to standard therapy hn bean ragiatared for••••
o Vaccine.a vbich uy treat and s>revnt lepro•J are tn the· early stage• of teating in man. Howe•er. the teat• vill take ft•• to eight yeat"a to coaplete because of the alo• natural history of the diaeaae.
o Simple kits to ••••ure the aen•it1Yity of aalaria para•it•• to druge to a1eure the correct choice of treataeat ar• belaa ••eel wfdel'y.
o A 1iaple teat to dtagnoae eleepiaa •1ckneaa (Afrt~ trypaaoaoaia•ia) at th• -.Ulage l•••·l. a11d thaa penait earl7 inter•eation, ie ready for vide•pread applicatioa ..
-
•••
It.I.I. Priace AW&llah Iba .AWel Aa1a 1 rtrat 1>e,.c, rr1 .. Kia1ater of the lia&dGII of SallCli Ara~ia 1
li:, ..
Aaoaa eipiftcat achin .... u at earlier ataaea of dnelo,...t are tbe followiq:
o Vaccillff apiaat ularia are now a real pouibU.itJ followtna the 1'eatifieati• aa4 proclacti• of tile a.-uae .. la tbe paruit• re•pcmaible for ua'• imnne reactiou qaiaat thn.
o A totally new faailJ of coa,....~• f~ the tr .. t ... t of .. 1ar1a, baaed on a tradiUoul Chia ... r ... dJ callu Qtaallao••• baa b•• aynthut&u au tfftiq bu bepa.
0
0
Drvga for the trutllellt of ri•u blia4a•••, critical for the control of thia .tta ... •, are beiq a:,athffi&N-' teate4.
»atural bioloaical •a••U are beiq teate4 1a tbe f1el4, aucb u !aclllua apbaaricu. wblcb will deatro, the lan .. of c:Ua ... .traa .. itttna iaaecta an4 recycle tbeaa•l• .. and la tbia way proloa., their effectbaua.
Staple au effectin diapoetic tuta - •ital to all dieede coatrol progr .... a - are beiq dnelopecl for Chapa' dlNae, achiatoa.-iaata, malaria aa4 leproay.
Sctntiata and insUtut1ou iD over 120 c•vatri•• partic.ipat• l• TDI and pro•id• the •teion, k.novledae and faeUitiea reqvire4 for the wort. So far, their proar••• h.a been o•t•taaclia,, while tha Procr .... '• catalytic effec:u have kept coats low. Ia abort. ve beline TDl to 'be cme of th• a.oat coat-effecti-.e 1n.•eataeata in bealtll ad dnelo,-.t aN ~ vbicll aertu your au,port. Bove-t•er, brin1tn1 a new clnia or •ac:c1»• fToa the la~oratory to the a .. dy faaily ia the< vill•a• tak .. 11a11y year• of work, and tor this TDI. require• botb ade411a&te aAd auatained f1naac1al aopport.
TDI. depeada eat1rely upo11 TOlUlltary contrihuttoaa. Fl'oa 1975 until 31 Aupet 1984, 27 ao•er .... t• aad 11 othar orsaataattoaa, toaetbeT vtth the tbr .. co-apoueort111 aaeaeiea, have coatribvted over uat 1,, a1111oa to the Proar .... (•H attached table). lowe...r, ava.Ual>l• fn4e 11••• fallea abort of tu. •1•1- req•irN {abolat ost 33 aillioa per year) to keep the Proar .... ~iq a~. tJnl .. • coatrikt1oea are iacrea ... ••• all&taiaed., Tl)I. will have to abudoa uay proaid.q iaitiati. .. tonra Iles a11cl effectiY• tool• to c01ltrol. the die .. •••• Malaria, aleepia& atcb .. •, riffr bltacm.u alNI laproay wUl coattaue to apreu au thwart ••J ho,. of eelf reliance for tbe people 11Yilll ia the troptca.
We are coa•iace4 that the partaer•hip of llNHR acince aacl tile Special Proar .... can 10 far to break tbe cycle of di ... •• ancf ~rty. Scienttata froa both the po~lic aDd pri••t• aectora are already 4oiq their part••• it la now ap to iovernae1lta aao •a .. ci•• to provide !DI with the fanda neceeaar, to coaplete the werk.
Saaclt Araltin edntteta are partidpatiq ia the work of Tia. Ve are very grateful to ,oar Go••r .... t aa4 aci•ttata for tbeir partictpa.tt• au
-n.1..1. Priace AWallaa. I1m AWel !mi.a, rtrat De,-ty
Prf.Jla lliaiater of the liaatl• of s..11 •••ta, 11,-•
•• hope it will iacr ..... Bow•••r, 1• •1 .. of the taella to be accoeplialaecl u4 the o,,.rtuJU•• before ua, ware ukt .. ,- to aep,ort na finaactally •• .. 11 •• tecbatcallJ aa4. 1• tbia waJ to vorll vitb a• at all 1•••18 of the Pr-oar•- to traaafora tbe op,erta1ti•• of tNaJ 1ato the nn dr.p aa4 •acciau of toaorrOW'.
V. ataeerely hope that 10• •1111!•• aerio11a coaaiaeratioa to 011r
r84(nat tor the financial partictpat1oa of JOU' C:O•erta11e11t. in the Special ProST .... and loot forwar4 to bariq fr• yoe at you earli .. t cou•eatence. We should be crateful 1f ,oa vovlcl and you reply to Dr Ralf.ta Mahler, l>irector-Gellual of tk w.ru Bealtll Oraaaiaact ...
S1acerely,
(Signed) A. W. Cl"usen ( ...., .. , ,,..J ) !,J :\"Ir-,·.. ._ \ --- . ~ . ' ~ ~ -· . . ~ .
4
Bradford MorH AdaiDiatrator, U.itN BaUou Deyelopaot Progr ....
A. W. Cla••• Pr••t••at, The World Bast
B.. llal:ller, M.D. Director-e:..aral, Worlcl Bealtb Or .. nt&atioa
-
Tbe World Health Organisation 1211 Geneva 21
Mr L1 Xianniaa Preaident of the People'• Republic
of China SVitzerland
•••
•••
Beijin' People I Republic of China
December 12, 1984
Dear Mr Preaideat,
We take the liberty of aolicitin& your support for a unique venture in international collaboration. Thi• venture in research and development ia an inveatment in the future of mankind and vill require year• of work and sustained financial aupport. However, we are convinced that the re1ult1 will have a profouftd impact on the health and well-being of humanity.
The Special Pl:ogratae for Reaearcb and Tra1n1na in Tropical D1seaae• (TDR) - co-sponaored by the United Nation• Developaent Prograstme, the World Bank and the World Health 01::ganization - seek• to develop the aeana to control six major tropical diaeaaea which today afflict or threaten over one thouaand million people living in developina countries. We attach for your information a booklet deacribing in more detail the work and achievement• of the Special Programme.
In spite of the explosive growth of knowledge in the bioloaical aciencea over the pa1t 30 year•, little proar••• haa been ude toward• the control of these di••••••• In fact the menace ia increaaina.
Million• of children die. from malaria before reachina their fifth birthday, and millions of tho•• who reach adulthood are incapacitated by one or more tropical infectioaa. They are sentenced to spud their live• on the treadaill of illneaa aud poverty with no hope of improving the lot of their families or their coaaunitiee.
cc& The Minieter of Public Health of the People'• Republic of China, Minbtry of Public Health, Beijing
Bia Excellency Waaa Bina,1an. State Counaellor and Minister of Finance, Beijing
The Permanent RaprHenUtive of the People.' a Republic of China· to the United NaUou Office at Geneva and other International Oraaniaat1oaa in Svtuerland
The Miniatry of roreiau Econoaic Relation• and Trade Departaeat of Relation.a with International Organizatioaa. ~iJina
EJCLS: Aa stated
bccl tJNDf (2) World Bank WlltO (2) Att: COi. and Dr A. Sbirait TDI. Wa&Pc. People'• Republic of China mw
ii
Mr Li liannian, Preaide11t of the People'• hpublic of Chiu, Beijiq
2
The devaatat1na blow, to the individual alld th• family, of an acute attack ot aalaria at harvHt u .. or of peraaae11t lo•• of dght by the •a• of 25 froa river blindne•• (onchocerciaaia) ia eaay to under1tand. However, the social and economic impact• upon a COllllUDity and• count~y vbea tropical di•••••• strike down hundred• of thouaande of people, go far l>eyend the individual or gro•• etatiatica. Ia fact, epld .. ica of aalaria, aleepina aickn••• and river blindne•• often drive aelf-aufficien.t coaamaiti .. inte state• of dependent poverty.
The deatructive symbiosis of dilease and poverty 11u1t, and can be replaced by the &ynergism of health and productivity. To brina thi• about, the tropical countries require both the tools for preventiOD and treatment of the tropical diseases and the ecientific and technical capabiliti .. to assure their effective application. Theae are the goal• of TDl.
Over the past ,even ye~r,, TDR ha• challenged and •tiaulated researchers at institutions throughout the world to work tocether toward these end1. Thousands of scientists in universities. reaearch institutions, government miniatries and induatry have responded and are nov working aa members of !DR teams - in fuudamental raaearch laboratorie•, in hospital clinics and in village ·health centres - to build tbe nev tools and prepare them for uae in the village, of the tropics. TDR baa catalysed the linking of research activities into an effective worldwide network and baa focueed the new methods and knowledge of the bioloatcal ttdenc:ea upon the tropical di1easea.
The results have been renarka.ble and ro1earch carried out both within and outside the Special Programs• has brought about 1iauificaut progreaa. Some new tools for diaease control have already reached the 1taae of actual applicatiOD in the field, while others are cloae to it. !:umplea of major developments towards the control of the diaeaees include:
o A biological agent, Bacillus thurinsienah 11-14, to control the fliea that spread river blindness is being used extonsively in \Jest Africa and ia being teated againat malaria-carrying moaquitoe.
o A new drug, mefloquine, for the treataent of malari~ infection• resistant to standard therapy baa been registered for uae.
o Vaccines which may treat and prevent leproay are in the early staae• of teatina in man. However, the teata will take five to eight years to complete becauae of the llow natural biltory of the disease.
o Simple kite to measure the sensitivity of malaria parHitea to drugs to a1aure the correct choice of treataent are beins ueed widely.
o A simple teat to diagnose aleepina sickaeae {African trypano1oaiada) at the vill•a• level, and thua permit early intervention, ia ready for widetpread application.
Aaena sianificant achieveaent• at earlier ataae• of developaeat are the followiD31
•••
Mr Li Xiannian, President of the People's Republic of China, Beijing
0
0
0
0
0
Vaccines against malaria are now a real possibility following the identification and production of the substances in the parasite responsible for man's immune reactions against them.
A totally new family of compounds for the treatment of malaria, based on a traditional Chineae remedy called Qinghaosu, baa been synthesized and testing baa begun. We are very grateful for your collaboration in this endeavour.
Drugs for the treatment of river blindness, critical for the control of this disease, are being synthesized and tested.
Natural biological agents are being teated in the field, such as Bacillus sphaericus, which will destroy the larvae of diseasetransmitting insects and recycle themaelvea and in this way prolong their effectiveness.
Simple and effective diagnostic tests - vital to all disease control programmes - are being developed for Chagas' disease, schistosomiasis, malaria and leprosy.
Scientists and institutions in over 120 countries participate in TDR and provide the vision, knowledge and facilities required for the work. So far, their progress has been outstanding, while the Programme's catalytic effects have kept costs low. In short, we believe TDR to be one of the most cost-effective investments in health and development and one which merits your support. However, bringing a new drug or vaccine from the laboratory to the needy family in the village takes many years of work, and for this TDR requires both adequate and sustained financial support.
TDR depends entirely upon voluntary contributions. From 1974 until 31 August 1984, 27 governments and 11 other organizations, together with the three co-sponsoring agencies, have contributed over US$ 155 million to the Programme (see attached table). However, available funds have fallen short of the minimum required (about US$ 33 million per year) to keep the Programme moving ahead. Unless contributions are increased and sustained, TDR will have to abandon many promising initiatives towards new and effective tools to control the diseases. Malaria, sleeping sickness, river blindness and leprosy will continue to spread and thwart any hope of self reliance for the people living in the tropics.
We are convinced that the partnership of modern science and the Special Programme can go far to break the cycle of disease and poverty. Scientists from both the public and private sectors are already doing their part and it is now up to governments and agencies to provide TDR with the funds necessary to complete the work.
Chinese institutions and scientists are participating in the work of TDR. They have carried out 25 research and development projects and the Special Programme has supported 26 training and institution strengthening projects in China at a total cost of US$ 1 517 000 to the Programme. The People's Republic of China has al10 taken an active part in the management of the Special Programme as a member of its Joint Coordinating Board from 1981 - 1983. We are very grateful to the Chinese institutions and scientists for their important participation, and to the Government of the
3
Mr Li Xiannian, Preeident of the People'• Republic of ~tu, hijing
People'• a.public ot China for ita financial contribution• to TDR which aaount to ust 150 000 up to 31 Augut 1984. However, in view of the taeb to be accospli•hed and the opporttrnitiea before ua, ve are askin1 you to conaider increaaiaa the level of China'• financial auppert to TDI ancl to work with ua to tranafor11 the opportuniti .. of today into the new drua• and vaccine• of tomorrow.
We sincerely hope that you will aiYe aerioua cona1deratiOD to our requeat for the increaaed financial participation of your Ccrrernllftt in the Special Progra111118 and look forward to hearina fro• you at your earlieat conYeuience. We ahould be grateful if 70a would aend your reply to Dr Ralfdan Mahler. Director-General of the World Health Organization.
Bradford Morse Administrator. United Nation• Deve.lopment ProgTamme
Sincttely,
A. W. Clauaen Preaident, The World Bank
H. Mahler, M.D. Director-General, World Health Organ iza tioa
4
. -
special programme for research and training in tr(JJ)ical diseases The World Health Organization 1211 Geneva 27 Switzerland
December 12, 1984
Dear Dr Al Shawi,
Dr Nizar Al Shawi Secretary General Union of Arab Councils for
Scientific Research P.O. Box 13027 Baghdad Iraq
We take the liberty of soliciting your support for a unique venture in international collaboration. This venture in research and development is an investment in the future of mankind and will require years of work and sustained financial support . However, we are convinced that the results will have a profound impact on the health and well-being of humanity .
The Special Programme for Research and Training in Tropical Diseases (TDR) - co-sponsored by the United Nations Development Programme, the World Bank and the World Health Organization - seeks to develop the means to control six major tropical diseases which today afflict or threaten over one thousand million people living in developing countries. We attach for your information a booklet describing in more detail the work and achievements of the Special Programme .
In spite of the explosive growth of knowledge in the biological sciences over the past 30 years, little progress has been made towards the control of these diseases. In fact the menace is increasing.
Millions of children die from malaria before reaching their fifth birthdays, and millions of those who reach adulthood are incapacitated by one or more tropical infections. They are sentenced to spend their lives on the ~readmill of illness and poverty with no hope of improving the lot of their families or their communities.
The devastating blow, to the individual and the family, of an acute attack of malaria at harvest time or of permanent loss of sight by the age of 25 from river blindness (onchocerciasis) is easy to understand . However, the social and economic impacts upon a community and a country when tropical diseases strike down hundreds of thousands of people, go far beyond the individual or gross statistics. In fact, epidemics of malaria , sleeping sickness and river blindness often drive self-sufficient communities into states of dependent poverty.
ENCLS: As stated
bee: World Bank (2) UNDP (2) EMRO (2) Att: TDR
UNDP!WORLD BANK/WHO
EMS/HQ
Dr Nizar Al Shawi, Secretary General, Union of Arab Councils for Scientific Research, Baghdad
Page ........ i ............ .
The destructive symbiosis of disease and poverty must, and can be replaced by the synergism of health and productivity. To bring this about, the tropical countries require both the tools for prevention and treat ent of the tropical diseases and the scientific and technical capabilities to assure their effective application. These are the goals of TDR.
Over the past six years, TDR has challenged and stimulated researchers at institutions throughout the world to work together toward these ends . Thousands of scientists in universities, research institutions, government ministries and industry have responded and are now working as members of TDR teams - in fundamental research laboratories, in hospital clinics and in village health centres - to build the new tools and prepare them for use in the villages of the tropics . TDR has catalysed the linking of research activities into an effective worldwide network and has focused the new methods and knowledge of the biological sciences upon the tropical disease.s .
The results have been remarkable and research carried out both within and outside the Special Progra e has brought about significant progress. Some new tools for disease control have already reached the stage of actual application in the field , while others are close to it. Examples .of major developments towards the control of the diseases include:
o A biological agent, Bacillus tburingiensis H-14, to control the flies that spread river blindness is being used extensively in West Africa and is being tested against malaria-carrying mosquitos.
o A new dru • mefloquine, for the treatment of malaria infections resistant to standard therapy has been registered for use .
o Vaccine which may treat and prevent leprosy are in the early stages of testing in man. However , the tests will take five to eight years to complete because of the slo natural history of the disease.
o Simple kits to measure the sensitivity of malaria parasites to drugs to assure the correct choice of treatment are being used widely.
o A simple test to diagnose sleeping sickness (African trypanoso iasis) at t e village level , and thus permit early intervention, is ready for widespread application.
Among significant achievements at earlier stages of development are the following .:
o Vaccines against malaria are now a real possibility following the identification and production of the substances in the parasite responsible for man's innn.une reactions against them.
o A totally new family of compounds for the treatment of malaria , based on a traditional Chinese remedy called Qinghaosu, has been synthesiz.ed and testing has begun.
...
Dr Nizar Al Shawi, Secretary General, Union of Arab Councils for Scientific Research, Baghdad
3 Page··············----·-······
0
0
0
Drugs for the treatment of river blindness, critical for the control of this disease, are being synthesized and tested.
Natural biological agents are being tested in the field, such as Bacillus sphaericus, which will destroy the larvae of diseasetransmitting insects and recycle t hemselves and in this way prolong their effectiveness.
Simple and effective diagnostic tests - vital to all disease control programmes - are being developed for Chagas ' disease, schistosomiasis, malaria and leprosy.
Scientists and institutions in over 120 countries participate in TDR and provide the vision, knowledge and facilities required for the work. So far, their progress has been outstanding, while the Programme's catalytic effects have kept costs low·. In short, we believe TDR to be one of the most cost-effective investments in health and development and one which merits your support. However, bringing a new drug or vaccine from the laboratory to the needy family in the village takes many years of work, and for this TDR requires both adequate and sustained f i nancial support.
TDR depends entirely upon voluntary contributions. From 1975 until 31 August 1984, 27 governments and 11 other organizations, together with the three co-sponsoring agencies, have contributed over US$ 155 million to the Programme (see attached table). However, available funds have fallen short of the minimum required (about US$ 33 million per year) to keep the Programme moving ahead . Unless contributions are increased and sustained, TDR will have to abandon many promising initiatives towards new and effective tools to control the diseases. Malaria, sleeping sickness, river blindness and leprosy will continue to spread and thwart any hope of self reliance f or the people living in the tropics.
We are convinced that the partnership of modern science and the Special Programme can go far to break the cycle of disease and poverty. Scientists from both the public and private sectors are already doing their part and it is now up to governments and agencies t o provide TDR with the funds necessary to complete the work.
We sincerely hope that you will give serious consideration to our request for the financial participation of your Union in the Special Programme and look f orward to hearing from you at your earliest , convenience. We should be grateful if you would send your reply to Dr Half dan Mahler, Director-General of t he World Health Organization.
Bradford Morse. . . Administrator, United Nations Development Programme
Sincerely,
(Signed) A. W. r.1;Juscn
A. W. Clausen President, The World Bank
(Sgd.) H. Mahler
H. Mahler, M. D. Director-General, World Health Organization
special programme for research and training in trapical diseases The World ft alth Organization 1211 Geneva 27
R. R. H. Prince Khalid .Al-Faisal D1rec tor-General
Switzerland King Faisal Foundation P. O. &>x 352 liyad Saudi Arabia
December 12, 1984
Your oyal Hi ghness,
We tak the liberty of soliciting your sup ort for a unique venture in international c()llaboration. This venture in research and develo ent is an investment in the future of ankind and ~ill r quire years of work and sustain d financial support . Ho ever , we are convinced that the results will have a profound itnpaet QJ.l the h alth and ell- being o.f h anity.
The Sp cia.l Progra e for Research and Trainin in Tropical Diseases ( TDR.) - co-epon ored by the Unite.d ations Develop nt Progra , tl e orld Bank and the World Health Organization - seeks to dev~.l.op th-e eans to control six maj r tropical di eases ht.ch today afflict or threaten over one
• • • thoUEland million people livi\1g in developing eountrie • We attacll f or your info ation a booklet describin in ore oetail the work and achiev ents of the Special Pro gr e.
•••
In spite of the explosi ve growth of kno ledge in the biologic.al s ciences over the past 30 years , little progress has been tnade t owards the control oft eee disea es . Inf ct the enace 1s increasing .
Millions of children die fro malaria before reaching their fifth birthdays , and illions of those who reach adulthood are inca ae.1tated by one or more tro ical infections. They are sentenced to spend their lives on the treadmill o-f illness and poverty with no hope of impr ov ing t.he lot of t heir families or theil:' co nities .
The devastating blow, to the individual and the family , of an acute attack of malaria at harvest ti e or of perlllanent loss of sight by t h age of 25 fro river blindness (onchocerciasis) is easy to undexstaud . HoweveJ:" , the social and e c.onomic impac ts upon a community and a country when tropical diseases strike down hundreds of t housands of people , go far beyond t h individual or gross s t atistics . In fact, epi demics of mal aria , sleeping sickness nd river blindness often dri e self- sufficient communiti es into s t a~es of dependent poverty.
ENCLS: As stated
bee; .world Bank (2) UNDP (2) RO ( 2) At t : TDR EMS/HQ WR&PC, Saudi Arabia
UNDP! W ORLD BANK/WHO
Tb d repl - d y t tropical co of tb t.ropic•l die a
e ur t :lr eff c ti\!'
0 A
0
0
- ai 1 1 Dir eter-Ce er.al, yad
t
Page __ ___ __ _ __ __ ______ _
8 to
•
to control t sed xte si J. t -
l _t:1a-c rrytn
f na
•
a ur th s n 1t1 ity o al ri per i to nutt the cor ct cbo1ce of trea t r bin u ed
0
sign! fi e.ant the followin -:
0 A totally n -_ eci o tr
synth au d a
(Afric 1 vel 11 and th permit early
d ppltcati • ·
elo t ue
la:d ., e en
. )
•••
B ••• Prine lid Al- isal, D!r ctor n Faisal Foundation, fliya
0
0
0
labor f r t
us fr t tr t ontrol -of this dis e ,
Si
i cerely ,
A. • Cl us n Pr ai nt,, 'Ih orld
Page ......... .3 ............ .
, critical for ~h iz d t t d .
y
it l . 11 for Cha.gas "'
"
r t -es ial t.
to io .
ir
(Sgct .) H. rvlahler.
hl r , ir ctor--Ge rld I 1th
Or .anb tion
• • ral,.
special programme for research and training in trOJ)ical diseases
o 1d Belt -Or an1z t1 n 1211 Geneva 21
i'ts l an
....
•••
December 12, 1984
co trol t hou.and inlor ()f t he
I a i t ft e sci cee ov~r t h past co t~ol of t ea dio~~~ca:t .
'CLS : As etat d.
bee: World Bank (2) UNDP {2 ) WR&PC, Saudi Arabia EMS
;r bib tt · ecr tary- Gener.al Oranisation of the 1 l ii!
C.onf ere c ... lox 17
J~dd h udi Arabia
1th n ho
EMRO (2) Att: TDR
ift b
V NDPIWORLD BANK/WHO
t h
t
ib at y , of t Isl
0
0
0
0
Aa try int
ani ti 2 Page ......................... .
tio
rl
t
..
...
bib tty. of t Isl ic
ti
0 8 f r t tro,alNO.,,,n
conttol ft i
0
... i cer ly.
(Signed) A. W. Clausen
• critic 1 f .r iz and te t d .
Page ....... ..,, .............. .
a
eir
-I • h
1 ,
,N.,~., r,~.,,~ ST ATE of ISRAEL
7/C~ ~ny-/:ment.J ~ ! ;t.tM'rhd- ~ 1 , s {'-LU w-~ 1-o ; ND,
}W; , u~I p( l1'f s
Beit Hanassi Jerusalem
•
S1 w11b ca.-. I f rtfl
he
of
OFFIOE OF THE PRESIDENT OF ISRAEL
, ....
1
1o •
~I c_ C : )1Y. >(n'-t ( '-
1 /o J
rld
your • t
ffi 11"1
ptes to: 1. • r dford "'• acn,1n·tatr1tor. U • De loMffl P,ofNGIII.
2. , Mr. • • Cla s • std t. •
6Z :S Ud 8- NVr S861
031'{1~83
:..
The World Health Organization 1211 Geneva 27 Switzerland
December 10, 1984
Dear Nr President,
Mr Chaim Herzog President of the State of Israel Jerusalem Israel
We take the liberty of soliciting your support for a unique venture in international collaboration. This venture in research and development is an investment in the future of mankind and will require years of work and sustained financial support. However, we are convinced that the results will have a profound impact on the heal t h and we ll-being of humanity .
The Special Programme for Research and Training in Tropical Diseases ( TDR) - co-sponsored by the t:nited Ka tions Development Programme, the World Bank and t he World Health Or ganization - seeks to develop the means to control six major tropical diseas es which today afflict or threaten over one thousand million people living in developing countries. We attach for your information a booklet describing in more detail the work and achieve!I'ents of t he Special Programme.
In spite of the explosive growth of knowledge in the biological sciences over the past 30 years, li ttle progress has been made towards the cen tral ·of t :1ese d iseases. In fact the .menace is increasing .
Millions of children die from malaria before r eaching their fifth LirthcJay , and mil lions of those i,ho reach ac!ultr.ood are incapacitated by one or more tropical infec tions . They are sen..tericed to spend their lives on t he treadmill of illness and poverty with no hope of impr oving the lot of their families or their communities.
cc: The Minis ter of Health , Government of Israel, Jerusalem The Minister for Foreign Affa irs, Division of International
Organizations, Government of Israel, Jerusalem Dr Moshe Y. Mandelbaum, Governor, Bank of Israel , Jerusalem The Permanent Representative of Israel to the United Na tions Office and
the International Organizations at Geneva
ENCLS: As stated
bee : Professor B. Lunenfeld, Counsellor for External Re lations, Minis try of Health, Jerusalem
UNDP World Bank EMRO (2) Att: TDR EMS/HQ
Mr Chai• Herzog. Preeideot of the State of Ierael, Jeruaal•
2
The dev .. tating blow. to the individual and the family, of an acute attack of aalaTia at harvest Ua or of pen.anent loss of eight by the age of 25 from ri•er blindne•s (onchocerciasis) is easy to understand . However, the social and economic impacts upon a community and a couutry vhen tropical diseases strike down hundreds of thousands of people, go far beyond the individual or gross statistics. In fact. epidemics of 11111laria, sleeping sickness and river blindness often drive self-sufficient communities Into states of dependent poverty.
The destructive S)'Tabiosis of disease and poverty must, and can be replaced by the synergism of health and productivity. To bring this about, the tropical countries require both t he tools for prevention and treatment of the tropical diseases and the scientific and technical capabilities to nssure their effective applic.ation. These a re the goals of TDR.
Over the past six years, TDR has challenged and sti1BUlated reaearchers at institutions throughout the world to work together toward theae ends. Thousands of scientists in universities, research institutions, go'f'ernment ministries and industry have res ponded and are nou working as members of TDR teama - in fw:idamental research laboratories, in hospital clinics and in village health centres - to build the new tools and prepare t hem for use in the villages of the tropics. TDR bas catalysed the linking of research activities into an effective worldwide network and has focused t he new methods and knowledge of the biological sciencas upon the tropical diseases.
The resolts have been ret:'l4rkable and research carried out both within and outside the Special Programme has brought about significant progress. Some new tcola f or disease control have already reached the stage of actual application in the field, while others are close to. it. Examples of iaajor developments towards the control of t ti e diseases i.nclude:
o A biological agent, Bacillus thuringiensis H-14, to control the flies that spread river b lindness is be ing used exte~sively in W~st Africa and i s being tested against malaria-carrying mosquitos.
o A new drug , mefloquine, for the treatment of malaria infections resistant to standard therapy has been registered for use.
o Vaccines wh ich ~ay treat and prevent leprosy are in the early stages of testing in man . However. the tests will take five to eight years to con:plcte because of the slow na tural his tory of the d 1sease.
o Simple kits to roeasure t he sensitivity of malar ia parasites to drugs to assure the correct choice of treatment are being uaed videly.
o A simple test to dia6nose sleeping sickness (African trypanosomiasis) at the village level, and thus permit early intervention, is ready for widespread application.
::.
...
Mr Chaia Herao1. Pre•ident of the State of Iarael. Jerwaal ..
Among significant achievements at earlier stages of developwent are the following:
o Vaccine• against malaria are now a real posaibility following the identification and production of the aubatances in the parasite responsible for man'• immune reactions againat thea.
o A totally new family cf compounds for the treatment of malaria, based on a traditional Chinese rel!ledy called Qinghaosu 11 has been synthesized and testing haa begun.
o Drugs for the treatment of river blindness, critical for the control of this disease, are being synthesized and tested.
0 Natural biological agents are being tested in the field, such as Bacillus sphaericua. which will destroy the larvae of diseasetransmitting insects and recycle themselves and io this way prolong their effectivenes1.
o Simple and effective diagnostic tests - vital to all disease control programmes - are being developed for Chagas' disease, achistosomiasis, malaria and leprosy.
Scientists and institutions in over 120 countries participate in TDR and provide t he vision, knowledge and facilities required for the work. So far, their progress haa been outstanding, while t he Programme's cataiytic effects have kept costs low. In short. we believe TDR to be one of the most cost-effective investments in health and development and one which merits your support. Rowever, bringing a new drug or vaccine from the l aboratory to the needy family in the village takes many years of work. an(i for this TDR requires both adequate an<l sustained financial support.
TDR depends entirely upon voluntary contributions. From 1974 until 31 Augus t 19 £4 , 27 governments and 11 otler organizations, toge lhcr with the three co-sponsoring agencies, have contributed over US$ 155 million to the Programme (see attached table). However, available funds have fallen short of the ~inimum required (about US$ 33 million per year) to keep the Progra~.me ~oving ar.ead. Unless contributions are increased and sustained, TDR will have to abandon many proraising initiative• towards new ancl effective tools to control the diseases. Halaria, sleeping sickness, river blindness and leprosy will continue to spread and thwart any hope of self reliance for the people living in t he tropics.
We are convinced t ha t the partnership of modern science and the Special Prot ramme can go far to break the cycle of disease and poverty . Scientists from both the publi c and private sectors are already doing their part and it is now up to governments and agencies to provide TDR with t he funds necessary to complete the work.
Israeli institutions and scientists are participating in tbe work of TDR. They have carried out 26 research and development projects at a total
3
. .
:..
Mr Chaim Herzog, President of the State of Israel, Jerusalea
Page .... .4. ....... ........ .
cost of USS 1 099 000 to TDR, and are participating in the scientific management of the Programme. We are very grateful to your Government, its institutions and scientists for their important participation. However, in view of the tasks to be accomplished and the opportunities before us, we are asking you to support TDR financially as well as technically and in this way to work with us at all levels of the Programme to transform the opportunities of today into the new drugs and vaccines of tomorrow.
We sincerely hope that you will give serious consideration to our request for the financial participation of your Government in the Special Programme and look forward to hearing from you at your earliest convenience. we should be grateful if you would send your reply to Dr Halfdan Mahler, Director-General of the World Health Organization.
Bradford Horse Administrator, United Nations Development Programme
Sincerely,
President, The World Bank
H. Mahler, M.D. Director-General, World Health Organization
,.
special programme for research and training in tropical diseases
The World Health Organization 1211 Geneva 27 Switzerland
December 10, 1984
Dear Mr President,
Mr Chaim Herzog President of the State of Israel Jerusalem Israel
We take the liberty of soliciting your support for a unique venture in international collaboration. This venture in research and development is an investment in the future of mankind and will require years of work and sustained financial support. However, we are convinced that the results will have a profound impact on the health and well-being of humanity.
The Special Programme for Research and Training in Tropical Diseases (TDR) - co-sponsored by the United Nations Development Programme, the World Bank and the World Health Organization - seeks to develop the means to control six major tro ical diseases which today afflict or threaten over one thousand million people living in developing countries. We attach for your information a booklet describing in more detail the work and achievements of the Special Programme.
In spite of the explosive growth of knowledge in the biological sciences over the past 30 years, little progress has been made towards the control of these diseases. In fact the menace is increasing. --Millions of children die from malaria before reaching their fifth birthday, and millions of those who reach adulthood are incapacitated by one or more tropical infections. They are sentenced to spend their lives on the treadmill of illness and poverty with no hope of improving the lot of their families or their communities. ·
cc: The Minister of Health, Government of Israel, Jerusalem The Minister for Foreign Affairs, Division of International
Organizations, Government of Israel, Jerusalem Dr Moshe Y. Mandelbaum, Governor, Bank of Israel, Jerusalem The Permanent Representative of Israel to the United Nations Office and
the International Organizations at Geneva
ENCLS: As stated
t .; l
~I I
,;
f
Mr Chaim Herzog, President of the State of Israel, Jerusalem
Page ..... 2 ................ .
The devastating blow, to the individual and the family, of an acute attack of malaria rvest time or of permanent loss of sight by the age of 25 from r r blindness (onchocerciasis) is easy to understand. However, the social and economic impacts upon a community and a country when tropical diseases strike down hundreds of thousands of people, go far beyond the individual or gross statistics. In fact, epidemics of malaria, sleeping -sickness and river blindness often drive self-sufficient communities into states of dependent poverty.
The destructive symbiosis of disease and poverty must, and can be replaced by the synergism of health and productivity. To bring this about, the tropical countries require both the tools for prevention and treatment of the tropical diseases and the scientific and technical capabilities to assure their effective application. These are the goals of TDR.
Over the past six years, TDR has challenged and stimulated researchers at institutions throughout the world to work together toward these ends. Thousands of scientists in universities, research institutions, government ministries and industry have responded and are now working as members of TDR teams - in fundamental research laboratories, in hospital clinics and in village health centres - to build the new tools and prepare them for use in the villages of the tropics. TDR has catalysed the linking of research activities into an effective worldwide network and has focused the new methods and knowledge of the biological sciences upon the tropical diseases.
The results have been remarkable and research carried out both within and outside the Special Programme has brought about significant progress. Some new tools for disease control have already reached the stage of actual application in the field, while others are close to it. Examples of major developments towards the control of the diseases include:
• A biological agent, Bacillus thuringiensis H-14, to control the flies that spread river blindness is being used extensively in West Africa and is being tested against malaria-carrying mosquitos.
• A new drug mefloquine, for the treatment of malaria infections resistant to standard therapy has been registered for use.
• Vaccines which may treat and prevent leprosy are in the early stages of testing in man. However, the tests will take five to eight years to complete because of the slow natural history of the disease.
• Simple kits to measure the sensitivity of malaria parasites to drugs to assure the correct choice of treatment are being used widely.
• A simple test to diagnose sleeping sickness (African trypanosomiasis) at the village level, and thus permit early intervention, is ready for widespread application.
Mr Chaim Herzog, President of the State of Israel, Jerusalem
Page ..... :1 ................ .
Among significant achievements at earlier stages of development are the following:
•
•
•
•
•
Vaccines against malaria are now a real possibility following the identification and production of the substances in the parasite responsible for man's immune reactions against them.
A totally new family of compounds for the treatment of malaria, based on a traditional Chinese remedy called Qinghaosu, has been synthesized and testing has begun.
Drugs for the treatment of river blindness, critical for the control of this disease, are being synthesized and tested.
Natural biological agents are being tested in the field, such as Bacillus sphaericus, which will destroy the larvae of diseasetransmitting insects and recycle themselves and in this way prolong their effectiveness.
Simple and effective diagnostic tests - vital to all disease control programmes - are being developed for Chagas' disease, schistosomiasis, malaria and leprosy.
Scientists and institutions in over 120 countries participate in TDR and provide the vision, knowledge and facilities required for the work. So far, their progress has been outstanding, while the Programme's catalytic effects have kept costs low. In short, we eLieve TDR to be one of the most cost-effective investments in health and development and one which me ifs your support. However, bringing a new drug or vaccine from t he laboratory to the needy family in the village takes many years of wor k, and for this TDR requires both adequate and sustained financial support.
TDR depends entirely upon voluntary contributions. From 1974 until 31 August 1984, 27 governments and 11 other organizations, together with the three co-sponsoring agencies, have contributed over US$ 155 million to the Programme (see attached table). However, available funds have fallen short of the minimum required (about US$ 33 million per year) to keep the Programme moving ahead. Unless contributions are increased and sustained, TDR will have to abandon many promising initiatives towards new and effective tools to control the diseases. Malaria, sleeping sickness, river blindness and leprosy will continue to spread and thwart any hope of self reliance for the people living in the tropics.
We are convinced that the partnership of modern science and the Special Programme can go far to break the cycle of disease and poverty. Scientists from both the public and private sectors are already doing their part and it is now up to governments and agencies to provide TDR with the funds necessary to complete the work.
Israeli institutions and scientists are participating in the work of TDR. They have carried out 26 research and development projects at a total
Mr Chaim Herzog, President of the State of Israel, Jerusalem
Page .... A ............... .
cost of USS 1 099 000 to TDR, and are participating in the scientific management of the Programme. We are very grateful to your Government, its institutions and scientists for their important participation. However, in view of the tasks to be accomplished and the opportunities before us, we are asking you to support TDR financially as well as technically and in this way to work with us at all levels of the Programme to transform the opportunities of today into the new drugs and vaccines of tomorrow.
We sincerely hope that you will give serious consideration to our request fo~ t e financial participation of your Government in the Special Programme and look forward to hearing from you at your earliest convenience. We should be grateful if you would send your reply to Dr Halfdan Mahler, Director-General of the World Health Organization.
Bradford Morse Administrator, United Nations Development Programme
Sincerely,
President, The World Bank
/ _)_~ 4 aLl.~er, M.D~
Director-General, World Health Organization
ATTACHMENTS TO EACH LETTER
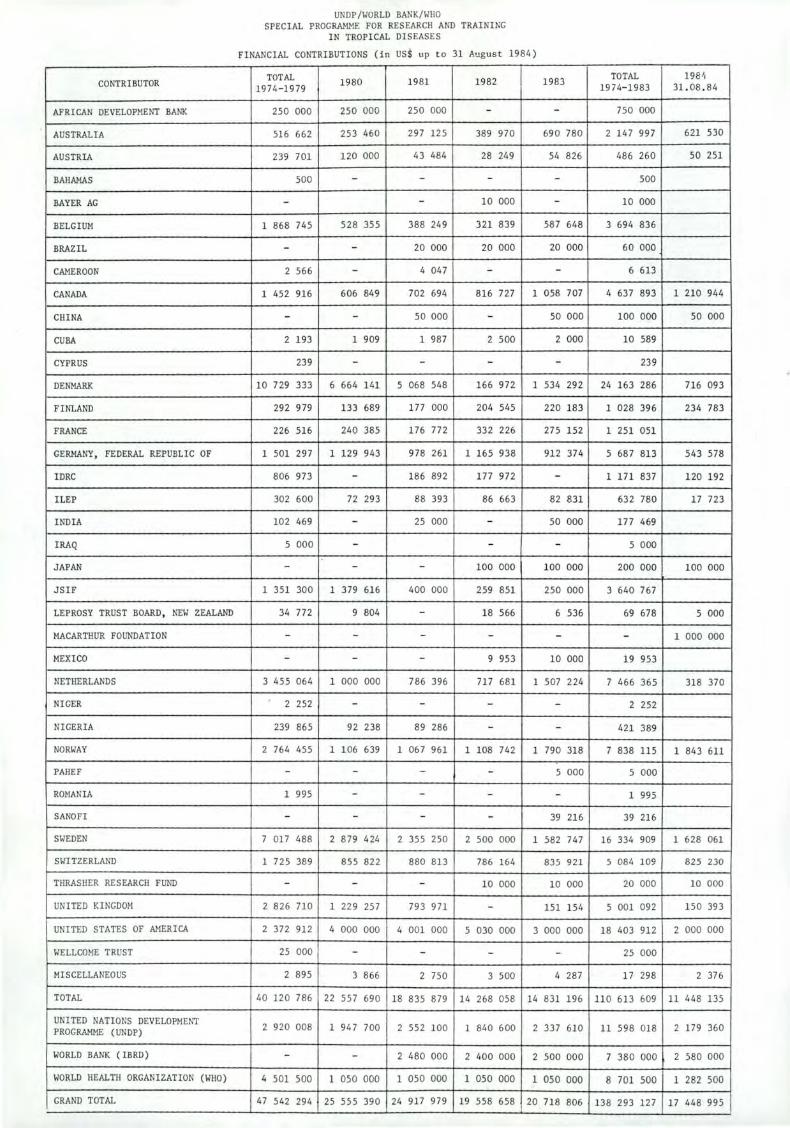
CONTRIBUTOR
AFRICAN DEVELOPMENT BANK
AUSTRALIA
AUSTRIA
BAHAMAS
BAYER AG
BELGIUM
BRAZ IL
CAMEROON
CANADA
CHINA
CUBA
CYPRUS
DENMARK
FINLAND
FRANCE
GERMANY, FEDERAL REPUBLIC OF
IDRC
ILEP
INDIA
IRAQ
JAPAN
JSIF
LEPROSY TRUST BOARD , NEW ZEALAND
MACARTHUR FOUNDATION
MEXICO
NETHERLANDS
NIGER
NIGERIA
NORWAY
PAHEF
ROMANIA
SANOFI
SWEDEN
SWITZERLAND
THRASHER RESEARCH FUND
UNITED KINGDOM
UNITED STATES OF AMERICA
WELLCOME TRUST
MISCELLANEOUS
TOTAL
UNITED NATIONS DEVELOPME~"f PROGRAMME (UNDP)
WORLD BANK (IBRD)
WORLD HEALTH ORGANIZATION (WHO)
GRAND TOTAL
UNDP/WORLD BANK/WHO SPECIAL PROGRAMME FOR RESEARCH AND TRAINING
IN TROPICAL DISEASES
FINANCIAL CONTRIBUTIONS (in US$ up to 31 August 1984)
TOTAL 1980 1974-1979
1981 1982 1983
250 000 250 000 250 000 - -
516 662 253 460 297 125 389 970 690 780
239 701 120 000 43 484 28 249 54 826
500 - - - -
- - 10 000 -
1 868 745 528 355 388 249 321 839 587 648
- - 20 000 20 000 20 000
2 566 - 4 047 - -
1 452 916 606 849 702 694 816 727 1 058 707
- - so 000 - so 000
2 193 1 909 1 987 2 500 2 000
239 - - - -10 729 333 6 664 141 5 068 548 166 972 1 534 292
292 979 133 689 177 000 204 545 220 183
226 516 240 385 176 772 332 226 27 5 152
1 501 29 7 1 129 94 3 978 261 1 165 938 912 374
806 973 - 186 892 177 972 -302 600 72 293 88 393 86 663 82 831
102 469 - 25 000 - so 000
5 000 - - -- - - 100 000 100 000
1 351 300 1 379 616 400 000 259 851 250 000
34 77 2 9 804 - 18 566 6 536
- - - - -- - - 9 953 10 000
3 455 064 1 000 000 786 396 71 7 681 1 507 224
2 252 - - - -239 865 92 238 89 286 - -
2 764 455 1 106 639 1 067 961 1 108 742 1 790 318
- - - - 5 000
1 995 - - - -- - - - 39 216
7 017 488 2 879 424 2 355 250 2 500 000 1 582 747
1 725 389 855 822 880 813 786 164 835 921
- - - 10 000 10 000
2 826 710 1 229 257 793 971 - 151 154
2 372 912 4 000 000 4 001 000 5 030 000 3 000 000
25 000 - - - -
2 895 3 866 2 750 3 500 4 287
40 120 786 22 557 690 18 835 879 14 268 058 14 831 196
2 920 008 1 947 700 2 552 100 1 840 600 2 337 610
- - 2 480 000 2 400 000 2 500 000
4 501 500 1 050 000 1 050 000 1 050 000 1 050 000
47 542 294 25 555 390 24 917 979 19 558 658 20 718 806
TOTAL 198 1,
1974- 1983 31.08 . 84
750 000
2 147 997 621 530
486 260 so 251
500
10 000
3 694 836
60 000
6 613
4 63 7 893 1 210 944
100 000 so 000
10 589
23 9
24 163 286 716 093
1 028 396 23 4 783
1 251 051
5 68 7 813 543 578
1 171 837 1 20 192
632 780 17 723
177 469
5 000
200 000 100 000
3 640 76 7
69 678 5 000
- 1 000 000
19 953
7 466 365 318 370
2 252
421 389
7 838 115 1 843 611
5 000
1 995
39 216
16 334 909 1 628 061
5 084 109 825 230
20 000 10 000
5 001 092 150 393
18 403 912 2 000 000
25 000
17 298 2 376
110 613 609 11 448 135
11 598 018 2 179 360
7 380 000 2 580 000
8 701 500 1 282 500
138 293 127 17 448 995
VENTURI fDR
HEALTH
VENTURE FOR
HEALTH UNDP/WORLD BANK/WHO Special Programme for Research
and Training in Tropical Diseases
WORLD HEAL TH ORGANIZATION
1211 GENEVA 27-SWITZERLAND
1984
PREFACE
I t is difficult for those living in temperate climates to comprehend the immense burden of disease carried by the people of the tropics. Children born and raised in rural Africa
are liable to be infected by four or more different diseaseproducing parasites by the time they reach adulthood. Every village child at times suffers the paroxysms of malaria fever, and most families will mourn the death of one or two children from this disease. Mothers are not surprised when their children pass blood in their urine, as a result of schistosomiasis transmitted by snails in the village pond. Those living near the rivers where blackflies breed and spread onchocerciasis, or "river blindness", know that one in ten of their neighbours may be blind in the prime of life. The ravages of disease are an integral part of every day life, but the ways which are available to prevent or treat these diseases in the hundreds of millions of people affected by them are grossly inadequate.
The Special Programme for Research and Training in Tropical Diseases (TDR) is a coordinated attack by the world's scientific community upon diseases of the tropics. Under the sponsorship of the United Nations Development Programme, the World Bank and the World Health Organization, the Spf!cial Programme has stimulated and supported a worldwide research eff art towards new and improved methods to control six major tropical diseases. The Programme is also strengthening the scientific and technical resources of the tropical countries to enable them to study the scope and nature of the diseases and participate fully in the development and effective application of new methods for their control.
This book describes some of the diseases and their impact upon the lives of those threatened and affected by them. It also describes some of the efforts of the thousands of scientists who are working with the Special Programme and who have created the opportunities to build the tools needed to control the diseases.
2 However, a great deal still remains to be done to transform these
opportunities into safe and effective means for the prevention and treatment of the tropical diseases.
We believe that the success of these efforts now depends not so much upon human ingenuity and technology, for there is good evidence that the necessary scientific skills are available, as upon the resources which mankind is prepared to devote to solving some of its oldest, most severe, but often least known problems. Success depends further upon the commitment of governments, organizations and individuals in many countries, both temperate and tropical, to provide the support which is required. After eight years of steadily increasing activity the Programme has now generated more promising leads than can be financed by its current annual income of less than $25 million. This income is derived almost entirely from voluntary contributions by governments and other agencies and additional funds must be made available if the Programme is to succeed. We sincerely hope that you will help us to bring this about.
Mr A. W. Clausen The World Bank
Dr H. Mahler World Health Organization
Mr B. Morse United Nations Development Programme
3
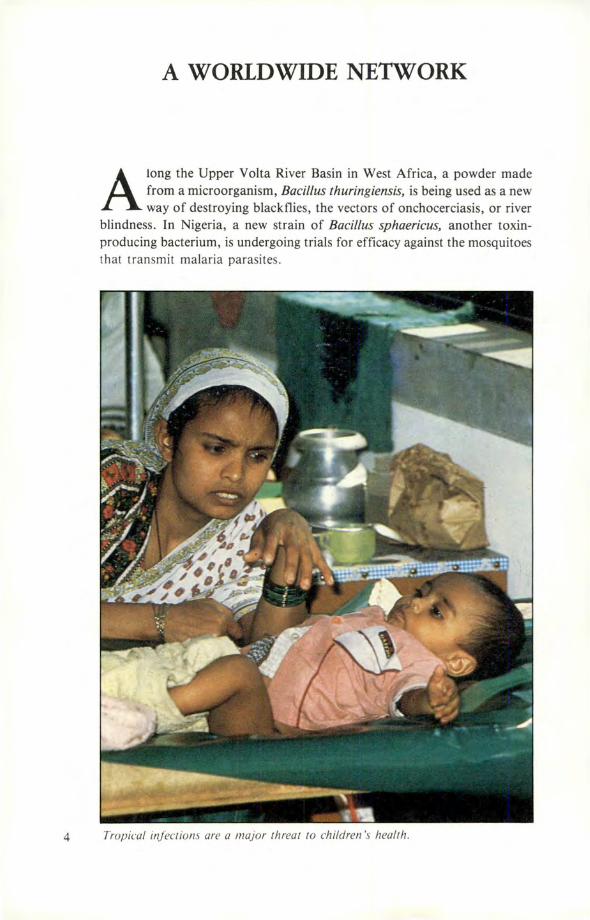
A WORLDWIDE NETWORK
A long the Upper Volta River Basin in West Africa, a powder made from a microorganism, Bacillus thuringiensis, is being used as a new way of destroying blackflies, the vectors of onchocerciasis, or river
blindness. In Nigeria, a new strain of Bacillus sphaericus, another toxinproducing bacterium, is undergoing trials for efficacy against the mosquitoes that transmit malaria parasites.
4 Tropical infections are a major threat to children's health.
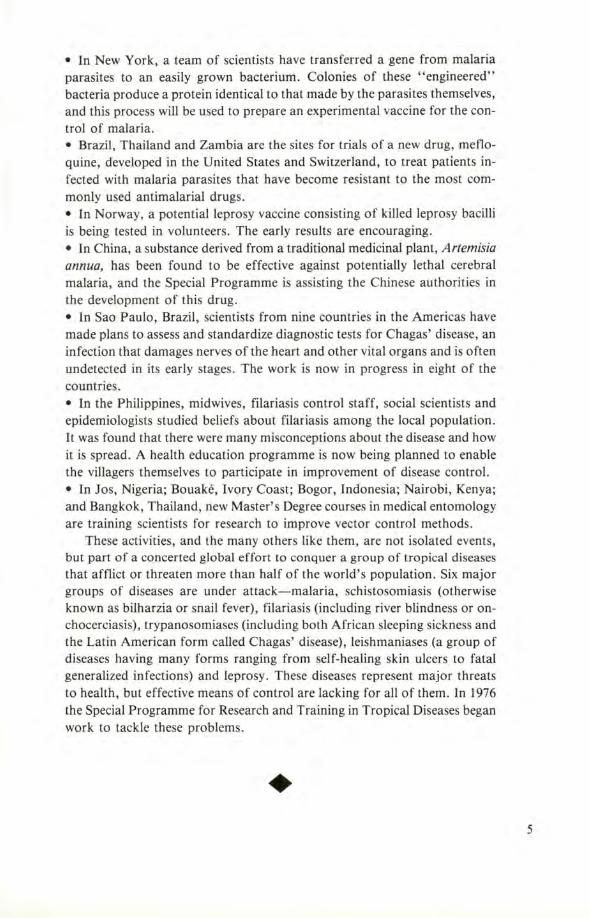
• In New York, a team of scientists have transferred a gene from malaria parasites to an easily grown bacterium. Colonies of these "engineered" bacteria produce a protein identical to that made by the parasites themselves, and this process will be used to prepare an experimental vaccine for the control of malaria. • Brazil, Thailand and Zambia are the sites for trials of a new drug, mefloquine, developed in the United States and Switzerland, to treat patients infected with malaria parasites that have become resistant to the most commonly used antimalarial drugs. • In Norway, a potential leprosy vaccine consisting of killed leprosy bacilli is being tested in volunteers. The early results are encouraging. • In China, a substance derived from a traditional medicinal plant, Artemisia annua, has been found to be effective against potentially lethal cerebral malaria, and the Special Programme is assisting the Chinese authorities in the development of this drug. • In Sao Paulo, Brazil, scientists from nine countries in the Americas have made plans to assess and standardize diagnostic tests for Chagas' disease, an infection that damages nerves of the heart and other vital organs and is often undetected in its early stages. The work is now in progress in eight of the countries. • In the Philippines, midwives, filariasis control staff, social scientists and epidemiologists studied beliefs about filariasis among the local population. It was found that there were many misconceptions about the disease and how it is spread. A health education programme is now being planned to enable the villagers themselves to participate in improvement of disease control. • In Jos, Nigeria; Bouake, Ivory Coast; Bogor, Indonesia; Nairobi, Kenya; and Bangkok, Thailand, new Master's Degree courses in medical entomology are training scientists for research to improve vector control methods.
These activities, and the many others like them, are not isolated events, but part of a concerted global effort to conquer a group of tropical diseases that afflict or threaten more than half of the world's population. Six major groups of diseases are under attack-malaria, schistosomiasis (otherwise known as bilharzia or snail fever), filariasis (including river blindness or onchocerciasis), trypanosomiases (including both African sleeping sickness and the Latin American form called Chagas' disease), leishmaniases (a group of diseases having many forms ranging from self-healing skin ulcers to fatal generalized infections) and leprosy. These diseases represent major threats to health, but effective means of control are lacking for all of them. In 1976 the Special Programme for Research and Training in Tropical Diseases began work to tackle these problems .
• 5
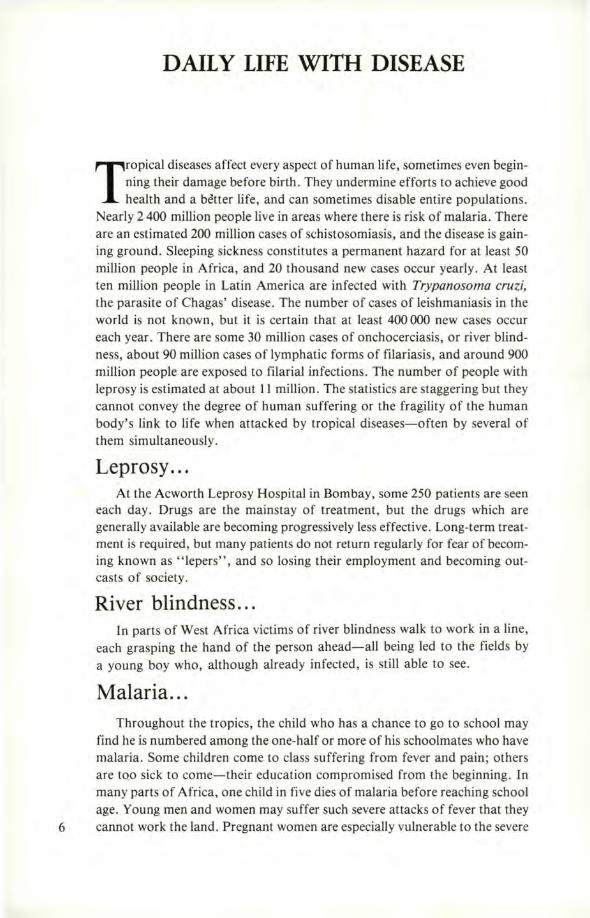
DAILY LIFE WITH DISEASE
Tropical diseases affect every aspect of human life, sometimes even beginning their damage before birth. They undermine efforts to achieve good health and a better life, and can sometimes disable entire populations.
Nearly 2 400 million people live in areas where there is risk of malaria. There are an estimated 200 million cases of schistosomiasis, and the disease is gaining ground . Sleeping sickness constitutes a permanent hazard for at least 50 million people in Africa, and 20 thousand new cases occur yearly. At least ten million people in Latin America are infected with Trypanosoma cruzi, the parasite of Chagas' disease. The number of cases of leishmaniasis in the world is not known , but it is certain that at least 400 000 new cases occur each year. There are some 30 million cases of onchocerciasis, or river blindness, about 90 million cases of lymphatic forms of filariasis, and around 900 million people are exposed to filarial infections . The number of people with leprosy is estimated at about 11 million . The statistics are staggering but they cannot convey the degree of human suffering or the fragility of the human body's link to life when attacked by tropical diseases-often by several of them simultaneously.
Leprosy ... At the Acworth Leprosy Hospital in Bombay, some 250 patients are seen
each day. Drugs are the mainstay of treatment, but the drugs which are generally available are becoming progressively less effective. Long-term treatment is required, but many patients do not return regularly for fear of becoming known as "lepers", and so losing their employment and becoming outcasts of society.
River blindness ... In parts of West Africa victims of river blindness walk to work in a line,
each grasping the hand of the person ahead-all being led to the fields by a young boy who, although already infected, is still able to see.
Malaria ... Throughout the tropics, the child who has a chance to go to school may
find he is numbered among the one-half or more of his schoolmates who have malaria. Some children come to class suffering from fever and pain; others are too sick to come-their education compromised from the beginning. In many parts of Africa, one child in five dies of malaria before reaching school age. Young men and women may suffer such severe attacks of fever that they
6 cannot work the land. Pregnant women are especially vulnerable to the severe
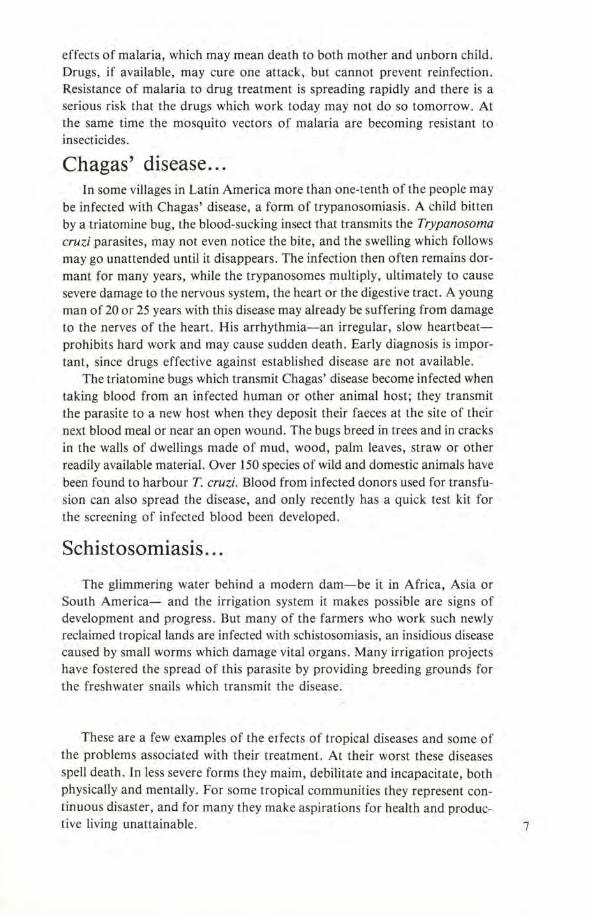
effects of malaria, which may mean death to both mother and unborn child . Drugs, if available, may cure one attack, but cannot prevent reinfection . Resistance of malaria to drug treatment is spreading rapidly and there is a serious risk that the drugs which work today may not do so tomorrow. At the same time the mosquito vectors of malaria are becoming resistant to insecticides.
Chagas' disease . .. In some villages in Latin America more than one-tenth of the people may
be infected with Chagas' disease, a form of trypanosomiasis. A child bitten by a triatomine bug, the blood-sucking insect that transmits the Trypanosoma cruzi parasites, may not even notice the bite, and the swelling which follows may go unattended until it disappears. The infection then often remains dormant for many years, while the trypanosomes multiply, ultimately to cause severe damage to the nervous system, the heart or the digestive tract. A young man of 20 or 25 years with this disease may already be suffering from damage to the nerves of the heart. His arrhythmia-an irregular, slow heartbeatprohibits hard work and may cause sudden death. Early diagnosis is important, since drugs effective against established disease are not available.
The triatomine bugs which transmit Chagas' disease become infected when taking blood from an infected human or other animal host; they transmit the parasite to a new host when they deposit their faeces at the site of their next blood meal or near an open wound. The bugs breed in trees and in cracks in the walls of dwellings made of mud, wood, palm leaves, straw or other readily available material. Over 150 species of wild and domestic animals have been found to harbour T. cruzi. Blood from infected donors used for transfusion can also spread the disease, and only recently has a quick test kit for the screening of infected blood been developed .
Schistosomiasis ...
The glimmering water behind a modern dam-be it in Africa, Asia or South America- and the irrigation system it makes possible are signs of development and progress . But many of the farmers who work such newly reclaimed tropical lands are infected with schistosomiasis, an insidious disease caused by small worms which damage vital organs. Many irrigation projects have fostered the spread of this parasite by providing breeding grounds for the freshwater snails which transmit the disease.
These are a few examples of the erfects of tropical diseases and some of the problems associated with their treatment. At their worst these diseases spell death. In less severe forms they maim, debilitate and incapacitate, both physically and mentally. For some tropical communities they represent continuous disaster, and for many they make aspirations for health and produc-tive living unattainable . 7
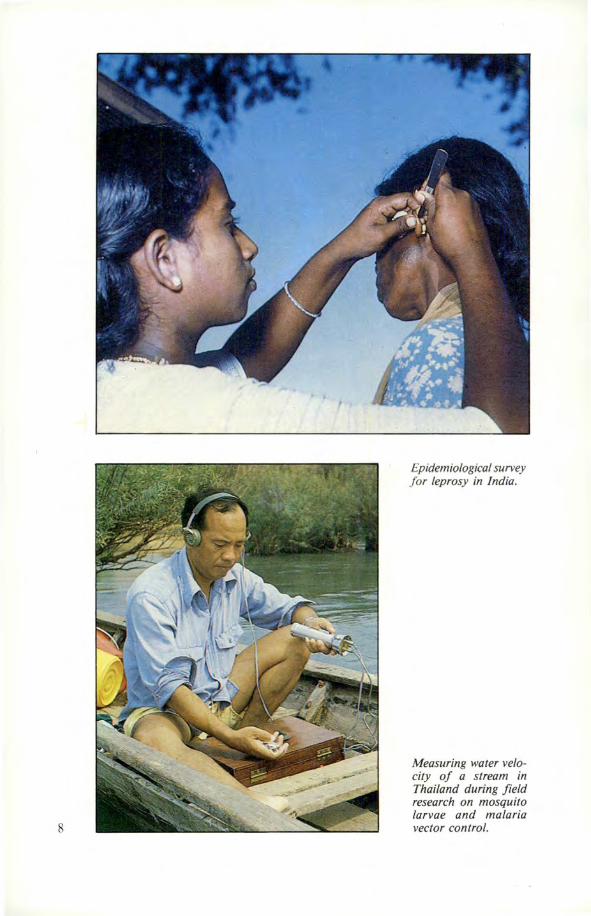
8
Epidemiological survey for leprosy in India.
Measuring water velocity of a stream in Thailand during field research on mosquito larvae and malaria vector control.

INTERNATIONAL SCIENTIFIC COLLABORATION
A few years ago research on tropical diseases was a neglected area.
Few scientists were involved, and these came chiefly from temperate developed countries where interest in such research had waned follow
ing the end of colonial eras. The tropical countries themselves lacked the scientific and technical resources needed for _this work. Thus, although tropical diseases presented some of the world's most severe health hazards there was no prospect of improvement, and indeed the situation has continued to deteriorate. Although these diseases chiefly affect the people of tropical countries, in a world where travel is increasing they also threaten the people and interests of non-tropical nations. For example, the rapid spread of drugresistant malaria is now a matter of worldwide concern, since all those who enter these regions are at risk.
Research to design better disease control strategies and to develop and test new tools for control, such as drugs, vaccines and diagnostic tests, must necessarily take place in tropical countries where the diseases can be studied in their natural environments. Research is also needed in advanced biomedical centres to deploy the latest advances of biomedical sciences to develop new disease control tools . For maximum effectiveness these two very different types of research must be linked so as to stimulate scientific resourcefulness and ingenuity, whilst at the same time keeping the target of disease control firmly in view.
This task and challenge was recognized by the World Health Assembly in 1974 and led in 1976 to the establishment of the Special Programme for Research and Training in Tropical Diseases. The Programme is sponsored by the United Nations Development Programme, the World Bank and WHO, and executed by WHO.
The Programme's objectives
The Programme has two main objectives. The first is to harness all available technology to develop new tools and methods to improve disease control. The second is to strengthen research in tropical diseases in the countries where these diseases are endemic. Under the Programme over 3 000 scientists are working in multinational .and multidisciplinary groups on the planing and conduct of research and development. In parallel an international group of experts works with institutions and governments of tropical countries to strengthen the foundations of national programmes of research on tropical diseases . The integration of so many efforts, and striking the right balance between activities, is the task of a small independent group of highly 9
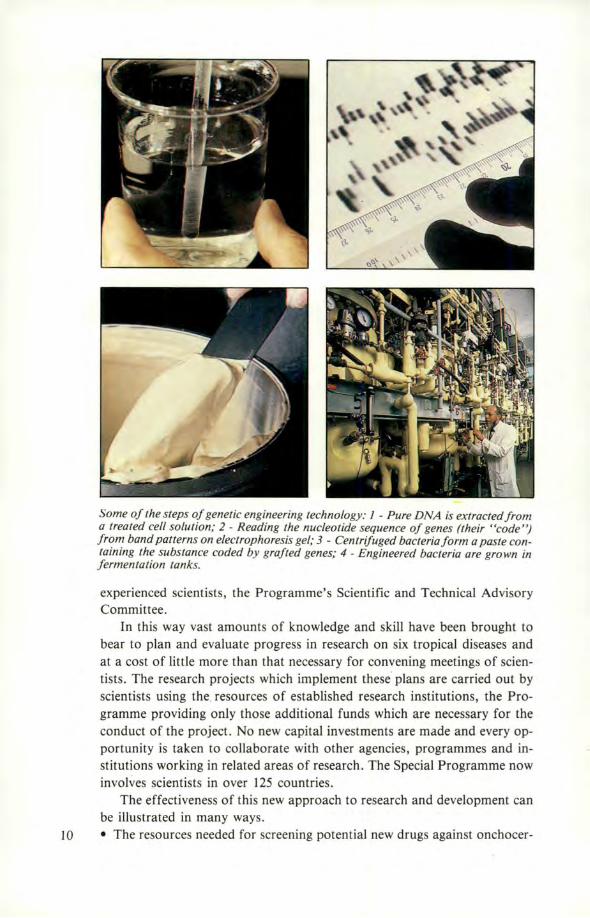
Some of the steps of genetic engineering technology: 1 - Pure DNA is extracted from a treated cell solution; 2 - Reading the nucleotide sequence of genes (their "code") from band patterns on electrophoresis gel; 3 - Centrifuged bacteria form a paste containing the substance coded by grafted genes; 4 - Engineered bacteria are grown in fermentation tanks.
experienced scientists, the Programme's Scientific and Technical Advisory Committee.
In this way vast amounts of knowledge and skill have been brought to bear to plan and evaluate progress in research on six tropical diseases and at a cost of little more than that necessary for convening meetings of scientists. The research projects which implement these plans are carried out by scientists using the. resources of established research institutions, the Programme providing only those additional funds which are necessary fo r the conduct of the project. No new capital investments are made and every opportunity is taken to collaborate with other agencies, programmes and institutions working in related areas of research . The Special Programme now involves scientists in over 125 countries.
The effectiveness of this new approach to research and development can be illustrated in many ways.
IO • The resources needed for screening potential new drugs against onchocer-
ciasis, or "river blindness", are scattered through many continents. New compounds are synthesized in Europe and Japan, and undergo a first stage of screening for effectiveness in Europe and America. The second stage of screening takes place in Australia using a local variety of cattle which have proven to be the best models for human disease. Finally, those compounds which pass the screens and safety tests are tested against human disease in Africa. • The distribution and spread of drug-resistant malaria is monitored by scientists in dozens of countries using standardized tests and protocols developed by the Special Programme. • The Special Programme acts as a source of biological materials which would otherwise be very difficult to obtain. For example, leprosy bacilli are needed for a variety of specialized studies; the Programme has established a bank of bacilli, and supplies scientists throughout the world. • Much of the value of epidemiological disease surveys depends upon their comparability from one country and from one study to another. The Programme has standardized research protocols for such surveys and for the diagnostic tests used in them.
The Special Programme is pleased to acknowledge the collaboration of the pharmaceutical industry in the planning and execution of research. By the end of 1983 seventy-eight scientists from 41 companies had been involved in Special Programme projects and in planning the development of new drugs and vaccines. The Programme complements the skills and experience of industry in drug and vaccine development through the provision of facilities for the determination of effectiveness against disease in animal models, and through collaboration with tropical countries to provide facilities for essential pharmacological and clinical studies in man.
Training grants
Under its policy of strengthening research in endemic countries the Programme has awarded over 500 training grants and is providing financial and other support to more than 60 national institutions to strengthen their research capability according to their individual needs . The effects of these efforts are now becoming apparent. The proportion of Programme funding going to scientists and institutions in developing countries in the tropics has risen steadily from 29% in 1977 to over 55% in 1983 , and more than one-third of the publications resulting from Programme research projects have come from scientists working in institutions of tropical countries .
• 11
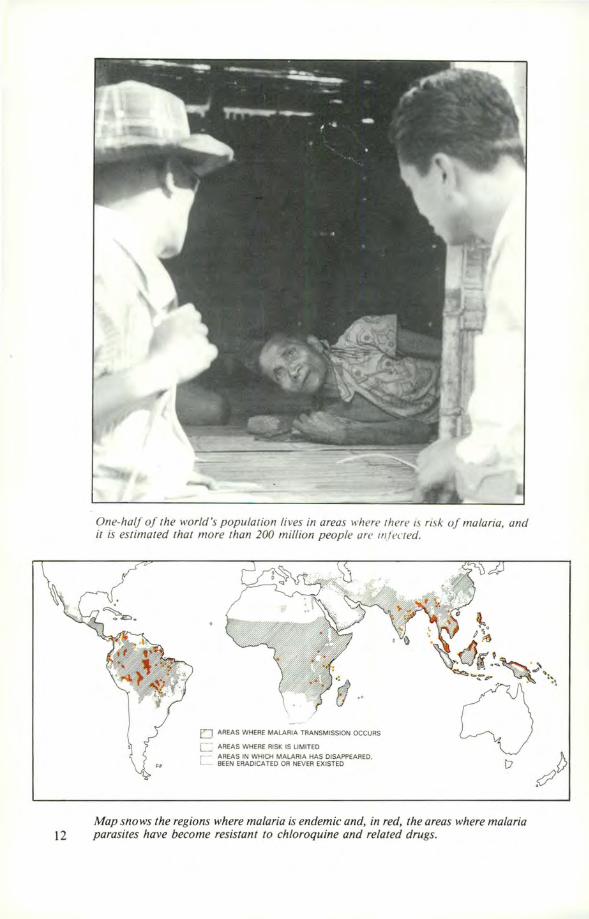
One-half of the world's population lives in areas where 1here is risk of malaria, and it is estimated that more than 200 million people are 111fec1ed.
"
eJ AREAS WHERE MALARIA TRANSMISSION OCCURS
C:::: AREAS WHERE RISK IS LIMITED
C :~i:i~~rii't!~~D~~~CE~AE~~~:;PEAREO. D
Map snows the regions where malaria is endemic and, in red, the areas where malaria 12 parasites have become resistant to chloroquine and related drugs.

THE KING OF DISEASES
I n ancient India, malaria was known as the "King of diseases" . One of the world's most widespread and severe diseases, it has plagued mankind since prehistoric times. In recent years, the relaxation of
control measures, the resistance of malaria parasites to antimalarial drugs, and the resistance of the mosquito vectors to insecticides have combined to create a dangerous and potentially explosive resurgence of the disease.
For centuries malaria has been treated with various medicinal plants, notably the bark of cinchona, a tropical tree from which quinine was isolated in 1820. Chloroquine, a major antimalarial drug, was synthesized almost half a century ago, and other related compounds followed. With the advent of
' ' DDT as an effective and inexpensive insecticide, total eradication, even in tropical areas outside Africa, appeared feasible and became the objective of a World Health Organization programme started in the late 1950s.
More than 50 countries undertook eradication programmes. Mosquitokilling insecticides were used to interrupt the cycle of transmission and drugs were employed to destroy the parasites in their human hosts. By the early 1960s, the disease had been eradicated in a number of countries in Europe and the Middle East and in parts of South America and the southern United States. By 1965, India had reduced the number of cases from tens of millions to about 100 000, and in Sri Lanka only 17 cases· were reported in' 1963.
Then malaria struck back. In 1969 about half a million cases were reported in a total population of 12 million in Sri Lanka, and in 1976 some 6.5 million cases were reported in India. In the WHO South-East Asian Region the number of reported cases rose from 1.8 million in 1972 to 3. 7 million in 1980. In tropical Africa, where the infrastructure for an eradication programme was lacking, the disease has always remained highly endemic, and it is estimated that more than 200 million people are infected.
What are the reasons for these severe setbacks? Large numbers of mosquitoes were out of reach of the DDT spraying cam
paigns and others gradually became resistant to this insecticide, which was also widely used in agriculture. Some sought new breeding places or began to avoid the places sprayed with DDT. Spraying campaigns were often too difficult or costly to carry out. Other insecticides came into use-usually more expensive chemicals such as dieldrin, malathion, temephos and permethrin, but resistance has now become widespread to these agents. Sometimes initial success was followed by a relaxation of efforts, leaving the door open to renewed breeding of mosquitoes and resurgence of disease.
Just as mosquitoes became resistant to insecticides, parasites became resis-tant to drugs. A number of antimalarials-quinine, chloroquine and other 13
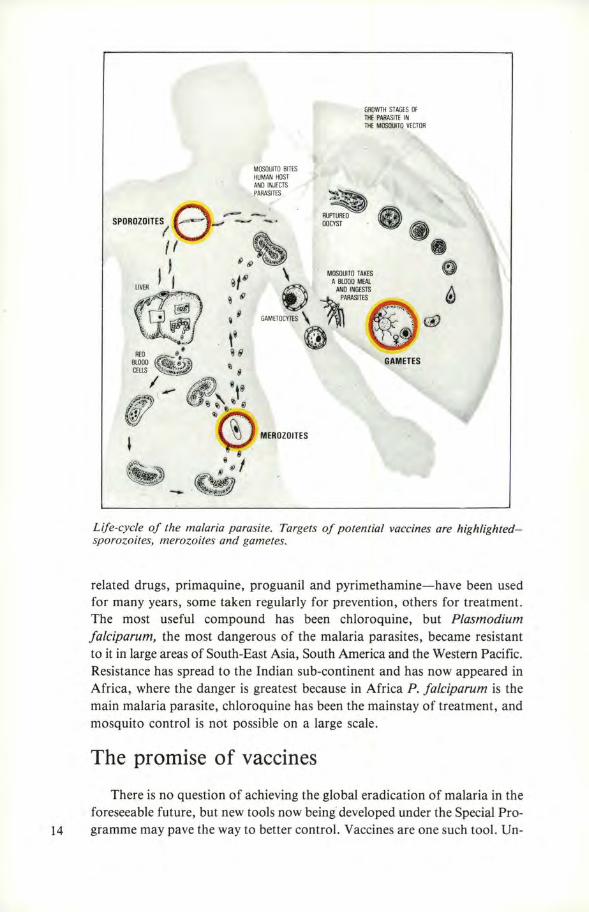
MOSQUITO BITES HUMAN HOST ANO INJECTS PARASITES
SPOROZO;TES/ e-----:.:.. f I .
\
GROWTH STAGES OF THE PARASITE IN THE MOSQUITO VECTOR
--. MOSQUITO TAKES
A BLOOD MEAL
@ I ' LIVER I ~ . ANO INGESTS A
~ ~ARASITES ~
ow"o=;o 7'11 ~ ~ ·~ .
GAMETES
-Life-cycle of the malaria parasite. Targets of potential vaccines are highlightedsporozoites, merozoites and gametes.
related drugs, primaquine, proguanil and pyrimethamine-have been used for many years, some taken regularly for prevention, others for treatment. The most useful compound has been chloroquine, but P/asmodium falciparum, the most dangerous of the malaria parasites, became resistant to it in large areas of South-East Asia, South America and the Western Pacific. Resistance has spread to the Indian sub-continent and has now appeared in Africa, where the danger is greatest because in Africa P. f alciparum is the main malaria parasite, chloroquine has been the mainstay of treatment, and mosquito control is not possible on a large scale.
The promise of vaccines
There is no question of achieving the global eradication of malaria in the foreseeable future, but new tools now being developed under the Special Pro-
14 gramme may pave the way to better control. Vaccines are one such tool. Un-
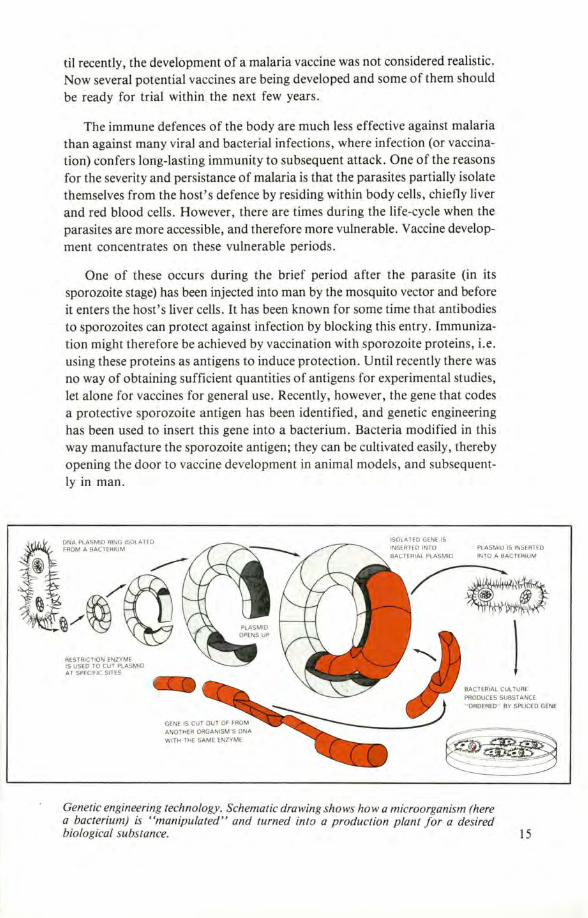
til recently, the development of a malaria vaccine was not considered realistic. Now several potential vaccines are being developed and some of them should be ready for trial within the next few years .
The immune defences of the body are much less effective against malaria than against many viral and bacterial infections, where infection (or vaccination) confers long-lasting immunity to subsequent attack . One of the reasons for the severity and persistance of malaria is that the parasites partially isolate themselves from the host ' s defence by residing within body cells, chiefly liver and red blood cells. However, there are times during the life-cycle when the parasites are more accessible, and therefore more vulnerable. Vaccine development concentrates on these vulnerable periods.
One of these occurs during the brief period after the parasite (in its sporozoite stage) has been injected into man by the mosquito vector and before it enters the host ' s liver cells. It has been known for some time that antibodies to sporozoites can protect against infection by blocking this entry. Immunization might therefore be achieved by vaccination with sporozoite proteins, i.e . using these proteins as antigens to induce protection. Until recently there was no way of obtaining sufficient quantities of antigens for experimental studies, let alone for vaccines for general use. Recently, however, the gene that codes a protective sporozoite antigen has been identified, and genetic engineering has been used to insert this gene into a bacterium. Bacteria modified in this way manufacture the sporozoite antigen; they can be cultivated easily, thereby opening the door to vaccine development in animal models, and subsequently in man.
ISOLATED GENE IS DNA PLASMID AlNG ISOLATED FROM A BACTEHIUM PLASMIU IS INSERTED
INTO A BACTERIUM
RESTRICTION ENZYME IS USED TO CUT PLASMID AT SPECIFIC SITES
ANOTHER ORGANISM 'S ONA WITH THE SAME ENZYME
~ l
BACTERIAL CUL TUAE PRODUCES SUBSTANCE " ORDERED" BY SPLICED GENE
Genetic engineering technology . Schematic drawing shows how a microorganism (here a bacterium) is "manipulated" and turned into a production plant for a desired biological substance. 15
Antimalarial drugs may be added to ordinary kitchen salt, but such systematic use may lead to parasite resistance to these drugs. Different strategies, new drugs and drug combinations must be studied to avoid, or at least delay, resistance.
The microbiologists at New York University Medical Center who did this work used as a model the sporozoite of Plasmodium knowlesi, a monkey malaria parasite. The chemical structure of the immunogenic part of the major sporozoite antigen has now been worked out and it can be produced by chemical synthesis. Studies on the corresponding antigen of the human malaria parasite, Plasmodium f alciparum, are under way. Similar principles are being applied to the search and production of protective antigens from malaria parasites at other phases of their life-cycle.
The merozoite stage, which results from a multiplication of the parasite in the liver and in red blood cells, is another focus of vaccine research. Merozoites invade red blood cells and so perpetuate the blood phase of the infection that provokes the major symptoms of malaria-high fever and rigor. Merozoite antigens have recently been isolated and found to induce immunity to malaria in mice, and similar studies are in progress on the merozoites of human malaria parasites. A successful merozoite vaccine could prevent the severe clinical effects of disease .
Another possible vaccine would be one that acts against the gametes (sex-16 ual stage) of the parasite. Gametes mature in the mosquito's stomach after
A malaria patient being carried to the dispensary.
ingestion of infected blood; there they fuse, and further development leads ultimately to the production of the sporozoites that transmit the infection when the mosquito bites again. The fusion of gametes in the mosquito can be prevented by antibodies to gametes in the ingested human blood. Vaccination causing the production of such antibodies by the human host therefore carries the potential of interrupting malaria transmission by the mosquito. Such vaccination would be entirely novel in concept; it would not prevent disease in the vaccinated person, but would prevent the transfer of his infection to others.
It is not known what type of vaccine will become available first for human trials but it is now clear that immunization against malaria is a realistic goal. A sporozoite vaccine could potentially prevent infection by attacking the parasite at its earliest stage of development in man . A merozoite vaccine could be used to reduce morbidity and the mortality associated with falciparum malaria, particularly in children and pregnant women. A gamete vaccine could reduce or interrupt transmission of the disease. Several types of vaccines, or vaccines combining several antigens, may eventually be required.
Dr. Adetokunbo 0. Lucas, Director of the Special Programme, believes that "from a public health point of view, a vaccine preventing severe illness and death among the highly susceptible would be a major boon, especially if the protection were to last a year or so. But even a short period of protection would help, since in some parts of the world, the transmission season lasts only a few months each year'' . The Nigerian epidemiologist concludes: "Therefore, a vaccine effective for six months could protect during the en-tire transmission season. Of course, there are problems of logistics in deliver- 17
ing any of these new tools to the community. But at present we have to give people drugs which they must take daily or weekly, and something that would need to be administered only once a year or even every six months would be a lot simpler''.
The mefloquine story
A new antimalarial drug will be available sooner than a vaccine. The development of mefloquine, a much needed replacement for drugs against which malaria parasites have developed resistance, has been an outstanding example of collaboration among the Special Progamme, several research institutes and the pharmaceutical industry.
The story starts soon after the advent of chloroquine resistance in Plasmodiumfalciparum, when the Walter Reed Army Institute of Research (WRAIR) scaled up its extensive research programme during which more than 300 000 compounds were synthesized and tested for antimalarial activity. In 1971 an active compound was discovered, selected for further development, and given the name mefloquine.
In 1975, research scientists from the Swiss pharmaceutical company Hoffmann-La Roche and representatives of WRAIR participated in a Special Programme planning meeting on the chemotherapy of malaria. Interest was expressed in the rapid development of mefloquine, but neither the Special Programme nor WRAIR were in a position to develop the drug alone. Hoffmann-La Roche offered to produce a mefloquine preparation and to provide amounts sufficient for clinical trials free of charge to the World Health Organization. It took about two years to develop a process of synthesis on an industrial scale and to achieve an acceptable formulation of mefloquine, a costly and complex multi-stage process. The Special Programme and Hoffmann-La Roche then collaborated in a series of clinical trials in Brazil, Zambia and Thailand, which confirmed the compound's safety and efficacy in man. It was found that infections with falciparum malaria, even when resistant to commonly used drugs, could usually be cured with a single dose.
But just as resistance developed to chloroquine, so it is likely to appear to mefloquine. Two steps are being taken to delay this: firstly, combinations of mefloquine with other antimalarials are being developed, and a pharmaceutical formulation of mefloquine with sulphadoxine and pyrimethamine will be registered very soon; secondly, WHO is advising countries on the rational use of mefloquine and mefloquine combinations and cautioning against indiscriminate use which can lead to resistance.
Qinghaosu
Another promising antimalarial drug is undergoing trials in China. The use of the herb qinghao (Artemisia annua) for the treatment of malaria was
18 first recorded in the Zhou hou beiji fang, "Handbook of Prescriptions for
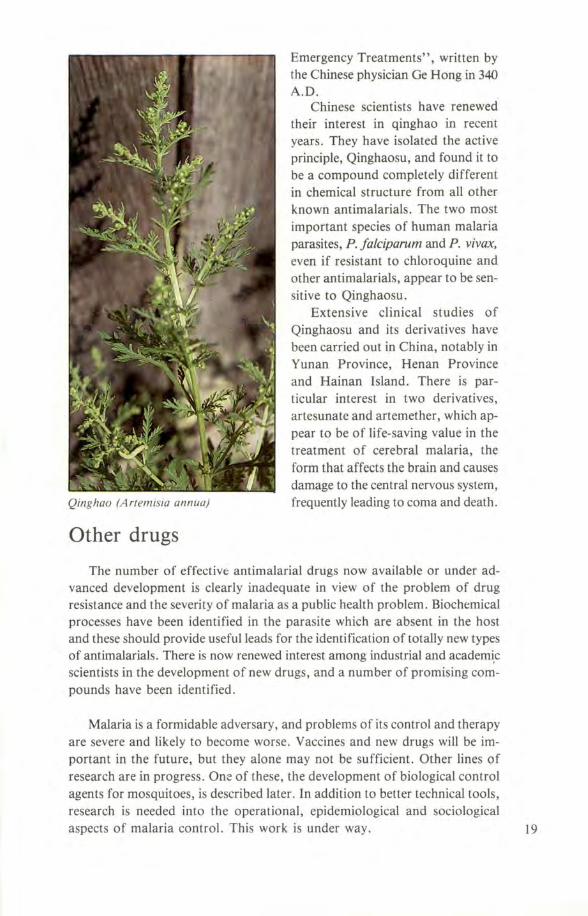
Qinghao (Artemisia annua)
Other drugs
Emergency Treatments", written by the Chinese physician Ge Hong in 340 A.D.
Chinese scientists have renewed their interest in qinghao in recent years. They have isolated the active principle, Qinghaosu, and found it to be a compound completely different in chemical structure from all other known antimalarials. The two most important species of human malaria parasites, P. falciparum and P. vivax, even if resistant to chloroquine and other antimalarials, appear to be sensitive to Qinghaosu.
Extensive clinical studies of Qinghaosu and its derivatives have been carried out in China, notably in Yunan Province, Henan Province and Hainan Island. There is particular interest in two derivatives, artesunate and artemether, which appear to be of life-saving value in the treatment of cerebral malaria, the form that affects the brain and causes damage to the central nervous system, frequently leading to coma and death.
The number of effective antimalarial drugs now available or under advanced development is clearly inadequate in view of the problem of drug resistance and the severity of malaria as a public health problem. Biochemical processes have been identified in the parasite which are absent in the host and these should provide useful leads for the identification of totally new types of antimalarials. There is now renewed interest among industrial and academ~c scientists in the development of new drugs, and a number of promising compounds have been identified .
Malaria is a formidable adversary, and problems of its control and therapy are severe and likely to become worse. Vaccines and new drugs will be important in the future, but they alone may not be sufficient. Other lines of research are in progress. Orn: of these, the development of biological control agents for mosquitoes, is described later. In addition to better technical tools , research is needed into the operational, epidemiological and sociological aspects of malaria control. This work is under way. 19
Instruction in simple physiotherapy and group exercise are organized for leprosy patients whose hands are affected.
A Burmese child being examined for loss of sensitivity of the skin, which is an early 20 sign of leprosy.

LEPROSY: NEW HOPE
F or the public, leprosy is one of the most misunderstood of the infectious diseases; and for the patient, one of the most tragic. Throughout the ages the disease has been looked upon with horror and in 18th
century Europe, leprosy patients were still liable to be locked up in leprosaria, or had to wear bells to warn people of their approach. To this day leprosy patients are often ostracized from society and made to feel guilty for having the disease. Because of these attitudes there has been an attempt to abandon the term "leprosy" in favor of "Hansen's disease", after the Norwegian physician Armauer Hansen who first identified Mycobacterium leprae more than
. a century ago. One misconception about leprosy is the notion that it is a disease only
of the past. There are more than 11 million people with this disease in the world today, mostly in tropical regions of Africa, Asia, especially India, and Latin America. Another erroneous belief is that the disease is easily contracted. In fact, few persons exposed to patients develop the disease, even though the infective agent may have been transmitted to them.
For the past thirty years leprosy has been treated effectively with the drug dapsone administered over very long courses, often for the lifetime of the patient. This advance has benefited millions, but there are now severe problems. Resistance of Mycobacterium leprae to dapsone has appeared on a worldwide scale, and in some studies resistance has been found in as many as one-third of new patients. Another problem is that drugs, even when they do work, cannot restore the mutilations caused by disease. There is also the chilling fact that only one in four leprosy patients ever receives systematic treatment and, since leprosy does not kill directly, most patients have to live out their lives as best they can without the benefit of effective therapy. Research is in progress to improve drug treatment, to develop tests for the diagnosis of infection before the appearance of disease and to develop a vaccine. People's attitudes and perceptions of leprosy are also under study, in the expectation that improved understanding of the disease will help to remove the stigma which is so great a barrier to treatment and control.
To improve chemotherapy, several different combinations of drugs have been assessed and have shown varying degrees of effectiveness. The effective combinations are more costly, but they are also more cost-effective than dapsone and they do not require life-long administration. The new multi-drug regimens are now recommended by WHO for use in leprosy control programmes. In addition the activity of several new compounds is being assessed in animal models.
Immunological studies have shown that there are constituents of M. leprae 21
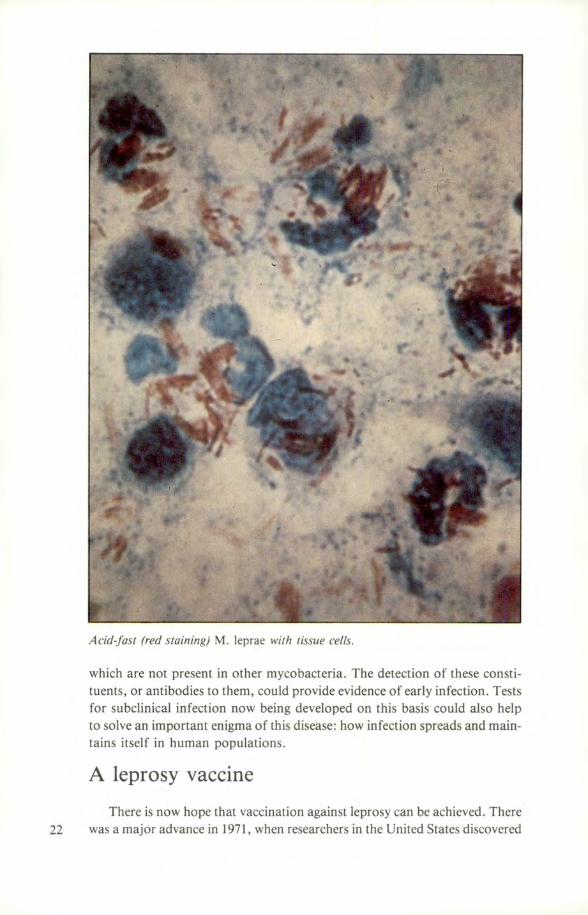
Acid-fast (red staining) M. leprae with tissue cells.
which are not present in other mycobacteria. The detection of these constituents, or antibodies to them, could provide evidence of early infection . Tests for subclinical infection now being developed on this basis could also help to solve an important enigma of this disease: how infection spreads and maintains itself in human populations.
A leprosy vaccine
There is now hope that vaccination against leprosy can be achieved. There 22 was a major advance in 1971, when researchers in the United States discovered
that injection of M. leprae into nine-banded armadillos caused massive infection, especially of the liver. A single gram of armadillo liver tissue can yield as many as 10 billion bacilli, which may be enough to produce from 100 to 1 000 doses of vaccine.
M. leprae in these amounts was sufficient to begin a worldwide research effort in vaccine development. The Special Programme has supplied researchers with leprosy bacilli, funded and coordinated their efforts, and made it possible for them to meet to compare results and explore new ideas .
"Armadillo farms" were established to grow M. leprae, ways were found to harvest and extract the bacilli from armadillo tissues , and the protective properties of killed bacilli were studied in animal models. There is now good evidence that a preparation of killed M. leprae does protect animals from infection.
A vaccine comprising killed M. leprae, prepared by the W ellcome Research Laboratories in England under contract with the Special Programme, is now undergoing trials in volunteers in Norway. Such tests are conducted in areas remote from the disease so that the results are not confused by previous exposure and possible immunity to infection. Studies focus on the immune response, the determination of the most appropriate dose and, of course, on the safety of the vaccine.
There is very encouraging evidence from recent research that a leprosy vaccine could be used for treatment as well as prevention . Dr. Jacinto Convit in Caracas, Venezuela, found that inoculation of killed M. leprae with the tuberculosis vaccine (BCG), together with chemotherapy, was effective in treatment of patients with severe lepromatous leprosy. Dr. Convit feels that if existing disease can be arrested in this way, there is even more hope that a vaccine may be effective in preventing the disease.
The Special Programme is now entering the phase of field trials of leprosy vaccines. Leprosy is a disease of low incidence, with a long incubation period, so that assessment of the protective efficacy of vaccines will require observations on large populations over many years . For this reason as much information as possible about vaccine efficacy will be obtained from preliminary small-scale studies, and the design of large-scale trials will be based upon these initial findings.
The development of leprosy vaccines to their present stage is the direct result of collaboration between scientists in many different disciplines, which include cell biology and fractionation, the immunology of infectious processes and clinical immunology, vaccine design and safety, and epidemiology. To conduct this research the Programme by the end of 1983 had provided research contracts to 65 scientists in 23 countries, and vaccine development is progressing on schedule, according to a plan originally drawn up in 1974. This is both a tribute to the foresight of the scientists who made the plan, and a practical example of what can be achieved by an international collaborative research network. 23
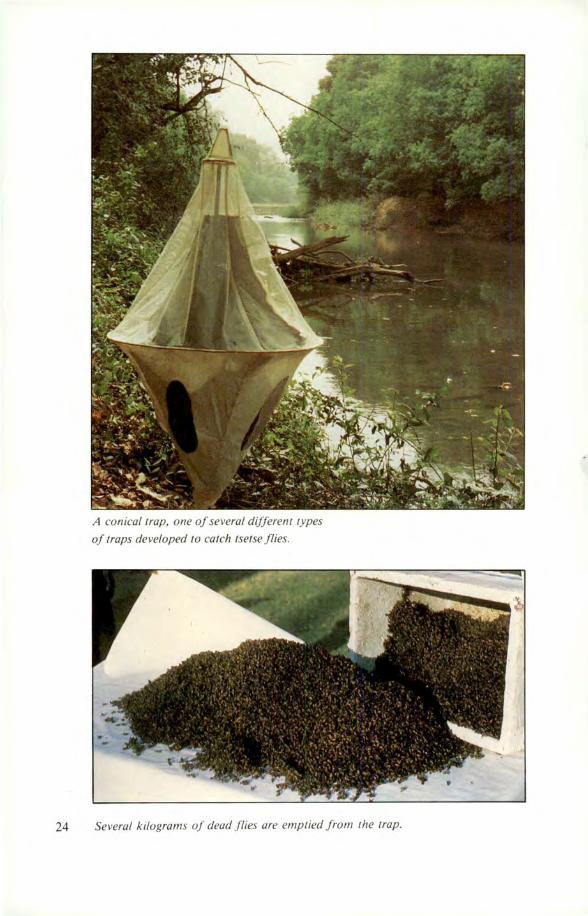
A conical trap, one of several differenl types
of traps developed to catch tsetse flies .
24 Several kilograms of dead flies are emptied from 1he trap.

NATURE'S OWN TOOLS
The infective agents of the six tropical diseases, with the exception of leprosy, are transmitted from one individual to another by various animal vectors, which include mosquitoes and other blood-sucking in
sects, and freshwater snails. Control of vectors can be a practical way to slow or stop the transmission of infection and is therefore an essential part of disease control.
Vectors such as mosquitoes, blackflies and snails can be killed by chemical pesticides, and insecticides such as DDT have been widely used with considerable success. But there are disadvantages: chemicals can be expensive, the target vectors can develop resistance, a variety of non-target organisms may be affected, and the intensive use of chemicals (particularly for agricultural purposes) has given rise to concern for damage to the environment.
An alternative approach to vector control is to use a biological agent, that is, an organism or its product which preys on or destroys insect vectors under natural circumstances. Such an agent is less likely to be an environmental danger and may have other advantages such as low cost and the possibility of being produced locally.
The two dozen or so organisms now being studied as potential vector control agents include viruses, bacteria, fungi, protozoa, nematodes, flatworms, fish, and insects such as predatory mosquitoes. Top priority has been given to one bacillus that has now become the object of worldwide research: Bacillus thuringiensis Serotype H-14, or B.t. H-14. This agent was developed to a great extent by industry and the Special Programme and has been tested in both temperate and tropical environments. It has been found to be remarkably safe, yet it is highly toxic to the larvae of two important disease vectors, the blackflies which transmit river blindness and the mosquitoes which transmit malaria and filariasis .
These effects are due to a specific toxin of the bacillus, present in bacillary spores. (Spores are the forms of bacilli especially adapted to withstand drying and other environmental hazards). The B. t. H-14 vector control agent consists of spores which are produced by large-scale fermentation, and then appropriately formulated to reach the vector under attack.
B.t. H-14 came to the attention of the Special Programme after Israeli scientists isolated a bacillus from ponds where mosquitoes were breeding. The spores of the bacillus were found to be highly toxic to mosquito larvae. The bacillus was subsequently identified at the Pasteur Institute, Paris, as B. t. H-14. Further research, sponsored in part by the Special Programme, confirmed the efficacy of B.t. H-14 against the larvae of mosquitoes and blackflies, and showed that the spores were specific in their attack on these 25
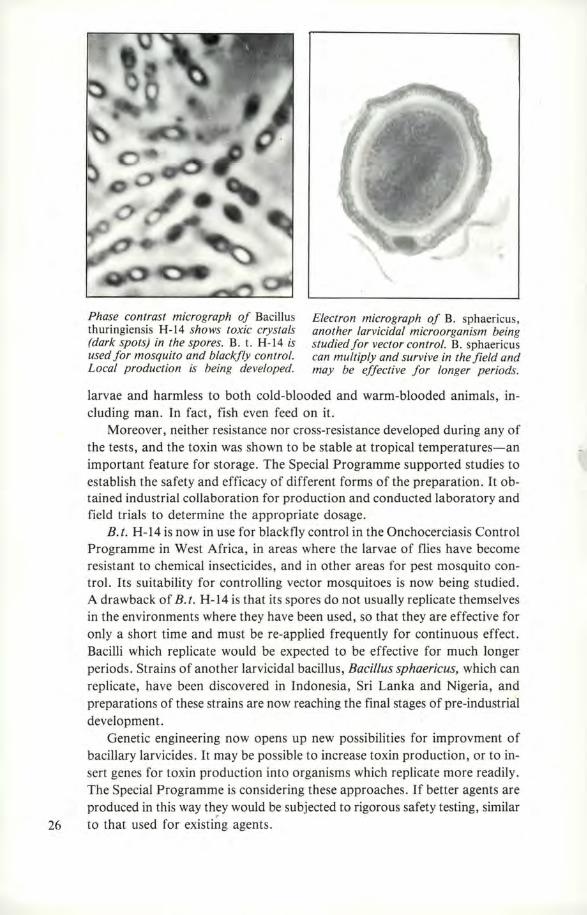
Phase contrast micrograph of Bacillus thuringiensis H-14 shows toxic crystals (dark spots) in the spores. B. t. H-14 is used for mosquito and blackfly control. Local production is being developed.
Electron micrograph of B. sphaericus, another larvicidal microorganism being studied for vector control. B. sphaericus can multiply and survive in the field and may be effective for longer periods.
larvae and harmless to both cold-blooded and warm-blooded animals, including man . In fact, fish even feed on it.
Moreover, neither resistance nor cross-resistance developed during any of the tests, and the toxin was shown to be stable at tropical temperatures-an important feature for storage. The Special Programme supported studies to establish the safety and efficacy of different forms of the preparation. It obtained industrial collaboration for production and conducted laboratory and field trials to determine the appropriate dosage.
B.t. H-14 is now in use for blackfly control in the Onchocerciasis Control Programme in West Africa, in areas where the larvae of flies have become resistant to chemical insecticides, and in other areas for pest mosquito control. Its suitability for controlling vector mosquitoes is now being studied. A drawback of B.t. H-14 is that its spores do not usually replicate themselves in the environments where they have been used, so that they are effective for only a short time and must be re-applied frequently for continuous effect. Bacilli which replicate would be expected to be effective for much longer periods. Strains of another larvicidal bacillus, Bacillus sphaericus, which can replicate, have been discovered in Indonesia, Sri Lanka and Nigeria, and preparations of these strains are now reaching the final stages of pre-industrial development.
Genetic engineering now opens up new possibilities for improvment of bacillary larvicides. It may be possible to increase toxin production, or to insert genes for toxin production into organisms which replicate more readily. The Special Programme is considering these approaches. If better agents are produced in this way they would be subjected to rigorous safety testing, similar
26 to that used for existi~g agents.
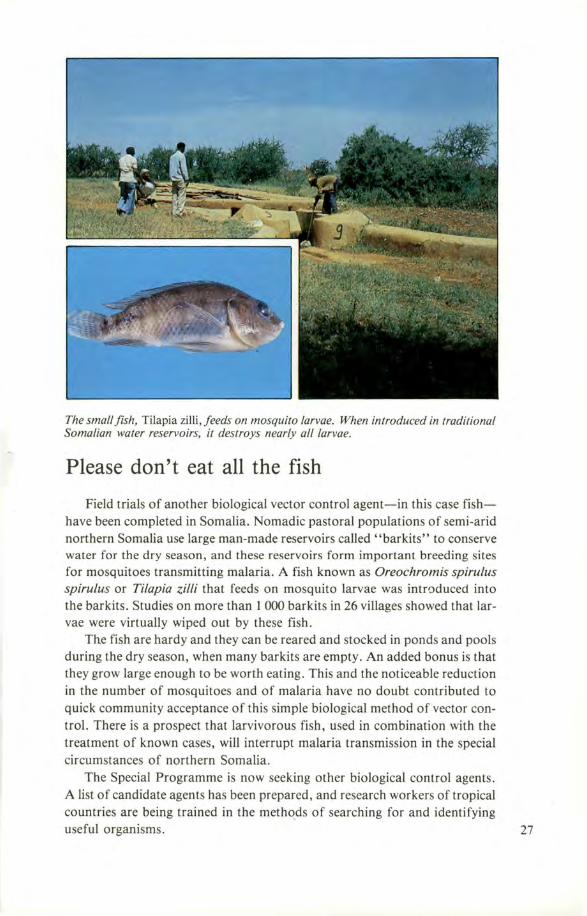
The small fish, Tilapia zilli, feeds on mosquito larvae. When introduced in traditional Somalian water reservoirs, it destroys nearly all larvae.
Please don't eat all the fish
Field trials of another biological vector control agent-in this case fishhave been completed in Somalia. Nomadic pastoral populations of semi-arid northern Somalia use large man-made reservoirs called "barkits" to conserve water for the dry season, and these reservoirs form important breeding sites for mosquitoes transmitting malaria. A fish known as Oreochromis spirulus spirulus or Tilapia zil/i that feeds on mosquito larvae was intraduced into the bar kits. Studies on more than I 000 barkits in 26 villages showed that larvae were virtually wiped out by these fish.
The fish are hardy and they can be reared and stocked in ponds and pools during the dry season, when many barkits are empty. An added bonus is that they grow large enough to be worth eating. This and the noticeable reduction in the number of mosquitoes and of malaria have no doubt contributed to quick community acceptance of this simple biological method of vector control. There is a prospect that larvivorous fish, used in combination with the treatment of known cases, will interrupt malaria transmission in the special circumstances of northern Somalia.
The Special Programme is now seeking other biological control agents. A list of candidate agents has been prepared, and research workers of tropical countries are being trained in the methods of searching for and identifying useful organisms. 27
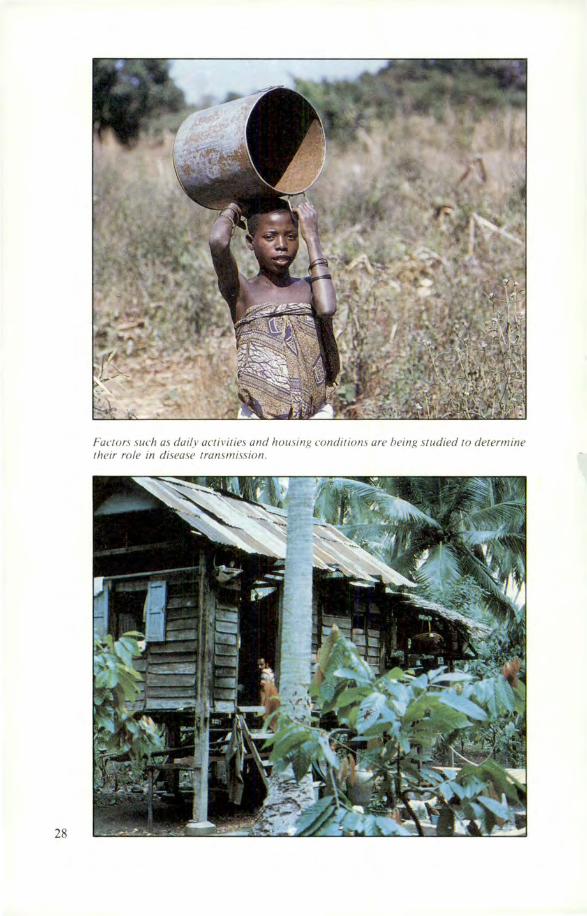
28
Fauors such as daily activities and housing condirions are being studied to determine their role in disease transmission.
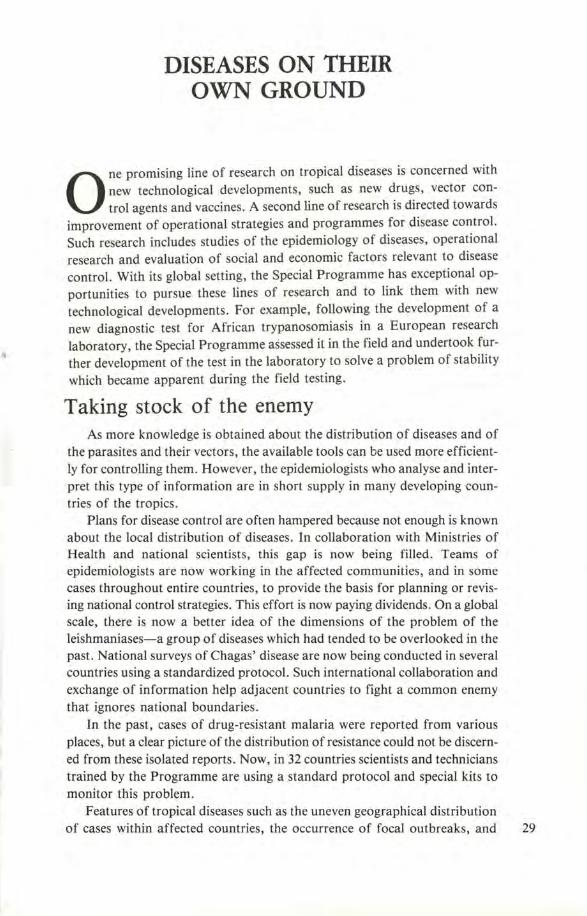
DISEASES ON THEIR OWN GROUND
0 ne promising line of research on tropical diseases is concerned with new technological developments, such as new drugs, vector control agents and vaccines. A second line of research is directed towards
improvement of operational strategies and programmes for disease control. Such research includes studies of the epidemiology of diseases, operational research and evaluation of social and economic factors relevant to disease control. With its global setting, the Special Programme has exceptional opportunities to pursue these lines of research and to link them with new technological developments. For example, following the development of a new diagnostic test for African trypanosomiasis in a European research laboratory, the Special Programme assessed it in the field and undertook further development of the test in the laboratory to solve a problem of stability which became apparent during the field testing.
Taking stock of the enemy As more knowledge is obtained about the distribution of diseases and of
the parasites and their vectors, the available tools can be used more efficiently for controlling them. However, the epidemiologists who analyse and interpret this type of information are in short supply in many developing countries of the tropics.
Plans for disease control are often hampered beqmse not enough is known about the local distribution of diseases. In collaboration with Ministries of Health and national scientists, this gap is now being filled. Teams of epidemiologists are now working in the affected communities, and in some cases throughout entire countries, to provide the basis for planning or revising national control strategies. This effort is now paying dividends. On a global scale, there is now a better idea of the dimensions of the problem of the leishmaniases-a group of diseases which had tended to be overlooked in the past. National surveys of Chagas' disease are now being conducted in several countries using a standardized protocol. Such international collaboration and exchange of information help adjacent countries to fight a common enemy that ignores national boundaries.
In the past, cases of drug-resistant malaria were reported from various places, but a clear picture of the distribution of resistance could not be discerned from these isolated reports. Now, in 32 countries scientists and technicians trained by the Programme are using a standard protocol and special kits to monitor this problem.
Features of tropical diseases such as the uneven geographical distribution of cases within affected countries, the occurrence of focal outbreaks, and 29
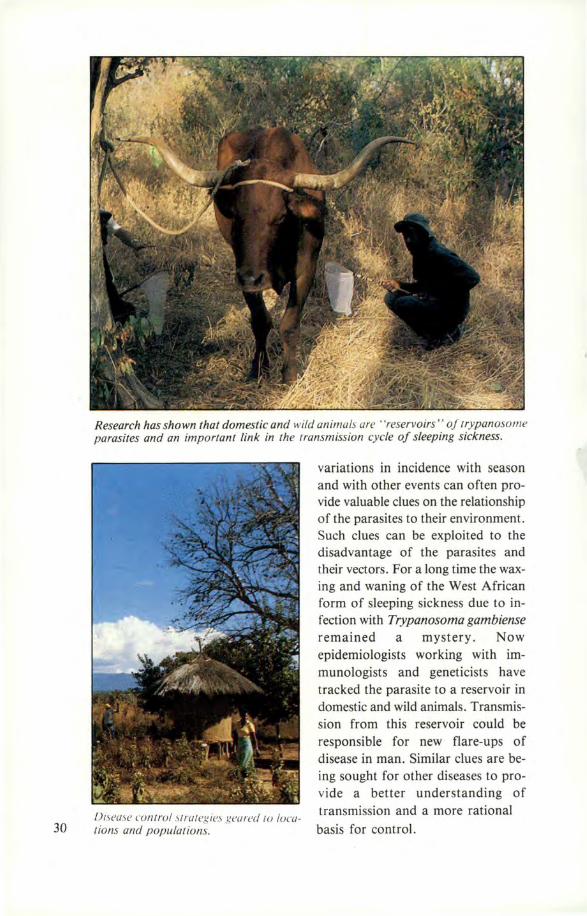
30
Research has shown that domestic and wild animals are · 'reservoirs " of 1rypanoso111e parasites and an important link in the lransmission cycle of sleeping sickness.
Di,ease cu111rul , trategies grnrecl lU local ions and populalions.
variations in incidence with season and with other events can often provide valuable clues on the relationship of the parasites to their environment. Such clues can be exploited to the disadvantage of the parasites and their vectors. For a long time the waxing and waning of the West African form of sleeping sickness due to infection with Trypanosoma gambiense remained a mystery. Now epidemiologists working with immunologists and geneticists have tracked the parasite to a reservoir in domestic and wild animals. Transmission from this reservoir could be responsible for new flare-ups of disease in man. Similar clues are being sought for other diseases to provide a better understanding of transmission and a more rational
basis for control.

Working with the people
Sometimes disease control programmes fail because of lack of understanding and cooperation by the local population. In the Philippines social scientists found that people gave various names and ascribed various causes to the different symptoms of filar;iasis, and that in general they associated the disease with working in water and carrying heavy loads . Based on this finding a local health education programme has been set up to increase community participation in the work of detection and treatment.
In Nigeria sociologists, local health workers and traditional healers are studying people's knowledge and understanding of different tropical diseases and the ways used to control them. Based on the findings appropriate health education is being planned for children and adults, including the preparation of an educational primer .
Better strategies for control
In Thailand an economist worked with the malaria control programme to evaluate the costs and effectiveness of different procedures for malaria surveillance. It was found that on both counts malaria clinics were much superior to home visiting, and a method for costing of surveillance was developed for future use.
In the Dominican Republic social scientists are working with the Malaria Division of the Ministry of Health to study social and economic factors associated with the transmission of malaria. Findings will be used to improve the strategies of control programmes; these are already being reviewed in the light of special problems which were found to be associated with migration and economic status.
Research on disease control strategies, which are often specific to locations and populations, will require many different studies in different countries. The Special Programme faces this challenge in several ways. Firstly, it considers that research must be regarded as an essential part of every disease control programme and encourages national authorities to appreciate its importance. Secondly, in view of the great shortage of epidemiologists, sociologists and economists working in the health sector in tropical countries, it has instituted postgraduate training programmes in these disciplines. Thirdly, it conducts its own research on these topics, both to obtain information directly relevant to disease control in certain locations and to develop and improve research methods for more general application .
• 31
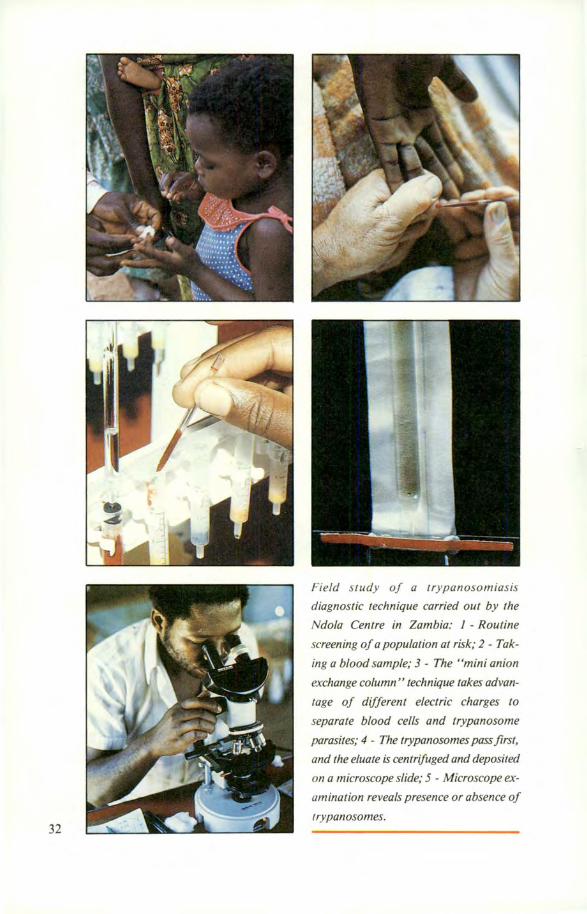
32
Field study of a trypanosomiasis
diagnostic technique carried out by the
Ndola Centre in Zambia: 1 - Routine
screening of a population at risk; 2 - Tak
ing a blood sample; 3 - The "mini anion
exchange column" technique takes advan
tage of different electric charges to
separate blood cells and trypanosome
parasites; 4 - The trypanosomes pass first,
and the eluate is centrifuged and deposited
on a microscope slide; 5 - Microscope ex
amination reveals presence or absence of
trypanosomes.

PARTNERS IN RESEARCH
A great variety of studies are required to improve the control of tropical diseases and many of these must necessarily take place in the countries where the diseases are endemic. New tools for control must be
field-tested; clinical, epidemiological, human behavioural and vector control studies are examples of work which can only be conducted on site in tropical countries. The conduct of such research is the responsibility of tropical countries and their scientists. Moreover, diseases and populations at risk are not unchanging. If disease control is to be achieved and maintained, tropical countries themselves must be competent to tackle new problems as they arise. The Special Programme has from its beginning recognized the importance of assisting tropical countries to acquire the competence in research which is needed to undertake these tasks.
How best can this assistance be provided, in view of the magnitude and diversity of the needs? The Special Programme has adopted the following policies and guidelines: • The Programme seeks to create a network of research institutions in tropical countries which jointly possess expertise in all the areas of research which are required to improve disease control. • The Programme identifies institutions for membership of the network on the basis of their resources and the institutional and national commitment to research. • In the first stage of building the network the Special Programme has assisted a number of institutions which already possessed a degree of scientific competence. Now in the second stage, these strengthened institutions are beginning to assist in the strengthening of other institutions in tropical countries. • The Programme provides support to institutions in two general ways: through financial grants and by training of scientists, research managers and other staff. The Programme especially aims to reduce the scientific isolation which hampers research in many institutions. • Because the development of capability in research is a long-term endeavour, all major institutional support is based on a long-term institutional development plan endorsed by both institutional and national authorities. An agreement is also reached for a progressive transfer of financial responsibility for the new activities from the Special Programme to national authorities. • Scientists of tropical countries receive priority under the Programme for support for research and development projects that are consistent with quality and rapid progress in research.
A period of a few years is a very short time to assess the success of such policies . There are, however, encouraging signs of progress. National 33
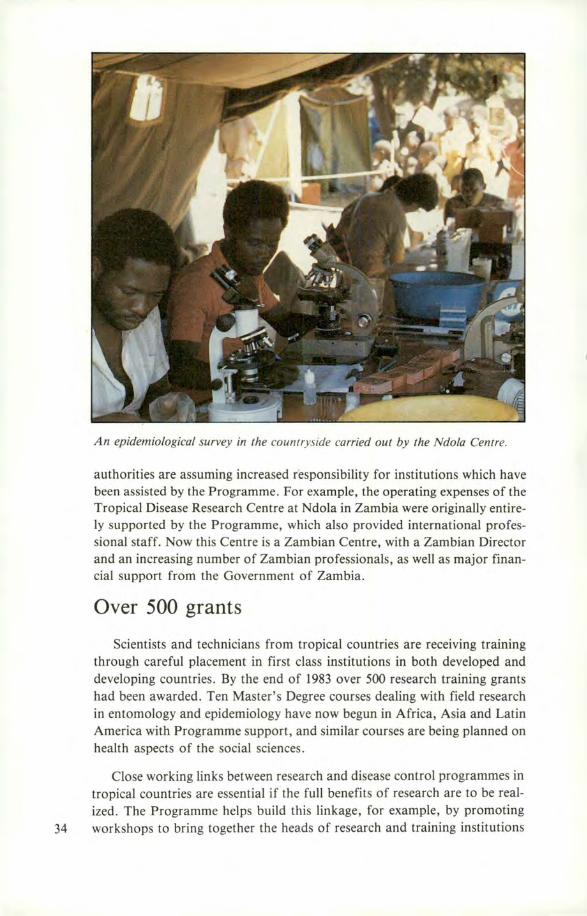
An epidemiological survey in the countryside carried out by the Ndola Centre.
authorities are assuming increased responsibility for institutions which have been assisted by the Programme. For example, the operating expenses of the Tropical Disease Research Centre at Ndola in Zambia were originally entirely supported by the Programme, which also provided international professional staff. Now this Centre is a Zambian Centre, with a Zambian Director and an increasing number of Zambian professionals, as well as major financial support from the Government of Zambia.
Over 500 grants
Scientists and technicians from tropical countries are receiving training through careful placement in first class institutions in both developed and developing countries. By the end of 1983 over 500 research training grants had been awarded. Ten Master's Degree courses dealing with field research in entomology and epidemiology have now begun in Africa, Asia and Latin America with Programme support, and similar courses are being planned on health aspects of the social sciences.
Close working links between research and disease control programmes in tropical countries are essential if the full benefits of research are to be realized. The Programme helps build this linkage, for example, by promoting
34 workshops to bring together the heads of research and training institutions
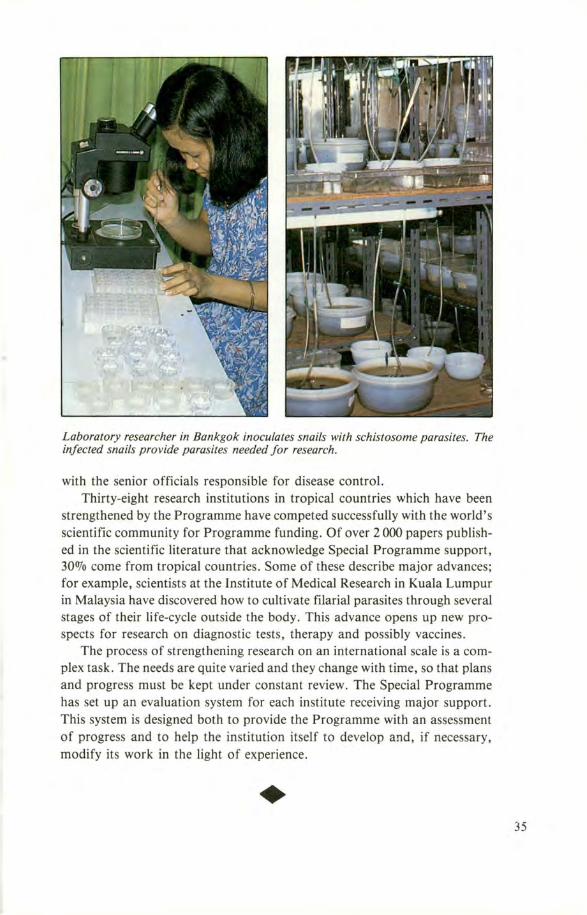
Laboratory researcher in Bankgok inoculates snails with schistosome parasites. The infected snails provide parasites needed for research.
with the senior officials responsible for disease control. Thirty-eight research institutions in tropical countries which have been
strengthened by the Programme have competed successfully with the world's scientific community for Programme funding. Of over 2 000 papers published in the scientific literature that acknowledge Special Programme support, 300Jo come from tropical countries. Some of these describe major advances; for example, scientists at the Institute of Medical Research in Kuala Lumpur in Malaysia have discovered how to cultivate filarial parasites through several stages of their life-cycle outside the body. This advance opens up new prospects for research on diagnostic tests, therapy and possibly vaccines.
The process of strengthening research on an international scale is a complex task. The needs are quite varied and they change with time, so that plans and progress must be kept under constant review. The Special Programme has set up an evaluation system for each institute receiving major support. This system is designed both to provide the Programme with an assessment of progress and to help the institution itself to develop and, if necessary, modify its work in the light of experience .
• 35
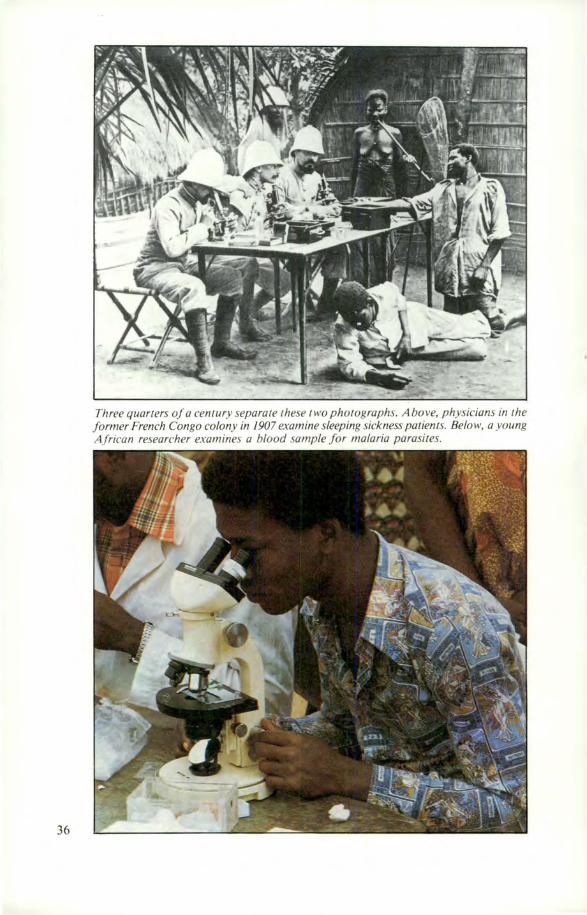
36
Three quarters of a century separate these two photographs. Above, physicians in the former French Congo colony in 1907 examine sleeping sickness patients. Below, a young African researcher examines a blood sample for malaria parasires.
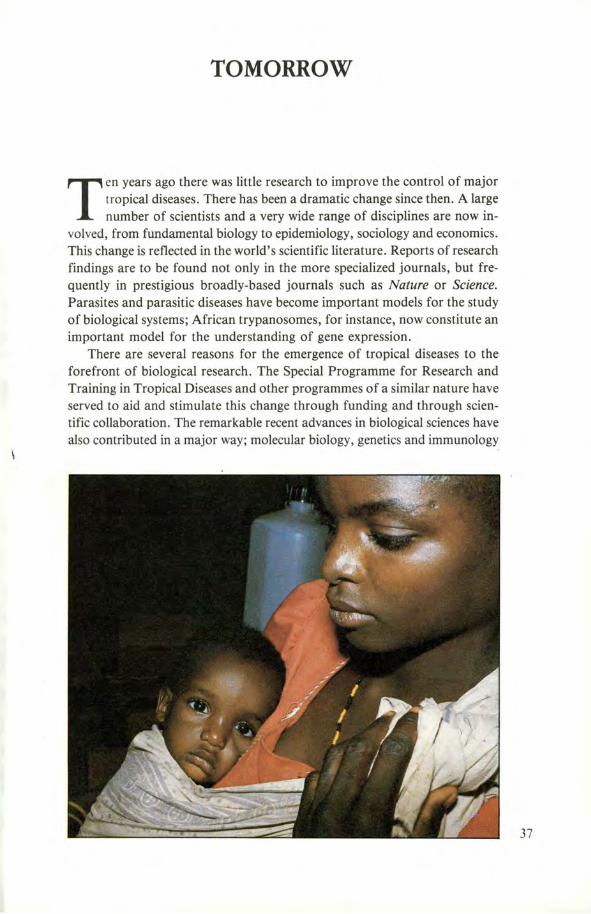
TOMORROW
Ten years ago there was little research to improve the control of major tropical diseases. There has been a dramatic change since then. A large number of scientists and a very wide range of disciplines are now in
volved, from fundamental biology to epidemiology, sociology and economics. This change is reflected in the world's scientific literature. Reports of research findings are to be found not only in the more specialized journals, but frequently in prestigious broadly-based journals such as Nature or Science. Parasites and parasitic diseases have become important models for the study of biological systems; African trypanosomes, for instance, now constitute an important model for the understanding of gene expression.
There are several reasons for the emergence of tropical ·diseases to the forefront of biological research. The Special Programme for Research and Training in Tropical Diseases and other programmes of a similar nature have served to aid and stimulate this change through funding and through scientific collaboration. The remarkable recent advances in biological sciences have also contributed in a major way; molecular biology, genetics and immunology
37

38
in particular have recently developed concepts and technologies which have proven especially relevant to the study of tropical diseases. The future for technological advance has never seemed brighter.
What will be the impact of these remarkable changes? It is now very probable that, given sufficient financial resources, a whole variety of new control tools and methods can be developed to the stage of proven efficacy. Will they serve to improve the health of deprived tropical populations, or will they serve only to make the tropics a healthier place for a privileged minority or for affluent visitors? To achieve radical improvements the products of research, and the research process itself, must be fully integrated into plans and systems for disease control in the endemic countries.
The World Health Organization has adopted as its objective "Health for All by the Year 2000". By that time all people should have access to health care systems which are relevant to their needs and appropriate to their circumstances, and which can deliver effective methods for disease control , including both prevention and therapy.
The scope of research in the Special Programme reflects the breadth of approach which is required. It would be a mistake, however, to imagine that once these methods are established diseases will rapidly and permanently be brought under control. Changes in infectious agents, vectors and human populations will inevitably produce changes in disease which will call for further research . As many countries now well appreciate, disease control programmes are inadequate without a continuing research component. A necessary condition for the long-term promotion of health of the peoples of tropical countries is that research on tropical diseases continue, and that the tropical countries themselves acquire a research capability which is appropriate to their needs and resources .
•
CREDITS
This publication was financed under a grant from the United Nations Development Programme.
Produced by the World Health Organization in collaboration with Mr A. Dorozynski.
Design and layout by S. Clerget-Vaucouleurs.
Photos and drawings:
Cover (clockwise from top right): (1), WHO, Mr F. Kuzoe; (2, 3, 5), WHO; (4, 6), MEDDIA: Royal Tropical Institute (Amsterdam) - World Health Organization -London School of Hygiene and Tropical Medicine - Liverpool School of Tropical Medicine ((4), Dr H.P. Striebel, Ciba-Geigy AG, Basel; (6), Dr H. Zaiman, Yonkers, N.Y.); (7), WHO, Dr P. de Raadt.
Pp.: 10 (1), Carlsberg Laboratory, Copenhagen; 10 (2-4), Hoffmann-La Roche Inc., Nutley, N. J.; 12, 14, 15 (drawings), S. Clerget-Vaucouleurs; 17, MEDDIA: Royal Tropical Institute (Professor L. J. Bruce-Chwatt, Wellcome Museum of Medical Science); 19, Professor W. Peters, London School of Hygiene and Tropical Medicine; 20 (top), MEDDIA: Royal Tropical Institute; 24 (bottom), WHO, Mr F. Kuzoe; 26 (left & right), Pasteur Institute, Paris; 27 (top), WHO, Dr N. Rishikesh (insert, WHO); 30 (top), WHO, Mr F. Kuzoe; 32 (1-5), WHO, Dr P. de Raadt; 34, WHO, Dr L. R. Rickman; 36 (top), Roger-Viollet Agence de Presse, Paris; 36 (bottom), WHO, Dr P. de Raadt; all others, WHO.
Printed by lmprimerie Barthelemy, Avignon 39