
Fitness and Gender-Related Differences in Heart Period Variability
9
Fitness and Gender-Related Differences in Heart Period Variability LYNN A. ROSSY, MA, AND JULIAN F. THAYER, PHD Objective: The purpose of this study was to elucidate the processes of autonomic nervous system control of the heart in high fit and low fit men and women by examining indices of vagally mediated cardiac control. Method: There were 40 participants (19 women and 21 men) classified as either high fit or low fit on the basis of scores from the University of Houston Non-Exercise Tcst (N-EX). Both time domain and frequency domain cardiovascular measures were calculated during a resting baseline period (BL), a facial cooling task (FCT) designed to elicit parasympathetic activity, a reaction time task (RT) designed to elicit pri~uarily sympathetic activity, and a combination task (COMBO) designed to elicit a combination of both parasympathetic and sympathetic activation and recovery periods after each task. Results: Both time and frequency domain indices of heart period variability (HPV) indicated that high fit individuals exhibited greater vagal control of the heart relative to low fit individuals at baseline and across all tasks. In addition, the results suggest greater relative vagal control of the heart in women compared with men. Reactivity scorcs revealed significant main effects for condition for both time and frequency domain measures of HPV, but no main effects or interactions involving fitness or gender. Conclusions: First, small differences in aerobic capacity result in meaningful differences in cardiac autonomic control, with high fit individuals clearly demonstrating greater vagally mediated cardiac control. Second, important gender-related differences in HPV indicate that women exhibit greater vagal control and men exhibit more sympathetic cardiac control even though heart period (HP) did not differ. Third, the mechanisms underlying the beneficial effects of fitness and those placing women at a reduced risk for coronary heart disease (CHD) seem to be similar. Key words: autonomic nervous system, fitness, gender, heart period variability, parasympathetic. N-EX = University of Houston Non-Exercise Test; FCT = facial cooling task; RT = reaction time task; COMBO = combination task; HPV = heart period variability; HP = heart period; CHD = coronary heart disease; CVD = cardiovascular disease; ANS = autonomic nervous system; %BB50 = percentage of HP differences greater than 50 msec; MSD = mean successive differences; HF = high frequency spectral power; %HF = percentage of total power related to HF; LFMF = ratio of low frequency to high frequency spectral power; ECG = electrocardiogram; LARA = leistungskontrollierender adaptiver Regelalgorithumus; BL = baseline period; FCT-R = recovery from FCT; RT-R = recovery from RT; COMBO-R = recovery from COMBO; VAR = variance of average HP in msec2; SD = standard deviation of the HP; LF = low frequency spectral power; LFP = low frequency peak; HFP = high frequency peak; %LF = percentage low frequency power; TSP = total spectral power; BMI = body mass index; ANOVAs = analyses of variance; ANCOVAs = analyses of covariance. INTRODUCTION CHD is a leadine; cause of death in the United States and other highly induscialized countries. The large number of behavioral risk factors for this disease (ie, smoking, body composition, and physical inactivity) have led people to refer to CHD as a disease of lifestyle. In particular, a sedentary lifestyle is a risk factor with nearly the same odds ratio as the known risk factors, such as hypercholesterolemia and smoking (1). Because of the large number of epidemiological studies that have evaluated the increased risk of CVD due to a From the University of Missouri-Columbia, Columbia, Missouri. Address reprint requests lo: Julian F. Thayer, PhD. 210 McAlesler Hall, University of Missouri-Columbia. Columbia. MO 6521 1. Email: psyjthay @showme.missouri.edu. Received for publication May 28, 1997: revision received July 6, 1998. sedentary lifestyle, it has been suggested that there is a causal relationship between sedentary habits and CHD (2). Powell et al. (l), in a review of 43 epidemiological studies, found that CHD occurred almost twice as oftenin sedentary individuals as opposed to physically active individuals. When the large number of sedentary people in the general population is taken into account, the total impact of physical inactivity on CHD becomes much larger than all other risk factors (1, 3). Not all risk factors for CHD fall into the category of behavior or lifestyle. For instance, a person's gender can be very predictive of future heart disease, such that women seem to be protected from CHD relative to men (4). In fact, men are two to three times more likely to develop CHD than premeno- pausal women, even when risk factors such as resting blood pressure, smoking, serum cholesterol level, relative weight, and glucose intolerance are taken into account (5-7). Two major hypotheses about why men are at higher risk for CHD morbidity and mortality (7) include the protective effect of reproductive hormones in women, especially estrogen (8), as well as the belief that men engage more often in behaviors that are potentially health darnaging instead of health promoting (4). Despite the relevance of gender and cardiovascular health, few studies have examined the effects of gender on cardio- vascular dynamics (9). The development of a noninvasive assessment of ANS activity has been a topic of great interest in medicine and physiology. Both time- and frequency-domain indices of ANS function have been investigated. Power spectral analysis was first used in the early 1970s to measure spontaneous heart rate variability in normal humans (10) and has become a method that has been widely recommended and used in research to assess ANS activitv. From beat-to-beat variations in HP. this technique extract; spectral components that differentially reflect autonomic mediators of cardiovascular variability (1 1). Due to the differential frequency components that arise from sympathetic and parasympathetic nervous system activity, heart period modulation by these two branches of the ANS can be examined by spectral analysis of the resulting time series. Frequencies from approximately 0.03 to 0.15 Hz are defined as the low frequency component and correspond primarily to baroreceptor-mediated regulation of blood pressure (12). Al- though this low frequency component is primarily indicative of sympathetic influence, substantial parasympathetic influ- Psychosomatic Medicine 60:773-781 (1998) 0033-3 174/98/6006-0773$03.00/0 Copyright O 1998 by the American Psychoso~natic Society
Transcript of Fitness and Gender-Related Differences in Heart Period Variability

Fitness and Gender-Related Differences in Heart Period Variability LYNN A. ROSSY, MA, AND JULIAN F. THAYER, PHD
Objective: The purpose of this study was to elucidate the processes of autonomic nervous system control of the heart in high fit and low fit men and women by examining indices of vagally mediated cardiac control. Method: There were 40 participants (19 women and 21 men) classified as either high fit or low fit on the basis of scores from the University of Houston Non-Exercise Tcst (N-EX). Both time domain and frequency domain cardiovascular measures were calculated during a resting baseline period (BL), a facial cooling task (FCT) designed to elicit parasympathetic activity, a reaction time task (RT) designed to elicit pri~uarily sympathetic activity, and a combination task (COMBO) designed to elicit a combination of both parasympathetic and sympathetic activation and recovery periods after each task. Results: Both time and frequency domain indices of heart period variability (HPV) indicated that high fit individuals exhibited greater vagal control of the heart relative to low fit individuals at baseline and across all tasks. In addition, the results suggest greater relative vagal control of the heart in women compared with men. Reactivity scorcs revealed significant main effects for condition for both time and frequency domain measures of HPV, but no main effects or interactions involving fitness or gender. Conclusions: First, small differences in aerobic capacity result in meaningful differences in cardiac autonomic control, with high fit individuals clearly demonstrating greater vagally mediated cardiac control. Second, important gender-related differences in HPV indicate that women exhibit greater vagal control and men exhibit more sympathetic cardiac control even though heart period (HP) did not differ. Third, the mechanisms underlying the beneficial effects of fitness and those placing women at a reduced risk for coronary heart disease (CHD) seem to be similar. Key words: autonomic nervous system, fitness, gender, heart period variability, parasympathetic.
N-EX = University of Houston Non-Exercise Test; FCT = facial cooling task; RT = reaction time task; COMBO = combination task; HPV = heart period variability; HP = heart period; CHD = coronary heart disease; CVD = cardiovascular disease; ANS =
autonomic nervous system; %BB50 = percentage of HP differences greater than 50 msec; MSD = mean successive differences; HF = high frequency spectral power; %HF = percentage of total power related to HF; LFMF = ratio of low frequency to high frequency spectral power; ECG = electrocardiogram; LARA =
leistungskontrollierender adaptiver Regelalgorithumus; BL = baseline period; FCT-R = recovery from FCT; RT-R = recovery from RT; COMBO-R = recovery from COMBO; VAR = variance of average HP in msec2; SD = standard deviation of the HP; LF = low frequency spectral power; LFP = low frequency peak; HFP = high frequency peak; %LF = percentage low frequency power; TSP = total spectral power; BMI =
body mass index; ANOVAs = analyses of variance; ANCOVAs = analyses of covariance.
INTRODUCTION CHD is a leadine; cause of death in the United States and
other highly induscialized countries. The large number of behavioral risk factors for this disease (ie, smoking, body composition, and physical inactivity) have led people to refer to CHD as a disease of lifestyle. In particular, a sedentary lifestyle is a risk factor with nearly the same odds ratio as the known risk factors, such as hypercholesterolemia and smoking (1). Because of the large number of epidemiological studies that have evaluated the increased risk of CVD due to a
From the University of Missouri-Columbia, Columbia, Missouri. Address reprint requests lo: Julian F. Thayer, PhD. 210 McAlesler Hall, University of
Missouri-Columbia. Columbia. MO 6521 1 . Email: psyjthay @showme.missouri.edu. Received for publication May 28, 1997: revision received July 6, 1998.
sedentary lifestyle, it has been suggested that there is a causal relationship between sedentary habits and CHD (2).
Powell et al. ( l) , in a review of 43 epidemiological studies, found that CHD occurred almost twice as oftenin sedentary individuals as opposed to physically active individuals. When the large number of sedentary people in the general population is taken into account, the total impact of physical inactivity on CHD becomes much larger than all other risk factors (1, 3).
Not all risk factors for CHD fall into the category of behavior or lifestyle. For instance, a person's gender can be very predictive of future heart disease, such that women seem to be protected from CHD relative to men (4). In fact, men are two to three times more likely to develop CHD than premeno- pausal women, even when risk factors such as resting blood pressure, smoking, serum cholesterol level, relative weight, and glucose intolerance are taken into account (5-7). Two major hypotheses about why men are at higher risk for CHD morbidity and mortality (7) include the protective effect of reproductive hormones in women, especially estrogen (8), as well as the belief that men engage more often in behaviors that are potentially health darnaging instead of health promoting (4). Despite the relevance of gender and cardiovascular health, few studies have examined the effects of gender on cardio- vascular dynamics (9).
The development of a noninvasive assessment of ANS activity has been a topic of great interest in medicine and physiology. Both time- and frequency-domain indices of ANS function have been investigated. Power spectral analysis was first used in the early 1970s to measure spontaneous heart rate variability in normal humans (10) and has become a method that has been widely recommended and used in research to assess ANS activitv. From beat-to-beat variations in HP. this technique extract; spectral components that differentially reflect autonomic mediators of cardiovascular variability (1 1). Due to the differential frequency components that arise from sympathetic and parasympathetic nervous system activity, heart period modulation by these two branches of the ANS can be examined by spectral analysis of the resulting time series. Frequencies from approximately 0.03 to 0.15 Hz are defined as the low frequency component and correspond primarily to baroreceptor-mediated regulation of blood pressure (12). Al- though this low frequency component is primarily indicative of sympathetic influence, substantial parasympathetic influ-
Psychosomatic Medicine 60:773-781 (1998)
0033-3 174/98/6006-0773$03.00/0 Copyright O 1998 by the American Psychoso~natic Society

L. A. ROSSY AND J. F. THAYER
ence has been found at this frequency under certain conditions(10, 12). Frequencies greater than 0.15 Hz are defined as thehigh frequency component and correspond to respiratory-mediated HPV. As the vagus is the only autonomic inputknown to exist at this frequency, resulting fluctuations of HPare the result of respiratory modulation of cardiac vagalactivity and indicate parasympathetic influence (13, 14).
From the large number of time- and frequency-domainmeasures of HPV, several have been shown to reflect primar-ily vagal activity. In the time domain, the percentage of HPdifferences greater than 50 msec (%BB50) and the mean ofsuccessive HP differences (MSD) are most closely reflectiveof vagal influences (15). In the frequency domain, HF and thepercentage of total power related to HF (%HF) are mostreflective of vagal activity (13). Moreover, the ratio of LF/HFhas been suggested as an index of relative ANS balance suchthat smaller values reflect greater vagal dominance (13).
Given the scarcity of literature that has investigated cardiacautonomic control in high and low fit men and womensimultaneously, the present study used measures of HPV toexamine autonomic control of the heart in these populations.Specifically, we sought to clarify the underlying cardiaccontrol mechanisms at work in the physically fit and womento better understand the relative cardiovascular health benefitsthat these individuals enjoy. To this end, time- and frequency-domain indices of vagally mediated cardiac control wereexamined, using spectral analysis of the HP time series in highfit and low fit men and women. HPV measurements wereobtained during a baseline condition and during a range oftasks designed to elicit combinations of autonomic activity tomore completely evaluate the dynamic cardiac control pro-cess. Cardiac vagal activity can be stimulated by eliciting thedive reflex through the use of a facial cooling task (16). Thedive reflex is mediated through trigeminal-brainstem-vagalpathways (17, 18).
Several types of psychologically challenging stressors havebeen developed for use in laboratory studies (19). A reactiontime task was used in this study to elicit sympathetic activity.A third task that combines the simultaneous use of the facialcooling task and the reaction time task was used to elicit bothparasympathetic and sympathetic activation. We have shownpreviously that this type of paradigm produces task-relatedresponses that reflect a range of ANS influences (16). Inaddition, reactivity (defined as the change in activity betweena resting baseline and a task period) was calculated toadditionally examine the relative influence of situationalfactors (task and person by task effects—state-like influences)compared with dispositional factors (person effects reflectingstable individual difference characteristics—trait-like influ-ences) in ANS activity to these tasks.
In summary, physical inactivity and male gender are bothwell known independent risk factors for CHD. However, themechanisms underlying the beneficial effects of exercise andfemale gender on cardiovascular health are not fully under-stood. The purpose of the present study was to elucidate theANS activity found in physically active participants andwomen to more fully understand the protective benefits thatthey confer. In particular, measures of HPV were examinedbecause of their suspected role in cardiovascular health (20).Spectral analysis of the HP time series was used to examinethe extent to which vagal influences contribute to autonomiccontrol of the heart.
We hypothesized that high fit individuals and womenwould show more vagally mediated cardiac control at baselineand across all tasks than low fit individuals and men. Thishypothesis would be reflected in high fit individuals andwomen showing greater time-domain (%BB50 and MSD) andfrequency-domain (HF and %HF) HPV at rest and across alltasks relative to low fit individuals and men.
A secondary aim of this study was to examine the extent towhich situational versus dispositional factors contribute toANS cardiac control. Reactivity scores reflect the influence ofsituational factors relatively devoid of dispositional factors(21). Given that ANS control mechanisms may be useful asindices of cardiovascular disease risk only if they generalizeacross diverse situations or tasks, we hypothesized that reac-tivity scores that remove baseline scores (and therefore mostdispositional influences) would result in the main effects ofthe experimental condition on our dependent variables but notthe main effects of or interactions with fitness and gender.
METHODParticipantsThe participants were recruited from students enrolled in an
introductory psychology course at a large midwestern university.After group administration and scoring of the University of HoustonNon-Exercise Test (N-EX), the invited sample consisted of studentswho classified as high fit (high active) or low fit (low active) basedon their extreme scores. Students were asked to complete a healthquestionnaire, and those indicating a history of cardiovascularproblems or students taking antihypertensive medication would notbe included in the final sample. The final sample consisted of 20 highfit participants (11 men, 9 women) and 20 low fit participants (10men, 10 women) between the ages of 17 and 25 (mean age = 19).Groups did not differ significantly in age. All participants abstainedfrom caffeine, nicotine, and alcohol for at least 12 hours before theexperiment. The study procedures were reviewed and approved bythe psychology department Internal Review Board.
ApparatusECG. The ECG was recorded using Ag-AgCl electrodes (UFI
Corp., Mono Bay, CA), with all electrode impedances reduced toless than 10 kohms by Omniprep skin prep (Omniprep, Inc., Aurora,CO). ECG signals were amplified using Grass 7P3 preamplifiers andGrass 7DA driver amplifiers (Grass Instruments, Inc., Quincy, MA).
QuestionnairesN-EX. The N-EX is a method used to estimate VO2,,,OJ[ based on
subjective interpretation of physical activity in combination with age,body composition, and gender (22, 23). This method uses a multipleregression equation that has been shown to produce scores that havea correlation of .78 with actual VO2max scores. This accuracy isevident in approximately 96% of the population with VO2max scoresless than or equal to 55 ml/kg/min. The remaining 4% of thepopulation are very highly fit individuals for which this model is lessaccurate.
Health Questionnaire. This self-report health questionnaire con-sisted of three items that asked about the recent use of caffeine,nicotine, or alcohol; current medication; and history of heart trouble.
Experimental TasksFCT. This task involved preparing a plastic bag containing ice and
water such that the temperature of the water was between 5 and 10°Cat the beginning of the task period. The use of water temperatures inthis range has been shown to stimulate the dive reflex without aconcomitant stimulation of pain receptors (16). The bag was placedon the participants' foreheads for 5 minutes.
RT. The forced choice RT being used for this study was based on
Psychosomatic Medicine 60:773-781 (1998)

FITNESS, GENDER, AND HPV
a computerized visual search (24). During this task, a 4 X 4 matrixof two-digit numbers was presented to each participant on a computerscreen. Participants were asked to scan the matrix of numbers for twotarget numbers (43 and 63) and to respond by pressing one of thekeys numbered one to four that corresponds with the combination oftarget numbers observed. The combination of target numbers was: 43only, 63 only, 43 and 63, and neither 43 nor 63. All combinations hadan equal probability of occurring.
This computer task, known as LARA, is defined as a closed-loopalgorithm controlled performance task. The response time deadlinechanges according to a pre-set success ratio. Therefore, if a partici-pant failed to respond within a certain window of time, the matrixdisappeared and the next matrix was presented. When a participant'srate of success exceeded the criterion (one correct response), theresponse time deadline for the next matrix was shortened by 0.12seconds. After an incorrect response, the response deadline wasincreased by 0.36 seconds. Thus, the task difficulty was determinedby the accuracy and speed of the response of each participant so thatperformance was held equivalent across participants.
Participants were instructed to respond as quickly as possible toeach stimulus. They were told that the speed of their responses wouldbe used in determining the recipient of a $25.00 prize at the end ofthe study. This contingency was incorporated to provide an incentivefor participants to remain motivated and attentive to the task.
After the task was explained to each participant, there was onedemonstration trial consisting of six matrices. The experimental trialwas performed immediately after the demonstration trial This triallasted 5 minutes.
COMBO. This task is a combination of the FCT and RT tasks. For5 minutes, a bag of cool water and ice was placed on the participantsforehead while they were engaged in the reaction time task.
ProceduresTesting took place in a small, sound-attenuated room with
participants seated in a comfortable lounge chair. After a completeexplanation of the experimental procedures, each participant wasasked to complete the self-report health questionnaire and sign aninformed consent form. Height, age, and weight information wasobtained. Electrodes were attached. One ECG lead was placedbeneath the center of the left collarbone, one was placed on the rightside beneath the floating rib directly above the hip. and one wasplaced in the middle of the left ribcage.
The participant was then seated in the lounge chair and allowed torelax and acclimate to the laboratory for an average of 20 minutes,during which time sample readings were taken. They were then askedto relax for a 5-minute rest period which preceded the presentation ofthe tasks. This rest period was designated as the BL. The order of thefirst two tasks (FCT and RT) was counterbalanced within groupsacross subjects. Each task was 5 minutes in duration and wasfollowed by a 5-minute recovery period (FCT-R and RT-R) similar tothe baseline period. The last task, the COMBO, was 5 minutes induration and was followed by a 5-minute recovery period (COMBO-R).
Quantification of Dependent MeasuresThe time domain cardiovascular measures calculated on each
5-minute condition included the following: 1) average cardiac period(HP = mean duration of R spike to R spike interval in msec), 2)variance of average HP in msec2 (VAR = a measure of the total heartperiod variability that is equivalent to total spectral power in allfrequencies), 3) standard deviation of the HP (SD), 4) the average ofthe absolute values of successive differences in R-R intervals in msec(MSD), and 5) the percentage of successive intcrbeat intervaldifferences greater than 50 msec (%BB50). The latter two measureswere chosen to reflect primarily vagal influences.
Frequency domain cardiovascular measures calculated on each5-minute condition were derived from an autoregressive programused for spectral analysis of the heart period time series (25).
According to this well-established method, a given signal is modeledby a set of parameters from which the frequency spectra arecomputed (26). The procedure yields power values for each spectralcomponent and sharply defined peaks in each power spectrum thatallows quantitative measurements of frequency shifts. The lowfrequency component (O.O3-.15 Hz) is primarily due to baroreceptor-mediated regulation of blood pressure and served mainly as indicesof sympathetic control. Although this low frequency component hasbeen thought to reflect primarily sympathetic activity (13), parasym-pathetic activity has been found at this frequency under certainconditions (10). The peak of the low frequency component isconsidered to be important in autonomic balance, such that the lowerthe peak frequency the more likely it is to reflect sympatheticinfluences (10). The high frequency component (.18-.40 Hz) servedas an index of parasympathetic control. The peak of the highfrequency component corresponds to the respiratory frequency (27).From the values for the low frequency component and the highfrequency component, the ratio of low frequency to high frequencyactivity was derived as an index of cardiac autonomic balance. Powervalues are given in power spectral density units (ms2 X Hz~').
The frequency domain cardiovascular measures that resulted fromthe method described above were 1) low frequency power (LF), 2)high frequency power (HF), 3) low frequency/high frequency ratio(LF/HF), 4) low frequency peak (LFP), 5) high frequency peak(HFP), 6) percentage low frequency power (%LF, representing thepercentage of total variability due to the low frequency componentand calculated as LF/TSP), 7) percentage high frequency power(%HF, representing the percentage of total variability due to the highfrequency component and calculated as HF/TSP), and 8) totalspectral power (TSP). Because TSP is equivalent to VAR it will notbe discussed additionally.
BM1 was calculated using the weight and height of each partici-pant (ie, weight/height2 where weight is in kilograms and height is inmeters). Thereafter, an estimated VO2ma( was calculated with aformula that uses the calculated BMI, activity level as reported on theN-EX, age, and gender (22, 23).
Statistical AnalysesThe first analysis was a manipulation check of group fitness
classification by conducting directional t tests for fitness (high andlow), using estimated VO2m.lN and activity level as the dependentvariables. Data for this and all following analyses were reported asmeans and SDs.
To test the hypothesis that high fit individuals and women wouldshow more vagally mediated cardiac control at baseline than low fitindividuals and men, analyses of baseline HPV measures wereconducted for fitness and gender effects in a series of directional /tests, after a series of fitness (high and low) by gender (men andwomen) ANOVAs revealed that fitness and gender did not interactfor any dependent variable. Furthermore, to adjust for the differencesin height and weight between men and women and the effects thesecharacteristics have on cardiac indices, ANCOVAs using body massindex as the covariate were conducted for both gender and fitnesseffects at baseline.
To test the hypothesis that high fit individuals and women wouldshow more vagally mediated cardiac control across all tasks than lowfit individuals and men, analyses of HPV measures were conductedfor fitness, gender, and condition effects using a series of 2 (fitness:high and low) X 2 (gender: male and female) X 7 (condition:baseline, FCT, recovery, RT, recovery, COMBO, recovery) repeated-measures ANOVAs. Again, repeated-measures ANCOVAs usingbody mass index as the covariate were used to adjust for weight andheight differences between men and women.
To test the hypothesis that main effects of condition, but not maineffects of or interactions with fitness and gender, would be found onmeasures of HPV reactivity, analyses of HPV reactivity wereconducted for fitness, gender, and condition effects using a series of2 (fitness: high and low) X 2 (gender; male and female) X 6
Psychosomatic Medicine 60:773-781 (1998)

(condition: FCT, recovery, RT, recovery, COMBO, recovery) repeat-ed-measures ANOVAs. HPV reactivity scores were calculated as theHPV measure for each condition minus the corresponding baselineHPV measure. Repeated-measures ANCOVAs using BMI as thecovariate were used to adjust for weight and height differencesbetween men and women.
In all of the above analyses, an a level of .05 was used for allstatistical tests. Effect sizes for single degree of freedom tests arereported as point-biserial correlations between the independent vari-able and the dependent variable. Effect sizes for multiple degree offreedom tests are reported as TJ. In both cases, the formula is [(dfn XF)l{dfn X F) + dfd] . When the sphericity assumption is violated forthe repeated-measures condition, degrees of freedom were adjusted,using the Greenhouse-Geisser or Huyhn and Feldt correction proce-dures or a multivariate approach was used and the Wilks' A teststatistic reported (28). Effect sizes for the multivariate test werecalculated as (1-Wilks' A)"2. Furthermore, no covariate analyses wasconducted on VO2lT1;lx, inasmuch as this dependent variable wascalculated with a formula that adjusts for BMI.
RESULTSManipulation Check of FitnessAnalyses indicated that the groups classified as high fit and
low fit were significantly different from one another in termsof activity level [ high fit, 6.6 (.5); low fit, 0.9 (l.0)-(t(36) =21.81 ,p< .001, r b = .96)] and VO2max [high fit, 51 (5); lowfit, 39 (6)-(r(36) = 10.61, p < .001, rpb = .87)].
Baseline MeasuresIn Table 1, significant main effects of fitness at baseline
were found for HP (f(36) = 2.25, p = .015, r b = .35),%BB50 W36) = 3.02, p = .0025, rpb = .45), SD (r(36) =1.78,p = .04, r b = .28), MSD « 3 6 ) = 1.93, p = .03, rpb =.31), and HF (r(36) = 1.80, p = .04, rpb = .29). Relative to thelow fit group, the high fit group was characterized by longerHP, larger SD, larger MSD, more %BB50, and higher HF. Allresults were identical, using BMI as a covariate.
In Table 2, significant main effects of gender at baselinewere found for %HF (f(33) = 2.00, p = .025, rh = .33; BMIas a covariate: f(32) = 2.20, p = .02, r b = .36), and VO2max
(r(35) - 4.21, p < .001, rpb = .58). Also as shown in Table2, significant main effects of gender at baseline were foundonly when using BMI as a covariate for LF (t(35) = 1.73, p =.045, rpb = .28) and %LF (f(32) = 1.84, p = .035, rpb = .31).Relative to men. women were characterized by smaller LF,
L. A. ROSSY AND J. F. THAYER
smaller %LF, larger %HF, and lower VO2max. In addition,there were no significant interactions between fitness andgender for any dependent variable.
Repeated-Measures Analyses of Raw ScoresIn Table 3, significant main effects of fitness were found
for HP (F(l,33) = 5.18, p = .03, rpb = .37; BMI as acovariate: F(l,32) = 4.9, p = .03, rpb = .36), VAR F(l,30) =4.17, p = .05, r b = .35; BMI as a covariate: F(l ,29) = 4.02,p = .05, r b = .35), SD (F(l,33) = 7.84, p = .008, r b = .44;BMI as covariate: F(l,32) = 7.48, p = .01, r b = .44), MSD(F(l,33) = 7.15, p = .01, rph = .42; BMI as covariate: F(l,32)= 6.81,/? = .01,r b = .42), and %BB50(F( 1,33) = 7.84,/? =.008, rpb = .44; BMI as covariate: F(l,32) = 7.47,/? = .01, rpb
= .44). A significant main effect of fitness was also found forHF (F(l,30) = 4.2, p = .05, rpb = .35); however, HF was onlymarginally significant when using BMI as a covariate (F(l,29)= 3.97, p = .06, rpb = .35). Relative to the low fit group, thehigh fit group was characterized by longer HP, larger VAR,larger SD, larger MSD, more %BB50, and higher HF.
Marginally significant main effects of gender were foundfor %BB50 (F(l,33) = 3.3, p = .08, r b = .30), and LF/HF(F(3,3O) = 3.89, p = .06, rpb = .34); however, %BB50 andLF/HF were not significant when using BMI as a covariate(Table 4). Relative to men, women were characterized bymore %BB50, and smaller LF/HF.
As shown in Table 5, which reports time domain cardio-vascular measures, significant main effects of condition werefound for HP (Wilks' A (6, 28) = .45, p = .0005, hm = .74;BMI as a covariate:Wilks' A (6, 22) = .45, p = .003, hm =.74), and %BB50 (F(6,198) = 3.66, p = .003, ehf = .82, h =.32). A significant effect for condition was found for SD(Wilks' A (6, 28) = .61, p = .02, hm = .62) and SD wasmarginally significant when using BMI as covariate (Wilks' A(6, 22) = .61, p = .07, hm = .62). A marginally significanteffect for condition was found for MSD (F(6,198) = 2.17,/? =.10, e = .46, h = .24). All significant main effects that reportGreenhouse and Geisser or Huynh and Feldt tests remainedthe same when using BMI as a covariate and are, therefore,not reported twice.
In Table 6, which reports frequency domain cardiovascularmeasures, a significant main effect of condition was found for
TABLE 1. Mean (SD) at Baseline for Fitness
Variable
HP"VARSD°MSD0
%BB50a
LFHF"LF/HFLFPHFP%LF%HF
Mean
7815486
655711
23351313
4.98.11.29
5338
Low Fit
SD
1046863
364210
34261788
12.4.03.04
2525
N
202020202020202020191818
Mean
8998573
858421
22842710
2.24.11.27
4344
High Fit
SD
2067052
364510
25322884
4.2.01.04
2523
N
202020202020202019201919
" p < .05. based on t tests.
Psychosomatic Medicine 60:773-781 (1998)

FITNESS, GENDER, AND HPV
TABLE 2. Mean (SD) at Baseline for Gender
Variable
HPVARSDMSD%BB50LFa
HFLF/HFLFPHFP%LFa
%HF"-b
V02 l m xb
Mean
8697402
766814
30131720
3.2.11.27
543349
"p < .05. using BMI as covariate.b p < .05, based on I tests.
Variable
Hpa.b
VAR"'b
SD"b
MSDab
%BB50"-b
LFHF"C
LF/HFLFPHFP%LF%HF
Mean
7594417
605111
13531213
1.99.11.29
5341
Men
SD
1648272
414810
38152241
4.0.02.03
21217
TABLE 3.
Low Fit
SD
834216
263110
16681666
1.56.02.04
1916
N
21212121212121212120202021
Mean
8116657
747318
16062303
4.0.12.29
414841
Mean (SD) for Main Effects of Fitness
N
1818181818161616101456
Mean
8607019
878519
22072724
1.90.11.28
4247
Women
SD
1795558
334312
13722731
12.9.03.04
28256
High Fit
SD
1965393
435311
24123073
3.89.02.04
2722
N
19191919191919191819171719
N
191619191918181816181414
" p < .05, based on ANOVAs.b p < .05, based on ANCOVAs using BMI as a covariate.c Marginally significant, based on ANCOVAs using BMI as a covariate.
LF/HF (Wilks' A (6, 25) = .26, p = .000003, hm = .86; BMIas a covariate:Wilks' A (6, 19) = .26, p = .0001, hm = .86)and %HF (Wilks' A (6, 11) = .17, p = .001, hm = .91).Percentage high frequency (%HF) was marginally significantwhen using BMI as a covariate (Wilks' A (6, 5) = .17, p =.08, hm = .91). No significant main effects of condition werefound for VAR, LFP, HFP, or %LF. In addition, there were nointeractions involving fitness or gender.
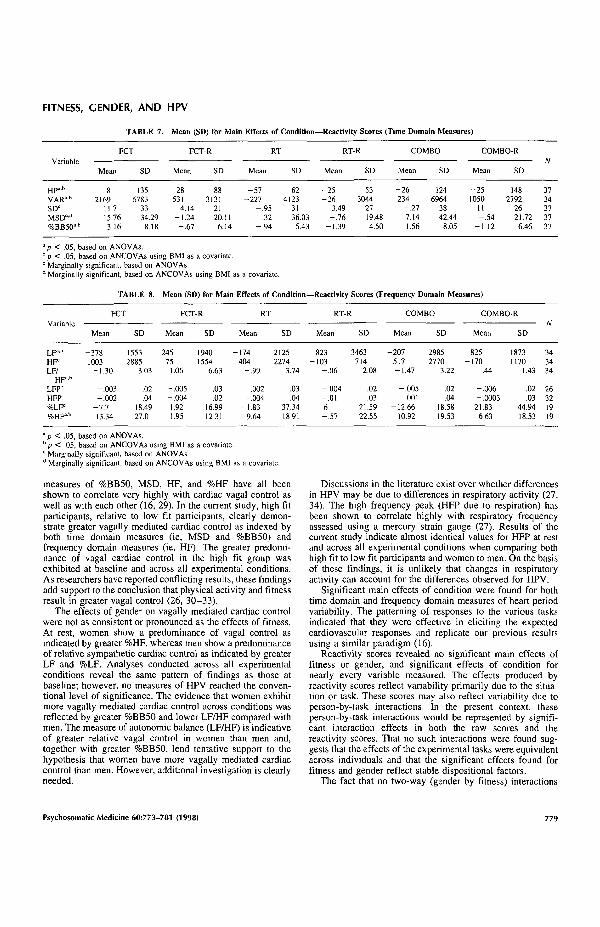
Repeated-Measures Analyses of Reactivity ScoresAnalyses on reactivity scores revealed no significant main
effects or interactions involving fitness or gender for anydependent variable. As shown in Table 7, which reports timedomain cardiovascular measures, significant main effects ofcondition were found for HP (Wilks' A (5, 29) = .63, p = .02,h = 61; BMI as a covariate: Wilks' A (5, 24) = .63, p = .04,h2
m = 61), VAR (Wilks' A (5, 26) = .57, p = .01, hm = .66;BMI as a covariate: Wilks' A (5, 21) = .57, p = .03, hm =.66), and %BB50 (F(5,165) = 3.99, p = .01, egg = .69, h =.33). All significant main effects that report Greenhouse andGeisser or Huynh and Feldt tests remained the same when
using BMI as a covariate and are, therefore, not reportedtwice.
Table 8 reports frequency domain cardiovascular measures,significant main effects of condition were found for LF(Wilks' A (5, 26) = .46, p = .0008, hm = .73; BMI as acovariate: Wilks' A (5, 21) = .46, p = .004, hm = .73), LF/HF(Wilks' A (5, 26) = .28, p = .000002, hm = .85; BMI as acovariate: Wilks' A (5, 21) = .28, p = .000036, hm = .85) and%HF (Wilks' A (5, 11) = .19, p = .001, hm = .90; BMI as acovariate: Wilks' A (5, 6) = .19, p = .03, hm = .90). Inaddition, no significant effects of condition were found forHFP. Taken together, these results support the hypothesis thatreactivity scores reflect primarily situational factors and thatcardiac control in this experiment was primarily due todispositional factors.
DISCUSSIONThe main purpose of this study was to investigate cardiac
control mechanisms in high fit and low fit men and women.Women relative to men, and high fit relative to low fit
Psychosomatic Medicine 60:773-781 (1998)
L A. ROSSY AND J. F. THAYER
TABLE 4. Mean (SD) for Main Effects of Gender
Variable
HPVARSDMSD%BB50"LFHFLF/HFb
LFPHFP%LF%HF
Mean
8275485
726111
20231552
2.85.11.28
5738
Men
SD
1545513
404710
25292605
3.96.02.03
3124
N
191819191919191916171314
Mean
7925951
767519
15372385
1.04.11.29
3949
Women
SD
1664540
364612
17092659
.91
.02
.041915
N
1816181818151515101566
> < .05, based on ANOVAs.b Marginally significant, based on ANOVAs.
TABLE 5. Mean (SD) for Main Effects of Condition (Time Domain Measures)
Variable
Hpa.b
VARSD"d
MSDcd
%BB50"-b
BL
Mean
8345056
706515
SD
1723812
314011
FCT
Mean
8427224
818018
SD
1827765
425513
FCT-R
Mean
8055587
746414
SD
1834065
314211
RT
Mean
7764829
696614
SD
1485189
435511
RT-R
Mean
8085030
736514
SD
1543907
394310
COMBO
Mean
8075290
707317
SD
1336708
415212
COMBO-R
Mean
8096106
816514
SD
1473922
404010
N
3734373737
° p < .05, based on ANOVAs.b p < .05, based on ANCOVAs using BMI as a covariate.c Marginally significant, based on ANOVAs.d Marginally significant, based on ANCOVAs using BMI as a covariate.
TABLE 6. Mean (SD) for Main Effects of Condition (Frequency Domain Measures)
Variable
LF=d
H F d
LFPHFPLF/
HP'"%LF%HFad
BL
Mean
16721718
.11
.282.4
4738
SD
16582313
.02
.043.4
2421
FCT
Mean
12932720
.11
.281.1
3951
SD
11703229
.03
.041.2
2332
FCT-R
Mean
19171792
.11
.283.4
4940
SD
19662722
.02
.0494
2320
RT
Mean
14982122
.11
.281.4
4550
SD
22533725
.02
.041.9
4022
RT-R
Mean
24951614
.11
.272.3
5339
SD
39142224
.02
.042.1
2126
COMBO
Mean
14652235
.11
.28
.9
3448
SD
26992729
.02
.04
.7
1617
COMBO-R
Mean
24961547
.11
.282.8
6932
SD
23081690
.02
.043.5
5514
N
3434263234
1920
" p < .05, based on ANOVAs.b p < .05, based on ANCOVAs using BMI as a covariate.c Marginally significant, based on ANOVAs.d Marginally significant, based on ANCOVAs using BMI as a covariate.
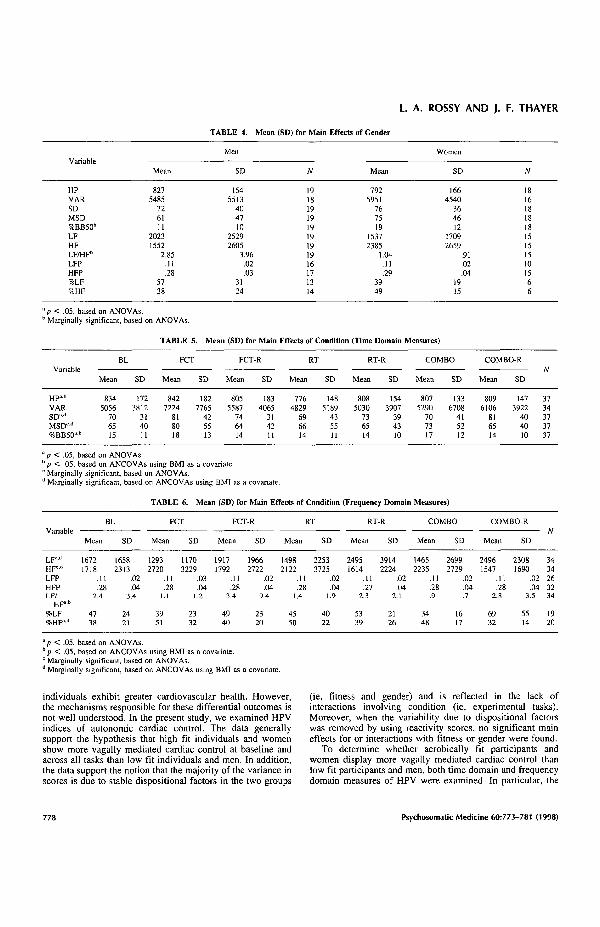
individuals exhibit greater cardiovascular health. However,the mechanisms responsible for these differential outcomes isnot well understood. In the present study, we examined HPVindices of autonomic cardiac control. The data generallysupport the hypothesis that high fit individuals and womenshow more vagally mediated cardiac control at baseline andacross all tasks than low fit individuals and men. In addition,the data support the notion that the majority of the variance inscores is due to stable dispositional factors in the two groups
(ie, fitness and gender) and is reflected in the lack ofinteractions involving condition (ie, experimental tasks).Moreover, when the variability due to dispositional factorswas removed by using reactivity scores, no significant maineffects for or interactions with fitness or gender were found.
To determine whether aerobically fit participants andwomen display more vagally mediated cardiac control thanlow fit participants and men, both time domain and frequencydomain measures of HPV were examined. In particular, the
Psychosomatic Medicine 60:773-781 (1998)
FITNESS, GENDER, AND HPV
TABLE 7. Mean (SD) for Main Effects of Condition—Reactivity Scores (Time Domain Measures)
Variable
Hpa.b
VAR"b
SD°MSDc'd
%BB50°-b
FCT
Mean
82169
11.715.763.16
SD
1356783
3334.29
8.18
FCT-R
Mean
- 2 8531
4.14-1.24
-.67
SD
883131
2120.11
6.14
RT
Mean
-57-227
- .95.32
- .94
SD
624123
3136.035.43
RT-R
Mean
-25-26
3.49- .76
-1.39
SD
533044
2719.484.50
COMBO
Mean
- 2 6234
-.277.141.56
SD
1246964
3842.44
8.05
COMBO-R
Mean
-251050
11-.54
- 1 12
SD
1482792
2621.726.46
N
3734373737
° p < .05, based on ANOVAs.b p < .05, based on ANCOVAs using BMI as a covariate.c Marginally significant, based on ANOVAs.d Marginally significant, based on ANCOVAs using BMI as a covariate.
TABLE 8. Mean (SD) for Main Effects of Condition—Reactivity Scores (Frequency Domain Measures)
FCT FCT-R COMBO COMBO-RVariable
Mean SD Mean SD Mean SD SD Mean SD Mean SD
LFJ b
HF=LF/
HF°'b
LFP°HFP%LP%HF°-b
-3781003
-1.30
-.003-.002
-7.713.34
15532885
3 03
.02
.0418.4927.0
24575
1.06
-.005-.0041.921.95
19401554
6.63
.03
.0216.9912.31
-174404
-.99
.002-.004
-1.839.64
21252274
3.74
.03
.0437.3418.91
823-103
- .06
- 0 0 4-.016-.57
3463714
2.08
.02
.0321.5922.55
-207517-1.47
-.005.001
-12.6610.92
29852770
3.22
.02
.0418.5819.53
825 1873 34-170 1170 34
.44 1.43 34
-.006 .02 26-.0003 .03 32
21.83 44.94 19- 6 63 18.53 19
a p < .05, based on ANOVAs.b p < .05, based on ANCOVAs using BMI as a covariate.c Marginally significant, based on ANOVAsd Marginally significant, based on ANCOVAs using BMI as a covariate.
measures of %BB50, MSD, HF, and %HF have all beenshown to correlate very highly with cardiac vagal control aswell as with each other (16, 29). In the current study, high fitparticipants, relative to low fit participants, clearly demon-strate greater vagally mediated cardiac control as indexed byboth time domain measures (ie, MSD and %BB50) andfrequency domain measures (ie, HF). The greater predomi-nance of vagal cardiac control in the high fit group wasexhibited at baseline and across all experimental conditions.As researchers have reported conflicting results, these findingsadd support to the conclusion that physical activity and fitnessresult in greater vagal control (26, 30-33).
The effects of gender on vagally mediated cardiac controlwere not as consistent or pronounced as the effects of fitness.At rest, women show a predominance of vagal control asindicated by greater %HF, whereas men show a predominanceof relative sympathetic cardiac control as indicated by greaterLF and %LF. Analyses conducted across all experimentalconditions reveal the same pattern of findings as those atbaseline; however, no measures of HPV reached the conven-tional level of significance. The evidence that women exhibitmore vagally mediated cardiac control across conditions wasreflected by greater %BB50 and lower LF/HF compared withmen. The measure of autonomic balance (LF/HF) is indicativeof greater relative vagal control in women than men and,together with greater %BB50, lend tentative support to thehypothesis that women have more vagally mediated cardiaccontrol than men. However, additional investigation is clearlyneeded.
Discussions in the literature exist over whether differencesin HPV may be due to differences in respiratory activity (27,34). The high frequency peak (HFP due to respiration) hasbeen shown to correlate highly with respiratory frequencyassessed using a mercury strain gauge (27). Results of thecurrent study indicate almost identical values for HFP at restand across all experimental conditions when comparing bothhigh fit to low fit participants and women to men. On the basisof these findings, it is unlikely that changes in respiratoryactivity can account for the differences observed for HPV.
Significant main effects of condition were found for bothtime domain and frequency domain measures of heart periodvariability. The patterning of responses to the various tasksindicated that they were effective in eliciting the expectedcardiovascular responses and replicate our previous resultsusing a similar paradigm (16).
Reactivity scores revealed no significant main effects offitness or gender, and significant effects of condition fornearly every variable measured. The effects produced byreactivity scores reflect variability primarily due to the situa-tion or task. These scores may also reflect variability due toperson-by-task interactions. In the present context, (heseperson-by-task interactions would be represented by signifi-cant interaction effects in both the raw scores and thereactivity scores. That no such interactions were found sug-gests that the effects of the experimental tasks were equivalentacross individuals and that the significant effects found forfitness and gender reflect stable dispositional factors.
The fact that no two-way (gender by fitness) interactions
Psychosomatic Medicine 60:773-781 (1998) 779

L. A. ROSSY AND J. F. THAYER
were found is interesting. This finding implies that the positivebenefits of exercise are the same across gender in this sample.To date, mechanisms underlying the protective effect ofexercise on cardiovascular health have not been studied inequal samples of men and women. Moreover, despite moststudies exclusively using men in their sample populations,cardiac control mechanisms are not fully understood in eithergender. The current study adds an important component—namely, gender—to the body of literature studying the effectsof exercise and fitness.
The links between fitness and gender effects seem to berelated to differences in parasympathetic activity as indexedby measures of HPV with high fit individuals showingsignificantly more HPV and women showing a trend towardmore HPV (based on a larger %BB50, smaller LF/HF, andlarger %HF). Although the evidence for more vagally medi-ated cardiac control in women compared with men is notexhibited in some measures of HPV (eg, HF and MSD), thesmaller LF/HF for women indicates that there is a predomi-nance of parasympathetic activity in the balance between thetwo branches of the ANS. Furthermore, this predominance isexhibited across a variety of experimental tasks designed toelicit activity of both branches separately and simultaneously.Conversely, men exhibit a relative sympathetic dominance asindexed by a larger LF and larger %LF, particularly atbaseline. An elevated LF, coupled with reduced HF, is apattern that has been associated with a variety of cardio-pathologies (16). Therefore, the presence of greater relativesympathetic control in the young, healthy men in the currentstudy is worthy of additional investigation.
Results from this study also serve to validate the use of theN-EX as a viable and practical research instrument forassessing and grouping individuals into meaningful fitnesscategories. The manipulation checks of activity level asreported on the N-EX and estimated VO2max both indicate asignificant effect of fitness. Moreover, standards have beendeveloped for evaluating aerobic fitness by VO2max that divideVO2 m a x values into five categories of low, fair, average, good,and high aerobic fitness (22). Using these standards to definethe level of aerobic fitness of individuals in this study, low fitand high fit participants fell into adjacent categories ofaverage and good, respectively. These findings suggest that,although there are significant effects of fitness between thetwo groups, the low fit and high fit participants comprise afairly homogenous group of individuals. As opposed to anumber of fitness studies that have compared trained athletes(eg, runners, swimmers, and cyclists) to sedentary individuals,the significant fitness effects found in this study may be morereflective of the general population.
The significant main effect of fitness at baseline forestimated VO2max is reflected in larger values for high fitcompared with low fit participants. The significant main effectof gender at baseline for estimated VO2max is reflected in asmaller mean VO2max for women than men. Women, as agroup, are known to have a VO2max approximately 20% lessthan men of a similar age group, primarily due to hormonaldifferences that cause women to have a lower concentration ofhemoglobin in their blood and a higher percentage of body fat(23). In the current study, additional analyses revealed that thedifferences in VO2max between the high fit and low fit menand the high fit and low fit women were not different. Thus,
there was no significant interaction between fitness andgender.
The most common finding in the literature on the effects offitness on the heart is a lower resting heart rate (longer HP)thought to be a result of an increase in vagal tone (30). Insupport of that conclusion, high fit individuals in this studyexhibit a longer resting HP than low fit individuals in thebaseline condition. The bradycardia displayed by high fitindividuals remains significant even after adjusting for BMI.Conversely, women and men show no differences in HP atbaseline. This finding does not support the conclusions of themeta-analytic review conducted by Stoney et al. (35) of sexdifferences in cardiovascular responses, which reported thatwomen exhibit higher heart rates at rest than men. In addition,the same pattern of HP exhibited at baseline was found acrossall experimental tasks (ie, FCT, RT, and COMBO). High fitindividuals continue to display significantly longer HP thanlow fit individuals and women and men continue to display nodifferences in HP.
CONCLUSIONSThere are three main conclusions of this study. First, small
differences in aerobic capacity result in meaningful differ-ences in autonomic cardiac control as indexed by both timedomain and frequency domain measurements of HPV. Thevagal dominance of high fit individuals is clearly demon-strated across a variety of laboratory stressors. Second, im-portant gender-related differences in HPV indicate that oppos-ing branches of the ANS predominate in men and women withwomen exhibiting more vagal control and men exhibitinggreater relative sympathetic control, even though HP did notdiffer. Third, the mechanisms underlying the beneficial effectsof fitness and those placing women at a reduced risk for CHDseem to be similar. However, the common vagal component inboth high fit individuals and women may be a product ofdifferent influences on the cardiovascular system. Findingsfrom experimental studies suggest that the effects of estrogenpromote vagal cardiac control in women (36), whereas theeffects of aerobic fitness promote vagal control in physicallyactive individuals, (26. 33). Inasmuch as both physical activityand female gender are related to greater cardiovascular health,research that investigates gender and fitness simultaneously,as in the present study, will be needed to additionally clarifythe mechanisms for the beneficial effects of fitness and thereduced risk for CHD in women.
REFERENCES1. Powell KE, Thompson PD, Caspersen CJ, et al: Physical activity
and the incidence of coronary heart disease. Annu Rev PublicHealth 8:253-257, 1987
2. Blair SN, Kohl HW, Gordon NF, et al: How much physicalactivity is good for health? Annu Rev Public Health 13:99-126,1992
3. Bovens AM. Van Baak MA, Vrencken JG, et al: Physicalactivity, fitness, and selected risk factors for CHD in active menand women. Med Sci Sports Exerc 25:572-576, 1993
4. Matthews KA: Interactive effects of behavior and reproductivehormones on sex differences in risk for coronary heart disease.Health Psychol 8:373-387, 1989
5. Lash SJ, Gillespie BL, Eisler RM, et al: Sex differences incardiovascular reactivity: Effects of the gender relevance of thestressor. Health Psychol 10:392-398, 1991
Psychosomatic Medicine 60:773-781 (1998)

FITNESS, GENDER, AND HPV
6. Truett J, Cornfield J, Kannel W: Multivariate analysis of the riskof coronary disease in Framingham. J Chronic Dis 20:511-524,1967
7. Wingard DL, Suarez L, Barret-Connor E: The sex differential inmortality from all causes and ischemic heart disease. Am JEpidemiol 177:165-172, 1983
8. Hazzard WR: Biological basis of the sex differential in longev-ity. J Am Geriatr Soc 34:445-471, 1986
9. Ryan SM, Goldberger AL, Pincus SM, et al: Gender- andage-related differences in heart rate dynamics: Are women morecomplex than men? J Am Coll Cardiol 24:1700-1707, 1994
10. Saul JP: Beat-to-beat variations of heart rate reflect modulationof cardiac autonomic outflow. News Physiol Sci 5:32-37, 1990
11. Thayer JF, Friedman BH, Borkovec TD: Autonomic character-istics of generalized anxiety disorder and worry. Biol Psychiatry39:255-266, 1996
12. Pomeranz B, Macaulay RJB, Caudill MA, et al: Assessment ofautonomic function in humans by heart rate spectral analysis.Am J Physiol 248:H15l-H153, 1985
13. Pagani M, Lombardi F, Guzzetti S, et al: Power spectral analysisof heart rate and arterial pressure variabilities as a marker ofsympatho-vagal interaction in man and conscious dog. Circ Res59:178-193, 1986
14. Sato N, Miyake S, Akatsu J, et al: Power spectral analysis ofheart rate variability in healthy young women during the normalmenstrual cycle. Psychosom Med 57: 331-335, 1995
15. Bigger JT Jr, Fleiss JL, Steinman RC, et al: Correlations amongtime and frequency domain measures of heart period variabilitytwo weeks after acute myocardial infarction. Am J Cardiol69:891-898, 1992
16. Friedman BH, Thayer JF, Tyrrell RA: Spectral characteristic ofheart period variability during cold face stress and shockavoidance in normal subjects. Clin Auton Res 6:147-152, 1996
17. Khurana R, Watabiki S, Garcia J, et al: Cold face test in vagaldysfunction. Trans Am Neurol Assoc 102:142-146, 1979
18. Khurana RK, Watabiki S, Hebel JR, et al: Cold face test in theassessment of trigeminal-brainstem-vagal function in humans.Ann Neurol 7:144-149, 1980
19. Turner JR: Cardiovascular reactivity and stress: Patterns ofphysiological response. New York and London, Plenum Press 1994
20. Kautzner J, Camm AJ: Clinical relevance of heart rate variabil-ity. Clin Cardiol 20:162-168, 1997
21. Cattell RB: The data box: Its ordering of total resources in termsof possible relational systems. In Cattell RB (ed), Handbook ofMultivariate Experimental Psychology. Chicago, Rand McNally,1966, 67-128
22. Jackson AS, Blair SN, Mahar MT, et al: Prediction of functionalaerobic capacity without exercise testing. Med Sci Sports Exerc22:863-870, 1990
23. Ross RM, Jackson AS: The role of exercise on health. In GladishK (ed), Exercise Concepts, Calculations, and Computer Appli-cations. Carmel, IN, Benchmark Press, 1990
24. Kuhmann W, Lachnit H, Vaitl, D: The quantification of exper-imental load: Methodological and empirical issues. In Steptoe A,Ruddel H, Neus H (eds), Clinical and Methodological Issues inCardiovascular Psychophysiology. Berlin, Springer, 1985
25. Colombo R, Mazzuero G, Soffiatino F, et al: A comprehensivePC solution to heart rate variability analysis in mental stress.1989 IEEE Comp Cardiol 475-478, 1990
26. Dixon EM, Kamath MV, McCartney N, et al: Neural regulationof heart rate variability in endurance athletes and sedentarycontrols. Cardiovasc Res 26:713-719, 1992
27. Thayer JF, Peasley C, Muth ER: Estimation of respiratoryfrequency from autoregressive spectral analysis of heart period.Biomed Sci Instrum 32:93-99, 1996
28. Vasey MW, Thayer JF: The continuing problem of false posi-tives in repeated measures ANOVA in psychophysiology: Amultivariate solution. Psychophysiology 24:479-486, 1987
29. Jennings JR, McKnight JD: Inferring vagal tone from heart ratevariability. Psychosom Med 56:194-196, 1994
30. Kenney WL: Parasympathetic control of resting heart rate:relationship to aerobic power. Med Sci Sports Exerc 17:451-455, 1985
31. DeMeersman RE: Heart rate variability and aerobic fitness. AmHeart J 125:726-731, 1992
32. Gallagher D, Terenzi T, DeMeersman R: Heart rate variability insmokers, sedentary and aerobically fit individuals. Clin AutonRes 2:383-387, 1992
33. Seals DR, Chase PB: Influence of physical training on heart ratevariability and baroreflex circulatory control. J Appl Physiol66:1886-1895, 1989
34. Grossman P, Svebak S: Respiratory sinus arrhythmia as an indexof parasympathetic cardiac control during active coping. Psycho-physiology 24:228-235, 1987
35. Stoney CM, Davis MC, Matthews, KA: Sex differences inphysiological responses to stress and in coronary heart disease: Acausal link? Psychophysiology 24:127-131, 1987
36. Du X, Riemersma RA, Dart AM: Cardiovascular protection byestrogen is partly mediated through modulation of autonomicnervous function. Cardiovasc Res 26:713-719, 1995
Psychosomatic Medicine 60:773-781 (1998)




















