Fertility and Adaptation: Indochinese Refugees in the United States
40
Fertility and Adaptation: Indochinese Refugees in the United States Author(s): Ruben G. Rumbaut and John R. Weeks Source: International Migration Review, Vol. 20, No. 2, Special Issue: Refugees: Issues and Directions (Summer, 1986), pp. 428-466 Published by: The Center for Migration Studies of New York, Inc. Stable URL: http://www.jstor.org/stable/2546043 Accessed: 05/04/2010 17:13 Your use of the JSTOR archive indicates your acceptance of JSTOR's Terms and Conditions of Use, available at http://www.jstor.org/page/info/about/policies/terms.jsp. JSTOR's Terms and Conditions of Use provides, in part, that unless you have obtained prior permission, you may not download an entire issue of a journal or multiple copies of articles, and you may use content in the JSTOR archive only for your personal, non-commercial use. Please contact the publisher regarding any further use of this work. Publisher contact information may be obtained at http://www.jstor.org/action/showPublisher?publisherCode=cmigrations. Each copy of any part of a JSTOR transmission must contain the same copyright notice that appears on the screen or printed page of such transmission. JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range of content in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new forms of scholarship. For more information about JSTOR, please contact [email protected]. The Center for Migration Studies of New York, Inc. is collaborating with JSTOR to digitize, preserve and extend access to International Migration Review. http://www.jstor.org
Transcript of Fertility and Adaptation: Indochinese Refugees in the United States

Fertility and Adaptation: Indochinese Refugees in the United StatesAuthor(s): Ruben G. Rumbaut and John R. WeeksSource: International Migration Review, Vol. 20, No. 2, Special Issue: Refugees: Issues andDirections (Summer, 1986), pp. 428-466Published by: The Center for Migration Studies of New York, Inc.Stable URL: http://www.jstor.org/stable/2546043Accessed: 05/04/2010 17:13
Your use of the JSTOR archive indicates your acceptance of JSTOR's Terms and Conditions of Use, available athttp://www.jstor.org/page/info/about/policies/terms.jsp. JSTOR's Terms and Conditions of Use provides, in part, that unlessyou have obtained prior permission, you may not download an entire issue of a journal or multiple copies of articles, and youmay use content in the JSTOR archive only for your personal, non-commercial use.
Please contact the publisher regarding any further use of this work. Publisher contact information may be obtained athttp://www.jstor.org/action/showPublisher?publisherCode=cmigrations.
Each copy of any part of a JSTOR transmission must contain the same copyright notice that appears on the screen or printedpage of such transmission.
JSTOR is a not-for-profit service that helps scholars, researchers, and students discover, use, and build upon a wide range ofcontent in a trusted digital archive. We use information technology and tools to increase productivity and facilitate new formsof scholarship. For more information about JSTOR, please contact [email protected].
The Center for Migration Studies of New York, Inc. is collaborating with JSTOR to digitize, preserve andextend access to International Migration Review.
http://www.jstor.org

Fertility and Adaptation:
Indochinese Refugees
in the
United States
Ruben G. Rumbaut, Principal Investigator/Director Indochinese Health & Adaptation Research Project1 San Diego State University
John R. Weeks, Administrative Director, International Population Center
San Diego State University
Levels of fertility among Indochinese refugees in the United States are
explored in the context of a highly compressed demographic transition
implicit in the move from high-fertility Southeast Asian societies to a
low-fertility resettlement region. A theoretical model is developed to
explain the effect on refugee fertility of social background charac?
teristics, migration history and patterns of adaptation to a different
economic and cultural environment controlling for marital history and length of residence in the U.S. Multiple regression techniques are
used to test the model which was found to account for nearly half of the
variation in refugee fertility levels in the United States. Fertility is
much higher for all Indochinese ethnic groups than it is for American
women; the number of children in refugee families is in turn a major determinant of welfare dependency. Adjustments for rates of natural increase indicate a total 1985 Indochinese population of over one
million, making it one of the largest Asian-origin populations in the United States. This remarkable phenomenon has occurred in less than
a decade. Implications of these findings for public policy are discussed,
focusing on family planning, maternal and child health needs, and the
attainment of refugee economic self-sufficiency.
The Indochinese exodus is one of the largest refugee movements in modern
history. Since the collapse in 1975 of U.S.-backed regimes in South Vietnam, Cambodia (now Kampuchea) and Laos, nearly two million refugees are known to have fled Indochina in search of asylum. Of these, 807,321 persons had been resettled in the United States as of September 30, 1985 (Gordon, 1985; ORR, 1985; ACNS, 1984). Two-thirds of this population are Vietnamese
1 This research was supported by Grant No. R01-HD15699 from the National Institute of Child Health and Human Development.
428 IMR Volume xx, No. 2

Indochinese Refugees in the United States 429
(including ethnic Chinese), followed by Cambodians (16%), lowland Lao
(12%) and Laotian hilltribes, mostly Hmong (7%). About 40 percent of the
refugees (over 300,000) have resettled in California; Texas is next among the 50 states with an Indochinese population of over 50,000. There are significant Indochinese concentrations in Washington, New York, Pennsylvania, Illi?
nois, Minnesota, Virginia, Massachusetts and Oregon, with smaller numbers scattered throughout each of the remaining states. These new migrant groups are socioeconomically as well as ethnoculturally diverse. Fewer than one in five of these refugees arrived in the U.S. during 1975-77 (the "first wave" of
immigration); most have arrived since 1980 (the peak year of a "second wave" of immigration which is still continuing). First-wave refugees were predo? minantly South Vietnamese urban residents and significantly more educated,
occupationally skilled and Westernized than the refugees who have arrived since 1978 (including the Vietnamese and ethnic Chinese "boat people", the survivors of the Pol Pot period in Kampuchea, and almost all of the Hmong), many of whom come from rural areas of Southeast Asia and most of whom have endured prolonged stays in refugee camps overseas prior to their resettlement in the United States.
In the process of adapting to the U.S. economy and society, one factor that has both advantages and disadvantages for the refugees is that they typically have large families. Extensive kinship networks founded on traditional values of filial piety provide the refugees with much-needed social and economic support as they attempt to cope with the extraordinarily stressful demands of their resettlement. On the other hand, the refugees' meager resources are further depleted by the need to provide for large families with many dependent children. This article explores the role of
fertility in the adaptation process, and aims to estimate the levels of fertility in the Indochinese refugee population in the United States, to explain the main determinants of refugee fertility, and to examine some significant implications of these findings for public policy.
Fertility rates in Southeast Asia are significantly higher than in the United States. For example, the Population Reference Bureau (1985) estimates the crude birth rate (CBR) in Vietnam to be 34 per 1,000, with a total fertility rate (TFR) of 4.7; in Laos the CBR is estimated at 41 per 1,000 with a TFR of
6.0; and in Democratic Kampuchea (Cambodia) the CBR is estimated at 32
per 1,000 with a TFR estimated to be 4.7. By comparison, the CBR in the United States is 16 per 1,000 and the TFR is 1.8. We should note that in the
mid-1970s, when the exodus of the refugees began in earnest, the fertility rates in the countries of origin were at least as high, or higher, than at the
present time. These averages conceal regional variations within each country, of course, especially the urban/rural differential. In Vietnam it has been estimated that completed family size in rural areas has been consistently 7-8 children (Fraser, 1980). Studies of Hmong highlanders in Thailand have
reported crude birth rates ranging from 49 to 76 per 1,000 (Geddes, 1976;

430 International Migration Review
Kunstadter, 1983,1984), and indeed Kunstadter has observed that the Hmong are "at the upper limits of human reproductive capacity" (1984:24). It is
clear, then, that the refugee population has come from a background of high
fertility. There is also evidence that countries of origin had relatively little
governmental commitment to family planning and that contraceptive utilization was probably quite low (Population Reference Bureau, 1976),
although since 1977 the government of Vietnam has been moderately
supportive of family planning (World Bank, 1984). The level of contraceptive utilization has probably been highest in Vietnam (Monnier, 1981), and the
urban Vietnamese, in particular, probably exhibit the lowest average levels of fertility in Southeast Asia (Jones, 1982).
Data from the refugee camps in Thailand are also suggestive of both the
relatively high levels of fertility and the cultural diversity in fertility patterns within the Indochinese population. Hoick and Cates (1982) found that in one
of two camps populated primarily by Khmer (Cambodian) refugees in 1979, the population was largely young adult with a balanced sex ratio and the
birth rate was very high (55 per 1,000). In a second camp in which the
proportion of young single women was high and the proportion of males was
fairly low, the birth rate was much lower, as would be expected. By 1981, the
average crude birth rate in all refugee camps in Thailand was 42 per 1,000
(Dewey, 1982). Among all Thai camps, those in which Cambodian refugees
predominate tend to have the highest crude birth rates (range = 46 to
64) ?rates which, if standardized, would probably be similar to those
prevailing in Cambodia prior to the fall of the Lon Nol government in 1975
(Meng-Try, 1981). Those camps in which the Hmong and Lao predominate have lower birth rates (range = 22 to 31), and those in which the Vietnamese
predominate tend to have the lowest levels (range = 21 to 25)(Dewey, 1982). These differences are at least partially explicable in terms of the different sex
ratios in the refugee camps. In Cambodian camps, for example, there were
nearly equal numbers of males and females, while the predominantly Vietnamese camps averaged more than twice as many men as women (Dewey, 1982). Consequently, age and sex standardized crude birth rates would
probably show high rates throughout the refugee camps. Because they come
from countries in which fertility is typically high and contraceptive utilization
is probably quite low, we can anticipate that fertility among Southeast Asian
refugees is well above the average for American women.
The main purpose in this article is to estimate the level of fertility among Indochinese refugees, and to place the fertility of the refugee population within the context of a highly compressed demographic transition implicit in the move from a high fertility homeland to a low fertility resettlement
region. The traditional explanation for the transition from high to low
fertility is that couples respond to economic development by trading quality in children for quantity of children (See, Weeks, 1986). Caldwell (1982) has
explained this phenomenon as representing a change in the direction in

Indochinese Refugees in the United States 431
which family income flows. In less developed societies children are economic
assets who contribute to their parents' well-being from early childhood until
the parents' death. A crucial change occurs in the process of economic
development, however, as a market economy replaces the family economy and the flow of income reverses ?parents now contributing to the child's
well-being from birth until the parents' death. Other researchers suggest that economic development is a sufficient but unnecessary cause of the
decline in a society's fertility. The important component of a fertility decline
is the change that occurs in the way that people view the world. In particular, it is argued that modernization, or more specifically, secularization, is causally linked to changing attitudes about family size (Lesthaeghe, 1977; Leasure,
1982). A key element in secularization is the growth in personal autonomy that leads people to believe that they have the ability to control their own
fertility (Coale, 1973). Indeed, this transformation of consciousness has been
characterized more broadly as a "movement from fate to choice"; that is, whereas the pre-modern individual tends to experience traditional social
life as a "world of fate", the modern individual in secular societies is confronted
with multiple options for both action and thought, such that every aspect of
life (including beliefs and values about sexuality, marriage and childbearing) becomes increasingly experienced as an "arena of choices" (Berger, 1979). Since this attitudinal shift invariably accompanies economic development, the latter is always associated with a decline in fertility, but a series of
regional demographic histories produced by the European Fertility History
Project at Princeton University suggest that secularization can occur and can
affect fertility even in the absence of widescale economic development. All of these influences on fertility are potentially observable within the
Indochinese refugee population. The refugees are going through the process of economic development in a very compressed time, with a speed the
equivalent of a time warp. In this process they are exposed clearly to the risk
that the traditional direction of income flow within the family will reverse
direction. Additionally, they are being exposed to Western, modern, secular
attitudes that are bound to have an impact on family size preference. Indochinese refugees in the United States are primarily from five different
broadly defined ethnic groups ?the Vietnamese, the ethnic Chinese (pri?
marily from Vietnam), the Khmer (people of Cambodian descent), the Lao
(the dominant ethnic group in Laos), and the Hmong (tribal highlanders from the northern mountain regions of Laos). Although all these ethnocul?
tural groups have shared a geographic region for centuries, their histories
have often been adversarial. Furthermore, there are distinct socioeconomic
and cultural differences among the groups that are likely to have influenced
past fertility patterns and, to the extent that people remain integrated into
the ethnic community, may also affect fertility (indeed, these differences
also influence the larger process of refugee adaptation to the American
economy and society).

432 International Migration Review
CONCEPTUAL MODEL
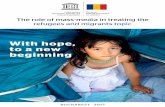
While it is beyond the scope of this article to test all of the possible explanations of the demographic transition, it is our goal to use these perspectives on the
demographic transition to attempt to explain the levels of fertility that
currently prevail in the United States within the Indochinese refugee
population. Our conceptual framework links social background characteristics
in the homeland (including urban/rural residence and education) to the
migration history of the refugees (the only anomaly with respect to the usual
pattern of in situ fertility shifts) to patterns of adaptation to a different
economic and cultural environment, as predictors of fertility in the United
States. Marital history (including years married and the number of children
already born prior to coming to the United States) will independently influence the level of childbearing in the United States, and the number of
years in the U.S. will obviously influence the extent to which adaptation has
occurred. These relationships are shown in Figure I.
FIGURE I
Conceptual Model
MARITAL HISTORY
SOCIAL BACKGROUND
YEARS IN THE U.S
\ ECONOMIC /'ADAPTATION
MIGRATION HISTORY
v^J CULTURAL W / ADAPTATION
.FERTILITY /OUTCOME
Sociodemographic Background
The Vietnamese have a patriarchal, patrilineal, patrilocal extended kin
system, with polygamy being practiced fairly commonly until the 1960s
(Haines, 1982; Van Deusen etal, 1981). The age at marriage appears to have been later than in other Southeast Asian cultures (18-25 for women) ?a fairly recent phenomenon (Crawford, 1966) that may help to account for the widely accepted perception (in the absence of much hard data) that fertility levels are lowest among the Vietnamese. There is no prescribed postpartum taboo on intercourse, and the usual period of breastfeeding prior to weaning appears to have been about two years (Van Deusen et al, 1981). Furthermore,

Indochinese Refugees in the United States 433
the Vietnamese have been sufficiently westernized over time that dating has
been permitted in urban areas. The Vietnamese are more urban than most of
the other groups, and educational levels accordingly tend to be somewhat
higher. The ethnic Chinese from Vietnam, who have played an important
"middleman minority" economic role in the history of Vietnam, are estimated
to have represented a substantial fraction of the population that fled Vietnam
(Fraser, 1980). Like the Vietnamese, the social organization of the ethnic
Chinese is basically patriarchal, patrilineal, and patrilocal. Also in common
with the Vietnamese, the family is the most powerful social unit, and the
status of women is clearly inferior to that of men (Schrock et al, 1966).
Further, like the Vietnamese, the ethnic Chinese are predominantly urban
and more educated relative to other Indochinese groups. In contrast to the Vietnamese and ethnic Chinese, the Khmer culture is
characterized by a nuclear, neolocal family system, with a typically young
age at marriage (16 is not uncommon) (Van Deusen et al, 1981; Khoa, 1981). The position of women has traditionally been stronger than among the
Vietnamese, and women are traditionally the controllers of the family budget in Khmer households (Schrock, et al, 1966). After the birth of a child there is
typically a period of 1-12 weeks of postpartum isolation from the husband
and children are usually weaned at about age three. The Khmer are typically rural in origin with consequent low levels of education.
The Lao are also organized around a nuclear family form although it is
usually matrilocal (as is actually often true among the Khmer for financial
reasons). Age at marriage is young (16-22), and a one-month postpartum period of isolation is usual, with weaning occurring after about two years (Van Deusen et al, 1981). The Hmong of northern Laos differ in important
respects from Laotians. The basic form of social organization is an extended
clan system that is patriarchal, patrilocal, and patrilineal, but sharing of
responsibilities by all family members is usual (Schrock etal, 1966; Dunnigan, 1982). Polygamy is still occasionally practiced; indeed, polygamy has ensured
that marriage is virtually universal for Hmong women throughout their
reproductive years even in small villages where the sex ratio is unbalanced
during marriageable ages (Kunstadter, 1983, 1984; Vang, 1982). For the
Hmong, age at marriage is youngest of all the ethnic groups (13-18), and
premarital intercourse and pregnancy are not normally punished. The birth
of a child is followed by a three-week period of postpartum abstinence, and
weaning typically occurs about a year and a half after birth (Chindarsi, 1976). The Hmong are almost universally from remote mountainous rural areas, and illiteracy in their native language (for which no alphabet existed until
after WWII) has been the norm among this group of Indochinese.
In general, then, although the family holds central importance for each
of these groups, the specific character of their family and traditions is
variable. Thus, whereas the Vietnamese and Chinese family system favors

434 International Migration Review
the extended family, the Hmong possess a clan system and the Lao and
Khmer emphasize nuclear ties. Average ages at marriage vary among the
groups, as do postpartum taboos and lactation periods. These cultural
differences may well have influenced past fertility levels and, to the extent
that they are transplanted to American society, may also influence current
and future levels of childbearing.
Migration History
The process of flight and the (often traumatic) nature of refugee migration
may variously affect fertility-regulating behavior. For both the current and
emerging population of adults in the Indochinese refugee population, the
scars of the flight from Asia are bound to heal only slowly. It is apparent from
most work on refugees, moreover, that the timing of flight affects how
penetrating its impact will be. In a summary of social theories of the refugee
experience, Stein (1981) suggests that anticipatory flight is somewhat similar
to voluntary migration (except that it involves a "push" not a "pull"), and
usually involves the better educated and economically well-to-do. Acute
flight at a time of crisis, however, can cause severe problems of adjustment because of the haste in which the move was made. Furthermore, in the case of
Indochinese refugees, acute-flight refugees were far more likely than others
to wind up in refugee camps prior to their entry into the United States and
that, too, has often been a brutalizing experience. As political refugees
escaping persecution, many Southeast Asians have experienced extreme
hardships, trauma and tragedy, including separation from and loss of family members (Huyck and Fields, 1981; Rumbaut, 1985).
Two fertility-related phenomena may be taking place in reaction to these
experiences; one we shall call "catching up", the other "rebuilding". Although
fertility levels are generally high in the refugee camps, some women may have been forced or may have elected to postpone childbearing during their
stay in or escape from the refugee camps. Similarly, many families have lost
one or more members. Certain cultural and psychological factors that help them cope with their loss make it probable that high fertility rates will result.
For example, the Buddhist belief in the cycle of life, including reincarnation,
encourages people to have children. The dependency of deceased ancestors
on the living for honor and sustenance in the spirit world requires future
generations of relatives. The survival of the family and of the people as a
whole requires the individual survivors to rebuild by reproduction. Con?
fucianism and its stress on filial piety and the maintenance of the family heritage also encourages family-building. Cambodians, in particular, are
likely to have experienced heavy loss of family members (Meng-Try, 1981; Ima et al, 1983), and may thus be influenced by the desire to rebuild the
family by bearing children (Ellis, 1982). Children, moreover, provide the

Indochinese Refugees in the United States 435
older refugees ?who, having lost home and homeland, often harbor little little hope for their own generation ?with their deepest source of present life
satisfaction and their best hopes for the future (Rumbaut, 1985).
Economic Adaptation
We have already mentioned that the timing of migration is related to the
socioeconomic status of migrants at the place of origin. Clearly, status at
origin will affect status or potential status in the United States. More
importantly, status in the United States will influence the speed and extent
of adaptation to the new economic environment. Learning English, getting a
job, earning an adequate income and owning a car so that geographic
mobility and independence can be enhanced are all factors that are bound to
be an influence on the processes of personal economic development and
secularization, leading to a new view about preferred family size. There is at
least anecdotal evidence that education is highly valued among some of the
Indochinese ethnic groups, especially the Vietnamese. Over time such a
phenomenon should have the effect of raising the age of marriage and
substantially delaying the birth of the first child (McDonald and Rindfuss,
1981; Rindfuss, Bumpass and St.John, 1980; Rhodes and Woodrum, 1980; Rindfuss and St. John, 1983). Education is also a source of family breakup, to
a certain extent, because it prepares people for non-family market labor (cf.
Jain. 1981). It is also part of the process of individual modernization. As
Caldwell (1981) has commented, "the study of fertility transition is the study of the transition of familial production into production through the labor
market, of traditional society into modern society" (p. 27).
It may be reasonable to assume that males will be the initial entrants into
the American labor force, and that the family's economic adaptation will be
heavily dependent upon the behavior of the male. Over time, however,
fertility is likely to be especially influenced by the labor force participation of women, especially that which clearly lifts her above the level in the labor
market that allows easy entrance and exit. In relatively unskilled work
requiring little education or training, a woman's employment need not have
a depressive effect on fertility because she can leave and reenter the labor
market freely so long as child care is available (Gurak and Kritz, 1982). The
principal adjustment that such mothers must make to their employment is to
substantially reduce the length of breastfeeding (Ward, Pridmore and Cox,
1981; Hollingsworth, Brown and Brooten, 1980). Only if the occupational demands of the wife are substantial enough to prevent easy movement into
and out of the labor force would we expect to notice an influence on fertility, at least in the short run. In the long run, it may be that work of any kind,
especially if the employer is a non-relative, may lead to greater levels of
economic integration into the dominant culture and thus to downward
pressure on fertility.

436 International Migration Review
Cultural Adaptation
When the sociocultural context of the refugee's life changes radically as a
consequence of resettlement in the United States, the framework of individual
decision-making is restructured, often having an influence on family-building
activity (Tabah, 1980; McNicoll, 1980). Particularly important in this regard is the extent to which a person is integrated (or is in the process of integrating) into the dominant culture. Language facility, networks of friends, reference
group identification, and acceptance of some of the symbols of the dominant
culture such as food and music are indicators of subtle, but important influences on a person's daily life, and there is increasing evidence that
present social circumstances are more important in determining fertility than has previously been thought (Smith, 1981; Janssen and Hauser, 1981).
Indochinese refugees find themselves in a bicultural setting with com?
peting demands and pressures. Their strategy for coping with these aspects of their life will likely have an important bearing on their decisions about
reproduction. Migrants may choose to integrate themselves into the local
ethnic community, in which case sociocultural background characteristics
may continue to affect role relationships and behavior, with the potential for
pronatalist pressures to be exerted. Or, they may choose to become more
integrated into the dominant culture, in which case new role relationships
may emerge with the potential for downward pressure on fertility.
Particularly important in maintaining strong ties to the traditional culture
is residence within an extended kin network (Davis, 1948). This theme has
existed for decades in the literature (Burch and Gendell, 1971), and in a
study of fertility in Sierra Leone it has recently been concluded that "the
prevalence of the extended family system is found to increase the demand
for children" (Ketkar, 1979:487). The presence of other relatives, especially older ones, increases the pressures to maintain traditional roles and to
strengthen ties through reproduction.. This may have the same effect in
other cultures as has been observed in Puerto Rico: "Status differences
between husband and wife, the taboos on discussion of sex, and the modesty of women in general combine to make many Puerto Ricans reticent when
facing problems of goal-setting with respect to family size, of mutuality in sex
relations, of seeking the means for fertility control and of putting these
means to work" (Hill et al, 1959:62-63). The obverse of this is that neolocal
nuclear families may be those in which the status and roles of women will
adapt most quickly to American norms and values. We should note, however, that the process of migration tends, in and of itself, to undermine the
existence of the extended family. We might expect, then, that those individuals who identify with their
cultural heritage will demonstrate behavior patterns that reflect that culture.
If having many children is the "Khmer" or "Hmong" way, then the more
"Khmer" or "Hmong" a woman is, the more children she might have.

Indochinese Refugees in the United States 437
However, the exact nature of the relationship between cultural adaptation and fertility is still muddy (Scrimshaw, 1975). It is likely that this is because
adaptation has both cultural and structural aspects (Frisbie and Bean, 1978). Some aspects of behavior are deeply ingrained in cultural values and
traditions and are unlikely to change in one or even two generations, whereas other aspects of behavior are a function of a group's status in society and if social mobility occurs then behavioral changes will follow suit (Beaujot, Krotki, and Krishan, 1982; Bean and Swicegood, 1982). The uncertainty about fertility and adaptation is evident in the literature. Day (1984) has used
census data from Australia to suggest that the decline of fertility among ethnic immigrant groups may be due less to assimilation into a new culture
than to 1) a mirroring of fertility trends in the country of origin (with which
immigrants may stay in contact and thus be influenced in their behavior); 2) the striving to take advantage of opportunities for economic and social
advancement; and 3) more information about and greater access to birth
control. Other data from Australia (Carlson, 1985) suggest further that, whatever the disruptive effect of migration on marriage and childbearing, the impact is short-term. Thus, long-term shifts in fertility may be seen as a
reaction to processes that transcend the migration experience itself, such as
adaptation (See, e.g., Lee and Farber's [1984] discussion of rural-urban
migration in Korea) or the factors identified by Day, as discussed above.
The ability of Asian immigrant populations to limit fertility has been
amply illustrated in Canada. Basavarajappa and Halli (1984) have used
indirectly age-standardized general fertility rates to show that in 1926-1931
the Chinese and Japanese immigrants to Canada had fertility rates that were
97 and 65 percent above the Canadian average, respectively. By 1946-1951, the Japanese-Canadians had already dropped below the Canadian average, and by 1966-1971 the fertility of the Chinese ethnic group was only 9 percent above the national average. In both cases, the decline of fertility in a new
setting was, in fact, occurring at the same time the high fertility was yielding to lower levels in the countries of origin.
Although immigrants may not assimilate into the new culture, they must,
nevertheless, cope with a new social and economic environment, and it is
worth noting that previous research suggests that, in a bicultural setting,
fluency in the dominant language is one of the most predictive indicators of
both economic and cultural adaptation, since it is the key to learning the
norms and expectations of the dominant cultural group (Cuellar and Weeks,
1980). Ability in English has been found, in particular, to be associated with
lower fertility among Puerto Rican migrants to New York (Rindfuss, 1976).
SAMPLE
Data for this analysis are drawn primarily from the first (Tl) of two sets of
interviews conducted by the Indochinese Health & Adaptation Research

438 International Migration Review
Project (IHARP) at the University of California, San Diego (now relocated
to San Diego State University). Since its inception in 1982, IHARP has
entailed a comprehensive three-year longitudinal study of the migration and resettlement of Southeast Asian refugees, based on interviews with
randomly selected samples of adult men and women of the Hmong, Khmer,
Lao, Chinese-Vietnamese, and Vietnamese communities of San Diego
County. The sampling process began with a systematic enumeration of the
Indochinese refugee population in San Diego County, which we found to
number nearly 40,000 persons as of April 1983. This enumeration was
stratified by the five major ethnic groupings, and, using heads of household
as the unit of selection, a random sample of householders and their spouses was drawn from within each ethnic group, producing a sample of 739 adults
(366 men, 373 women) residing in 437 households. Complete household
listings were obtained for each household, yielding basic demographic information on a total of 3,003 persons. This latter set of data was used for
this calculation of child-woman ratios, discussed in the next section.
Structured Tl interviews (with many open-ended questions) lasting an
average of nearly three hours were conducted during 1983 with the 739 adult
respondents, and were repeated a year later in 1984 (T2) for all but the Lao
sample. Interviews were conducted by skilled, extensively trained, indigenous interviewers in the home and language of the respondent. The refusal rate
was 6 percent (lower for the Hmong, Lao and Khmer, higher for the Chinese
and Vietnamese). Respondents were selected if they were between the ages of
25 and 65, and their spouses were included even if they were under 25 or over
65. The age limitation makes our data somewhat conservative with respect to
fertility behavior, since it effectively reduces the influence on our results of
those younger members of a group whose reproductive behavior does not
span both the homeland and the new area of resettlement. Still, given that
wives were nearly always younger than their husbands, the sample yielded a
total of 38 women under age 25. For our analysis of fertility and adaptation, most of the data reported in this paper are drawn from the 313 interviews
conducted with women of childbearing age (between the ages of 18 and 49 at
Tl, and under 45 years of age at arrival in the U.S.), including 63 Hmong, 54
Khmer, 61 Lao, 53 Chinese-Vietnamese, and 82 Vietnamese. Of these 313
women, 86.9 percent were married at Tl, 5.4 percent were single (signifi?
cantly, no Hmong women were single), 2.9 percent were divorced or separated
(mostly the Lao), and 4.8 percent were widowed (mostly the Khmer, who
evidence by far the greatest degree of family disorganization as a result of
post-1975 events in Kampuchea).
FINDINGS
Descriptive data for the adult sample (N=739) are shown in Table 1. It is
particularly noteworthy that the majority of respondents are second-wave

Indochinese Refugees in the United States 439
refugees, as are the majority of Indochinese refugees nationally. Little has
heretofore been known about this group. In comparison with the first-wave
migrants (N=115), those in the second wave (N=624) are significantly (p < .001) more rural in background, less educated, less fluent in English, live in
larger households with fewer employed family members, have higher rates
of poverty and welfare dependency, earn much less income from jobs, and
have higher levels of fertility. This latter fact, in particular, leads to a very
young age structure among second-wave refugees, especially among the
Hmong, who, as we will discuss, have by far the highest level of fertility. Since the majority of the refugees are part of the second wave, the char?
acteristics of this group tend to dominate the overall statistics.
Data from the total household sample (N=3,003) show that 43.8 percent of the Indochinese population consists of children under age 15; the median
age of this population is 18 (and for the Hmong, the median age is 12.7), much younger than the median age of 31 for the U.S. population. These
demographic differences are illustrated in Figure 2, which presents age-sex
pyramids for the San Diego Indochinese population and for the general San
Diego County population (the latter based on 1980 Census data). The older,
constrictive age structure of the San Diego population stands in sharp contrast to the young, expansive profile of the Indochinese population ? a
contrast typical of the respective population patterns of affluent countries
and developing regions. The youthful age structure of the Indochinese
population, combined with current high levels of fertility, suggests, of
course, a substantial rate of natural increase for a considerable length of time
in the future?a pattern which, although essentially similar to that of a less
developed nation, carries with it the added twist of exposure to the risk of
adaptation to a new environment in which low fertility rates prevails.
Fertility Levels
Our findings reveal that fertility is substantially higher in each of the
Indochinese communities than in the U.S. population. In the United States
in 1980, the child-woman ratio (CWR) was 309 children aged 0-4 per 1,000 women aged 15-44. By comparison, our household sample of 635 Indochinese
women aged 15-44 produced a CWR of 824. As can be seen in Table 2, the
child-woman ratios were lowest for the ethnic Chinese-Vietnamese (511), followed by the Lao (553) and Vietnamese (574). The Khmer had a higher ratio (816), while the Hmong evidenced an exceptionally high level of
fertility (1,769). We calculated age-standardized rates (using the indirect
method, based on age-specific fertility rates for the U.S. in 1980), and found
that age structure accounted for only a negligible proportion of the differences
in fertility.

4^ O
TABLE 1
Characteristics of the Indochinese Refugee Population, by Ethnic Group and Immigration Waves*
IHARP 1983 Adult Sample, N=73g (366 men, 373 women)
ETHNIC GROUP IMMIGRATION WAVE
CHARACTERISTICS (Means or Percents)
Hmong Khmer Lao Chinese Vietnamese
(N=144) (N=124) (N=139) (N=131) (N=201)
1st WAVE: 2nd WAVE: Pre-1978 Post-1978 (N=115) (N=624)
TIME AND AGE:
Months in Refugee Camps 34.3
Years in the U.S. 3.6
Age at Tl (1983) 37.0
SOCIAL BACKGROUND:
% Urban 8.3
% Writing Illiteracy 70.8
Years of Education 1.6
ENGLISH PROFICIENCY (Tl):
% Cannot Speak English 34.0
% Cannot Read English 54.2
% Cannot Write English 73.6
EMPLOYMENT STATUS (Tl)
Never Employed in U.S. 71.5
% Homemakers in Sample 49.6
% Time Employed in U.S. 11.4
25.5
2.8
35.6
46.3
34.2
5.0
54.5
55.3
61.7
69.9
42.3
12.2
23.0
3.6
39.2
79.1
26.6
4.9
46.8
48.9
55.7
71.2
25.2
11.9
10.3
3.6
41.8
95.4
17.6
6.7
54.9
58.9
61.8
60.3
33.6
18.2
7.8
4.1
35.9
94.0
1.0
9.8
24.9
25.4
30.8
42.3
26.9
27.8
6.6
7.1
37.8
88.9
7.8
9.5
13.9
15.7
27.0
4.2
19.7
66.7
19.1
3.0
37.3
71.9
23.5
6.3
42.9
46.9
53.0
50.9
36.4
20.6

z s r> X z M M
z H K M
o
H
TABLE 1 (continued) Characteristics of the Indochinese Refugee Population, by Ethnic Group and Immigration Waves*
IHARP 1983 Adult Sample, N=739 (366 men, 373 women)
ETHNIC GROUP IMMIGRATION WAVE
CHARACTERISTICS (Means or Percents)
Hmong Khmer Lao Chinese Vietnamese
(N=144) (N=124) (N=139) (N=131) (N=201)
1st WAVE: 2nd WAVE: Pre-1978 Post-1978 (N=115) (N=624)
Wage-Earners in Family** 0.38
% Both Spouses Working** 5.1
% Welfare Dependent** 65.0
FAMILY INCOME (Tl):
Annual Family Job Income** $2,231
Annual Welfare Income** 6,242
Total Annual Income** 8,485
Per Capita Income** 1,529
% Below Poverty Line** 93.8
% Owns Car** 27.5
Household Size** 8.7
0.41
4.9
69.2
$3,046
4,666
7,849
2,881
80.8
37.0
8.3
0.38
9.4
69.5
$2,925
5,721
8,717
2,447
82.4
51.8
6.3
0.49
9.6
57.5
$4,143
4,533
8,582
2,276
76.7
58.9
5.8
0.73
17.4
40.5
$7,294
4,155
11,522
3,881
57.0
69.4
5.5
1.12
33.1
15.3
$15,378
2,116
17,500
5,362
33.7
93.5
6.0
0.42
7.2
63.4
$ 2,643
5,409
8,113
2,498
80.0
45.0
6.5
* All differences between groups are significant at p < .001 for all variables listed, except Age of Respondent, which is not significantly differ? ent between immigration waves. Totals for immigration waves are weighted to reflect the actual proportion of each ethnic group in the total Indochinese population of San Diego County. ** Data are reported by family, not by individual (N=437 households, including 70 female heads of household).
SOURCE: Indochinese Health & Adaptation Research Project (IHARP), San Diego State University.

442 International Migration Review
FIGURE II
Age-Sex Structures: San Diego County Population (1980 Census, N ?*? 1,862,126) VS. Indochinese
Population (IHARP 1983 Household Sample, N ?*? 3,003)*
SAN DIEGO COUNTY TOTAL
75+ 70-74 65-69 60-64 55-59 50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5- 9 0- 4
MALES LL2Z
?X rm
[4^r AJL 4.4
14.0 WA
jn JE
1477
15
110.5
10
\hr VTJT
^
533
El
4.6
FEMALES
5,01 , 6.1 I
PERCENT
-Hhn
8.7 ITT 6.6 xa
10 15
TOTAL INDOCHINESE
75+ 70-74 65-69 60-64 55-59 50-54 45-49 40-44 35-39 30-34 25-29 20-24 15-19 10-14 5- 9 0- 4
MALES
Trf Er
no~ I 11.0
?Er 113.9
0.4 0.3
1.3 r ?6
M
j?z
JSjl 3.6
QX
TO^
11.2 TV2l
331
fi.
FEMALES
TT Ttt
"ZTT 11.5
13X1 CT
J5JD
15 10 0 PERCEOT
10 15
* Data for the Indochinese populationi s weighted to reflect the actual proportion of each ethnic group (Hmong, Khmer, Lao, Chinese-Vietnamese and Vietnamese) in the total Indochinese population of San Die to County. The asymmetry among males aged 18 to 29 in the general San Diego County population reflects the influence of U.S. Navy and Marine ases in the area. The gap in the 20-24 age group among the Indochinese (especially among males) may be due to migration selection, wartime mortalirty and/or conscription in the countries of origin, sampling procedures, or a combination of all of these factors. The gap is present in the age-sex structures of each of the five major Indochinese ethnic groups. SOURCE: Indochinese Health Adaptation Research Project (IHARP), San Diego State

Indochinese Refugees in the United States 443
TABLE 2
Child-Woman Ratios (CWR) by Ethnic Groups, San Diego County Indochinese Refugee Population (IHARP 1983 Household Sample N = 3,003)
Vietna- Age Groups Hmong Khmer Lao Chinese mese
(N=651) (N=693) (N=517) (N=430) (N=642) TOTAL
(N=2,933)
Total Children: 0 to 4 Years 184 142 68 48 78
(28.3%) (20.5%) (13.2%) (11.2%) (12.1%) 520
(17.7%)
Women: 15 to 19
20 to 24
25 to 29
30 to 34
35 to 39
40 to 44
Total: 15 to 44
24
20
25
11
16
_8 104
42
29
42
25
14
22
174
35
21
27
18
8
14
123
23
4
23
20
9
15
94
33
27
21
28
19
12
140
157
101
138
102
66
71
635
Child-Woman Ratios:
1,769 816 553 511 574 824
* CWR = (Total Children 0 to 4 Years)/(Total Women of Childbearing Age, 15 to 44) x 1,000
Data from the 1980 Census suggest a CWR of 386 for the Vietnamese (in? cluding Chinese-Vietnamese) population in the United States as of April 1, 1980. This is a figure well below the number derived for our Vietnamese
samples. The difference is explained principally by the fact that the Viet? namese who were enumerated in the United States early in 1980 were first-wave immigrants. They tended to be highly educated, from high status urban backgrounds, and thus typically prone to low fertility. Closer ex? amination of geographic pattern (by state) of child-woman ratios for the Vietnamese population revealed lowest fertility in those states in which Vietnamese had settled earliest (including especially Washington, D.C./
Virginia and California) and highest fertility levels among Vietnamese in those states that were resettlement sites for the earliest of the second-wave
immigrants (including especially Arkansas, Kansas, Louisiana, Minnesota, and Utah). In San Diego, the child-woman ratio for Vietnamese in 1980 (377) was also above the average for the total American population but still well below the level found in our data since the majority of the refugees arrived in San Diego after the census enumeration. Not unexpectedly, the child-woman ratios for the Indochinese refugees in San Diego are comparable to high- fertility Third World nations. In 1980, Thailand had an estimated CWR of

444 International Migration Review
683, while the rate for the Philippines was 637, and for Pakistan it was 888
(U.S. Bureau of the Census, 1979). A second measure of fertility provided by our data is the total number of
children ever born by age, shown in Table 3. The number of children ever
born to women 45-49, which may be taken as completed family size, confirm
the fact that the Hmong have the highest fertility level among the refugee
groups (8.63) followed by the Khmer (5.50), then the Chinese (5.29), the Lao
(5.25) and the Vietnamese (4.63). The total for all Indochinese women 45-49 in
Table 3 (5.26) is weighted to reflect the actual proportions of the various
ethnic groups in the total U.S. Indochinese population. In fact, the Hmong have extremely high fertility (our data practically replicating the findings of
Kunstadter [1984] concerning non-refugee Hmong in northern Thailand), while all of the other groups exhibit completed fertility which is only slightly
higher than that prevailing in the Southeast Asian region of origin where the
regional average fertility rate in 1985 was 4.5).
Using data on children born during the year prior to Tl and during the
T1-T2 interval, we have calculated the average number of children born
during the previous year at Tl and T2. We averaged the two time periods because the sample size was small enough that we felt that the average of two
dates would yield a more reliable estimate of current fertility. Furthermore, since the T1-T2 interval was just under a year, we did not feel that differences
in current fertility between the two dates could be interpreted as a trend.
Table 4 shows our estimates of the age-specific fertility rates (ASFR) for the
IHARP sample of Indochinese women of childbearing age (N = 313), broken down by ethnic group: again, the overall Indochinese totals are
weighted at each age for the proportion of the total U.S. Indochinese
population represented by each ethnic group. Our sample did not include
women at the youngest ages, so we extrapolated a rate for the 15-19 age
group, based on the data calculated from the other ages and from patterns of
age-specific birth rates in Asian nations (U.S. Bureau of the Census, 1979).
From these rates, we derived a total fertility rate (TFR) of 5.61 children per Indochinese woman. By combining the age-specific fertility rates with
children-ever-born by age, we used the Trussell modification of the Brass
fertility estimation methods (See, United Nations, 1983; Arriaga etal, 1976) to
produce a corrected estimated TFR of 5.75 children per Indochinese woman
in the United States. By comparison, the total fertility rate in the United
States in 1985 was 1.8 per woman (Population Reference Bureau, 1985).
Sample sizes within each ethnic group were too small to calculate corrected
TFRs, but it may be of interest to report the unadjusted rates, which are
included in Table 4: Hmong (11.90), Khmer (7.40), Lao (6.55), Chinese-
Vietnamese (4.65) and Vietnamese (3.40). The fact that all groups except the ethnic Chinese-Vietnamese and the Vietnamese have current total fertility levels that are higher even than cumulative fertility for each group (as

Indochinese Refugees in the United States 445
TABLE 3
Children Ever Born, by Ethnic Group
(IHARP 1983 Sample of Women of Childbearing Age. N=3i3)
Age Groups
Viet- Hmong Khmer Lao Chinese namese (N=63) (N=54) (N=61 (N=53) (N=82)
TOTAL* (weighted)
20 to 24
25 to 29
30 to 34
35 to 39
40 to 44
45 to 49
2.50
3.93
5.11
5.13
6.75
8.63
1.78
2.00
3.45
3.83
3.88
5.50
1.67
2.16
3.30
4.71
4.75
5.25
1.00
2.14
2.82
3.33
4.77
5.29
1.22
1.79
3.27
3.63
5.60
4.63
1.41
2.09
3.34
3.83
5.14
5.26
* Totals are weighted to reflect the proportion of each ethnic group in the overall Indochinese population of the United States as of September 1985.
TABLE 4
Age-Specific Birth Rates (Children Born in Previous Year), by Ethnic Group
(IHARP 1983 Sample of Women of Childbearing Age N=3i3)
Age Groups
Viet- Hmong Khmer Lao Chinese namese (N=63) (N=54) (N=61) (N=53) (N=82)
TOTAL* (weighted)
20 to 24
25 to 29
30 to 34
35 to 39
40 to 44
45 to 49
0.31
0.47
0.66
0.52
0.25
0.17
0.40
0.46
0.38
0.10
0.14
0
0.50
0.39
0.20
0.14
0.08
0
0.21
0.33
0.26
0.13
0
0
0.17
0.27
0.13
0.11
0
0
0.26
0.34
0.24
0.14
0.05
0.01
TFR* 11.90 7.40 6.55 4.65 3.40 5.61
* Totals are weighted to reflect the proportion of each ethnic group in the overall Indochinese population of the United States as of September 1985. ** TFR (Total Fertility Rate) = (Sum of Age-Specific Birth Rates) x 5. The overall rate of 5.61 includes an extrapolated estimate for ages 15 to 19.

446 International Migration Review
reflected by the total number of children born to women aged 45-49 in Table
3) could reasonably be a consequence of two phenomena: 1) a self-selection
of lower-parity women in the migration process ?those women who already had numerous children being less likely to migrate, thus leading to artificially low numbers of children-ever-born at the older ages of refugee respondents; and/or 2) a temporarily high level of current fertility, reflecting a "catch-up"
period of reproduction, which will last only for a short period of time. The
latter explanation seems preferable, for two reasons: 1) the Vietnamese, who
have been in the U.S. the longest, also have lower current fertility than
would be suggested by the number of children ever born to older women; and 2) the current pace of childbearing among the Hmong, especially, is
almost unbelievably high, and were it to continue would equal the level of
the Hutterites?acknowledged to be the world's most fertile group. It is also instructive to compare our results with another study of
Indochinese fertility in the United States. Hopkins and Clarke (1983) matched
birth records in Oregon with lists of known refugees in that state. They then
calculated age-specific birth rates and a general fertility rate for the popula? tion of Indochinese refugees in Oregon. Their observed rate of 127 births
per 1,000 women of childbearing age (15-44) was lower than our weighted
figure of 209 (using ages 15-49), but it was still twice the average for the
United States as a whole. Their data also reveal that a substantial proportion of births in the Indochinese population were higher order births, signaling the maintenance of large families. Among the Hmong, for example, Hop? kins and Clarke found that 35 percent of all women giving birth in 1981 had
already borne four or more children. Among the Khmer the percentage was
18, and among the Vietnamese it was 11, compared to only 4 percent for all
U.S. births.
Testing the Conceptual Model
Our review of the literature led to the development of a conceptual model
(Figure I) showing the relationship between fertility and its antecedent and
intermediate causes, while controlling for certain proximate determinants
of fertility. Antecedent factors include pre-migration social background characteristics of the refugees and various aspects of their migration history. Intermediate factors emphasize the roles that economic and cultural adap? tation to the United States have played in shaping fertility levels. The
proximate determinants of fertility in the United States include the number
of years married, the number of children born prior to arrival in the United
States and the length of residence in the United States.
Differences Between Means
As a first step in testing the model, we examined what turned out to be

Indochinese Refugees in the United States 447
largely linear relationships between fertility and each of these factors for our
sample of 313 Indochinese women of childbearing age. The results are
summarized in Table 5. We used the number of children born per year in the
United States as the primary fertility index. This measure has the advantage of directly controlling for length of time in the United States, which obviously will affect how many children will have been born. The Hmong, on average, have borne 0.46 children per year in the United States, whereas the Khmer have been bearing children at the pace of 0.27 per year, the Vietnamese at a
rate of 0.21 per year, the Lao at the rate of 0.20 per year, and the Chinese
respondents (with the oldest average age) at a rate of 0.16 per year. Note that
the data in Table 5 are weighted to reflect the actual proportion of each
ethnic group in the total Indochinese population in the United States (thus
relatively increasing the effect of the Vietnamese and decreasing the influence
of the Hmong in the results); unweighted results (not shown) show sharper differences between means.
Individually, the social background antecedents that distinguish mem?
bers of the two immigration waves also distinguish their fertility levels.
Table 5 shows the mean number of children born per year in the United
States according to two of the most important background characteristics of
migrants: urban/rural residence and education. Respondents from a rural
background are reproducing at a significantly higher rate in the United
States than those from an urban background. Those with no education in
their homeland have higher fertility rates in the United States than do those
with an elementary education (grades 1-6), who in turn have higher fertility than those with more advanced levels of education. In fact, the fertility of
women with less than six years of education is twice as high as that of women
with 12 years or more of education.
Migration history was another set of antecedent factors hypothesized to
affect fertility in the United States. Those who had suffered the greatest hard?
ships, as measured by length of time in refugee camps and the recent death
of family members (especially the deaths of children), were expected to
exhibit the higher levels of fertility. This expected relationship was explained as a function of the predisposing background characteristics (such as ethnicity, urban/rural residence, and education) of people who spent differing lengths of time in camps, and also as a function of the "making up" of births that may have been postponed due to encampment or may be viewed as a replacement for lost family members. The data in Table 5 show that the amount of time
spent in camps is positively associated with fertility in the United States.
Those respondents who spent more than one year in refugee camps were
averaging substantially more children than were those who had spent less
than one year in the camps. This is partly a consequence of the fact that the
Hmong and the Khmer, who have the highest fertility, also spent the
greatest amount of time in the camps. The number of child deaths in the

00
> H 0 Z
TABLE 5
Children Born Per Year in the United States, by Selected Migration and Adaptation Variables
(IHARP 1983 Sample of Women of Childbearing Age, N=3i3)*
Variable Variable Variable
ANTECEDENT VARIABLES:
Ethnicity:**
Hmong
Khmer
Lao
Chinese-Vietnamese
Vietnamese
Background: ***
Rural
Urban
Education:**
None
1 to 6 years
7 to 11 Years
12 Years or More
.46
.27
.20
.16
.21
.29
.21
.31
.26
.20
.14
63
54
61
53
82
105
208
95
109
62
47
ECONOMIC ADAPTATION:
Wage-Earners in Family:**
None Working .28 186
One Wage-Earner .17 89
Both Spouses Work .13 38
Percent of Time Employed in U.S.:**
Never Employed .27 225
Under 50% of Time .15 60
Over 50% of Time .11 28
Family Job Income:**
None .27 189
Under $7,500 .18 58
Over $7,500 .16 66
Welfare Dependency:*
CULTURAL ADAPTATION:
English Literacy Level:**
None or Poor .28
Some or Fair .20
Good or Fluent .15
Related Families in Household :*???
One Family
Two Families
Three or More
PROXIMATE VARIABLES:
Years in the U.S.:
Under 3 Years
.23
.21
.23
.28
.20
169
91
53
156
100
57
114
156 3 to 5 Yrs.

o
53
o
H E w
z H w O
4^ CO
TABLE 5 (continued)
Children Born Per Year in the United States, by Selected Migration and Adaptation Variables
(IHARP 1983 Sample of Women of Childbearing Age, N=3i3)*
Variable Variable Variable
MIGRATION HISTORY:
Time in Refugee Camps:***
Under 2 Months
2 to 12 Months
Over 12 Months
Children Lost:****
None
One or More
.17
.19
.28
.22
.29
31
105
177
284 29
Full Dependency .27
Some Dependency .22
None . 14
Poverty/Income
Level:***
Below Poverty Line .25 Low Incomes .17
Moderate Incomes .15
182
47
80
244 27
39
Over 5 years . 18 43
Children Born Before Arrival in U.S.
0 to 1 Child .33 115
2 to 4 Children .20 130
5 or More .07 66
Years Married:**
Under 5 Years .49 35
5 to 10 Years .32 62 10 to 20 Years .18 111
Over 20 Years .06 54
* N = unweighted frequencies, reflecting the actual sample size (a total of 313 women). ** p < .0001 _
??? p = ( .01 x = mean number of children born per year in the U. S., weighted to reflect the actual proportion **** ? = p = Not Significant of each ethnic group in the total Indochinese population in the U.S.
SOURCE: Indochinese Health & Adaptation Research Project (IHARP), San Diego State University

450 International Migration Review
family since the 1975 revolutions is also found to be positively related to
fertility, although the differences are not significant at the .05 level. As will
be shown below, however, multivariate analyses show that, controlling for
the influence of other factors, the number of children lost enters our regression
equation as a predictor of the number of children born in the United States.
The Hmong and the Khmer, with high fertility backgrounds, also suffered
the greatest amount of family loss and infant mortality, and their higher
fertility undoubtedly reflects the interaction of both background charac?
teristics and migration history. We measured economic adaptation by examining whether or not the
respondent had been employed in the United States, and if so, the proportion and type of employment of the respondent: and by looking at the number of
wage-earners in the family and the family's level of job income, poverty and
welfare dependency. Table 5 shows that on each of the measures, fertility is
lower as socioeconomic adaptation is greater. Respondents who are employed have lower fertility than those who are not; and among those who are or have
been employed, fertility decreases as the percent of time that the respondent has been employed in the United States increases. Moreover, families where
neither the husband nor the wife are working have a level of fertility more
than twice as high as that in families where both spouses are employed; and
respondents with the lowest level of family income have the highest fertility, as do those with the highest level of poverty and welfare dependency.
Cultural adaptation was measured mainly by the level of English language
proficiency, and by the household structure of the respondent (e.g., whether
or not the respondent lived with extended families). We noted earlier that
English proficiency in an Anglocultural setting is a central resource in the
social and economic integration of these newcomers, affecting such factors as
access to health care and family planning services, the number of American
friends and acquaintances, the ability to get a job or a driver's license and to
learn basic information about U.S. culture. As can be seen in Table 5,
fertility significantly decreases as the level of English reading and writing
literacy increases (p < .0001). However, tied as English proficiency is to
formal education, this effect may be as much a measure of background characteristics as it is expressly of adaptation processes.
On the other hand, contrary to expectations, we found no significant bivariate relationship (r = -.013) between fertility and the presence of
extended kin in the houshold, despite the fact that the two highest fertility
groups, the Hmong and the Khmer, are most likely to reside in multiple
family households. What is more, multiple regression results show that,
controlling for other factors, the number of families who share a household
is negatively related to fertility (as shown in Table 6, the standardized
regression coefficient is -.115), although the effect is small and accounts for
only one percent of the explained variance in the dependent variable (the

There TABLE 6
Multiple Regression Analysis, Predicting Level of Fertility in the United States* (IHARP Ti Sample of Women of Childbearing Age, N=3i3)
Predictor Variables BETA Correlation Significance R2 Change Analytical Category
# Years in the U.S. .593 .294 14.79 .0000 .089
# Children Pre-Arrival -.338 -.417 -7.04 .0000 .174
# Years Married -.304 -.377 -6.31 .0000 .034
English Literacy Level -.211 -.030 - 5.73 .0000 .028
# Wage-Earners in Family -.181 -.004 -4.59 .0000 .065
Family Job Income -.153 .059 -3.33 .0009 .010
# Families in Household -.115 -.013 -3.70 .0002 .009
# Children Lost .101 .058 3.26 .0012 .009
Hmong Ethnicity .210 .247 6.80 .0000 .072
Chinese Ethnicity -.068 -.137 -2.21 .0275 .004
Time (covariate)
Marital History (covariate)
Adaptation Variables (economic, cultural)
Migration History
Ethnocultural Group
Multiple Correlation = .704 R2 = .496 Standard Error = .644
* The regression is weighted to reflect the proportion of each ethnic group in the total U.S. Indochinese population. The weighted mean of the dependent variable (# of children born in the U.S.) is 0.827; the unweighted mean is 0.905.

452 International Migration Review
number of children born in the United States). It may be that extended kin
relations, while normally promotive of pronatalism, can also in this type of resettlement context encourage families to place limits on fertility and
choose an antinatalist position as an adaptive response. There is some
evidence that the presence of a grandparent in the household who is available
to take care of preschool children serves to free women of childbearing age to
enter the labor force, a decision that tends to have a depressive influence on
fertility. To unravel the complex sociocultural dynamics involved will
probably require further in-depth ethnographic research. We have, in any case, found no evidence to support a pronatalist hypothesis in this regard.
Finally, Table 5 shows the expected covariance of recent fertility with key
proximate determinants. Clearly, the more children a woman had born
prior to arrival in the U.S., and the longer a woman has been married (and hence the older she is and the more children she is likely to have already
had), the less likely she is to bear children in this country. More noteworthy is the finding that the number of children born per year in the U.S. declines
steadily and significantly with length of residence in and thus exposure to
the United States. Only in part is this a function of the socioeconomic
characteristics differentiating the two immigrant waves; that is, first-wave
refugees were also more urban, educated and prone to lower fertility than
more recent arrivals. However, among second-wave refugees, women who
had lived 3 to 5 years in the U.S. were bearing children at a significantly lower rate (.20) than those with less than 3 years of U.S. residence (.28). This
pattern of a general decline in childbearing over time in the host society is
observable among all the ethnic groups and suggests a cumulative depressive
impact on fertility as a result of economic and cultural adaptation processes.
Multivariate Analysis
We utilized multiple regression techniques to provide a more complete test
of the model shown in Figure I. The objective, of course, is to identify the main determinants of refugee fertility. Table 6 summarizes the ordinary least
squares (OLS) model with number of children born in the United States as
the criterion variable. Not unexpectedly, the single most important direct factor is the length of time in the United States, followed by the other two
proximate covariates: the number of children born prior to arrival in the
U.S. and the number of years married (a proxy for age). Current childbearing declines as the number of years married increases (and implicitly as fecundity declines as a function of age) and as parity increases. Together, these three
factors account for nearly 30 percent of the explained variance in the
dependent variable (R2 = .297). It is of some consequence, then, that there are several additional variables that are significantly related to fertility, net of the influence of years in the U.S., years married, and number of
children born prior to arrival.

Indochinese Refugees in the United States 453
Pre-migration social background variables (urban/rural residence and
education) do not enter the regression equation. Rather, their effects are
mediated by other variables, mainly adaptation and ethnicity measures.
English literacy level, the number of wage-earners in the family, and family
job income emerge as significant predictors of lower fertility, together
accounting for over 10 percent of the explained variance in the OLS model.
We have already noted the modest but negative contribution to fertility of
the number of families sharing the household. Among migration history variables, the number of children lost is positively related to fertility, as
hypothesized, but length of time in refugee camps does not achieve signifi? cance; its effects are mediated through more predictive factors. Of these,
Hmong ethnicity (entered as a dummy variable) is the strongest predictor reflecting the extraordinarily elevated levels of fertility among the Hmong.
Interestingly, controlling for other variables, Chinese-Vietnamese ethnicity enters into the equation as a negative but negligible correlate; Khmer, Lao
and Vietnamese ethnicity do not enter into the equation at all. Thus, except for the unique situation of the Hmong, the effect of ethnicity per se on
fertility is almost entirely accounted for by the influence of other variables in
the model.
As can be seen in Table 6, the final OLS model accounts rather remarkably for nearly half (R2 = .496) of the variation in fertility levels in the United
States within the Indochinese refugee population, and generally confirms
the conceptual model discussed earlier in this article. In particular the data
highlight the relative importance of economic and cultural adaptation as a
downward pressure on fertility in the United States.
DISCUSSION AND CONCLUSION
This article presents an analysis of fertility levels among Indochinese refugees to the United States, and examines the influence of adaptation and adjustment
processes on those levels of fertility. An important finding is that most of our
expectations about fertility differentials, drawn from a review of the literature
on the relationship between fertility and migration and on ethnographic data about each of the ethnic groups, were borne out in our analysis: first-wave
migrants do have lower fertility than second-wave; the Hmong do have the
highest levels of fertility, followed by the Khmer, the Lao, the Chinese-
Vietnamese and the Vietnamese; background characteristics such as urban
residence and education play subtle but important roles in determining
subsequent fertility levels; those respondents who have made the greatest
progress in terms of economic and cultural adjustment to their new environ?
ment have the lowest levels of fertility. The presence of extended kin rela?
tions in the household was found, however, to be negatively associated with
fertility. In general, then, our analysis confirms existing conceptual frame?
works.

454 International Migration Review
Without a doubt, the single most important finding is that the levels of
fertility within the Indochinese community are so high. This fact has important significance on at least three fronts: 1) it calls for an adjustment for natural
increase to be made in the estimates of the size of the Indochinese population; 2) it calls for a public policy to deal with the substantial maternal and child
health and family planning needs within the Indochinese community; and
3) it calls for an increased recognition of the effects of fertility on the
achievement of refugee economic self-sufficiency, which is the principal
goal of U. S. refugee policy?as formulated in the Refugee Act of 1980 (Public Law 96-212), and in subsequent amendments and extensions of this landmark
legislation.
Adjustment of the Size of the Indochinese Population
As we discussed in the introduction to this article, from 1975 to the end of
September 1985, a total of 807,321 Indochinese were admitted to the United
States (765,731 as refugees and 41,590 as immigrants). This total is in addition
to the 21,956 Vietnamese immigrants who had settled in the U.S. prior to
1975, and who will be excluded from our calculations for purposes of
estimating the natural increase of the post-1975 refugee population. Like
most migrant groups, young adults of childbearing age are disproportionately represented in the Indochinese population. Because of the higher than
average level of fertility, it is probable that the rate of natural increase in this
population is substantially higher than the rate for the U.S. population, and
that in the near future the Indochinese population in the U.S. will continue
to increase as a fraction of the total population through natural increase
alone. We have used data on number of children born per person in the
IHARP sample to estimate the likely augmentation of the total Indochinese
population in the United States. We judge our data to be generally repre? sentative of the Indochinese population in the entire United States, and so
our estimates should provide a reasonable approximation of national data.
Given the way in which IHARP data were collected, we based our
calculations on the number of children born in the U.S. per person for
people of each Indochinese ethnic group aged 25-64. We then multiplied that rate times the proportion of the total ethnic population that was between
those ages, yielding an estimate of the number of children born in the United
States per person in the total ethnic population. This preliminary step was
necessary because very young and very old persons were not included in the
respondent sample. Multiplying the estimated number of children born in
the United States per person in each ethnic population times the number of
refugees admitted from each ethnic group produced the estimates of the
likely total number of Indochinese refugees (See, Appendix for calculations). The method automatically adjusts for average length of time in the United

Indochinese Refugees in the United States 455
States. Note that we did not make an adjustment for mortality, but since the
age structure is so young, loss through death is probably negligible in
comparison to the contribution made to natural increase by fertility. As of
September 30, 1985, then, the results of our adjustments for natural increase
indicate a total Vietnamese and Chinese-Vitnamese population in the U.S.
of 665,755 (much higher than the sum of the 526,652 post-1975 admissions
plus the 21,956 pre-1975 immigrants).2 a total Khmer population of 159,739
(compared to 129,848 admissions),3 a Lao population of 122,572 (compared to
93,445 admissions); and a Hmong population of 80,223 (more than 40% greater than the 57,376 admissions).
Our calculations thus lead to an estimated total Indochinese population of 1,028,289 on September 30, 1985 ? 25 percent greater than the number of
admissions into the country. At its current rate of growth the Indochinese
population has probably overtaken the Cuban-American population as the
largest refugee population in the United States. In fact, the Indochinese as a
whole now constitute one of the largest Asian-origin groups in the United
States.4 This remarkable phenomenon has occurred in less than a decade.
Maternal and Child Health and Family Planning Needs
The second phase of IHARP questionnaires was conducted in mid-1984,
slightly less than a year after the Tl interviews. In that short interval, 22
percent of Hmong respondents of childbearing age had borne a child, while
19 percent of the Khmer had done so, as had 11 percent of the Chinese and 7
percent of the Vietnamese. Furthermore, in mid-1984, 16 percent of Hmong
respondents indicated that they were pregnant, while 9 percent of the Khmer
were pregnant, as were 4 percent of the Chinese, and 3 percent of the
Vietnamese. We should also note that 41 percent of Hmong female re-
2 Federal data do not distinguish the ethnic Chinese-Vietnamese among total Vietnamese admissions. IHARP data, however, suggest that the proportion of ethnic Chinese is no less than 20% and no more than 33% of the total Vietnamese population in the United States, with practically all Chinese-Vietnamese coming in the post-1978 second wave of immigration. For our calculations here we have used a proportion of 30% Chinese-Vietnamese among the total number of Vietnamese refugees (excluding pre-1975 admissions and post-1975 immigrants, whom we assume to be predominantly non-Chinese).
3 IHARP data indicate that at least 15% of all Cambodian refugee admissions are ethnic Chinese-Cambodians. The number of Chinese-Cambodians in the IHARP sample (N = 21) was too small to treat separately in our analyses, but no significant differences were found in the fertility behavior of the Chinese-Cambodian subsample compared to the ethnic Khmer.
4 Among Asian-origin groups, the 1980 U.S. Census enumerated a Chinese population of 806,040 persons, followed by the Filipino (774,652), Japanese (700,974), Korean (354,593) and Asian Indian (361,531) populations. All of these Asian-origin groups have also been growing rapidly in the 1980s and it is estimated that the Chinese and Filipino groups had each passed the one million mark by 1985{cf. Bouvier and Agresta, 1985).

456 International Migration Review
spondents of childbearing age indicated that they plan to have more children, as do 33 percent of the Khmer, 22 percent of the Lao, 19 percent of the
Chinese and 27 percent of the Vietnamese respondents. These data point out clearly the magnitude of need for maternal and
child health services to be continually made available to the Indochinese
refugee population at least for the near term (Rumbaut et al, forthcoming). Of course, such services do currently exist in San Diego and are nearly
universally known about by women of reproductive age. However, our data
indicate that the provision of such services cannot be thought of as a temporary
phenomenon, but rather is a need within the community that will exist for
several years to come.
We can infer the potential need for family planning services within the
Indochinese community by comparing the completed family size with the
average number of children born to women who say they plan to have no
more, which we call the "implicit stopping rule". For example, the average number of children born to Hmong women who say they plan to have no
more is 5.6. Since this is well below the average number ever born to older
women in the sample, women will have to begin utilizing fertility limitation
methods in their early thirties if they are to have an average of no more than
5.6 children. The "implicit stopping rule" among Khmer women is only 3.2
children ? the average number of children already born to women who plan no more children. The current rapid pace of childbearing among the Khmer
means that it will take considerable motivation as well as availability of
services to limit family size to 3.2 children.
Among the Chinese and Vietnamese the already lower levels of fertility indicate the already fairly widespread use of contraception; and the implied
stopping rules of 4.6 children and 3.9 children, respectively, do not indicate
any particular shift in current behavior to achieve the family-size goals
implied in these data. Nonetheless, the levels of fertility for all groups are
well above the average for the United States, and to the extent that socio-
economic and sociocultural adaptation is accompanied by declining fertility, the demand for family planning services will almost surely be on the rise
during the next several years. In this context, the findings of a recent study of family planning
knowledge, attitudes and practices of Indochinese refugees in San Francisco
(Minkler et al, 1985) are especially relevant. Those investigators found that
only 70 percent of the respondents who were not currently pregnant, and
who did not want to become pregnant, were actually using contraceptive methods ?a significant "knowledge-practice gap". Of those using contra?
ception, one third were found to be using methods which were not considered
"highly effective". Lack of English language proficiency and a limited
knowledge of reproductive physiology were identified as the main barriers
to family planning information and services. The study concluded that

Indochinese Refugees in the United States 457
"significant numbers of the refugee population undergoing resettlement are
unlikely to realize their fertility aspirations and are thereby less likely to
attain self-sufficiency as rapidly without continued special access services as
adjuncts to routine family planning clinic care" (pp. iii, 95). Moreover, this
study included a cost-benefit analysis of subsidized family planning services, based on California data, which found a 17 to 1 ratio of benefits to costs ? i.e., that "for every public dollar spent on family planning services to Southeast
Asian couples not intending to have a child, the present value of expected
public costs avoided would be 17 dollars" (pp. iv, 79-83). This is a conclusion of
considerable policy significance.
Fertility and Refugee Economic Self-Sufficiency
Finally, the data clearly underscore the relationship between fertility and
poverty in the refugee communities. In our conceptual model, we emphasized the positive side of that relationship ?that higher family income from jobs is
predictive of lower levels of fertility. But the other side of the coin is that
families with larger numbers of children are heavily dependent upon public assistance income, for which they are eligible on the same basis as U.S.
citizens. Indeed, for the entire adult sample of Indochinese refugees, the
major predictors of welfare dependency are the length of time in the United
States (the shorter the time the greater the dependency), age (the older the
person the more dependent on welfare income), English proficiency (the less
proficient in English the more dependent on welfare income), and the
number of dependent children in the family (the greater the number of
children the greater the dependency). Using welfare dependency as the
crierion variable (the ratio of family welfare income to total annual income), we ran ordinary least squares models separately for each of the ethnic
groups, and separately for each sex. The results confirm that no matter how
the data are organized, the number of children in the family is a major determinant of welfare dependency.
Specifically, Table 7 presents OLS results predicting the level of welfare
dependency among our sample of women of childbearing age (N=313). Net
of the influence of length of residence in the United States (the strongest
predictor), the two fertility variables (children born in the U.S. and children
born before arrival in the U.S. but residing with the respondent) together account for 13 percent of the variation in welfare dependency levels among Indochinese women in these relatively younger age groups. Of course,
eligibility for public assistance (especially for the principal welfare program, Aid to Families with Dependent Children), as well as the levels of such
assistance, are conditioned in part on the number of dependent children
residing with indigent applicants. But such rules and programs cannot
adequately explain, nor do they produce, the complex cycle of fertility, poverty and dependency.

4^ at 00
TABLE 7
Multiple Regression Analysis, Predicting Level of Welfare Dependency in the United States
(IHARP Ti Sample of Women of Childbearing Age, N =313)
Predictor Variables BETA Correlation Significance R2 Change Comment
# Years in the U.S. -.597 .506
# Children Born in U.S. .306 -.024
# Children Born Pre-U.S. .273 .221 (and living at home)
Age of Respondent .132 .114
English Literacy Level -.080 -.389
Lao Ethnicity .141 .117
Khmer Ethnicity .098 .145 Vietnamese Ethnicity .080 -.162
-16.04
8.30
6.78
3.33
- 2.20
4.14
2.78 2.08
.0000
.0000
.0000
.0009
.0280
.0000
.0057
.0379
.256
.066
.063
.011
.003
.012
.005
.004
Welfare Dependency decreases over time
Fertility variables account for 13% of the variance in welfare dependency level
The older the person and the less proficient in Eng? lish the more dependent on welfare
Weak positive associations with welfare dependency
Multiple Correlation = .648 R2 = .419 Standard Error = .346
* The regression is weighted to reflect the proportion of each ethnic group in the total U.S. Indochinese population. The weighted mean of the
dependent variable (the ratio of family welfare income to total annual income) is 0.620; the unweighted mean is 0.673.

Indochinese Refugees in the United States 459
Our basic position with respect to the relationship between welfare
dependency and fertility?as implied by the double-arrow in Figure I between
fertility and "economic adaptation" ? is that it is a dynamic process, differing at different stages of family-building (cf. Hout, 1978). For refugee families
that were already large upon arrival, welfare income has been a safety net
required because the large size of the family depletes the refugees' already scarce resources and hampers the family's ability to become economically self-sufficient. This is especially true when the children are young, on
average. As children age and enter the labor force, the family's welfare
dependency should lessen. In the meantime, those couples who are most
successful in their economic adaptation may also be those who have the
strongest motivation for small families.
In the demographic literature concerning the impact of government
policy on fertility, we find little to support the often-cited but ill-considered
unilinear belief that welfare is a stimulus to high fertility. Although the
current welfare system does, in fact, "reward" high fertility in the sense that
relief is provided in accordance with family size, there is virtually no evidence
that the modest size of welfare payments (which in the U.S. generally keeps families below the federal poverty threshhold while conferring a stigmatized status on the recipient) is viewed as an inducement to have large families
(See, Leroy, 1978, for a review; cf. also World Bank, 1984). The posited
positive relationship between welfare and fertility has a rich history and was
prominently featured long ago in Malthus' discussion of the Poor Law in
England. He argued that the Poor Law was a poor idea because it only
encouraged childbearing among the already miserable lower classes, and
created rather than protected surplus populations. However, historical
evidence has revealed that between 1801 and 1835 those English parishes that
administered Poor Law allowances did not have higher birth, marriage, or
total population growth rates than those in which the Poor Law assistance
was not available (Huzel, 1969). A further analysis examined out-migration rates to parishes which paid both Poor Law allowances-in-aid-of-wages and
child allowances on a scale geared to family size, and compared them to rates
in parishes which paid neither of these allowances; no evidence was found
that the allowances rooted the laborer to his parish of settlement and thus
restricted labor mobility (Huzel, 1980). These data, moreover, supported
precisely an opposite interpretation: namely, that high poverty levels even
in parishes where Poor Law allowances were paid encouraged rather than
restricted labor mobility, and more generally that the allowance system was
a reaction to population increase (and associated social and economic
conditions) rather than a stimulus. Huzel concluded that "Although the
Malthusian Poor Law-population theory was ideally suited to contemporaries who wished to explain away the problems of poverty by shifting the blame on

460 International Migration Review
to the shoulders of the procreating poor, its merit in explaining early
nineteenth-century demographic trends is extremely dubious" (1969:451). In a related vein, a contemporary study of economic adaptation among
Vietnamese, Chinese-Vietnamese and Lao refugees in five U.S. regions
(Boston, Chicago, Houston, Seattle and Orange County, California) found
no evidence that transfer income constituted a powerful disincentive to
seeking earned income, but rather that only with earned income can a
household expect to rise above the poverty level (Caplan et al, 1985). That
study identified household composition as the strongest predictor of economic
self-sufficiency, with two-wage-earner families showing by far the most
dramatic gains in economic status, and suggested that a key to self-sufficiency is the entry of the second spouse into the labor force. We have earlier shown
that the number of wage-earners in the family is also strongly predictive of
lower fertility. For those Indochinese parents who already have a large number of children, welfare income may be a fact of life at least until the
children are grown and economically self-sufficient; but for those with small
families, or those who have not yet begun family-building activity, the
conclusion seems clear that motivation to limit family size ill be positively associated with an ability to avoid later dependence on welfare. The provision of birth control methods to minority groups is always a policy fraught with
potential controversy, but for the Indochinese refugee community the
relationship between family size and welfare dependency is unequivocal. Our findings suggest the need to take family planning services ? and related
support services, including child care ? into account as part of a larger policy aimed to economic self-sufficiency. Refugee resettlement policy, accordingly, should be based on a comprehensive multidimensional and long-term
understanding of the complex process of adaptation ? including the recog? nition that the attainment of economic self-sufficiency by these refugee
groups is shaped by their reproductive behavior as it is by their productive human capital and by the structure of the labor market in which they are
struggling to rebuild their lives.
REFERENCES
ACNS (American Council for Nationalities Service) 1984 Refugee Reports V. 23-24 (December 28, 1984).
Arriaga, E., P. Anderson and L. Heligman 1976 Computer Programs for Demographic Analysis. Washington, DC: U.S. Bureau of
the Census.
Basavarajappa, K. and S. Halli 1984 "Ethnic Fertility Differences in Canada, 1926-71: An Examination of Assimilation
Hypotheses", lournal of Biosocial Science, 16(l):45-54.
Bean, F., and G. Swicegood 1982 "Generation, Female Education and Mexican-American Fertility", Social Science Quarterly,
63(1):1311-1344.

Indochinese Refugees in the United States 461
Beaujot, R., K. Krotki and P. Krishnan 1982 "An Analysis of Ethnic Fertility Differentials Through the Consideration of Assimilation",
International fournal of Comparative Sociology, 23(l-2):62-70.
Berger, P.L. 1979 The Heretical Imperative. Garden City, NY: Doubleday-Anchor.
Bouvier, L. and A.J. Agresta 1985 "The Fastest Growing Minority", American Demographics, May 1985, pp. 31-46.
Burch, T. and M. Gendell 1971 "Extended Family Structure and Fertility: Some Conceptual and Methodological
Issues". In Culture and Population, edited by S. Polgar, Cambridge, MA: Schenkman Publishing Company.
Caldwell, J. 1982 Theory of Fertility Decline. New York: Academic Press.
1981 "The Mechanisms of Demographic Change in Historical Perspective", Population Studies, 35(l):5-27.
Caplan, N. J.K. Whitmore and Q.L. Bui 1985 Southeast Asian Refugee Self-Sufficiency Study. Final Report to the Office of Refugee
Resettlement. DHHS. Ann Arbor: Institute for Social Research, University of Michigan.
Carlson, E. 1985 "The Impact of International Migration upon the Timing of Marriage and Childbearing",
Demography, 22(l):61-72.
Chindarsi, N. 1976 The Religion of the Hmong Njua. Bankok: The Siam Society.
Coale, A. 1973 "The Demographic Transition". Proceedings of the International Population Conference.
Liege. Volume 1, pp. 53-72.
Crawford, A. 1966 Customs and Cultures of Vietnam. Rutland, VA: Charles E. Tuttle Company.
Cuellar, J. and J. Weeks 1980 Minority Elderly Americans: A Prototype for Area Agencies on Aging. Final Report to the
U.S. Administration on Aging. San Diego: San Diego Area Agency on Aging and Allied Home Health Association.
Davis, K. 1948 Human Society. New York: MacMillan k Company.
Day, L. 1984 "Minority-Group Status and Fertility: A More Detailed Test of the Hypothesis", The So?
ciological Quarterly, 25(4):456-472.
Dewey, R. 1982 "Annual Summary of Medical and Public Health Reports From Indochinese Refugee
Camps in Thailand: 1 Dec. 80 - 30 Nov. 81". New York: United Nations High Commissioner for Refugees.
Dunnigan, T. 1982 "Segmentary Kinship in an Urban Society: The Hmong of St. Paul-Minneapolis",
Anthropological Quarterly, 55(3):126-134.
Ellis, J. 1982 "Southeast Asian Refugees and Maternity Care: The Oakland Experience", Birth.
9(3):191-194.
Fraser, S. 1980 "Vietnam's First Census", Intercom, 8:8-10.

462 International Migration Review
Frisbee, W. and F. Bean 1978 "Some Issues in the Demographic Study of Racial and Ethnic Groups". In The Demography
of Racial and Ethnic Groups. Edited by F. Bean and W. Frisbee. New York: Academic Press.
Geddes, W. 1976 Migrants of the Mountain: The Cultural Ecology of the Blue Miao (Hmong Njua) of Thailand.
London: Oxford University Press.
Gordon, L. 1985 U.S. Office of Refugee Resettlement and State Department data on Indochinese refugee
and immigrant arrivals, 1975-1985. Personal communication.
Gurak, D. and M. Kritz 1982 "Female Employment and Fertility in the Dominican Republic", American Sociological
Review. 47(6):810-818.
Haines, D. 1982 "Southeast Asian Refugees in the United States: The Interaction of Kinship and Public
Policy", Anthropological Quarterly. 55(3):170-181.
Hill, R., etal. 1959 The Family and Population Control. Chapel Hill: University of North Carolina Press.
Hirschman, C, and R. Rindfuss 1982 "Family Formation Events in Asia", American Sociological Review, 47(5):660-680.
Hoick, S. and W. Cates 1982 "Fertility and Population Dynamics in Two Kampuchean Refugee Camps", Studies in
Family Planning, 13(4):118-124.
Hollingsworth, A., L. Brown and D. Brooten 1980 "The Refugees and Childbearing: What to Expect", RN (November):45-48.
Hopkins, D. and N. Clarke 1983 "Indochinese Refugee Fertility Rates and Pregnancy Risk Factors. Oregon", American
fournal of Public Health. 73(11):1307-1309.
Hout, M. 1978 "The Determinants of Marital Fertility in the United States, 1968-1970: Influences from a
Dynamic Model", Demography. 15(2):139-160.
Huyck, E. and R. Fields 1981 "Impact of Resettlement on Refugee Children", International Migration Review,
15(l-2):246-254.
Huzel, J.P. 1980 "The Demographic Impact of the Old Poor Law: More Reflections on Malthus", Economic
History Review. 33(3):367-381.
1969 "Malthus, the Poor Law, and Population in Early Nineteenth-Century England", Economic History Review. 22:430-452.
Ima, K., A. Velasco, K. Ou and B. Yip 1983 "Adjustments Strategies of the Khmer Refugees in San Diego. California: Six Ethnographic
Histories". Report to the Union of Pan Asian Communities, San Diego.
Jain, M. 1981 "The Effect of Female Education on Fertility: A Simple Explanation", Demography. 18(4):
577-596.
Janssen, S. and R. Hauser 1981 "Religion, Socialization and Fertility", Demography. 18(4):511-528.
Jones, G. 1982 "Population Trends and Policies in Vietnam", Population and Development Review. (4):783-
810.

Indochinese Refugees in the United States 463
Ketkar, S. 1979 "Determinants of Fertility in a Developing Society: The Case of Sierra Leone", Population
Studies. 33(3):479-488.
Khoa, L.X. 1981 "Southeast Asian Social and Cultural Customs: Similarities and Differences Part 2", Jour-
nal of Refugee Resettlement. l{2):27-47.
Kunstadter, P. 1984 Demographic Differentials in a Rapidly Changing Mixed Ethnic Population in
Northwestern Thailand", NUPRI Research Paper Series No. 19. Tokyo, Japan: Nihon University Population Research Institute.
1983 "Highland Populations in Northern Thailand". In Highlanders of Thailand. Edited by J. McKinnon and W. Bhruksasri. Kuala Lumpur: Oxford University Press.
Leasure, J.W. 1982 "La Baisse de la Fecondite aux Etats-Unis de 1800 a 1860", Population, 30:607-622.
Lee, B. and S. Farber 1984 "Fertility Adaptation by Rural-Urban Migrants in Developing Countries: The Case of
Korea", Population Studies, 38(1):141-156.
Leroy, M. 1978 Population and World Politics. Leiden: Martinus Nijhoff.
Lesthaeghe, R. 1977 The Decline of Belgian Fertility, 1800-1970. Princeton University Press.
McDonald, M. and R. Rindfuss 1981 "Earnings, Relative Income, and Family Formation", Demography. 18(2):123-136.
McNicoll, G. 1980 "Institutional Determinants of Fertility Change". Population and Development Review. 6(3):
441-462.
Meng-Try, E.A. 1981 "Kampuchea: A Country Adrift", Population and Development Review. 7(2):209-228.
Minkler, D., C. Korenbrot, C. Brindis and F. Mitchell 1985 Improving Family Planning Services to Southeast Asian Refugees: A Study of Their Knowledge,
Attitudes and Practices. Final Report to the Office of Population Affairs, DHHS. San Francisco: Institute for Health Policy Studies. University of California. San Francisco.
Monnier, A. 1981 "Donnes Recentes sur la Population du Vietnam", Population. 36(3):609-641. Office of Refugee Resettlement 1985 Refugee Resettlement Program: Report to Congress. Washington, DC: U.S. Government Print?
ing Office.
Population Reference Bureau 1985 World Population Data Sheet. Washington, DC: Population Reference Bureau.
1976 World Population Growth and Response 1965-1975: A Decade of Global Actions. Washington, DC: Population Reference Bureau.
Rhodes, C. and E. Woodrum 1980 "Contending Hypotheses of Minority Fertility: Three Generations of Japanese-
Americans", Califoria Sociologist. 3(2):166-183.
Rindfuss, R. 1976 "Fertility and Migration: The Case of Puerto Rico", International Migration Review. 10(Sum-
mer):191-203.

464 International Migration Review
Rindfuss, R., L. Bumpass and C. St. John 1980 "Education and Fertility: Implications for the Roles Women Occupy", American Sociological
Review. 45(3):431-447.
Rindfuss, R. and C. St. John 1983 "Social Determinants of Age at First Birth'', fournal of Marriage and the Family. 45(3): 553-565.
Rumbaut, R.G. 1985 "Mental Health and the Refugee Experience: A Comparative Study of Southeast Asian Re?
fugees". In Southeast Asian Mental Health: Treatment, Prevention, Services, Training and Research Edited by T. Owan. National Institute of Mental Health. DHHS Publication No. (ADM) 85-1399. Washington, DC: U.S. Government Printing Office.
Rumbaut, R.G., L. Chavez, R. Moser, S. Pickwell and S. Wishik Forthcoming "The Politics of Migrant Health Care: A Comparative Study of Mexican Immi?
grants and Indochinese Refugees". In Research in the Sociology of Health Care, Volume 7. Edited by D. Wertz. Greenwich, CT: JAI Press. Forthcoming, 1987.
Schrock, J., W. Stockton, Jr., E. Murphy and M. Fromme 1966 Minority Groups in the Republic of Vietnam. Washington, DC: The American University.
Scrimshaw, S. 1975 "Families to the City: A Study of Changing Values, Fertility and Socioeconomic Status
Among Urban In-Migrants". In Population and Social Organization. Edited by M. Nag. Paris: Mouton Publishers.
Smith, S. 1981 "Women's Work, Fertility and Competing Time Use in Mexico City". In Research in Popula?
tion Economics. Volume 3. Edited by J. Simon and P. Lindert. Greenwich, CT: JAI Press. Pp. 167-187.
Stein, B. 1981 "The Refugee Experience: Defining the Parameters of a Field of Study", International Mi?
gration Review. 15(l):320-330.
Stolzenberg, R. and L. Waite 1977 "Age, Fertility and Plans for Employment", American Sociological Review. 42(5):769-783.
Tabah, L. 1980 "World Population. A Stocktaking", Population and Development Review. 6(3):355-390.
United Nations 1983 Indirect Techniques for Demographic Estimation. Population Studies, No. 81. Manual X. New
York: United Nations.
United States Bureau of the Census 1979 "Illustrative Projections of World Populations to the 21st Century", Current Population Re?
ports, Series P-23. No. 79.
1979 A Compilation of Age-Specific Fertility Rates for Developing Countries. International Research Document, No. 7. Washington, DC: U.S. Government Printing Office.
Van Deusen, J., C. Coleman and L. Khoa 1981 "Southeast Asian Social and Cultural Customs: Similarities and Differences. Part 1", four?
nal of Refugee Settlement. l(l):20-40.
Vang, K.N. 1982 "Hmong Marriage Customs: A Current Assessment". In The Hmong in the West. Edited by
B.T. Downing and D.P. Olney. Minneapolis: Center for Urban and Regional Affairs, Uni? versity of Minnesota.
Ward, B., B. Pridmore and C. Cox 1981 "Vietnamese Refugees in Adelaide: An Obstetric Analysis", The Medical fournal of
Australia. 24(January):72-75.

Indochinese Refugees in the United States 465
Weeks, J. 1986 Population: Introduction to Concepts and Issues. Third Edition. Belmont, CA:
Wadsworth Publishing Co.
World Bank 1984 World Development Report 1984. New York: Oxford University Press.

4^ 0>
H W 50
0 > r
g
o
APPENDIX
Estimation of Natural Increase Within the Indochinese Population of the United States
ETHNIC GROUP
Step in Estimation Procedure HMONG KHMER LAO
VIETNAMESE (incl. ethnic Chinese)*
3.
4.
6.
7.
Children Born in the U.S. Per 1,417 0.577 People Aged 25-64 Years (IHARP Sample, N=739)
Proportion of Ethnic Population .281 .399 that is Aged 25-64 (IHARP House? hold Sample, N=3,003) Estimate of Children Born in U.S. .3982 Per Person of All Ages (1x2) Number of Refugees and 57,376 Immigrants Admitted to U.S. Since 1975
Estimate of Post-1975 Natural 22,847 29,891 Increase (3x4) Pre-1975 Immigrants ? ?
Estimate of Population of 80,223 159,739 Indochinese Origin as of 30 September 1985 (4 + 5 + 6)
0.511
.372
.2302 .3117
129,848 93,445
29,127
122,572
0.566
.395
.2224
526,652
117,147
21,956
665,755
TOTAL INDOCHINESE POPULATION: (as of 30 Sept. 1985)
1,028,289
* Totals are weighted: Vietnamese (0.7) + Chinese-Vietnamese (0.3). Separate figures for these two groups are as follows: Children Born in U.S. Per people Aged 25-64 = 0.632 for Vietnamese and 0.412 for Chinese. Proportion of Ethnic Population that is 25-64 = .389 for Vietnamese and .401 for Chinese.