FALL 12 News.qxd - MDS Foundation
44
fall/winter 2012: volume 18, issue 2 newsletter of the myelodysplastic syndromes foundation www.mds-foundation.org REVISED INTERNATIONAL PROGNOSTIC SCORING SYSTEM FOR MDS The manuscript describing the Revised IPSS (IPSS-R) for MDS is available now in the September 23, 2012 issue of Blood (vol. 120, p. 2454). MDS News Highlights ASH 2012 – MDS FOUNDATION SYMPOSIUM ■ Myelodysplastic Syndromes: Current Understanding and Management Approaches Effective management of MDS requires understanding of underlying disease-specific abnormalities as well as patient-related features. These issues as well as current standard and recent novel therapeutic advances for MDS patients will be discussed. FROM THE GUEST EDITOR’S DESK 2 REVISED INTERNATIONAL PROGNOSTIC SCORING SYSTEM FOR MDS 3 Meeting Highlights/Announcements ASH 2012: MDS FOUNDATION SYMPOSIUM 6 37th Annual ONS Congress 8 12th International MDS 14 MDS Resources: Literature Highlights 16 News Briefs 18 From The Foundation 19 Patient Initiatives Worldwide Patient Forums/Support Groups 20 Patient Contributions 23 Nursing in MDS 28 MDS Centers of Excellence 29 Information on Clinical Trials 32 Contributions to the Foundation Thank You 33 In Memoriam 35 Living Endowments 43 MDS Foundation Board of Directors 44 TABLE OF CONTENTS FROM THE GUEST EDITOR’S DESK ■ Recent Molecular Abnormalities in MDS Presented by Luca Malcovati, MD
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of FALL 12 News.qxd - MDS Foundation

fall/winter 2012: volume 18, issue 2
newsletter of the myelodysplastic syndromes foundation
www.mds-foundation.org
REVISED INTERNATIONAL PROGNOSTIC SCORING SYSTEM FOR MDSThe manuscript describing the Revised IPSS (IPSS-R) for MDS is available nowin the September 23, 2012 issue of Blood (vol. 120, p. 2454).
MDS News Highlights
ASH 2012 – MDS FOUNDATION SYMPOSIUM ■ Myelodysplastic Syndromes: Current Understanding and Management Approaches
Effective management of MDS requires understanding of underlying disease-specificabnormalities as well as patient-related features. These issues as well as current standardand recent novel therapeutic advances for MDS patients will be discussed.
TABLE OF CONTENTS
FROM THE GUEST EDITOR’S DESK 2
REVISED INTERNATIONAL PROGNOSTIC SCORING SYSTEM FOR MDS 3
Meeting Highlights/Announcements
ASH 2012: MDS FOUNDATION SYMPOSIUM 6
37th Annual ONS Congress 8
12th International MDS 14
MDS Resources: Literature Highlights 16
News Briefs 18
From The Foundation 19
Patient Initiatives
Worldwide Patient Forums/Support Groups 20
Patient Contributions 23
Nursing in MDS 28
MDS Centers of Excellence 29
Information on Clinical Trials 32
Contributions to the Foundation
Thank You 33
In Memoriam 35
Living Endowments 43
MDS Foundation Board of Directors 44
TABLE OF CONTENTS
FROM THE GUEST EDITOR’S DESK■ Recent Molecular Abnormalities in MDS
Presented by Luca Malcovati, MD

2
Subsequent investigations showed thatribosomal deficiency in 5q− syndromeresults in activation of p53 and defectiveerythropoiesis.8 Other data from mousemodels suggested that haploinsufficiencyof the microRNA genes miR-145 and miR-146a may contribute to the dysregulatedmegakaryopoesis and thrombocytosis seenin this disorder.9
Acquired Somatic Mutations
Acquired somatic mutations have beenrecently detected in several genes. Thegenes mutated in MDS can be classifiedaccording to the function of the proteinsthey encode. The most commonly mutatedclass of genes in MDS encode splicingfactors (SF3B1, U2AF1/U2AF35, ZRSR2,SRSF2, SF3A1, PRPF40B, U2AF2/U2AF65,and SF1).10,11 Genes encoding epigeneticregulators are also commonly mutated inMDS, including TET2, DNMT3A, IDH1/2,ASXL1, and EZH2.12,13 Transcription factorsinvolved in hematopoietic progenitor cellsare also mutated, including RUNX1 andETV6.14 Mutations that lead to activatedtyrosine kinase signaling occur in thegenes encoding JAK2, NRAS/KRAS,PTPN11, MPL, and CBL.15 Mutations of thetumor suppressor gene TP53, involved inDNA damage repair pathway, are alsocommon.16
Recently, two groups have publishedindependent reports of mutations involvingmultiple components of the RNA splicingmachinery. Somatic mutations of SF3B1, agene encoding subunit 1 of the splicing factor3b protein complex, were first described byinvestigators from the Chronic MyeloidDisorders Working Group (CMD-WG) of theInternational Cancer Genome Consortium.10
Using massively parallel sequencing, theCMD-WG investigators found somaticmutations of SF3B1 in six of eight patientswith refractory anemia with ring sidero-blasts. A targeted resequencing of the genein hematologic malignancies and solidtumors showed SF3B1 mutations inapproximately 30% of patients with MDS,and 20% of patients with myelodysplastic/myeloproliferative neoplasm (MDS/MPN).
From the Guest Editor’s Desk
in one or more cell lineages, whereasperipheral blood cells are variably reduced.With time, differentiation and maturation ofhematopoietic cells are progressively impaired,and there is an increasingly high risk ofevolution to overt AML.
Unravelling the Molecular Basis of MDS
Until recently, the molecular basis of MDShad remained elusive. Recurrent chromo-somal abnormalities, in particular deletionsor amplifications of large chromosomalsegments, were reported in approximately50% of MDS patients using standardchromosomal banding analysis. Among themost frequent are –5/del(5q), –7/del(7q),trisomy 8, del(20q), and a complex karyo-type.4 However, the last few years have seenimportant progress in this field.
Gene Haploinsufficiency
Deletions of the long arm of chromosome5 are the most frequent single chromosomalabnormality in MDS. Patients with isolateddel(5q) may present a peculiar clinicalphenotype, first described by Van denBerghe et al. in 1974 and defined as the5q- syndrome.5 Patients with the 5q-syndrome have a macrocytic anemia, withnormal or elevated platelet countsassociated with hypolobulated megakaryo-cytes in the bone marrow.
The determination of the commonlydeleted region located at 5q33 was the firststep towards clarifying the molecular basisof MDS.6 Sequencing and high-resolutiontechniques failed to identify mutations in thecommonly deleted region, whereas afunctional screening of all these genes by anRNA-mediated interference-based approachdetermined that haploinsufficiency ofRPS14, encoding a component of the 40Sribosomal subunit, is likely the cause of theerythropoietic defect in the 5q− syndrome.7
Interestingly, heterozygous inactivatingmutations in RPS19 and other ribosomalproteins were previously described inDiamond Blackfan Anemia, an inheritedbone marrow failure syndrome.
Myelodysplastic syndromes (MDS) are aheterogeneous group of hematologic disorderscharacterized by ineffective hematopoiesis,peripheral cytopenias and increased riskof evolution into acute myeloid leukemia(AML).1 MDS are included in the categoryof myeloid neoplasms in the World HealthOrganization (WHO) classification of tumorsof hematopoietic and lymphoid tissues,together with myeloproliferative neoplasms(MPN), myelodysplastic/myeloproliferativeneoplasms (MDS/MPN), and AML.2
MDS represent some of the most commonhematologic malignancies in Westerncountries. They occur mainly in elderlypeople with a median age at diagnosis of70–75 years. Incidence is approximately 5per 100,000 persons per year in the generalpopulation, but increases to 20–50 per100,000 persons per year over the age of60.3 Considering the progressive aging ofthe population in Western countries, thenumber of MDS patients is destined toincrease over the next decades, makingMDS one of the most challenging issues forhematologists and health care providers inthe near future.
MDS are characterized by clonal prolif-eration of hematopoietic cells that differentiateinefficiently as a result of excessive apoptosisof hematopoietic precursors. The bonemarrow is generally hypercellular and severalmorphological abnormalities are observed
Recent MolecularAbnormalities in MDS
Luca Malcovati, MDDepartment of Hematology/OncologyUniversity of Pavia School of MedicineSan Matteo Hospital, Pavia, Italy
2

3
The gene was also found to be mutated insmaller proportions of patients with othertypes of tumor.
In patients with MDS, a close relationshipwas found between ring sideroblasts andSF3B1 mutations. Interestingly, a highprevalence of SF3B1 mutations was found inpatients with 15% or greater bone marrowring sideroblasts as well as in those with lessthan 15%.17 SF3B1 mutations wereassociated with downregulation of key genenetworks, including core mitochondrialpathways.10 The association between SF3B1mutation and ring sideroblasts wasconfirmed across all the myeloid neoplasms,including myeloproliferative neoplasms(MPN) and MDS/MPN. In fact, amongMDS/MPN, a high prevalence of SF3B1mutations was also observed in patientswith RARS associated with markedthrombocytosis.17 In addition, somaticmutations of SF3B1 were also observed in asmall fraction of patients with primarymyelofibrosis, and in all cases sideroblastswere detected in the bone marrow.18
In the same period, the CMD-WGdescribed SF3B1 mutation in MDS with ringsideroblasts. Yoshida et al. performed wholeexome sequencing in various subtypes ofMDS and described mutations in multiplecomponents of the spliceosome, includingU2AF1, ZRSR2, and SRSF2, mainly inmyeloid disorders without ring sideroblasts.11
In particular, approximately one-third ofpatients with chronic myelomonocyticleukemia (CMML) had a somatic mutation ofSRSF2. Although little is currently knownabout the downstream processes that areaffected by spliceosome mutations, thesedata clearly suggest that genes encodingcore components of the RNA splicingmachinery play a major role in MDSpathophysiology.
Epigenetic modifications mediatechanges in gene expression throughchemical modifications of DNA, includingmethylation of dinucleotides, and methyl-ation or acetylation of histone proteins.Aberrant DNA methylation has beenimplicated in the pathogenesis of MDS and
AML, and aberrant methylation profiles wereobserved in both disorders. In addition,hypomethylating agents, such as azacitidineand decitabine, are effective in the treatmentof MDS, and are indeed associated withchanges in genome-wide methylationpatterns in bone marrow cells of treatedpatients. However, no key genes ormethylation signatures that may predictresponse to therapy have been recognized.
TET2 mutations have been identified inapproximately 25% of patients with MDS.19
These mutations cause a loss of functionof the TET2 enzyme that converts 5-methyl-cytosine to 5-hydroxymethylcytosine.Additional evidence suggests that TET2 isimportant for normal myelopoiesis, and thatdisruption of TET2 enzymatic activity favorsmyeloid tumorigenesis.20
Mutations in DNA methyltransferase 3A(DNMT3A) were first discovered by wholegenome sequencing in AML cases, andsubsequently identified in 5–10% of MDSpatients. DNMT3A adds a methyl group tothe 5’ position of CpG dinucleotides.Experiments in mice showed that disruptionof DNMT3A results in impaired hemato-poietic differentiation but not in hematologicmalignancy, suggesting that transformationrequires co-operating mutations.21
Mutations in genes involved in theregulation of histone function were alsorecognized, including EZH2, and ASXL1.Mutations in ASXL1 have been found in10–15% of MDS patients. Loss of functionof ASXL1 leads to increased expression ofHOX genes and defective differentiation ofhematopoietic progenitors.22 Somatic
The manuscript describing the RevisedIPSS (IPSS-R) for MDS is available now inthe September 23, 2012 issue ofBlood (vol. 120, p. 2454).
Under the aegis of the MDSFoundation, the International WorkingGroup for Prognosis in MDS (IWG-PM)analyzed clinical features and outcomedata from over 7000 patients andgenerated an improved methodanalyzing MDS patient prognosis moreprecisely than the initial IPSS.
Novel components of this prognosticsystem include: five rather than threecytogenetic prognostic subgroups withspecific and new classifications of anumber of less common cytogenetic
Revised International Prognostic Scoring System for MDS
INTERNATIONAL PROGNOSTIC SCORING
subsets, splitting the low marrow blastpercentage value, and assessing depthof cytopenias. In addition to the majorprognostic variables of marrow blasts,cytogenetics and peripheral cytopenias,additive features for survival includepatient age, performance status, serumferritin and LDH.
URLs for a web-based calculator tool tocalculate the IPSS-R are located at theMDS Foundation website:http://www.mdsfoundation.org/ipss-r-calculator or http://www.ipss-r.com.
This IPSS-R should prove beneficial forpredicting the clinical outcomes of un-treated MDS patients and aiding design andanalysis of clinical trials in this disease.Copies of this manuscript are availableupon request from the MDS Foundationand can also be accessed online at:
http://www.mdsfoundation.org/revisedprognostic-system-for-mds/.

4
mutations in EZH2 were detected in 2–6%of MDS patients. EZH2 is part of amethyltransferase responsible for methyl-ation of histone 3. Inactivating mutations inmembers of this complex result in activatedgene expression.13
Additional studies will be required toclarify the specific mechanisms by whichthese mutated genes contribute to MDSpathogenesis and the patterns ofassociation between mutations. Furtherstudies will also help us understand theclinical implications of these mutations interms of disease course, treatment responseand survival.
Integrating Somatic Mutations inthe Diagnosis and Classificationof MDS
The current diagnostic approach to MDSincludes morphological analysis to detectabnormalities of peripheral blood cells andhematopoietic precursors, bone marrowbiopsy to evaluate marrow cellularity andtopography, and cytogenetics to detectclonal chromosomal abnormalities. Thecombination of marrow dysplasia and clonalcytogenetic abnormalities allows aconclusive diagnosis of MDS to be made,but this is found in only a fraction ofpatients. In many instances, the diagnosis ofMDS is exclusively based on clinical andmorphological criteria, and may beparticularly difficult in patients who do nothave robust morphological markers, such asring sideroblasts or excess of blasts.
A major effort should be made to identifynovel diagnostic tools that may improve theaccuracy of MDS diagnosis.
Although most of the genes recurrentlymutated in MDS can be detected in differentmyeloid neoplasms and are not, therefore,specific for MDS, they may be a valuablemeans of obtaining evidence of a clonaldisorder in patients with suspected MDS. Ina recent comprehensive report, 52% ofpatients with normal cytogenetics had atleast one point mutation.14 These figures areeven higher for mutations of the genesencoding for splicing factors.
Recent studies in chronic myelo-monocytic leukemia reported cytogeneticaberrations in approximately 20% ofpatients, whereas a comprehensivemutation analysis revealed that 93% ofpatients with this disorder carried at leastone somatic mutation.23
Although, at this stage, the screening ofsuch molecular defects cannot berecommended on a routine basis, the spreadof massive genotyping methods will soonmake it possible for clinicians to detect abroad range of cytogenetic aberrations inperipheral blood at a reasonable cost,making it easier to confirm diagnosis inpatients with suspected MDS.
Genotype-phenotype Correlations:The Foundation Stone for a MolecularClassification of MDS
In a group of disorders classified on thebasis of morphological criteria, identifyingspecific associations between genotype anddisease phenotype is essential forrecognizing disease entities according todistinctive genetic profiles.
This genotype-phenotype correlation inMDS is illustrated by the 5q- syndrome. Thetypical hematologic phenotype includesmacrocytic anemia, normal or elevated plateletcount with hypolobated megakaryocytes,and a low rate of progression to AML. In2001, the WHO classification recognized MDSwith isolated del(5q) as a distinct diseaseentity. Although cases classified in this subtypeshow different morphological features, andmost patients do not have the specificcombination of signs that constitute the 5q-syndrome, this represents the first subtypeof MDS defined by a genetic abnormality.2
A major step forward in genotype-phenotype correlation has been theidentification of somatically acquiredmutations in SF3B1 in MDS patients withring sideroblasts. The specific associationbetween SF3B1 and ring sideroblasts wasunequivocally demonstrated by the analysisof a subgroup of patients in whom anaccurate quantitative enumeration of ringsideroblasts was performed using recentlyestablished consensus criteria, irrespective
of WHO categories. Overall, the SF3B1mutation status had a positive predictivevalue for disease phenotype with ringsideroblasts of 97.7%, while the absence ofring sideroblasts had a negative predictivevalue for SF3B1 mutation of 97.8%. Thecausal relationship between SF3B1mutation and ring sideroblasts was alsosupported by the significant associationbetween the SF3B1 mutant allele burdenand the percentage of ring sideroblasts.17
Although several issues still remain to beclarified, these observations are importantfor MDS classification. The RCMD-RScategory was created in the 2001 WHOclassification of myeloid neoplasms, but wasthen incorporated into the RCMD category inthe updated 2008 WHO classification. Thesefindings suggest that RCMD and RCMD-RSshould instead be considered as separatecategories, or a distinction should at least bemade between patients with wild-type ormutated SF3B1.
In addition, the observation that SF3B1mutations were found in patients with 15%or greater bone marrow ring sideroblasts aswell as in those with less than 15%,suggests that this threshold, first adopted bythe FAB and then by the WHO classification,does not recognize separate entities, andthat, instead, the proportion of ring sidero-blasts in the bone marrow appears to be acontinuum of a unique biological process.
Prognostic Relevance of Somatic Mutations in MDS:Toward Next-GenerationPrognostic Scoring Systems
Myelodysplastic syndromes are aheterogeneous group of disorders rangingfrom indolent conditions with a near-normallife expectancy to forms close to AML.A risk-adapted treatment strategy ismandatory for conditions showing such ahighly variable clinical course. Prognosticassessment in patients with MDS iscurrently based on stratification systemsthat combine multiple clinical and hema-tologic variables, including the InternationalPrognostic Scoring System (IPSS),24 which

5
has been the reference for clinical decision-making as well as for design and analysis ofclinical trials in these disorders, the WHOclassification-based prognostic scoringsystem (WPSS),25 the M.D. AndersonPrognostic Scoring System (MPSS)26 and,more recently, the revised IPSS.27
The available evidence clearly indicatesthat a greater understanding of themolecular basis of MDS may improve ourability to stratify the prognosis of patientswith MDS.
Mutations in several genes have beenreported to influence overall survival and riskof disease progression in MDS. Recently, acomprehensive analysis of patients withMDS identified mutations in five genes(ASXL1, RUNX1, TP53, EZH2, and ETV6) thatwere significantly associated with poorsurvival after adjustment for demographicfactors and IPSS risk groups.14 A prognosticmodel was then developed to integrate themutational analysis results into the IPSS, byincluding a variable for mutations in one ormore of these five prognostic genes. Morerecently, SF3B1 mutations were found to beindependent predictors of favorable clinicaloutcome after adjusting for IPSS or WPSS.17
Taken together, this evidence suggeststhat the integration of somatic mutations innext-generation prognostic scoring systemsis resulting in more accurate stratification ofindividual patient risk, and further refinesclinical decision making in MDS.
ConclusionOur understanding of the molecular basis
of MDS is improving rapidly. Theidentification of genetic defects and therecognition of their association to clinicalfeatures and outcome is going to have amajor impact on our approach to MDSpatients. The more widespread use ofmassive genotyping technology will soonenable us to detect a broad range of genemutations at a reasonable cost. This willmake diagnosis of these disorders easier,and will improve our assessment ofindividual patient risk, the selection ofappropriate therapy and the monitoring ofresponse to treatment.
References01. Cazzola M, Malcovati L. Myelodysplastic
syndromes–coping with ineffective hemato-poiesis. N Engl J Med. 2005;352:536-538.
02. Swerdlow SH CE, Harris NL, Jaffe ES, PileriSA, Stein H, Thiele J, Vardiman JW. WHOClassification of Tumors Of Haematopoietic andLymphoid Tissues. Lyon (France): IARC;2008:89-107.
03. Rollison DE, Howlader N, Smith MT, et al.Epidemiology of myelodysplastic syndromesand chronic myeloproliferative disorders in theUnited States, 2001–2004, using data from theNAACCR and SEER programs. Blood. 2008;112:45-52.
04. Schanz J, Tuchler H, Sole F, et al. NewComprehensive Cytogenetic Scoring Systemfor Primary Myelodysplastic Syndromes (MDS)and Oligoblastic Acute Myeloid Leukemia AfterMDS Derived From an International DatabaseMerge. J Clin Oncol. 2012.
05. Van den Berghe H, Cassiman JJ, David G, FrynsJP, Michaux JL, Sokal G. Distinct haemato-logical disorder with deletion of long arm of no.5 chromosome. Nature. 1974;251:437-438.
06. Boultwood J, Fidler C, Strickson AJ, et al.Narrowing and genomic annotation of thecommonly deleted region of the 5q- syndrome.Blood. 2002;99:4638-4641.
07. Ebert BL, Pretz J, Bosco J, et al. Identification ofRPS14 as a 5q- syndrome gene by RNA inter-ference screen. Nature. 2008;451:335-339.
08. Barlow JL, Drynan LF, Hewett DR, et al. A p53-dependent mechanism underlies macrocyticanemia in a mouse model of human 5q-syndrome. Nat Med. 2010;16:59-66.
09. Starczynowski DT, Kuchenbauer F, ArgiropoulosB, et al. Identification of miR-145 and miR-146aas mediators of the 5q- syndrome phenotype.Nat Med. 2010;16:49-58.
10. Papaemmanuil E, Cazzola M, Boultwood J, et al.Somatic SF3B1 mutation in myelodysplasia withring sideroblasts. N Engl J Med. 2011;365:1384-1395.
11. Yoshida K, Sanada M, Shiraishi Y, et al. Frequentpathway mutations of splicing machinery inmyelodysplasia. Nature. 2011;478:64-69.
12. Jansen AJ, Essink-Bot ML, Beckers EA, HopWC, Schipperus MR, Van Rhenen DJ. Quality oflife measurement in patients with transfusion-dependent myelodysplastic syndromes. Br JHaematol. 2003;121:270-274.
13. Nikoloski G, Langemeijer SM, Kuiper RP, et al.Somatic mutations of the histone methyl-transferase gene EZH2 in myelodysplasticsyndromes. Nat Genet. 2010;42:665-667.
14. Bejar R, Stevenson K, Abdel-Wahab O, et al.Clinical effect of point mutations in myelo-dysplastic syndromes. N Engl J Med. 2011;364:2496-2506.
15. Makishima H, Cazzolli H, Szpurka H, et al.Mutations of e3 ubiquitin ligase cbl familymembers constitute a novel common patho-genic lesion in myeloid malignancies. J ClinOncol. 2009;27:6109-6116.
16. Jadersten M, Saft L, Smith A, et al. TP53mutations in low-risk myelodysplastic syndromeswith del(5q) predict disease progression. J ClinOncol. 2011;29:1971-1979.
17. Malcovati L, Papaemmanuil E, Bowen DT, et al.Clinical significance of SF3B1 mutations inmyelodysplastic syndromes and myelodysplastic/myeloproliferative neoplasms. Blood. 2011;118:6239-6246.
18. Lasho TL, Finke CM, Hanson CA, et al. SF3B1mutations in primary myelofibrosis: clinical,histopathology and genetic correlates among155 patients. Leukemia. 2012;26:1135-1137.
19. Langemeijer SM, Kuiper RP, Berends M, et al.Acquired mutations in TET2 are common inmyelodysplastic syndromes. Nat Genet. 2009;41:838-842.
20. Ko M, Huang Y, Jankowska AM, et al. Impairedhydroxylation of 5-methylcytosine in myeloidcancers with mutant TET2. Nature. 2010;468:839-843.
21. Challen GA, Sun D, Jeong M, et al. Dnmt3a isessential for hematopoietic stem cell differen-tiation. Nat Genet. 2011;44:23-31.
22. Boultwood J, Perry J, Pellagatti A, et al.Frequent mutation of the polycomb-associatedgene ASXL1 in the myelodysplastic syndromesand in acute myeloid leukemia. Leukemia. 2010;24:1062-1065.
23. Meggendorfer M, Roller A, Haferlach T, et al.SRSF2 mutations in 275 cases with chronicmyelomonocytic leukemia (CMML). Blood. 2012.
24. Greenberg P, Cox C, LeBeau MM, et al.International scoring system for evaluatingprognosis in myelodysplastic syndromes. Blood.1997;89:2079-2088.
25. Malcovati L, Germing U, Kuendgen A, et al.Time-Dependent Prognostic Scoring System forPredicting Survival and Leukemic Evolutionin Myelodysplastic Syndromes. J Clin Oncol.2007;25:3503-3510.
26. Kantarjian H, O’Brien S, Ravandi F, et al.Proposal for a new risk model in myelodys-plastic syndrome that accounts for events notconsidered in the original InternationalPrognostic Scoring System. Cancer. 2008;113:1351-1361.
27. Greenberg PL, Tuechler H, Schanz J, et al.Revised International Prognostic Scoring System(IPSS-R) for myelodysplastic syndromes.Blood. 2012.

6
Meeting Highlights and Announcements

7
AGENDAPROGRAM OVERVIEWEffective management of MDS requiresunderstanding of underlying disease-specificabnormalities as well as patient-relatedfeatures. These issues as well as currentstandard and recent novel therapeuticadvances for MDS patients will be discussed.
7:30 am – 7:40 am■ Program Overview and Objectives
Stephen D. Nimer, MDSylvester Comprehensive Cancer CenterUniversity of Miami
Advances in UnderstandingDisease Pathogenesis7:40 am – 8:15 am■ Bone Marrow Failure in MDS:
Role of Abnormal Telomere DynamicsNeal S. Young, MD, MACPNHLBI, NIH
8:15 am – 8:50 am■ Somatic Mutations in MDS:
Insight into their Prognostic and Biological ImportanceTimothy Graubert, MDWashington University
Therapeutic Advances 8:50 am – 9:25 am■ Impact of Co-Morbidities and
Treatment in Lower Risk MDS: InterimResults from the EU MDS RegistryTheo de Witte, MD, PhDUniversity of Nijmegen
9:25 am – 10:00 am■ Biomarker-Directed Treatment
Approaches for MDSAlan F. List, MDMoffitt Cancer Center
10:00 am – 10:35 am■ Progress in Reduced Intensity
Hematopoietic Stem CellTransplantation in MDSMary M. Horowitz, MD, MSMedical College of Wisconsin, CIBMTR
10:35 am – 11:00 am■ Questions/Answers/Discussion
MDS SYMPOSIUM: 37TH ANNUAL MEETING AMERCIAN SOCIETY OF HEMATOLOGISTS
PLAN TO ATTEND: ASH 2012 SYMPOSIUM
Myelodysplastic Syndromes:Current Understanding and Management Approaches December 7, 2012 • Georgia World Congress Center
Stay Connected...Follow us on:
Get Involved! Join the MDSF Development Committee!
The MDS Foundation is seeking members to join our Development Committee.Whether your contribution is time, skills, funds, or ideas you can make a difference!For more information contact Tracey Iraca at [email protected] or call800.637.0839.
Support the MDSF!Please make a tax-deductible donation today. Kindly use the enclosed donationenvelope or go to www.mds-foundation.org to make your donation.
Please think of the MDS Foundation in your holiday giving this year and help people living with MDS.
Thank you for your continued support!
Sign up to volunteer!If you are interested in helping out in the MDS Foundation office or in attending eventsas a representative of the MDSF, please call us at 800-MDS(637)-0839.
Thank You to OurPharmaceuticalSupporters
We would like to thank ourpharmaceutical supporters for theircommitment to the Foundation andits work. They have contributed inthe form of educational grants, whichmaintain not only this newsletter butalso the development of continuingmedical education programs, and thedissemination of patient information.

8
MDS MISSION FOR NURSING EDUCATION: 37TH ANNUAL ONS CONGRESS
The Myelodysplastic Syndromes: Challenges and Strategies for Effective Outpatient ManagementEducational Symposium Held in New Orleans, LA
The MDS Foundation was pleased toparticipate in this year’s Oncology NursingSociety (ONS) annual meeting held inconjunction with its 37th Annual Congresson May 3, 2012. More than 300 nurses fromacross the country joined us to learn moreabout MDS and its treatments.
Our distinguished faculty included 4illustrious members of our Nurse LeadershipBoard: Sandra E. Kurtin, Jean A. Ridgeway,Jayshree Shah, and Sara M. Tinsley. Ourpresenters provided the oncology nursingprofessional with the tools to assist patientsand their families in meeting the challengeof living with MDS. Learning objectivesimparted by our presenters included recentadvances in strategies for the treatment ofMDS from prognosis to treatment; practicaltools for effective management; web-basedresources for patients and nurses; as well asinformation developed from our Patient andFamily Forums that have been held aroundthe world which formed the basis for thepresentation on patient and family supportthroughout the continuum of care.
During this congress the International NurseLeadership Board for the MDS Foundationintroduced a supplement to the ClinicalJournal of Oncology Nursing whichincorporates an update on the science ofMDS, practical tools for clinical managementof MDS including iron overload, a discussionof quality of life in the patient living withMDS, and a review of strategies andresources for support. Copies of this CJONSupplement are available upon request fromthe MDS Foundation and can also beaccessed online at http://www.mds-foundation.org/cjon-supplement/.
On behalf of the MDS Foundation and our Board of Directors, thank you for joining us for our recent Satellite Symposium:

9
MDS MISSION FOR NURSING EDUCATION: 37TH ANNUAL ONS CONGRESS
The Myelodysplastic Syndromes: Challenges and Strategies for Effective Outpatient ManagementReprinted with the permission of the Oncology Nursing Society
Laura J. Pinchot, BA
At A GlanceMyelodysplastic syndromes are a categoryof incurable malignancies that affect mainlyolder adults. Cytogenetic testing andadvances in targeted therapies haveprovided a means to extend and improve thequality of life for these patients. However,patient education and overcoming barriers,such as ageism, complex and expensivetreatment regimens, and adverse events, arecritical to ensuring that patients with amyelodysplastic syndrome can fully benefitfrom evolving therapy options.
Myelodysplastic syndromes are a classof incurable diseases that originate in thebone marrow. The disease processes arequite complex and often difficult forhealthcare professionals to articulate topatients and family caregivers. Sandra E.Kurtin, RN, MS, AOCN®, ANP-C, simplifiedthe process by comparing myelodysplasticsyndromes to a “broken factory.” This groupof disorders is associated with the bonemarrow’s inability to produce healthyleukocytes, erythrocytes, and platelets.Myelodysplastic syndromes are malignantprocesses that can be a precursor for acutemyeloid leukemia (AML). Although nocomplete cure is currently available,treatments are available to support patienthealth for months to several years afterdiagnosis.
Kurtin noted that nurses must embracethe fact that treatment selection formyelodysplastic syndromes is movingtoward molecular-driven models. Thecomplexity of disease and treatment can bedifficult for even seasoned healthprofessionals to grasp, which poses achallenge for patient and family education.
Cytogenetic EvaluationJean A. Ridgeway, MSN, APN, NP-C,
AOCN®, reported thatmapping the patho-physiology of this class of hematologicdiseases has come a long way since theywere first classified in the 1970s. Earlyclassification models, including the French-American-British (FAB) classification in1976 and the World Health Organization’slate-1990s revision of this system focusedon cell morphology and myeloblast (blast)counts. These systems describe thedisease progression based on extent ofrefractory anemia and increase in blastswithin the marrow.
Ridgeway noted that, also in the 1990s,advances in genetic research allowedclinicians to move toward a cytogeneticevaluation of myelodysplastic syndromes,and this shift in focus greatly enhanced theunderstanding of the disease process andtreatment effects. In addition to thepreviously defined parameters of cellmorphology, researchers discovered thatthese syndromes involve multiple cytogeneticdefects. This discovery has allowed cliniciansto use cytogenetics to drive diagnosis,prognosis, and treatment selection(Vardiman et al., 2009; Westers et al., 2011).
Conventional metaphase cytogeneticanalysis is the gold standard for analyzingkaryotypes associated with myelodysplasticdiseases. This process uses an aspiratedsample of bone marrow to examine 20 cellsthat are in the metaphase stage of celldivision. Clinicians are then able to map themalignant defects within chromosomes. Onedrawback to the process is that the cellsmust be in active cell division because theerrors are not apparent when this process isused on non-dividing cells.
Emerging technologies are overcominglimitations to metaphase cytogenetic analysis.For example, use of the singlenucleotide
polymorphism (SNP, pronounced “snip”)array analysis is able to identify abnor-malities in non-dividing cells. In addition tohelping in diagnosis and prognosis, the SNParray also can track response to treatment,particularly therapies that target the TET2and TP53 genes (Garcia-Manero, 2010;Gondek et al., 2008; Graubert, 2011;Maciejewski & Mufti, 2008; Tiu, Visconte,Traina, Schwandt, & Maciejewski, 2011).
Flow cytometry is another emergingtechnology that may be useful in identifyingprognostic features of myelodysplasticsyndromes. This technology analyzes cellreceptor and internal protein expression. Theclinician can use this to evaluate cells fromboth qualitative and quantitative perspectives.Although flow cytometry has potential uses,studies indicate that standardization andrefinement of quantification measures isneeded (Vardiman et al., 2009; Westers etal., 2011).
Emerging technologies such as flowcytometry and SNP array analysis arehelping researchers study potential targetedtherapies that can be tailored to a patient’sspecific genetic makeup. Studies are underway to identify novel agents and targets inaddition to TET2 and TP53 (Bejar, Levine, &Ebert, 2011; Kurtin,2011; Tiu et al., 2011).
ComprehensivePrognostic Indicator
The International Prognostic ScoringSystem (IPSS) takes variables from cyto-genetic evaluation and cell morphologyindicators identified by early classificationsystems (e.g., cytopenias and number of bonemarrow blasts) to create a comprehensivescore to predict survival. Patients’ scoresare then placed in four risk categories:low, intermediate-1, intermediate-2, andhigh. Low-risk patients are expected to live5.7 years, intermediaterisk patients have a
10
prognosis of 1.2–2.5 years, and high-riskpatients are expected to live only a fewmonths (0.4 years) (Greenberg et al., 2011).
Ridgeway noted that IPSS also serves tohelp clinicians to form a treatment strategy.In low-risk patients, the priorities are tomanage cytopenias and their associatedsymptoms by administering packed redblood cells and thrombopoietin receptoragonists, as well as erythropoiesis-stimulating, immunomodulatory, andimmunosuppressive agents (Ridgeway,Fechter, Murray, & Borràs, 2012). Prolongingsurvival is the focus of treating high-riskpatients. These patients typically receivehypomethylating agents. Also, the onlyknown “cure” for myelodysplastic syndromesis allogeneic hematopoietic stem celltransplantation; therefore, patients who fallinto the high-risk category should beevaluated as potential candidates fortransplantation (Ridgeway et al., 2012).Ridgeway and Kurtin both hesitated to usethe word “cure” because myelodysplasticsyndromes behave differently than othermalignancies in that stem cell transplantationmay not offer a complete response.
Complete Patient CareAlthough the IPSS indicator is a handy
tool that helps determine treatment strategyand risk, Kurtin noted that these prognosticcategories were determined before currenttreatments were available. Therefore, high-risk patients have a prognosis of only a fewmonths without treatment. The implicationsof this are that clinicians must identify andadminister treatment quickly once amyelodysplastic syndrome is diagnosed.
In addition, Kurtin noted that althoughthis is a disease that occurs in mostly olderadults with the average age at diagnosisbeing aged 73, chronological age should notbe the only indicator of treatment planningand prognosis evaluation. Performancestatus, frailty (failure to thrive), andcomorbidities also should be considered(Balducci & Exermann, 2000; Pal, Katheria,& Hurria, 2010). Kurtin illustrated this pointby noting that the average life expectancy
for a 75-year-old in the United States is 12.5years, and low-risk patients have an averagetime to progression to AML of 9.4 years(Greenberg et al., 1997). A diagnosis atolder age does not indicate a deathsentence. With proper treatment, an olderadult can live an active life despitemyelodysplastic diseases.
Family caregivers have an important rolein ongoing care. Kurtin likes to call them her“truth squad” because family members andfriends often can see things that the patientdoes not realize are occurring regarding thepatient’s health, such as cognitive problemsand mood or personality changes. In
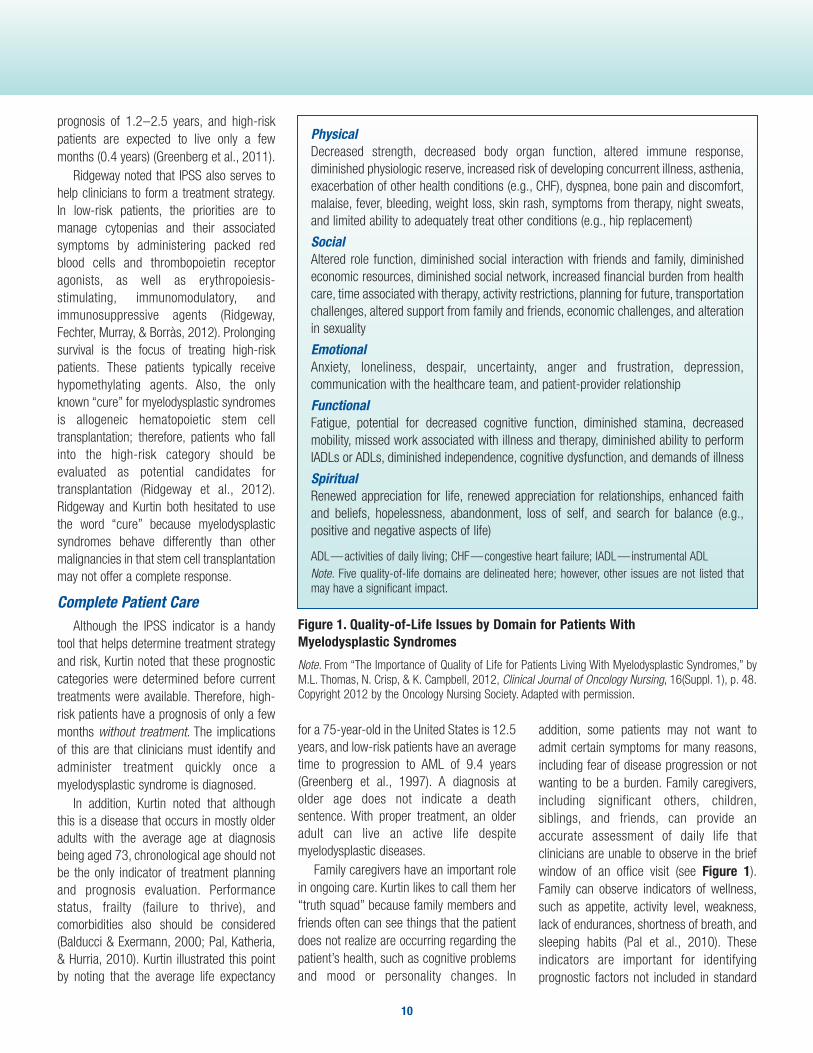
addition, some patients may not want toadmit certain symptoms for many reasons,including fear of disease progression or notwanting to be a burden. Family caregivers,including significant others, children,siblings, and friends, can provide anaccurate assessment of daily life thatclinicians are unable to observe in the briefwindow of an office visit (see Figure 1).Family can observe indicators of wellness,such as appetite, activity level, weakness,lack of endurances, shortness of breath, andsleeping habits (Pal et al., 2010). Theseindicators are important for identifyingprognostic factors not included in standard
PhysicalDecreased strength, decreased body organ function, altered immune response,diminished physiologic reserve, increased risk of developing concurrent illness, asthenia,exacerbation of other health conditions (e.g., CHF), dyspnea, bone pain and discomfort,malaise, fever, bleeding, weight loss, skin rash, symptoms from therapy, night sweats,and limited ability to adequately treat other conditions (e.g., hip replacement)
SocialAltered role function, diminished social interaction with friends and family, diminishedeconomic resources, diminished social network, increased financial burden from healthcare, time associated with therapy, activity restrictions, planning for future, transportationchallenges, altered support from family and friends, economic challenges, and alterationin sexuality
EmotionalAnxiety, loneliness, despair, uncertainty, anger and frustration, depression,communication with the healthcare team, and patient-provider relationship
FunctionalFatigue, potential for decreased cognitive function, diminished stamina, decreasedmobility, missed work associated with illness and therapy, diminished ability to performIADLs or ADLs, diminished independence, cognitive dysfunction, and demands of illness
SpiritualRenewed appreciation for life, renewed appreciation for relationships, enhanced faithand beliefs, hopelessness, abandonment, loss of self, and search for balance (e.g.,positive and negative aspects of life)
ADL—activities of daily living; CHF—congestive heart failure; IADL—instrumental ADLNote. Five quality-of-life domains are delineated here; however, other issues are not listed thatmay have a significant impact.
Figure 1. Quality-of-Life Issues by Domain for Patients With Myelodysplastic Syndromes
Note. From “The Importance of Quality of Life for Patients Living With Myelodysplastic Syndromes,” byM.L. Thomas, N. Crisp, & K. Campbell, 2012, Clinical Journal of Oncology Nursing, 16(Suppl. 1), p. 48.Copyright 2012 by the Oncology Nursing Society. Adapted with permission.

11
laboratory or physical examinations, such asundiagnosed comorbidities, quantifyingfunctional status, and determining frailty.
Treatment OptionsUnlike other cancers, such as lymphoma,
where clinicians have a multitude of agentsin their arsenal, Kurtin likened thetreatments for myelodysplastic disorders asa tasting menu rather than an extensivebuffet. Although research for novel therapiesis ongoing, currently only three agents areapproved by the U.S. Food and DrugAdministration for treatment of myelo-dysplastic disorders: azacitidine, lenalidomide,and decitabine (Kurtin & Demakos, 2010).Therefore, clinicians need to adequatelypace themselves so they do not run out oftreatment options.
Although allogeneic stem cell trans-plantation offers hope for a cure, this is notan option for most patients, and not everypatient who undergoes transplantation willexperience a complete response (Kurtin,2011; Kurtin & Demakos, 2010). However,stem cell transplantation does offer thebenefits of stabilizing disease, improvinghematologic status, and minimizing the needfor transfusions.
In regard to treating older adults withmyelodysplastic syndromes, treatmentusually aligns with the National Compre-hensive Cancer Network’s approach tooncology care. This guideline provides arange of characteristics that encompassolder adults who are functionally independentand are candidates for most treatmentoptions to those with poor prognosis andfunctional status where the focus oftreatment is supportive care and symptommanagement (National ComprehensiveCancer Network, 2011, 2012). However, oneformula does not apply to all patients withmyelodysplastic diseases, and treatmentplans can change throughout the diseasetrajectory. Kurtin noted that treatmenttriggers can alert clinicians as to the need tomodify therapy. These triggers include whena patient becomes dependent ontransfusions, progression or increased
symptom burden of cytopenias, increasedblasts, and progression to high-risk disease.
Patient and Caregiver EducationSara M. Tinsley, ARNP, AOCN®,
expressed the importance of clearcommunication and patient and familyeducation when treating myelodysplasticsyndromes. “Patients really want clearinformation about what their diagnosis is. It’snot like when patients with breast cancer telltheir friends, and everyone knows what theyhave, so they don’t have to go into a lot ofexplanation. Patients with myelodysplasticsyndromes have the task of explaining whattheir disorder is, not only to their friends andfamily, but also to other healthcare providerswho may not care for many patients withthese syndromes.”
Jayshree Shah, APN-C, AOCN®, MSN,BSN, BS, RN, CCRP, indicated that nursesare in a position to empower patients andfamilies to be active participants in theircare. Oncology nurses can directly affectoutcomes by thoroughly understanding thedisease state and available treatmentoptions, educating patients and families inplain language about elements of treatmentsuch as duration of therapy and potentialadverse events, and providing strategies forhow the patients can positively affectoutcomes through healthy lifestyle choices(Kurtin, 2012). Shah also reminds nursesthat a multidisciplinary approach to careusing effective communication strategiesamong all healthcare professionals (e.g.,specialists, primary care physicians,pharmacists, other nurses) results in betterpatient outcomes (Kurtin, 2012).
Healthcare professionals also can help byconsidering lifestyle factors, such as olderadults who are able to drive but need toschedule appointments in the daytimebecause they have poor night vision.Although some older adults are retired,many still may need to schedule treatmentsaround work schedules or socialcommitments. Offering this flexibility will notonly allow patients to maintain activelifestyles but also will help motivate them tostick with the treatment schedule.
Kurtin said that it is important for patientsand families to understand that, unlike manycancers that have a definitive beginningand end to treatment, myelodysplasticsyndromes are chronic illnesses that requiremanagement for the remainder of thepatient’s life span. Patients may expressfrustration with this, and nurses shouldfrequently remind them that treatment is “amarathon, not a sprint.”
Although life-sustaining, treatment formyelodysplastic syndromes is difficult andtime intensive. Patients can be subjected tomany transfusions over the course of theirlifetime. “Unfortunately, cytopenias areexpected to become worse before they getbetter because treatment cleans the marrowto allow for the new growth of healthy cells,”Kurtin explained. Worsening cytopenias willnaturally lead to a more intense symptomexperience. In addition, treatments also willsuppress patients’ immune systems, thusrequiring them to take extra precautions toavoid infections. Kurtin stressed thatpatients and families need to thoroughlyunderstand this trajectory at the outset oftreatment so that they avoid frustration anddiscouragement. Patients who understandthe disease process and that they need to“get to the other side of the [cytopenias]ravine” before their condition can improveare more likely to comply with thetreatment regimen.
In addition to the effects of immuno-suppressive therapies and worseningcytopenias, patients also will have to dealwith toxicities related to multipletransfusions. Shah noted that healthcareprofessionals should be aware of thepotential for iron overload because each unitof packed red blood cells that a patientreceives contains 25 mg of inextricable iron.This extra iron cumulates in the heart, liver,and endocrine system, which can lead totoxicities in these organs. Iron chelationtherapy can correct this, but Shah warnsthat this is not without side effects. Patientswho undergo chelation therapy canexperience pancytopenia, high-frequencyhearing loss, and ocular disorders, such as

12
cataracts and increased pressure (Jabbour,Garcia-Manero, Taher, & Kantarjian, 2009;Kurtin, 2007; Malcovati et al., 2005).
Reliable Resources for PatientsShah noted that the International Nursing
Leadership Board of the MyelodysplasticSyndromes Foundation has created a patienteducation tool called Building Blocks ofHope: A Patient and Care Giver Guide forLIVING With MDS. The guide answersquestions about the syndromes and theirtreatment options, and offers suggestionsabout how patients can adopt healthystrategies and be an active part of thetreatment team. The guide encouragespatients to continue with usual activitieswhile using common sense to avoidillnesses associated with suppressedimmunity.
Tinsley suggested that, in addition toinformation nurses can provide during appoint-ments, a wealth of resources are availableon the Internet from many organizations,such as the Myelodysplastic SyndromesFoundation (www.mds-foundation.org), theLeukemia and Lymphoma Society(www.lls.org), and the American CancerSociety (www.cancer.org). These sites offerpatient-specific information written in clearlanguage that helps to cut through medicaljargon. Some sites offer access to supportgroups, message boards, and clinicaltrial information.
SummaryTo effectively manage myelodysplastic
syndromes, clinicians must have a thoroughgrasp of the disease state, treatmenttrajectory, and expected side effects. Inaddition, effective communication, boththrough patient education and amongmultidisciplinary team members, will helpimprove treatment compliance and patientoutcomes.
Kurtin stressed that continued treatmentprovides the best opportunity for positiveresponses. She noted that barriers totreatment, including clinicians’ ageismtoward patients, patients’ and caregivers’
perceptions of lack of treatment benefit,treatment noncompliance, and toxicities andadverse events, can be overcome by clearexpectations and care plans, rapididentification and management of sideeffects and adverse events, and apartnership with the patient and family(Eliasson, Clifford, Barber, & Marin, 2011).Overcoming these barriers can help toensure that patients with myelodysplasticsyndromes can live full, active lives despitetheir illness.
– Reporting by Laura J. Pinchot, BA
ReferencesBalducci, L., & Extermann, M. (2000).Management of cancer in the older person: Apractical approach. Oncologist, 5, 224–237.doi:10.1634/theoncologist. 5-3-224
Bejar, R., Levine, R., & Ebert, B.L. (2011).Unraveling the molecular pathophysiologyof myelodysplastic syndromes. Journal ofClinical Oncology, 29, 504–515. doi:10.1200/JCO.2010.31.1175
Eliasson, L., Clifford, S., Barber, N., & Marin,D. (2011). Exploring chronic myeloid leukemiapatients’ reasons for not adhering to the oralanticancer drug imatinib as prescribed.Leukemia Research, 35, 626–630.doi:10.1016/j.leukres.2010.10.017
Garcia-Manero, G. (2010). Prognosis ofmyelodysplastic syndromes. HematologyAmerican Society of Hematology EducationProgram, 330–337. doi:10.1182/asheducation-2010.1.330
Gondek, L.P., Tiu, R., O’Keefe, C.L., Sekeres,M.A., Theil, K.S., & Maciejewski, J.P. (2008).Chromosomal lesions and uniparental disomydetected by SNP arrays in MDS, MDS/MPD, andMDS-derived AML. Blood, 111, 1534–1542.doi:10.1182/blood-2007-05-092304
Graubert, T. (2011). Molecular analysis as adiagnostic tool in myelodysplastic syndromes[Abstract 13]. Leukemia Research, 35(Suppl. 1), S5.
Greenberg, P., Cox, C., LeBeau, M.M.,Fenaux, P., Morel, P., Sanz, G., Bennett, J.(1997). International scoring system forevaluating prognosis in myelodysplasticsyndromes. Blood, 89, 2079–2088.
Greenberg, P., Tuechler, H., Schanz, J., Sole,F., Bennett, J.M., Garcia-Manero, G., Haase,D. (2011). Revised International PrognosticScoring System (IPSS-R), developed by theInternational Prognostic Working Group forPrognosis in MDS (IWG-PM) [Abstract 14].Leukemia Research, 35(Suppl. 1), S6.
Jabbour, E., Garcia-Manero, G., Taher, A., &Kantarjian, H.M. (2009). Managing ironoverload in patients with MDS with oraldeferasirox therapy. Oncologist, 14, 489–496.doi:10.1634/ theoncologist.2008-0154
Kurtin, S. (2011). Current approaches to thediagnosis and management of myelodys-plastic syndromes. Journal of the AdvancedPractitioner in Oncology, 2(Suppl. 2), 7–18.
Kurtin, S.E. (2007). Myelodysplasticsyndromes: Diagnosis, treatment planning,and clinical management. Oncology, 21(11,Suppl. Nurse Ed.), 41–48.
Kurtin, S.E. (2012). Myelodysplastic syn-dromes: The challenge of developing clinicalguidelines and supportive care strategies fora rare disease. Clinical Journal of OncologyNursing, 16(Suppl. 1), 5–7. doi:10.1118/12.CJON.S1.5-7
Kurtin, S.E., & Demakos, E.P. (2010). Anupdate on the treatment of myelodysplasticsyndromes [Online exclusive]. Clinical Journalof Oncology Nursing, 14, E24–E39.doi:10.1188/10.CJON.E24-E39
Maciejewski, J.P., & Mufti, G.J. (2008). Wholegenome scanning as a cytogenetic toolin hematologic malignancies. Blood,112, 965–974. doi:10.1182/blood-2008-02-130435
Malcovati, L., Porta, M.G., Pascutto, C.,Invernizzi, R., Boni, M., Travaglino, E., Cazzola,M. (2005). Prognostic factors and lifeexpectancy in myelodysplastic syndromesclassified according to WHO criteria: A basisfor clinical decision making. Journal ofClinical Oncology, 23, 7594–7603.doi:10.1200/JCO.2005.01.7038
National Comprehensive Cancer Network(2011). NCCN Clinical Practice Guidelines inOncology: Myelodysplastic syndromes[v.2.2011]. Retrieved from http://www.nccn.org/professionals/ physician_gls/pdf/mds.pdf

13
National Comprehensive Cancer Network.(2012). NCCN Clinical Practice Guidelines inOncology: Senior adult oncology [v.2.2012].Retrieved from http://www.nccn.org/professionals/physician_gls/pdf/senior.pdf
Pal, S.K., Katheria, V., & Hurria, A. (2010).Evaluating the older patient with cancer:Understanding frailty and the geriatricassessment. CA: A Cancer Journal forClinicians, 60, 120–132. doi:10.3322/caac.20059
Ridgeway, J.A., Fechter, L., Murray, C., &Borràs, N. (2012). Update on the science ofmyelodysplastic syndromes. Clinical Journalof Oncology Nursing, 16(Suppl. 1), 9–22.doi:10.1188/12.CJON.S1.9-22
Tiu, R.V., Visconte, V., Traina, F., Schwandt, A.,& Maciejewski, J.P. (2011). Updates incytogenetics and molecular markers in MDS.Current Hematologic Malignancy Reports, 6,126–135. doi:10.1007/s11899-011-0081-2
Vardiman, J.W., Thiele, J., Arber, D.A.,Brunning, R.D., Borowitz, M.J., Porwit, A.,Bloomfield, C.D. (2009). The 2008 revision ofthe World Health Organization (WHO)classification of myeloid neoplasms and acuteleukemia: Rationale and important changes.Blood, 114, 937–951. doi:10.1182/blood-2009-03-209262
Westers, T., Ireland, R., Kern, W., Alhan, C.,Balleisen, J., Bene, M.C., van de Loosdrecht,A.A. (2011). Standardization of flow cytometryin myelodysplastic syndromes: A report froman international consortium and the EuropeanLeukemiaNet Working Group [Abstract 137].Leukemia Research, 35(Suppl. 1), S53.
JUST BACK: AARP National Eventin New OrleansA special thank you to Joan Weidenfeld,a member of our MDSF DevelopmentCommittee, for suggesting that weattend the AARP Convention to spreadMDS awareness. Our booth was wellattended and we were able to distributea great amount of information. It wasthe first time that we had an MDSpatient joining us at our exhibit booth.We look forward to another successfulevent next year.
Her idea made a difference!
Pinchot, Laura J. (reporter). Spotlight onSymposia From Oncology Nursing Society37th Annual Congress: The MyelodysplasticSyndromes: Challenges and Strategies forEffective Outpatient Management. 2012;5–8.

14
THE 12TH INTERNATIONAL SYMPOSIUM ON MYELODYSPLASTIC SYNDROMES

15
THE 12TH INTERNATIONAL SYMPOSIUM ON MYELODYSPLASTIC SYNDROMES

16
Highlights of LatestLiterature in MDS Suneel D. Mundle, PhD
Listed below are citations of some newpublications relevant to MDS (pathogenesis,clinical characterization, management, etc.).To access the complete article log on towww.pubmed.gov.
EPIDEMIOLOGY:1. Maynadie M et al. Survival of European
patients diagnosed with myeloid malig-nancies: a HAEMACARE study. Haematologica.2012, Sep 14. [Epub ahead of print]The report presented analysis of 58,800cases incidence between 1995-2002 from48 population-based cancer registries in 20European countries. Among myeloid malig-nancies, the five-year overall survivalestimates were 17% for AML, 20% for MDS/MPD neoplasms, 31% MDS and 63% MPD.
2. Zandberg DP et al. Tertiary center referralpatterns for patients with myelodysplasticsyndrome are indicative of age and racedisparities: a single-institution experience.Leukemia Lymphoma. 2012, Sep 8. [Epubahead of print]A retrospective chart review of MDS patients(N=252) seen between 2000–2010 at asingle large American academic institutiondemonstrated that the median age of blackmen at diagnosis was remarkably youngerthan the white men (62 vs. 68 yearsrespectively, p=0.03) and a longer time toreferral was noted with the black men as well(9 mo vs. 1.5 months in white men, p=0.03).No such differences were noted in women.
3. Foran JM and Shammo JM. Clinicalpresentation, diagnosis and prognosis ofmyelodysplastic syndromes. Am J Med.2012;125(7, suppl):S6-13.The article describes a flow chart for aprimary care physician with differentindicators of the need for differentialdiagnosis of MDS. This flow chart suggestsimmediate referral to specialty physician ifbi- or multi-lineage cytopenias are seen. For amono-lineage cytopenia the referral isadvised after ruling out the common causesof cytopenia.
4. Kurtin SE et al. Patient and family resourcesfor living with myelodysplastic syndromes.Clin J Onc Nursing. 2012;16:58-64.The authors have identified a commun-ication gap between MDS treaters, patients
and their caregiver and have provided listingof valuable knowledge resources to assist inbridging the gap.
5. Niscola P et al. Transfusions at home inpatients with myelodysplastic syndromes.Leukemia Res. 2012;36(6):684-688.
A 5-year home care program evaluating 211patients treated during its implementation hasunderscored the feasibility of at-hometransfusions preserving the quality of life. Thereport however, warrants regarding theprovision of a dedicated home care service forthis purpose.
DIAGNOSIS/PROGNOSIS:1. Greenberg PL et al. Revised international
prognostic scoring system for myelodysplasticsyndromes. Blood. 2012;120(12):2454-2465.Combining MDS patient databases fromseveral international institutions offered a poolof 7012 MDS patients in the revised analysis(IPSS-R) compared to 816 patients includedin IPSS. Cytopenias, cytogenetics and marrowblast counts remained foundational in IPSS-R,albeit with more detailed categorizationand addition of several new entities. Thenew model recommends five prognosticcategories as opposed to the original four.The new categories are very low, low,intermediate, high and very high risk withoverall survival of 8.8, 5.3, 3, 1.6 and 0.8years respectively.
2. Shukron O et al. Analyzing transformation ofmyelodysplastic syndrome to secondary acutemyeloid leukemia using a large patient data-base. Am J Hematol. 2012;87(9):853-860.
By using a model to estimate the risk ofleukemic transformation as a function oftime from the diagnosis in 1079 patientrecords from Düsseldorf MDS registry, theauthors have demonstrated the risk oftransformation remained constant especiallyin low, int-1 and int-2 IPSS categories. As aresult the report concluded that there may bea single random genetic event that causes aleukemic transformation as opposed to amulti-event process.
3. Westers TM et al. Standardization of flowcytometry in myelodysplastic syndromes: areport from an international consortium andthe European LeukemiaNet working group.Leukemia. 2012;26(7):1730-1741.A multi-national working group tasked in2008 to propose standards for flow cytometryhas refined the minimum criteria to assessdysplasia by flow cytometry to potentiallycategorize subjects as normal, or suggestiveof MDS or diagnosed of MDS. The working
group has suggested that flow cytometryshould be a part of the integrated diagnosticpanel for MDS rather than being a stand-alone technique.
4. Germing U et al. Survival, prognostic factorsand rates of leukemic transformation in 381untreated patients with MDS and del(5q): amulticenter study. Leukemia. 2012;26(6):1286-1292.The median survival for the entire group was74 months (44 months in transfusiondependent vs. 97 months in transfusion-independent, p<0.0001). Of the total of 381,48% progressed to AML with a calculated riskof transformation being 4.9% at 2 years and17.6% at 5 years. The associated prognosticfactors were transfusion dependency, >5%marrow blasts and high WPSS score.
TREATMENT:Hematopoietic Cell Transplantation (HCT):1. Gyurcocza B and Deeg HJ. Allogeneic
hematopoietic cell transplantation for MDS:For whom, when and how? Blood Rev. 2012,Sep 13 [Epub ahead of print].Treatment-related mortality and relapse havecontinually posed barrier to the success ofHCT therapy. To this end, with the availabilityof cord blood stem cells and success withHLA-haploidentical donors, authors suggesteda possibility of offering HCT to all patients andexpressed optimism for cure in 25–75%based on the disease burden with 70%experiencing good to excellent quality of life.
2. Gerds AT et al. Pretransplantation therapywith azacitidine vs. induction chemotherapyand posttransplantation outcome in patientswith MDS. Biol Blood Marrow Transplantation.2012;18(8):1211-1218.A retrospective review of 68 cases of MDS orMDS AML with high-dose (40%) or reduceddose (60%) azacitidine in 35 patients andinduction chemotherapy in 33 patients prior toHCT, showed 1 year post transplant survival of57% with azacitidine vs. 36% with inductionchemotherapy. The risk of post-HCT mortality,non-relapse mortality and relapse rates werelower with azacitidine.
Hematopoietic Growth Factors:1. Crisà E et al. Long-term follow-up of
myelodysplastic syndrome patients withmoderate/severe anaemia receiving erythro-poietin+ 13-cis-retinoic acid anddihydroxylated vitamin D3: independentpositive impact of erythroid response onsurvival. Brit J Haematol. 2012;158(1):99.Previously authors reported 60% erythroidresponse rate with the above combination in
MDS Resources

17
63 elderly patients with clinical featuresotherwise unfavorable to erythroid response.The present update with a 7-year follow upshowed that especially in non-RAEB patients,the median duration of response was 22months, overall survival was 55 months andamong the erythroid responder subset thesurvival at 3-year from diagnosis was 90%.
Iron Chelation:1. Neukirchen J et al. Improved survival in MDS
patients receiving iron-chelation therapy–amatched pair analysis of 188 patients fromthe Düsseldorf MDS registry. Leukemia Res.2012;36(8):1067-1070. A comparison of two groups of 94 MDSpatients each with or without iron chelationtreatment for transfusion related iron overloaddemonstrated a significant overall survivaldifference in favor of chelation (74 months intreated vs. 49 months untreated patients,p=0.002).
2. List AF et al. Deferasirox reduces serumferritin and labile plasma iron in RBCtransfusion-dependent patients with myelo-dysplastic syndrome. J Clin Oncol. 2012;30(17):2134-2139.A three year prospective multicenter trialtreated 173 patients with iron overload(serum ferritin ≥1000 g/L and had received≥20 RBC transfusions with a continuedrequirement) with deferasirox (20 mg/kg/day–escalation allowed to 40 mg/kg/day).Mean serum ferritin decreased with a 23%,36.7% and 36.5% among those treated for alength of 1 year, 2 year or 3 year respectively.In addition, in all patients with abnormalbaseline labile plasma iron, normalization wasseen by week 13. Overall, 28% patientsshowed hematologic improvement (HI)response. The common drug-related adverseevents included gastro-intestinal disturbancesand elevated serum creatinine.
3. Gatterman N et al. Hematologic responses todeferasirox therapy in transfusion-dependentpatients with myelodysplastic syndromes.Haematologica. 2012;97(9):1364-1371.A post-hoc analysis of the EPIC study in aneligible subset of patients without anyconcomitant medications demonstratedhematologic improvement; 21.5% erythroidresponse, 13% platelet response, and22% neutrophil response after 109, 169 and226 days of treatment with deferasiroxrespectively. Labile plasma iron reduction≤0.4 M/L was observed starting fromweek 12.
IMiDs:1. Komrokji RS et al. Combined treatment with
lenalidomide and epoetin alfa in lower riskpatients with myelodysplastic syndrome.Blood. 2012, Aug 30 [Epub ahead of print].Low/Int-1 patients failing prior EPO weretreated with 10 or 15 mg/day lenalidomidefirst (N=39). At week 16 non-erythroidresponders were initiated on additionaltreatment with 40,000 IU/week rhu-EPO. Withlenalidomide monotherapy, erythroidresponse (HI-E) was higher in del 5q patients(86%) than the others (25%). Among 23 non-responders to monotherapy and receivingcombined treatment the eventual HI-E ratewas 26%. The combination is being studiedfurther in a phase III study by ECOG.
2. Sekeres MA et al. Phase 2 study of thelenalidomide and azacitidine combination inpatients with higher-risk myelodysplasticsyndromes. Blood. 2012, Aug 22 [Epub aheadof print]A combination of azacitidine (75 mg/m2/day x5 day) and lenalidomide (10 mg/day x 21days) in a 28 day cycle was administered to agroup of Int-1/Int-2 and high-risk MDSpatients (N=36). The most common grade3/4 adverse event was febrile neutropenia(22%). Overall response rate was 72% (CR-44%, HI-28%). Median CR duration was 17+months and median overall survival for allpatients was 13.6 months.
Demethylating Agents:1. Wang R et al. The impact of hypomethylating
agents on the cost of care and survival ofelderly patients with myelodysplastic syndromes.Leukemia Res. 2012;36(11): 1370-1375.A model comparing 6556 MDS patientsdiagnosed between 2001–2007 (≥66.5years) and taking into account MDS survivalprobability, estimated MDS-related-5 yearcost to be higher than 18 most prevalentcancers in the USA. Furthermore for MDS,when a time period prior to the availability ofhypomethylating agents (Jan 2001–Jun2004) was compared to period after theiravailability (Jul 2004–Dec 2007), in parallelwith an improvement in 24-month survival,the cost of patient management for 24months was also found to be increased($97,977 after, 2004–2207, vs. $42,628before, 2001–2004, the availability ofhypomethylating agents)
2. Greenberg PL et al. A randomized controlledtrial of romiplostim in patients with low- orintermediate-risk myelodysplastic syndromes(MDS) receiving decitabine. Leukemia Lym-phoma. 2012, Aug 20 [Epub ahead of print]
Development of thrombocytopenia is commonwith hypomethylating agents. The presentstudy tested romiplostim (n=15) vs. placebo(n=14) given concomitantly with decitabine.Mean platelet counts at the beginning of eachnew cycle of decitabine were higher. Also, thebleeding events and platelet transfusion rateswere notably lower in romiplostim treatedpatients. The overall therapeutic response toowas better with simultaneous administrationof romiplostim.
Other Agents:1. Sokol L et al. Randomized, dose-escalation
study of the p38α MAPK inhibitor SCIO-469in patients with myelodysplastic syndrome.Leukemia. 2012, Sep 11. [Epub ahead of print].SCIO-469 was tested at four total oral dailydose levels 90, 180,270,360 mg/day inlow/int-1 MDS patients who previously did notrespond to EPO (N=62). Hematologicimprovement was seen in 29% patients witha median time to respond as 72 days andduration of response ranging from 63 days to>2 years. One patient each had complete orpartial response and 58% patients had stabledisease. Approximately 18% (11 patients)discontinued treatment due to adverse events.
2. Natarajan-Amé S et al. Bortezomib combinedwith low-dose cytarabine in intermediate-2and high risk myelodysplastic syndromes. Aphase I/II study by the GFM. Brit J Haematol.2012; 158(2):232-237.Forty three higher-risk MDS patients receivedbortezomib (1.5 mg/m2 on days 1,4,8,11)and low dose cytarabine arabinoside(10 mg/m2, then 20 mg/m2 on days 1–14)every 28 days for four cycles. With a median29.7 months follow up, overall 28% responsewas seen including 1 CR. Response seemedto be limited to previously untreated patientsand the responders had a superior overallsurvival (18.2 months) as compared to thenon-responders (10 months). Major side-effects included hematologic toxicities andneuropathy.
3. Olnes MJ et al. Directed therapy for patientswith myelodysplastic syndromes (MDS) bysuppression of cyclin D1 with ON01910.Na.Leukemia Res. 2012;36(8):982-989.In a preclinical part of the study, ON01910.Nasuppressed cyclin D1 expression in MDSpatients’ bone marrow mononuclear cells.Additionally in the Phase I clinical study with12 higher risk MDS and 8 AMLs with trisomy8, three patients showed ≥50% decrease inmarrow blast counts (15%) and 3 hadhematologic improvement (15%). The latter

18
responders showed drop in cyclin D1expression in their marrow CD34+ cells.
PATHOBIOLOGY:1. Zhao Y et al. Methylation of the p73 gene in
patients with myelodysplastic syndromes:correlations with apoptosis and prognosis.Tumour Biol. 2012, Sep 28. [Epub aheadof print].A methylation-specific PCR in 126 de novoMDS patients demonstrated p73 genemethylation in the bone marrow mononuclearcells of 36.5% patients, which correlated withblast count and WHO classification. In vitro,decitabine restored p73 expression via itsdemethylation activity and increased Ara-Cinduced apoptosis of the bone marrow cells.The median survival was shorter in patientswith methylated p73gene as compared tothose without methylation (15 vs. >33months respectively, p=0.002).
2. Ohba R et al. Clinical and geneticcharacteristics of congenital sideroblasticanemia: comparison with myelodysplasticsyndrome with ring sideroblast (MDS-RS). AnnHematol. 2012, Sep 16. [Epub ahead of print]
A nationwide survey in Japan for sideroblasticanemia collected records of 137 patients withRCMD (n=72), RARS (n=47) or congenitalsideroblastic anemia (CSA, n=18). Thegenetic analysis data demonstrated distinctgenetic mutations in CSA. The SF3B1mutation common to MDS with ringedsideroblasts was absent in CSA and 70%cases of the latter had ALAS2 gene mutation.
3. Mailloux AW et al. Expansion of effectormemory regulatory T cells represents a novelprognostic factor in lower risk myelodys-plastic syndrome. J Immunol. 2012;189(6):3198-208T-regulatory (Treg) cell compartment wasfound to be altered in 34.6% of a total of 52MDS patients with low risk of leukemictransformation. Expansion of Treg may beindicative of a change in bone marrowmicroenvironment. An increase in theabsolute count of CD4(+) FOXP3(+) CD25(+)CD127 (low) CD45RA(–) CD27(–) Tregs(effector memory Tregs) was significantlyassociated with anemia (p=0.046), reducedhemoglobin (p=0.038), and blast counts≥5% (p=0.006).
REVIEWS AND PERSPECTIVES:The following articles provide significant reviewof literature and/or innovative perspective on thestate-of-the-art in MDS and identify need foradditional prospective studies.
1. Steensma DP. Dysplasia has a differentialdiagnosis: Distinguishing genuine myelodys-plastic syndromes (MDS) from mimics,imitators, copycats and impostors. CurrHematol Malig Rep. 2012, Sep 27. [Epubahead of print]
2. Steensma DP. Historical perspectives onmyelodysplastic syndromes. Leukemia Res.2012, Aug 23. [Epub ahead of print]
3. List AF. New therapeutics for myelodysplasticsyndromes. Leukemia Res. 2012, Sep 7.[Epub ahead of print]
4. Vardiman J. The classification of MDS: FromFAB to WHO and beyond. Leukemia Res.2012, Aug 30 [Epub ahead of print]
We would like to thank Suneel Mundle, amember of the MDS Foundation, for hisassistance in monitoring these importantpeer-review publications on MDS.
MDS News Briefs New Published MDSSupplement in the AmericanJournal of Medicine
View the recently published,supplement on MDS in the AmericanJournal of Medicine. These articlesare available on the internet throughopen access, allowing interestedparties to download the entiresupplement for free.
http://www.amjmed.com/supplements
New Website Resource forIron Overload Management
Iron Health Alliance is a newglobal initiative dedicated toincreasing awareness and sharingup-to-date information about irontoxicity with physicians and patientsaround the world.
http://www.ironhealthalliance.com/index.jsp
Launch of Fast Track for FirstPrescription Service throughCelgene Patient Support
Fast Track for First Prescription™ is anew opt-in service from Celgene PatientSupport® which helps patients on an oralCelgene product receive their firstprescription faster.
Which patients are eligible for this program?■ Patients on an oral Celgene product
receiving their first prescription ■ Patients with documented proof of
insurance■ Patients who are registered in a Celgene
risk management (REMS) program andhave a valid authorization number
How are eligible patients enrolled inthis program?■ Prescriber must fax the Fast Track Cover
Sheet and the Patient Prescription Form
with the authorization number and thepatient risk category (i.e., adult female ofchildbearing potential, adult male, etc) to1-800-822-2496
■ Patient’s contact information andinsurance
■ Prescriber must ensure patient hascompleted their Celgene risk management(REMS) survey
What can a patient expect after beingenrolled in this program?The specialty pharmacy will contact thepatient to:■ Review their insurance benefits for the
prescribed product (i.e., co-pay respon-sibilities and potential financial co-payassistance options)
■ Provide appropriate counseling (ifapplicable)
■ Set up a delivery date for shipment of themedication
For more information, or for any questions,call Celgene Patient Support® at 1-800-931-8691.

19
From The Foundation

20
Worldwide Patient Forums and Support Groups
SPREADING THE NEWS WORLDWIDE
Lakeland Patient Support Group Lakeland, Florida
“It was a great opportunity for each person to express their expectations for thegroup, not just for now, but for the future. As this cancer is rare, many patients feelisolated and singular. Our goals for the group are to encourage and support oneanother and to gain more knowledge about this rare disease. Everyone felt that theabove goals were accomplished and are looking forward to meeting again!”
Katherine Dempster
(L to R) Linda and Richard Brackett, Bonnie and Arnold Henig, Don and Katherine Dempster, Dave Paul. Vivian Paul, photographer
Southern California MDS Patient Support Group
NOW FORMING: MDS PATIENT AND FAMILYSUPPORT GROUPSWhether you are interested in starting amuch needed support group in your areaor looking to join one, please contactthe MDS Foundation at: 800-MDS(637)-0839 or [email protected].
The MDS Foundation has developed astrategy for setting up patient groups andassistance is now available to organizesupport groups for MDS patients. Anymember of the Foundation, patients, friends,family members, and caregivers are invitedto join with us to move this project forward.
“People started talking, asking questions and before weknew it 2 hours had gone by. It seemed like everyone thathad questions got the answers that they were looking for.”
Susan Urban
The Southern California MDS Support Group meets every thirdSaturday of the month at St. Mary Star of the Sea Church, 609 PierView Way in Oceanside, California at 2:30 PM. For more information,contact Susan Urban at (760) 966-0895 or [email protected] the following link to view their website:http://robnixonii.wix.com/socalmdssupport#!home/mainPage
PLEASE MAKE SURE TOREGULARLY CHECK OUR ONLINEUPCOMING EVENTS CALENDARFOR MEETINGS TAKING PLACE
IN A CITY NEAR YOU!
Our goals for the groupare to encourage andsupport one another andto gain more knowledge...
The Lakeland Regional MDSSupport Group was held at the homeof Dave and Vivian Paul in Lakeland,Florida. For more information, contactthe Dempsters at (863) 816-8482 orthe Pauls at (863) 698-5137.

21
SPREADING THE NEWS WORLDWIDE
Patient and Family Education ForumsFREE One-Day Conferences for MDS Patients and their Families
Thank you to all who have attended our MDS Patient andFamily Conferences in 2012. Ongoing meetings addressingquality of life issues for MDS patients will be planned and theseconferences will occur in ten cities around the world in 2013.A global patient forum will be held alongside our 12th Inter-national Symposium on MDS in Berlin, Germany. Check ourwebsite and facebook for updates. We look forward to anothersuccessful year!
Toronto, Canada MDS Patient Support Group“...we had 41 attendees (much larger than we had
expected)... Dr. Karen Yee did a presentation for the firsthour. She presented a general overview of MDS and thenspent a lot of time talking about the different treatmentoptions with a great overview of current clinical trials.Participants had an opportunity to ask questions. In thesecond hour, David Walkup facilitated a support/educationalsession using an MDS tool that his company (HealthyInteractions) has developed with some health care providersand a patient. It was a very powerful, engaging session.He was asking for participants’ feedback prior tofinalizing the tool.”
Cindy MurrayNurse Group LeaderPrincess Margaret Hospital
The Toronto, Ontario MDS Support Group has 4 meetings a year; every3 months at Trinity Presbyterian Church, 2737 Bayview Avenue, NorthYork 10:00 am to 12:00 pm. For more information, contact CindyMurray at (416) 946-4501 Ext. 5919 [email protected] or Nancy-Ann Pringle at (416) 946-4501 Ext. 5337 [email protected]
Request Your FREE PatientInformation Packet Today
The MDS Foundation has many resources on MDS-related topics,straight from leading experts in the field of MDS. Request your FREEpatient information packet from the MDSF, containing up to dateeducation on MDS in patient-friendly language. Many are alsoavailable in other languages. Order your patient packet today bycalling 800-MDS-0839 or email [email protected].

22
Hamilton, Ontario MDS Patient Support Group“Our attendance was the best ever, 40 people. My MDS
hand outs were well received. The excitement surroundingour webpage was unbelievable. Dr. Leber hopes we canget it up and running before year end. He also wants toknow if videos can be attached. People were in awe aboutthe webpage.”
William PearsonHamilton, Ontario MDS Patient Support Group
The Hamilton, Ontario group meets at the Emmanuel UnitedChurch, 871 Upper Ottawa Street, Hamilton 10:00 am to 12:00 noon.For more information, contact Tammy DeGelder, RN at (905) 521-2100,ext. 73435 or William Pearson (905) 561.6999 or e-mail to:[email protected].
SPREADING THE NEWS WORLDWIDE
NEW YORK CITYMDS PATIENT SUPPORT GROUP
– Now Being Formed –
Would you like to join anMDS Support Group in New York City?
Meet others with similar challenges,share hopes, and frustrations,
gather information to better understand MDS,listen to healthcare professional presentations,
and socialize!
Contact [email protected] more information.

NEW ITEM ADDED – MDS SILICONE BRACELETSHelp Spread Awareness of MDS and Order Your Silicone Bracelets Today!
For a donation of your choice, receive your custom silicone bracelet(s) as a “Thank You” foryour generosity. To order, call 800-MDS(637)-0839 or order by mail with check enclosed to:
The MDS Foundation, Inc.4573 South Broad StreetSuite 150Yardville, NJ 08620
Thank you for your support!
23
Patient Contributions
PATIENT TESTIMONIALS
Our Patients Speak Out...“Thank you for all of your help.”We are moving along with good advice andinformation now and a lot less fear!
John Custer
“You have been so encouragingto Nancy and I over the years andyou have helped so many otherpatients.”Your referrals of other Jehovah’s Witnessesto me have been very encouraging to all ofus fighting MDS. I feel that I’ve known youfor years. Thanks for all your help over thelast almost 8 years that I’ve battled MDSsuccessfully. Keep up your good work.
Nancy and Kirby Stone
“It was so kind of you to callback when you did.”Life has been so challenging lately for anumber of reasons and you made me smile...For you to have acknowledged ourconversation and to have implemented ideasimmediately is truly commendable... Our firstintroduction to the nitty gritty of MDS was theunbelievable combination of your mostwelcome dissemination of informationcoupled with our relationship with Dr. Nimer...Jerry and I thank you and your entire staff whohas always been welcoming, informativeand generously supportive! Of course, wewould want to attend each and everysymposium that you sponsor; however, theone in Miami in particular pulls at our heartstrings due to Dr. Nimer’s participation and theall inclusive participation of quite a roster ofspecialists... In appreciation of your courtesyalways...and, the compassion each and everyone of you at your offices have alwaysextended to us... we are eternally grateful.
Randy and Jerry Genet
“THANK YOU!!!”
From the first meeting with Dr. Mesa I knewI was going to be provided excellent care and
understanding of me and my concerns. Heand the staff at Mayo have been great athelping me with my cancer treatments, fatigueand dealing with the impact on my life.
Diane Johnson
“Thanks so much for sendingthe slides from the presentationlast week.”Again I have to tell you how much Iappreciated having the opportunity toattend; it was educational and affirming,telling me that the treatment my mom isgetting is pretty much on target. My motherand father were very happy to hear that Iattended and they are really looking forwardto reading all the handouts that were sogenerously provided (thanks again for thesecond book!). My mom was also glad to besigned up as a member of the Foundationand looks forward to receiving in the mailwhatever is sent over the course of the year.
“Thank you and the Foundationfor the terrific work you are doing,especially with so little money.” Susan Luciano
“Tom and I were extremelyimpressed with our first MDS Conference.”We realized that there is so much we didn’tknow about MDS. You did a great job.Thank you.
Joan and Tom Weidenfeld
“I’d like to thank you so verymuch for a WONDERFUL andhelpful seminar.”I was sad to see the number of people therewith MDS... I wouldn’t wish this on my worstenemy. I think for the number of us, wefound that we “aren’t” alone.
Richard Brackett
MDS FOUNDATION STORE

24
PATIENT STORIES
When the Doctor Tells Your Wife, “You Have Blood Cancer”John Bugay
When your doctor tells you, “you haveblood cancer,” it’s certainly one of the majorchallenges in life. I was with my wifeBethany when she heard those words.
She is a fighter, and thanks to a bonemarrow transplant at Pittsburgh’s West PennHospital, most of the fight is behind us. But Iwanted to share, from a family member’spoint of view, what’s involved with thosechallenges.
The Road to LeukemiaOn an early summer day last year, Beth
had to call off work because she was simplytoo tired to get out of bed. That wasn’t likeher at all. A veteran of the Iraq war, who gotthere just a month after the lead invasion in2003, she was not a person to back downfrom any challenge.
For a little over a year, I’d been workingdays, and she had been working full-timenights. Our youngest daughter was inschool, and this work schedule enabled usto avoid daycare expenses. Plus, we neededtwo incomes to make up for the eightmonths I had been unemployed duringthe recession.
But over the previous several months,Beth had been coming home more tired thanusual, and complaining of headaches. Onthis Sunday morning, she came home andwent right to bed. That afternoon, she hadto call off work, something she never did.She couldn’t get out of bed. She had aheadache, body aches, swelling of the legs.Her supervisor said, “why don’t you go toMedExpress and get yourself checked?”So we did.
The practitioner on duty that nightexamined her, came back in and said, “Youneed to have some tests tonight that I can’tgive you. I’m going to send you up to theemergency room”.
They brought her in and took some moretests. Her hemoglobin level was 5.7,
dangerously low. (The normal range is12–15). They gave her some bloodtransfusions and admitted her for moretests. One of the nurses told us that if shehad cut herself and bled out to that level,she’d be unconscious. But because shedropped slowly to that level, her bodygradually adapted to it.
Challenge 1: The Diagnosis Takes Time
At the hospital, there were a number oftests, one of which was a bone marrowbiopsy. After all the tests that had been doneand the bone marrow biopsy was headed forthe lab, her hematology/oncology physiciansaid he thought that it was most likely a viralinfection causing her severe anemia.
A follow-up visit to our GP came backwith the news: “you have a form of bloodcancer”. It was awkward for him and anincredible shock to us. He gave us a copy ofthe lab results, which said “Acute MyeloidLeukemia (AML) is indicated.”
Her immediate thoughts turned toquestions such as, “what’s going to happento me physically?” And the spiritualquestions came up. “Am I prepared to die?”“Am I right with God?” As a family member,I was certainly concerned with her spiritual
well-being. But in addition, we have sixchildren, some of them young, and it wasimportant to me to understand how to moveforward through these challenges.
One of the hardest things about hearingthe diagnosis “you have a blood cancer” issimply putting it into perspective. I spentsome time Googling “AML”, and found someexcellent information, but it was certainlydiscouraging for us, because, as it turnedout, I wasn’t looking in the right ballpark.
But at that point, we didn’t even have agood understanding of the diagnosis.
Challenge 2: Understanding MDS and Leukemia
A few days later, a brief talk with ourhem/onc physician helped us to betterunderstand where Beth’s diagnosis fit withinthe world of leukemia. Science has greatlyenhanced the medical field’s understandingof the disease and its many differentvariations, especially from a geneticstandpoint, but that doesn’t make it anyeasier for the patient to understand what’sgoing on.
Nevertheless, it was a conversation thatenabled me to narrow the focus of mysearches.
There are four types of “blood cancers”:chronic and acute myeloid leukemia, andchronic and acute lymphoma. Of course,these are just terms that set the four typesin contrast with each other, for the purposeof categorization; there are really a numberof different subvariations in each of thesecategories, each with a broad range ofthings that can go wrong.
The particular group of leukemias thatBeth had, AML, is a very nasty one. Thepreliminary diagnosis turned out to havebeen for a “pre-leukemia” version, one ofthe “myelodysplastic syndromes” (MDS).
We were scheduled to see yet anotherspecialist, Dr. James Rossetti from WestPenn Hospital in Pittsburgh.
Bethany Bugay with husband John Bugay,March 2012, at a school event.

25
He told us that the diagnosis was prettyclear about “what” it was but somewhatinconclusive on the severity continuum.There is a “risk factor” chart called the IPSSchart, and Beth was either at a “high” risklevel (the highest of the four) for developingAML, or she actually had moved into AML.Dr. Rossetti did another bone marrowbiopsy, and admitted her to the hospital forfurther testing.
What came back was something calledCMML, or chronic myelomonocytic leukemia,a sort of hybrid kind of disease, betweenMDS and a “myeloproliferative” variation ofthe disease. More specifically, Beth wasfound to have “dysplastic CMML-2”, whichis not as bad as having the “myeloprolif-erative” version of CMML, but it is not agood thing.
Untreated, the prognosis for CMML wasa lifespan of about 12–24 months. Dr.Rossetti was very clear that because of herage (50) and relative good health, she was aprime candidate for what they called a “bonemarrow transplant” (BMT).
That in itself opened up a whole newworld to have to understand. As it turnedout, the hardest part was yet to come.
Challenge 3: The TreatmentAfter learning about the diagnosis, we
finally got a complete overview of thetreatment plan:
1. Two or three courses of Vidaza to try toslow or mitigate the effects of thedisease. It was key to prevent theCMML from developing into AML.
2. A search for a donor.3. Upon finding a donor, a period of
“conditioning,” intense chemo and full-body radiation, essentially to destroyher existing, damaged bone marrow.
4. The transplant itself, an infusion of adultstem cells from an anonymous donor.
5. Follow-up to check on the effects of thetransplant.
The expectation was that the Vidazawould reduce her overall “risk level” (that herdisease would progress into full-blown AML)and strengthen her body for “conditioning”,
which would kill most if not all of the cancer-causing function in her bone marrow.
The “transplant” would do two things.First, the new stem cells would take upresidence in her bones and repopulate hernow-destroyed bone marrow. Second, thedifferences in the DNA match would provide a“the graft-vs.-tumor effect” to suppress andkill any latent cancer function within her body.
Prior to the transplant, Beth’s possibleoutcomes were:
– 30% cure;– 20% immediate complications;– 15% major longer-term complications;– 35% chance of relapse.
Challenge 4: The Transplant ItselfBeth actually ended up having six
courses of Vidaza, which had the intendedeffect of controlling the spread of thedisease and actually reducing the cellularityin her bone marrow (from 50% down toabout 20%), partially doing the job of the“conditioning” step.
By November 9th a donor had beenselected, and on December 14, 2011, thestem cells from our adult female donor wereflown into Pittsburgh on an internationalflight. Beth received her transplant fromapproximately 9:45 pm until around 10:35.
This was “Day Zero” of her new life. Andwhile the transplant itself may have beenuneventful, as it turned out, there was aMRSA infection on her central line (used toinput the stem cells). So the night of thetransplant and for several days following,Beth experienced some of those “immediatecomplications”: a fever as high as 103°F,violent chills and shakes.
At one point, she said, “It hurts Johnny”.“What?” I said.“Everything,” she said.She was very frightened by the reaction.
They treated her with a number of fevermedications as well as ice packs.Meanwhile, I had taken off a great deal oftime from work to spend time with her in thehospital. During that time, I had to run backand forth between home, to check on thekids, and hospital, to be with Beth.
In all, she spent the better part of threemonths in the hospital, and in the followingweeks and months, Beth managed to getalmost every type of complication you canget, including the ongoing MRSA infection,and a number of viral infections (treatmentsfor which caused her body to swelluncomfortably with retained fluids), and shecame very close to death.
Fortunately, that phase came to an end.Ongoing Chimerism tests have confirmedthat her leukemia has not made a reap-pearance. As I write this, we are about 10months out from the transplant. And thegood news is, her body has healed overtime. I told her shortly after the transplant,“you may feel terrible, but you don’t haveleukemia any more”.
We are grateful to live at a time whenmedical science can offer such a promising,if complicated cure to what would surelyhave been a deadly disease.
Challenge 5: The Financial Complications
The various leukemia organizationsoffered plenty of helpful advice for dealingwith insurance and other financial issues,but there are no easy solutions. Myemployer, Black Box Corporation inPittsburgh, PA offered an excellent healthinsurance package. They also worked withme to obtain the necessary Family MedicalLeave Act (FMLA) time off.
Bethany with daughter Danielle (7), ouryoungest of six children, January 2012, at the height of complications.

26
Through this whole process, Beth did notwork because she was physically not strongenough, and I had to take a great deal oftime off, to take her back and forth todoctor’s appointments, and to spend time inthe hospital. That meant we were goingwithout of one of our two incomes for a longtime, and both of our two incomes for atleast several months.
Apart from the notion that my wife coulddie from this process, the financial challengeswere the most frightening for me. And Ihave to say, frankly, that most of thefinancial advice that was offered was, whilewell-intentioned, not very helpful.
After the transplant, the Social Workerat the Hospital worked with us to file forSocial Security disability payments. It didn’ttake long for this application to beprocessed (although you must wait fivemonths after your last day of work beforeyou can apply for it). This amounted to halfof what she had been earning whileworking full time. Beth has also applied tothe Veterans Administration for disabilitybenefits; as I write, this application is stillbeing processed some 10 months later.
But it was the people who knew us andwho we interacted with on a regular basiswho helped us the most.
The vast majority of the financial helpthat we received came from private donations,after I had asked for it. My co-workers tookup several collections. I had a personal blog,and I set up a Paypal account through whichwe could take private donations. Otherbloggers as well helped us make our appealfor financial help.
Some teachers in the local elementaryschool our daughter attends chipped in withsome fundraising activities. The schoolpurchased Christmas gifts for our family,and a “Bowling for Bethany” event in Aprilraised several thousand dollars for us.
Several churches made financial contri-butions to us. Our own home church wasprobably the biggest financial help throughoutthe process. In addition to helping us withrides to various appointments, they actuallypurchased a freezer for us, brought prepared,frozen meals on a regular basis, and made
our mortgage payment for us for the betterpart of a year.
Concluding Considerations“You have a blood tumor” is not the kind
of thing anyone wants to hear. In just the last10 years, advances in genetic science havegreatly increased what is known about thevarious types of leukemias, and their varioustreatments. And MDS, formerly simplyknown as “pre-leukemia,” itself nowunderstood to be a complex of maladies witha bewildering array of possible causes,symptoms, and treatment options.
Organizations such as the MDSFoundation, the Leukemia and LymphomaSociety, and the National Marrow DonorProgram (marrow.org) all provide informationthat helps people to sort through all theramifications of this unsettling diagnosis andgive hope to patients and their families.
The greatest amount of help still camefrom the doctors and nurses we dealt withon a daily basis, and the friends andchurches in our various communities whotook up our cause and spread the word,“Bethany Bugay, an Iraq war veteran, has aform of leukemia, and she needs your help.”
Thanks to their help, we now havehope for the future.
Don’t miss out on our MDSPatient Forum! This featurehosted by the MDS Foundationand monitored by healthprofessionals is a free onlinediscussion board of informationexchanged between patients,caregivers, and family members.
Connect today at www.mds-foundation.org
Connect on our PATIENT FORUM
Organizations such as the MDS Foundation... provideinformation that helps peopleto sort through all theramifications of this unsettlingdiagnosis and give hope...

27
My MDS StoryMy name is Keith Hennig and on February
22, 1993 my father died of acute leukemia.He had refractory anemia that summer andmy mother was a nurses’ aid and her friend,the local doctor, told her that this was whathis father had died from and to anticipate thatthis would be Dad’s last Christmas. Therefractory anemia would manifest into acuteleukemia and he would die very soon afterthat. I received this information after Christmasand Dad got sick in early February. His directinvolvement in our lives ended that February.However, as many people may haveexperienced, when you lose a parent you sortof re-evaluate your life and tell yourself thatwhen you get the chance to do things for thegroups that have helped or could have helpedyou make an effort to do so. My Dad’s firstwife died of breast cancer and he and mymom were always the neighborhood AmericanCancer Society drive leaders. You can sort ofsay that I have followed in their footsteps andhave done the same thing now that I ammarried and have a family of my own.
I live in a small town in Wisconsin, prettymuch like the one in Iowa I grew up in, and Ilove them both. This is the first place I havereally called home since leaving my parents. Iserved on several city boards and madefriends with other board members. One ofthose board members was Ron Carlsen. Ronand I served on the City Park Board for about5 years together. I eventually moved out of thecity limits but still live in the great community,and Ron and I go to the same church. Oneday he was on the prayer list, and when Ifound out it was MDS it was a real gut punch.I knew what comes next, you just die. So thenext summer when Ron was putting togethera benefit to sign up marrow donors, and wasstill alive and kicking, I went in and got on thelist as a donor and asked him how it worked.I found out about the amazing network ofMDS donors and the MDS Foundation. I haveto say I was and still am impressed.
If my father had gotten sick in 2010 ratherthan 1993, I am much more confident hewould be here today.
I like to volunteer. I am a Boy Scout andVenture Crew leader, a swim coach, and oneof the youth leaders at St. John’s LutheranChurch (sort of the un-churchy youth leader).This past summer while working on getting inbetter shape for my scouts’ backpacking tripto Glacier National Park, my wife managed toget me signed up for a local version of “TheBiggest Loser”. I needed it. Not being one tonot take advantage of a good opportunity, Igot sponsors to help me pay for what isactually a fairly expensive little weight lossprogram. Once involved in this program, Iwanted to see what I could do to raise somemoney for a good cause. The first one thatcame to mind was the MDS Foundation – thegroup that helped my friend Ron, and thatcould have quite likely saved my dad if they,and the technology, had been available then.I sent out emails to all the groups I help withand got several to pledge dollars for poundsof weight lost. With donations ranging from$.25 per pound to “Put me down and we’llsee how you do” I was eventually raisingmoney for MDS. I did not get involved with allthis to lose weight, just to get in shape tomake it over the mountains without keelingover. My idea of teaching boy scouts first aidis not having a heart attack 10 miles from thenearest road! However, I found that knowingthat I was finally able to do something forDad, even after he was dead, was prettyinspiring. I had lost about 9 lbs. before I gotinvolved with the other “Fat Losers” (I thoughtit was a funny nickname but I am not sure allmy compatriots were amused) and then lost
another 51.4 lbs., 21.13% of my body weightduring the competition. I managed to raisejust over $1,000.00 for MDS. I have a coupleof friends with the audacity to challenge methat they will double their pledge if I keep theweight off for the next 6 months! Well, I amdown a couple more pounds and don’t planon stopping my fitness journey. I am signedup to do a 5K on Thanksgiving Day. I figurethat way I can have mashed potatoes andgravy with my turkey! Dad liked taters andgravy and I think he would appreciate that.
Everybody dies but not everybody trulylives. My father died when he was 68 yearsold and I was 26. He had made it to 68 withan 8th grade education and left my mothera widow for the second time in her life. Sincehe died she has not wanted for anything.Finances have never been a worry for her. Toput it into perspective, Dad heated our homewith wood that he cut, and after his death ittook almost 8 years before Mom burnedthrough all he had cut, split and prepared.She spends her time enjoying the love andrespect of her children, grandchildren, greatgrandchildren, and other friends andrelatives. That is an impressive legacy and Ihave a responsibility to live up to it.
Thank you MDS Foundation for beingthere for all the parents and for their childrenwho will get to have another Christmas withone another as a result of your work. On aslightly more personal note, thank you forhelping me to eliminate some of thehelplessness, both mine and that of thefamilies of those stricken with MDS. I prefer alife sentence to a death sentence any day!
This is a “before” and “after” shot of me.
This is a picture of Dad and my brothers and Icutting wood with an antique gasoline enginewith a buzz saw that he restored and loved.
FAMILY STORIES

28
International MDSFoundation NurseLeadership BoardErik Aerts, RNNurse ManagerUniversity Hospital ZürichInternal Medicine-OncologyStem Cell Transplantation Ward and
Polyclinic Hematology/Apherese/Stem Cell Transplantation
Zürich, Switzerland
Louise Arnold, RNClinical Nurse SpecialistDepartment of HaematologySt James’s Institute of Clinical OncologyLeeds, United Kingdom
Angelika Bitter, RNUniversitätsklinikum Carl Gustav CarusDresden, Germany
Claudia Boglione, RNStem Cell Transplantation Nurse MentorUniversity Hospital CareggiFlorence, Italy
Núria Borràs, RNHemato-Oncology NurseICMHO Hospital ClinicBarcelona, Spain
Karen Campbell, BSc(Hons), RN, MN, PGcertMacmillan Lecturer/Practitioner
in Cancer NursingTeaching FellowEdinburgh Napier UniversityEdinburgh, Scotland, United Kingdom
Debbie Carr, RN, Ba OH&SNursing Unit ManagerHaematology Day UnitCalvary Mater HospitalNewcastle, Australia
Nicole Crisp, MN, NPNurse Practitioner, HematologyUniversity of Alberta HospitalEdmonton, Alberta, Canada
Erin Demakos, RN, CCRNAdministrative DirectorMyelodysplastic Disease Center
and MPD ProgramMount Sinai School of MedicineNew York, New York, United States
Corien Eeltink, RN, MA ANPNurse PractitionerDepartment of HaematologyVU University Medical CenterAmsterdam, The Netherlands
Lenn Fechter, RNNurse Coordinator, Department of HematologyStanford Hospital and ClinicsStanford, California, United States
Janet Hayden, RN, BSc(hons), MPHMyeloid Clinical Nurse SpecialistHaematological MedicineKings College NHS Foundation TrustLondon, United Kingdom
Emily A. Knight, RN, BSN, OCNHematology Registered Nurse CoordinatorMayo ClinicScottsdale, Arizona, United States
Sandra E. Kurtin, RN, MS, AOCN, ANP-CHematology/Oncology Nurse PractitionerThe University of Arizona Cancer CenterAdjunct Clinical Assistant Professor of NursingClinical Assistant Professor of MedicineUniversity of ArizonaTucson, Arizona, United States
Petra Lindroos Kolqvist, RNTeamleader, Anemia Leukemia TeamDepartment of Hemathology and CoagulationSahlgrenska University HospitalGoteborg, Sweden
Arno Mank, RNPresident EBMT Nurses GroupEuropean Group for Blood and
Marrow TransplantationNurse ResearcherAcademic Medical CentreAmsterdam, The Netherlands
Cindy Murray RN, MN, NP-adultMalignant Hematology, Princess Margaret HospitalClinical AppointeeUniversity of Toronto, Lawrence S. Bloomberg Faculty of NursingToronto, Ontario, Canada
Phyllis Paterson, RN, RSCN, Dip OncMDS Clinical Nurse SpecialistCambridge University Hospitals
NHS Foundation TrustAddenbrooke’s HospitalCambridge, United Kingdom
Jean A Ridgeway, MSN, APN, NP-C, AOCNLeukemia/Stem Cell Transplant
Nurse PractitionerUniversity of Chicago Medical CenterDepartment of Hematology OncologyChicago, Illinois, United States
Jayshree Shah, APN-C, AOCN, RN, MSN, BSN, BS, CCRPNurse PractitionerJohn Theurer Cancer CenterHackensack University Medical CenterHackensack, New Jersey, United States
Natalie Singer, MSc, RN,BSc(Hons) Macmillan Haemato/Oncology CNSThe Beatson West of Scotland
Cancer CentreGlasgow, Scotland, United Kingdom
Mary L. Thomas, RN, MS, AOCNHematology Clinical Nurse SpecialistVA Palo Alto Health Care SystemPalo Alto, California, United StatesAssociate Clinical ProfessorUniversity of California, San FranciscoSan Francisco, California, United States
Sara M. Tinsley, ARNP, AOCNMalignant Hematology
Nurse PractitionerH. Lee Moffitt Cancer CenterTampa, Florida, United States
Nursing in MDS
New Resourcesfor NursesWe are pleased to announce thelaunch of our Nursing Portal on the MDSFoundation website, a free resourcedeveloped to provide the nursingcommunity with materials to helpcommunicate with and support theirpatients with MDS. Access http://www.mds-foundation.org/nursing-portal toview our comprehensive set ofresources. Here you can view thepresentation slides and audio presen-tations of our educational symposiumpresented in New Orleans.
29
Would you like your treatment center to become part of the referral system for MDS patients and be designated as a Center of Excellence? To be recognized as a Center of Excellence, an institution must have the following:■ An established university (or equivalent) program■ Recognized morphologic expertise in MDS■ Available cytogenetics and/or molecular genetics
UNITED STATESARIZONAMayo Clinic HospitalScottsdale, ArizonaRuben Mesa, MD/James Slack, MD/Raoul Tibes, MD, PhD
The University of ArizonaCancer CenterTucson, ArizonaRavi Krishnadasan, MO, FACP
CALIFORNIACedars-Sinai Medical CenterUCLA School of MedicineLos Angeles, CaliforniaH. Phillip Koeffler, MD
City of Hope National Medical CenterDuarte, CaliforniaStephen J. Forman, MD
Moores Cancer Center at theUniversity of California, San DiegoRafael Bejar, MD, PhDPeter Curtin, MD
Stanford University Medical CenterStanford, CaliforniaPeter L. Greenberg, MD
UCLA Center for Health SciencesLos Angeles, CaliforniaGary J. Schiller, MD
University of Southern CaliforniaKeck School of MedicineLos Angeles, CaliforniaCasey L. O’Connell, MD
FLORIDAAll Children’s HospitalSt. Petersburg, FloridaGregory Hale, MD
Mayo ClinicJacksonville, FloridaJames M. Foran, MD Alvaro Moreno-Aspitia, MD
Sylvester Comprehensive Cancer CenterUniversity of Miami Miller School of MedicineMiami, FloridaStephen D. Nimer, MD
University of Florida Shands HospitalGainesville, FloridaChristopher R. Cogle, MD
University of South FloridaH. Lee Moffitt Cancer CenterTampa, FloridaAlan F. List, MD
GEORGIAEmory Winship Cancer InstituteEmory University School of MedicineAtlanta, GeorgiaAmelia Langston, MD
The Blood and Marrow Transplant Program at Northside HospitalAtlanta, GeorgiaAsad Bashey, MD
ILLINOISLoyola University ChicagoCardinal Bernardin Cancer CenterMaywood, IllinoisScott E. Smith, MD, PhD
Robert H. Lurie Comprehensive Cancer Center ofNorthwestern UniversityFeinberg School of MedicineChicago, IllinoisOlga Frankfurt, MD
Rush University Medical CenterChicago, IllinoisJamile Shammo, MD
University of Chicago Medical CenterChicago, IllinoisRichard A. Larson, MD
INDIANAIndiana University Simon Cancer CenterIndianapolis, IndianaLarry Cripe, MDHamid Sayar, MD, MS
MARYLANDJohns Hopkins University School of MedicineBaltimore, MarylandSteven D. Gore, MD
University of MarylandGreenebaum Cancer CenterBaltimore, MarylandMaria R. Baer, MD
MASSACHUSETTSChildren’s Hospital BostonBoston, MassachusettsInga Hofmann, MD
Dana-Farber Cancer InstituteBoston, MassachusettsRichard M. Stone, MD/David P. Steensma, MD
Tufts University School of MedicineTufts Medical CenterBoston, MassachusettsKellie Sprague, MD
MICHIGANBarbara Ann KarmanosCancer InstituteWayne State UniversityDetroit, Michigan Charles A. Schiffer, MD
William Beaumont HospitalCancer CenterRoyal Oak, MichiganIshmael Jaiyesimi, DO
MINNESOTAMayo ClinicRochester, MinnesotaMark R. Litzow, MD
University of Minnesota Medical CenterFairview University of Minnesota Medical SchoolMinneapolis, Minnesota Erica D. Warlick, MD
MISSOURIWashington University School of MedicineSiteman Cancer CenterSt. Louis, MissouriJohn F. DiPersio, MD, PhD
NEBRASKAUniversity of Nebraska Medical CenterOmaha, NebraskaLori Maness, MD
NEW JERSEYThe Cancer Center of Hackensack University Medical CenterHackensack, New JerseyStuart Goldberg, MD
■ Ongoing research, includingInstitutional Review
■ Board–approved clinical trials
■ Documentation of peer-reviewedpublications in the field
Please contact the Foundation for further information and an application form for your center.
The following centers have qualified as MDS Centers of Excellence:
NEW YORKAlbert Einstein College of MedicineCancer CenterBronx, New YorkAmit Verma, MD
Columbia University Medical CenterNew York, New YorkAzra Raza, MD
Memorial Sloan-Kettering Cancer CenterNew York, New YorkVirginia M. Klimek, MD
Monter Cancer Center/NSLIJ Cancer InstituteLake Success, New YorkSteven L. Allen, MD
Mount Sinai School of MedicineNew York, New YorkLewis R. Silverman, MD
New York Medical College/ Westchester Medical CenterZalmen A. Arlin Cancer CenterValhalla, New YorkKaren Seiter, MD
Roswell Park Cancer CenterBuffalo, New YorkJames E. Thompson, MD
University of Rochester Medical CenterRochester, New YorkJane L. Liesveld, MD
Weill Medical College of Cornell UniversityNew York Presbyterian HospitalNew York, New YorkEric J. Feldman, MD
NORTH CAROLINADuke University Medical CenterDurham, North CarolinaCarlos M. deCastro, MD
Wake Forest UniversitySchool of MedicineComprehensive Cancer CenterWinston-Salem, North CarolinaBayard L. Powell, MD
OHIOCleveland Clinic FoundationTaussig Cancer CenterCleveland, OhioJaroslaw Maciejewski, MD, PhD

30
The Ohio State ComprehensiveCancer Center, James Cancer Hospital and Solove Research InstituteColumbus, OhioAlison R. Walker, MD
PENNSYLVANIAThe Western Pennsylvania Cancer InstitutePittsburgh, PennsylvaniaJames M. Rossetti, DO
Thomas Jefferson UniversityKimmel Cancer CenterPhiladelphia, PennsylvaniaEmmanuel C. Besa, MD
University of Pennsylvania Cancer CenterPhiladelphia, PennsylvaniaSelina Luger, MD
TENNESSEEVanderbilt University Medical CenterNashville, TennesseeMadan Jagasia, MDStephen Strickland, MD
TEXASCancer Care Centers
of South TexasSan Antonio, TexasRoger Lyons, MD
Southwest Regional Cancer CenterAustin, TexasRichard Helmer, III, MD
University of TexasMD Anderson Cancer CenterHouston, TexasGuillermo Garcia-Manero, MDHagop Kantarjian, MD
WASHINGTONFred HutchinsonCancer Research CenterUniversity of WashingtonSeattle Cancer Care AllianceSeattle, WashingtonJoachim Deeg, MD/Elihu Estey, MD
WASHINGTON, DCGeorgetown University HospitalLombardi Comprehensive Cancer CenterWashington, D.C.Catherine Broome, MD
WISCONSINMedical College of WisconsinBone Marrow Transplant ProgramMilwaukee, WisconsinParameswaran Hari, MD
University of WisconsinMadison Medical SchoolMadison, WisconsinMark B. Juckett, MD
OUTSIDE THE UNITED STATESARGENTINASanatorio Sagrado del CorazónBuenos Aires, ArgentinaMarcelo Iastrebner, MD
AUSTRALIAPeter MacCallum Cancer InstituteUniversity of MelbourneEast Melbourne, AustraliaJohn F. Seymour, MD
University of TasmaniaRoyal Hobart HospitalHobart, Tasmania, AustraliaRaymond M. Lowenthal, MD
AUSTRIAUniversity Hospital of InnsbruckInnsbruck, AustriaReinhard Stauder, MD
Medical University of ViennaVienna, AustriaPeter Valent, MD
BELGIUMAZ Sint-Jan AVBrugge, BelgiumDominik Selleslag, MD
University Hospital LeuvenLeuven, BelgiumMichel Delforge, MD, PhD
BRAZILAC Camargo Hospital –Cancer CenterSão Paulo, BrazilLuiz Fernando Lopes, MD, PhD
Hemocentro da UNICAMPUniversity of CampinasCampinas, Brazil Irene Lorand-Metze, MD
Servico de Hematologia do Hospital das Clinicasda Faculdade de Medicina da Universidadede São PauloSão Paulo, BrazilElvira R.P. Velloso, MD, PhD
Universidade Federal de CearáCeará, BrazilSilvia Maria M. Magalhães, MD, PhD
Universidade Federal de São PauloSão Paulo, BrazilMaria de Lourdes Chauffaille, MD, PhD
CANADAPrincess Margaret HospitalToronto, Ontario, CanadaKaren Yee, MD
Toronto SunnybrookRegional Cancer CentreToronto, Ontario, CanadaRichard A. Wells, MD
University of TorontoHospital for Sick ChildrenToronto, Ontario, CanadaYigal Dror, MD
CHINAInstitute of Hematology and Blood Diseases HospitalChinese Academy of Medical SciencesTianjin, ChinaZhijian Xiao, MD
CZECH REPUBLICInstitute of Hematology& Blood TransfusionPrague, Czech RepublicJaroslav Cermák, MD, PhD
DENMARKOdense University HospitalThe University of Southern DenmarkOdense, DenmarkGitte Birk Kerndrup, MD
Rigshospitalet National University HospitalCopenhagen, DenmarkLars Kjeldsen, MD, PhD
University of ÅrhusThe University HospitalÅrhus, DenmarkMette Skov Holm, MD, PhD
FRANCECentre Henri BecquerelRouen University School of MedicineRouen, FranceAspasia Stamatoullas, MD
Centre Hospitalier Universitaire (CHU) de Angers Service des Maladies du SangAngers, FranceNorbert Ifrah, MD
Centre Hospitalier Universitaire(CHU) de GrenobleGrenoble, FranceJean-Yves Cahn, MD
Centre Hospitalier Universitaire (CHU) de LimogesHôpital DupuytrenLimoges, FranceDominique Bordessoule, MD
Centre HospitalierUniversitaire (CHU) de NancyNancy, FranceAgnés Guerci-Bresler, MD, PhD
Centre Hospitalier Universitaire (CHU) de Tours Höpital BretonneauTours, FranceEmmanuel Gyan, MD, PhD
Hôpital Avicenne/University Paris XIIIBobigny, FrancePierre Fenaux, MD
Hôpital Cochin/University Paris VParis, FranceFrancois Dreyfus, MD
Hôpital Saint Louis/University Paris VIIParis, FranceChristine Chomienne, MD, PhD
Institut Paoli-CalmettesMarseille, FranceNorbert Vey, MDService des Maladies du SangHôpital Claude HuriezLille, FranceBruno Quesnel, MD
GERMANYGeorg-August-Universität GöttingenGöttingen, GermanyDetlef Haase, MD, PhD
Hannover Medical SchoolMedizinische Hochschule HannoverHannover, GermanyArnold Ganser, MD
Heinrich-Heine Universität DüsseldorfUniversity HospitalDüsseldorf, GermanyUlrich Germing, MD
Johann Wolfgang Goethe UniversitätFrankfurt Main, GermanyGesine Bug, MD
Klinikum Rechts der IsarTechnical University of MunichMunich, GermanyKatharina Götze, MD
MLL Münchner Leukämielabor Munich, GermanyTorsten Haferlach, MD
St. Johannes HospitalHeinrich-Heine Universität Duisburg, GermanyCarlo Aul, MD, PhD
31
Albert-Ludwigs-Universität FreiburgFreiburg, GermanyMichael Lübbert, MD, PhD
Universität HamburgHamburg, GermanyNicolaus Kröger, MD, PhD
UniversitätsklinikumCarl Gustav CarusDresden, GermanyUwe Platzbecker, MD
University Children’s HospitalFreiburg, GermanyCharlotte Niemeyer, MD
University of CologneCologne, GermanyKarl-Anton Kreuzer, MD
Universitätsklinikum Benjamin FranklinBerlin, GermanyOlaf Hopfer, MD
University Hospital MannheimMannheim, GermanyWolf-Karsten Hofmann, MD, PhD
GREECEG. Papanikolaou GeneralHospital of ThessalonikiUniversity of ThessalonikiThessaloniki, GreeceCharikleia Kelaidi, MD
Patras University HospitalPatras, GreeceArgiris Symeonidis, MD
University of Athens Laikon HospitalAthens, GreeceNora Viniou, MD
University General Hospital AttikonAthens, GreeceVassiliki Pappa, MD
HUNGARYSemmelweis University School of MedicineBudapest, HungaryJudit Várkonyi, MD, PhD
INDIATata Medical Centre Kolkata, IndiaCol (Dr.) Deepak Kumar Mishra, MD
Tata Memorial HospitalMumbai, IndiaPurvish Parikh, MD
IRELANDAdelaide and Meath HospitalDublin, IrelandHelen Enright, MD
ISRAELTel-Aviv Sourasky Medical CenterTel-Aviv, IsraelMoshe Mittelman, MD
Chaim Sheba Medical CenterTel Hashomer, IsraelDrorit Grizim Merkel, MD
ITALYCentro di RiferimentoOncologico di Basilicata (CROB)Rionero in Vulture (PZ), ItalyPellegrino Musto, MD
Istituto di EmatologiaUniversita’ Cattolica Sacro CuoreRoma, ItalyGiuseppe Leone, MDMaria Teresa Voso, MD
University of FlorenceAzienda OSP CareggiFlorence, ItalyValeria Santini, MD
University of Pavia School of MedicineFondazione IRCCS Policlinico San MatteoPavia, ItalyMario Cazzola, MD
JAPANKyoto University HospitalKyoto, JapanAkifumi Takaori, MD
Nagasaki University HospitalSchool of MedicineAtomic Bomb Disease InstituteNagasaki City, JapanMasao Tomonaga, MD
Nippon Medical SchoolTokyo, JapanKiyoyuki Ogata, MD, PhD
Saitama International Medical CenterSaitama Medical UniversityHidaka, Saitama, JapanAkira Matsuda, MD
Tokyo Medical CollegeTokyo, JapanKazuma Ohyashiki, MD, PhD
KOREACatholic Blood and Marrow Transplantation CenterThe Catholic University of KoreaSeoul, KoreaYoo-Jin Kim, MD
Seoul National University HospitalSeoul National University College of MedicineSeoul, KoreaDong Soon Lee, MD, PhD
THE NETHERLANDSUniversity Medical CenterNijmegen St. RadboudNijmegen, The NetherlandsG.A. Huls, MD
Vrije Universiteit Medical CenterAmsterdam, The NetherlandsGert J. Ossenkoppele, MD, PhD
POLANDJagiellonian University Collegium MedicumKraków, PolandAleksander Skotnicki, MD, PhD
PORTUGALHospital de Santa MariaLisbon, PortugalJoao F. Lacerda, MD
SAUDI ARABIAKing Faisal Specialist Hospital & Research CentreRiyadh, Saudi ArabiaMahmoud Deeb Aljurf, MD
King Khaled University HospitalKing Saud UniversityRiyadh, Saudi ArabiaAk Almomen, MD
SINGAPORESingapore General HospitalSingaporeLay-Cheng Lim, MD
SOUTH AFRICAUniversity of Cape TownGroote Schuur HospitalCape Town, South AfricaNicolas Novitzky, MD, PhD
SPAINHospital Universitario de SalamancaSalamanca, SpainConsuelo del Cañizo, MD, PhD
Hospital Universitario La FeValencia, SpainMiguel A. Sanz, MD, PhD
Hospital UniversitarioVall d’Hebron Laboratorio del Citologia-CitogéneticaBarcelona, SpainMaria Teresa Vallespi-Sole, MD, PhD
SWEDENKarolinska InstitutetHuddinge University HospitalStockholm, SwedenEva Hellström-Lindberg, MD, PhD
TAIWANNational Taiwan University HospitalTaipei, TaiwanHwei-Fang Tien, MD, PhD
THAILANDKing Chulalongkorn Memorial HospitalPathumwan, Bangkok, ThailandTanin Intragumtornchai, MD
TUNISIAHospital Aziza OthmanaTunis, TunisiaBalkis Meddeb, MD
TURKEYAnkara University School of Medicine HospitalAnkara, TurkeyOsman Ilhan, MD
UKRAINEResearch Center for Radiation MedicineKiev, UkraineDimitry Bazyka, MD
UNITED KINGDOMAberdeen Royal InfirmaryAberdeen University School of MedicineForesterhill, Aberdeen, ScotlandDominic Culligan, MD
Addenbrooke’s HospitalCambridge University HospitalsNHS Foundation TrustCambridge, United KingdomAlan J. Warren, PhD, FRCP, FRCPath
King’s College London &King’s College HospitalLondon, United KingdomGhulam J. Mufti, DM, FRCP, FRCPath
Queen Elizabeth HospitalUniversity Hospital BirminghamNHS TrustBirmingham, United KingdomCharles Craddock, MD
Radcliffe Hospitals and University of OxfordOxford, United KingdomParesh Vyas, MD
Royal Bournemouth HospitalBournemouth, United KingdomSally Killick, MD
St. James’s University HospitalSt. James’s Institute of OncologyLeeds, United KingdomDavid T. Bowen, MD
University Hospital of WalesCardiff, WalesJonathan Kell, MD

32
Announcing New Clinical TrialsNAME OF INSTITUTION:Novartis Pharmaceuticals
TRIAL NUMBER: NCT00940602Title of Trial or Description:Myelodysplastic Syndromes (MDS) EventFree Survival With Iron Chelation TherapyStudy (TELESTO) A Multi-center, Randomized, Double-blind, Placebo-controlled Clinical Trial ofDeferasirox in Patients With Myelodys-plastic Syndromes (Low/Int-1 Risk) andTransfusional Iron Overload
Currently Recruiting Participants.The primary purpose of this study is toprospectively assess the efficacy and safetyof iron chelation therapy with deferasiroxcompared to placebo in patients withmyelodysplastic syndromes (low/int-1 risk)and transfusional iron overload.
Contact the Novartis Clinical TrialsHotline at 800-340-6843 or go towww.clinicaltrials.gov for additionalinformation and to view the active sites.
New ResearchProtocol ListingNATIONAL CANCER INSTITUTE TRIALS
As we go to press the National CancerInstitute (NCI) has listed more than 100clinical trials that focus on myelodysplasticsyndromes. Full study information on thesetrials is available at www.cancer.gov. Thisinformation includes basic study information,study lead organizations, study sites, andcontact information. To access the information:■ Log on to www.cancer.gov■ Click on “Search for Clinical Trials”■ Click on “Type of Cancer” and type in
‘myelodysplastic syndromes’■ Hit search
This search will provide you with all thetrials currently underway in MDS. You mayalso sort by trials that only focus on treatmentor trials that only focus on supportive care.
To view listings of additional studiesyou can log onto www.clinicaltrials.gov.For telephone support, call the NationalCancer Institute at 1-800-4-CANCER.
Information on Clinical Trials
NAME OF INSTITUTION:Celgene CorporationTRIAL NUMBER: NCT01029262Title of Trial or Description:A Study of Lenalidomide Versus Placeboin Subjects With Transfusion DependentAnemia in Low Risk Myelodysplastic Syn-drome (MDS) Without Del 5Q (MDS-005)
Currently Recruiting Participants.The primary purpose of this study is tocompare the efficacy of Lenalidomide(Revlimid®) versus placebo in achievingred blood cell transfusion independencein the overall study population and in apre-specified subgroup of patients withan erythroid differentiation geneexpression signature predictive ofLenalidomide response.
Access
www.clinicaltrials.govfor additional information.
Access is Key to Treatment The MDS Foundation Will Provide Location Information for the Rigosertib (ESTYBON®
ON 01910.Na) MDS Clinical Trial
ONTIME: Study Description (ON 01910.Na TRIAL INMYELODYSPLASTIC SYNDROME)
A phase III study of rigosertib(Estybon®, ON 01910.Na) in myelo-dysplastic syndrome (MDS) patients afterVidaza® (azacitidine) or Dacogen®
(decitabine) treatment. Rigosertib is anovel mitotic inhibitor of PLK and PI-3kinase pathways.
Learn more at
ASH 2012Georgia World
Congress CenterAtlanta Georgia
December 8 –11thVisit BOOTH 2307!
The ONTIME MDS clinical trial is accessibleat a wide variety of locations and keymedical centers.
To find a trial site in your area wherethis study is being conducted, please visithttp://mdsclinicaltrial.com/oncology-trials/ontime-study/site-locations/.
Consider the ONTIME Trial for theTreatment of MDS Patients afterAzacitidine or Decitabine
– Accrual of patients is ongoingIf you are a physician or nurse and would
like to refer a patient for enrollment into thisclinical trial please contact the MDSFoundation at 800-MDS(637)-0839.
Learn More –More information can be found at www.mdstrial.com orclinicaltrials.gov, the identifier is NCT01241500

33
Contributions to the MDS Foundation
Thank You!Elizabeth PecknoldVancouver, BC, Canada
Milford & Zita DesenbergSarasota, FL
Mariana DagattiNewton, MA
James DowdStuart, FL
Hildred C. PehrsonLivermore, CA
Eileen DunneKingston, MA
Peter FinielloJamaica, NY
Thomas & Joanne KubiakCentennial, CO
Lorenzo & Filomena DiurnoWilton, CT
Jim & Chris MaierPalos Verdes Pnsla, CA
Audrey H. GabelSalinas, CA
Ross Jackson, Carmi, IL
FINRA Employees, WPG SOLUTIONS,INC. on behalf of FINRATacoma, WA
Meredith BruceMill Valley, CA
Dr. Kathleen De LorenzoMaumelle, AR
Larry SchneiderAventura, FL
Stephanie Ross-EvansSuperior, WI
The Kaliher FamilyBlaine, MI
Lynn RossNew Brighton, MN
John VoglandHudson, WI
Ernest UlrichNew York, NY
Mary Ellen KellyInverness, IL
West Boca Raton Comm. High SchoolThe School District of Palm BeachCounty, FloridaBoca Raton, FL
Marjourie L. MannCarla MercadoSan Antonio, TX
Ronald J. VanskiverNothingham, MD
Frederic LeverenzGilbert, AZ
Jay Biggs, Greenwood, DE
Jerry OliverGranville, OH
Nathan CedarsStephenville, TX
Stephen and Catherine Heft
Blair and Noreen NovyBoca Raton, FL
John M. Sweet and Nicola BoydHeadwaters FarmMiddlebrook, VA
James B. HarrisBarrie, ON, Canada
Lorraine B. GleixnerGreenwood, IN
Stephanie Ross-EvansSuperior, WI
Delos R. GoddardColorado Springs, CO
Kevin J. LawlorWarrington, PA
Yilmaz HassanHowell, NJ
Wayne SetherSt. Paul, MN
Augustus Harrison TullossRocky Mount, NC
West Boca Raton Comm. High School Boca Raton, FL
Jalil FardaneshFolsom, CA
Grifols Therapeutics, Inc., RTPNorth Caroline
Tracey L. Hill
Alexandra SchwartzNew York, NY
Audrey HassanHowell, NJ
Marilyn J. LitvinFramingham, MA
Mary BensonOrem, UT
John WilhelmiBoston, MA
Adept Consumer TestingBeverly Hills, CA
Isabel Calderon
John CazierIrvine, CA
Leopold LeBlancSilver Springs, FL
William A. RobertsNaples, FL
Rose RobustelliniLodi, NJ
Florence GilmartinSanford, FL
Maureen Pavlik, Odell, NE
Barbara LeonardoSebastian, FL
David and Carol UsherColchester, VT
Gifts to the FoundationThe MDS Foundation relies entirely on gifts and membership fees to further its work.
We would like to acknowledge the generosity of the following individuals and organizationsthat have recently provided gifts to the Foundation:
34
Jonathan A. SteeleNorth Charleston, SC
Delos R. GoddardColorado Springs, CO
Joseph J. CostaSleepy Hollow, NY
Robert CohnPalm Beach Gardens, FL
David HenselOak Forest, IL
Ross Jackson, Carmi, IL
Angela SudolElmwood Park, NJ
D.O. Totty, Collierville TN
Gerald C. ClementsNaples, ME
Robert Bryson, San Diego, CA
Leonard BiniFallbrook, CA
Judith Klick, Myrtle Beach, SC
Adrian E. RiccaWeirton, WV
Edward Carmody, Carson, CA
Thomas J. O’KeefeNewport Beach, CA
Joan R. Dorf, Rockville, MD
Clement & Joan RancourtPlantsville, CT
Caterina CaronJacksonville, FL
Marilyn S. GouldSt. Petersburg, FL
Joni Sitko, Elysburg, PA
Robert M. WesterDestin, FL
Richard A. OsborneKingwood, TX
Ron Ferrara, Pasadena, CA
Sheila MartinFairfax, VA
Ernest Ulrich, New York, NY
Armando R. RuizHuntington Beach, CA
V.R. “Spin” Nelson, Lakewood, CO
Allison MyslinskiMaryland Heights, MO
William Shulevitz, New York, NY
Chris and Tara KillgorePortland, OR
Ronald L. RapaportPotomac, MD
Pat Shirley, Golden CO
Edward DanielsRaleigh, NC
Mary ImperioliSandy Hook, CT
Carol FullSpringfield, VA
Nancy D. ArtleyTowson, MD
Tom MastandreaLincolnshire, IL
Michael & Sharon TierConshohocken, PA
Ina Block, Napa, CA
Rita Paul, Naples, FL
Martina WiedmayerCollegeville, PA
Marjourie L. Mann
Karen Werner, West Islip, NY
Jerry McMurrayKnoxville, TN
William VaultWashington, DC
Margaret H. WiedmayerPhiladelphia, PA
Daniel and Andrea ReeseCataula, GA
Nora Wrzesinski, Greenville, NC
Jean C. Forsell, Forest Lake, MN
Duane R. BogenschneiderMequon, WI
Tom and Joanne KubiakCentennial, CO
Stanley Rudick, Sparks, MD
Roger R. Hewitt, Smithville, TX
Redencion Bote LustreThe Villages, FL
R. George and Genevieve AnguloSun Lakes, AZ
Eunice Edgington, Rohnert Park, CA
Victoria SadlerHarwinton, CT
Joe Artuso, Berwyn, PA
Frances Gillen, Sparta, TN
Jalil FardaneshFolsom, CA
Marlene Strohl, San Marcos, CA
Congregation (Jacobs Ladder)Maple Glen, PA
Richard and Carolyn SendlerColumbia, SC
Barbara Bryson YoungWaxahachie, TX
Emily RubensteinWinter Park, FL
Gayle Leitman, Mtn. Brook, AL
Margaret HaskellGrantham, NH
Mariette Van EngelenThornton, CO
Clement & Joan RancourtPlantsville, CT
Tracey L. Hill
Steven Pepperman, New York, NY
Dr. Sol and Trudy KliozeEast Lyme, CT
Steve Gold, Glenmont, NY
Rob Skirboll, Greensboro, NC
Colleen Vevang
NationalNurses Day
A tribute gift has been made tothe MDS Foundation in honor of
Nurse Sandra E. Kurtin
Donated by Max AtwellTucson, AZ
who appreciates your skill,care and commitment.

35
In Memoriam
Vanessa CatanzaroTownship of Washington, NJ
A memorial fund has been established in the name of
Doctor Vincent J. CatanzaroDonations have been made in Dr. Catanzaro’s memory by:
Abbie C. CarterPhiladelphia, PA
A memorial fund has been established in the name of
Mr. Roy C. CarterDonations have been made in Mr. Carter’s memory by:
Mark and Leah Ralph, Vergennes, IL
A memorial fund has been established in the name of
Mr. Joseph “Joe” CalandroDonations have been made in Mr. Calandro’s memory by:
Claire-Elizabeth SloanPortland, OR
A memorial fund has been established in the name of
Mr. Clem CahallDonations have been made in Mr. Cahall’s memory by:
Candice Stark, Los Altos, CA
A memorial fund has been established in the name of
Ms. Harriet BrennerDonations have been made in Ms. Brenner’s memory by:
William Hanson, Eagan, MN
A memorial fund has been established in the name of
Mr. Jack BrennanDonations have been made in Mr. Brennan’s memory by:
Judy ArmstrongHamden, CT
A memorial fund has been established in the name of
Mr. John M. BlasiakDonations have been made in Mr. Blasiak’s memory by:
Dona Sue Black CoolColumbia, MO
A memorial fund has been established in the name of
Mr. Wayne Vincent BlackDonations have been made in Mr. Black’s memory by:
Ruth NicollSouth Ealing, London, UK
A memorial fund has been established in the name of
Ms. Bea BesetteDonations have been made in Ms. Besette’s memory by:
Paula Gevaudan, Annapolis, MD
A memorial fund has been established in the name of
Mr. Wayne J. BenderDonations have been made in Mr. Bender’s memory by:
Ricky Barnhart, Hilliard, OH
A memorial fund has been established in the name of
Mr. John L. Barnhart, Jr.Donations have been made in Mr. Barnhart’s memory by:
Mary Barr, Gardendale, AL
A memorial fund has been established in the name of
Mr. Freddie Arnold “Jerry” BarrDonations have been made in Mr. Barr’s memory by:
Peter and Mary Navarro, Downingtown, PA
A memorial fund has been established in the name of
Mr. William BallDonations have been made in Mr. Ball’s memory by:
Mary Warner-Bartella, Sun City, AZ
A memorial fund has been established in the name of
Mrs. Cathy Jean AvantsDonations have been made in Mrs. Avants’ memory by:
Jerry and Renee Green, Wildwood Crest, NJ
A memorial fund has been established in the name of
Aunt SaraDonations have been made in Aunt Sara’s memory by:
Robert and Barbara McGhee, Ocala, FL
A memorial fund has been established in the name of
Dr. John D. AndersonDonations have been made in Dr. Anderson’s memory by:
Robert and Theresa Sheldon, Geneva, OH
A memorial fund has been established in the name of
Mr. Edward AgoliaDonations have been made in Mr. Agolia’s memory by:
Widener UniversityChester, PA
Victoria AlfeBrookhaven, PA
Joseph and Lisa WolfingtonPhiladelphia, PA
Frank & Dolores CastellucciPhiladelphia, PA
A memorial fund has been established in the name of
Mr. Patrick M. AlfeDonations have been made in Mr. Alfe’s memory by:
Rich and Eileen WeaverCoastesville, PA
Fred and Regina HelmEast Fallowfield, PA
Marge KellyLansdowne, PA
George and Nancy HasselGlenolden, PA
Robert and Marie RedfernBrookhaven, PA
Jim and Brenda BarryPinopolis, SC
Victoria BudreauSummerville, SC
Ruby H. PreacherCharleston, SC
Billy and Sharon CatoMoncks Corner, SC
A memorial fund has been established in the name of
Mr. Jesse H. “Red” BrownDonations have been made in Mr. Brown’s memory by:
Bill and Betty MilnerCharlotte, NC
Cohen and Susie GaskinsAlvin, SC
Richard W. Salmons, Jr.Charleston, SC
John and Lila SmithBonneau, SC
Ronnie and Elaine HewittBonneau, SC
Curt and Connie KruegerLincolnshire, IL
A memorial fund has been established in the name of
Mr. Robert BrodyDonations have been made in Mr. Brody’s memory by:
Bruce and Ede WeinerHouston, TX
John and Mary WhiteAndover, KS
Heribert and Inge BlumenfurthScottsdale, AZ
Don and Arlene OgdenBranson, MO
Lindsay & Marilyn MillerScottsdale, AZ
William and Barbara PorterTopeka, KS
Jeffrey and Betty DeanScottsdale, AZ
Ernie and Wynona LorensonGower, MO
Roger and Carolyn BenefielWichita, KS
Robin BumgarnerScottsdale, AZ
Jim and Jacqueline SkeltonLee’s Summit, MO
Ken and Elender JahdeSavannah, GA
Larry and Rosalee WilsonSedalia, MO
Charles GuessSt. Joseph, MO
Ron and Marcia BrownWichita, KS
Kathleen RileScottsdale, AZ
David and Jill PattersonScottsdale, AZ
A memorial fund has been established in the name of
Mrs. Sandra Lynn “Sandy” BolarDonations have been made in Mrs. Bolar’s memory by:
Marc and Amy RileCincinnati, OH
Gary and Suzanne HattenBethany, MO
James and Janis ErlandLawrence, KS
Weldon and Neva WhiteakerSchaumburg, IL
Kent and Martha WhiteCedarburg, WI
Audrey E. ThorkelsonPhoenix, AZ
Elyzbeth EllmerGilbert, AZ
Jack and Kay Ann FeidenWichita, KS
Dick Anderson & Fran BeldenWichita, KS
Charles and Rita McCallMarcia Graul, Lincoln, NE
Larry & George Ann SeymourBella Vista, AR
Janice E. StitesWichita, KS
Gene McMichaelKansas City, MO
Julia MacLachlanPrairie Village, KS
Jean ScottTaipa, MACAU
Ray and Susan FritzemeyerWichita, KS
Lois HubbardWichita, KS
Dean and Paula SquiresMidlothian, VA
A memorial fund has been established in the name of
Mr. George J. BalintDonations have been made in Mr. Balint’s memory by:
Stephen and Barbara WheelerBuckingham, VA
Karen Boyd, St. Louis, MO
A memorial fund has been established in the name of
Mr. Joe BoydDonations have been made in Mr. Boyd’s memory by:
Dennis & Terri HirschbrunnerColumbus, NE
A memorial fund has been established in the name of
Mrs. Ruth BorchardtDonations have been made in Mrs. Borchardt’s memory by:
Lawrence DolanHelena, MT

William M. Harris, Burlington, NC
A memorial fund has been established in the name of
Mrs. Peggy CruseDonations have been made in Mrs. Cruse’s memory by:
Barbara Hunt,Wolfeboro, NH
A memorial fund has been established in the name of
Ms. Marie CooneyDonations have been made in Ms. Cooney’s memory by:
Peter McMahonLake Katrine, NY
BAE Systems, Endicott, NY
A memorial fund has been established in the name of
Ms. Elizabeth FlissDonations have been made in Ms. Fliss’ memory by:
Arden Down, New York, NY
A memorial fund has been established in the name of
Ms. Yeta FinkeDonations have been made in Ms. Finke’s memory by:
Alison McDowell, Vincennes, IN
A memorial fund has been established in the name of
Mrs. Edith Mae FarrisDonations have been made in Mrs. Farris’ memory by:
Patricia Everett, Wilmington, NC
A memorial fund has been established in the name of
Mr. Alfred J. EverettDonations have been made in Mr. Everett’s memory by:
Barbara YarbroughArcadia, CA
A memorial fund has been established in the name of
Mrs. Winnie GreenDonations have been made in Mrs. Green’s memory by:
Sara Edith Gallagher, Dayton, OH
A memorial fund has been established in the name of
Ms. Jennifer Sharon Gallagher-WelchDonations have been made in Ms. Welch’s memory by:
Ilene Lynch, Plantation, FL
A memorial fund has been established in the name of
Mr. Jake Edward FrougDonations have been made in Mr. Froug’s memory by:
Wm. Mark FriedmanDelray Beach, FL
A memorial fund has been established in the name of
Mr. Sam FriedmanDonations have been made in Mr. Friedman’s memory by:
Edward and Judith Lasher, Akron, OH
A memorial fund has been established in the name of
Mr. Michael FriedmanDonations have been made in Mr. Friedman’s memory by:
James E. Frye, Palestine, TX
A memorial fund has been established in the name of
Ms. Elaine FryeDonations have been made in Ms. Frye’s memory by:
Ekaterini Fokas, Astoria, NY
A memorial fund has been established in the name of
Mr. Andreas FokasDonations have been made in Mr. Fokas’ memory by:
Joseph and Julia Vassalluzzo
A memorial fund has been established in the name of
Ms. Eleanor Z. FalcoDonations have been made in Ms. Falco’s memory by:
Brian and Laura BeckerWest Hartford, CT
A memorial fund has been established in the name of
Mr. Arthur H. “Bushy” EpsteinDonations have been made in Mr. Epstein’s memory by:
Rodney and Joni Falk, Newton, MA
A memorial fund has been established in the name of
Mr. Leonard DicksteinDonations have been made in Mr. Dickstein’s memory by:
Roberto Degl’InnocentiMiami, FL
A memorial fund has been established in the name of
Mr. Alessandro Degl’InnocentiDonations have been made in Mr. Degl’Innocenti’s memory by:
M.S. DuFore, San Mateo, CA
A memorial fund has been established in the name of
Mr. Robert DuForeDonations have been made in Mr. DuFore’s memory by:
William McGahernCenter Moriches, NY
A memorial fund has been established in the name of
Mr. Edward S. DaleDonations have been made in Mr. Dale’s memory by:
Holly CrawfordWebster, NY
Cary and Suzy JensenRochester, NY
Deirdre FlynnRochester, NY
Diane CaselliPittsford, NY
Robert and Christine KalbFairport, NY
Sue StewartVictor, NY
Louis and Kathy ParkerRochester, NY
A memorial fund has been established in the name of
Mr. Murray CrumminsDonations have been made in Mr. Crummins’ memory by:
Bud & Roberta GeisenheimerFort Lee, NJ
Susan WormerVictor, NY
Nicholas and Janette NicksonRochester, NY
Susan LeahyRochester, NY
Richard FeldmanRochester, NY
George and Jennifer CleverStockton, NY
Aileen ShinamanRochester, NY
Diana HerbeCincinnati, OH
A memorial fund has been established in the name of
Mrs. Evelyn ForneyDonations have been made in Mrs. Forney’s memory by:
Forest Park Women’s ClubCincinnati, OH
Susan CameraShort Hills, NJ
Paul & Kathleen LeonardelliAndover, NJ
Jeff and Peggy MetzgerBangor, PA
Northwest SCORE 24Morristown, NJ
Thomas and Patricia ZickMount Sinai, NY
Harold and Jessie JenkinsStanhope, NJ
Monroe and Arlene SpiegelVerona, NJ
A memorial fund has been established in the name of
Mr. Alfred A. GianniMr. Gianni’s family made the decision to honor their lovedone by establishing this fund to be used for research.
Donations have been made in his memory by:
David M. IndykeHackettstown, NJ
Ajay and Rajni MisraLloyd Harbor, NY
Maryellen CheastyCornwall, PA
Tom and Sheila ThomasDekalb, IL
Patricia ThomasEast Stroudsburg, PA
John and Margaret PostTranquility, NJ
Darlene R. MontanaEaston, PA
Mountain 1st Bank & Trust CompanyHendersonville, NC
J. Martin RicheyBoston, MA
A memorial fund has been established in the name of
Mr. James “Jim” David GarrickDonations have been made in Mr. Garrick’s memory by:
Gene and Mary ShumateSuwanee, GA
Gary and Hazel NaborsEasley, SC
Julie DwyerElk Grove Village, IL
Gene and Gaile BorchartArlington Heights, IL
A memorial fund has been established in the name of
Mr. James W. FrejdDonations have been made in Mr. Frejd’s memory by:
Susan F. Burgess and StaffElmhurst, IL
Howard RennerElk Grove Village, IL
Paula BozzettiNew Lenox, IL
36
Florence C. SmithMillsboro, DE
Ruth Hudson, Millsboro, DE
Ann T. BradleyGeorgetown, DE
Theresa GibbonsPalm Harbor, FL
Lisa HuttoTarpon Springs, FL
Debbie ReynoldsHalethorpe, MD
A memorial fund has been established in the name of
Ms. Sarah T. CecilDonations have been made in Ms. Cecil’s memory by:
Jenny’s Friends & Co-WorkersGambrills, MD
Karen MolloySykesville, MD
Karen HamiltonCatonsville, MD
Marilyn NewtonCatonsville, MD
Barbara A. RobinsonParkton, MD

37
Shelley Lovell, Portland, OR
A memorial fund has been established in the name of
Mrs. Rebecca H. HubbardDonations have been made in Mrs. Hubbard’s memory by:
Eric and Alexis ScherrerMuncie, IN
A memorial fund has been established in the name of
Mr. Robert Michael HillgroveDonations have been made in Mr. Hillgrove’s memory by:
Carl and Bonnie HoseaErlanger, KY
Nancy S. Hewison, West Lafayette, IN
Marilyn J. Litvin, Framingham, MA
A memorial fund has been established in the name of
Mr. Barry LevinDonations have been made in Mr. Levin’s memory by:
Orville and Judy McKinney, Holiday Island, AR
A memorial fund has been established in the name of
Mrs. Arlene Marie LennoxDonations have been made in Mrs. Lennox’ memory by:
Leopold LeBlanc, Silver Springs, FL
A memorial fund has been established in the name of
Mrs. Edith LeBlancDonations have been made in Mrs. LeBlanc’s memory by:
Motorcycle Club of Sun City Carolina Lakes, Indian Land, SC
A memorial fund has been established in the name of
Mr. Roy KussnerDonations have been made in Mr. Kussner’s memory by:
Dr. and Mrs. Geoffrey and Sandy Goldworm, Cherry Hill, NJ
A memorial fund has been established in the name of
Dr. Leonard KleimanDonations have been made in Dr. Kleiman’s memory by:
Irma Blumenthal, Longboat Key, FL
A memorial fund has been established in the name of
Ms. Bunny KendallDonations have been made in Ms. Kendall’s memory by:
David Karam, Tully, NY
A memorial fund has been established in the name of
Mrs. Kathryn KaramDonations have been made in Mrs. Karam’s memory by:
Jimmy and Cecilia Bingham, Calhoun, LA
A memorial fund has been established in the name of
Mrs. Sallie Ammons JonesDonations have been made in Mrs. Jones’ memory by:
Nina Caplin and Laurie Edelman, New York, NY
A memorial fund has been established in the name of
Mr. James JonesDonations have been made in Mr. Jones’ memory by:
Mary Paris, Alexandria, VA
A memorial fund has been established in the name of
Ms. Chantal JaouenDonations have been made in Ms. Jaouen’s memory by:
Geoffrey and Sandy Goldworm, Cherry Hill, NJ
A memorial fund has been established in the name of
Mr. George IsenbergDonations have been made in Mr. Isenberg’s memory by:
Gerald and Barbara ValleeGallipolis, OH
A memorial fund has been established in the name of
Mrs. Rosenna Marie (Huff) Irwin Donations have been made in Mrs. Irwin’s memory by:
Woodloch Pines Inc. andthe Kiesendahl FamilyHawley, PA
Peter J. O’BrienMount Pocono, PA
Bob and Dru ScekeresMechanicsburg, PA
The Armillei FamilyOrlando, FL
Michael and Vincetta NestorLake Ariel, PA
Kevin and Dr. Kristen HollshwandnerEast Stroudsburg, PA
A memorial fund has been established in the name of
Mr. Ronald LoganDonations have been made in Mr. Logan’s memory by:
Frank and Michele CaliDunmore, PA
Norma Pritchard and FamilyHonesdale, PA
Glenair, Inc., Glendale, CA
Gordon, Maryann and Natalie OlsommerGreentown, PA
Jim and Phyllis CunninghamClarks Summit, PA
Madeleine Reilly, Macungie, PA
RBLA of PA, Inc.Stroudsburg, PA
John and Martha HelgersonReston, VA
Phillip and Charlotte CallifVienna, VA
A memorial fund has been established in the name of
Mrs. Barbara Pilch-Kuett LatchfordDonations have been made in Mrs. Latchford’s memory by:
COFCU Accounting Dept.Alexandria, VA
CommonWealth One FCUAlexandria, VA
John StackBasking Ridge, NJ
A memorial fund has been established in the name of
Mr. Francis “Al” LagowskiDonations have been made in Mr. Lagowski’s memory by:
Mr. and Mrs. Edward RonkEdison, NJ
John and Mary SchererGranger, IN
Kroc Institue of International Peace StudiesUniversity of Notre DameNotre Dame, IN
MA Class of 2012University of Notre DameNotre Dame, IN
Mr. amd Mrs. M.J. Van BruaeneGranger, IN
Catherine GoforthClarksville, IN
Joel Lamp and Rebecca GoforthBurlingame, CA
Adam Good, Granger, IN
Sandra J. HollowellGranger, IN
Maryann PajotSouth Bend, IN
Anne F. RiordanSouth Bend, IN
Robert and Linda Howerton, Carterville, IL
Thomas and Cheri GoforthThree Forks, MT
A memorial fund has been established in the name of
Mr. Patrick B. LaakeDonations have been made in Mr. Laake’s memory by:
Don & Gail HemlerUnion, MI
Carol ZirkWaukegan, IL
A memorial fund has been established in the name of
Mr. Francis B. JeddaDonations have been made in Mr. Jedda’s memory by:
Virginia JeddaBlacksburg, VA
Diane WeinreichNew York, NY
A memorial fund has been established in the name of
Ms. Miriam Hyams’ BrotherDonations have been made in Ms. Hyams’ Brother’s memory by:
Doctor and Mrs. Daniel SilbertPort Washington, NY
Culver Center PartnersMichigan LLCCulver City, CA
A memorial fund has been established in the name of
Mr. HockerDonations have been made in Mr. Hocker’s memory by:
Peter and Julie ByrneBirmingham, MI
P.J. ThibodeauRoyal Oaks, MI
Katharine Pease, McFarland, WI
A memorial fund has been established in the name of
Mr. James P. HellenbrandDonations have been made in Mr. Hellenbrand’s memory by:
Steven and Rebecca Heggemann Healthcare Fraud ShieldEmployees, Elkridge, MD
A memorial fund has been established in the name of
Ms. Patricia Anne HeggemannDonations have been made in Ms. Heggemann’s memory by:
Alessio Filippi, Los Angeles, CA
A memorial fund has been established in the name of
Ms. Susan Hartman FilippiDonations have been made in Ms. Filippi’s memory by:
Christine Cosenza, Branford, CT
A memorial fund has been established in the name of
Mrs. Ann Leslie Cosenza HallbergDonations have been made in Mrs. Hallberg’s memory by:
Harold C. RyderMechanicsburg, PA
A memorial fund has been established in the name of
Mr. Jesse GunderDonations have been made in Mr. Gunder’s memory by:
Geoffrey and Sandy Goldworm, Jupiter, FL
A memorial fund has been established in the name of
Mr. Willy GrossmanDonations have been made in Mr. Grossman’s memory by:

38
Carol Ann Weiss, Staten Island, NY
A memorial fund has been established in the name of
Ms. Ruth Glogow LublinDonations have been made in Ms. Lublin’s memory by:
Jerry and Liddy LatterNorthport, NY
Heidi McGoughCommack, NY
Brice FukumotoSummit, NJ
Michael and Mary MartinPort Jefferson, NY
Bill and Nancy MallioWinchester, MA
A memorial fund has been established in the name of
Mr. Ralph ManheimDonations have been made in Mr. Manheim’s memory by:
Bensonnhurst OPD/SouthBeach Psychiatric CenterBrooklyn, NY
Sheila CavoorisSt. James, NY
Jens MatthesNew York, NY
Richard and Marie HamiltonPhiladelphia, PA
David and Karen ViarCentreville, VA
David BarberoCentreville, VA
Richard AvidanoLevittown, NY
A memorial fund has been established in the name of
Mr. Robert LongDonations have been made in Mr. Long’s memory by:
Tedd & Linda Avidano HopeNaples, FL
Michael & Sherry RoithmayrSeffner, FL
Mariko Chouinard, Topanga, CA
Susan Martin, Herndon, VA
Ben HoleCollege Park, MD
A memorial fund has been established in the name of
Mrs. Rosalie MarcusDonations have been made in Mrs. Marcus’ memory by:
Donna HowertonSebring, FL
A memorial fund has been established in the name of
Mrs. Patricia J. MarshDonations have been made in Mrs. Marsh’s memory by:
Richard A. FehrmanSebring, FL
John FehrmanSebring, FL
A Tribute to ViViva Lee Barnard McDaniels1922–2012
Vi was born on October 6,1922 in Paris,Arkansas and came to Merced, CA withMom, Dad, Brother and Sister in 1931. Viattended Merced schools and graduatedfrom Merced High School in 1941.
Vi married almost immediately afterhigh school and worked in the retailsector during the war. From this marriage,Vi had a daughter and a son. She alsowas a volunteer airplane spotter for thethen Merced Army Airfield.
Vi trained as a dental assistant andworked in that field during the 50’s and60’s. That period was before x-rayeducation and the assistant would stay inthe exam room while taking the x-rays.She often mentioned that while takingx-rays on small children, she would holdthe film in the child’s mouth while the x-rayswere taken.
Vi and I were married in January, 1962,and although she was thirteen years olderthen I, everyone said and still says, thatwe were the perfect couple who adoredeach other. We must have been – as themarriage lasted over fifty years. What ajoy she was.
Although we never had children of ourown, there was often a baby or young child,
Vi passed away on June 10, 2012,peacefully and with family at her bedside,of sepsis brought on by a constantbladder infection and the transformationof the MDS into leukemia.
What else did this amazing woman doin her life time? She painted in oil,landscapes and animals mostly, withcows a big favorite. She worked inceramics and was a gourmet cook.
She was a first class seamstress whomade most of her own clothes and theclothes of whatever child was in thehouse at the time.
She was a hospital “Pink Lady” and atrout fisherman who could really catch them.
She was an antiques collector and aNotary Public who never charged for herservices as “people need the money fortheir family.”
And, in her last years, she knitted over150 caps for the young cancer patientsat Children’s Hospital, Central California“because there was a need.”
That’s what she did.
I will close with a short piece by Edna St. Vincent Millay:
“Where you used to be, there is a hole in the world, which I findmyself walking around in thedaytime, and falling in at night. I miss you like hell.”
Phil McDaniels, Merced, CA
who had been neglected in some fashion, inour home for periods of up to a year.
In my profession as a police investigator,we had the opportunity to live in severallocations in California, and I retired in SanLuis Obispo, CA. Shortly after, we movedback to Merced to be closer to Vi’s family.
In late 2006, Vi was found to have a largeaortic aneurysm and, after multiple CTscans and x-rays, and multiple refusals bycardiothoracic surgeons for surgery, shewas accepted into a trial at Tucson FranciscoMedical Center. That brought about more CTscans and x-rays, both before and aftersurgery on December 7, 2007, during whichshe had two Bates Graft Stents placed in theaorta. She often said it was a wonder shedidn’t glow in the dark.
In April, 2010, Vi was hospitalized withpneumonia and found to be anemic. Shereceived two units of blood along withantibiotics for the pneumonia. In May, shewas again found to be anemic and wasreferred to an oncology center with the resultsfinding she had MDS. We often wondered ifall the x-ray exposure she had contributed tohaving MDS. Vi had a round of chemo andher blood counts improved for severalmonths before starting a downhill slide.
M.J. Hollinger, Willamina, OR
A memorial fund has been established in the name of
Mrs. Viva Lee Barnad McDanielsDonations have been made in Mrs. McDaniels’ memory by:
Phil McDaniels, Merced, CA

39
Crown Realty Professionals, Inc.Conyers, GA
Charlie and Audrey WolfeSavannah, GA
Jimmy and Patsy WhitlockLilburn, GA
William M. HarrisBurlington, NC
A memorial fund has been established in the name of
Mrs. Peggy MozzoneDonations have been made in Mrs. Mozzone’s memory by:
Ron and Ann MickweeFremont, CA
Cathleen JonesAtlanta, GA
Harry and Deanna CrewsSnellville, GA
Joseph CohenNew York, NY
Albert and Tina Small, Bethesda, MD
A memorial fund has been established in the name of
Mr. NathanDonations have been made in Mr. Nathan’s memory by:
Robert Parker and Nancy GordonChevy Chase, MD
Dr. and Mrs. Sol and TrudyKlioze, East Lyme, CT
A memorial fund has been established in the name of
Mr. Hersh MuchnickDonations have been made in Mr. Muchnick’s memory by:
Irv and Sheila GoldmanS Burlington, VT
Stewart and Karen Hani,Rachael and Lauren CohenWynnewood, PA
Alexander & Marjorie MoonCalgary, AB, Canada
A memorial fund has been established in the name of
Mr. Garvin MorrisDonations have been made in Mr. Morris’ memory by:
Art and Bonnie HosieRegina, SK, Canada
Ernie and Diane AvramRegina, Sask, Canada
Robert MinardCentral Point, OR
Dennis WilsonBattle Ground, WA
Mr. & Mrs. Charles PickettMedford, OR
Dick and Terry BonneyTiller, OR
Bob and Barbara GilkeyCentral Point, OR
Randy LoydJacksonville, OR
Marshall & Kathy CymbalukEverett WA
Larry MartinCentral Point, OR
Tom and Cynthia PricePost Falls, ID
James & Kathleen WilliamsLongview, WA
Marylee VuylstekeBeaverton, OR
A memorial fund has been established in the name of
Mr. Richard B. “Dick” MoormanDonations have been made in Mr. Moorman’s memory by:
James and Nancy PrussackPost Falls, ID
Larry and Kiki HousePost Falls, ID
Mitch and Karen WindsorAnthem, AZ
Thomas Jarrett, Jr.San Antonio, TX
Rommel MirandaNaperville, IL
Richard and Linda CarneySalem, OR
Donald and Janet RuettgersStayton, OR
John W. KronenbergerCentral Point, OR
John D. HilkeyCentral Point, OR
Jim and Helen RuettgersStayton, OR
Larry and Judy HarringtonDorris, CA
Dick FitzgeraldMedford, OR
Mary Miyawaki, Honolulu, HI
A memorial fund has been established in the name of
Ms. Mary MiyawakiDonations have been made in Ms. Miyawaki’s memory by:
Bernard, Will, Tim, John M, Larry, Kevin, Tom, Todd and ChrisAnnapolis, MD
A memorial fund has been established in the name of
Mr. Howard McCannDonations have been made in Mr. McCann’s memory by:
Karen Mattern, Spokane Valley, WA
A memorial fund has been established in the name of
Mr. Floyd H. MatternDonations have been made in Mr. Mattern’s memory by:
Margaret Errico, Stone Ridge, VA
A memorial fund has been established in the name of
Mr. Anthony MassoneDonations have been made in Mr. Massone’s memory by:
CB and Emily GebhardSt. Louis, MO
Brock M. LutzSaint Louis, MO
Les and Wendy BorowskySt. Louis, MO
David E. StedelinCentralia, IL
D. M. and Karen ShuppTomball, TX
C. W. Holmes, St. Louis, MO
David E. StedelinCentralia, IL
A memorial fund has been established in the name of
Mr. A. Clay MollmanDonations have been made in Mr. Mollman’s memory by:
Jerry and Joan KaskowitzSt. Louis, MO
Barbara Steps, St. Louis, MO
Carol RossChesterfield, MO
Roy Pfautch, St. Louis, MO
Phil and Caroline LoughlinCambridge, MA
James and Mary BarnesSt. Louis, MO
Walter and Marilyn SharkoJacksonville, FL
Julie Linihan, St. Louis, MO
Dawn R. WayJanesville, WI
A memorial fund has been established in the name of
Mr. Don MoeDonations have been made in Mr. Moe’s memory by:
Truax Fire DepartmentMadison, WI
Phyllis L. LeeMadison, WI
Joyce Campbell, Newton, NJ
James and Patricia CoatesApollo Beach, FL
Jack Harris, Lafayette, NJ
Pauline SeretisLedgewood, NJ
Steve Baldwin & Eileen WyssHackettstown, NJ
A memorial fund has been established in the name of
Mr. George MilonasDonations have been made in Mr. Milonas’ memory by:
Jeffrey and Kitty PhilipsWest Palm Beach, FL
Jeff and Jennifer CzyzewskiPonte Vedra Beach, FL
Patricia, Judy, Valerie, Nyle,Marriette, Christa, Zabrina,Odetta, Melani, Karen, Vivian,Reggie and TimJacksonville, FL
Cumberland Insurance GroupBridgeton, NJ
Linda D’AmbrosioOradell, NJ
Independent InsuranceAgents & Brokers of New Jersey, Inc.Trenton, NJ
A memorial fund has been established in the name of
Mrs. Minnie F. MerulloDonations have been made in Mrs. Merullo’s memory by:
Jeffrey and Elizabeth BoltonRochester, MN
Plymouth Rock Assurance of NJBerkeley Heights, NJ
Associated Risk Managersof New Jersey, Latham, NY
Brad and Alison PatkochisPittstown, NJ
Andrew and Kay MyersLancaster, PA
A memorial fund has been established in the name of
Mr. Charles R. MertzDonations have been made in Mr. Mertz’ memory by:
Richard and Claire AshbyLititz, PA
Arthur and Dottie Ponzio, Galloway, NJ
Degia Piano StudioShakopee, MN
A memorial fund has been established in the name of
Mrs. Ruth MerfeldDonations have been made in Mrs. Merfeld’s memory by:
Robert and Clare KreuserShakopee, MN
Nancy A. Depaz, Burnsville, MN
Dick Rank and Mary KanakSt. Paul, MN
Eric and Sandra HorsmanCottage Grove, MN
A memorial fund has been established in the name of
Mrs. Maria- Luise “Diane” McDonaldDonations have been made in Mrs. McDonald’s memory by:
Deb NormanNorthfield, MN
Eugene and Christa TunickRexford, MT
Leslie HightPinehurst, NC
A memorial fund has been established in the name of
Mr. Edward L. McCarthyDonations have been made in Mr. McCarthy’s memory by:
Michael and Kristen McCarthyElk Grove, CA
Jon and Cheryl BearBurke, VA
A memorial fund has been established in the name of
Mrs. Marlene MaunderDonations have been made in Mrs. Maunder’s memory by:
Robert CoffmanWoodbine, MD
Patti O’BrienGeneva, IL
Phil and Colleen VevangBuffalo Grove, IL
Keith and Doris NicodemusNaperville, IL
Navistar Foundation,Navistar, Inc.Lisle, IL
Michael and MarySatterthwaite, Worth, IL
Thom and Linda BondWinfield, IL
A memorial fund has been established in the name of
Mr. Ronald H. MartensonDonations have been made in Mr. Martenson’s memory by:
Jason SandersChicago, IL
Jack and Mary RidgesNaperville, IL
Carrie Galles, Clive, IA
Catherine RooneyChicago, IL
Charles W. FultzLisle, IL
Mel and RosemarieDi Carlo-CottoneWest Chicago, IL
Carol Welch, Elmhurst, IL

40
Geoffrey and Sandy Goldworm, Cherry Hill, NJ
A memorial fund has been established in the name of
Mr. Jerome RichterDonations have been made in Mr. Richter’s memory by:
Korn/Ferry InternationalMcLean, VA
The Robison Family FundGabriel and Lillian BatarsehFlorence, SC
John and Judy HarrisonAustin, TX
A memorial fund has been established in the name of
Mr. Jon Arthur ReuscherDonations have been made in Mr. Reuscher’s memory by:
Colleagues of Mark BatarsehReston, VA
David and Cathy ChaseFalls Church, VA
Leanne WellsLaurel, MD
Doris Romas and FamilyBrazil, IN
Dawn Maeder, Brazil, IN
Mr. & Mrs. Leroy KerstiensFerdinand, IN
Ginny Hayes-BennettIndianapolis, IN
Leroy KerstiensFerdinand, IN
A memorial fund has been established in the name of
Mr. Edward J. RuheDonations have been made in Mr. Ruhe’s memory by:
Justin SchaferMeridianville, AL
Jerry and Kay PovazsayTerre Haute, IN
J and Goldie Hicks, Brazil, IN
Thomas C. MartinRockville, TN
Shawn and Chris BeckerFerdinand, IN
Eddy J. Rogers, Jr.Wimberley, TX
A memorial fund has been established in the name of
Mr. Rudy Rodriguez, Jr.Donations have been made in Mr. Rodriguez’ memory by:
Edward Main, Houston, TX
Ann Morgan, Houston, TX
Caroline WithersFayetteville, NC
Alan and Ruth GreenthalJohn Hardey, Palatine, IL
Rick and Cindy BeauregardLucas, TX
Brent and Leslie HradekGrapevine, TX
A memorial fund has been established in the name of
Mr. Ronald D. PiacentiDonations have been made in Mr. Piacenti’s memory by:
Matt and Joni SickingRichardson, TX
Paul Chow, Plano, TX
Robbie Marshall, Dallas, TX
Kevin and Carla LibbyDallas, TX
Diane Menza,Oak Park, IL
Libby York, Dallas, TX
Mary MillsHendersonville, TN
Charley and Betty HayesCoffeyville, KS
Gloria BuchananSeabrook, TX
A memorial fund has been established in the name of
Mrs. Lovella Ann Hayes RalstinDonations have been made in Mrs. Ralstin’s memory by:
Robin RolstonIrvine, CA
Royanne Holy, Houston, TX
Dr. Frost, Dr. Safdar and thePulmonary Hypertension StaffHouston, TX
Ralph and Maxine MarshallSpringfield, VA
Elizabeth BolanPurcellville, VA
A memorial fund has been established in the name of
Mr. Elmer (Bill) Rawls, Jr.Donations have been made in Mr. Rawls’ memory by:
Therese KalbacherCenterville, OH
Betty J. SoedlerLocust Grove, VA
Barbara MillerLocust Grove, VA
Iris MunizWood Ridge, NJ
A memorial fund has been established in the name of
Mr. Johnny RamosDonations have been made in Mr. Ramos’ memory by:
Everett and Lois HornigWood-Ridge, NJ
Renaissance Mens Club, Manchester, NJ
A memorial fund has been established in the name of
Mr. Donato ParisiDonations have been made in Mr. Parisi’s memory by:
Jim and Debbie Madonna, Oak Ridge, NJ
A memorial fund has been established in the name of
Mrs. Cecilia A. OtterbeinDonations have been made in Mrs. Otterbein’s memory by:
Francis and Jacquelyn Imada, Kailua, HI
A memorial fund has been established in the name of
Mr. Chris OkuharaDonations have been made in Mr. Okuhara’s memory by:
James J. O’Donnell, III, Ocean City, NJ
A memorial fund has been established in the name of
Mrs. Arlene O’DonnellDonations have been made in Mrs. O’Donnell’s memory by:
Margaret O’Connor, Lewisburg, PA
A memorial fund has been established in the name of
Ms. Barbara K. O’ConnorDonations have been made in Ms. O’Connor’s memory by:
Joan E. Nichols, Millis, MA
A memorial fund has been established in the name of
Mr. Kenneth NicholsDonations have been made in Mr. Nichols’ memory by:
Bonnie A. StewartEast Lansing, MI
John and Barbara MartelSt. Clair Shores, MI
Phyllis R. WeirSarasota, FL
Dorothy SprovieroRochester Hills, MI
Bill and Joanne SissonRochester, MI
Nancy MooneyhamRochester Hills, MI
Larry and Marilyn MillsRoyal Oak, MI
Christine M. PelleritoFrerndale, MI
A memorial fund has been established in the name of
Mr. Vincenzo “Vince” PelleritoDonations have been made in Mr. Pellerito’s memory by:
Brett and Mary FeolaBeverly Hills, MI
Toby and Kim TheodorePlymouth, MI
Theresa ZiskeSt. Clair Shores, MI
Gregory and Leah LeflerChesterfield, MI
Mary HickeyShelby Twp., MI
Thomas & Denise WurmlingerChesterfield, MI
Brian and Judith MeiningerCasco, MI
Frederick & Mary Ann MakinenAlgonac, MI
Concetta Pellerito, Richmond, MI
Lauren and Thomas BakerAltamonte Springs, FL
A memorial fund has been established in the name of
Mr. Victor J. PalumboDonations have been made in Mr. Palumbo’s memory by:
Joan PalumboCrawfordville, FL
Victor Andre PalumboCrawfordville, FL
John and Audrey BaglianiTowson, MD
Moe LiuThe City College of New YorkNew York, NY
A memorial fund has been established in the name of
Dr. Antonio K. OlmedoDonations have been made in Dr. Olmedo’s memory by:
Marcia WolfSparks, MD
Credo Capital ManagementBaltimore, MD
Orems Elementary School Faculty & Staff, Baltimore, MD
Anthony WickenheiserJoppatowne, MD
Brian Schmitt, Pasco, WA
Dennis and Bev ChristineArvada, CO
Bill and Karen KisicAurora, CO
Pam BartholomayLittleton, CO
Linda ArnesonLittleton, CO
Rose Community FoundationDenver, CO
Joan E. PayneGolden, CO
Carol S. HealdDenver, CO
Joyce A. TiptonWestminster, CO
Ronald E. StanislawLakewood, CO
Marilyn E. CoombsDenver, CO
Vicki Greivel, Golden, CO
Frances F. MyersArvada, CO
Shari A. RaymondMorrison, CO
Mark and Marilyn NorwalkDenver, CO
Judy AltenbergEnglewood, CO
Lisa Cohn, Denver, CO
Ed and Elizabeth TomsicDenver, CO
New West Physicians (Friends)Golden, CO
A memorial fund has been established in the name of
Mrs. Julie O’HanlonDonations have been made in Mrs. O’Hanlon’s memory by:
Catherine HodgeTampa, FL
Corbin and Marcel OttoLittleton, CO
Brown and Caldwell Denver Office, Golden, CO
Bill PedrickZephyr Cove, NV
Michelle BellowsFort Collins, CO
Mary Garey-OrrOverland Park, KS
Kevin and Cheryl BierbaumArvada, CO
Barbara WalzLakewood, CO
Patrick KeeganCentennial, CO
Dave Richards (and Brad)Lexington, KY
Jack and Kathryn HarrowerDenver, CO
Jean BierwirthTucson, AZ
David and Judith MillerErie, CO
Pat and Arlene MylesDenver, CO
URS Energy & ConstructionInc., Boise, ID
Leonard andMartha (Martina) JohnsonLakewood, CO
Greg and Susan MahieuHighlands Ranch, CO
Duane and MarjanneClaassenDenver, CO

41
VAACE, Alberta, VA
A memorial fund has been established in the name of
Mr. Landon “Butch” Scott Temple, Jr.Donations have been made in Mr. Temple’s memory by:
Howard Stephenson, Lakeside, MT
A memorial fund has been established in the name of
Mrs. Virginia R. StephensonDonations have been made in Mrs. Stephenson’s memory by:
David Stierle, Louisville, KY
A memorial fund has been established in the name of
Mr. Billie StierleDonations have been made in Mr. Stierle’s memory by:
Victor Arias, Irving, TX
A memorial fund has been established in the name of
Mr. Bob SpearDonations have been made in Mr. Spear’s memory by:
Frank and Kathleen BoccutiClayton, NJ
Louise Amato, West Berlin, NJ
Joseph & Margaret MuoioWest Chester, PA
Mr. and Mrs. Leonard Mac Adams, Woodbury, NJ
Mr. and Mrs. Carmen VisalliNorristown, PA
Lisa SeverinoCherry Hill, NJ
Roger, Kathleen and Angelina BoccutiPhiladelphia, PA
Maureen Musumeci and Family,Philadelphia, PA
Jesse and Cynthia StoopFarmingdale, NJ
Joseph & Kathleen MancanoHaddon Township, NJ
A memorial fund has been established in the name of
Mrs. Lucy TerranovaDonations have been made in Mrs. Terranova’s memory by:
Art and Sue SmithNorristown, PA
Paul and Betty VagedesFairfield Bay, AR
Linda, Michelle, Laura, Erika,Emma, Nicole, Ted and MattGlenolden, PA
Warren and Linda CohnNorristown, PA
Russ and Joan ThayerTroy, OH
Gerard and Patricia GiuffridaEagleville, PA
Benjamin and Lillian RisiliaPhiladelphia, PA
Terry and Dolores HertzbergWest Berlin, NJ
Marie RidolfoPhiladelphia, PA
Dolores Boccuti, Glendora, NJ
Robert and Pat HendrickRichmond, VA
Belle Ann ApodacaSandston, VA
James Warren PearmanRichmond, VA
Parker and Beverly DillardRichmond, VA
Spectrum of Richmond, Inc.Richmond, VA
Indiana Amateur SoftballAssoc., Bloomington, IN
George and Joy BaynesHenrico, VA
A memorial fund has been established in the name of
Mr. H. Franklin Taylor, IIIDonations have been made in Mr. Taylor’s memory by:
Craig FollisRichmond, VA
Richard and Sallie CrossRichmond, VA
Doug and Gloria WetmoreMidlothian, VA
Deborah Mauzy, Maidens, VA
Lee and Patti BourneMontpelier, VA
Elliot and Tim MerialRichmond, VA
Mr. and Mrs. Edward B. EvansMechanicsville, VA
Linda F. Young, Glen Allen, VA
Carmen J. ShorttRichmond, VA
Barry HodgesRichmond, VA
Adams, Jenkins andCheathamMidthothian, VA
Dave and Wendy AmesMechanicsville, VA
Allen Taylor, Richmond, VA
Bonnie and Polly CulleyMidlothian, VA
Elizabeth A. GallanisRochester, MN
Vipers Softball Clubfor VeteransAlexandria, VA
A. E. Robertson, Jr.Montgomery, AL
Mitch and Sue ForresterKilmarnock, VA
Steve and Martha StokesGlen Allen, VA
Anne N. M. JohnsonMidlothian, VA
Robert S. Brockmeier, Jr.Henrico, VA
W. R. and Joan BranchAshland, VA
Base Crawlers, Full Force,Junton & WilliamsRichmond, VA
Robert and Jayne UkropRichmond, VA
Jimmy and Nancy CallCustom Ornamental Iron, Inc.Glen Allen, VA
Grace E. GulickMechanicsville, VA
John and Jeannine MillerHopewell, VA
The 2012 Granger LeagueMidlothian, VA
Barbara I. YoungMechanicsville, VA
Earline B. BaylissRichmond, VA
William W. KingNorfolk, VA
Barbara G. WhitecottonMontpelier, VA
James F. RobinsonSt. Cloud, FL
Virginia FaulknerRichmond, VA
William J. EdwardsRichmond, VA
Sandra L. ClementsHampton, VA
Janice R. MillerDoswell, VA
Nancy S. BoyerRichmond, VA
James & Savilla PleasantsDeltaville, VA
Gaye Sakaguchi-YeeGlendale, CA
Ed & Jodi Felt, Turlock, CA
A memorial fund has been established in the name of
Mr. Satoru “Sat” SugiuraDonations have been made in Mr. Sugiura’s memory by:
Kathy (Sakaguchi) MarquardtElk Grove, CA
Janet T. Tashima, Turlock, CA
Marjorie Sudimack, Warren, OH
A memorial fund has been established in the name of
Mr. Robert SudimackDonations have been made in Mr. Sudimack’s memory by:
Tricia CowlesWestminster, CA
A memorial fund has been established in the name of
Mr. Paul StutzmanDonations have been made in Mr. Stutzman’s memory by:
Jerry, Gae and KevinMonaghan, Surprise, AZ
Martin and Deborah Segal, Suga Land, TX
A memorial fund has been established in the name of
Mr. Abraham (Abe) RosenthalDonations have been made in Mr. Rosenthal’s memory by:
Ed and Carole Johnson, Great Mills, MD
A memorial fund has been established in the name of
Mr. Paul RosinskiDonations have been made in Mr. Rosinski’s memory by:
Konnie Selch, Centennial, CO
A memorial fund has been established in the name of
Mr. Philip J. SelchDonations have been made in Mr. Selch’s memory by:
Carol Kosberg, Palm Beach, FL
A memorial fund has been established in the name of
Mr. Frank SamuelsDonations have been made in Mr. Samuels’ memory by:
Yvette Schmalz-Riedt, Earlysville, VA
A memorial fund has been established in the name of
Mr. Fred E. Schmalz-RiedtDonations have been made in Mr. Schmalz-Riedt’s memory by:
Robert Schieres, Centerville, OH
A memorial fund has been established in the name of
Mrs. Sue SchieresDonations have been made in Mrs. Schieres’ memory by:
Barry Rynk, Boca Raton, FL
A memorial fund has been established in the name of
Mr. Kenneth Larry SmithDonations have been made in Mr. Smith’s memory by:
Ron and Kim Thomason, Franklin, TN
A memorial fund has been established in the name of
Mr. Robert “Dewey” SmartDonations have been made in Mr. Smart’s memory by:
Delores J. Urdang, KathyMuleahy and Leonard andMarcia MolleyShaker Heights, OH
Edward and Adele BolsonRedmond, WA
Norman & Barbara WalkerFreeland, WA
Len and Esther MortonTulsa, OK
A memorial fund has been established in the name of
Mrs. Suzanne ShultzDonations have been made in Mrs. Shultz’ memory by:
Velva SternLake Forest Park, WA
Lawrence and Rosanna KahnRedmond, WA
Don and Jean KirshnerBellevue, WA
Ronald and Henrietta KleinRedmond, WA
Larry Jacobs, Leawood, KSAndy and Carol HarrisMercer Island, WA
Scott and Robin PaulDoylestown, PA
Stanley C. RombergOcala, FL
Charlotte J. ThielenSun City, CA
Shirley Ann Cox, Solon, IA
Helen M. RombergOcala, FL
Bradley & Kathleen McGowanKalona, IA
Jack and Marcia BedellSpirit Lake, IA
A memorial fund has been established in the name of
Lt. Col. (ret) Robert G. ShainDonations have been made in Lt. Col. Shain’s memory by:
Lisa LaFontaineWashington, DC
Larry Wisneski, U. S. ArmyExecutive Flight DetachmentCollege Station, TX
Claude and Toni BardPueblo West, CO
Rox Shain, Parker, CO
Art and Deb PescatoreHartsville, PA
Harry Charles LymnMcLean, VA

42
Angelo and Rose Staikos, Hazlet, NJ
A memorial fund has been established in the name of
Ms. Nellie WhiteDonations have been made in Ms. White’s memory by:
Lawrence and Melinda ZackLondon, Ontario, Canada
A memorial fund has been established in the name of
Ms. Alicia WhiteDonations have been made in Ms. White’s memory by:
Ann M. Thomas, Wichita Falls, TX
A memorial fund has been established in the name of
(Lt. Col. Ret.) USAF Timothy Louis ThomasDonations have been made in Lt. Col. Thomas’ memory by:
John and Nancy RivkinUniondale, NY
“Operations Department” ofPC Construction CompanyEssex Junction, VT
PC Construction CompanySouth Burlington, VT
A memorial fund has been established in the name of
Ms. Barbara Fayette TowneDonations have been made in Ms. Towne’s memory by:
Angelo and Lynn PizzagalliSouth Burlington, VT
Tom McCabeSouth Burlington, VT
James and Judy PizzagalliShelburne, VT
Alan TowneWinthrop, MA
James J. Handy, CLUBurlington, VT
Carolyn WarrenSt. Petersburg, FL
A memorial fund has been established in the name of
Mr. Jim WarrenDonations have been made in Mr. Warren’s memory by:
Larry and Stephanie SeipleOakland, CA
A memorial fund has been established in the name of
Mr. Thomas Earl WalrathDonations have been made in Mr. Walrath’s memory by:
Harry E. GlesnerGilson, IL
James M. andMary Lou OliverRoseville, IL
Bradley and Jamie BeckerMacomb, IL
William and Shirley WilsonElmwood, IL
Janie FarquharRoseville, IL
William and Marcia BrooksRoseville, IL
Robert K. SullivanRoseville, IL
Lyle H. NelsonAbingdon, IL
Wayne and MarilynBoydstunSt. Augustine, IL
Gary and Shirley PringleGalesburg, IL
Gary and Donna HayesRoseville, IL
Charlotte DowninGalesburg, IL
Lyle and Norma GoedekeMaquon, IL
Carl and LuAnn JohnsonGalesburg, IL
Robert J. and D.M. HartzellGerlaw, IL
Bradley andBarbara TillotsonLoveland, OH
A memorial fund has been established in the name of
Mr. N. Eugene “Whitey” WhiteDonations have been made in Mr. White’s memory by:
Daryl E. JohnsonCameron, IL
Mary H. TurnerRoseville, IL
James M. andWilla Deane MooreKnoxville, IL
M. Elouise SwisherRoseville, IL
Edward R. amdDiane C. WinklessTinley Park, IL
Gary and Linda JohnsonGerman Valley
Delbert and Shirley PriceAlexis, IL
Eldon R. andVirginia E. AupperleToulon, IL
Penny L. FlesnerKnoxville, IL
Robert and Kim StricklerRoseville, IL
Riley R. & Shirley J. JohnsonMonmouth, IL
Raymond C. BaldwinKnoxville, IL
Barbara HopkinsKnoxville, IL
James andVirginia Jean NorrisTennessee, IL
Edwin and Lois StricklerRoseville, IL
Harold G. and Mary K. LainCameron, IL
Karen I. FergusonRoseville, IL
Carl and Marjorie GoreWilmington, NC
Page WingfieldGoldsborog, NC
A memorial fund has been established in the name of
Mr. Neal Eddins WingfieldDonations have been made in Mr. Wingfield’s memory by:
E. Joan RollinsOklahoma City, OK
Rev. and Mrs. Robert ShieldsNew Bern, NC
Dr. and Mrs. AbrahamYurkofsky
A memorial fund has been established in the name of
Mrs. Joan ZimetbaumDonations have been made in Mrs. Zimetbaum’s memory by:
Nancy StraussScarsdale, NY
Lee RiffaterreNew York, NY
A memorial fund has been established in the name of
Mr. Fred ZuckerDonations have been made in Mr. Zucker’s memory by:
Kenneth RichieriNew York, NY
Ronee HerzDelray Beach, FL
Joanne ShaerBoca Raton, FL
A memorial fund has been established in the name of
Ms. Selma WeinerDonations have been made in Ms. Weiner’s memory by:
Bert and Marci BlicherDelray Beach, FL
Luxury Partners LLCDelray Beach, FL
Allen and Glenna LongCarmichael, CA
Arthur and Corinna BilottiHollywood, FL
Billie E. HugginsSt. Simons Island, GA
A memorial fund has been established in the name of
Mr. Richard (Rick) WarnerDonations have been made in Mr. Warnerx’s memory by:
Donald and Susan KahHollywood, FL
Mike and Barbara SantomasoHollywood, FL
Wade and Lindsey CoxOviedo, FL
Jeannette KiehlPalatine, IL
A memorial fund has been established in the name of
Mr. Paul M. VukelicDonations have been made in Mr. Vukelic’S memory by:
Alan and Cynthia Stoeckel and Family, Palatine, IL
Nick and Arlene DelmonacoEdison, NJ
Charles and Marie BreussaWyckoff, NJ
A memorial fund has been established in the name of
Mrs. Anita TremaroliDonations have been made in Mrs. Tremaroli’s memory by:
Frank and Terri TroicEast Meadow, NY
Steve and Marianne TremaroliHuntington, NY
Paula M. DaneseEast Meadow, NY
Donna, Dave, Davy BuntonArlington, VA
A memorial fund has been established in the name of
Mrs. Jeanette TothDonations have been made in Mrs. Toth’s memory by:
Joseph TothManalapan, NJ
Dale R. TanisGeneseo, IL
A memorial fund has been established in the name of
Mrs. Faith Darlene TogamiDonations have been made in Mrs. Togami’s memory by:
Nino MNorthbrook, IL
Mike and Rhonda WhitneyTaylor Ridge, IL
Tommie and Cindy WattsGarden City Beach, SC
A memorial fund has been established in the name of
Ms. Margaret D. (Peggy) TimmonsDonations have been made in Ms. Timmons’s memory by:
Dorothy D. ZeekSumter, SC
Suzanne FleischmanMemorial Fund
for Patient AdvocacyA fund has been established by the
MDS Foundation in memory of SuzanneFleischman. Contributions may besent to the Foundation with a notationdesignating the Suzanne FleischmanMemorial Fund for Patient Advocacy.
Roslyn Raney, Menlo Park, CA
Fay Wanetick, Pittsburgh, PA
Lisa SeverinoCherry Hill, NJ
A memorial fund has been established in the name of
Mrs. Doris Kjersgaard ThomasDonations have been made in Mrs. Thomas’ memory by:
Irene K. RobertsBroomfield, CO

43
A Living EndowmentMany families are affected by living with the reality of MDS. There is an extraordinary way to contribute to the MDS Foundation and
support our mission of working as a resource for patients, families, and healthcare professionals.
A commitment to donate to the Foundation on occasions of loss, birthdays, and anniversary remembrances can be made. Honor yourfriends or family members on these occasions with a donation, and the MDS Foundation will send an acknowledgment to the recipient,recognizing the occasion.
A Living Endowment donationhas been made in honor of:
Seth Cohen
This donation was submitted by: Geoffrey & Sandy Goldworm, Jupiter, FL
A Living Endowment donationhas been made in honor of:
Jonathan Cohn
This donation was submitted by: Dr. Robert Cohn and Ruth Cohn
Family Foundation
A Living Endowment donationhas been made in honor of:
Robert W. Cook
This donation was submitted by: Suzanne Demartini, Plymouth, MA
A Living Endowment donationhas been made in honor of:
Gerald Duehr
This donation was submitted by: Thomas Means, New Berlin, WI
Living Endowment donationshave been made in honor of:
Benny F. Evatt
These donations were submitted by: June M. Evatt, Pendleton, SC
Maureen Maughan, Cranbury, NJ
Peggy Cherkasky, Pittsford, NY
A Living Endowment donationhas been made in honor of:
Irv Glickman
This donation was submitted by: Geoffrey and Sandy Goldworm
Jupiter, FL
A Living Endowment donationhas been made in honor of:
Joan Kane
This donation was submitted by: Betty Jo Vail
Lititz, PA
A Living Endowment donationhas been made in honor of:
Mahaveer Prabhakar
This donation was submitted by:
Rajeev B. and Elizabeth PrabhakarWalnut Creek, CA
A Living Endowment donationhas been made in honor of:
Arnold Schwartz
This donation was submitted by: Gloria Schwartz
Woodland Hills, CA
Living Endowment donationshave been made in honor of:
Elizabeth Schwartz
These donations were submitted by:
Candace D. MorganPortland, OR
Elizabeth TouchonPortland, OR
Christine R. SchwartzMadison, WI
A Living Endowment donationhas been made in honor of:
Angelo Staikos
This donation was submitted by:
Angelo and RoseHazlet, NY
Living Endowment donationshave been made in honor of:
Morey Storck
These donations were submitted by: Newt & Lois Alterman, Tarrytown, NY
Herb & Gloria PortnoyBriarcliff Manor, NY
Mel and Dr. Cynthia ChesnerTarrytown, NY
Rita Wexler, Tarrytown, NY
Living Endowment donationshave been made in honor of:
Diana Termine
These donations were submitted by: Ronald and Linda Jaffe
Aurora, IL
George Zander, Palos Hills, IL
Patricia Adesso, Bloomingdale, IL
Carol Olivo, Elmwood Park, IL
Dave and Rhonda MeyerSaint Charles, IL
Scott Termine, Plainfield, IL
Jean Laumann, Naperville, IL
A Living Endowment donationhas been made in honor of:
Remo Tersolo
This donation was submitted by: Susan Urban, Oceanside, CA
A Living Endowment donationhas been made in honor of:
Ronald J. Vanskiver
This donation was submitted by:
Helen VanskiverNottingham, MD

44
The Foundation’s Board of DirectorsSandra E. Kurtin, RN, MS, AOCN, ANP-CHematology/Oncology Nurse PractitionerThe University of Arizona Cancer CenterAdjunct Clinical Assistant Professor of NursingClinical Assistant Professor of MedicineUniversity of ArizonaTucson, Arizona, U.S.A.
Alan F. List, MDPresident and CEOand Frank and Carol Morsani Endowed Chair
H. Lee Moffitt Cancer Center& Research Institute
Tampa, Florida, U.S.A.
Silvia M.M. Magalhães, MD, PhDProfessor of Clinical Medicine–Hematology
Federal University of CearáHospital Universitário Walter CantídioCeará, Brazil
Yasushi Miyazaki, MDChief, Dept. of HematologyNagasaki University Graduate School of Biomedical Sciences
Atomic Bomb Disease InstituteNagasaki, Japan
John Molle, CPAJRM Financial Associates, LLCFlemington, New Jersey, U.S.A.
Ghulam J. Mufti, DM, FRCP, FRCPathProfessor of Haemato-oncology and Head of DepartmentHaematological MedicineKing’s College London &King’s College HospitalLondon, United Kingdom
Charlotte M. Niemeyer, MDProfessor of PediatricsUniversity Children’s HospitalFreiburg, Germany
Stephen D. Nimer, MD, Chairman The MDS Foundation, Inc.Director, Sylvester ComprehensiveCancer Center
Professor of Medicine, Biochemistry & Molecular Biology
University of Miami Miller School of MedicineMiami, Florida, U.S.A
David P. Steensma, MDAssociate ProfessorDepartment of MedicineHarvard Medical SchoolDana-Farber Cancer InstituteBoston, Massachusetts, U.S.A.
Robert J. Weinberg, Esq.Pepper Hamilton LLPPhiladelphia, Pennsylvania, U.S.A.
Emeritus Member
Franz Schmalzl, MDInnsbruck, Austria
MDS Foundation Information
Become a MemberThe MDS Foundation would like to
have you as a member. Membershipis $50 a year for physicians and otherprofessionals. Patients, their families,and others interested in MDS may joinat the reduced rate of $35.
Membership benefits includeissues of the MDS News, a specialsubscription rate of $135.00 forLeukemia Research (a substantialdiscount from the current institutionalsubscription rate of $2,373), andthe worldwide Centers of Excellencepatient referral service.
Please visit us at:www.mds-foundation.org.
the myelodysplastic syndromes foundation, inc.
John M. Bennett, MDProfessor of Medicine, EmeritusLaboratory Medicine and PathologyUniversity of Rochester Medical CenterRochester, New York, U.S.A.
Mario Cazzola, MDProfessor of HematologyUniversity of Pavia School of MedicineHead, Department of HematologyFondazione IRCCS Policlinico San MatteoPavia, Italy
Erin Demakos, RN, CCRNAdministrative DirectorMyelodysplastic Disease Center and MPD Program
Mount Sinai School of MedicineNew York, New York, U.S.A.
Theo J.M. de Witte, MD, PhDProfessor of HematologyUniversity Medical Center Nijmegen St. RadboudNijmegen, The Netherlands
Pierre Fenaux, MDProfessor of HematologyHôpital Avicenne, University Paris 13Bobigny, France
Peter L. Greenberg, MDProfessor of Medicine/HematologyStanford UniversitySchool of MedicineStanford, California, U.S.A.
Eva Hellström-Lindberg, MD, PhDAssociate Professor of HematologyKarolinska InstitutetInstitution for MedicineHuddinge University HospitalStockholm, Sweden