
Factors influencing the development of evidence-based practice: a research tool
11
Factors influencing the development of evidence-based practice: a research tool Kate Gerrish 1 , Peter Ashworth 2 , Anne Lacey 3 , Jeff Bailey 4 , Jo Cooke 5 , Sally Kendall 6 & Elaine McNeilly 7 Accepted for publication 5 September 2006 1 Kate Gerrish BN MSc PhD RN Professor of Nursing Centre for Health and Social Care Research, Sheffield Hallam University, Sheffield Teaching Hospitals NHS Trust, Sheffield, UK 2 Peter Ashworth PhD FBPsS Professor of Educational Research Faculty of Development and Society, Sheffield Hallam University, Sheffield, UK 3 Anne Lacey MSc RN Senior Research Fellow/Director (Sheffield) Trent RDSU, ICOSS, University of Sheffield, Sheffield, UK 4 Jeff Bailey BSc Research Co-ordinator Barnsley Hospital NHS Foundation Trust, R&D Department, Barnsley, UK 5 Jo Cooke MA RN HV Primary and Social Care Lead Trent RDSU, University of Sheffield, Sheffield, UK 6 Sally Kendall BSc PhD RN HV Professor of Primary Health Care Nursing Faculty of Health and Human Sciences, University of Hertfordshire, Hatfield, UK 7 Elaine McNeilly BSc Research Assistant Faculty of Health and Human Sciences, University of Hertfordshire, Hatfield, UK Correspondence to Kate Gerrish: e-mail: [email protected] GERRISH K., ASHWORTH P., LACEY A., BAILEY J., COOKE J., KENDALL S. & GERRISH K., ASHWORTH P., LACEY A., BAILEY J., COOKE J., KENDALL S. & MCNEILLY E. (2007) MCNEILLY E. (2007) Factors influencing the development of evidence-based practice: a research tool. Journal of Advanced Nursing 57(3), 328–338 doi: 10.1111/j.1365-2648.2006.04112.x Abstract Title. Factors influencing the development of evidence-based practice: a research tool Aim. The paper reports a study to develop and test a tool for assessing a range of factors influencing the development of evidence-based practice among clinical nurses. Background. Achieving evidence-based practice is a goal in nursing frequently cited by the profession and in government health policy directives. Assessing factors influencing the achievement of this goal, however, is complex. Consideration needs to be given to a range of factors, including different types of evidence used to inform practice, barriers to achieving evidence-based practice, and the skills required by nurses to implement evidence-based care. Methods. Measurement scales currently available to investigate the use of evidence in nursing practice focus on nurses’ sources of knowledge and on barriers to the use of research evidence. A new, wider ranging Developing Evidence-Based Practice questionnaire was developed and tested for its measurement properties in two studies. In study 1, a sample of 598 nurses working at two hospitals in one strategic health authority in northern England was surveyed. In study 2, a slightly expanded version of the questionnaire was employed in a survey of 689 community nurses in 12 primary care organizations in two strategic health authorities, one in northern England and the other in southern England. Findings. The measurement characteristics of the new questionnaire were shown to be acceptable. Ten significant, and readily interpretable, factors were seen to underlie nurses’ relation to evidence-based practice. Conclusion. Strategies to promote evidence-based practice need to take account of the differing needs of nurses and focus on a range of sources of evidence. The Developing Evidence-Based Practice questionnaire can assist in assessing the specific ‘evidencing’ tendencies of any given group of nurses. Keywords: evidence-based practice, instrument development, nursing, research implementation, survey design RESEARCH METHODOLOGY JAN 328 Ó 2007 The Authors. Journal compilation Ó 2007 Blackwell Publishing Ltd
Transcript of Factors influencing the development of evidence-based practice: a research tool

Factors influencing the development of evidence-based practice:
a research tool
Kate Gerrish1, Peter Ashworth2, Anne Lacey3, Jeff Bailey4, Jo Cooke5, Sally Kendall6 &
Elaine McNeilly7
Accepted for publication 5 September 2006
1Kate Gerrish BN MSc PhD RN
Professor of Nursing
Centre for Health and Social Care Research,
Sheffield Hallam University, Sheffield
Teaching Hospitals NHS Trust, Sheffield, UK
2Peter Ashworth PhD FBPsS
Professor of Educational Research
Faculty of Development and Society,
Sheffield Hallam University, Sheffield, UK
3Anne Lacey MSc RN
Senior Research Fellow/Director (Sheffield)
Trent RDSU, ICOSS, University of Sheffield,
Sheffield, UK
4Jeff Bailey BSc
Research Co-ordinator
Barnsley Hospital NHS Foundation Trust,
R&D Department, Barnsley, UK
5Jo Cooke MA RN HV
Primary and Social Care Lead
Trent RDSU, University of Sheffield,
Sheffield, UK
6Sally Kendall BSc PhD RN HV
Professor of Primary Health Care Nursing
Faculty of Health and Human Sciences,
University of Hertfordshire, Hatfield, UK
7Elaine McNeilly BSc
Research Assistant
Faculty of Health and Human Sciences,
University of Hertfordshire, Hatfield, UK
Correspondence to Kate Gerrish:
e-mail: [email protected]
GERRISH K. , ASHWORTH P. , LACEY A. , BAILEY J. , COOKE J. , KENDALL S. &GERRISH K. , ASHWORTH P. , LACEY A. , BAILEY J. , COOKE J. , KENDALL S. &
MCNEILLY E. (2007)MCNEILLY E. (2007) Factors influencing the development of evidence-based
practice: a research tool. Journal of Advanced Nursing 57(3), 328–338
doi: 10.1111/j.1365-2648.2006.04112.x
AbstractTitle. Factors influencing the development of evidence-based practice: a research
tool
Aim. The paper reports a study to develop and test a tool for assessing a range of
factors influencing the development of evidence-based practice among clinical
nurses.
Background. Achieving evidence-based practice is a goal in nursing frequently cited
by the profession and in government health policy directives. Assessing factors
influencing the achievement of this goal, however, is complex. Consideration needs
to be given to a range of factors, including different types of evidence used to inform
practice, barriers to achieving evidence-based practice, and the skills required by
nurses to implement evidence-based care.
Methods. Measurement scales currently available to investigate the use of evidence
in nursing practice focus on nurses’ sources of knowledge and on barriers to the use
of research evidence. A new, wider ranging Developing Evidence-Based Practice
questionnaire was developed and tested for its measurement properties in two
studies. In study 1, a sample of 598 nurses working at two hospitals in one strategic
health authority in northern England was surveyed. In study 2, a slightly expanded
version of the questionnaire was employed in a survey of 689 community nurses in
12 primary care organizations in two strategic health authorities, one in northern
England and the other in southern England.
Findings. The measurement characteristics of the new questionnaire were shown to
be acceptable. Ten significant, and readily interpretable, factors were seen to
underlie nurses’ relation to evidence-based practice.
Conclusion. Strategies to promote evidence-based practice need to take account of
the differing needs of nurses and focus on a range of sources of evidence. The
Developing Evidence-Based Practice questionnaire can assist in assessing the specific
‘evidencing’ tendencies of any given group of nurses.
Keywords: evidence-based practice, instrument development, nursing, research
implementation, survey design
RESEARCH METHODOLOGYJAN
328 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

Introduction
Over the past 15 years, evidence-based practice has emerged
as a major policy theme in Western healthcare systems. The
increased emphasis internationally on clinical and cost-
effectiveness in health policy has highlighted the need for
quality health services to be built upon the use of best
evidence (McKenna et al. 2004). Various governments have
introduced initiatives to support the development of evi-
dence-based healthcare systems in which decisions made by
healthcare practitioners, managers, policy makers and
patients are based on high quality evidence. Activity has
focused on developing evidence-based guidelines for clinical
interventions. For example, in the United States of America
(USA) the Agency for Healthcare Research and Quality
(http://www.ahrq.gov) leads national efforts in the use of
evidence to guide healthcare decisions. The establishment of
the National Institute for Health and Clinical Excellence
(http://www.nice.org.uk) in England, the Scottish Intercol-
legiate Guidelines Network (http://www.sign.ac.uk), and the
National Institute for Clinical Studies (http://www.nicsl.co-
m.au) in Australia have similar responsibilities for developing
evidence-based guidelines and providing information on the
clinical and cost-effectiveness of interventions.
Developing evidence-based guidelines is just one step in a
complex process of ensuring that nurses actually base their
practice on evidence. Achieving evidence-based practice
requires skill on the part of nurses to appraise research
evidence in order to decide whether it is appropriate to use.
The evidence then needs to be translated into a form that can
be implemented in practice and following implementation,
the change needs to be evaluated (Gerrish 2006). Whereas the
publication of systematic reviews of research and national
clinical guidelines makes some aspects of the process easier,
implementing change can still be challenging (Collett & Elliot
2000). In recognizing the importance of evidence-based
practice to contemporary health care this paper reports on
the development and testing of a questionnaire designed to
identify factors which influence the development of evidence-
based practice in nursing.
Background
Despite widespread calls for nursing to be evidence-based,
there is a lack of clarity regarding the concept of evidence-
based practice. Sackett et al.’s (1996) definition of evidence-
based medicine is one of the most widely cited:
Evidence-based medicine is the conscientious, explicit, and judicious
use of current best evidence in making decisions about the care of
individual patients. The practice of evidence-based medicine means
integrating individual clinical expertise with the best available
external evidence from systematic research. (p. 71)
More recently, Sackett et al. (2000) acknowledged the need
also to take account of patient values.
Whereas Sackett’s definition of evidence-based medicine
has been applied to evidence-based practice in nursing (for
example, Ingersoll 2000, DiCenso et al. 2004), there is some
concern that the definition is too restrictive. Debates focus on
the perceived over-emphasis on research evidence, especially
that derived from randomized controlled trials, to the neglect
of other sources of evidence, the devaluing of patient
experiences and values, and the largely atheoretical medically
dominated model of evidence which is contrary to nursing’s
disciplinary focus on theory-guided practice (DiCenso et al.
2004).
There is general consensus that a broader definition of
evidence should be considered which takes account of other
ways of knowing that inform nursing practice (Lomas et al.
2005). For example, although Rycroft-Malone et al. (2004)
acknowledge the relationship of research, clinical experience
and patient experience as the core of evidence-based practice,
they argue that the evidence-base for nursing should also
include information derived from the local context. Clinical
experience as a source of evidence is elaborated by Gerrish
(2003) who, in drawing upon the work of Liaschenko and
Fisher (1999), differentiates between scientific, empirically
based knowledge, patient knowledge developed through an
understanding of how patients are located within the health-
care system and knowledge derived from the personal
biography of individual patients.
Nolan (2005) draws attention to the international growth
of policies promoting user participation which are under-
pinned by a belief that users should be active shapers of
knowledge and subsequent action. He argues that evidence-
based practice should encompass this tacit expertise of
patients in addition to that of professionals and research –
this moves beyond taking account of patient preferences to
valuing the knowledge that patients bring to the nurse–
patient interaction.
Fawcett et al. (2001) argue for a more theory-guided
approach to evidence-based practice in which multiple
patterns of knowing in nursing are acknowledged. Drawing
upon Carper’s typology of ways of knowing (empirical,
ethical, personal and aesthetic) they caution against the
virtually exclusive emphasis on empirical theories in evi-
dence-based practice and argue for a more holistic approach
in which different ways of knowing provide different lenses
for critiquing and interpreting different kinds of evidence.
JAN: RESEARCH METHODOLOGY Factors influencing the development of evidence-based practice
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 329

Research examining the implementation of evidence-
based practice in nursing has focused primarily on research
evidence, in particular on the barriers nurses encounter in
using research. These studies have consistently identified
that the major obstacles that nurses experience in seeking
to implement research findings relate to insufficient time to
access and review research reports, a shortfall in critical
appraisal skills together with lack of authority and support
to implement findings (Funk et al. 1991a, Bryar et al.
2003, McKenna et al. 2004). Researchers have also come
under criticism for not presenting their research to clinical
audiences in a way that is easy to understand and in which
the implications for practice are made clear (Nolan et al.
1998).
Much of the responsibility for evidence-based practice has
been placed on individual practising nurses. However,
although it is recognized that all nurses have a professional
responsibility to base their care on the best available
evidence, implementing evidence-based practice in healthcare
settings is a complex undertaking (Royle & Blythe 1998). It
has been argued that healthcare organizations should support
the development of a culture of evidence-based practice and
provide resources for its implementation (DiCenso & Cullum
1998, Gerrish & Clayton 2004). Consideration of this
broader context has highlighted the importance of the
leadership styles of senior clinical nurses in promoting a
ward/team culture that is patient-centred, values members
and promotes a learning environment to support evidence-
based practice (McCormack et al. 2002). Some models for
promoting evidence-based practice also emphasize the need
for facilitation by external and internal change agents to
support the process of change and identify the importance of
the personal characteristics of the facilitator, the style of
facilitation and the role of the facilitator in terms of authority
(Harvey et al. 2002).
Existing questionnaires used to examine evidence-based
practice have focused on research utilization, in particular
nurses’ ability to access and appraise research reports and
implement research findings in practice. The Barriers to
Research Utilization Questionnaire developed in the USA
by Funk et al. (1991a) has been used extensively over the
past 15 years in a number of countries including Australia
(Retsas & Nolan 1999, Hutchinson & Johnson 2004),
Finland (Oranta et al. 2002, Kuuppelomaki & Tuomi
2005), Ireland (Glacken & Chaney 2004), Sweden
(Kajermo et al. 1998), and the United Kingdom (UK)
(Dunn et al. 1998, Nolan et al. 1998, Closs & Bryar
2001). It has also been used to examine research utilization
in specific groups of nurses, for example, community nurses
(Bryar et al. 2003), specialist breast care nurses (Kirshbaum
et al. 2004) and forensic mental health nurses (Carrion
et al. 2004). The questionnaire identifies 29 items consid-
ered to be barriers to research utilization. Respondents are
asked to rate on a 5 point Likert scale the extent to which
they perceive each item to be a barrier. Factor analysis
grouped the items around four factors, the nurse’s research
values, skills and awareness, the quality of the research, the
way in which research is communicated and the charac-
teristics of the organization (Funk et al. 1991b). Inter-
national comparisons of published findings indicate that
nurses experience broadly similar barriers to using research
in terms of the ranking of individual items.
Some studies have sought to replicate the factor analysis.
Whereas the original four factors identified by Funk et al.
were confirmed by Hutchinson and Johnson (2004), other
studies have identified different groupings of items: Retsas
and Nolan (1999) – three factors, Marsh et al. (2001) – three
factors, Kirshbaum et al. (2004) – three factors, Ku-
uppelomaki and Tuomi (2005) – six factors. Closs and Bryar
(2001) and Marsh et al. (2001) undertook extensive testing of
the instrument and independently raised questions about the
content and construct validity of the scale for use in the UK.
Several other questionnaires have been developed to
examine research utilization, however, they have not been
used as extensively as the Barriers questionnaire in order to
test the validity and reliability of the instruments in other
settings (for example Lacey 1994, Rodgers 1994, Hicks
1996, Estabrooks 1998, McKenna et al. 2004). Moreover,
within the context of evidence-based practice they focus on
the use of research findings rather than a broader definition
of evidence identified as important in the literature and
referred to above. Although Estabrooks (1998) considered
a broad range of sources of information that nurses draw
upon, including professional and patient expertise, this was
in order to examine the extent to which sources of research
evidence were used rather than to acknowledge the
contribution of diverse sources of evidence. Nevertheless,
parts of Estabrooks instrument have the potential to be
used to examine a broader definition of evidence-based
practice.
From a review of the literature and existing instruments,
there appeared to be a need for a questionnaire which would
examine factors influencing evidence-based practice where in
addition to research evidence, other forms of evidence were
considered. The definition of evidence-based practice which
informed the development of the questionnaire in this study
was adapted from Sackett’s definition referred to above
which emphasizes the interplay of research evidence, clinical
expertise and patient preferences. However, the definition of
evidence was extended to include research products such as
K. Gerrish et al.
330 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

national guidelines and local information such as protocols
and audit reports.
This paper reports the design and testing of the psycho-
metric properties of a wide-ranging questionnaire designed to
measure several aspects of evidence-based practice. Two
surveys were undertaken in order to test the instrument, one
involving hospital nurses and the second nurses working in
the community.
The studies
Aims
The aim of the two studies was
• to develop and validate the Developing Evidence-Based
Practice (DEBP) questionnaire as a comprehensive measure
of evidence-based practice in England;
• to determine the important factors influencing the devel-
opment of evidence-based practice, using a composite
measuring tool, the DEBP questionnaire.
The results of the first aim are presented in this paper.
Results based on the application of the questionnaire will be
published elsewhere.
Study 1: Hospital nurses
Study 1 provided an opportunity to survey two contrasting
hospital sites. The nurse respondents were located in two
acute hospitals in northern England [a university teaching
hospital and a district general hospital (DGH)], within the
same strategic health authority. It built upon earlier research
(Nolan et al. 1998) undertaken in the teaching hospital which
had developed an anglicized version of the ‘Barriers to
Research Utilization’ scale. However, the current study took
a much broader view of evidence-based practice and included
the use of different sources of evidence and a self-appraisal of
skills in finding and using evidence. Data were collected
during 2002–2003.
Participants
The sample was drawn from the records of qualified nursing
staff at each hospital. All nurses were included in the sample
except those from two directorates at the teaching hospital
that were participating in another research study related to
evidence-based practice. This resulted in a sample of 728 at
the teaching hospital, and 683 at the DGH. Of these, 330
were returned at the teaching hospital, and 274 at the DGH,
a response rate of 45% and 40%, respectively. The useable
achieved sample was 598, after the exclusion of question-
naires without information about the respondents’ grades.
Study 2: Community health nurses
In the second study, a slightly expanded version of the
questionnaire was used, with an additional eight items which
in each case simply increased the lists of sources of evidence;
barriers and facilitators to employing evidence in practice,
and personal skills (see Table 2 for all items including the
additions, which are italicized). These minor modifications
arose from testing the content validity of the instrument
originally used for hospital nurses for use with community
health nurses. The respondents were community health
nurses in 12 primary care trusts (PCTs) in two strategic
health authorities, one in northern England and the other in
southern England. Data were collected during 2005.
Participants
A random sample of 1600 community health nurses was
drawn from the records of qualified staff in the 12 PCTs.
Equal numbers of health visitors, district nurses, community
nurses, practice nurses and school nurses were sampled. The
overall response rate was 47% with responses for each of the
five community health nursing groups as follows: health
visitors 57%, district nurses 55%, community nurses 40%,
practice nurses 37%, school nurses 43%. The usable sample
was 689, after the exclusion of questionnaires without
information about the respondents’ post.
Construction of the questionnaire
The DEBP questionnaire has five main parts, each one derived
from somewhat different sources. Twenty-two items, 16 of
which are anglicized versions of items of the Estabrooks scale
(Estabrooks 1998) about sources of knowledge, constitute the
first section of the questionnaire. Each item was scored on a
5-point scale from never (score 1) to always (score 5).
Permission to use these items was obtained from the author.
The second, third and fourth sections of the DEBP
questionnaire examine barriers to achieving evidence-based
practice. Feedback from the earlier study in the teaching
hospital that had utilized an anglicized version of the North
American ‘Barriers’ questionnaire identified a number of
problems with this instrument that necessitated the develop-
ment of a quite different set of items, albeit ones that still
examined barriers. The new items took account of a broader
understanding of evidence by including questions on organ-
izational information (defined as care pathways, clinical
protocols and guidelines) in addition to questions on research
evidence. Emphasis was also placed on changing practice
based on evidence rather than just the implementation of
research findings. Additionally, in contrast to the original
JAN: RESEARCH METHODOLOGY Factors influencing the development of evidence-based practice
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 331

Barriers scale which asked respondents to comment on ‘the
nurse’ in a generic sense, the new items used a personal ‘I’ or
‘my’ to ensure respondents were reporting their own experi-
ence rather than that of nurses in general. This new ‘Barriers’
scale consisted of 19 items with 5-point response scales.
These are divided into two groups of barriers and one group
concerned with colleague relations which facilitate evidence-
based practice (scored in the opposite direction to the other
two groups, but intended to reduce the apparent negativity of
the ‘barriers’ items of the questionnaire). The scoring used the
5-point scale technique of section 1, with a score of 1 for
‘agree strongly’.
Finally, a fifth section was devised consisting of eight items
asking nurses to rate themselves on skills of finding and
reviewing evidence, and using evidence to effect change.
Ratings on a 5-point scale ranged from ‘complete beginner’
(score 1) to ‘expert’ (score 5).
So the DEBP tool consisted of
• Section 1. Bases of practice knowledge (22 items).
• Section 2. Barriers to finding and reviewing evidence (10
items).
• Section 3. Barriers to changing practice on the basis of
evidence (five items).
• Section 4. Facilitation and support in changing practice
(four items).
• Section 5. Skills in finding and reviewing evidence (eight
items).
The core of the DEBP questionnaire hence consists of 49
items, designed as a paper-based tool for self-completion. It
was initially piloted with 20 nurses who worked in hospital
settings and minor modifications were subsequently made to
two items to improve clarity. Prior to study 2 the content
validity of the questionnaire was considered by a panel of four
experts in community health nursing and minor modifications
made to the questionnaire. This included four additional
sources of knowledge, two additional barriers and two further
skills considered to be relevant to the practice of community
health nursing. The revised questionnaire was piloted with
five community health nurses but no changes were required.
Data collection
Questionnaires were addressed individually and distributed
via the external post or internal mail system at each site,
depending on the preference of the organization. An
addressed envelope was enclosed for return of the question-
naire. In study 1, reminders were posted around the hospital
site to maximize response, but no individual reminders were
sent to maintain anonymity of responders. Ward managers
were asked to encourage completion of the questionnaires,
but it was stressed that this was entirely voluntary. In study 2
targeted reminders were sent to non-respondents to maximize
the response rate.
Ethical considerations
The study was approved by the relevant research ethics and
governance committees at each site. A participant informa-
tion sheet giving details of the study accompanied the
questionnaire. Consent to participate was assumed on the
basis of a returned, completed questionnaire.
Data analysis
The data for all items employed in both studies 1 and 2 were
analysed using SPSS version 13. Initial analysis suggested no
alteration in the structure of results over the timespan in
which data were collected; this justified bringing together the
findings of the two studies in validating the instrument.
Results
Measurement characteristics of the ‘Developing Evidence-
Based Practice’ Questionnaire
Responses were treated as five-point scale items, with ‘high’
and ‘low’ being assigned, as indicated above. The question-
naire has five major sections. The measurement features of
the sections are given in Table 1. To be noted in particular is
the column of values of reliability. Reliability in this context
means internal consistency. It refers to the extent to which the
scores on the items correlate with each other and, if they do,
this means that we can regard the items within a scale as all
being about the same thing. It then becomes justifiable to
treat the items as constituting a Likert scale, since it is
meaningful to sum up the scores of each item to give a scale
score for the individual. The questionnaire was tested as to
coherence of scales and subscales using intercorrelation of
items and Cronbach’s Alpha as indicators of reliability. The
most widely used index of internal consistency, Cronbach’s
Alpha is equivalent to the average of all possible split-half
correlation coefficients. The values of a for each scale and
subscale can be seen in Table 1a. All a values are acceptable
as estimates of reliability (the conventional value of a
regarded as indicating a level which avoids false positive
reliability estimates is 0Æ7). The five sections of the question-
naire can be assumed to be reliable. However, the pattern of
intercorrelations in Table 1b is such that it would be
inappropriate to employ all 49 items as a ‘scale’ (see also
factor analytic evidence below).
K. Gerrish et al.
332 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd
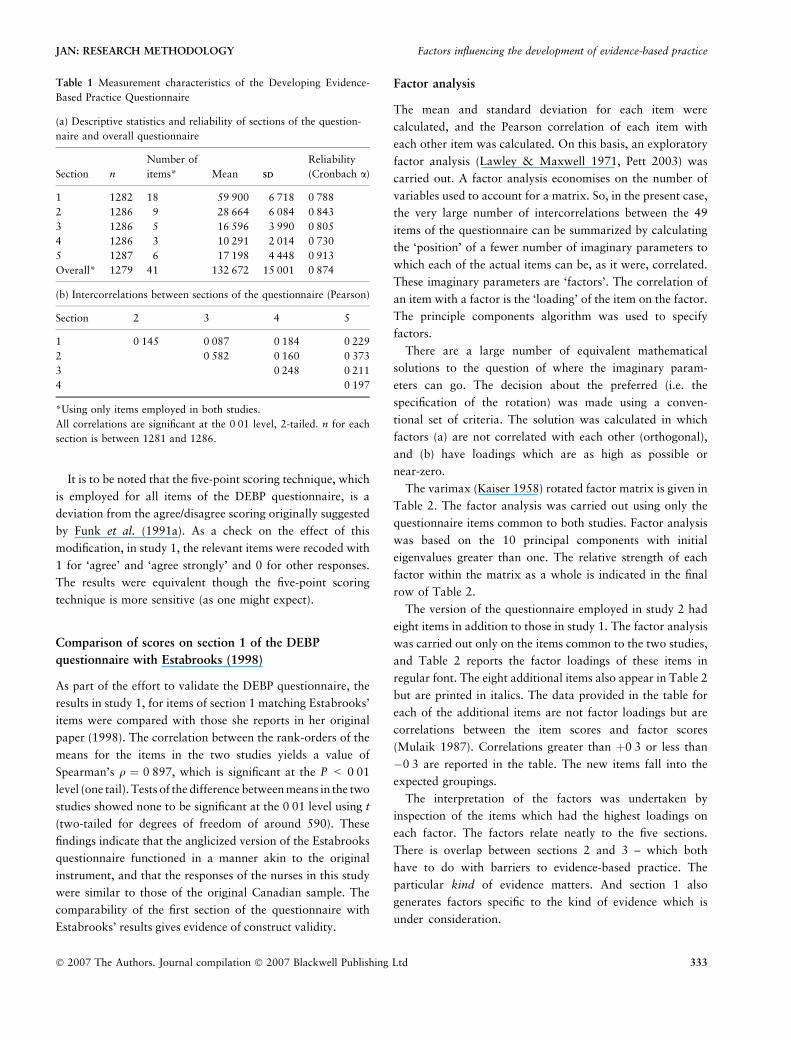
It is to be noted that the five-point scoring technique, which
is employed for all items of the DEBP questionnaire, is a
deviation from the agree/disagree scoring originally suggested
by Funk et al. (1991a). As a check on the effect of this
modification, in study 1, the relevant items were recoded with
1 for ‘agree’ and ‘agree strongly’ and 0 for other responses.
The results were equivalent though the five-point scoring
technique is more sensitive (as one might expect).
Comparison of scores on section 1 of the DEBP
questionnaire with Estabrooks (1998)
As part of the effort to validate the DEBP questionnaire, the
results in study 1, for items of section 1 matching Estabrooks’
items were compared with those she reports in her original
paper (1998). The correlation between the rank-orders of the
means for the items in the two studies yields a value of
Spearman’s q ¼ 0Æ897, which is significant at the P < 0Æ01
level (one tail). Tests of the difference between means in the two
studies showed none to be significant at the 0Æ01 level using t
(two-tailed for degrees of freedom of around 590). These
findings indicate that the anglicized version of the Estabrooks
questionnaire functioned in a manner akin to the original
instrument, and that the responses of the nurses in this study
were similar to those of the original Canadian sample. The
comparability of the first section of the questionnaire with
Estabrooks’ results gives evidence of construct validity.
Factor analysis
The mean and standard deviation for each item were
calculated, and the Pearson correlation of each item with
each other item was calculated. On this basis, an exploratory
factor analysis (Lawley & Maxwell 1971, Pett 2003) was
carried out. A factor analysis economises on the number of
variables used to account for a matrix. So, in the present case,
the very large number of intercorrelations between the 49
items of the questionnaire can be summarized by calculating
the ‘position’ of a fewer number of imaginary parameters to
which each of the actual items can be, as it were, correlated.
These imaginary parameters are ‘factors’. The correlation of
an item with a factor is the ‘loading’ of the item on the factor.
The principle components algorithm was used to specify
factors.
There are a large number of equivalent mathematical
solutions to the question of where the imaginary param-
eters can go. The decision about the preferred (i.e. the
specification of the rotation) was made using a conven-
tional set of criteria. The solution was calculated in which
factors (a) are not correlated with each other (orthogonal),
and (b) have loadings which are as high as possible or
near-zero.
The varimax (Kaiser 1958) rotated factor matrix is given in
Table 2. The factor analysis was carried out using only the
questionnaire items common to both studies. Factor analysis
was based on the 10 principal components with initial
eigenvalues greater than one. The relative strength of each
factor within the matrix as a whole is indicated in the final
row of Table 2.
The version of the questionnaire employed in study 2 had
eight items in addition to those in study 1. The factor analysis
was carried out only on the items common to the two studies,
and Table 2 reports the factor loadings of these items in
regular font. The eight additional items also appear in Table 2
but are printed in italics. The data provided in the table for
each of the additional items are not factor loadings but are
correlations between the item scores and factor scores
(Mulaik 1987). Correlations greater than þ0Æ3 or less than
�0Æ3 are reported in the table. The new items fall into the
expected groupings.
The interpretation of the factors was undertaken by
inspection of the items which had the highest loadings on
each factor. The factors relate neatly to the five sections.
There is overlap between sections 2 and 3 – which both
have to do with barriers to evidence-based practice. The
particular kind of evidence matters. And section 1 also
generates factors specific to the kind of evidence which is
under consideration.
Table 1 Measurement characteristics of the Developing Evidence-
Based Practice Questionnaire
(a) Descriptive statistics and reliability of sections of the question-
naire and overall questionnaire
Section n
Number of
items* Mean SDSD
Reliability
(Cronbach a)
1 1282 18 59Æ900 6Æ718 0Æ788
2 1286 9 28Æ664 6Æ084 0Æ843
3 1286 5 16Æ596 3Æ990 0Æ805
4 1286 3 10Æ291 2Æ014 0Æ730
5 1287 6 17Æ198 4Æ448 0Æ913
Overall* 1279 41 132Æ672 15Æ001 0Æ874
(b) Intercorrelations between sections of the questionnaire (Pearson)
Section 2 3 4 5
1 0Æ145 0Æ087 0Æ184 0Æ229
2 0Æ582 0Æ160 0Æ373
3 0Æ248 0Æ211
4 0Æ197
*Using only items employed in both studies.
All correlations are significant at the 0Æ01 level, 2-tailed. n for each
section is between 1281 and 1286.
JAN: RESEARCH METHODOLOGY Factors influencing the development of evidence-based practice
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 333
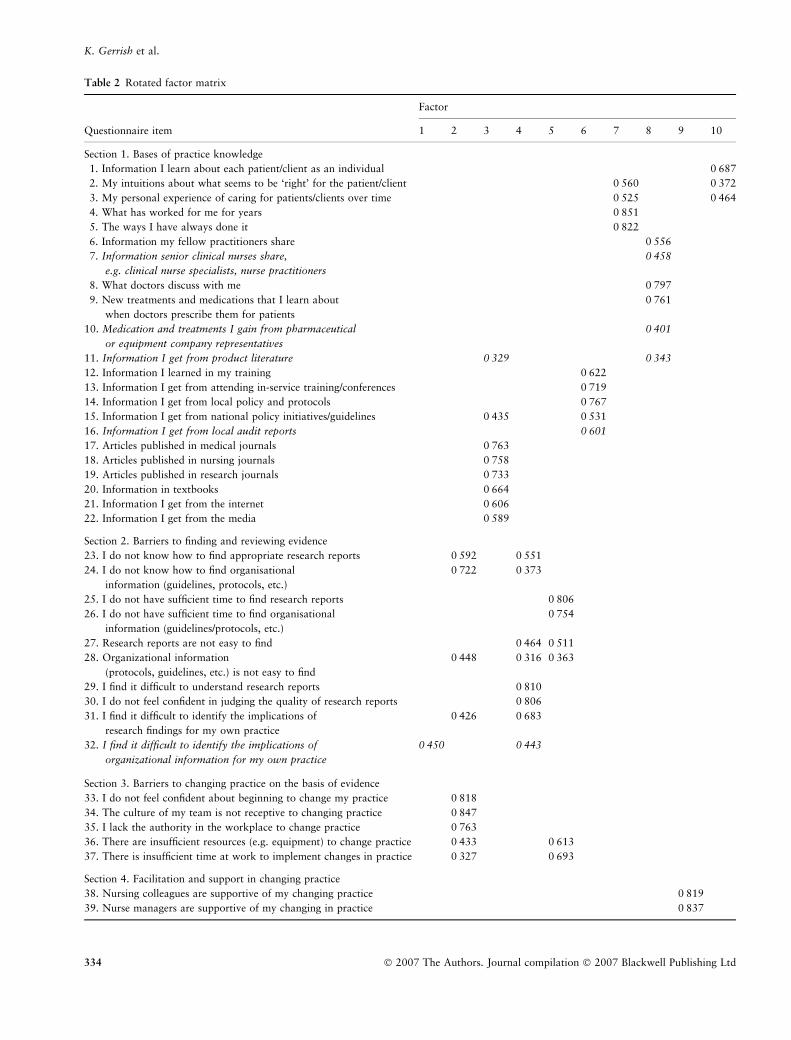
Table 2 Rotated factor matrix
Factor
Questionnaire item 1 2 3 4 5 6 7 8 9 10
Section 1. Bases of practice knowledge
1. Information I learn about each patient/client as an individual 0Æ687
2. My intuitions about what seems to be ‘right’ for the patient/client 0Æ560 0Æ372
3. My personal experience of caring for patients/clients over time 0Æ525 0Æ464
4. What has worked for me for years 0Æ851
5. The ways I have always done it 0Æ822
6. Information my fellow practitioners share 0Æ556
7. Information senior clinical nurses share,
e.g. clinical nurse specialists, nurse practitioners
0Æ458
8. What doctors discuss with me 0Æ797
9. New treatments and medications that I learn about
when doctors prescribe them for patients
0Æ761
10. Medication and treatments I gain from pharmaceutical
or equipment company representatives
0Æ401
11. Information I get from product literature 0Æ329 0Æ343
12. Information I learned in my training 0Æ622
13. Information I get from attending in-service training/conferences 0Æ719
14. Information I get from local policy and protocols 0Æ767
15. Information I get from national policy initiatives/guidelines 0Æ435 0Æ531
16. Information I get from local audit reports 0Æ601
17. Articles published in medical journals 0Æ763
18. Articles published in nursing journals 0Æ758
19. Articles published in research journals 0Æ733
20. Information in textbooks 0Æ664
21. Information I get from the internet 0Æ606
22. Information I get from the media 0Æ589
Section 2. Barriers to finding and reviewing evidence
23. I do not know how to find appropriate research reports 0Æ592 0Æ551
24. I do not know how to find organisational
information (guidelines, protocols, etc.)
0Æ722 0Æ373
25. I do not have sufficient time to find research reports 0Æ806
26. I do not have sufficient time to find organisational
information (guidelines/protocols, etc.)
0Æ754
27. Research reports are not easy to find 0Æ464 0Æ511
28. Organizational information
(protocols, guidelines, etc.) is not easy to find
0Æ448 0Æ316 0Æ363
29. I find it difficult to understand research reports 0Æ810
30. I do not feel confident in judging the quality of research reports 0Æ806
31. I find it difficult to identify the implications of
research findings for my own practice
0Æ426 0Æ683
32. I find it difficult to identify the implications of
organizational information for my own practice
0Æ450 0Æ443
Section 3. Barriers to changing practice on the basis of evidence
33. I do not feel confident about beginning to change my practice 0Æ818
34. The culture of my team is not receptive to changing practice 0Æ847
35. I lack the authority in the workplace to change practice 0Æ763
36. There are insufficient resources (e.g. equipment) to change practice 0Æ433 0Æ613
37. There is insufficient time at work to implement changes in practice 0Æ327 0Æ693
Section 4. Facilitation and support in changing practice
38. Nursing colleagues are supportive of my changing practice 0Æ819
39. Nurse managers are supportive of my changing in practice 0Æ837
K. Gerrish et al.
334 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd
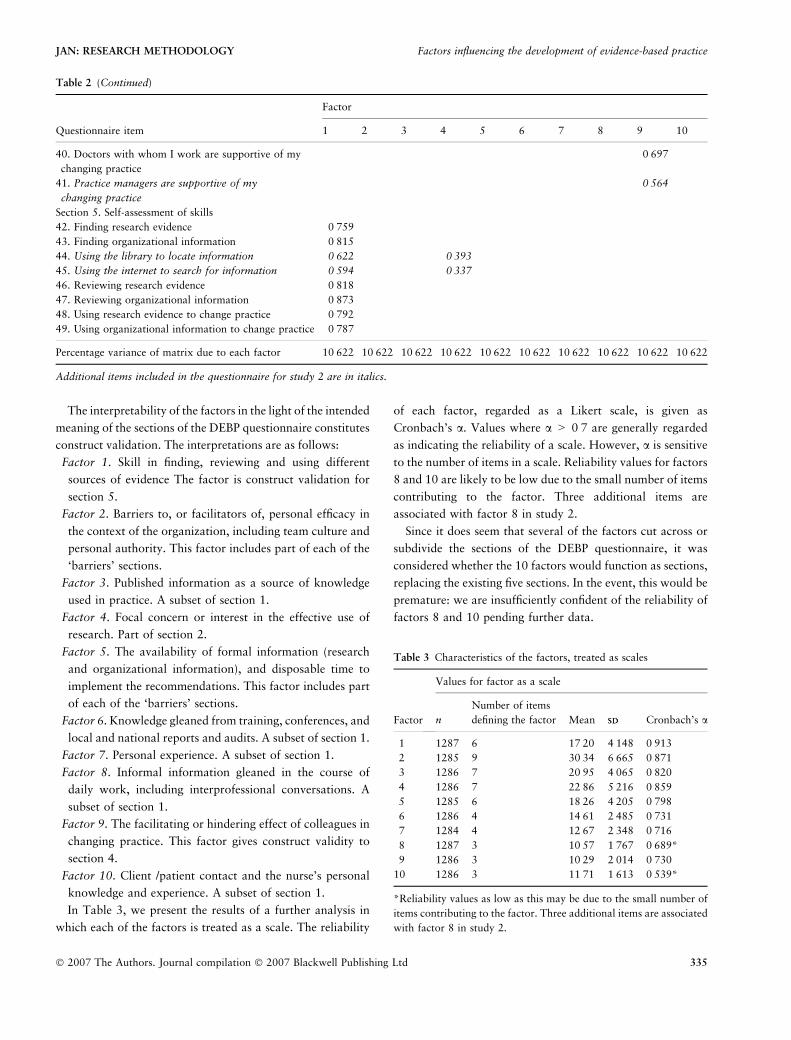
The interpretability of the factors in the light of the intended
meaning of the sections of the DEBP questionnaire constitutes
construct validation. The interpretations are as follows:
Factor 1. Skill in finding, reviewing and using different
sources of evidence The factor is construct validation for
section 5.
Factor 2. Barriers to, or facilitators of, personal efficacy in
the context of the organization, including team culture and
personal authority. This factor includes part of each of the
‘barriers’ sections.
Factor 3. Published information as a source of knowledge
used in practice. A subset of section 1.
Factor 4. Focal concern or interest in the effective use of
research. Part of section 2.
Factor 5. The availability of formal information (research
and organizational information), and disposable time to
implement the recommendations. This factor includes part
of each of the ‘barriers’ sections.
Factor 6. Knowledge gleaned from training, conferences, and
local and national reports and audits. A subset of section 1.
Factor 7. Personal experience. A subset of section 1.
Factor 8. Informal information gleaned in the course of
daily work, including interprofessional conversations. A
subset of section 1.
Factor 9. The facilitating or hindering effect of colleagues in
changing practice. This factor gives construct validity to
section 4.
Factor 10. Client /patient contact and the nurse’s personal
knowledge and experience. A subset of section 1.
In Table 3, we present the results of a further analysis in
which each of the factors is treated as a scale. The reliability
of each factor, regarded as a Likert scale, is given as
Cronbach’s a. Values where a > 0Æ7 are generally regarded
as indicating the reliability of a scale. However, a is sensitive
to the number of items in a scale. Reliability values for factors
8 and 10 are likely to be low due to the small number of items
contributing to the factor. Three additional items are
associated with factor 8 in study 2.
Since it does seem that several of the factors cut across or
subdivide the sections of the DEBP questionnaire, it was
considered whether the 10 factors would function as sections,
replacing the existing five sections. In the event, this would be
premature: we are insufficiently confident of the reliability of
factors 8 and 10 pending further data.
Table 2 (Continued)
Factor
Questionnaire item 1 2 3 4 5 6 7 8 9 10
40. Doctors with whom I work are supportive of my
changing practice
0Æ697
41. Practice managers are supportive of my
changing practice
0Æ564
Section 5. Self-assessment of skills
42. Finding research evidence 0Æ759
43. Finding organizational information 0Æ815
44. Using the library to locate information 0Æ622 0Æ393
45. Using the internet to search for information 0Æ594 0Æ337
46. Reviewing research evidence 0Æ818
47. Reviewing organizational information 0Æ873
48. Using research evidence to change practice 0Æ792
49. Using organizational information to change practice 0Æ787
Percentage variance of matrix due to each factor 10Æ622 10Æ622 10Æ622 10Æ622 10Æ622 10Æ622 10Æ622 10Æ622 10Æ622 10Æ622
Additional items included in the questionnaire for study 2 are in italics.
Table 3 Characteristics of the factors, treated as scales
Factor
Values for factor as a scale
n
Number of items
defining the factor Mean SDSD Cronbach’s a
1 1287 6 17Æ20 4Æ148 0Æ913
2 1285 9 30Æ34 6Æ665 0Æ871
3 1286 7 20Æ95 4Æ065 0Æ820
4 1286 7 22Æ86 5Æ216 0Æ859
5 1285 6 18Æ26 4Æ205 0Æ798
6 1286 4 14Æ61 2Æ485 0Æ731
7 1284 4 12Æ67 2Æ348 0Æ716
8 1287 3 10Æ57 1Æ767 0Æ689*
9 1286 3 10Æ29 2Æ014 0Æ730
10 1286 3 11Æ71 1Æ613 0Æ539*
*Reliability values as low as this may be due to the small number of
items contributing to the factor. Three additional items are associated
with factor 8 in study 2.
JAN: RESEARCH METHODOLOGY Factors influencing the development of evidence-based practice
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 335

Discussion
Study limitations
One of the main disadvantages of using a self-completed
postal questionnaire is the potential for a low response rate
(Robson 2002). Previous surveys examining barriers to
research utilization have experienced relatively poor response
rates. In study 1, the response rate of 45% for the teaching
hospital and 40% for the DGH are not dissimilar to the
response rate of 44% reported by Bryar et al. (2003) in a
large study involving two hospitals and four community
settings and the 40% response rate achieved by Funk et al.
(1991b) in their original study of barriers to research
utilization. In study 2 response rates were slightly higher at
47% which may reflect the effect of targeted reminders to
non-respondents.
Although the response rates compared favourably with
many similar studies, they may nevertheless conceal some
response bias. It was noted, for example, that in the
community study the response rate between different profes-
sional groups varied considerably (57% for health visitors
compared with 37% for practice nurses). It is possible that
nurses who were less favourable towards using evidence in
their practice might have been less likely to respond, thus
biasing the achieved sample. However, such response bias
would be more of a concern in interpreting the overall
findings of the study (to be reported elsewhere) rather than in
assessing the reliability and validity of the tool.
A further limitation might be that the DEBP questionnaire
was changed slightly between the two studies by the addition
of some items. Although these changes were made to enhance
face validity, after consulting users from community settings,
it might be suggested that such changes would have altered
the psychometric properties of the questionnaire. However,
this was not found to be the case. The new items related well
to the established factor structure.
Discussion of results
A large enough sample size (n ¼ 1287 in total) was achieved
for adequate testing of the tool. The psychometric properties
of the DEBP suggest that it is a reliable instrument with 10
identifiable factors, although it is not a single scale. The
conventions used to test the psychometric properties of the
questionnaire were drawn from well-established sources and
demonstrate high reliability (>0Æ7) for each of the five
sections and for eight of the 10 factors when treated as scales.
The lower values for the two remaining factors (8 and 10) are
likely to be due to the small number of items defining the
factors.
The 10 factors are in some cases consistent with the
different elements and sub-sections of the tool, but in some
cases provide over-arching concepts that are drawn from
different elements of the tool. Factor 2, for example,
highlights personal and organizational difficulties in using
evidence-based practice which range from a lack of personal
knowledge to a lack of empowerment to challenge estab-
lished practice. Factors 7 and 8 emphasize the role of
personal experience and informal sources of information in
nurses’ application of evidence-based practice. This aspect of
knowledge utilization has been disregarded in many previous
tools measuring evidence-based practice.
The need to promote the use of appropriate evidence in
nursing practice has been widely acknowledged, along with
an associated need to test and evaluate the extent of evidence-
based practice. As pointed out earlier in the paper, a variety
of instruments have been used to do this, particularly the
‘Barriers’ scale (Funk et al. 1991a) but these tools have been
either untested or found to be lacking in validity (Closs &
Bryar 2001, Marsh et al. 2001). Many of the previously
developed tools are also historically located in a time when
information technology and access to electronic information
in clinical settings was limited. Much has changed in the last
decade, with computer access close to patient care increas-
ingly available, and protocol-based care now integrated into
many clinical areas. We therefore set out to develop and test a
more comprehensive tool (DEBP).
The study has provided evidence of validation of the DEBP
questionnaire for investigating factors associated with evi-
dence-based practice among nurses in England. Notwith-
standing the need for additional studies in the UK and beyond
to further validate of the instrument, the inclusion of sources
of knowledge and skills ratings alongside the ‘barriers’ scale
adds considerably to its usefulness, and factor analysis
suggests that the scales are consistent. Whereas the DEBP
questionnaire has been shown in this study to be a valid
instrument, with reliable scales, the questionnaire as a whole
does not constitute a scale – the component sections are too
diverse in meaning for this. One significant modification to
earlier ‘barriers to research utilization’ questionnaires is the
inclusion in the current questionnaire of organizational
information as a source of evidence. This reflects the
increased emphasis placed on nurses in the UK to draw upon
national and local evidence-based guidelines and clinical
protocols rather than assuming that nurses would, or indeed
should, interpret the significance of findings in published
research papers for their practice.
K. Gerrish et al.
336 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd

Conclusion
The development and testing of the DEBP questionnaire
reported in this article suggest that the instrument is a valid
and reliable measure, although further testing is required to
fully establish its validity and reliability. The generalizability
of the DEBP questionnaire has been shown to extend to nurses
in hospital and community settings in England. However, its
validity in other countries remains to be demonstrated. Before
adoption elsewhere it will be important to review the cultural
appropriateness and content validity of items in the different
sections of the questionnaire as different barriers to evidence-
based practice may be important in some countries. For
example, Oranta et al. (2002) identified that one of the
greatest barriers to evidence-based practice for nurses in
Finland was the fact that most research papers were published
in a language other than Finnish (section 2 of questionnaire).
Indeed, the preponderance of English language journals may
present particular challenges for those whose first language is
not English. Moreover, the high turnover of staff in some
parts of South Africa is seen to mitigate against sustaining
change in respect of evidence-based practice (section 3 of
questionnaire) (Garner et al. (2004), McInerney 2004).
The questionnaire could be used as an outcome measure in
‘before and after’ intervention studies that aim to assess the
impact of service development, training or other innovations
on the extent of evidence-based practice. Organizations
wishing to build research capacity will also find the tool
useful in measuring progress. Because the tool has five
sections and 10 identifiable factors, it may be possible to
analyse the nature of the change being measured over time.
Policies can then be tailored to address the particular barriers
and organizational factors highlighted as being problematic.
It would also be interesting to test its relevance to other
professions such as allied health professions and social work.
Comparisons between the professions regarding the imple-
mentation of evidence-based practice would then be possible.
Author contributions
KG and AL were responsible for the study conception and
design of the manuscript and KG, PA and AL were
responsible for the drafting of the manuscript. KG, AL, JB,
JC, SK and EM performed the data collection and KG, PA
and AL performed the data analysis. KG, AL, JB and SK
obtained funding and JB, EM and JC provided administrative
support. PA provided statistical expertise. KG, PA, AL, JC,
SK and EM made critical revisions to the paper.
Acknowledgements
We are grateful to Professor Carole Estabrooks, University of
Alberta, Canada, for granting permission to adapt and use
some questions from an instrument she had developed to
examine research utilisation.
References
Bryar R., Closs S., Baum G., Cooke J., Griffiths J., Hostick T., Kelly
S., Knight S., Marshall K. & Thompson D. (2003) The Yorkshire
BARRIERS project: diagnostic analysis of barriers to research
utilisation. International Journal of Nursing Studies 40, 73–85.
Carrion M., Woods P. & Norman I. (2004) Barriers to research
utilisation among forensic mental health nurses. International
Journal of Nursing Studies 41, 613–619.
Closs J. & Bryar R. (2001) The BARRIERS scale: does it ‘fit’ the
current NHS research culture. NT Research 6, 853–865.
Collett S. & Elliot P. (2000) Implementing clinical guidelines in
primary care. In Implementing Evidence-Based Changes in
What is already known about this topic
• Existing instruments for assessing evidence-based prac-
tice have focused on examining research utilization ra-
ther than taking a broader view of different sources of
evidence that can inform practice.
• Nurses experience major barriers to implementing re-
search findings due to insufficient time to access and
review research reports, a shortfall in critical appraisal
skills, together with lack of authority and support to
implement findings.
• Whereas evidence-based guidelines and protocols are
increasingly available to support evidence-based prac-
tice, the extent to which nurses use these various forms
of evidence is not clear, nor is how skilled they are in
accessing them.
What this paper adds
• The development and initial validation data for a new
measure of a range of factors involved in evidence-based
practice for use with hospital and community nurses in
England.
• The questionnaire could be used as an outcome measure
in ‘before and after’ intervention studies that aim to assess
the impact of service development, training or other
innovations on the extent of evidence-based practice.
• Further research is needed to test the validity of the
instrument in other countries, and it would also be
interesting to test its relevance to other professions such
as allied healthcare professions and social work.
JAN: RESEARCH METHODOLOGY Factors influencing the development of evidence-based practice
� 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd 337

Healthcare (Evans D. & Haines A., eds), Radcliffe Medical Press,
Abingdon, pp. 235–256.
DiCenso A. & Cullum N. (1998) Implementing evidence-based
nursing: some misconceptions. Evidence-Based Nursing 1, 38–40.
DiCenso A., Prevost S., Benefield L., Bingle J., Ciliska D., Driever M.,
Lock S. & Titler M. (2004) Evidence-based nursing: rationale and
resources. Worldviews on Evidence-Based Nursing First Quarter
2004, 69–75.
Dunn V., Crichton N., Roe B., Seers K., & Williams K. (1998) Using
research for practice: a UK experience of the BARRIERS Scale.
Journal of Advanced Nursing 27, 1203–1210.
Estabrooks C. (1998) Will evidence-based nursing practice make
practice perfect? Canadian Journal of Nursing Research 30, 15–36.
Fawcett J., Watson J., Neuman B., Hinton Walker P. & Fitzpatrick J.
(2001) On nursing theories and evidence. Journal of Nursing
Scholarship Second Quarter 2001, 115–119.
Funk S.G., Champagne M.T., Wiese R.A. & Tornquist E.M. (1991a)
The Barriers to Research Utilization Scale. Applied Nursing
Research 4, 39–45.
Funk S.G., Champagne M.T., Wiese R.A. & Tornquist E.M. (1991b)
Barriers to using research findings in practice: the clinician’s per-
spective. Applied Nursing Research 4, 90–95.
Garner P., Meremikwu M., Volmink J., Xu, Q. & Smith H. (2004)
Putting evidence into practice: how middle and low income countries
‘get it together’. British Medical Journal 329, 1036–1039.
Gerrish K. (2003) Evidence-based practice: unravelling the rhetoric
and making it real. Practice Development in Health Care 2, 99–113.
Gerrish K. (2006) Evidence-based practice. In The Research Process
in Nursing (Gerrish K. & Lacey A., eds), 5th edn Blackwell Sci-
ence, London, pp. 491–505.
Gerrish K. & Clayton J. (2004) Promoting evidence-based practice:
an organisational approach. Journal of Nursing Management 12,
114–123.
Glacken M. & Chaney D. (2004) Perceived barriers and facilitators
to implementing research findings in the Irish practice setting.
Journal of Clinical Nursing 13, 731–740.
Harvey G., Loftus-Hill A., Rycroft-Malone J., Titchen A., Kitson A.,
McCormack B. & Seers K. (2002) Getting evidence into practice:
the role and function of facilitation. Journal of Advanced Nursing
37, 577–588.
Hicks C. (1996) A study of nurses’ attitudes towards research: a factor
analytic approach. Journal of Advanced Nursing 23, 373–379.
HutchinsonA.&JohnsonL. (2004)Bridging thedivide: a surveyofnurses’
opinions regarding barriers to, and facilitators of, research utilisation in
the practice setting. Journal of Clinical Nursing 13, 304–315.
Ingersoll G. (2000) Evidence-based nursing: what it is and what it
isn’t. Nursing Outlook 48, 151–152.
Kaiser H.F. (1958) The varimax criterion for analytic rotation in
factor analysis. Psychometrika 23, 187–200.
Kajermo K., Nordstrom G., Krusebrant A. & Bjorvell H. (1998) Barriers
to and facilitators of research utilisation, as perceived by a group of
registeredNurses inSweden. JournalofAdvancedNursing27, 798–807.
Kirshbaum M., Beaver K. & Luker K. (2004) Perspectives of breast
care nurses on research dissemination and utilisation. Clinical
Effectiveness in Nursing 8, 47–58.
Kuuppelomaki M. & Tuomi J. (2005) Finnish nurses’ attitudes
towards nursing research and related factors. International Journal
of Nursing Studies 42, 187–196.
Lacey E.A. (1994) Research utilisation in nursing practice: a pilot
study. Journal of Advanced Nursing 19, 987–995.
Lawley D.N. & Maxwell A.E. (1971) Factor Analysis as a Statistical
Method, 2nd edn. Butterworth, Oxford.
Liaschenko J. & Fisher A. (1999) Theorizing the knowledge that
nurses use in the conduct of their work. Scholarly Inquiry for
Nursing Practice. An International Journal 13, 29–40.
Lomas J., Culyer T., McCutcheon C., McAuley L., Law S. (2005)
Conceptualizing and Combining Evidence for Health System
Guidance. Canadian Health Services Research Foundation
(CHSRF). Retrieved from: http://www.chsrf.ca.
Marsh G., Nolan M. & Hopkins S. (2001) Testing the revised
barriers to research utilisation scale for use in the UK. Clinical
Effectiveness in Nursing 5, 66–72.
McCormack B., Kitson A., Harvey G., Rycroft-Malone J., Titchen A.
& Seers K. (2002) Getting evidence into practice: the meaning of
‘context’. Journal of Advanced Nursing 38, 94–104.
McInerney P. (2004) Evidence-based nursing and midwifery: the state
of the science in South Africa. Worldviews on Evidence-Based
Nursing 1, 4207.
McKenna H., Ashton S. & Keeney S. (2004): Barriers to evidence-
based practice in primary care. Journal of Advanced Nursing 45,
178–189.
Mulaik, S.A. (1987) A brief history of the philosophical foundations
of exploratory factor analysis. Multivariate Behavioural Research
22, 267–305
Nolan M. (2005) Reconciling tensions between research, evidence-
based practice and user participation: time for nursing to take the
lead. International Journal of Nursing Studies 42, 503–505.
Nolan M., Morgan L., Curran M., Clayton J., Gerrish K. & Parker
K. (1998) Evidence-based care: can we overcome the barriers?
British Journal of Nursing 7, 1273–1278.
Oranta O., Routasolo P. & Hupli M. (2002) Barriers to and facil-
itators of research utilisation among Finnish Registered Nurses.
Journal of Clinical Nursing 11, 205–213.
Pett M.A. (2003) Making Sense of Factor Analysis in Health Care
Research: A Practical Guide. Sage, London.
Retsas A. & Nolan M. (1999) Barriers to nurses’ use of research: an
Australian hospital study. International Journal of Nursing Studies
36, 335–343.
Robson C. (2002) Real World Research: A Resource for Social
Scientists and Practitioners. Blackwell, Oxford.
Rodgers S. (1994) An exploratory study of research utilisation by
nurses in general medical and surgical wards. Journal of Advanced
Nursing 20, 904–911.
Royle J. & Blythe J. (1998) Promoting research utilisation in nursing:
the role of the individual, organisation, and environment. Evi-
dence-Based Nursing 1, 71–72.
Rycroft-Malone J., Seers K., Titchen A., Harvey G., Kitson A. &
McCormack B. (2004) What counts as evidence in evidence into
practice? Journal of Advanced Nursing 47, 81–90.
Sackett D., Rosenburg W., Muir Gray J., Haynes R. & Richardson
W. (1996) Evidence-based medicine: what it is and what it isn’t.
British Medical Journal, 312, 71–72.
Sackett D., Richardson S., Richardson S., Rosenberg W. & Haynes B.
(2000) Evidence-Based Medicine: How to Practice and Teach
EBM. Churchill Livingstone, Edinburgh.
K. Gerrish et al.
338 � 2007 The Authors. Journal compilation � 2007 Blackwell Publishing Ltd




















