“Exploring the sexual and reproductive health of refugee ...
124
Hamburg University of Applied Sciences Faculty of Life Sciences, Department of Health Sciences “Exploring the sexual and reproductive health of refugee women in Hamburg, Germany” Master thesis 1 st SUPERVISOR: Prof. Dr. (mult.) Dr. h.c. (mult.) Walter Leal (HAW-Hamburg) 2 nd SUPERVISOR: Dipl. Ges.wirtinWiebkeBendt, MSc. (HAW-Hamburg) DATE OF SUBMISSION: 28.02.2019 SUBMITTED BY: Sona Sainju MATRICULATION NUMBER:
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of “Exploring the sexual and reproductive health of refugee ...

Hamburg University of Applied Sciences
Faculty of Life Sciences, Department of Health Sciences
“Exploring the sexual and reproductive health of refugee
women in Hamburg, Germany”
Master thesis
1st SUPERVISOR: Prof. Dr. (mult.) Dr. h.c. (mult.) Walter Leal (HAW-Hamburg)
2nd SUPERVISOR: Dipl. Ges.wirtinWiebkeBendt, MSc. (HAW-Hamburg)
DATE OF SUBMISSION: 28.02.2019
SUBMITTED BY: Sona Sainju
MATRICULATION NUMBER:
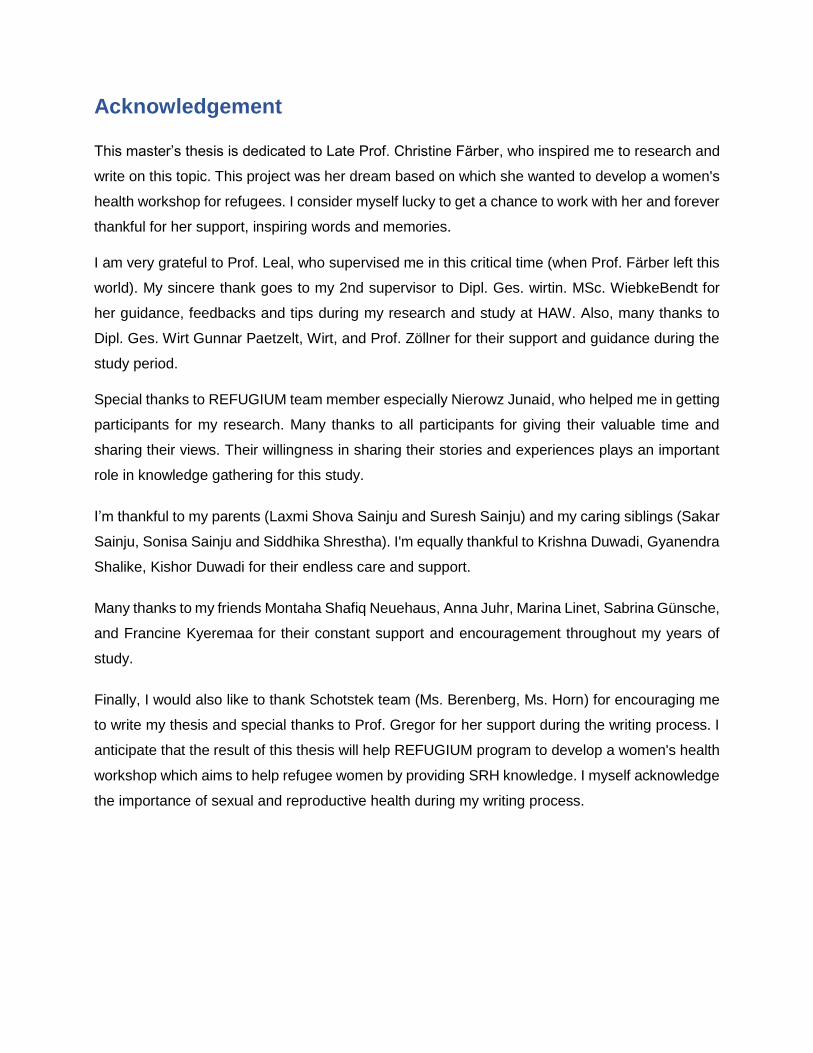
Acknowledgement
This master’s thesis is dedicated to Late Prof. Christine Färber, who inspired me to research and
write on this topic. This project was her dream based on which she wanted to develop a women's
health workshop for refugees. I consider myself lucky to get a chance to work with her and forever
thankful for her support, inspiring words and memories.
I am very grateful to Prof. Leal, who supervised me in this critical time (when Prof. Färber left this
world). My sincere thank goes to my 2nd supervisor to Dipl. Ges. wirtin. MSc. WiebkeBendt for
her guidance, feedbacks and tips during my research and study at HAW. Also, many thanks to
Dipl. Ges. Wirt Gunnar Paetzelt, Wirt, and Prof. Zöllner for their support and guidance during the
study period.
Special thanks to REFUGIUM team member especially Nierowz Junaid, who helped me in getting
participants for my research. Many thanks to all participants for giving their valuable time and
sharing their views. Their willingness in sharing their stories and experiences plays an important
role in knowledge gathering for this study.
I’m thankful to my parents (Laxmi Shova Sainju and Suresh Sainju) and my caring siblings (Sakar
Sainju, Sonisa Sainju and Siddhika Shrestha). I'm equally thankful to Krishna Duwadi, Gyanendra
Shalike, Kishor Duwadi for their endless care and support.
Many thanks to my friends Montaha Shafiq Neuehaus, Anna Juhr, Marina Linet, Sabrina Günsche,
and Francine Kyeremaa for their constant support and encouragement throughout my years of
study.
Finally, I would also like to thank Schotstek team (Ms. Berenberg, Ms. Horn) for encouraging me
to write my thesis and special thanks to Prof. Gregor for her support during the writing process. I
anticipate that the result of this thesis will help REFUGIUM program to develop a women's health
workshop which aims to help refugee women by providing SRH knowledge. I myself acknowledge
the importance of sexual and reproductive health during my writing process.
II
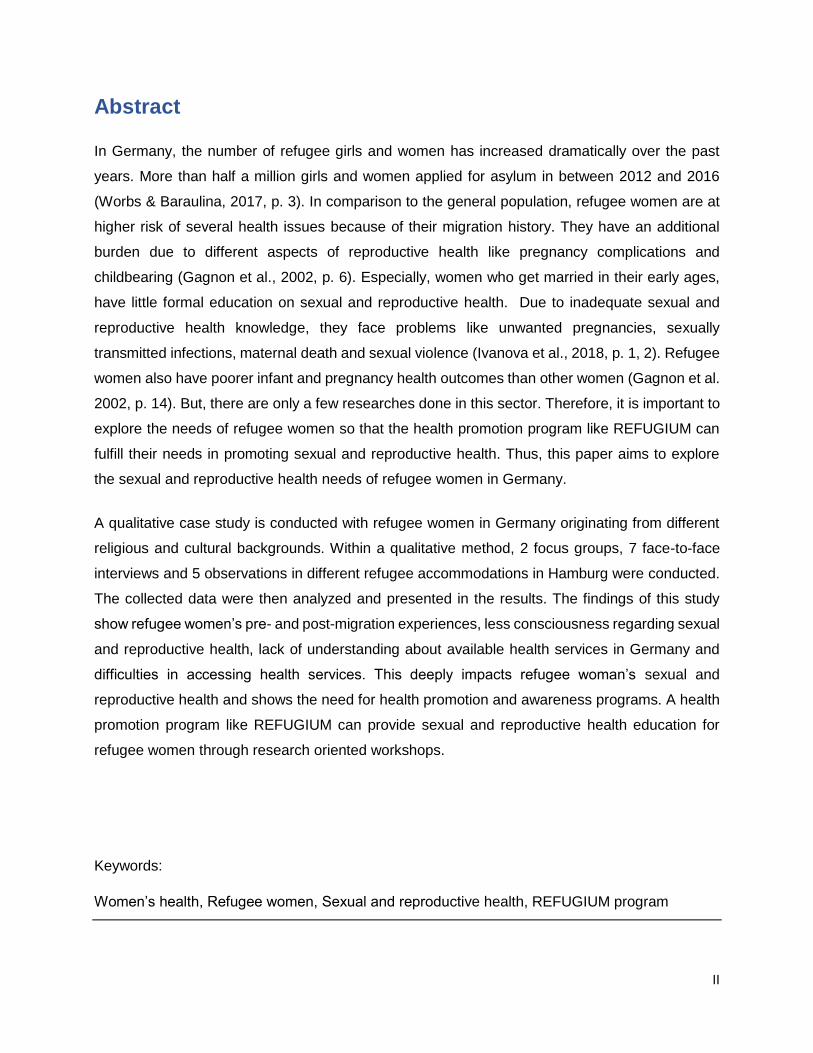
Abstract
In Germany, the number of refugee girls and women has increased dramatically over the past
years. More than half a million girls and women applied for asylum in between 2012 and 2016
(Worbs & Baraulina, 2017, p. 3). In comparison to the general population, refugee women are at
higher risk of several health issues because of their migration history. They have an additional
burden due to different aspects of reproductive health like pregnancy complications and
childbearing (Gagnon et al., 2002, p. 6). Especially, women who get married in their early ages,
have little formal education on sexual and reproductive health. Due to inadequate sexual and
reproductive health knowledge, they face problems like unwanted pregnancies, sexually
transmitted infections, maternal death and sexual violence (Ivanova et al., 2018, p. 1, 2). Refugee
women also have poorer infant and pregnancy health outcomes than other women (Gagnon et al.
2002, p. 14). But, there are only a few researches done in this sector. Therefore, it is important to
explore the needs of refugee women so that the health promotion program like REFUGIUM can
fulfill their needs in promoting sexual and reproductive health. Thus, this paper aims to explore
the sexual and reproductive health needs of refugee women in Germany.
A qualitative case study is conducted with refugee women in Germany originating from different
religious and cultural backgrounds. Within a qualitative method, 2 focus groups, 7 face-to-face
interviews and 5 observations in different refugee accommodations in Hamburg were conducted.
The collected data were then analyzed and presented in the results. The findings of this study
show refugee women’s pre- and post-migration experiences, less consciousness regarding sexual
and reproductive health, lack of understanding about available health services in Germany and
difficulties in accessing health services. This deeply impacts refugee woman’s sexual and
reproductive health and shows the need for health promotion and awareness programs. A health
promotion program like REFUGIUM can provide sexual and reproductive health education for
refugee women through research oriented workshops.
Keywords:
Women’s health, Refugee women, Sexual and reproductive health, REFUGIUM program

III
Table of Contents
Acknowledgement ........................................................................................................................ I
Abstract ....................................................................................................................................... II
Table of Contents ....................................................................................................................... III
List of Figures ............................................................................................................................. V
List of Tables ............................................................................................................................. VI
List of Appendices .................................................................................................................... VII
List of Abbreviations ................................................................................................................ VIII
1 Introduction .............................................................................................................................. 1
2 Sexual and reproductive health of refugee women in Germany ................................................ 4
2.1 Refugee women in Germany.............................................................................................. 4
2.2 Sexual and reproductive health .......................................................................................... 7
2.3 Refugee’s women sexual and reproductive health ........................................................... 10
2.4 Sexual and reproductive health service in Germany ........................................................ 15
2.5 Health promotion and awareness programs in Germany .................................................. 18
2.5.1 Zanzu ........................................................................................................................ 18
2.5.2 REFUGIUM program ................................................................................................. 20
3 Method ................................................................................................................................... 23
3.1 Qualitative approach ........................................................................................................ 23
3.2 Development of interview guide ....................................................................................... 25
3.3 Data collection ................................................................................................................. 27
3.3.1 Sampling and recruitment .......................................................................................... 27
3.3.2 Conducting focus-group ............................................................................................. 29
3.3.3 Conducting face-to-face interview .............................................................................. 31
3.3.4 Observation ............................................................................................................... 32
3.4 Data analysis ................................................................................................................... 34
3.4.1 Transcription .............................................................................................................. 34
3.4.2 Content analysis ........................................................................................................ 35
4. Results .................................................................................................................................. 39
4.1 Participants ...................................................................................................................... 39
4.2 Perception towards health ................................................................................................ 41
4.3 Perception towards sexual and reproductive health ......................................................... 44
4.4 Sexual and reproductive health knowledge ...................................................................... 46
4.5 Sexual and reproductive health issues ............................................................................. 48
4.5.1 Menstruation .............................................................................................................. 48

IV
4.5.2 Early and forced marriage ......................................................................................... 50
4.5.3 Pregnancy and childbirth ........................................................................................... 52
4.5.4 Abortion ..................................................................................................................... 53
4.5.5 Family planning and contraceptives ........................................................................... 54
4.5.6 Sexual transmitted infections ..................................................................................... 56
4.5.7 Sexual and gender-based violence ............................................................................ 57
4.6 Awareness about sexual and reproductive health services .............................................. 60
4.6.1 Health services in refugee camps .............................................................................. 60
4.6.2 Health care services in Germany ............................................................................... 60
4.6.3 Health promotion and awareness program ................................................................ 61
4.6.4 Health services in the country of origin ...................................................................... 63
4.7 Barriers in accessing health services ............................................................................... 64
4.7.1 Communication ......................................................................................................... 64
4.7.2 Gender aspects ......................................................................................................... 66
4.7.3 Different health care system ...................................................................................... 68
4.7.4 Social and financial support ....................................................................................... 69
4.7.5 Culture and tradition .................................................................................................. 70
4.7.6 Living conditions in refugee accommodation ............................................................. 71
4.7.7 Stress factors ............................................................................................................ 74
4.8. Advice and suggestions for women health workshop ...................................................... 75
4.8.1 General suggestions for a workshop.......................................................................... 75
4.8.2 Suggested SRH topics .............................................................................................. 76
5 Discussion .............................................................................................................................. 78
5.1 Summary of the findings .................................................................................................. 78
5.2 Discussion of results ........................................................................................................ 82
5.3 Discussion of method ....................................................................................................... 84
6 Recommendations ................................................................................................................. 87
6.1 General recommendations for REFUGIUM workshop ...................................................... 87
6.2 Specific sexual and reproductive health topics for women's health workshop .................. 88
7 Conclusion ............................................................................................................................. 97
8 References ........................................................................................................................... 100
9 Appendix .............................................................................................................................. 107
Declaration of Authorship

V
List of Figures
Figure 1 Number of asylum application in different regions of Germany in 2018 .......................... 4
Figure 2 Origin of Refugees in Germany ..................................................................................... 5
Figure 3 Contraceptive prevalence rate ..................................................................................... 11
Figure 4 Consequences of partner abuse, sexual assault, and child sexual abuse .................... 13
Figure 5 Logo of the campaign “Violence against women” ........................................................ 17
Figure 6 Six main themes of Zanzu ........................................................................................... 19
Figure 7 Zanzu information illustrated through pictograms ........................................................ 20
Figure 8 REFUGIUM health workshop topics ............................................................................ 21
Figure 9 Interview question types .............................................................................................. 25
VI
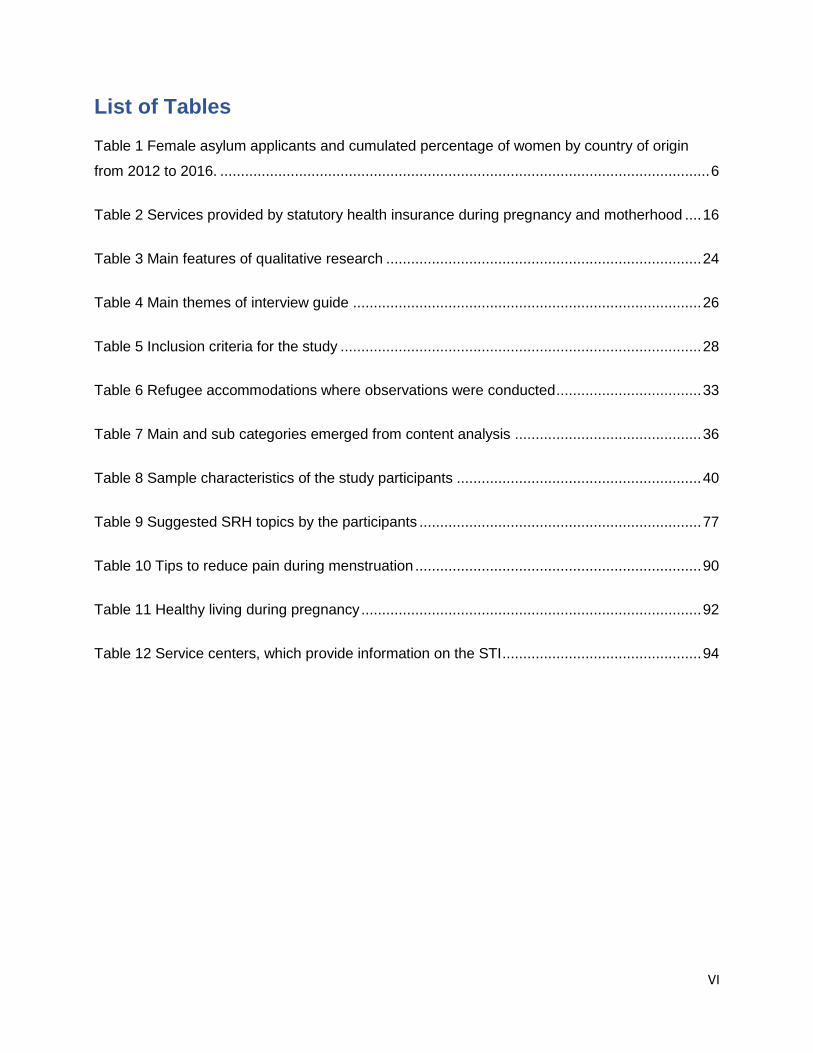
List of Tables
Table 1 Female asylum applicants and cumulated percentage of women by country of origin
from 2012 to 2016. ...................................................................................................................... 6
Table 2 Services provided by statutory health insurance during pregnancy and motherhood .... 16
Table 3 Main features of qualitative research ............................................................................ 24
Table 4 Main themes of interview guide .................................................................................... 26
Table 5 Inclusion criteria for the study ....................................................................................... 28
Table 6 Refugee accommodations where observations were conducted ................................... 33
Table 7 Main and sub categories emerged from content analysis ............................................. 36
Table 8 Sample characteristics of the study participants ........................................................... 40
Table 9 Suggested SRH topics by the participants .................................................................... 77
Table 10 Tips to reduce pain during menstruation ..................................................................... 90
Table 11 Healthy living during pregnancy .................................................................................. 92
Table 12 Service centers, which provide information on the STI ................................................ 94

VII
List of Appendices
Appendix A: Recruitment Script ............................................................................................... 107
Appendix B: Interview Guideline .............................................................................................. 108
Appendix C: Consent form ..................................................................................................... 111
Appendix D: Observation protocol ........................................................................................... 112
Appendix E: Interview Fieldnote .............................................................................................. 113
Appendix F: Focus group setting ............................................................................................. 114
VIII
List of Abbreviations
AIDA Asylum Information Database
AIDS Acquired immune deficiency syndrome
BAMF Bundesamtfür Migration und Flüchtlinge
(Federal Office for Migration and Refugees
BZgA Bundeszentralefür gesundheitliche Aufklärung
ECRE European Council on Refugees and Exiles
HAW Hamburg University of Applied Sciences
HIV Human immunodeficiency virus
MCWH Multicultural Centre For Women's Health
NGOs Non-governmental organizations
REFUGIUM Rat mit Erfahrung: Flucht Und Gesundheit, Information Und Multiplikation
(Experienced Advice: Refuge and Health, Information and Peer-Facilitation)
RHTAC The Refugee Health Technical Assistance Centre
SRH Sexual and Reproductive Health
STI Sexually Transmitted Infection
UNFPA United Nations Population Fund
UNHCR The United Nations Refugee Agency
WHO World Health Organization

1 Introduction
1
1 Introduction
Germany is one of the European countries that received the highest number of refugees for the
last years (Sönmez et al., 2017). In the year 2017, around 1.7 million people seeking protection
were registered in the Central Register of Foreigners (AZR) (Statistisches Bundesamt (Destatis),
2019). The majority of the people that claimed asylum in Germany are from Syria, Afghanistan,
Iraq and Iran. Among refugees, women and children constitute the most vulnerable groups from
war and conflicts (Sönmez et al., 2017). The number of refugee girls and women has also
increased dramatically over the past years. There were more than half a million girls and women
who applied for asylum in Germany between 2012 and 2016. Most of the refugee girls and women
are in the reproductive age (Worbs & Baraulina, 2017, p. 4).
A systematic review of refugee women’s reproductive health show that resettled women are at
higher risk than others for several harmful reproductive health outcomes because of their
migration experience (Gagnon et al., 2002, p. 6). Refugee women experienced many problems
in their home country, during their migration and in the host country (World Future Council, 2016,
p. 4). Especially, women and girls are exposed to sexual and gender-based violence, such as
rape, sexual exploitation and abuse, sexual harassment, psychological violence, trafficking, early
and forced marriage, transactional sex and domestic violence (Kurmeyer, Abels, & Merkle, 2017,
p.5). This gender-based violence, including forced marriage is one of the reasons for migration
for some refugee women (World Future Council, 2016, p. 4). Further on, female refugees have
an additional burden due to different aspects of reproductive health like pregnancy complications,
childbearing, which places them in a particularly disadvantaged position (Gagnon et al., 2002, p.
6). Especially, women who get married in their early age have little formal education on SRH
(Crossland et al., 2015, p. 397). Due to low SRH knowledge, they have to face problems like
unwanted pregnancies, sexually transmitted infections, maternal death and sexual violence
(Ivanova et al., 2018, p. 2). Refugee women have also poorer infant and pregnancy health
outcomes than other women (Gagnon et al., 2002, p. 14).
All these health-related problems, including gender-specific traumatization and the child care
responsibility of married women, language barrier, woman's changing role within the traditional
family context and loss of social support hinder refugee women to get access to medical care in
the host country (Charite, 2017). These kinds of pre- and post-resettlement factors can have
profound effects on women's reproductive health. Further on, only a few types of researches
have been done in the field of SRH care for refugee women with a focus on the provision of family
planning, SRH and maternity care (Mengesha et al., 2017). Thus, there is need of health
promotion programs, which helps refugee women to benefit and live a better life than they were
able to do before.

1 Introduction
2
REFUGIUM program in Hamburg is one of the health promotion and awareness programs, which
aim to promote refugee health by providing them knowledge of healthy lifestyle and information
on access to health services. REFUGIUM program is offering different health workshops in
refugee accommodations in cooperation with other organizations. To improve the sexual and
reproductive health of refugee women, REFUGIUM program aims to develop a women’s health
workshop (REFUGIUM program). Before the development of women’s health workshop for
refugees, their SRH issues and needs, and existing level of knowledge and their understanding
should be explored. Thus, this paper aims to study such needs, which should further help
REFUGIUM program to develop a women’s health workshop focusing on SRH. Therefore, the
research question is “What are the sexual and reproductive health needs of refugee women living
in Germany?”
Answering this question involves several steps. At first, some data regarding refugee women in
Germany are presented. Following it, sexual and reproductive health is described briefly including
some aspects such as pregnancy, family planning, contraceptive, STI, sexual and gender-based
violence. After that, refugee women’s SRH problems are presented based on literature research.
Further on, a brief description of SRH services in Germany and the health promotion and
awareness programs, i.e. Zanzu and REFUGIUM program are also introduced. This gives an
overview of the sexual and reproductive health of the refugee women in Germany. Then each
step of the applied method for the research is described. It starts with choosing a qualitative case
study design and the development of the interview guide. The data collection process involves
the recruitment of participants, conducting a focus group and face-to-face interviews based on a
semi-structured interview guide. The data analysis process includes transcriptions and content
analysis. During the research process, ethical aspects were also considered and a self-reflexivity
is also provided. Finally, the obtained data are interpreted and portrayed in results. Following
that, a summary of findings, some limitation of the results and applied method are also discussed.
At last, some recommendations are given to REFUGIUM program to conduct a women’s health
workshop. There is a general recommendation for conducting a women’s health workshop and
specific recommendations which provide relevant SRH information as a content for women’s
health workshop.
This paper explores refugee women's perception towards health, their health conscious and
health-related behaviors. It discusses their specific SRH issues such as early marriage, the
problems during menstruation, difficulties during pregnancy, low awareness about STI, and
contraception, high risk for sexual violence etc. The paper also explores the reason behind poor
sexual and reproductive health knowledge among refugee women. It also illustrates refugee
women’s awareness of health services in Germany, as well as their utilization of health services
in their home country. The results also present the barriers such as a communication barrier,
1 Introduction
3
gender aspects, the difference in health care systems, poor living conditions, lack of social and
financial support, stress factors, etc.
In this way, the paper presents different SRH issues that refugee women are experiencing and
emphasizes the need for public health intervention to promote their health as well as minimize
negative impacts on family and the economy. The results of this study will certainly help
REFUGIUM program to develop women’s health workshop modules. Further on, the finding from
this study could also help policymakers, educators and health care providers in promoting the
sexual and reproductive health of refugee women.
2 Sexual and reproductive health of refugee women in Germany
4
2 Sexual and reproductive health of refugee women in Germany
This chapter provides insight into the relevance of the topic by presenting some key facts about
refugee women in Germany, a description about sexual and reproductive health (SRH) and
refugee women’s SRH problems. It also provides information on different health services that
Germany is offering concerning SRH. Along with it, there is also a brief description of health
promotion and awareness program like Zanzu and REFUGIUM.
2.1 Refugee women in Germany
In recent years, Europe has encountered a refugee crisis due to continuing conflicts, war and
human rights violations in many countries. This has resulted in the displacement of millions of
people, who seek refuge in different countries (Entre Nous, WHO & UNFPA, 2016, p. 26).
European countries are currently the main recipient of immigrants as refugees. Among them,
Germany has become a popular destination for many refugees. There were more than 1 million
people who have migrated Germany since 2015 (BAMF, 2016). The immigrated refugees are
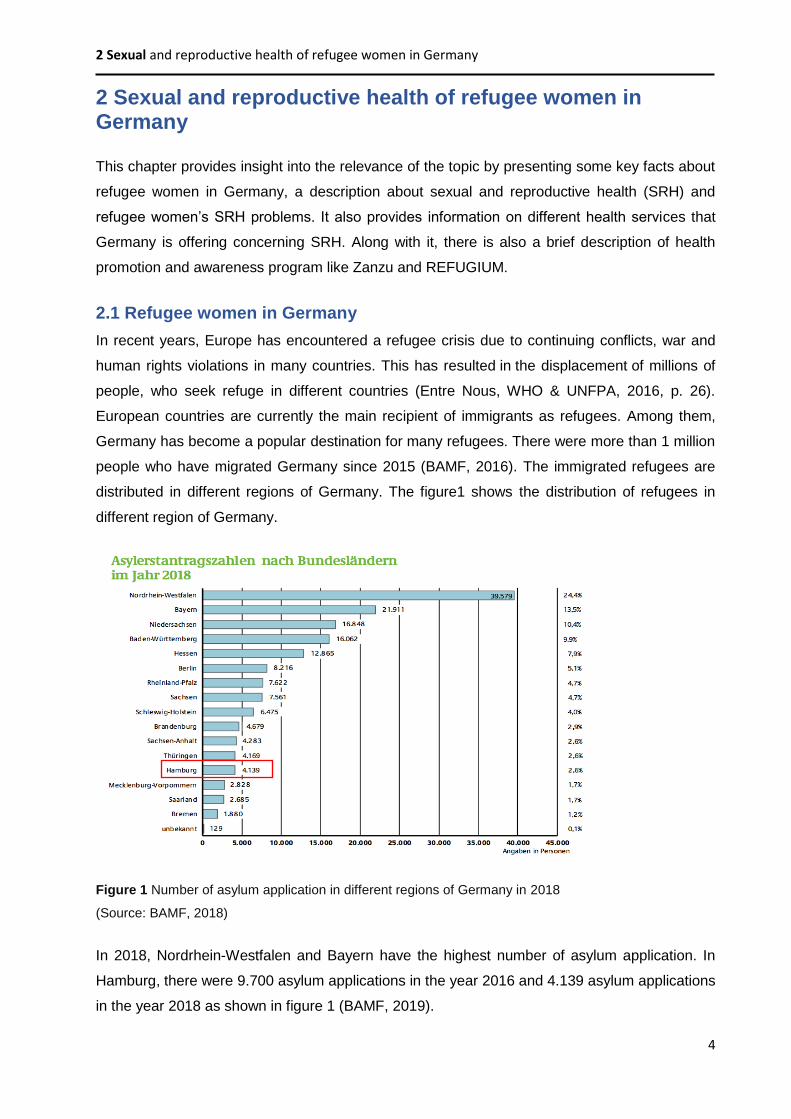
distributed in different regions of Germany. The figure1 shows the distribution of refugees in
different region of Germany.
Figure 1 Number of asylum application in different regions of Germany in 2018
(Source: BAMF, 2018)
In 2018, Nordrhein-Westfalen and Bayern have the highest number of asylum application. In
Hamburg, there were 9.700 asylum applications in the year 2016 and 4.139 asylum applications
in the year 2018 as shown in figure 1 (BAMF, 2019).
2 Sexual and reproductive health of refugee women in Germany
5
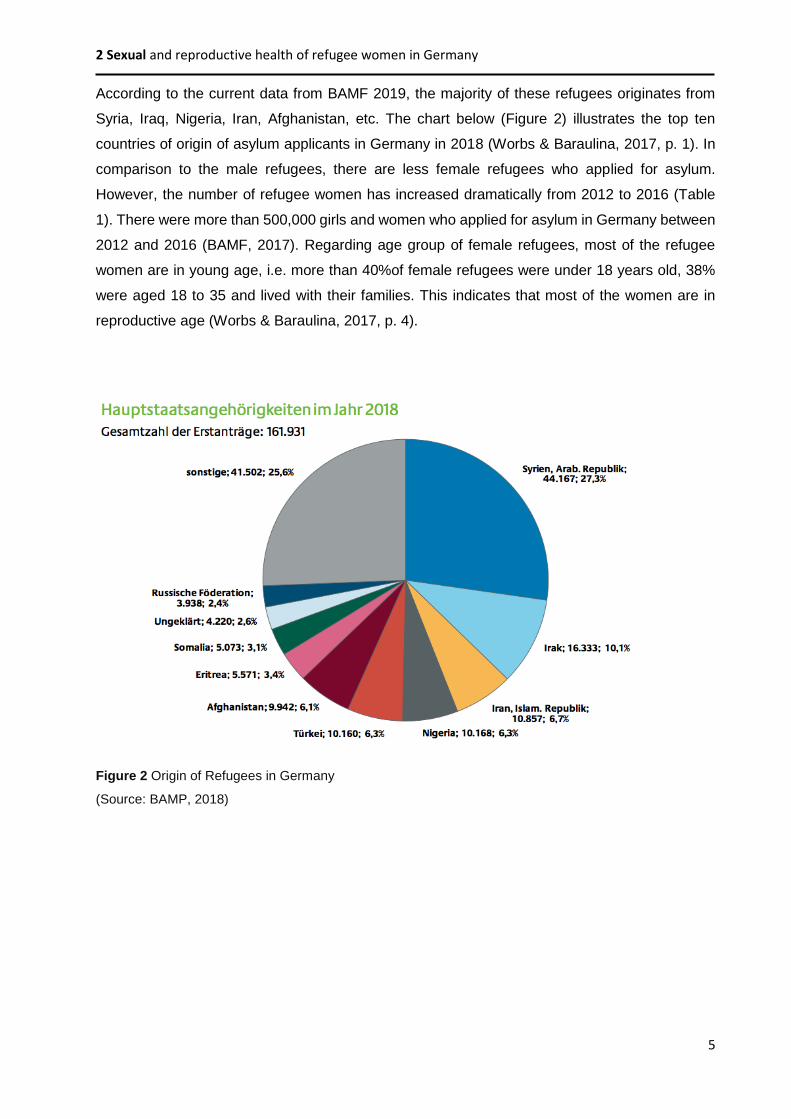
According to the current data from BAMF 2019, the majority of these refugees originates from
Syria, Iraq, Nigeria, Iran, Afghanistan, etc. The chart below (Figure 2) illustrates the top ten
countries of origin of asylum applicants in Germany in 2018 (Worbs & Baraulina, 2017, p. 1). In
comparison to the male refugees, there are less female refugees who applied for asylum.
However, the number of refugee women has increased dramatically from 2012 to 2016 (Table
1). There were more than 500,000 girls and women who applied for asylum in Germany between
2012 and 2016 (BAMF, 2017). Regarding age group of female refugees, most of the refugee
women are in young age, i.e. more than 40%of female refugees were under 18 years old, 38%
were aged 18 to 35 and lived with their families. This indicates that most of the women are in
reproductive age (Worbs & Baraulina, 2017, p. 4).
Figure 2 Origin of Refugees in Germany
(Source: BAMP, 2018)
2 Sexual and reproductive health of refugee women in Germany
6
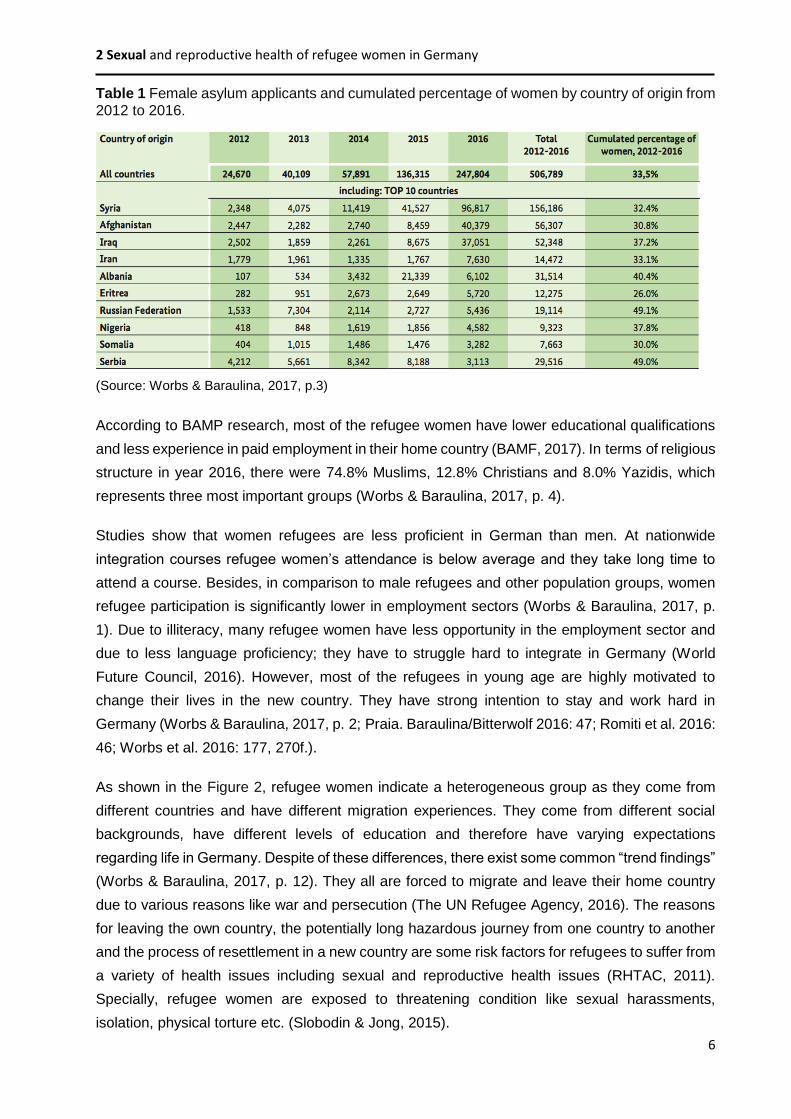
Table 1 Female asylum applicants and cumulated percentage of women by country of origin from 2012 to 2016.
(Source: Worbs & Baraulina, 2017, p.3)
According to BAMP research, most of the refugee women have lower educational qualifications
and less experience in paid employment in their home country (BAMF, 2017). In terms of religious
structure in year 2016, there were 74.8% Muslims, 12.8% Christians and 8.0% Yazidis, which
represents three most important groups (Worbs & Baraulina, 2017, p. 4).
Studies show that women refugees are less proficient in German than men. At nationwide
integration courses refugee women’s attendance is below average and they take long time to
attend a course. Besides, in comparison to male refugees and other population groups, women
refugee participation is significantly lower in employment sectors (Worbs & Baraulina, 2017, p.
1). Due to illiteracy, many refugee women have less opportunity in the employment sector and
due to less language proficiency; they have to struggle hard to integrate in Germany (World
Future Council, 2016). However, most of the refugees in young age are highly motivated to
change their lives in the new country. They have strong intention to stay and work hard in
Germany (Worbs & Baraulina, 2017, p. 2; Praia. Baraulina/Bitterwolf 2016: 47; Romiti et al. 2016:
46; Worbs et al. 2016: 177, 270f.).
As shown in the Figure 2, refugee women indicate a heterogeneous group as they come from
different countries and have different migration experiences. They come from different social
backgrounds, have different levels of education and therefore have varying expectations
regarding life in Germany. Despite of these differences, there exist some common “trend findings”
(Worbs & Baraulina, 2017, p. 12). They all are forced to migrate and leave their home country
due to various reasons like war and persecution (The UN Refugee Agency, 2016). The reasons
for leaving the own country, the potentially long hazardous journey from one country to another
and the process of resettlement in a new country are some risk factors for refugees to suffer from
a variety of health issues including sexual and reproductive health issues (RHTAC, 2011).
Specially, refugee women are exposed to threatening condition like sexual harassments,
isolation, physical torture etc. (Slobodin & Jong, 2015).

2 Sexual and reproductive health of refugee women in Germany
7
2.2 Sexual and reproductive health
According to World Health Organization (WHO) sexual and reproductive health (SRH) is defined
as “a state of complete physical, mental and social well-being in all matters relating to the
reproductive system” (WHO, 2018a). It implies that every individual is able to have a responsible,
satisfying and safe sex life and they have the rights to make their own choices about their sexual
and reproductive health (WHO, 2018c). In a comprehensive way, SRH refers to the ability to
have a voluntary sexual relationship, fertility regulation, disease protection and treatment, and
right for pregnancy support and delivery, abortion and post-abortion care and early child health
(Blanc, 2001, p. 190).
However, health advocates from developing countries have the opinion that the globally used
concept of reproductive health is not always applicable to all cultures as the concept of
reproductive health is culturally constructed. It is a product of specific historical, ethical and legal
transformations (Kaddour et al., 2005, p. 35). For example, the Reproductive Health Working
Group (RHWG) which is comprised of researchers, particularly from Egypt, Lebanon, Palestine,
Syria and Turkey defines reproductive health as ‘‘the ability of women to live through the
reproductive years and beyond with reproductive choice, dignity, and successful childbearing,
and to be free of gynecological disease and risk’’ (Kaddour et al., 2005, p. 35).
Nevertheless, SRH includes a wide range of aspects such as family planning, contraceptive, STI,
post-abortion care, menopause, female genital mutilation, sexual and gender-based violence
(Gagnon et al., 2002, p. 9). Another important subject area of SRH is maternal-health, which
encompasses pre-pregnancy, antenatal, childbirth and after birth supports which has profound
effect on mother and their child health (Commonwealth of Australia, 2010, p. 24). Furthermore, it
is also concerned with issues like human rights related to sexual health, sexual pleasure,
eroticism and sexual satisfaction, sexual dysfunction, and mental health related to sexual health
(WHO, 2018c). Following paragraphs provides some important aspects of SRH such as family
planning, contraceptive, pregnancy, STI and violence.
Family planning is an important aspect of SRH. Family planning enables individuals to make
informed choices about their SRH (WHO, 2018e). It is the information, means and methods that
allow individuals to decide if and when to have children (UNFPA, 2018). There are many benefits
of family planning. Firstly, family planning allows individuals to attain their desired number of
children and determine the spacing of pregnancies by contraceptive methods. Family planning
can delay pregnancies in young women and thus decrease the risk of health problems and death
from early childbearing. It prevents unintended pregnancies, mostly in case of older women who
face increased risks related to pregnancy. By reducing rates of unintended pregnancies, it also

2 Sexual and reproductive health of refugee women in Germany
8
reduces the need for unsafe abortion (WHO, 2018e). Family planning also empowers women
through efficient planning of their childbearing, education and employment (UNFPA, 2018).
Contraceptive is another major aspect of SRH. The use of the contraceptive method helps to
prevent the transmission of HIV and other STI. Contraceptive helps in decreasing unwanted
pregnancy and abortion (Entre Nous, WHO & UNFPA, 2016, p. 10). Due to lack of proper
education, there are millions of women, especially in developing countries, who are not using any
of these contraceptive methods. Mostly the adolescent girls from the age 15-19 died due to
complications from pregnancy and childbirth (UNFPA, 2018). It has also consequences of
neonatal mortality (WHO, 2019). SRH also deals with pregnancy related topics such as prenatal
care which helps to identify possible risks for mother and child that can be reduced by providing
appropriate medical, nutritional, and educational interventions. This helps further on to reduce
the adverse pregnancy conditions and outcomes (WHO, 2018c). An abortion is another aspect
of SRH. According to WHO statistic, there are around 25 million abortion cases in the world which
are not safe (Narasimhan, 2018). An abortion is legal in most of the countries within certain
circumstances, however different countries have different rules and regulations (BZgA, 2017b, p.
84).
Sexually transmitted infection (STI) is another important aspect of SRH. Worldwide, there are
more than 30 different types of STI. Some common STI are chlamydia, syphilis, gonorrhea,
hepatitis A, HIV and Aids (BZgA, 2018e). Among them, the prevalence of the most frequently
occurring STIs like chlamydia and gonorrhea has increased in several European countries (Entre
Nous, WHO & UNFPA, 2016, p. 13). The WHO world report states that there are around 1 million
women and girls who acquired HIV, which illustrate huge gaps in access to basic services
regarding STI (Narasimhan, 2018). Many STIs can have dreadful long-term consequences. The
STIs like chlamydia and gonorrhea may lead to complications such as infertility, chronic illness
and can also lead to life-threatening conditions in fetuses and newborn babies (WHO, 2018c).
But most of the STI can be treated if it is diagnosed early (BZgA, 2018e).
Violence is one of the sensitive topics of SRH. In today’s world, violence against women is
perceived as a public problem (BZgA, 2018a). Violence can take the form of physical assault,
sexual abuse, verbal abuse, psychological or emotional abuse, economic abuse, social abuse,
and spiritual abuse (MCWH, 2009, p. 36). The gender-based violence and sexual violence has a
multitude of negative effects on women’s SRH. Results from almost 50 population-based surveys
in worldwide show that between 10 and 67 % of women report being physically harmed by a male
partner at some point of their lives excluding psychological or sexual abuse (Blanc, 2001, p. 195).
This further on results to unwanted pregnancies leading to gynecological problems, pregnancy
complications and miscarriages, unsafe abortions, rejection and harassment in their families, and

2 Sexual and reproductive health of refugee women in Germany
9
STI (Ivanova et al. 2018, p. 2, 8; Blanc, 2001, p. 195). In addition, it can adversely affect the
mental and physical health of women and lead to post-traumatic stress disorder, anxiety and
depression. Due to sexual violence women in some culture experienced social rejection, stigma,
suicide or even murder by a family or community members (Entre Nous, WHO & UNFPA, 2016,
p. 27).
The social determinants of health play a key role in SRH, which impacts the development of
individuals, their families and communities’ at large level (Entre Nous, WHO & UNFPA, 2016, p.
12). The factors like education, employment, income, social connection, safety and security,
including freedom from violence have a huge effect on women SRH and their overall health
outcomes and their access to health care services (Commonwealth of Australia, 2010, p. 26). For
e.g. women who are socioeconomically disadvantaged suffer from poor health and have a high
risk of having children with poor health (Commonwealth of Australia, 2010, p. 25). Indeed, poor
SRH has the consequence of poor physical, psychological and social health and wellbeing of
women and their families (Mengesha et al., 2017). According to WHO, this kind of SRH problems
is responsible for one- third of health issues for women between the ages of 15 and 44 years
(WHO, 2017a). Looking at wide range, poor SRH leads to increase morbidity and mortality,
gender inequity, financial strain, and even decreasing national development and progress rate in
a large scale (Crossland et al., 2015, p. 393).
To maintain the SRH of an individual, the sexual rights of all individuals must be respected,
protected and fulfilled (WHO, 2018d; WHO, 2006a). In order to promote the sexual health of
individuals, all individuals should get an education about sexuality and they should be aware
about sexual health problems. The health sector of each community can play a significant role in
assessment and in providing counseling and care on SRH (Alexander & Korenbrot, 1995).
Therefore, all the women around the world should get equal access to information and services
relating to sexual health, reproductive health, and safe sex practices, screening and maternal
health for a better SRH (Commonwealth of Australia, 2010, p. 8).

2 Sexual and reproductive health of refugee women in Germany
10
2.3 Refugee’s women sexual and reproductive health
Most of the refugee women currently living in Germany originate from Arab countries that have
recently seen several conflicts and political upheavals. This not only caused death and
disabilities, but disrupted the provision of health and education services too. These have also led
to differential implications for SRH (DeJong et al., 2005, p. 50). The study on Syrian refugees has
shown that women’s health and specifically their SRH are disproportionately affected due to
limited access to contraception, difficulties in accessing health care services, increasing gender-
based violence, early marriage, lack of access to emergency obstetric care, etc. (Yasmine &
Moughalian, 2016, p. 27). In addition to that, most of the married women experienced
childbearing, parenting and domestic violence issues (MCWH, 2009, p. 38). The following
paragraphs demonstrate major SRH issues among refugee women.
Sexual and reproductive health education
In most of the Arabic countries, sexual education is not really given a priority (Mengesha et al.,
2017). To discuss the sexuality topic is even a taboo in the surrounding and public places in many
Arabic countries (DeJong et al., 2005). The study about SRH situation of young people in the
Arab states and Iran address that young people in Arab countries lack access to information. The
education curricula in the school levels rarely include SRH topics and if they are included, the
teachers are not prepared well or embarrassed to teach about SRH topics. Hence, some of the
teachers even skip SRH topics. Neither, the parents being the first source of information discuss
SRH with their young ones. Because of this, most of the younger generations people in Arab
countries lack SRH education (DeJong et al., 2005, p. 52). Studies on refugee women reported
that the majority of women lacks knowledge on different areas of SRH such as the body changes,
pregnancy, information on HIV/AIDS, sexuality, abortion (Ivanova et al., 2018, p. 8). Further on,
there is a huge gender disparity in social opportunities. More than half of Arab women lack
literacy, and thus have lowest participation rate in the labor market (DeJong et al., 2005, p. 51).
This largely influences on health awareness among women.
Family planning, contraception and STI
SRH is an important aspect of women’s quality of life, but the utilization of family planning
methods and STI prevention are lower among refugee women (Mengesha et al., 2017). Available
evidence from UNFPA indicates that, the use of contraceptive methods in south-west Asian
countries like Syria, Afghanistan, and Iraq are very low from where most of
the refugees originated (UNFPA, 2018). The contraceptive prevalence rate in different countries
can be seen in Figure 3 below. Looking at the worldwide statistics presented from WHO 2018,
there are around 214 million women in reproductive age in developing countries who want to
avoid pregnancy, but they are not using a modern contraceptive method (WHO, 2018b). Some
possible reasons are social barriers in some culture, such as opposition by partners, families or

2 Sexual and reproductive health of refugee women in Germany
11
communities (Ivanova et al., 2018, p. 8). Lack of knowledge plays a big role, as women do not
know what kind of contraceptive methods are available or having incorrect perceptions about the
health risks of modern methods. There are also some logistical problems, such as difficulty in
travelling to health facilities or supplies running out at health clinics, especially in developing and
underdeveloped countries (UNFPA, 2018).
In comparison to adults, many adolescents were less aware of modern methods of contraception
from the same group and culture (Ivanova et al., 2018, p. 5). There is also lack of proper services
regarding contraceptives and family planning like a counseling center. Due to lack of knowledge
about SRH and inadequate utilization of family planning methods among refugee women there
is a high rate of morbidity and mortality cases in women via pregnancy-related complications
(Ivanova et al. 2018, p. 9). Especially, women in younger age groups are at high risk. Their
emotional immaturity and lack of negotiation skills put many young girls in vulnerable positions
(Crossland, 2015, p. 394).
Figure 3 Contraceptive prevalence rate
(Source: UNFPA, 2018)
Regarding STI, a systematic review of the SRH knowledge among refugees demonstrated
that the majority of refugees did not know any correct route of HIV transmission and effective
means of avoiding HIV or other STI (Ivanova et al., 2018, p. 5). Particularly, young girls are more
susceptible to STIs (Crossland, 2015, p. 394). Studies also showed enormous stigma and rights
issues surrounding HIV in the Arab states (DeJong et al., 2005, p. 55).

2 Sexual and reproductive health of refugee women in Germany
12
Pregnancy and childbirth
According to WHO, adolescent girls, migrants and women with low socioeconomic status or
education have a higher risk of adverse outcomes of pregnancy and birth (WHO, 2019). Most of
the refugee women experience higher rates of unplanned pregnancy, obstetric complications and
induced abortion than women in the host population (WHO, 2001). Globally looking, the
complication in pregnancy and childbirth is one of the main causes of death for 15–19 years old
girls (Entre Nous, WHO & UNFPA, 2016, p. 12). In some developing countries, most of the
adolescent girls even lack access to SRH commodities like menstrual hygiene products (Ivanova
et al., 2018, p. 9).
Furthermore, there are still many early marriage cases and high incidence of
consanguineous marriages in many Arab countries. Particularly women are pressured to marry
at an early age and after marriage, they are pressurized to reproduce children (DeJong et al.,
2005, p. 52) which is further seen as a barrier to pursue education (Ivanova et al. 2018, p. 8).
There is also a higher number of single women and the resurgence of forms of non-conventional
marriage. However, there is a decline in polygamy in some Arab countries (DeJong et al., 2005,
p. 52).
Sexual and gender-based violence
Refugee women have high risk of sexual violence in combination with physical, emotional
or socioeconomic violence. A study in 2014 estimated that around 21% of women in 14 conflict
countries reported experiencing sexual violence (Entre Nous, WHO & UNFPA, 2016, p. 26).
Refugee women experience sexual violence not only in their country, but also on their journey
and even after their arrival in Europe (Entre Nous, WHO & UNFPA, 2016, p. 26). During the
journey, there are cases, where refugee women have been victims of violence from police and
border guards, as well as smugglers, who are demanding high prices to facilitate entry to the EU
(Keygnaert et al., 2012, p. 516). Some studies also address that refugee women are victims
from transactions and commercial sex, which is also called as “survival sex” in exchange for
goods, food, menstrual hygiene products and money or even in exchange for documents or
transport to Europe. Even after arriving in a new country, women and girls living in refugee camps
are experiencing violence as there is not enough security in camps (Entre Nous, WHO & UNFPA,
2016, p. 26).
Many studies demonstrated different forms of violence which refugee women have experienced
such as rape, unwanted physical touching, sexual exploitation, commercial sex, early marriage
and trafficking (Kurmeyer et al., 2017, p. 5; Multicultural Centre for Women’s Health, 2009, p. 36).
Moreover, a systematic review of Ivanova et al. reported that refugee women are suffering from
sexual exploitations and harassments by their family members and close relatives apart from

2 Sexual and reproductive health of refugee women in Germany
13
their partners which is quite difficult to assess as the victims may not be willing to open up to
report such incidences (Ivanova et al., 2018, p. 9). This kind of violence results to a negative
impact on women physical and mental health and their ability to access health services (MCWH,
2009, p. 36). The sexual abuse and violence have many other negative consequences such as
maternal mortality, suicide because of unwanted pregnancy, high risk of STIs, neonatal morbidity
due to transmission of STIs which are illustrated clearly in the diagram below (Garcia-Moreno &
Stöckl, 2009).
This violence in refugee population is rooted in gender and power imbalances (MCWH, 2009, p.
36, 37). Usually, women have less power in a relationship which gives men greater sexual
freedom and rights of sexual determination than women (Blanc, 2001, p. 190; Mason 1994, Riley
1997). In a family, gender-based power relations can also effect on the ability of partners to
acquire information relevant to reproductive health, on their ability to make decisions related to
their health, and on their ability to act to protect health or improve their health or health of those
who depend upon them. Due to imbalance in power among men and women, most of the women
can hardly negotiate about SRH concerns such as contraceptive use with their partners (Blanc,
2001, p. 190). Thus, this power relation has a direct causal link with violence or the threat of
violence and it in turn influences the health of the women in many ways.
Figure 4 Consequences of partner abuse, sexual assault, and child sexual abuse
(Source: Garcia-Moreno & Stöckl, 2009)

2 Sexual and reproductive health of refugee women in Germany
14
Barriers in accessing sexual and reproductive health service
There are numerous barriers which hinder refugee women to seek SRH services in the new
country. Some of them are pre- and post-migration experience, lack of understanding about
available services and difficulty navigating the health care system (Mengesha et al. 2017). As
refugees came from different country and were grown up with different culture, it is hard for them
to deal with sexuality and contraception in new countries (BZgA, 2017, p. 17). Along with this,
most of the refugee women from Middle East Asia feel ashamed to visit gynecologist and to ask
women health related questions (Charite, 2017).
Refugee women's health is also highly influenced by their relationship with the family. The study
on refugee health shows that husbands or male member of the family has a big role in the family.
Normally a man acts as decision making person. Also, in the context of SRH, husbands involved
in family planning consultations and decision making for their wives (Mengesha et al., 2017).
Therefore, men’s lack of knowledge on SRH can affect women’s health. For e.g. men‘s lack of
knowledge of the contraceptives can affect the couple’s choice of method (Blanc, 2001, p. 197).
Further on, women are not supposed to be knowledgeable about sex and are expected to be
passive in sexual matters. They feel uncomfortable in discussing sexual matters with their own
partner and hence women communicate indirectly or nonverbally or partially with their partner
(Blanc, 2001, p. 194).
Moreover, Muslim women prefer to undergo medical examination by the health professional who
belongs to same gender. This culture even tends to continue after the resettlement in new
countries like Germany, where they prefer to visit doctors from the same cultural and linguistic
backgrounds as their own as this allows for better communication and longer consultation times
(MCWH, 2010, p. 45). Communication barrier is another big problem for most of the refugee
women, who cannot speak the native language. There is also a problem in finding a professional
interpreter especially female interpreter. Women are very concerned about the gender of
interpreters too. Some women take relatives as a professional interpreter as they feel
uncomfortable to talk about the sensitive topics like sexual health in front of unknown people. The
scarcity of health interpreters may cause frustration in some women, who are left with no choice
but to use family members as interpreters (MCWH, 2010, p. 48, 49).
Further on, refugee women are not active in seeking health services and the utilization and
experiences in accessing health services also vary among refugee women. According to a study
conducted with refugee women in Australia, refugee women’s experiences in accessing health
care in their country of origin influenced their access and utilization of care after resettlement
in the new place.These all cultural, educational, societal factors indicate that there is a dynamic
interrelationship between women and their surroundings (Mengesha et al., 2017). Thus, it is very
crucial to empower refugee women, to educate refugee women about SRH and to inform them
personally about the available health services in their surroundings.

2 Sexual and reproductive health of refugee women in Germany
15
2.4 Sexual and reproductive health service in Germany
In Germany, there are different health care services regarding SRH such as gynecologist’s
service where women can get help if they have problems such as pain during menstruation and
pregnancy issues. They also offer consultations and preventive examinations during pregnancy
(BZgA, 2017, p. 11). There are also counseling services on abortion, STI, contraceptives, etc.
Further on, gynecologists and urologists help with the problem related to sexual organs,
prevention and sexuality (BZgA, 2017, p. 11). Some important SRH services in Germany are
described in following paragraphs.
Pregnancy and childbirth services
In the context of pregnancy, there is available of different services during pregnancy, childbirth,
for maternal care from clinic, midwives or gynecologist (BzgA, 2018). There are medical
examinations on a regular basis to monitor the child's development and maternal health. This
helps to detect risk and prevent from risks (BZgA, 2014). There are also pregnancy counseling
centers that help women to get answers to their questions about sexuality, contraception, the
desire to have children, etc. (Federal Ministry for Family Affairs, Senior Citizens, Women and
Youth, 2016; BZgA, 2017, p. 90). They also provide information about the possibilities of financial
support if required. Especially, the Federal Foundation known as “Mother and Child- Protection
of Unborn Life” support women with financial issues (Federal Ministry for Family Affairs, Senior
Citizens, Women and Youth, 2016).
There are also birth preparation courses conducted by midwives or physiotherapists, which aims
to accompany women during pregnancy and to prepare them comprehensively for the birth. The
course provides basic knowledge about pregnancy and childbirth and help pregnant women by
sharing tips regarding childbirth, to take care of the newborn baby and about breastfeeding
(BzgA, 2014). After the birth of a newborn, the newborn health and maternal health is regularly
examined. The newborn gets a first pediatrician's examination, which is known as U-
Untersuchung. Along with this, the pregnant mother also gets medical care and advisory support
from midwives on breastfeeding, to recover from birth injuries, to live a new life with a new child
(BZgA, 2016). There are also some other services like family-midwives (Familienhebammen) and
family health and child nurses (Familien-Gesundheits- und Kinderkrankenpflegerinnen).They
help women in difficult cases like if the newborn baby has some chronic diseases, or if parents
are disabled. These all above mentioned services are funded by statutory health insurance in
Germany (Federal Ministry for Family Affairs, Senior Citizens, Women and Youth, 2016). The
following table provides the list of services that are covered by statutory health insurance in
Germany.
2 Sexual and reproductive health of refugee women in Germany
16
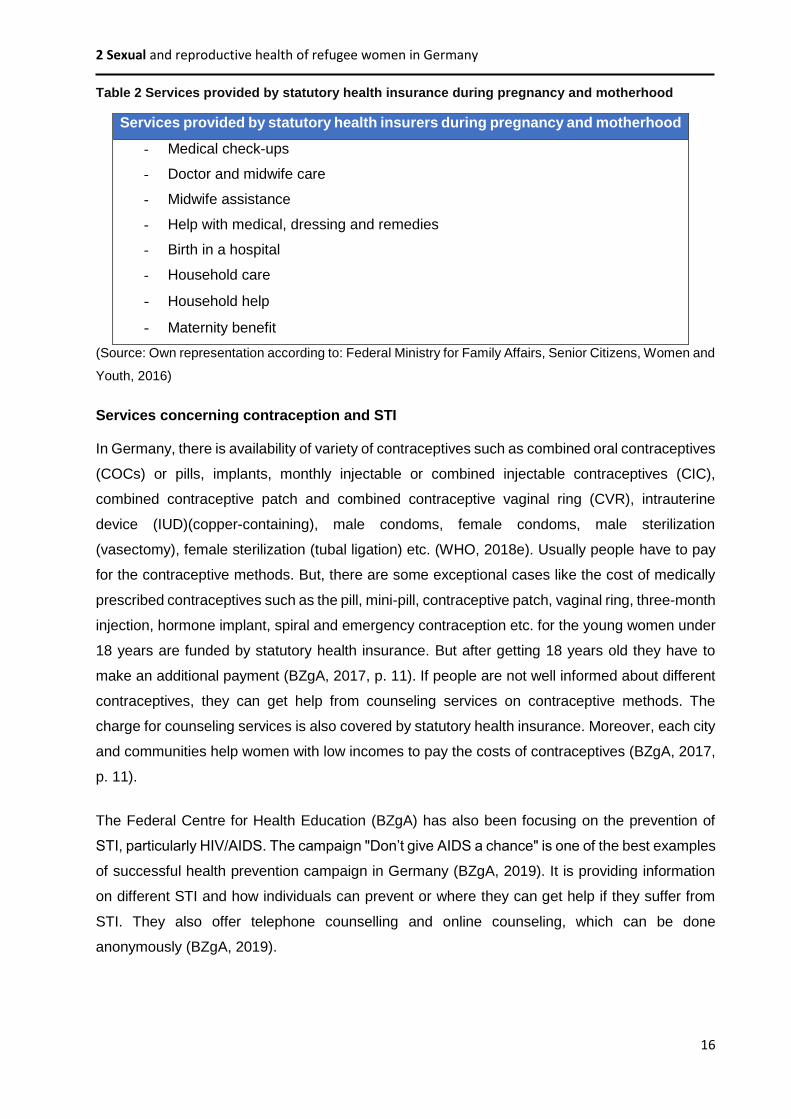
Table 2 Services provided by statutory health insurance during pregnancy and motherhood
Services provided by statutory health insurers during pregnancy and motherhood
- Medical check-ups
- Doctor and midwife care
- Midwife assistance
- Help with medical, dressing and remedies
- Birth in a hospital
- Household care
- Household help
- Maternity benefit
(Source: Own representation according to: Federal Ministry for Family Affairs, Senior Citizens, Women and
Youth, 2016)
Services concerning contraception and STI
In Germany, there is availability of variety of contraceptives such as combined oral contraceptives
(COCs) or pills, implants, monthly injectable or combined injectable contraceptives (CIC),
combined contraceptive patch and combined contraceptive vaginal ring (CVR), intrauterine
device (IUD)(copper-containing), male condoms, female condoms, male sterilization
(vasectomy), female sterilization (tubal ligation) etc. (WHO, 2018e). Usually people have to pay
for the contraceptive methods. But, there are some exceptional cases like the cost of medically
prescribed contraceptives such as the pill, mini-pill, contraceptive patch, vaginal ring, three-month
injection, hormone implant, spiral and emergency contraception etc. for the young women under
18 years are funded by statutory health insurance. But after getting 18 years old they have to
make an additional payment (BZgA, 2017, p. 11). If people are not well informed about different
contraceptives, they can get help from counseling services on contraceptive methods. The
charge for counseling services is also covered by statutory health insurance. Moreover, each city
and communities help women with low incomes to pay the costs of contraceptives (BZgA, 2017,
p. 11).
The Federal Centre for Health Education (BZgA) has also been focusing on the prevention of
STI, particularly HIV/AIDS. The campaign "Don’t give AIDS a chance" is one of the best examples
of successful health prevention campaign in Germany (BZgA, 2019). It is providing information
on different STI and how individuals can prevent or where they can get help if they suffer from
STI. They also offer telephone counselling and online counseling, which can be done
anonymously (BZgA, 2019).
2 Sexual and reproductive health of refugee women in Germany
17
Support for victim of sexual and gender-based violence
Violence against women occurs across all cultures and strata (Blanc, 2001, p. 190). Even in the
developed country like Germany, around 40% of women experience violence in their life. So, the
Federal Family Minister of Germany made a helpline service called 'Violence against women' to
help women who are victims of violence (BZgA, 2018). This helpline "Violence against women"
is a nationwide counseling service for women. Women can call the number 08000 116 016 or
contact via online. They offer direct service or online consultation anonymously in 17 different
languages for women with and without migration background. They give advice and consultation
on all forms of violence against women like domestic violence, mental, physical and sexual
violence outside of relationships, stalking, mobbing, digital violence, forced marriage, sexual
harassment in the workplace and in public places etc. They are available 24 hours a day and
throughout the whole year (Bundesamt für Familie und zivilgesellschaftliche Aufgaben, 2018).
Figure 5 below shows the logo of the helpline of violence against women.
Figure 5 Logo of the campaign “Violence against women”
(Source: Bundesamt für Familie und zivilgesellschaftliche Aufgaben, 2018)
These are some SRH services which are offered for the host citizenship as well for refugees and
migrants in Germany.
2 Sexual and reproductive health of refugee women in Germany
18
2.5 Health promotion and awareness programs in Germany
In Germany, there are several organizations which are working in the field of SRH to address its
importance and to raise awareness about the problems. Among several organizations, some of
them are pro-families which offer counseling on sexuality, pregnancy or partnership (pro familia).
There is Caritas Deutschland which provides counseling and advices on pregnancy (Caritas
Deutschland), Diakonie Deutschland which supports women that are victims of sexual violence
(Diakonie Deutschland, 2019). In the context of STI, there are Aids-Hilfe and CASA Blanca, which
provides counseling. The Federal Centre for Health Education (BZgA) is working in cooperation
with the Federal Ministry of Health in raising awareness program on overall SRH. They provide
information on different areas such as pregnancy, STI, family planning and contraception, and
even about screening of cancer etc. (BZgA, 2019). Currently, BZgA has developed an online
website which provides key information on the topic SRH. This website is known as “Zanzu”
which is described below in the upcoming paragraphs.
Moreover, there are some health promotion and awareness programs in Germany that are
working in the area of SRH and especially for the refugee population (World Future Council, 2016,
p. 4). Among them REFUGIUM program in Hamburg is one and it is also discussed in the
following paragraphs.
2.5.1 Zanzu
Zanzu is a multilingual online portal which is developed by German Federal Centre for Health
Education (BZgA) and Sensoa, the Flemish Expertise Centre for Sexual Health. This portal is
available in Germany since February 2016 (World Future Council, 20, p. 24). Zanzu provides
comprehensive information on SRH and rights in 13 different languages which are spoken by a
majority of migrant and refugee groups such as English, Arabic, Farsi, Russian etc. (BZgA &
Sensoa, 2019). This is an important element of Zanzu that migrant and refugee women living in
Germany can get information regarding SRH in their own native language. The website is also
intended to assist medical professionals in individual counseling sessions when there are
language barriers (World Future Council, 20, p. 24). The SRH topics are divided into 6 main
themes, i.e. Body, Family planning and pregnancy, infections, sexuality, relationships and
feelings and rights and law (BZgA & Sensoa, 2019). These topics are shown in the very first page
of the website a snapshot of which is shown below in the figure 6 below.

2 Sexual and reproductive health of refugee women in Germany
19
Figure 6 Six main themes of Zanzu
(Source: BZgA & Sensoa, 2019)
These six main topics are further divided into sub-topics. According to individual interest they can
get information on different SRH education in the language in which they can understand. For
each topic, it provides the important information illustrated by pictograms as shown in the figure
7 below. In addition to that, the website has a text-to-speech function, which allows the users to
have each page read out if they have difficulties in reading. The website also includes a dictionary
for most important terms such as STI connected to sexual health. These terms and its definition
can be translated and read out (BZgA & Sensoa, 2019). Overall, the information is provided in a
simple language.
2 Sexual and reproductive health of refugee women in Germany
20
Figure 7 Zanzu information illustrated through pictograms
(Source: BZgA & Sensoa, 2019)
2.5.2 REFUGIUM program
REFUGIUM is a health promotion and awareness program, which helps refugees to gain
knowledge of basic healthy living needs like nutrition, physical activity, hygiene, health care, etc.
REFUGIUM stands for “Rat mit Erfahrung: Flucht und Gesundheit – Information und
Multiplikation” (REFUGIUM). The program was developed by Late Prof. Dr. Christine Färber in
the year 2015 at the HAW Hamburg together with the health scientist Nita Kama, HAW Life
Science Department students and refugees. The aim of this program is to promote health
awareness and improve knowledge and capability of refugees through training, active
involvement and participation (REFUGIUM Flyer). Health trainings are provided in the form of
workshops to interested participants. The trained people are also refugee health facilitators who
are qualified to carry out interactive and activating themed health workshops for other refugees.
These health facilitators further conduct health workshops in different refugee accommodations
and in different settings like university, church etc. Thus, REFUGIUM works as a peer-to-peer
approach so that an adequate number of target groups can gain knowledge about health.
Furthermore, in REFUGIUM program the target group (refugees) is involved actively as peer
health facilitator in the continuous development process of the program, hence it follows the
participatory action research as researched cease to be objects and become partners in the
whole process (Baum et al. 2006).
2 Sexual and reproductive health of refugee women in Germany
21
The REFUGIUM health workshops consist of six different topics; nutrition, physical activity,
hygiene, oral health, mental health and health care in Hamburg as shown in the figure 8. For
each topic, there are flyers and manuals available which help to guide peer health facilitators to
conduct workshops. The flyers and manuals are available in eight different languages, i.e.
German, English, Albanian, Arabic, Bulgarian, Dari / Farsi, Russian and Turkish. Depending on
the participants, the workshops are conducted in their mother language, e.g. for Arabic speaking
participants, the workshops are given in Arabic language. A health workshop takes normally 90
minutes. The health facilitator provides the information about the workshop orally.
Figure 8 REFUGIUM health workshop topics
(Source: Own representation)
REFUGIUM program aims to enlarge the workshop topics, which are important and relevant for
refugees. As there is very little done in the sector of refugee women’s health, especially SRH,
REFUGIUM aims to conduct workshops focusing on SRH. For this, REFUGIUM needs to develop
a content, a manual i.e. workshops guide and flyers. The content of the workshop is SRH
information based on the needs of refugee women, which will be gained from refugees. As
REFUGIUM program work as peer to peer approach the needs of the refugees should be come
from refugees. Their unspoken voices or unheard voices should be explored. Thus, refugee
women were integrated in the development of a REFUGIUM workshop.
This paper presents the research study conducted with refugee women in the topic SRH. Through
a qualitative study, refugee women were asked to share their understanding towards SRH, their
issues and concerns and interest in SRH subjects. Based on their needs and problem,
REFUGIUM program can prepare a workshop content, manual and flyers. Through women health
workshop REFUGIUM program can provide SRH education to refugee women in Germany. Thus,
this paper aims to explore the SRH needs of refugee women in Hamburg, Germany. Based on
it, the research question of this study is formulated as “What are sexual and reproductive
Nutrition
Physical activity
Hygiene
Oral health
Mental health
Health care

2 Sexual and reproductive health of refugee women in Germany
22
health need of refugee women in Germany?” This study also aims to propose
recommendations for conducting women's health workshop for REFUGIUM program. To fulfill
these aims, some specific goals are made which are mentioned below:
To develop semi- structured interview guide
To contact refugee women and request for their participation in the research
To collect data from refugee women through focus groups as well as face-to-face
interviews (if focus groups do not meet the objectives)
To conduct observations in different refugee camps and look what kind of SRH services
are available
To explore the perceptions of female refugees towards health and SRH
To explore SRH issues and problems among refugee women
To find out the gap in knowledge on SRH
Some of these specific goals are as well part of the research data collection procedure which will
be further described in the method part of this paper in detail. Through these specific goals it is
possible to identify and explore the SRH needs of refugee women in Germany, which in turn
helps to achieve the main aim of this research.

3 Method
23
3 Method
The following chapter outlines the applied research design that was chosen to examine the
research questions. In the beginning, qualitative method as an appropriate method for this study
is discussed. Following that, a developed interview guideline as a data collection instrument is
described. The data collection procedures, which are implemented in this study such as focus
groups, in-depth interview and observations are also presented. Subsequently, the data analysis
strategies and self-reflexivity of the researcher during the research process will be illustrated.
During the whole research process, ethical aspects were also considered which are mentioned
in different phase of data collection and data analysis.
3.1 Qualitative approach
A qualitative study design was chosen to answer the research question as it helps in
exploring, understanding, describing and identifying different issues within the phenomenon of
interest (Lewis & Nicholls, 2014, p.51). According to Creswell (2013), a qualitative research is
appropriate to use when the issues of an individual or group needs to be explored or there is
need of complex, detailed understanding of the issues, which are hard to quantify and which
cannot be observed directly (Creswell, 2013, p.65). Such issues can be sexual activity, drug
addiction, childhood discipline, violence, death, etc. (Tracy, 2013, p.132). Qualitative study
especially deals with the issues of gender, culture and marginalized groups such as refugee
women (Creswell, 2013, p.51). Thus, qualitative approach is often used to open-up a new subject
area and helps to explore unanticipated topics like refugee women’s SRH (Lewis & Nicholls,
2014, p.47).
The qualitative approach allows examining people’s experiences in detail by using a specific set
of research method like in-depth interviews, focus group discussion, life histories, biographies,
etc. The qualitative approach helps to identify issues from the perspective of study participants
and understand the meanings and interpretations that they give to behavior, objects or events
(Hennik, Hutter & Bailey, 2010, p.8). For example, to understand refugee women`s perception
towards SRH, to know their health-related behavior, or to identify their social and cultural norms,
which are affecting their access to health services. Hence, it is a method that helps to understand
the knowledge and the behavior of individuals because it describes the world from the inner
perspective, e.g. of the individuals who experience the problems (Flick, 2016, p. 28; Creswell,
2013, p. 44).
The following table illustrates the main features of qualitative research which shows its objectives
and purpose. It also includes the data collection method, data analysis and outcome. While
planning the qualitative research, along with these features, it is also important to anticipate and

3 Method
24
consider ethical issues that might arise during several phases of the research process such as
at the beginning of the study, during data collection, in data analysis, in reporting the data, and
in publishing a study (Creswell, 2013, p.56, 57).
Table 3 Main features of qualitative research
Qualitative research
Objectives To gain a detailed understanding of underlying reasons, beliefs,
motivation
Purpose
To understand why, how?
What is the process?
What are the influences or contexts?
Data Data are words (textual data)
Study population Small number of participants or interviewees
Selected purposively (non-randomly)
Data collection In-depth interviews, observation, group discussion
Analysis Analysis is interpretive
Outcome To develop an initial understanding to identify and explain behavior,
beliefs or actions
(Source: Hennik, Hutter & Bailey, 2010, p.16)
Within qualitative research, there are many different approaches, namely: Narrative Research,
Phenomenology, Grounded Theory, Ethnography and Case Studies (Creswell, 2013, p.104).
Among these approaches, this research follows the case study approach since case studies
enable us to develop an in-depth description and analysis of a real-life case, or to explore an
issue or problem using the case as a specific illustration (Creswell, 2013, p.97). In this research,
the intent to choose a case study is to understand the SRH concern among refugee women who
recently settled in Germany. In a case study, the case may be a concrete entity like an individual,
a small group, an organization or even a community, a specific project etc. (Creswell, 2013, p.98).
Case studies are also distinguished by the size of the bounded case, such as if it involves one
individual it is a single case study and if it involves several individuals it is a collective case study
(Creswell, 2013, p.99). In this research study, a collective case is chosen which focuses on SRH
3 Method
25
issues of several refugee women. The intention to choose collective case study is to explore
different perspectives on SRH issues from different cases. The cases are the female refugee
women in reproductive age, who came to Germany recently and live in refugee accommodation.
The issues are the SRH needs among refugee women.
3.2 Development of interview guide
As a data collection tool, a semi-structured interview guide was developed which will be used to
conduct focus group and face-to-face interview. The interview guideline contains open-ended
questionnaires as it helps in exploring the issues from the participant’s perspective (Creswell,
2013, p.52). While developing the interview guide, some tips and tools for interview question
types and its right placement provided by Tracy in the literature were considered which is shown
in the Figure below.
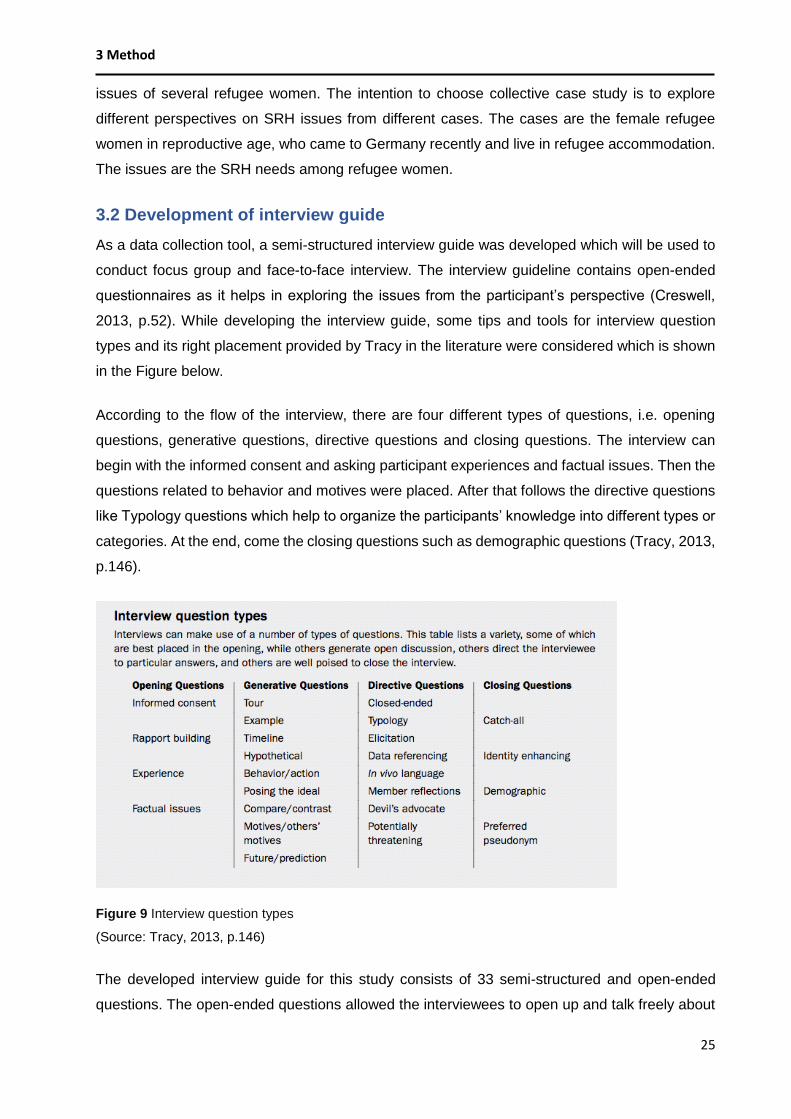
According to the flow of the interview, there are four different types of questions, i.e. opening
questions, generative questions, directive questions and closing questions. The interview can
begin with the informed consent and asking participant experiences and factual issues. Then the
questions related to behavior and motives were placed. After that follows the directive questions
like Typology questions which help to organize the participants’ knowledge into different types or
categories. At the end, come the closing questions such as demographic questions (Tracy, 2013,
p.146).
Figure 9 Interview question types
(Source: Tracy, 2013, p.146)
The developed interview guide for this study consists of 33 semi-structured and open-ended
questions. The open-ended questions allowed the interviewees to open up and talk freely about

3 Method
26
their views and experiences (Creswell, 2013, p.164; Flick, 2016, 221f). Furthermore, the
sequence of the interview questions was taken into consideration. General questions, which were
less sensitive, were put at the beginning of the interview so that the participants do not feel
uncomfortable. Therefore, the first questions start with general background information about
women in their home country to give impulse to the participants. More sensitive questions related
to sexual health and violence were put after the general questions (Flick, 2016, p. 222 f.). Some
questions also consist sub-questions. The socio-demographic questionnaires were put at the end
so that interview participants do not hesitate to share their personal things like age, family status,
etc. There are also some feedback questions at the end where participants have an opportunity
to share their ideas and their interested subjects on SRH. Almost all the questions are formulated
in a possible simple and clear way so that participants could easily understand it. While phrasing
questions, the use of acronyms, abbreviations are also avoided (Tracy, 2013, p.144).
The developed interview guideline is shown below in the Appendix . The interview questions were
divided into six main themes, which are shown below in the table:
Table 4 Main themes of interview guide
Main themes of interview guide
• Background information about women in own home country
• Current situation of refugee’s women who are living in refugee accommodation
• Women’s health in the perspective of refugee’s women
• Reproductive and sexual health in the perspective of refugee’s women
• Ideas gaining for conducting reproductive and sexual health workshop
• Socio-demographic Questionnaire
(Source: Own representation)
Pretest:
Before conducting the actual interviews, the questions from the interview guide had to be
reviewed and tested. Many researchers recommend a pilot test to refine the interview questions
and develop relevant lines of questions (Creswell, 2013, p.165). Pilot testing also helps to ensure
the use of proper language comprehensible to women (Kaddour, Hafez & Zurayk, 2005, p. 37).
Two sample face-to-face interviews were conducted with a questionnaire in order to check the
time frame, the comprehensibility of the questions, the order of the questions, the meaning of the
questions, the simplicity of the questions etc. One pre-test was conducted with a female member
of REFUGIUM program. She had also a migration background and can understand the condition
of refugee women living in Germany. However, she has been living in Germany for more than 2

3 Method
27
years. The second pre-test was conducted with a woman from Nepal who came as a student to
Germany. She is living in Germany for a few years and belongs to a migrant group. After the pre-
test, the order of some questions was changed. Some questions were then formulated in a simple
way and neutral way. Redundant questions were deleted after the pre-test or two questions were
combined to one. Furthermore, some technical terms were changed into everyday words. In
addition, the interview questions were formulated in a comprehensible and grammatically correct
way. The revised and rearranged interview guide is shown in the Appendix B.
3.3 Data collection
The data collection on a qualitative study is the procedure of gathering data, which
includes a series of interrelated activities such as gaining permissions, conducting a good
sampling strategy, preparing equipment for recording both digitally and on paper, and anticipating
ethical issues that may arise during data collection (Creswell, 2013, p.145). In this study, data
collection procedure starts with access to target group, i.e. sampling and recruitment process. In
qualitative approach, there are multiple data collection methods such as interviews, field notes,
conversations, photographs, observation, etc. The researcher can even combine two or more
methods, rather than relying on a single data source (Creswell, 2013, p. 44). For this study, it
was planned only to conduct focus group at the beginning. But there were difficulties in finding
appropriate time where all the participants could join. Therefore, after conducting 2 focus groups,
7 face-to-face interviews were conducted. Aside from that, an observation was also done in 5
different refugee accommodations.
3.3.1 Sampling and recruitment
Sampling is a necessary step in terms of choosing individual for study as a source for research
data. It is not only finding people who are willing to talk on the topic SRH, it is also finding people
who are prepared to share their time and stories (Tracy, 2013, p.134). This research follows the
purposeful sampling, which means that the individuals for research are selected in a way that
they can purposefully inform an understanding of the research problem and they fit into the
parameters of the research questions, goals, and purposes (Creswell, 2013, p.156: Tracy, 2013,
p.134). The target group of this study are refugee women living in different refugee’s camps in
Hamburg. Eligible in regarding our defined inclusion criteria are refugee women of reproductive
age, i.e. aged between 15-59. Furthermore, the origin of target group should be from most
common countries with greater number of refugees such as Syria, Afghanistan, Iraq, Iran, etc. In
addition, either proper English or German language skills were considered. Religious background
was not considered.
Further on, the snowball sampling method is also practiced to get more participants. The
participants were asked to suggest a colleague, a friend, or a family member to take part in the

3 Method
28
study, who fit into the same study’s criteria (Tracy, 2013, p.156). In this collective case study
diverse sample were selected such as single refugee women, married refugee women, refugee
women from different origin and cultural background so that they can provide different
perspectives on SRH concern.
Table 5 Inclusion criteria for the study
Inclusion criteria for the study
• Female refugee in reproductive age (women aged 15–59)
• Female refugee women living in Germany for 2-3 years
• Female refugee who are living in Hamburg in refugee
accommodation
• Female refugee who can speak either English or Germany
(Source: Own representation)
As researcher being a part of REFUGIUM program, the researcher first contacted the female
refugee participants of REFUGIUM program. Before contacting the female participants of
REFUGIUM program, the permission was taken from Project coordinator (Professor Färber) to
get contact data from female REFUGIUM participants. While accessing the target group of the
study, it is important to disclose the purpose of the study to them (Creswell, 2013, p.57).
Therefore, the contacted participants were at first informed orally about the purpose of the study
in English or in German. The gatekeeper helped in translation in Arabic and Kurdish languages.
Other REFUGIUM team member also helped in communication in Farsi.
During the study time frame, REFUGIUM had just completed its second-generation health
facilitator training program. In 2nd generation health facilitator program, there were two groups,
i.e. an Arabic group and a Farsi group. In the Arabic group, there were 4 female refugees and in
the Farsi group, there were 5 female refugees. All the female refugees were contacted. At first,
it was planned to conduct two focus groups, i.e. one focus group with an Arabic speaking female
participant and one with Farsi speaking female participants. But, among four only two women
from Arabic group showed up in the first focus group. From the Farsi group, none of the female
refugee showed their interest to take part in this study.
After some months, REFUGIUM program conducted 3rd generation health facilitator training
program, in which there were three women in the Arabic group and 3 women in a Russian group.
None of the Russian women could speak either English or German. Thus, it couldn’t meet the

3 Method
29
sample criteria. Unfortunately, there were no female refugees in the Farsi group. Thus, a second
focus group was conducted with two women from an Arabic group. Following that, REFUGIUM
program conducted 4 h generation training program, where there was one female participant in
Farsi group and 3 female participants in Arabic group. Among them, two face-to face interviews
were conducted with two female participants, one woman belonged to Farsi group and other
belonged to Arabic group.
As it was very hard to get participants for this study, another organization called
“Patenschaftsproject of BergedorferVölkerverständigung” was contacted. From there, the
researcher got to know some more women from Iran, Afghanistan, Syria and Pakistan. Among
them a woman from Iran and one from Pakistan managed to take part in this study. The
researcher also contacted 5th generation REFUGIUM participants. Only one of them took part in
the study. Afterwards the researcher joined in the workshop, which was conducted in cooperation
with Mut Café Afrika and Aids Hilfe Hamburg. From there, one woman from Iraq took part in the
study. She further suggested her friend and another woman from Syria took part in the study. At
the end, there were 11 refugee women who took part in the study.
3.3.2 Conducting focus-group
At the very beginning, only focus groups were planned to conduct. In the focus group the
participants who have similar characters are put in one group. The first focus group was
conducted with female refugees who speak the same language so that if one cannot speak
fluently English or German, other participants could help in translation and interpretation. It was
planned to conduct second focus group with Farsi speaking refugee women from Afghanistan.
But none of the contacted women showed up for a focus group. Few months later another focus
was conducted with women who spoke Arabic. In the first focus group, there were two participants
(out of 4 agreed). In the second focus group, there were also two participants (out of 3 agreed).
Before conducting focus group, the location/ setting and the equipment for recording were
prepared. It was made sure that the voices are audible, and the recording technology is
functioning correctly. The questionnaire and some papers and pen were prepared for taking field
notes. At first, the participants were greeted warmly. They were offered drinks and snacks.
Participants were also asked about their health condition, their travel etc. so that they could feel
more comfortable.
At the beginning, the participants were informed about the general purpose of the research, and
the specific objectives for the day. Then they were given a consent form. The consent form
includes the purpose of the study and the procedure to be used in data collection, the protection
of confidentiality of the respondents, the signature of the participant (see Appendix C) (Creswell,

3 Method
30
2013, p. 153). The informed consent was written in two languages: English and German. The
consent form is written in a short and simple way so that participants can understand it easily.
Moreover, the participants were not pressured to sign the consent form.
For conducting a focus group, the developed interview guide was used. During focus group, it
was made sure that all the participants got equal opportunity to share their views and
experiences. The participant’s nonverbal communications during focus group were also noted in
the field notes. Participants were not forced to answer all questions if they feel uncomfortable or
hesitation. During the focus group, participants were not discriminated because of different
culture, religion, gender and/or other differences. The researcher also tried to establish a
supportive, respectful relationship without stereotyping and using labels so that participants do
not have to face embarrassing moments.
Both focus groups took more time than planned. As most of the participants are not fluent in
English or in German, they need more time to translate some words (sometimes using Google
translator). The whole conversations during focus group were tape recorded for the data analysis
process. At the end, the focus group participants were requested to keep the focus group
conversations confidential. Lastly, all the participants were thanked for their time and
participation.
Focus group setting:
To conduct a focus group, it is very important to find a quiet location, which is free from noise and
any kind of distractions. For a focus group, there is need of extra room with chairs and desk.
While conducting focus group, the confidentiality, the privacy of the participants should be
respected from an ethical point of view (Webster, Lewis & Brown, 2014, p. 78). Therefore, both
focus groups were planned to conduct in a closed room in the absence of any male member and
outsiders. The group work room available in HAW Berliner Tor library have chairs and desks and
the rooms are quiet, small and free from disturbance. Thus, the first focus group with two Arabic
female refugees was conducted in a group work room at HAW Berliner Tor (see Appendix F).
The second focus group with other female refugees was planned in the same room, but as the
participants arrived late, half of the focus group was conducted in the group work room and the
other half on a corner of the canteen. As it was conducted in the afternoon, there were only a few
students in the canteen thus the surrounding area didn’t have a lot of disturbance. However, as
it had to move in between from the library group work room to canteen, it might have some impact
on consistent communication flow. During the focus group, the researcher and participants sat in
a round/circular position so that researcher could see all participants and it makes the
communication easier.

3 Method
31
3.3.3 Conducting face-to-face interview
As qualitative interviews elucidate subjectively lived experiences and viewpoints from the
respondent’s perspective (Tracy, 2013, p.132) seven face-to-face interviews were conducted with
refugee women. As the participants could not manage to join in the focus groups which were
conducted few weeks before, they were requested to choose their preferred time for the
interviews. Therefore, it made easier to conduct face-to-face interviews with all 7 refugee women.
Likewise, in conducting focus group, the setting and required equipment for conducting an
interview were prepared beforehand. While conducting interviews, participants were greeted
nicely at first and thanked for their presence. Participants were also offered drinks and snacks
and made comfortable. All the interviews begin with a briefing that includes a description of the
interview’s purpose, the amount of time that will be needed to complete and the plans for using
the findings from the interview. Participants were informed that they have the right to refuse to
answer any question which makes them uncomfortable. And they also have the right to stop their
participation at any time without any consequences. They were made sure that participating this
study will not put them at undue risk (Creswell, 2013, p.57). Then the informed consent was
handed over to the participants. An adequate time (around 4-5 minutes) were provided to read
over the inform consent form and ask questions if needed. While the interviewees are reading
over the consent form some field notes about the nonverbal communication, the appearance of
the interview such as looking nervous or, whether the interviewee arrived on time, when and
where the interview occurred, where the interviewee chose to sit, and other interesting data that
will not emerge in an audio recording were written down. One of the field notes taken during the
interview is shown in Appendix E. This type of notes about nonverbal communication enhances
the transcription (Tracy, 2013, p.161).
In comparison to the focus groups, the face-to face interviews were relaxed and pleasant.
Participants were more open and were ready to share their experiences. Thus, face-to face
interviews serve as an efficient method to “get to the heart of the matter” (Tracy, 2013, p.133).
Beside this, it also provides opportunity to openly verify, refute, defend, or expand certain points
(Tracy, 2013, p. 133.). During the interview, the researcher tried to create a logistically feasible
and comfortable interaction to encourage an honest and engaging conversation. When
participants were feeling uncomfortable about sharing their experiences, they were not forced to
answer the questions. During the interview, the imbalanced power relation between researcher
and the interviewee was also considered. Special attention was given when participants were
being emotional or talking about emotional subject matters. At the end, interviewees were
thanked and appreciated for their time and for sharing their experiences and opinions.

3 Method
32
Interview setting:
As an interview setting the HAW Campus in Berliner Tor and HAW Library in Alexander street in
Hamburg was chosen as it lies in the center of Hamburg and is not far away for the participants
to reach there (compared to HAW Campus Bergedorf). Out of seven face-to face interviews, two
were conducted in a closed room, i.e. group work room at Alexander street HAW library. Three
interviews were conducted in the corner of the canteen at HAW Berliner Tor where there was
presence of other students, but it was made sure that they could not hear the conversation. Rests
of the two interviews were conducted in participants home because they had to look after their
children. Thus, there was presence of participant’s children, which is considerable in this case.
But prior to conducting an interview, participants were asked for their permission to conduct an
interview at their home as researcher needs to seek permission to conduct research on site
(Creswell, 2013, p.57).
The settings of the interviews which were conducted in the canteen at HAW Berliner Tor were
little bit noisy and disturbing from other students. Whereas the interview conducted in the group
work room in library on Alexander Street was free from distractions. In the interviews conducted
at home, it had to be stopped quite a few times due to children crying or coming to play with their
mother. However, in all cases there was no presence of any third person except the children
during interviews with married women. During the interview, the researcher and the interviewee
sat in face-to-face position. In all the cases, there were required equipment for interviews like
comfortable chairs and desk. Almost all the interviews were conducted in the afternoon (around
4 pm) as most of the participants had German language class in the morning.
3.3.4 Observation
Observation is one of the data collection methods in qualitative research, which helps the
researcher to get a greater understanding of the phenomenon (Creswell, 2013, p. 166).
Observation is based on research purpose and questions. Like interviewing, observation also
includes a series of steps. At first, the site to be observed should be selected. Then the
observation object should be determined, including the time frame and time duration for
observation. The observation objects can be participants, activities, physical setting, interactions,
conversation, etc. The observer should also determine the role of an observer such as observer
as participant or non-participant. The observation protocol should be designed as a method for
recording notes in the field. The observed objects are written down and at the end presented in
which the researcher can also reflect own personal impression and ideas (Creswell, 2013, p.
166).

3 Method
33
In this research, the main observation objects are physical setting, i.e. different refugee
accommodations in Hamburg. The observation objects are available information on SRH services
in refugee accommodations. Such information could be in the form of flyer, brochure, poster, etc.
which are available in refugee camps. The observations took place in winter 2017, till 2018. Three
Observations were done during the time when REFUGIUM program was offering health
workshops in different refugee accommodations: Schnackenburgallee 81-83, Brookkehre 20, and
in Harburger Poststraße 1. The other two observations were done in Schmiedekoppel29/30 and
in August Kirchstraße 17. These two observations were conducted while visiting the camp for
interviews with two refugee women who had children. In total, five observations were done to
examine the health care facilities offered at the camps. The observed refugee accommodations
are situated in different region in Hamburg. Following are the list of refugee accommodation, with
its address (Table 6).
Table 6 Refugee accommodations where observations were conducted
No. Name of the refugee camp Region Address
1.
FlüchtlingsunterkunftSchnackenburgallee
Altona Schnackenburgallee 81-83
22525 Hamburg
2. WohnunterkunftBrookkehre
Bergedorf
Brookkehre 18-20
21029 Hamburg
3. ErstaufnahmeHarburgerPoststraße
Harburg
HarburgerPoststraße 1
21079 Hamburg
4. ErstaufnahmestelleSchmiedekoppel
Eimsbüttel
Schmiedekoppel 29/30
22453 Hamburg
5. Wohnunterkunft August-Kirch-Straße in
Bahrenfeld
Bahrenfeld
August-Kirch-Straße 17 a
22525 Hamburg
(Source: Own representation)
During the observation in refugee accommodation the main focus was more to observe the
facilities that are offered to refugees who are living there (Creswell 2013: 166) such as what kind
of health care facilities especially regarding SRH services are available at that certain refugee
accommodation? An observation protocol was made which include the name of refugee
accommodation, date and time, as shown in Appendix D.

3 Method
34
3.4 Data analysis
The data analysis in qualitative study involves several steps like organizing the data, conducting
a preliminary read through of the database, coding and organizing themes, representing the data,
and lastly forming an interpretation of them. Before that the audio recorded data are transcript.
Ultimately, it also includes representing the data in the form of a discussion, table, charts, etc.
These are the core elements of data analysis in qualitative study which will be discussed in
upcoming paragraphs (Creswell, 2013, p.179, 180).
3.4.1 Transcription
The first step of data analysis is to organize the data, which means the audio recorded interviews
and focus group data are organized in computer files and transcribed, which is one of the most
important parts of transforming embodied interviews into usable data (Tracy, 2013, p. 177).There
are numerous transcription rules in qualitative research such as transcription according to Ralf
Bohnsack, Udo Kuckartz, etc. (Fuß & Karbach 2014, p.27). In this study, the collected data are
transcribed according to Kuckartz. This means that every spoken word is literally transcribed, but
not transmitted in a summary form. The dialects of the participants are not transcribed, but
translated as precisely as possible into the general language. If there were long breaks in
between the interview, they were marked by mentioning the brackets, which include dots.
Incomprehensible words were identified by (unv.). Also, the individual pronunciation or
vocalizations such as "Mhm, Na" etc. are not indicated in the transcript. The vocal expression of
the interviewee supporting the statement like smiles or coughing are noted in brackets. Any kinds
of disruptions during the interview are also noted in brackets stating the cause like (Telephone
ringing). Incomplete sentences, wrong grammar etc. are corrected without changing the meaning
of the sentences. The original meaning, intent and ideas of the interviewee were reflected while
transcribing (Fuß & Karbach 2014, p.28).
To ensure anonymity, an individual name was assigned to each interviewee (Fuß & Karbach
2014, p.29). In this study, interviewees were also given a pseudonym like Nele, Zahra, Diva, etc.
which are presented in the results. The researcher is named as “Anna” in the transcripts. Some
interviews were conducted in half German language and half English language. The statements
in German languages are translated into English for the analysis. After the completion of
research, all recorded interviews will be deleted, and the transcript texts will not be utilized for
other purposes.

3 Method
35
3.4.2 Content analysis
For the analysis of verbal data, there are various qualitative content analyses available
(Bortz & Döring 2006, p.31). The present research follows the traditional methods of qualitative
content analysis according to Mayring, which dealt intensively with the formation of the category
(Diekmann 2006, S.481). The core and central tool of content analysis is its system of categories,
where every unit of analysis must be coded or allocated to one or more categories. These
categories are understood as the operational definitions of variables (Kohlbacher, 2006, p.10).
In the content analysis, the transcripts were first read several times to get an overview of the data
and sense of interview before breaking it into parts. The next step consists of describing,
classifying and interpreting the data (Creswell, 2013, p.183, 184). The data collected in this study
are analyzed inductively from particular to more general perspectives. These perspectives
emerged from the data are named as codes or categories (Creswell, 2013, p.52). At first, the
text data are reduced into smaller categories of information and then a label is assigned to it
(Flick, 2006, p. 315). For that, meaningful text passages are identified and assigned to a category.
That particular section of text is marked and stored in another document simultaneously. In this
way, a long list of coded segments will be created from which emerge categories or themes
(Kuckartz 1999, p. 90f.). Throughout the coding process, the constant comparative method will
be used to compare the data applicable to each code and to modify code definitions to fit new
data. This constant comparative method is circular, iterative, and reflexive (Tracy, 2016, p. 190).
After the formation of themes or categories from the codes, follows the process of organization
of themes into larger units of abstraction to make sense of the data. This process is known as
classification process and it helps further on interpretation of data. An interpretation involves
abstracting out beyond the codes and themes to the larger meaning of the data to make sense
of the data (Creswell, 2013, p.187). Thus, the researcher builds detailed descriptions, develop
themes and provide an interpretation considering their own views or views of perspectives in
literature (Creswell, 2013, p.183). The final phase of data analysis involves representing the data
using narratives, tables, charts, etc. While presenting a result, the confidentiality, the privacy and
anonymity of participants should be respected (Webster, Lewis & Brown, 2014, p. 78). Therefore,
participants were given pseudonyms in presenting their statements in results (Creswell, 2013, p.
175). There will also be no such information published which will potentially harm participants in
the present or future.
In this study, the categories are developed based on the interview guideline and specifically
contents of the transcribed interviews (Flick, 2006, p. 315). The data analysis process in this
research was purely inductive by which codes and themes were identified from the data and not

3 Method
36
from another theory. After analyzing the dataset following main categories have emerged. The
table below gives an overview about the main categories and the associated sub-themes.
Table 7 Main and sub categories emerged from content analysis
No. Main Categories Sub-Categories
1. Perception towards health • Understanding of health and women’s health
• Health consciousness
• Health-related behaviors
2. Perception towards SRH • Understanding of SRH
• Consciousness towards SRH
3. Sexual and reproductive health
knowledge
• Formal knowledge
• Informal knowledge
4. Sexual and reproductive health issues • Menstruation
• Early and forced marriage
• Pregnancy and childbirth
• Abortion
• Family planning and contraceptives
• Sexual transmitted diseases
• Sexual and gender-based violence
5. Awareness about health care services • Healthcare services in refugee camp
• Healthcare services in Germany
• Health promotion and awareness program
• Healthcare services in country of origin
6. Barriers in accessing health services • Communication
• Gender aspects
• Different health care system
• Social and financial support
• Culture and tradition
• Living conditions in refugee accommodation
• Stress factors
7. Advice and suggestions for REFUGIUM
workshop • General suggestions for a workshop
• Suggested SRH topics
(Source: Own representation)
3 Method
37
3.5 Self-reflexivity
In the qualitative approach, the researchers can bring their own subjective influence on the
research process particularly during data collection and interpretation. Thus, the researcher’s
background, position, or emotions are also integrated in the process of producing data (Hennik,
Hutter & Bailey, 2010, p. 19). Therefore, it is important to acknowledge the researcher’s
subjectivity. Creswell also emphasized the importance of describing the researcher’s perspective
in qualitative research that contains information about conceptions of researcher self and those
who are being researched (Creswell, 2013, p. 15-17). Research is created by the researcher
and is not the reality. Therefore, the positioning of the researcher is crucial in order to understand
how much is the influence of the researcher in the research process (Creswell, 2013, p.20).
A student doing a master’s degree with the major in Health Sciences is involved as a researcher
in this study. The researcher herself is a migrant from Nepal, who was grown up in different
religious and cultural environment. So, the researcher can view the things from different
perspectives. During the master 2nd semester, the researcher took part in the module “Advanced
Qualitative Study design” from Prof. Färber where she got in contact with refugees taking part in
REFUGIUM training program at HAW. At that time, she was involved in conducting a qualitative
research study about risks and resources of refugee’s mental health in Germany. For that, she
along with her group members conducted a narrative interview with different refugees. Through
that narrative research, she got to know about the critical living conditions of refugees, their
terrible migration experiences, their health-related problems, etc. All these factors had inspired
to discuss more on refugee’s topic and to help them to stay healthy in their upcoming life in
Germany.
According to the researcher’s experiences as a foreigner in Germany, she was able to understand
and research about refugees’ challenges and obstacles in accessing health care services in new
places as an outsider. The researcher being a female student with migration background had
experienced similar difficulties in the beginning to access information and locations for healthcare
services. Furthermore, she did her master internship in REFUGIUM program from February 2017
to July 2017. During her internship, she got close contact with lots of refugees. From them, she
got to know that female refugee are bearing more health burden than male refugees as they have
issues like pregnancy related complications, menstrual problems etc. These experiences added
to her interest in work on this project directly related to SRH in refugee women.
In course of the research, it was easier for the researcher to connect as a migrant and get close
as well as gain trust to conduct the whole research. On the other side, studying in a multi-cultural
and diverse team throughout the master’s program made her more culturally sensitive and very
open to different perspectives and belief systems. In addition to that, internship and working in a

3 Method
38
diverse team in REFUGIUM program improved her intercultural competence and communication
skills. This tremendously helped her in conducting research, especially conducting interviews and
focus groups with refugee women from different background. The researcher can also relate to
some extent different perspectives and views of refugee women from their origin which further
helps in the interpretation of their statements.
4. Results
39
4. Results
In this chapter, the results of analyzed data from 2 focus groups, 7 face-to-face in-depth
interviews are presented. Overall, seven main-categories have emerged from the data analysis.
At first, the participant characteristics are described in detail. Afterward, the main categories and
the associated sub-themes are described comprehensively. Each category and the according
themes will be described consistent with the participant's experiences and opinions which also
includes the statements of the participants. The statements of participants help in understanding
about the perception of target group regarding different subjects related to SRH.
The description of main categories starts with the perception of refugee women towards overall
health and then towards SRH. The consciousness of refugee women, their understanding of
health, their health-related behavior, and understanding of SRH are presented under this section.
After that, SRH knowledge among refugee women is explained. Then the SRH issues mentioned
by participants are presented in detail. Further on, awareness about the health care services on
SRH among refugee women is explored which present, the awareness about the health care
service in Germany, in the refugee camp as well as in the country of origin. For more detail
information regarding health care services offered in refugee accommodations, an observation
was also conducted. The findings from 5 observations are also included in the results.
The barriers mentioned by participants which hinder them to get access to health care services
in Germany are also presented in detail. At last, participant's suggestion for conducting women’s
health workshops are presented. In this way, refugee women’s perception towards SRH, their
SRH knowledge, SRH problems and issues and their awareness about health care services are
analyzed. Along with these, factors that are affecting refugee women in getting access to health
care services are also examined. These all together help in exploring the SRH needs of refugee.
4.1 Participants
Altogether, 11 refugee women participated in this study. There were 4 participants in the focus
group and 7 participants in a face-to-face interview. All the participants in this study were female
refugees, who live in Hamburg, Germany. During the study time frame, all the participants were
living in different refugee accommodations in Hamburg. The age of the participants ranges from
24 to 45. The participants are originated from different nations. There were six participants from
Syria, two from Iran, one from Pakistan, one from Iraq and one from Nigeria. Thus, the
participants have different cultural background and speak different languages. The women from
Syria and Iraq speak Arabic as their primary language. The participants from Iran speak Farsi as
their mother language and a participant from Pakistan speaks Urdu as her primary language and
a woman from Nigeria speak Igbo as her native language. All the participants could speak either

4. Results
40
German or English, which made the communication during the interview and focus group quite
easier. All the participants took part in the research process voluntarily and without any pressure.
Among 11 participants, there were four married women who have children and living with their
family in the refugee accommodation. Among them, one woman from Nigeria is divorced and has
three children. She is living in Germany with her two daughters in the refugee camp. The married
woman from Iran (Lena) has two children. One of the married women from Syria (Diva) has a son
and the other (Abba) has a son and a daughter. The four unmarried women (Nele, Celine, Zahra,
and Usma) are living with their family in the camp. Whereas the three unmarried women (Mona,
Ina, and Selli) are living in the camp, which is especially installed for female refugees.
Among 11 participants, 5 of them have graduated in their home country and want to study further
and work in the same field in Germany. Most of the married women have a comparatively lower
education level than the unmarried women. This indicates that most of the participants of this
study are educated. Participants have been living in Germany since 1 to 2 years. All of them are
learning German. Among 11 participants, 8 participants had participated in the REFUGIUM
program and are familiar with different REFUGIUM workshops. The two participants who were
contacted through the organization BergedorferVolkerverständingung did not know about the
REFUGIUM program. One woman was contacted through participant contacts. She had heard
about REFUGIUM but had not participated yet in the program. Some characteristics of the
participants are presented in the table below:
Table 8 Sample characteristics of the study participants
No. ID Age Nationality Family
status
Native
language
Refugee accommodation
1 Nele 29 Syria Single Arabic Accommodation for Family
2 Celine 26 Syria Single Arabic Accommodation for Family
3 Mona 31 Iran Single Farsi Accommodation for single
women
4 Abba 40 Syria Married Arabic Accommodation for family
5 Zahra 24 Pakistan Single Urdu Living with family
6 Diva 35 Syria Married Arabic In mixed accommodation
7 Usma 28 Syria Single Arabic Accommodation for Family

4. Results
41
8. Selli 25 Syria Single Arabic Accommodation for single
women
9. Lena 44 Iran Married Farsi In mixed accommodation
10. Bella 32 Nigeria Divorced Igbo In mixed accommodation
11. Ina 45 Iraq Single Arabic Accommodation for single
women
(Source: Own representation)
4.2 Perception towards health
Understanding of health and women’s health
Health is understood in a different way from refugee women from different countries. The women
from Syria, Pakistan and Nigeria understand good health as being free from diseases. However,
the women from Iran and Iraq associate good health along with good looking or women having
beautiful body and face. In this context Mona from Iran shared that:
“Women take care about their health. They always want to be fit, physically fit and look beautiful
and charming. If they feel they are beautiful then they feel good. So, they give lots of time for
making their hair, for make-up, for making nails. They also spend lots of money to be beautiful.
Lots of women do plastic surgery, operation of their nose, operation of breast, making big or small
as they wish. Actually, they do all kinds of operation” (Mona, 43-47).
Most of the participants of this study related women’s health with care during pregnancy, hygiene,
making body fit and fine, care during menstruation period, typical women’s health problems.
Some of them also linked women health as getting free from women diseases like breast cancer,
ovarian cancer. One of the participants reported that:
“I think the topic related to women’s health are all about the personal hygiene, birth control,
various female cancers like breast cancer, ovarian cancer, gynecological health problem,
pregnancy issues and many more” (Diva, 99-101)
Some participants also linked “age of the women” as one aspect of women’s health, as women
get older, she suffered from different problems like back pain, pain in shoulder, etc. Some
participants also mentioned other factors affecting women’s health like overweight and the
problems arising due to overweight like high blood pressure, diabetes etc. There were also some
typical women’s problem such as hair loss, stress due to children which are related to women’s
health.
4. Results
42
Health consciousness
Among refugee women from five different countries, women from Syria and Pakistan are less
conscious about their health. Especially, the Syrian women who had succeeded to escape from
the war in their home country and thus give more importance to save their life than to live a
healthy life. Some women are even not in a mentally stable condition to think about their health
as they had experienced horrible things in their home country due to war, and some of them are
still in trauma being far away from their family members, relatives and being forced to leave their
own home. In this context, one of the participants shared that:
“I don’t think women in our country care too much about their health. Well, talking in this
generation, I mean now where we have no peace in our country. I know health is very important.
But to survive is more important. You know I have seen many people in my life who struggle very
hard to survive and to escape from the country. I have even seen people who died in the war.
Those people’s faces still come in my mind. I left my home. But my parents, my family and friends
are there. I am here physically, but my mind is there. Whenever I hear bad news, I cannot sleep.
I even do not have an appetite to eat something. So, I am not in the condition to take care of my
health. I need time” (Selli, 35-42).
According to the participants, the women who are still living in Syria or in Pakistan are much less
conscious than the women who live in Germany because those women have to struggle almost
every day for the basic things like safe drinking water, to survive in extreme heat especially in
summer. These women lack knowledge of health. In contrast to these women, women from Iran,
Nigeria, and Iraq showed a little bit more consciousness about their health. They give value of a
healthy diet, being physically active, being mentally and socially fit.
The consciousness towards health is also influenced by education, economic condition, family
status etc. Most of the refugee women who are educated showed more consciousness towards
health than women with less education. They are conscious about healthy diet, physical exercise
and consequences of stress as a mental health problem. One of the participants shared that:“In
Iraq, the women from the big city are well educated. They take care of their health. They do sport.
They go to fitness.” (Ina, 24-26).
In contrast to these countries, women in Iran give more priority to their outlook and beauty than
their health. Women are also ready to spend huge amount of money for their beauty than their
health as one of the participants from Iran reported:
“In Iran, women are not much conscious about their health, but they are conscious about their
beauty. They do an operation like nose operation. But they do not care if they have broken teeth.
Really, women spent a lot of things for makeup, for clothes. And women are happy when they
4. Results
43
have gold. They spent lots of money to buy gold jewelry. But if they have a stomach ache, they
do not want to spend for that, I mean for health” (Lena, 125-129).
Comparing between married and unmarried women, the married women gave less priority to their
health. The health of their family, especially their children’s health is more important than their
own health. In this context, Abba shared that “usually the women, as I know they didn’t care about
their health. She cares about her children, her husband, her family more than for herself” (Abba,
5-6).
According to the participants, most of the women in the refugee camp neglect their health
because they have lots of resettlement issues, such as integrating in Germany, learning the
language, uncertainty about their future etc. In concerned with this, Mona shared that:
“I don’t think most of the women take care of their health. Most of the women in my camp are
busy with mobiles. Some are busy in learning language, struggling to adjust here. Some women
in my camp, even don’t come out. I don’t know why, but they just sit in their room. They do not
do exercise. I don’t understand them” (Mona, 87-90).
The refugees who have settled down for a long time in Germany are more conscious about their
health than the women who are recently here in Germany. Celine reported that, “I think, those
women who came here as refugee, but are already here for a long time, they care about their
health, about their family health. My elder sister, she is here for more than 5 years. She goes to
fitness. She has joined yoga class. They visit the doctor regularly” (Celine, 85-88).
However, participants have the view that women are more conscious towards health than men
as reported by Diva. “Both men and women have similar health problems. But women are much
more conscious than men” (Diva, 42-43).
Health-related behaviors
The participants of this study were living in different refugee accommodations during the study
time. Six women were living in initial refugee accommodation where they are not allowed to cook
food. Food is provided in the canteen. Among six women, who are living in the initial camp, all of
them had reservations about the food. Even the food provided in the canteen is not good, they
tried to intake more fruits and vegetables than meat. However, most of the refugee lack proper
diet as most of them use to skip the lunch or dinner provided in the canteen. Therefore, one of
the participants regularly takes vitamin tablets as supplementary, which are available at the
drugstore.

4. Results
44
The woman from Nigeria has a kitchen, which she must share with other refugees. She cares
about her diet as she does not want to gain weight as she said, “I am conscious of the weight. I
don’t want to be fat. I am conscious of what I eat, how I eat” (Bella, 164-165).
The women from Iraq, Nigeria and Iran also know the importance of physical exercise. These
women perform some kinds of exercises to maintain their health. For e.g. the women from Iraq
had joined fitness and do regular exercise. In contrast to that, the women from Syria, Pakistan
are not active in doing physical exercise. To this point, Celine from Syria reported that:
“(...) women are not so active in such things. They do not like to do exercises (laugh). They care
too much about their family, their children, but not about their own health” (Celine, 134-136).
Refugee women are also passive in seeking health services. If they suffer from minor pain, then
they try to treat themselves taking some medicines. They usually visit the doctor when they are
seriously ill. As Bella reported: “They are not really conscious about their health. When they get
sick, then they go to the hospital. Only after getting sick, they become conscious, but not before”
(Bella, 80-81).
Most of the refugee women are not concerned with their health until they get some serious
diseases or problem. However, there are also some women who give value to their health and
engage them in something so that they can be mentally and physically fit as mentioned by Diva
“I try to be strong, I mean mentally strong. I don’t want to sit like passive. I am most of the time
busy with something” (Diva, 105-106).
In this way, refugee women from different countries portrayed different concepts towards health
and women’s health.
4.3 Perception towards sexual and reproductive health
Understanding of sexual and reproductive health
Almost all participants except a woman from Nigeria were uncomfortable to talk about SRH as it
is taken as a very sensitive topic in their culture. In the home countries of participants, i.e., Syria,
Iran, Iraq, and Pakistan, it is not normal to talk about the topics which are related to SRH. Due to
this, many participants hesitated to answer some questions regarding SRH. Even with hesitation,
participants mentioned different subject areas related to SRH. Mostly the married women have a
broad view on SRH and mentioned different aspects of SRH like pregnancy, care during
childbirth, maternal health, problems that may arise during pregnancy. Regarding this, Abba
shared that:

4. Results
45
“(….) how women can take care of her body when she is in pregnancy. And also, after having a
baby. Her body will be weak, and she needs a nutrient diet to be strong. She needs lots of vitamin
and minerals to be strong. This is the most important thing for women to be conscious that she
should take care of her body during pregnancy and also after giving birth to a child” (Abba, 164-
168).
Some participants also mentioned topics like breastfeeding, childbearing. Most of the unmarried
participants linked SRH with menstruation, pain during menstruation and female hygiene. Some
other topics mentioned by refugee women are early and forced marriage and the complication in
giving birth in early age or in late age, or consequence of giving birth to many children as shared
by one of the participants: “In our country, one woman gives birth to many children. I think that
might also affect the women’s health. My mom gave birth to 9 children and my uncle has 12
children. (....). For people in Syria, it is normal” (Nele, 141-144).
Some participants also linked SRH with women’s diseases such as cancer like breast cancer,
ovary cancer. But there were also participants who have no idea about SRH at all.
Consciousness towards sexual and reproductive health
Among the participants, married women showed more consciousness about SRH than unmarried
women, especially as married women have already dealt with some SRH issues such as
pregnancy and childbirth. Whereas unmarried participants shared more on menstruation. One
of the married participants shared about her own experience that she regularly visits the doctor
and she was conscious about her diet during her pregnancy.
“After I became pregnant, I visit her regularly and she gives advice on what to eat and what not
to eat. And she also told me to do exercise so that my body gets active. Well, I know I should not
do heavy exercise. I should practice some light exercise. My doctor told me that thing too.” (Abba,
284-287).
The married women from Iran was also conscious about SRH health consequences as she
shared that: “It is also important to do a check-up before women get pregnant. If she has some
serious illness, then she might give birth to a baby with an illness “(Mona, 123-124).
The woman from Nigeria was more conscious than other women. Bella from Nigeria shared that
they are aware of family planning or birth control which can be clearer by her statement:
“Lots of women are now being conscious about these things especially birth control. They do not
want to have many children. Most of them have maximum 4 children. Now people are controlling
their childbirth. Before, people have many children. Like my mum have eight children. We are 4
girls and 4 boys. But right now, it is no longer like that” (Bella, 170-173).
4. Results
46
According to the participants, most of the refugee women living in the camp do not care about
their SRH. Participants shared that they have seen some pregnant women who regularly smoke
and are not aware or conscious about its effect on theirs and unborn children health. Participants
also do agree that most of them do not care about their SRH.
4.4 Sexual and reproductive health knowledge
The participants have the opinion that most of the refugee women have a very little knowledge
on SRH. Therefore, they are not much conscious about their SRH. Related to this, Zahra shared
that: “I think women in accommodation or camp are not much conscious about their reproductive
and sexual health because of lack of education” (Zahra, 78-79).
The knowledge on SRH can be acquired through different ways, which can be divided as formal
and informal education. Formal education indicates the knowledge that is gained through school
and Universities. Informal education is the information obtained through other contacts/means
such as from their sisters, mothers, friends, etc. which is described in following paragraphs.
Formal education
Six women in this study are grown up in Syria and they had completed their higher education in
Syria. One participant came from Pakistan and did her study in Pakistan. One participant came
from Iraq and had finished her undergraduate in Iraq. All these participants shared that they did
not get adequate knowledge on SRH in their school in their country. There is the availability of
books and articles regarding this topic, but the teacher hesitates to teach about these things. In
this context, Nele shared that:
“In our country, we learn about reproductive and sexual health in 9th grade. And it was also only
one lesson. Normally the teacher used to tell us about it very fast. And no one dares to ask
questions about it. And if the teacher is a man then he will say that it is not so important. Our
teacher told us that we should read it at home. He did not explain anything. And he also said that
he will not ask questions from that part in the exam” (Nele, 203-207).
The participants from Pakistan and Iraq also reported that they were not enough informed and
educated about SRH and its consequences on women’s health in their school and higher schools.
In contrast to these countries, the participant of Iran and Nigeria reported that they were taught
on different contents related to SRH like physiology, menstruation, pregnancy and
contraceptives. A woman from Iran shared that, girls and boys are taught separately in school at
her school time. Therefore, girls didn’t hesitate to learn about those things. Besides this, women
in Iran can also get information on SRH through a gynecologist.

4. Results
47
“In Iran, when I was in school, SRH was in the curriculum. We are taught about a woman’s body,
a man’s body, how women get pregnant, I mean the changes in hormone and the development
of the baby inside the mother’s womb such things. I can’t remember all but those things (….) and
we were taught by a female teacher. At that time, boys and girls were taught separately so we
did not feel hesitant” (Lena, 153-157).
The statements of participants signify that women from Iran and Nigeria got a comparatively
better education regarding SRH than women from Syria, Pakistan and Iraq.
Informal Education
In Syria, Iran, Iraq, and Pakistan, people usually do not talk about SRH related topics in public
places. It is like a very private thing. People feel embarrassed to share their problems related to
SRH. Some of them even hesitate to talk to their mothers. According to the statements of study
participants, the main source of information regarding SRH is sisters, friends and cousins.
Another source of information is neighbour, relatives, and people who are close to them.
Regarding this Abba shared that:
“When we have a problem, we get help from sisters, neighbors, other girls, friends who share
about this girl’s problem. Normally we also feel shy to talk about it with our mother. I normally talk
with my cousins, sisters when I have a problem regarding menstruation, pain in stomach. They
told me then that I have to drink a lot of tea. We should not do a lot of work during menstruation”
(Abba 54-58).
After marriage, women also share their problems related to SRH to their husband. Abba shared
in this context that: “I know my husband for 8 years. So, after all this year, I discovered that your
husband is the only man to whom you can tell everything. You can share everything, your secrets
in a very comfortable way. You can be sure that he will not say that thing to anybody. And he will
help you without thinking too much. Well, he will take care of you. You can share everything.
Women should let her share emotions with her man. If I did not tell him, then to whom should I
tell and share my things. How should he know that I have pain, or I am suffering from a headache
or I have pain in my arm?” (Abba, 112-118).
Almost all participants mentioned internet as a big source of knowledge regarding SRH after their
settlement in Germany. As participants could hardly share and ask regarding SRH to others, they
search on the internet, especially in google if they want to know some information related to SRH
as reported by Celine:
“Here we usually search in Google. Before, we didn’t have an insurance card and if I want to
know something, I search it in Google” (Celine, 178-179).
Thus, refugee women get SRH information through informal way, i.e. through the person who is
close to them such as sister, husband, mother, and friend and an internet has become a major
source of knowledge in Germany.

4. Results
48
4.5 Sexual and reproductive health issues
4.5.1 Menstruation
For most of the participants, menstruation is an awkward condition. About more than half of the
participants, especially the unmarried participants experienced a strong pain during
menstruation. Some participants have lower abdominal pain, while some have back pain. Some
participants had also experienced mood swings during their period. One of the Syrian participants
shared that:
“During my period, I have so strong pain in my stomach. And it happens for 3-4 days. Every
month when I have my period, I just want to sit and lie in my bed. (….) till now I have not taken
any medicine for pain. Sometimes I take paracetamol. Sometimes, it helps me and sometimes it
does not help me. And you know, it is not only in my case. I know many girls in my friend's circle
who have to bear pain during menstruation. And since I am here in Germany, I have an irregular
period. Last year, after arriving here, I did not get a period for 2-3 months. I was just hoping that
I am fine because I do not want to go to the doctor” (Selli, 115-121).
Even though most of the participants suffer from acute pain during menstruation, they hesitate to
visit the doctor as they are very embarrassed to talk about it and especially, with the male doctors.
Participants also mentioned that they try to find another way to reduce the pain during
menstruation. The participant from Syria and Iran shared that women usually drink a lot of tea
during menstruation. They believe that tea helps in reducing pain during the period as Mona
shared: “During menstruation, we drink a lot of tea. In Iran, it is like a tradition that we drink a lot
of tea, especially during menstruation. We believe that tea helps in reducing pain during
menstruation” (Mona, 24-26).
Another participant from Iran shared that she uses a hot bag during menstruation, which helps in
reducing pain. Some participants also shared that they suffer from premenstrual syndrome like
feeling tired, feeling irritated, mood changes, stress, anxiety, etc. In this context, one of the
participants shared that:
“before menstruation and even during menstruation I feel some kind of tiredness. I get irritated
with small things which do not suit me. I have like a kind of a headache and a bad mood. Oh, I
get so angry and sometimes I feel like I am another person. I think, I even talk crudely with people.
My mother tells me that, I usually have a bad mood before I get my monthly cycle. And I know
she is saying the truth. But I can’t change. What I do is, I try to remain calm and I usually stay at
home. I didn’t want to meet other people at that time” (Usma, 158-164).

4. Results
49
In most of the Muslim countries, people normally do not talk about menstruation, so women tried
to hide their problem especially with a male member of the family. Regarding this Celine shared
that: “we did not even talk about this openly. We could not talk about our menstruation in front of
our father. Mothers use to tell us, but she does not give all information which we should know”
(Celine, 163-164).
Another participant from Syria added that women lack basic knowledge of menstruation, so she
is left alone to handle the problem when she experiences it. Nelereported that, “In our country,
we get to know about menstruation, when we experience it but not before. If we know what
happen before then, at least that girl has an idea what she should do, instead of crying” (Nele,
158-160).
In contrast to this, women from Nigeria shared that they do not hesitate to talk about menstruation
with other family members or neighbors, including a male member which she mentioned in her
following statement: “When I was having menstruation, the whole house will know that I am
having menstruation. Because it is so painful, I used to cry so loudly” (Bella, 96-97).
Use of menstrual hygienic products
Almost all the participants use sanitary pads as menstrual hygiene products in Germany. There
were participants who also do not know about the tampons and other hygienic material before
coming here in Germany. Women learn about the use of sanitary pads from their sister, and peers
as Celine said.
“During my first menstruation, I even don’t know how to use sanitation pad. I asked my elder
sister. She told me how to use it correctly. She is like my teacher. She told me which foods are
best to eat during menstruation and which are not good (....) (Celine, 172-175).
The participant also shared that the sanitary pads are generally expensive in their home country
so it was hard to afford them. The participants from Iran also mentioned that girls could get
sanitary pads without any charge in the schools if they get their period in school. (Mona, 26-27).
The use of sanitary pads is also hardly communicated with the girls. Even mothers hesitated to
talk about sanitary pads in front of her husband. Celine shared her experience like this:
“You know when I was small around 5 or 6 years old, I didn’t know about the use of sanitary pads.
I used to see it in the market or an advertisement on TV. But no one told me what we do with
sanitary pads at that time. I have no idea about that. Once I asked my mother in front of my father,
what is that thing. For what purpose we use it. At that time, my mum just laughed and didn’t tell
me anything in front of my father. But after having menstruation, whenever there comes an
advertisement of sanitary pads, I used to change the channel because most of the time, my father
used to sit behind us. It is so funny. At the same time, it is embarrassing” (Celine, 166-172).

4. Results
50
4.5.2 Early and forced marriage
Early and forced marriage was another theme mentioned by participants from Syria, Iran, Iraq
and Pakistan. According to society and cultural system, the refugee women got married at a
different age. In Syria, Iraq and Iran, most of the girls from the big cities get married in mid or late
20. In rural areas, many girls get married at the age of 16 or even earlier. In Pakistan, most of the
girls get married at an earlier age like 16 or 18. Also, in African country Nigeria, there is a trend
of early marriage, especially in the east and west part of Nigeria, where girls get married at the
age of 15 or 16.
One reason behind early marriage in Syria is due to war and conflicts. The family with daughter
wants to protect their daughter through marriage. They think that their daughter could get
protection from her husband and if the man is living outside the country, then it is easy for the
women to migrate from their home country and stay safe. Due to this, some women are even
forced to get married to someone. Abba from Syria shared like this:
“You know I think because of war, people start to think like they should give their daughters away
so that her husband will take care of her. Most of the young men are travelling away from Syria
and they think that if their daughter gets married someone, she can go away with her husband.
And her husband will take care of her. Or if the man has been already outside, the parents hurry
up to marry their daughter with that man so that she can go away from Syria”. (Abba 41-46).
Another reason for early and forced marriage is due to a lack of education. The participant from
Iraq mentioned that mostly the uneducated people get married at an early age in Iraq, which
further make them difficult to continue their study.
“Specially, the uneducated people they get married at an early age. There are girls who married
at the age of 16 years old or 18 years old. You know the girl, who was with me in the workshop.
She got married in 16 years old. She was studying in school when she got married. So, she could
not finish her school level” (Ina, 61-65).
Especially in Pakistan and some part of Syria, many people are still following the tradition of
arranged marriage where the family selects a man for a woman. Some women are even forced
to marry with the person. But in the city area, this trend of arranged marriage is changing. The
women and men meet before they get married. Regarding this Zahra from Pakistan shared that:
“Everyone is free to choose his partner, but unfortunately, it is not common in my culture. Girls
are mostly not allowed to choose her life partner without the permission or willingness of her
parents. Maybe you know, in our culture, we follow the arrange marriage where parents search

4. Results
51
life partner for us. And the girl and boy are even not allowed to meet before marriage” (Zahra,
119-123).
Along with arranged and forced marriage, there is also the tradition of polygamy in Iraq, where
the man has the right to get married to more than one woman as reported by Ina:
“if a man wants to marry a woman and if parents are also satisfied than women get married with
the man even women are not ready. And you know that there are some men who are already
married, and they marry another woman. But that man should have enough money. He should
afford a house for both wives. He should make both of them happy. There are also some men
who are older, and they marry a very young girl. But these cases are now decreasing” (Ina, 259-
264).
In opposite to Syria, Pakistan, and Iraq, the trend of forced marriage is decreasing in Nigeria and
Iran. The participants from Iran and Iraq also shared that most of the women in their country are
getting married at their later age in these days than in the past generation.
Consequence of early and forced marriage
Participants mentioned that women who got married at her early age get pregnant at an early
and lack adequate knowledge of childbearing, breastfeeding and thus could not properly take
care of their children. One participant shared this issue like this:
“Most of them, they do not know how to cook, how to take care of their baby. They are themselves
like a baby and (….) and after 9 or 10 months, they get baby and they don’t know how to take
care of her baby” (Abba, 38-41).
Further on, some participants also shared that women give birth to many children when they get
married at an early age. The participant from Nigeria also reported that women in Nigeria suffer
from a disease where women cannot control their urinary tract.
“(…) a lot of girls suffer from a disease in which girl passed out urine without any control. I forget
the medical name for it. After giving birth to a child, they cannot control their urinary tract because
they are not mature enough to give birth to the baby. They are too young to get pregnant” (Bella,
64-68).
These are some problems mentioned by participants during the pregnancy and childbirth due to
early and forced marriage.

4. Results
52
4.5.3 Pregnancy and childbirth
All the married participants of this study indicated pregnancy and problems during pregnancy as
an important subject concerning SRH. They also shared that they were more conscious of their
health when they were pregnant. In their home country, they usually get get support and care
from their family and relatives during pregnancy. Regarding this Lena shared that:
“Me, personally, I was very much serious about my health when I was pregnant. My mother and
grandmother took care of my health. My grandmother made special food for me when I was
pregnant. It is a kind of food mixed with lots of nuts. And my mother told me that I should not eat
a lot of beans such things. I also got tips from doctors what I should eat and what I should avoid
during pregnancy” (Lena, 145-149).
Among four married women with children, three of them had experienced many difficulties during
their pregnancy. A woman from Nigeria with four children had even lost one of her children due
to lack of proper care and diet and stress during her pregnancy. She had to stay for many days
in the hospital as her body was very weak since she could not digest any food.
“The first three months were really terrible. I was very sick. I used to vomit after eating something.
I can’t eat for three months. I could not sleep well. I used to take just liquids. I can’t swallow. I
can’t chew. Even I just take liquid, I vomited that. Anything I put in my mouth, after some minutes
it comes out. I think after four months, I started eating gradually like a baby. I ate very little at that
time. And the smell of food is different. Those foods which I like to eat before does not taste good
to me. I can’t eat them more. The taste is different in my mouth” (Bella, 220-226).
Further, she reported how she lost her child in Germany due to stress and lack of proper care.
“I was pregnant when I was travelling from Nigeria to Germany. Those days are my worst time in
my life. I divorced my ex-husband. I have a lot of stress. After arriving here in Germany, I did not
get proper care. There was no one to care for my child and of me. There were times when I had
no food to eat. Being pregnant, I worked as a dishwasher. I didn’t know about the medical services
at that time. It was so hard. Due to all these stresses, my baby boy died after his birth” (Bella, 33-
38).
Another participant reported over thinking as a major problem during her pregnancy. “When I was
pregnant for the first time, I used to think too much” (Abba, 286).
The married participants mentioned that all of them had their child delivery in hospitals. However,
participants also mentioned that in the remote areas in their country, women also give birth to
their child at home. After the delivery of child, women normally get help and care from midwives,
4. Results
53
relatives or neighbors. Some participants are also aware about medical and midwives’ services
during pregnancy and childbirth in Germany. But, participants also mentioned that refugee
women who live in camp lack healthy diet during pregnancy as refugee camp does not offer
special food for pregnant women.
The married woman from Iran also mentioned that some women in Iran have difficulties in giving
birth to a child or they give birth to an unhealthy child which she illustrated in this way:
“Nowadays, many women have a problem that they cannot give birth to a child or they bring an
unhealthy child into the world. So many women are afraid about that. And nowadays there are
many new diseases, which doctors also did not know well” (Lena, 174-176).
In this way, women shared their pain, suffer and difficult experiences in relation to pregnancy and
childbirth.
4.5.4 Abortion
The participants from the Middle East Islamic countries shared that abortion is normally not
allowed after knowing that the baby is already there as Celine shared “And in our country, we are
not allowed to do abortion except in some serious cases. For example, one of my Aunt in Syria
does not want to have a baby as she has already many children. But it was already too late. So
that was her last baby” (Celine, 258-260).
In Iraq too it is not legal to do an abortion, but some doctors perform it secretly. (normally it is not
allowed, but some doctors do it illegally (Ina, 225)).
Also, in Iran, there are some cases when girls get pregnant before marriage and sometimes, they
have to undergo an abortion, which is officially and from the religious point of view not allowed
but many people do it secretly. Lena shared on this topic like this:
“it is not allowed from religion, but people do it with a secret. When they notice that they are
pregnant, then they go to women doctor and do it. There are also women who are against
abortion. Women who are religious, who still follows an old tradition, they do not do abortion”
(Lena, 56-58).
However, there are also women who follow the old tradition and are religious and are against
abortion.
In Pakistan, abortion is allowed only when pregnancy is severely affecting women’s health.
Regarding this, Zahra shared that: “I think, abortion is also allowed, but under certain conditions
for e.g. if pregnant women health is in danger due to pregnancy, then the women are permitted
4. Results
54
to do abortion. But she alone cannot take the decision. Both husband and wife should take the
decision”. (Zahra, 102-104). However, pregnant women could not take the decision alone if they
want to do abortions.
4.5.5 Family planning and contraceptives
Among 11 participants, 7 participants are single and have not yet thought about family planning
and contraceptives. Among the four married women, only two of mentioned they knew about
family planning and contraceptives. The woman from Nigeria also reported that women in Nigeria
are now more conscious regarding family planning.
“Lots of women are now being conscious of these things. Especially birth control. They do not
want to have many children. Most of them have maximum 4 children. Now people are controlling
their childbirth. Before, people have many children. Like my mum have eight children. We are 4
girls and 4 boys. But right now, it is no longer like that” (Bella, 171-174)
Also, in Iraq, women are now aware about family planning. In the past women used to have many
children, but now they are reducing their childbirth as mentioned by Ina:
“In past, people in Iraq have a lot of children. For e.g. I have seven siblings. And one of my friends
has 9 siblings. But now the people have fewer children. One of my sisters has 4 children and my
brother has 3 children, another brother has 4 children. One of my sisters is engaged. She has
not yet a child. My dad died early before 30 years old. If he was alive then we were more children”
(Ina, 73-77).
According to participants, most of women in refugee camps are married and have comparatively
more children than native citizen. One of the participants further stated that some couple
intentionally wants to have many children as they get money from the government on behalf of
their children.
“you know there are some women who intentionally do not use contraceptive because they want
to have more children so that they can get money from the government for their children. You
know that in Germany if you have children you get Kinder geld from the government. So, they
want to have more children. That’s why they do not go to work. But I can’t think of that. I want to
work and earn money” (Bella, 211-215).
The participant from Iran and Syria reported that the new generation couples are practicing family
planning as they recognize that they need more money to grow a child and it also helps women
to involve in the employment sector.

4. Results
55
“In Iran, it is very expensive to grow up the children. If you have more children, then you need
lots of money. So, people use contraceptives not to have a baby” (Mona, 137-138).
The participants from Syria, Iraq, Pakistan and Iran also shared that mostly the highly educated
and wealthier people think about family planning and contraceptive use. One of the participants
stated: “You know, in our country, most of the rich people have only 2 or 3 children. And most of
the poor people have more than 8 children. And later, they said it is hard to grow up many
children” (Celine, 147-148).
The married participants also shared about the involvement of a husband and wife in a decision-
making role for family planning and contraceptive use. However, the couple should decide before
having a baby in the mother’s womb.
“Well, I can decide that I don’t want the baby but before being pregnant. After getting pregnant, I
cannot say that I don’t want this baby. I am not allowed to say I don’t want a baby after having a
test and when the baby is already there. It’s a big mistake in our culture. Abortion is normally not
allowed” (Abba, 294-297).
Regarding contraceptives, all the participants stated that there are different methods available in
their home country and uses of contraceptive are also acceptable in their culture and religion.
Normally, people have to buy contraceptives for themselves However, in Nigeria, married women
are not supposed to use contraceptives. “Well, in Nigeria when you are married, you are not
supposed to use any contraceptive. After marrying, if women say her husband to use a condom
than the husband will say why did you marry me. Are you my girl friend? The husband does not
want to use it. And it is very hard to negotiate on this topic” (Bella, 184-187).
Like other SRH topics, people normally do not talk about contraceptive in the Middle East Islamic
countries within the family and between siblings. Only husband and wife negotiate about the use
of contraceptive. Many single women get to know about contraceptives only after marriage.
Therefore, the unmarried participants have very little idea about contraceptive method. Some of
them know only condom as a contraceptive method.
Among four married participants, only two of them have already dealt with contraceptives in their
home country. They know about the contraceptives like a condom, injection of a drug, pills,
spirals, etc. The married women from Iran shared that she had used a spiral and she finds it very
effective. “Yes, contraceptives are acceptable in our religion. I have used the spiral after giving
birth to my second child. We can do that by a gynecologist. My mother also used a spiral. In my
view, a condom is not so effective. But spiral is more effective, but it is expensive” (Lena, 196-
198).
4. Results
56
Another participant from Syria shared that she had used some pills in Syria. But she had problems
like unbalance in hormone as a side effect of that contraceptive method. Now, after settling down
in Germany she is not using anymore. The participants further reported that many women don
not use contraceptives because of its negative side effects such as weight gain or skin damage.
“But most of the women are not using contraceptives because they think that they will be fat after
using contraceptives” (Bella, 177-179).
Concerning counseling center for family planning and contraceptive, none of the participants
know about it in their home country as well as here in Germany. The participants were also asked
if they know where they can get contraceptives. Most of them did not know where to get it and
only a few mentioned that they can get contraceptives through a gynecologist.
4.5.6 Sexual transmitted infections
The participants from Syria, Pakistan, Iran and Iraq reported that they should not have a sexual
relationship before marriage. Most of the participants think that this system prevents them from
getting sexually transmitted diseases. Therefore, most of the women do not see STI as a huge
problem, especially for the unmarried women.
The participants from Syria also shared that, most of the women and man should undergo a
different health check-up before they get married. This helps men and women know about each
other diseases and to prevent from STI as reported by Abba.
“In Syria, before you get married, you have to go through a test or health checkups. They do a
blood test. They test, how good is your health condition if he or she has some diseases. But they
are not forced to do that. Normally, most of the people do that. The most important is that you
should not have a relation before marriage. Before arranging papers for marrying, you should do
some kind of health check-up and analysis” (Abba, 329-333).
Among different STI, almost all the participants are well known about HIV and AIDS. But most of
them are unaware of other STI such as Chlamydia, Syphilis, Gonorrhea etc. Most of the
participants shared that they have learned about STI during their school life, but they did not get
comprehensive information on it. The topic like STI is also taught only superficially in Pakistan,
Iran, Iraq as well as in Syria.
The participant from Nigeria had graduated in Biochemistry and one woman from Syria had
studied pharmacy. These women have more knowledge of STI than others. The women from
Nigeria even knew close people who suffered from Gonorrhea. “I know women who suffer from
Gonorrhea. One of the friends of my husband had also this disease. My husband also has a
4. Results
57
urinary tract infection, I am not sure if it is STI” (Bella, 364-366).
The participant also mentioned that there are availability of a few health promotion and
awareness programs on STI in Televisions in their home country. But none of the participants
are aware of the counselling center about STI neither in their country nor in Germany.
4.5.7 Sexual and gender-based violence
All the participants do agree with the existence of sexual and gender-based violence in their home
country or in their culture. Among the 11 participants who live in refugee camps in Hamburg, 6 of
them had expressed their feeling of insecurity in living in refugee camps. They believe that there
is a high risk of getting sexually abused inside the camps, especially at night when they have to
go to the washroom. In most of the refugee camp, the toilets and bathrooms are outside the room
and the bathrooms are open, i.e. there are only curtains instead of doors. Due to this, women
always need someone to stay outside the bathroom for protection when they are taking a shower
as reported by Celine:
“(...) The bathrooms are also not clean. The bathrooms are open. I mean there is no door in the
bathroom, only a curtain. So, it’s so uncomfortable to take a shower. One must stand outside the
bathroom and look if someone enters there” (Celine, 10-12).
Further on the participant from Nigeria shared that she usually takes a shower at night when most
of the people are already in their beds. “whenever I take showers, I am afraid. As there are no
doors, there are only curtains in the bathrooms. Even the men and women’s bathrooms are
separate, I am afraid that someone might enter and grab me. That’s why I usually take shower
at late at night, when most of the people are already in their bed” (Bella, 383-386).
Nevertheless, there are also some participants who feel more secure inside the camp than
outside because of the 24 hour security in the camp. Abba shared that:
“Inside the camp, it is more secure. But outside the camp, it is very dangerous as on the other
side of the road there is also another camp for single refugee men. Some of them are drunk at
night and can do anything. And some are crazy and have a mental problem. So, I do not let my
children play outside the camp. Even the securities told me that I should not let my children play
outside” (Abba, 365-369).
The participants find positive that most of the camps in Germany have 24 hours security. Three
participants are living currently in the camp where only single women are permitted to live. In
those camps, men are not allowed to enter inside the camp. Therefore, they feel safe in the camp.
Regarding this Mona shared that: “All women are alone. They are single women. We don’t have
4. Results
58
women with children. Normally, men are not allowed to come inside our camp, except for a
caretaker and securities. That is good for us. It is very safe” (Mona, 69-71).
Some of the participants reported that besides having security, they hear from people
experiencing sexual abuse inside the camp. Some of them have even experienced unusual
behavior of men like starring in an unusual way which makes them feel insecure when they are
travelling alone. In this context Selli shared like this:
“I have not experienced so horrible thing. But I had experienced bad things. It was in the
summertime, last year summer when I was returning to my room, I mean to my camp there were
some men standing outside the camp and they were looking me from top to bottom and from
bottom to top. It is so weird. It seems like they have seen a woman for the first time (….) they are
not German, they are also a foreigner, like us but I have not seen them before. I walked from
there so quickly as I can. After that, I have not seen them again” (Selli, 171-175).
Almost all the participants have heard about some kind of sexual abuse or sexual violence cases
in their camps. Moreover, the participants shared that they hear sexual violence cases
comparatively more in their home country than in Germany. The participant from Iran shared that
in Iran, women are sexually abused in working place, in universities and the worse things are that
some police officers are involved in doing such things who are actually there to protect public
from crime. Furthermore, the women being the victim of sexual violence blame for her. Regarding
this Mona reported that:
“In Iran, we are growing up with the ideology that if something bad happens then it’s because of
women mistake. For e.g., if women experience sexual harassment or something like this, then
it’s because of her. Police or Government says, women might have shown their hair to the boy,
so it happens. So, many people believe in that. And many women do not dare to speak up. From
our childhood, girls learn in that way that if they show their hairs then they will experience
something bad. It’s fully nonsense. A boy or man does something bad and people said it’s the
woman’s fault” (Mona, 171-176).
Participants also shared that women being the victim of sexual violence have very bad
consequences in some culture like in Pakistan and in Syria. Even the victims do not dare to
complain about it at the police because they are afraid that the women might have to face many
difficulties in the future.
Some participants expressed that living in Germany is much more secure than in their home
country. In Syria, there are many sexual violence cases, which are under-reported. Related to
this topic, Celine shared that: “(....) there are some places in Syria or in Iraq, where ISS attack
4. Results
59
Yazidi people. And some Muslims man had raped Yazidi women. And in Iraq, there is one place,
where ISS were selling Yazidi girls” (Celine, 387-389).
Regarding sexual and gender violence, the participants shared a lot of sexual violence cases,
which they have heard about or experienced in their home country as well as after settling down
in Germany. Most of the participants also shared that they feel safer in Germany than in their
own country.
Domestic violence
The participants also shared their opinion on domestic violence due to which many women in
Muslim countries have to suffer the adverse mental health problem. Participants shared that men
are taken as superior and guardian in Muslim culture. Concerning this Celine said that: “I have
seen many Muslim men. They are so dominating. They think that he has the power and his wife
should follow everything that he wants (Celine, 392-393).
Another participant from Iran also mentioned unbalance power relation between husband and
wife by illustrating one example: “For e.g., my sister is younger than me, she is 28 years old and
already married. She has one son and she always has to do that what her husband says. And in
Iran, women cannot give divorce to her man, but a man can do that” (Mona, 160-163).
This kind of unbalance power relation is mostly present in the old generation population. “In Syria,
it depends on the family. Mostly in the family with the older generation, women have to do what
the man said. Women cannot speak up against their man. If a man wants to have sex, then it is
more probable that women must do sex. But now, in new generations, it is not like that. Women
can speak and say not to have sex if she is not interested” (Celine, 322-32).
The participant from Nigeria was open to share that she was herself a victim of domestic violence
(Bella).
In some regions, people, especially family member even were found to murder women in the
name of honor when she broke any rules and regulation of the culture or religion. Even if women
were victim of sexual violence, she suffers from its consequences and not the predator. In this
context, Zahra shared that:
“Yes, people kill women, I mean their wife or daughter from their own family member when she
breaks any rules or law. It happens in most of the remote area. Some people even feel proud
after killing (Zahra, 129-131).

4. Results
60
4.6 Awareness about sexual and reproductive health services
4.6.1 Health services in refugee camps
All the participants except one who lived in emergency shelter reported about the availability of
general physician in a refugee camp. Some camps even have a special doctor for children.
However, the participants reported that it is hard to get an appointment with a doctor in camp as
they have to wait long for their turn. Regarding this, one of the participants shared that:
“The doctor in the camp is also good, but she did not come regularly. Even it is written that every
Monday there is the appointment and availability of doctor and doctor for children are also there
for once in a week. But it is most of the time full or they take only a few children and we have to
wait for a long time or search for another time” (Abba, 214-217).
In some refugee accommodation, there are also midwives’ services. Bella mentioned in her
interview that: “We have midwives, they come every Wednesday. If you have a problem, then
you can talk to them. They will give advice then” (Bella, 190-191).
In some refugee camp, they also offer yoga and meditation once a week, especially for refugee
women. But, there is no information regarding family planning, STI, sexual violence and other
topics related to SRH. One participant stated that: “I have seen many flyers and information
regarding healthy foods, sport, and mental health but not about sexual and reproductive health.
There are programs like yoga course, women café such thing” (Ina, 195-197).
The participants also reported that they were not informed about SRH services which are
available in their surroundings as one of the participants shared that “Normally in the canteen,
there is an information board where they hang flyers and posters from different programs. But we
have not seen any flyer related to reproductive and sexual health” (Celine, 225 -226).
The findings from observation also present that there are available doctors and general
physicians and special doctors for children in the observed refugee camps. Furthermore, it
presents that some camp also offer counseling for mothers (Mutterberatung). In some camps,
they also have midwives’ services for pregnant women. However, there are not abundant
services and information regarding SRH in refugee accommodations.
4.6.2 Health care services in Germany
The study participants are not well informed about different SRH services that are available in
Germany. Most of the participants, mostly the unmarried group had not even sought for
information regarding SRH such as family planning, contraceptives, sexual violence, etc. Hence,
the unmarried women have not yet utilized any SRH services. The married participants know a
little bit more about SRH and had also utilized the services like counseling for mother and

4. Results
61
gynecologist services. One of the participants shared that she got good medical care in Germany
when she was pregnant, and her child was ill.
“When my second child was sick, they took me to the doctor who gave me service, medical
service. They provide us doctor. When I was pregnant, I visited gynecologist. I also told her my
history that I already lost my child” (Bella, 317-319).
Among 11 women, only one married participant knew some counselling center for pregnant
women, which gives advice on proper diet during pregnancy and negative effects of medicine
during pregnancy. But the participant could not name the counselling center.
In Germany, there is help and support called as “Violence against women” (Gewaltgegen Frauen)
which offers help for women who are victim of sexual and domestic violence. But none of the
participants knew about this. If in case women experienced sexual abuse, then most of them said
that they will go to the police for complaining. Few participants even don’t know what they have
to do if they experience sexual abuse in their life. Most of the participants expressed that they
have more trust in a police officer in Germany than in their own country. Regarding this, Usma
shared that: “Yes, I think we can trust police here in Germany. It is not like in our country. The
police do such bloody things like sexual harassment, rape” (Usma, 210-211).
Participants were also asked about rights regarding sexuality. Almost all participants shared that
they have not heard about this right before the interview. After explaining the rights regarding
sexuality, participants meant to know these rights. Some participants shared that they are written
in the paper, but people do not follow these rights in their country. “Yes, I know these things, but
I am not sure if people follow these rules” (Diva, 198).
Nevertheless, most of the participants were interested to know about different SRH services
which are available in Germany since they are going to stay in Germany as reported by Selli.
“I don’t know anything regarding this. But I would like to know. Because, if I am going to stay here
in Germany, then I have to know that. In future, if I get married and get pregnant then I should
know where to go for a check-up, where to go for childbirth, where I get care after giving birth to
a child. All these things are important, but we do not know about it” (Selli, 134-138).
4.6.3 Health promotion and awareness program
Among 10 participants, eight knew about the REFUGIUM health promotion program in Hamburg.
Participants were also asked if they knew any other health promotion organizations. One of them
knew about an organization like Caritas Hamburg which is working in the field of SRH. Two
participants also mentioned about the health care services which is offered by the Church of that

4. Results
62
community. Regarding this Nele shared that:
“There is also a doctors' service in the church, near our refugee camp. My mom also went there.
The doctor in the church also said that she needs to have an operation. Her waist problem is
getting worse. She is getting older, so it will be hard for her to do operation later” (Nele, 128-130).
Another participant from Nigeria got service and care from Adebar Hamburg in Bahrenfeld. From
there, she got tips for breastfeeding, which she has reported in this way:
“And I also got help from Adebar. I was having a problem with my breastfeeding. My child has a
problem with sucking milk. So, the doctor suggested me to visit Adebar in Bahrenfeld. The
midwives there teach me how to breastfeed her. When my child was sucking well then I don’t
have to go there more” (Bella, 336-339).
A woman from Iraq also engages in different activities in different programs such as Frauen café
in Aidshilfe Hamburg, Mut cafe, Refugium, and Roteskreuz. She shared that she got to know
about SRH through Aidshilfe Hamburg. “Day before yesterday, we had a lecture about sexual
health in Aidshilfe in Hauptbahnhof” (Ina, 177).
The participants of this study were shown Zanzu website from the BZgA. The website contains
different SRH aspects such as women and man's body, family planning and pregnancy,
infections, sexuality, relationships and feelings, and rights and law. These are the main topic
which also includes sub-topics. Participants were asked if they knew about the online web site,
where SRH were explained in different languages. None of the participants knew about the Zanzu
website before. After knowing Zanzu, participants also gave some feedback. One of the
feedbacks from a participant is mentioned below:
“In my view, Zanzu is a very informative website, where everyone can get information about
sexual life. The positive thing about this website is that the information is available in different
languages. But the people who have no Internet cannot use this program” (Zahra, 141-143).
Participants appreciate that Zanzu is providing a lot of helpful information in different languages.
It is also easy to access as they can open the website in their smartphone. They liked that Zanzu
website is designed in an understandable way, i.e. that they can have a glance in separate topics
and to each topic there are subtopics. Due to lack of time, participants did not read all the
information from Zanzu during the interview. But most of the participants were interested to read
Zanzu information when they get time after the interview or focus groups were done.
There were participants who also knew about Diakonie, but they are not aware of the program
for a refugee. About half of the participants knew some health programs while half of the
participants are not aware of these programs except REFUGIUM.

4. Results
63
4.6.4 Health services in the country of origin
The participants reported that there are only few SRH services in Syria, Pakistan, Iraq, and Iran.
In comparison to these countries, Nigeria has more services on SRH. Many communities in Syria,
Pakistan, and Iraq face severe limitations in their access to medical care and SRH services.
Some participants even shared that most of the hospitals in remote areas are not hygienic.
Therefore, they do not provide quality care as mentioned by Ina in her interview: “We have a
good hospital, but the condition of the hospital is not good. The hospitals are not clean, and, in
some hospital, you can even see animals walking inside the hospital (laugh)” (Ina, 45-47).
In Syria, many hospitals and health centers got destroyed due to war. Now, there are only a few
hospitals in Syria. One of the participants mentioned in her interview that: “we have now not so
many hospitals. It is very sad to say. Before, there were either hospitals or health clinics almost
everywhere in Syria” (Usma, 69-70).
Besides hospitals and health centers, there were also some health promotion programs in Syria
which are not running anymore.
Participants from Iraq, Pakistan and Iran mentioned there were a lot of good hospitals available
which could provide quality care but they were expensive. There are clinics and hospitals where
they can give birth to their baby and they provide quality care for mothers after giving birth. In
Iran, they have midwives, gynecology services in hospitals or outside the hospitals. Women also
get special care in case of miscarriage in Iran. However, the gynecologist is expensive than
midwives. So many people prefer to go to midwives in Iran. “We have hospitals, midwives and
health center. And we have also gynecology. But you know gynecology is very expensive. So
many people go to midwives. Midwives cost is not so expensive” (Lena, 61-63).
Nevertheless, there is a common trend in all these countries that in rural areas, access to SRH
services is difficult vs. say big cities like Damascus or Tehran.
None of the participants knew about the counseling centers for women regarding family planning,
STI etc. in their home country. But in Nigeria, many hospitals are now offering a special course
for pregnant women about childbearing, family planning, and contraceptives as there were high
maternal and infant mortality rates in the past. In this context, Bella reported that: “There are not
so many cases about the child dead like before. Also, the maternal death cases are decreasing.
We have still the cases like where the mother died, or a child died, but not so much like in the
past. There are also miscarriage cases, but not so much” (Bella, 75-78).
Regarding health promotion and awareness program, most of them shared that their country
lacks health promotion and awareness program. In Iraq, however, there are different

4. Results
64
organizations, which are working in the health sector, such Iraq Red Cross as mentioned by Ina:
“We have some organization like Iraq Red Cross, IFIC, ICIC such things but not so much. They
have a lot of programs like they go to pregnant women and talk about what to do and what not.
Like what should they eat” (Ina, 91-94).
Excluding organizations that are offering health care services, there are lots of organizations in
Syria, Iran, which help women to read and write who are not educated. There are organizations
which provide swimming courses, nurse training course for women, or even training in doing
makeup, and haircut. In this context, one Syrian participant reported this:
“we have organizations (laugh) lot of organizations, but to learn like how to write for women who
are not educated, how to swim, how to do make-up and to learn to do a professional haircut and
dress up. Also, like training for women to become a nurse. I think this nurse training help women
to become strong and to earn money. So, she can work in this field and can earn money. Even
she can earn only a little money and can live with that. Yes, only this kind of organization” (Abba,
88-93).
All the participants indicated hospitals as a main medical care provider in their home country.
Some women from Syria got even emotional while talking about hospitals as they have seen
many big hospitals which got destroyed due to war.
The entire participant shared that their country lacks good health care system and they have no
universal health insurance coverage system like in Germany. Therefore, people have to pay from
their own pocket, if they get any medical care. Participants also shared that many of them had
not utilized any SRH services in their own country and therefore, they are not seeking any of
these services in Germany too.
4.7 Barriers in accessing health services
There are different barriers, which are hindering refugee women in getting access SRH services
in Germany. Some of the major ones are communication barrier, unfamiliar health care system,
stress factors, poor living conditions in a refugee camp, social and financial support, etc. These
factors, which are making refugee women difficult in getting access to health services are
described in detail in the following paragraphs.
4.7.1 Communication
For all the participants the native language of the country, i.e. German language as one of the
challenging factors in integrating and in seeking health care and other services. Almost all the
participants could not speak German fluently at the time of the interview and focus group. About

4. Results
65
more than half of the participants are joining language classes at the time. Some participants,
especially married women with children have less German proficiency. Due to low language
proficiency, they do not trust themselves to search doctors outside the camp. If in case they find
a doctor outside the camp, they need a translator. And to find a translator is another big challenge
for them. One of the participants shared her story while visiting the doctor like this: “(….) the nurse
and doctor don't speak good English and it was difficult for us. I visited doctor many times, but it
is hard to tell everything” (Abba, 217-218).
Further on participants reported that they hardly find doctors who speak their native language in
Germany as reported by Abba: “We tried to find doctors, a woman's doctor who speaks Arabic,
but we couldn't find. We find a doctor who speaks English. But still, it is not your mother language.
In other languages, it is hard to explain everything, so you summarize a lot of things. Also, some
medical terms and medical things are not found in our mother language or I don't know that in
English nor in German” (Abba, 222-226).
Due to insufficient language skills, participants faced difficulties in sharing and explaining the
problems to doctors or related person. At the same time, they are afraid that they will understand
the wrong thing and get wrong advice or medicine. One of the participants expressed her feeling
like this:
“To be honest, now I am also afraid to visit a doctor because I cannot speak good German. And
if I tell them something in broken German, they might understand the thing in another way. And
the doctor might give me the wrong medicine. And it might again affect my health. My health
condition might go worse. So, I don't want to take a risk” (Selli, 103-106).
Moreover, due to low language skills, refugee women in the camp have few social contacts. Abba
illustrates this problem like this:
"The first problem is language. People speak a different language and when people speak a
different language, it makes us hard to communicate. And this camp is for the family so most of
the family stay in their single room. And most of the time the man is also in the room. And we
come from a different country, different culture, different city and we have different views and
thinking. Sometimes it is very hard to see the people's behavior here” (Abba, 125-129).
The women not only have problem in communication with others but among own cultural groups
as well since SRH is considered a taboo. Even within a family, women usually share their
problems only with women as reported by Ina: “Menstruation (….) No, such things we don’t tell
4. Results
66
father or brother. They know somehow, but they pretend like they don’t know about our problem
and we pretend like we don’t know that they know (laugh)” (Ina, 112-114).
Due to this communication problem, participants reported that they lack knowledge on SRH as
Nelle said: “In our culture, the married women should somehow know what they have to do with
pregnancy and when they give birth to their child. We get this information from sisters, family
members, relatives, and friends. But before marriage, you do not have to know about these
things. It is also not good. Then after marriage, we have to know everything suddenly. Now, we
are over 20 and we don’t know anything about reproductive and sexual health” (Nele, 190-195).
Participants also shared that they are ashamed to share their problems with others, including
health workers. So, even if they suffer from pain and different diseases, they do not want to seek
health care and their condition gets worse as reported by Usma: “In the place where I came from,
most of the women are ashamed of talking about personal health care. If there are any facilities
available, they will not be using any of them. So, the conditions of women remain always the
same” (Usma, 80-82).
In contrast to Middle Eastern countries, women in Nigeria can freely share their problems with
others including male members of the family. Bella from Nigeria reported that:
“Yes, we share our problem with our family, especially with mother and with father. When I was
having menstruation, the whole house will know that I am having menstruation. Because it is so
painful, I used to cry so loudly. Even my dad felt very sad that he could not help me. We do not
keep quiet. We share our problem” (Bella, 95-98).
In this way, participants mentioned different kinds of problems which occurs due to low language
skill and due to own culture belief system.
4.7.2 Gender aspects
In terms of gender aspects, participants shared that men and women have a different role within
the family and in the community. Women are deprived of many social and public functions that
men do. In many Islamic countries, women are not allowed to do certain things in public place
like joggings, cycling, etc. “Women in our country follow what their parents and husband said.
They follow their words, not these rights" (Usma, 199-200).
Within the family, the unmarried girls have a different role in their family. The unmarried girls live
with their family till they get married. The unmarried women have the responsibility to take care
of her parents and to help her mother in the household. The unmarried woman's decision in term
of choosing a life partner is accepted, but the father has more decision-making power. The
4. Results
67
parents should accept the man first. Only after that, women can get married to that certain person.
In case of decision-making within a couple, generally, men are the one who takes a decision. Ina
shared the problem that women in Iraq are facing: "there are some cases, where women are
forced to marry, and some women are forced to do sex. (…)" (Ina, 253-254)
However, the educated women seem to have more decision make freedom than the uneducated
women. Those educated women can speak up and share their opinion and views. In this context,
Abba shared like this:
“It depends on the person. I think, to have sexual intercourse, both men and women should agree
first. And I think, if people are educated, then they won't do that. Most uneducated people act on
those things. Some people force their wife to do that. Actually, there is law in Syria that if women
are forced to do sex then she can complain about it to a lawyer and go to court. Unfortunately,
lots of women do not know about it. They do not stand against these things” (Abba, 350-354).
In Syria, women can even complain to the court, if she is forced to do sexual intercourse without
her willingness. Unfortunately, most of the uneducated women, especially from older generations
are not aware of this rule and have not so much power in decision making.
“Mostly in the family with the older generation, women have to do what the man said. Women
cannot speak up against their man. If a man wants to have sex, then women can do nothing
except than having sex. But now, in new generations, it is not like that. Women can speak and
say not to have sex if she is not interested” (Celine, 324-327).
The gender of the doctor or any health care provider or an interpreter also plays a significant role
among the refugee women's group. Mostly the women of Iran have shown very much concerned
about the gender of the doctor. They prefer to go to a female doctor when they want to do health
checkups as reported by Mona: “If I find a female doctor, then I go to her. But sometimes, it is
hard to find a female doctor, so I have to go to a male doctor. But I prefer to go to a female doctor”
(Mona, 38-39).
The women from Pakistan reported that women in Pakistan in conservative society are even
more disadvantaged as they are not allowed to undergo medical treatment by others. Zahra
shared in this context that:“(....) they are not able to get proper medical attention. Women are not
even allowed by others to undergo medical treatment or visit a doctor” (Zahra, 27-28).
As refugee women have low language proficiency, most of them need support from professional
Interpreter for performing different tasks. Women expressed the needs of professional Interpreter
of the same gender while visiting the doctor in Germany because most of them feel uncomfortable

4. Results
68
in translating in presence of an unknown male. And this can lead to miscommunication. Selli
expressed her feelings like this:
“In our refugee camp, we can also ask social management to arrange an interpreter while visiting
the doctor. But the problem is, it is hard to find a female Interpreter. If you are suffering from a
female problem, like menstruation, then think how we can describe it to a male interpreter and to
that person whom we meet the first time. I personally cannot do it. I feel very shy to talk about
my body parts in front of unknown male” (Selli, 109-113).
4.7.3 Different health care system
The health care system in Germany is different in many ways from the health care system in
Middle Eastern Islamic countries and Africa. Most of the participants find difficult to understand
the health care system in Germany. In most of the countries, from where participants are
originated, they go to hospitals, when they get injured or have some health problems. They are
not used to undergo a regular health checkup by a general physician. In most of the countries,
people do not have health insurance coverage. In case of Syria, Iran and Iraq only well educated,
wealthy people and people who work for the government have insurance. People without
insurance have to pay cash whenever they visit doctors or hospitals. Regarding this, Diva shared
that: “But we do not have an insurance card. Most of the rich people or who are employed, have
insurance. Most of the people, who work for the government have also insurance. And when
people do not have work or a job, they do not have insurance. Every time you visit a doctor, you
have to pay” (Diva, 71-74).
Participants further mentioned that health care service is very expensive in their home country
due to which lot of people could not afford to get treatment or diagnosed. Regarding this Ina
shared that:
“you know, if you want to do some check-up in a hospital, first you have to make payment. Only
after payment, the doctor will perform diagnosis or the operation or such things. Even if the patient
is going to die, first you must pay and then you will get treatment. There is no humanity. They
treat people like an animal. No respect, no value. The hospitals run after money. It's all about
money” (Ina, 49-53).
The participants from Syria, Iran, Pakistan also mentioned that they have to pay cash from their
own pocket to get health services. Due to this, most of them seek health services only when they
are seriously ill as reported by Nele: “In our culture, if you are in normal condition, then you won't
take care of your health. If something happens, and your health condition goes worse than only
people start to take care about it” (Nele, 188-189).

4. Results
69
In the beginning of their resettlement, some participants did not have their health insurance card.
Due to which, they could not visit doctors outside the camp. Even the refugee women can get
medical service from the doctor available in the camp, the doctor in camp does not have required
equipment’s for the treatment and therefore suggest them to search doctor outside the camp.
This further on leads refugee woman in frustration. In this context, one participant shared this:
“my mum used to visit there. But they said that they cannot treat her there as it is not like clinics.
They do not have equipment there to treat. Therefore, they suggested my mum to search a doctor
outside the camp. Every time when my mom visits her, she said she should visit the doctor
outside. The problem is, my mum does not have an insurance card till now. If we take her to
doctor outside, then she needs insurance card, so we cannot take her to doctor outside the camp”
(Nele, 96-101).
For most of the participants, unfamiliar with the German health care system and lack of insurance
card is a barrier in accessing proper health services at this initial stage of resettlement.
4.7.4 Social and financial support
Most of the participants feel isolated in the refugee accommodation as they do not have good
social contacts. Thus, a lot could not communicate with their neighbors due to language barriers.
Some of them experienced that they could not get immediate help as in their home country. As
Bella shared her experiences in the interview:
“When I was pregnant last time, I was here in Germany. And there was nobody to take care of
me. I have to be strong. I have to take care of my girl. I have to take her to school. I have to cook
food for her. And side-by-side, I have to take care of myself. I used to carry juice always in my
bag. When I feel exhausted, then I had something with me to drink. I was struggling. Once when
I was on the bus, I had a strong pain. Actually, I have to get out from the bus, but I could not. And
no one was there to help me” (Bella, 235-240).
In their home country, most of them live in a big family and if they need any help regarding their
health problems, including SRH, they can ask their family members, relatives, and neighbors. In
their countries of origin, women frequently visit each other. This interaction is vital as a source of
support, as it allows community members to get attached to each other. The family who need
help get support from neighbors and communities. Thus, most of the women are missing the
tradition of sharing and supporting each other in the community. In this context, Abba shared
that:
“In our country, we get help from neighbors and relatives. The neighbors and relatives live very
near to each other. My uncle lives very near us. My cousins live very near us. We have a very

4. Results
70
close bonding with our relatives, cousins, and neighbors. Our relatives, cousins, sibling helps in
such condition. And we have friends. Most girls have a good friendship. So, when we have some
problems, or pain in the body, we talk with friends. And my uncle's daughters, cousins are still
like teachers for me. When we talk about such things, we talk in our circle. Till now, I share my
things with them” (Abba, 64-70).
One of the reasons for poor social connection in the refugee camp is due to the refugee
resettlement process. Many refugees are busy with learning the German language, arranging
things for resettlement. That's why people normally do not have time to think of the next person.
Bella clarified this statement like this: “Everybody is busy here. Some are working. Some have
language class. And most of them, they have their own problem. So, they don’t come to help me.
I have to do everything by myself” (Bella, 243-245).
Some participants, particularly the married women are suffering from being far away from family
and relatives and are worried about childcare if they get ill. “It’s very hard to live alone or far away
from family and relatives. Now I think, what will happen to my children when I am ill?” (Abba, 198-
199).
Along with these, some refugee women also suffer from a financial problem. One of the
participants shared that she had to struggle hard during her pregnancy to know about the medical
service, to know the rules and regulation and as well as earn money because, at the initial stage,
she was not aware that she could get financial support and help from German Government. So,
she had to work hard during her pregnancy. “(…) I don’t have food to eat. If I get food, I gave it
to my daughter. Me I was pregnant, but I could not eat because she has to eat. I have to sleep
with an empty stomach. I called the father of my child and told the things. I asked him if he could
send me some money. But you know what he said. It's not his problem. I said to him, I am
pregnant with your child and I need to eat. He said I don't care if you are pregnant or not” (Bella,
267-271).
Bella further reported that she worked as a dishwasher when she was pregnant so that she can
earn some money and feed herself: "When I got pregnant with my last child, I even worked in
Reeperbahn as a dishwasher” (Bella, 303-304).
4.7.5 Culture and tradition
In most of the Muslim countries like Syria, Iran, and Pakistan women are dominated and hindered
from getting various services. Many women lack good education. There are certain rules and
regulation for women such as in Iran, girls are not allowed to do sports in public place. This all
demotivates women to involvement in public activities. One of the participants of Iran shared that:

4. Results
71
“there are also some disadvantages like I cannot go swimming in public places without covering
my whole body (…). And the police and government control you all the time. You have the feeling
like you are living in a big jail. There are certain rules and regulations, which you have to follow.
But for boys it is good. They can go as they like” (Mona, 9-13).
Even after settling down in Germany, some women from Syria, Pakistan or Iran still follow their
own cultural system. This cultural system is linked with health-related behavior and women are
active in doing physical activities like sports which is good for health.
The married women in Iran, Iraq, Syria, and Pakistan are not as independent as women in
Europe. Most of the married women depend on their husband and family. Before seeking any
health services, they have to communicate with their partner. One participant from Pakistan
shared that some women must get permission from their family member before seeking any
health care services or before performing medical care. In concerned in this context, Zahra
reported that: “Women are not even allowed by others to undergo medical treatment or visit a
doctor” (Zahra, 28).
There are also certain cultural things which influence women's health. For instance, in some
cultural belief in Syria, it is not good to take showers when women have their menstruation cycle.
Related to this, Celine shared that: “But you know in our culture, people say that it is not good to
take a shower during menstruation. It is not good when the warm blood flows out of the body and
get mixed with cold water or something like that” (Celine 51-53).
The African women from Nigeria also reported that there is some cultural belief which had
established the wrong concept in people's mind. For e.g. in Nigeria, women who are fat or
overweight are seen as better than women who are thin and slim. Fat women are seen as women
with proper diet. This leads many women to gain weight to have a better image in the society.
4.7.6 Living conditions in refugee accommodation
All the participants mentioned about the unhygienic living condition in the refugee camps. Most
of the participants have their own room, but they must share bathrooms and toilets with others.
Normally only one toilet and bathroom is available for 25-30 people. Due to this, the toilets and
bathrooms in the camps are not clean and hygienic as reported by Nele:
“Well, we are 5 women in our family and our neighbor has also 5 girls. I think around 25 people.
But sometimes there are some people from outside. I will say around with 30 people, we have to
share toilets and bathroom” (Nele, 19-21).
4. Results
72
Participants further stated that people in the camp do not feel responsible to clean the toilets and
bathroom after using it. There are some women who throw toilet papers and even sanitation pads
on the floor. Regarding this Celine shared that:
“The biggest problem is toilet area. Even though there is sanitation bag available where women
can throw their used menstruation pads, they do not use it well. Instead, they throw it on the floor
or left as it is on the side. Sometimes there are also small blood spots on the floor. It is so
disgusting. There are also some women in our camp who left their fallen hairs in the bathroom
as it is. It’s so disgusting” (Celine 12-17).
Because of unhygienic toilets and bathroom, one participant shared that she always takes
cleaning paper with disinfection whenever she had to use the toilet (Ina, 15-17). Nevertheless,
the participants of this study try to be healthy by following basic hygiene rules by taking shower
regularly. But most of the participants have seen other refugee women in camp who are not
utilizing the things in a hygienic way such as sharing razors. Related to this Celine also shared
another incident:
“in the morning, one woman was shaving her armpit in the sink. And she just left the dirt as it is.
We were brushing the teeth and it is so disgusting. Can you imagine that, how can we brush our
teeth seeing that thing? For us, this is the biggest problem” (Celine, 37-39).
Another important reason for the poor living condition is a lack of proper food. The participants
who are living in the initial refugee camp are not allowed to cook food as they have not their own
kitchen in camps. They get food from the canteen. Most of the participants are not satisfied with
the foods that are offered as they offer the same menu on a regular basis. Besides that, they
usually offer such foods that are prepared for local environment, but not from the people from the
Middle Eastern countries Related to this Abba shared that:
“We always have the same food. I go only for breakfast and for dinner. For lunch, I don't like to
go there because the food is always the same” (Abba, 146-147).
Due to inadequate food intake, one participant from Syria regularly takes vitamin B tablets, which
are available in the market.
Furthermore, in refugee camp it is not allowed to put Refrigerator in their room where they can
put fresh fruits for them. Due to this, participants also lack healthy fruits “We don't eat too much
healthy food here because we don't have a fridge where we can put fresh fruits and meat here.
And we are not allowed to cook” (Abba, 184-185).
4. Results
73
The participants are also not satisfied with the living conditions in the refugee camp. Foremost,
they have to share their room with others. They have to adjust with other unknown people from
other different culture. The environment in the refugee camp is normally noisy and some people
are disrespectful to others. Related to this Ina shared her story like this:
“I have to share the room with others. My neighbor from Palestine, she used to smoke inside the
room. And the smoke comes to my rooms also. I also complain about it, but she did not stop
smoking. Then I shift to another room. And the women are very loud. I need peace sometimes,
but there is no peace. Some women are crying. Some are talking so loudly. The women living in
the camp do not respect or think about others. If they talk in telephone, they use to talk loudly.
They don't think for others. And the problem is we are from a different country and we could not
communicate well” (Ina, 121-127).
Some women have even problems with their neighbors. They could not make a good relationship
with their neighbors. One of the participants had already fought several times with her neighbors.
“Sometimes, the children from neighbor play in the corridor, in front of my room. They hit my door
while playing. I am pretty sure that they are doing it intentionally. I almost beat her once when
she was so crude. She was very crude. I asked the little girl, who told you to hit in my door? The
little girl said that her big sister told her to do that. I asked her why she said to hit at the door of
my room. Then she said that after I use the toilets, the toilet smells so bad. Then I said, you don't
go to the toilet then. I even said to her that it is normal, and toilets do not smell like Gucci perfume.
I said she, do your toilet smell like Gucci perfume? I really do not want to quarrel in such a
nonsense thing” (Bella, 139-145).
Most of the refugee camp does not have a big room where children can play in winter. A married
participant with two children shared that whenever she allows her children to play outside, she
gets complaints from her neighbor which she illustrated in this way:
“We were most of the time in the room and for children it is boring just to sit inside the room. And
sometimes I let my children play outside, and my neighbors, they complain and tell me that they
are making noise. They even called security. We really need a place to sit and to play, which we
don't have” (Abba, 139-142)
Almost all the participants were unsatisfied with their unhygienic living condition. They all
expressed their problem having a bad social connection with their neighbors and having
difficulties to have proper food in the refugee camp.
4. Results
74
4.7.7 Stress factors
Most of the refugee women are mentally and physically tired due to their long journey. Most of
them had experienced terrible things in their life and journey to Germany. On the one hand, they
had to leave their own home country due to war. Most of them are sad to be far away from own
family, relatives, and friends. On the other hand, they must struggle hard for their resettlement.
As Diva shared:
“Some women are still traumatized with their long journey and what they have experienced in
their life” (Diva, 121-122).
Some women are afraid for their future. Mostly the women with children expressed their fear
regarding their children's health. In addition to that, most of the refugees could not decide
themselves where they want to live. The refugee center decides for them where to live, in which
city, etc. Thus, they are fully depending on others due to which some of them are in frustration.
“There are also women who get mentally and physically injured during their journey. They need
rest. They need time to recover and the most difficult thing is that they cannot do their things
themselves. They are depending on others, as they do not understand the German language.
And they must do all that immigration office says” (Diva, 127-130)
Another factor for stress is adjusting in a different society with a different culture. Most of them
already got a cultural shock as there are vast differences Middle East and European Society.
“Most of the women are struggling to adjust in the new society. Most of the women need time to
get into German culture. Some of them have got a cultural shock. Most of the women came from
another culture where they are not used to see women working together with men, shaking
hands. They need time to get into it. I don't think they are taking care of their health” (Usma, 123-
126)
Except resettlement issues, refugee women have many more other issues in their life which
makes them mentally in a stressed as one participant shared her stressful condition like this:
“At that time, I was very new here. I don't know where I could get medical care. I was stressed
with my ex-husband. I am divorced now. He never accepted the child. He never accepted the
pregnancy. I was in terrible condition. Unfortunately, the child died, which was a boy. So, it was
a really bad time. Whenever I think about it, I feel really bad” (Bella, 249-253).
Other participants also expressed their stress and worries regarding the new beginning of their
life in a new country. They are worried about the present condition of their country as well as their
future regarding safe shelter, job opportunity, etc.

4. Results
75
Some refugee women also shared that they are discriminated by other cultural groups. The
woman from Africa expressed that her neighbors in a refugee camp discriminated her in a several
ways because of color of her skin. On this subject, she shared her story like this:
“The problem is everywhere in refugee accommodation. There are people from Iraq, Iran,
Afghanistan. And they do not like us. Even though we have the same status as a refugee, they
hate us. They are really racist. You are in another country. They are providing us with shelter and
taking care of us. We are in the same group. They also came as I do, but we black people are
treated in a different way. They treat them like superior” (Bella, 152-156).
This kind of discrimination along with their own personal problems, health problems, traumatic
experiences in their home country, during the journey and resettlement process in Germany are
some stress factors for refugee women which make them difficult to get access to health services.
4.8. Advice and suggestions for women health workshop
The participants of this study were also asked for suggestions for conducting a women's health
workshop by REFUGIUM program, which focuses on SRH. Participants gave several advices
and commentaries for conducting SRH workshop.
4.8.1 General suggestions for a workshop
Participants provided some suggestions on conducting women's health workshops for
REFUGIUM program. They mentioned that women's health workshop should be first conducted
with the women participants of REFUGIUM program because they know each other well and how
REFUGIUM workshop functions. Regarding this, Nele reported that:
“If we do this women health workshop, then we should first begin with the women who are in the
program. Then we can know more or get the idea of how we can conduct the workshop in a better
way” (Nele, 418-419).
Another participant Celine suggested conducting a workshop in a small group so that women
won't feel uncomfortable or hesitate to share their personal things in a workshop with a few
people. As the topic SRH is taken as a very sensitive topic by refugee women, most of the refugee
women might feel discomfort to talk about their individual experiences. So, the workshop should
start with topics like female hygiene, but not with sensitive topic like sexual violence.
One of the participants suggested that the workshop should be conducted only by a women
health facilitator. And only female REFUGIUM team members should be allowed to enter in the
workshop room, as most of the women won't feel comfortable to talk in the presence of an
unknown man. Related to this, Abba said:

4. Results
76
“Most of the women feel shy to share their problems. They hide their problem as they feel it is a
very private thing. We are very shy to share our intimate things and problems. We feel so
uncomfortable, so if you want to conduct a workshop for women, it should be only for women”
(Abba, 422-425).
Some of the participants of this study think it will be very helpful for refugee women if REFUGIUM
program could develop flyers in different languages and distribute to the women who are living in
the refugee camp. Some participants predicted that women might not take part in the program
due to various reasons, but they can at least learn something from the flyer. Zahra shared like
this in this context: “At least if you can distribute the flyer about women's health, they get a lot of
things to know. The flyer should contain all important topics like help during pregnancy, maternal
health, STI, help for women who experience violence etc.” (Zahra, 157-159).
Mostly the participants who already took part in other workshops conducted by REFUGIUM
program suggested that the women's health workshops should have more content, unlike other
REFUGIUM workshops which contained basic relevant information for refugee women. Ina
expressed her views in this way: “The workshop should contain more information because most
of the workshops like nutrition, physical activity, they contain only a few things, I mean
information. You can provide a little bit more information. They are very basic. Me, I really want
to know more. So, I expected a little bit more from REFUGIUM workshops” (Ina, 306-309).
These are some specific suggestions of study participants for REFUGIUM program to conduct a
women's health workshop.
4.8.2 Suggested SRH topics
Participants were asked what topics they find relevant to women's health workshop. Participants
suggested different topics such as female hygiene, pregnancy, menstruation, rights and law and
help for women who experienced violence. Among these topics, almost all participants were not
aware of the rights and laws regarding sexuality, about the help and support for women who
experience violence. Therefore, they suggested including these topics in the workshop.
The other highly recommended topics are to mention some organizations which help women in
Germany, as well as the medical care and services during pregnancy, including childcare and
maternal care, such as organizations like “Adebar program”, midwives help, pregnancy care, etc.
“The information about midwives help, Adebar program, medical service free of charge, such
information help women like me during pregnancy” (Bella, 414-415).
Further on, Bella suggested including the topic of breastfeeding and child parenting in the
workshop. She also mentioned the points how women can take care of themselves during
pregnancy like being free from any kind of stress “It is also important to tell women that during
pregnancy women should not take a lot of stress. If women suffer from stress, it directly affects
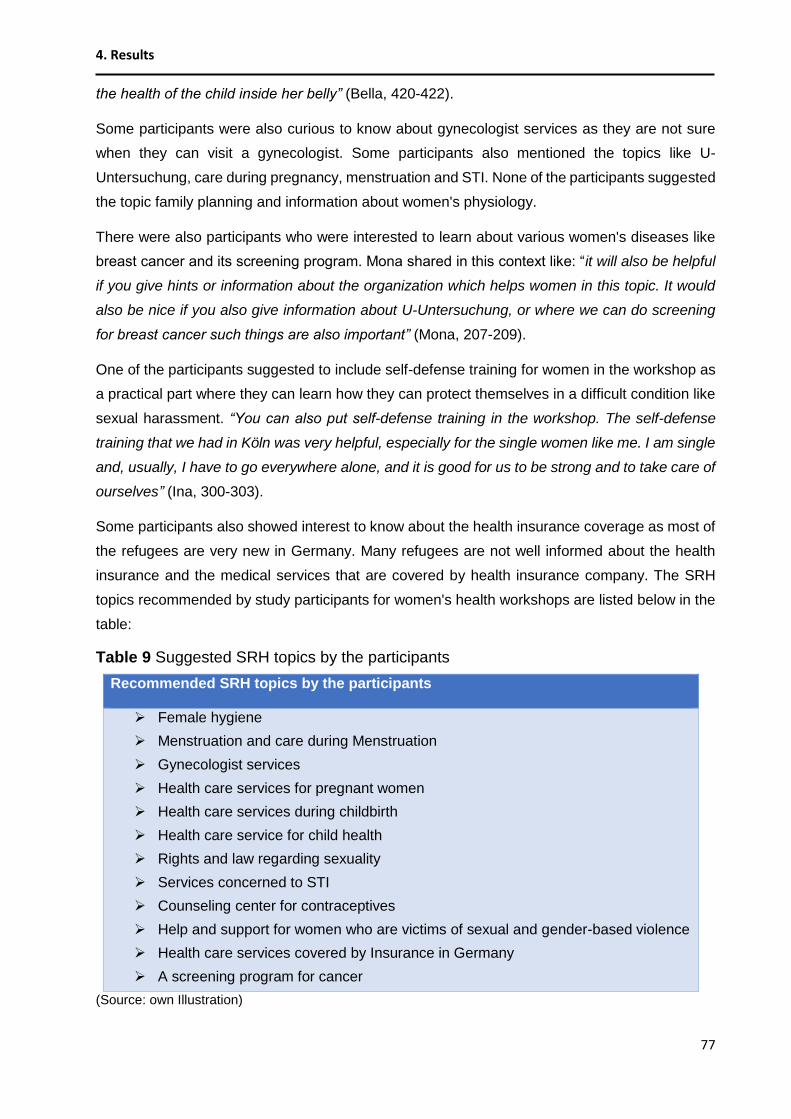
4. Results
77
the health of the child inside her belly” (Bella, 420-422).
Some participants were also curious to know about gynecologist services as they are not sure
when they can visit a gynecologist. Some participants also mentioned the topics like U-
Untersuchung, care during pregnancy, menstruation and STI. None of the participants suggested
the topic family planning and information about women's physiology.
There were also participants who were interested to learn about various women's diseases like
breast cancer and its screening program. Mona shared in this context like: “it will also be helpful
if you give hints or information about the organization which helps women in this topic. It would
also be nice if you also give information about U-Untersuchung, or where we can do screening
for breast cancer such things are also important” (Mona, 207-209).
One of the participants suggested to include self-defense training for women in the workshop as
a practical part where they can learn how they can protect themselves in a difficult condition like
sexual harassment. “You can also put self-defense training in the workshop. The self-defense
training that we had in Köln was very helpful, especially for the single women like me. I am single
and, usually, I have to go everywhere alone, and it is good for us to be strong and to take care of
ourselves” (Ina, 300-303).
Some participants also showed interest to know about the health insurance coverage as most of
the refugees are very new in Germany. Many refugees are not well informed about the health
insurance and the medical services that are covered by health insurance company. The SRH
topics recommended by study participants for women's health workshops are listed below in the
table:
Table 9 Suggested SRH topics by the participants
Recommended SRH topics by the participants
Female hygiene
Menstruation and care during Menstruation
Gynecologist services
Health care services for pregnant women
Health care services during childbirth
Health care service for child health
Rights and law regarding sexuality
Services concerned to STI
Counseling center for contraceptives
Help and support for women who are victims of sexual and gender-based violence
Health care services covered by Insurance in Germany
A screening program for cancer
(Source: own Illustration)

5 Discussion
78
5 Discussion
5.1 Summary of the findings
Refugee women in Germany belong to a diverse group as they come from countries with different
cultural backgrounds. The refugees participated in this study originated from Syria, Iran, Iraq,
Pakistan and Nigeria. These women have varied perceptions towards the state of “being healthy”.
Women from Syria, Pakistan, Iraq and Nigeria related good health with being free from diseases,
whereas women from Iran associated good health also reflects in their beauty and outlook. Most
of the refugee women do not give huge priority to their health. Due to horrible experiences from
conflicts and dysfunction in their home country and their long, difficult journey and resettlement
process in the new country, refugee women are not in a condition to “think” about their health.
For some of them, to be alive and to see their family well is highly prioritized than their own health.
Specially, the married women with children are more conscious about their family and children
but unfortunately, not their own health. However, some educated refugee women showed more
consciousness and practiced healthy behavior such as sports, healthy diet etc.
Refugee women in overall were not found to be conscious about their sexual and reproductive
health (SRH). The topic SRH is taken as a very sensitive topic in most of the Islamic countries.
Thus, most of the refugee women feel uncomfortable to talk about SRH except the women from
Nigeria. Most of the women related SRH with pregnancy, care during childbirth, maternal health,
menstruation, female hygiene, childcare, breastfeeding as well as diseases like breast cancer,
ovarian cancer etc. The married women were found to have a wide view on SRH in comparison
to single women as they already experienced pregnancy and know the importance of care during
the pregnancy.
Comparing the women from five different countries, refugee women from Syria, Pakistan, Iraq
have comparatively less knowledge on SRH than women from Iran and Nigeria. One of the
reasons is lack of any forms of SRH education in their home country. Many women in remote
areas are deprived of education. Even in the areas with access to schools SRH is not included
in curriculum as teachers hesitated to talk about those topics. Thus, women generally get
information from their sister, mothers and friends. Mostly in Muslim countries, women do not
share their SRH problems with a male member of their family. In contrast to that, women in
Nigeria could openly share their problems with male member of their family. These days, refugee
women are also found to using internet to get information regarding SRH especially after their
resettlement in Germany. Thus, there is both need and demand of SRH education among refugee
women.
5 Discussion
79
Although participants have very little idea about SRH, they shared their different problems during
this study. Most of the unmarried participants have pain during menstruation. Despite having
severe pain, they hesitate to visit a doctor. Instead they rely on bed rest, drinking hot tea etc.
which sometimes helped to alleviate the situation, but in many cases it didn’t. Some women also
shared about pre-menstrual syndromes like irritation, mood swings, etc. Most of the women are,
however aware of female hygiene especially during menstruation.
Another SRH issue among the refugee group is early and forced marriage where most of the girls
from poor social background are affected (at the age of 15/16). Especially in Syrian girls, early
and forced marriages have been associated with the conflicts. In many cases family were known
to get their daughters married in the hope of protection from their husband. In some remote area
of Syria and Pakistan, there is still the tradition of arranged marriage where the family member
chose a life partner for a girl. In Iraq, there are still some people who follow the polygamy i.e. a
man gets married to many women. Thus, some women are deprived of their rights to choose
their own life partner. They are neither aware about the rights regarding sexuality.
Because of early marriage, women get pregnant at an early age. These pregnant women might
face complication during their pregnancy and childbirth. These women also lack sufficient
knowledge of childbearing, breastfeeding and thus could not properly take care of their children
and their own health. There are many women in Nigeria, who suffer from urinary tract infection
due to childbirth at an early age. Furthermore, women suffer many difficulties during pregnancy
like having severe physical pain, mental stress etc. These further on, have bad impacts on the
health of newborn and the mother. Refugee women at the initial stage are unfamiliar with the
health care system in Germany and thus lack proper medical care and support. Due to this, a
woman from Nigeria also lost her child. In comparison to single women, married women with
children have better knowledge on the care during pregnancy from their own pregnancy
experience.
Abortion is another SRH issue, which is not legal in most of the Islamic countries except when a
woman’s health is in danger due to pregnancy. But there are also cases, where women got
pregnant before marriage. In such cases, abortion is mostly performed in secrecy. However, a
woman cannot take the decision alone, for an abortion, both husband and wife should decide
together. Nowadays women in Muslim countries are also following the family planning concept.
Mostly educated and employed group is aware of family planning and contraceptive methods.
However, women’s decision about family planning and contraceptive use is based on her
partner’s decision. Therefore, men’s knowledge on SRH also influences the women SRH
behavior. There are also some married women who do not use contraceptives because of its
negative side effects such as weight gain, skin damage etc.

5 Discussion
80
Regarding Sexually transmitted infections, refugee women have very inadequate knowledge.
Most of them are only familiar to HIV and Aids. Only few of them know about other STIs such as
Gonorrhea, Syphilis etc. Other important issue regarding SRH is sexual and gender-based
violence. Refugee women also expressed concerns that there are high risks of sexual violence
inside the camp as well as outside the camp, even with the security. Few refugee women in this
study had also experienced some kinds of sexual abuse outside the camp. However, it was
mentioned they feel comparatively safer here in Germany. Refugee women also admit the
existence of domestic violence in their culture due to unbalance power relation between men and
women. They also mentioned women who are victim of violence are blamed for herself and there
is no help and support for such victims in their home countries.
Refugee women who are living in Germany for a short time (1-2 years) do not get enough
information about different health care services including the SRH services. Most of them knew
about the availability of general physician in their camp and gynecologist service. Only few
married refugees were aware about some medical care and service for pregnant women. Most
of them were not aware about the pregnancy counseling center, counseling for STI, counseling
for family planning and contraceptive, help and support for victim who experience sexual and
gender-based violence. Similarly, women are also not aware of other health promotion programs
like REFUGIUM. Only a few of them know about Caritas Hamburg, Adebar Hamburg and
Aidshilfe Hamburg. None of them knew about BZgA and its website Zanzu which provide SRH
information in different languages. That signifies that refugee women need to be informed about
the available health care services in Germany. In addition to that, refugee women have only a
few SRH services in their home country and hence behavioral aspect may have led to low
utilization of such services here in Germany.
There are different barriers, which hinder refugee women in getting access to health care services
in Germany. For most of the women communication is a huge barrier. As most of them could not
speak German fluently, they are afraid to seek health care services. Moreover, SRH is taken as
taboo topic, and they find it very hard to communicate about it with others. The gender of the
health care workers also plays a significant role among the refugee women’s group. Most of the
refugee women preferred to get medical checkups from the same gender. As most of them have
low language skill, they needed help from an Interpreter for translation. Even the Interpreter was
expected to belong to the same gender, as women feel ashamed to tell their problem with other
unknown men. Beside this, for many refugees the health care system in Germany is very new.
They first have to know how the health care system works. Most of them still do not know about
the health insurance coverage and some of them even have not got health insurance card which
inhibits them to undergo medical checkups.

5 Discussion
81
The next challenging factor for refugee women is the poor living condition in refugee camps.
Many refugee camps have turned out to be unhygienic. Mainly the toilets and bathrooms are not
clean as around 25 to 30 people normally use single toilet and bathroom thought the day. The
overall environment and surrounding of refugee accommodations are unpleasant, noisy and
crowded. Most of the initial camps for refugee do not offer kitchen, so the foods are offered in the
canteen. Most of the refugees are not satisfied with the food that is offered in the canteen. That’s
why many were found to skip the lunch or dinner, and they admit that they are not getting a proper
diet. Even the refugee women, who have a kitchen in the refugee camp must share their kitchen
with others. But the women find very hard to share the kitchen with others as she could not build
good relationship with her neighbour in camp. Due to this, most of the refugee women feel
isolated in the new place, and they lack help and support from their relatives, friends and
neighbors which they used to get in their home country. Some women are also mentally stressed
with their private issues so that they could not focus on their health. Some women even
mentioned that they are discriminated in many ways, especially inside the camp. Thus, all these
factors are stressing them so much that they are not actively utilizing the available health care
services or seeking health care services regarding SRH in the new place.
Apart from this, only few services are offered in refugee camps to promote refugee’s health. There
are availability of general physician, counseling for mothers, special doctors for children, activities
such as Yoga class, German language course, support for finding a professional interpreter, etc.
But there has been very little done in the field of SRH in refugee camps. Hence, there is need of
services related to SRH in refugee accommodations.
Refugee women also showed their interest to gain some information regarding SRH. As most of
them lack information about different SRH services, they are curious to know about the services
during pregnancy, childbirth etc. Some women were interested to know about care during
menstruation, female hygiene, women’s rights, rights and law regarding sexuality, STI, help and
support for women, especially regarding gender-based violence, diseases like cancer etc. Some
of them desired to know more about insurance coverage in Germany. Only a few women showed
their interest in family planning and contraceptives. Hence, it seems very crucial to discuss on
different issues of SRH among refugee women.

5 Discussion
82
5.2 Discussion of results
The main aim of this paper is to find out the needs of refugee women regarding SRH. The result
of this study presents that refugee women living in the camp are not very conscious about SRH.
It is clear from the findings that they lack SRH education and not an adequate background from
their home country. Due to this, they are not giving priority to SRH even if they are experiencing
many chronic and new issues. They are not seeking help and support to as well as a lot of women
are also not aware of the health services that are available in the new country. Furthermore, they
go through many barriers which are hindering their access to SRH care. However, the results of
this study do not include the topic like parenting, family formation, breastfeeding, menopause etc.
Some of these findings obtained from the study resembles with many other previous researches.
The study conducted by Common health welfare in Australia also presents similar results like the
low utilization of health care services by refugee groups. They also present the challenges that
refugees faced such as communication problem, cultural differences etc. (Commonwealth of
Australia, 2010). Refugee women being a vulnerable group are a victim of sexual and gender-
based violence is also presented in this study, which resembles with other scientific researches
conducted with refugee women such as from Ivanova et al. (Ivanova, Rai & Kemigisha, 2018).
As the topic SRH is taken as very sensitive and a taboo especially in the Middle Eastern Islamic
countries, it was very challenging to communicate about it with the women who arrived mostly
from those countries. Therefore, the participants of this study also showed hesitation and
discomfort in talking about SRH topics. Apart from this, if the researcher also belonged to the
same cultural group, the participants might have expressed their views and opinion more openly.
Thus, the researcher being from a different culture background might have also played some role
for not being able to completely open them up during the interviews.
The result of this study could be more representative if the study could include a large sample
size. Altogether we were able to gather 11 participants, which is a small size. The sample of this
study consists of refugee women from different countries namely Syria, Iran, Iraq, Pakistan and
Nigeria. But there are also many refugee women in Germany from other countries like
Afghanistan, Eritrea, Turkey and Somalia etc. But this study does not include the participants
from these countries. Thus, the result gained from this study could not be valid for another refugee
group living in Germany. Further on, more than half of the participants in this study are well
educated. There might be further emerging themes related to SRH when the study had included
other participants with low education level. It is also important to consider that it might be more
challenging to get contact with the refugee women who are not well educated due to the language
barrier and their low participation in integration activities. All the participants of this study are
living currently in Hamburg. So, there might be another need and demand of refugee women

5 Discussion
83
living in other places as health care services, living condition of refugee women may vary in
different city. Moreover, most of the women are from the age group 20 to 45. So, there might be
other needs if the study will be conducted with wider age group as well (older generation).
Among eleven participants, there were only four refugee women who are married and have
children. If there were more women with children, there might be another SRH issue and the
results might explore more issues in the topic like family planning, contraceptive, domestic
violence etc. More than half of the participants in this study are unmarried and haven’t
experienced any sexual relationship. Therefore, they haven’t dealt with family planning,
contraceptives, pregnancy. This might be one of the reasons that, most of them don’t have
knowledge about the availability of counselling center regarding contraceptives, family planning,
services during the pregnancy. Hence, the results of this paper need to be studied in a larger
sample for validity including different women from different age group, different countries,
religious group, sharing different culture etc.
The participants were also asked about the health consciousness and health related behavior of
other refugee women living in the camp. But, most of them could not provide information about
the other refugee women as they have no good contacts or hesitation to talk about others.
However, they were able to provide some information generalizing the women from their home
country. Regarding consciousness about SRH, most of the participants were silent at the
beginning and they needed time to think what is meant by sexual and reproductive health.
Therefore, in some interviews the researcher made easier by explaining about SRH. Some of the
participants were also not familiar with the term family planning, contraceptive, STI, sexual rights.
These terms need to be explained or translated in their native language through Google translator
before the participants could share their views on it. Before answering, some participants took
time to come out with shyness and share their views and problems like problem during
menstruation, experience of sexual violence etc. Regardless, participants were very enthusiastic
while sharing their problems, which they are facing in the refugee camp such as unhygienic
condition of toilets and bathrooms, unsuitable foods, feeling of unsecure environment in the
camp, difficulties to know German health care system etc.
As most of the participants were not native German or English speaker, Google translator was
used for translating the interview questions. It could be better, if there was a professional
interpreter. But due to limited financial resources, it was not possible to get a translator. Also, the
team member of REFUGIUM program who is native Farsi or Arabic speaker could not manage
time at the time of interview. With Google translator there is a high chance that the sentences or
some words might have not translated accurately. Therefore, there might be some
misunderstanding in understanding the question. Some answers from the participants showed

5 Discussion
84
that the questions were translated making another sense that the participants gave the answer
in another subject area. Thus, the result interpreted from such statements might make bias in the
findings. Another point to be noted is the present paper is written in English although some
interviews were conducted in half German, half English. It is sometimes difficult to translate the
content of the interview without losing the actual meaning.
Being a researcher, it was sometimes difficult to be in a neutral position as there were some
moments when participants shared their problems regarding their unpleasant living condition.
Some of them are still traumatized from what they experienced in their country or during migration
and the participants were very sensitive while sharing their stories and experiences. Despite such
limitations, this paper contributes to know gap in the knowledge regarding SRH among refugee
women and to explore the SRH issues this under-researched vulnerable group.
5.3 Discussion of method
For this research, the chosen qualitative approach was appropriate to explore the needs of
refugee women regarding SRH which helps to provide the real-life phenomenon of the target
group (Flick, 2016, p.28). The interview with refugee women helps in gaining a detailed
understanding of their living conditions, their health consciousness about SRH and available
services.
Within a qualitative method, 2 focus groups and 7 face-to-face interviews were conducted in a
different time. The first challenging factor is the development of an interview guideline. As the
topic sexual and reproductive health is entrusted with the private matter of an individual and not
openly communicated in the Arabic-Asian culture, the questions should be formulated in a way
that participant can share their views, experiences without any hesitation. To reduce the
hesitation and discomfort among the participants, the interviews and the focus groups were
started in form of small talk. Secondly, as most of the refugees could not speak fluent German or
English, the interview questions were formulated in simple ways so that the participants could
understand easily. However, the interview questions consist of some terms, which are not familiar
to participants. The terms like SRH, family planning, STI, contraceptive had to be explained or
translated first in participants native language before they could share their views on it.
The REFUGIUM program follows the participatory action research in which the target group is
involved in the research process. The same was the concept of this study. To get access to
refugee women, all the female participants of REFUGIUM program were contacted either
personally or through a phone call or sending messages. They were informed about the research
and requested to take part in the study, but only a few showed their interest. Most of the female
refugees feel uncomfortable to talk about this topic. This might be the reason that the participants

5 Discussion
85
came up with excuses for some appointments. Another reason could be due to language barrier
and trust issue. The researcher also contacted another organization “Patenschaftsproject of
BergedorferfürVölkerverständigung” to get more participants for research. Moreover, the
researcher also joined in the workshops, which were conducted in cooperation with Mut Café
Afrika and Aids Hilfe Hamburg to get access to target groups. But the recruitment process turned
out to be one of the difficult part of this study.
As it was hard to get participants for this research, it could not work as planned. At first, it was
planned to conduct only focus group i.e. one focus group with an Arabic speaking participant and
one focus group with Farsi speaking participant. But it was hard to fix the date and time suitable
for all participants. In the first focus group, four participants had planned to join in the study but
only two of them showed up. For the second focus group, three participants intended to come
but at the end only two of them were present. Therefore, face-to-face interviews were conducted
later so that the researcher could meet one participant at one certain time and it was easier easy
to fix the appointments. Hence, face-to face interview turned out to be reliable, appropriate and
efficient in this study. But the whole data collection phase was highly time consuming which
resembles to one of the features of a qualitative study (Creswell 2013, 96).
Another problematic issue in this research was conducting focus group alone. For conducting
focus group, a researcher had to manage suitable room and devices to record the interviews.
The group room available at HAW Library in Berliner tor 5 or in Alexander Street 1 Hamburg were
booked for around 1 and half hour for the focus group. But most of the participants did not come
punctually so some interviews could not start as planned and the booked room for interviews
could not be used for full hours. Therefore, in some interviews there were breaks in between. At
the same time, there was difficulty in finding a replacement room or a suitable other place in a
short time. In case of 2 interviews conducted at the participant home, there was presence of
children who required more attention. Thus, the interview had to be stopped for 2-3 times in
between. Therefore, there was no consistent flow of communication during the interview which
might also have an indirect impact on transferring information.
Another tough part of this study is the topic itself. As the topic related to SRH is not communicated
well in the countries like Syria, Iran, Iraq, Pakistan, participants could not freely share their views,
opinions on this topic. Even as all the questions for the focus group and interviews were open-
ended, which was meant to motivate the individuals to share their ideas and views freely, the
participants felt uncomfortable in sharing their views. From the researcher’s point of view, it was
easier to communicate with participants who had already taken part in REFUGIUM program as
they were acquainted before. While comparing, the participants in the focus group were more

5 Discussion
86
passive and silent than in face-to-face interviews. In addition, the later one was more open and
provided a lot of information.
In terms of analyzing collected information, the systematic approach of the qualitative content
analysis by Mayring (2014) was appropriate. The inductive approach of working through the
transcripts, developing appropriate categories and assigning relevant paraphrasers to the
categories was suitable to explore the research question. However, the data analysis took a long
time as the collected notes and recording from interviews and focus groups had to be transcribed
and saved in the computer.
Hence, there were some limitations in the data collection and analysis procedure of this study.
However, the interview and focus group with refugee women helped in gaining a depth
understanding on the different perceptions of refugee women towards SRH, their awareness
level, SRH issues, awareness about available health services and their difficulties in accessing
those services.

6 Recommendations
87
6 Recommendations
The less knowledge about SRH and less awareness about health care services among refugee
women signifies that there is a need for SRH education. REFUGIUM program as a health
promotion program can provide SRH education in form of heath workshops which it is offering in
different subjects such as mental health, nutrition, etc. As Murphy (2004) stated that access to
information and education is a powerful determinant of health” (Murphy, 2004, p. 187).
REFUGIUM program can implement this idea to promote the sexual and reproductive health of
refugee women. The important and relevant information for refugee women regarding SRH is
provided in this chapter as a recommendation. At first the general recommendation for conducting
women's health workshops focusing on SRH is given. The second part of this chapter provides
the relevant SRH topics such as different services during pregnancy, service regarding STI etc.
6.1 General recommendations for REFUGIUM workshop
The women's health workshop, which focuses mainly on SRH is intended to develop, especially
for refugee women living in Germany. The large proportion of refugee women is originated from
Arabic culture with Muslim religion (BAMF, 2018) who feel very shy to share their problems and
issues regarding SRH in front of strangers, especially with unknown men. Thus, the workshop
should be conducted by a female health facilitator. To build a trustful atmosphere during the
workshop, no male member should be present in the workshop.
The workshop participants can consist of single as well as married women. Therefore, the
workshop should also offer childcare facility so that it motivates the women with children to take
part in the workshop. The workshop participants could be from different countries, different
religion, different ethnicity, culture, etc. Therefore, in the workshop the health facilitator should
respect all the participants equally and there should not be discrimination in the name of religion,
skin color, education level etc. All the participants should be given equal chance to share their
experiences, problems and views. Along with this, the workshop should be conducted in a non-
hierarchical manner where the health facilitator as a moderator should not treat herself as
qualified person than the participants. This also helps in building trust from participants and due
to this, participants might feel comfortable to contribute their knowledge and experiences. Beside
this, the health facilitator of the workshop should be interculturally competent.
As the workshop is dealing with a very sensitive topic SRH, that’s why the workshop activities
should be dealt very carefully. The results of this study have illustrated that the women normally
do not communicate openly about the problems and issues regarding SRH. Thus, the workshop
should not start with sensitive topics like sexual violence right at the beginning. It should rather
begin with the topic like female hygiene, care during pregnancy, contraceptive, maternal care

6 Recommendations
88
where women won’t feel much discomfort. If there is a large number of participants in the
workshop, women might not dare to share their views and opinion. So, it would be better if the
workshop takes place in a small group (for e.g. maximum 8 people). In a small group it is also
easy to create a peaceful environment and the health facilitator can also build trust among the
participants. Building a trust between the facilitator and participants helps to increase the
communications level among them.
The materials like flyers and manuals are the key elements of the REFUGIUM workshop. While
developing flyer and manual, the aspects of culture sensibility should be considered. For e.g. the
flyer should contain a woman with dark color hair instead of faired hair women. The symbols,
pictures which will be published on the flyer and manual should represent the refugee women.
While developing a flyer and manual, the use of scientific terms should also be neglected. The
flyer and the manual should be developed in simple language and if there is any scientific terms
or difficult terms, then it should be explained well. The explanation can be either done orally by a
health facilitator or by giving explanation in the flyer or manual.
While conducting workshop, participants should be integrated into the discussion. The workshop
should provide a platform for refugee women where they can share their problems and issues
and discuss about it. Thus, the workshop should provide sufficient time for discussion so that
participants can clarify questions if they have questions that have not been answered. At the end
of the workshop the participants should also get time to give feedback about the workshop as
well as health facilitator. From the feedback obtained from participants, the workshop could be
improved further.
As public health interventions can be highly effective when it is implemented in the setting where
the target group lives, thus it is highly recommendable to conduct refugee workshop in different
refugee camps. Therefore, REFUGIUM program should cooperate with different refugee
accommodations to get access to the target group.
6.2 Specific sexual and reproductive health topics for women's health
workshop
Based on refugee woman needs, desires, and their interest and curiosity to gain the information
regarding SRH topics, following topics are selected and recommended to include them as a
workshop content in a women's health workshop on REFUGIUM program.
Women's rights in Germany
Most of the refugee women belong to the culture, where women have not equal rights as men.
There is a power imbalance between the women and men thus refugee women should be
informed about the women's rights to empower women. They should be informed that they have
6 Recommendations
89
the right to access affordable and culturally appropriate SRH care. They should know that they
receive the same services regardless of their level of need in Germany i.e. equity where people's
access to services is based on the need for those services. Regarding this, the workshop should
provide following messages:
Every woman has the same rights as a man
Every woman has the right to be treated in a way that respects her dignity
Every woman has the right to make her own life decisions, to speak freely, to act on her
own behalf and in her own interest
Every woman has the right to choose her partner freely and to have sexual self-
determination
The refugee women have equal rights as other women living in Germany also regarding
SRH
(World Future Council, 2016, p. 24)
Gynecologist services in Germany
Even most of the refugee women know about the gynecologist service in their own country and
in Germany, but they are not sure when to visit a gynecologist. It will be very helpful for women
to know when they can visit a gynecologist and what kind of services they can get from the
gynecologist. Through workshop the refugee women should be informed that if women have
following symptoms, they can get service from a gynecologist:
If women have pain in the abdomen
If women have problems with urination or defecation
If women have bleeding without menstruation
If the menstrual period lasts more than ten days
If the periods often occur in too short intervals (less than 25 days)
If the menstrual period is very severe/painful
If the menstrual period is absent for more than 30 days
If the menstrual period is absent for more than 30 days
If puberty has not started by the age of 15 (there was no menstrual period till the age of
15)
If women experience itching and unusually strong or smelling discharge from the vagina
If women feel pain during or after sexual intercourse
If women have bleeding after intercourse
If women suffer from a headache and blurred vision or other side effects when taking
contraceptive method
(BZgA, 2017, p. 18)

6 Recommendations
90
Women should also know that the gynecologist is the responsible person to look for cancer
screening, reproductive health, urinary tract infections, STI, etc. (BZgA, 2017, p. 19).
Service and care during menstruation
According to the statements from study participants, refugee women feel shy to talk about the
menstruation. Due to this, they do not share their problems like pain during menstruation to others
and try to hide the problem. They do not seek help to get rid of the problems like by visiting a
doctor or gynecologist. Thus, refugee women need to be informed about the following points:
Menstruation is a natural process and every woman has it. Therefore, there is no need
to hide and feel shy
Women can get help from the gynecologist when they have strong pain during
menstruation
During menstruation, women should put their body clean, eat a healthy diet, do light
exercise, avoid alcohol or caffeine, get enough sleep
Women should change tampons or sanitary pads regularly
Women should avoid wearing tight pants as it may cause a bacterial infection
Women must not shave pubic hair for the good health
Women can have sexual intercourse, but unprotected sexual intercourse has high risk
for HIV
If the menstrual period stops, but the pregnancy test is repeatedly negative, women
should go for an examination in a medical practice or gynecologist
(BZgA / Sensoa, 2019)
If women have pain during menstruation, they can reduce the pain by the methods mentioned in
the table below:
Table 10 Tips to reduce pain during menstruation
Tips to reduce pain during menstruation
- Women can take a hot bath or hot shower
- Women can place a heat pad or a hot water bottle on her stomach or on her back
- They can drink a relaxing tea (chamomile tea) which helps in reducing pain
- Women can also do a light workout or some relaxation exercises
- In acute pain, women can ask in a pharmacy for an appropriate medicine or visit the
gynecologist.
(Source: BZgA & Sensoa, 2019)

6 Recommendations
91
Service and care during pregnancy in Germany
Being pregnant is one of the turning points in the life for every woman. But, most of the refugee
women are not aware about the services offered for pregnant women in Germany. Therefore, it
is important to inform them about the available services during pregnancy and childbirth.
Following information might help refugee women to know about the different services provided
during pregnancy and childbirth:
Every pregnant woman in Germany has a legal right to adequate medical examination
and counselling
Women can do a pregnancy test by themselves in their home with a pregnancy test
device which are available at drugstore
To get accurate results, women can do a pregnancy test by the gynecologist or in
clinic, or by midwives
Pregnant women should regularly visit the gynecologist (at the beginning, every four
weeks and from the 32nd week of pregnancy, every two weeks)
Pregnant women should follow the gynecologist’s tips like eating healthy food,
avoiding food that harms pregnancy like raw meat, raw fish, raw egg, etc.
Pregnant women can do prenatal diagnosis to determine whether the child has certain
diseases or malformations which can be treated during pregnancy.
Pregnant women can do ultrasound examinations at 10, 20 and 30 pregnancy weeks
After the child birth, women can get midwives service for the newborn
Pregnant women have the right to search pregnancy counseling center, which helps
woman for all non-medical questions such as social and legal matters both before and
during pregnancy
Pregnant women should take medicines only after consultation with their doctor even
though they are taking regular medicine, or they are taking any herbal remedies due
to any chronic illness. Medicines can affect the birth process or development process
of the child and milk production in the mother
The costs of prenatal care will be paid by health insurance companies
In Germany refugee women can also get financial support if they have insufficient
funds to meet the expenses of pregnancy and birth and for growing up the child. In
case of working women, they get maternity leave which begins six weeks before the
birth and ends eight weeks thereafter
(BzgA, 2019; BZgA, 2014; BZgA, 2017c; Caritas Deutschland, 2019)
Pregnancy is a long journey in which maternal, perinatal and newborn health should be given a
huge priority. Parents’ overall health and their lifestyle before and during pregnancy can affect

6 Recommendations
92
fertility, infant’s health as well as maternal health (WHO, 2019). Thus, the workshop can provide
basic healthy living tips for pregnant women, which are mentioned in following table.
Table 11 Healthy living during pregnancy
Healthy living during pregnancy
Avoid smoking and alcohol
Stay physically active
Have balance diet (take diet supplemented with iodine and folic acid)
Take small meals frequently, if women feel hungry often
Avoid harmful food during pregnancy, such as raw meat, fish, egg etc.
Avoid heavy physical work
Avoid stress
(Source: BzgA, 2017b)
Pregnancy at early age in Germany
Refugee women have often high risk to get married at an early age. Hence, they should be
informed if a woman aged under 20 is pregnant then she has a higher risk of having a difficult
delivery. The baby might risk premature birth, or low birth weight, which has further on risk for
illness (BZgA, 2017). Moreover, if a girl or woman gets unintentionally pregnant or if she is against
pregnancy, then she can get help from a pregnancy conflict counseling center. They help women
in such condition showing different possibilities. They inform about the services that help women
in pregnancy and to grow up a child and live with a new child (BZgA, 2018c).
Abortion in Germany
Following information regarding an abortion can be relevant for some refugee women:
If a woman has unintended pregnancy and does not want to have a baby, then she can do an
abortion. In Germany, an abortion within the first twelve weeks after conception is legal if a
woman can prove that she was in pregnancy counseling before (BZgA, 2017, p. 84). Except that,
there must be at least three days between counseling and abortion date. An abortion in Germany
must be performed by a doctor, who may not have been responsible for the consultation (BZgA,
2017, p. 85). In some cases, abortion is not illegal if the girl is not yet 14 years old at the beginning
of her pregnancy or if a pregnancy is the consequence of a sexual offense like rape and sexual
abuse. An abortion beyond the twelfth week of pregnancy is also allowed in Germany if there is
medical indication like if the pregnancy is seriously damaging the physical or mental health of the
pregnant woman and if the danger cannot be averted in another way except abortion (BZgA,
2017, p. 85).
6 Recommendations
93
Services regarding contraception in Germany
Contraceptives help women to prevent from getting pregnant, especially unintended pregnancy.
Refugee women have generally negative perception towards contraceptive. They are afraid to
use contraceptive. Thus, it is important to inform the refugee women that contraception is not bad
for health. To each person suits a contraception based on a person’s lifestyle, age and physical
condition, etc. For that, a woman can ask a health professional for advice (BZgA, 2018d).
Following information concerning contraceptives might help refugee women to enhance their
knowledge:
In Germany, people can trust health professional (gynecologist) and share their
problem as they are obliged by law to respect the privacy of people and cannot misuse
any information
All usual methods of contraception are easily available in Germany
Every individual has rights to choose certain methods which suits to them
Contraceptives such as hormonal contraceptives (the birth control pill, implants,
injections), IUDs (intrauterine devices such as the spiral), and diaphragms can be
taken only when they are prescribed by a gynecologist
Contraceptives like condom are easily accessible at every drugstore or pharmacy
Condom is one method of contraception that also protects against HIV and reduces
the risk of STI
(BZgA, 2018d)
In Germany, people usually have to pay themselves for contraceptives. But there are some
exceptions: In the case of young women who are insured by a statutory health insurance, the
health fund covers the costs of medically prescribed contraceptives (the pill, the mini-pill, the
contraceptive patch, vaginal ring, three-month injection, hormonal implant, spiral and emergency
contraception). There are also counselling centers for contraceptive in Germany. Many refugees
are not informed about it. So, it is important to aware them about counselling centers and the
services provided by counselling center (BZgA, 2018d).
Information regarding STI
As most of the refugee women know about HIV and Aids but do not have sufficient knowledge of
other STIs. It is important to share knowledge about other STIs such as Herpes, fungal,
Gonorrhea, syphilis, genital warts which are becoming common nowadays. Following information
regarding STI can be shared in the women's health workshop:
STIs are triggered by different pathogens such as bacteria, viruses, fungi or parasites
STIs are spread primarily through person-to-person sexual contact
6 Recommendations
94
A mother with STI can transfer the infection to her newborn during pregnancy, or delivery
or through breastfeeding
People can also get the STI by sharing injection
The disease like hepatitis B can be transferred by sharing toothbrush, towels and bed
linen with someone else
Unsafe sexual intercourse increases the risk of STIs
Most STIs can be treated and cured
Condom is one of the cheapest and easiest means to protect against many STIs,
especially against infection with HIV
Depending on STI, vaccines can also protect against many infections
(BZgA /Sensoa, 2019); WHO, 2018; BZgA, 2018e)
Furthermore, it is important to share them that, different STI can be treated differently. For the
therapy and treatment people should seek the health professionals. People can also get
information without any charge from the responsible counselling agencies or from local health
office in Germany. Some of them are listed below.
Table 12 Service centers, which provide information on the STI
(Source: Federal Office for Migration and Refugees, 2015)
Services regarding sexual violence in Germany
Refugee women often experience sexual violence, including domestic violence. And they are
also not aware of their rights and available support services in relation to domestic and sexual
violence. In this study, none of the participants knew about the helpline “violence against women”.
Therefore, it is very important to inform refugee women about the help and support services
available in Germany. The REFUGIUM workshop can provide following message through the
workshop.
Service centers, which provide information on the STI
General practitioners
Health insurance funds
Local health office
Pro Familia
AIDS counselling Center
The Migration Advisory Service for Adult Immigrants and the Youth Advisory Service.
6 Recommendations
95
If women get victim of sexual and domestic violence
She should not hide it
She should seek for help and support
She can call in the helpline violence against women
She can also get help from police
The violence against women help all women with and without migration background
This “Violence Against Women” provide free, anonymous, confidential, barrier-free,
multilingual advice by phone, email or chat
(BZgA /Sensoa, 2019)
Further on, women should know that all victims of sexual violence, particularly women and girls,
have equal protection and access to justice and they have the right to make decisions about
reproduction, free of discrimination, coercion or violence (Garcia-Moreno & Heikl, 2009, p.146).
The workshop can also provide self-defense training as a practical part which was mentioned by
one of the participants of the study.
Cancer Screenings in Germany
For every woman over the age of 20, both state-funded and private health insurance in Germany
covers an annual exam at her gynecologist to check for early symptoms of cervical cancer, ovary
cancer, breast cancer, and similar cancers of the reproductive organs.
- Breast exam (usually for women over 30)
- Rectal exam (for women over 45)
The German health insurance provider should pay for this yearly examination since it is part of
basic medical care in Germany (BZgA /Sensoa, 2019).
Organizations supporting refugee women in Germany
Here are some organizations which are working to promote refugee’s health in Germany.
Refugee women can get different kinds of help and support from these organizations. Therefore,
refugee women should be informed about these organizations.
Caritas Deutschland: They provide counselling for migrant women about pregnancy, medical
service, financial support, etc. (Caritas Deutschland, 2019).
ADEBAR Beratung und Begleitung von Schwangeren und Familien (Hamburg): ADEBAR
supports the family with a special burden in coping with their everyday life. They help mothers by
providing parenting skills, good parent-child bond, in improving the health of the child such as
with breastfeeding, etc. (ADEBAR Beratung und Begleitung von Schwangeren und Familien).

6 Recommendations
96
CASA blanca: They offer free and anonymous HIV/AIDS test (CASA blanca).
The Deutsche AIDS-Hilfe: They provide HIV therapy and counselling for people infected with HIV.
The counselling can be directly with the person, or over the phone as well as online. Normally
the counselling is provided anonymously (The Deutsche AIDS-Hilfe).
The Hamburg protection plan: It targets to protect refugee women from violence, especially
gender-based violence in refugee accommodation centers. The protection plan lays out a
minimum set of infrastructural measures that needs to be implemented in all facilities. These
include separate rooms and sleeping areas with lockable doors, gender-segregated and lockable
sanitation and health facilities and the possibility of gender-separated accommodation facilities
for particularly vulnerable persons (World Future Council, 2016, p. 17).
Campaign: “No Camps for Women and Children / Abolish all Camps”: They organize
empowerment training and peer education workshops “from refugee women to refugee women”
(World Future Council, 2016).
EmpowerVan – Mobile Information and Advice Service: The EmpowerVan is a mobile information
and advice service in a multi-van that regularly visits initial reception centers and accommodation
in Hamburg. Its goal is to counteract the isolation of girls and women in reception and
accommodation centers. The van is used as a safe space to assist women with everything from
medical appointments to finding new accommodation if a woman has experienced abuse. It also
provides an area for women to meet, interact and share experiences (World Future Council, 2016,
p. 36).
MiMi – Violence Prevention with Migrants for Migrants: Capacity Building for Violence Prevention,
Self-Protection and Empowerment for Refugee Women and Girls in Germany: This project aims
to inform refugee women and girl about the different forms of violence and possibilities for
protection in a way that is culture, language and gender–sensitive through intercultural mediators
(World Future Council, 2016, p. 25).
Zanzu – The multilingual online portal for sexual and reproductive health: Zanzu is a web portal
that provides comprehensive information on SRH in 13 different languages which is free of cost
(Zanzu, 2018).

7 Conclusion
97
7 Conclusion
In Germany, there is a high inflow of refugees since last few years. Due to overwhelming refugee
population, Germany is facing challenges in providing adequate health services (Entre Nous,
WHO & UNFPA, 2016, p. 27). The increasing number of refugee also demands the need for
health promotion and awareness and especially regarding women’s health. Generally, refugee
women have been found to have poor health conditions affected due to many physical, social
and mental factors. Concerning SRH, refugee women have inadequate knowledge and the topic
is generally considered a taboo among refugees from majority Muslim nations. Thus, even after
the resettlement, many refugee women face difficulties to negotiate and access services on SRH.
Many refugee women in their home country were victims of forced and early marriage due to
which several of them got pregnant in an early age. Refugee women have also low level of
awareness on family planning, modern contraceptives and sexually transmitted infections (STIs).
This knowledge deficit may put refugee women at greater risk of unwanted pregnancies,
complications during childbirth and STIs. Further on, they also have a high risk of sexual and
gender-based violence including domestic violence.
The findings from this study also show that refugee women’s previous experiences in accessing
health services influenced how they access the services in the new country. As there are a
comparatively low numbers of health care providers and less access to SRH services in their
home country, they don’t utilize these services regularly. Even in the refugee accommodations
here, there are not enough health care services addressing SRH. Due to this, they have to seek
health care services outside the camp. But, there are lots of challenges which hinder refugee
women to seek SRH services in a new country such as communication difficulties, cultural
difference, unfamiliarity with the health system, lack of support and gender role of health provider
also shows to play a vital role. Due to these challenges, refugee women hesitate to seek health
care services and hence cannot improve their health condition.
Thus, refugee women need educational programs which should inform them about the
importance of SRH in people's life. Most of the women need to be aware of women rights and
sexual and reproductive health rights, as well as support and convincing of their male partner or
member of the family. The SRH education should include information about family planning,
benefits of contraception, STI, the consequence of early childbirth etc. Refugee women need to
be aware of the available health care services in Germany such as gynecologist services,
midwives' services during childbirth, counseling regarding family planning and contraception and
services regarding STI test. They need to be informed about availability of support and service
for women who are the victim of sexual and gender-based violence including domestic violence.

7 Conclusion
98
They also should get information about programs and projects which are involved to promote
SRH of refugees such as Zanzu portal from BZgA, MIMI project, Aids Hilfe Hamburg etc. Some
of these topics were also suggested by refugee women who participated in this study to include
in the REFUGIUM women’s health workshop.
The findings from this study will help REFUGIUM program to develop a women’s health workshop
focusing on SRH for refugee women. The suggested SRH topics from refugee women should be
highly respected, valued and should be included in REFUGIUM women’s health workshop.
Moreover, the recommended SRH topics of this paper can be utilized as a workshop content.
The general recommendations provided in this study will also help REFUGIUM program to
conduct a women’s health workshop efficiently. Through health workshop, REFUGIUM program
can fulfill the needs of refugee women to some extent and increase the utilization of health. The
proper utilization of SRH care can improve SRH, overall health as well as positive social and
economic outcomes for women. It can reduce the rates of STI and unplanned pregnancy. Thus,
it is important to educate refugee women about SRH aspects to improve their health and well
being.
Based on the finding of this study many other health education interventions can be implemented
for refugee women. There should be cooperation, collaboration and strong policy coherence
between the education, social and health sectors to provide comprehensive sexual and
reproductive health education and services for refugee women. Further on, there should be
multiple and multidimensional intersectoral approaches or interventions for providing effective
SRH education for refugee women and increase the utilization of SRH services by refugees.
The SRH health of refugee women is also influenced by her partner. Partner’s SRH knowledge
also influences the SRH behavior of women such as men’s interest in seeking health care service
in the new country tends to increase the utilization of health services by the couple. Therefore,
there is also need of in-depth understanding of refugee men's perception and consciousness
towards SRH. Both refugee women and men are now part of German society. So, the SRH needs
of both women and men should be understood and fulfilled. For an effective result, this SRH
education should be part of early resettlement services for both refugee women and men.
Therefore, there is a need of a good quality program about sexuality for refugee women as well
as for men.
Findings from this study signify that SRH care provision for refugee women can be complex due
to the sensitive and culture-bound nature of SRH. Therefore, the health care provider should be
intercultural competent to deal with refugee women from different backgrounds and to understand
also from their perspective. The health care provider should also offer more time to refugee

7 Conclusion
99
women because of the use of interpreters, and they should keep in mind that most of the refugee
women might hesitate to negotiate on SRH topic.
This result of this study included the refugee women from Syria, Iraq, Iran, Pakistan and Nigeria.
To get a detailed understanding of other large refugee groups such as from Eritrea, Somalia, and
Russia, there is a need for further study those groups as well. This will help policymaker and
education provider to get an overview of the sexual and reproductive health needs of other
refugee group too.

8 References
100
8 References
ADEBAR Beratung und Begleitung von Schwangeren und Familien (Hamburg). (o.D.).
Unterstützung. Hamburg. Retrieved 14.12.2018, from URL https://www.adebar-
hh.de/unterstuetzung/
Alexander, G.R. and Carol C. Korenbrot, C.C. (1995). The Role of Prenatal Care in Preventing
Low Birth Weight. The Future of Children Vol. 5, No. 1, Low Birth Weight Spring, pp. 103-120
Retrieved 14.09.2018, from DOI: 10.2307/1602510
https://www.jstor.org/stable/1602510?seq=1#page_scan_tab_contents
Asylum Information Database (AIDA) & European Council on Refugees and Exiles (ECRE).
(2018). Health Care Germany. Retrieved 08.08.2018, from URL
http://www.asylumineurope.org/reports/country/germany/reception-conditions/health-care
BAMF. (2019). Aktuelle Zahlen zu Asyl. Retrieved 12.01.2019, from URL
file:///C:/Users/User/Desktop/asyl%20antrag%20statistik%20.pdf
BAMF. (2019). BAMF-Kurzanalyse. Ausgabe 01|2019 der Kurzanalysen des
Forschungszentrums Migration, Integration und Asyl des Bundesamtes für Migration und
Flüchtlinge. Retrieved 12.01.2019, from URL
http://www.bamf.de/SharedDocs/Anlagen/EN/Publikationen/Kurzanalysen/kurzanalyse1-2019-
fortschritte-sprache-beschaeftigung.pdf?__blob=publicationFile
BAMF. (2018). Aktuelle Zahlen zu Asyl (12/2018). Retrieved 22.11.2018, from
URLhttp://www.bamf.de/SharedDocs/Anlagen/DE/Downloads/Infothek/Statistik/Asyl/aktuelle-
zahlen-zu-asyl-dezember-2018.pdf?__blob=publicationFile
BAMF. (2017). Bundesamt für Migration und Flüchtlinge. Retrieved 07.07.2018, from URL
http://www.asylumineurope.org/sites/default/files/resources/bundesamt-in- zahlen-2016-asyl.pdf
BAMF (Federal Office for Migration and Refugees). (2017). Refugee women in Germany:
language, education and employment. Brief analysis. Retrieved 5.8.2018, from URL
http://www.bamf.de/SharedDocs/Anlagen/EN/Publikationen/Kurzanalysen/kurzanalyse7_gefluc
hetete-frauen.html
BAMF. (2015). Bundesamt für Migration und Flüchtlinge. Retrieved 28.11.2017, from URL
https://www.bamf.de/SharedDocs/Anlagen/DE/Downloads/Infothek/DasBAMF/2015-08- 20-
prognoseschreiben-asylantraege.html
BAMF. (2015). HIV/AIDS counselling/Information on sexually-transmitted infections (STI).
Retrieved 16.11.2017, from URL
http://www.bamf.de/EN/Willkommen/GesundheitVorsorge/Aidsberatung/aidsberatung-
node.html
Baum, F., MacDougall, C., & Smith, D. (2006). Participatory action research. Journal of
Epidemiology and Community Health, 60(10), 854–857. Retrieved 31.08.2017, from URL
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2566051/

8 References
101
Blanc, A.K. (2001). The effect of power in sexual relationships on sexual and reproductive
health: An examination of Evidence. In: Studies in family Planning. Vol. 32. Retrieved
12.08.2018, from URL https://onlinelibrary.wiley.com/doi/epdf/10.1111/j.1728-
4465.2001.00189.x
Bortz, J. & Döring, N. (2006). Forschungsmethoden und Evaluation für Human und
Sozialwissenschaftler, 4. überarbeitete Auflage. Springer Medizin Verlag. Heidelberg
Bundesamt für Familie und zivilgesellschaftliche Aufgaben, (2018). Das Hilfetelefon –
Beratung und Hilfe für Frauen. Retrieved 26.10.2017, from URL https://www.hilfetelefon.de/
Bundesamt für Familie und zivilgesellschaftliche Aufgaben. (2018). HIV/AIDS
counselling/Information on sexually-transmitted infections (STI). Retrieved 23.10.2018 from
URL www.bamf.de/EN/Willkommen/GesundheitVorsorge/Aidsberatung/aidsberatung-node.html
Bundeszentrale für gesundheitliche Aufklärung (BZgA). (2016). Wissen: Safer Sex. Retrieved
26.10.2018, from
http://www.gibaidskeinechance.de/wissen/safer_sex.php?L=0%3Fbg%3DMethode_300%3Fbg
%3DMethode_468%3Fbg%3DBeratung_468%3Fbg%3DMethode_160%3Fbg%3DMethode_30
0%3Fbg%3DBeratung_728%3Fbg%3DWissen_728%3Fbg%3DKampagne_160 Accessed on
10.07.2016
BZgA (2019). Recht und Amt nach der Geburt. Retrieved 15.10.2018, from URL
https://www.familienplanung.de/schwangerschaft/nach-der-geburt/recht-und-amt/
BZgA /Sensoa. (2019). Zanzu, my body in words and images. Retrieved 28.10.2018, from URL
https://www.zanzu.de/en/
BZgA. (2018a). Gewalt. Retrieved 28.10.2018, from URL
https://www.frauengesundheitsportal.de/themen/gewalt/
BZgA. (2018b). Sexuell übertragbare Infektionen. In:Frauengesundheitsportal. Retrieved
26.10.2018, from URL https://www.frauengesundheitsportal.de/themen/sexuell-uebertragbare-
infektionen-sti/mehr-zum-thema/
BZgA. (2018c). Schwangerschaft. Retrieved 25.10.2018, from URL
https://www.familienplanung.de/
BZgA. (2018d). Sichergehen. Verhütung für sie und ihn. Retrieved 15.10.2018, from URL
file:///C:/Users/User/AppData/Local/Packages/Microsoft.MicrosoftEdge_8wekyb3d8bbwe/Temp
State/Downloads/13060000%20(1).pdf
BZgA. (2018e). STI- Was ist das? Retrieved 15.10.2018, from URL
https://www.liebesleben.de/fuer-alle/sexuell-uebertragbare-infektionen/sti-was-ist-das/
BzgA, (2017a). Die ersten Tage in der Klinik. Retrieved 26.10.2018, from URL
https://www.familienplanung.de/schwangerschaft/nach-der-geburt/die-ersten-tage/die-ersten-
tage-in-der-klinik/
BZgA. (2017b). Gesund leben in der Schwangerschaft. Retrieved 25.10.2018, from URL
https://www.familienplanung.de/schwangerschaft/gesundheit-und-ernaehrung/gesund-leben/

8 References
102
BZgA. (2017c). Medikamente in der Schwangerschaft. Retrieved 25.10.2018, from URL
https://www.familienplanung.de/schwangerschaft/das-baby-vor-gefahren-
schuetzen/medikamente/
BZgA. (2017d). Welche Verhütungsmethode passt zu mir? Retrieved 14.10.2018, from URL
https://www.familienplanung.de/verhuetung/passende-methode-finden/
BZgA. (2016). Die Zeit im Wochenbett. Retrieved 27.10.2018, from
URLhttps://www.familienplanung.de/schwangerschaft/nach-der-geburt/das-wochenbett/die-zeit-
im-wochenbett/
BZgA. (2014). Vorsorgeuntersuchungen: Sicherheit für Mutter und Kind. Retrieved 26.10.2018,
from
URLhttps://www.familienplanung.de/schwangerschaft/schwangerschaftsvorsorge/vorsorge-zur-
sicherheit/#c24911
Caritas Deutschland. (2019). ONLINE-BERATUNG. Schwangerschaftsberatung. Retrieved
Retrieved 25.10.2018, from URL https://www.caritas.de/hilfeundberatung/hilfeundberatung
Centrum für AIDS und sexuell übertragbare Krankheiten in Altona (CASA blanca).(2018).
HIV/AIDS-Beratung und -Test. Retrieved Retrieved 25.10.2018, from URL
https://www.hamburg.de/casablanca/
Charite. (2017): Charité für geflüchtete Frauen. Universitätsmedizin Berlin. Retrieved
02.07.2017, from URL https://femalerefugees.charite.de/
Creswell, J.W. (2013). Qualitative Inquiry and research design. Choosing among five
approaches. 3rd Edition. SAGE publication.
Crossland, N. Hadden, W.C., Vargas, W.E., Valadez, J. Jeffery, C. (2015). Sexual and
Reproductive Health Among Ugandan Youth: 2003-04 to 2012 In: Journal of Adolescent Health.
Elsevier 393-398 Retrieved 08.07.2017, from https://doi.org/10.1016/j.jadohealth.2015.06.015
Commonwealth of Australia, 2010. National Women's Health Policy 2010. Retrieved 25.9.2018,
from URL
https://www.health.gov.au/internet/main/publishing.nsf/Content/3BC776B3C331D5EECA257BF
0001A8D46/$File/NWHP.pdf
DeJong, J., Jawad, R., Mortagy, I. & Shepard, B. (2005). The Sexual and Reproductive Health
of Young People in the Arab Countries and Iran, Reproductive Health Matters. Retrieved
17.09.2018, from URL https://www.tandfonline.com/doi/full/10.1016/S0968-
8080%2805%2925181 9?scroll=top&needAccess=true
Diakonie Deutschland. (2019). Flucht und Migration. Retrieved 22.11.2018, from URL
https://www.diakonie.de/unbegleitete-minderjaehrige-fluechtlinge/
Diekmann, A. (2006). Empirische Sozialforschung. Grundlagen, Methoden, Anwendungen. 16.
Auflage. Rowohlts Enzyklopädie im Rowohlt Taschenbuch Verlag. Reinbek bei Hamburg
Entre Nous, WHO & UNFPA (2016). Together for a better sexual and Reproductive health.
No.84. Retrieved 15.10.2018, from URL
http://www.euro.who.int/__data/assets/pdf_file/0017/319301/Entre-Nous-84-full-book.pdf?ua=1
8 References
103
Flick U. (2016). Qualitative Sozialforschung. Eine Einführung.7th ed. Reinbek: Rowohlt.
Flick U. (2006). An Introduction to Qualitative Research. 3rd Ed. Sage: London
Fuß, S. & Karbach, U. (2014). Grundlagen der Transkription, Eine praktische Einführung,
Barbara Budrich Verlag. Opladen und Toronto
Garcia-Moreno, C. & Stöckl, H. (2009). Protection of sexual and reproductive health rights:
Addressing violence against women. In: International Journal of gynecology and Obstetrics.
Retrieved 12.10.2018, from https://doi.org/10.1016/j.ijgo.2009.03.053
Gagnon, A.J., Merry, L. & Robinson, C. (2002). A Systematic Review of Refugee Women’s
Reproductive Health. Retrieved 06.06.2018, from URL http://www.evidenceaid.org/wp-
content/uploads/2016/08/Gagnon-et-al-Refugee-Womens-reproductive-health-Can-J-Refugees-
2002.pdf
Hennink, M., Hutter,I., & Bailey,A. (2011). Qualitative Research Methods. London. SAGE
publication Ldt. Retrieved 17.10.2018, from URL
https://books.google.de/books?hl=de&lr=&id=zN70kC0E3XQC&oi=fnd&pg=PP2&dq=qualitative
+research+methods&ots=HXW8ZxpIzu&sig=9oC78RE4rlZ5dFjmDXuGJw9Tin8#v=onepage&q
=qualitative%20research%20methods&f=false
Ivanova, O., Rai, M., & Kemigisha, E. (2018). A Systematic Review of Sexual and Reproductive
Health Knowledge, Experiences and Access to Services among Refugee, Migrant and
Displaced Girls and Young Women in Africa. International Journal of Environmental Research
and Public Health, 15(8), 1583. Retrieved 14.09.2018, from
http://doi.org/10.3390/ijerph15081583
Kaddour, A. Hafez, R., & Zurayk, H. (2005). Women's Perceptions of Reproductive Health in
Three Communities around Beirut, Lebanon, Reproductive Health Matters, Retrieved
04.11.2018, from DOI: 10.1016/S0968-8080(05)25170-4
Keygnaert, I., Vettenburg, N., & Temmerman, M. (2012). Hidden violence is silent rape: sexual
and gender-based violence in refugees, asylum seekers and undocumented migrants in
Belgium and the Netherlands, Culture, Health & Sexuality. Retrieved 06.06.2018, from DOI:
10.1080/13691058.2012.671961
Keygnaert, I., Vettenburg, N., Roelens, K., & Temmerman, M. (2014). Sexual health is dead in
my body: participatory assessment of sexual health determinants by refugees, asylum seekers
and undocumented migrants in Belgium and The Netherlands. BMC public health, Retrieved
06.06.2018, from doi:10.1186/1471-2458- 14-416
Kohlbacher, F. (2006). The Use of Qualitative Content Analysis in Case Study Research.
Volume 7.Retrieved 29.09.2018, from
URL.https://pdfs.semanticscholar.org/33a6/2dcbb00f86d99b1e10e4fad4fc9983e1a247.pdf
Kuckartz, U. (2005). Einführung in die computergestützte Analyse qualitativer Daten. 1.
Auflage. VS Verlag für Sozialwissenschaft/ GWV Fachverlage GmbH, Wiesbaden.

8 References
104
Kuckartz, U. (1999). Computergestützte Analyse Qualitativer Daten. Eine Einführung in
Methoden und Arbeitstechniken. Westdeutscher Verlag GmbH, Opladen/ Wiesbaden.
Kurmeyer, C., Abels, I., & Merkle, I., (2017). Charité für geflüchtete Frauen. Women for
Women. Jahresbericht 2016. Frauen- und Gleichstellungsbeauftragte der Charité. Berlin.
Retrieved from
URL:https://femalerefugees.charite.de/fileadmin/user_upload/microsites/sonstige/mentoring/pdf
s/Jahresbericht_femalerefugees_2016_final-1.pdf
Lewis, J., and Nicholls, Mc. C. (2014). Design Issues. In: Qualitative Research Practice: A
Guide for Social Science Students and Reserachers. SAGE Publication. Los Angeles.
Retrieved from
URL:https://books.google.de/books?hl=de&lr=&id=EQSIAwAAQBAJ&oi=fnd&pg=PP1&dq=ethic
al+aspects+in+scientific+reserach+&ots=l_POmwSs0O&sig=1G8YoprMtbmwhRSJurJHWQbJC
XI#v=onepage&q&f=false
Mayring, P. (2008). Qualitative Inhaltsanalyse. Grundlage und Techniken. 10. Auflage. Beltz
Verlag. Weinheim und Basel.
Mengesha, Z. B., Perz, J., Dune, T., & Ussher, J. (2017). Refugee and migrant women’s
engagement with sexual and reproductive health care in Australia: A socio-ecological analysis
of health care professional perspectives. Retrieved 08.10.2018, from URL.
http://doi.org/10.1371/journal.pone.0181421
Multicultural Centre for Women's Health (MCWC) (2012). Best Practice Guide. COMMON
THREADS, COMMON PRACTICE. WORKING WITH IMMIGRANT & REFUGEE WOMEN IN
SEXUAL & REPRODUCTIVE HEALTH. Retrieved 25.10.2018, from URL
http://www.mcwh.com.au/downloads/publications/MCWH_CommonThreads_BestPracticeGuid
e_WEB.pdf
MCWH. (2010). Points of Departure. An Advocacy Toolkit for Immigrant and Refugee Women.
Melbourne: Multicultural Centre for Women’s Health. Retrieved 25.10.2018, from URL
http://www.mcwh.com.au/downloads/publications/MCWH_POD_Advocacy_Toolkit.pdf
Multicultural Centre for Women’s Health. (2010). Points of Departure Project. Discussion Paper
National Issues for Immigrant and Refugee Women. Australia. Retrieved 25.10.2018, from URL
http://www.mcwh.com.au/downloads/publications/MCWH_POD_Advocacy_Toolkit.pdf
Murphy, B. (2004). Health education and communication strategies. In H. Kele- her & B.
Murphy (Eds.), Understanding health. A determinants approach (pp. 187–203). South
Melbourne, Vic., New York: Oxford University Press.
Narasimhan, M., Pillay, Y., García, P.J., Allotey,P., Gorna, R., Welbourn, A., Remme, M.,
Askew, L., Nordström,A., Haufikuon, B. (2018). Investing in sexual and reproductive health
and rights of women and girls to reach HIV and UHC goals In: the Lancet Global Health.
Retrieved 30.10.2018, from https://www.thelancet.com/journals/langlo/article/PIIS2214-
109X%2818%2930316-4/fulltext

8 References
105
pro familia Deutsche Gesellschaft für Familienplanung, Sexualpädagogik und Sexualberatung
e.V. Bundesverband.(o.D). Schwangerschaft und Geburt. Retrieved 12.10.2018, from
https://www.profamilia.de/themen/schwangerschaft.html
REFUGIUM: Rat mit Erfahrung: Flucht und Gesundheit – Information und Multiplikation.
Retrieved from www.refugium.agency
RHTAC (Refugee Health Technical Assistance Center). (2011). Women’s Health. Retrieved
25.10.2018, from http://refugeehealthta.org/physical-mental-health/health-conditions/womens-
health/ (Access on: 07.07.2017
Slobodin O., de Jong J. T. (2015). Mental health interventions for traumatized asylum seekers
and refugees. What do we know about their efficacy? In: International Journal of Social
Psychiatry. Vol. 61(1) 17–26. SAGE publication. Retrieved 15.08.2018, from
http://isp.sagepub.com/content/61/1/17.long
Sönmez, E.J., Jesuthasan, J., Abels, I., Nassar, R., Kurmeyer, C., & Schouler-Ocak, M. (2017).
Study on female refugees – A representative research study on refugee women in Germany.
European Psychiatry. Volume 41, Supplement. Retrieved 22.10.2018, from
https://doi.org/10.1016/j.eurpsy.2017.02.038
Statistisches Bundesamt (Destatis). (2018). Bevölkerung und Erwerbstätigkeit.
Schutzsuchende Ergebnisse des Ausländerzentralregisters. Retrieved 14.09.2018, from URL
https://www.destatis.de/DE/Publikationen/Thematisch/Bevoelkerung/MigrationIntegration/Schut
zsuchende2010240167004.pdf?__blob=publicationFile
The Deutsche AIDS-Hilfe. (o.D). HIV and Aids. Retrieved 14.09.2018, from URL
https://www.aidshilfe.de/hiv-aids
The UN Refugee Agency. (2017). Figures at a Glance. Retrieved 17.08.2018, from:
http://www.unhcr.org/figures-at-a-glance.html
Tracy, S.J. (2013). Qualitative Research Methods. Collecting Evidence, Crafting Analysis,
Communicating Impact, First Edition. Blackwell Publishing Ltd. Retrieved from
URLhttp://okt.kmf.uz.ua/atc/oktatatc/Basics_of_research_methodology/Tracy_2013_qualitative
_research_methods_collecting_evidence_crafting_analysis_communication.pdf
United Nation Population Fund (UNFPA). (2018). Family planning. Retrieved 14.09.2018, from
URL https://www.unfpa.org/family-planning
UNFPA. (2016). Reproductive health and development. Retrieved 14.09.2018, from URL
https://www.unfpa.org/sexual-reproductive-health
Webster, S., Lewis, J. and Brown, A. (2014). Ethical Considerations in Qualitative Research. In:
Qualitative Research Practice: A Guide for Social Science Students and Reserachers. SAGE
Publication. Los Angeles. Retrieved from URL
https://books.google.de/books?hl=de&lr=&id=EQSIAwAAQBAJ&oi=fnd&pg=PP1&dq=ethical+a
8 References
106
spects+in+scientific+reserach+&ots=l_POmwSs0O&sig=1G8YoprMtbmwhRSJurJHWQbJCXI#
v=onepage&q&f=false (Access on: 18.07.2017)
WHO (2019). Maternal and newborn health. Retrieved 14.09.2018, from URL
http://www.euro.who.int/en/health-topics/Life-stages/maternal-and-newborn-health/maternal-
and-newborn-health
WHO. (2018a). Sexual and reproductive health. Retrieved 14.09.2018, from URL
https://www.who.int/reproductivehealth/en/
WHO. (2018b). Family planning/Contraception. Retrieved 15.09.2018, from URL
http://www.who.int/en/news-room/fact-sheets/detail/family-planning-contraception
WHO. (2018c): Sexual and reproductive health. Strengthening the health system response to
violence against women. Retrieved 15.09.2018, from URL
http://www.who.int/reproductivehealth/topics/violence/en/
WHO. (2018d). Health topics. Reproductive Health. Retrieved 14.09.2018, from URL
http://www.who.int/topics/reproductive_health/en/
WHO. (2018e). Refugee and migrant health. Retrieved 14.09.2018, from URL
http://www.who.int/migrants/en/
WHO. (2017a). Promoting health through the life-course. Ten top issues for women's health.
URL: http://www.who.int/life-course/news/commentaries/2015-intl-womens-day/en/
WHO. (2017b). Health topics. Women’s health. Retrieved 14.09.2018, from URL
http://www.who.int/topics/womens_health/en/
WHO. (2001). WHO REGIONAL STRATEGY ON SEXUAL AND REPRODUCTIVE HEALTH.
Copenhagen, Denmark: World Health Organization, 2001.
Worbs, S., & Baraulina, T. (2017). Female Refugees in Germany: Language, Education and
Employment. BAMF Brief Analysis. Issue 1|2017 of the Brief Analyses by the Migration,
Integration and Asylum Research Centre at the Federal Office for Migration and Refugees.
Retrieved 08.08.2018, from URL
https://www.bamf.de/SharedDocs/Anlagen/EN/Publikationen/Kurzanalysen/kurzanalyse7_geflu
chetetefrauen.pdf;jsessionid=8BC00E77BA0758B9DB1D806B94515782.1_cid286?__blob=pub
licationFile
World Future Council. (2016). PROTECTING REFUGEE WOMEN AND GIRLS FROM
VIOLENCE. A Collection of Good Practices. Retrieved 20.09.2018, from URL
https://www.worldfuturecouncil.org/file/2016/12/WF_2016_Protecting-refugee-women-and-
girls.pdf (Accessed on: 17.07.2017)
Yasmine, R., & Moughalian, C. (2016). Systemic violence against Syrian refugee women and
the myth of effective intrapersonal interventions, Reproductive Health Matters, 24:47, 27-35.
Retrieved 20.09.2018, from URL DOI: 10.1016/j.rhm.2016.04.008
9 Appendix
107
9 Appendix
Appendix A: Recruitment Script
Project Information
Hello...........,
My name is Sona Sainju, a student of Health Sciences in the University of Applied Sciences
in Hamburg and a research peer facilitator in REFUGIUM program.
I would like to invite you to participate in a focus group/ interview for a research study on
“Exploring the sexual and reproductive health needs of refugee women in Germany”. The
study aims to investigate the sexual and reproductive health problems and issues of refugee
women to better understand their needs regarding sexual and reproductive health. The
results gained from this study will help REFUGIUM program to develop a women's health
workshop for refugee women.
If you agree to participate, you will be invited to a focus group or face-to-face interview. The
focus group / interview will have 11 open-ended semi-structured questions and will take
around 1 hour. The interview will be recorded with an electronic device if you agree to do so.
You may feel uncomfortable in answering some of the questions. You have the right to refuse
to answer any question that makes you uncomfortable. You also have the right to stop your
participation in the study at any time without any consequences.
There may be a potential breach of confidentiality because private stories could not be
identified or recognized by third parties. In addition, the consent form will not be connected to
the data. A pseudonym will be given to you to reduce the chance of identifying information in
the interviews. Data will be recorded and stored in a secure and password protected
computer.
Your participation is completely voluntary. You can choose to be in the study or not.
Participation or non-participation will not affect any services, benefits or any other personal
consideration or right you usually expect.
If you have any questions or if you like to participate then please contact me at
or email me at
Thank you very much.

9 Appendix
108
Appendix B: Interview Guideline
Interview Guideline (Questionnaire) about Women’s Health focusing on reproductive and
sexual health
Background information about women in own home country
1. Could you please tell me from which country are you from?
2. How is the condition of women /girls in your country regarding health, education, equality,
freedom?
3. When can a girl called as women in your country/culture?
4. What is the average marriage age of women in your country/culture?
5. How are health care services for women in your country?
6. How much importance do women give to their health?
7. How openly can women share their health problems with others (life partner, parents, and
siblings)?#
Current situation of refugee’s women living in refugee accommodation
8.In Which type of refugee accommodation are you living now?
9.Are there lots of single women or women with children?
10. How many children does one married woman have in average?
Women’s health in the perspective of refugee’s women
11. What comes in your mind, when I said, today we will talk about women’s health. /What is
women’s health in your perspective/in your view? / What do you think, what kind of topic
are related to women’s health?
12. How important is women’s health to you? / How much conscious are you about women
health
13. Could you please tell us what do you do to maintain your women’s health’ in good
condition?
14. Could you please share us, how is women’s health in general in refugee accommodation?
15. How much conscious are women in refugee accommodation about women’s health
For e.g. Feminine hygiene, violence, pregnancy, childcare, no privacy to have intimate
moments with your partner etc.
16. If you have some problem, regarding women problem, to whom you will share this
problem at first?
9 Appendix
109
17. Are there any health care facilities special for women in refugee accommodation? If yes,
are you using those facilities?
18. Do you know any health care facilities that are provided specially for women in Hamburg?
Are you utilising it?
19. How much conscious are you with diseases, which most of the women suffers from?
Reproductive and sexual health in the perspective of refugee’s women
20. How much conscious are you with reproductive health or sexual health?
21. What do you think, how much conscious are women in accommodation camp about
reproductive and sexual health?
22. What kind of health care facilities/services do you know in Germany regarding
reproductive health?
For e.g. Family planning counselling, Frühe Hilfen(BZGA)
- During pregnancy
- Before pregnancy
- After birth of new born baby
23. Are you using any health care services for sexual and reproductive health in Germany?
(Adults can get information from counselling centres or doctors. Moreover, the German
Federal Centre for Health Education (BZgA) offers brochures and online resources)
24. What opinion do you have concerning contraceptives?
25. Are contraceptives acceptable in your religion / culture? If no, why do you think it’s not
acceptable? Or how openly can you talk about contraceptives methods with your partner
or other family member?
26. What do you think do married women use any contraceptives methods in your culture?
27. How much conscious are you with sexually transmitted diseases like HIV, human
papillomavirus (HPV) infection (the world’s most common STI)
28. Like human rights there are also certain rights regarding sexuality. Are you aware with
rights concerned to sexuality?
(People can decide for themselves whether and how you want to live out your sexuality.
No one can force you into carrying out sexual acts.
You are free to choose your partner.
No one can discriminate against you or attack you because of your sexuality.
(source: zanzu.de))
29. Do you know anyone or Have you heard from anyone who had experienced sexual
violence during the migration and after settling down in Germany?

9 Appendix
110
30. What do you think, where women can get help in Germany if they are having problem due
to sexual violence?
(If women are affected by violence in their relationship or marriage, they can go to a or directly
to the police or Women's refuges (facilities that take in women who are mistreated by their
partners/husbands and offer them protection and help. If the women have children, the children
are also taken in with them. In most cases, women's refuges are managed by women or a
women's group) "Gewalt gegen Frauen (Violence Against Women)", telephone number 08000 -
116 016, is available all over Germany 24 hours a day
31. Regarding sexual and reproductive health, there are lot of prevention and awareness
program like zanzu
Do you know about it?
What are the things that you like from zanzu portal? And which things you didn’t like it?
Ideas gaining for conducting reproductive and sexual health workshop
32. We want to conduct workshop about women health, could you please suggest us, which
topic should we cover in Refugium? or which topics are important to discuss to promote
women health.
33. Is there anything else you would like to share how women’s health including sexual and
reproductive health can be promoted for those women living in refugee accommodation?
Socio-demographic Questionnaire
o Age:
o Home country
o Status: Single / married
o Native language:
o Education level:
9 Appendix
111
Appendix C: Consent form
Consent form:
I declare my willingness to participate in an interview /focus group as part of the mentioned
REFUGIUM Program. I have been well informed about the purpose and the process of the
research project. I can stop the interview at anytime, decline participation in further interviews
and withdraw my consent to recording and transcription without causing any irregularities.
I agree that the interview can be recorded using a recording device so that it can be then put
into a written form. For further scientific evaluation of the interview, all indication to my
personal details will be removed from the transcript or anonymised. Furthermore, I am also
assured that in scientific publications, the interview will only be cited in excerpts, to ensure
that it will not be identified by a third party through the sequence of the events reported.
Date: Signature:
Einverständniserklärung
Ich erkläre mich dazu bereit, im Rahmen des genannten REFUGIUM Program an einem
Interview/ Fokus group teilzunehmen. Ich wurde über das Ziel und den Verlauf des
Forschungsprojekts informiert. Ich kann das Interview jederzeit abbrechen, weitere Interviews
ablehnen und meine Einwilligung in eine Aufzeichnung und Niederschrift des/der Interviews
zurückziehen, ohne dass mir dadurch irgendwelche Nachteile entstehen.
Ich bin damit einverstanden, dass das Interview mit einem Aufnahmegerät aufgezeichnet und
sodann in Schriftform gebracht wird. Für die weitere wissenschaftliche Auswertung des
Interviewtextes werden alle Angaben zu meiner Person aus dem Text entfernt und/oder
anonymisiert. Mir wird außerdem versichert, dass das Interview in wissenschaftlichen
Veröffentlichungen nur in Ausschnitten zitiert wird, um sicherzustellen, dass ich auch durch
die in den Interviews erzählte Reihenfolge von Ereignissen nicht für Dritte erkennbar werde.
Datum: Unterschrift:
9 Appendix
112
Appendix D: Observation protocol
Observation protocol
Date:
Time:
Observation Site: Name of refugee camp:
Description of camp:
Healthcare services available in refugee accommodations
General health care service for refugee: For e.g. General physician
Health care service special for refugee women: For e.g. Sports, Consultation for mothers
Service regarding sexual and reproductive health: Like Midwives service, Information regarding STI, contraceptive, family planning, sexual and gender-based violence
Other services, or programs or activities: Like REFUGIUM workshop, Information about different organizations

9 Appendix
113
Appendix E: Interview Fieldnote

9 Appendix
114
Appendix F: Focus group setting

Declaration of Authorship
I hereby declare that the thesis submitted is my own unaided work. All direct or indirect sources
used are acknowledged as references.
I am aware that the thesis in digital form can be examined for the use of unauthorized aid and in
order to determine whether the thesis as a whole or parts incorporated in it may be deemed as
plagiarism. For the comparison of my work with existing sources I agree that it shall be entered
in a database where it shall also remain after examination, to enable comparison with future
theses submitted. Further rights of reproduction and usage, however, are not granted here.
This paper was not previously presented to another examination board and has not been
published.
Hamburg, 28.02.2019