exploring the sexual and reproductive health of adolescents in ...
242
Towards adulthood: exploring the sexual and reproductive health of adolescents in South Asia Edited by Sarah Bott Shireen Jejeebhoy Iqbal Shah Chander Puri World Health Organization Department of Reproductive Health and Research
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of exploring the sexual and reproductive health of adolescents in ...
i
Towards adulthood: exploring the
sexual and reproductive health of
adolescents in South Asia
Edited by
Sarah Bott
Shireen Jejeebhoy
Iqbal Shah
Chander Puri
World Health Organization
Department of Reproductive Health and Research
II
WHO Library Cataloguing-in-Publication Data
Towards adulthood : exploring the sexual and reproductive health of adolescents inSouth Asia / edited by Sarah Bott … [et al.]
1.Adolescent behavior 2.Sex behavior 3.Risk-taking 4.Knowledge, attitudes,practice 5.Reproductive health services 6.Adolescent health services 7.AsiaI.International Conference on Reproductive Health (2000 : Mumbai, India)II.Bott, Sarah.
ISBN 92 4 156250 1 (NLM classification: WS 462)
CreditsCover design: Máire Ní MhearáinCover photo: POPULATION COUNCIL/BONNIE HAZURIA
Back cover photo: CENTER FOR COMMUNICATION PROGRAMS, JOHNS HOPKINS UNIVERSITY
© World Health Organization 2003
All rights reserved. Publications of the World Health Organization can be obtained from Marketingand Dissemination, World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel:+41 22 791 2476; fax: +41 22 791 4857; email: [email protected]). Requests for permission toreproduce or translate WHO publications – whether for sale or for noncommercial distribution –should be addressed to Publications, at the above address (fax: +41 22 791 4806; email:[email protected]).
The designations employed and the presentation of the material in this publication do not imply theexpression of any opinion whatsoever on the part of the World Health Organization concerning thelegal status of any country, territory, city or area or of its authorities, or concerning the delimitation ofits frontiers or boundaries. Dotted lines on maps represent approximate border lines for which theremay not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they areendorsed or recommended by the World Health Organization in preference to others of a similarnature that are not mentioned. Errors and omissions excepted, the names of proprietary productsare distinguished by initial capital letters.
The World Health Organization does not warrant that the information contained in this publication iscomplete and correct and shall not be liable for any damages incurred as a result of its use.
The named authors alone are responsible for the views expressed in each chapter of this publication.
Printed in
IIntroduction

2
SARAH BOTT AND SHIREEN J. JEJEEBHOY

3
Adolescent sexual and reproductive health in South Asia: an overview
in school, experiencing puberty at younger ages,marrying and having children later than in the past.Neglect of this population has major implicationsfor the future, since reproductive and sexualbehaviours during adolescence have far-reachingconsequences for people’s lives as they developinto adulthood.
In South Asia, by the end of the 1990s, bothresearchers and governments had begun to shedtheir traditional ambivalence towards youngpeople’s sexual and reproductive health, and agrowing body of empirical evidence and governmentinterest provided an opportunity to take stock ofthe sexual and reproductive health situation ofyouth in the region. In response, HRP1 , ISRRF2
and IRR3 jointly organized an internationalconference in November 2000 entitled: “AdolescentReproductive Health: Evidence and ProgrammeImplications for South Asia”, held in Mumbai, India.Although international organizations subdivide Asiain different ways, this conference focused on fiveSouth Asian countries, namely, Bangladesh, India,Nepal, Pakistan and Sri Lanka. Insights from otherAsian settings were also presented, notably fromChina and Thailand.
Conference background
The World Health Organization (WHO) definesadolescents as the age group 10–19, a definitionused throughout this volume. The meaning ofadolescence as a cultural construct has beenunderstood in many different ways throughout theworld, however. In general terms, it is considereda time of transition from childhood to adulthood,during which young people experience changesfollowing puberty, but do not immediately assumethe roles, privileges and responsibilities ofadulthood. The nature of adolescence variestremendously by age, sex, marital status, class,region and cultural context. As a group, however,adolescents have sexual and reproductive healthneeds that differ from those of adults in importantways and which remain poorly understood or servedin much of the world.
Moreover, social, economic and political forces arerapidly changing the ways that young people mustprepare for adult life. These changes haveenormous implications for adolescents’ education,employment, marriage, childbearing and health.Adolescents are increasingly spending more time
1 HRP stands for the UNDP/UNFPA/WHO/World Bank Special Programme of Research, Development and ResearchTraining in Human Reproduction.
2 ISRRF stands for the Indian Society for Research on Reproduction and Fertility.3 IRR stands for the Institute for Research in Reproduction.
Adolescent sexual and reproductive health inSouth Asia: an overview of findings from the2000 Mumbai conference
Sarah Bott and Shireen J. Jejeebhoy
4
SARAH BOTT AND SHIREEN J. JEJEEBHOY
The conference aimed to review the evidence onadolescents’ sexual and reproductive healthsituation, needs and perspectives in South Asia,to learn from programme successes and failuresin the region, and to identify acceptable yet effectiveways to respond to adolescents’ unique needs.The conference addressed a number of centralquestions, including: What are adolescents’ needsin regards to sexual and reproductive health? Howcan we increase their ability to make informedreproductive choices? How do we enhance theiraccess to reproductive health services that areacceptable, unthreatening, and affordable? Whatkind of information do they need in order toexercise these choices and access services? Howcan we tailor programmes to deliver informationand services? And, how can programmes improvecommunication between adolescents and adults?
This conference brought together researchers fromdifferent disciplines, as well as service providers,programme managers, government representa-tives, policy-makers, representatives frominternational and donor agencies and, mostimportantly, young people themselves. Participantscame from more than 13 countries, including SouthAsia, other Asian countries such as China,Indonesia, and Thailand, and countries beyond the
region such as Chile, Colombia, several Europeancountries and the United States of America. Theagenda included 42 full presentations, 12 briefabstract presentations, comments from ninediscussants and 72 poster presentations,supplemented by panel discussions among youngpeople themselves and policy-makers.
In an attempt to record the evidence and insightsthat emerged from the conference, organizersasked the conference participants to writesummaries of their presentations. As a result, thisvolume contains summaries of 40 of the 42 majorpresentations and two of the three panel sessions.This overview chapter provides a brief social anddemographic profile of adolescents in South Asia,together, where possible, with information on otherAsian countries—China, Indonesia, thePhilippines, Thailand and Viet Nam—to enablereaders to place South Asia within the larger Asiancontext. This is followed by a review of the entirecollection of papers contained in this volume.
Profile of adolescents in South Asia
Of the estimated 1.2 billion adolescents in the worldtoday, nearly half live in Asia, and nearly one in
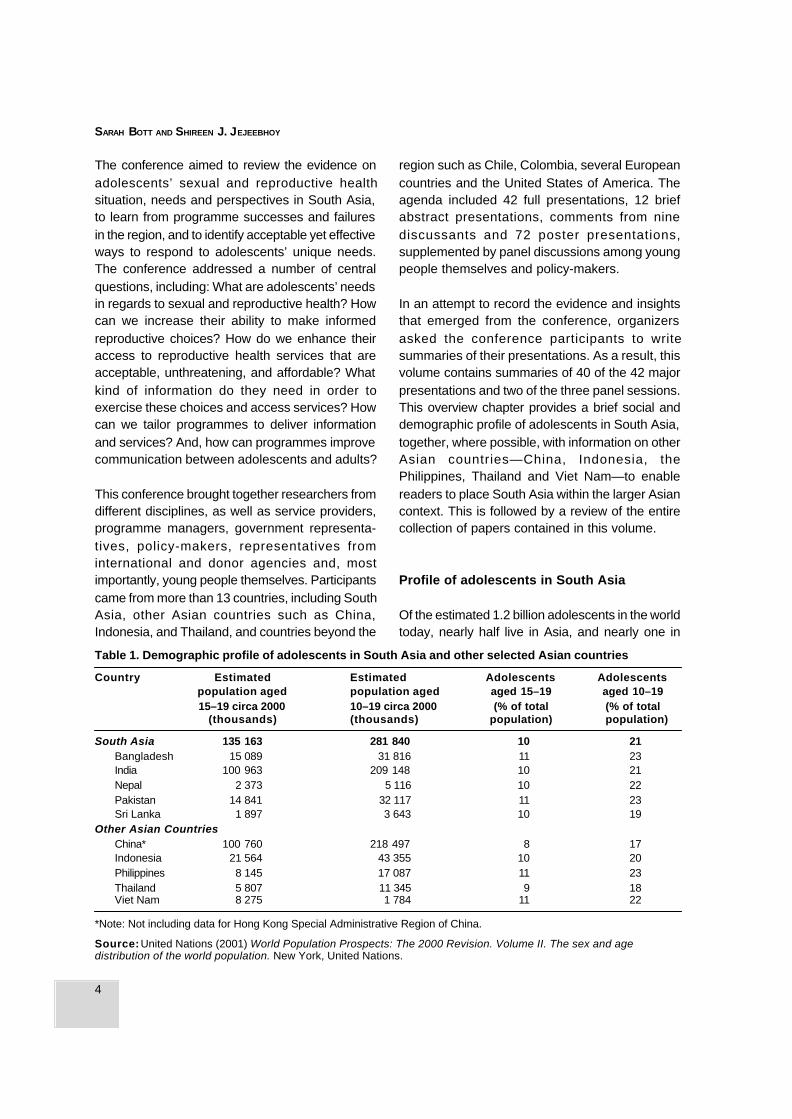
Table 1. Demographic profile of adolescents in South Asia and other selected Asian countries
Country Estimated Estimated Adolescents Adolescentspopulation aged population aged aged 15–19 aged 10–1915–19 circa 2000 10–19 circa 2000 (% of total (% of total
(thousands) (thousands) population) population)
South Asia 135 163 281 840 10 21Bangladesh 15 089 31 816 11 23India 100 963 209 148 10 21Nepal 2 373 5 116 10 22Pakistan 14 841 32 117 11 23Sri Lanka 1 897 3 643 10 19
Other Asian CountriesChina* 100 760 218 497 8 17Indonesia 21 564 43 355 10 20Philippines 8 145 17 087 11 23Thailand 5 807 11 345 9 18Viet Nam 8 275 1 784 11 22
*Note: Not including data for Hong Kong Special Administrative Region of China.
Source: United Nations (2001) World Population Prospects: The 2000 Revision. Volume II. The sex and agedistribution of the world population. New York, United Nations.
5
Adolescent sexual and reproductive health in South Asia: an overview
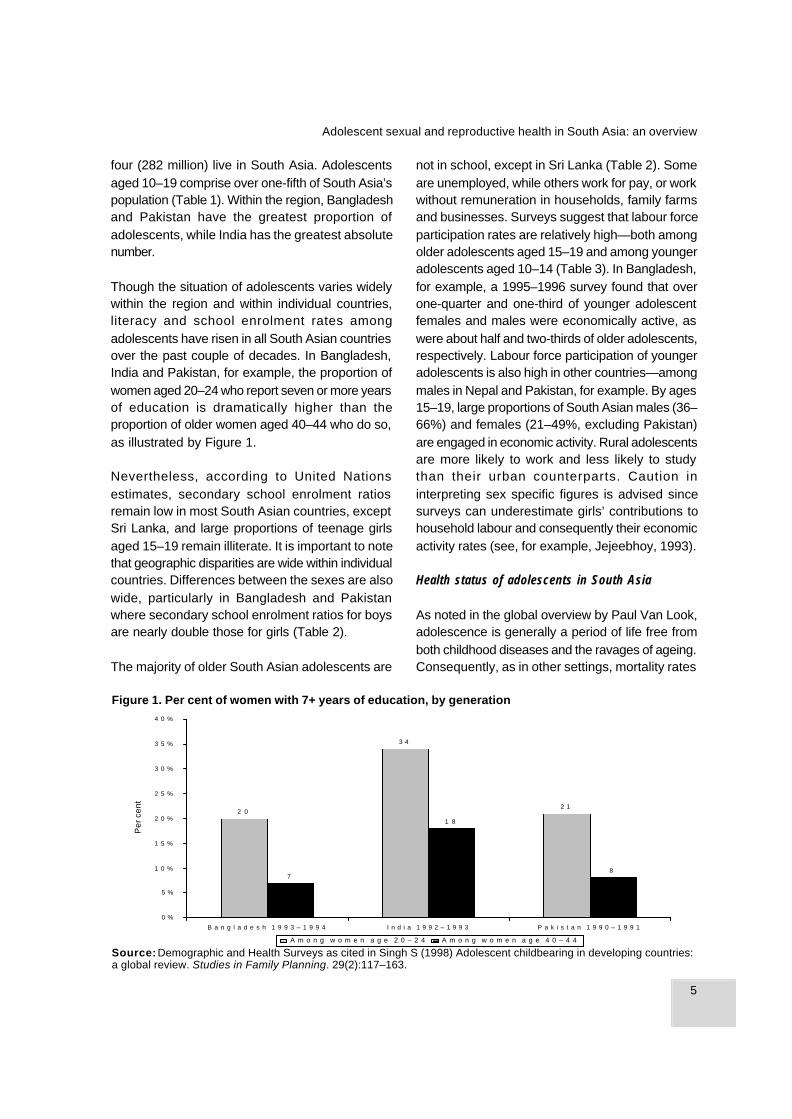
Figure 1. Per cent of women with 7+ years of education, by generation
four (282 million) live in South Asia. Adolescentsaged 10–19 comprise over one-fifth of South Asia’spopulation (Table 1). Within the region, Bangladeshand Pakistan have the greatest proportion ofadolescents, while India has the greatest absolutenumber.
Though the situation of adolescents varies widelywithin the region and within individual countries,literacy and school enrolment rates amongadolescents have risen in all South Asian countriesover the past couple of decades. In Bangladesh,India and Pakistan, for example, the proportion ofwomen aged 20–24 who report seven or more yearsof education is dramatically higher than theproportion of older women aged 40–44 who do so,as illustrated by Figure 1.
Nevertheless, according to United Nationsestimates, secondary school enrolment ratiosremain low in most South Asian countries, exceptSri Lanka, and large proportions of teenage girlsaged 15–19 remain illiterate. It is important to notethat geographic disparities are wide within individualcountries. Differences between the sexes are alsowide, particularly in Bangladesh and Pakistanwhere secondary school enrolment ratios for boysare nearly double those for girls (Table 2).
The majority of older South Asian adolescents are
not in school, except in Sri Lanka (Table 2). Someare unemployed, while others work for pay, or workwithout remuneration in households, family farmsand businesses. Surveys suggest that labour forceparticipation rates are relatively high—both amongolder adolescents aged 15–19 and among youngeradolescents aged 10–14 (Table 3). In Bangladesh,for example, a 1995–1996 survey found that overone-quarter and one-third of younger adolescentfemales and males were economically active, aswere about half and two-thirds of older adolescents,respectively. Labour force participation of youngeradolescents is also high in other countries—amongmales in Nepal and Pakistan, for example. By ages15–19, large proportions of South Asian males (36–66%) and females (21–49%, excluding Pakistan)are engaged in economic activity. Rural adolescentsare more likely to work and less likely to studythan their urban counterparts. Caution ininterpreting sex specific figures is advised sincesurveys can underestimate girls’ contributions tohousehold labour and consequently their economicactivity rates (see, for example, Jejeebhoy, 1993).
Health status of adolescents in South Asia
As noted in the global overview by Paul Van Look,adolescence is generally a period of life free fromboth childhood diseases and the ravages of ageing.Consequently, as in other settings, mortality rates
Source: Demographic and Health Surveys as cited in Singh S (1998) Adolescent childbearing in developing countries:a global review. Studies in Family Planning. 29(2):117–163.
2 1
3 4
2 0
8
1 8
7
0 %
5 %
1 0 %
1 5 %
2 0 %
2 5 %
3 0 %
3 5 %
4 0 %
B a n g l a d e s h 1 9 9 3 – 1 9 9 4 I n d i a 1 9 9 2 – 1 9 9 3 P a k i s t a n 1 9 9 0 – 1 9 9 1
Per
cen
t
A m o n g w o m e n a g e 2 0 – 2 4 A m o n g w o m e n a g e 4 0 – 4 4

6
SARAH BOTT AND SHIREEN J. JEJEEBHOY
* International Labour Organisation (1998) Yearbook of Labour Statistics 1998. Geneva, ILO.** International Labour Organisation (1999) Yearbook of Labour Statistics 1999. Geneva, ILO.***International Labour Organisation (2000) Yearbook of Labour Statistics 2000. Geneva, ILO.+ Aged 5–14; ++ aged 13–14.na: not available.
among adolescents and young people in thisregion are generally lower than those observed atyounger and older ages. However, unlike in othercountries, adolescent and young women in the
countries of South Asia, with the exception of SriLanka, experience somewhat higher mortality ratesthan males at the same ages (Table 4). Disparitiesare particularly evident among young people aged
Table 3. Labour force participation rates of adolescents and youth by sex and age group
Females (%) Males (%)
Aged Aged Aged Aged Aged AgedCountry and year 10–14 15–19 20–24 10–14 15–19 20–24
South Asia
Bangladesh (1995–96)* 28.1 47.8 58.7 37.8 65.5 82.0
India (1991)* 5.1+ 26.2 33.5 5.7+ 43.8 74.7
Nepal (1991)* 28.0 49.0 54.0 18.1 49.2 80.0
Pakistan (1999)** 5.8 9.6 11.7 16.5 51.1 85.5
Sri Lanka (1999)*** 3.1 21.2 50.6 3.3 35.8 87.1
Other Asian countries
China (1990)* na 68.3 89.6 na 61.5 92.6
Indonesia (1999)*** na 90.6 53.8 na 45.5 33.6
Philippines (1999)*** na 25.8 52.7 na 45.1 81.0
Thailand (1999)*** 8.3++ 29.1 67.9 9.0++ 37.7 77.9
Viet Nam (1989)* 37.4++ 73.3 88.8 29.5++ 67.4 94.4
Table 2. Secondary school enrolment and illiteracy rates among adolescents in South Asia and otherselected Asian countries, 1995–1997
Secondary school enrolment Per cent of teens aged 15–19ratios (% of # enrolled who are illiterate
to # in applicable age groups
Country Boys Girls Boys Girls
South AsiaBangladesh 25 13 58 71India 59 39 20 44Nepal 51 33 26 51Pakistan 33 17 56 74Sri Lanka 72 78 9 10
Other Asian CountriesChina 74 67 3 8Indonesia 55 48 2 3Philippines 77 78 4 1Thailand 38 37 1 2Viet Nam 48 46 7 7
Source: Population Reference Bureau (2000) The World’s Youth 2000. Washington, DC, Population ReferenceBureau, Measure Communication.
7
Adolescent sexual and reproductive health in South Asia: an overview
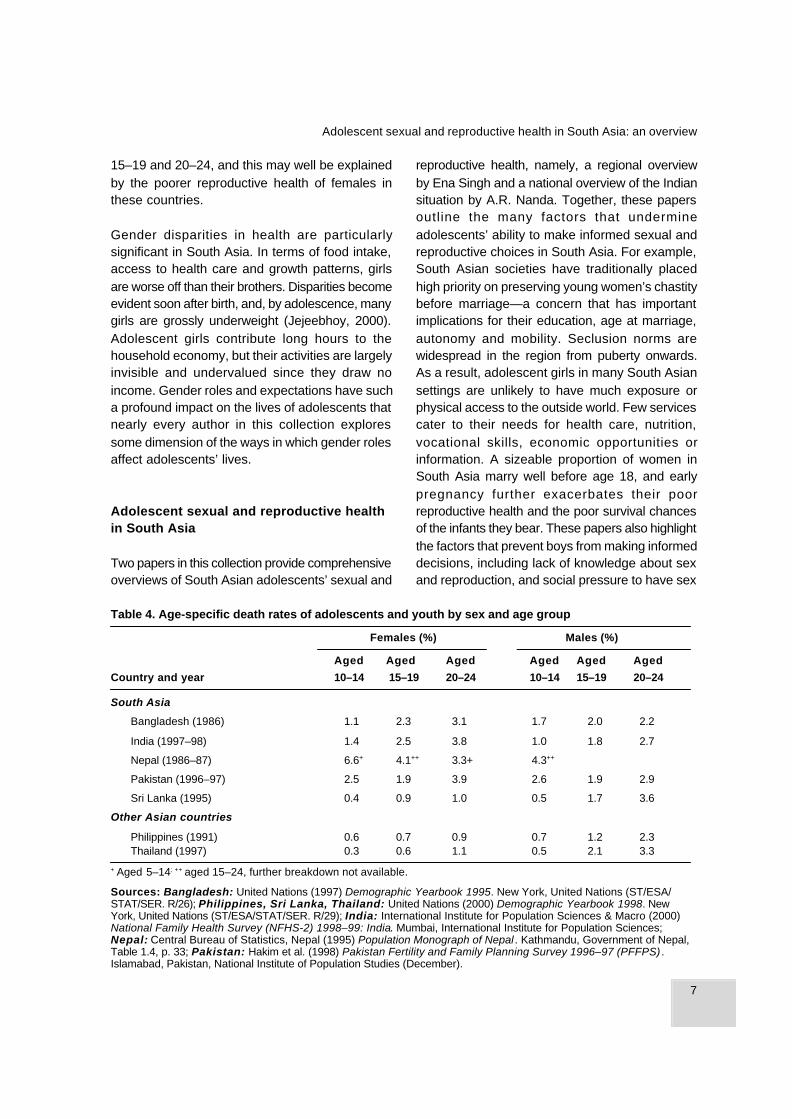
15–19 and 20–24, and this may well be explainedby the poorer reproductive health of females inthese countries.
Gender disparities in health are particularlysignificant in South Asia. In terms of food intake,access to health care and growth patterns, girlsare worse off than their brothers. Disparities becomeevident soon after birth, and, by adolescence, manygirls are grossly underweight (Jejeebhoy, 2000).Adolescent girls contribute long hours to thehousehold economy, but their activities are largelyinvisible and undervalued since they draw noincome. Gender roles and expectations have sucha profound impact on the lives of adolescents thatnearly every author in this collection exploressome dimension of the ways in which gender rolesaffect adolescents’ lives.
Adolescent sexual and reproductive healthin South Asia
Two papers in this collection provide comprehensiveoverviews of South Asian adolescents’ sexual and
reproductive health, namely, a regional overviewby Ena Singh and a national overview of the Indiansituation by A.R. Nanda. Together, these papersoutline the many factors that undermineadolescents’ ability to make informed sexual andreproductive choices in South Asia. For example,South Asian societies have traditionally placedhigh priority on preserving young women’s chastitybefore marriage—a concern that has importantimplications for their education, age at marriage,autonomy and mobility. Seclusion norms arewidespread in the region from puberty onwards.As a result, adolescent girls in many South Asiansettings are unlikely to have much exposure orphysical access to the outside world. Few servicescater to their needs for health care, nutrition,vocational skills, economic opportunities orinformation. A sizeable proportion of women inSouth Asia marry well before age 18, and earlypregnancy further exacerbates their poorreproductive health and the poor survival chancesof the infants they bear. These papers also highlightthe factors that prevent boys from making informeddecisions, including lack of knowledge about sexand reproduction, and social pressure to have sex
+ Aged 5–14; ++ aged 15–24, further breakdown not available.
Sources: Bangladesh: United Nations (1997) Demographic Yearbook 1995. New York, United Nations (ST/ESA/STAT/SER. R/26); Philippines, Sri Lanka, Thailand: United Nations (2000) Demographic Yearbook 1998. NewYork, United Nations (ST/ESA/STAT/SER. R/29); India: International Institute for Population Sciences & Macro (2000)National Family Health Survey (NFHS-2) 1998–99: India. Mumbai, International Institute for Population Sciences;Nepal: Central Bureau of Statistics, Nepal (1995) Population Monograph of Nepal . Kathmandu, Government of Nepal,Table 1.4, p. 33; Pakistan: Hakim et al. (1998) Pakistan Fertility and Family Planning Survey 1996–97 (PFFPS) .Islamabad, Pakistan, National Institute of Population Studies (December).
Table 4. Age-specific death rates of adolescents and youth by sex and age group
Females (%) Males (%)
Aged Aged Aged Aged Aged Aged
Country and year 10–14 15–19 20–24 10–14 15–19 20–24
South Asia
Bangladesh (1986) 1.1 2.3 3.1 1.7 2.0 2.2
India (1997–98) 1.4 2.5 3.8 1.0 1.8 2.7
Nepal (1986–87) 6.6+ 4.1++ 3.3+ 4.3++
Pakistan (1996–97) 2.5 1.9 3.9 2.6 1.9 2.9
Sri Lanka (1995) 0.4 0.9 1.0 0.5 1.7 3.6
Other Asian countries
Philippines (1991) 0.6 0.7 0.9 0.7 1.2 2.3Thailand (1997) 0.3 0.6 1.1 0.5 2.1 3.3
8
SARAH BOTT AND SHIREEN J. JEJEEBHOY
9
20
14
31
12
60
32
50
73
0%
10%
20%
30%
40%
50%
60%
70%
80%
Bangladesh93-4
India 98-9
Pakistan90-1
Nepal 96
Sri Lanka 93
Indonesia94
Philippines93
Thailand 87
Viet Nam 98
Per
cen
t
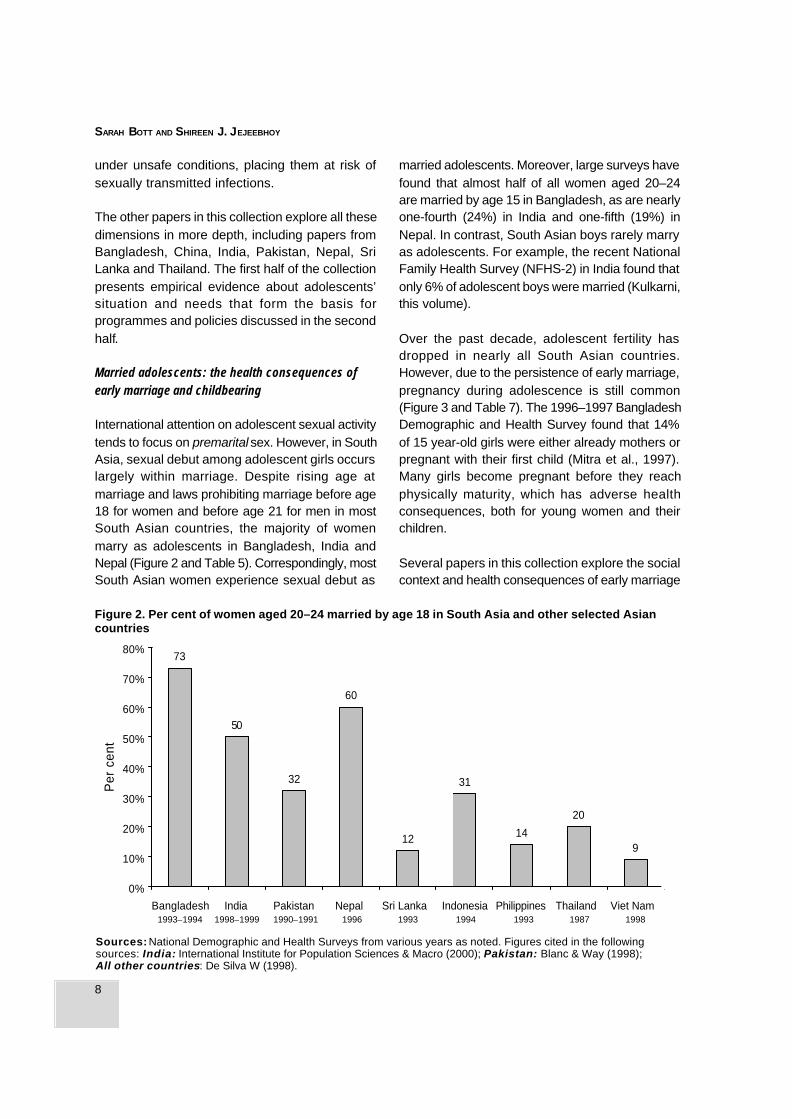
Figure 2. Per cent of women aged 20–24 married by age 18 in South Asia and other selected Asiancountries
Sources: National Demographic and Health Surveys from various years as noted. Figures cited in the followingsources: India: International Institute for Population Sciences & Macro (2000); Pakistan: Blanc & Way (1998);All other countries: De Silva W (1998).
under unsafe conditions, placing them at risk ofsexually transmitted infections.
The other papers in this collection explore all thesedimensions in more depth, including papers fromBangladesh, China, India, Pakistan, Nepal, SriLanka and Thailand. The first half of the collectionpresents empirical evidence about adolescents’situation and needs that form the basis forprogrammes and policies discussed in the secondhalf.
Married adolescents: the health consequences ofearly marriage and childbearing
International attention on adolescent sexual activitytends to focus on premarital sex. However, in SouthAsia, sexual debut among adolescent girls occurslargely within marriage. Despite rising age atmarriage and laws prohibiting marriage before age18 for women and before age 21 for men in mostSouth Asian countries, the majority of womenmarry as adolescents in Bangladesh, India andNepal (Figure 2 and Table 5). Correspondingly, mostSouth Asian women experience sexual debut as
married adolescents. Moreover, large surveys havefound that almost half of all women aged 20–24are married by age 15 in Bangladesh, as are nearlyone-fourth (24%) in India and one-fifth (19%) inNepal. In contrast, South Asian boys rarely marryas adolescents. For example, the recent NationalFamily Health Survey (NFHS-2) in India found thatonly 6% of adolescent boys were married (Kulkarni,this volume).
Over the past decade, adolescent fertility hasdropped in nearly all South Asian countries.However, due to the persistence of early marriage,pregnancy during adolescence is still common(Figure 3 and Table 7). The 1996–1997 BangladeshDemographic and Health Survey found that 14%of 15 year-old girls were either already mothers orpregnant with their first child (Mitra et al., 1997).Many girls become pregnant before they reachphysically maturity, which has adverse healthconsequences, both for young women and theirchildren.
Several papers in this collection explore the socialcontext and health consequences of early marriage
1993–1994 1998–1999 1990–1991 1996 1993 1994 1993 1987 1998
9
Adolescent sexual and reproductive health in South Asia: an overview
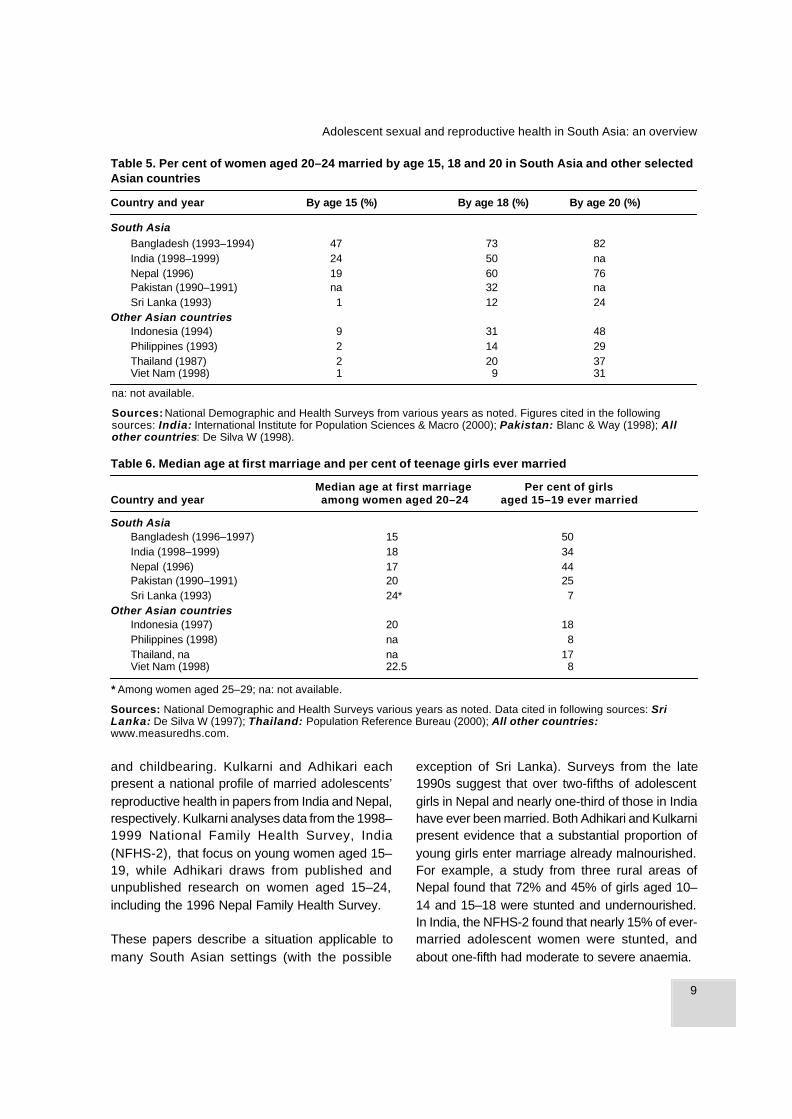
Table 5. Per cent of women aged 20–24 married by age 15, 18 and 20 in South Asia and other selectedAsian countries
Country and year By age 15 (%) By age 18 (%) By age 20 (%)
South AsiaBangladesh (1993–1994) 47 73 82India (1998–1999) 24 50 naNepal (1996) 19 60 76Pakistan (1990–1991) na 32 naSri Lanka (1993) 1 12 24
Other Asian countriesIndonesia (1994) 9 31 48Philippines (1993) 2 14 29Thailand (1987) 2 20 37Viet Nam (1998) 1 9 31
na: not available.
Sources: National Demographic and Health Surveys from various years as noted. Figures cited in the followingsources: India: International Institute for Population Sciences & Macro (2000); Pakistan: Blanc & Way (1998); Allother countries: De Silva W (1998).
Table 6. Median age at first marriage and per cent of teenage girls ever married
Median age at first marriage Per cent of girlsCountry and year among women aged 20–24 aged 15–19 ever married
South AsiaBangladesh (1996–1997) 15 50India (1998–1999) 18 34Nepal (1996) 17 44Pakistan (1990–1991) 20 25Sri Lanka (1993) 24* 7
Other Asian countriesIndonesia (1997) 20 18Philippines (1998) na 8Thailand, na na 17Viet Nam (1998) 22.5 8
* Among women aged 25–29; na: not available.
Sources: National Demographic and Health Surveys various years as noted. Data cited in following sources: SriLanka: De Silva W (1997); Thailand: Population Reference Bureau (2000); All other countries:www.measuredhs.com.
and childbearing. Kulkarni and Adhikari eachpresent a national profile of married adolescents’reproductive health in papers from India and Nepal,respectively. Kulkarni analyses data from the 1998–1999 National Family Health Survey, India(NFHS-2), that focus on young women aged 15–19, while Adhikari draws from published andunpublished research on women aged 15–24,including the 1996 Nepal Family Health Survey.
These papers describe a situation applicable tomany South Asian settings (with the possible
exception of Sri Lanka). Surveys from the late1990s suggest that over two-fifths of adolescentgirls in Nepal and nearly one-third of those in Indiahave ever been married. Both Adhikari and Kulkarnipresent evidence that a substantial proportion ofyoung girls enter marriage already malnourished.For example, a study from three rural areas ofNepal found that 72% and 45% of girls aged 10–14 and 15–18 were stunted and undernourished.In India, the NFHS-2 found that nearly 15% of ever-married adolescent women were stunted, andabout one-fifth had moderate to severe anaemia.

10
SARAH BOTT AND SHIREEN J. JEJEEBHOY
Figure 3. Per cent of married women aged 20–24 who gave birth by age 20, from national surveys in the1990s.
Source: Population Reference Bureau (2000) The World’s Youth 2000. Washington, DC, Population ReferenceBureau, Measure Communication.
Table 7.Childbearing among adolescents in South Asia and other selected Asian countries
Per cent of Per cent of TFR Teenage fertility Per cent of birthswomen aged attributed to rate (births per to women aged 15–
20–24 who births by 1000 girls 19 attended bygave birth by mothers aged aged 15–19) trained personnel*
Country aged 20* 15–19* circa 1999**
South AsiaBangladesh 63 18 140 14India 49 18 107 34Nepal 52 13 117 14Pakistan 31 9 100 17Sri Lanka 16 5 21 82
Other Asian countriesChina 8 1 15 naIndonesia 31 11 57 32Philippines 21 6 43 51Thailand 24 20 76 61Viet Nam 19 5 na 76
na: not available; TFR: total fertility rate
Sources: *Population Reference Bureau (2000) The World’s Youth 2000. Washington, DC, Population Reference Bureau,Measure Communication. **World Bank (2001) World Development Indicators. Washington, DC, World Bank.
The combination of poor nutrition and earlychildbearing expose young women to serioushealth risks during pregnancy and childbirth,including damage to the reproductive tract, maternalmortality, pregnancy complications, perinatal andneonatal mortality and low birth weight.International analyses suggest that, at the globallevel, girls aged 15–19 are twice as likely to diefrom childbirth as are women in their twenties, while
girls younger than age 15 face a risk that is fivetimes as great (United Nations Children’s Fund,2001). These sources report that more adolescentgirls die from pregnancy-related causes than fromany other cause (Population Reference Bureau,2000). Kulkarni and Adhikari support such findingswith data from India and Nepal. For example, studiesfrom Nepal found higher rates of obstetric morbidityamong adolescents than among adult women, as
16
31
5249
63
0%
10%
20%
30%
40%
50%
60%
70%
Bangladesh India Nepal Pakistan Sri Lanka
Per
cen
t

11
Adolescent sexual and reproductive health in South Asia: an overview
well as a 25–66% higher incidence of low birthweight among children of adolescent mothers. Bothauthors report considerably higher rates of neonataland infant mortality among children of adolescentmothers. Despite greater risks, both authors citeevidence that adolescents do not receive moreantenatal or intrapartum care than older women.Adhikari argues that adolescent girls in Nepalactually receive less prenatal care than olderwomen.
The social context of early marriage
Within the age- and gender-stratified familystructure that characterizes much of South Asia,young, newly married women are particularlypowerless. The average adolescent bride is unlikelyto have had a say in the decision about whom orwhen to marry, whether or not to have sexualrelations, and when to bear children. On thecontrary, society often places strong pressures onyoung women to prove their fertility, and, in manysettings, bearing sons is the only means by whichyoung women can establish social acceptance andeconomic security in their marital homes. Lack ofautonomy within their marital homes often meansthat married girls have limited access to healthcare or participation in decisions about their ownhealth. For example, Kulkarni notes that in someIndian states, such as Maharashtra and MadhyaPradesh, fewer than one-third of adolescent womensurveyed reported any involvement in decision-making about their own health.
Two papers in this collection focus on the socialcontext of married adolescents. Both Chowdhury(Bangladesh) and George (India) present qualitativefindings from small-scale, in-depth studies withselect groups. Findings from these studies are notnecessarily representative of larger populations,but they provide an important complement to thequantitative evidence, by describing experiencesof new wives and mothers in their own words.
George highlights young wives’ lack of sexualautonomy in a review of two qualitative studiesamong poor urban women in India. Those studies
gathered retrospective data from women whomarried as adolescents. Most women in thesestudies reported that they were unprepared for, andignorant about, sexual intercourse until the firstnight with their husbands. Many experienced someform of sexual coercion, and many described theirfirst sexual experience as traumatic, distasteful,painful and involving the use of physical force.
Chowdhury presents preliminary findings from astudy on first-time parents in Bangladesh. Womenreported that they did not have a choice as to whomor when to marry, or when to begin childbearing.As echoed by many papers in this collection (forexample, see Rashid), many male and femalerespondents told researchers that they would haveliked to have waited longer before getting married.Lack of decision-making authority permeated allaspects of young women’s lives—including foodintake during pregnancy, workload, mobility, andaccess to health care. Young women reportedheavy workloads during pregnancy, which onlyincreased after the birth of their child, and someexpressed great unhappiness about their situation.
Other papers in this collection explore the contextof early marriage as one among many issues thatconcern adolescents. Though it was not the centralfocus of their research, Waszak, Thapa and Daveydescribe similar experiences involving youngmarried women in Nepal, based on 71 focus groupdiscussions. Young women suggested that youngpregnant girls often have low priority when food isdistributed in their husbands’ family. Heavyworkloads are common and supported by localbeliefs such as: “the more you work, the lighteryour body becomes and easier it is at delivery”.Newly married girls are expected to tolerate sexualcoercion from their husbands, to prove their fertilityas soon as possible after marriage, and to allowfamily elders to limit their food intake and healthcare during pregnancy.
Many authors in this collection argue that girls whopostpone marriage and stay in school longer arebetter off than those who marry early. This is notonly because they will reach physical maturity

12
SARAH BOTT AND SHIREEN J. JEJEEBHOY
before childbearing, but also because they maybe better able to negotiate with their in-laws andvoice their own needs.
Social and economic factors behind earlymarriage
Many papers in this collection examine why earlymarriage persists in South Asia. Again, suchresearch findings tend to emerge from qualitativestudies that cannot be generalized to thetremendously diverse population of South Asia asa whole. Furthermore, it is important to note thatmarriage trends are in flux, and average age atwhich girls marry in South Asia is rising.Nevertheless, this collection of studies offersimportant insights into the factors that contributeto early marriage among girls—in the words of bothadolescents and their parents.
Rashid presents findings that emerged from focusgroup discussions in the Nilphamari district ofBangladesh. In this district, girls still marry asyoung as age 11. Mothers explained that the mainreason for early marriage was parents’ fear thatdaughters would be raped, become pregnant orelope. The knowledge that a girl has had premaritalsex (even resulting from rape) can ruin the statusand reputation of the entire family. Respondentssuggest that attitudes towards early marriage maybe changing, as parents increasingly appreciatethe value of education and the negative healthconsequences of early childbearing. Nevertheless,they noted that parents who wait too long to marrytheir daughters often face community pressure,including derogatory comments from communityelders. Chowdhury also cites evidence that earlymarriage of girls in Bangladesh may stem fromfinancial pressures, a father’s death or a large ofnumber of daughters.
Waszak, Thapa and Davey analysed focus groupdiscussions (FGDs) held in 11 districts in Nepal.During FGDs stratified by age, sex, marital statusand residence, researchers explored gender normsthat affect work, education, marriage andchildbearing among young people aged 14–22. On
the one hand, respondents suggested that familieshave increasingly recognized the benefits ofeducation for girls (though parents still generallyinvest more resources in sons). On the other hand,families face social pressure to marry theirdaughters early as a way to protect their“character”. The longer a girl stays at home, thelonger she is at risk of running away or having alove marriage—all of which could bring dishonouron the family. Adolescents described norms thatcondone premarital sexual activity among boys,but ruin girls who do the same. Parents’ fear abouttheir daughters’ sexual chastity often pressuresthem to end their schooling and arrange earlymarriages. Marriage usually ends a girls’education, because her increased householdresponsibilities are generally incompatible withattending school. The respondents also describedhow gender norms pose different challenges foryoung men. Pressure to achieve financial stabilitybefore marriage often forces them to delaymarriage, increasing pressures and opportunitiesfor young men to engage in unsafe sexual activity.
Attitudes and risk behaviours of unmarriedadolescents
Given highly conservative attitudes about sex inSouth Asia, few studies have successfully elicitedinformation on sexual behaviour. Most explorepremarital rather than marital sex, men’s behaviourrather than women’s, and young people’s currentexperiences or retrospective experiences of adults.Samples tend to be small and drawn from urbanareas rather than rural communities or slums.Results, therefore, tend to be unrepresentative ofthe general population. While generalization isdifficult, findings of the few available studies (seefor example, Jejeebhoy, 2000, for India; or Abraham,this volume) generally suggest that between 20%and 30% of young men and between 0% and 10%of young women report premarital sexualexperience. Sexual initiation occurs earlier thanmany assume, and is often unplanned andunprotected. Moreover, as noted in many papersin this volume, substantial proportions of youngmen report having sex with sex workers—usuallywithout condoms.

13
Adolescent sexual and reproductive health in South Asia: an overview
Several papers in this collection present findingson the sexual behaviour and attitudes of SouthAsian adolescents before marriage, includingstudies from Bangladesh, India, Nepal, Pakistanand Sri Lanka. Understandably, these studies arequite diverse, having used different methodologiesamong diverse populations. Study populationsincluded low-income urban college students inIndia, young people from provincial settings inPakistan and a nationwide sample in Nepal.Methodologies ranged from a combination ofqualitative and quantitative in India and Sri Lanka,to a pilot survey in Pakistan, and focus groupdiscussions in Nepal and Bangladesh.
Studies suggest that most South Asianadolescents have conservative attitudes towardsmarriage and sex. For example, in studies fromBangladesh, Nepal and Sri Lanka, young peopletold researchers that they generally disapprove oflove marriages, premarital sex (particularly bygirls), and often for that matter, social interactionbetween unrelated women and men. In somecases even the hint of a friendship with a boy canruin a girl’s reputation, her marriage prospects andthe social status of her entire family. While fewstudies have considered social constraints onadolescent boys, it is clear that their behaviour isless closely supervised than that of girls. Manyyoung people feel that society condones premaritalsexual activity among boys and even puts socialpressure on boys to become sexually active at anearly age.
Rashid presents findings from discussions withadolescents in Bangladesh about love andromance. Most adolescents did not approve of“love” (prem) and instead felt that young peopleshould marry whomever their parents chose forthem. They described heavy sanctions andpunishments that befall girls discovered to beinvolved in sexual relationships. Nevertheless,some respondents expressed attitudes that—inthe author’s view—were “considered unthinkablefor previous generations”. For example, some hadsecretly fallen “in love”. Many distinguishedbetween “pure” love as a relationship that leads to
marriage, and “impure” love as a relationship thatdoes not lead to marriage or involves sex.
Abraham presents focus group discussion andsurvey data gathered among low-income, urbancollege students aged 16–18 and 20–22 inMumbai. Young respondents reported friendshipswith members of the opposite sex, despite strongparental disapproval of such behaviour. The authordescribes different categories of friendship,including platonic (bhai-behen), romantic with theintention of marriage (“true love”) and transitorysexual relationships (“time pass”). The boundariesof these categories are fuzzy, as is the extent ofphysical intimacy. Authors note that manyresearchers have not adequately explored differentkinds of sexual activity. While only 26% of youngmen and 3% of young women reported penetrativesex, as many as 49% and 13%, respectively,reported other forms of physical intimacy. Youngwomen almost unanimously reported monogamousand committed relationships. By contrast, youngmen reported a range of partners, including sexworkers and “aunties” (older married women in theneighbourhood).
Silva and Schensul report considerable premaritalrelationships between young men and women inSri Lanka, according to survey data gatheredamong low-income youth and university studentsaged 17–28. Contrary to what the authorsexpected, this study found that university studentswere somewhat more likely than less educatedyoung people to oppose premarital sex amongwomen. Similar to the study among Indian collegestudents, young men were considerably morelikely than young women to approve of premaritalsexual activity. Unlike the Indian case, however,differences between women and men reporting a“love partner” (not necessarily a sexual partner)were marginal. Over 50% of both young womenand young men reported having such a partner.This study found that young people generallypreferred behaviours perceived to protect femalevirginity, such as inter-femoral and other forms ofnon-penetrative sex. Even so, as in India, a large

14
SARAH BOTT AND SHIREEN J. JEJEEBHOY
number of young boys and men reported sexualrelations with commercial sex workers.
Bhuiya and colleagues present findings from acommunity-based survey in two rural sites inBangladesh, which found relatively lower rates ofpremarital sexual activity among 2626 unmarriedadolescents aged 13–19. In this study, 9% of 1462boys and three of 1164 girls had ever engaged inpremarital sexual relations. (Two of the three girlsreported forced sex.) Once again, evidencesuggests that sexual relations are often unsafeand sometimes non-consensual. Two-fifths of thesexually experienced males reported sex withcommercial sex workers. Less than one-quarterof sexually experienced males reported condomuse at first sex. Twelve per cent reported a sexuallytransmitted infection (STI) symptom in the previoussix months, and 6% (7 adolescents) reported havingexperienced coerced sex.
Non-consensual sexual activity among adolescents
As a taboo subject, sexual violence is rarelyreported or studied. Hence it is difficult to estimatehow many young people suffer from sexual abuse,violence, coercion, incest, rape or sexualtrafficking. Nevertheless, evidence suggests thata disturbingly large number of adolescent girls andboys are subjected to coercion in South Asia.Several small studies suggest that sexual coercionand rape often occur within marriage, andadolescents may be more likely to experience suchviolence than older women. Sexual coercion canhave considerable health consequences, includingsequelae related to unsafe abortion.
Many papers in this collection cite evidence ofsexual coercion against young people, includingWaszak, Thapa and Davey (Nepal), George (India),Bhuiya et al. (Bangladesh), and Qazi (Pakistan).Three papers from India explore sexual coercionin more depth, including papers by Ramakrishnaet al. among street boys in Bangalore, by Sodhiand Verma among young people in a low-incomearea of Delhi, and by Patel et al. among school-going adolescents in Goa. None of these studies
was designed to explore sexual coercionexclusively; instead they focused on coercion asone of several risk behaviours. Given the sensitivenature of the topic, researchers typically learnedthe most about these experiences from in-depthinterviews rather than surveys.
As one might expect, evidence suggests that streetchildren are highly vulnerable to coercion.Ramakrishna and colleagues offer insight into thecontext of coercion among street boys inBangalore, a city with an estimated 85 000–100 000 street children. Using a variety ofqualitative methods and sample recruitmentstrategies, their study found that some 74 of 121street boys aged 9–21 were sexually experienced.Forty had their first sexual experience by age 12.A large proportion of boys reported coerciveexperiences, both as victims and perpetrators,often involving exchange of money, gifts or otherfavours, as well as physical force. Sexual coercionis so pervasive on the streets that street boysrated rape and forced sex as among the mostp leasurab le ways o f seek ing sexua lgrat i f icat ion. Authors argue that socia lcondit ions, poverty and drug use shapeconcepts of sexuality and coercion amongstreet boys.
Sodhi and Verma’s study among low-incomeadolescents in Delhi, India, supplements this profileof coercion. During 71 in-depth interviews withyouth, respondents described widespread verbalharassment of women as well as 32 instances ofsexual coercion, including forced sex. Both girlsand boys reported experiences of coercion,including cases in which girls were forced toengage in sex against their will, sometimes withmultiple partners. Double standards are pervasive,and young women who experience forced sex oftenface severe reprisals should their experience bedisclosed. Some are even forced to continuecoercive relationships under threat of disclosurefrom the perpetrator. Echoing other studies in thiscollection, young married women also reportedwidespread marital rape, which they tended to viewas “normal” male behaviour.

15
Adolescent sexual and reproductive health in South Asia: an overview
Patel and colleagues present the findings of asurvey that explored the prevalence andconsequences of abuse and violence among 811students in the first year of higher secondary school(average age 16). Researchers asked adolescentsabout forced or unwanted verbal or physical sexualcoercion in the last 12 months. As many as one-third of students—both male and female—reporteda coercive experience in the past year, and 6%reported forced sexual intercourse. Nearly half ofall adolescents who experienced coercion reportedmore than one such experience. Students andfriends were the most commonly reportedperpetrators, followed by strangers, neighbours andothers; abuse by parents and teachers was alsoreported. Most suffered the abuse in silence. Theauthors found strong associations between forcedsex and and a number of variables, including poorschool performance, self-reported mental andphysical health and subsequent consensual sexualrelations.
Together these studies suggest that for many youngpeople, homes, schools and neighbourhoods do notprovide a safe and supportive environment. Societalnorms and double standards often perpetuateviolence by condoning harassment and abuseperpetrated by young men, while blaming victims.Their findings suggests that researchers andservice providers need to pay more attention tofactors such as violence and sexual abuse thatimpact young people’s mental and emotionalhealth.
Adolescents’ use of condoms and contraceptives
In light of evidence that substantial proportions ofSouth Asian adolescents are sexually active, manypapers in this collection explored the extent towhich adolescents take measures to protectthemselves from unwanted pregnancy and STIs.At the global level, adolescents are far less likelythan adults to use contraception, either in or outof marriage. Not all contraceptive methods aresuitable for adolescents, and those that areappropriate may be inaccessible or simplyunavailable. Not surprisingly therefore, a
substantial proportion of sexually activeadolescents—both married and unmarried—havean unmet need for contraception and are at risk ofSTIs, including HIV/AIDS.
While an array of contraceptive methods exists,evidence of their suitability, safety and efficacyamong adolescents is incomplete. Questionsremain about their clinical performance and theireffects on adolescents who have not reachedphysical maturity. Meirik reviews the existingliterature on these issues, which suggests thatcertain methods, such as Depot-medroxyprogestrone acetate (DMPA) and theintrauterine device (IUD), are not advisable foradolescents. While evidence is still inconclusive,some data suggest that DMPA may reduceadolescents’ bone mass, thereby increasing therisk of fracture later in life. Concerns about theIUD arise from its possible link with increased riskof pelvic inflammatory disease (PID), to whichyoung women are at higher risk than adult women.In contrast, recent evidence demonstrates thatcombined oral contraceptives do not adverselyaffect either the maturation of the hypothalamic-pituitary-ovarian system or the risk of breast cancerlater in life, as was previously feared. The authorargues that combined oral contraceptives andmale condoms are clearly safe for adolescents.However, he notes that only condoms offer dualprotection against unwanted pregnancy and STIs,including HIV.
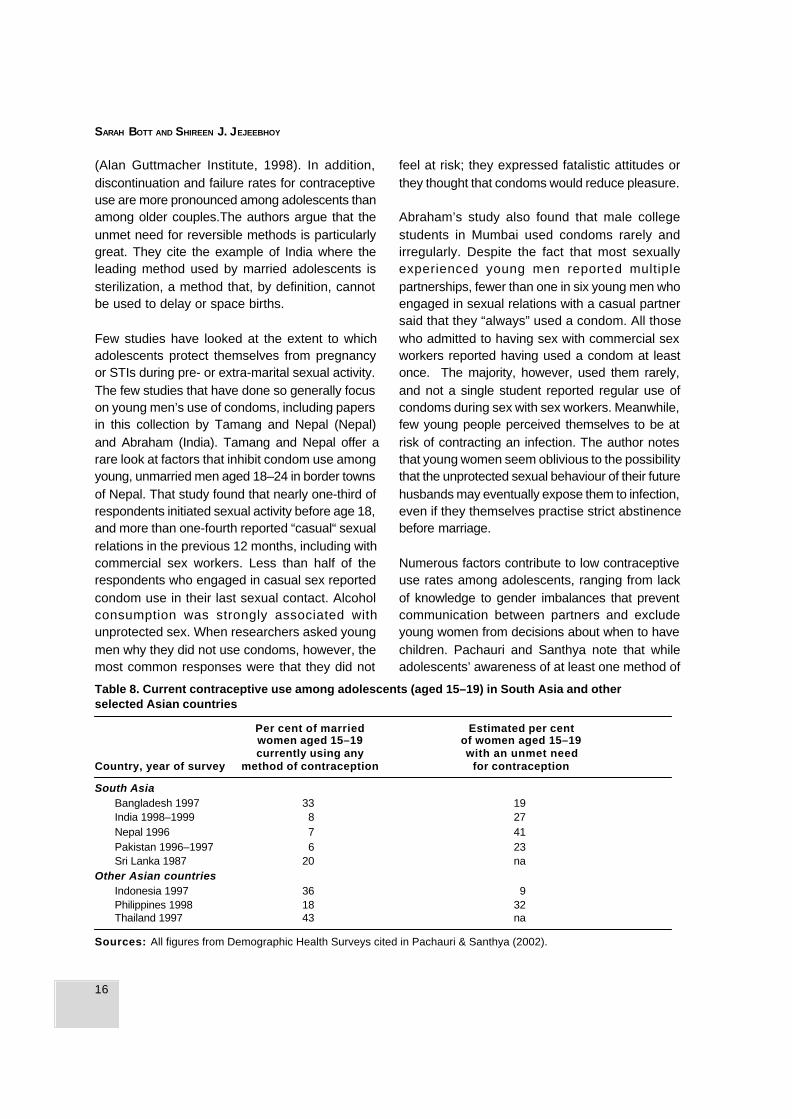
Pachauri and Santhya’s review of available dataon married adolescents’ contraceptive use in SouthAsia confirms that the proportion of marriedadolescents who use contraception in thesecountries remains low, even though significantminorities of young women say they want to delayor space births. In large surveys, 41% of sexuallyactive married adolescents aged 15–19 in Nepalreported an unmet need, as did 16% inBangladesh, 14% in India and 8% in Pakistan(Table 8). In India, Nepal and Pakistan, fewer than10% of married adolescent women or their partnerspractise contraception, compared to about one-quarter in Bangladesh and one-fifth in Sri Lanka
16
SARAH BOTT AND SHIREEN J. JEJEEBHOY
(Alan Guttmacher Institute, 1998). In addition,discontinuation and failure rates for contraceptiveuse are more pronounced among adolescents thanamong older couples.The authors argue that theunmet need for reversible methods is particularlygreat. They cite the example of India where theleading method used by married adolescents issterilization, a method that, by definition, cannotbe used to delay or space births.
Few studies have looked at the extent to whichadolescents protect themselves from pregnancyor STIs during pre- or extra-marital sexual activity.The few studies that have done so generally focuson young men’s use of condoms, including papersin this collection by Tamang and Nepal (Nepal)and Abraham (India). Tamang and Nepal offer arare look at factors that inhibit condom use amongyoung, unmarried men aged 18–24 in border townsof Nepal. That study found that nearly one-third ofrespondents initiated sexual activity before age 18,and more than one-fourth reported “casual“ sexualrelations in the previous 12 months, including withcommercial sex workers. Less than half of therespondents who engaged in casual sex reportedcondom use in their last sexual contact. Alcoholconsumption was strongly associated withunprotected sex. When researchers asked youngmen why they did not use condoms, however, themost common responses were that they did not
feel at risk; they expressed fatalistic attitudes orthey thought that condoms would reduce pleasure.
Abraham’s study also found that male collegestudents in Mumbai used condoms rarely andirregularly. Despite the fact that most sexuallyexperienced young men reported multiplepartnerships, fewer than one in six young men whoengaged in sexual relations with a casual partnersaid that they “always” used a condom. All thosewho admitted to having sex with commercial sexworkers reported having used a condom at leastonce. The majority, however, used them rarely,and not a single student reported regular use ofcondoms during sex with sex workers. Meanwhile,few young people perceived themselves to be atrisk of contracting an infection. The author notesthat young women seem oblivious to the possibilitythat the unprotected sexual behaviour of their futurehusbands may eventually expose them to infection,even if they themselves practise strict abstinencebefore marriage.
Numerous factors contribute to low contraceptiveuse rates among adolescents, ranging from lackof knowledge to gender imbalances that preventcommunication between partners and excludeyoung women from decisions about when to havechildren. Pachauri and Santhya note that whileadolescents’ awareness of at least one method of
Table 8. Current contraceptive use among adolescents (aged 15–19) in South Asia and otherselected Asian countries
Per cent of married Estimated per centwomen aged 15–19 of women aged 15–19currently using any with an unmet need
Country, year of survey method of contraception for contraception
South AsiaBangladesh 1997 33 19India 1998–1999 8 27Nepal 1996 7 41Pakistan 1996–1997 6 23Sri Lanka 1987 20 na
Other Asian countriesIndonesia 1997 36 9Philippines 1998 18 32Thailand 1997 43 na
Sources: All figures from Demographic Health Surveys cited in Pachauri & Santhya (2002).

17
Adolescent sexual and reproductive health in South Asia: an overview
contraception is nearly universal in South Asiancountries (with the exception of Pakistan),adolescents are not necessarily aware of reversiblemethods that might be most appropriate for theirsituation, such as oral contraceptives or condoms.Furthermore, many young couples do not knowhow to obtain such methods or understand how touse them correctly. As many papers in this volumeillustrate, adolescents who want to protectthemselves from pregnancy and STIs/HIV face ahost of obstacles including lack of access toservices, poor quality of care, and provider attitudesthat adolescents find threatening, disrespectful orindiscrete.
Few studies have explored the ways that providerattitudes may inhibit contraceptive use amongunmarried adolescents. Two papers in thiscollection shed light on this issue, including Gaoet al. (China) and Naravage (Thailand). Gao andcolleagues provide a rare look at provider attitudesin China. They report that as many as 40% ofproviders disapproved of supplying contraceptivesto unmarried young people. Their findings suggestthat even in settings such as China, where familyplanning is so well accepted, provider attitudes maydiscourage sexually active unmarried youth fromusing methods to protect themselves againstunwanted pregnancy or STIs.
Emergency contraception (EC) has increasinglybeen recognized as a useful backup method foradolescents who have unprotected sex, but fewstudies have explored the acceptability or use ofEC among youth in South Asia. The paper byNaravage suggests that misinformation andbarriers to access may undermine the potentialbenefits of EC. The study found that bothdistributors and purchasers had a poorunderstanding of how to use EC correctly.Furthermore, young women told researchers thatthey were reluctant to purchase EC for fear ofdisclosing the fact that they were sexually active.Many purchasers reported using EC incorrectly orusing it on a regular basis, which is contrary to itsintended purpose. These findings suggest that theintroduction of EC must be accompanied by clear
and accurate instructions, as well as efforts to raiseawareness among both potential users anddistributors about how to use EC correctly andhow to choose a contraceptive method that isappropriate for regular or long-term use.
Unplanned births and induced abortion amongadolescents
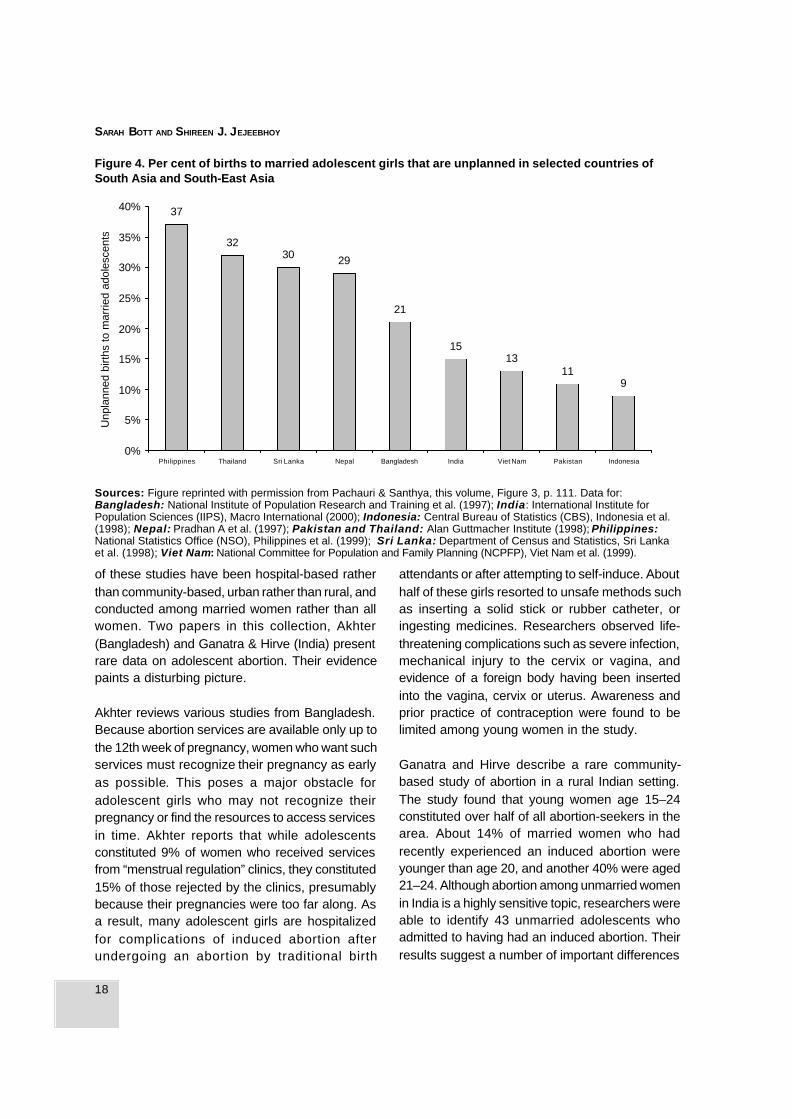
Because so many adolescents have sex withoutprotection (both in and out of marriage), theproportion of adolescent births that are unplanned,unwanted or mistimed is relatively high, asillustrated by Figure 4, reprinted from Pachauri andSanthya (this volume).
Worldwide, many unplanned births end in inducedabortion, often under unsafe conditions. Data onthe numbers of adolescent abortions are scarce,but estimates for developing countries range from1 to 4.4 million (McCauley & Salter, 1995). Someevidence suggests that adolescents—particularlyunmarried adolescents—are more likely than olderwomen to seek abortions from untrained providers,to undergo second trimester abortions and to suffercomplications. Fear, shame and lack of access toboth services and resources inhibit adolescentsfrom seeking safe and early abortions on the onehand, and from seeking care in case ofcomplications on the other (Bott, 2000).
The abortion scenario varies considerably withinSouth Asia. In India, abortion has been legal since1972, but limited availability and poor servicequality keep safe abortion beyond the reach ofmost poor women. In Bangladesh, abortion hasbeen available since 1999 for up to 12 weeks ofgestational age in the form of “menstrualregulation”, and large proportions of women usethese services. In Sri Lanka, abortion is legallyrestricted, but available, and women have accessto relatively safe services. In Nepal and Pakistan,it remains severely restricted and women whoundergo an abortion are liable to prosecution.
Few studies have explored the context of abortionamong young women in South Asia. The majority
18
SARAH BOTT AND SHIREEN J. JEJEEBHOY
of these studies have been hospital-based ratherthan community-based, urban rather than rural, andconducted among married women rather than allwomen. Two papers in this collection, Akhter(Bangladesh) and Ganatra & Hirve (India) presentrare data on adolescent abortion. Their evidencepaints a disturbing picture.
Akhter reviews various studies from Bangladesh.Because abortion services are available only up tothe 12th week of pregnancy, women who want suchservices must recognize their pregnancy as earlyas possible. This poses a major obstacle foradolescent girls who may not recognize theirpregnancy or find the resources to access servicesin time. Akhter reports that while adolescentsconstituted 9% of women who received servicesfrom “menstrual regulation” clinics, they constituted15% of those rejected by the clinics, presumablybecause their pregnancies were too far along. Asa result, many adolescent girls are hospitalizedfor complications of induced abortion afterundergoing an abortion by traditional birth
attendants or after attempting to self-induce. Abouthalf of these girls resorted to unsafe methods suchas inserting a solid stick or rubber catheter, oringesting medicines. Researchers observed life-threatening complications such as severe infection,mechanical injury to the cervix or vagina, andevidence of a foreign body having been insertedinto the vagina, cervix or uterus. Awareness andprior practice of contraception were found to belimited among young women in the study.
Ganatra and Hirve describe a rare community-based study of abortion in a rural Indian setting.The study found that young women age 15–24constituted over half of all abortion-seekers in thearea. About 14% of married women who hadrecently experienced an induced abortion wereyounger than age 20, and another 40% were aged21–24. Although abortion among unmarried womenin India is a highly sensitive topic, researchers wereable to identify 43 unmarried adolescents whoadmitted to having had an induced abortion. Theirresults suggest a number of important differences
Figure 4. Per cent of births to married adolescent girls that are unplanned in selected countries ofSouth Asia and South-East Asia
Sources: Figure reprinted with permission from Pachauri & Santhya, this volume, Figure 3, p. 111. Data for:Bangladesh: National Institute of Population Research and Training et al. (1997); India: International Institute forPopulation Sciences (IIPS), Macro International (2000); Indonesia: Central Bureau of Statistics (CBS), Indonesia et al.(1998); Nepal: Pradhan A et al. (1997); Pakistan and Thailand: Alan Guttmacher Institute (1998); Philippines:National Statistics Office (NSO), Philippines et al. (1999); Sri Lanka: Department of Census and Statistics, Sri Lankaet al. (1998); Viet Nam: National Committee for Population and Family Planning (NCPFP), Viet Nam et al. (1999).
37
3230 29
21
1513
119
0%
5%
10%
15%
20%
25%
30%
35%
40%
Philippines Thailand Sri Lanka Nepal Bangladesh India Viet Nam Pakistan Indonesia
Unp
lann
ed b
irths
to m
arrie
d ad
oles
cent
s

19
Adolescent sexual and reproductive health in South Asia: an overview
between married adolescent and adult abortion-seekers. First, adolescents reported considerablyless decision-making authority than older abortion-seekers. They were less likely to have been alloweda major role in the decision, more likely to havebeen coerced into an abortion, and conversely,more likely to have faced opposition from theirfamilies. As in Bangladesh, young women’sknowledge about and use of contraception werelimited, yet their need to space births was a leadingreason for seeking abortion. Finally, providers weremore likely to insist on spousal consent fromyounger abortion-seekers than from adult women,even though such consent is not legally required.
The study found several important differencesbetween married and unmarried adolescentabortion-seekers. While no evidence indicated thatmarried adolescents delayed seeking servicescompared to older married women, it was clearthat unmarried adolescents sought abortionsfurther along in their pregnancy than their marriedcounterparts. While married adolescents preferredthe private sector, unmarried adolescent abortion-seekers reported higher use of traditional providersas a result of less family support, less money,and concerns about confidentiality and providerattitudes. Adolescents tended to believe thatabortion services were not legally available tounmarried women. Researchers also found thatsome providers charged unmarried women a higherprice for their services. Regardless of maritalstatus, however, almost three-quarters ofadolescent abortion-seekers reported post-abortionmorbidity. Drawing on findings from other studies,the authors suggest that deaths related toabortions and unwanted pregnancies account fora significantly larger proportion of pregnancy-relateddeaths among adolescents than among olderwomen. They also noted that suicides related tounwanted pregnancy constitute a substantialportion of maternal deaths in the area.
Reproductive tract and sexually transmittedinfections among adolescents
In his address to the 6th International Congress
on AIDS in Asia and the Pacific, Peter Piot, theExecutive Director of the Joint United NationsProgramme on HIV/AIDS (UNAIDS), stated hisconviction that, “Asia and the Pacific hold the keyto the global future of the epidemic”. Compared tothe African region, many Asian countries have seenonly limited spread of HIV. Nonetheless, severalworrisome indicators suggest that South Asia isat risk of sharp future increases in the numbers ofHIV/AIDS cases. Estimates suggest that nearlyfour million people were living with HIV/AIDS in Indiaby the end of 2000, and some surveillance sites inSouthern India have found that more than 2% ofpregnant women are infected with HIV (Monitoringthe AIDS Pandemic & Joint United NationsProgramme on HIV/AIDS, 2001). Sex workersthroughout the region are at higher risk, as aremen who purchase sex, and their wives. As severalstudies in this collection suggest, this situationposes a serious concern for male adolescents,young men and their future wives.
In their global overview, Mane and McCauleydiscuss the physiological, behavioural and socialrisk factors surrounding STIs/HIV amongadolescents. They point out that physiologically,adolescents are more vulnerable to STIs thanadults, and girls are more vulnerable than boys.Gender power imbalances, societal norms, povertyand economic dependence all contribute to youngpeople’s risk of STIs. Many young people lackcontrol over the choice of their marital and sexualpartners, how many partners they have, thecircumstances and nature of sexual activity andthe extent to which sex is consensual or protected.Many lack information about condoms or areunaware of the risk. It is not surprising, therefore,that global estimates suggest that more than halfof all new HIV infections occur among young peopleage 15–24. Mane and McCauley note that thepandemic also has an impact on young peoplewho live with an HIV-infected parent. For theseyoung people, adolescence ends prematurely. Theyoften face early withdrawal from school and entryinto economic activity, stigma, poverty andpsychological suffering from losing a parent.
Few researchers have studied reproductive tract

20
SARAH BOTT AND SHIREEN J. JEJEEBHOY
infections (RTIs) or STIs among South Asianadolescents. Nonetheless, evidence suggests thatyoung people constitute a neglected but high-riskgroup. The typical STI patient is a young man barelyout of adolescence (modal ages are 20–25), ofrelatively low socioeconomic status. Likewise, theproportion of young women attending STI clinicshas been increasing (see, for example,Ramasubban, 2000).
Girls who marry early begin sexual activity whenthey are physiologically more vulnerable toinfection. Boys who have unprotected sex exposenot only themselves but also their future wives toinfection. Since discussion of sex is taboo, youngpeople often lack reliable information andmisconceptions abound. Gender imbalancesensure that girls are particularly uninformed abouttheir bodies and STIs. With limited power tonegotiate safer sex, young women in South Asiaare at risk of STIs/HIV no less than young men.Young people who experience an STI suffer notonly health consequences, but also shame andsocial stigma. Fear of reprisal often prevents youngpeople from getting timely treatment for an STI,thus worsening the situation and facilitating HIVinfection.
Several studies in this collection highlight theprevalence of reproductive tract infections, includingSTIs among adolescents, particularly among girls.Kulkarni and Adhikari cite evidence from India andNepal that adolescent women report relatively highrates of gynaecological morbidities—of particularconcern in settings where girls have limited accessto adequate health care. The 1998-1999 NFHS-2in India found that nearly two in five ever-marriedadolescent women reported some reproductivehealth problem.
Joseph and colleagues present a rare community-based study of RTI prevalence among 451 marriedwomen aged 16–22 in rural Tamil Nadu, India. Thisstudy found alarming levels of morbidity. As manyas 49% of women in the study suffered from oneor more RTI, not counting cases of infertility,urinary tract infections and prolapse. Clinical and
laboratory examination diagnosed 18% with anSTI, including chlamydia, trichomoniasis andsyphilis. Researchers found that wives of truckdrivers and army personnel seemed more likelythan other women to experience sexuallytransmitted morbidity, although the multivariateanalysis found that length of marriage was the onlystatistically significant variable. These data clearlysuggest that husbands’ unsafe sexual behaviourstransmit infections to their young wives—analarming finding, given that many infected womenare asymptomatic and are unlikely to seek medicalcare even when symptoms do appear. In fact, theauthors report that two-thirds of women withsymptoms did not seek care, and among thosewho did, over three in four sought treatment fromunqualified sources, such as home treatment oruntrained private practitioners.
Even when adolescents seek care, a host ofbarriers may prevent them from receivingappropriate care. Ranjha and Hussain carried outresearch on the Hakims who provide services at“Sex Clinics” throughout Pakistan and much ofSouth Asia. These clinics are more accessible andperceived to be less judgmental than public sectorfacilities. They are often the first place thatadolescents seek care. A nongovernmentalorganization (SAHIL) in the area found that morethan half of the adolescents seeking counsellingservices at their centres had previously sought carefrom Hakims at local sex clinics. Researchersfound that Hakims were poorly informed aboutsexual and reproductive health matters and lackedeven the vocabulary to address sexual andreproductive health issues. They knew little aboutSTIs, their diagnosis or treatments. Their servicesreinforced myths and misinformation and borderedon outright quackery. The medicine they prescribedcontained potentially dangerous substances suchas appetite stimulants, steroids, male and femalehormones, and narcotics. Additionally, researchersposing as mystery clients reported incidents ofsexual harassment by the Hakims.
Awasthi, Nichter and Pande report findings froman innovative, interactive programme designed to

21
Adolescent sexual and reproductive health in South Asia: an overview
raise awareness of risk behaviours and sexuallytransmitted infection among some 377 boysresiding in a slum in Kanpur in north India. As otherstudies have shown, a sizeable proportion of boyshad engaged in sexual activity, some with casualpartners and some with sex workers.Misperceptions concerning disease transmissionwere widespread, and condom use minimal. Theintervention included three educational sessionsusing a host of communication strategies, suchas “teaching by analogy” and responding toquestions dropped anonymously in a sealed letterbox. Messages drew upon previously conductedqualitative research with young males and usedanalogies drawn from events that were familiar tothese urban slum residents. Exposure to theintervention succeeded in significantly reducingmisconceptions about STI transmission amongparticipants—for example, that one can only beinfected by having sex with a prostitute. Theintervention also raised awareness of basic factssuch as the asymptomatic nature of STIs and thedays during a woman’s cycle when she is leastlikely to become pregnant. The intervention madesome headway in changing the misconception thattaking medicines before or after sex, using a vaginalbirth control tablet or washing the penis after sexwith disinfectant would reduce chances of acquiringsexually transmitted infections. In short, the studydemonstrated that to be effective and acceptableto young men, STI education requires innovativeand confidential approaches that address bothmedical and cultural concerns.
Communication between adolescents and adultsabout sexual and reproductive health
Adolescents in South Asia tend to be poorlyinformed about their own bodies and matters relatedto sexuality and health. The information they haveis often incomplete and confused. Low rates ofschooling, limited access to sex education andattitudes that prohibit discussion of sex exacerbatetheir ignorance. As gatekeepers who should playa central role in enabling adolescents to protecttheir health, parents often obstruct rather thanfacilitate informed choice. Adolescents commonly
report that discussions with parents about sex orreproduction are taboo. In both rural areas andurban slums, parents often want and expect theiradolescent children, particularly daughters, toremain uninformed about sex. Educational systemsalso tend to be ambivalent about sex education,though this has begun to change in the wake ofthe HIV/AIDS pandemic. In many cases, sexeducation continues to stress biological andscientific information over broader issues ofsexuality. Teachers often find the topicembarrassing or shameful, and may avoid suchissues, even in schools that supposedly teach afamily life/sex education curriculum. As a result ofadults’ reticence to address these issues, youngpeople tend to rely on peers and mass media forinformation about sex, reproduction and STIsincluding HIV/AIDS.
Qazi presents data from a pilot survey in Pakistanthat explored knowledge about sex andreproduction among adolescents aged 13–21 . Thesurvey found that adolescents’ knowledge tendedto be limited, with many misconceptions regardingpregnancy, contraception and STIs (including HIV/AIDS). The study also found that although sex andpregnancy were considered taboo topics ofdiscussion, many young people do indeed discussthem, often with peers. Qazi points out that in theconservative setting of Pakistan, parents are oftenreluctant to discuss matters of sex andreproductive health with their adolescent children,and many young people do not turn to their parentsfor such information.
Bhuiya and colleagues cite similar survey datasuggesting that communication between parentsand children on topics of sexuality and reproductionin Bangladesh is limited—particularly between parentsand boys. The study found that although a majority ofgirls had discussed reproductive health issues withtheir mothers, very few boys had discussed suchmatters with their parents or other family members,(2% with fathers, 3% with mothers and 6% withother family members).
Three papers, namely those by Rashid

22
SARAH BOTT AND SHIREEN J. JEJEEBHOY
(Bangladesh), ul Haque and Faizunnisa (Pakistan)and Masilamani (India), explore communicationbetween adolescents and adults based on focusgroup discussions in Bangladesh and Pakistan,and more informal discussions and programmeexperience in India. In all three settings, parentsreported embarrassment about discussing issueswith adolescent children—including menstruation.They generally preferred to leave this responsibilityto textbooks, teachers and others. In all threesettings, parents argued that they themselveslacked the knowledge and even the vocabulary todiscuss such sensitive issues. As a result, Rashidreports that many young girls knew nothing aboutmenstruation before it began. Unable to ask forhelp from their parents, many believed that theywere sick or dying. Concern for the sexual securityand chastity of daughters dominates parentalrelationships with adolescent girls. This concernleads to close supervision of daughters and strictlimits on their mobility. In contrast, sexual activityamong adolescent sons tends to be condoned. Inmany cases, as Masilamani notes, parents believethat talking to adolescents about these matterswill imply approval of premarital sexual activity.Adolescents perceive discussions with parentsabout sexual and reproductive topics to be tabooand express embarrassment at the prospect. Asa result, adolescents tend to get their informationfrom peers and the media, despite the fact thatadolescents often express a desire to be able toturn to parents for information and counsel. Thesepapers clearly suggest a need for educators andparents to improve their ability to communicate withyoung people.
A fourth paper describes family relationships andthe extent to which these can be dominated byfear and violence. Bella Patel Uttekar andcolleagues present findings from a study ofdomestic violence in the homes of 382 adolescentsaged 10–19 living in a slum area of Allahabad,India. The authors describe a situation in whichadolescents’ home environments are frequentlycharacterized by high levels of physical and verbalviolence perpetrated by fathers against mothersand children. As many as 49% of boys and 16% of
girls reported that they themselves had been beaten bytheir fathers, and a quarter reported that their motherswere verbally abused or beaten. Clearly, intra-familydynamics of this nature can severely impede theabil ity and wil l ingness of adolescents tocommunicate with parents on any threateningtopic, let alone sexual issues.
Programmes that address the sexual andreproductive health of adolescents
Equipping adolescents to make informed sexualand reproductive choices requires multi-prongedactivities, including efforts to enhance knowledgeand awareness, change attitudes and strengthenskills, such as the ability to negotiate with peers,partners and family members. At the facility level,programmes have tried to design “youth-friendly”services. At the household and community level,programmes have tried to enhance parents’ abilityand willingness to communicate with adolescents.Through a multitude of ways, programmes havetried to educate young people, build life skills andaddress the myriad of concerns that young peopleexpress that go beyond sexual and reproductivehealth.
Authors in this collection highlight several broad,but important lessons learned from adolescentprogrammes. First, evidence suggests that youthare reluctant to patronize clinics. Hence, theprogrammes that do not reach out beyond the clinicfacility are unlikely to reach many young people.Second, in the process of preparing for adulthood,young people face a plethora of challenges andconcerns, and projects intended to enhance theexercise of informed sexual and reproductivechoices among them need to be delivered withinthe context of other issues that adolescentsconsider to be relevant to their immediate needs.Finally, effective programmes need to use multiplestrategies. Most effective programmes have notlimited themselves to family planning, clinicalservices or education alone. They combinedmultiple strategies, including education,counselling, and building links with services, to

23
Adolescent sexual and reproductive health in South Asia: an overview
name but a few. The rest of this chapter reviewsthe papers in this collection that focus onprogramme experiences and recommendations.
Family life and sex education programmes
A variety of educational programmes are under wayin the region, implemented by both the public andnongovernmental sectors. According to a recentUNAIDS report, in the wake of new epidemiologicalevidence about the spread of HIV/AIDS, as manyas 25% of schools in India will have launched AIDSeducation programmes by 2001 (Monitoring theAIDS Pandemic-MAP & the Joint United NationsProgramme on HIV/AIDS, 2001). Chakrabartireviews population and sex education programmeswithin the formal and informal educational sectorsin India. With UNFPA funding and governmentcollaboration, the National Population EducationProject reached about 154 million students in 2000.She argues that such programmes mustcomplement sex education with strategies suchas telephone counselling, peer counselling, lifeskills education, health camps, and efforts tochange attitudes and awareness among teachersand parents.
In addition to governmental efforts to educate youth,the nongovernmental sector has designed manyinnovative sexuality education programmesthroughout South Asia, many of which use thestrategies that Chakrabarti recommends. Casestudies in this collection illustrate such efforts,including programmes run by Indiannongovernmental organizations (NGOs), such asthe Family Planning Association of India(Brahmbhatt) and Parivar Seva Sanstha (Tewari &Taneja), that work in schools, colleges, non-formaleducation sectors and community-based centres.Activities include counselling centres that offerservices individually, in groups, by correspondence,telephone hotlines and a variety of peer-ledactivities. In addition, they direct their programmesat gatekeepers, such as parents, teachers andservice providers. Both programmes underscorethe importance of flexibility to youth-friendlyservices. Aside from convenient locations,
affordable fees, and specially trained staff, centralelements of programmes aiming to communicatewith youth are anonymity and drop-in hours.
Rashid describes the efforts of BRAC, an NGO inBangladesh that provides reproductive healtheducation in conjunction with a three-year non-formal education programme conducted foradolescents who have never attended school.Introduced in the last year of the three-yearprogramme (and corresponding to the governmentsecondary school programme), the curriculuminforms adolescents about puberty, reproductionand contraception and sensitizes them aboutgender equity and responsible relationships.Tiedemann and DasGupta describe similar effortsamong youth organizations (namely the Scoutsand Guides Associations) in West Bengal, India.This programme is designed to use the “learning-by-doing” approach of the Associations. Theprogramme involves providing education, buildinglinks with local health providers and training Scoutsand Guides to become peer leaders. Since largenumbers of youth sign up to become Scouts andGuides in West Bengal, the programme hopes toreach thousands of young people.
In short, all these programmes include a range ofactivities intended to enhance young people’sknowledge and communication skills, changeattitudes, dispel misconceptions, prevent riskybehaviour and address traditional gender norms. Atypical curriculum addresses physiologicalchanges during puberty, menstrual hygiene,reproduction, contraception, gender equity, andskills needed to manage relationships. Incommunities where early marriage for girls iscommon, programmes often provide premaritalcounselling and sensitization on responsibleparenthood. Nearly all organize peer education,along with strategies to reach parents, teachersand service providers. Many emphasizecounselling services, including face-to-facecounselling, written correspondence and telephonecounselling. They all aim to communicate withyoung people in direct, non-judgmental yetculturally sensitive ways.

24
SARAH BOTT AND SHIREEN J. JEJEEBHOY
A number of papers in this collection describeevaluations of programmes that inform adolescentsabout sexual and reproductive health issues.Tiedemann and DasGupta describe the evaluationplans—including a study/control design—that willbe used to evaluate the programme among Scoutsand Guides in West Bengal. Papers by Teiwari &Taneja and by Rashid report tentative observationsof changes in awareness among adolescentsexposed to education programmes. Both report aconsiderable increase in awareness of issuesrelating to sex, contraception and infection. Inaddition, Rashid describes how adolescentsexposed to the programme reported improvedmenstrual hygiene as well as attempts to breakdown communication barriers between themselvesand their parents—in particular about their requestto delaying early marriage. Nevertheless, severalconference participants noted that programmeevaluation remains a weakness of many NGOs.They argued that policy-makers and donors needrigorous evidence about which strategies haveproduced results and are therefore worth scalingup.
Building self-efficacy among adolescents
Many programmes include “life skills” either as onecomponent or as the central focus of their work. Inthe early 1990s, the World Health Organizationdefined life skills (World Health Organization, 1993;1994) as the “abilities for adaptive and positivebehaviour that enable individuals to deal effectivelywith the demands and challenges of everyday life”.WHO identified a group of core life skills thatinclude problem-solving, decision-making, goalsetting, critical and creative thinking, valuesclarification, communication skills, inter-personaland negotiation skills, as well as self-awareness,self-esteem and understanding how to cope withstress.
Papers by Seth, and Levitt-Dayal and colleaguesdescribe life skills programmes in India. Sethdescribes a programme that trains teachers toconduct life skills programmes among youth inrural Rajasthan. Anecdotal feedback from
participating teachers suggested that such trainingempowered trainers to communicate sexual andreproductive health information more effectively andwith fewer inhibitions. Preliminary observations alsosuggest that such training may benefit teachersthemselves, as well as young people. Levitt-Dayalet al. describe programmes in rural Gujarat, ruralMadhya Pradesh and periurban areas of Delhi thataim to enhance life skills among young women.These programmes use a combination ofnonformal, family life and vocational education,combined with the provision of services. They giveyoung women the opportunity to learn to use banksand public transport, to participate in recreationalactivities and to receive leadership training. Theseprogrammes are among the few that have evaluatedthe impact of their efforts by gathering follow-updata among their alumnae and among a controlgroup of girls who did not participate in theirprogrammes. Compared to controls, alumnae weremore likely to remain in school and to have greaterdecision-making authority within their families,particularly with respect to decisions about whento marry and whether to continue their education.The alumnae demonstrated higher levels of self-esteem, assertiveness, mobility and exposure tomedia and new ideas. Married alumnae were alsomore likely to have married at age 18 years orolder, and were more likely to obtain appropriatecare during pregnancy, compared to those whohad not participated in the programmes.
Making health services accessible and friendly
While the need to provide accessible and friendlyservices to youth is generally acknowledged, thereis less clarity about what is meant by “youth-friendly” services. What is evident is that in mostsettings, adolescents face obstacles in accessinghealth services. Reviewing the global situation,Epstein, and Chandra Mouli highlight the manyobstacles that may discourage young people fromseeking health care. These include an inability toaccess services independently from their families,fear of discovery by family or community members,inconvenient locations and hours, long waits atclinics, high costs, and providers whom

25
Adolescent sexual and reproductive health in South Asia: an overview
adolescents perceive to be threatening, judgmentalor unwilling to respect their confidentiality. Usingsurvey data from Bangladesh, Bhuiya andcolleagues underline adolescents’ reluctance touse health services. They hold the perceivedunfriendliness of providers responsible for much ofthis reluctance. Only 1% of adolescents surveyedhad visited a facility in the prior six months, andconcerns about how they would be treated wereclearly an issue. Only 15% of boys and 1% ofgirls believed that providers would treat them withrespect if they sought contraceptive services, and26% and 7%, respectively, believed that providerswould treat them respectfully if they sought carefor STI symptoms. The adolescents’ perceptionsof pharmacies were similar, if not worse.
The literature often mentions the need for servicesto be “youth-friendly”, but this term is not alwaysclearly defined. However many authors (such asEpstein, Mehta, Poonkhum, Brahmbhatt, Tewari& Taneja and Chandra Mouli) note that, whenasked, adolescents generally cite a number offundamental characteristics that make services“youth-friendly”. These include special hours orsettings for adolescents, convenient access, aplace that does not look like a clinic, a place usedby their peers, affordable fees, drop-in hours, staffwho are empathetic, knowledgeable andtrustworthy, staff that are non-judgmental and non-punitive, and services geared towards youngpeople’s needs and interests. Epstein points toadolescents’ need for related services such ascounselling in managing friendships, partner andfamily relationships, and life skills developmentactivities that help young people develop practicaland applied skills in many areas of life.
Few organizations in South Asia haveimplemented, let alone evaluated, models fordelivering such “youth-friendly” services—althoughsuch efforts seem to be on the rise. Chandra Moulidescribes a number of models of youth-friendlyservices: integrated comprehensive services thatoffer a range of services including sexual andreproductive; community-based health facilitiesthat provide stand-alone sexual and reproductive
health services (such as those offered by MarieStopes International or Profamilia) or those thatare offered through a district or municipal healthsystem; community-based centres that offer anarray of personal development activities and alimited health focus; and outreach activitiesdesigned to enhance access to services. ChandraMouli stresses that priorities in adolescent-friendlyhealth services need to vary according to thenature of the health services provided and to thespecific adolescent group to be reached. Forexample, approaches that make services friendlyto sexually active males may not be whollyadaptable to girls in their early adolescent years.In short, programmes must be tailored to meetthe special needs of the adolescents who are beingaddressed, keeping in mind such issues as socialand cultural sensitivit ies, feasibil ity andsustainability. Clearly, strategies should be adaptedto different sociocultural and programme settings,but what is needed are supportive policies,involvement of the community and adolescents inthe design of services, and competent andcommitted providers.
This volume includes several case studies of youth-friendly services. Bhuiya and colleagues describeefforts to establish “youth-friendly” services inexisting NGO clinics, complemented with otheroutreach efforts in north-west Bangladesh. Thatproject introduced designated hours for adolescentclients, strengthened privacy and confidentiality,expanded the range of services offered, and madean effort to ensure that physicians have the skillsto provided counselling. They supplemented theseservices with efforts to educate communitymembers, provide telephone counselling andestablish community-based reproductive healthprogrammes for young people.
Two case studies from Thailand (Poonkhum) andIndia (Mehta) describe efforts to set up “youth-friendly” services in specially designated areaswithin government hospitals. These programmesinvolved remarkably similar preparatory steps,activities and experiences. Both designed theprojects based on discussions with adolescents.

26
SARAH BOTT AND SHIREEN J. JEJEEBHOY
Counselling on a variety of topics was thecornerstone of the projects. To avoid using the term“clinic”, the project in Thailand delivered servicesin “adolescent-friendly rooms”. Services were freeand offered during extended hours. Both maintainedconfidentiality through anonymous record-keeping.The projects developed training materials and factsheets (India) or manuals containing frequentlyasked questions (Thailand). In addition, theytrained peers, teachers and parents on reproductivehealth knowledge and life skills. In Thailand, theproject promoted its services with the help of radioDJs who had a wide following among adolescents.
Preliminary findings from both interventionssuggest that establishing adolescent-friendlyservices at government hospitals is feasible andsustainable. However, both found it difficult toattract adolescents to the hospital setting, despiteefforts to promote the services widely. Both foundthat adolescents preferred telephone counsellingrather than face-to-face services, probably becauseit provided greater privacy and anonymity. InThailand, the Department of Health has consideredsetting up services in sites outside hospitals thatwould be more acceptable to adolescents.
Reflecting on lessons learned from experiencesaround the world, Epstein suggests that the publicsector may not be the best entity to deliver suchservices. In many settings, adolescents perceiveNGO services to be less threatening and moreacceptable than public services. Furthermore, thepublic sector tends to take the clinic-basedapproach, the limitations of which are illustratedby examples in this collection. Several innovativeprogrammes have explored alternatives in theprivate and NGO sectors, such as trainingpharmacists or doctors in the private, for-profitsector to serve adolescents, providing counsellingand contraceptive services at workplaces andmilitary sites, setting up emergency drop-incentres, offering special hours or facilities for boys,developing long-term adult/adolescent mentoringprogrammes, and providing discussionopportunities for young couples on marriage andparenthood. Given the limited success of public
sector programmes, Epstein argues for a modelin which governments support NGOs to scale upsuccessful adolescent reproductive health services.
Regardless of the approach used, Epstein arguesthat cross-referrals are crucial, becauseadolescents’ needs go beyond the capacity of anyone sector. For example, hotline services need toestablish formal agreements with other services,such as pharmacies, private physicians,neighbourhood depot holders, abuse/violence crisiscentres, mental health counsellors, lawyers andlegal services centres, micro-credit facilities, or jobtraining programmes in order to best serve theneeds of adolescents. Such cross-referrals requireconsiderable cooperation across public and privatesectors and between organizations that providedifferent services to youth.
Finally, Epstein points out that existingprogrammes are rarely designed in ways thatfacilitate rigorous evaluation. Evaluations ofadolescent programmes tend to rely on pre- andpost-intervention assessments of reproductivehealth awareness. Because most programmesfocus on small populations and evaluations do notinclude comparisons or controls, it remains difficultto determine whether an outcome is directlyattributable to the programme alone, and therefore,whether a finding has programme or policyimplications. Furthermore, while manyprogrammes measure changes in knowledge, feware able to measure behaviour change, which wouldbe a more important indicator of success. Epsteinargues for building rigorous evaluations into allstages of programmes—a recommendation thathas major implications for those who fundprogrammes, because it would require investingsubstantial resources in evaluation.
Conclusions
This overview has sought to provide a profile of thesociodemographic and sexual and reproductivehealth situation of adolescents in South Asia. Moresignificantly, it has attempted to record the

27
Adolescent sexual and reproductive health in South Asia: an overview
evidence and insights that emerged at theconference and to synthesize from these asummary of what is currently known about thesexual and reproductive health risks and challengesfaced by adolescents and young people in theregion. The findings generally emphasize theconsiderable risks that adolescents continue toface, extending from unsafe or unwanted sexualactivity to such consequences as unwantedpregnancy, abortion and infection, and frommisperceptions to a lack of life skills and widegender power imbalances. They also underscorethe vast obstacles that must be overcome in orderto access contraceptive and other reproductivehealth information and services.
At the same time, however, several encouragingsigns are evident. The sexual and reproductivehealth needs of adolescents and young people arefirmly on national agendas in the South Asianregion. There is growing recognition thatadolescents themselves must be given a role inarticulating and designing such programmes.Finally, a growing number of programmeexperiences already exist that appear to respondsuccessfully to young people’s sexual andreproductive health needs in innovative andacceptable ways.
Nonetheless, throughout this volume, authorssuggest ways in which policy-makers, programmemanagers, researchers and service providers coulddo more to improve the lives of South Asianadolescents. The final chapter of this collectionsummarizes their recommendations—both forresearch and programmes. These recommenda-tions should be seen as a call to action by allthose who care about the well-being of the nextgeneration.
References
Alan Guttmacher Institute (1998) Into a New World:Young Women’s Sexual and Reproductive Lives. NewYork, Alan Guttmacher Institute.
Blanc A, Way A (1998) Sexual behavior andcontraceptive knowledge and use amongadolescents in developing countries. Studies inFamily Planning, 29(2):106-116.
Bott S (2000) Unwanted pregnancy and inducedabortion among adolescents in developing countries:Findings from WHO case studies. In: Puri CP andVan Look PFA, eds. Sexual and Reproductive Health:Recent Advances, Future Directions. Mumbai, NewAge International (P) Limited, Publishers.
Brown A, Jejeebhoy SJ, Shah I, Yount KM (2001)Sexual Relations Among Young People inDeveloping Countries: Evidence from WHO CaseStudies. Geneva, World Health Organization, Departmentof Reproductive Health and Research (WHO/RHR/01.8).
Central Bureau of Statistics (CBS), Indonesia et al.(1998) Indonesia Demograhic and Health Survey1997. Calverton MD, USA, Macro International.
De Silva W (1997) The Ireland of Asia: Trends inmarriage timing in Sri Lanka. Asia-Pacific PopulationJournal, 12(2):3–24.
De Silva W (1998) Socio-economic change andadolescent issues in the Asian and Pacific region,Report and Recommendations of the Expert GroupMeeting on Adolescents: Implications of PopulationTrends, Environment, and Development. Bangkok,ESCAP (Asian Population Studies Series, No. 149).
Department of Census and Statistics, Sri Lanka(1988) Sri Lanka Demographic and Health Survey1987. Columbia MD, USA, Institute for ResourceDevelopment/Westinghouse.
Department of Census and Statistics, Sri Lanka(1995) Demographic and Health Survey 1993 SriLanka . Colombo, Department of Census andStatistics, Sri Lanka.
Hakim A, Cleland J, Bhatti MH (1998) Pakistan Fertilityand Family Planning Survey 1996–1997. PreliminaryReport. Islamabad, Pakistan, National Institute ofPopulation Studies and London School of Hygieneand Tropical Medicine.
International Institute for Population Sciences, Macro(2000) National Family Health Survey (NFHS-2)1998–1999: India. Mumbai, International Institute forPopulation Sciences.

28
SARAH BOTT AND SHIREEN J. JEJEEBHOY
International Labour Organisation (1998) Yearbookof Labour Statistics 1998. Geneva, InternationalLabour Organisation.
International Labour Organisation (1999) Yearbookof Labour Statistics 1999. Geneva, InternationalLabour Organisation.
International Labour Organisation (2000) Yearbookof Labour Statistics 2000. Geneva, InternationalLabour Organisation.
Jejeebhoy S (1993) Family size, outcomes for childrenand gender disparities: A case of rural Maharashtra.Economic and Political Weekly, 28(35):1811–1822.
Jejeebhoy S (2000) Adolescent sexual andreproductive behaviour: A review of the evidence fromIndia. In: Ramasubban R, Jejeebhoy S, eds. Women’sReproductive Health in India. Jaipur, RawatPublications.
Macro International (2002) Demographic HealthSurveys, Stat Compiler [Online data base available athttp://www.measuredhs.com].
McCauley AP, Salter C (1995) Meeting the needs ofyoung adults. Population Reports, Series J, No. 41,Vol. XXIII, 3 (October).
Mitra SN, Al-Sabir A, Cross AR, Jamil K (1997)Bangladesh Demographic and Health Survey 1996-1997. Dhaka, Bangladesh, National Institute ofPopulation Research and Training (NIPORT).
Monitoring the AIDS Pandemic (MAP), Joint UnitedNations Programme on HIV/AIDS (2001) The Statusand Trends of HIV/AIDS/STI Epidemics in Asia andthe Pacific, Provisional Report. Melbourne, Australia,MAP, UNAIDS. [Available at: www.unaids.org/hivaidsinfo/statistics/MAP/index.html]
National Statistics Office (NSO), Republic of thePhilippines (1999) Philippines National Demographicand Health Survey 1998, Manila, NSO and MacroInternational.
National Committee for Population and FamilyPlanning (NCPFP), Viet Nam (1999) Viet NamDemographic and Health Survey 1997. Hanoi,NCPFP.
Nepal Central Bureau of Statistics (1995) PopulationMonograph of Nepal. Kathmandu, Central Bureau ofStatistics.
Pachauri S, Santhya KG (2002) Reproductive choicesfor Asian adolescents: a focus on contraceptivebehaviour . International Family PlanningPerspectives, 28(4):186–195.
Population Reference Bureau (2000) The World’sYouth 2000. Washington, DC, Population ReferenceBureau, Measure Communication.
Pradhan A et al. (1997) Nepal Family Health Survey1996. Kathmandu and Calverton, MD, Nepal Ministryof Health, New ERA and Macro International, Inc.
Ramasubban R (2000) Women’s vulnerability: Therecent evidence on sexually transmitted infections.In: Ramasubban R, Jejeebhoy S, eds. Women’sReproductive Health in India. Jaipur, RawatPublications:280–330.
Singh S (1998) Adolescent childbearing in developingcountries: a global review. Studies in Family Planning,29(2):117–163.
United Nations (1997) Demographic Yearbook 1995.New York, United Nations (ST/ESA/STAT/SER. R/26).
United Nations (1999) World Population Prospects:the 1998 Revision. Volume II: The Sex and AgeDistribution of the World Population. New York, UnitedNations.
United Nations (2000) Demographic Yearbook 1998.New York, United Nations (ST/ESA/STAT/SER. R/29).
United Nations Children’s Fund (2001) The Progressof Nations 2001. New York, UNICEF.
World Health Organization (1993) Increasing theRelevance of Education for Health Professionals.Geneva, World Health Organization (WHO TechnicalReport Series, No. 838).
World Health Organization (1994) The Developmentand Dissemination of Life Skills Education: anOverview. Geneva, World Health Organization (MNH/PSF/94.7).
IIInaugural presentations
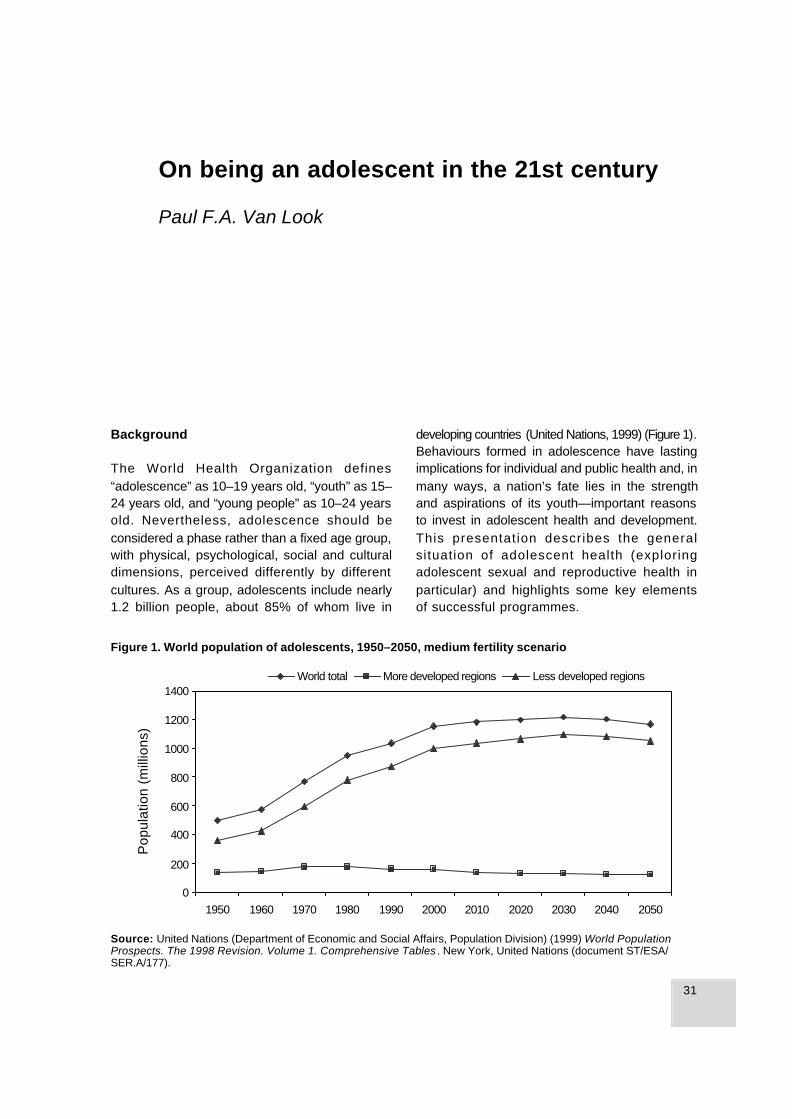
31
On being an adolescent in the 21st century
Background
The World Health Organization defines“adolescence” as 10–19 years old, “youth” as 15–24 years old, and “young people” as 10–24 yearsold. Nevertheless, adolescence should beconsidered a phase rather than a fixed age group,with physical, psychological, social and culturaldimensions, perceived differently by differentcultures. As a group, adolescents include nearly1.2 billion people, about 85% of whom live in
developing countries (United Nations, 1999) (Figure 1).Behaviours formed in adolescence have lastingimplications for individual and public health and, inmany ways, a nation’s fate lies in the strengthand aspirations of its youth—important reasonsto invest in adolescent health and development.This presentation describes the generalsituation of adolescent health (exploringadolescent sexual and reproductive health inparticular) and highlights some key elementsof successful programmes.
Source: United Nations (Department of Economic and Social Affairs, Population Division) (1999) World PopulationProspects. The 1998 Revision. Volume 1. Comprehensive Tables . New York, United Nations (document ST/ESA/SER.A/177).
0
200
400
600
800
1000
1200
1400
1950 1960 1970 1980 1990 2000 2010 2020 2030 2040 2050
Pop
ulat
ion
(mill
ions
)
World total More developed regions Less developed regions
Figure 1. World population of adolescents, 1950–2050, medium fertility scenario
On being an adolescent in the 21st century
Paul F.A. Van Look

32
PAUL F. A. VAN LOOK
The health status of adolescents
In the absence of a single measure that canexpress the health status of a population in ageneral sense, it is difficult to assess the health ofa population group. About ten years ago,researchers attempted to create such ameasurement unit, called the DALY (Disability-Adjusted Life Years), in order to quantify the globalburden of disease throughout the world (Murray &Lopez, 1996). This measure tries to capture twoelements at once—years of life lost due topremature mortality and years of healthy life lostfrom disability, adjusted for severity of the disability.For example, DALYs lost due to heart attack mayinclude years lost as a result of premature death,as well as healthy years lost due to disability suchas becoming bedridden.
Researchers have used DALYs to quantify theburden of each disease in the world in specificregions and in different population groups. Forexample, Chris Murray and Catherine Michaudattempted to quantify the degree of ill-health inadolescents in terms of DALYs in both developingand developed regions of the world. At the globallevel, they found that adolescents bore nearly 10%(6.6% in developed regions) of the ill-health presentin the world in 1990. We typically think ofadolescence as being the prime of life—relativelyfree from infectious diseases of childhood and fromconditions associated with ageing. Thus, one wouldexpect that the proportion of ill-health attributableto adolescents would be small. But clearly it isnot the case. In 1990, most DALYs (92.0%) amongadolescents were lost in developing regions, whichis not surprising, since that is where mostadolescents live. Adolescents in developed regionswere slightly healthier in terms of DALYs than theircounterparts in developing regions.
Table 1 presents the 10 most common factors thatled to death and disability among adolescentsglobally in 1990, as measured in terms of DALYs.The worldwide list mirrors the conditions that affectdeveloping countries, including infectiousdiseases, diarrhoeal diseases, iron-deficiency
Table 1. Causes of DALYs (per cent of total) indescending order among adolescents globally,1990 (Total DALYs in thousands = 132 562)
Rank Disease or injury Per cent of total
1 Unipolar major depression 6.92 Road traffic accidents 4.93 Falls 4.04 Iron-deficiency anaemia 3.75 War 3.56 Lower respiratory infections 3.37 Drowning 2.88 Self-inflicted injuries 2.79 Alcohol use 2.3
10 Diarrhoeal diseases 2.3 Total: 36.3
Source: Murray & Michaud (1996, unpublished data).
anaemia, accidents, injuries, war and suicideattempts. Perhaps surprisingly, the top rankedcondition is a mental health problem—unipolarmajor depression. Altogether the top ten conditionsrepresent more than one-third of DALYs lost amongadolescents worldwide (Table 1).
Looking at developed and developing regionsseparately, factors leading to death or disability indeveloping regions are the same as for the worldas a whole, but the pattern is quite different indeveloped regions. Only three factors appear onboth lists. Instead of infectious diseases andanaemia that are prominent in developing regions,the list for developed regions includes several othermental health problems, such bipolar disorders,obsessive-compulsive disorders (which include, forinstance, anorexia and bulimia) and schizophrenia.Drug and alcohol use, which are often associatedwith mental health disorders, are also high on thelist. Altogether, the top ten factors represent morethan 50% of the total amount of DALYs lost amongadolescents in developed regions (Table 2).
One major limitation of using DALYs to measureill-health among adolescents is that DALYs onlycapture those problems that are manifest at thatmoment in time. However, many events andbehaviours that begin during adolescence lead toserious problems later in life. Substance abusepatterns, such as smoking and drinking, often
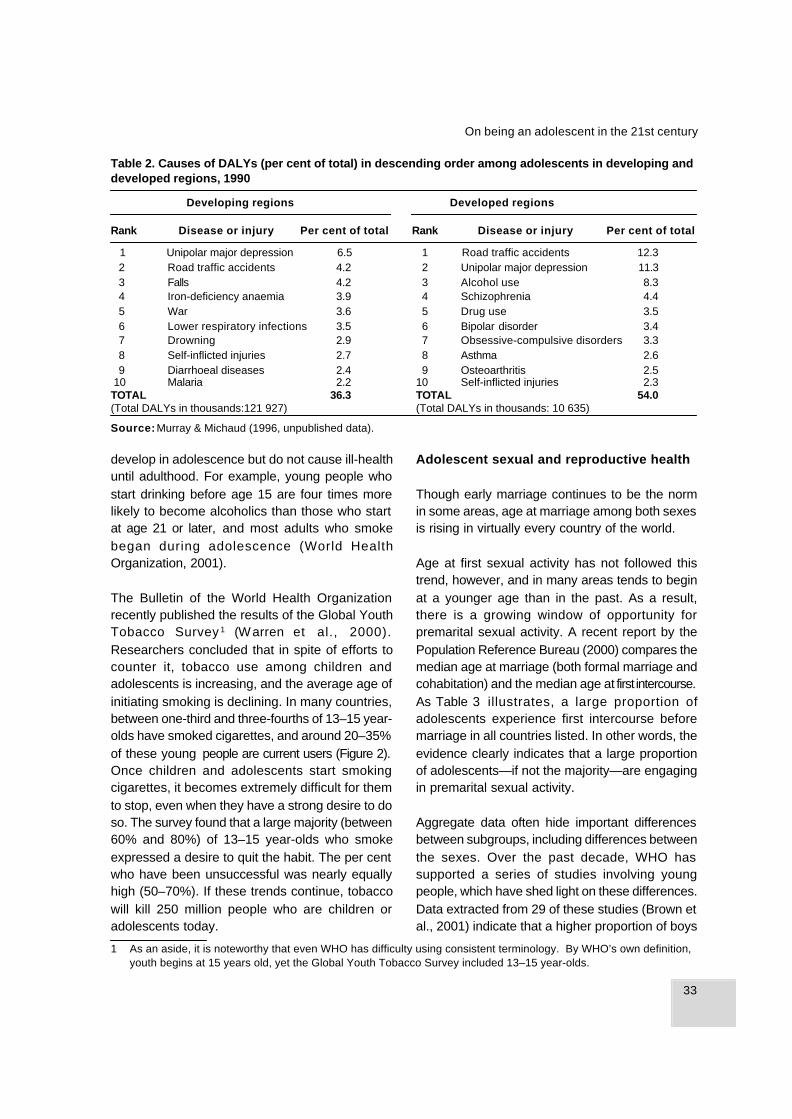
33
On being an adolescent in the 21st century
1 As an aside, it is noteworthy that even WHO has difficulty using consistent terminology. By WHO’s own definition,youth begins at 15 years old, yet the Global Youth Tobacco Survey included 13–15 year-olds.
Table 2. Causes of DALYs (per cent of total) in descending order among adolescents in developing anddeveloped regions, 1990
Developing regions Developed regions
Rank Disease or injury Per cent of total Rank Disease or injury Per cent of total
1 Unipolar major depression 6.5 1 Road traffic accidents 12.32 Road traffic accidents 4.2 2 Unipolar major depression 11.33 Falls 4.2 3 Alcohol use 8.34 Iron-deficiency anaemia 3.9 4 Schizophrenia 4.45 War 3.6 5 Drug use 3.56 Lower respiratory infections 3.5 6 Bipolar disorder 3.47 Drowning 2.9 7 Obsessive-compulsive disorders 3.38 Self-inflicted injuries 2.7 8 Asthma 2.69 Diarrhoeal diseases 2.4 9 Osteoarthritis 2.5
10 Malaria 2.2 10 Self-inflicted injuries 2.3TOTAL 36.3 TOTAL 54.0(Total DALYs in thousands:121 927) (Total DALYs in thousands: 10 635)
Source: Murray & Michaud (1996, unpublished data).
develop in adolescence but do not cause ill-healthuntil adulthood. For example, young people whostart drinking before age 15 are four times morelikely to become alcoholics than those who startat age 21 or later, and most adults who smokebegan during adolescence (World HealthOrganization, 2001).
The Bulletin of the World Health Organizationrecently published the results of the Global YouthTobacco Survey 1 (Warren et al., 2000).Researchers concluded that in spite of efforts tocounter it, tobacco use among children andadolescents is increasing, and the average age ofinitiating smoking is declining. In many countries,between one-third and three-fourths of 13–15 year-olds have smoked cigarettes, and around 20–35%of these young people are current users (Figure 2).Once children and adolescents start smokingcigarettes, it becomes extremely difficult for themto stop, even when they have a strong desire to doso. The survey found that a large majority (between60% and 80%) of 13–15 year-olds who smokeexpressed a desire to quit the habit. The per centwho have been unsuccessful was nearly equallyhigh (50–70%). If these trends continue, tobaccowill kill 250 million people who are children oradolescents today.
Adolescent sexual and reproductive health
Though early marriage continues to be the normin some areas, age at marriage among both sexesis rising in virtually every country of the world.
Age at first sexual activity has not followed thistrend, however, and in many areas tends to beginat a younger age than in the past. As a result,there is a growing window of opportunity forpremarital sexual activity. A recent report by thePopulation Reference Bureau (2000) compares themedian age at marriage (both formal marriage andcohabitation) and the median age at first intercourse.As Table 3 illustrates, a large proportion ofadolescents experience first intercourse beforemarriage in all countries listed. In other words, theevidence clearly indicates that a large proportionof adolescents—if not the majority—are engagingin premarital sexual activity.
Aggregate data often hide important differencesbetween subgroups, including differences betweenthe sexes. Over the past decade, WHO hassupported a series of studies involving youngpeople, which have shed light on these differences.Data extracted from 29 of these studies (Brown etal., 2001) indicate that a higher proportion of boys
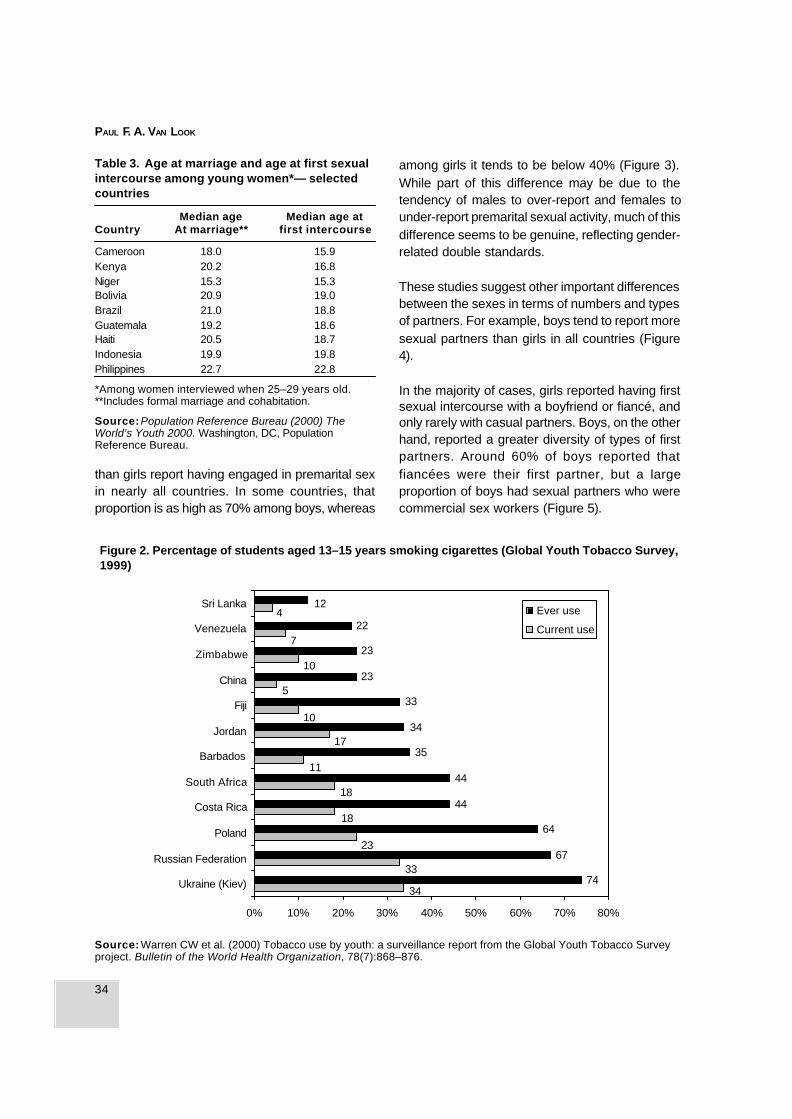
34
PAUL F. A. VAN LOOK
Source: Warren CW et al. (2000) Tobacco use by youth: a surveillance report from the Global Youth Tobacco Surveyproject. Bulletin of the World Health Organization, 78(7):868–876.
Table 3. Age at marriage and age at first sexualintercourse among young women*— selectedcountries
Median age Median age atCountry At marriage** first intercourse
Cameroon 18.0 15.9Kenya 20.2 16.8Niger 15.3 15.3Bolivia 20.9 19.0Brazil 21.0 18.8Guatemala 19.2 18.6Haiti 20.5 18.7Indonesia 19.9 19.8Philippines 22.7 22.8
*Among women interviewed when 25–29 years old.**Includes formal marriage and cohabitation.
Source: Population Reference Bureau (2000) TheWorld’s Youth 2000. Washington, DC, PopulationReference Bureau.
among girls it tends to be below 40% (Figure 3).While part of this difference may be due to thetendency of males to over-report and females tounder-report premarital sexual activity, much of thisdifference seems to be genuine, reflecting gender-related double standards.
These studies suggest other important differencesbetween the sexes in terms of numbers and typesof partners. For example, boys tend to report moresexual partners than girls in all countries (Figure4).
In the majority of cases, girls reported having firstsexual intercourse with a boyfriend or fiancé, andonly rarely with casual partners. Boys, on the otherhand, reported a greater diversity of types of firstpartners. Around 60% of boys reported thatfiancées were their first partner, but a largeproportion of boys had sexual partners who werecommercial sex workers (Figure 5).
23
34
33
7
10
5
10
17
11
18
18
412
22
23
23
33
34
35
44
44
64
67
74
0% 10% 20% 30% 40% 50% 60% 70% 80%
Ukraine (Kiev)
Russian Federation
Poland
Costa Rica
South Africa
Barbados
Jordan
Fiji
China
Zimbabwe
Venezuela
Sri LankaEver use
Current use
Figure 2. Percentage of students aged 13–15 years smoking cigarettes (Global Youth Tobacco Survey,1999)
than girls report having engaged in premarital sexin nearly all countries. In some countries, thatproportion is as high as 70% among boys, whereas

35
On being an adolescent in the 21st century
Figure 3. Proportion of young people reporting premarital sexual activity during the 1990s — selectedstudies*
Figure 4. Proportion of young people reporting two or more sexual partners—selected studies
*Note: The studies were not designed to be similar. Hence the samples, methodologies and age ranges varied.
Source : Brown A et al. (2001) Sexual relations among young people in developing countries. Evidence from WHOcase studies. Geneva, World Health Organization ( WHO/RHR/01.8).
Source: Brown A et al. (2001) Sexual relations among young people in developing countries. Evidence from WHOcase studies. Geneva, World Health Organization (WHO/RHR/01.8).
20
13
2520
1011
52 5050
24
73
15
55
36
0%
10%
20%
30%
40%
50%
60%
70%
80%
Nigeria Republic ofKorea
Philippines Thailand Viet Nam Argentina Peru
Sex
ually
exp
erie
nced
you
ng p
eopl
e
Female Male
0
24
36
19
33
15
53
31
19
6869 72
0%
10%
20%
30%
40%
50%
60%
70%
80%
Nigeria Republic ofKorea
Philippines Thailand Argentina Peru
You
ng p
eopl
e re
port
ing
two
or m
ore
part
ners
Female Male
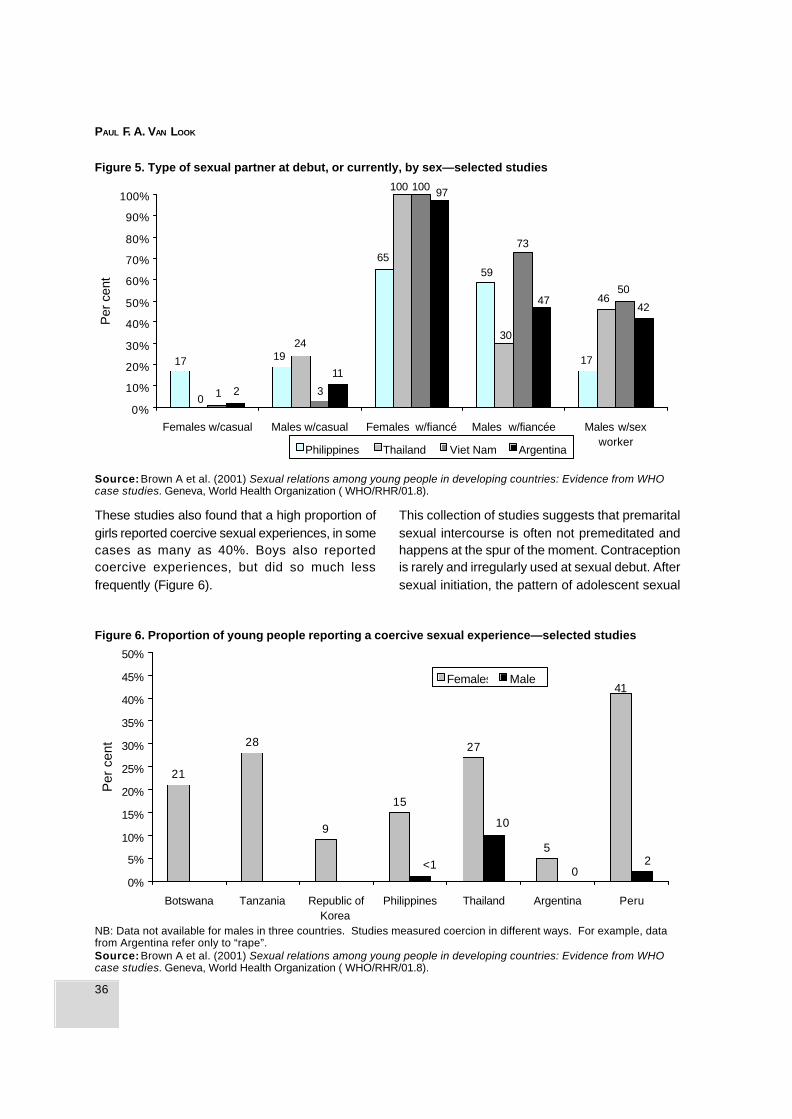
36
PAUL F. A. VAN LOOK
These studies also found that a high proportion ofgirls reported coercive sexual experiences, in somecases as many as 40%. Boys also reportedcoercive experiences, but did so much lessfrequently (Figure 6).
This collection of studies suggests that premaritalsexual intercourse is often not premeditated andhappens at the spur of the moment. Contraceptionis rarely and irregularly used at sexual debut. Aftersexual initiation, the pattern of adolescent sexual
Figure 5. Type of sexual partner at debut, or currently, by sex—selected studies
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Females w/casual Males w/casual Females w/fiancé Males w/fiancée Males w/sexworker
Per
cen
t
Philippines Thailand Viet Nam Argentina
17
0 1 2
1924
3
11
65
100 100 97
42
59
30
73
47
17
4650
Source: Brown A et al. (2001) Sexual relations among young people in developing countries: Evidence from WHOcase studies. Geneva, World Health Organization ( WHO/RHR/01.8).
41
5
27
15
9
28
21
20<1
10
0%
5%
10%
15%
20%
25%
30%
35%
40%
45%
50%
Botswana Tanzania Republic ofKorea
Philippines Thailand Argentina Peru
Per
cen
t
Females Males
Source: Brown A et al. (2001) Sexual relations among young people in developing countries: Evidence from WHOcase studies. Geneva, World Health Organization ( WHO/RHR/01.8).
Figure 6. Proportion of young people reporting a coercive sexual experience—selected studies
NB: Data not available for males in three countries. Studies measured coercion in different ways. For example, datafrom Argentina refer only to “rape”.
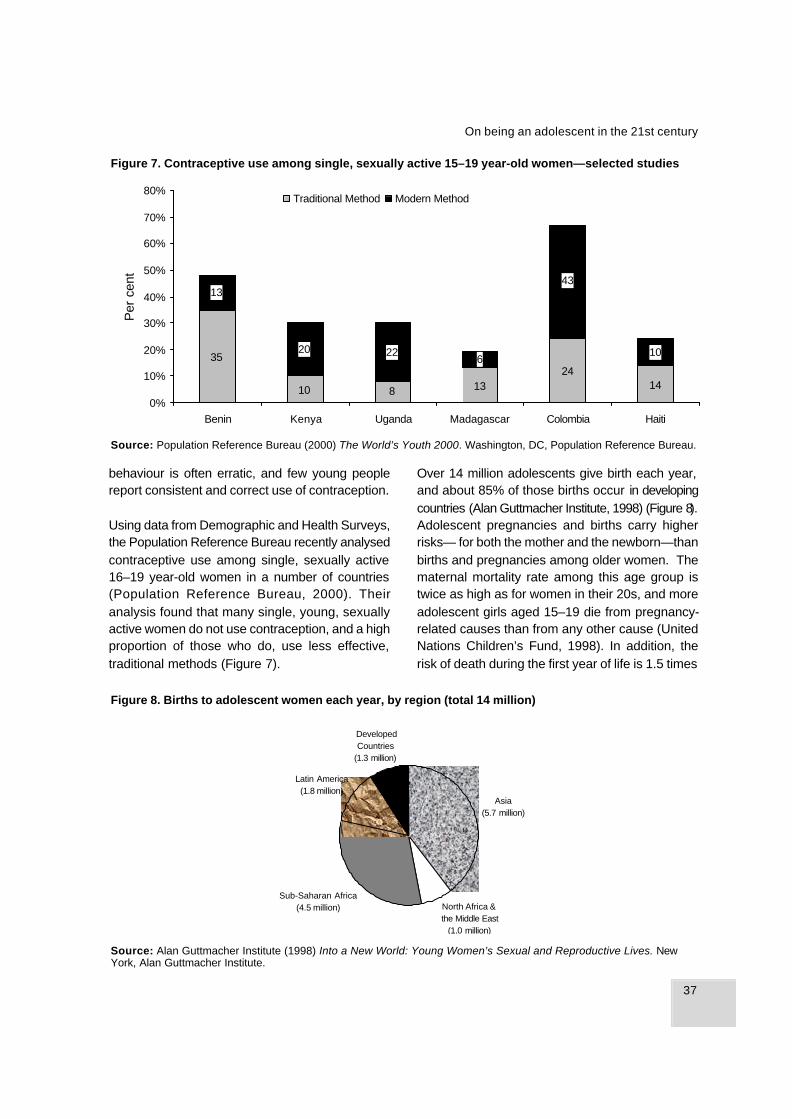
37
On being an adolescent in the 21st century
behaviour is often erratic, and few young peoplereport consistent and correct use of contraception.
Using data from Demographic and Health Surveys,the Population Reference Bureau recently analysedcontraceptive use among single, sexually active16–19 year-old women in a number of countries(Population Reference Bureau, 2000). Theiranalysis found that many single, young, sexuallyactive women do not use contraception, and a highproportion of those who do, use less effective,traditional methods (Figure 7).
Over 14 million adolescents give birth each year,and about 85% of those births occur in developingcountries (Alan Guttmacher Institute, 1998) (Figure 8).Adolescent pregnancies and births carry higherrisks— for both the mother and the newborn—thanbirths and pregnancies among older women. Thematernal mortality rate among this age group istwice as high as for women in their 20s, and moreadolescent girls aged 15–19 die from pregnancy-related causes than from any other cause (UnitedNations Children’s Fund, 1998). In addition, therisk of death during the first year of life is 1.5 times
Source: Alan Guttmacher Institute (1998) Into a New World: Young Women’s Sexual and Reproductive Lives. NewYork, Alan Guttmacher Institute.
Latin America (1.8 million)
Sub-Saharan Africa (4.5 million) North Africa &
the Middle East (1.0 million)
Asia (5.7 million)
Developed Countries
(1.3 million)
Figure 8. Births to adolescent women each year, by region (total 14 million)
35
10 8 1324
14
43
6
13
20 22 10
0%
10%
20%
30%
40%
50%
60%
70%
80%
Benin Kenya Uganda Madagascar Colombia Haiti
Per
cen
t
Traditional Method Modern Method
Figure 7. Contraceptive use among single, sexually active 15–19 year-old women—selected studies
Source: Population Reference Bureau (2000) The World’s Youth 2000. Washington, DC, Population Reference Bureau.
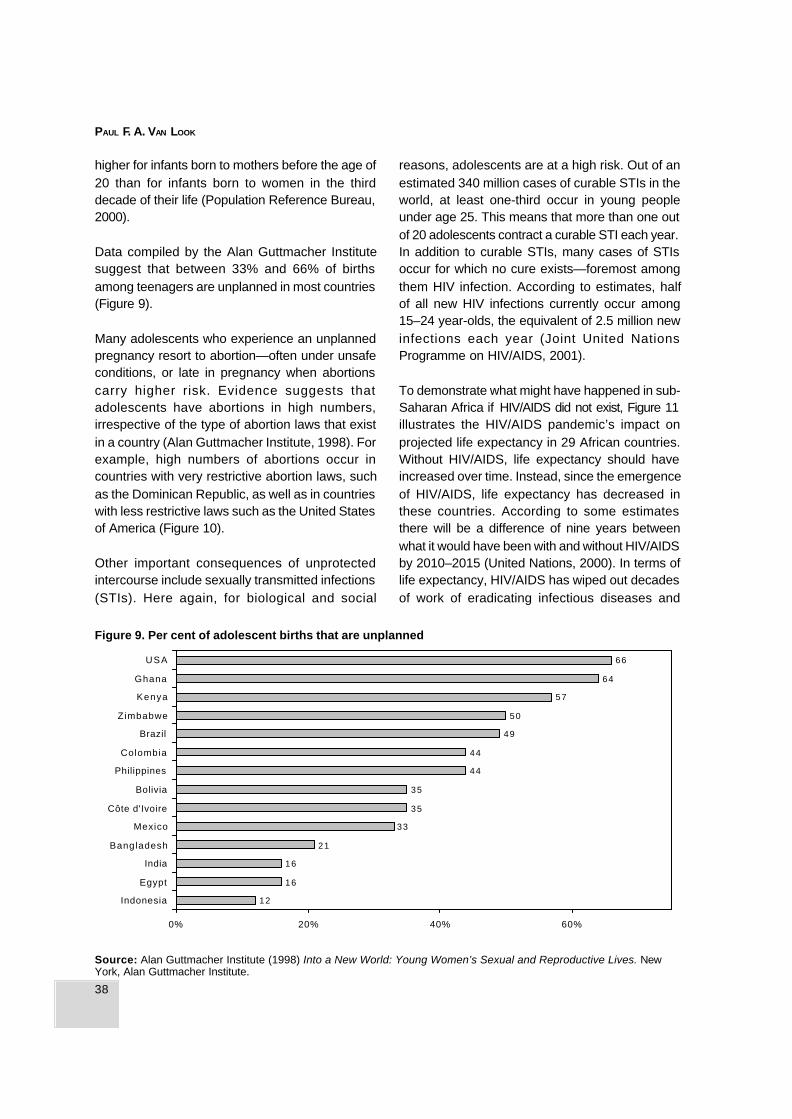
38
PAUL F. A. VAN LOOK
higher for infants born to mothers before the age of20 than for infants born to women in the thirddecade of their life (Population Reference Bureau,2000).
Data compiled by the Alan Guttmacher Institutesuggest that between 33% and 66% of birthsamong teenagers are unplanned in most countries(Figure 9).
Many adolescents who experience an unplannedpregnancy resort to abortion—often under unsafeconditions, or late in pregnancy when abortionscarry higher risk. Evidence suggests thatadolescents have abortions in high numbers,irrespective of the type of abortion laws that existin a country (Alan Guttmacher Institute, 1998). Forexample, high numbers of abortions occur incountries with very restrictive abortion laws, suchas the Dominican Republic, as well as in countrieswith less restrictive laws such as the United Statesof America (Figure 10).
Other important consequences of unprotectedintercourse include sexually transmitted infections(STIs). Here again, for biological and social
reasons, adolescents are at a high risk. Out of anestimated 340 million cases of curable STIs in theworld, at least one-third occur in young peopleunder age 25. This means that more than one outof 20 adolescents contract a curable STI each year.In addition to curable STIs, many cases of STIsoccur for which no cure exists—foremost amongthem HIV infection. According to estimates, halfof all new HIV infections currently occur among15–24 year-olds, the equivalent of 2.5 million newinfections each year (Joint United NationsProgramme on HIV/AIDS, 2001).
To demonstrate what might have happened in sub-Saharan Africa if HIV/AIDS did not exist, Figure 11illustrates the HIV/AIDS pandemic’s impact onprojected life expectancy in 29 African countries.Without HIV/AIDS, life expectancy should haveincreased over time. Instead, since the emergenceof HIV/AIDS, life expectancy has decreased inthese countries. According to some estimatesthere will be a difference of nine years betweenwhat it would have been with and without HIV/AIDSby 2010–2015 (United Nations, 2000). In terms oflife expectancy, HIV/AIDS has wiped out decadesof work of eradicating infectious diseases and
Figure 9. Per cent of adolescent births that are unplanned
Source: Alan Guttmacher Institute (1998) Into a New World: Young Women’s Sexual and Reproductive Lives. NewYork, Alan Guttmacher Institute.
12
16
16
21
33
35
35
44
44
49
50
57
64
66
0% 20% 40% 60%
Indonesia
Egypt
India
Bangladesh
Mexico
Côte d'Ivoire
Bolivia
Philippines
Colombia
Brazil
Zimbabwe
Kenya
Ghana
USA
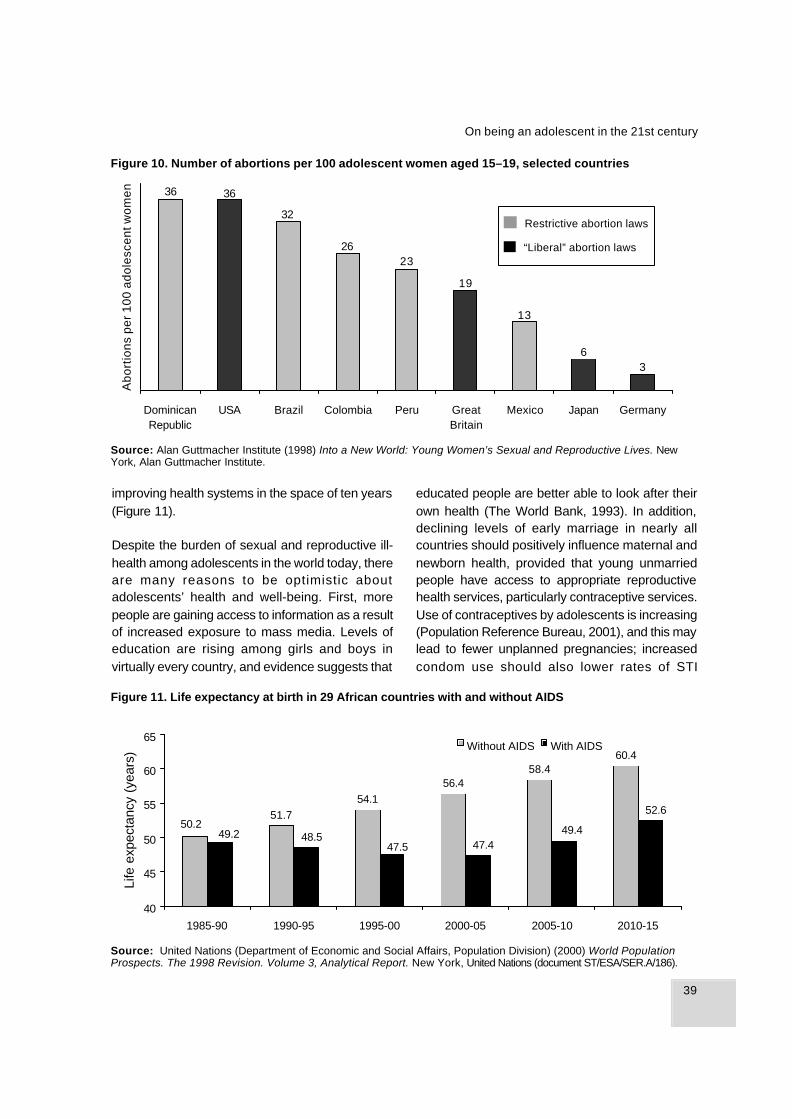
39
On being an adolescent in the 21st century
36
13
19
2326
32
3636
DominicanRepublic
USA Brazil Colombia Peru GreatBritain
Mexico Japan Germany
Source: Alan Guttmacher Institute (1998) Into a New World: Young Women’s Sexual and Reproductive Lives. NewYork, Alan Guttmacher Institute.
Source: United Nations (Department of Economic and Social Affairs, Population Division) (2000) World PopulationProspects. The 1998 Revision. Volume 3, Analytical Report. New York, United Nations (document ST/ESA/SER.A/186).
improving health systems in the space of ten years(Figure 11).
Despite the burden of sexual and reproductive ill-health among adolescents in the world today, thereare many reasons to be optimistic aboutadolescents’ health and well-being. First, morepeople are gaining access to information as a resultof increased exposure to mass media. Levels ofeducation are rising among girls and boys invirtually every country, and evidence suggests that
educated people are better able to look after theirown health (The World Bank, 1993). In addition,declining levels of early marriage in nearly allcountries should positively influence maternal andnewborn health, provided that young unmarriedpeople have access to appropriate reproductivehealth services, particularly contraceptive services.Use of contraceptives by adolescents is increasing(Population Reference Bureau, 2001), and this maylead to fewer unplanned pregnancies; increasedcondom use should also lower rates of STI
Figure 10. Number of abortions per 100 adolescent women aged 15–19, selected countries
Restrictive abortion laws
“Liberal” abortion laws
51.754.1
56.458.4
60.4
50.252.6
47.447.548.5
49.449.2
40
45
50
55
60
65
1985-90 1990-95 1995-00 2000-05 2005-10 2010-15
Life
exp
ecta
ncy
(yea
rs) Without AIDS With AIDS
Figure 11. Life expectancy at birth in 29 African countries with and without AIDS
Abo
rtio
ns p
er 1
00 a
dole
scen
t wom
en
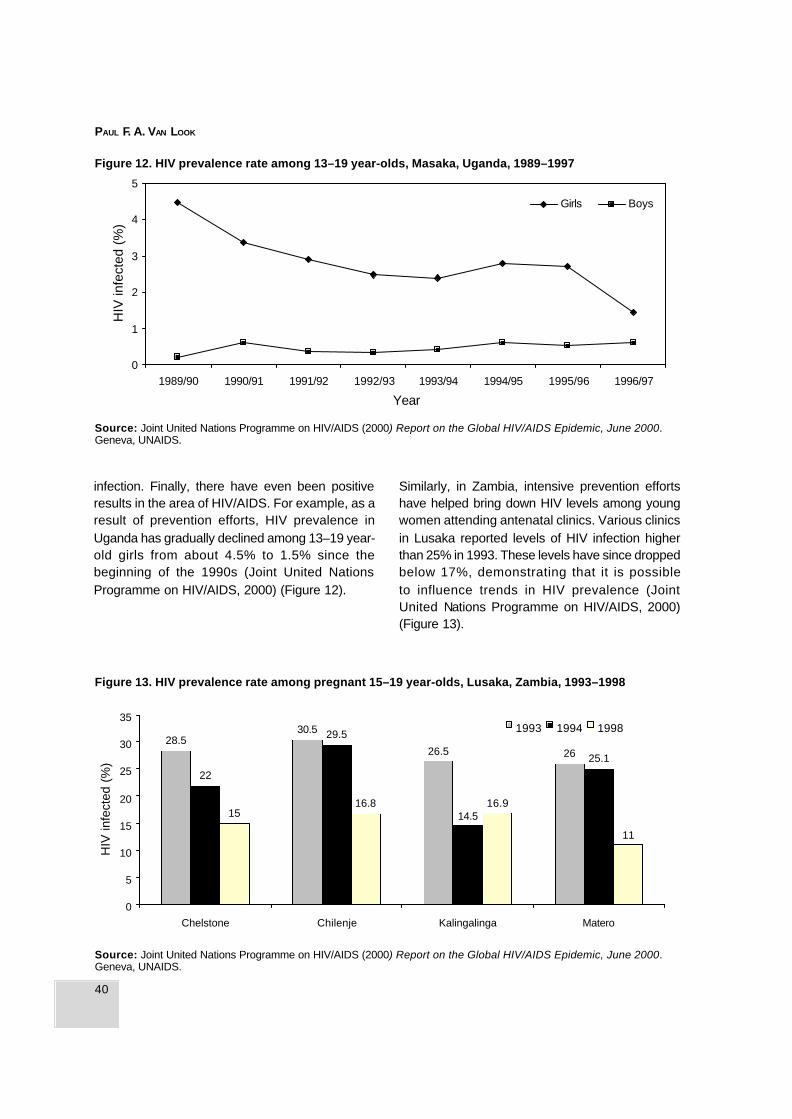
40
PAUL F. A. VAN LOOK
infection. Finally, there have even been positiveresults in the area of HIV/AIDS. For example, as aresult of prevention efforts, HIV prevalence inUganda has gradually declined among 13–19 year-old girls from about 4.5% to 1.5% since thebeginning of the 1990s (Joint United NationsProgramme on HIV/AIDS, 2000) (Figure 12).
Similarly, in Zambia, intensive prevention effortshave helped bring down HIV levels among youngwomen attending antenatal clinics. Various clinicsin Lusaka reported levels of HIV infection higherthan 25% in 1993. These levels have since droppedbelow 17%, demonstrating that it is possibleto influence trends in HIV prevalence (JointUnited Nations Programme on HIV/AIDS, 2000)(Figure 13).
Source: Joint United Nations Programme on HIV/AIDS (2000) Report on the Global HIV/AIDS Epidemic, June 2000.Geneva, UNAIDS.
0
1
2
3
4
5
1989/90 1990/91 1991/92 1992/93 1993/94 1994/95 1995/96 1996/97
Year
HIV
infe
cted
(%
)
Girls Boys
Figure 12. HIV prevalence rate among 13–19 year-olds, Masaka, Uganda, 1989–1997
Figure 13. HIV prevalence rate among pregnant 15–19 year-olds, Lusaka, Zambia, 1993–1998
28.530.5
26.5 26
22
29.5
14.5
25.1
1516.8 16.9
11
0
5
10
15
20
25
30
35
Chelstone Chilenje Kalingalinga Matero
HIV
infe
cted
(%
)
1993 1994 1998
Source: Joint United Nations Programme on HIV/AIDS (2000) Report on the Global HIV/AIDS Epidemic, June 2000.Geneva, UNAIDS.

41
On being an adolescent in the 21st century
Conclusions: key elements of successfulprogrammes
In 1999, Dr Gro Harlem Brundtland, DirectorGeneral of WHO, addressed the ICPD + 5 in TheHague. During her address, she argued that, “thereis a deep-seated discomfort when dealing withadolescent sexuality. We need to change this.”As researchers, policy-makers and programmemanagers address adolescent sexuality andsearch for ways to improve young people’s lives,they should consider a number of elements thatseem to be key to successful programmes. First,adolescents themselves need to participate inprogramme planning and design. Second,programmes need to address health problems ina comprehensive manner. Many problems thatadolescents experience have common roots andcommon determinants. It makes little sense toaddress one particular health problem whileignoring others.
In addition, programmes should combineinterventions from different areas, such as health,education and life skills development, micro-credit,small business development and safe environmentsfor entertainment. Whenever possible, programmesshould build links with existing services in order toachieve cost-effectiveness and avoid duplication.To reinforce services, ways need to be found toprovide young people with more supportiveenvironments within their families, schools andcommunities.
All these recommendations require strongprogramme management. It is not easy to developcomprehensive programmes for adolescents thatare able to deal with many facets of adolescentlife. To meet the needs of different categories ofadolescents in ways that respect cultural diversityrequires great skill from service providers andprogramme managers.
The above recommendations have emerged fromlessons learned or current thinking aboutprogramming for young people, but more work isneeded to define the elements of successful
programmes on the basis of empirical evidence.We hope that this Conference contributes to thateffort.
References
Alan Guttmacher Institute (1998) Into a New World:Young Women’s Sexual and Reproductive Lives. NewYork, Alan Guttmacher Institute.
Brown A, Jejeebhoy SJ, Shah I, Yount KM (2001)Sexual Relations Among Young People inDeveloping Countries: Evidence from WHO CaseStudies. Geneva, World Health Organization (WHO/RHR/01.8).
Joint United Nations Programme on HIV/AIDS (2000)Report on the Global HIV/AIDS Epidemic, June 2000.Geneva, UNAIDS.
Joint United Nations Programme on HIV/AIDS (2001)Children and Young People in the World of AIDS.Geneva, UNAIDS.
Murray CJL, Lopez AD, eds. (1996) The Global Burdenof Disease: A Comprehensive Assessment of Mortalityand Disability from Diseases, Injuries and RiskFactors in 1990 and Projected to 2020. Global Burdenof Disease and Injury Series, Vol. 1. Cambridge, MA,Harvard School of Public Health on behalf of the WorldHealth Organization and the World Bank.
Murray CJL, Michaud C (1996) Recalculation ofDALYs according to age groups pertaining toadolescents, youth, and young people—Descriptionof methodology and data used for calculation(unpublished paper).
Population Reference Bureau (2000) The World’sYouth 2000. Washington, DC, Population ReferenceBureau.
Population Reference Bureau (2001) Youth in Sub-Saharan Africa: A Chartbook on Sexual Experienceand Reproductive Health . Washington, DC,Population Reference Bureau.
United Nations (Department of Economic and SocialAffairs, Population Division) (1999) World PopulationProspects. The 1998 Revision. Volume 1:Comprehensive Tables. New York, United Nations(ST/ESA/SER.A/177).
United Nations (Department of Economic and Social

42
PAUL F. A. VAN LOOK
Affairs, Population Division) (2000) World PopulationProspects. The 1998 Revision. Volume 3: AnalyticalReport. New York, United Nations (ST/ESA/SER.A/186).
United Nations Children’s Fund (1998) Progress ofNations 1998. New York, UNICEF.
Warren CW et al. (2000) Tobacco use by youth: asurveillance report from the Global Youth TobaccoSurvey project. Bulletin of the World HealthOrganization, 78(7):868–876.
The World Bank (1993) World Development Report1993—Investing in Health . Oxford, Oxford UniversityPress on behalf of the World Bank.
World Health Organization (2001) Briefing note 3 onadolescent health—Provision of health services.Briefing Notes on Selected Adolescent Health Issues.Geneva, World Health Organization, Department ofChild and Adolescent Health and Development.
Paul F.A. Van Look, MD, PhD, FRCOGDirectorDepartment of Reproductive Health andResearchWorld Health Organization1211 Geneva 27Switzerland

43
Addressing the reproductive health needs of adolescents in India
Background
The World Health Organization defines “youngpeople” as those between the ages of 10 and 24.This age group is composed of two overlappingsubgroups, namely “adolescents” (aged 10–19)and “youth” (aged 15–24). The PlanningCommission of India estimates that as of March2000, adolescents aged 10–19 comprised 23% ofthe Indian population, i.e. almost 230 million. Sucha large group represents a major human resourcethat can and must contribute to the overalldevelopment of the country. Addressing their needswill contribute not only to social and economicdevelopment, but also to social harmony, gender parity,population stabilization and improved quality of lifefor all Indians.
Health programmes generally make provisions foradults and young children, but adolescents havelargely been overlooked. Adolescence is a periodof tremendous opportunity as well as of risk,characterized by physical, psychological andsocial change. While adolescents are not yetadults, neither are they completely out ofchildhood. The 1994 International Conference onPopulation and Development held in Cairorecommended that governments focus moreattention on adolescents through an integratedapproach to their health, education and social needs.
Official statistics in India do not completelycorrespond with emerging international definitions.Much information about the age group 15–19 needsto be estimated or disaggregated from informationabout the age group 15–24. Better quality dataare available for older adolescents (age 15–19) thanfor younger adolescents (age 10–14). Gender-disaggregated data for adolescents are limited andare generally available only for recent years. Morequalitative data are also needed, especially toexplore issues of gender discrimination andreproductive behaviour. Nevertheless, this paperreviews the data that are available on adolescents’situation in India in terms of employment, literacyand health. The paper goes on to makerecommendations for programming and reviewsongoing government policies and programmesaimed at young people.
Employment, education and literacy
Data from the Ministry of Human ResourceDevelopment indicate that nearly 90% of childrenaged 6–11 are enrolled in school, but enrolmentfalls to 59% among 11–14 year-olds. An obviousgender bias operates in the education sector; two-thirds of boys aged 11–14 are enrolled in schoolcompared with less than half of girls in that agegroup. The dropout rate for girls in high school is as
Addressing the reproductive health needs ofadolescents in India: directions forprogrammes
A.R. Nanda

44
A. R. NANDA
high as 72% (Government of India, Ministry of HumanResource Development, Department of Education,1999).
There is a close association between educationalattainment and age at marriage, fertility regulationand health-seeking behaviour. Studies from Indiareveal that while age at marriage among illiteratewomen is 15 years, age at marriage among girlswho have completed high school is significantlyhigher, at 22 years (United Nations PopulationFund, 1998). Globally, women with seven or moreyears of education tend to marry four years laterand have 2.2 fewer children than women with noschooling (United Nations Population Fund, 1996).
A large proportion of adolescents are employed.The 1994–95 National Sample Survey Organisationfound that the work participation rate among ruraladolescents aged 15–20 years was 77% for youngmen and 31% for young women. Manyadolescents, including those younger than age 14,work in occupations such as bidi-making, gem-polishing, coir-making, paper bag manufacturing,embroidery, zari embroidery, and the lock, glassand carpet industries. Many adolescents work inthe agricultural sector or for local village industriesas a part of a family labour force. In urban areas,girls form a large part of the unorganized sectorworking as domestic help. Besides receivingunequal wages, working girls are more vulnerableto sexual abuse and violence than older women.
Adolescent marriage and childbearing
In many parts of India, early marriage for girls is areligious and social imperative. Despite laws thatspecify the legal age of marriage for girls as 18years, cultural pressures often force parents tomarry off their daughters at a younger age. In 1996,an average of 38% of girls aged 15–19 were married(Jejeebhoy, 1998). This rate was significantly higherin rural areas where 46% of girls in this age groupwere married, compared with 22% of girls aged15–19 in urban areas. Age at marriage varies fromstate to state, however. Early marriages are
common in Madhya Pradesh, Andhra Pradesh,Rajasthan and Bihar, where more than 50% ofyoung women aged 15–19 are married. In Haryanaand Uttar Pradesh, 40–44% of young women aged15–19 are married. Women in Kerala, Punjab, Goa,Manipur, Mizoram and Nagaland tend to marry later,and in those states fewer than 15% of girls aged15–19 are married.
Because of early marriage, adolescent fertility inIndia is relatively high. This should be a cause forconcern since many younger adolescents arephysiologically immature for reproduction.Compared to adult women, childbearing duringadolescence poses greater health risks to boththe mother and the newborn. Fertility during thisperiod contributes to maternal morbidity andmortality, high incidence of low birth weight babiesand neonatal morbidity and mortality (Jejeebhoy,1998). Not surprisingly, 1997 age-specificfertility rates (ASFR) among 15–19 year-oldsreveal a major urban–rural differential. At 20.3 perthousand, the rural ASFR was more than doublethe urban ASFR of 9.8 per thousand (InternationalInstitute for Population Sciences, 1995).
Sexual behaviour and knowledge amongadolescents
Studies suggest that adolescents have limitedknowledge about sexual and reproductive health,and know little about the natural processes ofpuberty, sexual health, pregnancy or reproduction.This lack of knowledge about reproductive health—including the emerging threat of HIV/AIDS—mayhave grave consequences for the country.
Countrywide information on adolescents’ sexualbehaviour is not available. However, contrary togeneral expectations, small-scale studies suggestthat sexual activity begins at a relatively early age.As reported in a review of adolescent sexual andreproductive behaviour in India, a 1993–94 studyconducted by the Family Planning Association ofIndia among educated urban youth revealed thatthe average age of first sexual experience among

45
Addressing the reproductive health needs of adolescents in India
15–19 year-olds was age 14.8 for males and age16.1 for females; another 1995 study found thatonly 38% of young men and 63% of young womendisapproved of premarital sexual relationships(Jejeebhoy, 1998). While these studies are notrepresentative of the entire country, they dosuggest that a substantial proportion ofadolescents are sexually active. The need of thehour is to obtain more culturally and contextspecific data for formulating interventions thataddress sexual decision-making, gender roles andpower relations between the sexes.
Knowledge and use of contraception
Large-scale studies such as the National FamilyHealth Survey suggest that at least half of all youngwomen in India are sexually active by age 18—mostly within marriage—and almost one in five arepregnant by age 15. Well over half of all marriedwomen aged 15–19 have experienced a pregnancyor given birth (United Nations Population Fund,1998). Nevertheless, the 1995 National Survey onFerti l i ty and Family Planning Practices(International Institute of Population Sciences,1995) found that adolescents had relatively lowlevels of knowledge about reversible contraceptivemethods. The study revealed that while 89% ofadolescents were aware of sterilization, less than50% were aware of oral contraception and only39% knew about IUDs. In view of the previousdiscussion about sexual activity among youngerage groups, it is disheartening to note that such asmall percentage of adolescents are aware ofspacing methods that would be most suitable fortheir contraceptive needs.
Evidence suggests that contraceptive use riseswith age. The 1992–93 National Family and HealthSurvey (International Institute for PopulationSciences, 1995) indicated that no more than 5%of married women aged 13–14 and no more than7% of married women aged 15–19 were practicingcontraception. These low levels contrast with 21%of women aged 20–24 and 61% of women aged35–39 using contraceptives.
Programme recommendations
Many health programmes view the needs ofadolescents with a narrow focus on reproductivehealth. While reproductive health is undoubtedlyimportant, programmes need a wider perspectivethat considers adolescents’ broader emotional andphysical needs as well. For example, risk-takingbehaviour and employment in hazardous industriesplace young people at risk of physical injury.Adolescent health programmes also need toconsider relatively high rates of substance abuse,violence—especially sexual violence—andtrafficking of children and adolescents forcommercial sex work.
A programme’s willingness to address issues thatmay not relate directly to health can have aprofound effect on both the acceptability and cost-effectiveness of those interventions. Programmesshould focus not only on counselling services,contraception, nutrition, and rehabilitation of theabused or exploited, but also on factors such aslife skills, protection from abuse and vocationalguidance.
Programmes for adolescents also need torecognize the vast diversity among this segmentof the population. Adolescents include a widespectrum of categories: in-school and out-of-school; married and unmarried; tribal, rural andurban; the employed and the unemployed; thosewho have been sexually exploited; those ininstitutions; those who are disabled and those inconflict with the law.
Finally, programmes need to involve adolescentsthemselves and other stakeholders at every stage—from conceptualization to programme design andevaluation. Because adolescent sexual andreproductive health is such a sensitive issue,programmes must consult community leaders,religious groups, parents and teachers in order toensure the acceptability and effectiveness of theirinterventions.

46
A. R. NANDA
Institutional versus outreach models
Services for adolescents can be delivered throughinstitutions or through outreach schemes. Atpresent, hospital services do not cater toadolescents. To become more acceptable toadolescents, hospital services need to giveadequate attention to their particular concerns, suchas privacy. Although this may not require manyadditional resources, it does require sensitivity andreorganization of clinical services in some healthfacilities. The Safdarjung Hospital in New Delhi,which is one of the largest public hospitals in thecountry, has begun a two-year pilot project to testthe feasibility of such an approach.
Because a vast majority of the Indian populationlives in rural areas, outreach efforts are also neededto reach many adolescents. For example, healthcamps held at regular intervals in remote and far-flung areas can provide basic reproductive healthservices, as well as services such as counselling,nutritional advice, rehabilitative services, life skills,and vocational guidance. Ideally, governmental andnongovernmental organizations (NGOs) wouldcollaborate in this endeavour.
Government programmes for adolescents
While the Government of India has not yetformulated specific programmes for adolescents,several ongoing programmes have componentsthat address their needs. For example, the NationalPopulation Policy has recognized adolescents asan underserved category that will have a centralrole in determining the size of the population incoming decades. The policy aims to provide foradolescents’ nutritional, contraceptive andinformation needs. Other policy documents havealso addressed adolescents’ diverse needs: forexample, the National Nutrition Policy (1983)identified adolescent girls as a vulnerable group;the National Education Policy (1986) reaffirmed thecommitment of the government to eradicatingilliteracy in the age group 13–35; and the NationalPlan of Action for Children devoted a separate
section to adolescent girls. The draft National YouthPolicy 2000 calls for a multi-dimensional integratedapproach to youth development. This policyfocuses on youth empowerment, gender justice,youth participation in decision-making,establishment of a strong intersectoral approachand building a robust information and researchnetwork to address needs of the young population.
Several government schemes provide vocationaltraining, education, social development andempowerment of girls, including Training of RuralYouth for Self Employment (TRYSEM), VocationalGuidance and Employment Scheme, Balika andSarv Sksha Ahiyan, adolescent girls’ scheme underthe Integrated Child Development Scheme (ICDS),Nehru Yuvak Kendra Sangthan and the NationalService Scheme, among others. In addition, NGOprogrammes in several parts of the country addressadolescents’ needs, including reproductive health,rehabilitation of sexually abused children, streetchildren, gender equity, employment and otherissues.
Conclusions
This Conference on reproductive health is takingplace at an opportune moment for the Ministry ofHealth and Family Welfare. The Ministry is in theearly stages of formulating future strategies thatwill succeed the current Reproductive and ChildHealth Programme. The deliberations andrecommenda-tions of this Conference willundoubtedly help in this task.
References
Government of India, Ministry of Human ResourceDevelopment, Department of Education (1999)Selected Educational Statistics . New Delhi,Government of India.
International Institute for Population Sciences (1995)National Family Health Survey (MCH and FamilyPlanning), India 1992–93. Mumbai, InternationalInstitute for Population Sciences.

47
Addressing the reproductive health needs of adolescents in India
Jejeebhoy S (1998) Adolescent sexual andreproductive behaviour: a review of the evidence fromIndia. Social Science and Medicine, 10:1275–1290.
United Nations Population Fund (1996) The State ofthe World’s Population. New York, UNFPA.
United Nations Population Fund (1998) India CountryPaper. Paper presented at the South Asia Conferenceon the Adolescent, New Delhi.
A.R. NandaSecretary, Family WelfareMinistry of Health and Family WelfareGovernment of IndiaNirman BhavanNew Delhi 110011India
48
ENA S INGH
Background
Adolescents make up one-fifth of the world’spopulation—over a billion people. In South Asiathat proportion is even greater. Programmes aimedat adolescents affect not only their lives and thelives of their future offspring, but also the lives oftheir younger siblings, mothers and fathers—in fact,all of society. No matter which “sector” we comefrom—whether reproductive health, education,gender, violence, drug abuse or indeed any area ofserious concern to society today—we must realizethe importance of working with adolescents. Thatis why so many national policies include referencesto adolescents, including policies related to youth,women, children, population, education, health,nutrition and HIV/AIDS. This paper reviews thesituation of adolescents in South Asia in terms ofeducation, labour participation, sexual andreproductive health and violence. The paper thenexplores recommendations for designingsuccessful programmes to address the wide rangeof issues that adolescents face.
Education and employment of adolescents
Despite improved educational opportunities inrecent decades, a sizeable proportion ofadolescents remain illiterate in South Asiancountries; Sri Lanka and the Maldives are the
exceptions. In much of the rest of the region,between one-third and two-thirds of youngeradolescent girls are illiterate, as are one-fifth toone-half of younger adolescent boys. Moreover, inmany countries in the region, secondary schoolenrolments are low, and a large proportion of olderadolescents aged 15–19 engage in economicallyproductive activities. For example, olderadolescents’ labour participation rates range from18% in Sri Lanka, to 49% in Nepal, to 67% inBangladesh, while they average 33% for the restof the region (United Nations Population Fund,1998). Adolescents, especially girls, are subjectto many types of exploitation—including sexualexploitation and trafficking as well as economicexploitation such as organized begging (see, forexample, Mundigo & Indriso, 1999).
Sexual and reproductive health
Adolescents in South Asia often lack reproductivechoice, such as whether, when and whom to marry;whether and when to have children and how manyto have; whether to abort a female fetus; whetherto use contraceptives and where to get them. Morebroadly, adolescents often lack choice aboutwhether they can study and learn, work and earn,keep their own earnings or have to give them totheir elders or spouses, and whether they can sendtheir children to school. In many cases,
Adolescent reproductive health in South Asia:key issues and priorities for action
Ena Singh

49
Adolescent reproductive health: implications for South Asia programme
adolescents have dreams and aspirations, but littlefreedom to shape their own lives.
The age at which young girls marry is distressinglylow in most of South Asia. Early marriage for girlsis the norm in most countries of the region, despitelaws prohibiting marriage before age 18 for girls,and before age 21–24 for boys. Nearly two-thirdsof girls in most South Asian countries marry byage 18, while one-fourth marry by age 15. Again,Sri Lanka is an exception (United NationsPopulation Fund, 1998).
Nevertheless, age at marriage is rising throughoutthe region (see, for example, United NationsPopulation Fund, 2000). This trend raises its ownset of issues and concerns. South Asia societiesgenerally consider sex outside marriage immoraland condemn adolescents—girls in particular—who engage in it. However, rising age at marriageand more schooling, combined with increasedmigration and urbanization have led to moreopportunities for premarital sex. In Bangladesh,for example, one survey found that 60% ofunmarried urban adolescent boys and 10% ofunmarried urban girls reported sexual experiences(United Nations Population Fund, 1998). In India,one study found that 20–25% of unmarriedadolescent boys reported engaging in sexualrelations (United Nations Population Fund, 1998).
More opportunities for premarital sex combinedwith a lack of knowledge about the body andcontraception may be responsible for increasingthe number of unwanted pregnancies and abortionsamong adolescent girls. Studies suggest that notonly do many unmarried girls lack knowledge ofcontraceptives, but many hesitate to use them,because this would conflict with their self-imageas moral beings (United Nations Population Fund,1998). Sadly, “Had I known...” is a phrase oftenheard from young women who did not have basicknowledge of contraception and did not fullyunderstand the consequences of unprotected sex,the risks of pregnancy, or the dangers of unsafeabortion.
Because of delays in making a decision orreaching a service provider, adolescent abortionsare often second trimester, illegal and unsafe.Unfortunately, service providers are known to takeadvantage of adolescents’ vulnerability, oftenasking for money or favours that they would notask from older, married women. Abortion thusremains an urgent issue for young people. Optionssuch as increasing adolescents’ access toemergency contraception must be seriouslyexplored.
Young people are not only at high risk forpregnancy, but also for sexually transmittedinfections (STIs). The available data show highprevalence levels of reproductive tract infections(RTIs) and STIs among married and unmarriedadolescent girls and boys. For example, a studyin Bangladesh found that 40% of adolescent girls(including both married and unmarried) and 20%of unmarried adolescent boys reported symptomsof RTIs and STIs (United Nations Population Fund,1998). A study in Sri Lanka found that 7% ofadolescent boys had an STI (United NationsPopulation Fund, 1998).
Many adolescents, particularly girls, experienceviolence, such as sexual abuse, trafficking, rapeand “honour killings”. In Bangladesh, one thousandrapes were reported in 1995, 20% of which werecommitted against minors (United NationsPopulation Fund, 1998). This is only the tip of theiceberg. Most often, the perpetrators are boys ormen whom adolescents know and trust. In additionto the trauma of violence, young girls often sufferadditional shame and guilt inflicted by society uponthe victim.
Programmes
Because education, work, sex and violence areall part of adolescents’ lives, those who work withadolescents must let the boundaries of theirspecializations blur. Effective programmes foradolescents quickly become trans-sectoral,meaning that they integrate different sectors into

50
ENA S INGH
a single programme, rather than beingmultisectoral, which implies the mere inclusion ofmany separate interventions. Because adolescentswill not accept programmes that do not relate totheir lives, most successful programmes addresslife skills such as self-esteem, self-awareness,communication and negotiation. Indeed, inprogrammatic jargon, adolescents and life skillsseem to have become synonymous.
This conference has provided an opportunity todiscuss how to design, initiate and sustain life skillsprogrammes. In this context, the most importantquestion is what we teach young people in theseprogrammes. In a book entitled Conversations withGod, Book I, Neale Donald Walsch (1995) states:
Most people have misunderstood the meaning,the purpose, and the function of education, tosay nothing of the process by which it is bestundertaken. People think that the purpose ofeducation is to pass on knowledge; that to edu-cate someone is to give them knowledge. Yet,education has very little to do with knowledge.It has to do with Wisdom. Wisdom is knowl-edge applied… we mustn’t ignore wisdom infavour of knowledge… It would kill education.It is killing it. We are teaching our children whatto think instead of how to think. Lessons incritical thinking, problem solving, and logic areconsidered by many parents to be threatening.And well they might. Because children who areallowed to develop their own critical thinking pro-cess are very much likely to abandon theirparent’s morals, standards and entire way of life.
This quote addresses the perpetual question ofhow to balance parents’ responsibilities withadolescents’ rights, a question that generatedmuch heated debate at ICPD + 5 (5-Year Reviewand Appraisal of Implementation of the ICPDProgramme of Action) and other fora. No other topicin these debates evokes more intense discussionthan the topic of sexuality and sex education. Wehave a great deal of evidence that when sexualityis openly discussed and when young people learnabout their bodies and their emotions, they are
better able to cope with sexual maturation. Sexualcrimes, RTIs and unwanted births would not poseproblems of such magnitude if such issues weremore openly discussed. If each birth is to beconsidered a blessing and each sexual encounteran expression of love, not an irresponsibleexperiment or an act of aggression, then we musttalk openly about sex.
Because most reproductive health programmesoriginated from concern about population growth,they viewed adolescent fertility with concern. Froma demographic perspective, one-fifth of births occurin adolescence, and adolescent girls have shorterbirth intervals than older women. As a society,however, we have had to ask whether it isacceptable to tell unmarried adolescents aboutcontraception. Even if we can agree that it isacceptable to tell them about contraception, whatabout giving them contraception? Many argue thatwe might let unmarried boys have access tocondoms, but are more ambivalent about givingpills to unmarried girls. Health workers are oftenleft to sort out these dilemmas according to theirown value systems or the administrators’preferences.
There is a solution, however. First, each countryor state must make clear choices and must acton those choices. Second, we must not proposesolutions that do not match the problem. Denyingcontraception will not mandate morality. Moralitydepends on the way that men and women treateach other, the way that the media createsaspirations, and the way that society definessuccess—issues that should be tackled at theirown levels. Responsible sex education andcontraceptives should not be denied to people whoare at risk of disease or unwanted pregnancies.
Many countries have begun to provide sexual andreproductive information in a responsible andsensitive way, though often in response toconcerns about HIV/AIDS rather than unwantedpregnancy or unsafe abortion. Those who designeducation, services and counselling programmesfor adolescents must consider that young people

51
Adolescent reproductive health: implications for South Asia programme
have their own language about the body, sex andpregnancy. It is crucial to understand whoinfluences girls’ decisions to have sex or to aborta pregnancy, and what role their partners play. Canthey turn to a mother, sister, aunt or friend when introuble? Who will pay? Lack of money is acommon theme in young girls’ stories, includinglack of money to raise the child they carry, or lackof money to pay for a safe abortion.
Programmes for adolescents confront issues ascomplex as life itself—education, nutrition,contraception, disease control, reproductivechoices and rights, reproductive safety,employment, skills and mental health. They allmerit priority. Although this conference focuses onreproductive health, we must remember thatprogrammes cannot improve adolescents’reproductive health if they ignore the rest ofadolescents’ often turbulent lives.
A few broad principles should guide those of uswho work with adolescents from a reproductivehealth perspective. First, help adolescents to knowtheir potential to become knowledgeable, confident,responsible, and caring adults, whether this isachieved through camps, life skills programmesor regular education. Healthy reproductive healthchoices will follow. Such programmes may beexpensive, but failure to help adolescents achievetheir potential will be even more costly.
Second, we need to think beyond the scope of ourparticular sectors for a while. Programmes foradolescents can begin with focus on a singleissue, but they need to grow into broaderprogrammes covering the issues that are the wantsand needs of young people. If individual reproductivehealth issues are important, their turn will come.Most adolescents want information about love, sex,marriage and children. With time, reproductivehealth issues emerge as a priority—though notnecessarily the highest priority.
Third, we should collaborate with all those whowork with adolescents. Reproductive healthprogrammes do not have to start from scratch or
work in isolation. We can help professionals fromother sectors to address reproductive health issueseffectively. Often they ignore reproductive issuesnot because they discount their importance, butbecause they may not know how to talk aboutreproductive and sexual health concerns insensitive and engaging ways.
Fourth, we need to work with young people, not“work at” them. The conference session on youth-friendly services sheds light on how this can bedone. One lesson is that young people’s comfortwith their own sexuality is a prerequisite toresponsible and caring reproductive behaviour. Butas counsellors, service providers or managers, weneed to be comfortable with our own sexualitybefore trying to teach young people to becomfortable with theirs.
Finally, do not forget boys. Many initiatives havebeen preoccupied with girls, perhaps because theyemerged from efforts devoted to girls’ education,reproductive health or women’s empowerment. Itis good for programmes to concentrate on girls.However, I recall several occasions whenorganizations denied funding for boys simplybecause they had defined girls as a priority.Interventions for boys and girls do not need to bemutually exclusive.
In this regard, we need to remember that educatingand sensitizing boys are not shortcuts orsubstitutes for empowering girls, though suchefforts may support that objective. We mustpreserve the spaces that have been carved out forgirls and women at great cost. Involving men andboys can be a double-edged sword; it can cutthrough centuries of bias and patriarchy, but suchinvolvement can also threaten the tender ropes thatwomen have so recently woven to pull themselvesout of prison. We need to exercise the utmost carenot to allow this to happen.
Before closing, I would like to recall the collectivewords of the young people who attended a SouthAsia Conference on Adolescents held in New Delhiin 1998 (United Nations Population Fund, 1998):

52
ENA S INGH
We adolescents are not only conscious of ourrights but we also feel responsible for movingaway from the “me” decade in which we are liv-ing, to a decade where adolescents will proveto be an important human resource for the bet-terment of the region. We pledge to make thisa reality.
Our perspective is that we feel neglected, andso we need more attention, care and supportfrom all. We feel we do not have the right tomake our own choices, even after learningabout all the alternatives and choices relatedto our careers, friends, movements and lifepartners. We greatly lack proper and correctinformation and guidance, especially related toour bodies’ physiological and psychologicalchanges. We are not allowed to express ouremotions and our thoughts. We feel increas-ingly ‘self abused’ through frequent exposure topornography, blue films, sex shops and obsceneadvertisements.
To our parents, we say that we need you to lis-ten to us, to our dreams, our experiences, ourexplanations. Give us your time—you gave uslife, now we want your time. Don’t hide thingsfrom us, especially when they are related to us.Give us the privacy and the space to grow. Guideus; don’t drive us.
To our Governments, we say that our biggestdilemma is why girls are discriminated against.Do something. Review the education system,especially the way you evaluate us. Don’texperiment with us and change curriculafrequently. Make education more relevant andinteresting. Provide non-formal educationprogrammes for adolescents who can’t go toschool. Include lessons on life skills and sexeducation in formal and non-formal educationprogrammes. Provide adolescents withprofessional and confidential counsellingservices on sexual and reproductive healthissues. Eliminate child labour, child abuse and
all types of violence against adolescents,including trafficking. Take legal action againstimmoral acts such as pornography, blue films,sex shops, and obscene advertisements. Don’tjust make laws; enforce them. Require lawenforcement agencies to be more sensitivetowards physical abuse cases. Let us supportyou and join hands to fight the menace of drugs.
Our declaration ends here, but not our desireto do something for millions of adolescents werepresent.
With such a force on our side, is change notinevitable? Often I have heard people say that theylove working with adolescents because their effortsare met with enthusiasm, and because thetransformation of young people is fast and dramatic.It is a very rewarding experience. How fortunatethat it is so. Under such circumstances, surelywe will succeed.
References
Mundigo I, Indriso C, eds. (1999) Abortion in theDeveloping World. Delhi, World Health Organizationand Vistaar Publications.
United Nations Population Fund (1998) Report of theSouth Asia Conference on Adolescents. New Delhi,July 1998. Kathmandu, UNFPA Country Support Teamfor Central and South Asia.
United Nations Population Fund (2000) Adolescentsin India: A Profile. New Delhi, UNFPA for the UnitedNations System in India.
Walsch ND (1995) Conversations with God, Book I.London, Hodder and Stoughton.
Ena SinghUNFPA55 Lodi EstateNew Delhi 110013India

IIISexual and reproductivehealth of marriedadolescents

54
SUMATI KULKARNI
55
The reproductive health status of married adolescents as assessed by NFHS-2, India
The reproductive health status of marriedadolescents as assessed by NFHS-2, India
Sumati Kulkarni
Background
Adolescence is the transition period betweenchildhood and adulthood. However, in many Asiancountries, early marriage and childbearing deprivegirls of this transitional phase and push them toshoulder responsibilities for which they are not fullyequipped. As a result, married adolescents formone of the most vulnerable sections of thepopulation in a country like India. In order toformulate policies and programmes for this group,it is essential to know about the risks that theyface and the extent to which the present healthsystem meets their needs. This paper presentsfindings of the second National Family HealthSurvey (NFHS-2) that pertain to ever-marriedwomen in the age group 15–19, defined asadolescents in this paper.
Methods
The International Institute for Population Sciences(IIPS) undertook the NFHS-2 in 1998–1999, incollaboration with ORC Macro, USA. The studycovered a representative sample of 89 199 eligiblewomen aged 15–49, from 91 196 households in26 states. The survey included 8182 marriedadolescent women (aged 15–19), who formednearly 9.2% of the women interviewed in the survey.During two phases of data collection in November
1998 and March 1999, the survey gathered dataon fertility, family planning, maternal and childhealth, utilization of health services, women’sautonomy, reproductive health and nutritionalstatus. One unique feature of the survey was bloodtesting for haemoglobin levels, which made itpossible to measure levels of anaemia among therespondents.
Key findings
The survey revealed that nearly one-third of femaleadolescents were ever married compared to only6% of male adolescents. In addition, one-third ofever-married women aged 25–49 were married byage 15, while two-thirds were married by age 18.This situation remained unchanged since theNFHS-1 was conducted in 1991–1992. For themajority of women in the age group 25–49, theage at first cohabitation with their husbands was17 years, but it varied from 15 years in AndhraPradesh to 23 years in Goa.
During the last 15 years, there has been a 33%decline in adolescent fertility. Nevertheless,currently married adolescent women (aged 15–19at the time of the survey) reported 4209 birthsduring the three years preceding the survey, one-fourth of which were second or higher order births.This indicates the extent of physical strain on these
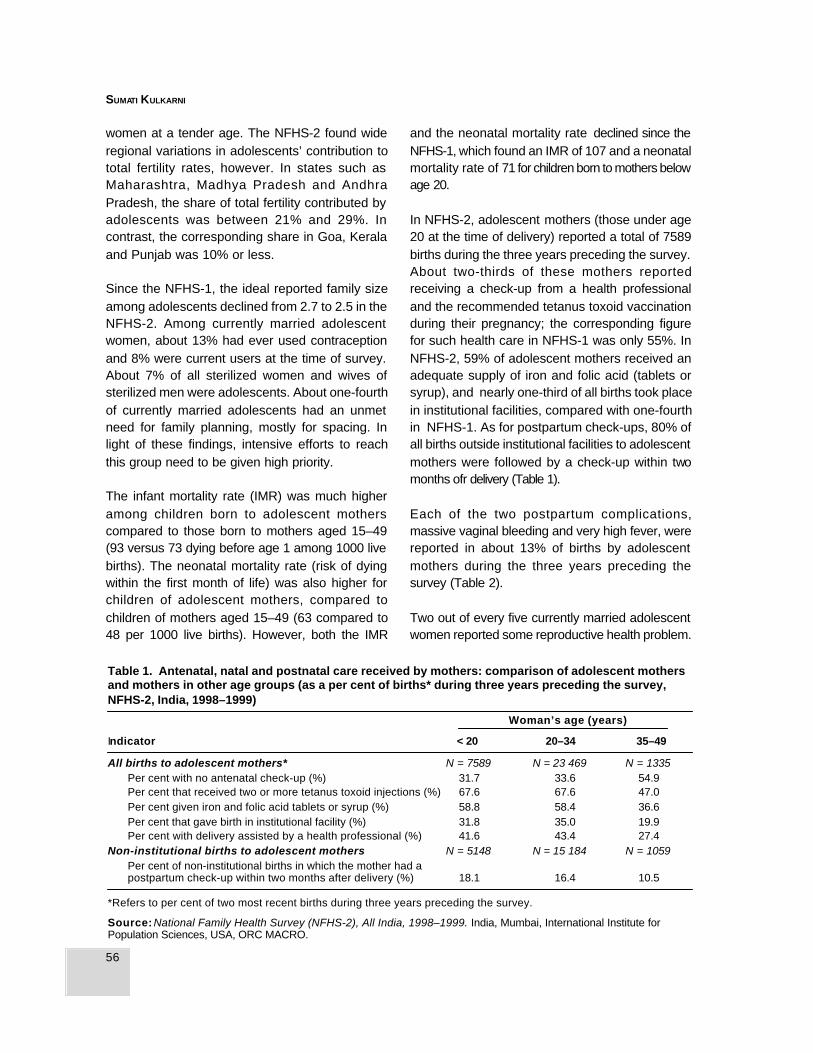
56
SUMATI KULKARNI
women at a tender age. The NFHS-2 found wideregional variations in adolescents’ contribution tototal fertility rates, however. In states such asMaharashtra, Madhya Pradesh and AndhraPradesh, the share of total fertility contributed byadolescents was between 21% and 29%. Incontrast, the corresponding share in Goa, Keralaand Punjab was 10% or less.
Since the NFHS-1, the ideal reported family sizeamong adolescents declined from 2.7 to 2.5 in theNFHS-2. Among currently married adolescentwomen, about 13% had ever used contraceptionand 8% were current users at the time of survey.About 7% of all sterilized women and wives ofsterilized men were adolescents. About one-fourthof currently married adolescents had an unmetneed for family planning, mostly for spacing. Inlight of these findings, intensive efforts to reachthis group need to be given high priority.
The infant mortality rate (IMR) was much higheramong children born to adolescent motherscompared to those born to mothers aged 15–49(93 versus 73 dying before age 1 among 1000 livebirths). The neonatal mortality rate (risk of dyingwithin the first month of life) was also higher forchildren of adolescent mothers, compared tochildren of mothers aged 15–49 (63 compared to48 per 1000 live births). However, both the IMR
and the neonatal mortality rate declined since theNFHS-1, which found an IMR of 107 and a neonatalmortality rate of 71 for children born to mothers belowage 20.
In NFHS-2, adolescent mothers (those under age20 at the time of delivery) reported a total of 7589births during the three years preceding the survey.About two-thirds of these mothers reportedreceiving a check-up from a health professionaland the recommended tetanus toxoid vaccinationduring their pregnancy; the corresponding figurefor such health care in NFHS-1 was only 55%. InNFHS-2, 59% of adolescent mothers received anadequate supply of iron and folic acid (tablets orsyrup), and nearly one-third of all births took placein institutional facilities, compared with one-fourthin NFHS-1. As for postpartum check-ups, 80% ofall births outside institutional facilities to adolescentmothers were followed by a check-up within twomonths ofr delivery (Table 1).
Each of the two postpartum complications,massive vaginal bleeding and very high fever, werereported in about 13% of births by adolescentmothers during the three years preceding thesurvey (Table 2).
Two out of every five currently married adolescentwomen reported some reproductive health problem.
Table 1. Antenatal, natal and postnatal care received by mothers: comparison of adolescent mothersand mothers in other age groups (as a per cent of births* during three years preceding the survey,NFHS-2, India, 1998–1999)
Woman’s age (years)
Indicator < 20 20–34 35–49
All births to adolescent mothers* N = 7589 N = 23 469 N = 1335Per cent with no antenatal check-up (%) 31.7 33.6 54.9Per cent that received two or more tetanus toxoid injections (%) 67.6 67.6 47.0Per cent given iron and folic acid tablets or syrup (%) 58.8 58.4 36.6Per cent that gave birth in institutional facility (%) 31.8 35.0 19.9Per cent with delivery assisted by a health professional (%) 41.6 43.4 27.4
Non-institutional births to adolescent mothers N = 5148 N = 15 184 N = 1059Per cent of non-institutional births in which the mother had apostpartum check-up within two months after delivery (%) 18.1 16.4 10.5
*Refers to per cent of two most recent births during three years preceding the survey.
Source: National Family Health Survey (NFHS-2), All India, 1998–1999. India, Mumbai, International Institute forPopulation Sciences, USA, ORC MACRO.
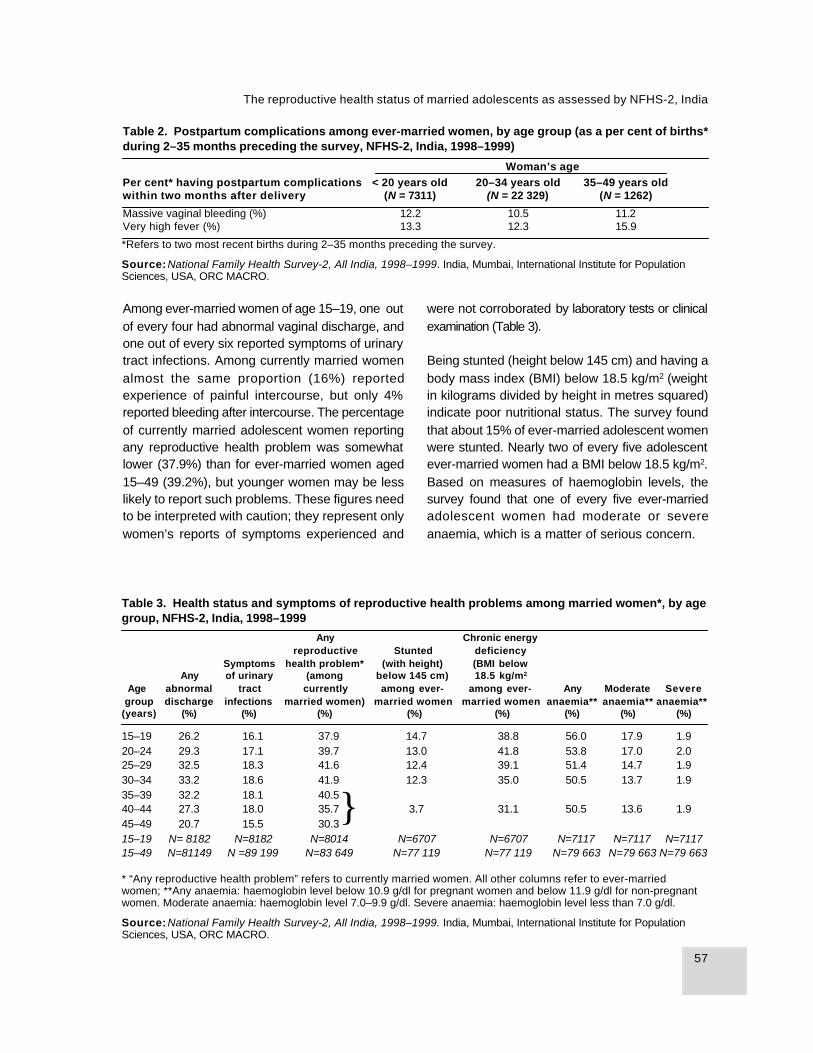
57
The reproductive health status of married adolescents as assessed by NFHS-2, India
Among ever-married women of age 15–19, one outof every four had abnormal vaginal discharge, andone out of every six reported symptoms of urinarytract infections. Among currently married womenalmost the same proportion (16%) reportedexperience of painful intercourse, but only 4%reported bleeding after intercourse. The percentageof currently married adolescent women reportingany reproductive health problem was somewhatlower (37.9%) than for ever-married women aged15–49 (39.2%), but younger women may be lesslikely to report such problems. These figures needto be interpreted with caution; they represent onlywomen’s reports of symptoms experienced and
were not corroborated by laboratory tests or clinicalexamination (Table 3).
Being stunted (height below 145 cm) and having abody mass index (BMI) below 18.5 kg/m2 (weightin kilograms divided by height in metres squared)indicate poor nutritional status. The survey foundthat about 15% of ever-married adolescent womenwere stunted. Nearly two of every five adolescentever-married women had a BMI below 18.5 kg/m2.Based on measures of haemoglobin levels, thesurvey found that one of every five ever-marriedadolescent women had moderate or severeanaemia, which is a matter of serious concern.
Table 3. Health status and symptoms of reproductive health problems among married women*, by agegroup, NFHS-2, India, 1998–1999
Any Chronic energyreproductive Stunted deficiency
Symptoms health problem* (with height) (BMI belowAny of urinary (among below 145 cm) 18.5 kg/m2
Age abnormal tract currently among ever- among ever- Any Moderate Severe group discharge infections married women) married women married women anaemia** anaemia** anaemia**(years) (%) (%) (%) (%) (%) (%) (%) (%)
15–19 26.2 16.1 37.9 14.7 38.8 56.0 17.9 1.920–24 29.3 17.1 39.7 13.0 41.8 53.8 17.0 2.025–29 32.5 18.3 41.6 12.4 39.1 51.4 14.7 1.930–34 33.2 18.6 41.9 12.3 35.0 50.5 13.7 1.935–39 32.2 18.1 40.540–44 27.3 18.0 35.7 3.7 31.1 50.5 13.6 1.945–49 20.7 15.5 30.315–19 N= 8182 N=8182 N=8014 N=6707 N=6707 N=7117 N=7117 N=711715–49 N=81149 N =89 199 N=83 649 N=77 119 N=77 119 N=79 663 N=79 663 N=79 663
* “Any reproductive health problem” refers to currently married women. All other columns refer to ever-marriedwomen; **Any anaemia: haemoglobin level below 10.9 g/dl for pregnant women and below 11.9 g/dl for non-pregnantwomen. Moderate anaemia: haemoglobin level 7.0–9.9 g/dl. Severe anaemia: haemoglobin level less than 7.0 g/dl.
Source: National Family Health Survey-2, All India, 1998–1999. India, Mumbai, International Institute for PopulationSciences, USA, ORC MACRO.
Table 2. Postpartum complications among ever-married women, by age group (as a per cent of births*during 2–35 months preceding the survey, NFHS-2, India, 1998–1999)
Woman’s agePer cent* having postpartum complications < 20 years old 20–34 years old 35–49 years oldwithin two months after delivery (N = 7311) (N = 22 329) (N = 1262)
Massive vaginal bleeding (%) 12.2 10.5 11.2Very high fever (%) 13.3 12.3 15.9
*Refers to two most recent births during 2–35 months preceding the survey.
Source: National Family Health Survey-2, All India, 1998–1999. India, Mumbai, International Institute for PopulationSciences, USA, ORC MACRO.
}

58
SUMATI KULKARNI
Fewer than two out of every five adolescent ever-married women had heard about AIDS. Amongthose who had heard of it, 80% had heard about itfrom television; however, 45% of ever-marriedadolescent women had not been exposed to anymedia. One-third of those who had heard of AIDScould not state how to avoid the infection. Thissuggests that intensive information, education andcommunication (IEC) activities for this vulnerablegroup should be given high priority.
Nearly one out of every three female adolescentswas illiterate, while one out of five had completedat least a high school education. Nearly one-fourthwere not involved in any decision-making in thehousehold, and only two out of five were involvedin decision-making about their own health care,which reflects the low level of autonomy that marriedadolescent women have in the Indian setting.
Conclusion
The NFHS-2 revealed many ways in which thereproductive health of married adolescent womenneeds to be improved. However, a single uniformstrategy across India would not be successful,owing to extreme inter-state variations inreproductive health, average age at marriage,contraceptive use and decision-making. Forexample, among all ever-married women aged 15–49, only 2–3% were in the age group 15–19 yearsin Kerala and Himachal Pradesh. In contrast, thecorresponding percentage in Madhya Pradesh andBihar was as high as 12–13%.The proportion ofadolescent women using contraception ranged
from 2–4% in Bihar and Rajasthan to 33% in WestBengal. In Maharashtra and Madhya Pradesh,fewer than one-third (31%) of married adolescentswere involved in decision-making about their ownhealth care, but in Himachal Pradesh and Punjabas many as 74–84% were involved. State-specificstrategies targeted at married adolescent womenare urgently required to ensure that young womenreceive antenatal, natal and postnatal services, aswell as clinical testing for reproductive tractinfections. Apart from these direct measures, whatwould really bring about change would be aneffective strategy to empower married adolescents.Ideally, no adolescent girl would marry. Strictimplementation of the law regarding legal minimumage at marriage as well as IEC activities to createawareness about reproductive health issues andto change attitudes are long-term solutions.
References
International Institute for Population Sciences (1995)National Family Health Survey (NFHS), 1992–1993.India, Mumbai, IIPS.
International Institute for Population Sciences, ORCMACRO (2000) National Family Health Survey(NFHS-2), All India 1998–1999. India, Mumbai, IIPS,USA, ORC MACRO.
Professor Sumati KulkarniConsultant to ORC-MACRO & PRBRetd. Professor, IIPS. Mumbai,E-2, Himachal Housing Society,Sector 17, Plot 22, Vashi,Navi Mumbai - 400 703

59
Pregnancy and postpartum experience among first time young parents in Bangladesh
The majority of adolescents in South Asia who bearchildren do so within marriage, and young couplesgenerally face social pressure to have a child soonafter marriage. As relatively new family members,young mothers are isolated and vulnerable. Theyhave limited control over their lives and lack socialsupport. However, the first birth may offer a uniqueopportunity to improve the prospects of youngmothers. Because the young women are about togive birth to the next generation, husbands andhusbands’ families may be open to new informationand behaviour change.
This paper presents preliminary findings from thefirst phase of a study that was designed to increaseunderstanding of the sociology of the first birth.The second phase will use these findings to developand test interventions to make services moreresponsive to young mothers’ needs. During thequalitative phase of this research, we focused onthe roles and influence of spouses, mothers-in-law, and other family members, in an attempt tounderstand why young women do not accesshealth services, breastfeed, or have safe sex. Thestudy also focused on the vulnerability that comeswith girls’ young age and position in the familyand how the young women’s social status affectsthe first birth and vice versa.
Methods
The study is being carried out in 24 villages insoutheast Bangladesh. The area is predominantlyMuslim and has a population of over 28 000 people.Researchers randomly selected eight of the 24villages and identified all 40 households in thosevillages that had young, first-time pregnant orpostpartum women. In-depth interviews were thenconducted with the young women, their husbands,senior women in the household including sisters-in-law and mothers-in-law, peers, and serviceproviders. In addition, researchers conducted focusgroup discussions with husbands and peers. Thestudy gathered information on issues such asmarriage patterns; knowledge, attitude, andpractices related to family planning, pregnancyand workload; food intake; mobility; social support;and health-seeking behaviours during pregnancy,delivery and post-partum.
Key findings
The young women interviewed included girlsbetween the ages of 13 and 19. All had a few yearsof school education, but not all were married toliterate men. Nearly all respondents, both men andwomen, mentioned that they would have liked tohave married later, and some women had evenpursued this issue with their parents or guardians.
Pregnancy and postpartum experience amongfirst time young parents in Bangladesh:preliminary observations
Syeda Nahid M. Chowdhury
Background

60
SYEDA NAHID M. CHOWDHURY
In most cases, however, their requests wereignored. A father’s death, a large number ofdaughters, and poor financial conditions influencedfamilies’ decision to marry their daughters early.Parents arranged the marriages, and girls did notget an opportunity to meet their prospectivehusband before marriage. Some men had had achance to see their prospective bride, but againthe decision depended on the parents. Dowriesare common in this area and can involve cash orin-kind payments, as well as promises to helpobtain jobs within or outside the country. To marrytheir daughters, families often agreed to thedemands of the husband’s family, which they thenoften failed to meet. Their inability to meet suchdemands affected the girls’ relationships andposition within the marital family.
In general, the young women in the study did notplan their pregnancies. All young women knew thename of some family planning methods, but nonehad actually used them. Their perception was thatonce they were married, they would have a baby.Many believed that getting pregnant soon aftermarriage was god’s will. Mothers-in-law were awarethat their daughters-in-law were not using familyplanning, but we found that they did not activelytry to influence the young couples’ decision-making. As one mother-in-law said, the “husbandand wife must decide, but they must take intoconsideration the opinion of the elders ”.Nevertheless, in-laws had a general expectationthat couples should have a baby soon aftermarriage. Even when young women expressed adesire to postpone childbearing, they did notnecessarily delay pregnancy. One respondent said,“I wanted a child after two or three years, but afterone year when I did not conceive, my sister-in-lawand neighbour started taunting me, saying that Iwas barren. That is why I wanted to have a baby. ”
The study gathered information on what changesoccurred once girls conceived, especially in termsof food intake, workload and mobility. We foundmany food taboos in the community, but noevidence that young women were given extra food
or particularly nutritious food during pregnancy. Theyoung women tended to be in charge of cooking,but other family members were responsible fordishing out the food. As a result, pregnant girlshad little control over their own food intake. Apartfrom work that required heavy lifting, young motherscontinued to have a heavy workload duringpregnancy. After delivery, their workload actuallyincreased because they had to take care of thenew child as well as do all the household work.The young women in the study expressed greatunhappiness about this situation.
In general the young women had limited mobility,as these villages are fairly conservative. There aremany taboos surrounding mobility duringpregnancy. For example, pregnant women are notsupposed to go out during the afternoon orevenings; nor are they supposed to go into thebackyard of the house for fear that they mightbecome possessed by evil spirits.
The study found that young women went to spiritualhealers to protect them against possession by evilspirits, but none of the young women had gone forantenatal check-ups during their pregnancy,despite the presence of NGOs and governmentfacilities in the area. In comparison, the 1996–1997Demographic and Health Survey found thatnationally, 71% of pregnancy women below age20 received no prenatal care (Mitra et al., 1997).Young women in this study were not aware of theneed for medical care during pregnancy or delivery.They had little idea about what to expect duringpregnancy and delivery, and only vague ideas aboutpossible complications.
Objections of in-laws and financial concerns weremajor barriers to seeking health care. The negativeattitude of one mother-in-law towards prenatal carewas captured in the following quote:
To go to a doctor you need money, after takingmoney they do not provide medicine… Every-where there is a doctor. They only take money,but they know nothing.

61
Pregnancy and postpartum experience among first time young parents in Bangladesh
Most women expected to deliver at the maritalhome aided by a traditional birth attendant, as isthe norm in these communities. Mothers-in-lawmake this decision, however, and young womendo not have any say in the matter.
Conclusions
Researchers hope that this study will shed lighton the sociology of first birth in rural Bangladesh.Preliminary findings reinforce the need forinterventions to take into consideration youngwomen’s social networks. Once researchers finishanalysing the qualitative data, they will design anintervention to investigate whether they can a)increase the level of agency through social supportand health programmes, and b) adapt healthservices to reflect the realities and needs of firsttime mothers.
Reference
Mitra SN, Al-Sabir A, Cross AR, Jamil K (1997)Bangladesh Demographic and Health Survey 1996–1997. Dhaka, Bangladesh, National Institute ofPopulation Research and Training [NIPORT].
Dr Syeda Nahid M.ChowdhuryProgramme ManagerOperations ResearchReproductive Health Alliance Europe443 Highgate Studios53–79 Highgate RoadLondon NW5 1TLUnited Kingdom
62
RAMESH K. ADHIKARI
Background
In South Asia, early marriage is a social norm,and marriages are expected to result in childbirthwithin a few years of couples living together. It isimportant to review how this influences the physicaland social well-being of young women in order todevelop relevant policies and programmes. Thispaper reviews several studies from Nepal, includingthe 1996 Nepal Family Health Survey (NFHS)(Nepal Ministry of Health et al., 1996), a 1994longitudinal study of factors influencing thenutritional status of adolescents, several hospital-based studies on outcomes of adolescentpregnancy, as well as information from theinternational literature. The paper highlights thephysical and social consequences of earlymarriage and childbearing among women aged 15–24 and puts forward some recommendations forpolicy consideration. For the purpose of this paper,adolescents are defined as the age group 15–19years, young adults as the age group 20–24 yearsand youth as the age group 15–24 years.
Adolescents and the youth population inNepal: some characteristics
Historically, child marriages were common inNepal, and the 1971 census noted that 2.4% ofchildren aged 6–9 were married. After 1962, thelegal minimum age for marriage was raised to 16
and 18 years for women and men, respectively,with parental consent, and 18 and 21 years withoutconsent. Mean age at marriage has increased from15.4 years in 1961 to 18.1 years in 1991, thoughthere is great geographic variation among districtsin Nepal, ranging from 15.1 to 23 years (Thapa etal., 1997). According to the 1996 NFHS, nearlyhalf (44%) of all female adolescents were marriedin 1996. Early marriage almost always leads toearly childbearing. Over half (54.3%) of the marriedadolescent girls in the 1996 NFHS were alreadymothers or were pregnant, as were 90% of marriedyoung adult women aged 20–24.
Nationwide information about the nutritional statusof adolescents is not available; however, one studyconducted in three remote rural areas found thatthe majority of adolescent girls were stunted andundernourished, including 72% of girls aged 10–14 and 45% of girls aged 15–18. The majority (70%)of younger girls had a body mass index (BMI) lessthan 5%, as did 15% of girls aged 15–18. The samestudy found that adolescent girls achievedmenarche later and continued to grow beyond theperiod when girls in the reference populationstopped gaining height, and the final height attainedby the majority of girls remained below the thirdpercentile (Regmi & Adhikari, 1994). Similarobservations have been reported from otherdeveloping countries, including Colombia,Guatemala and India (Kurz, 1996).
Early marriage and childbearing: risks andconsequences
Ramesh K. Adhikari

63
Early marriage and childbearing: risks and consequences
Health consequences of early marriage andchildbearing
It is generally accepted that childbearing amongwomen aged 15–19 doubles the risk of death dueto pregnancy-related causes compared to womenin their twenties (Population Reference Bureau,2000). Hospital-based studies from Nepal haveshown an association between teenage pregnancy,pregnancy-induced hypertension and anaemia. Thesame studies found that fetal loss and abnormaldeliveries were higher among teen mothers (Malla& Shrestha, 1996). The percentage of pregnantwomen attending antenatal care (ANC) is low inNepal, probably due to a lack of adequate services.Even in urban areas, where health facilities arewithin easy reach, pregnant adolescents attendantenatal facilities at lower rates than adult women(Adhikari & Amatya, 1996).
Several studies from Nepal have documentedpoorer outcomes for children born to adolescentmothers compared to older mothers. The NFHSfound that neonatal mortality among children ofadolescent mothers was 73% higher than childrenof older mothers, and 25% higher than children ofmothers aged 30–39. Studies have also found a25%–66% higher incidence of low birth weightamong children of adolescent mothers (Dali etal., 1989; Adhikari & Amatya, 1996). One hospital-based study found a perinatal mortality rate thatwas twice as high among children of adolescentmothers compared to children whose mothers wereolder than age 19 (40.5 versus 18 per 1000 births)(Adhikari & Amatya, 1996). In addition, evidencesuggests that children of older adolescents (aged17–19) fare better than those born to youngeradolescents (aged 16 or younger), when outcomessuch as low birth weight and pre-term birth arecompared (Dali & Pradhan, 1992).
Social consequences of early marriage andchildbearing
In addition to health consequences, early marriageand childbearing have consequences for women’s
education. Although literacy among youth hasgradually increased over the years, only 55% ofadolescents and 44% of young adults were literateas of 1991, according to the National Census(Central Bureau of Statistics, Nepal, 1995). The1996 NFHS found a gender difference in schoolinglevels. Only 15% of male adolescents had neverattended school compared to 53% of femaleadolescents. Women who marry “early” in theirteens tend to have even fewer educationalopportunities and a higher dropout rate. In the 1996NFHS, 32% of women who had dropped out ofschool cited marriage as the reason fordiscontinuing school. The 1996 NFHS also revealeda close relation between education andchildbearing among adolescents. Thirty-two percent of illiterate adolescents had already begunchildbearing, compared to only 10% of those whohad secondary education.
Finally, women who marry early and beginchildbearing in adolescence are expected to havea higher total fertility rate (TFR), thoughcontraceptive use may offset this. For example,although the teenage contribution to TFR is highin Bangladesh (18%) relative to Nepal (13%) andPakistan (9%), the overall TFR in Bangladesh isrelatively low (3.3) compared to Nepal (4.6) andPakistan (5.6). The lower TFR among youngBangladeshi women is apparently due to the higherprevalence of contraceptive use amongadolescents in that country (33%) compared toNepal, India (both 7%) and Pakistan (3%)(Population Reference Bureau, 2000). Thus, untiladolescent marriages can be delayed, adolescent-friendly contraceptive services may help keep downfertility rates.
International comparisons
Studies from Nepal seem to confirm thatadolescent pregnancy confers higher risk formothers and infants. Most studies from developingcountries—including Dali & Pradhan (1992), Malla &Shrestha (1996) and Adhikari & Amatya (1996)from Nepal; Ambedkar et al. (1999) and Verma &

64
RAMESH K. ADHIKARI
Das (1997) from India; Alam (2000) fromBangladesh; Weerasekara (1997) from Sri Lanka;Kumbi & Isehek (1999) from Ethiopia; andAdedoyin & Adetoro (1989) from Nigeria—also showthat pregnancy in adolescence results in poorerobstetric outcomes compared to pregnancy duringadulthood. However, studies from developedcountries are not so definite. While some studieshave reported poorer outcomes among youngeradolescents, such as Amini et al. (1996), Brownet al. (1991) and Satin et al. (1994) from the UnitedStates of America, others have shown no differenceor even better outcomes among late adolescentscompared to older women. The latter includesYoder & Young (1997) from the United States ofAmerica; Bradford & Giles (1989) from Australia;and Mukasa (1992) and Ncayiyana & ter Haar(1989) from South Africa.
Possible explanations for the difference betweendeveloping and developed country findings includethe availability and quality of prenatal care and thepoor nutritional status of adolescent girls indeveloping countries. A literature review by Kurz(1997) concluded that primiparity, continued growthduring pregnancy, quality of obstetric antenatal careand poor socioeconomic status are major riskfactors associated with poor outcomes ofadolescent pregnancy. This was supported by aWorld Health Organization analysis of 25 studies,which found an association between pre-term birthand the mother’s nutritional status. That analysisconcluded that women with a pre-pregnancy weightand height of less than 45 kg and 145 cm,respectively, were more likely to bear low birth-weight or premature infants (World HealthOrganization, 1995).
A few studies—including some from developedcountries—have reported that pregnantadolescents continue to grow during theirpregnancy, and apparently their growth competeswith the fetus for nutrients (Scholl et al., 1994).Thus, continued growth during pregnancy due tostunting may be one reason there is a higherincidence of low birth weight and pre-term birth
occurs among adolescent mothers compared toadult mothers in developing countries but not indeveloped countries. Low gynaecological age(defined as conception within two completed yearsof menarche), in particular, has been reported asan important factor responsible for almost doublethe risk of having a preterm birth and low birthweight babies (Scholl et al., 1989). Given that largenumbers of girls in Nepal are malnourished andreach menarche at an average age of 13.2 years,these research findings suggest that girls whobecome pregnant before age 15 are at higher riskof having a premature or low birth weight baby.
Another important explanation for poor obstetricoutcomes among adolescent mothers is the loweruse of prenatal care compared with use by adultwomen. Findings from Nepal consistently showthat the percentage of adolescents seekingantenatal care is lower compared to adult mothers,even though most adolescents have children withinwedlock. The reasons for this are unclear, but couldinclude poor social status of young women in theirhusbands’ families, or a tendency for adolescentsto hide their pregnancies. It is essential to identifythese factors so that obstetric services can bemade more adolescent friendly.
Conclusions
Adolescent girls who delay marriage andchildbearing benefit by completing their own growthfirst. They avoid putting themselves and their babiesat risk of nutritional deprivation. This evidencepoints to a need for programmes such as thefollowing:
a. Because early marriage and childbearing areassociated with less education and lower futureincome for young mothers, programmes thatkeep girls in school should be promoted. Theattainment of higher levels of education byyoung women can be expected to yield agreater use of reproductive health services andbetter employment prospects.

65
Early marriage and childbearing: risks and consequences
b. Parents and community members need to beinformed about the adverse health and socialconsequences of early childbearing, as well asthe benefits of delaying marriage andchildbearing until at least two completed yearsafter menarche.
c. Where marriage in adolescence continues,promoting contraceptive use can delaychildbirth until the couple is physically, sociallyand emotionally ready to bear a child. Therefore,there is a need for reproductive health services,particularly adolescent-friendly family planning.
d. Programmes to improve the economic statusof adolescent women can bring about positivechange, since economic factors may lie behindearly marriage and childbearing.
References
Adedoyin MA, Adetoro O (1989) Pregnancy and itsoutcome among teenage mother in Ilorin, Nigeria.East African Medical Journal, 66(7):448–452.
Adhikari N, Amatya A (1996) Outcome of adolescentpregnancy. Paper presented at 8th Congress ofPediatrics, Kathmandu, Nepal.
Alam N (2000) Teenage motherhood and infantmortality in Bangladesh: maternal age dependenteffect of parity one. Journal of Biosocial Science,32(2):229–236.
Ambedkar NN et al. (1999) Teenage pregnancyoutcome: a record based study. Indian Journal ofMedical Science, 53(1):14–17.
Amini SB et al. (1996) Births to teenagers: trends andobstetric outcomes. Obstetrics and Gynaecology,87(5):668–674
Bradford JA, Giles WB (1989) Teenage pregnancy inwestern Sydney. Australian and New Zealand Journalof Obstetrics and Gynaecology, 29(1):1–4.
Brown HL, Fan YD, Gonsoulin WJ (1991) Obstetriccomplications in young teenagers. Southern MedicalJournal, 84(1):46–48.
Central Bureau of Statistics, Nepal (1995) PopulationMonograph of Nepal. Kathmandu, Nepal.
Dali S et al. (1989) A Study of Low Birth Weight atTUTH. Kathmandu, TU Institute of Medicine.
Dali SM, Pradhan N (1992) Obstetric performance ofadolescent pregnancy at TUTH. Journal of the Instituteof Medicine, 14(1):13–19.
Kumbi S, Isehek A (1999) Obstetric outcomes ofteenage pregnancy in northwestern Ethiopia. EastAfrican Medical Journal, 76(3):138–140.
Kurz K (1996) Adolescent nutritional status indeveloping countries. The Proceedings of the NutritionSociety, 55:321–331.
Kurz K (1997) Health Consequences of AdolescentChildbearing in Developing Countries, ICRW workingpaper number 4. Washington, DC, InternationalCenter for Research on Women.
Malla DS, Shrestha PL (1996) Adolescent Pregnancyand Its Outcome. Mimeograph published by MaternityHospital, Kathmandu, Nepal.
Mukasa FM (1992) Comparison of pregnancy andlabour in teenagers and primigravidas aged 21–25years in Transkai. South African Medical Journal, 18;81(8):21–23.
Ncayiyana DJ, ter Haar G (1989) Pregnantadolescents in rural Transkai: age per se does notconfer high-risk status. South African Medical Journal,March 4; 75(5):231–232.
Nepal Ministry of Health, New Era, Macro InternationalInc. (1996) Nepal Family Health Survey. Kathmandu,Nepal Ministry of Health, Department of HealthServices, Family Health Division and New Era, MacroInternational Inc.
Population Reference Bureau (2000) The World’sYouth 2000. Washington, DC, Population ReferenceBureau.
Regmi SC, Adhikari R (1994) A Study on the FactorsInfluencing Nutritional Status of Adolescent Girls inNepal, Research paper ser ies number 6.Washington, DC, International Center for Researchon Women.
Satin AJ et al. (1994) Maternal youth and pregnancyoutcomes: middle school versus high school agegroups compared with women beyond the teen years.American Journal of Obstetrics and Gynecology,171(1):184–187.

66
RAMESH K. ADHIKARI
Scholl TO, Hediger ML, Ances IG (1990) Maternalgrowth during pregnancy and decreased infant birthweight. American Journal of Clinical Nutrition ,51(5):790–793.
Scholl TO et al. (1989) Association between lowgynaecological age and preterm birth. PaediatricPerinatal Epidemiology, 3(4):357–366.
Scholl TO et al. (1993) Maternal growth duringpregnancy and lactation. Hormone Research,39(Suppl. 3):59–67.
Scholl TO et al. (1994) Maternal growth duringpregnancy and the competition for nutrients. AmericanJournal of Clinical Nutrition, 60(2):183–188.
Thapa S, Acharya LB, Aryal RH (1997) Schooling,marriage, work and childbearing among the youthpopulat ion of Nepal: Emerging insights andchallenges. Mimeograph presented at the 1997Workshop on Youth Across Asia, Kathmandu.
Verma V, Das KB (1997) Teenage primigravidae:comparative study. Indian Journal of Public Health ,42(2):52–55.
Weerasekara DS (1997) Adolescent pregnancies—is the outcome different? Ceylon Medical Journal,42(1):16–17.
Yoder BA, Young MK (1997) Neonatal outcomes ofteenage pregnancy in a military population. Obstetricsand Gynaecology, 90(4):500–506.
World Health Organization (1995) Maternal weightgain and pregnancy outcomes. Bulletin of the WorldHealth Organization, Suppl. Vol. 73.
Ramesh K. AdhikariProfessor in Child HealthInstitute of MedicineMaharajgunj CampusPost Box No. 2533KathmanduNepal
67
Newly married adolescent women: experiences from case studies in urban india
Background
Newly married women in India are, by and large,adolescent women. As Jejeebhoy (1998) noted inher review of literature on adolescents, the situationof adolescent women is particularly precarious, asthey tend to have limited education, skills andopportunities for employment. They have relativelypoor health and limited access to good nutrition,and many are caught in a cycle of early marriageand child- bearing. Marriage adds dramatic changesto their lives that involve their bodies, emotions,and daily life experiences. These changes oftenoccur in unfamiliar surroundings among virtualstrangers, as a large proportion of marriages inIndia are patrilocal and arranged by family elders.Yet, as marriage is customarily accorded centralsignificance in the lives of Indian women, newlymarried adolescent women are aware that theyhave to “adjust” to the multiple changes in theirlives. How do they deal with marriage and thechanges it brings? What do they know of, and howdo they handle new bodily experiences? Whatactions do they take to be subjects of their newbodily experiences? In this paper, in an attempt toanswer some of these questions, I present andinterpret adult women’s recollections of theirexperiences as newly married adolescents.
Methods
This paper is based on two qualitative data setswith similar methods and participants. Both studiesgathered information about the adult sexual livesof working class women in Mumbai, and bothasked women about their early marital lives.However, this was not the focus of either studyand it required recall of events that happened manyyears in the past. Hence, the data have certainlimitations with respect to adolescent maritalexperiences. One study gathered data in 1991–1992, using repeated focus group discussions with35 women, divided into 6 groups (George & Jaswal,1995). The participants in the focus groups wereclients or employees of various nongovernmentalorganizations (NGOs) that worked for poor peoplein Mumbai. The women’s ages ranged from 20 to40 years, and the average age at marriage was 15years. Sixteen were illiterate; the rest had at leastfive years of schooling and one was a graduate. Atthe time of the study, 25 out of 35 women weremarried and the rest were widowed, deserted,separated or divorced. Nineteen women wereHindu, 11 women were Buddhist, and the rest hadother religious affiliations. Twenty-two women wereengaged in wage-earning activities like rag picking,cleaning homes and offices, and working ascommunity workers for NGOs.
Newly married adolescent women:experiences from case studies in urban India
Annie George

68
ANNIE GEORGE
The second data set was gathered in 1996–1997using repeated in-depth interviews with 65 women(George, 1997). Each respondent was interviewedan average of three times, with interviews lastinghalf an hour to two hours each. Participants in thein-depth interviews were purposively selected withthe help of NGOs. The 65 participants ranged inage from 20 to 38 years. Forty-seven were literate;on average, they had five years of schooling. Thirty-six women were gainfully employed and one inthree was the primary wage earner. The averageage at marriage was 16 years. On average, eachhad been married for twelve years and had threechildren. Marital discord had led 22 of the 65 womento be separated from their husbands at least onceduring the marriage.
Key findings
In narratives of their first sexual experiences,women typically present themselves as one of fourtypes of brides: reluctant, shy, fearful or pragmatic.Elements of each scenario overlap, and I makethese distinctions merely for analytical purposes.Each of these scenarios is presented below.
Reluctant brides: “I was tricked into it.” In thistype of narrative, women describe themselves asinnocents who were tricked into sex. In most cases,the typical story is that the woman had noknowledge about sexual relations, and had to be“tricked”, usually by older kinswomen from thehusband’s family, into being in the room where herhusband was waiting for her. In some narratives,older women are portrayed as “accomplices” ofthe husband, helping the eager husbandconsummate the marriage. In other narratives olderwomen were presented as the decision-makers,who decided when a married couple could startcohabiting. In these cases, the newly marriedwomen had either just attained, or not yet attainedpuberty. These narratives can be read in multipleways. On the one hand, the narratives suggestthat if the women were knowledgeable about sex,
they probably would not consent to it; they had tobe forced into sex through trickery. On the otherhand, the narratives also suggest that, followingthe dominant discourse on ideal womanhood, thewomen wanted to present themselves as goodwomen, who had to be robbed of their innocence.However, such processes are not totally violating,and some narratives portray husbands asresponsive to their wives’ wishes and experiencesof pain, fear and shyness.
Shy brides: “Daily sharam.” In these narratives,women used the word ‘sharam’ and ‘laaj vatene’,translated here as ‘shyness’ and ‘being or feelingshy’ to describe their feelings about sexualrelations. The word ‘shy’ does not capture thecomplexity of the term ‘sharam’, which containsconnotations of sexual modesty, femininity, virtueand honour. Shyness did not stem from lack ofsexual knowledge alone, although most womendid not know the details about sexual intercourseprior to marriage. Shyness also arose from thesocial situations in which newly marriedadolescent women found themselves. For instance,SEM1 had her first sexual relations in the in-laws’house in the village. Everybody was around, andso she felt strange, scared and shy. Culturalpractices, such as sharing the same room andhaving a bath after sexual activity, were means bywhich family members could easily know whethera couple had had sexual relations. This invasioninto their privacy, along with restricted privatespace, and the presence of family members whowere strangers to the newly married adolescentwomen, all added to their sense of ‘sharam’ .Families often exerted pressure on the couples tobe sexually active, adding to their sense ofshyness.
Fearful brides: “What will happen? How will itbe?” The word ‘darr’ or ‘bhiti’, translated as ‘fear’,were frequently used in the narratives to describea newly married adolescent woman’s sexualexperience. One woman from the focus groupdiscussion study described her experience by
1 All names are pseudonyms.

69
Newly married adolescent women: experiences from case studies in urban india
saying: “I was scared. I felt he would beat me if Irefused. I did not like sleeping with him, right undermy mother-in-law’s cot. I felt he was using forceon me. There was no need to sleep so soon infront of everyone. But he never experienced anyshame, and my mother-in-law would tell me that Ishould go to my husband, I am no longer small.”Participants in the in-depth interview study spokeabout the conditions that caused newly marriedadolescent women to fear sexual life. As oneparticipant described, “When I am with someunknown person, then one is going to feel fearisn’t it? I felt fear. I had pain and bleeding the firsttime. ” Another condition causing fear wasignorance of exactly what sexual relations entail.Even when women had information about sexualrelations, however, it did not necessarily decreasetheir fear. Most women said that their fear vanishedas sex became a ‘habit’. Fear of the unknownperson, bodily experience, and its consequencesdecreased over time with increasing familiarity.
Pragmatic brides: “This is married life.”Although the sexual experiences of newly marriedadolescent women may or may not have beenframed by fear or shyness, all the women learnedthat sexual intercourse was a necessarycomponent of marriage and of their identities asmarried women. As one woman described, “Manywomen explained to me that if you do this, awoman has a life [emphasis added] or else hewill move away from you. They would all say this.”This woman narrated clearly what many otherwomen also learnt—that if a woman complies andprovides sex whenever the man wants, then she“has a life”. “My friends and family told me (rightbefore her first sexual experience), don’t make anoise, you must bear the touch of a man. Thisman has married and brought you here for this.”These narratives show the disciplining nature ofearly sexual experience, which enjoys socialsanction and which married women learn throughfrequent bodily experience. Women in the focusgroup expressed the precarious nature of theirexistence, which one woman expressed as follows:“A woman needs some support. How long will herparents support her? So, a woman like me will
say, ‘if I’ve got to have clothes to wear and food toeat, then you do whatever you want (with my body)but keep me as a wife should be kept.’ “ If womendo not live up to the expectations of a wife,including being sexually available, then husbandscan move their attention to other women who maybe more willing. So, in order to have “a life”, status,esteem and honour, married woman had to submitto the demands of their husbands.
Conclusions
The broader social context of newly married womenof both data sets indicates that they weredependent on their husbands for social status andeconomic support, although they may also havebeen financial contributors to the household. Theyhad limited contact with their birth families, andmay have had limited social contacts and supportsin their marital home. During the early days ofmarriage, newly married adolescent women andtheir husbands may have been under the authorityof the husbands’ parents and other older relatives,and thus had relatively limited autonomy to makedecisions about their personal lives. The women’sresponses to their early married lives, when seenfrom these overlapping frames, shows a range ofresponses from selective compliance to selectiveresistance. However, I also argue that pragmatism,resulting from the precarious, tenuous nature oftheir social situation may be the dominantresponse of these women.
In summary, theories of the body can be used toread the sexual experiences of newly marriedadolescent women in Mumbai and point to thefollowing general patterns. First, newly marriedadolescent women are disciplined into normal adultwomanhood through embodied experiences ofsexual relations. Second, women tend to bepragmatic and use such regulation to fashion theiridentities as normal, good wives. Third, women’semotions mediate between their social contextsand their sense of control over their life situations.Finally, newly married women’s bodies are siteswhere individual, cultural and political conditions

70
ANNIE GEORGE
meet and are expressed in the form of bodilyexperience of pleasure, pain, illness or health.Women’s bodies, therefore, have the potential forpersonal and social transformations. Theseobservations are all reasons for undertaking morerigorous, culturally appropriate social scienceinvestigations into the sexual behaviour, knowledgeand reproductive health decision-making authorityof differently situated adolescent women and men.
References
George A (1997) Sexual Negotiation and SexualDecision-making among Poor Women and Men inMumbai. An Exploratory Study. Baroda, Sahaj Societyfor Health Alternatives.
George A, Jaswal S (1995) Understanding Sexuality:Ethnographic Study of Poor Women in Bombay.Women and AIDS Program Research Report SeriesNo. 12. Washington, DC, International Center forResearch on Women.
Jejeebhoy SJ (1998) Adolescent sexual andreproductive behavior: a review of the evidence fromIndia. Social Science and Medicine, 46(10):1275–1290.
Further Reading
Bourdieu P (1990) The Logic of Practice. (Translatedby Richard Nice). Stanford, California, StanfordUniversity Press.
Bourdieu P (1997) Outline of a Theory of Practice.(Translated by Richard Nice). Cambridge, CambridgeUniversity Press.
Butler JP (1993) Bodies that Matter: On the DiscursiveLimits of “Sex”. New York, Routledge.
Foucault M (1979) Discipline and Punishment: TheBirth of Prison. (Translated by Alan Sheridan).New York, Vintage.
Foucault M (1980) The History of Sexuality, Vol. 1.New York, Vintage.
George A (1998) Differential perspectives of men andwomen in Mumbai, India, on sexual relations and
negotiations within marriage. Reproductive HealthMatters, 6(12):87–96.
Goffman E (1969) Strategic Interaction. Philadelphia,University of Pennsylvania Press.
Grosz EA (1994) Volatile Bodies: Towards a CorporealFeminism . Bloomington, Indiana University Press.
Hochschild AR (1983) The Managed Heart:Commercialization of Human Feeling. Berkeley,University of California Press.
Holloway W (1984) Gender differences and theproduction of subjectivity. In: Henriques J, HollowayW, Urwin C, Venn C, Walkerdine V, eds. Changing theSubject: Psychology, Social Regulation andSubjectivity. London, Metheun:228–252.
Lock M, Kaufert P (1998) Introduction. In: Lock M,Kaufert P, eds. Pragmatic Women and Body Politics.Cambridge, Cambridge University Press.
Lyon L (1996) C. Wright Mills meets Prozac: therelevance of ‘social emotion’ to the sociology ofhealth and illness. In: James V, Gabe J, eds. Healthand Sociology of Emotions . Cambridge,Massachusetts, Blackwell Publishers:55–78.
Mauss M (1985) Category of the human mind: thenotion of person; the notion of self. In: Carrithers M,Collins S, Lukes S, eds. Category of the Person.Cambridge, England, Cambridge University Press:1–25.
Riessman CK (1993) Narrative Analysis. NewburyPark, California, Sage.
Scheper-Hughes N, Lock M (1987) Mindful body: aprolegomenon to future work in medical anthropology.Medical Anthropology Quarterly, New series, 1(1):6–41.
Scheper-Hughes N, Lock M (1991) The message inthe bottle: illness and the micropolitics of resistance.Journal of Psychohistory, 18(4):409–32.
Turner B (1996) The Body and Society, 2nd ed.Thousand Oaks, Sage Publications.
Annie GeorgeDepartment of Social & Behavioural SciencesUniversity of California, San FranciscoSan Francisco, CA 94143USA

IVSexual risk behaviours,perceptions and normsamong unmarriedadolescents: evidencefrom case studies

72
LEENA ABRAHAM
73
Risk behaviour and misperceptions among low-income college students of Mumbai
Background
Sexual behaviour studies of unmarried youthin India estimate that 19-28% of young menand 1–9% of young women have had (penetrative)sexual experience (Family Planning Associationof India, n.d.; Watsa, 1993; Goparaju, 1993;Bhende, 1994; Rangaiyan, 1996; Abraham, 1998;Jejeebhoy, 1998). These studies indicate thatpremarital sex among young men is not as rareas commonly believed, while it continues to becomparatively rare among young women. Genderdifferences in sexual behaviour are not merely theresult of over-reporting by men and under-reportingby women, but rather are the outcome of a sexualideology that promotes male sexuality and controlsfemale sexuality in India (Abraham, 1999). Studieshave reported that young people form a significantsegment of those attending sexually transmittedinfection (STI) clinics and those infected by HIV(AIDS Research and Control Organisation, 1995;National AIDS Control Organisation, 1994;Ramasubban, 1992; Urmil et al., 1989); it is,therefore, important to understand the risk behaviourof young men and women. This article discussesdata on sexual behaviour gathered amongunmarried, low-income youth attending college inMumbai during 1996–1998.
Methods
As sexual behaviour studies tend to focus onEnglish-speaking students of ‘elite’ colleges, ourstudy aimed to gather data from low-incomestudents. The study was conducted in and aroundthe premises of four colleges with co-ed, low-income student bodies. The colleges included bothhigher secondary (Junior College) andundergraduate courses (Senior College) in the arts,science and commerce streams. The sampleconsisted of students in their first year of highersecondary, who had just entered college, as wellas students in their third year of Senior College,who had spent a minimum of four years in college.A majority of juniors were aged 16–18, and amajority of seniors were aged 20–22. This studydesign was chosen to ensure coverage of studentswith and without sexual experience.
In the first phase, researchers gathered qualitativedata through focus group discussions (FGDs) andin-depth interviews with students from two of thefour colleges. In the second phase, they conducteda survey among students from the other twocolleges. A total of 75 students distributed in 10groups took part in the FGDs, and each groupparticipated in at least two 1– 1½ hour sessions.The FGDs explored students’ social interaction,views on marriage, partners and premarital sex,
Risk behaviour and misperceptions amonglow-income college students of Mumbai
Leena Abraham

74
LEENA ABRAHAM
sexual experiences and sources of information.The FGDs were followed by in-depth interviews with87 students to gain more detailed information abouttheir personal views and experiences. Thequalitative data gathered in the first phase wereused to design the structured, self-administeredquestionnaire, which was applied among arepresentative sample of boys and girls from thetwo classes mentioned. The final sample consistedof 966 students (625 boys and 341 girls).Researchers made the questionnaire available inboth English and Marathi, the local language.
As stated above, the students in our studybelonged to families of low socioeconomicbackground. The families lived in poor and crowdedliving conditions, very often in single-roomtenements located in slums. The studentsbelonged to different religious and ethnic groups.For instance, one college had a sizeable Muslimpopulation, while the remaining three had a majorityof Hindu students from various middle and lowercastes. Students from middle class familiesconstituted a minority in all four colleges. Thestudents did not consider themselves to be “veryreligious”, but considered their families to be“religious”.
Key findings
Mixed sex peer groups were not common, andfewer girls than boys said they were members ofmixed sex peer groups. However, friendships withthe opposite sex can be established in differentways. Respondents distinguished three types offriendships with opposite sex peers: bhai-behen,‘true love’ and ‘time pass’. Bhai-behen is said tobe a platonic relationship; ‘true love’ is a romanticone with the intention of marriage; and ‘time pass’is a transitory sexual relationship (Abraham, 2000).The boundaries of these categories are fuzzy, andthere are times when partners perceive therelationship differently, as well as instances whenbhai-behen is used as a cover for other types offriendship. The extent of physical intimacy variesbetween each type of relationship from minimal
physical intimacy (hath masti — ‘hitting’, ‘shakinghands’) in bhai-behen to sexual intercourse in ‘timepass’ relationships. In general, ‘true love’ does notinvolve intercourse but includes holding hands,touching, kissing and hugging.
In our study, we used the term ‘any sexualexperience’ to refer to any of the following acts:kissing, hugging, touching genitals, sexualintercourse, anal or oral sex. According to FGDdata, however, students did not consider kissingand hugging as ‘sexual acts’. For most students,sexual behaviour or ‘sex’ meant vaginal intercourse,or oral and anal sex. Many students alsoconsidered ‘touching’ sex organs or being ‘touched’by the opposite sex as a sexual act.
The survey data showed that many boys and girlshad engaged in sexual acts of varying degrees ofphysical intimacy, but there were marked genderdifferences. While “any sexual experience” wasreported by nearly half the boys (49%), only 26%reported sexual (vaginal) intercourse. Comparativelyfewer girls reported either “any sexual experience”(13%) or sexual intercourse (3%) (Table 1).
Sexual partners of girls were peers, either as ‘truelove’ or ‘time pass’ partners. Girls tended to bemonogamous, except in some instances of ‘timepass’ relationships. Boys’ sexual partners includedpeers (as both ‘time pass’ and ‘true love’ partners),commercial sex workers (CSWs) and olderwomen, whom they called ‘aunties’. Boys not onlyengaged in multiple partnerships but also exploreddifferent types of sex through these partnerships(Abraham, 1999). The sexual networks of boysdepended on opportunities to meet differentpartners, peer influence, personal income, eroticexposure and leisure time available. The qualitativedata showed five sets of sexual partnerships amongboys, including: 1) only CSWs; 2) only ‘time pass’partners; 3) ‘true love’ partners and CSWs; 4) ‘timepass’ partners, aunties and CSWs; and 5) a ‘truelove’ partner. Except for the last category, whichwas the only reported monogamous relationship,all were multiple partner relationships, either
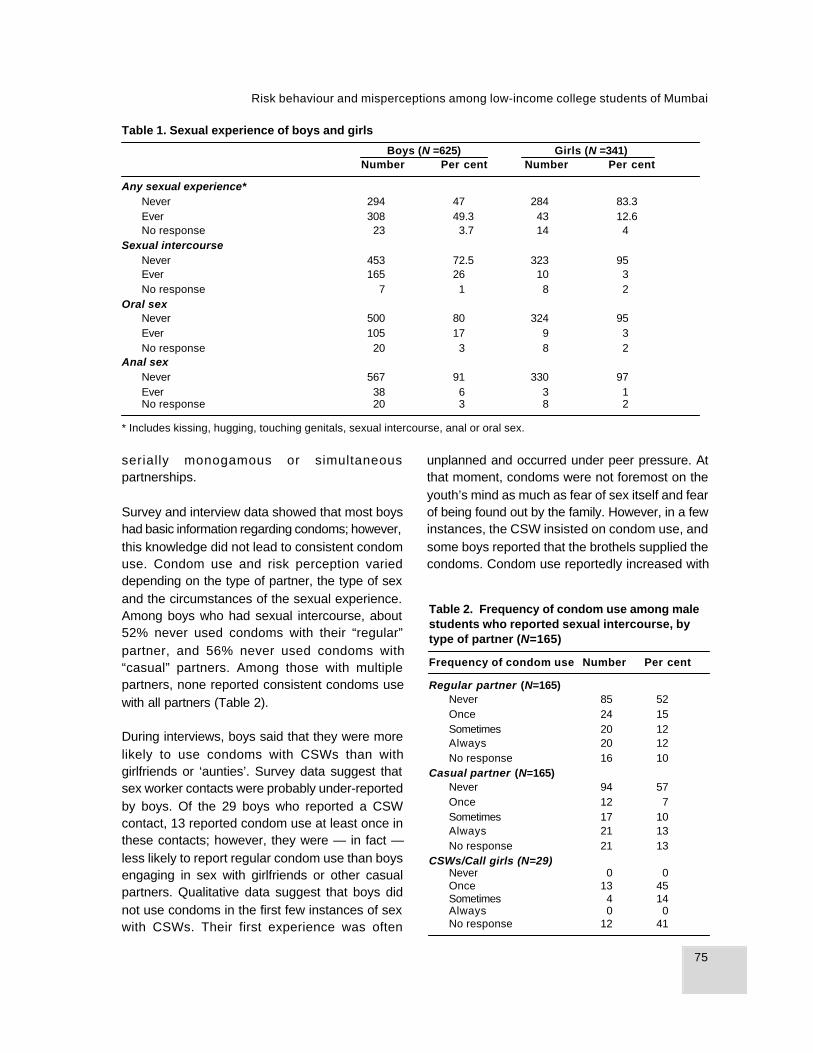
75
Risk behaviour and misperceptions among low-income college students of Mumbai
serially monogamous or simultaneouspartnerships.
Survey and interview data showed that most boyshad basic information regarding condoms; however,this knowledge did not lead to consistent condomuse. Condom use and risk perception varieddepending on the type of partner, the type of sexand the circumstances of the sexual experience.Among boys who had sexual intercourse, about52% never used condoms with their “regular”partner, and 56% never used condoms with“casual” partners. Among those with multiplepartners, none reported consistent condoms usewith all partners (Table 2).
During interviews, boys said that they were morelikely to use condoms with CSWs than withgirlfriends or ‘aunties’. Survey data suggest thatsex worker contacts were probably under-reportedby boys. Of the 29 boys who reported a CSWcontact, 13 reported condom use at least once inthese contacts; however, they were — in fact —less likely to report regular condom use than boysengaging in sex with girlfriends or other casualpartners. Qualitative data suggest that boys didnot use condoms in the first few instances of sexwith CSWs. Their first experience was often
* Includes kissing, hugging, touching genitals, sexual intercourse, anal or oral sex.
Table 2. Frequency of condom use among malestudents who reported sexual intercourse, bytype of partner (N=165)
Frequency of condom use Number Per cent
Regular partner (N=165)Never 85 52Once 24 15Sometimes 20 12Always 20 12No response 16 10
Casual partner (N=165)Never 94 57Once 12 7Sometimes 17 10Always 21 13No response 21 13
CSWs/Call girls (N=29)Never 0 0Once 13 45Sometimes 4 14Always 0 0No response 12 41
unplanned and occurred under peer pressure. Atthat moment, condoms were not foremost on theyouth’s mind as much as fear of sex itself and fearof being found out by the family. However, in a fewinstances, the CSW insisted on condom use, andsome boys reported that the brothels supplied thecondoms. Condom use reportedly increased with
Table 1. Sexual experience of boys and girls
Boys (N =625) Girls (N =341)Number Per cent Number Per cent
Any sexual experience*Never 294 47 284 83.3Ever 308 49.3 43 12.6No response 23 3.7 14 4
Sexual intercourseNever 453 72.5 323 95Ever 165 26 10 3No response 7 1 8 2
Oral sexNever 500 80 324 95Ever 105 17 9 3No response 20 3 8 2
Anal sexNever 567 91 330 97Ever 38 6 3 1No response 20 3 8 2

76
LEENA ABRAHAM
subsequent experiences with CSWs, mainly outof fear of AIDS.
The survey explored boys’ reasons for not usingcondoms (Table 3). Of the 125 boys who reportednot using condoms, just over 23% did not give anyreason. Others said that “sex suddenly happened”(21%), they were “not aware of condoms” (16%),or “condom reduces pleasure” (15%). Qualitativedata suggest that low use of condoms could bedue to situational factors, lack of information —particularly at the time of first sexual experience— and low risk perception associated with certainkinds of sexual partners.
Young men did not fear infection from sex withpeers, although they did fear pregnancy. Sexualintercourse was rare in ‘true love’ relationships,and if it occurred, young people generally tookprecautions against pregnancy. Condom use in‘time pass’ relationships was inconsistent. Boyssaid that they generally planned sex within a ‘timepass’ relationship and used condoms for fear ofpregnancy, unless “sex suddenly happened” orthey “got an unexpected chance for sex”. Boysconsidered sex with ‘aunties’ to be the least risky,since the woman initiated the relationship and —in their view — was responsible for contraception.As a result, boys did not usually use condoms,according to focus group discussion data fromthird-year boys. They did not report using condomsduring oral or anal sex with other males (thoughthere were very few cases reported); nor did mostboys think it was necessary to use condomsduring oral or anal sex. In general, students did
not have information about the potential risks ofHIV/AIDS from unprotected sexual relationshipswith another male.
More than half the students who engaged in sexdid not perceive any risk of contracting STIs,including HIV. This seemed to reflect ignoranceabout STIs as well as different perceptions of riskfrom different types of relationships. Boys who werenot sexually active considered those who wereactive to be ”at risk” and those who were sexuallyactive considered those who visited CSWs to be“at risk”. Some younger students mentioned sexualabstinence before marriage and avoiding certainpartners such as CSWs or ‘time pass’ friends aseffective measures of protection against HIV. Girlsseemed to believe that abstaining from premaritalsex not only preserved their izzat (honour) andensured marital bliss, but also provided insuranceagainst HIV. Projecting risks onto others andbelieving oneself to be immune from risks couldincrease their vulnerability to STIs by making youngpeople less likely to take preventive measuresagainst possible infection.
Conclusions
About one-fourth of boys in this particular samplehad engaged in risky premarital sex, and theirsexual networks included multiple partners andunsafe sex. They carried misperceptions aboutwhat constituted risky behaviour and therefore didnot consider themselves at risk. Although manygirls were aware that some boys had sexualrelations with their peers and that some went to“red light areas”, they did not perceive any risk ofcontracting HIV from their future partner or spouse.However, as long as boys continue to haveunprotected sex within multiple, transitoryrelationships, including relationships with ‘aunties’,‘time pass’ friends and CSWs, they are at risk ofcontracting STIs, including HIV, and are likely topass on the infection to their spouse or otherpartners.
Table 3. Reasons for non use of condoms amongboys (N=125)
Reason Number Per cent
Not aware of condom 20 16Sex suddenly happened 26 21Condom reduces pleasure 19 15Partner married, it is her responsibility 6 5Condom not available 6 5Feel shy to buy 7 6Partner insisted not to use 2 2Do not know how to use a condom 10 8No response 29 23

77
Risk behaviour and misperceptions among low-income college students of Mumbai
Acknowledgements: This study was funded bythe Rockefeller Foundation and supported by theInternational Center for Research on Women. Iacknowledge the cooperation of the students andthe sincere efforts of the research staff.
References
Abraham L (1998) Understanding youth sexuality: Astudy of college students in Mumbai. Mumbai, TataInstitute of Social Sciences (unpublished report).
Abraham L (1999) Drawing the Lakshman Rekha:Gender dimensions of youth sexuality in urban India.Paper presented at the International Conference onSexualities, Masculinities and Culture in South Asia:Knowledge, Practices, Popular Culture, and the State ,organized by the School of Literary andCommunication Studies, Deakin University,Melbourne, Australia.
Abraham L (2000) Bhai Behen, True love, Time-pass…friendships and sexual partnerships amongyouth in an Indian Metropolis . Paper presented at theWorkshop on Reproductive Health in India: NewEvidence and Issues. Pune, India, Feb. 28–March 1 .
Abraham L, Kumar KA (1999) Sexual experiences andtheir correlates among college students in MumbaiCity, India. International Family PlanningPerspectives, 25(3):139–146.
AIDS Research and Control Organization (1995)Summary Report of HIV Positive Cases. Bombay,ARCON.
Bhende A (1994) A study of sexuality of adolescentgirls and boys in underprivileged groups in Bombay.The Indian Journal of Social Work , LV(4)557– 571.
Family Planning Association of India (n.d.) YouthSexuality: A Study of Knowledge, Attitudes, Beliefsand Practices among Urban Educated Indian Youth,1993–94. Bombay, FPAI and SECRT.
Goparaju L (1993) Unplanned, unsafe: Male student’ssexual behaviour. Paper presented at the Workshopon Sexual Aspects of AIDS/STD Prevention in India.Bombay, Tata Institute of Social Sciences.
Jejeebhoy S (1998) Adolescent sexual andreproductive behaviour: A review of the evidence fromIndia. Social Science and Medicine, 10:1275–1290.
National AIDS Control Organisation (1994) CountryScenario: An Update. New Delhi, Government of India,Ministry of Health and Family Welfare.
Ramasubban R (1992) Sexual behaviour andconditions of health care: Potential risks for HIVtransmission in India. In: Dyson T, ed. SexualBehaviour and Networking: Anthropological andSocio-Cultural Studies on Transmission of HIV.Belgium, Deronaux – ordine:75–201.
Rangaiyan R (1996) Sexuality and sexual behaviourin the age of AIDS: A study among college youth inMumbai [Doctoral Dissertation]. Mumbai, InternationalInstitute of Population Sciences.
Urmil AC, Dutta PK, Sharma KK, Ganguly SS (1989)Medico-social profile of male teenager STD patientsattending a clinic in Pune. Indian Journal of PublicHealth , 33(4):176–182.
Watsa MC (1993) Premarital sexual behaviour ofurban educated youth in India. Paper presented atthe Workshop on Sexual Aspects of AIDS/STDPrevention in India. Bombay, Tata Institute of SocialSciences.
Leena AbrahamTata Institute of Social Sciences, MumbaiPost Box No. 8313Sion-Trombay HighwayDeonarMumbai 400 088India
78
YASMEEN SABEEH QAZI
Background
Adolescence is a formative time of transition toadulthood, roughly concurrent with the seconddecade of life. What happens between ages 10and 19 shapes how girls and boys live out theirlives as women and men—not only in thereproductive arena, but also in the social andeconomic realms. Throughout the world, girls andboys are treated differently from birth onward, butat puberty this gender divide widens. Boys enjoynew privileges, while girls endure new restrictions(Mensch, Bruce & Greene, 1998). In Pakistan,boys gain autonomy, freedom of movement,opportunity, and power (including power over sexualand reproductive lives of girls), while girls aresystematically deprived of freedom and independentaction. Only recently have the sexual andreproductive health needs of adolescents receivedattention in Pakistan. As part of an initial situationanalysis, investigators conducted a study toexplore unmarried adolescents’ knowledge,attitudes and sources of information about sexualand reproductive health, as well as to assess levelsof physical and sexual abuse.
Methods
Researchers conducted a pilot survey using face-to-face interviews among 310 unmarried young
people aged 13 to 21 years. In addition to applyinga structured questionnaire, interviewers wereencouraged to discuss a series of issues withyoung respondents, and they recorded qualitativenotes on these in-depth discussions. Respondentsincluded 177 girls and 133 boys who were attendingschool, working or doing neither. Respondents wereselected with the help of NGO (nongovernmentalorganization) staff working in the communities. Inaddition, researchers interviewed 110 parents andguardians about their perceptions of adolescents’behaviour and their suggestions for helpingadolescents become responsible adults. To allowfor regional comparisons, researchers gathereddata in four provincial cities, including Karachi,Quetta, Swabi and Gujranwala, as well as fromurban, periurban and rural areas.
Key findings
A majority of girls and boys reported that they haddiscussed “bodily changes” during puberty andmenstruation with friends or family members.Those who did not tended to be youngerrespondents. More boys than girls seemed to knowabout changes during puberty among the oppositesex. One finding with implications for hygieneeducation was that girls reported feeling “dirty”during menstruation, which may reflect the
Adolescent reproductive health in Pakistan
Yasmeen Sabeeh Qazi

79
Adolescent reproductive health in Pakistan
common practice of refraining from washing duringthis time.
A majority of boys and girls reported having heardabout or discussed pregnancy. Despite the factthat unmarried girls are not expected to talk aboutpregnancy in Pakistani culture, 81% of girlsreported having done so. Not surprisingly, oldergirls were better informed. Fewer femalerespondents reported knowing how a womanbecomes pregnant: 66% of girls versus 77% ofboys. However, an awareness of the connectionbetween pregnancy and menstruation did notnecessarily mean that they understood the actualmechanics of pregnancy. For example, only halfthe boys knew that, after puberty, girls could getpregnant through a sexual relationship, and youngergirls reported misconceptions such as the beliefthat kissing could cause pregnancy. In fact, only58% of girls surveyed had discussed sexualintercourse, although researchers considered thisfigure relatively high given that sex is not oftendiscussed openly in Pakistani society. A muchhigher percentage of boys (72%) than girls reportedhaving discussed sexual intercourse (Table 1).
A majority of both boys and girls had discussedcontraceptive methods, but twice as many boys(32%) as girls (15%) had not heard about ordiscussed contraceptive methods. The genderdifference may reflect girls being told about theimportance of marriage or having heard women inthe family talk about contraceptives. However, girlsand boys who had heard about contraceptives maynot necessarily know how to use them.Contraceptive use (mainly condoms and pills) wasextremely low—reported by about 5% of both girlsand boys.
The young people were also asked about theirknowledge of HIV/AIDS. Probably due to massawareness campaigns, most respondents hadheard of AIDS in a general sense, but they reportedmany misconceptions. For example, they thoughtthat touching, kissing, holding hands, and usingcommon washrooms could transmit HIV/AIDS.
When asked about information sources, about half(51%) of the girls stated that information about sexcould be “most” effectively provided by a mother,father or guardian, while 40% said the same abouta sister or brother. In contrast, only 30% of boysconsidered parents to be among the mostinformative sources, and a large proportion (41%)considered them to be among the least informative.Even fewer boys (21%) felt that siblings are amongthe most informative sources of information. Thisgender difference may reflect girls’ tendency to discussintimate matters with their mothers, while boyslook outside their families for information. Onefinding that has relevance for sex education in theschools was that many young people (43% of girlsand 36% of boys) perceived teachers to be the leastinformative about sex.
The survey also asked adolescents about physicaland sexual abuse. About 66% of boys and 28% ofgirls said that they had experienced physicalabuse, either by a family member or someone else.Of those who reported physical abuse, a majoritysaid that their abuser was someone living withthem—an adult, sibling or another teenager. Moreboys than girls reported physical abuse, but ahigher proportion of cases among girls (65%) wereperpetrated by adults living in the house, comparedto 33% of the cases among boys. About 19% ofgirls and 14% of boys reported some kind of sexual
Table 1. Knowledge among young people of selected reproductive health topics
Boys GirlsHealth topic (N = 133) (N = 177)
Had discussed pregnancy (%) 86 81Had discussed sexual intercourse (%) 72 58Had discussed contraceptive use (%) 61 80Said they knew how a woman becomes pregnant (%) 77 66

80
YASMEEN SABEEH QAZI
abuse. Given the sensitivity of the topic, this isprobably an underestimate.
Conclusion
These study findings suggest that both male andfemale adolescents in Pakistan often lackknowledge about sexuality and reproduction, andare unprepared for the physical and emotionalchanges that take place during this period of life.During what is already a vulnerable time oftransition, many young people experience physicaland sexual abuse. Ideally, parents should provideinformation and guidance about sexual matters.However, given the social and cultural context inPakistan, parents are often reluctant to discuss“sensitive” issues with their children. Policies andprogrammes could take several approaches toaddress the need for more education on sexualityand reproductive health. One way to do this maybe to provide counselling to parents, to help themcommunicate more effectively with their children.
Second, they can prepare other responsiblepersons such as teachers and health careproviders to understand adolescent developmentand be able to provide appropriate information aboutsexuality and reproduction to adolescents.
Reference
Mensch BS, Bruce J, Greene ME (1998) TheUncharted Passage: Girls’ Adolescence in theDeveloping World. New York, Population Council.
Yasmeen Sabeeh QaziExecutive DirectorPAVHNA (Pakistan Voluntary Health & NutritionAssociation)9C, 18th Commercial StreetDefence Phase II Extension, D.H.A.Karachi-75500Pakistan
81
Influence of gender norms on the reproductive health of adolescents in Nepal
Background
Gender norms are social rules for how femalesand males are supposed to behave within a givenculture. In Nepal, as in other South Asian countries,these norms perpetuate a cycle in which manygirls leave school early to become young wives.The 1996 Nepal Family Health Survey found thatonly 50% of girls had ever been enrolled in school,compared to over 80% of boys. Among the girlswho did not complete secondary education, 57%cited marriage or pregnancy as reason for leavingschool. In Nepal, 50% of girls marry before age18, and early childbearing follows early marriage,usually within 18 months (Pradhan et al., 1997).
The effect of gender norms on reproductive healthemerged as an important theme in focus groupdiscussions (FGDs) conducted in 1999 as onecomponent of the Nepal Adolescent and YoungAdult (NAYA) study. The study focused on theeffect of gender norms on access to schooling,work and familial expectations related to marriageand parenthood. This paper describes these normsand their effects from the perspective of Nepaliyouth.
Methods
Researchers held 72 focus group discussions in11 districts with married and unmarried youth
aged 14–22. FGDs were stratified by gender andmarital status. In rural settings, researchersstratified the groups further by literacy/educationlevel, whereas for urban settings, they stratified thesample by age group (14–17 and 18–22). Researcherspurposively selected the 11 districts to encompasstwo major ecological regions (Hill and Terai), fivedevelopment regions and urban–rural settings. Thestudy districts represented diverse ethnic groupswith Brahman and Chhetri having the largest shares(about 17% each). During FGDs, participantsdiscussed issues relevant to the reproductivehealth of young people, including schooling, work,love, marriage, pregnancy, childbirth and their needfor services (Thapa, Davey & Waszak, 2000).Researchers held the FGDs in school classrooms,hotel rooms and private homes. The FGDs wereconducted in Nepali and generally lasted aboutone hour. Every effort was made to capture theessence of the young people’s perspectives andto preserve the flavour of their expressions, proverbsand idiomatic phrases.
Key findings
Both girls and boys reported gender inequalitiesin decisions about schooling. They explained thatparents were more likely to educate sons thandaughters and often kept girls home to help withdomestic chores or to look after younger siblings.
The Influence of gender norms on thereproductive health of adolescentsin Nepal—perspectives of youth
Cynthia Waszak, Shyam Thapa and Jessica Davey

82
CYNTHIA WASZAK, SHYAM THAPA AND JESSICA DAVEY
Girls were often kept at home to ensure that theyremain chaste until marriage. Even when familieshad the economic means to educate both sonsand daughters, they often sent boys to “goodboarding schools” and kept daughters in localschools. One respondent explained why parentspreferred to invest in sons’ educations as follows:
People have the idea that if they educate a son,he will earn money and look after them later.Some parents feel that there is no use educat-ing a girl, because one day she has to go off toher husband’s place. (Uneducated woman fromurban Baitadi)
Some respondents suggested that attitudes maybe changing in communities where girls were not“allowed to go to school” in the past. Many parentsmay actually want their daughters to go to school,but economic and social pressures are often toogreat. Female FGD participants spoke about thevalue of education for girls, saying for example:
We believe that if girls are educated, then theycan support themselves and be independent.Also, if they are mistreated by their husbands,they will know about their rights and can seekhelp from them from the law. Likewise, they willbe able to take care of their families properly.(Married woman from rural Dhanusa)
Girls with no education were wistful about theirlack of opportunity. A young woman with limitededucation from Dhankuta said, “We could havelearned many things if we were given the chanceto study. Then we would not have to cut grass andcollect firewood. We could teach others as well.”
According to FGD participants, many parents tooktheir daughters out of school in order for them tomarry. Even when girls were not compelled to leaveschool upon marriage, increased household workand responsibilities inherent in early marriage andmotherhood often made it difficult for girls tocontinue in school. In contrast, when boysdiscussed reasons for having to leave school, theywere more likely to mention economic reasons
rather than marriage. In fact, they suggested boysin poor circumstances were more likely to marrylate, because they were expected to be financiallyindependent before marriage.
Many parents experienced anxiety about gettingtheir daughters married, according to the FGDrespondents. In some cases, parents believed thatthey would fulfil their religious duties (dharmakamaiencha) by marrying their daughters early(kanyadaan). Others worried that if girls delayedmarriage, it would become “hard to find a suitablebridegroom”. In addition, much pressure for earlymarriage came from concern over a girl’s‘character’. The longer girls remained unmarried,the more chances there were of ruining theircharacter and of reducing their chances ofmarriage. As one respondent described, many“parents fear that she might run away with a manor have a love marriage, which will lead to theirdishonour in the society.” There is a proverb aboutwhy daughters should marry early:
Chori lai dherai rakhnu bhaneko dhoka ma panibharnu jastai ho. Spilled water on the doorstepis very dangerous: anything can happen. Like-wise, keeping daughters at home too long isvery risky and dangerous. (Young uneducatedwoman from Kapilbastu)
The young people in this study acknowledged adouble standard in expectations for girls and boys,not only on the part of parents, but also of theirpeers. One participant explained why boys wantedto marry young girls, saying:
The boys do not want to get married to girlsolder than that as they think that older girls arenot virgins. There is a greater chance of oldergirls having premarital sex. The boys alwayswant to marry virgin [chokho] girls whether ornot they are virgins themselves. (Young manfrom urban Chitwan)
Because few parents allowed open courtship priorto choosing a spouse, adolescents who spent timewith members of the opposite sex did so

83
Influence of gender norms on the reproductive health of adolescents in Nepal
clandestinely. Girls “caught” talking to boys inpublic were criticized and sometimes punished byparents and the community for being characterlessor “randi”. An educated young woman from Bataidisaid, “If the boy and girl meet in an isolated place,then society blames the girl and says she has abad character.” Adolescents reported thatpremarital sex did take place, but out of the viewof parents and the community. During the FGDs,more boys than girls discussed sex in the contextof premarital romances. As one young man fromJhapa said, “After the youth fall in love, they doeverything married couples do. After they meet,they have sexual relationships and feel good whenthey meet each other.”
Girls who engaged in a sexual relationship beforemarriage were unlikely to know how to protectthemselves against pregnancy or sexuallytransmitted infections (STIs), since suchinformation was considered inappropriate forunmarried girls. The consequences of unprotectedpremarital sex for girls in Nepal were often severe,especially if they got pregnant. The respondentssaid that a boy who fathered a premarital pregnancywas normally asked to marry the girl, and if he didnot, “… the girl’s life is ruined. The news will spreadfast in the village and the girl is helpless. It is hardfor her to get married.” In some cases, girls whoget pregnant before marriage were “married off toa widower or old man. Those men are given moneyto marry such girls.”
Opinions varied among the focus group participantsabout the “ideal” age for marriage, but there wasconsensus that girls and boys needed to be olderat marriage than they typically were. Regardlessof the age at marriage, adolescents described thesituation in Nepal as one in which girls and womenwere often powerless to make reproductivedecisions. The participants explained that, unlikeboys, girls did not generally have any choice aboutwhom they would marry. More educated parentswere more likely to give their daughters a say inmarital decisions. Moreover, girls had little to sayin decisions regarding sex or childbearing. As oneeducated woman from Dhankuta explained:
… if a woman does not feel like having sex,she has to do it anyhow if the man feels like it.Similarly, if the husband or the in-laws want ason, the woman has to keep giving birth untilshe has one. The decision depends entirelyupon the family.
When girls got married, they were often pressuredto begin childbearing right away and were criticizedif they did not. As a young woman in Jhapadescribed:
If the couples do not have children for a fewyears, the girl is called tharangi [infertile] and isconsidered unlucky. The community memberswill not even look at such a woman before do-ing something important for fear she will causemisfortune.
The FGD participants described how earlymotherhood brought physical and social difficulties.They expressed particular concern about thetreatment of young pregnant wives. While mostadolescents in our study understood the need forgood nutrition during the prenatal period, they notedthat young pregnant wives from poor familiessuffered from a lack of food and mistreatment bytheir in-laws, especially mothers-in-law. As oneunmarried woman from Dhankuta said:
Pregnant women are not cared for during theirpregnancies as they are daughters-in-law. It isbelieved that the daughter-in-law should eat onlyafter she feeds all the family members… Thepregnant women have to go through a lot ofhardships and sometimes sleep without havinganything to eat.
The participants described practices thatcontributed to poor health for pregnant girls,including the belief that “the more you work, thelighter your body becomes and the easier it is indelivery”.
Though marriage practices and arrangementshad more disadvantages for girls, maritalexpectations also posed challenges for boys. Boys

84
CYNTHIA WASZAK, SHYAM THAPA AND JESSICA DAVEY
faced difficulties in establishing their financialindependence, considered necessary preparationfor marriage. The need to find work before marriageresulted in longer periods of remaining single forboys than for girls. Financial pressures could resultin boys having to migrate out of the area, evenafter marriage. The longer boys remained single,the more likely they were to engage in sex outsideof marriage, placing themselves at risk of STIs inan environment that lacked adequate STIprevention education.
Conclusion
Worldwide data show a clear relationship betweeneducation and age at marriage (Singh & Samara,1996), but the direction of causation is not clear.The findings of this study suggest that the causalrelationships between lack of education, earlymarriage, low social status and poverty may becircular rather than linear. The family economicsituation determines which families send childrento school; gender norms then may determinewhich, if any, children in the family go to school.Even when schooling is available for girls, parentsfear that more education will reduce their daughters’chances of finding suitable husbands. And formany, the well-being of the family is dependent onthe marriage of their daughters according to localnorms.
Regardless of the precise causal relationships, theconsequences of early childbirth exacerbated bypoverty include poor health outcomes for both themother and the child (Hobcraft, 1987; Mensch,Bruce & Greene, 1998; Senderowitz, 1995). Therealso are health risks for girls who do not marryearly (Singh & Samara, 1996). A longer period ofbeing single may create risks of premaritalpregnancy and STIs, especially in an environmentin which information and services are not availableto unmarried girls and boys, and in which thereare severe social sanctions for girls whoexperience premarital pregnancy. Greater accessto education for girls is a logical step towards
delaying childbearing and creating better lives forgirls.
Acknowledgements: Financial support for theNepal Adolescent and Young Adult study wasprovided by the United States Agency forInternational Development (USAID) through FamilyHealth International headquarters. The conclusionsreached in this paper do not necessarily representthe views of USAID, the reviewers or theorganizations with which the authors are affiliated.
References
Hobcraft J (1987) Does family planning save lives?Technical background paper prepared for theInternational Conference on Better Health for Womenand Children through Family Planning, Nairobi,Kenya.
Mensch B, Bruce J, Greene M (1998) The UnchartedPassage: Girls’ Adolescence in the Developing World.New York, The Population Council.
Pradhan A, Aryal Ram H, Regmi G, Ban B,Govindasamy P (1997) Nepal Family Health Survey1996, Kathmandu, Nepal and Calverton, Maryland,Ministry of Health [Nepal], New ERA and MacroInternational Inc.
Senderowitz J (1995) Adolescent health: reassessingthe passage to adulthood. World Bank DiscussionPaper No. 272. Washington, DC, World Bank.
Singh S, Samara R (1996) Early marriage amongwomen in developing countries. International FamilyPlanning Perspectives, 22:148–157.
Thapa S, Davey J, Waszak C (2000) ReproductiveHealth Needs of Adolescents and Youth in Nepal:Results from a Focus Group Study. Kathmandu, FamilyHealth International.
Further reading
Amin S, Sedgh G (1998) Incentive Schemes for
School Attendance in Rural Bangladesh. Working
Paper No. 106. New York, The Population Council.

85
Influence of gender norms on the reproductive health of adolescents in Nepal
Assaad M, Bruce J (1997) Empowering the nextgeneration: girls of the Maqattam garbage settlement.Seeds, 119.
Barnett B, Stein J (1998) Women’s Voices, Women’sLives: The Impact of Family Planning. ResearchTriangle Park, NC, Family Health International.
Jejeebhoy S (1998) Adolescent sexual andreproductive behavior: a review of the evidence fromIndia. Social Science and Medicine, 46:1275–1290.
Luther N, Thapa S (1999) Infant and Child Mortality inNepal. Kathmandu, Nepal, Family Health International.
Thapa S (1996) Girl child marriage in Nepal: Itsprevalence and correlates. Contributions to NepaleseStudies, 23:361–375.
Thapa S, Acharya LB, Aryal RH (1997) Schooling,marriage, work, and childbearing among the youth
populat ion of Nepal: Emerging insights andchallenges. Report prepared for the Workshop onYouth Across Asia, Kathmandu, Nepal, 23–25September 1997.
Thapa S, Chhetry D, Aryal R (1996) Poverty, literacyand child labour in Nepal: A district-level analysis.Asia-Pacific Population Journal, 11:3–12.
Shyam Thapa, PhDDirector and Senior ScientistPopulation and Reproductive HealthFamily Health InternationalGPO Box 20520KathmanduNepal

86
KALINGA TUDOR S ILVA AND STEPHEN SCHENSUL
Background
In Sri Lanka, as in other societies in this region,strong norms persist that prohibit premarital sexualcontact between young men and women. Thetaboo on sex has been particularly rigid for youngwomen who are traditionally expected to maintainvirginity until marriage and even to prove it as partof the marriage ceremony. However, this taboo hascome under severe strain due to increasing age atmarriage, increased opportunities for male–femalecontact in educational institutions, workplaces,etc. and greater exposure to new ideas about loveand sex transmitted through the media.
Sri Lanka is characterized by relatively late age atmarriage and has witnessed a considerableincrease in marital age over the last 50 years,especially among women. At present, age atmarriage is typically around 29 years for men and27 years for women (Dissanayake, 2000). Alongwith this evidence of marital postponement, thereis some indication of a decline in age at sexualdebut (Silva et al., 1997). This study explored theways in which young unmarried youth in Sri Lankareconcile new ideas about love and premarital sexwith traditional norms that disallow thesebehaviours. Specifically, the study explored theways in which young unmarried people perceivelove and sex, the extent to which young men andwomen hold different attitudes with regard to
premarital sex, and the implications of theseattitudes and behaviours for sexual healthprogrammes targeted at youth.
Methods
To compare differences in the perceptions of low-and middle-income, and poorly and well educatedyoung people, this study gathered data amongrespondents from two groups: youth from a low-income urban community, and university studentsfrom faculties of liberal arts and medicine. Thesample consisted entirely of never-married youthand adults aged 17 to 28. The mean age for theurban community sample was 21 years, comparedto 25 years for the university sample. Researcherschose this study design to ensure that the sampleincluded respondents from a broad range ofsocioeconomic backgrounds. As education wasconsidered an important factor leading to thepostponement of marriage (Caldwell et al., 1989),the inclusion of community and university samplesallowed researchers to study the impact of highereducation on perceptions about sexuality andmarriage.
The study used a mix of qualitative and quantitativeresearch techniques. In the first phase, researchersgathered qualitative data through key informantinterviews, open-ended interviews and pile
Differences in male and female attitudestowards premarital sex in a sample of SriLankan youth
Kalinga Tudor Silva and Stephen Schensul

87
Attitude towards sex in a sample of Sri Lankan youth: differences in male and female responses
sorting. The open-ended interviews involved atotal of 156 youth includ ing 93 universitystudents (42 males and 51 females) and 63community youth (30 males and 33 females). Inthe second phase, a larger and randomly chosensample of youth participated in a self-administeredsurvey. The survey sample consisted of 615respondents, including 303 from the community(151 males and 152 female respondents) and 312from the university (163 males and 149 females).Following the survey, a peer education interventionprogramme was implemented with a view toaddressing the problems identified throughqualitative and quantitative investigations. Findingsof the larger study are presented in Silva et al.(1997) and Silva, Sivayoganathan & Lewis (1998).The results of the intervention programme have beendiscussed in Nastasi et al. (1999). Using surveyfindings and results of qualitative investigations,the present paper explores the attitudes of maleand female respondents with regard to premarital sex.
Key findings
The study inquired of young respondents whetherthey were currently “in love”. This group includedthose who were sexually active as well as thosewho were not. While 50% of the sample reportedhaving a current love partner, this proportion variedfrom 30% and 49% among female and maleuniversity students respectively, to 51% and 63%among low-income female and male youth fromthe community.
While gender differences in the proportions of youthreporting a current love partner were apparent, theywere not statistically significant. In contrast,attitudes towards premarital sexual activity differedsignificantly by gender even more widely than byclass. For example, compared to femalerespondents, male respondents reported morefavourable attitudes towards premarital sex (Table1), and nearly half (46%) of male respondentsagreed that it is acceptable to have sex if it doesnot destroy a girl’s virginity, compared to only 14%of female respondents.
These findings clearly illustrate the intensity withwhich gender double standards persist. Virginityat marriage continues to be highly valued. It istherefore not surprising that young women—forwhom the consequences of premarital sex are mostprofound—are more likely than young men toadhere to these norms. As revealed in keyinformant and semi-structured interviews, youngmen, on the other hand, while refraining frompenetrative sex with their “love” partners, are indeedengaging in penetrative sex with casual partners,including older women and commercial sexworkers.
Observed differences between the attitudes ofuniversity students and those of low-income youthwere somewhat unexpected, although they werenarrower than gender differences. The hypothesisthat highly educated youth are less likely to holdtraditional attitudes towards the acceptability ofpremarital sex than less educated youth is not
* Difference between the two groups is significant at the 0.05 level.
**Difference between the two groups is significant at the 0.01 level.
Table 1. Attitudes towards premarital sexual activity, by sex and study group
Sex Study groupPer cent who agree or strongly agree Female Male Low-income Universitywith the following statements (N=301) (N=314) (N=303) (N=312)
I would like to marry/be a virgin at marriage (%) 82** 57 68 70
It is wrong to destroy virginity before marriage (%) 76** 65 67* 73
It is acceptable to have sex if it does not destroythe virginity of a girl (%) 14** 46 33* 28

88
KALINGA TUDOR S ILVA AND STEPHEN SCHENSUL
borne out in these data. Indeed, the data suggestthat low-income and less educated young peopleare somewhat more likely than university studentsto approve of premarital sexual activity.
Finally, the study findings suggest that youngpeople stop short of approving penetrative sexualactivity with a committed or “love” partner. Evenamong those who approved of premarital sex, thevast majority was in favour of non-penetrative sexualpractices that preserve female virginity.
Conclusions
Evidence from the study suggests that while youngpeople in Sri Lanka do indeed engage in datingand establish committed “love” relationships, theyalso remain ambivalent about the nature of theserelationships and the acceptability of premaritalsex. Double standards persist and premarital sexamong women continues to be consideredunacceptable, especially by young women.Typically, young people resolve this conflict in twoways—either by engaging in non-penetrative sexualrelations with “love” partners, or, in the case ofyoung men, resorting to penetrative sexual activitywith casual partners, including older women andsex workers. The extent to which these sexualbehaviours are risky or protected remains an openquestion. Relations with casual partners and/orsex workers must certainly put young men at riskof infection and in a position to transmit infectionto their “love” partners and future spouses. Sexualhealth programmes targeted at youth in Sri Lankaneed to pay greater attention to issues such asnon-penetrative sex, risks of sex with casualpartners and the implications of the concept offemale virginity in relation to sexual risks.
Acknowledgements: This study was supportedby a grant from the International Centre forResearch on Women. It was implemented by amultidisciplinary and international team from theUniversities of Peradeniya (Sri Lanka) andConnecticut (USA).
References
Caldwell J et al. (1989) Is marriage delay a multiphasicresponse to pressures for fertility decline? The caseof Sri Lanka. Journal of Marriage and Family, 51:327–335.
Dissanayake L (2000) Factors influencingstabil ization of women’s age at marriage. In:Demography of Sri Lanka. Colombo, Sri Lanka,Department of Demography, University ofColombo:45–58.
Nastasi BK et al. (1999) Community-based sexualrisk prevention program for Sri Lankan youth:influencing sexual decision making. InternationalQuarterly of Community Health Education 18(1):139–155.
Silva KT, Sivayoganathan C, Lewis J (1998) Love, sexand peer activity in a sample of youth in Sri Lanka. In:Hettige S, ed., Globalization, Social Change andYouth. Colombo, Sri Lanka, German CulturalInstitute:34–52.
Silva KT et al. (1997) Youth and Sexual Risk in SriLanka. Women and AIDS Research Program Phase11: Research Report Series No. 3. Washington, DC,International Center for Research on Women.
Dr Kalinga Tudor SilvaProfessor of SociologyUniversity of PeradeniyaPeradeniyaSri Lanka
Dr Stephen SchensulAssociate ProfessorDepartment of Community MedicineCenter for International Community HealthStudiesUniversity of Connecticut270 Farmington Avenue, Suite 260 MC 6330Farmington, CT 06030-6330USA

VUnwanted sex: sexualviolence and coercion
91
Sexual coercion among unmarried adolescents of an urban slum
Background
While carrying out programmes in the Tigri area ofDelhi, Swaasthya, a nongovernmental organi-zation, identified adolescents as a particularlyvulnerable group in terms of sexual and reproductivehealth (SRH). In order to design appropriateprogrammes, Swaasthya recognized the need tounderstand better the social context that influencesadolescent sexual behaviour. Therefore, in 1996–1997, they conducted a qualitative study in anurban resettlement colony called Shantibaug (apseudonym). The research objectives were to studyunmarried adolescents’ sexual behaviour,information needs and networks. In the course ofthe research, sexual coercion emerged as animportant issue, even though this was not theoriginal focus of the research. This paper describesthe kinds of coercion faced by adolescents andthe sociocultural factors that lead to coercion.
Methods
The sensitive topic of sexuality demanded a studywith an ‘emic’ perspective, that is, from the pointof view of adolescents themselves. To do this,researchers recruited adolescents from thecommunity to collect ethnographic data from theirpeers. The study began with 5 – 10 key informantinterviews, and researchers used these findings
to develop in-depth interview and focus groupdiscussion guidelines. They then conducted 71 in-depth interviews, 11 case studies (detailed lifehistories), and 15 follow-up interviews with boysand girls, most of whom were unmarried. Finally,researchers held eight focus groups to gatherinformation on normative behaviour: four with boysand four with girls. Researchers translated the datafrom Hindi into English and coded the issues thatemerged at the time of translation.
Key findings
The Shantibaug colony is home to about 15 000people, generally from the lower socioeconomicbracket. A majority are Hindus with some Muslims,Christians and Sikhs. The prevailing culture ispatriarchal, in which girls are seen as the family’sizzat (honour) and are sometimes referred to as‘paraya dhan’ or someone else’s property (i.e. theirfuture husband’s). Arranged marriages are thenorm, and any perceived ‘misdemeanour’ on thegirls’ part may compromise their prospects of a‘good’ marriage. As a result, families restrict girls’mobility and limit interactions with boys who arenot part of the family.
Researchers chose the term “coercion” toencompass not only physical violation of individualsbut also lesser (but often traumatic) manifestations
Sexual coercion among unmarriedadolescents of an urban slum in India
Geeta Sodhi and Manish Verma

92
GEETA SODHI AND MANISH VERMA
such as teasing and harassment. During 71 in-depth interviews, respondents mentioned teasing198 times and described 32 separate instances ofmore serious kinds of sexual coercion. Typically,groups of two to four boys tease girls who pass onthe street. Teasing includes comments, singingfilm songs, whistling, shouting, waving, and makinglewd sounds, suggestive hand gestures and facialexpressions. Boys who lack other opportunitiesuse teasing as a way to interact with girls. Whileteasing is mild compared to other issuesdiscussed in this paper, it may reinforce attitudesabout male dominance as boys become aware thatsociety tolerates this behaviour. Most teasing goes‘unrewarded’, but in a few cases it leads tofriendships between boys and girls.
Girls in the study described matrimony and thedesire for “true love”, not sex, as reasons forentering relationships. A 14 year-old girl who hada boyfriend who was interested in her since shewas 12 years old said, “when one loves somebodyfrom childhood and later marries that person thenit is called true love and in false love everything isdone (have sex) and then he leaves her...” Another19 year-old girl had a relationship with a boy whoshe says had loved her since she was young. Whenhe asked her to have sex, she said, “It doesn’tlook good, doing all this before marriage. My didi[older sister] says that those who do true love theynever ask from a girl for all this.” In contrast, mostboys interviewed felt that boys befriend girls withphysical relationships foremost in their minds. An18 year-old boy remarked, “mostly, boys dofriendship for the sake of physical relations…someboys keep friendship till friendship, but mostly boyswant…[to] establish physical relations as early aspossible.” An 18 year-old boy remarked, “Boysmostly…do ashiqui [romance] to have chut [femalegenitals].”
The interviews suggested that cinema plays amajor role in adolescents’ lives and serves toperpetuate gender stereotypes. Girls embrace thenotions of romantic love and “happily-living-after”scenarios from Hindi films, while boys watchpornographic films that objectify women andreinforce boys’ desire to seek sexual satisfaction.
Respondents described a number of relationshipsthat began as consensual but led to sexualcoercion, ranging from forced kissing to forcedsexual intercourse. In some cases coercionbecame progressively more violent. For example,one 15 year-old girl described how her boyfriend“kissed me forcefully on top in my bhabhi’s [sister-in-law’s] room. He took me there on the pretextthat he had to talk to me.” Subjugation at the startof the relationship led to more severe violence. Thisgirl explained:
...he gets angry if I talk to anyone in the lane.One day he saw me talking to my brother...hecame in the evening and beat me up. He wassaying that boy was my year [friend]...he beatme so much even then I did not say anything tohim because I love him so much.
An important factor that places girls at risk is thatrevelation of a relationship may lead to severerepercussions. Armed with this knowledge, boyscan use blackmail to demand sex. A 19 year-oldboy told of his sexual relationship with a marriedgirl during which he became violent. He said, “Shewas feeling the pain. I did this till I was satisfied.”When the girl tried to get out of the relationship,coercion progressed to blackmail. In his own words,he:
…gave her Dhamki [threat] that if she will notdo then I will tell everybody. Then I started tak-ing money for each sexual intercourse. I usedto threaten her that I will tell everybody. Sheused to give me Rs 20, sometimes Rs 50 or100.
Sometimes boys use the threat of defamation todemand sex for their friends. A 19 year-old studentremarked, “...friends also help in establishingphysical relations with his girlfriend…. And if thegirl says no then boys defame her in her gali [lane]and colony. Because there is no effect on boy’scharacter.”
This situation does not necessarily improve afterthe girl is married. The cultural context condones

93
Sexual coercion among unmarried adolescents of an urban slum
sexual coercion within marriage. An 18 year-oldgirl described her sister’s wedding night, saying,“She did not want to celebrate first night but herhusband was annoyed...he didn’t agree and did itforcefully. She was having a lot of pain so herBhabhi took her to the dispensary the nextmorning. ” This non-consensual sex/rape isconsidered part of a girl’s life. When asked whathappens on a wedding night one 18 year-old girlsaid, “the girl knows that on first night the boy willhave sex with her. Even if the girl refuses, he willdo sex forcefully. ” A 19 year-old painter spoke ofhow he overrode the will of his new wife “...At night,I asked her to take off her clothes. She refused.When I asked her two–three times, she startedcrying. I made her keep quiet, and after that I tookher clothes off and did my work.” Older women tellgirls to accept this situation as normal. Accordingto one girl, they say, “If you won’t give him then hewould force and you will have pain.”
Male respondents also described using violencewith commercial sex workers (CSWs). A 16 year-old boy related an incident in which his friend helda CSW down while he had anal sex with her. Hedescribed how, “she said it was paining and refusedto do it…she started screaming and tried tomove away… I asked my friend to hold her andnot to let her move forward. She screamed andbit my hand.”
Respondents described other acts of sexualviolence, including threats, rape and attemptedrape. One respondent described a friend whoexperienced incest by a brother. She spoke of herfriend’s helplessness saying, “She feels likerunning away. But where could she go?” One 16year-old boy described raping a girl who had runaway from home because her parents wanted tomarry her off. When he met her in the street, helured her to a friend’s home, saying, “ ‘Where wouldyou sleep—on the road? You come with me to myhome and sleep. You could leave in the morning.’…I talked to her for some time and then I kissedher, pressed her breasts, that girl was refusing.But I did it forcefully. I f—-ed her a lot.”
Girls are not the only ones coerced. Interviewsrevealed two instances in which older boys forced12 and 13 year-old boys to have anal sex. One 16year-old boy described how, “elder boys used toask me for Gandh [anal sex]. At that time, weused to feel very bad, but after some time, wealso started asking from our age boys for analsex.” A 19 year-old married adolescent said,“...when we were young, we used to have anal sexwith large numbers of boys.... We all together usedto go to the latrines. Whosoever we would seethere, we used to snatch his container and f—him. We couldn’t put it inside but used to touch iton the skin only. ”
These encounters are straightforward cases of rapeor molestation, which carry harsh legal penalties.However, society often tolerates coercion andplaces blame squarely on the victim, as thefollowing instance illustrates. A 14-year-old girlnarrated how a boy on the street assaulted her.“Once I was coming through the street...and thisboy came from the front, pressed my breasts, andran away. I had not wrapped a chunni [scarf] . ”Chunni is a symbol of modesty in the Indian socialcontext, and without it, women are often said tohave loose morals for exhibiting their breasts. Thegirl’s mother beat up the boy, but the neighbourcommented, “fault lies in your daughter who didnot wear a chunni.” The neighbour’s commentreflected tolerance of the boy’s behaviour, byplacing blame on the girl’s lack of character.
Conclusions
These research findings suggest that boys andgirls are at polar opposites regarding what theywant from relationships. Boys are outspoken abouttheir desire for sex, while girls speak aboutromantic and matrimonial aspirations in arelationship. Cinema plays a role in perpetuatinggender stereotypes, by encouraging girls toidealize the notion of ‘true love’ and encouragingboys to seek sexual gratification. Societyperpetuates abuse by tolerating certain kinds of

94
GEETA SODHI AND MANISH VERMA
coercion, which emboldens boys to become evenmore aggressive and violent. While boys havelicense from society to take advantage of sexualopportunities, girls risk defamation.
These research findings suggested a number ofimplications for interventions and programming thatSwaasthya incorporated into their work. First, itwas clear that there was a need for perspectivebuilding and sensitization about coercion andgender stereotypes. Because cinema has such astrong influence on young people, Swaasthyahelped young people from the community todevelop video programmes on these topics, whichit screens on street corners and local cableprogrammes. Second, because girls whoexperience coercion often lack social support,Swaasthya created opportunities within itsprogrammes for greater interaction betweenadolescent girls and gatekeepers, includingparents. In addition, it organized girls’ groups forpeer support and collective action. Third, given thatgirls’ lack of life skills increases their vulnerability,Swaasthya established a skill-building programmethat addressed decision-making, problem-solvingand communication and negotiation skills. Thepreliminary evaluation of these programmesindicates that they appear to be achieving somesuccess.
Further reading
Heise L, Moore K, Toubia N (1995) Sexual Coercionand Reproductive Health: A Focus on Research, NewYork, Population Council.
Jejeebhoy S (1996) Adolescent Sexual andReproductive Behaviour: A Review of the Evidencefrom India. Working Paper No. 3. Washington, DC,International Center for Research on Women.
Mehta S, Groenen R, Roque F (1998) Adolescents inchanging t imes: issues and perspectives foradolescent reproductive health in the ESCAP region.Background paper for High-level Meeting to Reviewthe Implementation of the Programme of Action ofthe International Conference on Population andDevelopment and Bali Declaration on Population andSustainable Development and to MakeRecommendations for Further Action. Bangkok,United Nations Economic and Social Commissionfor the Asia and the Pacific.
Segala UA (1999) Family violence: A focus on India.Aggression and Violent Behaviour 4(2) (Summer).[Available at: www.asiamedia.ucla.edu]
Zillmann D (1998) Sexual Behaviour Researchamong Adolescents in Tigri. Report submitted to theRockefeller Foundation, New Delhi, Swaasthya.
Zillmann D (2000) Influence of unrestrained accessto erotica on adolescents’ and young adults’dispositions toward sexuality. Journal of AdolescentHealth 27(2, Suppl. 1):41–44.
Dr Geeta SodhiFounder and DirectorSWAASTHYALower ground floor G1323Chittaranjan ParkNew DelhiIndia
95
Experiences of sexual coercion among street boys in Bangalore, India
Background
There are an estimated 100 million street childrenworldwide, including 40 million in Latin America,30 million in Asia and 10 million in Africa. Streetchildren as a group can be hard to define, but mayinclude children who are “of” the street and thosewho live “on” the street (de la Barra, 1998). Bysome estimates, India has over 414 700 streetchildren, mainly in big cities (Pinto, 1993). Manyare homeless and must fend for themselves withoutadult care. In such situations, children are oftenforced into “survival sex”, i.e. sex for protection,food, drugs and shelter (Inciardi & Surratt, 1998;Swart-Kruger & Richter, 1997). Street life ishierarchical, with well-developed power structures,and sexual coercion is a common way of exercisingpower. Sexual coercion encompasses behavioursthat range from physical and mental coercion toenticement with economic and psychologicalrewards.
BOSCO, a nongovernmental organization, hasworked with street children in Bangalore since1980. An estimated 85 000–100 000 street childrenlive in Bangalore alone (BOSCO, 1998; Reddy,1992). After a study for developing a drugprevention programme (BOSCO, 1999) found thatmore than 50% of children with a drug habit alsopractised unsafe sex, BOSCO carried out a studyto examine high-risk sexual behaviour among
street children in Bangalore. The research did notspecifically aim to study coercive sexualbehaviours, but this emerged as a dominant themeduring data analysis.
Methods
The study employed a combination of qualitativeand quantitative research methods. Using socialmapping, free listing, pile sorting and rating,researchers gathered information on boys’perceptions of sexual behaviour and coercion. Theyconducted in-depth interviews with children and keyinformants. In addition to qualitative data,researchers gathered quantitative information from121 boys on socio-demographic profiles, familyhistory, sleeping arrangements, alcohol/drug useand sexual activity. Study participants came fromfour of seven areas where BOSCO has outreachprogrammes. All members of the research teamhad more than five years experience working withstreet children, and their rapport with respondentswas essential to the success of the study.
Key findings
Boys in the study ranged from age 9 to 23.A majority (45%) were 14–17 years old, and themedian age was 16 years. On average, boys had
Experiences of sexual coercion among streetboys in Bangalore, India
Jayashree Ramakrishna, Mani Karott andRadha Srinivasa Murthy

96
JAYASHREE RAMAKRISHNA, MANI KAROTT AND RADHA SRINIVASA MURTHY
been on the street for five to six years. Boys citedpoverty as the major reason for leaving home.Nearly one-fourth did not have a father or mother,and a large per cent had an alcoholic parent. One-fourth never went home, and 40% went home onlyfor festivals, even though their parents lived in thesame town. Most boys did not have closeassociations with adults.
Life on the street is fraught with danger. Policeand local hoodlums (goondas) are feared by all.Living in a gang offers some protection fromoutsiders, though older gang members may takeadvantage of younger boys. Groups of boys work,sleep and play together. Drug and alcohol use iscommon. Half the boys inhaled “solution”(typewriter correcting whitener), and nearly half(46%) consumed alcohol. Street boys areextremely mobile; they change jobs and sleepingplaces frequently. Apart from a group of 16 boys inthe study who lived at home, the other boys sleptat the BOSCO shelter, in the streets, parks andworkplaces. In the social stratification of streetboys, rag pickers are at the bottom, coolies arehigher up, and parking attendants or those whosell cinema tickets are at the top. Although someboys earn a good wage, they do not have a way tosave money and are often robbed.
The boys in the study were quite comfortabletalking about sex with a trusted adult. Children onthe street use the English word “sex” or “sexu”when talking of sex-related themes. Twenty-threeboys free-listed words that came to mind whenthey heard the term “sexu”. Sex was commonlyseen as “work” (khelsa). For instance,masturbation is referred to as “hand work” (kaikhelsa), oral sex as “mouth work” (bai khelsa) andanal intercourse as “back work” (hinde khelsa).Street boys have a negative attitude towards sexand often refer to it as “bad work” (ketta khelsa)and “dirty work” (galeej khelsa). Anal sex and oralsex between same-sex partners were clearlydistinguished as “doing” and “getting done”. Boysdid not use the term “rape” in regards to boys, butthe English word “force” (force madduvadu).
Sixty-one boys rated 26 items according to howpleasurable and how dangerous they consideredeach sexual act. Overall, they rated consensualsex with girls as the most pleasurable activity,followed by raping a girl. When asked how theyknew that rape was pleasurable, they replied thatmen in movies seemed to enjoy it. Forcing boysto have anal sex was not thought to be aspleasurable as coercing girls, nevertheless theysaid that it gives some pleasure.
The major reasons boys cited for having sexincluded pleasure (maja), excitement/arousal(udhvega/choolu ), desire (asé), and feelingdepressed/bored (béjaar). Two spoke of falling inlove. Some street boys expressed fond feelingsfor “girl friends”, such as vendors or girls involvedin casual sex work. During the study period a boycommitted suicide because he thought a girl whosold peanuts had rejected him. Many boys saidthat they had a lot of “feeling” towards the sexworker with whom they had had their first sexualexperience. They had wanted to have a long-termrelationship, and many said they intended to marrythem. But these women told them to just finishtheir “work” quickly and were not interested in “talk”or feelings. After several such encounters, streetboys began to view women on the street in anegative light. They referred to sex workers asprostitutes (sulé), vehicle/carts (gaadi/vandi) andthings or goods (maal).
Sexual coercion needs to be viewed in the broadercontext of street life. According to the quantitativedata gathered in this study, 74 (61%) out of 121boys were sexually active. Four were initiated atage nine or younger. Most (36) were initiatedbetween ages 10 and 12; twenty-one were 13–14years old. Anal sex, which is usually a boy-to-boyactivity, was the most commonly reported sexualbehaviour, followed by vaginal sex. Few (8)practised solely vaginal or solely anal sex; themajority mentioned at least two behaviours. Olderboys tend to have sex with girls as well as analsex with boys. At times friends have anal sex, oralsex or practise mutual masturbation (Table 1).

97
Experiences of sexual coercion among street boys in Bangalore, India
Older boys, 15 years and above, often force orentice younger boys, some as young as 6 yearsold, to have anal sex. Younger boys are afraid andupset when they are “forced”, but do not see howthey can avoid the older boys. The older boysthreaten to beat them or ostracize them. In manycases the younger boys are dependent on the olderboys for protection. Older boys also entice youngerboys with money, food or empty bottles that canbe sold. They may also take them to a movie orgive them “solution”. Street boys hesitated toexpress fear, and some said that over time theyhad become used to the idea of being forced. Inone narrative, a 12 year-old boy described how heis no longer afraid when boys “force” him. In hisown words:
…older boys come and force us, when we refusethey beat us. They tell me that they will givemoney. Initially when others “call” us we areafraid. They also did it from the back [anal sex].Initially it was a little painful, but afterwards therewas no pain. Now, I have no fear.
Later, however, he said that when he thinks of boysforcing him, he is afraid. Perhaps the denial of fearis a way of coping with pain and trauma. This boyalso described having relations with adult porterswho give him food and money and beat other boyswho trouble him. The porters show affection but atthe same time they have sex with him. He said, “Idon’t like any of them.”
Younger boys perceive that the older boys mustbe getting pleasure (maja) from “forcing” them, andthey are eager to experience this maja. They are
not averse to forcing younger boys, so there areno clear distinctions between coercers and thecoerced. The younger boys said they wanted tohave sex with girls, but were too afraid and shy toapproach women. One uneducated 16 year-old saidthat he and other youngsters felt ashamed to visitsex workers, as they are very young. They weremore comfortable with young street girls or drunkensleeping women. Drunken sleeping women areeasy targets. They may wake up and scold theboys, or they may cooperate. Others show noreaction, or appear “dead”, as one boy remarked.Young street girls are sometimes willing toexchange sex for money and food. According toone informant, young girls call them saying, “giveus food and money and you can sleep with us.” Sohe and some young boys have had sexualrelationship with girls who are 8–12 years old.
Conclusions
In summary, social conditions, poverty and druguse shape concepts of sexuality and coercionamong street boys. Pleasure or maja is a dominanttheme associated with sex. Sex with girls isdeemed to be most pleasurable, even if it is rape.Sex with boys also gives pleasure, although “doing”anal sex is much more pleasurable than having it“done”. All things being equal, however, boys preferconsensual sex. Despite the pleasure boys derivefrom sex, they hold a negative view of sex: that itis bad, dirty and shameful. Nevertheless, they arewilling to talk about sexual matters.
Sexual coercion on the street is an exercise ofpower, a way to maintain status and subdue asubordinate. Boys who have been forced, in turnwant to be in positions of command. Just as sexmay express power, it may also be interpreted asan expression of affection and protection. Boyswho are “forced” may feel they will receiveprotection from hazards of street life. The natureof street life—including the lack of food, shelter,protection and emotional support combined withstrong power structures—sustains sexuallycoercive behaviours.
Table 1. Number and per cent of sexually activestreet boys reporting selected sexualbehaviours (N=74)
Sexual behaviours Number Per cent
Anal intercourse 46 62Vaginal intercourse 42 57Self masturbation 30 41Mutual masturbation 24 32Oral sex 10 14Sex with eunuchs (Hijra) 4 5

98
JAYASHREE RAMAKRISHNA, MANI KAROTT AND RADHA SRINIVASA MURTHY
Programmes must consider multiple risk factorswhen carrying out interventions (Richter, 1997).BOSCO is drawing upon these research findingsto modify the street boys’ environment by providingsafe places to sleep, healthy recreation options,safe ways to save money and opportunities to buildrelationships with caring adults. In addition, BOSCOis providing life-skills training, counselling andhealth education to help street boys adopt safersex behaviours.
Acknowledgements: We gratefully acknowledgethe cont r ibu t ions o f s t ree t educatorsMr Basavaraju, Mr Ramaswamy, Mr Ramesh,Ms Sheeba Thomas and Mr Shivamallu, and thesupport of Fr K.D. Varghese Kootungal, ExecutiveDirector, BOSCO, Bangalore, and Fr VarghesePallipuram, Project Holder, BOSCO; and theresearch guides, Dr Shekhar Sheshadri, andDr Vivek Benegal; Dr Pushpinder Pelia Lubana,and Professor Pertti Pelto, NIMHANS Small GrantsProgramme for Research on Sexuality and SexualBehaviour.
References
BOSCO (1998) Annual Report 1997–1998.Bangalore, BOSCO.
BOSCO (1999) Report of the Drug Abuse PreventionProgramme. Bangalore, BOSCO.
de la Barra X (1998) Poverty: the main cause of ill-health in urban children. Health Education andBehavior, 25(1):46–59.
Inciardi JA, Surratt HL (1998) Children in the streetsof Brazil: drug use, crime, violence, and HIV risks.Substance Use & Misuse, 33(7):1461–1480.
Pinto G (1993) Street children an urban phenomenon.In: Kanth A, Verma RM, eds. Neglected Child—Changing Perspectives. Delhi, Prayas.
Reddy N (1992) Situational Analysis of Street Childrenin Bangalore. NOIDA, Delhi, National Labour Institute.
Richter L (1997) Street children and HIV/AIDS. AIDSBulletin, 6(4):4–6.
Swart-Kruger J, Richter LM (1997) AIDS-relatedknowledge, attitudes and behaviour among SouthAfrican street youth: reflections on power, sexualityand the autonomous self. Social Science andMedicine, 45(6):957–966.
Jayashree Ramakrishna, PhD MPHAdditional ProfessorDepartment of Health EducationNational Institute of Mental Health and NeuroSciencesPost Bag 2900Bangalore 560 029India
99
Gender, sexual abuse and risk behaviours of adolescents in Goan schools
Background
There is growing evidence that the broader contextof reproductive health pertaining to adolescenceneeds attention. For example, in developingcountries, mental disorders such as depressionand substance abuse are among the most importantcauses of morbidity and disability in adolescents.Attempted suicide is the single most importantcause of death and hospitalization amongadolescents in South Asia (Eddleston et al., 1998).Girls are more likely to attempt suicide than boys,and this seems to be linked with their lack of controlover reproductive decision-making. Studies showthat violence against women is a serious socialand public health issue in India (Jejeebhoy, 1998).Sexual abuse of adolescents may also be awidespread problem with serious implications fortheir mental health. This paper describes findingsfrom a survey focusing on the prevalence andcorrelates of abuse among school-goingadolescents in Goa, India. The researchersexamined numerous issues related to abuse,drawn from the broader context of adolescentdevelopment, including sexual behaviour, mentalhealth, parental relationships and educationalachievements.
Methods
The project had two stages. The first stagegathered qualitative data on adolescents’ needsamong adolescents and adult key informants. Thesecond stage involved a cross-sectional surveyconducted in eight Goan schools. All students inthe survey sample were in their first year of highersecondary school (i.e. their 11th year of schooling).Researchers collected data through self-administered questionnaires in classroomsettings. The questionnaire was developed usingqualitative data from the first phase of the projectand existing instruments, such as the 12-itemGeneral Health Questionnaire (used to measuremental health).
The study defined sexual abuse as being any verbalor physical sexual experience in the previous 12months that was forced or against the wishes ofthe individual. Five key aspects of abuse weremeasured using the following questions: Have youexperienced any of these in the past 12 months:Someone talking to you about sex in a mannerthat made you uncomfortable? Someone purposelybrushing their private parts against you? Someoneforcing you to touch their body parts against yourwishes? Someone touching you in a sexual mannerwithout your permission? Someone forcing you tohave sex with them?
Gender, sexual abuse and risk behaviours inadolescents: a cross-sectional survey inschools in Goa, India
Vikram Patel, Gracy Andrews, Tereze Pierre andNimisha Kamat
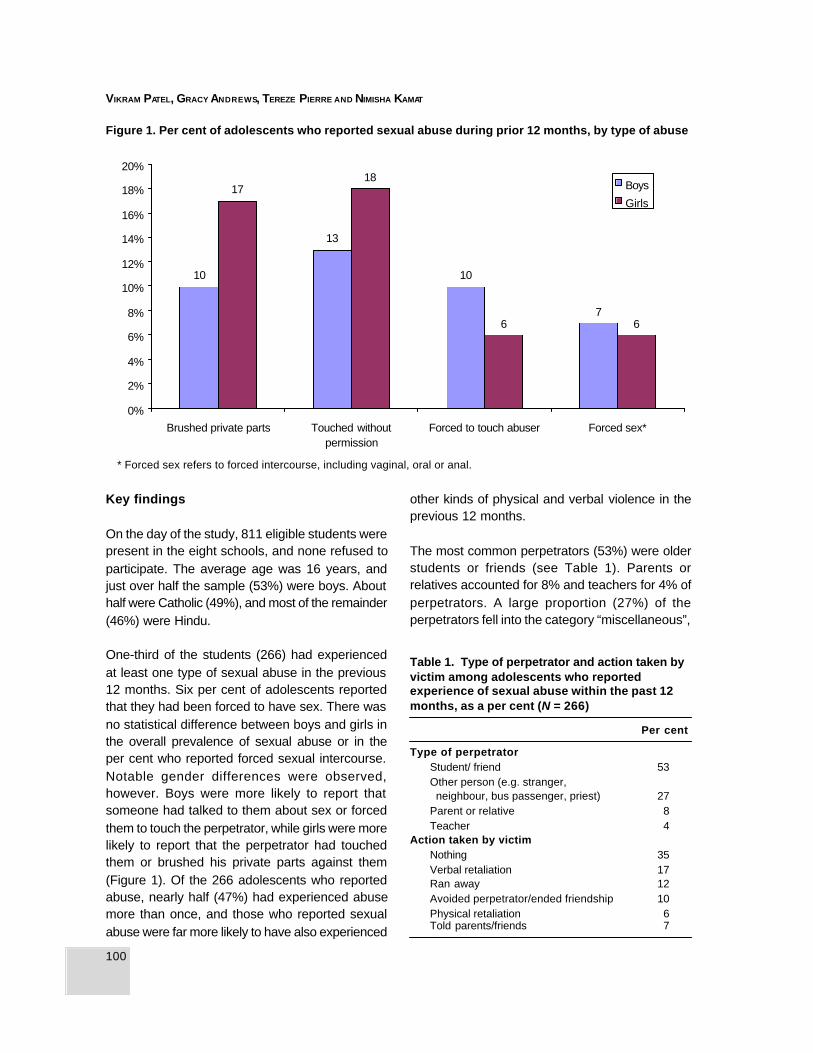
100
VIKRAM PATEL, GRACY ANDREWS, TEREZE PIERRE AND NIMISHA KAMAT
Key findings
On the day of the study, 811 eligible students werepresent in the eight schools, and none refused toparticipate. The average age was 16 years, andjust over half the sample (53%) were boys. Abouthalf were Catholic (49%), and most of the remainder(46%) were Hindu.
One-third of the students (266) had experiencedat least one type of sexual abuse in the previous12 months. Six per cent of adolescents reportedthat they had been forced to have sex. There wasno statistical difference between boys and girls inthe overall prevalence of sexual abuse or in theper cent who reported forced sexual intercourse.Notable gender differences were observed,however. Boys were more likely to report thatsomeone had talked to them about sex or forcedthem to touch the perpetrator, while girls were morelikely to report that the perpetrator had touchedthem or brushed his private parts against them(Figure 1). Of the 266 adolescents who reportedabuse, nearly half (47%) had experienced abusemore than once, and those who reported sexualabuse were far more likely to have also experienced
other kinds of physical and verbal violence in theprevious 12 months.
The most common perpetrators (53%) were olderstudents or friends (see Table 1). Parents orrelatives accounted for 8% and teachers for 4% ofperpetrators. A large proportion (27%) of theperpetrators fell into the category “miscellaneous”,
Table 1. Type of perpetrator and action taken byvictim among adolescents who reportedexperience of sexual abuse within the past 12months, as a per cent (N = 266)
Per cent
Type of perpetratorStudent/ friend 53Other person (e.g. stranger, neighbour, bus passenger, priest) 27Parent or relative 8Teacher 4
Action taken by victimNothing 35Verbal retaliation 17Ran away 12Avoided perpetrator/ended friendship 10Physical retaliation 6Told parents/friends 7
Figure 1. Per cent of adolescents who reported sexual abuse during prior 12 months, by type of abuse
* Forced sex refers to forced intercourse, including vaginal, oral or anal.
7
10
13
10
66
1817
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
Brushed private parts Touched withoutpermission
Forced to touch abuser Forced sex*
Boys
Girls
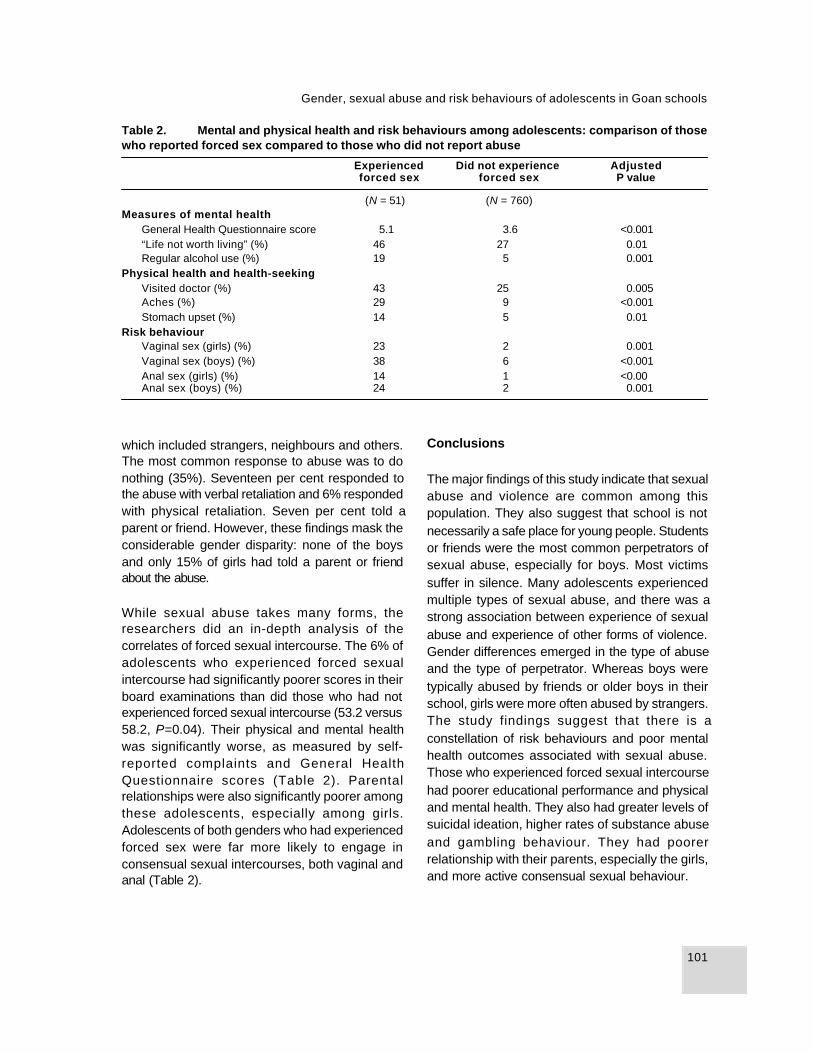
101
Gender, sexual abuse and risk behaviours of adolescents in Goan schools
which included strangers, neighbours and others.The most common response to abuse was to donothing (35%). Seventeen per cent responded tothe abuse with verbal retaliation and 6% respondedwith physical retaliation. Seven per cent told aparent or friend. However, these findings mask theconsiderable gender disparity: none of the boysand only 15% of girls had told a parent or friendabout the abuse.
While sexual abuse takes many forms, theresearchers did an in-depth analysis of thecorrelates of forced sexual intercourse. The 6% ofadolescents who experienced forced sexualintercourse had significantly poorer scores in theirboard examinations than did those who had notexperienced forced sexual intercourse (53.2 versus58.2, P=0.04). Their physical and mental healthwas significantly worse, as measured by self-reported complaints and General HealthQuestionnaire scores (Table 2). Parentalrelationships were also significantly poorer amongthese adolescents, especially among girls.Adolescents of both genders who had experiencedforced sex were far more likely to engage inconsensual sexual intercourses, both vaginal andanal (Table 2).
Conclusions
The major findings of this study indicate that sexualabuse and violence are common among thispopulation. They also suggest that school is notnecessarily a safe place for young people. Studentsor friends were the most common perpetrators ofsexual abuse, especially for boys. Most victimssuffer in silence. Many adolescents experiencedmultiple types of sexual abuse, and there was astrong association between experience of sexualabuse and experience of other forms of violence.Gender differences emerged in the type of abuseand the type of perpetrator. Whereas boys weretypically abused by friends or older boys in theirschool, girls were more often abused by strangers.The study findings suggest that there is aconstellation of risk behaviours and poor mentalhealth outcomes associated with sexual abuse.Those who experienced forced sexual intercoursehad poorer educational performance and physicaland mental health. They also had greater levels ofsuicidal ideation, higher rates of substance abuseand gambling behaviour. They had poorerrelationship with their parents, especially the girls,and more active consensual sexual behaviour.
Table 2. Mental and physical health and risk behaviours among adolescents: comparison of thosewho reported forced sex compared to those who did not report abuse
Experienced Did not experience Adjustedforced sex forced sex P value
(N = 51) (N = 760)Measures of mental health
General Health Questionnaire score 5.1 3.6 <0.001“Life not worth living” (%) 46 27 0.01Regular alcohol use (%) 19 5 0.001
Physical health and health-seekingVisited doctor (%) 43 25 0.005Aches (%) 29 9 <0.001Stomach upset (%) 14 5 0.01
Risk behaviourVaginal sex (girls) (%) 23 2 0.001Vaginal sex (boys) (%) 38 6 <0.001Anal sex (girls) (%) 14 1 <0.00Anal sex (boys) (%) 24 2 0.001
102
VIKRAM PATEL, GRACY ANDREWS, TEREZE PIERRE AND NIMISHA KAMAT
The implications for policy and programmes areclear. Health workers who care for adolescentsmust be trained in the assessment of abuse andmental health, communication skil ls andpsychosocial interventions. Interventions aimed atimproving reproductive health must address issuessuch as personal safety and prevention of abuse,mental health and self-esteem, substance abuseand communication skills (e.g. with parents).Gender-sensitive programmes for boys and girlsare needed, and programmes should focus onteachers and parents. Given the limitations of thecross-sectional study design, it was not possibleto identify which correlates were possible causalfactors and which were consequences of theabuse. Cohort studies are needed to examinecausal associations and outcomes of abuse, aswell as to evaluate possible interventions. Theseshould be priorities for future research.
This summary has been adapted from the full articleby Patel V and Andrew G (2001) entitled “Gender,sexual abuse and risk behaviours in adolescents:
a cross-sectional survey in schools in Goa“,published in The National Medical Journal of India,14:263–267.
References
Eddleston M, Rezvi Sheriff MH, Hawton K (1998)Deliberate self-harm in Sri Lanka: an overlookedtragedy in the developing world. British MedicalJournal, 317:133–135.
Jejeebhoy S (1998) Associations between wife-beating and foetal and infant death: impressions fromrural India. Studies in Family Planning, 29(3):300–308.
Vikram Patel, MRCPsych, PhDSenior LecturerLondon School of Hygiene & Tropical MedicineUnited Kingdom
Sangath Centre841/1 Alto PorvorimGoa 403521India

VIMeeting adolescents’needs for contraception

104
OLAV MEIRIK
105
Adolescence and safety of contraceptives
Most studies of safety and efficacy ofcontraceptives have been done in adult women,and equivalent data for adolescents are scarce.While much of the information from studies inadults is also valid for adolescents, there areparticular concerns about the clinical performanceof specific contraceptives in adolescents and theirpossible effects on development and maturation.Moreover, user-dependent methods that requireconsistency of use (e.g. contraceptive pills,condom) may be less effective when used byadolescents.
One specific concern for hormonal contraceptiveshas been that these methods might interfere withthe maturation of the hypothalamic-pituitary-ovariansystem of postmenarchial adolescents. Rey-Stocker et al. (1981) examined healthy adolescentwomen 1–6 years after menarche for the secretionof gonadotropins, thyrotropin, prolactin, estradiol,progesterone and thyroid hormones in the follicularand luteal phase of the menstrual cycle. They alsostudied the same hormones in adolescent womenof similar postmenarchial age who had takencombined oral contraceptive pills continuously for3–24 months. There were no differences in theendocrine profiles of never users and past users oforal contraceptives. The authors concluded thatcombined oral contraceptives do not adverselyaffect the maturation of the hypothalamic-pituitary-ovarian system in adolescents.
Another recent concern is the effect of suppressionby hormonal contraceptives of ovarian functionincluding estradiol, and the effect of thissuppression on bone mass in adolescent women.More than 90% of bone mass of the skeleton isacquired before age 20 (Theintz et al.,1992); andestrogens are essential for bone acquisition (Rizzoli& Bonjour, 1997). Depot-medroxyprogesteroneacetate (DMPA) suppresses the excretion ofestradiol by the ovary to low levels (Ortiz et al.,1977). Combined oral contraceptives and combinedmonthly injectables also suppress ovarianestradiol, but contain estrogens that compensatefor the suppression. The implantable contraceptiveNorplant suppresses ovarian estradiol to alesser extent than other hormonal methods(Croxatto et al., 1988). It is established that theuse of DMPA reduces bone mass, albeitreversibly, in adult women (Meirik, 2000). Tworelatively small studies indicate that use of DMPAduring adolescence is associated with a lower rateof bone accumulation or even reduction of bonemass (Cromer et al., 1996; Scholes et al., 1999).For adolescents, who are still at a stage whenthey are accumulating bone mass, this is ofconcern since it is not known whether low bonemass in early adult life is associated with increasedrisk of fracture later in life. For these reasons DMPAshould not be a first contraceptive choice foradolescent women.
Adolescence and safety of contraceptives
Olav Meirik

106
OLAV MEIRIK
Concerns about increased risk of cancer, and inparticular breast cancer, have negatively influencedthe acceptability of combined oral contraceptives.Recent data illustrate that, for women younger than20 years, the excess risk of breast cancerassociated with use of combined oralcontraceptives is in the order of 1 per 1 000 000woman-years and that the excess risk disappears10 years after stopping use (Collaborative Groupon Hormonal Factors in Breast Cancer, 1996).
Use of intrauterine devices (IUDs) amongadolescents is controversial. The main concern isthe increased risk of pelvic inflammatory disease(PID) associated with IUD use (World HealthOrganization, 1987), although modern IUDs andcurrent clinical practice attenuate the risk (Grimes,2000). Young women are at higher risk of PID thanadult women; Bell & Holmes (1984) estimated age-specific incidence rates of PID in sexually activewomen and reported that the rate was highest inadolescent women and declined exponentially withincreasing age. Relatively small clinical studiesfound high rates of expulsion of IUDs amongnulliparous adolescent women (Weiner, Berg &Johansson, 1978; Kulig et al, 1980), andindications of an increased risk of PID among them(Weiner, Berg & Johansson, 1978). However, astudy of IUD use in parous adolescent womenfound that the clinical performance of the methodwas similar to that in adult women (Diaz et al.,1993). Until more evidence is available on thesafety of IUD use in nulliparous adolescents, thismethod should not be a first choice for them.
Hormonal contraceptive methods have highcontraceptive efficacy, but do not protect againstsexually transmitted infections including humanimmunodeficiency virus (STI/HIV). Only for the malecondom is there good documentation of STI/HIVprevention (Hatcher et al., 1994; World HealthOrganization, 2000). Sexually active adolescentshave behavioural patterns that place them at higherrisk of STI/HIV than the average adult, and theirnaïve immunological system probably contributesto the higher risk. The male condom is a goodchoice for contraception and STI/HIV prevention,
but requires consistent and correct use to achieveeffective prevention against pregnancy and STI/HIV(Hatcher et al., 1994; World Health Organization,2000). To provide adolescents with knowledge,skills and motivation to protect themselves fromunwanted pregnancy and STI/HIV is a challengeto which communities and health services areobliged to respond.
References
Bell T, Holmes KK (1984) Age-specific risks of syphilis,gonorrhoea, and hospitalised pelvic inflammatorydisease in sexually experienced U.S. women.Sexually Transmitted Diseases, 11:291–295.
Collaborative Group on Hormonal Factors in BreastCancer (1996) Breast cancer and hormonalcontraceptives: collaborative reanalysis of individualdata on 53 297 women with breast cancer and100 239 women without breast cancer from 54epidemiological studies. Lancet, 347:1713–1727.
Cromer BA, MacArdle Blair J, Mahan JD, Zibners L,Naumovski Z (1996) A prospective comparison ofbone density in adolescent girls receiving depotmedroxyprogesterone acetate (Depo-Provera),levonorgestrel (Norplant), or oral contraceptives. TheJournal of Pediatrics, 129:671–676.
Croxatto HB, Diaz S, Pavez M, Brandeis A (1988)Estradiol plasma levels during long-term treatmentwith Norplant subdermal implants. Contraception,38:465–475.
Diaz J, Pinto Neta AM, Bahamondes L, Diaz M. ArceXE, Castro S (1993) Performance of the Copper T200 in parous adolescents: are copper IUDs suitablefor these women? Contraception, 48:23–28.
Grimes D (2000) Intrauterine device and upper-genital-tract infection. Lancet, 356:1013–1019.
Hatcher RA, Trussel J, Stewart F et al. (1994)Contraceptive Technology, 16th revised ed. New York,Irvington Publishers Inc.
Kulig JW, Rauh JL, Burket RL, Cabot HM, BrookmanRR (1980) Experience with the copper 7 intrauterinedevice in an adolescent population. Journal ofPediatrics, 96:746–759.
Meirik O (2000) Hormonal contraceptives and bonemass. IPPF Medical Bulletin, 34:1–3.

107
Adolescence and safety of contraceptives
Ortiz H, Hirol M, Stancyk FZ, Goebelsman U, MishellDR (1977) Serum medroxyprogesterone acetate(MPA) concentrations and ovarian function followingintramuscular injection of depo-MPA. Journal ofClinical Endocrinology and Metabolism , 44:32–38.
Rey-Stocker I, Zufferey MM, Lemarchand MT, Rais M(1981) The sensibility of the hypophysis, the gonadsand the thyroid of adolescents before and after theadministration of oral contraceptives. A resume.Pediatric Annals, 10:480–485.
Rizzoli R, Bonjour JP (1997) Hormones and bones.Lancet, 349 (Suppl. 1):SI 20–23.
Scholes D, Lacroix AZ, Ott SM, Ichikawa LE, BarlowWE (1999) Bone mineral density in women usingdepot medroxyprogesterone acetate for contraception.Obstetrics and Gynecology, 93:233–238.
Theintz G, Buchs B, Rizzoli R, Solsman D, Clavien H,Sizonenko PC, Bonjour JP (1992) Longitudinalmonitoring of bonemass in healthy adolescents:Evidence for a marked reduction after 16 years of ageat the level of lumbar spine and femoral neck in femalesubjects. Journal of Clinical Endocrinology andMetabolism, 75:1060–1065.
Weiner E, Berg AA, Johansson I (1978) Copperintrauterine contraceptive devices in adolescentnull iparae. British Journal of Obstetrics andGynaecology, 85:204–206.
World Health Organization (1987) Mechanism ofaction, safety and efficacy of intrauterine devices.Geneva, World Health Organization (WHO TechnicalReport Series No. 753).
World Health Organization (2000) Improving accessto quality care in family planning; medical eligibilitycriteria for contraceptive use, 2nd ed. Geneva, WorldHealth Organization (WHO/RHR/00.02).
Olav Meirik, MD, PhDInstituto Chileno de Medicina ReproductivaAve Luis Thayer Ojeda 1303Dto 402Providencia, SantiagoChile
108
SAROJ PACHAURI AND K.G. SANTHYA
Background
With the widespread acceptance of family planning,nearly every Asian country has experienced a dropin birth rates. However, national populations areexpected to continue to grow for some yearsbecause of population momentum—aconsequence of the large number of adolescentsand young people in Asia. Of the 1.15 billionadolescents in the world, over 700 million live inAsia (United Nations, 2000). Although adolescentsin Asia have several common concerns, there istremendous diversity in this region. This diversity,coupled with the paucity of data on adolescents,makes it difficult to carry out a comprehensiveanalysis of the challenges faced by adolescentsin Asia and the nature and scope of efforts requiredto address them.
Adolescents form one of the largest groups withunmet needs for reproductive health services. Oneof the most important challenges facingreproductive health programmes in Asia is toaddress the needs of adolescents as they initiatesexual activity and are exposed to the risk ofunwanted pregnancy and infection. Understandingthe extent to which young people know about anduse contraceptives is, therefore, a significant issuefor research and policy.
This paper examines contraceptive behaviours of
adolescents in Asia. The analysis is limited toBangladesh, India, Nepal, Pakistan and Sri Lankain South Asia and to Indonesia, the Philippines,Thailand and Viet Nam in South-East Asia. Wehave drawn data from Demographic and HealthSurveys, several national surveys conducted duringthe past decade and some small-scale studies. Itis important to bear in mind that, as these surveyshave a number of drawbacks, it is difficult to presenta truly representative and comprehensive pictureof adolescent behaviours, and results have to beinterpreted with caution.
An understanding of the context that determinesreproductive attitudes and behaviours is importantfor analysing contraceptive behaviours ofadolescents. First, it is important to note that maleand female gender roles typically create animbalance in negotiating positions betweenpartners in Asian cultures. Such imbalances areexacerbated for younger women since they aremore vulnerable. Second, adolescents do notconstitute a homogeneous entity. There aresignificant social, economic and genderdifferences. For example, girls do not have thesame education and employment opportunities asboys, and they face family and societal pressuresfor early marriage and early childbearing. Sexualcoercion within and outside marriage is the norm(Pachauri, 1996). Third, there has been a significantshift towards delayed marriage among adolescent
Contraceptive behaviours of adolescents inAsia: issues and challenges
Saroj Pachauri and K.G. Santhya

109
Contraceptive behaviours of adolescents in Asia
women in all the countries discussed in this paper.However, early marriage continues to be the normin Bangladesh, India and Nepal where betweenone-third and one-half of girls aged 15–19 yearsare married (National Institute of PopulationResearch and Training, Mitra & Associates, 1997;Pradhan et al., 1997; International Institute forPopulation Sciences & Macro International, 2000).
Consistent with early marriage, early childbearingis the norm in these countries. For example, inBangladesh more than three out of five (63%), inIndia nearly one-half (48%), and in Nepal more thantwo out of five (43%) of currently married 15–19year-old girls had a child (National Institute ofPopulation Research and Training, Mitra andAssociates, 1997; Pradhan et al., 1997;International Institute for Population Sciences &Macro International, 2000).
Finally, available evidence from these countriessuggests that an increasing proportion of unmarriedadolescent boys and girls are becoming sexuallyactive. A review in India showed that between 20%and 30% of boys and up to 10% of girls weresexually active before marriage (Jejeebhoy, 1996).A study in rural Bangladesh showed that by age18, 38% of unmarried boys and 6% of unmarriedgirls were sexually active (United NationsPopulation Fund, 1998a). Thus, contraceptivebehaviours of adolescents in these countries mustbe examined against this backdrop of prevailinggender power differentials, early marriage andchildbearing among adolescent girls in somecountries, and rising premarital sexual activityamong adolescent boys and girls in almost allcountries.
Knowledge and use of contraceptivesamong adolescents
In all the countries discussed in this paper, almostall married adolescents had knowledge ofcontraception (Pradhan et al., 1997; InternationalInstitute for Population Sciences & MacroInternational, 2000; Macro International, 2001).
Pakistan is an exception as only 75% of currentlymarried adolescent girls reported knowledge of atleast one modern contraceptive method(Population Council et al., 1998). However,knowledge about specific modern spacingmethods, such as oral contraceptives, injectables,intrauterine devices (IUDs), and implants, is lowamong married adolescent girls— 59% in Pakistanand 63% in India. It is, however, very high (99%) inBangladesh and Thailand (Alan GuttmacherInstitute, 1998). Knowledge of condoms amongadolescent girls is even lower in many countries(Figure 1).
In addition, knowledge of the sources of supply ofcontraceptive methods is not universal in many ofthese countries (Alan Guttmacher Institute, 1998;Population Council et al., 1998; United NationsPopulation Fund, 1998b).
There is a large gap between knowledge and useof contraception among 15–19 year-old marriedadolescents in these countries. While contra-ceptive use among currently married adolescentshas increased in many of these countries, lessthan 10% report using a traditional or moderncontraceptive method in India (8%), Nepal (7%)and Pakistan (6%) (International Institute forPopulation Sciences & Macro International, 2000;Pradhan et al., 1997; Hakim, Cleland & Bhatti,1998). In comparison, between one-fifth and two-fifths of married adolescent girls report using acontraceptive method in Viet Nam (18%), Sri Lanka(20%), the Philippines (22%), Bangladesh (33%),Thailand (43%), and Indonesia (45%) (NationalInstitute of Population Research and Training, Mitraand Associates, 1997; Pradhan et al., 1997;Hakim, Cleland & Bhatti, 1998; InternationalInstitute for Population Sciences & MacroInternational, 2000; Macro International, 2001)(Figure 2).
Married adolescents use modern contraceptivemethods more frequently than traditional methods,although the specific methods most commonlyused vary among countries. Oral contraceptivesare most commonly used in Bangladesh (18%),
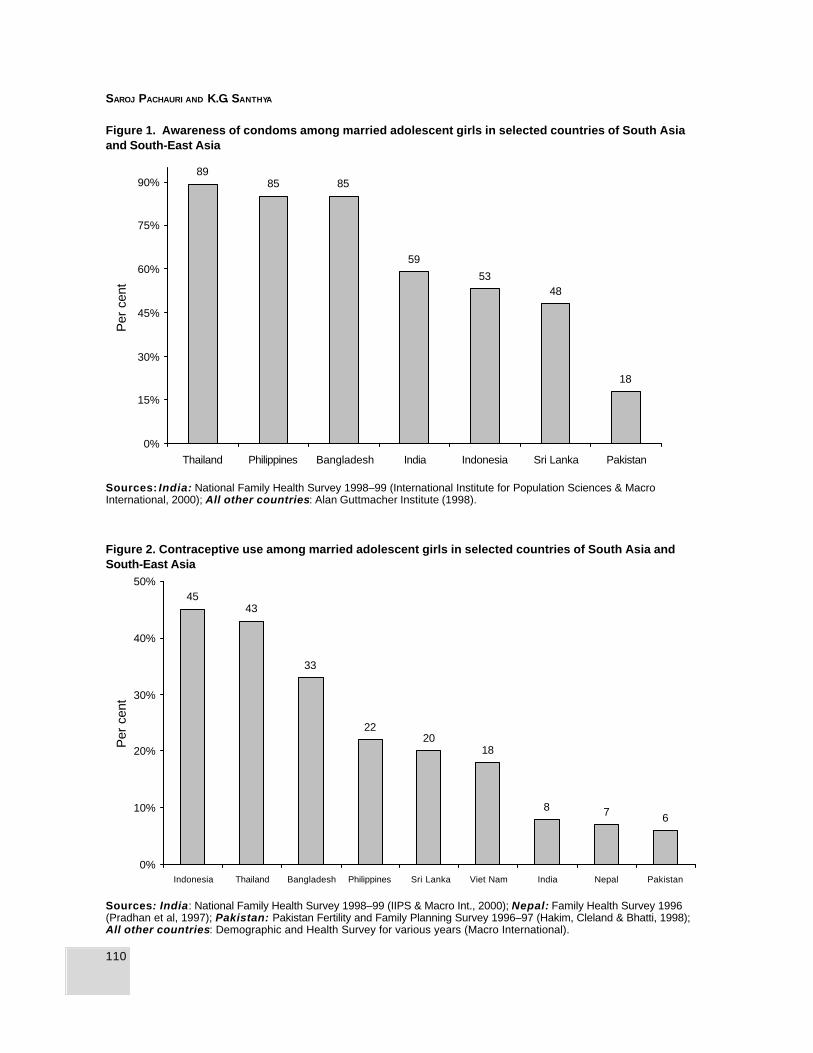
110
SAROJ PACHAURI AND K.G. SANTHYA
18
4853
59
858589
0%
15%
30%
45%
60%
75%
90%
Thailand Philippines Bangladesh India Indonesia Sri Lanka Pakistan
Per
cen
tFigure 1. Awareness of condoms among married adolescent girls in selected countries of South Asiaand South-East Asia
Sources: India: National Family Health Survey 1998–99 (International Institute for Population Sciences & MacroInternational, 2000); All other countries: Alan Guttmacher Institute (1998).
678
1820
22
33
4345
0%
10%
20%
30%
40%
50%
Indonesia Thailand Bangladesh Philippines Sri Lanka Viet Nam India Nepal Pakistan
Per
cen
t
Figure 2. Contraceptive use among married adolescent girls in selected countries of South Asia andSouth-East Asia
Sources: India: National Family Health Survey 1998–99 (IIPS & Macro Int., 2000); Nepal: Family Health Survey 1996(Pradhan et al, 1997); Pakistan: Pakistan Fertility and Family Planning Survey 1996–97 (Hakim, Cleland & Bhatti, 1998);All other countries: Demographic and Health Survey for various years (Macro International).
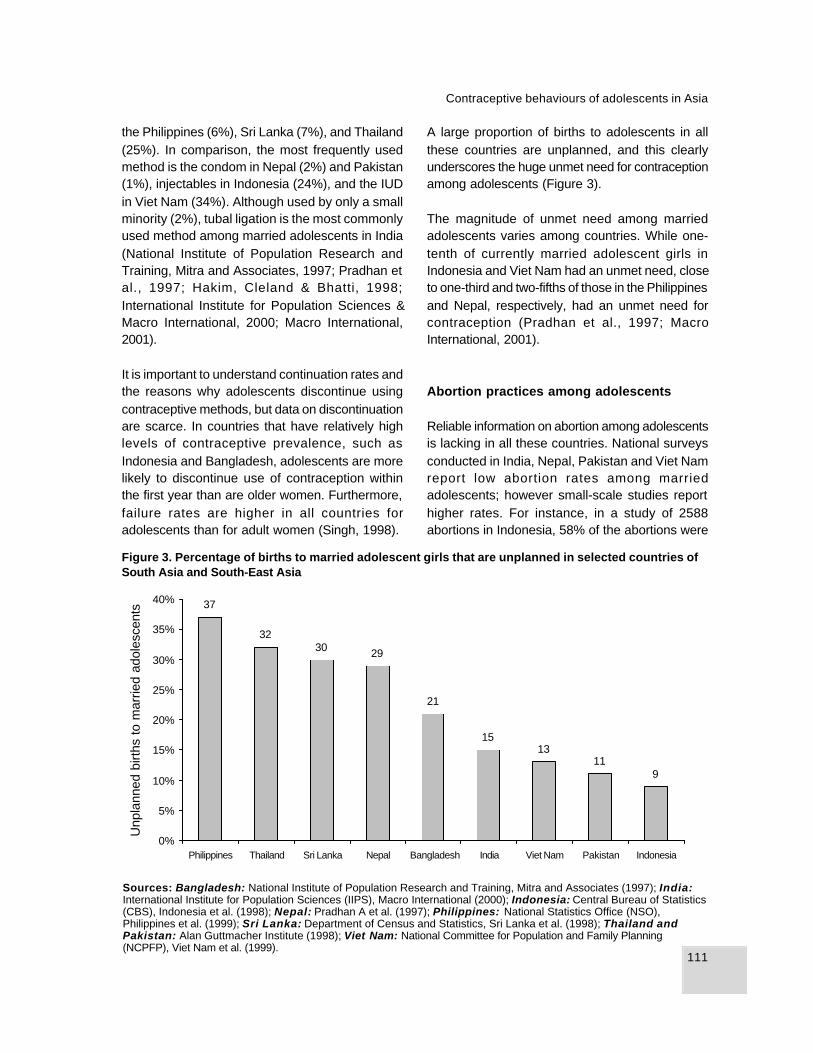
111
Contraceptive behaviours of adolescents in Asia
the Philippines (6%), Sri Lanka (7%), and Thailand(25%). In comparison, the most frequently usedmethod is the condom in Nepal (2%) and Pakistan(1%), injectables in Indonesia (24%), and the IUDin Viet Nam (34%). Although used by only a smallminority (2%), tubal ligation is the most commonlyused method among married adolescents in India(National Institute of Population Research andTraining, Mitra and Associates, 1997; Pradhan etal., 1997; Hakim, Cleland & Bhatti, 1998;International Institute for Population Sciences &Macro International, 2000; Macro International,2001).
It is important to understand continuation rates andthe reasons why adolescents discontinue usingcontraceptive methods, but data on discontinuationare scarce. In countries that have relatively highlevels of contraceptive prevalence, such asIndonesia and Bangladesh, adolescents are morelikely to discontinue use of contraception withinthe first year than are older women. Furthermore,failure rates are higher in all countries foradolescents than for adult women (Singh, 1998).
A large proportion of births to adolescents in allthese countries are unplanned, and this clearlyunderscores the huge unmet need for contraceptionamong adolescents (Figure 3).
The magnitude of unmet need among marriedadolescents varies among countries. While one-tenth of currently married adolescent girls inIndonesia and Viet Nam had an unmet need, closeto one-third and two-fifths of those in the Philippinesand Nepal, respectively, had an unmet need forcontraception (Pradhan et al., 1997; MacroInternational, 2001).
Abortion practices among adolescents
Reliable information on abortion among adolescentsis lacking in all these countries. National surveysconducted in India, Nepal, Pakistan and Viet Namreport low abortion rates among marriedadolescents; however small-scale studies reporthigher rates. For instance, in a study of 2588abortions in Indonesia, 58% of the abortions were
Figure 3. Percentage of births to married adolescent girls that are unplanned in selected countries ofSouth Asia and South-East Asia
Sources: Bangladesh: National Institute of Population Research and Training, Mitra and Associates (1997); India:International Institute for Population Sciences (IIPS), Macro International (2000); Indonesia: Central Bureau of Statistics(CBS), Indonesia et al. (1998); Nepal: Pradhan A et al. (1997); Philippines: National Statistics Office (NSO),Philippines et al. (1999); Sri Lanka: Department of Census and Statistics, Sri Lanka et al. (1998); Thailand andPakistan: Alan Guttmacher Institute (1998); Viet Nam: National Committee for Population and Family Planning(NCPFP), Viet Nam et al. (1999).
911
1315
21
293032
37
0%
5%
10%
15%
20%
25%
30%
35%
40%
Philippines Thailand Sri Lanka Nepal Bangladesh India Viet Nam Pakistan Indonesia
Unp
lann
ed b
irths
to m
arrie
d ad
oles
cent
s

112
SAROJ PACHAURI AND K.G. SANTHYA
among young women aged 15–24, and as manyas 38% of those women were married (Rosdiana,1998). Far less is known about the prevalence ofabortion among unmarried adolescents. Findingsfrom a number of small-scale studies in rural andurban settings in India suggest that unmarriedadolescents constitute a disproportionately largepercentage of those who seek abortion. Thesestudies also suggest that at least one-half ofunmarried women seeking abortions areadolescents, many of whom are below age 15(Jejeebhoy, 1996).
Conclusions
The results of our analysis show that whileknowledge of contraception is almost universalamong married adolescents, understanding ofspecific methods and their sources is limited.Although rates vary among countries, there hasbeen a significant increase in contraceptive useamong married adolescents, but a large unmetneed for contraceptives remains. Data oncontraceptive use by unmarried adolescents arerare, but suggest even lower rates of use thanamong their married counterparts.
Discussions in Asian countries are beginning tofocus on how reproductive health programmes foradolescents should be designed and implemented.A few studies are under way to test interventions.At present there is a poor fit between the design ofreproductive health programmes and the needs ofadolescents. Strategies should be designed toaddress the needs of subgroups of adolescents,disaggregated by their distinct characteristics.Policy prescriptions need to challenge social normsthat devalue girls. The answers lie in finding routesto economic and social survival for girls, andproviding information that is honest and timely. Inaddition, there is a need to recognize the powerdifferentials in relationships that prevent informationand services from reaching adolescents.
Although the availability of data on adolescentshas increased in recent years, there are several
gaps in knowledge. Available evidence suggeststhat an increasing proportion of unmarriedadolescent boys and girls are becoming sexuallyactive. However, data on contraceptive behavioursof unmarried adolescents are grossly inadequateand much less is known about the behaviours ofadolescent boys than adolescent girls. Anunderstanding of contraceptive discontinuationcould provide important information for the designof services for adolescents, but these data are notcurrently available. Data on abortion amongadolescents, especially unmarried adolescents,are lacking. Finally, a better understanding aboutthe circumstances surrounding sexual initiationand the decision to practise contraception isneeded to design user-friendly programmes foradolescents.
References
Alan Guttmacher Institute (1998) Into the New World:Young Women’s Sexual and Reproductive Lives. NewYork, Alan Guttmacher Institute.
Boyd A, Haub C, Cornelius D (2000) The World’s Youth2000 Data Sheet. Washington, DC, PopulationReference Bureau.
Central Bureau of Statistics (CBS), Indonesia et al.(1998) Indonesia Demographic and Health Survey,1997. Calverton, MD, CBS and Macro International.
Department of Census and Statistics, Sri Lanka,Ministry of Plan Implementation, Sri Lanka, Institutefor Resource Development (1988) Sri LankaDemographic and Health Survey, 1987. Columbia,MD, Institute for Resource Development.
Hakim A, Cleland J, Bhatti MH (1998) Pakistan Fertilityand Family Planning Survey 1996–1997, PreliminaryReport. Islamabad, National Institute of PopulationStudies and the London School of Hygiene andTropical Medicine.
International Institute for Population Sciences, MacroInternational (2000) National Family Health Survey-2 India, 1998–1999. Mumbai, International Institutefor Population Sciences.
Jejeebhoy SJ (1996) Adolescent Sexual andReproductive Behaviour—A Review of the Evidence

113
Contraceptive behaviours of adolescents in Asia
from India. Working Paper No. 3. Washington, DC,International Center for Research on Women.
Macro International (2001) Demographic HealthSurveys. [Available at: http//www.measuredhs.com]
National Committee for Population and FamilyPlanning (NCPFP), Viet Nam, Population and FamilyHealth Project and Macro International (1999) VietNam Demographic and Health Survey, 1997. Hanoi,NCPFP.
National Institute of Population Research andTraining, Mitra and Associates (1997) BangladeshDemographic and Health Survey 1996–1997. Dhaka,Bangladesh, NIPORT, Macro International Inc.
National Statistics Office (NSO), Philippines,Department of Health, Philippines, Macro International(1999) Philippines National Demographic and HealthSurvey, 1998. Manila, NSO and Macro International.
Pachauri S (1996) Reproductive health: the concept,ideology and operational issues. In: Sengupta J,Ghosh D, eds. Perspectives in Reproductive Health .New Delhi, New Age Publishers Ltd.
Population Council, Ministry of Population Welfare,Pakistan, and UNFPA (1998) Pakistan ContraceptivePrevalence Survey 1994–1995. Final Report.Islamabad, Population Council.
Pradhan A, Aryal RH, Regmi G, Ban B, Pavalavalli G(1997) Nepal Family Health Survey 1996. Kathmandu,
Nepal and Calverton, Maryland, Ministry of Health (Nepal),New ERA, and Macro International Inc.
Rosdiana D (1998) Pokok-Pokok Pikiran PendidikaanPendidikan Seks untuk Remaja. In: Kollman N, ed.Kesehatan Reproduksi Remaja. Jakarta, Indonesia,Yayasan Lembaga Konsumen.
Singh S (1998) Adolescent childbearing. Studies inFamily Planning, 29(2):117–136.
United Nations (2000) The World’s Women 2000Trends and Statistics. New York, United Nations.
United Nations Population Fund (1998a) Adolescenthealth and development: Issues and strategies.Country Paper, Bangladesh. UNFPA South AsiaConference on the Adolescent, New Delhi, 21–23 July.
United Nations Population Fund (1998b)Socioeconomic, demographic and reproductivehealth profiles of adolescents in SAARC countries.UNFPA South Asia Conference on the Adolescent,New Delhi, 21–23 July.
Saroj Pachauri, PhDRegional Director, South and East AsiaThe Population CouncilZone 5A, Ground FloorIndia Habitat CentreLodi RoadNew Delhi 110003India
114
Background
Over 1500 AIDS cases have been reported inNepal, and the numbers are rising, particularlyamong young people aged 14–29. As of May2000, 1077 (70%) of all reported humanimmunodeficiency virus (HIV) infections wereamong adolescents and young adults betweenages 14 and 29 (National Centre for AIDS andSTD Control, 2000). Given the hidden natureof the problem, the actual size of the infectedpopulation is likely to be considerably larger.Heterosexual sex, including commercial sex,is a major route of HIV transmission. Littleresearch has been done on the sexualbehaviour of young men in border towns,despi te the fact that commercial sex iscommon in those areas. To address this gapin knowledge, we carried out a qualitative andquantitative study in five border towns between1997 and 1999. The research questionsincluded: (1) To what extent do sexually activeyoung men residing in border towns engage incasual sexual relations, use condoms andconsider themselves to be at risk of contractingsexually transmitted infections (STIs ), includingHIV? (2) What factors constrain young men whoengage in risky sex from wearing condoms?This paper presents data from the subsample ofstudy participants who fell into the age group 18–24 years.
Methods
The study involved a survey among men residingin border towns. The subsample of young menbetween the ages of 18 and 24 included 242respondents, of whom 40% were 18 or 19 yearsold. Most (80%) were unmarried. We usedmultivariate analysis to identify variables correlatedwith casual sex, such as alcohol consumption. Inaddition, we calculated odds ratios for having hadcasual sex, according to education, occupationand other variables. The quantitative data weresupplemented with qualitative, in-depth casestudies.
Key findings
A majority of unmarried young men reported sexualexperience, including 54% who said that they weresexually active. Nearly one-third (30%) of all menin the subsample had their first sexual experiencebefore age 18. Casual sex among respondents wascommon; over one-fourth (27%) of all respondentsreported having casual sex within the previous 12months. This proportion was slightly lower (20%)among 18–19 year-old respondents than in thesubsample as a whole. Of those who reportedhaving casual sex in the past year, about one-third(31%) also reported having sex with a commercialsex worker.
Constraints on condom use among youngmen in border towns of Nepal
Anand Tamang and Binod Nepal

115
Constraints on condom use among young men in Nepal
Over half the young men surveyed said that theyconsumed alcohol. Out of 133 alcohol users (55%),nearly three-quarters (74% or 98 men) weresexually active. The multivariate analysis found thatyoung men who drank were almost four times morelikely to be involved in casual sex than those whodid not drink. Many young men reported consumingalcohol before having sex as a way to overcomeshame and fear. As one 19 year-old explained,“Without a drink, I feel ashamed to talk to a girl.But after drinking, I can do anything in mood.”
All respondents in the sample knew aboutcondoms. However, nearly half (62) of the 131sexually active young men had never used one,and even those who had used condoms reportedinconsistent use with non-regular sex partners(Table 1).
not carrying any diseases, how can I be at risk ofgett ing AIDS?” Even those who perceivethemselves to be at risk may not use condoms forvarious reasons. For example, a 19 year-oldunmarried man who reported having sex withcommercial sex workers explained, “There is noenjoyment in using condoms. Someday a man hasto die, so why not enjoy and die?”
Conclusions
In summary, casual sex is common in bordertowns of Nepal. Alcohol consumption is associatedwith increased involvement in casual sex. There isa large gap between knowledge, attitudes andpractice regarding condom use among young men.Most young men surveyed who reported havingcasual sex did not perceive themselves to be atrisk of contracting STIs, including HIV. Theseresearch findings suggest that more HIV/STIprevention efforts are needed among young menin border towns. Programme planners and policy-makers need to find ways to improve riskperception and increase preventive behaviour.
Reference
National Centre for AIDS and STD Control (2000)Cumulative HIV/AIDS Situation of Nepal (monthlybulletin). National Centre for AIDS and STD Control,Ministry of Health, Nepal.
Anand TamangCentre for Research on EnvironmentHealth and Population Activities (CREHPA)P.O. Box 9626KathmanduNepal
Table 1. Condom use by men in border townswho had engaged in casual sex during theprevious 12 months (N = 65)
Number
Number who had ever used a condomwith a casual sex partner 39Number who had used a condomduring last sex with a casual sex partner 31
In the survey, young men cited a number ofreasons for not using condoms with non-regularsex partners, including that they did not carry acondom with them, that there was no time for acondom, that their partners did not have sex withothers or were not infected with HIV, that sex withcondoms was less enjoyable, or simply that theydid not feel like using one.
In-depth interviews with young men provided moredetail about their attitudes towards condoms andtheir perceptions of their own risk. As the followingquote exemplifies, most (58 out of 65) young meninvolved in casual sex did not perceive themselvesto be at risk of contracting STIs, including HIV.One 21 year-old unmarried policemen explained,“I did not use condom during last time I had sex,since I did not carry one. Since my partners are
116
WANAPA NARAVAGE AND SIRIPORN YONGPANICHKUL
Background
In Thailand, studies estimate that one out of threepregnancies is unwanted (Chayovan & Knodel,1991) and 200 000–300 000 women terminate theirpregnancies each year (Koetsawang, 1993).Adolescents are more likely than adults to hide apregnancy, seek late-term abortion, and have theprocedure performed by untrained providers underunsafe conditions, which often leads to permanentdisability or death (Sertthapongkul & Phonprasert,1993; Koetsawang, 1993; Griensven, 2000).
Emergency contraception (EC) first becameavailable in Thailand in the form of two Ovral® orEugynon® pills taken within 48–72 hours aftersexual intercourse. Because of side-effects, thisregimen was not popular. An alternative form ofEC became available in 1984 when a dedicatedproduct, Postinor® (and later Madonna®), wasintroduced. Few studies have assessed patternsof EC use in Thailand; so in 1999, PATH (Programfor Appropriate Technology in Health) conducted astudy to assess users’ knowledge, attitudes anduse patterns, drugstore delivery of EC andstakeholders’ opinions.
Methods
This study gathered qualitative and quantitative
data among purchasers and users, drugstorepersonnel, stakeholders and potential providers inBangkok. First, data were gathered on purchaserand user attitudes, perceptions and experiences.Focus group discussions (FGDs) and in-depthinterviews were conducted with communitymembers who had used or purchased EC withinthe previous six months, including three FGDs withmen, and one FGD and four in-depth interviewswith women. In addition, men and women whopurchased EC at six drugstores were asked tocomplete anonymous, self-administeredquestionnaires on a voluntary basis. All selecteddrugstores were located in business areas, closeto factory dormitories and entertainment areas inBangkok. During a 6-week period, 36 men and 33women completed questionnaires. Most wereworking adults, but young people aged 18–24made up about one-third (22) of those who filledout questionnaires. Drugstore personnel reportedthat some adolescents did not want to participatein the purchaser survey even though it wasanonymous, so these data may not berepresentative.
Second, data were gathered on the perceptionsand experiences of providers and stakeholdersthrough a survey, in-depth interviews and the useof simulated clients. Self-administeredquestionnaires were distributed among 106drugstore personnel attending a meeting. This
Situation analysis of emergencycontraceptive use among young people inThailand
Wanapa Naravage and Siriporn Yongpanichkul

117
Situation analysis of emergency contraceptive use among young people in Thailand
questionnaire asked whether their drugstores solddedicated packages of EC, how frequently theymade such sales, and their perceptions of ECclients. In addition, researchers conducted 10 in-depth interviews with drugstore personnel to gathermore in-depth information about their attitudestowards young people seeking EC and theirpractices related to dispensing EC. Simulatedclients were also used to assess the practices ofdispensing EC in 20 stores. Finally, 18 in-depthinterviews were conducted with stakeholders,including policy-makers, family planning experts,representatives from women’s nongovernmentalorganizations (NGOs) and family planningproviders.
Key findings
FGD respondents offered several common localnames for EC, including ya kum chua crow,meaning temporary control of pregnancy, ya kumlang rum, meaning control of pregnancy afterunprotected sex, ya ka asuji meaning pills thatkill sperm, and ya kum dheb plan, meaning pillsthat have an immediate effect protecting frompregnancy. All these meanings reflect theperception that the pills are used as a post-coitalmethod, but none specifically refers to emergencysituations.
According to FGD respondents and drugstorepersonnel, the majority of purchasers are menbuying EC for women, and it is generally men whoselect the method for their girlfriends. Women,especially adolescents, said that they feel ashamedto purchase EC themselves. Women often lackinformation about the pill, and during thediscussions, women raised many questions aboutshort-term and long-term effects.
The majority of young people who filled out thepurchaser questionnaire learned about EC throughfriends (17 of 22) or drugstore personnel (5 of 22),similar to reports from the FGDs. Among the 22young purchasers, more men than women hadmade the decision to choose EC (13 versus 9).
When asked why they used EC, the most commonreason was that they had sex infrequently (8 outof 22). The majority said that if EC failed, theywould keep the baby; less than half said they wouldseek an abortion. Most young people hadpurchased EC more than once (17 out of 22). Whenasked whether they would keep using EC, themajority (15 of 22) said that they would. In termsof past contraceptive use, the majority of youngpeople or their partners (12 out of 22) had usedoral contraceptives or condoms before switchingto EC. Nearly half (10 out of 22) the young peoplesaid they had used EC in combination with othermethods. In FGDs, some men mentioned that theyused EC with temporary partners whom theybelieved were free of STDs/HIV, but used condomswith women who might have more than one partner,such as prostitutes. In general, married men saidthat their wives did not use EC.
Few respondents reported knowledge of the correctuse of EC. The majority (12 out of 22) said thatthey planned to take only one tablet after havingsex. Four of the 22 said that they planned to takeone tablet before sex. Only two reported planningto take two tablets after sex, the correct use ofEC. This practice was confirmed in FGDs with menand women, who said that they or their partner didnot consider taking the second tablet. Nine out of17 respondents who had purchased EC in the pastreported that they or their partners used more thantwo tablets of EC per month, which suggests thatthey may use it regularly, contrary to its intendedpurpose (Table 1).
A majority of purchasers said that they had receivedsome information from drugstore personnel.However, more than half of purchasers felt that theinformation was inadequate, and they wanted toknow more about side-effects, contraindicationsand long-term consequences. The information theyreceived consisted mainly of instructions on howto take the pills and a warning not to take morethan four tablets per month. Purchasers did notmention receiving important messages such asefficacy of the pills, not to use EC regularly, thatthe pills cannot prevent STIs/HIV, or information

118
WANAPA NARAVAGE AND SIRIPORN YONGPANICHKUL
about side-effects. It is noteworthy that nothing inthe package mentions the importance of takingthe second pill. Furthermore, drugstore staff wereaware of the study’s subject matter, and may havegiven more information than usual. This wasconfirmed through the use of simulated clients,who found that less than half of the drugstorepersonnel provided any information to purchasers.
Stakeholders were generally aware of the growinguse of EC among young people. They felt that ECis needed as an alternative choice for women;however, they felt that both the general public andservice providers lack adequate knowledge aboutthe method. Medical and family planning expertssaid that provision of EC through drugstores isappropriate and ensures easy access, but somestakeholders felt that this encouragesirresponsible sexual behaviour and/or incorrect useof EC. Many stakeholders mentioned the need tointegrate sex education in schools and the needto train health personnel at every level about EC.
Conclusions
These study findings suggest that both purchasersand providers lack adequate information about EC,
which points to a number of policy and programmeimplications. First, there is an urgent need toformulate standard guidelines for EC use that mirrorthose of the World Health Organization and otherinternational bodies. Instructions in the insert leafletshould include key messages such as: (a) EC isfor emergency use only, and should not be usedas a regular method; (b) EC cannot prevent STI/HIV infection; and (c) users should complete thetwo-tablet dose.
Public and private health professionals, drugstorepersonnel and representatives from women’snongovernmental organizations need additionaltraining on EC. For example, academic institutesthat train health professionals should include ECin their curriculum. Manuals and other educationalmaterials on EC should be produced for familyplanning providers, particularly drugstorepersonnel. And drugstore networks, such asPharmacist Associations and the Drugstore Clubof Thailand, should promote awareness of ECamong their members.
Finally, young people need to be convinced to useother contraceptive methods rather than EC astheir regular method. They should be informed thatEC is for “emergency” use only. Counsellingservices should provide accurate information onEC and related topics to young people. In the longrun, sex education for young people needs to beintegrated into formal education. Such programmesshould aim to give young people a comprehensiveunderstanding of contraceptive methods, includingEC, as well as to produce attitude changes ongender issues.
References
Chayovan N, Knodel J (1991) Coital activity amongmarried Thai women: evidence from the 1987Thailand Demographic and Health Survey. PopulationStudies Center Research Report No. 91-221(translated into Thai). Ann Arbor, Michigan, Universityof Michigan, Population Studies Center.
Griensven F (2000) Sex, drugs and HIV/STD amongadolescents in Northern Thailand: an innovative,
Table 1. EC use patterns among youngpurchasers (aged 18–24) surveyed in Bangkokdrugstores (N=22)
Number
Frequency of EC purchaseFirst time purchase 5Had purchased EC more than once 17
EC use per month (among thosewho had purchased EC in the past)
1 tablet per month 12 tablets per month 63 tablets per month 14 tablets per month 65 tablets per month 16 tablets or more per month 1Don’t know 1
How takenOne tablet after having sex 12One tablet before having sex 4Two tablets after having sex 2

119
Situation analysis of emergency contraceptive use among young people in Thailand
rapid, biological and behavioural assessment. Paperpresented at the XIII International AIDS Conference,Durban, South Africa, 9–14 July.
Koetsawang S (1993) Illegally induced abortion inThailand, Paper presented at the IPPF SEARORegional Programme Advisory Panel Meeting onAbortion, Bali, Indonesia, 29–30 October.
Sertthapongkul S, Phonprasert P (1993) Causes ofunplanned pregnancy and decision process forabortion: a case study at Bangkok private clinic.
Journal of Development Administration, Bangkok,Thailand.
Wanapa Naravage and Siriporn YongpanichkulPATH (Program for Appropriate Technology inHealth)37/1 Soi Petchburi15, Petchburi RoadBangkok 10400Thailand

VIIThe context of abortionamong adolescents

122
HALIDA HANUM AKHTER
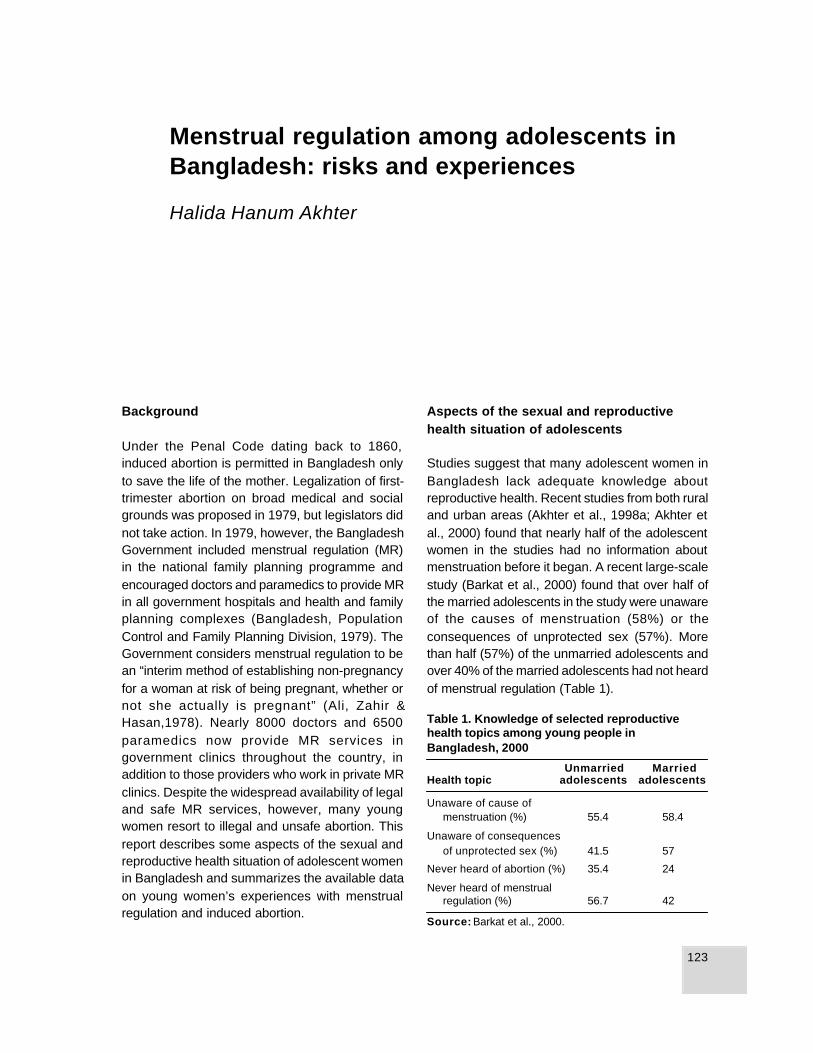
123
Menstrual regulation among adolescents in Bangladesh: risks and experiences
Background
Under the Penal Code dating back to 1860,induced abortion is permitted in Bangladesh onlyto save the life of the mother. Legalization of first-trimester abortion on broad medical and socialgrounds was proposed in 1979, but legislators didnot take action. In 1979, however, the BangladeshGovernment included menstrual regulation (MR)in the national family planning programme andencouraged doctors and paramedics to provide MRin all government hospitals and health and familyplanning complexes (Bangladesh, PopulationControl and Family Planning Division, 1979). TheGovernment considers menstrual regulation to bean “interim method of establishing non-pregnancyfor a woman at risk of being pregnant, whether ornot she actually is pregnant” (Ali, Zahir &Hasan,1978). Nearly 8000 doctors and 6500paramedics now provide MR services ingovernment clinics throughout the country, inaddition to those providers who work in private MRclinics. Despite the widespread availability of legaland safe MR services, however, many youngwomen resort to illegal and unsafe abortion. Thisreport describes some aspects of the sexual andreproductive health situation of adolescent womenin Bangladesh and summarizes the available dataon young women’s experiences with menstrualregulation and induced abortion.
Aspects of the sexual and reproductivehealth situation of adolescents
Studies suggest that many adolescent women inBangladesh lack adequate knowledge aboutreproductive health. Recent studies from both ruraland urban areas (Akhter et al., 1998a; Akhter etal., 2000) found that nearly half of the adolescentwomen in the studies had no information aboutmenstruation before it began. A recent large-scalestudy (Barkat et al., 2000) found that over half ofthe married adolescents in the study were unawareof the causes of menstruation (58%) or theconsequences of unprotected sex (57%). Morethan half (57%) of the unmarried adolescents andover 40% of the married adolescents had not heardof menstrual regulation (Table 1).
Table 1. Knowledge of selected reproductivehealth topics among young people inBangladesh, 2000
Unmarried MarriedHealth topic adolescents adolescents
Unaware of cause ofmenstruation (%) 55.4 58.4
Unaware of consequencesof unprotected sex (%) 41.5 57
Never heard of abortion (%) 35.4 24
Never heard of menstrualregulation (%) 56.7 42
Source: Barkat et al., 2000.
Menstrual regulation among adolescents inBangladesh: risks and experiences
Halida Hanum Akhter
124
HALIDA HANUM AKHTER
About half of all women in Bangladesh marry beforeage 20, and on average, women become pregnantwithin 13 months after marriage (Khan et al., 1997).According to the 1997 Demographic and HealthSurvey (DHS), nearly 15% of all 16–19 year-oldmarried women were pregnant at the time of thesurvey, and 58% had begun childbearing by age19 (NIPORT et al., 1997). At 31%, the contraceptiveprevalence rate among married adolescents ismuch lower than the national average for marriedwomen of 51%. Contraceptive use is increasingamong married adolescents, but estimates ofunmet need remain high. According to the Centrefor Health and Population Research, unmet needamong married women aged 10–14 and 15–19 is33% and 22% respectively (Quamrun et al., 1999).
Use of menstrual regulation amongadolescents
Several large- and small-scale studies havemeasured the magnitude of MR use amongadolescent women. The 1997 DHS found that 1.6%of currently married adolescents reportedundergoing menstrual regulation. Some evidencesuggests that about 19% of women who undergoMR are aged 15–19 (Koenig et al, 1988).
One study (Akhter et al., 1998b) collected dataamong women hospitalized for delivery of anunwanted pregnancy or complications of induced
abortion, as well as those who sought MR. Womenwho had no knowledge of MR were more likely tobe hospitalized for complications of unsafe abortionthan those who knew about MR. The study foundthat adolescents constituted 6% of women givingbirth to an unwanted child, 8% of womenhospitalized for complications of induced abortion,9% of those who received MR services and 15%of women rejected by MR providers (Table 2).
It is noteworthy that adolescents constituted alarger proportion of women rejected by MR clinicsthan of those accepted. Typically, providers rejectwomen for two main reasons. In some casesproviders reject women who are pregnant for thefirst time because they are concerned aboutinfection or future infertility. In other cases, providersreject women who are too far along in theirpregnancy to undergo the procedure. Adolescents— particularly unmarried adolescents — may bemore likely to be too late in recognizing theirpregnancy and/or seeking services.
This study found that a majority of adolescentwomen seeking to terminate a pregnancy did sofor their first pregnancy, including 81% hospitalizedfor complications of induced abortion, 46% of thosewho underwent MR, and 67% of those rejected byMR services. The majority of adolescents had notused a contraceptive method in the six monthsprior to seeking pregnancy termination (Table 2).When adolescents were asked why they had not
Source: Akhter et al., 1998b.
Table 2. Proportion of adolescents among women with unwanted pregnancy, and their history ofcontraceptive use
Sought services atHospitalized for: an MR clinic:
Delivery of an Complicationsunwanted of inducedpregnancy abortion Accepted Rejected(N = 726) (N = 628) (N = 1288) (N = 175)
Per cent of women <20 years old 5.5 8.4 8.8 15.4
Per cent of women <20 years old reporting nocontraceptive use within the six monthsprior to becoming pregnant 85 75.5 69 63

125
Menstrual regulation among adolescents in Bangladesh: risks and experiences
used contraception, approximately one-third saidthat they were unaware of contraceptive methodsor did not know where to obtain them. An additionalone-third mentioned that their husband did not wantthem to use contraception.
When 38 young women hospitalized for abortioncomplications were asked what kind of providerhad induced the abortion, respondents mentionedphysicians (7), nurses (7), traditional birthattendants (7), the woman herself (5), familyplanning workers (3), and allopathic village doctors(2). Seven women did not respond. The mostfrequently used methods of inducing abortionincluded MR syringes (18), insertion of solid sticks(7), insertion of rubber catheters (4), and ingestionof medicine (6) (Table 3).
Health consequences of abortion amongadolescents
A national study (Akhter et al., submitted forpublication) investigated abortion-related morbidityand mortality in 1996–1997 and found that of 30 668reported cases of complicated induced abortion,1415 (5%) resulted in death. Adolescentsconstituted 7% of those who experiencedcomplications and 8.1% of those who died. Nearly1% of women who died and 0.2% of those whoexperienced a reported complication wereunmarried. Using medical records from fivehospitals, Rochat & Akhter (1999) documented 52abortion-related tetanus deaths occurring in 1996and found that 10 cases were in women aged 10–19. The study by Akhter et al. (1998b) found that13% of adolescents hospitalized for induced
abortion had life-threatening complications. Halfhad symptoms of severe infection. Over 21% hadmechanical injury to the cervix or vagina. About16% had evidence of a foreign body having beeninserted into the vagina, cervix or uterus.
Conclusions
These research findings highlight numerous issues.First, studies suggest that adolescents lack anadequate understanding about the maturationprocess, fertile periods, and the risks of unprotectedsex. The majority do not use contraceptives toprevent unwanted pregnancies. Adolescents lackknowledge about the risks and consequences ofpregnancy termination, and many are unaware thatmenstrual regulation services are available.Because they do not have the information neededto recognize their pregnancy and seek MR quickly,they are often rejected by MR clinics because theirpregnancy is too far advanced. In many cases,these factors lead young women to resort to unsafemethods of abortion.
To address this situation, adolescents need to beprovided with better information and services to helpthem understand their sexuality and protect themfrom unwanted pregnancy. Greater awareness ofthe availability of MR services could reduce thenumbers of young women who resort to unsafeabortion. Policy-makers could also addressbarriers that influence the numbers of adolescentswho are rejected by MR clinics. Finally, socialbarriers such as the need to have a male escortneed to be addressed to facilitate adolescentwomen’s access to reproductive health care.
References
Akhter HH, Rochat R, Chowdhury M, Shah R, Yusuf H(submitted for publication) Complications frominduced abortion in Bangladesh and impact onmortality related to types of practitioner and methodin 1996.
Akhter HH, Karim F, Chowdhury ME, Rahman MH
Table 3. Method used to induce abortion that ledto complications (N = 38)
Type of method used Number of cases
MR procedure/syringe 18Rubber catheter 4Solid stick inserted 7Taking medicine 6Other 3
Source: Akhter et al., 1998b.

126
HALIDA HANUM AKHTER
(1998a) A study to identify the risk factors affectingnutritional status of adolescent girls in Bangladesh..Dhaka, Bangladesh, BIRPERHT (BIRPERHTPublication No. 119, Technical Report No. 67).
Akhter HH, Ahmed YH, Chowdhury ME, Rahman MH,Khan AR (1998b) A study to assess the determinantsand consequences of abortion in Bangladesh,Dhaka, Bangladesh, Development AssistanceCouncil and BIRPERHT (BIRPERHT PublicationNo. 118, Technical Report No. 66).
Akhter HH, Hossain MM, Akhter M, Desai SN, RahmanMH (2000) Report on needs assessments onreproductive health information and care amongadolescents in Paurashava schools and colleges.Dhaka, BIRPERHT (BIRPERHT Publication No. 123;Technical Report No. 71).
Ali MS, Zahir M, Hasan KM (1978) Report on LegalAspects of Population Planning in Bangladesh. Dhaka,The Bangladesh Institute of Law and InternationalAffairs.
Bangladesh, Population Control and Family PlanningDivision (1979) Circular No. FP/Misc-26/79/278 (600),issued on 31 May 1979. Government of People’sRepublic of Bangladesh, Population Control andFamily Planning Division Memo No. 5-14/MCH-FP/Trg/79.
Barkat A, Khan SH, Majid H, Sabina N (2000)Adolescent Sexual and Reproductive Health inBangladesh: A Needs Assessment. Dhaka,Bangladesh, Human Development Research Centre,prepared for Family Planning Association ofBangladesh .
Khan MA, Rahman M, Khanam PA, Barkat-e-Khuda,Kane TT, Ashraf A (1997) Awareness of sexuallytransmitted diseases among women and serviceproviders in rural Bangladesh. In: Kane TT, Barkat-e-Khuda, Phillips JF, eds. Reproductive Health in RuralBangladesh, Policy and Programmatic Implications,Volume 1. Dhaka, MCH-FP Extension Project (Rural),International Centre for Diarrhoeal DiseaseResearch, Bangladesh:1–20.
Koenig MA, Fauveau V, Chowdhury AI, Chakraborty J,Khan MA (1988) Maternal mortality in Matlab,Bangladesh: 1976–1985. Studies in Family Planning19(2):69–80.
Quamrun N et al. (1999) Strategies to Meet the HealthNeeds of Adolescents: A Review. Special Publication.Bangladesh, Operations Research Project, Healthand Population Extension Division, Centre for Healthand Population Research, International Centre forDiarrhoeal Disease Research, Bangladesh.
National Institute of Population Research andTraining, et al. (1997) Bangladesh Demographic andHealth Survey 1996–1997 . Dhaka, NIPORT,Calverton, Maryland, Mitra and Associates, MacroInternational Inc.
Rochat R, Akhter HH (1999) Tetanus and pregnancy-related mortality in Bangladesh. Lancet,354(9178):565 (letter).
Halida Hanum Akhter, MBBS, MCPS, MPH,Dr PHDirectorBangladesh Institute of Research for Promotionof Essential & Reproductive Health andTechnologies (BIRPERHT)House # 105, Road # 9/A, Dhanmondi R/ADhaka-1209Bangladesh

127
Induced abortions among rural adolescents in India
Background
An estimated six million abortions take place inIndia each year. However, gaps remain in ourunderstanding of the context of abortion, thedecision-making process, the reasons why womenseek abortion and choose different types ofproviders, and the extent to which abortions resultin complications. The information that is availableis drawn largely from urban hospital populationsor secondary analysis of case records. During1996–1998, researchers with the KEM HospitalResearch Centre in Pune, India carried out acommunity-based study on induced abortion in apredefined rural area of western Maharashtra. Thispaper presents the research findings that relate toadolescent abortion-seekers from that study.
Methods
Exploring such a sensitive issue throughcommunity-based research posed complexchallenges (Ganatra & Hirve, 2001). To identifywomen who had an induced abortion in an 18-monthreference period, the abortion study used amultiple-source community and provider-basedcase-finding process. Of the 1717 married womenidentified, 1409 acknowledged that their abortionwas induced and agreed to talk about it, including197 (14%) aged 20 or less, and 570 (41%) between
the ages of 21 and 24. In addition, researchersidentified 43 unmarried adolescent abortion-seekers, including 25 who had never married, 18who were separated and 2 who were widowed.Finally, researchers interviewed 159 abortionproviders in and around the study area.
Information on abortion-related mortality came froma separate population-based study on maternalmortality, also done by the KEM Hospital ResearchCentre in the same general region and in the samevillages that were part of the induced abortion study.That study screened all post-childhood femaledeaths in order to determine those that werepregnancy-related (Ganatra, Coyaji & Rao, 1998;Ganatra, 2001).
Key findings
As seen in Table 1, despite having a higher level ofeducation, young married women in the abortionstudy had a lower status in the household thanolder women. Younger women had significantlylower decision-making powers, less mobility andless likelihood of having an independent source ofincome or control over money earned (Table 1).
Young women’s lower status was reflected in theabortion decision-making process. Marriedadolescents were less likely to have played a major
Induced abortions: decision-making, providerchoice and morbidity experience among ruraladolescents in India
Bela Ganatra and S.S. Hirve
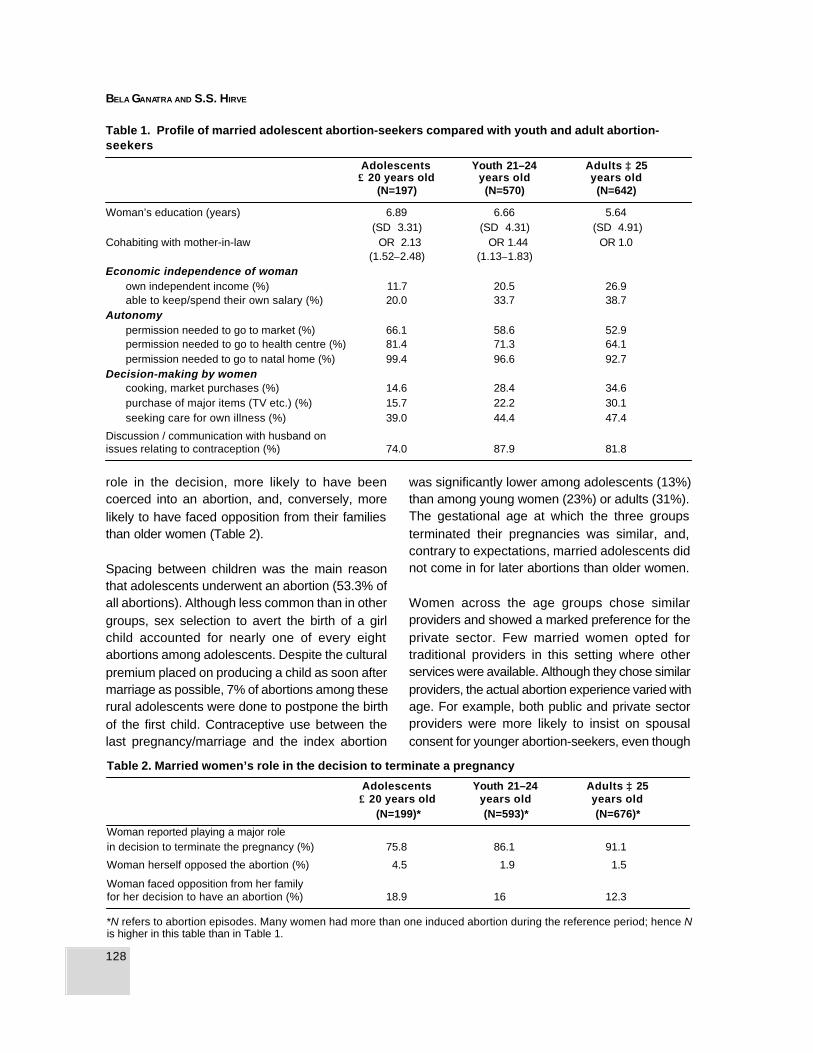
128
BELA GANATRA AND S.S. HIRVE
role in the decision, more likely to have beencoerced into an abortion, and, conversely, morelikely to have faced opposition from their familiesthan older women (Table 2).
Spacing between children was the main reasonthat adolescents underwent an abortion (53.3% ofall abortions). Although less common than in othergroups, sex selection to avert the birth of a girlchild accounted for nearly one of every eightabortions among adolescents. Despite the culturalpremium placed on producing a child as soon aftermarriage as possible, 7% of abortions among theserural adolescents were done to postpone the birthof the first child. Contraceptive use between thelast pregnancy/marriage and the index abortion
was significantly lower among adolescents (13%)than among young women (23%) or adults (31%).The gestational age at which the three groupsterminated their pregnancies was similar, and,contrary to expectations, married adolescents didnot come in for later abortions than older women.
Women across the age groups chose similarproviders and showed a marked preference for theprivate sector. Few married women opted fortraditional providers in this setting where otherservices were available. Although they chose similarproviders, the actual abortion experience varied withage. For example, both public and private sectorproviders were more likely to insist on spousalconsent for younger abortion-seekers, even though
Table 1. Profile of married adolescent abortion-seekers compared with youth and adult abortion-seekers
Adolescents Youth 21–24 Adults ≥ 25≤ 20 years old years old years old
(N=197) (N=570) (N=642)
Woman’s education (years) 6.89 6.66 5.64(SD 3.31) (SD 4.31) (SD 4.91)
Cohabiting with mother-in-law OR 2.13 OR 1.44 OR 1.0(1.52–2.48) (1.13–1.83)
Economic independence of womanown independent income (%) 11.7 20.5 26.9able to keep/spend their own salary (%) 20.0 33.7 38.7
Autonomypermission needed to go to market (%) 66.1 58.6 52.9permission needed to go to health centre (%) 81.4 71.3 64.1permission needed to go to natal home (%) 99.4 96.6 92.7
Decision-making by womencooking, market purchases (%) 14.6 28.4 34.6purchase of major items (TV etc.) (%) 15.7 22.2 30.1seeking care for own illness (%) 39.0 44.4 47.4
Discussion / communication with husband onissues relating to contraception (%) 74.0 87.9 81.8
Table 2. Married women’s role in the decision to terminate a pregnancy
Adolescents Youth 21–24 Adults ≥ 25≤ 20 years old years old years old
(N=199)* (N=593)* (N=676)*
Woman reported playing a major rolein decision to terminate the pregnancy (%) 75.8 86.1 91.1
Woman herself opposed the abortion (%) 4.5 1.9 1.5
Woman faced opposition from her familyfor her decision to have an abortion (%) 18.9 16 12.3
*N refers to abortion episodes. Many women had more than one induced abortion during the reference period; hence Nis higher in this table than in Table 1.

129
Induced abortions among rural adolescents in India
Table 3. Choice of provider, gestational age and perceived morbidity among unmarried and marriedadolescent abortion-seekers
Married adolescents Unmarried adolescents
(N=199)* (N=46)*
Number Per cent Number Per cent
Choice of providerTraditional provider 2 1 12 26.1Private practitioner 161 80.5 30 65.2Public hospital 37 18.5 4 8.7
Mean gestational age at abortion (weeks) 10.8 12.7Morbidity experienced 143 71.9 33 72.2**
it is not a legal requirement. Adolescents weresignificantly less likely to be counselled aboutcontraceptive use and were subsequently lesslikely than older women to adopt a contraceptiveafter abortion (36% of adolescents compared with58% of women aged 25 or older). Perceived post-abortion morbidity was higher among adolescents;however, life-threatening complications weresimilarly low across all age groups and were relatedto provider type and gestational age rather thanthe woman’s age.
Unmarried adolescent abortion-seekers reporteda markedly higher use of traditional providers thanmarried women, despite the availability of otherabortion services (Table 3). The principal factorsinfluencing provider choice were the level of supportfrom the family and/or the concerned man, needfor anonymity and provider attitudes. Cost may playa role as well, since the mean cost of a second-trimester private-sector abortion for an unmarriedadolescent was three times that of a similarabortion for a married adolescent. In-depth casestudies revealed that providers charged higherprices for unmarried clients. It is noteworthy thatnearly 60% of adolescents who had undergone anabortion were unaware that abortions amongunmarried women were legal. Similarly, of the 159abortion providers interviewed, 40% selectivelyrefused services to unmarried or separated women.
The population-based study on maternal mortalityfrom the same region found that abortion-related
mortality accounted for only four of the 140pregnancy-related deaths identified during a 35-month reference period. However, three of thesefour deaths were among adolescents. In addition,four unmarried pregnant adolescents committedsuicide in order to preserve family honour and diedwithout accessing any sort of abortion services.Thus, deaths related to abortions and unwantedpregnancies accounted for 18% of pregnancy-related deaths among adolescents as comparedwith 2% of deaths among older women.
Conclusions
While the state of Maharashtra has bettergeographic access to abortion services than manyother parts of India, these study findings suggestthat for adolescents, access is impeded by theirlow autonomy, mobility and status within thehousehold. These findings clearly demonstrate theneed for existing family planning programmes tofocus on the needs of young, recently marriedwomen, especially those who wish to delay thebirth of the first child or postpone a subsequentbirth. Post-abortion contraceptive counsellingcurrently targets older women who have finishedchildbearing. Such counselling needs to expandto both married as well as unmarried adolescents.
Being unmarried compounds the vulnerability ofbeing young and poses strong cultural, provider
* N: number of abortion episodes in reference period.**Includes one death.

130
BELA GANATRA AND S.S. HIRVE
and legal barriers. The most telling indicator of thisvulnerability is the substantial contribution ofsuicides due to unwanted pregnancies to maternaldeaths in the area. There is a compelling need tospread legal awareness among adolescents andproviders to ensure that barriers such as spousalconsent and higher costs do not make access toservices more difficult than it already is. The findingthat lower costs, provider sensitivity and concernsabout confidentiality led unmarried adolescents touse traditional providers even where safer optionswere available argues for technically sound servicesto improve quality of care and, in particular, providerattitudes. Abortion providers need to explore waysto make their services more anonymous, perhapsby mainstreaming them with other medicalservices. This would reduce the extent to whichthe stigma associated with illegitimate pregnanciesbecomes a barrier to the ability to respond towomen’s needs.
Acknowledgements: This study was funded bya grant from the Ford Foundation to the KEMHospital Research Centre, Pune. The study onMaternal Mortality was funded by a WHO grant(No.M/183/263 Safe Motherhood Research, Div.of Family Health) to the KEM Hospital ResearchCentre, Pune. A grant from the Institute ofReproductive Health, Department of Population and
Family Health, Johns Hopkins School of PublicHealth, provided the opportunity for preparation ofthis paper.
References
Ganatra BR (2001) Induced abortions: programmaticand policy implications of data emerging from anongoing study in rural Maharashtra. In: Puri C, VanLook P, eds. Sexual and Reproductive Health: RecentAdvances, Future Directions. New Delhi, New AgeInternational Limited Publishers:249–261.
Ganatra BR, Coyaji KJ, Rao VN (1998) Too little, toofar, too late: a community-based case control studyon maternal mortality. Bulletin of the World HealthOrganization, 76(6):591–598.
Ganatra BR, Hirve SS (2001) Ethical dilemmas insocial science research — a field study on inducedabortion. Issues in Medical Ethics, January, 9(1).
Bela Ganatra and S.S. HirveResearch FellowsDepartment of Population and Family HealthJohns Hopkins School of Public Health615 N Wolfe StreetBaltimore, MD 21205USA

VIIIReproductive tract andsexually transmittedinfections

132
PURNIMA MANE AND ANN P. MCCAULEY
133
Impact of sexually transmitted infections including AIDS on adolescents
Background
In recent years, the reproductive and sexual healthof adolescents has drawn increasing attention.Rates of sexually transmitted infections (STIs) aresoaring among young people, with one-third of the333 million new STI infections each year occurringamong young people under the age of 25 (WorldHealth Organization, 1999). Each year, more thanone out of 20 adolescents contracts a curable STI,not including viral infections (World HealthOrganization, 1997). Most importantly, younger agegroups are hardest hit by the pandemic of acquiredimmunodeficiency syndrome (AIDS). More than halfof all new human immunodeficiency virus (HIV)infections today occur in young people betweenthe ages of 15 and 24. This situation persists in apolicy climate that continues to deny adolescentsinformation and services that they need to makeinformed choices about their sexual andreproductive health, despite evidence thatadolescents show a remarkable capacity to adoptsafer behaviours when given access to suchknowledge, skills and services (Aggleton et al.,2000b; Joint United Nations Programme on HIV/AIDS, 1997). This paper describes thephysiological, behavioural and social factors thatmake adolescents more vulnerable than adults to
STIs, the consequences of STIs, including HIV,and the policy implications that follow.
Vulnerability of adolescents to STIs and HIV
Physiology is the first factor that makesadolescents—particularly girls—more vulnerablethan adults to STIs. Because girls have a largemucosal surface area exposed to infection andhave not developed mature mucosal defencesystems, the cells that line the opening of the cervixare more susceptible to chlamydia, gonorrhoea andHIV than those of adult women (Population Council,1999; Van Dam, 1995). This fact argues for latersexual initiation for girls. Yet, research carried outby the International Center for Research on Women(ICRW) partners in Brazil, Malawi and Papua NewGuinea indicates that many girls have intercoursebefore menarche (Weiss, Whelan, & Rao Gupta,1996). Not surprisingly, in some countries infectionrates among girls are higher than among boys. InKenya, for instance, nearly one girl in four betweenthe ages of 15 and 19 is believed to be living withHIV compared with one boy in 25; in Zambia, inthe same age group, 16% of girls versus 1% ofboys are HIV-infected (Joint United NationsProgramme on HIV/AIDS, 1998).
Impact of sexually transmitted infectionsincluding AIDS on adolescents: a globalperspective
Purnima Mane and Ann P. McCauley

134
PURNIMA MANE AND ANN P. MCCAULEY
Social powerlessness, poverty and economicdependence contribute to the vulnerability of youth.Many young people lack control over who theirsexual partners are, how many partners they have,or the circumstances and nature of sexual activity.Immediate needs for shelter, food, lodging, clothes,or even school fees may prevent young people fromchoosing safe sex, which increases the likelihoodof infection. Research indicates that young peopleworldwide suffer from sexual abuse andexploitation. Although this is more common forgirls, many boys are also sexually abused orcoerced (Heise, Moore & Toubia, 1995).Adolescents in situations such as armed conflict,social upheaval, refugee and migrant situations,and those who are homeless, drug users, orphans,or living with HIV may be highly vulnerable toinfection resulting from sexual exploitation.Unfortunately, they are often outside the reach ofgovernment programmes and policies. Their needsmust therefore be given special attention.
In some cases, social norms put young people atrisk by encouraging them to have sex in unsafecircumstances. For example, social approval ofearly marriage forces girls into early sexual activity.Unmarried girls often face pressures to have sex,such as in Zimbabwe, where girls report that theyhave to have sex with their boyfriend in order notto lose him (Bassett & Sherman, 1994). Socialnorms often push boys into early sexual initiationand risky behaviour. Deprived of reliable informationand access to preventive methods, boys are oftenill-equipped to protect themselves from STIs (JointUnited Nations Programme on HIV/AIDS, 1999c).Young gay men face even more difficulties ina world that favours heterosexuality (Aggletonet al., 2000a).
Social norms often forbid discussion of sex, despiteevidence that information prevents unwantedpregnancies, lowers rates of STI transmission anddelays sexual initiation (Joint United NationsProgramme on HIV/AIDS, 1997). In focus groupdiscussions with low-income Indian adolescents,researchers found that no one had explained toany of the girls about menstruation, sexual
intercourse, or childbearing (Bhende, 1995). Adultsoften justify this harmful refusal to inform youngpeople about sexuality as a way to maintain their“purity”. For girls in particular, just knowing orasking about sex may cause others to criticizethem because it is interpreted as a sign of beingsexually active. This social norm cuts girls off fromaccurate and useful information and the ability toprotect themselves (Weiss, Whelan & Rao Gupta,1996). To maintain the image of innocence, girlsin Thai factories said that, even if they knew aboutsex, they pretended they did not, so that they wereseen as virgins. This was the reason that theycould not carry condoms or suggest condom use(Cash & Anasuchatkul, 1995). In some ways theHIV pandemic has increased the amount ofinformation that adults give young people aboutsex. However, the Population Council’s Horizonsstudies among school youth in Mexico, SouthAfrica and Thailand indicate that many youngpeople have only superficial knowledge about HIV.The young people in those studies knew basicinformation about HIV, but they also believed thatmosquitoes and toilet seats could transmit HIV.
In all these factors, gender acts as a majordifferential. Data show that more girls than boysare uninformed about their bodies and STIs. Manyare not in a position to negotiate safer sex and aremore susceptible to rape or coerced sex. Clearlythe impact of STIs and HIV on girls is likely to bemore significant (Bassett & Sherman, 1994).
Consequences of STIs and HIV for youngpeople
Many STIs can be cured or treated. However, theconsequences of untreated or incurable STIsinclude infertility, illness and death—both for thoseyoung people who are infected and their children.The social and emotional costs of infertility areespecially high for women in contexts whereparenthood is highly valued. Failure to producechildren can result in emotional trauma, familyneglect, abuse or abandonment. STIs can also leadto the illness or death of a young person or a

135
Impact of sexually transmitted infections including AIDS on adolescents
neonate. STIs cause many young people to sufferchronic morbidity, including painful ulcers or warts,and skin lesions. STIs such as HIV, humanpapillomavirus (HPV), and hepatitis B may alleventually lead to death. Shame and fear of reprisaloften prevent young people from getting timelytreatment for an STI, thus worsening the situation.One serious consequence of STIs is that they mayfacilitate HIV infection. Evidence suggests thatSTIs, including syphilis, herpes and gonorrhoea,can increase the risk of HIV transmission 2–9-fold(Population Council, 1999). While shame adds tothe misery of having a curable STI, the stigma ofHIV can drastically affect young people’s mentaland emotional health.
As the global HIV pandemic spreads, growingnumbers of young people who are not infectedsuffer consequences because people close to themhave either died or are ill with AIDS. The Joint UnitedNations Programme on HIV/AIDS (UNAIDS)estimates that 16 million young people have alreadybeen orphaned by AIDS (Joint United NationsProgramme on HIV/AIDS, 2000b). For many, theloss of a parent was preceded by years of livingwith an ill parent. These children experience notonly the grief of losing a parent and the possibilityof being stigmatized by others in the community,but also a high likelihood of having a series ofcaregivers, receiving less food to eat and having toend their education (United Nations Children’sFund, 1999). Studies from Côte d’Ivoire, Haiti, India,and Thailand found that children were taken out ofschool as one means through which affectedfamilies reduced expenditures (Joint United NationsProgramme on HIV/AIDS, 1999d). The first to leaveschool are likely to be the older children who canearn income or care for others, particularly girls. Astudy in Mumbai found that in families with an HIV-positive member, income fell, children were takenfrom school and put into the labour market, andthe burden of care fell on the women. Because ofthe stigma associated with HIV, households werecareful to keep secret the HIV status of the familymember, thus cutting them off from communityresources (Joint United Nations Programme onHIV/AIDS, 1999d). In these settings, adolescents
have been compelled to take on adult rolesprematurely and the period of transition to adulthooddisappears. They care for ill parents, and manyeventually become the head of the household(Foster et al., 1997).
Long-term structural changes in high prevalencecountries will also affect adolescents. In areas ofhigh HIV prevalence, AIDS affects the wholeeducational system. As teachers become ill, classsizes grow and the quality of the educationdiminishes. In 1998, for example, Zambia lost 1300teachers—about 70% of the number of newteachers who finished training and started to teachthat year (Joint United Nations Programme on HIV/AIDS, 2000a). Demographers who used to talkabout population pyramids now talk aboutpopulation chimneys, because of the lack of adultsin the most productive years between 35 and 60.This loss will weaken institutions such asgovernments and inhibit the growth of private-sectorenterprises. As a result, poverty will become morewidespread (Joint United Nations Programme onHIV/AIDS, 2000c), further threatening theeconomic and social security of young people. Insum, adolescents in regions greatly affected byHIV face a bleak future if action is not taken.Researchers have noted the changes in adolescentopportunities and expectations, and haveadvocated policies and programmes that will assistthem to face some of the challenges, but little isknown or said about the psychological impact ofHIV on these young people.
Conclusions
To address the impact of STIs on adolescents, weneed to ensure access to information and services,and protection from discrimination. The examplesof Switzerland and Uganda demonstrate that,where governments acknowledge the problem ofHIV and provide access to information, servicesand protection from discrimination, they can reducethe rate of new infections among young people.We also need to ensure that young people haveaccess to new technologies now being developed.

136
PURNIMA MANE AND ANN P. MCCAULEY
Scientists are working on new treatments,microbicides and vaccines for STIs including HIV.If we continue to deny young people access toinformation and services, however, these will dolittle good.
To address long-term structural changes in society,new approaches must be multisectoral and includeplanning for continuity in education, public safety,health care and other institutions that are likely tobe impaired by high morbidity and mortality rates.In addition, policies and programmes need torecognize the heterogeneity of adolescents’ lives.Finally, both rhetoric and action should emphasizepositive aspects of sexual health. Adolescentsneed to appreciate that reproduction and sexualityare not just about unpleasant aspects ofpregnancy, disease and death, but about pleasure,fulfilment and living a full life. We need anapproach that is understanding without beingcondescending, acknowledges their potential,provides access to what is needed for a healthytransition to adulthood, and prepares them tocreatively face a challenging future.
In 1993, the Director of the STD and AIDS ControlProgram of a state in India visited an industrialtownship where he talked to local sex workersabout their experiences with STIs. The sex workerstold him that insisting on condoms was particularlydifficult during seasons when their business wasdown. When asked what these seasons were, theyidentified the period when thousands of 15 year-olds take the 10th standard All-State examinations.Policy-makers need to accept and deal with thisreality, not in a moralistic fashion, but in an openmanner that gives adolescents the means andsocial environment to ensure that they can enjoya safe and healthy future.
References
Aggleton P, Ball A, Mane P (2000a) Young people,sexuality and relationships. Sexual and MaritalRelationship Therapy, Special Issue, 15(3):213–220(editorial).
Aggleton P, Chase E, Rivers K, Tyler P (2000b)Innovative Approaches to HIV Prevention: SelectedCase Studies Prepared for the Joint United NationsProgramme on HIV/AIDS. Geneva, UNAIDS.
Bassett M, Sherman J (1994) Female SexualBehavior and the Risk of HIV Infection: AnEthnographic Study in Harare, Zimbabwe. Womenand AIDS Program Research Report Series.Washington, DC, International Center for Researchon Women.
Bhende A (1995) Evolving a Model for AIDSPrevention Education among UnderprivilegedAdolescent Girls in Urban India. Women and AIDSProgram Research Report Series. Washington, DC,International Center for Research on Women.
Cash K, Anasuchatkul B (1995) ExperimentalEducational Interventions for AIDS Prevention amongNorthern Thai Single Female Migratory Adolescents.Women and AIDS Program Research Report Series.Washington, DC, International Center for Researchon Women.
Foster G, Makufa C, Drew R, Kralovec E (1997)Factors leading to the establishment of child-headedhouseholds: the case of Zimbabwe. Health TransitionSupplement, 2(7):155–168.
Heise L, Moore K, Toubia N (1995) Sexual Coercionand Reproductive Health: A Focus on Research. NewYork, Population Council.
Joint United Nations Programme on HIV/AIDS (1997)Impact of HIV and Sexual Health Education on theSexual Behaviour of Young People: A Review Update.Geneva, UNAIDS.
Joint United Nations Programme on HIV/AIDS (1998)Report on the Global HIV/AIDS Epidemic. Geneva,UNAIDS.
Joint United Nations Programme on HIV/AIDS (1999a)AIDS Epidemic Update: December 1999. Geneva,UNAIDS.
Joint United Nations Programme on HIV/AIDS (1999b)A Review of Household and Community Responsesto the HIV/AIDS Epidemic in the Rural Areas of Sub-Saharan Africa. Geneva, UNAIDS.
Joint United Nations Programme on HIV/AIDS (1999c)Sex and Youth: Contextual Factors affecting Risk forHIV/AIDS. Geneva, UNAIDS.

137
Impact of sexually transmitted infections including AIDS on adolescents
Joint United Nations Programme on HIV/AIDS (1999d)Report on a Consultation on the Socio-EconomicImpact of HIV/AIDS on Households, Chiang Mai,Thailand. Geneva, UNAIDS.
Joint United Nations Programme on HIV/AIDS (2000a)HIV/AIDS and Development. Geneva, UNAIDS.
Joint United Nations Programme on HIV/AIDS (2000b)Report on the Global HIV/AIDS Epidemic. Geneva,UNAIDS.
Joint United Nations Programme on HIV/AIDS (2000c)Socio-Economic Impact of HIV/AIDS in Africa .Geneva, UNAIDS.
Population Council (1999) Reproductive TractInfections: A Set of Fact Sheets. Bangkok, PopulationCouncil, South and East Asia—Thailand Office.
United Nations Children’s Fund (1999) The Progressof Nations 1999. New York, UNICEF.
Van Dam CJ (1995) HIV, STD and their current impacton reproductive health: the need for control of sexuallytransmitted diseases. International Journal ofGynecology & Obstetrics, Suppl. 2:S121–S129.
Weiss E, Whelan D, Rao Gupta G (1996) Vulnerabilityand Opportunity: Adolescents and HIV/AIDS in the
Developing World. Washington, DC, InternationalCenter for Research on Women.
World Health Organization (1997) Young People andSexually Transmitted Diseases, Fact Sheet #186.Geneva, World Health Organization.
World Health Organization (1999) Programming forAdolescent Health and Development.. Geneva, WorldHealth Organization (WHO Technical Report SeriesNo. 886).
Purnima Mane, PhDVice President and DirectorInternational Programs DivisionPopulation CouncilOne Dag Hammarskjold PlazaNew York, NY 10017USA
Ann P. McCauley, PhDHorizons Project/International Center forResearch on WomenPopulation Council4301 Connecticut Avenue, # 280Washington, DC 20008USA
138
ABRAHAM JOSEPH, JASMIN PRASAD AND SULOCHANA ABRAHAM
Background
It is increasingly accepted that adolescentreproductive health deserves special attention.While a few studies have been done (Bang et al.,1989; Brabin et al., 1995), little is known aboutthe prevalence of reproductive tract infections (RTIs)or sexually transmitted infections (STIs) amongadolescents in the developing world. Becauselaboratory facilities are not available in manyresource-poor settings, the World HealthOrganization (WHO) has developed clinicalalgorithms (called the Syndromic Approach) todiagnose and treat RTIs based on easilyrecognizable signs and symptoms (WHO, 2000;WHO, 2001). To determine the nature and extentof gynaecological morbidity in young marriedwomen and to test the validity of the syndromicapproach, researchers from the Community Healthand Development Program (CHAD) of ChristianMedical College undertook a population-based,cross-sectional study in 13 South Indian villages.
Methods
The study was conducted in 13 villages ofKaniyambadi Block, a rural area of Vellore Districtin south India. Because of the communities’ trustin CHAD’s work, almost all (92%) eligible womenliving in the villages agreed to participate in the
study. Researchers enrolled 451 non-pregnantmarried women aged 16–22 (mean age of 20.7years). Information was collected on the women’smenstrual and obstetric histories, perceivedgynaecological symptoms, health care-seekingbehaviour and contraceptive practices. All womengave blood and urine samples and underwent amedical (speculum) examination for RTI. If thelaboratory tests or clinical examination detectedany signs suggestive of infection, then the womenwere asked a second round of questions aboutsymptoms they might have experienced.
Key findings
Among all young women in the study, 240 (53%)reported a symptom suggestive of an RTI, includingwhite discharge (44%), burning sensation whilepassing urine (19%) and vaginal itch (12%). Amongthose reporting symptoms, 171 women (38%) hadone symptom, 45 women (10%) had twosymptoms and 23 women (5%) had all three.
Clinical and laboratory diagnoses indicated that59% (265) of respondents had one or moregynaecological problem. This included 48.5% whosuffered from an RTI, 9% with infertility (defined asinability to conceive after two years of married lifewithout contraception), and 7% with a urinary tractinfection. The prevalence of STIs in this study group
Gynaecological problems among youngmarried women in Tamil Nadu, India
Abraham Joseph, Jasmin Prasad and Sulochana Abraham
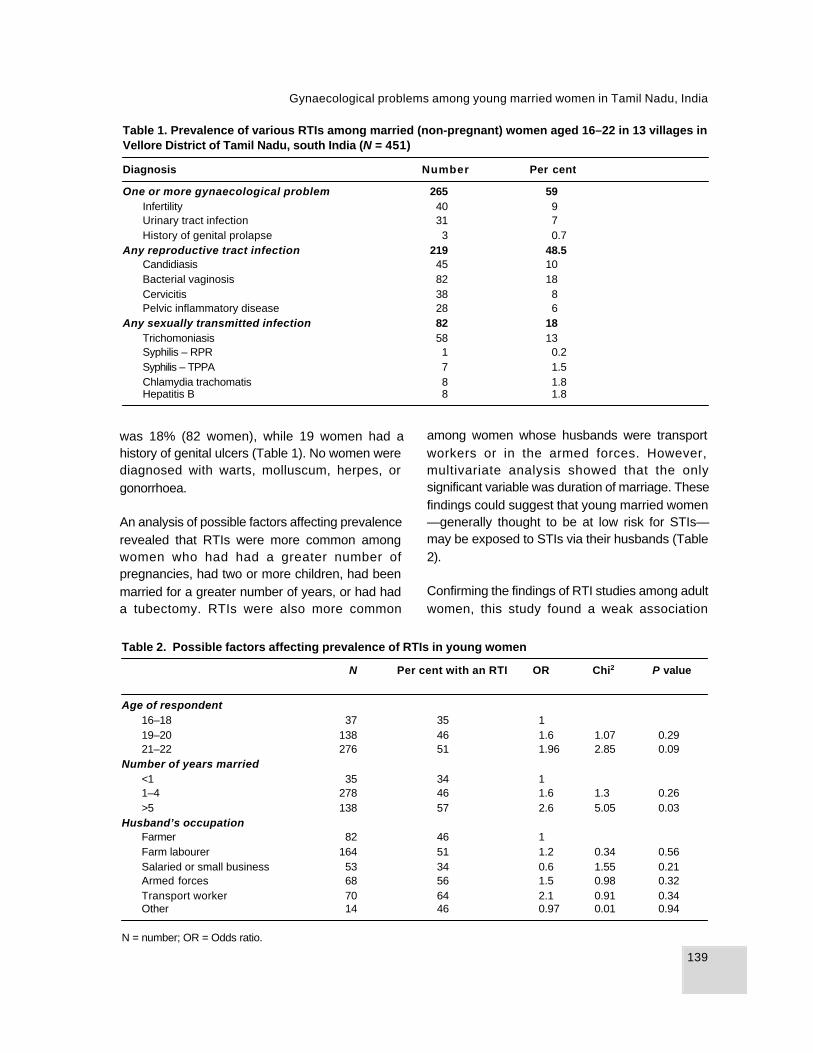
139
Gynaecological problems among young married women in Tamil Nadu, India
was 18% (82 women), while 19 women had ahistory of genital ulcers (Table 1). No women werediagnosed with warts, molluscum, herpes, orgonorrhoea.
An analysis of possible factors affecting prevalencerevealed that RTIs were more common amongwomen who had had a greater number ofpregnancies, had two or more children, had beenmarried for a greater number of years, or had hada tubectomy. RTIs were also more common
Table 1. Prevalence of various RTIs among married (non-pregnant) women aged 16–22 in 13 villages inVellore District of Tamil Nadu, south India (N = 451)
Diagnosis Number Per cent
One or more gynaecological problem 265 59Infertility 40 9Urinary tract infection 31 7History of genital prolapse 3 0.7
Any reproductive tract infection 219 48.5Candidiasis 45 10Bacterial vaginosis 82 18Cervicitis 38 8Pelvic inflammatory disease 28 6
Any sexually transmitted infection 82 18Trichomoniasis 58 13Syphilis – RPR 1 0.2Syphilis – TPPA 7 1.5Chlamydia trachomatis 8 1.8Hepatitis B 8 1.8
among women whose husbands were transportworkers or in the armed forces. However,multivariate analysis showed that the onlysignificant variable was duration of marriage. Thesefindings could suggest that young married women—generally thought to be at low risk for STIs—may be exposed to STIs via their husbands (Table2).
Confirming the findings of RTI studies among adultwomen, this study found a weak association
Table 2. Possible factors affecting prevalence of RTIs in young women
N Per cent with an RTI OR Chi2 P value
Age of respondent16–18 37 35 119–20 138 46 1.6 1.07 0.2921–22 276 51 1.96 2.85 0.09
Number of years married<1 35 34 11–4 278 46 1.6 1.3 0.26>5 138 57 2.6 5.05 0.03
Husband’s occupationFarmer 82 46 1Farm labourer 164 51 1.2 0.34 0.56Salaried or small business 53 34 0.6 1.55 0.21Armed forces 68 56 1.5 0.98 0.32Transport worker 70 64 2.1 0.91 0.34Other 14 46 0.97 0.01 0.94
N = number; OR = Odds ratio.

140
ABRAHAM JOSEPH, JASMIN PRASAD AND SULOCHANA ABRAHAM
between self-reported symptoms and clinical/laboratory diagnosis among young women. Of the240 young women who reported symptomssuggestive of an RTI, only 58% (138) werediagnosed with an infection. At the same time,among women who reported no symptoms, 38%(81) were diagnosed with an RTI.1 The study founda stronger association between laboratorydiagnosis and the WHO algorithms for diagnosingRTIs on the basis of clinic signs (using a speculumexamination).2 This finding suggests that evenwithout sophisticated laboratory facilities, primaryhealth centres could do more to diagnose and treatRTIs.
Data on health-seeking behaviour revealed thatonly 35% of women who reported gynaecologicalsymptoms had ever sought treatment. Mostwomen (78%) who did so tried home remedies orsought help from traditional medicine or unqualifiedprivate practitioners. Only 9% of women whoreported symptoms had sought medical care atthe government primary health centres. It isnoteworthy that most (50 out of 81) “asymptomatic”women diagnosed with an RTI were in fact awareof symptoms but had not reported them during thefirst round of questions because they regardedthese symptoms as normal or of trivial importance.
Conclusions
Women face many barriers to accessing RTIservices. In this area, laboratory facilities todiagnose and treat RTIs and STIs are currentlyavailable only in District and Taluk hospitals orperhaps private facilities. To access these services,many women from these villages would have totravel long distances.
The high prevalence of RTIs (48.5%) and STIs(18%) and the poor utilization of health services
among young married women, hitherto consideredto be at low risk of infection, should be of greatconcern. Not only do RTIs pose a threat to health,but they also impose an economic and socialburden due to the stigma associated with theseinfections. These study findings highlight the needto raise awareness of RTIs and STIs and to expandservices for prevention and treatment for youngwomen. To do this effectively, however, it may benecessary to improve the quality of care providedat the community level.
References
Bang RA, Bang AT, Baitule M, Choudhary T,Sarumukadda S, Tale O (1989) High prevalence ofgynaecological diseases in rural Indian women.Lancet, 1:85–88.
Brabin L et al. (1995) Reproductive tract infectionsand abortion among adolescent girls in rural Nigeria.The Lancet, 345:300–304.
WHO (2000) Women and sexually transmitteddiseases. Geneva, World Health Organization (WHOinitiative on HIV/AIDS and Sexually TransmittedInfections. Division of AIDS and STD. Fact SheetNo. 249).
WHO (2001) Guidelines for the management ofsexually transmitted infections. Geneva, World HealthOrganization (Document No. WHO/RHR/01.10).
Further reading
Amsel R, Totten PA, Spigel CA, Chen KCS,Eschenbach D, Holmes KK (1983) Non specificvaginitis: Diagnostic criteria and microbial andepidemiologic association. American Journal ofMedicine, 74:14–22.
Bhatia CJ, Cleland J (1995) Self-reported symptoms
1 The study found that the WHO algorithms based on reported vaginal discharge alone also had poor sensitivity (50%),specificity (60%) and predictive value (47%).
2 The WHO algorithm using clinical signs for diagnosis of RTIs (including speculum examination) had a high sensitivity(95%) and specificity (93%).

141
Gynaecological problems among young married women in Tamil Nadu, India
of gynaecological morbidity and their treatment inSouth India. Studies in Family Planning, 26(4):203–216.
Chakraborty S, Munni M (1989) Serological surveysfor syphilis amongst antenatal cases in selectedhospitals of Delhi. Indian Journal of Public Health , 33.
Dhall K, Sarkar A, Sokhey C, Dhall CL, Ganguly NK(1990) Incidence of gonococcal infection and itsclinico-pathological correlation in patients attendinggynaecological outpatient department. Journal ofObstetrics and Gynaecology of India:410–414.
Heine P, McGregor JA (1993) Trichomonas vaginalis:A re-emerging pathogen. Clinical Obstetrics andGynaecology, 36(1):137–143.
La Ruche G, Lorougnon F, Digbeu N (1995)Therapeutic algorithms for the management ofsexually transmitted diseases at the peripheral levelin Cote d’Ivoire: assessment of efficacy and cost.Bulletin of the World Health Organization, 73:305–313.
Lee HH et al. (1995) Diagnosis of Chlamydiatrachomatis genito-urinary infection in women byligase chain reaction assay of urine. Lancet, 345:213–216.
Ndinya-Achola JO, Kihara AN, Fisher LD, Krone MR,Plummer FA, Ronald A, Holmes KK (1996)Presumptive specific clinical diagnosis of genitalulcer disease in a primary health care setting inNairobi. International Journal of STD and AIDS,7:201–205.
Nugent RP, Krohn MA, Hillier SL (1991) Reliability ofdiagnosing bacterial vaginosis is improved by astandardised method of gram staining interpretation.Journal of Clinical Microbiology, 29(2):297–301.
Pels RJ et al. (1985) Dipstick urinalysis screening ofadults for urinary tract disorders. JAMA, 254:240–245.
Ridgway GL et al. (1996) Comparison of the ligasechain reaction with cell culture for the diagnosis ofChlamydia trachomatis infection in women. Journalof Clinical Pathology, 49:116–119.
Sobar JD (1993) Candidal vulvovaginitis. ClinicalObstetrics and Gynaecology, 36(1):153–165.
Tramont EC (1995) Treponema pallidum. In: Mandell,Douglas, Bennett, eds. Principles and Practices ofInfectious Diseases . New York, ChurchillLivingstone:2117–2132.
Wasserheit JN (1992) Epidemiological synergy.Interrelationships between human immunodeficiencyvirus infection and other sexually transmitteddiseases. Sexually Transmitted Diseases, March–April; 19(2):61–77.
Wasserheit JN, Harris JR, Chakraborty J, Kay BA,Mason KJ (1989) Reproductive tract infections in afamily planning population in rural Bangladesh.Studies in Family Planning, 20(2):69–80.
World Health Organization (1985a) Program ofresearch, development and research training inhuman reproduction, 1985, Annual Technical Report.Geneva, World Health Organization.
World Health Organization (1985b) Neisseriagonorrhoea and gonococcal infections: Report of aWHO scientific group. Geneva, World HealthOrganization:65—75 (Technical Report SeriesNo. 616).
Younis N, Khattab H, Zurayk H, El-muethy M, Amin MF,Faraq M (1993) A community study of gynaecologicaland related morbidity in rural Egypt. Studies in FamilyPlanning 24(3):175–176.
Dr Abraham JosephCommunity Health DepartmentChristian Medical CollegeVellore 632002Tamil NaduIndia
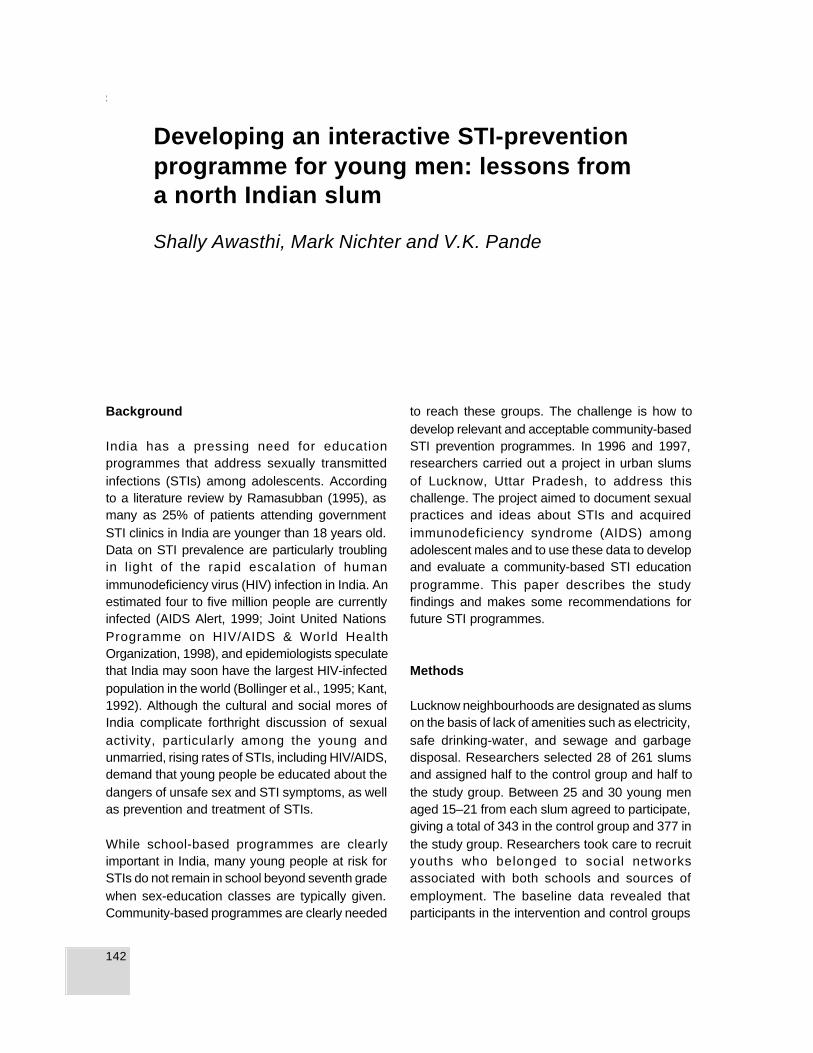
142
SHALLY AW ASTHI, MARK NICHTER AND V.K. PANDE
Background
India has a pressing need for educationprogrammes that address sexually transmittedinfections (STIs) among adolescents. Accordingto a literature review by Ramasubban (1995), asmany as 25% of patients attending governmentSTI clinics in India are younger than 18 years old.Data on STI prevalence are particularly troublingin light of the rapid escalation of humanimmunodeficiency virus (HIV) infection in India. Anestimated four to five million people are currentlyinfected (AIDS Alert, 1999; Joint United NationsProgramme on HIV/AIDS & World HealthOrganization, 1998), and epidemiologists speculatethat India may soon have the largest HIV-infectedpopulation in the world (Bollinger et al., 1995; Kant,1992). Although the cultural and social mores ofIndia complicate forthright discussion of sexualactivity, particularly among the young andunmarried, rising rates of STIs, including HIV/AIDS,demand that young people be educated about thedangers of unsafe sex and STI symptoms, as wellas prevention and treatment of STIs.
While school-based programmes are clearlyimportant in India, many young people at risk forSTIs do not remain in school beyond seventh gradewhen sex-education classes are typically given.Community-based programmes are clearly needed
to reach these groups. The challenge is how todevelop relevant and acceptable community-basedSTI prevention programmes. In 1996 and 1997,researchers carried out a project in urban slumsof Lucknow, Uttar Pradesh, to address thischallenge. The project aimed to document sexualpractices and ideas about STIs and acquiredimmunodeficiency syndrome (AIDS) amongadolescent males and to use these data to developand evaluate a community-based STI educationprogramme. This paper describes the studyfindings and makes some recommendations forfuture STI programmes.
Methods
Lucknow neighbourhoods are designated as slumson the basis of lack of amenities such as electricity,safe drinking-water, and sewage and garbagedisposal. Researchers selected 28 of 261 slumsand assigned half to the control group and half tothe study group. Between 25 and 30 young menaged 15–21 from each slum agreed to participate,giving a total of 343 in the control group and 377 inthe study group. Researchers took care to recruityouths who belonged to social networksassociated with both schools and sources ofemployment. The baseline data revealed thatparticipants in the intervention and control groups
Developing an interactive STI-preventionprogramme for young men: lessons froma north Indian slum
Shally Awasthi, Mark Nichter and V.K. Pande

143
Developing an interactive STI-prevention programme for young men
were well matched, with a slightly higher proportionof married youths in the intervention slums. Lossto follow-up was 14 boys (4%) in the interventiongroup and 0% in the control group.
During the formative stage of the project, 47adolescents were interviewed individually or as partof focus group discussions (FGDs) about theirknowledge of STIs and sexual behaviour of youngpeople in their slums. These data were used todevelop both the survey and the intervention.Following the pilot research, male project staffadministered the pretested questionnaire to youngmen in each intervention and control slum. Stafffilled out questionnaires for the youth after assuringthem of confidentiality. These pre-intervention datawere compared with post-intervention data collected6–8 weeks later using the same survey instrument.
The intervention consisted of three educationalsessions held at two-week intervals. Facilitatorspresented scientific information as well ascommonly held beliefs identified during the formativeresearch phase, and then opened up the sessionfor questions. Facilitators invited participants towrite questions and place them in a locked boxmarked with a sign that read, “Tell your problemsand get rid of the hidden disease”. The programmeprovided basic information about: (a) reproductivephysiology, fertility and conception; (b) STItransmission, types and symptoms, gupt roga (alocal name for STIs meaning “hidden disease”),and the nature of asymptomatic infections; (c) thelink between STIs and HIV infection; (d) HIV tests;and (e) STI prevention and “harm reduction”—meaning local practices meant to reduce negativeeffects of risky sex before, during, or after sex.
Facilitators employed and evaluated differentcommunication strategies, including teaching byanalogy. For example, to illustrate how AIDS harmsthe body gradually rather than all at once, facilitatorscompared it to termites eating a tree slowly fromwithin. Only when the tree falls does one realizethat the roots have been devoured. Each hour-longsession was prepared in Hindi and pretested amongyoung men of the same age in a slum not included
in the project. The session facilitator was supportedby three male assistants, who made themselvesavailable to participants for individual privateconsultations about sensitive issues. During thelast 15 minutes, facilitators played a taped set ofeducational messages that repeated key pointsmade in the live session. Some participantslistened to these messages while others discussedissues related to the session with friends or staff.At the end of the project, three FGDs were held toevaluate the programme from the perspective ofthe young men.
Key findings
During the project, participants placed more than150 questions in the question box. One-thirdfocused on HIV/AIDS, including questions suchas: could one get AIDS from kissing, sharing acigarette, or mosquito bites? And, does AIDSalways end in death? One-quarter of all questionsrelated to gupt roga. Some wanted to know howone could tell if girls they were about to marry hada condition that could give them gupt roga. Follow-up ethnographic research revealed that young menimagined causes of STIs unrelated to contagion ina biomedical sense, including having sex with agirl who has a “heaty” body (referring to bodytemperature in a humoral sense) or with a girlwhose blood is not complementary. Youths wantedto know whether a man could get gupt roga if awoman was menstruating or had discharge. Theyalso wanted to know if someone could develop STIsfrom too much sex. Youths wanted to know howto protect themselves before, during and after sex,including whether there were medicines one couldtake, or measures one could adopt, such aswashing the penis after sex. They also wanted toknow how a condom prevents sickness—is it justby enclosing the penis or is there some chemicalin the condom? A few sought advice on how totreat “male” symptoms such as cloudy or colouredurine.
Many questions concerned masturbation. Ismasturbation a sickness or addiction? How often

144
SHALLY AW ASTHI, MARK NICHTER AND V.K. PANDE
can the body lose semen without becoming sickor weak? Does masturbation alter the size of one’spenis or cause it to hang to one side? Does itaffect one’s virility or ability to impregnate one’swife later in life? Can one develop gupt roga orsome other illness from excessive masturbation?Boys also asked about the causes of nocturnalejaculation and how to prevent it. They wanted toknow whether it was a sign of sickness. Theyasked more than a dozen questions about the effectof smoking or chewing pan masala (betel leaf andnut), including whether smoking affects sex driveor performance.
Although the study did not aim to establish levelsof adolescent sexual activity, it did provide crudedata on sexual activity. At baseline, approximately15–17% of youths reported intercourse outside ofmarriage, including about 3% (22 youths) whoreported intercourse with a prostitute and 3% (20youths) who reported oral or anal sex with anothermale. When asked whether they anticipated havinga sexual encounter in the next six months, 18%of unmarried youths stated that the likelihood wasvery high, 20% stated that they probably would,and 62% replied that they would not. Of the 22youths who said they had visited a prostitute, seven(32%) reported having used a condom, whereas42 (56%) of those who said they had hadintercourse with a friend or relative reported havingused a condom. Protection against pregnancyseemed to motivate most condom use. Ten out of20 youths who reported sex with another malestated that they had a condom at least once, andall these young men also reported using a condomwith a woman.
Two issues related to sexual behaviour invite furtherresearch. First, the analysis suggests a possiblerelationship between sex with prostitutes and sexwith another male, given that eight out of 22 youthswho visited prostitutes also reported sex withanother male. Second, youths who engaged inweekly or daily alcohol use were significantly morelikely to engage in unsafe sex than were light ornon-drinkers (OR: 3.53; 95% CI: 1.64–7.61;P value < 0.0002). Eighteen per cent of the
intervention group and 13% of the control groupdefined themselves as weekly drinkers, and 1–2%defined themselves as daily drinkers.
Before the intervention, between 59% and 66% ofyouths in both study and control groups reportedknowing that there is more than one type of STI,but few participants were able to describe symptomclusters. In the follow-up survey, knowledge thatmultiple STIs exist had increased in both groups,but the increase was statistically significant onlyin the intervention group (from 66% to 83%). Atbaseline, between 30% and 40% of youths believedthat women and men with an STI always showsymptoms of their illness. Young men in theintervention group scored a statistically significantincrease in the knowledge that symptoms maynot always appear. They also registered significantincreases in their knowledge of STI symptoms andin their knowledge about how long symptoms ofAIDS (and associated diseases) take to becomeapparent. However, a majority of youths continuedto be confused about how long other STIs took tobecome symptomatic (Table 1).
After the intervention, awareness that STIs includingHIV/AIDS could be acquired from women other thanprostitutes jumped significantly from 50% to 76%in the intervention group. However, young men’sawareness that they were personally at risk ofacquiring STIs changed little during the intervention.Population-based data about STI risk did nottranslate into increased recognition that theirimmediate environment rendered them vulnerableto STIs. Fewer than 25% of those surveyed beforeor after the intervention thought that STIs were abig problem where they lived. Perhaps due tosecrecy surrounding the “hidden disease”, few saidthat they knew anyone who had experienced suchan illness.
The intervention made moderate headway ineducating youth about ineffective “harm-reduction”practices. A statistically significant decrease wasfound in the proportion of the intervention groupwho thought that taking medicines before or aftersex could prevent STIs (from 58% to 21%) or that
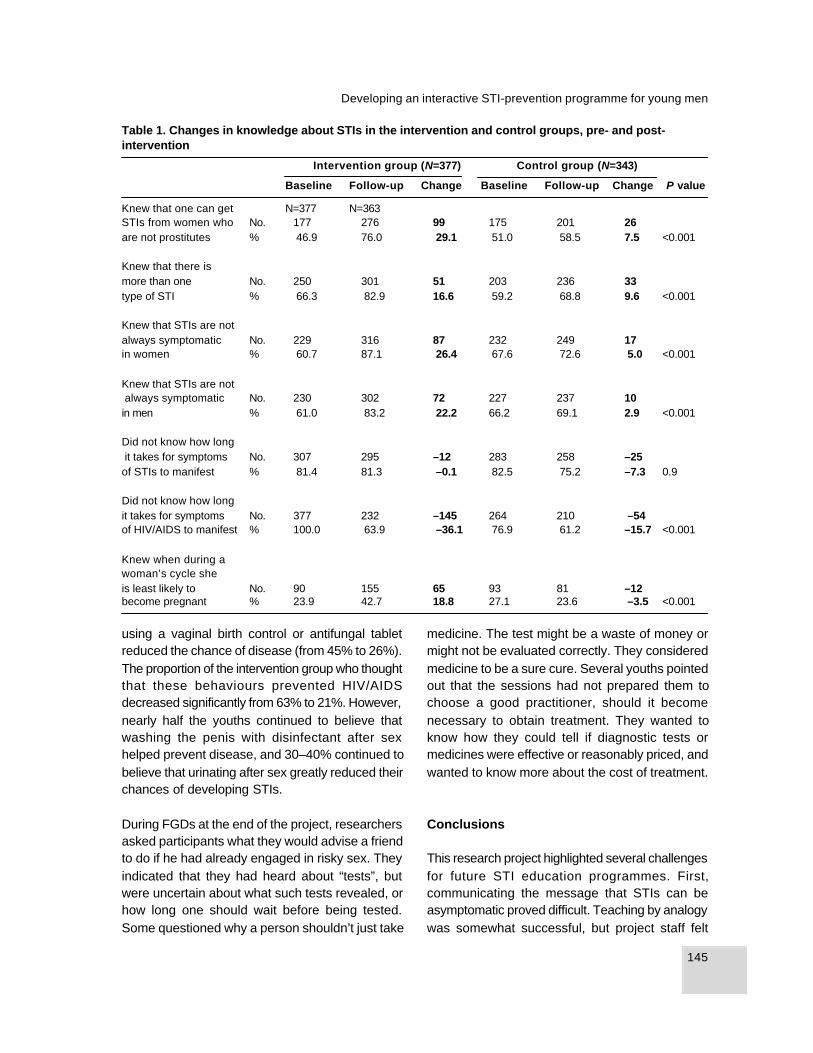
145
Developing an interactive STI-prevention programme for young men
using a vaginal birth control or antifungal tabletreduced the chance of disease (from 45% to 26%).The proportion of the intervention group who thoughtthat these behaviours prevented HIV/AIDSdecreased significantly from 63% to 21%. However,nearly half the youths continued to believe thatwashing the penis with disinfectant after sexhelped prevent disease, and 30–40% continued tobelieve that urinating after sex greatly reduced theirchances of developing STIs.
During FGDs at the end of the project, researchersasked participants what they would advise a friendto do if he had already engaged in risky sex. Theyindicated that they had heard about “tests”, butwere uncertain about what such tests revealed, orhow long one should wait before being tested.Some questioned why a person shouldn’t just take
medicine. The test might be a waste of money ormight not be evaluated correctly. They consideredmedicine to be a sure cure. Several youths pointedout that the sessions had not prepared them tochoose a good practitioner, should it becomenecessary to obtain treatment. They wanted toknow how they could tell if diagnostic tests ormedicines were effective or reasonably priced, andwanted to know more about the cost of treatment.
Conclusions
This research project highlighted several challengesfor future STI education programmes. First,communicating the message that STIs can beasymptomatic proved difficult. Teaching by analogywas somewhat successful, but project staff felt
Table 1. Changes in knowledge about STIs in the intervention and control groups, pre- and post-intervention
Intervention group (N=377) Control group (N=343)
Baseline Follow-up Change Baseline Follow-up Change P value
Knew that one can get N=377 N=363STIs from women who No. 177 276 99 175 201 26are not prostitutes % 46.9 76.0 29.1 51.0 58.5 7.5 <0.001
Knew that there ismore than one No. 250 301 51 203 236 33type of STI % 66.3 82.9 16.6 59.2 68.8 9.6 <0.001
Knew that STIs are notalways symptomatic No. 229 316 87 232 249 17in women % 60.7 87.1 26.4 67.6 72.6 5.0 <0.001
Knew that STIs are not always symptomatic No. 230 302 72 227 237 10in men % 61.0 83.2 22.2 66.2 69.1 2.9 <0.001
Did not know how long it takes for symptoms No. 307 295 –12 283 258 –25of STIs to manifest % 81.4 81.3 –0.1 82.5 75.2 –7.3 0.9
Did not know how longit takes for symptoms No. 377 232 –145 264 210 –54of HIV/AIDS to manifest % 100.0 63.9 –36.1 76.9 61.2 –15.7 <0.001
Knew when during awoman’s cycle sheis least likely to No. 90 155 65 93 81 –12become pregnant % 23.9 42.7 18.8 27.1 23.6 –3.5 <0.001

146
SHALLY AW ASTHI, MARK NICHTER AND V.K. PANDE
that better messages should be developed, takinginto account popular notions of STIs and the needfor gender sensitivity. Gender sensitivity is animportant issue as it became apparent in an FGDwith young Hindu men that some men associatedSTIs with women’s impurity and inherentdangerousness. As a result, researchers decidednot to explain that women tend to be asymptomaticmore often than men to avoid supporting negativestereotypes of women as primary disseminatorsof STIs. Another future challenge is the need toaddress sexual behaviours other than coitus. Thefinding that many youths who engaged in high-risk sex with prostitutes also engaged in sex withother males highlights the need for more researchon male-to-male sex in India, and the need todevelop new educational messages. The challengeis how to prepare communities for frankdiscussions about hidden sexual behaviours.Finally, because researchers had not investigatedthe medicines that local practitioners prescribed,the team felt at a loss to offer advice to participantsabout locally available STI treatment. In the future,researchers need to investigate what young mendo and whom they consult when they think theymight be developing an STI. Future programmesmust offer practical, reality-based recommen-dations about where to turn for testing andtreatment.
Despite these challenges, however, the studydemonstrated that STI education could beintroduced to young people in a community settingusing innovative approaches grounded in anunderstanding of local realities. Communityacceptance of STI education may increase ifeducators address cultural as well as medicalconcerns, and the study demonstrated theusefulness of programmes that are informed byanthropological research.
This summary has been adapted from the full articleentitled “Developing an interactive STD-preventionprogramme for youth: Lessons from a north Indianslum”, published in Studies in Family Planning,2000, 31(2):138–150.
Acknowledgements: The authors acknowledgethe technical inputs of Professor Gail Slap. Thestudy was funded by the International ClinicalEpidemiology Network (INCLEN)—Institute forResearch on Women and Gender, Small GrantsProgram.
References
AIDS Alert (1999) AIDS hits Indian population withmonsoon force. AIDS Alert-International Supplement,14(5):1.
Awasthi S, Nichter M, Pande VK (2000) Developingan interactive STD-prevention programme for youth:Lessons from a north Indian slum. Studies in FamilyPlanning, 31(2):138–150.
Bollinger RC, Tripathy SP, Quinn TC (1995) Thehuman immunodeficiency virus epidemic in India:Current magnitude and future projections. Medicine,74(2):97–106.
Joint United Nations Programme on HIV/AIDS, WorldHealth Organization (1998) Epidemiology fact sheeton HIV/AIDS and sexually transmitted diseases: India.Geneva, UNAIDS/WHO Working Group on Global HIV/AIDS and STD Surveillance.
Kant L (1992) HIV infection: Current dimensions andfuture implications. Council of Medical ResearchBulletin, 22:113–126.
Ramasubban R (1995) Patriarchy and the risks ofSTD and HIV transmission to women. In: Das GuptaM, Chen L, Krishnan TN, eds. Women’s Health inIndia. Oxford, Oxford University Press:212–239.
Further reading
Jejeebhoy SJ (1998) Adolescent sexual andreproductive behavior: A review of the evidence fromIndia. Social Science and Medicine, 46(10):1275–1290.
Khanna N, Nadkarni V, Bhutani L (1998) India. In:Plummer D et al., eds. Sexually Transmitted Diseasesin Asia and the Pacific. New South Wales, Australia,Venerology Publishing:115–137.

147
Developing an interactive STI-prevention programme for young men
Nichter M, Nichter M (1996) Education by appropriateanalogy. In: Nichter M, Nichter M, eds. Anthropologyand International Health: Asian Case Studies. NewYork, Gordon and Breach:401–426.
Watsa MC (1993) Premarital sexual behaviour inurban educated youth in India. Paper presented atthe Workshop on Sexual Aspects of AIDS/STDPrevention in India, Bombay, 23–27 November.
Dr. Shally AwasthiProfessorDepartment of Pediatrics and Clinical Epidemi-ology UnitKing George’s Medical CollegeLucknow UniversityLucknow, Uttar PradeshIndia

148
SHAHID MAQSOOD RANJHA AND ANUSHEH HUSSAIN
Background
In Pakistan, like many countries in South Asia,talking about sexuality is perceived as taboo orimmoral, and sex outside of marriage is stronglycondemned. As a result, many people, includinghealth providers, lack the vocabulary to addressissues related to sexual and reproductive health.Sexually active unmarried adolescents are oftenafraid to access reproductive health services, andservices that are available to adolescents oftenreinforce myths and misinformation. Adolescents(defined in this presentation as the age group 12–21years) make up nearly one-fourth of the Pakistanipopulation (Pakistan Integrated Household Survey,1995). However, the lack of adequate nationalpolicies has led to the neglect of adolescents’reproductive health needs. Several non-governmental organizations (such as PAVHNA,FPAP and ROZAN) provide adolescent reproductivehealth services, but they are not sufficient to meetthe need given the population size and the barriersto access that adolescents face.
Among the few providers of sexual and reproductivehealth services in Pakistan are the Hakim Sahibs,who practise herbal medicine in “sex clinics”, whichhave been present in the subcontinent since herbalmedicine began. These practitioners often claimto be specialists in sexual or other health matters,and they typically use the Ayurvedic or
homoeopathic system of medication. They havegenerally learned this skill from their forefathers,and usually have no degree or certificate from anyuniversity or medical college. In the 1960s, theGovernment of Pakistan legalized and registeredherbal clinics, including sex clinics. Some HakimSahibs are legally registered as practitioners ofhomoeopathic or Greek systems of medicine, butthe majority are unregistered and work illegally.
At least two reasons explain the popularity of sexclinics in Pakistan. First, much of the Pakistanipopulation lives in rural areas where basic healthservices are either unavailable or inaccessible tomost of the population. Sex clinics, on the otherhand, are abundant in both rural and urban areas,and can be found in every other street and mohalla(community). In many places, there are no obviousalternatives. Second, many people prefer the kindof herbal medicine practised in the sex clinics toallopathic medicine available elsewhere.
Sexual health services for adolescents at sexclinics in Rawalpindi, Pakistan
Shahid Maqsood Ranjha and Anusheh Hussain
1 SAHIL is the only major organization in Pakistan that fo-cuses on child sexual abuse (CSA) and child prostitution inPakistan. Our work includes sensitizing the media, con-ducting research on issues surrounding CSA, developingeducational materials for schools on prevention of CSA,and providing a healing centre for adult survivors whowere sexually abused as children or were forced intochild prostitution.

149
Sexual health services for adolescents at sex clinics in Rawalpindi, Pakistan
SAHIL1 , a registered voluntary organization,counsels children and adolescents on a broadrange of topics, including issues related tosexuality. As many as 80% of adolescentsattending SAHIL’s counselling programme seekhelp for issues related to sexual health, includingmasturbation, nocturnal emissions, menstrualbleeding and the condition of the hymen. Male andfemale homosexuality have also emerged asserious concerns. These concerns areexacerbated by myths and misconceptions, guiltand perceived associations with abnormality. SAHILfound that, among the adolescents with sexualhealth concerns, almost 50% had sought care fromHakim Sahibs in local sex clinics before comingto SAHIL. To gain a better understanding ofadolescents’ experiences at these sex clinics,SAHIL sought to investigate the servicesprovided by the Hakim Sahibs, including theirknowledge, att i tudes and pract ices, theinformation they provide, the terminology they use,and the medications they prescribe.
Methods
The study was carried out in Rawalpindi, the twincity of Islamabad. SAHIL is based in Islamabad,but most clients come from Rawalpindi. SAHILresearchers conducted an inventory of sex clinicsoperating in Rawalpindi. We visited 15 sex clinicswhere we interviewed 15 Hakims and five maleclients about their knowledge, attitudes andpractices. In addition, we conducted seven casestudies using a “mystery client” methodology.SAHIL researchers (five men and two women)sought services from Hakim Sahibs, based onthe most frequently heard concerns in ourcounsell ing programme. These concernsincluded: (1) hymen rupture; (2) masturbation;(3) nocturnal emission; (4) impotence; (5)premature ejaculation; and (6) homosexuality.Because no Hakim was willing to give ussamples of their medicines, we used the casestudies to obtain samples and conductedlaboratory tests to determine the contents.
Key findings
SAHIL found that Rawalpindi, a city of over 10 lakhs(one million people), had over 250 herbal clinics,of which over 50 were specifically sex clinicsadvertising services for sexual health problems,and over 200 others offered sexual health servicesamong a range of other services. The majority ofHakims interviewed claimed to have passed theirmatriculation equivalent to Class 10. Most saidthat they were in the business because their fathersand forefathers had done the same thing. The studyfound that the Hakims ’ knowledge aboutreproductive health, HIV, hepatitis C and othersexually transmitted infections (STIs) wasinsufficient and myth-ridden. For example, theygenerally believed that all reproductive and sexualhealth problems could be fixed by medicines, thatsemen is a major source of energy, that the directionof the penis plays a major role in sexual healthissues, and that masturbation can cause infertility,impotence and premature ejaculation. The majorityreported that the hymen could be reconstructedby taking oral medicines, that the absence of ahymen means “sexual corruption”, and thathomosexuality could cause a decrease in spermcount, leading to permanent infertility.
During the case studies, four out of seven Hakimstouched or spoke to our male and femaleresearchers in ways that were sexually suggestiveor harassing. For example, during check-ups offemale clients they said things such as: “you areso young”, “your wrists are very beautiful”, “you are apretty girl”, etc. Physical check-ups involvedattempts to massage the penis or in another caseto caress a woman’s wrist while pretending tocheck her pulse. (The latter case was for hymenreconstruction, so it was not clear why the Hakimwanted to take a pulse.) On the other hand, wefound that Hakims were uncomfortable with thelanguage of sexuality. Just like the general public,they used words that were indirect and obscure. Forexample, they asked women and men if pain wasfelt in the “lower area”, meaning the vagina or penis.

150
SHAHID MAQSOOD RANJHA AND ANUSHEH HUSSAIN
The instruments used during the check-upsseemed to be plastic toys and were mostly self-made. Some Hakims took urine samples, eventhough they had no laboratory equipment. Toanalyse the urine, they looked at it and prescribeda combination of medicines based on this visualassessment. All Hakims demanded their fee beforethe check-up, and they generally charged Rs 200,not including the cost of medicines.
When asked about the ingredients of themedication they dispensed, all Hakims claimedthat they used bear testicles, lioness fat, monkeybrains, sparrows’ kidneys, exotic herbs, beasts’organs, gold and silver. After conducting laboratorytest of these medicines, we found that they includedappetite stimulants such as Carmina, as well asspices, steroids and narcotics, such as opium andsynthetic morphine. Additional laboratory testsfound testosterone and progesterone (male andfemale hormones) in five out of seven samples.The cost of medicines varied between Rs 500 andRs 60 000, but the majority of Hakims demandedover Rs 12 000. Our researchers were told thatthe reason that the medicines were so expensivewas that they contained costly ingredients suchas “beasts’” organs, gold and silver.
The five adolescent clients interviewed had visitedHakims for reproductive health problems orperceived sexual problems, such as prematureejaculation, impotence and nocturnal emission.We found that the clients lacked the same kindsof knowledge as Hakims regarding sexual healthand sexual diseases. Our major finding, however,was that every adolescent client said that afterusing medicines they felt better than before visitingthe Hakim. We can only speculate about why theyfelt improvement, but perhaps the narcotics usedin these medicines reduce anxiety, fear or stress,thereby enhancing sexual activities. In addition,opiates and other narcotics block the senses andthereby help control premature ejaculation. Or, the
medicine may lead to perceived improvement byinducing a placebo effect that makes clients feelthat they have been treated.
Conclusions
In conclusion, the study found that both Hakimsand clients reported misconceptions and mythsabout sexual and reproductive health. Many of theHakims used sexually harassing language andtouch. Although clients reported feeling someimprovement after taking the costly medicinesdispensed by Hakims, such medicines containedingredients such as narcotics and hormones thatcould be dangerous for their health. These studyfindings illustrate how denying adolescents sexualhealth services and basic information aboutreproductive health has created even moremisinformation, trauma, and suffering for them.Quacks continue to thrive, while healthprofessionals turn their backs to the sexual healthneeds of adolescents. The choice between dogmaand adolescent safety and health is clear. Thisresearch demonstrates the need to change thebehaviour of service providers, as well as the needfor adolescents to adopt safe health behaviours.
References
Government of Pakistan (1998) National Survey ofPakistan [Unpublished Census data, available fromthe Government of Pakistan, Statistics Division].
Pakistan Integrated Household Survey (1995)Pakistan Institute of Development Economics.[Available at: www.pide.org.pk/serv04.html]
SAHIL#13, First FloorAl Babar Centre, F-8 MarkazIslamabadPakistan

IXCommunication betweenadolescents and adultsabout sexual andreproductive health

152
MINHAJ UL HAQUE AND AZEEMA FAIZUNNISA
153
Access to reproductive health information in Punjab and Sindh, Pakistan
Background
Pakistan has an adolescent population of nearly30 million, two-thirds (66%) of whom live in urbanareas and one-third (34%) in rural areas(Government of Pakistan, 1998). Pakistaniadolescents can be categorized into a number ofbroad groups—those who are employed, those inschool, those married, those in one or none of theabove groups (Durrant, 2001). Large genderdifferences exist within these groups. Fifty-two percent of adolescent boys are in school comparedwith only 31% of girls, for example, and 45% ofgirls are neither married, nor employed nor inschool, compared with only 13% of boys.
To obtain more information about the perspectivesof young unmarried adolescents, the PopulationCouncil carried out a qualitative study using focusgroup discussions (FGDs) with adolescents andparents. The FGDs covered education,employment, skill-building, autonomy, marriageand health. This paper presents findings related toreproductive health knowledge, practice anddeterminants, from the perspectives of bothadolescents and parents.
Methods
Researchers carried out the study in two stages.
In the first stage, they held 13 FGDs withadolescent girls and boys from Punjab. In thesecond stage, they conducted an additional 12FGDs with adolescent girls and boys and 12 FGDswith parents from Punjab and Sindh. Adolescentrespondents ranged in age from 10 to 19 years;separate FGDs were held for girls and boys.Respondents came from rural and periurban areas,including Sargodha, Rawalpindi, Bahawlapur,Sialkot and Chakwal districts in Punjab, andKhairpur, Hyderabad and Karachi districts in Sindh.The study included only unmarried adolescentsand their parents.
Key findings
Through FGDs, researchers explored the channelsand mechanisms that young people and theirparents use to seek and share reproductive healthinformation. Respondents discussed their preferredsources of information and the ways in whichparents and adolescents interact with each otherabout these issues.
Findings from FGDs with parents suggested thatparents, especially fathers, shied away fromdiscussing reproductive health issues with theirchildren. Most parents thought that adolescentswould learn about puberty and other reproductivehealth issues by themselves when the time came.
Access to reproductive health information inPunjab and Sindh, Pakistan: the perspectivesof adolescents and parents
Minhaj ul Haque and Azeema Faizunnisa

154
MINHAJ UL HAQUE AND AZEEMA FAIZUNNISA
Reflecting a cultural tendency to seek curative carefor an ailment after it strikes rather than takepreventive measures, parents described a generalapathy towards discussing reproductive healthissues with their children before there was a clearneed. Parents were aware of the media as aninfluential source of information and expressedconcerns about its negative impact on youngpeople. Parents considered schools and skilldevelopment centres as “safe” places foradolescents to learn about reproductive healthissues.
Researchers asked young people about theirinformation networks related to reproductive health.FGDs with girls and boys suggested that girls hadbetter personal networks of information among theirfamilies than boys. Girls’ sources of knowledgeincluded mothers, elder sisters and relatives. Incontrast, boys said that they tended to rely ontelevision, films, videos, books, hakims and friendsas primary sources of information aboutreproductive health, rather than family members.Boys described their reluctance to talk to parentsabout puberty, saying for example, “Boys are tooembarrassed to discuss these matters with theirfathers. We mostly talk about these things with aclose friend or older brother” (Boys’ FGD, ruralPunjab).
Nevertheless, both girls and boys felt that therewas a need for more information, especiallyregarding puberty. For example, girls said that theywere not given enough information aboutmenstruation. As one respondent described, “Noone tells us, it just happens, and then either anolder sister or the mother tells us to take propermeasures during the 4–5 days” (Girls’ FGD, ruralPunjab). Both girls and boys felt that teachersshould provide reproductive health information. Ingeneral, adolescents said that they wanted moreparental guidance to help prepare them foradulthood.
Girls generally felt that they faced more problemsduring adolescence than boys, because of limitson their freedom of movement, lack of say in major
life decisions, early marriage, lack of educationand lack of health care. In FGDs, parentsacknowledged that there are gender differences inhealth-seeking behaviour because of poor accessand social barriers. For example, fathers describedbarriers to taking their daughters to health carefacilities saying:
People ask embarrassing questions and drawunnecessary conclusions if a young girl fallssick. Therefore, we avoid taking her to the healthfacility, unless there is a dire need. (Fathers’FGD, rural Punjab).
Researchers asked adolescents about issuesrelated to marriage. As in much of South Asia,marriage occurs relatively early, and adolescentshave almost no say about whom and when to marry.FGD participants discussed this practice andidentified early marriage as a problem for manyadolescents, particularly rural girls. In FGDs, bothgirls and boys said that they would like more sayin choosing their life partner. Most girls and boysconsidered 20–25 to be the ideal age for marriage.
Conclusions
In conclusion, girls seem to have better personalinformation networks, but they also have lessaccess to health services and face greater socialconstraints. The results of this study suggest thatadolescents need more information aboutreproductive health, including physiologicalchanges during puberty, sex and reproduction.Both young people and parents consider parents,teachers and school textbooks as “safe” anddependable sources of reproductive healthinformation. Most parents say they prefer thatothers, such as relatives, teachers or elders,discuss reproductive health issues with theirchildren. Parents also suggest that schoolprogrammes should provide this information,pointing to a critical opportunity for reproductivehealth education programmes that want to reachadolescents.

155
Access to reproductive health information in Punjab and Sindh, Pakistan
These research findings raise a number ofimplications for research, policies andprogrammes. Given that data on adolescents arepaltry and often anecdotal, Pakistan needs morein-depth and representative data on the situationof adolescents in various strata of society.Programmes for youth need to evolve at thecommunity level involving local people and needto be integrated with life-skills development. Finally,because the influence of media is so strong, print,electronic and digital media need to address theseissues in a culturally sensitive way.
References
Durrant V (2001) Adolescent Girls and Boys inPakistan: Opportunities and Constraints in theTransition to Adulthood, Research Report No. 12.Islamabad, Population Council.
Government of Pakistan (1998) Population andHousing Census 1998: Advance Tabulation on Sex,Age Group, Marital Status, Literacy and EducationalAttainment (Bulletin 6). Islamabad, Government ofPakistan, Statistics Division.
Azeema FaizunnisaChief, Information ServicesPopulation Council7, Street 62Sector F 6/3, IslamabadPakistan
156
REKHA MASILAMANI
Background
Pathfinder and its partner organizations havelaunched adolescent reproductive healthprogrammes in several Indian states. One objectiveof these programmes is to influence parents,families and teachers of adolescents as a way toimprove the general environment in whichadolescents enter into sexual activity andmarriage. This presentation describes theseprogrammes and the barriers they must overcomein order to improve adolescent sexual andreproductive health.
Programme description
Community-based programmes are under way inthree slum areas of Delhi, one rural block in TamilNadu and nine villages in Rajasthan. Theseprogrammes involve community outreach andeducation, building of referral linkages to servicesand training of service providers. In Delhi, they alsocarry out school-based sexuality educationprogrammes that include efforts to sensitizeparents and teachers. These programmes focuson adolescent boys and girls, including youngmarried couples.
Their overall intent is to enable young people tochoose responsible and healthy behaviours as they
enter into sexual activity and marriage. Theyspecifically aim to help young people delay sexualdebut, to increase the age at marriage for girls, toencourage young couples to delay first births andto space subsequent births, and to increase theuse of spacing methods of contraception. Finally,they aim to prevent sexually transmitted infectionsand to lower rates of unsafe abortion.
To win over gatekeepers such as parents andteachers, programme staff emphasize the scope,importance and benefits of their efforts. To do this,the programmes have invested resources instrengthening the skills that field staff need in orderto communicate with and persuade these groups.In addition, the programmes try to empowerparents and adolescents to communicate with eachother, by increasing their knowledge,understanding, vocabulary and general comfortlevel related to sexual and reproductive health.
Barriers to improving sexual andreproductive health
Programme experiences suggest that severalbarriers impede efforts to help adolescentspostpone their sexual debut. Boys describenumerous factors that push them into early sexualactivity, including simple curiosity or adventurism,what they call “uncontrollable urges”, peer pressure,
Building a supportive environment foradolescent reproductive health programmesin India: essential programme components
Rekha Masilamani

157
Building a supportive environment for adolescent reproductive health programmes in India
parental attitudes disapproving interaction betweenyoung females and males and favouring earlymarriage for sons and especially daughters, whatboys believe to be tacit “permission” from society,and the common belief that masturbation isharmful. In contrast, girls cite coercion and abuseas the main barriers to delaying sexual debut.
Efforts to increase the age at marriage for girlsmust overcome parents’ fears about the sexualsecurity of their daughters. That is to say, parentsfear that until daughters are safely married, theyremain at risk of rape, coercion, or elopement—any of which could spell ruin for both the girl andher family.
Programme experiences suggest that efforts toencourage young couples to delay the first birthand space subsequent births using spacingcontraception must overcome a number of barriers.First, young couples often feel pressure to have achild soon after marriage in order to prove that theyare fertile. In addition, many young people lackadequate knowledge about spacing methods ofcontraception. Many have concerns aboutcontraceptive safety, diminished pleasure ordiminished sexual performance that outweigh thedesire to delay pregnancy. Many feel uncomfortablespeaking about such issues, lack the vocabularyto discuss them, or feel too shy to initiate suchdiscussions. Many girls believe that boys shouldinitiate discussions about contraception, whilemany boys believe that responsibility forcontraception belongs to girls. Other issues thatprevent young people from delaying or spacingpregnancies include the desire to please familiesand in-laws, as well as age differences betweenhusbands and wives that make it difficult for themto discuss sensitive issues.
Programme experience shows that several barriershamper efforts to prevent sexually transmittedinfections among young people. First, young menoften use condoms incorrectly or inconsistently.Second, many object to condoms because theysay that they interfere with pleasure or sexual
performance. Finally, the common belief thatmasturbation is harmful may make some boys andyoung men more likely to have sex with girls orwomen under circumstances that put them at riskfor infection.
Adolescents often feel guilt and shame aboutsexual matters and say that discussing thesetopics with parents is taboo. At the same time,many adolescents believe that their families knowwhat is best for sons and daughters, and theytherefore entrust their families with responsibilityfor important life decisions. They generally expressa strong desire to please and consult their parents.
Parents and family members say that boys andgirls prefer to talk to peers rather than parents.They describe feeling acutely embarrassed at thethought of discussing sexual matters with theirchildren. They also lack the vocabulary and thebasic information about sexuality that would helpthem talk about these matters with their adolescentchildren. Furthermore, they express concern thatdiscussing such matters might appear to give tacit“permission” to engage in sex. They associateknowledge of sexual matters with promiscuity anda loss of parental control. They are generallyconcerned for the sexual security of theirdaughters, but indifferent about their sons’behaviour.
Conclusions
These barriers have important implications foradolescent reproductive health programmes. Asgatekeepers, parents, families and teachers havea strong influence on adolescents’ behaviour.Together they comprise the social environment inwhich adolescents make decisions and in whichreproductive health programmes must work.Adolescents are not independent adults, but areheavily dependent upon family guidance andapproval. For all these reasons, programmes mustaddress the parents, families and teachers whoinfluence adolescents.
158
REKHA MASILAMANI
Rekha MasilamaniCountry RepresentativePathfinder International102 Adishwar Apartments34 Feroze Shah RoadNew DelhiIndia

159
Experience of family violence: reflections from adolescents in Uttar Pradesh, India
Background
It is increasingly being recognized that violencehas adverse effects on the physical and mentalhealth of adolescents. In addition, exposure toviolence can have implications for their subsequentbehaviour (Jejeebhoy, 1998; Centre for OperationsResearch and Training, 2000). Violence againstadolescents is an area that has not beenadequately addressed in the existing literature,policies or programmes. To address this gap inknowledge, researchers at the Centre forOperations Research and Training (CORT) inBaroda, India, carried out a study that aimed tounderstand forms of violence and perpetrators asperceived by adolescents, the actual reportedexperiences of violence against adolescents andtheir mothers, the determinants of violence, theconsequences and the coping mechanisms thatadolescents adopt.
Methods
These data were collected as part of a study carriedout in slum areas of Allahabad, Uttar Pradesh,using both qualitative and quantitative researchmethods. Researchers interviewed 382adolescents aged 10–18 years (178 boys and 204girls) using semi-structured questionnaires. Duringthese interviews, the adolescents were asked about
quarrels among their parents and about violencethat they may have experienced directly. Fourteenrespondents (seven boys and seven girls) had lostone parent and hence could not reflect on theirparents’ behaviour. Researchers also conductedin-depth interviews and a free-listing exerciseamong a subsample of 42 randomly selectedrespondents (32 boys and 10 girls).
Key findings
During the free-listing exercise, researchers askedadolescents to list different forms of violence. Maleadolescents mentioned: “verbal abuse” (16),beating (7), asking someone to leave the house (3),domestic violence, slapping, throwing out the foodplate, tearing clothes and physical fighting. Whenresearchers asked 10 girls to do the same, theyreported examples such as arguments andbeatings. Girls reported more examples of verbalabuse rather than physical violence whencompared with the boys. For example, girlsreported scolding, arguments and withholding offood, while boys were more likely to report beingslapped or beaten, having objects thrown at themand other forms of physical abuse. Adolescentsdid not mention sexual harassment during the free-listing exercise, but the topic did come up duringin-depth interviews.
Experience of family violence: reflectionsfrom adolescents in Uttar Pradesh, India
Bella Patel Uttekar, M.E. Khan, Nayan Kumar, Sandhya Bargeand Hemlata Sadhwani
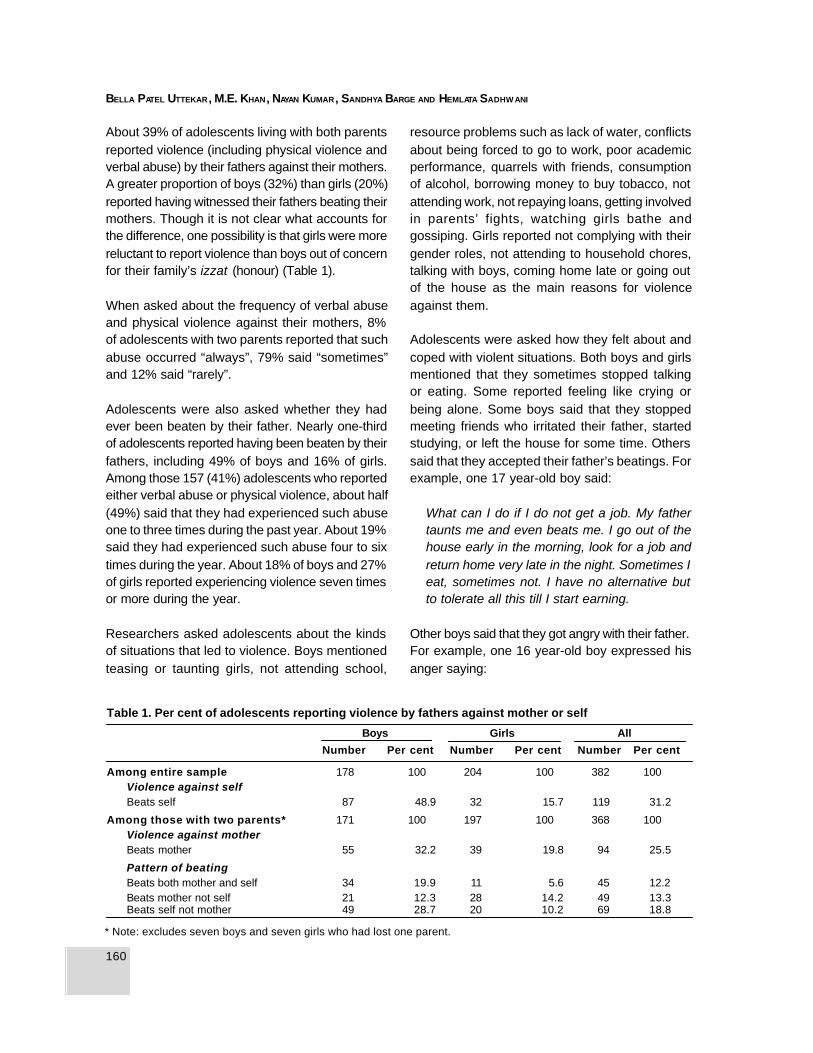
160
BELLA PATEL UTTEKAR, M.E. KHAN, NAYAN KUMAR , SANDHYA BARGE AND HEMLATA SADHW ANI
About 39% of adolescents living with both parentsreported violence (including physical violence andverbal abuse) by their fathers against their mothers.A greater proportion of boys (32%) than girls (20%)reported having witnessed their fathers beating theirmothers. Though it is not clear what accounts forthe difference, one possibility is that girls were morereluctant to report violence than boys out of concernfor their family’s izzat (honour) (Table 1).
When asked about the frequency of verbal abuseand physical violence against their mothers, 8%of adolescents with two parents reported that suchabuse occurred “always”, 79% said “sometimes”and 12% said “rarely”.
Adolescents were also asked whether they hadever been beaten by their father. Nearly one-thirdof adolescents reported having been beaten by theirfathers, including 49% of boys and 16% of girls.Among those 157 (41%) adolescents who reportedeither verbal abuse or physical violence, about half(49%) said that they had experienced such abuseone to three times during the past year. About 19%said they had experienced such abuse four to sixtimes during the year. About 18% of boys and 27%of girls reported experiencing violence seven timesor more during the year.
Researchers asked adolescents about the kindsof situations that led to violence. Boys mentionedteasing or taunting girls, not attending school,
* Note: excludes seven boys and seven girls who had lost one parent.
resource problems such as lack of water, conflictsabout being forced to go to work, poor academicperformance, quarrels with friends, consumptionof alcohol, borrowing money to buy tobacco, notattending work, not repaying loans, getting involvedin parents’ fights, watching girls bathe andgossiping. Girls reported not complying with theirgender roles, not attending to household chores,talking with boys, coming home late or going outof the house as the main reasons for violenceagainst them.
Adolescents were asked how they felt about andcoped with violent situations. Both boys and girlsmentioned that they sometimes stopped talkingor eating. Some reported feeling like crying orbeing alone. Some boys said that they stoppedmeeting friends who irritated their father, startedstudying, or left the house for some time. Otherssaid that they accepted their father’s beatings. Forexample, one 17 year-old boy said:
What can I do if I do not get a job. My fathertaunts me and even beats me. I go out of thehouse early in the morning, look for a job andreturn home very late in the night. Sometimes Ieat, sometimes not. I have no alternative butto tolerate all this till I start earning.
Other boys said that they got angry with their father.For example, one 16 year-old boy expressed hisanger saying:
Table 1. Per cent of adolescents reporting violence by fathers against mother or self
Boys Girls All
Number Per cent Number Per cent Number Per cent
Among entire sample 178 100 204 100 382 100Violence against selfBeats self 87 48.9 32 15.7 119 31.2
Among those with two parents* 171 100 197 100 368 100Violence against motherBeats mother 55 32.2 39 19.8 94 25.5
Pattern of beatingBeats both mother and self 34 19.9 11 5.6 45 12.2Beats mother not self 21 12.3 28 14.2 49 13.3Beats self not mother 49 28.7 20 10.2 69 18.8

161
Experience of family violence: reflections from adolescents in Uttar Pradesh, India
My father beats me, my sister and my mother.He comes home after drinking and abuses usfor no reason. I feel he should die so that wecan have some peace in our lives.
Conclusions
This study provides a glimpse into the violencewitnessed and experienced by adolescents in theslum areas of Uttar Pradesh. There is a need for adeeper understanding of the dynamics andconsequences of violence, including sexualviolence, which may have both short-term and long-term implications for both victims and perpetrators.In addition, an in-depth understanding of the factorsthat lead to violent behaviour could help point tostrategies to curb such violence. To achieve this,more in-depth research is needed in varioussettings.
References
Centre for Operations Research and Training (CORT)(2000) Baseline Survey for Action for Slum Dwellers’Reproductive Health Project. (Monograph). Baroda,CORT.
Jejeebhoy S (1998) Association between wife-beatingand fetal and infant death: Impressions from a surveyin rural India. Studies in Family Planning, 29(3):300–308.
Bella Patel UtterkarCORT402 Woodland AptRace CourseBaroda 390 007India


XFamily life and sexeducation

164
VANDANA CHAKRABARTI

165
Population education in formal and non-formal sectors in India
Background
Since 1980, the United Nations Population Fund(UNFPA) has supported the National PopulationEducation Project (NPEP) in India, which has beenimplemented in three sectors: school education,higher education and adult education. Theprogramme began with a focus on demographicissues but shifted its concern following the 1994Cairo International Conference on Population andDevelopment. The project now concentrates ongender equity, women’s empowerment,reproductive health and rights, adolescent sexualbehaviour, health education, family life education,drug addiction, HIV/AIDS and sustainabledevelopment. This paper describes the project andmakes a number of recommendations for thefuture, which may be relevant not only to thisproject, but to other adolescent programmes aswell.
Programme description
In 1980, the project began working in schools, andnow reaches 154 million students all over thecountry in grades I to XII, as well as 4.2 millionteachers. It is believed that an effective populationeducation programme in the formal school systemwill produce a generation of adults capable of
making informed and responsible decisionsregarding population and development issues. TheNPEP was implemented in the higher educationsector in 1986 and now reaches 6.7 millionstudents enrolled in more than 225 universities and400 colleges. This part of the project is designedfor unmarried students of reproductive age. In 1986the NPEP was also implemented in the non-formaladult education sector. It aims to reach 150 millionstudents aged 9–35, of whom about 62% arewomen or girls. The project is implemented in theadult education sector with technical support from18 State Resource Centres for Adult Literacy andthe National Population Education ResourceCentre.
In all three sectors, the project aims to increaseawareness, build positive attitudes and changebehaviour, through strategies such as integratingpopulation education into the school curriculum,carrying out non-curricular activities, developingmaterials, conducting advocacy, training andorientation, extension activities, research andevaluation. Because of its scale, the programmehas enormous potential for impact; however thescale may also impose certain limits on quality.Everyone from the top manager to the grass-rootsvolunteer must be inspired in order for the projectto achieve its potential.
Population education in formal andnon-formal sectors in India
Vandana Chakrabarti
166
VANDANA CHAKRABARTI
Recommendations for improvingprogrammes for adolescents
An evaluation of NPEP was conducted at the endof each phase by external agencies. Theirrecommendations have helped redefine prioritiesand revise strategies to attain the expectedoutcomes. On the basis of discussions with theimplementers of NPEP in different sectors and withexperts who conducted the mid-term review of thecurrent phase, this paper offers the followingsuggestions for making the project more useful inthe future.
1. Unlike in most other countries, adolescentfertility in India occurs largely within marriage.About half of all young women are sexuallyactive before they reach age 18. Presently, ageat marriage is discussed only in the primersused by adult learners. Efforts are needed inthe school and higher education sectors toeducate people about the need to marry later.
2. Although millions of teachers have been trainedon population issues, it is unclear how muchreproductive health information has actuallybeen imparted to students. Adolescent boysand girls need more education on topics suchas anatomy and physiology, changes inpuberty, menstruation, conception, infections,sexuality, contraception and sexuallytransmitted infections.
3. The project needs to include activities focusedon increasing the self-esteem and confidenceof young women and girls, given that they oftenfeel powerless, particularly when they aremarried early and sent to live with in-laws. Oftenthey have no say in reproductive matters.
4. The project should also work to develop lifeskills among adolescents, such as thinkingskills (problem-solving, examining choices,decision- making and goal-setting), socialskills (building positive relationships, listeningand communicating effectively, takingresponsibility and coping with stress) and
negotiating skills, which require both thinkingand social skills. These skills are important inall areas of life, but especially in the area ofsexuality and reproductive health.
In terms of recommended strategies, schoolteachers, college teachers and literacy workerswho implement the project need to be involved fromthe planning stage to ensure that they feel ownershipover the programme. The project could strengthenor expand a number of areas, including counsellingservices in formal education sectors, telephonecounselling services, peer education and healthcamps. The project should help parents and in-laws to understand adolescents better and to workmore closely with teachers and literacy workersin order to educate adolescents about reproductivehealth issues. In addition, adolescent programmesmust be supported by research. Only whenrelevant research is communicated to policy-makers, administrators and project functionarieswill more meaningful programmes for adolescentsand young adults be developed. Finally, it isimportant to mention that a project of thismagnitude needs to engage in frequent dialoguewith stakeholders and to build in monitoring andevaluation systems.
Further reading
Government of India (1997) Populat ion andDevelopment Education in Schools, ProjectAgreement between the Government of India andthe UNFPA. New Delhi, Ministry of Human ResourceDevelopment, Government of India.
Government of India (1998) Populat ion andDevelopment Education in Higher Education System,Project Agreement between the Government of Indiaand the UNFPA . New Delhi, University GrantsCommission, Ministry of Human ResourceDevelopment, Government of India.
Mohankumar V (1999) Population education in theadult education sector. Indian Journal of PopulationEducation. April–September (9):338.
Shirur RR (1999) Reproductive and sexual healtheducation for adolescents—a survey report. Indian
167
Population education in formal and non-formal sectors in India
Journal of Population Education. New Delhi, October–March (8):48–55.
United Nations Population Fund (1999) Populationand Development Education—Inter-sectoralResearch Consultation Report. New Delhi, UNFPA.
Dr Vandana ChakrabartiDirectorPopulation Education Resource CentreSNDT Women’s UniversityNew Marine LinesMumbai 400 020India
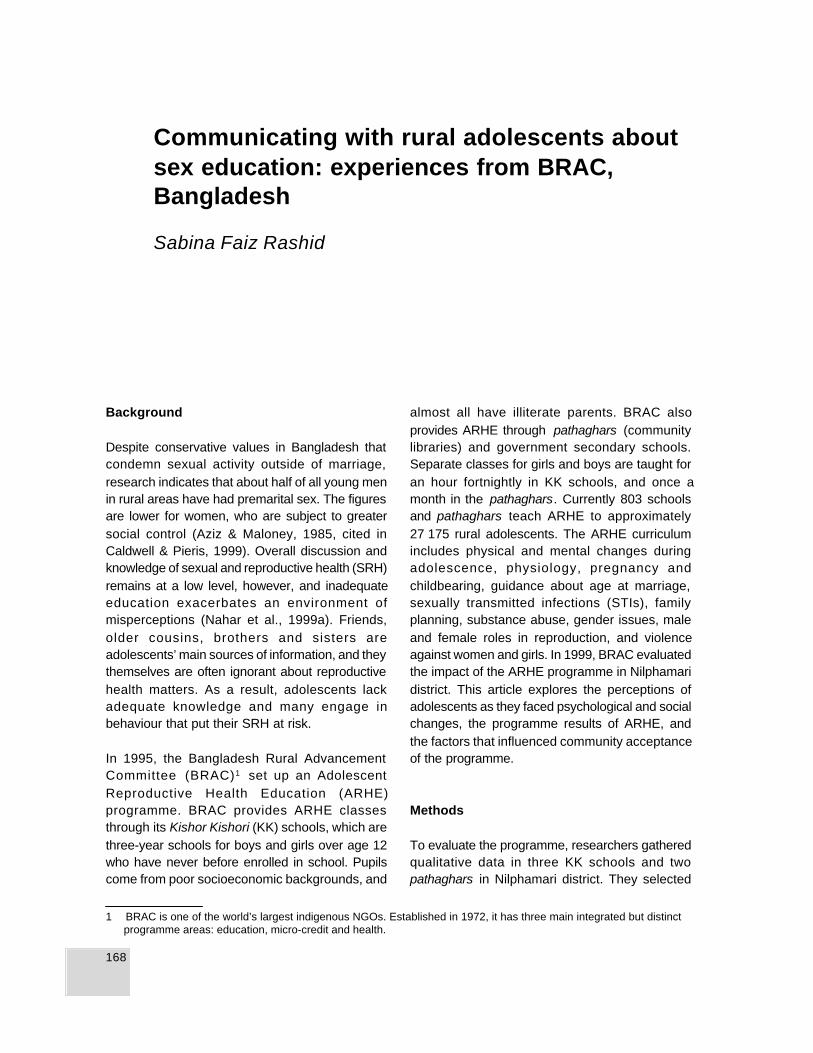
168
SABINA FAIZ RASHID
Background
Despite conservative values in Bangladesh thatcondemn sexual activity outside of marriage,research indicates that about half of all young menin rural areas have had premarital sex. The figuresare lower for women, who are subject to greatersocial control (Aziz & Maloney, 1985, cited inCaldwell & Pieris, 1999). Overall discussion andknowledge of sexual and reproductive health (SRH)remains at a low level, however, and inadequateeducation exacerbates an environment ofmisperceptions (Nahar et al., 1999a). Friends,older cousins, brothers and sisters areadolescents’ main sources of information, and theythemselves are often ignorant about reproductivehealth matters. As a result, adolescents lackadequate knowledge and many engage inbehaviour that put their SRH at risk.
In 1995, the Bangladesh Rural AdvancementCommittee (BRAC)1 set up an AdolescentReproductive Health Education (ARHE)programme. BRAC provides ARHE classesthrough its Kishor Kishori (KK) schools, which arethree-year schools for boys and girls over age 12who have never before enrolled in school. Pupilscome from poor socioeconomic backgrounds, and
almost all have illiterate parents. BRAC alsoprovides ARHE through pathaghars (communitylibraries) and government secondary schools.Separate classes for girls and boys are taught foran hour fortnightly in KK schools, and once amonth in the pathaghars. Currently 803 schoolsand pathaghars teach ARHE to approximately27 175 rural adolescents. The ARHE curriculumincludes physical and mental changes duringadolescence, physiology, pregnancy andchildbearing, guidance about age at marriage,sexually transmitted infections (STIs), familyplanning, substance abuse, gender issues, maleand female roles in reproduction, and violenceagainst women and girls. In 1999, BRAC evaluatedthe impact of the ARHE programme in Nilphamaridistrict. This article explores the perceptions ofadolescents as they faced psychological and socialchanges, the programme results of ARHE, andthe factors that influenced community acceptanceof the programme.
Methods
To evaluate the programme, researchers gatheredqualitative data in three KK schools and twopathaghars in Nilphamari district. They selected
1 BRAC is one of the world’s largest indigenous NGOs. Established in 1972, it has three main integrated but distinctprogramme areas: education, micro-credit and health.
Communicating with rural adolescents aboutsex education: experiences from BRAC,Bangladesh
Sabina Faiz Rashid

169
Communicating with rural adolescents about sex education: Bangladesh
this site because it had one of the longest-runningARHE programmes, having begun in 1995, andbecause it was one of the first to implement bothphase 1 and phase 2 of the ARHE programme.2
Respondents included young unmarried studentsaged 13–15, parents, guardians and teachers.
Researchers held eight focus group discussions(FGDs) with students—five FGDs with a total of46 girls, and three FGDs with a total of 18 boys.The two extra FGDs for girls were needed aspathaghars have only female students in theirARHE classes. Researchers then conducted semi-structured, open-ended interviews with 10 femalestudents and 8 male students. The interview guideallowed various topics to emerge and be pursued.Male researchers interviewed the boys, and femaleresearchers interviewed the girls. Interviewers wereyoung since it was felt that girls and boys wouldbe more likely to open up to someone closer totheir age than they would to older interviewers. Theycarried out the interviews privately and individuallyto allow respondents to speak freely on sensitivetopics.
Researchers interviewed 18 parents and guardians,including mothers and in some cases aunts. Theyalso held four FGDs with a total of 21 mothers andguardians, who had not previously been interviewed.Researchers held informal discussions with seventeachers and 16 programme staff. In addition, oneresearcher attended ARHE classes in order toobserve the teaching style and the level ofinteraction between teachers and students.
Key findings
Adolescent girls felt that menstruation was themost significant topic covered in the ARHEclasses. In Bangladesh, menstruation isassociated with sexuality, fertility and “pollution”.It is considered a shameful subject that girls rarelydiscuss, even with their mothers. A recent study
found that the majority of girls did not know aboutmenstruation before it began (Nahar et al., 1999b).Interviews confirmed that the onset of menstruationcould be traumatic for girls. One girl said, “I hadmy menses when I was 12 years old… I was reallyvery scared. I thought I was dying.”
Family planning was another popular topic withboth girls and boys. Family planning is a sensitivesubject that is rarely discussed between olderwomen and unmarried girls in the traditional ruralculture (Mita & Simmons, 1995). Boys said theyparticularly wanted information related to sex,including sexually transmitted infections (STIs)/AIDS and family planning.
Interviews suggested that those who attendedARHE classes became an important source ofbasic health knowledge for peers and familymembers. Girls shared their new knowledge withother girls in the village, after school and in thecommunity library. One girl explained:
We usually sit and talk together with the othergirls in the village. That is when they ask meabout what I am learning in class. One girlcame…and I told her what I know—use a cleancloth, wash it, and don’t worry, it is natural—it isnothing to be scared of.
Some girls also shared newly acquired knowledgeon hygiene during menstruation with their mothers.One mother remarked, “I am learning from her now. ”Other mothers knew about their daughters’ newknowledge without discussing it openly. Onemother explained, “I buy her soap as she said sheneeds to wash her things with it…but I don’t sayanything to her…what is there to say? As long asshe is learning all this, it is less worry for me.”Girls tended to share family planning informationwith sisters-in-law and close friends. They said theyhad discussed STIs among themselves, but hadnot generally talked about the issue with adults.
2 In the first phase the curricula emphasized primary health care education; this changed to an emphasis on reproductivehealth matters in phase 2.

170
SABINA FAIZ RASHID
Adolescent boys also reported sharing what theyhad learned in ARHE classes with friends and malecousins. One boy described the eagerness of otherboys who approached him for answers saying:
When my friends found out I was learning all ofthis in the school they came and asked me alot of questions like, “how does a girl getpregnant?” and “why does menses [period]happen?” … I answered some of the questions,not all, as I don’t know many of the answers.
In general, the ARHE programme seems to havegenerated a new consciousness about reproductivehealth matters and broken the shame and silencesurrounding girls’ and boys’ bodies. Nevertheless,the evaluation found that many adolescents whoparticipated in ARHE still lacked knowledge ofSTIs, including HIV/AIDS. During FGDs it appearedthat some adolescents saw AIDS as a potentialthreat to the community, but not to themselves.Almost all were aware of the link betweenunprotected sexual intercourse and STIs/AIDS, andalmost all knew that condoms were an effectivemeans of prevention. However, a majority of girlsand boys appeared confused about transmissionroutes and symptoms of HIV/AIDS and other STIs.Both adolescents and teachers said that if a personwere infected with HIV, she/he would show signsof illness. Adolescents reported that teacherspreferred to focus on topics such as menstruation,early marriage and family planning, while skimmingover STIs/HIV/AIDS. In part, this may reflect theshame that persists around reproductive healthmatters. More importantly, teachers acknowledgedthat their own knowledge was weak, and theyblamed lack of detailed information in thecurriculum.
One important topic addressed during ARHE isearly marriage. Although some adolescents saidthey wanted to choose their own marriage partners,many admitted that parents were the main decision-makers. In Nilphamari district, many girls aremarried at age 11–13 or younger. In one school,six out of 14 girls in the ARHE programme werealready married, with two expecting their first child.
According to the mothers, the main reason for earlymarriage is fear that their daughters would be raped,fall pregnant or elope. Knowledge that a girl hashad premarital sex affects the social status of herentire family. Thus, families continue to practiseearly marriage, despite awareness of its detrimentaleffects on the health of girls and their babies.
Many girls who participated in ARHE used theirnew knowledge to argue against early marriage.One girl implored her mother, “See—they are BRACpeople and they say early marriage is bad.” Someattitudes may be changing as parents realize theadvantages of more schooling and the dangers ofearly pregnancy, but some mothers confided thatthey faced derogatory comments from communityelders who said, “your girl has become big now,you should get her married… You are poor. Whatwill she do with all this education?”
In this context, ARHE classes provide anopportunity for girls and boys to share feelings about‘love’ and ‘romance’ that would have beenconsidered unthinkable for previous generations.A common remark by girls was, “Prem [love] isimpure and we should marry who our parents havechosen for us. Doing prem is bad!” Nonetheless,a number of adolescents said they had “fallen inlove” secretly, in the hope of finding a partner tomarry. However, these statements were alwaysaccompanied by remarks such as, “There isnothing wrong with the prem as long as it is notbad prem [involving sex].” Good love was definedas leading to marriage, while “impure” love wasdefined as involving sex before marriage or arelationship that does not lead to marriage (even ifit is “pure”). Though social norms are more relaxedfor boys, they were still reluctant to share personalstories of romance with researchers.
Some adolescents said that boys initiaterelationships with girls through letters, and manydescribed encounters influenced by films andtelevision. As Pelto (1999) argues, sinceadolescents have few opportunities to practiseheterosexual conversations, popular films provideinspiration. A few boys and girls went beyond letters

171
Communicating with rural adolescents about sex education: Bangladesh
and shared a kiss; one couple went into town tohave a photograph taken of themselves; andanother went to the cinema together. Most couplesresorted to meeting secretly in the evenings, whenit was dark and their families were asleep.
Only a few girls and boys mentioned cases of premwith happy endings. Girls are particularly vulnerableto coercive and unsafe sexual intimacy. Many girls’narratives centred on betrayal and punishment fromvillage elders, jail and unmarried girls gettingpregnant. Some centred on revenge, in which thegirl was gang-raped, or had acid thrown on herface. Parents’ stories mirrored those ofadolescents and were tinged with anxiety. As oneparent said, “What to do if they run off and do badwork? How will we show our face in the village?We worry about our girls!”
Adolescent girls spoke to researchers about theirsexual desires, displaying unusual openness in asociety that views women as good and pure if theyare sexually passive and considers overtexpressions of sexuality as shameful. One girlsaid, “Both men and women have equal rights inthe sexual relationship. If one wants to mix [havesex] then she can have pleasure from it, but if it isforced then one cannot enjoy it.” Much of thelanguage used by adolescents implied that youngpeople are not fully responsible for their actionsbecause they are driven by “too much desire/needs”. Both girls and boys described“uncontrollable urges” that lead to extramaritalactivities, saying for example, “Boys and girls getinvolved in sexual relations to meet their sexualneeds.”
A number of boys admitted to masturbatingregularly and saw it as something for “jonnomithano” (satisfying one’s needs), in contrast toanother study that found that boys consideredmasturbation a sin (Hashima-e-Nasreen et al.,1998). Some boys mentioned watchingpornographic films with friends, saying, “We feelgood, and we sit and masturbate to satisfy ourdesires.” Boys said that they would often rent avideo player and watch the movies in the privacy
of a cousin’s or a friend’s room, or in villagerecreation centres. Interviews with boys suggestedthat this is quite a common practice. Somemothers complained about this practice in FGDs,but said they could not control their sons’ behaviour.In one FGD , a mother mentioned that shesuspected that her son watched blue films withfriends, saying, “Sometimes I get angry and thenthey listen, but most of the time they do what theywant.” It appears from the FGDs that these womenknew what their sons were up to but largely choseto ignore it. When asked whether her daughterwatched blue films, the women looked horrified andthe mother stated, “They would never do suchthings.”
Boys appear aware that they have more sexualfreedom than girls. While some felt that theirbehaviour was justified as they had “more desires”,many boys and girls said that girls share similarfeelings, but due to social pressures “...even if sheis bursting to say or do something, she will not doit.”
Researchers explored parents’, teachers’ andcommunity members’ acceptance of the ARHEprogramme. With increasing exposure to outsideinfluences, many mothers worried that they wereunable to control their adolescent boys and girls,and they felt that life skills and ‘health education’were important for their children. However, somemothers were unaware of the details of the ARHEcurriculum. A majority thought that their childrenwere being taught proiyojon (necessary) life skillsto prepare them for the future, but did not knowwhat these supposed life skills were. Boys tendedto be too embarrassed to discuss sensitivesubjects with their mothers, and a majority of girlsdiscussed only the “safer” topics with their mothers.One adolescent explained, “My parents don’t reallyknow in detail what we are being taught. We remaincareful about what we say to them.” Power relationsalso play a role. Most families of ARHEparticipants depend on BRAC to educate theirchildren. One boy explained why his mother didnot protest saying, “She is scared—what if theyask me to leave the school?… She doesn’t want

172
SABINA FAIZ RASHID
to anger the programme staff.” Furthermore, someteachers come from rich families, with links to villageauthority figures. Many poor people feeluncomfortable questioning the authority ofteachers, who are educated and have a highersocial status.
While female teachers said they have graduallybecome comfortable teaching ARHE to girls(saying it feels like a duty of an older sister), someare still uncomfortable about teaching boys. As aresult, some teachers have held classes lessfrequently than BRAC guidelines require. Whenresearchers raised this issue with two teachers,they admitted to having reservations about teachingsensitive subjects to boys. One commented, “Icannot teach the boys all these things. I feelashamed. And what will the community say if theyfind out?”
Conclusions
In a strongly conservative environment, the ARHEprogramme provides adolescents with basicinformation on sexuality and reproductive health—a major achievement. Community acceptanceof the ARHE classes may reflect the growingurbanization of rural areas, the influence ofelectronic media, and increasing exposure tonongovernmental organizations such as BRAC. Inaddition, community involvement in the schools,power relations, uneven awareness of coursecontent and the fact that ARHE teachers comefrom the community may also have helped buildacceptance of ARHE by rural communities.
Overall, this research highlights the importance andfeasibility of ARHE in rural areas. The programmenot only provides information to participating girlsand boys, but also indirectly to other adolescentsand adults in the villages. ARHE has broken thesilence on sensitive topics. Future research needsto focus on what happens to programmeparticipants when they marry. Will husband andwife decide on contraceptive methods together?
To what extent will knowledge of reproductivehealth have a positive effect on their lives?
This summary has been excerpted from an articlethat first appeared under the title “Providing sexeducation to rural adolescents in Bangladesh:Experiences from BRAC”, published in Gender andDevelopment, 2000 (July) 8(2).
Acknowledgements: I would like to thank mycolleagues for their assistance during projectdesign and data collection. I am grateful to myresearch colleague Nusrat Chowdhury and myhusband Safi Rahman Khan for their usefulcomments and critical feedback. I would also liketo thank my field researcher assistants, BRAC fieldoffice staff and the participants in the research fortheir time and patience.
References
Caldwell BK, Pieris I (1999) Continued high-riskbehaviour among Bangladeshi males. In: CaldwellJC, Caldwell P, Anarfi J, Awusabo-Asare K, Ntozi J,March J et al., eds. Resistances to BehaviouralChange to Reduce HIV/AIDS in PredominantlyHeterosexual Epidemics in Third World Countries.Canberra, Health Transition Centre.
Hashima-e-Nasreen, Chowdhury M, Bhuiya A,Chowdhury S, Ahmed SM (1998) IntegratingReproductive and Sexual Health into a GrassrootDevelopment Programme. Dhaka, Bangladesh RuralAdvancement Committee—International Centre forDiarrhoeal Diseases Research, Bangladesh.
Mita R, Simmons R (1995) Diffusion of the culture ofcontraception: programme effects on young womenin rural Bangladesh. Studies in Family Planning,26(1):1–13.
Nahar Q, Amin S, Sultan R, Nazrul H, Islam M, KaneTT et al. (1999a) Strategies to Meet the Health Needsof Adolescents: A Review. Operations ResearchProject, Health and Population Extension Division,Special Publications No. 91. Dhaka, InternationalCentre for Diarrhoeal Diseases Research,Bangladesh.

173
Communicating with rural adolescents about sex education: Bangladesh
Nahar Q, Huq NL, Reza, M, Ahmed, F (1999b)Perceptions of Adolescents on Physical ChangesDuring Puberty, ICDDR,B Working Paper. Dhaka,International Centre for Diarrhoeal DiseasesResearch, Bangladesh and Concerned Women forFamily Development.
Pelto PJ (1999) Sexuality and sexual behaviour: thecurrent discourse. In: Pachauri S, Subramanian S,eds. Implementing a Reproductive Health Agendain India: The Beginning. New Delhi, PopulationCouncil.
Sabina Faiz RashidResearch and Evaluation DivisionBRAC (Bangladesh Rural AdvancementCommittee)
Mailing address:A23 Century EstateBara MaghbazaarDhaka 1217Bangladesh

174
SUDHA TEW ARI AND SUMITA TANEJA
Background
Parivar Seva Sanstha (PSS), a nongovernmentalorganization (NGO), is an affiliate of Marie StopesInternational and has provided reproductive healthcare in India since 1978. The mission of PSS is toenable couples to have “Children by Choice notChance”, through clinic-based services, socialmarketing of reproductive health products and otheroutreach programmes. In the course of its work atthe clinics in the mid-1980s, PSS observed thatyoung adults were seeking abortion services andlacked accurate information on important aspectsof life such as health, nutrition, hygiene,reproduction, motherhood, maturation and familyplanning.
To address young people’s needs, PSS hasdesigned a series of reproductive health education(RHE) programmes for boys and girls between theages of 10 and 24, adopting a definition of youththat extends from puberty to early adulthood. PSSoffers multifaceted programmes for youth thatprovide sexual and reproductive health (SRH)information and services. Recognizing theimportant role played by peers and other serviceproviders, such as auxiliary nurse midwives andanganwari workers at the village level, PSS trainspeer educators and providers to address youngpeople’s needs in acceptable and affordable ways.Because subgroups—such as out-of-school youth,
young people about to be married and those whoare physically or mentally challenged—havedifferent needs, PSS offers programmes that arespecifically tailored for these groups. This paperdescribes different strategies that PSS has usedwhen working with youth.
Description of reproductive healtheducation programmes
PSS programmes address rural and urban youthin school and out of school, including streetchildren, volunteers of Bharat Scouts and Guidesand Nehru Yuva Kendra, college students, thosewho are married or about to be married, as well asthose who are mentally or physically challenged.PSS is currently undertaking RHE interventions inschools and colleges in Bhubaneshwar, Balasore,Cuttock, Bangalore, Calcutta, Lucknow and Delhi.A new 6.5-year project funded by the BuffettFoundation in the United States of America hasalso been launched covering 10 districts in the stateof Rajasthan. A team of young educators are beingtrained to undertake RHE sessions in a sensitiveand friendly manner. A curriculum developed byPSS in Hindi and English serves as a broadguideline that educators adapt based on localneeds and type of audience. Educators cover asix-session curriculum using participatory teachingtechniques and special audiovisual and print
Reproductive health education: experiencesof Parivar Seva Sanstha in communicatingwith youth in India
Sudha Tewari and Sumita Taneja

175
Reproductive health education in India
materials. Recognizing the importance ofaddressing gatekeepers and sensitizing themabout the need for such education, PSS alsoinvolves parents, school authorities and communityleaders in its RHE programmes.
During the sessions, educators encouragestudents to ask questions either orally or by writingthem on pieces of paper (to maintainconfidentiality). Girls often ask about menstruation,how babies are made, pregnancy, childbirth andpersonal grooming. For example, a typical set ofquestions includes: “We have periods, what doboys have?” “Can I ride a bicycle or bathe in apond during my periods?” “Why are girls asked tosit separately during menstruation? ” “Whathappens on the wedding night?” “What are test-tube babies?” “How are twins born?” “If only onesperm is needed for conception, what happens toall the others that enter the body?” Boys often askabout attraction to the opposite sex, masturbation,ejaculation, nocturnal emissions, anatomy andphysiology. Typical questions include: “Do girls alsohave the same amount of interest in boys?” “Beingattracted to one girl is okay, but why do I find allgirls attractive?” “I have read somewhere that onedrop of semen is equal to a 100 drops of blood, isit true?” “Do girls also masturbate and how?” “Whatshould be the size of a normal penis?” “Dopregnancies occur without intercourse?”
In addition, PSS provides medical services inschool settings, usually linked with educationsessions. Through its existing network of MarieStopes clinics, PSS organizes health camps inschools, which, besides providing general healthcheck-ups, doctors and counsellors, addressadolescents’ psychosexual problems, such asconcerns about menstruation and masturbation.
To control anaemia, staff promote iron supplemen-tation among adolescent girls.
Initially PSS had planned to undertake a longitudinalsurvey to measure the impact of RHE interventionsin schools and colleges over a five-year period,but it proved difficult to follow up students oncethey left school for further studies or marriage. Asan alternative, PSS carries out assessmentsbefore and after they follow the curriculum. Whengroups are illiterate, PSS organizes focus groupdiscussions. While limited as research tools, thesetests measure improvement in students’knowledge and allow PSS to gather practicalfeedback on course content and methodology.An analysis of test results from selectedschools in Bhubaneshwar shows a wide range ofscores (Table 1).
PSS also conducts programmes for out-of-schoolyouth and those who are mentally or physicallychallenged. To address the needs of these groups,PSS has developed special teaching and learningtechniques, such as clay models, body mappingand exercises. Educators adapt the curriculum foreach group and sometimes bring in specialistssuch as psychologists, nutritionists, doctors andother resource persons.
Training educators and service providers
To expand outreach and reinforce messages, PSSworks with peer educators and conducts “trainingof trainers” programmes for school teachers andcounsellors. PSS selects 4 or 5 volunteer youth(often National Service Scheme volunteers) fromeach school or college for a 3-day training course.Once trained, these peer educators organize
Table 1. Selected pre- and post-intervention test scores among students aged 16–18
Pre-intervention (%)Post-intervention (%)
Name of school Batch students Stream Lowest Highest Lowest Highest
City Women’s College +2 (girls) 30 Arts 0 42 78 100Kamala Nehru Women’s College +2 (girls) 30 Science 15 55 90 100Acharya Harihar College +2 (boys) 30 Arts 0 38 27 85Patia College +2 (boys) 30 Science 20 58 43 90
No. of

176
SUDHA TEW ARI AND SUMITA TANEJA
programmes during events such as World AIDSDay, Women’s Day and Independence Day. PSSalso trains teachers and counsellors so that thereis a trained cadre of persons available on schoolpremises to answer adolescents’ queries.
PSS realized that a significant number ofadolescents could not be reached througheducational institutions, since many children dropout of school because they marry or becomepregnant, particularly girls in rural areas. To reachthese marginalized groups, PSS identifies andtrains other NGO staff and other grass-rootsservice providers who have access to theseadolescents. For example, in four districts of UttarPradesh, PSS reached rural adolescent girls andwomen by training anganwari workers on issuesrelated to adolescent sexuality. Anganwari workersare community-based, village level workers whoprovide education and nutritional supplements topreschool children and lactating and pregnantmothers. Once trained, these workers helpedmobilize adolescents for community educationprogrammes, which were jointly conducted by thePSS RHE team and the anganwari workers.
Because the demand for reproductive healthinformation exceeds what PSS can handle alone,it continues to provide training to those working inschools, health services and NGOs. For example,PSS initiated a “training of trainers” programmewith Bharat Scouts and Guides, Volunteers of theNational Service Scheme, Teachers TrainingInstitutes and other NGOs. To achieve financialsustainability, PSS charges a token fee to theschools and colleges that can afford to pay.
Some innovative initiatives of PSS
Because so many young people enter marriagewithout any knowledge of sexuality orcontraception, PSS launched an effort to reachyoung people who were about to be married. Inthis programme, called Adhaar (meaningfoundation for marriage), educators covered topicssuch as courtship, emotional, psychological and
physical preparation for marriage, sexuality andcontraception, personal grooming, legal issuesrelated to marriage, home management, bankingand finance, first aid and crisis management.
In an effort to reach a broad range of youth andadults who are difficult to reach throughconventional channels, PSS established atelephone hotline service in Delhi in 1993. Thishotline, called “Sparsh” or “sensitive touch”,answers questions on delicate issues ranging fromcontraception and sexually transmitted infectionsto drug and alcohol problems. In addition, thehotline provided counselling to those in distressand referred callers to appropriately qualifiedprofessionals. This service received anoverwhelming response from the general public(receiving 17 074 phone calls in one year) and themedia. When PSS first introduced Sparsh, therewas no dearth of questions such as: “Can kissingmake me pregnant?” “Will using my boyfriend’shandkerchief frequently lead to AIDS?” “What is acondom?”
During the course of PSS’s work with youth, aneed for a Distance Learning Course in Family LifeEducation (FLE) was expressed by many NGOrepresentatives, doctors, counsellors, schoolteachers and principals. PSS therefore introduceda one-year Distance Learning Course in FLE. Inaddition to sending course modules on RH tostudents against which they submittedassignments, PSS held personal contactprogrammes twice a year and asked students towork on projects under PSS guidance. Certificateswere awarded to students who were successful inthe written examination and interview held at theend of the course.
Future strategies
PSS has gained considerable experience indesigning innovative programmes to communicatewith youth and proposes to adapt the lessonslearned to programmes for larger audiences. Forexample, PSS programmes that addressed

177
Reproductive health education in India
adolescents who had just married or were aboutto do so (i.e. Adhaar) focused on urbanadolescents. These could be adapted to meet theneeds of adolescents in rural areas as well, wheremarriage continues to occur at an early age. PSSfeels that if the programme were packaged as“preparing your girls for marriage”, it would faceless resistance at the community level and wouldbe widely accepted. In addition, PSS hasrecognized an unmet need for distance learningcourses on SRH that target grass-roots governmentfunctionaries and NGO staff such as auxiliarynurse midwives and anganwari workers, as wellas other NGO functionaries. PSS is consideringdeveloping short courses of up to three monthsinstead of one year.
PSS consciously tries to build sustainability intoall its projects. However, since RHE programmesare targeted at youth who have little ability to pay,particularly in rural areas, partial cost recoveryalone cannot make the programme self-sustaining.
Realizing the importance of investing inadolescents today to create responsible adults oftomorrow, PSS stands committed to addressingthe needs of youth by integrating adolescent healthinterventions in all its ongoing reproductive healthprojects.
Sudha TewariManaging DirectorParivar Seva SansthaC374 Defence ColonyNew Delhi 110024India

178
RAJ BRAHMBHATT
Background
Adolescents, who constitute over one-fifth of India’spopulation (International Institute for PopulationSciences, 2000), have limited access to vitalinformation and services pertaining to sexual andreproductive health (SRH). Cultural taboossurrounding communication about sexual matterspersist in the parent–child relationship, and youngpeople have few opportunities outside their peergroup to talk about their feelings and anxieties.
Founded in 1949, the Family Planning Associationof India (FPAI) is the country’s largestnongovernmental organization (NGO) providingfamily planning and other reproductive healthservices. In addition to clinical services, training andresearch, FPAI carries out extensive information,education and communications programmesthroughout India. The FPAI has experimented withnumerous programmes to meet the needs of bothurban and rural youth, including campaigns toincrease the age at marriage, sexuality andreproductive health education programmes, andcounselling services. This paper describes aselection of these programmes.
Selected programme activities for youth
In the late 1960s, FPAI began educating young
people in schools, colleges and non-formaleducational institutions on issues related topopulation and family life. These programmesprovide an orientation for young people regardingsexuality, reproductive health, the prevention ofunplanned pregnancies and sexually transmittedinfections (STIs). In designing these programmes,the FPAI kept in view that adolescents have needsthat are distinct from those of adults. Theseeducation programmes do not merely provideinformation, but also aim to enhance youngpeople’s communication skills, clarify values,change attitudes and prevent risky behaviour.
In 1978, FPAI established Sexuality EducationCounselling Research Therapy/Training (SECRT)centres, which provide sexuality education andcounselling. Today 37 SECRT centres havereached over 120 000 young people. SECRTcentres offer counselling services to both marriedand unmarried adults and adolescents, on a rangeof topics, including premarital counselling, familyplanning, and marital and infertility counselling.FPAI offers these services individually, in groups,by correspondence and over the telephone.
FPAI has developed several innovative approachesin partnership with young people to promotesexual and reproductive health. The organizationworks through youth clubs in many settings toprovide accurate information on family life and
Counselling young people on sexual andreproductive health: individual and peerprogrammes
Raj Brahmbhatt

179
Counselling young people on sexual reproductive health: individual and peer programmes
adolescent health matters, including the preventionof sexually transmitted infections, including humanimmmunodeficiency virus infection (STIs/HIV). Inaddition, FPAI branches have developed peereducator initiatives in collaboration with other youthprogrammes, such as Youth Parliament, YoungWomen Information Centres and thespianprogrammes. In addition, FPAI has developed“Young Inspirers Clubs” in rural and urban areas.These clubs use folk media to raise awarenessabout STIs/HIV/AIDS, to eradicate myths andmisconceptions related to sexuality, and topromote reproductive health. The “Young Inspirers”publish a Hindi newsletter, called YASH (Youth andSexual Health), to spread life-planning informationamong their peers. In 1997, FPAI-SECRT initiated“Spearhead Youth Health Leadership TrainingProgramme”. This programme has trained nearly1000 youth leaders, many of whom have servedas peer counsellors in the FPAI Young Inspirers Clubs.
In 1999, the FPAI implemented a project on“Enhancing Sexual and Reproductive Health ofYoung Persons”. This project aimed to extendinformation and counselling on issues related tohuman sexuality, preparation for marriage,responsible parenthood, gender issues,contraception and prevention of STIs/HIV/AIDS. Aspart of the project, the six FPAI branches carriedout sensitization programmes, organized medicalcheck-up camps and provided counselling andtraining for teachers and peer educators. Theproject reached out to rural and urban youth, andthe response was overwhelming. For example, theSTI/HIV prevention programme reached 7065 youngpeople, including 3391 out-of-school, illiterateyouth. In Dharwad (Karnataka), the projectestablished a strong network of young peopletrained to impart knowledge on sexuality and STIs/HIV/AIDS. Its peer group leaders’ training led tothe establishment of eight community counsellingcentres in six villages where four to five peer groupleaders provide counselling on a regular basis.
Conclusions
From our experience we have learned manylessons regarding adolescent SRH programmes,a few of which are highlighted below. First, youngpeople are not a homogeneous group, andprogrammes need to consider economic, social,cultural and religious differences. Culturalsensitivity is essential, and for this reason, no singleprogramme can work for all India. Second, in theabsence of other information and services, quackshave taken advantage of adolescents’ sexualconcerns throughout India. On every street corner,such people advertise services for sexual problems.Young people need services and counselling thatdo not perpetuate misconceptions. Third,adolescents are more concerned about sex thanabout reproduction. Programmes need to gobeyond limited kinds of “sex education” that focusprimarily on anatomy, to “sexuality education”which addresses broader dimensions. Humour andfun are essential elements in gaining a rapport withyoung people.
Finally, in addition to elements of youth-friendlyservices such as convenient hours, convenientlocations, affordable fees and specially trained staff,FPAI has found that anonymity and drop-in hoursare particularly important. FPAI centres usenumbers instead of names to identify clinic records,so that young people do not have to reveal theiridentity. Welcoming drop-in clients is essential,because many young people have fewopportunities to come to the clinic. Allowing themthe freedom to drop into the clinic without aprearranged appointment has proven to be animportant way to increase access. It is these kindsof counselling and awareness-building strategiesthat can help young people get the education,health care and skills that they need early in life toensure their well-being as adults.

180
RAJ BRAHMBHATT
Reference
International Institute for Population Sciences (2000)National Family Health Survey (NFHS-2), India 1998–1999, Health and Family Welfare Wallchart. Mumbai,International Institute for Population Sciences, andWashington, DC, Population Reference Bureau.
Dr Raj BrahmbhattFPAIBaja BhavanNariman PointMumbai 400 020India

181
The Healthy Adolescent Project in India (HAPI)
Background
As in many Asian countries, there is an urgentneed to improve reproductive health knowledge andbehaviour among adolescents and young adultsin India. Over 20% of the population in India isbetween the ages of 10 and 19. Young people tendto marry early, and experience high fertility rates,low levels of contraceptive use, high abortion rates,and high levels of violence and sexual coercion(International Institute for Population Sciences,2000). To address these issues, Family HealthInternational (FHI), the World Association of GirlGuides and Girls Scouts (WAGGGS) and theBharat Scouts and Guides Association (BSG), thelargest youth organization in India, havecollaborated on a two-year project called theHealthy Adolescent Project in India (HAPI), withfunding from the David and Lucile PackardFoundation. The purpose of HAPI is to addressgaps in reproductive health knowledge andservices for adolescents and young adults byenhancing young people’s knowledge and skills,using a life-skills approach. The project also aimsto help participants develop healthy values andattitudes, and to establish links between Scoutsand Guides and local health providers. The FamilyPlanning Association of India/Calcutta Branch(FPAI) selected and supervises a team ofcommunity health workers who are charged withestablishing this link with local health providers.
The project has its headquarters in Kolkata andfocuses on West Bengal, where the Guide andScout associations have a strong presence andhave expressed considerable interest in activitiesintended to enhance adolescent sexual andreproductive health.
Project description
To improve the reproductive health of adolescents,the project incorporates a reproductive and generalhealth curriculum into girl guide and boy scoutprogrammes in seven project communities in WestBengal along the Eastern and South-EasternRailways. Through a series of health educationactivities, guides and scouts learn basic factsabout their health and how to convey thisinformation to their peers. By aiming to train 900peer educators, each of whom would make 25contacts, the project hopes to reach as many as22 500 young people. The HAPI project relies onthe BSG’s existing volunteer structure. The projecthas three coordinators (the only full-time paidstaff), 12 BSG trainers and 17 FPAI health workers,all of whom work with leaders of 30 BSG units,evenly split between boy scouts and girl guides.
The collaborating organizations have developed acurriculum that the scouts and guides will followto earn their HAPI merit badges. Merit badges are
The Healthy Adolescent Project in India(HAPI)
Matthew Tiedemann and Shakuntala DasGupta

182
MATTHEW TIEDEMANN AND SHAKUNTALA DASGUPTA
a key motivational tool in scouting and guiding.After completing a series of activities on a particulartopic, as outlined in the BSG curriculum, the scoutor guide earns a badge symbolizing the skillacquired. This badge is worn on the uniformand is a public sign of the young person’saccomplishments. The HAPI badge is larger thanthe typical BSG badge, in recognition of the factthat the curriculum is much more demanding thanothers, and as a way to enhance awareness ofthe project. After earning the badge, the scoutsand guides earn peer education achievementcertificates.
The HAPI curriculum draws on other adolescentcurricula adapted for the specific conditions in India.In addition, the project has developed anaccompanying handbook for unit leaders, whichprovides detailed instructions for leading scoutsand guides through each part of the badgecurriculum. The project has also supplied a rangeof other resource and reference materials for thetrainers, unit leaders and adolescents.
The project curriculum takes a holistic approachto adolescent health, covering reproductive healthtopics as well as broader health and other issuesrelated to the transition to adulthood. This approachtries to put sensitive reproductive health informationinto a positive, non-threatening context, byemphasizing the effects on the adolescents’ overallhealth. Specifically, the project addresses topicssuch as the human body and physical changes,female and male reproductive systems, sexuallytransmitted infections (STIs), contraception,pregnancy, gender roles, self-esteem, hygiene,nutrition, disease prevention and healthyrelationships. The curriculum is divided into twolevels, for ages 10–13 and ages 14–25. HAPI usesa participatory, interactive training methodology,both for adult trainers and for adolescent scoutsand guides. The approach emphasizes “learningby doing”, or experiential learning. Participantswork in small groups and learn by taking part inactivities rather than passively receivinginformation through lectures or reading. Suchactivities include skits, dance, drama and games.
The curriculum provides age-specific information,and topics progress from basic to more challenging.
One strength of the project is that it linkseducational programmes with locally availableclinical services. To earn their HAPI badge,adolescents must meet with the community healthworker assigned to their unit and visit local healthclinics. To build links with health care providers,the FPAI community health workers arrange talksby local physicians and other health care providers.Health workers lead sessions that coverreproductive health topics. In addition, the projectplans to hold special events at health centres,clinics and hospitals to introduce adolescents tothe health providers in their area. In this way, healthproviders become familiar with adolescents’ needs,while young people learn about what services areavailable. We anticipate that this interactionbetween adolescents and local clinics will makeyoung people more familiar and comfortable withthe services provided, and thereby increase theiruse of the services. We also anticipate that, asclinicians become more familiar with adolescentclients, their services will become more sensitiveto adolescents’ needs.
Project evaluation
At the beginning of the project, FHI, WAGGGSand BSG conducted a needs assessment in eacharea to determine local needs and to identify whatothers have done in the area of adolescentreproductive health. This information was used toadapt the project to the local context. BSG,WAGGGS and FHI have been regularly monitoringthe project’s progress, by collecting processindicators and conducting two formal monitoringvisits. In addition, the project has contracted witha research firm to collaborate with FHI on aquantitative pre- and post-intervention survey usinga quasi-experimental design. Evaluators willconduct the survey among scouts and guides in30 experimental units that participated in theproject and 30 control units that did not, matchedas closely as possible. In this way it is hoped to

183
The Healthy Adolescent Project in India (HAPI)
assess the impact of the project on participants interms of reproductive health knowledge andbehaviours, perceptions of the future and self-image. Because the effects of the intervention maybe mediated by variables such as the level ofproject participation (e.g., levels of achievement,number of meetings attended, etc.), sex, age, unitand BSG branch, these variables will be includedin the multivariate analyses comparing BSG unitsthat did and did not participate in the HAPI project.
FHI and WAGGGS have provided the initial trainingfor coordinators, community health workers,trainers who are responsible for training adult scoutand guide leaders, and members of the supportcommittee. The project is also in the process oforganizing an awareness camp for personnel.Coordinators are working with schools and localinstitutions to gain their support for the project,and to gain parental consent for adolescents totake part. In addition, a baseline survey is underway to assess the knowledge, skills, values andattitudes of both intervention and control groups.
Conclusions
The project faces a number of challenges. Thesechallenges include the need to gain the support ofparents, communities, and schools, as well as theneed to address the very low knowledge levels ofyounger participants. Given the sensitivity of someof the topics addressed, the project cannot takeplace without the support of communities, parents,schools and other local institutions. The projecthas great potential, however. Because the numberof young people participating in guiding andscouting activities totals nearly 20 000 in WestBengal and over three million across all of India(figures from BSG Annual Report 1998/1999), ifthe HAPI project is successful, it could beexpanded in the future to reach a large number ofadolescents.
Reference
International Institute for Population Sciences (IIPS)(2000) National Family Health Survey (NFHS-2),1998–1999 . Mumbai, International Institute forPopulation Sciences and ORC Macro.
Matthew TiedemannFamily Health InternationalPO Box 13950Research Triangle Park, NC 27709USA

XIBuilding self-efficacyamong adolescents

186
MARTA LEVITT-DAYAL, RENUKA MOTIHAR, SHUBHADA KANANI AND ARUNDHATI MISHRA

187
Adolescent girls in India choose a better future: an impact assessment
Background
Over the last decade, the Centre for Developmentand Population Activities (CEDPA) has beenworking to challenge gender inequities, expand lifeoptions and empower girls aged 12–20 through anintegrated programme called the “Better LifeOptions Program” (BLP). The programme providescourses for girls in non-formal education, vocationalskills, personality development, and family lifeeducation, and teaches them basic skills for living,such as how to use the post office, bank andtransport system. The programme also providesopportunities for recreation and focuses ondeveloping leadership skills. To carry out theseactivities, CEDPA has used the centre-basedapproach and has established village trainingcentres run by local literate women. In addition, ittrains alumni girls as peer educators and motivatesthem to open their own learning centres.
As part of an evaluation, CEDPA carried out a studyto assess the impact of the BLP on the lives ofgirls who participated between 1996 and 1999. Thestudy objectives were to compare BLP alumni witha similar control group of girls who had notparticipated in the programme, in terms ofeducational attainment, income generation,decision-making, mobility, self-esteem, fertility, ageat marriage, child-spacing, use of contraceptivesand health-seeking behaviours. This paper presents
the study findings and discusses CEDPA’s futurestrategies.
Methods
A comparative cross-sectional design was usedin three intervention areas—periurban Delhi, ruralMadhya Pradesh, and rural Gujarat—where theprojects had been implemented by the threepartner organizations, Prerana, BharatiyaGrameen Mahila Sangh (BGMS) and Gujarat StateCrime Prevention Trust (GSCPT). A random sampleof 1693 young women aged 15–26 was surveyed,including 858 controls and 835 BLP alumni.Respondents included both married and unmarriedwomen. Control areas were similar to interventionsites in terms of access to health facilities andethnic groups. Researchers adapted surveyquestions from the Demographic and HealthSurvey, and included questions about education,economic empowerment, health-seeking behaviourand related topics.
The study had limitations. First, many alumni hadmarried and moved away and were not available toparticipate in the survey. Second, the programmedid not collect baseline data; therefore, researchersselected a post-test-only control groupexperimental design. Since participation wasvoluntary, it is possible that self-selection bias may
Adolescent girls in India choose a betterfuture: an impact assessment of aneducational programme
Marta Levitt-Dayal, Renuka Motihar, Shubhada Kanani andArundhati Mishra

188
MARTA LEVITT-DAYAL, RENUKA MOTIHAR, SHUBHADA KANANI AND ARUNDHATI MISHRA
have accounted for some differences between thealumni and control groups. To reduce this, wecontrolled for two critical variables—girls’ educationand parents’ education. Finally, there may be agap between reported and actual behaviour.
Key findings
The study found significant differences betweenthe controls and BLP alumni in terms of education,vocational skills, economic empowerment,autonomy, self-confidence, reproductive behaviourand health-seeking behaviour. BLP alumni weresignificantly more likely to be literate, to havecompleted secondary education, to be employedand to have learned a vocational skill. They weremore likely to have travelled outside their villageand to have gone to a health centre alone in theprevious six months. In addition, BLP alumni weremore likely to have the autonomy to make theirown decisions about going to the market, spendingwhat they earned and deciding when to marry.These differences in autonomy were significanteven after controlling for education of girls and theirparents (Table 1).
In terms of reproductive health-seeking behaviour,married alumni (N=292) reported significantly morepositive behaviours than married controls (N=269)in a number of indicators related to reproductivehealth and child survival. BLP alumni weresignificantly more likely to have married at age 18or above and to use contraception. Amongrespondents who had experienced a pregnancy,
alumni (N=179) were more likely than controls(N=223) to have received prenatal and postnatalcare and to have delivered their baby in a healthinstitution. Girls’ education seemed to be thecritical factor in many of these positive reproductivehealth behaviours. However, receiving prenatalcare, two doses of tetanus toxoid (TT2) andpostnatal care remained significant when wecontrolled for the girls’ education (Figure 1).
In terms of child survival practices among marriedrespondents with children, BLP alumni reportedhigher rates of complete primary vaccinationsamong children over one year old compared withcontrols (63% versus 32%), and higher rates ofhaving given oral rehydration solution during boutsof diarrhoea (42% versus 12%). These practicesremained highly significant even after controllingfor girls’ education.
Conclusions
This programme evaluation found significantdifferences between girls who had participated inthe “Better Life Options Program” and girls fromthe control group, in terms of economicempowerment and health. Though differencesbetween these groups may reflect a certain amountof self-selection, survey findings suggest that theBLP integrated model can have a significant impacton participants’ economic empowerment, self-esteem, autonomous decision-making,reproductive health and child survival practices. Twoadditional lessons learned from the programme
Table 1. Selected indicators of education, autonomy, and mobility among alumni and controls
Control group (%) BLP alumni (%)Indicator (N = 858) (N = 835)
Illiterate 32 5Completed secondary education 46 66Had learned a vocational skill 22 99Employed/self-employed 8 35Could decide when to marry 7 25Could decide how to spend money earned 12 42Could decide to go to market 27 52Travelled alone to health centre in past six months 6 25Travelled alone outside village in past six months 21 68
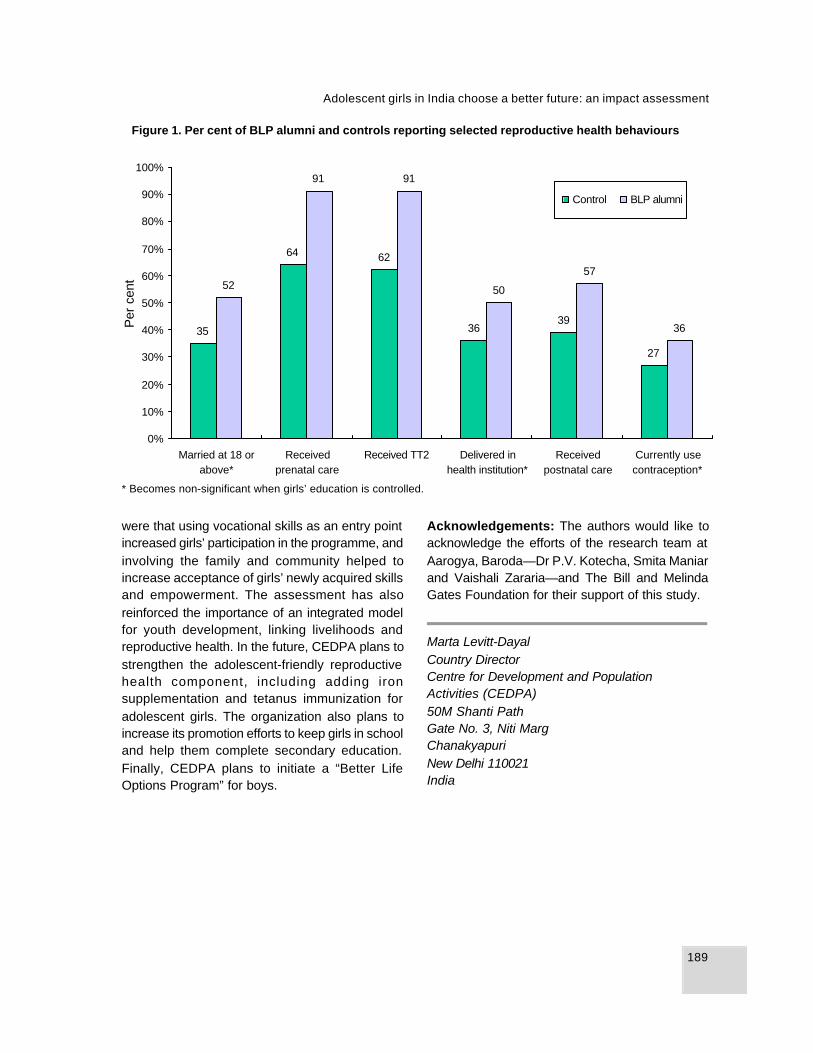
189
Adolescent girls in India choose a better future: an impact assessment
were that using vocational skills as an entry pointincreased girls’ participation in the programme, andinvolving the family and community helped toincrease acceptance of girls’ newly acquired skillsand empowerment. The assessment has alsoreinforced the importance of an integrated modelfor youth development, linking livelihoods andreproductive health. In the future, CEDPA plans tostrengthen the adolescent-friendly reproductivehealth component, including adding ironsupplementation and tetanus immunization foradolescent girls. The organization also plans toincrease its promotion efforts to keep girls in schooland help them complete secondary education.Finally, CEDPA plans to initiate a “Better LifeOptions Program” for boys.
Figure 1. Per cent of BLP alumni and controls reporting selected reproductive health behaviours
* Becomes non-significant when girls’ education is controlled.
Acknowledgements: The authors would like toacknowledge the efforts of the research team atAarogya, Baroda—Dr P.V. Kotecha, Smita Maniarand Vaishali Zararia—and The Bill and MelindaGates Foundation for their support of this study.
Marta Levitt-DayalCountry DirectorCentre for Development and PopulationActivities (CEDPA)50M Shanti PathGate No. 3, Niti MargChanakyapuriNew Delhi 110021India
27
393635
6264
36
57
50
9191
52
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Married at 18 orabove*
Receivedprenatal care
Received TT2 Delivered inhealth institution*
Receivedpostnatal care
Currently usecontraception*
Per
cen
t
Control BLP alumni
190
MRIDULA SETH
Background
The education and health needs of adolescents inremote villages of Rajasthan are not adequatelyserved through the existing government system.Moreover, reaching these adolescents directly isdifficult since many are not part of the formaleducation system. As a result, programmes needto explore alternative strategies for reaching thispopulation.
The Shiksha Karma project is currently pursuingone such strategy to reach rural youth. The ShikshaKarmi project works to expand primary schooleducation in rural villages of Rajasthan. Men andwomen selected as Shiksha Karmis (SKs) havefew educational qualifications and no teachingexperience when they begin, but they undergoextensive training and preparation to becomeprimary school teachers. As primary schoolteachers, they do not work directly withadolescents. Nonetheless, they represent apotential channel for spreading information andserving as change agents in areas that generallylack other organized groups or educated persons.As a result, the Shiksha Karmi Board and theUnited Nations Population Fund (UNFPA) identifiedthe SKs as an important resource to improve theskills and the health—particularly the reproductivehealth—of rural youth. To achieve this, UNFPA and
the Shiksha Karmi Board have undertaken a pilotproject to introduce health education and “lifeskills” into the SK training.
The World Health Organization (WHO) (1993)defines “life skills” as “the abilities for adaptive andpositive behaviour that enable individuals to dealeffectively with the demands and challenges ofeveryday life”. WHO (1994) identified a core set oflife skills that included problem-solving, decision-making, goal-setting, crit ical thinking,communication skills, assertiveness, self-awareness and skills for coping with stress. Interms of reproductive health, for example, suchskills can influence women’s fertility even withoutformal education, by helping them make informeddecisions and negotiate with their families.
In this paper, life skills have been conceptualizedin terms of thinking, social and negotiation skills.Self-awareness and social awareness, planningand problem-solving are considered to be thinkingskills. Establishing relationships and communi-cating effectively are considered social skills.Negotiation skills are an outcome of thinking andsocial skills. This paper describes the preliminaryexperiences with life skills education from theShiksha Karmi project and discusses somepreliminary lessons learned.
Training school teachers to pass on life skillsto adolescents
Mridula Seth

191
Training school teachers to pass on life skills to adolescents
Project description
The project provided training in life skills educationto women preparing to become SKs. The aim wasto build the life skills of the SK trainees andsimultaneously prepare them to build such skillsamong members of the communities in which theywould work. The project developed a framework toaddress a number of issues, including: (a) self-awareness; (b) social awareness such as socialnorms, gender discrimination and values; (c)problem-solving; (d) working with others; (e)communication skills; and (f) negotiation skills,including how to be assertive and how to resistpeer pressure. In terms of health concepts, theframework addressed topics such as physical andemotional changes during adolescence, locallyavailable services, and information related to sexdetermination, abortion, infertility, HIV/AIDS,reproductive tract infections (RTIs)/sexuallytransmitted infections (STIs), menstrual hygiene,fertility awareness and other health issues.
The project developed and field-tested a trainingmanual using participatory methods such as bodymapping, role-plays, questions boxes, casestudies, brainstorming, games and songs (UnitedNations Population Fund, 2000). To enhance long-term sustainability, the project trained 13 resourcepersons, who trained as many as 185 SKs in sevendistricts during 2000.
Programme evaluation
Life skills education has become an integral partof the residential training of SKs. Assessing theeffectiveness of life skills interventions poses achallenge, however. While measuring gains inknowledge is difficult enough, it is even moredifficult to measure changes in thinking, social andnegotiation skills. The project has receivedfeedback through group discussions, case studiesand the “critical incidence technique”. The criticalincidence technique allows information to be
collected about an incident that had a markedinfluence on a respondent’s life. By analysing theincident, the researcher can draw inferences aboutthe impact or effectiveness of an intervention onthe respondent’s personal, social and/orprofessional life.
This feedback clearly suggested a positive impacton participants, particularly among those selectedas “Master Trainers”. In general, SK traineesreported a greater ability to resist peer pressure,to convince their husbands and mothers-in-law tosupport family planning, and to share informationon sex discrimination with others. In terms of healthissues, SK trainees reported that the most relevantcontent of training included information about RTIs/STIs, contraceptives and menstrual hygiene. Atthe time of reporting, SKs had not yet had a chanceto hold sessions with adolescents in their villages,but they had reported sharing information withvillage women. Trainees also reported giving moreimportance to their own health and having fewerinhibitions about discussing sexual andreproductive health issues.
Conclusions
Many lessons were learned from the pilot projectabout life skills interventions, a few of which arehighlighted below. First, each group must choosewhich life skills are relevant to its own needs andsituation. It is essential to identify the skills andresources that already exist among those whoreceive training. Second, teachers need toenhance their own life skills before they caneffectively develop such skills in their students.Third, life skills interventions need to useexperiential, participatory methods, and they arenot effective if participants simply sit passivelytaking in information. Finally, there is a need forbetter indicators to evaluate life skills interventions.

192
MRIDULA SETH
References
World Health Organization (1993) Increasing theRelevance of Education for Health Professionals.Geneva, World Health Organization (WHO TechnicalReport Series No. 838).
World Health Organization (1994) The Developmentand Dissemination of Life Skills Education: AnOverview. Geneva, MNH/PSF, World HealthOrganization.
United Nations Population Fund (2000) Building lifeskills for better health—the Rajasthan experience.Delhi, UNFPA (unpublished report available from theUNFPA Delhi office: http://www.unfpa.org.in)
Mridula SethUNFPA55 Lodi EstateNew Delhi 110013India
XIIAccess to and quality ofreproductive healthservices

194
V. CHANDRA MOULI

195
Adolescent-friendly health services
Background
Adolescence, the second decade of life, is a periodin which an individual undergoes major physicaland psychological changes. Alongside this, thereare enormous changes in the person’s socialinteractions and relationships. It is more of a phasein an individual’s life than a fixed time period; aphase in which the individual is no longer a childbut is not yet an adult; a time of both opportunityand risk.
Adolescence presents a window of opportunity inseveral ways. Health problems “carried over” fromchildhood could be addressed during this period.Actions could be taken to set the stage for healthyadulthood and reduce the likelihood of problems(such as heart disease) in the years that lie ahead.At the same time, it is a period of risk, oftenmarked by such health problems as too early andunwanted pregnancies, and such behaviours assmoking that have serious immediate or longer-term consequences.
The World Health Organization (WHO), inconjunction with the United Nations Children’sFund (UNICEF) and the United Nations PopulationFund (UNFPA) has developed a common agendafor action in adolescent health and development.This common agenda is aimed at providing a safeand supportive environment, health and counselling
services (World Health Organization, UnitedNations Children’s Fund & United NationsPopulation Fund, 1997)
In examining the different elements of thiscomprehensive approach, a useful analogy is thatof a 7 year old child who needs to cross the roadevery day to get to school. She needs informationand skills—where to look, what to look for, whento walk across and when not to do so. She needsa safe and supportive environment—a pedestriancrossing, traffic lights that work or a traffic wardenin position, drivers who respect traffic rules or arepunished if they do not do so. She may also needhealth and counselling services, if she stumblesand falls, or is struck by a vehicle.
Many individuals and institutions have importantcontributions to make to the health anddevelopment of adolescents. It may be useful tothink of them in concentric circles of contact andinfluence. At the centre is the adolescent himselfor herself. Parents, siblings and some other familymembers are in immediate contact with theadolescent and constitute the first circle. Thesecond circle includes people in regular contactwith them such as personal friends, family friends,teachers, religious leaders and others. The thirdcircle includes musicians, film stars and sportsfigures, who can have a tremendous influence onthem from afar. Finally in the fourth circle,
Adolescent-friendly health services
V. Chandra Mouli

196
V. CHANDRA MOULI
politicians, journalists and bureaucrats (within thegovernment and private sectors) affect their livesin small and big ways, through their words anddeeds.
Health workers and facilities fit within the secondcircle in this scheme. Clearly, they play animportant role in helping ill adolescents get backto good health (by diagnosing health problems,detecting problem behaviours and managing orreferring them elsewhere). They also play animportant role in helping healthy adolescents staywell and develop into healthy adults, by providinginformation, advice and preventive services (orproducts). Services are provided in a range of healthfacilities or recognized institutions that providehealth services. For example, facilities includesmall clinics providing a limited range of (primarylevel) health services to large hospital complexesproviding a wide range of (tertiary level) health andsocial services. Health facilities may be operatedby the public, private (profit-seeking) or non-profit,nongovernmental sector. They may exist asindependent entities or be located within institutionsproviding other services to adolescents, includingschools, correctional institutions and residentialinstitutions such as youth hostels. They may alsobe established through social marketingprogrammes in shops, or provided in the communityby outreach programmes. And they may beprovided on a temporary basis in sites where largenumbers of people are forced to live in camp-likeconditions, for example in the aftermath of a naturaldisaster, civil strife or war.
Obstacles adolescents face in seeking care
Generally speaking, adolescents tend to behealthy and make the transition into adulthood ingood health. Although they may develop some ofthe health problems of children, such as intestinaland respiratory infections, and others that are moreprevalent in adulthood, such as anaemia andsexually transmitted infections (STIs), by and large,the illnesses of childhood have been overcome and
left behind, and the diseases and disorders of olderyears appear far away. The feeling of invulnerabilitythat their general good health engenders may,however, lead them to ignore or underestimatehealth threats, such as the adverse consequencesof risky sexual activity or drug use.
Adolescents are a diverse group. For example, aboy of 12 is at a very different stage of personaldevelopment than a boy of 18. Similarly, he isdifferent in psychological and social terms from agirl of 12, in addition to obvious physical differences.Social circumstances can also influence personaldevelopment, so that the health and developmentof a boy of 12 who is part of a caring middle classfamily are likely to be very different from those of aboy of the same age who is fending for himself onthe street. Finally, even two boys of the same age,growing up in very similar circumstances mayproceed through adolescence in different ways,and at different “speeds”.
The sexual and reproductive health service needsof adolescents are correspondingly heterogeneous.Adolescents who are not yet sexually active havedifferent needs from those who are; sexually activeadolescents in stable, monogamous relationshipsmay have different needs from those in more casualrelationships. A different set of needs characterizesthose faced with unwanted pregnancy or infection,or those who have been coerced into sex. It isimportant therefore for health providers to be awareof the diversity of sexual and reproductive healthneeds of adolescents. It is also important for themto be aware of the fact that adolescents are indeedat risk of developing health problems prevalentamong adults, such as anaemia and STIs, and insome cases, may be more vulnerable than adults.For example, adolescent girls may be moresusceptible than adult women to STIs for bothbiological and social reasons. When they acquirean infection, they are also more likely to developlong-term complications (Brabin et al., 2001).Finally, it is important to note that many healthproblems and problem behaviours are interlinked,such as drug use and depression, alcohol use and

197
Adolescent-friendly health services
injuries resulting from road traffic accidents, andundernutrition and complications in pregnancy andchildbirth (World Health Organization, 1999).
Adolescents who perceive themselves to be wellare unlikely to seek health care. They may seekhealth care at hospitals and clinics only if they areinjured or suffer from conditions that are not relatedto sexual or reproductive health. In many casesthey do not recognize that they are ill (e.g. manySTIs are asymptomatic). Those who do recognizethe need may not want to draw attention tothemselves and may try to solve the problemthemselves or turn to their friends, siblings orparents (especially girls) for help.
Even when adolescents choose to seek care, inmany parts of the world, there are important barrierspreventing access to care. First, in many places,health services such as emergency contraceptionand safe abortion are not available, either toadolescents or to adults. In many other places,where these health services are available,restrictive laws and policies may prevent them frombeing provided to some groups, such as unmarriedadolescents. Even when laws and policies are notan obstacle, judgemental health workers maywithhold services from unmarried adolescents. Thismeans that for all practical purposes, some of thehealth services that adolescents need are notavailable to them.
Second, even where they are available,adolescents may not be able to obtain the healthservices they need for several reasons. Forexample, they may not know where to go; facilitiesmay be located a long distance away from wherethey live, study or work, or in places that are difficultto reach; and facilities may not be open at timesof the day when they can get away from their study/work. In short, health services are not accessibleto them.
Third, health services may be delivered in waysthat adolescents perceive to be threatening or ofpoor quality (see for example, Senderowitz, 2000).Experience suggests that adolescents are
reluctant to use available services for fear that theymay be: observed by acquaintances also awaitingservices; required to go through a long bureaucraticprocedure before they get to see a health worker;or obliged to wait for lengthy periods before theysee a health worker or obtain the health servicesthey need. Of greater concern are their fearsconcerning interaction with health workers. Forexample, adolescents may fear that they will behumiliated by health workers who ask awkwardquestions or subject them to unpleasant and painfulprocedures, that health workers will demand theconsent of parents or guardians or will not respectconfidentiality. Finally, lack of affordability posesyet another obstacle to access. In short, healthservices are not acceptable to adolescents.
In summary, adolescents face a number ofobstacles relating to availability, accessibility andacceptability of services.
Adolescent-friendly services
There is a growing recognition of the pressing needto overcome these obstacles, and a number ofinitiatives are under way in both developed anddeveloping countries that focus on making existinghealth facilities more “adolescent-friendly”. Basedon these initiatives, there is growing evidence ofwhat constitutes the essential elements ofadolescent-friendly health services (World HealthOrganization, 1999). These include:
• policies that guarantee confidentiality, do notrequire parental consent and do not withholdservices and products from adolescents;
• procedures that allow simple registration orretrieval processes, short waiting times,facilities to “drop in” without prior appointment,strong linkages to other health and socialservice providers, affordable services withflexible payment requirements, etc.;
• staff who are technically competent, willing todevote adequate time to clients, interested in,understanding of and considerate of adolescent

198
V. CHANDRA MOULI
needs, able to relate to adolescents andperceived as trustworthy; a mechanismwhereby adolescents may see a particularprovider at repeat visits;
• an environment that is physically appealing andaccessible, offering convenient working hoursand location, as well as privacy in theexamination or consultation room, as well asin the waiting room and entrance, and one thatis not perceived as stigmatizing—for examplelabelled or identified as an STI clinic.
Adolescent-friendly services also require inputs fromthe community and from adolescent. Communitiesneed to be well informed about and supportive ofthe work that is under way. At the same time,adolescents must be well informed about availableservices and their quality, and must be able toparticipate actively in the design of appropriateservices.
Conclusion
Priorities in adolescent-friendly health services willundoubtedly vary according to the nature of thehealth services provided and the population groupto be reached. For example, privacy is likely to behigh on the list of concerns for an adolescentseeking treatment for a sexually transmittedinfection, but it may not be an issue at all for anadolescent seeking treatment for a twisted ankle.Further, approaches that make services friendlyto one group of adolescents (such as adolescentmales) may not make them any friendlier—or mayeven make them less friendly—to another group(such as girls in their early adolescent years). Inother words, although the elements listed abovemust be considered, the priority assigned to eachwill have to be tailored to meet the special needsof adolescents who are being addressed. They willalso need to offer these services in ways that
respect social and cultural sensitivities, yet arefeasible and sustainable. Providing adolescentswith services that are of good quality and areprovided in a client-centred manner is an enormousand difficult task, yet one that has huge publichealth implications for the prevention of healthproblems of adolescents and their prompt detectionand management.
References
Brabin L, Chandra Mouli V, Ferguson J, Ndowa F(2001) Tailoring clinical management practices tomeet the special needs of adolescents: Sexuallytransmitted infections. International Journal ofGynaecology and Obstetrics, 75(2):123–136.
Senderowitz J (2000) A Review of ProgrammeApproaches to Adolescent Reproductive Health. Paperprepared for the US Agency for InternationalDevelopment. Washington, DC, USAID.
World Health Organization (1999) Programming foradolescent health and development. Geneva,World Health Organization.
World Health Organization (2000) Synthesis of thefindings of the assessment phase of action researchprojects aimed at improving the access of school-going adolescents to the health services they need(unpublished draft). Geneva, World HealthOrganization.
World Health Organization, United Nations Children’sFund and United Nations Population Fund (1997)Action for adolescent health. Towards a commonagenda. Recommendations from a joint study group.Geneva, World Health Organization.
V. Chandra MouliDepartment of Child and Adolescent Health andDevelopmentWorld Health Organization1211 Geneva 27Switzerland

199
Making nongovernmental organization initiatives “youth-friendly”
Background
In recent years, there has been heightened interestin adolescent reproductive health (ARH) around theworld, including South Asia. This interest stemsin part from the large numbers of young peoplealready in or due to enter the 10–24 year age group,as well as growing concern about the impact ofHIV/AIDS. In addition, relatively small studies inSouth Asia indicate the number of boys and girlswho have sex before marriage may beunderestimated or increasing. Lacking accurateinformation and adequate services, young peopleface the risk of early, frequent, or unwantedpregnancies, increased morbidity, both personallyand in their children, and the spread of sexuallytransmitted infections (STIs) including HIV/AIDS.
Over the past ten years, the number and types ofstrategies for influencing adolescent behavioursand reproductive health outcomes have rapidlyincreased. The Focus on Young Adults (FOCUS)programme reviewed and synthesized evaluationdata from hundreds of ARH programmes andstudies from around the world. As FOCUSconcluded its work in 2001, the programme putout a summary of findings containing practical andactionable policy and programmerecommendations. Because ARH studies havemainly focused on small populations and
interventions without comparisons or controls, ithas sometimes been difficult to determine whetheran outcome is valid or whether a finding hasprogramme or policy implications. Nevertheless,many common findings have emerged. This paperdiscusses the characteristics that make areproductive health programme “youth-friendly”, theresults of research and evaluation data from ARHprogrammes, and the comparative advantages thatnongovernmental organizations (NGOs) andgovernments have in working with youth.
Adolescent reproductive health programmeexperience: results of research andevaluation
Senderowitz (1999) reviewed the literature andfound that young people typically cite the followingcharacteristics of “youth-friendly” reproductivehealth services: special hours or settings foradolescents; convenient access; a place that doesnot look like a clinic; a place used by their peers;empathetic, knowledgeable and trustworthycounsellors; good humane treatment that is non-judgemental and non-punitive; and counsellinglinked to services designed with young people’sneeds and interests in mind. In most studies, thecharacteristics of providers ranked among the mostimportant factors determining use of services.
Making nongovernmental organizationinitiatives “youth-friendly”
Sharon Epstein

200
SHARON EPSTEIN
Nevertheless, it is difficult to get adolescents touse clinics. In some cases young people lack theability to access services apart from their family.In other cases they are concerned that a family orcommunity member will discover their visit to aclinic. Protecting privacy and confidentiality istherefore of the utmost importance for both marriedand unmarried youth. Because adolescents do notgo to clinics, reproductive health programmes needto reach out to them where they congregate. Insome cases, programmes have to createopportunities for young people to gather together, withor without adults present.
Many reproductive health programmes have triedto reach out to adolescents by working throughthe school system. This remains difficult in manySouth Asian countries, however, because manyyoung people drop out of school at an early age ordo not attend regularly, and the schools may notbe open regularly or fully functioning. Teachers areoften uncomfortable with the topic of sexuality andreproductive health. In some cases, conservativeopposition prevents sexuality and reproductivehealth education in schools, although healthprofessionals can counter this by using theirinfluence to stimulate open and informeddiscussion of ARH.
Ample evidence suggests that neither informationnor services alone are enough to produce changesin young people’s behaviour. For example, evenwhere both are available, non-use, variable use orineffective use of contraceptives remain problems.One reason for this may be that young people arenot as free as adults to make and carry throughindependent decisions. Young people cite a needfor counselling and support in managingfriendships, and partner and family relationships.Programmes need to commit time and resourcesto this kind of counselling. Many organizationshave set up peer counselling programmes, althoughsuch programmes require careful planning, adultsupervision and operational support. They can alsobe quite costly, as young people who have beentrained grow out of adolescence or lose interest.
Young people have requested programmes thatuse the “life skills approach”, which includes butalso goes beyond reproductive health to help youngpeople develop practical and applied skills in otherareas of life. Other examples of innovativeprogrammes include efforts to train service providersin the private, for-profit sector (such as pharmaciesor private doctors) to serve adolescents, providecounselling and contraceptive services atworkplace or military sites where adolescents areemployed or serve as recruits, set up emergencydrop-in centres, offer special hours or facilities forboys, develop long-term adult/adolescent mentoringprogrammes, and provide discussion opportunitiesfor young unmarried couples and newly-weds onmarriage and parenthood.
The public–private partnership
In many cases, young people do not identifyreproductive health as a need, much less as theironly or most important need. A multisectoralapproach to adolescent interests seems mostlikely to convince young people that adults careabout them as “whole persons”, and are ready toaddress the full range of issues in their lives. ARHprogrammes, therefore, have to build closerrelationships with other parts of the health system,as well as with programmes that offer youth otherservices such as basic literacy and numeracy,education, employment training, job counsellingand placement, and housing.
Because adolescents’ needs go beyondreproductive health and even health in general, noone organization—be it public or private—shouldattempt to serve all their needs. Healthorganizations are not terribly good at providing non-health services. Public and private organizationsneed to recognize their distinct comparativeadvantages and collaborate more closely. Whilegovernments in principle have the ability to deployresources for ARH on a long-term and nationalbasis, the public sector may not be the best entityto deliver such tailored services. Public servicestend to be clinic-based, which have the limitations

201
Making nongovernmental organization initiatives “youth-friendly”
mentioned earlier. The funding that would beneeded to make government clinics “youth-friendly”may be more effectively used in outsourcing toand commissioning NGOs to scale-up ARHservices at the community level. Also, NGOs excelin serving married and unmarried adolescents whoare “outside the system” and are likely to remainfearful and suspicious of government officials. Forsensitive issues such as homosexuality, divorce,abuse and violence, rape, bride-burning and incest,which can present threats to young people fromfamily and community authorities, NGOs have adistinct advantage in responding to quickly andmaintaining privacy.
There is a tremendous need for more cross-referral,joint planning and complementary delivery ofservices among organizations that want to meetyoung people’s needs. For example, if counsellingis offered through a hotline in one location, thehotline needs to establish formal agreements withother services, such as pharmacies, privatephysicians, abuse/violence crisis centres, mentalhealth counsellors, lawyers and legal servicescentres, micro credit facilities, or job trainingprogrammes. To build this kind of collaboration anddevelop and implement mutually acceptableservice standards, NGOs need to overcome theirhistorical competitiveness with one another. Theyneed to find ways to do joint planning, facilitatecross-referrals, and submit collaborative proposalsfor funding. Governments and donors that supportreproductive health services should considerfunding “ARH consortia” of private and publicorganizations, rather than individual organizations.
The literature points to a series of strategies thathave not worked well for NGOs or governments,including programmes that have focused only on“family planning”, making no allowances for thedifferent needs of adults and adolescents. Someprogrammes fail to involve young people inplanning, implementation and evaluation. Somefocus solely on negative reproductive healthbehaviours and outcomes, as if every adolescentis dangerous, antisocial and ill-intentioned. Someprogrammes have failed to address young people’s
physical and emotional concerns about sexualityand development compared with peers. Others havenot understood or acknowledged violent situationswithin families and communities that putadolescents at great risk. Programmes have triedto change too many behaviours at once. They haveassumed (without gathering data) that unmarriedyoung people and married women are not sexuallyactive outside the bounds of marriage. Issues ofsame-sex relationships are generally notacknowledged. Programmes have focused only onthe adolescent/parent relationship and failed toconsider adolescents’ relationships within theextended family structure, particularly those ofmarried adolescents. Programmes haveoverestimated the contribution that youth centrescan make in the area of reproductive health, andhave underestimated how much youth centres costto establish and operate. Finally, programmes havefailed to pay enough attention to building coalitionsor alliances with other organizations.
Given the limitations of past efforts to evaluate ARHprogrammes, it is important to ensure that rigorousevaluation is built into all stages of ARHprogrammes. Ideally, cost-effective,methodologically sound evaluation designs shouldbe built into projects before they begin. Programmestaff can draw on the services of evaluation andresearch experts in their own countries or referdirectly to new evaluation workbooks and tools thathave recently become available (for example, seeNelson, MacLaren & Magnani, 2000; Adamchaket al., 2000).
Conclusions
More research and evaluation on some issuesrelated to ARH are no doubt genuinely needed.However, as this paper has attempted to illustrate,there is a substantial and growing body of evidencefrom developing countries that indicates thedirections that programmes and resource allocationshould take. It is time for all of us working inreproductive health to expand youth-friendlyprogrammes on the basis of what we already know.

202
SHARON EPSTEIN
This is equally true for national-level and othergovernment decision-makers, reproductive healthprogramme managers and reproductive healthdonors.
References
Adamchak S, Bond K, MacLaren L, Magnani R,Nelson K and Seltzer J (2000) A Guide to Monitoringand Evaluating Adolescent Reproductive HealthPrograms. Washington, DC, FOCUS on Young Adults.[Available from the FOCUS Web site: http://www.pathfind.org/focus.htm]
Nelson K, MacLaren L, Magnani R (2000) Assessingand Planning for Youth Friendly Reproductive HealthServices. FOCUS on Young Adults Tool Series (4Workbooks). [Available from the FOCUS Web site:http://www.pathfind.org/focus.htm]
Senderowitz J (1999) Making Reproductive HealthServices Youth Friendly. Washington, DC, FOCUS onYoung Adults. [Available from the FOCUS Web site:http://www.pathfind.org/focus.htm]
Further reading
Alauddin M, MacLaren L (1999) Reaching Newlywedand Married Adolescents . In FOCUS Series.Washington, DC, FOCUS on Young Adults.
Dickson-Tetteh K and the University ResearchCorporation (2000) National Adolescent FriendlyClinic Initiative (NAFCI) of South Africa: Standardsand Criteria. Washington, DC, University ResearchCorporation.
Population Reference Bureau (2000) The World’sYouth 2000. Washington, DC, Population ReferenceBureau.
Population Reports (1998) New GATHER Guide toCounselling. The Population Information Program,Center for Communication Programs, The JohnsHopkins University School of Public Health.
Stewart L (2000) Presentation on AdolescentReproductive Health at Tulane University, School ofPublic Health and Tropical Medicine. New Orleans,Louisiana, Focus on Young Adults.
United Nations Population Fund (1999) Implementingthe Reproductive Health Vision—Progress andFuture Challenges for UNFPA: Adolescents and Youth.UNFPA Evaluation Findings. New York, UNFPA.[Available from the UNFPA Country Office or from DeliaBarcelona, Youth RH Task Force Leader, UNFPAHeadquarters, New York, USA]
Sharon Epstein, MA, MPHProgramme DirectorFOCUS on Young Adults1201 Connecticut Avenue, NW, Suite 501Washington, DC 20036USA

203
Reproductive health services for adolescents: recent experiences from Bangladesh
Background
Adolescents represent approximately one-fourthof the Bangladesh population. This large group isnot adequately prepared for reproductive and sexuallife, since its members lack basic information abouttheir bodies, sexuality, contraception and sexuallytransmitted infections (STIs) including HIV/AIDS.Despite the persistence of early marriage amongwomen in Bangladesh, the gap between age atmenarche and age at marriage is growing (Mitraet al., 1997). Though social customs discouragepremarital sexual relationships, small-scalestudies suggest that, by age 19, a considerableproportion of young men have experiencedpremarital sex, and such experience is notunknown among girls (Haider et al., 1997; Naharet al., 1999).
Adolescents in Bangladesh have limited accessto reproductive health (RH) services, and theservices that do exist are often unresponsive tothe broader needs of adolescents, especially thosewho are unmarried (Nahar et al., 1999). Knowledgeabout sexuality and reproductive health is generallylow. For example, one study (Rob et al., 2001)found that the majority of adolescents had no ideaabout changes associated with puberty, such asmenstruation or wet dreams, until they occurred.Other studies have found that adolescents haveinadequate knowledge about STIs including HIV/
AIDS (Bhuiya et al., 2000). In a national survey(Haider et al., 1997), few female adolescents couldanswer questions about STIs correctly, and only5% could identify any symptom of an STI.
To address these issues, the Population Councildesigned a multicountry operations research projectto determine the feasibility, effectiveness and costof creating sustainable ‘adolescent-friendly’reproductive health care services through apackage of interventions. In collaboration with theUrban Family Health Partnership (UFHP), thePopulation Council is implementing this project innorth-western areas—Pabna and Dinajpur areexperimental, while Rangpur is a control area.Participating clinics are open to married andunmarried adolescents, but the project focusesmainly on the needs of unmarried adolescents. Inpreparation for the intervention, the PopulationCouncil conducted a baseline survey onadolescents’ knowledge, attitudes and practicesrelated to sexual and reproductive health. Thoughthe project is ongoing, this paper describes thebaseline survey results and preliminaryexperiences from the project intervention.
Methods
To evaluate the intervention, researchers are usinga quasi-experimental, pre-post design in two study
Reproductive health services for adolescents:recent experiences from a pilot project inBangladesh
Ismat Bhuiya, Ubaidur Rob, M.E. Khan and Ahmed Al Kabir
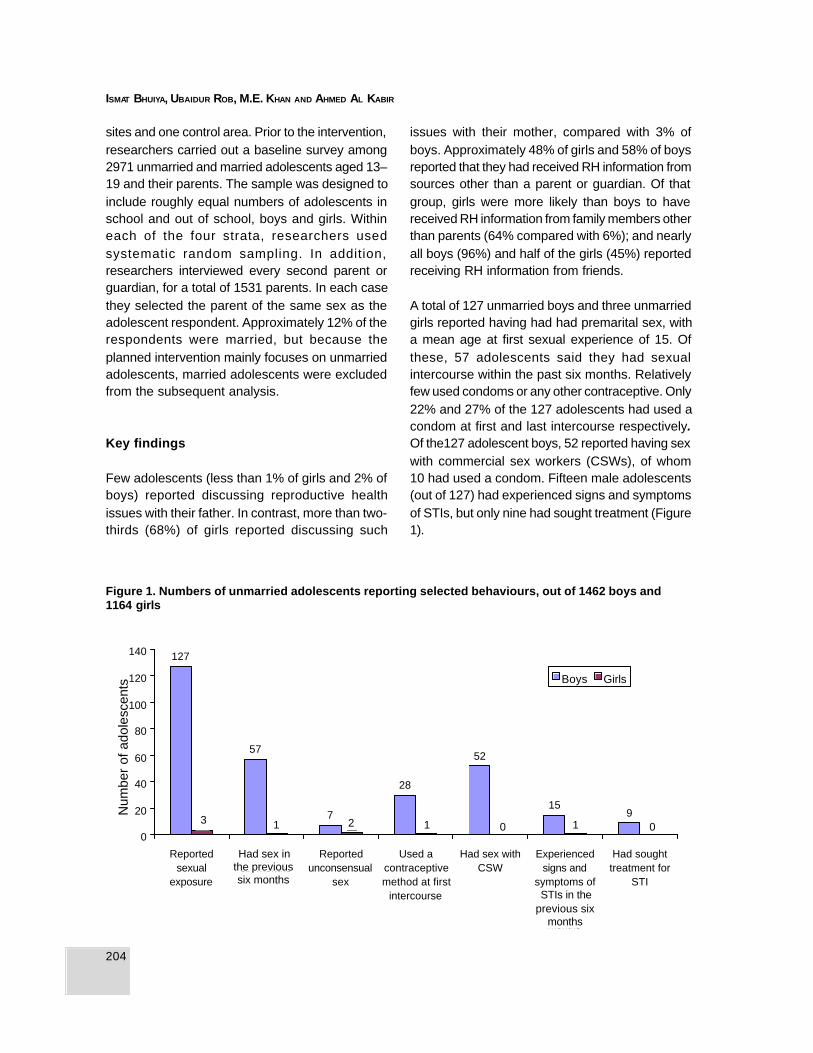
204
ISMAT BHUIYA, UBAIDUR ROB, M.E. KHAN AND AHMED AL KABIR
127
57
7
52
159
3 1 2 1 0 1 0
28
0
20
40
60
80
100
120
140
Reportedsexual
exposure
Had sex in lastsix months
Reportedunconsensual
sex
Used acontraceptivemethod at first
intercourse
Had sex withCSW
Experiencedsigns and
symptoms ofSTIs in the
past sixmonths
Had soughttreatment for
STI
Num
ber
of a
dole
scen
ts Boys Girls
1
sites and one control area. Prior to the intervention,researchers carried out a baseline survey among2971 unmarried and married adolescents aged 13–19 and their parents. The sample was designed toinclude roughly equal numbers of adolescents inschool and out of school, boys and girls. Withineach of the four strata, researchers usedsystematic random sampling. In addition,researchers interviewed every second parent orguardian, for a total of 1531 parents. In each casethey selected the parent of the same sex as theadolescent respondent. Approximately 12% of therespondents were married, but because theplanned intervention mainly focuses on unmarriedadolescents, married adolescents were excludedfrom the subsequent analysis.
Key findings
Few adolescents (less than 1% of girls and 2% ofboys) reported discussing reproductive healthissues with their father. In contrast, more than two-thirds (68%) of girls reported discussing such
issues with their mother, compared with 3% ofboys. Approximately 48% of girls and 58% of boysreported that they had received RH information fromsources other than a parent or guardian. Of thatgroup, girls were more likely than boys to havereceived RH information from family members otherthan parents (64% compared with 6%); and nearlyall boys (96%) and half of the girls (45%) reportedreceiving RH information from friends.
A total of 127 unmarried boys and three unmarriedgirls reported having had had premarital sex, witha mean age at first sexual experience of 15. Ofthese, 57 adolescents said they had sexualintercourse within the past six months. Relativelyfew used condoms or any other contraceptive. Only22% and 27% of the 127 adolescents had used acondom at first and last intercourse respectively.Of the127 adolescent boys, 52 reported having sexwith commercial sex workers (CSWs), of whom10 had used a condom. Fifteen male adolescents(out of 127) had experienced signs and symptomsof STIs, but only nine had sought treatment (Figure1).
Figure 1. Numbers of unmarried adolescents reporting selected behaviours, out of 1462 boys and1164 girls
Had sex inthe previoussix months
STIs in theprevious six
months
3 2 1 1 00

205
Reproductive health services for adolescents: recent experiences from Bangladesh
To assess the extent to which young people usedservices, researchers asked unmarriedadolescents whether they had visited healthfacilities for RH services in relation to any problemsof menstruation, discharge from penis or vagina,itching in the genital area, or ulcer in the genitalarea in the previous six months. Over 90% ofadolescents reported that they had not. Of the 22adolescents who had visited a health facility (15girls and 7 boys), girls visited government facilitiesmore than boys, and boys visited private facilitiesmore than girls. Researchers asked all unmarriedadolescents whether they thought they would betreated in a respectful manner if they visited clinicsor pharmacies for family planning services. Most(85%) felt that they would not be treatedrespectfully. A larger proportion of boys than girls(15% versus 1%) thought that they would be treatedwell if they visited a family planning clinic. Whenasked about STI services, only 26% of boys and7% of girls thought that they would be treated wellif they visited a clinic, and a similarly low proportion(24% and 6%) thought that they would be treatedwell if they visited a pharmacy.
Programme description
Using the findings from the baseline survey, theproject is trying to modify existing services atUFHP clinics to be more “adolescent-friendly” byintroducing several interventions. These include:training staff to treat adolescent clients withrespect, introducing designated hours specificallyfor adolescent clients, and increasing privacy andconfidentiality by ensuring that doctors who takeclinical histories and perform physicalexaminations also provide counselling. Theparticipating clinics offer reproductive healthservices, treatment for general adolescent healthissues, prevention and treatment of RTIs and STIs,including HIV/AIDS, family planning services,antenatal care, postnatal care, treatment foranxiety and depression, counselling and referrals.
To increase access, UFHP introduced a specialpre-paid health card for adolescents, which costs
Taka 20 (US$ 0.27). Young people can use thiscard to consult doctors at UFHP clinics withoutpaying fees for one year. Adolescents whoparticipate in the project’s reproductive healtheducation sessions receive a free health card. Inaddition, the project has established a telephonehotline and post-box facilities for adolescents whoare not comfortable visiting the clinic. Counsellorsanswer all queries over the phone without askingcallers to identify themselves. To answer queriesreceived at the post-box, staff print answers in theadolescents’ column of a local newspaper. Tocreate an enabling environment for theseinterventions, the project distributed educationalmaterials and undertook sensitization meetings todiscuss adolescents’ RH needs with gatekeeperssuch as parents, teachers, religious leaders,community leaders, health providers, politicalleaders and government officials.
In addition, the project developed a 20-hourreproductive health education curriculum foradolescents that addresses personal hygiene,nutrition, sanitation, changes during adolescence,child health and immunizations, marriage and legalrights, gender roles, drug abuse, sexualrelationships, sexual abuse, STIs including HIV/AIDS, childbirth process, antenatal care, postnatalcare, population growth and family planning. Theproject designed the curriculum with simplelanguage, stories and case studies.
To reach adolescents who are no longer in schoolwith the RH curriculum, the project used householdlistings to identify out-of-school girls and boys aged13–19, whom they formed into groups of 12 to 15adolescents, grouped by age, sex, employmentstatus and marital status. To teach these groups,the project selected facilitators among young adultsaged 21–28, who had at least 14 years ofeducation. Facilitators received a five-day trainingcourse on adolescent reproductive health issuesand facilitation skills.
The project has also used the school system toreach adolescents. Seven secondary schoolsagreed to introduce RH courses in classes 8 and

206
ISMAT BHUIYA, UBAIDUR ROB, M.E. KHAN AND AHMED AL KABIR
9. From each school, the project selected twoteachers to receive a four-day training on the RHcurriculum. The teachers prepared a lesson planbased on the RH curriculum for conductingsessions. They also planned to meet once a monthto share their experiences. During training sessionsand monthly meetings, teachers said that theywere comfortable with the curriculum, althoughthey expressed reservations about promotingcondoms.
Conclusions
The baseline study found evidence of sexual activityamong unmarried adolescents, particularly amongboys. However, sexually active, unmarriedadolescents reported that they did not feelcomfortable seeking advice or buying condomsfrom nearby clinics or pharmacies and few hadactually sought a service. In addition, theyperceived providers to be judgemental andunfriendly. Preliminary findings from the survey andinitial project experiences suggest the following.First, health services in Bangladesh should providereproductive health services for both married andunmarried young people. Second, to increaseaccess to services, it is important to address thesocial environment and increase communitysupport for information and services foradolescents. Finally, organizations that provideservices should introduce special hours foradolescent clients and train their providers toreceive, counsel and provide care for adolescents.
References
Bhuiya I, Rob U, Khan ME, Al Kabir A (2000)Reproductive health related KAPB of adolescents.Paper presented in a Workshop in Dinajpur.
Haider SJ, Saleh N, Kamal N, Gray A (1997) Study ofAdolescents: Dynamics of Perception, Attitude,Knowledge and Use of Reproductive Health Care.Dhaka, Population Council.
Mitra SN, Al-Sabir A, Cross AR, Jamil K (1997)Bangladesh Demographic and Health Survey 1996–1997. Dhaka and Calverton, Maryland: NationalInstitute of Population Research and Training(NIPORT), Mitra and Associates and MacroInternational Inc.
Nahar et al. (1999) Strategies to Meet the HealthNeeds of Adolescents: A Review. Dhaka, InternationalCentre for Diarrhoeal Diseases Research,Bangladesh. .
Rob U, Khan ME, Bhuiya I, Kabir M (2001) Factorsinfluencing adolescent sexual activity andcontraception in Bangladesh. Paper presented at thePopulation Association of America, Washington, DC,March 2001.
Ismat BhuiyaFRONTIERS in Reproductive Health ProgramPopulation CouncilHouse CES(B) 21, Road 118Gulshan, DhakaBangladesh
207
Attitudes of family planning workers toward providing contraceptive services in China
Background
With the opening of the system and generalsocioeconomic development in China, attitudestowards premarital sexual behaviour have changed,especially among adolescents. Sexual activityamong young unmarried men and women hasincreased rapidly during the past decade. A surveyconducted in seven Chinese provinces found thatthe proportion of married women who had had apremarital pregnancy was 16.8% in urban areasand 12.2% in rural areas. The proportions of urbanand rural married women who had premaritalinduced abortions were 2.4% and 1.9%,respectively, between 1987 and 1991. The studyalso found that rates of premarital pregnancyamong this group had increased between 1987 and1991 (Xu, 1998). Surveys conducted amongunmarried women visiting maternal and child healthcentres in Shanghai, Nanjing and other cities inthe 1990s for the required premarital physicalexamination showed that about 70% of womenwere sexually experienced (Gao, Tu & Yuan, 1997;Dai et al., 1996). Many of these sexuallyexperienced women were younger than 24 yearsat the time of first intercourse (Gao, 1997).
Although the proportion of sexually activeunmarried young adults is high, their contraceptiveuse rate is low, which places them at high risk ofunplanned pregnancy and induced abortion (Xu,
1998; Sun, 1994; Li et al., 1998; Liu et al., 1992).Lack of information about fertility and contraceptionand lack of access to contraceptive methods, aretwo important reasons for low contraceptive useamong young unmarried people in China (Gao, Tu& Yuan, 1997). Their lack of knowledge about sexand reproductive health combined with increasedpremarital sex has also put unmarried youth atincreased risk of sexually transmitted infections(STIs). Studies have found that between 25% and35% of STI patients are young and unmarried (Hu,1996; Xia, 1995; Li et al., 1997; Xu, 1997).
There is an urgent need to provide sex educationto raise awareness about self-protection as wellas to promote use of contraceptive services amongunmarried young adults in China. However, currentfamily planning (FP) services in China are mainlyfor married couples and pay little attention to theneeds of the unmarried. Meeting the reproductivehealth needs of young unmarried people hasbecome a challenge for the Chinese governmentand relevant departments.
This paper describes a multicentre study that wasdesigned to determine the attitudes towardproviding contraceptive and sexual/reproductivehealth services to sexually active unmarried youngadults, among different groups. Respondentsincluded sexually active, unmarried young adults,their parents, service providers and policy-makers
Attitudes of family planning workers towardsproviding contraceptive services forunmarried young adults in eightcentres in China
Gao Ersheng, Tu Xiaowen and Lou Chaohua

208
GAO ERSHENG, TU XIAOWEN AND LOU CHAOHUA
in different areas in China. The purpose of the studywas: 1) to identify unmet needs and barriers toprovision of contraceptive, sexual and reproductivehealth services; 2) to find acceptable and feasibleways to provide services for young adults; and 3)to ascertain the views of policy-makers and otherson providing services. This paper focuses onattitudes of family planning workers towardscontraceptive services for sexually active,unmarried young adults.
Methods
This study was carried out in eight cities, namelyShanghai, Fujian, Henan, Hebei, Jiangsu, Zhejiang,Sichuan and Chongqing. From May to December1998, researchers recruited 1927 family planningworkers to participate in a survey, including 965contraceptive providers and 962 contraceptivedistributors.1 In addition, they conducted focusgroup discussions with family planning staff andcontraceptive providers in eight centres.
Key findings
Attitudes towards providing contraceptive andsexual/reproductive health services to unmarriedyoung adults vary between areas and populationgroups. About 60% of respondents approved of theidea that the Government should providecontraceptive services for unmarried young adults,a figure that ranged from 28.3% to 80% amongthe eight centres. Thirty-six per cent of respondentsdisapproved, and another 4% said that they didnot have an opinion. Family planning workers fromurban areas were more likely to oppose providingsuch services. One important reason why someFP workers objected to actively providingcontraceptive services for young unmarried peoplewas that they did not consider them to be theirtarget population.
1 Contraceptive providers are defined as family planning staff in stations of contraceptive services and family planningoffices, while contraceptive distributors are defined as family planning workers in residential areas and work units.
The results of logistic regression indicated thatwhere respondents came from, their income, andtheir awareness of the magnitude andconsequences of sexual intercourse amongunmarried young adults were significantly relatedto their attitudes towards active governmentprovision of contraceptive services for unmarriedyoung adults. Whether the respondents werecontraceptive providers or distributors had nosignificant relation to their attitudes towards activegovernment provision of contraceptive services forunmarried young adults.
Family planning workers’ suggestions foracceptable and feasible ways to providecontraceptive services varied from one centre toanother. Generally speaking, however, FP workersfrom all eight centres considered drug stores themost acceptable place to provide contraceptiveservices for unmarried young adults, especially inurban areas. In rural areas, respondents alsoconsidered the FP network among the mostacceptable ways to provide contraceptive servicesfor unmarried young adults, because the customof engagement before marriage is common insome rural areas, and because there are fewerdrug stores in rural areas than in urban areas.Respondents recommended doctors or FP workersas the most suitable people for providingcontraceptive services for unmarried young adults,and they recommended condoms as the mostsuitable contraceptive method for this group.
Conclusions
The study findings point to a number of policyrecommendations, including the following:
• The study highlighted the urgent need tochange the attitudes of FP workers towardsprovision of contraceptive services for unmarriedyoung adults, especially in some areas inChina.

209
Attitudes of family planning workers toward providing contraceptive services in China
• The Government should develop clear policiesto include young unmarried people in familyplanning programmes.
• It is important to find acceptable and feasibleways to serve different target populations indifferent provinces and cities, in particular, toexplore ways suited to urban and rural areas.It is also important to consider strengtheningthe supervision of drug stores, training drug storeclerks and setting up condom vending machinesin public places to increase access forunmarried young adults.
Acknowledgements: This study was supportedby WHO. The institutes that participated in thestudy and the principal investigators of eachinstitute were: Shanghai Institute of PlannedParenthood Research (SIPPR): Tu XW, Lou CH;Hebei Family Planning Research Institute (FPRI):Yu JR; Henan FPRI: Gan SX; Jiangsu FPRI: DingJH; Zhejiang Academy of Medical Sciences FPRI:Sun DL; Fujian FPRI: Zhang YL; Sichuan FPRI:Cui N; Chongqing FPRI: Li H. SIPPR was thecoordinating centre and Dr Gao E the coordinatorof this multicentre study.
References
Dai MJ et al. (1996) The relationship between attitudestowards premarital sexual behavior and premaritalsexual behavior among adolescents, SchoolMedicine of China, 17(1):17–19.
Gao ES (1997) Study on the needs and unmet needsfor newly married women in Shanghai. Final report.
Gao ES, Tu XW, Yuan W (1997) Factors influencingpremarital contraceptive use at time of first intercourseamong women in Shanghai. Chinese PopulationScience, 61(4):57–64.
Hu XG (1996) The study of STDs among 429unmarried adolescents. Chinese Journal ofPrevention and Therapy of STDs/AIDS, 2(5):206–207.
Li CL et al. (1997) STDs epidemic of Shandongprovince in 1996. Chinese Journal of Prevention andTherapy of STDs/AIDS, 3(4):152.
Li DM et al. (1998) The survey of 1010 inducedabortions among unmarried women in Shanghai.Population Studies, 22(3):31–34.
Liu YR et al. (1992) The analysis of family backgroundamong unmarried female youth who had inducedabortion. Reproduction and Contraception, 12(5):82–83.
Sun RD (1994) Survey on premarital pregnancies.Population and Eugenics, 1:4–5.
Xia ZL (1995) Epidemiology analysis of 9687 STDpatients from 1989 to 1993 in Yunnan province.Chinese Journal of Prevention and Therapy of STDs/AIDS, 1(2):17–18.
Xu L (1998) Trends, outcomes and influences ofpremarital pregnancy in seven Chinese provinces.Population Studies, 21(1):51–54.
Xu YP (1997) Epidemiology analysis of syphilisbetween 1991 and 1995 in Zhejiang province.Chinese Journal of Prevention and Therapy of STDs/AIDS, 3(2):58–59.
Dr Gao ErshengShanghai Institute of Planned ParenthoodResearch2140 Xie Tu RoadShanghai 200030China
210
YUPA POONKHUM
Background
Evidence suggests that many Thai youth havepremarital sex. The first sexual experience is oftenunprotected, which can lead to sexuallytransmitted infections (STIs), including HIV/AIDS,unwanted pregnancies and illegal abortion.Although the Government has a policy to promotefamily life/sex education in schools, adolescentsface many barriers to obtaining information andservices related to sexual and reproductive health.To address this situation, the Thai Department ofHealth began a project in 1997 entitled“Development Model to Improve AdolescentReproductive Health Services for ThaiAdolescents”, supported by the World HealthOrganization Regional Office for South-East Asia(WHO/SEARO). This paper describes the projectand presents preliminary findings and lessonslearned.
Methods
The first phase of this project was to assess thestatus of adolescents’ reproductive health (RH) inThailand and to identify their needs for reproductivehealth services. This situation analysis included areview of the existing research literature and focusgroup discussions (FGDs) with adolescents inschools. In addition, the Department of Health held
a “grid workshop” with experts in adolescentprogrammes. During this workshop, experts wereasked to brainstorm ideas that could contribute toguidelines and recommendations for policy-makersand relevant stakeholders. Information obtainedfrom this first phase was used to design the secondphase of the project, which aims to improve theaccessibility and quality of RH services foradolescents, and to increase RH knowledge andlife skills among adolescents.
Key findings
The situation analysis highlighted the need for“adolescent-friendly” counselling and healthservices. During focus group discussions,adolescents expressed preferences regarding thedelivery of RH services, including a preference forproviders of the same sex, who are friendly,generous and know how to communicate withadolescents. In terms of atmosphere, FGDrespondents emphasized a private, relaxedatmosphere that protects confidentiality, isdecorated in an “adolescent style” and is not calleda clinic. They suggested that such services beconveniently located in towns and near destinationssuch as cinemas, discotheques, shopping mallsand department stores. When asked aboutpreferred hours and days of operation, adolescentssuggested that services be available every day,
Providing adolescent-friendly reproductivehealth services: the Thai experience
Yupa Poonkhum

211
Providing adolescent-friendly reproductive health services: the Thai experience
24 hours a day, but especially after office hours.They mentioned a need for both face-to-face andtelephone counselling, preferably free of cost.Finally, they recommended that the services bepromoted through radio programmes, as well asposters, leaflets and stickers.
Project design
This pilot project targeted in-school adolescents,as more than 60% of Thai adolescents are in theschool system. The second phase of the projectpromotes four main strategies, namely RH life skillseducation in schools, peer education, training ofparents and counselling services at selected healthsites. The Department of Health is carrying outthis phase in two districts of Nakorn Sri-ThammaratProvince, in southern Thailand. The fourparticipating organizations are: 1) the ProvincialPublic Health Office, an administrative andimplementing agency in the areas of healthpromotion, health prevention, surveillance andbasic medical treatment; 2) the Maharaj ProvincialHospital; 3) the Pakpanung District Hospital; and4) the Buddhists Association, a provincialnongovernmental organization whose mission isto promote good mental health among all agegroups.
The first three of these organizations haveestablished “adolescent-friendly rooms” in whichthey provide counselling services. The Departmentof Health installed telephones in each of the “rooms”so that staff could also counsel adolescents overthe phone. The first adolescent-friendly room atthe Provincial Hospital is near the outpatientdepartment. The second adolescent-friendly roomis located at the Provincial Public Health Office,which stands apart from the clinic building. Thelast adolescent-friendly room is behind theoutpatient department at the District Hospital. TheBuddhists Association provides only telephonecounselling during the evening (18:00–21:00)
To ensure the quality of services, a working groupwas created to monitor the project and provide
ongoing training in counselling skills to the staff.To promote the services, participants met with discjockeys from local radio programmes and askedthem to help advertise the services. They alsoproduced training materials, such as manuals onfrequently asked questions and on how to providecounselling, as well as promotional material suchas posters, stickers, calendar cards andsignboards, which were disseminated in schoolsand public places. The final component of thisproject was to train peers, teachers and parentsto help increase RH knowledge and life skillsamong adolescents.
The project has incorporated many of the findingsfrom the focus group discussions. For example,training in counselling skills was a centrepiece ofthe project. Services are not offered in a “clinic”,but in an adolescent-friendly “room”. Efforts aremade to protect confidentiality through anonymousrecord-keeping. In three sites, telephone servicesare offered from 09:00 to 21:00, while the BuddhistsAssociation provides telephone counselling duringthe evening. Counselling and family planningmethods are offered free of charge. The projecthas followed the recommendation that the servicesbe promoted by radio.
However, the project has not been able toincorporate all of the adolescents’ suggestions.For example, it did not set up adolescent-friendlyrooms in commercial areas, because it tried touse existing government resources in an effort tokeep costs low. Moreover, it has been impossibleto ensure that all counsellors are the same sex asthe clients, as most counsellors are women.
Lessons learned
The Department of Health has not yet undertakenthe final evaluation, but several preliminary lessonshave been learned, based on client records,discussions and observations during supervisionand monitoring activities. First, the projectdemonstrated that establishing adolescent-friendlyservices at government hospitals is feasible and

212
YUPA POONKHUM
sustainable. Using their government budgets, thesehospitals managed to set up adolescent-friendlyservices and to support counsellors throughovertime payments. Second, in the process ofconducting the focus group discussions, healthproviders began to realize the magnitude andseverity of RH problems among adolescents in theirprovincial area, and most expressed a newwillingness to devote themselves to prevention ofadolescent RH problems.
However, the project has found that hospitals maynot be the best location for adolescent-friendlyrooms because of low acceptability amongadolescents. The majority of adolescent clientshave preferred telephone counselling to face-to-facecounselling, probably because it gives them moreprivacy and confidentiality. Most call after officehours or around noon. Few adolescents have comefor face-to-face counselling services. As a result,the project may need to find more acceptable sitesthat will attract adolescents.
Finally, the project experience suggests that,despite training, not all staff can be goodcounsellors. Some have not followed counsellingprocedures, have tried to dominate clients’decision-making, or conversely, have lackedconfidence in their skills. Refresher courses, caseconferences, supervision and back-up have provenessential to ensuring quality services.
The project found that a variety of means is neededto communicate with adolescents. Client recordsrevealed that radio programmes, friends, teachersand other advertising efforts such as posters,stickers and signboards played a significant role
in promoting the services among adolescents.Radio broadcasting is the most expensive means,but it seems to reach the majority of adolescents.
Conclusions
Based on experiences gained from this project,the relevant research, as well as a recognition ofthe magnitude of RH problems among Thaiadolescents, the Director General of theDepartment of Health has declared that adolescent-friendly services are the Department’s top priority.He aims to improve the accessibility, availabilityand quality of counselling and health services forThai adolescents, with an emphasis on outreachservices. To achieve these objectives, theDepartment of Health will collaborate with healthpromoting centres, provincial public health offices,provincial hospitals, district hospitals and otherrelevant governmental and nongovernmentalorganizations to gain more experience withadolescent-friendly services in various settings. Theplan is to establish at least 24 adolescent-friendlycorners”(called “Friend Corners”) in the year 2001,and 51 more by the year 2002, at attractive locationssuch as department stores, youth centres,colleges and universities.
Yupa Poonkhum, MPHSenior Public Health Technical OfficerFamily Planning and Population DivisionDepartment of HealthMinistry of Public HealthNonthaburi 11000Thailand
213
Establishing adolescent health services in a general health facility
Establishing adolescent health services in ageneral health facility
Rajesh Mehta
Background
It has increasingly been recognized thatadolescents form a specific group in society andhave their own specific needs. Adolescence hasbecome a more clearly defined developmental stagein human life, and there is currently a greaterrecognition of this group’s biological, psychosocialand health needs than before (Senderowitz, 1999).Exploration and experimentation, the hallmark ofadolescent behaviour (Sigel & Emans, 1997), oftenpropel adolescents towards risk-taking andexposure to unwanted pregnancy, HIV/AIDS andother sexually transmitted infections, substanceabuse and unintended injuries. At the same time,adolescents often face constraints in seekingservices, including misperceptions about their ownneeds, fear of disclosure and service provider’snegative attitudes (Senderowitz, 1999). Toovercome these constraints, it is imperative todevelop specifically designated services foradolescents.
Adolescent-friendly services should be able toattract young people, meet their needs comfortablyand with sensitivity, and retain young clients forcontinuing care. The most important attributes ofadolescent-friendly services are specially trainedstaff whose attitudes respect privacy andconfidentiality, and a comfortable clinic
environment. Ideally, the holistic package ofservices should include reproductive healthservices, nutrition counselling, counselling topromote responsible sexual behaviour and preventsubstance abuse, and services such asimmunizations and life skills education. Althoughoutreach services such as school-linked clinics,workplace clinics, satellite clinics and mobileclinics have proven to be more successful andcost-effective, services for adolescents can beprovided from fixed sites such as hospitals andclinics (Advocates for Youth, 1995; Action HealthIncorporated, 1998a, 1998b; Association forReproductive and Family Health, 1998; JohnsHopkins University/Population CommunicationServices, 1998).
Safdarjang Hospital is a government hospital inNew Delhi that has 1500 beds and provides servicesfree of cost to the public. Until now, no specificservices have existed for adolescents. Children upto 12 years of age are seen in the PaediatricsOutpatient Department, and those above 12 yearsof age are seen in the Medical OutpatientDepartment or other specialty clinics. However, withthe increased recognition of adolescents’ needs,the Safdarjang Hospital is planning to implementa specially designed set of services foradolescents. This paper describes the effort thatis under way.

214
RAJESH MEHTA
Project description
To achieve the objectives of the project, the hospitalwill take the following steps. First, it will assessthe felt needs of adolescents. Second, it willadvocate for adolescent health care and work togenerate demand in the community for adolescentservices. Third, it will establish an Adolescent Clinicthat will provide clinic-based preventive, promotiveand curative services. Finally, the hospital plansto build linkages with schools, colleges andnongovernmental organizations (NGOs).
To assess the health care needs of adolescents,researchers will carry out a survey of healthawareness and health care needs among schooland college students using a self-administeredquestionnaire. This will give us an idea about theneeds as perceived by adolescents themselves.We then plan to develop IEC (information,education and communication) materials, includingfact sheets on relevant issues to provide informationto adolescents. This material will be available atthe clinic, where clients can read it while they waitor take copies home with them to read later.
The hospital will also build networks with localschools and colleges in the vicinity, and develop atraining curriculum for school and college teachers.Two teachers from each partner school and collegewill be trained as school counsellors so that theycan deal with day-to-day problems of their studentsand refer students to the hospital clinic whenneeded.
In preparation for the opening of the AdolescentClinic, doctors and other clinic staff will receivetraining in counselling skills and adolescent-friendlycharacteristics. Once the clinic opens, staff willprovide the following services: (i) curative servicesprovided by a multi-specialty team consisting of apaediatrician, an obstetrician, a psychiatrist andcounsellors; (ii) referrals to other specialtyservices, by providing referral cards that entitlethem to preferential services the next morning; and(iii) preventive and promotive services, includinggrowth and development monitoring, vaccinations,
nutrition counselling and counselling to prevent risk-taking behaviour and encourage healthy behaviour.
The Adolescent Clinic will aim to provide servicesthat respect young people, honour their privacy,allow adequate time for client–provider interactions,and are convenient in terms of hours and location.The hospital will monitor the quality of servicesprovided at the Adolescent Clinic through the useof exit-interviews among a random sample of clientsattending the clinic. The “mystery client” methodwill also be applied periodically.
Finally, the hospital will develop linkages andpartnerships with NGOs that provide services toout-of-school adolescents. A two-way arrangementwill be developed whereby adolescents who needspecialist services will be referred to the hospital,and clinic clients who need social support will bereferred to the NGOs. To accomplish this, thehospital will provide training to NGO personnel.
References
Action Health Incorporated (1998a) Mobile clinic goesto school. Growing Up, March, vol. 6, No. 1.
Action Health Incorporated (1998b) The youth clinic.Growing Up, June, vol. 6 No. 2
Advocates for Youth (1995) School Based and School-Linked Health Center: The Facts. Washington, DC,Advocates for Youth.
Association for Reproductive and Family Health(1998) ARFH and Youth Friendly Services: TheSatellite Experience. Ibadan, Nigeria, ARFH.
Johns Hopkins University/Population Communica-tion Services (1998) “Your Electronic Counselor”makes Sex Education accessible to Young People inPeru. Baltimore, Maryland, JHU/PCS.
Senderowitz J (1999) Making Reproductive HealthServices Youth Friendly: Research, Program andPolicy Series. Washington, DC, FOCUS on YoungAdults. [Available from the FOCUS Website: http://www.pathfind.org/focus.htm]
Sigel EJ, Emans SJ (1997) In: Gellis Kagan, eds .Current Pediatric Therapy:856–861.
215
Establishing adolescent health services in a general health facility
Dr Rajesh MehtaSenior Paediatrician and CoordinatorSHAHN (Safdarjang Hospital AdolescentHealthcare Network)Department of PaediatricsSafdarjang HospitalNew Delhi 110029India
XIIIPanel discussions:views of young people,governments andinterested agencies

218
PANEL DISCUSSION
219
Putting reproductive health within the wider contexts of adolescent lives
Five young people from South Asia participated inthe panel discussion entitled “Putting ReproductiveHealth within the Wider Context of AdolescentLives: Challenges and Experiences”. Panellistspresented their perceptions and experiences ofadolescents’ reproductive and sexual health needs,drawing from both their work and their personallives. They discussed the challenges they face,and identified areas for further work. Ms PoonamMuttreja moderated the session and stressed theimportance of listening to young people and learningfrom their insights. The panellists had a variety ofexperiences and backgrounds, including those ofa peer educator, a law student/volunteer, a highschool student/volunteer, a trainer/puppeteer anda social science researcher who presented theperspectives of rural adolescents. Four of the fivepresenters were from India, and one was fromBangladesh.1
Each of the five presenters had been involved inadolescent sexual and reproductive health (ASRH)programmes, and each spoke from both theirprofessional and personal experience. While theyhad diverse backgrounds and experiences, theirpresentations emphasized similar themes. Allpanellists argued that it is essential to considerthe “young people behind the numbers” (Namit
Kapoor—FPAI, Jabalpur, India) and to recognizethe diverse sociocultural milieus within South Asia,which shape young people’s perceptions andbehaviours (Priyanka Debnath—FPAB, Dhaka,Bangladesh). All panellists expressed concernabout unsafe and unwanted sexual activity amongSouth Asian adolescents. They argued that manyyoung people’s sexual and reproductive healthneeds remain unmet, and they identified a rangeof innovative strategies for meeting those needs inways that would be acceptable to youth.
Issues and concerns
Panellists highlighted a range of factors thatundermine sexual and reproductive health in theregion, including the following. Premarital sexualrelations among young people are not rare, butthey tend to occur secretly, without full informationand without protection. Meanwhile, traditionalnorms make it nearly impossible for many youngpeople to talk with their parents or teachers aboutsex or puberty. Panellists argued that althoughadolescents represent a large segment of thepopulation, they remain invisible in many ways—unable to speak out about their intimate concernsand unable to get adults to recognize or meet their
Putting reproductive health within the widercontext of adolescent lives: challenges andexperiences
1 The lack of representation of other countries was noted by the Chair and was attributed to the inability of youngpeople to attend due to other commitments, largely academic examinations.

220
PANEL DISCUSSION
reproductive health needs. Panellists lamented thetendency of policy-makers to perceive young peopleas a homogeneous group, a perception that mayobscure the unique needs of different groups—forexample, girls versus boys, or those from poorerversus more affluent economic backgrounds.
Panellists presented many examples of youngpeople who lack even the most basic informationabout bodily changes during puberty or the risksof unprotected sexual behaviour. They suggestedthat myths, misconceptions and a lack ofawareness about ASRH are widespread amongSouth Asian youth—irrespective of socioeconomicstatus, religion, sex and residence. Panellistsexpressed concern that this situation has seriousadverse consequences for the mental, physical andemotional health of adolescent girls and boys. Onepanellist narrated the experience of a young,educated, urban girl who feared that she haddeveloped cancer when she experienced her firstmenstrual period (Priyanka Debnath—FPAB,Dhaka, Bangladesh). Another panellist describedhow misconceptions about pregnancy, conceptionand pubertal changes exacerbated risk-takingbehaviours among rural youth (Laboni Jana—CINI,West Bengal, India).
Panellists argued that because young people lackreliable sources of information and counselling onsex and reproduction, they rely instead on media,peers and pornographic material for information.One panellist pointed out that young people turnto these sources not out of choice, but becausethey lack other options (Imran Haidar—IFSHA, NewDelhi, India). Not only do these sources oftenprovide misleading and inaccurate information, theyoften promote gender stereotypes, inequality andmisconceptions. Many young people would preferto get their information from parents and teachers;however, many parents and teachers are tooembarrassed to discuss these issues withadolescents. Furthermore, many parents,teachers, service providers and even health trainersare themselves poorly informed. In some cases,these adults perpetuate old myths andmisconceptions. For example, one panel member
narrated an incident in which a health trainerconducting an information session for adolescentsexpressed the view that masturbation was wrongand should not be practised (Imran Haidar—IFSHA,New Delhi, India). Panellists suggested that thelack of sensitive, trusted and knowledgeable adultsis a major concern for adolescents.
Panellists also discussed adolescents’ inability toaccess health services. They described a rangeof concerns—including the general lack of services,providers’ judgemental attitudes and youngpeople’s fears about confidentiality. Panellistsnoted that young people generally perceive serviceproviders to be unresponsive to their physical andemotional needs, unwilling to provide relevant andsensitive information, and lacking the practicalskills and knowledge necessary to help youngpeople make informed decisions (Namit Kapoor—FPAI, Jabalpur, India; Laboni Jana—CINI, WestBengal, India).
Panellists also highlighted the failure ofgovernments to address young people’s needs.They argued that while governments generallyrecognize that adolescents constitute a significantproportion of national populations, they neglect to“look beyond the numbers”. It is imperative,panellists argued, that South Asian governmentsrecognize the varied needs of young people, breakthe silence around those needs and provideinformation and services in a sensitive, confidentialand respectful manner. Panellists made theimportant point that many programmes designedto provide information or services to adolescentshave not adopted priorities or approachesacceptable to youth. Panellists urged governmentsto listen to youth when designing programmesintended to serve young people. They argued thatprogrammes must be flexible and take intoconsideration the fact that young people are aheterogeneous group with concerns that vary byresidence, marital status, age and sex, as well assexual lifestyle.
Finally, panellists argued that programmes andpolicies must consider sexual and reproductive

221
Putting reproductive health within the wider contexts of adolescent lives
health in the context of adolescent developmentmore generally and address young people’s needsin a holistic and comprehensive manner (PriyankaDebnath—FPAB, Dhaka, Bangladesh). Panellistsalso discussed the issue of adolescents’ rights.They pointed out that their rights remain poorlyunderstood and poorly articulated in governmentprogrammes in South Asia.
Strategies
Panellists identified a host of strategies thatprogrammes can use to address adolescent sexualand reproductive health—at the level of families,communities and governments. Many of theircomments reflected their personal experiences.Above all, panellists argued, programmes musttreat adolescents as active and equal partnersrather than passive recipients of services. Onceagain, they argued that young people mustparticipate in programme planning andimplementation (Priyanka Debnath—FPAB,Dhaka, Bangladesh).
At the family level, panellists pointed out that closeinteraction with parents has a protective influenceon young people (Laboni Jana – CINI, West Bengal,India). Reflecting on her personal experience, onepanellist highlighted her close and open relationshipwith her mother including communication aboutsexual health issues. She attributed her self-confidence, her overall feeling of security and herability to communicate with other young people inher work and personal life to this close parentalinvolvement (Urvashi Gupta – FPAI, Bhopal, India).More generally, panellists underscored the needfor communication between a range of trustedadults and young people.
Panellists called for the development of innovativeways of raising young people’s awareness of theirhealth and their rights. They strongly supportedthe idea of providing information on sexuality froma young age, building appropriately on thiseducation from childhood all the way throughadolescence. Panellists suggested that there is
no magic age at which society should initiatesexuality education, since young people’s needsvary throughout their life. Rather, they argued,messages need to be tailored to young people’sconcerns as they arise. Child sexual abuseillustrates the need to educate children from anearly age—for example, by making childrenunderstand appropriate behaviour, their own rightsand how to deal with abuse when it occurs (ImranHaidar—IFSHA, New Delhi, India). Others in theaudience concurred with this view.
With regard to strategies for imparting informationand delivering services, panellists made severalsuggestions. They repeatedly mentioned the needto present information to adolescents in creativeways that open safe avenues for discussion andrespect confidentiality. Specifically, they mentionedthe following examples:
• The “Young Inspirers” Programme in Lucknowforms youth groups that participate inprogramme planning and implementation;young people have found these activities highlyacceptable as evidenced by high rates of youthparticipation (Namit Kapoor—FPAI, Jabalpur,India).
• A talk show entitled “Interaction” providesaccurate information to urban girls. Thisexample illustrates the positive role that mediacan play in disseminating sexual andreproductive health messages to adolescentsas well as to the larger community (PriyankaDebnath—FPAB, Dhaka, Bangladesh).
• One panellist discussed puppets and theatreas a way to demystify sensitive topics andprovide information to adolescents in acaptivating and non-threatening way (ImranHaidar—IFSHA, New Delhi, India).
• Another panellist shared her experience ofproviding confidential information using aletterbox approach. Adolescents “posted” theirquestions anonymously in a box after aworkshop session, and workshop facilitators
222
PANEL DISCUSSION
provided the answers to the whole group(Urvashi Gupta—FPAI, Bhopal, India).
• Panellists also mentioned talks, street playsand periodic bulletins as ways to create informalfora for discussion and information provision(Namit Kapoor—FPAI, Jabalpur, India).
• Panellists argued that mixed-sex trainingsessions with peer educators and adolescentshave helped reduce levels of sexual harassmentamong both rural and urban participants (LaboniJana—CINI, West Bengal, India; Namit Kapoor—FPAI, Jabalpur, India).
Panellists suggested that interaction betweenyoung people and adult researchers, programmemanagers, trainers and service providers canprovide important new directions for adolescentsexual and reproductive health programmes. Theyrepeatedly stressed peer educators and youthinvolvement as necessary components of youthprogrammes, and they recommended expandingthe pool of peer educators and building networksof young people to exchange ideas and designnew programmes. Whatever strategy a programmeuses, panellists argued that success ultimatelydepends on the skills of the educator or provider— including their gender sensitivity, knowledge,training and communication skills. There is nosubstitute for skilled educators, whether they areteachers, service providers or peers.
Finally, panellists were acutely aware of the culturaland programmatic milieu in which South Asianadolescents are socialized and the implicationsof this context for adolescent sexual andreproductive health. They argued that strategiesmust be both realistic and acceptable—realisticin that they must consider sociocultural
sensitivities at the community level, and acceptablein that they must respond to adolescents’ needs,raise awareness and enhance young people’sability to make informed choices.
The panellists:
Priyanka DebnathStudent/volunteerFamily Planning Association of Bangladesh(FPAB)DhakaBangladesh
Urvashi GuptaPeer educator/volunteerFamily Planning Association of India (FPAI)Bhopal, Madhya PradeshIndia
Imran HaidarTrainer and puppeteer with Interventions forSupport Healing and Awareness (IFSHA)New DelhiIndia
Laboni JanaAdolescent Resource CenterChild in Need Institute (CINI)West BengalIndia
Namit KapoorPeer educator/volunteerFPAIJabalpur, Madhya PradeshIndia
The session moderator was Ms PoonamMuttreja, Regional Director, MacArthurFoundation, New Delhi, India.
223
Enhancing adolescents’ reproductive health: strategies and challenges
Representatives from governments, non-governmental organizations (NGOs) andinternational agencies participated in a paneldiscussion entitled “Enhancing Adolescents’Reproductive Health: Strategies and Challenges”,moderated by Dr Iqbal Shah. The objective of thisdiscussion was to share information aboutadolescent sexual and reproductive health (ASRH)programmes from different sectors and differentcountries. Panellists were asked to draw from theirpersonal and institutional experiences indiscussing strategies and approaches used byASRH programmes, as well as challenges andopportunities confronting those who work in thisarea. Panellists included governmentrepresentatives from India, Nepal and Sri Lanka,as well as NGO representatives from Bangladesh1
and Pakistan, and representatives from internationalagencies with a wide regional presence, includingUNAIDS (the Joint United Nations Programme onHIV/AIDS) and the World Health OrganizationRegional Office for South-East Asia (WHO/SEARO).
Despite their different perspectives, all panellistsstressed several similar themes, many of whichcoincided with those expressed by young people
themselves in an earlier panel discussion. Everypanellist called for youth involvement in the designand implementation of programmes: the need toplan with rather than for young people. They arguedthat strategies for youth must be different from thosefor adults, which requires innovative programmingat both the macro and grassroots levels. Panellistsalso agreed on the need for comprehensive policiesfor youth at the national level. In terms ofprogramme priorities, all panellists mentioned theneed to raise young people’s awareness of risksthrough both school-based sex education and non-formal, community-based programmes.Participants outlined a range of approaches,reflecting different social, cultural and politicalcontexts in the region. Finally, there was aconsensus among panel members thatoperationalizing ASRH policies and programmespresents a major challenge in each of theircountries.
Dr Firoza Mehrotra highlighted the Government ofIndia’s commitment to issues concerning youngpeople—including their sexual and reproductivehealth. She described a variety of policies andprogrammes that address young people’s needs—notably the National Population Policy, the National
1 The moderator noted Dr Halida Hanum Akhter’s extensive experience and involvement in government committees onreproductive health issues and her current involvement in a quasi-government organization in Bangladesh, and askedher to provide an overview of the Bangladesh Government’s programmes and perspectives on adolescent sexual andreproductive health issues.
Enhancing adolescents’ reproductive health:strategies and challenges

224
PANEL DISCUSSION
Youth Policy, the National AIDS Policy, the NinthFive Year Plan and the Reproductive and ChildHealth Programme. The National Youth Policy, forexample, emphasizes youth participation,empowerment of young people, gender equity andrights. In addition, the policy calls for anintersectoral approach grounded in a realisticneeds assessment. Both the National PopulationPolicy and the National AIDS Policy recognizeyouth as an underserved population and devoteconsiderable attention to strategies for this group.Central tenets of these policies include youthparticipation and well-being, along with acommitment to address youth in a holistic andcomprehensive way. Dr Mehrotra discussed theurgent need to translate macro-level policies to thegrassroots level. Finally, she reiterated theGovernment’s commitment to engage youth inprogramme design and programmeimplementation. Referring to the Delhi Declaration,a statement by youth made at the South AsiaConference on Adolescents held in New Delhi ayear earlier, she highlighted the multifaceted needsof adolescents—for education, employment, andhealth-related information, counselling andservices. She also highlighted their eloquent callfor parents, school systems and Governments toaddress these needs.
Dr Deepthi Perera presented the ways in whichthe Government of Sri Lanka has addressed youngpeople’s sexual and reproductive health. Youngpeople in Sri Lanka face many of the same risksand sociocultural obstacles to sexual andreproductive health as young people in India. Animportant difference, however, lies in theireducational attainment. Because large numbersof young people in Sri Lanka complete secondaryeducation, the Government has taken measuresto address sexual and reproductive health needsthrough schools. Dr Perera described howprogrammes have taken a multi-pronged approach,including training teachers to deliver appropriateinformation in friendly and non-threatening ways,
and incorporating sex education into the schoolcurriculum. At the same time, the Government hasbuilt partnerships with NGOs, universities and civilsociety for implementing ASRH programmes.
In Nepal, the focus has been somewhat different.Dr Pathak highlighted three ways that theGovernment of Nepal serves young people’s sexualand reproductive health needs. These include:fostering a safe and supportive environment,providing health services and counselling, andproviding information. The Government implementsa range of interventions in schools and incommunity settings. Programmes address youngpeople themselves as well as adults who playimportant roles in the socialization of young people—parents, teachers and others. Theseprogrammes use innovative measures to reachyouth, including youth groups, telephonecounselling, camps and training programmes.Finally, they attempt to address adolescent sexualand reproductive health needs in a comprehensiveand integrated way.
In Bangladesh, the Government has incorporatedadolescent sexual and reproductive health issuesinto the health policy and essential servicespackages programme. Dr Halida Akhter describedhow the Government of Bangladesh hasoperationalized its commitment to achieving ICPD2
goals. The Government has focused on meetingadolescents’ needs through the provision ofservices and information, as well as througheducation programmes and campaigns to changebehaviour. It has implemented programmes inschools as well as in community settings, inpartnership with NGOs, bilateral and donoragencies, and civil society. Efforts are currentlyunder way to translate national policy into a set ofachievable goals and activities.
In contrast to these experiences, national policiesin Pakistan rarely mention young people’s sexualand reproductive health, and Government input on
2 The objectives outlined at the 1994 International Conference on Population and Development held in Cairo, Egypt(United Nations 1994).

225
Enhancing adolescents’ reproductive health: strategies and challenges
the topic is minimal. Ms Yasmeen Qazi outlinedthis situation and identified several challenges thatconfront programmes for young people, includingweak commitment at the highest level, limitedresources, lack of a national policy and the paucityof research that might indicate how best to moveforward. Despite these challenges, Ms YasmeenQazi described how networking through media,policy-makers, NGOs and communities hasencouraged a shift in Government thinking. As aresult, various stakeholders have begun to discussprogramme development in the area of adolescenthealth and development.
Representatives of international agencies engagedin addressing the sexual and reproductive healthof young people outlined priorities facing nationalprogrammes. Dr Swaroop Sarkar, UNAIDS, NewDelhi, highlighted the need for programmes to moveforward on several fronts, including mobilizingresources, making existing networks sustainable,forging new partnerships, scaling up programmesand mobilizing gatekeepers. He argued thatinternational agencies can play a pivotal role infostering networks and dialogue among differentsectors. Dr Neena Raina, WHO/SEARO,discussed the need to review existing policies andprogrammes. She also outlined essentialingredients of successful programmes, includinggenerating a sense of ownership and forgingpartnerships among stakeholders, developingindicators for evaluation, and most important,involving adolescents at all stages of programmedesign and implementation.
The discussion was summarized by one panellist(Dr Firoza Mehrotra) who outlined some lessonsthat Governments could learn from the Conferenceabout programmes for young people:
• Involve young people in the design andimplementation of all programmes.
• Gain rapport with, orient and sensitize trustedadults—including parents and teachers—toincrease their support for youth programmes.
• Orient parents to communicate better with theirchildren on sensitive issues relating toadolescent sexual and reproductive health.
• Develop materials in consultation withadolescents, and field-test them for feasibilityand acceptability.
• Maintain the confidentiality of young clients andoffer them services that are accessible, non-threatening, and non-judgemental.
• Take into consideration the suggestion that peereducators can make better teachers thanadults.
• Understand that life skills and coping skills arean integral part of adolescents’ needs;sexuality education is only one, albeitimportant component of these needs.
• Influence the media to provide positive rolemodels, address gender stereotypes andprovide accurate information on sexual andreproductive health issues.
• Forge partnerships with NGOs and other civilsociety groups.
Finally, all panellists recognized the familiarchallenges facing adolescent sexual andreproductive health programmes, including:balancing priorities vis-à-vis resources, scaling upprogrammes and sustaining them, and buildingeffective partnerships. Despite the diverse contextsand strategies in the region, the panel discussionconveyed a strong message that all countries ofthe region have made an increased commitmentto address the sexual and reproductive healthneeds of young people.
Reference
United Nations (1994). Programme of actionadopted at the International Conference onPopulation and Development, Cairo, 5-13
226
PANEL DISCUSSION
September, 1994. New York, United Nations(document No. A/CONF. 171/13).
The panellists:
Dr Halida Hanum AkhterDirectorBangladesh Institute of Research for Promotionof Essential & Reproductive Health andTechnologies (BIRPERHT)DhakaBangladesh
Dr Firoza MehrotraPlanning CommissionGovernment of IndiaNew DelhiIndia
Dr Laxmi R. PathakMinistry of HealthGovernment of NepalKathmanduNepal
Dr Deepthi PereraDirector of Youth, Elderly and DisplacedPersonsDept of Health – Ministry of HealthGovernment of Sri LankaColomboSri Lanka
Ms Yasmeen QaziExecutive DirectorPAVHNA (Pakistan Voluntary Health & NutritionAssociation)KarachiPakistan
Dr Neena RainaWHO/SEARONew DelhiIndia
Dr Swaroop SarkarUNAIDSNew DelhiIndia
The session moderator was Dr Iqbal Shah, WorldHealth Organization, Geneva, Switzerland.
XIVLooking forward:recommendations of theconference

228
SARAH BOTT, IQBAL SHAH AND SHIREEN J. JEJEEBHOY

229
Looking forward: recommendatons for policies, programmes and research
Programme recommendations
This Conference brought together over 250 peoplefrom many different disciplines, sectors andcountries. A central aim of the Conference was toencourage dialogue among governmentrepresentatives, researchers, programmemanagers and service providers. The Conferenceorganizers hoped that after participants sharedtheir perspectives, knowledge and experience,service providers would return to their practiceswith more sensitivity towards adolescents,researchers would identify future lines of researchmost likely to benefit young people, and decision-makers would design policies and programmesbased on a more informed understanding ofadolescents’ needs and successful public healthstrategies. Indeed, in his inaugural speech on thefirst day of the Conference, Mr Nanda, Secretaryof Family Welfare, Government of India, affirmedthe Government of India’s interest in theConference recommendations with a view towardsincorporating them in strategies currently beingformulated for adolescent reproductive health.
In general terms, participants called forgovernments and nongovernmental organizations(NGOs) in South Asia (and elsewhere) to addressyoung people’s sexual and reproductive healthneeds and concerns, including the spread of HIV/
AIDS and other sexually transmitted infections(STIs), high rates of unwanted pregnancy, obstetriccomplications and unsafe abortion. To accomplishthis, they argued for a twofold approach: investmentin prevention and services for specific healthproblems, as well as investment in young people’sbroader needs—for education, jobs, and supportivefamilies and communities.
As a group, adolescents have diverse lifeexperiences; they include married and unmarriedindividuals, male and female, those who are notyet sexually active, those who are sexuallyexperienced but have suffered no adverseconsequences, and those who have engaged inrisky sex and suffered health consequences.Services designed for one group may not beacceptable or appropriate for another. Participantsnoted that NGOs have been innovators indeveloping “youth-friendly” services, and theirefforts provide important lessons about how todesign programmes for youth. In most cases,however, their coverage is limited and theirexperiences tend to be poorly documented andevaluated. To overcome these challenges,participants called for programmes to forgepartnerships among governmental, non-governmental and private sectors, to build onexisting systems and to reach beyond the clinicto where young people actually spend their time.
Looking forward: recommendations forpolicies, programmes and research
Sarah Bott, Iqbal Shah and Shireen J. Jejeebhoy

230
SARAH BOTT, IQBAL SHAH AND SHIREEN J. JEJEEBHOY
Papers in this collection include many other specificpolicy and programme recommendations, assummarized in the following pages.
• Intensify efforts to postpone early marriage andchildbearing among adolescent girls
Papers in this collection highlight the great genderdivide that exists with regard to adolescentreproductive health. As many as 1 in 10 adolescentSouth Asian women (aged 15–19) gives birth eachyear, often before reaching physical maturity, andoften without adequate obstetric care. A numberof authors call for efforts to raise awareness amonggirls, parents, teachers and community leadersabout the negative impact of early marriage andpregnancy on the health of women and children.They suggest several ways to address this issue,including community-based education, changingthe laws where necessary, holding governmentsaccountable for enforcing the legal age of marriagefor girls, and expanding educational andoccupational opportunities for young women.Simultaneously, programmes need to find waysto enhance married girls’ autonomy within theirmarital homes, perhaps by encouraging education,strengthening girls’ life skills and generatingemployment opportunities. Given the low statusof married adolescent girls in many communities,some authors suggest that programmes musttarget not only young married women, but alsomore powerful family decision-makers, such ashusbands and mothers-in-law.
• Train providers to recognize married girls as ahigh-risk group and to understand the negativehealth consequences of their social status
In many parts of South Asia, married adolescentwomen have little autonomy over their sexual andreproductive lives. As a result, many experiencerisky pregnancies, forced sex and STIs. Theevidence suggests that providers should be trainedto recognize married adolescent girls as a high-risk group. Providers need to offer information,
counselling and services in ways that considergirls’ lack of power within their husbands’ families.They should reach out beyond the clinic toencourage young women and families to seekprenatal visits and adequate obstetric care. Underthe right circumstances and with careful training,providers could also be encouraged to ask aboutyoung women’s experiences of coercion andviolence, as well as STI symptoms. In general,many providers need to learn how to provide carethat takes into consideration the social andeconomic constraints that young women face.
• Prioritize public health strategies that prevent the spread of sexuallytransmitted infections, including HIV/AIDS among young people
Studies in this collection suggest that premaritalsex among young people in South Asia is bothmore common than generally assumed andincreasing. Typically, South Asian societies haveplaced great value on young women’s chastitybefore marriage, but have not placed strict socialcontrols on the sexual behaviour of young men.As a result, not only are many young men at riskof STI/HIV infection, but young women who abstainfrom sex before marriage are often exposed to STIsthrough their husband’s behaviour. The growingseverity of the HIV/AIDS epidemic in South Asiashould compel every sector of society to considerwhat it can do. Authors in this collection suggesta host of measures, including: (a) increase accessto information and particularly risk awarenessthrough education programmes in the schools andthrough community-based efforts; (b) increaseaccess to quality health care for young people;and (c) carry out targeted campaigns to increasecondom use among high-risk groups, such as boysand young men who have sex with commercial sexworkers.
• Enhance young people’s ability to make informed choices about theirown health and risk behaviour
As has been observed in many settings, thiscollection of papers notes that young people need

231
Looking forward: recommendatons for policies, programmes and research
basic knowledge about sex, negotiation skills andthe ability to communicate with both peers andadults in order to make informed decisions aboutsexual and reproductive health. Studies presentedat this Conference suggest that relatively fewadolescents in South Asia are fortunate enoughto experience these protective circumstances.Adolescents across virtually all South Asiancountries face barriers to information and services.Adults such as parents, teachers, service providersand government officials have great influence overadolescents’ access to information and services,but the attitudes of these groups have often notkept pace with rapid social and economic change.Meanwhile, mass media have an increasinglypowerful, but not always positive, role in spreadinginformation and messages about how young peopleshould behave. Programmes that effectivelyincrease young people’s knowledge and life skillsmay offer one way to combat the spread of STIs,including HIV/AIDS among both young women andyoung men. While there is consensus thatadolescents need more (and better quality) sexeducation, there is often controversy over whatcontent is appropriate for adolescents at differentages, and who can best deliver this information.As a result, programmes must involve a wideconstituency—including parents, teachers, peers,religious leaders, community leaders and others.Papers in this collection suggest that such effortsare most likely to succeed when: (a) they addressa broad array of topics and skills that young peoplevalue; (b) they use a curriculum adapted to localbelief systems and behaviour patterns; (c) theycollaborate with groups within the community tobuild support for their work, including parents,community leaders and service providers; and (d)they ensure that staff are well trained and sensitiveto the perspectives of young people.
• Sensitize adults to provide a more supportiveenvironment for youth
Studies in this collection point out that good rapportand communication with trusted adults—especially parents—may help protect young
people from risky or non-consensual sex. Mostyoung people in these studies say that they wantmore information from adults in their lives, and manyspecifically say they wish they could discusssexual and reproductive health matters more openlywith their parents. These findings suggest a needto devise, implement and scale up activities thatstrengthen these ties. Programmes need to giveparents, teachers and other trusted adults theskills to understand adolescent development, todiscuss sensitive issues without embarrassment,and to provide a supportive environment moregenerally. Such interventions need to be rigorouslyevaluated, and strategies that prove effective needto be more widely applied.
• Increase access to high-quality “youth-friendly”health services drawing from the internationalexperience
Many studies in this collection describe barriersthat prevent young people from gaining access tohigh quality health services. Many young peopledo not have money to pay for services, do not wantto raise suspicion of sexual activity, or in manycases—particularly in the case of young girls—donot have authority within their families to makedecisions about their own health. Other barriersinclude: inconvenient locations and hours, longwaits, high costs and providers whom adolescentsperceive to be threatening, judgemental, or unwillingto respect young clients’ confidentiality.
Studies suggest that adolescents throughout theworld define youth-friendly services in broadlysimilar ways. For example, young people typicallymention special hours or sites for adolescents,convenient locations and hours, drop-in hours, aplace that does not look like a clinic, affordablefees and respect for confidentiality. Several authorsemphasize the importance of services such ascounselling and life skills development that helpyoung people manage their relationships withfriends, partners and families. Others highlight theneed for providers to understand the physiologicaldifferences between adolescents and adults,

232
SARAH BOTT, IQBAL SHAH AND SHIREEN J. JEJEEBHOY
differences that increase obstetric risk and makecertain contraceptive methods more or lessappropriate for young people. Perhaps mostimportant, young people say that they want staffto be empathetic, trustworthy and non-judgemental. Evidence from some communities(see Bhuiya et al., this volume) suggests that theperceived unfriendliness of providers deservesresponsibility for much of their reluctance to usehealth services.
There is now sufficient evidence—both from theinternational literature and from South Asia—tojustify widespread efforts to increase access tohealth care by making services more “youth-friendly” along the lines described here. Experiencefrom existing programmes suggests that toaccomplish this objective on a national scale, publicsector programmes need to build partnerships withboth private and nongovernmental sectors.
Recommendations for research
During the Conference, several participantsremarked that just a few years ago, it would havebeen difficult to predict the wealth of informationshared during this Conference. Nevertheless,important knowledge gaps remain. The Conferencehighlighted many areas that merit additionalresearch. There is much that we still do not knowabout South Asian adolescents’ lives or abouteffective strategies to address their sexual andreproductive health needs. This sectionsummarizes some key research priorities thatConference participants identified.
• Investigate sexual and reproductive choiceamong married youth
Given that a large proportion of South Asian womencontinue to marry in adolescence, there is a needfor better understanding of areas such as: (a) whyparents continue to marry their daughters early;(b) what factors constrain married adolescents’ability to make sexual and reproductive choices;
(c) how programmes and policies can ease socialpressure on girls to bear children before they arephysically mature; (d) what are the experiencesand needs of young first-time parents; and (e) whatare the circumstances surrounding young marriedwomen’s exposure to unsafe pregnancy, STIs andsexual coercion more generally. This Conferencehighlighted the need for both social science andoperations research to explore the effectivenessof interventions designed to enhance the autonomyand well-being of married adolescent women.
• Investigate pre- and extramarital sexualbehaviour, awareness and attitudes, includinghow adolescents form sexual partnerships andwhat factors increase or protect them from risk
The severity of HIV/AIDS in South Asia calls forspecial efforts to understand the levels and patternsof sexual activity, the ways in which sexualpartnerships are formed, and the social and culturalfactors that facilitate or hinder healthy behaviour.For example, more research on the magnitude andsocial context of unprotected sex with commercialsex workers could raise awareness about youngpeople’s vulnerability and could help identify publichealth strategies that could protect young peoplefrom HIV/AIDS and other STIs. More generally,many settings need a better understanding ofpremarital behaviour patterns, norms and genderroles among women and men, including how youngpeople form relationships, how they makedecisions about sex and how they communicatewith adult gatekeepers. Papers presented at thisConference reflect the limitations of the broaderresearch literature from this region; most focus onsmall samples or particular groups such as collegestudents or street children. To achieve a morecomplete picture of adolescents’ extramaritalexperiences, we need research that is both morerepresentative and more in-depth.
• Explore the levels, patterns and context ofunwanted pregnancy and abortion among youngwomen

233
Looking forward: recommendatons for policies, programmes and research
Studies in this collection suggest that unwantedpregnancy and abortion are observed amongdisturbingly high proportions of adolescent women.Evidence suggests that sexually active girls aremore likely than adult women to have an unmetneed for contraception, to experience an unwantedpregnancy, to delay seeking abortion, to seekabortion services from unqualified providers, to lackfamily support and to experience post-abortioncomplications. Despite the serious implications ofthese findings, there is limited information aboutunwanted pregnancy and abortion amongadolescents—in part due to the practical difficultiesof studying such a sensitive issue. To address theproblem, we need more information about howadolescents deal with unwanted pregnancy, howthey make decisions, what factors limit theiraccess to health care, what providers they chooseand why, what consequences they experience,and—in the case of abortion-seekers—whetherthey receive counselling on post-abortioncontraception.
• Explore sexual coercion and rape suffered byadolescent girls and boys, both married andunmarried
This collection highlights adolescent girls’ andboys’ vulnerability to sexual harassment, coercionand violence. Such coercion may involve physicalforce, threats or blackmail, as well as behaviourssuch as offers of money or favours in exchange forsex. Several authors note that, in some cases,parents curtail educational opportunities for girlsprecisely because they want to protect theirunmarried daughters from such coercion. At thesame time, the experience of forced sex withinmarriage is reported by women in several studiesin South Asia, and even considered normal bysome. Given the dearth of data on this topic,however, more research is needed to documentlevels and patterns of sexual coercion and violence,their nature and extent, the factors that protectadolescents or render them more vulnerable tocoercion, and the consequences of coercion forcontraceptive use, reproductive choices and broad
efforts to protect their own health. In particular,authors note that not enough is known about theextent to which adolescents as a group suffer frommental health problems associated with suchcoercion.
• Investigate adolescents’ access to health careand the quality of that care
Several papers in this collection call for researchersto help identify ways to increase young people’saccess to high quality care. First, authors notethat those who wish to make services “youth-friendly” need to understand the specific factors ineach community that prevent young people fromobtaining appropriate information and services. Thisenables programmes to be adapted to the localsocial and cultural setting. Second, studiessuggest that young people in South Asia often turnto unqualified providers, because of a lack ofaccessible alternatives. More evidence aboutinadequate care could build political will to reformthe informal health sector and increase access tobetter-quality services. Third, Conferenceparticipants suggested that we need moreresearch on quality of care in “youth-friendly”services. How should evaluators measure qualityof care for young people? What approaches havesuccessfully changed provider attitudes? How canprogrammes increase quality of care and sustainit as they scale up? Are some models of “youth-friendly” services better than others? How muchdo they cost? Fourth, authors note a number ofspecific operations research questions that remainunanswered. For example, can programmes thatprovide services in places where adolescentsactually spend their time (e.g. mobile clinics, malls,schools, etc.) attract more clients than traditionalclinic facilities? Are drugstores equipped to serveyoung people’s contraceptive needs? What are thestrengths and weaknesses of peer counsellorscompared with adult counsellors?
• Investigate the needs and attitudes among dif-ferent subgroups and settings

234
SARAH BOTT, IQBAL SHAH AND SHIREEN J. JEJEEBHOY
Several Conference participants note the dearth ofinformation about selected subgroups and settings.For example, how can services and programmesreach out-of-school adolescents? What are theparticular needs of subgroups within the broad agerange of 10 to 19? What do youth aged 13 to 15need compared to those who are aged 16 to 19?How do attitudes, needs and behaviour vary bysetting, by rural and urban residence, by maritalstatus, and socioeconomic situation? Such datacould contribute to more effective policies andprogrammes, at both the local and national levels.
• Methodological innovations
This Conference highlighted the need for certainmethodological innovations in research onadolescent sexual and reproductive health (ASRH).Researchers must overcome several limitations ofexisting designs. First, study samples need to bemore representative of the populations from whichthey are drawn. Second, the sensitive nature ofadolescent sexuality calls for greater reliance onqualitative methods, either on their own, or toprovide more insights into quantitative findings.Third, research questions must be carefully framedand pilot-tested to allow for as much insight aspossible. Whatever methodology they use,researchers must go beyond simple descriptionsof data to more rigorous analyses of behaviouralrelationships and the social and cultural correlatesof adolescent reproductive health. Researchersshould also consider how to ensure informedconsent among young people—both in researchand in service provision.
• The need for more rigorous operations researchand programme evaluation
Finally, many papers in this collection argue thatwe need to invest more resources in operationsresearch and programme evaluation. Most ASRHprogrammes in South Asia have not had a strongevaluation component. Donors and programmemanagers need rigorous evidence about the
feasibility, effectiveness and acceptability ofinterventions designed to provide sexual andreproductive health information and services toyoung people in different settings in order to identifywhich strategies are effective, and therefore worthscaling up. Too often, however, programmeshesitate to invest money in evaluation, and simplyhope that their efforts produced results. Authorsidentified a number of specific programmeevaluation questions that merit attention. Forexample, to what extent do life skills programmesaffect adolescents’ decision-making, negotiationand communication skills and (where applicable)sexual and reproductive behaviour? Also, whilemany have recommended that programmes trainproviders to deliver “youth-friendly” services, fewprogrammes have evaluated the extent to whichsuch training has actually changed providerattitudes, knowledge, counselling skills, treatmentof their clients, or respect for adolescents’confidentiality.
Conclusion
Conference participants described many innovativeprogrammes and approaches from different partsof South Asia, and they suggest that themomentum to address these issues is gainingstrength. During the Panel session “PuttingReproductive Health within the Wider Context ofAdolescents’ Lives: Challenges and Experiences”,young panellists from Bangladesh and India sharedtheir recommendations, their vision and theircommitment. The young panellists and the papersin this collection emphasize the extent to whichadolescents’ broader needs—e.g. for education,employment, health care, self-esteem and familysupport—are inextricably linked to sexual andreproductive health. Society cannot adequatelyaddress one set of needs without considering theother.
Finally, although this collection provides a wealthof information about adolescent sexual andreproductive health in South Asia, it also highlightsthe knowledge gaps that remain. To make informed

235
Looking forward: recommendatons for policies, programmes and research
policy decisions, we need more social science andoperations research to understand whyadolescents’ sexual and reproductive health needsremain unmet and how services should bestructured given the social, cultural and economicconstraints that adolescents face. At the sametime, programmes need to learn from documentedsuccesses from other settings. As John Townsend(FRONTIERS Project, Population Council, USA)noted during the Conference, to date there havebeen more diagnostic studies than interventionsresearch, more experience with informationprovision than service provision, more resourcesinvested in developing service delivery models thanin evaluating programmes, and little research onquality of services for adolescents. Ultimately,developing and sustaining youth-centredprogrammes require an understanding of whatyoung people need and want, a willingness toinnovate and a commitment to adapt to youngpeople instead of expecting young people to useservice delivery models intended for either childrenor older adults.
Papers from this Conference portray adolescenceas a complex transition period with great potentialand risks. Adolescents differ by age, ethnic group,culture, religion and socioeconomic status.Nonetheless, South Asian adolescents have muchin common. Whether urban or rural, whethermarried or unmarried, whether living in Bangladesh,
India, Nepal, Pakistan, or Sri Lanka, adolescentsface many sexual and reproductive health problemsthat are not being adequately addressed bysociety.
There is an urgent need for programme managersand researcher to act in three related areas:
• At the level of the adolescent, there is a needto enhance young people’s awareness, self-efficacy and autonomy to enable informeddecision-making and reduce unsafe andunwanted sexual activity.
• At the same time, parents, teachers and theadult community more generally must facilitatethis decision-making, whether through free andopen communication, or by creating anenvironment that protects adolescents fromabuse, and enables them to access informationand services without fear.
• Finally, health services and providers must learnto welcome and serve young people’s sexualand reproductive health concerns and needs.
Such actions taken by governments, NGOs andindividual communities to promote adolescentsexual and reproductive health will have far-reachingimplications for young people, communities andnations.
Annex 1
238
239
Annex 1
International Conference on AdolescentReproductive Health: Evidence andProgramme Implications for South Asia1–4 November 2000, Mumbai, India
CONFERENCE AGENDA
Registration
Inauguration
Perspectives on key issuesChairperson: Nirmal K. Ganguly (Indian Council of Medical Research, New Delhi, India)
On being an adolescent in the 21st centuryPaul F.A. Van Look (World Health Organization, Geneva, Switzerland)
Programming for adolescents: Indian perspectivesA.R. Nanda (Ministry of Health and Family Welfare, New Delhi, India)
Key concerns and priorities for actionEna Singh (United Nations Population Fund, New Delhi, India)
Session 1: Sexual and reproductive health of married adolescentsChairperson: Gunvanti Goding (Welcome Trust, UK)
Sexual and reproductive health of married adolescents: findings from NFHS-IISumati Kulkarni (International Institute for Population Sciences, Mumbai, India)
When marriage occurs in adolescents: the sexual and reproductive health needs of marriedadolescents in Bangladesh
Syeda Nahid Mukith Chowdhury (Population Council, Bangladesh)
Early marriage and childbearing: risks and consequencesRamesh K. Adhikari (Institute of Medicine, Kathmandu, Nepal)
Newly married adolescent women: experiences from a case study in urban IndiaAnnie George (University of California, San Francisco, CA, USA)
Reproductive health status of married adolescentsSandhya Barge (Centre of Operations Research and Training, Vadodara, India)
Analysing adolescent pregnancy and its outcomeShivani Sachdev* (JJ Hospital, Mumbai, India)
Discussant’s commentsLeela Visaria (New Delhi, India)
* Abstract presentation.
240
Session 2: Panel discussion—Putting reproductive health within the wider context of adolescents’lives: challenges and experiencesModerator : Poonam Muttreja (MacArthur Foundation, India)
Panellists: Priyanka Debnath (Family Planning Association, Dhaka, Bangladesh); Urvashi Gupta (FamilyPlanning Association, Bhopal, India); Imran Haidar (Interventions for Support, Healing and Awareness(IFSHA), New Delhi, India); Laboni Jana (Child In Need Institute, Kolkata, India); Namit Kapoor (FamilyPlanning Association, Jabalpur, India).
Session 3: Sexual risk behaviours, perceptions and norms among unmarried adolescents: evidencefrom case studiesChairperson: Padam Singh (Indian Council for Medical Research, New Delhi, India)
Risk behaviours and misperceptions among low-income college students of MumbaiLeena Abraham (Tata Institute of Social Sciences, Mumbai, India)
Adolescent reproductive and sexual health: an exploration of trends in PakistanYasmeen Sabeeh Qazi (Pakistan Voluntary Health and Nutrition Association, Karachi, Pakistan)
Youth perspectives on the influence of gender norms on the reproductive health of adolescents in NepalShyam Thapa (Family Health International, Kathmandu, Nepal)
A study of reproductive health awareness and sex behaviour among adolescents in IndiaAzad S. Kundu (Indian Council of Medical Research, New Delhi, India) (Summary not available)
Youth and sexuality in Sri LankaKalinga Tudor Silva (University of Peradeniya, Peradeniya, Sri Lanka)
Adolescent sexual and reproductive health in Bangladesh: a needs assessmentLeena Choudhary* (International Planned Parenthood Federation, London, UK)
Discussant’s commentsRavi Verma (International Institute for Population Sciences, Mumbai, India)
Session 4: Meeting adolescents’ needs for contraceptionChairperson: Badri Saxena (New Delhi, India)
Adolescence and safety of contraceptivesOlav Meirik (Santiago, Chile)
Contraceptive behaviours among adolescents in Asia: issues and challengesSaroj Pachauri (Population Council, New Delhi, India)
Constraints to condom use among young men engaged in risky sexual behaviour inborder towns of Nepal
Anand Tamang (Centre for Research on Environment, Health and Population Activities, Kathmandu,Nepal)
Attitude of family planning workers towards providing contraceptive services for unmarriedyoung adults in eight provinces/cities of China
Gao Ersheng (Shanghai Institute of Planned Parenthood Research, Shanghai, China)
* Abstract presentation.
241
Annex 1
Evaluation of reproductive and contraceptive knowledge and sexual behaviour of undergraduateuniversity students
Lata Dandekar* (Gourai Maternity and Nursing Home, Mumbai, India)
Discussant’s commentsRoger Ingham (University of Southampton, Southampton, UK)
Session 5: Reproductive tract and sexually transmitted infectionsChairperson: Somnath Roy (India)
The risk of infections: gynaecological problems among young married women in Tamil NaduAbraham Joseph (Christian Medical College, Vellore, India)
Impact of STIs and AIDS on adolescents: a global perspectivePurnima Mane (Population Council, Washington, DC, USA)
Developing an interactive STD-prevention programme for youth: lessons from a north Indian slumShally Awasthi (King George’s Medical College, Lucknow, India)
Adolescents attending STI clinics: case study from PakistanShahid Maqsood Ranjha (SAHIL, Islamabad, Pakistan)
Gynaecological morbidity among teenage mothers: a study based on rural women of Uttar PradeshSampurna Singh* (International Institute for Population Sciences, Mumbai, India)
Discussant’s commentsRadhika Ramasubban (SOCTEC, Mumbai, India)
Session 6: Panel discussion—Sexual and reproductive health of young people: problems andinterventionsModerator: Mahinder Watsa (Family Planning Association India, Mumbai)
Panellists: Halida H. Akhter (Bangladesh Institute of Research for Promotion of Essential and Reproduc-tive Health and Technologies, Dhaka, Bangladesh); Daphney Conco (Addinston Hospital, Durban, SouthAfrica); Gao Ersheng (Shanghai Institute of Planned Parenthood Research, Shanghai, China); RogerIngham (University of Southampton, Southampton, UK); Vijay Kulkarni (Mumbai, India); Duru Shah(Mumbai, India); Vihang Vahia (Pune, India).
Session 7: Emergency contraception and termination of pregnancyChairperson: N.C. Saxena (ICMR, New Delhi, India)
Menstrual regulation among adolescents in Bangladesh: risks and experiencesHalida H. Akhter (Bangladesh Institute of Research for Promotion of Essential and ReproductiveHealth and Technologies, Dhaka, Bangladesh)
Induced abortions: decision-making, provider choice and morbidity experience in rural adolescentsBela Ganatra (Johns Hopkins University, Baltimore, MD, USA)
Terminating unwanted pregnancies among adolescents: magnitude and experiencesNozer Sheriyar (Family Planning Association India, Mumbai) (Summary not available)
Situation analysis of emergency contraceptive drug use among young people in Thailand: a Bangkokcase study
Wanapa Naravage (Program for Appropriate Technology in Health, Bangkok, Thailand)* Abstract presentation.

242
Adolescent abortion: a view from rural BangladeshM. Kapil Ahmed* (International Centre for Diarrhoeal Disease Research, Dhaka, Bangladesh)
Abortion among young married women in Colombo districtP. Hewage* (University of Ruhuna, Colombo, Sri Lanka)
Discussant’s commentsDale Huntington (Population Council, New Delhi, India)
Session 8: Unwanted sex: sexual violence and coercionChairperson: Azeema Faizunnisa (Population Council, Islamabad, Pakistan)
Adolescents and sexual coercionGeeta Sodhi (Swaasthya, New Delhi, India)
Experience of sexual coercion among street boys in BangaloreJayashree Ramakrishna (National Institute of Mental Health and Neuro Sciences, Bangalore, India)
Prevalence and correlates of abuse in adolescents in higher secondary schools in GoaVikram Patel (Sangath Centre for Child Development and Family Guidance, Goa, India)
Experience of violence: Reflections from male adolescentsBella Patel Uttekar (Centre of Operations Research and Training, Vadodara, India)
Discussant’s commentsSurinder Jaswal (Tata Institute of Social Sciences, Mumbai, India)
Session 9: Communicating with adolescentsChairperson: Nina Puri (FPA India)
Educational strategies in family life and sex education: non-formal, school and higher education levels—how far does it go and how much further does it need to go?
Vandana Chakrabarti (SNDT Women’s University, Mumbai, India)
Counselling youth on sexual and reproductive health: individual and peer programmesRaj Brahmbhatt (Family Planning Association of India, Mumbai, India)
Reproductive health education: experiences of Privar Seva Sanstha in communicating with youthSudha Tewari (Parivar Seva Sanstha, New Delhi, India)
Providing sex education to rural adolescents in Bangladesh: experiences from BRACSabina Rashid (Bangladesh Rural Advancement Committee, Dhaka, Bangladesh)
The Healthy Adolescent Project in IndiaMatthew Tiedemann (Family Health International, Research Triangle Park, NC, USA)
Barriers in reproductive health services in school based family life education programmesRama Sivaram* (KEM Hospital Research Centre, Pune, India)
Impact of IEC on AIDS awareness among adolescents in Haryana, IndiaRajesh Kumar* (Post Graduate Institute of Medical Education and Research, Chandigarh, India)
Discussant’s commentsSabiha Syed (United Nations Educational, Scientific and Cultural Organization, Paris, France)
* Abstract presentation.
243
Annex 1
Session 10: Poster presentations
Session 11: Building a safe and supportive environmentChairperson: Sharon Epstein (FOCUS on Young Adults, Washington, DC, USA)
Adolescent girls in India choose a better future: an impact assessmentMarta Levitt-Dayal (the Centre for Development and Population Activities, New Delhi, India)
Connections with parents, families and teachers: the views from both sidesRekha Masilamani (Pathfinder International, New Delhi, India)
A gender-sensitive perspective from two generations: motives and seekers of reproductive health knowl-edge in Pakistan
Minhaj ul Haque (Population Council, Islamabad, Pakistan)
Enabling adolescents to build life skills: capacity building of facilitatorsMridula Seth (United Nations Population Fund, New Delhi, India)
Integrating adolescent reproductive health into public health services in Bawal Block, HaryanaSunil Mehra* (Mamta, New Delhi, India)
Adolescent girl’s initiative in MumbaiParimala Subramanian* (KEM Hospital, Mumbai, India)
Discussant’s commentsHally Mahler (Family Health International, Research Triangle Park, NC, USA)
Session 12: Access to and quality of reproductive health services: adolescent perspectivesChairperson: Meenakshi Datta-Ghosh (Ministry of Health and Family Welfare, New Delhi, India)
What is adolescent friendly?V. Chandra Mouli (World Health Organization, Geneva, Switzerland)
Reproductive health services for adolescents: recent experience from a pilot projectIsmat Bhuiya (Population Council, Dhaka, Bangladesh)
Making NGO initiatives youth friendlySharon Epstein (FOCUS on Young Adults, Washington, DC, USA)
Establishing adolescent health services in a general health facilityRajesh Mehta (Safdarjang Hospital, New Delhi, India)
Providing adolescent-friendly health services: the Thai experienceYupa Poonkhum (Family Planning and Population Division, Ministry of Public Health, Nonthaburi,Thailand)
Adolescent friendly reproductive health servicesA.K.M. Alamgir* (Bangladesh Open University, Gazipur, Bangladesh)
Discussant’s commentsJohn Townsend (FRONTIERS Project, Population Council, Washington, DC, USA)
* Abstract presentation.
244
Session 13: Panel discussion—Enhancing adolescent reproductive health:strategies and challengesModerator : Iqbal Shah (World Health Organization, Geneva, Switzerland)
Panellists: Yasmeen Qazi (Karachi, Pakistan); Halida Hanum Akhter (Bangladesh Institute of Research forPromotion of Essential and Reproductive Health and Technologies, Dhaka, Bangladesh); Firoza Mehrotra(Planning Commission, Government of India, New Delhi); Laxmi R. Pathak (Family Health Division, HMG ofNepal, Kathmandu); Deepthi Perera (Department of Health Services, Ministry of Health, Colombo, Sri Lanka);Neena Raina (World Health Organization, New Delhi, India); Swaroop Sarkar (UNAIDS, New Delhi).
VALEDICTORY FUNCTIONChairperson: Meenakshi Datta-Ghosh
Iqbal ShahHarbans S. JunejaPurnima ManeV. Chandra MouliPadam SinghShireen JejeebhoyChander Puri
Note: Institutional affiliations of presenters reflect the situation at the time of the Conference.