
Results of Caregiver Survey: Where do we go from here? Moving ...

http://heb.sagepub.com/Health Education & Behavior
http://heb.sagepub.com/content/early/2014/09/04/1090198114547817The online version of this article can be found at:
DOI: 10.1177/1090198114547817
published online 5 September 2014Health Educ BehavTracy Chu, Martine Hackett and Navpreet Kaur
Exploring Caregiver Behavior and Knowledge About Unsafe Sleep Surfaces in Infant Injury Death Cases
Published by:
http://www.sagepublications.com
On behalf of:
Society for Public Health Education
can be found at:Health Education & BehaviorAdditional services and information for
http://heb.sagepub.com/cgi/alertsEmail Alerts:
http://heb.sagepub.com/subscriptionsSubscriptions:
http://www.sagepub.com/journalsReprints.navReprints:
http://www.sagepub.com/journalsPermissions.navPermissions:
at AXINN LIBRARY*E on September 8, 2014heb.sagepub.comDownloaded from at AXINN LIBRARY*E on September 8, 2014heb.sagepub.comDownloaded from

Health Education & Behavior 1 –9© 2014 Society for PublicHealth EducationReprints and permissions: sagepub.com/journalsPermissions.navDOI: 10.1177/1090198114547817heb.sagepub.com
The United States has experienced a dramatic decline in sudden infant death syndrome (SIDS) in the past 20 years (Hauck & Tanabe, 2010; Shapiro-Mendoza, Kimball, Tomashek, Anderson, & Blanding, 2009), due in part to widespread safe sleep Back to Sleep education efforts. However, though there is a downward trend in infant mortal-ity overall (MacDorman, Hoyert, & Mathews, 2013), the decline in SIDS in particular is also partially due to shifting diagnostic criteria, such that many infant deaths are now more likely to be attributed to causes such as injury, with the majority of injury deaths occurring during infant sleep (Krous, 2010; Senter, Sackoff, Landi, & Boyd, 2011; Shapiro-Mendoza et al., 2009). As a result, sleep-related infant injury deaths have quadrupled over the same time period (Shapiro-Mendoza et al., 2009) and are now a leading cause in infant death nationwide (MacDorman et al., 2013).
A primary risk factor for sleep-related infant injury death is the use of an unsafe sleep surface, that is, a surface other than a crib or bassinet. This risk factor is most commonly
discussed in the context of bed-sharing, that is, sharing a sleep surface with another person (Schnitzer, Covington, & Dykstra, 2012). However, infant injury deaths may also occur while sleeping alone on an unsafe sleep surface, as risk factors such as soft mattresses and excessive bedding still pose a hazard (Fortin et al., 2011).
Both quantitative and qualitative studies in the United States have sought to understand how caregivers make deci-sions with regard to many aspects of infant sleep, such as sleep position (Moon, Oden, Joyner, & Ajao, 2010) and bed-sharing (Krouse et al., 2012). Some reasons indicated by
547817 HEBXXX10.1177/1090198114547817Health Education & BehaviorChu et al.research-article2014
1Brooklyn College, City University of New York, Brooklyn, NY, USA2Hofstra University, Hempstead, NY, USA
Corresponding Author:Tracy Chu, Department of Health and Nutrition Sciences, Brooklyn College, City University of New York, 2900 Bedford Avenue, Brooklyn, NY 11210, USA. Email: [email protected]
Exploring Caregiver Behavior and Knowledge About Unsafe Sleep Surfaces in Infant Injury Death Cases
Tracy Chu, PhD, MPH1, Martine Hackett, PhD, MPH2, and Navpreet Kaur, BS2
AbstractObjectives. In the United States, infant deaths due to sleep-related injuries have quadrupled over the past two decades. One of the major risk factors is the placement of an infant to sleep on a surface other than a crib or bassinet. This study examines contextual circumstances and knowledge and behaviors that may contribute to the placement of infants on an unsafe sleep surface in infant injury death cases. Method. This study employed a retrospective review of 255 sleep-related injury death cases in New York City from 2004 to 2010 where an infant was found sleeping on an unsafe sleep surface. Mixed-methods analyses, employing both quantitative analysis of vital statistics data and risk variables extracted from the medical examiner files and qualitative analysis of the narrative content of the files, were conducted. Results. In 48% of cases, a crib or bassinet was identified in the home. Quantitative analysis revealed no significant differences in demographic or risk factor characteristics between infants who had a crib or bassinet and those who did not. Qualitative analysis highlighted factors in caregivers’ decision making related to situational convenience, preference, and misconceptions concerning safe infant sleep. The health belief model (HBM), specifically the constructs of perceived susceptibility, severity, benefits, and barriers, was used as a lens to understand factors associated with caregiver behavior. Conclusions. This study provides evidence that infants are at risk of sleep-related injury death even when a crib or bassinet is present. Understanding the factors that may influence safe sleep behaviors can help produce more appropriate interventions.
Keywordscribs, infant injury deaths, infant mortality, parent education, safe sleep, suffocation
at AXINN LIBRARY*E on September 8, 2014heb.sagepub.comDownloaded from

2 Health Education & Behavior
research include the facilitation of breast-feeding infants during the night (Buswell & Spatz, 2007), infant safety and comfort (Joyner, Oden, Ajao, & Moon, 2010), and cultural traditions (Nelson et al., 2001; Rice & Naksook, 1998). In addition, some anthropological research has demonstrated protective advantages to mother–infant bed-sharing, high-lighting the evolutionary need for bed-sharing (see McKenna & McDade, 2005; Volpe, Ball, & McKenna, 2013). Based on similar theories of mother–infant bonding, attachment par-enting philosophy (Sears, Sears, Sears, & Sears, 2013) advo-cates for bed-sharing and on-demand breast-feeding during the early months of life to promote maternal and infant well-being. These perspectives argue that current recommenda-tions are overly broad and advocate for a less restrictive approach that is based on assessment of risk profiles for sleep-related death. Indeed, the overall national trend for regular bed-sharing has been rising over the past decade (Colson et al., 2013).
Although extensive epidemiological research has been conducted using retrospective reviews of death scene inves-tigations to establish risk factors for sleep-related infant deaths (Fu, Moon, & Hauck, 2010; Lahr, Rosenberg, & Lapidus, 2007; Moon, Tanabe, Yang, Young, & Hauck, 2012; Ostfeld, Esposito, Pen, & Hegyi, 2010; Vennemann et al., 2007), and both quantitative and qualitative research have been conducted to determine the behaviors of the parents and caregivers of live infants in order to understand the reasoning behind the risk factors for sleep-related deaths such as bed-sharing (Ball et al., 2012; Fu, Colson, Corwin, & Moon, 2008; Moon et al., 2010; Norton & Grellner, 2011), no study has used qualitative analysis of death scene investigation records to retrospectively examine the factors that influenced the decision-making behaviors among caregivers whose infants have died. In New York City (NYC), sleep-related infant injury death is a leading cause of infant mortality, with infants found on an unsafe sleep surface in more than three quarters (76%) of cases (Fortin et al., 2011). To better under-stand caregiver behaviors, this retrospective study examined the vital statistics and medical examiner investigation data in cases of sleep-related infant injury deaths where infants were placed to sleep on an unsafe sleep surface. Additionally, this study examined circumstances that may have led to caregiv-ers’ use of unsafe sleep surfaces when a crib or a bassinet was available.
Method
This study employed a retrospective review of vital statistics data and medical examiner documentation, including death scene investigations, for 255 deaths in NYC from 2004 to 2010 of infants younger than 1 year. The cases selected for review were those that were attributed to International Classification of Diseases, Version 10 (ICD-10) codes encompassing asphyxia and undetermined injuries (ICD-10 codes W75, W84, Y33, Y34), where the infant was known to
be sleeping when last seen alive and where the infant was found to be sleeping on an unsafe sleep surface. Quantitative and qualitative analyses of vital statistics data and medical examiner documentation—including autopsy reports, med-ico-legal investigator reports based on investigation at the death scene and supplemental notes—were conducted to investigate factors that may have influenced caregiver deci-sion making and behaviors. This research was approved by the NYC Department of Health and Mental Hygiene’s Institutional Review Board.
Variables Examined
In this study, birth and death certificate records were accessed to provide overall demographic data such as mother’s age, race/ethnicity, nativity, health insurance status, infant age at death, and infant’s gestational age. Quantitative data extracted from Office of the Chief Medical Examiner (OCME) records included variables related to the context of the death, such as sleep location, sleep positioning, bed-shar-ing, and type and quantity of bedding used.
Qualitative data were extracted from the narrative sec-tions of the investigative reports and supplemental follow-up memos and additional documentation from the other sources (e.g., autopsy reports, medical records) compiled in the OCME files. In these narratives, investigators report on aspects of the physical environment, including the presence of a crib or bassinet. These notations may be found in an investigator’s narrative description of the home, in the sketch of the room where the infant was found, or in photos.
Data Analysis
Variables were extracted from medical examiner records into a Microsoft Access file. The quantitative variables were then exported to the software package SPSS, Version 20 (IBM Corporation, 2011) and matched by OCME case number to corresponding data from birth and death records. Quantitative analysis, primarily chi-square (χ2) analysis, was employed to compare the key demographic and risk factor characteristics.
The qualitative data were exported to the software pack-age Atlas.ti, Version 6.2 (Scientific Software Development GmbH, 2011). First the open-ended responses from the med-ical examiner files in cases where a crib or a bassinet was in the home were collected and aggregated into a database that maintained individual case identification. To identify poten-tial codes, we began with a review of existing literature on sleep-related infant care practices and then conducted a sum-mative content analysis using Atlas.ti in order to identify codes that related to why the crib or bassinet was not used for the infant’s last sleep. Using a summative content analysis approach (Babbie, 1992), themes were developed by first quantifying non–mutually exclusive codes. The themes that had more than five codes associated with them were
at AXINN LIBRARY*E on September 8, 2014heb.sagepub.comDownloaded from

Chu et al. 3
considered robust enough for further analysis. Then latent content analysis was performed by the authors in an iterative process to discover and determine the underlying meanings of the words and phrases being used (Hsieh & Shannon, 2005). The themes identified were assessed by the authors to determine if they were able to explain the behavioral reasons why caregivers chose to place infants to sleep on an unsafe sleep surface when an alternative was available. Finally, we matched identified themes to the domains of the HBM (Hochbaum, 1958; Rosenstock, 1966) as a lens to understand the factors associated with caregiver behaviors.
Results
In an initial qualitative examination of the 255 cases where infants were found dead on an unsafe sleep surface, the pres-ence of a crib or bassinet in the home was reported in inves-tigator notes in 47.8% of cases (n = 122). In 17.6% (n = 45) of the 255 total cases, it was noted that there was no crib or bassinet in the home. As the presence of a crib or bassinet was not a discrete, standardized variable recorded by investi-gators, in 34.5% (n = 88) of the cases it was unknown or undocumented whether there was one in the household. Excluding these cases with “missing” data, only those cases where the presence of a safe sleep surface in the household was clearly known (n = 167) were subsequently explored further in quantitative and qualitative analysis.
Maternal, Infant, and Behavioral Risk Factor Characteristics
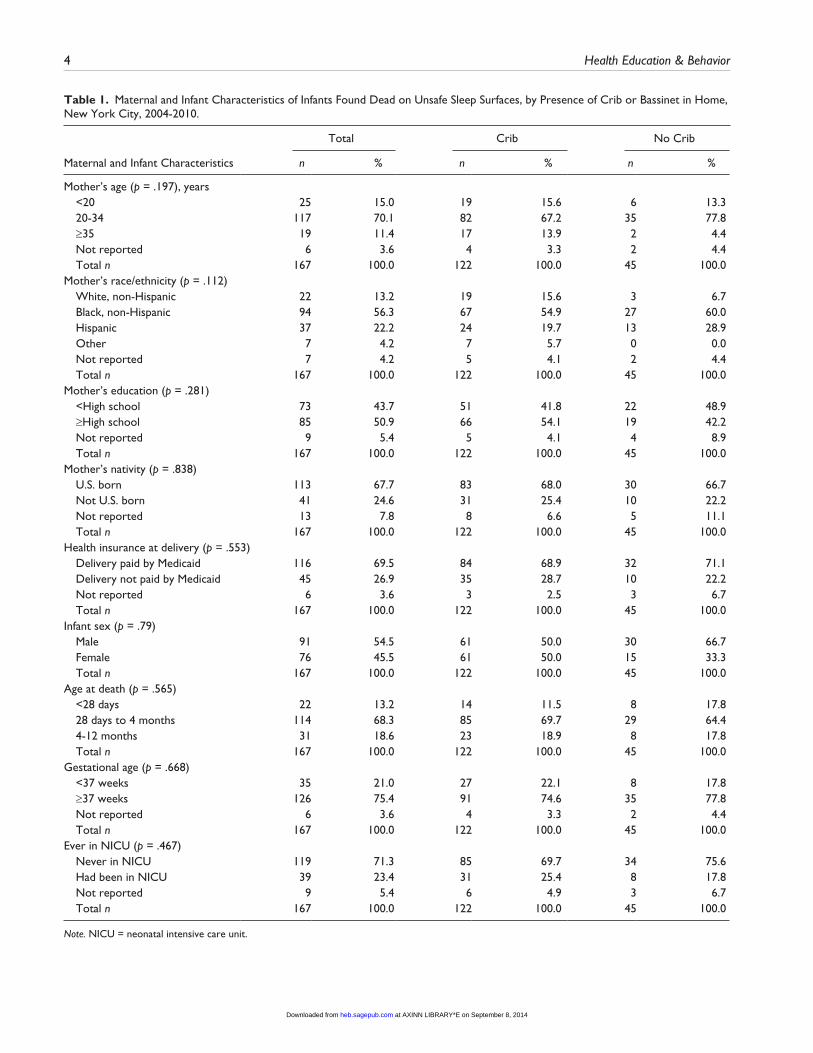
The maternal and infant characteristics of 167 cases of sleep-related infant deaths where the decedent was found in an unsafe sleep surface, and where the presence or absence of a crib or bassinet was documented, are presented in Table 1. Chi-square (χ2) analysis comparing the 122 cases where there was known to be a crib or bassinet in the home and the 45 cases where there was not indicated that there was no statisti-cal significance associated with any of these characteristics.
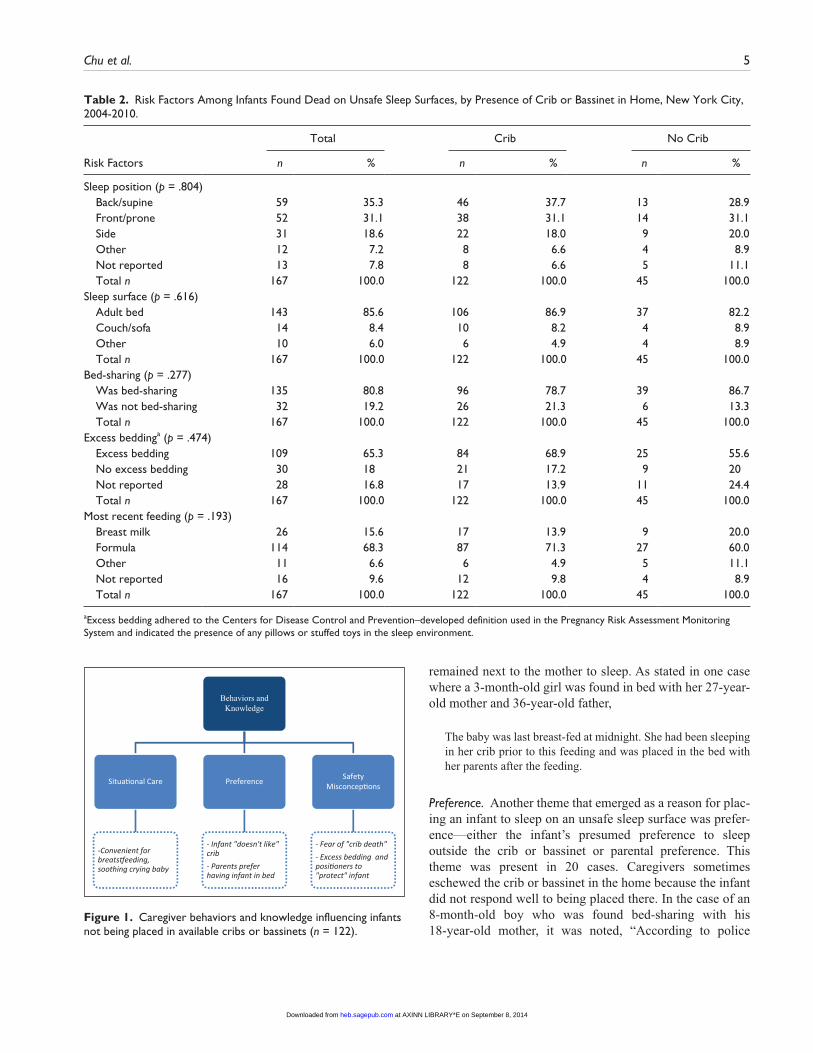
Other than placing infants on unsafe sleep surfaces such as adult beds or couches, there are a number of other known or suspected risk factors for sleep-related infant injury death connected to the sleep environment. These include placing the infant in prone or side sleep position, bed-sharing, and the presence of excess and soft bedding (American Academy of Pediatrics, 2000; Fortin et al., 2011). Table 2 presents these risk factors among the 167 infants found dead on an unsafe sleep surface, by presence of a crib or bassinet in the household. Overall, almost half of the infants were found in the prone or side position (49.7%), and most were found sleeping on an adult bed (85.6%), were bed-sharing (80.8%), or had excess bedding (65.3%). As a possible correlate to bed-sharing, infant breast-feeding status (i.e., whether the infant breast-fed during his or her last feeding) was also examined; in total, 15.6% of infants were breast-fed at their
last feeding. As with the maternal and infant characteristics, chi-square (χ2) analysis comparing those 122 infants who were known to have a crib or bassinet in the home and the 45 who did not revealed that there was no statistically signifi-cant difference associated with these risk factors.
In sum, among those infants who died while sleeping on an unsafe sleep surface, there was no statistically significant difference between those who were known to have a crib or bassinet in the home and those who did not, neither in terms of maternal and child characteristics nor in terms of behav-ioral risk factors associated with infant injury deaths. Because the quantitative data did not offer significant insight into the phenomena, we narrowed our focus to comprehensively examine those 122 cases where infants were placed on an unsafe sleep surface despite the presence of a crib or bassinet in the home.
Emerging Qualitative Themes Related to Caregiver Behaviors and Knowledge
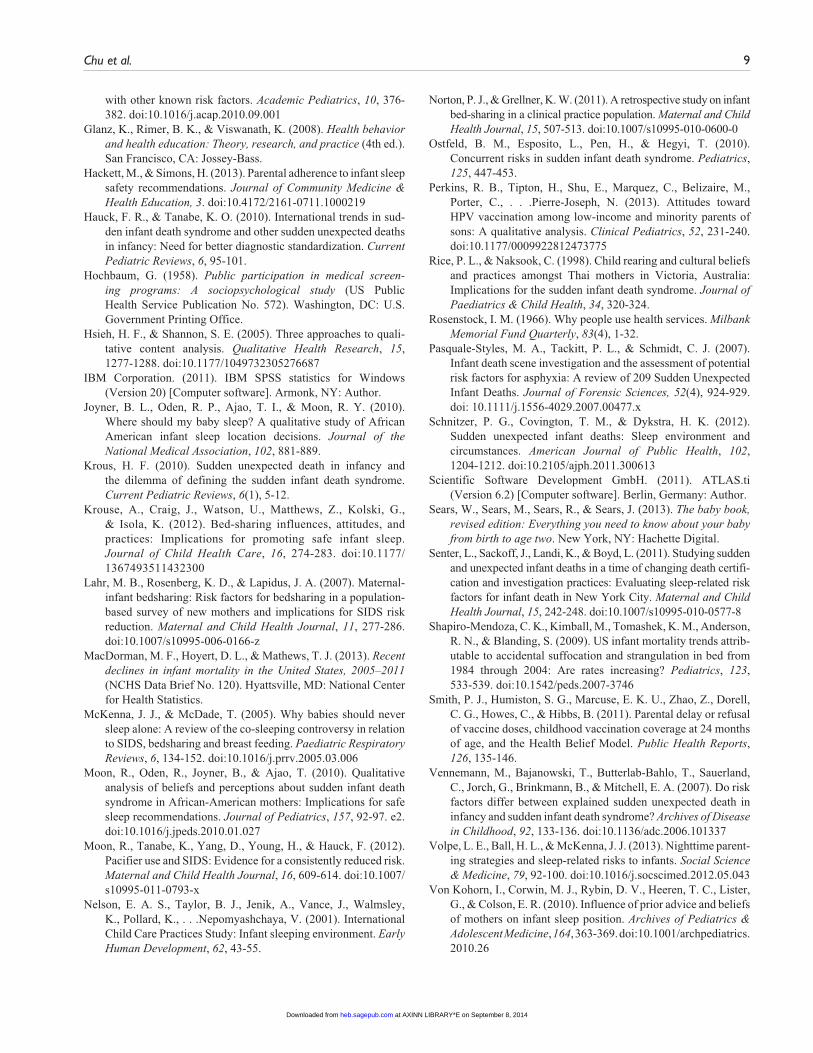
To better understand why infants were placed on unsafe sleep surfaces despite the availability of a crib or bassinet, we conducted a comprehensive qualitative analysis of those 122 cases. All of the cases had some narrative component. However, depending on how fully the investigator report and notes were completed, there may have been minimal detail available. Three themes that related to caregiver behavior and knowledge emerged: (a) caregivers often made decisions based on situational infant care needs, (b) caregivers often made decisions as a result of preference (either the infant’s or their own), and (c) choices often evidenced a lack of knowl-edge about safe sleep practices. Figure 1 presents these themes and examples.
Situational Infant Care. In some cases the crib or bassinet that was present in the home was never or rarely used; however, there were 11 instances where infants were outside the crib or bassinet temporarily, most often because they needed to be comforted or cared for. In these cases, the infant usually slept in a crib or bassinet but was taken out, for example, because they were crying or needed to be fed. The caregiver then often fell asleep with the infant on an adult bed or couch. For example, in the case of a 9-day-old girl and her 31-year-old father, the following was reported.
Father picked up baby because she was crying at 2 a.m. and held her as he lay on couch until she fell back asleep (between 2 and 3 a.m.). He ultimately fell asleep and wound up on top of her.
As indicated in the quantitative findings, the proportion of infants who breast-fed did not differ significantly between those infants who had a crib or bassinet in the home and those who did not. However, the qualitative analysis revealed a number of cases in which the infant was sleeping outside their crib or bassinet because they were nursing and then
at AXINN LIBRARY*E on September 8, 2014heb.sagepub.comDownloaded from
4 Health Education & Behavior
Table 1. Maternal and Infant Characteristics of Infants Found Dead on Unsafe Sleep Surfaces, by Presence of Crib or Bassinet in Home, New York City, 2004-2010.
Total Crib No Crib
Maternal and Infant Characteristics n % n % n %
Mother’s age (p = .197), years <20 25 15.0 19 15.6 6 13.3 20-34 117 70.1 82 67.2 35 77.8 ≥35 19 11.4 17 13.9 2 4.4 Not reported 6 3.6 4 3.3 2 4.4 Total n 167 100.0 122 100.0 45 100.0Mother’s race/ethnicity (p = .112) White, non-Hispanic 22 13.2 19 15.6 3 6.7 Black, non-Hispanic 94 56.3 67 54.9 27 60.0 Hispanic 37 22.2 24 19.7 13 28.9 Other 7 4.2 7 5.7 0 0.0 Not reported 7 4.2 5 4.1 2 4.4 Total n 167 100.0 122 100.0 45 100.0Mother’s education (p = .281) <High school 73 43.7 51 41.8 22 48.9 ≥High school 85 50.9 66 54.1 19 42.2 Not reported 9 5.4 5 4.1 4 8.9 Total n 167 100.0 122 100.0 45 100.0Mother’s nativity (p = .838) U.S. born 113 67.7 83 68.0 30 66.7 Not U.S. born 41 24.6 31 25.4 10 22.2 Not reported 13 7.8 8 6.6 5 11.1 Total n 167 100.0 122 100.0 45 100.0Health insurance at delivery (p = .553) Delivery paid by Medicaid 116 69.5 84 68.9 32 71.1 Delivery not paid by Medicaid 45 26.9 35 28.7 10 22.2 Not reported 6 3.6 3 2.5 3 6.7 Total n 167 100.0 122 100.0 45 100.0Infant sex (p = .79) Male 91 54.5 61 50.0 30 66.7 Female 76 45.5 61 50.0 15 33.3 Total n 167 100.0 122 100.0 45 100.0Age at death (p = .565) <28 days 22 13.2 14 11.5 8 17.8 28 days to 4 months 114 68.3 85 69.7 29 64.4 4-12 months 31 18.6 23 18.9 8 17.8 Total n 167 100.0 122 100.0 45 100.0Gestational age (p = .668) <37 weeks 35 21.0 27 22.1 8 17.8 ≥37 weeks 126 75.4 91 74.6 35 77.8 Not reported 6 3.6 4 3.3 2 4.4 Total n 167 100.0 122 100.0 45 100.0Ever in NICU (p = .467) Never in NICU 119 71.3 85 69.7 34 75.6 Had been in NICU 39 23.4 31 25.4 8 17.8 Not reported 9 5.4 6 4.9 3 6.7 Total n 167 100.0 122 100.0 45 100.0
Note. NICU = neonatal intensive care unit.
at AXINN LIBRARY*E on September 8, 2014heb.sagepub.comDownloaded from
Chu et al. 5
remained next to the mother to sleep. As stated in one case where a 3-month-old girl was found in bed with her 27-year-old mother and 36-year-old father,
The baby was last breast-fed at midnight. She had been sleeping in her crib prior to this feeding and was placed in the bed with her parents after the feeding.
Preference. Another theme that emerged as a reason for plac-ing an infant to sleep on an unsafe sleep surface was prefer-ence—either the infant’s presumed preference to sleep outside the crib or bassinet or parental preference. This theme was present in 20 cases. Caregivers sometimes eschewed the crib or bassinet in the home because the infant did not respond well to being placed there. In the case of an 8-month-old boy who was found bed-sharing with his 18-year-old mother, it was noted, “According to police
Table 2. Risk Factors Among Infants Found Dead on Unsafe Sleep Surfaces, by Presence of Crib or Bassinet in Home, New York City, 2004-2010.
Total Crib No Crib
Risk Factors n % n % n %
Sleep position (p = .804) Back/supine 59 35.3 46 37.7 13 28.9 Front/prone 52 31.1 38 31.1 14 31.1 Side 31 18.6 22 18.0 9 20.0 Other 12 7.2 8 6.6 4 8.9 Not reported 13 7.8 8 6.6 5 11.1 Total n 167 100.0 122 100.0 45 100.0Sleep surface (p = .616) Adult bed 143 85.6 106 86.9 37 82.2 Couch/sofa 14 8.4 10 8.2 4 8.9 Other 10 6.0 6 4.9 4 8.9 Total n 167 100.0 122 100.0 45 100.0Bed-sharing (p = .277) Was bed-sharing 135 80.8 96 78.7 39 86.7 Was not bed-sharing 32 19.2 26 21.3 6 13.3 Total n 167 100.0 122 100.0 45 100.0Excess beddinga (p = .474) Excess bedding 109 65.3 84 68.9 25 55.6 No excess bedding 30 18 21 17.2 9 20 Not reported 28 16.8 17 13.9 11 24.4 Total n 167 100.0 122 100.0 45 100.0Most recent feeding (p = .193) Breast milk 26 15.6 17 13.9 9 20.0 Formula 114 68.3 87 71.3 27 60.0 Other 11 6.6 6 4.9 5 11.1 Not reported 16 9.6 12 9.8 4 8.9 Total n 167 100.0 122 100.0 45 100.0
aExcess bedding adhered to the Centers for Disease Control and Prevention–developed definition used in the Pregnancy Risk Assessment Monitoring System and indicated the presence of any pillows or stuffed toys in the sleep environment.
Behaviors andKnowledge
Situa�onal Care
-Convenient forbreats�eeding,soothing crying baby
Preference
- Infant "doesn't like"crib- Parents preferhaving infant in bed
SafetyMisconcep�ons
- Fear of "crib death"- Excess bedding andposi�oners to"protect" infant
Figure 1. Caregiver behaviors and knowledge influencing infants not being placed in available cribs or bassinets (n = 122).
at AXINN LIBRARY*E on September 8, 2014heb.sagepub.comDownloaded from

6 Health Education & Behavior
report, crib was in bedroom but was never used because baby cried when put in there; thus bed-shared routinely.”
Parents’ preference, often influenced by a desire to bond with the infant, also factored into the decision making in many of these cases. For example, in the case of a 13-day-old girl found bed-sharing with her 35-year-old mother it was noted that the infant “was co-sleeping on couch, but there was a crib in apartment . . . Mother said she was co-sleeping because ‘she loved having the baby with her.’” In the case of a 10-week-old girl who was found bed-sharing with her 23-year-old mother and 34-year-old father, it was reported that “baby had crib in separate bedroom but mother didn’t put her in it because she wanted to ‘keep an eye on her.’”
Safety Misconceptions. As implied by the 10-week-old girl’s mother’s statement that she wanted to “keep an eye on” her infant, parents were often very mindful about safety. Miscon-ceptions about the best ways to protect infants during sleep, and the resulting efforts made to keep them safe while sleep-ing, was a theme that emerged in 13 of the cases reviewed. In these cases, caregivers placed their infants to sleep outside of their crib or bassinet explicitly because of concerns for their safety and/or, once outside the crib, they took precautions to safeguard their infant’s safety in ways that were, in fact, potentially harmful.
Some caregivers expressed a general sense of unease about placing their infant in their crib or bassinet. For exam-ple, in the case of a 4-month-old boy found dead while bed-sharing with his 21-year-old mother and 25-year-old father, it was noted that the parents “had a crib that they never put together. They felt decedent was ‘safer’ sleeping with them.” However, specific misconceptions about the risk of SIDS were also identified from the death scene investigations. In at least three cases, parents explicitly stated a fear of SIDS or “crib death” as their reason for not using the crib or bassinet that was in the home. In the case of a 2-month-old boy found bed-sharing with his 20-year old mother in a family shelter (where, by law, bassinets and cribs are supplied), the follow-ing was reported:
The mother stated that the baby did not like the crib, and she also needed to hold onto him, “to prevent him from rolling.” Moreover, the mother reported that “a baby of a cousin had died of ‘crib death,” so she was leery of using the crib.
In another case, the parents of a 4-month-old girl had a crib in their bedroom; however, she was found sleeping alone the time of her death and usually bed-shared with her 39-year old-mother and 45-year-old father. It was reported, “Apparently decedent always slept in adult bed with the par-ents. They were concerned with SIDS.”
Regardless of why caregivers placed infants to sleep out-side of their crib or bassinet, in some cases caregivers attempted to keep the infant safe while they slept. Some sur-rounded the infant with pillows to prevent them from rolling
off the bed or couch or coming into contact with an adjacent wall. Others attempted to keep the infant from changing positions by fashioning homemade “wedges” or positioners out of clothing or bedding or using commercial products in an adult bed. In the case of a 3-month-old boy found dead while sleeping alone in an adult bed despite a bassinet noted in the same room, his father surrounded him with pillows to prevent him from rolling. Moreover, he was placed in prone position, and it was noted that the father had “placed baby on stomach because he had just fed him and ‘he did not want the baby to spit up and choke’ if he placed him face up.” Thus in this instance there were multiple misconceptions concerning infant safety that motivated the caregiver’s decisions.
Discussion
As a study of sleep-related infant injury death cases, it is per-haps not surprising that the parents and caregivers in this sample were largely not compliant with the latest infant sleep safety recommendations from the American Academy of Pediatrics (2011). However, it is important to understand the factors that influenced these behaviors in order to intervene better and ultimately prevent these types of deaths.
The HBM posits that individuals’ beliefs about whether they are susceptible to deleterious health outcomes and the perceptions of the benefits of trying to avoid it influence their readiness to act (Hochbaum, 1958; Rosenstock, 1966). The HBM has been applied to understand parental decision making on a diversity of topics, such as vaccinations (Flood et al., 2010; Perkins et al., 2013; Smith et al., 2011), sun-screen use (De Vries, Van Osch, Eijmael, Smerecnik, & Candel, 2012), and asthma medication adherence (Armstrong, Duncan, Stokes, & Pereira, 2014). Our analysis of the factors that influenced caregivers’ behaviors used the domains of the HBM to understand the barriers to infant safe sleep behaviors.
Table 3 applies the major concepts of the model to the three qualitative themes that emerged in this research (situa-tion care, preference, and safety misconceptions), using infant death as the outcome and use of a safe sleep surface as the desired conduct.
Four of the six major constructs of the theory were directly relevant to the data. For example, perceived susceptibility of infant death was expressed through the mindfulness to safety that caregivers evidenced, even though their protective strat-egies were often flawed. In contrast, perceived severity of the risk of infant death was diminished. Caregivers had awareness that their infants were susceptible to infant death but did not appreciate the heightened risk that their sleep practices proffered. Perceived benefits and perceived barri-ers to using a safe sleep surface were expressed prominently in the data through all three of the major themes. Caregivers either did not perceive any benefits to using the crib or bas-sinet or were diminished or de-prioritized in the face of situ-ational needs or preference. Moreover, as expressed through
at AXINN LIBRARY*E on September 8, 2014heb.sagepub.comDownloaded from

Chu et al. 7
the safety misconceptions theme, some viewed the crib or bassinet as a threat rather than as a strategy to ameliorate the risk of infant death. Relatedly, the perceived barriers to using a safe sleep surface were heightened, specifically in cases where using the crib or bassinet came at the “cost” of incon-veniencing situational care needs or countermanding infant or parental preference.
Previous cross-sectional studies about barriers to follow-ing infant safe sleep recommendations have found that par-ents’ beliefs are crucial predictors of infant sleep position (Colson et al., 2006; Hackett & Simons, 2013). In particular, surveys with low-income African American mothers have found that beliefs about infant comfort and safety are signifi-cant predictors of infant sleep position: If mothers believed that infants were not comfortable or safe sleeping on their backs, they were less likely to place them in the recom-mended supine position (Von Kohorn et al., 2010). Though these studies focused on the predicted behaviors of parents, our analysis of the behavioral influences on sleep location choice among caregivers of infants who died similarly reflected how beliefs about comfort and safety are related to behaviors.
The misconceptions that caregivers had about the risks associated with infant sleep location aligned with the HBM concepts of perceived susceptibility and perceived severity. In particular, the connection between deleterious outcome, that is, SIDS or other infant death, and the severity of risk that they may have introduced through their care practices was not understood. This supports focus group research con-ducted with African American mothers that found mothers did not necessarily believe the link between sleep position and risk for SIDS, in part because SIDS was perceived to be a random occurrence (Moon et al., 2010). Moreover, incon-sistency of infant sleep recommendations contributed to the belief that SIDS could be prevented only by extreme vigi-lance, for example, watching the baby sleep (Moon et al., 2010).
Conclusion
The findings in this study have a number of important impli-cations for health educators and public health practitioners. One predominant intervention strategy to encourage the use of safe sleep surfaces has been the distribution of cribs and bassinets to at-risk populations, coupled with safe sleep edu-cation for clients who receive them (Carlins & Collins, 2007; Cribs for Kids, n.d.). Though these interventions are undoubt-edly important, they are also limited in their reach, and more important, this study indicates that there are factors, above and beyond actual access to a crib or bassinet, that influence the decision to use a safe surface appropriately.
One intervention approach suggested by our findings is that health educators and health professionals should explic-itly communicate the connections between infant sleep behaviors and infant death, that is, perceived susceptibility and perceived severity of risk. These communications should include significant explanation of the details and processes by which conclusions about these connections were reached, because caregivers may not otherwise appreciate the risk that infant sleep environments can pose to safety. It is only within the past few years that these types of suffocation-related injuries have been recognized as being different causes of death than SIDS deaths. Furthermore, in promoting safe sleep practices, health educators should address perceived effectiveness by clarifying the benefits of the safe sleep sur-face, and emphasizing its consistent use for every sleep, as well as heightened attentiveness to accidentally falling asleep with the infant. Perceived barriers related to situational care and preferences also need to be addressed. For example, in response to the sentiment that some babies don’t “like” the crib, health educators can inform caregivers of infants’ higher susceptibility to risk when sleeping in an adult bed, as compared to in a crib with a firm mattress and no excess bed-ding, and emphasize the notion that infant preferences are subjective. Overall, the findings from this study suggest that
Table 3. Health Belief Model Concepts Applied to Qualitative Findings.
Concept Definition Presence in ThemeWas Concept Heightened
(+) or Diminished (−)
Perceived susceptibility
Beliefs about the chances of infant death occurring
Safety misconceptions (+)
Perceived severity Beliefs about the seriousness of the risk of infant death
Safety misconceptions (−)
Perceived benefits Beliefs about the effectiveness of using a safe sleep surface to reduce risk of infant death
Situational care (−) Preference Safety misconceptions Perceived barriers Beliefs about the material and psychological
costs of using a safe sleep surface Situational care (+)
Preference Cues to action Factors that activate “readiness to change” Not applicable Not applicableSelf-efficacy Confidence in one’s ability Not applicable Not applicable
Source. Adapted from Glanz, Rimer, and Viswanath (2008).
at AXINN LIBRARY*E on September 8, 2014heb.sagepub.comDownloaded from

8 Health Education & Behavior
messages should reinforce an understanding of the severity of the risk to infant safety as compared to the transitory and navigable nature of the perceived barriers.
This study was exploratory in nature and limited in sev-eral ways. First, as a retrospective analysis of a sample of deceased infants without a live comparison group, we cannot be certain of the contribution of these factors to the deaths of the infants in our population. Second, as data that were not explicitly collected for research purposes, medical examiner records are necessarily limited in their scope. The death scene investigations involved lengthy, in-depth questioning, and examination, and subsequent reporting of many man-dated, standardized variables. However, nonstandardized, open-ended notes, observations, and other qualitative data, including reasons for not using the crib or bassinet in the home, were captured inconsistently. Most important, the context in which these data were collected must be acknowl-edged. They do not represent a “first-person account” of caregivers’ beliefs and knowledge. Rather, they are observa-tions filtered through third parties, for example, medico-legal investigators, and may both introduce bias and overlook subtle nuances as a result. Moreover, the context in which caregivers offer accounts of their actions and motivations, that is, in retrospect after an infant has died, must be factored in when interpreting these data. Beyond the possible unreli-ability of these narratives, how parents and caregivers frame reasons for not using a safe sleep surface—for example, as a safety concern—may be significantly affected, consciously or unconsciously, by the event itself and their consequent feelings of guilt and loss.
However, this study’s major strengths included the use of death scene investigation documents to understand caregiver behavior and knowledge in cases where their behaviors may have contributed to preventable sleep-related infant deaths. Another strength was the use of both quantitative and quali-tative analysis. The presence of cribs or bassinets in the homes of infants found on unsafe sleep surfaces and possible reasons why they were not used were identified through a qualitative examination of the medical examiner notes. Other research has indicated that the analysis of death scene inves-tigations has been crucial in identifying previously unknown risk factors for asphyxia in infants (Pasquale-Styles, Tackitt, & Schmidt, 2007). Our findings suggest that examining these investigative reports can also yield additional insights into caregiver decision making, insights that can ultimately inform more meaningful interventions to educate caregivers about risk factors for these deaths.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, author-ship, and/or publication of this article.
References
American Academy of Pediatrics. (2000). Changing concepts of sudden infant death syndrome: Implications for infant sleep-ing environment and sleep position. Pediatrics, 105(3 Pt. 1), 650-656.
American Academy of Pediatrics. (2011). SIDS and other sleep-related infant deaths: Expansion of recommendations for a safe infant sleeping environment. Pediatrics, 128, 1030-1039. doi:10.1542/peds.2011-2284
Armstrong, M. L., Duncan, C. L., Stokes, J. O., & Pereira, D. (2014). Association of caregiver health beliefs and parenting stress with medication adherence in preschoolers with asthma. Journal of Asthma, 51, 366-372. doi:10.3109/02770903.2013.876431
Babbie, E. (1992). The practice of social research. New York, NY: Macmillan.
Ball, H. L., Moya, E., Fairley, L., Westman, J., Oddie, S., & Wright, J. (2012). Bed- and sofa-sharing practices in a UK biethnic population. Pediatrics, 129, e673-e681. doi:10.1542/peds.2011-1964
Buswell, S. D., & Spatz, D. L. (2007). Parent-infant co-sleeping and its relationship to breastfeeding. Journal of Pediatric Health Care, 21(1), 22-28. doi:http://dx.doi.org/10.1016/j.pedhc.2006.04.006
Carlins, E. M., & Collins, K. S. (2007). Cribs for Kids: Risk and reduction of sudden infant death syndrome and accidental suf-focation. Health & Social Work, 32, 225-229.
Colson, E. R., Levenson, S., Rybin, D., Calianos, C., Margolis, A., Colton, T., . . .Corwin, M. J. (2006). Barriers to following the supine sleep recommendation among mothers at four centers for the Women, Infants, and Children Program. Pediatrics, 118, e243-250. doi:10.1542/peds.2005-2517
Colson, E. R., Willinger, M., Rybin, D., Heeren, T., Smith, L. A., Lister, G., & Corwin, M. J. (2013). Trends and factors associ-ated with infant bed sharing, 1993-2010: The National Infant Sleep Position Study. JAMA Pediatrics, 167, 1032-1037. doi:10.1001/jamapediatrics.2013.2560
Cribs for Kids. (n.d.). About us. Retrieved from http://www.cribsforkids.org/about-us/
De Vries, H., Van Osch, L., Eijmael, K., Smerecnik, C., & Candel, M. (2012). The role of risk perception in explaining parental sunscreen use. Psychology & Health, 27, 1342-1358. doi:10. 1080/08870446.2012.684059
Flood, E. M., Rousculp, M. D., Ryan, K. J., Beusterien, K. M., Divino, V. M., Toback, S. L., . . .Mahadevia, P. J. (2010). Parents’ decision-making regarding vaccinating their children against influenza: A web-based survey. Clinical Therapeutics, 32, 1448-1467. doi:10.1016/j.clinthera.2010.06.020
Fortin, P., Stayton, C., DiGrande, L., Yau, R., Hackett, M., & the New York City Child Fatality Review Team. (2011). Report from the Child Fatality Review team: Understanding child injury deaths. New York, NY: Department of Health and Mental Hygiene.
Fu, L. Y., Colson, E. R., Corwin, M. J., & Moon, R. Y. (2008). Infant sleep location: Associated maternal and infant charac-teristics with sudden infant death syndrome prevention recom-mendations. Journal of Pediatrics, 153, 503-508. doi:10.1016/j.jpeds.2008.05.004
Fu, L. Y., Moon, R. Y., & Hauck, F. R. (2010). Bed sharing among black infants and sudden infant death syndrome: Interactions
at AXINN LIBRARY*E on September 8, 2014heb.sagepub.comDownloaded from
Chu et al. 9
with other known risk factors. Academic Pediatrics, 10, 376-382. doi:10.1016/j.acap.2010.09.001
Glanz, K., Rimer, B. K., & Viswanath, K. (2008). Health behavior and health education: Theory, research, and practice (4th ed.). San Francisco, CA: Jossey-Bass.
Hackett, M., & Simons, H. (2013). Parental adherence to infant sleep safety recommendations. Journal of Community Medicine & Health Education, 3. doi:10.4172/2161-0711.1000219
Hauck, F. R., & Tanabe, K. O. (2010). International trends in sud-den infant death syndrome and other sudden unexpected deaths in infancy: Need for better diagnostic standardization. Current Pediatric Reviews, 6, 95-101.
Hochbaum, G. (1958). Public participation in medical screen-ing programs: A sociopsychological study (US Public Health Service Publication No. 572). Washington, DC: U.S. Government Printing Office.
Hsieh, H. F., & Shannon, S. E. (2005). Three approaches to quali-tative content analysis. Qualitative Health Research, 15, 1277-1288. doi:10.1177/1049732305276687
IBM Corporation. (2011). IBM SPSS statistics for Windows (Version 20) [Computer software]. Armonk, NY: Author.
Joyner, B. L., Oden, R. P., Ajao, T. I., & Moon, R. Y. (2010). Where should my baby sleep? A qualitative study of African American infant sleep location decisions. Journal of the National Medical Association, 102, 881-889.
Krous, H. F. (2010). Sudden unexpected death in infancy and the dilemma of defining the sudden infant death syndrome. Current Pediatric Reviews, 6(1), 5-12.
Krouse, A., Craig, J., Watson, U., Matthews, Z., Kolski, G., & Isola, K. (2012). Bed-sharing influences, attitudes, and practices: Implications for promoting safe infant sleep. Journal of Child Health Care, 16, 274-283. doi:10.1177/ 1367493511432300
Lahr, M. B., Rosenberg, K. D., & Lapidus, J. A. (2007). Maternal-infant bedsharing: Risk factors for bedsharing in a population-based survey of new mothers and implications for SIDS risk reduction. Maternal and Child Health Journal, 11, 277-286. doi:10.1007/s10995-006-0166-z
MacDorman, M. F., Hoyert, D. L., & Mathews, T. J. (2013). Recent declines in infant mortality in the United States, 2005–2011 (NCHS Data Brief No. 120). Hyattsville, MD: National Center for Health Statistics.
McKenna, J. J., & McDade, T. (2005). Why babies should never sleep alone: A review of the co-sleeping controversy in relation to SIDS, bedsharing and breast feeding. Paediatric Respiratory Reviews, 6, 134-152. doi:10.1016/j.prrv.2005.03.006
Moon, R., Oden, R., Joyner, B., & Ajao, T. (2010). Qualitative analysis of beliefs and perceptions about sudden infant death syndrome in African-American mothers: Implications for safe sleep recommendations. Journal of Pediatrics, 157, 92-97. e2. doi:10.1016/j.jpeds.2010.01.027
Moon, R., Tanabe, K., Yang, D., Young, H., & Hauck, F. (2012). Pacifier use and SIDS: Evidence for a consistently reduced risk. Maternal and Child Health Journal, 16, 609-614. doi:10.1007/s10995-011-0793-x
Nelson, E. A. S., Taylor, B. J., Jenik, A., Vance, J., Walmsley, K., Pollard, K., . . .Nepomyashchaya, V. (2001). International Child Care Practices Study: Infant sleeping environment. Early Human Development, 62, 43-55.
Norton, P. J., & Grellner, K. W. (2011). A retrospective study on infant bed-sharing in a clinical practice population. Maternal and Child Health Journal, 15, 507-513. doi:10.1007/s10995-010-0600-0
Ostfeld, B. M., Esposito, L., Pen, H., & Hegyi, T. (2010). Concurrent risks in sudden infant death syndrome. Pediatrics, 125, 447-453.
Perkins, R. B., Tipton, H., Shu, E., Marquez, C., Belizaire, M., Porter, C., . . .Pierre-Joseph, N. (2013). Attitudes toward HPV vaccination among low-income and minority parents of sons: A qualitative analysis. Clinical Pediatrics, 52, 231-240. doi:10.1177/0009922812473775
Rice, P. L., & Naksook, C. (1998). Child rearing and cultural beliefs and practices amongst Thai mothers in Victoria, Australia: Implications for the sudden infant death syndrome. Journal of Paediatrics & Child Health, 34, 320-324.
Rosenstock, I. M. (1966). Why people use health services. Milbank Memorial Fund Quarterly, 83(4), 1-32.
Pasquale-Styles, M. A., Tackitt, P. L., & Schmidt, C. J. (2007). Infant death scene investigation and the assessment of potential risk factors for asphyxia: A review of 209 Sudden Unexpected Infant Deaths. Journal of Forensic Sciences, 52(4), 924-929. doi: 10.1111/j.1556-4029.2007.00477.x
Schnitzer, P. G., Covington, T. M., & Dykstra, H. K. (2012). Sudden unexpected infant deaths: Sleep environment and circumstances. American Journal of Public Health, 102, 1204-1212. doi:10.2105/ajph.2011.300613
Scientific Software Development GmbH. (2011). ATLAS.ti (Version 6.2) [Computer software]. Berlin, Germany: Author.
Sears, W., Sears, M., Sears, R., & Sears, J. (2013). The baby book, revised edition: Everything you need to know about your baby from birth to age two. New York, NY: Hachette Digital.
Senter, L., Sackoff, J., Landi, K., & Boyd, L. (2011). Studying sudden and unexpected infant deaths in a time of changing death certifi-cation and investigation practices: Evaluating sleep-related risk factors for infant death in New York City. Maternal and Child Health Journal, 15, 242-248. doi:10.1007/s10995-010-0577-8
Shapiro-Mendoza, C. K., Kimball, M., Tomashek, K. M., Anderson, R. N., & Blanding, S. (2009). US infant mortality trends attrib-utable to accidental suffocation and strangulation in bed from 1984 through 2004: Are rates increasing? Pediatrics, 123, 533-539. doi:10.1542/peds.2007-3746
Smith, P. J., Humiston, S. G., Marcuse, E. K. U., Zhao, Z., Dorell, C. G., Howes, C., & Hibbs, B. (2011). Parental delay or refusal of vaccine doses, childhood vaccination coverage at 24 months of age, and the Health Belief Model. Public Health Reports, 126, 135-146.
Vennemann, M., Bajanowski, T., Butterlab-Bahlo, T., Sauerland, C., Jorch, G., Brinkmann, B., & Mitchell, E. A. (2007). Do risk factors differ between explained sudden unexpected death in infancy and sudden infant death syndrome? Archives of Disease in Childhood, 92, 133-136. doi:10.1136/adc.2006.101337
Volpe, L. E., Ball, H. L., & McKenna, J. J. (2013). Nighttime parent-ing strategies and sleep-related risks to infants. Social Science & Medicine, 79, 92-100. doi:10.1016/j.socscimed.2012.05.043
Von Kohorn, I., Corwin, M. J., Rybin, D. V., Heeren, T. C., Lister, G., & Colson, E. R. (2010). Influence of prior advice and beliefs of mothers on infant sleep position. Archives of Pediatrics & Adolescent Medicine, 164, 363-369. doi:10.1001/archpediatrics. 2010.26
at AXINN LIBRARY*E on September 8, 2014heb.sagepub.comDownloaded from
Copyright © 2022 FDOKUMEN




















