
Experimental transient bacteraemias in human subjects with varying degrees of plaque accumulation...
9
Journal of Clinical Periodontology: 1977: 4: 92-99 Key words: Bacieiaeinia - hiimati experimenial'on - periodonial health flatus. Accepted for publication: July 16, 1976. Experimental transient bacteraemias in human subjects with varying degrees of plaque accumulation and gingival inflammation JOHN G. SILVER, ALEXIS W. MARTIN AND BARRY C. MCBRIDE Departments of Oral Medicine and MicrobioJogy, University of British Columbia, Vancouver, British Columbia, Canada Abstraci. Ninety-six subjects were assigned to one of four groups according to severity of gingiva] inflamimation and bacterial plaque accumulation on the teeth. Following a standardized toothbrushing procedure, blood specimens from a vein in the antecubital fossa were cultured under aerobic and stringent anaerobic conditions. The percentage of positive cultures increased significantly with increasing severity of gingival inflammation, as did the number of species of organisms isolated. Thirty different microbial species indigenous to the oral cavity, including many strict anaerobes, were recovered. The study has implications for standards of oral health which might be considered necessary in patients with congenital or acquired endocardial defects or cardiovascular prostheses. Over forty years ago it was found that dental extractions produced a transitory bacteraemia and it was suggested that this phenomenon had a bearing on the aetio- logy of infective endocarditis in patients with rheumatic and congenital heart disease (Okell & Elliott 1935). It is known now that most dental manipulations including extractions (Jones et al. 1970), scaling (Bandt et al. 1964, Conner et al. 1967), surgical periodontal procedures (Korn & Schaffer 1962, Bender et al. 1963), filling of teeth (Harvey & Capone 1961) and root canal treatment (Farrington 1973) intro- duce bacteria into the blood stream as do such patient performed procedures as chew- ing (Cobe 1954), oral irrigation (Romans & App 1971, Berger et al. 1974) and tooth- brushing (Cobe 1954, Rise et al. 1969, Sco- nyers et al. 1973, Madsen 1974). There is thus sufficient circumstantial evidence to recommend certain precautions be taken during oral manipulative proce- dures in patients with congenital and ac- quired heart defects (Cooke 1970) and specific recommendation for antibiotic cover has been made (American Heart As- sociation 1965). Patients who have suc- cumbed to one attack of infective endocar- ditis have been advised to have their re- maining teeth extracted to prevetit further occurrence (Hobsen & Juel-Jensen 1956, Beeley 1969). It has been pointed out, how- ever, that further information is needed before dental clearance can be advised (Croxson et al. 1971) and the current un-
-
Upload
independent -
Category
Documents
-
view
4 -
download
0
Transcript of Experimental transient bacteraemias in human subjects with varying degrees of plaque accumulation...

Journal of Clinical Periodontology: 1977: 4: 92-99
Key words: Bacieiaeinia - hiimati experimenial'on - periodonial health flatus.Accepted for publication: July 16, 1976.
Experimental transient bacteraemiasin human subjects with varying
degrees of plaque accumulation andgingival inflammation
JOHN G. SILVER, ALEXIS W. MARTIN AND BARRY C. MCBRIDE
Departments of Oral Medicine and MicrobioJogy, University of British Columbia,Vancouver, British Columbia, Canada
Abstraci. Ninety-six subjects were assigned to one of four groups according to severityof gingiva] inflamimation and bacterial plaque accumulation on the teeth. Following astandardized toothbrushing procedure, blood specimens from a vein in the antecubitalfossa were cultured under aerobic and stringent anaerobic conditions. The percentage ofpositive cultures increased significantly with increasing severity of gingival inflammation,as did the number of species of organisms isolated. Thirty different microbial speciesindigenous to the oral cavity, including many strict anaerobes, were recovered. The studyhas implications for standards of oral health which might be considered necessary inpatients with congenital or acquired endocardial defects or cardiovascular prostheses.
Over forty years ago it was found thatdental extractions produced a transitorybacteraemia and it was suggested that thisphenomenon had a bearing on the aetio-logy of infective endocarditis in patientswith rheumatic and congenital heart disease(Okell & Elliott 1935). It is known nowthat most dental manipulations includingextractions (Jones et al. 1970), scaling(Bandt et al. 1964, Conner et al. 1967),surgical periodontal procedures (Korn &Schaffer 1962, Bender et al. 1963), fillingof teeth (Harvey & Capone 1961) and rootcanal treatment (Farrington 1973) intro-duce bacteria into the blood stream as dosuch patient performed procedures as chew-ing (Cobe 1954), oral irrigation (Romans &App 1971, Berger et al. 1974) and tooth-
brushing (Cobe 1954, Rise et al. 1969, Sco-nyers et al. 1973, Madsen 1974).
There is thus sufficient circumstantialevidence to recommend certain precautionsbe taken during oral manipulative proce-dures in patients with congenital and ac-quired heart defects (Cooke 1970) andspecific recommendation for antibioticcover has been made (American Heart As-sociation 1965). Patients who have suc-cumbed to one attack of infective endocar-ditis have been advised to have their re-maining teeth extracted to prevetit furtheroccurrence (Hobsen & Juel-Jensen 1956,Beeley 1969). It has been pointed out, how-ever, that further information is neededbefore dental clearance can be advised(Croxson et al. 1971) and the current un-

BACTERAEMIAS AND VARYING PERIODONTAL HEALTH
certainty of the dental assessment of pa-tients with valvular defects and the needfor further research also has been stated(Editorial, Lancet 1971).
Bearing in mind tbe above points, thepresent study of experimental bacteraemiaswas undertaken. The study differed fromprevious investigations by utilizing a samplesize suitable for statistical analysis and byemploying strict epidemiological criteria forcategorization of subjects. The methodchosen for attempted creation of the bac-teraemia was toothbrushing, the rationalefor this method being its everyday occur-rence in tbe hves of many persons andthe relative paucity of previous researchusing a timed, specified technique of brush-ing. Additionally, correlations betweenbacteraemias and specified parameters ofgingival health had not been proven (Cobe1954, Rise et al. 1969, Tamini et al. 1969,Sconyers et al. 1973, Madsen 1974).
Methods
A total of 96 subjects (44 male, 52 female)aged 17-61 years were assigned to one offour groups according to modified criteriafor the Gingival and Plaque Indices (Loe &Silness 1963, Silness & Loe 1964). The mod-ifications involved omission of instrumenta-tion within the gingival sulcus, thus reducingthe possibility of inadvertent pre-experi-mental bacteraemias. Bleeding on brusbingresulted in tbe assignation of a score of 2for the Gingival Index. All subjects werein good general health with no history ofany antibiotic therapy within the precedingmonth.
Each subject's mouth was divided intothree segments for both mandibular andmaxillary teeth. The gingival sulci of eachsegment were brushed by one of the in-vestigators using an electric toothbrush(Touch-Tronic,®, Teledyne Aqua Tec, Ltd.,Rexdale, Ont.) which started automatic
vibration by the application of pressure tothe brush head.
All brush heads, which were pre-ste-rilized in ethylene oxide, were of thesame soft nylon texture and the pres-sure applied to the brush was just suf-ficient to start the automatic action. Thebuccal and lingual gingival sulci of eachsegment were brushed for 10 sec restiltingin a total brushing time of 2 min for eachsubject. Immediately prior to brushing, 5 mlof blood were withdrawn from a vein inthe antecubital fossa of one arm and,during the last 30-60 sec of brushing, 10 mlwere withdrawn from a similar vein in theapposite arm. (Previous studies on dogshad shown that peak bacteraemia occurred30-60 sec after introduction of bacteriainto the circulation (Silver et al. 1975)).Prior to obtaining the blood samples, theskin of the antecubital fossae was cleansedthoroughly using, in succession, severalswabs soaked in 70 % ethyl alcohol.
The preoperative blood sample wasdivided equally and placed into 50 ml ofprereduced anaerobically sterile (PRAS)"B" medium (McMinn & Crawford 1970)contained in an anaerobic flask, and 50 mlof aerobic trypticase soy broth. Three mlof the postoperative blood sample wereplaced into 100 ml of trypticase soy hrotband 1 ml was mixed with 15 ml of pre-melted trypticase soy agar for aerobic in-cubation. The remaining 6 ml of blood wasdivided equally and placed into anaerobiccontainers holding respectively 100 ml ofPRAS "E" broth; 50 ml of brain heart in-fusion broth supplemented with 0.3 % yeastextract, 1.0 % trypticase, 0.0005 % haemin,0.05 % cysteine hydrochloride, and 25 mlof PRAS "E" broth supplemented with 2 %agar.
Blood cultures were incubated at 37°Cand inspected at intervals for growth.Aerobic cultures were maintained for a min-imum of 5 days and anaerobic cultures

94 SILVER, MARTIN AND McBRlDE
Table 1. Relationship of positive blood cultures to groupings of the Ginglval IndexVerhdltnis positlver Blutkulturen zu verschiedenen Gruppen des Gingival-JndexesRelation des cultures positives de sang et des groupes d'index gingival
Subjects
No. in groupNo. with positiveblood culturesPer cent with positivebiood cultures
0-0.75
25
4
1 6 %
Gingival
0.76-1.50
24
8
3 3 %
Index
1.51-2.25
25
14
5 6 %
2.26-3.00
22
15
6 8 %
No. in group (Anzahl Probanden in der Gruppe, nombre dans le groupe). No. with positive bloodcultures (Anzahl Probanden mit positiven Blutkulturen, nombre avec culture de sang positive).Per cent witb positive blood cultures (Anzahl Probanden mit positiven Blutkulturen in Pro-lent, potircentage de cultures de sang positives)
for 21 days. Samples were subciiltured ontoblood agar plates, anaerobic cultures being ^^" ^plated and incubated in an anaerobic The relationships between numbers andchamber (Coy Mfg. Co., Ann Arbor, Michi- percentages of subjects with positive bloodgan). Identification of microorganisms was cultures following toothbrushing and Gin-in accordance with criteria specified in gival and Plaque Indices are shown inBuchanan & Gibbons (1974) and Holde- Tables 1 and 2. As can be seen, the per-man & Moore (1975). centage of subjects demonstrating bactera-
Results were analyzed and significant emia increased with increasing severity ofdifferences determined by utilization of a gingival inflammation. Significant differ-critical ratio test. ences were found between those groupings
of the Gingival Index shown in Table 3,
Table 2. Relationship of positive blood cultures to groupings of the Plaque IndexVerhdltnis positiver Blutkulturen zu verschiedenen Gruppen des Plaque-IndexesRelation des cultures positives de sang et des groupes d'index de plaque
Subjects
No. in groupNo. with positiveblood culturesPer cent with positiveblood cultures
0-0.75
40
14
3 5 %
Plaque
0.76-1.50
26
9
3 5 %
Index
1.51-2.25
16
10
6 3 %
2.26-3.00
14
.8
5 7 %
Subjects (Probanden, Sujets), No. in group (Anzahl Probanden in der Gruppe, nonibre dansle groupe). No. with positive blood cultures (Anzahl Probanden mit positiven Blutkulturen,nombre avec culture de sang positive). Percent positive blood cultures (Anzahl Probanden mitpositiven Blutkulturen in Prozent, pourcentage de cultures de sang positives).
BACTERAEMIAS AND VARYING PERIODONTAL HEALTH
Table 3. Groupings of the Gingival Indexshowing significant differences in occurrence ofbacteraemias utilizing a Critical Ratio TestGingival'Index-Gruppen. Gezeigt werden s'lg-nifikante Unterschiede betr. Vorkommen vonBakteriaemie, beslimmt miltels Crtlical-Ralio-TestGroiipes de rindex gingival montrant des dif-ferences significalivcs de frequence de bacterie-mies uiiiisanf un test de proportion critique
Groupings compared Significance
0-0.75 < 1.51-2.250-0.75 < 2.26-3.00
0.76-1.50 < 2.26-3.00
0.001 <P< 0.01P < 0.001
O.O;L < P < 0.02
Groupings compared {Vergleich zwischenGruppen. comparaison des groupes).
but there were no significant differencesin values for groupings of the Plaque In-dex. Two subjects had preoperativebacteraemias, both having scores of 2.26-3.00 for both Gingival and Piaque Indices.In each case the number of species oforganisms increased markedly followingbrushing.
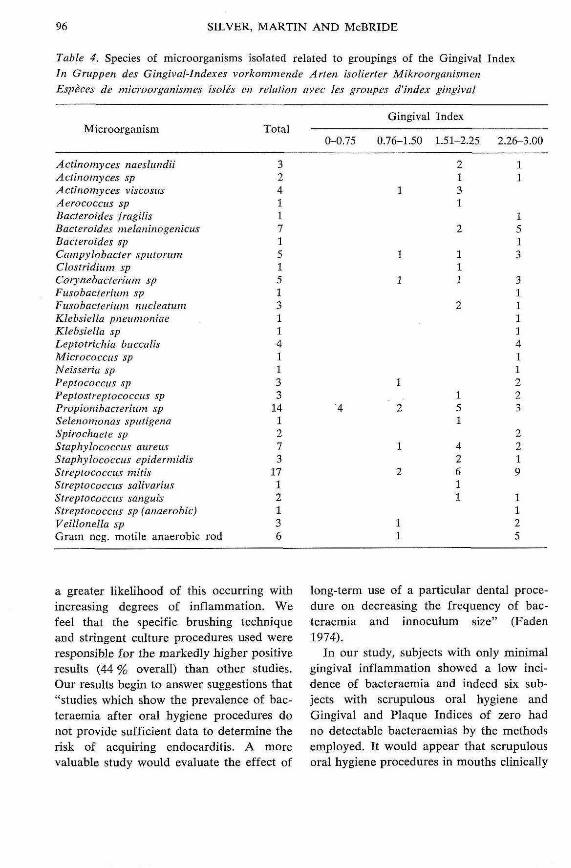
Species of organisms isolated were cor-related with the Gingival and Plaque In-dices; the results for the Gingival Indexare shown in Table 4. Although it was notpossible to determine total numbers of or-ganisms (see discussion), it was possible toassess the number of different species oforganisms In relation to the two indices.The higher the index for a particular sub-ject, the greater was the chance that morespecies of organisms would be isolated;again the results for the Gingivai Index arepresented (Table 5). In all cases the or-ganisms found were those indigenous tothe oral cavity of man.
Discussion
There is evidence that mild trauma suchas mastication or brushing of teeth can
cause a transitory bacteraemia from themouth (Cobe 1954, Rise et al. 1969, Sco-nyers et al. 1973, Madsen 1974). Cobe(1954) found 24.2 % of positive blood cul-tures with no differences between a groupneeding periodontal treatment and a groupwithout the need for treatment. Criteria forthese groupings were lacking. Rise et al.(1969) found 26% of 50 subjects with"clean mouths" to have bacteraemia fol-lowing toothbrushing, but there was nospecific definition of "clean mouths" norwas the nature of the bacteraemia. or thecontrols, if any, reported. Madsen (1974)was able to produce a Streptococcal bac-teraemia in 19 % of 16 subjects with gin-givitisj measured between 0.5-1.5 by theGingival Index, and in 54 % of 13 sub-jects with marginal period ontitis. Sur-prisingly no significant difference wasfound between these groups but it wassuggested that this may have been due toan inadequate sample size.
Sconyers et al.'s study (1973) differedfrom others in utilizing a standardizedbrushing technique and also an anaerobicculture technique which our own studyconfirmed to be superior for recovery ofanaerobic microorganisms. The 30 subjectswho participated in the toothbrushing as-pect of their study were assessed for peri-odontal pocket depths, tooth mobility andPlaque Index but not for Gingival Index.Our own feelings were that gingival inflam-mation was likely to be one of the mostimportant factors and this assessment wasa major consideration in our study. Scony-ers et al.'s (1973) results showed 16 % ofsubjects to have a bacteraemia followingbrushing but only two species of bacteriawere recovered, an aerobic and an an-aerobic Streptococcus.
Our study has confirmed that bactera-emia does occur following brushing of thegingival sulci in subjects with a wide rangeof gingival inflammation and that there is
96 SILVER, MARTIN AND McBRIDE
Table 4. Species of microorganisms isolated related to groupings of the Gingival IndexIn Gruppen des Gingival-Indexes vorkommende Arten isolierter MikroorganismenEspeces de microorganismes isoles en relation avec les groupes d'index gingival
Microorganism
Actinomyces naeslundiiActinoniyces spActinomyces viscosusAerococcus spBacteroides fragilisBacteroides melaninogenicusBacteroides spCampylobacter sputorumClostridium spCorynebacterium spFusobacterium spFusobacterium nucleatumKlebsiella pneumoniaeKlebsiella spLeptotrichia buccalisMicrococcus spNeisseria spPeptococcus spPeptostreptococciis spPropionibacterium spSelenomonas sputigenaSpirochaete spStaphylococcus aureusStaphylucoccus epidermidisStreptococcus mittsStreptococcus salivariusStreptococcus sanguisStreptococcus sp (anaerobic)Veillonella spGram neg. motile anaerobic rod
Total
3-24117151S13.114.1133
141213
171'2136
0-0.75
4
Gingival
0.76-1.50
U
1
1
1
2
1
2
11
Index
1.51-2.25
2X31
t111
"3
151
4
11
2.26-3.00
1:
1513
%%1Ii411223
2.21
1125
a greater likelihood of this occurring withincreasing degrees of inflammation. Wefeel that the specific brushing techniqueand stringent culture procedures used wereresponsible for the markedly higher positiveresults (44 % overall) than other studies.Our results begin to answer suggestions that"studies which show the prevalence of bac-teraemia after oral hygiene procedures donot provide sufficient data to determine therisk of acquiring endocarditis. A morevaluable study would evaluate the effect of
long-term use of a particular dental proce-dure on decreasing the frequency of bac-teraemia and innoculum size" (Faden1974).
In our study, subjects with only minimalgingival inflammation showed a low inci-dence of bacteraemia and indeed six sub-jects with scrupulous oral hygiene andGingival and Plaque Indices of zero hadno detectable bacteraemias by the methodsemployed. It would appear that scrupulousoral hygiene procedures in mouths clinically

BACTERAEMIAS AND VARYING PERIODONTAL HEALTH 97
Table 5. Numbers of species of microorgiinismsisolated related lo groupings of the GingivaiIndexZahl der in Gruppen des Gingival-Indexex vor-kommenden Arten isolierler MikroorganismenNombres d'especes de microorganismes isotesen relation avec les groupes d'index gingivai
Numbers ofspecies of -
micro-organisms
012
4567S'9
10
0-0.75
214-000
to,0Q0b0
Gingivai
0.76-1.50
165210000000
Index
1.51-2.25
116241000100
2.26-3.00
75311013001
Numbers of species of microorganisms {An-zahl Arten der Mikroorganismen, noinbred'especes de inicro-organisines).
free of gingivai inflammation markedlylessen the likelihood of bacteraemia follow-ing minor gingivai trauma such as tooth-brushing and indeed may prevent its oc-currence altogether. The imphcations forpatients susceptible to infective endocardi-tis are obvious. It should be appreciated,however, that the figures presented areminimal values and in reality the occur-rence of bacteraemia may be greater, par-ticularly in cases of marked gingivai in-flammation.
Our study is in agreement with others(Sconyers et al. 1973, Madsen 1974) infinding no correlation between bacteraemiaand degrees of plaque accumulation. Al-though the Gingivai and Plaque Indices areusually closely correlated (Silness & Loe1964), the absence of correlation betweenbacteraemia and plaque accumulation may
be explained by the modified assessmentused for the Plaque Index in this study.Instrumentation within the gingivai sulcusprior to the experimental procedure de-liberately was avoided and the resultingfigures thus are not directly comparable tothe Plaque Index as originally described.Also, on an individual basis there are likelyto be variations in the inflammatory re-sponse to plaque accumulation. The studytends to confirm our original hypothesisthat it is the severity of inflammationwhich is more likely to be a factor deter-mining the entry of microorganisms intothe circulation.
Another feature of the study was thelarge number of species of organismsisolated. Thirty different species were iso-lated including many anaerobes, this num-ber being even greater than numbers ofspecies recovered in studies assessing bac-teraemia following tooth extractions (Khai-rat 1966, Sconyers et al. 1973). The highnumber of anaerobes might be expectedwhen one considers the predominantly ana-erobic microflora of the gingivai sulcus andthe particular brushing and culture tech-niques used. The fact that such organismsenter the circulation must be consideredin patients susceptible to infective endo-carditis as anaerobic and mixed infectionshave been implicated in this disease (Lemer& Weinstein 1966, Felner & Dowell 1970)as well as the more classical oxygen toler-ant Streptococci which were the predomi-nant organisms of this study. Exact quanti-fication of microorganisms recoveredproved to be difficult as most growth oc-curred on primary isolation in broth. Inthese circumstances only identification oforganisms was possible giving rise to thefigures for the number of species of or-ganisms rather than specific numbers ofeach organism.
SILVER, MARTIN AND McBRIDE
Zu5amnienfassung
Experimentelle transitorische Bakteriaemie beimenschlichen Probanden mit unterschiedlichenPlaqueansanimlungen und Zahnfleischentziin-dungenEntsprechend der Schwere vorhandener Zahn-fleischentzundung und bakterieller Plaquean-sammlung an den Zahneii, wurden sechsund-neunzig Probanden einer von vier Versuchs-gruppen zugeordnet. Nach der Zahnretnigungmit standardisierten Methoden des Biirstens,wurden einer Vene der fossa cubiti Blut-proben entnommen, die unter aeroben undstrikt anaeroben Bedingungen kuUiviert wur-den. Der prozentuelle Anteil positiver Kultu-ren erhohte sich signifikant mit ansteigendengingivalen Entziindungsgraden, wie auch dieAnzahl tier isolierten Arten von Mikroorganis-men.
Es wurden dreissig verschiedene Arten ent-deckt die in der Mundhohle heimisch sind,unter ihnen viele strikt Anaerobe. Die vor-Iiegende Studie enthalt Hinweise auf die Hohedes Niveaus oraler Hygiene, die bei Patientenmit kongenitalen oder erworbenen endocardia-len Defekten oder cardiovascularen Prothesenals notwendig erachtet wird.
Bacteriemie passagere experimentale chez dessujets humains presentant differents degresd'accumulation de plaque bacterienne et d'in-flammation gingivaleQuatre-vingt seize sujets ont ete repartis enquatre groupes selon la severite de l'inflamraa-tion gingivale et I'accumulation de la plaquebacterienne sur les dents. Apres un brossagedes dents par un procede standardise, des prisesde sang ont ete faites au niveau d'une velne dupli du coude, et les specimens ont ete cultivesdans des conditions aerobies et dans des con-ditions strictement anaerobies. Le pourcentagede cultures positives augmentait de fafonsignificative avec la severity croissante de l'in-fiammation gingivale, ainsi que le nombred'especes des organismes isoles. Trente es-peces microbiennes differentes, hotes de lacavite buccale, parrai lesquelles un grandnombre d'anaerobies strlcts, ont ete trouvees.Cette etude semble indiquer qu'un certainniveau de sante buccale pourrait etre definicomme etant necessaire chez les patients pre-sentant des maladies congenitales ou acquises
de I'endocarde ou porteurs de protheses cardio-vasculaires.
Acknowledgements
This work was supported by a grant fromthe British Colutnbia Heart Foundation.
Statistical analysis was provided by JoyScott. Linda Devereaux was extremely pa-tient in typing many revisions of the manu-script.
References
American Heart Association (1965) Preventionof bacterial endocarditis. Circulation 31,953-954.
Bandt, C. L., Korn, N. A. & Schaffer, E. M.(1964) Bacteremias from ultrasonic and handinstrumentation. lournal of Periodontoiogy35, 214-215.
Beeley, L. (1969) Teeth, Streptococcus viridamand subacute bacterial endacarditis. BritishDental Journal 127, 424.
Bender, I. B., Seltzer, S., Tashman, S. & Me-loff, G. (1963) Dental procedures in patientswith rheumatic heart disease. Oral Surgery,Oral Medicine and Oral Pathology 16, 466-473.
Berger, S. A., Weitzmann, S., Edberg, S. C. &Casey, 3. I. (1974) Bacteremia after the useof an oral irrigation device. Annals of Inter-nal Medicine 80, 510-511.
Buchanan, R. E. & Gibbons, N. E. (eds.)(1974) Bergey's Manual of DeterntinativeBacteriology. 8th ed. Baltimore: Wiiliamsand Wilkins.
Cobe, H. M. (1954) Transitory bacteremia.Oral Surgery, Oral Medicine and OralPathology 1, 609-615.
Conner, H. D., Haberman, S., Collins, C. K.& Winford, T. E. (1967) Bacteremias follow-ing periodontal scaling in patients withhealthy appearing gingiva. Journal of Peri-odontology 38, 466-472.
Cooke, B. E. D. (1970) Relation between oraldisease and acute bacterial endocarditis.Proceedings of the Royal Society of Med-icine 63, 263-267.
Croxson, M. S., Altmann, M. M. & O'Brien,K. P. (1971) Dental status and recurrenceof Streptococcus viridans endocarditis. Lan-cet i, 1205-1207.

BACTERAEMIAS AND VARYING PERIODONTAL HEALTH 99
Editorial (1971) Prevention of infective endo-carditis. Lancet ii, 589-590.
Faden, S. H. (1974) Dental procedures andbacteremia. Annals of Internal Medicine 81,274.
Earrington, E. H. (1973) The incidence oftransient bacteremia pulpotomies on pri-mary teeth. Journal of Dentistry for Chil-dren 40, 175-184.
Felner, J. M. & Dowell Jr., V. R. (J970)Anaerobic bacterial endocarditis. New Eng-land Journal of Medicine 283, 1188-1192.
Harvey, W. P. & Capone, M. A. (1961) Bac-terial endocarditis related to cleaning andfiUing of teeth with particular reference tothe inadequacy of present day knowledgeand practice of antibiotic prophylaxis foraii dental procedures. American Journal ofCardiology 7, 793-798.
Hobson, F. G. & Juel-Jensen, B. E. (1956)Teeth, Streptococcus viridans and sub acutebacterial endocarditis. British Medical Jour-nal 1, 150J-1505.
Holdeman, L. V. & Moore, W. E. C. (eds,)(1975) Anaerobe Laboratory Manual. 3rd ed.Blacksburg, Va.: Virginia Polytechnic Insti-tute and State University.
Jones, J. C, Cutcher, J. L., Goldberg, J. R. &Lilly, G. E. (1970) Control of bacteremia as-sociated with extraction of teetb. Oral Sur-gery, Oral Medicine and Oral Pathology 30,454-459.
Khairat, O. (1966) An effective antibiotic coverfor the prevention of endocarditis followingdental and other postoperative bacteraemias.Journal of Clinical Pathology 19, 561-566.
Korn, N. A. & Scbaffer, E. M. (1962) A com-parison of postoperative bacteremias inducedfollowing different periodontal procedures.Journal of Pertodonlology 33, 226-231.
Lerner, P. I. & Weinstein, L. (1966) Infectiveendocarditis in the antibiotic era. New Eng-land Journal of Medicine 274. 199-206.
Loe, H. & Silness, J. (1963) Periodontal dis-ease in pregnancy. I. Prevalence and sever-ity. Acta Odontologica Scandinavica 21,533-551.
McMinn, M. T. & Crawford, J. J. (1970)
Recovery of anaerobic microorganisms fromclinical specimens in prereduced mediaversus recovery by routine clinical labora-tory metbods. Applied Microbiology 19,207-213.
Madsen, K. L. (1974) Effect of chlorbexidenemouthrinse and periodontal treatment uponbacteremia produced by oral hygiene proce-dures. Scandinavian Journal of Dental Re-search 82, 1-7.
Okell, C. C. & Elliott, S. D. (1935) Bactera-emia and oral sepsis with special referenceto the aetiology of subacute endocarditis.Lancet ii, 869-872.
Rise, E., Smith, J. F. & Bell, J. (1969) Reduc-tion of bacteremia after oral manipulations.Archives of Otolaiyngology 90, 198-201.
Romans, A. R. & App, G. R. (1971) Bacter-emia, a result from oral irrigation in sub-jects with gingivitis. Journal of Periodon-tology 42, 757-760.
Sconyers, J. R., Crawford, J. J. & Moriarty, J.D. (1973) Relationship of bacteremia totoothbrush! ng in patients with periodon-titis. Journal of the American Dental Asso-ciation 87, 616-622.
Silness, J. & Loe, H. (1964) Periodontal dis-ease in pregnancy. II. Correlation betweenoral hygiene and periodontal condition. ActaOdontologica Scandinavica 22, 121—135.
Silver, J. G., Martin, L. & McBride, B. C.(1975) Recovery and clearance rates of oralmicroorganisms following experimentalbacteraemias in dogs. Archives of OralBiology 20, 675-679.
Tamini, H. A., Thomassen, P. R. & Moser Jr.,E. H. (1969) Bacteremia study using a waterimgating device. Journal of Periodontology-Periodontics 40, 424^26.
Address:
/, a. SilverDepartment of Oral MedicineFaculty of DentistryUniversity of British ColumbiaVancouver, B.C.Canada, V6T 1W5





















