The Impact of an Intervention Taught by Trained Teachers on Childhood Overweight

International Journal of Pediatric Obesity, 2011; Early Online, 1–19
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
REVIEW ARTICLE
Evidence that the prevalence of childhood overweight is plateauing: data from nine countries
TIM OLDS 1 , CAROL MAHER 1 , SHI ZUMIN 2,3 , SANDRINE P É NEAU 4 , SANDRINE LIORET 5 , KATIA CASTETBON 6 , BELLISLE 4 , JEROEN DE WILDE 7 , MAEA HOHEPA 8 , RALPH MADDISON 9 , LAUREN LISSNER 10 , AGNETA SJ Ö BERG 10 , MICHAEL ZIMMERMANN 11 , ISABELLE AEBERLI 11,12 , CYNTHIA OGDEN 13 , KATHERINE FLEGAL 13 & CAROLYN SUMMERBELL 14
1 Health and Use of Time Group , Sansom Institute , University of South Australia , Adelaide , Australia ; 2 Jiangsu Provincial Center for Disease Control and Prevention , Nanjing , Jiangsu Province 210009 , China ; 3 School of Medicine , University of Adelaide , Adelaide , Australia ; 4 Unit é de Recherche en Epid é miologie Nutritionnelle , Bobigny , France ; 5 French Food Safety Agency, Dietary Survey Unit – Nutritional Epidemiology , Maisons-Alfort , France ; 6 French Institute for Health Surveillance ( InVS ), Universit é Paris 13 , Unit é de surveillance et d ’ é pid é miologie nutritionnelle , Bobigny , France ; 7 Municipal Health Service The Hague , Department of Epidemiology , Department of School Health Care , The Netherlands ; 8 Sport and Recreation New Zealand , Wellington , New Zealand ; 9 Clinical Trials Research Unit , Auckland University , Auckland , New Zealand ; 10 Department of Public Health and Community Medicine, Public Health Epidemiology Unit , Sahlgrenska Academy , University of Gothenburg , Gothenburg , Sweden ; 11 Laboratory for Human Nutrition , Institute of Food , Nutrition and Health , ETH Zurich , Switzerland ; 12 Clinic for Endocrinology , Diabetes and Clinical Nutrition , University Hospital Z ü rich , Switzerland ; 13 Centers for Disease Control and Prevention , Hyattsville , Maryland , USA ; 14 John Snow College , School of Medicine & Health , the Wolfson Research Institute , Stockton , UK
Abstract Until quite recently, there has been a widespread belief in the popular media and scientifi c literature that the prevalence of childhood obesity is rapidly increasing. However, high quality evidence has emerged from several countries suggesting that the rise in the prevalence has slowed appreciably, or even plateaued. This review brings together such data from nine countries (Australia, China, England, France, Netherlands, New Zealand, Sweden, Switzerland and USA), with data from 467,294 children aged 2 – 19 years. The mean unweighted rate of change in prevalence of overweight and obesity was � 0.00 (0.49)% per year across all age � sex groups and all countries between 1995 and 2008. For overweight alone, the fi gure was � 0.01 (0.56)%, and for obesity alone � 0.01 (0.24)%. Rates of change differed by sex, age, socioeconomic status and ethnicity. While the prevalence of overweight and obesity appears to be stabilizing at different levels in different countries, it remains high, and a signifi cant public health issue. Possible reasons for the apparent fl attening are hypothesised.
Key words: Child , adolescent , obesity , overweight , prevalence , international
Background
Paediatric obesity has been described as the primary childhood health problem in developed nations (1), having been linked to many serious physical, social and psychological consequences. These include increased risk of cardiovascular dysfunction (2), type 2 diabetes (3), and pulmonary (4), hepatic (5), renal (6) and musculoskeletal (7) complications; lower
Correspondence: Dr Carol Maher, Post Doctoral Research Fellow, Health and USouth Australia, 5001, Australia. Tel: � 61 8 8302 6558. E-mail: carol.maher@u
(Received 22 November 2010; fi nal version received 8 June 2011 )
ISSN Print 1747-7166 ISSN Online 1747-7174 © 2011 Informa HealthcareDOI: 10.3109/17477166.2011.605895
health-related quality of life (8); negative emotional states such as sadness, loneliness, and nervousness, and increased likelihood of engagement in high-risk behaviours (9); and undesirable stereotyping includ-ing perceptions of poor health, academic and social ineptness, poor hygiene and laziness (10).
There is widespread belief in the popular media that the prevalence of childhood obesity is escalating,
se of Time Group, University of South Australia, GPO Box 2471, Adelaide, nisa.edu.au.

2 T. Olds et al .
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
with ominous predictions about rapidly increasing rates in future decades. For example,
(The British Heart Foundation) claims that more than two thirds of British children will be overweight by 2050 and that Britain as a whole is heading for an obesity epidemic. … At this rate, … more than two thirds of all British kids will suffer from obesity by 2050. (11) Research indicates that if childhood obesity rates continue to soar, half of all Australian chil-dren will be overweight by the year 2025. (12)
These beliefs are echoed in the scientifi c health lit-erature, where it has become commonplace for child-hood obesity to be described as an epidemic or even a pandemic:
... there is growing interest in developing effective public health interventions to address the obesity pandemic. (13) The world-wide gravity of this health crisis is refl ected in data from a number of countries. The global trend of increasing childhood obe-sity makes this a health issue of concern to nurses throughout the world … Crisis level has been reached in a number of European coun-tries … (14)
While there is irrefutable evidence of historical increases in prevalence in recent decades, and strong evidence that prevalence continues to rise in certain countries and particular subgroups, evidence for con-tinuing rises is not universal. In contrast, high quality evidence from several countries around the world is emerging suggesting that the rise in the prevalence of childhood obesity has slowed appreciably, or even plateaued, which will be outlined in this paper.
The purpose of this paper is to show that high quality data from around the world suggest a slowing in the rate of rise of childhood obesity, in at least several countries. There is often great resistance to this idea. Reviewers treat studies suggesting a slow-down with some scepticism, public health experts may feel it will blunt the urgency of their message, and the media are aware that bad news sells better than good (15). Here we assemble evidence from Australia, China, England, France, The Netherlands, New Zealand, Sweden, Switzerland and the USA showing fl attening trends in childhood overweight and obesity.
Methods
This collaborative paper was instigated by the Aus-tralian co-authors (TO and CM). Other researchers
who had recently published or presented data indi-cating slowing or stabilization in the rate of child-hood obesity were identifi ed from literature auto-alerts and personal contacts. Contact details for these researchers were identifi ed either from the ‘ corre-sponding author ’ contact details published with their manuscript, or using an internet search engine. Rel-evant researchers were then sent an introductory email explaining the scope of the paper and inviting them to contribute. In this email, the researchers were also asked to identify any other research teams which they were aware of that were conducting research in the area. Any such additional researchers were then sent the introductory email.
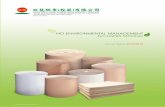
All contacted authors accepted the request to be involved in the manuscript and were invited to ask co-authors from their country if they considered it appropriate to do so. Authors were asked to review recent evidence from their country regarding preva-lence trends in childhood overweight and obesity. Descriptive data from each of the countries are pre-sented in the following sections Australia to the USA, in alphabetical order. With the exception of one French dataset (INCA 1) all height and mass were measured, rather than self-reported. Summary details of the sampling frames and protocols of the various included studies are provided in Appendix 1. Data from all countries were compi ed in Figure 1 and Table I using the International Obesity Task Force (IOTF) cut-offs (16) to allow cross-country com-parisons. Based on the IOTF centile curves for child BMI scores, throughout this manuscript, the term ‘ overweight including obesity ’ (OWOB) corresponds to an adult BMI � 25 kg/m 2 , ‘ overweight excluding obe-sity ’ (OW) corresponds to an adult BMI � 25 kg/m 2 and � 30 kg/m 2 , and ‘ obese ’ (OB) corresponds to an adult BMI � 30 kg/m 2 . The yearly rate of change in the prevalence of obesity (OB), overweight excluding obesity (OW) and/or overweight including obesity (OWOB) was calculated using linear regression. Visual inspection of the data in Figure 1 supports this functional form.
Results
Australia
In Australia, there have been offi cial national surveys of children ’ s weight status in 1985, 1995 and 2007. In addition, there have been many studies conducted at the national, state and regional level in the inter-vening years. A systematic review (17) located 41 Australian surveys of childhood weight status con-ducted between 1985 and 2008. The studies included data on 264,905 Australians aged 2 – 18 years, with raw data available on 70,758 children.

Pleateauing prevalence of childhood overweight 3
5-6 y
7-9 y10-11 y
14-15 y
6-10 y
05
1015202530354045
Stockholm
Gothenburg KarlstadUmeå
VästeråsYstad
05
1015202530354045
Dutch
Turkish
Moroccan
Surinamese
05
1015202530354045
1995 2000 2005 2010Year of measurement
2-19 y
2-5 y
6-11 y
12-19 y
05
1015202530354045
1995 2000 2005 2010
Year of measurement
05
101520253035404505
1015202530354045
05
1015202530354045
05
1015202530354045
05
1015202530354045
USA
Sweden 10-11 y
Netherlands 3-16 y
England 2-15y
China 12-14y
Australia 2-18y
Switzerland 6-13y
NZ 5-14y
France
% overweight or obese % overweight or obese
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
Figure 1. The prevalence of overweight and obesity in each country from 1995 – 2008. The broken line represents the mean rate of overweight including obesity for the entire sample (i.e., all countries across all years combined).

4 T. Olds et al .
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
Prevalence estimates for overweight and obese (IOTF criteria) were calculated for each study in age � sex categories, adjusted for age and sex, and plotted against measurement year. Where raw data were available, BMI z-scores (UK 1990 reference) (18) were plotted against measurement year. Two-linear-segment models were used to assess secular trends in prevalence estimates and BMI z-scores. The breakpoint for the two-linear-segment model (derived using the D max method) (19) was 1996. The slopes of linear segments pre- and post-1996 within age, gender and weight-status categories were compared using the method of Zar (20).
There has been a signifi cant deceleration in prev-alence in the years 1996 – 2008. The estimated preva-lence of overweight including obesity in boys rose from 10.2% in 1985 to 21.6% in 1996, to 23.7% in 2008. In girls, the estimated prevalence rose from 11.6% in 1985 to 24.3% in 1996, to 24.8% in 2008. The prevalence of overweight including obesity increased over the period 1985 – 1996 in boys at the rate of � 1.03 (95% CI: 0.69 – 1.37)% per annum, and in girls at the rate of � 1.16 (0.72 – 1.60)% per annum. However, from 1996 onwards, there was no signifi cant increase in prevalence in boys [ � 0.18 (CI: � 0.04 – 0.40)% per annum] or in girls [ � 0.04 ( � 0.20 – 0.28)% per annum]. There were similar trends in standardized BMI (z-scores). In boys, mean BMI z-score increased at the rate of � 0.28 (0.20 – 0.36) units per decade between 1985 and 1996, but slowed to � 0.04 ( � 0.02 – 0.10) units per decade between 1996 and 2008. In girls, it increased at the rate of � 0.33 (0.25 – 0.41) units per decade between 1985 and 1996, but only at � 0.07 ( � 0.01 – 0.15) units per decade between 1996 and 2008. These pat-terns were fairly consistent across the age span. Within each weight-status category, average BMI did not increase in the 1996 – 2008 period. Based on these data, the prevalence of overweight and obesity appears to have fl attened in Australia between 1996 and 2008.
China – Jiangsu Province
In China, under-nutrition was a major health concern prior to the 1980s. However, with economic develop-ment there has been a concurrent rapid change in the nutritional status of Chinese adolescents. Data from national nutrition surveys conducted in 1982, 1992 and 2002 show that the prevalence of overweight and obesity (IOTF c iteria) among adolescents aged 7 – 17 years rose from 1.3% in 1982 to 4.4% and 5.2%, respectively, in 1992 and 2002 (21).
More recent Chinese data concerning prevalence trends are available from two cross-sectional surveys of 824 and 1663 students conducted in the same
eight schools in 2002 and 2007, in Jiangsu Province (22). The province is one of the most affl uent prov-inces in China with a population of 76.2 million. The study locations included Zhenjiang, an affl uent pre-fecture, and Xuzhou, a relatively poor prefecture. In each, schools were randomly selected from each of four different areas: the inner city, a suburb of a city, a regional capital and a town. The age range of the study population was 12 – 14 years.
In total, 15.2% and 15.0% of the students were overweight or obese in 2002 and 2007, respectively (with no signifi cant difference; p � 0.90). Between 2002 and 2007, the increases in height and weight were � 2.1 cm ( p 0.001) and � 1.7 kg ( p � 0.01) in boys; the corresponding fi gures were � 0.7 cm ( p � 0.07) and � 0.3 ( p � 0.56) kg in girls. The sta-bility in the prevalence of overweight and obesity between 2002 and 2007 was observed in both urban and rural areas.
England
Prevalence of childhood obesity in England is rela-tively high in comparison to international reports (23), thus tackling the issue is a Government priority (24). In England, childhood obesity prevalence is monitored annually through two national surveys: the Health Survey for England (25) and the National Child Measurement Programme (26).
The Health Survey for England has measured the height and weight of 49,723 children aged 2 – 15 years, as part of a wider health survey, from a general population sample since 1995 (25). Annual trend data demonstrate an increase in the prevalence of childhood overweight and obesity over the entire 13 years of measurement. However, prevalence of obe-sity, and overweight including obesity appeared to peak around 2005 at 7.4% and 26.4%, respectively, and since appears to have levelled off. A similar lev-elling off trend has been reported for children aged 2 – 10 years and 11 – 18 years using the same Health Survey for England data (27).
The National Child Measurement Programme (26) was established in 2005, and annually weighs and measures the majority of school children in Reception (ages 4 – 5 years) and Year 6 (ages 10 – 11 years) across England. The programme, one of the largest of its kind, informs local planning and deliv-ery of services for children, and provides population-level surveillance data. In 2007/08, approximately 88% (973,073) of all eligible school children were measured. Due to low participation rates in the fi rst year (2005/06) of measurement and improvements in data quality over the early years of the programme, it is not yet possible to carry out detailed trend analyses. However, preliminary analyses comparing prevalence

Pleateauing prevalence of childhood overweight 5
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
data from the last three years (2006/07 and 2007/08) suggest no change (28). These data also demonstrate that obesity prevalence varies signifi cantly across the different regions of England and is higher in urban areas, and in children from deprived backgrounds and certain ethnic minorities including Black and Asian populations (29).
France
In France, numerous studies examining childhood weight status have been conducted in recent years. School-based studies carried out on a triennial basis with children aged 5 – 6 years, 10 – 11 years and 14 – 15 years (Triennial cycle of school surveys; Ministry of Health, Ministry of National Education, National Institute for Health Surveillance) (Direction de la Recherche des Etudes de l ’ Evaluation et des Statis-tiques) (30). Representative sampling is used, and the studies are based on compara le protocols, though the geographical coverage has not been strictly iden-tical from year to year . In 5 – 6-year-old children, the prevalence of overweight including obesity was stable between 1999 and 2000 ( n � 29,896) and 2005 – 2006 ( n � 22,143): 14.4% and 12.1%; as well as the prevalence of obesity: 3.9% and 3.1%, respectively. Similarly, in 10 – 11-year-olds, the prevalence of over-weight including obesity was stable between 2001 and 2002 ( n � 7851) and 2004 – 2005 ( n � 7255): 19.9% and 19.7%; as well as that of obesity: 4.1% and 3.7%, respectively. Finally, a stable prevalence was also observed in 14 – 15-year-old children between 2000 and 2001 ( n � 6590) and 2003 – 2004 ( n � 7229) for overweight including obesity: 15.7% and 16.8%; and obesity: 3.3% and 4.4%.
Another cross-sectional study based on the Euro-pean Childhood Obesity Group protocol (31) was carried out in 2000 ( n � 1582) and repeated in 2007 ( n � 1014) with 7 – 9-year-old children (32). Results showed that the prevalence of overweight including obesity was stable between 2000 (18.1% including 3.8% obesity) and 2007 (15.8%, including 2.8% obesity) (difference not signifi cant).
In addition to these data, yearly prevalence has been provided at a regional level (central/western part of France), in a standardized 6- to 15-year-old popu-lation between 1996 and 2006 (sample size across years � 26,600) (33). According to these data, the stabilization of overweight and obesity prevalence had already occurred in 1998 in most groups studied, and from 2001 in the disadvantaged SES group.
Two further national cross-sectional dietary sur-veys (Etudes Individuelles Nationales sur les Con-sommations Alimentaires, INCA1 and INCA2) (34), allow comparison of overweight rates in two repre-sentative samples of French children aged 3 – 14 y:
INCA 1 (1998 – 99, n � 1017) and INCA 2 (2006 – 07, n � 1030) (34). Weight and height were self-re-ported in INCA 1 and measured objectively in INCA 2. Socio-economic status (SES) was recorded on the basis of parent-reported occupation. In total, 14.5% of the children were overweight (including obesity) in 2006 – 07, which was not signifi cantly different from the 15.2% recorded in 1998 – 99. A strong inverse socio-economic gradient of overweight (including obesity) in French children was observed in both studies. Thus, after an increase in childhood overweight and obesity prevalence in the late 1990s, data from numerous cross-sectional studies con-ducted with French children suggest that rates are currently stabilizing.
The Netherlands – The Hague
Prevalence of overweight and obesity in children in The Netherlands has been among the lowest in Europe (35). Despite this however, prevalence rates have increased signifi cantly since the 1980s. The Fourth Dutch National Growth Study of 1997 showed an overweight prevalence including obesity of 13%, which is at least a two-fold increase since the Third National Growth Study of 1980 (36). Further increases were observed in 2002 – 2003 with cross-sectional data of several regions in The Netherlands showing prevalence rates for overweight including obesity in Dutch children, irrespective of ethnicity, of 14.5% in boys, and 17.5% in girls (37). When ethnicity is taken into account, however, the fi gures change.
An analysis over the years 1999 – 2007 in the city of The Hague shows the fi rst indications of a stabi-lization and even a decrease in certain ethnic groups. The study was based on a series of cross-sectional growth measurements in 3 – 16-year-old children that had been routinely collected by Child Health Care Services of the city of The Hague (37). In Dutch girls, a 14% decline in overweight e cluding obesity was found from 12.6% in 1999 to 10.9% in 2007. This decline was found to be due to a decrease of overweight excluding obesity in 3 – 6-year-olds girls. Age-specifi c analyses in Dutch boys showed a similar signifi cant decrease in 3 – 6-year-olds. Surinamese South Asian (15.0%) and Moroccan (23.0%) chil-dren, and Dutch boys (11.3%) showed an overall stabilization of overweight including obesity preva-lence between 1999 and 2007. There was however a strong and signifi cant increase in overweight includ-ing obesity prevalence in Turkish boys, from 22.4% (1999) to 34.5% (2007), and in Turkish girls, from 27.4 – 33.8%. Despite this unexplained increase of overweight including obesity in Turkish children, the prevalence of overweight including obesity in the

6 T. Olds et al .
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
other ethnic groups seems to have levelled off or even decreased.
New Zealand
In New Zealand, trend analysis has been conducted by comparing anthropometric data of children (aged 5 – 14 years) from two nationally representative sur-veys; the 2002 National Children ’ s Nutrition Survey (38) and the 2006/07 New Zealand Health Survey (39). Both surveys had a similar sample size of approximately 3,200 children and used identical stan-dardized methods to collect height and weight data.
These age-standardized data suggest there has been no change in the prevalence of childhood over-weight and obesity between 2002 (28.8%) and 2006/07 (28.5%). This pattern of stability was found for both boys (2002: 26.1%; 2006/07: 28.2%) and girls (2002: 31.7%; 2006/07: 28.8%) and for M a ori (2002: 38.8%; 2006/07: 37.3%) and Pacifi c Island (2002: 60.0%; 2006/07 57.2%) children; two ethnic groups that display signifi cantly higher rates of over-weight and obesity. Mean BMI among children also remained steady at 19.1 kg/m 2 in 2006/07. For Pacifi c children, however, a signifi cant decline in mean BMI of 2.2kg/m 2 was reported (39). Over a short time frame spanning 2002 – 2006/07, available evidence indicates that the prevalence of childhood overweight and obesity in New Zealand has remained stable.
Sweden
The World Health Organization MONICA Project (a 10-year survey monitoring trends and determi-nants in cardiovascular disease) showed Sweden to be a country with relatively low prevalence of obesity (40). However, Sweden has documented increasing rates of both adult and childhood obesity since the 1980s (41,42).
Recent trends in Swedish childhood obesity and overweight prevalence may be estimated on the basis of school health records from 10 – 11-year-olds. While there is presently no nationwide representative Swed-ish database on childhood obesity, most fourth-grad-ers undergo standardized health examinations by specialized nurses in the school setting.
In earlier studies from Gothenburg, 10-year-old children were examined in 1984 and 2000, and com-parisons of these two cohorts revealed two-fold increases in overweight including obesity and 3- to 4-fold increases in obesity alone. In boys, overweight including obesity increased from 7.2 – 17.1%, and in girls from 8.6 – 19.6% – corresponding increases for obesity were from 0.7 – 2.9% and from 0.8 – 3.0% among boys and girls, respectively (42 – 44). However, these trends did not continue into the 21st century.
In 2004, a new cohort of fourth-graders from Gothenburg was examined (44). Compared to the previously described cohort measured in 2000, prev-alence of overweight including obesity in girls decreased from 19.6 – 15.9% ( p � 0.01); no signifi -cant changes were observed in boys (total n � 8876 in both cohorts).
Similarly, in Stockholm, a total of 4,599 10 – 11-year-old schoolchildren were sampled from dif-ferent socioeconomic districts in academic years starting 1999 and 2003 (45). Obesity prevalence during this time appeare stable, with non-signifi cant decreases from 4.4 – 2.8% in girls, and non-signifi cant increases from 3.2 – 3.8% in boys.
Prevalence estimates from other areas representing various geographical regions of Sweden have recently been reported (Karlstad and Ume å , n � 3,111; and V ä ster å s and Ystad, n � 4473), and likewise sug-gested no change between 2003 and 2005 (46). Despite the overall stability in these four municipal-ities combined, increasing as well as decreasing trends could be observed within the individual municipalities.
Trends in childhood obesity according to SES were considered in the Gothenburg and Stockholm studies, with SES evaluated at the residential area level (44,45). Both of these studies confi rmed that overweight and obesity were more common in chil-dren from less advantaged environments. Among girls in both studies, the decreasing trends were con-sistent in all socioeconomic groups. However, in Stockholm the gap in obesity between boys from lower and higher socioeconomic groups appeared to be widening over time (45). In Gothenburg, increas-ing trends in overweight including obesity tended to occuring boys from middle-income areas, in contrast to decreasing trends in both high and low-income areas (44).
In summary, no signifi cant increases in overweight or obesity have been observed in recent studies of Swedish schoolchildren in six municipalities (47). The synthesized studies offer a consistent picture of stabilizing obesity rates particularly in urban Sweden, with some evidence that the trend is reversing in girls but not in boys.
Switzerland
A national study of 6 – 13-year-olds in Switzerland in 2002 ( n � 2431) suggested nearly 1 in 5 schoolchil-dren were overweight (48). In order to assess trends in Swiss childhood obesity, a 5-year follow-up study was carried out in 2007 with 2,222 6 – 13-year-old children (49). In both studies, a national representa-tive sample was obtained (48,49) and overweight and obesity were determined on the basis of Centres for

Pleateauing prevalence of childhood overweight 7
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
Disease Control and Prevention (CDC) BMI references (50). However, for the purposes of this review, IOTF cut-offs are used, and CDC cut-offs are provided in Appendix 2.
In 2007, the prevalence of overweight excluding obesity and obesity in boys were 11.4% and 2.3%, respectively, and in girls they were 11.2% and 2.1%. Compared to 2002, there were decreases in the prev-alence of overweight (excluding obesity) in girls ( � 4.2%) and boys ( � 1.4%) and obesity in both gen-ders ( � 1.6% in boys and � 1.6% in girls). In 2002, there were neither geographic nor demographic dif-ferences in prevalence rates. In contrast, in 2007 the prevalence of obesity was signifi cantly higher in com-munities with a population � 100,000 compared to smaller communities ( p � 0.05) and some regional differences were observed (please refer to [49] for further details).
Two other studies similarly provide evidence of recent stabilization in obesity and overweight preva-lence in Swiss children. In the canton of Geneva, there has been a small (not statistically signifi cant) decrease in the overweight and obesity prevalence in 5 – 6-year-old children from 2003 – 2008 (51). Also, a Swiss national study on iodine nutrition in 6 – 12-year-old children, which measured weight and height as a sec-ondary outcome measure, found stabilization in the prevalence of obesity between 2002 and 2009 (52). In summary, over the past 5 years, the prevalence of obe-sity has stabilized or decreased in Swiss children.
USA
Trend analyses in the USA are based on data from the National Health and Nutrition Examination Surveys (NHANES). NHANES is a cross-sectional survey, designed to monitor the health and nutritional status of the US civilian, non-institutionalized population (CDC/NCH ; National Health and Nutrition Exami-nation Survey 2009) (53). Starting in 1999 the survey became continuous with release and reporting of data every two years. The survey involves nationally repre-sentative samples, selected using a complex, multistage probability sample design. Oversampling is used to obtain reliable estimates of health and nutritional mea-sures for certain population subgroups. Sample weights account for differential probabilities of selection, non-response and non-coverage. Data are grouped into two-year cycles (1999 – 2000, 2001 – 2002, 2003 – 2004, 2005 – 2006 and 2007 – 2008). For the purpose of this review paper, analyses have been undertaken using IOTF defi nitions of obesity and overweight (16) rather than the usual CDC defi nitions.
Tests for trends between 1999 – 2000 and 2007 – 2008 were carried out using sex-specifi c logistic regression models adjusted for age and race-ethnicity.
Because previous analyses (54) have shown signifi -cant differences in prevalence of obesity by age and between non-Hispanic whites, non-Hispanic blacks and Mexican Americans in the USA, trend tests were adjusted for age group and race-ethnic group.
In analyses, survey period (1999 – 2000, 2001 – 2002, 2003 – 2004, 2005 – 2006 and 2007 – 2008) was treated as a continuous variable. All analyses were done with sample weights and were performed using the statistical packages SAS version 9.1 (SAS Insti-tute, Cary, NC, USA) and SUDAAN version 9.0 (RTI, Research Triangle Park, NC, USA) to account for the complex sample design.
In 2007 – 2008, 34.3% (SE 1.3) of children and adolescents 2 – 19 years of age were overweight (including obesity) while 15.7% (SE 1.0) were obese. In the same period, 15.7% (SE 1.1) of boys and 15.8% (SE 1.2) of girls were obese. Signifi cant age and race/ethnic differences in obesity prevalences exist (55). In 2007 – 2008, 2 – 5-year-old children were less likely to be obese compared to older children. In addition, sex specifi c analyses indicated that non-Hispanic black girls were more likely to be obese compared to non-Hispanic white girls and Mexican American boys were more likely to be obese com-pared to non-Hispanic white boys (54).
Trend tests showed no signifi cant trend in over-weight or obesity between 1999 – 2000 and 2007 – 08 among either boys ( p � 0.742 and p � 0.152) or girls ( p � 0.095 and p � 0.203) after adjusting for age and race-ethnicity. It appears that the rapid increase in obesity prevalence seen in the US during the 1980s and 1990s has slowed, especially among girls, during the most recent decade.
Aggregated data
Data from all the countries are compiled in Table I, and trends in summary prevalence data from each country are presented visually in Figure 1. Where available, data are presented in age, sex and weight status subgroups. All data were based upon objec-tively measured height and weight, with the excep-tion of the French INCA1 study, which obtained self-reported data for its 1,017 participants.
Linear regression was used to determine the annual rate of change in prevalence of obesity, over-weight including obesity and overweight excluding obesity, in each subgroup from each country. Overall, the mean (SD) unweighted rate of change in the prevalence of child and adolescent overweight and obesity (taking averages across all ethnicities for the Dutch data) from 112 reports (country specifi c age � sex categories) was � 0.00 (0.49)% per year. The mean rate of change in 40 reports of overweight including obesity combined was � 0.01 (0.58)% per

8 T. Olds et al .
Tab
le I
. P
reva
lenc
e of
ove
rwei
ght
and
obes
ity
in c
hild
ren
and
adol
esce
nts
in n
ine
coun
trie
s be
twee
n 19
95 a
nd 2
008.
Cou
ntry
Stu
dyA
geS
exS
ampl
e si
ze1
Wei
ght
stat
us19
9519
9619
9719
9819
9920
0020
0120
0220
0320
0420
0520
0620
0720
08S
lope
2
Aus
tral
ia(1
7)2–
18B
oys
1343
47O
W16
.218
.40.
182–
18B
oys
OB
5.4
5.3
–0.0
12–
18B
oys
OW
OB
21.6
23.7
0.18
2–18
Gir
ls13
0558
OW
18.6
18.9
0.02
2–18
Gir
lsO
B5.
75.
90.
022–
18G
irls
OW
OB
24.3
24.8
0.04
Chi
na(2
2)12
–14
Boy
s12
82O
WO
B19
.319
.0–0
.06
12–1
4G
irls
1205
OW
OB
10.7
10.7
0.00
Eng
land
(25)
& u
npub
lishe
d an
alys
is (
Din
sdal
e)2–
15B
oth
4972
3O
W15
.314
.915
.316
.717
.215
.718
.018
.318
.820
.119
.017
.717
.80.
33
2–15
Bot
hO
B3.
84.
64.
44.
25.
75.
25.
26.
55.
96.
77.
46.
06.
30.
24
2–15
Bot
hO
WO
B19
.119
.519
.720
.922
.920
.923
.224
.824
.726
.826
.423
.724
.10.
57F
ranc
e(3
0)5–
6B
oys
5203
93O
W8.
77.
6–0
.18
5–6
Boy
sO
B3.
62.
9–0
.12
5–6
Boy
sO
WO
B12
.310
.5–0
.30
5–6
Gir
lsO
W12
.210
.5–0
.28
5–6
Gir
lsO
B4.
33.
3–0
.17
5–6
Gir
lsO
WO
B16
.513
.8–0
.45
(32)
7–9
Boy
s25
963
OW
14.0
11.3
–0.3
97–
9B
oys
OB
3.9
2.8
–0.1
67–
9B
oys
OW
OB
17.9
14.1
–0.5
47–
9G
irls
OW
14.7
14.9
0.03
7–9
Gir
lsO
B3.
62.
8–0
.11
7–9
Gir
lsO
WO
B18
.317
.7–0
.09
(30)
10–1
1B
oys
1507
63O
W15
.515
.60.
0310
–11
Boy
sO
B4.
03.
5–0
.17
10–1
1B
oys
OW
OB
19.5
19.1
–0.1
310
–11
Gir
lsO
W16
.116
.50.
1310
–11
Gir
lsO
B4.
23.
9–0
.10
10–1
1G
irls
OW
OB
20.3
20.4
0.03
(30)
14–1
5B
oys
1381
93O
W12
.812
.7–0
.03
14–1
5B
oys
OB
3.5
4.8
0.43
14–1
5B
oys
OW
OB
16.3
17.5
0.40
14–1
5G
irls
OW
12.1
12.1
0.00
14–1
5G
irls
OB
3.2
3.9
0.23
14–1
5G
irls
OW
OB
15.3
16.0
0.23
INC
A 1
and
IN
CA
2
(34)
3–6
Bot
h56
0O
W9.
910
.50.
08
3–6
Bot
hO
B6.
33.
0–0
.41
(Con
tinue
d)
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.

Pleateauing prevalence of childhood overweight 9
Cou
ntry
Stu
dyA
geS
exS
ampl
e si
ze1
Wei
ght
stat
us19
9519
9619
9719
9819
9920
0020
0120
0220
0320
0420
0520
0620
0720
08S
lope
2
3–6
Bot
hO
WO
B16
.313
.5–0
.35
7–10
Bot
h64
4O
W14
.511
.1–0
.43
7–10
Bot
hO
B3.
03.
50.
067–
10B
oth
OW
OB
17.5
14.6
–0.3
611
–14
Bot
h76
8O
W10
.413
.10.
3411
–14
Bot
hO
B1.
22.
10.
1111
–14
Bot
hO
WO
B11
.715
.20.
44(6
5)6–
15B
oth
2660
0 O
WO
B10
.513
.615
.614
.715
.515
.715
.813
.515
.113
.714
.00.
13N
ethe
rlan
ds(3
7)3–
16B
oys
2558
8O
W8.
87.
78.
89.
88.
59.
69.
09.
38.
90.
09D
utch
ori
gin
3–16
Boy
sO
B2.
22.
42.
12.
42.
52.
52.
62.
52.
3
3–16
Boy
sO
WO
B11
.110
.110
.912
.211
.012
.111
.511
.811
.20.
113–
16G
irls
2480
5O
W12
.612
.612
.111
.911
.611
.511
.211
.110
.9–0
.23
3–16
Gir
lsO
B3.
73.
93.
43.
93.
32.
93.
13.
23.
3–0
.09
3–16
Gir
lsO
WO
B16
.316
.515
.515
.714
.914
.414
.314
.314
.2–0
.31
Tur
kish
or
igin
3–16
Boy
s73
50O
W14
.516
.314
.815
.716
.318
.217
.321
.321
.40.
84
3–16
Boy
sO
B7.
96.
98.
29.
811
.59.
910
.810
.813
.10.
633–
16B
oys
OW
OB
22.4
23.2
23.0
25.4
27.8
28.1
28.1
32.1
34.5
1.47
3–16
Gir
ls68
21O
W19
.418
.619
.117
.819
.520
.918
.622
.523
.20.
483–
16G
irls
OB
8.0
8.2
7.4
8.9
8.2
7.7
8.5
10.2
10.7
0.30
3–16
Gir
lsO
WO
B27
.426
.826
.526
.727
.728
.627
.232
.733
.80.
78M
oroc
can
orig
in3–
16B
oys
5452
OW
12.1
13.1
14.2
14.4
13.8
11.9
11.0
15.0
16.7
0.25
3–16
Boy
sO
B5.
66.
56.
84.
64.
75.
57.
55.
67.
20.
103–
16B
oys
OW
OB
17.8
19.6
21.0
19.0
18.6
17.4
18.5
20.6
23.9
0.35
3–16
Gir
ls55
45O
W20
.120
.214
.918
.815
.021
.018
.023
.220
.50.
323–
16G
irls
OB
7.2
9.1
7.6
6.3
6.7
6.9
5.8
7.2
6.6
–0.1
93–
16G
irls
OW
OB
27.3
29.3
22.4
25.0
21.7
27.9
23.8
30.3
27.1
0.13
Sur
inam
ese
Sou
th A
sian
3–16
Boy
s49
76O
W8.
96.
18.
97.
97.
410
.610
.410
.614
.50.
69
3–16
Boy
sO
B5.
15.
56.
25.
15.
45.
14.
15.
75.
4–0
.04
3–16
Boy
sO
WO
B14
.011
.615
.113
.012
.915
.714
.516
.319
.90.
653–
16G
irls
4697
OW
9.3
12.7
11.1
13.1
10.2
10.8
12.2
10.0
12.6
0.08
3–16
Gir
lsO
B4.
43.
84.
13.
63.
93.
02.
14.
54.
5–0
.04
3–16
Gir
lsO
WO
B13
.716
.515
.216
.614
.213
.814
.314
.617
.10.
06A
ll et
hnic
itie
s co
mbi
ned
3–16
Boy
s43
366
OW
10.1
9.8
10.6
11.1
10.3
11.5
10.7
12.1
13.0
0.32
3–16
Boy
sO
B3.
84.
14.
34.
24.
64.
54.
74.
55.
40.
153–
16B
oys
OW
OB
13.9
13.9
14.9
15.3
14.8
15.9
15.4
16.6
18.4
0.46
3–16
Gir
ls41
868
OW
14.1
14.7
13.6
13.8
13.1
14.3
13.3
14.4
14.7
0.02
Tab
le I
. (C
onti
nued
).
(Con
tinue
d)
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.

10 T. Olds et al .
Cou
ntry
Stu
dyA
geS
exS
ampl
e si
ze1
Wei
ght
stat
us19
9519
9619
9719
9819
9920
0020
0120
0220
0320
0420
0520
0620
0720
08S
lope
2
3–16
Gir
lsO
B4.
85.
34.
84.
94.
64.
34.
25.
05.
2–0
.02
3–16
Gir
lsO
WO
B18
.920
.018
.318
.717
.718
.617
.519
.419
.80.
00N
ew Z
eala
nd(3
8) a
nd (
39)
5–14
Boy
s64
923
OW
18.0
20.1
0.42
5–14
Boy
sO
B8.
18.
10.
00A
ll et
hnic
itie
s co
mbi
ned
5–14
Boy
sO
WO
B26
.128
.20.
42
5–14
Gir
lsO
W21
.720
.1–0
.32
5–14
Gir
lsO
B10
.08.
7–0
.26
5–14
Gir
lsO
WO
B31
.728
.8–0
.58
Mao
ri o
rigi
n45–
14B
oth
OW
24.4
24.6
0.04
5–14
Bot
hO
B14
.412
.7–0
.34
5–14
Bot
hO
WO
B38
.837
.3–0
.30
Pac
ifi c
orig
in4
5–14
Bot
hO
W32
.731
.0–0
.34
5–14
Bot
hO
B27
.326
.2–0
.22
5–14
Bot
hO
WO
B60
57.2
–0.5
6S
wed
en(4
5)10
–11
Boy
s23
19O
W18
.416
.7–0
.43
Sto
ckho
lm10
–11
Boy
sO
B3.
23.
80.
1510
–11
Boy
sO
WO
B21
.620
.5–0
.28
10–1
1G
irls
2260
OW
17.7
16.4
–0.3
310
–11
Gir
lsO
B4.
42.
8–0
.40
10–1
1G
irls
OW
OB
22.1
19.2
–0.7
3G
othe
nbur
g(4
4)10
–11
Boy
s44
40O
W14
.214
.80.
1510
–11
Boy
sO
B2.
92.
8–0
.03
10–1
1B
oys
OW
OB
17.1
17.6
0.13
10–1
1G
irls
4436
OW
16.6
13.4
–0.0
810
–11
Gir
lsO
B3.
02.
5–0
.13
10–1
1G
irls
OW
OB
19.6
15.9
–0.9
3K
arls
tad
(46)
10–1
1B
oth
1637
OW
15.1
17.5
2.40
10–1
1B
oth
OB
2.7
2.4
–0.3
010
–11
Bot
hO
WO
B17
.819
.92.
10U
meå
(46)
10–1
1B
oth
1474
OW
18.3
18.1
–0.2
010
–11
Bot
hO
B2.
32.
70.
4010
–11
Bot
hO
WO
B20
.620
.80.
20V
äste
rås
(46)
10–1
1B
oth
2379
OW
18.0
19.4
0.70
10–1
1B
oth
OB
5.3
4.7
–0.3
010
–11
Bot
hO
WO
B23
.324
.10.
40Y
stad
(46)
10–1
1B
oth
584
OW
18.5
15.8
–1.3
510
–11
Bot
hO
B4.
84.
7–0
.05
10–1
1B
oth
OW
OB
23.3
20.5
–1.4
0S
wit
zerl
and
(48,
49)
6–13
Boy
s22
52O
W12
.811
.4–0
.28
Tab
le I
. (C
onti
nued
).
(Con
tinue
d)
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.

Pleateauing prevalence of childhood overweight 11
Cou
ntry
Stu
dyA
geS
exS
ampl
e si
ze1
Wei
ght
stat
us19
9519
9619
9719
9819
9920
0020
0120
0220
0320
0420
0520
0620
0720
08S
lope
2
6–13
Boy
sO
B3.
92.
3–0
.32
6–13
Boy
sO
WO
B16
.713
.7–0
.60
6–13
Gir
ls23
74O
W15
.411
.2–0
.84
6–13
Gir
lsO
B3.
72.
1–0
.32
6–13
Gir
lsO
WO
B19
.113
.3–1
.16
US
A(5
3) &
unp
ublis
hed
anal
yses
2–19
Boy
s10
024
OW
18.4
16.3
20.3
17.4
18.5
0.07
2–19
Boy
sO
B12
.514
.515
.713
.615
.70.
282–
19B
oys
OW
OB
30.9
30.8
36.0
31.0
34.2
0.34
2–19
Gir
ls97
03O
W15
.517
.419
.916
.718
.50.
182–
19G
irls
OB
15.1
15.1
15.7
14.8
15.8
0.06
2–19
Gir
lsO
WO
B30
.632
.535
.631
.534
.30.
322–
5B
oys
OW
10.4
8.4
12.2
11.0
10.1
0.10
2–5
Boy
sO
B3.
44.
46.
84.
44.
40.
102–
5B
oys
OW
OB
13.8
12.8
19.0
15.4
14.5
0.20
2–5
Gir
lsO
W8.
910
.215
.610
.512
.00.
222–
5G
irls
OB
6.9
7.2
5.6
6.8
5.0
–0.2
12–
5G
irls
OW
OB
15.8
17.4
21.2
17.3
17.0
0.12
6–11
Boy
sO
W19
.016
.120
.017
.415
.9–0
.16
6–11
Boy
sO
B17
.718
.820
.316
.924
.20.
566–
11B
oys
OW
OB
36.7
34.9
40.3
34.3
40.1
0.31
6–11
Gir
lsO
W15
.320
.123
.515
.218
.90.
086–
11G
irls
OB
20.7
20.5
22.0
17.6
22.4
0.03
6–11
Gir
lsO
WO
B36
.040
.645
.532
.841
.30.
1412
–19
Boy
sO
W21
.819
.424
.120
.124
.30.
1912
–19
Boy
sO
B12
.714
.916
.215
.415
.40.
3012
–19
Boy
sO
WO
B34
.534
.340
.335
.539
.70.
5812
–19
Gir
lsO
W19
.018
.719
.220
.721
.50.
2312
–19
Gir
lsO
B14
.914
.615
.616
.416
.20.
2212
–19
Gir
lsO
WO
B33
.933
.334
.837
.137
.70.
57
OB
, obes
e; O
W,
over
wei
ght
(excl
udin
g o
bes
e);
OW
OB
, ov
erw
eight
(incl
udin
g o
bes
e);
Sam
ple
siz
e sh
ows
the
com
bin
ed s
ample
siz
es o
f th
e dif
fere
nt
surv
eys
in e
ach c
ountr
y f
rom
all
yea
rs c
om
bin
ed;
2L
inea
r re
gres
sion
was
use
d to
defi
ne
slop
e (s
ee M
etho
ds);
3S
ampl
e si
ze f
or b
oth
sexe
s co
mbi
ned;
4S
ampl
e si
ze f
or e
thni
c su
bgro
ups
not
avai
labl
e.
Tab
le I
. (C
onti
nued
).
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.

12 T. Olds et al .
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
year across all age � sex groups and all countries between 1995 and 2008. For overweight excluding obe-sity, the fi gure was 0.01 (0.56)% for 36 reports, and for obesity alone � 0.01 (0.24) for 36 reports. Overall, 50 of 112 reports (45%) showed declines, 60 (53%) showed increases and two (2%) showed no change.
When split by sex, the fl attening was more marked for girls than for boys. For overweight including obe-sity (taking average across all ethnicities for the Dutch data), the mean (SD) rate of change for boys (15 reports) was � 0.07 (0.37)% per year, while for girls (15 reports) it was � 0.16 (0.49)% per year. For obe-sity alone, the mean rate of change for boys was � 0.08 (0.25)% per year (14 reports), while for girls it was � 0.08 (0.19)% per year (14 reports). There were also differences by age, with the fl attening being more marked in younger children. The mean rate of change in overweight including obesity for preschoolers (age 2 – 5 or 6) was � 0.11 (0.29)% per year (six reports), compared to � 0.09 (0.69)% per year for primary school aged children (6 – 11 or 12 years; 17 reports) and � 0.25 (0.25)% per year for adolescents (12 – 19 years; nine reports). The corresponding fi gures for obesity alone were – 0.14 (0.17)% per year for pre-schoolers (6 reports), � 0.02 (0.26)% per year for primary school age (15 reports), and � 0.26 (0.11)% per year for adolescents (six reports).
Discussion
Main fi ndings
While this paper was not designed as a systematic review or meta-analysis of trends in the prevalence of childhood overweight and obesity, it does bring together data from nine countries showing a slowing plateau, and in some cases a decline in the prevalence of child-hood obesity and overweight in several countries in recent years. The countries involved in this paper rep-resent numerous regions around the globe including Western Europe, North America, Asia and Oceania. In addition, this trend for slowing or plateauing does not appear to be isolated to the countries reported in this paper. Recent studies from Russia (56), Greenland (57) and Scotland (58) have reported similar trends. In addi-tion, a major US Surveillance System based on low income children has also shown a stabilization in obe-sity levels (59). Thus it appears that there are many regions in the world where childhood obesity is not, as has been suggested, increasing exponentially, but is rather showing stabilizing trends.
Strengths and limitations
It is important to acknowledge the strengths and weaknesses of the current review. This paper is the
fi rst to bring together recent data from several coun-tries reporting stabilization in the rates of childhood obesity and/or overweight. In all cases, data arose from large, population-based studies, involving a total of over 500,000 children from nine countries. All the studies, with one exception (the INCA 1 data from France) used measured height and weight. In view of the fact the INCA 1 data provided baselines for trend analysis, and self-reported data usually underestimate BMI (60), it is likely that the data still support a stabilizing trend. The methodologies adopted in the different studies varied considerably in terms of the sampling frame, numbers of partici-pants, geographical spread of participants (in some cases representing entire nations, and in several cases representing specifi c geographical regions within countries) and parameters measured (e.g., some studies considered SES and ethnicity while most did not). In two countries, data came from geographi-cally narrow areas (Jiangsu Province for the China section, and The Hague for The Netherlands section) thus it is unclear whether the trends for stabilization in obesity rates reported in this paper are representa-tive of their entire nation. Calculation of average rates of change do not take into account varying sample sizes or the fact subgroup analyses within a country may be more alike than analyses across countries. In this study it was possible to overcome a seemingly trivial problem in the literature – the failure of some authors to specify if ‘ overweight ’ includes obesity or not. All of the authors contribut-ing to the present review have used the combined defi nition as defi ned by Cole et al. (16).
We quantifi ed trends in childhood overweight and obesity using BMI as a metric, rather than other measures of adiposity, such as skinfolds, because weight status is defi ned on the basis of BMI catego-ries by international convention (16), and there are very few comprehensive datasets available using skin-folds. One meta-analysis (61) found consistent increases in the skinfold thicknesses of children in the years up until 2004, a time we would expect BMIs to be plateauing (on the basis of the current paper). In the same study, Olds (61) showed there has been a shift towards central accumulation of body fat. So it is possible that children may be becoming fatter at the same BMI.
While the presentation of data from all countries according to IOTF cut-offs allows for valuable cross-country comparison, it also has limitations. Some countries routinely use alternative methods for defi n-ing overweight and obesity [for example, in England, they are usually defi ned on the basis of the UK1990 BMI growth reference (18), and in Switzerland and the US they are defi ned on the basis of CDC 2000 growth charts (62). Zimmermann and colleagues

Pleateauing prevalence of childhood overweight 13
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
(48) compared the sensitivity of CDC and IOTF defi nitions of overweight and obesity, and found that in Swiss children, the CDC defi nitions had superior ability over IOTF defi nitions to detect obesity determined on the basis of percentage body fat from skinfold tests. Furthermore, while the pat-terns of stabilization are similar across the nine countries, this study is not intended as a compre-hensive global survey of recent changes in chil-dren ’ s weight status. There are very likely countries where the prevalence of paediatric overweight and obesity is still increasing.
Different rates of change among subgroups
It is important to note that there are exceptions to this pattern for stabilization in particular subgroups of the pediatric population. In this review, data showed that rates of change at times differed accord-ing to sex, age, SES and ethnicity. For example, the trend for stabilization was more marked in girls than in boys. This was apparent in both aggregated data and data from New Zealand. Aggregated data also showed more marked stabilization in younger than in older children, which was also evident in the French, US and Australian data. In addition, the English and the French surveys reported differences according to socioeconomic status. In France, there was an increase in overweight prevalence in children with ‘ blue collar ’ parents, while there was a decrease in prevalence of overweight in children with ‘ white collar ’ parents (30).
In urban Sweden, decreasing prevalence in female obesity was observed across all socio-economic groups, whereas amongst Swedish boys decreases occurred consistently within the affl uent group, with inconsistent trends for lower and middle income groups. Variations on the basis of ethnicity were also reported in some cases. In The Netherlands, over-weight including obesity rates declined in children of Dutch origin between 1999 and 2007, but rose dramatically over the same period in children from Turkish backgrounds.
Stabilization at different prevalence levels
It is interesting to note that while stabilization appears to be occurring across the nine countries highlighted in this study, prevalence is not stabilizing at the same level. For roughly comparable age ranges (mid-points of range from 9 – 15 years), the average prevalence of overweight including obesity across the time periods reported ranges from 13.5% in France to 37.4% in the USA. The reasons for this are unclear; however, a combination of genetic and cultural factors s likely to be involved. While it is tempting to suggest that
initiatives aimed at preventing childhood obesity have been more successful at kerbing the increase in prevalence in certain countries than in others, this conclusion should be made with caution. It is equally possible that efforts across countries may be equally well designed, but are starting at a different base level. It may be that in countries with already high prevalence rates, it is easier to ‘ pick the low-hanging fruit ’ , that is to reduce overweight or obesity in chil-dren who are already substantially overweight or already obese. It could equally be argued that it may be harder to reverse trends in countries with already high prevalence. At the very least, the phenomenon of stabilization at different prevalences suggests that whatever the cause, factors in the social and physical environment probably play a role.
Potential causes
The intervention hypothesis
There are a number of possible reasons for the sta-bilization in childhood overweight and/or obesity rates. Childhood obesity has been recognized as a major public health concern in many countries for several years now, prompting public health cam-paigns and interventions aimed at promoting healthy eating and increased physical activity. It may be that the cumulative effect of such programs is now result-ing in stabilization of the prevalence of overweight and obesity in children.
Offering some support to the intervention hypoth-esis are dietary data collected in the French INCA surveys. These data showed that average energy intake in 3 – 14-year-old French children signifi cantly decreased from 1910 kcal/d in 1999 to 1739 kcal/d in 2006 – 07 ( p � 0.0001) (34). The link between this decrease in energy intake and the stabilization of overweight and obesity in the past decade deserves further investigation.
In particular, there have been numerous interven-tions aimed at addressing early risk factors of over-weight and obesity, such as birth weight, diet, growth-rates and transition from breast milk and/or formula to solid foods. As each of these factors has been associated with early childhood overweight and obesity (63), it is likely that interventions addressing them have contributed to the current trend towards stabilization of prevalence.
The saturation equilibrium hypothesis
An alternative explanation for stabilization in obesity rates may be that childhood overweight and/or obe-sity has now reached a point of saturation equilib-rium in many countries. Any given environment

14 T. Olds et al .
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
offers opportunities for children (and adults) to overeat and be inactive. The proportion of overweight children will depend on interactions between the dis-tribution of resilience (for example as a result of naturally high levels of physical activity or some other form of socially-programmed resilience) and the degree of ‘ obesogenicity ’ of the environment. It may be that today we live in societies which have become so obesogenic, which offer so many opportunities for high energy intake and sedentary pastimes, that any child who is predisposed to overweight has become overweight, and the remaining children are resistant to excessive adiposity. Differences in the levels of sta-bilization might refl ect different ‘ in-built ’ levels of resilience.
The self-selection hypothesis
A further explanation may be self-selection bias. While the data presented in this paper arose from major population-based studies in each of the nine countries, we cannot completely rule out sampling bias. It is possible that due to increased public aware-ness of childhood obesity and increased perceived stigmatization more parents of overweight and obese children declined participation in the latter measure-ment years compared to the baseline measurement years on which trend a alyses were based. However, some of the studies cited here are almost censuses of the population of interest, and selection bias is unlikely in these cases. Moreover, the assumption of increasing stigmatization in recent years may be questioned; it could be argued that severe stigmatiza-tion of childhood overweight and obesity has been recognized for many decades and that decreasing stigmatization may have also occurred in recent years due to high prevalences changing norms.
Conclusions
It is unclear whether the stabilization trends outlined in the countries in this paper presage a long-term change in the rates of childhood overweight and obe-sity, or whether it is a temporary lull, and overweight and obesity rates will soon begin to rise again. Future prevalence depends on many factors including immi-gration patterns, prevalence within age cohorts, and socio-demographic shifts. The fact that the stabiliza-tion of prevalence appears to be more marked in younger cohorts suggests that we might see a ‘ wash-through ’ effect as these groups age, with future decreases in prevalence. However, the experience of the inaccurate British forecasts [in which dire forecasts for the rates of overweight in 2 – 11-year-old girls in 2020 needed to be downgraded from 34% to 17%,
and the rate of obesity in 12 – 19-year-old girls revised from 30% to 9% (64)] should serve as a warning that projections should be treated with extreme caution.
Above all, the data presented in this paper should not be interpreted as meaning that childhood over-weight and obesity are not important public health issues. While rates of overweight and obesity appear to be stabilizing at present in many countries, they are still unacceptably high, with signifi cant ramifi ca-tions for the health and well-being of these children as they age. Moreover, the rates may still be increas-ing in some countries. Furthermore, it is possible that the ‘ adiposity gap ’ between the rich and poor in devel-oping countries is widening. If so, narrowcast inter-ventions targeting high-risk subgroups may be both more equitable and cost-effective than population-level broadcast interventions.
Acknowledgements
The authors would like to thank Marie-Fran ç oise Rolland-Cachera, for her contribution to the French descriptive section; Louisa Ells, Cathy Mulhall, Hywell Dinsdale and Carolyn Summerbell, for contributing the English data and description; and the Swedish Council for Social Research and Working Life, who were a major contributor to the Swedish work.
Declaration of interest : The authors report no confl icts of interest. The authors alone are respon-sible for the content and writing of the paper.
References
Ebbeling CB, Pawlak DB, Ludwig DS. Childhood obesity: 1. public-health crisis, common sense cure Lancet. 2002;360:473 – 82. Freedman D, Dietz W, Srinivasan S, Berenson G. The 2. relation of overweight to cardiovascular risk factors among children and adolescents: The Bogalusa Heart Study. Pediatrics. 1999;103:1175 – 82. Fagot-Campagna A, Pettitt D, Engelgau M et al. Type 2 dia-3. betes among North adolescents: an epidemiologic health perspective. J Pediatr. 2000;136:664 – 72. Figueroa-Mu ñ oz J, Chinn S, Rona R. Association between 4. obesity and asthma in 4 – 11 year old children in the UK. Thorax. 2001;56:133 – 7. Strauss R, Barlow S, Dietz W. Prevalence of abnormal serum 5. aminotransferase values in overweight and obese adolescents. J Pediatr. 2000;136:727 – 33. Adelman R, Restaino I, Alon U, Blowey D. Proteinuria and 6. focal segmental glomerulosclerosis in severely obese adoles-cents. J Pediatr. 2001;138:481 – 5 Chan G, Chen C. Musculoskeletal effects of obesity. Curr 7. Opin Pediatr. 2009;21:65 – 70. Tsiros MD, Olds T, Buckley J et al. Health-related quality of 8. life in obese children and adolescents. Int J Obes (Lond). 2009;33:387–400.

Pleateauing prevalence of childhood overweight 15
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
Strauss R. Childhood obesity and self-esteem. Pediatrics. 9. 2000;105:e15. Hill A, Silver E. Fat, friendless and unhealthy: 9 year old 10. childrens perception of body shape stereotypes. Int J Obes Relat Metab Disord. 1995;19:423 – 30. Millar J. Fat kids: British parents wake up call. Journal [serial 11. on the Internet]. 2009 Date: Available from: http://www.wcjb.co.uk/fat-kids-british-parents-wake-up-call-23460. Masters C. Working mums have fat kids Journal [serial on 12. the Internet]. 2007 Date: Available from: http://www.news.com.au/story/0,23599,21041424-36398,00.html. Ryan AS. Breastfeeding and the risk of childhood obesity. 13. Coll Antropol. 2007;31:19 – 28. Ben-Sefer E. The childhood obesity pandemic: promoting 14. knowledge for undergraduate nursing students. Nurse Educ Pract. 2009;9:159 – 65. Robinson MJ. Two decades of American news preferences. 15. Part 1: Analyzing what news the public follows – and doesn ’ t follow. Washington DC, USA: Pew Research Center for the People & the Press; 2007. Available from: http://pewresearch.org/assets/pdf/NewsInterest1986-2007.pdf. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a 16. standard defi nition for child overweight and obesity world-wide: international survey. BMJ. 2000;320:1240 – 3. Olds T, Tomkinson G, Maher C, Ferrar K. Trends in the 17. prevalence of childhood overweight and obesity in Australia between 1985 and 2008. Int J Obes. 2010;34:57 – 66. Cole TJ, Freeman JV, Preece MA. Body mass index reference 18. curves for the UK, 1990. Arch Dis Child. 1995;73:25 – 9. Cheng B, Kuipers H, Snyder AC, Keizer HA, Heukendrup 19. A, Hesselink M. A new approach to the determination of ventilatory and lactate thresholds. Int J Sports Med. 1992;13:518 – 22. Zar JH. Biostatistical Analysis. 4th ed. Upper Saddle River, 20. NJ: Prentice Hall; 1999. Li Y, Schouten E, Hu X, Cui Z, Luan D, Ma G. Obesity 21. prevalence and time trend among youngsters in China, 1982 – 2002. Asia Pac J Clin Nutr. 2008;17:131 – 7. Shi Z, Lien N, Kumar BN, Dalen I, Holmboe-Ottesen G. 22. The sociodemographic correlates of nutritional status of school adolescents in Jiangsu Province, China. J Adolesc Health. 2005;37:313 – 22. National Obesity Observatory. International comparisons of 23. obesity prevalence. Oxford: National Obesity Observatory; 2009. Available from: http://www.noo.org.uk/uploads/doc799_2_International_Comparisons_Obesity_Preva-lence2.pdf. Department of Health. Healthy weight, healthy lives: a cross 24. government strategy for England. London: Department of Health; 2008. Available from: http://www.dh.gov.uk/prod_consum_dh/groups/dh_digitalassets/documents/digitalasset/dh_084024.pdf. The NHS Information Centre for Health and Social Care. 25. Health Survey for England. Leeds: The Health and Social Care Information Centre; 2010. Available from: http://www.ic.nhs.uk/statistics-and-data-collections/health-and-life-styles-related-surveys/health-survey-for-england. National Health Service. National child measurement pro-26. gramme: Crown Copyright; 2010. Available from: http://www.dh.gov.uk/en/Publichealth/Healthimprovement/Healthyliving/DH_100123. Stamatakis E, Zaninotto P, Falaschetti E, Mindell J, Head J. 27. Time trends in childhood and adolescent obesity in England from 1995 to 2007 and projections of prevalence to 2015. J Epidemiol Community Health. 2010;64:167 – 74. The NHS Information Centre for Health and Social Care. 28. National Child Measurement Programme 2008/2009 school
year. Leeds, England: The Health and Social Care Informa-tion Centre; 2010. Available from: www.ic.nhs.uk/ncmp. The NHS Information Centre for Health and Social Care. 29. National Child Measurement Programme 2007/08 school year headline results. Leeds: IC; 2008. Available from: www.ic.nhs.uk. Direction de la Recherche, des Etudes, de l ’ Evaluation 30. et des Statistiques, Minist è re de la Sant é . Nutrition et activit é physique. Surpoids et ob é sit é chez l’enfant. L ’ é tat de sant é de la population en France: rapport 2009 – 2010. Paris; 2010. Lehingue Y. The European Childhood Obesity Group 31. (ECOG) project: the European collaborative study on the prevalence of obesity in children. Am J Clin Nutr. 1999;70:S166 – S8. Salanave B, P é neau S, Rolland-Cachera MF, Hercberg S, 32. Castetbon K. Stabilization of overweight prevalence in French children between 2000 and 2007. Int J Pediatr Obes. 2009;4:66 – 72. P é neau S, Salanave B, Maillard-Teyssier L et al. Prevalence 33. of overweight in 6- to 15-year-old children in central/western France from 1996 to 2006: trends toward stabilization. Int J Obes. 2009;33:401 – 7. Lioret S, Touvier M, Dubuisson C et al. Trends in child over-34. weight rates and energy intake in France from 1999 to 2007: relationships with socioeconomic status. Obesity (Silver Spring). 2009;15:1092 – 100. Lobstein T, Frelut M. Prevalence of overweight among chil-35. dren in Europe. Obes Rev. 2003;4:195 – 200. van den Hurk K, van Dommelen P, van Buuren S, Verkerk 36. PH, Hirasing RA. Prevalence of overweight and obesity in the Netherlands in 2003 compared to 1980 and 1997. Arch Dis Child. 2007;92:992 – 5. de Wilde JA, van Dommelen P, Middelkoop BJ, Verkerk PH. 37. Trends in overweight and obesity prevalence in Dutch, Turk-ish, Moroccan and Surinamese South Asian children in the Netherlands. Arch Dis Child. 2009;94:795 – 800. Ministry of Health. NZ Food, NZ Children: Findings of the 38. 2002 National Children ’ s Nutrition Survey. Wellington: Min-istry of Health; 2003. Available from: http://www.moh.govt.nz/moh.nsf/indexmh/obesity-publications. Ministry of Health. A portrait of health: key results of the 39. 2006/07 New Zealand Health Survey. Wellington: Ministry of Health; 2008. Keil U, Kuulasmaa K. WHO MONICA Project: risk factors. 40. Int J Epidemiol. 1989;18:S46 – 55. Berg C, Rosengren A, Aires N et al. Trends in overweight 41. and obesity from 1985 to 2002 in G ö teborg, West Sweden. Int J Obes. 2005;29:916 – 24. M å rild S, Bondestam M, Bergstr ö m R, Ehnberg S, Hollsing 42. A, Albertsson-Wikland K. Prevalence trends of obesity and overweight among 10-year-old children in western Sweden and relationship with parental body mass index. Acta Paedi-atr. 2004;93:1588 – 95. Karlberg J, Luo Z, Albertsson-Wikland K. Body mass index 43. reference values (mean and SD) for Swedish children. Acta Paediatr. 2001;90:1427 – 34. Sj ö berg A, Lissner L, Albertsson-Wikland K, M å rild S. 44. Recent anthropometric trends among Swedish school chil-dren: evidence for decreasing prevalence of overweight in girls. Acta Paediatr. 2008;97:118 – 23. Sundblom E, Petzold M, Rasmussen F, Callmer E, Lissner 45. L. Childhood overweight and obesity prevalences levelling off in Stockholm but socioeconomic differences persist. Int J Obes (Lond). 2008;32:1525 – 30. Lager AC, Fossum B, R ö rvall G, Bremberg SG. Children ’ s 46. overweight and obesity: local and national monitoring using

16 T. Olds et al .
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
electronic health records. Scand J Public Health. 2009;37:201 – 5. Lissner L, Sohlstr ö m A, Sundblom E, Sj ö berg A. Trends in 47. overweight and obesity in Swedish schoolchildren 1999 – 2005: has the epidemic reached a plateau? Obes Rev. 2010;11:553–9. Zimmermann M, G ü beli C, P ü ntener C, Molinari L. 48. Detection of overweight and obesity in a national sample of 6 – 12-y-old Swiss children: accuracy and validity of reference values for body mass index from the US Centers for Disease Control and Prevention and the International Obesity Task Force. Am J Clin Nutr. 2004;79:838 – 43. Aeberli I, Ammann R, Knabenhans M, Molinari L, 49. Zimmermann M. Decrease in the prevalence of paediatric adiposity in Switzerland from 2002 to 2007. Public Health Nutr. 2009:Sep 22:1 – 6. [Epub ahead of print]. Ogden CL, Carroll MD, Flegal KM. High body mass index 50. for age among US children and adolescents. JAMA. 2008;299:2401 – 5. Jeannot E, Mahler P, Duperrex O, Chastonay P. Evolution 51. of overweight and obesity among elementary school children in Geneva. Swiss Med Wkly. 2010;140:w13040. Aeberli I, Henschen I, Molinari L, Zimmermann M. Stabi-52. lization of the prevalence of childhood obesity in Switzerland. Swiss Med Wkly. 2010;140:w13046. Centres for Disease Control and Prevention. National Health 53. and Nutrition Examination Survey. Atlanta; 2008 [updated 2010 Sep 2; viewed 2010 Sep 14]; Available from: http://www.cdc.gov/nchs/nhanes.htm. Ogden C, Carroll M, Curtin L, Lamb M, Flegal K. Preva-54. lence of high body mass index in US children and adoles-cents, 2007 – 2008. JAMA. 2010;303:242 – 9. Kuczmarski R, Flegal K. Criteria for defi nition of overweight 55. in transition: background and recommendations for the United States. Am J Clin Nutr. 2000;72:1074 – 81.
Popkin B, Conde W, Hou N, Monteiro C. Is there a lag 56. globally in overweight trends for children compared with adults? Obesity (Silver Spring). 2006;14:1846 – 53. Schnohr C, S ø rensen T, Niclasen B. Changes since 1980 in 57. body mass index and the prevalence of overweight among inschooling children in Nuuk, Greenland. Int J Circumpolar Health. 2005;64:157 – 62. Mitchell R, McDougall C, Crum J. Decreasing prevalence of 58. obesity in primary schoolchildren. Arch Dis Child. 2007;92:153 – 4. Centers for Disease Control and Prevention. Obesity preva-59. lence among low-income, preschool-aged children – United States, 1998 – 2008. MMWR Morbidity and Mortality Weekly Report. 2009;58:769 – 73. Krul AJ, Daanen HA, Choi H. Self-reported and measured 60. weight, height and body mass index (BMI) in Italy, the Netherlands and North America. Eur J Public Health. 2011;21:414–9. Olds TS. One million skinfolds: secular trends in the fatness of 61. young people 1951 – 2004. Eur J Clin Nutr. 2009;63:934 – 46. Ogden C, Flegal K, Carroll M, Johnson C. Prevalence and 62. trends in overweight among US children and adolescents, 1999 – 2000. JAMA. 2002;288:1728 – 32. Hawkins SS, Cole TJ, Law C, the Millennium Cohort Study 63. Child Health Group. An ecological systems approach to examining risk factors for early childhood overweight: fi nd-ings from the UK Millennium Cohort Study. J Epidemiol Community Health. 2009;63:147 – 55. BBC news. Child obesity ‘ is levelling off ’ . 2009 [updated 64. 2009 Nov 3; viewed 2010 Sep 14]; Available from: http://news.bbc.co.uk/2/hi/health/8338456.stm. P é neau S, Salanave B, Maillard-Teyssier L et al. Prevalence 65. of overweight in 6- to 15-year-old children in central/western France from 1996 to 2006: trends toward stabilization. Int J Obes. 2009;33:401 – 7.

Pleateauing prevalence of childhood overweight 17
Appendix 1. Summary details of the sampling frames and protocols of the included studies.
Study Sampling frame Sampling exclusions Training of measurers Equipment calibrated Data weighting
Australia Variable, as meta analysis of 41 studies
Variable, as meta-analysis of 41 studies
Variable Unknown Variable
China – (Shi, Lien et al.
2005) (22)
Cluster, regional, same 8 schools in 2002, 2007
No Measured by trained health workers in local CDC
Yes No
England (The NHS Information Centre for Health and Social Care 2010) (25)
multi-stage stratifi ed probability
sampling design
Those living in institutions
Training and practical on interview and anthropometric measures
Yes Yes (to account for non-response), by age, gender, household type, number of children in household and geographic region
France – Triennial cycle of school surveys (Minst é re de al Sant é 2008) (30).
Two-stage random national sampling
No exclusions among children able to attend schools
Detailed instructions provided (nurses and physicians)
No Yes, by age, gender, regions, type of schools (education priority areas; public/private schools)
European Childhood Obesity Group protocol (Salanave, P é neau et al. 2009) (32)
Random national sampling
No exclusions among 7 – 9 years children who were able to attend schools
Detailed instructions provided (nurses and physicians)
No Yes, by age, gender, administrative school district, type of schools (education priority area, size of class by level)
INCA 1 The sample was made representative of the French population diversity through stratifi cation (region of residence, agglomeration size) and use of the quota method (age, gender, household size, head of household socioprofessional status)
Severely disabled and lack of literacy in French (caregiver)
One-day training on the questionnaires
Not applicable None
INCA 2 (Lioret, Touvier et
al. 2009) (34)
Random national Severely disabled and lack of literacy in French (caregiver)
One-day training for anthropometrics and questionnaires
No Yes, by unequal sampling probabilities and for differential non-responses by region, agglomeration size, age, gender, occupation of the head of household, size of the household, and season of the year
(P é neau, Salanave et al. 2009)
All children attending a regional health examination center
No exclusion among examined children at the center
Nurses trained when recruited
Scale: yes Height gauge: no
(fi xed)
Yes, by age, gender, economic status (deprived/non deprived)
(Continued)
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.

18 T. Olds et al .
Appendix 1. (Continued).
Study Sampling frame Sampling exclusions Training of measurers Equipment calibrated Data weighting
The Netherlands (de Wilde, van
Dommelen et al. 2009) (37)
Random, local City of the Hague,
routine health assessments of all children
None Youth Health Care professionals have been trained for several years
Yes No, analyses adjusted for age and/or gender
New Zealand (Ministry of Health
2003) (38)
Two staged sampling frame. A random sample of schools was selected, then children were randomly selected within these schools
Schools on the Chatham Islands, correspondence schools, and schools with less than 50 students, (note: all Te Kura Kaupapa schools were included regardless of size).
Fee-paying foreign students or foreign students on Ministry of Foreign Affairs and Trade scholarships were excluded
Anthropometric measurement training provided with interviewers tested before going into the fi eld
Yes Yes, by age, gender, ethnicity and region
(New Zealand Ministry of Health 2008)
(39)
Multi-stage, stratifi ed, probability proportionate to size (PPS) sample design, with increased sampling of some ethnic groups
Meshblocks with a very small number of households, and off-shore islands
Anthropometric measurement training provided with interviewers tested before going into the fi eld
Yes Yes, by age, gender, District Health Board area and ethnic group
Sweden – Stockholm (Sundblom, Petzold et al. 2008) (45)
8 SES areas, 10 schools from
each randomly selected
Very small schools Trained school nurses No Yes, by gender and place of residence
Gothenburg (Sj ö berg, Lissner et al. 2008)
� 80% coverage of population
None Trained school nurses Yes No
Karlstad (Lager, Fossum et al. 2009) (46)
94% coverage of population
None Trained school nurses Yes No
Ume å (Lager, Fossum et al. 2009) (46)
66 – 92% coverage of population
None Trained school nurses Yes No
V ä ster å s (Lager, Fossum et al. 2009) (46)
73 – 94% coverage of population
None Trained school nurses No No
Ystad (Lager, Fossum et al. 2009) (46)
96 – 99% coverage of population
None Trained school nur es Yes No
Switzerland – (Zimmermann, G ü beli et al. 2004) (48)
Random, national, probability-proportionate-to-size cluster sampling
None Individual training (2 examiners)
Yes No (PPS design instead of data weighting)
(Continued)
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.

Pleateauing prevalence of childhood overweight 19
Appendix 1. (Continued).
Study Sampling frame Sampling exclusions Training of measurers Equipment calibrated Data weighting
(Aeberli, Ammann et al. 2009) (49)
Random, national, probability-proportionate-to-size cluster sampling
None Individual training (2 examiners)
Yes No (PPS design instead of data weighting)
USA (Centres for Disease Control and Prevention 2008)
(53)
NHANES uses a complex, multistage, probability sampling design to select a representative sample of the resident civilian non-institutionalized population, including non-citizens
The sample does not include persons residing in nursing homes, members of the armed forces, institutionalized persons, or US nationals living abroad
NHANES staff are trained to follow standardized examination protocols, to calibrate equipment according to a prescribed schedule and method, and to measure and record the survey data with precision. Additionally, retraining sessions, gold standard examinations performed by expert examiners, and fi eld observations are conducted on a regular basis to reinforce the importance of measurement precision and standardized data collection methodology
Yes Yes, weights are created in NHANES to account for the complex survey design (including oversampling), survey non-response, and post-stratifi cation
Appendix 2 . Overweight and obesity prevalences in Swiss schoolchildren from two national studies conducted 2002 and 2007, reported according to Centers for Disease Control and Prevention (CDC) references.
Overweight % (SD) Obese % (SD) Overweight � obese % (SD)
2007 1 Boys ( n � 1083) 11.3 (0.94) 2 5.4 (0.67) 3 16.7 (1.1) 3 Girls ( n � 1139) 9.9 (0.87) 3 3.2 (0.52) 3 13.1 (0.98) 3
2002 1 Boys ( n � 1169) 12.5 (0.96) 7.4 (0.8) 19.9 (1.2)Girls ( n � 1235) 13.2 (0.96) 5.7 (0.7) 18.9 (1.1)
1 2007 and 2002: National study to determine the prevalence of overweight and obesity in schoolchildren in Switzerland (64,65); 2 in percentage (standard error), all such values; 3 signifi cantly different from 2002 ( p � 0.05).
Int J
Ped
iatr
Obe
s D
ownl
oade
d fr
om in
form
ahea
lthca
re.c
om b
y E
mm
a G
raha
m o
n 09
/07/
11Fo
r pe
rson
al u
se o
nly.
Copyright © 2022 FDOKUMEN