Evidence for low-grade systemic proinflammatory activity in patients with posttraumatic stress...
9
Evidence for low-grade systemic proinflammatory activity in patients with posttraumatic stress disorder Roland von Ka ¨nel a,b, * , Urs Hepp c , Bernd Kraemer c , Rafael Traber c , Marius Keel d , Ladislav Mica d , Ulrich Schnyder c a Department of General Internal Medicine, Division of Psychosomatic Medicine, University Hospital/INSELSPITAL, Freiburgstrasse 4, CH-3010 Berne, Switzerland b Psychocardiology Unit, Cardiovascular Prevention and Rehabilitation, Swiss Cardiovascular Center, University Hospital Berne, Switzerland c Department of Psychiatry, University Hospital Zurich, Switzerland d Department of Trauma Surgery, University Hospital Zurich, Switzerland Received 15 February 2006; received in revised form 4 May 2006; accepted 28 June 2006 Abstract Posttraumatic stress disorder (PTSD) may increase cardiovascular risk but the psychophysiological mechanisms involved are elusive. We hypothesized that proinflammatory activity is elevated in patients with PTSD as diagnosed by the Clinician Administered PTSD Scale (CAPS) interview. Plasma levels of proinflammatory C-reactive protein (CRP), interleukin (IL)-1b, IL-6, and tumor necrosis factor (TNF)-a, and of anti-inflammatory IL-4 and IL-10 were measured in 14 otherwise healthy PTSD patients and in 14 age- and gender- matched healthy non-PTSD controls. Levels of TNF-a (p = 0.038; effect size Cohen’s d = 0.58) and of IL-1b (p = 0.075, d = 0.68) were higher in patients than in controls. CRP (d = 0.10), IL-6 (d = 0.18), IL-4 (d = 0.42), and IL-10 (d = 0.37) were not significantly different between groups. Controlling for traditional cardiovascular risk factors, mood, and time since trauma revealed lower IL-4 in patients than in controls (p = 0.029) and rendered group differences in TNF-a and IL-1b insignificant. In all subjects, TNF-a correlated with total (frequency and intensity) PTSD symptom cluster of re-experiencing (r = 0.49, p = 0.008), avoidance (r = 0.37, p = 0.050), and hyper- arousal (r = 0.42, p = 0.026), and with PTSD total symptom score (r = 0.37, p = 0.054). Controlling for time since trauma attenuated these associations. The correlation between IL-1b and total avoidance symptoms (r = 0.42, p = 0.028) became insignificant when con- trolling for anxiety and depression. IL-4 correlated with total hyperarousal symptoms (r = 0.38, p = 0.047), and after controlling for systolic blood pressure and smoking status, with PTSD total symptom score (r = 0.41, p = 0.035). PTSD patients showed a low-grade systemic proinflammatory state, which, moreover, was related to PTSD symptom levels suggesting one mechanism by which PTSD could contribute to atherosclerotic disease. Ó 2006 Elsevier Ltd. All rights reserved. Keywords: Atherosclerosis; Cytokines; Inflammation; Posttraumatic stress disorder; Risk factor 1. Introduction Posttraumatic stress disorder (PTSD) may develop after exposure to a trauma that involves threat of injury or death (American Psychiatric Association, 1994). To meet diag- nostic criteria for PTSD, the traumatized person must have for at least 1 month three distinct types of symptoms con- sisting of re-experiencing the event, avoidance of reminders of the event, and hyperarousal (Yehuda, 2002). Life-time prevalence of PTSD is approximately 8% (Kessler et al., 1995) making PTSD the fourth most common mental dis- order (Yehuda, 2002). Common causes of PTSD are com- bat exposure, sexual assault, and accidents (Yehuda, 2002). However, clinicians are increasingly aware that PTSD may 0022-3956/$ - see front matter Ó 2006 Elsevier Ltd. All rights reserved. doi:10.1016/j.jpsychires.2006.06.009 * Corresponding author. Address: Department of General Internal Medicine, Division of Psychosomatic Medicine, University Hospital/ INSELSPITAL, Freiburgstrasse 4, CH-3010 Berne, Switzerland. Tel.: +41 31 632 20 19; fax: +41 31 382 11 84. E-mail address: [email protected] (R. von Ka ¨nel). J OURNAL OF P SYCHIATRIC RESEARCH Journal of Psychiatric Research 41 (2007) 744–752 www.elsevier.com/locate/jpsychires
Transcript of Evidence for low-grade systemic proinflammatory activity in patients with posttraumatic stress...

JOURNAL OF
PSYCHIATRIC
RESEARCHJournal of Psychiatric Research 41 (2007) 744–752
www.elsevier.com/locate/jpsychires
Evidence for low-grade systemic proinflammatory activity inpatients with posttraumatic stress disorder
Roland von Kanel a,b,*, Urs Hepp c, Bernd Kraemer c, Rafael Traber c,Marius Keel d, Ladislav Mica d, Ulrich Schnyder c
a Department of General Internal Medicine, Division of Psychosomatic Medicine, University Hospital/INSELSPITAL,
Freiburgstrasse 4, CH-3010 Berne, Switzerlandb Psychocardiology Unit, Cardiovascular Prevention and Rehabilitation, Swiss Cardiovascular Center, University Hospital Berne, Switzerland
c Department of Psychiatry, University Hospital Zurich, Switzerlandd Department of Trauma Surgery, University Hospital Zurich, Switzerland
Received 15 February 2006; received in revised form 4 May 2006; accepted 28 June 2006
Abstract
Posttraumatic stress disorder (PTSD) may increase cardiovascular risk but the psychophysiological mechanisms involved are elusive.We hypothesized that proinflammatory activity is elevated in patients with PTSD as diagnosed by the Clinician Administered PTSDScale (CAPS) interview. Plasma levels of proinflammatory C-reactive protein (CRP), interleukin (IL)-1b, IL-6, and tumor necrosis factor(TNF)-a, and of anti-inflammatory IL-4 and IL-10 were measured in 14 otherwise healthy PTSD patients and in 14 age- and gender-matched healthy non-PTSD controls. Levels of TNF-a (p = 0.038; effect size Cohen’s d = 0.58) and of IL-1b (p = 0.075, d = 0.68) werehigher in patients than in controls. CRP (d = 0.10), IL-6 (d = 0.18), IL-4 (d = 0.42), and IL-10 (d = 0.37) were not significantly differentbetween groups. Controlling for traditional cardiovascular risk factors, mood, and time since trauma revealed lower IL-4 in patients thanin controls (p = 0.029) and rendered group differences in TNF-a and IL-1b insignificant. In all subjects, TNF-a correlated with total(frequency and intensity) PTSD symptom cluster of re-experiencing (r = 0.49, p = 0.008), avoidance (r = 0.37, p = 0.050), and hyper-arousal (r = 0.42, p = 0.026), and with PTSD total symptom score (r = 0.37, p = 0.054). Controlling for time since trauma attenuatedthese associations. The correlation between IL-1b and total avoidance symptoms (r = 0.42, p = 0.028) became insignificant when con-trolling for anxiety and depression. IL-4 correlated with total hyperarousal symptoms (r = �0.38, p = 0.047), and after controllingfor systolic blood pressure and smoking status, with PTSD total symptom score (r = �0.41, p = 0.035). PTSD patients showed alow-grade systemic proinflammatory state, which, moreover, was related to PTSD symptom levels suggesting one mechanism by whichPTSD could contribute to atherosclerotic disease.� 2006 Elsevier Ltd. All rights reserved.
Keywords: Atherosclerosis; Cytokines; Inflammation; Posttraumatic stress disorder; Risk factor
1. Introduction
Posttraumatic stress disorder (PTSD) may develop afterexposure to a trauma that involves threat of injury or death
0022-3956/$ - see front matter � 2006 Elsevier Ltd. All rights reserved.
doi:10.1016/j.jpsychires.2006.06.009
* Corresponding author. Address: Department of General InternalMedicine, Division of Psychosomatic Medicine, University Hospital/INSELSPITAL, Freiburgstrasse 4, CH-3010 Berne, Switzerland. Tel.: +4131 632 20 19; fax: +41 31 382 11 84.
E-mail address: [email protected] (R. von Kanel).
(American Psychiatric Association, 1994). To meet diag-nostic criteria for PTSD, the traumatized person must havefor at least 1 month three distinct types of symptoms con-sisting of re-experiencing the event, avoidance of remindersof the event, and hyperarousal (Yehuda, 2002). Life-timeprevalence of PTSD is approximately 8% (Kessler et al.,1995) making PTSD the fourth most common mental dis-order (Yehuda, 2002). Common causes of PTSD are com-bat exposure, sexual assault, and accidents (Yehuda, 2002).However, clinicians are increasingly aware that PTSD may

R. von Kanel et al. / Journal of Psychiatric Research 41 (2007) 744–752 745
also occur in patients who are confronted with a potentiallylife-threatening disease. For instance, after myocardialinfarction, about 15% of patients present with PTSDrelated to the infarction (Gander and von Kanel, 2006).
Psychological distress is high in patients with PTSD(Yehuda, 2002) many of whom suffer from increased anxi-ety (Leskin and Sheikh, 2002) and depression (Fazel et al.,2005). The biological, namely cardiovascular consequencesof PTSD are equally devastating (Boscarino, 2004; Schnurrand Green, 2004). Vietnam veterans with PTSD showincreased all-cause mortality and death from cardiovascu-lar causes (Boscarino, 2006). Also, PTSD symptoms corre-lated with a higher rate of physician-diagnosed arterialdisease (Schnurr et al., 2000) and PTSD patients had moreelectrocardiographic signs of infarction than a non-PTSDcontrol group (Boscarino and Chang, 1999). In postmyo-cardial infarction patients, the diagnosis of PTSD pre-dicted the cardiovascular readmission rate at one-yearfollow up (Shemesh et al., 2004). Some of the relationshipbetween PTSD and increased risk of atherosclerotic dis-eases can be explained by relatively poor health behaviorand the clustering of traditional cardiovascular risk factorsin traumatized subjects (Rozanski et al., 2005). PTSD hasbeen associated with elevated blood pressure (Buckleyand Kaloupek, 2001), obesity (Dobie et al., 2004), dyslipi-demia (Kagan et al., 1999), diabetes (Goodwin and David-son, 2005), heavy smoking (Beckham et al., 1997), and lowphysical activity (Lang et al., 2003).
A direct pathophysiological consequence of PTSDpotentially contributing to atherosclerosis is chronic low-grade activation of systemic vascular inflammation (Willer-son and Ridker, 2004). Compared to controls, patientswith PTSD showed higher circulating levels of C-reactiveprotein (CRP) (Miller et al., 2001), interleukin (IL)-1b(Tucker et al., 2004; Spivak et al., 1997), and IL-6 (Maeset al., 1999), as well as lower levels of the anti-inflammatorycytokine IL-4 (Kawamura et al., 2001) though studies arenot uniform (Miller et al., 2001; Sondergaard et al.,2004). One study found higher IL-6 in PTSD patients thanin controls only after controlling for age (Baker et al.,2001) suggesting this research should consider commoncovariates of systemic inflammation (Gander and vonKanel, 2006). The inflammatory cascade is initiated bymonocyte-derived TNF-a and IL-1b both stimulating IL-6 production by various immune cells to ultimately inducehepatic synthesis of CRP (Yudkin et al., 2000). However, asimultaneous investigation of these cornerstone markers ofthe inflammatory pathway has not been performed inPTSD (Gander and von Kanel, 2006). Also, we lack studieswhich investigate the relationship of proinflammatory toanti-inflammatory cytokines being more informative interms of vascular consequences of PTSD than levels ofone single cytokine alone (Daxecker et al., 2002).
We measured a reasonable panel of proinflammatorymarkers (i.e. TNF-a, IL-1b, IL-6, CRP) and anti-inflam-matory cytokines (i.e. IL-4, IL-10) in otherwise healthypatients with PTSD and age- and gender-matched non-
PTSD controls with equal proportions of demographicand medical covariates of inflammation activity. Wehypothesized that, relative to controls, PTSD patientswould have higher plasma levels of proinflammatory mark-ers on the one hand, and lower levels of anti-inflammatorycytokines on the other. Controls had also experienced atrauma, in response to which they did not develop PTSD,allowing us to disentangle the specific effect of diagnosticPTSD from a more non-specific trauma effect on inflamma-tory markers. However, subthreshold levels of PTSD arefrequently observed in traumatized individuals (Marshallet al., 2001) and non-specific posttraumatic psychopathol-ogy has also been associated with TNF-a and soluble IL-6 receptor levels (Sutherland et al., 2003). Therefore, wefurther hypothesized that specific symptom clusters ofPTSD (i.e. re-experiencing, avoidance, hyperarousal) andtotal score of PTSD symptoms (i.e. PTSD severity) showa direct association with proinflammatory markers andan inverse association with anti-inflammatory cytokinesin our entire sample.
2. Materials and methods
2.1. Participants and recruitment procedure
The Ethics Committee of the State of Zurich, Switzer-land, approved the study protocol and all participants pro-vided written informed consent. A consecutive sample of14 subjects meeting Diagnostic and Statistical Manual ofMental Diseases (DSM-IV) diagnosis of PTSD (AmericanPsychiatric Association, 1994) was recruited from the psy-chiatric out-patient clinic of the Department of Psychiatry,University Hospital Zurich. Typically, causes of PTSDwere different types of accidents.
Patients were eligible for the study if they had no med-ical diseases as per a structured medical history. Specifi-cally, subjects were excluded if they reported a positivehistory of heart, liver, or renal diseases, or of any othersevere somatic disease. Further exclusion criteria were:accident or surgery within the previous month, currentrespiratory infection or fever within the previous 7 days,venous thrombosis or pulmonary embolism within the pre-vious 3 months, intake of aspirin within the previous 10days, intake of oral anticoagulants within the previous 3months, pregnancy, and any hormone therapy (note thatone female patient disclosed oral contraceptive use onlyafter she had been included in the protocol).
Fourteen gender- and age matched (±5 years) controlswere recruited from the Department of Trauma Surgery,University Hospital Zurich. Control subjects had experi-enced an accident that caused injuries requiring surgicalinpatient treatment but had not developed PTSD. Theyunderwent the same medical interview as PTSD patientsand were subject to the same exclusion criteria. Controlsubjects with major psychiatric disorders were excludedas per the Primary Care Evaluation of Mental Disorders(PRIME-MD) (Loerch et al., 2000).

746 R. von Kanel et al. / Journal of Psychiatric Research 41 (2007) 744–752
2.2. Assessment of cardiovascular risk factors and life style
We assessed traditional cardiovascular risk factors andhealth habits as potential covariates of inflammatory mark-ers. Subjects were asked whether they had ever been said bya physician to have high blood glucose levels or hypercho-lesterolemia, and whether they were currently smokers.Body mass index (BMI) was computed as the ratio betweenweight in kilograms and height in square meters. After arest of 5 min, three seated blood pressure (BP) measure-ments were obtained within 10 min by sphygmomanometryand the average BP was computed. Hypertension wasdefined as systolic BP P140 mm Hg and/or diastolic BPP90 mm Hg (Kjeldsen et al., 2002). We also asked subjectswhether they regularly drank alcohol and exercised.
2.3. Psychometric assessment
PTSD was diagnosed by a clinical interview using theGerman version of the Clinician-Administered PTSD Scale(CAPS) (Schnyder and Moergeli, 2002) tracking 17 specificsymptoms of PTSD across the three domains re-experienc-ing (DSM-IV Cluster B), avoidance and numbing (ClusterC), and hyperarousal (Cluster D). The instrument allowsfor the crude diagnosis of PTSD (yes/no) and for dimen-sional quantification of the frequency and intensity of eachPTSD symptom. In addition, the total score of each symp-tom cluster (frequency plus intensity) as well as the totalscore of all PTSD symptom clusters (i.e. ClustersB + C + D), the latter providing a measure of overallPTSD severity, can be used for calculation of correlationand regression analyses. Symptom levels of anxiety anddepression were assessed by the German Version of the14-item self-rating Hospital Anxiety and Depression Scale(HADS) (Herrmann et al., 1995).
2.4. Blood sampling and assays
For logistic reasons, patients and controls came to thelaboratory, either in the morning or in the afternoon(p = n.s. between groups). Venous blood was drawn byone-time venipuncture into glass tubes (BD VacutainerSystems, Plymouth, UK) containing 3.8% sodium citrate.Centrifugation was at 2000g for 20 min at 4 �C. Obtainedplasma was immediately aliquoted in polypropylene tubes(Nunc Cryo Tube Vials, Nunc, Roskilde, DK) and frozenat �80 �C until further analysis.
All determinations of proinflammatory measures wereperformed in the Thrombosis Research Laboratory, Uni-versity Hospital Bern (Andre Haeberli, PhD). Plasma levelsof IL-4 with sensitivity of <0.27 pg/ml, IL-6 <104 fg/ml,IL-10 <0.2 pg/ml, and TNF-a <0.09 pg/ml were all mea-sured by duplicates of ultra-sensitive enzyme-linked immu-nosorbent assays obtained from Biosource International(Camarillo, CA, USA). Quantikine HS immunoassay tomeasure plasma levels of IL-1b (detection limit <0.1 pg/ml) was from R&D Systems (Minneapolis, MN, USA).
Plasma levels of CRP with a senstivity <0.11 mg/l weredetermined by use of an immunoturbidimetric high-sensi-tivity assay (Roche, Mannheim, Germany). Samples frompatients and controls were randomly distributed across dif-ferent plates and assay runs to prevent systematic measure-ment errors. Inter- and intra-assay coefficients of variationfor all measures were <10%.
2.5. Statistical analyses
All data were analyzed using SPSS statistical softwarepackage (version 13.0; SPSS Inc. Chicago, IL). All testswere two-tailed at p 6 0.05 with p 6 0.10 defining border-line significance. Skewness and kurtosis of psychometricscales and inflammation marker values could not be nor-malized by logarithmic transformation. Therefore, distri-butions of inflammation measures, psychometric scores,and time since trauma were normalized by means of theBlom transformation (Blom, 1958). This procedurereplaces each raw score by its rank value and adjusts thescale distances between the ranks to achieve a normal dis-tribution. Accordingly, we show transformed data in fig-ures but provide means ± SD or medians withinterquartile ranges of original data in the text and Tables.We used Student’s t-test to compare differences betweentwo continuous variables and the Chi-square test to com-pare differences between categorical variables. Univariateanalysis of covariance (ANCOVA) was used to test for dif-ferences in inflammatory measures between groups control-ling for significant bivariate correlates of inflammatorymeasures. Pearson correlations quantified the bivariaterelationship between continuous variables. Partial correla-tion analysis was computed to control the continuous rela-tionship between levels of PTSD symptom domains andmeasures of inflammation controlling for bivariate corre-lates of inflammation measures.
3. Results
3.1. Subjects’ characteristics
Table 1 shows that demographic and medical data werenot significantly different between PTSD patients and con-trols. Screening systemic hypertension (systolic and/or dia-stolic BP P140/90 mm Hg) was diagnosed in each of fivepatients and controls. One patient indicated a positive his-tory of non-specific heart problems, whereas the history ofprevious liver disease, renal disease, or any other severesomatic disease was negative in all 28 subjects. In eachgroup, two subjects reported non-steroidal anti-inflamma-tory drug use.
As expected, patients who met diagnostic criteria forPTSD had higher scores in all PTSD symptom clustersthan controls (all p’s < 0.001). Compared to controls,PTSD-patients had also higher symptom levels of anxiety(14.2 ± 3.9 vs. 4.1 ± 2.9, p < 0.001) and depression(13.1 ± 5.5 vs. 2.4 ± 1.7, p < 0.001) indicating, on average,

Table 1Demographic and medical data of PTSD patients and controls(mean ± SD)
Patients(n = 14)
Controls(n = 14)
P-Value
Gender (male/female) 9/5 9/5 1.00Age (years) 33 ± 10 33 ± 11 0.955Body mass index (kg/m2) 24.8 ± 3.5 25.1 ± 4.6 0.896Systolic blood pressure (mmHg) 126 ± 13 130 ± 14 0.985Diastolic blood pressure (mmHg) 86 ± 12 87 ± 9 0.925Screening hypertension (y/n) 5/9 5/9 1.000Current smoker (y/n) 8/6 7/7 0.705History of high blood glucose (y/n) 0/9 0/9 1.00History of high cholesterol (y/n) 0/14 1/13 1.00Regular exercise (y/n) 4/10 5/9 0.686Regular alcohol consumption (y/n) 6/8 7/7 0.705Analgesic medication (y/n) 7/7 4/10 0.246
R. von Kanel et al. / Journal of Psychiatric Research 41 (2007) 744–752 747
moderate anxiety and depression. Patients had experiencedthe trauma significantly longer prior to investigation thancontrols (48 ± 35 months, range 6–102 vs. 21 ± 18 months,range 2–59; p = 0.017).
3.2. Correlations with inflammation measures
In all subjects, CRP was higher in hypertensives than innormotensives (3.1/1.0–10.0 mg/l vs. 0.8/0.3–2.1 mg/l,p = 0.004) and correlated with age (r = 0.44, p = 0.019)and BMI (r = 0.42, p = 0.028). IL-1b correlated with symp-toms of anxiety (r = 0.41, p = 0.030) and depression(r = 0.44, p = 0.019). TNF-a correlated with systolic BP(�0.43, p = 0.024) and time since trauma (r = 0.45,p = 0.017). IL-4 correlated with systolic BP (r = �0.42,p = 0.028) and was lower in smokers than in non-smokers(0.14/0.13–0.16 pg/ml vs. 0.16/0.14–0.18 pg/ml, p = 0.046).
3.3. PTSD diagnosis and inflammation
Table 2 shows that TNF-a was significantly higher inPTSD patients than in controls, with a similar trendtowards statistical significance observed for IL-1b. Aftercontrolling for all correlates of inflammatory markers (cf.legend to Table 2), IL-4 was significantly lower in patientsthan in controls, but the difference in TNF-a and IL-1bbetween groups became insignificant. CRP, IL-6, and IL-10 were not significantly different between groups. These
Table 2Inflammatory markers in PTSD patients and matched controls
PTSD patients (n = 14) C
CRP (mg/l) 1.09 (0.71–3.95) 1.IL-1b (pg/ml) 0.53 (0.34–0.75) 0.IL-6 (pg/ml) 0.21 (0.13–0.29) 0.TNF-a (pg/ml) 0.85 (0.85–0.94) 0.IL-4 (pg/ml) 0.14 (0.12–0.16) 0.IL-10 (pg/ml) 0.97 (0.88–1.23) 1.
Values are given as median and inter-quartile ranges. Control variables yieldanxiety and depression for IL-1b, systolic BP and time since trauma for TNF
results did not substantially change when the four subjectstaking non-steroidal anti-inflammatory drugs wereexcluded from analyses.
Crude differences in levels of inflammation markersbetween groups showed a medium to large effect size(Cohen’s d) for IL-1b (0.68) and TNF-a (0.58), a small tomedium effect size for IL-4 (0.42) and IL-10 (0.37), and anegligible effect size for IL-6 (0.18) and CRP (0.10). Thetotal required sample size to detect a significantly higherlevel of proinflammatory cytokines in PTSD patients com-pared to controls with a statistical power of 0.80 and alphaerror level of 0.05 (unequal variances assumed) was n = 58for IL-1b and n = 73 for TNF-a. Respective power calcula-tions yielded sample sizes of n = 103 for IL-4 and n = 179for IL-10 in order to detect a significantly lower level ofanti-inflammatory cytokines in PTSD patients comparedto controls. Power analyses suggest that, in spite of somecytokine levels showing close to or above medium effectsizes for mean differences between groups, our sample of28 subjects was too small to detect significances betweengroups.
3.4. Association of PTSD symptom clusters with
inflammation
Based on effect sizes, correlations between PTSD symp-tom domains and inflammation markers were computedfor IL-1b, TNF-a, IL-4, and IL-10 but not for CRPand IL-6. To account for spuriously significant associa-tions due to multiple comparisons, we computed onenet score of proinflammatory activity as follows (Babyak,2004): we aggregated standardized z-scores of normalizedIL-1b and TNF-a levels to one proinflammatory scoreand z-scores of IL-4 and IL-10 levels to one anti-inflam-matory score, respectively. The anti-inflammatory scorewas then subtracted from the proinflammatory score toyield a net proinflammatory activity score. This score cor-related positively with frequency, intensity, and total fre-quency and intensity scores of re-experiencing,avoidance, hyperarousal, and total PTSD symptom score(all r’s between 0.53 and 0.60, all p’s 6 0.004; p = 0.004for Bonferroni adjustment for 12 comparisons). Subse-quent correlation analyses were therefore considered aspost hoc tests and made no further adjustment for multi-ple testing.
ontrols (n = 14) p (crude) p (adjusted)
57 (0.41–3.01) 0.628 0.55834 (0.27–0.40) 0.075 0.95014 (0.10–0.29) 0.669 0.66982 (0.80–0.92) 0.038 0.18416 (0.14–0.18) 0.274 0.02908 (0.94–1.45) 0.335 0.335
ing adjusted P-values were age, BMI, and hypertension status for CRP;-a; and systolic BP and smoking status for IL-4.

748 R. von Kanel et al. / Journal of Psychiatric Research 41 (2007) 744–752
3.4.1. Symptoms of re-experiencing
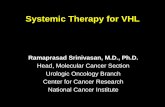
TNF-a correlated with re-experiencing frequency (r =0.44, p = 0.019), re-experiencing intensity (r = 0.51,p = 0.005), and total re-experiencing (r = 0.49, p = 0.008;Fig. 1a ). Controlling for systolic BP maintained these sig-nificances. However, additional adjustment for time sincetrauma rendered the associations between TNF-a and total
c Arousal and TNF-alpha
Total arousal symptoms3210-1-2
TN
F-a
lpha
leve
l
3
2
1
0
-1
-2
-3
Patients
Controls
Total sample
Rsq = 0,1766
a Re-experiencing and TNF-alpha
Total re-experiencing symptoms3210-1-2
TN
F-a
lpha
leve
l
3
2
1
0
-1
-2
-3
Patients
Controls
Total sample
Rsq = 0,2420
e Avoidance and IL-1beta
Total avoidance symptoms3210-1-2
IL-1
beta
leve
l
3
2
1
0
-1
-2
-3
Patients
Control
Total sample
Rsq = 0,1727
Fig. 1. Associations between PTSD symptom domains and cytokines. Scatter p(i.e. combined frequency and intensity scores) of posttraumatic stress disorder (d), interleukin (IL)-1beta (Panel e), and IL-4 (Panel f). Fit lines with variances eas normalized Blom scores.
re-experiencing (r = 0.36, p = 0.071) and re-experiencingintensity (r = 0.37, p = 0.066), respectively, of borderlinesignificance and the relationship with re-experiencing fre-quency insignificant. IL-1b correlated with re-experiencingfrequency (r = 0.34, p = 0.078) and, with borderline signif-icance, with total re-experiencing (r = 0.32, p = 0.10); theseassociations were not significant with adjustment for anxi-
f Arousal and IL-4
Total arousal symptoms
3210-1-2
IL-4
leve
ls
3
2
1
0
-1
-2
Patients
Controls
Total sample
Rsq = 0,1436
b Avoidance and TNF-alpha
Total avoidance symptoms3210-1-2
TN
F-a
lph
a le
vel
3
2
1
0
-1
-2
-3
Patients
Controls
Total sample
Rsq = 0,1393
d Total PTSD symptoms and TNF-alpha
Total PTSD symptom score3210-1-2
TN
F-a
lph
a le
vel
3
2
1
0
-1
-2
-3
Patients
Controls
Total sample
Rsq = 0,1359
lots illustrate relationships between different total symptom domain levelsPTSD) and plasma levels of tumor necrosis factor (TNF)-alpha (Panels a–xplained (rsq = r2) are shown for the entire sample (n = 28). Data are given

R. von Kanel et al. / Journal of Psychiatric Research 41 (2007) 744–752 749
ety and depression. Anxiety and depression were not signif-icantly associated with IL-1b when controlling for symp-toms of re-experiencing. IL-4 and IL-10 levels showed norelationship with symptoms of re-experiencing.
3.4.2. Symptoms of avoidanceTNF-a significantly correlated with avoidance frequency
(r = 0.39, p = 0.036), avoidance intensity (r = 0.39,p = 0.040), and total avoidance (r = 0.37, p = 0.050;Fig. 1b). These relationships showed borderline signifi-cance (r’s > 0.34, p’s < 0.09) when controlling for systolicBP and became insignificant when also controlling for timesince trauma. IL-1b showed a significant association withavoidance frequency (r = 0.38, p = 0.049), avoidance inten-sity (r = 0.43, p = 0.024), and total avoidance (r = 0.42,p = 0.028; Fig. 1e). Controlling for anxiety and depressionsymptoms yielded these relationships insignificant. Anxietyand depression were not significantly associated with IL-1bwhen controlling for symptoms of avoidance. IL-4 and IL-10 levels were not associated with avoidance symptoms.
3.4.3. Symptoms of hyperarousalTNF-a significantly correlated with hyperarousal fre-
quency (r = 0.43, p = 0.021), hyperarousal intensity(r = 0.44, p = 0.019), and total hyperarousal (r = 0.42,p = 0.026; Fig. 1c). These associations remained significantwhen controlling for systolic BP and time since trauma(r’s > 0.39, p’s 6 0.047). The relationship between IL-1band hyperarousal frequency was of borderline significance(r = 0.32, p = 0.095) and became insignificant with adjust-ment for anxiety and depression symptoms. Anxiety anddepression were not significantly associated with IL-1bwhen controlling for symptoms of hyperarousal. IL-4
showed significant associations with hyperarousal intensity(r = �0.41, p = 0.032) and total hyperarousal (r = �0.38,p = 0.047; Fig. 1f) and a trend towards statistical signifi-cance for an association with hyperarousal frequency(�0.36, p = 0.066). These relationships were all significantwhen controlling for systolic BP and smoking status(r’s P 0-.44, p’s 6 0.024). IL-10 was not associated withhyperarousal symptoms.
3.4.4. Total PTSD symptom score
TNF-a significantly correlated with total intensity score(r = 0.41, p = 0.029) and showed a trend towards a signif-icant correlation with total frequency score (r = 0.35,p = 0.070) and total frequency and intensity score(r = 0.37, p = 0.054; Fig. 1d). Controlling for systolic BPand time since trauma rendered the relationship betweenTNF-a and total intensity score of borderline significance(r = 0.33, p = 0.097) and those with total frequency andtotal frequency and intensity scores insignificant. IL-1bshowed a trend towards statistical significance with totalfrequency score (r = 0.33, p = 0.082), total intensity score(r = 0.34, p = 0.077), and total frequency and intensityscore (r = 0.33, p = 0.092). These associations becameinsignificant when controlling for symptoms of anxiety
and depression. Anxiety and depression were not signifi-cantly associated with IL-1b when controlling for totalPTSD symptom scores. In crude correlation analysis, IL-
4 was not significantly associated with any total PTSDsymptom score. However, when controlling for systolicBP and smoking status, IL-4 significantly correlated withtotal frequency score (r = �0.42, p = 0.033) and total fre-quency and intensity score (�0.41, p = 0.035) and, withborderline significance, with total intensity score(r = �0.38, p = 0.055). IL-10 showed no relationship withtotal PTSD symptom score.
4. Discussion
We confirmed our hypothesis in that we found evidencefor a proinflammatory state in patients with PTSD. Circu-lating levels of the proinflammatory cytokines TNF-a andIL-1b were higher and the level of the anti-inflammatorycytokine IL-4 was lower in PTSD patients than in controls.Some of these differences reached only marginal signifi-cance and were, moreover, affected by covariates. In addi-tion, continuous associations between the different PTSDsymptom domains and cytokines in the entire samplepointed in the hypothesized direction. More precisely,PTSD symptom severity showed a positive relationshipwith plasma TNF-a with total PTSD symptom intensitymaking a stronger contribution to this relationship thantotal PTSD symptom frequency. Moreover, individualPTSD symptom clusters re-experiencing, avoidance, andhyperarousal showed also a consistent and positive associ-ation with TNF-a. Apparently, some but not all associa-tions with TNF-a were affected by time since traumasuggesting the longer ago subjects had experienced thetrauma the higher their TNF-a levels. Characteristic sup-pression of the hypothalamic-pituitary adrenal axis withblunted cortisol secretion with sustained PTSD could mit-igate suppressive action of endogenous cortisol on proin-flammatory cytokine production (Yehuda et al., 1991;Gander and von Kanel, 2006). Such a mechanism couldhave kindled a proinflammatory response in our subjectsparticularly in those with higher PTSD symptom levels.Sympathomedullary hyperactivity and decreased vagaltone have also been described as typical alterations instress axes of PTSD patients with this sympathovagalimbalance possibly contributing to an inflammatoryresponse (Gander and von Kanel, 2006). We acknowledge,however, that we did not measure e.g. plasma catechola-mines, heart rate variability, and free salivary cortisol.We are therefore unable to state whether perturbation instress axes affected levels of TNF-a and of other inflamma-tion markers in our subjects.
In addition, total symptoms of avoidance correlatedpositively with IL-b levels. Symptoms of anxiety anddepression accounted for some of the positive associationsbetween PTSD symptom domain scores and IL-1b, and, inturn, PTSD symptoms accounted for some of the associa-tions of anxiety and depression with IL-1b. Plasma profiles

750 R. von Kanel et al. / Journal of Psychiatric Research 41 (2007) 744–752
of proinflammatory markers are quite similar in depression(i.e. elevated IL-1b, IL-6, TNF-a, and CRP) (Pasic et al.,2003) and PTSD (Gander and von Kanel, 2006). Our find-ings suggest that posttraumatic stress and depression mayelicit systemic inflammation not entirely independent ofeach other. A somewhat different picture emerged for IL-4. The continuous relationship between PTSD severityand IL-4 was significant only after controlling for covari-ates systolic BP and smoking status. On the whole, weinterpret that the more severe posttraumatic stress thegreater the proinflammatory activity along a continuumof severity. Importantly, PTSD symptomatology mighttherefore elicit proinflammatory activity before patientsmeet diagnostic criteria for full PTSD.
Our study is the first to show that TNF-a is associatedwith diagnostic PTSD. Moreover, the positive relationshipbetween PTSD symptom domains and TNF-a is in linewith a previous investigation showing that more generalposttraumatic psychological dysfunction was associatedwith higher levels of TNF-a (Sutherland et al., 2003). Incontrast to our novel findings for TNF-a, increased IL-1b levels and decreased IL-4 levels with more PTSDsymptoms confirm previous studies (Tucker et al., 2004;Spivak et al., 1997; Kawamura et al., 2001). Contraryto our hypothesis, however, IL-6 and CRP were not dif-ferent between PTSD patients and controls. We interpretthat PTSD significantly affected activation of initial stepsin the inflammatory cascade, but not later ones down-stream in the inflammatory pathway. However, the exactinterference of PTSD with the inflammatory cascaderemains incompletely understood, because previous find-ings on IL-6 and on CRP in PTSD were inconclusiveand, in part, different from those observed in our study.Compared to non-PTSD controls, PTSD patients hadhigher CRP in one study (Miller et al., 2001) and lowerCRP in another (Sondergaard et al., 2004). IL-6 wasfound both higher and unchanged in PTSD patients com-pared to controls (Miller et al., 2001; Maes et al., 1999;Baker et al., 2001).
Our findings suggest one psychobiological pathwayfrom posttraumatic stress to increased cardiovascular risk.A shift in the immunological response to chronically per-ceived traumatic stress towards a proinflammatory statemight contribute to atherosclerosis, thereby explainingsome of the increased prevalence of cardiovascular diseasesin patients with PTSD (Boscarino, 2006; Schnurr et al.,2000; Boscarino and Chang, 1999; Shemesh et al., 2004).Atherosclerosis is sustained by local and systemic inflam-matory processes resulting in unstable plaques to ulti-mately increase the risk of coronary artery disease andacute coronary events (Ross, 1999). IL-1 is a key playerin the atherogenic inflammatory response by virtue of acti-vating monocytes and of stimulating expression of adhe-sion molecules on endothelial cells, endothelial cellprocoagulant activity, and smooth muscle cell prolifera-tion, to name some of its mechanisms (Saadeddin et al.,2002). Plasma levels of IL-1b, the major active form of
IL-1 in circulation, were elevated in patients with minimalcoronary artery disease (Hasdai et al., 1996). TNF-a ispresent in atherosclerotic plaques (Barath et al., 1990),and its effects on systemic and local inflammation of thevasculature are similar to those of IL-1b (Dayer and Bur-ger, 1994). The clinical importance of TNF-a is demon-strated by a recent study showing that TNF-a predictedrecurrence of coronary events in patients with first-timemyocardial infarction (Ridker et al., 2000). Importantanti-inflammatory effects of IL-4 are mitigation of cellularadhesion molecule expression (Majewska et al., 1997) andof IL-1b and TNF-a production (Dayer and Burger,1994). Taken together, TNF-a, IL-1b, and IL-4, all show-ing altered plasma levels in relation to posttraumatic stressin our study, demonstrate pivotal proinflammatory andanti-inflammatory properties pertinent to atherosclerosisinitiation and progression.
The strengths of our study were the matching of patientsand controls in terms of age and gender, the inclusion ofpatients who were otherwise healthy and without majorpsychiatric co-morbidity, and the consideration of majorcovariates of inflammation markers for analyses. However,we also mention three limitations of our study. First, statis-tical power was low, and in spite of the fact that differencesin levels of TNF-a, IL-1b, IL-4, and IL-10 in patients com-pared to controls showed, on average, medium effect sizes,our results must be regarded as preliminary. Accordingly,we should also refrain from over-interpreting the lack ofdifference in IL6, CRP, and IL-10 between groups. Second,our study design raises methodological problems. Thesmall sample size precluded extensive statistical controlling.Demographics, medical variables, and medication althoughnot significantly different between groups, could exert sub-stantial effects on inflammation when controlled for togetherin a larger sample. In addition, although the same propor-tion of patients and controls had blood draws in either themorning or afternoon, diurnal variance in cytokine concen-trations could be a confounder of our data. Eventually,citrate (instead of EDTA) has not been validated as ananticoagulant in the assay we used to determine IL-1b.Third, our results and implications cannot be generalizedto populations with cardiovascular diseases and of moreadvanced age, both of which are positively associatedwith proinflammatory cytokines (Saadeddin et al., 2002;Bruunsgaard and Pedersen, 2003). However, given thatcarefully controlled studies on the issue are scarce, weunderstand our study as a first step to better understandingthe PTSD-inflammation link independent of its manymediators and moderators. Pending replication of ourfindings in larger samples, similar investigations seemwarranted in populations with atherosclerotic diseases.
To summarize, we found evidence for a positive relation-ship between PTSD diagnosis and symptomatology and acirculating cytokine profile indicative of a proinflammatorystate. Our finding of low-grade systemic inflammation in thevasculature of patients with PTSD provides evidence for onepsychobiological mechanism by which posttraumatic stress

R. von Kanel et al. / Journal of Psychiatric Research 41 (2007) 744–752 751
could promote atherosclerosis and increase cardiovascularrisk.
References
American Psychiatric Association. Diagnostic and statistical manual ofmental disorders. 4th ed. Washington (DC): APA; 1994.
Babyak MA. What you see may not be what you get: a brief, nontechnicalintroduction to overfitting in regression-type models. PsychosomaticMedicine 2004;66:411–21.
Baker DG, Ekhator NN, Kasckow JW, Hill KK, Zoumakis E, DashevskyBA, Chrousos GP, Geracioti Jr TD. Plasma and cerebrospinal fluidinterleukin-6 concentrations in posttraumatic stress disorder. Neuro-immunomodulation 2001;9:209–17.
Barath P, Fishbein MC, Cao J, Berenson J, Helfant RH, Forrester JS.Detection and localization of tumor necrosis factor in humanatheroma. American Journal of Cardiology 1990;65:297–302.
Beckham JC, Kirby AC, Feldman ME, Hertzberg MA, Moore SD,Crawford AL, Davidson JR, Fairbank JA. Prevalence and correlatesof heavy smoking in Vietnam veterans with chronic posttraumaticstress disorder. Addictive Behaviors 1997;22:637–47.
Blom G. Statistical estimates and transformed beta variables. NewYork: John Wiley & Sons; 1958.
Boscarino JA. Posttraumatic stress disorder and physical illness: resultsfrom clinical and epidemiologic studies. Annals of the New YorkAcademy of Science 2004;1032:141–53.
Boscarino JA. Posttraumatic stress disorder and mortality among U.S.army veterans 30 years after military service. Annals of Epidemiology2006;16:248–56.
Boscarino JA, Chang J. Electrocardiogram abnormalities among men withstress-related psychiatric disorders: implications for coronary heartdisease and clinical research. Ann Behavioral Medicine 1999;21:227–34.
Bruunsgaard H, Pedersen BK. Age-related inflammatory cytokines anddisease. Immunology and allergy clinics of North America 2003;23:15–39.
Buckley TC, Kaloupek DG. A meta-analytic examination of basalcardiovascular activity in posttraumatic stress disorder. PsychosomaticMedicine 2001;63:585–94.
Daxecker H, Raab M, Markovic S, Karimi A, Griesmacher A, MuellerMM. Endothelial adhesion molecule expression in an in vitro model ofinflammation. Clinica Chimica Acta 2002;325:171–5.
Dayer JM, Burger D. Interleukin-1, tumor necrosis factor and theirspecific inhibitors. European Cytokine Network 1994;5:563–71.
Dobie DJ, Kivlahan DR, Maynard C, Bush KR, Davis TM, Bradley KA.Posttraumatic stress disorder in female veterans: association with self-reported health problems and functional impairment. Archives ofInternal Medicine 2004;164:394–400.
Fazel M, Wheeler J, Danesh J. Prevalence of serious mental disorder in7000 refugees resettled in western countries: a systematic review.Lancet 2005;365:1309–14.
Gander ML, von Kanel R. Myocardial infarction and post-traumaticstress disorder: frequency, outcome, and atherosclerotic mechanisms.European Journal of Cardiovascular Prevention and Rehabilitation2006;13:165–72.
Goodwin RD, Davidson JR. Self-reported diabetes and posttraumaticstress disorder among adults in the community. Preventive Medicine2005;40:570–4.
Hasdai D, Scheinowitz M, Leibovitz E, Sclarovsky S, Eldar M, Barak V.Increased serum concentrations of interleukin-1 beta in patients withcoronary artery disease. Heart 1996;76:24–8.
Herrmann C, Buss U, Snaith RP. HADS-D Hospital Anxiety andDepression Scale-Deutsche Version. Ein Fragebogen zur Erfassungvon Angst und Depressivitat in der somatischen Medizin. Bern: Ver-lag Hans Huber; 1995.
Kagan BL, Leskin G, Haas B, Wilkins J, Foy D. Elevated lipid levels inVietnam veterans with chronic posttraumatic stress disorder. Biolog-ical Psychiatry 1999;45:374–7.
Kawamura N, Kim Y, Asukai N. Suppression of cellular immunity in menwith a past history of posttraumatic stress disorder. American Journalof Psychiatry 2001;158:484–6.
Kessler RC, Sonnega A, Bromet E, Hughes M, Nelson CB. Posttraumaticstress disorder in the National Comorbidity Survey. Archives ofGeneral Psychiatry 1995;52:1048–60.
Kjeldsen SE, Erdine S, Farsang C, Sleight P, Mancia G. 1999 WHO/ISHHypertension Guidelines subcommittee. 1999 WHO/ISH Hyperten-sion Guidelines—highlights & ESH update. Journal of Hypertension2002;20:153–5.
Lang AJ, Rodgers CS, Laffaye C, Satz LE, Dresselhaus TR, Stein MB.Sexual trauma, posttraumatic stress disorder, and health behavior.Behavioral Medicine 2003;28:150–8.
Leskin GA, Sheikh JI. Lifetime trauma history and panic disorder:findings from the National Comorbidity Survey. Journal of AnxietyDisorders 2002;16:599–603.
Loerch B, Szegedi A, Kohnen R, Benkert O. The primary care evaluationof mental disorders (PRIME-MD), German version: a comparisonwith the CIDI. Journal of Psychiatric Research 2000;34:211–20.
Maes M, Lin AH, Delmeire L, Van Gastel A, Kenis G, De JonghR, Bosmans E. Elevated serum interleukin-6 (IL-6) and IL-6receptor concentrations in posttraumatic stress disorder followingaccidental man-made traumatic events. Biological Psychiatry1999;45:833–9.
Majewska E, Paleolog E, Baj Z, Kralisz U, Feldmann M, Tchorzewski H.Role of tyrosine kinase enzymes in TNF-alpha and IL-1 inducedexpression of ICAM-1 and VCAM-1 on human umbilical veinendothelial cells. Scandinavian Journal of Immunology 1997;45:385–92.
Marshall RD, Olfson M, Hellman F, Blanco C, Guardino M, StrueningEL. Comorbidity, impairment, and suicidality in subthreshold PTSD.American Journal of Psychiatry 2001;158:1467–73.
Miller RJ, Sutherland AG, Hutchison JD, Alexander DA. C-reactiveprotein and interleukin- 6 receptor in post-traumatic stress disorder: apilot study. Cytokine 2001;13:253–5.
Pasic J, Levy WC, Sullivan MD. Cytokines in depression and heart failure.Psychosomatic Medicine 2003;65:181–93.
Ridker PM, Rifai N, Pfeffer M, Sacks F, Lepage S, Braunwald E.Elevation of tumor necrosis factor-alpha and increased risk ofrecurrent coronary events after myocardial infarction. Circulation2000;101:2149–53.
Ross R. Atherosclerosis–an inflammatory disease. New England Journalof Medicine 1999;340:115–26.
Rozanski A, Blumenthal JA, Davidson KW, Saab PG, Kubzansky L.The epidemiology, pathophysiology, and management of psychoso-cial risk factors in cardiac practice: the emerging field of behavioralcardiology. Journal of the American College of Cardiology 2005;45:637–51.
Saadeddin SM, Habbab MA, Ferns GA. Markers of inflammation andcoronary artery disease. Medical Science Monitor 2002;8:RA5–RA12.
Schnurr PP, Green BL. Trauma and health: physical health consequencesof extreme stress. Washington (DC): American Psychological Asso-ciation; 2004.
Schnurr PP, Spiro 3rd A, Paris AH. Physician-diagnosed medicaldisorders in relation to PTSD symptoms in older male militaryveterans. Health Psychology 2000;19:91–7.
Schnyder U, Moergeli H. German version of Clinician-AdministeredPTSD Scale. Journal of Traumatic Stress 2002;15:487–92.
Shemesh E, Yehuda R, Milo O, Dinur I, Rudnick A, Vered Z, Cotter G.Posttraumatic stress, nonadherence, and adverse outcome in survi-vors of a myocardial infarction. Psychosomatic Medicine 2004;66:521–6.
Sondergaard HP, Hansson LO, Theorell T. The inflammatory markersC-reactive protein and serum amyloid A in refugees with andwithout posttraumatic stress disorder. Clinica Chimica Acta2004;342:93–8.
Spivak B, Shohat B, Mester R, Avraham S, Gil-Ad I, Bleich A, ValevskiA, Weizman A. Elevated levels of serum interleukin-1 beta in combat-

752 R. von Kanel et al. / Journal of Psychiatric Research 41 (2007) 744–752
related posttraumatic stress disorder. Biological Psychiatry 2000;42:345–8.
Sutherland AG, Alexander DA, Hutchinson JD. Disturbance of pro-inflammatory cytokines in post-traumatic psychopathology. Cytokine2003;24:219–25.
Tucker P, Ruwe WD, Masters B, Parker DE, Hossain A, TrautmanRP, Wyatt DB. Neuroimmune and cortisol changes in selectiveserotonin reuptake inhibitor and placebo treatment of chronicposttraumatic stress disorder. Biological Psychiatry 2004;56:121–8.
Willerson JT, Ridker PM. Inflammation as a cardiovascular risk factor.Circulation 2004;109(21 Suppl. 1):2–10.
Yehuda R. Post-traumatic stress disorder. New England Journal ofMedicine 2002;346:108–14.
Yehuda R, Giller ER, Southwick SM, Lowy MT, Mason JW. Hypotha-lamic–pituitary–adrenal dysfunction in posttraumatic stress disorder.Biological Psychiatry 1991;30:1031–48.
Yudkin JS, Kumari M, Humphries SE, Mohamed-Ali V. Inflammation,obesity, stress and coronary heart disease: is interleukin-6 the link.Atherosclerosis 2000;148:209–14.