
EVIDENCE CORROBORATING MAY 19 TESTIMONY TO ...
51
EVIDENCE CORROBORATING MAY 19 TESTIMONY TO VICTORIAN CANNABIS INQUIRY In this document: 1. Lancet 2019 study on new psychosis diagnoses for London and Amsterdam 2. Journal study on cannabis and domestic violence 3. Study demonstrating mechanism for cannabis’ cause of cancers and congenital abnormalities 4. One of the worldwide media articles where cannabis was claimed to be the New Thalidomide 5. From the same Daily Mail media article corroboration of Gary Christian’s claim that cannabis is causal for 12 cancers which are not pediatric cancers 6. Cannabis and pediatric cancers study 7. Not in this pdf – Cannabis and congenital abnormalities study (could not copy into this pdf because it is a protected document)
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of EVIDENCE CORROBORATING MAY 19 TESTIMONY TO ...
EVIDENCE CORROBORATING MAY 19 TESTIMONY
TO VICTORIAN CANNABIS INQUIRY
In this document:
1. Lancet 2019 study on new psychosis diagnoses for London and Amsterdam
2. Journal study on cannabis and domestic violence
3. Study demonstrating mechanism for cannabis’ cause of cancers and congenital
abnormalities
4. One of the worldwide media articles where cannabis was claimed to be the New
Thalidomide
5. From the same Daily Mail media article corroboration of Gary Christian’s claim that cannabis
is causal for 12 cancers which are not pediatric cancers
6. Cannabis and pediatric cancers study
7. Not in this pdf – Cannabis and congenital abnormalities study (could not copy into this pdf
because it is a protected document)
www.thelancet.com/psychiatry Published online March 19, 2019 http://dx.doi.org/10.1016/S2215-0366(19)30048-3 1
Articles
The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control studyMarta Di Forti, Diego Quattrone, Tom P Freeman, Giada Tripoli, Charlotte Gayer-Anderson, Harriet Quigley, Victoria Rodriguez, Hannah E Jongsma, Laura Ferraro, Caterina La Cascia, Daniele La Barbera, Ilaria Tarricone, Domenico Berardi, Andrei Szöke, Celso Arango, Andrea Tortelli, Eva Velthorst, Miguel Bernardo, Cristina Marta Del-Ben, Paulo Rossi Menezes, Jean-Paul Selten, Peter B Jones, James B Kirkbride, Bart PF Rutten, Lieuwe de Haan, Pak C Sham, Jim van Os, Cathryn M Lewis, Michael Lynskey, Craig Morgan, Robin M Murray, and the EU-GEI WP2 Group*
SummaryBackground Cannabis use is associated with increased risk of later psychotic disorder but whether it affects incidence of the disorder remains unclear. We aimed to identify patterns of cannabis use with the strongest effect on odds of psychotic disorder across Europe and explore whether differences in such patterns contribute to variations in the incidence rates of psychotic disorder.
Methods We included patients aged 18–64 years who presented to psychiatric services in 17 sites across Europe and Brazil with first-episode psychosis and recruited controls representative of the local populations. We applied adjusted logistic regression models to the data to estimate which patterns of cannabis use carried the highest odds for psychotic disorder. Using Europe-wide and national data on the expected concentration of Δ⁹-tetrahydrocannabinol (THC) in the different types of cannabis available across the sites, we divided the types of cannabis used by participants into two categories: low potency (THC <10%) and high potency (THC ≥10%). Assuming causality, we calculated the population attributable fractions (PAFs) for the patterns of cannabis use associated with the highest odds of psychosis and the correlation between such patterns and the incidence rates for psychotic disorder across the study sites.
Findings Between May 1, 2010, and April 1, 2015, we obtained data from 901 patients with first-episode psychosis across 11 sites and 1237 population controls from those same sites. Daily cannabis use was associated with increased odds of psychotic disorder compared with never users (adjusted odds ratio [OR] 3·2, 95% CI 2·2–4·1), increasing to nearly five-times increased odds for daily use of high-potency types of cannabis (4·8, 2·5–6·3). The PAFs calculated indicated that if high-potency cannabis were no longer available, 12·2% (95% CI 3·0–16·1) of cases of first-episode psychosis could be prevented across the 11 sites, rising to 30·3% (15·2–40·0) in London and 50·3% (27·4–66·0) in Amsterdam. The adjusted incident rates for psychotic disorder were positively correlated with the prevalence in controls across the 11 sites of use of high-potency cannabis (r = 0·7; p=0·0286) and daily use (r = 0·8; p=0·0109).
Interpretation Differences in frequency of daily cannabis use and in use of high-potency cannabis contributed to the striking variation in the incidence of psychotic disorder across the 11 studied sites. Given the increasing availability of high-potency cannabis, this has important implications for public health.
Funding source Medical Research Council, the European Community’s Seventh Framework Program grant, São Paulo Research Foundation, National Institute for Health Research (NIHR) Biomedical Research Centre (BRC) at South London and Maudsley NHS Foundation Trust and King’s College London and the NIHR BRC at University College London, Wellcome Trust.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license.
IntroductionMany countries have legalised or decriminalised cannabis use, leading to concerns that this might result in an increase in cannabis use and associated harm,1,2 even if the latter only affects a minority of the population.3 Cross-sectional and prospective epidemiological studies4,5 as well as biological evidence6 support a causal link between cannabis use and psychotic disorder. Meta-analysis shows a dose–response association with the highest odds of
psychotic disorder in those with the heaviest cannabis use.7 Nevertheless, it is not clear whether, at a population level, patterns of cannabis use influence rates of psychotic disorder.8–10
A systematic review11 has described a five-times variation in the incidence of schizophrenia worldwide. A transnational case-control study (EU-GEI) has reported an eight-times difference in the incidence of psychotic disorder across 16 European sites plus one in Brazil.12
Lancet Psychiatry 2019
Published Online March 19, 2019 http://dx.doi.org/10.1016/ S2215-0366(19)30048-3
See Online/Comment http://dx.doi.org/10.1016/ PII
*Collaborators listed in the appendix
Social, Genetic and Developmental Psychiatry Centre (M Di Forti PhD, D Quattrone MD, Prof P C Sham PhD, Prof C M Lewis XX) and Department of Addiction (Prof M Lynskey PhD), Institute of Psychiatry, Psychology and Neuroscience and Department of Psychosis Studies (G Tripoli MSc , H Quigley MD, V Rodriguez MD, Prof J van Os PhD, Prof R M Murray FRS) and Department of Health Service and Population Research (C Gayer-Anderson PhD, Prof C Morgan PhD), Institute of Psychiatry, King’s College London, London, UK; National Institute for Health Research (NIHR) Mental Health Biomedical Research Centre at South London and Maudsley NHS Foundation Trust and King’s College London, UK (M Di Forti, D Quattrone, Prof C M Lewis); South London and Maudsley NHS Mental Health Foundation Trust, London, UK (M Di Forti, D Quattrone, Prof R M Murray); Society for the Study of Addiction, Department of Psychology, University of Bath, Bath, UK (T P Freeman PhD); Department of Psychiatry, University of Cambridge, Cambridge, UK (H E Jongsma PhD, Prof P B Jones PhD); Department of Experimental Biomedicine and Clinical Neuroscience,
This version saved: 15:10, 04-Mar-19
Guilia V
18TLP0389_DiFortiTHELANCETPSYCH-D-18-00389
S2215-0366(19)30048-3
Embargo: March 19, 2019–23:30 (GMT)
Doctopic: Primary Research
Gold OA TBC; Funding: Wellcome Trust + NIHR
Linked to 19TLP0164
vivaldig
Highlight
Please indicate preferred qualification
k1641103
Sticky Note
Please can you replace "Society for the Study of Addiction" with "Addiction and Mental Health Group (AIM)"
martadiforti
Sticky Note
PhD
martadiforti
Inserted Text
In agreement with the other authors we suggest to change 17 sites to 11 for consistency with the rest of the manuscript

1
5
10
15
20
25
30
35
40
45
50
55
Articles
2 www.thelancet.com/psychiatry Published online March 19, 2019 http://dx.doi.org/10.1016/S2215-0366(19)30048-3
Differences in the distribution of risk factors for psychosis, such as cannabis use, among the populations studied might contribute to these variations.
Therefore, using data from the EU-GEI case-control study of first-episode psychosis and the previously published data on incidence,12 we sought to describe differences in patterns of cannabis use across sites, identify the measure of cannabis use with the strongest impact on odds of psychotic disorder across sites, calculate the population attributable fraction (PAF) for the patterns of cannabis use associated with the highest odds for psychosis, and test whether differences in patterns of cannabis use contribute to variations in the incidence of psychotic disorder across sites.
MethodsStudy designThe EU-GEI project set out to estimate the incidence of psychosis and recruit first-episode psychosis cases and controls to investigate risk factors for psychotic disorder. First, incidence rates were estimated12 by identifying all individuals with a first episode of psychosis who presented to mental health services between May 1, 2010, and April 1, 2015, in 17 areas in England, France, the Netherlands, Italy, Spain, and Brazil (appendix). Second, to investigate risk factors, we attempted to assess
1000 first-episode cases and 1000 population-based controls during the same period.
ParticipantsPatients presenting with their first episode of psychosis were identified by trained researchers who carried out regular checks across the mental health services within the 17 catchment areas (one site per catchment area). Patients were eligible if they were aged 18–64 years and resident within the study areas at the time of their first presentation with a diagnosis of psychosis by ICD-10 criteria (F20–33); details are provided in the supple-mentary methods and in previous publications.12 Cases were approached via their clinical team and invited to participate. Using the Operational Criteria Checklist algorithm, all cases interviewed received a research-based diagnosis.13 Patients were excluded if they had been previously treated for psychosis or if they met criteria for organic psychosis (F09) or for psychotic symptoms resulting from acute intoxication (F1X.5).
We adopted quota sampling strategies to guide the recruitment of controls. Accurate local demographic data were used to set quotas for controls to ensure the samples’ representativeness of each catchment area’s population at risk in terms of age, gender, and ethnicity. Potential controls were initially identified on the basis of locally
University of Palermo, Palermo, Italy (L Ferraro PhD,
C La Cascia PhD, Prof D La Barbera MD);
Department of Medical and Surgical Science, Psychiatry
Unit, Alma Mater Studiorum Università di Bologna, Bologna,
Italy (I Tarricone PhD, Prof D Berardi MD);
INSERM U955, Equipe 15, Institut National de la Santé et
de la Recherche Médicale, Créteil, Paris, France
(Prof A Szöke PhD); Department of Child and Adolescent
Psychiatry, Hospital General Universitario Gregorio
Marañón, School of Medicine, Universidad Complutense,
IiSGM (CIBERSAM), Madrid, Spain (Prof C Arango PhD);
Etablissement Public de Santé Maison Blanche, Paris, France
(A Tortelli PhD); Department of Psychiatry, Early Psychosis Section, Academic Medical
Centre, University of Amsterdam, Amsterdam,
Netherlands (E Velthorst PhD, Prof L de Haan PhD); Barcelona
Clinic Schizophrenia Unit, Neuroscience Institute,
Hospital clinic, Department of Medicine, University of
Barcelona, IDIBAPS, CIBERSAM, Barcelona, Spain
(Prof M Bernardo PhD); Division of Psychiatry, Department of Neuroscience and Behaviour,
Ribeirão Preto Medical School (C M Del-Ben PhD) and
Department of Preventative Medicine, Faculdade de
Medicina FMUSP (Prof P R Menezes PhD),
University of São Paulo, São Paulo, Brazil; Rivierduinen
Institute for Mental Health Care, Leiden, Netherlands
(Prof J-P Selten PhD); CAMEO Early Intervention Service,
Cambridgeshire & Peterborough NHS Foundation
Trust, Cambridge, UK (Prof P B Jones); Psylife Group,
Division of Psychiatry, University College London,
London, UK (J B Kirkbride PhD, H E Jongsma); Department of
Psychiatry and Neuropsychology, School for
Mental Health and Neuroscience, South Limburg
Mental Health Research and Teaching Network, Maastricht
University Medical Centre, Maastricht, Netherlands
(Prof B P F Rutten PhD); Centre for Genomic Sciences, Li
KaShing Faculty of Medicine,
Research in context
Evidence before this studyThe evidence reporting the dose-dependent association between cannabis use and psychotic disorders has been summarised in the meta-analysis by Marconi and colleagues. We searched PubMed for studies published up to March 31, 2018, that had specifically measured the impact of high-potency cannabis use on the odds of psychotic disorder (not psychotic symptoms or psychosis in general) or that had calculated the proportion of new cases of psychotic disorder arising in specific populations that were attributable to the use of high-potency cannabis, using the terms “psychotic disorders” and “high potency cannabis” or “skunk-super skunk” or “high THC cannabis”; we also included the term “population attributable fraction”. Finally, we searched for studies that reported the impact of any use of cannabis on the incidence of psychotic disorder or schizophrenia. Three studies met our inclusion criteria. Boydell and colleagues speculated that an increase in the incidence rates of schizophrenia between 1965 and 1999 in south London might be related to the increase, over the same period, in the prevalence of cannabis use in the year before first presentation. Our two previous case-control studies showed that high-potency cannabis, especially when used daily, carries the highest risk for psychotic disorder and that, assuming causality, 24% of new cases of psychotic disorder in south London could be attributed to the use of high potency cannabis.
Added value of this studyThis multicentre case-control study across ten European and one Brazilian site replicates the strong effect of daily use of
high-potency cannabis on the odds for psychotic disorder in the whole sample—which, to our knowledge, is the largest to date to address this question. This effect was particularly visible in London and Amsterdam. Additionally, we show that, assuming causality, if high-potency cannabis types were no longer available, then 12% of cases of first-episode psychosis could be prevented across Europe, rising to 30% in London and 50% in Amsterdam. Most importantly, we provide the first direct evidence that cannabis use has an effect on variation in the incidence of psychotic disorders. We show that differences in the prevalence of daily use of cannabis, and in use of high-potency cannabis, among the controls from the different study sites made a major contribution to the striking variations in the incidence rates of psychotic disorder that we have previously reported across the same sites.
Implications of all available evidenceIn the context of the well reviewed epidemiological and biological evidence of a causal link between heavy cannabis use and psychotic disorders, our findings have substantial implications for mental health services and public health. Education is needed to inform the public about the mental health hazards of regular use of high-potency cannabis, which is becoming increasingly available worldwide.

1
5
10
15
20
25
30
35
40
45
50
55
Articles
www.thelancet.com/psychiatry Published online March 19, 2019 http://dx.doi.org/10.1016/S2215-0366(19)30048-3 3
available sampling strategies, most commonly random sampling from lists of all postal addresses and from general practitioner lists from randomly selected surgeries. To achieve representation of hard-to-reach groups (eg, young men), we then tried to oversample them using more ad-hoc approaches such as internet and newspaper advertisements, and leaflets at local stations, shops, and job centres. Controls were excluded if they had received a diagnosis of, or treatment for, psychotic disorder.
All participants provided informed, written consent. Ethical approval was provided by research ethics committees in each site.
MeasuresWe obtained sociodemographic data using the Medical Research Council Sociodemographic Schedule, as described previously.14 An updated version of the modified Cannabis Experience Questionnaire15 (CEQ
EU-GEI) was used
to gather detailed history of use of cannabis and other recreational drugs (appendix). To minimise recall bias, none of the recruitment materials for cases or controls mentioned cannabis or referred to its potential role as risk factor for psychotic disorder. Participants were asked if they had ever used cannabis in their lifetime; if the answer was yes, they were then asked to give details on their pattern of use. Questions on the type of cannabis used made no reference to its potency and allowed partici pants to report the colloquial name, in any language, of the cannabis they used.
We included six measures of cannabis use in the initial analyses, including lifetime cannabis use (ie, whether or not the individual had ever used cannabis), currently using cannabis, age at first use of cannabis,16 lifetime frequency of use (ie, the frequency that characterised the individual’s most consistent pattern of use), and money spent weekly on cannabis during their most consistent pattern of use. Using data published in the European Monitoring Centre for Drugs and Drug Addiction 2016 report17 that reported the concentration of Δ⁹-tetrahydrocannabinol (THC) in the types of cannabis available across Europe, supplemented by national data for each included country,18–26 we created the final measure of cannabis potency (appendix).
Statistical analysisWe used complete case analyses for all analyses using Stata version 14. We used inverse probability weights to account for any oversampling of controls relative to the populations at risk (appendix); we gave each control’s data a weight inversely proportional to their probability of selection given their key demographics (age, gender, and ethnicity) using census data on relevant populations. These weights were applied in all analyses.
To identify potential confounders, we used χ² and t tests to test for an association between sociodemographic data and the data on drug use with case-control status in the whole sample. On the basis of the χ² and t tests, data
on the use of other recreational drugs were included as confounders in the main analyses, with low or no use scored as 0 and use scored as 1 in categorical variables: tobacco (never used or smoked <10 cigarettes per day vs smoked ≥10 cigarettes or more per day); stimulants, hallucinogens, ketamine, and novel psychoactive substances (so-called legal highs; never tried vs ever tried); and mean number of alcoholic drinks consumed daily on an average week. All sociodemographic and drug-use variables associated with case-control status were controlled for in all analyses (appendix).
We applied adjusted logistic regression models to estimate the effect of each of the six measures of cannabis use on the odds of a psychotic disorder (ie, case status). The data have a multilevel structure because cases and controls are nested within sites. To take account of this clustering in the logistic regression analysis, we used the cluster option in Stata. We fitted interaction terms to logistic models. These interaction models, using likelihood ratio tests, were run to investigate whether individual measures of cannabis use interacted with each other to significantly increase the odds ratios (ORs) for psychotic disorder and whether the ORs for psychotic disorder of the individual measures of cannabis use varied significantly by site.
The STATA punafcc command was used to calculate the population attributable fraction (PAF) with 95% CIs for the two cannabis use measures that carried the largest adjusted OR for psychosis. The PAF measures the population effect of an exposure by providing an estimate of the proportion of disorder that would be prevented if the exposure were removed, assuming causality.
To account for potential selection bias, we did a probabilistic sensitivity analysis using the STATA episensi command.27 This analysis assumes that we can assign prior probability distributions for the bias parameters, which capture the uncertainty about those parameters, and use these distributions in a probabilistic sensitivity analysis (appendix).
Finally, we used Pearson’s correlation to test for an association between the incidence rates for psychotic disorder adjusted for ethnic minority status in each site and the prevalence of daily cannabis use and use of high-potency cannabis in the controls as representing the general population for each site.
Role of the funding sourceStudy funders contributed to the salaries of the re-search workers employed but did not participate in the study design, data analyses, data interpretation, or writing of the manuscript. All authors had full access to the study data and had final respon sibility for the decision to submit for publication.
ResultsBetween May 1, 2010, and April 1, 2015, we ap-proached 1519 patients with first-episode psychosis;
The University of Hong Kong, Hong Kong, China (Prof P C Sham); and Brain Centre Rudolf Magnus, Utrecht University Medical Centre, Utrecht, The Netherlands (Prof J van Os)
Correspondence to: Dr Marta Di Forti, Social, Genetic and Developmental Psychiatry Centre, Institute of Psychiatry, Psychology and Neuroscience, King’s College London, London SE5 8AF, UK [email protected]
See Online for appendix
1
5
10
15
20
25
30
35
40
45
50
55
Articles
4 www.thelancet.com/psychiatry Published online March 19, 2019 http://dx.doi.org/10.1016/S2215-0366(19)30048-3
356 (23%) refused to participate, 19 (1%) could not consent because of language barriers, and 14 (0·9%) were excluded because they did not meet the age inclusion criteria. Patients who refused to participate were older (p=0·0015), more likely to be women (p=0·0063) and of white European origin (p<0·0001; appendix).
Thus, 1130 cases took part. These cases were broadly representative for gender and ethnicity of the incidence sample, although younger (mean age 31·2 years [SD 10·6], median 29 years [IQR 23–37] for cases vs mean 34·5 years [12·0], median 31 years [23·0–41·0] for the
total incidence; p<0·0001; details by site are available in the appendix). All 17 sites contributed to the recruitment of 1499 population controls except for Maison Blanche, which was con sequently excluded from the analysis (appendix).
Most sites had minimal missing sociodemographic (≤3%) or CEQEU-GEI data (<5%). However, Verona, Santiago, Oviedo, Valencia, and Cuenca had at least 10% of data missing on the measures of cannabis use or on one or more of the main confounding variables; therefore, given their small sample sizes there was insufficient data to include these sites in the analysis. This resulted in 901 cases and 1237 controls for analysis.
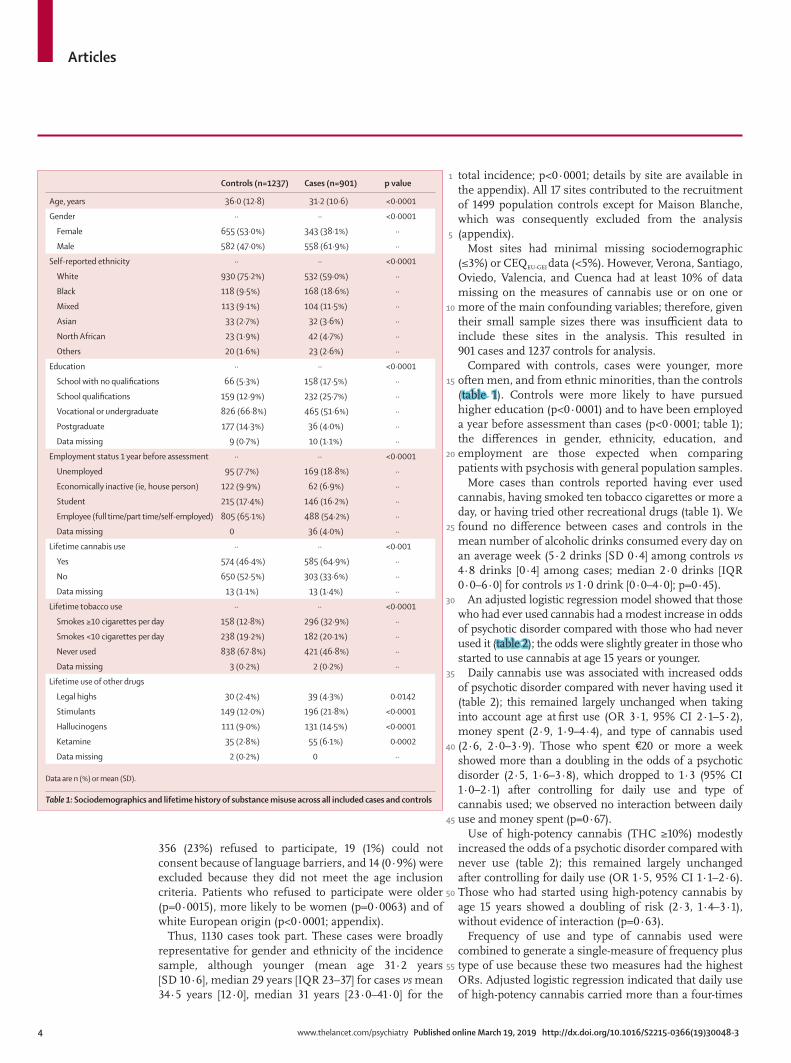
Compared with controls, cases were younger, more often men, and from ethnic minorities, than the controls (table 1). Controls were more likely to have pursued higher education (p<0·0001) and to have been employed a year before assessment than cases (p<0·0001; table 1); the differences in gender, ethnicity, education, and employment are those expected when comparing patients with psychosis with general population samples.
More cases than controls reported having ever used cannabis, having smoked ten tobacco cigarettes or more a day, or having tried other recreational drugs (table 1). We found no difference between cases and controls in the mean number of alcoholic drinks consumed every day on an average week (5·2 drinks [SD 0·4] among controls vs 4·8 drinks [0·4] among cases; median 2·0 drinks [IQR 0·0–6·0] for controls vs 1·0 drink [0·0–4·0]; p=0·45).
An adjusted logistic regression model showed that those who had ever used cannabis had a modest increase in odds of psychotic disorder compared with those who had never used it (table 2); the odds were slightly greater in those who started to use cannabis at age 15 years or younger.
Daily cannabis use was associated with increased odds of psychotic disorder compared with never having used it (table 2); this remained largely unchanged when taking into account age at first use (OR 3·1, 95% CI 2·1–5·2), money spent (2·9, 1·9–4·4), and type of cannabis used (2·6, 2·0–3·9). Those who spent €20 or more a week showed more than a doubling in the odds of a psychotic disorder (2·5, 1·6–3·8), which dropped to 1·3 (95% CI 1·0–2·1) after controlling for daily use and type of cannabis used; we observed no interaction between daily use and money spent (p=0·67).
Use of high-potency cannabis (THC ≥10%) modestly increased the odds of a psychotic disorder compared with never use (table 2); this remained largely unchanged after controlling for daily use (OR 1·5, 95% CI 1·1–2·6). Those who had started using high-potency cannabis by age 15 years showed a doubling of risk (2·3, 1·4–3·1), without evidence of interaction (p=0·63).
Frequency of use and type of cannabis used were combined to generate a single-measure of frequency plus type of use because these two measures had the highest ORs. Adjusted logistic regression indicated that daily use of high-potency cannabis carried more than a four-times
Controls (n=1237) Cases (n=901) p value
Age, years 36·0 (12·8) 31·2 (10·6) <0·0001
Gender ·· ·· <0·0001
Female 655 (53·0%) 343 (38·1%) ··
Male 582 (47·0%) 558 (61·9%) ··
Self-reported ethnicity ·· ·· <0·0001
White 930 (75·2%) 532 (59·0%) ··
Black 118 (9·5%) 168 (18·6%) ··
Mixed 113 (9·1%) 104 (11·5%) ··
Asian 33 (2·7%) 32 (3·6%) ··
North African 23 (1·9%) 42 (4·7%) ··
Others 20 (1·6%) 23 (2·6%) ··
Education ·· ·· <0·0001
School with no qualifications 66 (5·3%) 158 (17·5%) ··
School qualifications 159 (12·9%) 232 (25·7%) ··
Vocational or undergraduate 826 (66·8%) 465 (51·6%) ··
Postgraduate 177 (14·3%) 36 (4·0%) ··
Data missing 9 (0·7%) 10 (1·1%) ··
Employment status 1 year before assessment ·· ·· <0·0001
Unemployed 95 (7·7%) 169 (18·8%) ··
Economically inactive (ie, house person) 122 (9·9%) 62 (6·9%) ··
Student 215 (17·4%) 146 (16·2%) ··
Employee (full time/part time/self-employed) 805 (65·1%) 488 (54·2%) ··
Data missing 0 36 (4·0%) ··
Lifetime cannabis use ·· ·· <0·001
Yes 574 (46·4%) 585 (64·9%) ··
No 650 (52·5%) 303 (33·6%) ··
Data missing 13 (1·1%) 13 (1·4%) ··
Lifetime tobacco use ·· ·· <0·0001
Smokes ≥10 cigarettes per day 158 (12·8%) 296 (32·9%) ··
Smokes <10 cigarettes per day 238 (19·2%) 182 (20·1%) ··
Never used 838 (67·8%) 421 (46·8%) ··
Data missing 3 (0·2%) 2 (0·2%) ··
Lifetime use of other drugs
Legal highs 30 (2·4%) 39 (4·3%) 0·0142
Stimulants 149 (12·0%) 196 (21·8%) <0·0001
Hallucinogens 111 (9·0%) 131 (14·5%) <0·0001
Ketamine 35 (2·8%) 55 (6·1%) 0·0002
Data missing 2 (0·2%) 0 ··
Data are n (%) or mean (SD).
Table 1: Sociodemographics and lifetime history of substance misuse across all included cases and controls
1
5
10
15
20
25
30
35
40
45
50
55
Articles
www.thelancet.com/psychiatry Published online March 19, 2019 http://dx.doi.org/10.1016/S2215-0366(19)30048-3 5
Never used(reference)
OR
Rare use of THC<10%
Rare use of THC≥10%
Used THC<10% morethan once a week
Frequency and type of cannabis use
Used THC≥10% morethan once a week
Daily use of THC<10%
Daily use of THC≥10%
1
2
4
6
8
10
0
0·93 0·841·11 0·96
1·711·36
2·121·57
3·08
2·19
4·78
5·81
Crude ORAdjusted OR
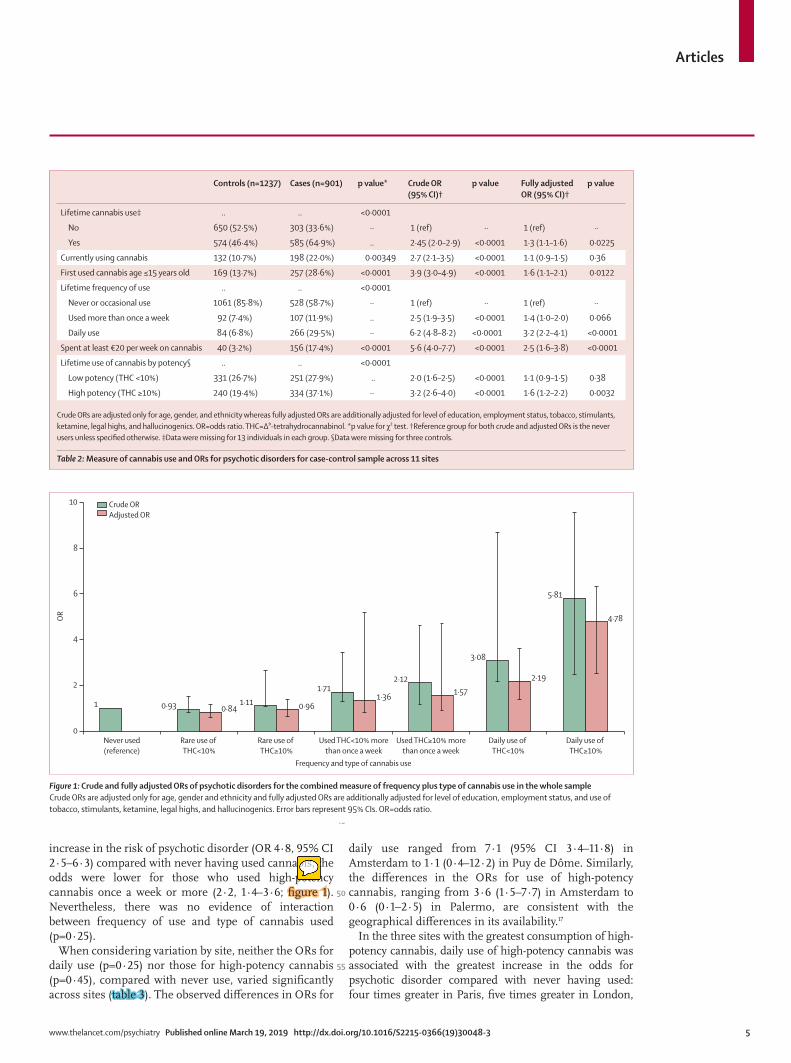
increase in the risk of psychotic disorder (OR 4·8, 95% CI 2·5–6·3) compared with never having used cannabis; the odds were lower for those who used high-potency cannabis once a week or more (2·2, 1·4–3·6; figure 1). Nevertheless, there was no evidence of interaction between frequency of use and type of cannabis used (p=0·25).
When considering variation by site, neither the ORs for daily use (p=0·25) nor those for high-potency cannabis (p=0·45), compared with never use, varied significantly across sites (table 3). The observed differences in ORs for
daily use ranged from 7·1 (95% CI 3·4–11·8) in Amsterdam to 1·1 (0·4–12·2) in Puy de Dôme. Similarly, the differences in the ORs for use of high-potency cannabis, ranging from 3·6 (1·5–7·7) in Amsterdam to 0·6 (0·1–2·5) in Palermo, are consistent with the geographical differences in its availability.17
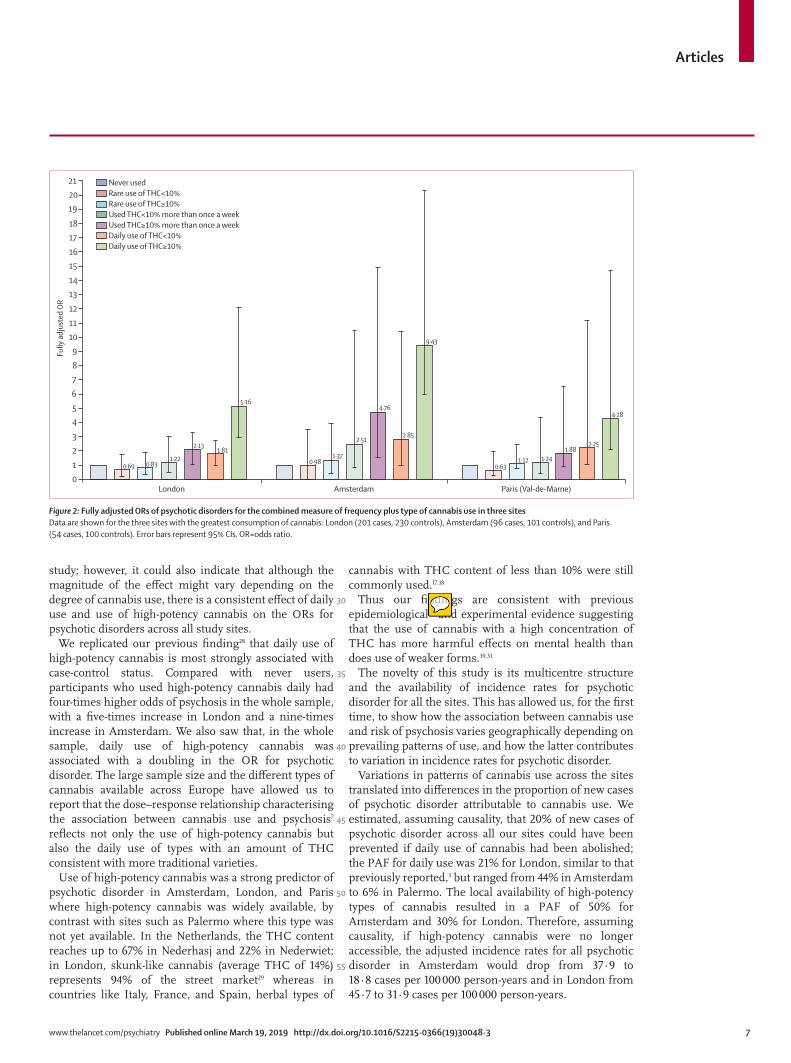
In the three sites with the greatest consumption of high-potency cannabis, daily use of high-potency cannabis was associated with the greatest increase in the odds for psychotic disorder compared with never having used: four times greater in Paris, five times greater in London,
Controls (n=1237) Cases (n=901) p value* Crude OR (95% CI)†
p value Fully adjusted OR (95% CI)†
p value
Lifetime cannabis use‡ .. .. <0·0001
No 650 (52·5%) 303 (33·6%) ·· 1 (ref) ·· 1 (ref) ··
Yes 574 (46·4%) 585 (64·9%) .. 2·45 (2·0–2·9) <0·0001 1·3 (1·1–1·6) 0·0225
Currently using cannabis 132 (10·7%) 198 (22·0%) 0·00349 2·7 (2·1–3·5) <0·0001 1·1 (0·9–1·5) 0·36
First used cannabis age ≤15 years old 169 (13·7%) 257 (28·6%) <0·0001 3·9 (3·0–4·9) <0·0001 1·6 (1·1–2·1) 0·0122
Lifetime frequency of use .. .. <0·0001
Never or occasional use 1061 (85·8%) 528 (58·7%) ·· 1 (ref) ·· 1 (ref) ··
Used more than once a week 92 (7·4%) 107 (11·9%) .. 2·5 (1·9–3·5) <0·0001 1·4 (1·0–2·0) 0·066
Daily use 84 (6·8%) 266 (29·5%) ·· 6·2 (4·8–8·2) <0·0001 3·2 (2·2–4·1) <0·0001
Spent at least €20 per week on cannabis 40 (3·2%) 156 (17·4%) <0·0001 5·6 (4·0–7·7) <0·0001 2·5 (1·6–3·8) <0·0001
Lifetime use of cannabis by potency§ .. .. <0·0001
Low potency (THC <10%) 331 (26·7%) 251 (27·9%) .. 2·0 (1·6–2·5) <0·0001 1·1 (0·9–1·5) 0·38
High potency (THC ≥10%) 240 (19·4%) 334 (37·1%) ·· 3·2 (2·6–4·0) <0·0001 1·6 (1·2–2·2) 0·0032
Crude ORs are adjusted only for age, gender, and ethnicity whereas fully adjusted ORs are additionally adjusted for level of education, employment status, tobacco, stimulants, ketamine, legal highs, and hallucinogenics. OR=odds ratio. THC=Δ⁹-tetrahydrocannabinol. *p value for χ² test. †Reference group for both crude and adjusted ORs is the never users unless specified otherwise. ‡Data were missing for 13 individuals in each group. §Data were missing for three controls.
Table 2: Measure of cannabis use and ORs for psychotic disorders for case-control sample across 11 sites
Figure 1: Crude and fully adjusted ORs of psychotic disorders for the combined measure of frequency plus type of cannabis use in the whole sampleCrude ORs are adjusted only for age, gender and ethnicity and fully adjusted ORs are additionally adjusted for level of education, employment status, and use of tobacco, stimulants, ketamine, legal highs, and hallucinogenics. Error bars represent 95% CIs. OR=odds ratio.
k1641103
Sticky Note
“the odds were lower for those who used high-potency cannabis once a week or more” – this should be changed to “the odds were lower for those who used low-potency cannabis daily” [you can see that this is the correct odds ratio of 2.2 based on Figure 1]
1
5
10
15
20
25
30
35
40
45
50
55
Articles
6 www.thelancet.com/psychiatry Published online March 19, 2019 http://dx.doi.org/10.1016/S2215-0366(19)30048-3
and more than nine times greater in Amsterdam (figure 2).Based on the prevalence of daily cannabis use, and use
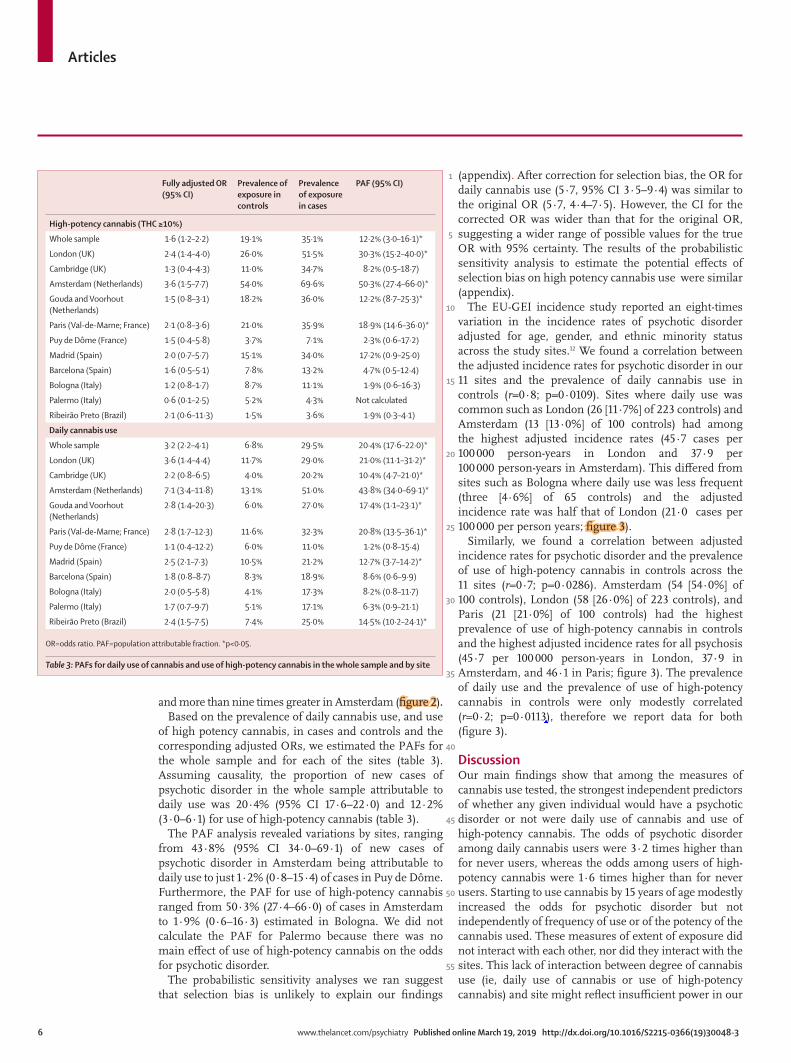
of high potency cannabis, in cases and controls and the corresponding adjusted ORs, we estimated the PAFs for the whole sample and for each of the sites (table 3). Assuming causality, the proportion of new cases of psychotic disorder in the whole sample attributable to daily use was 20·4% (95% CI 17·6–22·0) and 12·2% (3·0–6·1) for use of high-potency cannabis (table 3).
The PAF analysis revealed variations by sites, ranging from 43·8% (95% CI 34·0–69·1) of new cases of psychotic disorder in Amsterdam being attributable to daily use to just 1·2% (0·8–15·4) of cases in Puy de Dôme. Furthermore, the PAF for use of high-potency cannabis ranged from 50·3% (27·4–66·0) of cases in Amsterdam to 1·9% (0·6–16·3) estimated in Bologna. We did not calculate the PAF for Palermo because there was no main effect of use of high-potency cannabis on the odds for psychotic disorder.
The probabilistic sensitivity analyses we ran suggest that selection bias is unlikely to explain our findings
(appendix). After correction for selection bias, the OR for daily cannabis use (5·7, 95% CI 3·5–9·4) was similar to the original OR (5·7, 4·4–7·5). However, the CI for the corrected OR was wider than that for the original OR, suggesting a wider range of possible values for the true OR with 95% certainty. The results of the probabilistic sensitivity analysis to estimate the potential effects of selection bias on high potency cannabis use were similar (appendix).
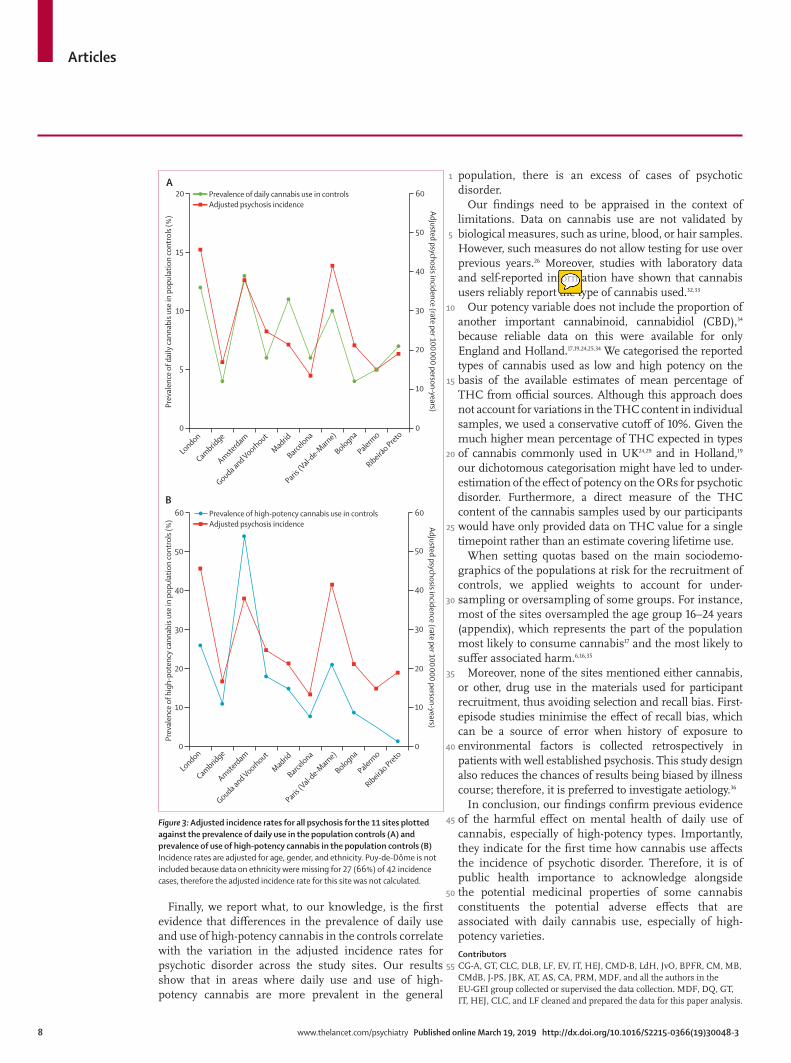
The EU-GEI incidence study reported an eight-times variation in the incidence rates of psychotic disorder adjusted for age, gender, and ethnic minority status across the study sites.12 We found a correlation between the adjusted incidence rates for psychotic disorder in our 11 sites and the prevalence of daily cannabis use in controls (r=0·8; p=0·0109). Sites where daily use was common such as London (26 [11·7%] of 223 controls) and Amsterdam (13 [13·0%] of 100 controls) had among the highest adjusted incidence rates (45·7 cases per 100 000 person-years in London and 37·9 per 100 000 person-years in Amsterdam). This differed from sites such as Bologna where daily use was less frequent (three [4·6%] of 65 controls) and the adjusted incidence rate was half that of London (21·0 cases per 100 000 per person years; figure 3).
Similarly, we found a correlation between adjusted incidence rates for psychotic disorder and the prevalence of use of high-potency cannabis in controls across the 11 sites (r=0·7; p=0·0286). Amsterdam (54 [54·0%] of 100 controls), London (58 [26·0%] of 223 controls), and Paris (21 [21·0%] of 100 controls) had the highest prevalence of use of high-potency cannabis in controls and the highest adjusted incidence rates for all psychosis (45·7 per 100 000 person-years in London, 37·9 in Amsterdam, and 46·1 in Paris; figure 3). The prevalence of daily use and the prevalence of use of high-potency cannabis in controls were only modestly correlated (r=0·2; p=0·0113), therefore we report data for both (figure 3).
DiscussionOur main findings show that among the measures of cannabis use tested, the strongest independent predictors of whether any given individual would have a psychotic disorder or not were daily use of cannabis and use of high-potency cannabis. The odds of psychotic disorder among daily cannabis users were 3·2 times higher than for never users, whereas the odds among users of high-potency cannabis were 1·6 times higher than for never users. Starting to use cannabis by 15 years of age modestly increased the odds for psychotic disorder but not independently of frequency of use or of the potency of the cannabis used. These measures of extent of exposure did not interact with each other, nor did they interact with the sites. This lack of interaction between degree of cannabis use (ie, daily use of cannabis or use of high-potency cannabis) and site might reflect insufficient power in our
Fully adjusted OR (95% CI)
Prevalence of exposure in controls
Prevalence of exposure in cases
PAF (95% CI)
High-potency cannabis (THC ≥10%)
Whole sample 1·6 (1·2–2·2) 19·1% 35·1% 12·2% (3·0–16·1)*
London (UK) 2·4 (1·4–4·0) 26·0% 51·5% 30·3% (15·2–40·0)*
Cambridge (UK) 1·3 (0·4–4·3) 11·0% 34·7% 8·2% (0·5–18·7)
Amsterdam (Netherlands) 3·6 (1·5–7·7) 54·0% 69·6% 50·3% (27·4–66·0)*
Gouda and Voorhout (Netherlands)
1·5 (0·8–3·1) 18·2% 36·0% 12·2% (8·7–25·3)*
Paris (Val-de-Marne; France) 2·1 (0·8–3·6) 21·0% 35·9% 18·9% (14·6–36·0)*
Puy de Dôme (France) 1·5 (0·4–5·8) 3·7% 7·1% 2·3% (0·6–17·2)
Madrid (Spain) 2·0 (0·7–5·7) 15·1% 34·0% 17·2% (0·9–25·0)
Barcelona (Spain) 1·6 (0·5–5·1) 7·8% 13·2% 4·7% (0·5–12·4)
Bologna (Italy) 1·2 (0·8–1·7) 8·7% 11·1% 1·9% (0·6–16·3)
Palermo (Italy) 0·6 (0·1–2·5) 5·2% 4·3% Not calculated
Ribeirão Preto (Brazil) 2·1 (0·6–11·3) 1·5% 3·6% 1·9% (0·3–4·1)
Daily cannabis use
Whole sample 3·2 (2·2–4·1) 6·8% 29·5% 20·4% (17·6–22·0)*
London (UK) 3·6 (1·4–4·4) 11·7% 29·0% 21·0% (11·1–31·2)*
Cambridge (UK) 2·2 (0·8–6·5) 4·0% 20·2% 10·4% (4·7–21·0)*
Amsterdam (Netherlands) 7·1 (3·4–11·8) 13·1% 51·0% 43·8% (34·0–69·1)*
Gouda and Voorhout (Netherlands)
2·8 (1·4–20·3) 6·0% 27·0% 17·4% (1·1–23·1)*
Paris (Val-de-Marne; France) 2·8 (1·7–12·3) 11·6% 32·3% 20·8% (13·5–36·1)*
Puy de Dôme (France) 1·1 (0·4–12·2) 6·0% 11·0% 1·2% (0·8–15·4)
Madrid (Spain) 2·5 (2·1–7·3) 10·5% 21·2% 12·7% (3·7–14·2)*
Barcelona (Spain) 1·8 (0·8–8·7) 8·3% 18·9% 8·6% (0·6–9·9)
Bologna (Italy) 2·0 (0·5–5·8) 4·1% 17·3% 8·2% (0·8–11·7)
Palermo (Italy) 1·7 (0·7–9·7) 5·1% 17·1% 6·3% (0·9–21·1)
Ribeirão Preto (Brazil) 2·4 (1·5–7·5) 7·4% 25·0% 14·5% (10·2–24·1)*
OR=odds ratio. PAF=population attributable fraction. *p<0·05.
Table 3: PAFs for daily use of cannabis and use of high-potency cannabis in the whole sample and by site
martadiforti
Inserted Text
My mistake the correct p value for this r=0.2 is p=0.0413
1
5
10
15
20
25
30
35
40
45
50
55
Articles
www.thelancet.com/psychiatry Published online March 19, 2019 http://dx.doi.org/10.1016/S2215-0366(19)30048-3 7
21
20
19
18
17
16
15
14
13
12
11
10
9
8
7
6
5
4
3
2
1
0London
Fully
adj
uste
d O
R
Amsterdam Paris (Val-de-Marne)
Never usedRare use of THC<10%Rare use of THC≥10%Used THC<10% more than once a weekUsed THC≥10% more than once a weekDaily use of THC<10%Daily use of THC≥10%
0·69 0·831·22
2·131·81
5·16
0·981·37
2·51
4·76
2·85
0·631·12 1·24
1·882·25
4·28
9·43
study; however, it could also indicate that although the magnitude of the effect might vary depending on the degree of cannabis use, there is a consistent effect of daily use and use of high-potency cannabis on the ORs for psychotic disorders across all study sites.
We replicated our previous finding28 that daily use of high-potency cannabis is most strongly associated with case-control status. Compared with never users, participants who used high-potency cannabis daily had four-times higher odds of psychosis in the whole sample, with a five-times increase in London and a nine-times increase in Amsterdam. We also saw that, in the whole sample, daily use of high-potency cannabis was associated with a doubling in the OR for psychotic disorder. The large sample size and the different types of cannabis available across Europe have allowed us to report that the dose–response relationship characterising the association between cannabis use and psychosis7 reflects not only the use of high-potency cannabis but also the daily use of types with an amount of THC consistent with more traditional varieties.
Use of high-potency cannabis was a strong predictor of psychotic disorder in Amsterdam, London, and Paris where high-potency cannabis was widely available, by contrast with sites such as Palermo where this type was not yet available. In the Netherlands, the THC content reaches up to 67% in Nederhasj and 22% in Nederwiet; in London, skunk-like cannabis (average THC of 14%) represents 94% of the street market29 whereas in countries like Italy, France, and Spain, herbal types of
cannabis with THC content of less than 10% were still commonly used.17,18
Thus our findings are consistent with previous epidemiological28 and experimental evidence suggesting that the use of cannabis with a high concentration of THC has more harmful effects on mental health than does use of weaker forms.30,31
The novelty of this study is its multicentre structure and the availability of incidence rates for psychotic disorder for all the sites. This has allowed us, for the first time, to show how the association between cannabis use and risk of psychosis varies geographically depending on prevailing patterns of use, and how the latter contributes to variation in incidence rates for psychotic disorder.
Variations in patterns of cannabis use across the sites translated into differences in the proportion of new cases of psychotic disorder attributable to cannabis use. We estimated, assuming causality, that 20% of new cases of psychotic disorder across all our sites could have been prevented if daily use of cannabis had been abolished; the PAF for daily use was 21% for London, similar to that previously reported,3 but ranged from 44% in Amsterdam to 6% in Palermo. The local availability of high-potency types of cannabis resulted in a PAF of 50% for Amsterdam and 30% for London. Therefore, assuming causality, if high-potency cannabis were no longer accessible, the adjusted incidence rates for all psychotic disorder in Amsterdam would drop from 37·9 to 18·8 cases per 100 000 person-years and in London from 45·7 to 31·9 cases per 100 000 person-years.
Figure 2: Fully adjusted ORs of psychotic disorders for the combined measure of frequency plus type of cannabis use in three sitesData are shown for the three sites with the greatest consumption of cannabis: London (201 cases, 230 controls), Amsterdam (96 cases, 101 controls), and Paris (54 cases, 100 controls). Error bars represent 95% CIs. OR=odds ratio.
k1641103
Sticky Note
Reference 28 should be moved to the end of the sentence with reference 30 and 31 for consistency, because refs 30 and 31 cover both epidemiological and experimental findings
1
5
10
15
20
25
30
35
40
45
50
55
Articles
8 www.thelancet.com/psychiatry Published online March 19, 2019 http://dx.doi.org/10.1016/S2215-0366(19)30048-3
Prev
alen
ce o
f dai
ly ca
nnab
is us
e in
pop
ulat
ion
cont
rols
(%)
Prev
alen
ce o
f hig
h-po
tenc
y ca
nnab
is us
e in
pop
ulat
ion
cont
rols
(%)
Adjusted psychosis incidence (rate per 100 000 person-years)
London
Cambridge
Amsterdam
Gouda and Voorhout
Madrid
Barcelona
Paris (V
al-de-M
arne)
Bologna
Palermo
Ribeirão Preto
London
Cambridge
Amsterdam
Gouda and Voorhout
Madrid
Barcelona
Paris (V
al-de-M
arne)
Bologna
Palermo
Ribeirão Preto
Adjusted psychosis incidence (rate per 100 000 person-years)
Prevalence of daily cannabis use in controlsAdjusted psychosis incidence
Prevalence of high-potency cannabis use in controlsAdjusted psychosis incidence
A
B
20
15
10
10
20
30
40
50
60
5
0 0
10
20
30
40
50
60
0
10
20
30
40
50
60
0
Finally, we report what, to our knowledge, is the first evidence that differences in the prevalence of daily use and use of high-potency cannabis in the controls correlate with the variation in the adjusted incidence rates for psychotic disorder across the study sites. Our results show that in areas where daily use and use of high-potency cannabis are more prevalent in the general
population, there is an excess of cases of psychotic disorder.
Our findings need to be appraised in the context of limitations. Data on cannabis use are not validated by biological measures, such as urine, blood, or hair samples. However, such measures do not allow testing for use over previous years.26 Moreover, studies with laboratory data and self-reported information have shown that cannabis users reliably report the type of cannabis used.32,33
Our potency variable does not include the proportion of another important cannabinoid, cannabidiol (CBD),34 because reliable data on this were available for only England and Holland.17,19,24,25,34 We categorised the reported types of cannabis used as low and high potency on the basis of the available estimates of mean percentage of THC from official sources. Although this approach does not account for variations in the THC content in individual samples, we used a conservative cutoff of 10%. Given the much higher mean percentage of THC expected in types of cannabis commonly used in UK24,29 and in Holland,19 our dichotomous categorisation might have led to under-estimation of the effect of potency on the ORs for psychotic disorder. Furthermore, a direct measure of the THC content of the cannabis samples used by our participants would have only provided data on THC value for a single timepoint rather than an estimate covering lifetime use.
When setting quotas based on the main sociodemo-graphics of the populations at risk for the recruitment of controls, we applied weights to account for under-sampling or oversampling of some groups. For instance, most of the sites oversampled the age group 16–24 years (appendix), which represents the part of the population most likely to consume cannabis17 and the most likely to suffer associated harm.6,16,35
Moreover, none of the sites mentioned either cannabis, or other, drug use in the materials used for participant recruitment, thus avoiding selection and recall bias. First-episode studies minimise the effect of recall bias, which can be a source of error when history of exposure to environmental factors is collected retrospectively in patients with well established psychosis. This study design also reduces the chances of results being biased by illness course; therefore, it is preferred to investigate aetiology.36
In conclusion, our findings confirm previous evidence of the harmful effect on mental health of daily use of cannabis, especially of high-potency types. Importantly, they indicate for the first time how cannabis use affects the incidence of psychotic disorder. Therefore, it is of public health importance to acknowledge alongside the potential medicinal properties of some cannabis constituents the potential adverse effects that are associated with daily cannabis use, especially of high-potency varieties.ContributorsCG-A, GT, CLC, DLB, LF, EV, IT, HEJ, CMD-B, LdH, JvO, BPFR, CM, MB, CMdB, J-PS, JBK, AT, AS, CA, PRM, MDF, and all the authors in the EU-GEI group collected or supervised the data collection. MDF, DQ, GT, IT, HEJ, CLC, and LF cleaned and prepared the data for this paper analysis.
Figure 3: Adjusted incidence rates for all psychosis for the 11 sites plotted against the prevalence of daily use in the population controls (A) and prevalence of use of high-potency cannabis in the population controls (B)Incidence rates are adjusted for age, gender, and ethnicity. Puy-de-Dôme is not included because data on ethnicity were missing for 27 (66%) of 42 incidence cases, therefore the adjusted incidence rate for this site was not calculated.
k1641103
Sticky Note
This should be changed to "reliably report frequency of use and the type of cannabis used"

1
5
10
15
20
25
30
35
40
45
50
55
Articles
www.thelancet.com/psychiatry Published online March 19, 2019 http://dx.doi.org/10.1016/S2215-0366(19)30048-3 9
MDF did the data analysis and wrote the findings in the initial manuscript. TPF, HEJ, DQ, and GT contributed to creation of the figures and tables. CM, CML, RMM, PCS, JvO, BPFR, LdH, J-PS, DB, IT, ML, TPF, JBK, CA, and PBJ provided a careful statistical and methodological revision of the manuscript and contributed to the final draft. RMM, ML, and CM contributed to the interpretation of the results. All authors had full access to all data (including statistical reports and tables) in the study and take responsibility for the integrity of the data and the accuracy of the data analysis.
Declaration of interestsRMM reports personal fees from Janssen, Lundbeck, Sunovion, and Otsuka, outside of the submitted work. MDF reports personal fees from Janssen, outside the submitted work. MB reports grants and personal fees from Adamed, Janssen-Cilag, Otsuka, and Abbiotics; personal fees from Angelini and Casen Recordati; and grants from Lundbeck and Takeda, outside of the submitted work. PBJ reports personal fees from being a member of the scientific advisory boards for Janssen and Ricordati, outside of the submitted work. CA reports personal fees from Acadia, Ambrosseti, Gedeon Richter, Janssen Cilag, Lundbeck, Merck, Otsuka, Roche, Servier, Shire, Schering Plough, Sumitomo Dainippon Pharma, Sunovion, and Takeda; and grants from CIBERSAM, Familia Alonso, Fundación Alicia Koplowitz, the European Commission, the Spanish Ministry of Science and Universities, and the Comunidad de Madrid, during the conduct of the study. All other authors declare no competing interests.
AcknowledgmentsThis study was funded by the Medical Research Council, the European Community’s Seventh Framework Program grant (agreement HEALTH-F2-2009-241909 [Project EU-GEI]), São Paulo Research Foundation (grant 2012/0417-0), the National Institute for Health Research (NIHR) Biomedical Research Centre (BRC) at South London and Maudsley NHS Foundation Trust and King’s College London, the NIHR BRC at University College London, and the Wellcome Trust (grant 101272/Z/12/Z).
References1 Grucza RA, Agrawal A, Krauss MJ, Cavazos-Rehg PA, Bierut LJ.
Recent trends in the prevalence of marijuana use and associated disorders in the united states. JAMA Psychiatry 2016; 73: 300–01.
2 Hall W, Lynskey M. Evaluating the public health impacts of legalizing recreational cannabis use in the United States. Addiction 2016; 111: 1764–73.
3 Wilkinson ST, Yarnell S, Radhakrishnan R, Ball SA, D’Souza DC. Marijuana legalization: impact on physicians and public health. Annu Rev Med 2016; 67: 453–66.
4 Gage SH, Hickman M, Zammit S. Association between cannabis and psychosis: epidemiologic evidence. Biol Psychiatry 2016; 79: 549–56.
5 Mustonen A, Niemelä S, Nordström T, et al. Adolescent cannabis use, baseline prodromal symptoms and the risk of psychosis. Br J Psychiatry 2018; 212: 227–33.
6 Murray RM, Englund A, Abi-Dargham A, et al. Cannabis-associated psychosis: neural substrate and clinical impact. Neuropharmacology 2017; 124: 89–104.
7 Marconi A, Di Forti M, Lewis CM, Murray RM, Vassos E. Meta-analysis of the association between the level of cannabis use and risk of psychosis. Schizophr Bull 2016; 42: 1262–69.
8 Ksir C, Hart CL. Cannabis and psychosis: a critical overview of the relationship. Curr Psychiatry Rep 2016; 18: 12.
9 Hill M. Perspective: be clear about the real risks. Nature 2015; 525: S14.10 Boydell J, van Os J, Caspi A, et al. Trends in cannabis use prior to
first presentation with schizophrenia, in South-East London between 1965 and 1999. Psychol Med 2006; 36: 1441–46.
11 McGrath J, Saha S, Welham J, El Saadi O, MacCauley C, Chant D. A systematic review of the incidence of schizophrenia: the distribution of rates and the influence of sex, urbanicity, migrant status and methodology. BMC Med 2004; 2: 13.
12 Jongsma HE, Gayer-Anderson C, Lasalvia A, et al. Treated incidence of psychotic disorders in the multinational EU-GEI study. JAMA Psychiatry 2018; 75: 36–46.
13 McGuffin P, Farmer A, Harvey I. A polydiagnostic application of operational criteria in studies of psychotic illness: development and reliability of the opcrit system. Arch Gen Psychiatry 1991; 48: 764–70.
14 Mallett R, Leff J, Bhugra D, Pang D, Zhao JH. Social environment, ethnicity and schizophrenia: a case-control study. Soc Psychiatry Psychiatr Epidemiol 2002; 37: 329–35.
15 Di Forti M, Morgan C, Dazzan P, et al. High-potency cannabis and the risk of psychosis. Br J Psychiatry 2009; 195: 488–91.
16 Casadio P, Fernandes C, Murray RM, Di Forti M. Cannabis use in young people: the risk for schizophrenia. Neurosci Biobehav Rev 2011; 35: 1779–87.
17 European Monitoring Centre for Drugs and Drug Addiction. European drug report 2016: trends and developments. Luxembourg: Publications Office of the European Union, 2016.
18 European Monitoring Centre for Drugs and Drug Addiction, Spanish Ministry of Health and Consumer Affairs. Spain national report (2011 data) to the EMCDDA 2012. Madrid: Government Delegation for National Plan on Drugs, 2012.
19 Niesink R, Rigter S. THC-concentraties in wiet, nederwiet en hasj in Nederlandse coffeeshops (2012–2013). AF1221. Utrecht: Trimbos-instituut, 2013.
20 Brisacier A-C, Cadet-Taïrou A, Díaz Gómez C, et al. Drogues, chiffres cles. Paris: Observatoire Francais des Drogues et des Toxicomanies, 2015.
21 Zamengo L, Frison G, Bettin C, Sciarrone R. Cannabis potency in the Venice area (Italy): update 2013. Drug Test Anal 2015; 7: 255–58.
22 Niesink RJM, Rigter S, Koeter MW, Brunt TM. Potency trends of Δ⁹-tetrahydrocannabinol, cannabidiol and cannabinol in cannabis in the Netherlands: 2005–15. Addiction 2015; 110: 1941–50.
23 de Oliveira GL, Voloch MH, Sztulman GB, Neto ON, Yonamine M. Cannabinoid contents in cannabis products seized in São Paulo, Brazil, 2006–2007. Forensic Toxicol 2008; 26: 31–35.
24 Potter DJ, Clark P, Brown MB. Potency of Δ⁹-THC and other cannabinoids in cannabis in England in 2005: implications for psychoactivity and pharmacology. J Forensic Sci 2008; 53: 90–94.
25 Hardwick S, King S. Home Office cannabis potency study 2008. London: Home Office Scientific Development Branch, 2008.
26 Taylor M, Sullivan J, Ring SM, Macleod J, Hickman M. Assessment of rates of recanting and hair testing as a biological measure of drug use in a general population sample of young people. Addiction 2016; 112: 477–85.
27 Orsini N, Bellocco R, Bottai M, Wolk A, Greenland S. A tool for deterministic and probabilistic sensitivity analysis of epidemiologic studies. Stata J 2008; 8: 29–48.
28 Di Forti M, Marconi A, Carra E, et al. Proportion of patients in south London with first-episode psychosis attributable to use of high potency cannabis: a case-control study. Lancet Psychiatry 2015; 2: 233–38.
29 Potter DJ, Hammond K, Tuffnell S, Walker C, Forti MD. Potency of Δ⁹-tetrahydrocannabinol and other cannabinoids in cannabis in England in 2016: implications for public health and pharmacology. Drug Test Anal 2018; 10: 628–35.
30 Freeman TP, van der Pol P, Kuijpers W, et al. Changes in cannabis potency and first-time admissions to drug treatment: a 16-year study in the Netherlands. Psychol Med 2018; 48: 2346–52.
31 Murray RM, Quigley H, Quattrone D, Englund A, Di Forti M. Traditional marijuana, high-potency cannabis and synthetic cannabinoids: increasing risk for psychosis. World Psychiatry 2016; 15: 195–204.
32 Freeman TP, Morgan CJA, Hindocha C, Schafer G, Das RK, Curran HV. Just say ‘know’: how do cannabinoid concentrations influence users’ estimates of cannabis potency and the amount they roll in joints? Addiction 2014; 109: 1686–94.
33 Meijer JH, Dekker N, Koeter MW, et al. Cannabis and cognitive performance in psychosis: a cross-sectional study in patients with non-affective psychotic illness and their unaffected siblings. Psychol Med 2012; 42: 705–16.
34 Englund A, Freeman TP, Murray RM, McGuire P. Can we make cannabis safer? Lancet Psychiatry 2017; 4: 643–48.
35 Mokrysz C, Freeman TP, Korkki S, Griffiths K, Curran HV. Are adolescents more vulnerable to the harmful effects of cannabis than adults? A placebo-controlled study in human males. Transl Psychiatry 2016; 6: e961.
36 Marshall M, Lewis S, Lockwood A, Drake R, Jones P, Croudace T. Association between duration of untreated psychosis and outcome in cohorts of first-episode patients: a systematic review. Arch Gen Psychiatry 2005; 62: 975–83.
k1641103
Sticky Note
Reference 33 should be changed to: Curran, H. V., Hindocha, C., Morgan, C. J., Shaban, N., Das, R. K., & Freeman, T. P. (2018). Which biological and self-report measures of cannabis use predict cannabis dependency and acute psychotic-like effects? Psychol Med 2018; 1-7. https://doi.org/ 10.1017/S003329171800226X�

Marijuana use is associated with intimate partner violence perpetration among men arrested for domestic violence
Ryan C. Shorey1, Ellen Haynes1, Meagan Brem2, Autumn Rae Florimbio2, Hannah Grigorian2, and Gregory L. Stuart2
1Ohio University
2University of Tennessee – Knoxville
Abstract
Intimate partner violence (IPV) is a serious public health problem. Substance use, particularly
alcohol, is a robust risk factor for IPV. There is a small but growing body of research
demonstrating that marijuana use is positively associated with IPV perpetration. However, research
on marijuana use and IPV has failed to control for other known predictors of IPV that may account
for the positive association between marijuana use and IPV perpetration. Therefore, the current
study examined whether marijuana use was associated with IPV perpetration after controlling for
alcohol use and problems, antisocial personality symptoms, and relationship satisfaction, all
known risk factors for IPV. Participants were men arrested for domestic violence and court-
referred to batterer intervention programs (N = 269). Findings demonstrated that marijuana use
was positively and significantly associated with psychological, physical, and sexual IPV
perpetration, even after controlling for alcohol use and problems, antisocial personality symptoms,
and relationship satisfaction. Moreover, marijuana use and alcohol use and problems interacted to
predict sexual IPV, such that marijuana use was associated with sexual IPV at high, but not low,
levels of alcohol use and problems. These findings lend additional support to the body of research
demonstrating that marijuana use is positively associated with IPV perpetration in a variety of
samples. Results suggest that additional, rigorous research is needed to further explore why and
under what conditions marijuana is associated with IPV perpetration.
Keywords
Marijuana; intimate partner violence; substance use; domestic violence
Intimate partner violence (IPV) is a difficult to treat and prevalent public health problem.
IPV includes psychological, physical, and sexual aggression (Straus, Hamby, Boney-McCoy,
& Sugarman, 1996). In the general population, annual prevalence rates of IPV are
approximately 80% for psychological IPV, 25% for physical IPV, and 20% for sexual IPV
(Archer, 2000; Shorey, Cornelius, & Bell, 2008). Not surprisingly, victims of IPV experience
numerous negative consequences, including depression (Devries et al., 2013), anxiety
(Nathanson, Shorey, Tirone, & Rhatigan, 2012), increased substance use (Devries et al.,
Corresponding Author: Ryan C. Shorey, Ph.D., Assistant Professor, Ohio University, Department of Psychology, 239 Porter Hall, Athens, Ohio 45701, Phone: (740) 597-3298, [email protected].
HHS Public AccessAuthor manuscriptTransl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Published in final edited form as:Transl Issues Psychol Sci. 2018 ; 4(1): 108–118. doi:10.1037/tps0000140.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
2014), physical injuries (Archer, 2000; Campbell, 2002), suicidal ideation (Devries et al.,
2013), and in the most severe cases, death (Davis, 2010). Unfortunately, psychosocial
intervention efforts aimed at reducing IPV perpetration among men arrested for domestic
violence have been largely unsuccessful. Meta-analyses on the effectiveness of batterer
intervention programs (BIPs), programs individuals who are arrested for domestic violence
are court-mandated to attend, demonstrate small effect sizes (Babcock, Green, & Robie,
2004) or no effect at all (Feder & Wilson, 2005). Thus, there is considerable room for
improving these programs.
Researchers have argued that interventions for IPV should include a focus on reducing
substance use (Stuart, Temple, & Moore, 2007), as substance use, particularly alcohol, is
known to be a robust risk factor for IPV perpetration across populations (Foran & O’Leary,
2008; Shorey, Stuart, & Cornelius, 2011). Indeed, preliminary evidence suggested that BIPs
have better short-term outcomes (i.e., reduced IPV) when adjunctive alcohol interventions
are included; however, the positive effects of this brief alcohol intervention fade over time
(Stuart et al., 2013). This may be due, in part, to extensive drug use among men arrested for
domestic violence (e.g., Stuart et al., 2004), which may have compromised IPV treatment
outcomes. Thus, researchers have recently advocated for additional research on substances
other than alcohol to determine their relations to IPV (Shorey, Haynes, Strauss, Temple, &
Stuart, 2017; Testa & Brown, 2015) since these substances may impact intervention
outcomes. Specifically, researchers have advocated for studies on the association between
marijuana and IPV, as well as the effects of combined alcohol and marijuana use on IPV
(Shorey et al., 2017; Testa & Brown, 2015).
Marijuana use is prevalent among men arrested for domestic violence and some research
suggests it is positively associated with IPV perpetration (Moore et al., 2008; Moore &
Stuart, 2004; Moore & Stuart, 2005; Testa & Brown, 2015). This research is particularly
important for a number of reasons, especially with the increasing legalization of marijuana
for both medical and recreational purposes in many US states, as it is imperative that public
health officials and policy makers have a clear understanding of how marijuana use
intersects with other important public health problems, such as IPV. Thus, the purpose of the
present study was to examine the association between marijuana use and IPV perpetration
among men arrested for domestic violence and court-referred to BIPs, controlling for known
IPV risk factors of alcohol use and problems, antisocial personality symptoms, and
relationship satisfaction.
Marijuana and IPV
The theoretical relationship between marijuana and IPV has received scant attention.
Although still underdeveloped, it has been theoretically postulated that, for some
individuals, marijuana may lead to increased negative effects (e.g., irritability, anxiety),
which may then lead to negative couple-related outcomes, such as IPV (Testa & Brown,
2015). A meta-analysis on the association between marijuana and IPV perpetration
demonstrated that, across 14 studies, there was a positive association between marijuana use
and physical (d = .21) and psychological (d = .35), but not sexual, IPV (Moore et al., 2008).
Since this meta-analysis, a review of 30 studies concluded that marijuana use distally (e.g.,
Shorey et al. Page 2
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
frequency of use in the past year) demonstrated modest, but positive, associations with distal
reports of IPV (e.g., frequency of IPV perpetration in past year; Testa & Brown, 2015). In
addition, Moore and Stuart (2004) reported that 53% of their sample of men arrested for
domestic violence reported past year marijuana use. However, the majority of prior studies
examining marijuana and IPV failed to control for known risk factors for IPV that may
account for this relationship. Specifically, it has been postulated that the relationship
between marijuana and IPV may be due to third variables such as alcohol use, antisocial
personality, and relationship satisfaction (Moore & Stuart, 2005; Moore et al., 2008; Shorey
et al., 2017). Thus, it will be important for marijuana and IPV research to account for these
well-established IPV risk factors.
In addition to controlling for IPV risk factors, researchers have called for investigations on
the interaction between marijuana and alcohol use in predicting IPV perpetration (Shorey et
al., 2017). Research on simultaneous marijuana and alcohol use shows that it is associated
with a number of negative consequences, including more frequent use of either substance,
increased quantity of alcohol use, driving while under the influence, social conflicts (e.g.,
arguments; conflict with spouse), unprotected sex, arrests, and personal consequences (e.g.,
health, finances; Metrik, Caswell, Magill, Monti, & Kahler, 2016; Subbaraman & Kerr,
2015; Terry-McElrath, O’Malley, & Johnston, 2013). Not surprisingly, simultaneous use of
these substances produces greater impairment, disinhibition, and risk-taking relative to either
substance when used alone (Subbaraman & Kerr, 2015). From a theoretical standpoint, the
disinhibition caused by using alcohol and marijuana together may increase the risk for IPV,
as disinhibition, according to the alcohol myopia model (AMM; Steele & Josephs, 1990) is a
proposed mechanism for the relationship between alcohol and IPV (Giancola, 2002). Thus,
marijuana may further decrease disinhibition when alcohol is consumed, further increasing
the risk for IPV.
We are aware of only one study to date that has examined the impact of concurrent
marijuana and alcohol use on IPV. A recent cross-sectional study demonstrated that young
adult men who were marijuana and alcohol users were more likely to perpetrate sexual IPV
than men who only used alcohol (Low et al., 2017). Thus, continued research is needed to
examine whether marijuana and alcohol interact to increase the risk for IPV perpetration. In
all, knowledge of whether marijuana use is associated with IPV among men arrested for
domestic violence, or whether marijuana and alcohol use interact to predict IPV, may
provide important clinical information for the development of more effective BIPs. That is, it
is currently unknown whether marijuana use would be an important treatment target in BIPs,
and thus research in this area would provide initial information on whether these programs
should focus attention on reducing marijuana use.
Based on previous findings and theory regarding the role of marijuana use with IPV, we
examined whether marijuana use was associated with psychological, physical, and sexual
IPV perpetration in a sample of men arrested for domestic violence and court-referred to
BIPs. After controlling for alcohol use and problems, antisocial personality symptoms, and
relationship satisfaction, we expected marijuana use to be positively associated with IPV
perpetration. Antisocial personality symptoms and relationship satisfaction were chosen as
covariates due to prior research demonstrating their consistent associations with IPV
Shorey et al. Page 3
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
perpetration (Brem, Florimbio, Elmquist, Shorey, & Stuart, 2017; Stith, Green, Smith, &
Ward, 2008) and speculation that the association between marijuana and IPV may reflect the
influence of these confounding variables (e.g., Moore et al., 2008). Based on the combined
disinhibiting effects of marijuana and alcohol use, we also expected the strength of the
association between marijuana use and IPV perpetration to be stronger for men high in
alcohol use and problems, relative to men low in alcohol use and problems.
Method
Participants
Participants included men who were arrested for domestic violence and were court-referred
to BIPs (N = 269). These participants are a subsample of men reported on elsewhere (Brem,
Florimbio, Elmquist, Shorey, & Stuart, in press), and were chosen for inclusion in the
current study based on having completed all measures of interest. Participants reported a
mean age of 32.39 years (SD = 11.26). The majority of the sample identified as White
(63.2%). Participants also identified as Hispanic or Latino (12.3%), Black (8.6%), American
Indian or Alaska Native (4.1%), or other (6.3%); 5.6% of the sample did not report a race. In
regards to relationship status, most participants reported being in a current intimate
relationship (68.1%). In the entire sample, 27.9% reported being in a dating relationship,
26.4% of participants reported living with a partner but not being married, and 13.8%
reported being married. The average length of relationship reported by participants was 4.63
years (SD = 7.07).
Procedure
Participants were recruited for study participation at BIP locations. Study investigators
obtained informed consent from individuals interested in participating in the study.
Questionnaires were completed in paper and pencil format in a group setting during
participants’ regularly scheduled BIP sessions. All study participation was voluntary and all
information was kept confidential from the BIP group facilitators and courts. No
compensation for participating was provided. All procedures were approved by the
Institutional Review Board where the study took place. At the time of study participation,
the mean number of BIP sessions attended by participants was 11.28 (SD = 7.61).
Measures
Marijuana Use—Marijuana use was measured using a single marijuana use item from the
Drug Use Disorders Identification Test (DUDIT; Stuart et al., 2003a,b; Stuart et al., 2004), a
measure that captures a variety of different substances (e.g., marijuana, cocaine, opiates).
The marijuana item asked participants “How often do you use cannabis?”, with instructions
for participants to think of the year prior to entering their BIP. This is the only item on the
DUDIT that is specific to marijuana use. Participants were asked to rate their marijuana use
on a 7-point scale (0 = Never, 1 = less than monthly, 2 = monthly, 3 = 2–3 times a month, 4
= weekly, 5 = 2–3 times a week, 6 = 4 or more times a week). Higher scores correspond with
more frequent marijuana use. The DUDIT has demonstrated good psychometric properties
in prior research (Stuart et al., 2003a,b).
Shorey et al. Page 4
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
IPV Perpetration—Psychological, physical, and sexual IPV perpetration were measured
using the Revised Conflict Tactics Scales (CTS2; Straus et al., 1996), a 78-item self-report
measure that assesses the amount of negotiation, psychological aggression, physical assault,
sexual coercion, and injury within an intimate relationship. The psychological aggression,
physical assault, and sexual coercion perpetration subscales were included in the present
study. Participants are asked to rate the frequency of each item’s occurrence in the year prior
to entry into the BIP on a 7-point scale (0=Never; 6=more than 20 times). The psychological
perpetration subscale includes 8 questions, the physical perpetration subscale includes 12
questions, and the sexual perpetration subscale includes 7 questions. Total scores for each
subscale are obtained by summing the midpoints for each item (e.g., 3–5 times is recoded
into 4; Straus, Hamby, & Warren, 2003). Higher scores correspond to more frequent IPV
perpetration. Past research with the CTS2 has demonstrated good reliability (Straus, 2004)
and good construct and discriminant validity (Straus et al., 1996). For the present study, the
internal consistency for the physical perpetration subscale was good (α = .88), the
psychological perpetration subscale was good (α = .83), and the sexual subscale was
acceptable (α = .63).
Alcohol Use and Problems—The 10-item Alcohol Use Disorders Identification Test
(AUDIT; Saunders, Asaland, Babor, de la Fuente, & Grant, 1993) was used to measure
alcohol use and problems in the year prior to entry into the BIP. Participants rated their
agreement with the first seven items on a 5-point scale, and the final three items on a 3-point
scale. Possible scores range from 0–40 and were calculated by summing all items. Higher
scores correspond to more alcohol use and related problems. In past research the AUDIT
demonstrated high internal consistency (average α’s = .81–.93; Saunders, et al., 1993).
Internal consistency in the current sample was good (α = .87).
Antisocial Personality Symptoms—The Antisocial Personality Disorder (ASPD)
subscale of the Personality Diagnostic Questionnaire-4 (PDQ4; Hyler et al. 1988) was used
to measure antisocial personality symptoms. The PDQ4 is a brief screening instrument used
to assess possible personality disorders, and contains a subscale for symptoms of ASPD
(e.g., “Lying comes easily to me and I often do it”). Individuals were asked to rate each item
as true or false about their personality, and scores can range from 0–11. Higher scores on the
ASPD subscale indicate higher endorsement of symptoms associated with ASPD. In past
research, the PDQ4 has demonstrated good test re-test reliability (Trull, 1993), high internal
consistency (Hyler et al., 1989), and high sensitivity and specificity for detecting ASPD
(Hyler et al., 1989). Internal consistency in the present study was excellent (α = .90).
Relationship Satisfaction—Relationship satisfaction was measured using the
Relationship Assessment Scale (RAS; Hendrick, 1988). Participants indicated their
agreement with 7 questions about their current intimate relationship (or most recent intimate
relationship if not currently in a relationship) on a 5-point scale (e.g. “How well does your
partner meet your needs?”). Possible scores range from 7–35. Higher scores correspond to
higher levels of relationship satisfaction. Participants completed the RAS in reference to the
same partner they rated on the CTS2. In past research, the RAS has demonstrated good
convergent validity with other relationship satisfaction measures and high internal
Shorey et al. Page 5
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
consistency (Hendrick, Dicke, & Hendrick, 1998). In the present study, internal consistency
of the RAS was excellent (α = .90).
Data Analytic Strategy
We examined the relationship between marijuana and IPV perpetration utilizing SPSS
version 23.0. Prior to analyses, we log-transformed all IPV variables due to positive skew
and kurtosis, consistent with prior IPV research (e.g., Mattson, O’Farrell, Lofgreen,
Cunningham, & Murphy, 2012; Shorey, Brasfield, Febres, & Stuart, 2011). First, we
examined bivariate correlations among study variables. Second, three separate regression
analyses, one for each type of IPV, were conducted to determine whether the relationship
between marijuana use and IPV was present after controlling for alcohol use and problems,
antisocial personality symptoms, and relationship satisfaction. Finally, after main effect
analyses, we examined the interactive effects of alcohol use and problems and marijuana use
on IPV following recommendations for testing interactions by Aiken and West (1991). That
is, we mean centered independent variables to reduce multicollinearity and then formed an
interaction term between alcohol use and problems and marijuana use, which was entered
into the regression equations. Significant interactions were probed at high (+1 SD) and low
(−1 SD) levels of alcohol use and problems.
Results
Means, standard deviations, and correlations among study variables are presented in Table 1.
As displayed, psychological, physical, and sexual IPV perpetration were positively and
significantly associated with marijuana use. All three forms of IPV were positively and
significantly associated with alcohol use and problems and antisocial personality symptoms.
Psychological and physical IPV were negatively and significantly related to relationship
satisfaction. Marijuana use and alcohol use and problems positively and significantly related
to antisocial personality symptoms. Number of BIP sessions completed negatively related to
relationship satisfaction. Regarding marijuana use in the year prior to BIP entry, 40.5% of
the sample reported no marijuana use, 11.5% reported less than monthly use, 3% reported
monthly use, 5.6% reported use 2 to 3 times a month, 4.1% reported weekly use, 5.9%
reported use 2 to 3 times a week, and 29.4% reported use 4 or more times a week. Thus,
59.5% of the entire sample reported marijuana use in the previous year and 39.4% of the
entire sample reported at least weekly marijuana use.
Table 2 presents results of the regression analyses for each form of IPV perpetration. Semi-
partial (sr) correlations between marijuana and IPV perpetration, derived from the regression
analyses, are presented below. As displayed in Table 2, marijuana use frequency remained
positively associated with the psychological (sr = .17, p < .01), physical (sr = ..14, p < .05),
and sexual IPV (sr = .23, p < .001) perpetration frequency after accounting for alcohol use
and problems, antisocial personality symptoms, and relationship satisfaction. The main
effect of marijuana use on sexual IPV was qualified by a significant interaction between
alcohol use and problems and marijuana use. Specifically, marijuana use was positively
associated with IPV perpetration at high (β = .36, p < .001), but not low (β = .12, p > .05),
levels of alcohol use and problems (see Figure 1).
Shorey et al. Page 6
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Discussion
Recent research indicated that marijuana use positively associated with IPV perpetration
among men arrested for domestic violence, but did not examine this association in the
presence of other known risk factors for IPV. Therefore, we examined the association
between marijuana use and IPV perpetration while controlling for alcohol use and problems,
antisocial personality symptoms, and relationship satisfaction in a sample of men arrested
for domestic violence and court-referred to attend BIPs. After accounting for these risk
factors, our findings demonstrated marijuana use positively associated with all forms of IPV
(psychological, physical, and sexual). Moreover, the main effect of marijuana use on sexual
IPV was qualified by an interaction between marijuana use and alcohol use and problems,
such that marijuana use was associated with IPV at high, but not low, levels of alcohol use
and problems among men arrested for domestic violence.
That marijuana use positively related to all three forms of IPV in the present study is
noteworthy given previous meta-analytic findings indicating that marijuana use did not relate
to sexual IPV (Moore et al., 2008). However, this meta-analysis only included one study that
assessed the association between marijuana use and sexual IPV. Other studies show that
marijuana use is associated with increased odds for problematic sexual behavior, such as
condomless sex (Metrik et al., 2016). Our findings provide preliminary evidence that this
association may also extend to sexual IPV perpetration. Importantly, the present findings
demonstrated that the association between marijuana use and sexual IPV was stronger for
individuals with high levels of alcohol use and problems relative to those with low alcohol
use and problems. This finding is consistent with prior research which suggests that
polysubstance users report more frequent IPV than non-polysubstance users (e.g., Low et al.,
2017), suggesting polysubstance use is an indicator for increased IPV risk. Although our
study did not assess the acute effects of marijuana and alcohol use, this finding may also
suggest that co-ingestion of marijuana and alcohol could create a high-risk situation for
sexual IPV, as simultaneous use of these two substances creates greater disinhibition and
impairment than either substance alone (Subbaraman & Kerr, 2015). However, until future
research examines these relationships utilizing event-level data (e.g., daily diary studies),
firm conclusions about co-ingestion of these two substances on risk for IPV is limited to
speculation. Moreover, caution should be used when interpreting this interaction finding due
to the small percentage of variance accounted for in sexual IPV by the interaction between
marijuana use and alcohol.
Our findings provide important information for future research to build upon, since
increasing evidence suggests that marijuana use is positively associated with IPV
perpetration. However, the reasons for this association (i.e., mechanisms) remain unknown.
In order to understand this association, we believe that future research examining marijuana
use at the event-level is needed. Indeed, researchers previously advocated for daily diary
studies or ecological momentary assessment designs to explore the temporal association
between marijuana use and IPV perpetration (Testa & Brown, 2015; Shorey et al., 2017).
This design will allow for the examination of the events that immediately precede IPV, such
as marijuana use, and potential mechanisms underlying marijuana-related IPV. This design
would also allow for the examination of concordance of marijuana use between partners.
Shorey et al. Page 7
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Theory (e.g., Testa & Brown, 2015) and prior research (e.g., Homish et al., 2009) suggests
discordant marijuana use among intimate partners may increase the risk for negative couple
outcomes, such as IPV, to a greater degree than concordant marijuana use, as concordant
substance use may reflect shared behaviors and closeness among intimate partners.
The alcohol myopia model (AMM; Steele & Josephs, 1990), which provides theoretical
support for the relationship between alcohol use and IPV, may offer insight into the
association between marijuana use and IPV. According to the AMM, alcohol use causes
individuals to focus on the most salient aspects in their environment (Steele & Joseph,
1990). When the most salient environmental cue is negative (e.g., negative affect), alcohol
will intensify this myopic effect, which may increase the risk for IPV (Giancola, 2002). A
similar process may take place for marijuana-related IPV. Indeed, research suggested that
marijuana use may increase allocation of attentional resources to negative stimuli (Metrik et
al., 2015). Moreover, negative affect may precede, and be increased by, marijuana use
(Shadur, Hussong, & Haroon, 2015; Shrier, Ross, & Blood, 2014; Trull, Wycoff, Lane,
Carpenter, & Brown, 2016). Preliminary daily diary research with drinking college women
demonstrated that marijuana use was positively associated with psychological IPV
perpetration at high, but not low, levels of negative affect (Shorey, Stuart, Moore, &
McNulty, 2014). Thus, it is plausible that proximal negative affect may impact risk for
marijuana-related IPV among men arrested for domestic violence. Future research
incorporating event-level research methods should explore this theoretical supposition.
An additional area for future practitioners and researchers is to consider is whether
marijuana use negatively impacts intervention outcomes for IPV. As previously mentioned,
alcohol interventions for men in BIPs result in improved short-term outcomes relative to
BIPs alone although the positive effects of the alcohol intervention fade over time (Stuart et
al., 2013). Given the high prevalence of marijuana use among men in BIPs identified in the
present study, and our preliminary finding that marijuana and alcohol use and problems
interact to predict sexual IPV, it is plausible that marijuana use could negatively impact BIP
outcomes. Indeed, individuals who are in alcohol treatment have poorer outcomes when they
are using marijuana during treatment relative to individuals who do not use marijuana during
treatment (Subbaraman, Metrik, Patterson, & Swift, 2017). Therefore, BIPs should consider
targeting marijuana use in their programs in order to determine whether marijuana use
treatment impacts BIP outcomes.
There are several limitations to consider when interpreting the findings of the present study.
First, the sample was comprised of men arrested for domestic violence perpetration, limiting
the generalizability of these findings to men who may perpetrate less frequent or less severe
forms of IPV. In addition, the measure of marijuana use consisted of a single item and
assessed only the frequency of marijuana use. Utilizing an in-depth measure that extends
beyond one item and assesses for other characteristics of marijuana use (e.g., quantity,
problems associated with marijuana use) would allow for a more comprehensive
understanding of the relation between marijuana use and IPV. The cross-sectional nature of
the study design precludes making causal inferences about the study variables. Future
studies should employ a longitudinal design to further elucidate the relationship between
marijuana use and IPV, while also controlling for identified risk factors for IPV perpetration.
Shorey et al. Page 8
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Event-level data (e.g., daily diary designs) would also provide information on the acute
effects of marijuana, and the combined effects of marijuana and alcohol, on IPV, and future
research should utilize these types of designs. The generalizability of the findings is limited
given the sample was comprised of primarily non-Hispanic White men. Future studies
should include a more ethnically diverse sample, as well as include women. We also did not
collect information on the number of men who declined to participate in the current study
and whether they may have differed from men who agreed to participate. Finally, it should
be noted that because the sample consisted of men arrested and court-mandated to BIPs,
social desirability may have impacted study findings.
In summary, findings demonstrated marijuana use positively associated with psychological,
physical, and sexual IPV perpetration among men arrested for domestic violence and court-
referred to BIPs. These findings were present even after accounting for other known risk
factors for IPV perpetration. We believe continued investigation into the associations
between marijuana use and IPV is important due to the public health, legal policy, and
treatment implications that would result from this line of research. Continued research
utilizing rigorous methodological designs, such as daily diary designs, is needed to further
understand the association between marijuana and IPV perpetration. Finally, pending
replication and extension, findings suggest BIPs may want to target reductions in marijuana
use, which may have the concurrent benefit of reducing IPV.
References
Aiken, LS, West, SG. Multiple regression: Testing and interpreting interactions. Sage; Thousand Oaks, CA: 1991.
Archer J. 2000; Sex differences in aggression between heterosexual partners: a meta-analytic review. Psychological Bulletin. 126:651–680. DOI: 10.5042/jacpr.2010.0141 [PubMed: 10989615]
Babcock JC, Green CE, Robie C. 2004; Does batterers’ treatment work? A meta-analytic review of domestic violence treatment. Clinical Psychology Review. 23:1023–1053. DOI: 10.1016/j.cpr.2002.07.001 [PubMed: 14729422]
Brem MJ, Florimbio AR, Elmquist J, Shorey RC, Stuart GL. (in press)Antisocial traits, distress tolerance, and alcohol problems as predictors of intimate partner violence in men arrested for domestic violence. Psychology of Violence.
Campbell JC. 2002; Health consequences of intimate partner violence. The Lancet. 359:1331–1336. DOI: 10.1016/S0140-6736(02)08336-8
Davis R. 2010; Domestic violence-related deaths. Journal of Aggression, Conflict and Peace Research. 2:44–52. DOI: 10.5042/jacpr.2010.0141
Devries KM, Child JC, Bacchus LJ, Mak J, Falder G, Graham K, … Heise L. 2014; Intimate partner violence victimization and alcohol consumption in women: a systematic review and meta- analysis. Addiction. 109:379–391. DOI: 10.1111/add.12393 [PubMed: 24329907]
Devries KM, Mak JY, Bacchus LJ, Child JC, Falder G, Petzold M, … Watts CH. 2013; Intimate partner violence and incident depressive symptoms and suicide attempts: A systematic review of longitudinal studies. PLoS Medicine. 10:e1001439.doi: 10.1371/journal.pmed.1001439 [PubMed: 23671407]
Feder L, Wilson DB. 2005; A meta-analytic review of court-mandated batterer intervention programs: Can courts affect abusers’ behavior? Journal of Experimental Criminology. 1:239–262. DOI: 10.1007/s11292-005-1179-0
Foran HM, O’Leary KD. 2008; Alcohol and intimate partner violence: A meta-analytic review. Clinical Psychology Review. 28:1222–1234. DOI: 10.1016/j.cpr.2008.05.001 [PubMed: 18550239]
Shorey et al. Page 9
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Giancola PR. 2002; Alcohol-related aggression during the college years: Theories, risk factors and policy implications. Journal of Studies on Alcohol. :129–139. DOI: 10.15288/jsas.2002.s14.129 [PubMed: 12022718]
Hendrick SS. 1988; A generic measure of relationship satisfaction. Journal of Marriage and Family. 50:93–98. DOI: 10.22307/352430
Hendrick SS, Dicke A, Hendrick C. 1998; The Relationship Assessment Scale. Journal of Social and Personal Relationships. 15:137–142. DOI: 10.1177/0265407598151009
Homish GG, Leonard KE, Kozlowski LT, Cornelius JR. 2009; The longitudinal association between multiple substance use discrepancies and marital satisfaction. Addiction. 104:1201–1209. DOI: 10.1111/j.1360-0443.2009.02614.x [PubMed: 19563563]
Hyler SE, Rieder RO, Williams JBW, Spitzer RL, Hendler J, Lyons M. 1988; The personality diagnostic questionnaire: Development and preliminary results. Journal of Personality Disorders. 2:229–237. DOI: 10.1521/pedi.1988.2.3.229
Hyler SE, Rieder RO, Williams JBW, Spitzer RL, Lyons M, Hendler J. 1989; A comparison of clinical and self-report diagnoses of DSM-III personality disorders in 552 patients. Comprehensive Psychiatry. 30:170–178. DOI: 10.1016/0010-440X(89)90070-9 [PubMed: 2920552]
Low S, Tiberio SS, Shortt JW, Capaldi DM, Eddy JM. 2017; Associations of couples’ intimate partner violence in young adulthood and substance use: A dyadic approach. Psychology of Violence. 7:120–127. DOI: 10.1037/vio0000038
Mattson RE, O’Farrell TJ, Lofgreen AM, Cunningham K, Murphy CM. 2012; The role of illicit substance use in a conceptual model of intimate partner violence in men undergoing treatment for alcoholism. Psychology of Addictive Behaviors. 26:255–264. DOI: 10.1037/a0025030 [PubMed: 21875168]
Metrik J, Aston ER, Kahler CW, Rohsenow DJ, McGeary JE, Knopik VS. 2015; Marijuana’s acute effects on cognitive bias for affective and marijuana cues. Experimental and Clinical Psychopharmacology. 23:339–350. DOI: 10.1037/pha0000030 [PubMed: 26167716]
Metrik J, Caswell AJ, Magill M, Monti PM, Kahler CW. 2016; Sexual risk behavior and heavy drinking among weekly marijuana users. Journal of Studies on Alcohol and Drugs. 77:104–112. DOI: 10.15288/jsad.2016.77.104 [PubMed: 26751360]
Moore TM, Stuart GL. 2004; Illicit substance use and intimate partner violence among men in batterers’ intervention. Psychology of Addictive Behaviors. 18:385–389. DOI: 10.1037/0893-164X.18.4.385 [PubMed: 15631612]
Moore TM, Stuart GL. 2005; A review of the literature on marijuana use and interpersonal violence. Aggression and Violent Behavior. 10:171–192. DOI: 10.1016/j.avb.2003.10.002
Moore TM, Stuart GL, Meehan JC, Rhatigan DL, Hellmuth JC, Keen SM. 2008; Drug abuse and aggression between intimate partners: A meta-analytic review. Clinical Psychology Review. 28:247–274. DOI: 10.1016/j.cpr.2007.05.003 [PubMed: 17604891]
Nathanson AM, Shorey RC, Tirone V, Rhatigan DL. 2012; The prevalence of mental health disorders in a community sample of female victims of intimate partner violence. Partner Abuse. 3:59–75. DOI: 10.1891/1946-6560.3.1.59 [PubMed: 22741043]
Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. 1993; Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO collaborative project on early detection of persons with harmful alcohol consumption. Addiction. 88:791–804. DOI: 10.1111/j.1360-0443.1993.tb02093.x [PubMed: 8329970]
Shadur JM, Hussong AM, Haroon M. 2015; Negative affect variability and adolescent self-medication: The role of the peer context. Drug and Alcohol Review. 34:571–580. DOI: 10.1111/dar.12260 [PubMed: 25867550]
Shrier LA, Ross CS, Blood EA. 2014; Momentary positive and negative affect preceding marijuana use events in youth. Journal of Studies on Alcohol and Drugs. 75:781–789. DOI: 10.15288/jsad.2014.75.781 [PubMed: 25208196]
Shorey RC, Brasfield H, Febres J, Stuart GL. 2011; The association between impulsivity, trait anger, and the perpetration of intimate partner and general violence among women arrested for domestic violence. Journal of Interpersonal Violence. 26:2681–2697. DOI: 10.1177/0886260510388289 [PubMed: 21118862]
Shorey et al. Page 10
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Shorey RC, Cornelius TL, Bell KM. 2008; A critical review of theoretical frameworks for dating violence: Comparing the dating and marital fields. Aggression and Violent Behavior. 13:185–194. DOI: 10.1016/j.avb.2008.03.003
Shorey RC, Haynes E, Strauss C, Temple JR, Stuart GL. 2017; Cannabis use and dating violence among college students: A call for research. Drug and Alcohol Review. doi: 10.1111/dar.12457
Shorey RC, Stuart GL, Cornelius TL. 2011; Dating violence and substance use in college students: A review of the literature. Aggression and Violent Behavior. 16:541–550. [PubMed: 22125415]
Shorey RC, Stuart GL, Moore TM, McNulty JK. 2014; The temporal relationship between alcohol, marijuana, angry affect and dating violence perpetration: A daily diary study with female college students. Psychology of Addictive Behaviors. 28:516–523. DOI: 10.1037/a0034648 [PubMed: 24274434]
Steele CM, Josephs RA. 1990; Alcohol myopia: It’s prized and dangerous effects. American Psychologist. 45:921–933. DOI: 10.1037/0003-066X.45.8.921 [PubMed: 2221564]
Stith SM, Green NM, Smith DB, Ward DB. 2008; Marital satisfaction and marital discord as risk markers for intimate partner violence: A meta-analytic review. Journal of Family Violence. 23:149–160. DOI: 10.1007/s10896-007-9137-4
Straus MA. 2004; Cross-cultural reliability and validity of the Revised Conflict Tactics Scales: A study of university student dating couples in 17 nations. Cross-Cultural Research. 38:407–432. DOI: 10.1177/1069397104269543
Straus MA, Hamby SL, Boney-McCoy S, Sugarman DB. 1996; The revised conflict tactics scales (CTS2): Development and preliminary psychometric data. Journal of Family Issues. 17:283–316. DOI: 10.1177/019251396017003001
Straus, MA, Hamby, SL, Warren, WL. The conflict tactics scales handbook. Los Angeles, CA: Western Psychological Services; 2003.
Stuart GL, Moore TM, Kahler CW, Ramsey SE. 2003; Substance abuse and relationship violence among men court-referred to batterers’ intervention programs. Substance Abuse. 24:107–122. DOI: 10.1080/08897070309511539 [PubMed: 12766378]
Stuart GL, Moore TM, Ramsey SE, Kahler CW. 2003; Relationship aggression and substance use among women court-referred to domestic violence intervention programs. Addictive Behaviors. 28:1603–1610. DOI: 10.1016/j.addbeh.2003.08.038 [PubMed: 14656548]
Stuart GL, Moore TM, Ramsey SE, Kahler CW. 2004; Hazardous drinking and relationship violence perpetration and victimization in women arrested for domestic violence. Journal of Studies on Alcohol. 65:46–53. DOI: 10.15288/jsa.2004.65.46 [PubMed: 15000503]
Stuart GL, Temple JR, Moore TM. 2007; Improving batterer intervention programs through theory-based research. Journal of American Medical Association. 298:560–562. DOI: 10.1001/jama.298.5.560
Subbaraman MS, Kerr WC. 2015; Simultaneous versus concurrent use of alcohol and cannabis in the national alcohol survey. Alcoholism: Clinical and Experimental Research. 39:872–879.
Subbaraman MS, Metrik J, Patterson D, Swift R. 2017; Cannabis use during treatment for alcohol use disorders predicts alcohol treatment outcomes. Addiction. doi: 10.1111/acer.12698
Terry-McElrath YM, O’Malley PM, Johnston LD. 2013; Simultaneous alcohol and marijuana use among US high school seniors from 1976 to 2011: Trends, reasons, and situations. Drug and Alcohol Dependence. 133:71–79. DOI: 10.1016/j.drugalcdep.2013.05.031 [PubMed: 23806871]
Testa M, Brown WC. 2015; Does marijuana use contribute to intimate partner aggression? A brief review and directions for future research. Current Opinion in Psychology. 5:6–12. DOI: 10.1016/j.copsyc.2015.03.002 [PubMed: 25839050]
Trull TJ. 1993; Temporal stability and validity of two personality disorders. Psychological Assessment. 1:11–18. DOI: 10.1037/1040-3590.5.1.11
Trull TJ, Wycoff AM, Lane SP, Carpenter RW, Brown WC. 2016; Cannabis and alcohol use, affect and impulsivity in psychiatric out-patients’ daily lives. Addiction. 111:2052–2059. DOI: 10.1111/add.13471 [PubMed: 27270874]
Shorey et al. Page 11
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Public Significance Statement
Marijuana use is prevalent among men arrested for domestic violence. Our findings
demonstrated that marijuana use was positively associated with intimate partner violence
perpetration among men arrested for domestic violence. Treatment of men arrested for
domestic violence should consider reducing marijuana.
Shorey et al. Page 12
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
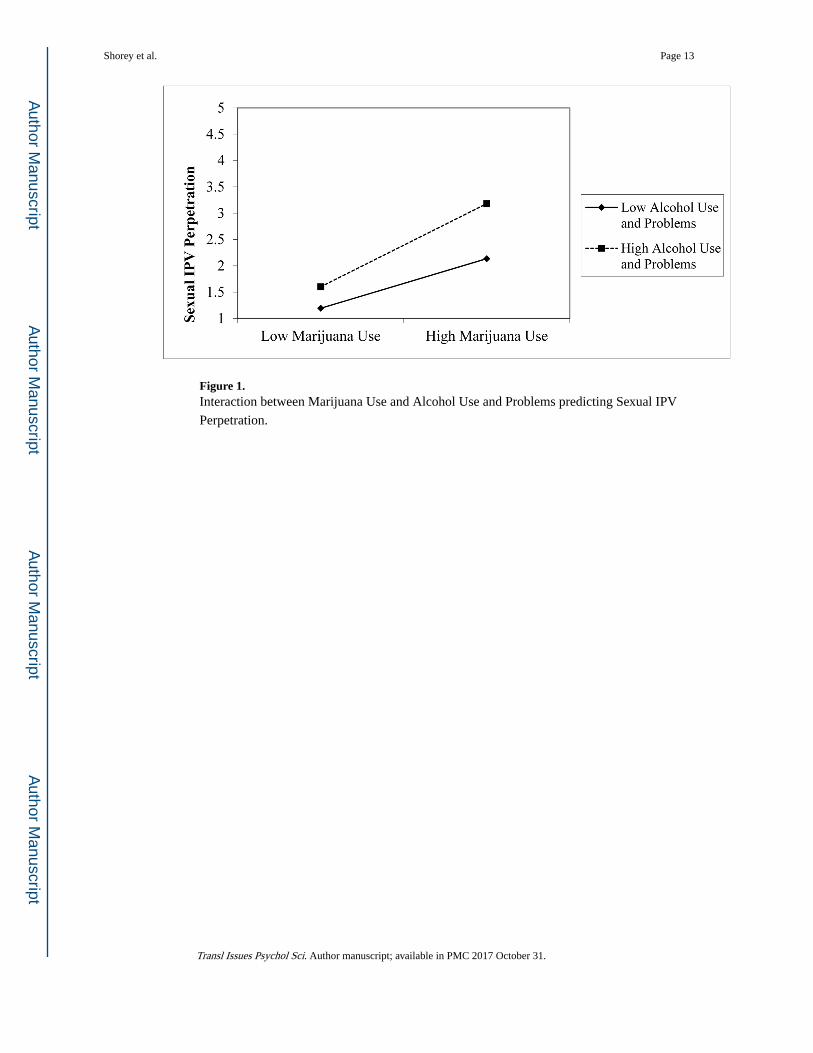
Figure 1. Interaction between Marijuana Use and Alcohol Use and Problems predicting Sexual IPV
Perpetration.
Shorey et al. Page 13
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript

Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Shorey et al. Page 14
Tab
le 1
Mea
ns, s
tand
ard
devi
atio
ns, a
nd b
ivar
iate
cor
rela
tions
am
ong
stud
y va
riab
les
12
34
56
78
1. P
sych
olog
ical
IPV
Per
petr
atio
n-
2. P
hysi
cal I
PV P
erpe
trat
ion
.55*
*-
3. S
exua
l IPV
Per
petr
atio
n.2
8**
.43*
*-
4. M
ariju
ana
Use
.17*
*.1
7**
.28*
*-
5. A
lcoh
ol U
se a
nd P
robl
ems
.27*
*.2
3**
.22*
*.0
6-
6. A
ntis
ocia
l Sym
ptom
s.1
8**
.28*
*.2
8**
.22*
*.3
4**
-
7. R
elat
ions
hip
Satis
fact
ion
−.3
7**
−.2
7**
−.1
1.0
7−
.02
−.0
7-
8. N
umbe
r of
BIP
Ses
sion
s.0
8.0
9.1
6**
.00
.10
−.0
7−
.17*
*-
Mea
n37
.46
10.8
16.
362.
579.
113.
1622
.96
11.2
8
Stan
dard
Dev
iatio
n38
.10
26.0
615
.50
2.63
8.65
2.23
7.49
7.61
Not
e. P
sych
olog
ical
, phy
sica
l, an
d se
xual
IPV
mea
n sc
ores
ref
lect
raw
val
ues;
log-
tran
sfor
med
sco
res
wer
e us
ed f
or c
orre
latio
n an
alys
es.
**p
< .0
1.
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.
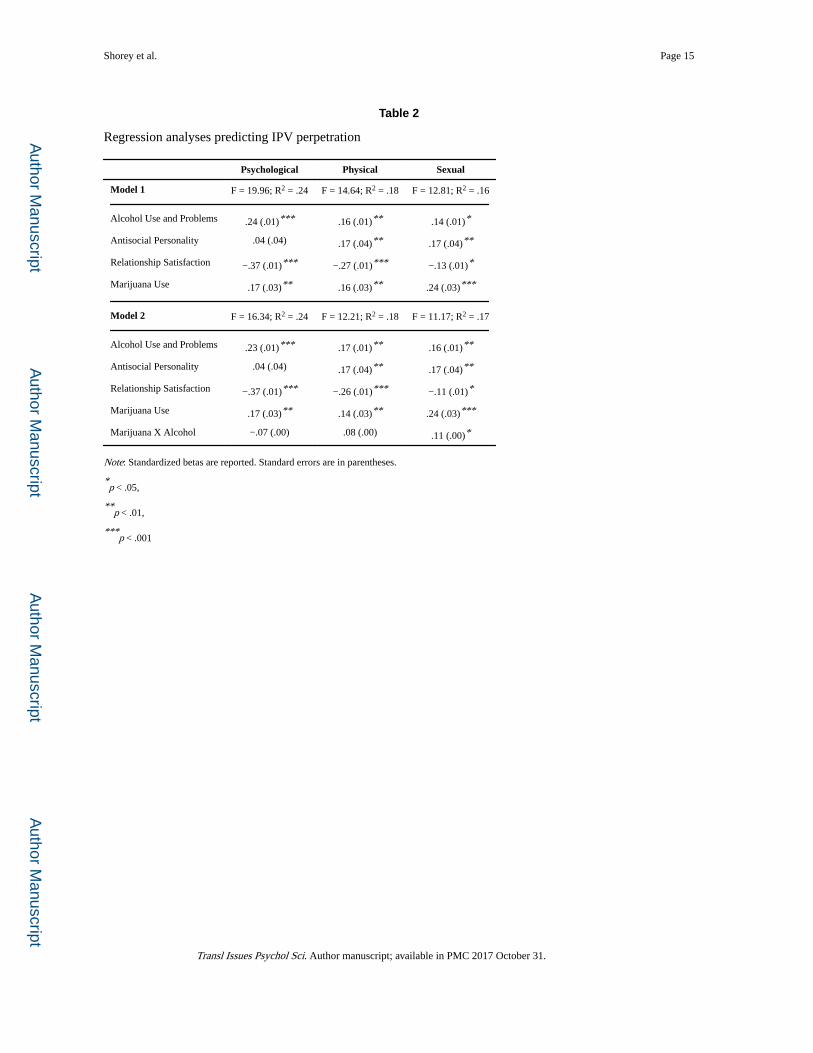
Author M
anuscriptA
uthor Manuscript
Author M
anuscriptA
uthor Manuscript
Shorey et al. Page 15
Table 2
Regression analyses predicting IPV perpetration
Psychological Physical Sexual
Model 1 F = 19.96; R2 = .24 F = 14.64; R2 = .18 F = 12.81; R2 = .16
Alcohol Use and Problems .24 (.01)*** .16 (.01)** .14 (.01)*
Antisocial Personality .04 (.04) .17 (.04)** .17 (.04)**
Relationship Satisfaction −.37 (.01)*** −.27 (.01)*** −.13 (.01)*
Marijuana Use .17 (.03)** .16 (.03)** .24 (.03)***
Model 2 F = 16.34; R2 = .24 F = 12.21; R2 = .18 F = 11.17; R2 = .17
Alcohol Use and Problems .23 (.01)*** .17 (.01)** .16 (.01)**
Antisocial Personality .04 (.04) .17 (.04)** .17 (.04)**
Relationship Satisfaction −.37 (.01)*** −.26 (.01)*** −.11 (.01)*
Marijuana Use .17 (.03)** .14 (.03)** .24 (.03)***
Marijuana X Alcohol −.07 (.00) .08 (.00) .11 (.00)*
Note: Standardized betas are reported. Standard errors are in parentheses.
*p < .05,
**p < .01,
***p < .001
Transl Issues Psychol Sci. Author manuscript; available in PMC 2017 October 31.

Mutation Research 789 (2016) 1–11
Contents lists available at ScienceDirect
Mutation Research/Fundamental and MolecularMechanisms of Mutagenesis
journa l homepage: www.e lsev ier .com/ locate /molmut
Communi ty address : www.e lsev ier .com/ locate /mutres
Review
Chromothripsis and epigenomics complete causality criteria forcannabis- and addiction-connected carcinogenicity, congenitaltoxicity and heritable genotoxicity
Albert Stuart Reece ∗, Gary Kenneth HulseSchool of Psychiatry and Clinical Neurosciences, University of Western Australia, Crawley, WA 6009, Australia
a r t i c l e i n f o
Article history:
Received 11 January 2016Received in revised form 17 April 2016Accepted 1 May 2016Available online 4 May 2016
Keywords:
CannabisMicrotubulesTubulinDose-response relationshipThreshold dosePopulation effectsOncogenesisFoetal malformationsChromothripsisEpigeneticsTransgenerationalHeritableInterdisciplinary
a b s t r a c t
The recent demonstration that massive scale chromosomal shattering or pulverization can occur abruptlydue to errors induced by interference with the microtubule machinery of the mitotic spindle followed byhaphazard chromosomal annealing, together with sophisticated insights from epigenetics, provide pro-found mechanistic insights into some of the most perplexing classical observations of addiction medicine,including cancerogenesis, the younger and aggressive onset of addiction-related carcinogenesis, the her-itability of addictive neurocircuitry and cancers, and foetal malformations. Tetrahydrocannabinol (THC)and other addictive agents have been shown to inhibit tubulin polymerization which perturbs the for-mation and function of the microtubules of the mitotic spindle. This disruption of the mitotic machineryperturbs proper chromosomal segregation during anaphase and causes micronucleus formation whichis the primary locus and cause of the chromosomal pulverization of chromothripsis and downstreamgenotoxic events including oncogene induction and tumour suppressor silencing. Moreover the comple-mentation of multiple positive cannabis-cancer epidemiological studies, and replicated dose-responserelationships with established mechanisms fulfils causal criteria. This information is also consistent withdata showing acceleration of the aging process by drugs of addiction including alcohol, tobacco, cannabis,stimulants and opioids. THC shows a non-linear sigmoidal dose-response relationship in multiple per-tinent in vitro and preclinical genotoxicity assays, and in this respect is similar to the serious majorhuman mutagen thalidomide. Rising community exposure, tissue storage of cannabinoids, and increas-ingly potent phytocannabinoid sources, suggests that the threshold mutagenic dose for cancerogenesiswill increasingly be crossed beyond the developing world, and raise transgenerational transmission ofteratogenicity as an increasing concern.
© 2016 Elsevier B.V. All rights reserved.
Contents
1. Introduction to seminal paper . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22. Dynamics of the cell cycle . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23. Mitotic spindle poisons . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34. Non-linear dose-response kinetics . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .55. Cannabis cancerogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56. Cannabis teratogenicity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 57. Cannabis-related mitochondrial inhibition . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 58. Cannabis-related gametotoxicity, zygote toxicity and reproductive impairment . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69. Other microtubule functions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 610. Other addictions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 611. Epigenetic contributions to mutagenicity . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
∗ Correspondence to: 39 Gladstone Rd., Highgate Hill, Brisbane, Queensland, Australia.E-mail addresses: [email protected], [email protected] (A.S. Reece).
http://dx.doi.org/10.1016/j.mrfmmm.2016.05.0020027-5107/© 2016 Elsevier B.V. All rights reserved.

2 A.S. Reece, G.K. Hulse / Mutation Research 789 (2016) 1–11
12. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Conflict interests . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Funding. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Fig. 1. Chromosomal Pulverization.Original Report of Chromosomal Pulverization. Figure 7 , Kato H., Sandberg AA(1967). “Chromosome Pulverization in Human Binucleate Cells. Following ColcemidTreatment.” J. Cell Biol. 34 (1): 35–45. Re-used by permission.
1. Introduction to seminal paper
In a remarkable and highly celebrated report, the Pellman labrecently showed that severe chromosomal fragmentation involvingdozens of double stranded breaks and subsequent apparently ran-dom and disordered repair of some of the fragments, could rapidlyoccur during the DNA synthetic phase (G2 and S-phases) of themitotic cell cycle, if chromosomes became isolated from the mainnuclear mass [1]. In this technical tour de force, high resolutionDNA sequencing of single cells and live cell imaging was deployedto show that chromosomes which had become detached fromthe mitotic spindle or chromosomes became isolated in micronu-clei, where, lacking the normal full complement of replication andrepair enzymes, the DNA became shattered in the process of dis-ordered and dysregulated replication. Such damage could becomepropagated through subsequent rounds of cell division, where theisolated chromosomes could also become joined up with those ofthe main nucleus. Where two or a few chromosomes were trappedtogether, in such a micronucleus random exchange could occurbetween them. Chromosome “pulverization” was first described in1967 due to experimental viral infection [2] (Figs. 1 and 2). The pro-cess has recently been named “chromothripsis” for chromosomalshattering at hundreds [3] or thousands [4] of loci; and a milderform was called “chromoplexy” (chromosomal tangles or braids,Fig. 3) [5]. Extraordinarily, this process was shown to proceed asrapidly as within 16 h [1].
This remarkable result immediately resolved a long standingparadox in cancer research as to how such dramatic event couldarise when the normal fidelity of DNA replication occurs with anerror (mutation) rate of only 10−8, and the rate in germ stem cellsis one hundred times lower. It also simultaneously provided an
elegant mechanism for the high rate of micronuclei, chromoso-mal fragments and abnormal chromosomes (truncated arms, chainand ring chromosomes and double minute circles [6]) which arefrequently seen in malignant tissues (Fig. 4)[7]. Tetraploidy itselfhas been shown to increase chromosomal instability, tolerance ofmitotic errors and the multidrug resistance typical of transformedand tumour cells and even the anchorage-independent growth ofnon-transformed cells [7].
In addition to cancer, such chromothriptic events have also beenshown in various congenital abnormality syndromes [8–14].
2. Dynamics of the cell cycle
The cell cycle has numerous check points which are designed toprevent such genetically catastrophic events from occurring. Themitotic spindle assembly checkpoint (SAC) in particular requiresall chromosomes to be attached to the spindle, and sister repli-cates to be attached at their kinetochores with opposing polarity(bi-orientation) to bundles of microtubules of the mitotic spindlewhich will draw them to opposite poles of the cell [15]. Mostlyerrors in this complicated machinery [16–19] generate cell cyclearrest, apoptosis, or the irreversible entry into cellular senescence[7]. But delay at the SAC is not indefinite [15]. Some cells slipback as tetraploid cells into interphase and a very few escape cellcycle controls altogether. This can particularly occur when chro-mothriptic events involve the functional silencing of such majortumour suppressor genes as TP53 (P53) and CDKN2A (P16INK4A),which normally sense and amplify such cellular and senescencecheckpoints [20]. Other genetic causes (mutations, insertions anddeletions) also exist for tumour suppressor gene silencing. Hencethe usual outcome of such events at the tissue level is; growth arrestvia apoptosis, senescence or cell cycle delay [21], and occasionallymalignant transformation where the malignant clone may have agrowth advantage [7,22].
The pathway described by the Boston group [1] wastherefore inhibition of spindle dynamics/failure of spindle attach-ment/micronuclear formation/chromosomal shattering or pulver-ization/haphazard chromosomal annealing by non-homologousend joining or microhomology-mediated break-induced repli-cation, then cell cycle arrest or occasionally and alternatively,oncogenic transformation [3,12,20,22–25]. Chromothripsis hasbeen described as occurring in about 2–3% of cancers includingmelanoma, sarcoma, lung, thyroid, oesophageal and renal cancers[4], although it is seen much more commonly in cancers of thebone (25%) [20,26], brain (39%) [27,28], bowel [29] and a majorityof prostate tumours [5]. It has also been said to be more com-mon in cancer per se, as the technical difficulties in unravellingthe enormous complexities in sequencing errors to which it givesrise are only beginning to be probed [5,22,24,26,27,29,30]. Its pres-ence and severity correlate with poor prognostic outcomes [27,30].Progressive chromosomal instability instigated or assisted by chro-mothriptic and disorderly mitotic mechanisms also explain theusual tendency of tumours to become increasingly aggressive [26].Curiously single cell chromothripsis has also been shown on occa-sion to cure rare genetic disorders [31].
The Boston work [1] also focussed attention on the extraordi-narily complicated machinery associated with the microtubulescomprising the mitotic spindle. Microtubules are primarily madeup of a- and b- tubulin dimers which, together with their numer-
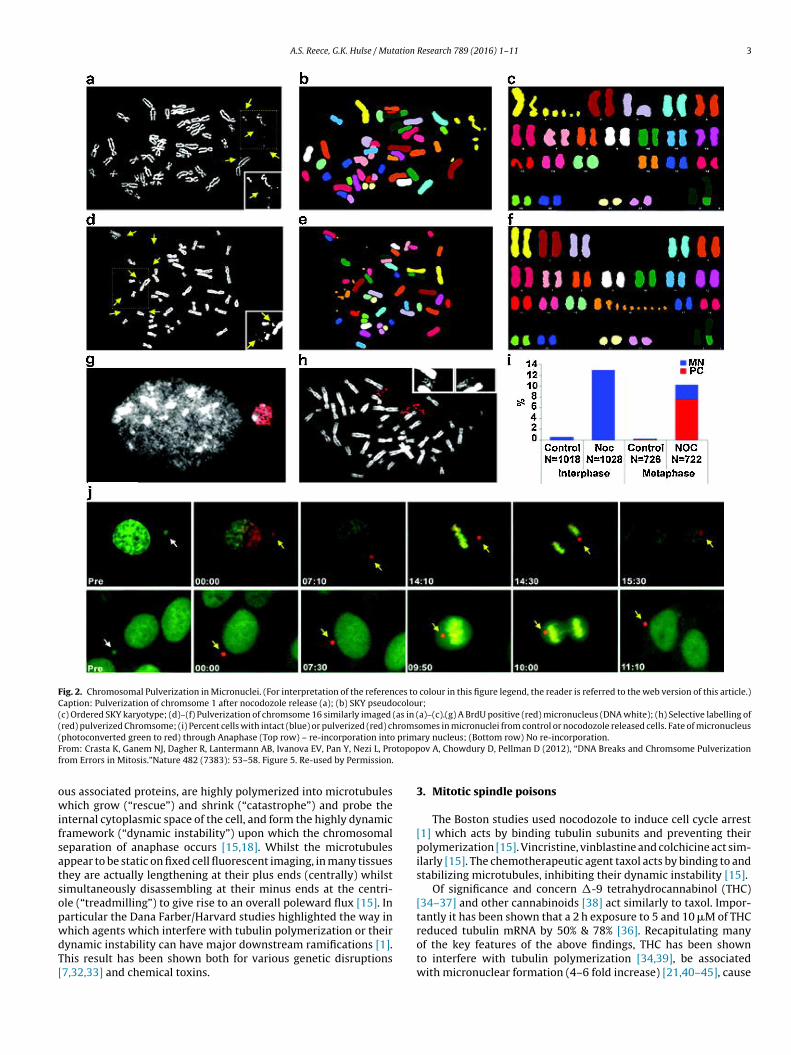
A.S. Reece, G.K. Hulse / Mutation Research 789 (2016) 1–11 3
Fig. 2. Chromosomal Pulverization in Micronuclei. (For interpretation of the references to colour in this figure legend, the reader is referred to the web version of this article.)Caption: Pulverization of chromsome 1 after nocodozole release (a); (b) SKY pseudocolour;(c) Ordered SKY karyotype; (d)–(f) Pulverization of chromsome 16 similarly imaged (as in (a)–(c).(g) A BrdU positive (red) micronucleus (DNA white); (h) Selective labelling of(red) pulverized Chromsome; (i) Percent cells with intact (blue) or pulverized (red) chromsomes in micronuclei from control or nocodozole released cells. Fate of micronucleus(photoconverted green to red) through Anaphase (Top row) – re-incorporation into primary nucleus; (Bottom row) No re-incorporation.From: Crasta K, Ganem NJ, Dagher R, Lantermann AB, Ivanova EV, Pan Y, Nezi L, Protopopov A, Chowdury D, Pellman D (2012), “DNA Breaks and Chromsome Pulverizationfrom Errors in Mitosis.”Nature 482 (7383): 53–58. Figure 5. Re-used by Permission.
ous associated proteins, are highly polymerized into microtubuleswhich grow (“rescue”) and shrink (“catastrophe”) and probe theinternal cytoplasmic space of the cell, and form the highly dynamicframework (“dynamic instability”) upon which the chromosomalseparation of anaphase occurs [15,18]. Whilst the microtubulesappear to be static on fixed cell fluorescent imaging, in many tissuesthey are actually lengthening at their plus ends (centrally) whilstsimultaneously disassembling at their minus ends at the centri-ole (“treadmilling”) to give rise to an overall poleward flux [15]. Inparticular the Dana Farber/Harvard studies highlighted the way inwhich agents which interfere with tubulin polymerization or theirdynamic instability can have major downstream ramifications [1].This result has been shown both for various genetic disruptions[7,32,33] and chemical toxins.
3. Mitotic spindle poisons
The Boston studies used nocodozole to induce cell cycle arrest[1] which acts by binding tubulin subunits and preventing theirpolymerization [15]. Vincristine, vinblastine and colchicine act sim-ilarly [15]. The chemotherapeutic agent taxol acts by binding to andstabilizing microtubules, inhibiting their dynamic instability [15].
Of significance and concern 1-9 tetrahydrocannabinol (THC)[34–37] and other cannabinoids [38] act similarly to taxol. Impor-tantly it has been shown that a 2 h exposure to 5 and 10 mM of THCreduced tubulin mRNA by 50% & 78% [36]. Recapitulating manyof the key features of the above findings, THC has been shownto interfere with tubulin polymerization [34,39], be associatedwith micronuclear formation (4–6 fold increase) [21,40–45], cause
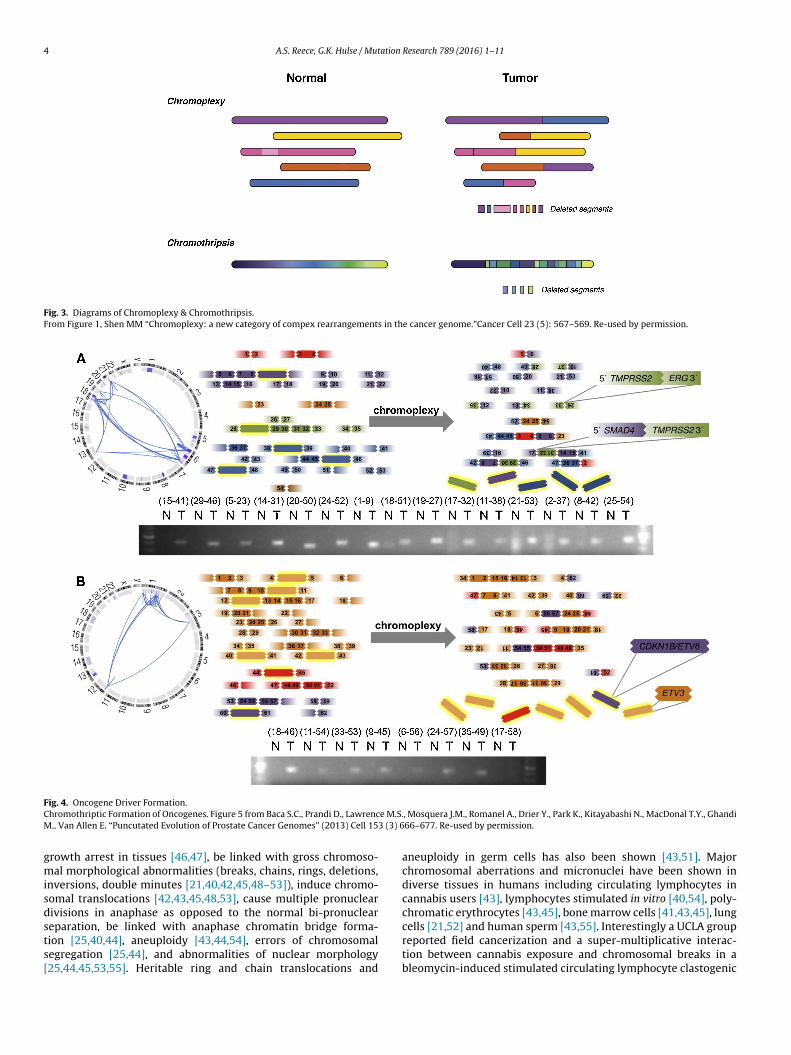
4 A.S. Reece, G.K. Hulse / Mutation Research 789 (2016) 1–11
Fig. 3. Diagrams of Chromoplexy & Chromothripsis.From Figure 1, Shen MM “Chromoplexy: a new category of compex rearrangements in the cancer genome.”Cancer Cell 23 (5): 567–569. Re-used by permission.
Fig. 4. Oncogene Driver Formation.Chromothriptic Formation of Oncogenes. Figure 5 from Baca S.C., Prandi D., Lawrence M.S., Mosquera J.M., Romanel A., Drier Y., Park K., Kitayabashi N., MacDonal T.Y., GhandiM., Van Allen E. “Puncutated Evolution of Prostate Cancer Genomes” (2013) Cell 153 (3) 666–677. Re-used by permission.
growth arrest in tissues [46,47], be linked with gross chromoso-mal morphological abnormalities (breaks, chains, rings, deletions,inversions, double minutes [21,40,42,45,48–53]), induce chromo-somal translocations [42,43,45,48,53], cause multiple pronucleardivisions in anaphase as opposed to the normal bi-pronuclearseparation, be linked with anaphase chromatin bridge forma-tion [25,40,44], aneuploidy [43,44,54], errors of chromosomalsegregation [25,44], and abnormalities of nuclear morphology[25,44,45,53,55]. Heritable ring and chain translocations and
aneuploidy in germ cells has also been shown [43,51]. Majorchromosomal aberrations and micronuclei have been shown indiverse tissues in humans including circulating lymphocytes incannabis users [43], lymphocytes stimulated in vitro [40,54], poly-chromatic erythrocytes [43,45], bone marrow cells [41,43,45], lungcells [21,52] and human sperm [43,55]. Interestingly a UCLA groupreported field cancerization and a super-multiplicative interac-tion between cannabis exposure and chromosomal breaks in ableomycin-induced stimulated circulating lymphocyte clastogenic
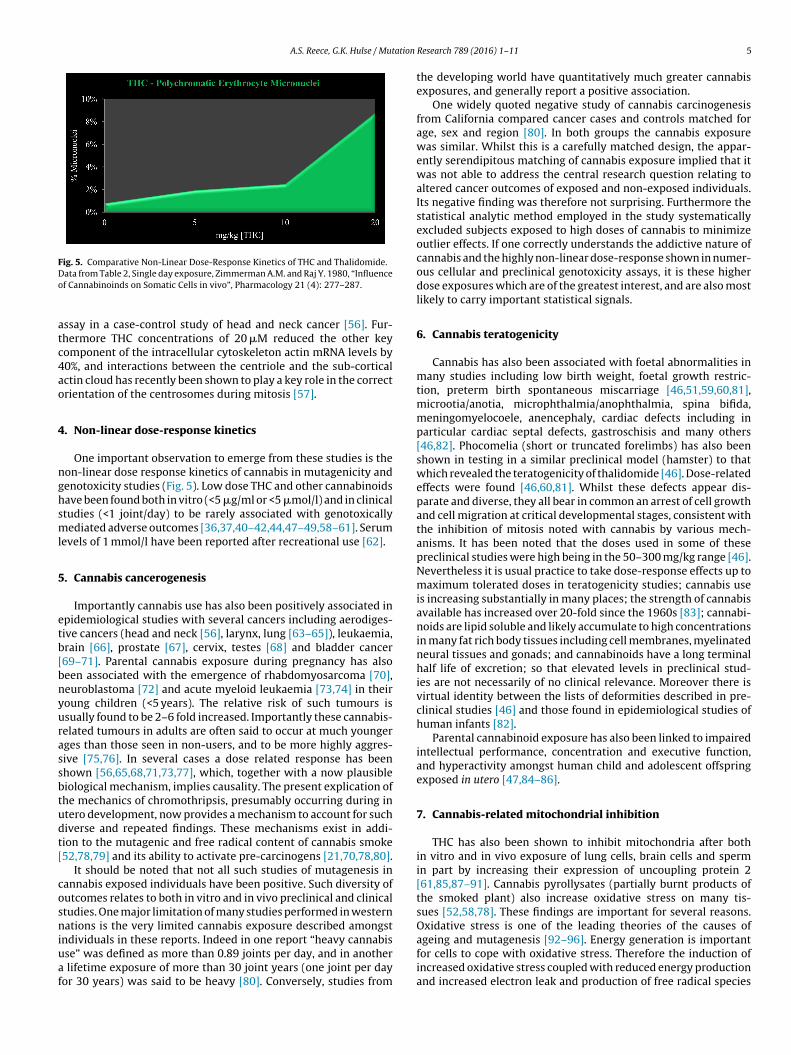
A.S. Reece, G.K. Hulse / Mutation Research 789 (2016) 1–11 5
Fig. 5. Comparative Non-Linear Dose-Response Kinetics of THC and Thalidomide.Data from Table 2, Single day exposure, Zimmerman A.M. and Raj Y. 1980, “Influenceof Cannabinoinds on Somatic Cells in vivo”, Pharmacology 21 (4): 277–287.
assay in a case-control study of head and neck cancer [56]. Fur-thermore THC concentrations of 20 mM reduced the other keycomponent of the intracellular cytoskeleton actin mRNA levels by40%, and interactions between the centriole and the sub-corticalactin cloud has recently been shown to play a key role in the correctorientation of the centrosomes during mitosis [57].
4. Non-linear dose-response kinetics
One important observation to emerge from these studies is thenon-linear dose response kinetics of cannabis in mutagenicity andgenotoxicity studies (Fig. 5). Low dose THC and other cannabinoidshave been found both in vitro (<5 mg/ml or <5 mmol/l) and in clinicalstudies (<1 joint/day) to be rarely associated with genotoxicallymediated adverse outcomes [36,37,40–42,44,47–49,58–61]. Serumlevels of 1 mmol/l have been reported after recreational use [62].
5. Cannabis cancerogenesis
Importantly cannabis use has also been positively associated inepidemiological studies with several cancers including aerodiges-tive cancers (head and neck [56], larynx, lung [63–65]), leukaemia,brain [66], prostate [67], cervix, testes [68] and bladder cancer[69–71]. Parental cannabis exposure during pregnancy has alsobeen associated with the emergence of rhabdomyosarcoma [70],neuroblastoma [72] and acute myeloid leukaemia [73,74] in theiryoung children (<5 years). The relative risk of such tumours isusually found to be 2–6 fold increased. Importantly these cannabis-related tumours in adults are often said to occur at much youngerages than those seen in non-users, and to be more highly aggres-sive [75,76]. In several cases a dose related response has beenshown [56,65,68,71,73,77], which, together with a now plausiblebiological mechanism, implies causality. The present explication ofthe mechanics of chromothripsis, presumably occurring during inutero development, now provides a mechanism to account for suchdiverse and repeated findings. These mechanisms exist in addi-tion to the mutagenic and free radical content of cannabis smoke[52,78,79] and its ability to activate pre-carcinogens [21,70,78,80].
It should be noted that not all such studies of mutagenesis incannabis exposed individuals have been positive. Such diversity ofoutcomes relates to both in vitro and in vivo preclinical and clinicalstudies. One major limitation of many studies performed in westernnations is the very limited cannabis exposure described amongstindividuals in these reports. Indeed in one report “heavy cannabisuse” was defined as more than 0.89 joints per day, and in anothera lifetime exposure of more than 30 joint years (one joint per dayfor 30 years) was said to be heavy [80]. Conversely, studies from
the developing world have quantitatively much greater cannabisexposures, and generally report a positive association.
One widely quoted negative study of cannabis carcinogenesisfrom California compared cancer cases and controls matched forage, sex and region [80]. In both groups the cannabis exposurewas similar. Whilst this is a carefully matched design, the appar-ently serendipitous matching of cannabis exposure implied that itwas not able to address the central research question relating toaltered cancer outcomes of exposed and non-exposed individuals.Its negative finding was therefore not surprising. Furthermore thestatistical analytic method employed in the study systematicallyexcluded subjects exposed to high doses of cannabis to minimizeoutlier effects. If one correctly understands the addictive nature ofcannabis and the highly non-linear dose-response shown in numer-ous cellular and preclinical genotoxicity assays, it is these higherdose exposures which are of the greatest interest, and are also mostlikely to carry important statistical signals.
6. Cannabis teratogenicity
Cannabis has also been associated with foetal abnormalities inmany studies including low birth weight, foetal growth restric-tion, preterm birth spontaneous miscarriage [46,51,59,60,81],microotia/anotia, microphthalmia/anophthalmia, spina bifida,meningomyelocoele, anencephaly, cardiac defects including inparticular cardiac septal defects, gastroschisis and many others[46,82]. Phocomelia (short or truncated forelimbs) has also beenshown in testing in a similar preclinical model (hamster) to thatwhich revealed the teratogenicity of thalidomide [46]. Dose-relatedeffects were found [46,60,81]. Whilst these defects appear dis-parate and diverse, they all bear in common an arrest of cell growthand cell migration at critical developmental stages, consistent withthe inhibition of mitosis noted with cannabis by various mech-anisms. It has been noted that the doses used in some of thesepreclinical studies were high being in the 50–300 mg/kg range [46].Nevertheless it is usual practice to take dose-response effects up tomaximum tolerated doses in teratogenicity studies; cannabis useis increasing substantially in many places; the strength of cannabisavailable has increased over 20-fold since the 1960s [83]; cannabi-noids are lipid soluble and likely accumulate to high concentrationsin many fat rich body tissues including cell membranes, myelinatedneural tissues and gonads; and cannabinoids have a long terminalhalf life of excretion; so that elevated levels in preclinical stud-ies are not necessarily of no clinical relevance. Moreover there isvirtual identity between the lists of deformities described in pre-clinical studies [46] and those found in epidemiological studies ofhuman infants [82].
Parental cannabinoid exposure has also been linked to impairedintellectual performance, concentration and executive function,and hyperactivity amongst human child and adolescent offspringexposed in utero [47,84–86].
7. Cannabis-related mitochondrial inhibition
THC has also been shown to inhibit mitochondria after bothin vitro and in vivo exposure of lung cells, brain cells and spermin part by increasing their expression of uncoupling protein 2[61,85,87–91]. Cannabis pyrollysates (partially burnt products ofthe smoked plant) also increase oxidative stress on many tis-sues [52,58,78]. These findings are important for several reasons.Oxidative stress is one of the leading theories of the causes ofageing and mutagenesis [92–96]. Energy generation is importantfor cells to cope with oxidative stress. Therefore the induction ofincreased oxidative stress coupled with reduced energy productionand increased electron leak and production of free radical species

6 A.S. Reece, G.K. Hulse / Mutation Research 789 (2016) 1–11
Fig. 6. Dividing Cell: Chromosomes, microtubules and mitochondria. (For interpre-tation of the references to colour in this figure legend, the reader is referred to theweb version of this article.)Dividing Cell; Tubulin in red; chromosomes in blue; mitochondria in green.National Cancer Institute, University of Pittsburgh Cancer Institute,Public Domain; https://visualsonline.cancer.gov/details.cfm?imageid=10708.
(and in many tissues reduced transcription of anti-oxidant defenceproteins [78]) is a powerful double edged pro-ageing insult. Mito-chondrial dysfunction is also one of the key hallmarks of cellularageing [97–99]. This is also consistent with our own unpublisheddata employing radial arterial tonometry of cardiovascular stiffness(by previously described techniques [100]) of increased cardio-vascular ageing (as a major surrogate for organismal aging) incannabis exposed patients compared to both control non-smokersand tobacco-only smokers in both cross-sectional and longitudinalstudies (unpublished data). This data in cannabis exposed patientsis consistent with other reports of accelerated aging after tobaccoand alcohol exposure [96] and after opioids [100–103].
8. Cannabis-related gametotoxicity, zygote toxicity and
reproductive impairment
Moreover cell division, and DNA and chromosomal replicationare very energy intensive processes. This point is well illustrated byFig. 6 which stains the mitotic spindle, chromosomes and the densenetwork of mitochondria surrounding the mitotic apparatus at theend of anaphase. Perhaps unsurprisingly mitotic errors includingchromosomal mis-segregation have been shown to be more com-mon in older cells [99]. Importantly it has also been shown thatimproved energy production from aged oocyte mitochondria isassociated with improved functional fidelity of the meiotic machin-ery and reduced errors of meiosis in female gametes and reducedsubsequent conceptus loss [99]. Meiosis in ova is relatively errorprone [17,99,104]. Cannabis has been shown to greatly increasethe rate of zygote death after the first cell division by 50% [25].The demonstration of sperm mitochondrial functional impairment[61] is similarly of great concern as it implies increased meioticerrors with the potential for transmission to subsequent genera-tion/s. Cannabinoids have also been shown to importantly mediateseveral sperm specific critical genetic functions via CB1R includ-ing DNA nicking in preparation for tight packing, the re-packagingof DNA from histones to transitional proteins and then to pro-tamines, and protection of packaged DNA [105,106]. Cannabinoidsalso play key functions in the reproductive tract, where they modifysperm activity, hypermotility and penetration, acrosome exocyto-
sis and egg penetration [61,107–109]. Cannabinoids and CB1R arepresent at high concentration in the oviduct and Graafian follicle[61]. Exogenous cannabinoids have been shown to act as partialfunctional antagonists and disruptors of these natural yet criticalendocannabinoid reactions [34,61,105,107].
9. Other microtubule functions
Microtubules are also essential to many other cell func-tions notably in stem cell niches and in neurons. It has beenshown that the cell cycle, particularly in S and G2 phases, gov-erns the human embryonic stem cell decision relating to theexit from pluripotency to cell differentiation (via a P53/ATM-ATR/CHEK2/CyclinB1/TGFb/Nanog spindle checkpoint pathway)[110], and that microtubule structures (nanotubes) mediate thespreading of deterministic molecular signals (bone morphogeneticprotein ligand decapentaplegic) from germ line niche cells to neigh-bouring stem cells (where it binds to its receptor Thickveins) andthus limit the stem cell maintenance signal to germ stem cells withwhich the hub support cells are in immediate contact [111]. Neu-ronal axons contain long microtubule bundles which can be up toone meter in length. Axons rapidly transport nutrients and pro-teins along using dynein and kinesin microtubule-based motors atspeeds of up to 1 mm/s [15]. Hence THC based disruption of micro-tubular function has been associated with loss of axonal directionfinding and an increase in target location errors, and errors of axonalsprouting [34,37].
The enzymes which metabolize cannabinoids in the brain(diacyl glyceryl lipase-a and monoacyl glyceryl lipase) and the dis-tribution of CB1R change dramatically during in utero and earlypost-natal development with important implications for axonalpathfinding and thus corticofugal tract definition, and this processis disrupted by exogenous cannabinoids [47]. As in sperm develop-ment, the endocannabinoid system plays a key role in such majorbrain developmental processes as cell proliferation, neurogenesis,migration and axon pathfinding via CB1R, CB2R, TRPV1R, GPR55and PPARa signalling and exophytocannabinoids act as partialantagonists and functional disruptors of this finely tuned system[47]. Hippocampal volume was found to be reduced in young ado-lescents following in utero exposure to cannabis, as have lastingalterations in glutamate, GABA, opioid serotonin and cholinergicmuscarinic and nicotinic brain signalling [47,112].
These effects of cannabinoids explain the confusing and para-doxical effects of cannabis in cancer. Various cannabinoids havebeen proposed to have possible therapeutic effects on tumoursand tumour growth in part by inhibition of DNA synthesis[43,50,113–116] but, as noted above, cannabinoids have alsobeen linked epidemiologically with carcinogenesis. The effects ofcannabis on tubulin and its association with cell growth inhibitionexplain these paradoxes – both can be true. Both cell cycle inhibi-tion and arrest of cell growth, and occasional mutant cell escapevia chromothriptic malignant induction can occur, both related tocannabis – tubulin interactions and in a dose dependent manner.Interestingly the function of the critical SAC checkpoint has beenshown to be reduced in tetraploid cells due to TP53 suppression,so such environments may make both error prone chromosomalreplication, and escape from the normal cell cycle controls, morecommon [7].
10. Other addictions
Interestingly similar comments can be made about severalother addictions. Dependency syndromes associated with alco-hol, tobacco, opioids and benzodiazepines have been associatedwith tumourigenesis [117–123]. Dependency on alcohol, benzo-
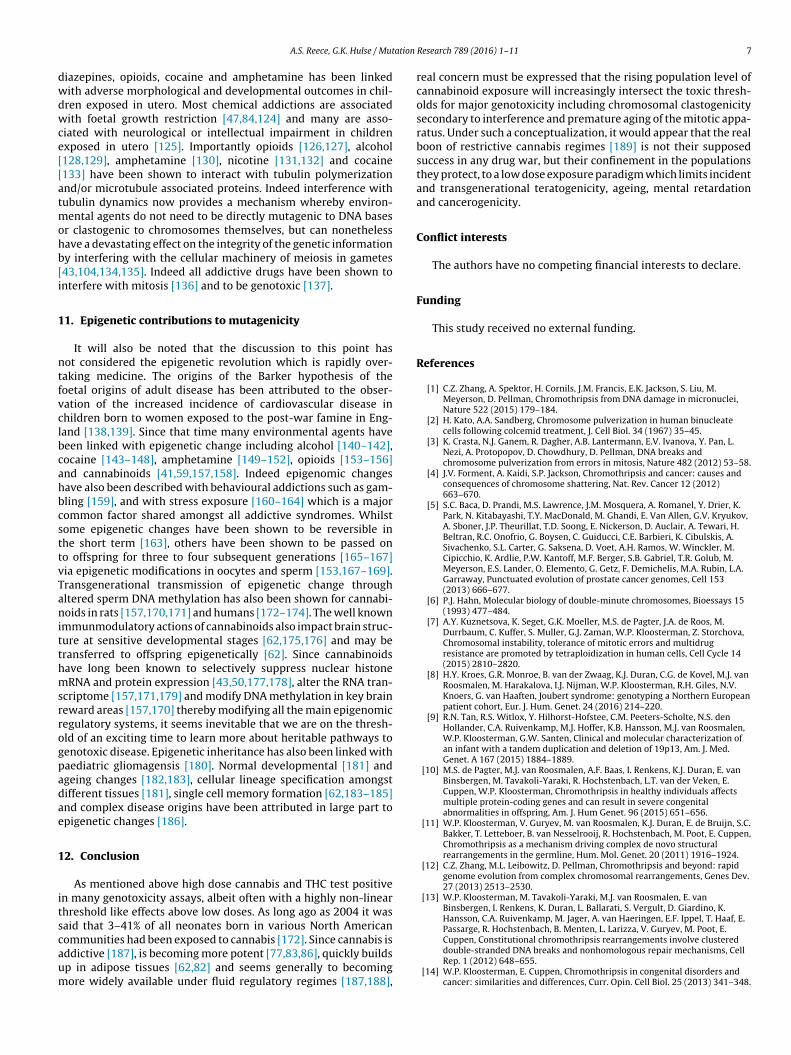
A.S. Reece, G.K. Hulse / Mutation Research 789 (2016) 1–11 7
diazepines, opioids, cocaine and amphetamine has been linkedwith adverse morphological and developmental outcomes in chil-dren exposed in utero. Most chemical addictions are associatedwith foetal growth restriction [47,84,124] and many are asso-ciated with neurological or intellectual impairment in childrenexposed in utero [125]. Importantly opioids [126,127], alcohol[128,129], amphetamine [130], nicotine [131,132] and cocaine[133] have been shown to interact with tubulin polymerizationand/or microtubule associated proteins. Indeed interference withtubulin dynamics now provides a mechanism whereby environ-mental agents do not need to be directly mutagenic to DNA basesor clastogenic to chromosomes themselves, but can nonethelesshave a devastating effect on the integrity of the genetic informationby interfering with the cellular machinery of meiosis in gametes[43,104,134,135]. Indeed all addictive drugs have been shown tointerfere with mitosis [136] and to be genotoxic [137].
11. Epigenetic contributions to mutagenicity
It will also be noted that the discussion to this point hasnot considered the epigenetic revolution which is rapidly over-taking medicine. The origins of the Barker hypothesis of thefoetal origins of adult disease has been attributed to the obser-vation of the increased incidence of cardiovascular disease inchildren born to women exposed to the post-war famine in Eng-land [138,139]. Since that time many environmental agents havebeen linked with epigenetic change including alcohol [140–142],cocaine [143–148], amphetamine [149–152], opioids [153–156]and cannabinoids [41,59,157,158]. Indeed epigenomic changeshave also been described with behavioural addictions such as gam-bling [159], and with stress exposure [160–164] which is a majorcommon factor shared amongst all addictive syndromes. Whilstsome epigenetic changes have been shown to be reversible inthe short term [163], others have been shown to be passed onto offspring for three to four subsequent generations [165–167]via epigenetic modifications in oocytes and sperm [153,167–169].Transgenerational transmission of epigenetic change throughaltered sperm DNA methylation has also been shown for cannabi-noids in rats [157,170,171] and humans [172–174]. The well knownimmunmodulatory actions of cannabinoids also impact brain struc-ture at sensitive developmental stages [62,175,176] and may betransferred to offspring epigenetically [62]. Since cannabinoidshave long been known to selectively suppress nuclear histonemRNA and protein expression [43,50,177,178], alter the RNA tran-scriptome [157,171,179] and modify DNA methylation in key brainreward areas [157,170] thereby modifying all the main epigenomicregulatory systems, it seems inevitable that we are on the thresh-old of an exciting time to learn more about heritable pathways togenotoxic disease. Epigenetic inheritance has also been linked withpaediatric gliomagensis [180]. Normal developmental [181] andageing changes [182,183], cellular lineage specification amongstdifferent tissues [181], single cell memory formation [62,183–185]and complex disease origins have been attributed in large part toepigenetic changes [186].
12. Conclusion
As mentioned above high dose cannabis and THC test positivein many genotoxicity assays, albeit often with a highly non-linearthreshold like effects above low doses. As long ago as 2004 it wassaid that 3–41% of all neonates born in various North Americancommunities had been exposed to cannabis [172]. Since cannabis isaddictive [187], is becoming more potent [77,83,86], quickly buildsup in adipose tissues [62,82] and seems generally to becomingmore widely available under fluid regulatory regimes [187,188],
real concern must be expressed that the rising population level ofcannabinoid exposure will increasingly intersect the toxic thresh-olds for major genotoxicity including chromosomal clastogenicitysecondary to interference and premature aging of the mitotic appa-ratus. Under such a conceptualization, it would appear that the realboon of restrictive cannabis regimes [189] is not their supposedsuccess in any drug war, but their confinement in the populationsthey protect, to a low dose exposure paradigm which limits incidentand transgenerational teratogenicity, ageing, mental retardationand cancerogenicity.
Conflict interests
The authors have no competing financial interests to declare.
Funding
This study received no external funding.
References
[1] C.Z. Zhang, A. Spektor, H. Cornils, J.M. Francis, E.K. Jackson, S. Liu, M.Meyerson, D. Pellman, Chromothripsis from DNA damage in micronuclei,Nature 522 (2015) 179–184.
[2] H. Kato, A.A. Sandberg, Chromosome pulverization in human binucleatecells following colcemid treatment, J. Cell Biol. 34 (1967) 35–45.
[3] K. Crasta, N.J. Ganem, R. Dagher, A.B. Lantermann, E.V. Ivanova, Y. Pan, L.Nezi, A. Protopopov, D. Chowdhury, D. Pellman, DNA breaks andchromosome pulverization from errors in mitosis, Nature 482 (2012) 53–58.
[4] J.V. Forment, A. Kaidi, S.P. Jackson, Chromothripsis and cancer: causes andconsequences of chromosome shattering, Nat. Rev. Cancer 12 (2012)663–670.
[5] S.C. Baca, D. Prandi, M.S. Lawrence, J.M. Mosquera, A. Romanel, Y. Drier, K.Park, N. Kitabayashi, T.Y. MacDonald, M. Ghandi, E. Van Allen, G.V. Kryukov,A. Sboner, J.P. Theurillat, T.D. Soong, E. Nickerson, D. Auclair, A. Tewari, H.Beltran, R.C. Onofrio, G. Boysen, C. Guiducci, C.E. Barbieri, K. Cibulskis, A.Sivachenko, S.L. Carter, G. Saksena, D. Voet, A.H. Ramos, W. Winckler, M.Cipicchio, K. Ardlie, P.W. Kantoff, M.F. Berger, S.B. Gabriel, T.R. Golub, M.Meyerson, E.S. Lander, O. Elemento, G. Getz, F. Demichelis, M.A. Rubin, L.A.Garraway, Punctuated evolution of prostate cancer genomes, Cell 153(2013) 666–677.
[6] P.J. Hahn, Molecular biology of double-minute chromosomes, Bioessays 15(1993) 477–484.
[7] A.Y. Kuznetsova, K. Seget, G.K. Moeller, M.S. de Pagter, J.A. de Roos, M.Durrbaum, C. Kuffer, S. Muller, G.J. Zaman, W.P. Kloosterman, Z. Storchova,Chromosomal instability, tolerance of mitotic errors and multidrugresistance are promoted by tetraploidization in human cells, Cell Cycle 14(2015) 2810–2820.
[8] H.Y. Kroes, G.R. Monroe, B. van der Zwaag, K.J. Duran, C.G. de Kovel, M.J. vanRoosmalen, M. Harakalova, I.J. Nijman, W.P. Kloosterman, R.H. Giles, N.V.Knoers, G. van Haaften, Joubert syndrome: genotyping a Northern Europeanpatient cohort, Eur. J. Hum. Genet. 24 (2016) 214–220.
[9] R.N. Tan, R.S. Witlox, Y. Hilhorst-Hofstee, C.M. Peeters-Scholte, N.S. denHollander, C.A. Ruivenkamp, M.J. Hoffer, K.B. Hansson, M.J. van Roosmalen,W.P. Kloosterman, G.W. Santen, Clinical and molecular characterization ofan infant with a tandem duplication and deletion of 19p13, Am. J. Med.Genet. A 167 (2015) 1884–1889.
[10] M.S. de Pagter, M.J. van Roosmalen, A.F. Baas, I. Renkens, K.J. Duran, E. vanBinsbergen, M. Tavakoli-Yaraki, R. Hochstenbach, L.T. van der Veken, E.Cuppen, W.P. Kloosterman, Chromothripsis in healthy individuals affectsmultiple protein-coding genes and can result in severe congenitalabnormalities in offspring, Am. J. Hum Genet. 96 (2015) 651–656.
[11] W.P. Kloosterman, V. Guryev, M. van Roosmalen, K.J. Duran, E. de Bruijn, S.C.Bakker, T. Letteboer, B. van Nesselrooij, R. Hochstenbach, M. Poot, E. Cuppen,Chromothripsis as a mechanism driving complex de novo structuralrearrangements in the germline, Hum. Mol. Genet. 20 (2011) 1916–1924.
[12] C.Z. Zhang, M.L. Leibowitz, D. Pellman, Chromothripsis and beyond: rapidgenome evolution from complex chromosomal rearrangements, Genes Dev.27 (2013) 2513–2530.
[13] W.P. Kloosterman, M. Tavakoli-Yaraki, M.J. van Roosmalen, E. vanBinsbergen, I. Renkens, K. Duran, L. Ballarati, S. Vergult, D. Giardino, K.Hansson, C.A. Ruivenkamp, M. Jager, A. van Haeringen, E.F. Ippel, T. Haaf, E.Passarge, R. Hochstenbach, B. Menten, L. Larizza, V. Guryev, M. Poot, E.Cuppen, Constitutional chromothripsis rearrangements involve clustereddouble-stranded DNA breaks and nonhomologous repair mechanisms, CellRep. 1 (2012) 648–655.
[14] W.P. Kloosterman, E. Cuppen, Chromothripsis in congenital disorders andcancer: similarities and differences, Curr. Opin. Cell Biol. 25 (2013) 341–348.
8 A.S. Reece, G.K. Hulse / Mutation Research 789 (2016) 1–11
[15] B. Alberts, A. Johnson, J. Lewis, M. Raff, K. Roberts, P. Walter, MolecularBiology of the Cell, 1601, Garland Science, New York, 2008.
[16] S. Ruchaud, M. Carmena, W.C. Earnshaw, Chromosomal passengers:conducting cell division, Nat. Rev. Mol. Cell Biol. 8 (2007) 798–812.
[17] A.Z. Balboula, P. Stein, R.M. Schultz, K. Schindler, Knockdown of RBBP7unveils a requirement of histone deacetylation for CPC function in mouseoocytes, Cell Cycle 13 (2014) 600–611.
[18] S. Lapenna, A. Giordano, Cell cycle kinases as therapeutic targets for cancer,Nat. Rev. 8 (2009) 547–566.
[19] L. Jia, S. Kim, H. Yu, Tracking spindle checkpoint signals from kinetochores toAPC/C, Trends Biochem. Sci. 38 (2013) 302–311.
[20] A.W. Wyatt, C.C. Collins, In brief: chromothripsis and cancer, J. Pathol. 231(2013) 1–3.
[21] R.M. Maertens, P.A. White, W. Rickert, G. Levasseur, G.R. Douglas, P.V.Bellier, J.P. McNamee, V. Thuppal, M. Walker, S. Desjardins, The genotoxicityof mainstream and sidestream marijuana and tobacco smoke condensates,Chem. Res. Toxicol. 22 (2009) 1406–1414.
[22] M.J. Jones, P.V. Jallepalli, Chromothripsis: chromosomes in crisis, Dev. Cell23 (2012) 908–917.
[23] N.J. Ganem, D. Pellman, Linking abnormal mitosis to the acquisition of DNAdamage, J. Cell Biol. 199 (2012) 871–881.
[24] G. Liu, J.B. Stevens, S.D. Horne, B.Y. Abdallah, K.J. Ye, S.W. Bremer, C.J. Ye, D.J.Chen, H.H. Heng, Genome chaos: survival strategy during crisis, Cell Cycle13 (2014) 528–537.
[25] A. Morishima, Effects of cannabis and natural cannabinoids onchromosomes and ova, NIDA Res. Monogr. 44 (1984) 25–45.
[26] P.J. Stephens, C.D. Greenman, B. Fu, F. Yang, G.R. Bignell, L.J. Mudie, E.D.Pleasance, K.W. Lau, D. Beare, L.A. Stebbings, S. McLaren, M.L. Lin, D.J.McBride, I. Varela, S. Nik-Zainal, C. Leroy, M. Jia, A. Menzies, A.P. Butler, J.W.Teague, M.A. Quail, J. Burton, H. Swerdlow, N.P. Carter, L.A. Morsberger, C.Iacobuzio-Donahue, G.A. Follows, A.R. Green, A.M. Flanagan, M.R. Stratton,P.A. Futreal, P.J. Campbell, Massive genomic rearrangement acquired in asingle catastrophic event during cancer development, Cell 144 (2011) 27–40.
[27] J.J. Molenaar, J. Koster, D.A. Zwijnenburg, P. van Sluis, L.J. Valentijn, I. van derPloeg, M. Hamdi, J. van Nes, B.A. Westerman, J. van Arkel, M.E. Ebus, F.Haneveld, A. Lakeman, L. Schild, P. Molenaar, P. Stroeken, M.M. van Noesel, I.Ora, E.E. Santo, H.N. Caron, E.M. Westerhout, R. Versteeg, Sequencing ofneuroblastoma identifies chromothripsis and defects in neuritogenesisgenes, Nature 483 (2012) 589–593.
[28] J.M. Furgason, R.F. Koncar, S.K. Michelhaugh, F.H. Sarkar, S. Mittal, A.E. Sloan,J.S. Barnholtz-Sloan, M. Bahassi el, Whole genome sequence analysis linkschromothripsis to EGFR, MDM2, MDM4, and CDK4 amplification inglioblastoma, Oncoscience 2 (2015) 618–628.
[29] W.P. Kloosterman, M. Hoogstraat, O. Paling, M. Tavakoli-Yaraki, I. Renkens,J.S. Vermaat, M.J. van Roosmalen, S. van Lieshout, I.J. Nijman, W. Roessingh,R. van ‘t Slot, J. van de Belt, V. Guryev, M. Koudijs, E. Voest, E. Cuppen,Chromothripsis is a common mechanism driving genomic rearrangementsin primary and metastatic colorectal cancer, Genome Biol. 12 (2011) R103.
[30] W.P. Kloosterman, J. Koster, J.J. Molenaar, Prevalence and clinicalimplications of chromothripsis in cancer genomes, Curr. Opin. Oncol. 26(2014) 64–72.
[31] D.H. McDermott, J.L. Gao, Q. Liu, M. Siwicki, C. Martens, P. Jacobs, D. Velez, E.Yim, C.R. Bryke, N. Hsu, Z. Dai, M.M. Marquesen, E. Stregevsky, N. Kwatemaa,N. Theobald, D.A. Long Priel, S. Pittaluga, M.A. Raffeld, K.R. Calvo, I. Maric, R.Desmond, K.L. Holmes, D.B. Kuhns, K. Balabanian, F. Bachelerie, S.F. Porcella,H.L. Malech, P.M. Murphy, Chromothriptic cure of WHIM syndrome, Cell 160(2015) 686–699.
[32] R. Sotillo, E. Hernando, E. Diaz-Rodriguez, J. Teruya-Feldstein, C.Cordon-Cardo, S.W. Lowe, R. Benezra, Mad2 overexpression promotesaneuploidy and tumorigenesis in mice, Cancer Cell 11 (2007) 9–23.
[33] R.M. Ricke, K.B. Jeganathan, J.M. van Deursen, Bub1 overexpression inducesaneuploidy and tumor formation through Aurora B kinase hyperactivation, J.Cell Biol. 193 (2011) 1049–1064.
[34] G. Tortoriello, C.V. Morris, A. Alpar, J. Fuzik, S.L. Shirran, D. Calvigioni, E.Keimpema, C.H. Botting, K. Reinecke, T. Herdegen, M. Courtney, Y.L. Hurd, T.Harkany, Miswiring the brain: delta9-tetrahydrocannabinol disruptscortical development by inducing an SCG10/stathmin-2 degradationpathway, EMBO J. 33 (2014) 668–685.
[35] S.L. Palmer, P.G. Meyehof, A.M. Zimmerman, Effects ofdelta-tetrahydrocannabinol on some aspects of mitotic organization, J. CellBiol. 91 (1981) 319a.
[36] S.K. Tahir, A.M. Zimmerman, Influence of marihuana on cellular structuresand biochemical activities, Pharmacol. Biochem. Behav. 40 (1991) 617–623.
[37] S.K. Tahir, J.E. Trogadis, J.K. Stevens, A.M. Zimmerman, Cytoskeletalorganization following cannabinoid treatment in undifferentiated anddifferentiated PC12 cells, Biochem. Cell Biol. 70 (1992) 1159–1173.
[38] R.G. Wilson Jr., S.K. Tahir, R. Mechoulam, S. Zimmerman, A.M. Zimmerman,Cannabinoid enantiomer action on the cytoarchitecture, Cell Biol. Int. 20(1996) 147–157.
[39] S.J. Parker, B.S. Zuckerman, A.M. Zimmermann, The effects of maternalmarijuana use during pregnancy on fetal growth, in: G.G. Nahas, K.M. Sutin,D.J. Harvey, S. Agurell (Eds.), Marijuana in Medicine, Humana PressTotowa,New York, 1999, pp. 461–468.
[40] V.J. Koller, F. Ferk, H. Al-Serori, M. Misik, A. Nersesyan, V. Auwarter, T.Grummt, S. Knasmuller, Genotoxic properties of representatives of
alkylindazoles and aminoalkyl-indoles which are consumed as syntheticcannabinoids, Food Chem. Toxicol. 80 (2015) 130–136.
[41] V.J. Koller, V. Auwarter, T. Grummt, B. Moosmann, M. Misik, S. Knasmuller,Investigation of the in vitro toxicological properties of the syntheticcannabimimetic drug CP-47,497-C8, Toxicol. Appl. Pharmacol. 277 (2014)164–171.
[42] A.M. Zimmerman, A.Y. Raj, Influence of cannabinoids on somatic cells invivo, Pharmacology 21 (1980) 277–287.
[43] S. Zimmerman, A.M. Zimmerman, Genetic effects of marijuana, Int. J. Addict.25 (1990) 19–33.
[44] R.T. Henrich, T. Nogawa, A. Morishima, In vitro induction of segregationalerrors of chromosomes by natural cannabinoids in normal humanlymphocytes, Environ. Mutagen. 2 (1980) 139–147.
[45] A.M. Zimmerman, S. Zimmerman, Cytogenetic studies of cannabinoideffects, in: M.C. Braude, A.M. Zimmerman (Eds.), Genetic and PerinatalEffects of Abused Substances, Academic Press Inc., Harcourt, BraceJovanovich, New York, 1987, pp. 95–112.
[46] W.F. Geber, L.C. Schramm, Teratogenicity of marihuana extract as influencedby plant origin and seasonal variation, Arch. Int. Pharmacodyn. Ther. 177(1969) 224–230.
[47] C.S. Wu, C.P. Jew, H.C. Lu, Lasting impacts of prenatal cannabis exposure andthe role of endogenous cannabinoids in the developing brain, Future Neurol.6 (2011) 459–480.
[48] D.G. Gilmour, A.D. Bloom, K.P. Lele, E.S. Robbins, C. Maximilian,Chromosomal aberrations in users of psychoactive drugs, Arch. Gen.Psychiatry 24 (1971) 268–272.
[49] M.A. Stenchever, T.J. Kunysz, M.A. Allen, Chromosome breakage in users ofmarihuana, Am. J. Obstet. Gynecol. 118 (1974) 106–113.
[50] M.J. Mon, R.L. Jansing, S. Doggett, J.L. Stein, G.S. Stein, Influence ofdelta9-tetrahydrocannabinol on cell proliferation and macromolecularbiosynthesis in human cells, Biochem. Pharmacol. 27 (1978) 1759–1765.
[51] S. Dalterio, F. Badr, A. Bartke, D. Mayfield, Cannabinoids in male mice:effects on fertility and spermatogenesis, Science 216 (1982) 315–316.
[52] H.R. Kim, B.H. Son, S.Y. Lee, K.H. Chung, S.M. Oh, The role of p53 in marijuanasmoke condensates-induced genotoxicity and apoptosis, Environ. HealthToxicol. 27 (2012) e2012017.
[53] A.M. Zimmerman, S. Zimmerman, A.Y. Raj, Effects of cannabinoids onspermatogensis in mice, in: G.G. Nahas, K.M. Sutin, D.J. Harvey, S. Agurell(Eds.), Marijuana and Medicine, Humana Press Totowa, New York, 1999, pp.347–358.
[54] A. Morishima, R.T. Henrich, J. Jayaraman, G.G. Nahas, Hypoploid metaphasesin cultured lymphocytes of marihuana smokers, Adv. Biosci. 22–23 (1978)371–376.
[55] W.C. Hembree Jr., G.G. Nahas, P. Zeidenberg, H.F.S. Huang, Changes inHuman Spermatozoa Associated with High Dose Marijuana Smoking, in:G.G. Nahas, K.M. Sutin, D.J. Harvey, S. Agurell (Eds.), Humana Press Totowa,New York, 1999, pp. 367–378.
[56] Z.F. Zhang, H. Morgenstern, M.R. Spitz, D.P. Tashkin, G.P. Yu, J.R. Marshall,T.C. Hsu, S.P. Schantz, Marijuana use and increased risk of squamous cellcarcinoma of the head and neck, Cancer Epidemiol. Biomarkers Prev. 8(1999) 1071–1078.
[57] M. Kwon, M. Bagonis, G. Danuser, D. Pellman, Direct microtubule-binding bymyosin-10 orients centrosomes toward retraction fibers and subcorticalactin clouds, Dev. Cell 34 (2015) 323–337.
[58] T. Sarafian, N. Habib, J.T. Mao, I.H. Tsu, M.L. Yamamoto, E. Hsu, D.P. Tashkin,M.D. Roth, Gene expression changes in human small airway epithelial cellsexposed to Delta9-tetrahydrocannabinol, Toxicol. Lett. 158 (2005) 95–107.
[59] M. Khare, A.H. Taylor, J.C. Konje, S.C. Bell, Delta9-tetrahydrocannabinolinhibits cytotrophoblast cell proliferation and modulates gene transcription,Mol. Hum. Reprod. 12 (2006) 321–333.
[60] J.D.P. Graham, Cannabis and health, in: J.D.P. Graham (Ed.), Cannabis andHealth, Academic PressLondon, New York, San Francisco, 1976, pp. 271–320.
[61] M. Rossato, F. Ion Popa, M. Ferigo, G. Clari, C. Foresta, Human sperm expresscannabinoid receptor Cb1, the activation of which inhibits motility,acrosome reaction, and mitochondrial function, J. Clin. Endocrinol. Metab.90 (2005) 984–991.
[62] C. Lombard, V.L. Hegde, M. Nagarkatti, P.S. Nagarkatti, Perinatal exposure toDelta9-tetrahydrocannabinol triggers profound defects in T celldifferentiation and function in fetal and postnatal stages of life, includingdecreased responsiveness to HIV antigens, J. Pharmacol. Exp. Ther. 339(2011) 607–617.
[63] S. Aldington, M. Harwood, B. Cox, M. Weatherall, L. Beckert, A. Hansell, A.Pritchard, G. Robinson, R. Beasley, Cannabis use and risk of lung cancer: acase-control study, Eur. Respir. J. 31 (2008) 280–286.
[64] N. Voirin, J. Berthiller, V. Benhaim-Luzon, M. Boniol, K. Straif, W.B. Ayoub,F.B. Ayed, A.J. Sasco, Risk of lung cancer and past use of cannabis in Tunisia, J.Thorac. Oncol. 1 (2006) 577–579.
[65] J. Berthiller, K. Straif, M. Boniol, N. Voirin, V. Benhaim-Luzon, W.B. Ayoub, I.Dari, S. Laouamri, M. Hamdi-Cherif, M. Bartal, F.B. Ayed, A.J. Sasco, Cannabissmoking and risk of lung cancer in men: a pooled analysis of three studies inMaghreb, J. Thorac. Oncol. 3 (2008) 1398–1403.
[66] J.T. Efird, G.D. Friedman, S. Sidney, A. Klatsky, L.A. Habel, N.V. Udaltsova, S.Van den Eeden, L.M. Nelson, The risk for malignant primary adult-onsetglioma in a large, multiethnic, managed-care cohort: cigarette smoking andother lifestyle behaviors, J. Neuro-Oncology. 68 (2004) 57–69.
A.S. Reece, G.K. Hulse / Mutation Research 789 (2016) 1–11 9
[67] S. Sidney, C.P. Quesenberry Jr., G.D. Friedman, I.S. Tekawa, Marijuana useand cancer incidence (California, United States), Cancer Causes Control 8(1997) 722–728.
[68] J.R. Daling, D.R. Doody, X. Sun, B.L. Trabert, N.S. Weiss, C. Chen, M.L. Biggs,J.R. Starr, S.K. Dey, S.M. Schwartz, Association of marijuana use and theincidence of testicular germ cell tumors, Cancer 115 (2009) 1215–1223.
[69] A.S. Reece, Chronic toxicology of cannabis, Clin. Toxicol. (2009) ()in press.[70] M. Hashibe, K. Straif, D.P. Tashkin, H. Morgenstern, S. Greenland, Z.F. Zhang,
Epidemiologic review of marijuana use and cancer risk, Alcohol (FayettevilleN.Y) 35 (2005) 265–275.
[71] J.A. Chacko, J.G. Heiner, W. Siu, M. Macy, M.K. Terris, Association betweenmarijuana use and transitional cell carcinoma, Urology 67 (2006) 100–104.
[72] E.C. Bluhm, J. Daniels, B.H. Pollock, A.F. Olshan, Maternal use of recreationaldrugs and neuroblastoma in offspring: a report from the Children’sOncology Group (United States), Cancer Causes Control 17 (2006) 663–669.
[73] L.L. Robison, J.D. Buckley, A.E. Daigle, R. Wells, D. Benjamin, D.C. Arthur, G.D.Hammond, Maternal drug use and risk of childhood nonlymphoblasticleukemia among offspring. An epidemiologic investigation implicatingmarijuana (a report from the Childrens Cancer Study Group), Cancer 63(1989) 1904–1911.
[74] W.Q. Wen, X.O. Shu, M. Steinbuch, R.K. Severson, G.H. Reaman, J.D. Buckley,L.L. Robison, Paternal military service and risk for childhood leukemia inoffspring, Am. J. Epidemiol. 151 (2000) 231–240.
[75] S. Bhattacharyya, S. Mandal, S. Banerjee, G.K. Mandal, A.K. Bhowmick, N.Murmu, Cannabis smoke can be a major risk factor for early-age laryngealcancer-a molecular signaling-based approach, Tumour. Biol. 36 (2015)6029–6036.
[76] M. Hashibe, D.E. Ford, Z.F. Zhang, Marijuana smoking and head and neckcancer, J. Clin. Pharmacol. 42 (2002) 103S–107S.
[77] W. Hall, The adverse health effects of cannabis use: what are they, and whatare their implications for policy? Int. J. Drug Policy 20 (2009) 458–466.
[78] R.M. Maertens, P.A. White, A. Williams, C.L. Yauk, A global toxicogenomicanalysis investigating the mechanistic differences between tobacco andmarijuana smoke condensates in vitro, Toxicology 308 (2013) 60–73.
[79] F.W. Busch, D.A. Seid, E.T. Wei, Mutagenic activity of marihuana smokecondensates, Cancer Lett. 6 (1979) 319–324.
[80] M. Hashibe, H. Morgenstern, Y. Cui, D.P. Tashkin, Z.F. Zhang, W. Cozen, T.M.Mack, S. Greenland, Marijuana use and the risk of lung and upperaerodigestive tract cancers: results of a population-based case-controlstudy, Cancer Epidemiol. Biomarkers Prev. 15 (2006) 1829–1834.
[81] W.F. Geber, L.C. Schramm, Effect of marihuana extract on fetal hamsters andrabbits, Toxicol. Appl. Pharmacol. 14 (1969) 276–282.
[82] M.B. Forrester, R.D. Merz, Risk of selected birth defects with prenatal illicitdrug use Hawaii, 1986–2002, J. Toxicol. Environ. Health 70 (2007) 7–18.
[83] W. Hall, L. Degenhardt, High potency cannabis: a risk factor for dependence,poor psychosocial outcomes, and psychosis, BMJ (Clinical research ed) 350(2015) h1205.
[84] N. Nora Volkow (Director, George Koob (Director, NIAAA), Alan Guttmacher(Director, NICHD), Bob Croyle (Director, Divison of Cancer Control andPopulation Sciences, NCI), National Longitudinal Study of theNeurodevelopmental Consequences of Substance Use, National Institutes ofHealth, Bethseda, Maryland, (2014).
[85] Adverse Health Effects of Marijuana Use, New England Journal of Medicine,371 (2014) 878–879.
[86] N.D. Volkow, R.D. Baler, W.M. Compton, S.R.B. Weiss, Adverse health effectsof marijuana use, N. Engl. J. Med. 370 (2014) 2219–2227.
[87] T.A. Sarafian, S. Kouyoumjian, F. Khoshaghideh, D.P. Tashkin, M.D. Roth,Delta 9-tetrahydrocannabinol disrupts mitochondrial function and cellenergetics, Am. J. Physiol. 284 (2003) L298–306.
[88] T.A. Sarafian, N. Habib, M. Oldham, N. Seeram, R.P. Lee, L. Lin, D.P. Tashkin,M.D. Roth, Inhaled marijuana smoke disrupts mitochondrial energetics inpulmonary epithelial cells in vivo, Am. J. Physiol. 290 (2006) L1202–1209.
[89] V. Wolff, O. Rouyer, A. Schlagowski, J. Zoll, J.S. Raul, C. Marescaux, Étude del’effet du THC sur la respiration mitochondriale du cerveau de rat. Une pistede réflexion pour expliquer le lien entre la consommation de cannabis et lasurvenue d’infarctus cérébral chez l’homme Study of the effect of THC onmitochondrial respiration of the rat brain. One line of thought to explain thelink between cannabis use and the occurrence of cerebral infarction in menRevue Neurologique, Neurol. Rev. 170 (2014) A19–A20.
[90] Z.S. Badawy, K.R. Chohan, D.A. Whyte, H.S. Penefsky, O.M. Brown, A.K. Souid,Cannabinoids inhibit the respiration of human sperm, Fertil. Steril. 91(2009) 2471–2476.
[91] B. Costa, M. Colleoni, Changes in rat brain energetic metabolism afterexposure to anandamide or Delta(9)-tetrahydrocannabinol, Eur. J.Pharmacol. 395 (2000) 1–7.
[92] C. Lopez-Otin, M.A. Blasco, L. Partridge, M. Serrano, G. Kroemer, Thehallmarks of aging, Cell 153 (2013) 1194–1217.
[93] R.S. Balaban, S. Nemoto, T. Finkel, Mitochondria, oxidants, and aging, Cell120 (2005) 483–495.
[94] E.C. Hadley, E.G. Lakatta, M. Morrison-Bogorad, H.R. Warner, R.J. Hodes, Thefuture of aging therapies, Cell 120 (2005) 557–567.
[95] T.B. Kirkwood, Understanding the odd science of aging, Cell 120 (2005)437–447.
[96] A.S. Fauci, E. Braunwald, D.L. Kapser, S.L. Hauser, D.L. Longo, J.L. Jameson,Harrison’s Principles of Internal Medicine, 17th edition, McGraw Hill, NewYork, 2008, pp. 2754.
[97] Secrets for Staying Young, Cell, 161, 1235.[98] P. Katajisto, J. Döhla, C.L. Chaffer, N. Pentinmikko, N. Marjanovic, S. Iqbal, R.
Zoncu, W. Chen, R.A. Weinberg, D.M. Sabatini, Asymmetric apportioning ofaged mitochondria between daughter cells is required for stemness, Science348 (2015) 340–343.
[99] A. Ben-Meir, E. Burstein, A. Borrego-Alvarez, J. Chong, E. Wong, T. Yavorska,T. Naranian, M. Chi, Y. Wang, Y. Bentov, J. Alexis, J. Meriano, H.K. Sung, D.L.Gasser, K.H. Moley, S. Hekimi, R.F. Casper, A. Jurisicova, Coenzyme Q10restores oocyte mitochondrial function and fertility during reproductiveaging, Aging Cell 14 (2015) 887–895.
[100] A.S. Reece, G.K. Hulse, impact of lifetime opioid exposure on arterialstiffness and vascular age: cross-sectional and longitudinal studies in menand women, BMJ Open 4 (2014) 1–19.
[101] A.S. Reece, G.K. Hulse, Impact of opioid pharmacotherapy on arterialstiffness and vascular ageing: cross-sectional and longitudinal studies,Cardiovasc. Toxicol. 13 (2013) 254–266.
[102] A.S. Reece, G.K. Hulse, Reduction in arterial stiffness and vascular age bynaltrexone-Induced interruption of opiate agonism, Br. Med. J. – Open 3(2013) (pii: e002610).
[103] G.L.F. Cheng, H. Zeng, M.K. Leung, H.J. Zhang, B.W.M. Lau, Y.P. Liu, G.X. Liu,P.C. Sham, C.C.H. Chan, K.F. So, T.M.C. Lee, Heroin abuse acceleratesbiological aging: a novel insight from telomerase and brain imaginginteraction, Transl. Psychiatry 3 (2013) e260.
[104] S. Pfender, V. Kuznetsov, M. Pasternak, T. Tischer, B. Santhanam, M. Schuh,Live imaging RNAi screen reveals genes essential for meiosis in mammalianoocytes, Nature 524 (2015) 239–242.
[105] T. Chioccarelli, G. Cacciola, L. Altucci, S.E. Lewis, L. Simon, G. Ricci, C. Ledent,R. Meccariello, S. Fasano, R. Pierantoni, G. Cobellis, Cannabinoid receptor 1influences chromatin remodeling in mouse spermatids by affecting contentof transition protein 2 mRNA and histone displacement, Endocrinology 151(2010) 5017–5029.
[106] G. Cacciola, T. Chioccarelli, L. Altucci, C. Ledent, J.I. Mason, S. Fasano, R.Pierantoni, G. Cobellis, Low 17beta-estradiol levels in CNR1 knock-out miceaffect spermatid chromatin remodeling by interfering with chromatinreorganization, Biol. Reprod. 88 (2013) 152.
[107] S.E. Lewis, M. Maccarrone, Endocannabinoids, sperm biology and humanfertility, Pharmacol. Res. 60 (2009) 126–131.
[108] N. Battista, C. Rapino, M. Di Tommaso, M. Bari, N. Pasquariello, M.Maccarrone, Regulation of male fertility by the endocannabinoid system,Mol. Cell. Endocrinol. 286 (2008) S17–23.
[109] M.R. Miller, N. Mannowetz, A.T. Iavarone, R. Safavi, E.O. Gracheva, J.F. Smith,R.Z. Hill, D.M. Bautista, Y. Kirichok, P.V. Lishko, Unconventionalendocannabinoid signaling governs sperm activation via the sex hormoneprogesterone, Science 352 (2016) 555–559.
[110] K.A. Gonzales, H. Liang, Y.S. Lim, Y.S. Chan, J.C. Yeo, C.P. Tan, B. Gao, B. Le, Z.Y.Tan, K.Y. Low, Y.C. Liou, F. Bard, H.H. Ng, Deterministic restriction onpluripotent state dissolution by cell-Cycle pathways, Cell 162 (2015)564–579.
[111] M. Inaba, M. Buszczak, Y.M. Yamashita, Nanotubes mediate niche-stem-cellsignalling in the Drosophila testis, Nature 523 (2015) 329–332.
[112] S. Navakkode, M. Korte, Pharmacological activation of CB1 receptormodulates long term potentiation by interfering with protein synthesis,Neuropharmacology 79 (2014) 525–533.
[113] A.E. Munson, L.S. Harris, M.A. Friedman, W.L. Dewey, R.A. Carchman,Antineoplastic activity of cannabinoids, J. Natl. Cancer Inst. 55 (1975)597–602.
[114] A. Preet, R.K. Ganju, J.E. Groopman, Delta9-Tetrahydrocannabinol inhibitsepithelial growth factor-induced lung cancer cell migration in vitro as wellas its growth and metastasis in vivo, Oncogene 27 (2008) 339–346.
[115] R.A. Carchman, L.S. Harris, A.E. Munson, The inhibition of DNA synthesis bycannabinoids, Cancer Res. 36 (1976) 95–100.
[116] S.K. Tilak, A.M. Zimmerman, Effects of cannabinoids on macromolecularsynthesis in isolated spermatogenic cells, Pharmacology 29 (1984) 343–350.
[117] E. Braunwald, A.S. Fauci, D.l Kasper., S.L. Hauser, D.L. Longo, J. J.L., Harrison’sPrinciples of Internal Medicine, 15th Edition, McGraw Hill New York (2001),pp. 1–2630.
[118] D.F. Kripke, R.D. Langer, L.E. Kline, Hypnotics’ association with mortality orcancer: a matched cohort study, BMJ Open 2 (2012) e000850.
[119] S. Behmard, A. Sadeghi, M.R. Mohareri, R. Kadivar, Positive association ofopium addiction and cancer of the bladder. Results of urine cytology in3,500 opium addicts, Acta Cytol. 25 (1981) 142–146.
[120] M.S. Fahmy, A. Sadeghi, S. Behmard, Epidemiologic study of oral cancer inFars Province, Iran, Community Dent. Oral Epidemiol. 11 (1983) 50–58.
[121] A. Ghavamzadeh, A. Moussavi, M. Jahani, M. Rastegarpanah, M. Iravani,Esophageal cancer in Iran, Semin. Oncol. 28 (2001) 153–157.
[122] M.R. Mousavi, M.A. Damghani, A.A. Haghdoust, A. Khamesipour, Opium andrisk of laryngeal cancer, Laryngoscope 113 (2003) 1939–1943.
[123] H. Khademi, R. Malekzadeh, A. Pourshams, E. Jafari, R. Salahi, S. Semnani, B.Abaie, F. Islami, S. Nasseri-Moghaddam, A. Etemadi, G. Byrnes, C.C. Abnet,S.M. Dawsey, N.E. Day, P.D. Pharoah, P. Boffetta, P. Brennan, F. Kamangar,Opium use and mortality in Golestan Cohort Study: prospective cohortstudy of 50 000 adults in Iran, BMJ (Clin. Res. ed.) 344 (2012) e2502.
[124] C. Davitian, M. Uzan, A. Tigaizin, G. Ducarme, H. Dauphin, C. Poncelet,[Maternal cannabis use and intra-uterine growth restriction], Gynecol.Obstet. Fertil. 34 (2006) 632–637.
10 A.S. Reece, G.K. Hulse / Mutation Research 789 (2016) 1–11
[125] T.M. Pinkert, Current research on the consequences of maternal drug abuse,NIDA Res. Monogr. 1 (1985) 1–113.
[126] C. Marie-Claire, C. Courtin, B.P. Roques, F. Noble, Cytoskeletal genesregulation by chronic morphine treatment in rat striatum,Neuropsychopharmacology 29 (2004) 2208–2215.
[127] R.Y. Tsai, Y.C. Cheng, C.S. Wong, (+)-Naloxone inhibits morphine-inducedchemotaxis via prevention of heat shock protein 90 cleavage in microglia, J.Formos Med. Assoc. 114 (2015) 446–455.
[128] A.M. Erdozain, B. Morentin, L. Bedford, E. King, D. Tooth, C. Brewer, D.Wayne, L. Johnson, H.K. Gerdes, P. Wigmore, L.F. Callado, W.G. Carter,Alcohol-related brain damage in humans, PLoS One 9 (2014) e93586.
[129] B.C. Feltes, J. de Faria Poloni, I.J. Nunes, D. Bonatto, Fetal alcohol syndrome,chemo-biology and OMICS: ethanol effects on vitamin metabolism duringneurodevelopment as measured by systems biology analysis, OMICS 18(2014) 344–363.
[130] S. Fernandes, S. Salta, T. Summavielle, Methamphetamine promotesalpha-tubulin deacetylation in endothelial cells: the protective role ofacetyl-l-carnitine, Toxicol. Lett. 234 (2015) 131–138.
[131] M.D. Minana, C. Montoliu, M. Llansola, S. Grisolia, V. Felipo, Nicotineprevents glutamate-induced proteolysis of the microtubule-associatedprotein MAP-2 and glutamate neurotoxicity in primary cultures ofcerebellar neurons, Neuropharmacology 37 (1998) 847–857.
[132] P. Poggi, M.T. Rota, R. Boratto, The volatile fraction of cigarette smokeinduces alterations in the human gingival fibroblast cytoskeleton, J.Periodontal Res. 37 (2002) 230–235.
[133] T.A. de Freitas, R.P. Palazzo, F.M. de Andrade, C.L. Reichert, F. Pechansky, F.Kessler, C.B. de Farias, G.G. de Andrade, S. Leistner-Segal, S.W. Maluf,Genomic instability in human lymphocytes from male users of crackcocaine, Int. J. Environ. Res. Public Health 11 (2014) 10003–10015.
[134] J. Dean, Exacting requirements for development of the egg, N. Engl. J. Med.374 (2016) 279–280.
[135] R. Feng, Q. Sang, Y. Kuang, X. Sun, Z. Yan, S. Zhang, J. Shi, G. Tian, A. Luchniak,Y. Fukuda, B. Li, M. Yu, J. Chen, Y. Xu, L. Guo, R. Qu, X. Wang, Z. Sun, M. Liu, H.Shi, H. Wang, Y. Feng, R. Shao, R. Chai, Q. Li, Q. Xing, R. Zhang, E. Nogales, L.Jin, L. He, M.L. Gupta, N.J. Cowan, L. Wang, Mutations in TUBB8 and humanoocyte meiotic arrest, New Engl. J. Med. 374 (2016) 223–232.
[136] A.J. Eisch, Adult neurogenesis: implications for psychiatry, Prog. Brain Res.138 (2002) 315–342.
[137] J.H. Li, L.F. Lin, Genetic toxicology of abused drugs: a brief review,Mutagenesis 13 (1998) 557–565.
[138] D.J. Barker, The fetal and infant origins of adult disease, B.M.J 301 (1990)1111.
[139] D.J. Barker, Fetal origins of cardiovascular disease, Ann. Med. 31 (Suppl. 1)(1999) 3–6.
[140] T. Hillemacher, H. Frieling, T. Hartl, J. Wilhelm, J. Kornhuber, S. Bleich,Promoter specific methylation of the dopamine transporter gene is alteredin alcohol dependence and associated with craving, J. Psychiatr. Res. 43(2009) 388–392.
[141] S. Rahman, Epigenetic mechanisms: targets for treatment of alcoholdependence and drug addiction, CNS Neurol. Disord. Drug Targets 11 (2012)101.
[142] I. Ponomarev, S. Wang, L. Zhang, R.A. Harris, R.D. Mayfield, Genecoexpression networks in human brain identify epigenetic modifications inalcohol dependence, J. Neurosci. 32 (2012) 1884–1897.
[143] F.M. Vassoler, S.L. White, H.D. Schmidt, G. Sadri-Vakili, R.C. Pierce,Epigenetic inheritance of a cocaine-resistance phenotype, Nat. Neurosci. 16(2013) 42–47.
[144] W. Renthal, A. Kumar, G. Xiao, M. Wilkinson, H.E. Covington 3rd, I. Maze, D.Sikder, A.J. Robison, Q. LaPlant, D.M. Dietz, S.J. Russo, V. Vialou, S.Chakravarty, T.J. Kodadek, A. Stack, M. Kabbaj, E.J. Nestler, Genome-wideanalysis of chromatin regulation by cocaine reveals a role for sirtuins,Neuron 62 (2009) 335–348.
[145] P.J. Kennedy, J. Feng, A.J. Robison, I. Maze, A. Badimon, E. Mouzon, D.Chaudhury, D.M. Damez-Werno, S.J. Haggarty, M.H. Han, R. Bassel-Duby,E.N. Olson, E.J. Nestler, Class I HDAC inhibition blocks cocaine-inducedplasticity by targeted changes in histone methylation, Nat. Neurosci. 16(2013) 434–440.
[146] H.E. Covington III., I. Maze, H. Sun, H.M. Bomze, K.D. DeMaio, E.Y. Wu, D.M.Dietz, M.K. Lobo, S. Ghose, E. Mouzon, R.L. Neve, C.A. Tamminga, E.J. Nestler,A role for repressive histone methylation in cocaine-Induced vulnerabilityto stress, Neuron 71 (2011) 656–670.
[147] F.F. Caputi, M. Di Benedetto, D. Carretta, S. Bastias del Carmen Candia, C.D’Addario, C. Cavina, S. Candeletti, P. Romualdi, Dynorphin/KOP andnociceptin/NOP gene expression and epigenetic changes by cocaine in ratstriatum and nucleus accumbens, Prog. Neuropsychopharmacol. Biol.Psychiatry. 49 (2014) 36–46.
[148] Q. Zhao, J. Hou, B. Chen, X. Shao, R. Zhu, Q. Bu, H. Gu, Y. Li, B. Zhang, C. Du, D.Fu, J. Kong, L. Luo, H. Long, H. Li, Y. Deng, Y. Zhao, X. Cen, Prenatal cocaineexposure impairs cognitive function of progeny via insulin growth factor IIepigenetic regulation, Neurobiol. Dis. 82 (2015) 54–65.
[149] A. Godino, S. Jayanthi, J.L. Cadet, Epigenetic landscape of amphetamine andmethamphetamine addiction in rodents, Epigenetics 10 (2015) 574–580.
[150] X. Li, F.J. Rubio, T. Zeric, J.M. Bossert, S. Kambhampati, H.M. Cates, P.J.Kennedy, Q.R. Liu, R. Cimbro, B.T. Hope, E.J. Nestler, Y. Shaham, Incubation ofmethamphetamine craving is associated with selective increases inexpression of Bdnf and trkb, glutamate receptors, and epigenetic enzymes in
cue-activated fos-expressing dorsal striatal neurons, J. Neurosci. 35 (2015)8232–8244.
[151] A. Aguilar-Valles, T. Vaissiere, E.M. Griggs, M.A. Mikaelsson, I.F. Takacs, E.J.Young, G. Rumbaugh, C.A. Miller, Methamphetamine-associated memory isregulated by a writer and an eraser of permissive histone methylation, Biol.Psychiatry 76 (2014) 57–65.
[152] A. Sadakierska-Chudy, M. Frankowska, M. Filip, Mitoepigenetics and drugaddiction, Pharmacol. Ther. 144 (2014) 226–233.
[153] D. Govorko, R.A. Bekdash, C. Zhang, D.K. Sarkar, Male germline transmitsfetal alcohol adverse effect on hypothalamic proopiomelanocortin geneacross generations, Biol. Psychiatry 72 (2012) 378–388.
[154] L.N. Wei, H.H. Loh, Transcriptional and epigenetic regulation of opioidreceptor genes: present and future, Annu. Rev. Pharmacol. Toxicol. 51(2011) 75–97.
[155] H. Sun, I. Maze, D.M. Dietz, K.N. Scobie, P.J. Kennedy, D. Damez-Werno, R.L.Neve, V. Zachariou, L. Shen, E.J. Nestler, Morphine epigenomically regulatesbehavior through alterations in histone H3 lysine 9 dimethylation in thenucleus accumbens, J. Neurosci. 32 (2012) 17454–17464.
[156] M.R. Chao, D. Fragou, P. Zanos, C.W. Hu, A. Bailey, S. Kouidou, L. Kovatsi,Epigenetically modified nucleotides in chronic heroin and cocaine treatedmice, Toxicol. Lett. 229 (2014) 451–457.
[157] J.A. DiNieri, X. Wang, H. Szutorisz, S.M. Spano, J. Kaur, P. Casaccia, D.Dow-Edwards, Y.L. Hurd, Maternal cannabis use alters ventral striataldopamine D2 gene regulation in the offspring, Biol. Psychiatry 70 (2011)763–769.
[158] H. Szutorisz, J.A. DiNieri, E. Sweet, G. Egervari, M. Michaelides, J.M. Carter, Y.Ren, M.L. Miller, R.D. Blitzer, Y.L. Hurd, Parental THC exposure leads tocompulsive heroin-seeking and altered striatal synaptic plasticity in thesubsequent generation, Neuropsychopharmacology 39 (2014) 1315–1323.
[159] T. Hillemacher, H. Frieling, V. Buchholz, R. Hussein, S. Bleich, C. Meyer, U.John, A. Bischof, H.J. Rumpf, Alterations in DNA-methylation of thedopamine-receptor 2 gene are associated with abstinence and health careutilization in individuals with a lifetime history of pathologic gambling,Prog. Neuropsychopharmacol. Biol. Psychiatry 63 (2015) 30–34.
[160] C. Dias, J. Feng, H. Sun, N.Y. Shao, M.S. Mazei-Robison, D. Damez-Werno, K.Scobie, R. Bagot, B. LaBonte, E. Ribeiro, X. Liu, P. Kennedy, V. Vialou, D.Ferguson, C. Pena, E.S. Calipari, J.W. Koo, E. Mouzon, S. Ghose, C. Tamminga,R. Neve, L. Shen, E.J. Nestler, beta-catenin mediates stress resilience throughDicer1/microRNA regulation, Nature 516 (2014) 51–55.
[161] J.J. Walsh, A.K. Friedman, H. Sun, E.A. Heller, S.M. Ku, B. Juarez, V.L. Burnham,M.S. Mazei-Robison, D. Ferguson, S.A. Golden, J.W. Koo, D. Chaudhury, D.J.Christoffel, L. Pomeranz, J.M. Friedman, S.J. Russo, E.J. Nestler, M.H. Han,Stress and CRF gate neural activation of BDNF in the mesolimbic rewardpathway, Nat. Neurosci. 17 (2014) 27–29.
[162] Y.N. Ohnishi, Y.H. Ohnishi, V. Vialou, E. Mouzon, Q. LaPlant, A. Nishi, E.J.Nestler, Functional role of the N-terminal domain of DeltaFosB in responseto stress and drugs of abuse, Neuroscience 284 (2015) 165–170.
[163] I.C. Weaver, N. Cervoni, F.A. Champagne, A.C. D’Alessio, S. Sharma, J.R. Seckl,S. Dymov, M. Szyf, M.J. Meaney, Epigenetic programming by maternalbehavior, Nat. Neurosci. 7 (2004) 847–854.
[164] S. St-Cyr, P.O. McGowan, Programming of stress-related behavior andepigenetic neural gene regulation in mice offspring through maternalexposure to predator odor, Front. Behav. Neurosci. 9 (2015) 145.
[165] M. Manikkam, C. Guerrero-Bosagna, R. Tracey, M.M. Haque, M.K. Skinner,Transgenerational actions of environmental compounds on reproductivedisease and identification of epigenetic biomarkers of ancestral exposures,PLoS One 7 (2012) e31901.
[166] V. Hughes, Epigenetics: the sins of the father, Nature 507 (2014) 22–24.[167] M. Manikkam, R. Tracey, C. Guerrero-Bosagna, M.K. Skinner, Dioxin (TCDD)
induces epigenetic transgenerational inheritance of adult onset disease andsperm epimutations, PLoS One 7 (2012) e46249.
[168] A. Ost, A. Lempradl, E. Casas, M. Weigert, T. Tiko, M. Deniz, L. Pantano, U.Boenisch, P.M. Itskov, M. Stoeckius, M. Ruf, N. Rajewsky, G. Reuter, N. Iovino,C. Ribeiro, M. Alenius, S. Heyne, T. Vavouri, J.A. Pospisilik, Paternal dietdefines offspring chromatin state and intergenerational obesity, Cell 159(2014) 1352–1364.
[169] T. Fullston, E.M. Ohlsson Teague, N.O. Palmer, M.J. DeBlasio, M. Mitchell, M.Corbett, C.G. Print, J.A. Owens, M. Lane, Paternal obesity initiates metabolicdisturbances in two generations of mice with incomplete penetrance to theF2 generation and alters the transcriptional profile of testis and spermmicroRNA content, FASEB J. 27 (2013) 4226–4243.
[170] C.T. Watson, H. Szutorisz, P. Garg, Q. Martin, J.A. Landry, A.J. Sharp, Y.L. Hurd,Genome-wide DNA methylation profiling reveals epigenetic changes in therat nucleus accumbens associated with cross-Generational effects ofadolescent THC exposure, Neuropsychopharmacology 40 (2015) 2993–3005.
[171] E.E. Zumbrun, J.M. Sido, P.S. Nagarkatti, M. Nagarkatti, Epigenetic regulationof immunological alterations following prenatal exposure to marijuanacannabinoids and its long term consequences in offspring, J. NeuroimmunePharmacol. 10 (2015) 245–254.
[172] X. Wang, D. Dow-Edwards, V. Anderson, H. Minkoff, Y.L. Hurd, In uteromarijuana exposure associated with abnormal amygdala dopamine D2 geneexpression in the human fetus, Biol. Psychiatry 56 (2004) 909–915.
[173] X. Wang, D. Dow-Edwards, E. Keller, Y.L. Hurd, Preferential limbicexpression of the cannabinoid receptor mRNA in the human fetal brain,Neuroscience 118 (2003) 681–694.

A.S. Reece, G.K. Hulse / Mutation Research 789 (2016) 1–11 11
[174] X. Wang, D. Dow-Edwards, V. Anderson, H. Minkoff, Y.L. Hurd, Discreteopioid gene expression impairment in the human fetal brain associatedwith maternal marijuana use, Pharmacogenomics J. 6 (2006) 255–264.
[175] B.E. Deverman, P.H. Patterson, Cytokines and CNS development, Neuron 64(2009) 61–78.
[176] L.M. Boulanger, Immune proteins in brain development and synapticplasticity, Neuron 64 (2009) 93–109.
[177] L.G. Green, J.L. Stein, G.S. Stein, Influence of delta 9-tetrahydrocannabinol onexpression of histone and ribosomal genes in normal and transformedhuman cells, Bioch. Pharmacol. 33 (1984) 1033–1040.
[178] G.S. Stein, J.L. Stein, Effects of cannabinoids on gene expression, NIDA Res.Monogr. 44 (1984) 5–24.
[179] M.S. Spano, M. Ellgren, X. Wang, Y.L. Hurd, Prenatal cannabis exposureincreases heroin seeking with allostatic changes in limbic enkephalinsystems in adulthood, Biol. Psychiatry 61 (2007) 554–563.
[180] P.W. Lewis, C.D. Allis, Poisoning the histone code in pediatric gliomagenesis,Cell Cycle 12 (2013) 3241–3242.
[181] K. Hochedlinger, K. Plath, Epigenetic reprogramming and inducedpluripotency, Development 136 (2009) 509–523.
[182] S. Horvath, DNA methylation age of human tissues and cell types, GenomeBiol. 14 (2013) R115.
[183] R.R. Kanherkar, N. Bhatia-Dey, A.B. Csoka, Epigenetics across the humanlifespan, Front Cell Dev. Biol. 2 (2014) 49.
[184] B.M. Turner, Cellular memory and the histone code, Cell 111 (2002)285–291.
[185] I.B. Zovkic, B.S. Paulukaitis, J.J. Day, D.M. Etikala, J.D. Sweatt, Histone H2A.Z.subunit exchange controls consolidation of recent and remote memory,Nature 515 (2014) 582–586.
[186] A. Petronis, Epigenetics as a unifying principle in the aetiology of complextraits and diseases, Nature 465 (2010) 721–727.
[187] N.D. Volkow, R.D. Baler, W.M. Compton, S.R. Weiss, Adverse health effects ofmarijuana use, N. Engl. J. Med. 370 (2014) 2219–2227.
[188] W. Hall, M. Weier, Assessing the public health impacts of legalizingrecreational cannabis use in the USA, Clin. Pharmacol. Ther. 97 (2015)607–615.
[189] W. Hall, Getting to grips with the cannabis problem: the evolvingcontributions and impact of Griffith Edwards, Addiction 110 (Suppl. 2)(2015) 36–39.

Could medical cannabis be the new THALIDOMIDE? Fears of a crisis as doctors consider doling marijuana-based medicines out to pregnant mothers despite evidence the drug can damage foetuses
• Pressure to loosen NHS guidelines on medical cannabis use is growing in the UK
• The British Medical Journal warned that widespread use could lead to disaster
• The potential crisis was compared to the thalidomide scandal of the 50s and 60s
By Guy Adams for the Daily Mail
Published: 10:31 AEST, 24 November 2018 | Updated: 05:36 AEST, 28 November 2018
Each of the 400 phone calls to the cannabis dispensaries followed a script. ‘Hi,’ said a female voice. ‘I’m eight weeks pregnant and feeling really nauseated. Are there any products recommended for morning sickness?’
In two-thirds of cases, the reply was: ‘Yes’.
Around half of those callers who’d received an affirmative answer were then advised to buy a specific ‘cure’ in a form they could eat.
Just under 40 per cent were told to get it in a form that could be inhaled or smoked. Most of the remainder were offered tinctures or drinks.
The recommended cure in question? Marijuana. But far from being genuine requests for help from expectant mothers, the phone calls were part of a research project by the University of Colorado.
The researchers were pretending to be pregnant to see how cannabis — legal for medical reasons in the U.S. state of Colorado since 2000 and fully legal since 2014 — was being dispensed. The answers they received offer a worrying insight into the booming medical marijuana industry.
When 400 phone calls were made to cannabis dispensaries from a supposedly pregnant woman, two thirds recommended cannabis products for morning sickness (stock image)
‘After eight weeks [of pregnancy], everything should be good with consuming alcohol and weed,’ one dispensary assistant replied.
‘When I was pregnant and started to feel nauseous, I did not smoke [cannabis] more than two times a day,’ recommended the proprietor of another clinic.
‘Edible [marijuana] would not hurt the child,’ reassured another, telling the woman, wrongly, that something ‘going through your digestional tract’ will have no effect on an unborn child.
Of the 277 dispensaries that recommended cannabis as a cure for morning sickness, three-quarters then attempted to sell a version of the drug containing THC, the chemical that gives users a ‘high’.
Many also advised their pregnant patients to keep their consumption of this intoxicating drug secret from their doctor.
‘The doctor will probably just tell you that marijuana is bad for kids and try pushing pills on you,’ said one. ‘I do not know if the baby doctors are chill or not, [so] do not go stoned when you talk to them,’ warned another.
Perhaps those doctors had good reason for their reservations about cannabis. For the Colorado research paper, published in the journal Obstetrics and Gynaecology earlier this year, highlights cannabis as a matter of growing concern to medical practitioners across the world.
Increasingly, marijuana is being sold for medical reasons. Yet this ‘medical’ marijuana is very far from being the safe, natural healthcare product its often-rapacious suppliers would have us believe.
‘After eight weeks [of pregnancy], everything should be good with consuming alcohol and weed,’ one dispensary assistant said (stock image)
In some circumstances, the product — which is becoming legal in growing numbers of countries, including Canada, the U.S. and most recently Britain in highly specific circumstances — can be dangerous and possibly fatal. Particularly when taken by pregnant women.
To blame is a simple fact: a multitude of studies over several years have shown all forms of cannabis to be ‘teratogenic’. Meaning that, like tobacco or excessive alcohol, they can harm a foetus.
The drug has been linked to a host of serious birth defects, including at least six life-threatening deformities.
They include two congenital heart problems; a neurological condition called anencephaly, in which a child is born with a large portion of the brain missing, often dying within hours; and the birth defect gastroschisis, where the intestines develop outside the body.
‘Babies exposed to marijuana in utero are at increased risk of admission to neonatal intensive care units,’ says Torri Metz, a University of Utah professor who was among the Colorado study’s authors.

‘There are also concerns about possible long-term effects on the developing brain, impacting cognitive function and decreasing academic ability later in childhood.’
Which brings us to the situation in Britain, where there is pressure on the Government from an increasingly powerful cannabis lobby to loosen the NHS guidelines on medical cannabis use.
In Britain, there is pressure on the Government from an increasingly powerful cannabis lobby to loosen the NHS guidelines on medical cannabis use (stock image, cannabis oil)
They were relaxed this year following two high-profile cases involving children who suffer from serious forms of epilepsy.
One, Alfie Dingley, found an unlicensed, technically illegal cannabis oil from Holland prevented his seizures. Another, Billy Caldwell, had medical marijuana from Canada confiscated at customs, causing him to be admitted to hospital with what his family described as ‘life-threatening’ seizures.
In response to the public outcry over both cases, the Home Office relaxed the law to allow specialist doctors to prescribe unlicensed cannabis-based drugs to patients.
Their use is still limited to three distinct conditions: epilepsy, nausea associated with chemotherapy, and muscle stiffness associated with multiple sclerosis. Even then, patients must first have tried conventional medicines.
But the cannabis lobby is calling for it to be made more widely available, claiming six million Britons would eventually use the product for a variety of ailments, including pain and nausea relief. It would almost certainly mean dispensaries handing it out over the counter, just like in Colorado.
The British Medical Journal (BMJ) recently published an article arguing that the widespread use of medical cannabis could eventually lead to a public health crisis bearing comparison with the thalidomide disaster.
‘When I was pregnant and started to feel nauseous, I did not smoke [cannabis] more than two times a day,’ recommended the proprietor of another clinic (stock image)
That scandal, one of the most notorious in modern history, came after the drug thalidomide was given to large numbers of pregnant women from the late Fifties to the early Sixties, mostly to treat morning sickness.
It caused hundreds of thousands of miscarriages, and resulted in around 10,000 babies being severely deformed. Many died.
‘Thalidomide was marketed for anxiety, morning sickness and pain relief. Very similar claims are now being made about cannabis, and we are being told that millions of people should take it,’ says the author of the BMJ article, Dr Albert Reece, a professor of medicine at Edith Cowan University in Perth, Australia.
‘But as with thalidomide, no one is properly looking at the side-effects. They are frightening.
‘During foetal development, the presence of it increases the chances of a child developing heart and intestinal defects. In the womb, it can also not only interfere with brain development but basically amputate the forebrain.’
Even for adults, there are serious side-effects, he adds: ‘Cannabis is linked to serious psychiatric symptoms, including depression, anxiety, bipolar disorder and schizophrenia. Plus stroke, heart attack and 12 kinds of cancer.’
The cannabis doctors can now prescribe in Britain — albeit only to certain very sick patients — can have intoxicating levels of the chemical THC. Most British patients who will take it are expected to be given it in the form of capsules or a highly concentrated oil. However, chemically speaking, there will be very little to distinguish these medical products from what recreational cannabis users might smoke.
For example, Bedrocan, a Dutch-made brand which is one of the world’s most popular varieties of medical cannabis, contains 22 per cent THC according to its manufacturer’s website, making it more intoxicating even than the ‘skunk’ (which ranges from around 14 per cent to 20 per cent THC for ‘superskunk’) that illegal dealers sell.
The difference, says the manufacturer, is that Bedrocan — which consists purely of dried cannabis flowers — is chemically standardised, so it is easier to regulate dosage, when taking the product.
Meanwhile, in California, where medical cannabis was first made available 20 years ago and has since been entirely legalised, a high-profile organisation called ‘Cannamommy’ advertises a range of what it terms ‘safe, organic natural products’ designed for mothers. One popular brand of medical marijuana is called ‘Trainwreck’, advertised as a cure for migraines, pain and arthritis.
In California, where medical cannabis was first made available 20 years ago and has since been entirely legalised, a high-profile organisation called ‘Cannamommy’ advertises a range of what it terms ‘safe, organic natural products’ designed for mothers (stock image)
According to the maker, the product, which is between 12 and 21 per cent THC and is sold in a dried form suitable for smoking, ‘begins its hurtle through the mind with a surge of euphoria, awakening creativity and happiness’.
Another Cannamommy product, ‘Green Crack’, which it recommends for housewives suffering ‘fatigue, stress and depression’, induces ‘an invigorating mental buzz’. A third, ‘Guerilla Glue’, will apparently ‘deliver heavy-handed euphoria and relaxation, leaving you feeling glued to the couch’.
To critics, this sales patter suggests many customers are as interested in enjoying a legal high as they are the medical benefits.
And when medical marijuana products are aimed at mothers, it’s a dangerous trend, they argue.
‘We are at ground zero of this new medical epidemic, which will lead to havoc,’ says one critic, Karen Randall, an emergency room physician in Colorado. ‘The number of babies testing positive for THC has increased dramatically.’
Randall says her local area contains 15 medical cannabis dispensaries. ‘When a breast-feeding mother uses marijuana, it gets concentrated in the breast milk.
‘There are many studies that show memory is decreased with constant use, so I guess that in five to ten years, we are going to see a lot of kids with learning issues.’
Someone who illustrates the potential hazards is Marie McKillop, 36, from the Australian city of Brisbane, who says smoking marijuana during pregnancy led to her daughter’s death.
This ‘medical’ marijuana is very far from being the safe, natural healthcare product its often-rapacious suppliers would have us believe (stock image)
Her baby, named Crystal, weighed just 2lb 9oz at birth and was unable to breathe or feed unaided because of a serious congenital heart defect. She underwent three major heart surgeries, but died aged eight months.
Adding to her mother’s trauma was the fact she’d previously had four miscarriages. ‘I felt totally broken,’ Marie says.
At the time the tragedy occurred, several years ago, McKillop was a troubled young woman battling substance abuse problems.
Though clinicians advised her to steer clear of the hardest illegal narcotics, they concluded that she should continue to take marijuana while pregnant. ‘The fear was that if I stopped, it would give me withdrawal symptoms, which could make me miscarry,’ she recalls.
Later, in hospital reports, marijuana was described as a ‘high contributing factor’ to Crystal’s subsequent health problems.
Thankfully, having weaned herself off drugs, Marie has since had three healthy children.
Others won’t be so lucky.
Her doctor, Stuart Reece, believes the drug affects three key organs of an unborn child: the brain, the heart and the intestines.
He cites a study in the Toxicology Journal last year in which pregnant laboratory mice were exposed to cannabis, which found that ‘smoking marijuana during pregnancy even at low doses can be embryotoxic and fetotoxic’; and a University of Arkansas study also from 2017 which associated pre-natal cannabis exposure with ‘lower birth weight, life-long smaller head circumference, reduced length of gestation, neonatal neurological disturbances, [and] reduced function in specific cognitive domains’.
Two studies by the American Center for Disease Control have linked it to anencephaly, while the American Heart Association and American Academy of Pediatrics believe it increases rates of ventricular septal defect and Ebstein’s anomaly, two heart defects.
The drug’s links to gastroschisis — when the intestines develop outside the body — are documented by, among others, a long-running Canadian study and a Hawaiian research project which has linked cannabis to no fewer than 21 birth defects.
‘Only once has a known teratogen like cannabis been marketed globally,’ Dr Reece says.
‘That was thalidomide. It’s the reason we have the entire modern drug approval system, but the medical cannabis lobby is saying that system should be abandoned and the drug should be given to millions of people. It’s incredibly dangerous.’
Sharing this view are 166 of Britain’s most eminent pain relief doctors. Last month, they wrote to The Times, saying medical cannabis ‘will provide little or no long-term benefit in improving pain and may be associated with significant long-term adverse cognitive and mental-health detriment.’
Until this year’s relaxation in the law, drugs in Britain that are made from cannabis had an identical status to those derived from other illegal narcotics such as heroin (stock image)
They argued there is no medical evidence that, in this field, cannabis works. There are, however, serious psychological problems associated with its regular use.
The 166 doctors cited a report from the International Association for the Study of Pain, which took in the results of 104 studies.
The report concluded that 24 patients in pain would need to be treated for just one to experience any benefit.
Yet one in six would suffer some form of ‘harm’ due to side-effects, including nausea, dizziness, insomnia and depression.
And the report concluded: ‘It seems unlikely cannabinoids are highly effective medicines for chronic non-cancer pain.’
‘As doctors, the first law is to “do no harm”,’ says author Dr Raj Munglani, a chronic pain expert who practises in Cambridge and London. ‘We could end up damaging more people than we help. We fear new rules in the UK could cause a major public health crisis.’
Until this year’s relaxation in the law, drugs in Britain that are made from cannabis had an identical status to those derived from other illegal narcotics such as heroin.
To be licensed for medical use, these products must undergo stringent testing to ensure that they are effective and safe.
Though the licensing process takes several years, it’s perfectly possible to negotiate it.
The UK firm GW Pharmaceuticals has done just that with marijuana, developing two licensed drugs: Sativex (with moderate levels of THC) which treats spasticity associated with multiple sclerosis, and Epidolex, for epilepsy (interestingly, patient notes make clear that they must never be taken by pregnant women).

In theory, there’s never been anything to stop other advocates of medical cannabis developing licensed products in this way to combat the myriad other conditions they say it can treat. But none have so far succeeded.
It seems it’s far easier to lobby politicians to relax the licensing laws. But the danger is that this could one day lead to a situation in Britain where, as in Colorado, cannabis is sold as a cure for morning sickness — with potentially terrifying consequences.
RESEARCH ARTICLE Open Access
A geospatiotemporal and causal inferenceepidemiological exploration of substanceand cannabinoid exposure as drivers ofrising US pediatric cancer ratesAlbert Stuart Reece1,2* and Gary Kenneth Hulse1,2
Abstract
Background: Age-adjusted US total pediatric cancer incidence rates (TPCIR) rose 49% 1975–2015 for unknownreasons. Prenatal cannabis exposure has been linked with several pediatric cancers which together comprise themajority of pediatric cancer types. We investigated whether cannabis use was related spatiotemporally and causallyto TPCIR.
Methods: State-based age-adjusted TPCIR data was taken from the CDC Surveillance, Epidemiology and EndResults cancer database 2003–2017. Drug exposure was taken from the nationally-representative National Survey ofDrug Use and Health, response rate 74.1%. Drugs included were: tobacco, alcohol, cannabis, opioid analgesics andcocaine. This was supplemented by cannabinoid concentration data from the Drug Enforcement Agency andethnicity and median household income data from US Census.
Results: TPCIR rose while all drug use nationally fell, except for cannabis which rose. TPCIR in the highest cannabisuse quintile was greater than in the lowest (β-estimate = 1.31 (95%C.I. 0.82, 1.80), P = 1.80 × 10− 7) and the time:highest two quintiles interaction was significant (β-estimate = 0.1395 (0.82, 1.80), P = 1.00 × 10− 14). In robust inverseprobability weighted additive regression models cannabis was independently associated with TPCIR (β-estimate =9.55 (3.95, 15.15), P = 0.0016). In interactive geospatiotemporal models including all drug, ethnic and incomevariables cannabis use was independently significant (β-estimate = 45.67 (18.77, 72.56), P = 0.0009). In geospatialmodels temporally lagged to 1,2,4 and 6 years interactive terms including cannabis were significant. Cannabisinteractive terms at one and two degrees of spatial lagging were significant (from β-estimate = 3954.04 (1565.01,6343.09), P = 0.0012). The interaction between the cannabinoids THC and cannabigerol was significant at zero, 2and 6 years lag (from β-estimate = 46.22 (30.06, 62.38), P = 2.10 × 10− 8). Cannabis legalization was associated withhigher TPCIR (β-estimate = 1.51 (0.68, 2.35), P = 0.0004) and cannabis-liberal regimes were associated with highertime:TPCIR interaction (β-estimate = 1.87 × 10− 4, (2.9 × 10− 5, 2.45 × 10− 4), P = 0.0208). 33/56 minimum e-Valueswere > 5 and 6 were infinite.
(Continued on next page)
© The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver (http://creativecommons.org/publicdomain/zero/1.0/) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
* Correspondence: [email protected] of Psychiatry, University of Western Australia, Crawley, WesternAustralia 6009, Australia2School of Medical and Health Sciences, Edith Cowan University, Joondalup,Western Australia 6027, Australia
Reece and Hulse BMC Cancer (2021) 21:197 https://doi.org/10.1186/s12885-021-07924-3

(Continued from previous page)
Conclusion: Data confirm a close relationship across space and lagged time between cannabis and TPCIR whichwas robust to adjustment, supported by inverse probability weighting procedures and accompanied by high e-Values making confounding unlikely and establishing the causal relationship. Cannabis-liberal jurisdictions wereassociated with higher rates of TPCIR and a faster rate of TPCIR increase. Data inform the broader generalconsideration of cannabinoid-induced genotoxicity.
Keywords: Cannabis, Cannabinoid, Δ9-tetrahydrocannabinol, Cannabigerol, Genotoxicity, Acute leukaemia, Pediatriccancer
BackgroundCDC Surveillance, Epidemiology and End Results (SEER)data from 9 US cancer registries indicates that the age-adjusted total Pediatric (age less than 20 years) cancerincidence rate (TPCIR) has risen 49.0% from 12.96 to19.32 / 100,000 from 1975 to 2015 [1]. Cancer incidenceis U-shaped across the pediatric age range being higherin the under 5 years and over 14 years age groups [2].Leukaemias, brain and nervous system, neuroblastoma,soft tissue sarcoma, lymphoma and testicular cancer areamongst the commonest pediatric cancers [2, 3].Notwithstanding a generally falling mortality rate from
childhood cancer, the TPCIR incidence is acknowledgedto be rising since the records of collated cancer registrieswere first published in 1975 [2]. The cause of this unpre-cedented increase is at present unclear. Moreover majorethnic differentials are evident for tumours such as AllChildhood Cancer (ACC), acute lymphatic leukaemia(ALL) and brain and testicular cancers where the ratesin African-American patients vary from 20 to 70% ofthose in the Caucasian-American community [2]. Againthe reasons for such large ethnic disparities are un-known. It therefore appears that several of the majorquestions relating to the aetiopathogenesis of pediatriccancer are outstanding.Whilst in adult populations the relationship between
cannabis use and cancer incidence is controversial withboth positive and negative reports in existence [4, 5],amongst pediatric populations the situation is muchclearer. It was noted by the California EnvironmentalProtection Agency in a very detailed literature reviewthat five of six studies reported a positive relationship[6–11]. Parental cannabis use has been linked with acutelymphatic leukaemia, acute myeloid leukaemia, child-hood astrocytoma, rhabdomyosarcoma and neuroblast-oma [2, 7–12]. Together these comprise 60–70% of thetotal cancers seen in children younger than 14 years andthose between 15 and 20 years [2]. In such a context itbecomes plausible that the rise in cannabis use since the1960’s may be a primary driver of total pediatric cancer.Testicular cancer is a particularly interesting case. It is
well established that testicular cancer occurs mainly inyounger men with an age peak at 30–34 years and 20%
of cases occur in the pediatric age range [1]. The tes-tes houses the germ cells and cannabinoids areknown to have myriad direct effects on the repro-ductive tract in both sexes [13–17]. There is greatuniformity in studies of the cannabis-testicular cancerlink as all four studies found a risk elevation of overtwo-fold [18–21] with an overall risk for current,weekly and chronic smokers of non-seminomatousgerm cell tumours estimated in meta-analysis of 2.59(95%C.I. 1.60–4.19) [22]. Since pediatric cancer oftenresults from inherited genetic errors [23, 24] thisimplies that major genetic errors in germ cells areinduced by parental cannabis exposure.Adding to concerns related to the potentially geno-
toxic actions of prenatal cannabinoid exposure (PCE) isan increasing interest in elevation of many birth defectsfollowing PCE in Hawaii, Colorado, Canada andAustralia [25–28]. A recent report noted a three-fold risein total congenital defects in the northern Territories ofCanada where more cannabis is smoked [28]. Downssyndrome, due to a major genetic trisomic error, hasalso been found to be elevated following PCE in Hawaii,Colorado and Australia [25–27] and this syndrome hasan established link with childhood ALL with 6–10% ofDowns syndrome children being affected by thismalignancy [29, 30].As discussed below the physiology and pathophysi-
ology of both the endocannabinoid system and theimpacts of diverse exogenous phytocannabinoids is pres-ently being studied in great detail and major impacts onreproductive health, genetic and physiological quality ofgametes, epigenetic effects on both DNA methylationand histone synthesis and signalling, immunomodulatoryand mitochondriopathic effects, and transgenerationalinheritable epigenetic effects in both man and mouse arewell established and have been demonstrated by a num-ber of investigators [15, 17, 31–38].Concerns are heightened by the recent demonstration
that 69% of cannabis dispensaries in Colorado recom-mended cannabis use to pregnant patients for varioussymptoms in a recent telephone survey [39] and that in2017 an estimated 161,000 women used cannabis whilstpregnant across USA [40, 41].
Reece and Hulse BMC Cancer (2021) 21:197 Page 2 of 33

Taken together these data suggest that an improvedunderstanding of cannabis-related carcinogenesis in theclosely defined pediatric context might well lead to im-portant insights into cannabis-related genotoxicity moregenerally [42, 43]. Moreover the advent of sophisticatedgeospatial analysis together with some of the formaltechniques of causal inference analysis implies that so-phisticated and modern analytical procedures could bebrought to bear on these important and increasinglytopical issues. Techniques such as inverse probabilityweighting and e-Values are designed to formally investi-gate causal, as opposed to merely associational,relationships.The objective of this study was to determine if the rise
in pediatric cancers across USA paralleled the recent risein the use of cannabis when considered formally acrossspace and time, and if the relationship met the criteriafor causal inference when assessed by strict quantitativecriteria.
MethodsDataAnnual data on age-adjusted rates of pediatric cancercases occurring in patients less than 20 years old wasaccessed from the publicly available SEER*Explorer web-site [1]. Data on state-based pediatric cancer rates wasaccessed via the SEER*Stat software from the SEER /NCI database [44]. Drug use data was accessed from thenationally representative National Survey of Drug Useand Health (NSDUH) conducted by the SubstanceAbuse and Mental Health Services Administration(SAMHSA) [45]. This survey reports a 74.1% responserate [46]. Data on the following drug variables was col-lated: monthly cigarette use; annual alcohol use disorder,monthly cannabis use, annual analgesic abuse and an-nual cocaine use. Data on ethnic composition and me-dian household income by state and year was accessedvia the tidycensus package in R from the US CensusBureau. The ethnicities for which data was collectedwere: Caucasian American, African American, HispanicAmerican, Asian American, American Indian / AlaskanNative American, Native Hawaiian / Pacific IslanderAmerican. Data on national cannabinoid concentrationsfor Δ9-tetrahydrocannabinol (THC), cannabinol, canna-bigerol and cannabichromene was obtained from variouspublished reports [47–49]. Data on cannabis legal statuswas adduced from an internet search [50].
Derived dataGiven the clear differences in drug use by ethnicity itwas considered important to formally take ethnic canna-bis use into account in regression modelling. Data onthe frequency of cannabis use by ethnicity was availableat the national level from the SAMHSA Substance
Abuse and Mental Health Data Archive (SAMHDA) Re-stricted Use Data Analysis System (RDAS) [45]. For eachethnicity and for each year the percentage of the ethni-city using cannabis at the midpoint of the indicated fre-quency were multiplied together and summed to gain anethnic cannabis use index. Hence if fraction x of an eth-nicity used cannabis from 20 to 30 days per month thenx would be multiplied by 25. This was repeated andsummed across all use frequencies to obtain a specificethnic cannabis use index for that year. This index wasmultiplied by the state cannabis use rate and the THCconcentration in that year to derive an estimate of theethnic exposure to THC in each state. Similarly the con-centration of selected cannabinoids was multiplied bythe state cannabis use rate to derive a state based expos-ure to that cannabinoid. Cannabis use quintiles were de-fined in each year and concatenated to form strataacross all years.
Missing dataThe total pediatric cancer rate for Wyoming 2008 wasabsent. This was imputed as the mean of its rate in 2007and 2009. The rate of analgesic use was missing for allstates in 2015. This was imputed as the mean of thestate rates for 2014 and 2016.
StatisticsR version 4.0.2 (2020-06-22) from CRAN was used fordata analysis and accessed via the RStudio 1.2.5042(2009–2020) GUI. Data analysis was performed in Sep-tember 2020. Graphs and map-graphs were drawn usingpackages ggplot, albersusa and sf. Covariates were log-transformed to approximate normality based on theShapiro-Wilks test. Linear, mixed effects, panel, robustmarginal structural models and spatial models werestudied using packages base, nlme, plm, survey and splm(spatial panel linear models) respectively [51–53]. Ineach case model reduction was performed by the clas-sical technique of serial deletion of the least significantterm. A variety of modelling procedures was employedfor the following reasons. Mixed effects regression wasuseful for state-wise study of data, for inverse probabilityweighted corrections, and for generation of standard de-viations which can be input to eValue calculations. Panelregression modelling was well suited to the time seriessequential nature of the dataset, can be inverse probabil-ity weighted and allowed the use of both lagging and in-strumental variables. Robust regression was conductedto examine the robust effects after inverse probabilityweighting. Spatiotemporal regression was performed asthe data are inherently distributed across space and timeand there was good evidence from the models for bothspatial and temporal autocorrelation (see Results). Asthe models also produce a variance estimate their output
Reece and Hulse BMC Cancer (2021) 21:197 Page 3 of 33

is well suited to the calculation of e-Values. Inverseprobability weighting was conducted with the ipw pack-age and e-Values for regression models were calculatedwith the package EValue. Tests for trend were con-ducted with the chi squared test in Base. T-tests wereconducted for parametric group comparisons and weretwo tailed. P < 0.05 was considered significantthroughout.Panel analysis utilized the pooling technique, a time ef-
fect, the random method of Swarmy, the instrumentalmethod of Amemiya and were inverse probabilityweighted. Robust structural models were conducted bystate and were inverse probability weighted.
Spatial analysisInterstate geospatial linkages were made on the “queen”basis of shared edges or corners and compiled with thepoly2nb function from package spdep. They were editedas described so that no state, such as Alaska or Hawaii,was left geospatially isolated (as shown in Results).Model specification of spatial models was undertakenfrom the general full model to the specific [54]. That isto say the standard spatiotemporal regression model wasconducted using the splm function spreml (spatial panelrandom effects maximum likelihood) including spatialautocorrelation after Kapoor, Kelejian and Prucha [55],random effects, serial correlation in the residual errorsand spatial autocorrelation, coded as sem2srre in spremlmodels [52]. Significance of the final model parametersphi, psi, rho and lambda which quantify random error,serial correlation in the residuals, spatial error correl-ation and spatial autocorrelation respectively, confirmedthat this maximal structure was appropriate (see Resultstables). The spatial error adjustment of Kapoor, Kelejianand Prucha takes into account spatial correlation in boththe exposure and the outcome and this was consideredto be reflective of the real world situation in this case[54]. spreml models do allow the use of both spatial andtemporal lagging which has been utilized as described.At the time of writing splm and spreml spatial modelsdo not allow the use of instrumental variables or inverseprobability weighting which implies the need for supple-mentary techniques.
Causal inferenceTwo techniques of causal inference were employed. In-verse probability weights were constructed for the ex-posure of interest, monthly cannabis exposure, as afunction of the other drug variables which were our pri-mary variables of interest. These weights were used toweight mixed effects, panel and robust regressionmodels appropriately. The effect of this procedure is toequalize exposure across study groups and has also beenvalidated for continuous exposures as considered here.
Such techniques are said to create pseudo-randomizedgroups from which causal inferences can properly bemade. We also calculated e-Values which are a measureof the association required of any unmeasured potentialconfounder variable with both the exposure and the out-come to discount the reported results. In the literatureminimum (of the two) e-Values above 1.25 are com-monly considered of relevance [56].
Data availabilityAll data, including R code, inverse probability weights,geospatial weights, and source datasets, has been madepublicly available through the Mendeley data base re-pository and may be accessed at this URL: https://doi.org/10.17632/cnwv9hdspd.1.
EthicsThe datasets used were all publicly available and de-identified. No reference has been made at any point toindividually identifiable data. The present work was ap-proved by the University of Western Australia HumanResearch Ethics Committee on June 7th 2019 (No. RA/4/20/4724).
ResultsInspection of the SEER*Explorer website shows that atthe national level that age-adjusted rates of several can-cers in the pediatric age group (younger than 20 years)are rising including all cancer and acute lymphatic leu-kaemia which is the commonest tumour. The annotationon the SEER website is made from the JoinPoint pro-gram which also comes from NCI and CDC. These tu-mours are listed in Table 1 and illustrated in Fig. 1 usingdata based on 9 US cancer registries 1975–2017. Supple-mentary Figure 1 shows other cancers which are mostlyrising utilizing data from 21 US cancer registries 2000–2017.Figure 2 shows national drug exposure data from
NSDUH 2003–2017 and US Census bureau medianhousehold income data. It is important to note that ex-posure to most classes of drugs is dropping with the not-able exception of cannabis. Since SAMHSA NSDUHdata could be temporally matched to the CDC SEERcancer database for the years 2003–2017, this becamethe period of analysis.Figure 3 shows the concentration of various cannabi-
noids found in federal cannabis seizures 1980–2017[47–49].Figure 4 shows the age-adjusted state-based TPCIR
plotted as a function of exposure to the various sub-stances listed. The regression line for cannabis is notedto be weakly and non-significantly positive.
Reece and Hulse BMC Cancer (2021) 21:197 Page 4 of 33
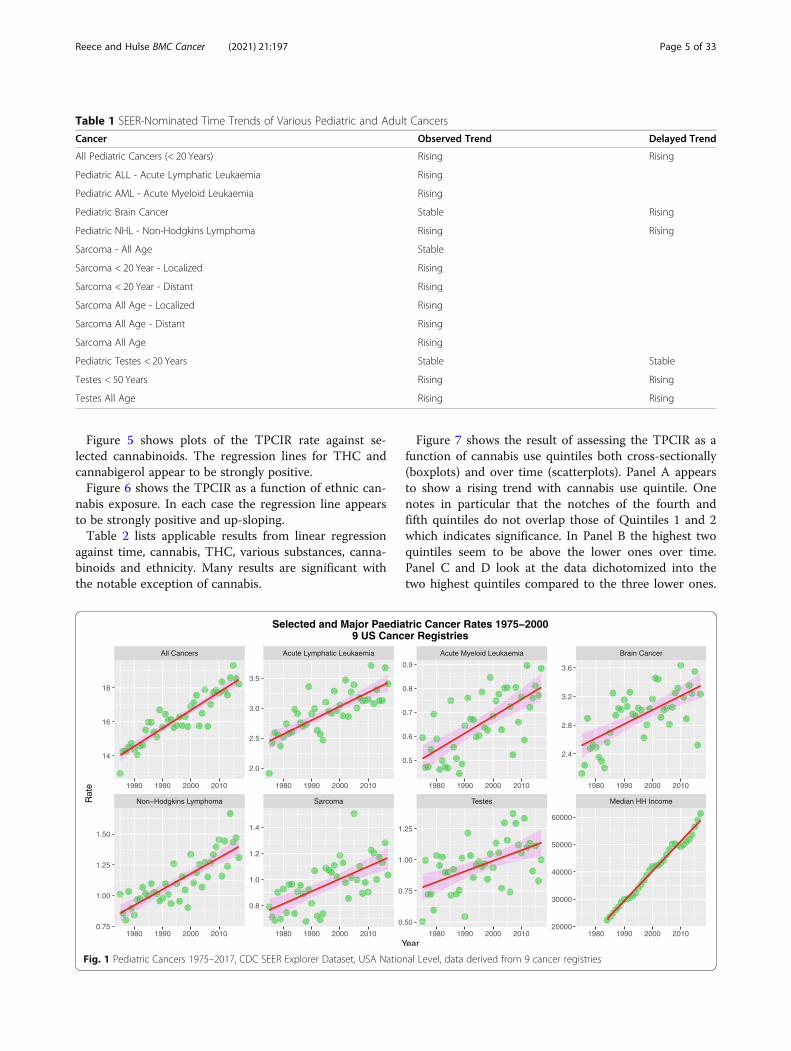
Figure 5 shows plots of the TPCIR rate against se-lected cannabinoids. The regression lines for THC andcannabigerol appear to be strongly positive.Figure 6 shows the TPCIR as a function of ethnic can-
nabis exposure. In each case the regression line appearsto be strongly positive and up-sloping.Table 2 lists applicable results from linear regression
against time, cannabis, THC, various substances, canna-binoids and ethnicity. Many results are significant withthe notable exception of cannabis.
Figure 7 shows the result of assessing the TPCIR as afunction of cannabis use quintiles both cross-sectionally(boxplots) and over time (scatterplots). Panel A appearsto show a rising trend with cannabis use quintile. Onenotes in particular that the notches of the fourth andfifth quintiles do not overlap those of Quintiles 1 and 2which indicates significance. In Panel B the highest twoquintiles seem to be above the lower ones over time.Panel C and D look at the data dichotomized into thetwo highest quintiles compared to the three lower ones.
Table 1 SEER-Nominated Time Trends of Various Pediatric and Adult Cancers
Cancer Observed Trend Delayed Trend
All Pediatric Cancers (< 20 Years) Rising Rising
Pediatric ALL - Acute Lymphatic Leukaemia Rising
Pediatric AML - Acute Myeloid Leukaemia Rising
Pediatric Brain Cancer Stable Rising
Pediatric NHL - Non-Hodgkins Lymphoma Rising Rising
Sarcoma - All Age Stable
Sarcoma < 20 Year - Localized Rising
Sarcoma < 20 Year - Distant Rising
Sarcoma All Age - Localized Rising
Sarcoma All Age - Distant Rising
Sarcoma All Age Rising
Pediatric Testes < 20 Years Stable Stable
Testes < 50 Years Rising Rising
Testes All Age Rising Rising
Fig. 1 Pediatric Cancers 1975–2017, CDC SEER Explorer Dataset, USA National Level, data derived from 9 cancer registries
Reece and Hulse BMC Cancer (2021) 21:197 Page 5 of 33
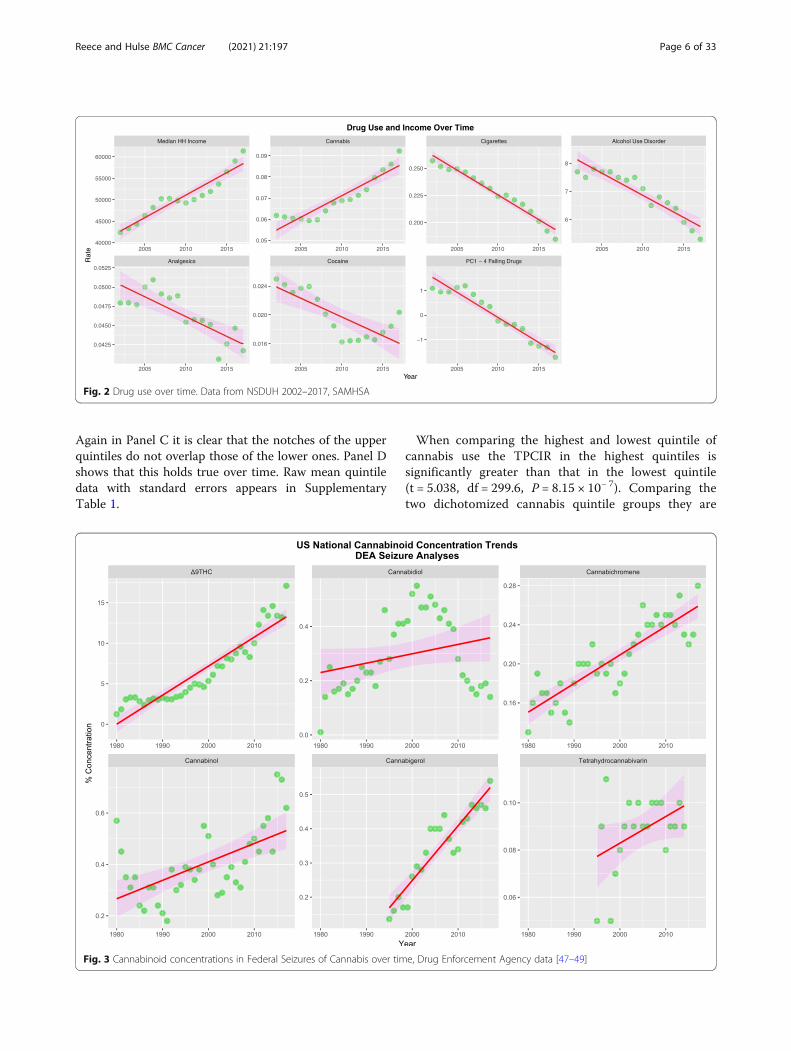
Again in Panel C it is clear that the notches of the upperquintiles do not overlap those of the lower ones. Panel Dshows that this holds true over time. Raw mean quintiledata with standard errors appears in SupplementaryTable 1.
When comparing the highest and lowest quintile ofcannabis use the TPCIR in the highest quintiles issignificantly greater than that in the lowest quintile(t = 5.038, df = 299.6, P = 8.15 × 10− 7). Comparing thetwo dichotomized cannabis quintile groups they are
Fig. 2 Drug use over time. Data from NSDUH 2002–2017, SAMHSA
Fig. 3 Cannabinoid concentrations in Federal Seizures of Cannabis over time, Drug Enforcement Agency data [47–49]
Reece and Hulse BMC Cancer (2021) 21:197 Page 6 of 33

also significantly different (t = 5.641, df = 673.6, P =2.4810− 8). The chi squared test for trend across thequintiles does not reach significance (Chi.Squ. = 465.4,df = 420, P = 0.0623). When these data are examinedby linear regression the significant results shown inTable 3 are found.Table 4 presents results from increasingly complex ro-
bust inverse probability weighted marginal structuralmodels. Results for additive, interactive with drugs only,
interactive including drugs, race and income and inter-active including cannabinoids, drugs, race and incomemodels are shown. It is particularly noteworthy that in asimple additive robust model (listed first in the table)cannabis is independently highly significant (β-esti-mate = 9.55 95%C.I. (3.95, 15.15), P = 0.0016).Since these robust models are not accompanied by a
model variance it is necessary to also use a mixed effectsmodel system in order to be able to calculate e-Values
Fig. 4 Total pediatric cancer incidence rate as a function of drug exposure
Reece and Hulse BMC Cancer (2021) 21:197 Page 7 of 33
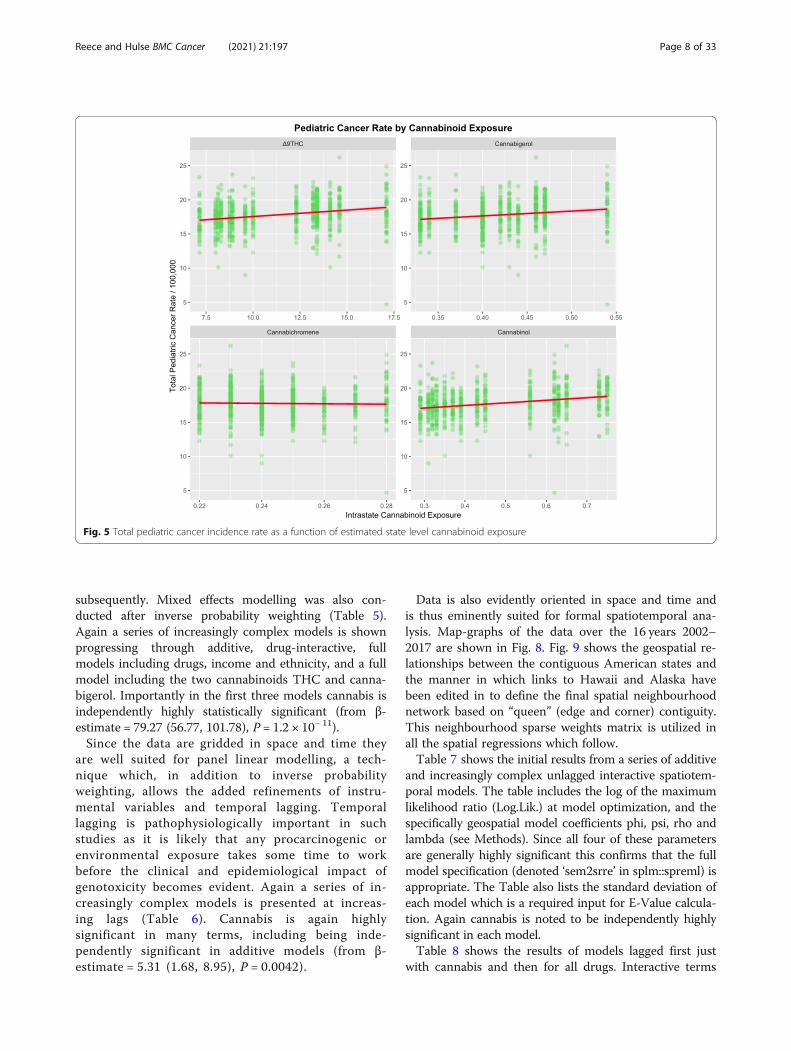
subsequently. Mixed effects modelling was also con-ducted after inverse probability weighting (Table 5).Again a series of increasingly complex models is shownprogressing through additive, drug-interactive, fullmodels including drugs, income and ethnicity, and a fullmodel including the two cannabinoids THC and canna-bigerol. Importantly in the first three models cannabis isindependently highly statistically significant (from β-estimate = 79.27 (56.77, 101.78), P = 1.2 × 10− 11).Since the data are gridded in space and time they
are well suited for panel linear modelling, a tech-nique which, in addition to inverse probabilityweighting, allows the added refinements of instru-mental variables and temporal lagging. Temporallagging is pathophysiologically important in suchstudies as it is likely that any procarcinogenic orenvironmental exposure takes some time to workbefore the clinical and epidemiological impact ofgenotoxicity becomes evident. Again a series of in-creasingly complex models is presented at increas-ing lags (Table 6). Cannabis is again highlysignificant in many terms, including being inde-pendently significant in additive models (from β-estimate = 5.31 (1.68, 8.95), P = 0.0042).
Data is also evidently oriented in space and time andis thus eminently suited for formal spatiotemporal ana-lysis. Map-graphs of the data over the 16 years 2002–2017 are shown in Fig. 8. Fig. 9 shows the geospatial re-lationships between the contiguous American states andthe manner in which links to Hawaii and Alaska havebeen edited in to define the final spatial neighbourhoodnetwork based on “queen” (edge and corner) contiguity.This neighbourhood sparse weights matrix is utilized inall the spatial regressions which follow.Table 7 shows the initial results from a series of additive
and increasingly complex unlagged interactive spatiotem-poral models. The table includes the log of the maximumlikelihood ratio (Log.Lik.) at model optimization, and thespecifically geospatial model coefficients phi, psi, rho andlambda (see Methods). Since all four of these parametersare generally highly significant this confirms that the fullmodel specification (denoted ‘sem2srre’ in splm::spreml) isappropriate. The Table also lists the standard deviation ofeach model which is a required input for E-Value calcula-tion. Again cannabis is noted to be independently highlysignificant in each model.Table 8 shows the results of models lagged first just
with cannabis and then for all drugs. Interactive terms
Fig. 5 Total pediatric cancer incidence rate as a function of estimated state level cannabinoid exposure
Reece and Hulse BMC Cancer (2021) 21:197 Page 8 of 33













![arXiv:2205.09704v1 [hep-th] 19 May 2022](https://static.fdokumen.com/doc/165x107/63317fd1ba79697da50fd393/arxiv220509704v1-hep-th-19-may-2022.jpg)




![arXiv:2105.08897v1 [astro-ph.EP] 19 May 2021](https://static.fdokumen.com/doc/165x107/63135794c72bc2f2dd03fd45/arxiv210508897v1-astro-phep-19-may-2021.jpg)

