Evaluation and management of language and speech disorders in preschool children
14
DOI: 10.1542/pir.26-4-131 2005;26;131-142 Pediatr. Rev. Heidi M. Feldman Children Evaluation and Management of Language and Speech Disorders in Preschool http://pedsinreview.aappublications.org/cgi/content/full/26/4/131 located on the World Wide Web at: The online version of this article, along with updated information and services, is Pediatrics. All rights reserved. Print ISSN: 0191-9601. Online ISSN: 1526-3347. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2005 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Point publication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.org Downloaded from
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Evaluation and management of language and speech disorders in preschool children

DOI: 10.1542/pir.26-4-131 2005;26;131-142 Pediatr. Rev.
Heidi M. Feldman Children
Evaluation and Management of Language and Speech Disorders in Preschool
http://pedsinreview.aappublications.org/cgi/content/full/26/4/131located on the World Wide Web at:
The online version of this article, along with updated information and services, is
Pediatrics. All rights reserved. Print ISSN: 0191-9601. Online ISSN: 1526-3347. Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2005 by the American Academy of published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1979. Pediatrics in Review is owned, Pediatrics in Review is the official journal of the American Academy of Pediatrics. A monthly
by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from

Evaluation and Management ofLanguage and Speech Disordersin Preschool ChildrenHeidi M. Feldman, MD,
PhD*
Author Disclosure
Dr Feldman received
gifts to Child
Development/Otitis
Study from
GlaxoSmithKline and
from Pfizer, Inc.
Objectives After completing this article, readers should be able to:
1. Describe key milestones in the development of language and speech.2. List indications for further evaluation of language and speech delays.3. Differentiate global delays, autism, and specific language impairment.4. Generate a differential diagnosis for language and speech delay.5. Evaluate management options for a child who has hearing loss.6. Justify referral to early intervention for children who have global delays.7. Discuss treatment of language impairments in autism.8. Evaluate the effectiveness of language and speech therapy for language and speech
disorders.
IntroductionLanguage is the expression of human communication through which ideas, information,emotions, and beliefs can be shared. Typically developing children master the fundamen-tals of language and speech in the toddler-preschool era. Language and speech skills servea pivotal role in learning and social relationships. Delays in the early development oflanguage and speech skills, which are prevalent in the population, may affect severaldomains of function. Management and treatment can improve language and speech skillssubstantially and reduce the functional impact of persistent disorders. Therefore, identify-ing children who have language and speech delays in the toddler-preschool period shouldbe a priority for the pediatric clinician. This article reviews the normal process of languagedevelopment up to school age, discusses the use of screening measures and parent reportinventories to verify parental reports of delays, provides a differential diagnosis of languageand speech delay, and suggests an approach to the child who has language or speechproblems in the absence of history or physical findings suggestive of a specific medicalcondition associated with language and speech disorders. In addition, the review discussesgeneral management of language and speech disorders and provides updates aboutmanagement of some of the underlying causes of speech and language delay.
DefinitionsLanguage is the use of systematic, arbitrary, and socially agreed upon signals (words andsentences) to convey meaning within a group or community. Receptive language refers tothe ability to understand and expressive language to produce this symbolic communica-tion. Speech is a manifestation of language that uses decodable vocal sounds as the mediumof exchange. Speech is created by a series of complex and coordinated movements of therespiratory, laryngeal, velopharyngeal, and oral systems. Natural sign languages are analternative method to convey meaning. Sign languages have underlying organizationcomparable with that of spoken language, but use a distinctive vocabulary and grammarbased on movements of the hands, body, and face. Children learn sign language atcomparable ages as they learn spoken language. There is no definitive evidence aboutwhether teaching sign language to hearing children confers any advantages or disadvan-tages to the children.
Developmental language disorders are persistent and significant limitations on theability to learn the language of the community. Characteristics of language disorders
*Ronald L. and Patricia M. Professor of Child Development, Children’s Hospital of Pittsburgh; Professor of Pediatrics, Universityof Pittsburgh School of Medicine, Pittsburgh, Pa.
Article cognition
Pediatrics in Review Vol.26 No.4 April 2005 131 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from

include limited understanding or production of vocabu-lary, misuse of words and their meanings, difficulty ex-pressing or following ideas, immature grammatical pat-terns, difficulty following directions, or altered patternsof conversation. Speech disorders are persistent delaysand deficits in the development of speech skills and voicequality. Speech disorders include problems in the pro-duction of speech sounds; disruptions in the flow orrhythm of speech; problems with voice pitch, volume, orquality; and poor intelligibility. Phonologic disorders(previously called articulation disorders) are commonspeech-sound disorders in childhood, in which the childis significantly less skilled than peers in articulating, se-quencing, or organizing the sounds of the language. Theerrors compromise the ability of strangers to interpret thechild’s speech, but are relatively consistent. Anotherspeech-sound disorder is verbal apraxia or developmentalverbal dyspraxia. This disorder is associated with diffi-culty in planning, programming,and producing speech sounds.Children who have this disorderusually make highly inconsistenterrors that severely compromiseintelligibility. Differentiationamong speech disorders requiresthe expertise of a speech-languagepathologist.
Children often present initiallyin the toddler-preschool periodwith a developmental delay in language or speech. Whendelays persist and affect communicative function, theybecome classified as disorders. The pediatric clinicianfrequently is called on to verify delays in the developmentof language and speech and to decide which affectedchildren warrant further evaluation and management.
EpidemiologyLanguage and speech disorders are features of manygenetic and chromosomal disorders. For example, chil-dren who have Down syndrome typically show verbalskills below those expected on the basis of cognitivefunctioning. Children who have fragile X and Klinefeltersyndromes may present with delayed language skills withor without characteristic physical features. Toddlers andpreschoolers who have William syndrome are delayed atearly stages of language development, although theyultimately exhibit communication and social skills inadvance of other aspects of their cognitive functioning.
Language and speech disorders also are features ofneurologic diseases. Children who have severe cerebralpalsy may have problems with language or the produc-
tion and coordination of speech sounds. Seizure disor-ders involving the left hemisphere, such as Landau-Kleffner syndrome, may interfere with the developmentand use of language. Boys who have Duchenne musculardystrophy may show early language and speech delayprior to or along with early signs of weakness.
In school-age children who have no obvious geneticor neurologic condition, the prevalence of language dis-orders is approximately 2% to 3%; the prevalence ofspeech disorders is between 3% and 6%. Some childrenhave both disorders. Speech and language disorders aremore common in boys than girls and more commonamong children who have a family history of language,speech, or reading disorders in a first-degree relative thanamong children who have a negative family history. Theprevalence of language and speech delays in the pre-school period is considerably higher, at about 15%, againwith considerable overlap. Children of low socioeco-
nomic standing are more likely to show delays in lan-guage and, in some studies, speech development than arechildren of upper and middle socioeconomic standing.
Clinical AspectsNormal Language Development
Table 1 summarizes language milestones from birth toschool age. From the neonatal period, children showinterest in human voices and faces in preference to otherstimuli, preferences that forge the building blocks ofcommunicative development. By about 2 to 3 months ofage, an infant begins to use his or her voice to makemelodic vowel sounds called cooing. Shortly thereafter,they begin to enter into reciprocal vocal exchanges withtheir caregivers. By about 6 months of age, the child addsconsonants to vowels, creating syllables known as babble.Also at about 6 months of age, children show emergingabilities to understand elements of the sound stream,responding appropriately to their name and to the word“no.” By 8 to 10 months of age, children can use verbalcues for practiced routines, such as “wave bye-bye.”Expressive communication at that age includes ma-ma or
Speech and language disorders aremore common in boys than girls and amongchildren who have a family history oflanguage, speech, or reading disorders.
cognition language and speech
132 Pediatrics in Review Vol.26 No.4 April 2005 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from

da-da, first used nonspecifically and then for the parent.Children begin to communicate nonverbally by point-ing.
At around the first birthday, babble becomes increas-ingly complex jargon, sounding like adult language interms of the variety of speech sounds and the intonationpatterns. Simultaneously, children begin to understandand use real words. Throughout the second year, they arecapable of understanding far more than they can pro-duce. They initially learn vocabulary slowly, at a rate ofapproximately two to three words per week. The earlywords are simple in structure, often repetitions of aconsonant and a vowel, such as wa-wa for water. Theearly words may be used too broadly, such as applyingthe label dog to all animals, or too narrowly, such asapplying the word dog only to the family pet.
Sometime usually between 18 and 24 months of age,when the child’s vocabulary reaches 30 to 60 words, thepace of language learning quickens dramatically. Chil-dren learn, on average, three to four words per day andbegin combining words into two-word phrases. As sen-tence length increases, the child masters language-
specific grammatical elements, including pronouns,question words, articles, and verb tense markings. At age3 years, comprehension is extremely good; sentences arethree or more words in length; children begin askingquestions, first “what” and then “why”; and they engagein short conversations. By 4 to 5 years of age, the child isable to construct complex sentences, participate in mean-ingful conversation, and tell short stories. After thatpoint, progress in language development is less obviousto the untrained listener. By school age, individual dif-ferences in language abilities are revealed in formal test-ing or laboratory studies.
Normal Speech DevelopmentSpeech development progresses in tandem with language(Table 1). The first eight consonant sounds that developare: m, b, y, n, w, d, p, and h. At age 2 years, a child whois developing typically can create speech that is intelligi-ble to an unfamiliar adult at least 50% of the time and atage 3 years, at least 75% of the time. Children maycontinue to have difficulty with pronouncing somesounds until about 7 years of age. The last eight conso-
Table 1. Normal Milestones in the Development of Language and SpeechAge Receptive Skills Expressive Skills
Birth Turns to source of soundShows preference for voicesShows interest in faces
Cries
2 to 4 months CoosTakes turns cooing
6 months Responds to name Babbles9 months Understands verbal routines (wave bye-bye) Points
Says ma-ma, da-da12 months Follows a verbal command Uses jargon
Says first words15 months Points to body parts by name Learns words slowly18 to 24 months Understands sentences Learns words quickly
Uses two-word phrases24 to 36 months Answers questions
Follows two-step commandsPhrases 50% intelligibleBuilds three- (or more) word sentencesAsks “what” questions
36 to 48 months Understands much of what is said Asks “why” questionsSentences 75% intelligibleMasters the early acquired speech sounds: m, b, y,
n, w, d, p, and h48 to 60 months Understands much of what is said,
commensurate with cognitive levelCreates well-formed sentencesTells stories100% intelligible
6 years Pronounces most speech sounds correctly; may havedifficulty with sh, th as in think, s, z, th as in the,l, r, and the s in treasure
7 years Pronounces speech sounds correctly, includingconsonant blends such as sp, tr, bl
cognition language and speech
Pediatrics in Review Vol.26 No.4 April 2005 133 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from

nants typically acquired are sh, th as in the word “think,”s, z, th as in the word “the,” l, r, and the zh sound usuallyspelled as s, as in the word “treasure.” Consonant blendssuch as sp, tr, and bl also may not emerge until earlyschool age. Nonetheless, 100% of speech should beintelligible by about age 4 years.
Fluency—the flow of output—also undergoes devel-opmental change. At around age 3 to 4 years, manychildren experience a period in which the fluency of theiroutput is poor. Developmental dysfluency is character-ized by repetition of whole words and syllables ratherthan individual sounds, seems to arise from poor coordi-nation of thoughts and words, and typically resolves byage 4 years. Stuttering is a long-term speech problemcharacterized by disruptions in fluency that create diffi-culties with communication. Stuttering consists of repe-titions of parts of words, prolongations of sounds, andcomplete blocks. Children who stutter may show evi-dence of tension and struggle as they attempt to formwords.
Detection of Language DelayToddlers rarely cooperate with a health care professionalto allow direct assessment of early language and speech ina short office visit. The Early Language Milestone, sec-ond edition, and the Clinical Adaptive Test/ClinicalLinguistic and Auditory Milestone Scale are brief screen-
ing measures that are appropriatefor use in the pediatric office. Gen-eral developmental screening testsprovide a pass-fail score and do notoffer information specifically aboutlanguage and speech.
Many pediatric practices assessdevelopment with history ratherthan with screening. Therefore, it isimperative that clinicians recognizeearly signs of disorder and delay.Table 2 describes abnormal find-ings on history (or developmentalobservation) at various ages thatshould prompt further evaluationof a child’s language or speech. Inaddition, a delay of 25% or greaterby 16 to 24 months of age is con-sidered significant. For example, a24-month-old child who functionsas a typical 18-month-old can beconsidered to have a clinically sig-nificant language delay.
Parental concerns about lan-guage or speech can be corroborated through the use ofparent report inventories, such as the Language Devel-opment Survey or the MacArthur Communicative De-velopment Inventories-Short Form. These measures, ob-tained when children are 18 months to 2 years old, havegood concurrent validity and predictive validity. Clini-cians should not wait until children are 3 years of age orolder to evaluate delayed language or speech.
Causes of Language DelaySignificant language delay (�25%) should not be disre-garded because the child is a boy, second- or third-bornin a family, or a member of a bilingual household. Studiesshow that boys function on average only 1 to 2 monthsbehind girls in vocabulary and grammar development.Birth order effects in language development are notconsistent across studies. Toddlers from bilingual house-holds may show minor delays at the initial phases oflanguage production and early mixing of the two lan-guage systems within a phrase or exchange. Theirprogress at differentiating languages occurs more quicklywhen the languages are associated with clear environ-mental contexts (language #1 at home, language #2 atschool) than when they are mixed within the context (theparent uses language #1 70% of the time and language #230% of the time). Children may develop uneven skills in
Table 2. Indications for Referral for Delays andDisorders of Language and Speech
Age Finding
Birth and at any age Lack of response to soundLack of interest in interaction with people
4 months Lack of any drive to communicate6 to 9 months Loss of the early ability to coo or babble
Poor sound localization or lack of responsiveness12 months No verbal routines
Failure to use ma-ma or da-daLoss of previous language or social milestones
15 to 18 months No single wordsPoor understanding of language
24 months Vocabulary less than 50 wordsNo two-word phrasesLess than 50% of speech intelligible to strangers
36 months Rote memorization of words or phrasesFrequent immediate or delayed repetition of others’ speechFlat or stilted intonationMore than 75% of speech unintelligible to strangers
48 months Inability to participate in conversationStuttering of initial sounds or parts of words
6 to 7 years Immature or inaccurate speech sound production
cognition language and speech
134 Pediatrics in Review Vol.26 No.4 April 2005 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from

the two languages as a function of the amount andquality of exposure to each language.
Significant delays in language development can resultfrom either biologic or environmental causes. The differ-ential diagnosis of language delays in children who haveno specific findings on history, physical examination, orneurologic examination includes hearing loss, global de-velopmental delay, autism, specific language impairment,and psychosocial deprivation. Hearing loss may be sus-pected based on the pattern of the child’s understandingand production. Speech sounds at the greatest risk forpoor reception and production in the context of moder-ate sensorineural hearing loss are s, th, and f, which arehigh-frequency sounds that have low energy (Fig. 1).Global developmental delay may be suspected on thebasis of other delays in cognitive or motor skills. If suchdevelopmental findings persist into school age, the childmay meet diagnostic criteria for mental retardation.
Autistic disorder should be suspected when language
not only is delayed but also is devi-ant, that is, different in terms ofvocabulary, grammar, or communi-cative pattern from the language ofyounger children. In autism, quali-tative impairments in communica-tion are accompanied by qualitativeimpairments in social interaction,such as a lack of eye-to-eye gaze andreciprocity, and by restrictive, re-petitive, and stereotyped patternsof behaviors, interests, or activities.Some children who have autism de-velop language and speech skills,but these higher functioning chil-dren show characteristic impair-ments in the ability to initiate orsustain conversation, a reliance onstereotyped or repetitive languagerather than truly novel construc-tions, and flat or stilted intonationpatterns. Longitudinal follow-up ofpreschool-age children who haveautistic features and do not meetdiagnostic criteria for autism at thatage often finds that they meet diag-nostic criteria at school age, al-though some children improveover time.
Specific language impairmentmay be suspected when languageskills are lower than other cognitive
abilities. Specific language impairment may affect onlyexpressive language or both receptive and expressivelanguage. Characteristics of the language include delaysor errors in the use of elements of the grammar that areinfrequent or unaccented in speech, such as accurateunderstanding or production of the plural (-s) or past-tense (-ed). In some children, social aspects of com-munication are affected, making differentiation of thesesemantic-pragmatic language impairments from autismchallenging.
Language delays also can result from a poor linguisticenvironment. Children who have suffered child abuse orsevere deprivation typically have delayed language andspeech. Under less extreme conditions, the size of chil-dren’s vocabulary and the maturity of their grammaticskills are associated with the quality and quantity ofparental input. The slow language development of chil-dren from low socioeconomic groups has been attributedto the relatively impoverished linguistic environment of
Figure 1. Audiogram with placement of common speech sounds at their averagefrequency and energy level. Adapted from Northen and Downs, 1984.
cognition language and speech
Pediatrics in Review Vol.26 No.4 April 2005 135 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from

children raised in poverty. Programs that encouragereading to infants and toddlers may improve languageskills in children by increasing the amount and diversityof language in their environment.
Evaluation of the Child Who Has Languageand Speech DelaysChildren presenting with language delay should receive afull audiologic assessment, using the assessment tech-niques that are appropriate for the child’s age. Universalnewborn hearing screening detects most children whohave moderate, severe, or profound sensorineural hear-ing loss in the newborn period because of the highsensitivity of the tests. However, the tests reliably misschildren who have mild-to-moderate, progressive, oracquired hearing loss. Therefore, children who have lan-guage or speech delay should be reassessed for hearingacuity.
Children who have normal hearing and indications ofimpairments of cognitive or social skills should receive acomprehensive developmental assessment. Early inter-vention services for children from birth to 3 years of agecan provide an assessment of the child’s level of function-ing in each developmental do-main. Advantages of referral toearly intervention for diagnosticpurposes are that the services areprovided at no charge to the fam-ily, and intervention can beginpromptly if delays are discov-ered. These evaluations typicallyprovide a description of levels offunctioning in developmentaldomains but do not offer an overriding or unifyingdiagnosis, such as cerebral palsy or autism. Psycholo-gists and medical specialists, such as developmental-behavioral pediatricians or neurologists, provide the di-agnostic formulation but may not, particularly in thecurrent fiscal climate, describe developmental levels in alldomains. Concurrent referral to early intervention ser-vices and medical subspecialists is sensible. The quality ofthe home environment can be assessed in several ways, asappropriate to the nature and degree of the concern.A careful interview may reveal poor parent-child interac-tions or a low level of stimulation in the home. Screeningtests for the home environment are available and oftenneed to be validated by a direct home assessment. Ifclinicians have serious concerns about the quality of thehome environment, options available include a referral tochild protective services, a mental health assessment ofparents, or a professional home assessment.
Children who otherwise seem to be progressing nor-mally may be referred to a speech-language pathologistfor verification of the degree and nature of language orspeech delay as well as recommendations for the fre-quency and type of treatment. The treatment of stutter-ing falls to the speech-language pathologist, as doesdifferentiation of developmental dysfluency and stutter-ing in difficult cases. Children who have language orspeech delays in addition to other developmental delaysor specific genetic or neurologic conditions also maybenefit from the speech-language pathologist’s evalua-tion. Early intervention programs typically include aspeech-language pathologist on the interdisciplinaryevaluation team.
ManagementGeneral Management Strategies
Speech and language disorders should be conceptualizedas chronic special health care needs for the purposes ofdesigning a management plan. Chronic concerns aremanaged best in the context of a meaningful, long-termrelationship between a proactive, prepared primary careteam and an informed, active family. A family-centered,
community-based “medical home” assumes responsibil-ity for coordinating services, facilitating communicationamong practitioners and family members, providing in-formation and direction, and offering emotional andinstrumental support. The child and family need accessto community-based therapeutic services within both themedical and the educational systems.
Evaluation of the child’s functional capacities is animportant component of chronic care for a developmen-tal disorder and should be used to set treatment goals,counsel families, and monitor progress. In this regard,the World Health Organization has created the Interna-tional Classification of Functioning, Disability andHealth (see Suggested Reading). This diagnostic manualprovides a useful conceptualization about the bidirec-tional relationships among impairments, functional ac-tivities, social participation, and environmental factors.The lists of functional activities and social participation
Concurrent referral to earlyintervention services and medicalsubspecialists is sensible.
cognition language and speech
136 Pediatrics in Review Vol.26 No.4 April 2005 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from

provide a schema for the comprehensive assessment ofrelevant domains that might be affected by the develop-mental disorder. Table 3 lists activities and participationthat may prove exceptional challenges to children whohave speech and language disorders, such as the ability tolearn and apply knowledge. The management planshould address the functional needs in these and relateddomains as they evolve over time.
Hearing LossThe management of hearing loss depends on both thedegree of loss and the preferences of families. Auditoryamplification is the mainstay of management formoderate-to-profound hearing loss. Referral to an audi-ologist is necessary to prescribe and fit hearing aidsproperly. An important decision for the family of a childwho has hearing loss is the mode of communication thechild will use. This decision must be considered on anindividual basis. Aural-oral education trains the child inthe conventional language of the community, but somechildren who are hearing impaired are very slow at learn-ing lip-reading and speech. Sign language may allow formeaningful communication at young ages. However, thesuccess of sign language depends on the adequacy of thelanguage environment. Parents and siblings of children
who are learning sign language alsoshould learn sign language and ide-ally serve as language models ratherthan coequal communication part-ners.
Cochlear implantation is a rela-tively new treatment for childrenwho have bilateral severe-to-profound sensorineural hearing lossand fail to show improvement withstandard hearing aids. Cochlear im-plantation allows for restoration ofthe perception of sound signals, al-though the nature of the percep-tion differs from normal hearing.Cochlear implantation is most suc-cessful when achieved early in life,possibly in the first year. Importantissues for the primary health careteam include providing informa-tion to families who are consideringthe procedure, assisting in the se-lection of appropriate candidates,emphasizing the importance ofpostprocedure auditory habilita-tion and language and speech ser-
vices, monitoring progress, and counseling families. Thesuccess of cochlear implantation is highly variable, evenamong children who receive the transplants at youngages and adhere to treatment. For children whose lan-guage and speech fail to develop adequately after areasonable trial, with or without cochlear implantation,consideration of alternative or augmentative methods isappropriate to meet functional needs for communicationand interpersonal interactions.
The most common cause of mild-to-moderate hear-ing loss in children is chronic otitis media with effusion.For many years, the prevailing dogma was that chronicotitis media with effusion was a cause of significantlanguage and speech delay. Therefore, the recommenda-tion was to insert tympanostomy tubes for bilateral effu-sions persisting 3 to 4 months. Recently, a large, careful,randomized clinical trial of tympanostomy tube insertionhas tested the hypothesis that compared with watchfulwaiting, early placement of tympanostomy tubes afterpersistent otitis media with effusion would lead to betteroutcomes in terms of speech, language, cognition, andpsychosocial development. The study participants werehealthy children who had no risk factors for developmen-tal delay except socioeconomic status and history of otitismedia. This study did not find an advantage for the early
Table 3. Functional Activities and SocialParticipation at Risk in Children Who HaveLanguage and Speech Disorders
Domain Specific Examples
Learning and applyingknowledge
Purposeful sensory experiences: listeningLearning to readLearning to write
General tasks and demands Undertaking a single taskUndertaking multiple tasksCarrying out daily routinesHandling stress and psychological demands
Communciation Communication—receivingCommunication—producingConversation and the use of communication
devices and techniquesInterpersonal interactions and
relationshipsBasic interpersonal interactions (respect,
tolerance, criticism, special cues)Complex interpersonal interactions (forming
and terminating relationships, regulatingbehavior within interactions, interactingwithin social rules)
Community, social, and civic life Recreation and leisureReligion and spirituality
Data from the World Health Organization, International Classification of Functioning, Disability, andHealth.
cognition language and speech
Pediatrics in Review Vol.26 No.4 April 2005 137 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from
tympanostomy group in any of the outcome variables(Paradise, 2001). Children who have tympanostomytube insertion are more likely to develop abnormal tym-panic membrane findings such as tympanosclerosis thanare children managed medically. Therefore, in otherwisehealthy children who have no other risk factors for de-velopmental compromise, watchful waiting for chronicotitis media with effusion appears to be a reasonabletactic. However, for children who have other develop-mental risk factors, the treatment should be individual-ized.
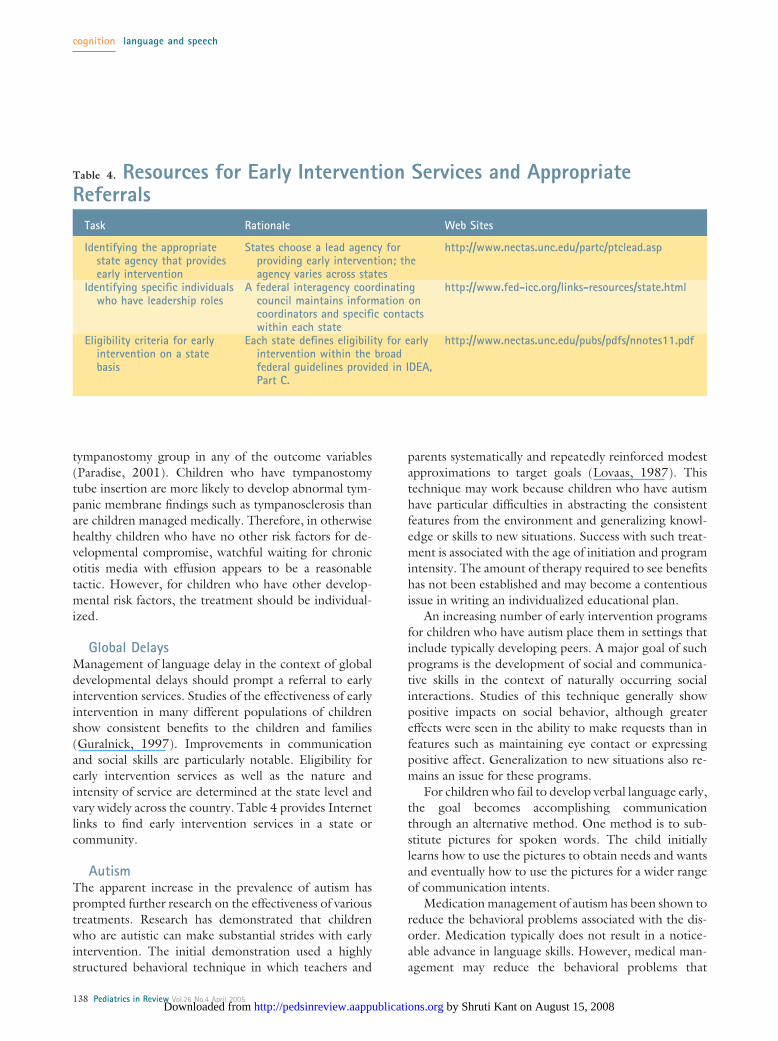
Global DelaysManagement of language delay in the context of globaldevelopmental delays should prompt a referral to earlyintervention services. Studies of the effectiveness of earlyintervention in many different populations of childrenshow consistent benefits to the children and families(Guralnick, 1997). Improvements in communicationand social skills are particularly notable. Eligibility forearly intervention services as well as the nature andintensity of service are determined at the state level andvary widely across the country. Table 4 provides Internetlinks to find early intervention services in a state orcommunity.
AutismThe apparent increase in the prevalence of autism hasprompted further research on the effectiveness of varioustreatments. Research has demonstrated that childrenwho are autistic can make substantial strides with earlyintervention. The initial demonstration used a highlystructured behavioral technique in which teachers and
parents systematically and repeatedly reinforced modestapproximations to target goals (Lovaas, 1987). Thistechnique may work because children who have autismhave particular difficulties in abstracting the consistentfeatures from the environment and generalizing knowl-edge or skills to new situations. Success with such treat-ment is associated with the age of initiation and programintensity. The amount of therapy required to see benefitshas not been established and may become a contentiousissue in writing an individualized educational plan.
An increasing number of early intervention programsfor children who have autism place them in settings thatinclude typically developing peers. A major goal of suchprograms is the development of social and communica-tive skills in the context of naturally occurring socialinteractions. Studies of this technique generally showpositive impacts on social behavior, although greatereffects were seen in the ability to make requests than infeatures such as maintaining eye contact or expressingpositive affect. Generalization to new situations also re-mains an issue for these programs.
For children who fail to develop verbal language early,the goal becomes accomplishing communicationthrough an alternative method. One method is to sub-stitute pictures for spoken words. The child initiallylearns how to use the pictures to obtain needs and wantsand eventually how to use the pictures for a wider rangeof communication intents.
Medication management of autism has been shown toreduce the behavioral problems associated with the dis-order. Medication typically does not result in a notice-able advance in language skills. However, medical man-agement may reduce the behavioral problems that
Table 4. Resources for Early Intervention Services and AppropriateReferrals
Task Rationale Web Sites
Identifying the appropriatestate agency that providesearly intervention
States choose a lead agency forproviding early intervention; theagency varies across states
http://www.nectas.unc.edu/partc/ptclead.asp
Identifying specific individualswho have leadership roles
A federal interagency coordinatingcouncil maintains information oncoordinators and specific contactswithin each state
http://www.fed-icc.org/links-resources/state.html
Eligibility criteria for earlyintervention on a statebasis
Each state defines eligibility for earlyintervention within the broadfederal guidelines provided in IDEA,Part C.
http://www.nectas.unc.edu/pubs/pdfs/nnotes11.pdf
cognition language and speech
138 Pediatrics in Review Vol.26 No.4 April 2005 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from
interfere with communication, thereby allowing thechild to use his or her skills more consistently or effec-tively.
Specific Language Impairment and SpeechDisorders
Speech-language pathologists treat the wide range oflanguage and speech disorders. In general, therapy iseffective for improving specific skills and communica-tion. For toddlers who have delayed development, sometreatments focus on the nature of adult input to the child,capitalizing on the importance of environmental input instimulating language development. Other approachestreat children in group settings or classrooms. Thesechildren generally benefit from participation with chil-dren who are developing typically and who provide goodmodels for communication.
Intervention for children who have speech-sound dis-
orders varies on the basis of thedisorder. The objective of the treat-ment is to help the child learn toproduce sounds correctly. Inter-ventions may focus on expandingthe child’s inventory of speechsounds and establishing situationsin which the new abilities can bepracticed. Children often need cueson how to shape the mouth orwhere to place the tongue. Practicefrequently builds from isolatedsounds to words to sentences.
Treatment of stuttering inyoung children is challenging. En-vironmental approaches, such ascoaching parents to reduce timepressures that contribute to achild’s dysfluency, rarely eliminatethe problem. Behavioral ap-proaches of rewarding fluentspeech may be effective in the shortterm, but long-term outcomes areless favorable. Current treatmentsusually combine a range of tech-niques aimed at both diminishingthe severity of individual stutteringevents and reducing the negativecognitive and affective responses tostuttering. In addition, medicationsmay play a role in the treatment ofstuttering. Risperidone has beenshown to be superior to placebo in
reducing stuttering. Paroxetine and sertraline may beuseful to reduce the anxiety associated with stuttering,but have substantial associated risks.
PrognosisLanguage and speech delays and disorders, treated earlyand appropriately, generally improve over time. The finalprognosis is a function of the nature and severity of theunderlying disorder. However, some children whose iso-lated language and speech delays at ages 3 or 4 yearsapparently resolved show difficulties in reading. Readingis a language-based skill that requires the child to appre-ciate the subtle differences among speech sounds andlink them to written symbols. Children who have readingdisorders are likely to have difficulties manipulatingspeech sounds, such as subtracting a syllable or soundfrom a word (eg, subtract the “sky” from “skyscraper” orthe “b” from “birthday”). It remains unclear whether
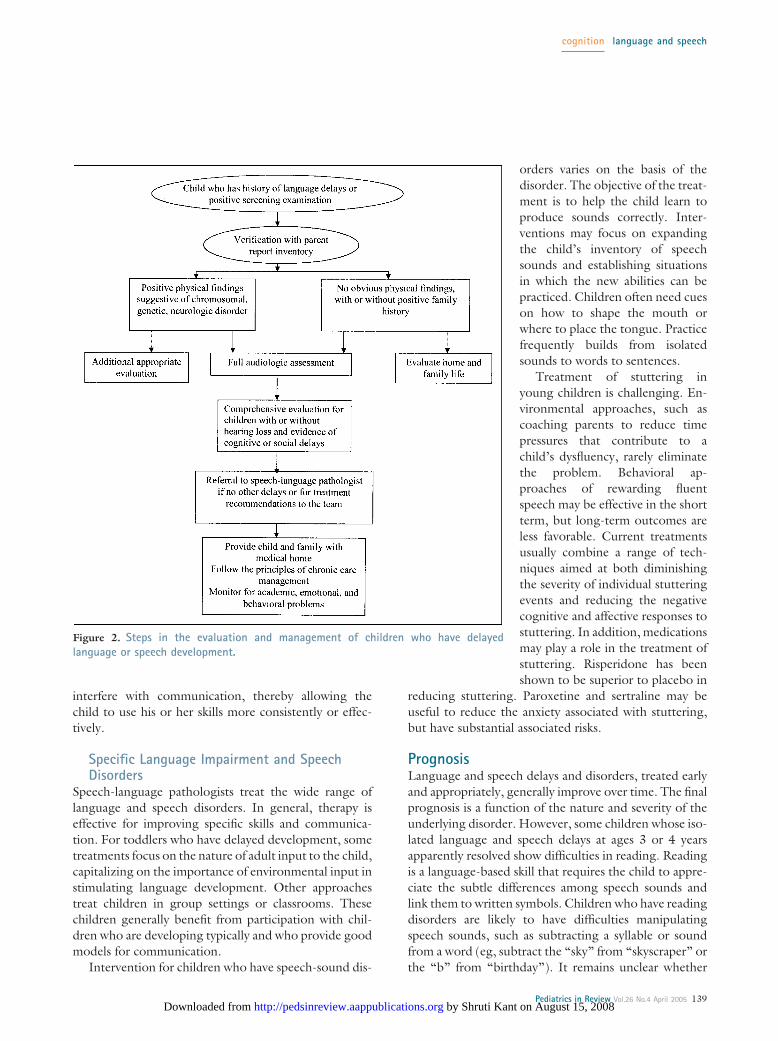
Figure 2. Steps in the evaluation and management of children who have delayedlanguage or speech development.
cognition language and speech
Pediatrics in Review Vol.26 No.4 April 2005 139 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from

early language and speech therapy can prevent or reducesubsequent reading problems.
Children who have language problems affectinggrammar, meaning, and conversational skills, but notisolated phonologic disorders, have a high prevalence ofmental health disorders over time. In addition, childrenpresenting with psychiatric disorders may have undiag-nosed problems of communication that warrant compre-hensive evaluation. Thus, the long-term management ofchildren who have language and speech delays shouldinclude close monitoring of academic, emotional, andbehavioral functioning.
ConclusionLanguage and speech disorders are prevalent in theschool-age population, and early delays are even moreprevalent in toddlers and preschoolers. The pediatricclinician plays a central role in the detection, evaluation,and management of children who have these delays anddisorders (Fig. 2). Initial and ongoing assessment oflanguage and speech use specific screening tests or acomprehensive history. Parent report inventories can beused to validate parental concerns. Children who havegenetic, chromosomal, or neurologic disorders requireevaluation and treatment appropriate to the underlyingcondition. For children who have no obvious underlyingdisorder, prediction of who will progress rapidly fromthose who will develop disorders is inaccurate. At aminimum, the evaluation of children who have signifi-cant delays in language or speech should include a fullaudiologic assessment, a comprehensive interdisciplinarydevelopmental assessment for children who have addi-tional cognitive or social problems, or a speech-languageevaluation for children who have no other issues. Themanagement of language and speech disorders shouldfollow the principles of chronic care management. Chil-dren who have language and speech disorders are at riskfor the development of academic and psychiatric disor-ders and, therefore, require regular long-term follow-up.
Suggested ReadingAmerican Academy of Pediatrics. The medical home. Pediatrics.
2002;110:184–186Coplan J, Gleason JR. Test-retest and interobserver reliability of the
Early Language Milestone Scale, second edition. J PediatrHealth Care. 1993;7:212–219
Fenson L, Pethick S, Renda C, Cox JL, Dale PS, Reznick JS. Shortform versions of the MacArthur Communicative DevelopmentInventories. Appl Psycholinguist. 2000;21:95–115
Gregg RB, Wiorek LS, Arvedson JC. Pediatric audiology: a review.Pediatr Rev. 2004;25:224–233
Guralnick MJ, ed. The Effectiveness of Early Intervention. Baltimore,Md: Paul H. Brookes Publishing Co, Inc; 1997
Hwang B, Hughes C. The effects of social interactive training onearly social communicative skills of children with autism. JAutism Dev Disord. 2000;30:331–343
Law J, Boyle J, Harris F, Harkness A, Nye C. Prevalence and naturalhistory of primary speech and language delay: findings from asystematic review of the literature. Int J Lang Commun Disord.2000;35:165–188
Lovaas OI. Behavioral treatment and normal educational and intel-lectual functioning in young autistic children. J Consult ClinPsychol. 1987;55:3–9
Maguire GA, Riley GD, Franklin DL, Gottschalk LA. Risperidonefor the treatment of stuttering. J Clin Psychopharmacol. 2000;20:479–482
McCracken JT, McGough J, Shah B, et al. Risperidone in childrenwith autism and serious behavioral problems. N Engl J Med.2002;347:314–321
Michelotti J, Charman T, Slonims V, Baird G. Follow-up ofchildren with language delay and features of autism frompreschool years to middle childhood. Dev Med Child Neurol.2002;44:812–819. (Commentary in AAP Grand Rounds,March 2003)
Northen JL, Downs MP. Hearing In Children. 3rd ed. Baltimore,Md: The Williams and Wilkins Co; 1984
Paradise JL, Bluestone CD. Consultation with the specialist: tym-panostomy tubes: a contemporary guide to judicious use. Pedi-atr Rev. 2005;26:60–66
Paradise JL, Feldman HM, Campbell TF, et al. Effect of early ordelayed insertion of tympanostomy tubes for persistent otitismedia on developmental outcomes at the age of three years.N Engl J Med. 2001;344:1179–1187
Rescorla L. The Language Development Survey: a screening toolfor delayed language in toddlers. J Speech Hear Dis. 1989;54:587–599
Shriberg LD, Tomblin JB, McSweeny JL. Prevalence of speechdelay in 6-year-old children and comorbidity with languageimpairment. J Speech Lang Hearing Res. 1999;42:1461–1481
Stool S, Berg A, Berman S, et al. Managing Otitis Media withEffusion in Young Children. Quick Reference Guide for Clini-cians. Rockville, Md: Agency for Health Care Policy and Re-search, Public Health Service, US Department of Health andHuman Services; 1994: Publication 94–0623
Toppelberg CO, Shapiro T. Language disorders: a 10-year researchupdate review. J Am Acad Child Adolesc Psychiatry. 2000;39:143–152
Wachtel RC, Shapiro BK, Palmer FB, Allen MC, Capute AJ.CAT/CLAMS. A tool for the pediatric evaluation of infants andyoung children with developmental delay. Clinical AdaptiveTest/Clinical Linguistic and Auditory Milestone Scale. ClinPediatr. 1994;33:410–415
Wagner E. Overview of the chronic care model. Improving ChronicIllness Care. Available at: http://www.improvingchroniccare.org/change/model/components.html. Accessed March 4, 2003
World Health Organization. International Classification of Func-tioning, Disability and Health. Available at: http://www3.who.int/icf/icftemplate.cfm. Accessed March 4, 2003
cognition language and speech
140 Pediatrics in Review Vol.26 No.4 April 2005 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from

PIR QuizQuiz also available online at www.pedsinreview.org.
9. What degree of language delay is considered clinically significant in an 18-month-old child?
A. 5%.B. 10%.C. 15%.D. 20%.E. 25%.
10. The most common cause of mild-to-moderate hearing loss in children is:
A. Chronic otitis media with effusion.B. Drug exposure.C. Genetics.D. Meningitis.E. Prenatal infection.
11. A 31⁄2-year-old boy is interested in communicating with others, asks “questions,” and can follow two-partinstructions. Approximately 50% of his language is understood by strangers. The best description of hisspeech/language ability is:
A. Developmental dysfluency.B. Expressive language delay.C. Normal development for age.D. Phonologic disorder.E. Receptive language delay.
12. Established reasons for a child to demonstrate clinically significant delays in language developmentinclude being:
A. A middle child.B. Male.C. Raised in a bilingual home.D. Raised in a poor linguistic environment.E. Taught sign language.
13. A 7-month-old child makes a variety of sounds that include both consonants and vowels. This ability isbest described as:
A. Babbling.B. Cooing.C. Jargoning.D. Reciprocating.E. Talking.
cognition language and speech
Pediatrics in Review Vol.26 No.4 April 2005 141 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from

ATTENTION ARTISTS AGES 5 TO 16 YEARSART CONTEST FOR COVERS OF THE
YEAR 2006 AND 2007 ISSUES OFPEDIATRICS IN REVIEW
INSTRUCTIONS TO ARTISTS:
Your drawing should be no smaller than 8.5� � 11� and no larger than 18� � 24�. Remember that your drawingwill be reduced to 5.5� � 6� on the cover of the journal, so:
Make your drawing COLORFUL. Try to make your drawing fit the space (vertical, not horizontal). Drawabout . . .
Your favorite thing to doYour dream of what you would like to happen somedayWhat you would like to be doing when you grow up
Entry Information (please fill in ALL information):
Name: Age:
Address:
City/State/Zip:
Social Security Number:
Pediatrician’s Name: Telephone #
Artwork should be submitted WITH THIS FORM TO:
Sydney SutherlandEditorial Assistant, PIRc/o Dept. of Pediatrics, Box 777University of Rochester Medical Center, Room 4-8104601 Elmwood AvenueRochester, NY 14642
ALL ENTRIES MUST BE RECEIVED BY DECEMBER 30, 2005
CLINICIANS: Please post this notice in your office FOR YOUR PATIENTS!
cognition language and speech
142 Pediatrics in Review Vol.26 No.4 April 2005 by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from

DOI: 10.1542/pir.26-4-131 2005;26;131-142 Pediatr. Rev.
Heidi M. Feldman Children
Evaluation and Management of Language and Speech Disorders in Preschool
& ServicesUpdated Information
http://pedsinreview.aappublications.org/cgi/content/full/26/4/131including high-resolution figures, can be found at:
Permissions & Licensing
http://pedsinreview.aappublications.org/misc/Permissions.shtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints http://pedsinreview.aappublications.org/misc/reprints.shtml
Information about ordering reprints can be found online:
by Shruti Kant on August 15, 2008 http://pedsinreview.aappublications.orgDownloaded from