Evaluating the Angina Plan in Patients Admitted to Hospital with Angina: A Randomized Controlled...
13
RESEARCH Evaluating the Angina Plan in Patients Admitted to Hospital with Angina: A Randomized Controlled Trial Stella Zetta, 1 Karen Smith, 1 Martyn Jones, 1 Paul Allcoat 2 & Frank Sullivan 3 1 School of Nursing and Midwifery, University of Dundee, Dundee, UK 2 Lynebank Hospital, Dunfermline, UK 3 Scottish School of Primary Care, University of Dundee, Dundee, UK Keywords Angina; Nurse-led; Randomized controlled trial; Self-help intervention. Correspondence Dr. Stella Zetta, Thettalon 19, Karditsa, 43100, Greece. Tel.: 00302441029380; E-mail: [email protected] doi: 10.1111/j.1755-5922.2009.00109.x The aim of this trial was to evaluate the Angina Plan (AP), a cognitive- behavioral nurse-facilitated self-help intervention against standard care (SC). A randomized controlled trial of 218 patients hospitalized with angina assessed participants predischarge and 6 months later. Data were collected during a structured interview using validated questionnaires, self-report, and physio- logical measurement to assess between group changes in mood, knowledge and misconceptions, cardiovascular risk, symptoms, quality of life, and health service utilization. The intention-to-treat (ITT) analysis found no reliable ef- fects on anxiety and depression at 6 months. AP participants reported increased knowledge, less misconceptions, reduced body mass index (BMI), an increase in self-reported exercise, less functional limitation, and improvements in gen- eral health perceptions and social and leisure activities compared to those re- ceiving SC. Sensitivity analysis excluding participants with high baseline de- pression revealed a statistical significant reduction in depression levels in AP compared to the SC participants. Analysis excluding participants receiving car- diac surgery or angioplasty removed the ITT effects on physical limitation, self-reported exercise and general health perceptions and the improvements seen in social and leisure activities, while adaptive effects on knowledge, mis- conceptions and BMI remained and between-group changes in depression ap- proached significance. Initiating the AP in a secondary care setting for patients with new and existing angina produces similar benefits to those reported in newly diagnosed primary care patients. Further evaluation is required to ex- amine the extent of observed effects in the longer term. Introduction International statistics show 9.8 million people in the USA and 1.98 million in the UK suffer from angina pec- toris and experience considerable mortality and morbid- ity [1,2] from this common clinical manifestation of coro- nary heart disease (CHD). It is estimated a further 96,000 and 785,000 new cases of stable angina are identified in the UK and USA, respectively [1,2]. This results in an annual increase in hospital admissions associated with angina; however, this group is not always included in tra- ditional rehabilitation and recovery programs [3]. Many patients with angina report psychological distress (anxiety and depression), which can influence the de- velopment and prognosis of CHD [4–6]. Symptoms in- cluding chest pain, fatigue, impaired physical function, and quality of life may affect recovery and may result in disability and increased hospital readmissions [4,7–11]. Therefore, when evaluating the effectiveness of health- care interventions that focus on angina, outcomes such as anxiety and depression, symptoms, physical function, quality of life, and service uptake should be assessed. Evaluation of cardiac rehabilitation (CR) and sec- ondary prevention programs targeting lifestyle modifi- cation following a cardiac event have shown improved knowledge and risk factor profiles, increased prescrip- tion and uptake of secondary prevention treatments, improved mood, clinical and physical status, all-cause mortality and cardiac mortality, quality of life, and a reduction in hospital admissions [12–14]. Traditionally, 112 Cardiovascular Therapeutics 29 (2011) 112–124 c 2009 Blackwell Publishing Ltd
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Evaluating the Angina Plan in Patients Admitted to Hospital with Angina: A Randomized Controlled...

RESEARCH
Evaluating the Angina Plan in Patients Admitted to Hospitalwith Angina: A Randomized Controlled TrialStella Zetta,1 Karen Smith,1 Martyn Jones,1 Paul Allcoat2 & Frank Sullivan3
1 School of Nursing and Midwifery, University of Dundee, Dundee, UK2 Lynebank Hospital, Dunfermline, UK3 Scottish School of Primary Care, University of Dundee, Dundee, UK
KeywordsAngina; Nurse-led; Randomized controlled trial;
Self-help intervention.
CorrespondenceDr. Stella Zetta, Thettalon 19, Karditsa,
43100, Greece.
Tel.: 00302441029380;
E-mail: [email protected]
doi: 10.1111/j.1755-5922.2009.00109.x
The aim of this trial was to evaluate the Angina Plan (AP), a cognitive-behavioral nurse-facilitated self-help intervention against standard care (SC).A randomized controlled trial of 218 patients hospitalized with angina assessedparticipants predischarge and 6 months later. Data were collected during astructured interview using validated questionnaires, self-report, and physio-logical measurement to assess between group changes in mood, knowledgeand misconceptions, cardiovascular risk, symptoms, quality of life, and healthservice utilization. The intention-to-treat (ITT) analysis found no reliable ef-fects on anxiety and depression at 6 months. AP participants reported increasedknowledge, less misconceptions, reduced body mass index (BMI), an increasein self-reported exercise, less functional limitation, and improvements in gen-eral health perceptions and social and leisure activities compared to those re-ceiving SC. Sensitivity analysis excluding participants with high baseline de-pression revealed a statistical significant reduction in depression levels in APcompared to the SC participants. Analysis excluding participants receiving car-diac surgery or angioplasty removed the ITT effects on physical limitation,self-reported exercise and general health perceptions and the improvementsseen in social and leisure activities, while adaptive effects on knowledge, mis-conceptions and BMI remained and between-group changes in depression ap-proached significance. Initiating the AP in a secondary care setting for patientswith new and existing angina produces similar benefits to those reported innewly diagnosed primary care patients. Further evaluation is required to ex-amine the extent of observed effects in the longer term.
Introduction
International statistics show 9.8 million people in theUSA and 1.98 million in the UK suffer from angina pec-toris and experience considerable mortality and morbid-ity [1,2] from this common clinical manifestation of coro-nary heart disease (CHD). It is estimated a further 96,000and 785,000 new cases of stable angina are identified inthe UK and USA, respectively [1,2]. This results in anannual increase in hospital admissions associated withangina; however, this group is not always included in tra-ditional rehabilitation and recovery programs [3].
Many patients with angina report psychological distress(anxiety and depression), which can influence the de-velopment and prognosis of CHD [4–6]. Symptoms in-
cluding chest pain, fatigue, impaired physical function,and quality of life may affect recovery and may result indisability and increased hospital readmissions [4,7–11].Therefore, when evaluating the effectiveness of health-care interventions that focus on angina, outcomes suchas anxiety and depression, symptoms, physical function,quality of life, and service uptake should be assessed.
Evaluation of cardiac rehabilitation (CR) and sec-ondary prevention programs targeting lifestyle modifi-cation following a cardiac event have shown improvedknowledge and risk factor profiles, increased prescrip-tion and uptake of secondary prevention treatments,improved mood, clinical and physical status, all-causemortality and cardiac mortality, quality of life, and areduction in hospital admissions [12–14]. Traditionally,
112 Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd

S. Zetta et al. Evaluating the Angina Plan
however, angina patients who are likely to gain sim-ilar benefit from such interventions have often beenexcluded from CR programs [3]. One trial, which eval-uated the health outcomes of patients with angina6 months after discharge from a chest pain service,showed that 58% of patients reported ongoing symptoms42% reported anxiety and 23% moderate depression [10]and limited change in risk factors postdischarge has beenreported [10,15].
Previous research has highlighted the need to iden-tify and correct misconceptions or maladaptive beliefs re-lated to CHD which are associated with increased levels ofanxiety, increased physical limitations, and more admis-sions to hospital [9,16]. Correcting misconceptions relat-ing to angina is thought to give patients the confidenceto engage in lifestyle changes and to enable more effec-tive self-management of their long-term condition [16].A randomized controlled trial (RCT) in selected primarycare patients has demonstrated that a brief cognitive-behavioral nurse-facilitated self-help intervention, theAngina Plan (AP), can reduce anxiety and depression,self-report of angina and physical disability when addedto a routine secondary prevention clinic in communitypatients [9]. However, such intervention is currently notwidely available to angina patients in the UK. There isa need, therefore, to offer structured support to anginapatients to target their educational needs, correct anymisconceptions, reduce anxiety and depression, optimizesymptom management, and encourage lifestyle modifica-tion [11].
The aim of this current trial was to establish the effec-tiveness of the AP in an unselected group of the CHD pop-ulation. This unselected population would reflect anginapatients who are being admitted every day into an acuteadmission or cardiology area. This may include patientswith a past history of cardiac disease or this may be theirfirst presentation with CHD. Since patients may be morewilling to change behavior at this time, there is an oppor-tunity to initiate this established intervention in a hospi-tal setting following an acute event and to continue thefollow-up in the community postdischarge. Anxiety asdetermined by the Hospital Anxiety and Depression Scale(HADS) [17] was the primary outcome measure in thistrial following the work of Lewin et al. (2002) [9]. Anabstract of this trial has been previously presented [18].
Methods
This pragmatic RCT with broad inclusion criteria targetedpatients who are commonly admitted to a medical admis-sions or coronary care unit in daily practice in two hospi-tals incorporating a teaching hospital and smaller districtgeneral hospital. This allowed the AP intervention to be
evaluated within the context of current clinical practiceover a 22-month period. Data were collected by a struc-tured interview predischarge and at 6-month follow-upusing a series of validated questionnaires, self-report andphysiological measurement. Ethical approval for this trialwas obtained from the local Committee on Medical Re-search Ethics. This trial was powered (98%) to be able todetect a difference of 1.5 units (SD = 3) on the HADSanxiety scale with a sample size of 260 participants at the6-month evaluation. This difference was comparable tothat shown by Lewin et al. (2002). Following screeningfor entry (see inclusion and exclusion criteria, Figure 1)written informed consent was obtained from 233 partici-pants who had been admitted to either the acute medicaladmissions wards or Coronary Care Units of either of thetwo hospitals (see Figure 2). Baseline data were collectedand participants were randomized to either:
1. Standard Care (SC): (N = 117) a minimal interven-tion by nurses during their admission which identifiedpatient’s risk factors, provided advice on their condi-tion and risk factor reduction where possible depend-ing on staff workload and skill mix.
2. Angina Plan (AP): (N = 116) participants re-ceived additional support in the form of a cognitive-behavioral nurse-facilitated self-help interventionover the following 12 weeks.
Random allocations were computer generated, allo-cated to permuted fixed blocks of 20 and stratified for site[19]. Following recruitment, the research officer in an offsite university research department initiated the random-ization. The research officer contacted the AP nurse whothen informed participants of their group allocation. Theresearcher (SZ) was blinded to group allocation through-out the trial.
The Angina Plan Intervention
The AP is a systematically developed intervention basedon theoretical principles of Cognitive Behavioral Therapy(CBT). The aim of CBT is to educate patients about thereciprocal relationship between thoughts, feelings andbehaviors and to increase awareness of the automaticthoughts that occur in response to situations, events, andinteractions. The aim of CBT is to allow the person totake control of his or her own problems and for him orher to manage his/her thoughts, feelings, and behaviorsin such a way that future problems are dealt with in anadaptive way [20]. The AP involves specific and struc-tured training for the nurses who provide the interven-tion and could potentially be replicated elsewhere. As itis short and does not require extensive resources it could
Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd 113

Evaluating the Angina Plan S. Zetta et al.
Figure 1 Inclusion, exclusion, and withdrawal criteria.
potentially be incorporated to existing rehabilitation ser-vices. During a 45-minute in-hospital consultation theAP nurse completed an assessment and initiated the APintervention, which was then facilitated over the next12 weeks. The patient’s cardiac misconceptions wereidentified using the brief questionnaire within the APpack at the start of the consultation to allow the nurse toproactively target and correct these misconceptions. Indi-vidual cardiovascular risk was assessed and advice on riskfactor modification given. Participants received the AP,which included a patient-held “work-book” and an au-diotaped relaxation and information program. The work-book provided information on angina and its manage-ment, cardiovascular risk, relaxation, exercise and goalsetting and pacing techniques. Over the following 12weeks a method of “goal setting and pacing” based onthe principles of CBT was used by the AP facilitator tointroduce lifestyle changes and support recovery duringtelephone follow-up at weeks 1, 4, 8, and 12 for all par-ticipants in the AP group [21].
Assessments
Data, including demographic and clinical information,cardiac risk factors, motivation to change, measures ofknowledge and misconceptions, mood, cardiovascular
symptoms, quality of life, health service utilization, andsatisfaction with care, were collected during a structuredinterview by the researcher at baseline (predischarge)and 6-month postdischarge in the research clinic. For par-ticipants unable to attend the follow-up clinic, these datawere collected in the participants’ home.
Mood was assessed using the Hospital Anxiety and De-pression Scale (HADS) a widely used and well-validated14-item tool with 2, seven item subscales to measure anx-iety and depression within a nonpsychiatric population[17]. A score from 0 to 3 for each item generated a totalscore (range 0 to 21) for each subscale. Scores between 8and 10 indicate borderline presence of anxiety or depres-sion and those above 10 suggest that these states may bepresent. Anxiety was the primary outcome measure inthis trial.
Knowledge and misconceptions were assessed usingthe 14-item York Angina Beliefs Questionnaire [22]. Thisuses a Likert scale response format ranging from “stronglyagree” to “strongly disagree” and has been reported to bereliable and valid in this client group. Items targeted thecause, physiology and coping with angina. Summationand transformation of the item scores generated a scaletotal ranging from 0–56 with higher numbers indicatingmore misconceptions.
Cardiovascular symptoms were measured using2 questionnaires. The first, Seattle Angina Questionnaire
114 Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd

S. Zetta et al. Evaluating the Angina Plan
Figure 2 Flowchart of participating patients.
(SAQ) [23] is a disease-specific health related quality oflife measure comprised of a 19 item questionnaire mea-suring five dimensions of coronary artery disease: physi-cal limitation, angina stability, anginal frequency, treat-ment satisfaction and disease perception. Each dimension
is scored separately on a 0–100 scale with higher scoresindicating better functioning. The Cardiovascular Limita-tions and Symptoms Profile (CLASP) [24] measures ninephysical and functional dimensions, including four symp-tom subscales (angina, shortness of breath, tiredness,
Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd 115

Evaluating the Angina Plan S. Zetta et al.
ankle swelling) and five subscales focusing on functionallimitations (mobility, social life and leisure activities,activities within the home, concerns and worries, sexualactivity). Each of the nine subscales is scored separatelyto calculate a specific measure of impairment. It is widelyused in clinical practice and research studies and itspsychometric validation has been published [24,25].
Quality of life (QoL) was measured using two instru-ments. The Short Form-36 Health Survey (SF-36) is a36-item questionnaire assessing general health and QoL,which has been used extensively with health and medicalpopulations and has demonstrated good validity, reliabil-ity and sensitivity to change over time. The eight dimen-sions of the SF-36 (physical functioning, role limitationscaused by physical problems, bodily pain, social function-ing, mental health, role limitations caused by emotionalproblems, vitality-energy/fatigue and general health per-ception) generate scores on each dimension between 0and 100, with higher scores representing better healthstatus [26]. The second the Schedule for the Evaluationof Individual Quality of Life – Direct Weighting (SEIQoL –DW) is an interview-based tool specifically designed forthe assessment of individual quality of life [27]. Using theSEIQoL – DW participants define five areas that comprisetheir individual ‘quality’ of life. These items are ratedin terms of level of importance. An overall score rang-ing from 0–100 is then calculated with higher scores re-flecting better quality of life. The SEIQoL-DW is totallysubjective and patient-centered and provides a relativelyunique measure of quality of life.
Individuals’ motivation to change behavior associatedwith cardiovascular risk was assessed using an adaptationof the stages of change model [28]. Individuals were cat-egorized into active or nonactive stages reflecting theirreadiness to change.
Cardiovascular risk assessment included blood pressure(BP) measurement, following British Hypertension Soci-ety Guidelines [29], plasma cholesterol levels and bodymass index (kg/m2). Current smoking, dietary and exer-cise habits were assessed by self-report questionnaires aspart of the structured interview. Smoking behavior wasverified using a calibrated Bedford EC50-piCO Smokerl-yser breath CO monitor.
Health service utilization was assessed by recording thefrequency and reasons for contact with primary and sec-ondary care during the 6-month follow-up period. Thiswas assessed by self-report and verified by screening GPand hospital case notes.
To control for order effects, questionnaires were ad-ministered sequentially to the participants in three dif-ferent agreed and preallocated orders. HADS was admin-istered first in each sequence as responses to the HADSmay be influenced by preceding questionnaires [30].
SEIQoL-DW was the last in each sequence as it was themost time consuming measure to complete. Data collec-tion took between 45 and 90 minutes per participant onaverage.
Data Analysis
Data were entered into the SPSS 11.5 (SPSS Inc.,Chicago, IL), cleaned and screened for normality of dis-tribution, presence of outliers and missing data. Charac-teristics of participants in each arm were compared de-scriptively. Two variables (HADS anxiety and depression)were transformed using square root transformation andone variable (CLASP concerns) was transformed usinglogarithmic transformation (log+1). Assessment of the ef-fect of the intervention was conducted using two-wayanalysis of variance (ANOVA) using two fixed factors,that is, the group (SC or AP) and sequence of ques-tionnaires (sequence 1, 2, and 3) for the YABQ, CLASP,SAQ, SF-36, and HEQ. Difference variables were createdby subtracting follow-up values from baseline. HADS,SEIQoL-DW, body mass index (BMI), and BP were anal-ysed using an independent samples t test because groupwas the only fixed factor. All tests were conducted usinga 2-tailed significance level of P < 0.05. A nonparamet-ric approach was adopted for variables (total cholesterol,HEQ-A, SAQ angina treatment satisfaction and anginalstability, SF-36 role emotional, role physical, social func-tioning and mental health and CLASP Home score) thatwere not normally distributed (see Table 3). The mainintention-to-treat (ITT) analysis included all participantsin the group to which they were randomly assigned, re-gardless of their adherence to the entry criteria, treatmentassignment and receipt, withdrawal from the program ordeviation from the protocol. The missing values strategyof replacing the mean of the other group for the patientgroup was adopted in order to minimize the type 1 er-ror since the dropout rate was less than 20% [31]. Twosensitivity analyses were performed. The first excludedparticipants who during the 6 months time being on thetrial, underwent either Coronary Artery Bypass Grafting(CABG) or Percutaneus Coronary Intervention (PCI). Thesecond excluded participants who scored more than 11on HADS depression at baseline (see Figure 3).
Results
Recruitment
Between August 2003 and October 2004, 566 eligible pa-tients were admitted to the two hospital sites. Four hun-dred and sixteen patients were available and approachedfor participation in the trial. A total of 233 patients
116 Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd

S. Zetta et al. Evaluating the Angina Plan
Figure 3 Data analysis process—sensitivity
analyses.
(56% of those available) agreed to participate in the trial(Figure 2), which ended in May 2005. During the first4 months of the recruitment period, patients were given24 hours or at least overnight to consider participation.However, this strategy resulted in approximate 60 eligi-ble patients being missed due to being discharged within24 hours (see Figure 2). The recruitment process wasthen changed with the approval of the Local Commit-tee on Medical Research Ethics to allow participants aminimum of 4 hours to consider their participation in thestudy, which improved the number of patients recruitedand reduced the number of patients being missed. How-ever capturing more patients earlier in their hospital stayalso increased the number of patients who refused to par-ticipate in the study.
The groups were similar at baseline (Table 1). Meanchange scores were calculated for mood, knowledge andmisconceptions, cardiovascular symptoms, QoL and car-diovascular risk. The results of the ITT analysis are pre-sented in Table 2 (parametric testing) and Table 3 (non-
parametric testing). The sequence x group interactionfor SF-36 energy and vitality (F (2,217) = 3.24, P =0.04) suggested that any significant results seen with thismeasure were influenced by the sequence of the ques-tionnaire administration and should be interpreted withcaution.
There was no significant difference in between-groupchange scores for anxiety or depression (Table 2). Therewas a highly significant difference in change scores be-tween groups in knowledge and misconceptions with theAP group demonstrating improved knowledge and fewermisconceptions (Table 2) than the control group.
Analysis of cardiovascular symptoms demonstratedthat there was a significant difference in change scoresbetween-groups in the social and leisure component ofthe CLASP [24]. Physical limitation due to angina mea-sured by the Seattle Angina Exertional Capacity Scale[23] showed a significant between-group change score.A single significant difference was shown in changescores between groups in general health perception in the
Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd 117

Evaluating the Angina Plan S. Zetta et al.
Table 1 Characteristics of the groups at baseline
SC AP
n = 109 n = 109
Mean age (SD) 65.94 (9.96) 64.8 (10.04)
n (%) n (%)
Number of males 71 (65%) 78 (72%)
Females 38 (35%) 31 (28%)
Lives alone 31 (28%) 34 (31%)
Lives with partner 78 (72%) 75 (69%)
Deprivation category 1–2 (most affluent) 30 (28%) 26 (24%)
Deprivation category 3–5 60 (55%) 64 (59%)
Deprivation category 6–7 (least affluent) 19 (17%) 19 (17%)
Presence of CHD and/or angina 87 (80%) 94 (86%)
Previous diagnosis of unstable angina 51 (47%) 57 (52%)
Previous myocardial infarction 48 (44%) 50 (46%)
Procedure performed in the past�PTCA 21 (19%) 25 (23%)�CABG 20 (18%) 22 (20%)
Presence of peripheral vascular disease 9 (8%) 6 (6%)
Previous cerebrovascular event 11 (10%) 12 (11%)
Previous attendance of cardiac rehabilitation 33 (30%) 29 (27%)
Diabetes 24 (22%) 18 (17%)
Smoking
Current 25 (23%) 21 (19%)
Ex-smoker 51 (47%) 53 (49%)
Nonsmoker 33 (30%) 35 (32%)
Family history of CHD 78 (72%) 67 (62%)
Hypertension diagnosis 70 (64%) 59 (54%)
Systolic blood pressure – mean (SD) 127.17 (19.97) 125.61 (18.14)
Diastolic blood pressure – mean (SD) 68.98 (11.15) 69.10 (10.41)
Total cholesterol
Up to 4.8 mmol/L 63 59
4.81 mmol/L and above 43 40
Body mass index mean (SD) 28.52 (4.66) 28.48 (4.80)
Units of alcohol / week mean (SD) 8.12 (11.37) 7.52 (9.35)
SF-36. No reliable differences were found in any otherdomains of the SF-36 nor the total QoL scores in theSEIQoL-DW.
In relation to cardiovascular risk factors, a significantdifference in change scores between-groups was foundfor BMI. Categorical assessment of BMI showed more APparticipants within the normal BMI category at follow-upin comparison with fewer SC participants (Table 4). Dif-ferences in patient movement between categories weresignificant between-groups with more participants in theAP group reducing their BMI and more in standard careincreasing their BMI (U = 5327.0, z = –2.27, P = 0.023)(see Table 4). Participants’ motivation to make behav-ioral changes was compared examining shifts betweenactive (maintenance and action) and nonactive (prepara-tion, contemplation and precontemplation) stages. A sig-
nificant difference in change scores between-groups wasfound for exercise, with more AP participants movingfrom the nonactive to active stage and more SC partic-ipants moving from active to nonactive stage over time(U = 5100.5, z = –2.28, P = 0.02). Dietary data althoughcollected using an adaptation from the Healthy EatingQuiz (HEQ) [32] have not been presented due to the lowreliability of the scale totals.
There were no significant between-group differencesin hospital admissions as assessed by either screening ofrecords (t(188) = 0.26, P = 0.79) or self-report (t(182) =–0.73, P = 0.47), contacts with primary care services us-ing records (t(186) = 0.87, P = 0.39) or patient self-report(t(184) = 1.75, P = 0.0.82), nor in participants satisfac-tion with the care they received (U = 3897.0, z = –0.05,P = 0.96).
118 Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd
S. Zetta et al. Evaluating the Angina Plan
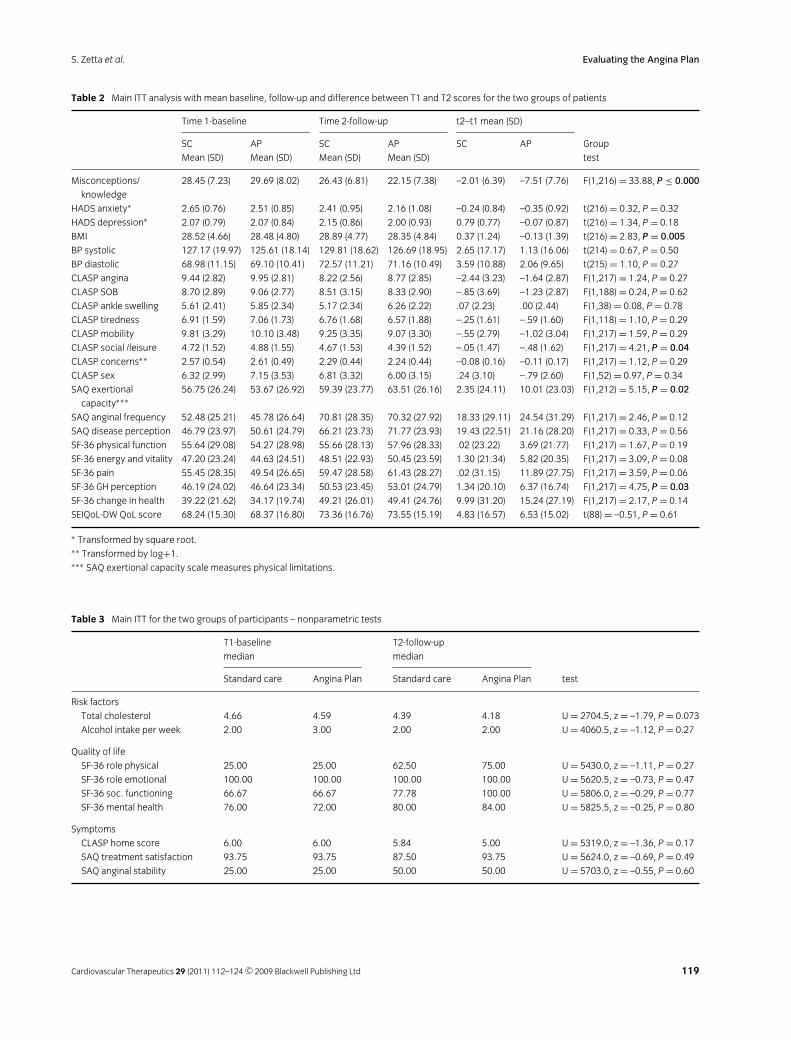
Table 2 Main ITT analysis with mean baseline, follow-up and difference between T1 and T2 scores for the two groups of patients
Time 1-baseline Time 2-follow-up t2–t1 mean (SD)
SC AP SC AP SC AP Group
Mean (SD) Mean (SD) Mean (SD) Mean (SD) test
Misconceptions/ 28.45 (7.23) 29.69 (8.02) 26.43 (6.81) 22.15 (7.38) –2.01 (6.39) –7.51 (7.76) F(1,216) = 33.88, P ≤ 0.000
knowledge
HADS anxiety∗ 2.65 (0.76) 2.51 (0.85) 2.41 (0.95) 2.16 (1.08) –0.24 (0.84) –0.35 (0.92) t(216) = 0.32, P = 0.32
HADS depression∗ 2.07 (0.79) 2.07 (0.84) 2.15 (0.86) 2.00 (0.93) 0.79 (0.77) –0.07 (0.87) t(216) = 1.34, P = 0.18
BMI 28.52 (4.66) 28.48 (4.80) 28.89 (4.77) 28.35 (4.84) 0.37 (1.24) –0.13 (1.39) t(216) = 2.83, P = 0.005
BP systolic 127.17 (19.97) 125.61 (18.14) 129.81 (18.62) 126.69 (18.95) 2.65 (17.17) 1.13 (16.06) t(214) = 0.67, P = 0.50
BP diastolic 68.98 (11.15) 69.10 (10.41) 72.57 (11.21) 71.16 (10.49) 3.59 (10.88) 2.06 (9.65) t(215) = 1.10, P = 0.27
CLASP angina 9.44 (2.82) 9.95 (2.81) 8.22 (2.56) 8.77 (2.85) –2.44 (3.23) –1.64 (2.87) F(1,217) = 1.24, P = 0.27
CLASP SOB 8.70 (2.89) 9.06 (2.77) 8.51 (3.15) 8.33 (2.90) –.85 (3.69) –1.23 (2.87) F(1,188) = 0.24, P = 0.62
CLASP ankle swelling 5.61 (2.41) 5.85 (2.34) 5.17 (2.34) 6.26 (2.22) .07 (2.23) .00 (2.44) F(1,38) = 0.08, P = 0.78
CLASP tiredness 6.91 (1.59) 7.06 (1.73) 6.76 (1.68) 6.57 (1.88) –.25 (1.61) –.59 (1.60) F(1,118) = 1.10, P = 0.29
CLASP mobility 9.81 (3.29) 10.10 (3.48) 9.25 (3.35) 9.07 (3.30) –.55 (2.79) –1.02 (3.04) F(1,217) = 1.59, P = 0.29
CLASP social /leisure 4.72 (1.52) 4.88 (1.55) 4.67 (1.53) 4.39 (1.52) –.05 (1.47) –.48 (1.62) F(1,217) = 4.21, P = 0.04
CLASP concerns∗∗ 2.57 (0.54) 2.61 (0.49) 2.29 (0.44) 2.24 (0.44) –0.08 (0.16) –0.11 (0.17) F(1,217) = 1.12, P = 0.29
CLASP sex 6.32 (2.99) 7.15 (3.53) 6.81 (3.32) 6.00 (3.15) .24 (3.10) –.79 (2.60) F(1,52) = 0.97, P = 0.34
SAQ exertional 56.75 (26.24) 53.67 (26.92) 59.39 (23.77) 63.51 (26.16) 2.35 (24.11) 10.01 (23.03) F(1,212) = 5.15, P = 0.02
capacity∗∗∗
SAQ anginal frequency 52.48 (25.21) 45.78 (26.64) 70.81 (28.35) 70.32 (27.92) 18.33 (29.11) 24.54 (31.29) F(1,217) = 2.46, P = 0.12
SAQ disease perception 46.79 (23.97) 50.61 (24.79) 66.21 (23.73) 71.77 (23.93) 19.43 (22.51) 21.16 (28.20) F(1,217) = 0.33, P = 0.56
SF-36 physical function 55.64 (29.08) 54.27 (28.98) 55.66 (28.13) 57.96 (28.33) .02 (23.22) 3.69 (21.77) F(1,217) = 1.67, P = 0.19
SF-36 energy and vitality 47.20 (23.24) 44.63 (24.51) 48.51 (22.93) 50.45 (23.59) 1.30 (21.34) 5.82 (20.35) F(1,217) = 3.09, P = 0.08
SF-36 pain 55.45 (28.35) 49.54 (26.65) 59.47 (28.58) 61.43 (28.27) .02 (31.15) 11.89 (27.75) F(1,217) = 3.59, P = 0.06
SF-36 GH perception 46.19 (24.02) 46.64 (23.34) 50.53 (23.45) 53.01 (24.79) 1.34 (20.10) 6.37 (16.74) F(1,217) = 4.75, P = 0.03
SF-36 change in health 39.22 (21.62) 34.17 (19.74) 49.21 (26.01) 49.41 (24.76) 9.99 (31.20) 15.24 (27.19) F(1,217) = 2.17, P = 0.14
SEIQoL-DW QoL score 68.24 (15.30) 68.37 (16.80) 73.36 (16.76) 73.55 (15.19) 4.83 (16.57) 6.53 (15.02) t(88) = –0.51, P = 0.61
∗ Transformed by square root.∗∗ Transformed by log+1.∗∗∗ SAQ exertional capacity scale measures physical limitations.
Table 3 Main ITT for the two groups of participants – nonparametric tests
T1-baseline T2-follow-up
median median
Standard care Angina Plan Standard care Angina Plan test
Risk factors
Total cholesterol 4.66 4.59 4.39 4.18 U = 2704.5, z = –1.79, P = 0.073
Alcohol intake per week 2.00 3.00 2.00 2.00 U = 4060.5, z = –1.12, P = 0.27
Quality of life
SF-36 role physical 25.00 25.00 62.50 75.00 U = 5430.0, z = –1.11, P = 0.27
SF-36 role emotional 100.00 100.00 100.00 100.00 U = 5620.5, z = –0.73, P = 0.47
SF-36 soc. functioning 66.67 66.67 77.78 100.00 U = 5806.0, z = –0.29, P = 0.77
SF-36 mental health 76.00 72.00 80.00 84.00 U = 5825.5, z = –0.25, P = 0.80
Symptoms
CLASP home score 6.00 6.00 5.84 5.00 U = 5319.0, z = –1.36, P = 0.17
SAQ treatment satisfaction 93.75 93.75 87.50 93.75 U = 5624.0, z = –0.69, P = 0.49
SAQ anginal stability 25.00 25.00 50.00 50.00 U = 5703.0, z = –0.55, P = 0.60
Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd 119

Evaluating the Angina Plan S. Zetta et al.
Table 4 Distribution of participants in BMI categories at two time points
Standard care Angina Plan
N (%) N (%)
T1 T2 T1 T2
BMI categories Baseline Follow-up Baseline Follow-up
Underweight 1 (0.9) 1 (0.9) 1 (0.9) 1 (0.9)
10–18.5
Normal 29 (26.6) 24 (22.0) 25 (22.9) 30 (27.5)
18.51–25
Preobese 43 (39.4) 44 (40.4) 50 (45.9) 43 (39.4)
25.1–30
Obese class I, II &III 36 (33.1) 40 (36.7) 33 (30.3) 35 (32.1)
30.1–60
Sensitivity Analyses
During this trial, 65 participants underwent further in-tervention through CABG or PCI. A sensitivity analy-sis was conducted to control for the potential effects ofthese interventions on outcomes. Once scores from theseparticipants had been removed, analysis on 77 SC par-ticipants and 76 AP participants confirmed the signifi-cant between-group differences on knowledge and mis-conceptions and BMI. In addition between-group differ-ence in depression approached significance (MAP = –0.16,SD = 0.78; MSC = 0.08, SD = 0.69; t(151) = 1.97, P =0.051). Although a significant result emerged in energyand vitality (SF-36) for the AP participants (MAP = 8.87,SD 19.82; MSC = 1.14 SD = 20.55; F(1,152) = 6.36, P =0.013), this result is likely to be an artifact of the se-quence by group effect reported previously. This sensi-tivity analysis also showed that the significant between-group differences seen in SAQ physical limitation, CLASPsocial and leisure activities, SF-36 general health percep-tion disappeared. Thus suggests that some improvementsreported in the ITT analysis may have been influencedby the positive effects of CABG/PCI on symptoms andrecovery.
When reviewing participants with probable presence ofclinical depression, that is, those with scores above 11, 13participants (6%) were identified 6 in the AP group and 7in the SC group. When reviewed individually, these par-ticipants had reported ongoing major life events, includ-ing bereavement, caring for a terminally ill relative andconsidering euthanasia, clinical depression on treatmentand factors unrelated to cardiac disease and that mayhave affected their mood. After removing those with ele-vated depression at baseline, a significant between-groupdifference was seen in change scores in depression. De-pression increased in the SC group (MSC = 0.77, SD =3.02) and decreased in the AP group (MAP = –0.20, SD =
3.18), and the between-group changes scores were reli-ably different t(203) = 2.23, P = 0.027). These resultssuggest that depression levels in AP participants improvedmarginally whilst depression levels in SC participants de-teriorated at 6 months although this effect was initiallyobscured by participants reporting high depression scoresat baseline.
Discussion
This pragmatic trial evaluated the effectiveness of the APin an unselected population of patients admitted to sec-ondary care with an acute exacerbation of angina. Theresults of this trial demonstrated that participants receiv-ing the AP reported improved knowledge and fewer mis-conceptions, improvements in some cardiac risk factors(BMI, self-reported exercise) and improvements in phys-ical limitation, general health perceptions and social andleisure activities. There were no reliable effects in the cur-rent trial on anxiety and depression in participants in theITT analysis.
The lack of significant difference in between-groupchange scores for anxiety or depression in the currenttrial was disappointing (Table 2). The current trial showedno significant differences in between -group changes foreither anxiety, the primary outcome measure, or depres-sion despite the trial having sufficient power to detectthese effects which was based on data in a similar pop-ulation of CHD patients [33]. Previous research has sug-gested that depression is a strong and independent riskfactor for mortality, recurrent cardiac events and lowerfunctional status in patients with unstable angina [6] andmyocardial infarction [5]. The prevalence of anxiety anddepression in this trial was similar to those reported byother researchers [34]. One possible explanation for thismay have been the reduction in anxiety reported in thestandard care groups, a finding not seen in the Lewinet al. (2002) [9] trial. This improvement in mood in thestandard care arm may be explained by improved follow-up and management of angina patients in primary care,which was not seen in the past.
No reliable differences were found in depression lev-els in the ITT analysis, yet Lewin et al. [9] previouslyreported that the most distressed participants showed asignificant improvement in mood. In contrast those withelevated depression at baseline in the current study didnot show improvement at follow-up. One possible expla-nation was that their depression may not have been re-lated to their cardiac condition therefore this interventionhad a limited effect in this group. After removing partic-ipants with elevated depression at baseline a significantbetween-group difference in change scores was seen in
120 Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd

S. Zetta et al. Evaluating the Angina Plan
depression, supporting this argument. Further researchmay illustrate whether the additional identification andtargeting of the underlying depression in those with ele-vated depression at baseline would allow such people tobenefit from the AP intervention.
The impact of knowledge and misconceptions in car-diac patients on functional and psychological status andas a potential barrier to lifestyle changes have been in-creasingly investigated by researchers [35–38]. Adap-tive change in angina beliefs over 1 year was the mostsignificant predictive factor for physical functioning at12-month follow-up [16]. Such belief based cognitiveinterventions can enable patients to participate activelyin recovery and lifestyle change thus improving self-management of CHD [38]. National guidelines now rec-ommend targeting misconceptions as part of CR andrecovery programs for cardiac patients as this has the po-tential to further enhance recovery [7]. The current trialshowed a highly significant improvement in knowledgeand a reduction in misconceptions for AP participantsin the ITT and sensitivity analyses, supporting previousstudies showing improvements in knowledge followingthe delivery of a targeted intervention [35,36]. This sug-gests that the AP may be useful in clinical practice to al-low the rapid identification of misconceptions and guideintervention to correct these beliefs, facilitating patientengagement in recovery and lifestyle modification.
Differences in cardiovascular symptoms were restrictedto the social and leisure dimension of the CLASP andphysical limitation as measured in the SAQ. A mean dif-ference of 10.01 in the SAQ physical limitation betweenbaseline and 6 months for the intervention group demon-strated clinically significant improvement with reductionin physical limitation in addition to the statistical dif-ference seen in the between group change scores [23].However these effects were lost after the sensitivity anal-ysis of interventions was completed. This suggests theeffect on symptoms and physical limitations may havestrongly influenced by the effects of PCI or surgery whichthemselves produce improvement in symptoms. Alterna-tively the smaller sample used for this analysis may thenhave been underpowered to detect the ITT effects withCABG/PCI patients removed.
The importance of QoL assessment in CR and recov-ery programs is well recognized [39]. Significant im-provements in QoL as measured by the SF-36 have beendemonstrated in other studies of angina patients awaitingcardiac surgery, however the intervention [40] was deliv-ered over a longer time period and involved face-to facecontact with the patient which may have affected results.Both groups in the current trial showed improved scoreson some domains of the SF36 as had been reported inother groups with Acute Coronary Syndrome [41]. Gen-
eral Health Perception was the only significant betweengroup difference shown in the current trial with the par-ticipants in the intervention group reporting better gen-eral health perception.
Cardiovascular risk profiles of the participants in thistrial were similar to those reported internationally, withsimilar baseline levels of obesity [42]. Previous work sug-gested that a 6-month period may be too short to detectmodification in such risk factors [9]. This trial, however,demonstrated a comparative reduction over 6 months inBMI for the AP group, both as a continuous and cate-gorical variable. This supports findings of a previous trialwhich demonstrated improvement in BMI following anintervention delivered on average for a 9-month periodfor angina patients on the waiting list for by pass surgery[40]. The reduction in BMI in the current trial may havebeen enhanced by the increase in self-reported activity inthe AP participants. In addition the AP participants weremore likely to be in the active stages of behavior changeat follow-up suggesting that the use of the AP may be auseful strategy to support client engagement in positivebehavioral change. Since obesity is becoming a major na-tional public health challenge [42] this type of interven-tion may be important in helping patients with CHD tomodify cardiovascular risk factors and prevent secondaryevents [43].
Although the previous trial on the AP did not reporton health service use [9], this outcome was measuredin the current trial by screening medical records and bypatient self-report and revealed no difference in healthservice use between-groups. The current trial results dif-fer from previous research evaluating a self-help, home-based program, based on the principles of CBT, on post-MI patients which demonstrated significantly less use ofhospital services by the intervention groups [33]. Onepossible explanation for the lack of difference seen in thecurrent trial may have been because the AP facilitatoridentified ongoing problems resulting in increased but ap-propriate contact with health services, a finding reportedin previous studies.
During the completion of this trial, 65 participants un-derwent further intervention through CABG or PCI. Theresults of the sensitivity analysis showed even after re-moving these participants the significant between-groupdifferences on knowledge and misconceptions, and BMIwere sustained, suggesting that the effects on these fac-tors are a result of the AP intervention. Interestinglya near significant reduction of depression was shown.The disappearance of the significant between-group dif-ferences seen in physical limitation, social and leisureactivities, general health perception suggests that theseimprovements reported in the ITT analysis may havebeen influenced by the positive effects of CABG/PCI on
Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd 121

Evaluating the Angina Plan S. Zetta et al.
symptoms and recovery and not resulting from the APintervention alone.
There is a number of limitations to this trial. This trialwas conducted in one UK, NHS Health Board Area andtherefore may not be typical of other settings. How-ever, as these sites included a large teaching hospitaland a smaller district general setting, this may strengthenthe applicability of these findings to a range of health-care settings. The evaluation of this trial was confined to6-month follow-up therefore we are unable to determineif any positive effects were sustained beyond this time.Longer-term evaluation would be useful. The SEIQoL-DW completion rate was lower than in other studies [44],which may have resulted from the number of question-naires administered. Self-reported physical activity datawithin the trial may also have been strengthened by ad-ditional objective measurement. A total of 56% of el-igible patients did not participate in the study as theywere either missed or refused to participate (Figure 2).Approaching patients earlier for inclusion in the studyresulted in less patients being missed due to early dis-charge. However, including more patients who werestaying 24 hours or less increased the number of patientswho refused to participate. From anecdotal information,a common reason for refusal to participate appeared tobe the patients’ imminent discharge and desire to leavehospital rather than participate in the trial.
One limitation of the trial potentially arises from theuse of multiple testing. The Bonferroni adjustment wasnot applied generally across this study. This conservativemethod reduces the risk of falsely rejecting a null hypoth-esis by dividing the significance level of 0.05 by N (thenumber of comparisons being undertaken). Antony [45]contends that if multiple tests are addressing different re-search questions, in this instance intervention effects onmood, BMI, and Health-Related Quality of Life, this ad-justment is not required. However, within our analysis ofbetween-group differences in Health Related Quality ofLife scores using the CLASP, SAQ, and SF 36, multipletesting may remain an issue. It is therefore possible, butunlikely that some of the four significant results in thiselement may have resulted by chance.
In conclusion, although the main results of this trial didnot detect any reliable effects on anxiety and depressionin participants at 6-month follow-up, the results haveshown that angina patients, with new and establishedCHD, admitted to an acute hospital setting who receivedthe AP reported improved knowledge, fewer misconcep-tions, improvements in some cardiac risk factors (BMI,self-reported exercise) improvements in physical limita-tion, general health perceptions and social and leisure ac-tivities. Past research has indicated that such people oftendo not engage in CR programs, even when they are avail-
able and may not wish to attend a hospital-based program[46]. One benefit of the AP is that unlike other mod-els of rehabilitation and support, the follow-up interven-tions may be delivered to the patients where it suits themeither at home by telephone support, as in the currenttrial, or at their GP practice [9] and thus is not resourceintensive.
These trial findings should be considered by cliniciansinvolved in the redesign and delivery of CR services lo-cally and nationally. The AP offers a short intervention(2.5 hours per patient) for the management of a cur-rently undertreated population of cardiac patients andhas shown benefits, which are sustained up to 6-monthfollow-up. Further research is needed to explore whetherthese benefits are sustained over a longer time period andwhether such effects are comparable to those that mightbe obtained through other CR programs offered to anginapatients. Further qualitative research is needed to exploreparticipants’ experiences of the AP in more detail. Thisprocess evaluation would enhance the current findingsand add to the understanding of patient experiences afteradmission to hospital with angina.
Acknowledgments
The authors would like to thank Connie Dunbar andCatherine Ryan, the Angina Plan facilitators for deliver-ing the intervention and Dr. Simon Ogston for his statis-tical advice. The study was supported by a grant providedby the Chief Scientist Office [CZH/4/99]. Stella Zetta wasin receipt of doctoral studentship provided by the Schoolof Nursing and Midwifery, University of Dundee.
Conflict of Interest
The authors have declared no conflict of interests.
References
1. Lloyd-Jones DM, Adams R, Carnethon M, et al., and for
the American Heart Association Statistics Committee and
Stroke Statistics Subcommittee. Heart Disease and Stroke
Statistics-2009 Update: A Report From the American
Heart Association Statistics Committee and Stroke
Statistics Subcommittee. Circulation 2009;119:e21–e181.
2. Allender S, Peto V, Scarborough P, Boxer A, Rayner M.
Coronary heart disease statistics 2007 edition. British
Heart Foundation Health Promotion Research Group.
Department of Public Health, University of Oxford, 2007.
3. NHS Scotland. Coronary heart disease/stroke task force
report. Edinburgh: Scottish Executive, 2001.
4. Martin CR, Thompson D. Depression in coronary heart
disease patients: Etiological and screening issues. Curr
Psychiatry Rev 2006;2:245–254.
122 Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd

S. Zetta et al. Evaluating the Angina Plan
5. Frasure-Smith N, Lesperance F. Depression and other
psychological risks following myocardial infarction. Arch
Gen Psychiatry 2003;60:627–636.
6. Rumsfeld JS, Magid DJ, Plomondon ME, Sales AE,
Grunwald GK, Every NR, Spertus JA. History of
depression, angina, and quality of life after acute
coronary syndromes. Am Heart J 2003;145:493–499.
7. SIGN. 57: Cardiac Rehabilitation – A national clinical
guideline. Edinburgh: Scottish Intercollegiate Guidelines
Network, 2002.
8. Spertus JA, McDonell M, Woodman CL, Fihn SD.
Association between depression and worse
disease-specific functional status in outpatients with
coronary artery disease. Am Heart J 2000;140:105–110.
9. Lewin B, Furze G, Robinson J, Griffith K, Wiseman S, Pye
M, Boyle R. A randomised controlled trial of a
self-management plan for patients with newly diagnosed
angina. Br J Gen Pract 2002;52:194–201.
10. Smith K, Ross D, Connolly E. Preliminary investigation of
the 6-month health outcomes of angina patients
discharged from a chest pain service. Eur Heart J
2001;22:623.
11. SIGN. 97-Risk estimation and the prevention of
cardiovascular disease. Edinburgh: Scottish Intercollegiate
Guidelines Network-NHS, 2007.
12. McAlister FA, Lawson FME, Teo KK, Armstrong PW.
Randomised trials of secondary prevention programmes
in coronary heart disease: systematic review. BMJ
2001;323:957–962.
13. Campbell N, Thain J, Deans H, Ritchie L, Rawles J, Squair
J. Secondary prevention clinics for coronary heart
disease: Randomised trial of effect on health. BMJ
1998;316:1434–1437.
14. Taylor R, Brown A, Ebrahim S, et al. Exercise-based
rehabilitation for patients with coronary heart disease:
Systematic review and meta-analysis of randomised
controlled trials. Am J Med 2004;116:682–692.
15. McCallum J, Lindsay G. Is there a need for cardiac
rehabilitation for patients admitted to hospital with
angina pectoris? Coron Health Care 2001;5:126–132.
16. Furze G, Lewin B, Murberg T, Bull P, Thompson D. Does
it matter what patients think? The relationship between
changes in patients’ beliefs about angina and their
psychological and functional status. J Psychosom Res
2005;59:323–329.
17. Zigmond AS, Snaith RP. The hospital anxiety
and depression scale. Acta Psychiatr Scand
1983;67:361–370.
18. Zetta S, Jones M, Smith K. Randomised controlled trial
comparing a self-help cognitive behavioural programme,
the Angina Plan, with standard care for angina patients
admitted to hospital. In 6th Annual Spring Meeting of the
Working Group on Cardiovascular Nursing of the
European Society of Cardiology and the Spring Meeting
of the Norwegian National Society of Cardiovascular
Nurses Bergen, Norway. Eur J Cardiovasc Nurs
2006;5S1:49–50.
19. Pocock S. Clinical trials: A practical approach. John Wiley
& Sons, Chicester, 1983.
20. Hobbis ICA, Sutton S. Are techniques used in cognitive
behaviour therapy applicable to behaviour change
interventions based on the theory of planned behaviour?
J Health Psychol 2005;10:7–18.
21. http://www.anginaplan.org.uk/training.htm.
22. Furze G, Bull P, Lewin B, Thompson D. Development of
the York Angina Beliefs Questionnaire. J Health Psychol
2003;8:307–315.
23. Spertus JA, Winder JA, Dewhurst TA, Deyo RA,
Prodzinski J, McDonnell M, Fihn SD. Development and
evaluation of the Seattle Angina Questionnaire, a new
functional status measure for coronary artery disease. J
Am Coll Cardiol 1995;25:333–341.
24. Devlen J, Michaelson S, Maguire P. Cardiovascular
limitations and symptoms profile. University of
Manchester, Manchester Centre for Primary Care
Research, 1989.
25. Lewin RJP, Thompson DR, Martin CR, Stuckey N, Devlen
J, Michaelson S, Maguire P. Validation of the
Cardiovascular Limitations and Symptoms Profile
(CLASP) in Chronic Stable Angina. J Cardiopulm Rehabil
2002;22:184–191.
26. Ware J, Sherbourne C. The MOS 36-item short-form
health survey (SF-36) I: Conceptual framework and item
selection. Med Care 1992;30:473–483.
27. O’Boyle C. The schedule for evaluation of individual
quality of life (SEIQoL). Int J Ment Health 1994;23:3–23.
28. Prochaska JO, DiClemente CC. Stages of change in the
modification of problems behaviours. In: Hersen M, Eisler
RS, Miller P, editors. Progress in behaviour modification,
vol 28. Sycamore Publishing, Sycamore, IL,
1992:183–218.
29. Williams B, Poulter N, Brown M, et al. The BHS
Guidelines working party guidelines for management of
hypertension: Report of the fourth working party of the
British Hypertension Society, 2004 – BHS IV. J Hum
Hypertens 2004;18:139–185.
30. Johnson NA, Heller RS. Prediction of patient
nonadherence with home-based exersise for cardiac
rehabilitation: The role of perceived bariers and perceived
benefits. Prev Med 1998;27:56–64.
31. Unnebrink K, Windeler J. Intention-to-treat: Methods for
dealing with missing values in clinical trials of
progressively deteriorating diseases. Stat Med
2001;20:3931–3946.
32. http://www.healthscotland.com/uploads/documents/
2973-Healthy Living Healthy Eating Quiz 4 pages.pdf.
33. Lewin B, Robertson IH, Cay EL, Irving JB, Campbell M.
Effects of self-help post-myocardial-infarction
rehabilitation on psychological adjustment and use of
health services. Lancet 1992;339:1036–1040.
Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd 123

Evaluating the Angina Plan S. Zetta et al.
34. Herrmann. International experiences with the hospital
anxiety and depression scale-a review of the validation
data and clinical results. J Psychosom Res 1997;42:17–41.
35. Johnston M, Foulkes J, Johnston DW, Pollard B,
Gudmundsdottir H. Impact on patients and partners of
inpatient and extended cardiac counselling and
rehabilitation: A controlled trial. Psychosom Med
1999;61:225–233.
36. Petrie K, Cameron LD, Ellis CJ, Buick D, Weinman J.
Changing illness perceptions after myocardial infarction:
An early intervention randomised controlled trial.
Psychosom Med 2002;64:580–586.
37. Karner A, Goransson A, Bergdahl B. Conceptions on
treatment and lifestyle in patients with coronary heart
disease—a phenomenographic analysis. Patient Educ Couns
2002;47:137–143.
38. Furze G, Lewin B, Roebuck A, Thompson D. Attributions
and misconceptions in angina: An exploratory study. J
Health Psychol 2001;6:501–510.
39. McGee H, Hevey D, Horgan J. Psychosocial outcome
assessments for use in cardiac rehabilitation service
evaluation: A 10-year systematic review. Soc Sci Med
1999;48:1373–1393.
40. McHugh F, Lindsay GM, Hanlon P, Hutton I, Brown MR,
Morrison C, Wheatley DJ. Nurse led shared care for
patients on the waiting list for coronary artery bypass
surgery: A randomised controlled trial. Heart
2001;86:317–323.
41. Chan DSK, Chau JPC, Chang AM. Acute coronary
syndromes: Cardiac rehabilitation programmes and
quality of life. J Adv Nurs 2005;49:591–599.
42. De Bacquer D, De Backer G, Cokkinos D, et al., for the
EUROASPIRE II Study Group. Overweight and obesity in
patients with established coronary heart disease: Are we
meeting the challenge? Eur Heart J 2004;25:121–128.
43. Hooper L, Summerbell CD, Higgins JPT, et al. Dietary fat
intake and prevention of cardiovascular disease:
Systematic review. BMJ 2001;322:757–763.
44. Campbell S, Whyte F. The quality of life of cancer
patients participating in phase I clinical trials using
SEIQoL-DW. J Adv Nurs 1999;30:335–343.
45. Antony D. Understanding advanced statistics. London:
Churchill Livingstone, 1999.
46. Tod AM, Read C, Lacey A, Abbott J. Barriers to uptake of
services for coronary heart disease: Qualitative. BMJ
2001;323:214.
124 Cardiovascular Therapeutics 29 (2011) 112–124 c© 2009 Blackwell Publishing Ltd