Evaluating community pharmacists’ perceptions of future generic substitution policy...
8
Health Policy 94 (2010) 68–75 Contents lists available at ScienceDirect Health Policy journal homepage: www.elsevier.com/locate/healthpol Evaluating community pharmacists’ perceptions of future generic substitution policy implementation: A national survey from Malaysia Chee Ping Chong a,∗ , Mohamed Azmi Hassali b , Mohd Baidi Bahari a , Asrul Akmal Shafie b a Discipline of Clinical Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia, 11800 Minden, Penang, Malaysia b Discipline of Social and Administrative Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia, 11800 Minden, Penang, Malaysia article info Keywords: Community pharmacist Perception Generic substitution Generic medicine Policy abstract Objectives: This study aims to provide baseline data to support the implementation of generic substitution policy in Malaysia by evaluating the community pharmacists’ per- ceptions and opinions on generic substitution and current substitution practices. Methods: A cross-sectional descriptive study involving the entire population of Malaysian community pharmacies (n = 1419) was undertaken using a self-completed anonymous mail questionnaire. Results: A total of 219 responses were received for a response rate of 15.4%. Majority of the respondents (93.6%) agreed that pharmacists should have generic substitution rights. Almost all pharmacists (96.8%) viewed Poison Class C (pharmacist only medicine) as most suitable class of controlled medicines for substitution. About half (51.6%) of the pharmacists preferred a policy which allowed substitution on any prescription. The pharmacists prefer to consult the physician when substituting narrow therapeutic index medicines (88.1%) and prescription only medicines (51.3%). Less than 25.0% of the pharmacists routinely keep the medication records and follow-up the patients who received substitution. Monitoring the efficacy (79.2%) and patient’s satisfaction with the generic medicines (74.9%) were the main reasons for following-up the patient if substitution occurs. Conclusions: Malaysian community pharmacists are generally in favour of generic substi- tution policy implementation. © 2009 Elsevier Ireland Ltd. All rights reserved. 1. Introduction In the recent years, escalating pharmaceutical cost has become a global challenge. Generic medicines provide the opportunity for savings in medicines expenditure due to their cheaper price [1,2]. Consequently, generic substitu- tion policy that aims to promote the utilization of generic medicines has been introduced in many developed [3–7] and developing countries [8–10]. This policy allows phar- macists to substitute generic for brand name medicine, unless the prescriber forbids or the patient declines the replacement. ∗ Corresponding author. Tel.: +60 12 5342685; fax: +60 4 6570017. E-mail address: [email protected] (C.P. Chong). Malaysia, like most developing countries, does not have a national public health insurance scheme to cover the citizens’ health expenditures [11]. Approximately 74% of funding in private Malaysian health sector is from consumers’ out-of-pocket money [12]. Therefore, the medicine’s price has become the major determination of access to affordable medicines. The Malaysian government does not control the prices of both innovator and generic medicines and believes that market force is capable to gen- erate reasonable price [13]. However, more than half of Malaysian consumers perceived medicines as expensive and urged that prices should be controlled [14]. Conversely, data from developed countries revealed that only 7–26% of citizens have medicines affordability problem [15]. Studies showed that innovator medicines sold in Malaysia were 27–90% more expensive than the generics 0168-8510/$ – see front matter © 2009 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.healthpol.2009.08.011
Transcript of Evaluating community pharmacists’ perceptions of future generic substitution policy...

Health Policy 94 (2010) 68–75
Contents lists available at ScienceDirect
Health Policy
journa l homepage: www.e lsev ier .com/ locate /hea l thpol
Evaluating community pharmacists’ perceptions of future genericsubstitution policy implementation: A national survey from Malaysia
Chee Ping Chonga,∗, Mohamed Azmi Hassalib, Mohd Baidi Baharia, Asrul Akmal Shafieb
a Discipline of Clinical Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia, 11800 Minden, Penang, Malaysiab Discipline of Social and Administrative Pharmacy, School of Pharmaceutical Sciences, Universiti Sains Malaysia, 11800 Minden, Penang, Malaysia
a r t i c l e i n f o
Keywords:Community pharmacistPerceptionGeneric substitutionGeneric medicinePolicy
a b s t r a c t
Objectives: This study aims to provide baseline data to support the implementation ofgeneric substitution policy in Malaysia by evaluating the community pharmacists’ per-ceptions and opinions on generic substitution and current substitution practices.Methods: A cross-sectional descriptive study involving the entire population of Malaysiancommunity pharmacies (n = 1419) was undertaken using a self-completed anonymous mailquestionnaire.Results: A total of 219 responses were received for a response rate of 15.4%. Majority ofthe respondents (93.6%) agreed that pharmacists should have generic substitution rights.Almost all pharmacists (96.8%) viewed Poison Class C (pharmacist only medicine) as mostsuitable class of controlled medicines for substitution. About half (51.6%) of the pharmacistspreferred a policy which allowed substitution on any prescription. The pharmacists preferto consult the physician when substituting narrow therapeutic index medicines (88.1%)
and prescription only medicines (51.3%). Less than 25.0% of the pharmacists routinely keepthe medication records and follow-up the patients who received substitution. Monitoringthe efficacy (79.2%) and patient’s satisfaction with the generic medicines (74.9%) were themain reasons for following-up the patient if substitution occurs.Conclusions: Malaysian community pharmacists are generally in favour of generic substi-menta
tution policy imple1. Introduction
In the recent years, escalating pharmaceutical cost hasbecome a global challenge. Generic medicines provide theopportunity for savings in medicines expenditure due totheir cheaper price [1,2]. Consequently, generic substitu-tion policy that aims to promote the utilization of genericmedicines has been introduced in many developed [3–7]
and developing countries [8–10]. This policy allows phar-macists to substitute generic for brand name medicine,unless the prescriber forbids or the patient declines thereplacement.∗ Corresponding author. Tel.: +60 12 5342685; fax: +60 4 6570017.E-mail address: [email protected] (C.P. Chong).
0168-8510/$ – see front matter © 2009 Elsevier Ireland Ltd. All rights reserved.doi:10.1016/j.healthpol.2009.08.011
tion.© 2009 Elsevier Ireland Ltd. All rights reserved.
Malaysia, like most developing countries, does nothave a national public health insurance scheme to coverthe citizens’ health expenditures [11]. Approximately74% of funding in private Malaysian health sector isfrom consumers’ out-of-pocket money [12]. Therefore, themedicine’s price has become the major determination ofaccess to affordable medicines. The Malaysian governmentdoes not control the prices of both innovator and genericmedicines and believes that market force is capable to gen-erate reasonable price [13]. However, more than half ofMalaysian consumers perceived medicines as expensive
and urged that prices should be controlled [14]. Conversely,data from developed countries revealed that only 7–26% ofcitizens have medicines affordability problem [15].Studies showed that innovator medicines sold inMalaysia were 27–90% more expensive than the generics

alth Poli
aN(gpfst2atNcp
dcspTomgwtPrPaeMpta
sptbts
2
snepqatmioae(aot
C.P. Chong et al. / He
nd hardly affordable for lowest income families [16–18].amely, a 1-month treatment of innovator omeprazole
20 mg daily) in private sector cost 2 weeks of lowestovernment wage while treatment using the lowest-rice generics cost 3–4 days’ wage [16]. Indeed, studiesrom others low- and middle-income countries showedimilar trend where patients were more able to affordo generic medicines than innovator brand [19,20]. In006, the Malaysian government reacted to this medicineffordability problem by documenting generic substitu-ion policy as one of the future plan under the Malaysianational Medicines Policy [21]. Nevertheless, there are nolearly defined frameworks and strategies for this futureolicy.
Currently, there was no separation of prescribing andispensing function between Malaysian private doctorlinics and community pharmacies. Despite this policy, atudy found that around 42% of the Malaysian consumersurchased medicine from community pharmacies [14].he government requires a pharmacy to be operated andwned at least 51% ownership by pharmacist(s) [22]. Theain opportunity for pharmacists to promote the use of
eneric medicines is when encountered with patients whoalked into a community pharmacy without a prescrip-
ion and requested for Class C Poisons. Under the Malaysianoison Act 1952, Class C Poison can be dispensed by aegistered pharmacist without a prescription order [23].oison Class C consists of medicines like antihistaminesnd NSAIDs which mainly cover mild to moderate dis-ases. However, under the National Medicine Policy, thealaysian government has attempted to implement dis-
ensing separation policy in the future [21]. Subsequently,he pharmacists as the sole medicines dispensers will havegreater role in enhancing generic medicines uptake.
An evaluation of the pharmacists’ views of generic sub-titution is crucial for the planning of generic substitutionolicy. Therefore, this study aims to provide baseline datao support the legislation of generic substitution policyy evaluating the community pharmacists’ perceptions ofhe suggested policy, opinions on substitution, and currentubstitution practices.
. Methods
This was a cross-sectional national survey using aelf-completed anonymous questionnaire. The question-aire was tested for face and content validity by twoxperts and 10 registered pharmacists and adjusted afterilot testing with 15 community pharmacists. The finaluestionnaire consisted of six sections. The first sectionssessed the demographic and practice characteristics ofhe pharmacists. The second section evaluated the phar-
acists’ perceptions of generic medicines (not presentedn this paper). The third section evaluated the pharmacists’pinions on types of prescriptions and medicines whichre suitable for substitution. The pharmacists’ knowl-
dge of generic medicines was assessed in section fournot presented in this paper). The fifth section evalu-ted pharmacists’ perceptions of future implementationf generic substitution policy. The final section evaluatedhe pharmacists’ current substitution practices, includingcy 94 (2010) 68–75 69
communication with the physician when performing sub-stitution, information provided to the physician and patientwhen recommending substitution, and documentation andfollow-up services for the patient who received substitu-tion.
The study population was the practicing communitypharmacists in Malaysia and the sampling unit was thecommunity pharmacy. The sampling frame was a listof 1419 community pharmacies in Malaysia which wasobtained from the Division of Pharmacy Services in eachstate government. Approximately 80% of the pharmacistsheld positive attitudes towards generic substitution, cal-culation using Raosoft® software showed that a total of210 pharmacies would provide a representative samplesize with 5% margin of error and 95% confidence level. Theentire population of 1419 pharmacies was recruited as theresponse rate was expected to be low. The respondentsreceived the survey questionnaires through mailing. Twoinvitation and two follow-ups reminder letters were usedto increase the response rate. The participation of phar-macists approached was strictly voluntary. The informedconsents of the participants were obtained and no personaldata of the participants were reported. Data were collectedfrom 1st May 2007 to 31st October 2007.
Data analysis was performed using SPSS® for Windows,version 11.5. Frequency and cross-tabulation were used fordescriptive analysis. Chi-square statistic was used to inves-tigate differences in the pharmacists’ responses betweendifferent groups of pharmacists (gender, age, employmentposition, type of pharmacy, number of working pharma-cists, region and location of pharmacy). A significance levelof less than 0.05 was used. Odds ratios were calculatedfor variables which demonstrated significant differencesbased on chi-square analysis.
3. Results
3.1. Demographics and practice characteristics
Of the 1419 questionnaires sent, 219 responses werereceived for a response rate of 15.4%, while 0.5% (n = 7) ofthe pharmacies were unreachable (either had moved or didnot exist any more). Majority of respondents were fromNorthern Region of West Malaysia (41.5%) (Table 1). Therespondents were mostly female (58.4%) and aged between31 and 40 years (48.0%). Most of the respondents (59.4%)practiced in a single outlet independent pharmacy settingand majorities (73.5%) were in urban area (Table 2).
3.2. Opinion on substitution
The pharmacists were asked to express their generalopinion of substituting generic medicines (Table 3). Majori-ties (87.2%) were in favour to generic substitution for mostcases, but they agreed that there are some situations inwhich substitution is not appropriate. About half (51.6%)
of the pharmacists indicated that generic substitution ismost suitable for any prescription in the Malaysian setting.When assessing the poison class which is suitable for sub-stitution in Malaysian scene, almost all (96.8%) respondentschose Class C Poison (pharmacist only medicine).
70 C.P. Chong et al. / Health Policy 94 (2010) 68–75
Table 1Total numbers of pharmacy outlets, response rate and distribution of respondents according to region in Malaysia.
Region Number of enrolled pharmacy outlets Respondents Response rate (%)
n % n %
(1) East Malaysia 202 14.2 32 14.6 15.8(2) Northern region of West Malaysia 414 29.2 91 41.5 22.0(3) Central region of West Malaysia 466 32.8 33 15.1 7.1
14.29.6
100.0
(4) Southern region of West Malaysia 201(5) East Coast of West Malaysia 136
Total 1419
3.3. Perception of future implementation of genericsubstitution policy
The majority (93.6%) of respondents agreed thatMalaysian community pharmacists should be given theright for substitution (Table 4). Most respondents (73.1%)preferred the standard of practice which required phar-macists to consult the prescribers only when substitutingcertain group of medicines. A great proportion (88.1%) ofthe respondents choose to consult the prescriber whensubstituting narrow therapeutic index (NTI) medicines,followed by Class B Poison (prescription only medicine)(51.3%) and Class A Poison (prescription narcotic) (42.5%).
3.4. Communication with the physician
The pharmacists’ current practices in relation to
communication with the physician when performing sub-stitution were assessed (Table 5). Majority of respondentswere either rarely (43.8%) or never (27.9%) consult thephysician when recommending substitution. When assess-ing the reasons for not consulting the physicians, a highTable 2Demographics and practices characteristics of respondents.
Characteristic n(%)
GenderMale 91(41.6)Female 128(58.4)
Age group (years)25–30 59(26.9)31–40 105(48.0)41–50 37(16.9)>50 18(8.2)
Employment positionSelf or part owner 131(59.8)Employee 87(39.8)Missing data 1(0.4)
Type of pharmacy where practicingSingle outlet independent 130(59.4)Multi-outlet independent 66(30.1)Chain 23(10.5)
Number of working pharmacists1 189(86.3)2 22(10.1)>2 6(2.7)Missing data 2(0.9)
Area where pharmacy locatedUrban 161(73.5)Rural 58(26.5)
40 18.3 19.923 10.5 16.9
219 100.0 15.4
proportion (80.5%) of respondents expressed that sub-stitution of non-prescription items (Poison Class C andnon-poison) do not require consultation with the pre-scriber. A few pharmacists expressed that consultingphysicians is not a trend in Malaysia and the physiciansmight not be interested and comfortable to discuss withpharmacists. One of the respondent felt inconvenienceto contact the prescriber each time substitution is madebecause the doctor may get annoyed if contacted toofrequently or because of alteration to the prescription.Besides, one pharmacist expressed that patient will makethe final decision about which brand to buy and is not nec-essary to consult the physician.
3.5. Information provided when performing substitution
The questionnaire further assessed the information pro-vided by the pharmacists to both the physicians andpatients when performing substitution (Table 5). Approxi-mately two-third of the pharmacists explained the reasonsfor substitution and choice of available generic drugs to thephysicians. In contrast, prices of generic medicines (76.3%)and cost-saving (65.3%) were the major information pro-vided to the patients.
3.6. Documentation and follow-up
In the current setting, pharmacists are not required tokeep the medication records and follow-up the patientswho received substitution. In this study, only 15.5% of therespondents always keep the records of the patient whoswitched to generics (Fig. 1). A high level of respondents(58.9%) claimed that the absence of a regulation is theirreason for not keeping the patient’s record. Other reasonsfor not keeping records were: “do not think it is neces-sary to keep the record” (36.8%), “patient refuses to keepthe record” (24.3%) and “too busy” (23.8%). Some respon-dents specified that they do not documented substitutionfor short-term cares, walk-in and non-regular consumers.
Majority of the respondents (40.2%) sometimes pro-vided follow-up services for patients who have switchedtheir therapy to generic medicines (Fig. 1). When assess-ing the reasons for following-up the patients, most of the
respondents intended to monitor the efficacy (79.2%) andpatient’s satisfaction with the generic (74.9%). Others mainreasons were: “to provide pharmaceutical care” (54.1%), “tomonitor safety” (48.6%), and “to monitor patient’s compli-ance with the generic medicines” (45.9%).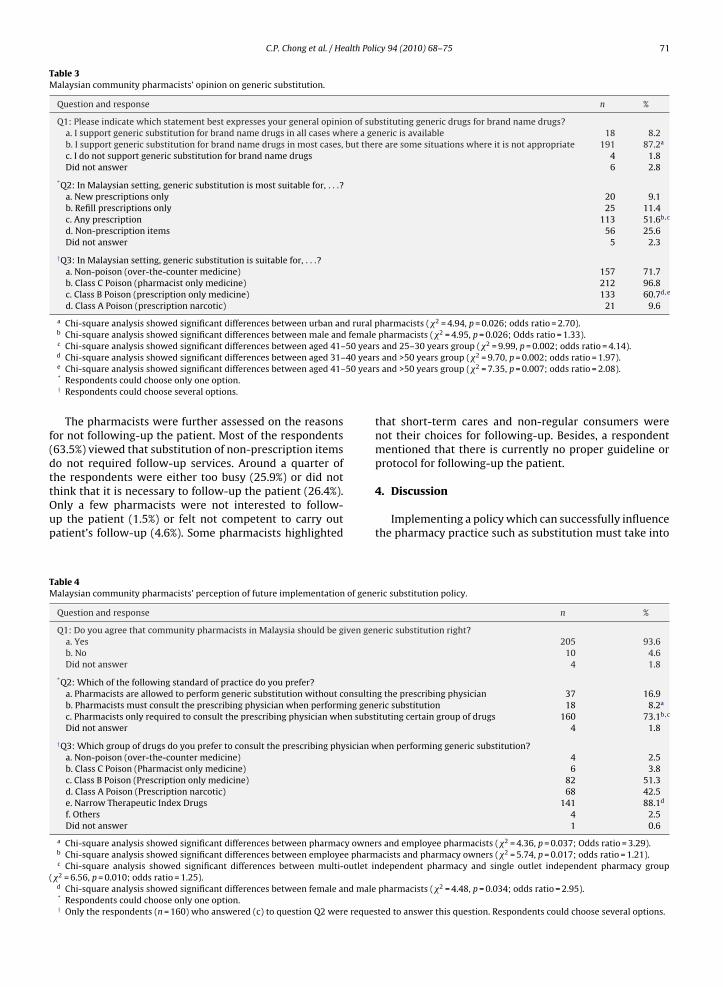
C.P. Chong et al. / Health Policy 94 (2010) 68–75 71
Table 3Malaysian community pharmacists’ opinion on generic substitution.
Question and response n %
Q1: Please indicate which statement best expresses your general opinion of substituting generic drugs for brand name drugs?a. I support generic substitution for brand name drugs in all cases where a generic is available 18 8.2b. I support generic substitution for brand name drugs in most cases, but there are some situations where it is not appropriate 191 87.2a
c. I do not support generic substitution for brand name drugs 4 1.8Did not answer 6 2.8
*Q2: In Malaysian setting, generic substitution is most suitable for, . . .?a. New prescriptions only 20 9.1b. Refill prescriptions only 25 11.4c. Any prescription 113 51.6b,c
d. Non-prescription items 56 25.6Did not answer 5 2.3
†Q3: In Malaysian setting, generic substitution is suitable for, . . .?a. Non-poison (over-the-counter medicine) 157 71.7b. Class C Poison (pharmacist only medicine) 212 96.8c. Class B Poison (prescription only medicine) 133 60.7d,e
d. Class A Poison (prescription narcotic) 21 9.6
a Chi-square analysis showed significant differences between urban and rural pharmacists (�2 = 4.94, p = 0.026; odds ratio = 2.70).b Chi-square analysis showed significant differences between male and female pharmacists (�2 = 4.95, p = 0.026; Odds ratio = 1.33).c Chi-square analysis showed significant differences between aged 41–50 years and 25–30 years group (�2 = 9.99, p = 0.002; odds ratio = 4.14).
40 year50 year
f(dttOup
TM
(
d Chi-square analysis showed significant differences between aged 31–e Chi-square analysis showed significant differences between aged 41–* Respondents could choose only one option.† Respondents could choose several options.
The pharmacists were further assessed on the reasonsor not following-up the patient. Most of the respondents63.5%) viewed that substitution of non-prescription itemso not required follow-up services. Around a quarter ofhe respondents were either too busy (25.9%) or did not
hink that it is necessary to follow-up the patient (26.4%).nly a few pharmacists were not interested to follow-p the patient (1.5%) or felt not competent to carry outatient’s follow-up (4.6%). Some pharmacists highlightedable 4alaysian community pharmacists’ perception of future implementation of gene
Question and response
Q1: Do you agree that community pharmacists in Malaysia should be given gena. Yesb. NoDid not answer
*Q2: Which of the following standard of practice do you prefer?a. Pharmacists are allowed to perform generic substitution without consultinb. Pharmacists must consult the prescribing physician when performing genec. Pharmacists only required to consult the prescribing physician when substDid not answer
†Q3: Which group of drugs do you prefer to consult the prescribing physician wa. Non-poison (over-the-counter medicine)b. Class C Poison (Pharmacist only medicine)c. Class B Poison (Prescription only medicine)d. Class A Poison (Prescription narcotic)e. Narrow Therapeutic Index Drugsf. OthersDid not answer
a Chi-square analysis showed significant differences between pharmacy ownerb Chi-square analysis showed significant differences between employee pharmc Chi-square analysis showed significant differences between multi-outlet in
�2 = 6.56, p = 0.010; odds ratio = 1.25).d Chi-square analysis showed significant differences between female and male* Respondents could choose only one option.† Only the respondents (n = 160) who answered (c) to question Q2 were reques
s and >50 years group (�2 = 9.70, p = 0.002; odds ratio = 1.97).s and >50 years group (�2 = 7.35, p = 0.007; odds ratio = 2.08).
that short-term cares and non-regular consumers werenot their choices for following-up. Besides, a respondentmentioned that there is currently no proper guideline orprotocol for following-up the patient.
4. Discussion
Implementing a policy which can successfully influencethe pharmacy practice such as substitution must take into
ric substitution policy.
n %
eric substitution right?205 93.6
10 4.64 1.8
g the prescribing physician 37 16.9ric substitution 18 8.2a
ituting certain group of drugs 160 73.1b,c
4 1.8
hen performing generic substitution?4 2.56 3.8
82 51.368 42.5
141 88.1d
4 2.51 0.6
s and employee pharmacists (�2 = 4.36, p = 0.037; Odds ratio = 3.29).acists and pharmacy owners (�2 = 5.74, p = 0.017; odds ratio = 1.21).dependent pharmacy and single outlet independent pharmacy group
pharmacists (�2 = 4.48, p = 0.034; odds ratio = 2.95).
ted to answer this question. Respondents could choose several options.

72 C.P. Chong et al. / Health Policy 94 (2010) 68–75
Table 5Malaysian community pharmacists’ current generic substitution practices.
Question and response n %
Q1: In your current practice, how often do you consult the physician when performing generic substitution?a. Never 61 27.9b. Rarely 96 43.8c. Sometimes 43 19.6a,b
d. Frequently 6 2.7e. Always 9 4.1Did not answer 4 1.9
*Q2: Please tell us your reason(s) for not consulting the physician when performing generic substitution?a. The drugs involved are non-prescription items (Poison group C and Non-poison) which do not require
consultation with the prescribing physician).169 80.5c
b. Do not have the contact numbers of the physician 77 36.7d,e
c. Too busy 13 6.2d. No confidence to communicate with the physician 2 1.0e. Not interested to consult the physician. 16 7.6f. Do not think it is necessary to consult the physician 85 40.5f
g. Others 29 13.8
†Q3: What types of information do you provide to the physician when performing generic substitution?a. Reasons for generic substitution 109 69.0b. Choices of generic drugs 107 67.7c. Prices of generic drugs 61 38.6d. How much is the cost-saving 54 34.2e. Quality of the generic drugs 65 41.1f. Patient’s satisfaction with the generic drugs 65 41.1g. Your own experiences with the generic drugs 64 40.5h. Others¶ 10 6.3
‡Q4: What types of information do you provide to the patient when performing generic substitution?a. Reasons for generic substitution 125 57.1b. Choices of generic drugs 117 53.4g
c. Prices of generic drugs 167 76.3d. How much is the cost-saving 143 65.3h,i , j
e. Quality of the generic drugs 138 63.0f. Physician’s satisfaction with the generic drugs 53 24.2g. Your own experiences with the generic drugs 115 52.5h. Others§ 5 2.3
a Chi-square analysis showed significant differences between male and female pharmacists (�2 = 5.51, p = 0.019; odds ratio = 2.24).b Chi-square analysis showed significant differences between urban and rural pharmacists (�2 = 6.11, p = 0.013; odds ratio = 3.29).c Chi-square analysis showed significant differences between urban and rural pharmacists (�2 = 5.72, p = 0.017; odds ratio = 2.48).d Chi-square analysis showed significant differences between aged 25–30 years and 41–50 years group (�2 = 8.40, p = 0.004; odds ratio = 4.12).e Chi-square analysis showed significant differences between multi-outlet independent pharmacy and chain pharmacy group (�2 = 7.48, p = 0.006; odds
ratio = 7.03).f Chi-square analysis showed significant differences between multi-outlet independent pharmacy and single outlet independent pharmacy group
(�2 = 7.21, p = 0.007; odds ratio = 2.33).g Chi-square analysis showed significant differences between rural and urban pharmacists (�2 = 4.39, p = 0.036; odds ratio = 1.98).h Chi-square analysis showed significant differences between single outlet independent pharmacy and chain pharmacy group (�2 = 13.25, p < 0.001; odds
ratio = 5.45).i Chi-square analysis showed significant differences between multi-outlet independent pharmacy and chain pharmacy group (�2 = 10.80, p = 0.001; odds
ratio = 5.30).j Chi-square analysis showed significant differences between East Malaysia and East Coast of West Malaysia group (�2 = 8.36, p = 0.004; odds ratio = 5.78).* A total of 210 respondents were requested to answer this question. Those who always consult the physician (n = 9) were asked to ignore this question.
Respondents could choose several options.† A total of 158 respondents were requested to answer this question. Those who never consult the physician (n = 61) were asked to ignore this question.
on. Respn, bioeqn.
Respondents could choose several options.‡ All of the respondents (n = 219) were requested to answer this questi¶ Cost-effectiveness of generic drugs, generic products’ country of origi§ Cost-effectiveness of generic drugs, generic products’ country of origi
account the views from all stakeholders. The present studywas an attempt to provide baseline data to support thegeneric substitution policy implementation based on whatpharmacists perceived and practiced. This study revealed
that the obstacle to future substitution policy implemen-tation was relatively low from the pharmacists as theiropinions and perceptions on substitution were positive onthe whole irrespective of their demographics and prac-tice characteristics. Majority of the pharmacists supportedondents could choose several options.uivalency and patient’s wealthy condition.
generic substitution and agreed that pharmacists should begiven substitution right. In addition, about half of the phar-macists indicated that generic substitution is suitable forany prescription. Although this percentage was lower than
a study result from United States (69.2%), it does shows thatthe pharmacists were unfavourable toward restriction onsubstitution based on type of prescriptions [24].Generic substitution is practiced on the basis of reducingmedicines expenditures while maintaining optimal patient

C.P. Chong et al. / Health Policy 94 (2010) 68–75 73
provided
cwtNmftftgaasCcisPasfiMactCNam(smCmoao
ptpoto
Fig. 1. Percentage of Malaysian pharmacists who documented and
are. There are countries with generic substitution lawhich prohibits certain groups of medicines from substitu-
ion, for instance, non-bioequivalent generic products andTI medicines in which small variation in bioavailabilityay be clinically significant [25,26]. In these countries, a
ormulary of interchangeable medicines was establishedo guide the substitution practice [7,25]. However, suchormulation was yet to be established in Malaysia [21]. Inhis study, most of the Malaysian pharmacists viewed thateneric substitution is suitable for most cases but therere some situations where it is not appropriate. Almostll respondents viewed Class C Poison as suitable for sub-titution. The pharmacists may prefer to substitute Class
Poison because of its wide therapeutic window. Theharacteristic of Class C Poison as pharmacists’ special-zed medicines may also contribute to its popularity inubstitution. Conversely, fewer pharmacists chose Class Boisons as preferable drugs for substitution. Class B Poisonsre prescription only medicines which are used for moreevere or critical illness. The pharmacists may lack of con-dence in substituting these medicines. Besides, under thealaysian Poison Law 1952, all NTI medicines like Digoxin
nd Warfarin are categorized under Class B Poison. Theomponent of NTI medicines in this class may also hinderhe pharmacists from substitution. Interestingly, althoughlass A Poison (prescription narcotics) does not consist ofTI medicines, only minority of the respondents viewed its appropriate for substitution. Currently, majority of theedicines in the Malaysian Poison List are Class B Poison
65.9%), followed by Class C Poison (28.9%), Class A Poi-on (3.3%) and others (1.9%) [23]. Based on this study, theost preferable controlled medicine for substitution was
lass C Poison, which is the second largest component ofedicines in the Malaysian Poison Lists. Nevertheless, in
rder to give a proper guidance on generic substitution,formulary of interchangeable medicines must be devel-ped.
Currently, there is no regulation that required Malaysianhysician to indicate generic substitution permissibility on
he prescription. There is also no legislation that requiredharmacist to obtain consent from prescriber when rec-mmending substitution. Within this context, the choiceo substitute generics and consult the prescriber dependsn the professional judgment of the pharmacist. A previousfollow-up services for patients who received generic substitution.
study found that 79.7% of Malaysian pharmacists’ substitu-tion recommendations did not involve consultation withprescriber, including Class B Poison (79.2%) and Class CPoison (80.6%) [18]. The present study further confirmedthat Malaysian pharmacists seldom consult the physicianwhen performing substitution. Most pharmacists preferreda model of practice in which consultation with the pre-scriber is needed only when substituting critical medicinesand medicines used for severe diseases (Class A and ClassB Poison). The concern about potential adverse conse-quences from substituting these medicines may influencethe pharmacists to communicate with the prescriber. Nev-ertheless, the Malaysian Government should consider thepracticality of requiring pharmacists to consult the physi-cian for each substitution involved Class A and B Poison.The heavy workload may restrict the pharmacists fromcontacting the prescriber. Indeed, a study showed thatgeneric interchange legislation which required pharma-cists to obtain consent from prescriber for each substitutioncan resulted in low substitution rate [27]. Another optionfor consideration is to adopt the generic substitution pol-icy in most countries, whereby pharmacists are allowed torecommend generic substitution, provided the prescriberdoes not designated on the prescription that substitutionis not permissible [6,28]. Alternatively, the governmentcan mandate that all prescriptions should be prescribedwith generic (International Non-proprietary) name onlyand the pharmacists can decide between supplying inno-vator brand or generic medicines. This option is basedon the basis of the Malaysian National Medicines Policywhich indicated that prescriptions should be written usinggeneric name [21].
The main factor in enhancing generic medicines uti-lization is to maintain the acceptability of generics byprescriber and patients [29]. This is where the pharma-cist can play a vital role as a medicines adviser. Studyshowed that advises from pharmacists can improve thegeneric prescription by the GPs [30]. Several countries inEurope have encouraged local pharmaco-therapeutic dis-
cussions between pharmacists and GPs to stimulate genericmedicines uptake [6]. Besides, adequate information pro-vided by pharmacists was capable to improve patients’confidence about consuming generic medicines [31]. Thepresent study found that the reasons for generic substi-
alth Poli
[
74 C.P. Chong et al. / He
tution and choices of generic products were the maintopics of discussion between Malaysian pharmacists andphysicians. Conversely, the pharmacists tend to explainmore about the prices of generics and amount of cost-savings to the patients. This reflected that the Malaysianphysicians’ acceptance toward generic substitution maybe more depended on the proper reasons for substitutionand availability of generic products. Meanwhile, the cost ofmedicines is the major concern of patients when selectingbetween brand name and generic medicines. These resultsare essential for the development of a guideline on genericsubstitution for Malaysian community pharmacists.
Documentation and follow-up of patients who receivedgeneric substitution are among the pharmacists’ practiceswhich rarely explored by the researchers in Malaysia. Itappears that that documentation and follow-up are notroutinely practiced by the Malaysian pharmacists whenperforming substitution. Majority of the respondents didnot document their substitution recommendations due tothe absence of a regulation which required them to do so.This suggested that the future generic substitution pol-icy may incorporate rules to require the pharmacists tokeep the medical and medication records of the patientswho received substitution therapy. These documentationswill assist pharmacists in following-up the patients. Thesuggested policy must also incorporate a guideline onfollowing-up the patients who received substitution ther-apy. This will guide the pharmacists in following-up thepatients to ensure that the patients are not confused anddoubling their medications.
Since 1999, Malaysia has included the bioequivalencestudies as requirement for the registration of genericmedicines [32]. The Malaysian Drug Control Authority(DCA) has gradually increased the number of generic prod-ucts which required to pass the bioequivalence test [33].Nevertheless, a recent survey found that more than halfof Malaysian community pharmacists were less confidentwith the Malaysian generic medicines approval system, inrelations to bioequivalence, quality and safety [34]. Theabsence of a formulary of interchangeable medicines mayfurther reduce the confidence of pharmacists in performingsubstitution. As noted in the present study, high propor-tion of pharmacists following-up the patients because ofconcerns about efficacy and safety of generic medicines.This finding further reflected that the Malaysian phar-macists are lacking confidence in the quality of genericmedicines. The Malaysian DCA needs to improve the con-fidence of pharmacists in the generic products approvalsystem through educational interventions. The establish-ment of a formulary of interchangeable drugs is anothergood strategy to improve this situation.
4.1. Study limitations
The overall response rate was sufficient to meet theminimum required representative sample size. Neverthe-
less, the skewed response rates from different regions ofMalaysia lead to over- and under-representative of phar-macists from Northern region and Central region of WestMalaysia, respectively. Additionally, the representative-ness of the respondent features could not be evaluated due[
[
cy 94 (2010) 68–75
to the absence of a national data on community pharma-cists’ demographic and practice characteristics. All thesefactors have limited the generalisability of the resultsfor Malaysian pharmacists. Therefore, this study is valu-able in providing a suggestive national baseline data onMalaysian community pharmacists’ perceptions and prac-tices of generic substitution.
5. Conclusions
The Malaysian community pharmacists generally sup-ported the implementation of generic substitution policy.However, the surveyed pharmacists were more preferredto substitute generics for brand name medicines which areused in mild to moderate diseases. A formulary of inter-changeable medicines must be established to guide andimprove the pharmacists’ confident in substitution. Addi-tionally, regulation and guideline are needed to encouragethe pharmacists for keeping the records and following-upthe patients who received generic substitution therapy.
Conflict of interest
None
Acknowledgement
The authors wish to thank all the pharmacists who vol-untarily participated in this study.
References
[1] King DR, Kanavos P. Encouraging the use of generic medicines:implications for transition economies. Croatian Medical Journal2002;43(4):462–9.
[2] Haas JS, Phillips KA, Gerstenberger EP, Seger AC. Potential savingsfrom substituting generic drugs for brand-name drugs: medicalexpenditure panel survey, 1997–2000. Annals of Internal Medicine2005;142(11):891–7.
[3] Kjoenniksen I, Lindbaek M. Patients’ attitudes towards and experi-ences of generic drug substitution in Norway. Pharmacy World andScience 2006;28(5):284–9.
[4] Heikkila R, Mantyselka P, Hartikainen-Herranen K, Ahonen R.Customers’ and physicians’ opinions of and experiences withgeneric substitution during the first year in Finland. Health Policy2007;82:366–74.
[5] Simoens S. Developing the Japanese generic medicines market:what can we learn from Europe? Journal of Generic Medicines2009;6(2):129–35.
[6] Simoens S, De Coster S. Sustaining generic medicines marketsin Europe. Belgia: Research Centre for Pharmaceutical Care andPharmaco-economics. Katholieke Universiteit Leuven; 2006.
[7] Suh DC. Trends of generic substitution in community pharmacies.Pharmacy World and Science 1999;21(6):260–5.
[8] Homedes N, Ugalde A. Multisource drug policies in Latin America:survey of 10 countries. Bulletin of the World Health Organization2005;83(1):64–70.
[9] Gossell-Williams M. Generic substitution: a 2005 survey of theacceptance and perceptions of physicians in Jamaica. West IndianMedical Journal 2007;56(5):458–63.
10] National Association of Pharmaceutical Manufacturers (NAPM). Thegeneric pharmaceutical market in South Africa: at the crossroads?Journal of Generic Medicines 2009;6(2):137–44.
11] World Health Organization. The World Health Report 2000. Healthsystem: improving performance. Geneva: World Health Organiza-tion; 2000.
12] World Health Organization. Country Health Information Pro-file: Malaysia, http://www.wpro.who.int/NR/rdonlyres/DB90A4E5-0963-4E00-B56C-E09C2AE01ECC/0/19Malaysia07.pdf; 2007.

alth Poli
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
C.P. Chong et al. / He
13] Pharmaceutical Service Division. My Medprice: Newsletter of theMedicine Price Monitoring System, no. 1/2007. Putrajaya: Ministryof Health Malaysia; 2007.
14] Babar ZUD, Ibrahim MIM. Affordability of medicines in Malaysia—consumer perceptions. Essential Drugs Monitor 2003;33:18–9.
15] Blendon RJ, Schoen C, DesRoches CM, Osborn R, Scoles KL, ZapertK. Inequities in health care: a five-country survey. Health Affairs2002;21(3):182–91.
16] Babar ZUD, Ibrahim MIM, Singh H, Bukahri NI, Creese A. Evaluat-ing drug prices, availability, affordability, and price components:implications for access to drugs in Malaysia. PLoS Medicine2007;4(3):0466–475.
17] Shafie AA, Hassali MA. Price comparison between innovator andgeneric medicines sold by community pharmacies in the stateof Penang, Malaysia. Journal of Generic Medicines 2008;6(1):35–42.
18] Chong CP, Bahari MB, Hassali MA. A pilot study on genericmedicine substitution practices among community pharmacists inthe State of Penang, Malaysia. Pharmacoepidemiology and DrugSafety 2008;17(1):82–9.
19] Cameron A, Ewen M, Ross-Degnan D, Ball D, Laing R. Medicineprices, availability, and affordability in 36 developing and middle-income countries: a secondary analysis. The Lancet 2009;373(9659):240–9.
20] Mendis S, Fukino K, Cameron A, Laing R, Filipe Jr A, Khatib O, et al.The availability and affordability of selected essential medicines forchronic diseases in six low- and middle-income countries. Bulletinof the World Health Organization 2007;85(4):279–88.
21] Ministry of Health Malaysia. National Medicines Policy of Malaysia.Putrajaya: Ministry of Health Malaysia; 2007.
22] Malaysian Community Pharmacists Association (MCPA). Pharmacyzoning and ownership, http://www.mcp.org.my/pharmzoning.html;2008.
23] Legal Research Board of Malaysia. Malaysian laws on poison and salesof drugs. Kuala Lumpur: International Law Books Services; 2006. pp.33–80.
[
cy 94 (2010) 68–75 75
24] Banahan B, Kolassa E. Generic substitution and narrow therapeu-tic index drugs: a national survey of retail and hospital pharmacies.Mississippi: The University of Mississippi; 1994.
25] Department of Health and Ageing. Schedule of pharmaceuticalbenefits, effective 1 July 2008–31 July 2008. Canberra: AustralianCommonwealth Government; 2008.
26] Murphy JE. Generic substitution and optimal patient care. Archivesof Internal Medicines 1999;159(5):429–33.
27] Karim SA, Pillai G, Ziqubu-Page TT, Cassimjee MH, Morar MS. Poten-tial savings from generic prescribing and generic substitution inSouth Africa. Health Policy and Planning 1996;11(2):198–205.
28] McManus P, Birkett DJ, Dudley J, Stevens A. Impact of the MinimumPricing Policy and introduction of brand (generic) substitution intothe Pharmaceutical Benefits Scheme in Australia. Pharmacoepidemi-ology and Drug Safety 2001;10(4):295–300.
29] Andersson K, Sonesson C, Petzold M, Carlsten A, Lonnroth K. Whatare the obstacles to generic substitution? An assessment of thebehaviour of prescribers, patients and pharmacies during the firstyear of generic substitution in Sweden. Pharmacoepidemiology andDrug Safety 2005;14(5):341–8.
30] Leach RH, Wakeman A. An evaluation of the effectiveness of commu-nity pharmacists working with GPs to increase the cost-effectivenessof prescribing. The Pharmaceutical Journal 1999;263(7057):206–9.
31] Hassali MA, Kong DCM, Stewart K. Generic medicines: perceptionsof consumers in Melbourne, Australia. International Journal of Phar-macy Practice 2005;13(4):257–64.
32] Ministry of Health Malaysia. Malaysian guidelines for the conduct ofbioavailability and bioequivalence studies. Kuala Lumpur: Ministryof Health Malaysia; 2000.
33] Drug Control Authority of Malaysia. List of test products, compara-
tor products and effective submission date for bioequivalence studyreport for year 2008-2009. Putrajaya: Ministry of Health Malaysia;2008.34] Babar ZUD, Awaisu A. Evaluating community pharmacists’ percep-tions and practices on generic medicines: a pilot study from Penin-sular Malaysia. Journal of Generic Medicines 2008;5(4):315–30.