
EUROPEAN COMMISSION GRANT AGREEMENT NUMBER ...
317
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019 H2020 General MGA — Multi: v5 EUROPEAN COMMISSION Directorate-General for Communications Networks, Content and Technology Digital Society, Trust and Cybersecurity eHealth, Well-Being and Ageing GRANT AGREEMENT NUMBER 875209 — ADLIFE This Agreement (‘the Agreement’) is between the following parties: on the one part, the European Union (‘the EU’), represented by the European Commission ('the Commission'), represented for the purposes of signature of this Agreement by head of unit, Directorate-General for Communications Networks, Content and Technology, Data, Administration and Finance, Mikaela FARR-DAVID, and on the other part, 1. ‘the coordinator’: ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD- KRONIKGUNE (KRONIKGUNE), established in RONDA DE AZKUE 1 TORRE DEL BILBAO EXHIBITION CENTRE, BARAKALDO 48902, Spain, VAT number: ESG95646014, represented for the purposes of signing the Agreement by Director, Esteban DE MANUEL KEENOY and the following other beneficiaries, if they sign their ‘Accession Form’ (see Annex 3 and Article 56): 2. UNIVERSITY OF STRATHCLYDE (USTRATH), established in Richmond Street 16, GLASGOW G1 1XQ, United Kingdom, VAT number: GB261339762, 3. THE UNIVERSITY OF WARWICK (WARWICK), established in Kirby Corner Road - University House, COVENTRY CV4 8UW, United Kingdom, VAT number: GB545270058, 4. ODENSE UNIVERSITETSHOSPITAL (OUH), established in Sdr. Boulevard 29, ODENSE 5000, Denmark, VAT number: DK35181628, 5. SZPITAL SPECJALISTYCZNY IM A FALKIEWICZA WE WROCLAWIU (FALKIEWICZ), established in UL. WARSZAWSKA 2, WROCLAW 52 114, Poland, VAT number: PL8992227939, 6. OPTIMEDIS AG (OM), established in BURCHARDSTRASSE 17, HAMBURG 20095, Germany, VAT number: DE227566961, 7. REGION JAMTLAND HARJEDALEN (RJH), established in KYRKGATAN 12, OSTERSUND 831 27, Sweden, VAT number: SE232100021401, 1 Associated with document Ref. Ares(2019)6450190 - 18/10/2019
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of EUROPEAN COMMISSION GRANT AGREEMENT NUMBER ...

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
EUROPEAN COMMISSIONDirectorate-General for Communications Networks, Content andTechnology
Digital Society, Trust and CybersecurityeHealth, Well-Being and Ageing
GRANT AGREEMENT
NUMBER 875209 — ADLIFE
This Agreement (‘the Agreement’) is between the following parties:
on the one part,
the European Union (‘the EU’), represented by the European Commission ('the Commission'),
represented for the purposes of signature of this Agreement by head of unit, Directorate-General forCommunications Networks, Content and Technology, Data, Administration and Finance, MikaelaFARR-DAVID,
and
on the other part,
1. ‘the coordinator’:
ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD-KRONIKGUNE (KRONIKGUNE), established in RONDA DE AZKUE 1 TORRE DEL BILBAOEXHIBITION CENTRE, BARAKALDO 48902, Spain, VAT number: ESG95646014, represented forthe purposes of signing the Agreement by Director, Esteban DE MANUEL KEENOY
and the following other beneficiaries, if they sign their ‘Accession Form’ (see Annex 3 and Article 56):
2. UNIVERSITY OF STRATHCLYDE (USTRATH), established in Richmond Street 16,GLASGOW G1 1XQ, United Kingdom, VAT number: GB261339762,
3. THE UNIVERSITY OF WARWICK (WARWICK), established in Kirby Corner Road -University House, COVENTRY CV4 8UW, United Kingdom, VAT number: GB545270058,
4. ODENSE UNIVERSITETSHOSPITAL (OUH), established in Sdr. Boulevard 29, ODENSE5000, Denmark, VAT number: DK35181628,
5. SZPITAL SPECJALISTYCZNY IM A FALKIEWICZA WE WROCLAWIU(FALKIEWICZ), established in UL. WARSZAWSKA 2, WROCLAW 52 114, Poland, VAT number:PL8992227939,
6. OPTIMEDIS AG (OM), established in BURCHARDSTRASSE 17, HAMBURG 20095,Germany, VAT number: DE227566961,
7. REGION JAMTLAND HARJEDALEN (RJH), established in KYRKGATAN 12,OSTERSUND 831 27, Sweden, VAT number: SE232100021401,
1
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
8. ASSUTA ASHDOD LTD (AMCA), established in HAREFUA 7, ASHDOD 7747629, Israel, VATnumber: IL514525591,
9. SRDC YAZILIM ARASTIRMA VE GELISTIRME VE DANISMANLIK TICARETANONIM SIRKETI (SRDC), established in SILIKON BINA 1 KAT NO 14 ODTU TEKNOKENTCANKAYA, ANKARA 06800, Turkey, VAT number: TR7810557732,
10. EVERIS SPAIN SL (EVERIS SPAIN SL), established in AVENIDA MANOTERAS 52,MADRID 28050, Spain, VAT number: ESB82387770,
11. THE EUROPEAN INSTITUTE FOR INNOVATION THROUGH HEALTH DATA (I-HD), established in OUDE MECHELSESTRAAT 165, STROMBEEK-BEVER 1853, Belgium, VATnumber: BE0628646310,
Unless otherwise specified, references to ‘beneficiary’ or ‘beneficiaries’ include the coordinator.
The parties referred to above have agreed to enter into the Agreement under the terms and conditionsbelow.
By signing the Agreement or the Accession Form, the beneficiaries accept the grant and agree toimplement it under their own responsibility and in accordance with the Agreement, with all theobligations and conditions it sets out.
The Agreement is composed of:
Terms and Conditions
Annex 1 Description of the action
Annex 2 Estimated budget for the action
2a Additional information on the estimated budget
Annex 3 Accession Forms
Annex 4 Model for the financial statements
Annex 5 Model for the certificate on the financial statements
Annex 6 Model for the certificate on the methodology
2
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
TERMS AND CONDITIONS
TABLE OF CONTENTS
CHAPTER 1 GENERAL..............................................................................................................................................11
ARTICLE 1 — SUBJECT OF THE AGREEMENT.......................................................................................11
CHAPTER 2 ACTION................................................................................................................................................. 11
ARTICLE 2 — ACTION TO BE IMPLEMENTED ......................................................................................11
ARTICLE 3 — DURATION AND STARTING DATE OF THE ACTION....................................................11
ARTICLE 4 — ESTIMATED BUDGET AND BUDGET TRANSFERS.......................................................11
4.1 Estimated budget................................................................................................................................ 11
4.2 Budget transfers..................................................................................................................................11
CHAPTER 3 GRANT...................................................................................................................................................11
ARTICLE 5 — GRANT AMOUNT, FORM OF GRANT, REIMBURSEMENT RATES AND FORMS OFCOSTS............................................................................................................................................11
5.1 Maximum grant amount..................................................................................................................... 11
5.2 Form of grant, reimbursement rates and forms of costs....................................................................11
5.3 Final grant amount — Calculation.....................................................................................................12
5.4 Revised final grant amount — Calculation....................................................................................... 14
ARTICLE 6 — ELIGIBLE AND INELIGIBLE COSTS................................................................................14
6.1 General conditions for costs to be eligible........................................................................................ 14
6.2 Specific conditions for costs to be eligible........................................................................................15
6.3 Conditions for costs of linked third parties to be eligible................................................................. 21
6.4 Conditions for in-kind contributions provided by third parties free of charge to be eligible............. 22
6.5 Ineligible costs....................................................................................................................................22
6.6 Consequences of declaration of ineligible costs................................................................................ 22
CHAPTER 4 RIGHTS AND OBLIGATIONS OF THE PARTIES........................................................................ 22
SECTION 1 RIGHTS AND OBLIGATIONS RELATED TO IMPLEMENTING THE ACTION................ 23
ARTICLE 7 — GENERAL OBLIGATION TO PROPERLY IMPLEMENT THE ACTION.........................23
7.1 General obligation to properly implement the action........................................................................ 23
7.2 Consequences of non-compliance...................................................................................................... 23
ARTICLE 8 — RESOURCES TO IMPLEMENT THE ACTION — THIRD PARTIES INVOLVED IN THEACTION.........................................................................................................................................23
ARTICLE 9 — IMPLEMENTATION OF ACTION TASKS BY BENEFICIARIES NOT RECEIVING EUFUNDING...................................................................................................................................... 23
ARTICLE 10 — PURCHASE OF GOODS, WORKS OR SERVICES..........................................................23
3
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
10.1 Rules for purchasing goods, works or services............................................................................... 23
10.2 Consequences of non-compliance.................................................................................................... 24
ARTICLE 11 — USE OF IN-KIND CONTRIBUTIONS PROVIDED BY THIRD PARTIES AGAINSTPAYMENT..................................................................................................................................... 24
11.1 Rules for the use of in-kind contributions against payment............................................................ 24
11.2 Consequences of non-compliance.................................................................................................... 25
ARTICLE 12 — USE OF IN-KIND CONTRIBUTIONS PROVIDED BY THIRD PARTIES FREE OFCHARGE........................................................................................................................................25
12.1 Rules for the use of in-kind contributions free of charge................................................................25
12.2 Consequences of non-compliance.................................................................................................... 25
ARTICLE 13 — IMPLEMENTATION OF ACTION TASKS BY SUBCONTRACTORS............................25
13.1 Rules for subcontracting action tasks.............................................................................................. 25
13.2 Consequences of non-compliance.................................................................................................... 26
ARTICLE 14 — IMPLEMENTATION OF ACTION TASKS BY LINKED THIRD PARTIES.................... 26
14.1 Rules for calling upon linked third parties to implement part of the action.................................... 26
14.2 Consequences of non-compliance.................................................................................................... 27
ARTICLE 14a — IMPLEMENTATION OF ACTION TASKS BY INTERNATIONAL PARTNERS...........27
ARTICLE 15 — FINANCIAL SUPPORT TO THIRD PARTIES.................................................................. 27
15.1 Rules for providing financial support to third parties......................................................................27
15.2 Financial support in the form of prizes........................................................................................... 27
15.3 Consequences of non-compliance.................................................................................................... 27
ARTICLE 16 — PROVISION OF TRANS-NATIONAL OR VIRTUAL ACCESS TO RESEARCHINFRASTRUCTURE.....................................................................................................................27
16.1 Rules for providing trans-national access to research infrastructure............................................... 28
16.2 Rules for providing virtual access to research infrastructure.......................................................... 28
16.3 Consequences of non-compliance.................................................................................................... 28
SECTION 2 RIGHTS AND OBLIGATIONS RELATED TO THE GRANT ADMINISTRATION.............. 28
ARTICLE 17 — GENERAL OBLIGATION TO INFORM............................................................................28
17.1 General obligation to provide information upon request.................................................................28
17.2 Obligation to keep information up to date and to inform about events and circumstances likely toaffect the Agreement........................................................................................................................28
17.3 Consequences of non-compliance.................................................................................................... 28
ARTICLE 18 — KEEPING RECORDS — SUPPORTING DOCUMENTATION.........................................29
18.1 Obligation to keep records and other supporting documentation.................................................... 29
18.2 Consequences of non-compliance.................................................................................................... 30
ARTICLE 19 — SUBMISSION OF DELIVERABLES................................................................................. 30
4
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
19.1 Obligation to submit deliverables.................................................................................................... 30
19.2 Consequences of non-compliance.................................................................................................... 30
ARTICLE 20 — REPORTING — PAYMENT REQUESTS.......................................................................... 30
20.1 Obligation to submit reports............................................................................................................ 30
20.2 Reporting periods............................................................................................................................. 31
20.3 Periodic reports — Requests for interim payments.........................................................................31
20.4 Final report — Request for payment of the balance....................................................................... 32
20.5 Information on cumulative expenditure incurred.............................................................................33
20.6 Currency for financial statements and conversion into euro........................................................... 33
20.7 Language of reports..........................................................................................................................33
20.8 Consequences of non-compliance.................................................................................................... 33
ARTICLE 21 — PAYMENTS AND PAYMENT ARRANGEMENTS...........................................................33
21.1 Payments to be made....................................................................................................................... 33
21.2 Pre-financing payment — Amount — Amount retained for the Guarantee Fund........................... 33
21.3 Interim payments — Amount — Calculation..................................................................................34
21.4 Payment of the balance — Amount — Calculation — Release of the amount retained for theGuarantee Fund................................................................................................................................ 34
21.5 Notification of amounts due.............................................................................................................35
21.6 Currency for payments..................................................................................................................... 35
21.7 Payments to the coordinator — Distribution to the beneficiaries....................................................36
21.8 Bank account for payments..............................................................................................................36
21.9 Costs of payment transfers...............................................................................................................36
21.10 Date of payment............................................................................................................................. 36
21.11 Consequences of non-compliance.................................................................................................. 36
ARTICLE 22 — CHECKS, REVIEWS, AUDITS AND INVESTIGATIONS — EXTENSION OFFINDINGS..................................................................................................................................... 37
22.1 Checks, reviews and audits by the Commission..............................................................................37
22.2 Investigations by the European Anti-Fraud Office (OLAF)............................................................39
22.3 Checks and audits by the European Court of Auditors (ECA)........................................................39
22.4 Checks, reviews, audits and investigations for international organisations..................................... 39
22.5 Consequences of findings in checks, reviews, audits and investigations — Extension offindings............................................................................................................................................. 39
22.6 Consequences of non-compliance.................................................................................................... 41
ARTICLE 23 — EVALUATION OF THE IMPACT OF THE ACTION....................................................... 41
23.1 Right to evaluate the impact of the action.......................................................................................41
23.2 Consequences of non-compliance.................................................................................................... 42
5
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
SECTION 3 RIGHTS AND OBLIGATIONS RELATED TO BACKGROUND AND RESULTS................. 42
SUBSECTION 1 GENERAL............................................................................................................................ 42
ARTICLE 23a — MANAGEMENT OF INTELLECTUAL PROPERTY......................................................42
23a.1 Obligation to take measures to implement the Commission Recommendation on the managementof intellectual property in knowledge transfer activities................................................................. 42
23a.2 Consequences of non-compliance.................................................................................................. 42
SUBSECTION 2 RIGHTS AND OBLIGATIONS RELATED TO BACKGROUND................................ 42
ARTICLE 24 — AGREEMENT ON BACKGROUND..................................................................................42
24.1 Agreement on background............................................................................................................... 42
24.2 Consequences of non-compliance.................................................................................................... 43
ARTICLE 25 — ACCESS RIGHTS TO BACKGROUND............................................................................ 43
25.1 Exercise of access rights — Waiving of access rights — No sub-licensing....................................43
25.2 Access rights for other beneficiaries, for implementing their own tasks under the action...............43
25.3 Access rights for other beneficiaries, for exploiting their own results............................................ 43
25.4 Access rights for affiliated entities.................................................................................................. 43
25.5 Access rights for third parties.......................................................................................................... 44
25.6 Consequences of non-compliance.................................................................................................... 44
SUBSECTION 3 RIGHTS AND OBLIGATIONS RELATED TO RESULTS............................................44
ARTICLE 26 — OWNERSHIP OF RESULTS...............................................................................................44
26.1 Ownership by the beneficiary that generates the results................................................................. 44
26.2 Joint ownership by several beneficiaries......................................................................................... 44
26.3 Rights of third parties (including personnel)................................................................................... 45
26.4 EU ownership, to protect results......................................................................................................45
26.5 Consequences of non-compliance.................................................................................................... 46
ARTICLE 27 — PROTECTION OF RESULTS — VISIBILITY OF EU FUNDING................................... 46
27.1 Obligation to protect the results.......................................................................................................46
27.2 EU ownership, to protect the results................................................................................................46
27.3 Information on EU funding..............................................................................................................46
27.4 Consequences of non-compliance.................................................................................................... 47
ARTICLE 28 — EXPLOITATION OF RESULTS..........................................................................................47
28.1 Obligation to exploit the results.......................................................................................................47
28.2 Results that could contribute to European or international standards — Information on EUfunding..............................................................................................................................................47
28.3 Consequences of non-compliance.................................................................................................... 47
ARTICLE 29 — DISSEMINATION OF RESULTS — OPEN ACCESS — VISIBILITY OF EUFUNDING...................................................................................................................................... 47
6
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
29.1 Obligation to disseminate results..................................................................................................... 47
29.2 Open access to scientific publications............................................................................................. 48
29.3 Open access to research data........................................................................................................... 48
29.4 Information on EU funding — Obligation and right to use the EU emblem ..................................49
29.5 Disclaimer excluding Commission responsibility............................................................................49
29.6 Consequences of non-compliance.................................................................................................... 49
ARTICLE 30 — TRANSFER AND LICENSING OF RESULTS..................................................................50
30.1 Transfer of ownership...................................................................................................................... 50
30.2 Granting licenses.............................................................................................................................. 50
30.3 Commission right to object to transfers or licensing.......................................................................50
30.4 Consequences of non-compliance.................................................................................................... 50
ARTICLE 31 — ACCESS RIGHTS TO RESULTS....................................................................................... 51
31.1 Exercise of access rights — Waiving of access rights — No sub-licensing....................................51
31.2 Access rights for other beneficiaries, for implementing their own tasks under the action...............51
31.3 Access rights for other beneficiaries, for exploiting their own results............................................ 51
31.4 Access rights of affiliated entities....................................................................................................51
31.5 Access rights for the EU institutions, bodies, offices or agencies and EU Member States..............51
31.6 Access rights for third parties.......................................................................................................... 51
31.7 Consequences of non-compliance.................................................................................................... 51
SECTION 4 OTHER RIGHTS AND OBLIGATIONS.......................................................................................52
ARTICLE 32 — RECRUITMENT AND WORKING CONDITIONS FOR RESEARCHERS..................... 52
32.1 Obligation to take measures to implement the European Charter for Researchers and Code ofConduct for the Recruitment of Researchers...................................................................................52
32.2 Consequences of non-compliance.................................................................................................... 52
ARTICLE 33 — GENDER EQUALITY.........................................................................................................52
33.1 Obligation to aim for gender equality..............................................................................................52
33.2 Consequences of non-compliance.................................................................................................... 52
ARTICLE 34 — ETHICS AND RESEARCH INTEGRITY.......................................................................... 52
34.1 Obligation to comply with ethical and research integrity principles............................................... 52
34.2 Activities raising ethical issues........................................................................................................ 53
34.3 Activities involving human embryos or human embryonic stem cells............................................54
34.4 Consequences of non-compliance.................................................................................................... 54
ARTICLE 35 — CONFLICT OF INTERESTS.............................................................................................. 54
35.1 Obligation to avoid a conflict of interests....................................................................................... 54
35.2 Consequences of non-compliance.................................................................................................... 54
7
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
ARTICLE 36 — CONFIDENTIALITY...........................................................................................................55
36.1 General obligation to maintain confidentiality................................................................................ 55
36.2 Consequences of non-compliance.................................................................................................... 56
ARTICLE 37 — SECURITY-RELATED OBLIGATIONS............................................................................. 56
37.1 Results with a security recommendation......................................................................................... 56
37.2 Classified information...................................................................................................................... 56
37.3 Activities involving dual-use goods or dangerous materials and substances...................................56
37.4 Consequences of non-compliance.................................................................................................... 56
ARTICLE 38 — PROMOTING THE ACTION — VISIBILITY OF EU FUNDING....................................56
38.1 Communication activities by beneficiaries...................................................................................... 56
38.2 Communication activities by the Commission................................................................................ 57
38.3 Consequences of non-compliance.................................................................................................... 58
ARTICLE 39 — PROCESSING OF PERSONAL DATA...............................................................................58
39.1 Processing of personal data by the Commission............................................................................. 58
39.2 Processing of personal data by the beneficiaries............................................................................. 59
39.3 Consequences of non-compliance.................................................................................................... 59
ARTICLE 40 — ASSIGNMENTS OF CLAIMS FOR PAYMENT AGAINST THE COMMISSION...........59
CHAPTER 5 DIVISION OF BENEFICIARIES’ ROLES AND RESPONSIBILITIES — RELATIONSHIPWITH COMPLEMENTARY BENEFICIARIES — RELATIONSHIP WITH PARTNERS OF AJOINT ACTION........................................................................................................................................ 59
ARTICLE 41 — DIVISION OF BENEFICIARIES’ ROLES AND RESPONSIBILITIES —RELATIONSHIP WITH COMPLEMENTARY BENEFICIARIES — RELATIONSHIP WITHPARTNERS OF A JOINT ACTION.............................................................................................59
41.1 Roles and responsibility towards the Commission.......................................................................... 59
41.2 Internal division of roles and responsibilities..................................................................................60
41.3 Internal arrangements between beneficiaries — Consortium agreement.........................................61
41.4 Relationship with complementary beneficiaries — Collaboration agreement.................................61
41.5 Relationship with partners of a joint action — Coordination agreement........................................ 61
CHAPTER 6 REJECTION OF COSTS — REDUCTION OF THE GRANT — RECOVERY — SANCTIONS— DAMAGES — SUSPENSION — TERMINATION — FORCE MAJEURE................................ 61
SECTION 1 REJECTION OF COSTS — REDUCTION OF THE GRANT — RECOVERY —SANCTIONS.............................................................................................................................................. 61
ARTICLE 42 — REJECTION OF INELIGIBLE COSTS.............................................................................. 61
42.1 Conditions......................................................................................................................................... 61
42.2 Ineligible costs to be rejected — Calculation — Procedure............................................................62
42.3 Effects............................................................................................................................................... 62
ARTICLE 43 — REDUCTION OF THE GRANT......................................................................................... 62
8
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
43.1 Conditions......................................................................................................................................... 62
43.2 Amount to be reduced — Calculation — Procedure.......................................................................63
43.3 Effects............................................................................................................................................... 63
ARTICLE 44 — RECOVERY OF UNDUE AMOUNTS............................................................................... 63
44.1 Amount to be recovered — Calculation — Procedure....................................................................63
ARTICLE 45 — ADMINISTRATIVE SANCTIONS..................................................................................... 67
SECTION 2 LIABILITY FOR DAMAGES.........................................................................................................67
ARTICLE 46 — LIABILITY FOR DAMAGES.............................................................................................67
46.1 Liability of the Commission............................................................................................................ 67
46.2 Liability of the beneficiaries............................................................................................................ 68
SECTION 3 SUSPENSION AND TERMINATION............................................................................................68
ARTICLE 47 — SUSPENSION OF PAYMENT DEADLINE....................................................................... 68
47.1 Conditions......................................................................................................................................... 68
47.2 Procedure.......................................................................................................................................... 68
ARTICLE 48 — SUSPENSION OF PAYMENTS.......................................................................................... 68
48.1 Conditions......................................................................................................................................... 68
48.2 Procedure.......................................................................................................................................... 69
ARTICLE 49 — SUSPENSION OF THE ACTION IMPLEMENTATION................................................... 69
49.1 Suspension of the action implementation, by the beneficiaries.......................................................70
49.2 Suspension of the action implementation, by the Commission....................................................... 70
ARTICLE 50 — TERMINATION OF THE AGREEMENT OR OF THE PARTICIPATION OF ONE ORMORE BENEFICIARIES..............................................................................................................71
50.1 Termination of the Agreement, by the beneficiaries........................................................................71
50.2 Termination of the participation of one or more beneficiaries, by the beneficiaries........................72
50.3 Termination of the Agreement or the participation of one or more beneficiaries, by theCommission...................................................................................................................................... 74
SECTION 4 FORCE MAJEURE.......................................................................................................................... 79
ARTICLE 51 — FORCE MAJEURE..............................................................................................................79
CHAPTER 7 FINAL PROVISIONS...........................................................................................................................79
ARTICLE 52 — COMMUNICATION BETWEEN THE PARTIES...............................................................79
52.1 Form and means of communication.................................................................................................79
52.2 Date of communication.................................................................................................................... 80
52.3 Addresses for communication.......................................................................................................... 80
ARTICLE 53 — INTERPRETATION OF THE AGREEMENT.....................................................................80
53.1 Precedence of the Terms and Conditions over the Annexes............................................................80
53.2 Privileges and immunities................................................................................................................ 81
9
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
ARTICLE 54 — CALCULATION OF PERIODS, DATES AND DEADLINES........................................... 81
ARTICLE 55 — AMENDMENTS TO THE AGREEMENT......................................................................... 81
55.1 Conditions......................................................................................................................................... 81
55.2 Procedure.......................................................................................................................................... 81
ARTICLE 56 — ACCESSION TO THE AGREEMENT............................................................................... 82
56.1 Accession of the beneficiaries mentioned in the Preamble............................................................. 82
56.2 Addition of new beneficiaries.......................................................................................................... 82
ARTICLE 57 — APPLICABLE LAW AND SETTLEMENT OF DISPUTES.............................................. 82
57.1 Applicable law..................................................................................................................................82
57.2 Dispute settlement............................................................................................................................ 82
ARTICLE 58 — ENTRY INTO FORCE OF THE AGREEMENT................................................................ 83
10
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
CHAPTER 1 GENERAL
ARTICLE 1 — SUBJECT OF THE AGREEMENT
This Agreement sets out the rights and obligations and the terms and conditions applicable to the grantawarded to the beneficiaries for implementing the action set out in Chapter 2.
CHAPTER 2 ACTION
ARTICLE 2 — ACTION TO BE IMPLEMENTED
The grant is awarded for the action entitled ‘INTEGRATED PERSONALIZED CARE FORPATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH ANDQUALITY OF LIFE’ — ‘ADLIFE’ (‘action’), as described in Annex 1.
ARTICLE 3 — DURATION AND STARTING DATE OF THE ACTION
The duration of the action will be 48 months as of 1 January 2020 (‘starting date of the action’).
ARTICLE 4 — ESTIMATED BUDGET AND BUDGET TRANSFERS
4.1 Estimated budget
The ‘estimated budget’ for the action is set out in Annex 2.
It contains the estimated eligible costs and the forms of costs, broken down by beneficiary (and linkedthird party) and budget category (see Articles 5, 6, and 14).
4.2 Budget transfers
The estimated budget breakdown indicated in Annex 2 may be adjusted — without an amendment(see Article 55) — by transfers of amounts between beneficiaries, budget categories and/or forms ofcosts set out in Annex 2, if the action is implemented as described in Annex 1.
However, the beneficiaries may not add costs relating to subcontracts not provided for in Annex 1,unless such additional subcontracts are approved by an amendment or in accordance with Article 13.
CHAPTER 3 GRANT
ARTICLE 5 — GRANT AMOUNT, FORM OF GRANT, REIMBURSEMENT RATES ANDFORMS OF COSTS
5.1 Maximum grant amount
The ‘maximum grant amount’ is EUR 6 379 670.88 (six million three hundred and seventy ninethousand six hundred and seventy EURO and eighty eight eurocents).
5.2 Form of grant, reimbursement rates and forms of costs
11
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The grant reimburses 100% of the eligible costs of the beneficiaries and the linked third partiesthat are non-profit legal entities and 70% of the eligible costs of the beneficiaries and the linkedthird parties that are profit legal entities (see Article 6) (‘reimbursement of eligible costs grant’)(see Annex 2).
The estimated eligible costs of the action are EUR 7 450 948.75 (seven million four hundred and fiftythousand nine hundred and forty eight EURO and seventy five eurocents).
Eligible costs (see Article 6) must be declared under the following forms ('forms of costs'):
(a) for direct personnel costs:
- as actually incurred costs (‘actual costs’) or
- on the basis of an amount per unit calculated by the beneficiary in accordance with itsusual cost accounting practices (‘unit costs’).
Personnel costs for SME owners or beneficiaries that are natural persons not receiving asalary (see Article 6.2, Points A.4 and A.5) must be declared on the basis of the amount perunit set out in Annex 2a (unit costs);
(b) for direct costs for subcontracting: as actually incurred costs (actual costs);
(c) for direct costs of providing financial support to third parties: not applicable;
(d) for other direct costs:
- for costs of internally invoiced goods and services: on the basis of an amount per unitcalculated by the beneficiary in accordance with its usual cost accounting practices (‘unitcosts’);
- for all other costs: as actually incurred costs (actual costs);
(e) for indirect costs: on the basis of a flat-rate applied as set out in Article 6.2, Point E (‘flat-ratecosts’);
(f) specific cost category(ies): not applicable.
5.3 Final grant amount — Calculation
The ‘final grant amount’ depends on the actual extent to which the action is implemented inaccordance with the Agreement’s terms and conditions.
This amount is calculated by the Commission — when the payment of the balance is made (seeArticle 21.4) — in the following steps:
Step 1 — Application of the reimbursement rates to the eligible costs
Step 2 — Limit to the maximum grant amount
Step 3 — Reduction due to the no-profit rule
12
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
Step 4 — Reduction due to substantial errors, irregularities or fraud or serious breach ofobligations
5.3.1 Step 1 — Application of the reimbursement rates to the eligible costs
The reimbursement rate(s) (see Article 5.2) are applied to the eligible costs (actual costs, unit costsand flat-rate costs; see Article 6) declared by the beneficiaries and linked third parties (see Article 20)and approved by the Commission (see Article 21).
5.3.2 Step 2 — Limit to the maximum grant amount
If the amount obtained following Step 1 is higher than the maximum grant amount set out inArticle 5.1, it will be limited to the latter.
5.3.3 Step 3 — Reduction due to the no-profit rule
The grant must not produce a profit.
‘Profit’ means the surplus of the amount obtained following Steps 1 and 2 plus the action’s totalreceipts, over the action’s total eligible costs.
The ‘action’s total eligible costs’ are the consolidated total eligible costs approved by theCommission.
The ‘action’s total receipts’ are the consolidated total receipts generated during its duration (seeArticle 3).
The following are considered receipts:
(a) income generated by the action; if the income is generated from selling equipment or otherassets purchased under the Agreement, the receipt is up to the amount declared as eligible underthe Agreement;
(b) financial contributions given by third parties to the beneficiary or to a linked third partyspecifically to be used for the action, and
(c) in-kind contributions provided by third parties free of charge and specifically to be used for theaction, if they have been declared as eligible costs.
The following are however not considered receipts:
(a) income generated by exploiting the action’s results (see Article 28);
(b) financial contributions by third parties, if they may be used to cover costs other than the eligiblecosts (see Article 6);
(c) financial contributions by third parties with no obligation to repay any amount unused at theend of the period set out in Article 3.
If there is a profit, it will be deducted from the amount obtained following Steps 1 and 2.
5.3.4 Step 4 — Reduction due to substantial errors, irregularities or fraud or serious breachof obligations — Reduced grant amount — Calculation
13
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
If the grant is reduced (see Article 43), the Commission will calculate the reduced grant amountby deducting the amount of the reduction (calculated in proportion to the seriousness of the errors,irregularities or fraud or breach of obligations, in accordance with Article 43.2) from the maximumgrant amount set out in Article 5.1.
The final grant amount will be the lower of the following two:
- the amount obtained following Steps 1 to 3 or
- the reduced grant amount following Step 4.
5.4 Revised final grant amount — Calculation
If — after the payment of the balance (in particular, after checks, reviews, audits or investigations;see Article 22) — the Commission rejects costs (see Article 42) or reduces the grant (see Article 43),it will calculate the ‘revised final grant amount’ for the beneficiary concerned by the findings.
This amount is calculated by the Commission on the basis of the findings, as follows:
- in case of rejection of costs: by applying the reimbursement rate to the revised eligible costsapproved by the Commission for the beneficiary concerned;
- in case of reduction of the grant: by calculating the concerned beneficiary’s share in the grantamount reduced in proportion to the seriousness of the errors, irregularities or fraud or breachof obligations (see Article 43.2).
In case of rejection of costs and reduction of the grant, the revised final grant amount for thebeneficiary concerned will be the lower of the two amounts above.
ARTICLE 6 — ELIGIBLE AND INELIGIBLE COSTS
6.1 General conditions for costs to be eligible
‘Eligible costs’ are costs that meet the following criteria:
(a) for actual costs:
(i) they must be actually incurred by the beneficiary;
(ii) they must be incurred in the period set out in Article 3, with the exception of costs relatingto the submission of the periodic report for the last reporting period and the final report(see Article 20);
(iii) they must be indicated in the estimated budget set out in Annex 2;
(iv) they must be incurred in connection with the action as described in Annex 1 and necessaryfor its implementation;
(v) they must be identifiable and verifiable, in particular recorded in the beneficiary’s accountsin accordance with the accounting standards applicable in the country where the beneficiaryis established and with the beneficiary’s usual cost accounting practices;
14
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
(vi) they must comply with the applicable national law on taxes, labour and social security, and
(vii) they must be reasonable, justified and must comply with the principle of sound financialmanagement, in particular regarding economy and efficiency;
(b) for unit costs:
(i) they must be calculated as follows:
{amounts per unit set out in Annex 2a or calculated by the beneficiary in accordance with its usualcost accounting practices (see Article 6.2, Point A and Article 6.2.D.5)
multiplied by
the number of actual units};
(ii) the number of actual units must comply with the following conditions:
- the units must be actually used or produced in the period set out in Article 3;
- the units must be necessary for implementing the action or produced by it, and
- the number of units must be identifiable and verifiable, in particular supported byrecords and documentation (see Article 18);
(c) for flat-rate costs:
(i) they must be calculated by applying the flat-rate set out in Annex 2, and
(ii) the costs (actual costs or unit costs) to which the flat-rate is applied must comply with theconditions for eligibility set out in this Article.
6.2 Specific conditions for costs to be eligible
Costs are eligible if they comply with the general conditions (see above) and the specific conditionsset out below for each of the following budget categories:
A. direct personnel costs;B. direct costs of subcontracting;C. not applicable;D. other direct costs;E. indirect costs;F. not applicable.
‘Direct costs’ are costs that are directly linked to the action implementation and can therefore beattributed to it directly. They must not include any indirect costs (see Point E below).
‘Indirect costs’ are costs that are not directly linked to the action implementation and therefore cannotbe attributed directly to it.
A. Direct personnel costs
Types of eligible personnel costs
15
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
A.1 Personnel costs are eligible, if they are related to personnel working for the beneficiary under anemployment contract (or equivalent appointing act) and assigned to the action (‘costs for employees(or equivalent)’). They must be limited to salaries (including during parental leave), social securitycontributions, taxes and other costs included in the remuneration, if they arise from national law orthe employment contract (or equivalent appointing act).
Beneficiaries that are non-profit legal entities1 may also declare as personnel costs additionalremuneration for personnel assigned to the action (including payments on the basis of supplementarycontracts regardless of their nature), if:
(a) it is part of the beneficiary’s usual remuneration practices and is paid in a consistent mannerwhenever the same kind of work or expertise is required;
(b) the criteria used to calculate the supplementary payments are objective and generally appliedby the beneficiary, regardless of the source of funding used.
‘Additional remuneration’ means any part of the remuneration which exceeds what the person wouldbe paid for time worked in projects funded by national schemes.
Additional remuneration for personnel assigned to the action is eligible up to the following amount:
(a) if the person works full time and exclusively on the action during the full year: up to EUR 8 000;
(b) if the person works exclusively on the action but not full-time or not for the full year: up to thecorresponding pro-rata amount of EUR 8 000, or
(c) if the person does not work exclusively on the action: up to a pro-rata amount calculated asfollows:
{{EUR 8 000
divided by
the number of annual productive hours (see below)},
multiplied by
the number of hours that the person has worked on the action during the year}.
A.2 The costs for natural persons working under a direct contract with the beneficiary other thanan employment contract are eligible personnel costs, if:
(a) the person works under conditions similar to those of an employee (in particular regardingthe way the work is organised, the tasks that are performed and the premises where they areperformed);
(b) the result of the work carried out belongs to the beneficiary (unless exceptionally agreedotherwise), and
1 For the definition, see Article 2.1(14) of the Rules for Participation Regulation No 1290/2013: ‘non-profit legal entity’means a legal entity which by its legal form is non-profit-making or which has a legal or statutory obligation not todistribute profits to its shareholders or individual members.
16
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
(c) the costs are not significantly different from those for personnel performing similar tasks underan employment contract with the beneficiary.
A.3 The costs of personnel seconded by a third party against payment are eligible personnel costs,if the conditions in Article 11.1 are met.
A.4 Costs of owners of beneficiaries that are small and medium-sized enterprises (‘SME owners’)who are working on the action and who do not receive a salary are eligible personnel costs, if theycorrespond to the amount per unit set out in Annex 2a multiplied by the number of actual hours workedon the action.
A.5 Costs of ‘beneficiaries that are natural persons’ not receiving a salary are eligible personnelcosts, if they correspond to the amount per unit set out in Annex 2a multiplied by the number of actualhours worked on the action.
Calculation
Personnel costs must be calculated by the beneficiaries as follows:
{{hourly rate
multiplied by
the number of actual hours worked on the action},
plus
for non-profit legal entities: additional remuneration to personnel assigned to the action under theconditions set out above (Point A.1)}.
The number of actual hours declared for a person must be identifiable and verifiable (see Article 18).
The total number of hours declared in EU or Euratom grants, for a person for a year, cannot be higherthan the annual productive hours used for the calculations of the hourly rate. Therefore, the maximumnumber of hours that can be declared for the grant are:
{number of annual productive hours for the year (see below)
minus
total number of hours declared by the beneficiary, for that person in that year, for other EU or Euratomgrants}.
The ‘hourly rate’ is one of the following:
(a) for personnel costs declared as actual costs (i.e. budget categories A.1, A.2, A.3): the hourly rateis calculated per full financial year, as follows:
{actual annual personnel costs (excluding additional remuneration) for the person
divided by
number of annual productive hours}.
using the personnel costs and the number of productive hours for each full financial yearcovered by the reporting period concerned. If a financial year is not closed at the end of the
17
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
reporting period, the beneficiaries must use the hourly rate of the last closed financial yearavailable.
For the ‘number of annual productive hours’, the beneficiaries may choose one of the following:
(i) ‘fixed number of hours’: 1 720 hours for persons working full time (or correspondingpro-rata for persons not working full time);
(ii) ‘individual annual productive hours’: the total number of hours worked by the person inthe year for the beneficiary, calculated as follows:
{annual workable hours of the person (according to the employment contract, applicablecollective labour agreement or national law)
plus
overtime worked
minus
absences (such as sick leave and special leave)}.
‘Annual workable hours’ means the period during which the personnel must beworking, at the employer’s disposal and carrying out his/her activity or duties under theemployment contract, applicable collective labour agreement or national working timelegislation.
If the contract (or applicable collective labour agreement or national working timelegislation) does not allow to determine the annual workable hours, this option cannotbe used;
(iii) ‘standard annual productive hours’: the ‘standard number of annual hours’ generallyapplied by the beneficiary for its personnel in accordance with its usual cost accountingpractices. This number must be at least 90% of the ‘standard annual workable hours’.
If there is no applicable reference for the standard annual workable hours, this optioncannot be used.
For all options, the actual time spent on parental leave by a person assigned to the actionmay be deducted from the number of annual productive hours.
As an alternative, beneficiaries may calculate the hourly rate per month, as follows:
{actual monthly personnel cost (excluding additional remuneration) for the person
divided by
{number of annual productive hours / 12}}
using the personnel costs for each month and (one twelfth of) the annual productive hourscalculated according to either option (i) or (iii) above, i.e.:
- fixed number of hours or
- standard annual productive hours.
18
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
Time spent on parental leave may not be deducted when calculating the hourly rate per month.However, beneficiaries may declare personnel costs incurred in periods of parental leave inproportion to the time the person worked on the action in that financial year.
If parts of a basic remuneration are generated over a period longer than a month, thebeneficiaries may include only the share which is generated in the month (irrespective of theamount actually paid for that month).
Each beneficiary must use only one option (per full financial year or per month) for each fullfinancial year;
(b) for personnel costs declared on the basis of unit costs (i.e. budget categories A.1, A.2, A.4, A.5):the hourly rate is one of the following:
(i) for SME owners or beneficiaries that are natural persons: the hourly rate set out in Annex 2a(see Points A.4 and A.5 above), or
(ii) for personnel costs declared on the basis of the beneficiary’s usual cost accounting practices:the hourly rate calculated by the beneficiary in accordance with its usual cost accountingpractices, if:
- the cost accounting practices used are applied in a consistent manner, based on objectivecriteria, regardless of the source of funding;
- the hourly rate is calculated using the actual personnel costs recorded in the beneficiary’saccounts, excluding any ineligible cost or costs included in other budget categories.
The actual personnel costs may be adjusted by the beneficiary on the basis of budgetedor estimated elements. Those elements must be relevant for calculating the personnelcosts, reasonable and correspond to objective and verifiable information;
and
- the hourly rate is calculated using the number of annual productive hours (see above).
B. Direct costs of subcontracting (including related duties, taxes and charges such as non-deductible value added tax (VAT) paid by the beneficiary) are eligible if the conditions in Article13.1.1 are met.
C. Direct costs of providing financial support to third parties
Not applicable
D. Other direct costs
D.1 Travel costs and related subsistence allowances (including related duties, taxes and chargessuch as non-deductible value added tax (VAT) paid by the beneficiary) are eligible if they are in linewith the beneficiary’s usual practices on travel.
D.2 The depreciation costs of equipment, infrastructure or other assets (new or second-hand)as recorded in the beneficiary’s accounts are eligible, if they were purchased in accordance with
19
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
Article 10.1.1 and written off in accordance with international accounting standards and thebeneficiary’s usual accounting practices.
The costs of renting or leasing equipment, infrastructure or other assets (including related duties,taxes and charges such as non-deductible value added tax (VAT) paid by the beneficiary) are alsoeligible, if they do not exceed the depreciation costs of similar equipment, infrastructure or assets anddo not include any financing fees.
The costs of equipment, infrastructure or other assets contributed in-kind against payment areeligible, if they do not exceed the depreciation costs of similar equipment, infrastructure or assets, donot include any financing fees and if the conditions in Article 11.1 are met.
The only portion of the costs that will be taken into account is that which corresponds to the durationof the action and rate of actual use for the purposes of the action.
D.3 Costs of other goods and services (including related duties, taxes and charges such asnon-deductible value added tax (VAT) paid by the beneficiary) are eligible, if they are:
(a) purchased specifically for the action and in accordance with Article 10.1.1 or
(b) contributed in kind against payment and in accordance with Article 11.1.
Such goods and services include, for instance, consumables and supplies, dissemination (includingopen access), protection of results, certificates on the financial statements (if they are required by theAgreement), certificates on the methodology, translations and publications.
D.4 Capitalised and operating costs of ‘large research infrastructure’2 directly used for the actionare eligible, if:
(a) the value of the large research infrastructure represents at least 75% of the total fixed assets (athistorical value in its last closed balance sheet before the date of the signature of the Agreementor as determined on the basis of the rental and leasing costs of the research infrastructure3);
(b) the beneficiary’s methodology for declaring the costs for large research infrastructure has beenpositively assessed by the Commission (‘ex-ante assessment’);
(c) the beneficiary declares as direct eligible costs only the portion which corresponds to theduration of the action and the rate of actual use for the purposes of the action, and
(d) they comply with the conditions as further detailed in the annotations to the H2020 grantagreements.
2 ‘Large research infrastructure’ means research infrastructure of a total value of at least EUR 20 million, for abeneficiary, calculated as the sum of historical asset values of each individual research infrastructure of that beneficiary,as they appear in its last closed balance sheet before the date of the signature of the Agreement or as determined on thebasis of the rental and leasing costs of the research infrastructure.
3 For the definition, see Article 2(6) of the H2020 Framework Programme Regulation No 1291/2013: ‘Researchinfrastructure’ are facilities, resources and services that are used by the research communities to conduct research andfoster innovation in their fields. Where relevant, they may be used beyond research, e.g. for education or public services.They include: major scientific equipment (or sets of instruments); knowledge-based resources such as collections,archives or scientific data; e-infrastructures such as data and computing systems and communication networks; and anyother infrastructure of a unique nature essential to achieve excellence in research and innovation. Such infrastructuresmay be ‘single-sited’, ‘virtual’ or ‘distributed’.
20
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
D.5 Costs of internally invoiced goods and services directly used for the action are eligible, if:
(a) they are declared on the basis of a unit cost calculated in accordance with the beneficiary’susual cost accounting practices;
(b) the cost accounting practices used are applied in a consistent manner, based on objectivecriteria, regardless of the source of funding;
(c) the unit cost is calculated using the actual costs for the good or service recorded in thebeneficiary’s accounts, excluding any ineligible cost or costs included in other budgetcategories.
The actual costs may be adjusted by the beneficiary on the basis of budgeted or estimatedelements. Those elements must be relevant for calculating the costs, reasonable and correspondto objective and verifiable information;
(d) the unit cost excludes any costs of items which are not directly linked to the production of theinvoiced goods or service.
‘Internally invoiced goods and services’ means goods or services which are provided by thebeneficiary directly for the action and which the beneficiary values on the basis of its usual costaccounting practices.
E. Indirect costs
Indirect costs are eligible if they are declared on the basis of the flat-rate of 25% of the eligible directcosts (see Article 5.2 and Points A to D above), from which are excluded:
(a) costs of subcontracting and
(b) costs of in-kind contributions provided by third parties which are not used on the beneficiary’spremises;
(c) not applicable;
(d) not applicable.
Beneficiaries receiving an operating grant4 financed by the EU or Euratom budget cannot declareindirect costs for the period covered by the operating grant, unless they can demonstrate that theoperating grant does not cover any costs of the action.
F. Specific cost category(ies)
Not applicable
6.3 Conditions for costs of linked third parties to be eligible
4 For the definition, see Article 121(1)(b) of Regulation (EU, Euratom) No 966/2012 of the European Parliament andof the Council of 25 October 2012 on the financial rules applicable to the general budget of the Union and repealingCouncil Regulation (EC, Euratom) No 1605/2002 (‘Financial Regulation No 966/2012’)(OJ L 218, 26.10.2012, p.1):‘operating grant’ means direct financial contribution, by way of donation, from the budget in order to finance thefunctioning of a body which pursues an aim of general EU interest or has an objective forming part of and supportingan EU policy.
21
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
Costs incurred by linked third parties are eligible if they fulfil — mutatis mutandis — the generaland specific conditions for eligibility set out in this Article (Article 6.1 and 6.2) and Article 14.1.1.
6.4 Conditions for in-kind contributions provided by third parties free of charge to beeligible
In-kind contributions provided free of charge are eligible direct costs (for the beneficiary or linkedthird party), if the costs incurred by the third party fulfil — mutatis mutandis — the general andspecific conditions for eligibility set out in this Article (Article 6.1 and 6.2) and Article 12.1.
6.5 Ineligible costs
‘Ineligible costs’ are:
(a) costs that do not comply with the conditions set out above (Article 6.1 to 6.4), in particular:
(i) costs related to return on capital;
(ii) debt and debt service charges;
(iii) provisions for future losses or debts;
(iv) interest owed;
(v) doubtful debts;
(vi) currency exchange losses;
(vii) bank costs charged by the beneficiary’s bank for transfers from the Commission;
(viii) excessive or reckless expenditure;
(ix) deductible VAT;
(x) costs incurred during suspension of the implementation of the action (see Article 49);
(b) costs declared under another EU or Euratom grant (including grants awarded by a MemberState and financed by the EU or Euratom budget and grants awarded by bodies other than theCommission for the purpose of implementing the EU or Euratom budget); in particular, indirectcosts if the beneficiary is already receiving an operating grant financed by the EU or Euratombudget in the same period, unless it can demonstrate that the operating grant does not coverany costs of the action.
6.6 Consequences of declaration of ineligible costs
Declared costs that are ineligible will be rejected (see Article 42).
This may also lead to any of the other measures described in Chapter 6.
CHAPTER 4 RIGHTS AND OBLIGATIONS OF THE PARTIES
22
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
SECTION 1 RIGHTS AND OBLIGATIONS RELATED TO IMPLEMENTING THEACTION
ARTICLE 7 — GENERAL OBLIGATION TO PROPERLY IMPLEMENT THE ACTION
7.1 General obligation to properly implement the action
The beneficiaries must implement the action as described in Annex 1 and in compliance with theprovisions of the Agreement and all legal obligations under applicable EU, international and nationallaw.
7.2 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 8 — RESOURCES TO IMPLEMENT THE ACTION — THIRD PARTIESINVOLVED IN THE ACTION
The beneficiaries must have the appropriate resources to implement the action.
If it is necessary to implement the action, the beneficiaries may:
- purchase goods, works and services (see Article 10);
- use in-kind contributions provided by third parties against payment (see Article 11);
- use in-kind contributions provided by third parties free of charge (see Article 12);
- call upon subcontractors to implement action tasks described in Annex 1 (see Article 13);
- call upon linked third parties to implement action tasks described in Annex 1 (see Article 14);
- call upon international partners to implement action tasks described in Annex 1 (seeArticle 14a).
In these cases, the beneficiaries retain sole responsibility towards the Commission and the otherbeneficiaries for implementing the action.
ARTICLE 9 — IMPLEMENTATION OF ACTION TASKS BY BENEFICIARIES NOTRECEIVING EU FUNDING
Not applicable
ARTICLE 10 — PURCHASE OF GOODS, WORKS OR SERVICES
10.1 Rules for purchasing goods, works or services
10.1.1 If necessary to implement the action, the beneficiaries may purchase goods, works or services.
23
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The beneficiaries must make such purchases ensuring the best value for money or, if appropriate, thelowest price. In doing so, they must avoid any conflict of interests (see Article 35).
The beneficiaries must ensure that the Commission, the European Court of Auditors (ECA) and theEuropean Anti-Fraud Office (OLAF) can exercise their rights under Articles 22 and 23 also towardstheir contractors.
10.1.2 Beneficiaries that are ‘contracting authorities’ within the meaning of Directive 2004/18/EC5 (or2014/24/EU6) or ‘contracting entities’ within the meaning of Directive 2004/17/EC7 (or 2014/25/EU8)must comply with the applicable national law on public procurement.
10.2 Consequences of non-compliance
If a beneficiary breaches any of its obligations under Article 10.1.1, the costs related to the contractconcerned will be ineligible (see Article 6) and will be rejected (see Article 42).
If a beneficiary breaches any of its obligations under Article 10.1.2, the grant may be reduced (seeArticle 43).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 11 — USE OF IN-KIND CONTRIBUTIONS PROVIDED BY THIRD PARTIESAGAINST PAYMENT
11.1 Rules for the use of in-kind contributions against payment
If necessary to implement the action, the beneficiaries may use in-kind contributions provided by thirdparties against payment.
The beneficiaries may declare costs related to the payment of in-kind contributions as eligible (seeArticle 6.1 and 6.2), up to the third parties’ costs for the seconded persons, contributed equipment,infrastructure or other assets or other contributed goods and services.
The third parties and their contributions must be set out in Annex 1. The Commission may howeverapprove in-kind contributions not set out in Annex 1 without amendment (see Article 55), if:
- they are specifically justified in the periodic technical report and
- their use does not entail changes to the Agreement which would call into question the decisionawarding the grant or breach the principle of equal treatment of applicants.
The beneficiaries must ensure that the Commission, the European Court of Auditors (ECA) and the
5 Directive 2004/18/EC of the European Parliament and of the Council of 31 March 2004 on the coordination ofprocedures for the award of public work contracts, public supply contracts and public service contracts (OJ L 134,30.04.2004, p. 114).
6 Directive 2014/24/EU of the European Parliament and of the Council of 26 February 2014 on public procurement andrepealing Directive 2004/18/EC. (OJ L 94, 28.03.2014, p. 65).
7 Directive 2004/17/EC of the European Parliament and of the Council of 31 March 2004 coordinating the procurementprocedures of entities operating in the water, energy, transport and postal services sectors (OJ L 134, 30.04.2004, p. 1)
8 Directive 2014/25/EU of the European Parliament and of the Council of 26 February 2014 on procurement by entitiesoperating in the water, energy, transport and postal services sectors and repealing Directive 2004/17/EC (OJ L 94,28.03.2014, p. 243).
24
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
European Anti-Fraud Office (OLAF) can exercise their rights under Articles 22 and 23 also towardsthe third parties.
11.2 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the costs related to the payment ofthe in-kind contribution will be ineligible (see Article 6) and will be rejected (see Article 42).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 12 — USE OF IN-KIND CONTRIBUTIONS PROVIDED BY THIRD PARTIESFREE OF CHARGE
12.1 Rules for the use of in-kind contributions free of charge
If necessary to implement the action, the beneficiaries may use in-kind contributions provided by thirdparties free of charge.
The beneficiaries may declare costs incurred by the third parties for the seconded persons, contributedequipment, infrastructure or other assets or other contributed goods and services as eligible inaccordance with Article 6.4.
The third parties and their contributions must be set out in Annex 1. The Commission may howeverapprove in-kind contributions not set out in Annex 1 without amendment (see Article 55), if:
- they are specifically justified in the periodic technical report and
- their use does not entail changes to the Agreement which would call into question the decisionawarding the grant or breach the principle of equal treatment of applicants.
The beneficiaries must ensure that the Commission, the European Court of Auditors (ECA) and theEuropean Anti-Fraud Office (OLAF) can exercise their rights under Articles 22 and 23 also towardsthe third parties.
12.2 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the costs incurred by the third partiesrelated to the in-kind contribution will be ineligible (see Article 6) and will be rejected (see Article 42).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 13 — IMPLEMENTATION OF ACTION TASKS BY SUBCONTRACTORS
13.1 Rules for subcontracting action tasks
13.1.1 If necessary to implement the action, the beneficiaries may award subcontracts covering theimplementation of certain action tasks described in Annex 1.
Subcontracting may cover only a limited part of the action.
The beneficiaries must award the subcontracts ensuring the best value for money or, if appropriate,the lowest price. In doing so, they must avoid any conflict of interests (see Article 35).
25
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The tasks to be implemented and the estimated cost for each subcontract must be set out in Annex 1 andthe total estimated costs of subcontracting per beneficiary must be set out in Annex 2. The Commissionmay however approve subcontracts not set out in Annex 1 and 2 without amendment (see Article 55),if:
- they are specifically justified in the periodic technical report and
- they do not entail changes to the Agreement which would call into question the decisionawarding the grant or breach the principle of equal treatment of applicants.
The beneficiaries must ensure that the Commission, the European Court of Auditors (ECA) and theEuropean Anti-Fraud Office (OLAF) can exercise their rights under Articles 22 and 23 also towardstheir subcontractors.
13.1.2 The beneficiaries must ensure that their obligations under Articles 35, 36, 38 and 46 also applyto the subcontractors.
Beneficiaries that are ‘contracting authorities’ within the meaning of Directive 2004/18/EC (or2014/24/EU) or ‘contracting entities’ within the meaning of Directive 2004/17/EC (or 2014/25/EU)must comply with the applicable national law on public procurement.
13.2 Consequences of non-compliance
If a beneficiary breaches any of its obligations under Article 13.1.1, the costs related to the subcontractconcerned will be ineligible (see Article 6) and will be rejected (see Article 42).
If a beneficiary breaches any of its obligations under Article 13.1.2, the grant may be reduced (seeArticle 43).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 14 — IMPLEMENTATION OF ACTION TASKS BY LINKED THIRD PARTIES
14.1 Rules for calling upon linked third parties to implement part of the action
14.1.1 The following affiliated entities10 and third parties with a legal link to a beneficiary11
(‘linked third parties’) may implement the action tasks attributed to them in Annex 1:
10 For the definition see Article 2.1(2) Rules for Participation Regulation No 1290/2013: ‘affiliated entity’ means anylegal entity that is:
- under the direct or indirect control of a participant, or- under the same direct or indirect control as the participant, or- directly or indirectly controlling a participant.
‘Control’ may take any of the following forms:(a) the direct or indirect holding of more than 50% of the nominal value of the issued share capital in the legal entity
concerned, or of a majority of the voting rights of the shareholders or associates of that entity;(b) the direct or indirect holding, in fact or in law, of decision-making powers in the legal entity concerned.
However the following relationships between legal entities shall not in themselves be deemed to constitute controllingrelationships:
(a) the same public investment corporation, institutional investor or venture-capital company has a direct or indirectholding of more than 50% of the nominal value of the issued share capital or a majority of voting rights of theshareholders or associates;
(b) the legal entities concerned are owned or supervised by the same public body.
26
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
- Servicio Vasco de Salud Osakidetza (OSAKIDETZA), affiliated or linked to KRONIKGUNE
- GESUNDER WERRA-MEISSNER-KREIS GMBH (GESUNDER), affiliated or linked to OM
- ASSUTA MEDICAL CENTERS LTD (AMCN), affiliated or linked to AMCA
- MACCABI SHEIRUTEI BRIUT FOUNDATION (MACCABI), affiliated or linked to AMCA
The linked third parties may declare as eligible the costs they incur for implementing the action tasksin accordance with Article 6.3.
The beneficiaries must ensure that the Commission, the European Court of Auditors (ECA) and theEuropean Anti-Fraud Office (OLAF) can exercise their rights under Articles 22 and 23 also towardstheir linked third parties.
14.1.2 The beneficiaries must ensure that their obligations under Articles 18, 20, 35, 36 and 38 alsoapply to their linked third parties.
14.2 Consequences of non-compliance
If any obligation under Article 14.1.1 is breached, the costs of the linked third party will be ineligible(see Article 6) and will be rejected (see Article 42).
If any obligation under Article 14.1.2 is breached, the grant may be reduced (see Article 43).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 14a — IMPLEMENTATION OF ACTION TASKS BY INTERNATIONALPARTNERS
Not applicable
ARTICLE 15 — FINANCIAL SUPPORT TO THIRD PARTIES
15.1 Rules for providing financial support to third parties
Not applicable
15.2 Financial support in the form of prizes
Not applicable
15.3 Consequences of non-compliance
Not applicable
ARTICLE 16 — PROVISION OF TRANS-NATIONAL OR VIRTUAL ACCESS TORESEARCH INFRASTRUCTURE
11 ‘Third party with a legal link to a beneficiary’ is any legal entity which has a legal link to the beneficiary implyingcollaboration that is not limited to the action.
27
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
16.1 Rules for providing trans-national access to research infrastructure
Not applicable
16.2 Rules for providing virtual access to research infrastructure
Not applicable
16.3 Consequences of non-compliance
Not applicable
SECTION 2 RIGHTS AND OBLIGATIONS RELATED TO THE GRANTADMINISTRATION
ARTICLE 17 — GENERAL OBLIGATION TO INFORM
17.1 General obligation to provide information upon request
The beneficiaries must provide — during implementation of the action or afterwards and in accordancewith Article 41.2 — any information requested in order to verify eligibility of the costs, properimplementation of the action and compliance with any other obligation under the Agreement.
17.2 Obligation to keep information up to date and to inform about events andcircumstances likely to affect the Agreement
Each beneficiary must keep information stored in the Participant Portal Beneficiary Register (viathe electronic exchange system; see Article 52) up to date, in particular, its name, address, legalrepresentatives, legal form and organisation type.
Each beneficiary must immediately inform the coordinator — which must immediately inform theCommission and the other beneficiaries — of any of the following:
(a) events which are likely to affect significantly or delay the implementation of the action or theEU's financial interests, in particular:
(i) changes in its legal, financial, technical, organisational or ownership situation or thoseof its linked third parties and
(ii) changes in the name, address, legal form, organisation type of its linked third parties;
(b) circumstances affecting:
(i) the decision to award the grant or
(ii) compliance with requirements under the Agreement.
17.3 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43).
28
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 18 — KEEPING RECORDS — SUPPORTING DOCUMENTATION
18.1 Obligation to keep records and other supporting documentation
The beneficiaries must — for a period of five years after the payment of the balance — keep recordsand other supporting documentation in order to prove the proper implementation of the action andthe costs they declare as eligible.
They must make them available upon request (see Article 17) or in the context of checks, reviews,audits or investigations (see Article 22).
If there are on-going checks, reviews, audits, investigations, litigation or other pursuits of claims underthe Agreement (including the extension of findings; see Article 22), the beneficiaries must keep therecords and other supporting documentation until the end of these procedures.
The beneficiaries must keep the original documents. Digital and digitalised documents are consideredoriginals if they are authorised by the applicable national law. The Commission may accept non-original documents if it considers that they offer a comparable level of assurance.
18.1.1 Records and other supporting documentation on the scientific and technicalimplementation
The beneficiaries must keep records and other supporting documentation on scientific and technicalimplementation of the action in line with the accepted standards in the respective field.
18.1.2 Records and other documentation to support the costs declared
The beneficiaries must keep the records and documentation supporting the costs declared, in particularthe following:
(a) for actual costs: adequate records and other supporting documentation to prove the costsdeclared, such as contracts, subcontracts, invoices and accounting records. In addition, thebeneficiaries' usual cost accounting practices and internal control procedures must enable directreconciliation between the amounts declared, the amounts recorded in their accounts and theamounts stated in the supporting documentation;
(b) for unit costs: adequate records and other supporting documentation to prove the number ofunits declared. Beneficiaries do not need to identify the actual eligible costs covered or to keepor provide supporting documentation (such as accounting statements) to prove the amount perunit.
In addition, for unit costs calculated in accordance with the beneficiary's usual costaccounting practices, the beneficiaries must keep adequate records and documentation toprove that the cost accounting practices used comply with the conditions set out in Article 6.2.
The beneficiaries and linked third parties may submit to the Commission, for approval, acertificate (drawn up in accordance with Annex 6) stating that their usual cost accountingpractices comply with these conditions (‘certificate on the methodology’). If the certificate
29
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
is approved, costs declared in line with this methodology will not be challenged subsequently,unless the beneficiaries have concealed information for the purpose of the approval.
(c) for flat-rate costs: adequate records and other supporting documentation to prove the eligibilityof the costs to which the flat-rate is applied. The beneficiaries do not need to identify the costscovered or provide supporting documentation (such as accounting statements) to prove theamount declared at a flat-rate.
In addition, for personnel costs (declared as actual costs or on the basis of unit costs), the beneficiariesmust keep time records for the number of hours declared. The time records must be in writing andapproved by the persons working on the action and their supervisors, at least monthly. In the absenceof reliable time records of the hours worked on the action, the Commission may accept alternativeevidence supporting the number of hours declared, if it considers that it offers an adequate level ofassurance.
As an exception, for persons working exclusively on the action, there is no need to keep time records,if the beneficiary signs a declaration confirming that the persons concerned have worked exclusivelyon the action.
For costs declared by linked third parties (see Article 14), it is the beneficiary that must keep theoriginals of the financial statements and the certificates on the financial statements of the linked thirdparties.
18.2 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, costs insufficiently substantiatedwill be ineligible (see Article 6) and will be rejected (see Article 42), and the grant may be reduced(see Article 43).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 19 — SUBMISSION OF DELIVERABLES
19.1 Obligation to submit deliverables
The coordinator must submit the ‘deliverables’ identified in Annex 1, in accordance with the timingand conditions set out in it.
19.2 Consequences of non-compliance
If the coordinator breaches any of its obligations under this Article, the Commission may apply anyof the measures described in Chapter 6.
ARTICLE 20 — REPORTING — PAYMENT REQUESTS
20.1 Obligation to submit reports
The coordinator must submit to the Commission (see Article 52) the technical and financial reportsset out in this Article. These reports include requests for payment and must be drawn up using theforms and templates provided in the electronic exchange system (see Article 52).
30
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
20.2 Reporting periods
The action is divided into the following ‘reporting periods’:
- RP1: from month 1 to month 18- RP2: from month 19 to month 36- RP3: from month 37 to month 48
20.3 Periodic reports — Requests for interim payments
The coordinator must submit a periodic report within 60 days following the end of each reportingperiod.
The periodic report must include the following:
(a) a ‘periodic technical report’ containing:
(i) an explanation of the work carried out by the beneficiaries;
(ii) an overview of the progress towards the objectives of the action, including milestonesand deliverables identified in Annex 1.
This report must include explanations justifying the differences between work expectedto be carried out in accordance with Annex 1 and that actually carried out.
The report must detail the exploitation and dissemination of the results and — if requiredin Annex 1 — an updated ‘plan for the exploitation and dissemination of the results’.
The report must indicate the communication activities;
(iii) a summary for publication by the Commission;
(iv) the answers to the ‘questionnaire’, covering issues related to the action implementationand the economic and societal impact, notably in the context of the Horizon 2020 keyperformance indicators and the Horizon 2020 monitoring requirements;
(b) a ‘periodic financial report’ containing:
(i) an ‘individual financial statement’ (see Annex 4) from each beneficiary and from eachlinked third party, for the reporting period concerned.
The individual financial statement must detail the eligible costs (actual costs, unit costsand flat-rate costs; see Article 6) for each budget category (see Annex 2).
The beneficiaries and linked third parties must declare all eligible costs, even if —for actual costs, unit costs and flat-rate costs — they exceed the amounts indicated inthe estimated budget (see Annex 2). Amounts which are not declared in the individualfinancial statement will not be taken into account by the Commission.
If an individual financial statement is not submitted for a reporting period, it may beincluded in the periodic financial report for the next reporting period.
31
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The individual financial statements of the last reporting period must also detail thereceipts of the action (see Article 5.3.3).
Each beneficiary and each linked third party must certify that:
- the information provided is full, reliable and true;
- the costs declared are eligible (see Article 6);
- the costs can be substantiated by adequate records and supporting documentation(see Article 18) that will be produced upon request (see Article 17) or in the contextof checks, reviews, audits and investigations (see Article 22), and
- for the last reporting period: that all the receipts have been declared (seeArticle 5.3.3);
(ii) an explanation of the use of resources and the information on subcontracting (seeArticle 13) and in-kind contributions provided by third parties (see Articles 11 and12) from each beneficiary and from each linked third party, for the reporting periodconcerned;
(iii) not applicable;
(iv) a ‘periodic summary financial statement’, created automatically by the electronicexchange system, consolidating the individual financial statements for the reportingperiod concerned and including — except for the last reporting period — the requestfor interim payment.
20.4 Final report — Request for payment of the balance
In addition to the periodic report for the last reporting period, the coordinator must submit the finalreport within 60 days following the end of the last reporting period.
The final report must include the following:
(a) a ‘final technical report’ with a summary for publication containing:
(i) an overview of the results and their exploitation and dissemination;
(ii) the conclusions on the action, and
(iii) the socio-economic impact of the action;
(b) a ‘final financial report’ containing:
(i) a ‘final summary financial statement’, created automatically by the electronicexchange system, consolidating the individual financial statements for all reportingperiods and including the request for payment of the balance and
(ii) a ‘certificate on the financial statements’ (drawn up in accordance with Annex 5) foreach beneficiary and for each linked third party, if it requests a total contribution of
32
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
EUR 325 000 or more, as reimbursement of actual costs and unit costs calculated on thebasis of its usual cost accounting practices (see Article 5.2 and Article 6.2).
20.5 Information on cumulative expenditure incurred
Not applicable
20.6 Currency for financial statements and conversion into euro
Financial statements must be drafted in euro.
Beneficiaries and linked third parties with accounting established in a currency other than the euromust convert the costs recorded in their accounts into euro, at the average of the daily exchangerates published in the C series of the Official Journal of the European Union, calculated over thecorresponding reporting period.
If no daily euro exchange rate is published in the Official Journal of the European Union for thecurrency in question, they must be converted at the average of the monthly accounting rates publishedon the Commission’s website, calculated over the corresponding reporting period.
Beneficiaries and linked third parties with accounting established in euro must convert costs incurredin another currency into euro according to their usual accounting practices.
20.7 Language of reports
All reports (technical and financial reports, including financial statements) must be submitted in thelanguage of the Agreement.
20.8 Consequences of non-compliance
If the reports submitted do not comply with this Article, the Commission may suspend the paymentdeadline (see Article 47) and apply any of the other measures described in Chapter 6.
If the coordinator breaches its obligation to submit the reports and if it fails to comply with thisobligation within 30 days following a written reminder, the Commission may terminate the Agreement(see Article 50) or apply any of the other measures described in Chapter 6.
ARTICLE 21 — PAYMENTS AND PAYMENT ARRANGEMENTS
21.1 Payments to be made
The following payments will be made to the coordinator:
- one pre-financing payment;
- one or more interim payments, on the basis of the request(s) for interim payment (seeArticle 20), and
- one payment of the balance, on the basis of the request for payment of the balance (seeArticle 20).
21.2 Pre-financing payment — Amount — Amount retained for the Guarantee Fund
33
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The aim of the pre-financing is to provide the beneficiaries with a float.
It remains the property of the EU until the payment of the balance.
The amount of the pre-financing payment will be EUR 3 402 491.14 (three million four hundred andtwo thousand four hundred and ninety one EURO and fourteen eurocents).
The Commission will — except if Article 48 applies — make the pre-financing payment to thecoordinator within 30 days, either from the entry into force of the Agreement (see Article 58) or from10 days before the starting date of the action (see Article 3), whichever is the latest.
An amount of EUR 318 983.54 (three hundred and eighteen thousand nine hundred and eighty threeEURO and fifty four eurocents), corresponding to 5% of the maximum grant amount (see Article 5.1),is retained by the Commission from the pre-financing payment and transferred into the ‘GuaranteeFund’.
21.3 Interim payments — Amount — Calculation
Interim payments reimburse the eligible costs incurred for the implementation of the action duringthe corresponding reporting periods.
The Commission will pay to the coordinator the amount due as interim payment within 90 days fromreceiving the periodic report (see Article 20.3), except if Articles 47 or 48 apply.
Payment is subject to the approval of the periodic report. Its approval does not imply recognition ofthe compliance, authenticity, completeness or correctness of its content.
The amount due as interim payment is calculated by the Commission in the following steps:
Step 1 — Application of the reimbursement rates
Step 2 — Limit to 90% of the maximum grant amount
21.3.1 Step 1 — Application of the reimbursement rates
The reimbursement rate(s) (see Article 5.2) are applied to the eligible costs (actual costs, unit costs andflat-rate costs; see Article 6) declared by the beneficiaries and the linked third parties (see Article 20)and approved by the Commission (see above) for the concerned reporting period.
21.3.2 Step 2 — Limit to 90% of the maximum grant amount
The total amount of pre-financing and interim payments must not exceed 90% of the maximum grantamount set out in Article 5.1. The maximum amount for the interim payment will be calculated asfollows:
{90% of the maximum grant amount (see Article 5.1)
minus
{pre-financing and previous interim payments}}.
21.4 Payment of the balance — Amount — Calculation — Release of the amount retainedfor the Guarantee Fund
34
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The payment of the balance reimburses the remaining part of the eligible costs incurred by thebeneficiaries for the implementation of the action.
If the total amount of earlier payments is greater than the final grant amount (see Article 5.3), thepayment of the balance takes the form of a recovery (see Article 44).
If the total amount of earlier payments is lower than the final grant amount, the Commission willpay the balance within 90 days from receiving the final report (see Article 20.4), except if Articles47 or 48 apply.
Payment is subject to the approval of the final report. Its approval does not imply recognition of thecompliance, authenticity, completeness or correctness of its content.
The amount due as the balance is calculated by the Commission by deducting the total amount ofpre-financing and interim payments (if any) already made, from the final grant amount determinedin accordance with Article 5.3:
{final grant amount (see Article 5.3)
minus
{pre-financing and interim payments (if any) made}}.
At the payment of the balance, the amount retained for the Guarantee Fund (see above) will be releasedand:
- if the balance is positive: the amount released will be paid in full to the coordinator togetherwith the amount due as the balance;
- if the balance is negative (payment of the balance taking the form of recovery): it will bededucted from the amount released (see Article 44.1.2). If the resulting amount:
- is positive, it will be paid to the coordinator
- is negative, it will be recovered.
The amount to be paid may however be offset — without the beneficiaries' consent — against anyother amount owed by a beneficiary to the Commission or an executive agency (under the EU orEuratom budget), up to the maximum EU contribution indicated, for that beneficiary, in the estimatedbudget (see Annex 2).
21.5 Notification of amounts due
When making payments, the Commission will formally notify to the coordinator the amount due,specifying whether it concerns an interim payment or the payment of the balance.
For the payment of the balance, the notification will also specify the final grant amount.
In the case of reduction of the grant or recovery of undue amounts, the notification will be precededby the contradictory procedure set out in Articles 43 and 44.
21.6 Currency for payments
35
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The Commission will make all payments in euro.
21.7 Payments to the coordinator — Distribution to the beneficiaries
Payments will be made to the coordinator.
Payments to the coordinator will discharge the Commission from its payment obligation.
The coordinator must distribute the payments between the beneficiaries without unjustified delay.
Pre-financing may however be distributed only:
(a) if the minimum number of beneficiaries set out in the call for proposals has acceded to theAgreement (see Article 56) and
(b) to beneficiaries that have acceded to the Agreement (see Article 56).
21.8 Bank account for payments
All payments will be made to the following bank account:
Name of bank: KUTXABANK, S.AFull name of the account holder: ASOCIACION CENTRO EXCEL INTERNACIONALINVESTIG SOBRE CRONICIDADIBAN code: ES4920950611009111334073
21.9 Costs of payment transfers
The cost of the payment transfers is borne as follows:
- the Commission bears the cost of transfers charged by its bank;
- the beneficiary bears the cost of transfers charged by its bank;
- the party causing a repetition of a transfer bears all costs of the repeated transfer.
21.10 Date of payment
Payments by the Commission are considered to have been carried out on the date when they aredebited to its account.
21.11 Consequences of non-compliance
21.11.1 If the Commission does not pay within the payment deadlines (see above), the beneficiariesare entitled to late-payment interest at the rate applied by the European Central Bank (ECB) for itsmain refinancing operations in euros (‘reference rate’), plus three and a half points. The reference rateis the rate in force on the first day of the month in which the payment deadline expires, as publishedin the C series of the Official Journal of the European Union.
If the late-payment interest is lower than or equal to EUR 200, it will be paid to the coordinator onlyupon request submitted within two months of receiving the late payment.
Late-payment interest is not due if all beneficiaries are EU Member States (including regional and
36
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
local government authorities or other public bodies acting on behalf of a Member State for the purposeof this Agreement).
Suspension of the payment deadline or payments (see Articles 47 and 48) will not be considered aslate payment.
Late-payment interest covers the period running from the day following the due date for payment (seeabove), up to and including the date of payment.
Late-payment interest is not considered for the purposes of calculating the final grant amount.
21.11.2 If the coordinator breaches any of its obligations under this Article, the grant may be reduced(see Article 43) and the Agreement or the participation of the coordinator may be terminated (seeArticle 50).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 22 — CHECKS, REVIEWS, AUDITS AND INVESTIGATIONS — EXTENSIONOF FINDINGS
22.1 Checks, reviews and audits by the Commission
22.1.1 Right to carry out checks
The Commission will — during the implementation of the action or afterwards — check the properimplementation of the action and compliance with the obligations under the Agreement, includingassessing deliverables and reports.
For this purpose the Commission may be assisted by external persons or bodies.
The Commission may also request additional information in accordance with Article 17. TheCommission may request beneficiaries to provide such information to it directly.
Information provided must be accurate, precise and complete and in the format requested, includingelectronic format.
22.1.2 Right to carry out reviews
The Commission may — during the implementation of the action or afterwards — carry out reviewson the proper implementation of the action (including assessment of deliverables and reports),compliance with the obligations under the Agreement and continued scientific or technologicalrelevance of the action.
Reviews may be started up to two years after the payment of the balance. They will be formallynotified to the coordinator or beneficiary concerned and will be considered to have started on the dateof the formal notification.
If the review is carried out on a third party (see Articles 10 to 16), the beneficiary concerned mustinform the third party.
The Commission may carry out reviews directly (using its own staff) or indirectly (using externalpersons or bodies appointed to do so). It will inform the coordinator or beneficiary concerned of the
37
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
identity of the external persons or bodies. They have the right to object to the appointment on groundsof commercial confidentiality.
The coordinator or beneficiary concerned must provide — within the deadline requested — anyinformation and data in addition to deliverables and reports already submitted (including informationon the use of resources). The Commission may request beneficiaries to provide such information toit directly.
The coordinator or beneficiary concerned may be requested to participate in meetings, including withexternal experts.
For on-the-spot reviews, the beneficiaries must allow access to their sites and premises, including toexternal persons or bodies, and must ensure that information requested is readily available.
Information provided must be accurate, precise and complete and in the format requested, includingelectronic format.
On the basis of the review findings, a ‘review report’ will be drawn up.
The Commission will formally notify the review report to the coordinator or beneficiary concerned,which has 30 days to formally notify observations (‘contradictory review procedure’).
Reviews (including review reports) are in the language of the Agreement.
22.1.3 Right to carry out audits
The Commission may — during the implementation of the action or afterwards — carry out audits onthe proper implementation of the action and compliance with the obligations under the Agreement.
Audits may be started up to two years after the payment of the balance. They will be formally notifiedto the coordinator or beneficiary concerned and will be considered to have started on the date of theformal notification.
If the audit is carried out on a third party (see Articles 10 to 16), the beneficiary concerned mustinform the third party.
The Commission may carry out audits directly (using its own staff) or indirectly (using externalpersons or bodies appointed to do so). It will inform the coordinator or beneficiary concerned of theidentity of the external persons or bodies. They have the right to object to the appointment on groundsof commercial confidentiality.
The coordinator or beneficiary concerned must provide — within the deadline requested — anyinformation (including complete accounts, individual salary statements or other personal data) toverify compliance with the Agreement. The Commission may request beneficiaries to provide suchinformation to it directly.
For on-the-spot audits, the beneficiaries must allow access to their sites and premises, including toexternal persons or bodies, and must ensure that information requested is readily available.
Information provided must be accurate, precise and complete and in the format requested, includingelectronic format.
On the basis of the audit findings, a ‘draft audit report’ will be drawn up.
38
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The Commission will formally notify the draft audit report to the coordinator or beneficiary concerned,which has 30 days to formally notify observations (‘contradictory audit procedure’). This periodmay be extended by the Commission in justified cases.
The ‘final audit report’ will take into account observations by the coordinator or beneficiaryconcerned. The report will be formally notified to it.
Audits (including audit reports) are in the language of the Agreement.
The Commission may also access the beneficiaries’ statutory records for the periodical assessmentof unit costs or flat-rate amounts.
22.2 Investigations by the European Anti-Fraud Office (OLAF)
Under Regulations No 883/201316 and No 2185/9617 (and in accordance with their provisions andprocedures), the European Anti-Fraud Office (OLAF) may — at any moment during implementationof the action or afterwards — carry out investigations, including on-the-spot checks and inspections,to establish whether there has been fraud, corruption or any other illegal activity affecting the financialinterests of the EU.
22.3 Checks and audits by the European Court of Auditors (ECA)
Under Article 287 of the Treaty on the Functioning of the European Union (TFEU) and Article 161of the Financial Regulation No 966/201218, the European Court of Auditors (ECA) may — at anymoment during implementation of the action or afterwards — carry out audits.
The ECA has the right of access for the purpose of checks and audits.
22.4 Checks, reviews, audits and investigations for international organisations
Not applicable
22.5 Consequences of findings in checks, reviews, audits and investigations — Extension offindings
22.5.1 Findings in this grant
Findings in checks, reviews, audits or investigations carried out in the context of this grant may leadto the rejection of ineligible costs (see Article 42), reduction of the grant (see Article 43), recovery ofundue amounts (see Article 44) or to any of the other measures described in Chapter 6.
16 Regulation (EU, Euratom) No 883/2013 of the European Parliament and of the Council of 11 September 2013concerning investigations conducted by the European Anti-Fraud Office (OLAF) and repealing Regulation (EC) No1073/1999 of the European Parliament and of the Council and Council Regulation (Euratom) No 1074/1999 (OJ L 248,18.09.2013, p. 1).
17 Council Regulation (Euratom, EC) No 2185/1996 of 11 November 1996 concerning on-the-spot checks and inspectionscarried out by the Commission in order to protect the European Communities' financial interests against fraud and otherirregularities (OJ L 292, 15.11.1996, p. 2).
18 Regulation (EU, Euratom) No 966/2012 of the European Parliament and of the Council of 25 October 2012 on thefinancial rules applicable to the general budget of the Union and repealing Council Regulation (EC, Euratom) No1605/2002 (OJ L 298, 26.10.2012, p. 1).
39
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
Rejection of costs or reduction of the grant after the payment of the balance will lead to a revised finalgrant amount (see Article 5.4).
Findings in checks, reviews, audits or investigations may lead to a request for amendment for themodification of Annex 1 (see Article 55).
Checks, reviews, audits or investigations that find systemic or recurrent errors, irregularities, fraud orbreach of obligations may also lead to consequences in other EU or Euratom grants awarded undersimilar conditions (‘extension of findings from this grant to other grants’).
Moreover, findings arising from an OLAF investigation may lead to criminal prosecution undernational law.
22.5.2 Findings in other grants
The Commission may extend findings from other grants to this grant (‘extension of findings fromother grants to this grant’), if:
(a) the beneficiary concerned is found, in other EU or Euratom grants awarded under similarconditions, to have committed systemic or recurrent errors, irregularities, fraud or breach ofobligations that have a material impact on this grant and
(b) those findings are formally notified to the beneficiary concerned — together with the list ofgrants affected by the findings — no later than two years after the payment of the balance ofthis grant.
The extension of findings may lead to the rejection of costs (see Article 42), reduction of the grant(see Article 43), recovery of undue amounts (see Article 44), suspension of payments (see Article 48),suspension of the action implementation (see Article 49) or termination (see Article 50).
22.5.3 Procedure
The Commission will formally notify the beneficiary concerned the systemic or recurrent errors andits intention to extend these audit findings, together with the list of grants affected.
22.5.3.1 If the findings concern eligibility of costs: the formal notification will include:
(a) an invitation to submit observations on the list of grants affected by the findings;
(b) the request to submit revised financial statements for all grants affected;
(c) the correction rate for extrapolation established by the Commission on the basis of thesystemic or recurrent errors, to calculate the amounts to be rejected if the beneficiary concerned:
(i) considers that the submission of revised financial statements is not possible or practicableor
(ii) does not submit revised financial statements.
The beneficiary concerned has 90 days from receiving notification to submit observations, revisedfinancial statements or to propose a duly substantiated alternative correction method. This periodmay be extended by the Commission in justified cases.
40
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The Commission may then start a rejection procedure in accordance with Article 42, on the basis of:
- the revised financial statements, if approved;
- the proposed alternative correction method, if accepted
or
- the initially notified correction rate for extrapolation, if it does not receive any observationsor revised financial statements, does not accept the observations or the proposed alternativecorrection method or does not approve the revised financial statements.
22.5.3.2 If the findings concern substantial errors, irregularities or fraud or serious breach ofobligations: the formal notification will include:
(a) an invitation to submit observations on the list of grants affected by the findings and
(b) the flat-rate the Commission intends to apply according to the principle of proportionality.
The beneficiary concerned has 90 days from receiving notification to submit observations or topropose a duly substantiated alternative flat-rate.
The Commission may then start a reduction procedure in accordance with Article 43, on the basis of:
- the proposed alternative flat-rate, if accepted
or
- the initially notified flat-rate, if it does not receive any observations or does not accept theobservations or the proposed alternative flat-rate.
22.6 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, any insufficiently substantiated costswill be ineligible (see Article 6) and will be rejected (see Article 42).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 23 — EVALUATION OF THE IMPACT OF THE ACTION
23.1 Right to evaluate the impact of the action
The Commission may carry out interim and final evaluations of the impact of the action measuredagainst the objective of the EU programme.
Evaluations may be started during implementation of the action and up to five years after the paymentof the balance. The evaluation is considered to start on the date of the formal notification to thecoordinator or beneficiaries.
The Commission may make these evaluations directly (using its own staff) or indirectly (using externalbodies or persons it has authorised to do so).
41
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The coordinator or beneficiaries must provide any information relevant to evaluate the impact of theaction, including information in electronic format.
23.2 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the Commission may apply themeasures described in Chapter 6.
SECTION 3 RIGHTS AND OBLIGATIONS RELATED TO BACKGROUND ANDRESULTS
SUBSECTION 1 GENERAL
ARTICLE 23a — MANAGEMENT OF INTELLECTUAL PROPERTY
23a.1 Obligation to take measures to implement the Commission Recommendation on themanagement of intellectual property in knowledge transfer activities
Beneficiaries that are universities or other public research organisations must take measures toimplement the principles set out in Points 1 and 2 of the Code of Practice annexed to the CommissionRecommendation on the management of intellectual property in knowledge transfer activities19.
This does not change the obligations set out in Subsections 2 and 3 of this Section.
The beneficiaries must ensure that researchers and third parties involved in the action are aware ofthem.
23a.2 Consequences of non-compliance
If a beneficiary breaches its obligations under this Article, the Commission may apply any of themeasures described in Chapter 6.
SUBSECTION 2 RIGHTS AND OBLIGATIONS RELATED TO BACKGROUND
ARTICLE 24 — AGREEMENT ON BACKGROUND
24.1 Agreement on background
The beneficiaries must identify and agree (in writing) on the background for the action (‘agreementon background’).
‘Background’ means any data, know-how or information — whatever its form or nature (tangible orintangible), including any rights such as intellectual property rights — that:
(a) is held by the beneficiaries before they acceded to the Agreement, and
19 Commission Recommendation C(2008) 1329 of 10.4.2008 on the management of intellectual property in knowledgetransfer activities and the Code of Practice for universities and other public research institutions attached to thisrecommendation.
42
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
(b) is needed to implement the action or exploit the results.
24.2 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 25 — ACCESS RIGHTS TO BACKGROUND
25.1 Exercise of access rights — Waiving of access rights — No sub-licensing
To exercise access rights, this must first be requested in writing (‘request for access’).
‘Access rights’ means rights to use results or background under the terms and conditions laid downin this Agreement.
Waivers of access rights are not valid unless in writing.
Unless agreed otherwise, access rights do not include the right to sub-license.
25.2 Access rights for other beneficiaries, for implementing their own tasks under the action
The beneficiaries must give each other access — on a royalty-free basis — to background needed toimplement their own tasks under the action, unless the beneficiary that holds the background has —before acceding to the Agreement —:
(a) informed the other beneficiaries that access to its background is subject to legal restrictions orlimits, including those imposed by the rights of third parties (including personnel), or
(b) agreed with the other beneficiaries that access would not be on a royalty-free basis.
25.3 Access rights for other beneficiaries, for exploiting their own results
The beneficiaries must give each other access — under fair and reasonable conditions — tobackground needed for exploiting their own results, unless the beneficiary that holds the backgroundhas — before acceding to the Agreement — informed the other beneficiaries that access to itsbackground is subject to legal restrictions or limits, including those imposed by the rights of thirdparties (including personnel).
‘Fair and reasonable conditions’ means appropriate conditions, including possible financial termsor royalty-free conditions, taking into account the specific circumstances of the request for access, forexample the actual or potential value of the results or background to which access is requested and/orthe scope, duration or other characteristics of the exploitation envisaged.
Requests for access may be made — unless agreed otherwise — up to one year after the period setout in Article 3.
25.4 Access rights for affiliated entities
Unless otherwise agreed in the consortium agreement, access to background must also be given
43
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
— under fair and reasonable conditions (see above; Article 25.3) and unless it is subject to legalrestrictions or limits, including those imposed by the rights of third parties (including personnel) —to affiliated entities20 established in an EU Member State or ‘associated country’21, if this is neededto exploit the results generated by the beneficiaries to which they are affiliated.
Unless agreed otherwise (see above; Article 25.1), the affiliated entity concerned must make therequest directly to the beneficiary that holds the background.
Requests for access may be made — unless agreed otherwise — up to one year after the period setout in Article 3.
25.5 Access rights for third parties
Not applicable
25.6 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43).
Such breaches may also lead to any of the other measures described in Chapter 6.
SUBSECTION 3 RIGHTS AND OBLIGATIONS RELATED TO RESULTS
ARTICLE 26 — OWNERSHIP OF RESULTS
26.1 Ownership by the beneficiary that generates the results
Results are owned by the beneficiary that generates them.
‘Results’ means any (tangible or intangible) output of the action such as data, knowledge orinformation — whatever its form or nature, whether it can be protected or not — that is generated inthe action, as well as any rights attached to it, including intellectual property rights.
26.2 Joint ownership by several beneficiaries
Two or more beneficiaries own results jointly if:
(a) they have jointly generated them and
(b) it is not possible to:
(i) establish the respective contribution of each beneficiary, or
(ii) separate them for the purpose of applying for, obtaining or maintaining their protection(see Article 27).
20 For the definition, see ‘affiliated entity’ footnote (Article 14.1).21 For the definition, see Article 2.1(3) of the Rules for Participation Regulation No 1290/2013: ‘associated country’
means a third country which is party to an international agreement with the Union, as identified in Article 7 ofHorizon 2020 Framework Programme Regulation No 1291/2013. Article 7 sets out the conditions for association ofnon-EU countries to Horizon 2020.
44
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The joint owners must agree (in writing) on the allocation and terms of exercise of their joint ownership(‘joint ownership agreement’), to ensure compliance with their obligations under this Agreement.
Unless otherwise agreed in the joint ownership agreement, each joint owner may grant non-exclusivelicences to third parties to exploit jointly-owned results (without any right to sub-license), if the otherjoint owners are given:
(a) at least 45 days advance notice and
(b) fair and reasonable compensation.
Once the results have been generated, joint owners may agree (in writing) to apply another regimethan joint ownership (such as, for instance, transfer to a single owner (see Article 30) with accessrights for the others).
26.3 Rights of third parties (including personnel)
If third parties (including personnel) may claim rights to the results, the beneficiary concerned mustensure that it complies with its obligations under the Agreement.
If a third party generates results, the beneficiary concerned must obtain all necessary rights (transfer,licences or other) from the third party, in order to be able to respect its obligations as if those resultswere generated by the beneficiary itself.
If obtaining the rights is impossible, the beneficiary must refrain from using the third party to generatethe results.
26.4 EU ownership, to protect results
26.4.1 The EU may — with the consent of the beneficiary concerned — assume ownership of resultsto protect them, if a beneficiary intends — up to four years after the period set out in Article 3 — todisseminate its results without protecting them, except in any of the following cases:
(a) the lack of protection is because protecting the results is not possible, reasonable or justified(given the circumstances);
(b) the lack of protection is because there is a lack of potential for commercial or industrialexploitation, or
(c) the beneficiary intends to transfer the results to another beneficiary or third party establishedin an EU Member State or associated country, which will protect them.
Before the results are disseminated and unless any of the cases above under Points (a), (b) or (c)applies, the beneficiary must formally notify the Commission and at the same time inform it of anyreasons for refusing consent. The beneficiary may refuse consent only if it can show that its legitimateinterests would suffer significant harm.
If the Commission decides to assume ownership, it will formally notify the beneficiary concernedwithin 45 days of receiving notification.
No dissemination relating to these results may take place before the end of this period or, if theCommission takes a positive decision, until it has taken the necessary steps to protect the results.
45
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
26.4.2 The EU may — with the consent of the beneficiary concerned — assume ownership of resultsto protect them, if a beneficiary intends — up to four years after the period set out in Article 3 — tostop protecting them or not to seek an extension of protection, except in any of the following cases:
(a) the protection is stopped because of a lack of potential for commercial or industrial exploitation;
(b) an extension would not be justified given the circumstances.
A beneficiary that intends to stop protecting results or not seek an extension must — unless any ofthe cases above under Points (a) or (b) applies — formally notify the Commission at least 60 daysbefore the protection lapses or its extension is no longer possible and at the same time inform it of anyreasons for refusing consent. The beneficiary may refuse consent only if it can show that its legitimateinterests would suffer significant harm.
If the Commission decides to assume ownership, it will formally notify the beneficiary concernedwithin 45 days of receiving notification.
26.5 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43).
Such breaches may also lead to the any of the other measures described in Chapter 6.
ARTICLE 27 — PROTECTION OF RESULTS — VISIBILITY OF EU FUNDING
27.1 Obligation to protect the results
Each beneficiary must examine the possibility of protecting its results and must adequately protectthem — for an appropriate period and with appropriate territorial coverage — if:
(a) the results can reasonably be expected to be commercially or industrially exploited and
(b) protecting them is possible, reasonable and justified (given the circumstances).
When deciding on protection, the beneficiary must consider its own legitimate interests and thelegitimate interests (especially commercial) of the other beneficiaries.
27.2 EU ownership, to protect the results
If a beneficiary intends not to protect its results, to stop protecting them or not seek an extension ofprotection, the EU may — under certain conditions (see Article 26.4) — assume ownership to ensuretheir (continued) protection.
27.3 Information on EU funding
Applications for protection of results (including patent applications) filed by or on behalf of abeneficiary must — unless the Commission requests or agrees otherwise or unless it is impossible— include the following:
“The project leading to this application has received funding from the European Union’s Horizon 2020research and innovation programme under grant agreement No 875209”.
46
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
27.4 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43).
Such a breach may also lead to any of the other measures described in Chapter 6.
ARTICLE 28 — EXPLOITATION OF RESULTS
28.1 Obligation to exploit the results
Each beneficiary must — up to four years after the period set out in Article 3 — take measures aimingto ensure ‘exploitation’ of its results (either directly or indirectly, in particular through transfer orlicensing; see Article 30) by:
(a) using them in further research activities (outside the action);
(b) developing, creating or marketing a product or process;
(c) creating and providing a service, or
(d) using them in standardisation activities.
This does not change the security obligations in Article 37, which still apply.
28.2 Results that could contribute to European or international standards — Information onEU funding
If results are incorporated in a standard, the beneficiary concerned must — unless the Commissionrequests or agrees otherwise or unless it is impossible — ask the standardisation body to include thefollowing statement in (information related to) the standard:
“Results incorporated in this standard received funding from the European Union’s Horizon 2020 researchand innovation programme under grant agreement No 875209”.
28.3 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced inaccordance with Article 43.
Such a breach may also lead to any of the other measures described in Chapter 6.
ARTICLE 29 — DISSEMINATION OF RESULTS — OPEN ACCESS — VISIBILITY OFEU FUNDING
29.1 Obligation to disseminate results
Unless it goes against their legitimate interests, each beneficiary must — as soon as possible —‘disseminate’ its results by disclosing them to the public by appropriate means (other than thoseresulting from protecting or exploiting the results), including in scientific publications (in anymedium).
47
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
This does not change the obligation to protect results in Article 27, the confidentiality obligations inArticle 36, the security obligations in Article 37 or the obligations to protect personal data in Article 39,all of which still apply.
A beneficiary that intends to disseminate its results must give advance notice to the other beneficiariesof — unless agreed otherwise — at least 45 days, together with sufficient information on the resultsit will disseminate.
Any other beneficiary may object within — unless agreed otherwise — 30 days of receivingnotification, if it can show that its legitimate interests in relation to the results or background wouldbe significantly harmed. In such cases, the dissemination may not take place unless appropriate stepsare taken to safeguard these legitimate interests.
If a beneficiary intends not to protect its results, it may — under certain conditions (see Article 26.4.1)— need to formally notify the Commission before dissemination takes place.
29.2 Open access to scientific publications
Each beneficiary must ensure open access (free of charge online access for any user) to allpeer-reviewed scientific publications relating to its results.
In particular, it must:
(a) as soon as possible and at the latest on publication, deposit a machine-readable electroniccopy of the published version or final peer-reviewed manuscript accepted for publication in arepository for scientific publications;
Moreover, the beneficiary must aim to deposit at the same time the research data needed tovalidate the results presented in the deposited scientific publications.
(b) ensure open access to the deposited publication — via the repository — at the latest:
(i) on publication, if an electronic version is available for free via the publisher, or
(ii) within six months of publication (twelve months for publications in the social sciencesand humanities) in any other case.
(c) ensure open access — via the repository — to the bibliographic metadata that identify thedeposited publication.
The bibliographic metadata must be in a standard format and must include all of the following:
- the terms “European Union (EU)” and “Horizon 2020”;
- the name of the action, acronym and grant number;
- the publication date, and length of embargo period if applicable, and
- a persistent identifier.
29.3 Open access to research data
Regarding the digital research data generated in the action (‘data’), the beneficiaries must:
48
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
(a) deposit in a research data repository and take measures to make it possible for third parties toaccess, mine, exploit, reproduce and disseminate — free of charge for any user — the following:
(i) the data, including associated metadata, needed to validate the results presented inscientific publications, as soon as possible;
(ii) not applicable;
(iii) other data, including associated metadata, as specified and within the deadlines laid downin the ‘data management plan’ (see Annex 1);
(b) provide information — via the repository — about tools and instruments at the disposal of thebeneficiaries and necessary for validating the results (and — where possible — provide thetools and instruments themselves).
This does not change the obligation to protect results in Article 27, the confidentiality obligations inArticle 36, the security obligations in Article 37 or the obligations to protect personal data in Article 39,all of which still apply.
As an exception, the beneficiaries do not have to ensure open access to specific parts of their researchdata under Point (a)(i) and (iii), if the achievement of the action's main objective (as described inAnnex 1) would be jeopardised by making those specific parts of the research data openly accessible.In this case, the data management plan must contain the reasons for not giving access.
29.4 Information on EU funding — Obligation and right to use the EU emblem
Unless the Commission requests or agrees otherwise or unless it is impossible, any dissemination ofresults (in any form, including electronic) must:
(a) display the EU emblem and
(b) include the following text:
“This project has received funding from the European Union’s Horizon 2020 research and innovationprogramme under grant agreement No 875209”.
When displayed together with another logo, the EU emblem must have appropriate prominence.
For the purposes of their obligations under this Article, the beneficiaries may use the EU emblemwithout first obtaining approval from the Commission.
This does not however give them the right to exclusive use.
Moreover, they may not appropriate the EU emblem or any similar trademark or logo, either byregistration or by any other means.
29.5 Disclaimer excluding Commission responsibility
Any dissemination of results must indicate that it reflects only the author's view and that theCommission is not responsible for any use that may be made of the information it contains.
29.6 Consequences of non-compliance
49
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43).
Such a breach may also lead to any of the other measures described in Chapter 6.
ARTICLE 30 — TRANSFER AND LICENSING OF RESULTS
30.1 Transfer of ownership
Each beneficiary may transfer ownership of its results.
It must however ensure that its obligations under Articles 26.2, 26.4, 27, 28, 29, 30 and 31 also applyto the new owner and that this owner has the obligation to pass them on in any subsequent transfer.
This does not change the security obligations in Article 37, which still apply.
Unless agreed otherwise (in writing) for specifically-identified third parties or unless impossible underapplicable EU and national laws on mergers and acquisitions, a beneficiary that intends to transferownership of results must give at least 45 days advance notice (or less if agreed in writing) to theother beneficiaries that still have (or still may request) access rights to the results. This notificationmust include sufficient information on the new owner to enable any beneficiary concerned to assessthe effects on its access rights.
Unless agreed otherwise (in writing) for specifically-identified third parties, any other beneficiarymay object within 30 days of receiving notification (or less if agreed in writing), if it can show thatthe transfer would adversely affect its access rights. In this case, the transfer may not take place untilagreement has been reached between the beneficiaries concerned.
30.2 Granting licenses
Each beneficiary may grant licences to its results (or otherwise give the right to exploit them), if:
(a) this does not impede the access rights under Article 31 and
(b) not applicable.
In addition to Points (a) and (b), exclusive licences for results may be granted only if all the otherbeneficiaries concerned have waived their access rights (see Article 31.1).
This does not change the dissemination obligations in Article 29 or security obligations in Article 37,which still apply.
30.3 Commission right to object to transfers or licensing
Not applicable
30.4 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43).
Such a breach may also lead to any of the other measures described in Chapter 6.
50
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
ARTICLE 31 — ACCESS RIGHTS TO RESULTS
31.1 Exercise of access rights — Waiving of access rights — No sub-licensing
The conditions set out in Article 25.1 apply.
The obligations set out in this Article do not change the security obligations in Article 37, which stillapply.
31.2 Access rights for other beneficiaries, for implementing their own tasks under the action
The beneficiaries must give each other access — on a royalty-free basis — to results needed forimplementing their own tasks under the action.
31.3 Access rights for other beneficiaries, for exploiting their own results
The beneficiaries must give each other — under fair and reasonable conditions (see Article 25.3) —access to results needed for exploiting their own results.
Requests for access may be made — unless agreed otherwise — up to one year after the period setout in Article 3.
31.4 Access rights of affiliated entities
Unless agreed otherwise in the consortium agreement, access to results must also be given — underfair and reasonable conditions (Article 25.3) — to affiliated entities established in an EU MemberState or associated country, if this is needed for those entities to exploit the results generated by thebeneficiaries to which they are affiliated.
Unless agreed otherwise (see above; Article 31.1), the affiliated entity concerned must make any suchrequest directly to the beneficiary that owns the results.
Requests for access may be made — unless agreed otherwise — up to one year after the period setout in Article 3.
31.5 Access rights for the EU institutions, bodies, offices or agencies and EU Member States
The beneficiaries must give access to their results — on a royalty-free basis — to EU institutions,bodies, offices or agencies, for developing, implementing or monitoring EU policies or programmes.
Such access rights are limited to non-commercial and non-competitive use.
This does not change the right to use any material, document or information received from thebeneficiaries for communication and publicising activities (see Article 38.2).
31.6 Access rights for third parties
Not applicable
31.7 Consequences of non-compliance
51
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43).
Such breaches may also lead to any of the other measures described in Chapter 6.
SECTION 4 OTHER RIGHTS AND OBLIGATIONS
ARTICLE 32 — RECRUITMENT AND WORKING CONDITIONS FOR RESEARCHERS
32.1 Obligation to take measures to implement the European Charter for Researchers andCode of Conduct for the Recruitment of Researchers
The beneficiaries must take all measures to implement the principles set out in the CommissionRecommendation on the European Charter for Researchers and the Code of Conduct for theRecruitment of Researchers23, in particular regarding:
- working conditions;
- transparent recruitment processes based on merit, and
- career development.
The beneficiaries must ensure that researchers and third parties involved in the action are aware ofthem.
32.2 Consequences of non-compliance
If a beneficiary breaches its obligations under this Article, the Commission may apply any of themeasures described in Chapter 6.
ARTICLE 33 — GENDER EQUALITY
33.1 Obligation to aim for gender equality
The beneficiaries must take all measures to promote equal opportunities between men and women inthe implementation of the action. They must aim, to the extent possible, for a gender balance at alllevels of personnel assigned to the action, including at supervisory and managerial level.
33.2 Consequences of non-compliance
If a beneficiary breaches its obligations under this Article, the Commission may apply any of themeasures described in Chapter 6.
ARTICLE 34 — ETHICS AND RESEARCH INTEGRITY
34.1 Obligation to comply with ethical and research integrity principles
23 Commission Recommendation 2005/251/EC of 11 March 2005 on the European Charter for Researchers and on a Codeof Conduct for the Recruitment of Researchers (OJ L 75, 22.3.2005, p. 67).
52
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The beneficiaries must carry out the action in compliance with:
(a) ethical principles (including the highest standards of research integrity)
and
(b) applicable international, EU and national law.
Funding will not be granted for activities carried out outside the EU if they are prohibited in allMember States or for activities which destroy human embryos (for example, for obtaining stem cells).
The beneficiaries must ensure that the activities under the action have an exclusive focus on civilapplications.
The beneficiaries must ensure that the activities under the action do not:
(a) aim at human cloning for reproductive purposes;
(b) intend to modify the genetic heritage of human beings which could make such changes heritable(with the exception of research relating to cancer treatment of the gonads, which may befinanced), or
(c) intend to create human embryos solely for the purpose of research or for the purpose of stemcell procurement, including by means of somatic cell nuclear transfer.
In addition, the beneficiaries must respect the fundamental principle of research integrity — as setout, for instance, in the European Code of Conduct for Research Integrity24.
This implies compliance with the following fundamental principles:
- reliability in ensuring the quality of research reflected in the design, the methodology, theanalysis and the use of resources;
- honesty in developing, undertaking, reviewing, reporting and communicating research in atransparent, fair and unbiased way;
- respect for colleagues, research participants, society, ecosystems, cultural heritage and theenvironment;
- accountability for the research from idea to publication, for its management and organisation,for training, supervision and mentoring, and for its wider impacts
and means that beneficiaries must ensure that persons carrying out research tasks follow the goodresearch practices and refrain from the research integrity violations described in this Code.
This does not change the other obligations under this Agreement or obligations under applicableinternational, EU or national law, all of which still apply.
34.2 Activities raising ethical issues
24 European Code of Conduct for Research Integrity of ALLEA (All European Academies)http://ec.europa.eu/research/participants/data/ref/h2020/other/hi/h2020-ethics_code-of-conduct_en.pdf
53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
Activities raising ethical issues must comply with the ‘ethics requirements’ set out as deliverablesin Annex 1.
Before the beginning of an activity raising an ethical issue, each beneficiary must have obtained:
(a) any ethics committee opinion required under national law and
(b) any notification or authorisation for activities raising ethical issues required under nationaland/or European law
needed for implementing the action tasks in question.
The documents must be kept on file and be submitted upon request by the coordinator to theCommission (see Article 52). If they are not in English, they must be submitted together withan English summary, which shows that the action tasks in question are covered and includes theconclusions of the committee or authority concerned (if available).
34.3 Activities involving human embryos or human embryonic stem cells
Activities involving research on human embryos or human embryonic stem cells may be carried out,in addition to Article 34.1, only if:
- they are set out in Annex 1 or
- the coordinator has obtained explicit approval (in writing) from the Commission (seeArticle 52).
34.4 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43) and the Agreement or participation of the beneficiary may be terminated (see Article 50).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 35 — CONFLICT OF INTERESTS
35.1 Obligation to avoid a conflict of interests
The beneficiaries must take all measures to prevent any situation where the impartial and objectiveimplementation of the action is compromised for reasons involving economic interest, political ornational affinity, family or emotional ties or any other shared interest (‘conflict of interests’).
They must formally notify to the Commission without delay any situation constituting or likely tolead to a conflict of interests and immediately take all the necessary steps to rectify this situation.
The Commission may verify that the measures taken are appropriate and may require additionalmeasures to be taken by a specified deadline.
35.2 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43) and the Agreement or participation of the beneficiary may be terminated (see Article 50).
54
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 36 — CONFIDENTIALITY
36.1 General obligation to maintain confidentiality
During implementation of the action and for four years after the period set out in Article 3, theparties must keep confidential any data, documents or other material (in any form) that is identifiedas confidential at the time it is disclosed (‘confidential information’).
If a beneficiary requests, the Commission may agree to keep such information confidential for anadditional period beyond the initial four years.
If information has been identified as confidential only orally, it will be considered to be confidentialonly if this is confirmed in writing within 15 days of the oral disclosure.
Unless otherwise agreed between the parties, they may use confidential information only to implementthe Agreement.
The beneficiaries may disclose confidential information to their personnel or third parties involvedin the action only if they:
(a) need to know to implement the Agreement and
(b) are bound by an obligation of confidentiality.
This does not change the security obligations in Article 37, which still apply.
The Commission may disclose confidential information to its staff, other EU institutions and bodies.It may disclose confidential information to third parties, if:
(a) this is necessary to implement the Agreement or safeguard the EU's financial interests and
(b) the recipients of the information are bound by an obligation of confidentiality.
Under the conditions set out in Article 4 of the Rules for Participation Regulation No 1290/201325,the Commission must moreover make available information on the results to other EU institutions,bodies, offices or agencies as well as Member States or associated countries.
The confidentiality obligations no longer apply if:
(a) the disclosing party agrees to release the other party;
(b) the information was already known by the recipient or is given to him without obligation ofconfidentiality by a third party that was not bound by any obligation of confidentiality;
(c) the recipient proves that the information was developed without the use of confidentialinformation;
25 Regulation (EU) No 1290/2013 of the European Parliament and of the Council of 11 December 2013 laying down therules for participation and dissemination in "Horizon 2020 - the Framework Programme for Research and Innovation(2014-2020)" (OJ L 347, 20.12.2013 p.81).
55
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
(d) the information becomes generally and publicly available, without breaching anyconfidentiality obligation, or
(e) the disclosure of the information is required by EU or national law.
36.2 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 37 — SECURITY-RELATED OBLIGATIONS
37.1 Results with a security recommendation
Not applicable
37.2 Classified information
Not applicable
37.3 Activities involving dual-use goods or dangerous materials and substances
Not applicable
37.4 Consequences of non-compliance
Not applicable
ARTICLE 38 — PROMOTING THE ACTION — VISIBILITY OF EU FUNDING
38.1 Communication activities by beneficiaries
38.1.1 Obligation to promote the action and its results
The beneficiaries must promote the action and its results, by providing targeted information to multipleaudiences (including the media and the public) in a strategic and effective manner.
This does not change the dissemination obligations in Article 29, the confidentiality obligations inArticle 36 or the security obligations in Article 37, all of which still apply.
Before engaging in a communication activity expected to have a major media impact, the beneficiariesmust inform the Commission (see Article 52).
38.1.2 Information on EU funding — Obligation and right to use the EU emblem
Unless the Commission requests or agrees otherwise or unless it is impossible, any communicationactivity related to the action (including in electronic form, via social media, etc.) and anyinfrastructure, equipment and major results funded by the grant must:
(a) display the EU emblem and
56
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
(b) include the following text:
For communication activities:
“This project has received funding from the European Union’s Horizon 2020 research and innovationprogramme under grant agreement No 875209”.
For infrastructure, equipment and major results:
“This [infrastructure][equipment][insert type of result] is part of a project that has received fundingfrom the European Union’s Horizon 2020 research and innovation programme under grant agreementNo 875209”.
When displayed together with another logo, the EU emblem must have appropriate prominence.
For the purposes of their obligations under this Article, the beneficiaries may use the EU emblemwithout first obtaining approval from the Commission.
This does not, however, give them the right to exclusive use.
Moreover, they may not appropriate the EU emblem or any similar trademark or logo, either byregistration or by any other means.
38.1.3 Disclaimer excluding Commission responsibility
Any communication activity related to the action must indicate that it reflects only the author's viewand that the Commission is not responsible for any use that may be made of the information it contains.
38.2 Communication activities by the Commission
38.2.1 Right to use beneficiaries’ materials, documents or information
The Commission may use, for its communication and publicising activities, information relatingto the action, documents notably summaries for publication and public deliverables as well as anyother material, such as pictures or audio-visual material received from any beneficiary (including inelectronic form).
This does not change the confidentiality obligations in Article 36 and the security obligations inArticle 37, all of which still apply.
If the Commission’s use of these materials, documents or information would risk compromisinglegitimate interests, the beneficiary concerned may request the Commission not to use it (seeArticle 52).
The right to use a beneficiary’s materials, documents and information includes:
(a) use for its own purposes (in particular, making them available to persons working for theCommission or any other EU institution, body, office or agency or body or institutions in EUMember States; and copying or reproducing them in whole or in part, in unlimited numbers);
(b) distribution to the public (in particular, publication as hard copies and in electronic or digitalformat, publication on the internet, as a downloadable or non-downloadable file, broadcastingby any channel, public display or presentation, communicating through press informationservices, or inclusion in widely accessible databases or indexes);
57
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
(c) editing or redrafting for communication and publicising activities (including shortening,summarising, inserting other elements (such as meta-data, legends, other graphic, visual, audioor text elements), extracting parts (e.g. audio or video files), dividing into parts, use in acompilation);
(d) translation;
(e) giving access in response to individual requests under Regulation No 1049/200127, withoutthe right to reproduce or exploit;
(f) storage in paper, electronic or other form;
(g) archiving, in line with applicable document-management rules, and
(h) the right to authorise third parties to act on its behalf or sub-license the modes of use set outin Points (b), (c), (d) and (f) to third parties if needed for the communication and publicisingactivities of the Commission.
If the right of use is subject to rights of a third party (including personnel of the beneficiary), thebeneficiary must ensure that it complies with its obligations under this Agreement (in particular, byobtaining the necessary approval from the third parties concerned).
Where applicable (and if provided by the beneficiaries), the Commission will insert the followinginformation:
“© – [year] – [name of the copyright owner]. All rights reserved. Licensed to the European Union (EU)under conditions.”
38.3 Consequences of non-compliance
If a beneficiary breaches any of its obligations under this Article, the grant may be reduced (seeArticle 43).
Such breaches may also lead to any of the other measures described in Chapter 6.
ARTICLE 39 — PROCESSING OF PERSONAL DATA
39.1 Processing of personal data by the Commission
Any personal data under the Agreement will be processed by the Commission under Regulation No45/200128 and according to the ‘notifications of the processing operations’ to the Data ProtectionOfficer (DPO) of the Commission (publicly accessible in the DPO register).
Such data will be processed by the ‘data controller’ of the Commission for the purposes ofimplementing, managing and monitoring the Agreement or protecting the financial interests of theEU or Euratom (including checks, reviews, audits and investigations; see Article 22).
27 Regulation (EC) No 1049/2001 of the European Parliament and of the Council of 30 May 2001 regarding public accessto European Parliament, Council and Commission documents, OJ L 145, 31.5.2001, p. 43.
28 Regulation (EC) No 45/2001 of the European Parliament and of the Council of 18 December 2000 on the protectionof individuals with regard to the processing of personal data by the Community institutions and bodies and on the freemovement of such data (OJ L 8, 12.01.2001, p. 1).
58
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The persons whose personal data are processed have the right to access and correct their own personaldata. For this purpose, they must send any queries about the processing of their personal data to thedata controller, via the contact point indicated in the privacy statement(s) that are published on theCommission websites.
They also have the right to have recourse at any time to the European Data Protection Supervisor(EDPS).
39.2 Processing of personal data by the beneficiaries
The beneficiaries must process personal data under the Agreement in compliance with applicable EUand national law on data protection (including authorisations or notification requirements).
The beneficiaries may grant their personnel access only to data that is strictly necessary forimplementing, managing and monitoring the Agreement.
The beneficiaries must inform the personnel whose personal data are collected and processed by theCommission. For this purpose, they must provide them with the privacy statement(s) (see above),before transmitting their data to the Commission.
39.3 Consequences of non-compliance
If a beneficiary breaches any of its obligations under Article 39.2, the Commission may apply any ofthe measures described in Chapter 6.
ARTICLE 40 — ASSIGNMENTS OF CLAIMS FOR PAYMENT AGAINST THECOMMISSION
The beneficiaries may not assign any of their claims for payment against the Commission to anythird party, except if approved by the Commission on the basis of a reasoned, written request by thecoordinator (on behalf of the beneficiary concerned).
If the Commission has not accepted the assignment or the terms of it are not observed, the assignmentwill have no effect on it.
In no circumstances will an assignment release the beneficiaries from their obligations towards theCommission.
CHAPTER 5 DIVISION OF BENEFICIARIES’ ROLES AND RESPONSIBILITIES— RELATIONSHIP WITH COMPLEMENTARY BENEFICIARIES —RELATIONSHIP WITH PARTNERS OF A JOINT ACTION
ARTICLE 41 — DIVISION OF BENEFICIARIES’ ROLES AND RESPONSIBILITIES— RELATIONSHIP WITH COMPLEMENTARY BENEFICIARIES —RELATIONSHIP WITH PARTNERS OF A JOINT ACTION
41.1 Roles and responsibility towards the Commission
The beneficiaries have full responsibility for implementing the action and complying with theAgreement.
59
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The beneficiaries are jointly and severally liable for the technical implementation of the action asdescribed in Annex 1. If a beneficiary fails to implement its part of the action, the other beneficiariesbecome responsible for implementing this part (without being entitled to any additional EU fundingfor doing so), unless the Commission expressly relieves them of this obligation.
The financial responsibility of each beneficiary is governed by Article 44.
41.2 Internal division of roles and responsibilities
The internal roles and responsibilities of the beneficiaries are divided as follows:
(a) Each beneficiary must:
(i) keep information stored in the Participant Portal Beneficiary Register (via the electronicexchange system) up to date (see Article 17);
(ii) inform the coordinator immediately of any events or circumstances likely to affectsignificantly or delay the implementation of the action (see Article 17);
(iii) submit to the coordinator in good time:
- individual financial statements for itself and its linked third parties and, if required,certificates on the financial statements (see Article 20);
- the data needed to draw up the technical reports (see Article 20);
- ethics committee opinions and notifications or authorisations for activities raisingethical issues (see Article 34);
- any other documents or information required by the Commission under the Agreement,unless the Agreement requires the beneficiary to submit this information directly to theCommission.
(b) The coordinator must:
(i) monitor that the action is implemented properly (see Article 7);
(ii) act as the intermediary for all communications between the beneficiaries and theCommission (in particular, providing the Commission with the information described inArticle 17), unless the Agreement specifies otherwise;
(iii) request and review any documents or information required by the Commission and verifytheir completeness and correctness before passing them on to the Commission;
(iv) submit the deliverables and reports to the Commission (see Articles 19 and 20);
(v) ensure that all payments are made to the other beneficiaries without unjustified delay (seeArticle 21);
(vi) inform the Commission of the amounts paid to each beneficiary, when required under theAgreement (see Articles 44 and 50) or requested by the Commission.
60
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The coordinator may not delegate or subcontract the above-mentioned tasks to any otherbeneficiary or third party (including linked third parties).
41.3 Internal arrangements between beneficiaries — Consortium agreement
The beneficiaries must have internal arrangements regarding their operation and co-ordination toensure that the action is implemented properly. These internal arrangements must be set out in a written‘consortium agreement’ between the beneficiaries, which may cover:
- internal organisation of the consortium;
- management of access to the electronic exchange system;
- distribution of EU funding;
- additional rules on rights and obligations related to background and results (including whetheraccess rights remain or not, if a beneficiary is in breach of its obligations) (see Section 3 ofChapter 4);
- settlement of internal disputes;
- liability, indemnification and confidentiality arrangements between the beneficiaries.
The consortium agreement must not contain any provision contrary to the Agreement.
41.4 Relationship with complementary beneficiaries — Collaboration agreement
Not applicable
41.5 Relationship with partners of a joint action — Coordination agreement
Not applicable
CHAPTER 6 REJECTION OF COSTS — REDUCTION OF THE GRANT —RECOVERY — SANCTIONS — DAMAGES — SUSPENSION —TERMINATION — FORCE MAJEURE
SECTION 1 REJECTION OF COSTS — REDUCTION OF THE GRANT — RECOVERY— SANCTIONS
ARTICLE 42 — REJECTION OF INELIGIBLE COSTS
42.1 Conditions
The Commission will — after termination of the participation of a beneficiary, at the time ofan interim payment, at the payment of the balance or afterwards — reject any costs which areineligible (see Article 6), in particular following checks, reviews, audits or investigations (see Article22).
61
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The rejection may also be based on the extension of findings from other grants to this grant (seeArticle 22.5.2).
42.2 Ineligible costs to be rejected — Calculation — Procedure
Ineligible costs will be rejected in full.
If the rejection of costs does not lead to a recovery (see Article 44), the Commission will formallynotify the coordinator or beneficiary concerned of the rejection of costs, the amounts and the reasonswhy (if applicable, together with the notification of amounts due; see Article 21.5). The coordinatoror beneficiary concerned may — within 30 days of receiving notification — formally notify theCommission of its disagreement and the reasons why.
If the rejection of costs leads to a recovery, the Commission will follow the contradictory procedurewith pre-information letter set out in Article 44.
42.3 Effects
If the Commission rejects costs at the time of an interim payment or the payment of the balance, itwill deduct them from the total eligible costs declared, for the action, in the periodic or final summaryfinancial statement (see Articles 20.3 and 20.4). It will then calculate the interim payment or paymentof the balance as set out in Articles 21.3 or 21.4.
If the Commission rejects costs after termination of the participation of a beneficiary, it will deductthem from the costs declared by the beneficiary in the termination report and include the rejection inthe calculation after termination (see Article 50.2 and 50.3).
If the Commission — after an interim payment but before the payment of the balance — rejectscosts declared in a periodic summary financial statement, it will deduct them from the total eligiblecosts declared, for the action, in the next periodic summary financial statement or in the final summaryfinancial statement. It will then calculate the interim payment or payment of the balance as set outin Articles 21.3 or 21.4.
If the Commission rejects costs after the payment of the balance, it will deduct the amount rejectedfrom the total eligible costs declared, by the beneficiary, in the final summary financial statement. Itwill then calculate the revised final grant amount as set out in Article 5.4.
ARTICLE 43 — REDUCTION OF THE GRANT
43.1 Conditions
The Commission may — after termination of the participation of a beneficiary, at the paymentof the balance or afterwards — reduce the grant amount (see Article 5.1), if :
(a) a beneficiary (or a natural person who has the power to represent or take decisions on its behalf)has committed:
(i) substantial errors, irregularities or fraud or
(ii) serious breach of obligations under the Agreement or during the award procedure
62
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
(including improper implementation of the action, submission of false information,failure to provide required information, breach of ethical principles) or
(b) a beneficiary (or a natural person who has the power to represent or take decision on its behalf)has committed — in other EU or Euratom grants awarded to it under similar conditions —systemic or recurrent errors, irregularities, fraud or serious breach of obligations that have amaterial impact on this grant (extension of findings from other grants to this grant; seeArticle 22.5.2).
43.2 Amount to be reduced — Calculation — Procedure
The amount of the reduction will be proportionate to the seriousness of the errors, irregularities orfraud or breach of obligations.
Before reduction of the grant, the Commission will formally notify a ‘pre-information letter’ to thecoordinator or beneficiary concerned:
- informing it of its intention to reduce the grant, the amount it intends to reduce and the reasonswhy and
- inviting it to submit observations within 30 days of receiving notification.
If the Commission does not receive any observations or decides to pursue reduction despite theobservations it has received, it will formally notify confirmation of the reduction (if applicable,together with the notification of amounts due; see Article 21).
43.3 Effects
If the Commission reduces the grant after termination of the participation of a beneficiary, it willcalculate the reduced grant amount for that beneficiary and then determine the amount due to thatbeneficiary (see Article 50.2 and 50.3).
If the Commission reduces the grant at the payment of the balance, it will calculate the reduced grantamount for the action and then determine the amount due as payment of the balance (see Articles 5.3.4and 21.4).
If the Commission reduces the grant after the payment of the balance, it will calculate the revisedfinal grant amount for the beneficiary concerned (see Article 5.4). If the revised final grant amountfor the beneficiary concerned is lower than its share of the final grant amount, the Commission willrecover the difference (see Article 44).
ARTICLE 44 — RECOVERY OF UNDUE AMOUNTS
44.1 Amount to be recovered — Calculation — Procedure
The Commission will — after termination of the participation of a beneficiary, at the paymentof the balance or afterwards — claim back any amount that was paid, but is not due under theAgreement.
Each beneficiary’s financial responsibility in case of recovery is limited to its own debt (including
63
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
undue amounts paid by the Commission for costs declared by its linked third parties), except for theamount retained for the Guarantee Fund (see Article 21.4).
44.1.1 Recovery after termination of a beneficiary’s participation
If recovery takes place after termination of a beneficiary’s participation (including the coordinator), theCommission will claim back the undue amount from the beneficiary concerned, by formally notifyingit a debit note (see Article 50.2 and 50.3). This note will specify the amount to be recovered, the termsand the date for payment.
If payment is not made by the date specified in the debit note, the Commission will recover theamount:
(a) by ‘offsetting’ it — without the beneficiary’s consent — against any amounts owed to thebeneficiary concerned by the Commission or an executive agency (from the EU or Euratombudget).
In exceptional circumstances, to safeguard the EU’s financial interests, the Commission mayoffset before the payment date specified in the debit note;
(b) not applicable;
(c) by taking legal action (see Article 57) or by adopting an enforceable decision underArticle 299 of the Treaty on the Functioning of the EU (TFEU) and Article 79(2) of theFinancial regulation No 966/2012.
If payment is not made by the date specified in the debit note, the amount to be recovered (see above)will be increased by late-payment interest at the rate set out in Article 21.11, from the day followingthe payment date in the debit note, up to and including the date the Commission receives full paymentof the amount.
Partial payments will be first credited against expenses, charges and late-payment interest and thenagainst the principal.
Bank charges incurred in the recovery process will be borne by the beneficiary, unlessDirective 2007/64/EC29 applies.
44.1.2 Recovery at payment of the balance
If the payment of the balance takes the form of a recovery (see Article 21.4), the Commission willformally notify a ‘pre-information letter’ to the coordinator:
- informing it of its intention to recover, the amount due as the balance and the reasons why;
- specifying that it intends to deduct the amount to be recovered from the amount retained forthe Guarantee Fund;
- requesting the coordinator to submit a report on the distribution of payments to the beneficiarieswithin 30 days of receiving notification, and
29 Directive 2007/64/EC of the European Parliament and of the Council of 13 November 2007 on payment servicesin the internal market amending Directives 97/7/EC, 2002/65/EC, 2005/60/EC and 2006/48/EC and repealingDirective 97/5/EC (OJ L 319, 05.12.2007, p. 1).
64
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
- inviting the coordinator to submit observations within 30 days of receiving notification.
If no observations are submitted or the Commission decides to pursue recovery despite theobservations it has received, it will confirm recovery (together with the notification of amounts due;see Article 21.5) and:
- pay the difference between the amount to be recovered and the amount retained for theGuarantee Fund, if the difference is positive or
- formally notify to the coordinator a debit note for the difference between the amount to berecovered and the amount retained for the Guarantee Fund, if the difference is negative. Thisnote will also specify the terms and the date for payment.
If the coordinator does not repay the Commission by the date in the debit note and has not submittedthe report on the distribution of payments: the Commission will recover the amount set out in thedebit note from the coordinator (see below).
If the coordinator does not repay the Commission by the date in the debit note, but has submitted thereport on the distribution of payments: the Commission will:
(a) identify the beneficiaries for which the amount calculated as follows is negative:
{{{{beneficiary’s costs declared in the final summary financial statement and approved by theCommission multiplied by the reimbursement rate set out in Article 5.2 for the beneficiary concerned
plus
its linked third parties’ costs declared in the final summary financial statement and approved by theCommission multiplied by the reimbursement rate set out in Article 5.2 for each linked third partyconcerned}
divided by
the EU contribution for the action calculated according to Article 5.3.1}multiplied by
the final grant amount (see Article 5.3)},
minus
{pre-financing and interim payments received by the beneficiary}}.
(b) formally notify to each beneficiary identified according to point (a) a debit note specifying theterms and date for payment. The amount of the debit note is calculated as follows:
{{amount calculated according to point (a) for the beneficiary concerned
divided by
the sum of the amounts calculated according to point (a) for all the beneficiaries identified accordingto point (a)}
multiplied by
the amount set out in the debit note formally notified to the coordinator}.
65
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
If payment is not made by the date specified in the debit note, the Commission will recover theamount:
(a) by offsetting it — without the beneficiary’s consent — against any amounts owed to thebeneficiary concerned by the Commission or an executive agency (from the EU or Euratombudget).
In exceptional circumstances, to safeguard the EU’s financial interests, the Commission mayoffset before the payment date specified in the debit note;
(b) by drawing on the Guarantee Fund. The Commission will formally notify the beneficiaryconcerned the debit note on behalf of the Guarantee Fund and recover the amount:
(i) not applicable;
(ii) by taking legal action (see Article 57) or by adopting an enforceable decision underArticle 299 of the Treaty on the Functioning of the EU (TFEU) and Article 79(2) of theFinancial Regulation No 966/2012.
If payment is not made by the date in the debit note, the amount to be recovered (see above) will beincreased by late-payment interest at the rate set out in Article 21.11, from the day following thepayment date in the debit note, up to and including the date the Commission receives full paymentof the amount.
Partial payments will be first credited against expenses, charges and late-payment interest and thenagainst the principal.
Bank charges incurred in the recovery process will be borne by the beneficiary, unlessDirective 2007/64/EC applies.
44.1.3 Recovery of amounts after payment of the balance
If, for a beneficiary, the revised final grant amount (see Article 5.4) is lower than its share of the finalgrant amount, it must repay the difference to the Commission.
The beneficiary’s share of the final grant amount is calculated as follows:
{{{beneficiary’s costs declared in the final summary financial statement and approved by the Commissionmultiplied by the reimbursement rate set out in Article 5.2 for the beneficiary concerned
plus
its linked third parties’ costs declared in the final summary financial statement and approved by the Commissionmultiplied by the reimbursement rate set out in Article 5.2 for each linked third party concerned}
divided by
the EU contribution for the action calculated according to Article 5.3.1}multiplied by
the final grant amount (see Article 5.3)}.
If the coordinator has not distributed amounts received (see Article 21.7), the Commission will alsorecover these amounts.
66
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The Commission will formally notify a pre-information letter to the beneficiary concerned:
- informing it of its intention to recover, the due amount and the reasons why and
- inviting it to submit observations within 30 days of receiving notification.
If no observations are submitted or the Commission decides to pursue recovery despite theobservations it has received, it will confirm the amount to be recovered and formally notify to thebeneficiary concerned a debit note. This note will also specify the terms and the date for payment.
If payment is not made by the date specified in the debit note, the Commission will recover theamount:
(a) by offsetting it — without the beneficiary’s consent — against any amounts owed to thebeneficiary concerned by the Commission or an executive agency (from the EU or Euratombudget).
In exceptional circumstances, to safeguard the EU’s financial interests, the Commission mayoffset before the payment date specified in the debit note;
(b) by drawing on the Guarantee Fund. The Commission will formally notify the beneficiaryconcerned the debit note on behalf of the Guarantee Fund and recover the amount:
(i) not applicable;
(ii) by taking legal action (see Article 57) or by adopting an enforceable decision underArticle 299 of the Treaty on the Functioning of the EU (TFEU) and Article 79(2) of theFinancial Regulation No 966/2012.
If payment is not made by the date in the debit note, the amount to be recovered (see above) will beincreased by late-payment interest at the rate set out in Article 21.11, from the day following thedate for payment in the debit note, up to and including the date the Commission receives full paymentof the amount.
Partial payments will be first credited against expenses, charges and late-payment interest and thenagainst the principal.
Bank charges incurred in the recovery process will be borne by the beneficiary, unlessDirective 2007/64/EC applies.
ARTICLE 45 — ADMINISTRATIVE SANCTIONS
In addition to contractual measures, the Commission may also adopt administrative sanctions underArticles 106 and 131(4) of the Financial Regulation No 966/2012 (i.e. exclusion from futureprocurement contracts, grants, prizes and expert contracts and/or financial penalties).
SECTION 2 LIABILITY FOR DAMAGES
ARTICLE 46 — LIABILITY FOR DAMAGES
46.1 Liability of the Commission
67
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The Commission cannot be held liable for any damage caused to the beneficiaries or to third partiesas a consequence of implementing the Agreement, including for gross negligence.
The Commission cannot be held liable for any damage caused by any of the beneficiaries or thirdparties involved in the action, as a consequence of implementing the Agreement.
46.2 Liability of the beneficiaries
Except in case of force majeure (see Article 51), the beneficiaries must compensate the Commissionfor any damage it sustains as a result of the implementation of the action or because the action wasnot implemented in full compliance with the Agreement.
SECTION 3 SUSPENSION AND TERMINATION
ARTICLE 47 — SUSPENSION OF PAYMENT DEADLINE
47.1 Conditions
The Commission may — at any moment — suspend the payment deadline (see Article 21.2 to 21.4)if a request for payment (see Article 20) cannot be approved because:
(a) it does not comply with the provisions of the Agreement (see Article 20);
(b) the technical or financial reports have not been submitted or are not complete or additionalinformation is needed, or
(c) there is doubt about the eligibility of the costs declared in the financial statements and additionalchecks, reviews, audits or investigations are necessary.
47.2 Procedure
The Commission will formally notify the coordinator of the suspension and the reasons why.
The suspension will take effect the day notification is sent by the Commission (see Article 52).
If the conditions for suspending the payment deadline are no longer met, the suspension will be lifted— and the remaining period will resume.
If the suspension exceeds two months, the coordinator may request the Commission if the suspensionwill continue.
If the payment deadline has been suspended due to the non-compliance of the technical or financialreports (see Article 20) and the revised report or statement is not submitted or was submitted but is alsorejected, the Commission may also terminate the Agreement or the participation of the beneficiary(see Article 50.3.1(l)).
ARTICLE 48 — SUSPENSION OF PAYMENTS
48.1 Conditions
68
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
The Commission may — at any moment — suspend payments, in whole or in part and interimpayments or the payment of the balance for one or more beneficiaries, if:
(a) a beneficiary (or a natural person who has the power to represent or take decision on its behalf)has committed or is suspected of having committed:
(i) substantial errors, irregularities or fraud or
(ii) serious breach of obligations under the Agreement or during the award procedure(including improper implementation of the action, submission of false information,failure to provide required information, breach of ethical principles) or
(b) a beneficiary (or a natural person who has the power to represent or take decision on its behalf)has committed — in other EU or Euratom grants awarded to it under similar conditions —systemic or recurrent errors, irregularities, fraud or serious breach of obligations that have amaterial impact on this grant (extension of findings from other grants to this grant; seeArticle 22.5.2).
If payments are suspended for one or more beneficiaries, the Commission will make partial payment(s)for the part(s) not suspended. If suspension concerns the payment of the balance, — once suspensionis lifted — the payment or the recovery of the amount(s) concerned will be considered the paymentof the balance that closes the action.
48.2 Procedure
Before suspending payments, the Commission will formally notify the coordinator or beneficiaryconcerned:
- informing it of its intention to suspend payments and the reasons why and
- inviting it to submit observations within 30 days of receiving notification.
If the Commission does not receive observations or decides to pursue the procedure despite theobservations it has received, it will formally notify confirmation of the suspension. Otherwise, it willformally notify that the suspension procedure is not continued.
The suspension will take effect the day the confirmation notification is sent by the Commission.
If the conditions for resuming payments are met, the suspension will be lifted. The Commission willformally notify the coordinator or beneficiary concerned.
During the suspension, the periodic report(s) for all reporting periods except the last one (seeArticle 20.3), must not contain any individual financial statements from the beneficiary concernedand its linked third parties. The coordinator must include them in the next periodic report after thesuspension is lifted or — if suspension is not lifted before the end of the action — in the last periodicreport.
The beneficiaries may suspend implementation of the action (see Article 49.1) or terminate theAgreement or the participation of the beneficiary concerned (see Article 50.1 and 50.2).
ARTICLE 49 — SUSPENSION OF THE ACTION IMPLEMENTATION
69
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
49.1 Suspension of the action implementation, by the beneficiaries
49.1.1 Conditions
The beneficiaries may suspend implementation of the action or any part of it, if exceptionalcircumstances — in particular force majeure (see Article 51) — make implementation impossible orexcessively difficult.
49.1.2 Procedure
The coordinator must immediately formally notify to the Commission the suspension (see Article 52),stating:
- the reasons why and
- the expected date of resumption.
The suspension will take effect the day this notification is received by the Commission.
Once circumstances allow for implementation to resume, the coordinator must immediately formallynotify the Commission and request an amendment of the Agreement to set the date on which theaction will be resumed, extend the duration of the action and make other changes necessary to adaptthe action to the new situation (see Article 55) — unless the Agreement or the participation of abeneficiary has been terminated (see Article 50).
The suspension will be lifted with effect from the resumption date set out in the amendment. Thisdate may be before the date on which the amendment enters into force.
Costs incurred during suspension of the action implementation are not eligible (see Article 6).
49.2 Suspension of the action implementation, by the Commission
49.2.1 Conditions
The Commission may suspend implementation of the action or any part of it, if:
(a) a beneficiary (or a natural person who has the power to represent or take decisions on its behalf)has committed or is suspected of having committed:
(i) substantial errors, irregularities or fraud or
(ii) serious breach of obligations under the Agreement or during the award procedure(including improper implementation of the action, submission of false information,failure to provide required information, breach of ethical principles);
(b) a beneficiary (or a natural person who has the power to represent or take decisions on its behalf)has committed — in other EU or Euratom grants awarded to it under similar conditions —systemic or recurrent errors, irregularities, fraud or serious breach of obligations that have amaterial impact on this grant (extension of findings from other grants to this grant; seeArticle 22.5.2), or
(c) the action is suspected of having lost its scientific or technological relevance.
70
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
49.2.2 Procedure
Before suspending implementation of the action, the Commission will formally notify the coordinatoror beneficiary concerned:
- informing it of its intention to suspend the implementation and the reasons why and
- inviting it to submit observations within 30 days of receiving notification.
If the Commission does not receive observations or decides to pursue the procedure despite theobservations it has received, it will formally notify confirmation of the suspension. Otherwise, it willformally notify that the procedure is not continued.
The suspension will take effect five days after confirmation notification is received (or on a later datespecified in the notification).
It will be lifted if the conditions for resuming implementation of the action are met.
The coordinator or beneficiary concerned will be formally notified of the lifting and the Agreementwill be amended to set the date on which the action will be resumed, extend the duration of the actionand make other changes necessary to adapt the action to the new situation (see Article 55) — unlessthe Agreement has already been terminated (see Article 50).
The suspension will be lifted with effect from the resumption date set out in the amendment. This datemay be before the date on which the amendment enters into force.
Costs incurred during suspension are not eligible (see Article 6).
The beneficiaries may not claim damages due to suspension by the Commission (see Article 46).
Suspension of the action implementation does not affect the Commission’s right to terminate theAgreement or participation of a beneficiary (see Article 50), reduce the grant or recover amountsunduly paid (see Articles 43 and 44).
ARTICLE 50 — TERMINATION OF THE AGREEMENT OR OF THE PARTICIPATIONOF ONE OR MORE BENEFICIARIES
50.1 Termination of the Agreement, by the beneficiaries
50.1.1 Conditions and procedure
The beneficiaries may terminate the Agreement.
The coordinator must formally notify termination to the Commission (see Article 52), stating:
- the reasons why and
- the date the termination will take effect. This date must be after the notification.
If no reasons are given or if the Commission considers the reasons do not justify termination, theAgreement will be considered to have been ‘terminated improperly’.
The termination will take effect on the day specified in the notification.
71
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
50.1.2 Effects
The coordinator must — within 60 days from when termination takes effect — submit:
(i) a periodic report (for the open reporting period until termination; see Article 20.3) and
(ii) the final report (see Article 20.4).
If the Commission does not receive the reports within the deadline (see above), only costs which areincluded in an approved periodic report will be taken into account.
The Commission will calculate the final grant amount (see Article 5.3) and the balance (seeArticle 21.4) on the basis of the reports submitted. Only costs incurred until termination are eligible(see Article 6). Costs relating to contracts due for execution only after termination are not eligible.
Improper termination may lead to a reduction of the grant (see Article 43).
After termination, the beneficiaries’ obligations (in particular Articles 20, 22, 23, Section 3 ofChapter 4, 36, 37, 38, 40, 42, 43 and 44) continue to apply.
50.2 Termination of the participation of one or more beneficiaries, by the beneficiaries
50.2.1 Conditions and procedure
The participation of one or more beneficiaries may be terminated by the coordinator, on request ofthe beneficiary concerned or on behalf of the other beneficiaries.
The coordinator must formally notify termination to the Commission (see Article 52) and inform thebeneficiary concerned.
If the coordinator’s participation is terminated without its agreement, the formal notification must bedone by another beneficiary (acting on behalf of the other beneficiaries).
The notification must include:
- the reasons why;
- the opinion of the beneficiary concerned (or proof that this opinion has been requested inwriting);
- the date the termination takes effect. This date must be after the notification, and
- a request for amendment (see Article 55), with a proposal for reallocation of the tasks and theestimated budget of the beneficiary concerned (see Annexes 1 and 2) and, if necessary, theaddition of one or more new beneficiaries (see Article 56). If termination takes effect after theperiod set out in Article 3, no request for amendment must be included unless the beneficiaryconcerned is the coordinator. In this case, the request for amendment must propose a newcoordinator.
If this information is not given or if the Commission considers that the reasons do not justifytermination, the participation will be considered to have been terminated improperly.
The termination will take effect on the day specified in the notification.
72
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
50.2.2 Effects
The coordinator must — within 30 days from when termination takes effect — submit:
(i) a report on the distribution of payments to the beneficiary concerned and
(ii) if termination takes effect during the period set out in Article 3, a ‘termination report’from the beneficiary concerned, for the open reporting period until termination, containingan overview of the progress of the work, an overview of the use of resources, theindividual financial statement and, if applicable, the certificate on the financial statement(see Articles 20.3 and 20.4).
The information in the termination report must also be included in the periodic report for the nextreporting period (see Article 20.3).
If the request for amendment is rejected by the Commission (because it calls into question the decisionawarding the grant or breaches the principle of equal treatment of applicants), the Agreement may beterminated according to Article 50.3.1(c).
If the request for amendment is accepted by the Commission, the Agreement is amended to introducethe necessary changes (see Article 55).
The Commission will — on the basis of the periodic reports, the termination report and the reporton the distribution of payments — calculate the amount which is due to the beneficiary and if the(pre-financing and interim) payments received by the beneficiary exceed this amount.
The amount which is due is calculated in the following steps:
Step 1 — Application of the reimbursement rate to the eligible costs
The grant amount for the beneficiary is calculated by applying the reimbursementrate(s) to the total eligible costs declared by the beneficiary and its linked third partiesin the termination report and approved by the Commission.
Only costs incurred by the beneficiary concerned until termination takes effect areeligible (see Article 6). Costs relating to contracts due for execution only aftertermination are not eligible.
Step 2 — Reduction due to substantial errors, irregularities or fraud or serious breach ofobligations
In case of a reduction (see Article 43), the Commission will calculate the reducedgrant amount for the beneficiary by deducting the amount of the reduction (calculatedin proportion to the seriousness of the errors, irregularities or fraud or breachof obligations, in accordance with Article 43.2) from the grant amount for thebeneficiary.
If the payments received exceed the amounts due:
- if termination takes effect during the period set out in Article 3 and the request foramendment is accepted, the beneficiary concerned must repay to the coordinator the amountunduly received. The Commission will formally notify the amount unduly received and
73
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
request the beneficiary concerned to repay it to the coordinator within 30 days of receivingnotification. If it does not repay the coordinator, the Commission will draw upon theGuarantee Fund to pay the coordinator and then notify a debit note on behalf of theGuarantee Fund to the beneficiary concerned (see Article 44);
- in all other cases, in particular if termination takes effect after the period set out in Article 3,the Commission will formally notify a debit note to the beneficiary concerned. If paymentis not made by the date in the debit note, the Guarantee Fund will pay to the Commission theamount due and the Commission will notify a debit note on behalf of the Guarantee Fundto the beneficiary concerned (see Article 44);
- if the beneficiary concerned is the former coordinator, it must repay the new coordinatoraccording to the procedure above, unless:
- termination takes effect after an interim payment and
- the former coordinator has not distributed amounts received as pre-financing orinterim payments (see Article 21.7).
In this case, the Commission will formally notify a debit note to the former coordinator.If payment is not made by the date in the debit note, the Guarantee Fund will pay to theCommission the amount due. The Commission will then pay the new coordinator and notifya debit note on behalf of the Guarantee Fund to the former coordinator (see Article 44).
If the payments received do not exceed the amounts due: amounts owed to the beneficiaryconcerned will be included in the next interim or final payment.
If the Commission does not receive the termination report within the deadline (see above), only costsincluded in an approved periodic report will be taken into account.
If the Commission does not receive the report on the distribution of payments within the deadline (seeabove), it will consider that:
- the coordinator did not distribute any payment to the beneficiary concerned and that
- the beneficiary concerned must not repay any amount to the coordinator.
Improper termination may lead to a reduction of the grant (see Article 43) or termination of theAgreement (see Article 50).
After termination, the concerned beneficiary’s obligations (in particular Articles 20, 22, 23, Section 3of Chapter 4, 36, 37, 38, 40, 42, 43 and 44) continue to apply.
50.3 Termination of the Agreement or the participation of one or more beneficiaries, by theCommission
50.3.1 Conditions
The Commission may terminate the Agreement or the participation of one or more beneficiaries, if:
(a) one or more beneficiaries do not accede to the Agreement (see Article 56);
(b) a change to their legal, financial, technical, organisational or ownership situation (or those
74
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
of its linked third parties) is likely to substantially affect or delay the implementation of theaction or calls into question the decision to award the grant;
(c) following termination of participation for one or more beneficiaries (see above), the necessarychanges to the Agreement would call into question the decision awarding the grant or breachthe principle of equal treatment of applicants (see Article 55);
(d) implementation of the action is prevented by force majeure (see Article 51) or suspended bythe coordinator (see Article 49.1) and either:
(i) resumption is impossible, or
(ii) the necessary changes to the Agreement would call into question the decision awardingthe grant or breach the principle of equal treatment of applicants;
(e) a beneficiary is declared bankrupt, being wound up, having its affairs administered by thecourts, has entered into an arrangement with creditors, has suspended business activities, oris subject to any other similar proceedings or procedures under national law;
(f) a beneficiary (or a natural person who has the power to represent or take decisions on itsbehalf) has been found guilty of professional misconduct, proven by any means;
(g) a beneficiary does not comply with the applicable national law on taxes and social security;
(h) the action has lost scientific or technological relevance;
(i) not applicable;
(j) not applicable;
(k) a beneficiary (or a natural person who has the power to represent or take decisions on itsbehalf) has committed fraud, corruption, or is involved in a criminal organisation, moneylaundering or any other illegal activity;
(l) a beneficiary (or a natural person who has the power to represent or take decisions on itsbehalf) has committed:
(i) substantial errors, irregularities or fraud or
(ii) serious breach of obligations under the Agreement or during the award procedure(including improper implementation of the action, submission of false information,failure to provide required information, breach of ethical principles);
(m) a beneficiary (or a natural person who has the power to represent or take decisions on itsbehalf) has committed — in other EU or Euratom grants awarded to it under similar conditions— systemic or recurrent errors, irregularities, fraud or serious breach of obligations that havea material impact on this grant (extension of findings from other grants to this grant; seeArticle 22.5.2);
(n) despite a specific request by the Commission, a beneficiary does not request — through thecoordinator — an amendment to the Agreement to end the participation of one of its linkedthird parties or international partners that is in one of the situations under points (e), (f), (g),(k), (l) or (m) and to reallocate its tasks.
75
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
50.3.2 Procedure
Before terminating the Agreement or participation of one or more beneficiaries, the Commission willformally notify the coordinator or beneficiary concerned:
- informing it of its intention to terminate and the reasons why and
- inviting it, within 30 days of receiving notification, to submit observations and — in case ofPoint (l.ii) above — to inform the Commission of the measures to ensure compliance with theobligations under the Agreement.
If the Commission does not receive observations or decides to pursue the procedure despite theobservations it has received, it will formally notify to the coordinator or beneficiary concernedconfirmation of the termination and the date it will take effect. Otherwise, it will formally notify thatthe procedure is not continued.
The termination will take effect:
- for terminations under Points (b), (c), (e), (g), (h), (j), (l.ii) and (n) above: on the day specifiedin the notification of the confirmation (see above);
- for terminations under Points (a), (d), (f), (i), (k), (l.i) and (m) above: on the day after thenotification of the confirmation is received.
50.3.3 Effects
(a) for termination of the Agreement:
The coordinator must — within 60 days from when termination takes effect — submit:
(i) a periodic report (for the last open reporting period until termination; see Article 20.3)and
(ii) a final report (see Article 20.4).
If the Agreement is terminated for breach of the obligation to submit reports (see Articles 20.8and 50.3.1(l)), the coordinator may not submit any reports after termination.
If the Commission does not receive the reports within the deadline (see above), only costswhich are included in an approved periodic report will be taken into account.
The Commission will calculate the final grant amount (see Article 5.3) and the balance (seeArticle 21.4) on the basis of the reports submitted. Only costs incurred until termination takeseffect are eligible (see Article 6). Costs relating to contracts due for execution only aftertermination are not eligible.
This does not affect the Commission’s right to reduce the grant (see Article 43) or to imposeadministrative sanctions (Article 45).
The beneficiaries may not claim damages due to termination by the Commission (seeArticle 46).
76
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
After termination, the beneficiaries’ obligations (in particular Articles 20, 22, 23, Section 3 ofChapter 4, 36, 37, 38, 40, 42, 43 and 44) continue to apply.
(b) for termination of the participation of one or more beneficiaries:
The coordinator must — within 60 days from when termination takes effect — submit:
(i) a report on the distribution of payments to the beneficiary concerned;
(ii) a request for amendment (see Article 55), with a proposal for reallocation of the tasks andestimated budget of the beneficiary concerned (see Annexes 1 and 2) and, if necessary,the addition of one or more new beneficiaries (see Article 56). If termination is notifiedafter the period set out in Article 3, no request for amendment must be submitted unlessthe beneficiary concerned is the coordinator. In this case the request for amendment mustpropose a new coordinator, and
(iii) if termination takes effect during the period set out in Article 3, a terminationreport from the beneficiary concerned, for the open reporting period until termination,containing an overview of the progress of the work, an overview of the use of resources,the individual financial statement and, if applicable, the certificate on the financialstatement (see Article 20).
The information in the termination report must also be included in the periodic report for thenext reporting period (see Article 20.3).
If the request for amendment is rejected by the Commission (because it calls into question thedecision awarding the grant or breaches the principle of equal treatment of applicants), theAgreement may be terminated according to Article 50.3.1(c).
If the request for amendment is accepted by the Commission, the Agreement is amended tointroduce the necessary changes (see Article 55).
The Commission will — on the basis of the periodic reports, the termination report and thereport on the distribution of payments — calculate the amount which is due to the beneficiaryand if the (pre-financing and interim) payments received by the beneficiary exceed this amount.
The amount which is due is calculated in the following steps:
Step 1 — Application of the reimbursement rate to the eligible costs
The grant amount for the beneficiary is calculated by applying thereimbursement rate(s) to the total eligible costs declared by the beneficiaryand its linked third parties in the termination report and approved by theCommission.
Only costs incurred by the beneficiary concerned until termination takes effectare eligible (see Article 6). Costs relating to contracts due for execution onlyafter termination are not eligible.
Step 2 — Reduction due to substantial errors, irregularities or fraud or serious breachof obligations
77
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
In case of a reduction (see Article 43), the Commission will calculatethe reduced grant amount for the beneficiary by deducting the amount ofthe reduction (calculated in proportion to the seriousness of the errors,irregularities or fraud or breach of obligations, in accordance with Article 43.2)from the grant amount for the beneficiary.
If the payments received exceed the amounts due:
- if termination takes effect during the period set out in Article 3 and the request foramendment is accepted, the beneficiary concerned must repay to the coordinator theamount unduly received. The Commission will formally notify the amount undulyreceived and request the beneficiary concerned to repay it to the coordinator within30 days of receiving notification. If it does not repay the coordinator, the Commissionwill draw upon the Guarantee Fund to pay the coordinator and then notify a debitnote on behalf of the Guarantee Fund to the beneficiary concerned (see Article 44);
- in all other cases, in particular if termination takes effect after the period set outin Article 3, the Commission will formally notify a debit note to the beneficiaryconcerned. If payment is not made by the date in the debit note, the Guarantee Fundwill pay to the Commission the amount due and the Commission will notify a debitnote on behalf of the Guarantee Fund to the beneficiary concerned (see Article 44);
- if the beneficiary concerned is the former coordinator, it must repay the newcoordinator according to the procedure above, unless:
- termination takes effect after an interim payment and
- the former coordinator has not distributed amounts received as pre-financingor interim payments (see Article 21.7).
In this case, the Commission will formally notify a debit note to the formercoordinator. If payment is not made by the date in the debit note, the Guarantee Fundwill pay to the Commission the amount due. The Commission will then pay the newcoordinator and notify a debit note on behalf of the Guarantee Fund to the formercoordinator (see Article 44).
If the payments received do not exceed the amounts due: amounts owed to the beneficiaryconcerned will be included in the next interim or final payment.
If the Commission does not receive the termination report within the deadline (see above), onlycosts included in an approved periodic report will be taken into account.
If the Commission does not receive the report on the distribution of payments within thedeadline (see above), it will consider that:
- the coordinator did not distribute any payment to the beneficiary concerned and that
- the beneficiary concerned must not repay any amount to the coordinator.
After termination, the concerned beneficiary’s obligations (in particular Articles 20, 22, 23,Section 3 of Chapter 4, 36, 37, 38, 40, 42, 43 and 44) continue to apply.
78
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
SECTION 4 FORCE MAJEURE
ARTICLE 51 — FORCE MAJEURE
‘Force majeure’ means any situation or event that:
- prevents either party from fulfilling their obligations under the Agreement,
- was unforeseeable, exceptional situation and beyond the parties’ control,
- was not due to error or negligence on their part (or on the part of third parties involved in theaction), and
- proves to be inevitable in spite of exercising all due diligence.
The following cannot be invoked as force majeure:
- any default of a service, defect in equipment or material or delays in making them available,unless they stem directly from a relevant case of force majeure,
- labour disputes or strikes, or
- financial difficulties.
Any situation constituting force majeure must be formally notified to the other party without delay,stating the nature, likely duration and foreseeable effects.
The parties must immediately take all the necessary steps to limit any damage due to force majeureand do their best to resume implementation of the action as soon as possible.
The party prevented by force majeure from fulfilling its obligations under the Agreement cannot beconsidered in breach of them.
CHAPTER 7 FINAL PROVISIONS
ARTICLE 52 — COMMUNICATION BETWEEN THE PARTIES
52.1 Form and means of communication
Communication under the Agreement (information, requests, submissions, ‘formal notifications’, etc.)must:
- be made in writing and
- bear the number of the Agreement.
All communication must be made through the Participant Portal electronic exchange system and usingthe forms and templates provided there.
If — after the payment of the balance — the Commission finds that a formal notification was not
79
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
accessed, a second formal notification will be made by registered post with proof of delivery (‘formalnotification on paper’). Deadlines will be calculated from the moment of the second notification.
Communications in the electronic exchange system must be made by persons authorised according tothe Participant Portal Terms & Conditions. For naming the authorised persons, each beneficiary musthave designated — before the signature of this Agreement — a ‘legal entity appointed representative(LEAR)’. The role and tasks of the LEAR are stipulated in his/her appointment letter (see ParticipantPortal Terms & Conditions).
If the electronic exchange system is temporarily unavailable, instructions will be given on theCommission website.
52.2 Date of communication
Communications are considered to have been made when they are sent by the sending party (i.e. onthe date and time they are sent through the electronic exchange system).
Formal notifications through the electronic exchange system are considered to have been made whenthey are received by the receiving party (i.e. on the date and time of acceptance by the receiving party,as indicated by the time stamp). A formal notification that has not been accepted within 10 days aftersending is considered to have been accepted.
Formal notifications on paper sent by registered post with proof of delivery (only after the paymentof the balance) are considered to have been made on either:
- the delivery date registered by the postal service or
- the deadline for collection at the post office.
If the electronic exchange system is temporarily unavailable, the sending party cannot be consideredin breach of its obligation to send a communication within a specified deadline.
52.3 Addresses for communication
The electronic exchange system must be accessed via the following URL:
https://ec.europa.eu/research/participants/portal/desktop/en/projects/
The Commission will formally notify the coordinator and beneficiaries in advance any changes tothis URL.
Formal notifications on paper (only after the payment of the balance) addressed to the Commissionmust be sent to the official mailing address indicated on the Commission’s website.
Formal notifications on paper (only after the payment of the balance) addressed to the beneficiariesmust be sent to their legal address as specified in the Participant Portal Beneficiary Register.
ARTICLE 53 — INTERPRETATION OF THE AGREEMENT
53.1 Precedence of the Terms and Conditions over the Annexes
The provisions in the Terms and Conditions of the Agreement take precedence over its Annexes.
80
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
Annex 2 takes precedence over Annex 1.
53.2 Privileges and immunities
Not applicable
ARTICLE 54 — CALCULATION OF PERIODS, DATES AND DEADLINES
In accordance with Regulation No 1182/7130, periods expressed in days, months or years are calculatedfrom the moment the triggering event occurs.
The day during which that event occurs is not considered as falling within the period.
ARTICLE 55 — AMENDMENTS TO THE AGREEMENT
55.1 Conditions
The Agreement may be amended, unless the amendment entails changes to the Agreement whichwould call into question the decision awarding the grant or breach the principle of equal treatmentof applicants.
Amendments may be requested by any of the parties.
55.2 Procedure
The party requesting an amendment must submit a request for amendment signed in the electronicexchange system (see Article 52).
The coordinator submits and receives requests for amendment on behalf of the beneficiaries (seeAnnex 3).
If a change of coordinator is requested without its agreement, the submission must be done by anotherbeneficiary (acting on behalf of the other beneficiaries).
The request for amendment must include:
- the reasons why;
- the appropriate supporting documents, and
- for a change of coordinator without its agreement: the opinion of the coordinator (or proof thatthis opinion has been requested in writing).
The Commission may request additional information.
If the party receiving the request agrees, it must sign the amendment in the electronic exchange systemwithin 45 days of receiving notification (or any additional information the Commission has requested).If it does not agree, it must formally notify its disagreement within the same deadline. The deadline
30 Regulation (EEC, Euratom) No 1182/71 of the Council of 3 June 1971 determining the rules applicable to periods, datesand time-limits (OJ L 124, 8.6.1971, p. 1).
81
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
may be extended, if necessary for the assessment of the request. If no notification is received withinthe deadline, the request is considered to have been rejected
An amendment enters into force on the day of the signature of the receiving party.
An amendment takes effect on the date agreed by the parties or, in the absence of such an agreement,on the date on which the amendment enters into force.
ARTICLE 56 — ACCESSION TO THE AGREEMENT
56.1 Accession of the beneficiaries mentioned in the Preamble
The other beneficiaries must accede to the Agreement by signing the Accession Form (see Annex 3) inthe electronic exchange system (see Article 52) within 30 days after its entry into force (see Article 58).
They will assume the rights and obligations under the Agreement with effect from the date of its entryinto force (see Article 58).
If a beneficiary does not accede to the Agreement within the above deadline, the coordinator must— within 30 days — request an amendment to make any changes necessary to ensure properimplementation of the action. This does not affect the Commission’s right to terminate the Agreement(see Article 50).
56.2 Addition of new beneficiaries
In justified cases, the beneficiaries may request the addition of a new beneficiary.
For this purpose, the coordinator must submit a request for amendment in accordance with Article 55.It must include an Accession Form (see Annex 3) signed by the new beneficiary in the electronicexchange system (see Article 52).
New beneficiaries must assume the rights and obligations under the Agreement with effect from thedate of their accession specified in the Accession Form (see Annex 3).
ARTICLE 57 — APPLICABLE LAW AND SETTLEMENT OF DISPUTES
57.1 Applicable law
The Agreement is governed by the applicable EU law, supplemented if necessary by the law ofBelgium.
57.2 Dispute settlement
If a dispute concerning the interpretation, application or validity of the Agreement cannot be settledamicably, the General Court — or, on appeal, the Court of Justice of the European Union — has solejurisdiction. Such actions must be brought under Article 272 of the Treaty on the Functioning of theEU (TFEU).
As an exception, if such a dispute is between the Commission and ASSUTA ASHDOD LTD, SRDCYAZILIM ARASTIRMA VE GELISTIRME VE DANISMANLIK TICARET ANONIM SIRKETI,the competent Belgian courts have sole jurisdiction.
82
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
H2020 General MGA — Multi: v5
If a dispute concerns administrative sanctions, offsetting or an enforceable decision under Article 299TFEU (see Articles 44, 45 and 46), the beneficiaries must bring action before the General Court —or, on appeal, the Court of Justice of the European Union — under Article 263 TFEU.
ARTICLE 58 — ENTRY INTO FORCE OF THE AGREEMENT
The Agreement will enter into force on the day of signature by the Commission or the coordinator,depending on which is later.
SIGNATURES
For the coordinator For the Commission
[--TGSMark#signature-955006420_75_210--] [--TGSMark#signature-service_75_210--]
83
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
EUROPEAN COMMISSIONDirectorate-General for Communications Networks, Content andTechnology
eHealth, Well-Being and Ageing
ANNEX 1 (part A)
Innovation action
NUMBER — 875209 — ADLIFE
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Table of Contents
1.1. The project summary................................................................................................................................. 3
1.2. The list of beneficiaries..............................................................................................................................4
1.3. Workplan Tables - Detailed implementation..............................................................................................5
1.3.1. WT1 List of work packages........................................................................................................... 5
1.3.2. WT2 List of deliverables................................................................................................................ 6
1.3.3. WT3 Work package descriptions...................................................................................................9
Work package 1........................................................................................................................... 9
Work package 2......................................................................................................................... 12
Work package 3......................................................................................................................... 15
Work package 4......................................................................................................................... 19
Work package 5......................................................................................................................... 22
Work package 6......................................................................................................................... 26
Work package 7......................................................................................................................... 30
Work package 8......................................................................................................................... 33
Work package 9......................................................................................................................... 37
Work package 10....................................................................................................................... 40
Work package 11....................................................................................................................... 43
1.3.4. WT4 List of milestones................................................................................................................ 45
1.3.5. WT5 Critical Implementation risks and mitigation actions........................................................... 47
1.3.6 WT6 Summary of project effort in person-months........................................................................52
1.3.7. WT7 Tentative schedule of project reviews.................................................................................53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
1.1. The project summary
Project Number 1 875209 Project Acronym 2 ADLIFE
One form per project
General information
Project title 3INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCEDCHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
Starting date 4 01/01/2020
Duration in months 5 48
Call (part) identifier 6 H2020-SC1-DTH-2019
Topic SC1-DTH-11-2019Large Scale pilots of personalised & outcome based integrated care
Fixed EC Keywords Quality of health care, Integrated care
Free keywords large scale deployment, personalized empowerment platforms, clinical decision supportsystems, advanced chronic diseases
Abstract 7
Due to population ageing and advances in medical science, people with chronic diseases –including advanced severelife-threatening chronic diseases- live longer. Challenges are how to sustain quality independent living for the patient;support caregivers facing an increasing burden; create sustainable healthcare and social care systems with limitedresources. ADLIFE aims to provide a solution for the integration of therapies and approaches targeting early detectionand assessment of deterioration, advanced and well-coordinated care planning and integrated supportive care toenhance quality of life, reduce suffering and accelerate recovery for these patients and their families. It will deploydeveloped and validated personalised digital solutions for integrated supportive care based on H2020 projects C3-Cloud and Power2DM, previously tested in two health systems.The ADLIFE Toolbox solutions include: a Personalised Care Plan Management Platform, Clinical Decision SupportServices; Interoperability Solutions and Patient Empowerment Platform with Just-In Time Adaptive InterventionDelivery Engine.The ADLIFE system will be deployed through large-scale pilots in 7 countries and Health Systems, involve577 healthcare professionals from 75 hospitals, clinics and primary care services. It will prove that intelligent,collaborative digital solutions can enable care teams, patients and caregivers to improve or better maintain health inpatients with advanced chronic disease (over 200,000 in the participating regions). It will test its effectiveness in 882patients and 1243 caregivers. ADLIFE will demonstrate significant outcomes-based efficiency gains in health and caredelivery enhancing seamless care coordination, avoiding gaps and overlaps in care.The ADLIFE ICT Toolbox and the evidence behind this digitally-enabled approach from the 7 reference sites will bestrongly disseminated to multiple stakeholders and decision makers in Europe both online and in-person actions
Page 3 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
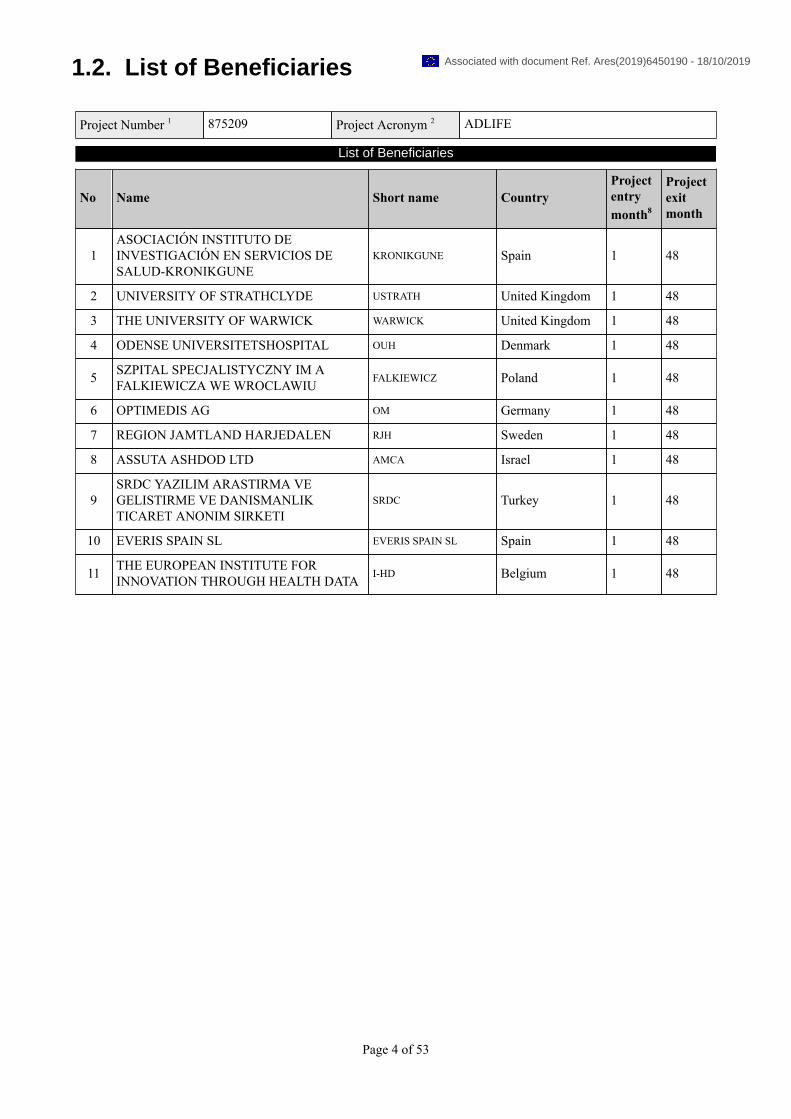
1.2. List of Beneficiaries
Project Number 1 875209 Project Acronym 2 ADLIFE
List of Beneficiaries
No Name Short name CountryProjectentrymonth8
Projectexitmonth
1ASOCIACIÓN INSTITUTO DEINVESTIGACIÓN EN SERVICIOS DESALUD-KRONIKGUNE
KRONIKGUNE Spain 1 48
2 UNIVERSITY OF STRATHCLYDE USTRATH United Kingdom 1 48
3 THE UNIVERSITY OF WARWICK WARWICK United Kingdom 1 48
4 ODENSE UNIVERSITETSHOSPITAL OUH Denmark 1 48
5 SZPITAL SPECJALISTYCZNY IM AFALKIEWICZA WE WROCLAWIU FALKIEWICZ Poland 1 48
6 OPTIMEDIS AG OM Germany 1 48
7 REGION JAMTLAND HARJEDALEN RJH Sweden 1 48
8 ASSUTA ASHDOD LTD AMCA Israel 1 48
9SRDC YAZILIM ARASTIRMA VEGELISTIRME VE DANISMANLIKTICARET ANONIM SIRKETI
SRDC Turkey 1 48
10 EVERIS SPAIN SL EVERIS SPAIN SL Spain 1 48
11 THE EUROPEAN INSTITUTE FORINNOVATION THROUGH HEALTH DATA I-HD Belgium 1 48
Page 4 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

1.3. Workplan Tables - Detailed implementation
1.3.1. WT1 List of work packages
WPNumber9 WP Title Lead beneficiary10 Person-
months11Startmonth12
Endmonth13
WP1 COORDINATION ANDMANAGEMENT 1 - KRONIKGUNE 36.00 1 48
WP2 DISSEMINATION ANDCOMMUNICATION 2 - USTRATH 33.00 1 48
WP3
DIGITAL TOOLS TO CREATEAND DELIVER PERSONALIZEDCARE PLAN MANAGEMENTPLATFORM
3 - WARWICK 100.50 1 26
WP4
PATIENT EMPOWERMENTPLATFORM ANDPERSONALIZED SELF-MANAGEMENT SUPPORTMECHANISMS
9 - SRDC 112.00 1 26
WP5CLINICAL DECISION SUPPORTSYSTEMS AND EARLYIDENTIFICATION TOOLS
10 - EVERIS SPAIN SL 150.50 1 30
WP6EVIDENCE BASEDPERSONALIZED CAREDELIVERY
7 - RJH 65.50 1 26
WP7EMPOWERMENT OFPATIENT, CAREGIVERS ANDCOMMUNITIES
4 - OUH 52.00 1 15
WP8 PILOT DESIGN ANDIMPLEMENTATION 8 - AMCA 102.00 1 44
WP9 EVALUATION 1 - KRONIKGUNE 83.50 1 48
WP10 EXPLOITATION 6 - OM 34.00 1 48
WP11 Ethics requirements 1 - KRONIKGUNE N/A 1 48
Total 769.00
Page 5 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

1.3.2. WT2 list of deliverables
DeliverableNumber14 Deliverable Title
WPnumber9 Lead beneficiary Type15 Dissemination
level16
DueDate (inmonths)17
D1.1 Data management plan WP1 11 - I-HD
ORDP:OpenResearchData Pilot
Public 6
D2.1
Communication anddissemination planand Communicationmaterial
WP2 2 - USTRATH Report Public 6
D2.2 Website WP2 2 - USTRATH Other Public 3
D2.3 Final report ondissemination activities WP2 2 - USTRATH Report Public 48
D3.1ADLIFE softwarerequirement andarchitectural description
WP3 3 - WARWICK Other
Confidential,only for membersof the consortium(including theCommissionServices)
8
D3.2Intelligent tools(PCPMP, TIS, SIS)customisation build
WP3 3 - WARWICK Other
Confidential,only for membersof the consortium(including theCommissionServices)
26
D3.3
Assurance reportincluding softwarequality plan, assessmentof certifiability againstMDR and GDPR.
WP3 3 - WARWICK Report
Confidential,only for membersof the consortium(including theCommissionServices)
26
D4.1ADLIFE PatientEmpowerment Platformsupporting PROMS
WP4 9 - SRDC Other
Confidential,only for membersof the consortium(including theCommissionServices)
18
D4.2Intelligent AdaptiveIntervention DeliveryMechanisms
WP4 9 - SRDC Other
Confidential,only for membersof the consortium(including theCommissionServices)
24
D5.1ADLIFE CDSS betaversion and technicalguide
WP5 10 - EVERIS SPAINSL Other
Confidential,only for membersof the consortium(including theCommissionServices)
23
Page 6 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
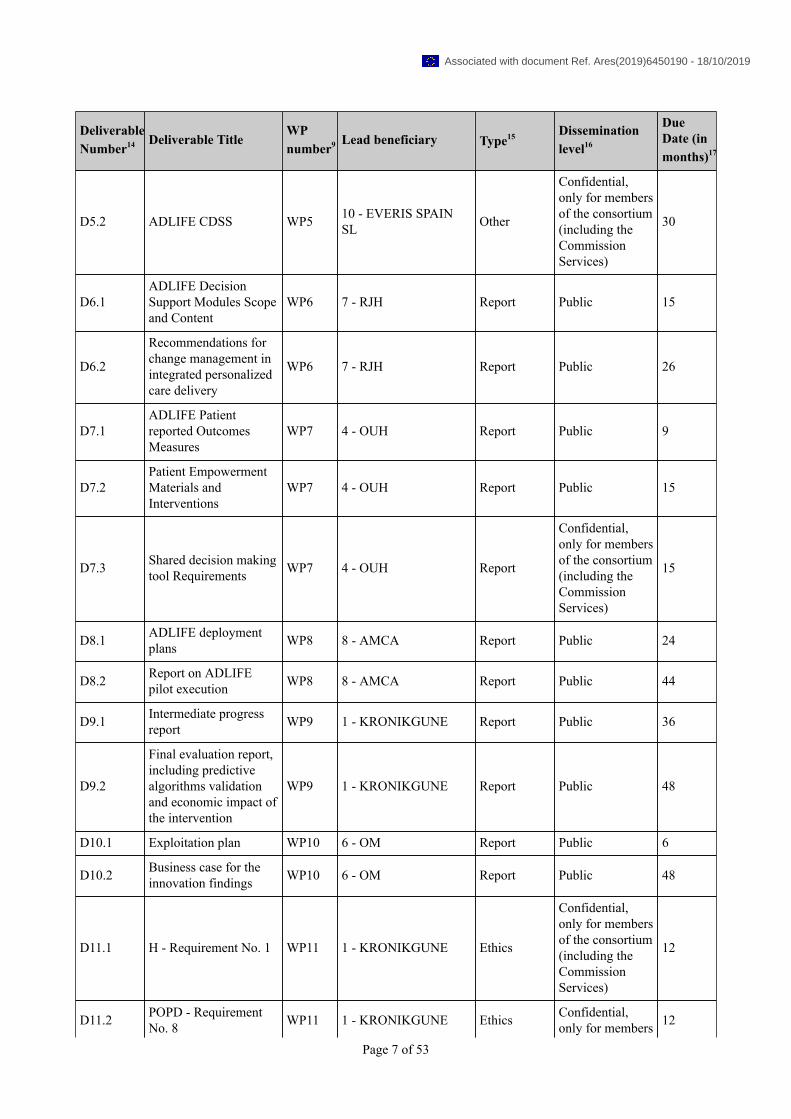
DeliverableNumber14 Deliverable Title
WPnumber9 Lead beneficiary Type15 Dissemination
level16
DueDate (inmonths)17
D5.2 ADLIFE CDSS WP5 10 - EVERIS SPAINSL Other
Confidential,only for membersof the consortium(including theCommissionServices)
30
D6.1ADLIFE DecisionSupport Modules Scopeand Content
WP6 7 - RJH Report Public 15
D6.2
Recommendations forchange management inintegrated personalizedcare delivery
WP6 7 - RJH Report Public 26
D7.1ADLIFE Patientreported OutcomesMeasures
WP7 4 - OUH Report Public 9
D7.2Patient EmpowermentMaterials andInterventions
WP7 4 - OUH Report Public 15
D7.3 Shared decision makingtool Requirements WP7 4 - OUH Report
Confidential,only for membersof the consortium(including theCommissionServices)
15
D8.1 ADLIFE deploymentplans WP8 8 - AMCA Report Public 24
D8.2 Report on ADLIFEpilot execution WP8 8 - AMCA Report Public 44
D9.1 Intermediate progressreport WP9 1 - KRONIKGUNE Report Public 36
D9.2
Final evaluation report,including predictivealgorithms validationand economic impact ofthe intervention
WP9 1 - KRONIKGUNE Report Public 48
D10.1 Exploitation plan WP10 6 - OM Report Public 6
D10.2 Business case for theinnovation findings WP10 6 - OM Report Public 48
D11.1 H - Requirement No. 1 WP11 1 - KRONIKGUNE Ethics
Confidential,only for membersof the consortium(including theCommissionServices)
12
D11.2 POPD - RequirementNo. 8 WP11 1 - KRONIKGUNE Ethics Confidential,
only for members 12
Page 7 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
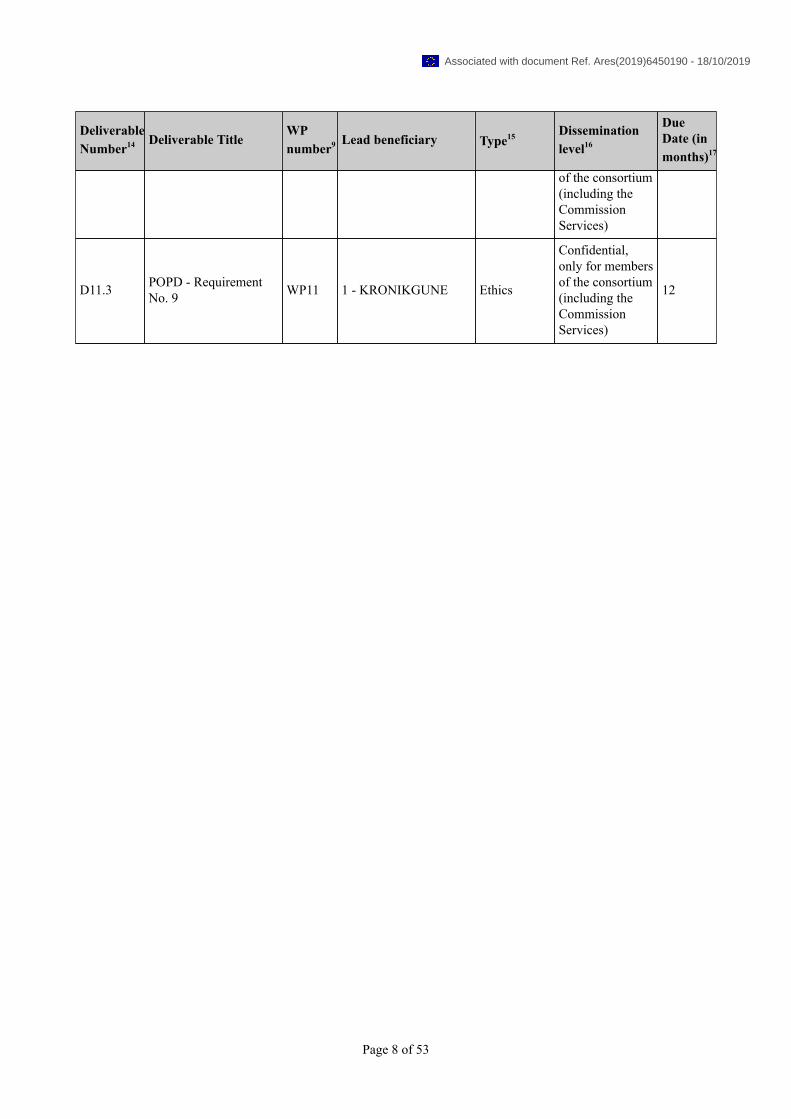
DeliverableNumber14 Deliverable Title
WPnumber9 Lead beneficiary Type15 Dissemination
level16
DueDate (inmonths)17
of the consortium(including theCommissionServices)
D11.3 POPD - RequirementNo. 9 WP11 1 - KRONIKGUNE Ethics
Confidential,only for membersof the consortium(including theCommissionServices)
12
Page 8 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
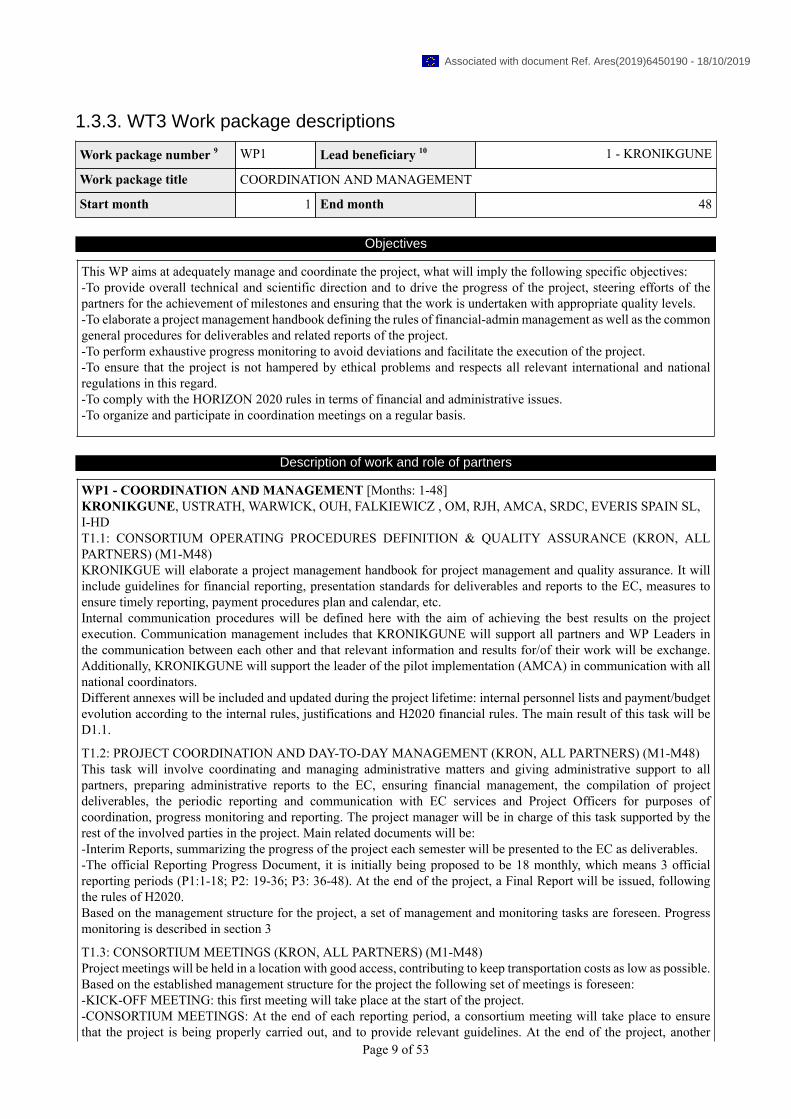
1.3.3. WT3 Work package descriptions
Work package number 9 WP1 Lead beneficiary 10 1 - KRONIKGUNE
Work package title COORDINATION AND MANAGEMENT
Start month 1 End month 48
Objectives
This WP aims at adequately manage and coordinate the project, what will imply the following specific objectives:-To provide overall technical and scientific direction and to drive the progress of the project, steering efforts of thepartners for the achievement of milestones and ensuring that the work is undertaken with appropriate quality levels.-To elaborate a project management handbook defining the rules of financial-admin management as well as the commongeneral procedures for deliverables and related reports of the project.-To perform exhaustive progress monitoring to avoid deviations and facilitate the execution of the project.-To ensure that the project is not hampered by ethical problems and respects all relevant international and nationalregulations in this regard.-To comply with the HORIZON 2020 rules in terms of financial and administrative issues.-To organize and participate in coordination meetings on a regular basis.
Description of work and role of partners
WP1 - COORDINATION AND MANAGEMENT [Months: 1-48]KRONIKGUNE, USTRATH, WARWICK, OUH, FALKIEWICZ , OM, RJH, AMCA, SRDC, EVERIS SPAIN SL,I-HDT1.1: CONSORTIUM OPERATING PROCEDURES DEFINITION & QUALITY ASSURANCE (KRON, ALLPARTNERS) (M1-M48)KRONIKGUE will elaborate a project management handbook for project management and quality assurance. It willinclude guidelines for financial reporting, presentation standards for deliverables and reports to the EC, measures toensure timely reporting, payment procedures plan and calendar, etc.Internal communication procedures will be defined here with the aim of achieving the best results on the projectexecution. Communication management includes that KRONIKGUNE will support all partners and WP Leaders inthe communication between each other and that relevant information and results for/of their work will be exchange.Additionally, KRONIKGUNE will support the leader of the pilot implementation (AMCA) in communication with allnational coordinators.Different annexes will be included and updated during the project lifetime: internal personnel lists and payment/budgetevolution according to the internal rules, justifications and H2020 financial rules. The main result of this task will beD1.1.
T1.2: PROJECT COORDINATION AND DAY-TO-DAY MANAGEMENT (KRON, ALL PARTNERS) (M1-M48)This task will involve coordinating and managing administrative matters and giving administrative support to allpartners, preparing administrative reports to the EC, ensuring financial management, the compilation of projectdeliverables, the periodic reporting and communication with EC services and Project Officers for purposes ofcoordination, progress monitoring and reporting. The project manager will be in charge of this task supported by therest of the involved parties in the project. Main related documents will be:-Interim Reports, summarizing the progress of the project each semester will be presented to the EC as deliverables.-The official Reporting Progress Document, it is initially being proposed to be 18 monthly, which means 3 officialreporting periods (P1:1-18; P2: 19-36; P3: 36-48). At the end of the project, a Final Report will be issued, followingthe rules of H2020.Based on the management structure for the project, a set of management and monitoring tasks are foreseen. Progressmonitoring is described in section 3
T1.3: CONSORTIUM MEETINGS (KRON, ALL PARTNERS) (M1-M48)Project meetings will be held in a location with good access, contributing to keep transportation costs as low as possible.Based on the established management structure for the project the following set of meetings is foreseen:-KICK-OFF MEETING: this first meeting will take place at the start of the project.-CONSORTIUM MEETINGS: At the end of each reporting period, a consortium meeting will take place to ensurethat the project is being properly carried out, and to provide relevant guidelines. At the end of the project, another
Page 9 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
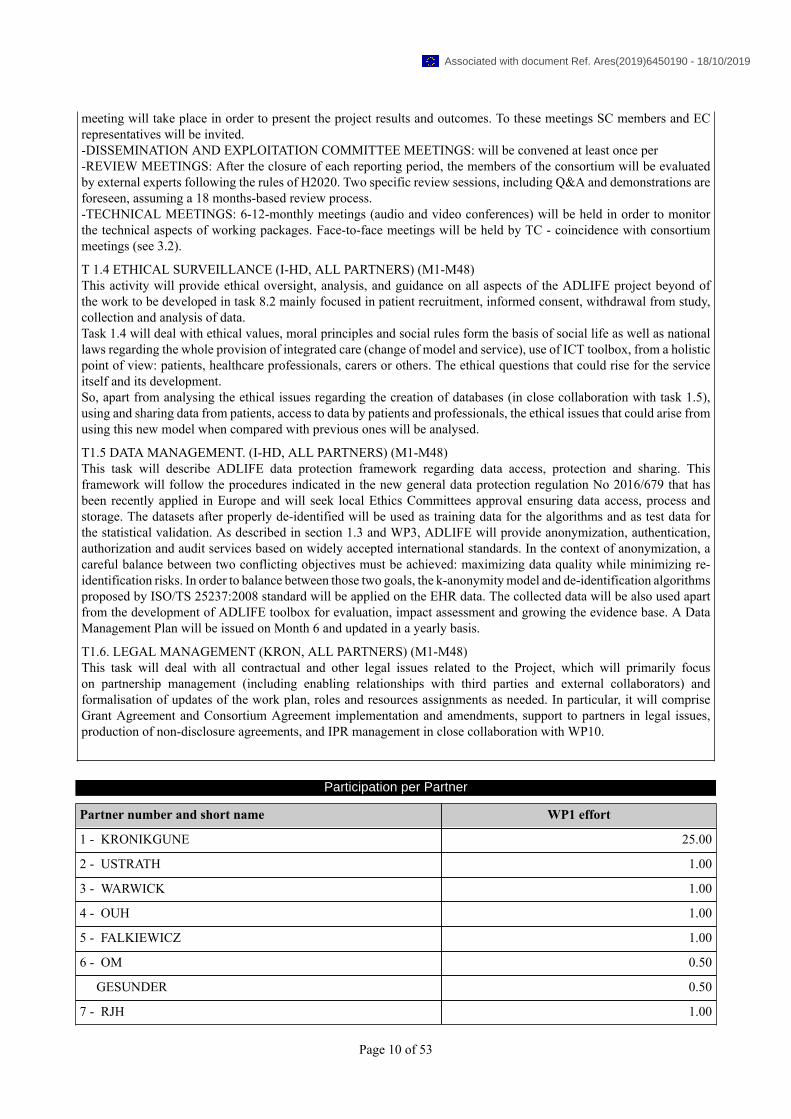
meeting will take place in order to present the project results and outcomes. To these meetings SC members and ECrepresentatives will be invited.-DISSEMINATION AND EXPLOITATION COMMITTEE MEETINGS: will be convened at least once per-REVIEW MEETINGS: After the closure of each reporting period, the members of the consortium will be evaluatedby external experts following the rules of H2020. Two specific review sessions, including Q&A and demonstrations areforeseen, assuming a 18 months-based review process.-TECHNICAL MEETINGS: 6-12-monthly meetings (audio and video conferences) will be held in order to monitorthe technical aspects of working packages. Face-to-face meetings will be held by TC - coincidence with consortiummeetings (see 3.2).
T 1.4 ETHICAL SURVEILLANCE (I-HD, ALL PARTNERS) (M1-M48)This activity will provide ethical oversight, analysis, and guidance on all aspects of the ADLIFE project beyond ofthe work to be developed in task 8.2 mainly focused in patient recruitment, informed consent, withdrawal from study,collection and analysis of data.Task 1.4 will deal with ethical values, moral principles and social rules form the basis of social life as well as nationallaws regarding the whole provision of integrated care (change of model and service), use of ICT toolbox, from a holisticpoint of view: patients, healthcare professionals, carers or others. The ethical questions that could rise for the serviceitself and its development.So, apart from analysing the ethical issues regarding the creation of databases (in close collaboration with task 1.5),using and sharing data from patients, access to data by patients and professionals, the ethical issues that could arise fromusing this new model when compared with previous ones will be analysed.
T1.5 DATA MANAGEMENT. (I-HD, ALL PARTNERS) (M1-M48)This task will describe ADLIFE data protection framework regarding data access, protection and sharing. Thisframework will follow the procedures indicated in the new general data protection regulation No 2016/679 that hasbeen recently applied in Europe and will seek local Ethics Committees approval ensuring data access, process andstorage. The datasets after properly de-identified will be used as training data for the algorithms and as test data forthe statistical validation. As described in section 1.3 and WP3, ADLIFE will provide anonymization, authentication,authorization and audit services based on widely accepted international standards. In the context of anonymization, acareful balance between two conflicting objectives must be achieved: maximizing data quality while minimizing re-identification risks. In order to balance between those two goals, the k-anonymity model and de-identification algorithmsproposed by ISO/TS 25237:2008 standard will be applied on the EHR data. The collected data will be also used apartfrom the development of ADLIFE toolbox for evaluation, impact assessment and growing the evidence base. A DataManagement Plan will be issued on Month 6 and updated in a yearly basis.
T1.6. LEGAL MANAGEMENT (KRON, ALL PARTNERS) (M1-M48)This task will deal with all contractual and other legal issues related to the Project, which will primarily focuson partnership management (including enabling relationships with third parties and external collaborators) andformalisation of updates of the work plan, roles and resources assignments as needed. In particular, it will compriseGrant Agreement and Consortium Agreement implementation and amendments, support to partners in legal issues,production of non-disclosure agreements, and IPR management in close collaboration with WP10.
Participation per Partner
Partner number and short name WP1 effort
1 - KRONIKGUNE 25.00
2 - USTRATH 1.00
3 - WARWICK 1.00
4 - OUH 1.00
5 - FALKIEWICZ 1.00
6 - OM 0.50
GESUNDER 0.50
7 - RJH 1.00
Page 10 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
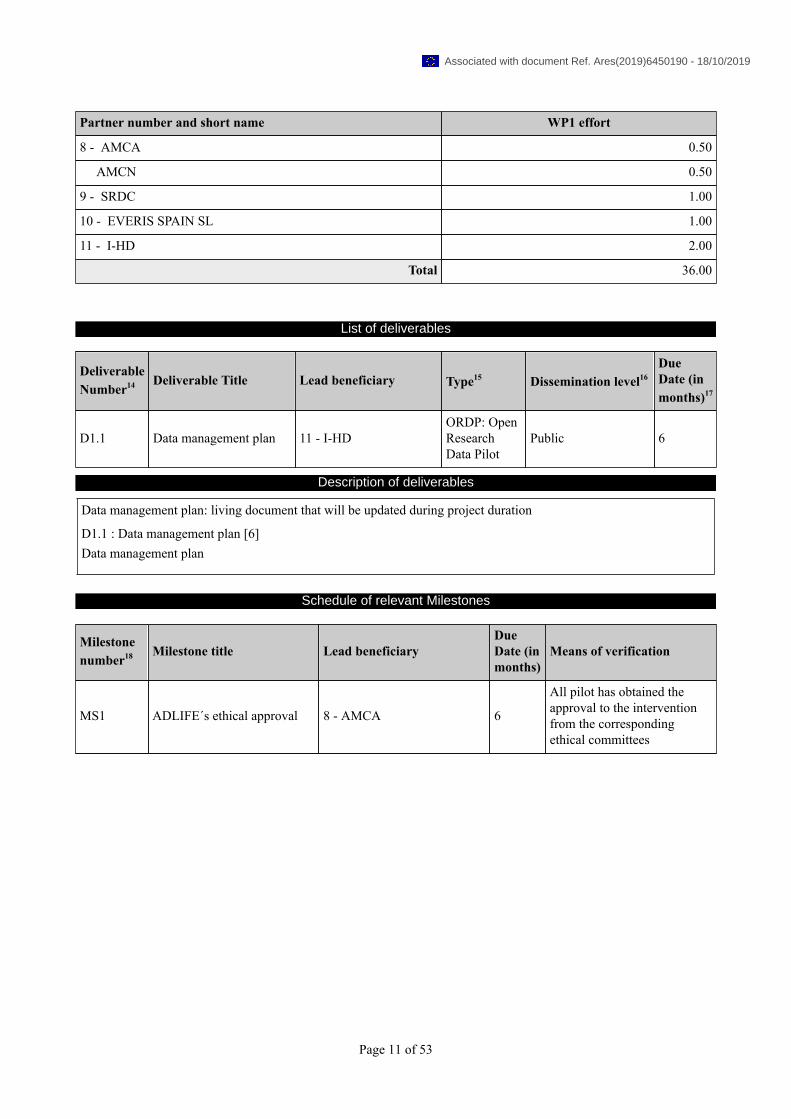
Partner number and short name WP1 effort
8 - AMCA 0.50
AMCN 0.50
9 - SRDC 1.00
10 - EVERIS SPAIN SL 1.00
11 - I-HD 2.00
Total 36.00
List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D1.1 Data management plan 11 - I-HDORDP: OpenResearchData Pilot
Public 6
Description of deliverables
Data management plan: living document that will be updated during project duration
D1.1 : Data management plan [6]Data management plan
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
MS1 ADLIFE´s ethical approval 8 - AMCA 6
All pilot has obtained theapproval to the interventionfrom the correspondingethical committees
Page 11 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Work package number 9 WP2 Lead beneficiary 10 2 - USTRATH
Work package title DISSEMINATION AND COMMUNICATION
Start month 1 End month 48
Objectives
WP2 will ensure timely and wide dissemination of the results of the ADLIFE integrated care toolbox and model to theappropriate audience through diffusion activities:-To develop and implement an ambitious but realistic Communication and Dissemination Plan-To facilitate networking and communication both to the scientific/technical community and the general public-To reach all the potential clinical, scientific, and non-scientific audiences (target groups)-To provide accurate and reliable results to inform evidence-based recommendations to improve the guidelines forproviding innovative integrated care-To ensure the transfer of the results of ADLIFE into care practice-To provide health-economic evaluations to governmental bodies and policy makers
Description of work and role of partners
WP2 - DISSEMINATION AND COMMUNICATION [Months: 1-48]USTRATH, KRONIKGUNE, WARWICK, OUH, FALKIEWICZ , OM, RJH, AMCA, SRDC, EVERIS SPAIN SL,I-HDT2.1: DISSEMINATION AND COMMUNICATION PLAN (STRAT, ALL PARTNERS) (M1-M48)An updated detailed dissemination and communication plan will be provided describing dissemination andcommunication strategies and planned actions at all levels together with a schedule of the most important disseminationevents. The dissemination and communication plan will continuously be updated and will include a report of the currentstatus.
T2.2: PROJECT WEBSITE AND EXTERNAL COMMUNICATION TOOLS (STRAT, ALL PARTNERS) (M1-M48)The project will set up a website that shall be used as the main interface towards the stakeholders and that will also act asa communication and dissemination channel for the project’s results and for involving and enlarging the stakeholders’community. The website will be designed and implemented by the University of Strathclyde. A dedicated section ofthe same or possibly a separate website will be set up as a SharePoint for the consortium, containing all institutionalinformation, including working documents and deliverables. The ADLIFE web strategy will merge traditional webdissemination tools, such as e-Newsletters, and advanced web communication features, based on 2.0 instruments, into aunique concept. This innovative approach will consider the most recent trends in web communication patterns, stronglysuggesting the adoption of 2.0 instruments, which are increasingly used by professional communities and not only byprivate citizens or young people. The project website will be designed and continuously updated in such a way to include:-Interface with web2.0 tools and the ADLIFE social network pages (e.g. LinkedIn, Twitter, Facebook, etc.); VideoStreaming facilities-Project’s public results, press releases, eNewsletters on ADLIFE related topics; specific RSS feeds and other automatednews services; links to major websites and portals, including those managed by the European Commission; articles andinterviews around the project and related topics written by professional journalists when available.The first complete version of the project website will be available by M3. All partners will also include a reference tothe project and provide links to the project site on their respective web sites. The website setup and maintenance willbe coordinated by STRAT, with the co-operation of all other partners for content provision and site population. It isforeseen that the website will be maintained (and even expanded) after the end of the project. Finally, as an added valueto the task profiles in social networks such as LinkedIn and a Twitter micro-blog system account will be created.
T2.3: DISSEMINATE ADLIFE RESULTS IN THE SCIENTIFIC COMMUNITY (STRAT, ALL PARTNERS) (M1-M48)To make the project results available at scientific level the consortium will disseminate them through articles in themain technical publications in the research fields tackled by the project (see point 2.2.1.1). The consortium will publishADLIFE objectives and results among a wide range of scientific media including high quality journals and mainworldwide conferences included in section 2 and linked also in social platforms such as ResearchGate. Disseminationactivities will be centralized by the scientific committee which will review the preliminary publications and plannedparticipations in conferences or marketing actions. For doing that, members of the consortium will share the information
Page 12 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

by mail with the steering committee, at least 15 days in advance. The scientific committee will give special attentionto IP matters or ethical aspects before agreeing to the proposal. The committee shall give an answer within one monthsince the reception of the proposal. Upcoming scientific and technical results will be reviewed by IP experts prior topublication.
T 2.4 DISSEMINATION TO THE PUBLIC AND OTHER TARGET GROUPS (I-HD, ALL PARTNERS) (M1-M48)The different target groups to be contacted (e.g. general public, healthcare decision makers, clinical, scientific and non-scientific audiences) will be identified and contacted via appropriate tools. For each target group, the route to establishcontact will be chosen according to the best “marketing” strategy as described in section 2Information material (e.g. posters) will be designed to be disseminated at meetings and conferences.Collaborations with other EU-funded projects in the field of integrated care (including the one funded in the same topic)will be sought for exchange of information and to maximize efficient communication and dissemination. The projectwebsite will be of course used to this aim.Dissemination plan for public awareness will involve more generalist communication channels and media also boostin WP7 where the empowerment of patient, caregivers and communities will be achieved. This dissemination planwill also include workshops, face to face meetings, and several media channels (on-line information multipliers, socialmedia, radio7tv media, EC dissemination channels).Near the end of ADLIFE, an international conference will be organized to communicate and disseminate the studyfindings. The conference will target key stakeholders including patients, clinicians, business, policy makers and otheraffiliated organisations. The scope will be to inform specific stakeholder groups about achievements and opportunitiesthat might derive from the project results and its exploitation to other research and industrial communities. The locationwill be decided during the project progress, and the option of embed them into major events (fairs, conferences, etc.)will also be explored.
T2.5. ROADMAP POR IMPROVING EUROPEAN AND NATIONAL GUIDELINES AND MODELS OFINTEGRATED CARE (I-HD, ALL PARTNERS) (M1-M48)A roadmap to change the recommendations by European and national associations and guidelines for integrated carewill be created. Members of the consortium belong to different health systems all around Europe and beyond so haveaccess to policy makers at regional and national level in each of the participating countries, that could participate inchanging the actual models and services of chronic and integrated care provided at regional. In addition, in the pilotingteam’s healthcare professionals belonging to relevant chronic and integrated care societies will be involved in the projectand will work in changing the actual guidelines. They will, as appropriate, disseminate the results (including the robustevaluation) of ADLIFE in the different forums at regional and national level together with the active participation ofthe coordinator and the rest of the partners in EIP-AHA.
T2.6. OPEN ACCESS STRATEGY (I-HD, ALL PARTNERS) (M1-M48)ADLIFE project is fully aware with the open access to scientific publications article as stated in the Article 29.2 of theH2020 Grant Agreement. All the peer reviewed publications arising from ADLIFE will try to provide an open access toscientific publications from the project, without jeopardizing the exploitability of project results as it has been describedin section 2.2.1 and 2.2.2. In addition, data obtained in the project are quite sensitive, so protection and privacy of thedata are of crucial importance in the project but the re-use of generate data of the project will be also included in the DMPtogether with the procedures to access to the guidelines generated, evaluation data and robustly anonymised raw data.
Participation per Partner
Partner number and short name WP2 effort
1 - KRONIKGUNE 1.00
OSAKIDETZA 1.00
2 - USTRATH 12.00
3 - WARWICK 1.00
4 - OUH 2.00
5 - FALKIEWICZ 2.00
6 - OM 1.00
7 - RJH 2.00
Page 13 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Partner number and short name WP2 effort
8 - AMCA 1.50
AMCN 1.50
9 - SRDC 2.00
10 - EVERIS SPAIN SL 2.00
11 - I-HD 4.00
Total 33.00
List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D2.1Communication anddissemination plan andCommunication material
2 - USTRATH Report Public 6
D2.2 Website 2 - USTRATH Other Public 3
D2.3 Final report ondissemination activities 2 - USTRATH Report Public 48
Description of deliverables
D2.1 : Communication and dissemination plan and Communication material [6]Communication and dissemination plan and Communication material
D2.2 : Website [3]Website
D2.3 : Final report on dissemination activities [48]Final report on dissemination activities
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
MS2 Website 2 - USTRATH 3 Website for the projectlaunched
Page 14 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Work package number 9 WP3 Lead beneficiary 10 3 - WARWICK
Work package title DIGITAL TOOLS TO CREATE AND DELIVER PERSONALIZED CARE PLANMANAGEMENT PLATFORM
Start month 1 End month 26
Objectives
The objectives of this work package are:-To identify new technical requirements for the architecture based on the particular clinical needs.-To adapt the existing Care Plan Management Platform provided by C3-Cloud architecture, to facilitate developmentand deployment of personalised care plans to local systems and the patient empowerment platform.-To provide the necessary interoperability adaptors for integration with local pilot settings-To assure the intelligent tools for data protection, safety and quality.
Description of work and role of partners
WP3 - DIGITAL TOOLS TO CREATE AND DELIVER PERSONALIZED CARE PLAN MANAGEMENTPLATFORM [Months: 1-26]WARWICK, KRONIKGUNE, USTRATH, OUH, FALKIEWICZ , OM, RJH, AMCA, SRDC, EVERIS SPAIN SL3.1 TECHNICAL REQUIREMENTS ANALYSIS AND CONCEPTUAL DESIGN FOR ADAPTATION OF THEINTEGRATED ICT INFRASTRUCTURE FOR ADLIFE (WARWICK; P: SRDC, EVERIS, KG, RJH, OUH, LWS,STRATH, OM,AMCA (M1-M7) ,This task will analyse the technical requirements of the ICT infrastructure for ADLIFE, encompassing the integratedPersonalized Care Plan Management Platform and its integration with the pilot sites and the Clinical Decision Supportmodules. The process will use input from WP6 identifying the specific clinical needs of the ADLIFE solution, toevaluate the pedigree components such as C3-Cloud and Power2DM. The IEEE standard IEEE std 828:2012 (Standardfor Configuration Management in Systems and Software Engineering) will be used where appropriate to create asoftware configuration management plan, which will document the adaptation. Using configuration management, asoftware baseline constituting of the legacy components will be identified, and change requests will be implemented,driven from the specific clinical needs. A requirements document specific to ADLIFE will be created, following theRecommendations of the well-established standard IEEE Std. 29148:2011 which incorporates guidelines providedby IEEE STD 830-1998 and IEEE STD 1233-1998 will be followed to document the requirement specifications forADLIFE pilot sites. ADLIFE legacy components already comply to the IEEE STD 830-1998.Finally, following the same method, the task will design and build the overall architecture of the integrated technicalsolution for ADLIFE, adapting the highly modular architecture of C3-Cloud, which will be documented in compliancewith IEEE STD 1016:2009 (Standard for Information Technology--Systems Design--Software Design Descriptions).Existing ICT components already comply with IEEE STD 1016:1998. All the interfaces between ADLIFE ICTInfrastructures modules, such as PCPMP, Clinical Decision Support systems, Semantic and Technical InteroperabilitySuite, Security and Privacy Suite and Patient Empowerment Platform will be documented in detail to guide thedevelopment tasks in WP3, WP4 and WP5.
T3.2 CUSTOMIZATION AND INTEGRATION OF THE PERSONALIZED CARE PLAN MANAGEMENTPLATFORM TO ADLIFE (SRDC; P:WARWICK, EVERIS (M8- M26):A Personalized Care Plan Management Platform (PCPMP) will enable creation, update and follow-up of personalizedintegrated care plans for patients. Interactions with the care model defined in WP4 (patient empowerment platformand personalisation) and WP6 (care pathway), will be analysed and necessary adaptations will be implemented. Allthe feedback from the Clinical reference Group in terms of personalized care plan requirements will guide ICT expertsin the final design of the PCPMP. The PCPMP lies at the heart of the integrated care solution, and is the componentaround which, the data repository, the Clinical Decision Support Services, and the Patient Empowerment Platform areintegrated. PCPMP. It will be updated and improved according to the needs of long-term care of patients with severechronic diseases with an expected progression in severity defined by the clinical experts of the ADLIFE project. PCPMPwill be integrated with several Clinical Decision Support Services (CDSS) for enabling predictive risk assessment,personalised goal recommendations and intervention recommendations. The task will implement the changes needed, asidentified in Task 3.1. This will include customisations for ADLIFE, such as the user interface layout, access to additionalFHIR resources such as patient reported outcome measures, as well as interfacing with the Patient EmpowermentPlatform, and predictive risk assessment algorithms to intelligently adapt the care plan of the patient. The task will also
Page 15 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

implement customisations needed for each pilot site based on their specific organisation models, as well as implementtranslated versions. The task is not expecting to implement major interface implementation, as the legacy componentsare already fully compliant with well-established standards (FHIR, cds-hooks and REST). The task will result in adeployable build. The actual deployment of PCPMP and CDS Services to the pilot sites and the integration of theplatforms in the local electronic health records will be carried out in Task 8.2.
T3.3 PILOT SITE INTEGRATION AND INTEROPERABILITY (WARWICK; P: SRDC, ALL PILOT SITES)(M6-26):This task is responsible with developing the drivers that will enable interfacing of the solution with local systems. Thiswill encompass technical, as well as semantic interoperability of the various local systems that will need to provide datato the integrated care ICT infrastructure. This will be achieved by the development of two components, the TechnicalInteroperability Suite (TIS) and the Semantic Interoperability Suite (SIS). The Technical Interoperability Suite (TIS)will be responsible for integration of PCPMP with the local electronic health record systems of the pilot sites forretrieving the relevant parts from the medical records of the patients and providing them to the HL7 FHIR® basedSecure Data Repository utilized by PCPMP. TIS will utilize the Semantic Interoperability Suite (SIS) to be developed inthis task for handling the structural transformation of local EHR content models to HL7 FHIR based data sets and codemapping activities. SIS will adopt a lightweight approach by creating quick access (hashed) ontology which will mapthe clinical concepts, following the guidance of ISO 11179 Metadata Registry (MDR) standard. Mapping of conceptswill be achieved by using reference mappings to the Unified Medical Language System (UMLS), individually verifiedby clinicians in T8.1. SRDC and Warwick teams will closely collaborate with IT personnel of local care sites to achievethis integration, based on their experience from the C3-Cloud Project, which successfully integrated three different pilotsites, using multiple systems. TIS and SIS will be developed as add-ons to existing components, further expanding thecapabilities of the legacy components (e.g., C3-Cloud), as they will provide new APIs for additional local systems.
T3.4 ASSURANCE OF THE SECURITY, PRIVACY AND QUALITY OF INTELLIGENT TOOLS SUITE (SRDC;P: WARWICK, ALL PILOT SITES (M8- M26):This task will focus on generating information that will support assurance that the technical solution is appropriateand fit for purpose. The scope of the task will encompass software quality, the General Data Protection Regulationand the Medical Devices Regulation. Within the scope of this task, necessary security and privacy mechanisms tosafeguard the secure access, processing, sharing and storing of patient’s personalized information including his/herelectronic health records and also other patient generated data (including sensor measurements, interactions with theirenvironments, feedback about their care plans and PROMs) in line with GDPR requirements will be implemented.Audit trails for electronic health records will be analysed and suitable profiles for integrated care will be selected. Opensource implementations of the common components such as audit repositories, open source libraries for sending auditmessages, and authentication and authorization services will be provided to be used by other ADLIFE components.Interoperability with the existing privacy protection and security mechanisms (e.g. health professional authentication& authorization systems) in the pilot settings will be achieved by supporting standard based adapters implementingOAUTH 2.0, OpenID Connect protocols. Furthermore, in collaboration with WP6, the consent and opt-out requirementsof GDPR, will be incorporated. The task will also deliver a data anonymization tool suite that can be adapted to the needsof predictive analytics algorithms to be developed and trained on top of anonymized data sets of pilot sites within thescope of WP5. Our aim will be maximizing data quality while minimizing re-identification risks, by providing a suiteof modular de-identification algorithms proposed by ISO/TS 25237:2008 standard ta such as generalization, redactionand fuzzing.In addition to data privacy, the infrastructure will provide recommendations to clinicians and patients, which isconsidered as a class of medical devices according to the new EU Medical Device Regulation (MDR). The task willlook into the requirements of the MDR (class IIa) and will inform Tasks 3.1, 3.2 and 3.3 as well as WP4, WP5 andWP6 specifying safety mechanisms at the CDSS and organizational level respectively, making the solution amenable tocompliance with the MDR. This will also increase the exploitability of the solution, as subsequent operators will be ableto comply with the MDR more easily and cost-effectively post-project. Finally, the task will create a quality assuranceplan for software development based on IEEE std 730-2014, and monitor its application, in collaboration of the overallproject quality assurance process in WP1.
Participation per Partner
Partner number and short name WP3 effort
1 - KRONIKGUNE 3.00
Page 16 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
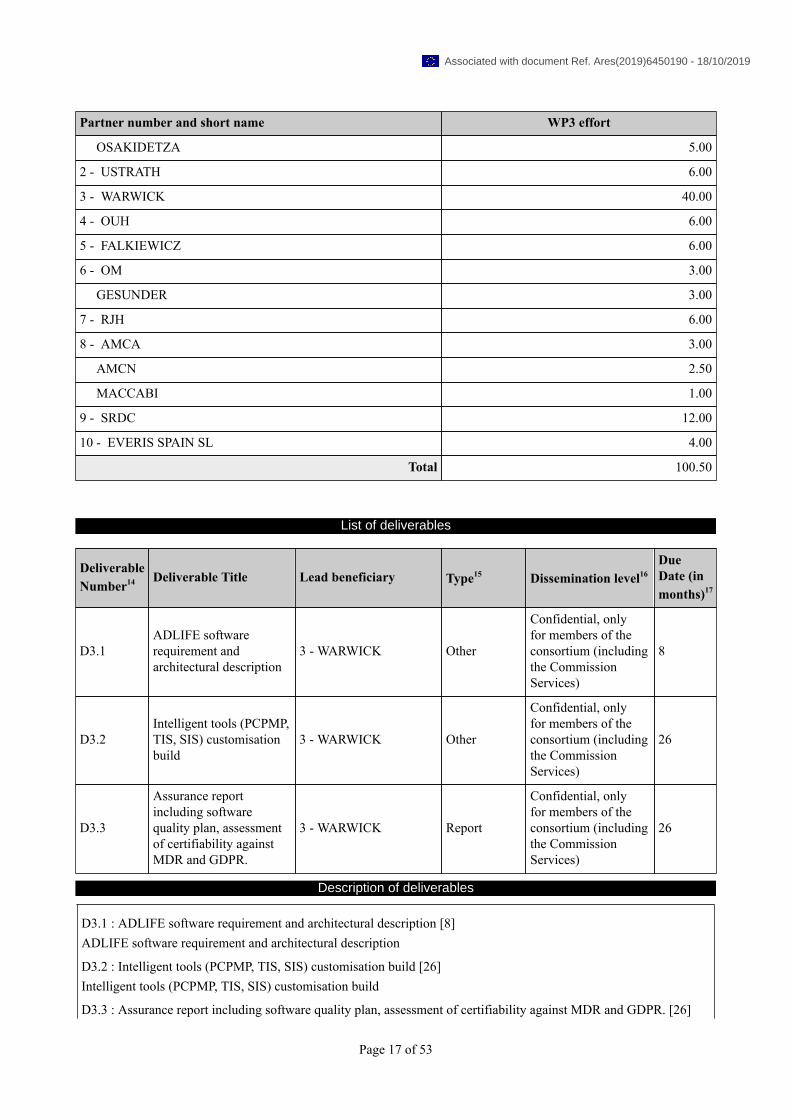
Partner number and short name WP3 effort
OSAKIDETZA 5.00
2 - USTRATH 6.00
3 - WARWICK 40.00
4 - OUH 6.00
5 - FALKIEWICZ 6.00
6 - OM 3.00
GESUNDER 3.00
7 - RJH 6.00
8 - AMCA 3.00
AMCN 2.50
MACCABI 1.00
9 - SRDC 12.00
10 - EVERIS SPAIN SL 4.00
Total 100.50
List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D3.1ADLIFE softwarerequirement andarchitectural description
3 - WARWICK Other
Confidential, onlyfor members of theconsortium (includingthe CommissionServices)
8
D3.2Intelligent tools (PCPMP,TIS, SIS) customisationbuild
3 - WARWICK Other
Confidential, onlyfor members of theconsortium (includingthe CommissionServices)
26
D3.3
Assurance reportincluding softwarequality plan, assessmentof certifiability againstMDR and GDPR.
3 - WARWICK Report
Confidential, onlyfor members of theconsortium (includingthe CommissionServices)
26
Description of deliverables
D3.1 : ADLIFE software requirement and architectural description [8]ADLIFE software requirement and architectural description
D3.2 : Intelligent tools (PCPMP, TIS, SIS) customisation build [26]Intelligent tools (PCPMP, TIS, SIS) customisation build
D3.3 : Assurance report including software quality plan, assessment of certifiability against MDR and GDPR. [26]
Page 17 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Assurance report including software quality plan, assessment of certifiability against MDR and GDPR.
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
MS3 ADLIFE´s software designand configuration description 3 - WARWICK 12
Task 3.1 done. Identificationof the technical requirementsand the adaptationrequirements for theintegration in each of the 7pilot sites.
MS4 ADLIFE interoperability andsecurity assurance of the tools 3 - WARWICK 18
Task 3.4 solved,interoperability, security,privacy and quality issuessolve in all the pilot sites
MS7 ADLIFE Pilot site builds forintelligent and secure tools 3 - WARWICK 25
Task 3.2 and 3.3done. Integration ofthe personalized caremanagement platform
MS8
ADLIFE patientempowerment platform andJTA mechanisms ready foreach pilot
9 - SRDC 26
Task 4.1, 4.2 and 4.3done. Personalized JTAIbuilt per site upon thePower 2DM intelligentcommunication engine. WP7done and patients, carers andcommunity empowered
MS11 Launch of ADLIFE pilots 8 - AMCA 30
ADLIFE´s participantsidentified and included inthe 7 pilots’ sites. WP 3-7finished
Page 18 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Work package number 9 WP4 Lead beneficiary 10 9 - SRDC
Work package title PATIENT EMPOWERMENT PLATFORM AND PERSONALIZED SELF-MANAGEMENT SUPPORT MECHANISMS
Start month 1 End month 26
Objectives
The objective of this work package is to deliver the Patient Empowerment Platform as the technical infrastructure toextent healthy and independent living and support patients and their informal care givers in their long term care journeywith the following functionalities:-Provide an online environment to the patient for reviewing his/her care plans including the details of the goals andactivities-Provide an online platform to the patient to communicate with his/her caregivers regarding his care plan, providefeedback, and outcomes of the activities assigned-Provide an online platform to the patient to fill in Patient Reported Outcome Measures-Provide an adaptive intervention delivery mechanism to present personalized behavioural change interventions to thepatient in a context aware manner to increase his/her adherence to the care plan
Description of work and role of partners
WP4 - PATIENT EMPOWERMENT PLATFORM AND PERSONALIZED SELF-MANAGEMENTSUPPORT MECHANISMS [Months: 1-26]SRDC, KRONIKGUNE, USTRATH, WARWICK, OUH, FALKIEWICZ , OM, RJH, AMCA, EVERIS SPAIN SLT4.1 PATIENT EMPOWERMENT PLATFORM INTEROPERABILITY/SAFETY (SRDC, P: ALL PILOT SITES)(M1-M26In this task, first of all the existing Patient Empowerment Platforms of all pilot sites and their existing features such ascare plan delivery, self-management support, integration with medical devices, access to care records will be thoroughlyanalysed for gap analysis, and to identify the integration interfaces required. At this step we will closely work withtechnical teams of pilot sites. Based on this analysis, this task will deliver the software interfaces to retrieve the mostrecent care plan of the patient from the PCPMP via international standards (HL7 FHIR Care Plan), and will deliver eventmanagement interfaces to establish continuous communication between PCPMP and existing Patient EmpowermentPlatforms (example events are care plan creation, care plan update, comment from a patient regarding his goals/activities,questionnaires assigned to patient, questionnaires finished by the patient, sensor measurements fulfilled by the patientetc. through HL7 FHIR based interfaces. Pilot sites who already have Patient Empowerment Platforms will integratethe interoperability services delivered by this task to get integrated with PCPMP. Support will be provided to local caresites for guiding the integration of these Restful interfaces to existing patient empowerment platforms. also). ADLIFEwill deliver a Patient Empowerment Platform as a web based portal to implement these interfaces to be integrated withPCPMP and also provide user interfaces to present the care plan to the patient, collect feedback, comments from thepatient, asynchronous messaging between patients and care givers, sensor measurement management, support onlinequestionnaires and assessments. This platform will build upon the existing Personal Health Record System of SRDC,‘eSaglikKaydım’. The pilot sites who do not have a Patient Empowerment Platform supporting these features will usethis platform during the ADLIFE Intervention implementation. This task will also implement the decision aids identifiedin WP7 and will deliver the information materials and self-management interventions designed in WP7. This task willutilize the security and privacy measures to be delivered in WP3 to achieve single sign-on, authentication, authorizationand audit to ensure trust of users with regard to data access, protection, sharing and storing.
T4.2 PATIENT REPORTED OUTCOME MEASURES (SRDC, P: OUH, KG, ALL PILOT SITES)) (M1-M26)This task will implement a functionality that allows online patient-reported outcome measures (PROM) questionnairesto be available from the Patient Empowerment Platform and feed the result to PCPMP and Clinical Decision SupportServices so that results flow into the care plan in real time in order to be actionable. This task will deliver theinteroperability interfaces in conformance to ‘Patient Reported Outcomes (PRO) FHIR Implementation Guide (IG)’ sothat PROMs can be seamlessly exchanged between PEP and legacy EHRs and also PCPMP and CDS services througha standard based interface. Through PROMs, it will be enabled to monitor and guide individual patient's treatmentbased on his/her care personalized plan. PROMs will be made actionable: They will be tracked over time in relationto ongoing care plan. Data generated by patients through the PROMs filled via PEP will be fed into PCPMP through
Page 19 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
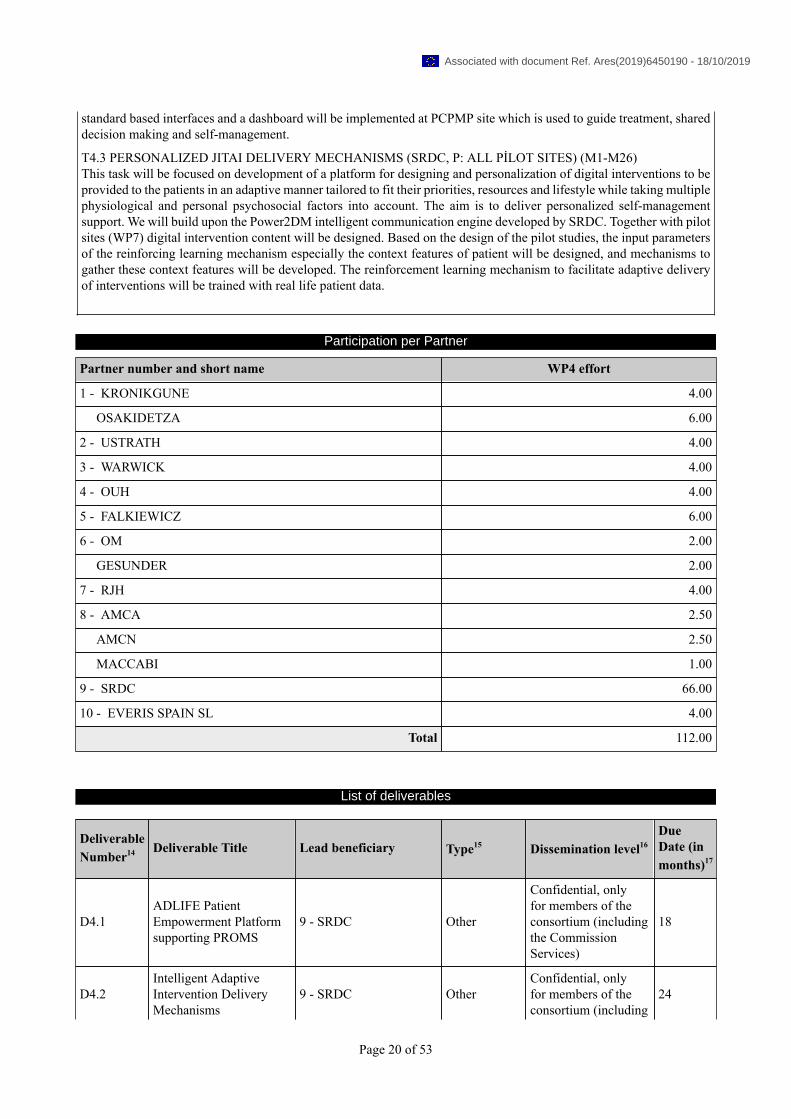
standard based interfaces and a dashboard will be implemented at PCPMP site which is used to guide treatment, shareddecision making and self-management.
T4.3 PERSONALIZED JITAI DELIVERY MECHANISMS (SRDC, P: ALL PİLOT SITES) (M1-M26)This task will be focused on development of a platform for designing and personalization of digital interventions to beprovided to the patients in an adaptive manner tailored to fit their priorities, resources and lifestyle while taking multiplephysiological and personal psychosocial factors into account. The aim is to deliver personalized self-managementsupport. We will build upon the Power2DM intelligent communication engine developed by SRDC. Together with pilotsites (WP7) digital intervention content will be designed. Based on the design of the pilot studies, the input parametersof the reinforcing learning mechanism especially the context features of patient will be designed, and mechanisms togather these context features will be developed. The reinforcement learning mechanism to facilitate adaptive deliveryof interventions will be trained with real life patient data.
Participation per Partner
Partner number and short name WP4 effort
1 - KRONIKGUNE 4.00
OSAKIDETZA 6.00
2 - USTRATH 4.00
3 - WARWICK 4.00
4 - OUH 4.00
5 - FALKIEWICZ 6.00
6 - OM 2.00
GESUNDER 2.00
7 - RJH 4.00
8 - AMCA 2.50
AMCN 2.50
MACCABI 1.00
9 - SRDC 66.00
10 - EVERIS SPAIN SL 4.00
Total 112.00
List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D4.1ADLIFE PatientEmpowerment Platformsupporting PROMS
9 - SRDC Other
Confidential, onlyfor members of theconsortium (includingthe CommissionServices)
18
D4.2Intelligent AdaptiveIntervention DeliveryMechanisms
9 - SRDC OtherConfidential, onlyfor members of theconsortium (including
24
Page 20 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
the CommissionServices)
Description of deliverables
D4.1 : ADLIFE Patient Empowerment Platform supporting PROMS [18]ADLIFE Patient Empowerment Platform supporting PROMS
D4.2 : Intelligent Adaptive Intervention Delivery Mechanisms [24]Intelligent Adaptive Intervention Delivery Mechanisms
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
MS6Tools for empowermentdelivered and ready to betested in WP8
9 - SRDC 15
Participants (patients,professionals, carers…)engaged and testing thebeta version of the tools andsupporting the launching ofthe pilots.
MS8
ADLIFE patientempowerment platform andJTA mechanisms ready foreach pilot
9 - SRDC 26
Task 4.1, 4.2 and 4.3done. Personalized JTAIbuilt per site upon thePower 2DM intelligentcommunication engine. WP7done and patients, carers andcommunity empowered
MS11 Launch of ADLIFE pilots 8 - AMCA 30
ADLIFE´s participantsidentified and included inthe 7 pilots’ sites. WP 3-7finished
Page 21 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
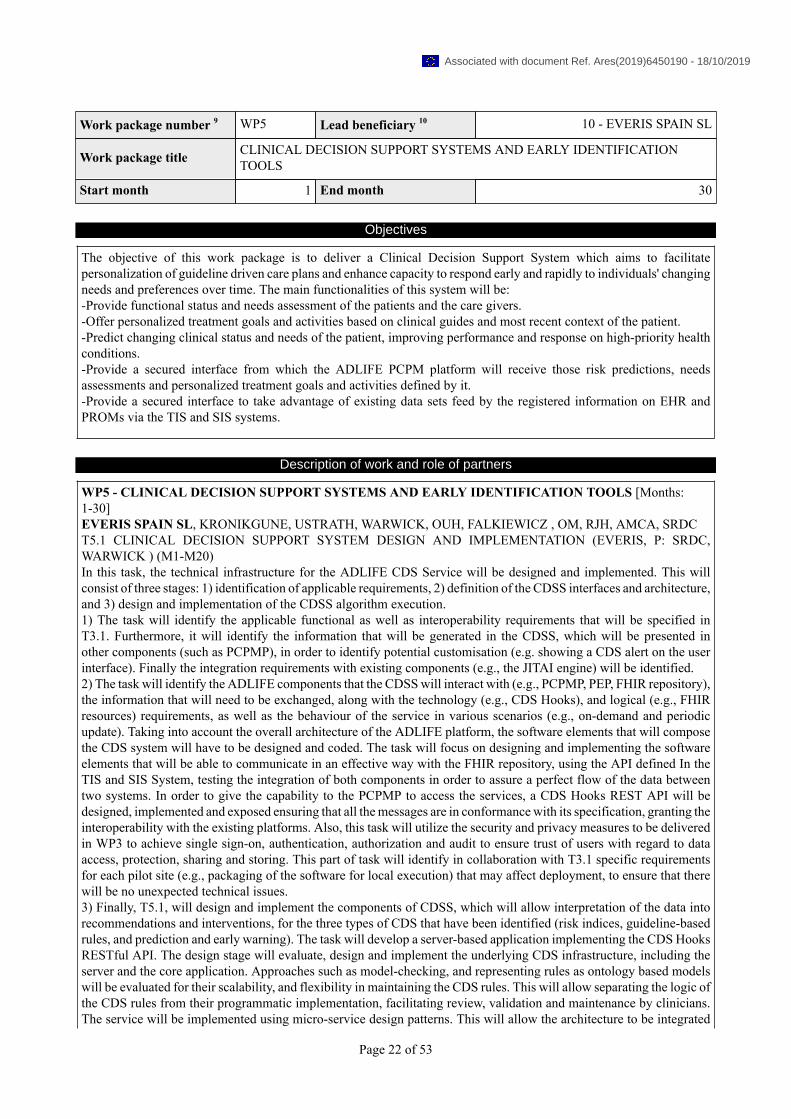
Work package number 9 WP5 Lead beneficiary 10 10 - EVERIS SPAIN SL
Work package title CLINICAL DECISION SUPPORT SYSTEMS AND EARLY IDENTIFICATIONTOOLS
Start month 1 End month 30
Objectives
The objective of this work package is to deliver a Clinical Decision Support System which aims to facilitatepersonalization of guideline driven care plans and enhance capacity to respond early and rapidly to individuals' changingneeds and preferences over time. The main functionalities of this system will be:-Provide functional status and needs assessment of the patients and the care givers.-Offer personalized treatment goals and activities based on clinical guides and most recent context of the patient.-Predict changing clinical status and needs of the patient, improving performance and response on high-priority healthconditions.-Provide a secured interface from which the ADLIFE PCPM platform will receive those risk predictions, needsassessments and personalized treatment goals and activities defined by it.-Provide a secured interface to take advantage of existing data sets feed by the registered information on EHR andPROMs via the TIS and SIS systems.
Description of work and role of partners
WP5 - CLINICAL DECISION SUPPORT SYSTEMS AND EARLY IDENTIFICATION TOOLS [Months:1-30]EVERIS SPAIN SL, KRONIKGUNE, USTRATH, WARWICK, OUH, FALKIEWICZ , OM, RJH, AMCA, SRDCT5.1 CLINICAL DECISION SUPPORT SYSTEM DESIGN AND IMPLEMENTATION (EVERIS, P: SRDC,WARWICK ) (M1-M20)In this task, the technical infrastructure for the ADLIFE CDS Service will be designed and implemented. This willconsist of three stages: 1) identification of applicable requirements, 2) definition of the CDSS interfaces and architecture,and 3) design and implementation of the CDSS algorithm execution.1) The task will identify the applicable functional as well as interoperability requirements that will be specified inT3.1. Furthermore, it will identify the information that will be generated in the CDSS, which will be presented inother components (such as PCPMP), in order to identify potential customisation (e.g. showing a CDS alert on the userinterface). Finally the integration requirements with existing components (e.g., the JITAI engine) will be identified.2) The task will identify the ADLIFE components that the CDSS will interact with (e.g., PCPMP, PEP, FHIR repository),the information that will need to be exchanged, along with the technology (e.g., CDS Hooks), and logical (e.g., FHIRresources) requirements, as well as the behaviour of the service in various scenarios (e.g., on-demand and periodicupdate). Taking into account the overall architecture of the ADLIFE platform, the software elements that will composethe CDS system will have to be designed and coded. The task will focus on designing and implementing the softwareelements that will be able to communicate in an effective way with the FHIR repository, using the API defined In theTIS and SIS System, testing the integration of both components in order to assure a perfect flow of the data betweentwo systems. In order to give the capability to the PCPMP to access the services, a CDS Hooks REST API will bedesigned, implemented and exposed ensuring that all the messages are in conformance with its specification, granting theinteroperability with the existing platforms. Also, this task will utilize the security and privacy measures to be deliveredin WP3 to achieve single sign-on, authentication, authorization and audit to ensure trust of users with regard to dataaccess, protection, sharing and storing. This part of task will identify in collaboration with T3.1 specific requirementsfor each pilot site (e.g., packaging of the software for local execution) that may affect deployment, to ensure that therewill be no unexpected technical issues.3) Finally, T5.1, will design and implement the components of CDSS, which will allow interpretation of the data intorecommendations and interventions, for the three types of CDS that have been identified (risk indices, guideline-basedrules, and prediction and early warning). The task will develop a server-based application implementing the CDS HooksRESTful API. The design stage will evaluate, design and implement the underlying CDS infrastructure, including theserver and the core application. Approaches such as model-checking, and representing rules as ontology based modelswill be evaluated for their scalability, and flexibility in maintaining the CDS rules. This will allow separating the logic ofthe CDS rules from their programmatic implementation, facilitating review, validation and maintenance by clinicians.The service will be implemented using micro-service design patterns. This will allow the architecture to be integrated
Page 22 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

and tested in parallel to the development of each CDSS sub-component (tasks 5.2, 5.3 and 5.4), and offer a fully modulararchitecture for ADLIFE that can be deployed as a distributed but also as a local system, covering all potential needsof the will be designed and implemented.
T5.2 INTEGRATION OF THE SCALES AND HEURISTIC RISK ALGORITHMS (EVERIS, P: OUH, RJH) (M12-M20)The main objective of this task is to design and develop the scales and the heuristic risk algorithms and rules basedon the patients’ clinical needs specified in WP6 and WP7, as a micro-service. This deliverable will interpret the scalesinto a computer algorithm. Interpretation of the scaled will include identification of the data needed in each scale, theFHIR resources where the data will be extracted from, and annotation of the algorithm with clinical terminologies. Thedefined algorithms will cover behaviour in unexpected conditions such as missing data. The task will also identify thecomputation requirements for each type of scales. The task will implement the specified algorithms as a micro-serviceto be integrated with the overall CDSS.
T5.3 INTEGRATION OF THE CLINICAL GUIDELINES (WARWICK, P:, SRDC EVERIS) ) (M12-M20)In this task, the recommendations from the evidence based clinical guidelines will be integrated into the CDS Systemas a micro-service. ADLIFE partners SRDC and WARWICK will implement rule based CDS services for automatingthe decision trees embedded in the selected NICE (National Institute for Health and Care Excellence) guidelines for themanagement of COPD and CHF. The guidelines will be customized for each pilot site, and the logic of the guidelineswill be represented as activity diagrams annotated with clinical codes and FHIR (data) resources. These CDS serviceswill be implemented as FHIR based the CDS Hooks services. The decision logic will be implemented using a modelbased approach, where the guideline logic will consist of constraints, rules and invariants, which will be applied duringa model validation step. EVERIS will integrate this solution in the final decision system granting the interoperabilitywith other components, the compatibility with the existing components and assuring that the final system satisfies theobjectives of the of the work package.
T5.4 RISK PREDICTION MODEL DESIGN AND IMPLEMENTATION (EVERIS, P: WARWICK, SRDC, KG,PILOT SITES ) (M1- -M23)In this task, a predictive model will be delivered allowing predictive and continuous risk assessment, improvingperformance and response on high-priority health conditions. This model will monitor specific clinical indicators andsymptoms changes and general indicators of decline and functional and dependency status. The objective is to identifyearly in patients risk of such acute events generating a set of predefined alarms that will be sent to the PCMP platform.It will be implemented using a machine learning supervised learning approach. CRISP-DM (CRoss-InduStry Processfor Data Mining) will be used. It will be divided in six iterative phases:-Business understanding: the desired outputs of the project will be established, defining the objectives, the availableresources, and the project plan and business success criteria.-Data understanding: in this stage an initial data collection report will be produced, exploring its characteristics andquality.-Data preparation: the data will be selected and cleaned. If necessary, new data will be inferred or generated bycombination.-Modelling: in this phase, the specific modelling tool will be selected and the model will be built along with the testsets in order to find the accuracy and generality of the model.-Evaluation: the degree to which the model meets the business objectives will be measured and reviewed, determiningthe next steps.-Deployment: in this stage, the evaluation results will be taken and a strategy for their deployment will be defined.The first task will be the analysis of the context and the number of different chronic conditions in which these risksituations are present. They will be diseases specific (COPD and CHF, taking into account comorbidities). With thisstudy completed, the characteristics and variables that define these situations will be listed and a complete analysis ofcorrelation between these variables will be done, in order to extract the most relevant ones.Feature selection methods can reduce the number of attributes, which can avoid the redundant features. PCA andminimum redundancy maximum relevance (mRMR) methods will be used to reduce the dimensionality and reducethe original multiple variables to one or more comprehensive ones. At the same time, the reduction of variables willfacilitate further calculation, analysis and evaluation.After the definition of the inputs and outputs of the system regarding the risk alerts defined in WP6, a first candidatemodel will be built. To build this model, different supervised algorithms will be revisited, looking for the bestperformance with the available data. Starting from previous regression algorithms described in WP6, various state-of-the-art approaches will be evaluated as decision trees, support vector machines with different kernels, random forestor artificial neural networks. Besides, ensemble methods will be tested in order to decrease bias (hypothesis boosting,variance (bootstrap aggregating) or improve predictions (stacked generalization). To evaluate the capability of the
Page 23 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
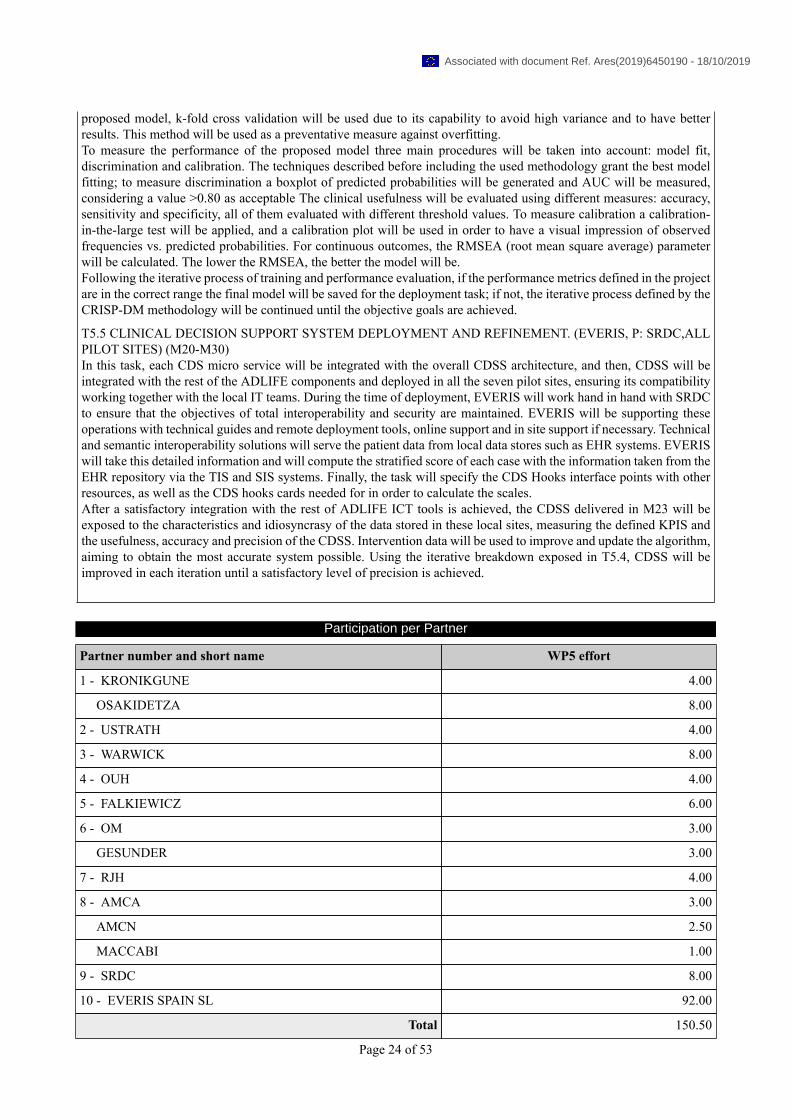
proposed model, k-fold cross validation will be used due to its capability to avoid high variance and to have betterresults. This method will be used as a preventative measure against overfitting.To measure the performance of the proposed model three main procedures will be taken into account: model fit,discrimination and calibration. The techniques described before including the used methodology grant the best modelfitting; to measure discrimination a boxplot of predicted probabilities will be generated and AUC will be measured,considering a value >0.80 as acceptable The clinical usefulness will be evaluated using different measures: accuracy,sensitivity and specificity, all of them evaluated with different threshold values. To measure calibration a calibration-in-the-large test will be applied, and a calibration plot will be used in order to have a visual impression of observedfrequencies vs. predicted probabilities. For continuous outcomes, the RMSEA (root mean square average) parameterwill be calculated. The lower the RMSEA, the better the model will be.Following the iterative process of training and performance evaluation, if the performance metrics defined in the projectare in the correct range the final model will be saved for the deployment task; if not, the iterative process defined by theCRISP-DM methodology will be continued until the objective goals are achieved.
T5.5 CLINICAL DECISION SUPPORT SYSTEM DEPLOYMENT AND REFINEMENT. (EVERIS, P: SRDC,ALLPILOT SITES) (M20-M30)In this task, each CDS micro service will be integrated with the overall CDSS architecture, and then, CDSS will beintegrated with the rest of the ADLIFE components and deployed in all the seven pilot sites, ensuring its compatibilityworking together with the local IT teams. During the time of deployment, EVERIS will work hand in hand with SRDCto ensure that the objectives of total interoperability and security are maintained. EVERIS will be supporting theseoperations with technical guides and remote deployment tools, online support and in site support if necessary. Technicaland semantic interoperability solutions will serve the patient data from local data stores such as EHR systems. EVERISwill take this detailed information and will compute the stratified score of each case with the information taken from theEHR repository via the TIS and SIS systems. Finally, the task will specify the CDS Hooks interface points with otherresources, as well as the CDS hooks cards needed for in order to calculate the scales.After a satisfactory integration with the rest of ADLIFE ICT tools is achieved, the CDSS delivered in M23 will beexposed to the characteristics and idiosyncrasy of the data stored in these local sites, measuring the defined KPIS andthe usefulness, accuracy and precision of the CDSS. Intervention data will be used to improve and update the algorithm,aiming to obtain the most accurate system possible. Using the iterative breakdown exposed in T5.4, CDSS will beimproved in each iteration until a satisfactory level of precision is achieved.
Participation per Partner
Partner number and short name WP5 effort
1 - KRONIKGUNE 4.00
OSAKIDETZA 8.00
2 - USTRATH 4.00
3 - WARWICK 8.00
4 - OUH 4.00
5 - FALKIEWICZ 6.00
6 - OM 3.00
GESUNDER 3.00
7 - RJH 4.00
8 - AMCA 3.00
AMCN 2.50
MACCABI 1.00
9 - SRDC 8.00
10 - EVERIS SPAIN SL 92.00
Total 150.50
Page 24 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
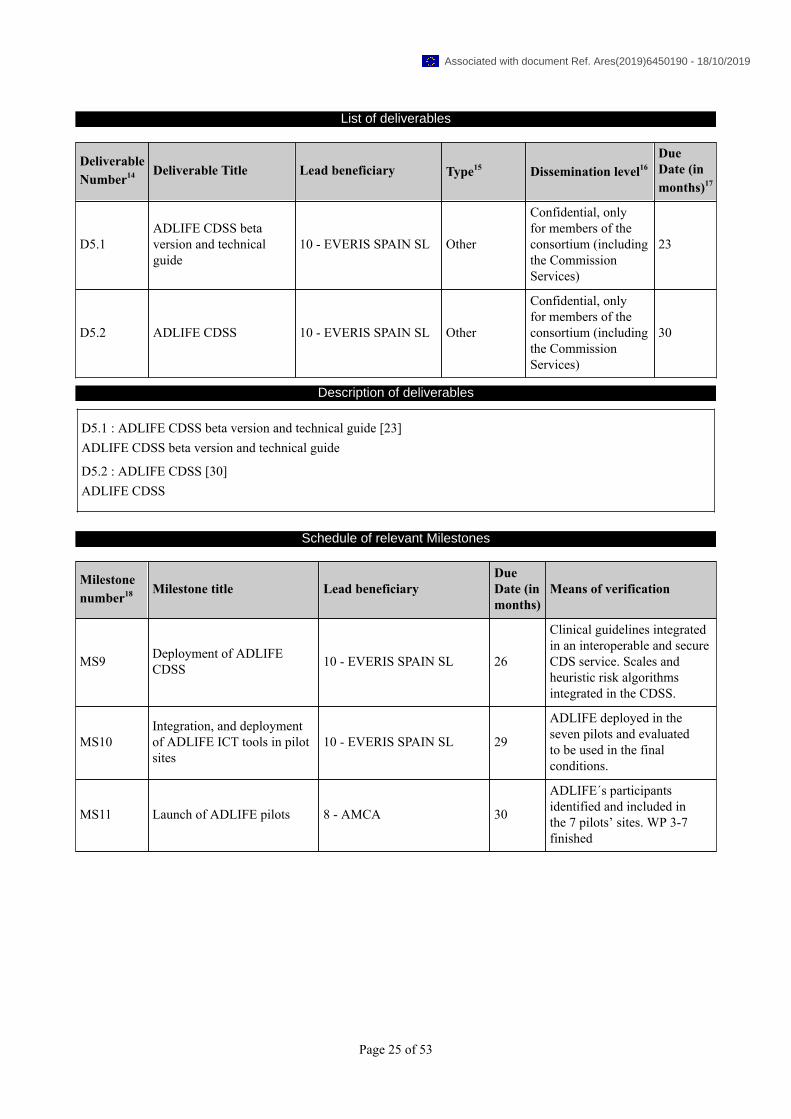
List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D5.1ADLIFE CDSS betaversion and technicalguide
10 - EVERIS SPAIN SL Other
Confidential, onlyfor members of theconsortium (includingthe CommissionServices)
23
D5.2 ADLIFE CDSS 10 - EVERIS SPAIN SL Other
Confidential, onlyfor members of theconsortium (includingthe CommissionServices)
30
Description of deliverables
D5.1 : ADLIFE CDSS beta version and technical guide [23]ADLIFE CDSS beta version and technical guide
D5.2 : ADLIFE CDSS [30]ADLIFE CDSS
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
MS9 Deployment of ADLIFECDSS 10 - EVERIS SPAIN SL 26
Clinical guidelines integratedin an interoperable and secureCDS service. Scales andheuristic risk algorithmsintegrated in the CDSS.
MS10Integration, and deploymentof ADLIFE ICT tools in pilotsites
10 - EVERIS SPAIN SL 29
ADLIFE deployed in theseven pilots and evaluatedto be used in the finalconditions.
MS11 Launch of ADLIFE pilots 8 - AMCA 30
ADLIFE´s participantsidentified and included inthe 7 pilots’ sites. WP 3-7finished
Page 25 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Work package number 9 WP6 Lead beneficiary 10 7 - RJH
Work package title EVIDENCE BASED PERSONALIZED CARE DELIVERY
Start month 1 End month 26
Objectives
The over-arching aim of the WP is to, based on best knowledge/practice, design the features of personalized care plans(PCP) for patients (Senior over 55, Heart failure (NYHA III-IV), COPD (FEV1<50) with or without comorbidities,that promote and facilitate a holistic case management addressing the multidimensional nature of their diseases whichincludes physical, psychological, social and spiritual domains. The objectives are:-To integrate and coordinate care in chronic threatening diseases into existing health care services by care pathways-To define the scope and contents of Clinical Decision Support services-To design and develop flexible Personalized Care Plans including shared decision making-To design a change management strategy taking into account the potential barriers to routine implementation andprovide solutions
Description of work and role of partners
WP6 - EVIDENCE BASED PERSONALIZED CARE DELIVERY [Months: 1-26]RJH, KRONIKGUNE, USTRATH, WARWICK, OUH, FALKIEWICZ , OM, AMCA, SRDC, EVERIS SPAIN SL, I-HDTASK 6.1. INTEGRATION AND COORDINATION OF CARE FOR ADVANCED CHRONIC DISEASES INEXISTING HEALTH-CARE SERVICES (RJH; KRON, AMCA, STRAT, OUH, FALKHOSP, OPTIMEDIS) (M1-M6):This task will analyze the present care deliverance model and level of care integration at each pilot site for patients withchronic severe diseases, using interviews and focus groups involving relevant stakeholders.In the explorative phase an emergent design will be used focusing on improvement areas and lack of seamlessnessin the existing care deliverance, from the patient´s perspective. Patients and informal care givers as well as doctors,nurses, social workers, from care organisations at different levels (home care/municipality care, primary and secondarycare) will be involved. ADLIFE will identify the most relevant improvement areas related to organizational aspects thatcould hinder the implementation (WP8). Special emphasis will be made on improvement of working conditions of allhealth care and social care providers involved, taking into account multi-disciplinary environment and constraints andincluding work time management and coordination. In co-operation, the information gathered, both regarding presentand future wished-for situation, will be used to co-design pathways for integrated supportive care in the PCP module.
TASK 6.2. DECISION SUPPORT MODULES SCOPE AND CONTENT (RJH; KRON, AMCA, STRAT, OUH,FALKHOSP, OPTIMEDIS (M2-M12):The Clinical Reference Group will, with healthcare professional representatives of all Pilot Sites guide the process ofdefining and refining CDSS. The CRG will identify and agree, based on an updated review of the literature, assessmentscales, the guidelines and the clinical prediction algorithms to be used for estimation risk and poor evolution (mortality,admission to ICU, re-admissions, complications...) for the selected pathologies. Review good quality guidelines andevidence, assessment scales and clinical predictive algorithms to identify key information to support decisions atdifferent levels decisions: capacity, goals for care, issue prioritization, therapeutic options, treatment choices consent,withholding, withdrawing therapy, hastened death, surrogate decision-making, advance directives, conflict resolution.It will provide guidance to recommend personalized treatment and actions. In this task the Clinical Reference Group,with clinical representatives of all Pilot sites will review and agree, based on an updated review of the literature, to:-Review the most adequate assessment scales and select those that will be computerized. They will include PROMsreviewed in WP7. They will agree on the actions and care strategies that can be activated according to the assessmentscales scores-Select the most adequate Guidelines to provide evidence-based input to these CDSS. The reference guidelines willbe the NICE guidelines on CHF and COPD. Recommendations will be reviewed through taking into account the Pilotsites´ reference Guidelines and a systematic process to reconcile conflicting recommendations for multimorbid patientsand adapt to local context and guides will be made. “If-else-then” programming flows will be developed and structuredin decision trees-Assess the clinical prediction algorithms selected for COPD and CHF, review the variables used, including output(mortality, admission to ICU, re-admissions, complications...).
Page 26 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

CRG will define the types of recommendations and alerts. They will select decision rules, scales and algorithms to beimplemented, identifying data needed. They will work with technical partners (WP5) defining their visualization. Thefinal ADLIFE CDSM rules and algorithm set will be assessed by local clinical expert groups (clinicians working in thePilot Sites) to ensure they support the continuous assessment and treatment of the physical, psychological, spiritual, andsocial consequences of the patients’ changing situation and condition.Pilot Sites will assess and map the variables identified in local care sites´ EHR systems. This will be an important stepfor the design of the interoperability adopters to be used to extract data from EHR sources and feed them to clinicaldecision support services (WP5).
TASK 6.3. DESIGN, DEVELOP AND TEST PERSONALIZED CARE PLAN (RJH; P: KRON, STRAT, OUH,AMCA, SRDC WARWICK, EVERIS AND ALL PILOTS) (M1-M26):Clinicians at all pilot sites will, together with technical partners, review and refine requirements for a personalised careplan, based on HL7 FHIR definitions, covering the patients´ needs from a holistic perspective and include evaluation,examination, information sharing, care planning and execution activities and monitoring of the care plan. A PCPMP willenable creation, update and follow-up of personalized integrated care plans for patients. Special focus will be on shareddecision making and on creating a “living” care plan, i.e. a flexible up-dateable document. Shared decision making aidtools identified in WP7 will be reviewed and completed.Clinical reference group supported by local experts will review the technical specification produced by TechnologicalPartners including data availability in different sites (WP3, 4 and 5), validate translation to local languages and testall functionalities of the ICT tools from a user perspective. Once final ICT platforms are deployed on the staging andproduction environments in each Pilot site, they will test them with fake patients with realistic data, to ensure realperformance complies with expected one. Test scripts guiding each functionality will be developed.
TASK 6.4. CHANGE MANAGEMENT FOR PERSONALIZED INTEGRATED CARE DELIVERY (AMCA; P: RJH,KRON, STRAT, OUH, SRDC) (M6-M26)A change management strategy will be designed (to be implemented in WP8). This task will analyse barriers and criticalsuccess factors for routine implementation of the patient- and family- centred care based on early detection of needsand a “living” personalized care plans. Second, guidelines or recommendations on organizational change managementwill be provided to facilitate the implementation of ADLIFE care model in real life.Key stakeholders for change, i.e. patient organisations, care personnel, care administrators, will be identified at each pilotsite. With results from focus groups and interviews a work plan for change including identified options and obstacleswill be produced.Local working teams will identify the changes needed by defining outcome-based pathways, depicting target groups,roles, sequencing of activities, quality of data/information exchange and multi-disciplinary coordination mechanismsdefined through a co-design approach. Once the most relevant improvement areas have been targeted, the local workingteams will recommend organizational implementation actions separately for each pilot site.One focus group per pilot site will be organized to identify gaps in knowledge and needs among the various clinicalprofessions. The outcomes will be used to deploy specific activities to increase awareness of prevalence and needs ofthe patients with advanced chronic disease amongst healthcare and identify and update care educational resources. Shorttraining programs addressing needs identified.Training activities will be organized to prepare participants for their involvement in the study, including informing,supporting, up-skilling and coaching. The training activities will ensure that key stakeholders have sufficient knowledge,confidence and practical understanding of both the study and the ADLIFE system to participate in, or to support, thestudy effectively.The training plan will be defined according to each stakeholder group. For each, a number of training activities willbe organised. Each will be defined in terms of the information provided, the materials and tools used, the trainers, andthe date and facility/place of the event. A set of core training materials /tools will be developed to support trainingevents (Introductory Video, Project Guide Books, User Manuals, On line video tutorial, Administrator Guide, TechnicalUser Manuals for ADLIFE components and Technical Webinar). The materials and tools must be tailored to the targetaudience and in will be concise and user friendly. Pilot sites will localise them (including translation and contextadaptation). The approach of the training will be pragmatic, minimising the time required for trainers and trainees andthe production/use of materials, tools and facilities. Self-directed learning and tools will be encouraged.
Participation per Partner
Partner number and short name WP6 effort
1 - KRONIKGUNE 4.00
Page 27 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Partner number and short name WP6 effort
OSAKIDETZA 4.00
2 - USTRATH 6.00
3 - WARWICK 2.00
4 - OUH 6.00
5 - FALKIEWICZ 6.00
6 - OM 3.00
GESUNDER 3.00
7 - RJH 18.00
8 - AMCA 3.00
AMCN 2.50
MACCABI 1.00
9 - SRDC 2.00
10 - EVERIS SPAIN SL 4.00
11 - I-HD 1.00
Total 65.50
List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D6.1ADLIFE DecisionSupport Modules Scopeand Content
7 - RJH Report Public 15
D6.2
Recommendations forchange management inintegrated personalizedcare delivery
7 - RJH Report Public 26
Description of deliverables
D6.1 : ADLIFE Decision Support Modules Scope and Content [15]ADLIFE Decision Support Modules Scope and Content
D6.2 : Recommendations for change management in integrated personalized care delivery [26]Recommendations for change management in integrated personalized care delivery
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
MS5 ADLIFE guidelines, scalesand PROMs final selection 7 - RJH 15 Task 6.2 Decision support
modules scope and contentPage 28 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
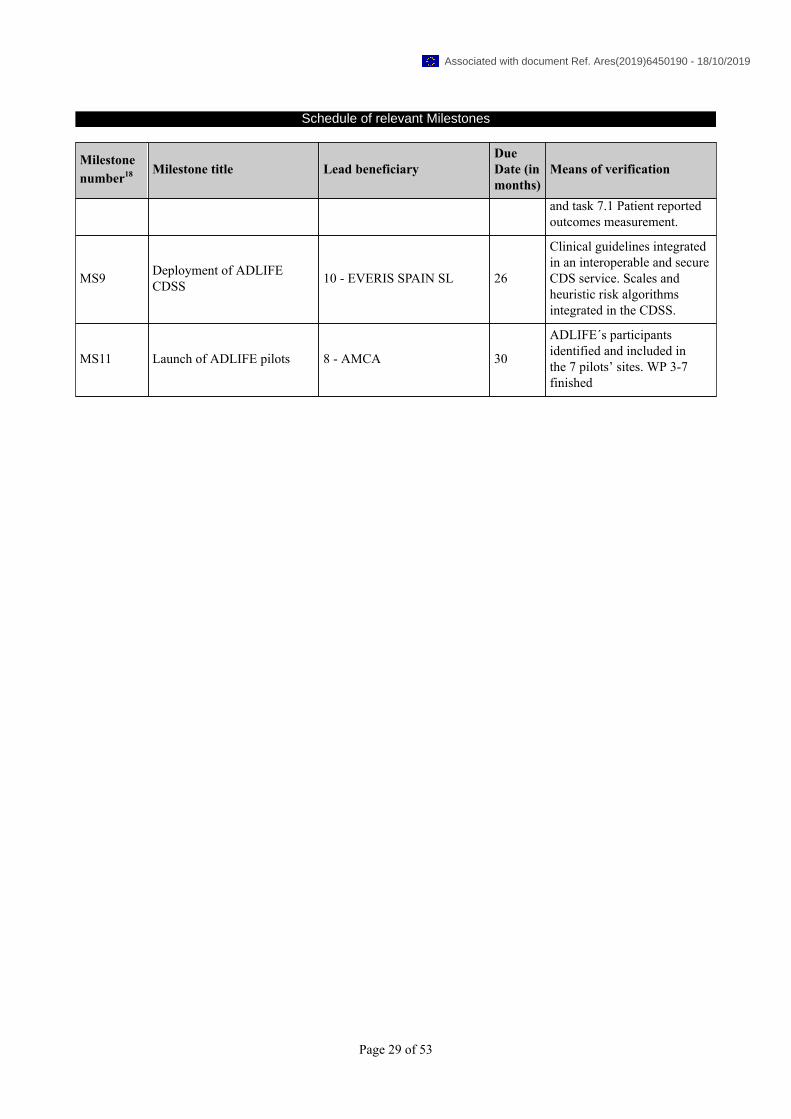
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
and task 7.1 Patient reportedoutcomes measurement.
MS9 Deployment of ADLIFECDSS 10 - EVERIS SPAIN SL 26
Clinical guidelines integratedin an interoperable and secureCDS service. Scales andheuristic risk algorithmsintegrated in the CDSS.
MS11 Launch of ADLIFE pilots 8 - AMCA 30
ADLIFE´s participantsidentified and included inthe 7 pilots’ sites. WP 3-7finished
Page 29 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
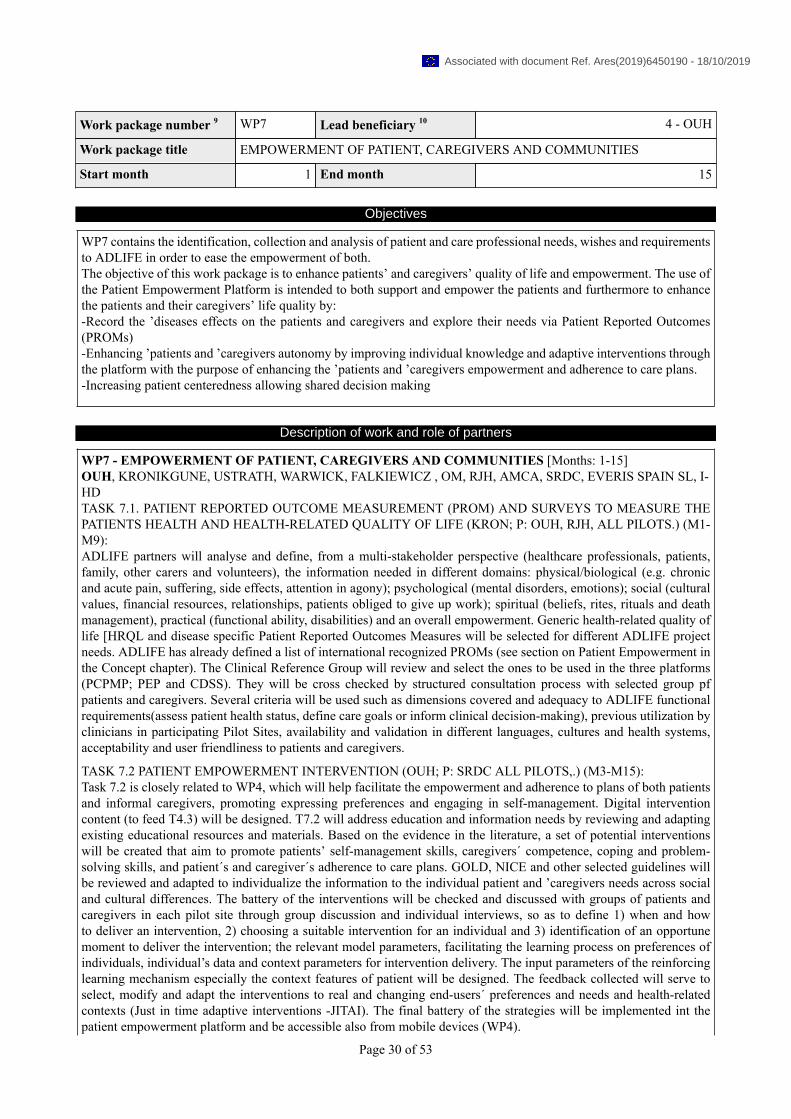
Work package number 9 WP7 Lead beneficiary 10 4 - OUH
Work package title EMPOWERMENT OF PATIENT, CAREGIVERS AND COMMUNITIES
Start month 1 End month 15
Objectives
WP7 contains the identification, collection and analysis of patient and care professional needs, wishes and requirementsto ADLIFE in order to ease the empowerment of both.The objective of this work package is to enhance patients’ and caregivers’ quality of life and empowerment. The use ofthe Patient Empowerment Platform is intended to both support and empower the patients and furthermore to enhancethe patients and their caregivers’ life quality by:-Record the ’diseases effects on the patients and caregivers and explore their needs via Patient Reported Outcomes(PROMs)-Enhancing ’patients and ’caregivers autonomy by improving individual knowledge and adaptive interventions throughthe platform with the purpose of enhancing the ’patients and ’caregivers empowerment and adherence to care plans.-Increasing patient centeredness allowing shared decision making
Description of work and role of partners
WP7 - EMPOWERMENT OF PATIENT, CAREGIVERS AND COMMUNITIES [Months: 1-15]OUH, KRONIKGUNE, USTRATH, WARWICK, FALKIEWICZ , OM, RJH, AMCA, SRDC, EVERIS SPAIN SL, I-HDTASK 7.1. PATIENT REPORTED OUTCOME MEASUREMENT (PROM) AND SURVEYS TO MEASURE THEPATIENTS HEALTH AND HEALTH-RELATED QUALITY OF LIFE (KRON; P: OUH, RJH, ALL PILOTS.) (M1-M9):ADLIFE partners will analyse and define, from a multi-stakeholder perspective (healthcare professionals, patients,family, other carers and volunteers), the information needed in different domains: physical/biological (e.g. chronicand acute pain, suffering, side effects, attention in agony); psychological (mental disorders, emotions); social (culturalvalues, financial resources, relationships, patients obliged to give up work); spiritual (beliefs, rites, rituals and deathmanagement), practical (functional ability, disabilities) and an overall empowerment. Generic health-related quality oflife [HRQL and disease specific Patient Reported Outcomes Measures will be selected for different ADLIFE projectneeds. ADLIFE has already defined a list of international recognized PROMs (see section on Patient Empowerment inthe Concept chapter). The Clinical Reference Group will review and select the ones to be used in the three platforms(PCPMP; PEP and CDSS). They will be cross checked by structured consultation process with selected group pfpatients and caregivers. Several criteria will be used such as dimensions covered and adequacy to ADLIFE functionalrequirements(assess patient health status, define care goals or inform clinical decision-making), previous utilization byclinicians in participating Pilot Sites, availability and validation in different languages, cultures and health systems,acceptability and user friendliness to patients and caregivers.
TASK 7.2 PATIENT EMPOWERMENT INTERVENTION (OUH; P: SRDC ALL PILOTS,.) (M3-M15):Task 7.2 is closely related to WP4, which will help facilitate the empowerment and adherence to plans of both patientsand informal caregivers, promoting expressing preferences and engaging in self-management. Digital interventioncontent (to feed T4.3) will be designed. T7.2 will address education and information needs by reviewing and adaptingexisting educational resources and materials. Based on the evidence in the literature, a set of potential interventionswill be created that aim to promote patients’ self-management skills, caregivers´ competence, coping and problem-solving skills, and patient´s and caregiver´s adherence to care plans. GOLD, NICE and other selected guidelines willbe reviewed and adapted to individualize the information to the individual patient and ’caregivers needs across socialand cultural differences. The battery of the interventions will be checked and discussed with groups of patients andcaregivers in each pilot site through group discussion and individual interviews, so as to define 1) when and howto deliver an intervention, 2) choosing a suitable intervention for an individual and 3) identification of an opportunemoment to deliver the intervention; the relevant model parameters, facilitating the learning process on preferences ofindividuals, individual’s data and context parameters for intervention delivery. The input parameters of the reinforcinglearning mechanism especially the context features of patient will be designed. The feedback collected will serve toselect, modify and adapt the interventions to real and changing end-users´ preferences and needs and health-relatedcontexts (Just in time adaptive interventions -JITAI). The final battery of the strategies will be implemented int thepatient empowerment platform and be accessible also from mobile devices (WP4).
Page 30 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
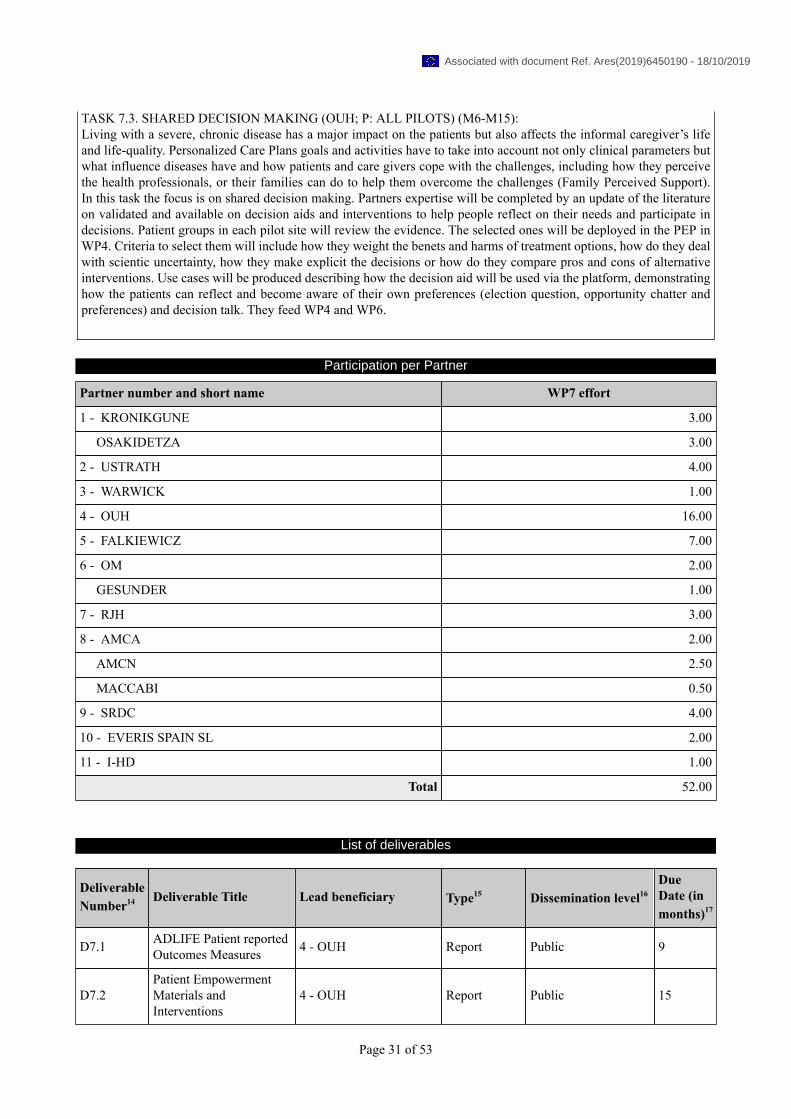
TASK 7.3. SHARED DECISION MAKING (OUH; P: ALL PILOTS) (M6-M15):Living with a severe, chronic disease has a major impact on the patients but also affects the informal caregiver’s lifeand life-quality. Personalized Care Plans goals and activities have to take into account not only clinical parameters butwhat influence diseases have and how patients and care givers cope with the challenges, including how they perceivethe health professionals, or their families can do to help them overcome the challenges (Family Perceived Support).In this task the focus is on shared decision making. Partners expertise will be completed by an update of the literatureon validated and available on decision aids and interventions to help people reflect on their needs and participate indecisions. Patient groups in each pilot site will review the evidence. The selected ones will be deployed in the PEP inWP4. Criteria to select them will include how they weight the benets and harms of treatment options, how do they dealwith scientic uncertainty, how they make explicit the decisions or how do they compare pros and cons of alternativeinterventions. Use cases will be produced describing how the decision aid will be used via the platform, demonstratinghow the patients can reflect and become aware of their own preferences (election question, opportunity chatter andpreferences) and decision talk. They feed WP4 and WP6.
Participation per Partner
Partner number and short name WP7 effort
1 - KRONIKGUNE 3.00
OSAKIDETZA 3.00
2 - USTRATH 4.00
3 - WARWICK 1.00
4 - OUH 16.00
5 - FALKIEWICZ 7.00
6 - OM 2.00
GESUNDER 1.00
7 - RJH 3.00
8 - AMCA 2.00
AMCN 2.50
MACCABI 0.50
9 - SRDC 4.00
10 - EVERIS SPAIN SL 2.00
11 - I-HD 1.00
Total 52.00
List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D7.1 ADLIFE Patient reportedOutcomes Measures 4 - OUH Report Public 9
D7.2Patient EmpowermentMaterials andInterventions
4 - OUH Report Public 15
Page 31 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D7.3 Shared decision makingtool Requirements 4 - OUH Report
Confidential, onlyfor members of theconsortium (includingthe CommissionServices)
15
Description of deliverables
D7.1 : ADLIFE Patient reported Outcomes Measures [9]ADLIFE Patient reported Outcomes Measures
D7.2 : Patient Empowerment Materials and Interventions [15]Patient Empowerment Materials and Interventions
D7.3 : Shared decision making tool Requirements [15]Shared decision making tool Requirements
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
MS5 ADLIFE guidelines, scalesand PROMs final selection 7 - RJH 15
Task 6.2 Decision supportmodules scope and contentand task 7.1 Patient reportedoutcomes measurement.
MS6Tools for empowermentdelivered and ready to betested in WP8
9 - SRDC 15
Participants (patients,professionals, carers…)engaged and testing thebeta version of the tools andsupporting the launching ofthe pilots.
MS8
ADLIFE patientempowerment platform andJTA mechanisms ready foreach pilot
9 - SRDC 26
Task 4.1, 4.2 and 4.3done. Personalized JTAIbuilt per site upon thePower 2DM intelligentcommunication engine. WP7done and patients, carers andcommunity empowered
MS11 Launch of ADLIFE pilots 8 - AMCA 30
ADLIFE´s participantsidentified and included inthe 7 pilots’ sites. WP 3-7finished
Page 32 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Work package number 9 WP8 Lead beneficiary 10 8 - AMCA
Work package title PILOT DESIGN AND IMPLEMENTATION
Start month 1 End month 44
Objectives
The main objectives of this WP are:-To engage all stakeholders (patients, families, formal caregivers, healthcare professionals, social workers, volunteers…)-To prepare and set up all materials and technical resources required for the intervention-To deploy the intervention focused on early detection of supportive care needs and personalized supportive care delivery-To ensure consistent and effective deployment of the intervention by early detection of difficulties or deviations anda prompt adjustment and solution.
Description of work and role of partners
WP8 - PILOT DESIGN AND IMPLEMENTATION [Months: 1-44]AMCA, KRONIKGUNE, USTRATH, WARWICK, OUH, FALKIEWICZ , OM, RJH, SRDC, EVERIS SPAIN SL, I-HDTASK 8.1 PREPARE THE IMPLEMENTATION OF THE INTERVENTION (AMCA; ALL PARTNERS) (M12-M30)The preparation of the ADLIFE intervention implementation is a critical step that needs special attention. ADLIFEintervention requires not only the deployment of innovative technological solutions (such as the PCPMP, PEP and theCDSS) but also the establishment of the required features in care pathway as well as the training of the professionalsinvolved. The activities to be performed at the site level, are:-Recruitment of healthcare professionals that will be responsible for implementing ADLIFE intervention. Each site willdecide the profile of the professionals that will be involved but building multidisciplinary team will be mandatory.-Training of professionals, based on the design and materials prepared in T.6.4, including the use of the PCPMP,understanding its functionalities and the scientific and evidence base behind the CDS Services. Case studies as wellas consensus groups will be included in the training methodology to ensure that professionals understand, accept andadopt both the clinical (T6.2 and 6.3) and technical dimensions of the PCPMP (T3.2)-Putting in place the organizational changes required in each site as defined in T6.1 to enable the incorporation of theADLIFE care pathways into real-life settings.-Set up the recommendations resulting from the change management analysis done in T6.4 to minimize as much aspossible the barriers that could hamper the successful implementation of ADLIFE intervention.-Prepare all the materials, logistics and infrastructure required to provide patients, families and communities withtraining on empowerment and shared decision making defined in T7.2-T7.3.-Each site will prepare a comprehensive Deployment Plan to organize and schedule all the activities aforementionedto ensure that they are carried out as expected. The deployment plan will also include the detailed Research Protocolsand processes (Standard Operation Procedures, SOP) that will be implemented and that will be included in the materialsubmitted to the Ethics Committee in each site (T. 8.3)-Each site will verify that they have Ethics Committee Approval as a result of the relevant tasks carried out in WP1and T.8.3.Once these activities and T8.2 are completed, the recruitment of patients can begin. Patients with Advanced ChronicDiseases complying with the inclusion and exclusion criteria will be identified approached, validated and recruited.
TASK 8.2 DEPLOYMENT AND OPERATION OF ADLIFE PILOT APPLICATION -(WARWICK,: ALL PARTNERS(M18-M30):This task will explore in detail how the solutions provided by ADLIFE ICT components can be deployed at each pilotsite. A High-level Deployment Design (HDD) will define the deployment requirements of the ADLIFE Componentsto be implemented at the pilot sites, defining the strategy on how the whole system can be deployed and used intheir real production scenarios. The HDD maps the components identified in the logical architecture to physicalservers and other network devices to create the deployment architecture, including the non-functional requirements andlogistical infrastructure. This task will ensure readiness of the pilot sites for the actual deployment. Integration of theADLIFE toolkit together with interoperability adapters into the local computer systems (e.g, computer desktop software,smartphone, electronic health record) of pilot sites will ease their daily use by healthcare professionals. Integration ofthe Personalized Care Plan Management Platform (PCPMP) into local systems following the instructions developedin Tasks 3.1, 3.4, 4.1 and 5.5, will ensure readiness of pilot sites. This preparation phase will include activities such
Page 33 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

as confirming data quality through manual interventions and semi-automatic tools, as well as securing physical/logicalinfrastructure for the deployment.
TASK 8.3 ETHICAL APPLICATIONS FOR ETHICAL COMMITTEE APPROVAL (AMCA; ALL PARTNERS) (M1-M44)This task will be focused on the submission for approval with all the details concerning the clinical studies to the EthicsCommittees for all sites including::-Submission of all necessary forms and documents including protocols for the pilot implementation studies to the EthicsCommittee.-This process needs to begin as early as possible in order to appraise the Ethics Committee about the project withcontinued updates until final approval.-Creating consent forms for the patient and the caregivers for approval by the Ethics Committee.-Preparing information and ultimately demonstration of those aspects of the PCP technology Platform that will be usedby and/or directly affect the patient and the Caregivers.-Assuring that the technology does not fall into the category of new medical devices requiring certification from otherbodies, at least during the period of the project and pilot implementation-Updates to the Ethics Committees as necessary before and during the implementation studies.The Guidance for applicants on informed consents provided by the EC H2020 will be used as well.Regular updates of this information will be promoted so that ethical issues are continuously being considered throughoutthe project and all relevant regulations are fully complied with.
TASK 8.4. DEPLOY THE ADLIFE INTEGRATED CARE INTERVENTION (AMCA; ALL PARTNERS) (M12-M41)Intervention will be built mainly on two pillars: Identification of patients with advanced chronic conditions requiringstructured supportive care, baseline assessment and stratification and provision of personalized care. The integrated careintervention will address patients´ and caregivers´ empowerment and professionals´ training as well. The interventionincludes not only the large scale deployment and use of the ADLIFE components but a trial to demonstrate how thedeployed ADLIFE application delivers on the objectives set out at the project. The trial involves actual users, i.e.professionals, patients and informal care givers (Table 1 in page 2 of this 1-3 Annex). The methodological approachto facilitate the implementation will be based on continuous improvement model that will enable the continuousassessment of the implementation process and ongoing adaptations in the intervention to better fit the needs of thepatients, families, professionals and organisation. Patients will be identified according to the inclusion and exclusioncriteria from the clinical and administrative data bases in each site. These patients will be reviewed and validated by thehealthcare professionals. Once the candidate patients are confirmed and selected, professionals will approach and theminform them that they are eligible for the new intervention, recruit them, and obtain signed informed consent forms.A baseline assessment and needs assessment will be made to provide the basis for a personalized care plan. Dates forthe intervention are: M30-M41 Intervention, M28-M31 Recruitment, M39-M42 Control Recruitment and M41-M30Retrospective Control AnalysisTASK 8.5 MONITOR THE IMPLEMENTATION AND PILOT DATA MANAGEMENT AND PREPARATION(AMCA; ALL PARTNERS) (M12-M44)This task will be focused on monitoring the ADLIFE implementation, both clinical, organizational and technical,process to promptly detect problems or deviations and propose corrective actions. An agile-like approach with frequentinteractions with pilot partners will be adopted, with regular virtual meetings to check on progress.The follow up for intervention group patients is up to 12 months in unless the patient drops out or dies. Control grouppatients will be retrospectively monitored for the same period of time. This task will monitor the ongoing collection ofdata at each deployment site, and the preparation of the datasets in accordance with the evaluation plan defined in WP9and guidelines stablished for ADLIFE data management at holistic level (WP1). A data manager will be appointed ineach pilot site responsible for: ensuring adequacy, accuracy and legitimacy of data collected; devising and implementingefficient and secure procedures for data management. The datasets will be transferred in accordance with the EvaluationPlan (T9.1) and the DMP (D 1.1)
Participation per Partner
Partner number and short name WP8 effort
1 - KRONIKGUNE 8.00
OSAKIDETZA 6.00
2 - USTRATH 8.00
Page 34 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Partner number and short name WP8 effort
3 - WARWICK 2.00
4 - OUH 12.00
5 - FALKIEWICZ 10.00
6 - OM 2.00
GESUNDER 6.00
7 - RJH 12.00
8 - AMCA 18.00
AMCN 4.00
MACCABI 9.00
9 - SRDC 2.00
10 - EVERIS SPAIN SL 2.00
11 - I-HD 1.00
Total 102.00
List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D8.1 ADLIFE deploymentplans 8 - AMCA Report Public 24
D8.2 Report on ADLIFE pilotexecution 8 - AMCA Report Public 44
Description of deliverables
D8.1 : ADLIFE deployment plans [24]ADLIFE deployment plans
D8.2 : Report on ADLIFE pilot execution [44]Report on ADLIFE pilot execution
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
MS1 ADLIFE´s ethical approval 8 - AMCA 6
All pilot has obtained theapproval to the interventionfrom the correspondingethical committees
MS4 ADLIFE interoperability andsecurity assurance of the tools 3 - WARWICK 18 Task 3.4 solved,
interoperability, security,
Page 35 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
privacy and quality issuessolve in all the pilot sites
MS6Tools for empowermentdelivered and ready to betested in WP8
9 - SRDC 15
Participants (patients,professionals, carers…)engaged and testing thebeta version of the tools andsupporting the launching ofthe pilots.
MS7 ADLIFE Pilot site builds forintelligent and secure tools 3 - WARWICK 25
Task 3.2 and 3.3done. Integration ofthe personalized caremanagement platform
MS8
ADLIFE patientempowerment platform andJTA mechanisms ready foreach pilot
9 - SRDC 26
Task 4.1, 4.2 and 4.3done. Personalized JTAIbuilt per site upon thePower 2DM intelligentcommunication engine. WP7done and patients, carers andcommunity empowered
MS10Integration, and deploymentof ADLIFE ICT tools in pilotsites
10 - EVERIS SPAIN SL 29
ADLIFE deployed in theseven pilots and evaluatedto be used in the finalconditions.
MS11 Launch of ADLIFE pilots 8 - AMCA 30
ADLIFE´s participantsidentified and included inthe 7 pilots’ sites. WP 3-7finished
MS12 Baseline data for evaluation 1 - KRONIKGUNE 30 Participants recruited, and theinitial situation evaluated
Page 36 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Work package number 9 WP9 Lead beneficiary 10 1 - KRONIKGUNE
Work package title EVALUATION
Start month 1 End month 48
Objectives
-To develop an evaluation strategy that includes a credible and feasible research design and analysis plan-To coordinate the evaluation process at project level-To analyze the results from quantitative and qualitative perspectives-To estimate the economic impact of the intervention at population level in mid-long term
Description of work and role of partners
WP9 - EVALUATION [Months: 1-48]KRONIKGUNE, USTRATH, WARWICK, OUH, FALKIEWICZ , OM, RJH, AMCA, SRDC, EVERIS SPAIN SLT9.1 DEVELOP THE EVALUATION FRAMEWORK AND PLANNING (KRON; ALL PARTNERS) (M1-M24)The evaluation framework will provide the detailed methodological operationalization for the project. It will contain theevaluation objectives (main and secondary variables), final indicators based on the list already produced, and evaluationand analysis design. Data gathering sources methods and tools (both quantitative and qualitative) will be specified. AData collection Sheet (DCS) as well as a database will be designed for the collection of the data by the sites (Task8.5). Data processing (including pseudonimization), uploading and quality control will be established. Reports will beprepared, reviewed and disseminated.The evaluation will start with the agreement of the minimum dataset to be evaluated across all pilot sites according to theevaluation indicators described in the Evaluation section above. Agreement of the consortium partners will be necessaryto access and to share data. Individual written informed consent will be obtained from all participants according to theauthorization granted by reference Clinical Ethics Committees (T8.3).
T9.2 EVALUATE OUTCOMES AT DIFFERENT TIME-POINTS LEAD: KRON; INVOLVED: ALL PARTNERS)(M24-M48)An individual follow up method will be used. For intervention group, each participant and their caregivers will beassessed at baseline, when recruited, and will be asked to fulfill a final assessment at the end of follow up period of whendeath occurs. Final assessment will be performed on caregivers and professionals and for patients, data about HRQLand satisfaction will be missed. Information regarding use of services, especially for the main variable (unplanned ERvisits) will be extracted systematically all along the follow up period.Control group will be selected at the end of the intervention period in order to be comparable to intervention group(matched) and to assure that this group has received usual care. Data of the main variable and use of services will becollected retrospectively for the same period of time than the intervention group.The main outcomes that will be assessed are: at patient’s level, unplanned ER visits, as a proxy of continuity andcoverage of care. HRQL and satisfaction will be also assessed; at caregiver’s level, burden of care and satisfaction;at professionals’ level, satisfaction with the care and at system’s level use of resources, expecting to observed a moreefficient use of services. A number of secondary variables will be assessed too as explained in the methodologysection (symptom management, impact on households, benefits and costs of early identification, cost effectiveness andfeasibility, among others). As has been described earlier in the document a mixed evaluation strategy will be performedcombining quantitative and qualitative analysis depending on the studied outcome.
T9.3 EVALUATION OF THE CLINICAL PREDICTIVE RULES (KRON; ALL PARTNERS) (M25-M48)The robustness of the clinical predictive rules (CPR) in the ALDIFE proposal will be evaluated at two distinct phases:(a) we will evaluate the general fitness, applicability in clinical practice and transferability to our samples after havingimplemented the rules in software and (b) a validation of the algorithms in the final evaluation step. In last period, theperformance of these CPRs will be assessed by means of their model fit and their model discrimination and calibrationabilities. To this end, the AUC values (an AUC > 0.80 will be considered acceptable) and the clinical screeningparameters such as sensitivity and specificity will be computed. Model calibration will be tested by means of thecalibration-in-the-large (ie, a comparison of the average predicted probability for the whole cohort and the proportion ofpatients with the event of interest) and by visually inspecting a calibration plot, in which groups of predicted probabilitiesare plotted against actually observed outcomes and perfect predictions should be on 45º line. Finally, in the (a) section,we will investigate whether new covariates (not been included in the original model) significantly improved the original
Page 37 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
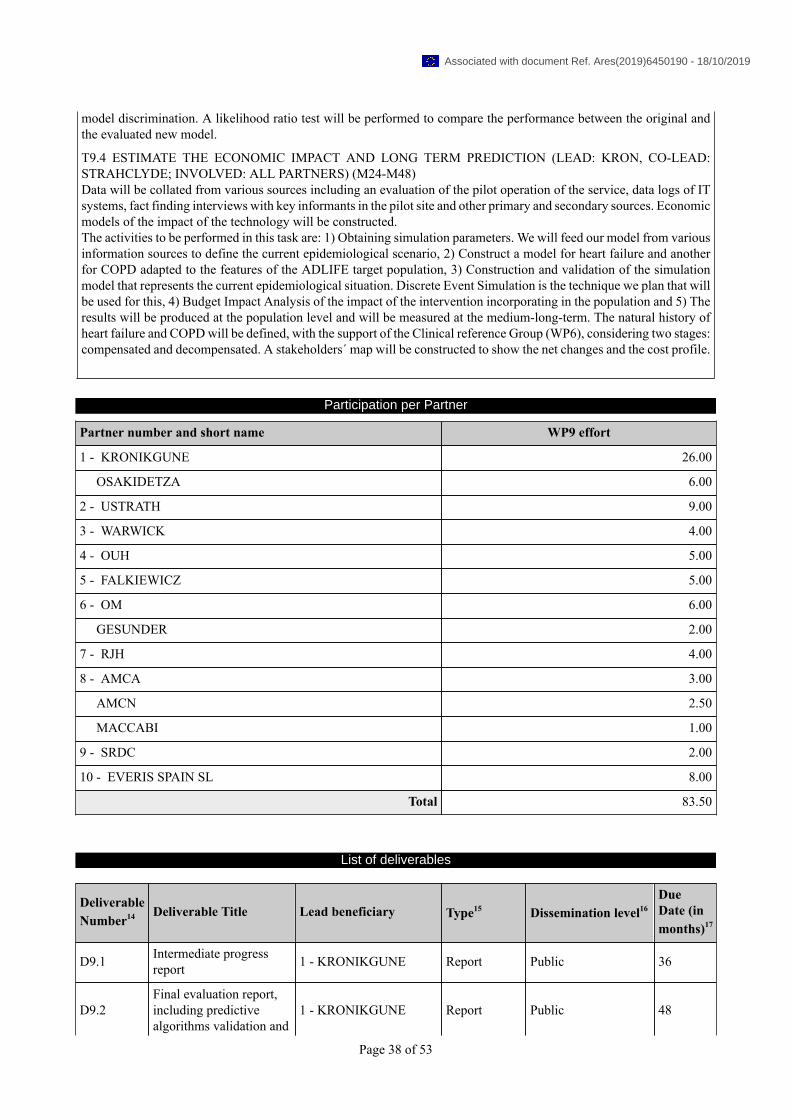
model discrimination. A likelihood ratio test will be performed to compare the performance between the original andthe evaluated new model.
T9.4 ESTIMATE THE ECONOMIC IMPACT AND LONG TERM PREDICTION (LEAD: KRON, CO-LEAD:STRAHCLYDE; INVOLVED: ALL PARTNERS) (M24-M48)Data will be collated from various sources including an evaluation of the pilot operation of the service, data logs of ITsystems, fact finding interviews with key informants in the pilot site and other primary and secondary sources. Economicmodels of the impact of the technology will be constructed.The activities to be performed in this task are: 1) Obtaining simulation parameters. We will feed our model from variousinformation sources to define the current epidemiological scenario, 2) Construct a model for heart failure and anotherfor COPD adapted to the features of the ADLIFE target population, 3) Construction and validation of the simulationmodel that represents the current epidemiological situation. Discrete Event Simulation is the technique we plan that willbe used for this, 4) Budget Impact Analysis of the impact of the intervention incorporating in the population and 5) Theresults will be produced at the population level and will be measured at the medium-long-term. The natural history ofheart failure and COPD will be defined, with the support of the Clinical reference Group (WP6), considering two stages:compensated and decompensated. A stakeholders´ map will be constructed to show the net changes and the cost profile.
Participation per Partner
Partner number and short name WP9 effort
1 - KRONIKGUNE 26.00
OSAKIDETZA 6.00
2 - USTRATH 9.00
3 - WARWICK 4.00
4 - OUH 5.00
5 - FALKIEWICZ 5.00
6 - OM 6.00
GESUNDER 2.00
7 - RJH 4.00
8 - AMCA 3.00
AMCN 2.50
MACCABI 1.00
9 - SRDC 2.00
10 - EVERIS SPAIN SL 8.00
Total 83.50
List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D9.1 Intermediate progressreport 1 - KRONIKGUNE Report Public 36
D9.2Final evaluation report,including predictivealgorithms validation and
1 - KRONIKGUNE Report Public 48
Page 38 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
economic impact of theintervention
Description of deliverables
D9.1 : Intermediate progress report [36]Intermediate progress report
D9.2 : Final evaluation report, including predictive algorithms validation and economic impact of the intervention[48]Final evaluation report, including predictive algorithms validation and economic impact of the intervention
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
MS12 Baseline data for evaluation 1 - KRONIKGUNE 30 Participants recruited, and theinitial situation evaluated
MS13 Final evaluation 1 - KRONIKGUNE 47
Control and interventionfollow up finished and dataobtained from 12 monthswhen possible.
Page 39 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
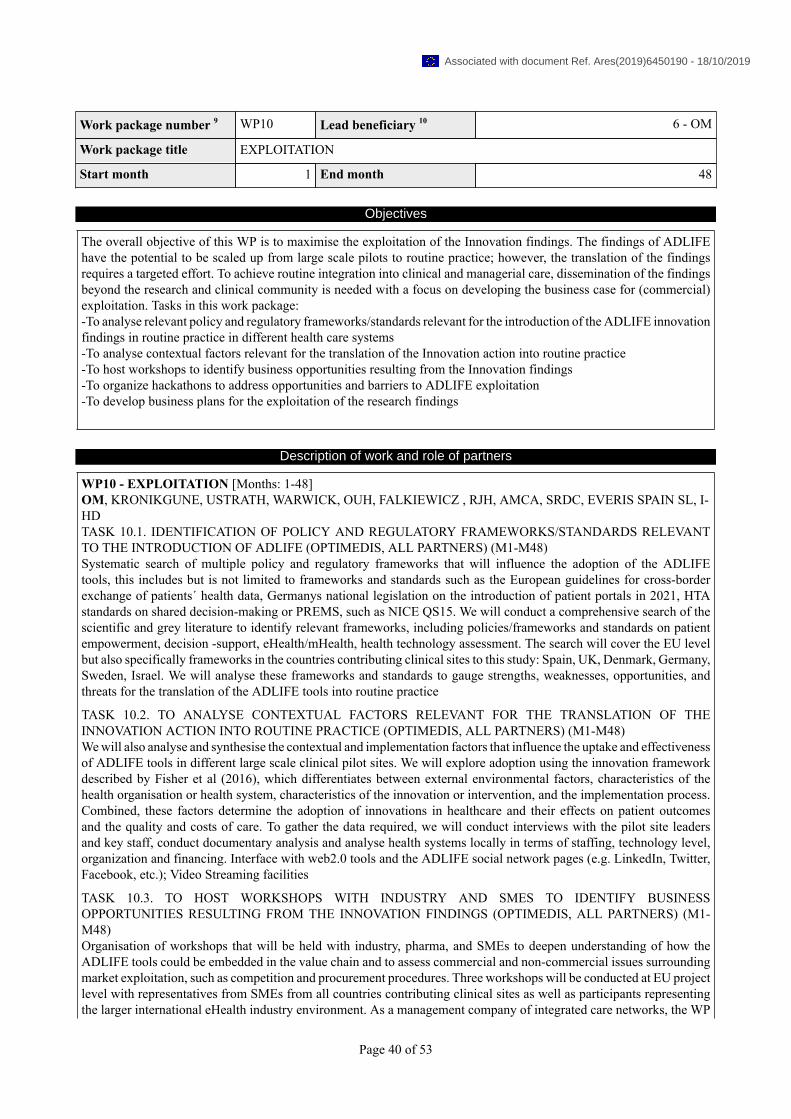
Work package number 9 WP10 Lead beneficiary 10 6 - OM
Work package title EXPLOITATION
Start month 1 End month 48
Objectives
The overall objective of this WP is to maximise the exploitation of the Innovation findings. The findings of ADLIFEhave the potential to be scaled up from large scale pilots to routine practice; however, the translation of the findingsrequires a targeted effort. To achieve routine integration into clinical and managerial care, dissemination of the findingsbeyond the research and clinical community is needed with a focus on developing the business case for (commercial)exploitation. Tasks in this work package:-To analyse relevant policy and regulatory frameworks/standards relevant for the introduction of the ADLIFE innovationfindings in routine practice in different health care systems-To analyse contextual factors relevant for the translation of the Innovation action into routine practice-To host workshops to identify business opportunities resulting from the Innovation findings-To organize hackathons to address opportunities and barriers to ADLIFE exploitation-To develop business plans for the exploitation of the research findings
Description of work and role of partners
WP10 - EXPLOITATION [Months: 1-48]OM, KRONIKGUNE, USTRATH, WARWICK, OUH, FALKIEWICZ , RJH, AMCA, SRDC, EVERIS SPAIN SL, I-HDTASK 10.1. IDENTIFICATION OF POLICY AND REGULATORY FRAMEWORKS/STANDARDS RELEVANTTO THE INTRODUCTION OF ADLIFE (OPTIMEDIS, ALL PARTNERS) (M1-M48)Systematic search of multiple policy and regulatory frameworks that will influence the adoption of the ADLIFEtools, this includes but is not limited to frameworks and standards such as the European guidelines for cross-borderexchange of patients´ health data, Germanys national legislation on the introduction of patient portals in 2021, HTAstandards on shared decision-making or PREMS, such as NICE QS15. We will conduct a comprehensive search of thescientific and grey literature to identify relevant frameworks, including policies/frameworks and standards on patientempowerment, decision -support, eHealth/mHealth, health technology assessment. The search will cover the EU levelbut also specifically frameworks in the countries contributing clinical sites to this study: Spain, UK, Denmark, Germany,Sweden, Israel. We will analyse these frameworks and standards to gauge strengths, weaknesses, opportunities, andthreats for the translation of the ADLIFE tools into routine practice
TASK 10.2. TO ANALYSE CONTEXTUAL FACTORS RELEVANT FOR THE TRANSLATION OF THEINNOVATION ACTION INTO ROUTINE PRACTICE (OPTIMEDIS, ALL PARTNERS) (M1-M48)We will also analyse and synthesise the contextual and implementation factors that influence the uptake and effectivenessof ADLIFE tools in different large scale clinical pilot sites. We will explore adoption using the innovation frameworkdescribed by Fisher et al (2016), which differentiates between external environmental factors, characteristics of thehealth organisation or health system, characteristics of the innovation or intervention, and the implementation process.Combined, these factors determine the adoption of innovations in healthcare and their effects on patient outcomesand the quality and costs of care. To gather the data required, we will conduct interviews with the pilot site leadersand key staff, conduct documentary analysis and analyse health systems locally in terms of staffing, technology level,organization and financing. Interface with web2.0 tools and the ADLIFE social network pages (e.g. LinkedIn, Twitter,Facebook, etc.); Video Streaming facilities
TASK 10.3. TO HOST WORKSHOPS WITH INDUSTRY AND SMES TO IDENTIFY BUSINESSOPPORTUNITIES RESULTING FROM THE INNOVATION FINDINGS (OPTIMEDIS, ALL PARTNERS) (M1-M48)Organisation of workshops that will be held with industry, pharma, and SMEs to deepen understanding of how theADLIFE tools could be embedded in the value chain and to assess commercial and non-commercial issues surroundingmarket exploitation, such as competition and procurement procedures. Three workshops will be conducted at EU projectlevel with representatives from SMEs from all countries contributing clinical sites as well as participants representingthe larger international eHealth industry environment. As a management company of integrated care networks, the WP
Page 40 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

leader OptiMedis AG has an excellent network of SMEs, Physician networks and commercial partners that can be drawnon to organise such workshops as part of the innovation strategy.
TASK 10.4 TO ORGANIZE HACKATONS TO ADDRESS OPPORTUNTIES AND BARRIERS TO ADLIFEEXPLOITATION (OPTIMEDIS, ALL PARTNERS) (M1-M48)As an innovative element we will organise 2 hackathons to address obstacles associated with research exploitation. Ahackathon is an event in which software designers and developers come together and intensively work on a project. Wewill organise 2 international events in a central location to draw young researchers and healthcare managers togetherto work on an interdisciplinary team to address very specific problems (resulting from the obstacles to implementation,as identified by experts and user groups, see tasks 10.1./10.2/10.3.) with the overall aim of developing solutions for theintegration of ADLIFE tools into daily clinical practice. OptiMedis is successfully organizing similar event as part ofthe EU funded HealthPros Marie-Curie Training Network.
TASK 10.5. TO DEVELOP BUSINESS PLANS FOR THE (COMERCIAL) EXPLOITATION OF THE RESEARCHFINDINGS (OPTIMEDIS, ALL PARTNERS) (M1-M48)The development of business plans for the ADLIFE tools will be key to the exploitation of research results. Our businessplans will address diverse market contexts and risks according to: Characteristics of national, regional, and local healthsystems (tax or insurance-based…), Characteristics of the market (open or highly regulated, extent of competition…),Purchasing arrangements (procurement and commissioning). Business plans will address national, regional and localhealth systems and provide a clear case for investment, specifying the prerequisites for implementation. To facilitate thisprocess, we will use the Business Model Canvas, a lean management template for developing new business models thatcharts key elements of business proposals, such as key partners, key activities, value proposition, customer relationships,customer segments, key resources and channels. The aim is to generate a business case that demonstrates why a regionalauthority, health care provider or statutory health insurance company should invest in the technology as proposed inthis project. The final business canvas templates will be prepared after the analysis of regulatory frameworks andcontextual factors and the workshops with the consortium members/members of industry, pharma and SMEs and willalso incorporate output from the IPT assessment and hackathons. A business canvas template will be produced for eachof the clinical sites/participating countries, supported by detailed documentation on the respective business proposals.
Participation per Partner
Partner number and short name WP10 effort
1 - KRONIKGUNE 3.00
2 - USTRATH 2.00
3 - WARWICK 2.00
4 - OUH 1.00
5 - FALKIEWICZ 2.00
6 - OM 10.00
GESUNDER 2.00
7 - RJH 1.00
8 - AMCA 1.00
AMCN 1.00
9 - SRDC 2.00
10 - EVERIS SPAIN SL 4.00
11 - I-HD 3.00
Total 34.00
Page 41 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D10.1 Exploitation plan 6 - OM Report Public 6
D10.2 Business case for theinnovation findings 6 - OM Report Public 48
Description of deliverables
D10.1 : Exploitation plan [6]Exploitation plan for ADLIFE project
D10.2 : Business case for the innovation findings [48]Business case for the innovation findings of ADLIFE project
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
Page 42 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
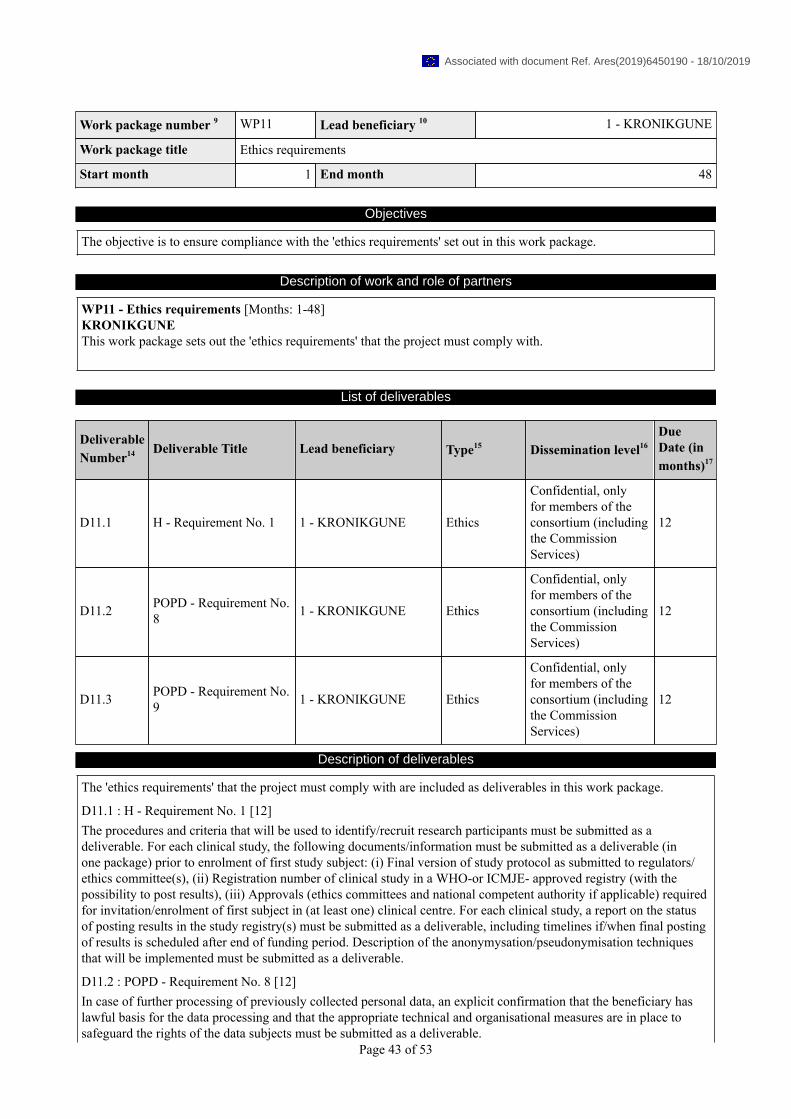
Work package number 9 WP11 Lead beneficiary 10 1 - KRONIKGUNE
Work package title Ethics requirements
Start month 1 End month 48
Objectives
The objective is to ensure compliance with the 'ethics requirements' set out in this work package.
Description of work and role of partners
WP11 - Ethics requirements [Months: 1-48]KRONIKGUNEThis work package sets out the 'ethics requirements' that the project must comply with.
List of deliverables
DeliverableNumber14 Deliverable Title Lead beneficiary Type15 Dissemination level16
DueDate (inmonths)17
D11.1 H - Requirement No. 1 1 - KRONIKGUNE Ethics
Confidential, onlyfor members of theconsortium (includingthe CommissionServices)
12
D11.2 POPD - Requirement No.8 1 - KRONIKGUNE Ethics
Confidential, onlyfor members of theconsortium (includingthe CommissionServices)
12
D11.3 POPD - Requirement No.9 1 - KRONIKGUNE Ethics
Confidential, onlyfor members of theconsortium (includingthe CommissionServices)
12
Description of deliverables
The 'ethics requirements' that the project must comply with are included as deliverables in this work package.
D11.1 : H - Requirement No. 1 [12]The procedures and criteria that will be used to identify/recruit research participants must be submitted as adeliverable. For each clinical study, the following documents/information must be submitted as a deliverable (inone package) prior to enrolment of first study subject: (i) Final version of study protocol as submitted to regulators/ethics committee(s), (ii) Registration number of clinical study in a WHO-or ICMJE- approved registry (with thepossibility to post results), (iii) Approvals (ethics committees and national competent authority if applicable) requiredfor invitation/enrolment of first subject in (at least one) clinical centre. For each clinical study, a report on the statusof posting results in the study registry(s) must be submitted as a deliverable, including timelines if/when final postingof results is scheduled after end of funding period. Description of the anonymysation/pseudonymisation techniquesthat will be implemented must be submitted as a deliverable.
D11.2 : POPD - Requirement No. 8 [12]In case of further processing of previously collected personal data, an explicit confirmation that the beneficiary haslawful basis for the data processing and that the appropriate technical and organisational measures are in place tosafeguard the rights of the data subjects must be submitted as a deliverable.
Page 43 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

D11.3 : POPD - Requirement No. 9 [12]The beneficiary must evaluate the ethics risks related to the data processing activities of the project. This includesalso an opinion if data protection impact assessment should be conducted under art.35 General Data ProtectionRegulation 2016/679. The risk evaluation and the opinion must be submitted as a deliverable.
Schedule of relevant Milestones
Milestonenumber18 Milestone title Lead beneficiary
DueDate (inmonths)
Means of verification
Page 44 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

1.3.4. WT4 List of milestones
Milestonenumber18 Milestone title
WPnumber9 Lead beneficiary
DueDate (inmonths)17
Means of verification
MS1 ADLIFE´s ethicalapproval
WP1,WP8 8 - AMCA 6
All pilot has obtained theapproval to the interventionfrom the correspondingethical committees
MS2 Website WP2 2 - USTRATH 3 Website for the projectlaunched
MS3
ADLIFE´ssoftware designand configurationdescription
WP3 3 - WARWICK 12
Task 3.1 done. Identificationof the technical requirementsand the adaptationrequirements for theintegration in each of the 7pilot sites.
MS4
ADLIFEinteroperability andsecurity assurance ofthe tools
WP3,WP8 3 - WARWICK 18
Task 3.4 solved,interoperability, security,privacy and quality issuessolve in all the pilot sites
MS5ADLIFE guidelines,scales and PROMsfinal selection
WP6,WP7 7 - RJH 15
Task 6.2 Decision supportmodules scope and contentand task 7.1 Patient reportedoutcomes measurement.
MS6Tools for empowermentdelivered and ready tobe tested in WP8
WP4,WP7,WP8
9 - SRDC 15
Participants (patients,professionals, carers…)engaged and testing thebeta version of the tools andsupporting the launching ofthe pilots.
MS7ADLIFE Pilot sitebuilds for intelligentand secure tools
WP3,WP8 3 - WARWICK 25
Task 3.2 and 3.3done. Integration ofthe personalized caremanagement platform
MS8
ADLIFE patientempowerment platformand JTA mechanismsready for each pilot
WP3,WP4,WP7,WP8
9 - SRDC 26
Task 4.1, 4.2 and 4.3done. Personalized JTAIbuilt per site upon thePower 2DM intelligentcommunication engine. WP7done and patients, carers andcommunity empowered
MS9 Deployment ofADLIFE CDSS
WP5,WP6 10 - EVERIS SPAIN SL 26
Clinical guidelines integratedin an interoperable and secureCDS service. Scales andheuristic risk algorithmsintegrated in the CDSS.
MS10
Integration, anddeployment ofADLIFE ICT tools inpilot sites
WP5,WP8 10 - EVERIS SPAIN SL 29
ADLIFE deployed in theseven pilots and evaluatedto be used in the finalconditions.
Page 45 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
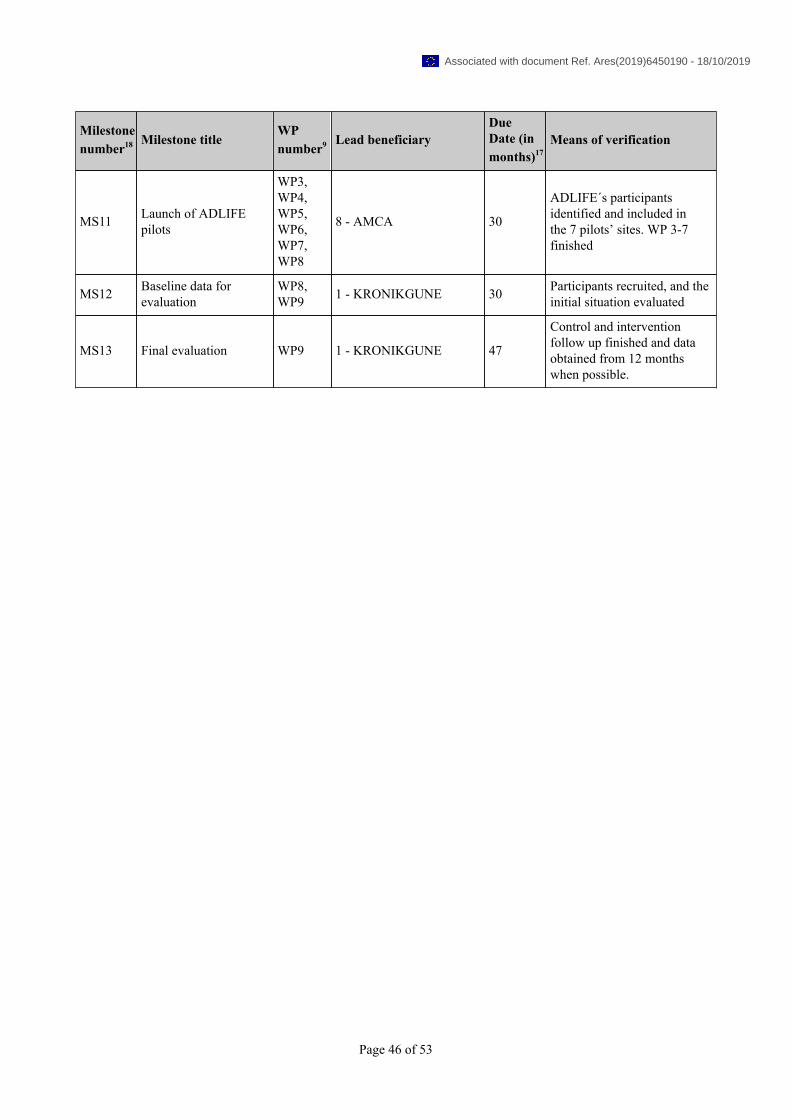
Milestonenumber18 Milestone title
WPnumber9 Lead beneficiary
DueDate (inmonths)17
Means of verification
MS11 Launch of ADLIFEpilots
WP3,WP4,WP5,WP6,WP7,WP8
8 - AMCA 30
ADLIFE´s participantsidentified and included inthe 7 pilots’ sites. WP 3-7finished
MS12 Baseline data forevaluation
WP8,WP9 1 - KRONIKGUNE 30 Participants recruited, and the
initial situation evaluated
MS13 Final evaluation WP9 1 - KRONIKGUNE 47
Control and interventionfollow up finished and dataobtained from 12 monthswhen possible.
Page 46 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

1.3.5. WT5 Critical Implementation risks and mitigation actions
Risknumber Description of risk WP Number Proposed risk-mitigation measures
1Progress starting too late inthe project resulting in poordelivery and project outcome
WP1
Help to create a project with stepwise projectprogress, realistic time-lines and resourceestimates based on industrial experience and bestpractice
2 A partner leaves the project WP1
The rest of the consortium will try to assume thepartner objectives, responsibilities and resources.In case the responsibilities reallocation is notpossible, the consortium will look for otherpartner with the same profile.
3Results of evaluation foreach WP are not goodenough
WP1Technical Committee has been planned to detectlosses of quality and implement correctivemeasures.
4Deliverables or officialnotifications to the EC arrivelate
WP1
The coordinator will check, 15 days earlier ofthe deadline the status of any of deliverable to besent to the EC. In case there is a delay, it will beinformed and justified beforehand establishing thereal deadline
5 No-deal scenario for Brexit WP1
The impact of no-deal Brexit for ADLIFE willbe very low, because WARWICK and STRAT,the only two partners from UK, have discussedthis issue with their entities and national contactpoints, that have assured that both universitiescan guarantee the funding to go-on in the project.In an even worse scenario the tasks that will bedeveloped by WARWICK could be brought intofruition by other partners (EVERIS and SRDC)and the number of participants to be recruited bySTRAT could be recruited in the other sites or theinclusion of other country could be analyzed.
6 Results not disseminated orexploited as expected WP10, WP2
Dissemination and exploitation plan will beupdated every six months in order to avoid thisrisk. In the update new ways of dissemination willbe planned
7 Unrealistic pilot siteinteroperability WP3, WP8
To avoid the potential medium impact, pilot sitesystems and compliant technologies inventoryhave been collected during the process preparationof the proposal. Initial plan has consideredintegration issues solved in C3Cloud.
8 Unclear clinical requirements WP3, WP6
Involvement of technical stakeholders in feedbackof the organizational models defined in WP6, willensure that they are documented in a way suitablefor technical requirement analysis and minimizethe medium impact of this risk.
9 Incorrect mapping ofterminology in SIS WP3, WP6
Mapping of terminology performed bothautomatically from UMLS mappings, butalso checked by clinicians to ensure validity.Involvement of the clinicians from the verybeginning of the project and preparation willminimize the high impact of this risk.
Page 47 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
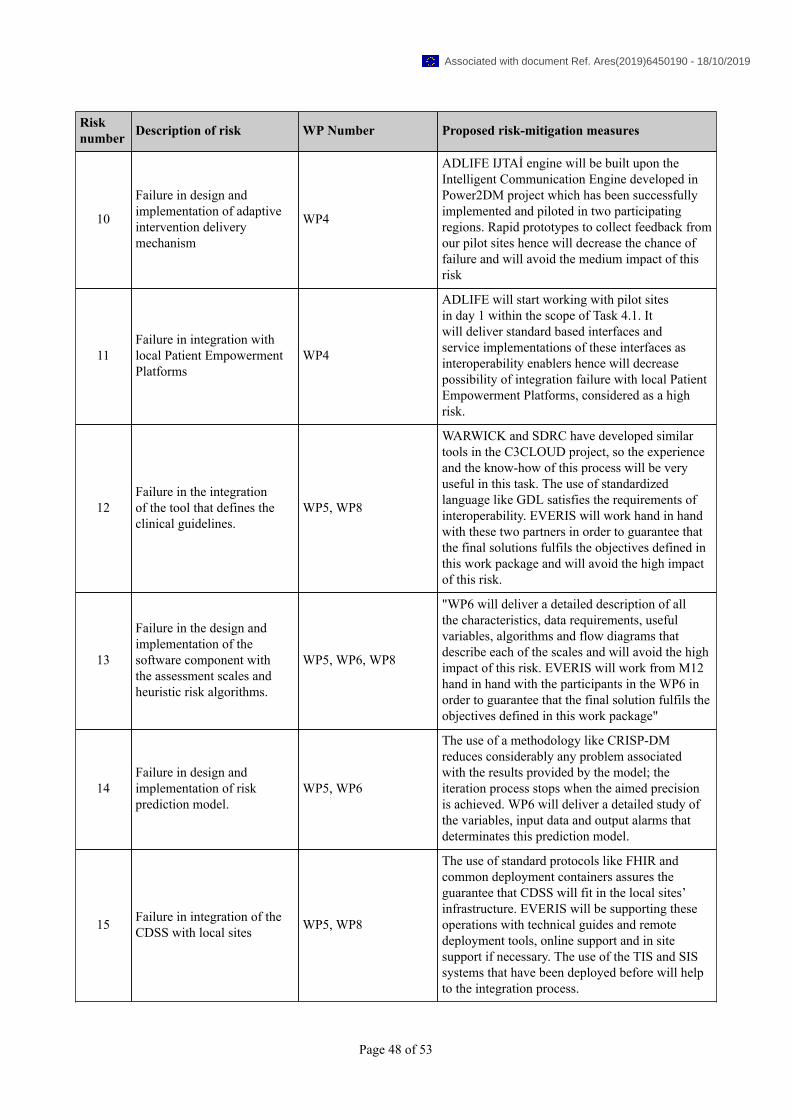
Risknumber Description of risk WP Number Proposed risk-mitigation measures
10
Failure in design andimplementation of adaptiveintervention deliverymechanism
WP4
ADLIFE IJTAİ engine will be built upon theIntelligent Communication Engine developed inPower2DM project which has been successfullyimplemented and piloted in two participatingregions. Rapid prototypes to collect feedback fromour pilot sites hence will decrease the chance offailure and will avoid the medium impact of thisrisk
11Failure in integration withlocal Patient EmpowermentPlatforms
WP4
ADLIFE will start working with pilot sitesin day 1 within the scope of Task 4.1. Itwill deliver standard based interfaces andservice implementations of these interfaces asinteroperability enablers hence will decreasepossibility of integration failure with local PatientEmpowerment Platforms, considered as a highrisk.
12Failure in the integrationof the tool that defines theclinical guidelines.
WP5, WP8
WARWICK and SDRC have developed similartools in the C3CLOUD project, so the experienceand the know-how of this process will be veryuseful in this task. The use of standardizedlanguage like GDL satisfies the requirements ofinteroperability. EVERIS will work hand in handwith these two partners in order to guarantee thatthe final solutions fulfils the objectives defined inthis work package and will avoid the high impactof this risk.
13
Failure in the design andimplementation of thesoftware component withthe assessment scales andheuristic risk algorithms.
WP5, WP6, WP8
"WP6 will deliver a detailed description of allthe characteristics, data requirements, usefulvariables, algorithms and flow diagrams thatdescribe each of the scales and will avoid the highimpact of this risk. EVERIS will work from M12hand in hand with the participants in the WP6 inorder to guarantee that the final solution fulfils theobjectives defined in this work package"
14Failure in design andimplementation of riskprediction model.
WP5, WP6
The use of a methodology like CRISP-DMreduces considerably any problem associatedwith the results provided by the model; theiteration process stops when the aimed precisionis achieved. WP6 will deliver a detailed study ofthe variables, input data and output alarms thatdeterminates this prediction model.
15 Failure in integration of theCDSS with local sites WP5, WP8
The use of standard protocols like FHIR andcommon deployment containers assures theguarantee that CDSS will fit in the local sites’infrastructure. EVERIS will be supporting theseoperations with technical guides and remotedeployment tools, online support and in sitesupport if necessary. The use of the TIS and SISsystems that have been deployed before will helpto the integration process.
Page 48 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
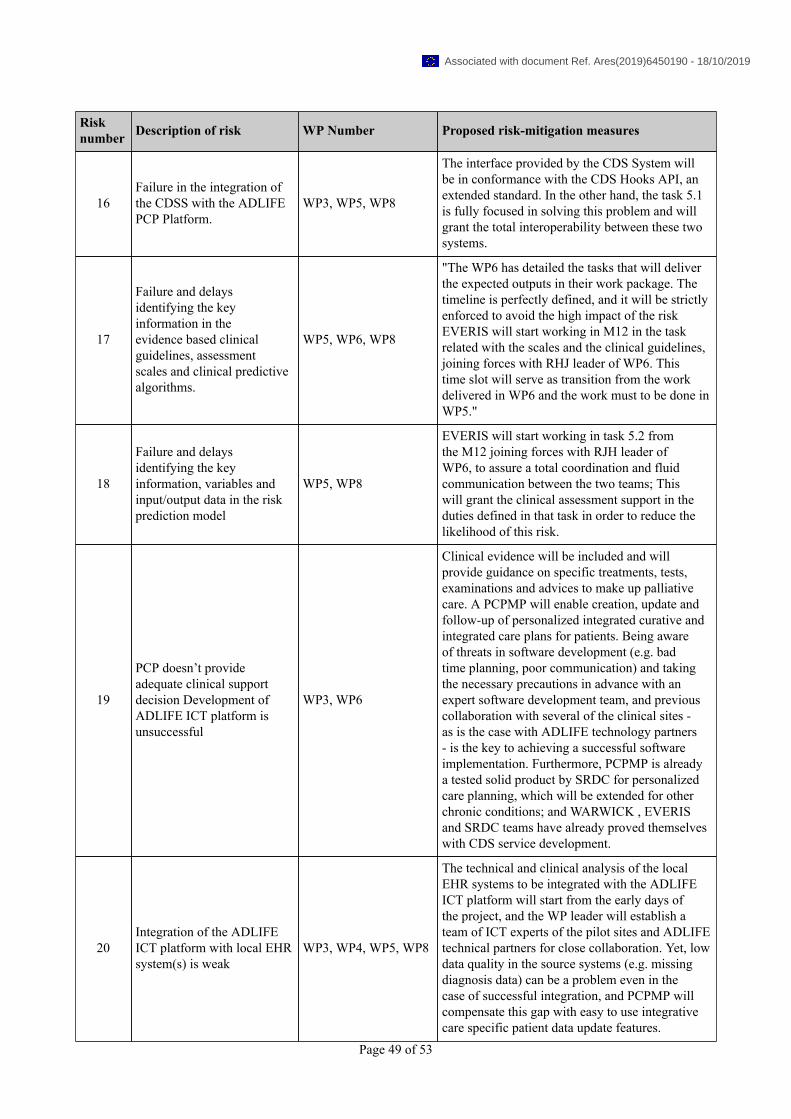
Risknumber Description of risk WP Number Proposed risk-mitigation measures
16Failure in the integration ofthe CDSS with the ADLIFEPCP Platform.
WP3, WP5, WP8
The interface provided by the CDS System willbe in conformance with the CDS Hooks API, anextended standard. In the other hand, the task 5.1is fully focused in solving this problem and willgrant the total interoperability between these twosystems.
17
Failure and delaysidentifying the keyinformation in theevidence based clinicalguidelines, assessmentscales and clinical predictivealgorithms.
WP5, WP6, WP8
"The WP6 has detailed the tasks that will deliverthe expected outputs in their work package. Thetimeline is perfectly defined, and it will be strictlyenforced to avoid the high impact of the riskEVERIS will start working in M12 in the taskrelated with the scales and the clinical guidelines,joining forces with RHJ leader of WP6. Thistime slot will serve as transition from the workdelivered in WP6 and the work must to be done inWP5."
18
Failure and delaysidentifying the keyinformation, variables andinput/output data in the riskprediction model
WP5, WP8
EVERIS will start working in task 5.2 fromthe M12 joining forces with RJH leader ofWP6, to assure a total coordination and fluidcommunication between the two teams; Thiswill grant the clinical assessment support in theduties defined in that task in order to reduce thelikelihood of this risk.
19
PCP doesn’t provideadequate clinical supportdecision Development ofADLIFE ICT platform isunsuccessful
WP3, WP6
Clinical evidence will be included and willprovide guidance on specific treatments, tests,examinations and advices to make up palliativecare. A PCPMP will enable creation, update andfollow-up of personalized integrated curative andintegrated care plans for patients. Being awareof threats in software development (e.g. badtime planning, poor communication) and takingthe necessary precautions in advance with anexpert software development team, and previouscollaboration with several of the clinical sites -as is the case with ADLIFE technology partners- is the key to achieving a successful softwareimplementation. Furthermore, PCPMP is alreadya tested solid product by SRDC for personalizedcare planning, which will be extended for otherchronic conditions; and WARWICK , EVERISand SRDC teams have already proved themselveswith CDS service development.
20Integration of the ADLIFEICT platform with local EHRsystem(s) is weak
WP3, WP4, WP5, WP8
The technical and clinical analysis of the localEHR systems to be integrated with the ADLIFEICT platform will start from the early days ofthe project, and the WP leader will establish ateam of ICT experts of the pilot sites and ADLIFEtechnical partners for close collaboration. Yet, lowdata quality in the source systems (e.g. missingdiagnosis data) can be a problem even in thecase of successful integration, and PCPMP willcompensate this gap with easy to use integrativecare specific patient data update features.
Page 49 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Risknumber Description of risk WP Number Proposed risk-mitigation measures
21Resistance by theprofessionals to the change inthe organizational model
WP6, WP8
To avoid the medium impact of this risk culturaland structural differences across the regions havetaken into account to make a coherent shareddecision tool requirement report. In addition,participant centres in the pilot regions have beenalready contacted and are committed to the changeand willing to participate in ADLIFE project,in fact two pilots (Basque and Sweden) havepreviously participated in piloting C3-Cloudproject and they have shared and will share theirexperience with the other professionals.
22 Challenges in recruitingpatients WP8
All pilots have identified a larger number ofpotential patients in each of the pilots that couldbe recruited to the intervention. To boost theparticipation and empower the participants WP8will be devoted to this work not only to clarifyany potential ethical issue, but also to make themmore active in self-management and decisionmaking. Additionally, it will be clearly stated thatpatients will receive personalized care accordingto their changing needs
23 Patients/caregivers are notempowered. WP4, WP7, WP8
Shared decision making tool will be tailored toeach group and each region taking into account allthe specific features.
24 Difficulties in getting ethicalcommittee´s approval WP1, WP8
To avoid this high impact risk that could leadto the rejection form committees very well-structured and evidence based protocols will beprepare emphasizing that communication betweenpatients and professionals will be key. All pilotshave a broad experience in the developing clinicaltrials and assays.
25 Pilots not implemented WP8Implementation process will be carefully monitorand the timelines and appropriateness of careintervention plans will be assessed.
26 Lack of recruitment andenrolment WP8
Pilots and participating centers have beencarefully selected and have accepted to participatein the project. All pilot leaders and participantsor healthcare providers or stakeholders with amain role in health care so they can guaranteethe inclusion of the participants in the project.All centers have confirmed they have enoughnumber of patients to reach the target of ADLIFE(126) taking into account the potential withdraws.All of them have previous experience in thedevelopment of interventions.
27Professionals are not ableto implement the ADLIFEintervention
WP8
Selected professionals are experts in the field ofintegrated care and are committed to the change.Professionals will be trained and empowered inWP8
Page 50 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Risknumber Description of risk WP Number Proposed risk-mitigation measures
28 No agreement on evaluationindicators WP9
Early discussion and refinement of evaluationtemplate with pilot sites, reducing number ofevaluation indicators where appropriate
29 Evaluation is not feasible WP9
The indicators will be reviewed every 6 weeksso enough data will be obtained from eachparticipant. In addition, data from formal andinformal caregivers and professionals will beobtained always after 12 months of trial.
Page 51 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

1.3.6. WT6 Summary of project effort in person-months
WP1 WP2 WP3 WP4 WP5 WP6 WP7 WP8 WP9 WP10 WP11 Total Person/Monthsper Participant
1 - KRONIKGUNE 25 1 3 4 4 4 3 8 26 3 ✓ 81
· OSAKIDETZA 0 1 5 6 8 4 3 6 6 0 39
2 - USTRATH 1 12 6 4 4 6 4 8 9 2 ✓ 56
3 - WARWICK 1 1 40 4 8 2 1 2 4 2 65
4 - OUH 1 2 6 4 4 6 16 12 5 1 ✓ 57
5 - FALKIEWICZ 1 2 6 6 6 6 7 10 5 2 ✓ 51
6 - OM 0.50 1 3 2 3 3 2 2 6 10 ✓ 32.50
· GESUNDER 0.50 0 3 2 3 3 1 6 2 2 22.50
7 - RJH 1 2 6 4 4 18 3 12 4 1 ✓ 55
8 - AMCA 0.50 1.50 3 2.50 3 3 2 18 3 1 ✓ 37.50
· AMCN 0.50 1.50 2.50 2.50 2.50 2.50 2.50 4 2.50 1 ✓ 22
· MACCABI 0 0 1 1 1 1 0.50 9 1 0 14.50
9 - SRDC 1 2 12 66 8 2 4 2 2 2 101
10 - EVERIS SPAIN SL 1 2 4 4 92 4 2 2 8 4 123
11 - I-HD 2 4 0 0 0 1 1 1 0 3 ✓ 12
Total Person/Months 36 33 100.50 112 150.50 65.50 52 102 83.50 34 769
Page 52 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
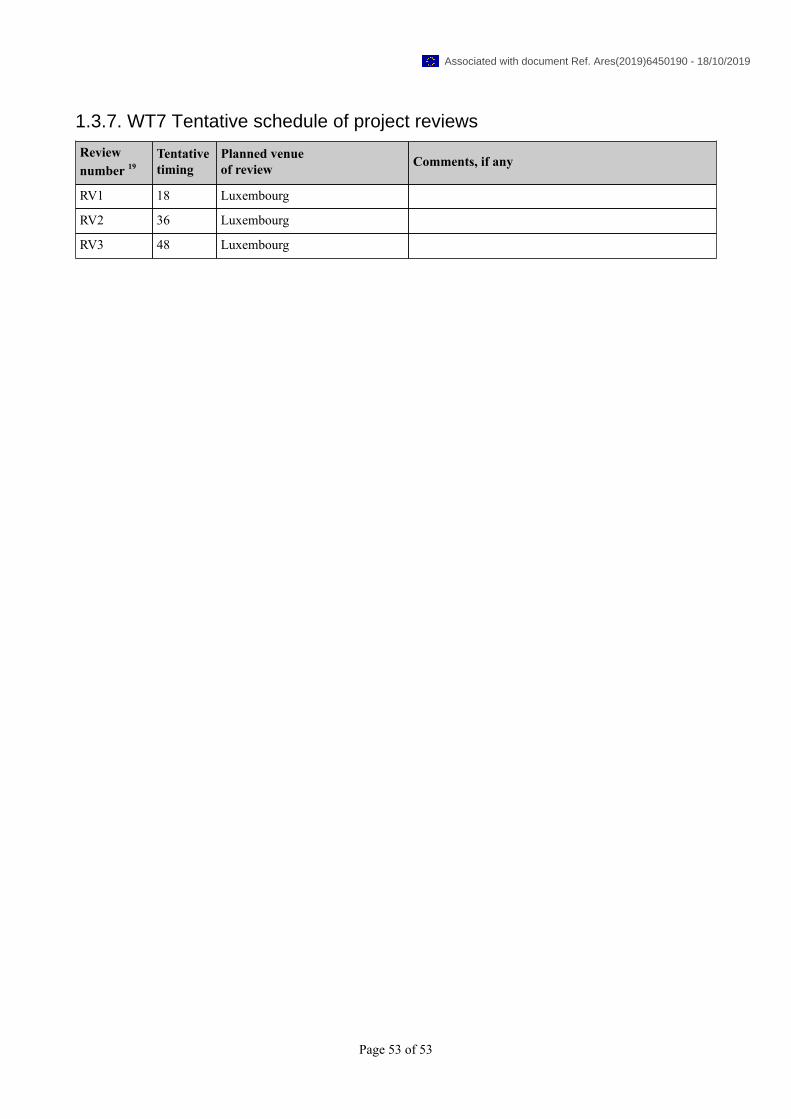
1.3.7. WT7 Tentative schedule of project reviews
Reviewnumber 19
Tentativetiming
Planned venueof review Comments, if any
RV1 18 Luxembourg
RV2 36 Luxembourg
RV3 48 Luxembourg
Page 53 of 53
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
1. Project number
The project number has been assigned by the Commission as the unique identifier for your project. It cannot bechanged. The project number should appear on each page of the grant agreement preparation documents (part Aand part B) to prevent errors during its handling.
2. Project acronym
Use the project acronym as given in the submitted proposal. It can generally not be changed. The same acronym shouldappear on each page of the grant agreement preparation documents (part A and part B) to prevent errors during itshandling.
3. Project title
Use the title (preferably no longer than 200 characters) as indicated in the submitted proposal. Minor corrections arepossible if agreed during the preparation of the grant agreement.
4. Starting date
Unless a specific (fixed) starting date is duly justified and agreed upon during the preparation of the Grant Agreement,the project will start on the first day of the month following the entry into force of the Grant Agreement (NB : entry intoforce = signature by the Commission). Please note that if a fixed starting date is used, you will be required to provide awritten justification.
5. Duration
Insert the duration of the project in full months.
6. Call (part) identifier
The Call (part) identifier is the reference number given in the call or part of the call you were addressing, as indicatedin the publication of the call in the Official Journal of the European Union. You have to use the identifier given by theCommission in the letter inviting to prepare the grant agreement.
7. Abstract
8. Project Entry Month
The month at which the participant joined the consortium, month 1 marking the start date of the project, and all other startdates being relative to this start date.
9. Work Package number
Work package number: WP1, WP2, WP3, ..., WPn
10. Lead beneficiary
This must be one of the beneficiaries in the grant (not a third party) - Number of the beneficiary leading the work in thiswork package
11. Person-months per work package
The total number of person-months allocated to each work package.
12. Start month
Relative start date for the work in the specific work packages, month 1 marking the start date of the project, and all otherstart dates being relative to this start date.
13. End month
Relative end date, month 1 marking the start date of the project, and all end dates being relative to this start date.
14. Deliverable number
Deliverable numbers: D1 - Dn
15. Type
Please indicate the type of the deliverable using one of the following codes:R Document, reportDEM Demonstrator, pilot, prototypeDEC Websites, patent fillings, videos, etc.OTHERETHICS Ethics requirementORDP Open Research Data PilotDATA data sets, microdata, etc.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
16. Dissemination level
Please indicate the dissemination level using one of the following codes:PU PublicCO Confidential, only for members of the consortium (including the Commission Services)EU-RES Classified Information: RESTREINT UE (Commission Decision 2005/444/EC)EU-CON Classified Information: CONFIDENTIEL UE (Commission Decision 2005/444/EC)EU-SEC Classified Information: SECRET UE (Commission Decision 2005/444/EC)
17. Delivery date for Deliverable
Month in which the deliverables will be available, month 1 marking the start date of the project, and all delivery datesbeing relative to this start date.
18. Milestone number
Milestone number:MS1, MS2, ..., MSn
19. Review number
Review number: RV1, RV2, ..., RVn
20. Installation Number
Number progressively the installations of a same infrastructure. An installation is a part of an infrastructure that could beused independently from the rest.
21. Installation country
Code of the country where the installation is located or IO if the access provider (the beneficiary or linked third party) isan international organization, an ERIC or a similar legal entity.
22. Type of access
VA if virtual access,TA-uc if trans-national access with access costs declared on the basis of unit cost,TA-ac if trans-national access with access costs declared as actual costs, andTA-cb if trans-national access with access costs declared as a combination of actual costs and costs on the basis of
unit cost.
23. Access costs
Cost of the access provided under the project. For virtual access fill only the second column. For trans-national accessfill one of the two columns or both according to the way access costs are declared. Trans-national access costs on thebasis of unit cost will result from the unit cost by the quantity of access to be provided.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 1
HISTORY OF CHANGES
# Original submitted part B Section 1-5
Response and/or content change made to the DoA to be submitted for the Grant Agreement
Part I: Changes related to the Ethics Summary Report
Pre-Grant Requirements
#1 P
rote
ctio
n o
f p
erso
nal
dat
a
4.3 Justification for the processing of sensitive personal data must be included in the grant agreement before signature.
The project will only collect essential data (clinical, health-related, use of resources, perception of participants) that will enable assessing the impact of the ADLIFE intervention in terms patient health status, functionality and autonomy and system efficiency. The collected data will be used only for the purposes of evaluation, impact assessment and growing the evidence base in the field of digitally-enabled personalized integrated care.
The project will only collect essential data (clinical, health-related, use of resources, perception of participants) that will enable assessing the impact of the ADLIFE intervention in terms patient health status, functionality and autonomy and system efficiency. The collected data will be used only for the purposes of evaluation, impact assessment and growing the evidence base in the field of digitally-enabled personalized integrated care.
Text included in 5.1.3 DATA PROTECTION AND PRIVACY section (page 114). “The project will only collect essential data (clinical, health-related, use of resources, perception of participants) that will enable assessing the impact of the ADLIFE intervention in terms patient health status, functionality and autonomy and system efficiency. The collected data will be used for the purposes of evaluation, impact assessment and growing the evidence base.” There is a paragraph already in the proposal ensuring that the collected data are strictly necessary for the study. PROTECTION AND PRIVACY section (page 115). “In addition, The D1.1 Data Management Plan will include the privacy impact assessment ensuring that the information collected is strictly necessary for the study. The Privacy Impact Assessment will include a description of how the project envisions processing the data and for what purpose. It will explain how processing this data could impact the rights and freedoms of the data subjects. And it will detail the measures that will be taken to mitigate the risks and the security safeguards and mechanisms that will be put into place to ensure the protection of personal data and comply with the EU Data Protection Regulation. “
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 2
#2
Pro
tect
ion
of
per
son
al d
ata
4.10 In case personal data are transferred from a non-EU country to the EU (or another third state), confirmation that such transfers comply with the laws of the country in which the data was collected must be specified in the grant agreement).
The task T1.5 Data management will describe the ADLIFE data protection framework regarding data access, protection and sharing. This framework will be based on the protection regulation No 2016/679. Two ADLIFE beneficiaries are from non-EU countries (Israel and Turkey).
The task T1.5 Data management will describe the ADLIFE data protection framework regarding data access, protection and sharing. This framework will be based on the protection regulation No 2016/679. Two ADLIFE beneficiaries are from non-EU countries (Israel and Turkey).
A specific section of how to share data between non-EU and EU countries will be included in the data protection framework and included in the D1.1. Data Management Plan.
Text included in 5.1.3.1 THIRD COUNTRIES section (Page 115)
“Two third countries participate in the project: Turkey and Israel. The procedure to share documentation between partners and with third parties, considering cross-border transfers, will be deeply described in D1.1 Data Management Plan. The data shared will include clinical and health-related information (anxiety, depression, functionality, quality of life, wellbeing, satisfaction, mortality, place of death, care burden), use of resources (admissions, emergency room visits) and perception of participants in terms of communication with patients, coordination of care and trust in in quality and security in data access, processing, sharing and storage. The information sources are local administrative databases (Electronic Health Record), interviews or focus groups and ADLIFE data logs. Detailed information will be provided in D7.1 and D11.1. The procedures will comply with the current EU legislation as well as the laws of the corresponding countries: Turkey and Israel. A Data Sharing Agreement and the corresponding templates will be included in the D1.1 Data Management Plan.”
#3 P
rote
ctio
n o
f p
erso
nal
dat
a 4.11 Detailed information on the informed consent procedures in regard to data processing must be kept on file (to be specified in the grant agreement)].
The description of the informed consent procedures are included in the section 5.1.2 INFORMED CONSENT (page 112). The deliverable D11.1 ADLIFE´s Study protocol will include the detailed procedures for obtaining informed consents.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 3
#4
Th
ird
Co
un
trie
s 6.3. Details on the materials which will be imported to/exported from the EU must be included in the grant agreement before signature#.
The data that will be shared are mainly clinical, health-related, use of resources and perception of participants with regards to communication, coordination, quality of care and security in data management. Text included in Text included in the 5.1.3.1 THIRD COUNTRIES section (Page 115) “Two third countries participate in the project: Turkey and Israel. The procedure to share documentation between partners and with third parties, considering cross-border transfers, will be thoroughly described in D1.1 Data Management Plan. The data shared will include clinical and health-related information (anxiety, depression, functionality, quality of life, wellbeing, satisfaction, mortality, place of death, care burden), use of resources (admissions, emergency room visits) and perception of participants in terms of communication with patients, coordination of care and trust in in quality and security in data access, processing, sharing and storage. The information sources are local administrative databases (Electronic Health Record), interviews or focus groups and ADLIFE data logs. Detailed information will be provided in D7.1 and D11.1.”
#5
Th
ird
Co
un
trie
s
6.4. Copies of import/export authorisations, as required by national/EU legislation must be kept on file (to be specified in the grant agreement).
No biological material will be imported or exported. Text included in the 5.1.3.1 THIRD COUNTRIES section (Page 115)
“No biological material will be imported or exported, so it is not necessary to have import/export authorisations for the development of the activities included in ADLIFE project.”
Post-Grant Requirements
#6 H
um
ans
2.1. The procedures and criteria that will be used to identify/recruit research participants must be submitted as a deliverable.
The detailed description of the inclusion criteria and how potential participants are approached and invited to take part in the study will be included in the D11.1.Study protocol. This document will include: General information
Protocol title, registration number in a WHO-or ICMJE- approved registry and date.
Name, title and contact of the investigator(s).
Rationale & background information Study goals and objectives Study design and duration Study population
Inclusion and exclusion criteria Recruitment procedures
Sample size Data sources Data analysis (quantitative and qualitative) Data management (including pseudonymisation techniques) Quality assurance Ethics
Procedures for informed consent Local ethical committee´s procedures Local ethical committee´s approvals
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 4
#7 H
um
ans
2.10. For each clinical study, the following documents/information must be submitted as a deliverable (in one package) prior to enrolment of first study subject: (i) Final version of study protocol as submitted to regulators/ethics committee(s), (ii) Registration number of clinical study in a WHO-or ICMJE- approved registry (with the possibility to post results), (iii) Approvals (ethics committees and national competent authority if applicable) required for invitation/enrolment of first subject in (at least one) clinical centre.
The detailed study protocol will be included in the D11.1. Study Protocol (see answer to 2.1).
#8 H
um
ans
2.11. For each clinical study, a report on the status of posting results in the study registry(s) must be submitted as a deliverable, including timelines if/when final posting of results is scheduled after end of funding period.
Information on the status of the result posting including timelines when final posting of results is scheduled after end of funding period will be included in D11.3. ADLIFE Status of posting results.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 5
#9
Pro
tect
ion
of
per
son
al d
ata 4.8 Description
of the anonymization and pseudonymization techniques that will be implemented must be submitted as a deliverable.
This information will be described in the D11.1. ADLIFE Study Protocol (see answer to 2.1).
#10
Pro
tect
ion
of
per
son
al d
ata
4.15 In case of further processing of previously collected personal data, an explicit confirmation that the beneficiary has lawful basis for the data processing and that the appropriate technical and organizational measures are in place to safeguard the rights of the data subjects must be submitted as a deliverable.
The description of the organizational processes planned to support privacy and other rights of the data subjects will be included in the D11.2. ADLIFE Impact Assessment.
This deliverable will explain in depth the mechanisms for authentication and authorization of users who access to sensitive data. It will include procedures based on widely accepted international standards that ensure the confidentiality and integrity of the data communication among ADLIFE components, eg. application of industry standard cryptographic algorithms and protocols, user accountability through audit trail mechanism etc.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 6
#11
Pro
tect
ion
of
per
son
al d
ata
4.16 The beneficiary must evaluate the ethics risks related to the data processing activities of the project. This includes also an opinion if data protection impact assessment should be conducted under art.35 General Data Protection Regulation 2016/679. The risk evaluation and the opinion must be submitted as a deliverable.
A Data Protection Officer (DPO) (from Kronikgune) will supervise compliance with the provisions of the Section 39.1.b) REGULATION (EU) 2016/679 OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL of 27 April 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data. The DPO will analyze whether pilot sites have to conduct an impact assessment. The detailed information related to the GDPR COMPLIANCE CHECK and the impact assessments required will be included in D11.2. ADLIFE Impact Assessment.
Part II: Other changes
#12 tables 3.1a, 3.1b and 3.1c
tables 3.2a and 3.2b
table 3.4a
As requested, moved these tables to the Part A of Annex 1 to the Grant Agreement.
#13 The Work package for ethics has been re-numbered.
In order to maintain the WP numbering of the whole proposal, we have assigned the number 11 to the ethical WP.
#14 Delivery date of the deliverables of the ethical Work Package
The delivery date of the D11.1, D11.2 and D11.3 are postponed until M12 (originally set for M6). To define the complete study protocol and give time to obtain approvals from local ethical committees, implement security measures for sensitive data access and sharing and assess impact and risks will require longer than 6 months.
#15 Responsible of D6.1 and 6.2 has been updated
RJH will be the responsible for deliverables 6.1 and 6.2 as leader of tasks included in this WP.
#16 Deliverables Aligned the Deliverables with the changes reported in a separate table enclosed below.
#17 Budget Other direct costs table has been updated due to the change of ICT adaptation to local settings from other costs to subcontracting activities developed by RJH and AMCA.
#18 Description of subcontractors and third parties
RJH and AMCA have added subcontracting activities for the ICT adaptation to local settings. AMCA has modified the participation of its third party: Maccabi healthcare services that will develop part of the work and has included a new Third Party Assuta Medical Centers, also as linked third party.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 7
Mapping of the original Deliverables (as per proposal) with the ones introduced in SyGMa
(for implementation)
Deliverable as listed in the original proposal
Deliverable as introduced in SyGMa
Explanation and justification
D1.1 Data management plan D1.1 Data management plan No modification.
D2.1 Communication and dissemination plan and communication material
D2.1 Communication and dissemination plan and communication material
No modification.
D2.2 Website D2.2 Website No modification.
D2.3 Final report on dissemination activities
D2.3 Final report on dissemination activities
No modification.
D3.1 ADLIFE software requirement and architectural description
D3.1 ADLIFE software requirement and architectural description
No modification.
D3.2 Intelligent tools (PCPMP, TIS, SIS) customization build
D3.2 Intelligent tools (PCPMP, TIS, SIS) customization build
No modification.
D3.3 Assurance report including software quality plan, assessment of certifiability against MDR and GDPR
D3.3 Assurance report including software quality plan, assessment of certifiability against MDR and GDPR
No modification.
D4.1 ADLIFE Patient Empowerment Platform supporting PROMS
D4.1 ADLIFE Patient Empowerment Platform supporting PROMS
No modification.
D4.2 Intelligent adaptive intervention delivery mechanisms
D4.2 Intelligent adaptive intervention delivery mechanisms
No modification.
D5.1 ADLIFE CDSS beta version and technical guide
D5.1 ADLIFE CDSS beta version and technical guide
No modification.
D5.2 ADLIFE CDSS D5.2 ADLIFE CDSS No modification.
D6.1 ADLIFE Decision Support Modules scope and content
D6.1 ADLIFE Decision Support Modules scope and content
Update of entity in charge: RJH instead of OUH
D6.2 Recommendations for change management in integrated personalized care delivery
D6.2 Recommendations for change management in integrated personalized care delivery
Update of entity in charge: RJH instead of OUH
D7.1 ADLIFE Patient Reported Outcomes Measures
D7.1 ADLIFE Patient Reported Outcomes Measures
No modification.
D7.2 Patient empowerment materials and interventions
D7.2 Patient empowerment materials and interventions
No modification.
D7.3 Shared decision making tools requirements
D7.3 Shared decision making tools requirements
No modification.
D8.1 ADLIFE deployment plans D8.1 ADLIFE deployment plans No modification.
D8.2 Report on ADLIFE pilot execution
D8.2 Report on ADLIFE pilot execution
No modification.
D9.1 ADLIFE´s evaluation framework
Deleted as the content of this original deliverable will be included in the D11.1 ADLIFE Study Protocol.
D9.2 Intermediate progress report D9.1 Intermediate progress report Re-numbered.
D9.3 Final evaluation report, including predictive algorithms
D9.2 Final evaluation report, including predictive algorithms
Re-numbered.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 8
validation and economic impact of the intervention
validation and economic impact of the intervention
D10.1 Exploitation plan D10.1 Exploitation plan No modification.
D10.2 Business case for innovation findings
D10.2 Business case for innovation findings
No modification.
H- Requirement No.1-D11.1 ADLIFE Study Protocol
New deliverable
POPD – Requirement No.-8-D11.2. ADLIFE Impact Assessment
New deliverable
POPD – Requirement No. 9 - D11.3. ADLIFE Status of posting results.
New deliverable
1. EXCELLENCE ................................................................................................................................................. 9
1.1 OBJECTIVES ....................................................................................................................................................... 10 1.2 RELATION TO THE WORK PROGRAMME .......................................................................................................... 11 1.3 CONCEPT AND METHODOLOGY ....................................................................................................................... 12 1.4 AMBITION ......................................................................................................................................................... 31
2. IMPACT ...................................................................................................................................................... 34 2.1 EXPECTED IMPACTS .......................................................................................................................................... 34 2.2 MEASURES TO MAXIMISE IMPACT ................................................................................................................... 37 2.3 COMMUNICATION ACTIVITIES .......................................................................................................................... 46
3. IMPLEMENTATION ..................................................................................................................................... 48 3.1 WORK PLAN – WORK PACKAGES, DELIVERABLES ............................................................................................. 48 3.2 MANAGEMENT STRUCTURE, MILESTONES AND PROCEDURES ....................................................................... 50 3.3 CONSORTIUM AS A WHOLE .............................................................................................................................. 55 3.4 RESOURCES TO BE COMMITTED ....................................................................................................................... 57
4. MEMBERS OF THE CONSORTIUM ................................................................................................................ 59 4.1 ASOCIACIÓN CENTRO DE EXCELENCIA INTERNACIONAL EN INVESTIGACIÓN SOBRE CRONICIDAD (KRONIKGUNE) ........................................................................................................................................................ 59 4.2 UNIVERSITY OF STRATHCLYDE (STRAT) ........................................................................................................... 66 4.3 UNIVERSITY OF WARWICK (WARWICK) ........................................................................................................... 69 4.4 ODENSE UNIVERSITY HOSPITAL (OUH) ............................................................................................................ 74 4.5 A.FALKIEWICZ SPECIALIST HOSPITAL IN WROCLAW (FALK-HOSP) .................................................................. 80 4.6 OPTIMEDIS AG ................................................................................................................................................. 82 4.7 REGION JÄMTLAND HÄRJEDALEN (RJH) ........................................................................................................... 85 4.8 ASSUTA ASHDOD LTD. (AMCA)........................................................................................................................ 91 4.9 SOFTWARE RESEARCH DEVELOPMENT AND CONSULTANCY CORP (SRDC) ..................................................... 96 4.10 EVERIS ........................................................................................................................................................... 101 4.11 I-HD ............................................................................................................................................................... 107 4.12 THIRD PARTIES INVOLVED IN THE PROJECT ................................................................................................. 110
5. ETHICS AND SECURITY .............................................................................................................................. 114 5.1 ETHICS ............................................................................................................................................................. 114 5.2 SECURITY ......................................................................................................................................................... 120
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 9
1. EXCELLENCE
Due to the aging of the population and advances in medical science, people with chronic diseases – even those with advanced severe life-threatening chronic diseases - are living longer. This has created new challenges: sustaining quality of life and independent living, providing support for caregivers who are shouldering an increasing burden, and creating sustainable healthcare and social care systems in the face of increasing demands and limited resources. Integrated care has been proposed as the key approach to meet these challenges1.
ADLIFE CHALLENGE: Persons with progressive Advanced Chronic Diseases are a special group who are facing permanently or temporarily reduced functionality and capabilities. They can greatly benefit of digitally supported interventions that can improve or maintain their health, avoid unnecessary deterioration, extend their independence and optimize health resources utilization2,3. Integrated supportive care can be an effective approach to enhance quality of life and may also positively influence the course of illness. It is applicable early in the course of illness. The impact of digitalisation of health services is expected to be profound but it is important to evaluate their impact4. ADLIFE aims to provide evidence to support decisions to adopt, use or reimburse new digital health services supporting integrated care at different levels of the health care system. ADLIFE UNIQUE SOLUTION: ADLIFE responds to the societal and health system challenge in Europe of an increasing number of persons with Advanced Chronic Diseases, often with accompanying co-morbidity, polypharmacy, frailty and sometimes isolation. ADLIFE will provide a solution for the integration of therapies and approaches targeting the early detection and assessment of deterioration, advanced and well-coordinated care planning and integrated supportive care to enhance quality of life, reduce suffering and accelerate recovery from an illness deterioration. ADLIFE LARGE SCALE: ADLIFE will deploy, through large scale pilots. Its intervention in seven different Countries and Health Systems, involving 577 healthcare professionals from 75 different hospitals, clinics and primary care services (Table 1). It will provide the evidence that intelligent, collaborative digital solutions can enable care teams, patients and caregivers to improve or better maintain health in patients with advanced chronic disease (more than 200,000 in the participating regions): avoid unnecessary deterioration, extend their independence and optimize health resource utilization (avoid unnecessary treatments, improve care at home and reduce hospital admissions).
ADLIFE EVIDENCE: It will evaluate its effectiveness in 882 patients (126 per site) and 1243 caregivers. ADLIFE will demonstrate significant outcomes-based efficiency gains in health and care delivery enhancing seamless care coordination and avoiding gaps and overlaps in care through large scale clinical care pilots and rigorous evaluation. ADLIFE CLINICAL: It will improve coverage, ensure earlier detection and multi-needs assessment and will provide high quality, effective and continued symptom management through evidence-based digital personalized care plans.
ADLIFE EMPWOERMENT: It will also provide intelligent mechanisms to deliver personalized self-management support through adaptive interventions. ADLIFE is grounded on the principle of self-determination and respect for autonomy, respecting different preferences for intervention and self-management. Being that the advanced chronic disease target group is one of the most complex and demanding ones, solutions that can be demonstrated effective and efficient and sustainable for them can be easily be extended to other patient groups.
ADLIFE is going to demonstrate that it is feasible to provide a personalized integrated care to improve the health situation, deliver more appropriate targeted and timely care for patients with Advanced Chronic Diseases by the means of the use of an innovative ADLIFE toolbox that will support early detection of care needs and dynamic
and personalized care provision..
The participants in ADLIFE PROJECT are a wide range of professionals; caregivers and healthcare providers from seven countries and different types of health systems ((Beveridge and Bismarckian) as seen in Table 1.
1 National Institutes of Health/World Health Organization. Global health and aging. http://www.who.int/ageing/ publications/global_health.pdf. 2 Lunney JR, Lynn J, Foley DJ, et al. Patterns of functional decline at the end of life. JAMA 2003;289(18):2387-2392. 3 Tanuseputro P, et al. (2015) The Health Care Cost of Dying: A Population-Based Retrospective Study of the Last Year of Life in Ontario. PLOS ONE 10(3): 4 Assessing the impact of digital transformation of health services. Report of the Expert Panel on effective ways of investing in Health (EXPH). European Union, 2019 https://ec.europa.eu/health/expert_panel/sites/expertpanel/files/docsdir/022_digitaltransformation_en.pdf
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 10
TABLE 1 ADLIFE LARGE SCALE DEPLOYMENT
PILOT (126+126 patients)
PARTICIPANTS IN ADLIFE PROJECT (professionals; caregivers (informal including families); healthcare
organizations)
DISSEMINATION/ EXPLOITATION
SUSTAINABILITY AND
REPLICABILITY AFTER-ADLIFE
PROJECT Health prof.
Care giver
s Healthcare organizations
Other professionals, citizens in the region
Basque Country (Osakidetza)
General practitioner (GP): 60 Nurse: 64 Specialist: 16 Total: 140
160 Integrated Healthcare Organizations (OSI) (9 centres): OSIAraba, OSI Donostialdea;OSI Barrualde-Galdakao;OSI Alto Deba;OSI Debabarrena ; OSI Tolosaldea;OSI Ezkerraldea-Enkarterri-Cruces; OSI Bidasoa; OSI Uribe
There are 13 OSI in the area that involve 4,500 professionals in primary care
Osakidetza will adopt ADLIFE as a corporative tool, to provide integrated care to more than 30,000 patients in the area
United Kingdom (NHSL Lanarkshire)
GP: 60 Nurse:100 Specialist: 40 Total: 200
250 NHSL Lanarkshire – 3 Acute Hospitals (Hairmyres, Monklands and University Hospital Wishaw) and over 100 sites in total
Primary care facilities include health centres and 15 community hospitals. More than 12,000 professionals
NHS will deploy solution in the health Boards in West Coast of Scotland. 50,000 professionals 90,000 patients
Denmark (Southern Denmark)
GP: 50 Nurse:40 Specialist: 10 Total: 100
400 OUH-Svendborg Hospital covers 50% of the Region of Southern Denmark 10 local municipalities and all relevant GPs in these municipalities OUH covers 10% of hospital capacity in Denmark
4 hospitals 785 general medical practices in Region 36 hospitals in Denmark 1900 General Practices in Denmark
RSYD will secure sustainable reimbursement models (high incentives) 25,000 patients
Poland (FALKHOSP Lower Silesia)
GP: 2 Nurse:4 Specialist: 4 Total: 10
200 Hospitals -2, primary care- 3, specialized ambulatory care-1, other health services (rehabilitation)
30 hospitals and primary care in the region 300 professionals
Change of geriatric competences in the region 20,000 patients
Germany (Werra-Meißner Kreis)
GP: 7 Nurse:4 Specialist: 4 Total: 15
63 2 Hospitals: 2, Hospital Werra-Meißner GmbH: two locations in Witzenhausen and Eschwege 5 centers of primary care and 4 homecare
2 Hospital in the region 10 primary care 100 professionals 1,500 patients
OptiMedis core activity (sustainable models of integrated care)
Sweden -RJH (Region Jämtland Härjedalen)
GP: 20 Nurse:10 Specialist: 15 Total:45
20 RJH: One hospital: Östersund hospital, 8 primary care health centres, two specialized ambulatory care services; Mobile team for “nearer” care, Storsjögläntan – specialized unit
4 private primary care 1,000 professionals (≈1% of Swedish population)
Inclusion in RJH catalogue 5,000 patients
Israel (Maccabi Healthcare Services)
GP: 15 Nurse:7 Specialist: 38 Total: 67
150 Assuta Ashdod Hospital Maccabi healthcare Services (includes over 250 GP, over 50 nurses, at least 50 other health professionals) Ashdod Municipality Social Services
4 Health Plans ≥10,000 professionals participate in the annual conferences of Ministry of Health
Inclusion in the catalogue of entity 20,000 patients
1.1 OBJECTIVES
The vision of ADLIFE is to improve the quality of life of senior people with Advanced Chronic Diseases by providing innovative integrated intelligent personalized care. ADLIFE will deploy a large-scale implementation of digitally enabled holistic and integrated supportive care. The ADLIFE ICT Toolbox solutions will use and extend in real life
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 11
settings already existing, validated and trusted personalised digital solutions, most of them developed in previous FPVII and Horizon 2020 project from the consortium partners. They will adopt international standards such as HL7 FHIR and PCHA device standards.
The ambition of ADLIFE is to:
Demonstrate that ICT supported ADLIFE intelligent and outcome-based personalized care model of integrated care is flexible and can be deployed and replicated at large scale in different environments and be trusted in regard to data access, protection and sharing.
Achieve quantified gains in patient health status, preventing unnecessary suffering, slowing down clinical and functional deterioration and improving Patient reported Outcomes (PROMs) (WP9).
Obtain improvements in efficiency by making a better use of resources, increasing the coordination among all the key stakeholders of care and improving working conditions of professionals (WP8,9).
Protect functionality and enhance autonomy, empowering patients to participate in decisions making on their own health and adapting to their changing conditions and context.
The digitally enabled operational objectives of ADLIFE are: To provide collaborative tools to create personalized care plans for multidisciplinary care team members to
efficiently manage the delivery of integrated care services improving working conditions of health care and social care providers, optimizing work time management and multi-disciplinary coordination (WP3 an WP6).
To implement intelligent tools for clinical decision-making support that seamlessly access and assess the most recent patient’s clinical context (EHR and PROMs), by automating evidence-based guidelines and need assessments scales and risk prediction algorithms to early detect health changes or undesired events (WP5).
To securely access, process, share and store patient’s data in electronic health records and also other patient generated data (including sensor measurements, interactions with their environments, feedback about their care plans and PROMs) in line with the requirements of GDPR (WP3-4).
To change the traditional care models for chronic patients with advanced chronic disease by integrating unconnected care tasks performed in different levels and settings addressing the multidimensional nature of their conditions and the secure and quality exchange of data and information (WP6).
To facilitate a more active role of patients and caregivers in managing their own health and symptoms encouraging shared decision making, deliver individualized adaptive interventions (WP4-7).
To deploy the new tools in 75 hospitals/clinics/primary care centres in seven different European and associated regions, involving 577 professionals (WP8).
To assess the effectiveness and efficiency of the intervention with a large-scale pilot involving 884 patients and 1243 caregivers, evaluating health gain, quality of life, use of resources and economic costs (WP9)
To have a direct impact by contacting/including in healthcare conferences/programmes in the Region on more than 102,900 professionals and 2,128 centres in the participating regions where more than 190,000 patients could benefit in a short-term with the project results (WP2).
To produce guidelines and policy recommendations providing financial sustainable, flexible and replicable solutions to disseminate results, transfer and deploy at large-scale to other patient groups in the EU and beyond and create further business and job creation opportunities (WP2, WP10).
1.2 RELATION TO THE WORK PROGRAMME SC1-DTH-11-2019 ALIGNMENT OF “ADLIFE” PROJECT “Senior people are statistically at greater risk of … multiple chronic health conditions …
ADLIFE will focus on senior people with advanced chronic and potentially life-threatening conditions. This group has been selected as a challenging group for the complex management of their pathologies that have serious consequences affecting their independence, quality of life (and their families) and an large costs for health systems (these group represent 75% of the mortality in middle-high income countries, have a prevalence of 1.5% of the general population and 35%–45% of hospital admissions5). ADLIFE solution will be easily transferred to other condition.
The challenge is now to foster secure, scalable and robust digital solutions for integrated care which will ensure….
ADLIFE is based on secure and robust digital solutions for management of chronic diseases, developed and implemented in previous projects such as C3-Cloud, Power2DM, ASSEHS and CAREWELL. ADLIFE personalized care plans goals and activities will be created and updated, considering patient-oriented outcomes, changing needs and risks (WP5) in a cooperative way between patients, and healthcare professionals (WP3, WP4, WP5). ADLIFE will deploy Security and Privacy Suite to pilot sites to enable single sign-on authentication, role-based authorization
5 Rosa Mertnoff et al the comprehensive care of people with advanced chronic diseases in acute hospitals.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 12
SC1-DTH-11-2019 ALIGNMENT OF “ADLIFE” PROJECT and anonymization. All data exchanged within and across ADLIFE components is encrypted and properly auditable. It is based on the work developed in -C3Cloud with a track record and unique knowhow regarding the barriers and obstacles and how to achieve secure health data acquisition, storage and sharing (WP3, 4 and 5).
The scope of this topic is to foster the large-scale pilots for deployment of trusted and personalised digital solutions dealing with Integrated Care,
ADLIFE will deploy an upgraded version of C3-Cloud, with more and improved functionalities, including intelligent tools for adaptive interventions and decisio0n making support. It will be tested in 7 different countries and health systems involving 75 hospitals, clinics and primary care centres, reaching at least 577 professionals and 1243 carers. Personal Care Management Platform (PCPMP) (WP3), patient empowerment platform (PEP) (WP4) and Clinical Decision Support Services (CDSS) support integrated personalized healthcare to prevent the deterioration and enhance healthy and independent living. ADLIFE will be applicable in any health systems in Europe or beyond, having been deployed in seven different countries. ADLIFE solution will be implemented in close collaboration with the ICT teams of the participating health services.
to contribute to a patient-centred and truly individualized strategy develop trusted, robust and financially sustainable
ADLIFE is patient-centred using Patient Reported Outcomes measures (PROM) and shared decision-making aids deployed in PEP as drivers of the personalized care plan development (PCPM) and patient follow up and clinical management (CDSS). ADLIFE intervention will demonstrate health gains, efficiency improvement and the socio-economic impact. Implementation drivers and barriers will be identified. WP10 will design and analyse the best business options feasible for the companies involved and others.
These approaches aim to enable people to remain independent…
PCPM will support coordinated care, CDSS will allow early needs assessment and early warning systems (EWS) and PEP will deploy just in time adaptive interventions (JITAI). Altogether the will increase the impactability of health and care activities, better targeting patients´ needs, acting earlier and optimizing resource utilization avoiding unnecessary hospital admission and deterioration of the patient conditions.
Expected outcomes are in priority: Efficiency gains; Flexibility and replicability; Ensuring secure and efficient sharing and processing of all data; Improvement of quality of life for the patient
ADLIFE will provide robust and scientific evidence of its outcomes (WP9). It will be provided using a quasi-experimental design (non-randomized, non-concurrent and controlled) and mixed method analysis. Data, 28 indicators including health quality of life, working conditions, service utilization and economic, will be collected from the intervention deployed in seven different health systems, all around Europe and Israel., with 882 patients (126 in each country) and comparing with a similar number of patients with care as usual. (WP9, WP8)
Data management (data access, process and storage) will follow the procedures indicated in the new general data protection regulation No 2016/679 and approved by local Ethics Committees (WP1). ADLIFE will provide anonymization, authentication, authorization and audit services based on widely accepted international standards.
Outcome indicators Recruitment of
professionals Quality of life... Measurement
of cost-efficiency …
A total set of 28 indicators including Patient Reported Outcomes measures (PROM) including quality of life (SF36) and other assessment tools), disease specific health parameters, satisfaction and working conditions, health services utilization and economic variables will be analysed (WP9). A socio-economic impact assessment based on cost-outcome and budget impact analysis and a simulation modelling methodology will be carried out to develop scenarios for the long-term sustainability of the project interventions.
… contribution from the EU of between EUR 4 and 6 …
ADLIFE is requesting 6,3 Million Euros. This investment can have a high return due to future scaling up. Not only ADLIFE technologies will be deployed in very different environments but sound evaluation will provide the evidence for easier acceptance by professionals. The generated impact and in the replication of the project this cost could be reduced around the 60% (taking into account the higher costs in this first approach of ICT tools and evaluation and dissemination/exploitation efforts).
1.3 CONCEPT AND METHODOLOGY
1.3.1 OVERALL CONCEPT UNDERPINNING THE PROJECT
AADLIFE will deploy trusted and personalised digital solutions for integrated supportive care capabilities: Personalized Care Plan Management Platform (PCPMP), intelligent Clinical Decision Support Services (CDSS);
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
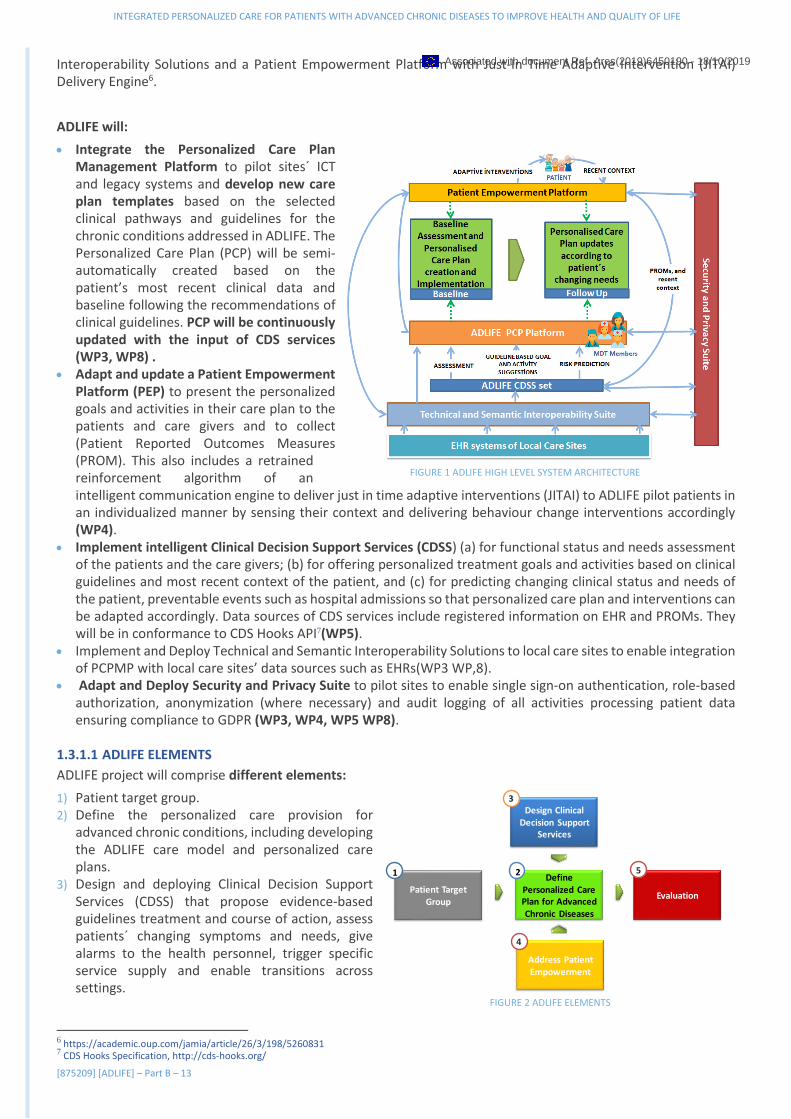
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 13
Interoperability Solutions and a Patient Empowerment Platform with Just-In Time Adaptive Intervention (JITAI) Delivery Engine6.
ADLIFE will:
• Integrate the Personalized Care Plan Management Platform to pilot sites´ ICT and legacy systems and develop new care plan templates based on the selected clinical pathways and guidelines for the chronic conditions addressed in ADLIFE. The Personalized Care Plan (PCP) will be semi-automatically created based on the patient’s most recent clinical data and baseline following the recommendations of clinical guidelines. PCP will be continuously updated with the input of CDS services (WP3, WP8) .
• Adapt and update a Patient Empowerment Platform (PEP) to present the personalized goals and activities in their care plan to the patients and care givers and to collect (Patient Reported Outcomes Measures (PROM). This also includes a retrained reinforcement algorithm of an intelligent communication engine to deliver just in time adaptive interventions (JITAI) to ADLIFE pilot patients in an individualized manner by sensing their context and delivering behaviour change interventions accordingly (WP4).
• Implement intelligent Clinical Decision Support Services (CDSS) (a) for functional status and needs assessment of the patients and the care givers; (b) for offering personalized treatment goals and activities based on clinical guidelines and most recent context of the patient, and (c) for predicting changing clinical status and needs of the patient, preventable events such as hospital admissions so that personalized care plan and interventions can be adapted accordingly. Data sources of CDS services include registered information on EHR and PROMs. They will be in conformance to CDS Hooks API7(WP5).
• Implement and Deploy Technical and Semantic Interoperability Solutions to local care sites to enable integration of PCPMP with local care sites’ data sources such as EHRs(WP3 WP,8).
• Adapt and Deploy Security and Privacy Suite to pilot sites to enable single sign-on authentication, role-based authorization, anonymization (where necessary) and audit logging of all activities processing patient data ensuring compliance to GDPR (WP3, WP4, WP5 WP8).
1.3.1.1 ADLIFE ELEMENTS
ADLIFE project will comprise different elements:
1) Patient target group. 2) Define the personalized care provision for
advanced chronic conditions, including developing the ADLIFE care model and personalized care plans.
3) Design and deploying Clinical Decision Support Services (CDSS) that propose evidence-based guidelines treatment and course of action, assess patients´ changing symptoms and needs, give alarms to the health personnel, trigger specific service supply and enable transitions across settings.
6 https://academic.oup.com/jamia/article/26/3/198/5260831 7 CDS Hooks Specification, http://cds-hooks.org/
Patient Target Group
Define Personalized Care Plan for Advanced Chronic Diseases
Evaluation
5
Design Clinical Decision Support
Services
3
1 2
Address PatientEmpowerment
4
FIGURE 2 ADLIFE ELEMENTS
FIGURE 1 ADLIFE HIGH LEVEL SYSTEM ARCHITECTURE
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 14
4) Address empowerment of patients and carers sharing the care plan, deploying adaptive interventions and supporting PROMs.
5) Intervention and evaluation, with quantitative, qualitative and socioeconomic impact analysis.
1) Patient Target Group
The challenge ADLIFE addresses is the supporting and improving quality of life patients with advanced chronic conditions, who can really benefit from the personalized dedicated integrated care. The target population is patients with a severe, chronic, and incurable disease, with an expected progression in severity and a potential reduction in life expectancy. Advanced chronic conditions include foreseeable; progressive conditions without curative treatments; as well as irreversible but non-progressive conditions causing severe disability, leading to susceptibility to health complications and the possibility of premature death.
Integrated Care is a highly complex issue that must be addressed holistically and personalized to each patient to optimize personal care and quality care planning8. The idea is to be able to adjust clinical practice with patients with chronic medical illnesses in advanced stages, trying, where possible, to slow down and even partially reverse the progression and prevent sequelae/disability, by intensifying technical-therapy interventions or, if not, to orient the care objectives towards global and integral comfort and avoid obstinacy and iatrogenesis with procedures of doubtful/no benefit.
Care coordination among multidisciplinary care teams is critical, in order to ensure the needs of the individual are met seamlessly across different stakeholders and healthcare settings9. The proper management of these often complex and multi-faceted patients requires continuous assessment10, effective and collaborative, multidisciplinary working within and between generalist and specialist teams, whether the person is at home, in hospital or elsewhere. Targeted interventions may reduce variability and align treatment with patient wishes11.
For ADLIFE, as representative of these increasing group of diseases, we have selected two of the more prevalent ones, Chronic Obstructive Pulmonary Disease (COPD) and Congestive Heart Failure (CHF)12. The criteria for recruiting patients to participate in the project are:
Inclusion criteria
• Senior (over 55) • Heart failure (NYHA III-IV) in functional stage III/IV according to the NYHA scale13 and stages C and D of the
ACCF/AHA classification14. Stable-phase (at least two months without decompensation) • And/or COPD (FEV1<50), >2 GOLD scale15. • With/without comorbidities: ± Diabetes ± Chronic renal failure ± Chronic hepatopathy ± Stroke ± Mild cognitive
disorder. Exclusion criteria:
• Presence of active malignant neoplastic disease. • Inclusion in the active list of cardiac, hepatic and/or renal transplantation. • No signature of Informed consent by a legally capable patient.
2) Deploying Personalized Care Provision for Advanced Chronic Conditions
ADLIFE will promote a shift to an outcomes-based, patient-centred multidisciplinary and multi-sectoral approach; adapted to the specific cultural, social and economic environments; and integrated into existing health systems, with emphasis on primary health care, community- and home-based care. It will be a flexible and replicable solution, financially sustainable, and deployable at large scale. It will allow business and job creation opportunities. ADLIFE is based on the care pathway concept16.
8 Jefford M, et al. Implementing improved post-treatment care for cancer survivors in England, with reflections from Australia, Canada and the USA. Br J Cancer. 2013;108:14-20. 9 NHS.Innovation to implementation: Stratifed pathways of care for people living with or beyond cancer A ‘how to guide’ 10 NIH-the-Science Conference Statement: Symptom Management in Cancer: Pain, Depression, and Fatigue, July 15–17, 2002. JNCI 11 MR Larochelle, et al. Hospital staff attributions of the causes of physician variation in end-of-life treatment intensity. Palliat Med. 2009;23(5):460-70 12 Hawkins NM, et al. Heart failure and chronic obstructive pulmonary disease: diagnostic pitfalls and epidemiology. Eur J Heart Fail. 2009;11(2):130–139. doi:10.1093/eurjhf/hfn013 13 III Marked limitation of physical activity. Comfortable at rest, but less than ordinary activity causes symptoms of HF. IV Unable to carry on any physical activity without symptoms of HF, or symptoms of HF at rest. he Criteria Committee of the New York Heart Association.Nomenclature and criteria for diagnosis of diseases of the heart and great vessels, 9th edition. Boston, Mass: Little & Brown; 1994.Google Scholar 14 C Structural heart disease with prior or current symptoms of HF D Refractory HF requiring specialized interventions Hunt SA, Abraham WT, Chin MH, et al.. 2009 Focused update incorporated into the ACC/AHA 2005 guidelines for the diagnosis and management of heart failure in adults: 15 https://goldcopd.org/ 16 European Pathway Association in http://e-p-a.org/care-pathways/
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 15
ADLIFE care plan is defined as a dynamic, personalized plan that identifies needed healthcare activities, health objectives and healthcare goals, relating to one or more specified health issues in a healthcare process17. It includes the patient´s wishes and decisions about their future health care.
We will be building upon the Personalized Care Plan Management Platform (PCPMP,) which has been developed and tested in real-life healthcare settings by some ADLIFE partners within the scope of the C3-Cloud European Project18. The current functionalities of the Personalized Care Plan Management Platform are:
I. Import and review of medical summary: PCPMP supports integration with interoperability APIs, in order to import all the patient data that is provided by the local electronic health records systems including conditions, medications, allergies, lab results, vital signs, procedures and social history to facilitate continuous synchronization. By default, it supports HL7 F ast Healthcare Interoperability Resources (FHIR) API and has a secure HL7 FHIR patient data repository. HL7 FHIR is an emerging ’standards framework, created by HL7, and combines the features of HL7's v2, HL7 v3 and CDA product lines, while leveraging the latest web standards and applying a tight focus on feasibility of implementation. In this way, PCPMP presents the medical summary to the care team members in a single location.
II. Management of the care plan building blocks: goals, activities and education materials: The tool allows creation and update of the integrated care plan which is mainly composed of goals to manage the health concerns and activities (i.e,. interventions) to achieve these goals and improve health concerns. It natively stores the care plan in conformance to HL7 Care Plan Domain Analysis Model as HL7 FHIR CarePlan resource19 and its associated resources. The Plan has associations to concepts for Health Concern, Health Goal, Health Risk, Care Barrier, Care Preference, Conversation, Plan Activity (including interventions), Acceptance Review, Plan Review and key care team participations through time and space between the Patient, Providers, Care Givers and other Supporting Members20.
III. Suggestion of Personalized goals and activities: PCPMP supports the CDS Hooks standard21, in order to facilitate integration with modular CDS services and implementing clinical guideline recommendations to suggest personalized goal and intervention recommendations to be included in the care plan of the patient based on their medical summary. Education materials for patients and families are also recommended as a part of the care plans.
IV. Update of the care plan: PCPMP is enabled to integrate with modular CDS services to monitor the changing needs and status of the patients, hence facilitates continuous follow-up of the patient to update the integrated care plan to adjust to the most recent patient context. Semi-automatic care plan update can also happen upon feedback from the patient, during and after planned and unplanned encounters after the patient context is updated and shared with PCPMP.
V. Enable Collaboration of Multi-disciplinary Care Teams: It is possible to create a care team and invite new care team members to a care plan. Communication among care team members and with the patient/informal care giver via asynchronous messaging or Organization of tele/video conferences (e.g,. for a virtual case review meeting). Updates in the care plan are notified to care team members to keep them up-to-date. It supports a Dashboard view to enables a signed in care team member to quickly go over the important updates in the care plans of all patients since the previous login, such as new messages received, awaiting appointments, new system notifications. The Activity calendar enables view and update of scheduled activities of a care team member on a calendar.
17 Pecoraro et al. An Integrated Model to Capture the Provision of Health and Social Care Services Based on the ContSys and FHIR Standards. EJBI Volume 13 18 http://c3-cloud.eu/ 19 HL7 FHIR CarePlan resource, http://hl7.org/fhir/careplan.html 20 HL7 Care PlanDomainAnalysis ModelDocuments, http://wiki.hl7.org/images/1/1d/PCWG_Care_Plan_DAM_Specification_-_Part_1_-_Draft_2015-11-04.pdf 21 https://cds-hooks.org/
FIGURE 3 PCPMP FUNCTIONALITIES
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
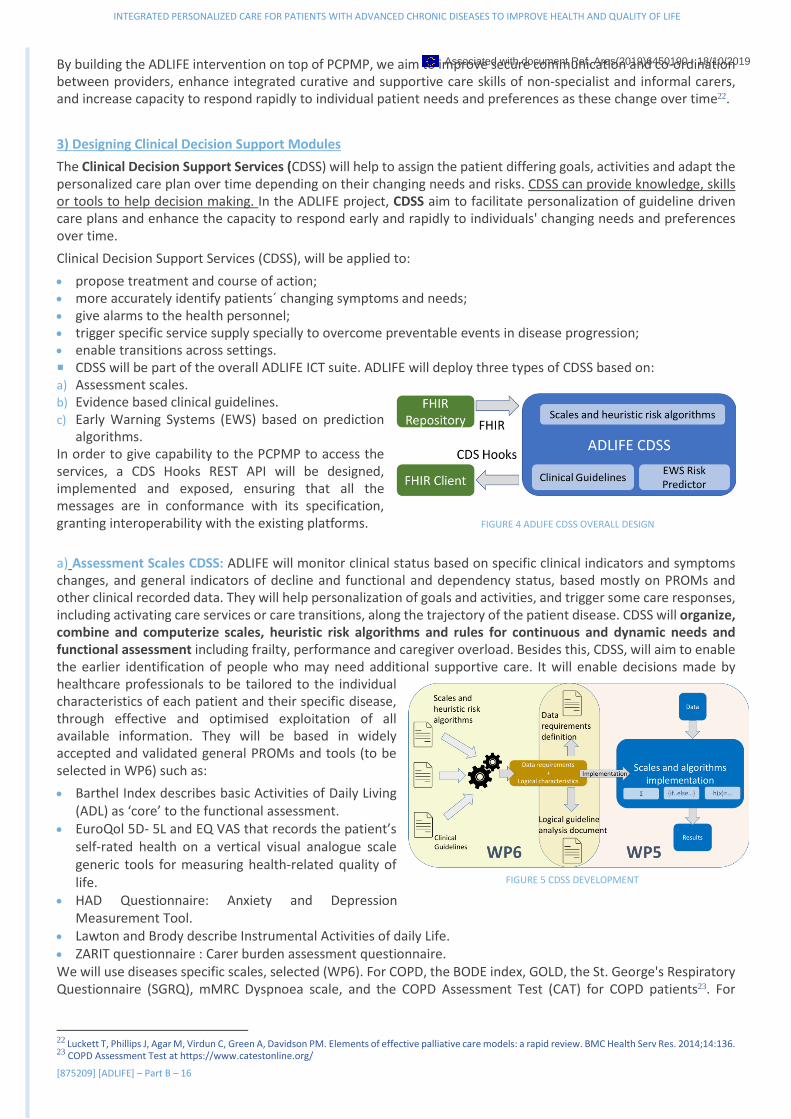
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 16
By building the ADLIFE intervention on top of PCPMP, we aim to improve secure communication and co-ordination between providers, enhance integrated curative and supportive care skills of non-specialist and informal carers, and increase capacity to respond rapidly to individual patient needs and preferences as these change over time22.
3) Designing Clinical Decision Support Modules
The Clinical Decision Support Services (CDSS) will help to assign the patient differing goals, activities and adapt the personalized care plan over time depending on their changing needs and risks. CDSS can provide knowledge, skills or tools to help decision making. In the ADLIFE project, CDSS aim to facilitate personalization of guideline driven care plans and enhance the capacity to respond early and rapidly to individuals' changing needs and preferences over time.
Clinical Decision Support Services (CDSS), will be applied to:
• propose treatment and course of action; • more accurately identify patients´ changing symptoms and needs; • give alarms to the health personnel; • trigger specific service supply specially to overcome preventable events in disease progression; • enable transitions across settings. CDSS will be part of the overall ADLIFE ICT suite. ADLIFE will deploy three types of CDSS based on: a) Assessment scales. b) Evidence based clinical guidelines. c) Early Warning Systems (EWS) based on prediction
algorithms. In order to give capability to the PCPMP to access the services, a CDS Hooks REST API will be designed, implemented and exposed, ensuring that all the messages are in conformance with its specification, granting interoperability with the existing platforms.
a) Assessment Scales CDSS: ADLIFE will monitor clinical status based on specific clinical indicators and symptoms changes, and general indicators of decline and functional and dependency status, based mostly on PROMs and other clinical recorded data. They will help personalization of goals and activities, and trigger some care responses, including activating care services or care transitions, along the trajectory of the patient disease. CDSS will organize, combine and computerize scales, heuristic risk algorithms and rules for continuous and dynamic needs and functional assessment including frailty, performance and caregiver overload. Besides this, CDSS, will aim to enable the earlier identification of people who may need additional supportive care. It will enable decisions made by healthcare professionals to be tailored to the individual characteristics of each patient and their specific disease, through effective and optimised exploitation of all available information. They will be based in widely accepted and validated general PROMs and tools (to be selected in WP6) such as:
• Barthel Index describes basic Activities of Daily Living (ADL) as ‘core’ to the functional assessment.
• EuroQol 5D- 5L and EQ VAS that records the patient’s self-rated health on a vertical visual analogue scale generic tools for measuring health-related quality of life.
• HAD Questionnaire: Anxiety and Depression Measurement Tool.
• Lawton and Brody describe Instrumental Activities of daily Life. • ZARIT questionnaire : Carer burden assessment questionnaire. We will use diseases specific scales, selected (WP6). For COPD, the BODE index, GOLD, the St. George's Respiratory Questionnaire (SGRQ), mMRC Dyspnoea scale, and the COPD Assessment Test (CAT) for COPD patients23. For
22 Luckett T, Phillips J, Agar M, Virdun C, Green A, Davidson PM. Elements of effective palliative care models: a rapid review. BMC Health Serv Res. 2014;14:136. 23 COPD Assessment Test at https://www.catestonline.org/
FIGURE 5 CDSS DEVELOPMENT
FIGURE 4 ADLIFE CDSS OVERALL DESIGN
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 17
Congestive Heart Failure, the NYHA, HeartQoL, Minnesota living with heart failure questionnaire and the ESC Guidelines for the diagnosis and treatment of heart failure.
Continuous assessment of the need of supportive care will be included, using the logical framework of Complexity assessment as ICD PAL, GSF PIG, NECPAL and others. The Clinical Reference Group will review the most adequate and select those that will be computerized. They will agree on the actions and care strategies that can be activated according to the assessment scales scores.
The Selected scales (WP6) will integrate the final CDSS . The variables will be defined in each scale. The prediction risk algorithm and the computation needed in each scale:
• If the scale is based on questionnaires, the sum of all elements. • If the scale is based on flow diagrams, an if-else programmatic structured. • If the scale is based on raw data, logistic regression algorithm. b) Evidence Based Clinical Guidelines CDSS: Clinical guidelines and protocols support health professionals, by facilitating and standardizing diagnosis, management and treatment in specific clinical specialties at different institutions24. Clinical Decision Support Services (CDSS) will integrate with PCPMP to enable personalised goal recommendations and intervention recommendations (e.g., medication therapies, guidance on contradicting medications, laboratory test requests, referrals to specialists, scheduling follow-up timings) for the care team members. These CDS services will automate the recommendations from the evidence based clinical guidelines. The Clinical Reference Group will select the most adequate Guidelines to provide evidence-based input to these CDSS. The reference guidelines will be the NICE guidelines on CHF and COPD. Recommendations will be reviewed through, taking into account the Pilot sites reference Guidelines and a systematic process to reconcile conflicting recommendations for multimorbid patients25. “if-else-then” programming flows will be developed and structured in decision trees.
Maccabi Healthcare Services has a fully functioning CDSS that performs functions, such as medication therapies, guidance on contradicting medications, laboratory test requests, referrals to specialists, or scheduling follow-up timings, based on adoption of internationally accepted guidelines. ADLIFE ’partners SRDC and University of Warwick have already implemented rule based CDS services for automating the decision trees embedded in the selected four NICE (National Institute for Health and Care Excellence) guidelines26 for the management of diabetes, renal failure, heart failure and depression, within the scope of C3-Cloud Project. These CDS services have been implemented as FHIR based the CDS Hooks services, with decision logic encoded in the Guideline Definition Language (GDL) version 2. Similarly, in the ADLIFE project, CDS services for the additional selected guidelines will be automated following the partners ‘experience and the C3-Cloud model.
(c) Early Warning Systems (EWS) EWS-based alert algorithms have the potential to facilitate appropriate alert management in clinical practice. EWS will allow predictive and continuous risk assessment. A EWS provides a dynamic score, representing a patients’ health condition at the given time and delivers risk using numerical values that indicate the need for assessment and interventions at certain critical thresholds. However, variety of clinical information is complex, wide and changes dynamically. The design of EHR-driven alerting systems that identifies the right patient at the right time so the clinician can manage a health risk remains a challenge. Clinically relevant and information driven criteria are particularly important for alerts activated by Early Warning Systems (EWS). The Clinical Reference Group (CRG), with healthcare professional representatives of all Pilot Sites, will guide the process of defining and refining CDSS. The CRG will identify and agree, based on an updated review of the literature, assessment scales, the guidelines and the clinical prediction algorithms to be used for estimation risk and poor evolution (mortality, admission to ICU, re-admissions, complications, etc.) for the selected pathologies. They will select decision rules, scales and algorithms to be implemented, identifying data needed. They will be validated in the different contexts of ADLIFE Pilot sites, checking local data sources. The final ADLIFE CDSM rules and algorithm set will be assessed by clinicians, working in the Pilot Sites. They will be implemented and applied in the dedicated software (WP5).
EWS will be implemented using a supervised learning approach. CRISP-DM (CRoss-InduStry Process for Data Mining) standard will be used. This methodology is robust and well-proven and provides a structured approach to planning a data mining project 27. It is divided in six iterative phases or stages: Business understanding, data understanding, data preparation, modelling, evaluation and deployment. The reference clinical predictive algorithms will be based
24 G-I-N international guideline library www.g-i-n.net/library/international-guidelines-library 25 G-I-N international guideline library www.g-i-n.net/library/international-guidelines-library GuíaSalud (España) www.guiasalud.es, NICE (National Institute for Health and Care Excellence) clinical guidelines (Reino Unido), www.nice.org.uk/about/what-we-do/our-programmes/nice-guidance/nice-guidelines/nice-clinicalguidelines, Scottish Intercollegiate Guidelines Network (SIGN) (Reino Unido) www.sign.ac.uk, CMA Infobase: Clinical Practice Guidelines Database (CPGs) (Canadá) www.cma.ca/En/Pages/clinical-practice-guidelines.aspx,Sweden https://www.socialstyrelsen.se/nationalguidelines, 26 NG28 Type 2 diabetes in adults: management (May 2017); CG182 Chronic kidney disease in adults: assessment and management (2015); CG108 Chronic heart failure in adults: management (2010) and CG90 Depression in adults: recognition and management (2018). 27 Kenneth Jensen. https://commons.wikimedia.org/wiki/File:CRISP-DM_Process_Diagram.png
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 18
on the ones produced by Kronikgune researchers for COPD28,29 and CHF30. The Clinical reference Group will review and refine them, during the Project’s lifetime, based on trustful sources.31. These CDS services will be redefined by statistical machine learning algorithms. A supervised learning approach, applied to retrospective datasets from participating regions, will be used. An initial and basic list of the symptoms/signs, which these early warning systems use, will be agreed by the CRG. The required data (such as of diagnoses, drug prescriptions, hospital care utilization, primary care visit, diagnostic tests and other demographic data) will be extracted, transformed and loaded into the environment. Validation checks will be undertaken, including the identification and imputation of missing data.
To build the first candidate model, different supervised algorithms will be revisited, looking for the best performance with the available data. Ensemble methods will be tested in order to decrease bias (hypothesis boosting)32, variance (bootstrap aggregating)33 or improve predictions (stacked generalization)34. To evaluate the capability of the proposed model, k-fold cross validation35 will be used due to its capability to avoid high variance and to have better results.
To measure the performance of the proposed model three main procedures will be taken into account: model fit, discrimination and calibration. The techniques described before including the used methodology grant the best model fitting; to measure discrimination a boxplot of predicted probabilities will be generated and AUC will be measured, considering a value >0.80 as acceptable The clinical usefulness will be evaluated using different measures: accuracy, sensitivity and specificity. All of them evaluated with different threshold values. To measure calibration a calibration-in-the-large test will be applied and a calibration plot will be used in order to have a visual impression of observed frequencies vs. predicted probabilities.
For continuous outcomes, the RMSEA (root mean square average) parameter will be calculated. The lower the RMSEA, the better the model will be. Technical and semantic interoperability with local care sites’ EHR systems will be ensured (WP3). An analytic environment will be set up at each site, in conformance with applicable data protection and security regulations. The use of the data will follow the new GDPR regulation and will seek local Ethics Committees approval ensuring data access, process and storage. Technical and semantic interoperability solutions will serve the patient data from local data stores such as EHR systems.
After the iterative process of training and performance evaluation, if the performance metrics defined are in the right range, the final model will be saved for deployment. If not, the iterative process in the CRISP-DM methodology will be continued until the objective is achieved. Within the study period, and every 4-5 months, the algorithms performance will be assessed. They will be updated (if feasible) using other variables, not initially considered in the original predictive rules but relevant for the study outcomes. The model update process will be: (1) the relationship between those exposure factors and the outcomes will be evaluated, (2) if there is an evidence of that relationship, this will be entered in the model and, we will evaluate the performance of the new model, compared to the latest one, (3) in case new variables are considered in the model, the algorithm will be recomputed. This procedure will be applied in both phases of the study.
28 Esteban C, Arostegui I, Garcia-Gutierrez S, Gonzalez N, Lafuente I, Bare M, Fernandez de Larrea N, Rivas F, Quintana JM; IRYSS-COPD Group. A decision tree to assess short-term mortality after an emergency department visit for an exacerbation of COPD: a cohort study. Respir Res. 2015 Dec 22;16:151. 29 Quintana JM, Esteban C, Unzurrunzaga A, Garcia-Gutierrez S, Gonzalez N, Barrio I, Arostegui I, Lafuente I, Bare M, Fernandez-de-Larrea N, Vidal S; IRYSS-COPD group. Predictive score for mortality in patients with COPD exacerbations attending hospital emergency departments. BMC Med. 2014 Apr 23;12:66. 30 Escobar A, García-Pérez L, Navarro G, Bilbao A, Quiros R;.A one-year mortality clinical prediction rule for patients with heart failure . CACE-HF Score group. Eur J Intern Med. 2017 Oct;44:49-54. doi: 10.1016/j.ejim.2017.06.013. Epub 2017Jun 19 31 http://www.guiasalud.es/egpc/EPOC/completa/apartado07/tratamiento_exacerbacion.html, https://www.atsjournals.org/doi/full/10.1164/rccm.201204-0596PP 32 Freund. https://cseweb.ucsd.edu/~yfreund/papers/IntroToBoosting.pdf 33 Breiman L. https://www.stat.berkeley.edu/~breiman/bagging.pdf 34 Wolpert H. http://www.machine-learning.martinsewell.com/ensembles/stacking/Wolpert1992.pdf 35 Kohavi http://ai.stanford.edu/~ronnyk/accEst.pdf
FIGURE 6 EWS DEVELOPMENT, DEPLOYMENT AND EVALUATION PROCESS
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 19
4) Addressing Empowerment of Patients and Carers
Living with a severe, chronic disease has a major impact on the patients but it also affects the caregiver’s life and life-quality36. The prioritization of patient-centred care in health care has resulted in an increased focus on patient empowerment, which is considered to facilitate patient independence, self-management, and self-efficacy. In ADLIFE, empowerment is defined as the capacity of individuals, groups and/or communities to take control of their circumstances, exercise power and achieve their own goals, and the process by which, individually and collectively, they are able to help themselves and others to maximize the quality of their lives37. ADLIFE approaches empowerment as a process: the mechanism by which people, organizations, and communities gain mastery over their lives. ADLIFE is based on the use of Patient Reported Outcomes as means to guide health care, empowerment adaptive interventions and share decision making.
• Patient Reported Outcome Measures (PROMs) are a means of collecting information on the effectiveness of care delivered to patients as perceived by the patients themselves. They capture quality-of-life issues that are the very reasons that most patients seek care: to address a bothersome symptom, limited function, or ailing mental health. A Patient Reported Outcome (PRO) is directly reported by the patient without interpretation of the patient’s response by a clinician or anyone else and pertains to the patient’s health, quality of life, or functional status associated with health care or treatment.
• Patient empowerment adaptive interventions: Patients and their informal care givers need to receive full information about the benefits and risks of
treatments; receive support to enhance resources to cope with the demands with their challenges and be involved in care, expressing preferences and engaging in self-management. ADLIFE interventions will be tailored to fit priorities, resources and lifestyle and adapting over time. A challenge for the success of long-term integrated care is adherence rates. In ADLIFE, we aim to deliver “Just in time adaptive intervention (JITAI)”. We aim to implement an intelligent support for personalized self-management to deal with a person’s varying adherence. Reinforcement learning (RL) will tailor the intervention: a) for deciding to deliver an intervention, b) choosing a suitable intervention for an individual and c) identification of an opportune moment to deliver the intervention.
Shared decision Making: ADLIFE is founded in the principle of self-determination and respect for autonomy38. It is critical that the individual has the capacity to understand, discuss options available and agree to what is then planned. Discussion should be focused on the views of the individual, although they may wish to invite their carers or another close family member or friend to participate. There is a need, not only to discuss and share decisions on treatment options, but to be able to agree on different goals and activities of the personalized care plan and be able to access them during the disease’s trajectory. Decision aids support the patient in formulating preferences, clarify decision and describe the course of decision.
ADLIFE will provide a Patient Empowerment Platform (PEP) as a part of the intervention for shared decision making and care plan management involving the patient and their caregivers. PEP will present the detailed information about the care plan and education materials. PCPMP will share the care plan with PEP, via a standard based interface based on HL7 FHIR Care Plan model. The PEP will be notified whenever the care plan is updated by the caregivers. The ADLIFE project will provide PEP functionalities, by extending the Web based Personal Health Record System SRDC has previously developed and used in a number of FP7 projects (https://www.srdc.com.tr/esaglikkaydim/). Pilot sites, who do not already have a legacy patient empowerment tool, will use this system. On the other hand, when pilot sites already have existing tools, such as the Personal Health Folder in the Basque Country and the Maccabi Personal Health Record in Israel, we aim to extend the features of these platforms to be integrated with PCPMP via the proposed standard based interface to exchange and visually present the care plan listing the related goals and activities to the patients and care givers.
PEP will implement a functionality that allows online PROM questionnaires, in order to continuously collect feedback from the patients about the outcome measures, and to monitor risk factors. PROMS will feed PCPMP and CDS Services. The results flow into the care plan in real time, support risk stratification assessment and EWS predictive algorithms. They will be put in context with graphical information, decision support, or shared decision-making tools. The Patient Reported Outcomes (PRO) FHIR Implementation Guide (IG) will be adopted. so that PROMs can be seamlessly exchanged through a standard based interface.
36 Wright LM, Leahey M. Nurses and families: a guide to family assessment and intervention. 6. ed. Philadelphia: F.A. Davis; 2013. 37 Adams, Robert. Empowerment, participation and social work. New York: Palgrave Macmillan, 2008, p.xvi 38 Kolarik RC, Arnold RM, Fischer GS, Tulsky JA. Objectives for Advance Care Planning. J Palliat Med. 2002;5(5):697-704.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 20
ADLIFE we will employ and adapt the Intelligent Communication Engine developed within the scope of H2020 Power2DM39 project. Personalization will sense and react to patients’ momentary and long-term contexts and adapting the intervention delivery strategy accordingly. Just-in-time adaptive interventions (JITAI) will be delivered via mobile devices, making them accessible all the time. The relevant model parameters, facilitating the learning process on preferences of individuals, will be identified. For example, momentary context parameters like location, time or phone activity will be used to identify the right moment for intervention delivery.
5) EVALUATION AND QUALITATIVE, QUANTITATIVE AND SOCIO-ECONOMIC IMPACT ANALYSIS
The aim of this project is to deploy at large scale and demonstrate the effectiveness of ADLIFE intervention when deployed in clinical real conditions. The project will generate evidence of benefits for the patients, the families and carers, the professionals and the health system.
Effectiveness evaluation (WP9) will be based on a quasi-experimental design40 (non-randomized, non-concurrent, controlled trial). The intervention group will be patients identified from clinical and administrative databases complying with ADLIFE inclusion and exclusion criteria.
Patients will be recruited by clinicians (intervention group) from months (M28-M31). Informed consent forms will be signed and followed up for a maximum period of 12 months (M30-41), or less if death occurs. The control group will be patients receiving usual care. It will be selected retrospectively and anonymously from administrative databases considering that patients included in this group should be comparable to the intervention group in demographic, socioeconomic and clinical terms. A mixed-methods approach will be employed41. Table 2 shows the proposed list of indicators to be used to measure the effectiveness of the ADLIFE intervention. The Clinical reference Group will revise the indicators and decide on the final list.
TABLE 2 ADLIFE EVALUATION INDICATORS
END USER INDICATOR TOOL SOURCE
Patient
Extended time at home Proxy (unplanned A&E visits,
reduced unnecessary admissions and LOS)
EHR Administrative databases
Clinical control Questionnaire EHR or interview
Anxiety/depression HADS, Hospital Anxiety and
Depression Scale EHR or Interview
Functionality Barthel, Lawton, EHR or Interview
Quality of life SF36 EHR or Interview
Patients´ trust in quality and security in data access, processing, sharing and storage
Questionnaire Interview or focus group
Satisfaction Questionnaire On-line or interview
Caregiver
Support network Gijon Questionnaire Interview
Satisfaction and support FAMCARE-2 Focus Group
Carer burden and Work limitation Zarit Interview
Wellbeing Carer burden and wellbeing
questionnaire Focus Group
Enhanced knowledge and ability to care Questionnaire Interview or focus groups
39 Gonul, S., et al. (2018). An Expandable Approach for Design and Personalization of Digital, Just-In-Time Adaptive Interventions. Journal of the American Medical Informatics Association. 40 Harris AD, , et al. The Use and Interpretation of Quasi-Experimental Studies in Medical Informatics. JAMIA. 2006;13(1):16-23. doi:10.1197/jamia.M1749. 41 Tariq S, Woodman J. Using mixed methods in health research. JRSM Short Reports. 2013;4(6):2042533313479197. doi:10.1177/2042533313479197.
FIGURE 7 OVERALL EVALUATION DESIGN
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 21
END USER INDICATOR TOOL SOURCE
Satisfaction, Working conditions
Overall Job Satisfaction scale. (SEHC) survey.
Person-centred Climate Questionnaire – PCQ-S
Time management, working time per patient IT systems data logs Administrative databases
Professional
Better communication with patients
Questionnaire Interview and focus group
Trust in quality and security in data access, processing, sharing and storage.
Competencies self-assess level of knowledge
Perceived improvement in means of providing coordinated care
Professional recruitment
System
Range of patients served IT systems data logs Administrative databases
Use and cost of services over time IT systems data logs Administrative databases
Reduced hospital death rate IT systems data logs Administrative databases
Early identification (>90 days before death) IT systems data logs Administrative databases
Quality of care during the last 12 months (≥2 emergency room visits, ≥2 hospital
admissions, ≥14 days of hospitalization) IT systems data logs Administrative databases
Increased death at home IT systems data logs Administrative databases
Communication between care levels Questionnaire Interview or focus group
Personalized care plans generated. EHR IT systems data logs ADLIFE data logs
Decision makers trust in quality and security in data access, processing, sharing and
storage Interviews Qualitative approach
The evaluation comprises five parts:
a) Sample size calculation
Sample size has been calculated using visits to A&E department as main primary outcome, as a good proxy indicator of several of the dimensions ADLIFE wants to impact (health gains, time at home, quality of life or utilization of health services). Assuming a conservative intra-cluster correlation coefficient42 of 0.06 in per year, with a standard deviation of 1.2, considering a loss to follow up rate of 30%, 1764 patients will be required (882 per branch) to measure the primary end-point (90% statistical power and α = 0.05). Each site will recruit 252 patients, 126 per branch, intervention recruited by clinicians and control from administrative data bases (being the intervention group data pseudonymized and the control group data anonymized).
b) Quantitative analysis
The quantitative analyses will be performed for the whole sample and for each subgroup (each pilot site). This approach will allow providing overall efficacy measurements, as well as a comparison between the pilot sites, for primary and secondary outcomes. Outcomes will be monitored at baseline and at the end of the follow-up period, according to each variable and data source. The analysis will be carried out on an intention-to-treat basis; the available data of all patients participating in the study will be assessed as part of their allocation group, even for those cases lost to follow up.
For the intervention group, baseline evaluation will be carried out before the intervention starts. This evaluation will be based on the information collected on the electronic health records (EHR) and, also, on quantitative data collected by means of validated questionnaires. These questionnaires will be available online. Final evaluation will be performed at the end of the defined follow-up period or at patient´s death if it occurs earlier. For the control clinical status at baseline and at the end of one year follow up period or death prior to end of follow-up period, will be collected from the EHR for a defined. Use of resources will be collected too.
Main variables will be obtained from the EHR for both, intervention and control groups, whereas HRQL and satisfaction questionnaires will be collected only for intervention group (control group data are retrospective and
42 Kul et al. Intraclass correlation coefficients for cluster randomized trials in care pathways and usual care: hospital treatment for heart failure. BMC Health Services Research 2014
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 22
anonymous). The effect of the intervention will be assessed by generalized mixed models for longitudinal data, taking into account the clustered structure of the data. Linear models will be used for continuous variables and logistic models for dichotomous variables. All models will be adjusted for potentially confounding factors.
c) Qualitative analysis
Qualitative techniques will generate a deeper understanding of the evaluation process, using patients, families and professionals’ experiences and perceptions to provide a multi-perspective approach to the phenomenon. Two main techniques will be used: semi-structured interviews and focus groups. They will be applied, according to Table 2 Indicators above to intervention stakeholders’ groups (patient, caregivers, professionals and managers). Stakeholders with similar characteristics as the Intervention ones, but not participating in ADLIFE, will be interviewed and asked to be part of dedicated focus groups. They will be identified not be related with the Control group in the quantitative analysis, as patients there cannot be identified.
The qualitative analysis will be carried out after the intervention. The semi-structured interviews will target patients, whereas focus groups will investigate professionals´, managers and families´ perception. The main areas to be studied will be: satisfaction, communication, quality of care, accessibility, decision making process and so on. Special emphasis will be made on healthcare professionals’ satisfaction and working conditions43. A thematic analysis of narratives will be made (using the “reading and re-coding” method) to generate an explanatory framework obtained from the empirical data. Finally, to validate the results, data will be triangulated with the site and the data sources.
d) Prediction rules evaluation and improvement
The algorithms will be evaluated and validated in different ways to ensure their general fitness, applicability in clinical practice and transferability to different populations and care settings. Prediction rules evaluation and improvement will require the close collaboration of the algorithm developers and the clinical experts. They will review, discuss and agree on the final parameters to include in the predictive risk tool. Besides from classifying the patients according to the mentioned developed risk-scores, an evaluation and the validation of these clinical prediction rules will be performed at two stages of this proposal:
I. After having implemented the prediction rules in software, as first step and for each individual in our cohort, we will evaluate the general fitness, applicability in clinical practice and transferability to our samples trough the linear predictor (LP) for predicting the moderate/severe stages, defined according to their main pathology, will be computed using the regression coefficients of the previously original published model. Three main procedures will be considered for the external validation of the risk prediction tools in our cohort: model fit, discrimination and calibration. First, to check the model fit, a logistic regression will be developed, considering the LP as the covariate to estimate its beta regression coefficient. If the beta regression coefficient of the slope is 1, a model is considered valid. Moreover, a likelihood-ratio test was performed to check that the slope was 1. Second, the predicted probabilities will be subsequently used to evaluate the discriminative ability. The discriminative ability (area under the ROC curve, AUC) refers to the model’s ability to discriminate between patients who will, and those who will not develop the event. An AUC value >0.8 with a high sensitivity is considered to indicate an acceptable accuracy. Third, the calibration of the model refers to the agreement between predicted probabilities and observed frequencies of the outcome. The calibration of a model is usually examined by computing the calibration in-the-large (i.e. a comparison of the average predicted probability for the whole cohort and the proportion of patients with the event of interest) and by visually inspecting a calibration plot, in which groups of predicted probabilities are plotted against actually observed outcomes and perfect predictions should be on a 45º line. Finally, we will investigate whether new covariates (not been included in the original model) significantly improved the original model discrimination. A likelihood ratio test will compare the performance between the original and the new model.
II. Validation of the algorithms at the final evaluation phase. Statistical procedures to assess the model discrimination and calibration will be computed. To measure the discrimination ability, the AUC (AUC>0.8 as acceptable) and the screening parameters such as sensitivity and specificity (for the clinical usefulness) will be computed. As regards to calibration, the calibration-in –the-large will used. For continuous outcomes, the RMSEA (root mean square average) parameter will be calculated. The lower the RMSEA, the better the model will be. This process would imply a more real stratification, more personalized, and more dynamic because we are constantly evaluating the robustness of these models
e) Socio-economic impact assessment
43 https://www.researchgate.net/figure/Satisfaction-of-Employees-in-Health-Care-SEHC-Survey-English_fig1_258504978
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 23
A socio-economic impact assessment will be carried out to develop scenarios for the long-term sustainability of the project interventions in each pilot region. The impact analysis will feed the business planning for the technology exploitation and sustainability. The simulations we propose will give insight into the price points and pricing models for a technology such as ADLIFE once it enters the commercialization phase. Any entity commercializing ADLIFE will have to recoup the investments involved in bringing the technology to market. Our vision of ADLIFE is that it will be priced at a level where it can be widely affordable throughout Europe and beyond, while still delivering a commercial return.
Data will be collated from various sources including an evaluation of the pilot operation of the service, data logs of IT systems, fact finding interviews with key informants in the pilot site and other primary and secondary sources such as EUROSTAT44, DG ECFIN45 and SHARE46. Economic models of the impact of the technology will be constructed. Fully accounting the benefits of ADLIFE, as quality of life in advanced chronic patients, personalization and empowerment are hard to monetize.
We will apply a cost-outcome analysis based on two steps. It will be applied to the intervention scenario (ADLIFE intervention) and standard scenario: measurement of program costs and measurement of program outcomes. We will analyze costs (budget impact analysis) in the two scenarios in terms of costs and outcomes. We will assign prices to the various categories of resources used by patients using both local price and also a standard “European” price-set, so that we can compare the cost situation in the different countries with the effect of local prices stripped out.
A simulation modelling methodology will be used to (i) represent the natural history of patients with advanced chronic disease that could benefit from integrated care defined, who move between two stages: compensated and decompensated and (ii) calculate the economic and epidemiological impact of the project in each region and in EU in the long term. For simulation Discrete Event Simulation will be used. This framework was developed and also tested within the European Projects Carewell47 and SmartCare48. Costs will be borne in a varying degree by different parties (e.g, .health service, local government or the patient or their extended family network) in each Pilot Site. We will map them to show the net changes and the cost profile.
1.3.1.2 TECHNICAL AND SEMANTIC INTEROPERABILITY SOLUTIONS
The ADLIFE Care Plan Model will be based on HL7 Fast Healthcare Interoperability Resources (FHIR) CarePlan resource49 and its associated resources. HL7 FHIR will also be used to model patient medical summary collected by PCPMP and shared with CDS services to personalize care plan goals and interventions. PCPMP is natively integrated with a FHIR repository which holds the medical summaries imported from with local care sites as FHIR resources.
As depicted in table 3, the EHR API, data representation, and operational environment vary amongst local care systems, which hinders the PCPMP and the integrated CDS services to seamlessly process these EHRs provided by care sites. In ADLIFE Project we will deploy Technical Interoperability Suite (TIS) services to local care sites which provides a standard-based data exchange protocol through RESTful FHIR interfaces, in order to enable information exchange with local care systems. We will build upon the TIS that has been developed in C3-Cloud Project as a flexible and extensible extract, transform and load (ETL) software development kit (SDK). TIS utilizes the ETL model to pull patient data out of a local EHR system, through its native API, convert the data into selected FHIR resources with the help of Semantic Interoperability Suite (SIS) adopters and stores them to FHIR Repository to be consumed by PCPMP and CDS services. While TIS enables syntactic interoperability to facilitate communication with local EHR APIs, SIS adopters transform the data into FHIR resources by also achieving terminology system mappings when necessary.
C3-Cloud TIS and SIS solutions already support import of HL7 CDA based medical summaries (supported by Basque and Lower Silesia sites) and the proprietary JSON format exposed by Swedish Care site. In ADLIFE project new ETL jobs and SIS services will be implemented as adaptors on top of HL7 V2 messaging and the other native EHR APIs provided by local care sites participating the pilot studies.
44 EUROSTAT (https://ec.europa.eu/eurostat/statistics-explained/index.php?title=People_in_the_EU_-_population_projections), 45 DG-ECFIN (https://ec.europa.eu/info/sites/info/files/economy-finance/ip065_en.pdf) 46 SHARE (http://www.share-project.org/home0.html) 47 Soto-Gordoa M, Arrospide A, Merino Hernández M, Mora Amengual J, Fullaondo Zabala A, Larrañaga I, de Manuel E, Mar J; [on behalf of the CareWell group]. Incorporating Budget Impact Analysis in the Implementation of Complex Interventions: A Case of an Integrated Intervention for Multimorbid Patients within the CareWell Study. Value Health. 2017 Jan;20(1):100-106 48 Larrañaga I, Stafylas P, Fullaondo A, Apuzzo GM, Mar J. Economic Evaluation of an Integrated Health and Social Care Program for Heart Failure Through 2 Different Modeling Techniques. Health Serv Res Manag Epidemiol. 2018 Dec 3;5:2333392818795795.. 49 HL7 FHIR CarePlan resource, http://hl7.org/fhir/careplan.html
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 24
TABLE 3 EHR AND DATA SETS PROVIDED BY PILOT CARE SITES
Region EHR Data Sources and structured EHR data that can be exploited in
pilot studies EHR APIs Provided
Basque Country (Spain)
Administrative databases and Electronic Health Record from the Public Basque Health Service (Osakidetza) including diagnosis, medication, treatment, use of resources from primary and hospital care and demographics.
SOAP and REST Services exposing HL7 CDA documents
Hamburg (Germany)
Administrative data from members of the Hamburg statutory health insurance for the North Rhine region. The data cover pseudonymised patient master data, diagnoses, medication prescription, lab results, procedure and treatment codes from all sectors and demographics.
The Hospitals in the region support standard based APIs (HL7) to access EHRs. Primary care systems do not offer standard based APIs.
South Denmark (Denmark)
Danish EHRs cover every aspect of the patients’ interaction with both primary and secondary health systems, and include details on diagnoses, treatments, medication, etc. Administrative and demographical data is available.
Access can be delivered in the form of CSV files, HL7 and EDI messages.
Ashdod (Israel)
Administrative databases and Electronic Health Record from Maccabi Healthcare Services and Assuta Ashdod Hospital including diagnosis, medication, treatment, lab test results, imaging test results, other tests result such as ECG, pathology, use of resources from primary and hospital care and demographics
HL7 messaging
Scotland (UK)
Electronic Health Record and related database information including demographics, diagnosis, medication, treatment, service use, symptoms and Patient Reported Outcome Measures (PROMs) data. It is anticipated that Electronic Health Record and related database information from NHS Lanarkshire will be available for this project.
HL7 V2 Messages and CDA documents
Region Jämtland (Sweden)
Sweden Administrative databases and a common Electronic Health Record (EHR) for all primary and secondary care in Region Jämtland which include diagnosis, medication, treatment, use of resources from primary and hospital care and demographics.
Web services exposing EHR data in a proprietary JSON format
FALKHOSP (Poland)
Demographics, Conditions, Lab results and Procedure Data are available.
HL7 CDA documents
1.3.1.3 SECURITY AND PRIVACY SOLUTIONS
The use of the data will follow the new GDPR regulation and ADLIFE will obtain local Ethics Committees approval for all intended data access, processing and storage as well as for the care intervention. The datasets will be used, only after formal de-identification, as training data for the prediction algorithms to be developed in WP5 and as test data for the statistical validation.
ADLIFE will implement anonymization, authentication, authorization and audit services based on widely accepted international standards such as OAUTH 2.0, OpenID Connect, ISO/DTS 27789 - Audit trails and According to the ISO/TS 25237:2008 standard for Pseudonymization. The Security and Privacy Suite (SPS) will be responsible for authentication and authorisation of the care team members, while they are managing personalised care plans of patients and ensuring that all data exchanged within and across ADLIFE components is encrypted and properly auditable. In ADLIFE, the patient's electronic health records received from the local EHR systems via the TIS, patient reported outcomes received from the PEP, and the care plan of the patient managed through PCPMP will be all stored in a secure FHIR Repository. Hence, each of these client apps, i.e. TIS, PEP and PCPMP will be authenticated and authorized to access (read, write, and update) patient data to the secure FHIR Repository, via the functionalities provided by SPS. All such operations will be logged for ensuring accountability via SPS. ADLIFE will provide an Audit Record Repository that maintains audit trail records, implemented as FHIR AuditEvent resource. ADLIFE SPS will be integrated with the existing privacy protection and security mechanisms in the pilot sites. As a result, SPS will enable authentication of the care team members into the ADLIFE applications via their already existing accounts (e.g., username-password) provided by the local authorities by integrating with the existing Identity Provider (IdP) systems of the pilot sites.
In the context of anonymization, a careful balance between two conflicting objectives will be achieved: maximizing data quality while minimizing re-identification risks. In order to balance between those two goals, the k-anonymity model and de-identification algorithms proposed by ISO/TS 25237:2008 standard will be applied on the EHR data
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 25
such as generalization, redaction and fuzzing. k-anonymity works against linking and disclosing attributes, by enforcing an upper bound on the re-identification risk of all records.
There is no single de-identification procedure that will meet the diverse needs of all the medical uses, while ensuring privacy of patient data. Therefore, the data anonymization, de-identification and re-identification software tools will be modularly designed to be able to adapt to disparate information systems, and the needs of data analysis tasks.
The ADLIFE SPS authentication, authorization and audit services will build upon the OnAuth Security and Privacy Manager, developed by SRDC, and validated within the scope of C3-Cloud and Power2DM projects. It will be deployed, configured for the needs of the project (e.g., new roles will be defined, authorization rule sets will be defined), and integrated with Single Sign-on mechanisms of pilot sites. For anonymization, the de-identification mechanisms, which have been developed and tested by SRDC within the scope of SALUS Project, will be used as a baseline and adapted where necessary.
1.3.2 SUMMARY OF THE EXISTING ICT INFRASTRUCTURES AND PLATFORMS TO BE EMPLOYED AND ADAPTED IN ADLIFE INTERVENTIONS
ADLIFE Intervention will be built upon several different existing successful research results. The PCPMP, which has been developed and tested in real-life healthcare settings by ADLIFE partners within the scope of the C3-Cloud Project50, will be adapted and implemented in ADLIFE pilot sites. Partners will collaborate to the deployment and tuning of the Clinical Decision Support Services implementing evidence-based guidelines advanced chronic patients to be integrated with the PCPMP. EVERIS will apply its experience using the CRISP-DM methodology. In addition to this, ADLIFE partner, SRDC, has implemented and piloted an Intelligent Communication Engine, within the scope of H2020 Power2DM51 project, to deliver personalized just in time adaptive interventions to support the treatment adherence of diabetic patients52. This intelligent communication engine will be adopted and tailored to the needs of ADLIFE projects within the scope of ADLIFE pilots. The table 4 below shows the existing tool sets that will be used and the functionalities they deliver, including the TRL.
TABLE 4 FUNCTIONALITIES DELIVERED AND TECHNOLOGY STATUS
Existing Toolsets to
re-use Functionalities delivered and Technology Status TRL
C3CLOUD Coordinated Care Cure Delivery Platform
Collaborative creation and monitoring of personalised care plans for patients with multiple chronic conditions by multi-disciplinary healthcare practitioners. Developed in C3-Cloud Project (H2020-689181) by SRDC, and being piloted in Basque Country (Spain), Region of Jamtland Harjedalen (Sweden) and South Warwickshire NHS Foundation Trust (UK) via a 12 months pilot study with approximately 62 health and social care workers and 526 patients.
6
OnFHIR Health Data Repository
The onFhir.io provides an HL7 FHIR based secure health data repository for managing patient data and care plans. Developed by SRDC and been validated in two H2020 projects, namely C3-Cloud (H2020-689181) and Power2DM (H2020-689444).
6
C3CLOUD Clinical Decision Support (CDS) Services
Personalized Clinical Decision Support providing suggestions for treatment goal and activities via clinical guideline automation. Within the scope of C3-Cloud (H2020-689181), ADLIFE partners Warwick and SRDC has developed CDS Services to automate the selected NICE guidelines for Diabetes Mellitus type 2, Renal Failure(excluding Glomerular Filtration rate or estimated (eGFR<30), Heart Failure NYHA I-II; excl. NYHA III-IV and Depression (mild/moderate conditions). Maccabi Healthcare Services have a fully functioning CDSS. On top of this SRDC has developed Clinical decision support services for automating Turkish clinical guidelines for the management of diabetes, hypertension and CVD Risk stratification.
6
POWER2DM Communication Engine
Continuous daily support by personalized adaptive notifications (reminders, motivations, etc.) via mobile phone based on personalized behavioural change techniques. Developed by SRDC within the scope of Power2DM (H2020-689444), and currently being piloted in two pilot studies in 2 different European countries (Netherlands and Spain) with 280 patients.
6
eSağlıkKaydım PHR Platform
This platform provides a personal health record system (PHR) that enables patients to access and manage their personal medical records securely over the web interface. The platform is developed by SRDC and has been validated in Palante Project (FP7- 297260), as a Patient Empowerment platform for the collaborative management of Rheumatoid Arthritis
7
50 http://c3-cloud.eu/ 51 Gonul, S., Namli, Huisman, S., Laleci Erturkmen, G. B., Toroslu, I. H & Cosar, A. (2018). An Expandable Approach for Design and Personalization of Digital, Just-In-Time Adaptive Interventions. Journal of the American Medical Informatics Association. (Accepted for publication)http://power2dm.eu/ 52 http://dx.doi.org/10.1093/jamia/ocy160
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
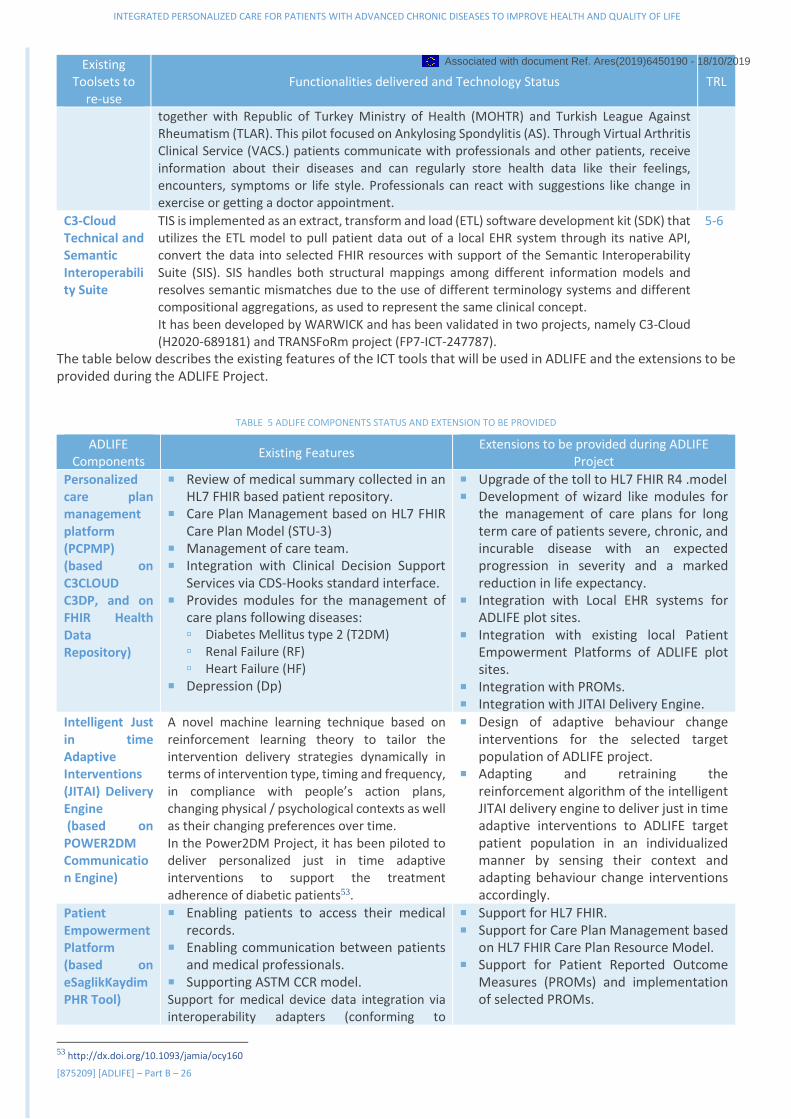
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 26
Existing Toolsets to
re-use Functionalities delivered and Technology Status TRL
together with Republic of Turkey Ministry of Health (MOHTR) and Turkish League Against Rheumatism (TLAR). This pilot focused on Ankylosing Spondylitis (AS). Through Virtual Arthritis Clinical Service (VACS.) patients communicate with professionals and other patients, receive information about their diseases and can regularly store health data like their feelings, encounters, symptoms or life style. Professionals can react with suggestions like change in exercise or getting a doctor appointment.
C3-Cloud Technical and Semantic Interoperability Suite
TIS is implemented as an extract, transform and load (ETL) software development kit (SDK) that utilizes the ETL model to pull patient data out of a local EHR system through its native API, convert the data into selected FHIR resources with support of the Semantic Interoperability Suite (SIS). SIS handles both structural mappings among different information models and resolves semantic mismatches due to the use of different terminology systems and different compositional aggregations, as used to represent the same clinical concept. It has been developed by WARWICK and has been validated in two projects, namely C3-Cloud (H2020-689181) and TRANSFoRm project (FP7-ICT-247787).
5-6
The table below describes the existing features of the ICT tools that will be used in ADLIFE and the extensions to be provided during the ADLIFE Project.
TABLE 5 ADLIFE COMPONENTS STATUS AND EXTENSION TO BE PROVIDED
ADLIFE Components
Existing Features Extensions to be provided during ADLIFE
Project
Personalized care plan management platform (PCPMP) (based on C3CLOUD C3DP, and on FHIR Health Data Repository)
Review of medical summary collected in an HL7 FHIR based patient repository.
Care Plan Management based on HL7 FHIR Care Plan Model (STU-3)
Management of care team. Integration with Clinical Decision Support
Services via CDS-Hooks standard interface. Provides modules for the management of
care plans following diseases: Diabetes Mellitus type 2 (T2DM) Renal Failure (RF) Heart Failure (HF)
Depression (Dp)
Upgrade of the toll to HL7 FHIR R4 .model Development of wizard like modules for
the management of care plans for long term care of patients severe, chronic, and incurable disease with an expected progression in severity and a marked reduction in life expectancy.
Integration with Local EHR systems for ADLIFE plot sites.
Integration with existing local Patient Empowerment Platforms of ADLIFE plot sites.
Integration with PROMs. Integration with JITAI Delivery Engine.
Intelligent Just in time Adaptive Interventions (JITAI) Delivery Engine (based on POWER2DM Communication Engine)
A novel machine learning technique based on reinforcement learning theory to tailor the intervention delivery strategies dynamically in terms of intervention type, timing and frequency, in compliance with people’s action plans, changing physical / psychological contexts as well as their changing preferences over time. In the Power2DM Project, it has been piloted to deliver personalized just in time adaptive interventions to support the treatment adherence of diabetic patients53.
Design of adaptive behaviour change interventions for the selected target population of ADLIFE project.
Adapting and retraining the reinforcement algorithm of the intelligent JITAI delivery engine to deliver just in time adaptive interventions to ADLIFE target patient population in an individualized manner by sensing their context and adapting behaviour change interventions accordingly.
Patient Empowerment Platform (based on eSaglikKaydim PHR Tool)
Enabling patients to access their medical records.
Enabling communication between patients and medical professionals.
Supporting ASTM CCR model. Support for medical device data integration via interoperability adapters (conforming to
Support for HL7 FHIR. Support for Care Plan Management based
on HL7 FHIR Care Plan Resource Model. Support for Patient Reported Outcome
Measures (PROMs) and implementation of selected PROMs.
53 http://dx.doi.org/10.1093/jamia/ocy160
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 27
ADLIFE Components
Existing Features Extensions to be provided during ADLIFE
Project Continua Health Alliance Specs and IHE Patient Care Devices profiles.)
Integration with Just in time Adaptive Intervention Delivery Engine.
Clinical Decision support systems
Provides suggestions for treatment goal and activities by automating clinical guidelines.
Implemented modules for Diabetes, Heart Failure, Renal Failure and Depression.
New clinical guidelines for CHF and COPD will be automated.
New CDS services for functional and need assessment will be implemented.
Existing predictive models (such as readmission to hospitals) will be reviewed, improved and localized to pilot sites.
New supervised learning approaches will be implemented using well probed big data solutions and industry standard infrastructures which includes these advanced data analytics capabilities (MLlib, tensorflow…)
Technical and Semantic Interoperability Suite
Provides an ETL Pipeline mechanism. Structural mapping to HL7 FHIR (already
supports HL7 CDA and proprietary format of Swedish pilot.)
Semantic mapping vi a terminology server (supports SNOMED-CT, ICD-10, Read codes and Spanish and Swedish versions of ICD-10 for conditions, LOINC and WHO ATC for drugs ad lab operations.)
New ETL pipelines will be developed for pilot sites.
New structural mappings will be defined for HL7 v2 messages and other local formats
New terminology mappings need to be added for local code systems.
Security and Privacy Suite
Provides authentication, role-based authorization and audit record functionalities.
Supports oAUTH2.0, OpenID Connect. Provides a flexible anonymization toolkit.
Configuration based on the needs of the project (new roles will be defined, authorization rule sets will be defined.)
Integrated with Single Sign-on mechanisms of pilot sites.
New rules, configuration for anonymization.
1.3.3 POSITIONING OF THE PROJECT
ADLIFE technologies and methodologies are not exactly at the same level of maturity. However, it can be considered that the TRL for the innovative ADLIFE model of integrated care will evolve from 5 to 8 so the model will be complete and qualified in the participating health systems. The evolution of the TRLs for the different components will be:
WP3 Personalized Care plans: as described in table 4 the PCP will be based in the knowledge generated in C3Cloud so the TRL will evolve from 6 to 8;
WP4 patient empowerment platform: As it is been described in table 4 the different ICT components of ADLIFE project are in the perfect status to be validated and supported by an Innovation Action instrument. The TRL will advance from 6/7 to 8;
WP5 CDSS: The aim of ADLIFE is to solve one of the most challenging issues related to the automation of information and analysis extracting from medical guidelines as well as generating predictive tools based on machine learning supervised learning approach based on EVERIS Healthcare BigData&Advanced Analytics previous work. So also, many information and work has been done in previous projects as C3Cloud in this field the TRL will go from 5 to 8;
1.3.4 NATIONAL OR INTERNATIONAL RESEARCH AND INNOVATION ACTIVITIES
Different initiatives have been previously developed and put in a unique position ADLIFE consortium to really tackle the challenges of integrative care:
C3-Cloud where Kronikgune, SRDC, Warwick and RJH participate, aims to establish an ICT infrastructure enabling a collaborative care and cure cloud to enable continuous coordination of patient-centred care activities by a multidisciplinary care team and patients/informal care givers. A Personalised Care Plan Development Platform allows, for the first time, collaborative creation and execution of personalised care plans for multi-morbid patients through systematic and semi-automatic reconciliation of clinical guidelines, with the help of Decision
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 28
Support Modules for risk prediction and stratification, recommendation reconciliation, poly-pharmacy management and goal setting.
Power2DM where SRDC participates, aims to reinforce the prevention sector in healthcare by raising the acceptance of self-management support system based on decision support system that use predictive models fed by data from personal devices. Within the scope of this project, SRDC has developed an Intelligent Communication Engine that delivers JITAIs to patients, in order to reinforce behavioural change interventions for the management of diabetes. Power2DM encourages individuals towards more frequent and long-term use of personal devices for self-monitoring, boosting the development of these devices. We will adapt the JITAI learning mechanism to the context of ADLIFE project for reinforcing the adherence of elderly population suffering from complex long-term conditions.
CAREWELL: The aim of Carewell was to propose, implement and validate new ICT supported integrated care models for patients with multiple comorbidities. Mainly focussed on improving care and care services for complex chronic patients (multiple co-morbidities) by two routes: (i) coordination and communication between healthcare professionals and (ii) empowering the patient and/or caregiver, and home-based care and support based on the use of information and communication technologies (ICT). Main design and implementation lessons will be applied in ADLIFE.
CONNECARE - Personalized Connected Care for Complex Chronic Patients (2016-2019) is an H2020 project to co-design, develop, deploy, and evaluate a novel smart, adaptive integrated care system for chronic care management that strongly relies on the capability of advanced ICT to support personalized care trajectories.
USECARE - an AAL project (2015-2017) to further develop the current prototype of a self-management system SENACA 3.0 (for Senior health Academy) to enable carers for remote-controlling of critical bio-markers of patients, therapy adherence (medication and lifestyle), aggregating information and social interaction and to field-test the prototype focusing on interaction between Carers and Elderly Patients, in a multicentre observational study in different cultural settings.
1.3.5 OVERALL METHODOLOGY
ADLIFE approach has been described above (section 1.3.1.1 ADLIFE elements). The detailed methodology will be organized in ten Work Packages (WP). Out of them, Seven WP (3 to 9) perform the development and innovation (D&I) activities aiming at completing, integrating, deploying and evaluating the ADLIFE personalized digital solution, care model and patient empowerment. Three WP (1, 2 and 10) are in charge of management, dissemination and communication related to future replication and change of policies and exploitation and generation of business models. Three phases can be identified:
Phase I – Organizational issues and ICT platforms implementation: This phase will be organized in 3 main blocks:
Clinical and organizational: a) Personalized care provision: Integration and Coordination of Care For Advanced Chronic Diseases In Existing
Health-Care Services. Ensure that the evidence base personalized care plan model covers and addresses different stakeholders´ needs across multidimensional domains. Review, select and process evidence based scales, guidelines and predictive algorithms for CDSS (WP6).
b) Select validated and available PROMs, shared decision aids and interventions to support patient centered care and self-management.
c) Recruitment of Professionals and establishment of organizational processes: Organization of the ADLIFE multidisciplinary and cross sectoral teams
d) Change package design and implementation for personalized integrated care delivery including implementation of improvement activities and training
e) Ethical Applications For Ethical Committee Approval ICT Platforms implementation:
a) PCPMP will be updated and customized to the needs of advanced chronic disease care management as defined by the clinical experts of the CRG. Technical requirements and Conceptual Design for adaptation of the Integrated ICT Infrastructure and assurance of the Security, Privacy and Quality will be implemented
FIGURE 8 ADLIFE METHODOLOGY
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 29
b) CDSS will be deigned, integrated and implemented, fed by evidence-based knowledge from guidelines and updated scientific sources. Assessment scales computerized. Predictive algorithms trained, refined, integrated, deployed and validated.
c) Patient Empowerment Platform (PEP) upgraded to all ADLIFE functionalities. Enabling patients to access their care plan and communication between patients and medical professionals, implementation Patient Reported Outcomes (PRO) following FHIR Implementation Guide, Intelligent Just in time Adaptive Interventions (JITAI) Delivery Engine (based on POWER2DM Communication Engine and Support for medical device data integration via interoperability adapters (conforming to Continua Health Alliance Specs and IHE Patient Care Devices profiles
d) Deployment of ADLIFE toolbox in different health systems: The ADLIFE platforms and tools will be integrated with the existing legacy system/EHRs an all of the pilot sites and tested so that , from the perspective of the clinicians and healthcare professionals, working with the PCPMP will be an extension of their normal routine use of their organizations' EHR This will also include training all professionals in the use of the PCMCP and all other ADLIFE tools
Phase II – Intervention large scale deployment: ADLIFE intervention is based on the creation of personalized care plans, which ARE shared by health professionals in different settings, and continuously adapted according to patients´ changing needs and preferences. ADLIFE intervention will be implemented in 7 Regions across Europe representing six different EU Countries and one Associated Country, involving 75 healthcare facilities, 577 healthcare professionals, 882 patients and 1243 caregivers.
ADLIFE is a complex intervention54. Once Phase I is completed, the intervention will be implemented from M30 up to M41. It includes:
Identify, validate and recruit patients, with Advanced Chronic Diseases complying with inclusion and exclusion criteria.
Assess patient´s and family´s baselines risks and multidimensional needs and create the Personalized Care Plans for each of patient.
Follow up: A multidisciplinary team manages the health and care needs of each patient the Personalized Care Plan, using the PCPM, the CDSS recommendations (including EWS) and PEP, with JITAI.
Deploy the adaptive digital intervention content and execute and manage the Patient Empowerment Platform. Follow up and review regularly the Personalized Care Plan and update when necessary using CDSS. A case study describing the intervention for patients and the multidimensional professional team (MDT) explains how ADLIFE will work.
ADLIFE PATIENT: My name is Agnes Jones, 83, with a COPD that has been accompanying me since I was 60, but my disease has been getting worse during the last 3 years, and it is now incapacitating me in my daily-life, due also to the complications and decline of my global health status. I grew two children that live far from my home (500 kms). Few weeks ago, I was invited to participate in a new program, ADLIFE that, as my GP, Dr. Börg and my nurse, Mr. Smith have explained to me, is going to accompany me till the end of my life, but they want me to spend these lasting days/months/years in the healthiest and best quality possible way. In my situation, being healthier means avoiding shortness of breath, fatigue, insomnia and chest pain and not having airways infections. I want to stay as long as possible living independently at home and not having to go in a hurry to the A&E Department each time I feel worse. In a first meeting, I have prepared, well, we have prepared with my team of doctors (MDT), Jacob and Mary a personalized care plan, where I have included my preferences for my spare time, and other interesting things that I want to state if anything happens to me. It has been a relief for me, being also able to explain that I would prefer to receive care at home. They have also updated my drug treatment. They have told me that with this new program they can be sure that I take the pills that I need and that my husband hasn´t need to pay attention to the changes in the doses or new recommendations because everything is connected; and if I go to the pneumologist, my general practitioner (GP) will know and of course, Mr. Smith, the nurse that usually come to visit me, will be always posted. So, everything is going to be connected and we don´t have to worry if my pneumologist knows or not, about if I have been in my primary care centre or if Mr. Smith has detected that something is not working correctly. In fact, we have (me, Jacob and my daughters) a group in a new internet page (the Patient Empowerment Platform they call it) with information on what to do and where we can contact “my team” and also a phone contact available 24/7, what a relief. I will be
54 Craig P, et al. M. Developing and evaluating complex interventions: the new Medical Research Council guidance. The BMJ. 2008;337:a1655. doi:10.1136/bmj.a1655.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 30
able to report on my situation, difficulties or symptoms through my phone. They call it PROMs! I will be given information on what to do thanks to the information I give them with my telephone! I also receive motivation messages about taking my drugs on time, carrying out regular light walks. Yesterday it motivated me by reminding last week’s positive performance. The messages are always friendly, never repeating and encouraging (they call it adaptive interventions), as if I have a personal assistant with me all the time. Although, at the beginning I didn’t know what to expect about this ADLIFE, after the first six months I am very glad of having been selected to the program. I have easily updated my plan after being hospitalized and after my recovery and I feel very active, I don´t feel pain or these attacks and nightmares for not being able to breath at nights, as I have answered in these questionnaires that I have had to complete.
ADLIFE MDT: Dr Börg is a GP working in the region. She has been approached by the ADLIFE Project and has accepted to participate and use the ADLIFE Personalized Care Management Platform (PCPMP). One of her patients, Agnes Jones, 83, with a COPD since many years ago, was identified as a potential candidate that could benefit of ADLIFE. The next time Agnes came to her office, she performed an assessment of the patient. She offered her to create a Personalized Care Plan (PCP). She discussed with Agnes (and her relatives) her concerns and set some health goals in different dimensions (physical, psychological, spiritual, social are set). The shared decision making tools available in the ADLIFE app were very helpful. The PCPMP automatically drew Patient data from the electronic health records (EHR). When completing the Care Plan, Dr. Börg was offered a risk assessment and evidence-based recommendation by the CDSS, according to the Patient status, on lab test needed and treatment options.
Dr Börg acts as Case Manager. She benefits of her previous knowledge and experience but has also the CDSS at her disposal supporting her decisions with evidence-based information, continuous assessment of changing needs and predict events that may be impactable or require further action. This way, Agnes had the opportunity to receive much more early adequate treatment and care option. Dr. Börg considered inviting other health professionals to become members of the Multidisciplinary team (MDT).
Dr Börg and Mr. Smith, the Primary Care Nurse, frequent re- assessed of Agnes health status using scales and tools offered in the PCPMP. They also have included some digital intervention content in the Patient Empowerment Platform, that Agnes and her carers use to examine her Personalized Care Plan and communicate with her MDT. Some weeks later, Agnes clinical condition deteriorated. She had more shortness of breath, anxiety and restlessness which are recorded via PEP. These are detected by CDSSs, and care team members are automatically advised to alter the care plan. Dr Börg decided to involve Dr. García, from the Neumology Department in the Reference Hospital in the team. Dr. García can access and edit the personalized plan in the PCPMP. Although Dr Börg is the ultimate responsible, he suggests changes in goals, adding new ones or modifying existing ones. He offers new care options, including physical rehabilitation, psychological support or adapted lifestyle and diet recommendations. Special emphasis is given to quality of life, targeting symptoms burden and suffering. CDSS offer different options in these new areas too. The JITAI functionality of the PEP offers adaptive interventions and enhances adherence to the recommendations.
Dr Börg discussed these new goals and treatment options with Agnes and her spouse. They updated the different care options. She is going to complete the PROMs questionnaires in a scheduled way allowing to assess her symptoms control and quality of life. They use the Advanced Care Template available in the PCPMP to write down Agnes´s wishes, in case it has to be invoked at some later stage.
Some months later, an alarm triggered by the Risk Predictive Algorithm warned Dr. Börg that Agnes clinical situation was deteriorating. Dr. Börg agreed with Dr. García that she would benefit of some days admission at the Local Hospital. The locus of responsibility shifts to Dr. García, who became the new Case Manager. Dr. Börg maintained access to the PCPMP and Agnes´s Care. After ten days, Agnes was discharged to her home with new goals and interventions in her PCP. Homecare and treatment was organized between Dr.García, the Hospital Liaison Nurse and Dr. Börg and Mr. Smith.
One night, a few weeks later, the dyspnoea worsens due to an acute respiratory infection. Jacob called the Out of Hours Emergency department. The Doctor in call accessed Agnes´s PCP, and adjusted her medication, using a dedicated CDSS. Agnes improved and avoids being admitted to Hospital. Fourteen months later, Agnes dies in peace at home, with her love ones as she had expressed in her advanced care plan.
Phase III. Evaluation: ADLIFE intervention is a complex innovation intervention. To assess the effectiveness on the health gain, quality of life, working conditions, health services utilization and economic impact, ADLIFE will use a quasi-experimental design (non-randomized, non-concurrent, controlled trial) (WP9). A mixed-methods approach will be used, including comparison between quantitative and qualitative analysis. A list of 28 indicators will be studied. The intervention group (882 patients) will be patients with Advanced Chronic Diseases (CHF and/or COPD
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 31
with/without co-morbidities. The control group will be 882 patients selected anonymously and retrospectively from administrative data bases having similar clinical and demographic characteristics. Data will be collected from the very beginning, to have a baseline in both control and intervention groups. Final and intermediate outcomes will be monitored at regular intervals (baseline, follow-up and final), according to each variable and data source. A socio-economic impact assessment will be carried out to develop scenarios for the long-term sustainability of the project interventions in each pilot region as well as on a larger scale in further regions of the EU and elsewhere Simulation-modelling methodology will be used.
SEX AND/OR GENDER ANALYSIS
Gender Aspects in ADLIFE Intervention and Tools
Taking into account the holistic approach of the project it is not expected to have any gender bias. On the contrary, ADLIFE addresses some of the gender disparities around healthcare, disease burden, communication between patients and professionals and care givers support. In average chronic diseases affect both women and men even though it is true that some diseases have more significance (or are exclusive) to a specific gender. In spite of the fact that women’s life expectancy is higher than men’s, it has been traditionally believed that women had poorer health, and higher morbidity and incapacity rates than men, and use health services much more often than men55.
It may be however, that gender affects the communication of information between health professionals and patients as well as caregivers. Women and men are known to utilize different communication styles and previous research has shown that male and female physicians tend to differ in the way they talk to patients. These gender differences in communication styles have been shown to exist within the patient-physician interaction, affected by both sex of the patient as well as the sex of the physician56.
Family-caregiving still remains a predominantly feminine activity despite the fact that with changing demographics and changes in social structures and norms, men are increasingly assuming roles as caregivers a trend that is likely to continue as family life is reconstructed alongside changing gender roles and expectation57. Nevertheless, nearly 70% to 80% of the older adults are cared for at home by their family members. Varying estimates across different countries indicate that 57% to 81% of all caregivers of the older adults are women. In most cases female caregivers are wives or adult daughters of the adult person58.
Gender Consortium Composition
The project consortium will ensure gender balance and to promote participation of women in the different tasks of the project. In fact, women will lead five of the ten work packages: WP2, WP4, WP7, WP8 and WP9. In addition, 53% of the personnel that will participate in the project are female. Some of the specific actions that will be taken in this context are: general management of the project will guarantee gender equality, i.e. equal consideration to the life patterns, needs and interests of both women and men; the consortium will encourage all partners to favour the hiring and nomination of female workers in the project; the ADLIFE project will make every possible effort to gender mainstreaming in order to give European women an equal chance of shaping, participating in, monitoring and evaluating EU supported scientific projects and programs; flexible working-time arrangements will be promoted among participating organizations for men and women to reconcile work and private life, not interfering in terms of income and carer perspective. In addition, it is important to highlight that gender balance is also an individual commitment for each one of the partners as it is included in their internal policies and in line with national regulations.
1.4 AMBITION
Digital Transformation of Health and Care for the Ageing Society59. ADLIFE is going to use the unique knowledge of the consortium to really take the integrated care services based in digital solutions to the next level of real implementation and revolution of healthcare systems and digital market. It can derive the learning of ongoing and completed pilots and implementation experiences and create an evidence-based roadmap for concerted actions by a diversity of stakeholders.
Providing person-centred and integrated supportive care and guaranteeing access will require systems to be organized around older people’s needs and preferences and will require services to be age-friendly and closely
55 Matud MP. Gender and Health. 2017; http://dx.doi.org/10.5772/65410 56 Nolen HA. Patient Preference for Physician Gender inthe Emergency Department Yale journal of biology and medicine 89 (2016), pp.131-142. 57 Washington et al. Gender differences in caregiving at end of life. Journal of palliative medicine:205: vol 18, 1048-1053. 58 Sharma N et al . Gender differences in family-caregiving. World J Psychiatr. 2016;6(1): 7-17 59 https://ec.europa.eu/digital-single-market/en/blueprint-digital-transformation-health-and-care-ageing-society
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 32
engaged with families and communities60. Integrated supportive care61 must be addressed holistically and personalized to each patient, based on assessment of individual risks, needs and preferences62. Patients with Advanced Chronic Diseases is a group considered to be one in where we can achieve more relative gains in health status (delaying deterioration, improving symptoms control and avoiding exacerbations and adverse events). It is a group where health services resources utilization can be greatly optimized preventing unplanned A&E visits, hospital admissions, inappropriate aggressive and costly diagnostic and therapeutic interventions or poly-medication side effects. There is a significant margin to enhance independent living, preventing unnecessary suffering and quality of life63. There is evidence to support implementation efforts64, but there remains no global consensus concerning actions required to upscale it at the service (meso) or system (macro) levels to achieve sustainable implementation of integrated care or how to transfer these experiences to other contexts65.
Altogether, the main limitations in the current state of the art for the successful implementation of integrated care are lack of Patient focus/empowerment; inadequate governance and organisational change; insufficient workforce education and training ; limited monitoring evaluation of the integrated care; lack of stakeholder engagement and limited political support and commitment.
To align and coordinate care across fragmented care teams and care settings, good communication and information sharing is needed. Without secure information exchange among the actors involved in health, social and informal care services, it is impossible to coordinate care and avoid gaps, duplications and unnecessary interventions. There are some ICT supported tools that support preparation of care plans, that can establish common goals and activities, although they are incomplete and not interoperable among different systems and organizations, hampering coordinated care66. They fall short in supporting patients in their long-term care journey, and not providing personalized interventions to reinforce their adherence to the often-complex care regimens. Clinical Decision Support Systems and Patient Reported Outcomes are being developed to measure health gain in patients undergoing different procedures but are not widely used.67 Digital health and care solutions remain mostly local, small-scale and unevenly distributed across the EU. The impact of digitalisation of health services is expected to be profound. However, there is growing evidence of low scalability of digital health and care approaches from pilots to large-scale deployment and widespread uptake. Despite the recognised potential of integrated, person-centred care models and the digital transformation of health and care provision, benefits have not come to fruition. In many cases initiatives remain at project stage and do not permeate health and care provision at scale, hindering supply of services to all citizens who can benefit from them. Among other factors that have hampered the update: Available digital solutions on the market have limited scope, are small-scale and unevenly distributed Lack of interoperability (need for an EU framework) and difficult to integrate to the existing healthcare
information systems; Lack of openness of the (proprietary) solutions for data sharing among the health and care providers and for the
2nd use of data for research and innovation purpose; Healthcare organisations usually prefer tailor-made solutions and decide to develop their own ones; The digital gap for ageing population still remains; Lack of user-friendly solutions.
ADLIFE ambition is to go beyond these limitations. It will build on the knowledge, experience and results of on previous initiatives and experiences and will address the main limitations that have been previously described.
60 Briggs AM et al. Actions required to implement integrated care for older people in the community using the World Health Organization’s ICOPE approach: A global Delphi consensus study. PLOS ONE, 2018, October. 61 https://www.cancer.gov/publications/dictionaries/cancer-terms/def/supportive-care 62 Jefford M, et al. Implementing improved post-treatment care for cancer survivors in England, with reflections from Australia, Canada and the USA. Br J Cancer. 2013;108:14-20. 63 Llobera J, , et al. Strengthening primary health care teams with palliative care leaders: protocol for a cluster randomized clinical trial. BMC Palliat Care. 2017;17(1): 64 6. Threapleton DE, et al. Integrated care for older populations and its implementation facilitators and barriers: A rapid scoping review. Int J Quality Health Care. 2017; 29:327–34 65 Leichsenring, Ke tal. Long-term care in Europe – improving policy and practice. Basingstoke: Palgrave Macmillan; 2013. 66 Cano et al. An adaptive case management system to support integrated care services: Lessons learned from the NEXES project. Journal of Biomedical Informatics 55 (2015) 11–22 67 NHS Digital, Patient Reported Outcome Measures (PROMs) https://digital.nhs.uk/data-and-information/data-tools-and-services/data-services/patient-reported-outcome-measures-proms#summary
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
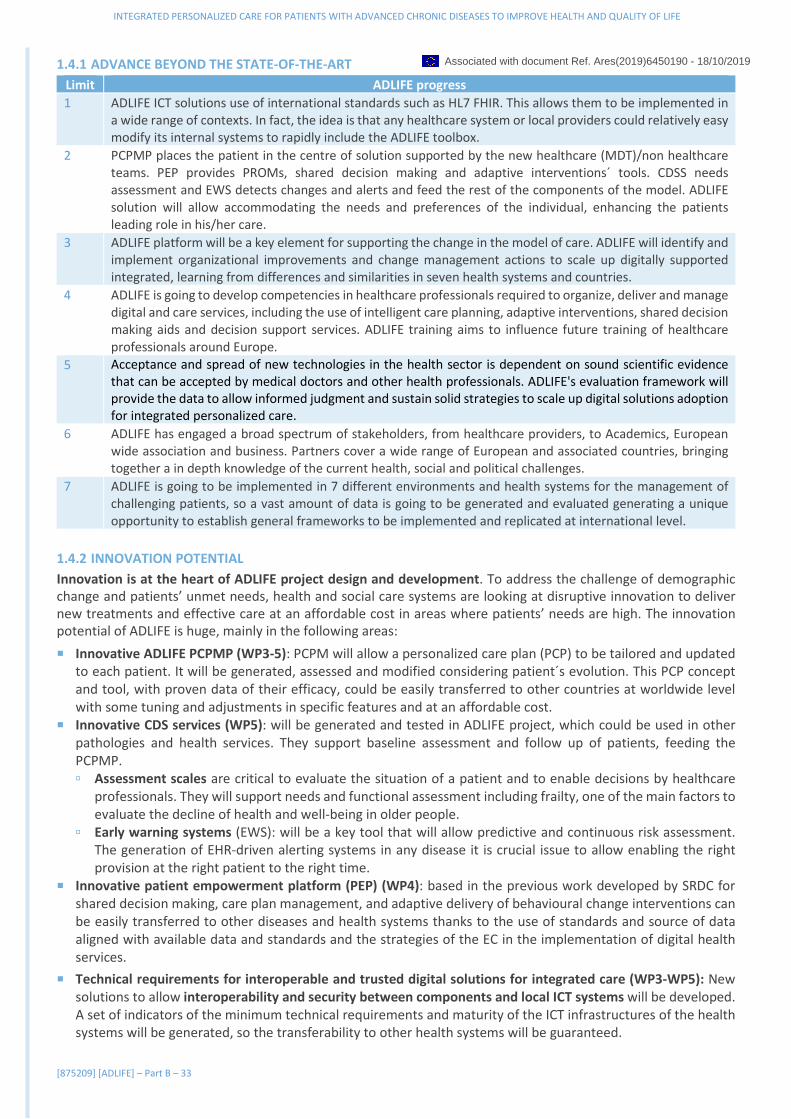
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 33
1.4.1 ADVANCE BEYOND THE STATE-OF-THE-ART
Limit ADLIFE progress
1 ADLIFE ICT solutions use of international standards such as HL7 FHIR. This allows them to be implemented in a wide range of contexts. In fact, the idea is that any healthcare system or local providers could relatively easy modify its internal systems to rapidly include the ADLIFE toolbox.
2 PCPMP places the patient in the centre of solution supported by the new healthcare (MDT)/non healthcare teams. PEP provides PROMs, shared decision making and adaptive interventions´ tools. CDSS needs assessment and EWS detects changes and alerts and feed the rest of the components of the model. ADLIFE solution will allow accommodating the needs and preferences of the individual, enhancing the patients leading role in his/her care.
3 ADLIFE platform will be a key element for supporting the change in the model of care. ADLIFE will identify and implement organizational improvements and change management actions to scale up digitally supported integrated, learning from differences and similarities in seven health systems and countries.
4 ADLIFE is going to develop competencies in healthcare professionals required to organize, deliver and manage digital and care services, including the use of intelligent care planning, adaptive interventions, shared decision making aids and decision support services. ADLIFE training aims to influence future training of healthcare professionals around Europe.
5 Acceptance and spread of new technologies in the health sector is dependent on sound scientific evidence that can be accepted by medical doctors and other health professionals. ADLIFE's evaluation framework will provide the data to allow informed judgment and sustain solid strategies to scale up digital solutions adoption for integrated personalized care.
6 ADLIFE has engaged a broad spectrum of stakeholders, from healthcare providers, to Academics, European wide association and business. Partners cover a wide range of European and associated countries, bringing together a in depth knowledge of the current health, social and political challenges.
7 ADLIFE is going to be implemented in 7 different environments and health systems for the management of challenging patients, so a vast amount of data is going to be generated and evaluated generating a unique opportunity to establish general frameworks to be implemented and replicated at international level.
1.4.2 INNOVATION POTENTIAL
Innovation is at the heart of ADLIFE project design and development. To address the challenge of demographic change and patients’ unmet needs, health and social care systems are looking at disruptive innovation to deliver new treatments and effective care at an affordable cost in areas where patients’ needs are high. The innovation potential of ADLIFE is huge, mainly in the following areas:
Innovative ADLIFE PCPMP (WP3-5): PCPM will allow a personalized care plan (PCP) to be tailored and updated to each patient. It will be generated, assessed and modified considering patient´s evolution. This PCP concept and tool, with proven data of their efficacy, could be easily transferred to other countries at worldwide level with some tuning and adjustments in specific features and at an affordable cost.
Innovative CDS services (WP5): will be generated and tested in ADLIFE project, which could be used in other pathologies and health services. They support baseline assessment and follow up of patients, feeding the PCPMP. Assessment scales are critical to evaluate the situation of a patient and to enable decisions by healthcare
professionals. They will support needs and functional assessment including frailty, one of the main factors to evaluate the decline of health and well-being in older people.
Early warning systems (EWS): will be a key tool that will allow predictive and continuous risk assessment. The generation of EHR-driven alerting systems in any disease it is crucial issue to allow enabling the right provision at the right patient to the right time.
Innovative patient empowerment platform (PEP) (WP4): based in the previous work developed by SRDC for shared decision making, care plan management, and adaptive delivery of behavioural change interventions can be easily transferred to other diseases and health systems thanks to the use of standards and source of data aligned with available data and standards and the strategies of the EC in the implementation of digital health services.
Technical requirements for interoperable and trusted digital solutions for integrated care (WP3-WP5): New solutions to allow interoperability and security between components and local ICT systems will be developed. A set of indicators of the minimum technical requirements and maturity of the ICT infrastructures of the health systems will be generated, so the transferability to other health systems will be guaranteed.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 34
Drivers implementing healthcare models (WP6 and 8): Digital solutions are enablers and can be implemented successfully only if they are based and support on adequate organizational models ADLIFE will provide new knowledge on barriers, facilitators and change management strategies trequired to successfully implement and scale up digital integrated care
Materials, tools and methodologies for empowerment and training (WP7): adaptive intervention, selected and dedicated PROM, and shared decision making aids, together with guidelines and training materials will be generated for the empowerment of formal and informal caregivers as well as for patients.
New evidence of care effectiveness and cost-effectiveness (WP9): ADLIFE is going to generate specific evidence to assess the effectiveness of the integrated care in long term ADVANCED CHRONIC DISEASES.
Evaluation framework: ADLIFE evaluation framework will generate conclusions that will support health systems in making decisions about not only the digitalization of the care but also the change of model for providing integrated care. The framework is aligned with methodologies used in health technology assessment (HTA) like MAST and also MAFEIP.
2. IMPACT
2.1 EXPECTED IMPACTS
Assessment and evaluation of Digital Health Services: Public expenditure on health and long-term care has been increasing over the last decades in all EU Member States and is expected to rise even further. In 2015, it accounted for 8.5% of GDP in the EU and could reach up to 12.5% of GDP in 206068. A substantial part of the increase has been attributed to the introduction and funding of new technologies in health care, including digital ones. In this context, there is a growing need for robust evidence to support arguments that digital health solutions69. The ADLIFE large scale and cost-effective deployment of digital innovation for professional and informal health and social care will support the Triple Win for Europe: Improve the health and quality of life of citizens; Support the long-term sustainability and efficiency of health and social care systems; Enhance the competitiveness of EU industry creating economic growth opportunities and jobs in the Silver Economy.
ADLIFE will deliver a systematic assessment and evaluation of the impact of digital health services. The ADLIFE framework for the assessment of the digital transformation of health services and its impact will generate the evidence that is required for decision-making on stimulating, using and/or funding digital health strategies at various levels in the health care system.
In addition, a growing share of the population in Europe (19,2% in 201670) is over 65 and expected to reach 26% by 203071. More than half of all older people have at least three chronic conditions and a significant proportion has five or more. The clinical management of patients suffering from multiple 72 chronic conditions is very complex, disconnected and time consuming with the traditional care settings. This is much more relevant for those patients with Advanced Chronic Diseases.
ADLIFE will make a vital difference through the demonstration of how the digital services for integrated care can increase the quality of life of patients, carers and relatives and at the same time minimize the impact of the costs related to healthcare of the worst scenario of long term chronic patients, ADVANCED CHRONIC DISEASES. ADLIFE will do this by providing the tools and data to healthcare managers and professionals on how resources and organizations have to be re-organized to maximize the benefit and the quality of the care and resources. ADLIFE is based in previously robust evidence generated among others in collaborative projects like C3-Cloud and CAREWELL, where limitations from health services have been identified and tackled. C3Cloud has been tested in two different countries Spain and Sweden, but in a less complex situation (not Advanced Chronic Diseases). The evaluation conducted in ADLIFE project (WP9) will generate robust health, social and economic data and indicators. ADLIFE will generate a framework for the assessment of the digital transformation of health services that will be useful to generate the evidence also in other projects.
Management of comorbidities: ADLIFE will improve the life of patients, families and carers of Advanced Chronic Diseases, that have an enormous impact on their quality of life and on health systems. Chronic obstructive pulmonary disease (COPD) is an important cause of morbidity and mortality with high social and economic costs. The prevalence of COPD has been reported to vary between 6 and 26.1% worldwide. COPD has also been associated with a high prevalence of one or more comorbid conditions, which have an impact on health status and mortality.
68 European Commission's Joint Report on Health Care and Long-term Care Systems and Fiscal Sustainability (7 October 2016) 69 WHO. Monitoring and Evaluating Digital Health interventions: A practical guide to conducting research and assessment. WHO 2016. 70People in the EU - statistics on an ageing society 71 https://ec.europa.eu/research/social-sciences/pdf/policy_reviews/kina26426enc.pdf 72 Integrated care models: an overview, Working document, Health Services Delivery Programme, Division of Health Systems and Public Health, WHO (2016).
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 35
In contrast to coronary heart diseases and stroke, it is the only leading cause of death that is still increasing73. The estimated the total cost in Europe for COPD is 141.4 billion euros74 (23.3€ bn direct costs; 25.1E bn indirect costs and 93 € bn monetised value of DALYs lost). Heart failure (HF) is a major and growing medical and economic problem worldwide as 1-2% of the healthcare budget is spent for heart failure75. The global economic burden of HF is estimated at $108 billion per annum, with $65 billion attributed to direct and $43 billion to indirect costs. Europe accounts for 6.83% of total global HF costs. The hospitalization costs are the greatest cost component of overall healthcare costs. Among total healthcare costs, expenditures for medication are the second largest issue. The direct impact that implementing ADLIFE integrated model care in both diseases, only with reducing the hospitalization rates in a 5% the impact in the costs can be enormous. ADLIFE will demonstrate the benefits of the digital integrated care in reducing the socio-economic burden and improved quality of life. It will provide evidence to support the sustainability of health systems by optimizing the available resources.
Real deployment of integrated healthcare services: ADLIFE is perfectly aligned with the strategy proposed by EIP on AHA76 Blueprint where it is stated that a shared vision is essential to mobilise investment and guarantee the commitment of all actors for the digital transformation of health and care for the ageing society. ADLIFE will demonstrate how Europe can configure more sustainable models for health and care delivery, as part of a process of health innovation, where the ongoing structural reforms that aim at increasing the effectiveness and resilience of health and care systems. ADLIFE is a coordinated approach led by the health systems participating in the project and including the point of view of the patients, society and the industrial sector.
2.1.1 EXPECTED IMPACTS SET OUT IN THE WORK PROGRAMME
A common vision of technical prerequisites and framework to ensure users trust with regard to health and social data and information in IT supported environment, in line with existing EU data protection regulation As it has been stated before and highlighted in different strategic documents published by EC and other initiatives76 Standards and regulation can affect demand and market outcomes leading to either customer trust (leading to acceleration of the diffusion of innovation) or distrust and uncertainty (leading to lower investment, less value created, further market fragmentation and the stagnation of innovation). Lack of interoperability is both a reason for and a result of market fragmentation. It perpetuates market fragmentation and creates significant barriers to entry, especially for innovators and SMEs. Better coordination of care requires open platforms and widely adopted standards on which each player can contribute, and innovations can thrive. This lack of standards has also limited the user trust at level of citizens or healthcare systems.
ADLIFE proposes (WP3) to conceive the digital solutions as “medical devices” so they can fulfil not only the General Data protection regulation but also the Medical Devices Regulation (MDR). Therefore, all the necessary security and privacy mechanisms will be implemented to safeguard the secure access, sharing and storing´s of patients ‘personalized information. ADLIFE the toolbox/platform can be considered as class IIa following the recently updated MDR as clinical recommendation provider. Audit trails for electronic health records will be analysed and suitable profiles for integrated care will be selected. ADLIFE will provide an Audit Record Repository that maintains audit trail records implemented as an FHIR AuditEvent resource. Following these MDR guidelines will increase the exploitability of the solution as subsequent operators will be able to comply with the MDR more easily and cost effectively post project.
ADLIFE will provide anonymization, authentication, authorization and audit services based on widely accepted international standards such as OAUTH 2.0, OpenID Connect, ISO/DTS 27789 - Audit trails and According to the ISO/TS 25237:2008 standard for Pseudonymization. The Security and Privacy Suite (SPS) will be responsible for authentication and authorisation of the care team members, while they are managing personalised care plans of patients and ensuring that all data exchanged within and across ADLIFE components is encrypted and properly auditable.
Regarding technical prerequisites all ADLIFE previous developments comply with IEEE STD 1016:1998 and well-established standards (FHIR, CDS-hooks and REST) as well as following the guidance of ISO 11197 Metadata Registry (MDR) standard for the semantic interoperability suite (SIS) and the Unified Medical Language System (UMLS). ADLIFE proposes to use the IEEE standard IEEE std 828:2012 (Standard for Configuration Management in Systems and Software Engineering) to create a software configuration management plan and a requirements document following the Recommendations of the well-established standard IEEE Std. 29148:2011 (Systems and Software engineering- Life cycle processes – Requirements engineering) which incorporates guidelines provided by
73 May S etal. Burden of chronic obstructive pulmonary disease: Healthcare costs and beyond. Allergy Asthma Proc. 2015 Jan-Feb; 36(1): 4–10. 74 https://www.europeanlung.org/assets/files/publications/lung_health_in_europe_facts_and_figures_web.pdf 75 Lesyuk W etal .Cost-of-illness studies in heart failure: a systematic review 2004–2016. BMC Cardiovasc Disord. 2018; 18: 74. 76 Blueprint Digital Transformation of health and care for the ageing society. Strategic Vision Developed by Stakeholders January 2017
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 36
IEEE STD 830-1998 and IEEE STD 1233-1998. And for adaptations, the IEEE STD 1016:2009 (Standard for Information Technology--Systems Design--Software Design Descriptions) will be followed.
WP3 will deliver an ‘Assurance report including software quality plan, assessment of certifiability against MDR and GDPR’ as D3.5. In addition to this, the trust/distrust in the ADLIFE toolbox/platform will be evaluated in WP9 and the problems/barriers to implement this minimum framework and technical requirements will be monitor also during the implementation and adjustment of the tools in the corresponding pilots. So, ADLIFE will generate a robust and large amount of data to support the recommendations in the digital health sector.
ADLIFE will follow the common innovation language indicated in the Blueprint strategy, that has been built on the availability of shared and widely recognised impact assessment tools for innovation in health and active and healthy ageing such MAFEIP. MAFEIP has already been adopted by the partners and References Sites of the European Innovation Partnership on Active and Healthy Ageing (EIP on AHA) like consortium coordinator Basque Country (Partner 1), and partners Scotland (Partner 2) and Southern Denmark (Partner 4) that are 4 stars Reference Sites in EIP-AHA. Combined with the evaluation methodology will support the framework.
Minimum data set: Clerical information: complete definition; Clinical information: generic definition Data and data sources are critical for integrated care from a holistic point of view. In fact, data are critical for managing multi-morbidity, through the current treatment methods, results in specialty silos involving multiple health and social care providers who are not effectively communicating and sharing information. As the number and complexity of health conditions increase over time and episodes of acute illness are superimposed, the type and number of care providers contributing to the care of individuals also increases. It becomes significantly more difficult to align and coordinate care across care teams and care settings. This results in fragmented care, due to poor communication and information sharing. Without secure information exchange among the actors involved in health, social and informal care services and a process to reconcile potentially connecting treatment plans, it is impossible to avoid redundant and potentially harmful interventions.
To guarantee an integrated care model of adequate quality a minimum set of data is necessary at two levels as it is described in the table 1 of section 1:
Clerical data: administrative information included in the EHR or obtained from administrative and demographical data Including age, gender, marital status, living situation, education, occupation (WP3-9).
Clinical data: included in the EHR but also from other sources including diagnosis, medication treatment, procedures, laboratory and imaging results, hospitalizations (number and duration of stay), emergency room visits. (WP3-10)
In ADLIFE we will identify the necessary minimum data sets for the care plans, we will implement and validate these through the ADLIFE Technical and Semantic Interoperability toolsets, and we will make these data sets available by building interoperability adaptors on top of pilot sites local EHR systems. The data will be available from the secure HL7 FHIR repository in a standard based format for the use of intelligent personalized care plan management platform. Similarly, anonymized data sets will be made available for the training of predictive risk models.
Harmonisation, certification, approval labelling or reliable identification of adequate solutions . Integrated care tends to raise high expectations for enhanced effectiveness and efficiency, and the sustainability of broader service delivery. There is an expectation for integrated care to support the achievement of the so-called ‘Triple Aim’ approach – a simultaneous focus on improving health outcomes, enhancing the patient care experience and reducing costs. In order to assess the extent to which the transformation to more integrated care systems meets these overarching goals, it will be necessary to collect evidence involving ongoing monitoring of progress to identify potential problems, support the further development of approaches and inform decision making within a framework that includes specific and measurable objectives.
Identifying indicators suitable for assessing the performance of integrated care systems faces the same challenges that for choosing measures capturing the quality of care77 more broadly. Fundamental to measurement is the notion that an observed change in a given indicator reflects something about the underlying care delivery and quality. Therefore, if measurement is to guide further improvement, indicators should meet certain criteria to allow for appropriate conclusions about cause and effect to be drawn or cause of action to be taken.
ADLIFE deliberately does not aim to create a certification programme for integrated care. ADLIFE will harmonize the minimum requisites from the technical point of view (data, ICT infrastructure), human resources, health
77 Tools and methodologies to assess integrated care in Europe. Report by the Expert Group on Health Systems Performance Assessment
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 37
systems and governance for a tool or a model to be adopted for integrated care. All technical WPS are focused in this strategy but specially WP8 and WP9. The pilots´intevention evaluation will generate a set of indicators that could be transferred to other models to “certified” the quality of the system.
Robust and reliable and replicable business models for IT supported solutions ADLIFE is based in previous exploitable IT supported solutions developed by members of the consortium in the C3-Cloud projects ,among others, where a SME like SRDC is currently exploiting generated results that are integrated in their portfolio of services and products (KronIQTM), as it is described in the following section 2.2.2 where the exploitation of the ADLIFE toolbox is described. In addition, EVERIS a leading company in the sector of IT supported solutions, is also participating in the project and ADLIFE toolbox will be integrated in the portfolio of EVERIS´ products. ADLIFE comes from and is directed to health systems to really change the available models of integrated care. But in this depicting of the change of models ADLIFE coordinator and rest of participants health systems are complete aware that to really achieve the change a new ecosystem of work should be created from the very beginning where health systems, industry (e.g. digital health services providers, ICT developers, ICT support and services), researchers, professionals, patients and citizens are involved and that is how ADLIFE has been designed. This truly personalized and multi-disciplinary environment will be the base for all technical WPs but also for WP10 devoted to the identification of a roadmap of business models for digital health solutions, thanks to the inclusion in the projects to other companies and entrepreneurs that could include new points of view to this ecosystem.
2.1.2 IMPROVING INNOVATION CAPACITY
The ADLIFE project will be based on the advanced ICT technologies (e.g. Artificial intelligence, Big Data, Interactive Technology, Interoperability, Security/Cybersecurity), intervention methodologies (e.g. patient empowerment, behavioural change interventions, change of organization methods) and evaluation methods (e.g. mixed methods). These technologies and methodologies are horizontal and could be used in very different sectors not only in health and with the specific target of integrated care. The horizontal technologies and methodologies will have the innovation capacity for being implemented in other sectors: education, administration among others. The events included in WP2 and WP10 and in the following section will help to exchange knowledge among the participants, and encourage new, collaborations in different domains.
ADLIFE digital services will allow other workers (not only healthcare) to expand their range of tasks as well as taking on others previously assigned to higher-level workers78 . They will raise their performance thanks to the availability of patients´ information as well as the instant contact with the resto the members of the team (MDT).
2.1.3 BARRIERS/OBSTACLES
Despite the expected benefits arising from the application of ADLIFE project, there are diverse barriers which need to be overcome to achieve all the expected impacts, that have also a direct relation with the main problems included in the state of the art:
Lack of infrastructures: ADLIFE is a large-scale pilot that includes 7 different health systems and more than 70 different centers, so apart from identifying the minimum pre-requisites and necessary infrastructures, the toolbox could be implemented in different contexts in Europe.
Lack of trust/security: ADLIFE is designed to have zero security issues as has been described and will evaluate the trust of the patients and health systems in the solutions and will identify the minimum gaps/issues.
Lack of resources/cost: ADLIFE will optimize the health system resources to really change the organizational model of integrated care. ADLIFE model improves communication among stakeholders and creation of interconnected teams and optimizes use of available facilities and services. The project will quantify the cost outcome of the intervention, leading to planning and reorganization of services.
Resistance to change of model/roles: ADLIFE will create training programmes/methodology to convince and explain the advantages of the care model and how to really change. In addition, the evaluation will quantify the advantages of the change and will compile the effect of the improvement of skills and how acquiring new responsibilities and working in teams is perceived by the health professionals and systems.
2.2 MEASURES TO MAXIMISE IMPACT
2.2.1 DISSEMINATION AND EXPLOITATION OF RESULTS
ADLIFE will play a significant role in large-scale sustainable deployment of digitally-enabled innovation for integrated care delivery to the ageing population in Europe. To do so, it needs a clear strategy and effort for dissemination and communication its activities, progress and results. But, to really do so, it is necessary to create
78 WHO guideline recommendations on digital interventions for health system strengthening. April 2019.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 38
the adequate market environment. Companies developing digitally tools and services need to understand and adapt to the complexity of a market where one of the main buyer is the public health sector. Health systems must see the opportunities of developing and including in their portfolio tools and platforms created for the management of integrated care. ADLIFE is aware of this fact so dissemination activities will be the cornerstone for generating a deep impact of the project results terms and attracting the interest of main stakeholders. WP2 be led by STRAT an university with a broad experience in participation in H2020 and leading dissemination strategies. STRAT together with all other partners is already working on a well-defined strategy for the dissemination and exploitation in this project. It is important to start right from the beginning so that the communication channels work effectively. A detailed dissemination plan will be provided as part of WP2 within the first six months of the project. It will be a “living document” which will be used, extended and adapted to the project needs during the whole duration of ADLIFE. STRAT will stay in close contact with all partners and use the expert advice from the Innovation and Exploitation Management Board and OPTIMEDIS, the leader of Exploitation WP. OPTIMEDIS a German company expert in developing and managing regional integrated healthcare by also including digitally-enabled innovation, will lead WP10. WP10 will coordinate the commercial exploitation activities directly involving partners of the project SRDC and EVERIS among others. SMEs and other industries from the sector will have the opportunity to participate in the events organized. Not only the exploitation of ADLIFE results will be guaranteed but also the creation of roadmaps and routes for other digital solutions related to integrated care or focused in health and care delivery to ageing population will be pursued.
All partners will play an active role, trying to disseminate the work using their individual means and channels: journals, participation in conferences, workshops, and using their own networks of contacts. Resources have been devoted to dissemination activities including a dedicated budget for open access publication.
The dissemination plan includes the branding of ADLIFE project (logo, templates and communication guidelines) to promote the awareness of the project within the consortium and at a European level. Moreover, the advances of the project will be public in the project website. The website will include a FAQ’s section, articles and reflection pieces on integrated care and large-scale implementation. Updated information of events, seminars and national and international conferences and specific events related to ADLIFE will be published in the website.
The consortium will ensure the publication of the results in a wide range of scientific and clinical media including high quality journals (preferably open access) and main worldwide conferences. Partners have an extensive record of scientific, technical, industrial, political and social publications and of events reaching the general public as can be seen in section 4-5. The ADLIFE consortium has already identified the following target groups (section 2.2.1) and types of information for dissemination of the project outputs.
2.2.1.1 PLAN FOR THE DISSEMINATION AND EXPLOITATION OF THE PROJECT’S RESULTS
DISSEMINATION PLAN FOR PROJECT STAKEHOLDERS
The first step for the set-up of the ADLIFE dissemination plan will be a “stakeholder/market analysis”. In order to assess the strategies that would be used to reach the relevant stakeholders and potential users of project results, these groups need to be re-defined and updated from the initial plan included here in this proposal. Only if these groups are known, together with their interest and behaviour in information search, clear ways and strategies on how to reach them can be defined. In the following table it is included an overview of the definition of stakeholders and the plan for the project to reach them.
Potential users of results/ Stakeholders
Channels of dissemination and interaction
Explanation of implementation and participation in the project
(A)R&D and academia in the field of integrated care from the point of view of health and ICT
Scientific publications in peer reviewed journals (Computational and Structural Biotechnology, Health policy, Value Health, BMC Health Service Research; IJIC…), congresses and conferences, summer school for
Stakeholders read scientific publications in international peer-reviewed scientific journals; they will be reached via presentations at National and international congresses and conferences (e.g. International Conference on Integrated Care (ICIC), HIMSS and health 2.0 European conference, Informatics for Health, Medical Information Europe (MIE), eHealth Forum, International Conference on Informatics, Management and Technology in Healthcare, eHealth Forum). EIP-AHA events and meeting will be an important forum for ADLIFE project discussion. Three ADLIFE partners project are 4 stars Reference Sites like Basque Country (KRON), Southern Denmark (OUH) and Scotland (STRAT). Young researchers and students participate in training courses (PhD and Master programs) and
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 39
Potential users of results/ Stakeholders
Channels of dissemination and interaction
Explanation of implementation and participation in the project
researcher/students
summer courses held in the participant entities (STRAT, WARWICK) and in linked ones (health systems). ADLIFE developments will be included.
(B)Healthcare professionals
Scientific publications, medical guidelines. General and specific training programs in hospitals. Congresses, Conferences i-HD networks
Professionals read scientific publications and guidelines for chronic and integrated care management. ADLIFE will include ADLIFE toolbox in the training programs designed by the participating health systems (Osakidetza, RMJ, AMCA as described in Technical annex 4-5) and delivered in the corresponding region, not only partners. i-HD has a network of healthcare professionals and hospitals (European Network of Excellence for Hospitals) working in the field of reuse of health data for research and semantic interoperability where the results of ADLIFE fit and will reach this large community. Healthcare professional societies develop clinical guidelines, other professional practice materials, development syllabus and examinations. ADLIFE best practices for our advanced disease and multi-morbidity population, which are presently not so well served by these bodies because excellent care often crosses the domains of multiple societies. We will therefore work across them to establish how they can each better shape professional practices for these patients.
(C)Formal and informal carers
Videos, project website, social media, articles, information leaflets, sessions in social services units (facilities) or primary care units
Formal and informal carers are not usually grouped in associations or have specific training programmes, but they collaborate with social services units/facilities and primary care where working days and seminars are normally held every trimester/semester. ADLIFE program and results will be advanced to the other formal and informal carers not participating in ADLIFE project. The experience of carers participating in ADLIFE will be used as an example of the benefits of the initiative to the third sector.
(D)Patients and patients’ organizations
Project website, videos, social media, articles in lay press, publications of healthcare systems for patients, information leaflets; I-HD patients ‘initiative
The project website will provide updated information on the projects background, aim and status and can be reached by advance chronic patients using appropriate search terms; videos (Power of storytelling will be used to communicate the ADLIFE project objectives and model of integrated care from the point of view of professionals and patients) will be recorded and uploaded; articles in lay press or publications by the participant Health Systems in their publications focused in patients. Information leaflets will be available for distribution in participating hospitals, primary health centres belonging to the regional health systems participating in the project and other health centres belonging to the networks of participants. The i-HD initiative in patient involvement will be a tool to engage and disseminate ADLIFE results to patients not directly involved in the project or belonging to participating regions. Specific patients ‘organization will be contacted when patients will be recruited because in the case of Advanced Chronic Diseases several patients ‘groups could be included (COPD, heart and/or kidney failure…). The representation of the patients is guaranteed thanks to the network of contacts of regional healthcare systems and specific partners like OptiMedis and i-HD that works at European level with different patients’ organizations.
(E)Industry: Digital health tools/services and platforms developers, ICT health sector.
Workshops with industry and SMEs, HACKATONs, participation in fairs and congresses (including stands)
ADLIFE will organize in WP10 (section 3) different workshops to analyse the environment and value chain of the marketable aspects (ADLIFE toolbox) and to identify the best market strategies and potential roadmaps for a complex market. SRDC and EVERIS will also show ADLIFE results and products in different fairs and congresses of the sector like ICIC conference where SRDC usually participates with a stand and others like HIMSS (HIMSS and
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 40
Potential users of results/ Stakeholders
Channels of dissemination and interaction
Explanation of implementation and participation in the project
Health 2.0 European conference) where EVERIS and SRDC usually participate with their whole portfolio of products.
(F)Healthcare decision makers
Personal communication, social media, articles in lay press, scientific publications in peer-reviewed journals, presentation at congresses and conferences
All measures of dissemination outlined above will be used to reach healthcare decision makers including personal communication within European, national or local advisory boards or expert testimonies and messages and updates sent via social media. ADLIFE’s pilot coordinators represent regional health systems that will present project results in the regular meetings (6 months, annual) that are held in the corresponding regions for the generation and update of chronic management strategies and plans that could be also presented in national strategies. In addition, OptiMedis (OptiMedis organizes discussion events with Ministers of Health i.e. Germany and Netherlands in the field of integrated care) and i-HD will use their contacts and networks with European, national and regional politician and healthcare decision makers to disseminate the project results and ensure rapid transfer into practice. ADLIFE will target those decision-makers responsible for using cost-effectiveness data to develop new infrastructure and workforce training strategies.
(G)Specialized media
To exploit the access to specialized media: relevant news.
Press meetings and releases (one per year) Electronic or paper updates sent to appropriate media i-HD webpage and resources will be used to boost the ADLIFE dissemination
(H)Other initiatives and projects related to ADLIFE
To guarantee an exchange of information and results; avoid duplication of work, boost use of tools
Contacting other projects funded in the area and inviting them to participate in events organized by ADLIFE. Partners are also participating in project related to ADLIFE like C3Cloud, Power2DM, BigMedilytics among others. The joint of synergy will be boost considering confidentiality and GDPR issues. Participating in events organized by EC.
(I)General public
To inform general population of the overall achievement of the project Advertise the latest developments/milestones
Press meetings and releases (one per year) Electronic or paper updates sent to media. Partners ‘webpages Webcasts and videos Posters in hospitals, primary care services, social services facilities in pilots’ sites EIP-AHA events: KRON usually participates in the conferences as a speaker. Basque Country, Sweden, UK are reference sites with the highest qualifications
TECHNICAL/SCIENTIFIC PUBLICATIONS AND PARTICIPATION IN INTERNATIONAL JOURNALS, CONGRESSES AND FAIRS
Technical and scientific publications: The partners will publish results of the project in high-impact peer-reviewed scientific journals in the area of digital health data, integrated care and clinical management of chronic diseases. The main papers describing the results of the ADLIFE toolbox will be submitted to general health technology papers of high impact (e.g. Studies health technology informatics, Healthcare informatics research, Computation and Structural Biotechnology, Journal of Medical Internet Research, Journal of Biomedical Informatics, Methods of Information in Medicine, Digital Health, JAMIA). ADLIFE clinical results (chronic diseases and integrated care) as well as intervention and evaluation results will be published not only in international journals (i.e. PEPs Group, PLoS One, Nurse Education Today, Journal of Professional Nursing) but also in specialized journals (i.e. Israel Journal of health policy Research,) in each region to boost the dissemination of the results. All manuscripts arising from the projects will be circulated to all partners before submission for their comments and approval. The consortium is committed to an open science policy and will seek to publish on open access journals whenever possible. Scientific publication will be fostered by the strong publication records held by ADLIFE consortium. The clinical and technical partners of ADLIFE have authored numerous clinical and scientific publications in high-ranked journals including Clinical Epidemiology, Health services research, PloS, Cancer Research, Cancer Nursing, Journal of Clinical Oncology, BMJ Open, Journal of Biomedical Informatics, European Journal of Bioinformatics, Journal of Integrated Care and International Journal of Integrated Care among others. Many consortium partners have published
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 41
together before with results generated in previous collaborative projects like C3-Cloud among others. Partners have Editor in Chief position and participate in editorial boards of key journals like Digital Health. Conferences, Congresses, Fairs: Project results will also be presented at international high-impact fairs and technical/scientific conferences, e.g. the International Conference on Integrated Care (ICIC), MIE, HIMSS events, International Conference on Informatics, Management and Technology in Healthcare, eHealth Forum and national conferences. The partners foresee attending and aiming to make presentations as key speakers at these conferences and fairs (including a stand when feasible) to disseminate the project results. For the first presentation of the main results, a European conference will be preferred, unless this will lead to inappropriate delay of the presentation. Clinical partners will also seek opportunities to increase the visibility of ADLIFE at national and regional congresses and conferences organized by relevant entities and associations. The regional forum for planning and development/update of strategic plans for chronic diseases management and personalized medicine inclusion in healthcare systems will be a key scenario to share ADLIFE results and socio-economic impact. PERFORMANCE INDICATORS (DISSEMINATION, CLUSTERING) Average events for academia (attendance): 3 per year. 1 top conference publications/year. Average events for industry (attendance): 3 per year. ADLIFE own events: 3 webinars, 3 hackathons, 1 final event. Journal/peer reviewed publications at international journals during the project: at least 6. Independent journalistic articles and interviews: 3. Citations to the project/publications by others: >1.000 references (2 years after the project). Press and news releases: 6. Newsletter: 4 releases per year to be distributed to registered web users (>100) and other stakeholders; each partner will have the possibility to spread project’s newsletter in PDF format to its contacts. Info-packs: 5, distributed to mini.60 contacts each; >300 downloads from website and other online repositories. Clustering activities: 2 meetings per year with project related to ADLIFE. Downloads from the open-source project repository: >250. Numbers of external contributors registered on the open-source repository (25). New SMEs and Industries contacted by company partners leveraging project developments and results,
generation of new business models: 5. Social media performance:
# of tweets and retweets: 2 tweets per week. # posts and forwards on LinkedIn: 1 post per week. # of followers on ADLIFE social media channels: +250.
2.2.2 STRATEGY FOR THE EXPLOITATION OF THE RESULTS
The consortium intends to turn their participation and the project outcomes into profit (building a common strategy based on the ADLIFE ecosystem including health systems market), and to launch new activities, thanks to the increased gained knowledge. Exploitation will be led by OPTIMEDIS and will ensure that partners will work towards a successful access to the market. It will ensure the high visibility and promotion of the project and its results during its execution and after its end (WP2) as well as the identification of the routes and business models to the market (WP10). Due to the different nature of the partners as well as of that of the results, the preliminary exploitation strategy will be different for the different types of organizations, since all of them expect to obtain different benefits and/or revenues from the exploitation of the different outcomes. The exploitation strategy will be twofold: (1) exploitation of the knowledge generated (non-commercial), (2) exploitation of the results (commercial).
1 NON-COMMERCIAL EXPLOITATION – RESEARCH AND ACADEMIA PARTNERS Since these partners are non-profit research entities, their exploitation strategy will be to add the know-how generated during the project execution into their background to improve their technological expertise and continue generating and transferring related knowledge to the industry. The exploitation strategy is the following:
OBJECTIVE Partner DESCRIPTION Change model of healthcare provision (integrated care) Enhance integrated care educational offer
KRON, STRAT, OUH, FALK,
KRONIKGUNE´s positioning in relation to research and management of chronic diseases and digital health will be reinforced. The know-how about integrated care (organizational model, indicators…) as well as the training materials will be directly transferred to the training programs for Osakidetza healthcare professionals. The ADLIFE toolbox could be included
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 42
Creation of new training content
RJH, AMCA,
in the portfolio of Osakidetza´s healthcare services. So, the work developed in ADLIFE will bolster the positioning of Basque Country as a reference site in the provision of innovative digital health services to the citizens. STRAT has significant know-how in digital health, health analytics and health interventions as well as business analysis in health developments. The project will gain experience in digital health in relation to integrated models of care which will be relevant to generate new publications, projects, collaborations, attract new students. This project will bring pioneering ideas and knowledge to students (undergraduate and postgraduate students in Biomedical Engineering, Computer Science, Digital Health, Data Analytics, Software Engineering, Business analysis and technology) that will impact their academic work (PhD dissertation, post-Doc, papers) along with the practical experience obtained. OUH, FALK, RJH, AMCA are experts in the management of chronic diseases in their corresponding regions so ADLIFE project will enhance their capabilities in changing the actual model of care into an integrated one. The ADLIFE toolbox, model, indicator and training material will be also used to train the new generation of healthcare professionals. In addition, ADLIFE model for integrated care and toolbox could be included in the portfolio of health services provided to the citizens in each area positioning also the regions as reference sites at worldwide level in the management of chronic diseases and inclusion of digital services. The project will boost their positioning at national and European level to weigh in the change of healthcare policies. WARWICK´s positioning as world leading research digital health and healthcare technologies will be consolidated by the participation in ADLIFE projects. The work in the field of interoperability and customization of digital tools that will be done in the project will be a key pillar for future research funding by public and industrial investors beyond the scope of ADLIFE. I-HD´s networks and steering committees will be increased by the participation in ADLIFE project leading to promote the role as an international centre of reference for health data re-use and management. I-HD will also promote the value and trustworthiness of the digital solutions across its stakeholders, and the importance of interoperability and data quality.
Increase & extend research expertise to: -Attract highly skilled staff and students. -Increase publications. -Attaching added value to on-going digital health innovation, research and health ecosystem transformation. -Create and maintain multi-professional health networks. -Demonstrating that public-private collaboration for the creation of new solutions for healthcare services is possible and can generate new business opportunities for companies and optimizing resources. -Create new research projects. -Create new direct collaboration with digital health industry. -Create IPRs: licensing, contract agreements,
KRON, STRAT, WARWICK, OUH, FALK, RJH, AMCA, I-HD
2 COMMERCIAL EXPLOITATION – INDUSTRIAL PARTNERS As it is described in WP10 exploitation of ADLIFE digital tools is a must for the project but also de creation of new opportunities for other companies in the digital health sector due to the nature/complexity of the health sector (interoperability, fragmentation, access, reimbursement). Business models for digital health solutions will be generated based in the experience of the consortium where industrial partners (EVERIS; SRDC and OPTIMEDIS) have previous experience and will establish an open dialogue (technical collaboration included) with healthcare systems from the seven participant regions including in the project central ICT supports team from the corresponding health systems, following the methodology included in the next image.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
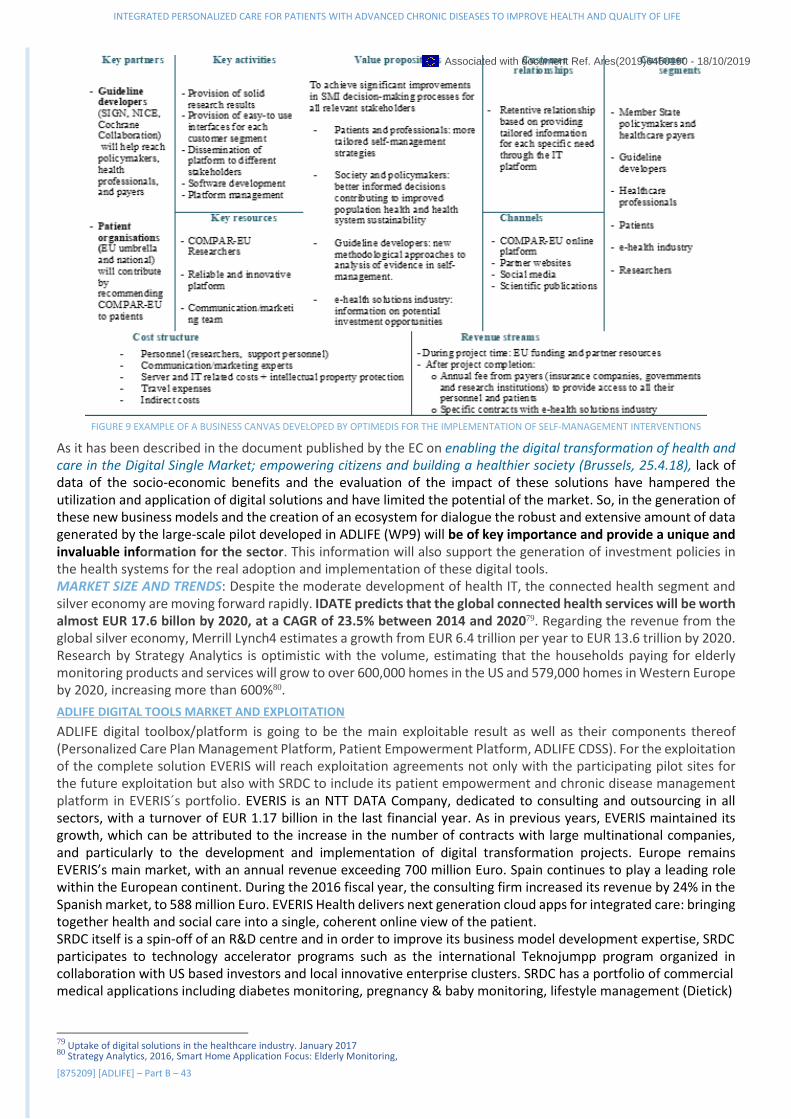
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 43
FIGURE 9 EXAMPLE OF A BUSINESS CANVAS DEVELOPED BY OPTIMEDIS FOR THE IMPLEMENTATION OF SELF-MANAGEMENT INTERVENTIONS
As it has been described in the document published by the EC on enabling the digital transformation of health and care in the Digital Single Market; empowering citizens and building a healthier society (Brussels, 25.4.18), lack of data of the socio-economic benefits and the evaluation of the impact of these solutions have hampered the utilization and application of digital solutions and have limited the potential of the market. So, in the generation of these new business models and the creation of an ecosystem for dialogue the robust and extensive amount of data generated by the large-scale pilot developed in ADLIFE (WP9) will be of key importance and provide a unique and invaluable information for the sector. This information will also support the generation of investment policies in the health systems for the real adoption and implementation of these digital tools. MARKET SIZE AND TRENDS: Despite the moderate development of health IT, the connected health segment and silver economy are moving forward rapidly. IDATE predicts that the global connected health services will be worth almost EUR 17.6 billon by 2020, at a CAGR of 23.5% between 2014 and 202079. Regarding the revenue from the global silver economy, Merrill Lynch4 estimates a growth from EUR 6.4 trillion per year to EUR 13.6 trillion by 2020. Research by Strategy Analytics is optimistic with the volume, estimating that the households paying for elderly monitoring products and services will grow to over 600,000 homes in the US and 579,000 homes in Western Europe by 2020, increasing more than 600%80.
ADLIFE DIGITAL TOOLS MARKET AND EXPLOITATION
ADLIFE digital toolbox/platform is going to be the main exploitable result as well as their components thereof (Personalized Care Plan Management Platform, Patient Empowerment Platform, ADLIFE CDSS). For the exploitation of the complete solution EVERIS will reach exploitation agreements not only with the participating pilot sites for the future exploitation but also with SRDC to include its patient empowerment and chronic disease management platform in EVERIS´s portfolio. EVERIS is an NTT DATA Company, dedicated to consulting and outsourcing in all sectors, with a turnover of EUR 1.17 billion in the last financial year. As in previous years, EVERIS maintained its growth, which can be attributed to the increase in the number of contracts with large multinational companies, and particularly to the development and implementation of digital transformation projects. Europe remains EVERIS’s main market, with an annual revenue exceeding 700 million Euro. Spain continues to play a leading role within the European continent. During the 2016 fiscal year, the consulting firm increased its revenue by 24% in the Spanish market, to 588 million Euro. EVERIS Health delivers next generation cloud apps for integrated care: bringing together health and social care into a single, coherent online view of the patient. SRDC itself is a spin-off of an R&D centre and in order to improve its business model development expertise, SRDC participates to technology accelerator programs such as the international Teknojumpp program organized in collaboration with US based investors and local innovative enterprise clusters. SRDC has a portfolio of commercial medical applications including diabetes monitoring, pregnancy & baby monitoring, lifestyle management (Dietick)
79 Uptake of digital solutions in the healthcare industry. January 2017 80 Strategy Analytics, 2016, Smart Home Application Focus: Elderly Monitoring,
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 44
and personal health record (PHR) systems (eSağlıkKaydım). SRDC has been investing on chronic disease management solutions for the past 15 years and has a product called KronIQTM, which delivers clinical decision supported guidance to medical doctors for the management of chronic diseases. The system has been built for Ministry of Health Turkey and will be operationalized in fall 2019 to be used by more than 20.000 Family Medicine Practitioners for management of the screening and monitoring of whole Turkish population (around 80 million patients). ADLIFE will provide SRDC with the opportunity to integrate the patient empowerment, behavior change interventions components into its chronic disease management platform KronIQTM. SRDC aims to extend its market base to Europe and serve to regional and national health services around Europe through the local partnerships it aims to establish during the lifetime of the project. As it explained in the following paragraphs where the exploitation of 3 main digital services/tools is explained, it can be estimated that the exploitation of the ADLIFE platform will be profitable at a short-term after the end of the project (2024) for the companies participating in the project. Considering that the platform alone could never obtain the same impact it is also necessary to include the cost of the interventions. In this project the estimated costs for interventions are around 6.9 million euros for the 75 centres the cost per centre is about 92,000 €, that is an affordable cost for health services around Europe, even more taking into account the enormous reduction of costs that the change to integrated care model will generate. In addition, for the future implementation of ADLIFE toolbox the cost related with facing interoperability issues, designing CDSS, working in patient empowerment or in changing the model of care will be reduced in around an 80%, so the real costs will be related with the final tuning and implementation in the new healthcare system conditions.
EXPLOITABLE RESULTS
R1 ADLIFE Toolbox/Platform: will belong to all partners and EVERIS will lead the exploitation strategy and will reach the corresponding agreements with the participant partners (IPR management, WP10). EVERIS will exploit the results of the project across EVERIS´s presence at 16 countries around the world, especially on health. EVERIS has a wide experience in developing and commercializing BigData and Artificial Intelligence solutions in different sectors but health is one of the most important. Therefore, the important market capabilities of EVERIS will contribute to the exploitation activities. In addition, EVERIS will contribute to the business perspective of the health sector where the company has a deep knowledge of customers’ requirements. According to a recent report81 , “Europe healthcare IT services market was valued at USD14.43 billion in 2016, and is forecast to grow at a CAGR of 7.63%, in value terms, during 2017-2022, to reach USD22.87 billion by 2022, on the back of growing demand for patient safety and data accuracy, increasing patient population base and increasing spending in healthcare industry”. In addition other report82 stablished that “the population of the EU-28 on 1 January 2017 was estimated at 511.5 million…Older persons (aged 65 or over) had a 19.4 % share (an increase of 0.2 percentage points compared with the previous year and an increase of 2.4 percentage points compared with 10 years earlier)”. The characteristics of ADLIFE platform will take benefit of this expected increase ratios and EVERIS will use its network and partnerships agreements in Europe trying to translate this numbers to concrete sales that will be included in the exploitation results of the project (WP10).
R2 ADLIFE CDSS: will belong to EVERIS that will include the three CDSS tools in their portfolio. The exploitation actions will be focused on delivering ADLIFE CDSS to the market. Basically, the expected impacts described at the beginning of this section will be accomplished if certain exploitation actions are also fulfilled. The relation between exploitation actions and their associated impacts can be depicted as it's shown in the following. Identification of related stakeholders and data sources Definition of the project's value proposition IP scouting, assessment and protection Presentation at specific venturing and industrial meetings, and other marketing activities Project's tests in relevant environment - data gathered & released Market size is expected to grow significantly in the next years. According to a recent report83, “the AI in healthcare market is expected to grow from USD 2.1 billion in 2018 to USD 36.1 billion by 2025, at a CAGR of 50.2% during the forecast period”. The market has a huge potential across various end users such as hospitals, healthcare payers, and pharmaceutical and biotechnology companies.
R3 ADLIFE PCMP and PEP will belong to SRDC that will extend their chronic disease platform. These chronic disease management services will include a variety of services, such as multidisciplinary care, guidelines for the self-management of the chronic disease condition, and guidance for healthy behavioral change, to increase
81https://www.techsciresearch.com/report/europe-healthcare-it-services-market-by-type-medical-imaging-managed-services-etc-by-application-healthcare-analytics-etc-by-platform-by-end-user-healthcare-provider-healthcare-payer-competition-forecast-opportunities/1149.html 82 https://ec.europa.eu/eurostat/statistics-explained/index.php/Population_structure_and_ageing#The_share_of_elderly_people_continues_to_increase 83 https://www.marketsandmarkets.com/Market-Reports/artificial-intelligence-healthcare-market-54679303.html
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 45
patient empowerment. After these pilot studies in ADLIFE, SRDC will approach regional and national health services providers, public and private payers all over the Europe through the local partnerships it aims to establish (5-8 per year). Two of the first partnerships will be through EVERIS in Spain and OPTIMEDIS in Germany. SRDC will initially utilize the extended dissemination channels of ADLIFE identified in Section 2.1.1.1 to reach potential customers. The envisioned licensing strategy is yearly subscription fees, which includes initial deployment, localization, integration with local systems. It is estimated that the cost of these initial deployment activities will be compensated after two years subscription, starting from third year we aim to obtain revenue from each deployment site.
In addition, economic exploitation of ADLIFE project will be related with the provision of services related to the ADLIFE digital toolbox/platform not only for EVERIS or SRDC that will provide consultancy services about the minimum requirements needed for the implementation and integration of integrated care services but also with services provided by OPTIMEDIS. OptiMedis is a small but very innovative population health management company operating in Germany, Belgium, the Netherlands, and the UK. Its work of developing population-based integrated care contracts with insurers and providers is internationally recognized as best-practice model (reference: https://healthpolicy.duke.edu/sites/default/files/atoms/files/germany_25jan2017.pdf). OptiMedis has through its financial modeling and shared savings contracts a particular expertise to contribute that facilitates market entry for products and services that generate value beyond the service that is deploying the service. An example is the introduction of a patient empowerment platform deployed by a hospital, generating costs for the hospitals for savings for another care sector or provider. This will be a key issue in the exploitation of the ADLIFE tools and OptiMedis will develop proposals for economic exploitation in such contexts. 2.2.3 HOW THE PARTICIPANTS WILL MANAGE THE RESEARCH DATA GENERATED AND/OR COLLECTED
ADLIFE will establish a customised Data Management Plan (DMP) D1.1, to determine which datasets can/cannot be considered open access, along with the following data sources that have been identified: Technical reports by the Project Technical Committee (PTC): project partners and WP leaders will jointly
produce technical reports. The Quality Assurance Plan will detail the management procedures required to guarantee that project documents are correctly and efficiently produced, updated, distributed and stored.
Generated data on main results: this data will reflect the quantified impacts that ADLIFE displays under real piloting conditions in the seven regional healthcare models (WP9). Key results will be disseminated among all involved stakeholders. Dissemination/sharing and/or exploitation/protection of results generated will be subjected to the decision of the consortium, with the supervision of the coordinator.
Scientific publications, conferences, EU Events, trade fairs and workshops: results and achievements in the project will be disseminated among the healthcare professionals, managers and regulators; scientific community; industry, and further key stakeholders. The publications shall include acknowledgements to the project and be communicated to the technical coordination.
Open Access (OA): prior to publishing any scientific publication, the partner involved will contact the SC for revision and validation. Partners will provide OA to all peer-reviewed scientific publications relating to its results84
The authors of all peer-reviewed scientific publications will choose the most appropriate way of publishing their results, and these publications will be stored in an OA repository, during and after the project’s life. The consortium will also select access research data (free of charge or restricted access and/or use).
ADLIFE Data collected/generated: as indicated in the section 1 and 5, ADLIFE is going to collect very sensitive data from the participants in the pilots and health systems. ADLIFE will provide anonymization, authentication, authorization and audit services based on widely accepted international standards. Anonymized data will be store in centralized repository so no direct access to participating health systems information will be feasible. The accession and re-use of this will store information (data sharing) will be analysed during the project but it is expected that partners will require that any use of these data by a third party must address a scientific question in ADLIFE research area that will be evaluated and approved/rejected by ADLIFE´s committee. Data collected from newsletters and website subscribers: The project and all partners are committed to
respect the personal data processing principles under the GDPR, and will be led by i-HD, expert in the area.
2.2.4 STRATEGY FOR KNOWLEDGE MANAGEMENT AND PROTECTION
ADLIFE proposes a complete range of activities leading to the optimal visibility of the project and its results, increasing the likelihood of market uptake and ensuring a smooth handling of the partners’ IPR, thus paving the way to knowledge transfer. Internal knowledge management will be facilitated through a web-based secure collaborative space for information and document sharing. IPR protection and strategy is completely integrated
84 Article 29.2. of the GA and H2020 Guidelines on OA to Scientific Publications (EC, 2013).
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
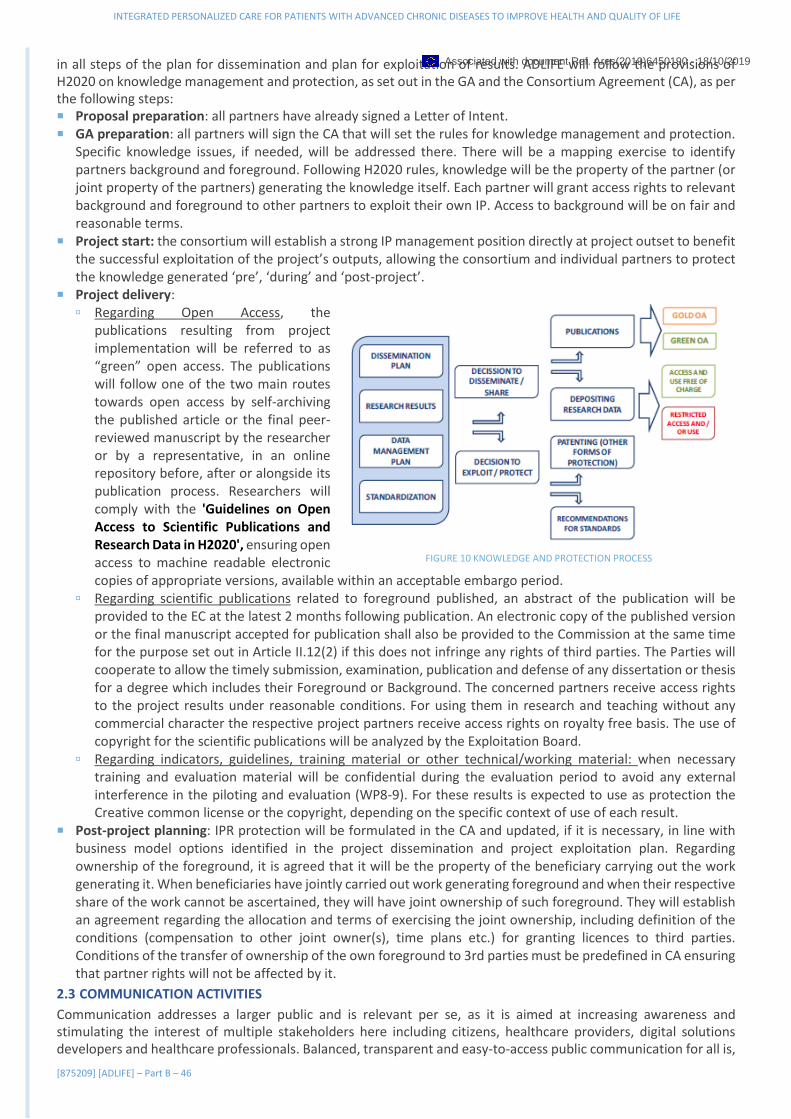
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 46
in all steps of the plan for dissemination and plan for exploitation of results. ADLIFE will follow the provisions of H2020 on knowledge management and protection, as set out in the GA and the Consortium Agreement (CA), as per the following steps: Proposal preparation: all partners have already signed a Letter of Intent. GA preparation: all partners will sign the CA that will set the rules for knowledge management and protection.
Specific knowledge issues, if needed, will be addressed there. There will be a mapping exercise to identify partners background and foreground. Following H2020 rules, knowledge will be the property of the partner (or joint property of the partners) generating the knowledge itself. Each partner will grant access rights to relevant background and foreground to other partners to exploit their own IP. Access to background will be on fair and reasonable terms.
Project start: the consortium will establish a strong IP management position directly at project outset to benefit the successful exploitation of the project’s outputs, allowing the consortium and individual partners to protect the knowledge generated ‘pre’, ‘during’ and ‘post-project’.
Project delivery: Regarding Open Access, the
publications resulting from project implementation will be referred to as “green” open access. The publications will follow one of the two main routes towards open access by self-archiving the published article or the final peer-reviewed manuscript by the researcher or by a representative, in an online repository before, after or alongside its publication process. Researchers will comply with the 'Guidelines on Open Access to Scientific Publications and Research Data in H2020', ensuring open access to machine readable electronic copies of appropriate versions, available within an acceptable embargo period.
Regarding scientific publications related to foreground published, an abstract of the publication will be provided to the EC at the latest 2 months following publication. An electronic copy of the published version or the final manuscript accepted for publication shall also be provided to the Commission at the same time for the purpose set out in Article II.12(2) if this does not infringe any rights of third parties. The Parties will cooperate to allow the timely submission, examination, publication and defense of any dissertation or thesis for a degree which includes their Foreground or Background. The concerned partners receive access rights to the project results under reasonable conditions. For using them in research and teaching without any commercial character the respective project partners receive access rights on royalty free basis. The use of copyright for the scientific publications will be analyzed by the Exploitation Board.
Regarding indicators, guidelines, training material or other technical/working material: when necessary training and evaluation material will be confidential during the evaluation period to avoid any external interference in the piloting and evaluation (WP8-9). For these results is expected to use as protection the Creative common license or the copyright, depending on the specific context of use of each result.
Post-project planning: IPR protection will be formulated in the CA and updated, if it is necessary, in line with business model options identified in the project dissemination and project exploitation plan. Regarding ownership of the foreground, it is agreed that it will be the property of the beneficiary carrying out the work generating it. When beneficiaries have jointly carried out work generating foreground and when their respective share of the work cannot be ascertained, they will have joint ownership of such foreground. They will establish an agreement regarding the allocation and terms of exercising the joint ownership, including definition of the conditions (compensation to other joint owner(s), time plans etc.) for granting licences to third parties. Conditions of the transfer of ownership of the own foreground to 3rd parties must be predefined in CA ensuring that partner rights will not be affected by it.
2.3 COMMUNICATION ACTIVITIES
Communication addresses a larger public and is relevant per se, as it is aimed at increasing awareness and stimulating the interest of multiple stakeholders here including citizens, healthcare providers, digital solutions developers and healthcare professionals. Balanced, transparent and easy-to-access public communication for all is,
FIGURE 10 KNOWLEDGE AND PROTECTION PROCESS
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 47
as a first, necessary step to generate engagement and social acceptance. Communication activities aim at promoting the project towards the broad public, thus they will necessarily focus on the scope and impacts of the project for society, transforming the more complex jargon into contents addressing less technical audiences with the objective to guarantee outreach and enhance its visibility as well as communicating the potential and real impact of how ADLIFE model of integrated are could really improve and change his life and how the chronic disease affects and alters their lives. Communication activities will start from the very beginning and will be carried out through a variety of different channels and formats to reach different target groups as effectively as possible. On site and face to face communication actions will be combined with digital actions; a 360-degree communication strategy that will be carefully designed to avoid creating false expectations in such a sensitive field like human health and wellbeing. The communication plan (D2.1) comprises activities for a proactive communications effort, which include maintaining a strategic calendar to prepare for important events, working with a network of communication contacts and strengthening the messaging both in terms of content and in the way, it is communicated. Active promotion and communication activities, including online and non-electronic communication methods and tools, special events as well as publications are core activities. The plan will include measures for dissemination and to actively engage stakeholders and enhance the buy-in of project results. Main specific activities (see WP2) are:
Development of the visual and content identity: logo, style guidelines, videos, communication kit, etc. The following communication materials will be produced: 1 Flyer, in English, (M8) describing the overall approach of the project, its innovation and the expected
impacts to be widely distributed by partners at meetings and events. 1 Roll-up to be displayed at fairs, conferences, events. Local versions will be produced by the local partners.
Online channels: website, periodically updated, will act as dissemination hub, central repository and news broadcast channel for all public information. Social media: the management of the website contents will be backed up by a social media strategy assessing the most efficient channels (mainly LinkedIn and Twitter) to reach different segments of the audience: LinkedIn: this social media is used by professionals and companies. It can be used to engage health
professionals and managers, industrial stakeholders, academic public and those who also offer formal carers services.
Twitter: mostly used by companies and stakeholders who have a better presence on the social media (public sector and industrial stakeholders). Tweets can be used to reach industrial stakeholders, research institute and general public. For a Twitter based communication activity to be effective, tweets need to be published regularly. STRAT and i-HD will be responsible of pursuing this task.
Media distribution: FORMATS TARGET AUDIENCE AND CHANNEL OBJECTIVE/MESSAGE
Independent journalistic articles and interviews (2) around the project and related topics produced.
Broad audience, specifically, companies & citizens. Articles will be distributed to online newspapers and magazines, dedicated portals and communication channels and promoted via the project social media networks.
To inform but also to stimulate interest and possibly raise debate, engagement and acceptance.
Social media weekly animation and 2 social media engagement campaigns.
A Twitter account will be opened and animated. Twitter Campaigns will be designed on occasion of project milestones and engagement initiatives through dedicated hashtags and Twitter cards.
Engagement of civil society at European and global level.
Press and news releases (at least 5)
General public. To inform and raise visibility on the project results at a European and global level as well as local level.
ADLIFE’s communication measures are also tightly coupled with the project’s dissemination activities:
Means Description KPIs
Target
Means Description KPIs Target KPIS Target
Logo and presentations
Logo and presentations template for all partners N/A ALL
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 48
Means Description KPIs
Target
Means Description KPIs Target KPIS Target
Project website and positioning
Project’s website, providing information about the project, demos and results, showcasing project's news and acting as a communication hub.
25,000 visits ALL
Videos and multimedia
3-4 promotional videos will be produced, focusing in the benefits of the ADLIFE toolbox/model from the different points of view of the users (patient, healthcare professionals, carers) and one focusing on the technological innovation and benefits of the technology for the market and healthcare providers. They will be presented at events, sent through the newsletter and shared across social networks to gain followers, increase visits to the site and thus strengthen the communication strategy
2,000 views on YouTube
ALL
Social media channels
Twitter account (information, general domain news & communicating with parties); LinkedIn community group to gather all interested stakeholders
>800 followers
ALL
Communication material
Project posters/Rollups; Flyers/Leaflets/Postcards that will contain general project information, and ad-hoc information for events
Hundreds of peopl
ALL
Written content Articles and interviews (3) on the project and related topics will be produced and distributed to the media, specialist press, technology websites, integrated care, digital healthcare, related portals and other relevant information outlets. At least 6 news releases on the project and its outcomes.
> 80.000 readers
ALL
ADLIFE events 1 final event will be organized SME events, hackatons
>300 participants >200 participants
ALL E
Joint events, workshops and networking
Events organised/co-organised by experts, researchers, potential technology users and industry audience. Project partners will be invited to present its work and vision. All events will be present on the project’s website and Twitter.
> 20 events attended/ hundreds of participants
A, B, E, H
In addition, constant contact with the Communication Team of the European Commission will be maintained to
ensure that continued progresses and milestones of the project reach the widest audience. The publications,
newsletters and websites mentioned in the H2020 Communication Guidelines will be considered for that.
3. IMPLEMENTATION
3.1 WORK PLAN – WORK PACKAGES, DELIVERABLES
3.1.1 BRIEF PRESENTATION OF THE OVERALL STRUCTURE OF THE WORK PLAN
ADLIFE is divided into 10 different WPs, three transversal (WP1, WP2, WP10) and seven technical ones. Three of the technical ones are devoted to the technical development of ADLIFE toolbox (WP3, WP4, WP5) and two of them for changing the model and empowering patients (WP6, WP7). Theses five WPs will allow completing the Phase 1 (Organisational issues and ICT platforms implementation) and lead to obtaining the ADLIFE toolbox and model that will be implemented in the Phase 2 (WP8) and
FIGURE 11 ADLIFE´S WORK PACKAGES
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
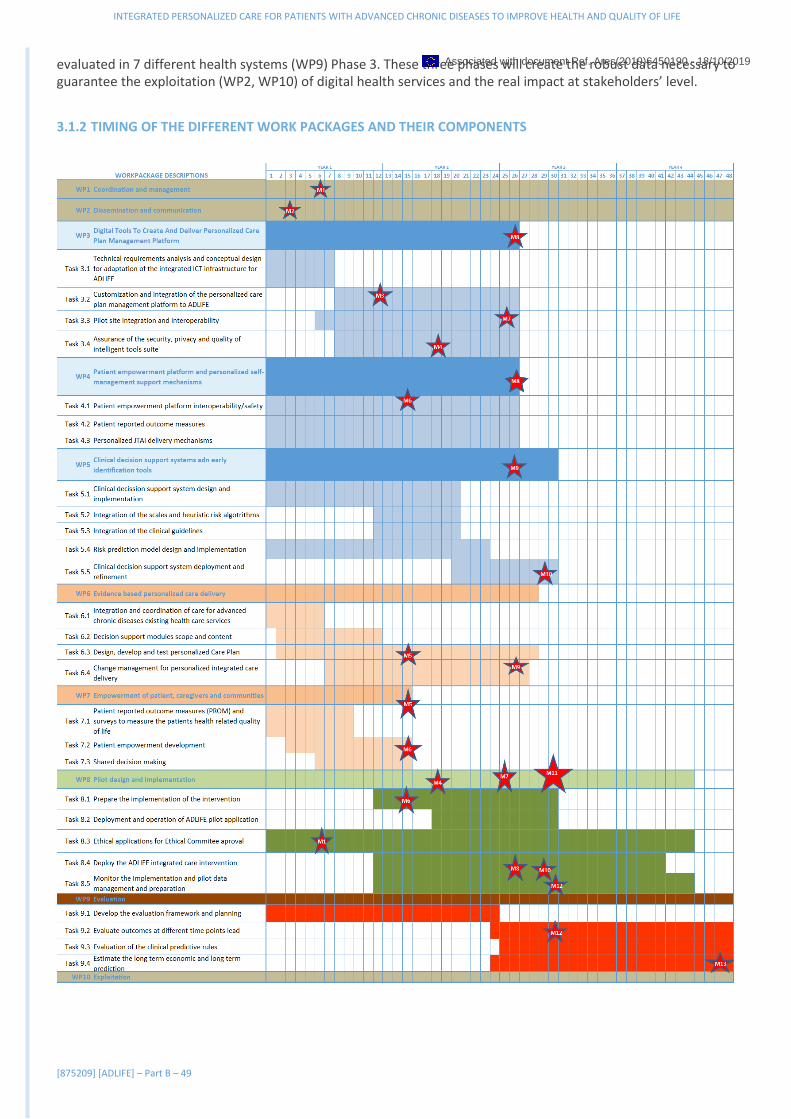
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 49
evaluated in 7 different health systems (WP9) Phase 3. These three phases will create the robust data necessary to guarantee the exploitation (WP2, WP10) of digital health services and the real impact at stakeholders’ level.
3.1.2 TIMING OF THE DIFFERENT WORK PACKAGES AND THEIR COMPONENTS
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 50
3.1.3 GRAPHICAL PRESENTATION OF THE COMPONENTS
3.2 MANAGEMENT STRUCTURE, MILESTONES AND PROCEDURES
3.2.1 ORGANISATIONAL STRUCTURE AND DECISION MAKING
The management structure of ADLIFE is organized into the following elements: [1] Project Coordinator; [2] Steering Committee - (contractual partners); [3] Project Technical Committee-Work Package leaders; [4] Advisory Boards (external experts and social awareness), [5] Clinical reference groups and regional intervention teams, [6] Ethical Advisory Board
PROJECT COORDINATOR (PC): KRONIKGUNE will assume the role of project coordinator – it will be the organization that represents the ADLIFE Consortium and is responsible for the achievement of the project goals and the contractual obligations towards the European Commission.
Dr. Esteban de Manuel will be the coordinating person. He is the Director of KRONIKGUNE and has a broad experience in the participation of cooperative projects at international level in H2020 and in the previous Framework Programmes but also in the area of Public Health.
KRONIKGUNE will also provide the administrative service for the project (every-day project running, assistance to the Project Coordinator in the administrative issues, execution of the organizational issues, etc.).
The Project Coordinator’s main managerial responsibilities include:
To monitor compliance of the beneficiaries with their obligations as described in the GA.
FIGURE 12 ADLIFE MANAGEMENT
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 51
Organising project management meetings; administration, preparation of minutes; Organising, steering, checking and assuring the reporting in time towards the Commission; Follow-up and adaptation of the project planning. The overall monitoring of progress on all work packages and
setting in place procedures for ensuring more detailed progress monitoring in consultation with the subgroups; Monitoring of the expenses and allocation of the budget; assistance towards the participants concerning
administrative aspects of the project; Communicating with the Commission & coordinating the payments to the partners; Providing assistance towards the participants concerning: the rules of the project, the project planning, giving
advice on all kind of matters, e.g. how to fill in cost statements, full cost system, rights.
STEERING COMMITTEE (SC): The Steering Committee will be composed of one representative of each partner of the consortium, which is chaired by the Project Coordinator. One main aim of this Board is to advise and support the decisions of the Project Coordinator on operational and management issues. Furthermore, the SC will be an effective and efficient communication hub. This committee will be responsible for all decisions of general nature within the frame of the EC Contract and the Consortium Agreement. The detailed responsibilities and tasks are described in the Project’s Consortium Agreement.
The Project Management Board will be convened every 12 months in face to face consortium meetings and whenever needed in audio conferences. The meetings will be organised by the Coordinator.
An effort will be made to celebrate the consortium meetings in some of the different regions where the interventions take place. This will allow to arrange simultaneous events and enable the assistance of members of the Regional Team, therefore promoting the dissemination of the project outcomes.
PROJECT TECHNICAL COMMITTEE-WORK PACKAGE LEADERS: The Work Package leaders will form the Technical Committee whose responsibilities are to ensure the coordination between the different staff within their work teams that collaborate to achieve concrete results. They will ensure the timely execution of tasks included in each WP and stimulate interaction between partners and the stakeholders involved. They are also responsible for consolidating the reports and executing the tasks required within each WP. They will be a person belonging to the organizations that are members of the Consortium: WP 1: KRONIKGUNE; WP 2: STRAT; WP 3: WARWICK; WP 4: SRDC; WP 5: EVERIS; WP 6: RJH; WP7: OUH; WP8: AMCA, WP9: KRONIKGUNE, WP10: OPTIMEDIS
The role of the WP Leaders will be:
Define, in coordination with the other Partners, the detailed planning of the tasks and activities identified. Monitor the technical quality of the work, in order to achieve the expected results. Organize timely (weekly, monthly…) calls with the rest of members to check the status of the work being done.
Convey those calls (either group calls or bilateral), propose an agenda and draft the minutes. Coordinate with other Work Package leaders the necessary information flow. Prepare the Progress Reports summarizing the work performed. Inform the Steering Committee, in advance of meetings, about progress achieved, results obtained, and
problems encountered. Coordinate, approve (preliminarily) and forward the Deliverables prepared in the related Work Package.
CLINICAL REFERENCE GROUPS: A clinical reference group will be created in each of the pilot sites including at least three different healthcare roles for professionals: General practitioners (GP), Nurses, Specialist at hospitals that will have access to other members of the healthcare system. RJH will coordinate the groups. This figure will have a key role in WP6 and WP7 and WP3 and 4, regarding semantic interoperability requirements and update of intersemantic mapping as well as the quality of translation of documents, requirements, programs, training among others and in the selection and revision of PROMS. In addition, the groups will be a key pillar in WP5 for the selection, revision and reconciliation of clinical guidelines and the definition and refinement of EWS.
REGIONAL INTERVENTION TEAMS (RIT): A Regional Intervention team will be created in each of the seven regions where the ADLIFE pilots take place (Sweden, Israel, Germany, Denmark, United Kingdom, Poland and Spain). Each regional team will be led by the ADLIFE partner in charge of the intervention in that particular country and will include all the clinical reference group and the rest professionals involved in the change of the organizational model of care, representatives of social and informal care, families and third sector and other stakeholders such as policy makers, etc. All pilot sites currently work with social services (Third sector) and carers, that will be involved in the project from the very beginning, for the final selection of the representatives that will participate in ADLIFE. Taking into account the nature of the intervention the final groups of patients will be recruited during the project.
All members of each regional team will meet regularly in order to share their experiences and learn from them, suggest improvements, receive and provide support, plan different measures, review objectives, and collect and
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 52
deliver good practices. During these meetings, the ADLIFE partner will inform the members of the team about the progress of the intervention in the other regions, highlighting any problematic situation or any issues raised.
A diffusion event will be celebrated simultaneously to the consortium meeting and all the members of the intervention team in that particular region will be encouraged to participate in order to facilitate the diffusion of the project outcomes.
In addition, the ADLIFE partners leading the interventions will have to report their respective progress to the work package Leader, AMCA (WP8 Leader), who will play a relevant coordination role among the different partners and the different activities carried out within the pilots. To summarize, the main roles of the regional teams will be to:
Define the specific determinants (barriers/facilitators) for the implementation of the intervention in each region. Implement the intervention Provide information of the current status of the intervention in each region. Participate in regular meetings and events Create regional forum to disseminate the results of the project to citizens
INNOVATION AND EXPLOITATION BOARD (IEB): The Innovation and Exploitation Board is responsible to ensure during the whole duration of ADLIFE that the project and its results are disseminated and exploited according to the exploitation plan set up in WP10 and section 2.2. The IEB will be led by OPTIMEDIS leader of WP10. They will ensure that the expected impact will be achieved as indicated. In order to ensure this, the IEB will have regular telephone conferences and will take part in the Steering Committee Meetings. During these meetings they will always have an agenda item reserved in order to give an update on the current activities and discuss further upcoming actions and events. During these meetings they can also assign tasks to the responsible project partners. The members of the board were selected based on their experience in dissemination and exploitation and are the following: OPTIMEDIS, SRDC, EVERIS, I-HD, KRONIKGUNE, WARWICK, STRAT.
ETHICS ADVISORY BOARD (EAB): An external Ethics Advisory Board will be created at the beginning of the project to ensure that the ethical regulations are respected along the project course and that all potential ethical issues are solved according to regulations. The members of the Board will have expertise and experience in ethical principles, methodology and research ethics. The ADLIFE consortium will discuss the persons and/or organizations best meet project´s requirements related to ethical aspects. Some candidate organizations to be approached are: National Ethical Committees of seven pilot sites and the European Network of Research Ethics Committees (EUREC). Also, representatives from the ethics committee of the hospitals and care centres involved in ADLIFE will participate in the EAB when defining the general intervention trial design and when adapting the trial to every region.
ADVISORY BOARD (AB) AND SOCIAL AWARENESS BOARD (SAB): The Advisory Board will be the organ through which external expert people recruited from relevant sectors to the project will give their advice and feedback on the main arising issues of the ADLIFE project. Members of International Foundation for Integrated Care, which last meeting in 2019 has been held in San Sebastian will be confirmed to participate in the AB as well as members of the different committees where members as i-HD are participating. The composition of the SAB will be selected from the regional teams as well as from the network of citizen and patients associations that are part of the General Assembly of i-HD.
3.2.2 APPROPRIATENESS TO THE COMPLEXITY AND SCALE OF THE PROJECT
The nature of the ADLIFE project requires a coherent and well-defined management structure. As such, it is necessary to consider the diverse composition of the consortium and the several working groups involved. It is required to also take into consideration the project’s duration of four years, and the variety of activities to be carried out - coordination, co-creation, pilot implementation, analysis of project results, networking, and global dissemination.
The ADLIFE consortium proposes a streamlined and effective management structure in order to effectively manage the project’s work plan. The overall management team will aim to:
Ensure the project runs smoothly and efficiently. Establish and follow decision making procedures. Ensure the achievement of optimal results within the established timeframe and budget. Ensure and/or establish a proper communication flow. Comply with the reporting requirements outlined in the project work plan and ensure that deliverables are
achieved on schedule. Solve any conflicts that might arise.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 53
In order to ensure the most effective coordination, the consortium has put great care into agreeing and defining a simple leadership hierarchy that ensures fast decision taking among all members of the team and smooth project management, while providing the necessary control and participation mechanisms. These management mechanisms are:
MONITORING AND PROGRESS REPORTING: Each WP Leader will report project progress to the Project Coordinator every 6-months. This will cover technical progress, results, deliverables and compliance with the WP, as well as the monitoring and updating of the possible identified risks. Progress of the tasks will be reported in terms of percentage of completion and estimated time to completion, deviations from agreed time scales and corrective actions. The PC will summarise the overall project progress, updating planning charts and manpower records, and will also establish a rolling financial plan to be annually updated, reviewing actual costs against the GA and forecast expenditure for the next period. Significant deviations will be reported as per EC’s requirements, together with corrective actions taken.
INFORMATION AND COMMUNICATION: To ensure collaboration, a good communication strategy is needed. ADLIFE will hold regular meetings. A project web site will be set up with a restricted area for consortium members, with a repository to upload and keep record of deliverables, meetings, events… as a workspace for information exchange. The consortium will also disseminate technical progress and assess project planning. Unanimity in decision-making is highly desirable, both for quality assurance and to ensure that partners’ interests are respected.
BACKGROUND KNOWLEDGE: Taking into account that it is an IA based on previous partners development and also collaborative projects, each partner will be considered as the exclusive owner of its background or in the joint conditions that have been stipulated in the other projects, the prior to the GA. Access rights to background will be further developed in the CA and will not contradict IPR regulations established by the standard GA from EC.
RESULTS IPR MANAGEMENT: IPR issues of the results and the exploitation plan are directly under the control of the EB. Unless otherwise stated, results intellectual property will be property of the partner that generates it. Should several partners have jointly developed results, it will be jointly owned, unless partners concerned agree upon another alternative. The CA shall include additional specific rules regarding exploitation of jointly developed results. QUALITY ASSURANCE To ensure project’s quality, a Project Management Handbook will be produced at the beginning of the project. Internal reviewing procedures to guarantee the quality of results will be adopted. Each WP Leader will be responsible for the technical excellence of their respective outcomes, with special focus on deliverables. RISK MANAGEMENT: The management process will identify and monitor, during project implementation, internal and external risks as well as any other issues that might affect the project progress. Each partner has the responsibility to report immediately to their respective WP leader and to the Project Coordinator any situation that may arise and may affect the project objectives or their successful completion. Any change in time schedule of deliverables or in the allocated budget must be reported to the corresponding WP leader or to the Project Coordinator. In case of problems or delays, the Steering Committee will be consulted, and it will establish mitigation plans to reduce the impact of risk occurring.
CONFLICT RESOLUTION: Default procedures will be provided in the CA. Conflicts will be solved at the lowest level possible, preferably amicably. If an agreement cannot be reached at task or WP level, the PC will mediate. If that is not satisfactory, the PMB will decide and, if need be, authorisation from the EC will be required.
3.2.3 HOW EFFECTIVE INNOVATION MANAGEMENT WILL BE
ADLIFE’s management structure has been specifically designed to be the most effective innovation management system in order to produce marketable products from RTD results and maximise its success rate. This structure has been designed following the first European Standard for Innovation Management, CEN/TS 16555-1, that defines the innovation management systematic processes.
The three main aspects that have been considered are:
Organizational structure: innovation requires organization at different stages: coordinating level, operational level and support level. That is the reason why the project coordinator, the steering committee, the project technical committee and WP leaders, the regional teams and the advisory board have been designated. No specific innovation figure has been defined due to the nature of the results, but the SC will also have a key role in innovation management.
Internal communication flow: having a good communication within the consortium is one of the key elements of innovation management and decision making, even more when the number of partners is high, complicating this task.
Dissemination and Exploitation: the definition of the work plan is essential to achieve an effective innovation management system. During the proposal preparation, all the partners have jointly defined the Work Packages,
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 54
its objectives and expected results, paying special attention to Dissemination and Exploitation tasks in order to achieve market objectives.
3.2.4 CRITICAL RISKS
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 55
FIGURE 13 ADLIFE´S RISK (L: LIKEHOOD; I:IMPACT)
3.3 CONSORTIUM AS A WHOLE
3.3.1 DESCRIPTION OF THE CONSORTIUM
The ADLIFE consortium is formed by 11 organisations from 9 different countries, being KRONIKGUNE the proposal coordinator. It includes 7 member-states (Spain, United Kingdom, Denmark, Germany, Poland, Sweden and Belgium) and 2 associated states (Israel and Turkey). The project will deploy a large-scale intervention in 7 pilot sites where more than 200,000 advanced chronic patients live. The ADLIFE project has been made possible thanks to a well-balanced consortium: healthcare providers, well-known Universities of international prestige, top EU Research Centres and international ICT companies.
FIGURE 14 - MAP OF THE CONSORTIUM
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 56
The consortium counts with:
• Healthcare services/providers/managers: All healthcare services/providers will provide access to healthcare professionals and centers, as well as to third sector, patients and carers in each of the participating regions. KRONIKGUNE is an Institute for Health Services Research, who entrusts the Basque Health System on international R&D&I projects aimed at developing services and organizational models and their deployment for the whole Basque Country (2,2M inhabitants). It leads the Basque Country 4 stars Reference Site in EIP-AHA. Kronikgune will work with healthcare professionals of Osakidetza (Third party) to deploy the large-scale pilot. STRAT will collaborate with clinicians from primary, secondary and tertiary care that are responsible for delivering healthcare services in NHS Lanarkshire. STRAT has a strong past and on-going research relationship with the health care teams participating in this project. OUH operates four academic and community hospitals located in the eastern part of the Region of Southern Denmark, including Svendborg Sygehus which has the largest medical department in Denmark. The region is one of the reference sites of EIP-AHA. FALKHOSP is a leading hospital in Lower Silesia (Poland) one of the most advances regions in the provision of digital healthcare services in the country. OPTIMEDIS is a private company aiming to develop and manage regional integrated care delivery systems together with physician networks and other providers. Two of the largest hospital in their region will participate in the pilot. RJH’s is the main responsible for primary and secondary healthcare in its County in Sweden. AMCA is the Israel´s newest public hospital with more than 650 beds and will also work with its third paryt Maccabi healthcare services Israel's second largest Health Insurer and Provider and operates comprehensive healthcare services in the Community. Maccabi is a member of the B3 Integrated Care Action in group of the European Innovation Partnership for Active and Healthy Aging.
• Experts in development of digital healthcare services: WARWICK, SRDC and everis have complementary roles and capabilities to deploy a successful ADLIFE toolbox. Interoperability, security, quality, integration issues will be solved by WARKICK in cross-collaboration with the rest of experts as well as the ICT services/teams of the pilots. SRDC will extend and adopt its existing Patient Empowerment Platform (eSaglıkKaydım) for the needs of ADLIFE Project. Both, WARWICK and SRDC have previously collaborated in the C3-Cloud project in the bases of ADLIFE project that has been tested in KRON and RJH regions. Everis is an international large company expert in artificial intelligent among other fields that have worked in the development of CDSS. I~HD is expert in health data protection, storage and management.
• Experts in intervention deployment and evaluation: All pilot sites have a large experience in developing clinical trials and interventions in large groups of patients where they have also previously worked together (patient recruitment, interaction with healthcare and social professionals, patients, carers, citizens, politicians, regulators, ethics committees). RJH’s unit oversees education, including parts of the training for all medical personnel. Considering this background, they are ideal to lead the “Evidence based Personalized Care Delivery” in WP6. OUH has an important centre for innovative medical technology where interdisciplinary teams work together foor bridging resarch and science in practical implementation and technology development. KRONIKGUNE is an expert in the field of evaluating healthcare and social interventions by using mixed-methods approach that will be complemented by the experience in the economic evaluation of the interventions provided by STRAT.
• Dissemination and exploitation experts: STRAT has a strong experience in involving and communicating with stakeholders (like patient associations) in the development and implementation of IT solutions in remote patient care. I~HD has a substantial experience in developing promotional materials and in working across stakeholders on complex health and health informatics messages and I~HD experts have experience of defining evidence and roadmap for sustaining for profit and not for profit initiatives arising from EC projects. OPTIMEDIS has formal joint ventures in different countries in the field of providing integrated healthcare services and work in the analysis of the business models for healthcare sector. SRDC and EVERIS are currently selling digital services and toolbox to different health systems.
3.3.2 CONTRIBUTION TO THE PROJECT
The following table details the partners involved in the ADLIFE project and their main role in it:
PARTNER MAIN ROLE IN ADLIFE KRONIKGUNE Project Coordinator (WP1), Evaluation leader (WP9) and Spanish pilot leader. STRAT Dissemination and Communication leader (WP2). UK pilot leader. WARWICK Leader of WP3: a) gather the technical requirements to guide the adaptation of personalized
care plan management platform to pilot sites´ particularities; b) adapt existing platforms to local contexts (interoperability); c) support clinical decision making with the IT tool
OUH Empowerment of patients, caregivers and communities’ leader (WP7). Danish pilot leader.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 57
PARTNER MAIN ROLE IN ADLIFE FALKHOSP Polish pilot leader. OptiMedis German pilot leader. Leader of WP10, ensuring the exploitation of ADLIFE’s results and the
creation of roadmaps and routes for exploitation of other digital solutions RJH Swedish Pilot Leader. Evidence based personalized care delivery leaders (WP6). Design and
develop personalized care based on clinical evidence. AMCA Israel Pilot Leader. Trial design and implementation leaders (WP8). . SRDC Leaders of WP4. They will be responsible for the delivering the Patient Empowerment Platform
as the technical infrastructure to extend healthy and independent living and support to patients and their informal care givers in the long term. Exploitation of digital solutions.
EVERIS Leaders of WP5, Clinical Decision Support Systems and Early Identification Tools. They will be closely involved in WP10: exploitation of CDSS and ADLIFE digital toolbox
i-HD Co-leader WP2. Roadmap for change of clinical management. Data protection and management
3.3.3 INDUSTRIAL/COMMERCIAL INVOLVEMENT IN THE PROJECT TO ENSURE EXPLOITATION OF THE RESULTS
The consortium has been structured to maximise the exploitation of the project’s outcomes (WP2 and WP10). As it is described in the section 2:
• Everis will lead the exploitation of ADLIFE toolbox including the product in the portfolio and reaching agreement with piloting and developers’ partners in the project for the exploitation and implementation of the solution in the health services.
• SRDC will include the new version of the empowerment platform in its portfolio of products and guarantee the future exploitation and implementation of the solution in other health services.
• OPTIMEDIS is going to generate business models (WP10) and exploitation routes for the exploitation and use of digital health services not only for integrated care.
Additionally, all partners of ADLIFE consortium, which involve 9 different countries, can reach a wide number of industrial stakeholders across Europe through their network of contacts in order to foster interactions with potential end-users. This network of stakeholders will enable new business opportunities, allowing the project developments to impact in a large number of healthcare services public and private at worldwide level and analysing the use of the digital tools in other contexts (education, administration…)
3.4 RESOURCES TO BE COMMITTED
As can be seen in the use of the resources, the development of the intervention of the digital tools in WP3-5 needs a high percentage of the total person months (almost 48% of resources) to guarantee also the commitment of all the healthcare professionals from pilot sites as well as technical developers and ICT team in the different pilot sites, that have not the same maturity of infrastructures an technology. The preparation of the pilot sites for intervention (WP6-7) and the intervention (WP8) account for a 28% of the resources. As detailed in section 4-5, in three pilots UK, Poland and Germany the integration of the healthcare professionals is also managed by subcontracting their participation in the project. All partners have included similar other direct costs: travels for participating in meetings and dissemination activities related to the project as well as costs for dissemination (open access, journals, congresses) and audit if necessary. Pilot sites have also included expenses for ICT adaptation to local settings and translation of manuals, questionnaires and scales among others.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 58
3.4.1 OTHER DIRECT COSTS
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 59
4. MEMBERS OF THE CONSORTIUM 4.1 ASOCIACIÓN CENTRO DE EXCELENCIA INTERNACIONAL EN INVESTIGACIÓN SOBRE CRONICIDAD (KRONIKGUNE) 4.1.1 DESCRIPTION OF THE LEGAL ENTITY AND ITS MAIN TASKS
Kronikgune (KG) is an Institute for Health Services Research that promotes and carries out management and organization research on health and socio-health services. Its scientific research programme is aligned with the policies of the Basque Department of Health, that pursue the continuous adaptation and transformation of the health system by keeping people at the center of the system and addressing the challenges derived from aging, chronicity and dependency.
Kronikgune will advance in health policies and services evaluation, intervention models development, dissemination and the analysis of health services’ change and implementation. Its expertise lies in the analyses for health promotion strategies; study of stratification models and their usefulness to predict patients’ needs and adequacy of resources; design of personalized care; best models and management services for integrated care; strategies and advanced methods of decision making, organisational transformation and innovation, including research in developing new products and technologies for e-health (diagnosis, support, monitoring, coordination).
Kronikgune is experienced in the coordination and management of European projects and Joint Actions mainly related to research and implementation of innovative health care delivery integration systems. Kronikgune has coordinated Carewell (CIP) 85 , also ASSEHS (2HP) and now is coordinating UPRIGHT (H2020). Other European projects are C3Cloud, Fi-STAR, Mastermind, SCIROCCO, ACT, ACT@Scale, Advantage, Chrodis-Plus, EIP on AHA (B3 Action Group on Integrated Care).
Kronikgune’s area of expertise comprises the development and implementation ICT enabled solutions for the management of chronic disease, evaluation of health services and identification of determinants in the management of chronicity, with a common framework that integrates both social and health aspects.
Overall, Kronikgune analyses strategies for health promotion, including individual and structural actions and action models in community health; studies stratification models and their usefulness to predict needs and adequacy of resources for chronic patients; the design of personalized care (care management for high-risk patients, chronic patient integrated, multidisciplinary collaborative care programs); best models and management services for chronicity, including funding, contracting services, integrated care systems, technologies or new professional roles; strategies and advanced methods of decision making, organisational transformation and innovation, including research
ROLE IN THE PROJECT
KRONIKGUNE will be involved in several WPs and tasks of the ADLIFE project. Kronikgune will lead WP1 Project Management, including the Administrative coordination, Financial management, Operational management, Quality assurance and performance monitoring, and the Ethic plan. From the most technical point of view, KRONIKGUNE will lead WP9 Evaluation and pilot outcome assessment. The main tasks within this WP will rely on the evaluation from a qualitative and quantitative point of view the success and effectiveness of the intervention. This duty is absolutely aligned with the expertise and experience of Kronikgune. In line with his broad experience in the field of health care evaluation and management by design and development of pilots, the team will also be involved in:
WP3: Define and integrate the personalized care plan management platform into the Basque system. WP4: Define and incorporate the PEP application in the Basque Country system. WP5: Outline and develop the clinical decision support system and to adapt it into the local context of Basque
Country of the core intervention. WP6: Support the development of healthcare pathways, organizational models and change management. WP7: Support the development of the patient empowerment platform.
85 https://ec.europa.eu/digital-single-market/en/news/top-25-influential-ict-active-and-healthy-ageing-projects
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 60
WP8: Develop the implementation and monitoring of the intervention to be developed in the Basque Country, as well as to stablish the ethical and socio-cultural endpoints.
Coordinate the regional team where schools (teachers, youths, families), experts and health services (Osakidetza) will participate.
4.1.2 CV OF THE PERSONS
Dr. Esteban de Manuel Keenoy
Gender Male
Qualification Doctor of Medicine
Staff Category Director of Kronikgune
Short description of work experience, relevant to the proposal
MD. Esteban de Manuel Keenoy, obtained MD University of Navarra holds a Master degree in Community Health, University of London (LSHTM) and a Specialist degree in Family Medicine, Autonomous University of Madrid. Has a career in management in health and scientific institutions. From 1983 to 2002 he was in Andalucía, first as Regional Director of Primary Health Care and Health Promotion and later, as Academic Director of the Andalucian School of Public Health. From 2003 to 2011 he has been CEO of the Institute of Health Sciences of Aragón, responsible for Health R&D and knowledge management in the Region of Aragon, in Northeast Spain. Since July 2011 he is in charge of Kronikgune, the Basque Centre for Health Services Research and Chronicity set up by the Basque Government within the R&D strategy to confront ageing, chronic diseases and healthy living. He has been involved in national and international projects advising public health and health systems development. His main expertise is on strategic management, human resources development and knowledge management in health services and research.
Dr. Ane Fullaondo
Gender Female
Qualification PhD in Genetics and Molecular Biology
Staff Category Coordinator of research projects in KRONIKGUNE
Short description of work experience, relevant to the proposal
Ane Fullaondo, obtained an MD in Biology at the Autonomous University of Madrid (2005) and PhD in Genetics and Molecular Biology at the University of the Basque Country (2009). Currently, she obtained a Masters in research methods and evaluation of health services health economics of the National Distance Education University (UNED). In 2015 she obtained the LEAD – The certificate of Specialization in Leadership and Transformation in Organizations and Health Systems from Deusto Business School. Since the end of 2012, she has been a researcher in KRONIKGUNE and from November 2015 until now, she has been coordinator of research projects in KRONIKGUNE.
Dr. Nerea González
Gender Female
Qualification PhD in Psychology
Staff Category Project Manager
Short description of work experience, relevant to the proposal
Nerea González, PhD in Psychology by the University of the Basque Country, is the Project Manager of REDISSEC (Health Services Research on Chronic Patients Network), where she gives support to the Networks’ coordinator managing the 14 groups, the main research areas, the activities around them and the documentation that is produced. Her main research lines focus on: health services research; patient reported outcomes; psychometrics, developing, adapting and validating questionnaires; and qualitative methodology, employing different techniques (focus groups, interviews,…) and analysing the resulting information. Also, she collaborates with national and international journals in reviewing scientific manuscripts.
Dr. Olatz Albaina
Gender Female
Qualification PhD in Pharmacy
Staff Category Researcher and project manager of European projects
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 61
Short description of work experience, relevant to the proposal
Olatz Albaina, holds a PhD in Pharmacy at the University of the Basque Country, a Bachelor degree in Science and Food Technology at the University of the Basque Country and a Master degree in Parasitology, Microbiology and Immunology at the University of the Basque Country. She has worked as researcher in Biosasun, and as R&D project consultant in Adigest. She joined KRONIKGUNE in November 2015 working as researcher and project manager of European projects.
Maider Mateo-Abad
Gender Female
Qualification MSc on Mathematical Modelling, Statistics and Computing Research
Staff Category Researcher in European projects
Short description of work experience, relevant to the proposal
Maider Mateo-Abad holds a degree in mathematics and a MSc on Mathematical Modelling, Statistics and Computing Research at the Basque Country University. She has worked as researcher in the university of the Basque Country and in the Basque health system-Osakidetza. From 2015 she works as researcher in Kronikgune for European projects, in collaboration with the Primary Care Research Unit in Gipuzkoa. She is member of the Research Group on Primary Care at Biodonostia Health Institute and also collaborates with the Biostatistics Research Group-Biostit at the University of the Basque Country.
Dolores Verdoy
Gender Female
Qualification Ph.D. in Biology
Staff Category Project Manager
Short description of work experience, relevant to the proposal
Dolores Verdoy is a Project Manager in Kronikgune, the International Centre of Excellence in Chronicity Research. Dolores joined Kronikgune in 2016. She has an extensive experience as a researcher in European projects. Dolores has a B.Sc. in Biology at the University of Navarra (1998) and obtained her Ph.D. in Biology at the Autonomous University of Madrid (2003). In 2017 she obtained the Certificate as Expert in Research in health services and chronic diseases from University of Alcala. She works currently as project manager of European projects.
Javier Mar
Gender Male
Qualification Ph.D.
Staff Category Head of Clinical Management Unit of the Hospital Alto Deba
Short description of work experience, relevant to the proposal
Javier Mar, Head of Clinical Management Unit of the Hospital Alto Deba and coordinator of the West Gipuzkoa Health Research Unit encompassing Zumarraga, Mendaro and Alto Deba hospitals from 1992 to 2013. His research line is the economic evaluation of clinical decisions both diagnostic and therapeutic. His latest publications deal with the epidemiology and economic evaluation in neurological and chronic diseases. He is specialized on the developing and applying population models built with discrete event simulation to calculate the budget impact analysis of health programs. He has applied this approach to thrombolysis for stroke, use of hyaluronic acid in knee osteoarthritis, Alzheimer’s disease, breast cancer screening and bariatric surgery. He has published 44 papers (26 in international journals and 18 in national journals) and two books in the last 12 years.
José María Quintana
Gender Male
Qualification Ph.D. in Medicine
Staff Category Head of the Research Unit of the Galdakao-Usansolo Hospital
Short description of work experience, relevant to the proposal
José María Quintana is a Doctor in Medicine, specialist in Preventive Medicine and Public Health, and also in Pediatrics, Master of Science in Epidemiology and, also, in Health Policy and Management by the School of Public
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 62
Health of Harvard University. Head of the Research Unit of the Galdakao-Usansolo Hospital for 25 years, and scientific coordinator of the Spanish Network for Research in Health Services in Chronic Diseases (REDISSEC). His research areas, within the scope of health services research, focuses on the study of the appropriateness, variability and patient safety; the evaluation of the effectiveness of different interventions, devices or treatments; development of predictive models and of clinical practice rules; development of assessment tools to measure health related quality of life as referred by the patient. He has participated and participates in various research projects, both regional, national and European. Among them, he has significant leadership and experience in the development and validation of clinical prediction rules projects as well as the development of applications derived from them with more than 70 publications on the field. Additionally, he is the author of more than 230 scientific articles, several of them on intervention studies. Data from the Web of Science indicates that he has an h-index of 33, has been cited 4180 times in 3512 articles. It has 10 products registered as copyright. He has directed 15 doctoral theses and 5 more are underway.
Urko Aguirre
Gender Male
Qualification MSc in Computer Science
Staff Category Biostatistician in the Research Unit of the Hospital Galdakao-Usansolo
Short description of work experience, relevant to the proposal
Urko Aguirre, BSc in Mathematics and MSc in Computer Science, University of the Basque Country. He
started his career as biostatistician in 2004 in the Research Unit of the Hospital Galdakao-Usansolo (Biscay, Spain). Since then, he has been involved (as collaborator and/or principal investigator) in many public competitive national and international research projects focused in the Health Services Research. His main research field is the development, validation and application of statistical methods, mainly in Health Related Quality of Life data, in longitudinal epidemiological studies. He is an expert in predictive modelling of longitudinal data, especially on the statistical strategies for handling missing data, and on the application of data mining techniques in medical sciences. He is an active member of the Health Services Research on Chronic Patients Network (REDISSEC) since its foundation and member of the Sociedad Española de Biometría (SEB) and of the BIOSTATNET (National Biostatistics Group).
Itziar Vergara
Gender Female
Qualification PhD
Staff Category Responsible of the Primary Care Research Unit of Gipuzkoa
Short description of work experience, relevant to the proposal
Itziar Vergara, MD, MPH (UC Berkeley CA, USA), PhD (EHU-UPV). Currently in charge of the Primary Care Research Unit of Gipuzkoa, at Osakidetza, the Basque Health System. She leads the Primary Care Research Group at Biodonostia Health Research Institute. She is member of the Spanish network of Health Services Research REDISSEC and coordinates the group of Healthy Ageing Research at Kronikgune. She is the principal investigator of several public founded research projects and has published papers in aging, frailty and health services research domains.
4.1.3 LIST OF RELEVANT PUBLICATIONS Arostegui I, Gonzalez N, Fernández-de-Larrea N, Lázaro-Aramburu S, Baré M, Redondo M, Sarasqueta C, Garcia-
Gutierrez S, Quintana JM; REDISSEC CARESS-CCR Group. Combining statistical techniques to predict postsurgical risk of 1-year mortality for patients with colon cancer. Clin Epidemiol. 2018 Mar 6;10:235-251. doi: 10.2147/CLEP.S146729. eCollection 2018. PubMed PMID: 29563837; PubMed Central PMCID: PMC5846756.
Uranga A, Quintana JM, Aguirre U, Artaraz A, Diez R, Pascual S, Ballaz A, España PP. Predicting 1-year mortality after hospitalization for community-acquired pneumonia. PLoS One. 2018 Feb 14;13(2):e0192750. doi: 10.1371/journal.pone.0192750. eCollection 2018. PubMed PMID: 29444151; PubMed Central PMCID: PMC5812619.
Baré M, Alcantara MJ, Gil MJ, Collera P, Pont M, Escobar A, Sarasqueta C, Redondo M, Briones E, Dujovne P, Quintana JM; CARESS-CCR Study Group. Validity of the CR-POSSUM model in surgery for colorectal cancer in Spain (CCR-CARESS study) and comparison with other models to predict operative mortality. BMC Health Serv. Res. 2018 Jan 29;18(1):49. doi: 10.1186/s12913-018-2839-x. PubMed PMID: 29378647; PubMed Central PMCID: PMC5789585.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 63
Zarcos-Pedrinaci I, Téllez T, Rivas-Ruiz F, Padilla-Ruiz MDC, Alcaide J, Rueda A, Baré ML, Suárez-Varela MMM, Briones E, Sarasqueta C, Fernández-Larrea N, Escobar A, Quintana JM, Redondo M; REDISSEC-CARESS/CCR group. Factors Associated with Prolonged Patient-Attributable Delay in the Diagnosis of Colorectal Cancer. Cancer Res Treat. 2018 Jan 2. doi: 10.4143/crt.2017.371. [Epub ahead of print] PubMed PMID: 29334608.
Esteban C, Garcia-Gutierrez S, Legarreta MJ, Anton-Ladislao A, Gonzalez N, Lafuente I, Fernandez de Larrea N, Vidal S, Bare M, Quintana JM, -Copd Group I. One-year Mortality in COPD After an Exacerbation: The Effect of Physical Activity Changes During the Event. COPD. 2016 Dec;13(6):718-725. Epub 2016 Jun 10. PubMed PMID: 27285279.
Bengoetxea,S. García, K. Vroutsou M J. Onaindia, JM. Quintana. Opioid Use at the End of Life and Survival in a Hospital al Home Unit. Journal Of Palliative Medicine. 2010. Vol 13 (9).
4.1.4 LIST OF RELEVANT PREVIOUS PROJECTS CAREWELL: The aim of Carewell was to propose, implement and validate new integrated care models for
patients with multiple comorbidities that are cost-effective, using different routes, such as improving home-based patient care, thereby preventing their hospitalisation, and improving communication channels between (healthcare and social) professionals and patients and/or care models to facilitate the exchange of information for each patient, thereby avoiding duplication of effort. Mainly focussed on improving care and care services for complex chronic patients (multiple co-morbidities) by two routes: coordination and communication between healthcare professionals and empowering the patient and/or caregiver, and home-based care and support based on the use of information and communication technologies (ICT). This allows patients or their caregivers to communicate with the doctor or advice centre using methods that do not require the patient to attend the health centre.
C3-CLOUD: aims to develop personalised care plans for complex multimorbid patients, supported by ICT tools and managed by a coordinated multidisciplinary team, that promotes integrated care and the involvement of the patient and/or caregiver. A Personalised Care Plan Development Platform will allow collaborative creation and execution of personalised care plans for multimorbid patients, through systematic and semi-automatic reconciliation of clinical guidelines. This will be realised with the help of Decision Support Modules, recommendation reconciliation, poly-pharmacy management and goal setting. Fusion of multimodal patient and provider data will be achieved via C3-Cloud Interoperability Middleware for seamless integration with existing information systems. A Terminology Service with advanced semantic functions will enable meaningful analysis of multimodal data and clinical rules. Active patient involvement and treatment adherence will be attained through a Patient Empowerment Platform.
The Interoperability Middleware contains three components: 1) The Technical Interoperability Suite enables seamless data exchange between the local care systems and the C3-Cloud components;2) The Semantic Interoperability Suite addresses the challenge of heterogeneous clinical data representation formats; 3) The Security and Privacy Suite has been developed, based on open source toolkits for authentication and authorization of care team members and for ensuring encrypted and auditable data exchange across C3-Cloud software components. The C3-Cloud platform and applications have been developed with interoperability in mind, and use popular interoperability standards to make it easier to connect with electronic health record systems. State of the art security measures protect patient privacy to an extent that meets information security requirements of health systems across Europe, and complies with the latest data protection legislation (including the GDPR). C3-Cloud aims to support clinical workflow and workload by making it easier to plan and to document care for patients with multi-morbidity, and to communicate with other care actors involved with a patient through a collaboration platform that supports secure messages for case conferences. The involvement of patients in more effective, clinician-guided and software supported self-care should reduce treatment complications and we hope it will reduce unscheduled care encounters. To demonstrate feasibility, pilot studies will focus on diabetes, heart failure, renal failure, depression in different comorbidity combinations. Pilots will operate for 15 months in 3 European regions with diverse health and social care systems and ICT landscape, which will allow for strengthening the evidence base on health outcomes and efficiency gains. C3-Cloud adaptive patient pathways and organisational models validated by patient organisations and a clinical reference group, change management and training guidelines will be shared with the European community. Commercial exploitation of C3-Cloud integrated care solutions will be facilitated through an Industry Vendor Forum and commercial EHR/PHR products of 3 leading SMEs.
ASSEHS (Activation of Stratification Strategies and Results of the interventions on frail patients of Healthcare Services). (Health Programme 2013, Executive Agency for Health and Consumers, EAHC (currently CHAFEA):
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 64
ASSEHS European project is an international effort to study current existing health risk stratification strategies and tools and the challenges to spread their use and the application on frail elderly patients. To face the challenge of active and healthy ageing (AHA), European Health Systems and services should move towards proactive, anticipatory and integrated care. Health care systems thus need to personalize services, put patients in the centre of care and provide services using the adequate resources. Population health risk management is emphasized through the use of tools to stratify people with chronic diseases according to their risk and offering support commensurate with this risk. Effective screening of frailty is key in optimizing care for frail population at risk. Risk Stratification tools can help to identify complex frail and high-risk patients and maintain these patients on the radar of the Health Services. Risk Stratification helps ensuring appropriate coverage of key secondary health risk prevention interventions, including managing disease stratification registers systematically by modelling expected versus actual prevalence and incidence, and thereby identifying practices where improvement is necessary. Systematic screening of groups of people in risk of suffering a disease constitutes a part of a broader area-level strategy on public health. A Health System is an intricate network of health care structures with multiple levels of governance. There is not a unique model for the screening and stratification of people at risk of suffering frailty and the different configuration of almost any Health System of the world creates even more alternatives. The analysis of Risk Stratification techniques in different Health Systems and the lessons learnt out of the implementation of stratification-based interventions on the four Health Services in ASSEHS will help in generating useful conclusions and risk stratification solutions transferable to a variety of regions in the future.
UPRIGHT (Project ID: 754919_Universal Preventive Resilience Intervention Globally implemented in schools to improve and promote mental Health for Teenagers) (EU-funded SC1-PM-07-2017). UPRIGHT general objective is to promote mental wellbeing and prevent mental disorders by enhancing resilience capacities in youths, through a holistic approach addressing early adolescents, families and education professionals. UPRIGHT conceptual framework is structured in four different domains (effective coping skills, self-efficacy; social emotional learning; mindfulness; positive parenting skills). Three of the domains target youths and teachers, whereas the last one is for families. The project consists of 4 main building blocks: 1) co-creation (co-design, co-production and co-customization) of the intervention in EU regions; 2) deployment of resilience interventions; 3) process and outcome evaluation; 4) transfer learning on implementation of positive culture of mental wellbeing to future regional, national and pan European programs. The UPRIGHT program will be implemented in 5 pilot sites across Europe representing different regions and income countries: Poland (Lower Silesian), Spain (Basque Country), Italy (Trento), Denmark (Denmark) and Iceland (Reykjavik capitol area). Schools of the pilot regions already have committed their participation (Letter of intent included in part4-5 of the proposal).
FI-STAR (Future Internet Social and Technological Alignment Research) is focused on promoting innovative and sustainable services focussing on active and healthy ageing and which make optimal use of technology. The creation of a learning community comprising partners of a different nature and from different European countries aimed at promoting innovative and sustainable services focussing on active and healthy ageing and which make optimal use of technology. The community formed will focus on the exchange of experiences and definition of routes to roll-out specific interventions aligned with the aims of the EIP-AHA action plans. The specific purpose of the Basque Country was to assess the efficacy and impact of an on-line model for the treatment of Bipolar disorder patients which are already being treated for this disease in the Basque Country Healthcare System. Data of the activity and use of the BTPM module plus the necessary clinical data related to the patient health (mood status, anxiety, functionality…), active treatment and some biological parameters will be managed in the experiment.
MASTERMIND aimed to make high quality treatment for depression more widely available for adults suffering from the illness by the use of ICT. The goal was to assess through implementation at scale (more than 5.000 patient overall) the impact of cCBT (computerised Cognitive Behavioural Therapy) and video conference for collaborative care and treatment for depression across 10 EU and Associated Countries. Regarding the identified barriers and success factors to implementing the two services on a large scale in different political, social, economic and technical health care contexts and from the perspective of different stakeholders such as patients, professionals and health insurances, the project aimed to provide recommendations for successful strategies for implementing the two services for depression in these different settings.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 65
4.1.5 DESCRIPTION OF ANY SIGNIFICANT INFRASTRUCTURE
4.1.5.1 NETWORKS – COLLABORATIONS - DISSEMINATION CAPACITY
Since 2016,the Basque Country is considered a 4-star Reference Site, which is the highest rating awarded by the European Commission to demonstrate excellence in the development, implementation and scaling-up of innovative practices, in line with the strategic aims of EIP on AHA. This recognition is also due to the commitment undertaken regarding an integral approach to active and healthy ageing and including new policies which place the person at the centre of all actions.
The Basque Government Health Department, through Kronikgune, Osakidetza and other organisations and institutions, has been part of the European EIP on AHA Association since 2012.
Kronikgune participed in The 6th EIP on AHA Partner Conference hold under the slogan: “Digital transformation of health and care for Active and Healthy Ageing in Europe”. The event has focused on reviewing the action plans defined within the Action Groups which come under the framework of the EIP on AHA strategy. The alignment of the plans and commitments undertaken by the partners in relation to the European Commission policies have been analysed, and in particular, regarding the “Transformation of Health” and “Care in the context of the Digital Single Market”. Kronikgune, representing the Basque Country, took part in.
4.1.5.2 DISSEMINATION CAPABILITY:
In 2017, a series of meetings have been held between the European reference regions with the aim of fostering the deployment of innovative solutions for active and healthy ageing.
• “Scale AHA” is an initiative of the European Innovation Partnership on Active and Healthy Ageing (EIP on AHA). It seeks to promote scaling-up, deployment and implementation of digitally-enabled innovative practices between European regions. For this purpose, activities have been jointly organised by EIP on AHA partners, reference sites and other national / regional / local organisations and ecosystems. These activities have fostered the transfer of knowledge related to healthcare, social care, health, Information and Communications Technology (ICTs) and finance.
• The reference sites of the 24 European countries took part on the call for Twinning collaboration between regions. Throughout 2017, 26 Reference Sites from 13 European countries received financial support for visits and twinning activities, to transfer knowledge and promote the deployment of innovative solutions.
• In 2016, Kronikgune, representing the Basque Country, was awarded four projects: one as a recipient region in relation patient empowerment; and three as a reference region on risk stratification. The empowerment twinning has provided deeper knowledge of innovative Good Practices implemented in Scotland around this area. Through the activities organised under this collaboration and based on the lessons learnt, Osakidetza along with other organisations, is already working to improve educational tools and programmes available. On the other hand, the Basque Country has shared knowledge on risk stratification Good Practices with three European regions: Liguria, Scotland and Aquitaine. This tool has been used in the Basque Health System since 2011. It serves to identify people more likely to require greater healthcare services in the future, and plan new actions adapted to the population needs.
• The final Scale AHA report provides an overview of all the different study activities and results, as well as recommendations proposed by participating regions. To download the report, click on the following link: Final Scale AHA study report.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 66
4.2 UNIVERSITY OF STRATHCLYDE (STRAT)
4.2.1 DESCRIPTION OF THE LEGAL ENTITY AND ITS MAIN TASKS
The University of Strathclyde (founded in 1796 as the Andersonian Institute) is one of the UK’s leading technological universities with a world class research profile and a reputation for excellence in teaching and research. The institution was awarded University of the Year 2012 and Entrepreneurial University of the year 2013 by Times Higher Education. Our areas of expertise include energy, future cities, health and manufacturing. We have a world-leading reputation for our work with businesses and organisations, large and small. We're ranked 7th in the UK for spin-out company creation. Our research is in the top 20 in the UK. Our new Technology & Innovation Centre is designed to increase our partnership working. It is the place where companies like GlaxoSmithKline, AstraZeneca, SSE, Scottish Power and the Weir Group work with us. Our Innovation Strategy confirms Strathclyde’s position as the UK’s leading university in the field of innovation.
The University of Strathclyde is a leading international technological university. Based on the results of REF 2014, the Times Higher Education ranked Strathclyde as one of the UK’s top 20 universities for research intensity. Strathclyde is a multi-award-winning university. Most recently the University received the accolade of Work Place of the Year at the 2017 Time Higher Education Leadership and Management Awards. This is one of seven THE awards received in seven years. The University’s £89m Technology and Innovation Centre is the cornerstone of the Glasgow Innovation District. The landmark centre houses shared and flexible facilities, where 700 world-class researchers work side-by-side with industrial partners.
Our seven strategic themes bring together research, teaching and innovation strengths from the whole University. Our Health & Wellbeing theme brings together cross-faculty expertise in Better Medicines; Biomedical Imaging and Biophysics; Digital Health and Health Analytics; Health Interventions and Population Growth; Living Well, Aging Well; Medical Devices and Technologies; Rehabilitation; and Sensor and Analysis Technologies. Strathclyde is a member of four of the UK’s seven Catapult Centres, which are transforming the UK’s capability for innovation.
ROLE IN THE PROJECT
The STRATHCLYDE partner will facilitate access to one of the most advanced healthcare structures and systems across our EU partners. Drawing on existing clinical networks from organized integrated care services and structures across Scotland, more specifically Glasgow, STRATHCLYDE will provide expertise in the context of integrated care and digital health. In fact, the NHSL Lanarkshire, as part of the team of STRATHCLYDE in the project, will provide the access to 3 Acute Hospitals and over 100 sites in the region. A region that it is included as a reference site in the EIP-AHA. STRATHCLYDE are experts in the remote monitoring and management of patients, having developed and evaluated the remote patient monitoring system, the Advanced Symptom Management System (ASyMS), in a series of large-scale observational trials. STRATHCLYDE have considerable experience of involving and communicating with stakeholders (including patients and patient associations and healthcare professionals) in the development and implementation of IT solutions in remote patient care. In addition, they develop different programs at the university to train the professionals of the future both in the field of health and digital technologies. Therefore, they will be in charge of the dissemination and communication activities (WP2), which are of great importance in ADLIFE. In addition, the economic department of the university will design in cross-collaboration with Kronkigune the socio economic evaluation of the tools and the integrated care of model.
STRATHCLYDE will also:
Be the UK pilot leader in collaboration with NHSL Lanarkshire. Develop the organizational model for the integrated care system. Adapt to local particularities existing ICT platforms that provide patients and caregivers with specific training for
better management of patients’ needs. Tailor the existing ICT solutions that best monitor and manage symptoms of patients at home to local
particularities. Define and implement face-to-face or technology-supported training programs for professionals.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 67
4.2.2 CV OF THE PERSONS
Prof. Roma Maguire
Gender Female
Qualification PhD
Staff Category Professor of Digital Health and Care
Short description of work experience, relevant to the proposal
Roma Maguire is a Professor of Digital Health and Care at the University of Strathclyde. She also holds an Honorary Nurse Consultant post in Cancer Care at NHS Lanarkshire. Her research interests include Digital Health, Cancer and Palliative Care, Dementia, LTC Management, Patient Experience, Supportive Care, Predictive Risk Modelling and Implementation Science. She has significant experience in the development and evaluation of supportive care and digital health interventions and has led several multi-site clinical trials in the UK and Europe. She is Principal Investigator of the €6 million EU FP7 eSMART study which is evaluating the impact of a mobile phone based remote patient monitoring system on chemotherapy related toxicity. Professor Maguire was also a co-investigator on the TIHM for dementia study which is a £5 million grant from the Department of Health and Innovate UK to evaluate an internet of things intervention for people with dementia.
Dr Lisa McCann
Gender Female
Qualification PhD
Staff Category Deputy Director of eSMART
Short description of work experience, relevant to the proposal
Dr Lisa McCann is a Senior Lecturer working within the Digital Health and Wellness Group at the University of Strathclyde. Dr McCann is the Deputy Director of the eSMART study and she has expertise in the development and evaluation of person-centered digital health interventions and working with people across the life course, including people with complex and palliative care needs. Dr McCann has experience of qualitative, mixed-methods and randomised controlled trial research methods.
4.2.3 LIST OF RELEVANT PUBLICATIONS
Maguire, R; Fox, P. A., McCann, L; Miaskowski, C., Kotronoulas, G., Miller, M.<https://pure.strath.ac.uk/portal/en/persons/morven-miller(ce9b8526-7112-4585-90bb-49744e088bb3).html>, Furlong, E., Ream, E., Armes, J., Patiraki, E., Gaiger, A., Berg, G. V., Flowerday, A., Donnan, P. T., McCrone, P., Apostolidis, K., Harris, J., Katsaragakis, S., Buick, A. R. & Kearney, N (2017) The eSMART study protocol: a randomised controlled trial to evaluate electronic symptom management using the advanced symptom management system (ASyMS) remote technology for patients with cancer<http://bmjopen.bmj.com/content/7/5/e015016> . BMJ Open May 2017, 7 (5) e015016
Papachristou Nikoloas , Barnaghi Payam, Cooper Bruce A., Hu Xiao, Maguire, R; Apostolidis Kathi, Armes Jo, Conley Yvette P., Hammer Marilyn , Katsaragakis Stylianos , Kober Kord M., Levine Jon D., McCann, L; Patiraki Elisabeth , Paul Steven M., Ream Emma, Wright Fay, Miaskowski Christine (2017) Congruence between latent class and k-modes analyses in the identification of oncology patients with distinct symptom experiences. Journal of Pain and Symptom Management, 55 (2), 318-333.
Maguire R, Ream E, Richardson A, Connaghan J, Johnston B, Kotronoulas G, Pedersen V, McPhelim J, Pattison N, Smith A, Webster L, Taylor A, Kearney N (2015) Development of a novel remote patient monitoring system: The advanced symptom management system for radiotherapy to improve the symptom experience of patients with lung cancer receiving radiotherapy. Cancer Nursing, 38 (2), pp. E37-E47
Kotronoulas, G; Kearney, N; Maguire, R; Harrow, A; Croy,S; McGillivray, S (2104) What is the Value of Routine Use of Patient-Reported Outcome Measures Towards Improvement of Patient Outcomes, Processes of Care and Health Service Outcomes in Cancer Care? A Systematic Review of Controlled Trials. Journal of Clinical Oncology, 32 (14), 1480-1501
McCall,K.; Keen,J.; Farrer,K.; Maguire,R.; McCann, L.; Johnston,B.; McGill,M.; Sage,M.; Kearney,N (2008) Perceptions of the use of a remote monitoring system in patients receiving palliative care at home. International Journal of Palliative Nursing 14 (9):426-431.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 68
4.2.4 LIST OF RELEVANT PREVIOUS PROJECTS
Strathclyde is actively involved in Horizon 2020 and has a portfolio of 81 projects with a value of over €26.5m. Under FP7 Strathclyde had a portfolio of 128 projects. The portfolio has a value of approximately €50m and involves collaboration with over 900 partners. Research and Knowledge Exchange Services at the University has been supporting academic staff with EU funding applications since the late 1980s, and therefore has significant experience of dealing with the management of contracts.
eSMART (Project ID: 602289_Randomised controlled trial to evaluate electronic Symptom Management using the Advanced Symptom Management System (ASyMS) Remote Technology for patients with cancers (The eSMART Study) (FP7: HEALTH.3013.2.4.1-3). The eSMART programme of work will demonstrate the effects of a real-time, mobile phone based, remote patient monitoring intervention on key patient outcomes and delivery of care provided to people with cancer during and after chemotherapy. Utilising the remote patient monitoring system, the Advanced Symptom Management System (ASyMS), will reduce the symptom burden experienced by patients receiving chemotherapy, improve their quality of life (QoL) during acute treatment and survivorship, and result in changes in clinical practice and improved delivery of care for patients with cancer. eSMART involves 11 European and one American partner as well as cancer care clinicians from all partner countries. A two-group, multicentre, repeated-measures randomised controlled trial (RCT) will be conducted across 16 sites in Europe, 1108 patients will be recruited. Adult (>18 years) patients diagnosed with breast, colorectal cancer or haematological cancers, commencing first-line chemotherapy and planned to receive at least 4 cycles of chemotherapy will be invited to participate. Work will take place in four consecutive phases. Members of the European Cancer Patient Coalition have an integral role as advisors at every stage of the programme to provide advice and feedback and ensure that work is conducted in line with patients’ perspectives and needs. eSMART will demonstrate how delivering patient focused, anticipatory care via technology can improve outcomes for people with cancer whilst simultaneously addressing the increasing demands on acute services across Europe by; enhancing patient outcomes and quality-of-life improvement; promoting of advances in cancer care; reducing social and economic barriers in cancer care; accelerating interoperability and collaboration across Europe and enhancing the economic stimulation of the National Health markets. eSMART clinical trial (https://clinicaltrials.gov/ct2/show/NCT02356081). In recruitment status.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 69
4.3 UNIVERSITY OF WARWICK (WARWICK)
4.3.1 DESCRIPTION OF THE LEGAL ENTITY AND ITS MAIN TASKS
University of Warwick (WARWICK) is one of the UK's leading research led universities, ranking 7th overall in the UK in the last Research Assessment Exercise, where 87% of its research was classed a world leading or internationally excellent. Warwick is also a member of the Russell Group of universities, committed to maintaining the very best research, an outstanding teaching and learning experience and unrivalled links with business and the public sector for its 25,615 students.
Warwick Manufacturing Group (WMG) is an academic department at the University of Warwick, providing research, education and knowledge transfer in engineering, manufacturing and technology. Founded in 1980, WMG’s mission has been to improve the competitiveness of organisations around the world through the application of value adding innovation, new technologies and skills deployment, bringing academic rigour to industrial and organisational practice.
WMG currently consists of five dedicated buildings on the University of Warwick campus near Coventry and hosts the Institute of Digital Healthcare (IDH). IDH’s objective is to enhance the quality, safety, accessibility and productivity of healthcare by supporting the implementation of digital solutions for the public, patients and professionals, underpinned by rigorous, multi-disciplinary research, development and evaluation. IDH has a 35-strong team including software engineers and health informaticians. IDH brings strength in the areas of technological solutions of connectivity within and across domains, building databases and applications, and developing training for end-users. It has an established track record of both national grants and NHS commissioned work (e.g., Electronic Healthcare Record Systems Connectivity, Semantic Interoperability and Integration of Healthcare Data, Secondary Clinical Research Databases for coordination of Clinical Trials, National Functional Imaging Database for the Children’s Cancer and Leukaemia Group, etc.), as well as a strong participation on number of EU grants; including currently as co-ordinator of a the C3-Cloud Horizon 2020 research programme. C3-Cloud (A Federated Collaborative Care Cure Cloud Architecture for Addressing the Needs of Multi-morbidity and Managing Poly-pharmacy) is a four-year (May 2016 – April 2020), 5 million euro EU Horizon 2020 Research and Innovation Action, as part of the PHC-25-2015 (Advanced ICT systems and services for integrated care) call. C3-Cloud establishes an extensive ICT infrastructure, enabling a collaborative care and cure cloud, to achieve continuous coordination of patient-centred care activities by a multidisciplinary care team and patients/informal caregivers, for chronic conditions that present multi-morbidity needs (e.g., diabetes, cardiovascular disease, renal failure, depression, etc.). The Institute of Digital healthcare is also part of the UK’s Health Data Research Initiative, which is funded by the UK Medical Research Council, Engineering and Physical Sciences Research Council, Economic and Social Research Council, Department of Health and Social Care (England), Chief Scientist Office of the Scottish Government Health and Social Care Directorates, Health and Social Care Research and Development Division (Welsh Government), Public Health Agency (Northern Ireland), British Heart Foundation and Wellcome Trust. Professor Theodoros N. Arvanitis, who is the lead contact for ADLIFE, is currently the Associate Director for the HDR UK’s Midlands Site.
ROLE IN THE PROJECT
In this project, WARWICK intends to expand and enhance its role as a world leading and research active academic institution in digital health and healthcare technologies in health (as delivered by WMG and its Institute of Digital Healthcare)
In ADLIFE, WARWICK will participate by leading in WP3 Intelligent Tools to create and deliver Personalized Care Plans and strongly supporting WP4 Patient Empowerment Platform and Personalized Self-Management Support Mechanisms and WP7 empowerment of patient, caregivers and communities. WARWICK is also involved in all 10 workplaces of the project in supporting roles.
In addition, WARWICK will have an important role in WP4 and WP5 in close collaboration with the other ICT experts of the project EVERIS and SRDC and of course with all the ICT teams from the pilots. WARWICK will be also an active partner in communication, dissemination and exploitation activities.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 70
4.3.2 CV OF THE PERSONS
Professor Theodoros N. Arvanitis
Gender Male
Qualification Medical Radiologic Technologist, DPhil Biomedical Engineering, Chartered Engineer
Staff Category Head of Research at The Institute of Digital Healthcare
Short description of work experience, relevant to the proposal
Professor Theodoros Arvanitis is currently the Chair of Digital Healthcare Innovation and Head of Research at The Institute of Digital Healthcare, WMG, at University of Warwick. He is also an Affiliate Professor at Warwick Medical School and Honorary Professor at the Institute of Cancer and Genomic Sciences, University of Birmingham. He has been recently part of the newly MRC-Wellcome Trust funded €35 million Health Data Research UK Initiative, where he is the Associate Director of the Midlands Substantive Site of the UK-wide network. Within Warwick, he leads the Biomedical Informatics, Imaging and Healthcare Technologies Research Group. He received his RT (BSc) degree (medical radiological technology) in 1990, from TEI of Athens, Greece, and his DPhil (biomedical engineering) in 1997 from the University of Sussex, UK. Prior to joining the University of Warwick in 2013, he held various posts at the Universities of Sussex and Birmingham. He has recently held the post of co-Director of the West Midlands Academic Health Science Network (WM AHSN) Digital Theme (2014-2016). His research interests span the areas of biomedical engineering, neuroimaging and health informatics (clinical systems interoperability and clinical decision support systems), with a strong academic and industrial experience in software engineering for healthcare applications. As a Research Leader, he has developed a substantial digital health team that encompasses experience across multiple disciplines, which brings together a rich and long pedigree of knowledge, in interconnectivity, interoperability and deployment of innovative solutions. He has delivered solutions at multiple maturity levels (from lab-based innovation to product deployment), and has established collaboration with major actors in the healthcare industry, including trusts, healthcare IT and medical device companies, as well as patient forums and regulators. He is currently the co-ordinator of the €5 million C3-Cloud H2020 Project: A Federated Collaborative Care Cure Cloud Architecture for Addressing the Needs of Multi-morbidity and Managing Poly-pharmacy (PHC-25-2015: 689181), which is high relevant to the ADLIFE project. Professor Arvanitis has a substantial academic publication record (h-index= 33 with a total of 4303 citations @ scholar google on 22/4/2019, 1 Book; 5 Book Chapters; 2 Patent filings; 110 full papers in refereed journals; 48 abstracts in refereed journals; 260 publications in refereed conference proceedings, 90 publications/keynote talks at unrefereed conferences and events, 12 guest editorials in journals, 27 published research reports and newsletters), while he has received research funding from national (UK), European and international governmental funding agencies, charities and industry. He has been involved in UK (BSI) and EU (CEN) standardisation work. He is a Charted Engineer (CEng), Fellow of the Royal Society of Medicine (FRSM) and a member of various scientific and professional groups (IET, AMIA, NYAS, RCS, ISMRM). He is also the Joint Editor-in-Chief at the Digital Health, open access peer-reviewed, journal, published by Sage Publications, UK. Professor Theodoros N. Arvanitis has the appropriate interdisciplinary research skills (clinical science, biomedical and software engineering), together with a long-standing senior management and leadership experience, that confirm his suitability to lead the Warwick team in this research programme. In ADLIFE, he will be the lead investigator from WARWICK involved in WP1, WP2, WP3, WP4, WP5, WP7, WP9 and WP10
Prof. Sudhesh Kumar
Gender Male
Qualification PhD in Computer Science
Staff Category Director of the Institute for Digital Healthcare
Short description of work experience, relevant to the proposal
Professor Sudhesh Kumar is currently Dean & Professor of Medicine at Warwick Medical School, University of Warwick and Honorary Consultant Physician at the University Hospital of Coventry and Warwickshire, NHS Trust. He is also Director of the Institute for Digital Healthcare. His research seeks to unravel the molecular basis of human body fat distribution, the defects that cause diabetes and heart disease, and to discover new ways of targeting treatment. He has also run a number of clinical studies including investigating novel approaches to delivery of care for obesity and new ways of delivering diabetes care to the Indo-Asian population and investigating new ways of empowering patients, particularly with type-2 diabetes, to look after themselves. For example, he was a co-founder of Counterweight and UKADS studies (which together included over 10,000
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 71
patients) and also the ICCD study that investigated intermediate care for diabetes. He has risen over £30m in grants over his career for various projects. He has published over 230 full papers, over 700 published abstracts relating to obesity and diabetes and edited 6 books.
Dr Sarah Lim Choi Keung
Gender Female
Qualification PhD in Computer Science
Staff Category Research Fellow in Health Informatics at the Institute of Digital Healthcare
Short description of work experience, relevant to the proposal
Dr Sarah Lim Choi Keung is a Senior Research Fellow in Health Informatics at the Institute of Digital Healthcare, University of Warwick. She works on several national and European research projects in the area of health informatics, particularly looking into semantic interoperability challenges in the health domain, the participatory requirements gathering process for stakeholders in clinical information systems, and the standardisation in health informatics. Sarah has experience of assessing technological solutions and considering requirements and needs of a range of stakeholders, in clinical, research and the public. Sarah is a co-investigator and researcher, with project management roles in several research projects. In the EU Horizon 2020 C3-Cloud project, Sarah is the scientific project manager working on the coordinating team and is, also, on the project Ethics Committee that oversees ethical and information governance issues. In ADLIFE, she will be involved in WP2, WP3, WP4, and WP8.
Dr George Despotou
Gender Male
Qualification PhD
Staff Category Assistant Professor at IDH
Short description of work experience, relevant to the proposal
is a Senior Research Fellow in Health Informatics at the Institute of Digital Healthcare, University of Warwick. She works on several national and European research projects in the area of health informatics, particularly looking into semantic interoperability challenges in the health domain, the participatory requirements gathering process for stakeholders in clinical information systems, and the standardisation in health informatics. Sarah has experience of assessing technological solutions and considering requirements and needs of a range of stakeholders, in clinical, research and the public. Sarah is a co-investigator and researcher, with project management roles in several research projects. In the EU Horizon 2020 C3-Cloud project, Sarah is the scientific project manager working on the coordinating team and is, also, on the project Ethics Committee that oversees ethical and information governance issues. In ADLIFE, she will be involved in WP2, WP3, WP4, and WP8.
Dr Tim Robbins
Gender Male
Qualification Doctor of Medicine
Staff Category Assistant Professor at Institute of Digital Health
Short description of work experience, relevant to the proposal
Dr Tim Robbins graduated from Brasenose College, Oxford in 2009 with a 1st Class Honours Degree in Medical Sciences, and subsequently in 2012 with the degree Bachelor of Medicine and Bachelor of Surgery. He now works as a National Institute of Health Research (NIHR) Academic Clinical Fellow in Endocrinology and Digital Health at Warwick University and South Warwickshire NHS Foundation Trust. He holds publications on the molecular basis of ageing, dignity in old age, communication between primary and secondary care, and the inpatient admissions process. He has won national awards in digital leadership, patient safety, change management, and education across care settings. In ADLIFE, he will be involved in WP5, WP6 and WP9
Dr Helen Muir
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 72
Gender Female
Qualification PhD in Engineering
Staff Category Management and RTD
Short description of work experience, relevant to the proposal
Dr Helen Muir has 12 years’ experience managing projects and is a Prince2 qualified practitioner. She has managed projects with values up to €11million and 28 project partners. She has extensive experience of working charities including Age UK, Teenage Cancer Trust, and The Nuffield Foundation, the NHS (NIHR, HIECs, Trusts, Deaneries), as well as other governmental and industry organisations. She is highly experienced in managing projects relating to digital health and cyber security, and has led projects, which have taken products and services from development through to operation. Dr Muir has led on the management of multi-million pound portfolios at university-wide and departmental level, leading teams of up to 22 project managers. She has particular expertise in maximising project outputs in terms of quality and impact, and has designed and implemented successful project, departmental, and university-level processes to achieve this. Dr Muir has won contracts to deliver project management training internationally and to undertake evaluations of European Commission funded projects. Dr Muir is involved in C3-Cloud Project, supporting the co-ordinator (Prof T. N. Arvanitis). She will be instrumental in the exploitation and project management elements of ADLIFE (WP1 and WP10).
4.3.3 LIST OF RELEVANT PUBLICATIONS
T. D. Robbins, S.N. Lim Choi Keung, S. Sankar, H. Randeva, and T.N. Arvanitis, Risk factors for readmission of inpatients with Diabetes: A systematic review, Journal of Diabetes and its Lead Applicant Information - Recent Relevant Publications Complications, 2019 (in press/online).
G. Laleci Erturkmen, M. Yuksel, B. Sarigul, P. Lindman, R. Chen, L. Zhao, J. Bouaud, M. Lilja, E. de Manuel, D. Verdoy, A. de Blas, C. Marguerie, G. Klein, S. N. Lim Choi Keung and T. N. Arvanitis, Management of Personalised Guideline-driven Care Plans Addressing the Needs of Multi-Morbidity via Clinical Decision Support Services, International Journal of Integrated Care, 18(S2: A132/1-8, 2018.
de Blas, N. González, M. Ogueta, D. Verdoy, M. Lilja, M. Holm Sherman, C. Marguerie, D. Roberts, M. Beach, M. Yuksel, G. Laleci Erturkmen, T. N. Arvanitis, Organizational and Care Model Analysis for C3-Cloud Deployment Preparation, International Journal of Integrated Care, 18(S2):A335/1-8, 2018
T. Robbins, S. N Lim Choi Keung, S. Sankar, H. Randeva, and T. N Arvanitis, Diabetes and the Direct Secondary Use of Electronic Health Records: Using Routinely Collected and Stored Data to Drive Research and Understanding, Digital Health, 4: 1-10, Article ID 2055207618804650, 2018.
E. Bilici, G. Despotou, and T.N. Arvanitis, The Use of Computer-Interpretable Clinical Guidelines to Manage Care Complexities of Patients with Multimorbid Conditions: A review, Digital Health, 4: 1-21, Article ID 2055207618804927, 2018.
4.3.4 LIST OF RELEVANT PREVIOUS PROJECTS
HDR UK (MRC HDR-3001) – Health Data Research UK Midlands Substantive Site, a programme that develops new health data science tools for managing complexity in chronic and multi-morbid diseases, modern e-trials systems and epidemiological research methodologies, among other data science in medicine innovations.
C3-Cloud (H2020-PHC-25-2015-689181) - A Federated Collaborative Care Cure Cloud Architecture for Addressing the Needs of Multi-morbidity and Managing Poly-pharmacy, a project that develops ICT and Clinical Decision Support tools for care pathway management and patient-centred self-management approached of multi-morbid chronic diseases.
I-CARE P (NIHR- PB-PG-0214-33092) - Integrated Care in Prostate Cancer, a project that develops digital patient-centric tools for the online holistic needs assessment and for supporting the link of the patient and the health care team
TRANSFoRm (FP7-ICT-247787) - Translational Research and Patient Safety in Europe, a project that developped the technology that facilitates a learning healthcare system in terms of syntactic and sematic interoperability.
eCRN (NIH-BAA-RM-04-23) - The electronic Primary Care Research Network (ePCRN) was an NIH funded roadmap project providing a sophisticated electronic infrastructure to facilitate translational research in primary care in the US. The project has developed tools facilitating syntactic and semantic interoperability between federated databases of clinical information and EHRs.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 73
CURe: A Framework and Web Application System for Secondary Care Research in the West Midlands, bridging the needs of research and care delivery, including palliative care. The framework is currently used as part of clinical research and care for children with brain tumours (funded by the Childhood Cancer and Leukaemia Group) and the UK National Centre for Miscarriage Research and Care (funded by the Tommy’s Charity).
4.3.5 DESCRIPTION OF ANY SIGNIFICANT INFRASTRUCTURE 4.3.5.1 INFRASTRUCTURE AND PLATFORMS
The Institute of Digital Healthcare, as an Institute of WMG at the University of Warwick, has access to advance GCP-compliant data centre and computational facilities, appropriate for health informatics related research. In addition, IDH hosts an integrated vocabulary services system, based on LexEVS technology. IDH will provide access to the ICT tools of person-centred integrated care of the C3-Cloud project, relevant to the ADLIFE project. These include infrastructure middleware for syntactic and semantic interoperability, clinical decision support modules, care pathway planning and implementation modules, etc.
4.3.5.2 NETWORKS – COLLABORATIONS:
WARWICK, through the Institute of Digital healthcare is an active partner of the NHS-funded West Midlands Academic Health Sciences Network (WM AHSN) in the UK. IDH is also part of the newly funded €35million Health Data Research UK Initiative, where Professor Arvanitis is the Associate Director of the Midlands Substantive Site for the UK-wide network. IDH researchers are involved in UK (BSI) and EU (CEN) standardisation work in the fields of biomedical informatics and imaging.
4.3.5.3 DISSEMINATION CAPABILITY:
WARWICK, being an academic institution, has a world-leading track record and experience in scientific/academic publications. The bulk work of its dissemination efforts will be mostly on scientific publications in academic journals (e.g., JAMIA, International Journal of Integrated Care, BMC Medical Informatics and Decision Making, BMJ, Digital Health, etc.), while the group will publish and present at national/international conferences and exhibitions, addressing both scientific and socio-technical aspects of the project. WARWICK will also be involved in the project’s website and social media delivery. Through IDH’s links to the UK’s regional and national NHS Academic Health Science Networks, the WARWICK group will disseminate open source knowledge, promoting adoption and clinical translation of the work, while it will get involved in local and national Public/Patient Partnership events. Prof. Theodoros N. Arvanitis, being the Joint Editor-in-Chief of the newly published academic journal Digital Health (by SAGE Publishers), will use his editorial capacity to disseminate further the academic, clinical and public results of the ADLIFE project.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 74
4.4 ODENSE UNIVERSITY HOSPITAL (OUH)
4.4.1 DESCRIPTION OF THE LEGAL ENTITY AND ITS MAIN TASKS
Odense University Hospital (OUH) operates four academic and community hospitals located in the eastern part of the Region of Southern Denmark, including Svendborg Sygehus which has the largest medical department in Denmark.
A 1,000+ bed medical centre, OUH annually has more than 100,000 inpatient admissions and handles in excess of 1.1 million outpatient visits in 50 different clinical departments. The hospital has a budget of €870 million and employs more than 8,700 people. In Denmark, 16 specialised care pathways are offered only at OUH, and the hospital serves patients from across Denmark, as well as from abroad. The hospital has an organisation-wide, distinct patient-centred culture where the patients’ and their relatives’ benefit and experience are of the highest importance. At all times, this core value is reflected in every aspect of the work done at OUH by every member of staff.
OUH is highly experienced and adept at cross border and international collaboration, often as lead coordinator on international high-profile projects. OUH is an international model in clinical innovation and telemedicine and has recently been awarded HIMSS Stage 6 recognition. OUH started to implement Electronic Health Records (EHR) 1999, making the hospital an early adopter in terms of electronic medical systems. Today, Denmark’s largest EHR installation is located in Odense where it has fully replaced traditional medical records. In addition, Southern Denmark is one of the references sites that have obtained the highest qualification by the EIP-AHA.
The new Odense University Hospital (New OUH) is expected to open in 2023 and will replace the current OUH. Every aspect of the new €1.06 billion hospital is designed with the future of health care in mind, incorporating a myriad of major and minor innovative technologies and workflows. Contiguous to the new Faculty of Health at the University of Southern Denmark (SDU), New OUH will be an epicentre of practical health care innovation, bridging the gap between research and clinical treatment. While the new hospital will be slightly smaller than the current OUH, all 849 beds will be in private wards, designed to accommodate the needs of patients and their relatives, who will become more independent and less reliable on the physical environment for their treatment. The new hospital is expected to run at full scale within a year from its initial opening. To accommodate this, OUH is currently going through a process of scaling the organisation and all technological processes to match the new environments currently being built just over a mile away. The new hospital will have easy access to regional infrastructure, including two stops on the currently-in-construction, city-wide tram system.
Innovation activities at Odense University Hospital are organised in CIMT (Centre for Innovative Medical Technology) (www.cimt.dk) by a highly skilled and experienced team of scientists, project managers, health IT researchers, and other experts. CIMT is a joint research and innovation centre for Odense University Hospital and University of Southern Denmark. The close cooperation between the hospital and the university is a unique partnership that adds a new dimension for health solutions by bridging research and science with practical implementation and technological development. All activities at CIMT have a practical aim with a short distance from idea to operations. CIMT works in close collaboration with other regional agencies in the field of health innovation and integrated care. Much of the work done at CIMT is intended for the in-construction New OUH, set to open in a few years.
ROLE IN THE PROJECT
OUH will lead WP7, which deals with the empowerment of patients, caregivers and communities through the identification and analysis of empowerment opportunities and the needs towards these. Expected tasks for the project includes designing strategies for patients’ and families’ self-perception of their situation and the physical and mental implications thereof; the co-designing of integrative care pathways that take into account the measures surrounding the treatment and perspectives of everyone involved; the definition of interventions for improved empowerment and proactive attitudes among patients and caregivers; and the preparation of the implementation of the intervention, particularly in regard to barriers and entries.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 75
They will also be in charge of:
Empowerment of patients, caregivers and communities (WP7); Pilot Danish trial where OUH-Svendborg Hospital and 10 local municipalities will participate in the project,
including the formal/informal carers and the social services, To design strategies to provide support of patients and families for their ewmpowerment; Co-Design integrated care pathways including the patient and its stakeholders; Prepare the implementation of the intervention with special emphasis on potential barriers/facilitators.
4.4.2 CV OF THE PERSONS
Claus Duedal Pedersen
Gender Male
Qualification Economist
Staff Category CIO of the Centre for Innovative Medical Technology at Odense University Hospital (OHU)
Short description of work experience, relevant to the proposal
Claus Duedal Pedersen (Male) graduated from University of Southern Denmark with a master degree in Economics in 1995. He is currently Chief Innovation Officer of the Centre for Innovative Medical Technology at OUH Odense University Hospital. In the hospital, he is in charge of CIMT (Centre for Innovative Medical Technology) a joint research centre between OUH and the University of Southern Denmark. In this position Claus Duedal Pedersen is in charge of development, testing and implementation of telemedicine and eHealth solutions in a wide range of areas within the hospital. These have primarily focused on improving the cooperation between the hospital, the primary care sector and the patients. Examples of solutions deployed are home-hospitalisation of COPD patients and a videoconference based language interpretation. Many of the solutions have been developed in EU projects and have been evaluated at large scale and in RCTs as part of the EU project Renewing Health. Claus was project manager of the Methotelemed project that developed the MAST evaluation model for telemedicine solutions. Claus is currently coordinator of the ImpleMentAll project.
Anne Dichmann Sorknæs
Gender Female
Qualification PhD
Staff Category Assistant professor at the Acute Medical Department and the Medical Department at OUH
Short description of work experience, relevant to the proposal
Anne Dichmann Sorknæs (Female) is a senior nurse, RN, MSc in Nursing, Ph.D. Anne is currently an assistant professor at the Acute Medical Department and the Medical Department, Odense University Hospital-Svendborg Hospital and at the University of Southern Denmark. The main focus of her research is eHealth and Family Nursing. Anne has been working a registered nurse at medical departments since 1980, and is an advanced nurse specialist in respiratory and pulmonary diseases. Anne’s Ph.D. focused on the effects of real-time telemedical video consultations between caregivers and patients with COPD (chronic obstructive pulmonary disease). Anne has been working in many national and international projects with focus e.g. on telemedicine, patient decision support, respiratory and severe chronic diseases, including the Renewing Health project.
4.4.3 LIST OF RELEVANT PUBLICATIONS
Sorknæs AD, Hounsgaard L, Olesen F, Jest P, Bech M, Østergaard B. (2015). Nurses’ and patients’ experiences of teleconsultations. Supplement to the International Journal of Integrated Care
Lange P, Tøttenborg SS, Sorknæs AD, Andersen JS, Søgaard M, Nielsen KA. (2015). Danish Register of Chronic Obstructive Pulmonary Disease. Journal of Clinical Epidemiology
Konradsen H, Dieperink KB, Lauridsen J, Perboell P, Sorknæs AD, Østergaard B (2015). Danish translation and validation of ICE-EFFQ: a questionnaire to assess the functioning of families. The Scandinavian Journal of Caring Sciences (Submitted)
Sorknæs AD, Bech M, Madsen H, Titlestad I, Hounsgaard L, Hansen-Nord M, Jest P, Olesen F, Lauridsen J, Østergaard B. (2013). The effects of real-time telemedicine consultations between hospital-based nurses and
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 76
patients with severe COPD discharged after exacerbation admissions. Journal of Telemedicine and Telecare, Dec;19(8):466-74. Epub 2013 Nov 13
Brandt, C.J.; Ellegaard, H.; Joensen, M.; Kallan, F.V.; Sorknæs, A.D.; Tougaard, L. (1997): Effect of diagnosis of smoker´s lung. The Lancet ( vol. 349, January 25, s. 253)
Tougaard, L.; Krone, T.; Sorknæs, A.; Ellegaard, H. and the PASTMA group ( 1992): Economic benefits of teaching patients with chronic Obstuctive pulmonary disease about their illness. The Lancet (vol. 339, June 20, s. 1517-1520)
4.4.4 LIST OF RELEVANT PREVIOUS PROJECTS
ImpleMentAll, (Project ID: 733025_Towards evidence-based tailored implementation strategies for eHealth) (SC1-PM-21-2016) January 2017 to March 2021 - €6m www.implementall.eu). ImpleMentAll will develop, apply, and evaluate tailored implementation strategies in the context of on-going eHealth implementation initiatives in the EU and beyond. Common mental health disorders account for an alarming proportion of the global burden of disease. Being regarded as an evidence-based psychotherapeutic eHealth intervention, Internet-based Cognitive Behavioural Therapy (iCBT), has the potential to answer to this societal challenge by providing an efficacious and efficient treatment from which more people can benefit. As a result, various iCBT implementation projects are currently conducted across the world. We propose to use this natural laboratory to develop and evaluate a toolkit for tailored implementation strategies that is expected to make implementation trajectories more efficient. The objectives for ImpleMentAll are:
o To develop a generic Integrated Theory-based Framework for Intervention Tailoring Strategies (the ItFits-toolkit) for data-driven tailored implementation of evidence-based eHealth services.
o To demonstrate the impact of the ItFits toolkit on the implementation of eHealth for common mental disorders, in 9 European countries, 2 LMIC, and Australia.
o To disseminate the validated toolkit in various healthcare contexts across Europe. ImpleMentAll is a true multidisciplinary international collaboration that unites key experts in clinical practice, health innovation, clinical research, and implementation science. Combined with it’s unique setup, ImpleMentAll will be able to test if tailoring implementation strategies lead to more efficient implementation. The resulting ItFits-toolkit will enable data driven evaluation of eHealth implementation projects in terms key performance indicators for process, effectiveness, and efficiency outcomes. Its methods, materials, and strategies will provide concrete guidance on tuning implementation interventions to local determinant of practice across a variety of health care systems.
MasterMind (Project ID: 621000_Management of mental health disorders through advanced technology and services-Telehealth for the Mind) (CIP-ICT-PSP-2013-7 - March 2014-February 2017 - €7m (plus €7m co-financing)) – www.mastermind-project.eu). The MasterMind Consortium to avoid dispersing efforts has narrowed the scope of the services to just one, non-organic, mental disorder: depression. This because of its high incidence, social cost and proven clinical effectiveness of ICT in its treatment. MasterMind intends to implement at scale: 1) evidence based computerised Cognitive Behavioural Therapy (cCBT) services for depressed adults (more than 5.000 patient overall) . 2) Video conference for Collaborative Care and treatment of depression (ccVC). Both services will be deployed across 10 EU and Associated Countries and from this implementation, the project will: identify the barriers and success factors to implement cCBT and ccVC on a large scale in different political, social, economic and technical health care contexts and from the perspective of different stakeholders such as patients, professionals and health insurances; recommend successful strategies for implementing cCBT and ccVC in these different contexts/settings. Using the lessons learnt, the Consortium will develop guidelines and a toolkit for promoting and facilitating the broader implementation across Europe of a safe, effective and efficient service which I supported by relevant stakeholders. The project will support the roll-out of cCBT in other (committed) regions of the EU. By involving regions and healthcare providers outside of the Consortium, the knowledge and experiences from the project will be transferred and re-used in their implementation of the services. This will extend the outreach of the deployment to more citizens in Europe. The outcome of the service will be evaluated using a widespread HTA-based rigorous multi-dimensional evaluation methodology, MAST, already in use in other Pilots A. The Consortium provides a balanced mix between pioneer and early followers and between Northern and Southern, Eastern and Western Europe
SmartCare – (Project ID: 325158_Joining up ICT and service processes for quality integrated care in Europe) (CIP-ICT-PSP-2012-6 – March 2013-August 2016 – www.pilotsmartcare.eu). Against the background of the European
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 77
Innovation Partnership on Active & Healthy Ageing, SmartCare aims to define a common set of standard functional specifications for an open ICT platform enabling the delivery of integrated care to older European citizens. A total of 24 regions and their key stakeholders will define a comprehensive set of integration building blocks around the challenges of data-sharing, coordination and communication. Ten regions will then pilot integrated health & social services to combat a range of threats to independent living commonly faced by older people while the other will prepare for early adoption. In a rigorous evaluation approach, the pilot will produce and document much needed evidence on the impact of integrated care, developing a common framework suitable for other regions in Europe. Guidelines and specifications for procuring, organising and implementing the service building blocks will be produced. The organisational and legal ramifications of integrated care will be analysed to support long term sustainability and upscaling of the services. SmartCare services will provide full support to cooperative delivery of care, integrated with self-care and across organisational silos, including essential coordination tools such as shared data access, care pathway design and execution as well as real time communication support to care teams and multi-organisation access to home platforms. The services build on advanced ICT already deployed in the pilot regions including high penetrations of telecare and telemonitoring home platforms. System integration will be based, whenever possible, on open standards and multivendor interoperability will be strongly encouraged. The common services will allow efficient cooperative care delivery and empower all older people according to their mental faculties to take part in effective management of their health, wellness, and chronic conditions and maintain their independence despite increasing frailty.
Renewing Health (Project ID: 250487_ Regions of Europe working together for health) (CIP-ICT-PSP-2009-3 – February 2010-December 2013 - €7m – www.renewinghealth.eu ) Renewing Health (REgioNs of Europea WorkINg together for HEALTH) aims at implementing, validating and evaluating innovative telemedicine solutions within the management of chronic diseases. The project brings together a consortium of nine European regions, where service solutions are operational for tele-monitoring and treatment of patients suffering from diabetes, chronic obstructive pulmonary and/or cardiovascular diseases. The services give patients a central role in the management of their own diseases: in fine-tuning the choice and dosage of medications, in following and adhering to their treatment, and in helping healthcare professionals to detect early signs of worsening.
Carewell (Project ID: 620983_Multi-level integration for patients with complex needs) (CIP-ICT-PSP-2013-7 - December 2013-February 2017 - €3m- www.carewell-project.eu ) CareWell will enable the delivery of integrated healthcare to frail elderly patients in a pilot setting through comprehensive multidisciplinary integrated care programmes where the role of ICTs can foster the coordination and patient centered delivery care. Carewell will focus in particular complex, multi-morbid elderly patients, who the patients most in need of health and social care resources (35% the total cost of Health Care System) and more complex interventions due to their frailty and comorbidities (health and social care coordination, monitoring, self-management of the patient and informal care giver). ICT platforms and communication channels that allow sharing information between healthcare and social care professionals involved in the delivery care of these patients, facilitating their coordination, increasing their resoluteness and avoiding duplicities when tackling patients´ diagnostic, therapeutic, rehabilitation or monitoring needs. Additionally, ICT-based platforms can improve the adherence to treatment, enhance self-care and increase patient awareness about their health status , as well as, improve the empowerment of informal caregivers, who usually take care of these patients. According to this, the benefit of integrated care programmes based on (1) integrated care coordination and (2) patient empowerment & home support pathways supported by ICT is greater and essential for these patients. Care pathways will cut across organisational boundaries and will activate the most appropriate resources across the entire spectrum of healthcare and social care services available for both scheduled and emergency care. CareWell aims to scale up the services in pioneer regions and share their approach, learning from and supporting the other pilot sites which are at different levels of maturity in respect to designing, developing and implementing new ways of providing integrated care services.
4.4.5 DESCRIPTION OF ANY SIGNIFICANT INFRASTRUCTURE
The Region of Southern Denmark (RSD) infrastructure comprises the Danish Health Data Network, electronic health
and care records, and the national online health portal (Sundhed.dk). The healthcare IT infrastructure is supported
by several organizations and strategies on national, regional, and municipal level. To ensure the further
development of the already well-established healthcare IT infrastructure, the region invests considerably in eHealth
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 78
related projects; regional, national, and international. The aim is to improve the quality of life for citizens with
health problems and allow for more flexible and efficient health care services in urban as well as rural areas. Also,
RSD works towards a higher degree of interoperability of health information systems and of electronic health
records.
In 2012 RSD deployed its first integrated care internet portal, the Shared Care Portal, for heart failure care. The
solution is generic and deployment is to be extended to care for other somatic diseases. The portal’s generic nature
allows it to also be extended to include mental disorders. Two existing services will be trialled as part of the project:
computerised cognitive behaviour therapy (cCBT) for depression and a collaborative care model with built-in video
conferencing for depression. The cCBT service consists of a treatment program accessible for the patient via a
website containing information and a preliminary test for depression. The patient can access the program without
referral from a GP. On the basis of the test, the patient is offered a video-based interview to determine whether
internet-based treatment is relevant. If this is the case, the patient gets access to a personalised treatment site and
goes through nine text and video-based modules. During the course of treatment, the patient receives written
support by affiliated healthcare professionals. The patient can access the treatment independently of time and
place, which increases flexibility of the treatment as well as opens up for opportunities within (cost) effectiveness
and empowerment. A follow-up depression test is carried out after three months. The cCBT program does not focus
on supplementary treatment, e.g. for anxiety or insomnia.
The second service consists of a collaborative care model with built-in video conferencing for depression patients.
The primary outcome is depression measured using Hamilton Depression Scale (Ham-D6)1. The intervention
consists of an intensified cooperation model between GPs and Mental Health Services in Esbjerg allocating care
managers (CM) for GPs and the use of video conferencing. The GP determines which services respectively the GP
and CM are to provide for the individual patient. Services include observation by the GP, medical treatment with
the GP, short-term therapy by the CM, supportive treatment with symptom assessment by the CM, and
psychoeducation conducted by the CM. A cluster randomised multicentre trial with cross-over design will be
conducted in which clusters are established on the basis of GP provider numbers. The study is conducted in five
Danish municipalities. This trial can contribute with new knowledge about more optimal utilisation of resources by
including video conferencing in the treatment of patients with depression.
My Patient Journey is a locally designed and developed app that helps the patients achieve information according
to their treatment course, record clinical parameters measured at home (such as blood pressure and weight) which
are instantly available to health care professionals in the patients’ electronic health journals. The tool (app) is used
to improve patient involvement.
IT tools that will be used in the project:
The electronic patient journal system at OUH is based on Cambio COSMIC, which is a comprehensive healthcare information system for all types of healthcare. It is a system that provides cohesive and patient-focused operational support, while ensuring that important patient information is readily available. Cambio COSMIC is built on a modern and powerful platform with a wide range of associated subsystems to support all types of healthcare. All layers in the system architecture are clearly separated and Cambio COSMIC can be scaled out on all layers to support very large installations with thousands of simultaneous users. Cambio COSMIC is very robust and has extremely high availability. MS SQL Server is used exclusively for the database and JBoss is used for the application layer. (http://www.cambiohealthcare.co.uk/).
My Patient Journey, which is an app developed by MedWare for Odense University Hospital. The app facilitates easy and efficient collection of PROMs. The app also helps patients find and keep track of information from the hospital and gives them a better overview and experience in communicating with the hospital. Since the app was created in 2014, it has become a personal access point for patients involved in a number of specific treatment processes as well as for patients with chronic conditions. Today, more than 26,000 patients use the app as a support tool in their communication with the hospital. The app helps patients become more active in their treatment and pro-active in their communication, and many say they feel more involved and have more options for being an active part in the dialogue around their condition and treatment process. (http://www.medware.dk/en/project/my-patient-journey/).
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 79
Involved patients will need to bring their own compatible ICT device for use with the hospital’s systems and digital services, for example for video conference purposes.
4.4.5.1 NETWORKS – COLLABORATIONS – DISSEMINATION CAPABILITY Odense University Hospital, through the Region of Southern Denmark and its other supporting partners, is a four-star reference state for active and healthy ageing. The coalition coverage and partners supporting the application and reference site consist of the quadruple helix: Academia (University of Southern Denmark – Institute of Sports Science and Clinical Biomechanics, University College Lillebaelt, University College Syd, CIMT – Centre for Innovative Medicine and Technology), Industry & Clusters (Welfare Tech, Healthcare Denmark, Enterprise Europe Network, MedCom), Healtcare Providers (all hospitals and GPs in the region), Citizens. The reference site is also supported through European Connected Health Alliance and participation in the Reference Sites Collaborative Network.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 80
4.5 A.FALKIEWICZ SPECIALIST HOSPITAL IN WROCLAW (FALK-HOSP)
4.5.1 DESCRIPTION OF THE LEGAL ENTITY AND ITS MAIN TASKS
The A. Falkiewicz Specialist Hospital is a leading centre in Lower Silesia in the field of care for the elderly. It has a geriatrics and internal diseases warp and has implemented the pilot of CareWell project in Lower Silesia. The Hospital is a Provider of healthcare services/facilities and professionals for the implementation of the Polish pilot site of the CareWell Project. It has been creating the Geriatric Competence Centre. This is why the Hospital is participating in one more project undertaken by the Lower Silesian Voivodeship Marshal Office – TITTAN (Interreg Europe). It will also take part in the eCare project (H2020 PCP), it is also participating in a project for youth - UPRIGHT (H2020).
The A. Falkiewicz Specialist Hospital, within his geriatrics and internal diseases warp activity, has experience and competences in the area of supportive care and chronic diseases as well as in telemonitoring of life parameters.
The Hospital is ready to integrate its HIS system and telemonitoring system as well as the Project’s platform.
ROLE IN THE PROJECT
The main role of FALK-HOSPITAL will be leading the ADLIFE pilot in Poland, that will also imply a close work with all the groups but specially with WARWICK, SDRC and EVERIS for solving the interoperability issues regarding the implementation of ADLIFE toolbox in the hospital and in the region. Although the region is an active partner in tele health and remote monitoring in the patients, the hospital has not been involved in the previous project C3-CLOUD, but has worked with other members of the consortium in piloting and deploying digital health solutions. In addition, FALK will have a key role in dissemination and communication activities, as its integration and direct contact with the region of Lower Silesia, where new policies for ageing population are being generated.
4.5.2 CV OF THE PERSONS
Janusz Wrobel
Gender Male
Qualification Doctor in Medicine
Staff Category Director of A. Falkiewicz Specialist Hospital
Short description of work experience, relevant to the proposal
Graduated from medical and postgraduate studies at the Medical University in Wroclaw. Professional experience gained working in the Railway District Hospital in Wrocław, Lower Silesia Health Department Marshal's Office and the Lower Silesian branch of the National Health Fund.
Antoni Zwiefka
Gender Male
Qualification PhD in Engineering
Staff Category Representative of Hospital Director for innovation and outer funds
Short description of work experience, relevant to the proposal
Representative of Hospital Director for innovation and outer funds. Graduated from Wroclaw University of Technology, employed by LSV Marshal Office in Health Department and A. Falkiewicz Specialist Hospital. He is used to applying Internet technologies for many subjects concerning health and elderly people care. As a former network administrator he has been involved in new information technologies implemented within European projects for healthcare funded under the Programmes: 6FP (RIGHT Project), LLL (4Leaf Clover Project) and CE (InTraMed C2C Project) ICT PSP (CareWell Project). The RIGHT Project was undertook by Lowe-Silesian Voivodeship to help Health Care Professionals in diagnosis and treatment and helped him to gain a remarkable knowledge and understanding of the different new technologies used in healthcare systems in the EU. What is more, he was also the author of numerous articles and presentations in the field of e-Health and Tele-Health. He
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 81
is involved in the implementation of new technologies in the medical sector. On daily basis, he is implementing the idea of innovation transfer by developing and acquiring ideas given by medical workers. This is due to the scientific passion for knowledge change management in innovation transfer.
4.5.3 LIST OF RELEVANT PUBLICATIONS
Mateo M. *, Fullaondo A., Merino M., Gris S., Marchet F., Avolio F., Graps E., Ravic M., Kovac M., Zwiefka A., Davies D. , Mancin S., Forestiero A. , Stafylas P., Hurtado M., d´Angelantonio M., Daugbjerg S., Pedersen C. D., Hammerschmidt R., Stroetmann V., Azkargorta L., Giné A., Verdoy D. , Soto M., Mora J., Mar J., Vergara I. and de Manuel Keenoy E. (in Preparation), Impact assesmentof an innovative integrated care model for complex patients with multimorbidity: the CareWell Project
Piotrowicz J., Soll A., Kielar U, Zwiefka A., Guligowska A., Pigłowska M, Kostka T., Kurpas D. , ICT and environmental support for patients with frailty syndrome: CareWell Project, Focus Project and SUNFRAIL Project. MSP (2017); 11, 1: 37–43.
Zwiefka A., (2013) Bariery wdrażania innowacji telemedycznych, Transgraniczna wymiana danych medycznych Dolnego Śląska i Saksonii, Schwarz A, Zwiefka A (Ed), ISBN 978-83-62276-10-3
Zwiefka A., Nycz M., Management of Knowledge Acquisition from Human Sources in Innovation Transfer In book: New Research on Knowledge Management Technology, InTech 2012
Zwiefka A., Frączkowski K., New trends in Diagnosis Support and role of Nurses based on RIGHT-like systems. Telenursing, Elsevier 2010
Zwiefka A., Wodoklis-Kaczyńska E., Frączkowski K., Redukcja ryzyka w diagnozie i leczeniu w oparciu o system RIGHT, 2008, Family Medicine and Primary Care Review, 10 (3), 1186-1190
4.5.4 LIST OF RELEVANT PREVIOUS PROJECTS
InTraMed C2C Project – Innovtion transfer in medical sector from Clinics to Companies– Interreg CE; CareWell Project - Multil-level Integration for Patients with Complex Needs (ICT PSP, 2014-2017) .The purpose
of the Project was measuring the impact of ICT-enabled integrated care with a multidimensional evaluation methodology. The project has recently undergone its Final Annual Review and has been rated "Excellent";
TITTAN Project - Network for Technology, Innovation and Translation in Ageing (Interreg Europe 2016 – 2020).
4.5.5 DESCRIPTION OF ANY SIGNIFICANT INFRASTRUCTURE
Falkiewicz Hospital is responsible for the telemonitoring system and devices. It is currently scaling up this system
for additional 1000 patients. It is part of the Geriatric Competence Centre.
4.5.5.1 NETWORKS – COLLABORATIONS:
The FALK-HOSPITAL, as a LSV Marshal Office healthcare unit, has strong cooperation with several gminas in the region (including Wroclaw municipality) which are responsible for social services. As well as it is also collaborating with other Marshal Office healthcare units. It is also participating in Network for Technology, Innovation and transfer in Ageing process- TITTAN project
4.5.5.2 DISSEMINATION CAPABILITY:
FALK-HOSPITAL has the possibility of dissemination by presenting the project's achievements in the form of scientific articles in national and foreign journals and conferences (Europe and the whole World). The hospital also participates in all activities of the Health Department of the LSV Marshal's Office - among others in the realization of the REGIONS4PERMED project - a conference on the personalization of me-Health will be organized in Lower Silesia. In addition, the ADLIFE project will be presented at seminars, workshops and exhibitions on both the scientific and socio-technical aspects of the project. It will be involved also in the project's website and providing information for social media.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 82
4.6 OPTIMEDIS AG
4.6.1 DESCRIPTION OF THE LEGAL ENTITY AND ITS MAIN TASKS
The OptiMedis AG is a management and health data analytics company registered in Germany. Its core business is to develop and manage regional integrated care delivery systems together with physician networks and other providers. OptiMedis analyses data from physician practices and health insurance funds in order to identify opportunities for quality and efficiency improvement. It also conducts regular population surveys to assess patients´ experience with care, levels of patient activation and health-related quality of life.
Together with regional medical networks, OptiMedis AG is building an integrated healthcare structure in which doctors, therapists, hospitals, pharmacies and many other partners work in association and overcome past constraints. They coordinate treatment and can access all important information at a glance through the electronic network. Insured patients will be actively involved and motivated for early disease prevention and participation in health and care programs. Clubs, schools, businesses and local authorities in the region will also be involved. In other words, the focus is on the whole person and its environment.
The work of OptiMedis is underpinned by a population-health contract financially rewarding long-term improvements to population health. OptiMedis´ approach to transforming health care systems has frequently been recognised by the EU, multiple EU research projects, the Commonwealth Fund, Duke Margolis Centre for Health Policy, WHO, the World Bank and others.
OptiMedis manages three Integrated Care Delivery Systems in Germany with a population of over 120,000 and involving over 150 health care providers. Its 30 staff members at OptiMedis Headquarters support the work of OptiMedis as a research and performance management institute to these regional delivery systems. OptiMedis is very well linked to health insurances, ministries, medical associations and public services. OptiMedis has formal joint ventures in the UK, the Netherlands and Belgium and currently collaborates with health care authorities, purchasers and providers in Austria, France, Switzerland, and Poland. OptiMedis is currently involved in competitive research and implementation projects with a volume of over 10 million Euros.
ROLE IN THE PROJECT
Coordinator of the German pilot site; WP leader on business exploitation (WP10); Task leader/contribute to tasks across WPs to support methodological developments and adaptations; Contributor to dissemination.
4.6.2 CV OF THE PERSONS
Dr Oliver Groene
Gender Male
Qualification PhD in Public Health
Staff Category Vice Chairman of the Board at Optimedis
Short description of work experience, relevant to the proposal
Dr Oliver Groene is Vice Chairman of the Board at Optimedis AG and Honorary Associate Professor at the London School of Hygiene and Tropical Medicine. He has extensive experience in applied health services and implementation research projects and has been awarded competitive research funding for example from the UK NHS Health Policy Research Programme, the German Innovation Fund, and the European Commission. He served as PI or co-PI on various multi-country research grants, with total research funding in PI/co-PI roles over 6 million EUROs. He has 15 years of experience in health services research, evidence-based healthcare management, outcomes research and statistical modelling. His H-Index is 33. He is an invited fellow to the 2019 Sciana Health Leaders Network. He holds a Masters Degrees in Medical Sociology (University of Bielefeld), a MSc in Public Health (London School of Hygiene and Tropical Medicine) and a PhD in Public Health (University Pompeu Fabra, Barcelona).
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 83
Dr Katja Stahl
Gender Female
Qualification PhD in Nursing Sciences
Staff Category Manager of Research & Development
Short description of work experience, relevant to the proposal
Dr Katja Stahl studied Nursing Science at the University of Bremen, Germany, and Midwifery Science at the University of Aberdeen, Scotland. She did her PhD at the University of Osnabrück, Germany, on the care experience of mothers who have given births in hospital. She worked for ten years at the German branch of the Picker Institute Europe where she was responsible for planning and managing patient and employee surveys as well as for the development of new survey instruments for measuring patient experience and work experience of health care staff. In her current position as Manager Research & Development at OptiMedis she is responsible for developing and implementing studies in healthcare research focussing on patient-centred care as well as for the development of concepts for integrating innovative care concepts into practice.
4.6.3 LIST OF RELEVANT PUBLICATIONS
Groene O. Patient and public involvement in developing patient-reported outcome measures: indispensable, desirable, challenging. PATIENT. 2012;5(2):75-7.
Groene O, Arah OA, Klazinga NS et al. Patient Experience Shows Little Relationship with Hospital Quality Management Strategies. PLOS ONE. 2015 Jul 7;10(7):e0131805;
Groene O. Patient centredness and quality improvement efforts in hospitals: rationale, measurement, implementation. INTERNATIONAL JOURNAL FOR QUALITY IN HEALTH CARE. 2011 Oct;23(5):531-7.
Taylor A, Groene O. European hospital managers' perceptions of patient-centred care. JOURNAL OF HEALTH ORGANIZATION AND MANAGEMENT. 2015;29(6):711-28.
Groene O, Pfaff H, Hildebrandt H. Scaling up a population-based integrated health care system: the case of ´Healthy Kinzigtal´ in Germany. In: Braithwaite , Matsuyama Y, Mannion R, Shekelle P(eds): HEALTH SYSTEMS IMPROVEMENT ACROSS THE GLOBE: SUCCESS STORIES FROM 60 COUNTRIES, 2017
4.6.4 LIST OF RELEVANT PREVIOUS PROJECTS
COMPAR-EU - Comparing the Effectiveness of Self-Management Interventions. EU Horizon 2020 – Research and Innovation Action. OptiMedis collaborates with NIVEL and FAD in the implementation of this research project, where OptiMedis is responsible for Dissemination and Exploitation of Research Findings.
HEALTH PROS - A Training Network for Health System Performance Professionals. EU Horizon 2020 - European Training Network. An international network of 13 PhDs, two under the direction of Oliver Groene, that conduct health services research, including PREMs and PROMs.
PSK - Nursing-home sensitive hospital admissions: development of an indicator set. OptiMedis analyses data of multiple German statutory health insurance funds and conducts consensus panels with providers.
BigMedilytics - Big Data Analytics in Medicine and Health Systems. EU Industrial Action. OptiMedis designs a performance dashboard including nudges to providers.
INVEST - A Population-Based Integrated Care Project for Deprived Urban Areas. German Innovations fond. OptiMedis set up a new integrated care system, including the first German health kiosk, a one-stop shop for patients for and health system navigation.
4.6.5 DESCRIPTION OF ANY SIGNIFICANT INFRASTRUCTURE
4.6.5.1 NETWORKS – COLLABORATIONS:
OptiMedis is managing and involved in a range of networks that can support scaling up of the ADLIFE technology. First, OptiMedis has various joint ventures in other EU countries: OptiMedis Netherlands, OptiMedis Belgium and OptiMedis-Cobic UK. Through its joint ventures, OptiMedis can elicit feedback on prototypes or pilot the technology in a range of health system contexts. The OptiMedis joint ventures are also a potential customer for the final technology. Secondly, OptiMedis collaborates with health care authorities and providers that aim deploy digital
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 84
health innovations, currently supporting a large-scale procurement within the NHS or collaborating with an IT partner in establishing the NHS Performance Dashboard. Thirdly, OptiMedis is involved in a wide range of academic and non-governmental networks, such as the International Foundation for Integrated Care or the International Network of Health Promoting Hospitals.
4.6.5.2 DISSEMINATION CAPABILITY:
OptiMedis can support the dissemination of the ADLIFE project through the following functions: On the one hand, OptiMedis is consortium partner in the H2020 funded research and innovation action Compar-EU (www.self-management.eu) where it is responsible for dissemination and exploitation. This project emphasizes a multi-prong approach to dissemination including both traditional media and a wide range of social media canals. The experience of this project, which started in 2018, will be very valuable to improving the dissemination efforts for ADLIFE. On the other hand, Dr Oliver Gröne, Vice-Chair of OptiMedis, has considerable experience in editorial functions (he was Deputy Editor of the International Journal for Quality in Health Care, 2014-2019) and an own publishing record (H-Index = 33). In addition, OptiMedis has its own communications department which has access to a substantial network of medial canals and experience in producing high impact press releases.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 85
4.7 REGION JÄMTLAND HÄRJEDALEN (RJH) 4.7.1 DESCRIPTION OF THE LEGAL ENTITY AND ITS MAIN TASKS
RJH’s legal status is a County Council. Its main responsibility is primary and secondary healthcare, as well as regional development in a region of approximately 130,000 inhabitants. RHJ also works with preventative measures and dentistry. Secondary healthcare is carried out at the sole hospital in the only town of the region - Östersund Hospital – where there are 416 beds and 51 out-patient clinics. Primary healthcare is carried out in 28 locations in the sparsely-populated region, while home and social care are the responsibilities of its eight municipalities. There are roughly 4,000 employees in 100 different professions in RJH, and around 93% of the total budget is allocated to healthcare. As a relatively small but pro-active healthcare organisation, RJH has the experience and advantage of deploying and implementing eHealth innovations on a wide-scale.
RJH has a well-established common EHR (e-prescriptions included) for all primary and secondary care. Other
activities in the eHealth area include video conference systems, video appointments from patients’ homes with
doctors at the hospital and primary care centres, as well as with nutritionists. In the southern part of the region,
there are three healthcare centres that run emergency rooms off-hours. These rooms employ digital solutions where a nurse and patient are remotely connected with a physician. Follow-ups have shown positive results as to medical quality, cost reductions and fewer transfers of patients to the hospital ER. RJH also administers patient self-managed eHealth rooms in some villages. Here, patients are able to do health check-ups (e.g. blood tests) and real-time video interaction, and results are entered into the EHR system. Large-scale self-measurements among primary care patients using electronic weight scales and blood pressure measurers communicating with the carers are being launched this year.
As part of RJH, the R&D unit oversees education, including parts of the training for all medical personnel. R&D and its Project Office are responsible for and collaborates mainly within EU developmental projects. The Project Office functions as a resource to internal and external project partners, and also acts as a networking resource in that it takes the project results onto a larger marketplace.
The R&D Project Office is located at the eHealth Centre of RJH. A Centre that was created to strengthen and speed up the transformation of the health care sector with the assistance of digital tools regarding products and services. Placed in an 850 square meter office and demonstration area, employees from health care and e-Health of RJH and municipalities work alongside SMEs and corporations -, regional, national and international, to enhance the development of e-Health.
ROLE IN THE PROJECT
Will lead and function as:
Coordinator of the Swedish pilot site; WP leader of Evidence-based personalised care delivery (WP6); Task leader in WP6 of: Integration and coordination of care for advanced chronic diseases in existing health care
services; Decision support modules scope and content; Design, develop and test personalised care CE. Pilot design and implementation and Policy recommendations; Will contribute to tasks across WPs to support methodological developments and adaptations as well as to
dissemination.
RJH is undertaking an organisational-wide initiative that entails a strategic transformation towards ”Good and near care”. This originates from a major national initiative ”Good quality, local health care – a joint roadmap and vision”. The focus of this RJH work on coordinating, integrating and personalising care shares much in common with the intentions of the ADLIFE project and is specifically relevant to WP6.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 86
4.7.2 CV OF THE PERSONS
Dr. Göran Larsson
Gender Male
Qualification Professor, PhD
Staff Category Head of R&D and Education
Short description of work experience, relevant to the proposal
Göran S. Larsson, Professor, Ph.D. Head of R&D and Education. Wenner-Gren Fellow since 2001. Associate professor and researcher at Umeå University, Sweden, where he was responsible for one of the pre-clinical semesters in its Medical education programme. Between 2001 and 2003 post-doctoral training at University of Cambridge, UK. Author of 25 peer reviewed papers in scientific journals, including Nature, PNAS, Allergy, among others.
Mikael Lilja, MD
Gender Male
Qualification Doctor in medicine, Specialist and Assistant professor in family medicine, PhD
Staff Category Head research physician at the R&D unit.
Short description of work experience, relevant to the proposal
Mikael Lilja, Assistant Professor, MD, specialist in Family medicine, PhD, lecturer at the Department of Family Medicine, Umeå University. Head physician for seven years at a palliative care unit of Östersund municipality. Member of the boards of the Swedish Society for Diabetolog+y. Previously worked as head of primary care centres in the counties of Västernorrland and Jämtland, Sweden, and as Medical Director at the regional level in the County of Västernorrland. Ongoing research within various fields of Family Medicine.
Marie Sherman
Gender Female
Qualification LLM degree
Staff Category Strategist / Team leader of EU projects
Short description of work experience, relevant to the proposal
Marie Sherman – Strategist / Team leader - Grants and Operations Development Office in Health promotion and healthcare with focus on innovation and R&D. Has initiated and developed collaboration works with research institutes and other partners in Sweden and the EU. Previous positions in RJH include Director of the Medical Department that included developmental work addressing multimorbidity, geriatrics and integrated care. Has an LLM degree from Uppsala School of Law, under- and graduate courses in Sociology, Social Psychology and Biology from Uppsala and Yale Universities. Has worked as an executive in Sweden and the USA for twelve years. She is senior project coordinator and functions as Deputy Manager in Horizon 2020 projects such as C3-Cloud, mHealth hub and HSMonitor. She has previous experience in major developmental projects on national, regional and international levels.
Eva-Pia Darsbo, MD
Gender Female
Qualification Doctor in Medicine
Staff Category Doctor in Medicine, Specialist in family medicine and geriatrics
Short description of work experience, relevant to the proposal
Eva-Pia Darsbo MD, Specialist in Family medicine and Geriatrics. Presently working within the Primary Care as medically responsible physician at nursing homes, as well as physician in the Mobile Team for “near care” placed in the Medical Department and Primary care. Coordinator of physicians responsible for care at nursing homes and the municipalities’ home care. Lecturer in Geriatrics
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 87
Kristine Bergström
Gender Female
Qualification Masters Degree in Public Health
Staff Category Nurse
Short description of work experience, relevant to the proposal
Kristine Bergström, Nurse. Masters Degree in Public Health. Has worked clinically for ten years in Orthopedics. Other works include head of an ER, project leader and operational developer in Primary care.
Elsy Bäckström
Gender Female
Qualification Specialist nurse in Medicine and Surgery
Staff Category Coordinator of cohesive care between RJH and the Municipalities
Short description of work experience, relevant to the proposal
Elsy Bäckström, Specialist nurse, in Medicine and Surgery. Has held many positions within elderly care as a nurse and manager and has led many implemented projects, some on a national level. Led a group of high-level health care managers in developing the collaboration between caregivers of Specialised and Primary care (RJH) and the municipalities’ Home care. The work focused on Palliative care and included the introduction of the Swedish National Palliative Register. Has served as the municipalities’ representative in the Northern Region’s Consultation group on Palliative Care, this included the production of web-based education on Palliative care. Presently engaged in the coordination of cohesive care between RJH and the Municipalities. Developed Geriatric support in the project “Ability to lead” and started the Mobile Team for “near care”. Presently working on the development of Personalised care on a regional and national levels.
Annette Boije
Gender Female
Qualification Nurse
Staff Category Operations developer in Primary care
Short description of work experience, relevant to the proposal
Annette Boije is experienced in many areas such as an examinator of quality assessment, as a controller of internal operations, clinical work in ambulatory care, the ER and medical Department. She has twenty years experience of project leadership, operations developer and has served as an executive in Primary and Secondary care. She functions as one of the project leaders in ”Good and near care”.
Kristine Bergström
Gender Female
Qualification Masters Degree in Public Health
Staff Category Nurse and project leader
Short description of work experience, relevant to the proposal
Kristine Bergström has worked clinically for ten years in Orthopedics. Other works include head of an ER, project leader and operational developer in Primary care. She functions as one of the project leaders in ”Good and near care”.
Anna Fremner
Gender Female
Qualification Nurse and project leader
Staff Category Assistant head of Primary care at RJH
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 88
Short description of work experience, relevant to the proposal
Anna Fremner has worked as an oncology nurse. She functions as one of the project leaders in ”Good and near care”.
Anna Granevärn
Gender Female
Qualification Economist
Staff Category Head of Primary care at RJH
Short description of work experience, relevant to the proposal
Anna Granevärn is head of the County Council driven primary care in RJH. She is also responsible for the process “Very Important Patients” (VIP), which includes mobile teams for frail patients, home monitoring and of patients with chronic diseases and a fast track to hospitalised care for patients characterised as VIP. Anna has a strong track record of change management and digitalisation in primary care processes.
Elsy Bäckström
Gender Female
Qualification Specialist nurse in Medicine and Surgery
Staff Category Coordinator of cohesive care between RJH and the Municipalities
Short description of work experience, relevant to the proposal
Elsy Bäckström, Specialist nurse, in Medicine and Surgery. Has held many positions within elderly care as a nurse and manager and has led many implemented projects, some on a national level. Led a group of high-level health care managers in developing the collaboration between caregivers of Specialised and Primary care (RJH) and the municipalities’ Home care. The work focused on Palliative care and included the introduction of the Swedish National Palliative Register. Has served as the municipalities’ representative in the Northern Region’s Consultation group on Palliative Care, this included the production of web-based education on Palliative care. Presently engaged in the coordination of cohesive care between RJH and the Municipalities. Developed Geriatric support in the project “Ability to lead” and started the Mobile Team for “near care”. Presently working on the development of Personalised care on a regional and national levels.
Maria Omberg
Gender Female
Qualification Nurse
Staff Category Head of the Patient safety unit at RJH
Short description of work experience, relevant to the proposal
Maria Omberg, Strategist. Nurse in primary and secondary care. Head and originator of the Patient safety unit at RJH. Representative of the Northern Region in the National Cooperation Group on Patient safety. Strategist in Patient safety with focus on “near care” and personalised care. Presently working on the development of Personalised care on a regional and national levels.
Dr. Rita Sjöström
Gender Female
Qualification PhD
Staff Category Physical Therapist
Short description of work experience, relevant to the proposal
Rita Sjöström, PhD. Registered Physical Therapist (RPT), Vasa, Finland, Master of Science in Physical Therapy. Umeå University, Sweden, Specialty Board in Physical Therapy with subspecialty of Primary Health Care. PhD, Department of Health Sciences, Mid Sweden University, Östersund, Sweden.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 89
4.7.3 LIST OF RELEVANT PUBLICATIONS
Gray S, Axelsson B. The prevalence of deranged C-reactive protein and albumin in patients with incurable cancer approaching death. PLoS One. 2018 Mar 13;13(3):e0193693. doi: 10.1371/journal.pone.0193693. eCollection 2018. PubMed PMID: 29534089; PubMed Central PMCID: PMC5849305.
Martinsson L, Heedman PA, Lundström S, Axelsson B. Improved data validity in the Swedish Register of Palliative Care. PLoS One. 2017 Oct 19;12(10):e0186804. doi: 10.1371/journal.pone.0186804. eCollection 2017. PubMed PMID: 29049396; PubMed Central PMCID: PMC5648220.
3: Martinsson L, Axelsson B, Melin-Johansson C. Patients' perspectives on information from physicians during palliative chemotherapy: A qualitative study. Palliat Support Care. 2016 Oct;14(5):495-502. doi: 10.1017/S1478951515001200. Epub 2015 Dec 14. PubMed PMID: 26653583.
Näppä U, Rasmussen BH, Axelsson B, Lindqvist O. Challenging situations when administering palliative chemotherapy - a nursing perspective. Eur J Oncol Nurs. 2014 Dec;18(6):591-7. doi: 10.1016/j.ejon.2014.06.008. Epub 2014 Jul 3. PubMed PMID: 24997518.
Näppä U, Lindqvist O, Axelsson B. Avoiding harmful palliative chemotherapy treatment in the end of life: development of a brief patient-completed questionnaire for routine assessment of performance status. J Support Oncol. 2012 Nov-Dec;10(6):230-7. doi: 10.1016/j.suponc.2012.06.003. Epub 2012 Aug 28. PubMed PMID: 22951048.
Willers C, Iderberg H, Axelsen M, Dahlström T, Julin B, Leksell J, Lindberg A, Lindgren P, Looström Muth K, Svensson AM, Lilja M. Sociodemographic determinants and health outcome variation in individuals with type 1 diabetes mellitus: A register-based study. PLoS One. 2018;13:e0199170.
4.7.4 LIST OF RELEVANT PREVIOUS PROJECTS
WelfareTechnology: Mixed Zone for welfare technological TestLabs. (Interreg / Sweden – Norway, The Nordic Green Belt, Category Innovative environments). Led by RJH in collaboration with Norway / Tröndelag. WPs consist of: Mobile health solutions / decentralised health rooms; Digitally connected homes; Emergency supports. European territorial cooperation. http://valtel.eu/
C3-Cloud (H2020-PHC-25-2015-689181) - A Federated Collaborative Care Cure Cloud Architecture for Addressing the Needs of Multi-morbidity and Managing Poly-pharmacy, a project that develops ICT and Clinical Decision Support tools for care pathway management and patient-centred self-management approached of multi-morbid chronic diseases.
Testbed for an active lifestyle in multimorbidity – VINNOVA, Sweden’s Innovation Agency. RJH leads the project in collaboration with Mid-Sweden University. Testing various e-health services and creating conditions for stroke patients’ Independent Living enhancing early rehabilitation to increase the probability of a fast recovery.
HSMonitor (SC1-DTH-10-2019-2020 - Digital health and care services). Pre-commercial Procurement of innovative ICT-enabled monitoring to improve health status and optimise hypertension care. In HSMonitor, RJH will be the public procurer for the region of Jämtland Härjedalen, as well as the health service provider and provider of site for requirements analysis, prototype tests and pilots. In addition, RJH leads the work on testing of the HSMonitor prototype systems (T5.2 and T5.4) and Quality Assurance (T9.5).
4.7.5 DESCRIPTION OF ANY SIGNIFICANT INFRASTRUCTURE
4.7.5.1 NETWORKS – COLLABORATIONS:
RJH is one of four regions participating in the nationwide project ”Orderly introduction of digital services and products in healthcare” led by the Swedish Association of Local Authorities and Regions and partly funded by the National Regional Fund Programme. As a pilot site, RJH will share its experience and knowledge to work towards full implementation of digital services and products in healthcare. The Regions´ eHealth Centre gives a unique opportunity to collaborate with national and international enterprises as well as SMEs.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 90
The eight municipalities of the region Jämtland Härjedalen are involved to varying degrees in the aforementioned internal and external developmental actions. This collaboration strengthens the ongoing efforts to improve integrated and personalised care.
4.7.5.2 DISSEMINATION CAPABILITY:
Researchers in RJH collaborate with national and international universities in a wide-range of subjects within the medical field. Many of the researches are also teachers at the medical faculty of Umeå University for medical students or at Mid-Sweden University for paramedics, making dissemination in medical journals and at congresses a natural part of RJH’s activities. Additionally, the Region’s eHealth Centre provides the opportunity to communicate with SMEs and national and international enterprises within eHealth.
RJH has strong and established regional, national and international networks. Each and every project initiative contributes to the ability to influence these networks by proactive dissemination of the project results.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 91
4.8 ASSUTA ASHDOD LTD. (AMCA)
4.8.1 DESCRIPTION OF THE LEGAL ENTITY AND ITS MAIN TASKS
Samson Assuta Ashdod University Hospital (AMCA) is Israel’s newest public hospital (began operation in June 2017), located in Ashdod, the fifth largest city in Israel. It is a 300-bed hospital with a potential for expansion to 650 beds. It has a state-of-the-art Emergency Department and two Internal Medicine Wards as well as a short stay Internal Medicine Unit, and 9 modern operating rooms. The unique mission of the new not-for-profit University Hospital is to create a fully integrated care system that links the hospital staff, community health care providers, social services, community support services, the patient and the patient's family by reengineering the care process supported by information and communication technologies.
Maccabi Healthcare Services, the owner of ASSUTA, is the second largest health plan in Israel and provides comprehensive primary and secondary community healthcare services to over 2 million people. Maccabi is AMCA's key partner in developing the model for integrating hospital and community care in Assuta Ashdod University Hospital and in the ADLIFE project.
The new Assuta Ashdod University Hospital's overall goal is the development of an integrated care system in collaboration with the Health Plans and the Municipality (social services). This is being developed by creating interfaces between the hospital and community EMRs predominantly with Maccabi Healthcare Services, and interfaces with Social Services of the Municipality. Samson Assuta Ashdod Hospital's focus on integration with community services has already fostered unique innovations such as joint workshops between the Emergency Room staff and primary care doctors in the community, and the establishment of a unique short-stay internal medicine war. Maccabi has set up an Integration Unit in the hospital that fosters joint discharge planning for coordinated care in the community post-discharge and thus a seamless transition back to the community.
ROLE IN THE PROJECT
The Ashod hospital is formally affiliated with the Ben Gurion University School of Medicine for training and research and has a clinical research unit that works closely with the hospital's innovation unit. The hospital is currently involved in a H2020 project – CONNECARE – that is focused on implementing digitally enabled integrated care.
The ASSUTA Ashdod Hospital is one of the sites in which ADLIFE will be implemented, in close collaboration with Maccabi Healthcare Services primary and secondary care services in the community in the Ashdod area. AMCA will be an active participant in all aspects of ADLIFE and will function as the Work Package leader for WP8 - the work package that guides the pilot design and implementation of the ADLIFE Care Model and Digital Platform in the pilot sites.
Other main tasks will be:
Israel Pilot Leader. Interaction with other EU consortia. Change management for new ways for integrated care delivery. Deployment of the integrated care intervention and monitoring the implementation.
4.8.2 CV OF THE PERSONS
Tal Patalon, M.D
Gender Female
Qualification Doctor in Medicine
Staff Category Director of the Department of Innovation and Ventures at Assuta Ashdod Hospital.
Short description of work experience, relevant to the proposal
Tal Patalon, M.D. is the Director of the Department of Innovation and Ventures at Assuta Ashdod Hospital. One of her primary focuses is on the development of digital tools for monitoring and intervention, both in the hospital
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 92
and after discharge to the community. She will be the primary contact person and coordinator for Assuta for this project. Dr.Patalon is a staff physician in the Short Stay Internal Medicine Unit as well as a senior physician in the Emergency Department. Prior to coming to AMCA, she directed the Home Hospitalization and Palliative Care programs and served as a senior physician in the Emergency Department at Wolfson Hospital Tel Aviv. Dr. Patalon is a family physician with additional training in Emergency Medicine and Pain Management. She received her M.D in Budapest, Hungary and completed her Residency Training in Family Medicine at the University of Tel Aviv Medical School.
Dr. Rachelle Kaye
Gender Female
Qualification PhD
Staff Category International Projects Coordinator
Short description of work experience, relevant to the proposal
Dr. Rachelle Kaye, PhD is the International Projects Coordinator for Assuta Medical Centers, as well as a member of the core team for implementing digitally enabled integrated care in Assuta Ashdod. Prior to joining Assuta Dr Kaye directed the Maccabi Institute for Health Services Research that has been an active participant In European Framework Projects (FP7 and AAL) such as KSERA, HELP, REMPARK, USEFIL all of which involved remote monitoring and coaching of elderly people in their homes. Dr. Kaye is a member of the Board of Directors of EHTEL (the European Health Telematics Association).
Asaf Peretz M.D.
Gender Male
Qualification Doctor in Medicine
Staff Category Director of Internal Medicine Short Stay Unit at Assuta Ashdod University Hospital
Short description of work experience, relevant to the proposal
Asaf Peretz M.D., is Director of Internal Medicine Short Stay Unit at Assuta Ashdod University Hospital that will be a key partner in the ADLIFE pilot. Before joining the Assuta Ashdod medical staff, Dr. Peretz was Deputy Medical Director at Maccabi Healthcare Services - Jerusalem & Shfela Region as well as a Senior Physician in the Emergency Department at Wolfson Medical Center. Dr. Peretz has led many international projects in the past, mainly in the field of emergency medical services. His current focus is on improving and promoting effective interactions between community health services and hospitals. Dr. Peretz received his MD from Ben-Gurion University, Beer-Sheva and completed his Internal Medicine Residency at Hadassah University Hospital. He received his MBA in Management Information Systems at Bar Ilan University, Israel
Barak Nahir M.D
Gender Male
Qualification Doctor in Medicine
Staff Category Specialist in Family Medicine as well as Emergency Medicine
Short description of work experience, relevant to the proposal
Barak Nahir M.D, MBA, is a specialist in Family Medicine as well as Emergency Medicine. He is a senior physician in Assuta Ashdod Hospital in the short stay internal medicine ward and the Emergency Department as well as a General Practitioner in Maccabi Health Services in Jerusalem, Israel. His current focus is minimizing the need for hospital care, while using available community resources wisely. Dr. Nahir received his MD from Ben-Gurion University, Beer-Sheva, completed his Family Medicine Residency at Maccabi Health Services and his Emergency Medicine Residency was completed in Wolfson Medical Center in Holon, Israel. He received his MBA in Management Information Systems at Bar Ilan University, Israel
Reut Ron M.D.
Gender Female
Qualification M.Sc in Epidemiology
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 93
Staff Category Researcher in the Assuta Health Services Research Institute
Short description of work experience, relevant to the proposal
Reut Ron, M.Sc is a researcher in the Assuta Health Services Research Institute. Reut holds a degree in Epidemiology from Tel Aviv University, and she has experience in promoting, designing and conducting research. Prior to her position in Assuta, Reut was a research coordinator in the Department of Child and Women's Health at the Gertner Institute for Epidemiology and Health policy research (2015-2017).
Dr. Erela Rotlevi
Gender Female
Qualification Doctor in Medicine
Staff Category Medical director of Maccabi's Southern region
Short description of work experience, relevant to the proposal
Dr. Erela Rotlevi, is the Medical director of Maccabi's Southern region, responsible for supervising all of Maccabi's Healthcare services in the Region. Dr. Rotlevi participated in the establishment of the integration process between Assuta Ashdod hospital and Maccabi. Prior to her position as regional medical director, Dr. Rotlevi was the Medical director of Gedera and Mazkeret Batya region (2013-2016) and coordinator of instruction and teaching in Maccabi's Department of Family Medicine (2014-2017). Dr. Rotlevi is a senior lecturer in the Medical School at Ben Gurion University. She continues to function as a family physician in the community, treating a diverse population from children to elderly patients (2007-present).
Dr. Shragit Greenberg
Gender Female
Qualification Doctor in Medicine
Staff Category Medical director of Maccabi's Home Palliative care unit
Short description of work experience, relevant to the proposal
Dr. Shragit Greenberg, is the Medical director of Maccabi's Home Palliative care unit in Beer-Sheva. As part of her daily job, Dr. Greenberg is responsible for the approval of a new patient to the unit, the patient's treatment and ongoing home visits, all in close cooperation with the rest of the unit's multi-disciplinary staff. Dr. Greenberg is also the Director of Roah Dromit, a voluntary association of complementary medicine for cancer patients and their families, and an Instructor in communication skills in the Family Practice Residency program at the Ben-Gurion University of the Negev. Prior to her position at Maccabi, Dr. Greenberg worked as pain management and palliative care consultant at the Pediatric Oncology Department in Soroka hospital (2000-2008) and as a family physician in the community at Clalit Health Services, during which time she also worked at Clalit's Home Palliative care unit. Dr. Greenberg did a Paliative Care fellowship at the University of British Columbia, Vancouver B.C. Canada (1979-1999), and has Israeli Board Certification in palliative care.
Dr. Michal Yeshayahu
Gender Female
Qualification Doctor in Medicine
Staff Category Medical director of the integrative care unit at the Assuta Ashdod University hospital
Short description of work experience, relevant to the proposal
Dr. Michal Yeshayahu is the medical director of Maccabi's Integrated Care Unit at the Assuta Ashdod University hospital which is responsible for the continuity of care for complex patients discharged from Assuta Ashdod hospital back to the community, and an active member of the Maccabi Health Services Faculty of Family Medicine. She graduated from Ben Gurion University Medical School in Israel in 2001, followed by a residency in family medicine, at Maccabi Health Services in Jerusalem. After her residency, she completed an academic fellowship in medical education at the University of Toronto., She is also a practicing family physician, teaching students and residents. Her main fields of interest are inter-professional education, collaboration and integrated care.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 94
4.8.3 LIST OF RELEVANT PUBLICATIONS
Kaye, Rachelle, Normie, Lawrence, Lemberger, John (2011). 21st Century Tools for Aging in Place. Home Care for Frail Older Adults: Issues, Services, Programs. ed. Ester Iecovich PhD. DC-Israel-Eshel with the Ministry for Senior Citizens, Jerusalem (Hebrew).
Kaye, Rachelle, Kokia, Ehud, Shalev, Varda, Idar, Dalia, Chinitz, David. 2010, E-Health and Health Information Technology: Barriers and Critical Success Factors: a practitioner's perspective. Journal of Management and Marketing in Healthcare. VOL. 3 NO. 2. PP 163–175. June, 2010).
Kaye R, Ron R, Azaria B, Bar-Ilan M, Rotlevi E, Iacubovsky T. Integrated Care for High Risk Surgical Patients – Before, During and After. International Journal of Integrated Care. 2018;18(s2):241.
Nahir B, Kovalski N, Zimmerman DR. Failure to radiologically confirm community-acquired pneumonia means antibiotic overtreatment. Clinical Infectious Diseases 2012; 54:1816.
Shiri Guy-Alfandary, PharmD; Barak Nahir, MD; Yifat Namer-Tal, MD; et al, Clinical Utilization Pattern and Effectiveness of Omalizumab for Asthma Patients in Israel. Chest. 2012;142
4.8.4 LIST OF RELEVANT PREVIOUS PROJECTS
CONNECARE - Personalized Connected Care for Complex Chronic Patients (2016-2019) is an H2020 project to co-design, develop, deploy, and evaluate a novel smart, adaptive integrated care system for chronic care management that strongly relies on the capability of advanced ICT to support personalized care trajectories.
USECARE - an AAL project (2015-2017) to further develop the current prototype of a self-management system SENACA 3.0 (for SENior health ACAdemy) to enable carers for remote-controlling of critical bio-markers of patients, therapy adherence (medication and lifestyle), aggregating information and social interaction and to to field-test the prototype focusing on interaction between Carers and Elderly Patients, in a multicentre observational study in different cultural settings.
USEFIL- Unobtrusive Smart Environments For Independent Living- (2011-2014) was an FP7 project to address the gap between technological research advances and the practical needs of elderly people by developing advanced but affordable in-home unobtrusive monitoring and web communication solutions. USEFIL used low cost "off-the-shelf" technology to develop immediately applicable services to assist the elderly in maintaining their independence and daily activities
REMPARK- Personal Health Device for the Remote and Autonomous Management of Parkinson’s Disease - (2013-2015) was an FP7 Project to develop a Personal Health System (PHS) with closed loop detection, response and treatment capabilities for management of Parkinson's Disease (PD) patients
KSERA (FP7) - Knowledgeable Service Robots for Aging (2010-2013). Development of a Robot Based Systems for Disease management of COPD, aiming to seamlessly integrate smart home technology with socially assistive robots.
4.8.5 DESCRIPTION OF ANY SIGNIFICANT INFRASTRUCTURE
4.8.5.1 INFRASTRUCTURES
Assuta Ashdod EMR system (Camillion) - including referrals prescriptions, closed loop system (referrals from the EMR and results back to the EMR) for laboratory, imaging, other diagnostic examinations, , interface with Operating Room system.
Maccabi EMR system (Cliks) – comprehensive integrated EMR used by all medical and healthcare professionals including referrals, prescriptions, test results supported by a sophisticated CDSS
Maccabi Patient Portal (Maccabi Online) that enables patients to see their medical information as well as to communicate with their primary care doctor. The portal is a web-based service accessible by computer as well as smart-phone app.
4.8.5.2 DISSEMINATION CAPABILITY
AMCA is extremely active not only at European and international level but also in the region and country where it
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 95
is very active in communicating and disseminating results in the healthcare and social care community as well as in the general population.
AMACA lectures at courses in the Schools of Public Health and Health care Systems Management in Ben Gurion University and Tel Aviv University. The Maccabi Research Institute is directly affiliated with the School of Public Health at Tel Aviv University and some of its staff are professors both in the school of public health and the Medical School. Likewise, with Assuta Ashdod Hospital and Maccabi at Ben-Gurion University – so this also give AMCA the opportunity to bring learnings from ADLIFE to students learning to be clinicians and healthcare professionals as well as managers.
In addition, AMCA actively participates in and organizes different conferences:
Annual Conference of the Israel National Institute for Health Policy Research Israel Association for Medical Informatics Annual Conference Israel Gerontology Association Annual Conference Annual Conference of Israel Heart Society Quarterly meetings of the Israel Association of Family Physicians Assuta – Maccabi Conference on Medical and Healthcare Research Annual conference of the Association of Public Health Physicians and Public Health Schools in Israel Annual Conference on Chronic Diseases Israel - MEDICAL Expo Annual conference of the Israeli Association for Patient Rights
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 96
4.9 SOFTWARE RESEARCH DEVELOPMENT AND CONSULTANCY CORP (SRDC)
4.9.1 DESCRIPTION OF THE LEGAL ENTITY AND ITS MAIN TASKS
SRDC Corp. was founded by a professional team of engineers directed by Prof. Asuman Dogac in Middle East Technical University (METU) Technopolis in 2007. SRDC is a spin-off company of the METU Software Research and Development Center, which was founded in 1991 with the support of The Scientific and Technological Research Council of Turkey (TUBITAK) and METU Faculty of Engineering. A majority of the team hold PhD and MSc degrees in Computer Engineering at METU, and the remaining are progressing.
SRDC enjoys strong backing from the university for transferring the R&D efforts to the industry and public administrations. SRDC performs R&D activities both for developing brand new products and services and for innovative improvement of existing products and services. SRDC team has extensive expertise in large-scale software development, interoperability standards and enabling technologies, semantic Web technologies, interoperability solutions for e-health, e-government and e-business domains, data analytics, conformance and interoperability testing, and mobile application development. SRDC team has been working in the e-health domain since 2003.
ROLE IN THE PROJECT
SRDC is the leader of WP4 Patient Empowerment Platform and Personalized Self-Management Support Mechanisms. SDRC will lead to the development of Patient Empowerment Platform to establish continuous communication with the patient to guide them about the care plan activities, for outcome and risk monitoring through PROMS, and finally for facilitating delivery of just-in-time personalized, adaptive interventions to reinforce adherence to personalized care plans. SRDC will extend and adopt its existing Patient Empowerment Platform (eSaglıkKaydım) for the needs of ADLIFE Project. In particular, SRDC will add HL7 FHIR support to this platform, extend the platform to support PROMs, and integrate it to the adaptive intervention engine. SRDC has already developed an intelligent adaptive intervention delivery mechanism within the scope of Power2DM (H2020-689444), which is currently being piloted in two pilot studies in 2 different European countries (Netherlands and Spain) with 280 patients. SRDC will design of adaptive behaviour change interventions for the selected target population of ADLIFE project, and adapt and retrain the reinforcement algorithm of the intelligent JTAI delivery engine to deliver just in time adaptive interventions to ADLIFE target patient population in an individualized manner by sensing their context and adapting behaviour change interventions accordingly.
In WP3, SRDC will lead Task 3.2 for adapting its Personalised Care Plan Management Platform (PCPMP) according to the needs of the ADLIFE project. PCPMP is a generic platform for collaborative personalised care planning that has been used so far for elderly multi-morbid patients with chronic diseases like diabetes, renal failure, heart failure and depression within the scope of C3-Cloud, a Horizon 2020 research and innovation project for achieving integrated care. As the owner of PCPMP, SRDC will develop wizard like modules for the management of care plans for long term care of patients severe, chronic, and incurable disease with an expected progression in severity and a marked reduction in life expectancy. SRDC has been investing on chronic disease management solutions for the past 15 years and has a product called KronIQTM, which delivers clinical decision supported guidance to medical doctors for the management of chronic diseases. The system has been built for Ministry of Health Turkey and will be operationalized in fall 2019 to be used by more than 20.000 Family Medicine Practitioners for management of the screening and monitoring of whole Turkish population (around 80 million patients).
SRDC will lead Task 3.4 for building the security and privacy mechanisms for ADLIFE Project. SRDC has extensive experience in this domain and has already a domain independent security and privacy tool, onAuth, as a security and privacy framework implementing modern Web authorization specifications like OAuth 2.0, OpenID Connect 1.0 and Smart App Authorization. SRDC will adapt the tool based on the needs of the project (new roles will be defined, authorization rule sets will be defined), will integrate it with the Single Sign-on mechanisms of pilot sites and will define new rules and configuration for anonymization.
SRDC will be involved in Task 3.3 (which is led by University of Warwick) for achieving interoperability between PCPMP and the patient data sources at the pilot sites, such as the EHR systems. The interoperability layer will be based on modern and widely used HL7 FHIR® specifications for both common data model and data exchange API. SRDC has extensive experience in achieving both structural and semantic interoperability in the health domain. In the SALUS project, which is coordinated by SRDC, SRDC has developed a scalable semantic interoperability
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 97
middleware integrating clinical care and clinical research domains, and on top of this middleware implemented several post market safety study tools. SALUS interoperability solutions and post market safety study tools have been deployed in real-life settings on top of enormous regional and institutional Electronic Health Record (EHR) systems. As an example, the data warehouse of Lombardy Region as one SALUS site contained 16 million patients with 1 billion patient records. SRDC has also implemented its own HL7 FHIR® repository, onFHIR, as a secure and high-performance health data repository. onFHIR will be reused in the ADLIFE project.
SRDC will also be actively involved in Task 5.3 for development of CDS services for implementing guideline-based goal and activity suggestions. SRDC has experience of working with clinical experts to extract implementable technical specifications from written clinical guidelines, and then implementing those specifications as CDS software services. In the C3-Cloud project, SRDC has first developed the technical specifications of 8 CDS services to cover the NICE "Type 2 Diabetes in Adults" (NG28) clinical guideline and then implemented them as CDS software services compliant to the CDS Hooks specification. In earlier work, SRDC has implemented several other clinical guidelines (e.g. cardiovascular diseases) as automated workflows and CDS services.
As a technical partner, SRDC will also be actively involved in Task 3.1 for gathering the technical requirements of the overall ADLIFE ICT solution.
Finally, as an SME who is experienced in transferring the knowledge generated in R&D projects to the industry, SRDC will strongly support exploitation activities the ADFLIFE outcomes beyond the project. SRDC is very much dedicated to the exploitation of the ICT tools that will be provided/improved to a wider audience. SRDC will also coordinate the consortium’s exploitation efforts for non-IT outcomes like integrated care pathways, organizational models, and the training approach.
4.9.2 CV OF THE PERSONS
Dr. Gokce Banu Laleci Erturkmen
Gender Female
Qualification PhD in Computer Engineering
Staff Category Deputy Manager
Short description of work experience, relevant to the proposal
Dr. Gokce Banu Laleci Erturkmen, Deputy Manager, Senior Researcher, BSc, MSc, PhD from the Computer Engineering Department of the Middle East Technical University. She has finalized her PhD study on Intelligent Healthcare Monitoring Systems based on Semantically Enriched Clinical Guidelines in June 2008. She has coordinated ICT-287800 SALUS project, which addresses standards based semantic interoperability in pharmacovigilance domain. She has worked as the principal researcher in many IST and ICT projects, including IST-027074-STP SAPHIRE, ICT-213031 iSURF, ICT-248240 iCARDEA, and as a researcher in many others. She is also the main author of the C3-Cloud project proposal. She has acted as the technical co-chair of IHE QRPH domain between 2013-2015, which is a standardization initiative in the field of quality reporting and public health domain. Currently she is giving a lecture on “Electronic Health Records: Representation, Standards and Coding” in the Medical Informatics Graduate Program of the Middle East Technical University.
Dr. Mustafa Yuksel
Gender Male
Qualification PhD in Computer Engineering
Staff Category Senior Researcher
Short description of work experience, relevant to the proposal
Dr. Mustafa Yuksel, Senior Researcher and Software Engineer, BSc, MSc, PhD from the Computer Engineering Department of the Middle East Technical University. His research areas include eHealth, eBusiness, Interoperability, Big Data Analytics, Semantic Web, Interoperability Testing and Service Oriented Architectures. He has participated in many EC supported projects including C3-Cloud, SALUS, WEB-RADR, epSOS, PALANTE, iCARDEA, iSURF, SAPHIRE and RIDE H2020/FP7/FP6 projects. Currently he leads the development of the Personalised Care Plan Management Platform and the overall software integration in the C3-Cloud project. In epSOS, he has developed the first and only open source implementation of the epSOS specifications for cross-border data exchange. He has provided consultancy services on the management of National Health Information System to the Ministry of Health, Turkey; as well as to Hospital Information System vendors for their standards-
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 98
based implementation and testing activities. He finalized his MSc thesis entitled “Sharing Electronic Healthcare Records Across Country Borders” in 2008, and PhD thesis entitled “A Semantic Interoperability Framework for Reinforcing Post Market Safety Studies” in 2013.
Bunyamin Sarigul
Gender Male
Qualification Bc in Computer Engineering
Staff Category Full-stack Web developer
Short description of work experience, relevant to the proposal
Bunyamin Sarigul, Software Engineer, BSc from the Computer Engineering Department of the Middle East Technical University. He is having his MSc study in the Medical Informatics Graduate Program of the Middle East Technical University. Bunyamin is a full-stack Web developer with strong skills in user interface development. He is one of the core technical members of the C3-Cloud project actively developing the Personalised Care Plan Management Platform.
4.9.3 LIST OF RELEVANT PUBLICATIONS
Suat Gonul, Tuncay Namli, Sasja Huisman, Gokce Banu Laleci Erturkmen, Ismail Hakki Toroslu, Ahmet Cosar. An expandable approach for design and personalization of digital, just-in-time adaptive interventions. Journal of the American Medical Informatics Association, Volume 26, Issue 3, March 2019, Pages 198–210, https://doi.org/10.1093/jamia/ocy160
Gokce Banu Laleci Erturkmen, Mustafa Yuksel, Bunyamin Sarigul, Mikael Lilja, Rong Chen, Theodoros N. Arvanitis. Personalised Care Plan Management Utilizing Guideline-Driven Clinical Decision Support Systems. Medical Informatics Europe (MIE2018), April, 2018, Gothenburg, Sweden
Laleci G.B. et al. Guideline-Driven Telemonitoring and Follow-up of Cardiovascular Implantable Electronic Devices using ISO/IEEE 11073, HL7 & IHE Profiles. In 33rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC ’11), August 30 - September 3, 2011, Boston, USA
Laleci G. B., Dogac A. A Semantically Enriched Clinical Guideline Model Enabling Deployment in Heterogeneous Healthcare Environments. In IEEE Transactions on Information Technology in Biomedicine, volume 13, no. 2, March 2009, pp. 263 - 273 (Science Citation Index Core, Impact Factor: 1.787)
4.9.4 LIST OF RELEVANT PREVIOUS PROJECTS
C3-Cloud (H2020, 2016-2020, SRDC author and core technical partner) - A Federated Collaborative Care & Cure Cloud Architecture for Addressing the Needs of Multi-morbidity and Managing Poly-pharmacy - C3-Cloud has established an ICT infrastructure enabling continuous coordination of patient-centred care activities by a multidisciplinary care team (MDT) and patients/informal care givers. The Coordinated Care and Cure Delivery Platform (C3DP) allows, collaborative creation and execution of personalised care plans for multi-morbid patients through systematic and semi-automatic reconciliation of clinical guidelines. Clinical decision support (CDS) systems implementing flowcharts from evidence based clinical guidelines are integrated to present suggestions for treatment goal and activities. As the author of the C3-Cloud project, SRDC is leading the development of the Personalised Care Plan Management Platform and the overall software integration.
POWER2DM (H2020, 2016-2019, SRDC author and core technical partner) - Predictive model-based decision support for diabetes patient empowerment - The main objective of the POWER2DM project is to develop and validate a personalized self-management support system for Type-1 and Type-2 diabetes patients that combines and integrates a decision support system (DSS) based on interlinked predictive computer models; automated e-coaching and advice functionalities based on Behavioural Change Theories; and real-time personal data processing and interpretation. SRDC has developed the pro-active personalized decision support services for patients and the HL7 FHIR based personal data storage.
epSOS (FP7 CIP PSP, 2008-2014, SRDC core technical partner) - Smart Open Services - Open eHealth Initiative for a European Large Scale Pilot of Patient Summary and Electronic Prescription - A large scale piloting project for pan-European exchange of electronic patient summary and prescriptions documents among 25 European
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 99
countries. SRDC realised the first and only open source implementation of the epSOS interoperability specifications, which turned into a multi-national open source effort named OpenNCP. SRDC also implemented the Turkish pilot on top of the National Health Information System of Turkey and led the global validation work package.
iCARDEA (FP7 ICT, 2010-2013, SRDC coordinator) - An Intelligent Platform for Personalized Remote Monitoring of the Cardiac Patients with Electronic Implant Devices (CIED) - SRDC implemented the clinical guideline automating adaptive care planner engine for patients with CIED, as well as the EHR interoperability layer and security and privacy mechanisms to ensure safe patient data exchange.
SAPHIRE (FP6 IST, 2006-2008, SRDC coordinator) - Intelligent Healthcare Monitoring based on Semantic Interoperability Platform - As the coordinator and leading technical partner, SRDC team developed a clinical guideline based intelligent monitoring and decision support system on a platform integrating
4.9.5 DESCRIPTION OF ANY SIGNIFICANT INFRASTRUCTURE
SRDC has the necessary software development tools and hardware to realise its activities in the ADLIFE project. SRDC prefers software development through open source and freely available frameworks, libraries, tools. Related to ADLIFE, SRDC has the following previous developed IT infrastructures and platforms:
Personalised Care Plan Management Platform (PCPMP): PCPMP enables creation, update and follow-up of personalized & integrated care plans for patients, especially the elderly patients with several chronic diseases. PCPMP enables collaborative care plan management with involvement of a multi-disciplinary care team composed of health professionals (GP, nurse, specialist, dietitian, physiotherapist, …) and social care workers. PCPMP is integrated with several Clinical Decision Support (CDS) services for enabling predictive risk assessment (e.g. QRISK2 algorithm), personalised goal recommendations (e.g. blood pressure targets, dietary targets) and intervention recommendations (medication therapies, guidance on contradicting medications, laboratory test requests, referrals to specialists, scheduling follow-up timings) to the care team members based on evidence based clinical guidelines. PCPMP has been developed by SRDC within the scope of C3-Cloud H2020 project and will soon be validated in 3 different European regions with the involvement of 60+ health professionals and 600 multi-morbid elderly patients.
KronIQTM: KnonIQ is a chronic disease management platform which provides clinical decision supported guidance to medical doctors for the management of chronic diseases. The system has been built for Ministry of Health Turkey and will be operationalized in fall 2019 to be used by more than 20.000 Family Medicine Practitioners for management of the screening and monitoring of whole Turkish population (around 80 million patients).
onFHIR is a secure and high-performance health data repository that is totally compliant with the HL7 FHIR® specifications for data models and data exchange APIs. onFHIR enables secure and standards compliant health data exchange among different parties in any health data exchange use case, such as between EHR systems and personalised care plan management applications, or clinical care and clinical research domains. onFHIR supports all HL7 FHIR versions and it has been successfully tested in a FHIR Connectathon event. onFHIR has also received the highest scores in FHIR compliance benchmarking tools.
eSaglikKaydim (myPHR in English) is a personal health platform consisting of various patient guidance applications that can be used by both patients and health professionals. eSaglikKaydim enables patients to manage their personal health data easily in a secure way. It also enables doctors, who are allowed by patients, to monitor data and status of the patients. eSaglikKaydim is compliant with well-accepted e-health standards (HL7/ASTM CCR, HL7 CCD, IHE PCC templates, HL7 Web Services) and has been integrated with the gigantic Turkish National Health Information System named SaglikNet.
Intelligent Just in time Adaptive Interventions (JTAI) Delivery Engine is a novel machine learning technique based on reinforcement learning theory. It is used to tailor the intervention delivery strategies dynamically in terms of intervention type, timing and frequency, in compliance with people’s action plans, changing physical / psychological contexts as well as their changing preferences over time. In Power2DM Project it has been piloted to deliver personalized just in time adaptive interventions to support the treatment adherence of diabetic patients.
4.9.5.1 DISSEMINATION CAPABILITY Being a spin-off of a university R&D Lab, and hence having an academic background, SRDC has a track record in publications and will pursue dissemination of the ADLIFE project through international journal and conference
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 100
publications, and exhibitions addressing both scientific and industrial events. SRDC has close collaboration with the Turkish Ministry of Health through consultancy services and project partnerships; SRDC will promote ADLIFE integrated care solutions at the highest level. SRDC is also actively involved in standardisation activities such as IHE, ISO and OASIS. SRDC will pursue possible standardization opportunities and aims to contribute to the development and improvement of standards for digital representation of integrated care plans.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 101
4.10 EVERIS
4.10.1 DESCRIPTION OF THE LEGAL ENTITY AND ITS MAIN TASKS
everis is an international large company that offers its clients comprehensive business solutions covering all aspects of the value chain, from business strategy to systems implementation. everis was established in Spain in 1996 as DMR Consulting, its name until October 2006. It started operating in Spain with the opening of an office in Madrid and Barcelona, soon followed by expansion in Europe and Latin America. At present, the company has a wide presence in Europe and America (LATAM and the USA), with offices in several locations in Spain, as well as in Brussels, Lisbon, Milan, Rome, Santiago de Chile, Buenos Aires, Mexico City, Sao Paulo, Rio de Janeiro and Bogotá, Washington, among others.
Currently, everis has over 18,000 employees in 25 offices in 15 countries and its annual turnover is more than 800 Million Euros. Since January 2014, became part of NTT Data group, which enables everis to offer a wider range of solutions and services through increased capacity, as well as technological, geographical, and financial resources, establishing the 5th worldwide ICT Company integrated by more than 70,000 employees and with presence in 41 countries.
As ICT provider, everis is organised by sectors, from the business point of view, and we count on several technological key lines (IoT to be underlined). Thanks to our dual nature, both technological and business oriented, we can act as facilitators, providing a common place for technology solutions and their potential end users.
everis is active on European funded projects (POLYCARE, V-Chain, iDetecT4ALL, INFRA, REACT, COM2REACT, GPM, X-MOB, Ecosell, M-to-Guide, OPTIMI, SafeCity, CROSS, INSEC, ARGOS, District of Future, Multisensor, RRI, BaaS, CaaS, HEARTEN), undertaking a wide range of innovative activities, such as technological developments, pilots implementations, industry reports and surveys, business plans, commercialisation and exploitation programs, integration developments and Coordination management.
From a business perspective, everis covers actions in economic sectors such as Industry, Utilities, Public Administration, Healthcare, Insurance, Media, Telecom and Banking. everis provides its clients with global business solutions covering all aspects of the value chain of any organization, from business strategy and reengineering, to implementation of technological solutions.
Some major everis clients, implying multi-site, multi-country and complex projects include: Banco Santander, TSB, Banque Paribas, Barclays Bank, and British Gas, Sanitas, Asisa, Altadis, Gas Natural, Endesa, Telefónica, SCH, La Caixa and Deutsche Bank, CEPSA, Gestamp, CHEP, Citroën, Peugeot, SEAT, REPSOL, Groupe Air France, Abbey National, Fortis AG, among others.
As result, the company gathers experts in project management, preparation and implementation of business and exploitation plans, IT development and dissemination. On the other hand, everis makes possible for clients to simplify technology without losing depth, therefore allowing these organizations to concentrate more their energy on business objectives.
everis health is a unit developed within everis to assist the health and social care sector; it is a strategic everis initiative with the vocation of leading the transformation of the sector, facing up to new health challenges in specific ways, on the basis of in-house knowledge and investment in the creation of new knowledge, services and assets.
Commitment to the client is the fundamental basis for any business. Based on this simple idea, we have organized our services into five primary departments to offer a full range of flexible and proactive services:
everis business consulting has ongoing projects involving corporate strategy, business practices, and process consulting. Our activity is based on business sector knowledge, innovation, and specialization.
everis BPO offers business process outsourcing service agreements, freeing our clients up to focus on things of more pressing concern, and giving our clients greater control over quality and costs relating to these services.
everis solutions is dedicated to designing and implementing technological solutions and management of outsourced services (applications, infrastructures and processes). Promoting the use of quality assurance methodologies, outsourcing work to high performance centers with a high degree of operational and technological specialization.
Outsourcing of Systems and Applications. Service unit specialized in strategy, consulting, design, management, and services related to outsourcing. This unit uses its experience, as well as best market practices, and tools to respond to each client’s needs.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 102
Software manufacture. everis centers manages the use of high performance centers. This business department has the structure and capacity to work at the pace of the industry with a high level of productivity and efficiency. There are currently high performance centers in Madrid, Barcelona, Seville, Murcia, Alicante, Buenos Aires, Santiago, and Sao Paulo.
Besides, there are two cross service lines focused on innovation and on its transfer to the market: everis innova systematizes innovation with the aim of helping to position consortium as a leader in transforming
innovation into a competitive advantage—individually and collectively, in business and in society, in a diversified and sustained manner. everis innova promotes innovation through Internet platforms where we can work with clients, providers, and others, to keep up with current tendencies.
everis initiatives is the cornerstone of our strategy to position us a company with an international presence, a leader in market strategies, promoting and encouraging entrepreneurial spirit and talent. With the goal to develop and launch new businesses, everis initiatives selects ideas with business potential and then offers everis capabilities and resources behind the concept, in order to turn those ideas into profitable businesses.
Excellence is a way of life at everis. It is accomplished through high levels of productivity and the quality of delivery. everis has developed a methodology called COM (Corporate Methods), which encompasses the experiences gained in projects carried out. COM transforms these experiences into easily applicable methods, which provides the most appropriate solutions to our clients. As a result of this way of working, everis has obtained the international ISO 9001 certification. Our teams are highly qualified, as our consultants have gained more than a thousand certificates (SAP, Oracle, Sun, IBM, PMI, Prince2, ITIL, etc.). We also have high performance centers with a CMMi-5 certification in several countries. This is the highest level of quality in the IT industry. In addition, everis has proven expertise in identifying business benefits and change processes, without forgetting business strategy development under co-creative spirit together with our partners and clients, as well as the management decisions required to achieve these objectives. This focus provides a methodological framework that guarantees that investments and projects are evaluated in line with business results. Our professionals are experts in applying this approach to the whole range of services we offer to our clients. From the technological perspective, everis counts on several key lines, subjects identified as core technologies which will transform the traditional IT business, implying our present and future value proposal to our clients.
ROLE IN THE PROJECT
everis will lead the WP5 CLINICAL DECISION SUPPORT SYSTEMS AND EARLY IDENTIFICATION TOOLS, which aims to facilitate personalization of guideline driven care plans and enhance capacity to respond early and rapidly to individuals' changing needs and preferences over time. everis will solve one of the most challenging issues related to the automatization of information and analysis extracting from medical guidelines as well as generating dynamics tools that will cover the needs of this project.
While the project is being executed, everis will manage these tasks:
Coordination and mediation between all entities involved in the work package. Assure the interoperability and securization of all the tools developed. Develop the intelligent tools that will include predictive models feeded by the available data sources. Supply the ICT architecture that will integrate the solutions delivered by the other partners involved in the work
package. Guarantee the future exploitation of ADLIFE results (WP10, WP2)
Everis has been active within the health and social services field for more than ten years and has wide experience in Big Data&Advanced Analytics, developing important projects for referent clients. To reinforce this strategic line, there is a specific unit in the Group dedicated to it, everis Healthcare Advanced Analytics. This unit will assume the main responsibilities of the tasks described before.
4.10.2 CV OF THE PERSONS
Gonzalo Vallejo Setién
Gender Male
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 103
Qualification Bc Computer Engineering
Staff Category Director
Short description of work experience, relevant to the proposal
Director at everis specialized in the Health and Innovation areas. He is a Computer Engineer with more than 19 years of experience in ICT services (always related to health projects). Since 2015, he has been leading the everis Health sector in the Basque Country office. Responsible for the health strategy in the office as well as responsible for clients such as Osakidetza (with a relevant project of maintenance the global platform of Business Intelligence and advanced analytics), Department of Health of the Basque Country, University Clinic of Navarra and Cantabrian Health Service. He is also responsible for the area of innovation in health in the Bilbao office with relevant projects in Artificial Intelligence such as personalized prescription in patients with bipolar disorder, financed by NTT Data.
Arkaitz Cámara Etxebarria
Gender Male
Qualification Bc Computer Engineering
Staff Category Project Manager
Short description of work experience, relevant to the proposal
Arkaitz Cámara Etxebarria project manager at EVERIS specialized in the Health and Innovation areas. He is a Computer Engineer, holds a PMP certification and he is also certified as Java Programmer (Sun Certified Java Programmer 1.4.2). He speaks Basque and Spanish as mother languages, English fluently (B2 certificate) and a little bit of French. With more than 15 years of experience in ICT services (always related to health projects), has conducted several innovative and financed projects like the SRT - Smart Remote Treatment for patients diagnosed with bipolar disorder, funded by the NTT Data. Since 2017 he manages projects execution in the health and innovation area at everis in the Basque Country. A relevant project managed at the moment is SRT, working with a distributed team set in different cities (Madrid, Bilbao, Barcelona, Zaragoza or Tokyo), sharing different cultures (Japanese and Spanish), with different time zones or speaking different languages (Spanish, Basque, English and Japanese) and in collaboration with the Public Health Provider in the Basque Country.
Andoni Martín Reboredo
Gender Male
Qualification Bc Computer Engineering
Staff Category Data analytics team leader
Short description of work experience, relevant to the proposal
Andoni Martín Reboredo, Data analytics team leader at EVERIS for the last two years. Specialized in Big Data and its applications in building mathematical and machine learning models for business specific needs. Certified system administrator with specific experience in deployment of Big Data on-premise and cloud infrastructures. Andoni has provided specific solutions to the health sector, acting as team leader in a project for the development of a decision support system (DSS) for the treatment of patients with bipolar disorder through the recommendation of a personalized posology; and he was the responsible for the quality assurance of a software for the management of animal facilities destined to medical research.
Aratz Setién Gutiérrez
Gender Male
Qualification Bc Telecommunications Engineering
Staff Category Specific Knowledge Analyst
Short description of work experience, relevant to the proposal
Aratz Setien Gutierrez works as Specific Knowledge Analyst at EVERIS since February. He holds a Master’s degree in Telecommunications Engineering and speaks Basque and Spanish as mother languages, English fluently (C1 certificate).With more than 11 years of experience in the ICT sector, he has been involved in diverse projects as R&D Engineer, including international (ICT FP7 - Collaborative Project: Embedded Computer Engineering Learning Platform E2LP), regional (VIRUSES - Visually Immersive Researching Unit for Scientific and Educational Scenarios.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 104
Patent ES2649789A1) or private funded (eVida©Knee). Focusing his activity in the health sector in the last years, he is certified in Machine Learning (Standford University) and Deep Learning (deeplearning.ai) technologies.
4.10.3 LIST OF RELEVANT PUBLICATIONS/PRODUCTS
Everis Health Division
One of everis strategic key lines is everis health, a unit developed within everis to assist the health and social care sector. It has delivered projects and services for notable customers within both the public and private sectors worldwide. Our wide experience in the sector, through projects carried out all over the world, and in all activities of the value chain (health authorities, health insurance, sanitary health providers, etc)., have given us a deep knowledge about its dynamics and tendencies.
Apart from that, everis health has specialized in innovation in the following areas: Collaborative Environments, Health Intelligence, Rehabilitation, Active Ageing, Training and learning, Interoperability, Personal Health Record, Management of Chronic Diseases and Mental Health.
ICT provider for Public Healthcare Provider of several Regional Health Services
everis provides maintenance and evolution of the main healthcare applications used in public health system in different regions in Spain. As the most important systems maintained and projects executed may be cited:
Expand the Electronic Health Record implementation (EHR) across the different assistance and improve its functionality
Extend the electronic prescription to Specialized Care and Emergency. EMPI (Enterprise Master Person Index) management Implement changes required in several applications: laboratories management, HCD, neonatal screening...
ehCOS
everis has developed ehCOS, an innovative process-oriented technology platform both for clinical and administrative process. Its functional and technological base provides a strong initial layer which reduces the development time and maintainability of the new solution.
The platform incorporates health industry concepts and standards:
Latest trends in interoperability: HL7, DICOM, IHE, CDA, etc. Coding Standards (CIE, NAND, etc.) Usability: WC3, MSCUI. Pre-built indicators: AHRQ, mortality, GRD. It incorporates both global best practices and recommendations from leading independent bodies in the field (HIMSS EMR Adoption Model, Gartner Criteria for Enterprise CPR, CCHIT, etc.) and supports new industry trends: Cloud, mHealth, Continua Health Alliance.
The ehCOS product suite responds to the main market challenges. It encapsulates the knowledge acquired by our professionals in more than twelve years of experience in the implementation of projects within the health sector, in addition to the main standards in clinical care processes established by major health organizations (WHO).
ehCOS facilitates continuous innovation and evolution in the needs of our customers and strengthens strategic partnerships with technology provider and university customers.
Everis Business
In addition everis has proven expertise in identifying business benefits and change processes as well as the management decisions required to achieve these objectives. This focus provides a methodological framework that guarantees that investments and projects are evaluated in line with business results. Our professionals are experts in applying this approach to the whole range of services we offer to our clients. As said before, there is a specific division for strategy and business projects.
4.10.4 LIST OF RELEVANT PREVIOUS PROJECTS
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 105
everis has already cooperated in several European funded projects (INFRA, REACT, COM2REACT, GPM, X-MOB, OPTIMI, SafeCity, CROSS, INSEC, District of Future, Multisensor, RRI, BaaS, CaaS) undertaking a wide range of activities such as industry reports and surveys, business plans, commercialisation programs, integration developments and Coordination management. The main references of relevant research projects are:
POLYCARE (H2020-PHC-25-2015) :Develop and test a model of comprehensive patient-centered care, supported by the use of information technology that enables the monitoring and care of chronic patients in acute phases at home including: Wereables use, detection of vital signs and other health measures out of range. Alert management, Alerts interactions in making medicines, Collaborative environment for caregivers (agendas, making manual entry steps, etc.), design gamification apps for patients and caregivers.
FOCUS PROJECT (Frailty management optimization through EIP AHA Commitments and Utilisation of Stakeholders input - 3rd Health Programme HP-PJ-04-2014): The purpose is to critically reduce the burden of frailty in Europe by assisting those partners within European Innovation Partnership for Active and Healthy Ageing with commitments focusing on early diagnosis/screening and/or management of frailty to achieve scalability.
HEARTEN (H2020-PHC-26-2014): HEARTEN is a H2020 project that aims to develop a pilot monitoring solution for heart disease with mobile technology and inclusion of mechanisms of adherence to prescribed treatment.
iSOPHIE project – FEDER INNTERCONECTA call (Spanish National Ministry of Economy – CDTI): iSOPHIE project aims to develop an eHealth platform for oncology services, following 4P medicine principles (personalized, participatory, predictive and preventive), the excellence and full quality.
RRI TOOLS PROJECT (Foster Responsible Research and Innovation for society, with society (FP7-SCIENCE-IN-SOCIETY-2013-1)): This project develops and uses a Training and Dissemination Toolkit on Responsible Research and Innovation (RRI). It is addressed and designed by representatives of all the stakeholders of the Research and Innovation (RI) value chain, including Researchers, Civil Society, Industry and Education but will specially focus on Policy Makers in order to impact significantly in the future governance of RI.
4.10.5 DESCRIPTION OF ANY SIGNIFICANT INFRASTRUCTURE
everis is a company with extensive possibilities in deploying all the resources necessary for the optimal development of their projects. Corporately, they have the following resources: the research unit everisInnova, Foundation everis, department of marketing and visibility, center of documentation and competence center of everis. It also has the ability to offer appropriate technical resources for development projects. everis has an IT support for all employees.
On the other hand, our office in Barcelona holds a new Open Innovation space, the everis Living Lab. Our Living lab is born with the aim of creating an ecosystem around the Open Innovation process, incorporating public administrations, companies, researchers and people in general. The Living lab is user-centered and provides the necessary tools for exploration, co-creation, experimentation and evaluation of innovative ideas, scenarios, concepts, technologies and, in general, methodologies for real life use cases.
Aligned with the objectives postulated in Open Science and Open Innovation, due to the immediacy in the testing of experimental methodologies, it adds the "landing" of these methodologies by involving the user in all this ecosystem.
One of the greatest advantages of Living Labs is the mitigation capacity of real life mistakes, and the fast absorption of results from the “quadruple helix” (universities/research centers, industry, governments and society). This is mainly because the living lab is a space where results feed themselves and where a dynamic balance between all parties is reached. It includes the following facilities:
Showroom (Observation phase) to show innovation and to identify trends, to inspect the market and to generate valuable insights for all stakeholders.
Co-Creation y Co-Design (Creation phase) where open innovation with partners, stakeholders and the innovation ecosystem is facilitated, fomented and developed. Its main aim is to generate innovation and to involve users in the process.
Laboratory (Prototyping and Validation phases) where experimentation and testing of concepts, methodologies and new solutions, as well as their iteration and evaluation in real contexts id facilitated.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 106
Feedback and Learning (Learning phase) both of all that has happened in this space and of the results of the process followed.
4.10.5.1 NETWORKS everis health makes available for the project its specific knowledge, partnership network and marketing activities:
Continuous observatory of health sector Special Report Elaboration of studies and specialized informs on the sector (on behalf of clients or internal reports) Member of the Bamberg Foundation: “Global Health Leaders” event // “Latin American Health leaders” event. HL7 and IHE Member – More than 50 certified professionals A network of consultants consisting of GPs, experts on system management and health units, etc. Partnership agreements with:
Leading health solutions companies. Universities and Investigation Centres. Scientific societies, clients and experts, with the aim of reuse best practices and solutions in other markets.
4.10.5.2 DISSEMINATION CAPABILITY Everis has presence at 16 countries around the world with wide presence in Europe and America (LATAM and the USA) and is an ICT provider for Public Healthcare Provider of several Regional Health Services. Everis will use his network capabilities to expose the project and to look for relevance, in order to provide new competences and solutions for health clients on the prediction of diseases and decision support systems. Therefore, the important market capabilities of everis will contribute to the dissemination activities.
In addition, everis is in charge of the organization and sponsorship of national and international events for the Health Sector, where the results of the project will be presented.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 107
4.11 I-HD
4.11.1 DESCRIPTION OF THE LEGAL ENTITY AND ITS MAIN TASKS
i~HD (www.i-hd.eu) is a not for profit institute registered in Belgium. It is a membership-based organisation with members from pharma, healthcare providers, academic organisations, and works closely with patient organisations, healthcare payers, the health ICT sector and standards development organisations. i~HD develops methods, solutions and services that can maximise the value obtained from health data, to support innovations in health, health care and knowledge discovery, while ensuring compliance with legal prerequisites, especially regarding patient’s privacy protection. It tackles areas of challenge in the successful scaling up of innovations that rely on high quality and interoperable health data. It collates, develops and supports adoption of best practices in information governance and data protection. Its activities include a Network of Excellence for healthcare providers, data quality assessment and improvement support, promoting codes of practice and expertise in sustainability and business modelling. i~HD benefits from core scientific and management staff who bring significant experience leading or being a partner in over 80 EC projects in the areas of electronic health records, interoperability, security and privacy protection.
ROLE IN THE PROJECT
Lead of task 1.5 on data management and data protection. I~HD has considerable expertise in defining codes of practice for managing and sharing health data for healthcare, learning health systems and research. Its team has been very active in examining the implications of the GDPR on these purposes of using health data, and on the legal bases that might be considered. It has also been very involved in the evolution of data sharing agreements across Europe. In ADLIFE i~HD will develop and oversee compliance with a code of practice for all personnel and sites handling data (personal including pseudonymised, and anonymous) and support all sites with standard text for the data sharing and data processing agreements they will need to co-operate on integrated personalised care and on the studies proposed. It will develop and govern the adoption of a data management plan.
Contributor to task 2.2 on external communication, bringing substantial experience in developing promotional materials and in working across stakeholders on complex health and health informatics messages.
Contributor to task 2.4 on interaction with other EU consortia, given that the i~HD network of experts are very involved in Horizon 2020, IMI and EIT Health initiatives and interact regularly with the leadership of these programmes.
Contributor to WP10 on exploitation, with a focus on business modelling. I~HD has considerable experience in the development of multi-stakeholder value chains and business models and can conduct cost benefit assessments if needed. I~HD experts have experience of defining evidence and roadmap for sustaining for profit and not for profit initiatives arising from EC projects. It is itself a not for profit sustainable entity arising from EC projects.
4.11.2 CV OF THE PERSONS
Professor Dipak Kalra
Gender Male
Qualification PhD, FRCGP, FBCS,
Staff Category President
Short description of work experience, relevant to the proposal
Dipak Kalra, is President of The European Institute for Innovation through Health Data (i~HD). He plays a leading international role in research and development of Electronic Health Records, including the development of ISO standards on EHR interoperability, personal health records, EHR requirements. He has contributed to several EHR security and confidentiality standards. Dipak has led multiple Horizon 2020 and IMI projects in these areas, alongside pharma companies, hospitals and ICT companies. He recently co-led a €16m project on the re-use of EHR information for clinical research, EHR4CR, alongside ten global pharma. He ws a partner in another IMI
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 108
project, EMIF, on the federating multiple population health and cohort studies. Dipak also led an EU Network of Excellence on semantic interoperability and is a partner in other EU projects on the sustainability of interoperability assets, the transatlantic sharing of patient summaries and quality labelling. Dipak is Professor of Health Informatics at University College London and Visiting Professor of Health Informatics at the University of Gent.
Professor Pascal Coorevits
Gender Male
Qualification BICT, MSc, PhD,
Staff Category Task force
Short description of work experience, relevant to the proposal
Pascal Coorevits, is Professor of Medical Informatics and Statistics at the Faculty of Medicine and Health Sciences of the Ghent University in Belgium. He has participated in many EU, national – and transatlantic eHealth research projects (e.g. ASSIST, EHR‐Implement, EHR‐QTN, ARGOS, HITCH, EHR4CR, SemanticHealthNet, EURECA,…). His primary research interests lie in the domain of Electronic Health Records (EHRs) and are oriented towards various aspects of quality labelling and certification of EHRs (EHR functional descriptive criteria, EU and US quality labelling and certification models, tools/methodologies for EHR evaluation and conformance testing). Pascal leads the data quality assessment Task Force of i~HD.
Dr Nathan Lea
Gender Male
Qualification PhD
Staff Category Task force
Short description of work experience, relevant to the proposal
Dr Nathan Lea leads i~HD’s task force on i~HD on the GDPR, the development of adaptive codes of practice and standard operating procedures to govern and secure the use of health and genetic data for research purposes and digital health innovation. He has focused his research on operational security and design implementation, and he has an interest in understanding the legal, ethical and societal impacts and concerns around novel health data uses, particularly in the area of Artificial Intelligence for health management and genomics research. Nathan is also a Senior Research Associate at UCL where his research and teaching focuses on understanding legal, ethical and security requirements for Big Data driven clinical research.
Mr Geert Thienpont
Gender Male
Qualification Computer Scientist
Staff Category President and director of RAMIT
Short description of work experience, relevant to the proposal
Mr Geert Thienpont is a computer scientist and studied at the Industrial School of the State B.M.E. GENT. Currently, he is president and director of RAMIT and Project manager of EuroRec, which includes coordination of software implementation, HR and financial management. Furthermore, he was or is involved in national and European associations such as the Microsoft Healthcare User Group Europe (MS-HUGe), MedNet, World of Health ICT: Education, Events and Exhibitions (WHIte³) and ProRec-Belgium.
4.11.3 LIST OF RELEVANT PUBLICATIONS/PRODUCTS
Floridi et al. Key Ethical Challenges in the European Medical Information Framework. Minds and Machines 2018. https://doi.org/10.1007/s11023-018-9467-4
Prodinger B, Rastall P, Kalra D, Wooldridge D, Carpenter I. Documenting Routinely What Matters to People: Standardized Headings for Health Records of Patients with Chronic Health Conditions. Applied Clinical Informatics 09(02):348-365. https://doi.org/10.1055/s-0038-1649488
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 109
Wise J, Möller A, Christie D, Kalra D, Brodsky E, Georgieva E, Jones G, Smith I, Greiffenberg L, McCarthy M, Arend M, Luttringer O, Kloss S, Arlington S. The positive impacts of Real-World Data on the challenges facing the evolution of biopharma. Drug Discovery Today 2018 Volume 23, Issue 4, April 2018, Pages 788-80. https://doi.org/10.1016/j.drudis.2018.01.034
Ohmann C, Banzi R, Canham S, Battaglia S, Matei M, Ariyo C, Becnel L, Bierer B, Bowers S, Clivio L, Dias M, Druml C, Faure H, Fenner M, Galvez J, Ghersi D, Gluud C, Groves T, Houston P, Karam G, Kalra D, Knowles RL, Krleæa-Jeriƒá K, Kubiak C, Kuchinke W, Kush R, Lukkarinen A, Marques PS, Newbigging A, O'Callaghan J, Ravaud P, Schl√ºnder I, Shanahan D, Sitter H, Spalding D, Tudur-Smith C, van Reusel P, van Veen EB, Visser GR, Wilson J, Demotes-Mainard J. Sharing and reuse of individual participant data from clinical trials: principles and recommendations. BMJ Open. 2017 Dec 14;7(12):e018647. https://doi.org/10.1136/bmjopen-2017-018647
Dupont D, Beresniak A, Sundgren M, Schmidt A, Ainsworth J, Coorevits P, Kalra D, Dewispelaere M, De Moor G. Business analysis for a sustainable, multi-stakeholder ecosystem for leveraging the Electronic Health Records for Clinical Research (EHR4CR) platform in Europe. Int J Med Inform 97:341-352 2017. http://dx.doi.org/10.1016/j.ijmedinf.2016.11.003
4.11.4 LIST OF RELEVANT PREVIOUS PROJECTS
C3-CLOUD (H2020 689181, 01.05.2016 - 30.04.2020), a federated Collaborative Care Cure Cloud architecture for addressing the needs of multi-morbidity and managing poly-pharmacy
VALUeHEALTH (H2020 643847, 01.04.2015 - 31.03.2017), Business model for sustainable eHealth services in Europe
SemanticHealthNet (FP7 288408; 01.12.2011 - 31.05.2015), Semantic Interoperability for Health Network EMIF (IMI-JU 115372; 01/01/2013 - 31/12/2018), European Medical Informatics Framework eHealth innovation (CIP 270986; 01.03.2011 - 28.02.2013), Scaling up eHealth facilitated personalised health
services.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 110
4.12 THIRD PARTIES INVOLVED IN THE PROJECT
1.KRONIKGUNE YES/NO
Does the participant plan to subcontract certain tasks (please note that core tasks of the project should not be sub-contracted)
NO
Does the participant envisage that part of its work is performed by linked third parties?
Name of the third party: OSAKIDETZA, BASQUE COUNTRY-SPAIN (OSAKIDETZA),
Description of the third party: Osakidetza is the public healthcare service of the Basque Country, a region located in the north of Spain. Osakidetza was created by the Health Department of the Basque Government in 1983. All the public hospitals and primary care centers of the Basque Region are under this organization. The Basque Health System includes 14 hospitals, more than 100 primary care clinics organized through four different geographical areas, apart from the Mental Health Centers, Emergencies and Basque Transfusions and Human Tissue Centre. More than 30.000 professionals work for Osakidetza, which could be considered the biggest organization of the Basque Country.
Link to the partner: affiliated entity linked to Kronikgune
Osakidetza will be strongly involved in all tasks of WP1, project coordination and management, WP2 Dissemination and communication, WP7 - empowerment of patient and caregivers, WP9 – Evaluation, and WP10 exploitation. In WP3 – Intelligent and secure tools to create and deliver personalised care plans, Osakidetza will be highly involved in the task 3.1, 3.2 and 3.3 (technical requirements analysis, customization and integration of the personalised care plan management, and pilot site integration and interoperability). Osakidetza will participate in the patient empowerment platform interoperability/safety (task 4.1) of WP4. In WP5 – Clinical decision support services, Osakidetza will be strongly involved in the risk prediction model design and implementation (task 5.3). Osakidetza will be participating in the task 6.1. integration and coordination of care for advanced chronic diseases in existing health-care services and task 6.3. design, develop and test personalized care. Finally, as one of the pilot sites of ADLIFE, Osakidetza will also strongly contribute to task 8.1, 8.2 and 8.3 (prepare the implementation of the intervention, ethical application and deploy the ADLIFE integrated supportive care intervention).
YES
Does the participant envisage the use of contributions in kind provided by third parties (Articles 11 and 12 of the General Model Grant Agreement)?
NO
2.STRAT YES/NO
Does the participant plan to subcontract certain tasks (please note that core tasks of the project should not be sub-contracted)?
STRAT will collaborate with clinicians from primary, secondary and tertiary care that are responsible for delivering healthcare services in NHS Lanarkshire. STRAT has a strong past and on-going research relationship with the health care teams participating in this project. All projects have access to a strong multi-disciplinary team of clinicians and representatives as partners and collaborators which has resulted in excellent relationships with and access to practices, professionals and patients for the optimal research process outcomes. In addition, the Centre ensures that evidence is applied in practice and works with professionals to develop appropriate pathways to implement improvements.
In relation to the ADLIFE project, STRAT has secured the support of clinical partners by subcontracting their services (staff dedication and all the resources needed for the implementation and the interventions to be developed in these health care centres). The subcontracting activities will include a payment of 250 euros per site per patient recruited to the trial (n=126), the time of experts’ clinicians to advise on educational material (80,000€).
YES
Does the participant envisage that part of its work is performed by linked third parties? NO
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 111
Does the participant envisage the use of contributions in kind provided by third parties (Articles 11 and 12 of the General Model Grant Agreement)?
NO
5.FALK YES/NO
Does the participant plan to subcontract certain tasks (please note that core tasks of the project should not be sub-contracted)?
Subcontract: FALK will need to subcontract some healthcare professionals as well as the implementation of the digital toolbox in the ICT infrastructure 45,000 €. Considering the ICT infrastructures in the hospital it is expected to devote internal effort from ICT developers in the region apart from the internal team.
YES
Does the participant envisage that part of its work is performed by linked third parties? NO
Does the participant envisage the use of contributions in kind provided by third parties (Articles 11 and 12 of the General Model Grant Agreement)?
NO
6. OPTIMEDIS YES/NO
Does the participant plan to subcontract certain tasks (please note that core tasks of the project should not be sub-contracted)?
Subcontract: OPTIMEDIS will collaborate with clinicians from primary, secondary and tertiary care that are responsible for delivering healthcare services in STRAT will collaborate with clinicians from primary, secondary and tertiary care that are responsible for delivering healthcare services in NHS Lanarkshire. OPTIMEDIS has a strong past and on-going research relationship with the health care teams participating in this project. All projects have access to a strong multi-disciplinary team of clinicians and representatives as partners and collaborators which has resulted in excellent relationships with and access to practices, professionals and patients for the optimal research process outcomes.
In relation to the ADLIFE project, OPTIMEDIS has secured the support of clinical partners by subcontracting their services (staff dedication and all the resources needed for the implementation and the interventions to be developed in these health care centres). The subcontracting activities will include a payment per site per patient recruited to the trial (n=126), the time of experts clinicians to advise on educational material (80,000). It would be also necessary to subcontract ICT support experts from the region to implement the tools in the pilot (25,000 €).
YES
Does the participant envisage that part of its work is performed by linked third parties?
Name of the third party: Werra-Meißner Kreis Gmbh is a 100% subsidiary ltd company of OptiMedis.
Werra-Meißner Kreis Gmbh would be the regional third party that will be in charge of piloting the ADLIFE intervention in the two locations (Witzenhausen and Eschwege) of the participating hospital Werra-Meißner Kreis Gmbh. Optimedis usually uses this model of work for the development of the different programs of integrated care al around the world. The expected budget is 289,931 €.
YES
Does the participant envisage the use of contributions in kind provided by third parties (Articles 11 and 12 of the General Model Grant Agreement)
NO
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 112
7. RJH YES/NO
Does the participant plan to subcontract certain tasks (please note that core tasks of the project should not be sub-contracted)?
RJH will need to subcontract part of the tasks related to ICT adaptation to local settings (20,000€)
YES
Does the participant envisage that part of its work is performed by linked third parties NO
Does the participant envisage the use of contributions in kind provided by third parties (Articles 11 and 12 of the General Model Grant Agreement)?
NO
8. AMCA YES/NO
Does the participant plan to subcontract certain tasks (please note that core tasks of the project should not be sub-contracted)?
AMCA will need to subcontract part of the tasks related to ICT adaptation to local settings (25,000€).
YES
Does the participant envisage that part of its work is performed by linked third parties?
AMCA will include two linked third parties in the project Maccabi Healthcare Services (Maccabi) and Assuta Medical Centers Network (AMCN). As can be seen in the following graph the three entities are linked as Maccabi healthcare Services owns Assuta Medical Centers which is the owner of AMCA. AMCA is a subsidiary organization of Maccabi.
Third party: Maccabi healthcare services
Description of the third party: Maccabi Healthcare Services will be AMCA's partner in this project. Maccabi (Israel’s second largest Health plan – both insurer and provider with over 2 million members) operates a comprehensive network of primary and secondary healthcare services in the community. Maccabi has been a pioneer in the development of comprehensive ICT systems for clinical and administrative management of medical services and patient health. Maccabi operates services for medical, nursing and rehabilitative home care in all of the country's districts that treat homebound people, who suffer from a wide variety of diseases and medical and functional conditions. Maccabi Healthcare Services is Israel's second largest Health Insurer and Provider and operates comprehensive healthcare services in the Community., including the development of parameters for early identification of patients needing integrative care. Maccabi is a member of the B3 Integrated Care Action in group of the European Innovation Partnership for Active and Healthy Aging.
Tasks in the project: Maccabi Healthcare Services will focus predominantly on WP8 in which Maccabi will be responsible for the primary care services in the community that will work in coordination with Assuta Ashdod Hospital to provide integrated supportive care to ADLIFE patients. Maccabi will also provide the database for selecting the control group as well as providing additional data about the intervention group. The expected budget is 164,437 € for the staff that it is going to participate in the project and for the necessary travels for the project.
YES
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 113
Third party: Assuta medical services (AMCN)
Description of the third party: AMCN is Israel’s largest and leading private medical services network comprising eleven clinics and hospitals across Israel and providing innovative surgeries, diagnostic procedures and specialty outpatient services in all fields of medicine, including cardiology, oncology, gynaecology, urology and more. Assuta-Ashdod Hospital, the project partner, is the newest member of the Assuta hospital network and its first public hospital. AMACA has been designed to be the model for the network as well as the rest of the Israeli hospital system for integrated care, forging new links for coordination with community health and social care as well as with the patient and his/her family. The AMCN central staff provides policy guidance and support to all of the hospitals and clinics in the network including clinical guidelines and policies, ICT support and support in the areas of research and development.
Tasks in the project: Considering the potential impact of the project at global level in the network of hospitals, it is crucial to involve the central institution, AMCN, that will support AMCA in the overall project management and administration issues related to the project (coordination of transversal teams, interaction with EC among others). AMCA staff will benefit of AMCN’s experience and expertise while avoiding unnecessary duplication of effort within the Network. his will include support from the central ICT staff and the Institute’s research staff. The expected budget is 247,500 € for the staff that it is going to participate in the project.
Does the participant envisage the use of contributions in kind provided by third parties (Articles 11 and 12 of the General Model Grant Agreement)
NO
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 114
5. ETHICS AND SECURITY 5.1 ETHICS
This section identifies the relevant ethical issues that are involved in the project and that are addressed in this
section:
TABLE 1 MAIN ETHICAL ISSUES ADRESSED IN ADLIFE PROJECT
Section 1: HUMAN EMBRYOS/FOETUSES Yes/No Page Does the proposed research involve human Embryos? No - Does the proposed research involve human Foetal Tissues/ Cells? No - Does the proposed research involve human Embryonic Stem Cells (hESCs)? No - If Yes -Will they be directly derived from embryos within this project? -
-Are they previously established cells lines? -
Section 2: HUMANS Yes/No Page Does your research involve human participants? Yes 3-58 If Yes - Are they volunteers for social or human sciences research? Yes 3-58
- Are they persons unable to give informed consent? No - Are they vulnerable individuals or groups? No - Are they children/minors? No
- Are they patients? Yes 3-58
- Are they healthy volunteers for medical studies? No Does your research involve physical interventions on the study participants? No If Yes
- Does it involve invasive techniques (e.g. collection of human cells or tissues, surgical or medical interventions, invasive studies on the brain, TMS etc.)?
No
- Does it involve collection of biological samples? No
If your research involves processing of genetic information, please also complete the section “Protection of Personal Data” i.e. Section 4.
Section 3: HUMAN CELLS / TISSUES Yes/No Page Does your research involve human cells or tissues? (Other than from “Human Embryos/Foetuses” i.e. Section 1)
No
If Yes - Are they available commercially?
- Are they obtained within this project? - Are they obtained within another project? - - Are they deposited in a biobank?
Section 4: PROTECTION OF PERSONAL DATA Yes/No Page Does your research involve personal data collection and/or processing? It should be noted that: 1. “Personal data” can be defined as identifiers: any information that could, in any way, lead to the specific identification of one unique person, such as name, social security numbers, date of birth, address, mails IPs etc. 2. Any data that you are using should be taken into account, regardless of the method by which they are/were collected: for example, through interviews, questionnaires, direct online retrieval etc. 3. Processing should be understood to not only include data usage, but also merging, transformation, transfer and, more generally, as all actions using data for research purposes.?
Yes 3-58
If Yes - Does it involve the collection and/or processing of sensitive personal data (e.g. health, sexual lifestyle, ethnicity, political opinion, religious or philosophical conviction)? It should be noted that this involvement applies, whatever the research topic or Programme. The above list is only indicative. If the type of data that you will be handling in your research is not included the list, it does not mean you should not take into consideration the subject of data
Yes 3-58
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 115
processing. - Does it involve processing of genetic information? No -
- Does it involve tracking or observation of participants? It should be noted that this issue is not limited to surveillance or localization data. It also applies to Wan data such as IP address, MACs, cookies etc.
Yes 3-58
Does your research involve further processing of previously collected personal data (secondary use)?
Yes 3-58
If Yes It should be noted that this question is threefold. If you answer YES to any of the 3 questions below, you fall within its scope: 1. Are you planning not to collect any data directly but rather to use pre-existing other data sets or sources and/or does your research involve further processing of previously collected data? 2. Does your research involve merging existing data sets? 3. Are you planning to share data with non-EU member states?
Yes 3-58 Yes 3-58 Yes 3-58
Section5: ANIMALS Yes/No Page
Does your research involve animals? No
If Yes No - Are they non-human primates (NHP)? - - Are they genetically modified? -
- Are they cloned farm animals? - -- Are they an endangered species? -
Please indicate the species involved (Maximum number of characters allowed: 1000)
Section 6: THIRD COUNTRIES Yes/No Page Does your research involve third countries? Countries:(Maximum number of characters allowed: 1000) Israel and Turkey
Yes 1, 56
Do you plan to use local resources (e.g. animal and/or human tissue samples, genetic material, live animals, human remains, materials of historical value, endangered fauna or flora samples, etc.)? If YES:
No -
Do you plan to import any material, including personal data, from non-EU/third countries into the EU? If your research involves importing data, please also complete the section “Protection of Personal Data” i.e. Section 4
Yes 3-58
If Yes Specify the materials and countries involved (maximum number of characters allowed: 1000) The project includes pseudonymized patient research data and pilot results
-
Do you plan to export any material, including personal data, from the EU to third/non-EU countries? If your research involves importing data, please also complete the section “Protection of Personal Data” i.e. Section
No -
If Yes Specify the materials and countries involved (maximum number of characters allowed: 1000)
-
If your research involves low and/or lower-middle income countries, are any benefit-sharing actions planned?
No -
Could the situation in the country put the individuals taking part in the research at risk?
No -
Section 7: ENVIRONMENTAL PROTECTION AND SAFETY Yes/No Page Does your research involve the use of elements that may cause harm to the environment, animals or plants? If YES:
No
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 116
Does your research deal with endangered fauna and/or flora /protected areas? :If YES:
No -
Does your research involve the use of elements that may cause harm to humans, including research staff? If YES::
No
If Yes Does your research involve harmful biological agents? Does your research involve harmful chemical and explosive agents? Does your research involve harmful radioactive agents? Does your research involve other harmful materials or equipment, e.g. high-powered laser systems?
Section 8: DUAL USE Yes/No Page
Does your research have the potential for military applications? No - If Yes Does your research have an exclusive civilian application focus? -
Will your research use or produce goods or information that will require export licenses in accordance with legislation on dual use items?
-
Does your research affect current standards in military ethics – e.g., global ban on weapons of mass destruction, issues of proportionality, discrimination of combatants and accountability in drone and autonomous robotics developments, incendiary or laser weapons?
-
Section 9: MISUSE Yes/No Page Does your research have the potential for malevolent/criminal/terrorist abuse? No -
If Yes Does your research involve information on/or the use of biological-, chemical-, nuclear/radiological-security sensitive materials and explosives, and means of their delivery?
-
Does your research involve the development of technologies or the creation of information that could have severe negative impacts on human rights standards (e.g. privacy, stigmatization, discrimination), if misapplied?
-
Does your research have the potential for terrorist or criminal abuse e.g. infrastructural vulnerability studies, cybersecurity related research?
-
Section 10: OTHER ETHICS ISSUES Yes/No Page Are there any other ethics issues that should be taken into consideration? Please specify: (Maximum number of characters allowed: 1000)
No -
5.1.1 GENERAL CONSIDERATIONS
The ADLIFE project has an intervention study evaluation (WP8), that aims to demonstrate that a holistic intervention in advanced chronic disease patients in a personalized integrated care program will relieve symptoms and suffering and will improve life quality of patients, will ameliorate caregivers burden and will optimize healthcare costs.
Although clinical interventions will not be developed in the project and the intervention does not involve any physical intervention on the patients, apart from routine care by their health care professionals, ethical issues are of crucial importance due to the data that are going to be collected and the extremely sensitive situation of the patients and their relatives. All measures have been taken to ensure compliance with the ethical standards of H2020 during the project preparation and development. Ethics standards and guidelines of Horizon2020 will be rigorously applied. These guidelines will be shared with the consortium and the D1.1 Data Management Plan will include specific requirements that all pilot sites will mandatorily comply with. Apart from the tasks included in WP8, T1.4 Ethical Surveillance will monitor the ethical issues of the project.
The project coordinator will oversee all the procedure related to the ethical issues. The pilot sites (Sweden, Israel, Germany, Denmark, United Kingdom, Poland and Spain) will provide the coordinator with all requirements from local ethical committees where the ADLIFE pilot studies will take place. The ADLIFE team will ensure that all the persons involved in research as subjects understand the information transmitted (note: the documents will be provided in their own language).
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 117
An external Ethics Advisory Board (EAB) will be created at the beginning of the project to ensure that the current ethical regulations are respected along the project course and that all potential ethical issues are solved according to regulations. The members of the Board will have expertise and experience in ethical principles and methodology and research ethics. The ADLIFE consortium will discuss the persons and/or organizations that best meet the project´s requirements related to ethical aspects. Some candidate organizations to be approached are: National Ethical Committees of the different pilot sites and the European Network of Research Ethics Committees (EUREC). Also, representatives from the ethics committee of the hospitals and care centres involved in ADLIFE will participate in the EAB when defining the general intervention trial design and when adapting the trial to every region.
5.1.2 INFORMED CONSENT
Obtaining the informed consent is a process of sharing information and addressing questions and concerns, rather than simply obtaining a signature on a prescribed form. In ADLIFE, researchers will:
Raise awareness on European Commission directives and national or regional specific guidelines among study participants to ensure they know their rights.
Follow an appropriate and culturally-sensitive process of information sharing leading up to obtaining the participant's signature on the informed consent form.
Informed consent of all participants (patients, formal and informal care givers and/or relatives) will be gathered. Despite the target group including patients with advanced chronic diseases, to enter in the trial patients will have to able to: a) personally give consent participation, b) understand the terms of the intervention c) consciously participate. It is possible that in the evolution of the patient during the trial, the cognitive abilities may diminish, in that case, legal representatives may be responsible to continue the participation. Data from intervention patients will be compared with anonymized data of similar demographic and clinical characteristics drawn from administrative data bases. The k-anonymity model and de-identification algorithms proposed by ISO/TS 25237:2008 standard will be applied.
Study participants and their caregivers will be informed accurately in advance on the aims of the project, its implications as well as the evaluation. This will be provided in both oral and written form and presented in accessible language. Clear information on confidentiality, anonymity, data management (collection, processing, storage, access, reuse or destruction) will be provided to all participants. The participants will be offered enough time to take the decision to participate or not in the study.
Study participants are free to decline to participate in the project and this statement will be included as an exclusion criterion. At the same time, participants that consent to take part in the intervention can withdraw at any time without providing any justification. In both cases (refusal or withdrawal), patients' data will not be neither collected nor analysed.
If incidental findings such as health problems (including mental health disorders) or social problems occur during the study, the hospitals/care places will follow their protocols already in place, irrespective of the ADLIFE project. These protocols (communication channels and coordination procedures) are mainly based on referrals of patients to healthcare care or social services according to the need identified.
Pilot sites are responsible for obtaining the approval of their local/regional Ethical Committees, who will act as external experts ensuring that the regulation in force is respected. The report to be submitted to these Committees will include the explanation of obtaining the informed consent among other.
The detailed process of obtaining the informed consent will be documented in D9.1 ADLIFE´s first study approvals package as part of the scientific protocol. Guidance note for researchers and evaluators of social sciences and humanities research (2010) will be used as a handbook to describe the process of obtaining the informed consent.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 118
5.1.3 DATA PROTECTION AND PRIVACY
A key aspect of the ADLIFE project is to protect the interests of the patients involved in the studies and their families. ADLIFE will involve no risk of physical or emotional harm to participants who take part in the users’ research. The work carried out will observe strict ethical standards, for example in relation to users’ privacy, confidentiality and consent. Research conducted within the ADLIFE project will respect fundamental ethical principles, including those reflected in the Charter of Fundamental Rights of the European Union: dignity, freedom, equality, solidarity, citizens’ rights and justice. Moreover, the project will act in accordance with the European Human Rights Convention, especially with regard to privacy and autonomy. Each test and intervention conducted within ADLIFE will follow the guidelines set out by the World Health Organization on its “Handbook for good clinical research practice (GCP)”, the Helsinki Declaration of 1964 (Recommendation for conduct of clinical research), the Convention for the Protection of Human Rights and Dignity of the Human Being with regard to the Application of Biology and Medicine: Convention on Human Rights and Biomedicine, the UNESCO Universal Declaration on Bioethics and Human Rights, and the recommendations from the UNESCO World Commission on the Ethics of Scientific Knowledge and Technology (COMEST), among others.
Each pilot will be in direct contact with the competent authorities in order to fulfil all the ethics requirements due to the sensitive nature of the subjects involved. Regional Study protocols will be created with explicit reference to the ADLIFE project title and will be submitted for ethics approval. All participants’ partners, have previous experience in the design and development of intervention in the project’s target groups and have a fluent communication with the corresponding committees. Specific documents may be requested in each region to be submitted in parallel with the study protocols, supporting the investigators in completing the requested application and drawing the feasibility study form at local level. Document consent, recruitment method, study code should not only include demographic data, but also data necessary for obtaining the indicators defined by WP9. Detailed reference to the pilot design and ethic management can be checked in the complementary document requesting information for proposal with clinical trials/studies/investigations. Informed consent will be necessary to participate in the intervention. Document consent will be obtained to participate in the project. As at first stage, all selected hospitals and care-centres involved in the pilots have accepted to participate in the project.
The Consortium (both the member countries of EU and the associated countries) will follow Good Clinical Practices (GCP) (Directive 2004/27/EC) and, from an ethical point of view, these rules are aimed at safeguarding the security of Subjects Included in the Research and ensure the accuracy, reliability and integrity of the data obtained in Research. The directive 2004/27/EC is, in turn, based on the Directive 95/46/EEC of the European Parliament and of the Council of 24 October 1995 on the protection of individuals regarding the processing of personal data. All measures will be taken to ensure the confidentiality of participants in the intervention. Specifically, the new General Data Protection Regulation (GPDR) (UE) 2016/679 (27th April 2016).
As it is described in the technical annex 1-3, ADLIFE will provide anonymization, authentication, authorization and audit services based on widely accepted international standards such as OAUTH 2.0, OpenID Connect, ISO/DTS 27789 - Audit trails and According to the ISO/TS 25237:2008 standard for Pseudonymization. The Security and Privacy Suite (SPS) will be responsible for authentication and authorisation of the care team members, while they are managing personalised care plans of patients and ensuring that all data exchanged within and across ADLIFE components is encrypted and properly auditable. In ADLIFE the patient's electronic health records received from the local EHR systems via the TIS, patient reported outcomes received from the PEP, and the care plan of the patient managed through PCPMP will be all stored in a secure FHIR Repository. Hence, each of these client apps, i.e. TIS, PEP and PCPMP will be authenticated and authorized to access (read, write, and update) patient data to the secure FHIR Repository, via the functionalities provided by SPS. All such operations will be logged for ensuring accountability via SPS. ADLIFE will provide an Audit Record Repository that maintains audit trail records implemented as FHIR AuditEvent resource. ADLIFE SPS will be integrated with the existing privacy protection and security mechanisms in the pilot sites. As a result, SPS will enable authentication of the care team members into the ADLIFE applications via their already existing accounts (e.g., username-password) provided by the local authorities by integrating with the existing Identity Provider (IdP) systems of the pilot sites.
In the context of anonymization, a careful balance between two conflicting objectives must be achieved: maximizing data quality while minimizing re-identification risks. In order to balance between those two goals, the k-anonymity model and de-identification algorithms proposed by ISO/TS 25237:2008 standard will be applied on the EHR data
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 119
such as generalization, redaction and fuzzing. k-anonymity works against linking and disclosing attributes by enforcing an upper bound on the re-identification risk of all records.
There is no single de-identification procedure that will meet the diverse needs of all the medical uses while ensuring privacy of patient data. Therefore, the data anonymization, de-identification and re-identification software tools will be modularly designed to be able to adapt to disparate information systems, and the needs of data analysis tasks.
The ADLIFE SPS authentication, authorization and audit services will build upon the OnAuth Security and Privacy Manager developed by SRDC and validated within the scope of C3-Cloud and Power2DM Projects. It will be deployed, configured for the needs of the project (new roles will be defined, authorization rule sets will be defined), and integrated with Single Sign-on mechanisms of pilot sites. For anonymization, the de-identification mechanisms that have been developed and tested by SRDC within the scope of SALUS Project will be used as a baseline and adapted where necessary.
Since ADLIFE is a user-centred project, the system is tested with real users who are included in the design process. Informed consent will be drawn on permanently for the ADLIFE interviews and trials. Data will be pseudonymized for the evaluation process. In ADLIFE, secondarily processed data will be obtained as a result of quantitative and qualitative analysis. Depending on the evaluation purpose, raw data (surveys, questionnaires, records of focus groups and interviews) will be manipulated accordingly. This data processing will be carried out following the data protection regulation No 2016/679. The project will only collect essential data (clinical, health-related, use of resources, perception of participants) that will enable assessing the impact of the ADLIFE intervention in terms patient health status, functionality and autonomy and system efficiency. The collected data will be used for the purposes of evaluation, impact assessment and growing the evidence base.
A member of Kronikgune (project coordinator) will be the Data Protection Officer and will work closely with Data and Safety Management Group (see below). This Officer will guarantee that the data collection and analysis are performed according to current EU and national legislation. The Data and Safety Management Group will be formed by representatives of 6 pilot sites. These local Data and Safety managers will assure that data collection is done according to the current legislation meaning that privacy, confidentiality and ethical approvals are covered. This Data and Safety Management Group will report in a regular basis to the Data Protection Officer and the documentation will be included in dedicated sections of the Periodic Report to the EC. The Data Management Plan will describe how this Data Protection Officer proceeds as well as the data sharing agreement and the corresponding permissions in relation to data import and export.
Considering the importance of data management, T1.5 Data management will manage the data protection of the project and D1.1 will provide a data management plan that could evolve and be updated during the project. D1.1 Data Management Plan will include the detailed information of the procedures in terms of data collection, storage, protection, reuse and/or destruction. These procedures will comply with the general data protection regulation No 2016/679 that has been recently incorporated and will be based on the Guidelines on FAIR Data Management in Horizon 2020 (http://ec.europa.eu/research/participants/data/ref/h2020/grants_manual/hi/oa_pilot/h2020-hi-oadata-mgt_en.pdf ).
The Data Protection Framework of the project will be based on this regulation. If the applicable law is not the EU General Data Protection Regulation (Regulation (EU) 2016/679) at the moment of defining the Data Protection Framework will take into account key elements of the existing drafts of the Regulation, particularly the need to ensure privacy and confidentiality, the processing personal data in the project, and the need for strong informed consent.
In addition, The D1.1 Data Management Plan will include the privacy impact assessment ensuring that the information collected is strictly necessary for the study. The Privacy Impact Assessment will include a description of how the project envisions processing the data and for what purpose. It will explain how processing this data could impact the rights and freedoms of the data subjects. And it will detail the measures that will be taken to mitigate the risks and the security safeguards and mechanisms that will be put into place to ensure the protection of personal data and comply with the EU Data Protection Regulation.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

INTEGRATED PERSONALIZED CARE FOR PATIENTS WITH ADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE
[875209] [ADLIFE] – Part B – 120
As explained above, a key aspect of ADLIFE, an IA project, is to protect the interests of users and patients. For this reason, task “T1.4 Ethical and legal surveillance” will be in charge of deeply considering all the ethical issues that the ADLIFE project involves including, gender balance, race, socioeconomic profile, religion and or personal beliefs. This task will also take into consideration all the ethical aspects that ICT supporting tools will comply with.
5.1.3.1 THIRD COUNTRIES
Two third countries participate in the project: Turkey and Israel. The procedure to share documentation between partners and with third parties, considering cross-border transfers, will be thoroughly described in D1.1 Data Management Plan. The data shared will include clinical and health-related information (anxiety, depression, functionality, quality of life, wellbeing, satisfaction, mortality, place of death, care burden), use of resources (admissions, emergency room visits) and perception of participants in terms of communication with patients, coordination of care and trust in in quality and security in data access, processing, sharing and storage. The information sources are local administrative databases (Electronic Health Record), interviews or focus groups and ADLIFE data logs. Detailed information will be provided in D7.1 D11.1. The procedures will comply with the current EU legislation as well as the laws of the corresponding countries: Turkey and Israel. A Data Sharing Agreement and the corresponding templates will be included in the D1.1 Data Management Plan.
No biological material will be imported/exported, so it is not necessary to have import/export authorisations for the development of the activities included in ADLIFE project.
5.2 SECURITY
• Activities or results raising security issues: NO
• EU-classified information' as background or results: NO
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
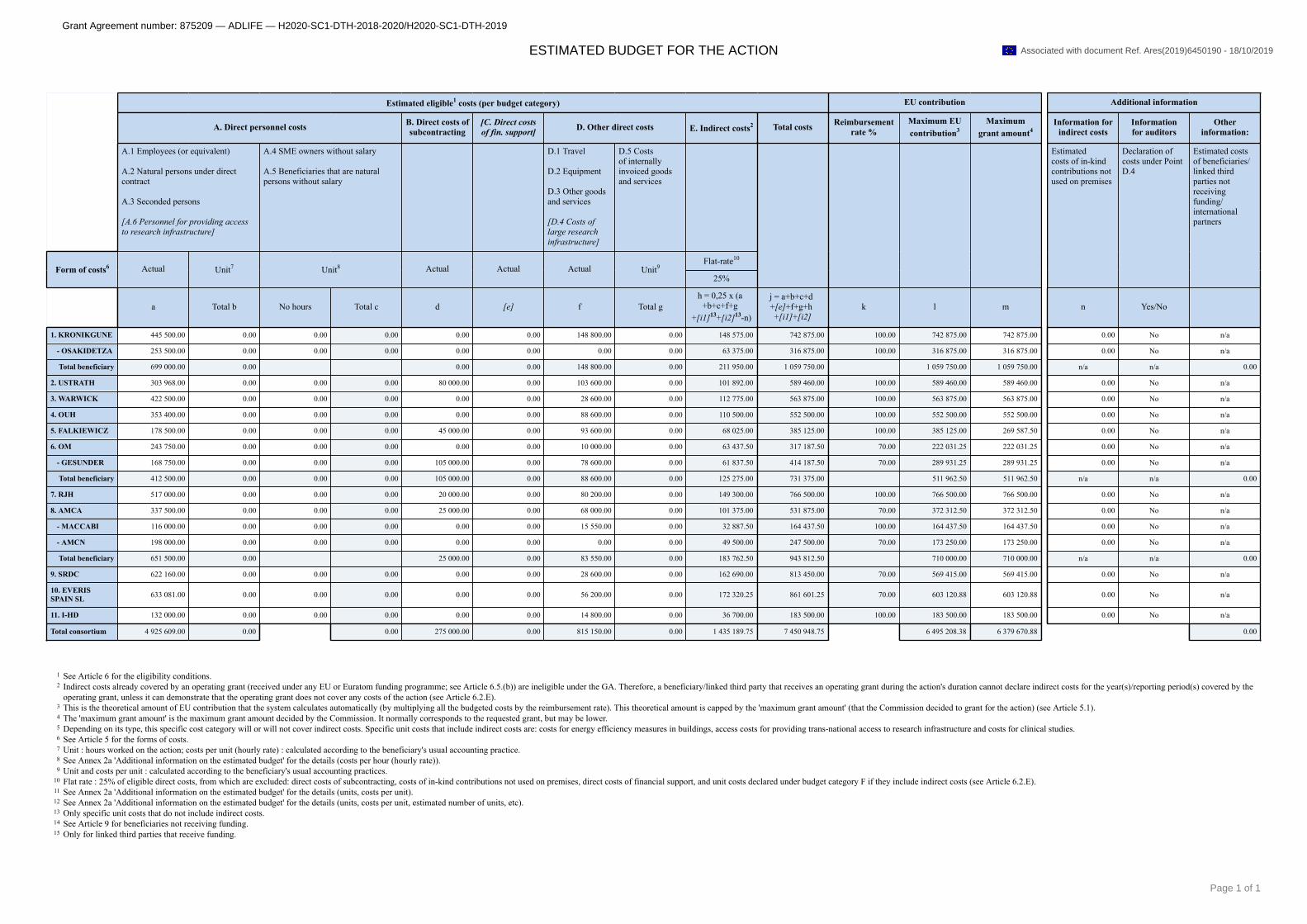
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
ESTIMATED BUDGET FOR THE ACTION
Estimated eligible1 costs (per budget category) EU contribution Additional information
A. Direct personnel costs B. Direct costs ofsubcontracting
[C. Direct costsof fin. support] D. Other direct costs E. Indirect costs2 Total costs Reimbursement
rate %Maximum EUcontribution3
Maximumgrant amount4
Information forindirect costs
Informationfor auditors
Otherinformation:
A.1 Employees (or equivalent)
A.2 Natural persons under directcontract
A.3 Seconded persons
[A.6 Personnel for providing accessto research infrastructure]
A.4 SME owners without salary
A.5 Beneficiaries that are naturalpersons without salary
D.1 Travel
D.2 Equipment
D.3 Other goodsand services
[D.4 Costs oflarge researchinfrastructure]
D.5 Costsof internallyinvoiced goodsand services
Flat-rate10
Form of costs6 Actual Unit7 Unit8 Actual Actual Actual Unit925%
Estimatedcosts of in-kindcontributions notused on premises
Declaration ofcosts under PointD.4
Estimated costsof beneficiaries/linked thirdparties notreceivingfunding/internationalpartners
a Total b No hours Total c d [e] f Total gh = 0,25 x (a
+b+c+f+g+[i1]13+[i2]13-n)
j = a+b+c+d+[e]+f+g+h+[i1]+[i2]
k l m n Yes/No
1. KRONIKGUNE 445 500.00 0.00 0.00 0.00 0.00 0.00 148 800.00 0.00 148 575.00 742 875.00 100.00 742 875.00 742 875.00 0.00 No n/a
- OSAKIDETZA 253 500.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 63 375.00 316 875.00 100.00 316 875.00 316 875.00 0.00 No n/a
Total beneficiary 699 000.00 0.00 0.00 0.00 148 800.00 0.00 211 950.00 1 059 750.00 1 059 750.00 1 059 750.00 n/a n/a 0.00
2. USTRATH 303 968.00 0.00 0.00 0.00 80 000.00 0.00 103 600.00 0.00 101 892.00 589 460.00 100.00 589 460.00 589 460.00 0.00 No n/a
3. WARWICK 422 500.00 0.00 0.00 0.00 0.00 0.00 28 600.00 0.00 112 775.00 563 875.00 100.00 563 875.00 563 875.00 0.00 No n/a
4. OUH 353 400.00 0.00 0.00 0.00 0.00 0.00 88 600.00 0.00 110 500.00 552 500.00 100.00 552 500.00 552 500.00 0.00 No n/a
5. FALKIEWICZ 178 500.00 0.00 0.00 0.00 45 000.00 0.00 93 600.00 0.00 68 025.00 385 125.00 100.00 385 125.00 269 587.50 0.00 No n/a
6. OM 243 750.00 0.00 0.00 0.00 0.00 0.00 10 000.00 0.00 63 437.50 317 187.50 70.00 222 031.25 222 031.25 0.00 No n/a
- GESUNDER 168 750.00 0.00 0.00 0.00 105 000.00 0.00 78 600.00 0.00 61 837.50 414 187.50 70.00 289 931.25 289 931.25 0.00 No n/a
Total beneficiary 412 500.00 0.00 0.00 0.00 105 000.00 0.00 88 600.00 0.00 125 275.00 731 375.00 511 962.50 511 962.50 n/a n/a 0.00
7. RJH 517 000.00 0.00 0.00 0.00 20 000.00 0.00 80 200.00 0.00 149 300.00 766 500.00 100.00 766 500.00 766 500.00 0.00 No n/a
8. AMCA 337 500.00 0.00 0.00 0.00 25 000.00 0.00 68 000.00 0.00 101 375.00 531 875.00 70.00 372 312.50 372 312.50 0.00 No n/a
- MACCABI 116 000.00 0.00 0.00 0.00 0.00 0.00 15 550.00 0.00 32 887.50 164 437.50 100.00 164 437.50 164 437.50 0.00 No n/a
- AMCN 198 000.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 49 500.00 247 500.00 70.00 173 250.00 173 250.00 0.00 No n/a
Total beneficiary 651 500.00 0.00 25 000.00 0.00 83 550.00 0.00 183 762.50 943 812.50 710 000.00 710 000.00 n/a n/a 0.00
9. SRDC 622 160.00 0.00 0.00 0.00 0.00 0.00 28 600.00 0.00 162 690.00 813 450.00 70.00 569 415.00 569 415.00 0.00 No n/a
10. EVERISSPAIN SL 633 081.00 0.00 0.00 0.00 0.00 0.00 56 200.00 0.00 172 320.25 861 601.25 70.00 603 120.88 603 120.88 0.00 No n/a
11. I-HD 132 000.00 0.00 0.00 0.00 0.00 0.00 14 800.00 0.00 36 700.00 183 500.00 100.00 183 500.00 183 500.00 0.00 No n/a
Total consortium 4 925 609.00 0.00 0.00 275 000.00 0.00 815 150.00 0.00 1 435 189.75 7 450 948.75 6 495 208.38 6 379 670.88 0.00
1 See Article 6 for the eligibility conditions.2 Indirect costs already covered by an operating grant (received under any EU or Euratom funding programme; see Article 6.5.(b)) are ineligible under the GA. Therefore, a beneficiary/linked third party that receives an operating grant during the action's duration cannot declare indirect costs for the year(s)/reporting period(s) covered by the
operating grant, unless it can demonstrate that the operating grant does not cover any costs of the action (see Article 6.2.E).3 This is the theoretical amount of EU contribution that the system calculates automatically (by multiplying all the budgeted costs by the reimbursement rate). This theoretical amount is capped by the 'maximum grant amount' (that the Commission decided to grant for the action) (see Article 5.1).4 The 'maximum grant amount' is the maximum grant amount decided by the Commission. It normally corresponds to the requested grant, but may be lower.5 Depending on its type, this specific cost category will or will not cover indirect costs. Specific unit costs that include indirect costs are: costs for energy efficiency measures in buildings, access costs for providing trans-national access to research infrastructure and costs for clinical studies.6 See Article 5 for the forms of costs.7 Unit : hours worked on the action; costs per unit (hourly rate) : calculated according to the beneficiary's usual accounting practice.8 See Annex 2a 'Additional information on the estimated budget' for the details (costs per hour (hourly rate)).9 Unit and costs per unit : calculated according to the beneficiary's usual accounting practices.
10 Flat rate : 25% of eligible direct costs, from which are excluded: direct costs of subcontracting, costs of in-kind contributions not used on premises, direct costs of financial support, and unit costs declared under budget category F if they include indirect costs (see Article 6.2.E).11 See Annex 2a 'Additional information on the estimated budget' for the details (units, costs per unit).12 See Annex 2a 'Additional information on the estimated budget' for the details (units, costs per unit, estimated number of units, etc).13 Only specific unit costs that do not include indirect costs.14 See Article 9 for beneficiaries not receiving funding.15 Only for linked third parties that receive funding.
Page 1 of 1
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Templates: Annex 2a (Additional information on the estimated budget)
1
ANNEX 2a
ADDITIONAL INFORMATION ON THE ESTIMATED BUDGET
Instructions and footnotes in blue will not appear in the text generated by the IT system (since they
are internal instructions only). For options [in square brackets]: the applicable option will be chosen by the IT system. Options not
chosen will automatically not appear. For fields in [grey in square brackets] (even if they are part of an option as specified in the previous
item): IT system will enter the appropriate data.
Transitory period: Until SyGMa fully supports Annex 2a, you must prepare it manually (using this template by choosing and deleting the options/entering the appropriate data). For the ‘unit cost tables’: either fill them out manually or use currently existing tables from Annex 1 or the proposal. The document can then be uploaded in SyGMa and attached to the grant agreement.
Unit cost for SME owners/natural beneficiaries without salary
1. Costs for a [SME owner][beneficiary that is a natural person] not receiving a salary
Units: hours worked on the action
Amount per unit (‘hourly rate’): calculated according to the following formula:
{the monthly living allowance for researchers in MSCA-IF actions / 143 hours}
multiplied by
{country-specific correction coefficient of the country where the beneficiary is established}
The monthly living allowance and the country-specific correction coefficients are set out in the Work
Programme (section 3 MSCA) in force at the time of the call:
- for calls before Work Programme 2018-2020:
- for the monthly living allowance: EUR 4 650
- for the country-specific correction coefficients: see Work Programme 2014-2015 and Work
Programme 2016-2017 (available on the Participant Portal Reference Documents page)
- for calls under Work Programme 2018-2020:
- for the monthly living allowance: EUR 4 880
- for the country-specific correction coefficients: see Work Programme 2018-2020 (available on the
Participant Portal Reference Documents page)
[additional OPTION for beneficiaries/linked third parties that have opted to use the unit cost (in the
proposal/with an amendment): For the following beneficiaries/linked third parties, the amounts per unit
(hourly rate) are fixed as follows:
- beneficiary/linked third party [short name]: EUR [insert amount]
- beneficiary/linked third party [short name]: EUR [insert amount]
[same for other beneficiaries/linked third parties, if necessary] ]
Estimated number of units: see Annex 2
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Templates: Annex 2a (Additional information on the estimated budget)
2
Energy efficiency measures unit cost
2. Costs for energy efficiency measures in buildings
Unit: m2 of eligible ‘conditioned’ (i.e. built or refurbished) floor area
Amount per unit*: see (for each beneficiary/linked third party and BEST table) the ‘unit cost table’ attached
* Amount calculated as follows:
{EUR 0.1 x estimated total kWh saved per m² per year x 10}
Estimated number of units: see (for each beneficiary/linked third party and BEST table) the ‘unit cost table’
attached
Unit cost table (energy efficiency measures unit cost)1
Short name beneficiary/linked
third party
BEST No Amount per unit Estimated No of
units
Total unit cost (cost per unit x
estimated no of units)
1 Data from the ‘building energy specification table (BEST)’ that is part of the proposal and Annex 1.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Templates: Annex 2a (Additional information on the estimated budget)
3
Research infrastructure unit cost
3. Access costs for providing trans-national access to research infrastructure
Units2: see (for each access provider and installation) the ‘unit cost table’ attached
Amount per unit*: see (for each access provider and installation) the ‘unit cost table’ attached
* Amount calculated as follows:
average annual total access cost to the installation (over past two years3) ________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________________
average annual total quantity of access to the installation (over past two years4)
Estimated number of units: see (for each access provider and installation) the ‘unit cost table’ attached
Unit cost table (access to research infrastructure unit cost)5
Short name
access
provider
Short
name
infrastru
cture
Installation Unit of
access
Amount per
unit
Estimated No
of units
Total unit
cost (cost per
unit x estimated
no of units) No Short name
Clinical studies unit cost
4. Costs for clinical studies
Units: patients/subjects that participate in the clinical study
Amount per unit*: see (for each sequence (if any), clinical study and beneficiary/linked third party) the ‘unit
cost table’ attached
* Amount calculated, for the cost components of each task, as follows:
For personnel costs:
For personnel costs of doctors: ‘average hourly cost for doctors’, i.e.:
{certified or auditable total personnel costs for doctors for year N-1 _________________________________________________________________________________________________________________________________________________________________________________
{1720 * number of full-time-equivalent for doctors for year N-1}
multiplied by
estimated number of hours to be worked by doctors for the task (per participant)}
For personnel costs of other medical personnel: ‘average hourly cost for other medical personnel’, i.e.:
{certified or auditable total personnel costs for other medical personnel for year N-1 ____________________________________________________________________________________________________________________________________________________________________________________
_
{1720 * number of full-time-equivalent for other medical personnel for year N-1}
2 Unit of access (e.g. beam hours, weeks of access, sample analysis) fixed by the access provider in proposal. 3 In exceptional and duly justified cases, the Commission/Agency may agree to a different reference period. 4 In exceptional and duly justified cases, the Commission/Agency may agree to a different reference period. 5 Data from the ‘table on estimated costs/quantity of access to be provided’ that is part of the proposal and
Annex 1.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Templates: Annex 2a (Additional information on the estimated budget)
4
multiplied by
estimated number of hours to be worked by other medical personnel for the task (per participant)}
For personnel costs of technical personnel: ‘average hourly cost for technical personnel’, i.e.:
{certified or auditable total personnel costs for technical personnel for year N-1 ____________________________________________________________________________________________________________________________________________________________________________________
_
{1720 * number of full-time-equivalent for technical personnel for year N-1}
multiplied by
estimated number of hours to be worked by technical personnel for the task (per participant)}
‘total personnel costs’ means actual salaries + actual social security contributions + actual taxes and other
costs included in the remuneration, provided they arise from national law or the employment
contract/equivalent appointing act
For consumables:
For each cost item: ‘average price of the consumable’, i.e.:
{{certified or auditable total costs of purchase of the consumable in year N-1 _______________________________________________________________________________________________________________________________________________________
total number of items purchased in year N-1}
multiplied by
estimated number of items to be used for the task (per participant)}
‘total costs of purchase of the consumable’ means total value of the supply contracts (including
related duties, taxes and charges such as non-deductible VAT) concluded by the beneficiary
for the consumable delivered in year N-1, provided the contracts were awarded according to
the principle of best value- for-money and without any conflict of interests
For medical equipment:
For each cost item: ‘average cost of depreciation and directly related services per unit of use’, i.e.:
{{ certified or auditable total depreciation costs in year N-1 + certified or auditable total costs of
purchase of services in year N-1 for the category of equipment concerned} ____________________________________________________________________________________________________________________________________________________
total capacity in year N-1
multiplied by
estimated number of units of use of the equipment for the task (per participant)}
‘total depreciation costs’ means total depreciation allowances as recorded in the beneficiary’s
accounts of year N-1 for the category of equipment concerned, provided the equipment was
purchased according to the principle of best value for money and without any conflict of
interests + total costs of renting or leasing contracts (including related duties, taxes and charges
such as non-deductible VAT) in year N-1 for the category of equipment concerned, provided
they do not exceed the depreciation costs of similar equipment and do not include finance fees
For services:
For each cost item: ‘average cost of the service per study participant’, i.e.:
{certified or auditable total costs of purchase of the service in year N-1 ______________________________________________________________________________________________________________________________________________________
total number of patients or subjects included in the clinical studies for which the service was
delivered in year N-1}
‘total costs of purchase of the service’ means total value of the contracts concluded by the
beneficiary (including related duties, taxes and charges such as non-deductible VAT) for the
specific service delivered in year N-1 for the conduct of clinical studies, provided the contracts
were awarded according to the principle of best value for money and without any conflict of
interests
For indirect costs:
{{{cost component ‘personnel costs’ + cost component ‘consumables’ + cost component ‘medical
equipment’}
minus
{costs of in-kind contributions provided by third parties which are not used on the beneficiary’s premises
+ costs of providing financial support to third parties (if any)}}
multiplied by
25%}
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Templates: Annex 2a (Additional information on the estimated budget)
5
The estimation of the resources to be used must be done on the basis of the study protocol and must be the
same for all beneficiaries/linked third parties/third parties involved.
The year N-1 to be used is the last closed financial year at the time of submission of the grant application.
Estimated number of units: see (for each clinical study and beneficiary/linked third party) the ‘unit cost table’
attached
Unit cost table: clinical studies unit cost6
Task, Direct cost
categories
Resource per
patient
Costs year
N-1
Beneficiary
1
[short
name]
Costs year
N-1
Linked
third party
1a
[short
name]
Costs year
N-1
Beneficiary
2
[short
name]
Costs year
N-1
Linked
third party
2a
[short
name]
Costs
year N-1
Third
party
giving in-
kind
contributi
ons 1
[short
name]
Sequence No. 1
Task No. 1
Blood sample
(a) Personnel costs:
- Doctors
n/a
- Other Medical
Personnel
Phlebotomy
(nurse), 10
minutes
8,33 EUR 11,59 EUR 10,30 EUR 11,00 EUR 9,49 EUR
- Technical Personnel Sample
Processing (lab
technician), 15
minutes
9,51 EUR 15,68 EUR 14,60 EUR 15,23 EUR 10,78
EUR
(b) Costs of
consumables: Syringe XX EUR XX EUR XX EUR XX EUR XX EUR
Cannula XX EUR XX EUR XX EUR XX EUR XX EUR
Blood container XX EUR XX EUR XX EUR XX EUR XX EUR
(c) Costs of medical
equipment:
Use of -80° deep
freezer, 60 days
XX EUR XX EUR XX EUR XX EUR XX EUR
Use of centrifuge,
15 minutes XX EUR XX EUR XX EUR XX EUR XX EUR
(d) Costs of services Cleaning of XXX XX EUR XX EUR XX EUR XX EUR XX EUR
(e) Indirect costs (25% flat-rate) XX EUR XX EUR XX EUR XX EUR XX EUR
Task No. 2
…
Amount per unit (unit cost sequence 1): XX EUR XX EUR XX EUR XX EUR XX EUR
Sequence No. 2
Task No. 1
6 Same table as in proposal and Annex 1.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Templates: Annex 2a (Additional information on the estimated budget)
6
XXX
(a) Personnel costs:
- Doctors
XXX
XX EUR
XX EUR
XX EUR
XX EUR
XX EUR
- Other Medical
Personnel XXX XX EUR XX EUR XX EUR XX EUR XX EUR
- Technical Personnel XXX XX EUR XX EUR XX EUR XX EUR XX EUR
(b) Costs of
consumables: XXX XX EUR XX EUR XX EUR XX EUR XX EUR
XXX XX EUR XX EUR XX EUR XX EUR XX EUR
XXX XX EUR XX EUR XX EUR XX EUR XX EUR
(c) Costs of medical
equipment:
XXX XX EUR XX EUR XX EUR XX EUR XX EUR
XXX XX EUR XX EUR XX EUR XX EUR XX EUR
(d) Costs of services XXX XX EUR XX EUR XX EUR XX EUR XX EUR
(e) Indirect costs (25% flat-rate) XX EUR XX EUR XX EUR XX EUR XX EUR
Task No. 2
…
Amount per unit (unit cost sequence 2): XX EUR XX EUR XX EUR XX EUR XX EUR
…
Amount per unit (unit cost entire study): XX EUR XX EUR XX EUR XX EUR XX EUR
]
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
ANNEX 3
ACCESSION FORM FOR BENEFICIARIES
UNIVERSITY OF STRATHCLYDE (USTRATH), established in Richmond Street 16,GLASGOW G1 1XQ, United Kingdom, VAT number: GB261339762, (‘the beneficiary’), representedfor the purpose of signing this Accession Form by the undersigned,
hereby agrees
to become beneficiary No (‘2’)
in Grant Agreement No 875209 (‘the Agreement’)
between ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD-KRONIKGUNE and the European Union (‘the EU’), represented by the European Commission ('theCommission'),
for the action entitled ‘INTEGRATED PERSONALIZED CARE FOR PATIENTS WITHADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE(ADLIFE)’.
and mandates
the coordinator to submit and sign in its name and on its behalf any amendments to the Agreement,in accordance with Article 55.
By signing this Accession Form, the beneficiary accepts the grant and agrees to implement it inaccordance with the Agreement, with all the obligations and conditions it sets out.
SIGNATURE
For the beneficiary[--TGSMark#signature-999974068_75_210--]
1
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
ANNEX 3
ACCESSION FORM FOR BENEFICIARIES
THE UNIVERSITY OF WARWICK (WARWICK), established in Kirby Corner Road - UniversityHouse, COVENTRY CV4 8UW, United Kingdom, VAT number: GB545270058, (‘the beneficiary’),represented for the purpose of signing this Accession Form by the undersigned,
hereby agrees
to become beneficiary No (‘3’)
in Grant Agreement No 875209 (‘the Agreement’)
between ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD-KRONIKGUNE and the European Union (‘the EU’), represented by the European Commission ('theCommission'),
for the action entitled ‘INTEGRATED PERSONALIZED CARE FOR PATIENTS WITHADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE(ADLIFE)’.
and mandates
the coordinator to submit and sign in its name and on its behalf any amendments to the Agreement,in accordance with Article 55.
By signing this Accession Form, the beneficiary accepts the grant and agrees to implement it inaccordance with the Agreement, with all the obligations and conditions it sets out.
SIGNATURE
For the beneficiary[--TGSMark#signature-999976784_75_210--]
2
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
ANNEX 3
ACCESSION FORM FOR BENEFICIARIES
ODENSE UNIVERSITETSHOSPITAL (OUH), established in Sdr. Boulevard 29, ODENSE 5000,Denmark, VAT number: DK35181628, (‘the beneficiary’), represented for the purpose of signing thisAccession Form by the undersigned,
hereby agrees
to become beneficiary No (‘4’)
in Grant Agreement No 875209 (‘the Agreement’)
between ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD-KRONIKGUNE and the European Union (‘the EU’), represented by the European Commission ('theCommission'),
for the action entitled ‘INTEGRATED PERSONALIZED CARE FOR PATIENTS WITHADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE(ADLIFE)’.
and mandates
the coordinator to submit and sign in its name and on its behalf any amendments to the Agreement,in accordance with Article 55.
By signing this Accession Form, the beneficiary accepts the grant and agrees to implement it inaccordance with the Agreement, with all the obligations and conditions it sets out.
SIGNATURE
For the beneficiary[--TGSMark#signature-999489553_75_210--]
3
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
ANNEX 3
ACCESSION FORM FOR BENEFICIARIES
SZPITAL SPECJALISTYCZNY IM A FALKIEWICZA WE WROCLAWIU (FALKIEWICZ),established in UL. WARSZAWSKA 2, WROCLAW 52 114, Poland, VAT number: PL8992227939,(‘the beneficiary’), represented for the purpose of signing this Accession Form by the undersigned,
hereby agrees
to become beneficiary No (‘5’)
in Grant Agreement No 875209 (‘the Agreement’)
between ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD-KRONIKGUNE and the European Union (‘the EU’), represented by the European Commission ('theCommission'),
for the action entitled ‘INTEGRATED PERSONALIZED CARE FOR PATIENTS WITHADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE(ADLIFE)’.
and mandates
the coordinator to submit and sign in its name and on its behalf any amendments to the Agreement,in accordance with Article 55.
By signing this Accession Form, the beneficiary accepts the grant and agrees to implement it inaccordance with the Agreement, with all the obligations and conditions it sets out.
SIGNATURE
For the beneficiary[--TGSMark#signature-910868801_75_210--]
4
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
ANNEX 3
ACCESSION FORM FOR BENEFICIARIES
OPTIMEDIS AG (OM), established in BURCHARDSTRASSE 17, HAMBURG 20095, Germany,VAT number: DE227566961, (‘the beneficiary’), represented for the purpose of signing this AccessionForm by the undersigned,
hereby agrees
to become beneficiary No (‘6’)
in Grant Agreement No 875209 (‘the Agreement’)
between ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD-KRONIKGUNE and the European Union (‘the EU’), represented by the European Commission ('theCommission'),
for the action entitled ‘INTEGRATED PERSONALIZED CARE FOR PATIENTS WITHADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE(ADLIFE)’.
and mandates
the coordinator to submit and sign in its name and on its behalf any amendments to the Agreement,in accordance with Article 55.
By signing this Accession Form, the beneficiary accepts the grant and agrees to implement it inaccordance with the Agreement, with all the obligations and conditions it sets out.
SIGNATURE
For the beneficiary[--TGSMark#signature-945709067_75_210--]
5
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
ANNEX 3
ACCESSION FORM FOR BENEFICIARIES
REGION JAMTLAND HARJEDALEN (RJH), established in KYRKGATAN 12, OSTERSUND831 27, Sweden, VAT number: SE232100021401, (‘the beneficiary’), represented for the purpose ofsigning this Accession Form by the undersigned,
hereby agrees
to become beneficiary No (‘7’)
in Grant Agreement No 875209 (‘the Agreement’)
between ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD-KRONIKGUNE and the European Union (‘the EU’), represented by the European Commission ('theCommission'),
for the action entitled ‘INTEGRATED PERSONALIZED CARE FOR PATIENTS WITHADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE(ADLIFE)’.
and mandates
the coordinator to submit and sign in its name and on its behalf any amendments to the Agreement,in accordance with Article 55.
By signing this Accession Form, the beneficiary accepts the grant and agrees to implement it inaccordance with the Agreement, with all the obligations and conditions it sets out.
SIGNATURE
For the beneficiary[--TGSMark#signature-929148645_75_210--]
6
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
ANNEX 3
ACCESSION FORM FOR BENEFICIARIES
ASSUTA ASHDOD LTD (AMCA), established in HAREFUA 7, ASHDOD 7747629, Israel, VATnumber: IL514525591, (‘the beneficiary’), represented for the purpose of signing this Accession Formby the undersigned,
hereby agrees
to become beneficiary No (‘8’)
in Grant Agreement No 875209 (‘the Agreement’)
between ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD-KRONIKGUNE and the European Union (‘the EU’), represented by the European Commission ('theCommission'),
for the action entitled ‘INTEGRATED PERSONALIZED CARE FOR PATIENTS WITHADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE(ADLIFE)’.
and mandates
the coordinator to submit and sign in its name and on its behalf any amendments to the Agreement,in accordance with Article 55.
By signing this Accession Form, the beneficiary accepts the grant and agrees to implement it inaccordance with the Agreement, with all the obligations and conditions it sets out.
SIGNATURE
For the beneficiary[--TGSMark#signature-904317906_75_210--]
7
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
ANNEX 3
ACCESSION FORM FOR BENEFICIARIES
SRDC YAZILIM ARASTIRMA VE GELISTIRME VE DANISMANLIK TICARET ANONIMSIRKETI (SRDC), established in SILIKON BINA 1 KAT NO 14 ODTU TEKNOKENTCANKAYA, ANKARA 06800, Turkey, VAT number: TR7810557732, (‘the beneficiary’),represented for the purpose of signing this Accession Form by the undersigned,
hereby agrees
to become beneficiary No (‘9’)
in Grant Agreement No 875209 (‘the Agreement’)
between ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD-KRONIKGUNE and the European Union (‘the EU’), represented by the European Commission ('theCommission'),
for the action entitled ‘INTEGRATED PERSONALIZED CARE FOR PATIENTS WITHADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE(ADLIFE)’.
and mandates
the coordinator to submit and sign in its name and on its behalf any amendments to the Agreement,in accordance with Article 55.
By signing this Accession Form, the beneficiary accepts the grant and agrees to implement it inaccordance with the Agreement, with all the obligations and conditions it sets out.
SIGNATURE
For the beneficiary[--TGSMark#signature-999683553_75_210--]
8
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
ANNEX 3
ACCESSION FORM FOR BENEFICIARIES
EVERIS SPAIN SL (EVERIS SPAIN SL), established in AVENIDA MANOTERAS 52, MADRID28050, Spain, VAT number: ESB82387770, (‘the beneficiary’), represented for the purpose of signingthis Accession Form by the undersigned,
hereby agrees
to become beneficiary No (‘10’)
in Grant Agreement No 875209 (‘the Agreement’)
between ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD-KRONIKGUNE and the European Union (‘the EU’), represented by the European Commission ('theCommission'),
for the action entitled ‘INTEGRATED PERSONALIZED CARE FOR PATIENTS WITHADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE(ADLIFE)’.
and mandates
the coordinator to submit and sign in its name and on its behalf any amendments to the Agreement,in accordance with Article 55.
By signing this Accession Form, the beneficiary accepts the grant and agrees to implement it inaccordance with the Agreement, with all the obligations and conditions it sets out.
SIGNATURE
For the beneficiary[--TGSMark#signature-999938081_75_210--]
9
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: 875209 — ADLIFE — H2020-SC1-DTH-2018-2020/H2020-SC1-DTH-2019
ANNEX 3
ACCESSION FORM FOR BENEFICIARIES
THE EUROPEAN INSTITUTE FOR INNOVATION THROUGH HEALTH DATA (I-HD),established in OUDE MECHELSESTRAAT 165, STROMBEEK-BEVER 1853, Belgium, VATnumber: BE0628646310, (‘the beneficiary’), represented for the purpose of signing this AccessionForm by the undersigned,
hereby agrees
to become beneficiary No (‘11’)
in Grant Agreement No 875209 (‘the Agreement’)
between ASOCIACIÓN INSTITUTO DE INVESTIGACIÓN EN SERVICIOS DE SALUD-KRONIKGUNE and the European Union (‘the EU’), represented by the European Commission ('theCommission'),
for the action entitled ‘INTEGRATED PERSONALIZED CARE FOR PATIENTS WITHADVANCED CHRONIC DISEASES TO IMPROVE HEALTH AND QUALITY OF LIFE(ADLIFE)’.
and mandates
the coordinator to submit and sign in its name and on its behalf any amendments to the Agreement,in accordance with Article 55.
By signing this Accession Form, the beneficiary accepts the grant and agrees to implement it inaccordance with the Agreement, with all the obligations and conditions it sets out.
SIGNATURE
For the beneficiary[--TGSMark#signature-923112723_75_210--]
10
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
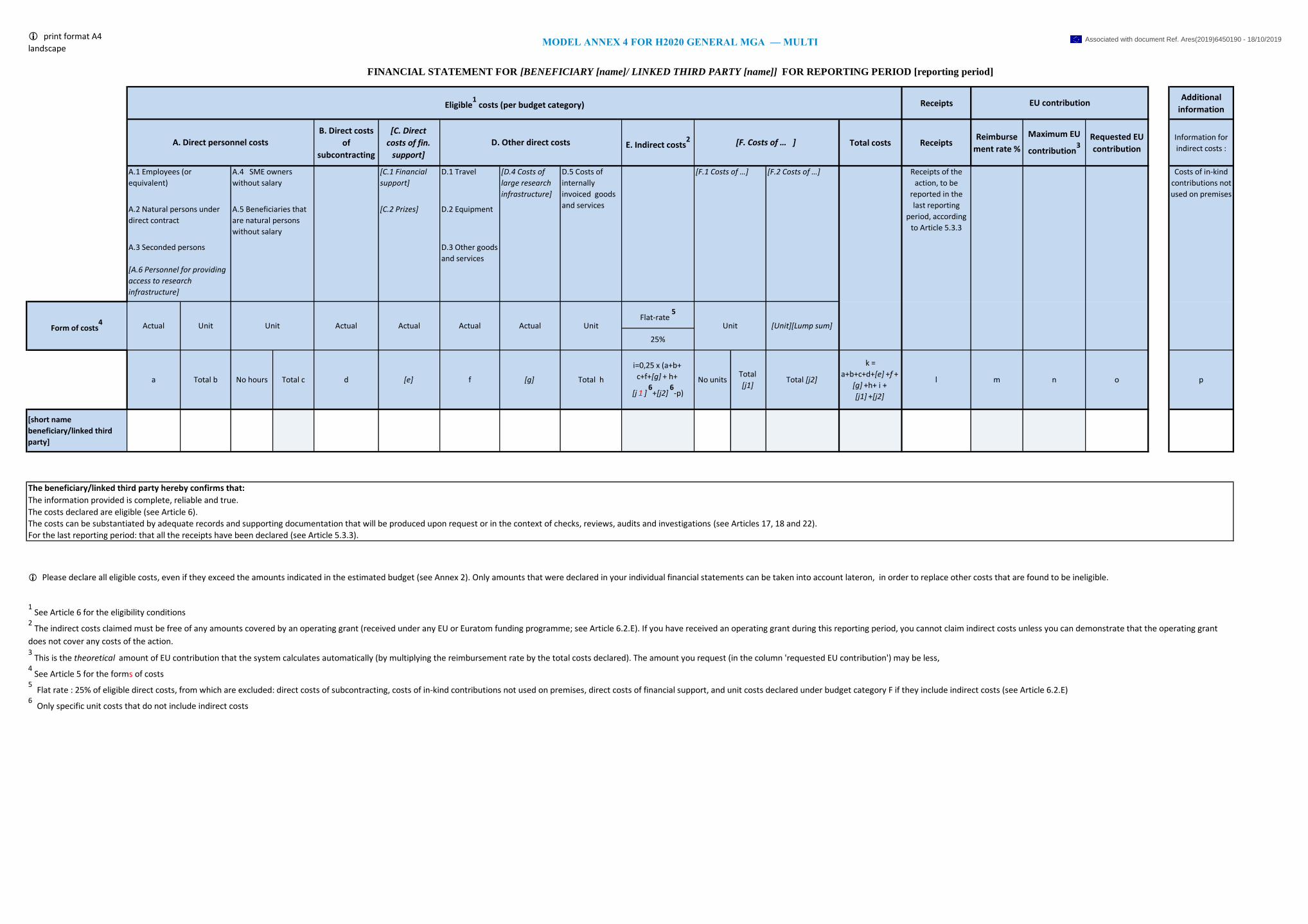
i print format A4
landscape
ReceiptsAdditional
information
B. Direct costs
of
subcontracting
[C. Direct
costs of fin.
support] E. Indirect costs
2 Total costs ReceiptsReimburse
ment rate %
Maximum EU
contribution3
Requested EU
contribution
Information for
indirect costs :
[C.1 Financial
support]
D.1 Travel
[C.2 Prizes] D.2 Equipment
Flat-rate 5
25%
[short name
beneficiary/linked third
party]
[F.1 Costs of …] [F.2 Costs of …]
Actual Actual Actual Unit Unit Unit [Unit][Lump sum]
For the last reporting period: that all the receipts have been declared (see Article 5.3.3).
ma [e]
i=0,25 x (a+b+
c+f+[g] + h+
[j 1 ]6
+[j2]6
-p)
[g] nTotal
[j1]
Receipts of the
action, to be
reported in the
last reporting
period, according
to Article 5.3.3
f oNo units
The costs can be substantiated by adequate records and supporting documentation that will be produced upon request or in the context of checks, reviews, audits and investigations (see Articles 17, 18 and 22).
ActualForm of costs4 Unit Actual
Total [j2]
k =
a+b+c+d+[e] +f +
[g] +h+ i +
[j1] +[j2]
lTotal b No hours Total c d Total h
MODEL ANNEX 4 FOR H2020 GENERAL MGA — MULTI
FINANCIAL STATEMENT FOR [BENEFICIARY [name]/ LINKED THIRD PARTY [name]] FOR REPORTING PERIOD [reporting period]
Eligible1 costs (per budget category) EU contribution
p
A. Direct personnel costs [F. Costs of … ]
Costs of in-kind
contributions not
used on premises
A.2 Natural persons under
direct contract
A.5 Beneficiaries that
are natural persons
without salary
A.4 SME owners
without salary
A.3 Seconded persons
[A.6 Personnel for providing
access to research
infrastructure]
D.3 Other goods
and services
A.1 Employees (or
equivalent)
D. Other direct costs
[D.4 Costs of
large research
infrastructure]
D.5 Costs of
internally
invoiced goods
and services
6 Only specific unit costs that do not include indirect costs
i Please declare all eligible costs, even if they exceed the amounts indicated in the estimated budget (see Annex 2). Only amounts that were declared in your individual financial statements can be taken into account lateron, in order to replace other costs that are found to be ineligible.
The beneficiary/linked third party hereby confirms that:
The information provided is complete, reliable and true.
The costs declared are eligible (see Article 6).
4 See Article 5 for the forms of costs
5 Flat rate : 25% of eligible direct costs, from which are excluded: direct costs of subcontracting, costs of in-kind contributions not used on premises, direct costs of financial support, and unit costs declared under budget category F if they include indirect costs (see Article 6.2.E)
1 See Article 6 for the eligibility conditions
2 The indirect costs claimed must be free of any amounts covered by an operating grant (received under any EU or Euratom funding programme; see Article 6.2.E). If you have received an operating grant during this reporting period, you cannot claim indirect costs unless you can demonstrate that the operating grant
does not cover any costs of the action.3 This is the theoretical amount of EU contribution that the system calculates automatically (by multiplying the reimbursement rate by the total costs declared). The amount you request (in the column 'requested EU contribution') may be less,
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
1
ANNEX 5
MODEL FOR THE CERTIFICATE ON THE FINANCIAL STATEMENTS
� For options [in italics in square brackets]: choose the applicable option. Options not chosen should
be deleted. � For fields in [grey in square brackets]: enter the appropriate data
TABLE OF CONTENTS
TERMS OF REFERENCE FOR AN INDEPENDENT REPORT OF FACTUAL FINDINGS ON COSTS
DECLARED UNDER A GRANT AGREEMENT FINANCED UNDER THE HORIZON 2020 RESEARCH
FRAMEWORK PROGRAMME
INDEPENDENT REPORT OF FACTUAL FINDINGS ON COSTS DECLARED UNDER A GRANT
AGREEMENT FINANCED UNDER THE HORIZON 2020 RESEARCH FRAMEWORK PROGRAMME
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
2
Terms of Reference for an Independent Report of Factual Findings on costs declared
under a Grant Agreement financed under the Horizon 2020 Research and Innovation
Framework Programme
This document sets out the ‘Terms of Reference (ToR)’ under which
[OPTION 1: [insert name of the beneficiary] (‘the Beneficiary’)] [OPTION 2: [insert name of the
linked third party] (‘the Linked Third Party’), third party linked to the Beneficiary [insert name of the
beneficiary] (‘the Beneficiary’)]
agrees to engage
[insert legal name of the auditor] (‘the Auditor’)
to produce an independent report of factual findings (‘the Report’) concerning the Financial
Statement(s)1 drawn up by the [Beneficiary] [Linked Third Party] for the Horizon 2020 grant
agreement [insert number of the grant agreement, title of the action, acronym and duration from/to]
(‘the Agreement’), and
to issue a Certificate on the Financial Statements’ (‘CFS’) referred to in Article 20.4 of the Agreement
based on the compulsory reporting template stipulated by the Commission.
The Agreement has been concluded under the Horizon 2020 Research and Innovation Framework
Programme (H2020) between the Beneficiary and [OPTION 1: the European Union, represented by
the European Commission (‘the Commission’)][ OPTION 2: the European Atomic Energy Community
(Euratom,) represented by the European Commission (‘the Commission’)][OPTION 3: the [Research
Executive Agency (REA)] [European Research Council Executive Agency (ERCEA)] [Innovation and
Networks Executive Agency (INEA)] [Executive Agency for Small and Medium-sized Enterprises
(EASME)] (‘the Agency’), under the powers delegated by the European Commission (‘the
Commission’).]
The [Commission] [Agency] is mentioned as a signatory of the Agreement with the Beneficiary only.
The [European Union][Euratom][Agency] is not a party to this engagement.
1.1 Subject of the engagement
The coordinator must submit to the [Commission][Agency] the final report within 60 days following
the end of the last reporting period which should include, amongst other documents, a CFS for each
beneficiary and for each linked third party that requests a total contribution of EUR 325 000 or more,
as reimbursement of actual costs and unit costs calculated on the basis of its usual cost accounting
practices (see Article 20.4 of the Agreement). The CFS must cover all reporting periods of the
beneficiary or linked third party indicated above.
The Beneficiary must submit to the coordinator the CFS for itself and for its linked third party(ies), if
the CFS must be included in the final report according to Article 20.4 of the Agreement.
The CFS is composed of two separate documents:
- The Terms of Reference (‘the ToR’) to be signed by the [Beneficiary] [Linked Third Party]
and the Auditor;
1 By which costs under the Agreement are declared (see template ‘Model Financial Statements’ in Annex 4 to
the Grant Agreement).
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
3
- The Auditor’s Independent Report of Factual Findings (‘the Report’) to be issued on the
Auditor’s letterhead, dated, stamped and signed by the Auditor (or the competent public
officer) which includes the agreed-upon procedures (‘the Procedures’) to be performed by the
Auditor, and the standard factual findings (‘the Findings’) to be confirmed by the Auditor.
If the CFS must be included in the final report according to Article 20.4 of the Agreement, the request
for payment of the balance relating to the Agreement cannot be made without the CFS. However, the
payment for reimbursement of costs covered by the CFS does not preclude the Commission [ Agency,]
the European Anti-Fraud Office and the European Court of Auditors from carrying out checks,
reviews, audits and investigations in accordance with Article 22 of the Agreement.
1.2 Responsibilities
The [Beneficiary] [Linked Third Party]:
• must draw up the Financial Statement(s) for the action financed by the Agreement in
compliance with the obligations under the Agreement. The Financial Statement(s) must be
drawn up according to the [Beneficiary’s] [Linked Third Party’s] accounting and book-
keeping system and the underlying accounts and records;
• must send the Financial Statement(s) to the Auditor;
• is responsible and liable for the accuracy of the Financial Statement(s);
• is responsible for the completeness and accuracy of the information provided to enable the
Auditor to carry out the Procedures. It must provide the Auditor with a written representation
letter supporting these statements. The written representation letter must state the period
covered by the statements and must be dated;
• accepts that the Auditor cannot carry out the Procedures unless it is given full access to the
[Beneficiary’s] [Linked Third Party’s] staff and accounting as well as any other relevant
records and documentation.
The Auditor:
• [Option 1 by default: is qualified to carry out statutory audits of accounting documents in
accordance with Directive 2006/43/EC of the European Parliament and of the Council of 17
May 2006 on statutory audits of annual accounts and consolidated accounts, amending
Council Directives 78/660/EEC and 83/349/EEC and repealing Council Directive 84/253/EEC
or similar national regulations].
• [Option 2 if the Beneficiary or Linked Third Party has an independent Public Officer: is a
competent and independent Public Officer for which the relevant national authorities have
established the legal capacity to audit the Beneficiary].
• [Option 3 if the Beneficiary or Linked Third Party is an international organisation: is an
[internal] [external] auditor in accordance with the internal financial regulations and
procedures of the international organisation].
The Auditor:
• must be independent from the Beneficiary [and the Linked Third Party], in particular, it must
not have been involved in preparing the [Beneficiary’s] [Linked Third Party’s] Financial
Statement(s);
• must plan work so that the Procedures may be carried out and the Findings may be assessed;
• must adhere to the Procedures laid down and the compulsory report format;
• must carry out the engagement in accordance with this ToR;
• must document matters which are important to support the Report;
• must base its Report on the evidence gathered;
• must submit the Report to the [Beneficiary] [Linked Third Party].
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
4
The Commission sets out the Procedures to be carried out by the Auditor. The Auditor is not
responsible for their suitability or pertinence. As this engagement is not an assurance engagement, the
Auditor does not provide an audit opinion or a statement of assurance.
1.3 Applicable Standards
The Auditor must comply with these Terms of Reference and with2:
- the International Standard on Related Services (‘ISRS’) 4400 Engagements to perform
Agreed-upon Procedures regarding Financial Information as issued by the International
Auditing and Assurance Standards Board (IAASB);
- the Code of Ethics for Professional Accountants issued by the International Ethics
Standards Board for Accountants (IESBA). Although ISRS 4400 states that independence
is not a requirement for engagements to carry out agreed-upon procedures, the
[Commission][Agency] requires that the Auditor also complies with the Code’s
independence requirements.
The Auditor’s Report must state that there is no conflict of interests in establishing this Report
between the Auditor and the Beneficiary [and the Linked Third Party], and must specify - if the
service is invoiced - the total fee paid to the Auditor for providing the Report.
1.4 Reporting
The Report must be written in the language of the Agreement (see Article 20.7).
Under Article 22 of the Agreement, the Commission[, the Agency], the European Anti-Fraud Office
and the Court of Auditors have the right to audit any work that is carried out under the action and for
which costs are declared from [the European Union] [Euratom] budget. This includes work related to
this engagement. The Auditor must provide access to all working papers (e.g. recalculation of hourly
rates, verification of the time declared for the action) related to this assignment if the Commission [,
the Agency], the European Anti-Fraud Office or the European Court of Auditors requests them.
1.5 Timing
The Report must be provided by [dd Month yyyy].
1.6 Other terms
[The [Beneficiary] [Linked Third Party] and the Auditor can use this section to agree other specific
terms, such as the Auditor’s fees, liability, applicable law, etc. Those specific terms must not
contradict the terms specified above.]
[legal name of the Auditor] [legal name of the [Beneficiary][Linked Third Party]]
[name & function of authorised representative] [name & function of authorised representative]
[dd Month yyyy] [dd Month yyyy]
Signature of the Auditor Signature of the [Beneficiary][Linked Third Party]
2 Supreme Audit Institutions applying INTOSAI-standards may carry out the Procedures according to the
corresponding International Standards of Supreme Audit Institutions and code of ethics issued by INTOSAI
instead of the International Standard on Related Services (‘ISRS’) 4400 and the Code of Ethics for
Professional Accountants issued by the IAASB and the IESBA.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
5
Independent Report of Factual Findings on costs declared
under Horizon 2020 Research and Innovation Framework Programme
(To be printed on the Auditor’s letterhead)
To
[ name of contact person(s)], [Position]
[ [Beneficiary’s] [Linked Third Party’s] name ]
[ Address]
[ dd Month yyyy]
Dear [Name of contact person(s)],
As agreed under the terms of reference dated [dd Month yyyy]
with [OPTION 1: [insert name of the beneficiary] (‘the Beneficiary’)] [OPTION 2: [insert name of
the linked third party] (‘the Linked Third Party’), third party linked to the Beneficiary [insert name of
the beneficiary] (‘the Beneficiary’)],
we
[name of the auditor ] (‘the Auditor’),
established at
[full address/city/state/province/country],
represented by
[name and function of an authorised representative],
have carried out the procedures agreed with you regarding the costs declared in the Financial
Statement(s)3 of the [Beneficiary] [Linked Third Party] concerning the grant agreement
[insert grant agreement reference: number, title of the action and acronym] (‘the Agreement’),
with a total cost declared of
[total amount] EUR,
and a total of actual costs and unit costs calculated in accordance with the [Beneficiary’s] [Linked
Third Party’s] usual cost accounting practices’ declared of
[sum of total actual costs and total direct personnel costs declared as unit costs calculated in
accordance with the [Beneficiary’s] [Linked Third Party’s] usual cost accounting practices] EUR
and hereby provide our Independent Report of Factual Findings (‘the Report’) using the
compulsory report format agreed with you.
The Report
Our engagement was carried out in accordance with the terms of reference (‘the ToR’) appended to
this Report. The Report includes the agreed-upon procedures (‘the Procedures’) carried out and the
standard factual findings (‘the Findings’) examined.
3 By which the Beneficiary declares costs under the Agreement (see template ‘Model Financial Statement’ in
Annex 4 to the Agreement).
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
6
The Procedures were carried out solely to assist the [Commission] [Agency] in evaluating whether the
[Beneficiary’s] [Linked Third Party’s] costs in the accompanying Financial Statement(s) were
declared in accordance with the Agreement. The [Commission] [Agency] draws its own conclusions
from the Report and any additional information it may require.
The scope of the Procedures was defined by the Commission. Therefore, the Auditor is not responsible
for their suitability or pertinence. Since the Procedures carried out constitute neither an audit nor a
review made in accordance with International Standards on Auditing or International Standards on
Review Engagements, the Auditor does not give a statement of assurance on the Financial Statements.
Had the Auditor carried out additional procedures or an audit of the [Beneficiary’s] [Linked Third
Party’s] Financial Statements in accordance with International Standards on Auditing or International
Standards on Review Engagements, other matters might have come to its attention and would have
been included in the Report.
Not applicable Findings
We examined the Financial Statement(s) stated above and considered the following Findings not
applicable:
Explanation (to be removed from the Report):
If a Finding was not applicable, it must be marked as ‘N.A.’ (‘Not applicable’) in the corresponding row on the
right-hand column of the table and means that the Finding did not have to be corroborated by the Auditor and
the related Procedure(s) did not have to be carried out.
The reasons of the non-application of a certain Finding must be obvious i.e.
i) if no cost was declared under a certain category then the related Finding(s) and Procedure(s) are
not applicable;
ii) if the condition set to apply certain Procedure(s) are not met the related Finding(s) and those
Procedure(s) are not applicable. For instance, for ‘beneficiaries with accounts established in a
currency other than euro’ the Procedure and Finding related to ‘beneficiaries with accounts
established in euro’ are not applicable. Similarly, if no additional remuneration is paid, the related
Finding(s) and Procedure(s) for additional remuneration are not applicable.
List here all Findings considered not applicable for the present engagement and explain the
reasons of the non-applicability.
….
Exceptions
Apart from the exceptions listed below, the [Beneficiary] [Linked Third Party] provided the Auditor
all the documentation and accounting information needed by the Auditor to carry out the requested
Procedures and evaluate the Findings.
Explanation (to be removed from the Report):
- If the Auditor was not able to successfully complete a procedure requested, it must be marked as ‘E’
(‘Exception’) in the corresponding row on the right-hand column of the table. The reason such as the
inability to reconcile key information or the unavailability of data that prevents the Auditor from
carrying out the Procedure must be indicated below.
- If the Auditor cannot corroborate a standard finding after having carried out the corresponding
procedure, it must also be marked as ‘E’ (‘Exception’) and, where possible, the reasons why the
Finding was not fulfilled and its possible impact must be explained here below.
List here any exceptions and add any information on the cause and possible consequences of
each exception, if known. If the exception is quantifiable, include the corresponding amount.
….
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
7
Example (to be removed from the Report):
1. The Beneficiary was unable to substantiate the Finding number 1 on … because ….
2. Finding number 30 was not fulfilled because the methodology used by the Beneficiary to
calculate unit costs was different from the one approved by the Commission. The differences
were as follows: …
3. After carrying out the agreed procedures to confirm the Finding number 31, the Auditor found a
difference of _____________ EUR. The difference can be explained by …
Further Remarks
In addition to reporting on the results of the specific procedures carried out, the Auditor would like to
make the following general remarks:
Example (to be removed from the Report):
1. Regarding Finding number 8 the conditions for additional remuneration were considered as
fulfilled because …
2. In order to be able to confirm the Finding number 15 we carried out the following additional
procedures: ….
Use of this Report
This Report may be used only for the purpose described in the above objective. It was prepared solely
for the confidential use of the [Beneficiary] [Linked Third Party] and the [Commission] [Agency], and
only to be submitted to the [Commission] [Agency] in connection with the requirements set out in
Article 20.4 of the Agreement. The Report may not be used by the [Beneficiary] [Linked Third Party]
or by the [Commission] [Agency] for any other purpose, nor may it be distributed to any other parties.
The [Commission] [Agency] may only disclose the Report to authorised parties, in particular to the
European Anti-Fraud Office (OLAF) and the European Court of Auditors.
This Report relates only to the Financial Statement(s) submitted to the [Commission] [Agency] by the
[Beneficiary] [Linked Third Party] for the Agreement. Therefore, it does not extend to any other of
the [Beneficiary’s] [Linked Third Party’s] Financial Statement(s).
There was no conflict of interest4 between the Auditor and the Beneficiary [and Linked Third Party]
in establishing this Report. The total fee paid to the Auditor for providing the Report was EUR ______
(including EUR______ of deductible VAT).
We look forward to discussing our Report with you and would be pleased to provide any further
information or assistance.
[legal name of the Auditor]
[name and function of an authorised representative]
[dd Month yyyy]
Signature of the Auditor
4 A conflict of interest arises when the Auditor's objectivity to establish the certificate is compromised in fact
or in appearance when the Auditor for instance:
- was involved in the preparation of the Financial Statements;
- stands to benefit directly should the certificate be accepted;
- has a close relationship with any person representing the beneficiary;
- is a director, trustee or partner of the beneficiary; or
- is in any other situation that compromises his or her independence or ability to establish the certificate
impartially.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
8
Agreed-upon procedures to be performed and standard factual findings to be confirmed by the Auditor
The European Commission reserves the right to i) provide the auditor with additional guidance regarding the procedures to be followed or the facts to be
ascertained and the way in which to present them (this may include sample coverage and findings) or to ii) change the procedures, by notifying the Beneficiary
in writing. The procedures carried out by the auditor to confirm the standard factual finding are listed in the table below.
If this certificate relates to a Linked Third Party, any reference here below to ‘the Beneficiary’ is to be considered as a reference to ‘the Linked Third Party’.
The ‘result’ column has three different options: ‘C’, ‘E’ and ‘N.A.’:
� ‘C’ stands for ‘confirmed’ and means that the auditor can confirm the ‘standard factual finding’ and, therefore, there is no exception to be reported.
� ‘E’ stands for ‘exception’ and means that the Auditor carried out the procedures but cannot confirm the ‘standard factual finding’, or that the Auditor
was not able to carry out a specific procedure (e.g. because it was impossible to reconcile key information or data were unavailable),
� ‘N.A.’ stands for ‘not applicable’ and means that the Finding did not have to be examined by the Auditor and the related Procedure(s) did not have to
be carried out. The reasons of the non-application of a certain Finding must be obvious i.e. i) if no cost was declared under a certain category then the
related Finding(s) and Procedure(s) are not applicable; ii) if the condition set to apply certain Procedure(s) are not met then the related Finding(s) and
Procedure(s) are not applicable. For instance, for ‘beneficiaries with accounts established in a currency other than the euro’ the Procedure related to
‘beneficiaries with accounts established in euro’ is not applicable. Similarly, if no additional remuneration is paid, the related Finding(s) and
Procedure(s) for additional remuneration are not applicable.
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
A ACTUAL PERSONNEL COSTS AND UNIT COSTS CALCULATED BY THE BENEFICIARY IN ACCORDANCE WITH ITS USUAL
COST ACCOUNTING PRACTICE
The Auditor draws a sample of persons whose costs were declared in the Financial Statement(s)
to carry out the procedures indicated in the consecutive points of this section A.
(The sample should be selected randomly so that it is representative. Full coverage is required if
there are fewer than 10 people (including employees, natural persons working under a direct
contract and personnel seconded by a third party), otherwise the sample should have a minimum
of 10 people, or 10% of the total, whichever number is the highest)
The Auditor sampled ______ people out of the total of ______ people.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
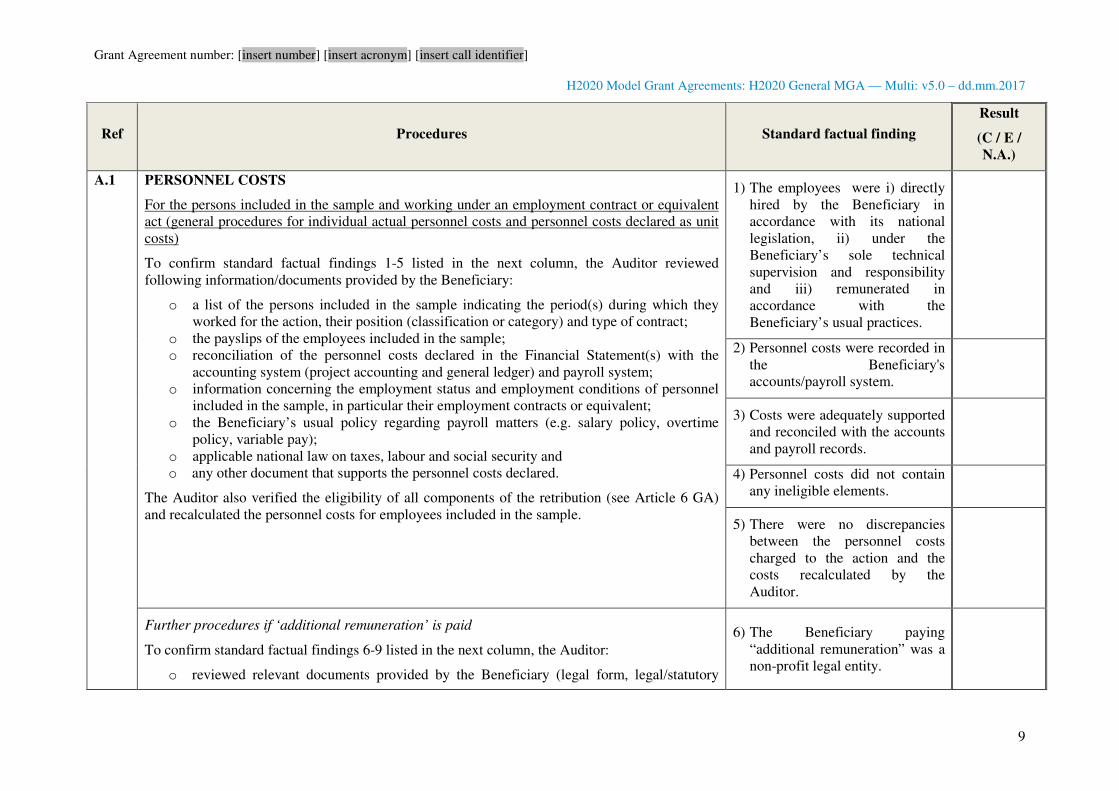
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
9
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
A.1 PERSONNEL COSTS
For the persons included in the sample and working under an employment contract or equivalent
act (general procedures for individual actual personnel costs and personnel costs declared as unit
costs)
To confirm standard factual findings 1-5 listed in the next column, the Auditor reviewed
following information/documents provided by the Beneficiary:
o a list of the persons included in the sample indicating the period(s) during which they
worked for the action, their position (classification or category) and type of contract;
o the payslips of the employees included in the sample;
o reconciliation of the personnel costs declared in the Financial Statement(s) with the
accounting system (project accounting and general ledger) and payroll system;
o information concerning the employment status and employment conditions of personnel
included in the sample, in particular their employment contracts or equivalent;
o the Beneficiary’s usual policy regarding payroll matters (e.g. salary policy, overtime
policy, variable pay);
o applicable national law on taxes, labour and social security and
o any other document that supports the personnel costs declared.
The Auditor also verified the eligibility of all components of the retribution (see Article 6 GA)
and recalculated the personnel costs for employees included in the sample.
1) The employees were i) directly
hired by the Beneficiary in
accordance with its national
legislation, ii) under the
Beneficiary’s sole technical
supervision and responsibility
and iii) remunerated in
accordance with the
Beneficiary’s usual practices.
2) Personnel costs were recorded in
the Beneficiary's
accounts/payroll system.
3) Costs were adequately supported
and reconciled with the accounts
and payroll records.
4) Personnel costs did not contain
any ineligible elements.
5) There were no discrepancies
between the personnel costs
charged to the action and the
costs recalculated by the
Auditor.
Further procedures if ‘additional remuneration’ is paid
To confirm standard factual findings 6-9 listed in the next column, the Auditor:
o reviewed relevant documents provided by the Beneficiary (legal form, legal/statutory
6) The Beneficiary paying
“additional remuneration” was a
non-profit legal entity.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
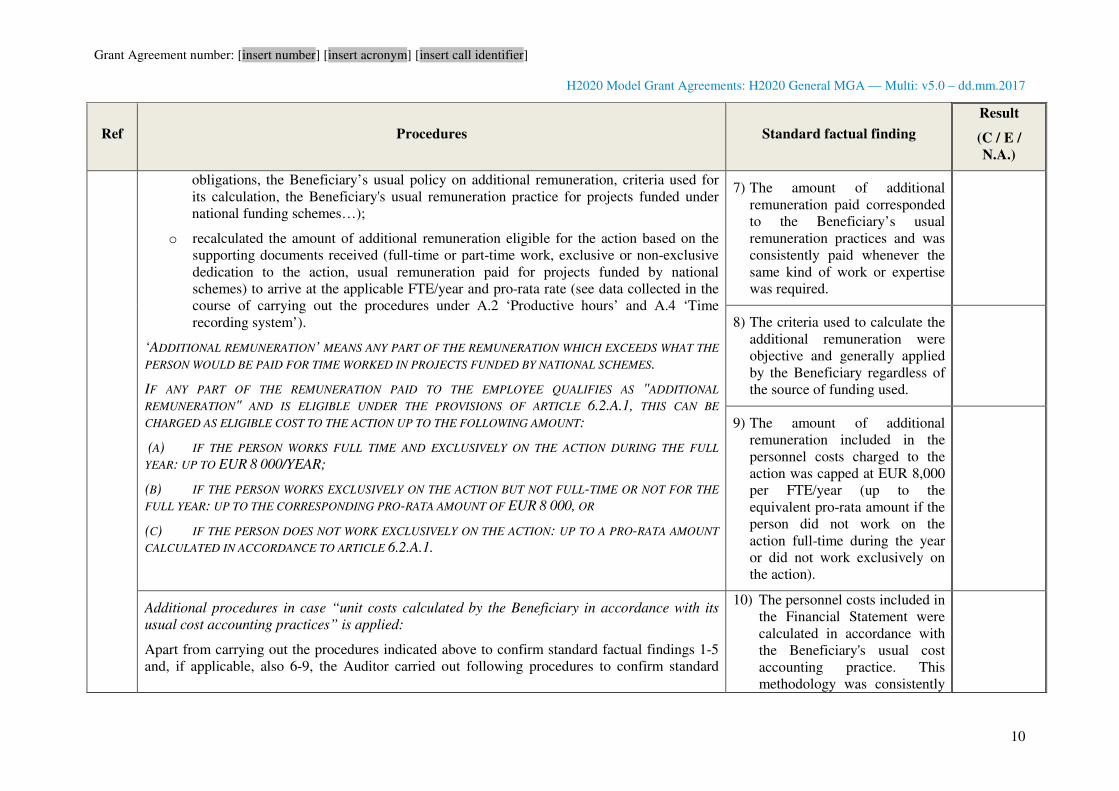
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
10
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
obligations, the Beneficiary’s usual policy on additional remuneration, criteria used for
its calculation, the Beneficiary's usual remuneration practice for projects funded under
national funding schemes…);
o recalculated the amount of additional remuneration eligible for the action based on the
supporting documents received (full-time or part-time work, exclusive or non-exclusive
dedication to the action, usual remuneration paid for projects funded by national
schemes) to arrive at the applicable FTE/year and pro-rata rate (see data collected in the
course of carrying out the procedures under A.2 ‘Productive hours’ and A.4 ‘Time
recording system’).
‘ADDITIONAL REMUNERATION’ MEANS ANY PART OF THE REMUNERATION WHICH EXCEEDS WHAT THE
PERSON WOULD BE PAID FOR TIME WORKED IN PROJECTS FUNDED BY NATIONAL SCHEMES.
IF ANY PART OF THE REMUNERATION PAID TO THE EMPLOYEE QUALIFIES AS "ADDITIONAL
REMUNERATION" AND IS ELIGIBLE UNDER THE PROVISIONS OF ARTICLE 6.2.A.1, THIS CAN BE
CHARGED AS ELIGIBLE COST TO THE ACTION UP TO THE FOLLOWING AMOUNT:
(A) IF THE PERSON WORKS FULL TIME AND EXCLUSIVELY ON THE ACTION DURING THE FULL
YEAR: UP TO EUR 8 000/YEAR;
(B) IF THE PERSON WORKS EXCLUSIVELY ON THE ACTION BUT NOT FULL-TIME OR NOT FOR THE
FULL YEAR: UP TO THE CORRESPONDING PRO-RATA AMOUNT OF EUR 8 000, OR
(C) IF THE PERSON DOES NOT WORK EXCLUSIVELY ON THE ACTION: UP TO A PRO-RATA AMOUNT
CALCULATED IN ACCORDANCE TO ARTICLE 6.2.A.1.
7) The amount of additional
remuneration paid corresponded
to the Beneficiary’s usual
remuneration practices and was
consistently paid whenever the
same kind of work or expertise
was required.
8) The criteria used to calculate the
additional remuneration were
objective and generally applied
by the Beneficiary regardless of
the source of funding used.
9) The amount of additional
remuneration included in the
personnel costs charged to the
action was capped at EUR 8,000
per FTE/year (up to the
equivalent pro-rata amount if the
person did not work on the
action full-time during the year
or did not work exclusively on
the action).
Additional procedures in case “unit costs calculated by the Beneficiary in accordance with its
usual cost accounting practices” is applied:
Apart from carrying out the procedures indicated above to confirm standard factual findings 1-5
and, if applicable, also 6-9, the Auditor carried out following procedures to confirm standard
10) The personnel costs included in
the Financial Statement were
calculated in accordance with
the Beneficiary's usual cost
accounting practice. This
methodology was consistently
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
11
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
factual findings 10-13 listed in the next column:
o obtained a description of the Beneficiary's usual cost accounting practice to calculate unit
costs;.
o reviewed whether the Beneficiary's usual cost accounting practice was applied for the
Financial Statements subject of the present CFS;
o verified the employees included in the sample were charged under the correct category
(in accordance with the criteria used by the Beneficiary to establish personnel categories)
by reviewing the contract/HR-record or analytical accounting records;
o verified that there is no difference between the total amount of personnel costs used in
calculating the cost per unit and the total amount of personnel costs recorded in the
statutory accounts;
o verified whether actual personnel costs were adjusted on the basis of budgeted or
estimated elements and, if so, verified whether those elements used are actually relevant
for the calculation, objective and supported by documents.
used in all H2020 actions.
11) The employees were charged
under the correct category.
12) Total personnel costs used in
calculating the unit costs were
consistent with the expenses
recorded in the statutory
accounts.
13) Any estimated or budgeted
element used by the
Beneficiary in its unit-cost
calculation were relevant for
calculating personnel costs and
corresponded to objective and
verifiable information.
For natural persons included in the sample and working with the Beneficiary under a direct
contract other than an employment contract, such as consultants (no subcontractors).
To confirm standard factual findings 14-17 listed in the next column the Auditor reviewed
following information/documents provided by the Beneficiary:
o the contracts, especially the cost, contract duration, work description, place of work,
ownership of the results and reporting obligations to the Beneficiary;
o the employment conditions of staff in the same category to compare costs and;
o any other document that supports the costs declared and its registration (e.g. invoices,
accounting records, etc.).
14) The natural persons worked
under conditions similar to
those of an employee, in
particular regarding the way
the work is organised, the tasks
that are performed and the
premises where they are
performed.
15) The results of work carried out
belong to the Beneficiary, or, if
not, the Beneficiary has
obtained all necessary rights to
fulfil its obligations as if those
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
12
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
results were generated by itself.
16) Their costs were not
significantly different from
those for staff who performed
similar tasks under an
employment contract with the
Beneficiary.
17) The costs were supported by
audit evidence and registered
in the accounts.
For personnel seconded by a third party and included in the sample (not subcontractors)
To confirm standard factual findings 18-21 listed in the next column, the Auditor reviewed
following information/documents provided by the Beneficiary:
o their secondment contract(s) notably regarding costs, duration, work description, place of
work and ownership of the results;
o if there is reimbursement by the Beneficiary to the third party for the resource made
available (in-kind contribution against payment): any documentation that supports the
costs declared (e.g. contract, invoice, bank payment, and proof of registration in its
accounting/payroll, etc.) and reconciliation of the Financial Statement(s) with the
accounting system (project accounting and general ledger) as well as any proof that the
amount invoiced by the third party did not include any profit;
o if there is no reimbursement by the Beneficiary to the third party for the resource made
available (in-kind contribution free of charge): a proof of the actual cost borne by the
Third Party for the resource made available free of charge to the Beneficiary such as a
statement of costs incurred by the Third Party and proof of the registration in the Third
Party's accounting/payroll;
18) Seconded personnel reported to
the Beneficiary and worked on
the Beneficiary’s premises
(unless otherwise agreed with
the Beneficiary).
19) The results of work carried out
belong to the Beneficiary, or, if
not, the Beneficiary has
obtained all necessary rights to
fulfil its obligations as if those
results were generated by
itself..
If personnel is seconded against
payment:
20) The costs declared were
supported with documentation
and recorded in the
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
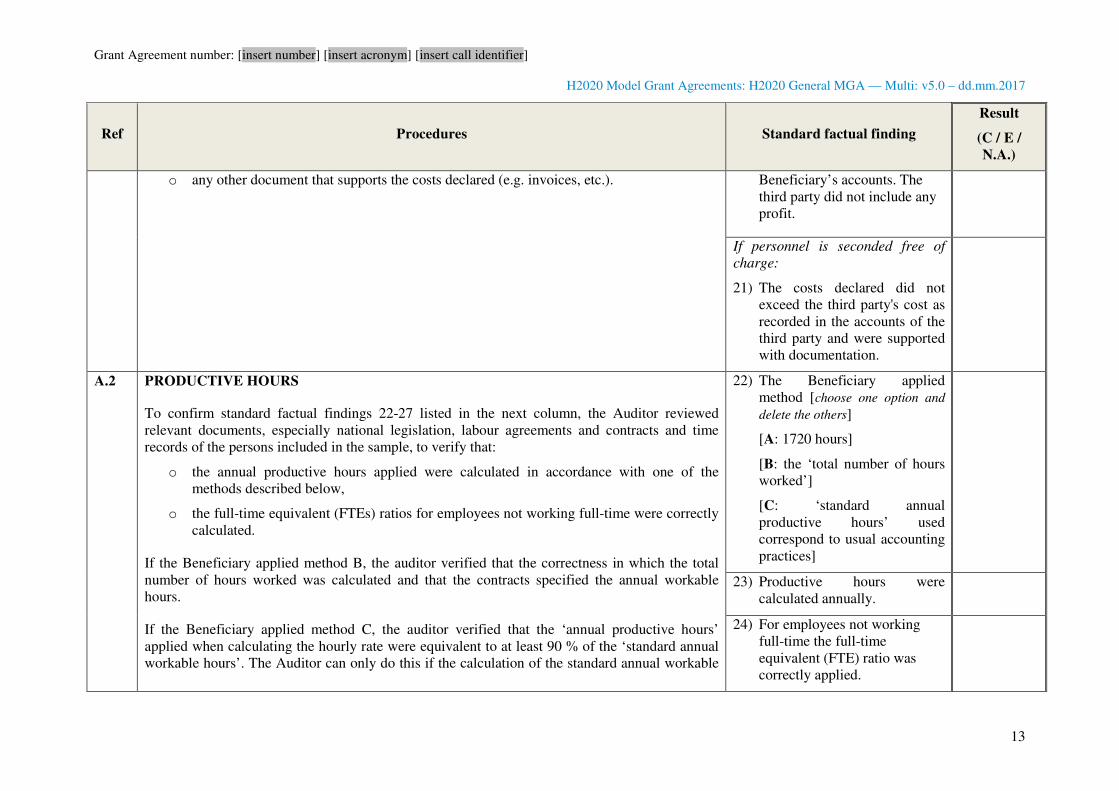
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
13
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
o any other document that supports the costs declared (e.g. invoices, etc.). Beneficiary’s accounts. The
third party did not include any
profit.
If personnel is seconded free of
charge:
21) The costs declared did not
exceed the third party's cost as
recorded in the accounts of the
third party and were supported
with documentation.
A.2 PRODUCTIVE HOURS
To confirm standard factual findings 22-27 listed in the next column, the Auditor reviewed
relevant documents, especially national legislation, labour agreements and contracts and time
records of the persons included in the sample, to verify that:
o the annual productive hours applied were calculated in accordance with one of the
methods described below,
o the full-time equivalent (FTEs) ratios for employees not working full-time were correctly
calculated.
If the Beneficiary applied method B, the auditor verified that the correctness in which the total
number of hours worked was calculated and that the contracts specified the annual workable
hours.
If the Beneficiary applied method C, the auditor verified that the ‘annual productive hours’
applied when calculating the hourly rate were equivalent to at least 90 % of the ‘standard annual
workable hours’. The Auditor can only do this if the calculation of the standard annual workable
22) The Beneficiary applied
method [choose one option and
delete the others]
[A: 1720 hours]
[B: the ‘total number of hours
worked’]
[C: ‘standard annual
productive hours’ used
correspond to usual accounting
practices]
23) Productive hours were
calculated annually.
24) For employees not working
full-time the full-time
equivalent (FTE) ratio was
correctly applied.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
14
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
hours can be supported by records, such as national legislation, labour agreements, and contracts.
BENEFICIARY'S PRODUCTIVE HOURS' FOR PERSONS WORKING FULL TIME SHALL BE ONE OF THE
FOLLOWING METHODS:
A. 1720 ANNUAL PRODUCTIVE HOURS (PRO-RATA FOR PERSONS NOT WORKING FULL-TIME)
B. THE TOTAL NUMBER OF HOURS WORKED BY THE PERSON FOR THE BENEFICIARY IN THE YEAR
(THIS METHOD IS ALSO REFERRED TO AS ‘TOTAL NUMBER OF HOURS WORKED’ IN THE NEXT
COLUMN). THE CALCULATION OF THE TOTAL NUMBER OF HOURS WORKED WAS DONE AS
FOLLOWS: ANNUAL WORKABLE HOURS OF THE PERSON ACCORDING TO THE EMPLOYMENT
CONTRACT, APPLICABLE LABOUR AGREEMENT OR NATIONAL LAW PLUS OVERTIME WORKED
MINUS ABSENCES (SUCH AS SICK LEAVE OR SPECIAL LEAVE).
C. THE STANDARD NUMBER OF ANNUAL HOURS GENERALLY APPLIED BY THE BENEFICIARY FOR ITS
PERSONNEL IN ACCORDANCE WITH ITS USUAL COST ACCOUNTING PRACTICES (THIS METHOD IS
ALSO REFERRED TO AS ‘STANDARD ANNUAL PRODUCTIVE HOURS’ IN THE NEXT COLUMN). THIS
NUMBER MUST BE AT LEAST 90% OF THE STANDARD ANNUAL WORKABLE HOURS.
‘ANNUAL WORKABLE HOURS’ MEANS THE PERIOD DURING WHICH THE PERSONNEL MUST BE
WORKING, AT THE EMPLOYER’S DISPOSAL AND CARRYING OUT HIS/HER ACTIVITY OR DUTIES UNDER
THE EMPLOYMENT CONTRACT, APPLICABLE COLLECTIVE LABOUR AGREEMENT OR NATIONAL
WORKING TIME LEGISLATION.
If the Beneficiary applied method
B.
25) The calculation of the number
of ‘annual workable hours’,
overtime and absences was
verifiable based on the
documents provided by the
Beneficiary.
25.1) The Beneficiary calculates
the hourly rates per full
financial year following
procedure A.3 (method B
is not allowed for
beneficiaries calculating
hourly rates per month).
If the Beneficiary applied method
C.
26) The calculation of the number
of ‘standard annual workable
hours’ was verifiable based on
the documents provided by the
Beneficiary.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
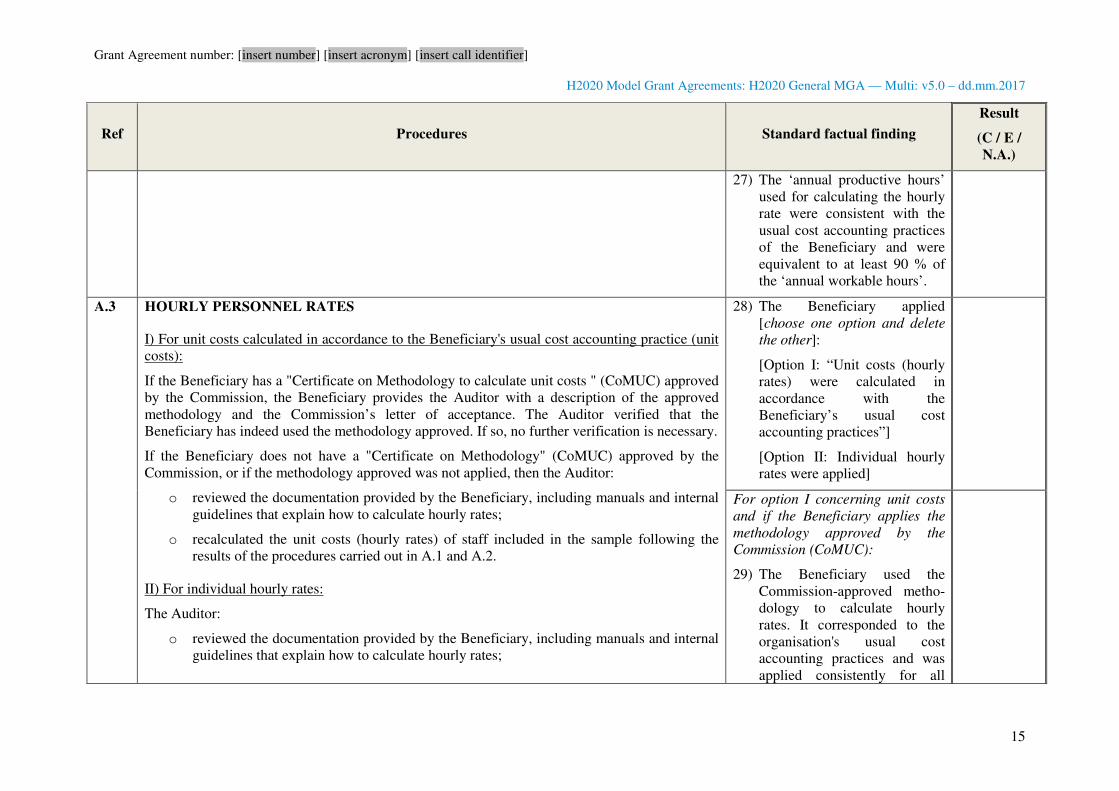
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
15
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
27) The ‘annual productive hours’
used for calculating the hourly
rate were consistent with the
usual cost accounting practices
of the Beneficiary and were
equivalent to at least 90 % of
the ‘annual workable hours’.
A.3 HOURLY PERSONNEL RATES
I) For unit costs calculated in accordance to the Beneficiary's usual cost accounting practice (unit
costs):
If the Beneficiary has a "Certificate on Methodology to calculate unit costs " (CoMUC) approved
by the Commission, the Beneficiary provides the Auditor with a description of the approved
methodology and the Commission’s letter of acceptance. The Auditor verified that the
Beneficiary has indeed used the methodology approved. If so, no further verification is necessary.
If the Beneficiary does not have a "Certificate on Methodology" (CoMUC) approved by the
Commission, or if the methodology approved was not applied, then the Auditor:
o reviewed the documentation provided by the Beneficiary, including manuals and internal
guidelines that explain how to calculate hourly rates;
o recalculated the unit costs (hourly rates) of staff included in the sample following the
results of the procedures carried out in A.1 and A.2.
II) For individual hourly rates:
The Auditor:
o reviewed the documentation provided by the Beneficiary, including manuals and internal
guidelines that explain how to calculate hourly rates;
28) The Beneficiary applied
[choose one option and delete
the other]:
[Option I: “Unit costs (hourly
rates) were calculated in
accordance with the
Beneficiary’s usual cost
accounting practices”]
[Option II: Individual hourly
rates were applied]
For option I concerning unit costs
and if the Beneficiary applies the
methodology approved by the
Commission (CoMUC):
29) The Beneficiary used the
Commission-approved metho-
dology to calculate hourly
rates. It corresponded to the
organisation's usual cost
accounting practices and was
applied consistently for all
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
16
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
o recalculated the hourly rates of staff included in the sample (recalculation of all hourly
rates if the Beneficiary uses annual rates, recalculation of three months selected randomly
for every year and person if the Beneficiary uses monthly rates) following the results of
the procedures carried out in A.1 and A.2;
o (only in case of monthly rates) confirmed that the time spent on parental leave is not
deducted, and that, if parts of the basic remuneration are generated over a period longer
than a month, the Beneficiary has included only the share which is generated in the
month.
“UNIT COSTS CALCULATED BY THE BENEFICIARY IN ACCORDANCE WITH ITS USUAL COST
ACCOUNTING PRACTICES”:
IT IS CALCULATED BY DIVIDING THE TOTAL AMOUNT OF PERSONNEL COSTS OF THE CATEGORY TO
WHICH THE EMPLOYEE BELONGS VERIFIED IN LINE WITH PROCEDURE A.1 BY THE NUMBER OF FTE
AND THE ANNUAL TOTAL PRODUCTIVE HOURS OF THE SAME CATEGORY CALCULATED BY THE
BENEFICIARY IN ACCORDANCE WITH PROCEDURE A.2.
HOURLY RATE FOR INDIVIDUAL ACTUAL PERSONAL COSTS:
IT IS CALCULATED FOLLOWING ONE OF THE TWO OPTIONS BELOW:
A) [OPTION BY DEFAULT] BY DIVIDING THE ACTUAL ANNUAL AMOUNT OF PERSONNEL COSTS OF AN
EMPLOYEE VERIFIED IN LINE WITH PROCEDURE A.1 BY THE NUMBER OF ANNUAL PRODUCTIVE HOURS
VERIFIED IN LINE WITH PROCEDURE A.2 (FULL FINANCIAL YEAR HOURLY RATE);
B) BY DIVIDING THE ACTUAL MONTHLY AMOUNT OF PERSONNEL COSTS OF AN EMPLOYEE VERIFIED IN
LINE WITH PROCEDURE A.1 BY 1/12 OF THE NUMBER OF ANNUAL PRODUCTIVE HOURS VERIFIED IN
LINE WITH PROCEDURE A.2.(MONTHLY HOURLY RATE).
activities irrespective of the
source of funding.
For option I concerning unit costs
and if the Beneficiary applies a
methodology not approved by the
Commission:
30) The unit costs re-calculated by
the Auditor were the same as
the rates applied by the
Beneficiary.
For option II concerning individual
hourly rates:
31) The individual rates re-
calculated by the Auditor were
the same as the rates applied by
the Beneficiary.
31.1) The Beneficiary used only
one option (per full financial
year or per month) throughout
each financial year examined.
31.2) The hourly rates do not
include additional
remuneration.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
17
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
A.4 TIME RECORDING SYSTEM
To verify that the time recording system ensures the fulfilment of all minimum requirements and
that the hours declared for the action were correct, accurate and properly authorised and
supported by documentation, the Auditor made the following checks for the persons included in
the sample that declare time as worked for the action on the basis of time records:
o description of the time recording system provided by the Beneficiary (registration,
authorisation, processing in the HR-system);
o its actual implementation;
o time records were signed at least monthly by the employees (on paper or electronically)
and authorised by the project manager or another manager;
o the hours declared were worked within the project period;
o there were no hours declared as worked for the action if HR-records showed absence due
to holidays or sickness (further cross-checks with travels are carried out in B.1 below) ;
o the hours charged to the action matched those in the time recording system.
ONLY THE HOURS WORKED ON THE ACTION CAN BE CHARGED. ALL WORKING TIME TO BE CHARGED
SHOULD BE RECORDED THROUGHOUT THE DURATION OF THE PROJECT, ADEQUATELY SUPPORTED BY
EVIDENCE OF THEIR REALITY AND RELIABILITY (SEE SPECIFIC PROVISIONS BELOW FOR PERSONS
WORKING EXCLUSIVELY FOR THE ACTION WITHOUT TIME RECORDS).
32) All persons recorded their time
dedicated to the action on a
daily/ weekly/ monthly basis
using a paper/computer-
based system. (delete the
answers that are not
applicable)
33) Their time-records were
authorised at least monthly by
the project manager or other
superior.
34) Hours declared were worked
within the project period and
were consistent with the
presences/absences recorded in
HR-records.
35) There were no discrepancies
between the number of hours
charged to the action and the
number of hours recorded.
If the persons are working exclusively for the action and without time records
For the persons selected that worked exclusively for the action without time records, the Auditor
verified evidence available demonstrating that they were in reality exclusively dedicated to the
action and that the Beneficiary signed a declaration confirming that they have worked exclusively
for the action.
36) The exclusive dedication is
supported by a declaration
signed by the Beneficiary and
by any other evidence
gathered.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
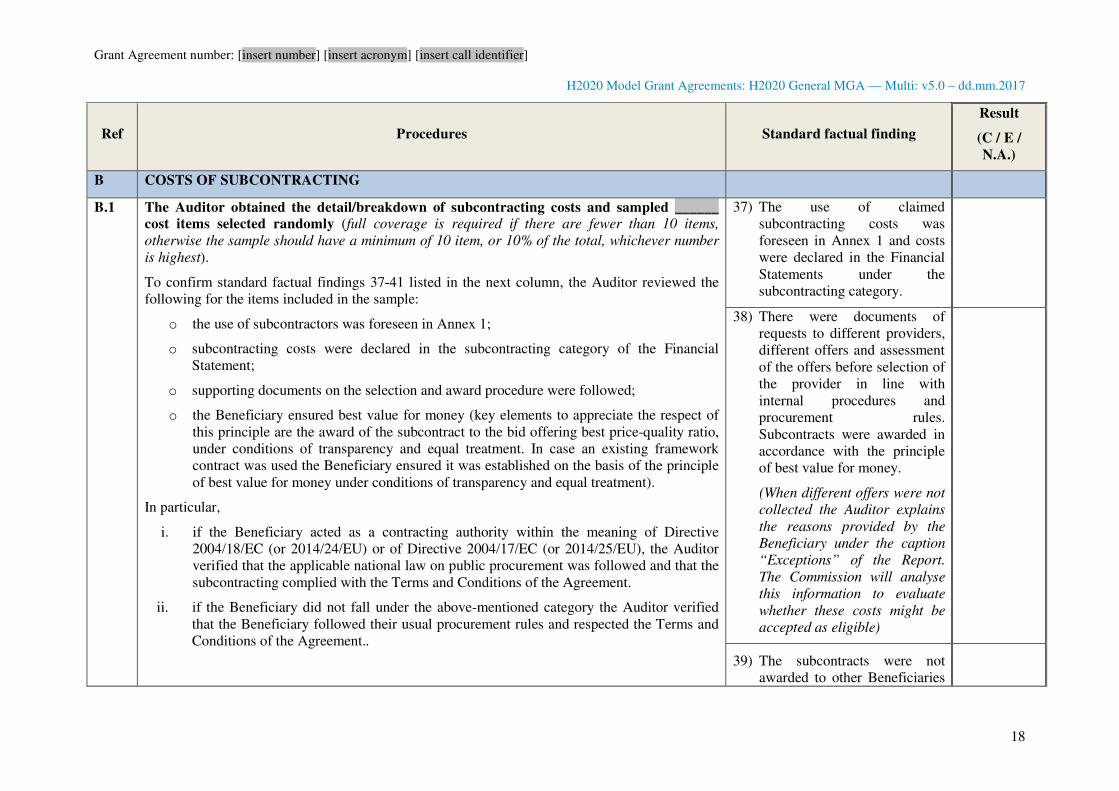
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
18
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
B COSTS OF SUBCONTRACTING
B.1 The Auditor obtained the detail/breakdown of subcontracting costs and sampled ______
cost items selected randomly (full coverage is required if there are fewer than 10 items,
otherwise the sample should have a minimum of 10 item, or 10% of the total, whichever number
is highest).
To confirm standard factual findings 37-41 listed in the next column, the Auditor reviewed the
following for the items included in the sample:
o the use of subcontractors was foreseen in Annex 1;
o subcontracting costs were declared in the subcontracting category of the Financial
Statement;
o supporting documents on the selection and award procedure were followed;
o the Beneficiary ensured best value for money (key elements to appreciate the respect of
this principle are the award of the subcontract to the bid offering best price-quality ratio,
under conditions of transparency and equal treatment. In case an existing framework
contract was used the Beneficiary ensured it was established on the basis of the principle
of best value for money under conditions of transparency and equal treatment).
In particular,
i. if the Beneficiary acted as a contracting authority within the meaning of Directive
2004/18/EC (or 2014/24/EU) or of Directive 2004/17/EC (or 2014/25/EU), the Auditor
verified that the applicable national law on public procurement was followed and that the
subcontracting complied with the Terms and Conditions of the Agreement.
ii. if the Beneficiary did not fall under the above-mentioned category the Auditor verified
that the Beneficiary followed their usual procurement rules and respected the Terms and
Conditions of the Agreement..
37) The use of claimed
subcontracting costs was
foreseen in Annex 1 and costs
were declared in the Financial
Statements under the
subcontracting category.
38) There were documents of
requests to different providers,
different offers and assessment
of the offers before selection of
the provider in line with
internal procedures and
procurement rules.
Subcontracts were awarded in
accordance with the principle
of best value for money.
(When different offers were not
collected the Auditor explains
the reasons provided by the
Beneficiary under the caption
“Exceptions” of the Report.
The Commission will analyse
this information to evaluate
whether these costs might be
accepted as eligible)
39) The subcontracts were not
awarded to other Beneficiaries
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
19
Ref Procedures Standard factual finding
Result
(C / E /
N.A.)
For the items included in the sample the Auditor also verified that:
o the subcontracts were not awarded to other Beneficiaries in the consortium;
o there were signed agreements between the Beneficiary and the subcontractor;
o there was evidence that the services were provided by subcontractor;
of the consortium.
40) All subcontracts were
supported by signed
agreements between the
Beneficiary and the
subcontractor.
41) There was evidence that the
services were provided by the
subcontractors.
C COSTS OF PROVIDING FINANCIAL SUPPORT TO THIRD PARTIES
C.1 The Auditor obtained the detail/breakdown of the costs of providing financial support to
third parties and sampled ______ cost items selected randomly (full coverage is required if
there are fewer than 10 items, otherwise the sample should have a minimum of 10 item, or 10% of
the total, whichever number is highest).
The Auditor verified that the following minimum conditions were met:
a) the maximum amount of financial support for each third party did not exceed EUR 60
000, unless explicitly mentioned in Annex 1;
b) the financial support to third parties was agreed in Annex 1 of the Agreement and the
other provisions on financial support to third parties included in Annex 1 were respected.
42) All minimum conditions were
met
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
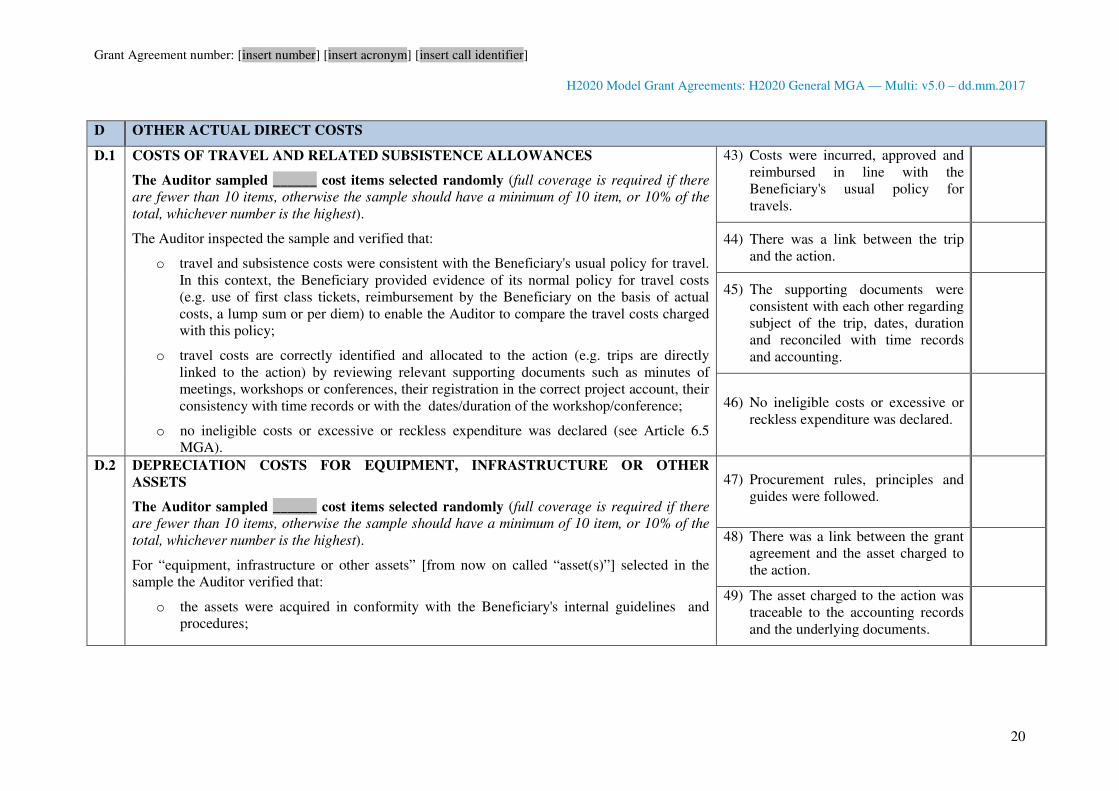
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
20
D OTHER ACTUAL DIRECT COSTS
D.1 COSTS OF TRAVEL AND RELATED SUBSISTENCE ALLOWANCES
The Auditor sampled ______ cost items selected randomly (full coverage is required if there
are fewer than 10 items, otherwise the sample should have a minimum of 10 item, or 10% of the
total, whichever number is the highest).
The Auditor inspected the sample and verified that:
o travel and subsistence costs were consistent with the Beneficiary's usual policy for travel.
In this context, the Beneficiary provided evidence of its normal policy for travel costs
(e.g. use of first class tickets, reimbursement by the Beneficiary on the basis of actual
costs, a lump sum or per diem) to enable the Auditor to compare the travel costs charged
with this policy;
o travel costs are correctly identified and allocated to the action (e.g. trips are directly
linked to the action) by reviewing relevant supporting documents such as minutes of
meetings, workshops or conferences, their registration in the correct project account, their
consistency with time records or with the dates/duration of the workshop/conference;
o no ineligible costs or excessive or reckless expenditure was declared (see Article 6.5
MGA).
43) Costs were incurred, approved and
reimbursed in line with the
Beneficiary's usual policy for
travels.
44) There was a link between the trip
and the action.
45) The supporting documents were
consistent with each other regarding
subject of the trip, dates, duration
and reconciled with time records
and accounting.
46) No ineligible costs or excessive or
reckless expenditure was declared.
D.2 DEPRECIATION COSTS FOR EQUIPMENT, INFRASTRUCTURE OR OTHER
ASSETS
The Auditor sampled ______ cost items selected randomly (full coverage is required if there
are fewer than 10 items, otherwise the sample should have a minimum of 10 item, or 10% of the
total, whichever number is the highest).
For “equipment, infrastructure or other assets” [from now on called “asset(s)”] selected in the
sample the Auditor verified that:
o the assets were acquired in conformity with the Beneficiary's internal guidelines and
procedures;
47) Procurement rules, principles and
guides were followed.
48) There was a link between the grant
agreement and the asset charged to
the action.
49) The asset charged to the action was
traceable to the accounting records
and the underlying documents.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
21
o they were correctly allocated to the action (with supporting documents such as delivery
note invoice or any other proof demonstrating the link to the action)
o they were entered in the accounting system;
o the extent to which the assets were used for the action (as a percentage) was supported by
reliable documentation (e.g. usage overview table);
The Auditor recalculated the depreciation costs and verified that they were in line with the
applicable rules in the Beneficiary’s country and with the Beneficiary’s usual accounting policy
(e.g. depreciation calculated on the acquisition value).
The Auditor verified that no ineligible costs such as deductible VAT, exchange rate losses,
excessive or reckless expenditure were declared (see Article 6.5 GA).
50) The depreciation method used to
charge the asset to the action was in
line with the applicable rules of the
Beneficiary's country and the
Beneficiary's usual accounting
policy.
51) The amount charged corresponded
to the actual usage for the action.
52) No ineligible costs or excessive or
reckless expenditure were declared.
D.3 COSTS OF OTHER GOODS AND SERVICES
The Auditor sampled ______ cost items selected randomly (full coverage is required if there
are fewer than 10 items, otherwise the sample should have a minimum of 10 item, or 10% of the
total, whichever number is highest).
For the purchase of goods, works or services included in the sample the Auditor verified that:
o the contracts did not cover tasks described in Annex 1;
o they were correctly identified, allocated to the proper action, entered in the accounting
system (traceable to underlying documents such as purchase orders, invoices and
accounting);
o the goods were not placed in the inventory of durable equipment;
o the costs charged to the action were accounted in line with the Beneficiary’s usual
accounting practices;
o no ineligible costs or excessive or reckless expenditure were declared (see Article 6 GA).
In addition, the Auditor verified that these goods and services were acquired in conformity with
53) Contracts for works or services did
not cover tasks described in Annex
1.
54) Costs were allocated to the correct
action and the goods were not
placed in the inventory of durable
equipment.
55) The costs were charged in line with
the Beneficiary’s accounting policy
and were adequately supported.
56) No ineligible costs or excessive or
reckless expenditure were declared.
For internal invoices/charges only
the cost element was charged,
without any mark-ups.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
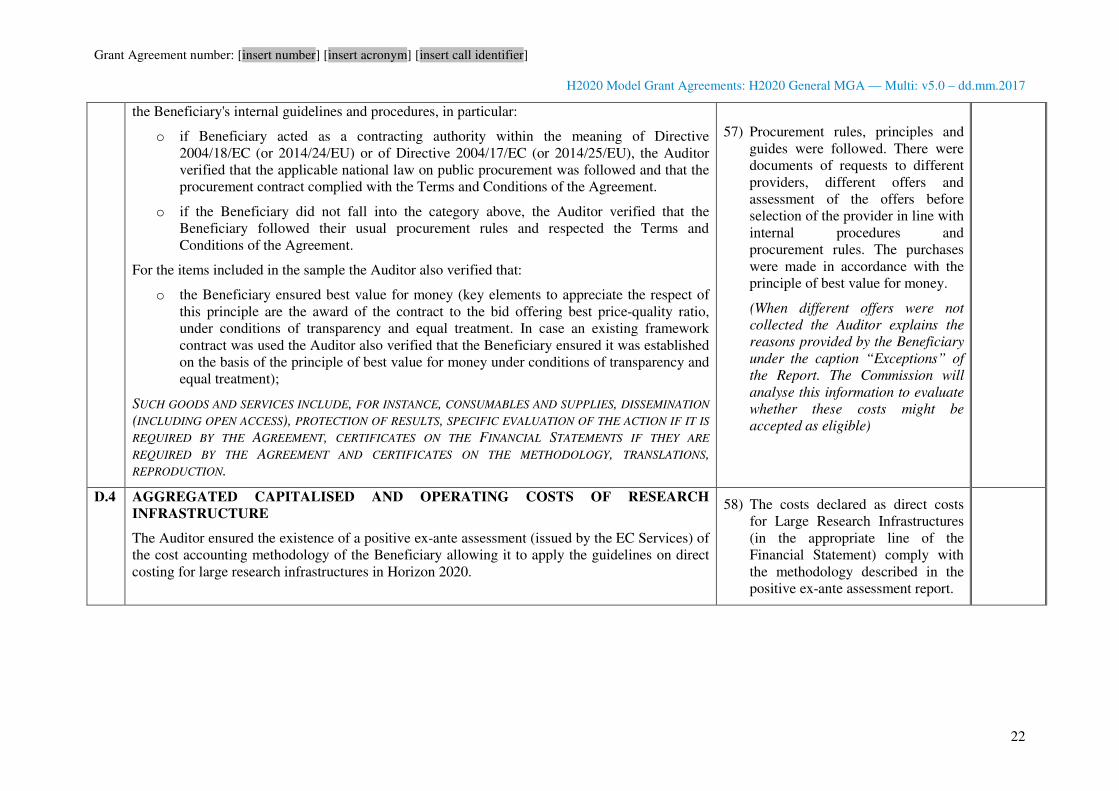
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
22
the Beneficiary's internal guidelines and procedures, in particular:
o if Beneficiary acted as a contracting authority within the meaning of Directive
2004/18/EC (or 2014/24/EU) or of Directive 2004/17/EC (or 2014/25/EU), the Auditor
verified that the applicable national law on public procurement was followed and that the
procurement contract complied with the Terms and Conditions of the Agreement.
o if the Beneficiary did not fall into the category above, the Auditor verified that the
Beneficiary followed their usual procurement rules and respected the Terms and
Conditions of the Agreement.
For the items included in the sample the Auditor also verified that:
o the Beneficiary ensured best value for money (key elements to appreciate the respect of
this principle are the award of the contract to the bid offering best price-quality ratio,
under conditions of transparency and equal treatment. In case an existing framework
contract was used the Auditor also verified that the Beneficiary ensured it was established
on the basis of the principle of best value for money under conditions of transparency and
equal treatment);
SUCH GOODS AND SERVICES INCLUDE, FOR INSTANCE, CONSUMABLES AND SUPPLIES, DISSEMINATION
(INCLUDING OPEN ACCESS), PROTECTION OF RESULTS, SPECIFIC EVALUATION OF THE ACTION IF IT IS
REQUIRED BY THE AGREEMENT, CERTIFICATES ON THE FINANCIAL STATEMENTS IF THEY ARE
REQUIRED BY THE AGREEMENT AND CERTIFICATES ON THE METHODOLOGY, TRANSLATIONS,
REPRODUCTION.
57) Procurement rules, principles and
guides were followed. There were
documents of requests to different
providers, different offers and
assessment of the offers before
selection of the provider in line with
internal procedures and
procurement rules. The purchases
were made in accordance with the
principle of best value for money.
(When different offers were not
collected the Auditor explains the
reasons provided by the Beneficiary
under the caption “Exceptions” of
the Report. The Commission will
analyse this information to evaluate
whether these costs might be
accepted as eligible)
D.4 AGGREGATED CAPITALISED AND OPERATING COSTS OF RESEARCH
INFRASTRUCTURE
The Auditor ensured the existence of a positive ex-ante assessment (issued by the EC Services) of
the cost accounting methodology of the Beneficiary allowing it to apply the guidelines on direct
costing for large research infrastructures in Horizon 2020.
58) The costs declared as direct costs
for Large Research Infrastructures
(in the appropriate line of the
Financial Statement) comply with
the methodology described in the
positive ex-ante assessment report.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
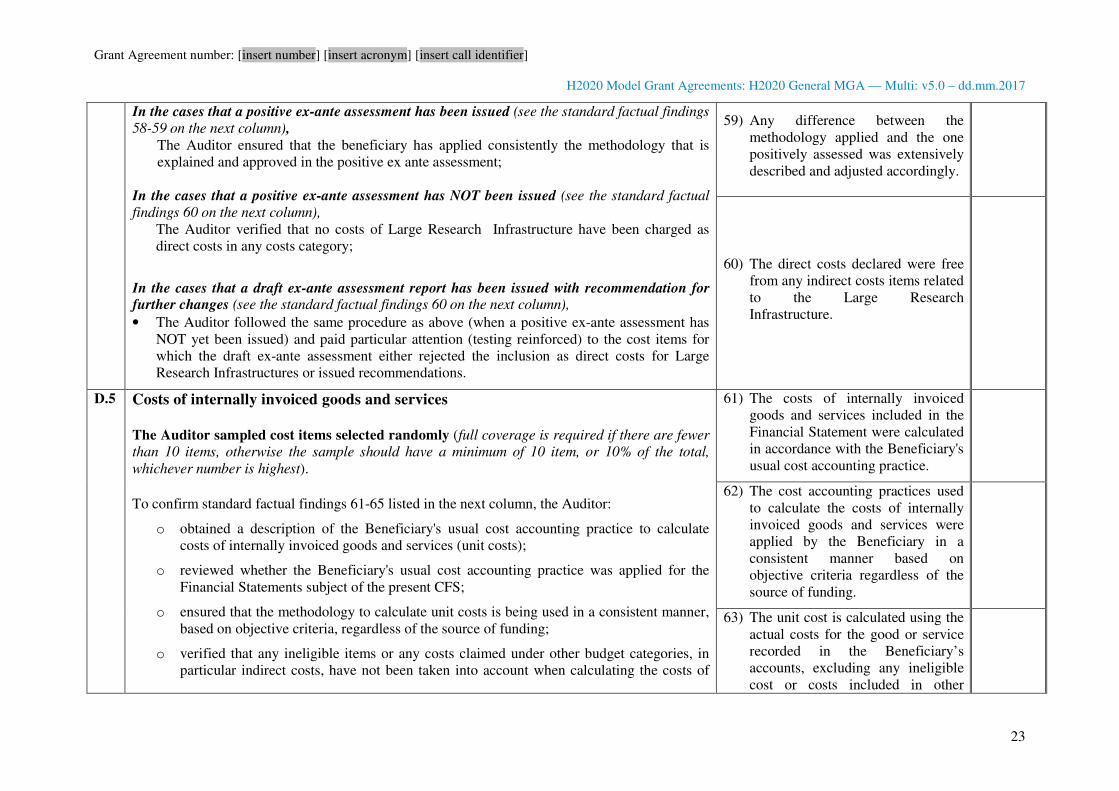
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
23
In the cases that a positive ex-ante assessment has been issued (see the standard factual findings
58-59 on the next column),
The Auditor ensured that the beneficiary has applied consistently the methodology that is
explained and approved in the positive ex ante assessment;
In the cases that a positive ex-ante assessment has NOT been issued (see the standard factual
findings 60 on the next column),
The Auditor verified that no costs of Large Research Infrastructure have been charged as
direct costs in any costs category;
In the cases that a draft ex-ante assessment report has been issued with recommendation for further changes (see the standard factual findings 60 on the next column),
• The Auditor followed the same procedure as above (when a positive ex-ante assessment has
NOT yet been issued) and paid particular attention (testing reinforced) to the cost items for
which the draft ex-ante assessment either rejected the inclusion as direct costs for Large
Research Infrastructures or issued recommendations.
59) Any difference between the
methodology applied and the one
positively assessed was extensively
described and adjusted accordingly.
60) The direct costs declared were free
from any indirect costs items related
to the Large Research
Infrastructure.
D.5
Costs of internally invoiced goods and services
The Auditor sampled cost items selected randomly (full coverage is required if there are fewer
than 10 items, otherwise the sample should have a minimum of 10 item, or 10% of the total,
whichever number is highest).
To confirm standard factual findings 61-65 listed in the next column, the Auditor:
o obtained a description of the Beneficiary's usual cost accounting practice to calculate
costs of internally invoiced goods and services (unit costs);
o reviewed whether the Beneficiary's usual cost accounting practice was applied for the
Financial Statements subject of the present CFS;
o ensured that the methodology to calculate unit costs is being used in a consistent manner,
based on objective criteria, regardless of the source of funding;
o verified that any ineligible items or any costs claimed under other budget categories, in
particular indirect costs, have not been taken into account when calculating the costs of
61) The costs of internally invoiced
goods and services included in the
Financial Statement were calculated
in accordance with the Beneficiary's
usual cost accounting practice.
62) The cost accounting practices used
to calculate the costs of internally
invoiced goods and services were
applied by the Beneficiary in a
consistent manner based on
objective criteria regardless of the
source of funding.
63) The unit cost is calculated using the
actual costs for the good or service
recorded in the Beneficiary’s
accounts, excluding any ineligible
cost or costs included in other
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
24
internally invoiced goods and services (see Article 6 GA);
o verified whether actual costs of internally invoiced goods and services were adjusted on
the basis of budgeted or estimated elements and, if so, verified whether those elements
used are actually relevant for the calculation, and correspond to objective and verifiable
information.
o verified that any costs of items which are not directly linked to the production of the
invoiced goods or service (e.g. supporting services like cleaning, general accountancy,
administrative support, etc. not directly used for production of the good or service) have
not been taken into account when calculating the costs of internally invoiced goods and
services.
o verified that any costs of items used for calculating the costs internally invoiced goods
and services are supported by audit evidence and registered in the accounts.
budget categories.
64) The unit cost excludes any costs of
items which are not directly linked
to the production of the invoiced
goods or service.
65) The costs items used for calculating
the actual costs of internally
invoiced goods and services were
relevant, reasonable and correspond
to objective and verifiable
information.
E USE OF EXCHANGE RATES
E.1 a) For Beneficiaries with accounts established in a currency other than euros
The Auditor sampled ______ cost items selected randomly and verified that the exchange
rates used for converting other currencies into euros were in accordance with the following
rules established in the Agreement ( full coverage is required if there are fewer than 10 items,
otherwise the sample should have a minimum of 10 item, or 10% of the total, whichever number is
highest):
COSTS RECORDED IN THE ACCOUNTS IN A CURRENCY OTHER THAN EURO SHALL BE CONVERTED INTO
EURO AT THE AVERAGE OF THE DAILY EXCHANGE RATES PUBLISHED IN THE C SERIES OF OFFICIAL
JOURNAL OF THE EUROPEAN UNION
(https://www.ecb.int/stats/exchange/eurofxref/html/index.en.html ), DETERMINED OVER THE
CORRESPONDING REPORTING PERIOD.
IF NO DAILY EURO EXCHANGE RATE IS PUBLISHED IN THE OFFICIAL JOURNAL OF THE EUROPEAN
UNION FOR THE CURRENCY IN QUESTION, CONVERSION SHALL BE MADE AT THE AVERAGE OF THE
MONTHLY ACCOUNTING RATES ESTABLISHED BY THE COMMISSION AND PUBLISHED ON ITS WEBSITE
(http://ec.europa.eu/budget/contracts_grants/info_contracts/inforeuro/inforeuro_en.cfm ),
66) The exchange rates used to convert
other currencies into Euros were in
accordance with the rules
established of the Grant Agreement
and there was no difference in the
final figures.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
25
DETERMINED OVER THE CORRESPONDING REPORTING PERIOD.
b) For Beneficiaries with accounts established in euros
The Auditor sampled ______ cost items selected randomly and verified that the exchange
rates used for converting other currencies into euros were in accordance with the following
rules established in the Agreement ( full coverage is required if there are fewer than 10 items,
otherwise the sample should have a minimum of 10 item, or 10% of the total, whichever number is
highest):
COSTS INCURRED IN ANOTHER CURRENCY SHALL BE CONVERTED INTO EURO BY APPLYING THE
BENEFICIARY’S USUAL ACCOUNTING PRACTICES.
67) The Beneficiary applied its usual
accounting practices.
[legal name of the audit firm]
[name and function of an authorised representative]
[dd Month yyyy]
<Signature of the Auditor>
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
1
ANNEX 6
MODEL FOR THE CERTIFICATE ON THE METHODOLOGY
� For options [in italics in square brackets]: choose the applicable option. Options not chosen should be deleted.
� For fields in [grey in square brackets]: enter the appropriate data.
TABLE OF CONTENTS
TERMS OF REFERENCE FOR AN AUDIT ENGAGEMENT FOR A METHODOLOGY CERTIFICATE IN
CONNECTION WITH ONE OR MORE GRANT AGREEMENTS FINANCED UNDER THE HORIZON 2020
RESEARCH AND INNOVATION FRAMEWORK PROGRAMME
INDEPENDENT REPORT OF FACTUAL FINDINGS ON THE METHODOLOGY CONCERNING GRANT
AGREEMENTS FINANCED UNDER THE HORIZON 2020 RESEARCH AND INNOVATION
FRAMEWORK PROGRAMME
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
2
Terms of reference for an audit engagement for a methodology certificate
in connection with one or more grant agreements financed
under the Horizon 2020 Research and Innovation Framework Programme
This document sets out the ‘Terms of Reference (ToR)’ under which
[OPTION 1: [insert name of the beneficiary] (‘the Beneficiary’)] [OPTION 2: [insert name of the
linked third party] (‘the Linked Third Party’), third party linked to the Beneficiary [insert name of the
beneficiary] (‘the Beneficiary’)]
agrees to engage
[insert legal name of the auditor] (‘the Auditor’)
to produce an independent report of factual findings (‘the Report’) concerning the [Beneficiary’s]
[Linked Third Party’s] usual accounting practices for calculating and claiming direct personnel costs
declared as unit costs (‘the Methodology’) in connection with grant agreements financed under the
Horizon 2020 Research and Innovation Framework Programme.
The procedures to be carried out for the assessment of the methodology will be based on the grant
agreement(s) detailed below:
[title and number of the grant agreement(s)] (‘the Agreement(s)’)
The Agreement(s) has(have) been concluded between the Beneficiary and [OPTION 1: the European
Union, represented by the European Commission (‘the Commission’)][ OPTION 2: the European
Atomic Energy Community (Euratom,) represented by the European Commission (‘the
Commission’)][OPTION 3: the [Research Executive Agency (REA)] [European Research Council
Executive Agency (ERCEA)] [Innovation and Networks Executive Agency (INEA)] [Executive Agency
for Small and Medium-sized Enterprises (EASME)] (‘the Agency’), under the powers delegated by the
European Commission (‘the Commission’).].
The [Commission] [Agency] is mentioned as a signatory of the Agreement with the Beneficiary only.
The [European Union] [Euratom] [Agency] is not a party to this engagement.
1.1 Subject of the engagement
According to Article 18.1.2 of the Agreement, beneficiaries [and linked third parties] that declare
direct personnel costs as unit costs calculated in accordance with their usual cost accounting practices
may submit to the [Commission] [Agency], for approval, a certificate on the methodology (‘CoMUC’)
stating that there are adequate records and documentation to prove that their cost accounting practices
used comply with the conditions set out in Point A of Article 6.2.
The subject of this engagement is the CoMUC which is composed of two separate documents:
- the Terms of Reference (‘the ToR’) to be signed by the [Beneficiary] [Linked Third Party]
and the Auditor;
- the Auditor’s Independent Report of Factual Findings (‘the Report’) issued on the Auditor’s
letterhead, dated, stamped and signed by the Auditor which includes; the standard statements
(‘the Statements’) evaluated and signed by the [Beneficiary] [Linked Third Party], the agreed-
upon procedures (‘the Procedures’) performed by the Auditor and the standard factual findings
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
3
(‘the Findings’) assessed by the Auditor. The Statements, Procedures and Findings are
summarised in the table that forms part of the Report.
The information provided through the Statements, the Procedures and the Findings will enable the
Commission to draw conclusions regarding the existence of the [Beneficiary’s] [Linked Third Party’s]
usual cost accounting practice and its suitability to ensure that direct personnel costs claimed on that
basis comply with the provisions of the Agreement. The Commission draws its own conclusions from
the Report and any additional information it may require.
1.2 Responsibilities
The parties to this agreement are the [Beneficiary] [Linked Third Party] and the Auditor.
The [Beneficiary] [Linked Third Party]:
• is responsible for preparing financial statements for the Agreement(s) (‘the Financial
Statements’) in compliance with those Agreements;
• is responsible for providing the Financial Statement(s) to the Auditor and enabling the Auditor
to reconcile them with the [Beneficiary’s] [Linked Third Party’s] accounting and
bookkeeping system and the underlying accounts and records. The Financial Statement(s) will
be used as a basis for the procedures which the Auditor will carry out under this ToR;
• is responsible for its Methodology and liable for the accuracy of the Financial Statement(s);
• is responsible for endorsing or refuting the Statements indicated under the heading
‘Statements to be made by the Beneficiary/ Linked Third Party’ in the first column of the table
that forms part of the Report;
• must provide the Auditor with a signed and dated representation letter;
• accepts that the ability of the Auditor to carry out the Procedures effectively depends upon the
[Beneficiary] [Linked Third Party] providing full and free access to the [Beneficiary’s]
[Linked Third Party’s] staff and to its accounting and other relevant records.
The Auditor:
• [Option 1 by default: is qualified to carry out statutory audits of accounting documents in
accordance with Directive 2006/43/EC of the European Parliament and of the Council of 17
May 2006 on statutory audits of annual accounts and consolidated accounts, amending
Council Directives 78/660/EEC and 83/349/EEC and repealing Council Directive
84/253/EEC or similar national regulations].
• [Option 2 if the Beneficiary or Linked Third Party has an independent Public Officer: is a
competent and independent Public Officer for which the relevant national authorities have
established the legal capacity to audit the Beneficiary].
• [Option 3 if the Beneficiary or Linked Third Party is an international organisation: is an
[internal] [external] auditor in accordance with the internal financial regulations and
procedures of the international organisation].
The Auditor:
• must be independent from the Beneficiary [and the Linked Third Party], in particular, it must
not have been involved in preparing the Beneficiary’s [and Linked Third Party’s] Financial
Statement(s);
• must plan work so that the Procedures may be carried out and the Findings may be assessed;
• must adhere to the Procedures laid down and the compulsory report format;
• must carry out the engagement in accordance with these ToR;
• must document matters which are important to support the Report;
• must base its Report on the evidence gathered;
• must submit the Report to the [Beneficiary] [Linked Third Party].
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
4
The Commission sets out the Procedures to be carried out and the Findings to be endorsed by the
Auditor. The Auditor is not responsible for their suitability or pertinence. As this engagement is not an
assurance engagement the Auditor does not provide an audit opinion or a statement of assurance.
1.3 Applicable Standards
The Auditor must comply with these Terms of Reference and with1:
- the International Standard on Related Services (‘ISRS’) 4400 Engagements to perform
Agreed-upon Procedures regarding Financial Information as issued by the International
Auditing and Assurance Standards Board (IAASB);
- the Code of Ethics for Professional Accountants issued by the International Ethics Standards
Board for Accountants (IESBA). Although ISRS 4400 states that independence is not a
requirement for engagements to carry out agreed-upon procedures, the Commission requires
that the Auditor also complies with the Code’s independence requirements.
The Auditor’s Report must state that there was no conflict of interests in establishing this Report
between the Auditor and the Beneficiary [and the Linked Third Party] that could have a bearing on the
Report, and must specify – if the service is invoiced - the total fee paid to the Auditor for providing the
Report.
1.4 Reporting
The Report must be written in the language of the Agreement (see Article 20.7 of the Agreement).
Under Article 22 of the Agreement, the Commission, [the Agency], the European Anti-Fraud Office
and the Court of Auditors have the right to audit any work that is carried out under the action and for
which costs are declared from [the European Union] [Euratom] budget. This includes work related to
this engagement. The Auditor must provide access to all working papers related to this assignment if
the Commission[, the Agency], the European Anti-Fraud Office or the European Court of Auditors
requests them.
1.5 Timing
The Report must be provided by [dd Month yyyy].
1.6 Other Terms
[The [Beneficiary] [Linked Third Party] and the Auditor can use this section to agree other specific
terms, such as the Auditor’s fees, liability, applicable law, etc. Those specific terms must not
contradict the terms specified above.]
[legal name of the Auditor] [legal name of the [Beneficiary] [Linked Third Party]]
[name & title of authorised representative] [name & title of authorised representative]
[dd Month yyyy] [dd Month yyyy]
Signature of the Auditor Signature of the [Beneficiary] [Linked Third Party]
1 Supreme Audit Institutions applying INTOSAI-standards may carry out the Procedures according to the
corresponding International Standards of Supreme Audit Institutions and code of ethics issued by INTOSAI
instead of the International Standard on Related Services (‘ISRS’) 4400 and the Code of Ethics for
Professional Accountants issued by the IAASB and the IESBA.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
5
Independent report of factual findings on the methodology concerning grant agreements
financed under the Horizon 2020 Research and Innovation Framework Programme (To be printed on letterhead paper of the auditor)
To
[ name of contact person(s)], [Position]
[[Beneficiary’s] [Linked Third Party’s] name]
[ Address]
[ dd Month yyyy]
Dear [Name of contact person(s)],
As agreed under the terms of reference dated [dd Month yyyy]
with [OPTION 1: [insert name of the beneficiary] (‘the Beneficiary’)] [OPTION 2: [insert name of
the linked third party] (‘the Linked Third Party’), third party linked to the Beneficiary [insert name of
the beneficiary] (‘the Beneficiary’)],
we
[ name of the auditor] (‘the Auditor’),
established at
[full address/city/state/province/country],
represented by
[name and function of an authorised representative],
have carried out the agreed-upon procedures (‘the Procedures’) and provide hereby our Independent
Report of Factual Findings (‘the Report’), concerning the [Beneficiary’s] [Linked Third Party’s] usual
accounting practices for calculating and declaring direct personnel costs declared as unit costs (‘the
Methodology’).
You requested certain procedures to be carried out in connection with the grant(s)
[title and number of the grant agreement(s)] (‘the Agreement(s)’).
The Report
Our engagement was carried out in accordance with the terms of reference (‘the ToR’) appended to
this Report. The Report includes: the standard statements (‘the Statements’) made by the [Beneficiary]
[Linked Third Party], the agreed-upon procedures (‘the Procedures’) carried out and the standard
factual findings (‘the Findings’) confirmed by us.
The engagement involved carrying out the Procedures and assessing the Findings and the
documentation requested appended to this Report, the results of which the Commission uses to draw
conclusions regarding the acceptability of the Methodology applied by the [Beneficiary] [Linked Third
Party].
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
6
The Report covers the methodology used from [dd Month yyyy]. In the event that the [Beneficiary]
[Linked Third Party] changes this methodology, the Report will not be applicable to any Financial
Statement1 submitted thereafter.
The scope of the Procedures and the definition of the standard statements and findings were
determined solely by the Commission. Therefore, the Auditor is not responsible for their suitability or
pertinence.
Since the Procedures carried out constitute neither an audit nor a review made in accordance with
International Standards on Auditing or International Standards on Review Engagements, we do not
give a statement of assurance on the costs declared on the basis of the [Beneficiary’s] [Linked Third
Party’s] Methodology. Had we carried out additional procedures or had we performed an audit or
review in accordance with these standards, other matters might have come to its attention and would
have been included in the Report.
Exceptions
Apart from the exceptions listed below, the [Beneficiary] [Linked Third Party] agreed with the
standard Statements and provided the Auditor all the documentation and accounting information
needed by the Auditor to carry out the requested Procedures and corroborate the standard Findings.
List here any exception and add any information on the cause and possible consequences of each
exception, if known. If the exception is quantifiable, also indicate the corresponding amount.
…..
Explanation of possible exceptions in the form of examples (to be removed from the Report):
i. the [Beneficiary] [Linked Third Party] did not agree with the standard Statement number … because…;
ii. the Auditor could not carry out the procedure … established because …. (e.g. due to the inability to
reconcile key information or the unavailability or inconsistency of data);
iii. the Auditor could not confirm or corroborate the standard Finding number … because ….
Remarks
We would like to add the following remarks relevant for the proper understanding of the Methodology
applied by the [Beneficiary] [Linked Third Party] or the results reported:
Example (to be removed from the Report):
Regarding the methodology applied to calculate hourly rates …
Regarding standard Finding 15 it has to be noted that …
The [Beneficiary] [Linked Third Party] explained the deviation from the benchmark statement XXIV
concerning time recording for personnel with no exclusive dedication to the action in the following manner:
…
Annexes
Please provide the following documents to the auditor and annex them to the report when submitting
this CoMUC to the Commission:
1 Financial Statement in this context refers solely to Annex 4 of the Agreement by which the Beneficiary
declares costs under the Agreement.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
7
1. Brief description of the methodology for calculating personnel costs, productive hours and
hourly rates;
2. Brief description of the time recording system in place;
3. An example of the time records used by the [Beneficiary] [Linked Third Party];
4. Description of any budgeted or estimated elements applied, together with an explanation as to
why they are relevant for calculating the personnel costs and how they are based on objective
and verifiable information;
5. A summary sheet with the hourly rate for direct personnel declared by the [Beneficiary]
[Linked Third Party] and recalculated by the Auditor for each staff member included in the
sample (the names do not need to be reported);
6. A comparative table summarising for each person selected in the sample a) the time claimed
by the [Beneficiary] [Linked Third Party] in the Financial Statement(s) and b) the time
according to the time record verified by the Auditor;
7. A copy of the letter of representation provided to the Auditor.
Use of this Report
This Report has been drawn up solely for the purpose given under Point 1.1 Reasons for the
engagement.
The Report:
- is confidential and is intended to be submitted to the Commission by the [Beneficiary] [Linked
Third Party] in connection with Article 18.1.2 of the Agreement;
- may not be used by the [Beneficiary] [Linked Third Party] or by the Commission for any other
purpose, nor distributed to any other parties;
- may be disclosed by the Commission only to authorised parties, in particular the European
Anti-Fraud Office (OLAF) and the European Court of Auditors.
- relates only to the usual cost accounting practices specified above and does not constitute a
report on the Financial Statements of the [Beneficiary] [Linked Third Party].
No conflict of interest2 exists between the Auditor and the Beneficiary [and the Linked Third Party]
that could have a bearing on the Report. The total fee paid to the Auditor for producing the Report was
EUR ______ (including EUR ______ of deductible VAT).
We look forward to discussing our Report with you and would be pleased to provide any further
information or assistance which may be required.
Yours sincerely
[legal name of the Auditor]
[name and title of the authorised representative]
[dd Month yyyy]
Signature of the Auditor
2 A conflict of interest arises when the Auditor's objectivity to establish the certificate is compromised in fact
or in appearance when the Auditor for instance:
- was involved in the preparation of the Financial Statements;
- stands to benefit directly should the certificate be accepted;
- has a close relationship with any person representing the beneficiary;
- is a director, trustee or partner of the beneficiary; or
- is in any other situation that compromises his or her independence or ability to establish the certificate
impartially.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
8
Statements to be made by the Beneficiary/Linked Third Party (‘the Statements’) and Procedures to be carried out by the Auditor (‘the
Procedures’) and standard factual findings (‘the Findings’) to be confirmed by the Auditor
The Commission reserves the right to provide the auditor with guidance regarding the Statements to be made, the Procedures to be carried out or the
Findings to be ascertained and the way in which to present them. The Commission reserves the right to vary the Statements, Procedures or Findings by
written notification to the Beneficiary/Linked Third Party to adapt the procedures to changes in the grant agreement(s) or to any other circumstances.
If this methodology certificate relates to the Linked Third Party’s usual accounting practices for calculating and claiming direct personnel costs declared as
unit costs any reference here below to ‘the Beneficiary’ is to be considered as a reference to ‘the Linked Third Party’.
Please explain any discrepancies in the body of the Report.
Statements to be made by Beneficiary Procedures to be carried out and Findings to be confirmed by the Auditor
A. Use of the Methodology
I. The cost accounting practice described below has been in use since [dd
Month yyyy].
II. The next planned alteration to the methodology used by the Beneficiary
will be from [dd Month yyyy].
Procedure:
� The Auditor checked these dates against the documentation the Beneficiary
has provided.
Factual finding:
1. The dates provided by the Beneficiary were consistent with the
documentation.
B. Description of the Methodology
III. The methodology to calculate unit costs is being used in a consistent
manner and is reflected in the relevant procedures.
[Please describe the methodology your entity uses to calculate personnel costs,
productive hours and hourly rates, present your description to the Auditor and
annex it to this certificate]
[If the statement of section “B. Description of the methodology” cannot be
endorsed by the Beneficiary or there is no written methodology to calculate unit
costs it should be listed here below and reported as exception by the Auditor in the
main Report of Factual Findings:
- …]
Procedure:
� The Auditor reviewed the description, the relevant manuals and/or internal
guidance documents describing the methodology.
Factual finding:
2. The brief description was consistent with the relevant manuals, internal
guidance and/or other documentary evidence the Auditor has reviewed.
3. The methodology was generally applied by the Beneficiary as part of its
usual costs accounting practices.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
9
Please explain any discrepancies in the body of the Report.
Statements to be made by Beneficiary Procedures to be carried out and Findings to be confirmed by the Auditor
C. Personnel costs
General
IV. The unit costs (hourly rates) are limited to salaries including during
parental leave, social security contributions, taxes and other costs included
in the remuneration required under national law and the employment
contract or equivalent appointing act;
V. Employees are hired directly by the Beneficiary in accordance with
national law, and work under its sole supervision and responsibility;
VI. The Beneficiary remunerates its employees in accordance with its usual
practices. This means that personnel costs are charged in line with the
Beneficiary’s usual payroll policy (e.g. salary policy, overtime policy,
variable pay) and no special conditions exist for employees assigned to
tasks relating to the European Union or Euratom, unless explicitly provided
for in the grant agreement(s);
VII. The Beneficiary allocates its employees to the relevant group/category/cost
centre for the purpose of the unit cost calculation in line with the usual cost
accounting practice;
VIII. Personnel costs are based on the payroll system and accounting system.
IX. Any exceptional adjustments of actual personnel costs resulted from
relevant budgeted or estimated elements and were based on objective and
verifiable information. [Please describe the ‘budgeted or estimated
elements’ and their relevance to personnel costs, and explain how they
were reasonable and based on objective and verifiable information, present
your explanation to the Auditor and annex it to this certificate].
X. Personnel costs claimed do not contain any of the following ineligible
costs: costs related to return on capital; debt and debt service charges;
provisions for future losses or debts; interest owed; doubtful debts;
currency exchange losses; bank costs charged by the Beneficiary’s bank for
transfers from the Commission/Agency; excessive or reckless expenditure;
deductible VAT or costs incurred during suspension of the implementation
of the action.
XI. Personnel costs were not declared under another EU or Euratom grant
Procedure:
The Auditor draws a sample of employees to carry out the procedures indicated in
this section C and the following sections D to F.
[The Auditor has drawn a random sample of 10 employees assigned to Horizon 2020
action(s). If fewer than 10 employees are assigned to the Horizon 2020 action(s), the
Auditor has selected all employees assigned to the Horizon 2020 action(s)
complemented by other employees irrespective of their assignments until he has
reached 10 employees.]. For this sample:
� the Auditor reviewed all documents relating to personnel costs such as
employment contracts, payslips, payroll policy (e.g. salary policy, overtime
policy, variable pay policy), accounting and payroll records, applicable
national tax , labour and social security law and any other documents
corroborating the personnel costs claimed;
� in particular, the Auditor reviewed the employment contracts of the
employees in the sample to verify that:
i. they were employed directly by the Beneficiary in accordance with
applicable national legislation;
ii. they were working under the sole technical supervision and
responsibility of the latter;
iii. they were remunerated in accordance with the Beneficiary’s usual
practices;
iv. they were allocated to the correct group/category/cost centre for the
purposes of calculating the unit cost in line with the Beneficiary’s
usual cost accounting practices;
� the Auditor verified that any ineligible items or any costs claimed under
other costs categories or costs covered by other types of grant or by other
grants financed from the European Union budget have not been taken into
account when calculating the personnel costs;
� the Auditor numerically reconciled the total amount of personnel costs used
to calculate the unit cost with the total amount of personnel costs recorded
in the statutory accounts and the payroll system.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
10
Please explain any discrepancies in the body of the Report.
Statements to be made by Beneficiary Procedures to be carried out and Findings to be confirmed by the Auditor
(including grants awarded by a Member State and financed by the EU
budget and grants awarded by bodies other than the Commission/Agency
for the purpose of implementing the EU or Euratom budget in the same
period, unless the Beneficiary can demonstrate that the operating grant
does not cover any costs of the action).
If additional remuneration as referred to in the grant agreement(s) is paid
XII. The Beneficiary is a non-profit legal entity;
XIII. The additional remuneration is part of the beneficiary’s usual remuneration
practices and paid consistently whenever the relevant work or expertise is
required;
XIV. The criteria used to calculate the additional remuneration are objective and
generally applied regardless of the source of funding;
XV. The additional remuneration included in the personnel costs used to
calculate the hourly rates for the grant agreement(s) is capped at
EUR 8 000 per full-time equivalent (reduced proportionately if the
employee is not assigned exclusively to the action).
[If certain statement(s) of section “C. Personnel costs” cannot be endorsed by the
Beneficiary they should be listed here below and reported as exception by the
Auditor in the main Report of Factual Findings:
- …]
� to the extent that actual personnel costs were adjusted on the basis of
budgeted or estimated elements, the Auditor carefully examined those
elements and checked the information source to confirm that they
correspond to objective and verifiable information;
� if additional remuneration has been claimed, the Auditor verified that the
Beneficiary was a non-profit legal entity, that the amount was capped at
EUR 8 000 per full-time equivalent and that it was reduced proportionately
for employees not assigned exclusively to the action(s).
� the Auditor recalculated the personnel costs for the employees in the
sample.
Factual finding:
4. All the components of the remuneration that have been claimed as personnel
costs are supported by underlying documentation.
5. The employees in the sample were employed directly by the Beneficiary in
accordance with applicable national law and were working under its sole
supervision and responsibility.
6. Their employment contracts were in line with the Beneficiary’s usual
policy;
7. Personnel costs were duly documented and consisted solely of salaries,
social security contributions (pension contributions, health insurance,
unemployment fund contributions, etc.), taxes and other statutory costs
included in the remuneration (holiday pay, thirteenth month’s pay, etc.);
8. The totals used to calculate the personnel unit costs are consistent with those
registered in the payroll and accounting records;
9. To the extent that actual personnel costs were adjusted on the basis of
budgeted or estimated elements, those elements were relevant for
calculating the personnel costs and correspond to objective and verifiable
information. The budgeted or estimated elements used are: — (indicate the
elements and their values).
10. Personnel costs contained no ineligible elements;
11. Specific conditions for eligibility were fulfilled when additional
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
11
Please explain any discrepancies in the body of the Report.
Statements to be made by Beneficiary Procedures to be carried out and Findings to be confirmed by the Auditor
remuneration was paid: a) the Beneficiary is registered in the grant
agreements as a non-profit legal entity; b) it was paid according to objective
criteria generally applied regardless of the source of funding used and c)
remuneration was capped at EUR 8 000 per full-time equivalent (or up to up
to the equivalent pro-rata amount if the person did not work on the action
full-time during the year or did not work exclusively on the action).
D. Productive hours
XVI. The number of productive hours per full-time employee applied is [delete
as appropriate]:
A. 1720 productive hours per year for a person working full-time
(corresponding pro-rata for persons not working full time).
B. the total number of hours worked in the year by a person for the
Beneficiary
C. the standard number of annual hours generally applied by the
beneficiary for its personnel in accordance with its usual cost
accounting practices. This number must be at least 90% of the
standard annual workable hours.
If method B is applied
XVII. The calculation of the total number of hours worked was done as
follows: annual workable hours of the person according to the
employment contract, applicable labour agreement or national law plus
overtime worked minus absences (such as sick leave and special leave).
XVIII. ‘Annual workable hours’ are hours during which the personnel must be
working, at the employer’s disposal and carrying out his/her activity or
duties under the employment contract, applicable collective labour
agreement or national working time legislation.
XIX. The contract (applicable collective labour agreement or national
working time legislation) do specify the working time enabling to
calculate the annual workable hours.
Procedure (same sample basis as for Section C: Personnel costs):
� The Auditor verified that the number of productive hours applied is in
accordance with method A, B or C.
� The Auditor checked that the number of productive hours per full-time
employee is correct.
� If method B is applied the Auditor verified i) the manner in which the total
number of hours worked was done and ii) that the contract specified the
annual workable hours by inspecting all the relevant documents, national
legislation, labour agreements and contracts.
� If method C is applied the Auditor reviewed the manner in which the
standard number of working hours per year has been calculated by
inspecting all the relevant documents, national legislation, labour
agreements and contracts and verified that the number of productive hours
per year used for these calculations was at least 90 % of the standard number
of working hours per year.
Factual finding:
General
12. The Beneficiary applied a number of productive hours consistent with
method A, B or C detailed in the left-hand column.
13. The number of productive hours per year per full-time employee was
accurate.
If method B is applied
14. The number of ‘annual workable hours’, overtime and absences was
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
12
Please explain any discrepancies in the body of the Report.
Statements to be made by Beneficiary Procedures to be carried out and Findings to be confirmed by the Auditor
If method C is applied
XX. The standard number of productive hours per year is that of a full-time
equivalent.
XXI. The number of productive hours per year on which the hourly rate is based
i) corresponds to the Beneficiary’s usual accounting practices; ii) is at least
90 % of the standard number of workable (working) hours per year.
XXII. Standard workable (working) hours are hours during which personnel are at
the Beneficiary’s disposal preforming the duties described in the relevant
employment contract, collective labour agreement or national labour
legislation. The number of standard annual workable (working) hours that
the Beneficiary claims is supported by labour contracts, national legislation
and other documentary evidence.
[If certain statement(s) of section “D. Productive hours” cannot be endorsed by the
Beneficiary they should be listed here below and reported as exception by the
Auditor:
- …]
verifiable based on the documents provided by the Beneficiary and the
calculation of the total number of hours worked was accurate.
15. The contract specified the working time enabling to calculate the annual
workable hours.
If method C is applied
16. The calculation of the number of productive hours per year corresponded to
the usual costs accounting practice of the Beneficiary.
17. The calculation of the standard number of workable (working) hours per
year was corroborated by the documents presented by the Beneficiary.
18. The number of productive hours per year used for the calculation of the
hourly rate was at least 90 % of the number of workable (working) hours per
year.
E. Hourly rates
The hourly rates are correct because:
XXIII. Hourly rates are correctly calculated since they result from dividing annual
personnel costs by the productive hours of a given year and group (e.g.
staff category or department or cost centre depending on the methodology
applied) and they are in line with the statements made in section C. and D.
above.
[If the statement of section ‘E. Hourly rates’ cannot be endorsed by the Beneficiary
they should be listed here below and reported as exception by the Auditor:
- …]
Procedure
� The Auditor has obtained a list of all personnel rates calculated by the
Beneficiary in accordance with the methodology used.
� The Auditor has obtained a list of all the relevant employees, based on
which the personnel rate(s) are calculated.
For 10 employees selected at random (same sample basis as Section C: Personnel
costs):
� The Auditor recalculated the hourly rates.
� The Auditor verified that the methodology applied corresponds to the usual
accounting practices of the organisation and is applied consistently for all
activities of the organisation on the basis of objective criteria irrespective of
the source of funding.
Factual finding:
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
13
Please explain any discrepancies in the body of the Report.
Statements to be made by Beneficiary Procedures to be carried out and Findings to be confirmed by the Auditor
19. No differences arose from the recalculation of the hourly rate for the
employees included in the sample.
F. Time recording
XXIV. Time recording is in place for all persons with no exclusive dedication to
one Horizon 2020 action. At least all hours worked in connection with the
grant agreement(s) are registered on a daily/weekly/monthly basis [delete
as appropriate] using a paper/computer-based system [delete as
appropriate];
XXV. For persons exclusively assigned to one Horizon 2020 activity the
Beneficiary has either signed a declaration to that effect or has put
arrangements in place to record their working time;
XXVI. Records of time worked have been signed by the person concerned (on
paper or electronically) and approved by the action manager or line
manager at least monthly;
XXVII. Measures are in place to prevent staff from:
i. recording the same hours twice,
ii. recording working hours during absence periods (e.g. holidays, sick
leave),
iii. recording more than the number of productive hours per year used to
calculate the hourly rates, and
iv. recording hours worked outside the action period.
XXVIII. No working time was recorded outside the action period;
XXIX. No more hours were claimed than the productive hours used to calculate
the hourly personnel rates.
[Please provide a brief description of the time recording system in place together
with the measures applied to ensure its reliability to the Auditor and annex it to the
Procedure
� The Auditor reviewed the brief description, all relevant manuals and/or
internal guidance describing the methodology used to record time.
The Auditor reviewed the time records of the random sample of 10 employees
referred to under Section C: Personnel costs, and verified in particular:
� that time records were available for all persons with not exclusive
assignment to the action;
� that time records were available for persons working exclusively for a
Horizon 2020 action, or, alternatively, that a declaration signed by the
Beneficiary was available for them certifying that they were working
exclusively for a Horizon 2020 action;
� that time records were signed and approved in due time and that all
minimum requirements were fulfilled;
� that the persons worked for the action in the periods claimed;
� that no more hours were claimed than the productive hours used to calculate
the hourly personnel rates;
� that internal controls were in place to prevent that time is recorded twice,
during absences for holidays or sick leave; that more hours are claimed per
person per year for Horizon 2020 actions than the number of productive
hours per year used to calculate the hourly rates; that working time is
recorded outside the action period;
� the Auditor cross-checked the information with human-resources records to
verify consistency and to ensure that the internal controls have been
effective. In addition, the Auditor has verified that no more hours were
charged to Horizon 2020 actions per person per year than the number of
productive hours per year used to calculate the hourly rates, and verified that
Associated with document Ref. Ares(2019)6450190 - 18/10/2019

Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
14
Please explain any discrepancies in the body of the Report.
Statements to be made by Beneficiary Procedures to be carried out and Findings to be confirmed by the Auditor
present certificate1].
[If certain statement(s) of section “F. Time recording” cannot be endorsed by the
Beneficiary they should be listed here below and reported as exception by the
Auditor:
- …]
no time worked outside the action period was charged to the action.
Factual finding:
20. The brief description, manuals and/or internal guidance on time recording
provided by the Beneficiary were consistent with management
reports/records and other documents reviewed and were generally applied
by the Beneficiary to produce the financial statements.
21. For the random sample time was recorded or, in the case of employees
working exclusively for the action, either a signed declaration or time
records were available;
22. For the random sample the time records were signed by the employee and
the action manager/line manager, at least monthly.
23. Working time claimed for the action occurred in the periods claimed;
24. No more hours were claimed than the number productive hours used to
calculate the hourly personnel rates;
25. There is proof that the Beneficiary has checked that working time has not
been claimed twice, that it is consistent with absence records and the
number of productive hours per year, and that no working time has been
claimed outside the action period.
26. Working time claimed is consistent with that on record at the human-
resources department.
1 The description of the time recording system must state among others information on the content of the time records, its coverage (full or action time-recording, for all
personnel or only for personnel involved in H2020 actions), its degree of detail (whether there is a reference to the particular tasks accomplished), its form, periodicity of
the time registration and authorisation (paper or a computer-based system; on a daily, weekly or monthly basis; signed and countersigned by whom), controls applied to
prevent double-charging of time or ensure consistency with HR-records such as absences and travels as well as it information flow up to its use for the preparation of the
Financial Statements.
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Grant Agreement number: [insert number] [insert acronym] [insert call identifier]
H2020 Model Grant Agreements: H2020 General MGA — Multi: v5.0 – dd.mm.2017
15
Please explain any discrepancies in the body of the Report.
Statements to be made by Beneficiary Procedures to be carried out and Findings to be confirmed by the Auditor
[official name of the [Beneficiary] [Linked Third Party]] [official name of the Auditor]
[name and title of authorised representative] [name and title of authorised representative]
[dd Month yyyy] [dd Month yyyy]
<Signature of the [Beneficiary] [Linked Third Party]> <Signature of the Auditor>
Associated with document Ref. Ares(2019)6450190 - 18/10/2019
Commission européenne/Europese Commissie, 1049 Bruxelles/Brussel, BELGIQUE/BELGIË - Tel. +32 22991111
This document is digitally sealed. The digital sealing mechanism uniquely binds the
document to the modules of the Funding & Tenders Portal of the European
Commission, to the transaction for which it was generated and ensures its integrity and
authenticity.
Any attempt to modify the content will lead to a breach of the electronic seal, which can
be verified at any time by clicking on the digital seal validation symbol.




















