‘Without Occupation You Don't Exist’: Occupational Engagement and Mental Illness

1
ETHOLOGY AND “MENTAL ILLNESS”
John Richer
Paediatric Psychology, Oxford University Hospitals
Department of Physiology, Anatomy and Genetics, University of Oxford
In Evolutionary Science of Human Behavior: An Interdisciplinary Approach. Eds P. LaFreniere and G Weisfeld 2014

2
Foreword The suffering of most people diagnosed with mental illnesses is undeniable, but what constitutes mental illness in general, and clear useful definitions of specific illnesses are far from agreed. Thoroughgoing ethologists step outside this debate; they simply study the range of behaviour of the species Homo sapiens. How people use the term “mental illness”, or the terms for specific illnesses, could be an object of study, but it is not what defines the research area itself. Such terms are best seen as clinicians’ tools, necessary but imprecise, influenced by cultural norms, professional and wider politics. They are risky to use as a starting point for scientific research. This the first section of this chapter. The second section looks at some of the work of ethologists and clinicians, who still have the mindset which largely accepts conventional categories but have applied many aspects of ethological thinking, especially evolutionary theory, to mental illness, frequently with interesting and useful results. In the third section the more complete application of ethological thinking to the range of human behaviour is discussed. Inevitably the relationship of this to conventional mental illness categories is discussed but with the mindset which assumes these conventional categories are not necessarily clear, fixed, useful or easily distinguishable from “normal” behaviour. Examples are drawn mainly from the study of the behaviour of children and young people.
1. Mental Disorders, Mental I l lness
Even a cursory glance at the history of mental illness will reveal that notions of what constitutes mental illness changes considerably over time and varies from place to place, culture to culture, (e.g. McGuire & Troisi, 1998; Claridge & Davis, 2003). But the definition of mental illness requires some idea of what is health. These are not, as we shall see, matters of science but are practical definitions resulting from negotiation within a society. As McGuire and Troisi (1998) amongst many others show, no criterion for defining either mental illness in generaloffers clear demarcations. In effect the definitions function as part of the job description of mental health workers, defining what they

3
may do. They are subject to many of the, often shifting and arbitary, demarcations to be expected from a job description. The various categories of mental illness are a little better defined than mental disorder in general. Attempts have been made to refine the definition of mental disorders notably in the Diagnostic and Statistical Manuals of the American Psychiatric Association, the latest being DSM-5 (APA, 2013), and the WHO’s International Classification of Diseases (WHO, 1994), but the definitions change from edition to edition. The previous versions of DSM have been widely criticised. Essentially, as many have argued, e.g. Claridge & Davis, 2003; Bentall (2007), Brune (2008), Kinderman et al. (2013),
• most patient’s problems do not fit well into the categories • there is overlap of categories • there are no clear boundaries between “disorder” and “normal” • the disorders do not correlate with causes • the disorders do not imply clear treatments • the disorders do not predict outcomes
Whilst each of these points could have been applied to other branches of medicine in the past, and perhaps still could in some, the problem seems especially acute in psychiatry. Just as in the evolution of any category system, terms come and go or change their meaning according to their usefulness. There is nothing wrong with this, ; vocabulary evolves, knowledge develops. However it must always be borne in mind that when scientists try to study, say, depression or conduct disorder or paranoid schizophrenia, they are focussing on a category which (i) is likely to change with societal changes and (ii) exists for a complex cluster of reasons (practical, cultural, moral, etc.) which are more than, and different from, the criteria for a good scientific category. But, the scientist could argue, one has to start somewhere. True. Existing categories are as good a place to start as any, as long as their fluid, non scientific status is kept in mind. Indeed, for all practical purposes, there is little choice. Many ethologically inclined psychiatrists, psychologists and other clinicians have offered explanations of mental illnesses and they, to varying extents,

4
use the diagnostic categories defined according to existing criteria. I shall call this the “ethologically influenced” approach. It usually emphasises evolutionary theory. But a thoroughgoing ethologist would say, “if I am going to study the behaviour of this species, Homo sapiens, then it would be unwise to use their concepts, however useful those concepts are to those humans, since there is no guarantee that concepts which are useful within a culture will be useful to describe that culture from the outside”. The linguist and anthropologist Pike (1967) discussed the same issue; a culture could be described in the concepts of the culture itself or in the scientist’s concepts. He called these “emic” and “etic” accounts respectively. When ethologists study non-human species there is no emic account (at least not one we are privy to!), just as for physicists or chemists, there is no emic account, only an etic one. This is the scientific approach and is a further step on the road away from anthropocentrism trodden by Copernicus, Gallileo, and Darwin. So the thoroughgoing ethologist must step outside the mindset of asking whether something is an illness or not, and just consider the range of human behaviour, its causes and consequences. Such knowledge of the range of human behaviour will probably inform the practical decision of whether something should be assessed and treated, i.e. whether it is classified as a “illness”, but it will not decide it. Pure science does not make moral decisions (although the facts can sometimes be so clear as to make a decision a “no-brainer”). So in the third part of this paper, I shall explore what happens when this fully ethological approach is adopted. Most of the “ethologically influenced” writers are practicing clinicians and have a wealth of direct experience and direct observation of their patients. I They are thus able to relate their observations to, say, analogous behaviour in other species (Price, 1967). In having this direct experience, they are but a small step away from the fully ethological approach which tries to put the existing diagnostic categories aside and just observe the range of behaviour. It may be the case that, after pursuing a fully ethological approach, something very close to the existing diagnostic categories are returned to, albeit somewhat differently defined and shaped. Stevens and Price (2000) are explicit that they started with scepticism but ended with their belief

5
reinforced in the broad validity of the existing diagnostic categories. However their reason, that evolutionary underpinnings of the categories could be deduced, is not a strong one.
2. Ethologically influenced approaches The “discovery” of evolutionary theory Throughout the history of ethology, a few ethologists have tentatively stepped into the field of mental disorders (e.g. Tinbergen & Tinbergen, 1972), and a few psychologists and psychiatrists have argued for an ethological or evolutionary approach (e.g. Bowlby, 1957, 1969, 1973, 1980; Ounsted, 1964; Price, 1967; Hutt & Hutt, 1970; Hutt & Ounsted 1970; McGuire & Fairbanks 1977; Richer, 1976, 1979a & b; Kramer & McKinney, 1979). But for a long time, up to even the 1980s, most psychologists and psychiatrists ignored ethological approaches. In the 1970s the main difference between most psychological / psychiatric disciplines and ethology was twofold: Ethology (i) embraced evolutionary theory and (ii) used direct observation. In most other respects relating to Tinbergen’s 4 Whys (Tinbergen, 1963), they were similar; they both researched causes, consequences and development. In the 1980s psychology “discovered” evolutionary theory and the disciplines of evolutionary psychology and evolutionary psychiatry got under way (e.g. Tooby & Cosmides, 1990; Stevens & Price, 2000; Nesse & Williams, 1996). Although there was still a failure adequately to observe behaviour in everyday environments, the use of evolutionary theory was a welcome advance; psychologists and psychiatrists had a proper biological theory to give a framework to their thinking. Furthermore the emphasis on looking at underlying functions, adaptive in some past environments and perhaps now, promised greatly to increase understanding and guide research into more fruitful avenues – after all, it is more likely that productive ( “good”) research questions will be asked, if there is a better notion of what a mechanism is for. Bowlby (1969) coined the term “environment of evolutionary adaptedness” (EEA), and he, like many ethologists, had in mind the environment and

6
lifestyle of hunter gatherers which existed for humans in the late Pleistocene period. Humans started to move out of this lifestyle only some 10,000 years ago, a few still live this way. Adaptation to the hunter gatherer environments and lifestyle led to genetically transmitted behavioural tendencies which still strongly influence human behaviour today, despite the environment in the developed world being very different. The major cause of this rapid change has been cultural evolution, with the creation of what Tinbergen (1972) calls the “anthropogenic environment”. Adaptations to the EEA and mental i l lness Depression Many depressive episodes, especially severe ones, currently have little adaptive value, ; depressed people risk “gross incapacity, suicide or social and financial ruin” (Stevens & Price, 2000), so a straightforward search for adaptive value in depression seems unpromising. But many authors have suggested motivational structures that underlie this behaviour. Price and others (Price, 1972; Price et al., 1994; Price et al. 2007) put forward the idea that depressive behaviour evolved as a “yielding behaviour” when an individual is moving down the social hierarchy. Like submissive behaviour in animals, it had adaptive value because it reduced aggression from competitors and reduced demands from those who expect the individual to fight on their behalf (Stevens & Price, 2000) and thus enabled the individual to remain in the group. Individuals who de-escalate are said to have reduced RHP (Resource Holding Potential) which is equated to self esteem. The opposite, “escalating strategy”, facilitates rising in the hierarchy. Just as the subjective experience during the de-escalation strategy is low mood. , so the escalating strategy is related to high self esteem, positive mood, and in the extreme, manic behaviour, where patients have an unrealistically elevated sense of their own power, popularity and importance. Nesse (2000) focusses on a slightly different, though not incompatible, function: depression reduces stress in the individual himself and helps to avoid futile or dangerous effort in unpropitious circumstances.

7
So this view bundles together (de-) escalation, avoidance of aggression or unpromising effort, hierarchy, status, group membership, mood, self esteem, and feelings of efficacy. These features co-vary. The bundle can be stimulated at many different points. Depression is heterogeneously caused. Understanding this is useful in therapy. In an update of the theory, Price et al. (2007) suggest that whilst the de-escalating and escalating strategies underlie depression and mania respectively, clinical depression seems mainly to arise when the de-escalating strategy is somehow blocked by external factors such as lack of acceptance by others of the appeasement, or more often, by internal factors, such as continued ambition, moral standards, and continued anger. This means that treatments, such as Cognitive Behaviour Therapy (Beck, 2008), aimed at removing these blocks are likely to be helpful in such cases, as they are. Schizophrenia Schizophrenia poses a problem for evolutionists. There is a strong genetic contribution to the aetiology, but people with schizophrenia, as a group, have fewer offspring. It might be expected therefore that the tendency to schizophrenia would be selected out. Yet its prevalence remains at about the same percentage of the population across many cultures. The exact percentage depends of on what is counted as schizophrenic, since there are recognised to be degrees of severity: schizoid, schizotypal, paranoid personality type and schizophrenia. That reveals a further feature, namely that there is a spectrum of disorders, which nevertheless share features: “eccentric thinking, speech and belief, the same self-referential sensitivity to outer events, and a highlighted awareness of unusual ideas and images emanating from their minds” (Stevens & Price, 2000, p 147). This range of severity would be consistent with the polygenic view of inheritance (e.g. Gottesman & Sheilds, 1982). So, as with a number of mental illnesses, the argument runs, relatives of schizophrenic people have some advantage which increases their adaptiveness and especially their reproductive success.
Depressive bundle • de-escalation • status in hierarchy • group membership • appeasement • avoid unpromising effort • low RHP • dearth of initiative Subjective • low mood, • negativity, pessimism • low self esteem • doubts about self efficacy

8
In contrast to “Disorders of Attachment and Rank” like depression, Stevens and Price see the schizophrenias as a “Spacing Disorder” related to ancestral group splitting (Price & Stevens, 1998; Stevens & Price, 2000, 2001). Outgrowing the ability of their immediate environment to support all group members would be a time of stress for a Hhunter Ggatherer group, but leaving a group with whom there would likely be strong bonds was difficult and venturing out into unknown territory would be dangerous. There needed to be an added impetus and that was putatively provided by a charismatic leader who offered a new ideology with its admixture of morals, beliefs, ideals, rituals and ways of perceiving and relating which made it easier to break bonds with the group, and who provided an image of unswerving certainty in the new ideology to inspire them to follow the leader to the “promised land”. Cult leaders in recent times, and phrophets, fall into this category. Price and Stevens (1998) describe them as pursuing the “schizotypal strategy”. When they are successful in persuading others to join them in their beliefs, they are cult leaders. But when they do not, and their self esteem is low, and they risk becoming a psychotic patient. Unlike those diagnosed with schizophrenia, cult leaders are often notoriously fecund, which may be one mechanism by which the genes promoting this behaviour remain in the gene pool (Stevens & Price, 2000). Other mechanisms by which the genes remain in the gene pool have been proposed: better adaptation to sparsely populated habitats (Slater & Roth, 1969), being less accepting of convention and thus being innovative (Simonton, 1994), and being less accepting of the honesty of others and therefore being less likely to be deceived (Jarvik & Chadwick ,1973). Again there is being proposed an evolved bundle of behavioural tendencies, a “strategy”, which can sometimes be adaptive, but at other times and in combination with other factors, can lead to psychotic breakdown. Crucially the bundle may be stimulated at many points. Understanding what the cluster of tendencies is and what their adaptive purpose might have been, can inform assessment and treatment.
Schizotypal bundle • group splitting • new belief system • new world view • unshakeable self belief • low trust • charismatic leader

9
3. Ethological approaches
In the previous section the theorists did not start from systematic direct observation of a range of individuals regardless of any diagnosis, although they were usually richly informed by the sensitive observations of experienced clinicians. In this section I shall look at work (i) which has employed direct observation of a wide range of individuals, as well as evolutionary theory, and (ii) which is much less tied to existing diagnostic categories although it can rarely avoid relating to them. Motivational systems Hierarchical organisation The bundles of behavioural tendencies so far discussed had some derivation in observation of patients, but were not closely tied to behaviour in a way traditional in ethology. An ethologist would probably call these bundles, “motivational systems” or “behavioural systems” (Hinde, 1982). These are usually understood to be organised hierarchically (Tinbergen, 1951; Baerends 1976).
Gathering Reproductive behaviour Nest
building
Sexual behaviour
Fighting Threatening Chasing Biting
etc.
etc.
etc.
Gluing
Zigzag dance Leading Trembling
Figure 1 Basis of a classificatory system for the reproductive activities of the male three spined stickleback. In Hinde (1970) modified from Tinbergen (1951)
10
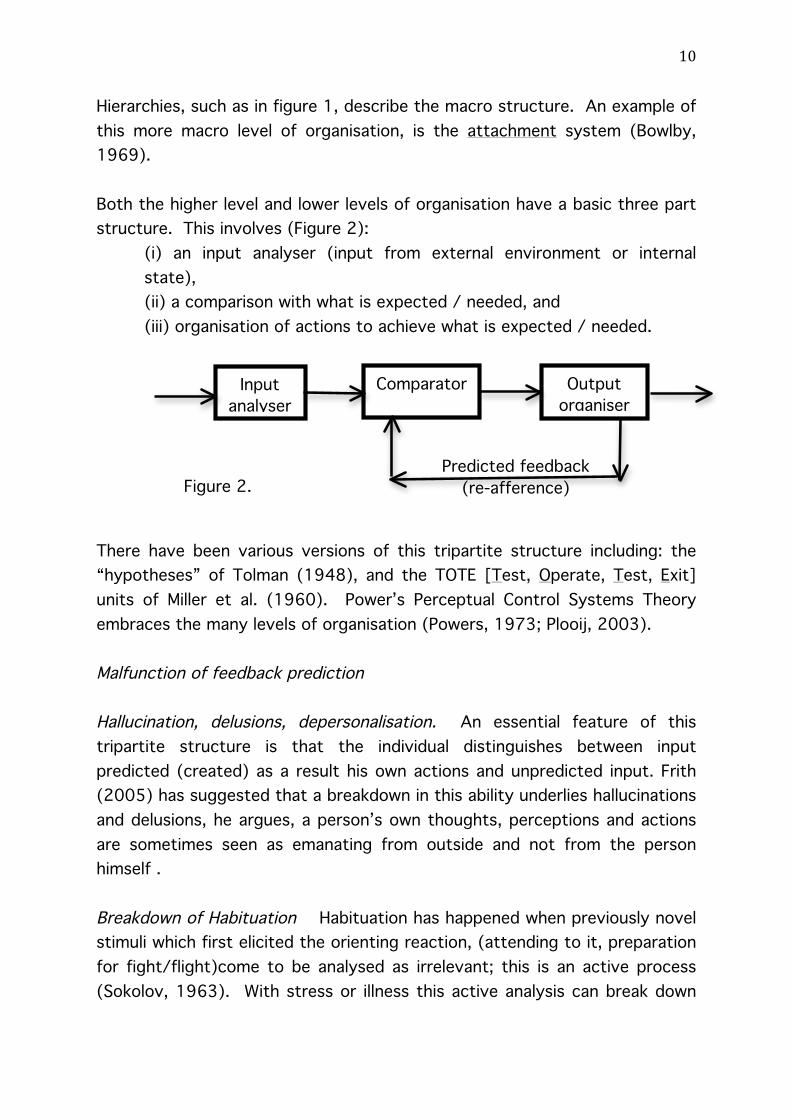
Hierarchies, such as in figure 1, describe the macro structure. An example of this more macro level of organisation, is the attachment system (Bowlby, 1969). Both the higher level and lower levels of organisation have a basic three part structure. This involves (Figure 2):
(i) an input analyser (input from external environment or internal state), (ii) a comparison with what is expected / needed, and (iii) organisation of actions to achieve what is expected / needed.
There have been various versions of this tripartite structure including: the “hypotheses” of Tolman (1948), and the TOTE [Test, Operate, Test, Exit] units of Miller et al. (1960). Power’s Perceptual Control Systems Theory embraces the many levels of organisation (Powers, 1973; Plooij, 2003). Malfunction of feedback prediction Hallucination, delusions, depersonalisation. An essential feature of this tripartite structure is that the individual distinguishes between input predicted (created) as a result his own actions and unpredicted input. Frith (2005) has suggested that a breakdown in this ability underlies hallucinations and delusions, he argues, a person’s own thoughts, perceptions and actions are sometimes seen as emanating from outside and not from the person himself . Breakdown of Habituation Habituation has happened when previously novel stimuli which first elicited the orienting reaction, (attending to it, preparation for fight/flight)come to be analysed as irrelevant; this is an active process (Sokolov, 1963). With stress or illness this active analysis can break down
Input analyser
Comparator Output organiser
Predicted feedback (re-afference) Figure 2.
11
and the orienting reaction again elicited. Using psychophysiological measures such as Galvanic Skin Response (GSR), Lader and Wing (1966), report that the high reactivity pattern (said to be typical of anxiety states) sometimes suddenly changes to a non reacting pattern (i.e. flat lines). At this point the patient describes a feeling of “depersonalisation/derealisation” (i.e he and the world seem unreal). When the patient resumes showing extreme anxiety (orienting) responses the depersonalisation / derealisation goes. In other words, the patients were over-reacting to stimuli (they were not habituating); then there was a defensive shut down of responding the subjective experience of which was depersonalisation / derealisation. Habituation is thought often to break down in children with autistic behaviour. Subjectively they describe sensory overload which is confusing and incapacitating. It is shown particularly in noisy bustling environments. Behaviour classification. Behaviour itself is classified either by morphology (spatiotemporal patterns of muscular contraction) or by consequences (Hinde, 1970). These behaviours can be clustered according to common causation or common function. At this stage, motivations begin to be induced from these clusters. Then the hierarchies of motivations begin to be inferred. The researcher should be careful of simply doing only statistical cluster or factor analyses of the behaviours, as this usually does not take account of function or environmental contingencies or motivational conflict (e.g. Richer, 2001a concerning Buitelaar et al., 1991) and is thus far too crude and misleading. One disincentive to direct observation is that simple patterns which are clinically useful, are rarely found at the level of behaviour itself, ; they are found at the level of motivations. A word of caution. The motivational category is induced from, and defined by, the clusters of behaviours and related causes and consequences. It is not “measured” by them as in psychology. It is worth noting Blurton Jones’ (1975) very succinct comment, "One could contrast the “lateral thinking” inductive work of ethologists and anthropologists with the dedication of psychology to the deductive method and its disdain for facts for their own sake" (page 72).

12
Blocking I have already discussed that, on a macro level, some theorists have argued that it is often the blocking of evolved motivational systems that leads to mental illness (e.g. in depression or schizophrenia, Price et al., 2007). I move now to a more micro level. Responses to the blocking of an activity either by external factors (frustration) or internal ones (conflicting motivations), are helpful in investigating “disordered” behaviour. The responses are very similar. The impact of one motivation, fear, has rewarded close investigation (e.g. Gray, 1976, 1987). Gray (1987) has argued for the causal and functional close similarity between fear and frustration. Indeed one could say that frustration, external blocking, leads to motivational conflict behaviour where the current motivation is in conflict with fear motivation. Fear / Avoidance motivation Fear, sometimes called avoidance, motivation is defined by a cluster of behaviours which, in children, include:
• attempts to distance or protect self from the putatively feared object: moving whole or part of body away, turning away, hunching up, pulling chin in, shielding with arm over head or face
• attempts to reduce input (e.g. gaze aversion, hands over the ears or eyes, hanging the head down)
• attempts to reduce output: still face (Grant, 1969), freezing,
• correlated expressions: fear grin (often mistaken for a sociable smile, Richer 1979a and see pictures in Figure 3), eyebrows strongly up, eyebrows strongly down (also protective)
What follows are some examples of the application of ethological approaches to issues relevant to clinical practice. Most will be taken from studies of children. I shall also try to relate the ethological analysis to clinical categories and to everyday descriptions which are encountered in clinic
Fear Grin Smile Figure 3

13
(clinicians are failing if they do not communicate with their patients or their patients’ caregivers) – but it must be borne in mind that the everyday descriptions given here may be specific to the UK or even to just one part of it. The clinician may need to translate differently. Reactions to frustration (external blocking) Let me start by looking at behaviour when an ongoing activity is blocked by some external factor, in other words, when there is frustration. The responses to frustration in numerous species are well described (e.g. Hinde, 1970) and include:
• Exploration • Overintensity (responding too fast, too intensely, to a narrowed range
of cues and stopping too soon) • Switch activity • Displacement activities • Aggression and re-directed aggression • Regressive behaviour • Attachment behaviour
An expanded description of these was developed into a leaflet and offered to parents in our clinic. It was similar to the indented text below. Most parents understood it very well and related it their child’s behaviour. Note that the structure is ethological but an attempt is made to relate the ethological description to everyday descriptions. I leave it in this format to illustrate one of the challenges for a clinician in this area – embracing simultaneously scientific and everyday language.
1. Exploration. This is the main adaptive reaction to frustration, but it requires the child to maintain attention on a problem even when failing. Frustration leads to switches of attention within the goal of trying to solve the problem, i.e. trying out different possible solutions. Children differ in the amount to frustration they can tolerate before they give up exploration, switch away from a focus on the problem and start the other types of behaviour.

14
2. Overintensity. The child still maintains some attention to the activity but tends to respond to a narrowed range of cues and he responds too quickly and with too great an intensity (he is impulsive and careless). Children sometimes appear loud and attention seeking, and sometimes appear to be aggressive (but the motivation is not aggressive) and "overconfident", (but this masks their “lack of confidence” at the time). Their behaviour is sometimes described as “Over The Top” (OTT). 3. Switch attention. The child gives up the activity. It is said he "cannot concentrate", is "easily frustrated", "doesn't try", etc. He may also switch attention from, or avoid, the person he is with. As frustration increases, children move from 1 to 2 to 3, first they concentrate, then get careless and impulsive, then give up, illustrated in Figure 4.
Figure 4. Schematic description of the inverted J curve This is seen in reverse as children become more confident in, say, a social situation. They are at first said to be shy or even avoidant, then they become loud and attention seeking and “silly”, and then they become calmer and more focussed and self-controlled.
Approach Avoidance
Fear / Frustration / Anxiety / Stress 1. OK
2.OTT
3.Avoid

15
The following frustration reactions imply some switching of attention from the task in hand. Some can be performed at the same time as the first three. 5. Displacement activities. Attention is switched to something irrelevant to the ongoing activity. Displacement activities are simple, often repetitive, activities, and so are very likely to be done successfully. Their function seems to be homeostatic. In other words, just as we shiver to warm ourselves, so at a time of frustration, the displacement activity gives some success. ("I may not be able to do this sum, but at least I'm succeeding in scratching my head"!) Displacement activities can occur with exploration - they seem to help the child to maintain concentration on the activity. They can occur before starting an activity (“plucking up courage”) or after the child has switched away from the activity (“calming down”). 6. Aggression. Frustration in an encounter with another child or an adult can lead to aggression directly against that person. (For example, Fred will not give Jamie a toy, so Jamie hits Fred to try and get it, or Fred hits Jamie to try and get rid of him!). 7. Re-directed aggression. Here, to continue the example, Jamie goes and hits Ben or smashes some thing. The aggression is not directed against the cause of the frustration, but at somebody or something else. At home “Ben” is very often mother or younger sibling, who often bear the brunt of re-directed aggression! People often say Jamie is venting his frustration on Ben. 8. Regression. This is when the child behaves in a way typical of a younger child. 9. Attachment behavior. The child seeks to get close to someone he trusts, usually a parent, and seek comfort. This is done either by the child moving towards the parent, or attracting the parent over by crying, calling etc.
16
These reactions to frustration are not confined to clinical groups, ; they, or at least some, are universal (and not just in humans but many other species, probably all mammals and some other classes of animal). Individuals differ in their thresholds, most particularly in how quickly they stop exploring (concentrating on) the task and move to overintensity, switching attention, aggression, regression etc. Displacement activities can sometimes be an aid to concentration (e.g. the well known pacing up and down whilst thinking through a difficult problem). Attention Deficit Hyperactivity Disorder (ADHD) Reactions to frustration are seen in all individuals and therefore in all clinical groups, but one clinical category is worth singling out, Attention Deficit Hyperactivity Disorder (ADHD). DSM-5 gives the following definition of ADHD (APA 2013)
A. Persistent inattention and/or hyperactivity-impulsivity, more frequent/severe than in developmental peers
B. Present before 12 years C. At least 2 settings D. Interference with social, academic, occupational functioning E. Not exclusively during the course of Schizophrenia, other Psychotic disorder and is
not better explained by other mental disorder Under the first part (A) DSM-5 gives some details of the behaviours involved, which can be summarised: Inattention: Often: inattentive, careless, does not listen, does not complete tasks, poor organisation, avoids sustained effort, loses things, easily distracted, forgetful. Hyperactivity & Impulsivity: Often: fidgets, leaves seat, runs climbs when inappropriate, noisy, talks excessively, on the go, not wait turn, interrupts. This definition has several shortcomings which illustrate the differences between conventional and ethological approaches.
17
1. Unclear boundaries The DSM-5 description, like in its predecessor DSMs, makes it unclear where the boundaries of the category are: How inattentive? How hyperactive? How much more severe or frequent? What is the behaviour of peers? And so on. The lack of clarity of boundaries is widely accepted (e.g. British Psychological Society Working Party Report, 2000, Claridge & Davis, 2003). Given this, it is unsurprising that prevalence estimates vary wildly from 3% to 12% (Wender et al., 2001; Brown et al., 2001) and even reach as high as 25% if parents are asked in a general clinic (Foreman et al., 2001). It lays open the possibility of diagnostic inflation that so many (e.g. Frances, 2013) have pointed out. 2. Muddled behaviour description. The behaviours defining ADHD are reactions to frustration. But they would not be arranged in the same way as in DSM-5. The impulsivity/hyperactivity category is a mixture of different types of behaviour:
• “hyperactivity”, “on the go”, is the sequence of switching activity, then acting overintensely (“rushing impulsively”), then switching again and rushing and so on (i.e. switch attention and overintensity alternate).
• “Fidgets” is usually a displacement activity. • “Interrupts” and “not waiting turn” are examples of overintensity, • “leaving seat” is switching attention plus perhaps overintensity.
The “inattention” category is much the same as the frustration response of switching activity. This illustrates how detailed ethological observation and analysis of behaviour shows up the inadequacies of using everyday categories of behaviour. 3. Re-description masquerading as explanation. There is also the frequent assertion, perhaps more by lay people than clinicians, that ADHD causes the behaviour, an assertion encouraged by the DSM-5’s definition of a disorder which includes: “disturbance in an individual’s cognition, emotion regulation, or behavior that reflects a dysfunction in the psychological, biological, or developmental processes underlying mental functioning.” (underlining mine). Scadding (1988) too discusses how, for many syndromes, this mistaken assumption - that there is a single underlying cause - is probably even more

18
prevalent in lay people than in clinicians. In short, ADHD is not the cause of the behaviour; it is the behaviour and only the behaviour. 4. Heterogeneous aetiology. Again given the universality of frustration reactions, it would be expected that the causation of ADHD would be highly heterogeneous, as indeed is the finding (e.g. Millichap, 2008). 5. A fuzzy category for research. When a category has unclear boundaries and is poorly defined, it becomes difficult to use it in research. Moreover, as Rettew and Hudziak (2009) argue, much information about causes and consequences is lost by the arbitrary cut off points in the diagnosis which prevent quantitative differences in behaviour being taking into account. 6. Comorbidity. Given that all humans show frustration behaviours, it might be expected that a diagnostic category, with which it seems to correlate closely, would be comorbid with many other diagnostic categories. This is the case; indeed there is little that ADHD has not found to be co-morbid with! (Watkins, 2002; Brown, 2009). One way of re-describing this is offered by Brown (2009, p.4), who describes ADHD as a “Foundational Disorder”, which “substantially increases a person’s risk of experiencing additional cognitive, emotional or behavior disorders across the life span”. Brown (2009), like Barkley (1998), sees ADHD as a “developmental impairment of executive functions”. It seems that there is an edging towards the idea which can be more coherently and economically expressed by simply talking about a low frustration tolerance, and taking that as a starting point for scientific study, rather than the diagnostic category of ADHD. 7. NOT a redefinition of ADHD. Am I saying that ADHD is co-extensive with having a low frustration tolerance? No. After all, how low is low? That misses the point. Frustration tolerance varies (within and between children) with a number of factors, but there are children who tend to stop exploring and to start showing overintensity and switching attention much sooner compared to other children in similar settings. It is probably the case that the more likely they are to show these frustration behaviours, the more likely they are to receive the diagnosis of ADHD. The diagnostic categories, like ADHD, have been tested in the real world. The enormous amount of work by thousands of intelligent and talented

19
people makes it very likely that there will be correlations between them and the ethological description. But what is being proposed is not a re-description or re-definition of ADHD but an altogether different and alternative approach. This approach determinedly starts from a description and analysis of observable behaviour of a wide variety of individuals in everyday settings, without prior assumptions, or premature classification. It will talk not about illness or disorders, but about, for instance, behavioural tendencies and thresholds. Motivational conflict behaviour (internal blocking) When two, or more, motivations are aroused simultaneously, one motivation may win out and behaviour be under the control of that motivational system. But sometimes the conflicting motivations are more evenly balanced and motivational conflict behaviours are seen. I shall focus on cases where one of the motivations in the conflict is fear. Most motivational conflict behaviours are similar to frustration behaviours and these include:
• Displacement activities • Aggression and re-directed aggression • Regressive behaviour • Attachment behaviour • Overintensity
Some examples of overintensity in children include:
• the child approaches but bashes hard into the person • the child starts to touch but then grabs very hard • the child speaks loudly or talks on and on • the child stares at the other person and gets very close
In addition to these reactions shared with frustration, there are intention movements and the alternating or simultaneous expression of the two motivations. Consider the example of a child who is motivated both to be sociable and to interact with someone, but is also fearful of doing so. Intention movements:
• sometimes just the beginning of a movement sequence is shown.

20
Alternating expression: • the child may alternate between looking at the other then looking
away, • the child may move towards the other then move away then towards
and this pattern is repeated, • the child may make alternating “intention movements” towards and
away (e.g. leaning towards then away) – the appearance is of “dithering”.
Simultaneous expression:
• the child may approach the other but with no gaze fixation, • the child may approach but facing away (i.e. approach backwards) • the child may speak but facing away • the child may approach someone, not look at him, take hold of him and
pull him to something, to get that thing, or so it seems,. Autistic Spectrum Disorder The behaviour of children diagnosed with Autistic Spectrum Disorder (ASD) can illustrate the value of looking at motivational conflict, but given its universality, the relevance of motivational conflict should always be borne in mind in observing any group. Essentially the behavioural criteria boil down to two main areas:
(i) severe difficulties in social interaction, communication and relationships (ii) a tendency to show extremely risk averse, stereotyped behaviour.
It is important to emphasise that, as with ADHD (and most other psychiatric diagnoses), the ASD diagnosis is of the behaviour, not the child. In this respect it is no different from most other medical diagnoses. We do not refer to someone as “a measles” or “a deep vein thrombosis”; she is a person who is currently suffering from a measles infection or deep vein thrombosis. This point becomes important when a clinician is asked (by social services, benefit agencies, educational authorities, etc.), “does this child ‘have ASD’?” The answer the clinician would like to give may well be of the form, “at home he tends not to show much ASD behaviour, but at school and in crowded public places he does, so in those situations he needs the relevant support”.
21
Reality, though perhaps not bureaucracies, is better served by such a nuanced answer. Avoidance dominated motivational conflict behaviour. Returning to the motivational conflict behaviours described above, where fear is in conflict with other motivations, these behaviours may be seen in all children, but they are particularly useful in describing children who receive the diagnosis of autistic spectrum disorder (Richer & Nicholl, 1971, Tinbergen & Tinbergen 1972, 1983, Richer, 1978, 2001a). If children who receive the ASD diagnosis are observed in their everyday environments, it is clear that they show frequent motivational conflict behaviour where fear (also called avoidance) motivation dominates other motivations much more than in other children (Tinbergen & Tinbergen 1972, 1983, Richer & Nicholl, 1971, Richer, 1976, 1978, 2001a). The more a child behaves like this, the more development is delayed, in part as a consequence of this predominant social avoidance (Richer 1978, 2001b). Development is delayed especially in those skills acquired from people, or related to communicating with people - essentially the skills of their culture. I have described these children as “dyscultural” (Richer, 1978). Misapprehensions A large number of false or meaningless statements have been applied to these children. I shall give a few examples to illustrate how ethological thinking differs from everyday thinking The contrast is more stark for this group who have acquired less of the culture of where they live.
• The child “uses people as objects” (as in: “the child may approach someone, not look at him, take hold of him and pull him to something, to get, or so it seems, that thing” - but a better description is that the child is showing simultaneous motivational conflict behaviour).
• The child “smiles and laughs inappropriately” (mistaking a fear grin, and the monotonous giggle that sometimes accompanies it, for sociable behaviour).
• The child is not “aware” of others (but what does that mean and how could the clinician know? In fact, the child behaves to avoid attracting the attention of others).
• The child is apparently indifferent to pain (see DSM-5 criteria) or worse, the child “does not feel pain”. This assertion is nonsense in its strong form, ; the children do not suffer the damage seen in children

22
with, say, congenital analgesia. Moreover close observation reveals that the children do react, in an albeit inhibited way, when they have accidently been hurt, but often not with attachment behaviour. In addition many children with autistic behaviour injure themselves, such as biting the back of their hands, banging their heads, pressing themselves against something very hot, but these are intense displacement activities done at times of great stress. (Self harm in troubled adolescent girls is analaogous.)
Immediate causes. It is possible to plot what factors reduce the fear behaviours in a social context, i.e. where the child with the ASD diagnosis could interact with others. These include:
• the joint activity the child is doing is easy • the situation and joint activity is predictable for the child • the other person is not too socially intrusive • the activity is with just one other person, not a group • the situation is quiet, not crowded, • if food intolerant, as many are, the child has not recently consumed
the non- tolerated food Individual differences in thresholds. It is also possible to observe that the threshold for showing this predominant social avoidance behaviour differs between children. Some children (child A in figure 5) show it in most situations they encounter (these are easily diagnosed as conforming to ASD if their behaviour also shows considerable stereotypy). On the other hand, most children (D) would not fall into this way of behaving in the presence of these causal factors. Some children (B and C) fall into this way of behaving only when the causal factors are sufficiently intense / numerous / long lasting.

23
Figure 5. Schematic representation of individual differences in thresholds for showing autistic behaviour with various causal factors. It needs to be remembered that a frequently repeated finding in ethological research is that motivations may be triggered by stimuli being sufficiently intense, and/or lasting a sufficient time, and/or acting together with a sufficient number of other (often called predisposing) stimuli (Hinde, 1970, 1982). Improvement course. The improvement of children away from severely autistic behaviour follows the pattern expected from this analysis, especially bearing in mind the inverted J curve (Figure 6). The children start to behave in an over-intense way first in situations characterised by the above causal factors minimising avoidance / fear, before behaving less overintensely. The over-intense behaviour is often more difficult to manage and some adults unwittingly try to discourage it, even punish it, thereby pushing the child back into autistic behaviour.
Improvement
Figure 6

24
Asperger’s syndrome Some, who often receive the diagnosis of Asperger’s syndrome, are frequently in this state (Figure 7): they often make intrusive social approaches to people, get too close, stare too hard, talk too loudly and too long, etc., whilst at other times they withdraw. Predictability seeking. Avoidance dominated motivational conflict social behaviour is only one aspect of what describes children who receive the ASD diagnosis. Many other children also show this conflict behaviour and may be colloquially or clinically described as timid, highly introverted, socially anxious, or even socially phobic. Children who get the ASD diagnosis also have a strong tendency to seek and create predictability (the second main criterion for ASD of stereotypy), which is the opposite of the tendency to explore and play. A dimension from Displacement Activities to Playfulness. So far I have discussed displacement activities in the context of reactions to frustration and motivational conflict. It is useful to see them in a wider context. Although they are often described as “goalless”, because they do not seem part of achieving adaptive goals, this is not the whole story; their execution, like the execution of most, if not all, activity, creates the expectation that particular feedback will be received. In that limited sense, each has a goal. Displacement activities are very likely to achieve their expected feedback - it is difficult to fail at scratching one’s head, or at rocking back and forth. They are simple activities, they are often repetitive and they require few specific environmental conditions – many are self grooming activities and so involve the individual’s own body (which is always there!). Their function is homeostatic. The more an individual seeks out novelty and is playful, the more that adaptive behaviour will be acquired. Children receiving the ASD diagnosis do the opposite and not only rarely play but also strive to create familiarity / predictability. This is to the severe detriment of their learning. Given their tendency to be avoidant of any but the simplest social interactions, their learning from other people and about other people is impaired. This
Figure 7
OK
Aspe
rger
Au
tistic
25
“dysculturalness” is their area of greatest disability (Richer, 1976, 1978, 2001a & b). Attachment Attachment theory is arguably the most fertile and useful ethological theory with widely recognized clinical applications. Because it is well known and discussed in Chapter 8 it will not be discussed here. Eating disorders Understanding eating disorders involves many of the issues and motivational levels that have already been discussed. 95% of people start their anorexic illness before 25 years, most in their teens, i.e. early in their reproductive careers. 95% are female (Södersten, Bergh, & Zandian, 2006) and these will be focussed on. They tend to come from higher social classes and from developed countries with low adult mortality rates. There are more socioecological stresses and unfavourable reproductive conditions than average (Voland & Voland, 1989). There is a relatively high risk of death in the short term and of irreversible physical complications associated with near self starvation in the long term. These demand clinical attention, but self starvation and body image distortions (Bruch, 1962) are not the key to understanding the behaviour or to its complete treatment (Hsu, 1991). As with depression and schizophrenia, it seems perverse to argue that anorexia is related to an adaptive function. But, as with many other disorders, there is a fairly high degree of heritability( perhaps 0.58-0.76, Ben-Dor et al 2002), although the data are not unequivocal (Fairburn et al., 1999). Anorexia is argued to involve behavioural systems which did, and maybe still do, have adaptive value. Most note that reduction of body fat and other consequences of reduced nutrition reduce fertility and postpone reproduction since the chances of successfully bearing and caring for a child when deficient in fat and other nutrients are reduced (Mealey, 2000). Here are some of the main suggested evolutionary explanations.
26
• This mechanism of reducing food consumption and fertility appears when the girl’s environment seems unpropitious for successful child rearing (e.g. Surbey, 1987).
• One example of an unpropitious environment would be when there was food scarcity which would trigger denial of hunger, restricted food intake and hyperactivity which would all facilitate migration to lands with more food (“flee from famine” hypothesis, Guisinger, 2003).
• Another example of an unpropitious environment is when the girl is losing out in female-female competition and so is less likely to attract “high quality mates” (Salmon & Crawford, 2008), so she postpones reproduction.
• Relatedly, Mealey (2000) saw anorexia a feature of intrasexual competition and as a manipulative strategy imposed on subordinates by dominant females.
• Gatward (2007) suggests that “social attention holding power” (SAHP) (Gilbert, 1992) is low in anorexic people. SAHP is a correlate of social rank, ; high ranking individuals have more and can get resources from others. Dietary restriction is a response to a perceived threat of exclusion from the group (exclusion would have probably been fatal for a hunter gatherer). About 75% of women with eating disorders are also diagnosed as depressed (Mitchell & Pyle, 1985) and depression is also seen as related to appeasement behaviour, allowing the individual to remain in the group whilst slipping down the hierarchy. Anorexia is a form of altruistic behaviour where the girl is foregoing reproduction and food for the sake of her kin and so improving her inclusive fitness, (Voland & Voland, 1989). These authors also suggest that parental manipulation by dominant and overprotective parents promotes such altruism in some cases.
There seem to be common components in these hypotheses 1. Reduced food intake reduces fertility (leading to amenorrhoea and thinness which reduces attractiveness to males). 2. Deciding that fertility should be postponed leads to reduced food intake. 3. This happens in environments seen as unpropitious to reproduction because of unavailability of nutrition, family / social support, or having low social rank, etc. 4. Anorexic girls feel devalued through a combination of domination by others and their own interpretations of events.

27
Is there a behavioural system that could have evolved because of the inclusive fitness it bestowed? If there is, it seems to have the following components:
• Reduced food intake • Postponement of reproduction (amenorrhoea, being thin and less
attractive to males, etc.) • Self-denial, altruism, caretaking. • A response to stress
This combination could increase inclusive fitness in a Hunter Gatherer group during times of food shortage, or when there were other stresses on the group. Young females are most likely to be affected since they potentially have the most time ahead of them and so can postpone child bearing. But why should this mechanism be most likely to be triggered in societies where food shortage is least likely? Here we need to look at the self denial / altruism / caretaking aspect. Attachment insecurity (Ainsworth et al., 1978) is expressed in two main strategies, ambivalent and avoidant. The avoidant strategy involves being caring and compliant, achievement oriented, emotionally independent and vigilant for the behaviour of others; the individual tends to deny her own wants and needs in order to fit in with others, notably the caregivers, again to maximise safety. The strategy is a response to a child’s needs not being sensitively responded to by their caretakers. This is the personality style, family functioning and history reported in most girls with anorexia. It would be predicted from this that the attachment style of girls with anorexia would be one of avoidant insecurity. This is the finding of the majority of studies (Dozier et al., 2008). Dozier et al. (p. 731) summarise the attachment findings by stating, “a picture generally emerges of an over controlling, perfectionist mother who communicates lack of support for her daughter’s autonomy striving; an emotionally rejecting father; and a daughter who feels rejected, controlled, and inadequate.” One feature of the avoidant strategy is to seek attention and nurturance by exaggerating minor injury or discomfort, in other words, creating a “real” or “objective” reason for getting nurturant attention. Self starvation gives a difficult-to-miss objective reason for receiving nurturant parental attention. Watanabe (1994) reports a successful strategy with hospitalised girls with anorexia, involving extreme nurturance, almost to the point of infantilising the girl. She discusses this in terms of the Japanese concept of Amae which involves both attachment and dependency (Doi, 1973).

28
So again, as with depression and schizophrenia, there seems to be a behavioural strategy, which can be argued to have had adaptive value, both because it immediately enhanced inclusive fitness and enhanced the individual’s chances of later raising her own viable offspring, during times of stress, especially food shortage, in the hunter gatherer period. This mechanism is now aroused by inputs primarily stimulating the self denial aspects, but the reduced food intake and fertility are also stimulated (Figure 8). It would be expected that this mechansism would be most likely to be stimulated when other factors stimulate reproductive motivation. These include puberty, first sexual experience, and the prevailing peer culture being oriented towards exploring sexual relationships (i.e. adolescence). It would be expected also that adequate supplies of food would not alleviate the condition, as they would have done in hunter gatherer times.
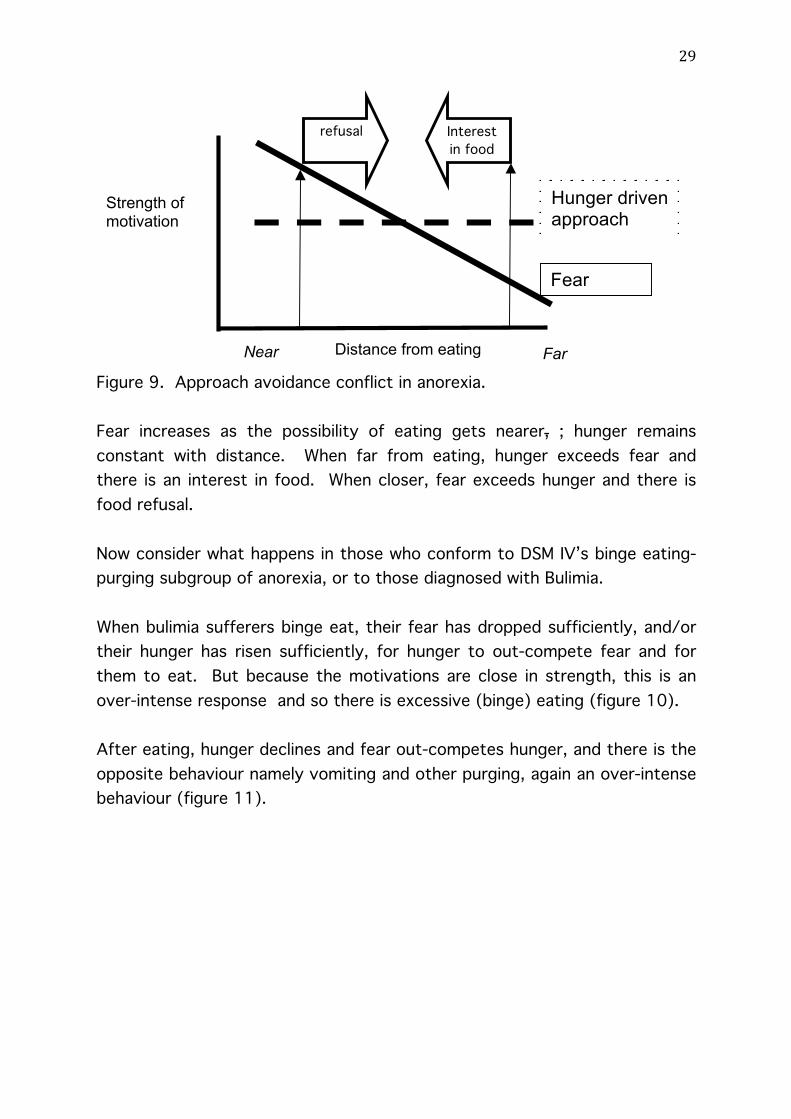
Figure 8. Hypothesised motivational system involved in anorexia. What about some other aspects of anorexia? A puzzling feature is that some anorexic girls have a great interest in preparing food and feeding others, but baulk at feeding themselves. This could be seen as an aspect of their altruism, but it is possible to go further into the likely mechanism. Here we shift levels and look at motivational conflict. Anorexic people can be seen as being in a state of conflict between a hunger driven approach to food and a fear of eating (figure 9).
food intake reduction
reduced fertility, amenorrhoea
self denial, altruism, caretaking
Food shortage Unpropitious time for child bearing Domineering family Low status Avoidant insecurity
29
Figure 9. Approach avoidance conflict in anorexia. Fear increases as the possibility of eating gets nearer, ; hunger remains constant with distance. When far from eating, hunger exceeds fear and there is an interest in food. When closer, fear exceeds hunger and there is food refusal. Now consider what happens in those who conform to DSM IV’s binge eating- purging subgroup of anorexia, or to those diagnosed with Bulimia. When bulimia sufferers binge eat, their fear has dropped sufficiently, and/or their hunger has risen sufficiently, for hunger to out-compete fear and for them to eat. But because the motivations are close in strength, this is an over-intense response and so there is excessive (binge) eating (figure 10). After eating, hunger declines and fear out-competes hunger, and there is the opposite behaviour namely vomiting and other purging, again an over-intense behaviour (figure 11).
Strength of motivation
Distance from eating Near Far
Fear
Hunger driven approach
Interest in food
refusal

30
Figure 10. Hunger out competiting fear
Figure 11. Reduced hunger being outcompeted by fear So here an ethological analysis combines higher order motivational systems (attachment and food scarcity module) to understand the structure of anorexia, with lower order motivational analysis (motivational conflict) to understand the detailed flow of behaviour. Body image perception distortions are simply by-products of the pressure not to eat. Whilst therapy must ensure adequate nutrition as an immediate necessity, that is only the beginning of treatment. Attending to the girl’s attachment relationships, her peer relationships and her self esteem are likely to lead to sustained improvement. The NICE commissioned report in the UK (NICE, 2004) is consistent with this conclusion, in that it understandably emphasises the focus on restoring eating as an immediate measure but also notes that later focus on other psychological aspects is usually necessary.
Distance from eating Near Far
Strength of motivation
Fear
Hunger driven approach
Interest in food
Binge
Strength of motivation
Distance from eating Near
Fear
Hunger driven approach
Interest in food
vomit

31
Conclusions: the Ethological contribution to Understanding Mental I l lness The range of human behaviour (not health or illness) So where does this different approach leave us? First of all let me repeat that we need to step outside the mindset of asking whether something is an illness or not. Instead we need to consider the range of human behaviour, “watching and wondering” as Niko Tinbergen put it, trying to describe and make sense of what is publicly observable in the everyday world.
Looking at the range of human behaviour has echoes in what many writers have advocated, namely a dimensional approach, albeit they accept diagnostic categories to a large extent, where mental illnesses can usually be seen as an exaggeration or an extreme of dimensions of difference in the whole population. Claridge and Davis (2003) do this, pointing to population dimensions in personality and other functioning. Claridge (1995) emphasises the “‘boundaries of uncertainty’ at the meeting-points of illness and behavioural variations”. It is understandable that clinicians want diagnostic categories, even when they know that reality is not quite like this. The pressure on them is to do something, and they need accepted criteria to trigger particular actions and communicate with colleagues and others. But it is important that this is explicitly acknowledged. In particular it is important that researchers do not try and use these categories as if they are good, precisely defined, scientific categories. The clinician’s toolkit, the researcher’s palette - Mentalistic concepts Might there be better concepts for the clinician’s “tool kit” or the researcher’s “palette” (with which a “picture of the world” is painted)? The well known ethological maxim for deciding on behaviour categories should always be borne in mind, “when in doubt, split don’t lump”. In the ethological account there would be strenuous attempts to distinguish the inside / emic / agent / mentalistic and the outside /etic / onlooker /
32
body views (Pike, 1967; Richer, 1975, 1993). An analogous distinction was made by Harré and Secord (1972) describing the two aspects to the study of human social behaviour:
1. “Negotiation of accounts” 2. “Micro sociological analysis”
The first, the “negotiation of accounts”, involves discussion with the people being studied, trying, through a process of to and fro conversation, to understand as well as possible what their viewpoints are. The second, what they call the “micro sociological analysis”, involves observing behaviour. This is how an ethologist would observe behaviour, using the observer’s own categories to describe the behaviour under investigation. Even if a good ethological description were available, this does not relieve clinicians from the need to empathise and communicate with those who consult them, and this requires the mentalistic language of everyday communication. So a translation is required of the sort I have illustrated when describing reactions to frustration. The clinician’s toolkit, the researcher’s palette - The “tool kit” or “palette” will likely be at several conceptual levels, including:
• Being able to recognise and understand the meaning of particular behaviours (e.g. fear grin”, which is often mistaken for a sociable smile).
• Recognising that patterns useful to clinicians (and researchers) are more likely to emerge at the level of motivational systems than at the level of behaviour. A motivation which is a likely contender for being relevant to many mental illnesses is fear.
• Seeing where behaviour control units (e.g. TOTE), the basic structural pattern of motivations, malfunction (e.g. habituation breakdown, delusions, hallucinations, depersonalisation).

33
• Understanding motivational conflict, frustration and the impact of the inverted J curve.
• Embracing the hypothesised higher order motivational bundles such as those discussed here (e.g. attachment, de-escalating strategies, group splitting leadership strategies, the food refusal / reproduction suspending / altruism cluster) which can guide thinking of about how apparently disparate patterns of behaviour causally and functionally cohere and so how therapy might proceed.).
This change will not happen quickly. Too many habitual ways of thinking and other impediments get in the way. But a first step is for clinicians and researchers to recognise the flaws in current approaches and aim to avoid them. With such self discipline, an ethological science which usefully informs the field of mental illness can be pursued.

34
References Ainsworth, M. D. S., Blehar, M. C., Waters, E., & Wall, S. (1978). Patterns of
attachment: A psychological study of the strange situation. Hillsdale, NJ: Erlbaum.
APA (2013): American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (2013) Arlington VA: American Psychiatric Association
Baerends G.P. The functional organisation of behaviour. Animal Behaviour 24, 726-38.
Barkley. R.A. (1998) Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment. New York, NY: Guilford Press.
Beck, AT (2008) "The Evolution of the Cognitive Model of Depression and Its Neurobiological Correlates". American Journal of Psychiatry 165:969
Ben-Dor, D.H., Laufer, N., Apter, A., Frisch, A., Weizman, A., (2002) Heritability, genetics and association findings in anorexia nervosa. Israeli Journal of Psychiatry and Related Sciences. 39(4):262-70.
Bentall, R.P (2007) Researching Psychotic Complaints. The Psychologist, 20 (5), 293-295
Blurton Jones, N. G. (1975). Ethology, anthropology and childhood. In R. Fox (Ed.) A.S.A. Studies-Biosocial Anthropology, London. Dent.
Bowlby, J (1957) An ethological approach to research in child development. British Journal of Medical Psychology 20, 230-240.
Bowlby, J (1969) Attachment. London, Hogarth press Bowlby, J (1973) Attachment and Loss. Volume 2 Separation: Anxiety and
Anger. London, Hogarth press Bowlby, J (1980) Attachment and Loss. Volume 3 Loss: sadness and
depression. London, Hogarth press British Psychological Society Working Party Report (2000) Attention
Deficit/Hyperactivity Disorder (ADHD). Guidelines and Principles for successful multi-agency working. Leicester.
Brown, R.T., Freeman, W.W. Perrin, J.M., Stein, M.T., Amler, R.W., Feldman, H.M., Pierce, K, and Wolraich, M. (2001) Prevalence and assessment of Attention-Deficit/Hyperactivity Disorder in Primary Care Settings. Paediatrics,107(3), 1-11
Brown, T.E. (2009) Developmental complexities of attentional disorders. In. Brown, T.E. (ed) ADHD Comorbidities: handbook of ADHD
35
complications in children and adults. Arlington VA: American Psychiatric Association.
Bruch, H. (1962). Perceptual and conceptual disturbances in anorexia nervosa. Psychosomatic Medicine, 24(2), 187-194
Brune, M (2008) Textbook of Evolutionary Psychiatry Oxford, Oxford University Press.
Buitelaar, J.K., van Engeland, H, de Kogel, K.H. and van Hooff J.A.R.A.M. (1991) Differences in the structure of social behaviour of autistic children and non autistic controls. Journal of Child Psychology and Psychiatry. 32. 995-1016
Claridge, G (1995) The origins of Mental Illness (2nd edition). Cambridge, Ma. ISHK.
Claridge, G and Davis, C. (2003) Personality and Psychological Disorders. London, Arnold
Doi, T. (1973). The anatomy of dependence: The key analysis of Japanese behavior (J. Bester, Trans.). Tokyo: Kodansha International.
Dozier, M., Stovall-McClough, KC, Albus, K.E. (2008) Attachment and Psychopathology in Adulthood. In: Cassidy, J. and Shaver, P.R. (eds) Handbook of Attachment. 2nd edition. New York, The Guildford Press
Fairburn, C. G. ; Cowen, P.J. ; Harrison, P. J.(1999) Twin studies and the etiology of eating disorders. International Journal of Eating Disorders, 26(4), pp. 349-358
Foreman, D., Foreman, D., Prendegast, M., Minty, B. (2001) Is clinic prevalence of ICD–10 hyperkinesis underestimated? Impact of increasing awareness by a questionnaire. European Child and Adolescent Psychiatry, 10, 130– 134.
Frances, A (2013) Saving Normal: An Insider's Revolt Against Out-of-Control Psychiatric Diagnosis, DSM-5, Big Pharma, and the Medicalization of Ordinary Life. New York: William Morrow.
Frith, C. D.(2005) The neural basis of hallucinations and delusions. C.R. Biologies 328. 170-175
Gatward, N. (2007) Anorexia Nervosa: an evolutionary puzzle. European Eating Disorders Review. 15, 1-12
Gilbert, P. (1992). Depression: The evolution of powerlessness. Hove, East Sussex: Lawrence Erlbaum
Gottesman, I.I. and Shields, J. (1982) Schizophrenia: The epigenetic Puzzle. Cambridge, Cambridge University Press.
Grant, E.C. (1969) Human facial expressions, Man 4, 525-536.

36
Gray, J. A. (1976). The behavioural inhibition system: A possible substrate for anxiety. In M. P. Feldman, & A. M. Broadhurst (Eds.), Theoretical and experimental bases of behaviour modification (pp. 3–41). London: Wiley.
Gray J.A. (1987) The psychology of fear and stress. London: Cambridge University Press.
Guisinger, S. (2003) Adapted to flee famine: Adding an evolutionary perspective on anorexia nervosa. Psychological Review 110, 745-761
Harré, R, and Secord, P. (1972) The Explanation of Social Behaviour. Oxford: Blackwell.
Hinde, R.A. (1970) Animal Behaviour. New York. McGraw Hill Hinde R.A. (1982) Ethology Fontana, London Hsu, L.K.G. ; Sobkiewicz, T.A. (1991) Body image disturbance: Time to
abandon the concept for eating disorders? International Journal of Eating Disorders, 1991, 10(1),15-30
Hutt, C and Ounsted, C (1970) Gaze Aversion and its significance in childhood autism. In Behaviour Studies in Psychiatry Hutt, S.J. and Hutt C (Eds.) Elmsford, New York, Pergamon.
Hutt, S.J. & C. (1970) Direct Observation and Measurement of Behavior. Springfield, IL: Charles C. Thomas, pp. 210-218.
Jarvik, L.F. and Chadwick, S.B. (1973) Schizophrenia and survival. In Psychopathology: Contributions from the Social, Behavioural and Biological Sciences. M. Hammer, K.Salzinger, and S. Sutton (Eds) New York, Wiley
Kinderman, P., Read, J., Moncrieff, J. and Bentall, R.P. (2013) 'Drop the language of disorder'. Evidence Based Mental Health 16, pp 2-3 doi:10.1136/eb-2012-100987
Kramer, D.A. and McKinney, W.T. (1979) The overlapping terretories of psychiatry and ethology. Journal of Nervous and Mental Disease. 167, 3- 22
Lader, M.H. and Wing, L. (1966). Physiological measures, sedative drugs and morbid anxiety (Maudsley Monographs No. 14). London, England: Oxford University Press.
McGuire, M. and Fairbanks, L. (1977) Ethology – psychiatry’s bridge to behavior. In: Ethological Psychiatry: Psychopathology in the context of Evolutionary Biology M.T. McGuire, and L.A. Fairbanks (eds) New York, Grune and Stratton

37
McGuire, M. and Troisi, A. (1998) Darwinian Psychiatry. New York, Oxford University Press
Mealey, L. (2000). Anorexia: A ‘losing’ strategy. Human Nature, 2, 31–57. Miller, G.A., Galanter, E. & Karl H. Pribram, K.H. (1960). Plans and the
Structure of Behavior. New York, Holt Millichap, J.G. (2008) Etiologic Classification of Attention-
Deficit/Hyperactivity Disorder. Pediatrics. 121, 358-365 Mitchell, J.E. and Pyle, R.L. (1985) Characteristics of Bulimia. In J.E.Mitchell
(Ed.) Anorexia nervosa and bulimia: Diagnosis and Treatment. Minneapolis. University of Minnesota Press
Nesse, R.M. and Williams, G.C. (1996) Evolution and Healing. The New Science of Darwinian Medicine. London. Phoenix
Nesse, R.M. (2000) Is depression and adaptation? Archives of General Psychiatry 57, 14-20 .
NICE (2004) Eating Disorders National Clinical Practice Guideline Number CG9 London. National Institute for Clinical Excellence
Ounsted, C (1964) The measurement of Children’s behaviour Proceedings of the Royal Society 1176 46-47
Pike, K.L. (1967) Language in Relation to a Unified Theory of the Structure of Human Behaviour. Mouton, Elmsford, New York: Glendale Summer Institute of Linguistics.
Plooij F. (2003) The Trilogy of Mind. In Heimann, M. Regression Periods in Human Infancy. London. Lawrence Erlbaum Associates.
Powers, W.T. (1973) Behaviour: the Control of Perception Chicago, Aldine. Price, J. (1967). Hypothesis: The Dominance Hierarchy and the Evolution of
Mental Illness. Lancet, ii, 243–246. Price, J. S. (1972). Genetic and phylogenetic aspects of mood variations.
International Journal of Mental Health, 1,124 -144. Price, J.S., Sloman, L., Gardner, R., Gilbert, P., and Rohde, P. (1994) The
social competition hypothesis of depression. British Journal of Psychiatry, 164, 309-335.
Price J.S. and Stevens, A (1998) The Human Male Socialisation Strategy set: Cooperation, Defection Individuation and Schizotypy. Evolution and Human Behaviour. 19, 57-70
Price, J.S. , Gardner, R., Wilson, D.R., Sloman, L., Rohde, P. Erikson, M. (2007) Territory, Rank and Mental Health: the history of an idea. Evolutionary Psychology 5(3).1474-7049

38
Rettew, D.C and Hudziak, J.J. (2009) Genetics of ADHD In ADHD Comorbidities: Handbook for ADHD Complications in Children and Adults (ed) Brown T.E. Arlington VA: American Psychiatric Association.
Richer, J.M. and Nicholl, S. (1971) A playroom for autistic children and its companion therapy project. British Journal of Mental Subnormality 17, 132-143.
Richer, J.M. (1975) Two types of agreement: two types of psychology. Bulletin of the British Psychological Society. 28. 342-345. (Reprinted in Readings in psychology for the Teacher Child D. (ed) Holt, Rinehart, and Winston, London 1977)
Richer, J.M. (1976) Social avoidance in autistic children Animal Behaviour 24. 898-906.
Richer, J.M. (1978) The partial non communication of culture to autistic children. In Rutter, M. and Schopler, E. (eds) Autism: reappraisal of concepts and treatment.. New York, Plenum Press
Richer, J.M. (1979a) Human ethology and mental handicap. In: James, F.C. and Snaith, R.P. (eds) Psychiatric Illness and Mental Handicap London Gaskell.
Richer, J.M. (1979b) Human ethology and psychiatry. In: van Praag et al (eds) Handbook of Biological Psychiatry Plenum press. New York.
Richer, J.M. (1993) Onlookers, agents, agreements, evolution, consciousness and intersubjectivity. paper read at Ethology and Cognition. Siena Italy
Richer, J.M. (2001a) An Ethological Approach to Autism: From Evolutionary Perspectives to Treatment In Richer, J.M. and Coates, S. (eds) (2001) Autism: The Search for Coherence. London: Jessica Kingsley.
Richer, J.M. (2001b) The Insufficient Integration of Self and Other in Autism In Richer, J.M. and Coates, S. (eds) (2001) Autism: The Search for Coherence. London; Jessica Kingsley.
Salmon, C, Crawford, C.B. and Walters, S. (2008) Anorexic behaviour, female competition and stress: developing a female competition stress test. Evolutionary Psychology 6(1) 96-112.
Scadding, J.G. (1988) Health and disease: what medicine do for philosophy? Journal of Medical Ethics. 14, 118-124
Simonton, D.K.(1994) Greatness: Who Makes History and Why. New York. Guildford Press
Slater E. and Roth M. (1969) Clinical Psychiatry. (3rd ed) London. Balliere, Tindall, Cassell

39
Södersten, P., Bergh, C., & Zandian, M. (2006). Understanding eating disorders. Hormones and Behavior, 50, 572-578.
Sokolov, Y.N. (1963).Higher nervous functions: The orienting reflex.. Annual Review of Physiology 25: 545–580.
Stevens, A and Price J. (2000) Evolutionary Psychiatry London Routledge Stevens, A and Price J. (2001) Prophets, Cults and Madness London
Duckworth Surbey, M.K. (1987) Anorexia nervosa, amenorrhea and adaptation. Ethology
and Sociobiology, 8 (3s), 47-62. Tinbergen N. (1951) The Study of Instinct Oxford, Oxford University Press Tinbergen, N. (1963) On the aims and methods of ethology. Zeitschrift
fur Tierpsychologie, 20, 410-33. Tinbergen N. (1972) The Croonian Lecture, 1972: Functional Ethology and
the Human Sciences. Proceedings of the Royal Society of London. Series B, Biological Sciences, 182 No 1069 (Dec 5 1972)
Tinbergen, E.A. and Tinbergen, N. (1972) Early childhood autism - an ethological approach. Advances in Ethology. 10.
Tinbergen, N. and Tinbergen, E.A. (1983) "Autistic" Children: New Hope for a Cure. George Allen and Unwin, London.
Tolman EC (1948) Cognitive maps in rats and men. Psychological Review 55:189–208
Tooby, J and Cosmides, L (1990)The past explains the present: emotional adaptations and the structure of ancestral environments. Ethology and Sociobiology 11(4/5): 375-424, 1990
Voland, E. & Voland, R. (1989) Evolutionary biology and psychiatry: the case for anorexia nervosa. Ethology and Sociobiology, 10, 223-240.
Watanabe, H. (1994) The application of “amae” in approaching clinical problems in Japan. Paper presented at IACAPAP International Congress. San Francisco.
Watkins, C. (2002) ADHD and Comorbidity. Northern County Psychiatric Associates. http://ncpamd.com/add-comorbidity/
Wender, P.H., Wolf, L.E., Wasserstein, J. (2001) Adults with ADHD. An overview. Annals of the New York Academy of Science. 931, 1-16
WHO (1994): World Health Organization The ICD-10 Classification of Mental and Behavioural Disorders Clinical descriptions and diagnostic guidelines http://www.who.int/classifications/icd/en/bluebook.pdf
Copyright © 2022 FDOKUMEN
















![[Routine Outcome Monitoring for patients with severe mental illness: a consensus document]](https://static.fdokumen.com/doc/165x107/633637c764d291d2a302cca6/routine-outcome-monitoring-for-patients-with-severe-mental-illness-a-consensus.jpg)