Essential Guide to Grant Applications - rds-sc.nihr.ac.uk
392
15 th - 17 th February 2022 Essential Guide to Grant Applications
-
Upload
khangminh22 -
Category
Documents
-
view
1 -
download
0
Transcript of Essential Guide to Grant Applications - rds-sc.nihr.ac.uk

15th - 17th February 2022
Essential Guide to Grant Applications

Contents Presentations
Foreword by Issy Reading, Director of RDS South Central ……………………………………… 1
EGGA 2022 Programme …………………………………………………………………………….. 2
Presentations
Day 1: Getting Your Message Across to Reviewers Quickly and Clearly
The Purpose of a Grant Application (Sophie Hyndman)
How Do Projects Get Funded? Processes & People (Issy Reading)
Developing a Research Question (and aims & objectives) (Lisa Douet)
Writing Tips: Story, Style & Sales Pitch (Sophie Hyndman)
The Importance of Plain English; How to Write a Plain English Summary (Paul Hewitson and Bernard Gudgin)
Day 2: Showing Reviewers You Can Deliver I: The Research Plan
(Sophie Hyndman)
Research Plan: Developing a Research Plan: A Worked Example (Mio Hu)
Writing Technical Sections: Introduction (Issy Reading)
Writing Technical Sections I: Health Economics (Maria Chorozoglou)
Writing Technical Sections II: Statistics (Joanna Moschandreas)
Writing Technical Sections III: Qualitative Studies (Jane Vennik)
Day 3: Showing Reviewers You Can Deliver II: Demonstrating Credible Support and Potential Impact
Research Processes & the Importance of Good Project Planning (Sophie Hyndman)
The Importance of Patient & Public Involvement (Heather Parsons, Paul Hewitson, Bernard Gudgin and Tracey Newman)
The Importance of Equality, Diversity and Inclusion (Rebecca Barnes and Chris Newby)
Dissemination - Demonstrating Potential for Tangible Outputs & Impact: Papers, Plus, Plus, Plus! (Dean Phillips)
Managing Intellectual Property (Philippa Christoforou)
The Importance of Good Pre-Submission Review (Sophie Hyndman)
Contributors ……………………………………………………………………………........................ 224
…………………………………….. 5
………………………. 15
………………….. 23
………………………………... 34
…………………………………………………………………. 55
…………………………………………………………………………………………. 147
…………………………………………………………. 166
……………………………………………………………………………………… 187
………………………………………………………………… 193
……………………………………… 207
…………………….. 218
Research Plan : Expectations, Reviewers’ Concerns & Common Confusions ………………………………………………………………………………. 70
…………….. 85
……………………………………… .……………………………………. 98
……………………. 102
… …………………………. 117
………………………….. 133
Contents Coursework, exercises, worksheets and redacted application examples
Coursework
Day 1: Writing techniques
Day 2: Reviewing a methods section
Worksheets and exercises
The worksheets are there to help you relate the content of EGGA to your own research project. The exercises provide an opportunity to apply the skills discussed in that particular session.
WORKSHEET …. The Purpose of a Grant Application (Sophie Hyndman)
WORKSHEET …. Developing a Research Question (Lisa Douet)
EXERCISE ……… Writing Tips: Story, Style and Sales Pitch (Sophie Hyndman)
WORKSHEET …. Writing Tips: Story, Style and Sales Pitch (Sophie Hyndman)
(Sophie Hyndman)
EXERCISE ……… Qualitative Studies (Jane Vennik)
WORKSHEET …. The Importance of Good Project Planning
WORKSHEET …. The Importance of Patient and Public Involvement (Paul Hewitson)
Redacted Application Examples
Redacted Application 1:
Redacted Application 2:
.………………………………………………………………………… 228
………………………………………………................... 233
………………… 239
....................................... 241
………….. 243
………….. 244
WORKSHEET …. Expectation s, Reviewers' Concerns and Common Confusions …………………………………………………………… 245
………………………………………….. 249
………………………………… 250
………………………………………………………………. 251
.………………………………………………………………………… 228
…….………………………………………………................... …….. 233

Foreword
Dear all,
On behalf of the Research Design Service (RDS) South Central, I warmly welcome you to our Essential Guide to Grant Applications (EGGA) masterclass.
RDS South Central is part of the National Institute for Health Research (NIHR), and one of ten RDSs nationally.
RDSs provide free advice on research design to researchers who are developing proposals for national, peer-reviewed funding competitions for applied health or social care research.
During this three-day event, we will cover all aspects of writing a typical application for research funding. This includes: the importance of getting a good research question; considerations for your chosen design; how to present your background and methods sections (including statistics, health economics and qualitative aspects); how best to involve patients and the public; advice on common pitfalls and how to reassure reviewers; how to bring this together and write an application that will be attractive to funders.
RDS South Central has considerable experience and expertise in improving and adding value to funding applications. I hope that you find the three days’ programme of presentations and coursework stimulating and helpful in enhancing your ability to develop high quality funding applications. Please do contribute to the discussions, make use of the worksheets to think about your own research funding applications, and if you have any questions, do not hesitate to ask our EGGA co-ordinators using the online chat function.
Professor Issy Reading
Director, RDS South Central
1

Programme: Day 1 15th February GETTING YOUR MESSAGE ACROSS TO REVIEWERS QUICKLY & CLEARLY
09.10-09.30 Welcome & Introduction. The Purpose of a Grant Application Sophie Hyndman, RDS South Central
09.30-10.00 How Do Projects Get Funded? Processes & People Issy Reading, RDS South Central
10.00-10.40 PANEL DISCUSSION: What do Funding Panels Love & Hate in the Applications They See? Sophie Hyndman (Chair) • Jane Appleton, Member, Clinical Doctoral Research Fellowship Committee• Sarah Brien, NIHR Pre-doctoral Fellowship Selection Committee• Issy Reading, Member, Programme Grants for Applied Research (PGfAR) Committee• Lisa Douet, Senior Research Manager, NIHR Evaluation, Trials & Studies Coordinating Centre
(NETSCC)• Paul Hewitson, Panel Member, Oxfordshire Health Services Research Committee• Nicola Melody, Assistant Director, Personal Awards, NIHR Academy• James Sheppard, Member, NIHR Research for Patient Benefit (RfPB) South East & Central
Regional Advisory Committee
10.40-11.00 COFFEE/TEA BREAK
11.00-11.40 Getting Your Foot in the Door I: Developing a Research Question (& Aims & Objectives) Lisa Douet, RDS South Central
11.40-11.55 Q&A Session Sarah Brien, RDS South Central (Chair), Sophie Hyndman, Dorit Kunkel, Ramon Luengo-Fernandez, Issy Reading, RDS South Central Advisers
11.55-12.30 Writing Tips: Story, Style & Sales Pitch Sophie Hyndman
12.30-12.45 COFFEE/TEA BREAK
12.45-13.25 Getting Your Foot in the Door II: The Importance of Plain English; How to Write a Plain English Summary Paul Hewitson, RDS South Central & Bernard Gudgin, PPI Representative for RDS South Central
13.25-13.30 Course Work Brief: Writing Techniques Sophie Hyndman
13.30-14.30 LUNCH
14.30-15.00 Q&A Session: Space to Ask Questions Arising from Today’s Sessions Sophie Hyndman (Chair) Dorit Kunkel, Sarah Brien, Ramon Luengo-Fernandez, Issy Reading, RDS South Central Advisers
From 15.00 One-to-Ones with RDS Advisers (scheduled)
2

Programme: Day 2
16th February SHOWING REVIEWERS YOU CAN DELIVER I: THE RESEARCH PLAN
09.10-09.30
Course Work Debrief Sophie Hyndman
09.30-10.20
Research Plan I: Expectations, Reviewers’ Concerns & Common Confusions Sophie Hyndman
10.20-10.40
Research Plan II: Developing a Research Plan: a Worked Example Mio Hu, RDS South Central
10.40-11.00
COFFEE/TEA BREAK
11.00-11.15 Q&A Session Heather Parsons, RDS South Central (Chair) Sarah Brien, Jane Wolstenholme, Jo Brett, Issy Reading, Sophie Hyndman, RDS South Central Advisers
11.15-11.20 Writing Technical Sections: Introduction Issy Reading
11.20-11.55 Writing Technical Sections I: Health Economics Maria Chorozoglou, RDS South Central
11.55-12.10 COFFEE/TEA BREAK
12.10-12.50
Writing Technical Sections II: Statistics Joanna Moschandreas, RDS South Central
12.50-13.25 Writing Technical Sections III: Qualitative Studies Jane Vennik, RDS South Central
13.25-13.30 Course Work Brief: Reviewing a Research Plan Sophie Hyndman
13.30-14.30 LUNCH
14.30-15.00 Q&A Groups: Space to Ask Questions Arising from Today’s Sessions Jane Vennik (Chair) Sarah Brien, Sophie Hyndman, Liz Stokes, RDS South Central Advisers
From 15.00 One-to-Ones with RDS Advisers (scheduled)
3

Programme: Day 3
17th February SHOWING REVIEWERS YOU CAN DELIVER II: DEMONSTRATING CREDIBLE SUPPORT & POTENTIAL IMPACT
09.10-09.30
Course Work Debrief Sophie Hyndman
09.30-10.10
Research Processes & the Importance of Good Project Planning Sophie Hyndman
10.10-10.25
COFFEE/TEA BREAK
10.25-11.30
The Importance of Patient & Public Involvement Heather Parsons, Paul Hewitson, Bernard Gudgin, RDS South Central, & Tracey Newman, Associate Professor of Neuroimmunology & Director of Graduate School (Medicine), University of Southampton
11.30-11.50
The Importance of Equality, Diversity & Inclusion (EDI) Rebecca Barnes & Chris Newby, National RDS Priority Leads for EDI
11.50-12.10 PPI & EDI Q&A Panel Sophie Hyndman (Chair) Heather Parsons, Paul Hewitson, Bernard Gudgin, Rebecca Barnes, Chris Newby
12.10-12.25 COFFEE/TEA BREAK
12.25-12.50 Dissemination - Demonstrating Potential for Tangible Outputs & Impact: Papers, Plus, Plus, Plus! Dean Phillips
12.50-13.20
Managing Intellectual Property Philippa Christoforou, Senior Licensing & Ventures Manager, and Werther Vecchiato, Assistant Licensing & Ventures Manager, Oxford University Innovation Ltd.
13.20-13.30 The Importance of Pre-submission Review, the Role of the RDS & Your Next Steps Issy Reading
13.30-14.30 LUNCH
14.30-15.00 Q&A Groups: Space to Ask Questions Arising from Today’s Sessions Lisa Douet (Chair) Maria Chorozoglou, Sophie Hyndman, Jane Vennik, Heather Parsons, Issy Reading, RDS South Central Advisers
From 15.00 One-to-Ones with RDS Advisers (scheduled)
4

EGGA 2022 (15th – 17th February 2022)
Day 1: Getting Your Message Across to Reviewers Quickly and Clearly
The Purpose of a Grant Application
Sophie Hyndman
5

Tuesday 15th February 2022 The Purpose of a Grant ApplicationSophie Hyndman
15th-17th February 2022
Sophie Hyndman
Research Design Service South Central
The Essential Guide to Grant Applications
EGGA, 15th February, 2022
Welcome & Introduction to EGGA
• ‘House-keeping’
• The NIHR Research Design Service
• Response to feedback & changes from last year
• The Essential Guide to Grant Applications
clipart-library.com
• One-to-Ones
DAY 1: Getting Your Message Across to Reviewers Quickly & Clearly
• What is a grant application?• How do projects get funded?• What do funding panels love & hate in the applications they
see?• Writing tips: the importance of story, style & sales pitch• The importance of the research question, title, aims &
objectives• The importance of plain English & the plain English summary
Course Content
1
2
3
6

Tuesday 15th February 2022 The Purpose of a Grant ApplicationSophie Hyndman
DAY 2: Showing Reviewers You Can Deliver I: the Methods Section
• Writing the methods section: reviewer expectations, likely questions, common confusions, worked example
• How to present health economics sections• How to present statistics sections• How to present qualitative sections
DAY 3: Showing Reviewers You Can Deliver II: Demonstrating Credible Support & Potential Impact
• The importance of good project planning• The importance of good patient & public involvement• Demonstrating the potential for tangible outputs & impact• Managing intellectual property• The importance of good pre-submission review• Way forward
Sophie Hyndman
Research Design Service South Central
The Purpose of a Grant Application
EGGA, 15th February, 2022
4
5
6
7
Tuesday 15th February 2022 The Purpose of a Grant ApplicationSophie Hyndman
What is a Research Grant Application?
IT IS NOT:
• A research paper
• A research protocol
• An ethics application
Clip Art
You must take your reader on an easy to understand, logical journey aimed at convincing them to spend
thousands or millions of pounds on you and your project
IT’S GOT TO BE GOOD!
IT IS:
• An application for money
• Competitive
• A ‘sales pitch’
So a research grant application is…
A ‘sales’ pitch aimed at convincing a particular funder that your idea is important enough to them, your suggested approach is good enough,what they get will be good value for money & your team are expert enough to successfully deliver the work
Aldridge & Derrington, 2012
What Does a Grant Application Look Like?
Pearson Scott Foresman via Wikimedia
7
8
9
8

Tuesday 15th February 2022 The Purpose of a Grant ApplicationSophie Hyndman
NIHR - Usual Headings (Stage 2)• Application summary information (includes title)• Lead applicant• Lead & co-applicant research backgrounds• Research team (roles)• Scientific abstract• Plain English summary• Changes from Stage 1• Detailed research plan
Background/ rationale Aims & objectives Research plan/ methods Dissemination, outputs, anticipated impact Timetable Project management Ethics/ regulatory approvals Project/ research expertise Success criteria/ barriers Gantt chart
• Patient & public involvement• Budget• Management & governance• Uploads• Administrative contact details• R&D office contact details
Useful Reference
J. Aldridge & A. Derrington (2012) The Research Funding Toolkit, Sage.
‘A general principle of grant writing is that you should give the reader the information that they want when they want it’
Aldridge & Derrington, 2012, p.78
10
11
12
9

Tuesday 15th February 2022 The Purpose of a Grant ApplicationSophie Hyndman
‘Four Key Propositions’
• Importance: this project is important
• Success: this project can answer the question
• Value: this project is good value for money
• Competence: this team can deliverEverything you include should support one or more of these
Aldridge & Derrington, 2012
What is a Good Research Idea?
• Novel
• Important
• Useful
• Researchable
Image: FreeDigitalPhotos.net
Public Domain
Important to Whom?To the Funder’s Remit
• ‘Mission’/ aims & objectives/ of funder
• Projects funded
• Eligibility criteria
• Guidance notes
13
14
15
10

Tuesday 15th February 2022 The Purpose of a Grant ApplicationSophie Hyndman
Will the Proposed Study Answer the Question?
• Will the research plan deliver?
• Is it appropriate & scientifically rigorous?
• Is the plan feasible?
• Will it deliver useful outputs?
Will the Work be Good Value for Money?
Toby Hudson, via Wikimedia
Are You a Credible Applicant?
• Applying for award at right level for you in terms of background, expertise & track record
• You have a team to cover all major methodological areas
• You have institutional support
16
17
18
11

Tuesday 15th February 2022 The Purpose of a Grant ApplicationSophie Hyndman
A research grant application is…A competitive ‘sales’ pitch aimed at convincing a particular funder that:
your idea is important to them
your suggested approach will successfully deliversomething meaningful
what they get will be good value for money
you and your team are eligible for funding and competent to undertake the work
BUT EVEN IF…
• You have an important question, a potentially successful project plan, offer good value for money & you are a credible, eligible applicant…
• …unless you can CONVEY these things to funders’ reviewers and panels through your writing, you will not get funded
Presenting the Idea
Image: FreeDigitalPhotos.net
Lienhard Schulz, Wikipedia
There is a BIG difference between…
Having the Idea
19
20
21
12

Tuesday 15th February 2022 The Purpose of a Grant ApplicationSophie Hyndman
Presenting the Idea
…should not be: It should be:
• Jumbled up• Unclear• Difficult to decipher• Confusing• Unconvincing
• Clear• Unambiguous• Easy on the eye• Easy on the brain• Convincing
Like a picture, a research grant application…
Leonardo da Vinci, Public Domain
A few Lots
A few A few
What the RDS Sees:
Image: FreeDigitalPhotos.net Leonardo da Vinci, Public Domain
Nota BeneIt does not matter how well your application is presented if:
Images: Wikimedia Commons, Wikipedia (by JJ), Office Online, European Space Agency, renjith krishnan (www.freedigitalphotos.net); clipartpanda.com
• You are not in scope
• Your team are not qualified to do the work
• You do not follow the guidance notes
• Your application is incomplete
• You miss the deadline (even by a minute!)
• You are being over-ambitious or unrealistic
• The research is not good value for money
• You have a poor research question
• Your employer is not eligible to hold the grant
22
23
24
13

Tuesday 15th February 2022 The Purpose of a Grant ApplicationSophie Hyndman
The Pre-requisites for a Successful Grant Application…
A competitive ‘sales’ pitch aimed at convincing a particular funder that:
your idea is important to them
you and your team are eligible for funding and competent to undertake the work
your suggested approach will successfully deliver something meaningful
what they get will be good value for money
You are able to write a well-crafted, understandable description of your work that will convince funders of the above
WORKSHEET
In your own time, thinking of the project you are planning, write down why your project is important.
• Is it important to patients &/or carers? In what way?
• Is it important to the NHS? In what way?
• Is it important to wider society? In what way?
• Is it important to the scientific community? In what way?
• What do you hope the impact of your work will be?
• If you have a funder in mind, have a look at their remit. Is your project important to the funder? In what way/s are you addressing their remit?
Page XXX in the handouts booklet
25
26
14
EGGA 2022 (15th – 17th February 2022)
Day 1: Getting Your Message Across to Reviewers Quickly and Clearly
How Do Projects Get Funded? Processes & People
Issy Reading
15

Tuesday 15th February 2022 How Do Projects Get Funded?Issy Reading
Issy Reading
Research Design Service South Central
How do Projects get Funded?Processes and People
Processes
A game of snakes and ladders
• Initial ‘scrutiny’
• Subject expert
review(s)
• Methodologist
review(s)
• Lay review(s)
• Prioritisation
panels
• Commissioning
panels
• Liaison with other
funding
programmes
• Pre-panel scoring
• Panel shortlisting to second stage with feedback
• Panel funding recommendation (with conditions)
1
2
3
16

Tuesday 15th February 2022 How Do Projects Get Funded?Issy Reading
Scrutiny
Remit
Completeness
Competitiveness
- Assessed by NIHR programme managers or a sub-group of the funding programme’s panel
Panels
Types of panels
Panel membership
Panel procedures
Types of Panels
Prioritisation (Stage 1 or pre-stage 1)
Commissioning (Stage 2)
Advisory Committee (Stage 1 and Stage 2)
4
5
6
17

Tuesday 15th February 2022 How Do Projects Get Funded?Issy Reading
Membership of Panels
A variety of expertise…..
…but no guarantee of specific subject knowledge
Panel Procedures
Lead assessors:- May provide pre-panel scores- Thorough but brief review of
application and indicative score- Present external reviewer comments- Help to compile feedback- HIGHLY INFLUENTIAL
The rest:- Speed readers- May look at lay summary (and
not much more)- Contribute to general discussion
The chair:- Summarises the discussion and the
‘sense’ of feeling in the room- Facilitates agreement (and a decision)
within the panel
Panel Procedures II
Stage 1 panel meeting:
- Looking to shortlist to stage 2- May have guidance as to proportion/number to
aim to take forward- May focus more weight on importance of the
research question, scientific merit of the work proposed and remit of the funding programme
- Aim to give feedback on these and on specific methods, team, and value for money
7
8
9
18

Tuesday 15th February 2022 How Do Projects Get Funded?Issy Reading
Panel Procedures III
Stage 2 panel meeting:
- Looking to recommend for funding- May have guidance as to number to aim to recommend- Will give particular attention to how feedback from Stage 1
and external reviewers has been addressed- Will look closely at each of:
- Importance of topic to the funding programme- Value for Money- Team- Scientific merit of the work plan and ability to answer the
research question, likelihood of impact
External Reviewers
Usually a combination of:
MethodologistsClinical/subject area expertsLay public/patient
May have external reviews for only Stage 2 applications, or for both stages
May be the only opportunity for a directly relevant subject expert to comment on the proposal
People
10
11
12
19

Tuesday 15th February 2022 How Do Projects Get Funded?Issy Reading
A few thoughts on panel members and reviewers…
- Real Human- Know what it’s like to
write a bid- Have expertise, but not
necessarily in your specific area
- Will know what the funder is (and isn’t) looking for
- Want to do a good job
- In general, will start off on your side
Credit: Milka Kostic kicking off peer review week 2016, http://crosstalk.cell.com/blog/kicking‐off‐peer‐review‐week‐2016‐with‐some‐tips‐for‐reviewers
- They will be busy!- They may not have much
time to devote to your proposal
- They will start forming an opinion of your application straight away
- They will have many other applications to review which are in competition with yours
Get to know your reviewer…
What the reviewer will do
- Head straight for a glass of wine your lay summary and/or scientific abstract (and will be delighted if this is clear, concise, complete and accurate)
- Look for the rationale and justification for all aspects of the study to be provided in the application (without needing to assume it or have prior knowledge)
- Carefully compare your aims with the work you are proposing
- Have in mind the remit of the funding stream- Will judge the strength of the proposal on the
strength of the writing, to a degree- Will think in terms of ‘fixable faults’ and ‘fatal
flaws’
Reviewers will give up if it’s taking too long
13
14
15
20

Tuesday 15th February 2022 How Do Projects Get Funded?Issy Reading
Reviewer expectations…
- That they can visualise your project plan, in detail
- That they will be convinced of the need for the work
- That they can see what the work will provide
- That they can see impact/benefit somewhere down the line
- That they will be persuaded that the team can deliver the work
- That the costs will be justified…and that they shouldn’t need to anything
…And the irritations
Reviewers don’t want to:- Try to make sense of your brain dump of
information in the background section- Read lots of dense text
They also don’t want to:- fight through a ‘blizzard of acronyms’- Spot numerous typos- Get annoyed by poor grammar
(especially misplaced apostrophes!)
…And some more irritations
Reviewers don’t want to be made to feel stupid, so
• Don’t try to ‘blind with science’• But don’t patronise either
• Guide your reader through your proposal
• Ensure a logical flow and argument • If your methods are unusual/
obscure/ novel, give assurances via references and team expertise
• Test out your proposal on colleagues, friends, family and your local RDS
16
17
18
21

Tuesday 15th February 2022 How Do Projects Get Funded?Issy Reading
19
22

EGGA 2022 (15th – 17th February 2022)
Day 1: Getting Your Message Across to Reviewers Quickly and Clearly
Developing a Research Question (& Aims & Objectives)
Lisa Douet
23

Tuesday 15th February 2022 Developing a Research QuestionLisa Douet
Developing a Research Question
(and aims and objectives)
Lisa Douet
Today we will discuss
Research questionTitleAims and objectives
How do we come up with a “good” question?
We need to consider:
• On what criteria will the question be judged
• How we articulate the question – ideally in a single sentence
1
2
3
24

Tuesday 15th February 2022 Developing a Research QuestionLisa Douet
NIHR criteria
Need for the evidence
• HOW BAD IS THE PROBLEM?
• WHAT DON’T WE KNOW YET?
• WHY MIGHT THIS WORK HELP?
• WILL THIS MAKE A NOTICEABLE CHANGE?
• WHO IS CALLING FOR THIS WORK?
Funder-specific criteria
NIHR criteria
Need for the evidence
• HOW BAD IS THE PROBLEM?
4
5
6
25

Tuesday 15th February 2022 Developing a Research QuestionLisa Douet
NIHR criteria
Need for the evidence
• WHAT DON’T WE KNOW YET?
NIHR criteria
Need for the evidence
• WHY MIGHT THIS WORK HELP?
Problem
• Underlying cause
Proposed solution
• Reason for thinking this tackles cause of problem
Proposed research
• Findings able to inform practice (or future work)
By changing X, we change Y
By changing Y, we impact Z
NIHR criteria
Need for the evidence
• WILL THIS MAKE A NOTICEABLE CHANGE?
7
8
9
26

Tuesday 15th February 2022 Developing a Research QuestionLisa Douet
NIHR criteria
Need for the evidence
• WHO IS CALLING FOR THIS WORK?
An example
• National COPD Audit Programme reported that uptake of pulmonary rehabilitation was 69%
• The report highlighted this as an area worth exploring: how can we improve uptake?
11
Check for relevant NICE guidance and any research recommendations made by NICE.
Develop the idea
• Talk to clinical colleagues – is this really a problem?
• Clinical colleagues are worried about the impact of wasted resources for missed appointments
12
• Talk to patients – what is the issue from their point of view.
• Patients felt a disconnect between their expectations of pulmonary rehabilitation and the reality.
10
11
12
27

Tuesday 15th February 2022 Developing a Research QuestionLisa Douet
13
National committee ‐ How can we improve uptake of pulmonary rehabilitation?
Consultation with patients and clinicians ‐Why don’t people attend pulmonary rehabilitation?
Consult literature • Referrers not reflecting positive
expectations• A perceived lack of information
relating to purpose and content of PR
• Lack of perceived benefit from attending
Develop the idea further
Develop the idea furtherMotivational interviewing to combat:• Lack of information (and/or issues with communication)• Lack of perceived benefit
Delivered by PR teams upon referral:• Most accessible path of referral pathway BUT requires investment
from PR teams (training = time required)• Some programmes familiar with it as some had used it in initial
appointments• Other work had developed training manual for healthcare
professionals
Consult patient group feedback on design, recruitment etc
14
15
• HOW BAD IS THE PROBLEM?
• Described in terms of the established benefits of Pulmonary Rehabilitation and the extent to which it was not being taken up
• WHAT DON’T WE KNOW YET?
• Whether Motivational Interviewing would improve uptake of Pulmonary Rehabilitation
• WHY MIGHT THIS WORK HELP?
• Work in other fields suggest MI could help people see the benefit of Pulmonary Rehabilitaion; may also overcome communication issues
• WILL THIS MAKE A NOTICEABLE CHANGE?
• Uptake has potential to make important difference, given that Pulmonary Rehabilitation is already recommended in NICE guidelines
• WHO IS CALLING FOR THIS WORK?
• Professional body, clinicians
13
14
15
28

Tuesday 15th February 2022 Developing a Research QuestionLisa Douet
Our research question• Does motivational interviewing improve uptake of pulmonary
rehabilitation?
• Could we refine this to be clearer about what we would like to investigate in the study?
• Does motivational interviewing improve uptake of pulmonary rehabilitation?
• Does motivational interviewing improve uptake of Pulmonary Rehabilitation compared to usual care?
• Does motivational interviewing improve uptake of Pulmonary Rehabilitation compared to usual care?
• Does motivational interviewing improve uptake of PR compared to usual care?
• What is the effectiveness of motivational interviewing compared to usual care in uptake of pulmonary rehabilitation?
16
Thought‐process followed PICO format
• Population (those referred to PR)
• Intervention (motivational interviewing)
• Comparator (usual care ‐ variable)
•Outcome (uptake of PR)
The aim of this study is:
To investigate the effect of motivational interviewing compared to usual care on uptake of pulmonary rehabilitation
Question to Aim
16
17
18
29

Tuesday 15th February 2022 Developing a Research QuestionLisa Douet
• Objectives now break down how we will achieve our aim
• Should use language appropriate to aim
– feasibility study should not discuss effectiveness or efficacy
– Qualitative: explore, understand…
– Quantitative: assess, measure…
• Conceptual rather than methodological
Aim to Objectives
• Act as ultimate “priming” for reader – they should identify the major parts of your study
• E.g., randomising is not a major part of a study but a method used to facilitate assessment of effectiveness
• Recruitment is not a major part of a study but a means of getting people onto your study
• A nested qualitative study is a major part of a study –this has many considerations (purpose, sampling, analysis etc.) associated with it
• Assessment of effectiveness or cost-effectiveness is a major part of a study, as per above
Objectives
The aim of this study is to investigate the effect of motivational interviewing (MI) compared to usual care on uptake of pulmonary rehabilitation (PR).
The objectives are to:
1. Refine the face-to-face MI intervention for use over the telephone
2. Determine the effectiveness of using clinician-delivered MI with respect to uptake and completion of PR amongst eligible patients
3. Assess the fidelity of the delivery of MI
4. Explore acceptability and perceived utility of MI among patients and clinicians
5. Explore barriers and facilitators to delivering MI
Objectives
19
20
21
30

Tuesday 15th February 2022 Developing a Research QuestionLisa Douet
Why this approach?
• One aim and limited number of objectives does not overload reader but still provides clear signal for what is to come
• Provides structure for project plan
• Makes it easy for reader to refer back to
Last but not least…
• Descriptive but concise
• Capture key components of study
Project title
Investigating motivational interviewing to improve uptake of pulmonary rehabilitation:
a randomised controlled trial
• Doesn’t have to form a catchy word…
Gosh, aRe you are having tOo much fun with AcroNyms
Title
22
23
24
31

Tuesday 15th February 2022 Developing a Research QuestionLisa Douet
Work on your one question/aim and make sure it is water-tight
Take your time crafting the objectives to lay out how you will achieve your aim
Consider your title carefully – this is the face of the application
Summary
NICE https://www.nice.org.uk/ – condition specific under “Tools and resources” derived from guidance development
James Lind Alliance http://www.jla.nihr.ac.uk/about-the-james-lind-alliance/
NIHR funding www.nihr.ac.uk/researchers/funding-opportunities/
MRC initiatives www.ukri.org/councils/mrc/guidance-for-applicants/types-of-funding-we-offer/
References
27
www.rds‐sc.nihr.ac.uk
25
26
27
32

Tuesday 15th February 2022 Developing a Research QuestionLisa Douet
WorksheetA worksheet is available in the resource pack giving a list of things to consider when refining your research question:
• Define the problem
• Need for evidence
• What do we need to know
• Who is calling for the evidence?
• Talk to colleagues
• Talk to patients
• Clearly define PICO
• Patients
• Intervention
• Comparator
• Outcomes
28
28
33

EGGA 2022 (15th – 17th February 2022)
Day 1: Getting Your Message Across to Reviewers Quickly and Clearly
Writing Tips: Story, Style & Sales Pitch
Sophie Hyndman
34

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
Writng Tips: Story, Style & Sale Pitch
Sophie Hyndman
Reserach Design Srvice South Central
EGGA, 15th February, 2022
Writing Tips: Story, Style & Sales Pitch
Sophie Hyndman
Research Design Service South Central
EGGA, 15th February, 2022
Tips from the top
‘The first draft of anything is ****’
Ernest Hemingway
‘Fill your paper with the breathings of your heart’
William Wordsworth
‘One day I will find the right words, and they will be simple’
Jack Kerouac
‘I love deadlines. I love the whooshing noise they make as they go by’
Douglas Adams
‘But for my own part, if a book is well written, I always find it too short.’
Jane Austen
All Wikimedia, including Douglas Adams (courtesy of Michael Hughes)
1
2
3
35

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
Useful Reference
J. Aldridge & A. Derrington (2012) The Research Funding Toolkit, Sage.
Used to inform this presentation
‘Four Key Propositions’
• Importance: this project is important
• Success: this project can answer the question
• Value: this project is good value for money
• Competence: this team can deliver
J. Aldridge & A. Derrington (2012) The Research Funding Toolkit, Sage.
Challenges
Rigid templates:• Page limits & word counts• Right information in the right place
Funding panels & reviewers:• Specialists• Non-specialists• ‘Detailed’ readers• Speed-readers
They need:• Clear pointers • Relevant information; no waffle• Arguments – appeal to funder, not necessarily discipline• Sufficient detail to assess quality & feasibility
4
5
6
36

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
Structure ‘The existing arrangement & mutual relation of the constituent parts of a material object.’
Symmetry ‘Due or just proportion; harmony of parts with each other & the whole; fitting, regular, or balanced arrangement & relation of parts or elements; the condition or quality of being well-proportioned or well-balanced.’
Oed.com
Brirush, Wikimedia
Importance of Overall Structure & ‘Symmetry’
Crucial role of plain English summary at start
Wikimedia [Public Domain]
Title
Plain English summary
Scientific abstract
Background/ rationale
Research plan/ methodsOutputs & impact
Project/ research expertise
Patient & public involvement
Budget
AIMS &OBJECTIVES
Franz Jüttner [Public domain]
STORY Extremely important!
• Background/ rationale
• Plain English summary
• Scientific summary
7
8
9
37
Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
• The literature Systematic/ other reviews Primary research papers Other
• Pilot & feasibility work
• Presentation – style, language, argument, coherence
STORY Your Tools
Franz Jüttner [Public domain]
STORY What’s the Argument?For example:
• … is a problem [give evidence for it, e.g. prevalence/ incidence, poor patient outcomes, cost]
• Its resolution would improve things [e.g. reduce prevalence/ incidence, improve patient outcomes, reduce costs]
• Previous work has shown …, but this is deficient in the following ways… [knowledge gap]
• This project will address [the knowledge gap], e.g. resolve uncertainty, provide necessary information/ solution]
• When the project is done, the problem will be resolved & the impact of this will be…
10
11
12
38

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
A Study to Evaluate the Impact of Jedi Force Staff Training on
the Mortality & Morbidity Associated with the
Dark Side
(IJeSt)
• The Dark Side is a problem. It causes death in large numbers of people every year, & has even been known to exterminate whole planetary populations. In addition it causes much anxiety & depression. The costs are enormous, both for victims, but also in rebuilding lives & civilisations affected.
• Removal of the Dark Side would be beneficial to many millions of people. It would reduce suffering & death & reduce costs to the NHS & other health & social welfare organisations.
• Current approaches to remove the Dark Side, such as attacks by small numbers of disorganised rebels have failed. There is a clear need for a more radical & magical solution. Preliminary studies indicate the potential of Force training for Jedi Knights in tackling the Dark Side, but its full efficacy/ effectiveness is unknown.
• This project will evaluate whether or not Force training of Jedi Knights is effective in fighting the Dark Side.
• If this approach is found to be beneficial, the Dark Side may be successfully defeated, with resulting improvements in quality of life & longevity throughout the Galaxy.
So:
(… until another Jedi Knight goes AWOL)
• Obesity has led to more Type 2 diabetes, which causes morbidity & premature mortality. It costs the NHS a great deal
• Reduction in obesity would reduce complications, even resolve diabetes.
• Current guidance suggests that for those under BMI 35kg/m2, dietary changes, exercise, behavioural changes or drugs should be used. These have some modest effects. Preliminary studies show the potential of bariatric surgery (BS) for those >30kg/m2. Results need confirming in a larger trial but we do not know if this is feasible.
• A feasibility study will enable us to see if BS is acceptable to this group of patients, & their clinicians.
• If this is successful, & a definitive study shows it works, BS could provide a cost-effective solution for this group.
OBESITY IS A PROBLEM
ITS RESOLUTION WOULD IMPROVE MANY THINGS
KNOWLEDGE GAPS – WE NEED BETTER INTERVENTIONS; BS IS A POSSIBILITY BUT WE NEED A TRIAL; WE DO NOT KNOW WHETHER A TRIAL IS FEASIBLE
THIS PROJECT WILL ADDRESS THE KNOWLEDGE GAP/ UNCERTAINTIES
IF BS WORKS FOR THIS GROUP, WE WILL HAVE A SOLUTION
Example, Paul Roderick et al., Successful RfPB Team, 2010
More Seriously – What’s the Argument?
13
14
15
39

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
What’s the Argument?• Currently the in-patient care on offer for children & young people (CYP) with
severe mental health problems is variable &, where they end up on adult wards, unsatisfactory.
Costs, outcomes and satisfaction for in-patient child and adolescent psychiatric services. Royal College of Psychiatristshttps://www.journalslibrary.nihr.ac.uk/programmes/hsdr/081304062/#/summary-of-research
SOME CYP ARE RECEIVING UNSATISFACTORY CARE
THIS PROJECT WILL ADDRESS THESE KNOWLEDGE GAPS
THIS STUDY WILL PROVIDE MUCH NEEDED INFORMATION TO PLAN BETTER SERVICES
• Currently we do not know how patients fare, whether different settings affect patients’ progress, and the cost implications of these different settings.
• This information will be vital to those responsible for ensuring that young people have access to high quality in-patient care when needed. It will also help staff in local services to make better use of their beds.
IMPROVED CARE WOULD LEAD TO BETTER OUTCOMES/ RESOURCE USE
• Improvements in care would lead to better patient outcomes & resource use.
• This project will provide information on patient experiences & the costs of different patient pathways.
KNOWLEDGE GAPS: WE DO NOT KNOW HOW DIFFERENT SETTINGS AFFECT OUTCOMES & COSTS
Convincing = supportive = remember
Defensive = deals with problems = forget
For example: ‘Although we are only collecting data from these two counties, data from the ONS show the socio-demographic profile to be very similar to national averages. Results from this study should therefore be generalisableto the broader UK population’
STORY ‘Convincing’ and ‘defensive’ arguments
STORY Adding Emphases & Refining Arguments
Make good use of connectives!
‘As well as…’
‘Despite this…’
‘In contrast…’
‘Consequently…’
‘In spite of…’
‘However…’
‘It appears…’
‘None…’
‘The majority…’
‘Undoubtedly…’
‘The fact is…’
‘In conclusion…’
‘Remarkably…’
‘Importantly…’
In addition
‘…and yet…’‘Accordingly…’
16
17
18
40

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
Using the literature:
• Define
• Justify
• Evidence of best design
• Show work fits remit
• Logical, convincing argument
STORY Pack a Punch!
Image: Wikimedia Commons [Public Domain]
‘Why haven’t we done this before?!’
E.g. NIHR sub-headings
Set scene: What is the problem being addressed?• Define problem • Impact - patients, health & care services • How research will fill evidence gap• How research fits remit
Why is this research important in terms of improving the health &/or wellbeing of the public &/or to patients & health and care services?• Importance for patients• Importance to NHS • Anticipated outcomes, outputs & impact• Pathway & timescale to patient benefit
Review of existing evidence - How does the existing literature support this proposal?• Evidence for need & rationale• Past & current research justifying work (‘add distinct value’) • Systematic review – do or update if necessary• Prior work of team (e.g. pilot or feasibility data)
STORY Fitting it on the Form
www.freeclipart.pw/clipart_images/yoda-outline-clipart-11286
STORY
19
20
21
41

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
• Headline messages, not convoluted arguments
• Use adjectives sparingly Slow the reader down Use for factual qualification only Avoid ‘exciting’, ‘profound’ – let reader ‘feel it’, not read it
• Use adverbs even more sparingly!
STYLE Keep it Easy to Read
‘May in Ayemenem is a hot, brooding month. The days are long and humid. The river shrinks and black crows gorge on bright mangoes in still, dustgreen trees. Red bananas ripen. Jackfuits burst. Dissolute bluebottles hum vacuouslyin the fruity air. Then they stun themselves against clearwindowpanes and die, fatly baffled in the sun.’
Arundhati Roy – The God of Small Things
Literary Interlude
Clipartpanda.com
• Do not use typography to emphasise too much text
• Bullet points & numbered lists
• Short sentences (c.10 words)
• Short paragraphs
• Simple punctuation (no colons & semi-colons 😒)
STYLE Keep it Easy to Read
22
23
24
42
Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
‘In consideration of the day and hour of my birth, it was declared by the nurse, and by some sage women in the neighbourhood who had taken a lively interest in me several months before there was any possibility of our becoming personally acquainted, first, that I was destined to be unlucky in life; and secondly, that I was privileged to see ghosts and spirits; both these gifts inevitably attaching, as they believed, to all unlucky infants of either gender, born towards the small hours on a Friday night.’
Dickens – David Copperfield
Walliams – Awful Auntie
Literary Interlude
Clipartpanda.com
‘Outside there was not a sound. The house had never been this quiet before. All was silent. From her bed Stella turned her head to look out of the window.’
LITERARY EXERCISE
Clipartpanda.com
Can you re-write this in a ‘Walliams’ style?
Mrs. Rachel Lynde lived just where the Avonlea main road dipped down into a little hollow, fringed with alders and ladies’ eardrops and traversed by a brook that had its source away back in the woods of the old Cuthbert place; it was reputed to be an intricate, headlong brook in its earlier course through those woods, with dark secrets of pool and cascade; but by the time it reached Lynde’s Hollow it was a quiet, well-conducted little stream, for not even a brook could run past Mrs. Rachel Lynde’s door without due regard for decency and decorum; it probably was conscious that Mrs. Rachel was sitting at her window, keeping a sharp eye on everything that passed, from brooks and children up, and that if she noticed anything odd or out of place she would never rest until she had ferreted out the whys and wherefores thereof.
Anne of Green Gables, L.M.Montgomery, 1908
https://en.wikisource.org/wiki/Anne_of_Green_Gables_(1908)/Chapter_IText is available under the Creative Commons Attribution-ShareAlike License
Mrs. Rachel Lynde lived just where the Avonlea main road dipped down into a little hollow. The hollow was fringed with alders and ladies’ eardrops. It was also traversed by a brook. The source of the brook was away back in the woods of the old Cuthbert place. The brook was reputed to be an intricate, headlong brook in its earlier course through those woods, with dark secrets of pool and cascade. By the time it reached Lynde’s Hollow, however, it was a quiet, well-conducted little stream. Not even a brook could run past Mrs. Rachel Lynde’s door without due regard for decency and decorum. It was probably conscious that Mrs. Rachel was sitting at her window. She was no doubt keeping a sharp eye on everything that passed, from brooks and children up. If she noticed anything odd or out of place she would never rest until she had ferreted out the whys and wherefores thereof.
With apologies to L.M.Montgomery
25
26
27
43

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
• Simple verb structures – present tense, active form Keeps word count down
E.g. ‘This project asks…’ = ‘The question to be asked by this project…’ ‘This project is asking the following question…’ ‘It is expected that the project will ask…’
• Have ‘breathing space’ in the text
• Use sub-headings
STYLE Keep it Easy to Read
In the UK, each year, about 100 healthy babies die(1) and about 1,100 sustain brain injury(2) during labour at term. Nearly 50% of the NHS litigation bill is due to obstetric claims (£3.1bn in 2000-10), most of which relate to shortcomings in labour management and CTG interpretation(3). During labour, materno-fetal respiratory exchange is transiently compromised by uterine contractions leading to reduced oxygen supply to the fetus. If the physiological state is overwhelmed, the fetushas to rely on adjusting its cardiac output, redistributing blood to prioritise the heart and brain, and adapting biochemically. Rarely, this leads to fetal decompensation (asphyxia) and permanent brain damage or death (1.5 per 1,000 births(2)). In the UK, during labours at low risk, fetal health is monitored by intermittent auscultation of the fetal heart using a handheld Doppler ultrasound device; while in the large proportion of women with associated risk factors, cardiotocography (CTG) is adopted, providing continuous monitoring of the fetal heart rate and uterine contractions. CTG is used worldwide to detect fetuses that may benefit from emergency operative delivery (Caesarean or instrumental vaginal birth). A few ‘classic’ CTG patterns have been empirically identified: baseline, variability, accelerations and decelerations, forming the basis for current clinical practice that has “remained static” over 40 years(4-6). CTG interpretation in labour is unreliable(7,8) and, for certain CTG patterns, the disagreement in visual interpretation between experts reaches 100%(8).
Research Plan – Background, Antoniya Georgieva, Successful NIHR CDF, 2016; edited to make a point
STYLE Example
In the UK, each year, about 100 healthy babies die(1) and about 1,100 sustain brain injury(2) during labour at term. Nearly 50% of the NHS litigation bill is due to obstetric claims (£3.1bn in 2000-10), most of which relate to shortcomings in labour management and CTG interpretation(3).
During labour, materno-fetal respiratory exchange is transiently compromised by uterine contractions leading to reduced oxygen supply to the fetus. If the physiological state is overwhelmed, the fetus has to rely on adjusting its cardiac output, redistributing blood to prioritise the heart and brain, and adapting biochemically. Rarely, this leads to fetal decompensation (asphyxia) and permanent brain damage or death (1.5 per 1,000 births(2)). In the UK, during labours at low risk, fetal health is monitored by intermittent auscultation of the fetal heart using a handheld Doppler ultrasound device; while in the large proportion of women with associated risk factors, cardiotocography (CTG) is adopted, providing continuous monitoring of the fetal heart rate and uterine contractions. CTG is used worldwide to detect fetuses that may benefit from emergency operative delivery (Caesarean or instrumental vaginal birth).
A few ‘classic’ CTG patterns have been empirically identified: baseline, variability, accelerations and decelerations, forming the basis for current clinical practice that has “remained static” over 40 years(4-6). CTG interpretation in labour is unreliable(7,8) and, for certain CTG patterns, the disagreement in visual interpretation between experts reaches 100%(8).
Edited to make a point
28
29
30
44

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
The Problem: Healthy Babies Die During LabourIn the UK, each year, about 100 healthy babies die(1) and about 1,100 sustain brain injury(2) during labour at term. Nearly 50% of the NHS litigation bill is due to obstetric claims (£3.1bn in 2000-10), most of which relate to shortcomings in labour management and CTG interpretation(3).
The Use of Cardiotocography (CTG)During labour, materno-fetal respiratory exchange is transiently compromised by uterine contractions leading to reduced oxygen supply to the fetus. If the physiological state is overwhelmed, the fetus has to rely on adjusting its cardiac output, redistributing blood to prioritise the heart and brain, and adapting biochemically. Rarely, this leads to fetal decompensation (asphyxia) and permanent brain damage or death (1.5 per 1,000 births(2)). In the UK, during labours at low risk, fetal health is monitored by intermittent auscultation of the fetal heart using a handheld Doppler ultrasound device; while in the large proportion of women with associated risk factors, cardiotocography (CTG) is adopted, providing continuous monitoring of the fetal heart rate and uterine contractions. CTG is used worldwide to detect fetuses that may benefit from emergency operative delivery (Caesarean or instrumental vaginal birth).
Current CTG Interpretation is Unreliable A few ‘classic’ CTG patterns have been empirically identified: baseline, variability, accelerations and decelerations, forming the basis for current clinical practice that has “remained static” over 40 years(4-6). CTG interpretation in labour is unreliable(7,8) and, for certain CTG patterns, the disagreement in visual interpretation between experts reaches 100%(8).
Edited to make a point
• Avoid new or specialist acronyms
• Define more than once
Alphabet soup
‘The case notes of CMHTs will be reviewed…’
‘We will compare mean PANSS scores…’
STYLE Keep it Easy to Understand
‘Bad Application’ by Helen Lloyd, RDS South Central
• Limit use of overly technical language, jargon & ‘buzzwords’
Tech Speak“Post colloquial discourse modulation protocol for user status enhancement. It's a referential system for functional-structural, microscopically specific macroscopic-object redesignation. It's a universal semantic transformation procedure. It's a holophrastic technocratic sociolect. It's a meta-semiotic mode for task specific nomenclature." Get the idea?
BuzzwordAn important-sounding word or phrase connected with a specialized field or group that is used primarily to impress laypersons: “‘Sensitivity’ is the buzzword in the beauty industry this fall.”
‘Tech Speak’ as defined by Edward Tenner (1986) Tech Speak, Random House
STYLE Keep it Easy to Understand
31
32
33
45

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
• Between sections, e.g. Common error: meandering objectives
• In use of terms
E.g. ‘Directorate’, ‘Unit’, ‘Ward’
STYLE Be Consistent
Picture: NASA
Literary Interlude
‘There was Eru, the One, who in Arda is called Illuvatar; and he made first the Ainur, the Holy Ones, that were the offspring of his thought, and they were with him before aught else was made…’
J.R.R. Tolkien – The Silmarillion
Clipartpanda.comhttps://www.wallpaperenginefree.com/2018/08/lord-of-rings-morgoth-and-fingolfin.html
Melkor or Morgoth?
Escher, Relativity, 1953 Wikimedia
STYLE Be Logical
• Logical arguments
• Logical flow of sentences, paragraphs, sections
• Don’t contradict yourself!
34
35
36
46

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
‘Twas a summer’s night in winterAnd the rain was snowing fast.A barefoot boy with shoes on
Stood sitting on the grass(Anon)
Yesterday upon the stairI met a man who wasn’t thereHe wasn’t there again todayI wish, I wish he’d go away
(from Antigonish, Hughes-Mearns)
Literary Interlude
Clipartpanda.com
STYLE Avoid Spelling Mistakes & Poor Grammar
Tom Goskar, Flickrhttps://creativecommons.org/licenses/by-nc-sa/2.0/
Michele Peters ©
STYLE Repeat Key Messages'This proposal arises from my extensive prior work…’ [Scientific Summary]
‘My preliminary results already show the feasibility & potential impact of my central research hypothesis… [Relevant Expertise & Experience]
‘This proposal builds on extensive prior work… [Introduction]
‘Prior work First key achievement: …Second key achievement: …’ [Background]
‘It is a pioneering and ambitious proposal with a strong chance of success because of …the existing system prototype’ [End of Research Plan]
‘This proposal arises from my extensive prior work…’ [Any prior work]
I have already gained approval for the CTG and clinical data… used for the first prototypes development…’ [Ethics Issues]
‘This proposal aims to improve on an existing diagnostic system prototype…[IP]
Example: Antoniya Georgieva, Successful NIHR CDF, 2016; edited slightly; my emphases
37
38
39
47

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
• Miller (1956) ‘the magical number seven’
• Helped by ‘chunking’ – grouping related information
‘The systematic review will include: The physiological variables that form each EWS and the
weights that are applied to each variable. The statistical methods used to develop and assess the
performance of each EWS. Whether the EWS was validated, what methods were used
and whether internal (using the dataset the EWS was derived from) or external (using separate data) validation occurred.
External validation of each EWS with my data to test its performance, measured by how well it predicts future outcomes.’
STYLE Keep it Memorable
Example, Steve Gerry, successful NIHR DRF, 2016
STYLE Keep it Formal
• Avoid abbreviations commonly used in informal writing, e.g. ‘we’ll’, ‘sha’n’t’
• Avoid informalities & over-personalisatione.g. ‘I’ & ‘We’, but not ‘I am not convinced …’ Let the evidence speak for itself
• Colloquialisms OK for Plain English Summary
http://www.hasslefreeclipart.com
Denicolo, P & Becker, L (2012) Developing Research Proposals; Sage
STYLE: Helpful Writing Techniques
• Key messages at start of paragraph • Make assertion, justify with evidence, rather than argue case & conclude
• Simple, direct communication• Assertions can be lifted out for summaries
E.g. ‘This area of work is under-researched …’
‘Current therapies do not address this area …’
‘Previous work is limited & lacks methodological rigour …’
‘This programme of work will address prior deficiencies & enable us to answer the research questions raised …’
1. Assert-Justify
40
41
42
48

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
Literary Interlude
‘It is a truth universally acknowledged, that a single man in possession of a good fortune, must be in want of a wife.’
Austen – Pride and Prejudice
‘All happy families are alike; each unhappy family is unhappy in its own way.’
Tolstoy – Anna Karenina
Clipartpanda.com
Ask yourself ‘if a speed-reading reviewer reads ONLY the first sentence in each paragraph, will they get the message?’
STYLE: Helpful Writing TechniquesAssert-Justify
I have developed my career in biomedical research, building on my expertise in signal processing, computing & mathematics …
I ALREADY HAVE A CAREER IN THIS AREA
After BSc in Applied Mathematics (2004) & PhD in Computer Science (2007), I took a post-doctoral position in Oxford …
I AM WELL QUALIFIED
My supervisors encouraged me to become independent early on …I AM AN INDEPENDENT RESEARCHER
My results have been published in peer-reviewed medical, biomedical & engineering journals & presented at international scientific meetings …
I HAVE A GOOD RESEARCH TRACK RECORD
I have already successfully supervised two PhD, two MSc… several undergraduate students …I AM ALREADY INVOLVED IN RESEARCH CAPACITY DEVELOPMENT
Together with colleagues from Prague & Lyon, I recently organised the ‘1st Workshop on Signal Processing & Monitoring in Labour’ … a newly emerging forum.
I HAVE INTERNATIONAL COLLABORATORS IN THIS NOVEL FIELD
My preliminary results already show the feasibility & potential impact of my central research hypothesis …
THIS PROJECT IS LIKELY TO SUCCEED
Example: Expertise & Experience Section, Antoniya Georgieva, Successful NIHR CDF, 2016; edited slightly; my emphases
STYLE: Helpful Writing TechniquesAssert-Justify
43
44
45
49

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
‘A systematic review published in 2007 found 33 Early Warning Score (EWS) algorithms in use, with a high degree of overlap in the vital signs included, but with considerable variability in the weighting systems used to obtain the score.(14) However, due to numerous deficiencies in the methods used to develop many of these EWSs, the authors concluded thatnone of the algorithms could be said to ‘perform well’ at identifying patients at increased risk of in-hospital death from those who were not.’
Current Early Warning Scores do not ‘perform well’ at identifying patients at increased risk of in-hospital death due to numerous deficiencies in the methods used to develop them. These were the conclusions of a systematic review published in 2007, which identified 33 EWS algorithms. There was a high degree of overlap in the vital signs included, but considerable variability in the weighting systems used to obtain the score…’
Example: Research Plan: Background, Steve Gerry, Successful DRF, 2016; edited to make a point
STYLE: Helpful Writing TechniquesAssert-Justify
Advance information that will make reader more likely to agree to your proposition
E.g.
‘Each year, 30,000 people suffer from …’ priming for work on it
‘There is a dearth of evidence concerning …’ priming for work later to remedy this
‘Data will be gathered using …’ priming for a later resource request
‘Previous relevant work by the co-applicant …’ priming choice of personnel for study detailed later
http://jimhorne.co.uk/falling-asleep-at-the-wheel/
motorwayservices.info
STYLE: Helpful Writing Techniques2. Priming
• Tells reader important information is coming
• Helps structure and highlight arguments
• Allows speed-readers to skip or take note
• Ensures detailed readers take note
STYLE: Helpful Writing Techniques
E.g. ‘In this section we describe …’
‘We now set out the state of the art …’
‘The following work-packages will answer these questions …’
‘For details, see section…’
3. Sign-posting
46
47
48
50

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
• Connects arguments & maintains narrative
• Allows reader to see logic of what you are doing clearly
• Counteracts ‘bitty’ nature of grant templates
E.g.
‘Whilst this previous work has shown encouraging results, there are only two studies that have looked specifically at this issue …’ [detailed next]
‘This work will answer one aspect of the question, however, there remains the issue of…’ [addressed next]
‘The intervention has been shown, in several studies, to work in the acute phase, furthermore, early evidence suggests it may also benefit patients in the chronic stage’
4. LinkingSTYLE: Helpful Writing Techniques
• Connects arguments & maintains narrative
• Allows reader to see logic of what you are doing clearly
• Counteracts ‘bitty’ nature of grant templates
E.g.
‘Whilst this previous work has shown encouraging results, there are only two studies that have looked specifically at this issue …’ [detailed next]
‘This work will answer one aspect of the question, however, there remains the issue of…’ [addressed next]
‘The intervention has been shown, in several studies, to work in the acute phase, furthermore, early evidence suggests it may also benefit patients in the chronic stage’
4. LinkingSTYLE: Helpful Writing Techniques
Remember your connectives!
Plain English Summary
There are several problems with the way Early Warning Scores have been developed. Good statistical techniques exist to develop a tool for predicting patient outcomes. However these have not generally been used in the past for the creation of Early Warning Scores, meaning that they do not perform as well as they could. In addition, the current Early Warning Scores do not include factors such as age and disease type (or severity), yet they are intended to be used across all types of patients, meaning that the predicted risks are unlikely to be accurate for all patients. Finally, and importantly, because current Early Warning Scores only take into account the most recent set of patient readings and ignore the previous ones, they will not notice a patient who is getting sicker as soon as they could do.
Steve Gerry, Successful NIHR DRF, 2016
However
In additionyet
Finally, and importantly,
49
50
51
51

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
• Highlights themes running through document
• Use identical sub-headings/ repeated phrases to label themes
• Repetition of key technical terms/ concepts helps reader feel they understand
[Objectives] ‘The project objectives are as follows:
1. Conduct a systematic review of the medical literature to identify current Early Warning Scores, examine the methodology used in their development and validation, and assess their performance …’
[Methods] ‘Objective 1: Conduct a systematic review of current Early Warning Scores …’
5. Use of ‘Tag Phrases’/ LabellingSTYLE: Helpful Writing Techniques
Example: Steve Gerry, Successful NIHR DRF, 2016, edited.
POLL(1) Thinking about the various writing techniques you have heard about today. Which
do you think will make the biggest difference to the way you approach your own
grant-writing?
• Linking• Assert-justify• Sign-posting• Priming• Using ‘tag phrases’
(2) If you were reviewing an application, which of the following would most annoy
you?
• Unexplained acronyms• Illogical structure• Jargon• Inconsistent use of language• Spelling mistakes• Long, complicated sentences
‘Know your customer ‘
• Scope & remit of funder• Follow guidance notes• Respond carefully to
commissioned calls
‘Know your product’
• Be on top of the literature• Know where what you are
offering fits in with the picture
‘Acknowledge the problems with existing products’
• Be on top of the literature• Know the evidence gaps
‘Offer solution to a problem’
• Produce an intervention/ study which addresses the problem & the limitations of previous interventions/ studies
‘Say why your product is better than others’
• Know the limitations of other studies/ interventions
• Produce an intervention/ study which addresses the problem & the limitations of previous interventions/ studies
SALES PITCH
Clipartpanda.com
52
53
54
52

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
‘Hook your customer’
‘Address objections up front’
‘Dazzle them’
‘Differentiate yourself’
‘Tell a story’
‘Make a good first impression’
‘Listen and respond to customer’
• Have a good title• Have a fantastic plain
English summary
• No typos in title!• Have a great team• Have a good title• Have a fantastic plain English
summary
• Acknowledge the limitations of your approach• Provide mitigation where possible
• Have logically argued background/ rationale
• Have a great team• Have an original idea/ project • Respond to reviewers’
comments for round 2/ next attempt/ at interview• Have a great team
• Have an original idea/ project• Have a fantastic grant proposal!
SALES PITCH
Clipartpanda.com
"Leonard Nimoy Spock 1967" by NBC Television - eBayfrontback. Licensed under Public Domain via Commons -https://commons.wikimedia.org/wiki/File:Leonard_Nimoy_Spock_1967.jpg#/media/File:Leonard_Nimoy_Spock_1967.jpg
Quote: Star Trek, Season 3, episode 7, 1968
"Star Trek William Shatner" by NBC Television - eBay itemphoto frontpublicity release. Licensed under Public Domain via Commons -https://commons.wikimedia.org/wiki/File:Star_Trek_William_Shatner.JPG#/media/File:Star_Trek_William_Shatner.JPGQuote: Star Trek, Season 1, episode 23, 1967
SPOCK VS
KIRK
Sometimes a feeling is all we humans have to
go on
I find their illogic and foolish emotions a constant irritant.
SALES PITCH
• Give yourself TIME to do a good job
• Include everything requested
• Proof read in & out of specialty area
• Keep tweaking, adjusting and re-drafting until your application is a thing of beauty
AND FINALLY…
Leonardo da Vinci [Public Domain]
55
56
57
53

Tuesday 15th February 2022 Writing Tips: Story, Style and Sales PitchSophie Hyndman
WORKSHEET In your own time, using just five brief bullet points, use the worksheet to summarise the argument for your proposed study.
• … is a problem [give evidence for it, e.g. prevalence/ incidence, poor patient outcomes, cost]
• Its resolution would improve things [e.g. reduce prevalence/ incidence, improve patient outcomes, reduce costs]
• Previous work has shown …, but this is deficient in the following ways… [knowledge gap]
• This project will address [the knowledge gap], e.g. resolve uncertainty, provide necessary information/ solution]
• When the project is done, the problem will be resolved & the impact of this will be…
For worksheets, see resource pack
58
54

EGGA 2022 (15th – 17th February 2022)
Day 1: Getting Your Message Across to Reviewers Quickly and Clearly
The Importance of Plain English; How to Write a Plain English Summary
Paul Hewitson & Bernard Gudgin
55

Tuesday 15th February 2022 The Importance of Plain EnglishPaul Hewitson
Dr Paul HewitsonRDS-SC Research Advisor and PPI Officer
University of Oxford
Importance of the PlainEnglish Summary and
Writing in Plain English
Overview
• Requirement for NIHR (and other funders) is to include a ‘lay’ or plain English summary
• Number of techniques available to improve the comprehension of your plain English summary
• Writing in plain English improves the readability and understanding of your application
Defining Plain English
• “It is a message, written with the reader in mind and with the right tone of voice, that is clear and concise” (Plain English Campaign)
• Primarily concerned with reducing complexity of written language to improve reader comprehension
“Writers of plain English let their audience concentrate on the message instead of being distracted by complicated
language” - R. Eagleson (1989)
1
2
3
56

Tuesday 15th February 2022 The Importance of Plain EnglishPaul Hewitson
Importance of the Summary
• Usually first (sometimes only) part of application read at committee
• Will ‘prime’ the reader in regards to content of the main application
• Poorly written plain English summary can have a negative effect on the reader
“If the plain English summary is well written, somehow the whole application seems easier to assess – I have an
idea of what it is about.” - Public Reviewer
Plain English Summary (pEs)
• Clear, brief summary of the research that has been written for members of the public, rather than researchers or professionals
• Following groups expected to read pEs:i. reviewers/committee members to have a
better understanding of the proposalii. the researchers funders to publicise research
they fundiii. members of the public, health professionals,
policy makers and the media
General Requirements
• Do not cut-and-paste your scientific abstract…not a good first impression
• Remove/avoid jargon and clearly explain technical/medical terms
• Explain all acronyms or abbreviations• Should describe the research accurately
“If it is felt that your plain English summary is not clear and of a good quality then you may be required to amend
it prior to final funding approval” - NIHR
4
5
6
57

Tuesday 15th February 2022 The Importance of Plain EnglishPaul Hewitson
NIHR Format
• NIHR suggests including the following subheadings:
i. Aim(s) of the researchii. Backgroundiii. Design and methods usediv. Patient and Public Involvementv. Dissemination
• The summary needs to be used on its own to describe the research, without the rest of the application
Six Writing Tips
• Keep it simple (use alternative words)• Ask your PPI contributors to help write
and refine the summary• Be concise and balanced• Use active phrases/verbs not passive• Keep sentences short (15 to 20 words)• Write for at the expected reading level
Quiz
7
8
9
58

Tuesday 15th February 2022 The Importance of Plain EnglishPaul Hewitson
Reading Ease/Grade Level
• Around 15% of the UK adult population have reading age of 9-11 years old
• GOV.UK recommends 9 year old• Majority bestsellers 9-11 years old• Flesch Reading Ease, Flesch Kincaid
Grade Level• Suggest aiming for score of 70+
Sentence Length
• Average sentence length 8 words = 100%• If 14 words = 90%; 43 words = 10%• When given choice, 80% of people
preferred plain English• As education increases, so does
preference for plain English• 86% of PhD versus 76% under College• 41% were ‘annoyed’ by complicated terms
with just 0.5% being ‘impressed’
Active Phrase/Verbs
• Active verbs are when the sentence’s subject does something
• Passive verbs are when the sentence’s subject has something done to it
• Will reduce length of sentences• Look for ‘by’ in sentence (passive) - “A trend is shown by the evidence” = passive
- “The evidence shows a trend” = active
10
11
12
59

Tuesday 15th February 2022 The Importance of Plain EnglishPaul Hewitson
Concise and Balanced
• Don’t exaggerate benefits• Remove superfluous information • Example:
“Participants will be recruited by the research team at the University of Somewhere who have a strong track record of conducting large-scale studies of a similar nature.”
• “We will recruit participants…”
Summary
• Writing in plain English is not as simple as you might expect
• First impressions count – summary should engage the reader, not enrage them
• PPI/proof-reading and using readability checkers
• Multiple resources available to help improve writing in plain English
Resources
• Local Research Design Service
• NIHR – Plain English Summarieshttps://www.nihr.ac.uk/documents/plain-english-summaries/27363
• Plain English Campaignhttp://www.plainenglish.co.uk/
• Office of National Statisticshttps://style.ons.gov.uk/category/writing-for-the-web/plain-english/
13
14
15
60

Tuesday 15th February 2022 The Importance of Plain EnglishPaul Hewitson
And now to the fun presentation…
16
61

Tuesday 15th February 2022 The Importance of Plain EnglishBernard Gudgin
Essential Guide to Grant Applications
15th February 2022
--
How Plane is your Ingerlish?
--
Dr Bernard Gudgin
My Background (apologies)
• I am a lay person with no medical training.
• I have been a Type 2 diabetic for 35 years and have taken part as a volunteer in several major trials.
• Member of the:– Thames Valley & South Midlands ARC Board
– Diabetic Eye Screening Research Advisory Committee
– TCC ICA Doctoral Research Fellowship Panel
– RDS South Central Pre-Submission Review Panel
– Co-applicant on the SuMMiT-D project
– Co-applicant on a project evaluating the NHS App
– Have been on i4i, HTA and HS&DR
No: 3
It’s obvious!
1
2
3
62

Tuesday 15th February 2022 The Importance of Plain EnglishBernard Gudgin
Fortune 500 company (Annual Report)
"Your management is fully incented to identify value-added enhancements as we build momentum byselectively outsourcing shareholder value in theinterest of maximising incentive compensation. As inevery year in our company’s history, once again thisyear we have eliminated waste and increasedmarket-leading growth potential by streamlining ourworld-class quality and innovation, using a widevalue mix to make major strides in integratingoperating strategies to realise all of the marginbenefits available."
West Hampshire Clinical Commissioning Group
In deciding whether a person has a primary health need the representatives will consider whether the nursing or other services required by that person are:-a) where the person is, or will be, accommodated in a care home, more than incidental or ancillary to the provision of accommodation which a Local Authority is, or would be, but for a person’s means, under a duty to provide; orb) of a nature beyond which a Local Authority whose primary responsibility is to provide social services could be expected to provide and if it decides that the nursing or other health services required do, when considered in their totality, fall within paragraph (a) or (b), it must decide that the person has a primary health need.
Getting the Message Across
• You are being invited to take part in the “Effect of Sitagliptin on glycaemiccontrol in type 1 diabetes” study that will take place in the Clinical Research Unit (CRU) at the Oxford Centre for Diabetes Endocrinology & Metabolism (OCDEM) Churchill Hospital Oxford would perform this study and which has been approved by a local ethics committee.
4
5
6
63

Tuesday 15th February 2022 The Importance of Plain EnglishBernard Gudgin
SummaryAims The aim of the study is to examine theimpact of statin or omega-3-acid ethyl esters 90 (omega-3EE90; omega-3-acid ethyl esters 90 refers to amixture of ethylesters of n-3 fatty acids) on estimated cardiovascular disease(CVD) risk in community-based people with type 2 diabetesbut without known CVD and not taking lipid-lowering therapy.Methods A central computer will randomise 800 patients in59 UK general practices to atorvastatin (n=401, 20 mg/day)or placebo (n=399) and omega-3 EE90 (n=397, 2 g/day) orplacebo (n=403) in a concealed factorial manner. Participantswith LDL-cholesterol <2.6 mmol/l, triacylglycerol<1.5 mmol/l and estimated 10-year CVD risk <20% werecompared at 4 months.
The Medical - Public divide!
SummaryAims The aim of the study is to examine theimpact of statin or omega-3-acid ethyl esters 90 (omega-3EE90; omega-3-acid ethyl esters 90 refers to amixture of ethylesters of n-3 fatty acids) on estimated cardiovascular disease(CVD) risk in community-based people with type 2 diabetesbut without known CVD and not taking lipid-lowering therapy.Methods A central computer will randomise 800 patients in59 UK general practices to atorvastatin (n=401, 20 mg/day)or placebo (n=399) and omega-3 EE90 (n=397, 2 g/day) orplacebo (n=403) in a concealed factorial manner. Participantswith LDL-cholesterol <2.6 mmol/l, triacylglycerol<1.5 mmol/l and estimated 10-year CVD risk <20% werecompared at 4 months.
The Medical - Public divide!
They’ll be queuingup for this one
SummaryAims The aim of the study is to examine theimpact of statin or omega-3-acid ethyl esters 90 (omega-3EE90; omega-3-acid ethyl esters 90 refers to amixture of ethylesters of n-3 fatty acids) on estimated cardiovascular disease(CVD) risk in community-based people with type 2 diabetesbut without known CVD and not taking lipid-lowering therapy.Methods A central computer will randomise 800 patients in59 UK general practices to atorvastatin (n=401, 20 mg/day)or placebo (n=399) and omega-3 EE90 (n=397, 2 g/day) orplacebo (n=403) in a concealed factorial manner. Participantswith LDL-cholesterol <2.6 mmol/l, triacylglycerol<1.5 mmol/l and estimated 10-year CVD risk <20% werecompared at 4 months.
The Medical - Public divide!
Yes doctor, it’s a very interesting study
7
8
9
64

Tuesday 15th February 2022 The Importance of Plain EnglishBernard Gudgin
SummaryAims The aim of the study is to examine theimpact of statin or omega-3-acid ethyl esters 90 (omega-3EE90; omega-3-acid ethyl esters 90 refers to amixture of ethylesters of n-3 fatty acids) on estimated cardiovascular disease(CVD) risk in community-based people with type 2 diabetesbut without known CVD and not taking lipid-lowering therapy.Methods A central computer will randomise 800 patients in59 UK general practices to atorvastatin (n=401, 20 mg/day)or placebo (n=399) and omega-3 EE90 (n=397, 2 g/day) orplacebo (n=403) in a concealed factorial manner. Participantswith LDL-cholesterol <2.6 mmol/l, triacylglycerol<1.5 mmol/l and estimated 10-year CVD risk <20% werecompared at 4 months.
The Medical - Public divide!
As a diabetic you are more at risk of a heart problem.Are you interested in taking part in a trial to see if statins
or fish oils may help you?
SummaryAims The aim of the study is to examine theimpact of statin or omega-3-acid ethyl esters 90 (omega-3EE90; omega-3-acid ethyl esters 90 refers to amixture of ethylesters of n-3 fatty acids) on estimated cardiovascular disease(CVD) risk in community-based people with type 2 diabetesbut without known CVD and not taking lipid-lowering therapy.Methods A central computer will randomise 800 patients in59 UK general practices to atorvastatin (n=401, 20 mg/day)or placebo (n=399) and omega-3 EE90 (n=397, 2 g/day) orplacebo (n=403) in a concealed factorial manner. Participantswith LDL-cholesterol <2.6 mmol/l, triacylglycerol<1.5 mmol/l and estimated 10-year CVD risk <20% werecompared at 4 months.
The Medical - Public divide!
That I can understand!
I hear what you say
Dear John
I want a man who knows what love is all aboutyou are generous kind thoughtful people whoare not like you admit to being useless andinferior you have ruined me for other men Iyearn for you I have no feelings whatsoeverwhen we're apart I can be forever happy willyou let me be yours
Gloria
10
11
12
65

Tuesday 15th February 2022 The Importance of Plain EnglishBernard Gudgin
Words Worth
Number of words in:
• Ten Commandments: 135
• The American Declaration of Independence: 300
• US Dept. of Agriculture, Directive on pricing of cabbages: 15,269
• European legislation on smoking: 24,942
• Brexit agreement: 586,108
Writing Plain English
My thanks to the Plain English Campaign http://www.plainenglish.co.uk
where you will find much information and many helpful guides
Some Tips - 1
• An average sentence should have a length of 15-20 words
• Be punchy
• Vary your writing style by mixing short sentences with longer ones
• Try to stick to one idea per sentence
• If you write a long sentence, try to break it up
13
14
15
66

Tuesday 15th February 2022 The Importance of Plain EnglishBernard Gudgin
Some Tips - 2
• Remember most sentences have a subject, a verb and an object
• Use active verbs
• Peter watched the television (active)
• The television was watched by Peter (passive)
• Use ‘you’ and ‘we’
• ‘You must send us…’, not ‘Applicants must send us…’
Some Tips - 3
• Don’t say: “The packet should be removed from the box. The contents should then be placed in the oven”
• Be direct: “Remove the packet from the box, then place it in the oven”
Some Tips - 4
• Avoid nominalizations! Examples:
Verb Nominalization
• Complete Completion
• Introduce Introduction
• Provide Provision
• Fail Failure
• Arrange Arrangement
• Investigate Investigation
16
17
18
67

Tuesday 15th February 2022 The Importance of Plain EnglishBernard Gudgin
Some Tips - 5
• Words to avoid
• Additional (extra)
• Applicant (you)
• Commence (start)
• Consequently (so)
• In respect of (for)
• Per annum (a year)
• Prior to (before)
• Intervention
• Procedure
Getting the Message Across
• What is it?, when is it?, where is it?, why is it?
• Write in simple English for, at least, both the “Plain English” summary and the PPI sections.
• Punctuation is free!
• The Gunning Fog index.
The Gunning fog index measures the readability of English writing. Texts for a wide audience need a fog index less than 12. Texts requiring near-universal understanding need an index less than 8.
The Gunning Fog Index
Fog Index
171312
96
Reading level
GraduateFresherSixth FormerHigh school fresher“Sun” reader
In the example we just saw it is 30!
19
20
21
68

Tuesday 15th February 2022 The Importance of Plain EnglishBernard Gudgin
Hywel Williams was brought up in the hillside village of Cymmer Afan in South Wales, where he attended the local comprehensive school. … Whilst training in dermatology at Kings, he published an article in the Lancet about a dog detecting skin cancer and was the first to suggest the possibility of canine cancer detection.
Sir Jonathan Van-Tam attended Boston Grammar School and graduated in medicine from the University of Nottingham. Why is he a good speaker? Partly it’s his manner – the gentleness and the composure – but also his language. He talks more simply and engagingly than other scientists (or the politicians standing alongside him). As far as possible he speaks in plain English. He uses metaphors and analogies drawn from everyday life (train journeys, football, etc). And on the rare occasion he does resort to scientific jargon, it’s in a wry way (“The South African variant – which, in the trade, we know as ‘B1.351’…”).
And Finally …
• I will be back on Thursday to speak about the importance of PPI
“Pray state, this day, on one side of a sheet of foolscap, how the Royal Navy is being adapted to meet the conditions of modern warfare.”
22
23
24
69

EGGA 2022 (15th – 17th February 2022)
Day 2: Showing Reviewers You Can Deliver I: The Research Plan
Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
70

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
The Research Plan:Expectations, Reviewers’ Concerns
& Common Confusions
Sophie Hyndman
Research Design Service South Central
EGGA, 16th February, 2022
‘Four Key Propositions’
• Importance: this project is important
• Success: this project can answer the question
• Value: this project is good value for money
• Competence: this team can deliver
RESEARCH PLAN
J. Aldridge & A. Derrington (2012) The Research Funding Toolkit, Sage
Research Plan
www.flickr.comRon Adams
www.flickr.comswiftjetsum626
By Vlastimil (originally posted to Flickr as Studentky) [CC BY-SA 2.0 (http://creativecommons.org/licenses/by-sa/2.0)], via Wikimedia Commons
By Kamyar Adl (Flickr) [CC BY 2.0 (http://creativecommons.org/licenses/by/2.0)], via Wikimedia Commons
By Jaykayfit (Own work) [CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
Public Domain via Wikimedia
Image: Leonardo da Vinci - Public Domain, courtesy of Wikimedia
Public Domain via Wikimedia
31st FW Balkan Operations Gantt chart. United States Air Force, 2000
NASA
RESEARCH PLAN
http://www.consort-statement.org/Media/Default/Downloads/CONSORT%202010%20Flow%20Diagram.pdf
1
2
3
71

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
Check specific guidance notes, but usually includes:
• Study design
Details of randomisation, allocation, blinding (If relevant)
• Setting, sampling & recruitment
• (if relevant) Intervention and comparator
• Data collection
• Outcome measures
• Data analysis
• Project management
Expected Sections
Referees need sufficient detail to gauge all this
What Referees Care About
• Will the research plan answer the research question?
• Is it appropriate & scientifically rigorous?
• Is it feasible?
• Will it deliver useful outputs?
Steindy (talk) 13:41, 18 November 2015 (UTC) [CC BY-SA 3.0 (https://creativecommons.org/licenses/by-sa/3.0)]
Literary Interlude
You don’t want this…
Clipartpanda.com
4
5
6
72

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
You want this…
• Funders don’t usually interview, so answer all questions that might be asked in your written application
Banksy; www.pixelstalk.net
Demonstrate Your Thinking
• Pre-empt criticism & confront it
Acknowledge weaknesses & remove or mitigate where possible
Discuss strengths over alternative approaches
There is rarely a perfect method!
Study DesignDetails
Public Domain via Wikimedia
http://www.consort-statement.org/Media/Default/Downloads/CONSORT%202010%20Flow%20Diagram.pdf
7
8
9
73

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
Will the design answer the research question?
What Referees Will Ask
What are the relative strengths & weaknesses?
How does the design compare to alternatives? Are the theoretical underpinnings of the
design suited to the nature of the question?
Might there be any practical implications in attempting to
implement the design?
Have patients/ service users/ carers/ relevant stakeholders been involved in the design?
Has a clear rationale been provided for the
study design?
Is the design clear?
Have the researchers consulted appropriate
methods experts?
What methods are used to ensure rigour?
What is the ontological & epistemological position of
the work?
Is randomisation procedure suitable?
Are relevant confounders accounted for?
Where relevant…
Are researchers familiar with the culture of the participating
organisations?
Is there any chance of contamination between
intervention & control arms?
Does the design use more than one method of data collection to facilitate
cross-checking (triangulation) of findings?
Is a clinical trials unit on board?
Are there any ethical issues in relation to the design that
need consideration?
ExamplesDescriptive study examining health beliefs based only on quantitative survey
An RCT involving sham surgery
An intervention run in 2 hospital wards compared to 2 ‘control’ wards in same hospital
A study of a nurse-patient interaction, where patients are consented before & interviewed after the interaction of interest
A before & after study of an intervention to reduce allergens in the home
A quasi-experiment of an intervention in one site compared with a control site
Lack of insight – need qualitative work
Will patients agree to take part?
Will intervention & control groups become contaminated?
Will there be systematic differences between sites affecting outcomes?
Are there seasonal patterns that will influence outcome?
Will researchers influence the intervention itself (Hawthorne Effect)?
What would you ask?
10
11
12
74

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
?Population
?Setting/ location
?Sampling method(s)
?Sample size
?Eligibility criteria
?Recruitment & Consent
Sampling & RecruitmentDetails
By Vlastimil (originally posted to Flickr as Studentky) [CC BY-SA 2.0 (http://creativecommons.org/licenses/by-sa/2.0)], via Wikimedia Commons
www.flickr.comRon Adams
By Kamyar Adl (Flickr) [CC BY 2.0 (http://creativecommons.org/licenses/by/2.0)], via Wikimedia Commons
Is the process of accessing, approaching, consenting &
enrolling potential participants ethical & suitable?
Does the stated population & setting relate sensibly to the research
question?
What Referees Will Ask
Is the sample size justified on a theoretical/ statistical basis?
Is recruitment likely to meet targets?
What are the eligibility criteria?
Have patients/ carers/ service users been consulted about
recruitment process?
How, when & by whom will eligibility criteria be applied?
Are sampling methods clearly stated & consistent with research
objectives?
Is the sample size clear?
ExamplesA study comparing two treatments with n=20
Study looking at barriers/ facilitators to quality improvement, interviewing only patients & nursing staff
A study of a rare disease in only three sites
A study looking at access to healthcare that has no plans to recruit non-English speakers
A study of carers of people with dementia
A study hoping to provide results to influence practice nationwide, based in one rural general practice
Need all key stakeholders
Need details of prevalence & likely will need many more sites
Need plans for outreach, interpretation and translation
Will this practice be representative of practices nationally?
Need clear process for how eligible people will be identified & consented
Likely to need a bigger sample; must be a proper sample size calculation
What would you ask?
13
14
15
75

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
?Product/ technology/
therapy
?Comparator
(Where relevant) Intervention Details
By Jaykayfit (Own work) [CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0)], via Wikimedia Commons
Is the intervention clearly described?
What is the current evidence to support it?
Can the intervention be applied properly &
consistently?
What is the rationale for the ‘dosing’ schedule?
What Referees Will Ask
Does it make sense for the group of interest?
Have the researchers considered the implications for the NHS?
Is the intervention novel?
What is the likelihood of effect relative to other
factors?
Can health/ social care professionals administer it?
Is the timing of the intervention clear?
Will participants adhere to the intervention?
Is the comparison group well described & sensible?
Will patients/ carers/ service users be happy
do it?
Will staff be happy to administer the intervention?
Is blinding/ a placebo necessary/
possible?
How will fidelity be ensured?
Are staff training plans adequate?
Are staff experiences or preferences an issue?
Are there any ethical issues in relation to the
intervention?
16
17
18
76

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
ExamplesA study using an evidence-based CBT intervention for a ‘new’ group of patients
The iterative development & testing of a training pack for nurses to help carers with patients with a long term condition
A study of an exercise package for patients with MS to be delivered over 6 months
An RCT of a novel surgical technique
A study of a new drug for children with considerable behavioural side effects
A comparison of an intervention with ‘treatment as usual’
Is the trail of causation clear & convincing?
Why the specific package? Why over 6 months? ‘Dose’ & rationale for it? Long term fidelity?
Evidence to support technique? Evidence that surgeons can use technique? Evidence that it is at RCT stage in research trajectory? Consideration of IDEAL Framework?
Will parents/ patients be willing to adhere to treatment?
Is this really novel & interesting enough to fund?
What is ‘treatment as usual’? What would you ask?
Data CollectionDetails
Public Domain via Wikimedia
What Referees Will AskAre the data types
appropriate for meeting the research objectives?
Are potential weaknesses of approaches identified &
addressed?
Is it clear what data collection methods are being used?
Are the data being collected at sensible times in relation to what
is being examined (e.g. intervention & follow-up)?
Have other potential options
been considered?
Is it clear what types of data are being
collected?
Is it clear who will collect the data, where & from
whom?
Is data collection sensible in relation to NHS structures &
pathways?
19
20
21
77

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
Have the ethical implications been considered?
Will missing data/ poor quality data be an issue?
If ‘big data’, are permissions& timelines accounted for?
Is the data collection process acceptable to patients/ carers/ service users?
Is data collection feasible?
Is blinding necessary/ feasible? Is sufficient expertise available to
ensure data of suitable quality?
ExamplesA prognostic study examining risk factors for knee osteoarthritis using a routine database
A study of risk factors for respiratory allergies using combined data from more than one routine dataset
Mixed staff & patient focus groups to explore implementation of a new multi-disciplinary intervention in an NHS rehabilitation setting
An intervention study requiring working age patients to attend hospital daily in the morning for a blood test
A survey of health & lifestyles using smartphones for data collectionHave issues of digital poverty been considered?
Will patients & different staff disciplines & grades be happy to share thoughts in mixed groups?
Can data be standardised across datasets?
Are all important risk factors & confounders reliably recorded in the database?Will the researchers have access to the data in time for the study start?
What would you ask?Will patients be able to attend clinics that regularly?
(Where relevant) Outcome MeasuresDetails
Image: Leonardo da Vinci - Public Domain, courtesy of Wikimedia
22
23
24
78

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
What Referees Will AskAre the outcome measures
appropriate for the research question?
Are the measures valid & reliable?
Are the measures relevant/ appropriate for the patient/
service user/ carer/ staff group of interest?
Are the outcome measures acceptable to patients/
service users/ carers/ staff ?
Do proxy measures correlate strongly with more important
outcomes?
Is the rationale for particular outcome measures clear?
Are outcome measures sensitive to the intervention
being evaluated?
Are the outcome measures properly
referenced?
Examples
A study using an activities of daily living measure for patients who are unable to walk
A comparison between two different interventions using an outcome measure derived from two others
A study using a tool developed for adults in a paediatric ward
A study requiring patients to have two extra biopsies for histological assessment
Using length of stay as the primary outcome in a study of a nursing quality intervention aimed at reducing pressure sores
Will the ADL measure be sensitive enough?
How valid & reliable will this measure be?
What would you ask?
Is length of stay, which is affected by many other things, a sensible primary outcome measure?
How valid & reliable will this measure be for children?
How acceptable would this be to patients?
Data AnalysisDetails
NASA
25
26
27
79

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
What Referees Will Ask
Will the analysis help achieve the aims & objectives?
Is specialist methodological input required?
Are the proposed methods suitable based on the type of data collected?
Is the analysis plan clear & thorough?Are the proposed methods suitable
based on the sampling approach?
Are appropriate guidelines or references highlighted?
Is blinding necessary/ feasible?
How will the data be prepared for analysis?
Examples
A randomised study comparing new & current treatment of bowel cancer based on percentage cancer-free at 6 months
A study comparing outcomes at 1, 3, 6, 9, 12, 24, 36 & 48 months post-randomisation
An interpretive phenomenological analysis to explore how participants experience an intervention
A natural experiment comparing the outcomes of a new exercise intervention for patients with COPD running in one trust compared with standard care in another
Does analysis suitably account for repeated measurements over time?
Is such a theoretical approach required to answer the question?
Would progression-free survival be preferable as primary outcome?
Will all potential confounding variables be accounted for in the analyses?
Does study account for stratification factors?
What would you ask?
31st FW Balkan Operations Gantt chart. United States Air Force, 2000
Project ManagementDetails
?Sponsorship & governance
?Ethics
?Management & advisory structures
?data management
?intellectual property
?timeline & milestones
28
29
30
80

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
What Referees Will Ask
Has the researcher given themselves enough time &
funding for each step?
Are stages of the study in a sensible order?
Is sponsorship appropriate & is it clear that ethics & governance
principles can be upheld?
Do they have the right researchers in the right place at the right time?
Have they got the right materials, equipment & space they need?
Are all other relevant permissions & approvals
in hand?
Is the proposed work feasible in the time
allocated?
How will data be entered & managed?
Have researchers considered the logistics of
sample transport & storage?
Do the arrangements for transcribing & storing interviews & focus groups meet the criteria for GDPR?
Do the researchers have ‘freedom to
operate’?
Do the Gantt charts & flow diagrams make sense?
Have all quality assurance issues been considered properly?
Have they got the support of other relevant
organisations?
Overall, will the project be well-managed? Will it
deliver?
Examples
One month set aside to obtain NHS ethics approval
A study of people with severe mental health difficulties
A study examining MRI images of the brain taken monthly over 6 months in 30 patients
An RCT followed by qualitative sub-study
A home-based physiotherapy intervention involving 100 patients and data collection over three weeks
Have consent procedures been thoroughly considered with reference to research ethics best practice?
Is access to the MRI planned appropriately & agreed?
Will the study fall behind schedule & have time to recruit/ analyse/ disseminate?
Is this logistically possible?Is the Clinical Research Network involved?
Could qualitative work run alongside RCT to reduce study length?
31
32
33
81

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
A clinical trial to evaluate a re-purposed drug for a new patient group
A study involving the regular collection of tissue samples
A study developing a new device for taking biopsies
Have MHRA costs & permissions been considered?Have researchers considered suppliers, packaging & placebo?Do they have a CTU involved?Is the pharmacy ‘on board’?Is there a Data Monitoring & Ethics Committee?
Have storage & transport issues been considered?Have issues related to the Human Tissue Act been considered?
Are there measures in place to capture intellectual property?Are appropriate regulatory requirements being addressed?
What would you ask?
More on project planning tomorrow
NASA via Wikipedia
Common Errors & Confusions
Clipart-Library.com
34
35
36
82

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
• Pilot versus feasibility studies - see: https://www.nihr.ac.uk/documents/nihr-research-for-patient-benefit-rfpb-programme-guidance-on-applying-for-feasibility-studies/20474
• A feasibility study for a trial versus testing the feasibility of an intervention
• Patient & Public Involvement ‘focus groups’ versus qualitative research
• Patient & Public Involvement versus patient participation (e.g. in co-design)
• ‘Quality of Life research’ versus ‘qualitative research’ versus ‘survey’
• Cost-effectiveness vs. cost-utility vs. cost-benefit vs. cost-consequence vs. cost-minimisation analysis
• Outcome measures versus ‘outcomes’
• ‘Outcomes’ versus ‘outputs’
• Primary outcome versus primary endpoint
• ‘Proof of principle’, ‘Proof of concept’
Worksheet
Use the list of questions provided, as you develop your own study, to help make your research plan reviewer-proof!
For list, see resource pack
37
38
39
83

Wednesday 16th February 2022 The Research Plan: Expectations, Reviewers’ Concerns & Common Confusions
Sophie Hyndman
40
84

EGGA 2022 (15th – 17th February 2022)
Day 2: Showing Reviewers You Can Deliver I: The Research Plan
Developing a Research Plan: a Worked Example
Mio Hu
85

Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
Developing a Research Plan: a Worked Example
Xiao-Yang (Mio) Hu
Research Design Service South Central
With acknowledgements to Sean Ewings, Southampton CTU
Study design
• Begin your project plan by stating your design, in a sentence
• “A double-blind, parallel randomised controlled trial”• “A prospective cohort study with nested qualitative study”
• The relevance to the objectives should be clear
• Level of justification required depends on:• Novelty of approach (or likely familiarity to audience)• Whether approach is the most obvious (at least initially)• Extent of limitations associated with the approach
What is the effectiveness of motivational interviewing compared
to usual care in uptake of pulmonary rehabilitation?
ExampleStudy design
1
2
3
86

Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
• Refine the face-to-face MI intervention for use over the telephone
Example
Objectives Design
• Determine the effectiveness of using clinician-delivered MI with respect to uptake and completion of PR amongst eligible patients
• Explore barriers and facilitators to delivering MI
• Assess the fidelity of the delivery of MI
• Explore acceptability and perceived utility of MI among patients and clinicians
• Determine the effectiveness of using clinician-delivered MI with respect to uptake and completion of PR amongst eligible patients
• INTERVENTION DEVELOPMENT
• Explore barriers and facilitators to delivering MI
• Assess the fidelity of the delivery of MI
• Explore acceptability and perceived utility of MI among patients and clinicians
Example
Objectives Design
• INTERVENTION DEVELOPMENT
• RANDOMISED CONTROLLED TRIAL
• Explore barriers and facilitators to delivering MI
• Assess the fidelity of the delivery of MI
• Explore acceptability and perceived utility of MI among patients and clinicians
Example
Objectives Design
4
5
6
87

Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
• INTERVENTION DEVELOPMENT
• PART OF RCT
• RANDOMISED CONTROLLED TRIAL
• Explore barriers and facilitators to delivering MI
• Explore acceptability and perceived utility of MI among patients and clinicians
Example
Objectives Design
• INTERVENTION DEVELOPMENT
• NESTED QUALITATIVE STUDY
• PART OF RCT
• RANDOMISED CONTROLLED TRIAL
• Explore barriers and facilitators to delivering MI
Example
Objectives Design
• INTERVENTION DEVELOPMENT
• NESTED QUALITATIVE STUDY
• NESTED QUALITATIVE STUDY
• PART OF RCT
• RANDOMISED CONTROLLED TRIAL
Example
Objectives Design
7
8
9
88

Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
This study is a RANDOMISED CONTROLLED TRIAL with NESTED QUALITATIVE STUDY and prior INTERVENTION DEVELOPMENT.
Example
Objectives Design
A simple statement of population of interest
• Supported by additional eligibility criteria and rationale
• Should include reference to setting of recruitment
Population
The population of interest are those referred to pulmonary rehabilitation via any route.
Inclusion criteria:• Telephone contact details (as this is how intervention is
delivered)• Able to converse in English
Individual PR programmes may not be able to deliver the intervention to non-English speakers; where this occurs, the individual will not be considered eligible for the study.
Example
Population
10
11
12
89

Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
Recruitment
Identification
Consent
Screening
Initial contact
Who will carry out these steps?
How does it fit in with current care
pathways?
CONSORT-style flow-chart
Identification
Consent
Screening
Initial contact
All people referred to participating PR programmes will be screened.
PR teams will identify those with telephone contact details.
Those who are eligible will be sent a participant information sheet by post detailing…
Consent will be audio-recorded over the phone.
Stages of recruitment example:
You should be realistic…
Lasagna’s law:
In clinical research the prevalence of any disease falls to about 10% of what you thought it was the day you start to look for cases for your study
Recruitment
13
14
15
90

Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
Required sample size: 350
“Easy!”
What is uptake likely to be?
Example
Recruitment
Required sample size: 350
“Previous work reported uptake of 50% and drop-out of 20%; this means we need to recruit 438 people and approach 876”
How many sites?
Example
Recruitment
Required number to approach: 876
“We see about 150 people per year; if we get 6 sites recruiting for 12 months, we’ll get our target”
But what about the
eligibility criteria?
Example
Recruitment
16
17
18
91

Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
“We see about 150 people per year; if we get 6 sites recruiting for 12 months, we’ll get our target”
“We see about 100 eligible people per year; if we get 9 sites recruiting for 12 months, we’ll get our target”
Do other sites see
similar figures?
Example
Recruitment
“We see about 150 people per year; if we get 6 sites recruiting for 12 months, we’ll get our target”
“We see about 100 eligible people per year; if we get 9 sites recruiting for 12 months, we’ll get our target”
“Overall, sites have a mean of 70 eligible people per year; if we get 11 sites recruiting for 14 months, we’ll get our target”
When will each site open?
Example
Recruitment
“We see about 150 people per year; if we get 6 sites recruiting for 12 months, we’ll get our target”
“We see about 100 eligible people per year; if we get 9 sites recruiting for 12 months, we’ll get our target”
“Overall, sites have a mean of 70 eligible people per year; if we get 11 sites recruiting for 14 months, we’ll get our target”
“With a staggered opening of two sites per month, we require 14 sites recruiting over 14 months.”
Example
Recruitment
19
20
21
92
Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
A local audit suggests 150 people per year come through our service. We will therefore recruit from 6 sites over 12 months in order to achieve our target sample size.
Based on previous studies, we anticipate uptake of 50% [REF] and retention of 80% [REF], suggesting we need to approach 876 to achieve a sample of size 438. A review of our study sites suggests a mean of 70 eligible people per year. We anticipate opening two sites per month, and will aim to open the larger sites earlier in the recruitment period; we will therefore recruit from 14 sites for 14 months.
versus
Example
Recruitment
CONSORT-style flow-chart
Identification
Study processes
Consent
Screening
Initial contact
What happens now a person is in
your study?
How does it fit in with current care
pathways?Data collection
E.g., randomisation
CONSORT-style flow-chart Study processes example
Screening
Randomisation
Consent
Intervention
Data collection
Control
Data collection
Allocation
Follow-up
Analysis
22
23
24
93

Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
Participants will be randomised to intervention or control.
How? When? In what ratio?
Example
Study processes: randomisation
Following consent, participants will be randomised to intervention or control in a 1:1 ratio, using an online randomisation service.
Example
Study processes: randomisation
Following consent, participants will be randomised to intervention or control in a 1:1 ratio, using an online randomisation service.
Allocation concealment and blinding upheld?
Example
Study processes: randomisation
25
26
27
94
Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
Following consent, participants will be randomised to intervention or control in a 1:1 ratio, using an online randomisation service to preserve allocation concealment. Blinding of participants, those delivering the intervention, and those collecting data will not be possible; however, given the objective nature of the primary outcome, we do not envisage this biasing the results.
Example
Study processes: blinding
Following consent, participants will be randomised to intervention or control in a 1:1 ratio, using an online randomisation service to preserve allocation concealment. Blinding of participants, those delivering the intervention, and those collecting data will not be possible; however, given the objective nature of the primary outcome, we do not envisage this biasing the results.
Example
Study processes: study arms
The intervention is a motivational interview.
How? When? Delivered by?
Example
Study processes: intervention
28
29
30
95

Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
The intervention is a motivational interview delivered over the phone by a trained healthcare professional. Consent for the call to be recorded will be requested (for fidelity-checking purposes); the call will continue unrecorded if consent is not obtained. Call times will vary, but are anticipated to last 15-20 minutes.
Example
Study processes: intervention
The control arm will follow usual care.
What does this look like?
Example
Study processes: control arm
The control arm will follow usual care, as practised by the participating PR programme. This is variable and may involve an appointment letter with or without a programme-specific information pack on PR.
Example
Study processes: control arm
31
32
33
96

Wednesday 16th February 2022 Developing a Research Plan: A Worked ExampleMio Hu
Outcome /Time Baseline First PR session Completion of PR
PR attendance X
PR completion X
MRC breathlessness
X X X
Is everything you are asking for justifiable?
Are the methods or tools you are using most
obviously suitable to answer your question?
Is it clear how the data will be collected?
Example
Study processes: data collection
Study processes
• Data analysis• Dissemination
• To be covered later…
Summary
• Design
• Which group of people are of interest?• Details of eligibility and rationale
• How will you get them into your study?• Are you clear this approach is feasible?
• What will happen to them once they are in your study?• Randomisation (where applicable)• Care received (where applicable; e.g., intervention)• Data collection
• What will you do with data?
• What will you do with results?
34
35
36
97

EGGA 2022 (15th – 17th February 2022)
Day 2: Showing Reviewers You Can Deliver I: The Research Plan
Writing Technical Sections: Introduction
Issy Reading
98

Wednesday 16th February 2022 Writing Technical Sections: IntroductionIssy Reading
Issy Reading
Research Design Service South Central
Writing Technical Sections
Technical sections?
Refers to methods to be used, i.e., descriptions of:
• Statistics
• Health economics
• Qualitative methods
The following sessions are about:
• Working with your methodologists:
– What to expect when working with a methodologist
– What the methodologists want from you
• Ensuring the technical details are adequately presented
The following sessions are not about:
• Teaching you methods
• Trying to replace the input from a methodologist
1
2
3
99

Wednesday 16th February 2022 Writing Technical Sections: IntroductionIssy Reading
Technical sections: funder’s guidance
Section Guidance
Plain English summary
Consider including design and methods used
Scientific abstract Potential headings/elements could include methods
Research plan Should provide “sufficient methodological detail” // Should address how the analysis will be conducted // Power calculation (where applicable) should be independently verifiable
Detailed project description
Methods heading. Can be considered as an extension to the Research Plan, allowing more details to be included and more discussion of choices.
Methodologists in the funding process
• All NIHR panels will have at least one each of a statistician, qualitative methodologist, and health economist
• The peer review process will include (at least one) methodological review
What are they looking for?
• Evidence that there is a sensible plan regarding anything related to their field: e.g., sampling, data collection, analysis
• Suitability of methodological input (co-applicants with suitable expertise; realistic costings)
4
5
6
100

Wednesday 16th February 2022 Writing Technical Sections: IntroductionIssy Reading
General points
• You should engage with your methodologists early – they generally prefer input early on
• It helps if you know (and can articulate) the literature - methodologists are often not clinical experts and will not know your area
• You have at least a vague idea of what you want to do
7
101

EGGA 2022 (15th – 17th February 2022)
Day 2: Showing Reviewers You Can Deliver I: The Research Plan
Writing Technical Sections I: Health Economics
Maria Chorozoglou
102

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
16th February 2022
Maria Chorozoglou, Senior Health EconomistResearch Design Service South Central
Writing Technical Sections I: Health Economics
◤
◤
📍 The concept of ‘health’ economics
📍 Economic study Examples
📍 Economic Evaluation (EE) with emphasis on EEACT
📍 CEA study Examples
📍 NIHR programmes and different HE work aspects
📍 Working with a HE
📍 Summary, Questions & Discussion
◤
◤
📍The concept of ‘health’ economics
1
2
3
103

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤Economic constraints on public sector budgets have increased the need for research on how best to allocate resources and deliver services that are efficient, equitable and offer good value for money.
The main economic concepts refer to two elements:
Scarcity + Opportunity cost
In a national health system, it is likely that the aim is to meet needs.
In the health care system however, there are not enough health care resources to meet all the health needs that people have (scarcity).
So, we have to choose which needs are met and which are not met (opportunity cost).
Common misconception
Costs in economics usually means opportunity costs.
This concept is quite different to the more familiar idea of financial costs, which is the cost of goods, services and scarce resources in terms of the money that must be paid to obtain them.
In practice, financial costs are very often used to measure opportunity costs, but this is not always the case.
HE refers to how society decides
◤
What do health economists do?
1
Conduct EE including decision analysis (modelling)
2
In the UK, NICE has a wider purview
3
Collect and assess information providing evidence to policy makers
4
Assess policy decisions -some time retrospectively
5
In a collectively-funded health care system, EA is grounded on the need to produce evidence to support decision-making
4
5
6
104

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
Economic Evaluation
(CEA, CUA, CBA, CCA)
Economic impact (COI)
analysis, Value of Information (VoI) analysis
Efficiency (or costs and benefits)
and
Equity
Policy Evaluation,
Implementation
◤
◤
📍Health Economic study Examples
Other Study design(s)
◤Publications in Southampton
Preschool hyperactivity is associated with long-term economic burden: evidence from a longitudinal health economic analysis of costs incurred across childhood, adolescence and young adulthood,
Association between 12-hr shifts and nursing resource use in an acute hospital: Longitudinal study,
.Societal costs of permanent childhood hearing loss at teen age: a cross-sectional cohort follow-up study of universal newborn hearing screening.
7
8
9
105

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤
Publications in Oxford
Health-related quality of life impact of minor and major bleeding events during dual antiplatelet therapy: a systematic literature review and patient preference elicitation study
Longitudinal medical resources and costs among type 2 diabetes patients participating in the Trial Evaluating Cardiovascular Outcomes with Sitagliptin (TECOS)
Accurate costs of blood transfusion: a micro-costing of administering blood
products in the United Kingdom National Health Service
◤
◤
📍Economic Evaluation (EE) with emphasis on EEACT
◤Economic case
Potential Economic RQs matching the Clinical need and supported by a strong economic argument
▪ Relevance to the needs and healthcare priorities of the NHS.
▪ How the proposed intervention or programme might influence clinical practice, for example:
▪ It is not sufficient to explore whether the technology works, it is equally important to explore how this will benefit the NHS and/or patients in real terms.
▪ Identifying challenges related to barriers and constraints to future uptake in the NHS, including implementation strategies.
10
11
12
106

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤
Health care is a massive ecosystem
Minimising Cost while Maximising benefits
EEACT - Economic Evaluation Alongside Clinical Trials
Typically, the first step in an EE is comparing intervention costs to
intervention outcomes, with the goal being to reduce costs and increase health
benefits
◤
Steps involved conducting EE within an RCT
1
Quantifying the cost and effect of care
2
Assessing whether and of how much average cost and effect differ among the treatment groups
3
Comparing the magnitude of differences in cost and effect an evaluation of the “value of the cost”, e.g., ICER
4
Identifying the population to whom the results apply
◤
Measuring Effect
Is the primary outcome suitable to be used for a CEA?
CUA - Quality of life instruments estimating QALYs -Is EQ-5D-5L suitable? Other? Children QoL?
When? at each follow-up visit (+ baseline)
Disease- or symptom-specific outcome measures?
QALYs have the advantage that they combine multiple dimensions of outcomes & understand how much we are willing to pay for a unit of effect.
13
14
15
107

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤
Measuring resource use and costs
▪ Explore resource use in healthcare
▪ Conduct cost analyses from different perspectives (health service, personal social services, social care, patient)
▪ Evaluate impact of interventions on days of lost productivity/education
▪Considerations:
▪ What - Healthcare resource use
▪ How - through questionnaires and e-records
▪ Intervention costs
▪ Other resource use and costs?
◤
Valuing Resource Use
Micro-costing vs PLICs vs NHS Reference Costs data
Health economics and quality of life in a feasibility study of paediatric acute appendicitis
Accurate costs of blood transfusion: a micro-costing of administering blood products in the United Kingdom National Health Service
Patient Level Information and Costing System (PLICS) Data
◤
◤
📍CEA study Examples
16
17
18
108

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤Cost-Effectiveness Publications
Cost-effectiveness of healthcare interventions for rare cancers: evidence from a systematic literature review and meta-analysis
Emollient bath additives for the treatment of childhood eczema (BATHE): multicentre pragmatic parallel group randomised controlled trial of clinical and cost effectiveness
Using “big data” in the cost-effectiveness analysis of next-generation sequencing technologies: challenges and potential solutions
The impact of hospital costing methods on cost-effectiveness analysis: a case study
Publications from Oxford & Southampton
◤
Aims and objectives section
▪ Describe the aims and objectives of the economic component
▪ Could be primary or secondary aims/objectives
▪ Case study:
▪ To evaluate the costs and health outcomes associated with high and low intensity physical exercise, and no exercise, for treating depression in adolescents
▪ To assess the cost-effectiveness, both within the trial period and extrapolating to the lifetime of patients, of these interventions, using a cost-utility analysis to determine the incremental cost per QALY gained
▪ Common error:
▪ No aim or objective related to the economic component of the work
◤Methods and analysis section (1)
• Describe what data will be collected and explain why
– Often need to collect secondary outcome measures related to the economic analysis
• Resource use (NHS, social care, patient personal resource use)
• Productivity data (e.g. time off work)
• Use of informal care
• Unit costs
• Health outcomes / quality of life
– How will this data be collected?
• Self-reported
• Questionnaires / instruments
• Interviews
• Routine data sources (medical notes, disease registries, Hospital Episode Statistics (HES), Clinical Practice Research Datalink (CPRD))
– When will this data be collected? Need to minimise patient burden
19
20
21
109

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤Methods and analysis section (3)
Explain how the health economics work will adhere to best practice guidelines
NICE guidance
Guide to the Methods of Technology Appraisal
Guide to the Methods for the Development of Public Health Guidance, NICE processes – Incorporating EE, using economic evidence to formulate guideline recommendations
Decision Support Unit Technical support document series
Consolidated health economic evaluation reporting standards (CHEERS) - Explanation and elaboration: A report of the ISPOR health economic evaluations publication guidelines good reporting practices task force
Case study: NICE guidelines and CHEERS guidelines should be referenced and followed
▪ Common error:
▪ Ignoring guidelines or not following them fully or correctly
◤
Methods and analysis section (4)
▪ When will the analysis be undertaken? Will there be an interim analysis e.g. feasibility/validity of methods?
▪ What will be done?
▪ Choice of analytical perspective & time horizon
▪ Dealing with missing data
▪ Sources of unit cost data
▪ Discounting – use of appropriate rates
▪ Reporting costs and outcomes
▪ Consideration of uncertainty
◤
Methods and analysis section (5)
▪Case study:
▪ NHS perspective
▪ Minimum one year follow-up; consider building in provision for longer-term follow-up (modelling?)
▪ Missing data – multiple imputation?
▪ Discount costs and health outcomes at 3.5%
▪ Sensitivity and subgroup analysis crucial:
▪ Does cost-effectiveness vary in patient subgroups (e.g. by presence of comorbidities)?
▪ Impact of adherence/uptake?
▪ Common error:
▪ Ignoring guidelines or not following them fully or correctly
22
23
24
110

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤
◤
📍 NIHR programmes and different HE work aspects
NIHR programmes
📍 Different programmes require highlighting different economic arguments in support of the proposed study. For example, CEA and CUA are commonly used alongside an RCT which is very common study design for clinical trials funded by the HTA programme.
While a broader and different perspective is taken when applying to the i4i programme. The key aim of the i4i programme is to encourage and provide support for projects which have a strong potential for commercialisation and acceptance for use within the NHS. This requires a different way of thinking for economic arguments to support the proposed study.
Equally SC and PH studies use a different approach too, heavily relying on observational, longitudinal or other quasi-experimental design(s).
This Photo by Unknown Author is licensed under CC BY‐NC
◤
Different programmes different HE input requirements
▪Health technology assessment (HTA)
▪ Health services and delivery research (HS&DR)
▪ The i4i programme
▪ Research for Patient Benefit (RfPB)
25
26
27
111

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤
◤
The economic
case for the i4i
programme
The application must contain an explanation of how adoption of the technology would change clinical practice and how the project will generate data to drive adoption - NICE guidelines (later in this slides).
RAND audit review states:
Encourage applicants to consider adoption, health economic analysis and product design issues at application and selection stages, …
Health economic analysis is increasingly important for product development and uptake but rarely visibly conducted at present by most funded projects.
… show whether the innovation is economically attractive ….
◤
Working with a health
economist
◤Where can you find a health economist?
• 7 health economists work as RDS advisors in the South Central region
Oxford:
– Elizabeth Stokes
– James Buchanan
– Jane Wolstenholme
– José Leal
– Ramón Luengo-Fernandez
– Rositsa Koleva-Kolarova
Southampton:
– James Raftery
– Maria Chorozoglou
28
29
30
112

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤
When to contact a health economist?▪ The earlier the better!
▪ If a health economist is involved from the start…
▪ Include most appropriate methods of collecting data on quality of life, resource use, costs
▪ Embed the health economics aspects of the project in the application
▪ Cost the health economist’s time appropriately
▪ In a full trial, all methods of data collection will need to be piloted and assessed for feasibility
▪ If in doubt, contact an RDS health economist
◤
What we need from you
▪You are the expert!
▪ You have more clinical expertise than us
▪ You know the clinical and scientific literature related to your topic better than us
▪ Be prepared to answer clinical and scientific queries to help us to refine plans for the health economics components of the application
◤
Study design - What preplanning should be done?
What medical service use should we measure?
In what form should the data be collected?
Which price weight (unit cost) estimates should be used for the study?
How naturalistic should the study design be?
What should we do if the full benefit and cost of therapy are not expected to be observed during the study period?
31
32
33
113

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤
How to work with your health economist: key tasks
▪ Ensure the economic question is stated clearly in the objectives
▪ Ensure that the question and choice of approach is justified in terms of what will be undertaken and delivered
▪ Ensure that the proposed data collection and analysis can be completed within the timeframe and budget of the grant
▪ Ensure that the proposed data collection will not be too much of a burden on patients
▪ Adhere to best practice guidelines
▪ Agree on the key milestones and deliverables
This Photoby Unknown Author is licensed under CC BY‐SA
◤
Budgeting for health economics
▪ Most health economists are project-funded – need to fully cover costs
▪ Sample costs:
▪ Salary for the lead HE and perhaps for a junior HE, fully costed for the study,
▪ Cost to allow for national and international conferences, e.g., £750 each for national conference, £2,000 each for international conference
▪ Training for junior researcher: £6,000
▪ Design of cost-effectiveness analysis (£3,000) and software (£500)
▪ Miscellaneous costs, including travel (£2,500)
◤
Reporting results and dissemination▪ How will you report the health
economics results?
▪ Will there be space in a combined paper with the clinical/scientific results?
▪ Reporting requirements for health economic work are increasingly strict
▪ In many cases, a separate publication to a specialist journal is the best solution
▪ Publication costs should be fully costed in the application and time should be set aside to prepare the publication
34
35
36
114

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤
Summary
Health Economics
Health economists can make a variety of valuable contributions to your grant application
Contact
Contact a health economist early in the grant writing process to maximise these benefits!
RDSMake an RDS health economist your first point of call
Work
Work with them collaboratively to ensure that the planned health economics is fully integrated with the other elements in the application
◤References Used in this presentation,University of Southampton
Griffiths, Peter, Saville, Christina, Ball, Jane E., Jones, Jeremy and Monks, Thomas , On behalf of the Safer Nursing Care Tool study team (2021) Beyond ratios - flexible and resilient nurse staffing options to deliver cost-effective hospital care and address staff shortages: a simulation and economic modelling study. International Journal of Nursing Studies, 117, [103901].(doi:10.1016/j.ijnurstu.2021.103901).
Griffiths, P., Saville, C., Ball, J. E., Jones, J., Monks, T., & On behalf of the Safer Nursing Care Tool study team (2021). Beyond ratios - flexible and resilient nurse staffing options to deliver cost-effective hospital care and address staff shortages: a simulation and economic modelling study. International Journal of Nursing Studies, 117, [103901]. https://doi.org/10.1016/j.ijnurstu.2021.103901
Santer, M., Ridd, M., Francis, N., Stuart, B., Rumsby, K., Chorozoglou, M., Becque, T., Roberts, A., Liddiard, L., Nollett, C., Hooper, J., Prude, M., Wood, W., Thomas, K., Thomas-Jones, E., Williams, H., & Little, P. (2018). Emollient bath additives for the treatment of childhood eczema (BATHE): multicentre pragmatic parallel group randomised controlled trial of clinical and cost effectiveness. BMJ, 361(8151), [k1332]. https://doi.org/10.1136/bmj.k1332
Chorozoglou, M., Reading, I., Eaton, S., Hutchings, N., & Hall, N. J. (2018). Health economics and quality of life in a feasibility RCT of paediatric acute appendicitis: a protocol study. BMJ Paediatrics Open, 2(1), [e000347]. https://doi.org/10.1136/bmjpo-2018-000347
Chorozoglou, M., Mahon, M., Pimperton, H., Worsfold, S., & Kennedy, C. (2018). Societal costs of permanent childhood hearing
loss at teen age: a cross-sectional cohort follow-up study of universal newborn hearing screening. BMJ Paediatrics
Open. https://doi.org/10.1136/bmjpo-2017-000228
Chorozoglou, M., Smith, E., Koerting, J., Thompson, M. J., Sayal, K., & Sonuga-Barke, E. J. S. (2015). Preschool hyperactivity is associated with long-term economic burden: evidence from a longitudinal health economic analysis of costs incurred across childhood, adolescence and young adulthood. Journal of Child Psychology and Psychiatry, 56(9), 966-975. https://doi.org/10.1111/jcpp.12437
◤References Used in this presentation,University of Oxford
Doble, B., Pufulete, M., Harris, J., Johnson, T., Lasserson, D., Reeves, B., & Wordsworth , S. (2018). Health-related quality of life impact of minor and major bleeding events during dual antiplatelet therapy: A systematic literature review and patient preference elicitation study. Health and Quality of Life Outcomes, 16, [191]. https://doi.org/10.1186/s12955-018-1019-3
Reed SD, Li Y, Leal J, Radican L, Adler AI, Alfredsson J, Buse JB, Green JB, Kaufman KD, Riefflin A, Van de Werf F, Peterson ED, Gray AM, Holman RR; TECOS Study Group. Longitudinal medical resources and costs among type 2 diabetes patients participating in the Trial Evaluating Cardiovascular Outcomes with Sitagliptin (TECOS). Diabetes Obes Metab. 2018 Jul;20(7):1732-1739. doi: 10.1111/dom.13292. Epub 2018 Apr 20. PMID: 29573215.
Stokes EA, Wordsworth S, Staves J, Mundy N, Skelly J, Radford K, Stanworth SJ. Accurate costs of blood transfusion: a microcosting of administering blood products in the United Kingdom National Health Service. Transfusion. 2018 Apr;58(4):846-853. doi: 10.1111/trf.14493. Epub 2018 Jan 30. PMID: 29380872.
Rodriguez-Martin, A.-M., Zacharopoulou, P., Hassan, A. B., & Tsiachristas, A. (2018). Cost-effectiveness of healthcare interventions for rare cancers: Evidence from a systematic literature review and meta-analysis. Journal of Cancer Policy, 18(2018), 1–10.
Wordsworth S, Doble B, Payne K, Buchanan J, Marshall DA, McCabe C, Regier DA. Using "Big Data" in the Cost-Effectiveness Analysis of Next-Generation Sequencing Technologies: Challenges and Potential Solutions. Value Health. 2018 Sep;21(9):1048-1053. doi: 10.1016/j.jval.2018.06.016. Epub 2018 Aug 17. Erratum in: Value Health. 2019 Apr;22(4):502. PMID: 30224108.
Leal J, Manetti S, Buchanan J. The Impact of Hospital Costing Methods on Cost-Effectiveness Analysis: A Case Study. Pharmacoeconomics. 2018 Oct;36(10):1263-1272. doi: 10.1007/s40273-018-0673-y. Erratum in: Pharmacoeconomics. 2019 Jun;37(6):867. PMID: 29785689; PMCID: PMC6132447.
37
38
39
115

Wednesday 16th February 2022 Writing Technical Sections I: Health EconomicsMaria Chorozoglou
◤Photos & Graphics:
Photos from Unknown Authors licensed under CC BY
Graphics from Glasgow Caledonian University
Any questions?
40
41
116

EGGA 2022 (15th – 17th February 2022)
Day 2: Showing Reviewers You Can Deliver I: The Research Plan
Writing Technical Sections II: Statistics
Joanna Moschandreas
117
Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Writing Technical Sections II: Statistics
Joanna MoschandreasResearch Design Service South Central
EGGA, 16th February 2022
With thanks to Amy Whitehead for the use of her slides
The statistician who supposes that his main contribution
to the planning of an experiment will involve statistical
theory, finds repeatedly that he makes his most valuable contribution simply by persuading the
investigator to explain why he wishes to do the experiment
- Gertrude M Cox1900-1978
Statistician
Two important statistical components in a grant application
• Calculate sample size and write up justification• Formulate a brief analysis plan
1
2
3
118
Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Calculating sample sizes:
What’s the question?Common types of questions:
• Comparative
– Is a strengthening and stretching programme for people with rheumatoid arthritis better than current care?
• Descriptive
– What is the prevalence of sedation in critical care units?
– What is the association between self-reported and measured physical activity?
– What are the recruitment and drop-out rates?
Sample size –Comparative Studies
Calculating sample sizes:
Comparative studiesA statistician needs to know:
• Study design
• Effect size
• Measure of variability
• Desired power
• Desired Type I error rate
Sample sizes for comparative studies are power-based
4
5
6
119

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Calculating sample sizes:
Study design
• Many issues here can feed into sample size calculation, e.g.
– Number of groups
– Whether the study involves repeated measures
or independent groups
– Type of randomisation e.g. individual or clustered
– Primary outcome
Calculating sample sizes - Comparative studies:
Effect sizeWhat is an effect size?
• In this situation, an effect size (“target difference”) is a difference between groups
• In a well-designed study, this is equivalent to the effect of the intervention or behaviour of interest
• It is expressed in the units of the primary outcome
• The choice of an effect size relates to the following:
• “Should this effect size exist, we want a good chance of
ruling out there being no effect”
Calculating sample sizes - Comparative studies:
Effect sizeWhere should it come from?
• This is a clinical decision• Ideally this is the smallest value that would lead to a change in
practice; i.e., what level of superiority is required of the new intervention or behaviour to convince us it is worth investing in (sometimes called the minimal clinically important difference)
• If you’re fortunate, someone will have researched into clinically meaningful changes already
• E.g., various work suggests changes between 15 and 60m in the 6-minute walk test for people with COPD is important
7
8
9
120

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Calculating sample sizes - Comparative studies:
Effect sizeWhere should it come from?
• If no literature…• Clinical judgement and reasoning may be an alternative, but
will need justifying
• Statisticians should not be responsible for this• In some circumstances, where a suitable effect size cannot be
found, a statistician can help you take a more generic approach that does not require this info
Calculating sample sizes - Comparative studies:
Effect size considerations
Difference
Sam
ple
size
req
uire
d
• The smaller the effect, the bigger the sample size
• A choice too small will raise questions about how important the difference really is
• A choice too large will raise questions about whether a useful difference could be missed
Calculating sample sizes - Comparative studies:
VariabilityWhat?• For a continuous outcome, this is the standard deviation (or variance) of your
primary outcome• For a binary outcome, all we need is the baseline rate/proportion
Where from?• Pilot data
• Other research in the literature (baseline data)• Would prioritise study quality, similarity of populations to
yours, sample size (larger is better)
• If an estimate cannot be found, a statistician can help with a generic approach to sample size calculation not requiring this info
10
11
12
121

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Calculating sample sizes - Comparative studies:
Variability considerations
• Estimates of variability can be combined across studies
• The larger the variability, the bigger the required sample size
Calculating sample sizes:
Comparative studiesA statistician needs to know:
• Study design
• Effect size
• Measure of variability
• Desired power
• Desired Type I error rate
Sample sizes for comparative studies are power-based
Calculating sample sizes - Comparative studies:
Power and error rates
What?
• Both relate to how willing you are to make a mistake
Where from?
• These are largely set by convention• Power commonly 80% or 90% (push for more
studies to use 90%)• Type I error rate 5%
• Only in very particular circumstances would you consider alternatives (e.g. phase II study); your statistician will advise
Type I ErrorFalse Positive
Type II ErrorFalse Negative
“There’s nothing to fear, it’s just a cat”
“There’s a fierce lion at the window!”
“Looking for a signal of danger”
13
14
15
122

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Calculating sample sizes - Comparative studies:
What to expect
• The considerations we’ve discussed are not always fixed in stone; there are often decisions to be made
• It is not uncommon to consider a range of scenarios; for example, your statistician may present you with:
Effect size Drop-out (%) Total sample size
0.3 10 524
20 588
0.4 10 296
20 334
Sample size –Descriptive Studies
Calculating sample sizes:
Descriptive studiesA statistician needs to know:
• What analysis will be performed (which they can advise on) and is of most interest
– These sorts of questions usually involve estimating a correlation or proportion
• A planning value for the statistic of interest
• A desired level of precision
Sample sizes for descriptive studies are precision-based
16
17
18
123

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Calculating sample sizes – Descriptive studies:
Planning valuesWhat is a planning value?• A prior belief in what the correlation or proportion of interest might
be• This is because precision depends on their value
Where should it come from?• Pilot data
• Relevant literature
• If no information at all, we can use what is the “worst-case scenario” in statistical (not clinical) terms (i.e., ensure that the precision is no worse than some desired level)
Calculating sample sizes – Descriptive studies:
Level of precisionWhat is precision?
• Precision is given by a confidence interval (formed by lower and upper limits), usually 95%
• We define what is an acceptable level of precision, equivalent to pre-specifying the width of the confidence interval
Where should it come from?
• This should be clinically-driven• The interval should be at least narrow enough to
meaningfully progress our knowledge
Calculating sample sizes - Descriptive studies:
What to expect
• It is again not uncommon to consider a range of scenarios; for example:
Planningvalue for
proportion
Desired 95% CI width
Approx. anticipated
95% CI
Sample size
0.5 0.1 0.45 to 0.55 385
0.2 0.40 to 0.60 97
0.3 0.1 0.25 to 0.35 323
0.2 0.20 to 0.40 81
19
20
21
124

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Calculating sample sizes:
Other info
• A sample size calculation may also include a precautionary inflation to account for drop-out• Estimates of drop-out would ideally come from previous literature
Other common considerations:• Studies using survival data require info on event rates, follow-up, type of
censoring…• Studies that are cluster-randomised require info on level of correlation
expected within clusters, number and size of clusters…
Calculating sample sizes:
Furthermore…
Sample size is inherently related to other considerations:
Consideration Source of information
No. of recruitment sites required
• Rates of eligible people per site
• Length of recruitment period
Review of site files; experience
Length of recruitment period• Number of sites
• Rates of uptake
Previous research; clinical judgement
Calculating sample sizes:
Putting it all together
• A sample size should be independently verifiable (and panels will check!)
• So any information your statistician used to inform the calculation should be presented• E.g., for a comparative study, you need an effect size, measure of variability, power and
type I error rate as a minimum
• You may include alternative scenarios (e.g., what happens if drop-out is higher than expected)
22
23
24
125

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Calculating sample sizes:
Putting it all together
Section Example
Plain English summary We will aim to recruit 387 participants.
Scientific abstract Based on a mean difference of 2, standard deviation of 4.4, 90% power and Type I error rate of 5%, and accounting for 20% drop-out, we require 129 participants per treatment group or 387 participants overall.
Calculating sample sizes:
Putting it all together
The research plan should go into more detail…
“After consultation with a statistician, the sample size was determined to be 387.”
Calculating sample sizes:
Putting it all together“The sample size is based on the primary analysis of comparing theintervention and control arms on the PHQ-A at one year post-randomisation. Based on a clinically important mean difference of 2 points[Ashworth et al., 2008], a standard deviation of 4.4 [Richardson et al.,2010], 90% power and Type I error rate of 5%, we require a total of 103participants per treatment group. Based on previous studies in similarpopulations, we will aim to recruit 387 participants in total to account forup to 20% drop-out. An average size centre will see approximately 9eligible patients per month, assuming we can recruit a third of thesepatients, over the 18 month recruitment period, we would require 10centres to recruit the required sample size”
25
26
27
126

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Calculating sample sizes:
Putting it all together“The sample size is based on the primary analysis of comparing theintervention and control arms on the PHQ-A at one year post-randomisation. Based on a clinically important mean difference of 2 points[Ashworth et al., 2008], a standard deviation of 4.4 [Richardson et al.,2010], 90% power and Type I error rate of 5%, we require a total of 103participants per treatment group. Based on previous studies in similarpopulations, we will aim to recruit 387 participants in total to account forup to 20% drop-out. An average size centre will see approximately 9eligible patients per month, assuming we can recruit a third of thesepatients, over the 18 month recruitment period, we would require 10centres to recruit the required sample size”
Useful reminder of primary purpose of study
Calculating sample sizes:
Putting it all together“The sample size is based on the primary analysis of comparing theintervention and control arms on the PHQ-A at one year post-randomisation. Based on a clinically important mean difference of 2 points[Ashworth et al., 2008], a standard deviation of 4.4 [Richardson et al.,2010], 90% power and Type I error rate of 5%, we require a total of 103participants per treatment group. Based on previous studies in similarpopulations, we will aim to recruit 387 participants in total to account forup to 20% drop-out. An average size centre will see approximately 9eligible patients per month, assuming we can recruit a third of thesepatients, over the 18 month recruitment period, we would require 10centres to recruit the required sample size”
Primary outcome (and timing)
Calculating sample sizes:
Putting it all together“The sample size is based on the primary analysis of comparing theintervention and control arms on the PHQ-A at one year post-randomisation. Based on a clinically important mean difference of 2 points[Ashworth et al., 2008], a standard deviation of 4.4 [Richardson et al.,2010], 90% power and Type I error rate of 5%, we require a total of 103participants per treatment group. Based on previous studies in similarpopulations, we will aim to recruit 387 participants in total to account forup to 20% drop-out. An average size centre will see approximately 9eligible patients per month, assuming we can recruit a third of thesepatients, over the 18 month recruitment period, we would require 10centres to recruit the required sample size”
Values necessary to recreate the calculation
28
29
30
127

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Calculating sample sizes:
Putting it all together“The sample size is based on the primary analysis of comparing theintervention and control arms on the PHQ-A at one year post-randomisation. Based on a clinically important mean difference of 2 points[Ashworth et al., 2008], a standard deviation of 4.4 [Richardson et al.,2010], 90% power and Type I error rate of 5%, we require a total of 103participants per treatment group. Based on previous studies in similarpopulations, we will aim to recruit 387 participants in total to account forup to 20% drop-out. An average size centre will see approximately 9eligible patients per month, assuming we can recruit a third of thesepatients, over the 18 month recruitment period, we would require 10centres to recruit the required sample size”
Extra information going into final target
Calculating sample sizes:
Putting it all together“The sample size is based on the primary analysis of comparing theintervention and control arms on the PHQ-A at one year post-randomisation. Based on a clinically important mean difference of 2 points[Ashworth et al., 2008], a standard deviation of 4.4 [Richardson et al.,2010], 90% power and Type I error rate of 5%, we require a total of 103participants per treatment group. Based on previous studies in similarpopulations, we will aim to recruit 387 participants in total to account forup to 20% drop-out. An average size centre will see approximately 9eligible patients per month, assuming we can recruit a third of thesepatients, over the 18 month recruitment period, we would require 10centres to recruit the required sample size”
Extra information for recruitment
Calculating sample sizes:
Putting it all together
• The detailed project description can go into more detail; e.g.,
• More comprehensive overview of the relevant literature (e.g., different recommended effect sizes) and justification
• Different scenarios that were considered
31
32
33
128

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Analysis Plan
Analysis description:
Putting it all together
• The analysis should be consistent with your study objectives and your sample size calculation
• If your objective is to compare groups, the sample size should be power-based and the main analysis should be about comparing the groups through a statistical test
• If your objectives are around estimation, the sample size should be based on this, perhaps precision-based and the appropriate analysis would be descriptive
Analysis section:
Putting it all together
Section Example
Plain English summaryParticipants will be randomly put into one of three groups: Group one will be usual care which will consist of contact with a psychologist, Group two will receive usual care plus a programme of high intensity exercise and Group three will receive usual care plus a programme of low intensity exercise. After following up the participants for one year we will compare the scores on a questionnaire measuring depression level between the groups to look at the effect of exercise on the participants.
34
35
36
129

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Analysis section:
Putting it all together
Section Example
Scientific abstractThis trial is a multicentre, three-arm, individually randomised, parallel-group, double blind, superiority randomised controlled trial, which intends to recruit from 10 centres over 18 months with one year of follow up. The primary analysis will use an ANCOVA model adjusted for stratification factors and baseline outcome measure. A two-sided p-value of 0.05 or less will be used to declare statistical significance for all analyses and results will be presented with 95% confidence intervals.
Analysis section:
Putting it all togetherThe research plan should go into more detail…“Three-arm, individually randomised, parallel-group, double-blind superiority randomised control trial recruiting over 10 centres for 18 months with one year follow up. Participants will be randomised on a 1:1:1 ratio to usual care (as defined above), usual care plus high intensity exercise or usual care plus low intensity exercise.
Randomisation will be conducted through an online system using stratified block randomisation with variable block sizes. Stratification factors will include, gender, previous pharmacological therapy use and baseline depression score.
The primary analysis will be conducted using an ANCOVA model adjusted for randomisation stratification factors on an intention-to-treat population. A two-sided p-value of 0.05 or less will be used to declare statistical significance for all analyses and results will be presented with 95% confidence intervals.
If missingness accounts for more than 10% of the sample, approaches for dealing with missing data (e.g. multiple imputation) will be discussed with the trial oversight committees.”
Time Commitment
37
38
39
130

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Time – Costing in a statisticianTrial development Trial set-up Trial management Trial close out
Attend trial development group meetings
Advise on method of randomisation
Write the analysis plan
Sample size calculation
Write the statistical sections of the grant application
Respond to reviewers/ boards comments
Attend trial management meetings
Input into the protocol development
Aid in the design of the database and case report forms
Help design and test the randomisation system
Prepare the randomisation and concealment lists
Attend trial management meetings
Prepare the reports and analysis for the DMEC
Attend DMEC meetings
Carry out any interim analyses
Write the statistical analysis plan
Help with any statistical queries
Involved in protocol amendments
Involved in central monitoring of accumulating data
Prepare statistical code for the final analysis
Support the process of data cleaning and final download from the database
Undertake the final analysis
Contribute to the study report
Contribute to publications of trial results
Common Problems
Common Problems
• Engaging with your statistician too late
• Repeatedly or belatedly changing the primary outcome (or any major component of the sample size calculation)
• Leaving a statistician with a clinical judgement call
• Removing details from the statistics sections without checking with your statistician first
40
41
42
131

Wednesday 16th February 2022 Writing Technical Sections II: StatisticsJoanna Moschandreas
Common Problems
• Sample size calculation based on continuous outcome when the primary outcome is in fact binary
• Wrong study design or within-group comparisons rather than between-group comparisons
• Estimated treatment effect too big – clinically unrealistic
• Sample size too big to be feasible within the time frame
• Have not taken into account losses to follow-up or even treatment cross-over
• Not enough details for others to replicate the calculation
Thank you
43
44
132
EGGA 2022 (15th – 17th February 2022)
Day 2: Showing Reviewers You Can Deliver I: The Research Plan
Writing Technical Sections III: Qualitative Studies
Jane Vennik
133

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
Essential Guide to Grant Applications 2022
Dr Jane Vennik on behalf of the qualitative research advisers from
Research Design Service South Central
Writing Technical Sections III: Qualitative Studies
What to expect from this session
When to use Qualitative research
Common funder criticisms
Writing technical sections
Practicalities (i.e. cost, ethics)
Questions and answers
Not a teaching session on qualitative methodologies
not
1. I’m not sure what qualitative research is
2. I have limited knowledge or experience of qualitative research
3. I have conducted some qualitative research
4. I have led qualitative research projects.
How much experience do you have with qualitative research?
1
2
3
134

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
What is qualitative research?
• A broad term which encompasses a range of approaches and methods
• Concerned with the meanings people attach to their experiences of the social world, and how they make sense of that world (Mays & Pope 2006;p3)
• Used to explore the behaviour, perspectives and experiences of people they study (Holloway, 1997;p2)
Why use qualitative approaches?
Types of Qualitative Questions
‘What’, ‘How’ and ‘Why’ questions- About patient voice and experience
Why do young people not adhere to their asthma medication?
- About complex organisations, events, processesHow do doctors communicate prognosis to people at the end of life?
- Exploring a new area or a sensitive topicHow do couples come to terms with a stillbirth?
- Optimising study processes, recruitment and implementationWhat factors affect patients’ decisions to participate in a trial?
- Developing and evaluating complex interventionsWhat do clinicians think about intervention components?How to patients engage with the intervention?
4
5
6
135

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
Quantitative Qualitative
• Objective • Subjective
• Purpose: generalisability; prediction; explanation
• Purpose: contextualising;interpreting; understanding
• Tests hypotheses, theories • Develops hypotheses, theories
• Questions: ‘how many?’, ‘how much?’, ‘how often?’
• Questions: ‘how?’, ‘why?’ ‘what?’
• Data type: numbers • Data type: words, objects, pictures, observations
Qualitative vs quantitative approaches
When to use Qualitative research
1. Qualitative on its own – exploring perceptions, attitudes, experiences, observing and analysing behaviour…describing, or building a theory.
2. Qualitative then quantitative (mixed methods – exploratory) – to discover the most comprehensible terms or important issues for a questionnaire. Or exploratory work prior to the main quantitative work.
3. Quantitative then qualitative (mixed methods – explanatory) – to expand and clarify on issues arising from quantitative data.
4. Qualitative plus quantitative (mixed methods - triangulation) –common in large-scale projects.
What are GPs’ views and experiences of prescribing antibiotics for acute respiratory tract infections?
9
How do patients perceive education on treatment options for chronic kidney disease?
Use appropriate question word
Identify participant group
Use qualitative wording
Identify broad topic of interest
Specify topic of interest
Formulating a qualitative research question
7
8
9
136

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
Research topic 1: Covid Vaccines and pregnancy
Research topic 2: Prehabilitation and hip/knee surgery
Comparing qualitative research and PPI
Participation Involvement
Taking part in a study as a research participant.
Involved in shaping research by being part of the research team or as a research collaborator
• Taking part in qualitative interviews or focus groups with the aim being research.
• User‐testing of interventions
• Co‐applicant• Stakeholder group member• Involved in priority setting,
reviewing documents, analysis, interpretation, dissemination activities.
• May include focus groups – with the aim of priority setting.
What to avoid - common pitfalls
10
11
12
137

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
Funder main Issues
2018 and 2019
A number of predominately quantitative‐focused research proposals included a warranted, but poorly developed, qualitative research element.
Qualitative and mixed methods project designs where the theoretical grounding and methodologies were not of the same high standard as those for quantitative research proposals.
Funder main IssuesSection Criticism
Rationale Poorly justified/inadequate
Methods Not aligned to research question/aims/objectives
Data collection Inadequate detail of method
Analysis No rationale/ missing detail for proposed analysis method
Timeline Unrealistic /not shown on Gantt chart
Ethics Lack of awareness/sensitivity of issues
Team Lack of qualitative expertise on team
Impact Over/understating impact
Inaccuracies Talking about generalisability/conflating QoL/Survey
Costs Over or under costed
Lack of understanding
Of types of qualitative approaches
PPI Confusing PPI with qualitative research
Rigour No or inadequate mention of approaches. Lack of, or inappropriate, quality criteria
How to write the technical sections for a qualitative study
13
14
15
138

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
Background, rationale, aims & objectives
• Why is this research important?
• What are the gaps in the literature?
• What type of study do you intend to do?
• Leading to specification of clear aims and objectives
Example:
Aim: To explore patients’ and clinicians’ views and perspectives of the [intervention] to inform a definitive trial.
Objective: To explore patient acceptability and adherence to the [intervention] through qualitative semi-structured interviews
Study Design
• Informed by question, aims and objectives
• (Philosophical underpinning)
• How it fits other work planned in the application
• Other practical considerations
Example: This is a feasibility study with a pragmatic nested qualitative component using semi-structured face-to-face interviews and thematic analysis.
Study population & recruitment
• Who is your study population?
• What are the eligibility criteria?
• How will potential participants be identified and by whom?
• What will the recruitment process be?
Example: Help-seeking adolescents with depression will be identified from primary care and purposively sampled from both interventions arms of the trial population. A letter, reply slip and participant information sheet from the research team will be sent by post or email to the adolescents inviting them to participate in a face-to-face semi-structured interview. Interested participants will return the reply slip to the research team who will then arrange an interview time.
16
17
18
139

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
Sampling strategy
• What sorts of participants are you looking for?• What sampling strategy will you use to achieve this?
• Convenience sampling (available)• Purposive sampling (with purpose)
• Maximum variation• Homogenous sampling• Snowball sampling (through referral)
• Theoretical sampling (grounded theory)
Purposive maximum variation sampling will be used to include participants with a range of ages, gender, co-morbidities and socio-demographics.
Sample size• Large numbers not needed
• emphasis is on richness and depth of data and analysis
• Depends on a number of factors• Data saturation– i.e. when the researcher is no longer hearing or
seeing new information• Information power – the more relevant information the sample
holds the fewer participants needed (i.e richness of data)
• Rule of thumb: • between 20 and 30 participants for individual interviews• around 3-5 focus groups (6-10 per group).
Example: We will conduct 20-30 in-depth semi-structured interviews which we consider will provide sufficient depth of data for analysis to answer our research question.
Data collection
• How will your data be collected?
• Who will collect the data, when and where?
• How will data be made available for analysis?
Example: Semi-structured face-to-face interviews will be conducted using an interview schedule to guide the interviews. The interview schedule was developed with patient and public involvement input, existing literature and input from clinicians. The interviews will be held in the GP surgery and will be approximately 45-60 minutes duration. The interviews will be digitally recorded and transcribed verbatim for analysis.
19
20
21
140

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
Data collection
The research question is about…. Source of dataBeliefs, feelings, perceptions, ideas about a topic, concept, intervention or illness
Interviews, focus groups, diaries,websites, media articles, open-ended sections in survey
Group norms and shared experiences, exploring socially marginalised
Focus groups, websites, media articles
Behaviours in natural settings, cultures, examining situations or process, impact of technologies or interventions
Observation e.g. ethnography, video recordings
Development of a validated questionnaire or set of core outcomes
Focus groups, cognitive interviews
Feasibility and acceptability of an intervention or study design or process and barriers and facilitators
Interview, focus group, diaries, observation
Developing and evaluating complex interventions Think aloud interviews, case vignettes, interviews
Data analysis and management
• Informed by research question, time & resources available
• Define and justify your chosen analytical method
• Describe how data is managed
• Describe the process of analysis• Six main analysis types: thematic, framework, grounded theory,
conversation, content and Interpretive Phenomenological Analysis
Example: Analysis & transcription of interviews will start as soon as data collection commences. Transcripts will be analysed using thematic analysis (Braun & Clarke, 2006). Analysis will involve familiarisation of the data, constant comparison, identification of initial codes anditerative development of themes and relationship between themes. NVivo qualitative data management software will facilitate management of the dataset.
Gantt chart and timeline
Month of study ‐4 to
‐1
1 2 3 4 5 6 7 8 9 10 11 12
Ethics and R&D approvals
Study set up
Recruitment
Data collection (Interviews)
Data analysis
Data interpretation
PPI meetings
Report/publication writing
22
23
24
141

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
Example: Written informed consent will be obtained before interviews are conducted. All interviews will be anonymisedon transcription. Any identifiable information will be removed from excerpts included in publications and all data stored on an encrypted hard drive.
• Consent • Anonymity and confidentiality• Data storage and data protection• Dealing with distress, need further information/
disclose illegal activity etc.
Ethical issues
Patient and Public Involvement
• Help develop the interview schedule • Identify recruitment and data collection strategies• Support data analysis (e.g. secondary coding, discuss
emerging themes, confirm findings)• Interpretation of findings• Support dissemination
Research Team• An experienced qualitative researcher as either lead or co–applicant on
your team
• specify the role, commitment and costs.
• State relevant expertise
• Consider who will actually carry out the qualitative research
• ensure that you cost for qualitative research assistant
Example: Dr Wood who is experienced in supervising and leading qualitative work in primary care and alcohol studies will lead the qualitative workstream and supervise the qualitative research assistant to undertake the interviews and analysis.
25
26
27
142

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
Role of a qualitative expert
Dissemination and Impact
Dissemination Uptake and Use Impact on Health Decisions and Outcomes
PresentationsPublications
Other metricsPatient/public websites
Adoption/IntegrationGuidelines
Policies
Changes in CareHealth decisions,
Outcomes
Example: A paper on the qualitative nested study will be submitted to the British Journal of General Practice, and presented at conferences. Findings from the study will be used to inform PPI group meetings when planning the main trial.
Costs
Staff costs and time Salaries for qualitative co‐applicant and research assistant
PPI costs Time, travel, subsistence, room hire, training
Data management software & training
Nvivo /Atlas
Recruitment costs Research and service support costs
Equipment Interviews & focus groups: Encrypted digital recorder, telephone adaptorObservational: Encrypted video recorder
Conducting interviews or focus groups
Travel/phone costs or location costs. Vouchers
Transcription Depth interviews, focus groups
Publication Open access, conference fees, etc
Archiving Institution/departmental costs for this
28
29
30
143

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
Summary sections
Section Example
Plain English summary
We will speak to 20‐30 adults from doctors surgeries who have been found to be drinking a harmful amount of alcohol. We will ask them what they think about receiving a questionnaire through the post that asks them about their drinking habits. We will also…
Scientific abstract
20‐30 adults who have been identified as drinking to harmful/hazardous levels in primary care will be purposively sampled using a maximum variation sampling. Face to face semi‐structured interviews will be conducted to explore experience and acceptability of taking part in the study and understanding of the brief intervention. Interviews will be recorded, transcribed and analysed using thematic analysis. To ensure rigour and minimise bias….
Quality criteria – methods for rigour
• How do you ensure the study is rigorous?• Reflexivity (reflection on biases & methodology)• Audit trail• Secondary/independent coding• Supporting verbatim quotes as evidence• Triangulation• Respondent/member validation
• Refer to quality checklists appropriate for your chosen design.
Example: Standard methods, e.g. audit trail and secondary analysis, will be employed to ensure rigour and minimise bias
31
32
33
144

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
Section Positive framing
Rationale Well justified
Methods Aligned to research question/aims/objectives
Data collection Adequate detail and justification of method
Analysis Rationale and detailed proposed analysis method
Timeline Realistic timeline, shown on Gantt chart
Ethics Awareness/sensitivity of issues
Team Evidence of qualitative expertise/input on team
Impact Realistic detailed impact outline
Costs Costs considered and justified
Understanding Of selected qualitative approaches demonstrated
PPI PPI input separated from research
Rigour Adequate detail of approaches and quality criteria
A strong application will be ….
Thinking about your project, will it be..
All quantitative
Mostly quantitative, some qualitative
Mostly qualitative, some quantitative
All qualitative
I don’t currently have a project
Thinking about your project, will you have a health economic element?
Yes
No
Still deciding
I don’t currently have a project
34
35
36
145

Wednesday 16th February 2022 Writing Technical Sections III: Qualitative StudiesJane Vennik
QUESTIONS!
Request RDS support. https://www.rds‐sc.nihr.ac.uk/
37
146

EGGA 2022 (15th – 17th February 2022)
Day 3: Showing Reviewers You Can Deliver II: Demonstrating Credible Support & Potential Impact
Research Processes & the Importance of Good Project Planning
Sophie Hyndman
147

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
Research Processes & the Importance of Good Project
Planning
Sophie Hyndman
Research Design Service South Central
EGGA, 17th February, 2022
Perseverance
Photograph: NASA
“Beagle 2 could have crashed into Mars because the atmosphere on the planet was less dense than expected”, explained Professor Pillinger. “The probe may have been going too
fast for its parachute and airbags to bring about a soft landing.”
Open University WebSite, March 2010 ; Picture: ESA
Beagle 2
1
2
3
148

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
• You need to consider the logistical aspects of your study BEFORE your application NOT afterwards!
• Many have cost & time implications that should be included in your grant application
• You won’t DO all of the following at application stage, but you should consider them in planning, timetabling & costing your study
The Importance of Logistics
‘Four Key Propositions’
• Importance: this project is important
• Success: this project can answer the question
• Value: this project is good value for money
• Competence: this team can deliver
PROJECT PLANNING
PROJECT PLANNING
PROJECT PLANNING
J. Aldridge & A. Derrington (2012) The Research Funding Toolkit, Sage.
RESEARCH PROCESSES
NASA/Bill IngallsAttribution-NonCommercial 2.0 Genericwww.flickr.com (via www.nasa.gov)
4
5
6
149

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
Context• Good Clinical Practice (GCP) & the UK Medicines for Human Use (Clinical
Trials) Regulations (2004) Responsibilities & accountabilities for clinical trials of investigational medicinal
products
• Research Governance Framework for Health & Social Care (2005) Informed by above, but for research more generally
• Best Research for Best Health (2006) Infrastructure & systems
• The NHS Constitution for England (2015) A commitment to promote, conduct & use research to improve health & care A commitment to inform patients of research studies in which they may be
eligible to participate, & to share anonymised data.
• NHS Five Year Forward View (2014) & NHS Long Term Plan (2019) Funding priorities
All research carried out in the NHS requires:
• A sponsor
• R&D (/R&I) approvals
Most research will require:
• Funding
• Ethics approval
(http://www.hra-decisiontools.org.uk/ethics/)
Some research will require:
• Other approvals (e.g. Clinical Trial Authorisation)
• Research passports (honorary contract or letter of access)
Hula hoop moment from Circus Smirkus performance 2006. http://smirkus.orgImage provided courtesy of Wikipedia. Permission is granted to copy, distribute and/or modify this document under the terms of the GNU Free Documentation License, Version 1.2
What You Need to Consider
POLLWhich of the following organisations
have you heard of?• Research Design Services (RDSs)• Health Research Authority (HRA)• Research & Development Offices• Clinical Research Networks (CRNs)• Clinical Trials Units (CTUs)• Technology Transfer Offices (TTOs)• Medicines and Healthcare products Regulatory Agency
(MHRA)• MedTech and In Vitro Diagnostics Co-operatives (MICs)• Academic Health Science Networks (AHSNs)• Applied Research Collaborations (ARCs)
7
8
9
150

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
NASA - APOD
You are NOT alone!
Supporting Organisations• Research Design Services (RDSs)
• Health Research Authority (HRA)
• Research & Development Offices (University & NHS Trust)
• Clinical Research Networks (CRNs)
• Clinical Trials Units (CTUs)
• Technology Transfer Offices (TTOs)
• Medicines and Healthcare products Regulatory Agency (MHRA)
• MedTech and In Vitro Diagnostics Co-operatives (MICs)
• Academic Health Science Networks (AHSNs)
• Applied Research Collaborations (ARCs)
FreeDigitalPhotos.netwww.pngall.com/wp-content/uploads/2016/05/Fireworks-PNG.png
Things to Do
Write proposal
Find a sponsor
Apply for Health Research Authority
(R&D, ethics & other) approval
(IRAS7)
Attend to research passports
Talk to CRN for cost attribution (ACoRD2
SoECAT3)
APPLY FOR RESEARCHFUNDING
Get sites on board (e.g. letters
of support)
Talk to your sponsor’s
R&D/ finance office (costs,
ETCs1)
Talk to RDS
Talk to clinical trials unit
Talk to TTO/ IP5 office
Talk to your CRN SSS4 to help ID sites
Talk to MHRA6
1 ETCs = Excess treatment costs
2 ACoRD = Attributing the Costs of health & social care Research & Development
3 SoECAT = Schedule of Events Cost Attribution Template
4 CRN SSS = Clinical Research Network Study Support Service
5 TTO/ IP office = technology transfer office/ intellectual property office
6 MHRA = Medical & Heathcareproducts Regulatory Agency
7 IRAS = Integrated Research Application System
With thanks to RDS colleagues & Carole Fogg for their help with this slide
10
11
12
151

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
“… this is not the end. It is not even the beginning of the end … it is, perhaps, the
end of the beginning.”
Winston Churchill (1942)
But …
Yousuf Karsh, Public domain, via Wikimedia Commons
PROJECT PLANNING
Clipart-library.com
Time
The people you needThe materials, equipment & space you need
The time you need
How you organise the above
Who?What?When?Where?
For how long?
Think about what will need to be done on a day-to-day basisThink about maximising benefits to all involved
13
14
15
152

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
‘The organisation of a tertiary cardiac surgery service in the UK presented several barriers to recruitment. Referral information was often inadequate to confirm eligibility. Limited surgeon participation at a centre, the need to meet referral-to-treatment performance targets and complex referral pathways did not support an expertise-based allocation. Urgent patients waiting for surgery in local 'feeder' hospitals were often not transferred until late the night before surgery, which limited the time available to take consent and organise the surgery on an expertise basis. Several elective patients declined to take part because they wanted the surgeon they had met when the surgery was first discussed in clinic to operate. Several initiatives were explored to boost recruitment. After 10 months of recruitment, the trial design was modified to permit both within-surgeon and expertise-based randomisation within a centre. However, this did not have sufficient impact and
Coronary artery bypass grafting in high-RISk patients randomised to off- or on-Pump surgery: a randomised controlled trial (the CRISP trial)
Health Technol Assess. 2014 Jul;18(44):v-xx, 1-157. doi: 10.3310/hta18440
the trial was stopped on the grounds of futility after 106 patients (< 2% of the target sample size) had been recruited in 18 months.’
Photograph: NASA
The People You Need
Applicants & Research Team
Principal Investigator• Award fits career stage• Experience & expertise• Track record & delivery experience• Previous grants held• Publications & impact
Co-applicants & Research Team• Right skill mix• Sensible FTE contribution
16
17
18
153

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
Collaborators• Bring the right skill mix to the research team• Varying degrees of involvement, e.g. site leads, consultants
Day-to-day project manager/ co-ordinator• Managing the study on a day-to-day basis
Patients/ public• Different levels of involvement, but important in design,
management & disseminationE.g. Consultation, collaboration, co-design
Research assistants/ nurses• Consenting patients• Data collection • Collection & processing of samples
Research Team
Administrative staff• Administrative support
Consultants• For specialist help & advice• Possible co-applicants
E.g. statisticians, economists, qualitative researchers, computing experts
Support staff• People external to the study, but whose help may be
needed.E.g. staff on wards, library, local data protection officer
Other Types of People
Steering Committee• Overseeing the work, ensuring that the study happens as
intended• Project team plus independent advisers
Data Safety Monitoring Board/ Data Monitoring & Ethics Committee• Some trials• Independent• Periodically check on data being collected for patient safety
purposes• Broad-ranging monitoring of data quality & integrity
Advisory groups• Depends on study, but could be patients, other stakeholders
etc.
Groups of People
19
20
21
154

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
• Who is in charge of what?
• Roles clearly designated
• Everyone involved must be committed in terms of interest & time
• Staff management crucial
Organising Personnel
A funding panel needs to see how the research team will function & that personnel
are justified
Patient & Public Involvement• RDS & other bodies provide help in recruiting PPI• Pre-application work on research idea & project
plan, including logistics, essential• PPI work timetabled & costed sensibly throughout
study
Staff• Liaison with personnel • Development of job descriptions• Advertisements• Interviewing• Getting proper references
Time
Logistics
Sites• Liaison with management• Liaison with health professionals• Information about the study, what it will entail for
the study site, the information being collected etc.
Time
22
23
24
155

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
‘…systematic reviews show that the originally specified sample size is recruited in a little more than half of clinical trials.’
http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(13)62297-7/fulltext
Participants
How might you ensure good recruitment in a study?
Pop some ideas in the chat!
I’ll give you 1 minute!
Recruiting Participants• Patient & Public Involvement
• Clear recruitment plan & sampling strategy
• Think through first contact, informed consent
• Realistic timing - use local data & apply eligibility criteria, look at throughput, variation in caseload, refusals, etc.
• Be inclusive: minority/ ‘under-served’/ disadvantaged/ particular socioeconomic groups Describe provision for overcoming poor
literacy, language & other barriers
• Feasibility work
http://news.joindementiaresearch.nihr.ac.uk
25
26
27
156

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
Photograph: NASA
Importance of Communication
• Who should be involved in the study?• Who should know about it?
• Formal agreements (e.g. sponsorship, financial arrangements, data ownership & authorship)
• Health Research Authority (ethics, global checks for R&D)• Medicines & Healthcare products Regulatory Authority• Local trust R&D offices – discussion of treatment costs/ confirmation of capacity/
capability• Clinical research networks – for cost attribution (ACoRD & SoECAT); study sites• Technology transfer offices (intellectual property, ‘innovations’ etc.)• Clinical trials units (if involved)• External communication (e.g. websites, press office)
Examples of who may need to know:• Senior managers• Health care professionals• Medical records officer• Pharmacy• Clinic/ ward clerks• GPs
Before the Study Starts
Start talking to people early on
If you have people ‘on board’ the funding application is more convincing
• Clearly defined roles between researchers – ‘chain of command’, appropriate support
• To ensure data quality, reaching of project milestones• With ethics committee (change in protocol, methods, dilemmas etc.)• With participants: contact person for everyone, whenever required
(e.g. everyday, or ‘on-call’, as necessary)• Complaints contact• Back-up information • With study sites & personnel: politics & facilitation• Clearly identified researchers on wards etc.• General information exchange • Query-answering• Trouble-shooting• Feedback & acknowledgement
On-going Communication
28
29
30
157

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
Photograph: NASA
The Other Resources You Need
Stationery
Printing
Postage
Travel
Samples/ TestsEquipment
Telephones
Miscellaneous, e.g. staff training
Images: Wikimedia & Jonathan Stilts, Flickr (computer code)
Software
Logistical Considerations in Study Design
NASA
31
32
33
158

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
• Can your proposal be operationalised?
• Sample selection & monitoring of recruitment
If applicable:
• Randomisation
• Arranging an intervention (e.g. obtaining funding, training, fitting around care pathways)
Assigning responsibility & ensuring time for these
Data collection on MarsPhotograph: NASA
Logistical Considerations in Data Collection & Data Management
• Measuring outcomes tools may need finding (N.B. permissions) tools may need developing (N.B. validity, reliability)
• Lay & non-English speaking issues
• Collecting other information, e.g. process, administrative, contextual
• Coding for the computer, development of database –expertise?
• Only collect what you need to answer the question
• ‘Dummy tables’ for ‘sanity check’
General Considerations
34
35
36
159

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
• How will the data be collected: by whom? Where? When?
• Application process for use of ‘Big Data’
• Holidays, bank holidays (postage)
• Data checking & quality control (e.g. double data entry)
• Data manager?
• Data security – appropriate storage
• Procedures for reporting adverse events
• Computing – coding & data entry
• Data cleaning
General Considerations
Biological Samples
• Analysis of samples – ‘in-house’ or central laboratory contract?
• Transport of samples – specialist courier?
• On-going transport elsewhere or local storage until study end – fridges/ freezers?
• Provision for long-term storage needed? E.g. biobank (Human Tissue Act)
Clinical Trials
• MHRA approvals & costs
• Preparation of study drug – packaging, supplier, labelling, use of placebo
• Who is responsible for pharmacovigilance –contract research organisation or clinical trials unit?
• Get specific advice from sponsor
37
38
39
160

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
Prior work demonstrates the viability of your study
Photograph: NASA
Feasibility & Pilot Studies (NIHR)
Costs & Time
PILOT STUDIES‘ask the same questions but also has a specific design feature: in a pilot study a future study, or part of a
future study, is conducted on a smaller scale.’
Internal/ external
FEASIBILITY STUDIES ‘ask whether something can be done, should we proceed with it, and if so, how’
https://www.nihr.ac.uk/documents/nihr-research-for-patient-benefit-rfpb-programme-guidance-on-applying-for-feasibility-studies/20474
Logistical Issues in Data Analysis
Cray 2 Supercomputer, NASAPhotograph: NASA
Planned before the study has started:
• Statistical, health economic, qualitative, other methods
• Equipment (hardware, software)
TIME & MONEY
40
41
42
161

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
Logistical Issues in Dissemination
Pigeon post; source: Wikipedia (Public Domain)
‘We know from follow up of registered clinical trials that about 50% are never published in full…’
At least 50% of published reports are not ‘sufficiently clear, complete, and accurate for others to interpret, use, or replicate the research correctly.’
TimeGlasziou & Chalmers, http://blogs.bmj.com/bmj/2016/01/14/
• Gantt charts
• Flow diagrams
• Draw on published guidance for studies/ trials to see what will be expected later in terms of protocols & reporting, e.g. SPIRIT, CONSORT
31st FW Balkan Operations Gantt chart. United States Air Force, 2000
Demonstrating Clear Planning
http://www.consort-statement.org/consort-statement/flow-diagram
If funders cannot understand your plans, & see they make sense, they will not fund the study
43
44
45
162

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
nuttakit, freedigitalphotos.net
Finances
• Local University/ NHS R&D Finance Officer
• Collaborators’ Finance Officers
• Clinical Research Networks
Photo: renjith krishnan, www.freedigitalphotos.net,http://www.freedigitalphotos.net/images/view_photog.php?photogid=721
The People You Will Need to Involve
Research costs & discussion of Excess Treatment Costs
Cost attribution (ACoRD & SoECAT), NHS Support Costs & Excess Treatment Costs
Happy with costs, & sorting out contracts
TIME
Always:
• Consult your Finance Office at an early stage
Be aware:
• Costs likely broken down by project year• Timings for university/ trust/ CRN approval/ PhD ‘windows’• Which organisation is responsible for project sign off• ‘System’ will not necessarily exist for sorting respective costs between
collaborating organisations• Participation/ costs of other collaborators also need sign off• Formal collaboration agreements/ contracts need to be in place before
funds distributed
The Finance Form
renjith krishnan, www.freedigitalphotos.net,http://www.freedigitalphotos.net/images/view_photog.php?photogid=721
46
47
48
163

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
• How will resources requested be used?
• How realistic/ accurate are costings?
• ‘Best price’ found for tests etc.?
• Anything ‘over-budgeted’?
• Requested resources justified?
• Efficient use of resources?
• Good value for money?
Overall Budget
Have you considered:
renjith krishnan, www.freedigitalphotos.net,http://www.freedigitalphotos.net/images/view_photog.php?photogid=721
If funders cannot understand your costs, or feel the study is not good value for money, they may not fund it
Give yourself some leeway
Useful linksAcademic Health Science Networks https://www.ahsnnetwork.com/
Applied Research Collaborations https://www.nihr.ac.uk/explore-nihr/support/collaborating-in-applied-health-research.htm
Clinical Research Networks https://www.nihr.ac.uk/explore-nihr/support/clinical-research-network.htm
Clinical Trials Units https://www.ukcrc.org/research-infrastructure/clinical-trials-units/registered-clinical-trials-units/
Medicines and Healthcare products Regulatory Agency
https://www.gov.uk/government/organisations/medicines-and-healthcare-products-regulatory-agency
MedTech and In Vitro Diagnostics Co-operatives (MICs)
https://www.nihr.ac.uk/partners-and-industry/industry/access-to-expertise/medtech.htm
NHS R&D Offices https://rdforum.nhs.uk/rd-contacts-directory/
Research Design Services https://www.nihr.ac.uk/explore-nihr/support/research-design-service.htm
WorksheetThink about your proposed project.
Using the worksheet in your resources pack, jot down:
1. The type of people* you may need as co-applicants.
2. The type of people you may need, in addition to co-applicants, as part of your broader research team.
3. Other types of people/ groups of people/ organisations you are likely to need to consult or work with to develop & deliver your research.
* experience, subject & methods expertise
For worksheet, see resource pack
49
50
51
164

Thursday 17th February 2022 Research Processes & the Importance of Good Project Planning
Sophie Hyndman
Photograph: NASA
52
165

EGGA 2022 (15th – 17th February 2022)
Day 3: Showing Reviewers You Can Deliver II: Demonstrating Credible Support & Potential Impact
The Importance of Patient & Public Involvement
Heather Parsons, Paul Hewitson,
Bernard Gudgin & Tracey Newman
166

Thursday 17th February 2022 Importance of Patient & Public InvolvementHeather Parsons
Patient & Public Involvement
A brief introduction
Heather Parsons
Research Design Service
Context
Patient and Public Involvement is an overarching principle and way of working, rather than a research method
Has been incorporated into NIHR research in an official capacity for well over 10 years
Now an expectation of all high quality health and social care research
The UK leads the way with PPI, but it is being adopted globally
UK Standards for Public Involvement
These are a set of six standards to support the quality and consistency of public involvement in research.
The RDS fully supports the use of these Standards when working with patients, carers, service users and other members of the public as partners in research.
1
2
3
167

Thursday 17th February 2022 Importance of Patient & Public InvolvementHeather Parsons
The Six UK Standards for Public Involvement
Inclusive OpportunitiesOffer public involvement opportunities that are accessible and that reach people and groups according to research needs.
Working TogetherWork together in a way that values all contributions, and that builds and sustains mutually respectful and productive relationships.
Support and LearningOffer and promote support and learning that builds confidence and skills for public involvement in research
The Six UK Standards for Public Involvement
CommunicationsUse plain language for well-timed and relevant communications, as part of involvement plans and activities
ImpactSeek improvement by identifying and sharing the difference that public involvement makes to research.
GovernanceInvolve the public in research management, regulation, leadership and decision making.
Relationships with the public in research
Participation
Is where patients are recruited into a study as ‘subjects’.
Engagement
Is where information and results about research and research findings are shared with patients and the public in a variety of ways
4
5
6
168

Thursday 17th February 2022 Importance of Patient & Public InvolvementHeather Parsons
Relationships with the public in research
• Is where there is a collaborative relationship between members of the public and research teams to inform all aspects of research
• The NIHR definition of public involvement in research is
“research being carried out ‘with’ or ‘by’ members of the public rather
than ‘to’, ‘about’ or ‘for’ them.”
Involvement
Consultation Collaboration Co-production
Patient or public provide feedback (though advisory groups or 1:1 discussions)
which is used to help improve, shape and
inform research plans and process.
Explicit and defined opportunities for certain PPI members to play a specific role in the research process and participate in decision
making.
PPI representatives are partners in the research
delivery; there is an ethos of equal ownership. Public members define and lead
on some initiatives.
Partnership
7
8
9
169

Thursday 17th February 2022 Importance of Patient & Public InvolvementHeather Parsons
It improves health and social care research(and ultimately health outcomes!)
• Provides a different perspective, understanding patients’ and carers point of view and needs
• Helps ensure research is relevant, manageable and implementable
• Ennis and Wykes (2013): studies involving patients to a greater extent were more likely to reach recruitment targets
• Allows identification of barriers in practical aspects of research
De-mystifying research
• Challenges societal preconceptions about health and social care research
• Part of a 2-way educational process
• Creates a sense of ownership of healthcare system, and subsequently ownership of health
10
11
170

Thursday 17th February 2022 Importance of Patient and Public Involvement
Paul Hewitson
Dr Paul HewitsonRDS-SC Research Advisor and PPI Officer
University of Oxford
Planning and Guidancefor Patient and Public
Involvement (PPI)
Overview
• NIHR (and most funders) have specific expectations for PPI in applications
• Require ‘pre-grant PPI activity’ prior to submission of application
• Also require a robust ‘PPI plan’ for the (if) funded research project
• Start early…seriously, start early
NIHR Definition of ‘Public’
“When using the term ‘public’ we include patients, potential patients, carers and people
who use health and social care services as well as people from organisations that represent people who use services. Whilst all of us are
actual, former or indeed potential users of health and social care services, there is an important
distinction to be made between the perspectives of the public and the perspectives of people who have a professional role in health and social care
services.”
1
2
3
171

Thursday 17th February 2022 Importance of Patient and Public Involvement
Paul Hewitson
The ‘Who’ of PPI…
• Patients (current, former, future)• Carers, parents, guardians• People who use healthcare or social
services• Patient/Public Advocacy Groups and
Charities
Perspectives of patients and the public (knowledge, experience, views, expectations) are different to doctors,
nurses, clinicians, researchers or managers.
‘Lived Experience’
• People who have personal knowledge gained through direct, first-hand involvement/experience
• Knowledge through own experience of care, or the care of others
• Lived experience insights valuable for design, conduct and communication
“Researchers may have textbook knowledge about different conditions, but unless they have also lived
thought it, there will be gaps in their knowledge.”
The ‘What’ of PPI…
• PPI are not research participants• PPI are ‘involved in discussions and
decisions’ about the research• PPI expected to be involved in:
o design of the researcho developing the funding applicationo undertaking the researcho interpreting the research findingso communication/dissemination
4
5
6
172

Thursday 17th February 2022 Importance of Patient and Public Involvement
Paul Hewitson
The Research Cycle (I)
Design /Pre-Grant
Identifying & Prioritising
Developing Proposal
Undertaking & Managing
Analysis & Interpretation
Disseminating Results
Impact / Implementing
Monitoring & Evaluation
The Research Cycle (II)
Design /Pre-Grant
Identifying & Prioritising
Developing Proposal
Undertaking & Managing
Analysis & Interpretation
Disseminating Results
Impact / Implementing
Monitoring & Evaluation
PPI
NIHR View of PPI
• For project and fellowship applications:i. Pre-grant PPI activityii. PPI plan for (if) funded researchiii. ‘embed’ PPI throughout application
• For project grants, requirement of a ‘PPI Lead’ as part of the research team
• Also requirement for evaluation of the impact PPI has on the research
“The NIHR expects appropriate and well designed involvement of patients/service users, carers, the public and other key stakeholders in the research it supports”
7
8
9
173

Thursday 17th February 2022 Importance of Patient and Public Involvement
Paul Hewitson
Design/Developing Stage
• Before/during writing your fundingapplication (initial draft) PPI can:
- clarify the research question and/or potential outcomes of the research
- identify potential problems with the design or data collection methods
- assist in developing a recruitment strategy (patient networks/charities)
- how involved in interpretation and dissemination of research findings
Pre-Grant PPI Activities
• Discussion prior to submission- meeting(s) between research team and PPI
representatives- draft ‘PPI plan’ outlining what PPI contributors
will be doing during the research- budgeting/costs for PPI contributors - draft ‘roles and responsibilities’ for the
research team (PPI Lead) and the PPI contributors
- facilitates recruitment and discussion
PPI Lead (Project)
• Named member of the research team- facilitate, liaise and support PPI throughout
research- leading and managing PPI plan; adequately
costed and resourced- can involve coordinating/delivering bespoke or
formal training to PPI contributors
“…has the relevant skills, experience and authority to be accountable, represent, manage and embed PPI in
all aspects of the research
10
11
12
174

Thursday 17th February 2022 Importance of Patient and Public Involvement
Paul Hewitson
Undertaking/Analysis
• During the course of your research, PPI can:
- give lay and patient perspectives throughout the research process
- contribute to steering groups- directly involved in gathering/analysing data- write clear participant information sheets- advise on the key patient messages and
recommendations arising from the research data
Dissemination Stage
• During the course of your research, PPI can:
- advise on different ways to disseminate findings to diverse audiences
- jointly present the findings with researchers
- help distribute findings through formal and informal networks
RDS PPI Support
• Review proposals and advise on PPI strategic plans
• Signposting and helping to advertise for PPI contributors
• Limited funding available for pre-grant PPI meetings/activities
13
14
15
175

Thursday 17th February 2022 Importance of Patient and Public Involvement
Paul Hewitson
Resources (General)
• UK Standards for Public Involvement -https://sites.google.com/nihr.ac.uk/pi-standards/home
• NIHR Briefing Notes for Researchers -https://www.nihr.ac.uk/documents/briefing-notes-for-researchers-public-involvement-in-nhs-health-and-social-care-research/27371
• RDS Brief Guide to Public Involvement -https://www.rdsblog.org.uk/Resources/A5_PPI_Pocket_Guide_V3%20(1).pdf
Resources (Specific)
• NIHR Costing Resources -https://www.nihr.ac.uk/documents/payment-guidance-for-researchers-and-professionals/27392
• Evaluating PPI in Research (UWE) -http://www.phwe.org.uk/wp-content/uploads/Guidance-on-evaluating-Public-Involvement-in-research.pdf
• Equality, Diversity and Inclusion Toolkit -https://www.trialforge.org/wp-content/uploads/2020/08/rds_edi_toolkit_pilot_may2021.pdf
Final Thoughts
• Start early…seriously, start early• Read the guidance literature• Limited pre-grant funding; need to be
creative• We are here to help
16
17
18
176

Thursday 17th February 2022 Importance of Patient and Public Involvement
Paul Hewitson
Worksheet
Thank you for your time
19
20
177

Thursday 17th February 2022 Importance of Patient & Public InvolvementBernard Gudgin
No: 1
No: 2
No: 3
1
2
3
178

Thursday 17th February 2022 Importance of Patient & Public InvolvementBernard Gudgin
No: 4
No: 5
No: 6
4
5
6
179

Thursday 17th February 2022 Importance of Patient & Public InvolvementBernard Gudgin
No: 7
No: 8
No: 9
7
8
9
180

Thursday 17th February 2022 Importance of Patient & Public InvolvementBernard Gudgin
No: 10
No: 11
No: 12
10
11
12
181

Thursday 17th February 2022 Importance of Patient & Public InvolvementBernard Gudgin
No: 13
No: 14
No: 15
13
14
15
182

Thursday 17th February 2022 Importance of Patient & Public InvolvementBernard Gudgin
No: 16
No: 17
No: 18
16
17
18
183

Thursday 17th February 2022 Importance of Patient & Public InvolvementBernard Gudgin
No: 19
No: 20
No: 21
19
20
21
184

Thursday 17th February 2022 Importance of Patient & Public InvolvementBernard Gudgin
No: 22
No: 24
22
23
24
185

Thursday 17th February 2022 Importance of Patient & Public InvolvementBernard Gudgin
No: 25
No: 26
25
26
186

EGGA 2022 (15th – 17th February 2022)
Day 3: Showing Reviewers You Can Deliver II: Demonstrating Credible Support & Potential Impact
The Importance of Equality, Diversity & Inclusion (EDI)
Rebecca Barnes & Chris Newby
187

Thursday 17th February 2022 The Importance of Equality, Diversity & InclusionBecky Barnes and Chris Newby
The importance of equality, diversity and inclusion (EDI)
17th February 2022
Dr Rebecca Barnes and Dr Chris Newby Research Design Service East Midlands
EDI and health and social care research: why it matters
Our research needs to identify and target the populations and geographies where need is greatest
Those who are most marginalised and underserved in health and social care services are least likely to participate in research: we need to engage with them and better meet their needs
We need to avoid research waste resulting from conducting studies with homogenous samples that are then not relevant to more diverse populations
We need to know whether some groups are adversely affected by a new intervention, even if it is effective for the majority of people
We need to avoid harm by developing interventions which have been tested on a diverse sample
1
2
3
188

Thursday 17th February 2022 The Importance of Equality, Diversity & InclusionBecky Barnes and Chris Newby
NIHR’s EDI requirements for grant/fellowship applicants
• Encompasses all nine protected characteristics in the Equality Act 2010 and factors such as socio-economic status, geographical location and access to health and social care
• Applicants need to demonstrate:• How you’ve considered and addressed EDI characteristics in your proposal• How you will ensure that your sample is representative of the target
population• Which groups you will recruit to ensure inclusivity, and what the justification
of for any exclusion criteria are e.g. English speakers only• How you will collect EDI data• That you’ve considered all potential recruiting locations
• See full wording (published May 2020): https://www.nihr.ac.uk/documents/strengthening-our-commitment-to-equality-diversity-inclusion-and-patient-and-public-involvement-and-engagement-ppie/24697
Historical Context and Structural Inequality
PPI
Research Team
Selection of Participants, Sites and Samples
Data Collection
Data Analysis and Presentation
Dissemination, Implementation and Impact
Budgeting for Inclusion
The RDS EDI Toolkit
Historical context and structural inequality
Has previous research excluded certain populations?
What historic and structural issues might affect research participation or involvement?
How will you navigate these issues?
4
5
6
189

Thursday 17th February 2022 The Importance of Equality, Diversity & InclusionBecky Barnes and Chris Newby
Patient and public involvement (PPI)
How aware are you of EDI issues in PPI?
How will your PPI strategy enable you to recruit and retain diverse public contributors?
How will you support and empower your diverse PPI group?
Research team
• How diverse is your team?
• How culturally competent is your team?
• How has incorporating diverse perspectives and lived experiences affected your research design?
Selection of participants, sites and samples
• How generalisable is your sample?
• Has geographical need informed your choice of site(s)?
• Are you excluding anyone, if so is this justified?
• How is data on EDI collected?
7
8
9
190

Thursday 17th February 2022 The Importance of Equality, Diversity & InclusionBecky Barnes and Chris Newby
Data collection
How equitable is your data collection strategy?
Do your methods address participants' protected characteristics, circumstances and needs?
What steps will you take to include 'seldom heard' groups?
Data analysisand presentation
How will you describe participants’ protected characteristics?
How will you analyse and report EDI characteristics?
Has diverse PPI been incorporated to support the interpretation of results?
Dissemination, implementation and impact
• Will findings be disseminated via accessible and inclusive formats?
• How will this research be taken forward to benefit all patients/service users?
• Does the research/intervention work across all settings?
10
11
12
191

Thursday 17th February 2022 The Importance of Equality, Diversity & InclusionBecky Barnes and Chris Newby
Budgeting for EDI
Any questions or comments?
Thank you for participating!
13
14
192

EGGA 2022 (15th – 17th February 2022)
Day 3: Showing Reviewers You Can Deliver II: Demonstrating Credible Support & Potential Impact
Dissemination - Demonstrating Potential for Tangible Outputs & Impact: Papers,
Plus, Plus, Plus!
Dean Phillips
193

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
DisseminationDemonstrating potential for tangible outputs
and impact: Papers, plus, plus, plus!
Dr Dean Phillips
Senior Research Design Adviser
Research Design Service South Central
“Research is of no use unless it gets to the people who need to use it.”
Professor Sir Chris WhittyChief Medical Officer for England & the UK
1
2
3
194

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
NIHR application form
Dissemination, outputs and anticipated impact− How and who you will talk to− Describe what the outputs of the research might be− What impact there might be
NIHR− Understands impact may take time− Difficult to provide definitive answers or guarantees
Impact
• Demonstratable contribution research makes to– Society and economy
• Benefits− Individuals, organisations & nations
• Impact is the outcome, not the process
• Process is knowledge mobilisation– Engagement, co-design, dissemination and
commercialisation
Generating meaningful impact
• Engage with people likely to use the research– Before the design stage– Every stage of the research process
• Planning for impact− What kind of impacts do you hope to achieve?− How will you engage with research users to
deliver impact from your research?
4
5
6
195

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
For impact think…….
• What are the expected impact goals (the real-life benefits)?
• Who is going to benefit?
• What engagement activities will enable you to deliver these impact goals to those who are going to benefit?
https://www.fasttrackimpact.com/resources
Ultimately for NIHR
“Impact is about making a meaningful difference to people’s lives, through research”
7
8
9
196

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
NIHR and dissemination
Effective dissemination is about:
• Getting your research findings– To people who can make use of them– Maximise the benefit and impact without delay
What does the NIHR mean by dissemination?
Dissemination is more than
• Just saying– Publish a paper– Will present at a conference
• Needs to be– Appropriate– Proportionate– Realistic
• Feasibility study unlikely to be published in or lead to a keynote address at a World Congress
Outputs from your research• Written outputs – press releases, research reports, papers,
presentation slides, posters, website, social media (blogs)
• Presentations – workshops, conferences, media interviews
• Software
• Training materials – manuals, DVDs
• Checklists, protocols, toolkits, questionnaires
• Guidelines (clinical, service)
• Research tools – data analysis techniques
• Patentable inventions – new therapeutics, diagnostics, medical device
• Potential new drug or health or social care intervention
Provide brief details of each anticipated output
10
11
12
197

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
How will your outputs be used
If your research is successful
• Describe how they will be used in the health and care service or wider society
• Might be through commercial exploitation
• Is further funding or support needed to maximise impact?
Any possible barriers
• To uptake of any likely output– Intellectual property issues– Regulatory hurdles
• To– Further research– Development of the research area– Adoption of the research findings– Implementation
Short, medium and long term impact
• Patient benefit
• Healthcare staff benefits
• Changes in service - efficiency savings?
• Commercial return - contribute to economic growth?
• Public wellbeing
• Anticipated timescale for the benefits to reach patients, the public and services
• If possible, provide a quantitative estimate of the scale of potential benefits
13
14
15
198

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
Dissemination plan
Create a dissemination plan
https://www.nihr.ac.uk/researchers/manage-your-funding/manage-your-project/outputs-and-branding.htm
https://www.nihr.ac.uk/documents/how-to-disseminate-your-research/19951
https://www.nihr.ac.uk/researchers/apply-for-funding/how-to-apply-for-project-funding/plan-for-impact.htm
Objectives
What do you want to achieve?
• Beginning of research– Engage with people to help shape your research
• End of research– Raise awareness and understanding– Change practice
• Be realistic and pragmatic
Your audience• Identify your audience
– Who might benefit from using your findings– Patients, clinicians, commissioners, funders
• Understand where and how– They look for or receive information
• Stay connected throughout your research
• Feedback to patients, clinicians etc., who might also participate in dissemination
16
17
18
199

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
Format of dissemination
• Targeted outputs
• Appropriate format for the user
• Consider range of tailored outputs for:– Decision makers– Patients– Researchers– Clinicians– Public
Timing of dissemination
• Identify and plan critical time points
• Should not be limited to the end of a study
• Where possible, share any interim findings
• Utilise existing opportunities– e.g. upcoming conferences
• Build momentum throughout project
Resources for dissemination
• Include costing in your application to enable you to deliver your planned dissemination activity
• What is the expertise in your team?
• Do you need additional help with dissemination?
• Would you benefit from liaising with others?– NIHR comms for a specific programme– Your institution’s press office can lead to
19
20
21
200
Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
PPI involvement in dissemination
• Help to review the results and pick out points of interest and relevance to the public
• Help to write up main points in plain English
• Assist in writing a press release
• Help to prepare and present at public events
22
23
24
201

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
Main message for dissemination
• Needs to resonate with your target audience
• Use the right language
• Focus on the possible impact of your research on your target audience– Their practice– Their daily life
Think about any potential risks and sensitivities
• Be aware of current cultural and political climate
• Consider how your dissemination might be perceived by different groups
• Possible risks e.g. intellectual property issues
• Is content aligned with your university, hospital and your funder
Channels of communication
• Use the most effective ways to communicate your message to your target audience
• Websites, social media, conferences, journals dissemination event, media,1:1 meetings; blogs, email, webinar, film, animation, infographics
• Identify and connect with influencers in your audience who can champion your findings
25
26
27
202

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
www.
• Web presence through a research group at work
• On line communities in diabetes, dementia, ageing– Voice www.voice-global.org– www.diabetes.co.uk
• Create a website– A starting point for getting information out– Different pages for each target audience– Make your messages short and succinct
New Scientist
28
29
30
203

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
Social media
To help you engage with patients, researchers, funders
• In an active conversation about the work you do
• Be careful with the content of your message
• Be clear about the message you want to say
• Twitter– Could use to direct people to your website / articles– Start small, then roll out to larger audiences
• YouTube video when an article is published
31
32
33
204

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
Useful resources• “Introduction to impact through the lens of NIHR”
• NIHR - Plan for Impact– https://www.nihr.ac.uk/researchers/apply-for-
funding/how-to-apply-for-project-funding/plan-for-impact.htm
• The Health Foundation toolkit– https://www.health.org.uk/publications/communicating-your-
research-a-toolkit
• Fast Track Impact– https://www.fasttrackimpact.com/resources
Summary
• Aim to get your research findings– To people who can make use of them, without
delay to maximise benefit
• Needs to be– Appropriate– Proportionate– Realistic
34
35
36
205

Thursday 17th February 2022 Dissemination - Demonstrating Potential for Tangible Outputs & Impact
Dean Phillips
ConclusionNot just publishing a paper and going to a conference
YES, but +++
Dissemination includes:
• Participants, patients, public, study sites, ethics, funder
• Policy makers and managers
• Engaging with guideline people e.g. NICE
• Professional bodies and colleagues
• Training courses
• Websites, other social media
• Anyone else who can shift research results into practice!
“Research is of no use unless it gets to the people who need to use it.”
“Impact is about making a meaningful difference to people’s lives, through research”
37
38
206

EGGA 2022 (15th – 17th February 2022)
Day 3: Showing Reviewers You Can Deliver II: Demonstrating Credible Support & Potential Impact
Managing Intellectual Property
Philippa Christoforou
207

Thursday 17th February 2022 Managing Intellectual PropertyPhilippa Christoforou
© Copyright 2017 Oxford University Innovation Ltd.
Intellectual Property
Dr Philippa Christoforou
Senior Licensing and Ventures ManagerDigital Health, Medical Devices and Bioinformatics team
Oxford University Innovation
© Copyright 2017 Oxford University Innovation Ltd.
Oxford University Innovation
• OUI is the Technology Transfer Office for the University of Oxford and OUH NHS Trust
• But IP management and support can take a variety of names...• Research Office• Research and Business Development Office• Research and Knowledge Transfer • Research and Innovation Services
© Copyright 2017 Oxford University Innovation Ltd.
The University assists those who wish to
commercialise their research
IDENTIFYRecognising ideas and technology with potential commercial value
PROTECTManage legal agreements (e.g. patents) and support academics
INCUBATEDevelop ideas and build value – funded through grant applications
EXPLOITMaterial sales, Licences, Spinout Companies
Our commodity is Intellectual Property (IP)
1
2
3
208

Thursday 17th February 2022 Managing Intellectual PropertyPhilippa Christoforou
What is Intellectual Property?
INTELLECTUAL…A creative product of the mind
PROPERTY…Has commercial value and can be bought,
sold and rented (like a house or car)
IP RIGHTSA legal framework exists throughout the world to protect
those who create, sell and buy IP
© Copyright 2017 Oxford University Innovation Ltd.
Why does the NIHR care about IP?
© Copyright 2017 Oxford University Innovation Ltd.
Look to the future…
4
5
6
209

Thursday 17th February 2022 Managing Intellectual PropertyPhilippa Christoforou
© Copyright 2017 Oxford University Innovation Ltd.
Avoiding IP barriers…
© Copyright 2017 Oxford University Innovation Ltd.
Why does the NIHR care about IP?
1) Avoiding IP barriers…a) Are there issues in securing permissions (expensive or not possible)?
b) Is it possible to licence a technology in an area subject to patent protection?
© Copyright 2017 Oxford University Innovation Ltd.
Research Output
Adding IP value
Grant Application + IP protection
7
8
9
210

Thursday 17th February 2022 Managing Intellectual PropertyPhilippa Christoforou
© Copyright 2017 Oxford University Innovation Ltd.
Why does the NIHR care about IP?
1) Avoiding IP barriers…a) Are there issues in securing permissions (expensive or not possible?)
b) Is it possible to licence a technology in an area subject to patent protection
2) Add IP value to your technology / idea…a) Able to defend technology against anyone copying your ideas
b) Minimise need for 3rd party permissions
c) Able to clearly identify ownership of a technology
d) Provides an explicit tradable commodity
e) Makes technology more attractive to commercial partners
...increasing the chance of achieving patient benefit
© Copyright 2017 Oxford University Innovation Ltd.
Patents
DesignsTrademarks Databases
Copyright
IP
© Copyright 2017 Oxford University Innovation Ltd.
• Agreement between the State and the inventor offering ashort term monopoly (20 years) in return for a fulldescription of the invention, which is published (after 18months).
• Protects technical innovation (anInvention) and requires a formalapplication process
• Gives the owner the right for a limited period to stop othersfrom making, selling or using the invention without thepermission of the owner (on a geographical basis)
10
11
12
211

Thursday 17th February 2022 Managing Intellectual PropertyPhilippa Christoforou
© Copyright 2017 Oxford University Innovation Ltd.
PatentsTo be awarded a patent, your invention must be 4 things:
Novel Inventive
Enabling
Never been disclosed or made public before the application (priority) date
Involve an inventive step (not obvious to somebody skilled in the art)
Sufficiently describes the invention for others to practise it (it teaches)
Applicable
Capable of industrial application
© Copyright 2017 Oxford University Innovation Ltd.
Protects the written word and images:
• Literary works, art, photography, films, TV, music, web content, sound recordings & questionnaires
• Protects only what is written, not the meaning or idea itdescribes
• Protection is automatic and lasts for 70 years after thedeath of the creator.
• Includes software source code and object code, as well asquestionnaires (ROMS/PROMS).
Copyright ©
© Copyright 2017 Oxford University Innovation Ltd.
Design Rights
• Can be unregistered or registered
• Protects appearance:
3D shape, colour, packaging, patterns etc.
Trademarks
• Protects names, logos and jingles.
Database Rights (EU)• If collation is original. Protects against copying of database
not data.
DesignsTrademarks Databases
13
14
15
212
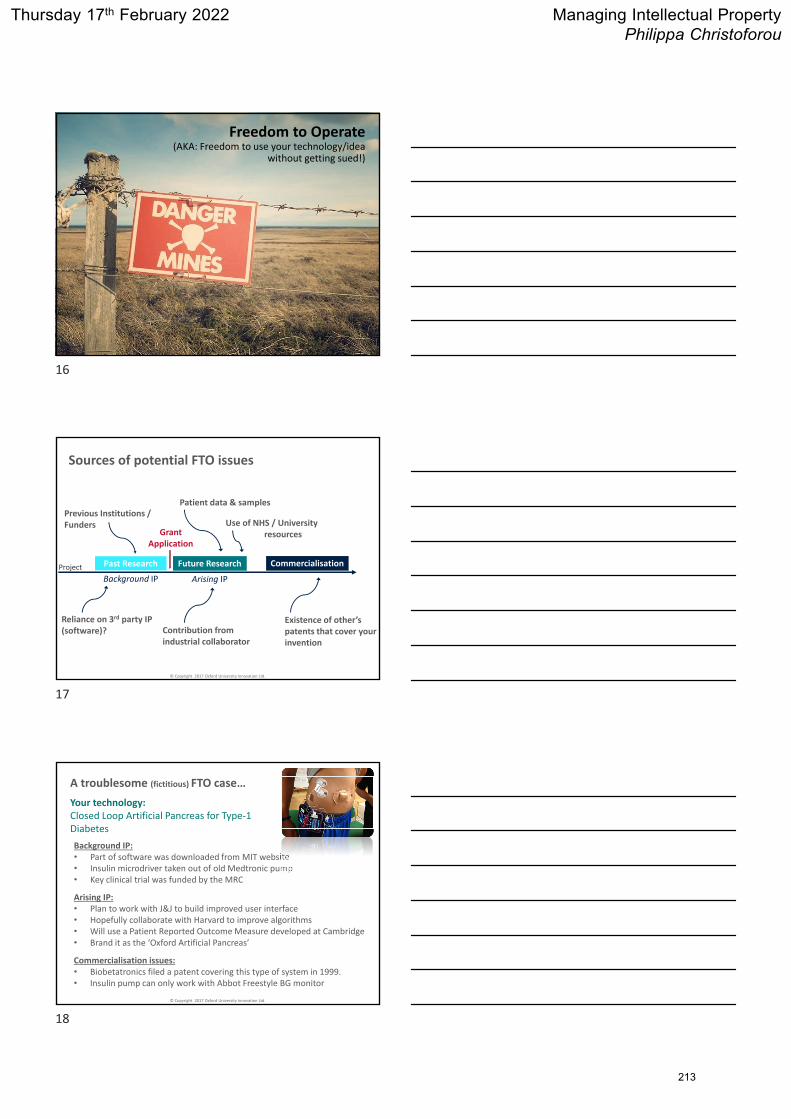
Thursday 17th February 2022 Managing Intellectual PropertyPhilippa Christoforou
© Copyright 2017 Oxford University Innovation Ltd.
Freedom to Operate(AKA: Freedom to use your technology/idea
without getting sued!)
© Copyright 2017 Oxford University Innovation Ltd.
Grant Application
Arising IPBackground IP
Past Research Future Research Commercialisation
Previous Institutions / Funders
Reliance on 3rd party IP (software)?
Existence of other’s patents that cover your invention
Sources of potential FTO issues
Patient data & samples
Contribution from industrial collaborator
Use of NHS / University resources
Project
© Copyright 2017 Oxford University Innovation Ltd.
A troublesome (fictitious) FTO case…
Your technology: Closed Loop Artificial Pancreas for Type‐1 Diabetes
Background IP: • Part of software was downloaded from MIT website• Insulin microdriver taken out of old Medtronic pump • Key clinical trial was funded by the MRC
Commercialisation issues: • Biobetatronics filed a patent covering this type of system in 1999. • Insulin pump can only work with Abbot Freestyle BG monitor
Arising IP: • Plan to work with J&J to build improved user interface • Hopefully collaborate with Harvard to improve algorithms• Will use a Patient Reported Outcome Measure developed at Cambridge• Brand it as the ‘Oxford Artificial Pancreas’
16
17
18
213

Thursday 17th February 2022 Managing Intellectual PropertyPhilippa Christoforou
© Copyright 2017 Oxford University Innovation Ltd.
Also consider legal ownership/rights to samples, data and materials
Who owns:
• Patient data?
• Blood samples?
• Medical scans?
• GM animal models?
• Antibodies?
• Cell lines?
Were these provided for non‐commercial purposes only?
© Copyright 2017 Oxford University Innovation Ltd.
The definition of Intellectual Property (IP) includes copyright(such as new software, checklists, scales, protocols,questionnaires, toolkits, guidelines or similar) and research tools(such as data analysis techniques, assays, cell lines, biomarkers,materials or equipment and devices) patents, trademarks anddesigns.
The mission of the NIHR is to improve the health and wealth of the nation through research. To achieve this goal, research funded by NIHR needs to be translated into improvements in treatments, technologies, services and expertise used by the National Health Service and allied organisations.
© Copyright 2017 Oxford University Innovation Ltd.
What is the Background IP?What relevant IP (patents, design right, copyrightetc.) is held by the applicants and how does itrelate to this application?
• Look backwards at all the IP that may exist within your research to date
• Only refer to IP that is owned by you (or your institution)
• The IP does not need to have any obvious commercial value
• Demonstrate that you have carried out due diligence and assessed whether you hold IP
19
20
21
214

Thursday 17th February 2022 Managing Intellectual PropertyPhilippa Christoforou
© Copyright 2017 Oxford University Innovation Ltd.
Do you have freedom to operate?Has a freedom to operate search been conducted and by whom?
• Demonstrate that you are surrounded by competent people!
• What patents are in the area you are working on – who might stop you
using your technology commercially?
• What IP exists within your technology that is not owned by you/your
institution? (3rd party software or hardware?)
• Who has funded your research? Has a revenue sharing agreement been
put in place?
• Who owns the data/materials that you have used in your research?
• Have other institutions contributed to your research? Has an IP
management agreement been put in place?
© Copyright 2017 Oxford University Innovation Ltd.
What will be the Arising IP?Will any IP be produced or improved during the proposed research?
• This is a look forward at arising IP
• What might you create during the proposed project?
• Improvements refer to both your own IP and other’s IP
• Not just patents!
• Again, ignore whether there is clear commercial value at this point
Don’t underestimate the “small stuff” – just because it’s not the cure for cancer doesn’t mean its not interesting. If its meaningful to the NHS then its of interest to NIHR.
© Copyright 2017 Oxford University Innovation Ltd.
Describe how any new IP generated through the proposed research will be managed, protected and exploited, either through adoption in the healthcare service or through commercial exploitation:
• Introduce your IP ‘expert’ here, and give them a seat on your steering
committee!
• IP‐management agreements (such as between collaborating institutions)
that will avoid downstream conflict
• Make sure everything has been thought through – avoid ambiguity
• Will you protect your IP with a patent application, or through copyright –
who will do this?
• Confidentiality agreements will protect against patent‐invalidating
disclosures
22
23
24
215

Thursday 17th February 2022 Managing Intellectual PropertyPhilippa Christoforou
© Copyright 2017 Oxford University Innovation Ltd.
Describe how any new IP generated through the proposed research will be managed, protected and exploited, either through adoption in the healthcare service or through commercial exploitation:
• Adoption within healthcare and commercial exploitation are both valid,
but need to provide evidence as to why this route is best
• What resources are needed to get tech to patients?
• What contacts/collaborators do you have that would facilitate this?
• Do you have any letters of interest from a commercial party?
• Is it best to licence technology, set up a spinout, engage in a trial?
• If you will not commercially exploit, why not?
© Copyright 2017 Oxford University Innovation Ltd.
What are the key current and future barriers to utilising any new IP/innovation through dissemination and adoption in the healthcare service or through commercial exploitation e.g. potential regulatory hurdles?
• Identify anything that might make getting your tech to patients ‘difficult’:
• What regulators might your technology be reviewed by?
• MHRA and CE marking? NHS Digital and Safety Risk Standards (SCCI0129)?
• Will you need health economics data to demonstrate cost utility to payers
and NICE?
• Will additional clinical studies be required?
• Will there be any cultural barriers (prescribing practice, care pathway
modification?)
• Which KOLs and stakeholders will you need to engage?
© Copyright 2017 Oxford University Innovation Ltd.
Summary
• Do not let the IP section be an afterthought
• Even if you don’t see commercial interest, anyone using your tech will want reassurance that they have all necessary rights
• Show you have identified competent staff who will manage existing and arising IP, as well as commercial exploitation
• Demonstrate that you have thought ahead, all the way to getting your tech into the hands of clinicians / patients
• Be clear on IP strategy and, if relevant, protect IPR before any publication
• Seek advice early – Ask for support from your technology transfer office or similar entity, or the RDS
25
26
27
216

Thursday 17th February 2022 Managing Intellectual PropertyPhilippa Christoforou
© Copyright 2017 Oxford University Innovation Ltd.
THANK YOU
www.innovation.ox.ac.uk
twitter.com/OxUInnovation
linkedin.com/company/oxford‐university‐innovation
28
217

EGGA 2022 (15th – 17th February 2022)
Day 3: Showing Reviewers You Can Deliver II: Demonstrating Credible Support & Potential Impact
The Importance of Pre-submission Review, the Role of the RDS & Your Next
Steps
Issy Reading
218

Thursday 17th February 2022 The Importance of Pre-submission Review, the Role of the RDS & Your Next Steps
Issy Reading
The Importance of Pre-Submission Review –
the Role of the RDS & Your Next Steps
Issy Reading
Research Design Service South Central
EGGA, 4th March, 2021
Rigid templates:• Page limits and word counts• Right information in the right place
Funding panels and reviewers:• Specialists• Non-specialists• ‘Detailed’ readers• Speed-readers
They need:• Clear pointers • Relevant information; no waffle• Arguments – appeal to funder, not necessarily discipline• Sufficient detail to assess quality and feasibility
From Day 1: Challenges
• Good for background and design
• Help prevent criticism from detailed peer reviewers/ subject specialists
• Less useful in assessing proposal from broad funding panel perspective
Funding panels like applications which:
• Are easy for non-specialists to understand
• Are easy for non-specialists to speed-read
• Will convince a critical, busy non-specialist
Role of Expert Review
J. Aldridge & A. Derrington (2012) The Research Funding Toolkit, Sage
www.freeclipart.pw/clipart_images/yoda-outline-clipart-11286
To understand easy it must be
1
2
3
219

Thursday 17th February 2022 The Importance of Pre-submission Review, the Role of the RDS & Your Next Steps
Issy Reading
• All experts in your area
• All enthusiasts
• Happy to spend time reading your/ local applications
• You/ they may not understand funding processes
• May not wish to hurt feelings
• May be too busy to provide good constructive feedback
Why You Can’t Depend on Yourself/ Immediate Colleagues for Comprehensive Review
J. Aldridge & A. Derrington (2012) The Research Funding Toolkit, Sage.
Pixabay.com
Useful People for General Review
• Academic colleagues outside of discipline
• Colleagues who sit on funding panels
• People who review for the scheme
• Colleagues with prior success in the scheme
• For NIHR and others – Patient and Public Involvement representatives
J. Aldridge & A. Derrington (2012) The Research Funding Toolkit, Sage
• Sources of funding
• Identifying and refining research question
• Designing a study
• Research methods including medical statistics, health economics, qualitative
• Patient and public involvement
• Identifying potential collaborators
• Advice on common pitfalls
• Interpreting feedback from funding panels
• Overall presentation & flow
Research Design Service
4
5
6
220

Thursday 17th February 2022 The Importance of Pre-submission Review, the Role of the RDS & Your Next Steps
Issy Reading
• Sources of funding
• Identifying and refining research question
• Designing a study
• Research methods including medical statistics, health economics, qualitative
• Patient and public involvement
• Identifying potential collaborators
• Advice on common pitfalls
• Interpreting feedback from funding panels
• Overall presentation & flow
Research Design Service
• Sources of funding
• Identifying and refining research question
• Designing a study
• Research methods including medical statistics, health economics, qualitative
• Patient and public involvement
• Identifying potential collaborators
• Advice on common pitfalls
• Interpreting feedback from funding panels
• Overall presentation & flow
FREE
Research Design Service
Is your study in scope: does it address the funding criteria explicitly?
Are you doing what the guidance asks?
Have you shown the relevance of the study to the funder?
Do you have a clear research question, aims and objectives?
Do you have clear lay and scientific summaries?
Have you demonstrated a need for thestudy / your knowledge of the area?
Do you have an appropriate study design?
Are your interventions (if applicable) clearly described, including ‘usual care’?
Are all aspects of the methods and procedures clear?
Do you link question/ aims & objectives, methods & analysis?
Have you consulted all appropriate experts
Has any necessary feasibility/ pilot work been undertaken/ planned?
Do you have adequate lay involvement?
What does the RDS look at?
7
8
9
221

Thursday 17th February 2022 The Importance of Pre-submission Review, the Role of the RDS & Your Next Steps
Issy Reading
What does the RDS look at?
Have you given yourself a realistic timetable?Is your study sensibly resourced & funded?
Are you being over-ambitious?
Do you have good dissemination plans?
Have you considered the short and long term impact of your work?
Is your proposal understandable to a diverse audience?
Have you given yourself enough time to develop the application properly?
Is your application ‘well-crafted’?
It your application complete?
Have you made the necessary research partnerships?
Do you have the right skill mix in your team?
Ways the RDS works
• One-to-one contact• Research design advisory panels (RDAPs)• Pre-submission review panels• Mock interviews• Events and workshops• Web – www.rds-sc.nihr.ac.uk – request support &
sign up to our mailing list
RDS regions across the nation
https://www.nihr.ac.uk/explore-nihr/support/research-design-service.htm
10
11
12
222

Thursday 17th February 2022 The Importance of Pre-submission Review, the Role of the RDS & Your Next Steps
Issy Reading
Useful Reference
J. Aldridge & A. Derrington (2012) The Research Funding Toolkit, Sage.
Suggest a series of ‘tests’ for your draft:
• Eligibility & strategy for funder• Project design• Readable• Understandable• Sufficient detail• Memorable• Convincing• Fundable• Speed-readable• Panel test• (Referee reports for future improvements)
Leonardo da Vinci: Public Domain
Evaluation form
13
14
15
223

EGGA 2022 (15th – 17th February 2022)
CONTRIBUTORS
224

Contributors
Jane Appleton Member, Clinical Doctoral Research Fellowship Committee & RDS South Central Adviser
Rebecca Barnes National RDS Priority Lead for EDI
Steven Blackburn One-to-one Adviser, RDS West Midlands
Jo Brett One-to-One Adviser, RDS South Central
Jackie Birks One-to-one Adviser, RDS South Central
Sarah Brien One-to-One Adviser, RDS South Central & member of NIHR PCAF Review Panel
Caroline Burgess One-to-one Adviser, RDS London
Maria Chorozoglou Senior Research Adviser, RDS South Central
Philippa Christoforou Senior Licensing & Venture Manager, Oxford University Innovation Ltd.
Lisa Douet Senior Adviser, RDS South Central & NIHR NETSCC Senior Research Manager/Scientific Adviser
Rachel Evley One-to-one Adviser, RDS East Midlands
Alexis Foster One-to-one Adviser, RDS Yorkshire and The Humber
Ushma Galal One-to-one Adviser, RDS South Central
Antoniya Georgieva NIHR Career Development Fellow & Scientific Director, Oxford Centre for Fetal Monitoring Technologies
Bernard Gudgin PPI Representative, RDS South Central & former panel member of several NIHR panels
Louise Hayes One-to-one Adviser, RDS North East and North Cumbria
Paul Hewitson PPI Manager (Oxford) and Senior Research Adviser, RDS South Central & panel member, Oxfordshire Health Services Research Committee
Kate Hill One-to-one Adviser, RDS Yorkshire and The Humber
Helen Hickey One-to-one Adviser, RDS North West
Mio Hu One-to-One Adviser, RDS South Central
Sophie Hyndman Deputy Director & Senior Research Adviser, RDS South Central
Dorit Kunkel Senior Research Adviser, RDS South Central
Brian Leask Administrator, RDS South Central
225

Paul Lott Operations & Information Officer, RDS South Central
Ramon Luengo-Fernandez Senior Adviser in Health Economics, RDS South Central
Anna Maguire-Elliott Research Administrator, RDS South Central
Nicola Melody Assistant Director, Personal Awards, NIHR Academy
Joanna Moschandreas Senior Statistician, RDS South Central
Chris Newby National RDS Priority Lead for EDI
Tracey Newman Associate Professor of Neuroimmunology & Director of Graduate School (Medicine), University of Southampton
Raquel Nunes One-to-one Adviser, RDS West Midlands
Heather Parsons Patient & Public Involvement Officer, RDS South Central
Dean Phillips Senior Research Design Adviser, RDS South Central
Issy Reading Director & Senior Adviser in Statistics, RDS South Central
Paul Roderick Professor of Public Health within Medicine, University of Southampton
Wanda Russell One-to-one Adviser, RDS West Midlands
Phil Saunders Administrator, RDS South Central
James Sheppard Member, NIHR RfPB South East & Central Regional Advisory Committee & University Research Lecturer, University of Oxford
Julius Sim One-to-one Adviser, RDS West Midlands
Ivonne Solis-Trapala One-to-one Adviser, RDS West Midlands
Liz Stokes One-to-One Adviser, RDS South Central
Neil Thomas One-to-one Adviser, RDS West Midlands
Sarah Thomas One-to-one Adviser, RDS South West
Dean Thompson One-to-one Adviser, RDS West Midlands
Werther Vecchiato Assistant Licensing & Ventures Manager, Oxford University Innovation Ltd.
Jane Vennik Senior Research Adviser, RDS South Central
Eila Watson One-to-one Adviser, RDS
Jane Wolstenholme One-to-One Adviser, RDS South Central
Tracey Young One-to-one Adviser, RDS Yorkshire and The Humber
With thanks also to Sean Ewings, Caroline Eyles and Mary Boulton for their contributions to the structure and content of EGGA over the years
226

EGGA 2022 (15th – 17th February 2022)
COURSEWORK
227

15th February 2022
Writing Tips: Story, Style & Sales Pitch
Practical: Writing techniques
1. What immediately obvious thing has been done to help the reader?
2. Find three examples of ASSERT-JUSTIFY.
3. Find two examples of where ASSERT-JUSTIFY might have been used, but was not. Can you find a sentence in the paragraph that could either be used or adapted for use for this purpose?
4. Find three examples of priming
5. Find three examples of linking
6. Find three examples of signposting
7. Can you identify any tag-phrases?
8. In five short bullet points, outline the argument being made to reviewers
9. Did you understand the importance of the proposed work?
COURSEWORK
228

EGGA 2022
Background & Rationale Section (Gerry, DRF, 2016) Developing a new early warning score to more accurately predict which hospital patients are in need of immediate care, using novel dynamic prediction methods Clinical problem Severe clinical deterioration of hospital patients is often preceded by changes in their physiological parameters, such as blood pressure, respiratory rate, pulse and level of consciousness.1-4 Chart reviews and a recent report from the National Confidential Enquiry into Patient Outcome and Death (NCEPOD) show that before serious events such as death, cardiac arrest and intensive care unit admission occur, there is often several hours of evidence of clinical deterioration. Many of these serious events could thus be prevented with appropriate action.3,5-8 Factors associated with failure to prevent deaths in hospital include poor patient monitoring, failure to recognise signs of deterioration, inadequate interpretation of physiological changes, and failure to take appropriate action.9-12 A recent review estimated that 12,000 deaths could have been prevented in English hospitals in 2009, whilst other sources estimate this number could reach 40,000 per year.3 Early Warning Scores are the existing solution Hospitals need tools to help staff recognise patients at risk of deterioration, enabling them to provide appropriate, timely care and prevent unnecessary serious events. Morgan proposed the Early Warning Score (EWS) as a solution in 1997.13 Many adaptations of the idea have since been proposed. These simple algorithms usually allocate points for each physiological vital sign, weighted according to the degree of departure from a range perceived as normal, then add up the weighted points to give a total score. The vital signs typically assessed are respiratory rate, systolic blood pressure, temperature, heart rate and level of consciousness. It is the total score that informs care. Particular scores trigger particular actions, such as increasing the frequency of vital sign monitoring, calling more experienced staff or calling a rapid response team. These simple tools can easily be implemented as part of traditional bedside observation charts. A systematic review published in 2007 found 33 EWS algorithms in use, with a high degree of overlap in the vital signs included, but with considerable variability in the weighting systems used to obtain the score.14 However, due to numerous deficiencies in the methods used to develop many of these EWSs, the authors concluded that none of the algorithms could be said to ‘perform well’ at identifying patients at increased risk of in-hospital death from those who were not. In the same year, NICE released guideline CG50 on recognising and responding to deterioration using EWSs.15 Recommendations from the guideline concluded that all adult patients in acute hospital settings should be monitored using an EWS, that there are six key physiological factors that should be included in an EWS, and that they should be used on admission, at least every twelve hours, and more frequently if an
229

EGGA 2022
abnormal physiology is detected. As a result, NHS hospitals in England could collect around 350 million sets of vital signs observations each year.16 In 2012 a group formed by the Royal College of Physicians published recommendations17 proposing a standardised EWS to be used across the NHS. This led to the development of the National Early Warning Score (NEWS). The NEWS incorporates the six physiological parameters recommended in NICE CG50: respiratory rate, oxygen saturations, temperature, systolic blood pressure, pulse rate and level of consciousness. The weighting for each vital sign is based on a recently developed EWS, called ViEWS18, and on the clinical consensus of the group. The NEWS is now seen as the gold standard EWS.17 Early Warning Scores have been developed using suboptimal methods Several approaches have been used to develop EWSs. The majority have been based wholly or partly on the clinical expertise of a committee and on a review of the literature. Others have used a ‘trial and error’ approach18, in which parameters are manipulated and weights assigned based on those that give the optimal results from a single dataset. This approach leads to ‘overfitting’ problems: the model fits idiosyncrasies in that particular dataset rather than any underlying generalisable patterns, meaning that the model fails to work in other data.19 Very few EWS models have been developed using robust statistical regression modelling, which is the most widely recommended approach for developing clinical risk prediction models. The inherent correlation between different vital signs is thus not typically accounted for in current EWS models. In contrast, if a statistical model were used, apparent predictive effects of one vital sign could be explained by other predictive variables, and a more robust and unbiased choice of which predictors to include in the model could be made. When data-driven methods have been used in the past, over-simplistic assumptions have been made. For example, when datasets have been used in which any one patient may contribute multiple sets of vital signs, these sets have been assumed to be independent. However, measurements are likely to be highly correlated within a patient, and therefore results from these approaches could be biased and over-confident. Further, although the link between vital signs and patient outcomes is of interest, it can often be confounded by treatment interventions. For example, hospital staff may notice that a patient is deteriorating, give appropriate medical care, and therefore prevent a serious event. Ignoring the occurrence of this treatment intervention will modify the apparent relationship between vital signs and outcome.
By definition, a model will generally fit better to the data that it is derived from than most other datasets. Models must therefore be evaluated on another, independent, dataset, which is known as external validation.20 As there is little evidence that EWSs generally undergo external validation, their performance is largely unknown, which raises questions about whether they should be used.21 The validation studies that do exist tend to have been
230

EGGA 2022
poorly designed, conducted and reported, show only limited usefulness, look at a very specific population, or have been carried out on a very similar population to the original derivation dataset.22,23 A further weakness of the current EWSs is the way they have been developed and delivered: in many cases the same algorithm is applied to all hospital patients, regardless of their illness (and severity), age or sex.24 There are a few exceptions, such as the development of paediatric- or antenatal-specific versions.25,26 However, EWSs are generally applied to highly variable populations. As one would expect different physiological factors to predict poor outcome in different illnesses, a generic algorithm is likely to perform badly in some groups.24,27 Furthermore, despite their broad target population, most algorithms do not contain patient-specific variables that could ‘individualise’ the prediction, such as age, sex and medical indication (and severity).28
As with all risk prediction algorithms, the aim is to have a system that flags the majority of those actually at risk (sensitivity) and correctly does not flag those not at risk (specificity). Once an algorithm has been chosen, a threshold score at which action will be taken is defined. The threshold creates a trade-off between sensitivity and specificity – improving one is to the detriment of the other. The NEWS has a recommended threshold for calling the critical care team of five points. This threshold results in a specificity of around 80%; 20% of alerts are false alerts17. However, the scores are meant to be calculated regularly. A patient who will not ultimately deteriorate has around a 60% chance of being flagged as at risk in any one day, assuming six hourly assessments. This creates a tremendous workload for clinical staff, resulting in protocols often not being followed.29,30 This may be part of the reason why randomised trials of EWSs have generally shown them to be ineffective in improving health outcomes.31 A fundamental problem with current methods for developing EWSs is that only a patient’s most recent information is considered. Current EWSs all aim to predict future risk of deterioration based on a single moment in time, the most recent vital signs measured for a particular patient. All observations of that patient made in the past are ignored when calculating the patient’s current risk. Any trends (or deterioration) in previous measurements are not captured, which is clearly wasteful. For example, a patient with oxygen saturation readings over the course of a day of 100%, 99%, 97% and 95% is showing a clear downward trend that may well increase their risk of deterioration. However, the most recent value alone, 95%, may not prompt a nurse to take appropriate action.
Electronic systems give the opportunity for next-generation Early Warning Scores Vital signs have traditionally been recorded on paper observation charts. An assessor, typically a nurse, applies weights to each vital sign and sums them to calculate the total EWS. Unsurprisingly, this approach is errorprone; incorrect scores are assigned to vital signs and individual scores are incorrectly summed.32 Electronic EWS systems have been
231
EGGA 2022
developed, partly to mitigate human-error flaws. An electronic system assigns scores to vital signs and computes the EWS automatically.33 These systems can send alerts, prompt appropriate action and give ward- or hospital-level oversight of the EWS status of all patients.
The Health Secretary delivered a mandate in 2013 that the NHS should be paperless by 2018.34 A 2013 audit reported that 27% of English NHS trusts were already using electronic systems to monitor vital signs.35 The majority of hospitals are likely to be using electronic EWS systems soon. As electronic systems become more widely available, they should be the subject of focused research. More sophisticated models can be devised now that scores are calculated automatically. Further, very large numbers of vital sign observations will be recorded. These datasets can be used to develop improved EWSs. Next-generation scores risk being developed using the same poor statistical methods Despite their enormous potential, there has been no obvious improvement in the methods used to develop EWSs in the five years since electronic systems became available. There is a real risk that the basic EWS algorithms developed to take into account the restrictions of paper observation charts will continue to be used if no concerted effort is made. In light of the lack of progress in this area, it seems likely that any new EWSs will continue to be developed using the same poor quality methods and will continue to be of little benefit to patients.
My research will provide a better solution The developments in electronic systems and their increasing use within hospitals present an opportunity and need for robust and novel methods to be applied to EWSs, to take them to the next stage of their development. My proposed research will take this step.
I will use statistical regression modelling techniques that are robust and unbiased, and will more accurately link vital signs to patient outcomes. Other patient characteristics may be included in the models, such as age and medical condition, allowing for individualisation of the risk prediction. Unlike previous attempts, I will not ignore the complexity of the problem. I will take into account the potential for multiple, correlated measurements within each patient. I will also recognise that any treatment interventions that occur could severely modify the relationship between vital signs and outcomes. I will validate any models that I develop using data from different hospitals, allowing for a better test of the models’ prediction. Finally, and perhaps most importantly, I will use dynamic prediction modelling methods to build prediction models that use both past and current measurements. This will allow individualised trends to be detected and therefore allow faster recognition of deterioration.
232

EGGA 2022
16th February, 2022
Writing the Research Plan
Practical: Reviewing a Research Plan
Task Read through this research plan with a critical eye. Does the research plan, as presented, convince you that:
• The researchers will be able to answer the research question? • That the methods being used are appropriate & scientifically rigorous? • That the proposed work is feasible?
What could be improved, e.g. in terms of structure, detail, presentation? Is the plan complete? The plain English summary and aims are included for background information. Plain English Summary: Weight loss surgery works by helping to reduce the number of calories in the body by either reducing the size of the stomach or by bypassing the small intestine. Studies have shown that such surgery leads to sustained weight loss over a long period of time. Surgery does, however, carry some mainly short term risks. In some patients with late onset (type 2) diabetes, surgery has cured their diabetes. However, surgery is normally only done on severely obese patients i.e. with a Body Mass Index greater than 40. Those with a lower BMI of less than 35 and diabetes must try other methods to reduce their weight. These methods have shown very limited effectiveness, particularly over the long term. More research is needed in order to understand the role surgery might play for those with diabetes who are not so severely obese. In order for such research to succeed it is crucial that we understand patients' willingness to participate in such a study and identify potential barriers to taking part. This study assesses the attitudes of patients with type 2 (or late onset) diabetes to having surgery to improve their weight and better manage or lead to resolution of their diabetes. The views of clinicians will also be sought and will help to identify whether they feel weight loss surgery is appropriate for this group of patients and if so, what type of surgery would be suitable for particular patient characteristics (e.g. age, BMI). If patients and clinicians do feel that surgery would be an appropriate part of their weight and diabetes management, then this research will show whether it is feasible to run a trial to compare weight loss surgery with non-surgical alternatives in such patients. We also aim to identify a patient advisory group to assist with the further development of the trial design and materials. (Taken from the RfPB website)
Aims i) To explore the attitudes and beliefs of patients with type 2 diabetes and non-morbid obesity
(BMI 30-40kg/m2), about the role of bariatric surgery and other weight loss interventions in their management. To ascertain whether they would consider entry to an RCT which randomised to BS.
ii) To identify the number of patients with BMI 30-40 kg/m2 and type 2 diabetes who might be potentially eligible for an RCT in a sample of GP diabetes registers in the South West (SW) and the Central England (CE) PCRNs.
iii) To assess the attitudes of bariatric surgeons, GPs, and diabetologists to BS as a treatment option for such patients; their opinions on participating in an RCT above and for which sub-groups of patients (e.g. HBA1c level), and their equipoise over gastric bypass and banding. (Taken from the RfPB website)
233

EGGA 2022
Optimum care for non-morbidly obese patients with type 2 diabetes: the perspectives of patients and clinicians on the role of bariatric surgery. (Roderick et al., 2010; edited to make points) GP practices who are members of the ***** and England PCRNs will be contacted and asked to see if they would be willing to participate in the study. Of those that reply positively, 40 practices will be selected to provide a variety of rural/urban, socio-economic and where possible, ethnic mix. (We recognise that such GPs may not be representative of all GPs but they would be likely recruitment sites for an RCT and their patients will be equally representative).
The Diabetic Lead GPs in these 40 practices will be asked to co-ordinate:
1.1 Database Search: A pro-forma will be developed to aid identification of the number of Type 2 diabetics with BMI 30-40 kg/m2 aged 18-74 with no obvious contraindications to BS (i.e. secondary diabetes, previous BS, drug/alcohol addiction, mental health problems, recent major CVD, recent /malignancy (though not non melanotic skin), advanced or severe CKD, liver fibrosis /portal hypertension, severe respiratory disease).
(We will sample patients with BMI 27.5-40 kg/m2 in south Asian patients, 27.5 is the WHO ‘s lower public health action point for south Asian patients who have more body fat than Caucasians at the same BMI level.) Clinical details (year of diagnosis, latest HbA1c, Framingham risk score if available and age) will allow calculation of the effect of various cut points on potential sample size. Details of the ethnic mix and the Index of Multiple Deprivation of their catchment area will be obtained if available (or derived for the practice’s Local authority using the practice postcode and Geo-convert system).
Preliminary work in one practice (***) revealed 220 registered patients with diabetes (2.8% of list) of whom 124 (56%) had a BMI>30. Of these 47 were aged below 65 and had a BMI in the 30-40 range. A further 7 were excluded due to medical contraindications or prior surgery leaving a potential sample of 40. However this would be reduced further if duration or diabetes control were restrictive entry criteria and we do not know how many would then be willing to accept surgery and entry to a randomised trial. Such data will be crucial in trial planning.
1.2 Qualitative Interviews:
Sampling:
In 5 practices from different demographic areas, a purposive sample (based on BMI, age, gender, ethnic and socioeconomic factors) of 60 patients (ie 12 per site) will be invited by their GP to participate in the qualitative interview study. From respondents, 30 patients will be selected to explore attitudes and beliefs about their diabetes, role of BS and other weight loss interventions, use of the private sector, willingness to enter an RCT or preferences for particular modes.
Current research by **** involves interviews with type 2 diabetics in low IMD areas and from the South Asian community in ******, so the proposed purposive sampling strategy is felt to be feasible.
234

EGGA 2022
Semi-structured interviews will explore:
• experiences of managing weight whilst living with type 2 diabetes, any weight loss interventions tried
• understanding preferences and attitudes to BS and different types of BS
• how BS might affect diet, exercise and self-management of their diabetes
• the support and information they would like, in what format, when and who from, to decide whether BS was appropriate for them
• whether they would consider being randomised to different types of BS or no surgery within an RCT and what information and support would help them to make an informed choice
• interest in participating in a patient advisory group.
Interviews will be digitally recorded and transcribed as soon after the interview as possible. A reflexive log will be kept to record the researcher’s perceptions of the interviews and to identify early themes to explore in later interviews.
1.3 Qualitative Interviews of Private Patients
Few patients with type 2 diabetes and BMI < 40kgm2 have undergone BS. Those that have are predominantly in the private sector. These patients will be identified from existing databases in ***** and ****. Explorative qualitative interviews will be conducted with a small group sampled at varying times post operation (n=10) to explore their decision to pay for surgery, experiences of surgery and how it has affected their lives and diabetes management.
Qualitative Analysis: the interview transcripts from patients in 1.2 and 1.3 above will be analysed using the Framework Approach.(19) This approach, through coding, charting and mapping allows the data to be explored deductively as well as inductively. In this way, findings can focus on the key questions outlined above, as well as emerging more inductively from the data.
The analysis of data will be conducted in parallel with data collection so the interview guide can be developed iteratively to explore emerging themes. The researcher will conduct the analysis. **** and other co-applicants, particularly the lay collaborator if she agrees, will code a selection of transcripts to provide inter-rater reliability.(20)
Participants will be asked if they would be interested in joining a patient advisory group to advise on:
• the development of the patient questionnaire (1.3 below)
• the content and style of information materials explaining the rationale for BS for BMI 30-40 kg/m2 and the hypothetical trial options
1.3 Questionnaire of Patient Views
235

EGGA 2022
Based on the findings of the qualitative phase, a questionnaire will be developed to quantify the views of patients towards the role of BS within the management of their diabetes, other weight loss strategies they have tried and their willingness to enter various designs (i.e. 2 arm, 3 arm, delayed preference) of a potential trial.
This will be mailed out to all those identified through the GPs’ databases. Information materials explaining the evidence for and rationale for BS for BMI 30-40 kg/m2 and the hypothetical trial options will be included.
Sample size for Patient Questionnaire:
Estimating that an average of 20 patients will be indentified in each of the 40 practices gives a total of 800 questionnaires (formatted for electronic scanning for efficient and accurate data entry).
Estimating a conservative response rate of 50%, 400 questionnaires will be returned. Taking the primary outcome as the proportion prepared to enter a hypothetical trial and assuming it is 25%, the true proportion can be estimated to within +-5% with 95% confidence with 289 completed questionnaires . Increasing the sample to 400 will allow us to look at associations with factors such as gender and BMI (<>35).
Analysis of patient questionnaire: we will use descriptive statistics and contingency tables to explore patients’ willingness to enter various designs of a hypothetical trial, their views on bariatric surgery and simple associations with ethnic, socio-demographic, age, gender and clinical factors (e.g. BMI).
Phase 2: Clinicians Views: Bariatric Surgeons, Diabetologists, GPs (Diabetic Leads) surveys 2.1)
Bariatric Surgeons: All bariatric surgeons in England will be sent the questionnaire n=100.
Consultant Diabetologists:
A random sample of 200 consultant diabetologists registered with the Association of British Clinical Diabetologists will be contacted. A previous survey had a 50% response rate. (21) With 100 responses, assuming 25% would agree to participate on a trial, the true proportion can be estimated to within +_ 8.5% with 95% confidence.
GPs Diabetic Leads: GPs from PCRNs in *** and *** n= 200
To help develop the questionnaire we will follow-up by short telephone call the lead GPs for diabetes in the 40 practices in phase 1 to elicit their views in a semi-structured interview.
The sample size has been calculated pragmatically to balance resource constraints against precision of any estimate of response rate.
Also included with the questionnaire will be:
• Information sheets presenting the evidence and uncertainties over BS in the BMI 30-40kg/m2 group with type 2 diabetes.
236

EGGA 2022
• Summary of findings of qualitative interviews and patient questionnaire to provide information of patients’ views of BS.
Questionnaires and information sheets will be piloted with a small group of surgeons, diabetologists and diabetic lead GPs in Southampton. The questionnaire will draw on the work of Young (22) in establishing equipoise among surgeons using a postal questionnaire.
The questionnaire will ask:
• opinions on the role of BS for type 2 diabetics with BMI 30-35 kg/m2, and/or 35-40 kg/m2, all or only those with HBA1c >7.5%, or with high CVD risk on Framingham or other criteria (eg microalbuminuria)
• whether they would recommend surgery and for which types of patient
• whether they would be prepared to enter patients into a hypothetical trial
• whether they would consider even lower BMI 27.5-30kg/m2 if patient was at higher risk
• which age groups they would consider for BS
• what support would be needed pre and post operatively for these patients
• whether they would consider participating in an RCT and reasons for their decision
• preferences for the design of the trial (3 arm, 2 arm i.e band or bypass vs best medical, which type of surgery), and the reasons for their preference
• whether they favour one arm over another, and reasons for their view
• additional capacity required to provide the operations
Analysis of Questionnaires: We will use descriptive statistics and contingency tables to explore clinicians‘ response rates, their willingness to participate and their views on trial design. Factors of interest include volume of operations for surgeons and geographical area or IMD 2007 of practices for GPs).
Phase 3: Stakeholder Conference
A stakeholder conference will be held to present the findings and agree whether an RCT of BS in this patient group is appropriate and feasible and if so to identify the next steps required to design such a study.
Participants (approx. 30):
• Patient advisory group
• Key bariatric surgeons, diabetologists and Diabetic lead GPs
• The research team
• Selected PCT Commissioners
237

EGGA 2022 (15th – 17th February 2022)
WORKSHEETS AND EXERCISES
238

The Purpose of a Grant Application Sophie Hyndman Why is your project important?
Is it important to patients &/or carers? In what way? Is it important to the NHS? In what way? Is it important to wider society? In what way?
WORKSHEET Essential Guide to Grant Applications 2022 Research Design Service South Central
239

Is it important to the scientific community? In what way? What do you hope the impact of your work will be? If you have a funder in mind, have a look at their remit. Is your project important to the funder? In what way/s are you addressing their remit?
240

Developing a Research Question (& Aims & Objectives) Lisa Douet Use the following as a reminder of things to consider when refining your request question, aims and objectives. Define the problem
In terms of scale, impact on person, carers, NHS, costs
Notes:
Need for evidence
What is the gap in the literature, what don’t we know?
Notes:
What do we need to
know? How will this study bridge the gap in the evidence
Notes:
Who is calling for
the evidence? • James Lind Alliance • NICE research
recommendations
Notes:
Talk to colleagues
Is it a problem for others?
Notes:
WORKSHEET Essential Guide to Grant Applications 2022 Research Design Service South Central
241

Talk to patients Is it a problem for them?
Notes:
Clearly define PICO Notes:
Patients Notes:
Intervention Notes:
Comparator Notes:
Outcomes Notes:
What is your research question (ideally in a single sentence):
242

Writing Tips: Story, Style & Sales Pitch Sophie Hyndman Tweak the following text so that it has more of a ‘David Walliams’ style Mrs. Rachel Lynde lived just where the Avonlea main road dipped down into a little hollow, fringed with alders and ladies’ eardrops and traversed by a brook that had its source away back in the woods of the old Cuthbert place; it was reputed to be an intricate, headlong brook in its earlier course through those woods, with dark secrets of pool and cascade; but by the time it reached Lynde’s Hollow it was a quiet, well-conducted little stream, for not even a brook could run past Mrs. Rachel Lynde’s door without due regard for decency and decorum; it probably was conscious that Mrs. Rachel was sitting at her window, keeping a sharp eye on everything that passed, from brooks and children up, and that if she noticed anything odd or out of place she would never rest until she had ferreted out the whys and wherefores thereof. Anne of Green Gables, L.M.Montgomery, 1908
https://en.wikisource.org/wiki/Anne_of_Green_Gables_(1908)/Chapter_I Text is available under the Creative Commons Attribution-ShareAlike License
EXERCISE Essential Guide to Grant Applications 2022 Research Design Service South Central
243

Writing Tips: Story, Style and Sales Pitch Sophie Hyndman Summarise the argument for your proposed study in five brief bullet points. … is a problem [give evidence for it, e.g. prevalence/ incidence, poor patient outcomes, cost]
Its resolution would improve things [e.g. reduce prevalence/ incidence, improve patient outcomes, reduce costs]
Previous work has shown …, but this is deficient in the following ways… [knowledge gap]
This project will address [the knowledge gap, e.g. resolve uncertainty, provide necessary information/ solution]
When the project is done, the problem will be resolved & the impact of this will be…
WORKSHEET Essential Guide to Grant Applications 2022 Research Design Service South Central
244

Research Plan I: Expectations, Reviewers’ Concerns & Common Confusions Sophie Hyndman THE RESEARCH PLAN: QUESTIONS REFEREES MAY ASK This is not a comprehensive list, but will ensure that you think about a number of important things that reviewers will be looking out for in the main research plan section of your application. Remember, you need to pre-empt possible criticism by answering any questions reviewers may think of, within your written application. Overall, consider:
Will the research plan answer the research question? Is it appropriate? Is it scientifically rigorous? Is it feasible? Will it deliver useful outputs? Have weaknesses been acknowledged & removed or mitigated where possible?
Importantly, do referees have sufficient detail to gauge the quality of your work? Consider an external review (e.g. from the RDS) to ascertain this.
STUDY DESIGN ISSUES Is the design clearly stated? Will the design answer the research question? Is the justification / rationale for the design clear? Are the theoretical underpinnings of the design suited to the nature of the question? Have the relative strengths & weaknesses of the design been considered? How does the design compare to alternatives? Have appropriate methodologists been consulted in deciding on the design? [Where necessary] Is a clinical trials unit on board? Have patients/ carers/ service users/ other relevant stakeholders been involved in the design? Have the practical aspects of implementing the design been considered? What methods are used to ensure rigour (‘trustworthiness’, validity, reliability, reproducibility etc.) in the
design? E.g. Where relevant, does the design use more than one method of data collection to facilitate cross-checking (triangulation) of findings?
[If comparative study] Is there any chance of contamination between intervention & control arms? [Where other things can influence outcomes] Are relevant confounders accounted for in the design (e.g.
through randomisation)? [Where used] Is the randomisation procedure suitable? [If qualitative] What is the ontological (nature of reality) & epistemological (theory of knowledge) position
of the work? Where necessary, are researchers familiar with the culture of the participating organisations? Are there any ethical issues in relation to the study design that need to be considered?
WORKSHEET Essential Guide to Grant Applications 2022 Research Design Service South Central
245

SAMPLING & RECRUITMENT Is the population of interest clearly stated? Is the setting of the research clearly stated? Does the stated population & setting relate sensibly to the research question? Are the sampling method/s clearly stated? Are the sampling methods consistent with the objectives? Is the sample size clearly stated? Is the rationale/ justification (statistical or theoretical) for the sample size clear? Are the eligibility criteria clearly stated? Is it clear how, when & by whom eligibility criteria will be applied? Is it clear how potential participants will be accessed, approached, consented & enrolled? Is the recruitment process ethical & suitable? Is recruitment likely to meet targets? Have the researchers presented any evidence to support the likely
recruitment rate stated? Have patients/ carers/ service users been consulted about the recruitment process?
INTERVENTION Is the intervention clearly described/ explained? Is the intervention novel? In what ways? What is the evidence to support the intervention? Does the intervention make sense for the patient/ carer/ service user group? What is the ‘dose’ for the intervention & the rationale for it? Is the timing of the intervention clear? What is the likelihood that the intervention will have an effect, relative to other factors? What are the implications of the intervention for the NHS? Can the intervention be applied properly & consistently? Can staff administer the intervention appropriately? Are staff training plans adequate & clear? Will staff be happy to administer the intervention? Are staff experiences & preferences an issue for the intervention? How will the fidelity of the intervention (ensuring it is delivered as intended) be ensured? Will patients/ carers/ service users be happy to do the intervention? Will patients/ carers/ service users adhere to the intervention? [Where relevant] Has the comparator been clearly explained, including ‘treatment as usual’? [Where relevant] Is the comparator sensible (e.g. in relation to potential biases/ confounders)? Should/ can participants be ‘blinded’ to the intervention? Is a placebo necessary/ possible? Are there any ethical issues in relation to the intervention that need to be considered?
246

DATA COLLECTION Is it clear what type of data are being collected? Are the data types appropriate for addressing the research question, aims & objectives? What methods are being used to collect data (e.g. postal, online, telephone)? Who will collect the data? From whom & where are data being collected? When are data being collected & does the timing make sense (e.g. in relation to intervention)? Is data collection sensible in relation to NHS structures & pathways? Have other options for data collection been considered? Have potential weaknesses in the data collection approach been identified & addressed? Is the data collection feasible? Can data be collected successfully (is there evidence to support this)? Have the ethical implications of data collection been considered? Will missing or poor quality data be an issue? [If routine data/ ‘big data’], have permission & timelines for these been considered? Are the data collection methods & schedule acceptable to patients? E.g. Are they burdensome? Are they
realistic with regard to continued participant involvement? [Where applicable] Should, & can, data collection be ‘blind’ to intervention group? Is there sufficient expertise on the team to ensure data of suitable quality?
OUTCOME MEASURES Are the outcome measures being used appropriate for the research question, aims & objectives? Are the outcome measures relevant/ appropriate to the patient/ carer/ service user/ staff to whom they will
be administered? Will the specific measures be acceptable to patients/ carers/ service users/ staff? Have patients/ carers/
service users/ staff been consulted? Are the outcome measures valid & reliable? Is there a good rationale (& is it explained) for using particular outcome measures (e.g. over
alternatives)? Will the outcome measures be sensitive to the intervention? If proxy measurements are being used, are they appropriately correlated to important outcomes? Are outcome measures properly referenced?
247

DATA ANALYSIS Will the data analysis proposed address the research question, aims & objectives? Are the methods suitable, based on the type of data collected? Are the methods suitable, based on the sampling approach? How will the data be prepared for analysis? Is the analysis plan thorough? Will relevant guidelines/ references be followed & are these highlighted? Has an appropriate methodologist been consulted? Should/ can the data analyst be blinded to the intervention group?
PROJECT MANAGEMENT Does the study have an appropriate sponsor? Is it clear that ethics & governance principles will be upheld? Are all other relevant permissions & approvals in hand? Is the proposed work feasible in the time allocated? Are the study stages in a sensible order? Has sufficient time & funding been allocated for each step? Are the right researchers in the right place at the right time? Will all the materials, equipment & space required be available? How will data be entered & managed (including storage)? Do all aspects of data processing (e.g. storage, transcription) meet GDPR? Have all quality assurance issues been considered appropriately? [Where necessary] Have the logistics of sample transport & storage been considered appropriately? Has provision been made for issues relating to intellectual property, e.g. do researchers have ‘freedom to
operate’? Have Gantt charts/ flowcharts been used where these will be helpful/ have been requested? Do they
make sense? Is appropriate support from other relevant organisations (e.g. collaborators, clinical research network)
assured? Overall, will the project be well-managed? Will it deliver?
248

Writing Technical Sections: Qualitative StudiesJane Vennik
Qualitative studies ask “what”, “how” and “why” questions. For each of the following areas, summarise the research topic into a “what”, “how” or “why” question.
Research topic 1: Literature has shown that adolescents (11-18 year olds) with asthma are 40% less likely to carry or use an inhaler compared to adults. Several reasons for this have been identified including stigma and embarrassment, potential side effects, and lack of routine/forgetfulness. This study will look at the key factors that prevent adolescents using their asthma medication and will identify the most prevalent.
Potential qualitative questions:
Research topic 2: COVID-19 vaccines offer protection against COVID-19 disease which can be serious in later pregnancy for some women. However, uptake of the vaccine in pregnant women remains low. This study aims to identify the reasons for vaccine hesitancy in pregnancy or those planning pregnancy, in order to develop an intervention for primary care professionals and midwives to promote uptake of vaccine in women who are pregnant or planning pregnancy.
Potential qualitative questions:
1. ___________________________________________________________________________________
2. ___________________________________________________________________________________
3. ___________________________________________________________________________________
Research topic 3: Osteoarthritis is a common condition and leading cause of joint pain and disability. Management includes pharmacological and non-pharmacological treatments, and surgery for the most severely affected. Preparing for surgery by identifying and addressing risk factors can potentially reduce length of hospital stay, reduce complications and speed recovery. This programme of work aims to develop and evaluate an individualised prehabilitation programme for patients waiting for hip/knee surgery.
Potential qualitative questions:
1. ___________________________________________________________________________________
2. ___________________________________________________________________________________
3. ___________________________________________________________________________________
EXERCISE Essential Guide to Grant Applications 2022 Research Design Service South Central
249
EXAMPLE: Why do adolescents not use their asthma inhaler? EXAMPLE: What factors might support the use of asthma inhalers in adolescents? EXAMPLE: What are the main barriers for using inhalers for adolescents with asthma?

Research Processes & the Importance of Good Project Planning Sophie Hyndman Think about the people you will need to involve in your research project.
The type of people* you may need as co-applicants. *experience, subject & methods expertise.
The type of people you may need, in addition to co-applicants, as part of your broader research team.
Other types of people / groups of people / organisations you are likely to need to consult or work with to develop & deliver your research.
WORKSHEET Essential Guide to Grant Applications 2022 Research Design Service South Central
250

The Importance of Patient & Public Involvement Paul Hewitson Planning for Patient and Public Involvement in NIHR Grant Applications: A Brief Overview Effective Patient and Public Involvement (PPI) in developing research applications requires planning. How you approach the planning stage of your PPI component will have a dramatic effect on the quality of the PPI information you will include in your application. Start early. The following provides a brief overview of the steps you will need to undertake in planning and delivering your PPI pre-grant activities (and beyond).
Guidance Familiarise yourself with the specific guidance for that particular grant. It is important that you understand what you are being asked to include about PPI in your application, and how you should be presenting this information in the application. This includes what you will be required to write in the PPI section of the application, and also, the content and format for the plain English summary. Notes: Draft PPI Plan Have you written a draft PPI plan, detailing what you will asking PPI contributors to do over the course of the research?
• The draft PPI plan should include the ‘what’, the ‘when’, and the ‘why’ for PPI contributors during the research (if you were funded…)
• This means ‘what’ are you asking them to do, ‘when’ are you asking them to do it, and ‘why’ is it important for the research
• This should include PPI representation for any steering/advisory group associated with the research
• The draft PPI plan should reflect the ‘milestones’, or most important points of your research where involving PPI will contribute to the research
• This can include: o Reviewing submissions ethics committees o Writing/commenting on participation information
materials o Assisting with developing questionnaires or semi-
structured interview schedules o Providing comments on the relevance of findings from a
patient/public perspective o Writing or presenting research findings as part of the
dissemination strategy o Opportunities for support and learning for PPI
contributors (e.g. bespoke training in research methods or formal courses)
Note: Your draft PPI plan does not have to be extensive, nor should it be the ‘final’ version. It is a good idea to give it to potential PPI contributors (before/during your pre-grant PPI activity) so you can discuss any potential changes that may be required. Discussion with the PPI contributors should result in a shared understanding of the roles, responsibilities and expectations of involvement in research.
Notes:
WORKSHEET Essential Guide to Grant Applications 2022 Research Design Service South Central
251
Role/Responsibilities Do you have a draft ‘roles and responsibilities’ document you can give potential PPI contributors?
• Drafting a brief ‘roles and responsibilities’ document outlining what the PPI contributors’ roles will be in the research, and what they will be responsible for during the research
• You should also include what the roles and responsibilities are for the research team (and specifically, the PPI Lead, if required)
• This is not a formal contract, and should be in draft, as any final decision on PPI roles and responsibilities should be negotiated and agreed with the PPI contributors
Notes:
Flexibility Have you considered whether there is some choice or flexibility in opportunities for PPI contributors?
• Not all potential PPI contributors will be interested or available for all aspects of the research. Giving people options for how they can be involved in your ‘roles and responsibilities’ document can facilitate pre-grant discussions and improve your chances of recruiting PPI contributors to your study
People Do the people you are approaching have a ‘lived experience’ of the condition you are researching?
• Ideally, you are looking to involve people who have personal, direct knowledge and experience of living with the condition you intend to investigate
• ‘Lived experience’ can include people with the condition, but also includes those who care for people with the condition (e.g. dementia), parents of children with a condition, or people who have experienced treatment, but no longer have the condition (e.g. cancer survivors)
• Note: Health professionals who treat, manage or care for people with a condition are not considered PPI contributors. They may have a wealth of experience in delivering services to people with the condition, but this is not viewed as ‘lived experience’ of the condition
Are the people you intend to approach representatives of all those who suffer from the condition?
• Diversity, inclusion and equality are at the centre of identifying and approaching potential PPI contributors. The people you are approaching should be representative of all the people with the condition, not a more accessible subset of people
Notes:
252

Recruiting What strategies do you have for recruiting PPI contributors for your pre-grant activity and your research?
• Direct Contact: If you are in direct contact with patients/public either through clinical practice or in another professional capacity, you can approach
• Advertisements: NIHR host a website (www.peopleinresearch.org) where you can advertise for potential PPI contributors
• Charity/patient advocacy groups: Contact national/regional charity or patient/public advocacy group(s) to ask for their help in identifying or being directly involvement as PPI contributors to your research
Notes:
Costings Have you budgeted for all costs associated with including PPI contributors in your research?
• Payment for PPI contributors’ time is currently (Feb 2022) set at £25 per/hour. This includes both direct contact with PPI contributors (e.g. meetings), but also payment for time performing other agreed duties (e.g. reading/commenting on documents). For example, if you have a two-hour steering group meeting, with two hours’ expected reading time prior to the meeting, then the cost for the PPI contribution would be £100 (2x2hr meeting + 2x2hr reading time)
• Payment for travel for the PPI contributor (and potentially payment for subsistence) also is required
• Payment may also be required to cover costs associated with childcare or carer support costs
• Note: see www.nihr.ac.uk/documents/payment-guidance-for-researchers-and-professionals/27392 for further guidance on the NIHR requirements for PPI costings
• It is important to include your PPI costings in your draft PPI plan
Notes:
Resources
• UK Standards for Public Involvement - sites.google.com/nihr.ac.uk/pi-standards/standards
• NIHR Briefing Notes for Researchers - www.nihr.ac.uk/documents/briefing-notes-for-researchers-public-involvement-in-nhs-health-and-social-care-research/27371
• RDS Brief Guide to Pubic Involvement in Funding Applications: How can the RDS Help? - www.rdsblog.org.uk/Resources/A5_PPI_ Pocket_Guide_V3%20(1).pdf
Notes:
253

EGGA 2022 (15th – 17th February 2022)
REDACTED APPLICATIONS
Following EGGA 2021, attendees requested more examples of successful grant writing. We have permission to share with you the following two redacted applications, which we hope will be useful.
254

Reference: Date submitted: Page 1 of 65
Summary
Reference NumberLead ApplicantResearch Title Understanding the role of intravenous iron to treat anaemia in survivors of critical
illness Plain English Summary Background of the research
Anaemia is also known as low red blood cell count or low haemoglobin. Haemoglobin carries oxygen and therefore anaemia reduces the amount of oxygen that is available to the body. Anaemia is very common in intensive care unit (ICU) patients and also in those who leave ICU alive. 164,000 patients are admitted to ICU per year in the United Kingdom. Nearly half of these who survive ICU will leave with a haemoglobin of less than 100 grams per liter (g/L), which is termed ‘moderate-severe’ anaemia. The body reacts to infection or injury by producing inflammation (an attempt to heal or mend the body). Inflammation is present in nearly all ICU patients. However, whilst doing this, the body is unable to use available iron to make haemoglobin resulting in anaemia because iron is essential to make haemoglobin. Current blood tests are not able to reliably tell us how much iron is available because of inflammation. A new blood test of the main hormone that controls iron in body - hepcidin, has become recently available and may be a better test. Patients who survive ICU often experience high levels of tiredness and weakness resulting in a poor quality of life. These could be symptoms of anaemia, but may also relate to other complications the patient may have experienced during their illness such as muscle wasting and nerve damage. Given that so many patients leave ICU with anaemia, it is important to see whether treating this aspect of their ill health improves their symptoms. To our knowledge, there is no research that has investigated treating anaemia with iron after the patient has left ICU. AimsThe aim of this research is to understand the role of intravenous (‘through a drip’) iron in treating anaemia in patients who are recovering from intensive care. Study designCurrently, patients do not routinely receive intravenous iron to treat anaemia after intensive care. I will compare a group of patients who have survived ICU to receive intravenous iron (treatment group) to a group that will not recieve iron (control or 'usual care' group). My objective is to see if this study is feasible. If so, the results would be used to facilitate a larger study involving other hospitals where we would investigate whether treating anaemia with intravenous iron after intensive care improves quality of the life after hospital by treating the symptoms mentioned above. I am using intravenous iron because it works more effectively than oral iron. A one-off injection, lasting 15 minutes, contains the equivalent of 2-3 months of oral iron. Oral iron also has unpleasant side effects such as constipation and nausea. Furthermore, the body is not able to use oral iron because of inflammation whereas it can use intravenous iron. In patients with cancer or kidney problems, who also have inflammation, intravenous iron has been shown to work very well. In this study, a computer will decide randomly (based on chance) which group a patient will be allocated to (randomisation). The control group will not receive any treatment from us. The treatment group will receive the intravenous iron within 72 hours of leaving ICU. I will collect information on how many patients are eligible for the study, how many agree to participate and how many I am able to follow-up after ICU. I will take blood tests, which will include hepciidn, prior to and 4 weeks, 3 months and 6 randomisation. These will be looking at the levels of inflammation and iron stores in the body which will further develop our understanding of anaemia after ICU. Patients in
255
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 2 of 65
both groups will also be asked about symptoms of faitgue and their quality of life using validated questionnaires. Patient and public involvementI have spoken to ICU survivors from our hosptial's ICU support group. Many of them felt weak and tired for a long time after leaving ICU. They were not aware of how common anaemia is after intensive care, the negative impact it could have and what little research into treatment exists for it. They understood why undertaking this research to treat a potentially easily treatable condition has the potential to improve quality of life after ICU. Dissemination of findings of this researchThe findings of this research will be shared with regional research groups, the local and international academic community through forums and conferences, and to our local and national patient groups. The findings will also be published in highly read intensive care medical journals.
Total Research Cost 422,466.00
256
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 3 of 65
The Department of Health, National Institute for Health Research (DH NIHR) is the Data Controller under the Data Protection Act 1998 (‘the Act’). Applicants for funding should be aware that information contained in this application might be shared with other DH NIHR bodies for the purposes of statistical analysis and other DH NIHR management purposes, including targeted communications with selected groups of researchers. Applicants may be assured that DH NIHR is committed to protecting privacy and to processing all personal information in a manner that meets the requirements of the Act.
Table Of Contents
1. Research Details
2. Applicant Details
3. Applicant CV
4. Research Degree
5. History of Previous Applications
6. Patient & Public Involvement
7. Case for Support - Part 1
8. Case for Support - Part 2
9. Case for Support - Part 3
10. Management & Governance
11. Intellectual Property & Innovation
12. Involvement with NIHR Infrastructure & Other Partner Organisations
13. Training and Development
14. Research Supervision
15. Finances
16. DH Monitoring Information
17. Research Design Service (RDS) Involvement
18. Participants
19. Declarations & Signatories
257
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 4 of 65
1. Research Details
Research title Understanding the role of intravenous iron to treat anaemia in survivors of critical illness
Research TypePlease select up to 3 responses which best reflect the type of research you are proposing in your application.
Feasibility study
Themed Call NamePlease indicate if the research you are proposing falls within any of the NIHR wide Themed Calls which the NIHR Fellowship Programme is taking part in for Round 10. Further details of the Themed Calls can be found in the guidance notes.
Not Applicable
Host organisation (which will administer any award)
Do you wish to hold a fellowship at 60%/75%/100%?
100%
What percentage of time is anticipated for the following activities within the time funded by the award?What percentage of time is anticipated for formal courses?
10
What percentage of time is anticipated for research?
83
What percentage of time is anticipated for other training?
2
What percentage of time is anticipated for clinical training/ service (Clinical Applicants Only)Maximum 20% can be entered
5
Proposed start date if grant awarded
258
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 5 of 65
2. Applicant Details
Title Address Line 1Forename(s) Address Line 2Surname Address Line 3ORCID iD County
PostcodeEmail Address
Are you an applicant from a Devolved Nation? No
Professional Background Medically Qualified
Specialty Intensive Care Medicine
Correspondence AddressAddress Line 1
Address Line 2
Address Line 3
City
County
Postcode
Country
Institution NHS Foundation Trust
Job title Specialist Registrar in Anaesthesia & Intensive Care
Department Intensive Care
% WTE commitment 100
Current grade ST4
Current salary 40090
259
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 6 of 65
Provide an approximate breakdown (%) of how your current appointment is divided between the following activities
%
Service/Clinical 75
Research 25
Teaching 0
Other
If applicable please specify the other activity.
Are you on a fixed term contract? No
Current research commitments
I have completed 9 months of protected academic training. During this time, I have carried out a pilot laboratory study, completed a systematic review and meta-analysis, published review articles and presented my work at various regional and international conferences. The focus of my work has been on anaemia after critical illness and blood and blood product transfusion in anaesthesia and critical care. As part of my ACF, I am undertaking a Diploma in Health Research at where I have completed modules in Evidence Based Practice, Introduction to Research Methods and Systematic Reviews. I have three upcoming modules on Essential Medical Statistics, Ethics for Bioscience and Randomized Controlled Trials.
where I have had the opportunity to review grant applications, shortlist research abstracts for conferences and I am currently working on methods to improve access to academic medicine for intensive care trainees.
Do you currently hold an NIHR award? Yes
Please specify NIHR Academic Clinical Fellowship
Date of commencement
Have you previously held an NIHR award? No
Are you currently or have you previously been an Academic Clinical Fellow?ACFs have 25% of their time protected for research training and their salary may be funded by NIHR. Please answer current/previous as appropriate to this question regardless of who funded your ACF and you should answer current/previous as appropriate if you have indicated above that you are currently or have previously been an NIHR ACF.
Current
Are you currently or have you previously been a Clinical Lecturer?CLs have 50% of their time protected for research training and their salary may be funded by NIHR. Please answer current/previous as appropriate to this question regardless of who funded your CL and you should answer current/previous as appropriate if you have indicated above that you are currently or have previously been an NIHR CL. Please only indicate if you are or have been a medical or dental NIHR Clinical Lecturer.
260
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 7 of 65
No
261
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 8 of 65
3. Applicant CV
A CV for the Applicant is a mandatory component of this application; please ensure this is completed fully.
Please note that the first few CV questions are automatically completed from information you have provided in the 'Update CV' section of the 'Manage My Details' page. These can be updated via the TCCi Home Page or by following this link https://tcci.nihr.ac.uk/MyAccount/UpdateCV.aspxDegrees(including details of dates, degree, subject/professional qualification(s) and institution)From To Degree Class Institution Department Country Subject
MSc Pass United KingdomMedical and Healthcare Simulation
MBBS 2:1 United Kingdom (England) Medicine
BMedSci (Hons) 2:1 United Kingdom Anaesthesia and
Intensive Care
Present and previous positions held (including from/to dates, job title and employer)
Start Date End Date WTE % Research Job Title Employer
- 25
NIHR Academic Clinical Fellow in Intensive Care, Specialist Registrar in Anaesthesia & Intensive Car
25NIHR Academic Clinical Fellow, Specialist Registrar in Anaethesia & Intensive Care
0 Core Trainee In Anaesthetics
0 Core Trainee in Anaesthetics
0 Clinical Fellow in Cardiac Intensive Care
0 Foundation Year 2 Doctor
0 Foundation Year 1 Doctor
Recent relevant publication(s)(including list of authors,article title, publication name,volume reference)Publications
262
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 9 of 65
Recent relevant publication(s)(including list of authors,article title, publication name,volume reference)Publications
Relevant Prizes, Awards and other Academic DistinctionsDate Title Awarding Body
Intensive Care Poster Prize - Most Original Poster
Intensive Care Prize for Best Case Summary
'Distinction' in Paediatrics
Research Grants
Title of Grant Role in the Research Grant
Total Grant £
Source of Grant (Organisation Name)
Duration (In Months)
Start Date of Funding
End Date of Funding
I was awarded this conference travel award through competitive selection to present
350
0
263
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 10 of 65
Title of Grant Role in the Research Grant
Total Grant £
Source of Grant (Organisation Name)
Duration (In Months)
Start Date of Funding
End Date of Funding
my BMedSci research project at the European Society of Anaesthesiology meeting
The funds were for accomodation, travelling, and conference fees.
I was awarded this small scale grant to pay for laboratory consumable costs to undertake my study of investigating hepcidin and iron profiles of critical care surivivors.
1000Clinical
Academic Graduate School
3
Employment Breaks
None
Professional bodiesMembership Reference Institution
General Medical CouncilThe Royal College of Anaesthetists
264
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 11 of 65
4. Research Degree
Are you registered for or undertaking a research doctorate (PhD/MD/Dphil) at the time of making this application (N.B. The NIHR reserves the right to change start dates prior to contracting depending on circumstance)
No
265
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 12 of 65
5. History of Previous Applications
Has this application, or a similar application, previously been submitted to this or any other funding body?
No
266
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 13 of 65
6. Patient & Public Involvement
The NIHR expects the active involvement of patients and the public in the research it supports. NIHR recognises that the nature and extent of active patient and public involvement (PPI) is likely to vary depending on the context of each study or award. In this section it is important that you describe in as much detail as possible how patients and the public have been involved in the development of the application as well as plans for involvement in the proposed research. Please see the Applicant Guidance Notes for more information on PPI in research. In addition: a definition of patient and public involvement in research, further information and resources are available from INVOLVE (www.invo.org.uk); the NIHR Research Design Service (www.rds.nihr.ac.uk) provides advice on applications and the James Lind Alliance (http://www.jla.nihr.ac.uk/) has a step-by-step guidebook on involvement in research identification and priority setting.
Were patients and the public actively involved? Yes
If Yes, please tick the appropriate boxes below
Involved in identifying the research topic/prioritising the research questions
Please further describe how patient and public involvement has informed and/or influenced the development of the application and how patients and the public have been actively involved
I presented my research idea to our local Critical Care Patient Forum Group which consists of previous intensive care unit (ICU) patients. They were a diverse group, with ages ranging from 21 to 75, both sexes, and with a broad range of medical problems causing their intensive care unit stay. I explained the prevalence and causes of anaemia during critical illness and highlighted the evidence gap in management of anaemia after intensive care. All of them complained about excessive blood sampling whilst they were in ICU. None were aware of being told they were anaemic when they eventually went home. A particular point they raised was that if there is a potentially simple treatment option like intravenous iron, why doesn't everyone get it? Hence they were strongly supportive of my proposed research. The importance of this research to patients and the public was further emphasised through the work of the James Lind Alliance Priority Setting Partnership and the NIHR, who set priorities for future research. Improving recovery and developing models to guide treatments for common conditions or complications of critical illness – of which anaemia can be classed as one - has been identified as a key priority by both.
Please indicate the ways in which the public will be actively involved in the proposed research, by ticking all relevant boxes
Design of the research, Management of the research (e.g. steering/advisory group), Developing participant information resources, Dissemination of research findings
Please give more details, including how patient and public involvement will benefit the research, the reasons for taking this approach and arrangements for training and support.
The Critical Care Patient Forum Group mentioned above thave assisted with the design of previous studies including
.
267
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 14 of 65
The group were very keen to be involved in my research. I will utilise their experience in designing the patient information leaflets, consent forms, and will also invite a member to be on the trial steering group. At the end, they will be involved in disemminating the results, as evidenced by this group, ICU survivors have little or no knowledge that they are anaemic.
268
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 15 of 65
7. Case for Support - Part 1
Plain English summary Please summarise your proposed research in plain English
Background of the researchAnaemia is also known as low red blood cell count or low haemoglobin. Haemoglobin carries oxygen and therefore anaemia reduces the amount of oxygen that is available to the body. Anaemia is very common in intensive care unit (ICU) patients and also in those who leave ICU alive. 164,000 patients are admitted to ICU per year in the United Kingdom. Nearly half of these who survive ICU will leave with a haemoglobin of less than 100 grams per liter (g/L), which is termed ‘moderate-severe’ anaemia. The body reacts to infection or injury by producing inflammation (an attempt to heal or mend the body). Inflammation is present in nearly all ICU patients. However, whilst doing this, the body is unable to use available iron to make haemoglobin resulting in anaemia because iron is essential to make haemoglobin. Current blood tests are not able to reliably tell us how much iron is available because of inflammation. A new blood test of the main hormone that controls iron in body - hepcidin, has become recently available and may be a better test. Patients who survive ICU often experience high levels of tiredness and weakness resulting in a poor quality of life. These could be symptoms of anaemia, but may also relate to other complications the patient may have experienced during their illness such as muscle wasting and nerve damage. Given that so many patients leave ICU with anaemia, it is important to see whether treating this aspect of their ill health improves their symptoms. To our knowledge, there is no research that has investigated treating anaemia with iron after the patient has left ICU. AimsThe aim of this research is to understand the role of intravenous (‘through a drip’) iron in treating anaemia in patients who are recovering from intensive care. Study designCurrently, patients do not routinely receive intravenous iron to treat anaemia after intensive care. I will compare a group of patients who have survived ICU to receive intravenous iron (treatment group) to a group that will not recieve iron (control or 'usual care' group). My objective is to see if this study is feasible. If so, the results would be used to facilitate a larger study involving other hospitals where we would investigate whether treating anaemia with intravenous iron after intensive care improves quality of the life after hospital by treating the symptoms mentioned above. I am using intravenous iron because it works more effectively than oral iron. A one-off injection, lasting 15 minutes, contains the equivalent of 2-3 months of oral iron. Oral iron also has unpleasant side effects such as constipation and nausea. Furthermore, the body is not able to use oral iron because of inflammation whereas it can use intravenous iron. In patients with cancer or kidney problems, who also have inflammation, intravenous iron has been shown to work very well. In this study, a computer will decide randomly (based on chance) which group a patient will be allocated to (randomisation). The control group will not receive any treatment from us. The treatment group will receive the intravenous iron within 72 hours of leaving ICU. I will collect information on how many patients are eligible for the study, how many agree to participate and how many I am able to follow-up after ICU. I will take blood tests, which will include hepciidn, prior to and 4 weeks, 3 months and 6 months after randomisation. These will be looking at the levels of inflammation and iron stores in the body which will further develop our understanding of anaemia after ICU. Patients in both groups will also be asked about symptoms of faitgue and their quality of life using validated questionnaires. Patient and public involvementI have spoken to ICU survivors from our hosptial's ICU support group. Many of them felt weak and tired for a long time after leaving ICU. They were not aware of how common anaemia is after intensive care, the negative impact it could have and what little research into treatment exists for it. They understood why undertaking this research to treat a potentially easily treatable condition has the potential to improve quality of life after ICU. Dissemination of findings of this research
269
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 16 of 65
The findings of this research will be shared with regional research groups, the local and international academic community through forums and conferences, and to our local and national patient groups. The findings will also be published in highly read intensive care medical journals.
Scientific Abstract of Research
BackgroundApproximately 30-50% of intensive care unit (ICU) survivors leave hospital with a haemoglobin (Hb) of ≤100 g.L-
1 which equates to ‘moderate / severe anaemia’. Patients surviving ICU often experience poor health-related quality of life, high levels of fatigue and weakness. Anaemia could be causing some of these symptoms, but the precise contribution it makes, over and above other causes such as deconditioning, muscle wasting and nerve damage, remains unclear.
Available evidence so far has not demonstrated any benefit in using iron to treat anaemia in ICU. This can partly be explained by study limitations but also becuase patients may have simply been too sick to utilise the iron. No trials have attempted to treat anaemia after critical illness where it is plausible that iron utilisation will be greater as inflammation regresses. AimsThe overall aim of this fellowship is to undertake a feasibility study to determine whether or not a large multicentre trial of intravenous iron versus placebo in ICU survivors with anaemia can be carried out.
2) To identify the patient characteristics and biological profiles of patients who respond to intravenous iron and whether or not biomarkers such as hepcidin predict response to iron. Research methodsTo answer these objectives I will use the following methods. 1) A feasibility open-label randomised trial of intravenous iron versus no iron (control) in ICU survivors with anaemia. Participants will receive a one-off dose of 1000mg of ferric carboxymaltose within 72 hours of leaving ICU. This contains the equivalent of 2-3 months of oral iron. Intravenous iron is also more efficacious than oral iron as it bypasses the hepcidin-block created by inflammation. Participants will be followed up at 4 weeks, 3 month and 6 months post-randomisation. 2) For all participants, I will analyse their biological (biochemistry, iron, inflammatory and bone marrow) profiles. Novel techniques developed in our institution are now able to provide a functional quantitative result of bone marrow function from a blood test, thereby avoiding the need for a bone marrow aspirate which is invasive and painful. In the group that received iron, I will explore if hepcidin can predict a rise in haemoglobin. Analysis of the control group will help determine which biological factors, if any, are associated with a spontaneous improvement (or lack of) in haemoglobin. Potential impact
Research objectives to be address in this fellowship 1) To estimate important feasibility and clinical outcomes, such as number of eligible participants, recruitment rates, follow-up rates, metrics of changes in haemoglobin concentration and quality of life scores, which would be required for the larger study.
Iron restriction is a major factor underlying anaemia in ICU either because of absolute iron deficiency, iron sequestration (impaired iron trafficking) or functional iron deficiency (imbalance between iron requirements of the bone marrow and availability). Standard biochemistry tests are unable to identify specific causes because of inflammation – which is present in nearly all ICU patients. The discovery of the iron hormone hepcidin has improved our understanding of iron metabolism. Hepcidin is elevated in inflammation where it blocks the duodenal absorption of iron (thereby limiting the efficacy of oral iron) and release from macrophages. Conversely, low hepcidin levels facilitate the absorption of iron and release of iron from body stores. Evidence from other patient groups has shown it can identify absolute iron deficiency in spite of inflammation and it can also predict responsiveness (increase in haemoglobin) to iron (i.e. lower the hepcidin the more likely a response).
270
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 17 of 65
This research has the potential to treat a common and potentially easily reversible condition, which could alleviate symptoms and improve quality of life in ICU survivors.
Select up to 5 MeSH terms to describe your project Please choose at least 1 and no more than 5 terms from the MeSH classification.Anemia Anemia, Hypochromic Anemia, Iron-Deficiency Clinical Laboratory Techniques
Relevant expertise and experience
Academic experience Medical schoolMy desire to pursue a career in academic medicine began as a medical student at the . I specifically chose an intercalated BMedSci degree project in the university’s Anaesthesia and Critical Care research group for its strong track record of academic excellence, provision of taught courses on research methodology, and for the opportunity to develop an independent project. My project evaluated the performance of various oxygen delivery devices on simulated models of airways disease patterns and led to a presentation at an international anaesthesia conference and a peer-reviewed publication. Through competitive process, I was awarded the annual BMedSci Conference Fund. In my final year, I was elected to be the Medical Student Representative on the Medical School’s Ethics Committee which regularly involved reviewing research proposals to ensure that the welfare and dignity of participants was protected. Senior house officer/core anaestheticsAfter foundation programme training, I spent a year as a Junior Clinical Fellow in cardiac intensive care where, in collaboration with , I led on a prospective observational study testing the use of validated cardiac post-operative morbidity tool to describe morbidity patterns in patients undergoing aortic valve surgery. From this experience, I learned how to lead and co-ordinate other team members in the process of carrying out a study, create confidential online databases, and perform basic statistical analysis on observational datasets. This work was presented at national and international conferences and resulted in a peer-reviewed publication. During my tenure there, I was also involved in devising a surveillance system to monitor for and reduce central venous catheter blood-stream infections, staff training of using thromboelastography to reduce blood product use, and setting up a sustainable, multidisciplinary simulation training day on cardiac surgical emergencies. During my core anaesthetics training, I took the lead in enrolling my local hospital onto a HTA funded large multicenter randomised controlled trial evaluating the effectiveness of intravenous iron to treat pre-operative anaemia (PREVENTT). This process involved close working with the hospital’s Research and Development team, pre-operative assessment clinic nurses, surgeons and pharmacy. Through collaboration, I devised a local pathway through which patients could be screened, recruited and if consented, receive the intervention or placebo in an appropriate environment. This experience provided me with an insight into the complexities and challenges of conducting clinical trial research. I was also involved locally in setting up and undertaking data collection for a regional audit investigating the prevalence of intraoperative hypotension, and for the Sprint National Anaesthesia Project (SNAP-1) evaluating patient reported outcomes after anaesthesia. Both these studies have been published recently. To develop my interest in medical education, I completed a part-time Masters in Medical and Healthcare Simulation over a 2-year period. Modules included Evidence Based Practice, Simulation – Design and Delivery, Healthcare Delivery and Human Error and Medical Emergencies. Through the various assignments I was able to further develop my skills in analytical writing, critical appraisal of best evidence and improve my understanding of patient safety and health systems. ACF, Registrar in Anaesthesia & Intensive CareSince 2014, I have been an NIHR Academic Clinical Fellow (ACF) in Intensive Care Medicine . During my time, I have completed and published a systematic review and meta-analysis on iron supplementation to
271
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 18 of 65
treat anaemia in critical care with the Systematic Review Initiative . I have also written review articles on transfusion of blood and blood products in anaesthesia and intensive care and on the current state of evidence on age on blood. From these experiences, I have developed skills in writing protocols, critically appraising research studies, using software such as RevMan, and preparing manuscripts. I utilized these skills when I updated our local ICU guideline on blood product transfusion. I also carried out a laboratory project at under the supervision
, . My work was on investigating the utility of hepcidin to diagnose iron deficiency in survivors of
critical illness. Having never carried out ‘wet’ laboratory research previously I quickly learned how to perform ELISAs, PCR and electrophoresis. I thoroughly enjoyed working with and learning from research assistants, basic scientists, DPhil students and post-doctoral fellows in the laboratory and learned the importance of attention to detail, patience and trouble-shooting when performing experiments. I am also undertaking a Diploma in Health Research . I have successfully completed three modules and the methods training provided has greatly complemented my research experiences above. For example, undertaking the Systematic Reviews module provided me with an opportunity to refine my research question and develop strategies to address limitations for the systematic review mentioned above
. Clinical experience I have been awarded dual training numbers in Anaesthesia & Intensive Care and am currently in my ST4 year of training. I have obtained both MRCP and FRCA qualifications at early stages in my training. My interest in medical education is maintained regularly by teaching junior doctors and allied healthcare professionals on regional simulation courses. Recently, I helped set up a transfusion medicine initiative (‘Transfusion Camp’) in
aimed at improving transfusion knowledge of haematology, anaesthetic and critical care trainees through a series of monthly tutorials. Better clinical care is often driven by improved understanding of the basic mechanisms of disease, performing high-quality trials and systematic review of developments in the evidence base. My research experiences have shown me that I am best suited to and enjoy these translational aspects. Balancing my academic training with the clinical commitments of anaesthesia and intensive care has always been challenging but I believe that the progression I have demonstrated so far provides evidence of my ability and dedication. This NIHR fellowship will build on the foundations of my ACF and provide me with excellent opportunities and research skills to fulfill my long-term aim of being a clinician scientist.
272
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 19 of 65
8. Case for Support - Part 2
273
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 20 of 65
Research Plan If you are proposing a clinical trial, you have a word limit of 5250 words.If you are not proposing a clinical trial, you have a word limit of 3500 words.All content included beyond the word limit will be removed by NIHR TCC prior to assessment.
Background
Observational studies have shown that anaemia (defined by World Health Organisation as haemoglobin concentration (Hb) ≤130 g.L-1 in men and ≤120 g.L-1 in women) affects 60-80% of patients in the intensive care unit (ICU). Of these, 50-70% develop moderate-severe anaemia defined as Hb ≤90 g.L-1 (Napolitano et al, 2009, Walsh & Stanworth, 2010). In a study of 283 ICU survivors, 85% of patients were anaemic at ICU discharge of which 52% had a Hb of ≤100 g.L-1 (Walsh et al, 2006). A recent audit of our own institution of 504 ICU survivors found that 97% were anaemic at hospital discharge, with 35% discharged home with a Hb of ≤100 g.L-1 and 19% with a Hb of ≤80 g.L-1 (Shah et al, 2016). There was also no mention of anaemia in any discharge summary and no patients recieved iron therapy. Critically ill patients develop anaemia as a result of blood loss, haemodilution, excessive blood sampling, dysregulated iron metabolism, blunted erythropoietin response and restrictive transfusion practices (Hayden et al, 2012). As highlighted above, this anaemia carries through to hospital discharge and at present there are no guidelines on managing this anaemia. The problem of anaemia after critical illnessTwo observational studies in survivors of critical illness have shown that a Hb of ≤100 g/L is associated with increasing fatigue at day 28 post-ICU and that survivors with anaemia have reduced Short Form-36 scores when compared to a national cohort of unselected former ICU survivors particularly in the physical function and role physical domains (Bateman et al, 2009, Lasocki et al, 2014). Evidence from postoperative studies suggests that anaemia is associated with fatigue, reduced exercise capacity and muscle strength particularly at a Hb of ≤100 g/L (Foss et al, 2008, Carson et al, 2013). A strong association also exists between poor outcomes and anaemia in a number of other chronic illnesses such as chronic obstructive pulmonary disease, chronic kidney disease, and heart failure (Hayden et al, 2012). These conditions are common amongst critically ill patients either as a comorbidity or as part of the reason for ICU admission. (Lone et al, 2016). Recent National Institute for Clinical Excellence guidance has reduced transfusion thresholds to 70 g.L-1 (80 g.L-
1 for patients with a history of ischaemic heart disease) in the absence of active bleeding. This change in practice is likely to lead to more patients being discharged from ICU, and subsequently hospital, with anaemia, with unknown consequences on recovery and long-term health in the community. The data available from ICU survivors and that extrapolated from other similar populations suggests that persistent anaemia after critical illness may carry important long-term consequences. Further detailed study of this patient group is therefore needed. I recently carried out a systematic review on iron supplementation to treat anaemia associated with critical illness and found no studies that treated anaemia after intensive care thereby highlighting a deficiency in the available evidence for this important patient group. Understanding of mechanisms of critical illness-related anaemia to date Iron is an essential component of haemoglobin and therefore restriction of iron delivery to red blood cell (RBC) precursors can limit their production (erythropoiesis). Iron restriction occurs through 4 main mechanisms:(i) Absolute iron deficiency (low total body iron stores) - this is the commonest cause of anaemia worldwide and is easily treatable with iron (Camaschella 2015)(ii) Functional iron deficiency (imbalance between increased iron requirements of the bone marrow and iron availability)(iii) Iron-restricted erythropoiesis (impaired iron trafficking regardless of the level of iron stores, which are usually replete)(iv) Hereditary conditions As a result of chronic diseases, inflammation, and infection, majority of ICU patients will have an anaemia of inflammation (AI) This refers to the collective processes leading to functional iron deficiency and/or iron-restricted erythropoiesis, increased cytokine production, and reduced RBC proliferation and life span. Overall around 90% of patients discharged from ICU and subsequently from hospital have an anaemia of inflammation (AI). (Walsh et al. ICM 2006, Lasocki et al, Crit Care 2014, Shah et al, 2015). Absolute iron deficiency may manifest itself later from the consequences of chronic blood loss (e.g. through frequent blood sampling) and poor oral intake. One study found that the prevalence of absolute iron deficiency in ICU survivors increased from 8% at hospital discharge to 35% after six months. Therefore during the acute phase of critical illness, patients
274
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 21 of 65
are more likely to have an iron-restricted erythropoiesis but during recovery, functional and absolute iron deficiency may become more prominent. Our understanding of iron metabolism has been improved by the discovery of the hepcidin - the chief hormone regulator of iron status. It is upregulated in inflammation and blocks both duodenal iron absorption and iron release from macrophages, a key step in iron transfer to the developing RBCs (Ganz 2013). This is thought to be an evolutionary response to sequester and deny iron to invading pathogens (Michels et al, 2015) as iron is also essential for microbial growth. Critically ill patients presenting with sepsis have elevated hepcidin levels that fall during recovery (Van Eijk LT et al, 2011). Hepcidin upregulation also limits iron availability for erythroid progenitor cells and impairs haemoglobin synthesis, leading to iron-restricted erythropoiesis (Ganz 2013). Conversely, low hepcidin levels facilitate the absorption of iron and the release of iron from body stores. Proinflammatory cytokines, such as IL-1, IL-6 and tumour necrosis factor, also impair iron homeostasis, decrease regulatory feedback between body iron needs and intestinal absorption, inhibit erythropoietin production and the marrow response to circulating erythropoietin leading to functional iron deficiency. Recent work has demonstrated a close relationship between vitamin D and iron metabolism. Vitamin D deficiency is very prevalent in ICU patients (Amrein et al, 2014). An inverse relationship between Vitamin D levels and hepcidin transcription has been observed and a recent pilot RCT showed that critically ill patients treated with high-dose vitamin D had increased haemoglobin concentrations over time coupled with acutely reduced serum hepcidin concentrations (Smith et al, 2016). Data from non-critically ill patients in the community shows that vitamin D deficiency is associated with worsening anaemia (Monlezun et al, 2015). Correction of Vitamin D deficiency may therefore lead to hepcidin suppression and improved iron absorption from the gut and release from macrophages, allowing more effective erythropoiesis. This relationship between Vitamin D replacement and improvement in anaemia should be confirmed in both acutely ill ICU patients and ICU survivors. Anaemia is difficult to characterise in ICU survivorsSerum ferritin, iron and transferrin saturation are the commonly used tests to identify absolute iron deficiency, where all would be reduced. However, inflammation and the acute phase response increase serum ferritin and reduce iron and serum transferrin. Various thresholds of ferritin have been proposed but there is no universal agreement. In a recent study of ICU suvivors, inflammation was still present in >59% of patients even 3 months after ICU after ICU discharge (Griffith et al, 2016). As a consequence, characterisation of the anaemia and trying to identify absolute iron deficiency in the context of inflammation is challenging. Measuring hepcidin has shown promise in this area where it has identified absolute iron deficiency in spite of inflammation but in addition, has also predicted responsiveness to iron therapy (i.e. the lower the hepcidin concentration, the more likely one is to absorb and utilise iron (Pasricha et al, 2014, Girelli et al, 2016). Patients’ responses to iron will necessitate not only a favourable biochemical prolife (eg adequate presence of iron and erythropoietin, low hepcidin), but in addition the bone marrow environment must be permissive for proliferation and differentiation of haematopoietic stem cells down the erythroid pathway to generate RBCs. One small study of 10 critically ill patients with sepsis has examined bone marrow function through direct sampling, and shown increased cell death of RBC precursors when compared to controls (Claessens Y et al, 2003). There are few functional assays of marrow function, the most readily non-invasive proxy being a measure of reticulocyte count in peripheral blood. This has been shown to be inappropriately reduced in ICU patients, even in the present of anaemia (Walsh et al, 2006). Using sophisticated multi-colour flow cytometry it is now possible to identify in the peripheral blood sub-populations of erythroid progenitors at different stages of differentiation. These provide a quantitative functional read-out of bone marrow function, and has been used in a variety of conditions to assess bone marrow function (Mead et al, 2013). During my Academic Clinical Fellowship, I undertook a laboratory and diagnostic accuracy study investigating the utility of hepcidin as a marker of iron deficiency in the context of inflammation in 117 patients discharged from critical care. We found that 94% (110/117) of patients were discharged home with anaemia and of those 55% had a Hb of ≤100 g.L-1. 91% (100/110) of the patients discharged with an anaemia of inflammation (inflammation defined as C-reactive protein 8 ≥mg.L-1). An important finding was that 40% of patients had low/inappropriately normal serum hepcidin concentrations despite the presence of inflammation. The identification of a sizable proportion of ICU patients with low hepcidin levels affords an opportunity for prospectively evaluating the use of hepcidin levels in predicting iron responsiveness in ICU survivors. Supporting this hypothesis, hepcidin levels have been shown to predict iron-responsiveness in other groups of patients with anaemia of inflammation (Pasricha et al, 2014, Girelli et al, 2016). Why intravenous iron may be a suitable treatment option
275
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 22 of 65
At present, blood transfusion is the mainstay for treating anaemia. Although it can be life-saving, this is a finite and costly resource which is associated with its own risks such as transfusion reactions (Isbister et al, 2011). Erythropoetin-stimulating agents have not been shown to be beneficial so far in critically ill patients (Zarychanski et al, 2007). Intravenous iron is the standard of care for treating anaemia in other conditions with co-existing inflammation such as inflammatory bowel disease and chronic renal failure. Trials are also underway in preoperative anaemic surgical patients with cancer (Onken et al, 2014, Richards et al, 2015). Intravenous administration of iron bypasses hepcidin-mediated restriction of the enteral absorption of iron and can therefore treat iron-restricted, functional and absolute iron deficiency syndromes effectively (Goodnough et al, 2010). New intravenous iron preparations can be administered safely as a single dose in a relatively short period of time (15-20 minutes) without the need for a test dose. Whilst oral iron is inexpensive, its side effects (such as constipation, nausea and vomiting) significantly limit patient compliance (Tolkien Z, 2015). Furthermore, hepcidin-mediated mechanisms described above reduce enteric absorption of iron. Our recent systematic review on iron supplementation to treat anaemia associated with critical illness identified only a small number of randomised trials (Shah et al, 2016). Although there was no evidence that iron supplementation to treat anaemia in critically ill patients reduced blood transfusion requirements or improved clinical outcomes there were many methodological problems, including heterogeneity of intervention and study population, small sample sizes, bias (only one trial was at low risk of bias), variable and limited follow-up and wide confidence intervals for all reported outcomes. The lack of evidence that iron supplementation improves outcomes for patients who are critically ill has not been improved by the most recently published Intravenous Iron or Placebo for Anaemia in Intensive Care (IRONMAN) trial which also found no reduction in blood transfusion requirements in critically ill patients treated with intravenous iron (Litton et al, 2016). Despite being underpowered, an interesting observation of this trial was that the intravenous iron group of patients had significantly higher haemoglobin at hospital discharge when compared to the placebo group. The median duration from initiation of intravenous iron to hospital discharge in this trial was 11 days and given that the maximal effect may not have occurred for 3-4 weeks, a time point which was not included in the trial, the observed differences may have been greater post-discharge in the recovery phase of critical illness. A potential mechanism for this could be increased utilisation of iron by a recovering bone marrow as inflammation resolves and marrow iron needs are met during the recovery phase of critical illness. Recent evidence has shown that a single 1000-mg dose of ferric carboxymaltose after major elective orthopaedic, intra-abdominal and genito-urinary surgery corrects anaemia and improves quality of life compared to oral iron (Bisbe et al, 2014, Khalafallah et al, 2016). Although a different group of patients, these patients were anaemic with functional iron deficiency. Why my research is neededImproving recovery and developing models to guide treatments for common conditions or complications of critical illness – of which anaemia can be classed as one - has been identified as a key priority by the NIHR critical care portfolio and the James Lind Alliance. So far, we have shown that anaemia after critical illness is associated with adverse outcomes, difficult to characterise, and therefore treat. Recent advances in iron metabolism and assessments of marrow function provide a unique opportunity for more detailed characterisation of anaemia after critical illness than standard blood tests. Iron supplementation to treat anaemia during critical illness has not improved outcomes. No major clinical trial has been conducted yet, addressing the correction of anaemia with intravenous iron in patients recovering from critical illness. Proposed designI propose a feasibility study which will be an open-label randomised trial. At present there is no accepted best practice for managing anaemia in patients recovering from critical illness. A randomised study is the best possible methodology to ascertain the effect of intravenous iron while balancing for baseline differences in age, sex, severity of critical illness, and pre-existing co-morbidities. All patients will be followed at 4 weeks, 3 months, and 6 months post-randomisation. It will allow me to assess important feasibility outcomes such as recruitment rate and determine the metrics of the primary and secondary outcomes that will be used in the larger study. An assessment of a primary clinical outcome will also be carried out. This will be the haemoglobin concentration at 3 months post-randomisation. How the results will be usedThe main purpose of this feasibility trial is to support an application to the NIHR Efficacy and Mechanism Evaluation (EME) programme for a phase II/III randomised controlled trial to investigate the clinical efficacy of intravenous iron for the treatment of anaemia after critical illness. The aim of this proposal is to pave the way for that future main trial by testing that the processes of recruitment, randomisation, treatment, and follow-up
276
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 23 of 65
assessments are achievable in this patient group. Through our clinical outcomes measures we will seek to develop minimal clinically important difference end-points for the main trial. The novel work on understanding mechanisms of anaemia in ICU survivors has the potential to stratify which patients may respond to iron and thereby allowing more targeted therapy. The results from this feasibility study will also be presented at national conferences to stimulate interest and enthusiasm for centres to participate in the intended future trial. To create the time necessary to run this larger study I would seek to apply for an NIHR Academic Clinical Lectureship award and/or take co-applicant role with a more senior tenured academic as the Chief Investigator. Principal research questions
1) To estimate important feasibility and clinical outcomes, such as number of eligible participants, recruitment rates, follow-up rates, metrics of changes in haemoglobin concentration and quality of life (QoL) scores, which would be required for the larger study. 2) What are the patient characteristics and biological (biochemistry, inflammation, iron and haematopoetic) profiles of patients who show a response to intravenous iron and can biomarkers such as hepcidin predict response to intravenous iron? Methodology to address research questions1) To estimate important feasibility and clinical outcomes, such as number of eligible participants, recruitment rates, follow-up rates, metrics of haemoglobin concentration and quality of life (QoL) scores, which would be required for the larger study. The key feasibility and clinical outcomes of this trial are summarised below. Feasibility outcomes
What proportion of participants that are suitable for ICU discharge have a haemoglobin of ≤ 100 g.L-1 and ICU length of stay of ≥ 48 hours?
What proportion of participants with capacity are able to consent? Of those that are unable to consent, what proportion have a personal legal consultee?
How many participatns have a contra-indication to ferric carboxymaltose? What is the burden of investigator time and what are the practicalities of delivering the intervention on
the hospital wards? How many participants recieved the intervention within 72 hours? What proportion of participants enter ICU with known pre-existing anaemia in the community (i.e. prior to
hospital admission)? This could be a potentially important sub-group who may demonstrate a greater response to iron therapy
Protocol adherence: number of participants who were followed up at all three time-points (4 weeks, 3 months, 6 months post-randomisation)
What is loss to follow-up rate?
Clinical outcomesPrimary outcome:The primary outcome is the mean (standard deviation (SD)) haemoglobin (Hb) concentration at 3 months post-randomisation. This data is missing from the current literature, as there are no trials of intravenous iron in survivors of critical illness. This would provide an estimate of the effect size but we acknowledge that the confidence limits will be wide due to a small sample size. Secondary outcomes include:
Mean (SD) haemoglobin concentration at 4 weeks and 6 months post-randomisation. Proportion of participants who demonstrate a Hb response of ≥20 g.L-1 from baseline to 3 months post-
intervention. This definition has been used previously (Henry et al, 2006). Comparisons of iron, inflammation, and haematopoetic profiles between participants who demonstrate a
response and those who do not based on the definitions above. In-hospital infection – defined as ‘commencement, escalation or change of antibiotics for a confirmed or
strongly suspected infection’. This definition is pragmatic and was used in the IRONMAN trial. Post-ICU Health-related quality of life (HRQoL) – Multidimensional Fatigue Inventory (MFI) and
European Quality of Life: 5 Dimensions (EQ-5D-5L) at 4 weeks, 3 months, and 6 months post-
277
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 24 of 65
randomisation. Hospital re-admissions following hospital discharge during the trial period. Proportion of participants receiving RBC transfusion between randomization and hospital discharge. Our
local data shows that approximately 20% of patients receive a blood transfusion in the period between ICU and hospital discharge.
Mortality at trial end-point (6 months post-intervention). Side effects of drug infusion – We are not expecting any serious adverse drug reactions. The UK
Summary of Product Characteristics (SPC) of ferric carboxymaltose states that side effects are minimal but include nausea, hypertension, injection site reactions and hypophophataemia. None have been associated with a serious adverse event in published trials, including the IRONMAN trial (Litton et al, 2016). We will assess for all these effects.
To increase certainty of the clinical outcome data, I will in parallel to the feasibility study, undertake a database study of the past 9 years of patient ICU discharge data available from Critical Care Research Group based in . Data collected will include ICU discharge Hb, ICU and hospital length of stay, and in-hospital post-ICU mortality. I will collect data on post-ICU hospital readmissions and mortality at 2 years that is available from the Intensive Care Outcomes Network (ICON) database – the world’s largest study of quality of life and functional outcomes in survivors of critical illness. I will also seek specific approval early on in order to analyse general practice records of ICU survivors for Hb measurements in the community (all samples are analysed in the same laboratory) without patients’ knowledge through the Health and Social Care Information Centre. This would lead to the development of a ‘safe haven’ that can be used for anonymised database linkage analysis. This would provide more data on the prevalence of anaemia in the community after hospital discharge, which would increase the certainty of feasibility outcome data. I will undertake a taught course on 'Big Data Epidemiology' to develop the required skills and knowledge to manage large datasets. Trial details ParticipantsAll ICU admissions will be screened for eligibility. Inclusion criteria will be ≥48 hours of ICU stay, the physician in charge of the patient considers them fit for discharge from the ICU and a Hb of ≤100 g.L-1 at, or the point closest to, ICU discharge. This threshold has been adopted from the limited data on post-ICU anaemia, as explained previously, where symptoms of anaemia appear to be more severe at Hb ≤100 g.L-1. The WHO grading on cancer-related anaemia also uses this threshold, where severity of anaemia has been linked to quality of life. A full list of the inclusion and exclusion criteria are shown in Table 1. ConsentPatients with mental capacity will be approached for consent to participate in the trial. For those lacking mental capacity, the next of kin, welfare attorney or a professional consultee will be approached for consent. Consent for ongoing participants will then be sought as soon as possible. RandomisationTo minimise selection bias, I will use a web-based system to support randomisation. Randomisation will be stratified according illness severity as defined by the Acute Physiology and Chronic Health Evaluation (APACHE) II score. Interventions and comparatorParticipants randomly assigned to the intervention arm will receive a one-off dose of 1000mg of intravenous ferric carboxymaltose (Ferinject) as an infusion over a minimum of 15 minutes. This dose is based on the maximum allowable dose per week as per the UK Summary of Product Characteristics. Participants in the placebo group will not receive any placebo drug. Following discussions with my supervisors and other senior ICU researchers, we believe that this is appropriate as it is ‘usual care’ and the costs of using a placebo for the purposes of a feasibility study would be too high. Participants will receive the intervention within 72 hours of ICU discharge (but whilst still an in-patient in hospital). This would be feasible based on previous data showing that the median (IQR) post-ICU hospital length of stay is 10 (6-23) days. (Walsh et al, 2015). It is also pragmatic to try minimise loss of patients over weekends. We have opted for a one-off dose of ferric carboxymaltose as it may adequately replenish iron stores (McDonagh, 2015) and because the maximum recommended single doses of other intravenous iron preparations are lower than that of ferric carboxymaltose thereby avoiding multiple doses (Keating, 2015).
278
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 25 of 65
Methods of recruitmentClinical staff will be notified of the study through presentations at the governance meetings, posters and email. The research team will work closely with the responsible clinical team to identify eligible participants on a regular basis. Eligible participants will be identified and approached first by the healthcare team. The ICU has a strong track-record of being involved in recruiting for multi-centre studies so I do not anticipate this to be a problem. Number of centresA single-centre study conducted in a research active environment of an Adult ICU at
. Data collection and follow up
Baseline, pre-randomisation data to be collected are shown in Table 2. Follow-up data in the community will be collected at 4 weeks, 3 months and 6 months post-randomisation. To minimise loss to follow-up, we will invite patients to return to our ICU follow-up clinic, which runs every Friday afternoon. The ICU follow-up clinic routinely invites discharged patients who were in ICU for ≥72 hours at 3 months. Therefore a proportion of patients would be returning anyway. If patients are unable to attend, we will undertake home visits to collect blood samples and administer questionnaires. This latter approach was successfully used in a recent ICU survivor trial (Walsh et al, 2016) which resulted in a 10% loss to follow-up rate at 3 months post-discharge. Quality of life measurements at 4 weeks , 3 and 6 months post-randomisation and health economics evaluationWe will measure HRQoL using two validated tools. The EuroQoL-5D-5L is a brief, standardised tool used as a measure of health outcome that has been validated and used in critical care (Oeyen et al, 2015). It consists of a descriptive system that measures health in five domains – mobility, self care, usual activities, pain/discomfort and anxiety/depression. On a visual analogue scale, participants can rate their overall health from 1-100.The Multidimensional Fatigue Inventory (MFI-20) is a 20-item self-reporting score designed and validated to measure fatigue (Smets et al, 1995) using five domains: general fatigue, physical fatigue, mental fatigue, reduced motivation and reduced activity. High MFI scores indicate high degrees of fatigue.I will also attempt to measure baseline (i.e. pre-ICU) QoL. This is challenging as most patient aren’t able to complete questionnaires on ICU admission and use of relatives, proxies or recovering patients is influenced by recall bias. To address this, I will use surrogate objective measures such as English Index of Multiple Deprivation (IMD), which is routinely recorded in GP records, and calculate the Charlson Comorbidity Index (CCI). IMD ranks every small area in England from 1 (most deprived) to 32,844 (least deprived). The CCI is a validated tool for predicting mortality by classifying or weighing co-morbidities in various disease groups including critical illness (Christensen et al, 2011). Following consultation with a health economist at the RDS, I have incorporated measuring the number of hospital re-admissions in order to perform basic health economics evaluations. This, in addition to mortality and QoL measurements, will enable us to potentially calculate Quality Adjusted Life Years. Statistical considerationsSample sizeAs this is a feasibility pilot study, we have not undertaken a formal power calculation. Using local case mix data for the ICU, 800 patients are admitted each year. 120 patients were elective post-operative admissions who would be expected to stay less than 48 hours. Of the remaining 680 patients, assuming unit mortality of 14%, 584 would be expected to survive ICU. Based on pretrial work and previous studies, 50% (292 patients) would leave ICU with a Hb of ≤100 g.L-1. Assuming 40% enrolment, we expect to enrol 116/year or 9/month (approximately 2 patients per week). The planned recruitment period is therefore 52 weeks. Data analysisFor feasibility outcomes, all enrolled participants will be included in the analysis. For clinical outcomes, analyses will be performed on all enrolled participants for whom an outcome is available. Continuous variables will be described using means and standard deviations or median and interquartile ranges as appropriate. Categorical variables will be summarised using frequencies and percentages. Analyses will be conduced on an intention-to-treat and per protocol basis. Linear regression techniques will be used to evaluate the association between anaemia and QoL scores at 4 weeks, 3 months and 6 months. I will use statistical support to estimate the minimally clinical important difference (MCID) of treatment with intravenous iron on QoL – which is likely to be the primary outcome for the main trial. Data management
279
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 26 of 65
All data will be recorded on paper case report forms which will then be entered into a secure trial database such as REDCap (https://projectredcap.org/about/). Trial management detailsI will be responsible for the undertaking the major day-to-day tasks in running the trial with oversight from the doctoral steering group. This group will consist of the academic supervisors
, Dr. , and a member from our local ICU patient forum group. Research Nurse support will also be sought from the NIHR Clinical Research Network. Regarding Clinical Trials Unit (CTU) support, I am currently in discussions with the CTU. They do not have the capacity to support me currently but I am reassured that discussions will progress depending on the outcome of this application. I have sought advice from the Research and Design Service who feel that statistical and administrator support should be adequate for my feasibility study and I have accounted for the salaries of this in my Finances section. Trials methodology trainingThis fellowship will provide me with training in designing and running a feasibility study - which can then be used to design the main RCT, laboratory techniques and handling routine healthcare data in a research setting. I will also develop skills in grant writing and delivering high-quality presentations. To enrich my training experience, I will undertake specific trials methodology training by completing taught modules from
on ‘Clinical Trial Management’, ‘Statistics for Clinical Trials’, and ‘Big Data Epidemiology'. 2) What are the characteristics and iron profile of patients who respond (and those who do not respond) to intravenous iron and can biomarkers such as hepcidin predict response to intravenous iron?
The overall aim of this work is to better characterise the anaemia in ICU survivors by exploring the predictive role of hepcidin in the treatment group, the possible interaction between Vitamin D and iron metabolism and the assessment of bone marrow function using established immunophenotyping techniques. I will evaluate full blood count, routine iron profiles (ferritin, serum iron, transferrin saturation), soluble transferrin receptor, and serum hepcidin concentrations in both study groups before and after randomisation. I will also evaluate routine biochemistry profiles (renal function, liver function tests, calcium and phosphate), C-reactive protein and Vitamin D concentrations. By measuring the Vitamin D levels of patients in our cohort, I intend to identify whether this is an independent variable in the persistence of anaemia in ICU survivors, which may inform the design of a future large RCT in which Vitamin D replacement may need to be considered alongside iron replacement. I will quantify marrow sub-populations (haematopoietic stem cells, multipotent progenitors, committed erythroid progenitors) and analyse the relationship between bone marrow activity as evidenced by these populations, and the response or otherwise to intravenous iron replacement. This will allow me to determine whether bone marrow function, independently of iron parameters, determines the natural evolution of anaemia in ICU survivors. Data analysisThis will be anexploratory analysis where I would use standard linear techniques such as univariate and multivariate analysis. In both groups, I will perform univariate associations first, using logistic regression, between response and indices of iron profiles (hepcidin, ferritin, and sTfR), vitamin D and inflammation (CRP). Analysis of the control group may identify factors associated with a spontaneous improvement in haemoglobin. For all variables demonstrating univariate association with Hb response, I will construct multivariate models. Regressions will be calculated separately for 4 week, 3 month and 6 month follow-ups and combined data. To explore specific patient and illness related factors associated to Hb response, we will also perform univariate and multivariate analyses between age, gender, ICU admission Hb, critical illness severity scores, organ-support days, ICU and hospital length of stay and Hb response. I would also use classification techniques such as latent class analysis to create models to predict why certain participants may demonstrate a response to iron and the consequences of mounting / not mounting a response. The benefits of this work include potential stratification and sample enrichment for the intended main trial as well as improving understanding of mechanisms of anaemia after critical illness. SummaryThe findings from this feasibility study can be used to test whether administering intravenous iron in survivors of
280
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 27 of 65
critical illness with anaemia, when compared to placebo, results in an improvement in haemoglobin leading to meaningful changes in quality of life in a large multi-centre trial. Improved understanding of iron metabolism and anaemia using novel biomarkers and techniques has the real potential for sample enrichment for the design of a larger trial, in order to target interventions for patients who may stand to benefit the most.
References
281
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

D
Reference: D Date submitted: 1 Page 28 of 65
282
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

D
Reference: D Date submitted: 1 Page 29 of 65
283
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
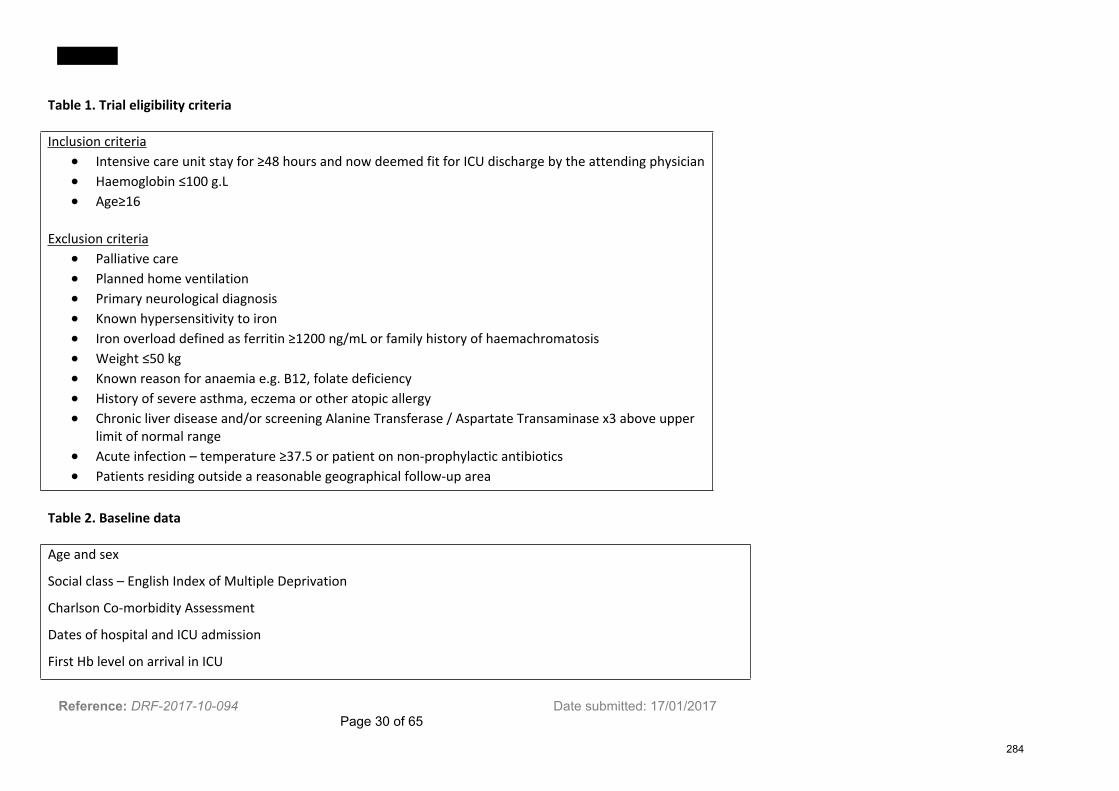
Reference: DRF-2017-10-094 Date submitted: 17/01/2017 Page 30 of 65
Table 1. Trial eligibility criteria
Inclusion criteria Intensive care unit stay for ≥48 hours and now deemed fit for ICU discharge by the attending physician Haemoglobin ≤100 g.L Age≥16
Exclusion criteria Palliative care Planned home ventilation Primary neurological diagnosis Known hypersensitivity to iron Iron overload defined as ferritin ≥1200 ng/mL or family history of haemachromatosis Weight ≤50 kg Known reason for anaemia e.g. B12, folate deficiency History of severe asthma, eczema or other atopic allergy Chronic liver disease and/or screening Alanine Transferase / Aspartate Transaminase x3 above upper
limit of normal range Acute infection – temperature ≥37.5 or patient on non-prophylactic antibiotics Patients residing outside a reasonable geographical follow-up area
Table 2. Baseline data
Age and sex
Social class – English Index of Multiple Deprivation
Charlson Co-morbidity Assessment
Dates of hospital and ICU admission
First Hb level on arrival in ICU
284
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

D
Reference: DRF-2017-10-094 Date submitted: 17/01/2017 Page 31 of 65
Source of ICU admission
APACHEII score and diagnostic code on ICU admission
Organ support required in ICU: mechanical ventilation, vasopressors, renal replacement therapy
Table 3. Flow chart of study assessments
Screening Baseline (pre-
randomisation)
Hospital discharge 4 weeks post-
randomisation
3 months post-
randomisation
6 months post-
randomisation
Full blood count x x x x x
Reticuloyte count x x x
Urea & Electrolytes x x x x
C-reactive protein x x x x
Liver function tests x x x x
Iron studies –
ferritin, iron, Tsat,
sTfR,
x x x x
Hepcidin x x x
Progenitor assay x x x
Vitamin D x x x
History and vital
signs
x
Infection x x
285
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

D
Reference: DRF-2017-10-094 Date submitted: 17/01/2017 Page 32 of 65
Transfusion use x
HRQoL
- MFI
- EQ-5D
x x x x
286
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 33 of 65
9. Case for Support - Part 3
Dissemination and projected outputs
I strongly believe that the findings from this fellowship will improve our understanding of anaemia after intensive care and further strengthen the call for a larger definitive trial. Therefore, the findings of this research will be shared as quickly as possible to the relevant people through the following mechanisms: International academic communityI intend to publish in high-impact peer reviewed journals and will ensure open access wherever possible. I will target the American Journal of Respiratory and Critical Care Medicine, Intensive Care Medicine and Critical Care. I will aim for oral and poster presentations at international conferences, specifically the annual UK Intensive Care Society State of the Art Meeting and the European Society of Intensive Care Medicine Meeting. Some of my laboratory research may also be novel to other anaemias associated with inflammation and I will aim to publish in haematology and/or general medical journals so that others can apply the methods in different fields. Local academic communityI will actively seek to present my work at the NIHR Trainee Meeting and at seminars within
. In addition to attending all weekly meetings with the research group, I will present my progress at 3-monthly intervals. Clinical trials groupsThere will be opportunities to present my work at and
research network biannual meetings. This will be crucial for generating interest in potential trial centres for the intended main trial. Patient groupsI will seek to present my work to our local patient forum group consisting of ICU survivors along with national support groups such as ICUsteps (www.icusteps.org).
Overview of Future Plans
Academic aimsMy overall career aim is to be a clinician scientist in intensive care medicine. I have so far been privileged to have trained in research-active departments which have given me the opportunity to develop specialist interests in transfusion medicine and outcomes following anaesthesia and critical illness. My current NIHR Academic Clinical Fellowship has provided me with the opportunity to obtain preliminary data to generate hypotheses for future research. Through studying for the Diploma in Health Research, I have received structured training in critically appraising evidence and applying health research techniques to answer research questions.
As a natural follow-on to this, I believe that the NIHR Doctoral Research Fellowship will provide me with the opportunity to utilise these skills to prospectively test the hypotheses derived from my preliminary data. In addition, this fellowship will also provide me with the opportunity to learn a wide variety of new skills in epidemiological analysis, laboratory assessment of erythropoetic function and importantly, how to design, manage and complete a clinical trial. Presentation and dissemination of our work will provide oppurtnities for learning from others and networking with the wider research community. I have already benefited from working with expert collaborators with a proven record in translational research and this will hold me in good stead for future collaborations and a future career in clinical research. If successful, I would builid on this doctoral fellowship and incorporate post-doctoral research into my final years of clinical training through a Clinical Lectureship award with the long-term goal of a career in academic intensive care medicine, such as through a Clinician Scientist award. To maintain and develop my interest in medical education, I would actively involve myself with the University in formal teaching of medical students as well as engaging with the relevant medical colleges to develop new educational initiatives for postgraduate trainees and when appropriate, involve myself in assessment of postgraduate examinations. Clinical aims
287
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 34 of 65
I would like to combine my academic interests with the clinical responsibilities as a Consultant Intensive Care with a specialist interest in tranfusion medicine and post-ICU outcomes. Through my work so far on the ICU-related anaemia, I have also developed a broad interest in more holistic patient rehabilitation and outcomes after critical iillness. I would seek opportunities to involve myself in post-intensive care follow-up clinics and to improve links between secondary and primary care for this challenging cohort of patients. Future workThe results of this research project have the potential to identify areas of focus for further research. Most importantly, the results of our feasibility trial will be used to design a larger study powered to detect differences in patient-relevant outcomes. The laboratory work aimed at identifying which patients respond to iron therapy can be used to advance beyond currently available iron profiles and generate hypotheses for testing in further clinical trials. Identifying the factors associated with persistence of anaemia in the community can be used to develop diagnostic pathways and algorithms to help standardise the management of anaemia in this cohort of patients. Intravenous iron has other pleiotropic effects such as improving skeletal muscle oxygen handling, reversing hypoxic pulmonary vasocontriction and improving exercise performance in other patient populations. Whether this hold true for survivors of critical illness also requires further exploration.
288
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 35 of 65
289
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 36 of 65
10. Management & Governance
Description: Research Timetable File Name: Screen Shot .png
290
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 37 of 65
Research management arrangements Please explain the practical arrangements for managing the research and its constituent components
I am a self-motivated individual and my experience of balancing clinical and academic commitments during the Academic Clinical Fellowship has helped me develop effective time-management and prioritisation skills.
My progress will be assessed on a frequent basis by the supervisors via monthly face-to-face research meetings. In addition, quarterly progress checks will be compared with the GANTT timeline of the project. I have worked with all my supervisors before and have very good relationships with them. I therefore anticipate that the supervision will be easily accessible and of high quality. All the supervisors have collaborated on projects so I do not anticipate any problems with disagreement. The doctoral steering group, all of whom have a proven track record in national and international clinical trials, will supervise the conduct of the trial. A trial specific monitoring plan will be established and the trial will be monitored according to this plan. All trial data will be available for trial related monitoring, audits and research ethics committee review. Financial management will be through detailed record keeping by myself with oversight from the supervisors and departmental administrators at
.
Has any work relevant to this proposal already commenced? No
Does your proposal include a clinical trial? Yes
A Sponsor is required to complete the Declarations and Signatories’ section of the application form.
Is Clinical Trials Authorisation required? Yes
Is a Clinical Trials Unit (CTU) involved with this research proposal? No
Please explain why and who/what will be involved instead of a CTU
Regarding Clinical Trials Unit (CTU) support, I am currently in discussions with the CTU. They do not have the capacity to support me currently but I am reassured that discussions will progress depending on the outcome of this application. I have sought advice from the Research and Design Service who feel that statistical and administrator support should be adequate for my feasibility study and I have accounted for the salaries of this in my Finances section.
Have you read the MRC Good Practice Guidelines for Clinical Trials? Yes
Will / does the trial appear on the UK Clinical Trials Gateway? Yes
Does the proposed research programme raise any ethical issues? Yes
If yes, discuss how these issues will be addressed.
We will require ethical approval for this research as we are conducting a Clinical Trial of an Investigative Medicinal Product (CTIMP). First we will seek positive approval from a research ethics committee. At the same time, we will also apply for clinical trial authorization from the Medicines Healthcare products Regulatory
291
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 38 of 65
Authority. As part of the database study analysing general practice records of ICU survivors for Hb measurements in the community (all samples are analysed in the same laboratory) we will seek approval from NHS Digital, previously known as the Health and Social Care Information Centre. This would lead to the development of a ‘safe haven’ that can be used for anonymised database linkage analysis. I will seek these approvals as early as possible in the first year of my fellowship.
Please detail how and when you intend to get ethical review completed
I intend to the ethical review completed within the first 9 months of my fellowship.
Have any appropriate regulatory bodies already granted the necessary approvals? No
Are you intending to undertake a systematic review? Yes
292
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 39 of 65
11. Intellectual Property & Innovation
The definition of Intellectual Property Rights (IP) includes copyright (such as new software, checklists, scales, protocols, questionnaires, toolkits, guidelines or similar) and research tools (such as data analysis techniques, assays, cell lines, biomarkers, materials or equipment and devices) patents, trademarks and designs.
Will any IP be produced or improved during the proposed research? Yes
If Yes, please describe what IP will be produced and/or improved
I have sought advice from a Research Contracts and IP specialist based in Research Services at who has provided advice on this application. Academic publications resulting from this work will be one
form of IP. Another potential form of IP could be the adoption of a questionnaire used to assess quality of life (QoL) specifically in ICU survivors. The two questionnaires we are going to use in this study are externally validated, freely available for non-commercial purposes and have been used in other ICU survivor studies but they are not specific for ICU patients. From our research, we may find that important outcomes for ICU survivors may be not be adequately addressed in the questionnaires. The patient dataset created from the findings of this trial will also be IP.
Please describe how any new IP generated through the proposed research will be recognised, captured, managed and utilised, either through dissemination and adoption in the healthcare service or through commercial exploitation.
Results will be published in open-access, peer-reviewed journals and the findings will be presented at conferences of the intensive care societies of UK and Europe. The patient dataset created as result of this trial will be stored on a secure University computer and password protected. It is anticipated that this will be freely available for publicly funded healthcare NHS professionals and for non-commercially funded academic purposes. IP from the intended main trial after this feasibilty study has the potential to develop guidelines and protocols for management of anaemia after intensive care.
What are the key current and future barriers to using any new IP/innovation through dissemination and adoption in the healthcare service or through commercial exploitation? e.g potential regulatory hurdles
I have not identified any current or potential barriers of using any new IP or innovation arising from this project. The assays we are using for our laboratory work have already been developed and are commercially available. In the future, if intravenous iron were to become the standard of care to treat anaemia after intensive care as part of a guideline, potential barriers would include seeking relevant local, regional and/or national governing committee approvals for adoption of the new guideline.
293
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 40 of 65
12. Involvement with NIHR Infrastructure & Other Partner Organisations
Network involvement Please describe links to NIHR networks, identifying, if appropriate, any benefits that have already accrued from working with networks
I will apply for NIHR Clinical Research Network (CRN) support so that the the study to be added to the NIHR CRN research portfolio. If adopted, specific supprt will be sought regarding NHS support service costs such as research nurses, achieving recruitment targets, and performance monitoring.
Two of the supervisors for this project have lead roles in the with specialist expertise in
. They have experience of running many multicentre randomised controlled trials. The collaborative approach within the NIHR CRNs has helped ensure the successful delivery of multiple haematology and critical care research studies. The primary supervisor is a senior group leader
Involvement with other partnersWhat, if any, other organisations will partner this research?
Will this application be supported by any other funding body? No
294
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 41 of 65
13. Training and Development
Proposed training and development programme
From my research experience so far, I have gained skills in undertaking observational studies, systematic review and meta-analysis, statistic analysis and basic laboratory skills. There are areas in which I have limited experience in such as randomized controlled trials, trial statistics and outcome measurements. As these areas are relevant to my research proposal, my training plan is focused on developing and expanding on these areas. Internal training
I am currently pursing a part-time Diploma in Health Research as part of my NIHR Academic Clinical Fellowship. This will be completed in . Prior to commencing the Doctoral Research Fellowship, if awarded, I will have completed a 5-day taught module on Randomized Controlled Trials ( ) as part of the Diploma. During the first year of my fellowship, I intend to complete the following modules: - Clinical Trials Management – this module will provide me with the skills necessary to set up and manage trials along with an understanding of the lifecycle of a clinical trial. - Big Data Epidemiology – this module will teach me about protocols, approvals, data management and longitudinal analysis of very large databases. The skills gained will complement the database linkage analysis work I plan on carrying out as part of my feasibility study. - Statistics for Clinical Trials – this module will allow me to gain competence in protocol development, statistical planning, statistical methods for testing and interpreting effect sizes and reporting of outcomes and presentation data. I will also attend courses run locally by the Medical Sciences Division such as 'Managing your supervisor' (Year 1) and 'Writing skills - papers and thesis' (Year 3). The skills gained from these courses will be invaluable for conducting my feasibility trial and designing the intended main trial to ensure that it is has a clear research question, relevant outcome measures and the appropriate trial infrastructure (e.g ethics, organisational approvals, statistical rigor). External training - Edinburgh Critical Care Research Methods Course – I will attend this 2-day course designed to provide an overview of research methods with a specific focus on the challenges of carrying out research in an acute health care setting. - Outcome Measurement and Valuation for Health Technology Assessment – this 3-day workshop at the University of York Centre for Health Economics will provide me with training in key principles of outcome measurement, and economic evaluation based on measures such as EQ-5D - a tool that I am using as part of this research. - John Hopkins Critical Care Rehabilitation Conference – this 3-day conference at the John Hopkins School of Medicine in Baltimore, USA, focuses on promoting interdisciplinary collaboration to bridge the gap between research and delivery at the bedside. Specific workshops that I would attend for my academic and clinical interests would include those on describing the impact and challenges of ICU survivorship on patients and families, appraising evidence on long-term outcomes after critical illness and developing quality improvement processes for early rehabilitation. I have spoken to senior ICU researchers involved in post-ICU outcomes research and they have said that is the best annual ICU outcomes meeting out there. The above courses will provide me with a detailed knowledge of the challenges specific to ICU survivor research methodologies and an training on health economics evaluations. My long-term career aim is to be a recognised clinical academic specialising in the field of improving outcomes after ICU and the courses, such as the one in
295
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 42 of 65
John Hopkins, will be a fantastic opportunity to develop international collaborations, develop and share new research ideas and learn about other healthcare systems pathways of ICU rehabilitation to see if they can be developed in the UK.
Host organisation support This section must be completed by the Head of Department or Senior Manager of the academic host organisation.
I am pleased to lend my full support to ’s application for an NIHR Doctoral Research Fellowship. is an NIHR Academic Clinical Fellow (ACF) in Intensive Care Medicine on
. He wishes to undertake a DPhil based in . He already has a number of publications and has previously received a small
research grant from the . ’s research aims to understand the role of intravenous iron to treat anaemia in survivors of critical illness. It is hoped that the research will improve the quality of life of people after treatment in intensive care. Intensive Care is an area of medicine that could benefit from greater research capacity and it would be highly desirable to see candidates such as supported in this fellowship scheme.
is a multi-disciplinary department with research interests that span
the translational spectrum, from basic biological research through to clinical application. We have internationally renowned programmes in a broad range of sciences related to medicine, from cardiovascular, diabetes, endocrinology, and stroke research, to molecular medicine, immunology, haematology and pathology, including programmes in stem cell and regenerative medicine. The Department employs in the region of 700 staff, has approximately 120 postgraduate research students and an annual turnover of around £59 million.
The Department strongly supports the career progression of all its researchers (students and staff) and we hold an Athena SWAN Silver Award in recognition of our efforts to support the careers of female students and staff. We run a dedicated mentoring programme for all students and staff, which provides an additional channel for personal and professional development. We also provide extensive training opportunities in a wide range of areas from management of staff, to grant writing workshops, to training on how to run a research group, how to handling conflict, and effective communication etc. Indeed we have a dedicated Career Development Committee in the Department whose aim is to support the career development of all staff and students across .In addition, tailored advice on career directions, support in identifying funding opportunities, and support with preparing grant applications is provided by the Research Strategy Coordinator in the Department. All Fellowship holders will have a formal mid-term review, by a panel of senior academics from the department, to ensure their research is progressing and that they are on track for renewing their fellowship or applying for a more senior award, as appropriate. We have an excellent track record in supporting early career researchers into senior fellowship positions and faculty positions.For Graduate Students there are additional support structures in place within the department: (1) There are a number of Graduate Advisors in the Department whose role is to oversee student supervision and monitor student progress. They also act as an additional source of advice and support. Graduate Advisors meet with each student once per year to review progress and training requirements and to discuss future career plans. Together with the supervisor, the Graduate Advisors will support the applicant to ensure they successfully complete their research and their specific training and develoment programme. (2) Termly reports on each student's progress are submitted by all supervisors through the University's Graduate Supervision System (GSS). GSS also facilitates self-reporting by students on their own progress or concerns. Reports can be viewed by the student and anyone with supervisory responsibility for the student, including the Graduate Advisor and the Director of Graduate Studies. (3) Students are allocated a who provides pastoral support for the student and can act as a further line of support where necessary. (4) As well as the specific training that will be offered in the lab, scientific skills training is available through various courses organised by the department and generic skills training is offered through the Medical Sciences Division's Skills Training Programme. This programme offers a comprehensive range of courses covering all domains of the Researcher Development Statement: knowledge and intellectual abilities, personal effectiveness, research governance and organisation, and engagement, influence and impact. Students are actively encouraged to take advantage of the training opportunities available to them. (5) All incoming students receive a comprehensive induction, which is followed by a welcome event where they will be able to meet existing students and selected PIs, helping them to integrate quickly into the research environment. As well as an active programme of research events, there are student-led academic and social events.In summary, I believe that our Department provides an excellent and supportive environment where all students and staff can develop and advance in their careers.
296
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 43 of 65
Proposed academic department
AddressAddress Line 1
Address Line 2
Address Line 3
City
Tel. No.
What percentage of the applicant's working time will be spent in this department?
100
Please summarise the department's record in your proposed research area
brings together
multidisciplinary clinical laboratory-based disciplines and hosts most of the haematology research within the University. The group has a national and international profile in clinical and applied research in Transfusion Medicine, based around the activities of lead investigators. The unit hosts the systematic reviews initiative (£0.25 million/ year), which has completed over 60 systematic and Cochrane reviews over 10 years, and supported the unique resource of .
Dissemination of evidence with significant and leadership by the
transfusion investigators has been undertaken through national and international guideline groups, including NICE, ICTMG and BSH.
Indicate in what ways your department demonstates excellence
is one of the largest
297
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 44 of 65
departments in the . Headed by is a multi-disciplinary department with research interests that span the translational spectrum, from basic biological research through to clinical application.The Department has internationally renowned programmes in a broad range of sciences related to medicine, from cardiovascular, diabetes, endocrinology, and stroke research, to molecular medicine, immunology, haematology and pathology, including programmes in stem cell & regenerative medicine. The Department employs in the region of 700 staff, has around 120 postgraduate research students and an annual turnover of around £59 million.In the 2014 Research Excellence Framework, the was part of the Clinical Medicine return and .
Insert a link to latest RAE/ REF rating
Number of research students currently in the departmentDoctorate: 120
Masters: 0
Collaborations
Local collaborations
The host group has strong exisiting links with NHS Blood and Transplant, NHS Foundation Trust and the Critical Care Research Group in the . These organisations have a strong research infrastructure and have conducted large multicentre studies in blood management, haemorrhage, and intensive care. Studies have included Age of Blood Evaluation (ABLE) trial; the TRACMAN trial which was the world's largest trial on the timing of tracheostomies; OSCAR, HTA funded trial to study high frequency oscillatory ventiation in Acute Respiratory Distress Syndrome; and the Intensive Care Study of Coagulopathy (ISOC-1 and -2). I intend to utilise the experience of these groups to use the data from my feasibility trial to design and deliver a large multicenter trial. This work also represents collaboration with and at the
. I have already worked in their laboratory and established good links with the scientists and research associates working there. The lab has been at the international forefront of iron and hepcidin-related research and collaboration will provide a unique mechanistic aspect to our feasibility trial. The lab are currently developing an assay for erythroferrone - a recently discovered hormone that inhibits the action of hepcidin thereby making more iron available for haemoglobin synthesis. This opens up another avenue for mechanistic research into critical illness anaemia. Having as a supervisor will form collaborations with the group based in the
. The group has a leading interest in the interplay between iron and oxygen at the molecular level the protective effect of iron on hypoxic vasoconstriction.
This can have potential benefits such as reduced ventilator days for patients with underlying lung disease. External collaborations
Two of my supervisors ) have strong links with Research Group led by . This group has carried out several large studies on ICU outcomes and recovery after critical illness with methodologies ranging from qualitative research to randomized controlled trials and big data. In collaboration with , the group has also led on large trials on transfusion. I have already collaborated with this group for my laboratory study. The samples analysed were from the ICU survivors recruited into their large randomized controlled trial assessing the effects of a physical and nutritional rehabilitation 'package' on quality of life after intensive care. During the first year of my Fellowship, I intend to spend some time there (1-2 weeks) learning more about the carrying out ICU outcomes research and
298
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 45 of 65
challenges associated with it. This will provide me with the opportunity to develop my own collaborations as well as strengthen the pre-exisiting ones.
299
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
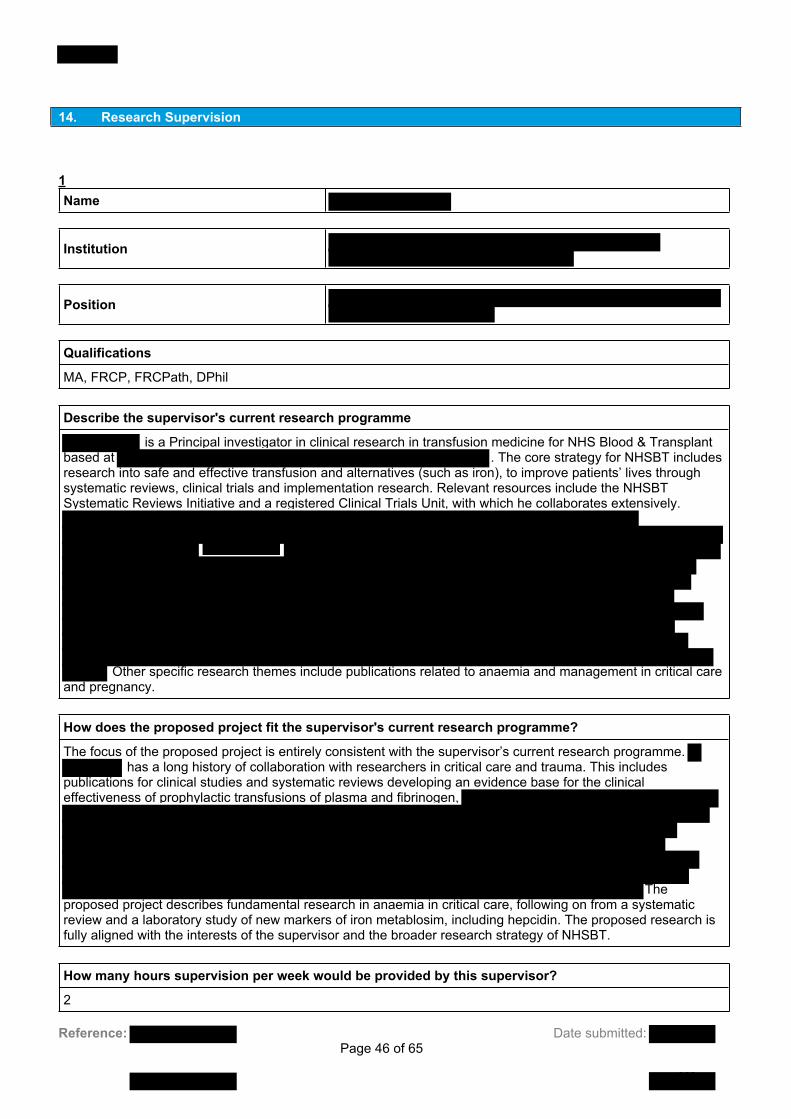
Reference: Date submitted: Page 46 of 65
14. Research Supervision
1Name
Institution
Position
Qualifications
MA, FRCP, FRCPath, DPhil
Describe the supervisor's current research programme
is a Principal investigator in clinical research in transfusion medicine for NHS Blood & Transplant based at . The core strategy for NHSBT includes research into safe and effective transfusion and alternatives (such as iron), to improve patients’ lives through systematic reviews, clinical trials and implementation research. Relevant resources include the NHSBT Systematic Reviews Initiative and a registered Clinical Trials Unit, with which he collaborates extensively.
Other specific research themes include publications related to anaemia and management in critical care and pregnancy.
How does the proposed project fit the supervisor's current research programme?
The focus of the proposed project is entirely consistent with the supervisor’s current research programme. has a long history of collaboration with researchers in critical care and trauma. This includes
publications for clinical studies and systematic reviews developing an evidence base for the clinical effectiveness of prophylactic transfusions of plasma and fibrinogen,
The proposed project describes fundamental research in anaemia in critical care, following on from a systematic review and a laboratory study of new markers of iron metablosim, including hepcidin. The proposed research is fully aligned with the interests of the supervisor and the broader research strategy of NHSBT.
How many hours supervision per week would be provided by this supervisor?
2
300
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 47 of 65
Number of research students supervised through to completion Masters
0
Doctoral 3
Number of research students currently supervised Masters
0
Doctoral 2
List three recent publications by the supervisor that are relevant to this application
2Name
Institution
Position
Qualifications
BSc (Hons), MBChB, FRCA, DICM, FFICM, PhD
Describe the supervisor's current research programme
is a Consultant in Intensive Care Medicine and Anaesthesia and an Honorary Research Fellow of . In recent years he has been principle investigator for a number of international and
national studies in critical care
’s current research programme builds upon collaborative links with haematology and NHSBT to
better understand the prevalence, characterisation and impact of the anemia associated with critical illness,
301
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 48 of 65
coagulopathy and it’s management and (red cell, plasma and platelet) transfusion practice. has co-supervised my studies investigating the use of hepcidin to characterize the anaemia following critical illness (publication pending) and is co-chief investigator of a study examining the role of desmopressin in critically ill patients with thrombocytopaenia undergoing interventional procedures.
is also
How does the proposed project fit the supervisor's current research programme?
has published widely in the area of anaemia and transfusion in critical care
has co-supervised my studies investigating the prevalence and characterization of anaemia
during recovery from critical illness (publication pending) and has played a central role in the development of this research proposal. The proposed project is fully aligned with the research interests of and builds on his current research programme and established collaborations.
He currently supervises one NIHR Academic Clinical Fellow (applicant, ) and is the educational supervisor and mentor for one DPhil student and one NIHR Academic Clinical Lecturer at the
How many hours supervision per week would be provided by this supervisor?
1
Number of research students supervised through to completion Masters
0
Doctoral 0
Number of research students currently supervised Masters
0
Doctoral 0
List three recent publications by the supervisor that are relevant to this application
3Name
302
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 49 of 65
Institution
Position
Qualifications
MA, DPhil, BM, BCh
Describe the supervisor's current research programme
How does the proposed project fit the supervisor's current research programme?
How many hours supervision per week would be provided by this supervisor?
1
Number of research students supervised through to completion Masters
1
Doctoral 27
Number of research students currently supervised Masters
0
Doctoral 5
List three recent publications by the supervisor that are relevant to this application
303
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 50 of 65
304
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

305

306
307

308
309

310

311

312

313

Reference: Date submitted: Page 60 of 65
16. DH Monitoring Information
Department of Health Monitoring Information - Please use the drop-down menus and tick boxes to provide the information requested. This will be used by the Department of Health solely for accountability, audit and monitoring purposes.Place of work of Applicant Acute Trust
Is the research multicentre? No
Please indicate in which region your host organisation is based
UKCRC Health Categories Please select a maximum of two classifications from the list below that are applicable.UKCRC Health Categories Blood
UKCRC Research Activities Please select a maximum of two classifications from the list below that are applicable.UKCRC Research Activities Aetiology 2.1 Biological and endogenous factors Evaluation of Treatments and Therapeutic Interventions 6.1 Pharmaceuticals
314
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 61 of 65
17. Research Design Service (RDS) Involvement
Did you contact the RDS? Yes
Please indicate in which region
Please describe the RDS’s input
The RDS reviewed my research proposal and plain English and scientific summaries. They provided trial methodology and statistical advice and provided useful suggestions on improving my plain English summary such as using the Gunning Fog index. When confronted with the possiblity of not having a Clinical Trials Unit on boad, the RDS provided suggestions on alternative CTUs and advice on proceeding without a CTU. They also refined the PPI section of my trial.
How satisfied overall were you with the input of the RDS?
Very satisfied
To what extent do you feel the quality of your proposal improved as a result of RDS involvement?
Improved greatly
Would you recommend the RDS to other people developing research applications?
Yes
Please expand on your responses above, explaining the reasons for your choices. Please also add any other comments about your experience of using the RDS.
The RDS were extremely helpful in adding more clarity to the background my research proposal, especially on being clear on the definitions of iron defiency. I had a face-to-face meeting with three research advisors, and regularly kept in touch over email.
315
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 62 of 65
18. Participants
Participants must complete their actions on your application prior to submission; signatories must also approve your application after you select the ‘submit’ option but BEFORE the application submission deadline. You are required to supply the names and email addresses (if not already registered on the TCCi application system) of the individuals who will be undertaking ‘participant’ roles as part of your application. Everyone named in this section will be acting as a ‘participant’ to your application and will need to agree to be part of this application. Participants are required to review the declaration for the role before confirming participation. By confirming participation, participants are acknowledging their involvement and input into this application and agree to be involved in it before it is submitted. You must ensure all participants are happy for your application to be submitted before submitting it on the online system. Details of the individuals who will be required to approve your application after submission (signatories) should be entered in the 'Declarations & Signatories' section. Please note it is often the case that one or more of the participants named in this section are also named in the "Declaration and Signatories" section of the form. Participants must confirm their participation on your application before you will be able to press the submit button. Please see the 'NIHR TCC Signatory Flow Diagram' in the guidance notes for further information.
Doctoral Primary Supervisor ParticipantTitleForename(s)SurnamePosition Consultant Haematologist
Supervisor ParticipantTitleForename(s)SurnamePosition Consultant
Supervisor ParticipantTitleForename(s)SurnamePosition
316
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 63 of 65
NHS Facilities and Staff ParticipantTitleForename(s)SurnamePosition
Research Contract Officer ParticipantTitleForename(s)SurnamePosition Research Contracts Manager
317
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 64 of 65
19. Declarations & Signatories
Applicant conflict of interest
None
By completing this form, the programme reserves the right to share, in confidence, details of your application with other parts of the NIHR and with the Department of Health.
ApplicantThis must be the applicant applying for the Award. You will also be required to supply the name and email address for all the people listed below who will be required to complete a declaration and in some cases part of the application form.How did you hear about this call? NIHR website
Applicant Declaration (Not registered for a research degree)I confirm that I have secured all necessary licences and ethical approvals in relation to the research and will abide by the terms of those licences and approvals in carrying out the research. I confirm that I have read the NIHR Carbon Reduction Guidelines and, where possible, taken steps to reduce the carbon emissions generated by this research. I confirm that, if required, I have submitted this application to the relevant Research and Development Office of my intended Devolved Nation. I undertake to conduct the research according to such guidelines for good research practice as the Host Organisation may from time to time lay down according to the NIHR research governance framework and the guidelines set out in ‘Good Clinical Practice in MRC-funded Trials’ (MRC 1998). In completing this, I declare that, to the best of my knowledge, the information provided in this application, is true, accurate and complete. I have read the Guidance Notes and agree to accept the process by which an application is assessed and agree to abide by the conditions under which an award may be granted. I agree that the NIHR may hold and process, by computer or otherwise, personal and other data supplied with this application and, if successful, additional data provided during the fellowship award. I understand that the application will be shared with members of the Expert Review Panel and may be sent for external peer review.
Confirmed
Signatories Participants must complete their actions on your application prior to submission; signatories must also approve your application after you select the ‘submit’ option but BEFORE the application submission deadline. You are required to supply the names and email addresses (if not already registered on the TCCi application system) of the individuals who will be ‘signing off’ your application. Once their contact details have been entered below, the signatories will be invited to log into the system and confirm their participation.
318
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE

Reference: Date submitted: Page 65 of 65
Once participation is confirmed, the Finance Officer will be able to access and edit the ‘Finance’ section (this should be completed in conjunction with the applicant) and the Head(s) of Department(s) must complete the relevant question in the ‘Training and Development’ section. These sections can be completed independently whilst the applicant works on the rest of the application. All signatories must have agreed to participate in your application and have completed their sections before the applicant is able to press the submit button and send the application for signatory approvals. The final signatory approval will result in the application being fully submitted to the NIHR. All parties (applicant, participants and signatories) will be notified of this via an automated system generated email. NIHR will not accept any applications unless fully approved by your signatories prior to
Signatories must confirm their participation and complete the relevant sections before you will be able to press the submit button.
SponsorTitleForename(s)SurnamePosition Head of Clinical Trials & Research Governance
Head of Department or Senior ManagerTitleForename(s)SurnamePosition Professor of Medicine and Head of
Department
Administrative Authority or Finance OfficerTitleSurnameForename(s)Position Research Funding Manager
319
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
MaguireE
Sticky Note
None set by MaguireE
MaguireE
Sticky Note
MigrationNone set by MaguireE
MaguireE
Sticky Note
Unmarked set by MaguireE
Page 1 of 70
Research for Patient Benefit
Reference number
Lead Applicant
Organisation
Research Title Early Video Assisted Thoracoscopic Surgery (VATS) or Intrapleural Enzyme Therapy (IET) in Pleural Infection - a feasibility randomised trial.
Plain English Summary
Pleural infection is a serious complication of pneumonia where infected fluid collects around the lung in a large abscess. It can affect anyone, and occurs in 40 patients every day in the UK. Treatment requires antibiotics and drainage of fluid using a chest tube inserted with local anaesthetic between the ribs, and admission to hospital for 2 weeks. When these treatments fail, patients either die (about 20% of cases) or are referred for major surgery (a further 20%). Surgery is important when initial treatment fails, but has several side effects and is not an option for elderly and sick patients, where the death rate is 40%. A new treatment (called Intrapleural Enzyme Therapy or IET) can be given through the chest tube early in treatment, which improves drainage and reduces the need for surgery and the time spent in hospital. Keyhole surgery is also now available to drain infected fluid (Video Assisted Thoracoscopic Surgery or VATS), and some people believe that this should occur early in treatment to prevent death and long hospital admissions, but this has not been proven. Early treatment with either IET or VATS may therefore improve care but we do not know the long-term effects (e.g. restriction in breathing) or impact on quality of life. We aim to consult with patients to understand what factors are important to them when treating this disease. This will help us to understand what should be measured in a study to best improve care. We will then use this information to conduct a study where patients are randomised (assigned by computer) to usual treatment (chest tube and antibiotics), early VATS or early IET. We will measure whether it is acceptable to patients to be randomised in this way and whether a larger study in the future is important and possible.
Total Research Cost 264,901.00
320

: Page 2 of 70
The Department of Health, National Institute for Health Research (DH NIHR) is the Data Controller under the Data Protection Act 1998 (‘the Act’). Applicants for funding should be aware that information contained in this application might be shared with other DH NIHR bodies for the purposes of statistical analysis and other DH NIHR management purposes, including targeted communications with selected groups of researchers. Applicants may be assured that DH NIHR is committed to protecting privacy and to processing all personal information in a manner that meets the requirements of the Act.
321

Page 3 of 70
Table Of Contents
1. Project Team
2. Research Details
3. Lead Applicant Details
4. Co-applicant Details
5. Research and Development Office Contact details
6. History of this application
7. Patient and Public Involvement
8. Case for Support - Part 1
9. Case for Support - Part 2
10. Case for Support - Part 3
11. Management and Governance
12. Intellectual Property and Innovation
13. Involvement with NIHR Infrastructure and Other Partner Organisations
14. Finance
15. Department of Health Monitoring information
16. Nominated/Suggested Reviewers
17. Supporting Documentation
18. Declarations & Signatures
19. Lead Applicant CV
20. Co-applicant CVs
322

Page 4 of 70
1. Project Team
Full NameOrganisation
Full NameOrganisation
Full NameOrganisation
Full NameOrganisation
Full NameOrganisation
Full NameOrganisation
Full NameOrganisation
Full NameOrganisation
Full NameOrganisation
323

: Page 5 of 70
2. Research Details
Research titleEarly Video Assisted Thoracoscopic Surgery (VATS) or Intrapleural Enzyme Therapy (IET) in Pleural Infection - a feasibility randomised trial.
Host organisation (which will administer any award)
Research duration 33
Proposed start date if awarded funding
Application type Feasibility Study
If your application is related to one of the past NIHR themed calls, please indicate which call here.
N/A
324

Page 6 of 70
3. Lead Applicant Details
Full Name ORCID iD
Position Address Line 1
Speciality Address Line 2Institution Address Line 3
City/TownEmail Address
Provide an approximate breakdown (%) of how your current appointment is divided between the following activities:
%
Service/Clinical 40
Research 55
Teaching 5
Other 0
If applicable, please specify what your 'other' research activity consists of.
not applicable
Administrative contact detailsAdministrative contact name
Administrative contact job title
Administrative contact email address
325

Page 7 of 70
4. Co-applicant Details
APPLICANT ROLE AND % FTE COMMITMENT 1Name of applicant
Is this a patient/public co-applicant? No
Specify role in research
Overall responsibilty for design, delivery and analysis of the study - Chief Investigator.
% FTE commitment 5
APPLICANT ROLE AND % FTE COMMITMENT 2Name of applicant
Is this a patient/public co-applicant? No
Specify role in research
Key Investigator and PI at recruiting centre
% FTE commitment 5
APPLICANT ROLE AND % FTE COMMITMENT 3Name of applicant
Is this a patient/public co-applicant? No
Specify role in research
Statistician for the study
% FTE commitment 25
APPLICANT ROLE AND % FTE COMMITMENT 4Name of applicant
Is this a patient/public co-applicant? No
Specify role in research
326

: Page 8 of 70
Key Investigator and PI at recruiting centre
% FTE commitment 5
APPLICANT ROLE AND % FTE COMMITMENT 5Name of applicant
Is this a patient/public co-applicant? No
Specify role in research
Key Investigator and PI at recruiting centre
% FTE commitment 5
APPLICANT ROLE AND % FTE COMMITMENT 6Name of applicant
Is this a patient/public co-applicant? No
Specify role in research
Thoracic surgical expertise, advice on quality assurance and surgical pathway
% FTE commitment 5
APPLICANT ROLE AND % FTE COMMITMENT 7Name of applicant
Is this a patient/public co-applicant? No
Specify role in research
Thoracic surgical expertise, advice on quality assurance and surgical pathway
% FTE commitment 5
APPLICANT ROLE AND % FTE COMMITMENT 8Name of applicant
Is this a patient/public co-applicant? No
Specify role in research
327

: Page 9 of 70
Director - oversight of quality assurance, trial delivery and regulatroy aspects.
% FTE commitment 15
APPLICANT ROLE AND % FTE COMMITMENT 9Name of applicant
Is this a patient/public co-applicant? No
Specify role in research
Key Investigator and PI at recruiting Centre
% FTE commitment 5
APPLICANT ROLE AND % FTE COMMITMENT 10Name of applicant
Is this a patient/public co-applicant? No
Specify role in research
Pleural expertise, PI for local centre, key role in establishment of patient interest group via previous study and current clinical practice.
% FTE commitment 5
APPLICANT ROLE AND % FTE COMMITMENT 11Name of applicant
Is this a patient/public co-applicant? No
Specify role in research
Expertise in health economic anlaysis which in this study will be used to assess the feasibility of assessment of important HE outcomes in this study population
% FTE commitment 6
328

Page 10 of 70
5. Research and Development Office Contact details
Please note we will notify the R&D office of the outcome of this application including any associated feedback.Host Institution (which will administer any award)
R&D contact name
R&D contact job title
R&D contact telephone number
R&D contact email address
329

Page 11 of 70
6. History of this application
Has this application, or a similar application previously been submitted to this or any other funding body?
Yes
Title of previous application
Name of Lead Applicant
Funding body to whom it was submitted NIHR Health Technology Assessment Programme
Please indicate whether this was a Stage 1 (outline) or Stage 2 (full) application. Stage 1
The reference number of previous application
Outcome Unsuccessful
If unsuccessful, please indicate why.
The HTA board rejected the previous application, which was for a full phase III randomised controlled trial comparison of Video Assisted Thoracoscopic Surgery (VATS) and Intrapleural Enzyme Therapy (IET), on the basis that "the proposal as presented was not deemed to be a priority for the NHS at this time".
Where a previous, related application was made, please indicate how this research proposal differs from the previous application.
We have taken on board the feedback of the HTA board, and considered several specific new aspects in this application, these being:1. Establishing the patient centred outcomes which are most important in assessing quality and optimal management in this disease. We will achieve this through establishing PPI structures as the first part of this application, which will inform further work. 2. Demonstrating the feasibilty and hurdles toward recruitment to a phase III randomised surgery versus no-surgery trial in pleural infection. We will achieve this through the second part of this application, which is for a feasiblilty randomised trial with the same intended patient population, interventions and outcomes as a larger trial, informed by PPI work in the first phase. 3. In light of the comments provided by this RFPB panel, we have also added a control group to the feasiblity trial which represents "standard care" to allow the clinical effect of interventions (IET or surgery) to be assessed against normal treatment (chest drainage via tube and antibiotics only) - please see later research details. 4. We have in addition conducted a review of the trial proposal by two patients who have personal experience of pleural disease, with positive feedback.
330

Page 12 of 70
7. Patient and Public Involvement
In this section it is important that you describe, in as much detail as possible, how patients and the public have been involved in the development of the application as well as plans for involvement in the proposed research.
Were patient and the public actively involved in either identifying the research topic/prioritising the research questions and/or preparing this application?
Yes
If yes, please tick all relevant boxes below.
Involved in identifying the research topic/prioritising the research questions, Involved in preparing the application
Please further describe how patient and public involvement has informed and/or influenced the development of the application and how patients and the public have been actively involved.
The has an established Patient and Public Involvement mechanism specific to respiratory / pleural disease. We curate an approved database of patient contacts with a range of respiratory disease (n>40) which is used to contact patients to gain views on proposed applications, research questions, relevance and patient acceptability. This mechanism will be used once funding has been obtained to create the proposed patient / carer group for pleural infection. Two patients with personal experience of pleural disease treated by our unit ( ) have assessed the current stage 2 application and both commented positively on the research idea, design of the study and the lay summary. To create the pleural infection patient / carer group, we will recruit 10 patients and carers who have survived pleural infection to capture the full experience of the disease process, as this illness is associated with prolonged hospital stay and recovery phase. The group will meet regularly (2 monthly) to discuss priorities in care and proposed outcomes for the later feasibility trial. Discussions will be recorded in a structured manner to ensure key themes are identified. The group will meet with physicians, surgeons and trial team in the first 3 months of this proposal as the feasibility study is being planned, to ensure that the study design remains aligned with patient and carer priorities and that key outcomes are captured. Two members will be offered full membership of the Trial Steering Committee and Trial Management Group for the feasibility trial. Members of the group will be asked to form a Patient Writing Group, which will input to patient material (information leaflets, consent forms) and academic outputs (manuscripts, presentations).
Please indicate the ways in which the public will be actively involved in the proposed research, by ticking all relevant boxes below.
Design of the research, Management of the research (e.g. steering/advisory group), Developing participant information resources, Undertaking/analysing the research (e.g. member of the research team), Contributing to the reporting of the study report, Dissemination of research findings
Please give more details, including how patient and public involvement will benefit the research, the reasons for taking this approach and arrangements for training and support.
There are no studies specifically addressing patient experience of pleural infection or the risks / benefits of invasive treatments and priorities in care. This is a reflection of there historically being only one treatment pathway (i.e. chest tube drainage and antibiotics, and then surgery in those failing treatment). The innovation of IET creates the opportunity for choice of intervention, and thus requires careful assessment of patient priorities. It is essential that research aimed at improving patient care prioritises outcomes of importance to patients who
331

Page 13 of 70
have experienced pleural infection to ensure study results are applicable to healthcare systems and clinical outcomes, and also patient experience. As no such data currently exists, the formation of the patient / carer group as the first step of this proposal is key to directing the outcomes and design of the feasibility trial. We propose that the patient / carer group will continue to meet throughout the research process.We have shown that collection of this specific patient reported data is possible; we have completed a pilot study assessing pain from pleural interventions in 33 patients (visual analogue scale (0-100mm), which demonstrated that chest tubes are painful and pain levels are comparable with more invasive procedures (thoracoscopy) (mean score of 21mm SD 8mm).During the feasibility trial, we propose continued assessment of patient experience and identification of outcomes for a phase III study, to occur via patient interviews in 20 individuals included in the randomised study, once the illness has resolved. Trained nurses will conduct structured interviews covering patient acceptability of randomisation and interventions, patient and carer experience, impact on quality of life and priorities in care. We have thus costed for:
Newspaper/radio advertising for members of the advisory group Fees for advisory group (2 monthly meetings plus associated travel & catering costs) TSC meeting (x3) attendance (travel and catering costs) Fees for 20 trial participants completing structured interviews
If this proposal is successful, we propose that members of this patient / carer group will be involved as key co-applicants in future grant applications for the larger definitive phase III study of interventions in pleural infection.
332

Page 14 of 70
8. Case for Support - Part 1
Aims and objectives Describe the overarching aims of the research, outlining the research question which the work will address.
Overall AimThe aim of our programme of work is to improve care of patients with pleural infection, by definitively identifying the optimal early treatment strategy in terms of real patient benefit. This proposalWe ultimately aim to perform a phase III randomised study comparing early use of the current “gold standard” treatment of Video Assisted Thoracoscopic Surgery (VATS) with a novel, less invasive treatment of intrapleural enzyme therapy (IET) which has been shown in phase IIb trials to be of potential benefit(1). Our landmark placebo controlled randomised trial in showed that IET (intrapleural tPA and DNase given early in treatment through a chest tube) is associated with better outcomes and a reduced need for surgery compared to placebo(1). IET may be associated with less hospital stay, lower costs, lower morbidity and lower mortality, and be applicable to a wider range of patients (pleural infection occurs in the elderly and frail, in whom surgery is high risk) than VATS. However, before undertaking a definitive and costly phase III trial, there are areas of uncertainty in the literature which include:
1. The feasibility of randomising patients to early surgery or less invasive treatment in pleural infection.2. Patient acceptability of the two treatments.3. The outcomes most important to patients with pleural infection.4. Feasibility of collecting resource use, quality of life and other outcomes data in this patient population.
This proposal is therefore for a feasibility study which will address the following objectives: Primary Objective:To assess the feasibility of randomising 75 patients with pleural infection to standard care, early VATS or early IET. Secondary Objectives:
1. Explore the costs and benefits from a patient perspective of a standard care, VATS or IET treatment strategy by creating a patient involvement group with personal experience of the disease process (patients and carers).
2. Assess the outcomes most important in pleural infection, by conducting structured interviews with patients who have experienced treatment for pleural infection.
3. Understand the acceptability of randomisation in a surgery versus non-surgery trial. This will be achieved through the randomised design, whereby those patients who do not accept randomisation are interviewed around their concerns.
4. Assess feasibility of collecting accurate long-term (6 month) outcomes in patients in accepting the randomised study including mortality, hospital stay, lung function, functional ability, patient reported outcomes and quality of life.
Deliverability and ExperienceThe study team has conducted 2 randomised controlled multicentre trials in pleural infection (n=660)(2, 3), and recently completed recruitment to an observational study (n=550) in pleural infection(4). HypothesisOur hypothesis is that it will be feasible to randomise patients to standard treatment, VATS or IET through our established UK network of pleural centres, that this will be acceptable to patients and that a sufficient recruitment rate will be achieved to render a larger trial feasible. We hypothesise that key patient related
333

: Page 15 of 70
outcome measures (such as quality of life, breathlessness and functional ability) which have not been studied in this disease area are key outcomes for the larger definitive study.
Scientific abstract of research Please provide a structured summary which outlines the background to the research, the aims of the work, including the question to be addressed by this research, the plan of investigation and a summary of the potential benefits to patients and the NHS.
Pleural Infection, where infected fluid develops between the lung and chest wall, is common(5-7) and increasing (5, 7). Treatment involves antibiotics and drainage of infected material using a chest tube (inserted between the ribs)(8). Despite treatment, the disease has a mortality of 20% (8) and 20% fail initial treatment which requires surgery, that is invasive, costly(2, 3, 9, 10) and associated with high morbidity (11, 12). Surgery is avoided in the most ill (7, 13), in whom mortality is 40%(14). Average length of hospital stay is 14 days(2, 3, 8) and treatment costs around £6000 / patient(3). Novel TreatmentNewer surgical “keyhole” techniques (Video Assisted Thoracoscopic Surgery, VATS) are now used when initial treatment fails after 3 to 5 days, as they are less invasive than traditional surgery(15). However, we do not know the role of early VATS treatment in this disease (8). A recent placebo-controlled trial(3) by the
suggests the non-surgical treatment of Intrapleural Enzyme Therapy (IET, which involves medications given through the chest tube as part of early treatment) improves drainage and reduces the need for surgery and hospital stay. IET is available to all patients, not requiring the patient to be “fit” enough for an operation. Aims of the Work and Questions to be addressed Assessing the early use of VATS or IET requires a randomised phase III direct comparison. Before undertaking a large trial, key outcomes of importance to patients require development, and feasibility of recruitment, patient acceptability and outcome collection requires assessment. We therefore propose a randomised study to address feasibility of randomising patients to standard care, early VATS or early IET, and we will create a patient involvement group with personal experience of the disease, to understand acceptability of randomisation and priorities in care. Plan of InvestigationOur aims will be achieved by: 1. Formation of a Patient / Carer Group (n=10) to allow exploration of the patient centred impact of this disease and priorities of care, via 2 monthly focus groups, meetings with the trial team, and membership for patients to key oversight committees for the feasibility trial. 2. In-depth Patient Interviews where 20 patients assessed for inclusion in the study (see below) will undergo structured interviews, exploring patient and carer experience, impact on quality of life and priority areas of care. 3. A Randomised Feasibility Trial will be conducted in 75 pleural infection patients treated in routine clinical care, in centres with a track record of delivery to previous pleural infection studies (n>1000). Patients will be randomised to:
1. Standard care (chest tube drainage and antibiotics)2. IET - through the chest tube, intrapleural tPA (10mg bd) and DNase (5mg bd) will be administered for
72 hours (3), immediately after randomisation.3. VATS - referred immediately after randomisation to local surgical services
The Primary outcome is the feasibility of randomizing 75 patients over 18 months recruitment in 5 UK centres. Exploratory secondary outcomes include trial related (proportion accepting randomization, patient acceptability), healthcare related (hospital stay, mortality, need for further surgery, adverse events) and patient outcomes (patient reported pain, breathlessness, health-related quality of life). Summary of the Potential Benefits An in-depth understanding of patient reported priorities and experience would provide the required outcome
334

Page 16 of 70
tools to conduct an applicable and important larger study. Demonstration of feasibility of recruitment is a vital step in conducting a larger, potentially practice changing study. Eventually, evidence demonstrating the utility of early treatment with VATS or IET has the potential to reduce mortality, reduce hospital stay, reduce suffering, improve quality of life and reduce healthcare costs.
Background and rationale What is the problem being addressed?Describe the background to the research, describing the limitations identified in the evidence base that the research is trying to address.
Pleural InfectionPleural infection, where infected fluid develops between the lung and chest wall forming an abscess, is common(5-7), affecting 18,000 patients / yr in the UK and USA(5, 16, 17). Forty patients / day are diagnosed with this condition in the UK, and it is increasing year on year in the UK, USA and Europe despite increased use of antibiotics, particularly in the elderly(5, 7). The condition develops as a complication of pneumonia, which results in 250,000 admissions / year (18), with 7% of patients developing pleural infection(19). Most patients have risk factors such as old age, diabetes and chronic disease, but 30% occur in otherwise healthy people(9). Impact on patients and healthcareTreatment for pleural infection involves the use of antibiotics to control the infection, and drainage of infected material using a chest tube (inserted between the ribs)(8). The patient is then monitored in hospital to assess if the infection resolves with these treatments. This disease is associated with high mortality and morbidity. Mortality is 20% and unchanged over the last 40 years(8). 20% of patients fail initial treatment (with a chest drain and antibiotics) over 3 to 5 days, and then require surgery to drain infected fluid, which is invasive, costly(2, 3, 9, 10) and associated with chronic pain, high morbidity and mortality (11, 12). Surgical treatment is avoided in the most ill, like the elderly(7, 13), in whom mortality is 40%(14). Patients who fail initial treatment and are unable to undergo surgery experience a chronic, wasting illness which results in death. Even with modern antibiotic treatment, drainage and surgery, the average length of hospital stay is 14 days(2, 3, 8). Treatment for pleural infection is costly, at around £6000 / patient(3). Reducing length of hospital stay and the need for surgery are likely to reduce costs. New treatment directions to improve careIn recent years, newer “keyhole” surgery (Video Assisted Thoracoscopic Surgery, VATS, using 3 small incisions in the chest under general anaesthetic) is used in patients who have failed initial treatment, as it is less invasive than traditional surgery such as thoracotomy(15) (which requires an up to 25cm incision in the chest under general anaesthetic). Its place in early treatment is not known. A recent placebo-controlled trial(3) conducted by suggests that a novel, non-surgical treatment of early Intrapleural Enzyme Therapy (IET, which is medications given through the chest tube as part of initial treatment) improves drainage and reduces the need for surgery and length of hospital stay. Importantly, IET is available to all patients immediately with this disease, and does not require the patient to be “fit” enough for an operation or to wait for a surgical slot. Review of the LiteratureThe evidence for early VATSEarly surgery has been advocated in pleural infection (20) on the basis of two randomised studies which compared standard care (antibiotics and chest tube) to early VATS(21, 22). Both demonstrate earlier hospital discharge and lower mortality with VATS, but are underpowered (90 patients total) and methodologically flawed (unclear criteria for medical failure, lack of objective decision making criteria, no blinding). There is no evidence which addresses when patients failing initial therapy should be referred for surgery, despite SIGN methodology searches via national guidelines(8); currently patients are referred between 3 and 7 days post initial treatment. The evidence for IET
335

: Page 17 of 70
The largest study in pleural infection to date ( (2)) demonstrated no benefit from fibrinolytic alone (streptokinase) above placebo, and meta-analysis showed fibrinolytics alone did not alter clinical outcomes(23). We have since developed combined IET as a potential treatment in pleural infection, culminating in the randomised, placebo controlled trial (3). In this study we identified a novel combination of enzymes given early in treatment through the chest tube (fibrinolytic (tPA) and DNase) which work by lysing fibrinous septations (pockets) within the infected space (tPA) and reducing viscosity(24) of the infected fluid (DNase). This study demonstrated that tPA+DNase significantly improved drainage (primary), reduced need for surgery (OR for surgery 0.17, 95% CI 0.03 to 0.87) and reduced hospital stay (6.7 days, 95% CI 12.0 to 1.9, p = 0.006)(10) compared to placebo. A meta-analysis including suggests potential benefit of intrapleural tPA + DNase(24) but suggested further studies are needed. Case series using tPA+DNase (25) have been published, demonstrating safety and efficacy as rescue therapy in selected patients; this treatment is now used in patients unfit for surgery(25). Cost analyses of demonstrates tPA+DNase treatment is cheaper than placebo, driven by reductions in hospital stay(26). We have conducted a search for current trials in this disease area, and there are no studies in pleural infection which conflict with this proposal. SummaryThe current data suggest that care in pleural infection could be significantly improved using early VATS or early IET. This requires a robust, head to head comparison to assess which intervention provides optimal treatment for patients. Reducing mortality, hospital stay and the need for surgery are clearly important, however, there have been no assessments of the impact of the disease or the two interventions on outcomes which should drive which intervention is considered “optimal”. These include:
1. Long-term effects on the chest x-ray.2. Quality of life.3. Return to normal activity.4. Lung function.5. Patient reported outcomes (e.g. pain).
None of these outcomes have been assessed over prolonged follow up after the infection has resolved. Our previous data demonstrates that most patients have residual chest x-ray changes for 3 months after discharge (27). We therefore need to address immediate “hospital” outcomes (e.g. need for surgery, length of stay) and longer term, patient focussed outcomes before conducting a full phase III trial. Although IET is cost saving compared to placebo (26), there are no direct cost comparisons with early VATS, nor any evaluations in which costs and outcomes of the two interventions have been compared jointly. This study will provide the opportunity to assess feasibility of conducting an economic evaluation alongside the definitive trial by collecting data on healthcare resource use and quality of life.
336

Page 18 of 70
9. Case for Support - Part 2
337

Research for Patient Benefit (RfPB) Programme: – Early Video Assisted Thoracoscopic Surgery (VATS) or Intrapleural Enzyme Therapy (IET) in Pleural Infection - a feasibility randomised trial Further to our previous correspondence, after review of all Stage 1 applications submitted to the RfPB Programme Competition 30, I am pleased to inform you that your application has been invited to progress to Stage 2 of the application process. However, the Panel has made the following comments on your proposal which should be addressed in Stage 2 of the application process:
The Panel considered the description of the interventions was lacking clarity and more detail was required for the justification of the study design.
The Panel noted that the study has two arms, however, if both are novel interventions then it was of the opinion that a third control should be included with the standard practice.
There was a lack of clarity regarding the randomisation procedure, as not all patients may be eligible for both treatments.
Further details were required for the planned number of patients being recruited. The costs allocated for patient groups were considered to be too low.
The Stage 2 application form is now available to complete on the Research Management System and the deadline for Stage 2 applications is . Further information on the RfPB programme, including the guidance for applicants, can be found on the RfPB website at The RfPB programme also encourages applicants to share the feedback and speak with the local NIHR Research Design Service (RDS) for further advice. RDS contact information can be found at
I wish you all the best for the rest of the competition. Yours sincerely
338

Page 20 of 70
Changes from Stage 1 Please address the attached feedback points about your Stage 1 application and explain how this application has changed as a result of the feedback received.
1. The Panel considered the description of the interventions was lacking clarity and more detail was required for the justification of the study design. We apologies for this lack of clarity, and would like to clarify as follows:
Standard treatment involves antibiotics and drainage of infected fluid using a chest tube, a small plastic tube inserted between the ribs using local anaesthetic and does not require an operation. Chest tubes are used in all patients (i.e. even if very unfit) and available in all hospitals. This standard treatment often fails due to the presence of “pockets” of fluid (septations) and thick or viscous fluid.
Intrapleural enzyme therapy (IET) is injected through the chest tube described above, and involves a combination of two enzymes (tPA and DNase) which break up septations and thins viscous fluid. This does not require an operation or further tube insertion. Each drug is given twice daily for 3 days (i.e. 12 doses of each drug).
Video Assisted Thoracoscopic Surgery (VATS) is “keyhole” surgery. Surgery is used when standard treatment (chest tube drainage and antibiotics) fails to resolve the infection over 3-5 days. Patients are then referred for VATS which involves a general anaesthetic, and the insertion of cameras through small incisions to remove infected material. Only certain patients are fit enough to undergo surgery. Around 15% of patients need the VATS treatment extending on the operating table to a much larger operation (thoracotomy, which requires an up to 25cm incision in the chest) if VATS fails.
The rationale for this study is therefore to compare the utility of early IET with early VATS. IET given early in treatment through a chest tube has been shown in our previous trial to improve drainage, reduce hospital stay and reduce failure leading to surgery, versus standard care (placebo). VATS early in treatment (i.e. within 1 day) has been shown in methodologically flawed trials to improve hospital stay. Therefore, skipping “standard care” of antibiotics and chest tube only and using early treatment with VATS or IET has never been compared. 2. The Panel noted that the study has two arms, however, if both are novel interventions then it was of the opinion that a third control should be included with the standard practice. The trial team has reflected on this aspect, and we agree that both IET and early VATS are novel treatments. IET is novel in that it is not “proven” in a phase III randomised trial. VATS is widely available but only used once standard treatment has failed after 3-5 days of treatment. We therefore agree that the use of early VATS constitutes novel therapy.We have therefore added a third arm to the feasibility study; a further 25 patients randomised to “standard treatment” – i.e. chest tube and antibiotics. Inclusion of this group allows precise calculation of study size for a subsequent larger study and provides information on expected outcomes. We propose comparisons of standard care to VATS, standard care to IET and IET to VATS. 3. There was a lack of clarity regarding the randomisation procedure, as not all patients may be eligible for both treatments. We agree that not all patients will be fit enough to undergo VATS. Many case series of VATS demonstrate good outcomes; however, comparing previous randomised trials of “all comers” in pleural infection with VATS series, patients included in VATS series were on average 10 years younger than those included in randomised trials. We therefore believe that younger, fitter patients are selected for VATS which may lead to better outcomes.IET can be given to any patient with a chest tube (i.e. everyone), and can be given immediately, whereas surgery may require waiting for a theatre slot. These are significant advantages of IET over VATS and key outcomes to capture.We therefore propose that ALL patients with pleural infection are randomised – those assigned “surgical management” will be assessed for fitness for surgery by surgeons, but analyses will be conducted using intention to treat, thus capturing the true effects of IET and VATS. We will record “fitness” (ASA grading) in all patients, to allow exploratory subgroup analyses. Crossovers will be permitted and recorded and a per-protocol analysis will be conducted. 4. Further details were required for the planned number of patients being recruited.As a feasibility trial, the main purpose is to assess the feasibility of randomising patients for a larger, subsequent and definitive trial. The primary outcome of the larger trial will be informed by this study, but we propose that an
339

Page 21 of 70
outcome such as hospital stay would be reasonable. Using this information encompassing a clinically meaningful difference in hospital stay (of 3 days) (mean hospital stay IET = 11.8 days, VATS = 8.5 days, assumed shared SD 10 days, 90% power, 5% significance), randomising 1:1 between IET and VATS requires 193 patients per arm = total 386 patients. Including 10% attrition, the estimated sample size for the larger definitive trial is 426 patients. We believe this is a strong basis for the conduct of a feasibility trial to measure recruitment rate as a key outcome. To achieve the 426 patient trial, 1 patient per month across 20 centres over a 48-month recruitment period are required. This rate has been achieved in our previous observational study of pleural infection (n=550 on identical diagnostic criteria), where assessment of recruitment rate in the best 5 centres demonstrates a mean monthly rate of 1.3 patients. 5. The costs allocated for patient groups were considered to be too low.We appreciate the importance for sufficient funding for patient / public involvement related research activity. We were unsure as to what the panel referred to in this comment, as breakdown costs of allocated funding were not provided in the first stage of the application. However, we have allocated a total of £15,000 costs to patient groups which includes costings for travel, hosting, interview costs, advertising and meeting costs (please see comprehensive breakdown in cost justification section).
Please detail any additional alterations to the application
The following changes to the application have been made:1. We have added a third arm to the study to include 25 patients randomised to standard care (chest tube
and antibiotics) who will be referred for surgery at day 3 to 5 on objective criteria if failing treatment, as per national current guidelines.
2. The associated costs of increasing recruitment from 50 patients to 75 patients to include the third arm have been added to the costings, which include extension of recruitment time to remain realistic.
3. We have included discussion around key trial parameters such as crossovers, clarification of intention to treat and how surgical patients unfit for surgery will be treated, and objective decision making criteria for referral for surgery in all 3 randomised groups to be applied equally.
4. Information on collection of "fitness for surgery" has been specified as an outcome which will be collected post randomisation.
5. Two patients with pleural disease from our PPI group have reviewed the study proposal and felt it was an important idea, and approved the design, outcomes and commented that the lay summary was well written.
6. The total cost of the requested funding has increased to reflect the above changes to a total of £302,979.
7. The detailed costs for PPI involvement have been specified and are detailed below.In response to further panel comments, we have in addition made the following changes / responses:
1. As requested, we have revised the trial budget to come within the suggested £280,000 limit (to £274k currently), and this includes a reduction in the statistician FTE as suggested by the Panel (to 0.025FTE for the senior statistician and 0.1 for the junior statistician).
2. We can confirm that all treatment modalities are available in all suggested treatment sites. Specifically, access to surgical treatment for pleural infection is an NHS requirement for all hospitals (whether on site or offsite), and the intrapleural treatment (tPA and DNase) will be provided by the trial team to the treating clinicians locally. This exact strategy has been successful in our previous placebo controlled trial of tPA and DNase ( ) and we have selected the best recruiting 5 centres from for this project. We are therefore confident that all treatments in the trial are available to all patients in all proposed centres.
3. We would like to thank the Panel for suggesting an appraisal of the research nurse time in this study. Follow up and assessment of recruited patients will occur via the Clinical Research Network local resource (as has proven successful in previous trials), and we have estimated total follow up time for all patients to be around 3.5 hours per patient (equating to 0.08 FTE) which will be split across all sites. In addition, we have allocated specific research nurse time of 20 hours to conduct interviews (10 patients, 2 hours per patient) and 30 hours training time for these nurses to be provided by our experienced trials nurse in who will travel to sites. On this basis, we have increased research nurse time to 0.1
340

Page 22 of 70
FTE and increased site payments (to £400 per patient per site) to cover some of these costs.4. We would like to thank the Panel for suggesting a PPI representative should be involved in the
randomisation process, which had not occurred to us. There are some challenges with this as pleural infection presents “out of hours” at any time and therefore a significant proportion of patients will be randomised by clinicians “out of hours”. In addition, if the results of this study are to be used to support a larger phase III trial (as we hope), requiring a PPI representative for all randomisations may be impractical in a larger trial. We therefore suggest that randomisations occurring in and which occur in hours will be supported by a PPI rep from who will discuss the study with the patient wherever possible. We will document these discussions as an outcome from the study to assess if this has helped the understanding of the patient and randomisation process.
Costs for Patient Advisory Group Ten individuals contributing to research design, conduct and delivery:
Advertising for group members = £675 for newspaper advertising Meetings every 2 months – 17 meetings x £50 x 10 members = £8,500 Travel costs 10 members x 17 meetings x £10 each = £1,700 Catering £100 x 17 meetings = £1,700 = £11,900
Two members of PAG group attending TSC meetings 3 meetings x £150 x 2 = £600 Travel £10 x 2 x 3 meetings = £60 Catering £100 x 3 meetings = £300 = £960
Patient structured interviews at 3 month follow up: 20 patients x £75 per interview = £1,500
Grand Total for PPI costs = £15,035
Research Plan Describe the proposed research plan, providing descriptions of the overall research design and a strong justification of sampling strategies, methods of data collection and analysis.It is vital to add as much detail as possible on design and methodology, including justification of sample size, power calculations and sample selection and exclusion criteria where applicable.
Research PlanTo achieve our research objectives, we aim to conduct 2 phases of work: 1. Formation of a Patient / Carer GroupWe will create a patient / carer group specific to pleural infection, to include any patient or relative who has experience of pleural infection. The involvement of both patients and carers / relatives is important to capture the patient experience, and also the experience of those caring for pleural infection patients on discharge from hospital over a potentially prolonged recovery phase (up to 3 months). This will allow exploration of the full patient centred impact of this disease in both the acute (in hospital) and recovery phases, and permit meaningful discussions of what priorities in care should be. Ethically approved advertising within key centres from our network will be used to recruit 10 individuals who will contribute to research design, conduct and delivery. A total of 10 members are required to allow a range of views to be represented (who have for example undergone different treatments) and to permit continuity in cases of absence. We propose the group to conduct the following areas of work:
1. Regular (2 monthly) meetings of the group assessing the patient view of proposed outcomes, the carer / relative perspective on the disease and exploring views of outcomes important in pleural infection. This will include video conferencing facilities to allow membership of the group in several geographic areas and minimise inconvenience to patient group members.
2. Meetings with the trial team, physicians and surgeons to discuss the on-going development of the study and permit continued engagement with the study process. We anticipate that this unique resource will
341

: Page 23 of 70
be valuable in the proposed study area, but also more widely for future pleural and serious lung infection research proposals.
3. Full membership of 2 patients to the Trial Management Group and Trial Steering Committee for the randomised study.
4. Establishment from this group of a Patient Writing Group who will input to patient information leaflets and academic outputs (e.g. manuscripts), assist in dissemination including presentation of results, and who will be co-applicants on future applications.
2. Randomised Feasibility Study with in-depth Patient InterviewsThe structure of the proposed study is as below. The key secondary exploratory outcomes will be finalised following the work in described above in the first phase of the project. The randomised trial is described first, and then details on the patient interview aspects is given. Randomised Controlled Trial - DesignThe study proposed is a randomised controlled trial which will be offered to all patients with pleural infection treated in routine clinical care in the selected centres. All centres proposed in this study were high recruiters in the studies which are all pleural infection studies conducted by . This collaboration therefore has significant experience in this disease area, and has delivered very high data completion using similar outcomes in these previous studies (primary outcome completion in 98%).All patients randomised will be carefully followed and outcomes collected in order to permit assessment of the feasibility of randomisation and trial recruitment. Factors which affect acceptance of randomisation will be explored by specific structured interviews in both those patients who decline those who accept participation. The randomised study itself will provide early signals of efficacy and outcomes which will power the subsequent phase III study. Target PopulationAdults (no maximum age) with pleural infection diagnosed on national and clinically accepted criteria (British Thoracic Society Guideline on pleural infection, (8)), requiring admission to hospital for antibiotics and chest tube drainage. Inclusion criteria As per our previous successful multicentre trials in pleural infection, inclusion criteria exactly reflect normal clinical practice in diagnosis:1) Clinical presentation of pleural infection.2) Pleural fluid requiring drainage, where pleural fluid is any of the following: purulent, culture positive or acidic (pH <7.2). Exclusion criteriaExclusion criteria are minimal to ensure external validity of the feasibility assessment:1) Known sensitivity to study medications2) Coincidental major bleed Specific consideration was given to the possibility of excluding patients who are considered “unfit for surgical intervention” from the randomised trial. However, including these patients is particularly important in this study for a number of reasons. Firstly, the study is assessing the feasibility and acceptability of randomising to surgical versus non-surgical treatment, rather than the actual performance of surgery. Secondly, IET has the specific advantage over surgery that it is applicable to “all comers” with pleural infection(25), including the frail and elderly in whom clinical outcomes are the poorest. As we envisage the larger phase III trial to include all comers with pleural infection, inclusion of all patients in the feasibility study is therefore scientifically required for consistency. Patients who are randomised to surgery but considered not fit enough for surgical treatment will have treatment according to standard best practice, protocolised care. RandomisationRandomisation will occur via our usual web-based system with minimisation for centre, which allows for control of varied surgical referral practices. Interventions for randomised patientsPatients will be randomised 1:1:1 to: Standard Care
342
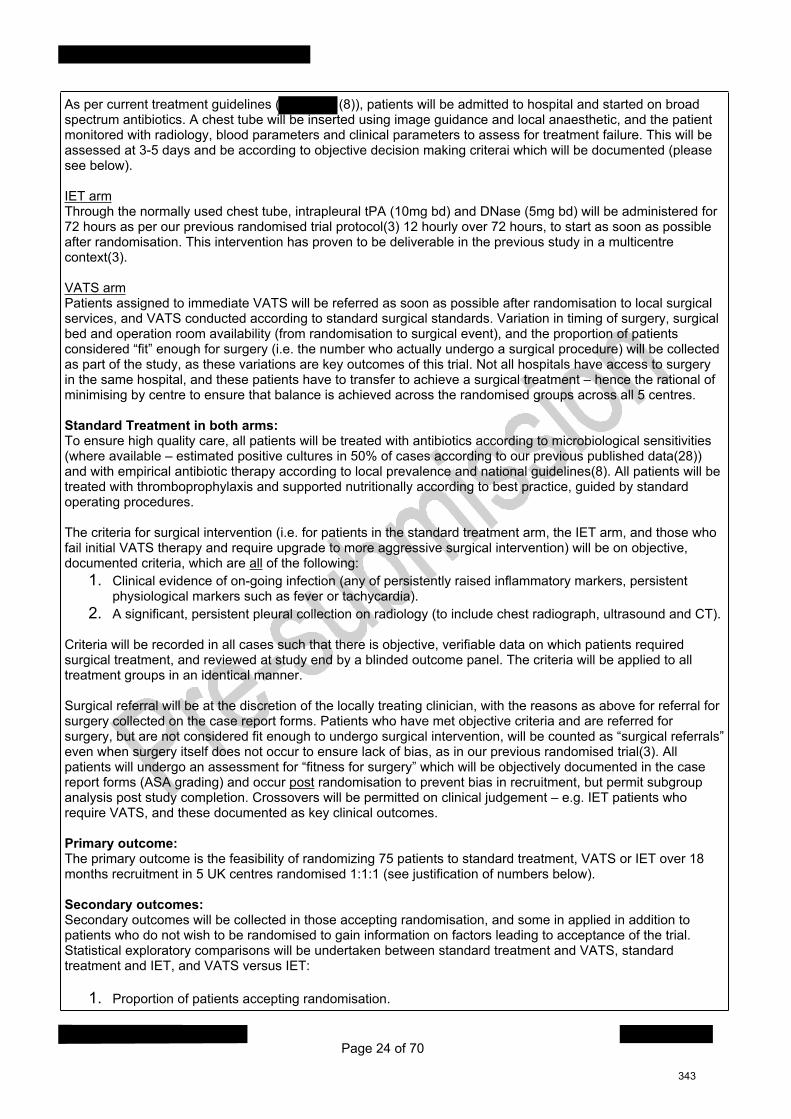
Page 24 of 70
As per current treatment guidelines ( (8)), patients will be admitted to hospital and started on broad spectrum antibiotics. A chest tube will be inserted using image guidance and local anaesthetic, and the patient monitored with radiology, blood parameters and clinical parameters to assess for treatment failure. This will be assessed at 3-5 days and be according to objective decision making criterai which will be documented (please see below). IET armThrough the normally used chest tube, intrapleural tPA (10mg bd) and DNase (5mg bd) will be administered for 72 hours as per our previous randomised trial protocol(3) 12 hourly over 72 hours, to start as soon as possible after randomisation. This intervention has proven to be deliverable in the previous study in a multicentre context(3). VATS armPatients assigned to immediate VATS will be referred as soon as possible after randomisation to local surgical services, and VATS conducted according to standard surgical standards. Variation in timing of surgery, surgical bed and operation room availability (from randomisation to surgical event), and the proportion of patients considered “fit” enough for surgery (i.e. the number who actually undergo a surgical procedure) will be collected as part of the study, as these variations are key outcomes of this trial. Not all hospitals have access to surgery in the same hospital, and these patients have to transfer to achieve a surgical treatment – hence the rational of minimising by centre to ensure that balance is achieved across the randomised groups across all 5 centres. Standard Treatment in both arms:To ensure high quality care, all patients will be treated with antibiotics according to microbiological sensitivities (where available – estimated positive cultures in 50% of cases according to our previous published data(28)) and with empirical antibiotic therapy according to local prevalence and national guidelines(8). All patients will be treated with thromboprophylaxis and supported nutritionally according to best practice, guided by standard operating procedures. The criteria for surgical intervention (i.e. for patients in the standard treatment arm, the IET arm, and those who fail initial VATS therapy and require upgrade to more aggressive surgical intervention) will be on objective, documented criteria, which are all of the following:
1. Clinical evidence of on-going infection (any of persistently raised inflammatory markers, persistent physiological markers such as fever or tachycardia).
2. A significant, persistent pleural collection on radiology (to include chest radiograph, ultrasound and CT). Criteria will be recorded in all cases such that there is objective, verifiable data on which patients required surgical treatment, and reviewed at study end by a blinded outcome panel. The criteria will be applied to all treatment groups in an identical manner. Surgical referral will be at the discretion of the locally treating clinician, with the reasons as above for referral for surgery collected on the case report forms. Patients who have met objective criteria and are referred for surgery, but are not considered fit enough to undergo surgical intervention, will be counted as “surgical referrals” even when surgery itself does not occur to ensure lack of bias, as in our previous randomised trial(3). All patients will undergo an assessment for “fitness for surgery” which will be objectively documented in the case report forms (ASA grading) and occur post randomisation to prevent bias in recruitment, but permit subgroup analysis post study completion. Crossovers will be permitted on clinical judgement – e.g. IET patients who require VATS, and these documented as key clinical outcomes. Primary outcome: The primary outcome is the feasibility of randomizing 75 patients to standard treatment, VATS or IET over 18 months recruitment in 5 UK centres randomised 1:1:1 (see justification of numbers below). Secondary outcomes:Secondary outcomes will be collected in those accepting randomisation, and some in applied in addition to patients who do not wish to be randomised to gain information on factors leading to acceptance of the trial. Statistical exploratory comparisons will be undertaken between standard treatment and VATS, standard treatment and IET, and VATS versus IET:
1. Proportion of patients accepting randomisation.
343

Page 25 of 70
2. Hospital stay from randomisation to discharge on objective criteria.3. Mortality over 6 months post randomization / inclusion.4. Total hospital stay post randomisation to 90 days (including re-admissions).5. Proportion requiring further surgery (VATs in standard and IET arm, thoracotomy or repeat VATS in
VATS arm).6. Proportion of “compliance” in each intervention arm (i.e. number of patients who complete IET therapy
or who actually undergo surgery).7. Type of surgery (VATS, thoracotomy) and delays in achieving surgery in the surgical arm.8. Adverse events, using a modified thoracic Clavien-Dindo classification for surgery, provided by our
surgical co-applicants.9. Patient acceptability of interventions (in all intervention groups).
10. Patient reported outcomes (pain and breathlessness on validated 100mm Visual Analogue Score(29, 30) at discharge, 1, 3 and 6 months.
11. Health-related quality of life (EQ-5D-5L 1, 3, 6 months).12. Lung function at 1,3 and 6 months.13. Time to return to normal functional status (to baseline), at 1,3 and 6 months.14. Chest x-rays (digital assessment of pleural involvement at 1,3 and 6 months as per our previous trial
methodologies(3, 31)).15. Costs of treatment including standard care, intrapleural drugs, surgery, initial and subsequent
hospitalisation, outpatient, A&E and primary care contacts. Costs of surgery will be assessed using a micro-costing study evaluating staff time, theatre time and consumables. Other healthcare resource use will be obtained from patients trial records; hospital records; and patient self-report through questionnaires (1, 3 and 6 months). Resource use will be costed using appropriate unit costs.
Sample sizeAs a feasibility trial, no formal sample size calculations were conducted. However, the primary purpose of this study is to assess if recruitment to a larger, definitive trial is feasible, and the recruitment target of 75 patients in 5 UK centres over 18 months has been chosen based on this aspect, and recent recruitment to our observational study in pleural infection (20 patients per month in 20 centres). Extrapolating data to be obtained from this study, if 75 patients can be randomised in 18 months from 5 centres, a future phase III study will be able to recruit 480 suitable patients from 20 centres over 2 years. This number of patients is sufficient for a definitive trial whose outcome is hospital stay, in which our current data suggests a total sample size of 432 patients are required randomised 1:1 (rationale: using information encompassing a clinically meaningful difference in hospital stay of more than 3 days (mean hospital stay in IET arm = 11.8 days(3), mean hospital stay in VATS arm = 8.5 days(21, 22), assumed both arms same SD of 10 days, 90% power, 5% significance level), randomising 1:1 between IET and VATS requires 194 patients per arm, totaling 388 patients. Allowing a 10% attrition rate, the estimated total sample size for the larger definitive trial is 432 (216 in each arm) patients randomised). Thus, demonstration of successful randomisation of 75 patients over 18 months of recruitment from 5 centres would demonstrate that a phase III trial of this size, in this population and with similar randomised groups, is feasible. The primary outcome(s) of a future phase III trial will be informed by work conducted in this feasiblity trial . Potential Confounders in the Randomised TrialThere are a number of potential confounders within this small randomised trial. Imbalance in baseline factors is to be expected in a feasibility (and not definitive) study, which include the known factors predictive of outcome in pleural infection To mitigate against this risk, all these factors (=baseline blood urea and albumin levels, infection source, diastolic blood pressure and age) will be recorded permitting assessment of imbalance and adjusted analysis for early efficacy signals which will be used to accurately power the subsequent randomised study.
Patient Interviews in the Randomised TrialPatients with pleural infection who have been assessed for inclusion in the randomised feasibility study (see below) and their relatives / carers will be approached during the conduct of the feasibility study. This will occur
344

Page 26 of 70
only once the illness has resolved, during routine 3-month clinical follow up. To ensure representative views, a range of patients (age, gender) will be approached, and patients included who refused randomisation, and those who have been randomised to standard medical treatment, intrapleural enzyme therapy (IET), VATS and other surgical techniques. The has significant experience in pleural infection studies, having included more than 1000 patients in multicentre studies in this disease over the last 10 years(2-4). has a research nurse with specific training in structured interviews who will train fellow nurses in different centres, and appropriately trained nurses will conduct the interviews within the following areas:
1. Patient experience of the illness in hospital, during interventions and in the recovery phase.2. Relative / carer experience and worries of the hospital and recovery phases of treatment.3. Impact on quality of life, daily living and on-going health issues.4. Which areas of care are considered the most important, and what the priorities to optimise care should
be from a patient perspective. A total of 20 such patients will be approached to provide a range of views, and to ensure a range of interventions and treatments are discussed in patient terms.
345

Page 27 of 70
10. Case for Support - Part 3
Dissemination Please describe your plans for disseminating the findings of this research.
Dissemination of the research findings of this study will occur through a number of routes which have been successfully used in the publication of our previous studies and will include:
1. The patient experience, and randomised trial findings will be submitted to major national and international scientific meetings as per our previous work. This will include i)
. This will allow dissemination and discussion of study results to clinicians and
academics involved in the care of patients with pleural infection, and will in addition access specialist nurses in respiratory medicine.
2. Results of both the patient experience and randomised trial work will be submitted to a major international peer-reviewed journal with an open access policy. We will submit the trial protocol to an open source journal prior to completion of the study.
3. Study results will be publicised across the UK and international pleural communities – the applicant and co-applicants are faculty members on a number of national and international course in pleural disease
4. The main applicant is chair of the current and will use this position to promote results of the study across the UK via the .
5. We will engage with disease specific and patient groups including the to disseminate patient experience and randomised trial results, and include our PPI group to help disseminate this information.
6. Once funded, we plan to engage with social media platforms providing up to date feeds on trial progress and study results as finalised results become available.
Expected Output of Research/Impact Please describe how the outcomes of this research could be translated into the NHS and wider healthcare community to provide improvements in service delivery, patient health and/or wellbeing.
Successful completion of this study will provide the first patient focused data on the experience, concerns and priorities of patients who experience pleural infection. This information will be highly valuable to our group and other researchers in the conduct of studies in this common disease to improve care in a patient focused manner. We anticipate that the patient focused study results (from initial focus group work) will be available to be published within 12 months of funding, and would have an immediate impact on future research in the UK in pleural infection. If this feasibility randomised trial is able to recruit 75 patients over 12 months, we will then apply (via ) to conduct a full phase III randomised trial to compare IET to VATS (estimated n=426). We anticipate the primary outcome measure to be important and clinically meaningful (e.g. mortality, hospital stay, quality of life), informed by results of the feasibility study. Information obtained on the statistical variation in these parameters will allow accurate sample size calculation for the phase III study. Key health economic (HE) outcomes are to be collected in the feasibility study, to allow a robust HE component in the phase III trial. Completion of the phase III trial providing robust evidence on patient and healthcare focused risks and benefits of IET or VATS early in treatment would be transformational for pleural infection treatment, with the potential to reduce mortality, reduce suffering and hospital stay, and treatment related costs. We anticipate that results of a phase III study would enter treatment guidelines (as have our previous studies(2, 8)), Cochrane reviews and NICE guidelines. The study results should be applicable in the UK as well as elsewhere, with pleural infection being a global health problem, and our previous IET data having been applied in many countries(25).
346

Page 28 of 70
Relevant expertise and experience Please outline the individual role of each member of the research team, highlighting the skills and experience of the team that make them well placed to carry out the work.
Team Expertise: The is uniquely placed to deliver this research. Our unit has conducted 6 randomised studies in pleural diseases (n=2200) in >50 UK centres with an established track record and results published in high profile journals and in national treatment guidelines(8, 32). has conducted the 3 largest prospective studies in pleural infection to date in the world literature(2-4), totalling 1210 patients through our established network of recruiting centres, and our studies have been key in developing intrapleural therapy in pleural infection. This experience provides expertise in the trial management and results in high quality data, with >95% primary data completion for all studies. The main applicant has published 4 randomised multicenter studies in pleural disease (n=770) which are published with first or senior authorship(3, 30, 33, 34). He directs the , has experience of methodology and design of clinical trials, with an MSc in Clinical Trials , and is chair for the
is Operations Director for the and has substantial regulatory and oversight experience,
with the currently conducting over 30 studies, including multi-centre randomised studies in the UK. is a Senior statistician at , and provides
expertise in trial design, analysis and statistics. Health Economic expertise is provided by from the , with experience in similar pleural trials. leads the , holds national grants for 4 randomised trials in pleural disease (no recruitment conflict) and was chair of the
lead busy pleural services and are the highest recruiting centres in pleural trials. provide thoracic surgical expertise and have conducted thoracic surgical trials including randomisation to surgery versus non-surgical treatment in other pleural diseases(35, 36).
347

Page 29 of 70
11. Management and Governance
Research timetable Please provide an overview of the research plan which includes specific milestones and deliverables.
Project Timetable:1) Establishment of a patient / relative group and analysis of outcomes to inform the subsequent trial – 3 months. Patients and carers will be recruited from our clinical service and in addition through advertising in local media (to identify patients with recovered pneumonia).2) In parallel to the above, protocol development, regulatory and ethical approval processes will be conducted for the multicenter study, and randomised trial centre set up (6 months) (key milestone 1 – ethical approval by 6 months).3) Recruitment – 18 months (5 centres, 1 patient / centre / month, total 75 patients) (key milestone 2 – 50% recruitment complete at 18 months)4) Follow up – 6 months to permit longer-term health outcomes to be assessed, in depth interviews to occur in this period.5) Database clean, lock and analysis / publication (3 months).6) TOTAL = 33 months.
Research management arrangements Please explain the practical arrangements for managing the research and its constituent components.
The Trial Manager based at will be responsible for the day-to-day set-up and ongoing management of the trial. They will work closely with the PI who will take responsibility for the clinical delivery of the trial and both will work to our established which cover all areas of trial set up, management and close out. The trial management group meets regularly and is in regular contact to discuss day-to-day issues. Senior management oversight will be provided by Operations Director who will also be responsible for managing the budget and ensuring that the overall project objectives and milestones are met in a timely manner. They regularly attend meetings with Finance to review budget status. Monthly senior management meetings take place to review progress of all studies being run by the unit and monthly reviews of trial progress are arranged with the Trial Managers. A trial steering committee and data monitoring committee will be set up to review trial progress and safety (see Gantt chart for proposed timing of meetings, which will be adapted according to trial specific requirements and risk assessments).
Has any work relevant to this proposal already commenced? Yes
If yes, please give details of any relevant work that has already commenced in the preparation of this research.
We have assembled the required trial team to conduct this research and included co-applicants from previously successful recruiting centres, and surgeons with an academic track record. The research and recruitment infrastructure is present within our UK pleural network, which has been setup over the last 10 years and recruited a total of 2200 patients with pleural disease to date. Work on the protocol and regulatory / ethics application will begin once key staff are in place dependant on successful funding from this application.
Success criteria and barriers to proposed work Please set out the measurements of success you intend to use and also the key risks to delivering this research and what contingencies you will put in place to deal with them.
The key measures of success in this trial will be successful creation of the patient advisory group, and subsequent recruitment to the feasibility trial with the provision of high quality data. The key risk in this study is lack of recruitment – however, has a track record of delivery to multicentre studies in pleural infection. We have recruited >2200 patients in to multicentre randomised pleural disease trials, and there is substantial experience in encouraging and driving both recruitment and high quality data completion in multicentre trials
348

Page 30 of 70
within the Trials Unit. The selected centres were high recruiters in our previous observational study, which achieved a recruitment of 550 patients with pleural infection from 25 centres(4). We have developed strategies to encourage recruitment which have proven successful. This includes regular centre contact from the trial team via phone, email shots / presentations, study days and site visits offering support. The proposed trial team includes two surgical colleagues with surgical and trial expertise to drive the surgical components of the study.
Does the proposed research raise ethical issues? Yes
If yes, discuss how these issues will be addressed.
Patients will be asked to undergo interventions (early IET, early VATS) which are not definitively proven to be of benefit, and this is the purpose this trial. All centres involved are highly experienced in treating pleural infection including IET, and in randomising patients in pleural studies. All trial participants will be fully consented to GCP standards. As pleural infection presents unexpectedly, and treatment must be started immediately, decisions to participate in the study have to be taken quickly on diagnosis, There is therefore sometimes not the usual “reflection time” (of 24 hours) to allow patients to consider participation. We will mitigate this risk by seeking specific ethics committee permission to shorten normal consideration time, and provide both detailed and summary information leaflets – all patients will discuss participation in the study with an experienced doctor or nurse trained in consent specific to this trial. This strategy has proven successful in our pleural infection randomised trials(1, 2, 4). All patients will be monitored for safety outcomes in all trial arms, with adverse events reported and reviewed according to standard operating procedures, and to GCP standards. Formal risk assessment will occur on receipt of funding as for all studies.
Please detail how and when you intend to get ethical review completed.
Ethical review will occur via the system once funding is confirmed and a finalised protocol is signed off by the Trial Steering Committee, according to standard operating procedures, and conducted by an experienced Trial Manager with support from the PI.
Have any appropriate regulatory bodies already granted a favourable opinion? No
Involvement of Clinical Trials UnitsIs Clinical Trials Authorisation required? Yes
Is a Clinical Trials Unit (CTU) involved with this research proposal? Yes
If yes, what is the name of the CTU?
Does the CTU hold a UKCRC registration number? No
Please describe how you have worked with the CTU in developing your application and what support they will provide if funding is approved.
This study is conceived and originated by staff in the ) which has a track record in delivering similar trials in pleural infection (n>1000). has reviewed the project from a feasibility and project management point of view. We have a substantial experience in the delivery of trials in multicentre randomised studies across more than 20 UK, and 7 international centres.
will provide oversight, trial management, database construction and management, data cleaning and verification, monitoring, oversight committee organisation, methodology and design support and randomisation
349

Page 31 of 70
according to our established standard operating procedures. The current Patient and Public Involvement Group will be expanded and used to create the Pleural infection Advisory Group for the first phase of the project, and continued throughout feasibility trial recruitment using our previous established infrastructure in other disease areas.
350

Page 32 of 70
12. Intellectual Property and Innovation
The definition of Intellectual Property (IP) includes copyright (such as new software, checklists, scales, protocols, questionnaires, toolkits, guidelines or similar) and research tools (such as data analysis techniques, assays, cell lines, biomarkers, materials or equipment and devices) patents, trademarks and designs.
What relevant IP (patents, design right, copyright etc.) is held by the applicants and how does it relate to this application?
There are no relevant IP issues releated to this proposal, as the novel intervention proposed (Intrapleural Enzyme Therapy) is previously published by our group and in clinical use in specific circumstances (e.g. rescue therapy in those unable to have surgery).
Has a freedom to operate search been conducted and by whom? No
If no search has been conducted please set out the rationale.
Not required
Will any IP be produced or improved during the proposed research? No
351

: Page 33 of 70
13. Involvement with NIHR Infrastructure and Other Partner Organisations
Network involvement Please describe links to NIHR networks, identifying, if appropriate, any benefits that have already accrued from working with networks.
Previous and current trials conducted by the have utilised the Clinical Research Network resource to provide nursing support to all multi-centre trials with appropriate funding. This support has been vital to the delivery of previous studies in and the recruitment centres across the UK, providing support to PIs to deliver research and improving quality of data and protocol adherence across all sites.
Please describe the RDS’s input.
The RDS has been approached to aid in the design of the study and this application, and has been incredibly responsive, helpful and highly valuable in guiding design, statistical and PPI issues relevant to the trial.
Research Design Services (RDS) InvolvementPlease indicate, if applicable, which organisations (e.g. NIHR Research Design Service) you have contacted in the course of preparing this application.
Involvement with other partnersWhat, if any, other organisations will partner this research?
Describe the role, if any, these will have in the research.
The main applicant is partly funded by the to Direct the and his time in conducting this study will be partly used via this funding mechanism.
352

: Page 34 of 70
14. Finance
STAFF DETAILS 1Name
Staff type Lead Applicant
Employing organisation
Role on this research Lead Applicant
Grade
Starting point on scale
Increment Date
Details of Posts and Salaries Total (£)
Salary (£) 76001
Geographical Weighting (£) 0
Other allowances (£) 0
Superannuation & Nat. Insurance (£) 23049
Current Annual Costs (£) 99050
STAFF DETAILS 2Name
Staff type Other
Employing organisation
Role on this research Operations Manager
Grade
Starting point on scale
Increment Date
Details of Posts and Salaries
353

: Page 35 of 70
Total (£)
Salary (£) 49772
Geographical Weighting (£) 0
Other allowances (£) 0
Superannuation & Nat. Insurance (£) 14708
Current Annual Costs (£) 64480
STAFF DETAILS 3Name
Staff type Co-applicant
Employing organisation
Role on this research Health Economist
Grade
Starting point on scale
Increment Date
Details of Posts and Salaries Total (£)
Salary (£) 51260
Geographical Weighting (£) 0
Other allowances (£) 0
Superannuation & Nat. Insurance (£) 15181
Current Annual Costs (£) 66441
STAFF DETAILS 4Name
Staff type Co-applicant
Employing organisation
Role on this research Co-applicant
Grade
Starting point on scale
354

Page 36 of 70
Increment Date
Details of Posts and Salaries Total (£)
Salary (£) 33943
Geographical Weighting (£) 0
Other allowances (£) 0
Superannuation & Nat. Insurance (£) 9675
Current Annual Costs (£) 43618
If there are any applicants whose costs are not being claimed then, for each person, state their name and explain briefly why costs are not being claimed and what resources are being used to cover their contribution.
are pleural physicians who will be PIs in their local centres for this study. They are fully funded from a combination of NHS and Research sources and will participate in the study as part of their interest in pleural disease, with clinical research network support.
are fully funded from the NHS as consultant surgeons, and do not require further financial support for their participation in this study, which will be in an advisory and coordination role.
Direct CostsThese are the costs that are specific to the research, which will be charged as the amount actually spent and can be supported by an audit record.
Staff Type:(Lead Applicant)Type of cost:HEI% Full-time on this research:10.0Total months on this research:33.0
Year 1 Year 2 Year 3 Total Cost (£)Basic Salary 10073 10388 7982 28443
Staff Type:(Co Applicant)-Type of cost:HEI% Full-time on this research:15.0Total months on this research:33.0
Year 1 Year 2 Year 3 Total Cost (£)Basic Salary 9708 9979 7503 27190
Staff Type:OtherName:Trial ManagerType of cost:HEI% Full-time on this research:20.0Total months on this research:31.0
Year 1 Year 2 Year 3 Total Cost (£)Basic Salary 8081 8330 4995 21406
355

Page 37 of 70
Staff Type:OtherName:Trial Nurse (Interviews)Type of cost:HEI% Full-time on this research:3.0Total months on this research:14.0
Year 1 Year 2 Year 3 Total Cost (£)Basic Salary 1412 239 0 1651
Staff Type:OtherName:Trial Nurse (Follow Up)Type of cost:HEI% Full-time on this research:10.0Total months on this research:24.0
Year 1 Year 2 Year 3 Total Cost (£)Basic Salary 1416 4367 2997 8780
Staff Type:OtherName:Database ManagerType of cost:HEI% Full-time on this research:2.0Total months on this research:33.0
Year 1 Year 2 Year 3 Total Cost (£)Basic Salary 749 770 595 2114
Staff Type:OtherName:Database CoordinatorType of cost:HEI% Full-time on this research:1.0Total months on this research:33.0
Year 1 Year 2 Year 3 Total Cost (£)Basic Salary 427 441 340 1208
Staff Type:OtherName:Senior StatisticianType of cost:HEI% Full-time on this research:5.0Total months on this research:33.0
Year 1 Year 2 Year 3 Total Cost (£)Basic Salary 2545 2618 2021 7184
Staff Type:OtherName:Junior StatisticianType of cost:HEI% Full-time on this research:10.0Total months on this research:33.0
Year 1 Year 2 Year 3 Total Cost (£)Basic Salary 3543 3643 2814 10000
Staff Type:(Co Applicant)-
356

Page 38 of 70
Type of cost:HEI% Full-time on this research:6.0Total months on this research:33.0
Year 1 Year 2 Year 3 Total Cost (£)Basic Salary 3428 3532 5463 12423
Year 1 Year 2 Year 3 Total Cost (£)Total HEI 41382 44307 34710 120399Total NHS 0 0 0 0Total Commercial 0 0 0 0Total Other 0 0 0 0
Travel, Subsistence and Conference FeesType of cost:HEIDescription:Journey Costs
Year 1 Year 2 Year 3 Total Cost (£)1818 5018 3789 10625
Type of cost:HEIDescription:Conference Fees
Year 1 Year 2 Year 3 Total Cost (£)0 2570 1930 4500
Year 1 Year 2 Year 3 Total Cost (£)Travel, Subsistence and Conference Fees Total 1818 7588 5719 15125
EquipmentNo costs have been added Consumables
Type of cost:HEIPlease describe fully:Research Consumables
Year 1 Year 2 Year 3 Total Cost (£)975 975 975 2925
Type of cost:HEIPlease describe fully:Blood Collection Kits
Year 1 Year 2 Year 3 Total Cost (£)685 515 0 1200
Year 1 Year 2 Year 3 Total Cost (£)Consumables Total 1660 1490 975 4125
Patient and Public Involvement
Type of cost:HEIPlease describe fully:PPI Costs
Year 1 Year 2 Year 3 Total Cost (£)8000 6500 2500 17000
Year 1 Year 2 Year 3 Total Cost (£)Patient and Public 8000 6500 2500 17000
357

Page 39 of 70
Involvement Total
Other Direct Costs
Type of cost:HEIPlease describe fully:CTA Application
Year 1 Year 2 Year 3 Total Cost (£)3448 0 0 3448
Type of cost:HEIPlease describe fully:Drug Packaging and Randomisation
Year 1 Year 2 Year 3 Total Cost (£)10000 0 0 10000
Type of cost:HEIPlease describe fully:Lung Function Test
Year 1 Year 2 Year 3 Total Cost (£)0 7700 5800 13500
Type of cost:HEIPlease describe fully:Database Hosting, Back up and Maintenance
Year 1 Year 2 Year 3 Total Cost (£)1091 1091 818 3000
Type of cost:HEIPlease describe fully:Publications
Year 1 Year 2 Year 3 Total Cost (£)0 0 1500 1500
Type of cost:HEIPlease describe fully:IDMC Meetings
Year 1 Year 2 Year 3 Total Cost (£)0 750 0 750
Type of cost:HEIPlease describe fully:Site Activities
Year 1 Year 2 Year 3 Total Cost (£)3273 3273 2454 9000
Year 1 Year 2 Year 3 Total Cost (£)Other Direct Costs Total 17812 12814 10572 41198
Year 1 Year 2 Year 3 Total Cost (£)
Total Direct Costs 70672 72699 54476 197847
Indirect Costs
HEI Indirect Costs
Type of cost:Estates ChargesName of Higher Education Institute:
358

Page 40 of 70
Year 1 Year 2 Year 3 Total Cost (£)13147 13850 9949 36946
Type of cost:Other Indirect CostsName of Higher Education Institute:
Year 1 Year 2 Year 3 Total Cost (£)34042 35811 26480 96333
Year 1 Year 2 Year 3 Total Cost (£)HEI Indirect Costs Total 47189 49661 36429 133279
Commercial Indirect CostsNo costs have been added Other Partner Organisation Indirect CostsNo costs have been added
Year 1 Year 2 Year 3 Total Cost (£)
Total Indirect Costs 47189 49661 36429 133279
NHS Support Costs
Description of expected additional procedures/resource requirements:Clinician time to consent patients to study Cost per patient (£):16
Year 1 Year 2 Year 3 Total Cost (£)280 882 0 1162
Description of expected additional procedures/resource requirements:Resaerch nurse time to consent patients for structured interviews Cost per patient (£):12
Year 1 Year 2 Year 3 Total Cost (£)0 180 60 240
Description of expected additional procedures/resource requirements:Cost of pharmacy time to dispense the trial drug (25 patients) Cost per patient (£):11
Year 1 Year 2 Year 3 Total Cost (£)0 178 100 278
Year 1 Year 2 Year 3 Total Cost (£)NHS Support Costs Total 280 1240 160 1680Have you discussed and agreed these costs with the Lead Network? Yes
Please expand on your above response including justification either for the costs entered or if relevant, why no costs will be required.
NHS support costs are for activities that will end with the end of the research: Nurse and clinician time for consenting the patients to the trial (x75patients) = £1,162 Consenting patients to participate in the interviews (x20 patients) = £240.
359

Page 41 of 70
Phamacy time for drug accountability (x 25 patients) = £278.
NHS Treatment CostsCost per patient (£):1632Description of expected resources required or released: Purchase of the IMP
Year 1 Year 2 Year 3 Total Cost (£)10000 30800 0 40800
Cost per patient (£):2933Description of expected resources required or released: VATS will be performed in in the early surgery treatment arm in 7 patients who would otherwise have not had this intervention
Year 1 Year 2 Year 3 Total Cost (£)5000 15531 0 20531
Cost per patient (£):19Description of expected resources required or released: Dispensing of the drug is a treatment cost as this is a cost that would continue if the intervention were to become standard care.
Year 1 Year 2 Year 3 Total Cost (£)100 375 0 475
Year 1 Year 2 Year 3 Total Cost (£)NHS Treatment Costs Total 15100 46706 0 61806
Have you discussed and agreed the NHS costs with the Lead Trust? Yes
Please expand on your above response including either justification for the costs entered or if relevant, why no costs will be required.
NHS treatment costs are costs for activities that would continue should the new intervention become standard care and include:
Supply and dispensing of the study drug/IMP (for 25 patients) (= intrapleural enzyme therapy) Performing VATS on 7 patients who would otherwise have not received this particular intervention.
Although there are treatment costs associated with the intervention arms (IMP and VATS) we expect to be to offset this with a cost saving by being able to discharge patients from hospital approximately 5 days earlier than those in the standard care arm. This could save up to £2000 per patient (based on average 25 patients, total = £50,000). If the treatment costs of £61,806 in total are accounted for, this bed day saving would offset the costs.
Is the patient care being provided different from the usual standard treatment for the condition? Yes
If yes, detail the costs of usual standard care below.
The care provided in the VATS and IET arm is different to that provided in the standard care arm as defined in the research plan section. Standard care involves:
Chest tube insertion Antibiotic therapy In patient treatment with the above for an average (from previous data) of 14 days
The costs are therefore largely related to the in patient bed stay.
Usual Treatment CostsCost per patient (£):2000Description of expected additional procedures/resource requirements: The bed day costs saved in 25 patients receiveing IET and VATs
Year 1 Year 2 Year 3 Total Cost (£)
360

Page 42 of 70
15000 35000 0 50000
Year 1 Year 2 Year 3 Total Cost (£)Usual Treatment Costs Total 15000 35000 0 50000
Excess Treatment costs/(savings) Cost perpatient(£) Year 1 Year 2 Year 3 Total Cost (£)
Total NHS Excess Treatment costs/(savings)
2584 100 11706 0 11806
NHS Support and Treatment Costs Total (£)
NHS Support Costs requested from networks 1680
NHS Excess Treatment costs/savings 11806
TOTAL NHS SUPPORT AND TREATMENT COSTS 13486
Research Costs Requested From Funder Direct costs
Indirect costs/Overheads
Total Costs
% of costs paid by NIHR 1-80% or 100%
Amount requested
Total Higher Education Institution Costs 197847 133279 331126 80.0 264901
Total Commercial Costs 0 0 0 100 0Total Other Parther Organisation Costs 0 0 0 100 0
Total NHS Research Costs 0 0 0 100.0 0
Total Research Costs Requested From Funder
197847 133279 331126 264901
Total Funding Required (including non-research costs) Total (£)
Total Research Costs Requested from Funder 264901
Total NHS (Support and Excess Treatment) Costs 13486
Total Funding Required 278387
Please explain how the research costs requested have been calculated and justify how they have been allocated.
Essential staff to provide oversight, scientific direction, organisation and researh related activity include: 10% of the main applicant’s time as Chief Investigator. 15% FTE is requested for the Operations Director of ) to to maintain an efficient
infrastructure and ensuring continuity and stability of trial delivery and ensure that a Quality Management System is in place to meet all appropriate regulations and legislation and that the capabilities, capacity and resources are available.
20% FTE of a Trial Manager is required to coordinate the multicentre study aspects, and conduct regulatory and ethics approval processes.
64 hours research nurse time to train/be trained in interviewing and conducting each interview (each
361

Page 43 of 70
interview expected to take up to 2 hours each (40hours in total)). 0.10 FTE of research nurse time is requested to cover the time needed to follow up the patients in the
trial. Equivalent to 264 hours or 3.5 hours follow up time per patient. Significant amounts of data wil be generated from the structured interviews and feasibility trial, and
construction, coordination and management of a bespoke trials database including electronic data capture (EDC) is required. We therefore request 1% of a data coordinator and 2% of a data manager.
Statistical input from planning to analysis phases of the study is conducted via , and costed at 5% of a senior statistician who will supervise a junior statisitician (10% FTE),
including the provision of reports for trial oversight committees and statistical anlayis plan writing. Health economic (HE) outcome collection feasibility is a key part of this study, and 6% FTE of a health
economist is costed to allow HE input during planning and analyis phases.Direct research costs includes the following:
Site set up visits (5 sites, costed at 3 visits per centre, total cost of £100 per visit) IDMC meetings (1 meeting, £750) Conferences - 3 conference visits for CI, £1500 per conference CRF consumables for printing (£30 per patient) - totalling £2,250 to include CRF printing for all papers
and all patients Blood collection bottles for central storage (£16 per patient) CTA application to conduct the study (£3,448) PI time at sites to screen potentially eligible patients for inclusion in this feasibilty study (estimated 200
patients to be screened, £45 per patient, total £9000) Patient travel expenses (£75 for extra visit per patient) PPI expenses, divided in to:
o 2-monthly meetings, over (£50 per meeting, 10 x 13.5 months = £6,750, plus associated travel costs of and catering of £1,450)
o 2 PPI member attendance at TSC meetings (3 meetings, £50 per person / meeting = £600, plus travel and catering of £400)
o Patient structured interviews (20 x £75 per interview = £1,500o Advertising and associated material = £6,300o Total = £17,000
Drug packaging costs to GCP standards and associated randomisation system, to allow smooth delivery in all centres of the IMP and include accountability = £10k
Lung function testing (£180 per patient at 3 months) IT infrastructure to host and backup clinical trials database, OpenClinica platform = £3k Statistician contribution to hardware and conference = £675 £1500 for open access publication
Please explain how the NHS Support and Treatment costs requested have been calculated and justify how they have been allocated.
NHS support costs are as follows: Taking informed consent for participation in the trial - 75 patients x 30mins @ £31/hour = £1162 Consenting patients to participate in the interviews - 20 patients x 30mins @ £24/hour = £240 Drug accountability = £11.10 per patient = £278 for 25 patients
NHS Treatment costs are as follows:
The IMP costs £1632 per patient x 25 patients = £40,800 7 extra patients will receive VATs - £2993 x 7 = £20,531
Please explain how the research provides value for money.
The costs of this research are substantial, but relatively modest for a feasibility trial which will provide key information on a further definitive phase III study and key information on patient experience and outcomes. Should the further phase III study be conducted, this is likely to demonstrate significant hospital stay reductions
362

Page 44 of 70
using either VATS or IET compared with current standard treatment. The cost of VATS is approximately £3000 and IET costs £1632 per patient. Our previous trial of IET therapy was associated with a 5-day reduction in hospital stay compared with standard care, which translates to a cost saving in bed days alone of £2000. Thus provision of evidence on the most efficacious treatment is potentially cost saving in the long term, but requires investment in the development of a high quality trial, and this feasibility trial is the first step in that development.
363

: Page 45 of 70
15. Department of Health Monitoring information
Department of Health Monitoring Information - Please use the drop-down menus and tick boxes to provide the information requested. This will be used by the Department of Health solely for accountability, audit and monitoring purposes.Place of work of Lead Applicant
Lead Applicant’s profession Clinical Academic
Is the research multicentre? Yes
UKCRC Health Categories Please select all classifications from the below list that are applicable.UKCRC Health Categories Respiratory
Programme monitoring data Programme Monitoring Data Research Design Clinical trial Feasibility study Research Participants Older people (65 yrs plus) Working age adults (18 - 65 yrs) Research Purpose Explanatory Research Setting (in which research will take place) Acute/emergency care Research Team Academic (clinical)
Research Team - If 'other' is selected please describe
Research Design - If 'other' is selected please describe
Research Setting (in which research will take place) - If 'other' is selected please describe
Research Participants - If 'other' is selected please describe
364

Page 46 of 70
Research Purpose - If 'other' is selected please describe
365

Page 47 of 70
16. Nominated/Suggested Reviewers
Please suggest three potential peer reviewers who have the relevant expertise to provide appropriate peer review for your application These reviewers should be independent (i.e. not have worked with you directly in the recent past) and should have no competing/conflicting interests with your application (such as being from your own institution/university). Your suggestions will be used as only one source of peer reviewers and these individuals may not be approached to undertake a review.
TitleForenameSurnameExpertiseDepartmentInstitutionTelephoneEmail
TitleForenameSurnameExpertiseDepartmentInstitutionTelephoneEmail
TitleForenameSurnameExpertiseDepartmentInstitutionTelephoneEmail
366

: Page 48 of 70
17. Supporting Documentation
367

Re:
Early video assisted thorascopic surgery (VATs) or intrapleural enzyme therapy (IET) in pleural infection – a feasibility randomised trial.
The NIHR are happy to support this application and have received the costs for this study and consider that they have been attributed appropriately Please do not hesitate to get in touch if we can be of further assistance at this time. Yours sincerely
368

GANTT CHART -‐ Early Video Assisted Thoracoscopic Surgery (VATS) or Intrapleural Enzyme Therapy (IET) in Pleural Infection -‐ a feasibility randomised trial
Task Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr MayTrial management group communication
Patient Advisory Group - set up and interviews
Advisory group meetings
Protocol review and finalisation
Create & Finalise Trial Specific Procedures
Create IRAS forms
Ethics application - submission
R&D application submission
Create study forms (PIC, consent, etc.)
Create & Finalise CRFs
Site specific approvals
Set up randomisation server
Set up database
Site initiation visits
Equipment
Patient recruitment
Follow-up 1 month
Follow up 6 months
Patient Interviews
Monitoring checks
Data entry
Data queries resolution
Ethics annual reports
Database lock
Finalise Statistical Analysis Plan
Data analysis
TSC meetings
DMC meetings
Study report
Key Milestones
Ethics app
roval
50% re
cruitm
ent com
plete
100%
recruitm
ent com
plete
369

Application Early Video Assisted Thoracoscopic Surgery (VATS) or Intrapleural Enzyme Therapy (IET) in
Pleural Infection -‐ a feasibility randomised trial.
References
370

371

372

373

Page 55 of 70
18. Declarations & Signatures
COI declaration Please declare any conflicts or potential conflicts of interest that you or your co-applicants may have in undertaking this research, including any relevant personal, non-personal and commercial interest that could be perceived as a conflict of interest.
Nil
In ticking this, you as Lead Applicant confirm that the information given on this form is complete and correct and that you will be actively engaged in this research and responsible for its overall management. Ticking this box constitutes an electronic signature of the supporting role with regard to this application
Confirmed
Director of Finance signature against declarationIn ticking this, you as the Director of Finance for the host NHS body or other provider of NHS services confirm that you have checked the financial details of this of application and that the named institution is prepared to carry out this research at the stated costs and to administer the award if made. You also confirm that the staff grades and salaries quoted are correct and in accordance with the normal practice of this organisation. Ticking this box constitutes an electronic signature of the supporting role with regard to this application.
Confirmed
Full Name Organisation
Head of Department or Senior Manager signature against declarationIn ticking this, you as Senior Manager, Director of Research, Grants and Contracts Manager, Clinical Director or Chief Executive for the host NHS body or other provider of NHS services confirm that you have read this application and that, if funded, the work will be accommodated and administered in the named NHS body or other provider of NHS services and that the body or other provider of NHS services is capable of fulfilling the role of research sponsor as set out in the Research Governance Framework for Health and Care. You also confirm that the applicants for whom you are responsible may undertake this work. Ticking this box constitutes an electronic signature of the supporting role with regard to this application.
Confirmed
Full Name Organisation
374

Page 56 of 70
19. Lead Applicant CV
Degrees(including details of dates, degree, subject/professional qualification(s) and institution)From To Degree Institution Department Subject
FRCP Medicine Medicine
Dphil Department of Medicine Clinical Medicine
MSc(Hons) Clinical Trials
Dphil Medical Sciences Clinical Medicine
MSc Clinical Trials
BM BCh Clinical Medicine Medical Degree
BM BCh Department of Medicine Clinical Medicine
MA Medical Sciences Division Physiological Sciences
MA Medical Sciences Physiology
Present and previous positions held (including from/to dates, job title and employer)Start Date End Date Job Title Employer
Associate Professor of Respiratory Medicine
Senior Lecturer and Consultant Respiratory Physician
Consultant and Senior Lecturer
Clinical Director,
Academic Clinical Lecturer
Academic Clinical Lecturer
Specialist Registrar Respiratory Medicine
Medical Research Council Clinical Training Fellow
Pleural Research Fellow
Specialist Registrar Respiratory Medicine
Selected relevant publication(s) (including list of authors,article title, publication name,volume reference)Publications
375

Page 57 of 70
Selected relevant publication(s) (including list of authors,article title, publication name,volume reference)Publications
376

Page 58 of 70
Selected relevant publication(s) (including list of authors,article title, publication name,volume reference)Publications
Research award(s) held
Start Date Duration Amount Source Title Role of Applicant
36 270,000.00
Chief Investigator
36 250,846.00
Co Applicant
36 230,882.00 Co Applicant
60 250,000.00 NIHR Chief Investigator
12 145,146.00 PI
24 27,663.00 Clinical Trials Unit Director
60 2,649,834.00 Co Applicant
377

Date submitted: Page 59 of 70
Research award(s) held
Start Date Duration Amount Source Title Role of Applicant
12 44,318.00 British Heart Foundation
Clinical Trials Unit Director and CI
36 344,811.00 CCF
Co Applicant
36 611,632.00 CCF
Co Applicant
54 350,000.00 CCF
Lead Applicant
36 350,000.00 Marie Curie Chief Investigator
36 350,000.00 Chief Investigator
41 149,301.00
Clinical Trials Unit Director
43 48,590.00 British Lung Foundation
Clinical Trials Unit Director
60 174,895.00Clinical Trials Unit Director and local PI
36 350,000.00 Medical Research Chief
378

: Page 60 of 70
Research award(s) held
Start Date Duration Amount Source Title Role of Applicant
Council Investigator
48 120,000.00
Chief Investigator
379

Page 61 of 70
20. Co-applicant CVs
Title Address Line 1
Forename(s) Address Line 2Surname Address Line 3Date of Birth CountyNationality Postcode
EducationFrom Degree Class Country Subject University/Institute
Doctorate in Medicine
Inflammatory pleural disease
MBBS(Hons) Medicine and Surgery
MBBS Medical degree
B Med Sci Medicine
BSc B Med Sci (hons)
EmploymentStart Date End Date Job Title Employer
Professor of Respiratory Medicine
Reader in Respiratory Medicine
Consultant Senior Lecturer
Respiratory Consultant
Senior Lecturer
Consultant Respiratory Physician
Consultant Physician
MRC Clinical Fellow
Specialist Registrar - Respiratory Rotation
PublicationsPublication Details Date Published
Grants
Start Date Duration Amount Source Title Role of Applicant
36 250,846.00 CCF
Co Applicant
380

: Page 62 of 70
Grants
Start Date Duration Amount Source Title Role of Applicant
24 287,465.00 CCF
Lead
Applicant
36 344,811.00 CCF
Lead Applicant
36 59,000.00 British Lung Foundation
Grant holder and chief investigator
54 350,000.00 CCF
Co Applicant
36 342,923.00
Co-applicant
12 141,500.00 Chief investigator
36 496,500.00 British Lung Foundation
Co-applicant, TSC member, local PI
36 670,000.00
Chief investigator
36 635,000.00
Chief investigator
381

Page 63 of 70
Grants
Start Date Duration Amount Source Title Role of Applicant
45 238,606.00 CCF
Lead Applicant
46 238,606.00
Chief Investigator
36 150,000.00
Chief Investigator
36 120,000.00
Co-applicant
48 250,000.00 Chief Investigator
Title Address Line 1Forename(s) Address Line 2Surname Address Line 3Date of Birth CountyNationality Postcode
EducationFrom Degree Class Country Subject University/Institute
Intercollegiate Speciality Board Examination in Cardiothoracic Surgery
PhD Oncology
382

Page 64 of 70
EducationFrom Degree Class Country Subject University/Institute
MBChB Medicine
EmploymentStart Date End Date Job Title Employer
- Honorary Senior Lecturer
- Consultant Thoracic Surgeon
PublicationsPublication Details Date Published
Grants
Start Date Duration Amount Source Title Role of Applicant
36 250,846.00 CCF
Co Applicant
12 54,557.00
Co-Applicant, Trial Management Group
36 50,000.00 Cancer Research UK
Co-applicant, Trial Steering Committee,
24 215,835.00
Co-Applicant, Site Principal Investigator
12 49,991.00
Co-Applicant, Trial Management Group Lead
383

: Page 65 of 70
Grants
Start Date Duration Amount Source Title Role of Applicant
Surgeon,
36 499,908.00 British Lung Foundation
Co-Applicant, Trial Management Group, Site Princip
60 243,211.00 CCF
Co Applicant
Title Address Line 1Forename(s) Address Line 2Surname Address Line 3Date of Birth CountyNationality Postcode
EducationFrom Degree Class Country Subject University/Institute
EmploymentStart Date End Date Job Title Employer
PublicationsPublication Details Date Published
Grants
Start Date Duration Amount Source Title Role of Applicant
Title Address Line 1Forename(s) Address Line 2Surname Address Line 3Date of Birth CountyNationality Postcode
EducationFrom Degree Class Country Subject University/Institute
384

Date submitted: Page 66 of 70
EducationFrom Degree Class Country Subject University/Institute
PhD Sepsis
MRCP (UK) Royal College of Physicians
MBBS Medicine
BScBasic Medical Sciences and Pharmacology
EmploymentStart Date End Date Job Title Employer
- Consultant Thoracic Surgeon
PublicationsPublication Details Date Published
Grants
Start Date Duration Amount Source Title Role of Applicant
Title Address Line 1Forename(s) Address Line 2Surname Address Line 3Date of Birth CountyNationality Postcode
EducationFrom Degree Class Country Subject University/Institute
BSc Pharmacology and Physiology
EmploymentStart Date End Date Job Title Employer
- Operations Director
Senior Business Operations Associate
Senior Business Operations Associate
Senior Business Development Executive
385

Date submitted: Page 67 of 70
EmploymentStart Date End Date Job Title Employer
Business Operations Executive
Business Operations Executive
Clinical Research Associate / Project Manager
PublicationsPublication Details Date Published
Grants
Start Date Duration Amount Source Title Role of Applicant
Title Address Line 1
Forename(s) Address Line 2
Surname Address Line 3Date of Birth CountyNationality Postcode
EducationFrom Degree Class Country Subject University/Institute
PhD
Content-Based Multisensory Signal Analysis and Fusion
MSc(Hons)Statistical Machine Learning
BSc Electronic Engineering
EmploymentStart Date End Date Job Title Employer
Medical Statistician
Post-doctoral Research Associate
386

Page 68 of 70
EmploymentStart Date End Date Job Title Employer
Post-doctoral Research Fellow
PublicationsPublication Details Date Published
Grants
Start Date Duration Amount Source Title Role of Applicant
Title Address Line 1Forename(s) Address Line 2Surname Address Line 3Date of Birth CountyNationality Postcode
EducationFrom Degree Class Country Subject University/Institute
MRCP Medicine
MBBS Medical Degree
EmploymentStart Date End Date Job Title Employer
Consultant
Consultant
PublicationsPublication Details Date Published
Grants
Start Date Duration Amount Source Title Role of Applicant
Title Address Line 1
387
: Page 69 of 70
Forename(s) Address Line 2
Surname Address Line 3Date of Birth CountyNationality Postcode
EducationFrom Degree Class Country Subject University/Institute
PhD
EmploymentStart Date End Date Job Title Employer
PublicationsPublication Details Date Published
Grants
Start Date Duration Amount Source Title Role of Applicant
Title Address Line 1Forename(s) Address Line 2Surname Address Line 3Date of Birth CountyNationality Postcode
EducationFrom Degree Class Country Subject University/Institute
Dphil Public Health/Health Economics
MSc Health Economics
MA(Hons) Economics andEuropean Studies
EmploymentStart Date End Date Job Title Employer
University Research Lecturer
Senior Researcher
Research Officer
388

: Page 70 of 70
PublicationsPublication Details Date Published
Grants
Start Date Duration Amount Source Title Role of Applicant
54 350,000.00 CCF Co Applicant
12 43,840.00 UK National Screening Committee Co-applicant
42 1,247,984.00 Co-applicant
60 5,298,179.00 NIHR Co-applicant
60 120,000.00
European Commission-Seventh Framework Programme
Health Economist
389