вбдгжеиз © £ ! # " $&%'©( )0©2 13 )¡5 4617©8¥9£ A @CB0 3 ...
Upload
khangminh22Category
view
2download
0
Centro Universitario Residenziale - Bertinoro
Drugs in pregnancyMario Regazzi – Pavia (I)
Postgraduate Education CourseInfectious Diseases in Pregnant Women, Fetuses and Newborns
Bertinoro, 25‐29 September 2016
ESCMID Online Lecture Library
© by author

Prescribing in pregnancy
Effect of the DRUG Effect of the ILLNESS
Potential adverse effectsof the drug (usually to the fetus)
Benefit (usually to themother) of treating the disease.
M.Regazzi, 2016
ESCMID Online Lecture Library
© by author
Karen Feibus,, 20113
Information needed by HCPs when prescribing for women of childbearing potential
• What is my patient’s underlying medical condition?
– Is pharmaceutical treatment essential for her health?
– Is her medical condition well managed on her current medications?
– What are the reproductive/developmental risks of her medications?• What is this based on?• Are there any other data available that are not in the drug labeling?
– Are there other medications that treat her underlying condition that have better developmental risk profiles?• Are these alternatives appropriate for her?
– Have I informed my patient about the reproductive risks of her medicines and discussed the relative risk/benefits of appropriate therapies?• If she was pregnant, what would I do differently?
ESCMID Online Lecture Library
© by author

Why a woman takes medication while pregnant:
There are three reasons:
1. Inadvertent exposure to medication
2. Intended continuation of treatment for a pre‐existing medicalcondition
3. Initiation of treatment in pregnancy for example, for infection or apregnancy‐specific problem such as pre‐eclampsia
ESCMID Online Lecture Library
© by author
Management principles
1. Inadvertent exposure tomedication
• Obtain accurate details of exposureand gestational age
• Check for confounding family andpersonal medical history
• Obtain up‐to‐date informationabout published risks of the drug inhumans
• Emphasize background risk incounselling
• Be clear what is known (absence ofdata does not equal no risk)
2. Intended continuation or 3. Initiation of medication in pregnancy
• Medication should only be used if theexpected benefits (usually to themother) are greater than thepotential risks (usually to the fetus)
• Try to avoid first trimester use• Use drugs that have been used
extensively in pregnancy, not newones
• Use the minimum dose required toobtain the desired effect
• Absence of data does not imply safetyESCMID Online Lecture Library
© by author
Women and Chronic Conditions
• Prevalence of chronic conditions is among women
• There has been an population of pregnant women whohave pre‐existing conditions due to the increasing age of thechildbearing population and new and improved treatmentsfor these conditions.
• An high percentage of women take an over‐the‐counter(OTC) or prescription medication during pregnancy; >50% ofwomen are prescribed these medications during pregnancy.
ESCMID Online Lecture Library
© by author
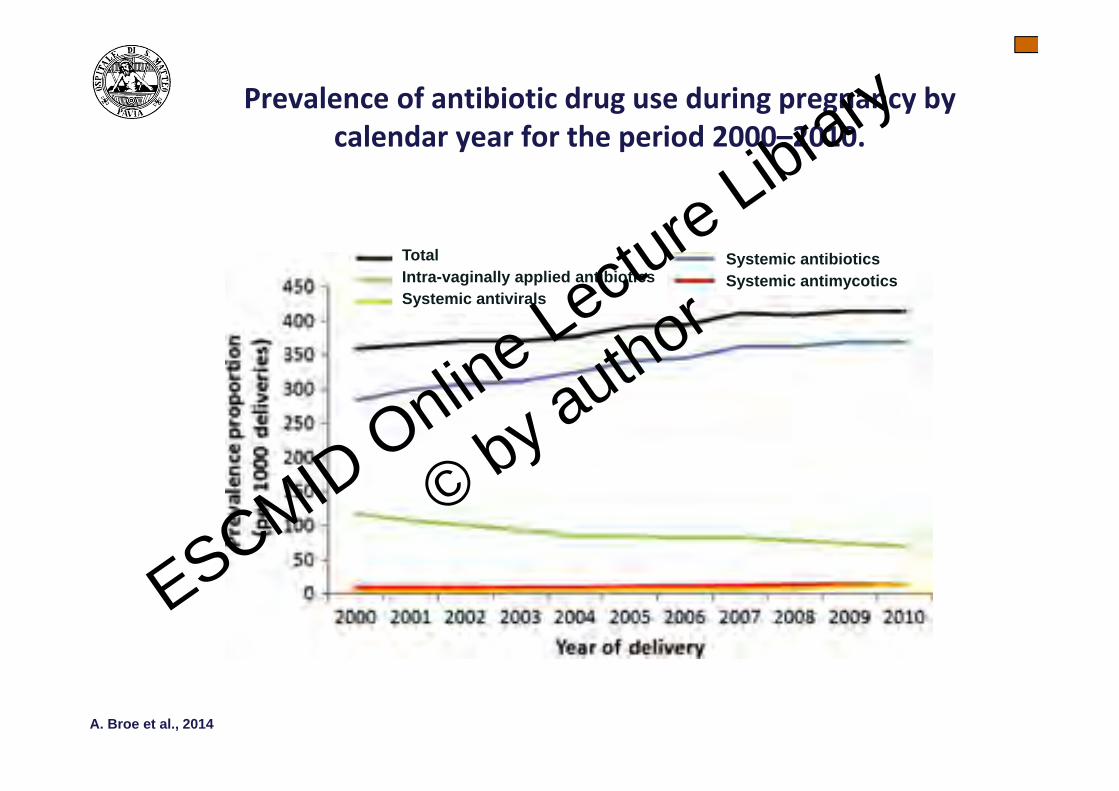
Increasing use of antibiotics in pregnancy during the period 2000–2010: prevalence, timing, category, and demographics
TotalIntra-vaginally applied antibioticsSystemic antivirals
Systemic antibioticsSystemic antimycotics
Prevalence of antibiotic drug use during pregnancy by calendar year for the period 2000–2010.
A. Broe et al., 2014
ESCMID Online Lecture Library
© by author
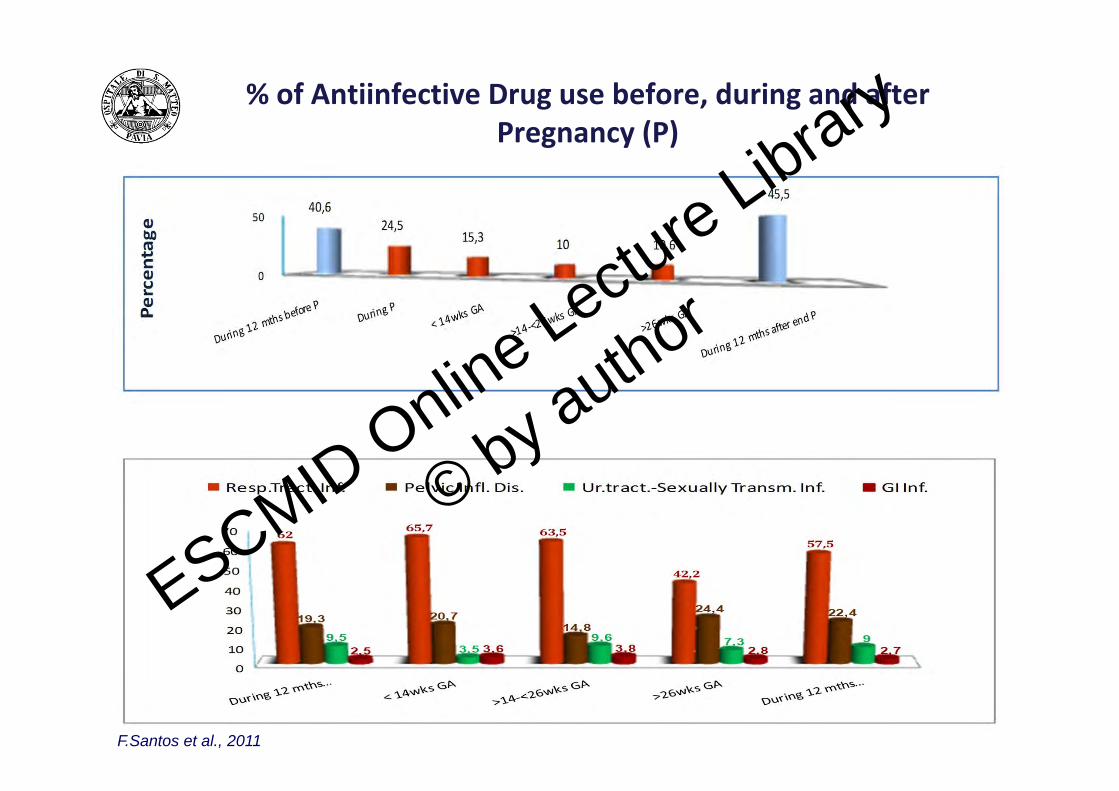
% of Antiinfective Drug use before, during and afterPregnancy (P)
F.Santos et al., 2011
ESCMID Online Lecture Library
© by author
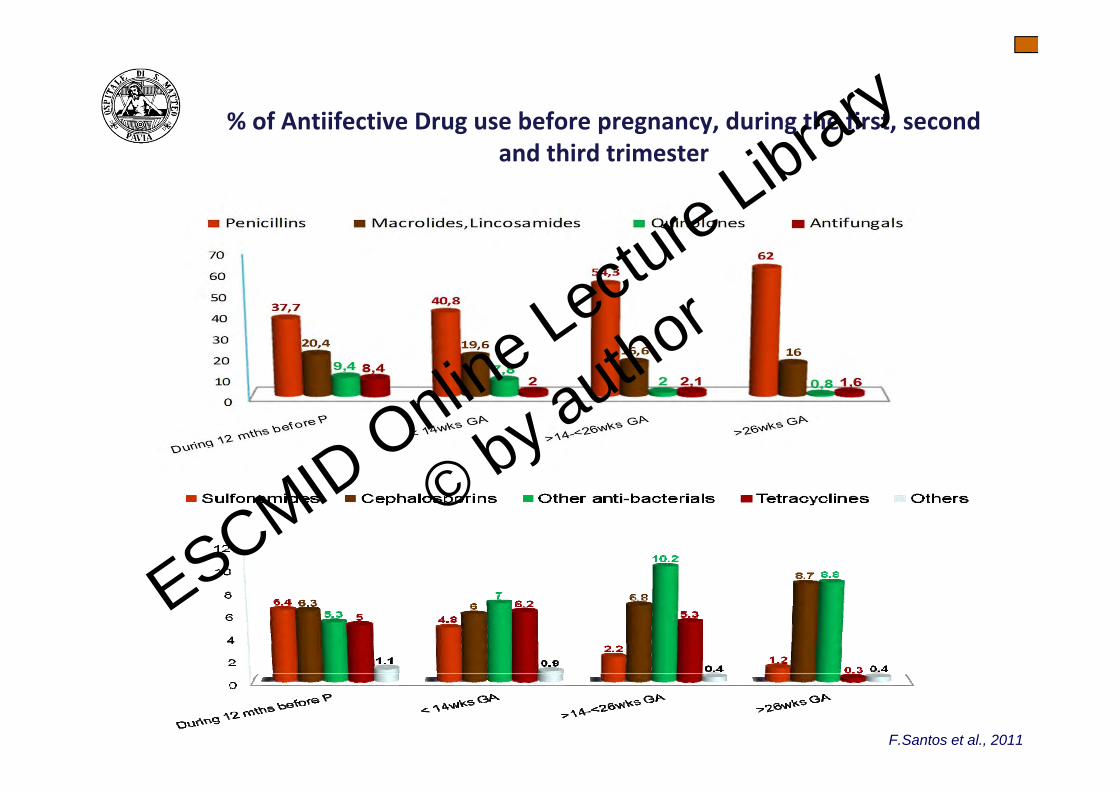
% of Antiifective Drug use before pregnancy, during the first, secondand third trimester
F.Santos et al., 2011
ESCMID Online Lecture Library
© by author
Pregnant women & medical research:
• Development of knowledge in understanding the use of antiinfective drugs during pregnancy has been limited by difficulties intesting medications in pregnant women and lack of evidence‐baseddata.
• Since studies so rarely include pregnant women, treatmentdecisions are “generally not evidence based.” That can meaninadequate dosing and uncertain risks.
• Absence of Evidence is not evidence of absenceESCMID Online Lecture Library
© by author
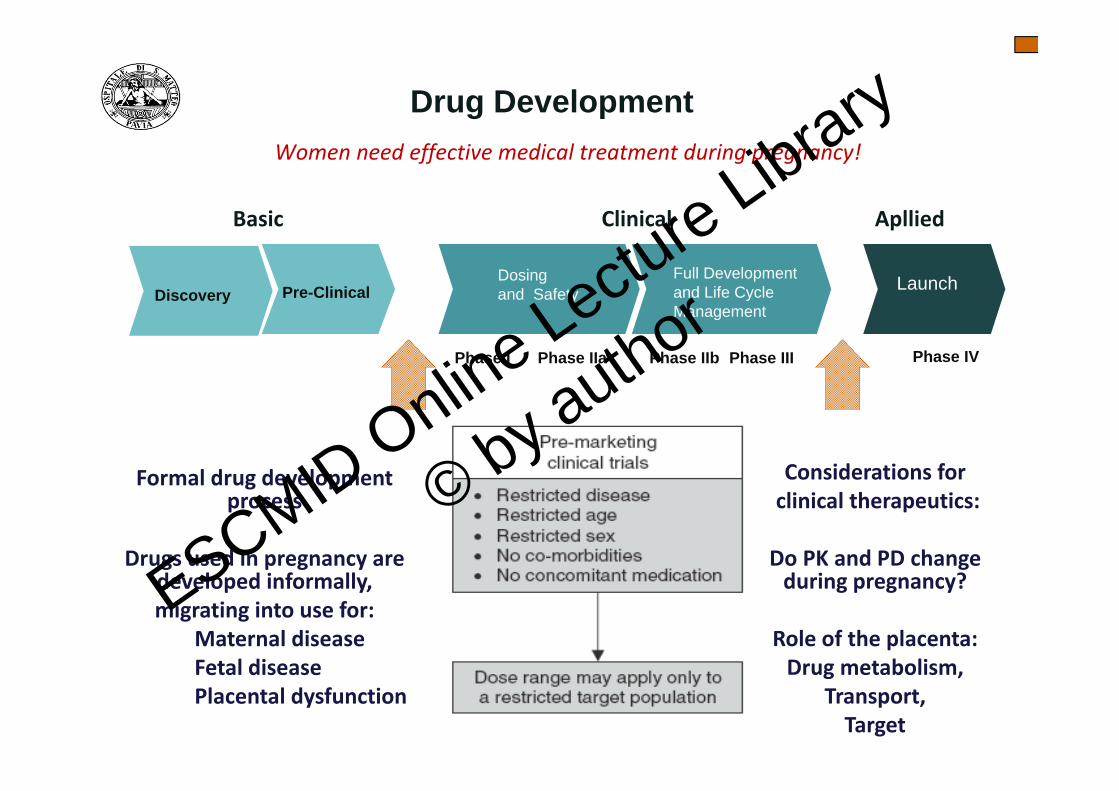
Formal drug development process
Drugs used in pregnancy are developed informally, migrating into use for:
Maternal diseaseFetal diseasePlacental dysfunction
Considerations forclinical therapeutics:
Do PK and PD change during pregnancy?
Role of the placenta:Drug metabolism,
Transport, Target
Basic Clinical Apllied
Phase I Phase IIa Phase IIb Phase III Phase IV
Discovery Pre-ClinicalDosingand Safety
Full Developmentand Life CycleManagement
Launch
Drug DevelopmentWomen need effective medical treatment during pregnancy!
ESCMID Online Lecture Library
© by author

Pregnant women & medical research:
• The costs of exclusion– 1. Fetal safety; 2.Reticence to use needed medication; 3. Access to the
benefits of research participation; 4. Effective treatment for pregnantwomen
• In the absence of information about the safety and efficacy ofmedications, pregnant women and their clinicians are left withtwo unsavory options– take a drug with unknown safety and efficacy or– fail to treat the condition,
M.O. Little et al., 2009
ESCMID Online Lecture Library
© by author
ESCMID Online Lecture Library
© by author
Study areas of specific interest
1. Foetal therapy studies
‐ Efficacy and safety information‐ Outcome measures: foetal loss and infant mortality rates, gestationalage at delivery, birth weight, premature rupture of membranes, neonatalcomplications, congenital malformations and developmental delay.
2. Pharmacokinetic studies
3. Pharmacogenetic studies
ESCMID Online Lecture Library
© by author

Different possibilities of drug and drug metabolite transferbetween mother and fetus
Parent drug (non polar)
Polar metabolite
Parent drug (non polar)
Mother Placenta Fetus
Mother Placenta Fetus
Elimination
Elimination
No drugParent drug (polar)ESCMID Online Lecture Library
© by author

Different possibilities of drug and drug metabolite transferbetween mother and fetus
Mother Placenta Fetus
Mother Placenta Fetus
Elimination Elimination
Elimination
Parent drug (non polar)
Non polar metabolite
Polar metabolite
Parent drug (non polar)
Non polar metabolite
Parent drug (non polar)
Non polar metabolite
Polar metabolite
Parent drug (non polar)
Non polar metabolite
Polar metabolite
ESCMID Online Lecture Library
© by author
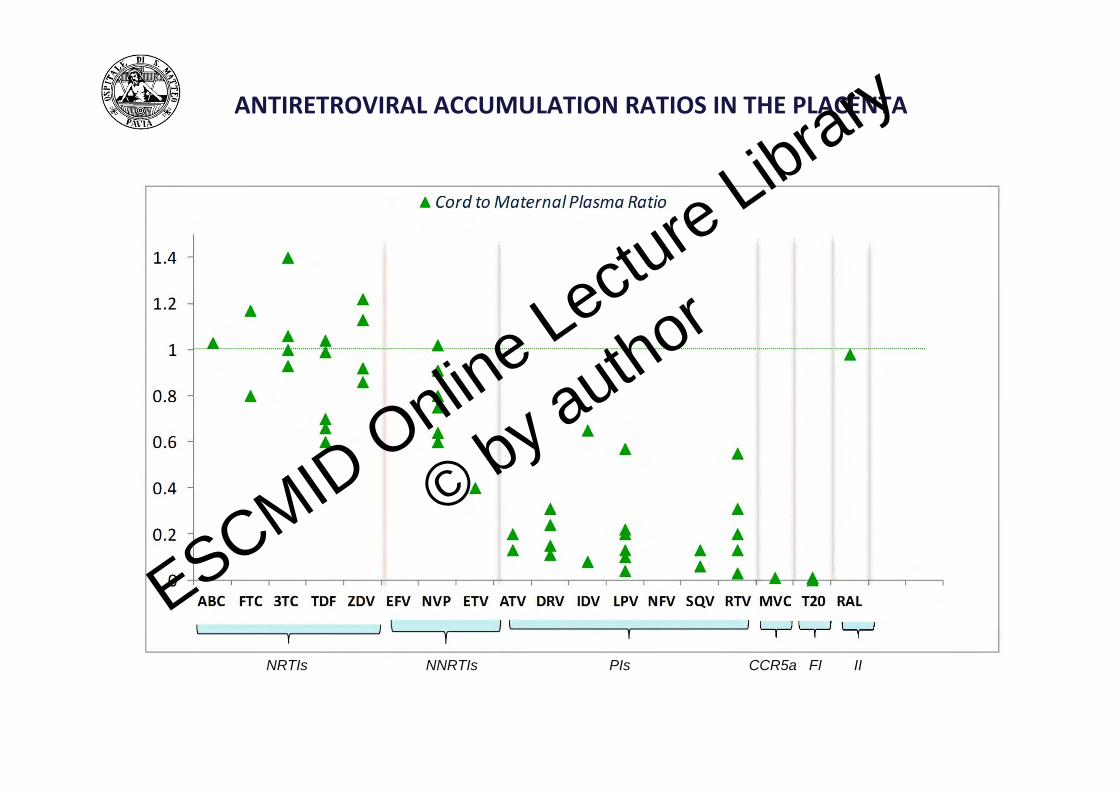
ANTIRETROVIRAL ACCUMULATION RATIOS IN THE PLACENTA
NRTIs NNRTIs PIs FICCR5a II
ESCMID Online Lecture Library
© by author
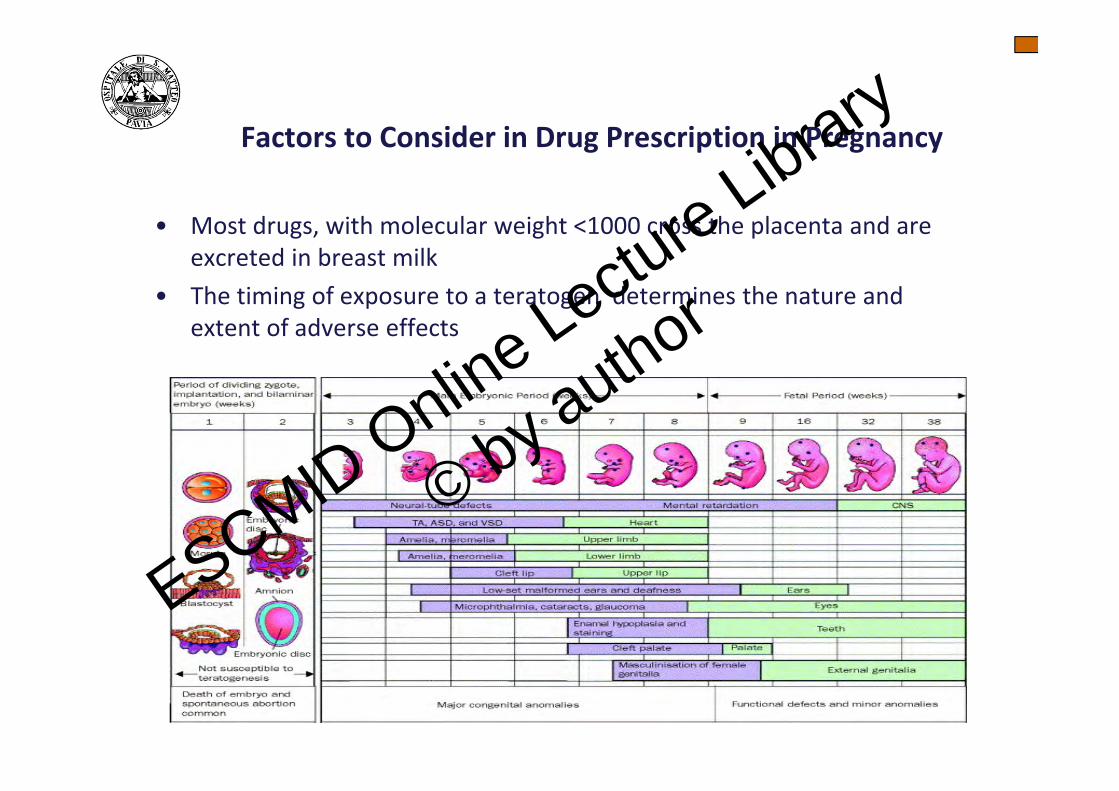
Factors to Consider in Drug Prescription in Pregnancy
• Most drugs, with molecular weight <1000 cross the placenta and are excreted in breast milk
• The timing of exposure to a teratogen determines the nature and extent of adverse effects
ESCMID Online Lecture Library
© by author
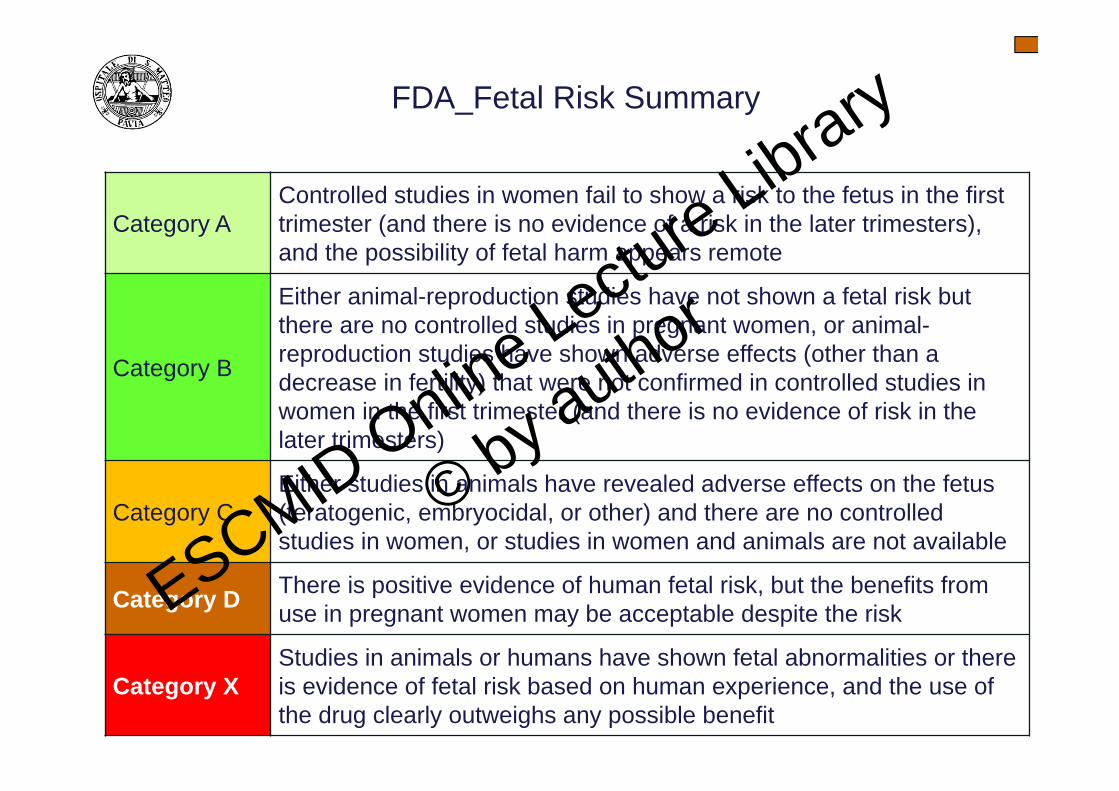
FDA_Fetal Risk Summary
Category AControlled studies in women fail to show a risk to the fetus in the first trimester (and there is no evidence of a risk in the later trimesters), and the possibility of fetal harm appears remote
Category B
Either animal-reproduction studies have not shown a fetal risk but there are no controlled studies in pregnant women, or animal-reproduction studies have shown adverse effects (other than a decrease in fertility) that were not confirmed in controlled studies in women in the first trimester (and there is no evidence of risk in the later trimesters)
Category CEither studies in animals have revealed adverse effects on the fetus (teratogenic, embryocidal, or other) and there are no controlled studies in women, or studies in women and animals are not available
Category D There is positive evidence of human fetal risk, but the benefits from use in pregnant women may be acceptable despite the risk
Category XStudies in animals or humans have shown fetal abnormalities or there is evidence of fetal risk based on human experience, and the use of the drug clearly outweighs any possible benefit
ESCMID Online Lecture Library
© by author
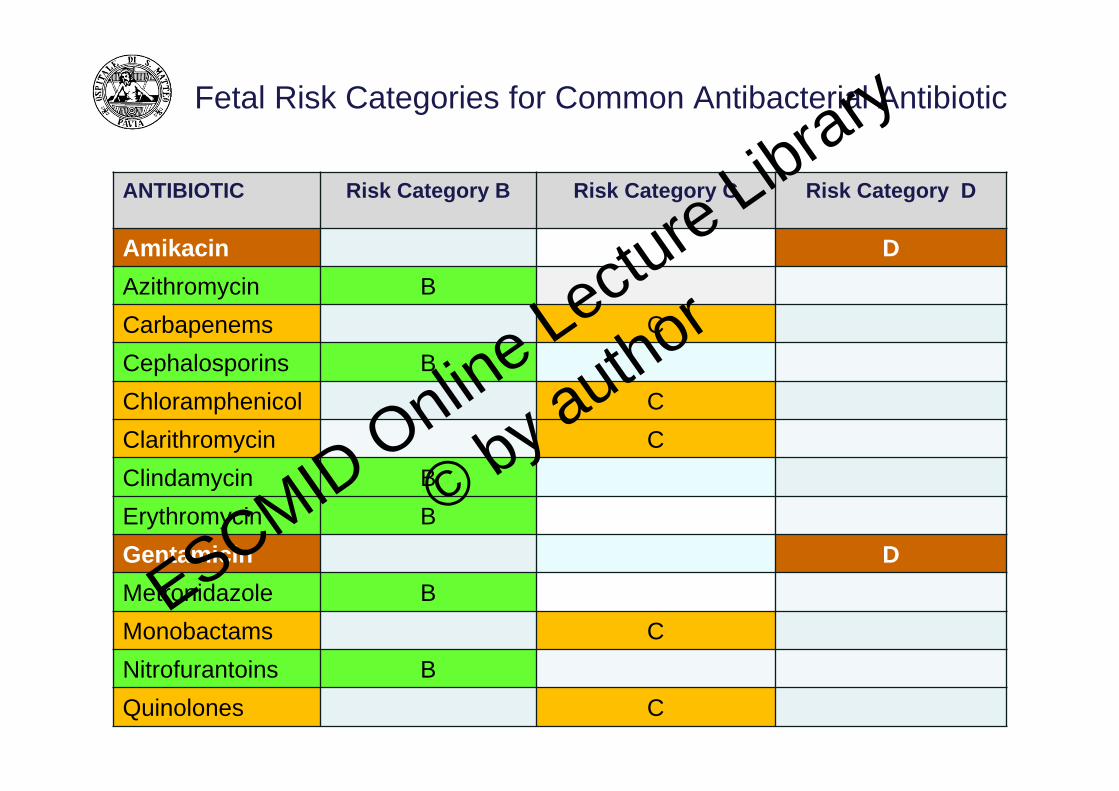
Fetal Risk Categories for Common Antibacterial Antibiotic
ANTIBIOTIC Risk Category B Risk Category C Risk Category D
Amikacin DAzithromycin BCarbapenems CCephalosporins BChloramphenicol CClarithromycin CClindamycin BErythromycin BGentamicin DMetronidazole BMonobactams CNitrofurantoins BQuinolones C
ESCMID Online Lecture Library
© by author

Fetal Risk Categories for Common Antibacterial Antibiotic
ANTIBIOTIC Risk Category B Risk Category C Risk Category D
Penicillins B
Spectinomycin B
Spiramycin B
Sulfonamides B
Tobramycin D
Trimethoprim C
Vancomycin C
ESCMID Online Lecture Library
© by author
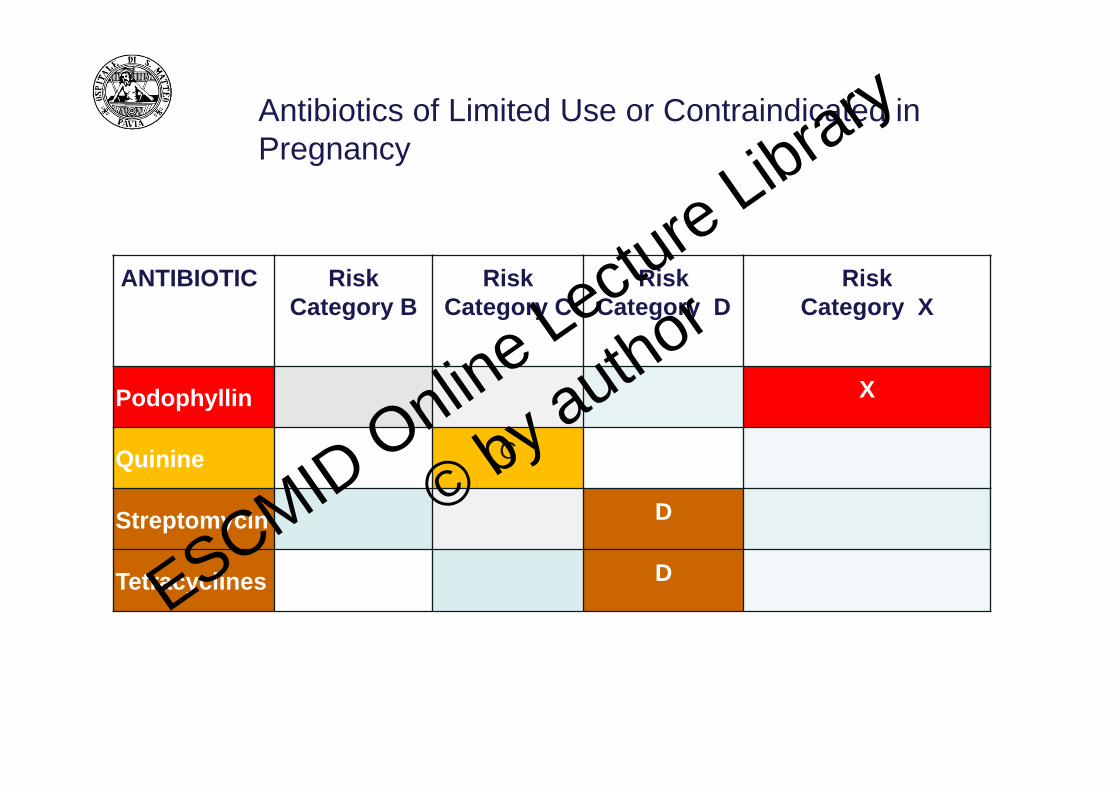
Antibiotics of Limited Use or Contraindicated in Pregnancy
ANTIBIOTIC RiskCategory B
RiskCategory C
RiskCategory D
RiskCategory X
Podophyllin X
Quinine C
Streptomycin D
Tetracyclines DESCMID Online Lecture Library
© by author
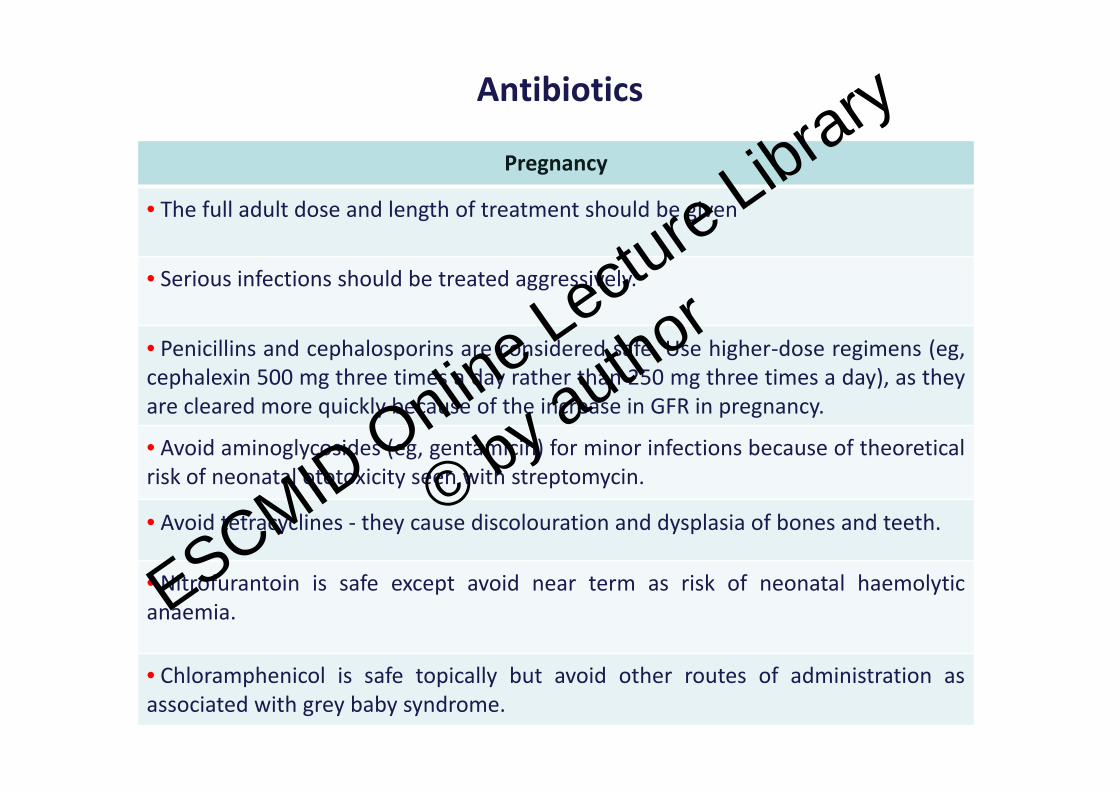
Antibiotics
Pregnancy
• The full adult dose and length of treatment should be given
• Serious infections should be treated aggressively.
• Penicillins and cephalosporins are considered safe. Use higher‐dose regimens (eg,cephalexin 500 mg three times a day rather than 250 mg three times a day), as theyare cleared more quickly because of the increase in GFR in pregnancy.
• Avoid aminoglycosides (eg, gentamicin) for minor infections because of theoreticalrisk of neonatal ototoxicity seen with streptomycin.
• Avoid tetracyclines ‐ they cause discolouration and dysplasia of bones and teeth.
• Nitrofurantoin is safe except avoid near term as risk of neonatal haemolyticanaemia.
• Chloramphenicol is safe topically but avoid other routes of administration asassociated with grey baby syndrome.
ESCMID Online Lecture Library
© by author
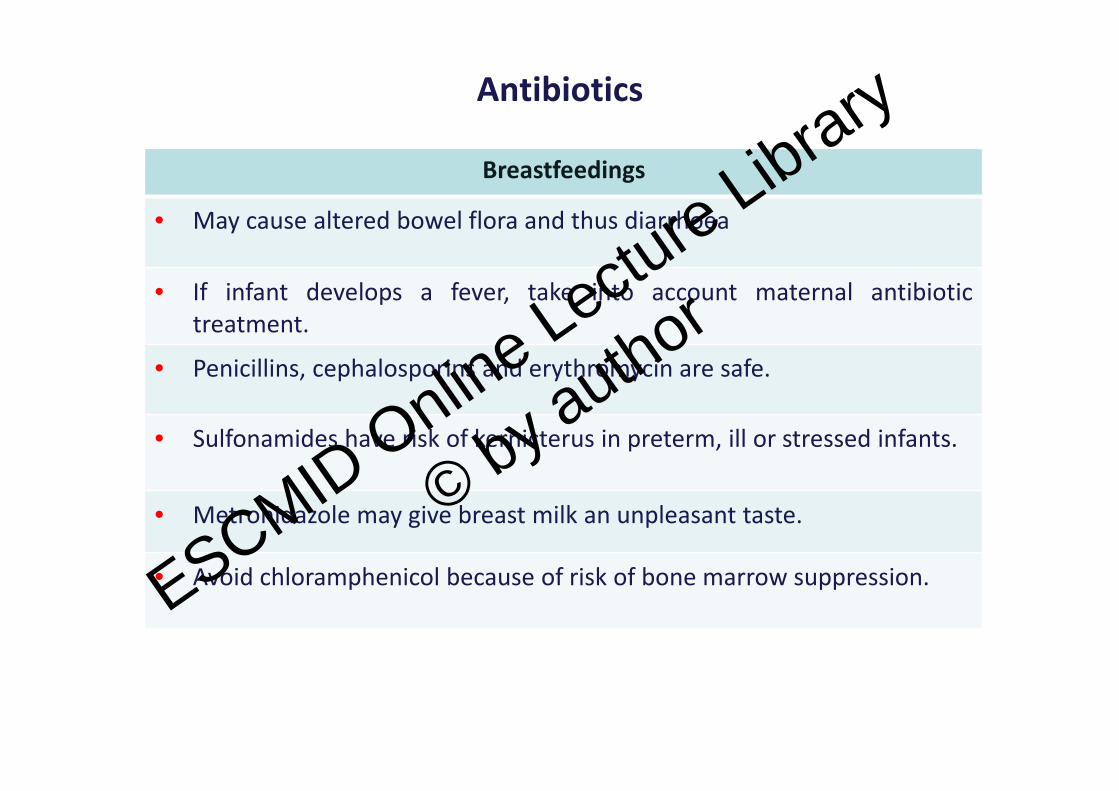
Antibiotics
Breastfeedings
• May cause altered bowel flora and thus diarrhoea
• If infant develops a fever, take into account maternal antibiotictreatment.
• Penicillins, cephalosporins and erythromycin are safe.
• Sulfonamides have risk of kernicterus in preterm, ill or stressed infants.
• Metronidazole may give breast milk an unpleasant taste.
• Avoid chloramphenicol because of risk of bone marrow suppression.ESCMID Online Lecture Library
© by author
ANT
• Antiretroviral Agents
No evidence of teratogenety has been observed inanimals (exception of indinavir)
Benfits outweigh risks.
Antiviral Drugs
ESCMID Online Lecture Library
© by author
Antiretroviral Therapy during Pregnancy
Antiretroviral therapy (ART) during pregnancy should focus on
• the reduction of perinatal transmission and
• the treatment of maternal human immunodeficiency virus (HIV) disease.
ART can reduce perinatal transmission by several mechanisms, including
• lowering maternal antepartum viral load and
• preexposure and postexposure prophylaxis of the infant.
For prevention of perinatal transmission of HIV, combined antepartum,intrapartum, and infant antiretroviral prophylaxis is recommended.
Combination drug regimens are considered the standard of care fortreatment of HIV infection and for prevention of perinatal HIVtransmission.ESCMID Online Lectu
re Library
© by author
Factors in Antiretroviral Therapy Selection
• Comorbidities
• Patient adherence and convenience of therapy
• Potential for adverse drug effects on the mother and drug interactions
• Results of genotypic resistance testing
• Pharmacokinetic changes in pregnancy
• Potential teratogenic effects on the fetus and other adverse effects on the fetus or newbornESCMID Online Lectu
re Library
© by author
Preferred Treatment Regimens
Preferred regimens have demonstrated optimal efficacy and durability with acceptable toxicity and ease of use. No evidence of teratogenic effects on the fetus or established association with teratogenic or clinically significant adverse outcomes for the mother, fetus, or newborn are present.
• Two–non‐nucleoside reverse transcriptase inhibitor backboneZidovudine with lamivudine (300 mg ZDV/150 mg 3TC) PO BID (combination
with most experience in pregnancy; can cause hematological toxicity) or
Tenofovir with emtricitabine (TDF/FTC) or lamivudine (3TC) once daily (use with caution in renal insufficiency) or
Abacavir with lamivudine (ABC/3TC) once daily (only if HLA‐B5701–negative)
• Non‐nucleoside reverse transcriptase inhibitors ̶ based regimenAfter the first 8 weeks of pregnancy, efavirenz (EFV) alone is used. Although
there are concerns of potential neural tube defects in women of childbearing age before pregnancy is detected, increasing data in pregnancy are reassuring.
ESCMID Online Lecture Library
© by author
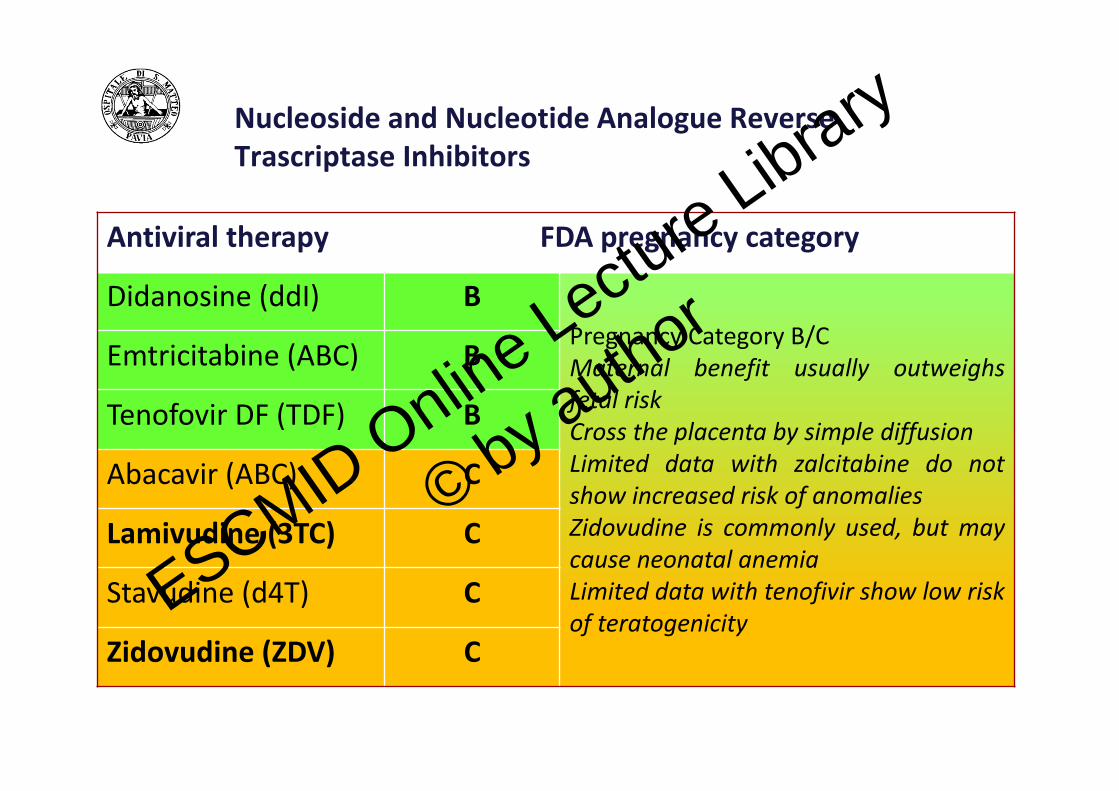
Nucleoside and Nucleotide Analogue Reverse Trascriptase Inhibitors
Antiviral therapy FDA pregnancy category
Didanosine (ddI) BPregnancy Category B/CMaternal benefit usually outweighsfetal riskCross the placenta by simple diffusionLimited data with zalcitabine do notshow increased risk of anomaliesZidovudine is commonly used, but maycause neonatal anemiaLimited data with tenofivir show low riskof teratogenicity
Emtricitabine (ABC) B
Tenofovir DF (TDF) B
Abacavir (ABC) C
Lamivudine (3TC) C
Stavudine (d4T) C
Zidovudine (ZDV) CESCMID Online Lectu
re Library
© by author
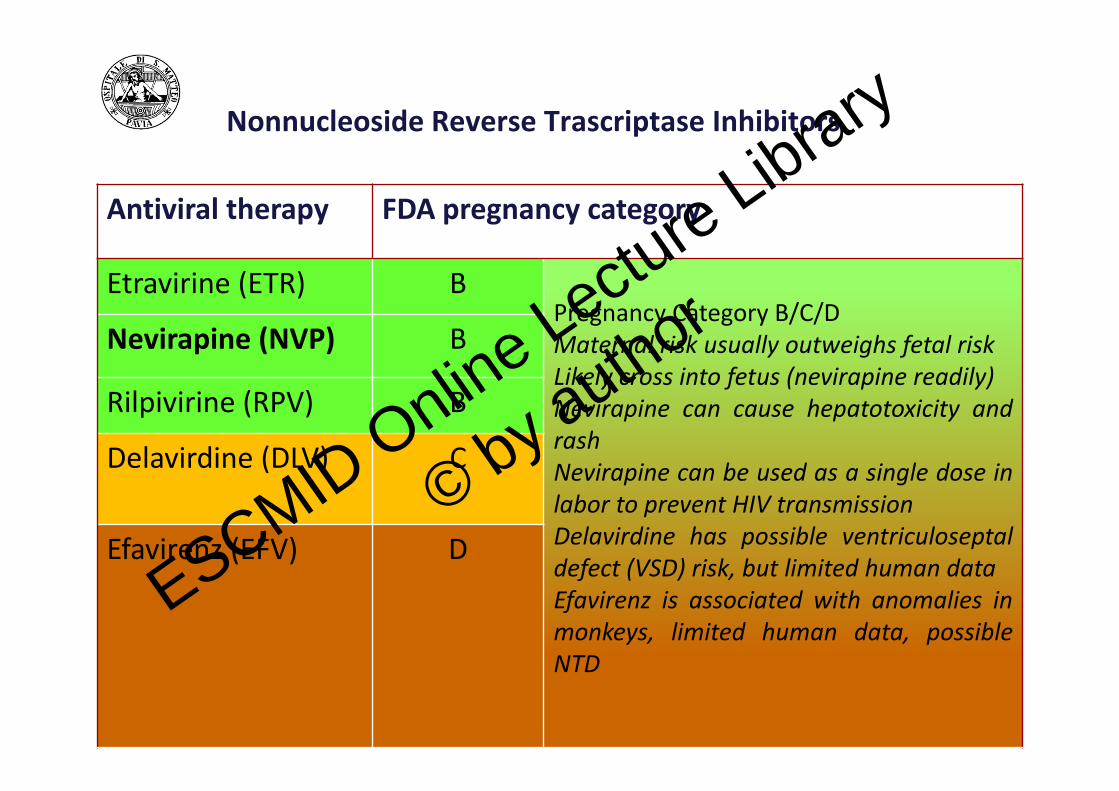
Nonnucleoside Reverse Trascriptase Inhibitors
Antiviral therapy FDA pregnancy category
Etravirine (ETR) BPregnancy Category B/C/DMaternal risk usually outweighs fetal riskLikely cross into fetus (nevirapine readily)Nevirapine can cause hepatotoxicity andrashNevirapine can be used as a single dose inlabor to prevent HIV transmissionDelavirdine has possible ventriculoseptaldefect (VSD) risk, but limited human dataEfavirenz is associated with anomalies inmonkeys, limited human data, possibleNTD
Nevirapine (NVP) B
Rilpivirine (RPV) B
Delavirdine (DLV) C
Efavirenz (EFV) D
ESCMID Online Lecture Library
© by author
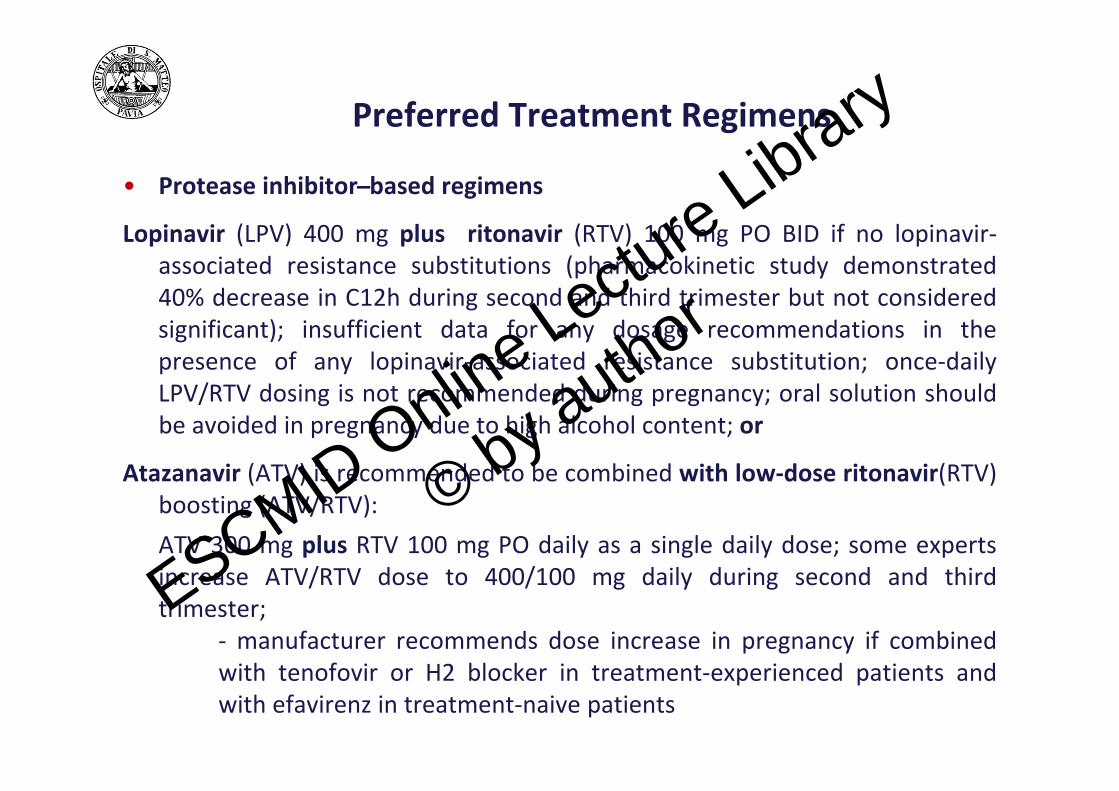
• Protease inhibitor ̶ based regimens
Lopinavir (LPV) 400 mg plus ritonavir (RTV) 100 mg PO BID if no lopinavir‐associated resistance substitutions (pharmacokinetic study demonstrated 40% decrease in C12h during second and third trimester but not considered significant); insufficient data for any dosage recommendations in the presence of any lopinavir‐associated resistance substitution; once‐daily LPV/RTV dosing is not recommended during pregnancy; oral solution should be avoided in pregnancy due to high alcohol content; or
Atazanavir (ATV) is recommended to be combined with low‐dose ritonavir(RTV) boosting (ATV/RTV): ATV 300 mg plus RTV 100 mg PO daily as a single daily dose; some experts increase ATV/RTV dose to 400/100 mg daily during second and third trimester;
‐ manufacturer recommends dose increase in pregnancy if combined with tenofovir or H2 blocker in treatment‐experienced patients and with efavirenz in treatment‐naive patients
Preferred Treatment Regimens
ESCMID Online Lecture Library
© by author
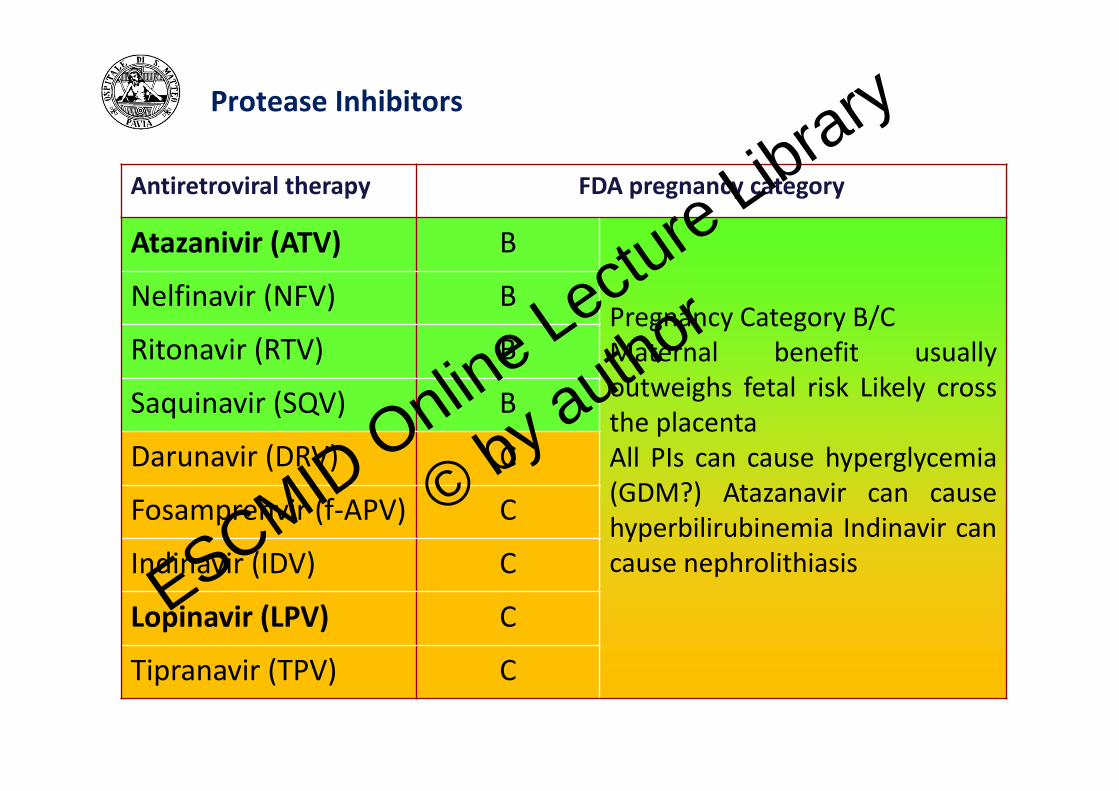
Protease Inhibitors
Antiretroviral therapy FDA pregnancy category
Atazanivir (ATV) B
Pregnancy Category B/CMaternal benefit usuallyoutweighs fetal risk Likely crossthe placentaAll PIs can cause hyperglycemia(GDM?) Atazanavir can causehyperbilirubinemia Indinavir cancause nephrolithiasis
Nelfinavir (NFV) B
Ritonavir (RTV) B
Saquinavir (SQV) B
Darunavir (DRV) C
Fosamprenvir (f‐APV) C
Indinavir (IDV) C
Lopinavir (LPV) C
Tipranavir (TPV) C
ESCMID Online Lecture Library
© by author

Antiretroviral Drugs (others)
Antiretroviral therapy FDA pregnancy category
Fusion Inhibitor
Enfuvirtide (T‐20) B
CCR% antagonist
Maraviroc (MVC) B
Integrase Inhibitor
Raltegravir (RAL) CESCMID Online Lecture Library
© by author
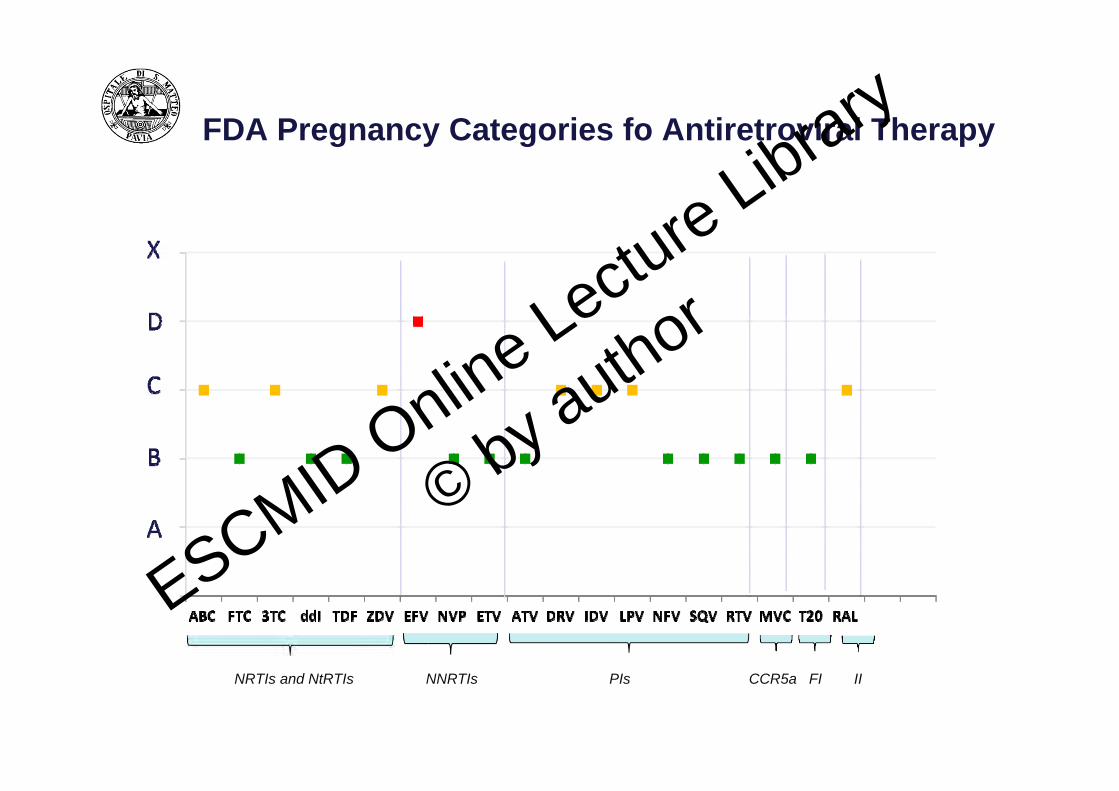
FDA Pregnancy Categories fo Antiretroviral Therapy
NRTIs and NtRTIs NNRTIs PIs FICCR5a II
ESCMID Online Lecture Library
© by author
FDA issues final rule on changes to pregnancy and lactation labeling information for prescription drug and
biological products.
• Until now, FDA of taking a drug or biological product during pregnancyunder a five‐letter system (A, B, C, D and X) based on what was knownabout that product.
• But
– comments received by FDA showed that the letter system wasoften confusing because it was overly simplistic, and did notreflect the available information. This system could lead to falseassumptions about medications based on their category.
ESCMID Online Lecture Library
© by author
FDA issues final rule on changes to pregnancy and lactation labeling information for prescription drug and biological products
‐ Limitations ‐
• The final rule replaces the current product letter categories – A, B, C, D andX – used to classify the risks of using prescription drugs during pregnancywith three detailed subsections that describe risks within the real‐worldcontext of caring for pregnant women who may need medication.
• The biggest default of this system is the misinterpretation by care providers,due to the impression that a letter‐based system gives. The teratogenic riskwas “undetermined” for 97.7 % of the medications approved between 2000and 2010.
• The amount of data available for assessing safety in pregnancy was rated as“none” for 73.3 % of these medications as well. For medications approvedfrom 1980 to 2000, only 5 percent had changed a full risk category or morein the previous 10 years.
• Only 30 medications have clearly demonstrated teratogenic effects
ESCMID Online Lecture Library
© by author

FDA issues final rule on changes to pregnancy and lactation labeling information for prescription drug and biological products
ESCMID Online Lecture Library
© by author

• The Pregnancy subsection will provide information relevant to the useof the drug in pregnant women, such as dosing and potential risks tothe developing fetus, and will require information about whether thereis a registry that collects and maintains data on how pregnant womenare affected when they use the drug or biological product. Informationin drug labeling about the existence of any pregnancy registries hasbeen previously recommended but not required until now.
FDA issues final rule on changes to pregnancy and lactation labeling information for prescription drug and biological products
ESCMID Online Lecture Library
© by author
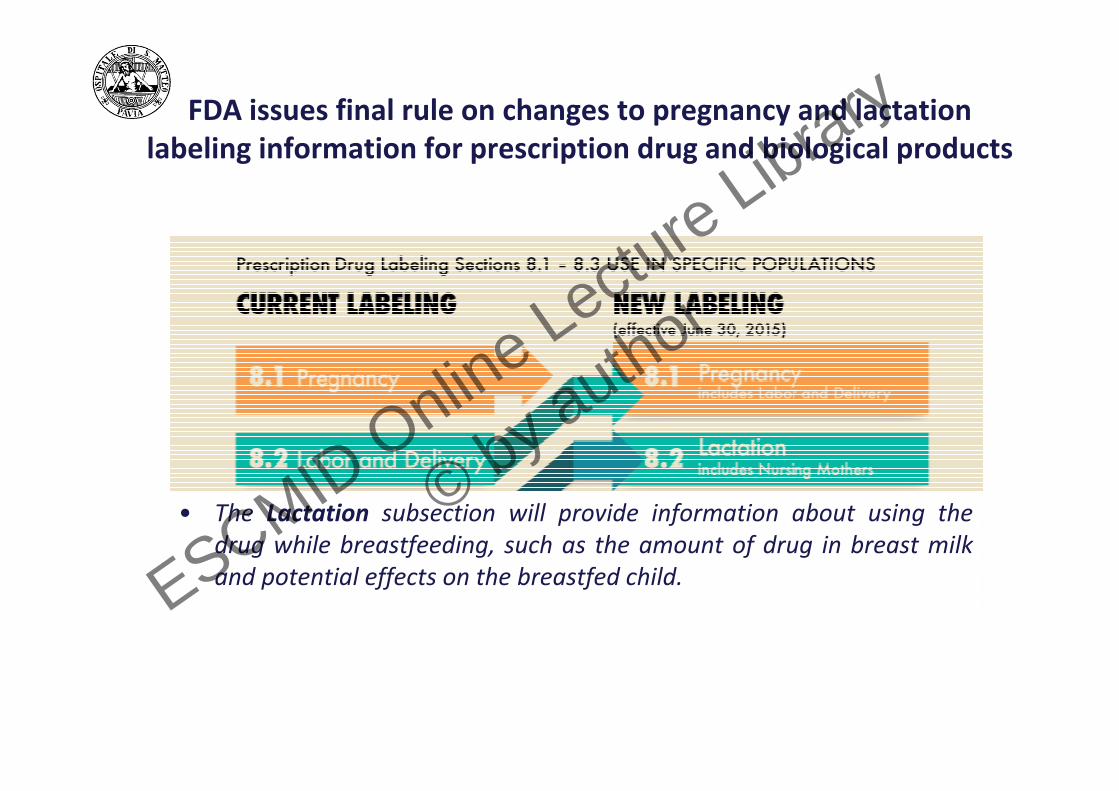
• The Lactation subsection will provide information about using thedrug while breastfeeding, such as the amount of drug in breast milkand potential effects on the breastfed child.
FDA issues final rule on changes to pregnancy and lactation labeling information for prescription drug and biological products
ESCMID Online Lecture Library
© by author

• The Females and Males of Reproductive Potential subsection will includeinformation about pregnancy testing, contraception and about infertility asit relates to the drug. This information has been included in labeling, butthere was no consistent placement for it until now.
FDA issues final rule on changes to pregnancy and lactation labeling information for prescription drug and biological products
ESCMID Online Lecture Library
© by author
Study areas of specific interest 1. Foetal therapy studies
‐ Efficacy and safety information‐ Outcome measures: foetal loss and infant mortality rates, gestationalage at delivery, birth weight, premature rupture of membranes, neonatalcomplications, congenital malformations and developmental delay.
2. Pharmacokinetic studies‐ A number of studies in the literature have addressed thepharmacokinetics (PK) of specific medicines in pregnancy (notablyantibiotics, valaciclovir, theophylline, methadone, antiepileptics,nortriptyline and enoxaparin).‐ PK of agents for which a benefit from therapy is known, late 2nd and 3rdtrimesters and early post‐partum period.
3. Pharmacogenetic studies‐ High maternal concentrations of both the active compound and poorelimination of toxic metabolites may be major determinants ofmalformations.
EMEA/CHMP/313666/2005
ESCMID Online Lecture Library
© by author

Pregnant women may be involved in PK studies if the following conditions are met:
• Preclinical studies, including studies on pregnantanimals, and clinical studies, including studies onnonpregnant women, have been conducted and providedata for assessing potential risk to pregnant women andfetuses; and
• The risk to the fetus is not greater than minimal and thepurpose of the research is the development ofimportant biomedical knowledge which cannot beobtained by any other means
EMEA/CHMP/313666/2005
ESCMID Online Lecture Library
© by author

PK studies be conducted in pregnant women in any of the following situations:
• The drug is known to be prescribed in or used by pregnant women, especially in the second and third trimesters.
• For a new drug or indication, if there is anticipated or actual use of the drug in pregnancy.
• Use is expected to be rare, but the consequences of uninformed dosages are great (e.g., narrow therapeutic range drugs, cancer chemotherapy). Drugs of this type can normally be studied in pregnant patients.
• Pregnancy is likely to alter significantly the PK of a drug (e.g., renally excreted drug) and any of the above apply.
EMEA/CHMP/313666/2005
ESCMID Online Lecture Library
© by author
Study Design
• Longitudinal Design – For drugs that are administered chronically or given for several treatment cyclesduring pregnancy, a longitudinal study design is most clinically meaningful.This allows for intensive PK studies in pregnant women conducted serially so that eachwoman serves as her own control,– avoiding the common criticism that PK/PD studies in pregnant women are flawedbecause of the comparison group employed (Reynolds 1991; Little 1999).Such a study would focus on comparing each pregnant woman enrolled at onetrimester of pregnancy to the same patient at a different trimester as well as duringthe postpartum period
• Population PK Design – A population PK approach with nonlinear mixed effects modeling techniques can beused as an alternate way to enroll pregnant women in PK studies and minimize thenumber of blood draws and PD assessments.The population PK approach can assess the impact on the PK of a drug on variouscovariates, such as maternal characteristics (e.g., age, gravity, parity, race, weeks ortrimester of gestation), concomitant medications, and underlying medical conditions.
EMEA/CHMP/313666/2005
ESCMID Online Lecture Library
© by author
Considerations for Therapy during Pregnancy
• Does the dose need to be altered
ESCMID Online Lecture Library
© by author

AUC Ratio forARV evaluated during Antepartum(3rd trimester, 3Tr) and Postpartum (PP)
Modified from K. Buckoreclall et al., 2012
ESCMID Online Lecture Library
© by author
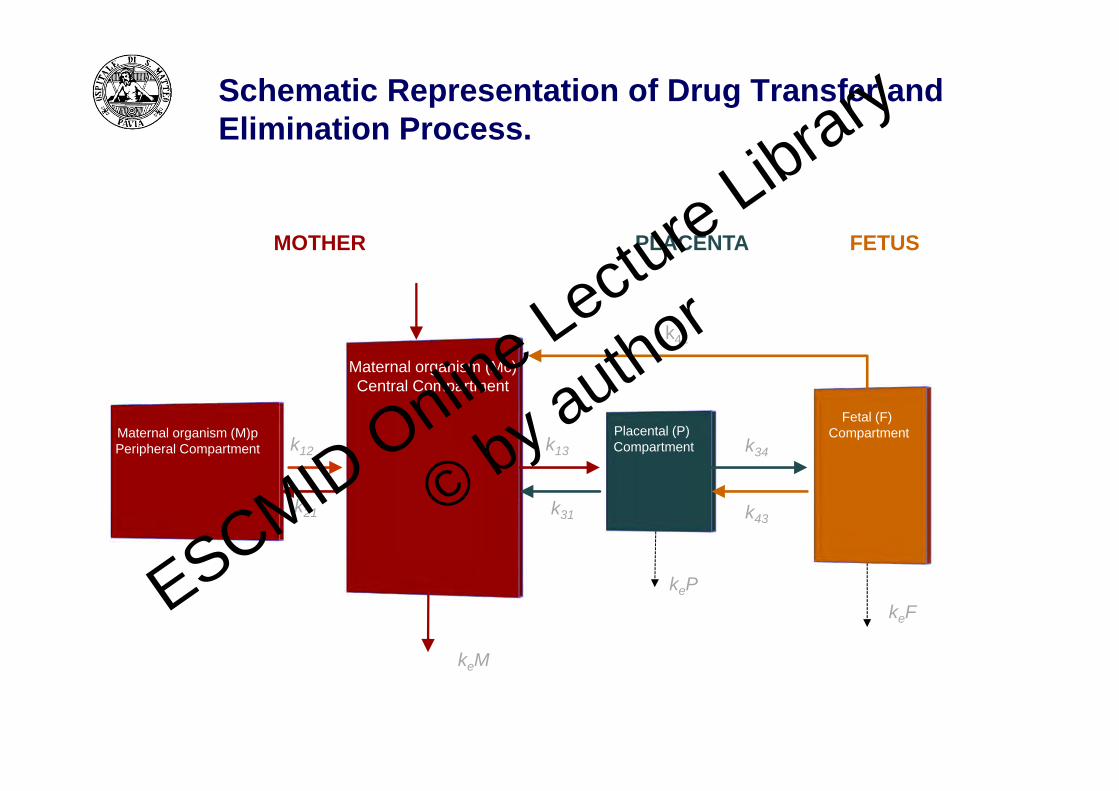
Schematic Representation of Drug Transfer and Elimination Process.
MOTHER PLACENTA FETUS
Maternal organism (Mc)Central Compartment
Maternal organism (M)pPeripheral Compartment
Placental (P)Compartment
Fetal (F)Compartment
k41
k34
k43
k13k12
k31k21
keM
kePkeFESCMID Online Lectu
re Library
© by author

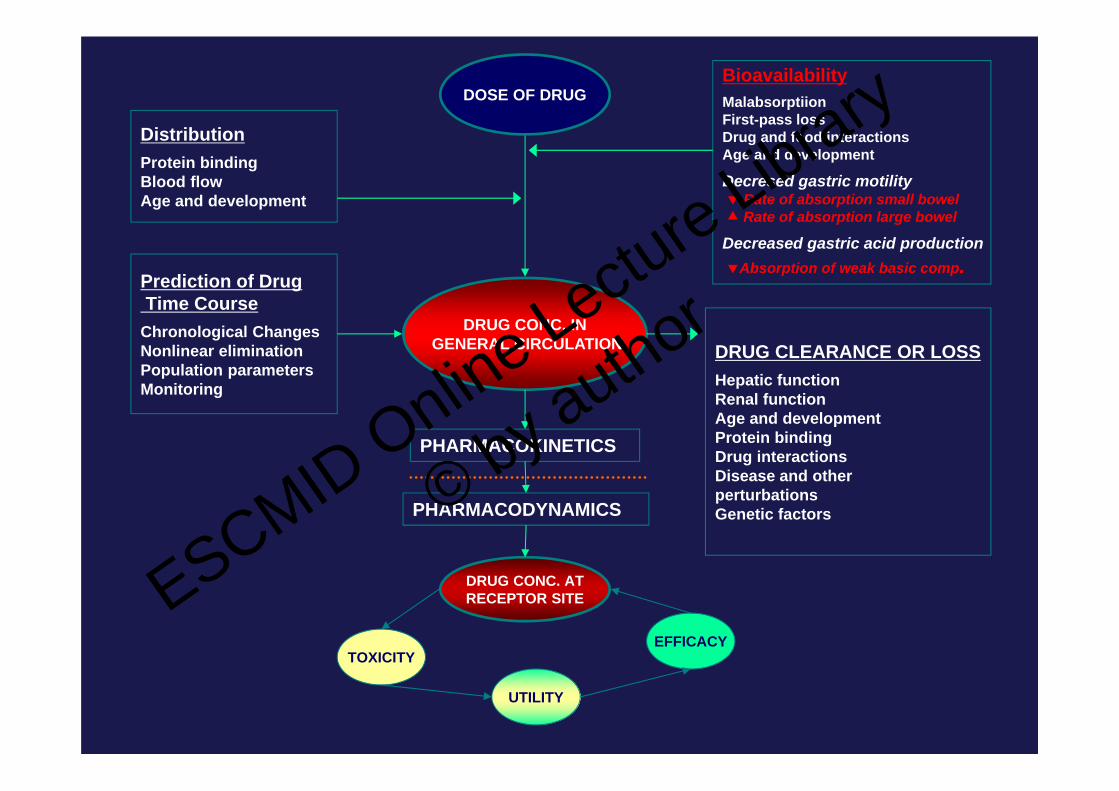
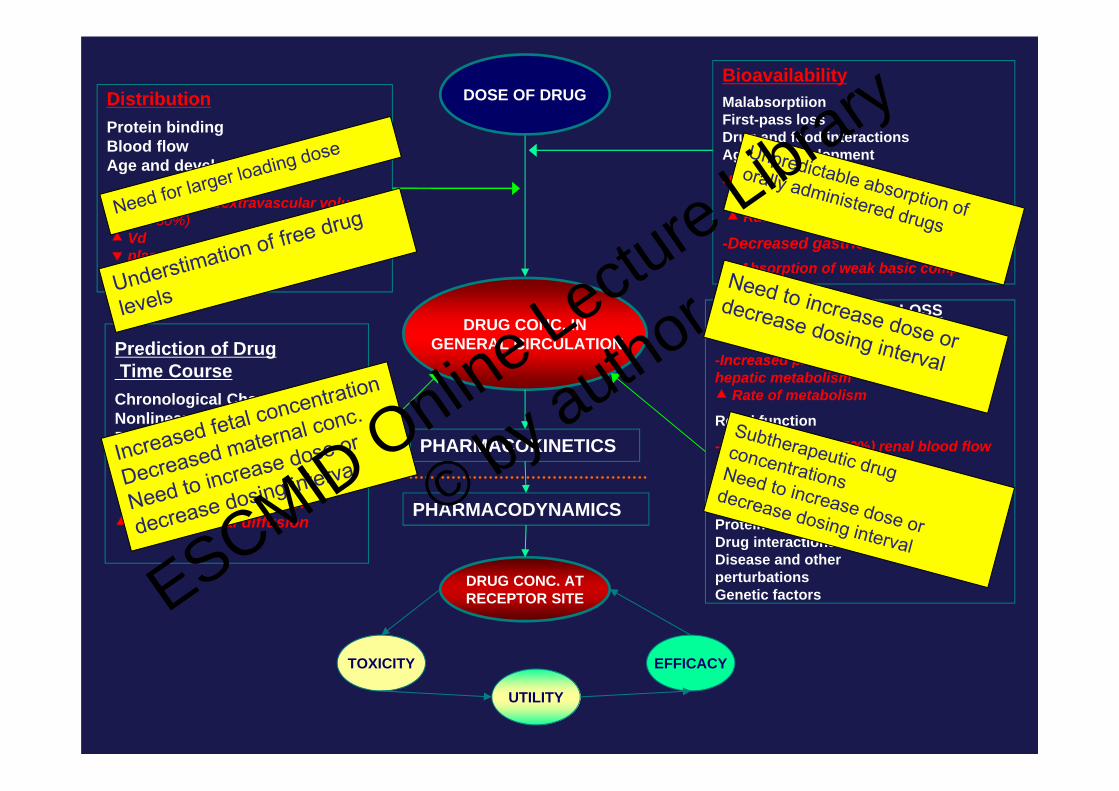
DRUG CONC. INGENERAL CIRCULATION
DOSE OF DRUG
DistributionProtein bindingBlood flowAge and development
Prediction of Drug Time CourseChronological ChangesNonlinear eliminationPopulation parametersMonitoring
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
DRUG CLEARANCE OR LOSSHepatic functionRenal functionAge and developmentProtein bindingDrug interactionsDisease and otherperturbationsGenetic factorsPHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author
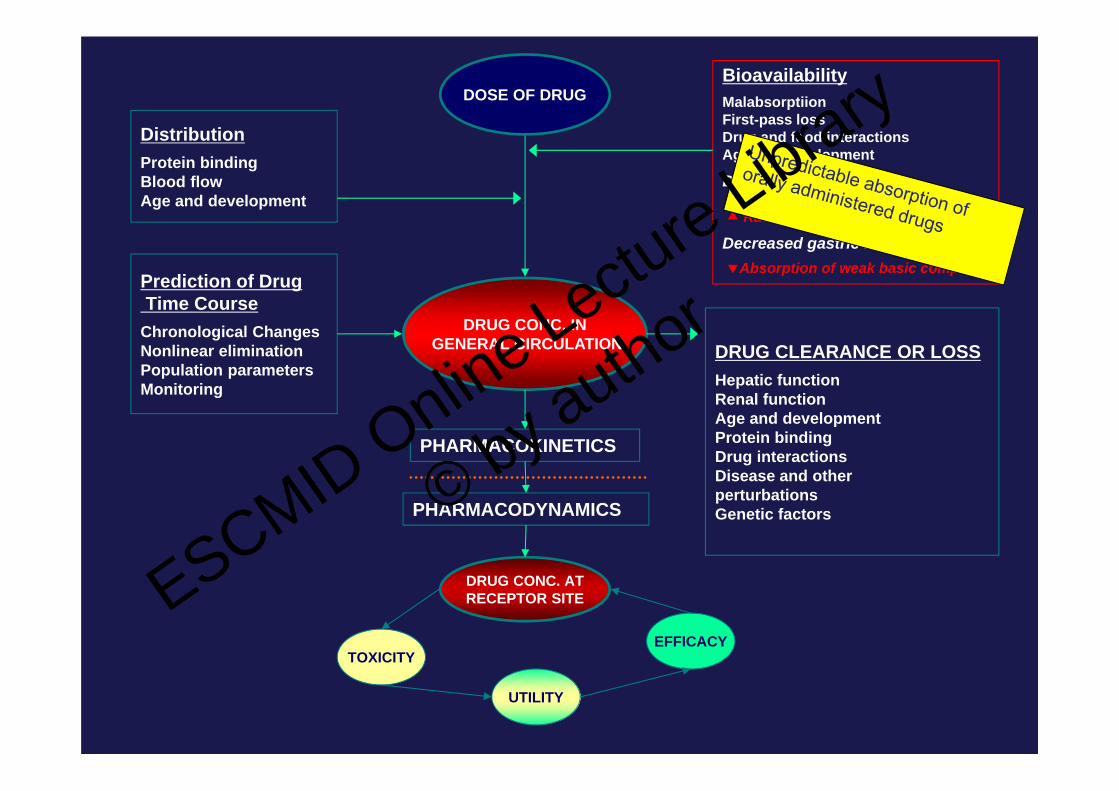
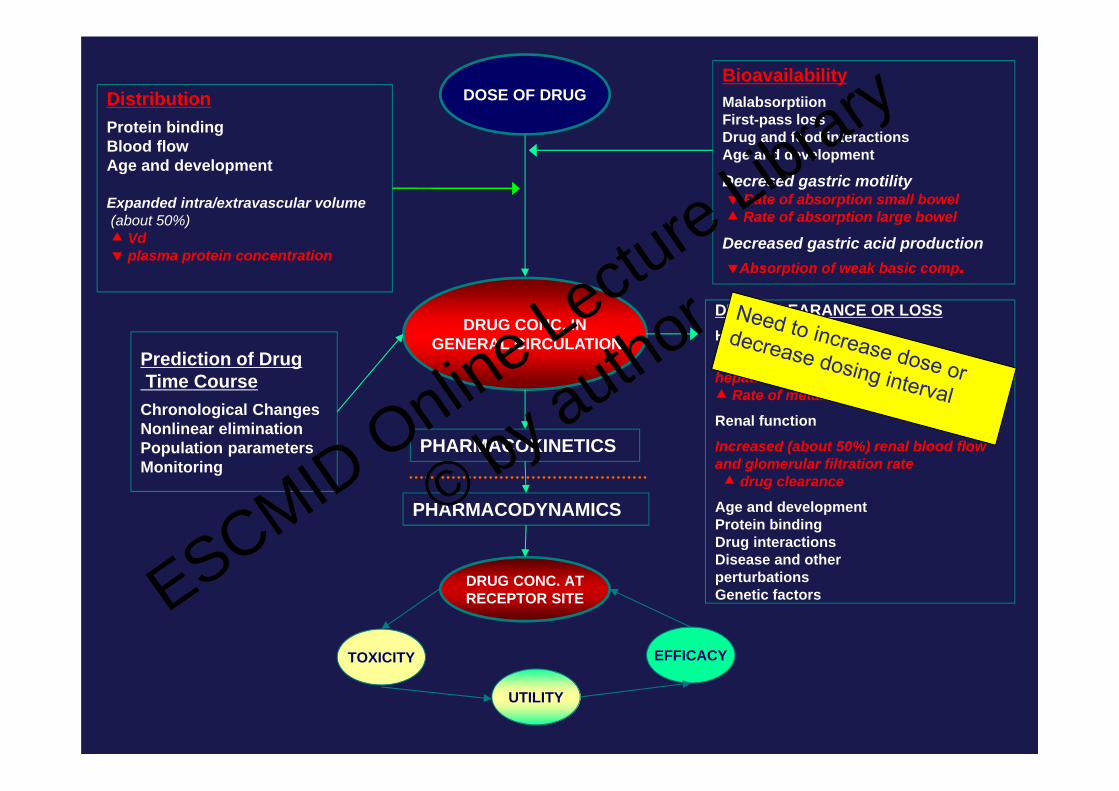
DRUG CONC. INGENERAL CIRCULATION
DOSE OF DRUG
DistributionProtein bindingBlood flowAge and development
Prediction of Drug Time CourseChronological ChangesNonlinear eliminationPopulation parametersMonitoring
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
Decreased gastric acid productionAbsorption of weak basic comp.
DRUG CLEARANCE OR LOSSHepatic functionRenal functionAge and developmentProtein bindingDrug interactionsDisease and otherperturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author
DRUG CONC. INGENERAL CIRCULATION
DOSE OF DRUG
DistributionProtein bindingBlood flowAge and development
Prediction of Drug Time CourseChronological ChangesNonlinear eliminationPopulation parametersMonitoring
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
Decreased gastric acid productionAbsorption of weak basic comp.
DRUG CLEARANCE OR LOSSHepatic functionRenal functionAge and developmentProtein bindingDrug interactionsDisease and otherperturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author
DRUG CONC. INGENERAL CIRCULATION
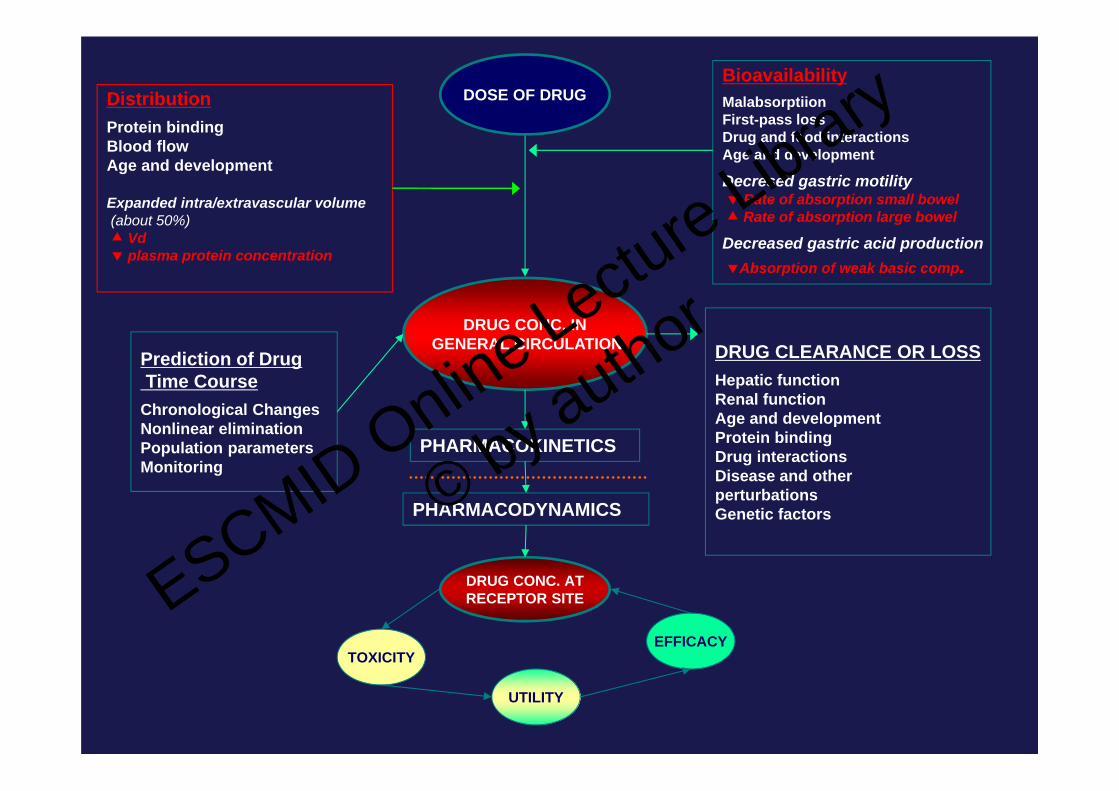
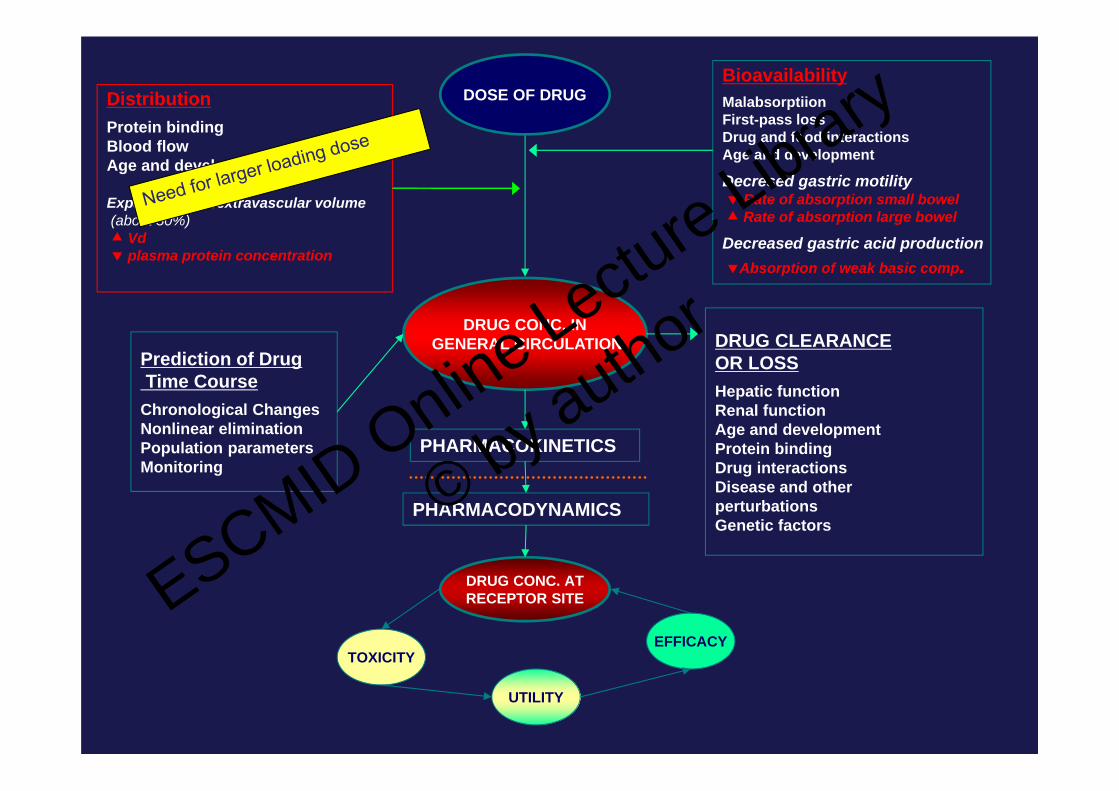
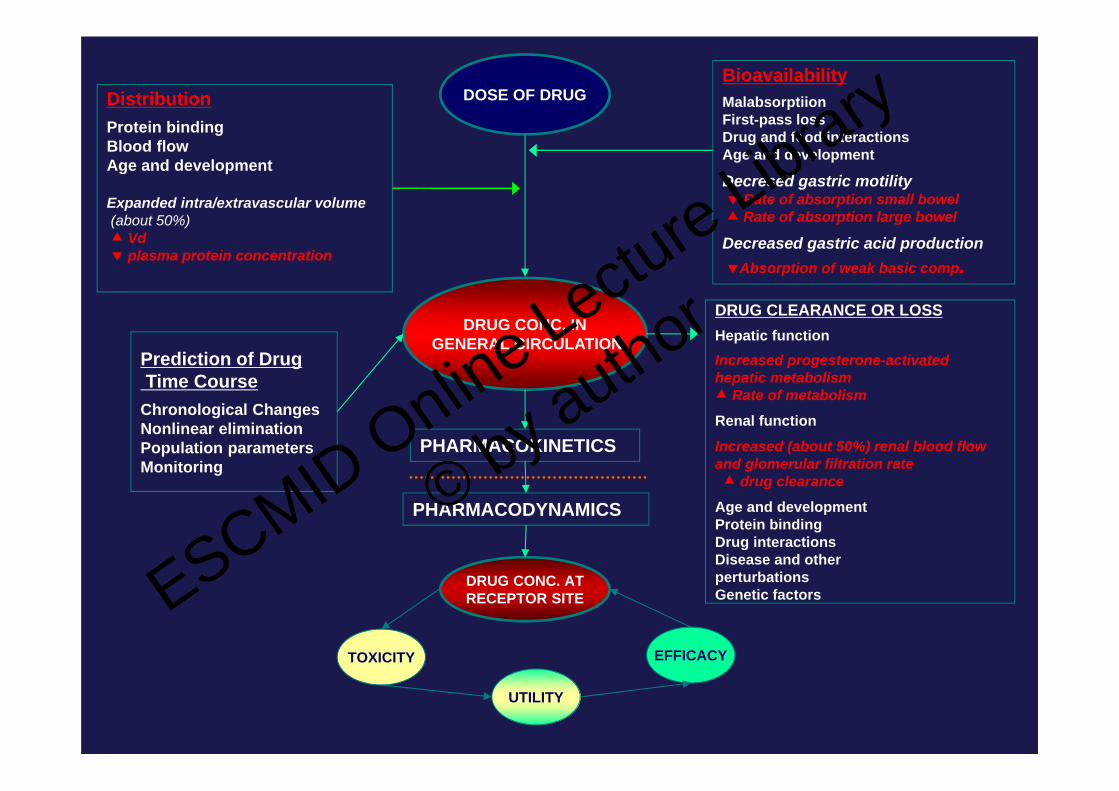
DOSE OF DRUGDistributionProtein bindingBlood flowAge and development
Expanded intra/extravascular volume (about 50%) Vd plasma protein concentration
Prediction of DrugTime Course
Chronological ChangesNonlinear eliminationPopulation parametersMonitoring
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
Decreased gastric acid productionAbsorption of weak basic comp.
DRUG CLEARANCE OR LOSSHepatic functionRenal functionAge and developmentProtein bindingDrug interactionsDisease and otherperturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author

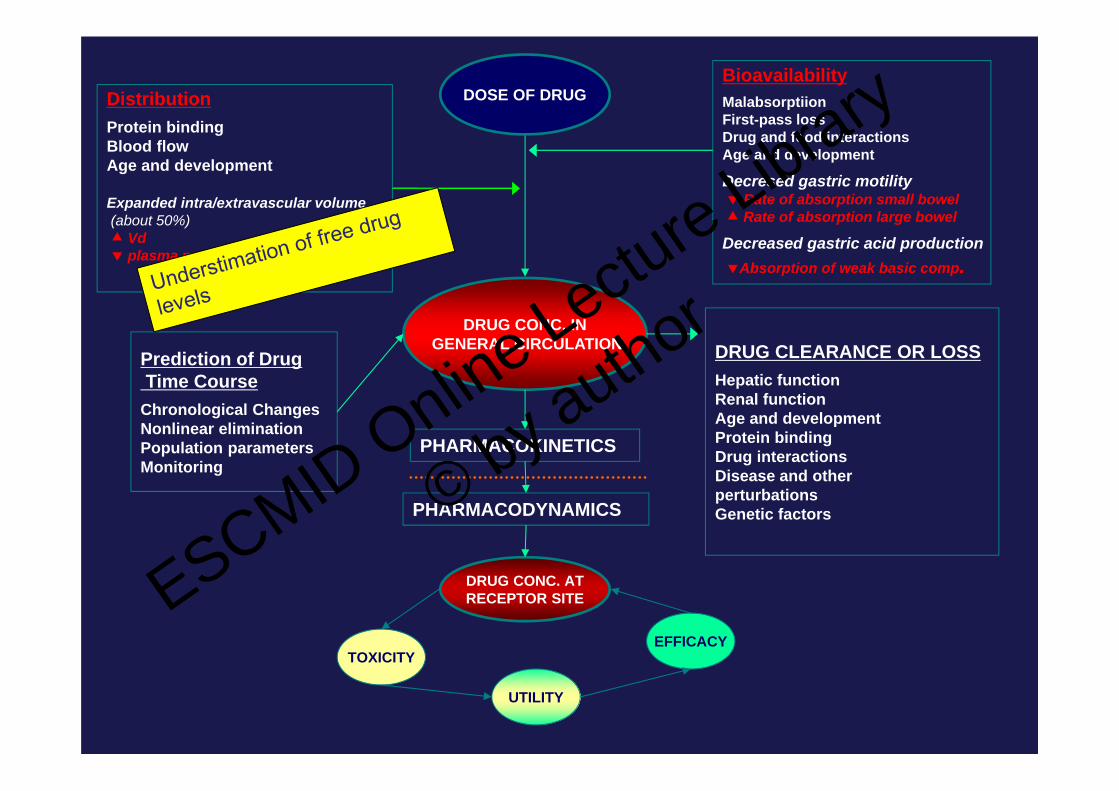
Changes Affecting Drug Distribution
• Body composition– Total body water increased by 8
liters
– Plasma volume increased by50%
– Increased body fat stores
• Protein Binding– Decreased albumin (dilution)
– Increased competitors in blood• Free fatty acids & steroids
• Increased volume of distribution (Vd)
• Decreased peak plasma concentrations (Cmax)
• Increased free or unbound drug ( Cu)
• Increased effect ( eff) ESCMID Online Lectu
re Library
© by author

Mean plasma concentration–time curves for total Darunavir (left),unbound darunavir (right) after administration of darunavir/ritonavir600/100 mg twice daily (bid), during the second and third trimestersand postpartum.
Total Darunavir Unbound Darunavir
Zorilla et al 2013
ESCMID Online Lecture Library
© by author
DRUG CONC. INGENERAL CIRCULATION
DOSE OF DRUG
Prediction of DrugTime Course
Chronological ChangesNonlinear eliminationPopulation parametersMonitoring
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
Decreased gastric acid production Absorption of weak basic comp.
DRUG CLEARANCEOR LOSSHepatic functionRenal functionAge and developmentProtein bindingDrug interactionsDisease and otherperturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
DistributionProtein bindingBlood flowAge and development
Expanded intra/extravascular volume (about 50%) Vd plasma protein concentration
ESCMID Online Lecture Library
© by author
DRUG CONC. INGENERAL CIRCULATION
DOSE OF DRUGDistributionProtein bindingBlood flowAge and development
Expanded intra/extravascular volume (about 50%) Vd plasma protein concentration
Prediction of DrugTime Course
Chronological ChangesNonlinear eliminationPopulation parametersMonitoring
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
Decreased gastric acid productionAbsorption of weak basic comp.
DRUG CLEARANCE OR LOSSHepatic functionRenal functionAge and developmentProtein bindingDrug interactionsDisease and otherperturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author
DRUG CONC. INGENERAL CIRCULATION
DOSE OF DRUGDistributionProtein bindingBlood flowAge and development
Expanded intra/extravascular volume(about 50%) Vd plasma protein concentration
Prediction of DrugTime Course
Chronological ChangesNonlinear eliminationPopulation parametersMonitoring
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
Decreased gastric acid productionAbsorption of weak basic comp.
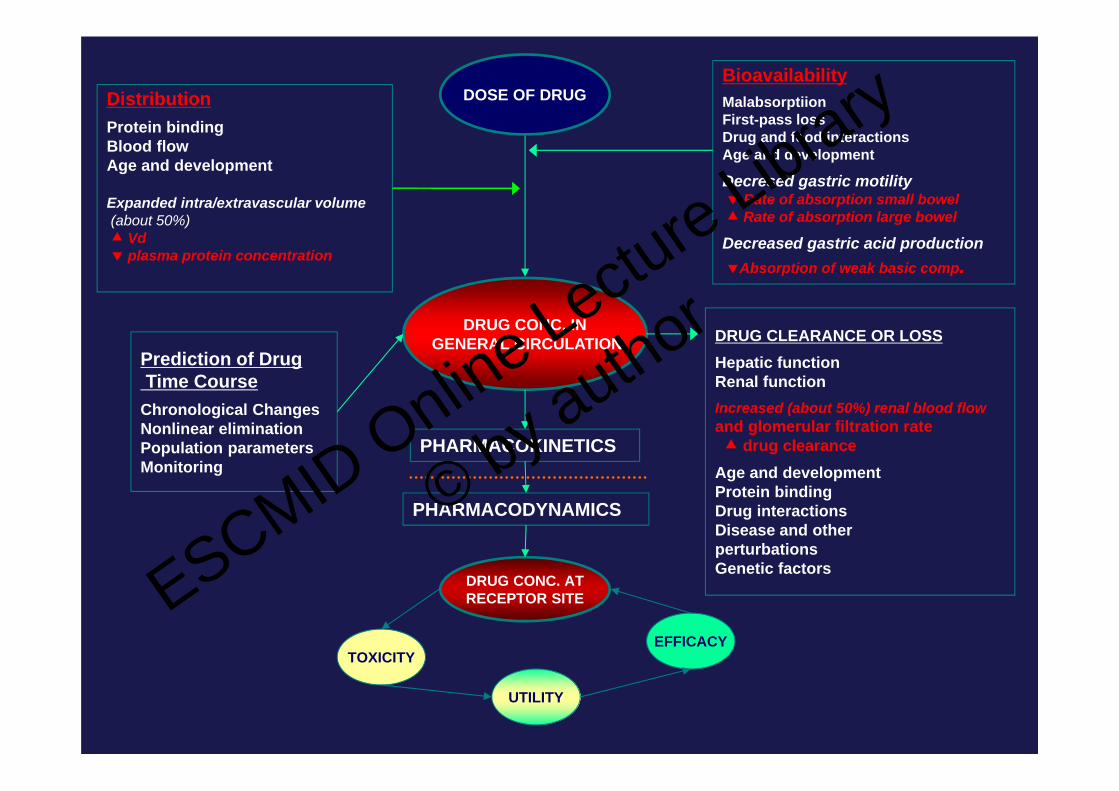
DRUG CLEARANCE OR LOSSHepatic functionRenal functionIncreased (about 50%) renal blood flowand glomerular filtration rate drug clearanceAge and developmentProtein bindingDrug interactionsDisease and other perturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author
Physiologic Changes in Pregnancy that AffectDrug Elimination
• Increased Cardiac Output– Renal plasma flow increase 25‐50%– GFR increases up to 50%
• Increased elimination of renally cleared drugs• Lower trough concentrations
• Cholestasis may reflect changes in transport activity• Changes in drug metabolizing enzyme activity‐dependent on isoform
ESCMID Online Lecture Library
© by author
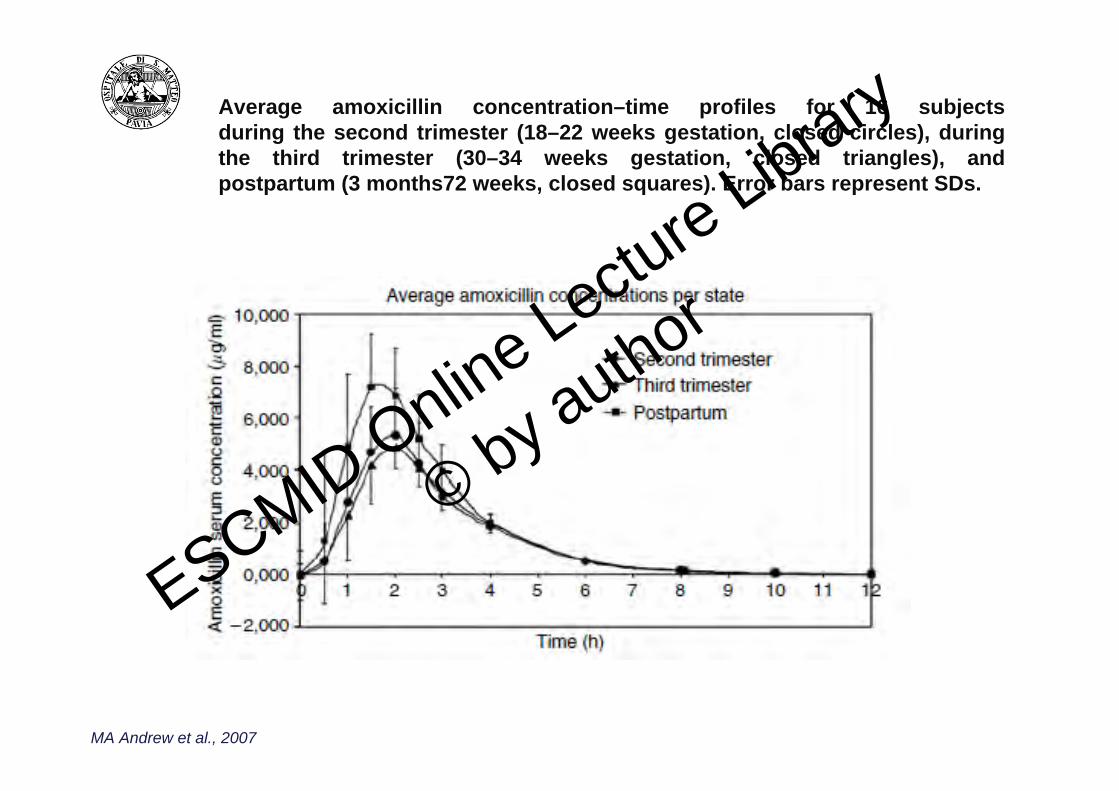
Average amoxicillin concentration–time profiles for 16 subjectsduring the second trimester (18–22 weeks gestation, closed circles), duringthe third trimester (30–34 weeks gestation, closed triangles), andpostpartum (3 months72 weeks, closed squares). Error bars represent SDs.
MA Andrew et al., 2007
ESCMID Online Lecture Library
© by author
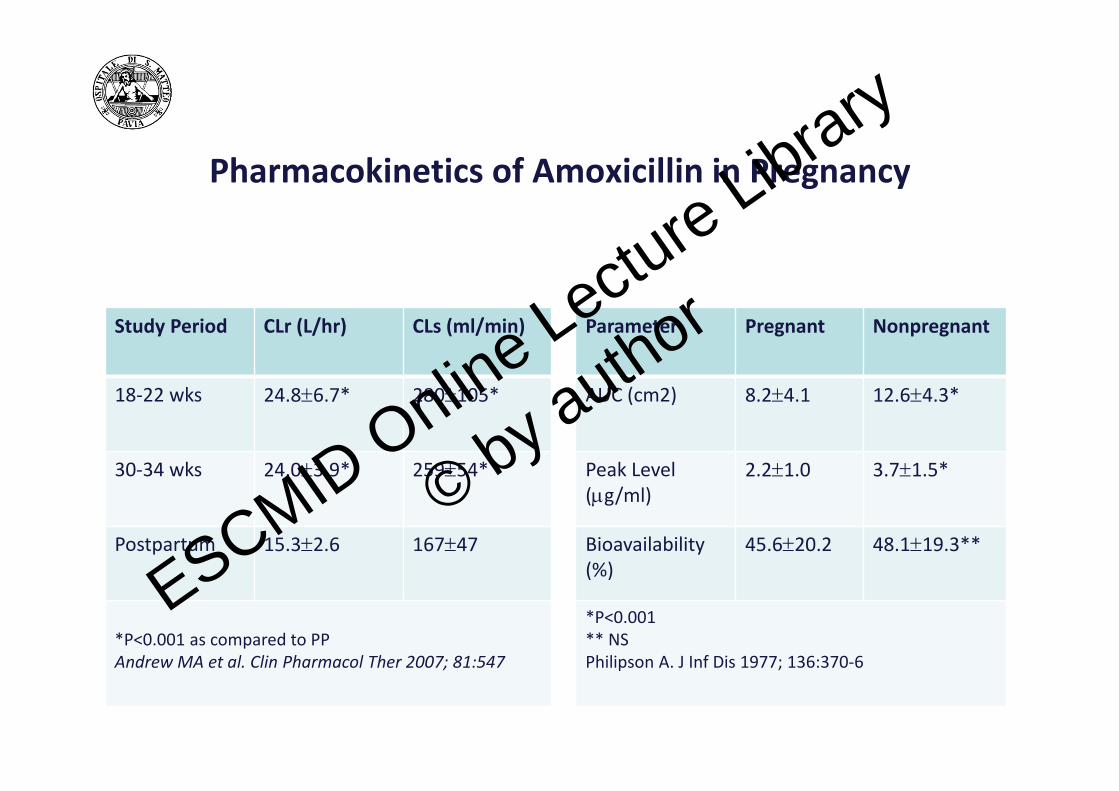
Pharmacokinetics of Amoxicillin in Pregnancy
Parameter Pregnant Nonpregnant
AUC (cm2) 8.24.1 12.64.3*
Peak Level(g/ml)
2.21.0 3.71.5*
Bioavailability(%)
45.620.2 48.119.3**
*P<0.001** NSPhilipson A. J Inf Dis 1977; 136:370‐6
Study Period CLr (L/hr) CLs (ml/min)
18‐22 wks 24.86.7* 280105*
30‐34 wks 24.03.9* 25954*
Postpartum 15.32.6 16747
*P<0.001 as compared to PPAndrew MA et al. Clin Pharmacol Ther 2007; 81:547
ESCMID Online Lecture Library
© by author

DRUG CONC. INGENERAL CIRCULATION
DOSE OF DRUGDistributionProtein bindingBlood flowAge and development
Expanded intra/extravascular volume (about 50%) Vd plasma protein concentration
Prediction of DrugTime Course
Chronological ChangesNonlinear eliminationPopulation parametersMonitoring
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
Decreased gastric acid productionAbsorption of weak basic comp.
DRUG CLEARANCE OR LOSSHepatic functionRenal functionIncreased (about 50%) renal blood flowand glomerular filtration rate drug clearance
Age and developmentProtein bindingDrug interactionsDisease and otherperturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author
DRUG CONC. INGENERAL CIRCULATION
DOSE OF DRUGDistributionProtein bindingBlood flowAge and development
Expanded intra/extravascular volume(about 50%) Vd plasma protein concentration
Prediction of DrugTime Course
Chronological ChangesNonlinear eliminationPopulation parametersMonitoring
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
Decreased gastric acid productionAbsorption of weak basic comp.
DRUG CLEARANCE OR LOSSHepatic functionIncreased progesterone-activated hepatic metabolism Rate of metabolism
Renal function
Increased (about 50%) renal blood flowand glomerular filtration rate drug clearance
Age and developmentProtein bindingDrug interactionsDisease and other perturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author

Physiologic Changes in Pregnancy that AffectDrug Elimination
• Increased Cardiac Output– Renal plasma flow increase 25‐50%– GFR increases up to 50%
• Increased elimination of renally cleared drugs• Lower trough concentrations
• Cholestasis may reflect changes in transport activity• Changes in drug metabolizing enzyme activity‐dependent on isoform
ESCMID Online Lecture Library
© by author
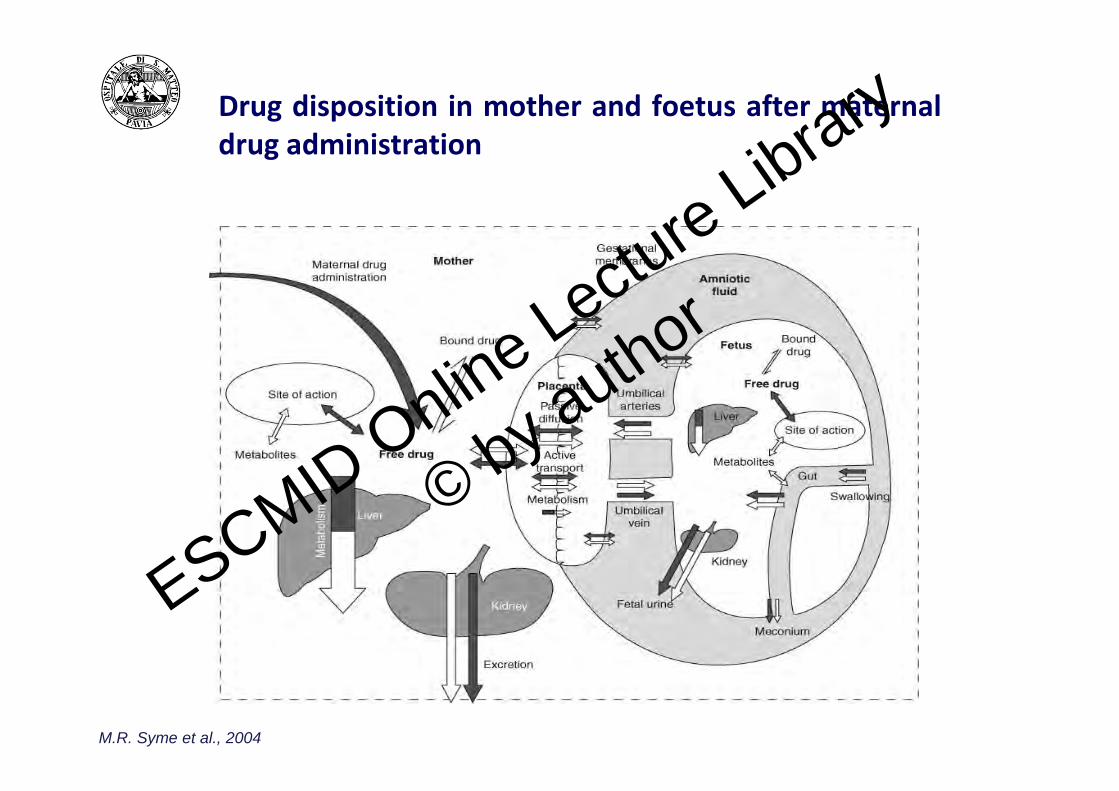
Drug disposition in mother and foetus after maternaldrug administration
M.R. Syme et al., 2004
ESCMID Online Lecture Library
© by author
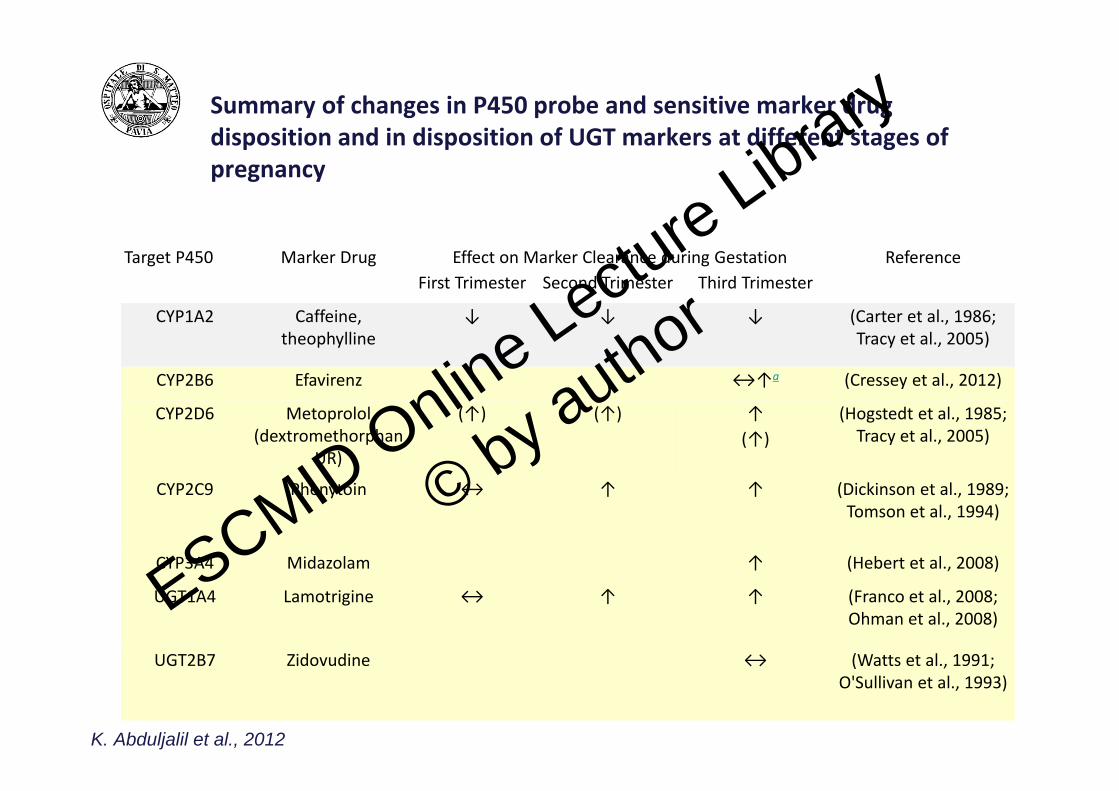
Summary of changes in P450 probe and sensitive marker drug disposition and in disposition of UGT markers at different stages of pregnancy
Target P450 Marker Drug Effect on Marker Clearance during Gestation ReferenceFirst Trimester Second Trimester Third Trimester
CYP1A2 Caffeine, theophylline
↓ ↓ ↓ (Carter et al., 1986; Tracy et al., 2005)
CYP2B6 Efavirenz ↔↑a (Cressey et al., 2012)
CYP2D6 Metoprolol (dextromethorphan
UR)
(↑) (↑) ↑ (Hogstedt et al., 1985; Tracy et al., 2005) (↑)
CYP2C9 Phenytoin ↔ ↑ ↑ (Dickinson et al., 1989; Tomson et al., 1994)
CYP3A4 Midazolam ↑ (Hebert et al., 2008)
UGT1A4 Lamotrigine ↔ ↑ ↑ (Franco et al., 2008; Ohman et al., 2008)
UGT2B7 Zidovudine ↔ (Watts et al., 1991; O'Sullivan et al., 1993)
K. Abduljalil et al., 2012
ESCMID Online Lecture Library
© by author
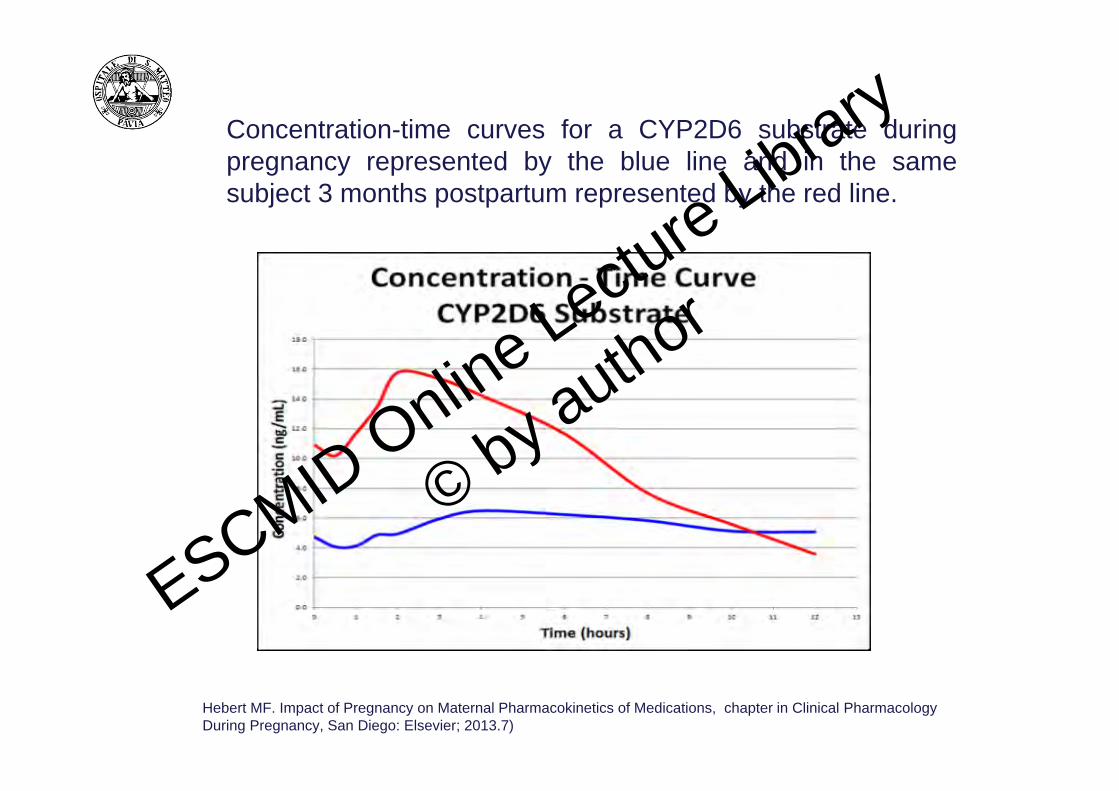
Concentration-time curves for a CYP2D6 substrate duringpregnancy represented by the blue line and in the samesubject 3 months postpartum represented by the red line.
Hebert MF. Impact of Pregnancy on Maternal Pharmacokinetics of Medications, chapter in Clinical Pharmacology During Pregnancy, San Diego: Elsevier; 2013.7)
ESCMID Online Lecture Library
© by author

Mean midazolam plasma concentration-time curves duringpregnancy and postpartum. Error bars represent SD.
ESCMID Online Lecture Library
© by author
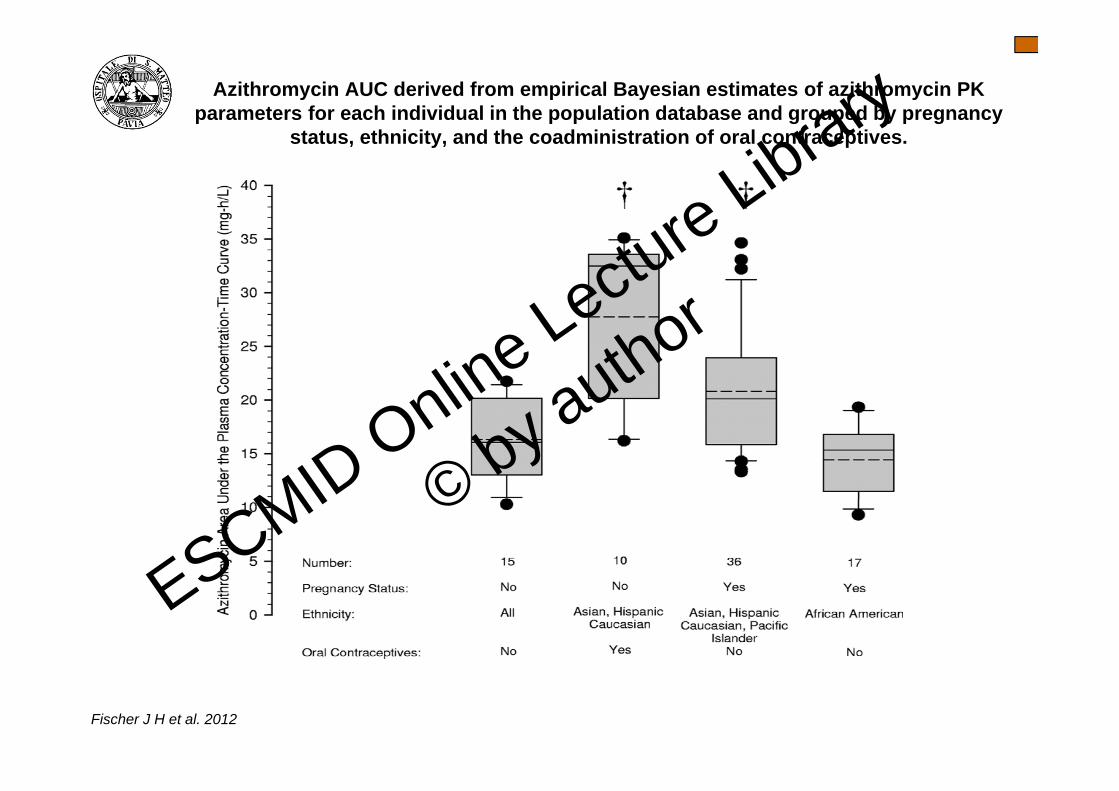
Azithromycin AUC derived from empirical Bayesian estimates of azithromycin PK parameters for each individual in the population database and grouped by pregnancy
status, ethnicity, and the coadministration of oral contraceptives.
Fischer J H et al. 2012
ESCMID Online Lecture Library
© by author
DRUG CONC. INGENERAL CIRCULATION
DOSE OF DRUGDistributionProtein bindingBlood flowAge and development
Expanded intra/extravascular volume(about 50%) Vd plasma protein concentration
Prediction of DrugTime Course
Chronological ChangesNonlinear eliminationPopulation parametersMonitoring
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
Decreased gastric acid productionAbsorption of weak basic comp.
DRUG CLEARANCE OR LOSSHepatic functionIncreased progesterone-activatedhepatic metabolism Rate of metabolism
Renal function
Increased (about 50%) renal blood flowand glomerular filtration rate drug clearance
Age and developmentProtein bindingDrug interactionsDisease and otherperturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author

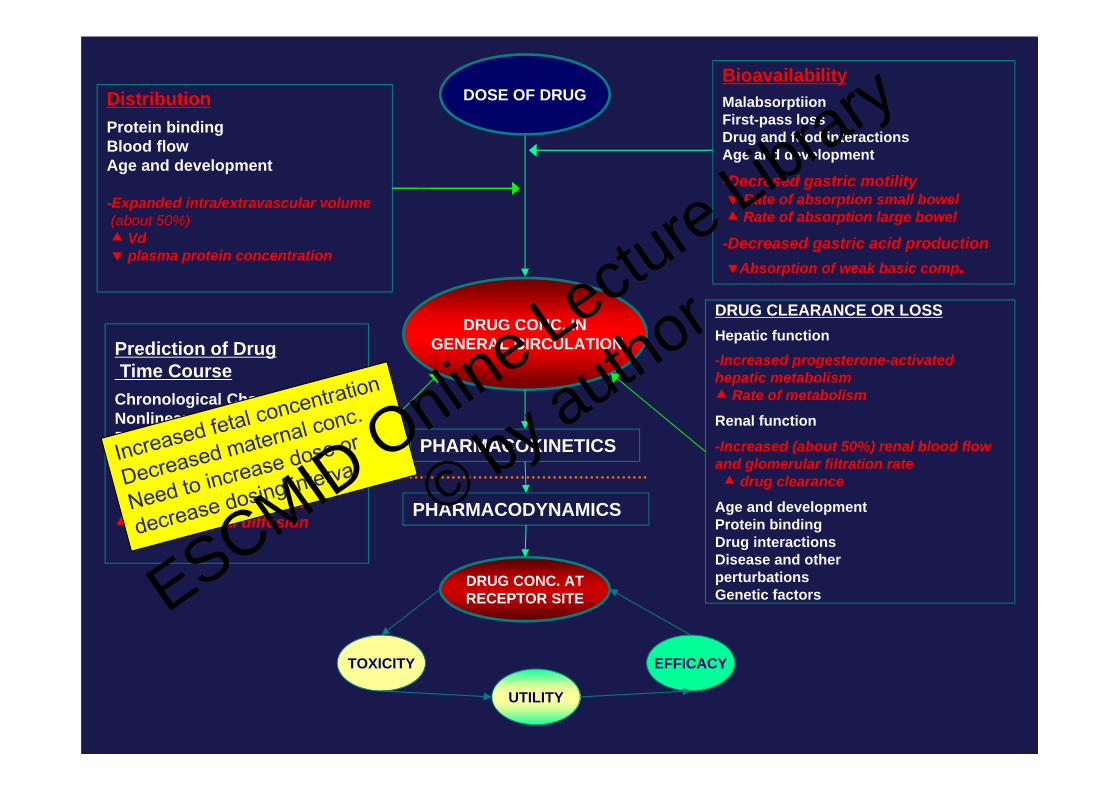
DRUG CONC. INGENERAL CIRCULATION
DOSE OF DRUGDistributionProtein bindingBlood flowAge and development
-Expanded intra/extravascular volume(about 50%) Vd plasma protein concentration
Prediction of DrugTime Course
Chronological ChangesNonlinear eliminationPopulation parametersMonitoring-Thinning of fetomaternal barrierwith advancing gestationtransplacental diffusion
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
-Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
-Decreased gastric acid production Absorption of weak basic comp.
DRUG CLEARANCE OR LOSSHepatic function-Increased progesterone-activatedhepatic metabolism Rate of metabolism
Renal function
-Increased (about 50%) renal blood flowand glomerular filtration rate drug clearance
Age and developmentProtein bindingDrug interactionsDisease and otherperturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author
DRUG CONC. IN GENERAL CIRCULATION
DOSE OF DRUGDistributionProtein bindingBlood flowAge and development
-Expanded intra/extravascular volume(about 50%) Vd plasma protein concentration
Prediction of DrugTime Course
Chronological ChangesNonlinear eliminationPopulation parametersMonitoring-Thinning of fetomaternal barrierwith advancing gestationtransplacental diffusion
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
-Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
-Decreased gastric acid productionAbsorption of weak basic comp.
DRUG CLEARANCE OR LOSSHepatic function-Increased progesterone-activated hepatic metabolism Rate of metabolism
Renal function
-Increased (about 50%) renal blood flowand glomerular filtration rate drug clearance
Age and developmentProtein bindingDrug interactionsDisease and other perturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author
DRUG CONC. IN GENERAL CIRCULATION
DOSE OF DRUGDistributionProtein bindingBlood flowAge and development
-Expanded intra/extravascular volume(about 50%) Vd plasma protein concentration
Prediction of Drug Time CourseChronological ChangesNonlinear eliminationPopulation parametersMonitoring-Thinning of fetomaternal barrier with advancing gestation transplacental diffusion
BioavailabilityMalabsorptiionFirst-pass lossDrug and food interactionsAge and development
-Decresed gastric motility Rate of absorption small bowel Rate of absorption large bowel
-Decreased gastric acid productionAbsorption of weak basic comp.
DRUG CLEARANCE OR LOSSHepatic function-Increased progesterone-activatedhepatic metabolism Rate of metabolism
Renal function
-Increased (about 50%) renal blood flowand glomerular filtration rate drug clearance
Age and developmentProtein bindingDrug interactionsDisease and otherperturbationsGenetic factors
PHARMACOKINETICS
PHARMACODYNAMICS
DRUG CONC. ATRECEPTOR SITE
TOXICITY
UTILITY
EFFICACY
ESCMID Online Lecture Library
© by author

Estimation of PK parameters
• The Agency recommends that total and unbound plasma concentration data (and urinary excretion data if collected) be used to estimate PK parameters of the parent drug and metabolite(s).
• Standard PK parameters of a drug include the area under the plasma concentration curve (AUC), peak concentration (Cmax), plasma clearance (CLT) or apparent oral clearance (CL/F), renal clearance (CLR), apparent volume of distribution (VZ/F or Vss/F), and terminal half‐life (t1/2).
• It is recommended that PK parameters be expressed in terms of total and unbound concentrations and when applicable (e.g., oral and renal clearance, expressed in terms of body weight, L/hr/kg).
• For drugs and metabolites with a relatively low extent of plasma protein binding (e.g., extent of binding less than 80 percent), description and analysis of the PK in terms of total concentrations can be sufficient.
• Noncompartmental and/or compartmental modeling approaches to parameter estimation can be employed.
ESCMID Online Lecture Library
© by author

For drugs whose PK is influenced by pregnancy, the statement similarto the following can be modified as appropriate and in accordance withwhat is known about the drug (e.g., active or toxic metabolite) andfrom the studies performed in accordance with this guidance:
• The disposition of [Drug X] was studied in [number of] pregnant patients [in ytrimester or from a through b weeks gestation]. Elimination of the drug (andmetabolite, if applicable) is significantly changed during pregnancy. Total bodyclearance of (unbound, if applicable)
• [Drug X]/metabolite was reduced/increased in pregnant patients compared to[healthy postpartum women, the same women prior to pregnancy or c weekspostpartum].
• The terminal half‐life of [Drug X]/metabolite is [prolonged/decreased] by Y‐, and Z‐fold in second and third trimesters, respectively.
• Protein binding of [Drug X]/metabolite [is/is not] affected by pregnancy. The[drug/metabolite accumulates/does not accumulate] in pregnant patients on chronicadministration resulting in increased/decreased plasma levels of drug/metabolite.The pharmacologic response [is/is not] affected by pregnancy. The dosage/dosinginterval should be [decreased/increased] in pregnant patients receiving
ESCMID Online Lecture Library
© by author
Dosage and Administration
As appropriate, the following information could be included:
• A statement describing the relationship between the drug’s clearance andpregnancy
• A statement describing how the dose would be adjusted during pregnancy, forexample:
The dose of [Drug X] should be [increased/decreased by _____%] during pregnancy.
• A statement describing how the dose would be adjusted in the postpartumtime period in nonlactating women, specifying the time period studied (e.g., 2weeks postpartum)
• If no dose adjustment is necessary the following statement is suggested: Theinfluence of pregnancy on [Drug X] pharmacokinetics is sufficiently small thatno dosing adjustment is needed.ESCMID Online Lectu
re Library
© by author
Conclusions
• Many factors alter drug disposition in pregnant patients and may require alteration in dosing
• Detailed knowledge of drug characteristics can help predict these differences
• Maintaining consistent and optimal antiinfetcive exposure is critical for long‐term treatment success
• PK, PD changes across pregnancy are likely to may make typical adult doses toxic or inadequate
• Understanding PK of maternal‐infant drug transfer can lead to effective therapies for antiinfective therapy
ESCMID Online Lecture Library
© by author
References
•KM Jose, FDA Pregnancy Categories for Antiretroviral Therapy. Medscape, Updated: Mar 26, 2014•Recommendations for Use of Antiretroviral Drugs in Pregnant HIV‐1‐Infected Women for Maternal Health and Interventions to Reduce Perinatal HIV Transmission in the United States. Available at http://aidsinfo.nih.gov/contentfiles/lvguidelines/PerinatalGL.pdf•British HIV Association guidelines for the management of HIV infection in pregnant women 2012 (2014 interim review). HIV Medicine , 15 (Suppl. 4), 1–77, 2014•Requirements for Pregnancy and Lactation Labeling. FDA http://federalregister.gov/a/2014‐28241, and on FDsys.gov•“Pregnancy and Lactation Labeling Rule (https://s3.amazonaws.com/publicinspection. federalregister.gov/2014 ‐ 28241. pdf)” (PLLR or final rule).•Guidance for Industry Pharmacokinetics in Pregnancy — Study Design, Data Analysis, and Impact on Dosing and Labeling. U.S. Department of Health and Human Services, Food and Drug Administration, Center for Drug Evaluation and Research (CDER), . Clinical Pharmacology, October 2004•E Henderson et al., Prescribing in pregnancy and during breast feeding: using principles in clinical practice. Postgrad Med J; 87:349‐354, 2011•A Broe et al., Increasing use of antibiotics in pregnancy during the period 2000–2010: prevalence, timing, category, and demographics. Royal College of Obstetricians and Gynaecologists 2014
ESCMID Online Lecture Library
© by author

THE END
ESCMID Online Lecture Library
© by author

Germany: categorisation system for prescribingmedicines in pregnancy
Group Description
Group 1 Extensive human tests and animal studies have not shown the drug to be embryotoxic/teratogenic.
Group 2 Extensive human tests of the drug have not shown the drug to be embryotoxic/teratogenic.
Group 3Extensive human tests of the drug have not shown the drug to be embryotoxic/teratogenic. However, the drug appears to be embryotoxic/teratogenic in animals.
Group 4 No adequate and well-controlled studies of the drug's effects on humans are available. Animal studies have shown no embryotoxic/teratogenic effects.
Group 5 No adequate and well-controlled studies of the drug's effects on humans are available.
Group 6 No adequate and well-controlled studies of the drug's effects on humans are available. Animal studies have shown embryotoxic/teratogenic effects.
Group 7 There is a risk that the drug is embryotoxic / teratogenic in humans, at least in the first trimester.
Group 8 There is a risk that the drug is toxic to fetuses throughout the second and third trimesters.
Group 9 There is a risk that the drug causes prenatal complications or abnormalities.
Group 10 There is a risk that the drug causes hormone specific action on the human fetus.
Group 11 There is a known risk that the drug is a mutagen/carcinogen.
ESCMID Online Lecture Library
© by author
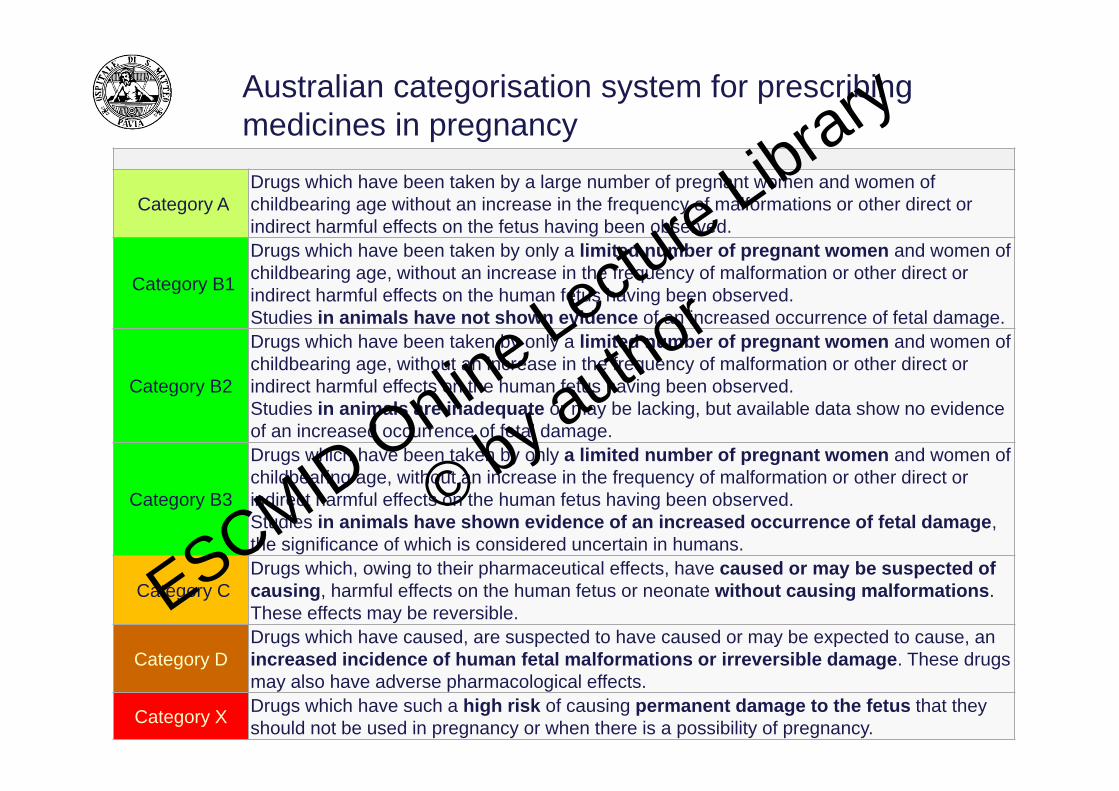
Australian categorisation system for prescribing medicines in pregnancy
Category ADrugs which have been taken by a large number of pregnant women and women of childbearing age without an increase in the frequency of malformations or other direct or indirect harmful effects on the fetus having been observed.
Category B1
Drugs which have been taken by only a limited number of pregnant women and women of childbearing age, without an increase in the frequency of malformation or other direct or indirect harmful effects on the human fetus having been observed.Studies in animals have not shown evidence of an increased occurrence of fetal damage.
Category B2
Drugs which have been taken by only a limited number of pregnant women and women of childbearing age, without an increase in the frequency of malformation or other direct or indirect harmful effects on the human fetus having been observed.Studies in animals are inadequate or may be lacking, but available data show no evidence of an increased occurrence of fetal damage.
Category B3
Drugs which have been taken by only a limited number of pregnant women and women of childbearing age, without an increase in the frequency of malformation or other direct or indirect harmful effects on the human fetus having been observed.Studies in animals have shown evidence of an increased occurrence of fetal damage, the significance of which is considered uncertain in humans.
Category CDrugs which, owing to their pharmaceutical effects, have caused or may be suspected of causing, harmful effects on the human fetus or neonate without causing malformations. These effects may be reversible.
Category DDrugs which have caused, are suspected to have caused or may be expected to cause, an increased incidence of human fetal malformations or irreversible damage. These drugs may also have adverse pharmacological effects.
Category X Drugs which have such a high risk of causing permanent damage to the fetus that they should not be used in pregnancy or when there is a possibility of pregnancy.
ESCMID Online Lecture Library
© by author

Fetal Risk Categories for Antiparasits
ANTIPARASITIC Risk Category B Risk Category C Risk Category D
Chloroquine C
Mebendazole C
Mefloquine C
Metronidazole B
Piperazine B
Primaquine C
Pyrimethamine C
ESCMID Online Lecture Library
© by author

Fetal Risk Categories for Antiparasits
ANTIVIRALS Risk Category B Risk Category C Risk Category D
Acyclovir B
Amantadine C
Ganciclovir C
Famciclovir B
Valacyclovir BESCMID Online Lecture Library
© by author
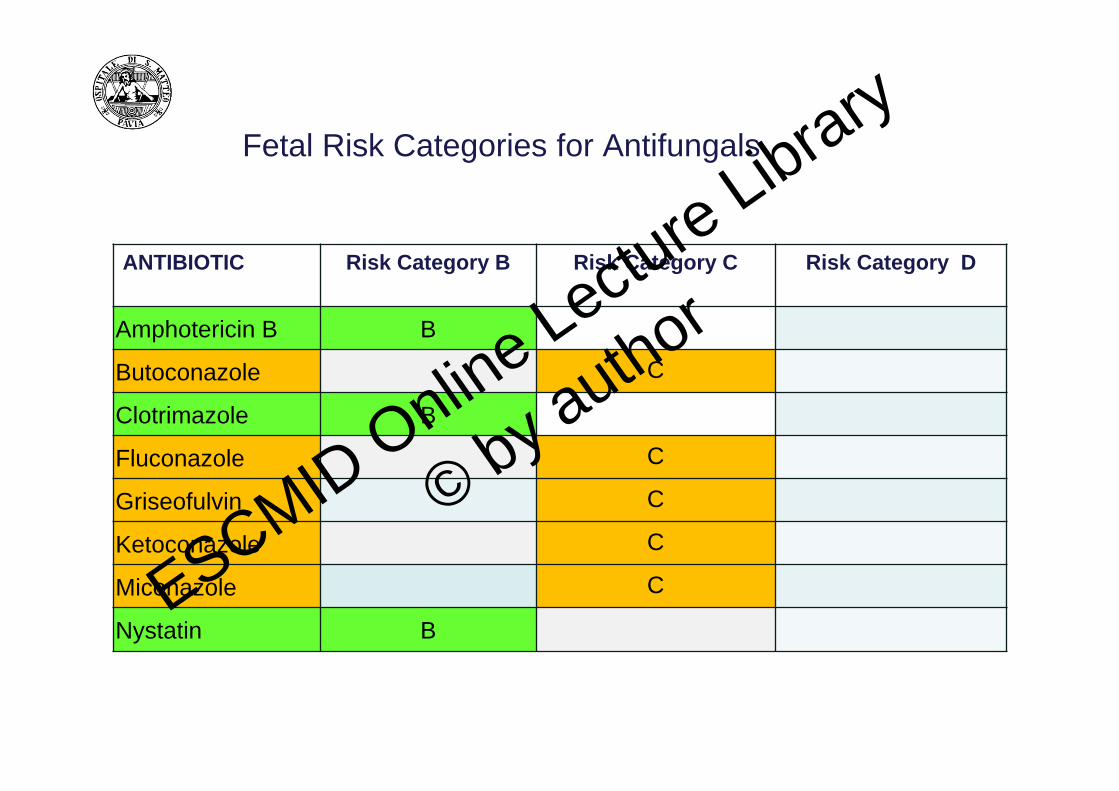
Fetal Risk Categories for Antifungals
ANTIBIOTIC Risk Category B Risk Category C Risk Category D
Amphotericin B B
Butoconazole C
Clotrimazole B
Fluconazole C
Griseofulvin C
Ketoconazole C
Miconazole C
Nystatin BESCMID Online Lectu
re Library
© by author

Antibiotics approved for restricted use during pregnancy
Category Comments RecommendationsAminoglycosides(C)
No teratogenic side effects have been reported to date. There is evidence of selective uptake of aminoglycosides by the foetal kidney resulting in damage to immature nephronsAlthough an impairment of the 8th cranial nerve has been proven only for streptomycin, this complication cannot be entirely ruled out for other aminoglycosides All aminoglycosidesmust be considered potentially nephrotoxicand ototoxic
Prescriptions are restricted to vital indicationsGentamicin is currently considered thesafest choice due to extensive andcomprehensive experience with this antibioticTherapeutic blood concentrations in themother do not equate with safetyfor the foetus
Metronidazole(B)
Animal experiments suggest mutagenic and carcinogenic effects, but no embryo‐toxic/teratogenic effects have been reported in humans For trichomonas and anaerobic infections
Metronidazole may also be used duringpregnancy for appropriate indicationsFor precautionary reasons, it is currentlyrecommended not to use metronidazole duringthe first trimester This also applies to systematic therapy, especially as there are doubts about the eVectiveness of vaginalapplication
ESCMID Online Lecture Library
© by author
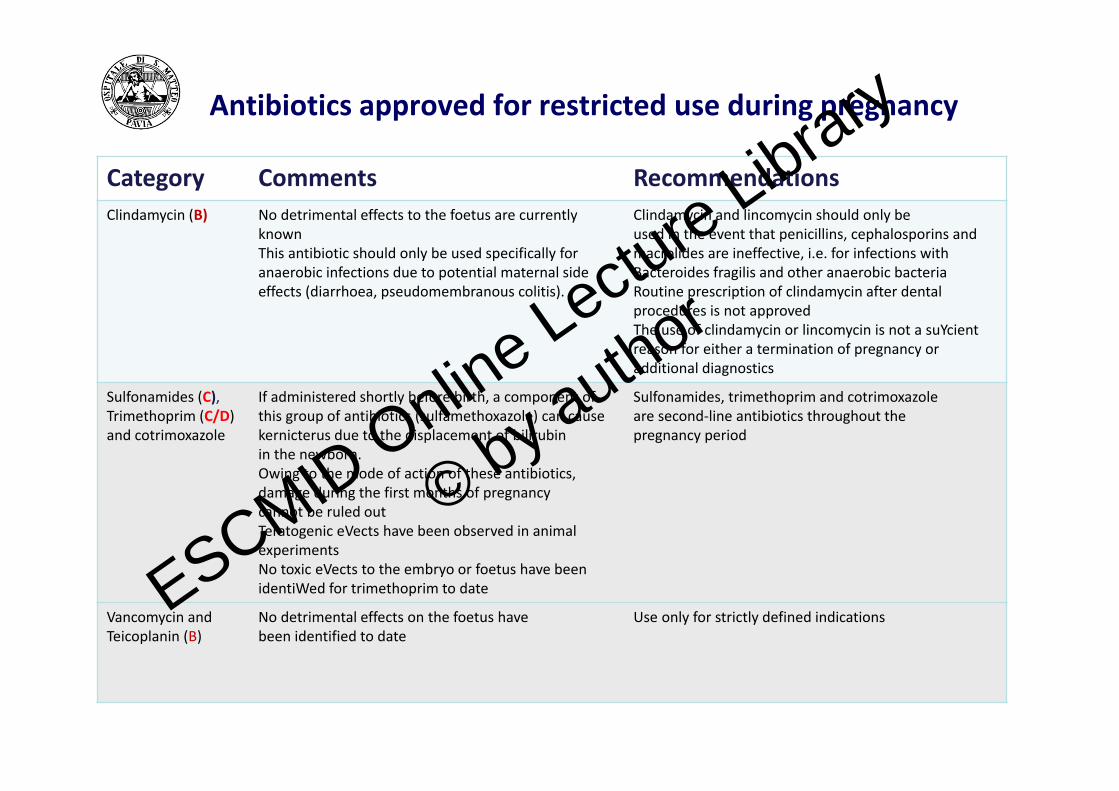
Antibiotics approved for restricted use during pregnancy
Category Comments RecommendationsClindamycin (B) No detrimental effects to the foetus are currently
knownThis antibiotic should only be used specifically foranaerobic infections due to potential maternal sideeffects (diarrhoea, pseudomembranous colitis).
Clindamycin and lincomycin should only beused in the event that penicillins, cephalosporins and macrolides are ineffective, i.e. for infections with Bacteroides fragilis and other anaerobic bacteriaRoutine prescription of clindamycin after dental procedures is not approvedThe use of clindamycin or lincomycin is not a suYcientreason for either a termination of pregnancy or additional diagnostics
Sulfonamides (C),Trimethoprim (C/D)and cotrimoxazole
If administered shortly before birth, a component of this group of antibiotics (sulfamethoxazole) can causekernicterus due to the displacement of bilirubinin the newborn.Owing to the mode of action of these antibiotics,damage during the first months of pregnancycannot be ruled outTeratogenic eVects have been observed in animal experimentsNo toxic eVects to the embryo or foetus have beenidentiWed for trimethoprim to date
Sulfonamides, trimethoprim and cotrimoxazoleare second‐line antibiotics throughout thepregnancy period
Vancomycin andTeicoplanin (B)
No detrimental effects on the foetus havebeen identified to date
Use only for strictly defined indicationsESCMID Online Lecture Library
© by author
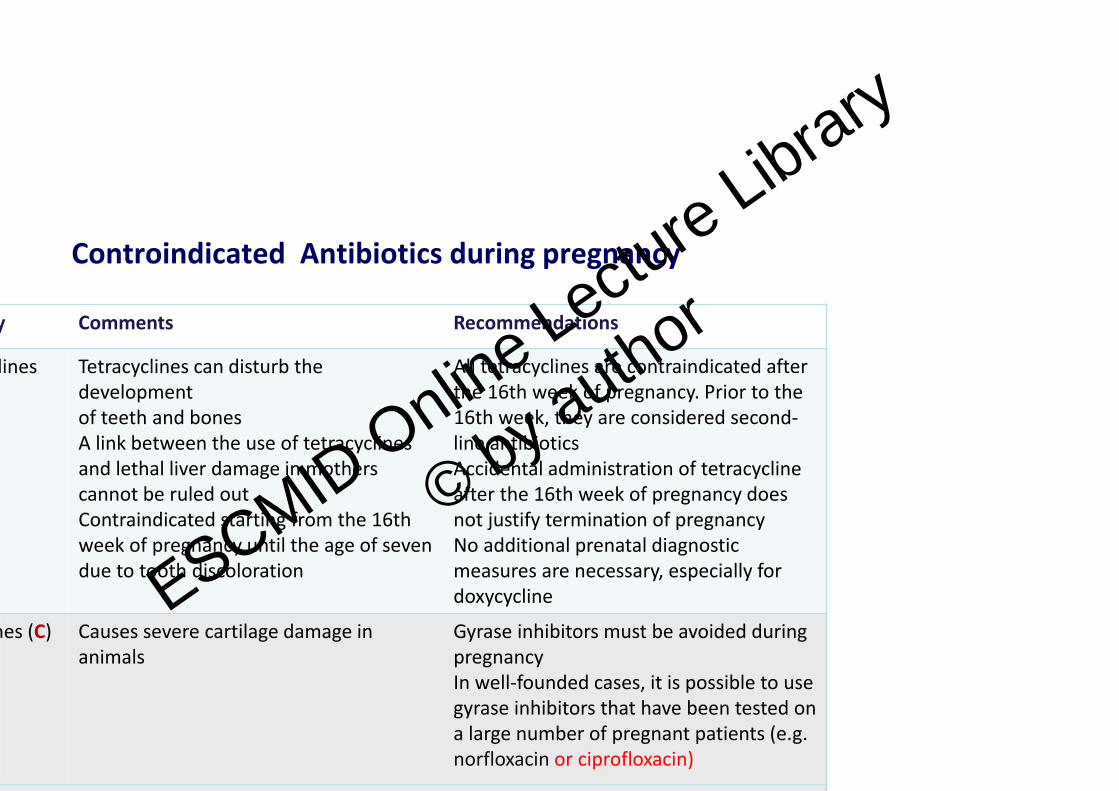
Controindicated Antibiotics during pregnancy
y Comments Recommendations
lines Tetracyclines can disturb the developmentof teeth and bonesA link between the use of tetracyclinesand lethal liver damage in mothers cannot be ruled outContraindicated starting from the 16th week of pregnancy until the age of seven due to tooth discoloration
All tetracyclines are contraindicated after the 16th week of pregnancy. Prior to the 16th week, they are considered second‐line antibioticsAccidental administration of tetracycline after the 16th week of pregnancy does not justify termination of pregnancyNo additional prenatal diagnosticmeasures are necessary, especially for doxycycline
nes (C) Causes severe cartilage damage in animals
Gyrase inhibitors must be avoided during pregnancyIn well‐founded cases, it is possible to use gyrase inhibitors that have been tested on a large number of pregnant patients (e.g. norfloxacin or ciprofloxacin)
ESCMID Online Lecture Library
© by author
• Amphotericin B ( B)
remains the drug of choice for systemic fungal infections in pregnancy although it has significant renal toxicity but not seen more frequently in pregnants and listed as safe drug.
• Griseofulvin (C )
is a known teratogen in laboratory animals
has been demonstrated to cross the human placenta
is controindicated during pregnancy
Pregnancy should be avoided for 1 month after treatment
Men shoul not attempt to father children within 6 months of treatment
ANTIFUNGALS
ESCMID Online Lecture Library
© by author

Ketoconazole ( C)
inhibits placental microsomal aromatase and cythochrome P‐450
should be avoided during pregnancy as there is not enough information toconfirm its safety.
Triazoles_fluconazole and itraconazole (C )
if tretament of these conditions is clinically indicated, other safer antifungalagents should be used
Terbinafine (B)
Approved for the treatment of onychromycosis & it is estimated that 4 milionpatients worldwide have been treated with oral terbinefine
ANTIFUNGALS
ESCMID Online Lecture Library
© by author
Atovaquone/Proguanil ( C)
no fetal harm in pregnant rats and rabbits
proguanil is considered to be the least toxic
women taking the drug either alone or in combination should be supplemented with folic acid
should be used with caution in the first trimester
ANTI‐MALARIAL AGENTS
ESCMID Online Lecture Library
© by author

Chloroquine( C)
at high doses, it is embryotoxic and teratogenic in rats
chloroquine should not be with held during pregnancybecause the risk of complications from malarial infection inpregnancy is increased
safe to breastfeed
ANTIMALARIAL AGENTS
ESCMID Online Lecture Library
© by author
ANTAcyclovir (B) Not found to be teartogenic in pregnant mice, rats and abbitts Probably safe in pregnancy and breastfeeding
Amantadine (C) Dose related teratogenicity in rats at doses equivalent to the human dose No fetal harm was observed in pregnant rabbits Birth defects have been observed in humans but the data are very limited A id d i l t ti
ANTIVIRAL DRUGS
ESCMID Online Lecture Library
© by author
BREAST FEEDING
ost drugs, the infant is exposed to a much higher concentration during pregnancy an during lactation. Therefore, if the drug was considered acceptable during egnancy, it is usually reasonable to continue it during breast feeding. However, ere are exceptions. The most important factors are the concentration of drug in the fant’s blood and the effects that this might have.molecules get into breast milk more easily than large molecules. For example,
eparin is not excreted in breast milk. It is often advocated that feeds should be med to occur just before the mother takes a dose of medication, which could eoretically minimise the amount of drug the baby will ingest. In practice, this is rely achievable, and counselling of the risks and benefits of a particular medication ould not rely on this unrealistic option. The half‐life of some drugs in the neonatal rculation is longer than in the mother, because infant liver metabolism is immature. his may lead to accumulation of drug in the infant.articularly applies to morphine, lamotrigine, phenobarbitone, benzodiazepines and pirin (in analgesic dose). Premature infants may be particularly sensitive to aternal medication through breast milk.en who need to take drugs with a high potential for toxicity, such as lithium and
ESCMID Online Lecture Library
© by author
BREAST FEEDING
contrast with the situation in pregnancy, warfarin, NSAIDs and b‐blockers are considered safe while breast feeding. As with pregnancy, it is necessary to consult up‐to‐date literature in order to counsel a woman about the risks associated with a specific drug taken while breast feeding. Table 1 highlights key medication considerations.
mprehensive information about each drug is beyond the scope of this review and can be found elsewhere.
ESCMID Online Lecture Library
© by author
Copyright © 2022 FDOKUMEN