Ergonomics in bed design: the effect of spinal alignment on sleep parameters
11
PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [Verbraecken, Johan] On: 18 May 2011 Access details: Access Details: [subscription number 933060208] Publisher Taylor & Francis Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37- 41 Mortimer Street, London W1T 3JH, UK Ergonomics Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713701117 Ergonomics in bed design: the effect of spinal alignment on sleep parameters Vincent Verhaert a ; Bart Haex a ; Tom De Wilde a ; Daniel Berckmans b ; Johan Verbraecken c ; Elke de Valck d ; Jos Vander Sloten a a Biomechanics and Engineering Design, Katholieke Universiteit Leuven, Heverlee, Belgium b M3- BIORES, Katholieke Universiteit Leuven, Heverlee, Belgium c Multidisciplinary Sleep Disorders Centre, Universitair Ziekenhuis Antwerpen, Edegem, Belgium d Biological Psychology, Vrije Universiteit Brussel, Brussels, Belgium Online publication date: 02 February 2011 To cite this Article Verhaert, Vincent , Haex, Bart , Wilde, Tom De , Berckmans, Daniel , Verbraecken, Johan , Valck, Elke de and Sloten, Jos Vander(2011) 'Ergonomics in bed design: the effect of spinal alignment on sleep parameters', Ergonomics, 54: 2, 169 — 178 To link to this Article: DOI: 10.1080/00140139.2010.538725 URL: http://dx.doi.org/10.1080/00140139.2010.538725 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of Ergonomics in bed design: the effect of spinal alignment on sleep parameters

PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Verbraecken, Johan]On: 18 May 2011Access details: Access Details: [subscription number 933060208]Publisher Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
ErgonomicsPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713701117
Ergonomics in bed design: the effect of spinal alignment on sleepparametersVincent Verhaerta; Bart Haexa; Tom De Wildea; Daniel Berckmansb; Johan Verbraeckenc; Elke de Valckd;Jos Vander Slotena
a Biomechanics and Engineering Design, Katholieke Universiteit Leuven, Heverlee, Belgium b M3-BIORES, Katholieke Universiteit Leuven, Heverlee, Belgium c Multidisciplinary Sleep Disorders Centre,Universitair Ziekenhuis Antwerpen, Edegem, Belgium d Biological Psychology, Vrije UniversiteitBrussel, Brussels, Belgium
Online publication date: 02 February 2011
To cite this Article Verhaert, Vincent , Haex, Bart , Wilde, Tom De , Berckmans, Daniel , Verbraecken, Johan , Valck, Elkede and Sloten, Jos Vander(2011) 'Ergonomics in bed design: the effect of spinal alignment on sleep parameters',Ergonomics, 54: 2, 169 — 178To link to this Article: DOI: 10.1080/00140139.2010.538725URL: http://dx.doi.org/10.1080/00140139.2010.538725
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

Ergonomics in bed design: the effect of spinal alignment on sleep parameters
Vincent Verhaerta*, Bart Haexa, Tom De Wildea, Daniel Berckmansb, Johan Verbraeckenc,Elke de Valckd and Jos Vander Slotena
aBiomechanics and Engineering Design, Katholieke Universiteit Leuven, Heverlee, Belgium; bM3- BIORES, Katholieke UniversiteitLeuven, Heverlee, Belgium; cMultidisciplinary Sleep Disorders Centre, Universitair Ziekenhuis Antwerpen, Edegem, Belgium;
dBiological Psychology, Vrije Universiteit Brussel, Brussels, Belgium
(Received 27 April 2010; final version received 20 September 2010)
This study combines concepts of bed design and sleep registrations to investigate how quality of spine support affectsthe manifestation of sleep in healthy subjects. Altogether, 17 normal sleepers (nine males, eight females; age24.3+ 7.1 years) participated in an anthropometric screening, prior to the actual sleep experiments, during whichpersonalised sleep system settings were determined according to individual body measures. Sleep systems (i.e.mattress and supporting structure) with an adjustable stiffness distribution were used. Subjects spent three nights of8 h in bed in the sleep laboratory in a counterbalanced order (adaptation, personalised support and saggingsupport). During these nights, polysomnography was performed. Subjective sleep data were gathered by means ofquestionnaires. Results show that individual posture preferences are a determinant factor in the extent that subjectsexperience a negative effect while sleeping on a sagging sleep system.
Statement of Relevance: This study investigated how spine support affects sleep in healthy subjects, finding that therelationship between bedding and sleep quality is affected by individual anthropometry and sleep posture. Inparticular, results indicate that a sagging sleep system negatively affects sleep quality for people sleeping in a prone orlateral posture.
Keywords: bed design; sleep posture; sleep quality; sleep system; spinal alignment
1. Introduction
Although the domains of both sleep research andergonomics are rapidly expanding, it is surprising tolearn how little research is at hand that combines theknowledge of both disciplines. A key issue in the designof current, state of the art sleep systems (i.e. mattressand supporting structure) is how the optimisation ofbed design affects the manifestation of sleep in healthyhuman beings. Whereas some research is available onthe influence of the mechanical characteristics ofmattresses and supporting structures on spinal align-ment (Lahm and Iaizzo 2002, DeVocht et al. 2006),very few ergonomists perform actual sleep registrationsto test whether their findings have an effect on howpeople sleep. Additionally, the available research thatlooks at sleep quality on different bedding systemsremains very vague on the actual bed properties, usingterms such as soft, firm, medium-firm, (un)comforta-ble, etc. without further specification (Bader andEngdal 2000, Lee and Park 2006, Jacobson et al.2008, 2010). This lack of quantification makes itdifficult to compare and interpret results.
The main function of sleep systems is to supportthe human body in a way that allows the muscles and
intervertebral discs to recover from nearly continuousloading by day (Nachemson and Elfstrom 1970). Thisrecovery can be achieved when the shape of the spine isin its natural physiological shape, yet with a slightlyflattened lumbar lordosis due to the changed workingaxis of gravity (Dolan et al. 1988). In general, themechanical characteristics of a sleep system shouldaccount for two anthropometrical aspects: bodycontours and weight distribution. Since both of thesefactors are highly individual, the allocation of anappropriate sleep system to a specific person should bedone on a personalised basis (Haex 2004).Furthermore, the body contours that are in contactwith the mattress surface are dependent on the adoptedsleep posture. Because healthy sleep requires thepresence of several major posture changes throughoutthe night (De Koninck et al. 1992, Coenen 2006), theideal sleep system should be able to cope with thesevariable loading conditions; for instance, by changingits characteristics according to the adopted posture atany moment during the night (Verhaert et al. 2009).
The objective assessment of a sleep system’ssupport qualities is generally done by evaluating eithercontact pressure or spinal alignment. A lot of research
*Corresponding author. Email: [email protected]
Ergonomics
Vol. 54, No. 2, February 2011, 169–178
ISSN 0014-0139 print/ISSN 1366-5847 online
� 2011 Taylor & Francis
DOI: 10.1080/00140139.2010.538725
http://www.informaworld.com
Downloaded By: [Verbraecken, Johan] At: 15:59 18 May 2011

has already been done in the field of pressuredistribution because of its clinical relevance in theprevention of pressure ulcers (Defloor 2000, Rithalia2005, Vanderwee et al. 2005). Little research howeverfocuses on the influence of spinal alignment on normalsleep quality and quantity. Lahm and Iaizzo (2002)studied the physiological response of 22 ‘back pain-free’ participants during a 30 min trial on a sleepsystem at three levels of firmness. They reported nodifference in electromyographic activity, heart rate,blood pressure and subjective comfort. In contrast,spinal alignment was significantly improved at mid-range and higher firmness levels. DeVocht et al. (2006)measured both contact pressure and spinal alignmentto evaluate four ‘top of the line’ mattresses in a malepopulation. They reported significant differencesbetween mattresses, but the pattern of results was notconsistent; the mattress with the highest maximalcontact pressure tended to have the lowest spinaldistortions. Again, the impact on sleep was notincorporated in the study.
The few scientific reports of sleep quality ondifferent mattress types yielded quite contradictoryfindings. Bader and Engdal (2000) investigated ninemen, sleeping in their homes for at least fiveconsecutive nights on a soft and a more firm mattress.They experienced no global preference for any of thetest beds. Jacobson et al. (2008) studied subjective sleepratings of 62 persons at home for 28 nights in their ownbeds (pre) and for 28 nights on a new ‘medium-firm’bedding system (post). Unfortunately, order effectswere not controlled by way of counterbalancing thetwo mattress conditions. They found immediate andsignificant improvements in all areas of physical pain,sleep comfort and sleep quality on the new beddingsystems. Kovacs et al. (2003) looked at 313 adults withchronic non-specific low back pain and randomlyassigned them a firm or medium-firm mattress. Painwhen lying in bed, pain on rising and the degree ofdisability after a period of 90 d were assessed andcompared to baseline. Results showed improvementsin all variables for both mattresses. Scharf et al. (1997)performed full polysomnographic recordings in 10normal subjects in a laboratory setting on both a high-quality innerspring mattress and a unique foamsupport mattress. The order of mattress conditionswas counterbalanced. No significant changes in sleeparchitecture were reported, but cyclic alternatingpattern rate was significantly reduced on the foamsupport mattress, suggesting better recuperation dur-ing sleep on this type of mattress. Lee and Park (2006),however, did find differences in sleep architecture, withsignificantly more slow wave sleep (SWS) and a highersleep efficiency on ‘comfortable’ than on ‘uncomfor-table’ mattresses. However, no quantitative
characteristics are provided that describe thedifference between ‘comfortable’ and ‘uncomfortable’.
The lack of consistency in the above findings mightbe due to the diversity of sleep systems that were usedin the different studies, with no specifications on theactual bed properties. Another possible explanation isthe lack of individualisation of the experimentalconditions. The interaction between a bed and its useris not only dependent on the properties of the bed, butalso on the anthropometric features of the sleeper.Neglecting such individual properties corresponds toapplying a different experimental condition for eachparticipant. This paper will assess sleep system qualityby measuring the spinal alignment of the sleeper,rather than by the characteristics of the sleep systemitself. This approach accounts intrinsically foranthropometric differences as well, because theresulting interaction between both sleep system andhuman body is measured. Since spinal alignment isinfluenced by the adopted sleep postures during thenight, the amount of time spent in each posture isconsidered as an independent factor in the analysis ofthe results.
2. Methods
2.1. Subjects
Altogether, 17 subjects (nine males, eight females; age24.3+ 7.1 years) were recruited throughadvertisement. Inclusion criteria were a regularsleep–wake schedule and a good general healthcondition. According to the Pittsburgh Sleep QualityIndex (Buysse et al. 1989) and a sleep diary, all subjectswere normal sleepers and did not suffer from insomnia.Exclusion criteria were medical problems that caninterfere with normal sleep, e.g. intake of sleepmedication, antidepressants, any form of back pain.All subjects signed an informed consent. The study wasapproved by the Ethics Committee of the VrijeUniversiteit Brussel.
2.2. Experimental design
After a baseline night, each subject underwent twoexperimental conditions: (1) a reference condition witha personalised stiffness distribution; (2) an inductionwith a stiffness distribution that simulates a saggingmattress. Counterbalancing was applied to avoidcarry-over effects between both conditions.
2.3. Procedure
Prior to the actual sleep experiments, the subjectsunderwent an anthropometric screening. The purposeof this screening was to determine the sleep system
170 V. Verhaert et al.
Downloaded By: [Verbraecken, Johan] At: 15:59 18 May 2011

configuration for each of the subjects that bestmatched their individual body dimensions and toobjectively validate the effect of both experimentalconditions on spinal alignment. In order to provideboth a personalised and a sagging support for a varietyof people, sleep systems with an adjustable stiffnessdistribution were used (DynaSleep; Custom8, Leuven,Belgium). The mattress core of these systems consistsof pocket springs and comprises 10 comfort zones.Eight of these comfort zones can be separatelyadjusted in stiffness by applying a verticaldisplacement of the zones’ spring bases, effectivelycreating positive or negative preloads.
The reference condition consists of an individua-lised sleep system configuration that minimises spinaldeformation in a lateral sleep posture (i.e. when thespine approximates a straight line in the frontal plane).A lateral posture was considered because it is the mostcommonly adopted sleep posture in the Western world(approximately 60% of time in bed is spent in a lateralsleep posture) (Haex 2004). Furthermore, this corre-sponds to how most modern sleep systems withcomfort zones are designed at present (Coenen 2006).The induction consists of a configuration with arelatively high stiffness of the shoulder zone and arelatively low stiffness of the waist and hip zonescompared to the reference condition. This simulates ahomogeneous sleep system that is worn down andsuffers from sagging of the most load-bearing zones.Subjects were blinded from the experimental condi-tions to eliminate expectation effects.
A night in the sleep laboratory consists ofapproximately 8 h in bed: subjects entered the sleeplaboratory at 19.00; bedtime was between 22.30 and23.30; subjects were awakened at 07.00 hours. In theevening, they were allowed to engage in recreationalactivities, such as watching television, reading andconversation. No caffeinated drinks or heavy mealswere allowed. Subjects completed the sleepiness, stateof arousal and mood scales at 22.15 and 07.20 hours.Subjective sleep quality was assessed at 07.20 hours.
2.4. Measurements and analysis
2.4.1. Anthropometric screening
During anthropometric screening, the following seriesof measurements was conducted. First, a set of 29 61-D body measurements was collected by means of acalliper and a tape measure. Height, width andcircumference were measured on the following anato-mical sites: acromion; shoulder; breast; waist; pelvis;hip; crotch. An additional depth measure was taken onthe acromion, shoulder, breast, waist and pelvis sites.Finally, body weight, total body length and neck base
height were also determined. Second, 2-D bodycontours in both the sagittal and frontal planes wereautomatically registered (Ikelo; Custom8). Finally,back surface measurements were done by means ofrasterstereography for a lateral sleep posture on boththe personalised and the sagging sleep system (3DVario; Vialux, Chemnitz, Germany). Thesemeasurements were used to validate spinal alignmentin both conditions (Drerup and Hierholzer 1994,Huysmans 2004).
The measurements of body dimensions and bodycontours serve as a basis to estimate the personalisedstiffness distribution for each of the participants. First,the location and size of three comfort zones (shoulderzone, waist zone and hip zone) are individuallydetermined with regard to the eight adjustable stiffnesszones. This first step allows the adaptation of the sleepsystem to longitudinal body measurements, such asshoulder height, waist height and hip height. Second,the estimation of the actual stiffness settings percomfort zone is done based on BMI, shoulderwidth:waist width ratio (SW) and hip width:waistwidth ratio (HW). The values of SW and HW arecompared to the percentiles (25th, 50th and 75th) of adataset of 64 subjects. This results in four differentstiffness settings per comfort zone. Finally, for peoplewith a BMI of �25 kg/m2, the general stiffness of thesleep system across the eight adjustable zones isincreased. Figure 1 illustrates the dimensions of thedifferent stiffness zones and their locations with regardto the sleep system. Table 1 lists the intrinsic stiffnesscoefficients for each mattress zone, together with thepossible preload values. Both stiffness and preloadvalues refer to the properties of the individual springs,rather than the entire zones. Positive and negativepreload values correspond to tensile and compressivepreload respectively. The sagging stiffness distributionis the same for all subjects, regardless of theiranthropometric features.
Figure 1. Dimensions (mm) and locations of the sleepsystem’s stiffness zones.
Ergonomics 171
Downloaded By: [Verbraecken, Johan] At: 15:59 18 May 2011

In order to objectively quantify the effect of bothconditions on spinal alignment, an algorithm is usedthat detects the line through the spinous processes,based on back shape data, with a mean accuracy of2.6 mm (Huysmans 2004). Four shape parameters arecalculated that objectively quantify spinal alignment inthe frontal plane (Haex 2004). Figure 2 clarifies thedefinition of the four shape parameters. The firstparameter is defined as the angle between thehorizontal axis and the straight line that connects thevertebra prominens with the midpoint of the dimplesof the posterior superior iliac spine. Second, the meandistance from the measured line to the least square linethrough the measured points is determined (parameter2). The third parameter is the angle between thehorizontal axis and the least square line through themeasured points. Finally, the angle between the leastsquare lines through the lumbar and the thoracic partof the measured points (parameter 4) completes thequantification of spine shape.
2.4.2. Objective and subjective sleep measures
The subjects underwent three full night polysomno-graphic recordings (DREAM; Medatec, Brussels,Belgium). Electrodes were attached according to thestandardised 10–20 system of electrode placement(Jasper 1958) at the F3, C3, O1, F4, C4 and O2positions, together with electrooculography, submentalelectromyography and electrocardiography. Further-more, video frames and chest orientation wererecorded in order to determine the adopted sleeppostures during the night. The nights were blinded andscored according to the Rechtschaffen and Kalescriteria and the modifications of the AmericanAcademy of Sleep Medicine (Rechtschaffen and Kales1968, Iber et al. 2007).
Further to this objective evaluation of sleep, severalsubjective measures were also determined. Subjectivesleep quality was evaluated on a visual analogue scaleof zero (extremely poor) to 20 (extremely good) in themorning following the test night. Furthermore, therestorative effect of sleep was determined by three
different scales, comparing the subjective level offunctioning the evening before and the morning afterthe test night. The first scale was the KarolinskaSleepiness Scale, which has been widely used inliterature to evaluate subjective sleepiness (Akerstedtand Gillberg 1990). Second, state of arousal wasdetermined by the arousal scale of Cox’s Stress/Arousal Adjective Check List (Mackay et al. 1978).Third, the fatigue scale of the Profile of Mood Stateswas used to evaluate subjective fatigue (Cluydts 1979).All three scores were scaled to five and sleepiness andfatigue were inversed to make sure that a positivedifference between morning and evening scores reflectsa more restorative night.
2.5. Statistical analysis
First, all grouped data were tested for normality usingLilliefors’ adaptation of the Kolmogorov–Smirnov test(Lilliefors 1967). Normal distributions were analysedusing parametric repeated measures ANOVA. For non-normal distributions, non-parametric FriedmanANOVAwere performed. Subjective datawere analysedusing non-parametric FriedmanANOVAbecause of theordinal nature of the subjective scales. Unsupervisedcluster analysis based on the k-means algorithm(MacQueen 1967) was performed to partition the dataon sleep postures into different categories. The amountof clusters was determined by means of clustersilhouettes (Rousseeuw 1987). The squared Euclideandistance was used as distance measure to perform thek-means clustering and to calculate silhouette values.Both experimental condition (personalised vs. saggingsupport) and the amount of time spent in each posture(cluster A vs. cluster B) were considered as independentfactors in the statistical analysis of the results of the sleepexperiments.
3. Results
3.1. Anthropometric screening
The calculated spine shape parameters for thereference and induction nights are listed in Table 2. All
Table 1. Possible settings for the sleep system’s stiffness zones in both experimental conditions.
Zone 1 Zones 2–4 Zones 5–6 Zones 7–9 Zone 10
Intrinsic spring stiffness coefficient (N/mm) 0.20 0.076 0.20 0.20 0.20Spring preload (N) Personalised stiffness distribution 0 70.76 72.00 72.00 0
0 0 0þ0.76 þ2.00 þ2.00þ1.52 þ4.00 þ4.00þ2.28 þ6.00þ3.04
Sagging stiffness distribution 0 71.52 þ4.00 þ4.00 0
172 V. Verhaert et al.
Downloaded By: [Verbraecken, Johan] At: 15:59 18 May 2011

parameters are significantly higher in the saggingcondition. This means that the change in stiffnessdistribution results in a changed spine shape and thatthe applied sagging induction corresponds to animpaired spinal alignment. Figure 3 visualises theeffect of both support conditions on the shape ofthe spine during lateral recumbency for one of thesubjects.
3.2. Sleep experiments
3.2.1. Sleep postures and cluster analysis
Three main sleep postures were considered: supine;lateral (left þ right); prone. Most time is spent in alateral posture (55.4+ 17.3%), followed by a supineposture (32.2+ 19.2%) and the least time is spent in aprone posture (12.4+ 13.7%). However, these meanvalues go along with a lot of variation and most of this
variation has to do with interpersonal rather thannight-to-night differences (Verhaert et al. 2009).Cluster analysis is performed considering two andthree clusters. The two-cluster solution reveals thehighest average silhouette width (0.66) and is thereforechosen to reorganise the dataset. Figure 4 shows theobtained clusters together with the correspondingsilhouette values. Cluster A consists of eight subjectswho spent most time in a lateral and prone posture(61.0+ 16.9% and 23.4+ 9.1%, respectively) and arelatively small amount of time in a supine posture(15.0+ 9.9%). Cluster B comprises nine subjects whospent most time in a lateral and supine posture(51.9+ 14.7% and 44.1+ 12.8%, respectively) andalmost no time in a prone posture (4.0+ 5.5%).Comparing the amount of time spent in each posturewithin subjects reveals no significant differencesbetween conditions (supine: p ¼ 0.92, lateral:p ¼ 0.88, prone: p ¼ 0.91), indicating that subjects did
Table 2. Spine shape parameters.
P1 (8) P2 (mm) P3 (8) P4 (8)
Reference condition (personalised support) 3.31+ 1.49 4.81+ 2.31 2.92+ 1.93 6.31+ 4.52Induction (sagging support) 7.77+ 2.68 6.10+ 2.56 7.69+ 3.25 8.53+ 5.61Significance 51075 0.01 51075 0.046
For details of parameters, see section 2.4.1.
Figure 2. Objective quantification of spinal alignment during lateral recumbency by four shape parameters. vp ¼ vertebraprominens; dm ¼ dimples of the posterior superior iliac spine.[] For details of parameters, see section 2.4.1.
Ergonomics 173
Downloaded By: [Verbraecken, Johan] At: 15:59 18 May 2011

not alter their postural habits during the course of theexperiment.
3.2.2. Subjective assessment
In general, subjective sleep quality is lower in thesagging induction condition compared to the referencecondition (12.1+ 3.8 vs. 14.4+ 1.8; w2(1) ¼ 4.57, p 50.05). However, it can be inferred from Figure 5(a) thata large variation exists in the subjective sleep qualityscores after the induction condition.
Taking into account the amount of time spent ineach posture as an independent factor in the analysis ofthe results reveals some new insights. In cluster A,subjective sleep quality is significantly lower during thesagging condition compared to reference (9.0+ 3.1 vs.
13.4+ 1.8; w2(1) ¼ 7, p 5 0.01). No such differencebetween conditions is present in cluster B (14.9+ 1.4vs. 15.2+ 1.4; w2(1) ¼ 0.14, p ¼ 0.71), indicating thatsubjects of cluster B did not report a lower sleepquality score on a sagging than on a personalised sleepsystem. Figure 5(b) shows the reported scores ofsubjective sleep quality for both conditions in bothposture groups.
The restorative effect of sleep is determined by thedifference in mood, sleepiness and arousal between themorning after and the evening before the test night.Figure 6 illustrates the interaction effects betweencondition and posture preference for these three scales.Statistically significant differences could only bedemonstrated for the arousal scale. Subjects in clusterA were less recuperated in terms of their state ofarousal after the night on the sagging sleep systemcompared to the personalised sleep system (morning–evening difference: –0.6+ 0.9 vs. 1.0+ 0.7; w2(1) ¼ 7,p 5 0.01). Cluster B showed no difference betweenboth conditions (morning–evening difference:0.6+ 1.1 vs. 0.8+ 0.8; w2(1) ¼ 0, p ¼ 0.99). Neitherthe sleepiness scale nor the fatigue scale revealed astatistically significant interaction effect.
3.2.3. Sleep architecture
No general effects of condition on the parametersderived from the sleep hypnogram have been found.Analogous to the results of the subjective assessment,the amount of time spent in each posture has beenconsidered as an independent factor influencing sleepon different sleep systems. Tables 3 and 4 list thecharacterising parameters of the scored nights for bothconditions in clusters A and B respectively. Similar tosubjective findings, differences between conditionswere dependent on the posture group.
Figure 4. Two-cluster solution and silhouette plot of sleep posture preference.
Figure 3. Effect of both conditions on the shape of the spineas determined from back shape measurements.
174 V. Verhaert et al.
Downloaded By: [Verbraecken, Johan] At: 15:59 18 May 2011

First, a significant difference in wake time is presentbetween conditions in clusterA. Subjects spentmore timeawake (as a percentage of time in bed) during the night on
the sagging system compared to the reference condition(12.1+ 5.1% vs. 8.8+ 5.8; w2(1) ¼ 6, p5 0.05). Forsubjects of cluster B, no difference in wake time is present
Table 3. Objective sleep data for cluster A.
Induction Reference condition Significance
TIB (min) 454.92+ 20.13 470.08+ 15.21 0.65SOL (min) 24.75+ 11.39 20.08+ 9.40 0.99PSL (min) 28.50+ 16.43 21.67+ 8.37 0.99TST (min) 374.33+ 18.39 408.5+ 25.57 0.10Awake (min) 55.83+ 25.44 41.50+ 28.34 0.01Awake (%TIB) 12.13+ 5.08 8.79+ 5.81 0.01REM sleep (%TIB) 11.53+ 6.24 17.09+ 6.36 0.01SWS (%TIB) 28.22+ 4.33 28.00+ 5.00 0.41SST (n) 144.17+ 30.49 138.17+ 16.99 0.41Awakenings (n) 21.17+ 7.52 25.50+ 4.85 0.10Awakening duration (min) 4.00+ 1.33 2.40+ 1.10 0.01REM latency (min) 150.83+ 62.11 101.42+ 34.49 0.01SWS latency (min) 12.17+ 10.75 13.83+ 4.25 0.41SEI (%) 84.2+ 5.50 86.97+ 5.95 0.10
TIB ¼ time in bed; SOL ¼ sleep onset latency; PSL ¼ persistent sleep latency; TST ¼ total sleep time; TWT ¼ total wake time; REM ¼rapid eye movement; SWS ¼ slow wave sleep; SST ¼ sleep stage transitions; SEI ¼ Sleep Efficiency Index (TST/TIB).
Figure 6. Estimated marginal means and standard deviations for morning–evening difference of sleepiness (KarolinskaSleepiness Scale [KSS]), state of arousal (Cox’s Stress Arousal Adjective Check List [SACL_A]) and fatigue (Profile of MoodStates [POMS_F]) with the independent variables condition (induction [in] vs. reference [re]) and posture preference (cluster Avs. cluster B).
Figure 5. Subjective ratings of sleep quality in general (a) and considering the two clusters (b) in the induction (in) andreference condition (re).
Ergonomics 175
Downloaded By: [Verbraecken, Johan] At: 15:59 18 May 2011
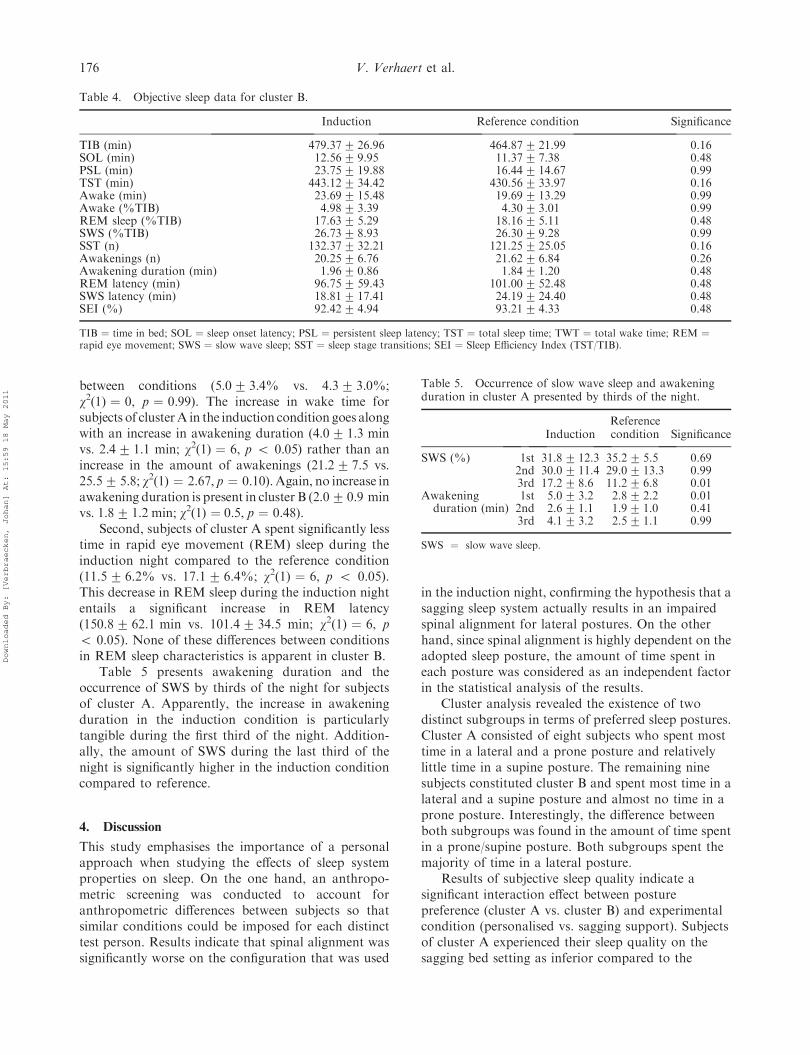
between conditions (5.0+ 3.4% vs. 4.3+ 3.0%;w2(1) ¼ 0, p ¼ 0.99). The increase in wake time forsubjects of clusterA in the induction condition goes alongwith an increase in awakening duration (4.0+ 1.3 minvs. 2.4+ 1.1 min; w2(1) ¼ 6, p 5 0.05) rather than anincrease in the amount of awakenings (21.2+ 7.5 vs.25.5+ 5.8; w2(1) ¼ 2.67, p ¼ 0.10).Again, no increase inawakening duration is present in cluster B (2.0+ 0.9 minvs. 1.8+ 1.2 min; w2(1) ¼ 0.5, p ¼ 0.48).
Second, subjects of cluster A spent significantly lesstime in rapid eye movement (REM) sleep during theinduction night compared to the reference condition(11.5+ 6.2% vs. 17.1+ 6.4%; w2(1) ¼ 6, p 5 0.05).This decrease in REM sleep during the induction nightentails a significant increase in REM latency(150.8+ 62.1 min vs. 101.4+ 34.5 min; w2(1) ¼ 6, p5 0.05). None of these differences between conditionsin REM sleep characteristics is apparent in cluster B.
Table 5 presents awakening duration and theoccurrence of SWS by thirds of the night for subjectsof cluster A. Apparently, the increase in awakeningduration in the induction condition is particularlytangible during the first third of the night. Addition-ally, the amount of SWS during the last third of thenight is significantly higher in the induction conditioncompared to reference.
4. Discussion
This study emphasises the importance of a personalapproach when studying the effects of sleep systemproperties on sleep. On the one hand, an anthropo-metric screening was conducted to account foranthropometric differences between subjects so thatsimilar conditions could be imposed for each distincttest person. Results indicate that spinal alignment wassignificantly worse on the configuration that was used
in the induction night, confirming the hypothesis that asagging sleep system actually results in an impairedspinal alignment for lateral postures. On the otherhand, since spinal alignment is highly dependent on theadopted sleep posture, the amount of time spent ineach posture was considered as an independent factorin the statistical analysis of the results.
Cluster analysis revealed the existence of twodistinct subgroups in terms of preferred sleep postures.Cluster A consisted of eight subjects who spent mosttime in a lateral and a prone posture and relativelylittle time in a supine posture. The remaining ninesubjects constituted cluster B and spent most time in alateral and a supine posture and almost no time in aprone posture. Interestingly, the difference betweenboth subgroups was found in the amount of time spentin a prone/supine posture. Both subgroups spent themajority of time in a lateral posture.
Results of subjective sleep quality indicate asignificant interaction effect between posturepreference (cluster A vs. cluster B) and experimentalcondition (personalised vs. sagging support). Subjectsof cluster A experienced their sleep quality on thesagging bed setting as inferior compared to the
Table 4. Objective sleep data for cluster B.
Induction Reference condition Significance
TIB (min) 479.37+ 26.96 464.87+ 21.99 0.16SOL (min) 12.56+ 9.95 11.37+ 7.38 0.48PSL (min) 23.75+ 19.88 16.44+ 14.67 0.99TST (min) 443.12+ 34.42 430.56+ 33.97 0.16Awake (min) 23.69+ 15.48 19.69+ 13.29 0.99Awake (%TIB) 4.98+ 3.39 4.30+ 3.01 0.99REM sleep (%TIB) 17.63+ 5.29 18.16+ 5.11 0.48SWS (%TIB) 26.73+ 8.93 26.30+ 9.28 0.99SST (n) 132.37+ 32.21 121.25+ 25.05 0.16Awakenings (n) 20.25+ 6.76 21.62+ 6.84 0.26Awakening duration (min) 1.96+ 0.86 1.84+ 1.20 0.48REM latency (min) 96.75+ 59.43 101.00+ 52.48 0.48SWS latency (min) 18.81+ 17.41 24.19+ 24.40 0.48SEI (%) 92.42+ 4.94 93.21+ 4.33 0.48
TIB ¼ time in bed; SOL ¼ sleep onset latency; PSL ¼ persistent sleep latency; TST ¼ total sleep time; TWT ¼ total wake time; REM ¼rapid eye movement; SWS ¼ slow wave sleep; SST ¼ sleep stage transitions; SEI ¼ Sleep Efficiency Index (TST/TIB).
Table 5. Occurrence of slow wave sleep and awakeningduration in cluster A presented by thirds of the night.
InductionReferencecondition Significance
SWS (%) 1st 31.8+ 12.3 35.2+ 5.5 0.692nd 30.0+ 11.4 29.0+ 13.3 0.993rd 17.2+ 8.6 11.2+ 6.8 0.01
Awakening 1st 5.0+ 3.2 2.8+ 2.2 0.01duration (min) 2nd 2.6+ 1.1 1.9+ 1.0 0.41
3rd 4.1+ 3.2 2.5+ 1.1 0.99
SWS ¼ slow wave sleep.
176 V. Verhaert et al.
Downloaded By: [Verbraecken, Johan] At: 15:59 18 May 2011

reference condition. No difference in sleep quality wasreported in cluster B between both support conditions.These results were also reflected in the outcome of theStress/Arousal Adjective Check List, administered inthe evening before and the morning following the testnight. Whereas the evening scores did not differsignificantly between both conditions, subjects ofcluster A reported being in a lower state of arousalthe morning following the induction night compared tothe reference night. This suggests that subjects whospend relatively little time in a supine posture show lessrecovery in terms of arousal after a nights’ sleep on asagging mattress in comparison with a non-saggingmattress.
Objective sleep data showed an interaction betweenposture preference and mattress type for parametersrelated to wake time and REM sleep. First, subjectswho preferred a prone and lateral posture spent moretime awake during the sagging induction than duringthe reference condition. The increased wake time wasdue to longer awakenings, rather than more awaken-ings. No differences in wake time were present in thegroup that preferred a supine and lateral posture. Priorresearch regarding the effects of aircraft noise on sleep(Basner et al. 2006) suggests that the risk of recalledawakenings increases with the duration of the awaken-ing and that recalled awakenings are correlated withthe subjective evaluation of sleep quality and sleepquantity. Consequently, a higher amount of recalledawakenings could be an explanation for the low sleepquality rating that prone/lateral sleepers reported afterthe night on the sagging sleep system. Second, thesesubjects spent less time in REM sleep during inductioncompared to reference. In addition to this decrease inREM sleep, a higher REM latency was also observed.Analysis by thirds of the night revealed two additionalfindings for prone/lateral sleepers. On the one hand,the increase in awakening duration during the induc-tion night was mainly present during the first third ofthe night. On the other hand, the amount of SWS inthe third part of the night was significantly higherduring the induction night compared to reference. Thepersistence of SWS in the later parts of the night incombination with suppression of REM sleep andincreased REM latency might indicate a recoveryfrom disturbed SWS episodes due to the prolongedawakenings in the first part of the night.
One of the underlying causes for the distinctreaction of both posture groups could be related tothe nature of the induction. Depending on the adoptedsleep posture, the sagging mattress setting will result ina different loading of the human spine and therefore adifferent spinal alignment. The induction is chosen soas to deteriorate spinal alignment in a lateral sleepposture, because this is the most commonly adopted
posture during sleep in the Western world. However,the effect of the sagging configuration on both a supineand a prone posture should also be taken into account.The range of motion of the spine in the sagittal plane isquite large for frontal bending, yet quite small forbackward bending. Therefore, lying in a supine postureon the sagging bed will cause little discomfort. A proneposture on the other hand will result in hyperlordosisof the lumbar spine. This hyperlordosis will becomemore explicit in the condition that simulates a saggingmattress. One can look at it in a similar way as lying ina hammock; in this case, it is not hard to see that asupine posture will cause less discomfort than a lateraland especially a prone posture.
A first limitation of the present study is that itinvolves short-term changes of body support. Thesedata suggest that people do not change their adoptedpostures during the course of one night; withinsubjects, the adopted postures were not different forboth conditions. On the one hand, it is possible that ifsubjects slept on the sagging sleep system during aprolonged period, they would alter their habits andadopt a supine posture more often. Another possibilityis the existence of an adaptation effect to thedeteriorated conditions. On the other hand, prolongedsagging support could also result in back and/or sleepcomplaints. Further research is necessary to test thesehypotheses. Second, the current study deals with younghealthy sleepers with no back or sleep problems. Apopulation with pre-existing back/sleep problemsmight be more affected by a sagging sleep system(Gracovetsky 1987, Jacobson et al. 2010). In thiscontext, Enck et al. (1999) showed in a field study with265 hotel guests that for those with chronic back painthe influence of mattress quality was more pronouncedcompared to subjects without chronic back pain.
In conclusion, the effect of bed design on sleepcannot be fully assessed by a mere comparison of twodifferent sleep systems in a population of normalsleepers without taking into account interpersonalvariability. This interpersonal variability does not onlyconcern anthropometric differences, but individualposture preferences as well. The results of this studyindicate that a sagging sleep system has a negativeeffect on sleep quality for people who spend most timein a lateral and prone posture. People who spend moretime in a supine posture do not experience this negativeeffect. Consequently, future research should considerthe amount of time spent in each posture as adetermining factor when studying the effect of bedproperties on sleep.
Currently, most sleep systems in the Westernworld are designed to optimise spinal alignment in alateral posture because it is the most commonlyadopted sleep posture in these regions. Some of the
Ergonomics 177
Downloaded By: [Verbraecken, Johan] At: 15:59 18 May 2011

high-end sleep systems have the option ofindividually adjusting mechanical characteristics tothe customer’s anthropometric features, which isalready an important step forward regardingpersonalisation. However, this approach does notaccount for the amount of time that is spent in eachposture. For instance, a high-end sleep system that ispersonalised based on a sleeper’s lateral bodycontours does not result in an optimal spinalalignment if this person sleeps most of the time ina prone and/or supine posture. Therefore, one couldthink of a future sleep system being able to detectposture changes (Verhaert et al. 2009) and, in asecond step, actively change its mechanical propertiesto optimise spine support for the recognised postureduring the night: a so-called ‘active’ sleep system. Infact, since sleep is commonly referred to as an activeprocess, the concept of an active sleep system doesnot seem that far-fetched.
References
Akerstedt, T. and Gillberg, M., 1990. Subjective andobjective sleepiness in the active individual. InternationalJournal of Neuroscience, 52, 29–37.
Bader, G.G. and Engdal, S., 2000. The influence of bedfirmness on sleep quality. Applied Ergonomics, 31, 487–497.
Basner, M., Samel, A., and Isermann, U., 2006. Aircraftnoise effects on sleep: application of the results of a largepolysomnographic field study. Journal of the AcousticalSociety of America, 111, 2772–2784.
Buysse, D.J., et al., 1989. The Pittsburgh Sleep Quality Index:a new instrument for psychiatric practice and research.Psychiatry Research, 21, 193–213.
Cluydts, R., 1979. Gemoedstoestanden en slaap. Thesis (PhD).Vrije Universiteit Brussels.
Coenen, A.M.L., 2006. De slaap en het bed: een psychobio-logische beschouwing. Medische Antropologie, 11, 133–148.
Defloor, T., 2000. The effect of position and mattress oninterface pressure. Applied Nursing Research, 11, 2–11.
De Koninck, J., Lorrain, D., and Gagnon, P., 1992. Sleeppositions and position shifts in five age groups: anontogenic picture. Sleep, 11, 143–149.
DeVocht, J.W., et al., 2006. Biomechanical evaluation offour different mattresses. Applied Ergonomics, 31, 297–304.
Dolan, P., Adams, M.A., and Hutton, W.C., 1988. Com-monly adopted postures and their effect on the lumbarspine. Spine, 11, 197–201.
Drerup, B. and Hierholzer, E., 1994. Back shape measure-ment using video rasterstereography and three-dimen-sional reconstruction of spinal shape. ClinicalBiomechanics, 1, 28–36.
Enck, P., Walten, T., and Traue, H.C., 1999. Associationsbetween back pain, quality of sleep and quality ofmattresses. Double-blind pilot study with hotel guests.Schmerz, 11, 205–207.
Gracovetsky, S.A., 1987. The resting spine. A conceptualapproach to the avoidance of spinal re-injury during rest.Physical Therapy, 61, 549–553.
Haex, B., 2004. Back and bed: ergonomic aspects of sleeping.Boca Raton: CRC Press.
Huysmans, T., 2004. Spine modeling from back shape data: anactive contour and active shape model approach. Thesis(PhD). Katholieke Universiteit Leuven.
Iber, C., et al., 2007. The AASM manual for the scoring ofsleep and associated events: rules, terminology, andtechnical specification. 1st ed. Westchester, IL: AmericanAcademy of Sleep Medicine.
Jacobson, B.H., et al., 2008. Grouped comparisons of sleepquality for new and personal bedding systems. AppliedErgonomics, 31, 247–254.
Jacobson, B.H., et al., 2010. Effect of prescribed sleepsurfaces on back pain and sleep quality in patientsdiagnosed with low back and shoulder pain. AppliedErgonomics, 42 (1), 91–97.
Jasper, H.H., 1958. Report of the committee on methods ofclinical examination in electroencephalography.Electroencephalography and Clinical Neurophysiology, 11,370–375.
Kovacs, F.M., et al., 2003. Effect of firmness of mattress onchronic non-specific low-back pain: randomized, double-blind, controlled, multicentre trial. The Lancet, 361,1599–1604.
Lahm, R. and Iaizzo, P.A., 2002. Physiologic responsesduring rest on a sleep system at varied degrees of firmnessin a normal population. Ergonomics, 41, 798–815.
Lee,H. andPark, S., 2006.Quantitative effects ofmattress types(comfortable vs. uncomfortable) on sleep quality throughpolysomnography and skin temperature. InternationalJournal of Industrial Ergonomics, 31, 943–949.
Lilliefors, H.W., 1967. On the Kolmogorov-Smirnov test fornormality with mean and variance unknown. Journal ofthe American Statistical Association, 61, 399–402.
Mackay, C., et al., 1978. An inventory for the measurementof self-reported stress and arousal. British Journal ofSocial & Clinical Psychology, 11, 283–284.
MacQueen, J.B., 1967. Some methods for classification andanalysis of multivariate observations. In: Proceedings ofthe 5th Berkeley Symposium on Mathematical Statisticsand Probability, Vol. 1, 281–297.
Nachemson, A. and Elfstrom, G., 1970. Intravital dynamicpressure measurements in lumbar discs. A study ofcommon movements, maneuvers and exercises.Scandinavian Journal of Rehabilitation Medicine, 1, 1–40.
Rechtschaffen, A. and Kales, A., 1968. A manual ofstandardized terminology, techniques and scoring system ofsleep stages in human subjects. Los Angeles: BrainInformation Service/Brain Research Institute, Universityof California.
Rousseeuw, P.J., 1987. Silhouettes: a graphical aid to theinterpretation and validation of cluster analysis.Computational and Applied Mathematics, 21, 53–65.
Rithalia, S., 2005. Assessment of patient support surfaces:principle, practice and limitations. Journal of MedicalEngineering & Technology, 21, 163–169.
Scharf, M.B., et al., 1997. Comparative effects of sleep on astandard mattress to an experimental foam surface onsleep architecture and CAP rates. Sleep, 21, 1197–1200.
Vanderwee, K., Grypdonck, M.H.F., and Defloor, T., 2005.Effectiveness of an alternating air mattress for theprevention of pressure ulcers. Age Ageing, 34, 261–267.
Verhaert, V., et al., 2009. Automatic posture recognitionduring sleep. In: Proceedings of the 17th world congress onergonomics. 9–14 August 2009. Beijing. InternationalErgonomics Association (IEA), CD ROM, 2PD0036.
178 V. Verhaert et al.
Downloaded By: [Verbraecken, Johan] At: 15:59 18 May 2011