
A Comparison of Entecavir and Lamivudine for HBeAg-Positive Chronic Hepatitis B

Entecavir Therapy for Lamivudine-Refractory ChronicHepatitis B: Improved Virologic, Biochemical, and
Serology Outcomes Through 96 WeeksMorris Sherman,1 Cihan Yurdaydin,2 Halis Simsek,3 Marcelo Silva,4 Yun-Fan Liaw,5 Vinod K. Rustgi,6 Hoel Sette,7
Naoky Tsai,8 Daniel J. Tenney,9 James Vaughan,9 Bruce Kreter10 and Robert Hindes9 for the AI463026 Benefits ofEntecavir for Hepatitis B Liver Disease (BEHoLD) Study Group
In hepatitis B e antigen (HBeAg)-positive chronic hepatitis B patients who were refractory to currentlamivudine therapy, switching to entecavir was superior to continued lamivudine at week 48 forhistologic improvement, viral load reduction by polymerase chain reaction and alanine aminotrans-ferase normalization. We assessed the efficacy, safety, and resistance profile of entecavir through 96weeksof treatment.Atotalof286patientswererandomizedandtreatedwithentecavir1mg(n�141)or continued lamivudine 100 mg (n � 145). At week 52, 77 entecavir-treated patients who had aprotocol-defined virologic response (HBV branched DNA [bDNA] < 0.7 MEq/mL but HBeAg-positive) continued blinded therapy for up to 96 weeks. Patients were assessed for efficacy, safety, andemerging resistance. Cumulative proportions of all treated patients who achieved confirmed efficacyendpoints were also analyzed. Between week 48 and the end of dosing, the proportions of patientswith HBV DNA <300 copies/mL by polymerase chain reaction increased from 21% to 40%, andalanineaminotransferasenormalization(<1�upper limitofnormal) increasedfrom65%to81%.Inthe second year, HBeAg seroconversion was achieved by 10% of patients. Of the 77 patients in thesecond year treatment cohort, entecavir resistance emerged in six patients, and seven experiencedvirologic breakthrough (five with genotypic resistance acquired before year 2). The safety profile ofentecavir in the second year of therapy was consistent with that reported during year 1. Conclusion:Through 96 weeks of treatment, 1 mg entecavir resulted in continued clinical benefit in lamivudine-refractoryHBeAg-positivechronichepatitisBpatientswithasafetyprofilecomparable to lamivudine.(HEPATOLOGY 2008;48:99-108.)
Chronic hepatitis B virus (CHB) infection is esti-mated to be the 10th leading cause of mortalityworldwide, responsible for the death of between
500,000 and 1.2 million people every year.1,2 Although
an effective vaccine exists, new infections are still frequentand there is a large reservoir of chronically infected indi-viduals.1 These individuals are at high risk of developingserious liver diseases such as cirrhosis and hepatocellular
Abbreviations: ALT, alanine aminotransferase; bDNA, branched-chain DNA; CHB, chronic hepatitis B; HBeAg, hepatitis B e antigen; HBsAg, hepatitis B surfaceantigen; HCC, hepatocellular carcinoma; PCR, polymerase chain reaction; ULN, upper limit of normal.
From the 1Department of Medicine, Toronto General Hospital, Toronto, Ontario, Canada; 2Ankara University Medical School, Ankara, Turkey; 3Medical FacultyInternal Diseases Department, Hacettepe University, Ankara, Turkey; 4Hospital Universitario Austral, Pilar, Argentina; 5Liver Research Unit, Chang Gung Universityand Memorial Hospital, Taipei, Taiwan; 6Metropolitan Research, Fairfax, VA; 7Faculty of Medicine, University of Sao Paulo, Sao Paulo, Brazil; 8John A. Burns Schoolof Medicine, University of Hawaii, Honolulu, HI; 9Bristol-Myers Squibb Company, Research & Development, Wallingford, CT; and 10Bristol-Myers Squibb Company,Research & Development, Princeton, NJ.
Received September 5, 2007; accepted March 4, 2008.Supported by Bristol-Myers Squibb.Address reprint requests to: Morris Sherman, Department of Medicine, Toronto General Hospital, Toronto, Ontario, Canada. E-mail: [email protected]; fax:
416-591-2107.Copyright © 2008 by the American Association for the Study of Liver Diseases.Published online in Wiley InterScience (www.interscience.wiley.com).DOI 10.1002/hep.22323Potential conflict of interest: Dr. Sherman is a consultant for, is on the speakers’ bureau of, and received grants from Bristol Myers Squibb. Dr. Yurdaydin is on the
speakers’ bureau of and received grants from Roche, Novartis, and Gilead. He is also on the speakers’ bureau of Bristol-Myers Squibb. Dr. Simsek is on the speakers’ bureauof and received grants from Bristol-Myers Squibb. Dr. Tsai is a consultant for, advises, is on the speakers’ bureau of, and received grants from Bristol-Myers Squibb, Gilead,and Idenix/Novartis. Drs. Tenney and Kreter own stock in Bristol-Myers Squibb.
99

carcinoma (HCC). Large cohort studies have demon-strated that the risk of liver disease progression in patientswith CHB is associated with elevated hepatitis B virus(HBV) DNA.3,4 There is now additional evidence that asustained reduction in HBV DNA can lead to a decreasein hepatic necroinflammatory response, and halt or re-verse liver disease progression.5-8 Therefore, virologic sup-pression is a major goal of treatment for CHB.9,10
Lamivudine was introduced as a treatment for CHBseveral years before any alternative nucleoside analogs be-came available, and initially proved to be effective in re-ducing HBV DNA.11,12 However, a major liability oflamivudine is the selection of drug-resistant HBV, whichhas been shown to occur in approximately 24% of pa-tients after 1 year of treatment and in as many as 70% ofpatients after 4 years of treatment.13 Lamivudine-resistantviruses carry substitutions in the reverse transcriptase do-main of HBV polymerase—typically involving a changefrom methionine to valine or isoleucine at amino acidposition 204 (M204 I/V) in the tyrosine-methionine-as-partate-aspartate (YMDD) active site motif.14 These sub-stitutions render the virus less replication competent; theM204V change is not observed clinically without an ad-ditional compensatory change (L180M) that allows thevirus to replicate more efficiently.14 Emergence of lami-vudine resistance results in loss of virologic suppression,which can lead to disease progression and, in patients withcirrhosis, to hepatic decompensation, HCC, and removalfrom liver transplantation lists.15,16 As a result, currenttreatment recommendations do not suggest using lamivu-dine in treatment-naive patients.9,10 Adefovir dipivoxil isalso approved for treatment of CHB infection and hasactivity against lamivudine-resistant virus. However, inpatients with lamivudine-resistant HBV, virologic sup-pression is not optimal and resistance to adefovir is in-creased.17,18 There is increasing evidence that addingadefovir to continued lamivudine therapy is associatedwith lower adefovir resistance rates,19 but does not resultin improved virologic suppression.20,21
Entecavir is a potent inhibitor of HBV DNA polymer-ase, which has been shown to be safe and effective for thetreatment of lamivudine-refractory patients with CHB ata dose of 1 mg daily.22,23 In the phase III study ETV-026,switching to entecavir was superior to continued lamivu-dine at week 48 as assessed by histologic improvement,HBV DNA �300 copies/mL, and alanine aminotransfer-ase (ALT) normalization (�1� upper limit of normal[ULN]) in lamivudine-refractory hepatitis B e antigen(HBeAg)-positive CHB patients.23 In this report, we de-scribe the cumulative efficacy, safety, and resistance ofentecavir and lamivudine in lamivudine-refractory pa-tients for up to 96 weeks of blinded treatment. The dura-
bility of treatment responses was also evaluated through24 weeks after treatment in patients who achieved a pro-tocol-defined response and discontinued study therapy.
Materials and Methods
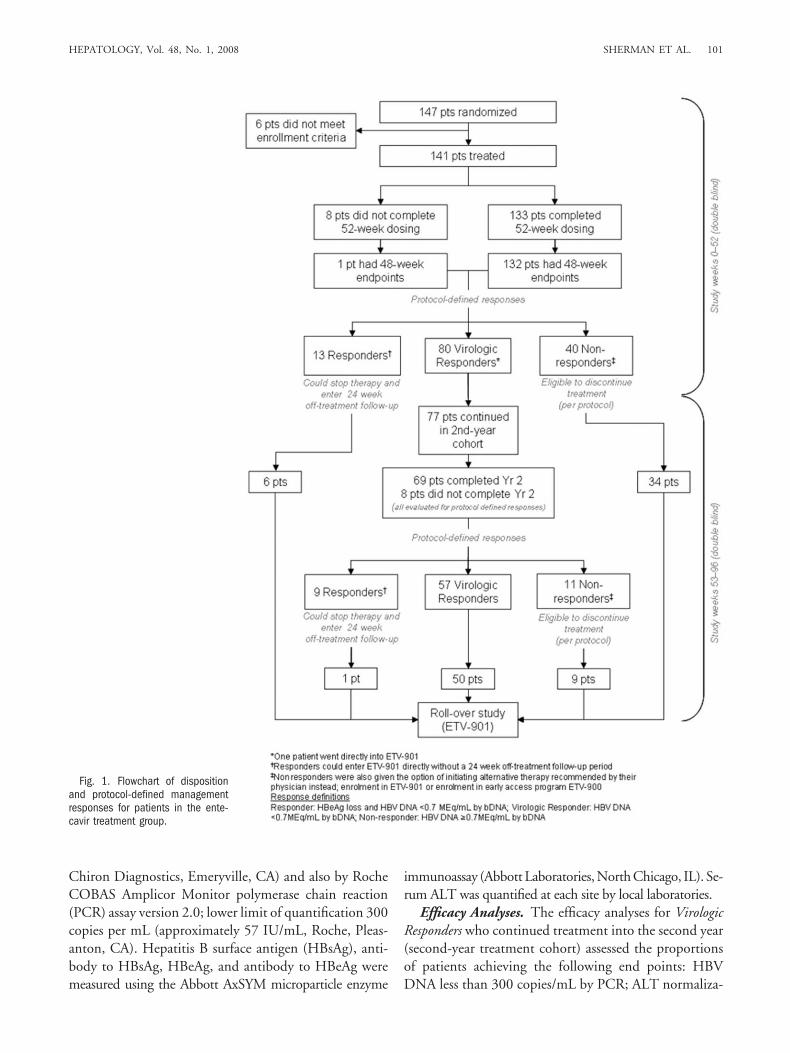
Study Design. This double-blind, double-dummy,randomized, controlled trial compared the safety and ef-ficacy of entecavir 1 mg once daily to continued lamivu-dine 100 mg once daily in HBeAg-positive CHB patientswho were refractory to lamivudine, defined by continuedor recurrent viremia or documented viral resistance dur-ing lamivudine therapy. The study had a 52-week blindedtreatment phase that was followed by an extended blindedtreatment phase for up to 44 additional weeks, for a totalof 96 weeks. The disposition of entecavir-treated patientsis shown in Figure 1. Between February 2002 and De-cember 2002, a total of 293 patients were recruited intothe study from 84 centers around the world.
To assess the hypothesis that finite antiviral therapycould be successful, patients either stopped therapy at theend of 52 weeks of treatment, or continued blinded treat-ment according to protocol-defined patient managementcriteria based on week 48 results for HBV DNA (bDNAassay) and HBeAg status. Efficacy and safety assessmentsfor all patients who completed the first year of blindedtherapy have been reported (23).
Patient management criteria grouped patients intothree distinct categories: Responders, Virologic Responders,and Nonresponders. Responders achieved HBV bDNA lessthan 0.7 MEq/mL and loss of HBeAg; these patients wereto discontinue therapy at week 52 and enter an off-treat-ment follow-up of up to 24 weeks. Nonresponders weredefined as patients whose HBV DNA was �0.7 MEq/mLby bDNA; they also were to discontinue study therapy atweek 52. Both Responders who relapsed during off-treat-ment follow-up and Nonresponders were offered enroll-ment in a rollover protocol (study AI463-901, entecavir 1mg) or were managed according to the discretion of theirphysician. Patients who achieved HBV DNA less than 0.7MEq/mL by bDNA, but who did not achieve HBeAgloss, were considered Virologic Responders and could con-tinue receiving blinded treatment up to week 96. VirologicResponders who became Responders or Nonresponders dur-ing the second year of treatment (week 52–96) discontin-ued study therapy and were managed as previouslydescribed. The management criteria described here aredistinct from the efficacy analyses of the second-year en-tecavir cohort that appear below.
Assay Methodology. Serum HBV DNA was quanti-fied using the Quantiplex bDNA assay, lower limit ofquantification 0.7 MEq/mL (Bayer Diagnostics, formerly
100 SHERMAN ET AL. HEPATOLOGY, July 2008
Chiron Diagnostics, Emeryville, CA) and also by RocheCOBAS Amplicor Monitor polymerase chain reaction(PCR) assay version 2.0; lower limit of quantification 300copies per mL (approximately 57 IU/mL, Roche, Pleas-anton, CA). Hepatitis B surface antigen (HBsAg), anti-body to HBsAg, HBeAg, and antibody to HBeAg weremeasured using the Abbott AxSYM microparticle enzyme
immunoassay (Abbott Laboratories, North Chicago, IL). Se-rum ALT was quantified at each site by local laboratories.
Efficacy Analyses. The efficacy analyses for VirologicResponders who continued treatment into the second year(second-year treatment cohort) assessed the proportionsof patients achieving the following end points: HBVDNA less than 300 copies/mL by PCR; ALT normaliza-
Fig. 1. Flowchart of dispositionand protocol-defined managementresponses for patients in the ente-cavir treatment group.
HEPATOLOGY, Vol. 48, No. 1, 2008 SHERMAN ET AL. 101

tion (�1.0� ULN); and HBeAg seroconversion (loss ofHBeAg and appearance of anti-HBe) at end of dosing (upto 96 weeks).
An efficacy analysis of the cumulative response rateswas also carried out using on-treatment data for all treatedpatients in year 1 and year 2 (entecavir, n � 141; lamivu-dine, n � 145). In this analysis, a cumulative confirmedresponse was defined as two sequential measurements orlast on-treatment measurement through week 96. Cumu-lative confirmed analyses are presented for proportions ofpatients with HBV DNA less than 300 copies/mL andALT normalization. A similar analysis is provided forHBeAg seroconversion through the last observation (on-treatment and 6 months post-treatment). This type ofanalysis does not imply maintenance of the response atweek 96 or during off-treatment follow-up; however, itprovides the cumulative probability of ever achieving aconfirmed end point.
Off-treatment efficacy was evaluated among patientswho were Responders (HBV DNA by bDNA �0.7MEq/mL and HBeAg loss) at week 52 or who becameResponders during the second year of treatment and dis-continued study therapy. Off-treatment efficacy end-points evaluated included HBV DNA �300 copies/mLby PCR, ALT normalization (�1.0� ULN), HBeAgloss, and HBeAg seroconversion at the time of treatmentdiscontinuation and through 24 weeks off treatment (sus-tained responses).
Safety Analysis. The safety analyses presented hereinclude adverse events, serious adverse events, discontinu-ations due to adverse events, and deaths. Cumulative datafor all treated patients during treatment are included inthe on-treatment safety analyses. On-treatment hepaticflares were defined as ALT elevations greater than 2�baseline and greater than 10� ULN. Safety informationfor the off-treatment observation period during which noalternative antiviral therapy was given (up to 24 weeks offollow-up) is described in the off-treatment safety analy-ses. Off-treatment hepatic flares were defined as ALT el-evations greater than 2� reference and greater than 10�ULN; the reference value was defined as the baseline orend-of-treatment ALT value, whichever was lower.
Resistance Analysis. As described elsewhere, geno-typic analysis of HBV polymerase was carried out on allavailable paired baseline and on-treatment samples fromentecavir-treated patients with detectable HBV DNA byPCR (�300 copies/mL, Roche COBAS Amplicor) atweeks 48 and 96, or at end of dosing (up to week 96).23,24
Virologic breakthrough was defined as an increase inHBV DNA of �1 log10 in copies/mL from the on-treat-ment nadir, as determined by at least two sequential mea-surements or the last on-treatment measurement. The
analysis presented here includes patients from the second-year treatment cohort.
Statistical Methods. Since the number of patientscontinuing treatment into the second year in the lamivu-dine group was small (n � 3), this report focuses on theentecavir treatment group and no statistical comparisonsare presented for the second-year cohort results. For thecumulative confirmed analysis, the proportions of pa-tients having achieved a confirmed end point were com-pared between the two treatment groups. Confidenceintervals for differences in proportions were based on thenormal approximation to the binomial distribution, withunpooled proportions used to calculate the standard errorof the difference. P values were based on two-sided tests.
Results
Patient Disposition. At the end of the first year of thestudy, 13/141 (9%) entecavir-treated patients and 1/145(�1%) lamivudine-treated patient achieved a protocol-defined Response (Fig. 1). At the same point in time, 40(28%) entecavir-treated patients and 121 (83%) lamivu-dine-treated patients were classified as Nonresponders. Atotal of 80 (57%) entecavir-treated patients and seven(5%) lamivudine-treated patients were classified as Viro-logic Responders at week 48 and were offered continuedblinded therapy for a second year. Of these, 77 entecavir-treated and three lamivudine-treated patients continuedinto year 2 (Fig. 1). Because only three patients continuedlamivudine therapy, efficacy analyses are not presented forthis treatment arm.
For entecavir patients continuing into the second year,the mean time on treatment through week 96 or end ofdosing was 94.8 weeks. During the second year, eightpatients discontinued blinded entecavir therapy: one pa-tient withdrew consent, there was one death (which wasunrelated to study treatment), and six patients were dis-continued for lack of efficacy (as assessed by the investi-gator). Two of the lamivudine-treated patientsdiscontinued during the second year of treatment: onewithdrew consent and one discontinued due to an adverseevent.
As previously reported, both treatment groups werewell balanced at baseline (pre-treatment) for disease anddemographic characteristics.23 The mean baseline HBVDNA for entecavir-treated patients who continued intothe second year of treatment was comparable to that of allentecavir-treated patients (9.59 log10 copies/mL and 9.48log10 copies/mL, respectively). Mean baseline ALT wasalso comparable between the second-year entecavir treat-ment cohort and all entecavir-treated patients (139.53U/L and 123.9 U/L, respectively).
102 SHERMAN ET AL. HEPATOLOGY, July 2008

Efficacy Results for the Second-Year Entecavir Co-hort. A total of 77 entecavir-treated patients continuedto the second year of blinded treatment. Within the sec-ond-year entecavir cohort, the proportion of patients whoachieved HBV DNA by PCR �300 copies/mL increasedfrom 16 of 77 (21%) at week 48 to 31 of 77 (40%) at theend of dosing (Fig. 2; Table 1). The mean change in HBVDNA from baseline to end of dosing was �5.9 log10
copies/mL. The proportion of patients with ALT normal-ization increased from 50 of 77 (65%) at week 48 to 62 of
77 (81%) at the end of dosing. HBeAg seroconversionwas achieved by 8 of 77 (10%) patients during the secondyear of treatment (Table 1).
Cumulative Confirmed Efficacy Analyses. For alltreated patients, the cumulative proportions of patientsachieving HBV DNA � 300 copies/mL by PCR, ALTnormalization, and HBeAg seroconversion through week96 were greater in the entecavir treatment group than inthe lamivudine treatment group (Table 2). Through year
Fig. 2. Distribution of HBV DNAlevels through week 96 in the sec-ond-year entecavir treatment cohort(n � 77). Circle diameters are pro-portional to the percentage of pa-tients at the specified HBV DNAlevel, with the circles in each columntotaling 100%. EOD, end-of dosing.
Table 1. Proportions of Patients Achieving Efficacy EndPoints at Week 48 and at End of Dosing for the Second-
Year Entecavir Treatment Cohort (n � 77)
Week 48(n � 77)
Week 96/Endof Dosing(n � 77)
HBV DNA by PCR �300 copies/mL, n (%) 16 (21) 31 (40)ALT normalization (�1 � ULN), n (%) 50 (65) 62 (81)HBeAg seroconversion, n (%) 0 (0) 8 (10)
Table 2. Cumulative Confirmed Proportions of PatientsAchieving Efficacy End Points Through Week 96: All Treated
Patients
Number of Patients (%)Entecavir
(n � 141)Lamivudine(n � 145) P value
HBV DNA by PCR �300 copies/mL,n (%) 42 (30) 1 (�1) �0.0001
ALT normalization (to �1 � ULN),n (%) 120 (85) 42 (29) �0.0001
HBeAg seroconversion, n (%) 22 (16) 6 (4) 0.0012
HEPATOLOGY, Vol. 48, No. 1, 2008 SHERMAN ET AL. 103

2, 30% of all entecavir-treated patients achieved HBVDNA �300 copies/mL and 85% had ALT �1� ULN(versus �1% and 29% of lamivudine-treated patients,respectively; P � 0.0001). Among all treated patientsthrough 96 weeks, including 6 months of posttreatmentobservation, 17% of all entecavir-treated patients (24/141) versus 6% of all lamivudine-treated patients (8/145)achieved a confirmed HBeAg seroconversion (P �0.0011). Two entecavir-treated patients also achieved aconfirmed HBsAg loss. This was accompanied by detec-tion of anti-HBs (HBsAg seroconversion) in one patient,and both events were sustained through the last observa-tion on study.
Off-Treatment Results. At week 48 of therapy, 13patients in the entecavir group met the protocol-definedResponse criteria (HBV DNA less than 0.7 MEq/mL andHBeAg loss). Among Responders who discontinued studytherapy, 10 entecavir-treated patients had HBV DNA�300 copies/mL, 11 had ALT normalization, and 11 hadachieved HBeAg seroconversion at the end of dosing.These results were sustained in 10%, 55%, and 45%,respectively, at 24 weeks off-treatment (Table 3).
Of the 77 entecavir patients treated in year 2, ninepatients met the protocol-defined criteria of Response. Atthe time of treatment discontinuation, eight patients hadHBV DNA � 300 copies/mL, eight patients had attainedALT normalization, and eight patients had achievedHBeAg seroconversion. These results were sustained in50%, 63%, and 75%, respectively, through 24 weeks off-treatment (Table 3).
Resistance. Entecavir resistance leading to virologicbreakthrough is associated with the lamivudine-resistancesubstitutions M204V/I and L180M in combination withan additional substitution at residues T184, S202, orM250 in the reverse transcriptase region of HBV poly-merase.24 Through 2 years of treatment in ETV-026, 23patients in the entecavir treatment arm had evidence ofentecavir-resistance substitutions and nine of these pa-tients experienced virologic breakthrough (Table 4). In
the original cohort of patients randomized to receive en-tecavir (n � 141), baseline virus samples from seven pa-tients (5%) had preexisting entecavir-resistancesubstitutions in addition to lamivudine-resistance substi-tutions. None of these seven patients experienced viro-logic breakthrough during year 1 and the specificsubstitutions present at baseline were not associated withhigh-level phenotypic resistance to entecavir in six out ofseven patients.25 Two of the seven patients subsequentlyexperienced breakthrough during year 2 after emergenceof additional entecavir-resistance substitutions, whichconferred high-level entecavir resistance (Table 4).26 Atotal of 10 patients with pre-existing lamivudine-resis-tance substitutions had emergence of genotypic entecavirresistance during the first year of treatment. Two of thesepatients experienced virologic breakthrough during year 1and three of them experienced virologic breakthroughduring year 2.
Of the 77 patients who continued on to a second yearof treatment, HBV DNA measurements by PCR assaywere available for 76 patients. Evidence of genotypic re-sistance to entecavir emerged in six of these patients, andvirologic breakthrough associated with entecavir resis-
Table 3. Proportions of Responders Who Exhibited Sustained Virologic, Biochemical, and Serologic End Points Through 24Weeks Off-Treatment
Number with SustainedEnd Point/Number withEnd Point at Response*
Year-1 Responders Year-2 Responders† Total
ETV(n � 13)
LVD(n � 1)
ETV(n � 9)
LVD(n � 0)
ETV(n � 22)
LVD(n � 1)
HBV DNA �300 copies/mL 1/10 1/1 4/8 0/0 5/18 1/1ALT �1� ULN 6/11 1/1 5/8 0/0 11/19 1/1HBeAg† seroconversion 5/11 0/0 6/8 0/0 11/19 0/0
*Not all patients who had a protocol-defined response (HBV DNA by bDNA � 0.7 MEq/mL and HBeAg loss) also achieved the end points listed in the table.†During the second year of treatment (weeks 52-96), patients could discontinue therapy once Response was identified. Thus, most of these individuals did not receive
a consolidation period after HBeAg loss/seroconversion.Abbreviations: ETV, entecavir; LVD, lamivudine.
Table 4. Genotypic Resistance to Entecavir and VirologicBreakthrough Due to Entecavir Resistance
Baseline Year 1 Year 2 Total
Genotypic resistance* to entecavir 7 10 6 23Virologic breakthrough†
Year 1 0 2 NA 2Year 2 2 3 2 7Total 9
*Genotypic resistance to entecavir was defined as the detection of any aminoacid substitution at positions T184, S202, or M250 in the reverse transcriptaseregion of HBV polymerase, in association with lamivudine-resistance substitutionsat positions M204 � L180.
†Virologic breakthrough was defined as an increase in HBV DNA of �1 log incopies/mL from the on-treatment nadir, as determined by at least two sequentialmeasurements or the last on-treatment measurement in the presence of genotypicresistance substitutions to entecavir.
NA, not applicable.
104 SHERMAN ET AL. HEPATOLOGY, July 2008

tance occurred in two of these patients during year 2. NoALT flares were seen in patients experiencing virologicbreakthrough associated with entecavir resistance.
Predictors of Entecavir Treatment Outcome. Todetermine if there were predictive factors that distin-guished patients who developed virologic breakthroughdue to entecavir resistance from those who achieved HBVDNA �300 copies/mL in the absence of entecavir resis-tance, a variety of baseline demographics and disease char-acteristics were compared, including: race, HBV DNAand ALT levels, Knodell necroinflammatory score, HBVphylogenic genotype, and prior interferon therapy. Pa-tients with HBV DNA �7 log10 copies/mL had a higherprobability of achieving HBV DNA �300 copies/mL onentecavir (8/11, 73%), compared to those with baselineHBV DNA �7 log10 copies/mL (21/130, 16%). A totalof 42 (30%) entecavir-treated patients achieved HBVDNA �300 copies/mL during the first 2 years of therapy,and only one patient who achieved HBV DNA �300copies/mL (at week 72) subsequently developed entecavirresistance (at week 90). No other baseline characteristicswere associated with virologic breakthrough due to ente-cavir resistance.
Examination of the HBV DNA levels at weeks 24 or 48of entecavir therapy showed a correlation between re-duced HBV DNA levels and subsequent maintenance orachievement of undetectable viral loads. Of 24 patientswho had HBV DNA �10,000 copies/mL at week 24, 20(83%) subsequently maintained or achieved HBV DNA�300 copies/mL in year 2 or at end-of-dosing, comparedwith 11 of 53 (21%) patients with HBV DNA �10,000copies/mL at week 24 (P � 0.0001). At week 48, 21 of 23patients (91%) who had achieved HBV DNA �1,000copies/mL subsequently maintained or achieved HBVDNA �300 copies/mL during year 2 or at end-of-dosing,compared with 10 of 54 patients (19%) whose HBVDNA remained above 1,000 copies/mL (P � 0.0001).
Safety Results. The on-treatment safety analyses in-cluded information for all 141 entecavir-treated and 145lamivudine-treated patients up to the point when theydiscontinued study treatment. The mean exposure tostudy drug was 77 weeks for entecavir and 53 weeks forlamivudine. The overall frequency of adverse events, re-gardless of severity or relationship to study therapy, wascomparable between the two groups (entecavir, 83%;lamivudine, 80%; Table 5). The frequency of on-treat-ment serious adverse events was low, and comparable be-tween treatment groups (entecavir, 11%; lamivudine,7%). ALT flare (ALT �2� baseline and �10� ULN)during treatment was observed in fewer entecavir-treatedthan lamivudine-treated patients (�1% versus 11%, re-spectively; Table 5). As previously described,23 the single
ALT flare in the entecavir group was associated with adecline in HBV DNA to �0.7 MEq/mL, which wasmaintained throughout the study, while all the flares inthe lamivudine group were associated with stable or risingHBV DNA levels. Discontinuations due to adverse eventswere less frequent in the entecavir group (two patients;1%) than in the lamivudine group (10 patients; 7%).
A total of 54 patients in the entecavir group and 19patients in the lamivudine group entered an off-treatmentfollow-up period. A total of 33 patients (61%) in theentecavir-treated group and 10 patients (53%) in thelamivudine-treated group had off-treatment adverseevents. The overall frequency of grade 3 to grade 4 adverseevents attributed to study therapy was comparable be-tween treatment groups (entecavir, 6%; lamivudine, 8%).Six patients in the entecavir group and no patients in thelamivudine group experienced an off-treatment ALT flare(ALT �2� reference and �10� ULN). In four of thesepatients—one week-48 Responder and three week-96 Vi-rologic Responders—the flare was associated with a returnof serum HBV DNA levels toward the baseline whentreatment was stopped. The remaining two patients wereNonresponders at the end of dosing.
A total of five deaths occurred during the study, two inthe entecavir treatment group (liver failure and lym-phoma) and three in the lamivudine treatment group(liver failure in two patients and septic shock in one); nodeaths were considered to be related to the study drug.
DiscussionProfound and durable suppression of HBV DNA is a
principal goal of CHB therapy.9,27 Data from the RiskEvaluation of Viral Load Elevation and Associated LiverDisease/Cancer (REVEAL) study demonstrated a clearassociation between elevated HBV DNA and subsequentprogression to cirrhosis and HCC.3,4 In addition, reduc-tion in HBV DNA is linked to improved treatment out-come8 and treatment with antiviral agents has been shown
Table 5. Cumulative On-Treatment Safety Summary ThroughWeek 96
Number of PatientsEntecavir
(n � 141)Lamivudine(n � 145)
Any adverse event (%) 117 (83) 116 (80)Any grade 3-4 adverse event (%) 23 (16) 22 (15)Serious adverse events (%) 15 (11) 10 (7)On-treatment ALT flare* (%) 1 (�1) 16 (11)Discontinuations due to adverse
events (%) 2 (1) 10 (7)Deaths 2 3
*On-treatment ALT flares were defined as ALT �2 � baseline levels and�10 � ULN.
HEPATOLOGY, Vol. 48, No. 1, 2008 SHERMAN ET AL. 105

to reduce the long-term risks of advanced liver disease anddeath among those with compensated cirrhosis.28
The patients included in this large, randomized, clini-cal trial represent a therapeutic challenge: all wereHBeAg-positive, viremic, and had failed prior long-termlamivudine treatment (median, 2.5 years); 85% had doc-umented lamivudine-resistance substitutions at study en-try; and just over 50% had also failed prior interferontherapy.23 In addition, 5% of the total entecavir-treatedcohort demonstrated entecavir-resistance substitutionsprior to any exposure to the drug.
Published year-1 results showed that switching therapyto entecavir was superior to continued lamivudine acrosshistologic, virologic, and biochemical endpoints.23 Theyear-2 results demonstrated that patients continue to ex-perience clinical benefit with entecavir therapy beyond 1year, while the safety profile remained stable. For the sec-ond-year treatment cohort, entecavir therapy increasedthe percentage of patients with HBV DNA �300 cop-ies/mL from 21% to 40% between week 48 and the end ofdosing.
In the current study, entecavir treatment of HBeAg-positive, lamivudine-refractory patients resulted in anoverall mean HBV DNA reduction from baseline of 5.1log10 copies/mL after 48 weeks of treatment. This reduc-tion compares favorably to the results of studies withother agents in lamivudine-refractory patients: 2.4 to 4.0log10 copies/mL with adefovir, and 5.0 to 5.6 log10 cop-ies/mL with tenofovir.29-31 In the second-year entecavirtreatment cohort, increases in viral suppression were ob-served with continued treatment, with patients achievinga mean reduction of 5.9 log10 copies/mL on-treatment atend of dosing. Consistent with greater HBV DNA sup-pression, increases in the proportions of patients achiev-ing ALT normalization and experiencing HBeAgseroconversion between weeks 49 and 96 were also ob-served, with one patient experiencing HBsAg seroconver-sion at the end of follow-up. Patients who achieved HBVDNA levels below 10,000 copies/mL at week 24 or 1,000copies/mL at week 48 were highly likely to maintain orachieve HBV DNA �300 copies/mL during year 2. Thisfinding of potent virologic response being predictive of afavorable outcome on therapy confirms findings withother HBV therapies.25,26
The baseline HBV DNA was higher in this study (9.5log10 copies/mL) than is currently encountered in clinicalpractice of lamivudine-refractory patients. Previous stud-ies on the treatment of lamivudine-refractory CHB havepredominantly examined HBeAg-negative patients withlower baseline HBV DNA levels, a population more likelyto achieve an undetectable HBV DNA and with reducedlikelihood for developing resistance.20,32-35 Although
some antivirals have shown antiviral activity in HBeAg-positive lamivudine-refractory patients, these studies haveinvolved small populations, with lower mean baselineHBV DNA than the patients described here.21,36 Withmore frequent monitoring and improved detection meth-ods, lamivudine resistance is typically identified when apatient’s circulating HBV DNA is less than 6 log10 copies/mL. The probability of achieving HBV DNA �300 cop-ies/mL at 96 weeks with entecavir was 73% in 11 patientswhose baseline HBV DNA was less than 7 log10 cop-ies/mL at study entry, and none of these patients subse-quently developed entecavir resistance. An earlier switchto entecavir in lamivudine-refractory patients while HBVDNA levels remain relatively low could result in HBVDNA reduction to �300 copies/mL in a higher propor-tion of patients, and lower rates of emerging resistancethan were observed in the current study.
Sustained off-treatment responses were evaluated inpatients achieving a protocol-defined Response (HBVDNA �0.7 MEq/mL and loss of HBeAg) who discontin-ued therapy at week 52, or immediately after achieving aResponse in year 2. HBeAg seroconversion was sustainedin 58% (11/19) of Responders. It is now widely recom-mended that nucleoside analog treatment be continuedfor at least 6 months after HBeAg seroconversion duringa consolidation period to increase the probability of sus-taining HBeAg seroconversion off-treatment.6,9,10,37 Thestudy described here was conducted before consolidationtherapy was a part of treatment guidelines and thus wasnot administered. Therefore, the current results may un-derestimate the rate of sustained responses that might beobserved following a consolidation period.
In this comparative study, the first in an exclusivelyHBeAg-positive lamivudine-refractory population, 40%of patients who continued entecavir therapy through 96weeks achieved HBV DNA �300 copies/mL at the endof dosing. Analysis of entecavir-treated patients identifiedseven patients in the total cohort with baseline entecavirresistance substitutions, 10 patients with resistanceemerging in year 1, and six patients with resistance emerg-ing in year 2. These observations suggest an incrementalincrease in the proportion of patients developing resis-tance during the first 2 years of treatment, and not asudden upward surge in the frequency of resistance be-yond year 1. Virologic breakthroughs, however, were onlynoted in two patients in year 1, but increased to sevenpatients through 2 years of treatment. The majority (5) ofthese breakthroughs occurred in patients in whom geno-typic resistance had emerged in prior years. Thus, there isa temporal lag between the time that genotypic resistanceemerges and virologic breakthrough occurs.
106 SHERMAN ET AL. HEPATOLOGY, July 2008

Patients enrolled in this study were part of a largerresistance cohort of 187 entecavir-treated lamivudine-re-fractory patients from three clinical studies.26 Data fromthis cohort predict a cumulative probability of genotypicresistance to entecavir emerging in 6.2% of patients inyear 1 and in 15.0% of patients through year 2. Thecumulative probability of virologic breakthrough associ-ated with genotypic resistance to entecavir was 1.1% inyear 1, and 10.7% through year 2.
The presence of M204V and L180M in patients withlamivudine resistance lowers the genetic barrier to ente-cavir resistance, since only one additional entecavir-resis-tance substitution is needed at T184, S202, and/orM250, compared to a requirement for multiple aminoacid substitutions in wild-type virus.26,38 The emergenceof entecavir resistance after 2 years of therapy is muchlower in the nucleoside-naive population (�1%),38 com-pared to the lamivudine-refractory population,26 due to agreater potency against wild-type HBV and a higher ge-netic barrier.
In this study, entecavir was shown to be less effective inHBeAg-positive lamivudine-refractory patients with highbaseline HBV DNA levels than in lamivudine-refractorypatients. The response in lamivudine-refractory patientsmay be improved by re-establishing a high genetic barrierto resistance by using the combination of potent antiviralswith non-overlapping resistance patterns, such as thecombination of entecavir with either adefovir or tenofo-vir.
The safety profile for entecavir in lamivudine-refrac-tory patients over the first 48 weeks of treatment has beenreported.23 The 96-week safety profile was consistent withchronic HBV infection and was comparable to that seenat 48 weeks. Long-term surveillance of entecavir efficacyand safety in lamivudine-refractory patients continues tobe assessed.
In summary, a second year of entecavir treatment inlamivudine-refractory patients with HBeAg-positiveCHB resulted in continued virologic, serologic, and bio-chemical improvement and a safety profile that was com-parable with the first year of therapy. A longer duration oftreatment and continued treatment of patients withHBeAg loss may lead to higher rates of virologic responseand seroconversion in lamivudine-refractory CHB pa-tients.
Acknowledgment: We acknowledge our colleaguesRichard Colonno, Ronald (Burt) Rose, and Kevin Pokor-nowski for their genotypic analysis of the resistance co-hort included in this work, and Joanna Yang and DongXu for providing data and analyses of treatment assess-ments. In addition to the authors, the EntecavirAI463026 Benefits of Entecavir for Hepatitis B Liver Dis-
ease (BEHoLD) Study Group includes the following in-vestigators: North America: F. Anderson, J. Bloomer, T.Boyer, R. Brown, K. Burak, S. Cotler, R. Gish, S. Gor-don, S. Han, D. Jensen, W. Lee, A. Lok, P. Martin, E.Martinez, P. Pockros, R. Rai, R. Rubin, V. Rustgi, E.Schiff, A.O. Shakil, M. Shiffman, T. Tran, N. Tsai, L.Tyrrell, and V. Yang; South America: F. Carrilho, H.Cheinquer, H. Coelho, and H. Sette; Europe/Middle East:Y. Batur, A. Boron-Kaczmarska, J. Cianciara, A. Gladysz,Z. Gonciarz, S. Hadziyannis, W. Halota, V. Isakov, S.Kaymakoglu, W. Kryczka, R. Modrzewska, F. Nevens, A.Nimer, D. Oguz, V. Pokrovsky, D. Prokopowicz, M.Raptopoulou-Gigi, M. Rizzetto, H. Senturk, D. Shouval,H. Simsek, G. Storozhakov, and E. Tsianos; and Asia/Australia: T.T. Chang, Y.C. Chao, S.K. Chin, G. Cook-sley, J. George, J. Lao-Tan, A. Lee, S.D. Lee, V. Leung,Y.F. Liaw, Y.W. Luk, G. Marinos, S.K. Menon, I. Meri-can, C Pramoolsinsap, S. Roberts, M. Rosmawati, S.Strasser, C.K. Tan, T. Tanwandee, S.S. Wu, and F. Zano.
References1. Lavanchy D. Hepatitis B virus epidemiology, disease burden, treatment,
and current and emerging prevention and control measures. J Viral Hepat2004;11:97-107.
2. Lee WM. Hepatitis B virus infection. N Engl J Med 1997;337:1733-1745.3. Chen C-J, Yang HI, Su J, Jen CL, You SL, Lu SN, et al. Risk of hepato-
cellular carcinoma across a biological gradient of serum hepatitis B virusDNA level. JAMA 2006;295:65-73.
4. Iloeje UH, Yang HI, Su J, Jen CL, You SL, Chen CJ. Predicting cirrhosisrisk based on the level of circulating hepatitis B viral load. Gastroenterology2006;130:678-686.
5. Dienstag JL, Goldin RD, Heathcote EJ, Hann HWL, Woessner M, Ste-phenson SL, et al. Histological outcome during long-term lamivudinetherapy. Gastroenterology 2003;124:105-117.
6. Liaw YF, Leung N, Guan R, Lau GK, Merican I, McCaughan G, et al.Asian-Pacific consensus statement on the management of chronic hepatitisB: a 2005 update. Liver Int 2005;25:472-489.
7. Leung NW, Lai CL, Chang TT, Guan R, Lee CM, Ng KY, et al. Extendedlamivudine treatment in patients with chronic hepatitis B enhances hepa-titis B e antigen seroconversion rates: results after 3 years of therapy. HEPA-TOLOGY 2001;33:1527-1532.
8. Mommeja-Marin H, Mondou E, Blum MR, Rousseau F. Serum HBVDNA as a marker of efficacy during therapy for chronic HBV infection:analysis and review of the literature. HEPATOLOGY 2003;37:1309-1319.
9. Keeffe EB, Dieterich DT, Han SH, Jacobson IM, Martin P, Schiff ER, etal. A treatment algorithm for the management of chronic hepatitis B virusinfection in the United States: an update. Clin Gastroenterol Hepatol2006;4:936-962.
10. Lok AS, McMahon BJ. Chronic hepatitis B. HEPATOLOGY 2007;45:507-539.
11. Dienstag JL, Schiff ER, Wright TL, Perrillo RP, Hann HW, Goodman Z,et al. Lamivudine as initial treatment for chronic hepatitis B in the UnitedStates. N Engl J Med 1999;341:1256-1263.
12. Lai CL, Chien RN, Leung NW, Chang TT, Guan R, Tai DI, et al. Aone-year trial of lamivudine for chronic hepatitis B. Asia Hepatitis Lami-vudine Study Group. N Engl J Med 1998;339:61-8.
13. Lai CL, Dienstag J, Schiff E, Leung NW, Atkins M, Hunt C, et al. Prev-alence and clinical correlates of YMDD variants during lamivudine ther-apy for patients with chronic hepatitis B. Clin Infect Dis 2003;36:687-696.
14. Locarnini S, Mason WS. Cellular and virological mechanisms of HBVdrug resistance. J Hepatol 2006;44:422-431.
HEPATOLOGY, Vol. 48, No. 1, 2008 SHERMAN ET AL. 107

15. Andreone P, Gramenzi A, Cursaro C, Biselli M, Camma C, Trevisani F, etal. High risk of hepatocellular carcinoma in anti-HBe positive liver cirrho-sis patients developing lamivudine resistance. J Viral Hepat 2004;11:439-442.
16. Di Marco V, Marzano A, Lampertico P, Andreone P, Santantonio T,Almasio PL, et al. Clinical outcome of HBeAg-negative chronic hepatitis Bin relation to virological response to lamivudine. HEPATOLOGY 2004;40:883-891.
17. Fung SK, Chae HB, Fontana RJ, Conjeevaram H, Marrero J, OberhelmanK, et al. Virologic response and resistance to adefovir in patients withchronic hepatitis B. J Hepatol 2006;44:283-290.
18. Lee YS, Suh DJ, Lim YS, Jung SW, Kim KM, Lee HC, et al. Increased riskof adefovir resistance in patients with lamivudine-resistant chronic hepati-tis B after 48 weeks of adefovir dipivoxil monotherapy. HEPATOLOGY
2006;43:1385-1391.19. Lampertico P, Vigano M, Manenti E, Iavarone M, Sablon E, Colombo M.
Low resistance to adefovir combined with lamivudine: a 3-year study of145 lamivudine-resistant hepatitis B patients. Gastroenterology 2007;133:1445-1451.
20. Rapti I, Dimou E, Mitsoula P, Hadziyannis SJ. Adding-on versus switch-ing to adefovir therapy in lamivudine-resistant HBeAg-negative chronichepatitis B. HEPATOLOGY 2007;45:307-313.
21. Peters MG, Hann HH, Martin P, Heathcote EJ, Buggisch P, Rubin R, etal. Adefovir dipivoxil alone or in combination with lamivudine in patientswith lamivudine-resistant chronic hepatitis B. Gastroenterology 2004;126:91-101.
22. Chang TT, Gish RG, Hadziyannis SJ, Cianciara J, Rizzetto M, Schiff ER,et al. A dose-ranging study of the efficacy and tolerability of entecavir inlamivudine-refractory chronic hepatitis B patients. Gastroenterology2005;129:1189-1209.
23. Sherman M, Yurdaydin C, Sollano J, Silva M, Liaw YF, Cianciara J, et al.Entecavir for treatment of lamivudine-refractory, HBeAg-positive chronichepatitis B. Gastroenterology 2006;130:2039-2049.
24. Tenney DJ, Levine SM, Rose RE, Walsh AW, Weinheimer SP, Discotto L,et al. Clinical emergence of entecavir-resistant hepatitis B virus requiresadditional substitutions in virus already resistant to lamivudine. Antimi-crob Agents Chemother 2004;48:3498-3507.
25. Baldick CJ, Eggers BJ, Fang J, Levine SM, Pokornowski KA, Rose RE, etal. Hepatitis B virus quasispecies susceptibility to entecavir confirms therelationship between genotypic resistance and patient virologic response. JHepatol 2008 (in press). Epub ahead of print. DOI 10.1016/j.jhep.2007.12.024
26. Tenney DJ, Rose RE, Baldick CJ, Levine SM, Pokornowski KA, WalshAW, et al. Two-year assessment of entecavir resistance in lamivudine-refractory hepatitis B virus patients reveals different clinical outcomes de-pending on the resistance substitutions present. Antimicrob AgentsChemother 2007;51:902-911.
27. Sherman M. Predicting survival in hepatitis B. Gut 2005;54:1521-1523.28. Liaw YF, Sung JJY, Chow WC, Farrell G, Lee CZ, Yuen H, et al. Lami-
vudine for patients with chronic hepatitis B and advanced liver disease.N Engl J Med 2004;351:1521-1531.
29. Peters MG, Hann HW, Martin P, Heathcote EJ, Buggisch P, Rubin R, etal. Adefovir dipivoxil alone or in combination with lamivudine in patientswith lamivudine-resistant chronic hepatitis B. Gastroenterology 2004;126:91-101.
30. van Bommel F, Wunsche T, Mauss S, Reinke P, Bergk A, Schurmann D,et al. Comparison of adefovir and tenofovir in the treatment of lamivudine-resistant hepatitis B virus infection. HEPATOLOGY 2004;40:1421-1425.
31. Hann HWL, Chae H, Dunn SR. Tenofovir (TNV) has a stronger antiviraleffect than adefovir dipivoxil (ADV) against lamivudine (LAM) resistanthepatitis B virus (HBV). Presented at Digestive Diseases Week (DDW).Gastroenterology 2006;130:4(Suppl 2): abstract T1841.
32. Lampertico P, Marzano A, Levrero M, Santantonio T, Di Marco V, Bru-netto M, et al. Adefovir and lamivudine combination therapy is superior toadefovir monotherapy for lamivudine-resistant patients with HBeAg-neg-ative chronic hepatitis b. Presented at the 57th Annual Meeting of theAmerican Association for the Study of Liver Diseases (AASLD). HEPATOL-OGY 2007;46 (Suppl): abstract LB5.
33. Lampertico P, Vigano M, Manenti F, Iavarone M, Lunghi G, Del NinnoE, et al. Three years of adefovir and lamivudine combination therapyminimizes the risk of genotypic resistance to adefovir in lamivudine resis-tant patients. Presented at the 42nd Annual Meeting of the EuropeanAssociation for the Study of the Liver (42nd EASL). J Hepatol 2007;44(Suppl 2): abstract 57.
34. Hann HW, Chae H, Dunn SR. Tenofovir has stronger antiviral effect thanadefovir dipivoxil against lamivudine-resistant hepatitis B virus. Presentedat the 41st Annual Meeting of the European Association for the Study ofthe Liver (41st EASL). J Hepatol 2006;44(Suppl 2): abstract 495.
35. Gane E, Safadi R, Xie Q, Chen Y, Yin Y, Wei L, et al. A randomized trialof telbivudine versus lamivudine in lamivudine experienced patients-week24 primary analysis. Presented at the 57th Annual Meeting of the Ameri-can Association for the Study of Liver Diseases (AASLD). HEPATOLOGY
2007;46(Suppl): abstract 1007.36. van Bommel F, Zollner B, Sarrazin C, Spengler U, Huppe D, Moller B, et
al. Tenofovir for patients with lamivudine-resistant hepatitis B virus(HBV) infection and high HBV DNA level during adefovir therapy. HEPA-TOLOGY 2006;44:318-325.
37. EASL Jury. EASL International consensus conference on hepatitis B.J Hepatol 2003;39:S3-S25.
38. Colonno RJ, Rose R, Baldick CJ, Levine S, Pokornowski K, Yu CF, et al.Entecavir resistance is rare in nucleoside naive patients with hepatitis B.HEPATOLOGY 2006;44:1656-1665.
108 SHERMAN ET AL. HEPATOLOGY, July 2008
Copyright © 2022 FDOKUMEN










