Enhancing a sector approach in health in the context of the New Deal for Somalia
54
Enhancing A Sector Approach in Health (05-03-2014) 1 Enhancing A Sector Approach In Health In the context of the New Deal for Somalia Review Report 5 March 2014 Analysis commissioned by the Somali Health Advisory Board in September 2013 Funded by the Department for International Development (DfID, UK). Conducted in November – December 2013. Authors: David Daniels Harry Jeene Marina Madeo
Transcript of Enhancing a sector approach in health in the context of the New Deal for Somalia
Enhancing A Sector Approach in Health (05-03-2014)
1
Enhancing A Sector Approach In Health
In the context of the New Deal for Somalia Review Report 5 March 2014
Analysis commissioned by the Somali Health Advisory Board in September 2013 Funded by the Department for International Development (DfID, UK). Conducted in November – December 2013.
Authors: David Daniels Harry Jeene Marina Madeo
Enhancing A Sector Approach in Health (05-03-2014)
2
Contents page
Executive Summary 4
1. Introduction 6
1.1 Background 1.2 The New Deal and the Compact
2. The implications of the New Deal on Health 8
2.1 The implications of the Compact, the new aid finance arrangements and aid principles on the health sector
2.2 The implications for the health sector of actions agreed in PSG 5 on Revenue and Service Delivery
2.3 The implications for the health sector of the draft Economic Recovery Plans.
2.4 Some concluding comments on the New Deal and its implications
3. Current Health Sector Context 13 3.1 Profile of the Health Sector 3.2 The Health Sector Strategic Plans (2013-2016) 3.3 Political context 3.4 Health Sector stakeholder analysis 3.5 Financing the Health Sector 3.6 Health Sector coordination 3.7 Transitioning from Humanitarian Assistance to development 3.8 Conclusions and potential for change
4. Options for a broader sector wide financing mechanism for the
Health Sector 29
5. Additional steps necessary to move towards a Sector Approach in Health, including the timeframe for this to take place. 35
6. Conclusion 39
Annexes 41 Annex 1 - People Consulted Annex 2 - Documents Reviewed Annex 3 - The New Deal at a glance Annex 4 - IHP+ Seven Behaviours Annex 5 - New Deal for Somalia – Pledges Annex 6 - Key Health Indicators Annex 7- Definitions - Health Sector Strategic Plans (HSSPs) Annex 8 - Definitions – Sector-Wide Approach (SWAp)
Enhancing A Sector Approach in Health (05-03-2014)
3
Acronyms AfDB African Development Bank AusAID Australian Agency for International Development CAP Consolidated Appeal Process CCM Country Coordinating Mechanism (for GFATM grants) DFID Department For International Development DoH Directorate of Health DPT-3 Diphtheria, Pertussis and Tetanus – 3 doses EPHS Essential Package of Health Services. EPI Expanded Programme of Immunization ERP Economic Recovery Plan EU European Union FGS Federal Government of Somalia GFATM Global Fund to fight AIDS, Tuberculosis & Malaria HAB Health Advisory Board HCS Health Consortium Somalia HIS Health Information System HMIS Health Management Information System HPA Health Poverty Action (INGO) HR Human Resources HSC Health Sector Committee HSS Health Systems Strengthening HSSP Health Sector Strategic Plan ICC Interagency Coordinating Committee (for GAVI grants) IHP+ International Health Partnership and related initiatives IMC International Medical Corps (INGO) INGO International NGO IRC International Rescue Committee (INGO) JANS Joint Assessment of National Strategy (IHP+) JAR Joint Annual Review JHNP Joint Health and Nutrition Programme JPLG Joint Programme of Local Governance MDTF Multi Donor Trust Fund MICS Multiple Indicators Cluster Survey MoH Ministry of Health MPTF Multi Partner Trust Fund NAC National AIDS Commission NGO Non-Governmental Organization NSA Non State Actors PFM Public Financial Management PR Principal Recipient (GFATM) PSG Peacebuilding and Statebuilding Goals PSI Population Service International (INGO) RMNCH Reproductive, Maternal, Neonatal and Child Health SCI Save the Children International (INGO) SDF Somaliland Development Fund SHA Somali Health Authorities SIDA Swedish International Development Agency SRCS Somali Red Crescent Society SRDF Somalia Reconstruction and Development Facility SSF Somalia Stability Fund SWAp Sector-Wide Approach THET Tropical Health & Education Trust (INGO) UN United Nations UNFPA United Nations Population Fund UNICEF United Nations Children’s Fund USAID United States Agency for International Development WHO World Health Organization
Enhancing A Sector Approach in Health (05-03-2014)
4
Executive Summary A review1 of the implications of the New Deal and Compact on the health sector was conducted in December 2013 and included an assessment on its implications for future health sector financing. The review looks at the options open to the health sector for moving towards a more developmental sector approach taking into account the wider context of political and social change across the country. Several health financing options exist or are emerging and their feasibility and suitability are assessed including wider issues of security, government legitimacy, access and stakeholder relationships and how these vary across the country. The review shows that the health sector has made good progress in the last few years on coordination, planning and systems development. The drafting and adoption of Health Sector Strategic Plans by health authorities is now being further underpinned by work on the HMIS, Joint Annual Review (JAR) process, M&E and Human Resource Development initiatives. There is also a growing debate and confidence about transitioning from humanitarian aid to more development approaches while recognising that the former still has an important role to play. The current financing mechanisms supporting the health sector include joint funded programmes such as the JHNP and JPLG, bilateral health programmes, humanitarian assistance in more conflict affected regions and severe environmental conditions, and social protection initiatives aimed at some of the more marginalised communities. The review supports a gradual move to a sector approach, being realistic about the time it will take and the challenges, risks and variation that exist across the country. A move towards on-budget support aligned to the country owned Health Sector Strategic Plans, annual work plans and budgets is now encouraged as well as the continued support and accelerated roll-out of existing joint funded programmes that contribute to the building of more robust central and regional systems. This could include limited on-treasury support to core systems development to stimulate government systems strengthening and increase confidence in future use of these systems. This measured move towards sector working can be supported through the new financing “Windows” under SRDF and through the SDF. The risks will be seen as high but these can be mitigated through careful planning and transparent processes. The review also encourages taking up the challenges of the New Deal principles that have been worked on in the health sector through IHP-like activities for the last few years. This will require further improvement of government ownership and leadership and more attention and commitment to mutual accountability around health sector pooled funding arrangements and aligned bilateral programmes. The location of future pooled fund arrangements requires more analysis and dialogue between donors and government on the options that are emerging. For example this type of arrangement could be organised through the WB MDTF Window, the UN MPTF Window, or the SDF for Somaliland, or alternatively, a new pooled funding arrangement outside these “Windows”. The role of more direct support to communities and households through bilateral programmes at regional or district levels or social protection programmes are also important complementary approaches that will help to improve access for the more marginalised people and those with limited access due to security. The review also highlights some of the wider opportunities, risks and challenges to progress in the health sector. The complex political discussions that surround the New Deal and pledged resources may or may not impact on the ability of health sector
1 The review team included: David Daniels, Dr Marina Madeo and Dr Harry Jeene.
Enhancing A Sector Approach in Health (05-03-2014)
5
stakeholders to maintain the current high levels of cooperation and dialogue across the country. This will depend on the diverse and shifting political processes taking place in the country and the dialogue between the FGS, Somaliland and Puntland authorities, as well as other regional and local authorities. It will also depend on the facilitation role expected from the international actors and their adherence to harmonization and alignment principles. Moves towards more transparency and on-budget support from donors is in line with the New Deal principles (and those of the IHP+) although this will be challenging given the push by many of these same donors for more tangible results in the short term and their attribution to specific investments. The review found that many stakeholders see the potential role of the health sector and improved basic services in peace-building, and the importance of establishing transparent and accountable systems in enhancing government legitimacy and state-building. The report provides an overview of funding modalities and the relevance of each to the health sector now and as progress is made in developing the SRDF financing “Windows” and the SDF mechanism. In summary the New Deal should allow sector Ministries to benefit from funding to develop government core functions, such as public sector financial, management, accounting and audit, human resources development and information systems. The health sector, building on its progresses so far, can be proposed as a pilot sector for the development of systems related to some of these government core functions. Budget support is unlikely for many years to come given the work ahead in establishing these core systems; however, some small budget support could be used to build trust, stimulate progress and test systems. Ministries of health and donors must work together to advocate for a share of general funds through the new financing windows being established, either as a share of the overall funding to systems, or through establishing earmarked, pooled funding for health. Pooled funding for donors that have compatible policies should be the preferred option. Bilateral programmes will no doubt continue and grow. Whatever the funding modalities and related management arrangements, the important issue is to ensure alignment to the HSSPs and respective Annual Work Plans and Budgets, and increasingly having all funds on-budget, i.e. planned and reported within health sector processes. The importance of maintaining progress in developing a sector approach is stressed and a number of steps are highlighted for government, donors, UN and implementing partners. Key to success in this transitional period is to ensure that development assistance encourages and underpins the steps being taken on peace-building and state-building. The New Deal with its promise of substantial new resources from the international community must aim to both build the legitimacy of the State and ensure equitable distribution of benefits across the country. This report suggests health has been at the vanguard of development and has a major role to play in the New Deal agenda.
Enhancing A Sector Approach in Health (05-03-2014)
6
1. Introduction 1.1 Background In September 2013, the Somali Health Donors proposed an analysis to look at the implications of the New Deal on Health and opportunities for enhancing a sector approach to the Somali health sector. The draft Terms of Reference (ToR) for the analysis were presented and discussed during the meetings of the Somali Health Sector coordination bodies (10th-13th September 2013 in Nairobi). The Health Advisory Board (HAB) welcomed the proposal, recognizing the opportunity to have a common understanding of the potential impact of the New Deal, the ways for involvement and benefit from the process, as well as contributing to it, based on the particular experience of the Somali health sector in the past few years. The report follows the order of the objectives as indicated in the ToR for the analysis:
A. To identify the implications of the New Deal on Health (see Section 2), including:
a) the implications of the Compact, the new aid finance arrangements and aid principles
b) the actions agreed in PSG 5 on revenue and service delivery c) the implications of the draft Economic Recovery Plan on the health sector
B. Conduct a sector wide analysis of the factors that affect the performance of the sector, including the interests and incentives at work (see Section 3)
C. Explore the options for a broader sector wide financing mechanism for the Health Sector (see Section 4)
D. Identify the additional steps necessary to move towards a Sector Approach in Health, including the timeframe for this to take place (see Section 5)
Key contextual elements supporting the rationale of this work include:
• The health status of the Somali population, with indicators among the worst in the world and less than positive trends.
• The needs of the Somali health sector for capacity building and for increased and more effective management and financing, in order to improve services and ultimately the health of the Somali population.
• The already existing understanding, among the Somali health sector partners, of the principles of aid effectiveness (IHP-like approach) and the need for transition from humanitarian to development approach.
• The current changing context – political, of international relationships, of willingness of Somali and external actors – providing great opportunities.
The report’s findings are based on a review of document, studies and reports (Annex 2) relating to National Development Plans, the Somali health sector, the New Deal, the Compact, PSGs and proposed actions and financial arrangements. The review team conducted consultations in Mogadishu, Garowe, Hargeisa and Nairobi with key stakeholders including representatives of the Somali authorities from Ministries of Finance, Planning and Health, Somali Non-State Actors, Donors, UN agencies, international NGOs, and academic institutions (Annex 1).
Enhancing A Sector Approach in Health (05-03-2014)
7
1.2 The New Deal and the Compact Global context The global “New Deal for Engagement in Fragile States” was developed through the forum of the International Dialogue for Peace building and State building2, presented at the Fourth High-Level Forum on Aid Effectiveness in Busan, Korea, in November 2011 and endorsed by over 44 countries (including Somalia) and multilateral partners. The New Deal is the agreement between fragile states and partners and represents the official commitment to realize the principles of the Paris Declaration (and subsequent statements) in fragile states. The New Deal defined five Peacebuilding and Statebuilding Goals (PSGs) as the foundation for progress and a guide for work in fragile and conflict-affected states. • PSG 1 – Legitimate Politics. Foster inclusive political settlements and conflict
resolution • PSG 2 – Security. Establish and strengthen people’s security • PSG 3 – Justice. Address injustices and increase people’s access to justice • PSG 4 – Economic Foundations. Generate employment and improve livelihoods • PSG 5 – Revenues and Services. Manage revenue and build capacity for fair and
accountable service delivery The New Deal defined the FOCUS, five elements in the new way for engagement, supporting inclusive, country-owned and country-led pathways out of fragility, and the TRUST, a set of commitments related to resources and financial management to enhance transparency, manage risk to use country systems, strengthen national capacities and improve the timeliness and predictability of aid. (Annex 3 – New Deal at a glance) In 2012 the New Deal implementation kicked off. Seven countries began piloting the New Deal: Afghanistan, Central African Republic, Democratic Republic of Congo, Liberia, Sierra Leone, South Sudan and Timor Leste; supported by Partner countries: Australia, Denmark, European Union, France, Netherlands, Sweden, UK and USA. The New Deal for Somalia On 16 September 2013 the Conference “A New Deal for Somalia” was held in Brussels, co-hosted by the Somali Federal Government and the European Union, with participation from Somali regions, Members of Parliament and civil society, and the international community. The Conference endorsed the Somali Compact, pledged support to enable its implementation and re-commit to the Somali political process. The financial pledges from development partners, as of September 2013, are over $2.4 billion (USD) with EU, UK and Norway as top donors, followed by Denmark, Sweden, Germany and 16 others (Annex 5 – New Deal for Somalia – Pledges). The Somali Compact The Compact priorities are drawn from existing plans and strategies: the Six Pillar Programme of the FGS, the Puntland second Five-year Development Plan and, by including a Special Arrangement for Somaliland, from the Somaliland National
2 The International Dialogue on Peacebuilding and Statebuilding is the first forum for political dialogue to
bring together conflict-affected and fragile countries, international partners and civil society. http://www.pbsbdialogue.org
Enhancing A Sector Approach in Health (05-03-2014)
8
Development Plan. These priorities and their objectives are framed according to the five PSGs, are agreed upon between Somalis and Partners and represent the commitment for aligning domestic and external efforts.
The Somali Compact acknowledges the complex and different challenges faced by Somalia and provides the strategic framework for coordinating political, security and development efforts as well as defining a set of priorities – for the next three years (2014-2016) – toward long-term peace and state-building. The New Deal is important as it raises the profile of Somalia on the international stage and represents a commitment to change and support by a broad section of the international community. With the signing of the Compact comes an expectation of continued progress in internal stability and security. The substantial pledging of support to institution building and social development also brings with it the need to demonstrate measurable progress both by national authorities and by the international community.
2. The implications of the New Deal on Health 2.1 The implications of the Compact, the new aid finance arrangements and aid
principles on the Health Sector The New Deal and Compact have both political and financial implications for the health sector. The political discussions have included concerns that the process has concentrated on the Federal Government and South Central regions of the country. This has raised concerns in Somaliland and Puntland about the effect on centralisation of powers in Mogadishu. These regional tensions have affected attendance at Conferences and led to the call for special arrangements for Somaliland. The implications of these political discussions on sectoral working are yet to be seen but commentators have highlighted both opportunities and threats for the health sector. The limited participation by sectoral stakeholders and others in the Compact and New Deal discussions, which were reported as too rushed, was seen by some commentators in government as a lost opportunity for ownership and understanding of these instruments. It was also noted that the level of engagement has increased since the Brussels Conference and is becoming more substantial with the establishment of PSG working groups. The New Deal profiles the health sector as an example of progress in policy, planning and service delivery, albeit modest. The New Deal can be an opportunity to reinforce the approach already present in the health sector and raise its profile with senior government officials, including those in Ministries of Finance and Planning, as an important element of peace-building and state legitimacy. With this higher profile there also comes the potential of more negative political involvement with health being brought into wider regional tensions that could alter the current productive approach between health authorities on coordinated and harmonised policy and planning. The increased external assistance that should materialise from the international pledges of $2.4m presents an obvious opportunity for the health sector to increase the flow of sectoral development funding. The Somalia Reconstruction and Development Facility (SRDF) is a new mechanism to support national priorities as highlighted in the Economic Recovery Plan (ERP). This financing umbrella is designed to work through four mechanisms, A World Bank Multi-Donor Trust Fund; a UN Multi-Partner Trust Fund; an
Enhancing A Sector Approach in Health (05-03-2014)
9
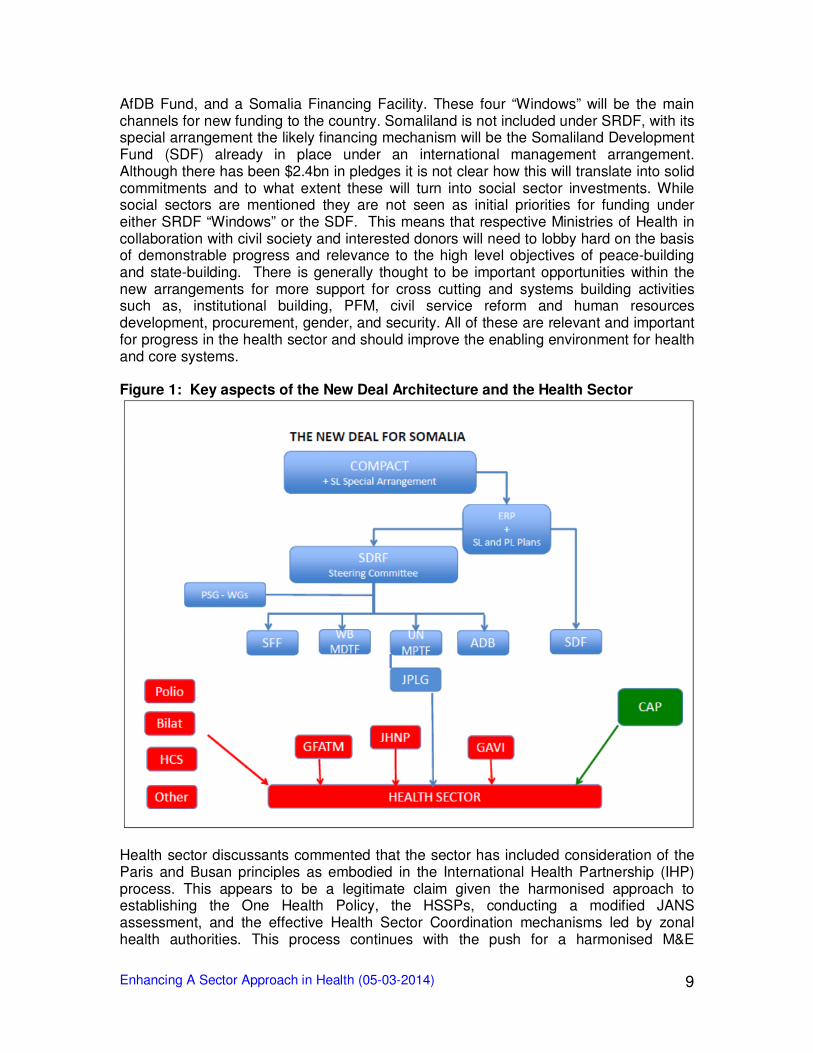
AfDB Fund, and a Somalia Financing Facility. These four “Windows” will be the main channels for new funding to the country. Somaliland is not included under SRDF, with its special arrangement the likely financing mechanism will be the Somaliland Development Fund (SDF) already in place under an international management arrangement. Although there has been $2.4bn in pledges it is not clear how this will translate into solid commitments and to what extent these will turn into social sector investments. While social sectors are mentioned they are not seen as initial priorities for funding under either SRDF “Windows” or the SDF. This means that respective Ministries of Health in collaboration with civil society and interested donors will need to lobby hard on the basis of demonstrable progress and relevance to the high level objectives of peace-building and state-building. There is generally thought to be important opportunities within the new arrangements for more support for cross cutting and systems building activities such as, institutional building, PFM, civil service reform and human resources development, procurement, gender, and security. All of these are relevant and important for progress in the health sector and should improve the enabling environment for health and core systems. Figure 1: Key aspects of the New Deal Architecture and the Health Sector
Health sector discussants commented that the sector has included consideration of the Paris and Busan principles as embodied in the International Health Partnership (IHP) process. This appears to be a legitimate claim given the harmonised approach to establishing the One Health Policy, the HSSPs, conducting a modified JANS assessment, and the effective Health Sector Coordination mechanisms led by zonal health authorities. This process continues with the push for a harmonised M&E
Enhancing A Sector Approach in Health (05-03-2014)
10
framework and the forthcoming first Joint Annual Review (JAR) of the HSSPs due in February 2014 facilitated by the WHO and other UN partners. One of the commonly quoted implications of the Compact is on accelerating the introduction of aid effectiveness principles into the relationship between government, donors and implementing agencies. Most non-health discussants interviewed also highlighted the efforts and progress made by the health sector, in the past few years, in pursuing the principles of aid effectiveness. This could be seen as a key starting point for positioning the health sector in the New Deal process, and one option is to propose the sector as a pilot for the implementation of core systems development through the new funding “Windows”. A process toward sectoral approach will link these “windows” in terms of funding modalities. According to the draft Terms of Reference of the UN MPTF, the existing UN joint programmes related to PSG5, such as JPLG and JHNP, would be phased into the Somalia UN MPTF over time, maintaining their funding channels and governance bodies but also subject to the common reporting standards required by the SRDF and under the same oversight mechanism. The impact of this provision if realized could be very positive in at least two aspects. Firstly, the alignment of JHNP with the wider aid coordination framework would bring benefits in terms of coordination and synergies with other initiatives in the health sector and beyond. Secondly, the JHNP experience in governance with the three MoHs of FGS, Puntland and Somaliland would be a living example, within the SDRF, of balanced technical collaboration among national and different regional authorities. In the longer term, subsequent phases of joint programmes could be fully under the new aid architecture also including funding channels and integrated governance structure. The principles and approaches expressed in the draft UN MPTF ToR could have a positive impact. It could mean that the trust fund is fully aligned under the SRDF and therefore accountable to a system wider than the UN and donors and tailored to the country context. In addition, it could mean that the MPTF will function as an alignment instrument within the UN system. If the UN agencies working in health will promote programmes and projects under the trust fund then this will create increasing funding opportunities for the sector. A challenge will be to have all new initiatives fully aligned to the HSSPs and country’s development plans, rather than the current more fragmented set of programmes managed by the UN. The role of the government and donors in endorsing all such initiatives will be critical. 2.2 The implications for the Health Sector of actions agreed in PSG 5 on Revenue
and Service Delivery The PSG 5 - Revenues and Services, includes in its strategic objective to “Increase the delivery of equitable, affordable, and sustainable services”. The critical role of non-state actors (private and NGOs) in the provision of services is recognised and expected to continue, but increasingly under the umbrella of the government and in a regulated and standardized framework. At the same time the role that service delivery plays in building trust between state and society and in increasing the legitimacy of public institutions is emphasized. The SRDF and four financing “Windows” discussed above are being established to fund priority actions under PSGs.
Enhancing A Sector Approach in Health (05-03-2014)
11
Based on sectoral workshops convened to discuss priorities in the ERP, five PSG Working Groups have been established with the involvement of the FGS’ Ministry of Human Development and its Directorate of Health (now Ministry of Health) in the PSG 5 WG. PSG 5 relates to core state functions and social sectors and includes three priority areas consistent with the Health Sector Strategic Plans: Leadership and Governance, Human Resources and Service Delivery. The overall partnership framework provided in the Compact, as well as a number of actions under other PSGs (1-4) and the cross-cutting issues, are also relevant for the health sector. The New Deal Fragility Assessment Somali’s Input Paper on PSG 5 raises a range of issues and challenges as well as drivers of fragility and resilience. One of the issues relevant to the health sector is the “fragmented delivery of humanitarian and development services” and the fact that these are “off-budget and therefore side-lining nascent and emerging country systems”. This is generally consistent with the health sector situation with limited “on-budget” programming especially for humanitarian aid. The JHNP is the only donor-funded support that appears to be proactively aligned with the HSSP and this was done retrospectively demonstrating commitment of the funding and implementing partners. The analysis also highlights the weaknesses in the public sector in terms of “managerial, technical and administrative skills” and the causative “absence of academic institutions, emigration of skilled human resources, overstaffing of institutions resulting in high recurrent costs, low productivity and an organizational culture that is not conducive for effective service delivery and public service”. These are major issues that have been recognised in the three HSSPs and prioritized in the first Annual Work Plans and Budgets (2103) for health. Unfortunately as yet little support has been provided to implementing this section of the Plans. The health and education sectors are recognised as showing signs of progress in service delivery through pragmatic approach that makes use of available resources and financing instruments, including humanitarian assistance channelled through a range of civil society organisations. This is all off-budget and mainly outside the decision-making of health authorities at zonal level although more engaged with local authorities and groups in control of disputed areas. In terms of financial systems it is widely recognised that across government, including the health sector, public financial management systems are very weak, this being a result of years of conflict, destructive of government systems. Revenues remain low as do skills and capacities. As such fiduciary risk is high across Somalia although significant variation exists. Risk in Somaliland and to a lesser extent Puntland is seen as lower, while high across South Central. In all HSSPs the option of greater contracting in and out of primary health services is included as a pragmatic approach to expanding EPHS services and improving quality. However to date contracting competencies and procurement systems are still lacking to allow any movement in this direction. The effect of the introduction of the SRDF could be that new funds do not reach the health sector and health sector specific funding is not increased. For this reason the health authorities will need to consider how to promote their sector as a recipient of funding for core PSG 5 priority actions under the financing “Windows” while keeping, as transitional, existing sector specific pooled funding instruments such as the JHNP. The review understood that the UN managed JHNP would stay as a pooled fund, even though possibly under the SRDF’s oversight mechanism, and so could continue to build
Enhancing A Sector Approach in Health (05-03-2014)
12
sector capacity and expand EPHS coverage through to 2016. The current debate as to the fate of the UN managed JPLG was not yet clear and this may be included in the UN Trust Fund. The implications of such a decision and the implications for allocation of district budgets for health are therefore also unclear. Given the scale of funding the fate of the JPLG should be seen as an area for advocacy for health sector stakeholders. 2.3 The implications for the Health Sector of the draft Economic Recovery Plans.
Different zonal Development plans exist for South Central Somalia (Economic Recovery Plan), Somaliland (Somaliland National Development Plan), and Puntland (draft 5 Year Development Plan). The ERP is focused on the 11 regions of SCS and this is important when considering wider issues of development, federalism and international cooperation in Somalia. ERP and the Health Sector The Economic Recovery Plan (ERP) was drafted by the FGS and this is proposed as the basis of an interim Poverty Reduction Strategy Paper (PRSP). It is meant as an instrument to guide the transition from emergency relief to early recovery and development and as such is an ambitious document. It looks to provide a basis for increasing the role of the Federal and Regional governments in managing and monitoring the development process. It was prepared with line Ministries and includes indicative costings. The ERP focuses on four main sectors: 1. Core State Functions; 2. Productive and Natural Resources; 3. Infrastructure; 4. Social. The ERP includes a number of flagship programmes to act as the vanguard for progress. One of these is on basic health services: “Basic Essential Package of Health Services available in all regions, and the full EPHS rolled out within accessible regions”; this provides an important entry point for health sector discussion. The ERP states that the government’s preferred implementation channel is the Somalia Reconstruction and Development Facility (SRDF) and using the four proposed funding “Windows” for new investments. The indicative Health and Nutrition budget under the ERP is stated as US$51,656,567, which includes a budget of US$30,000,000 for the flagship programme on basic health services. Economic Development Plans in the three zones have taken into account the HSSPs (likely the only sectoral plans defined from the consultation with a wide range of constituencies) and have incorporated their priorities in one way or another. The focus on EPHS as a flagship programme is a clear sign of this. The ERP funding does not include the funds received by Somalia through the CAP for humanitarian action. This is a substantial fund that mainly supports basic health services through NGOs in more conflict and harsh environmental area. 2.4 Some concluding comments on the New Deal and its implications Opinions are numerous and mixed about the impact that the New Deal will have on Somalia generally and on sectors such as health in particular. The process was perceived as too fast (or rushed), and opportunities for dialogue between government and international actors only occurred in short meetings, often called at short notice. The perception is also that the consultation process has improved since the September conference. The recently established PSG working groups include representatives from international actors and key persons from line ministries and regional authorities who are expected to play a major role in the definition of PSG work plans.
Enhancing A Sector Approach in Health (05-03-2014)
13
Perceptions on the New Deal as a process also varied and some consider the process driven by the international community and mainly giving power to “Mogadishu” without proper consideration of the wider regional / zonal situations and dynamics. This is manifest in the focus of the SRDF on South Central regions, the need for a Special Arrangement for Somaliland and on-going discussions with Puntland. Many expressed the need for strong coordination in both the process and the management of tools, wide inclusiveness of the SRDF Steering Committee (in terms of regional government) and the establishment of sectoral technical coordination bodies. The New Deal is described by some as a “security instrument with some development added”. While the “services” in PSG 5 are clearly not among the highest priorities, many interviewed expressed confidence in the opportunities that the New Deal process can provide to the health sector, by establishing – or more likely setting the direction toward – a wider health sector development approach and increased funding flows. From the discussion above it seems clear that this will require a proactive approach and active participation from different constituencies, especially in the next few months while the process is defined. The funds pledged by donors and the signing of the New Deal Compact has clearly create expectations within government at different levels and most likely amongst the public. However as yet there is still a lack of firm commitments, clear timeframe and clarity on what is really additional versus “re-packaged” existing commitments. 3. Current Health Sector Context. A sector wide analysis of the factors that affect the performance of the sector The health sector is influenced by a wide range of factors that affect its performance, current organizational structure and functions - how decisions are influenced and made, power relations and competition for resource and what the benefits are to people. This section provides an overview sector analysis to highlight these factors by looking at the current profile of the health sector, the HSSPs and the wider political context. A general stakeholder analysis looks at the different actors from their own perspective, incentives and priorities. A synthesis on current financing, external and domestic is included, based on available information. The transition from humanitarian assistance to a development approach is also briefly explained. Health sector coordination issues are addressed including the ongoing programmes and planned actions linked to change towards a sector approach and the alignment process already underway in the sector. 3.1 Profile of the Health Sector Somalia ranks amongst the Least Developed Countries and is considered the most fragile state in the world3 after 22 year of conflict, institutional, social and economic disruption and recurrent humanitarian emergencies. This reflects on the health status of the population and available data positions Somalia among the lowest ranking countries on all health indicators except life expectancy. Among the key indicators (Annex 6) maternal mortality ratio is estimated at 1,000 maternal deaths per 100,000 live births and the under-5 mortality at 180 child deaths per 1,000 live births in 2010. The availability, quality and utilization of public health services are low, while a fast growing private-
3 Failed States Index 2013. http://ffp.statesindex.org/somalia.
Enhancing A Sector Approach in Health (05-03-2014)
14
commercial sector increasingly provides health services. This unregulated private sector is filling the services gap for part of the population but leaving out the most vulnerable. Since 2012 the health sector has been considered a model sector in the Somali context: - Country-owned HSSPs in place and being implemented, framed according to the
WHO six building blocks for health systems strengthening - Focus on results and the M&E framework being defined - A defined plan for institutional capacity building to be implemented - Active participatory coordination under the leadership of the Somali Health
Authorities. A sound review of the coordination mechanism done, providing clear and agreed directions for improvement.
- Increasing alignment and harmonization of health partners - Increasing accountability of partners – and health authorities – based on wide and
consistent information sharing and ethical commitments (although still lacking formal accountability mechanisms).
- Some significant programmes in place, oriented to health sector development. 3.2 The Health Sector Strategic Plans (2013-2016) In 2012 the health authorities from South Central Somalia (TFG and later the FGS), Somaliland and Puntland undertook a coordinated strategic planning process and developed Health Sector Strategic Plans (HSSPs) for a four-year period (2013-2016). These plans (launched in March 2013) were costed and the process included more detailed annual plans and budgets for 2013. This, together with work undertaken on developing health policy frameworks for each zonal authority, signified a substantial step forward for the Somali health sector. The HSSP process was both pragmatic, in terms of establishing a set of common objectives (Annex 7) and priority interventions across the whole of the country, and timely, in terms of providing a government-owned framework for dialogue with the international community at a time of increasing interest in provision of development assistance. The HSSP process included careful consideration of aid effectiveness principles as embedded in IHP+. The process was government led and the HSSP government owned. The HSSPs strive for a focus on results both in terms of systems development but also in service provision. The HSSPs include a strong emphasis on building government’s capacity and legitimacy to lead and manage the sector as well as delivering the agreed Essential Package of Health Services (EPHS). The HSSPs include an emphasis on measurement and as part of this have made provision for Joint Annual Reviews (JARs) of the Sector. HSSPs are therefore well aligned to principles underpinning the New Deal and Compact. The HSSPs also recognise the fragility of government systems and capacities and provide a framework for building government’s ability to, incrementally, take over management of the sector. Many of the priorities of the respective national plans relate well to those highlighted in the HSSPs that recognise the importance of core functions of government such as leadership, public financial management, accountability and equitable service provision. The extent to which funding under the SRDF and SDF “Windows” can be accessed by sectoral Ministries for core functions is yet to be understood. 3.3 Political context The signing of the Compact and establishment of new financing mechanisms and increased resources will now require the various health actors to start looking more intensely at the wider political factors at play not least linked to regional development
Enhancing A Sector Approach in Health (05-03-2014)
15
plans and the new SRDF. The increasing move to development approaches will benefit from maintaining the current level of coordination and dialogue across the health sector and this will require concerted action by the Health Ministries and proactive support from donors and UN agencies. Under the New Deal and Compact the intention is for government to increasingly be managing resources as capacity and systems strengthen. This means a greater focus on government and donor (mutual) accountability not just for financial management but ultimately for making progress on peace-building and state-building. Ultimately the “donor” Government is accountable to its citizens for effective use of resources. The “recipient” Government is accountable primarily to its citizens and, according to a defined aid and partnership framework, to Partners contributing to the development of the Country.
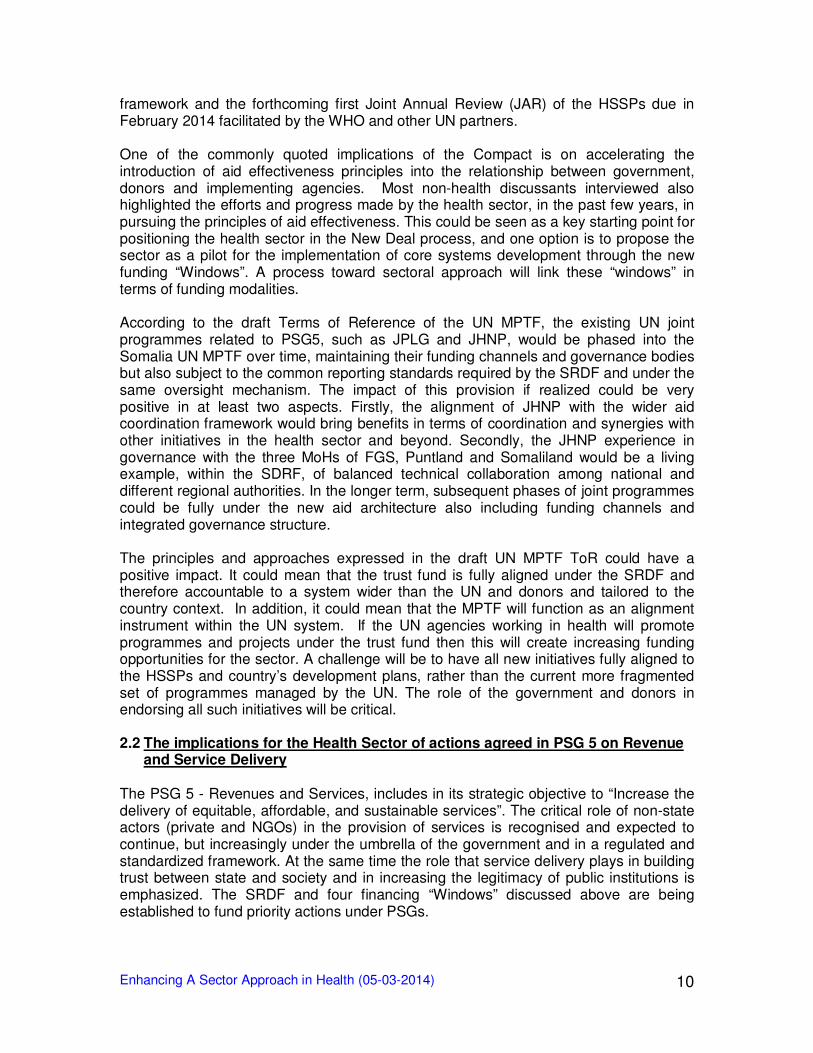
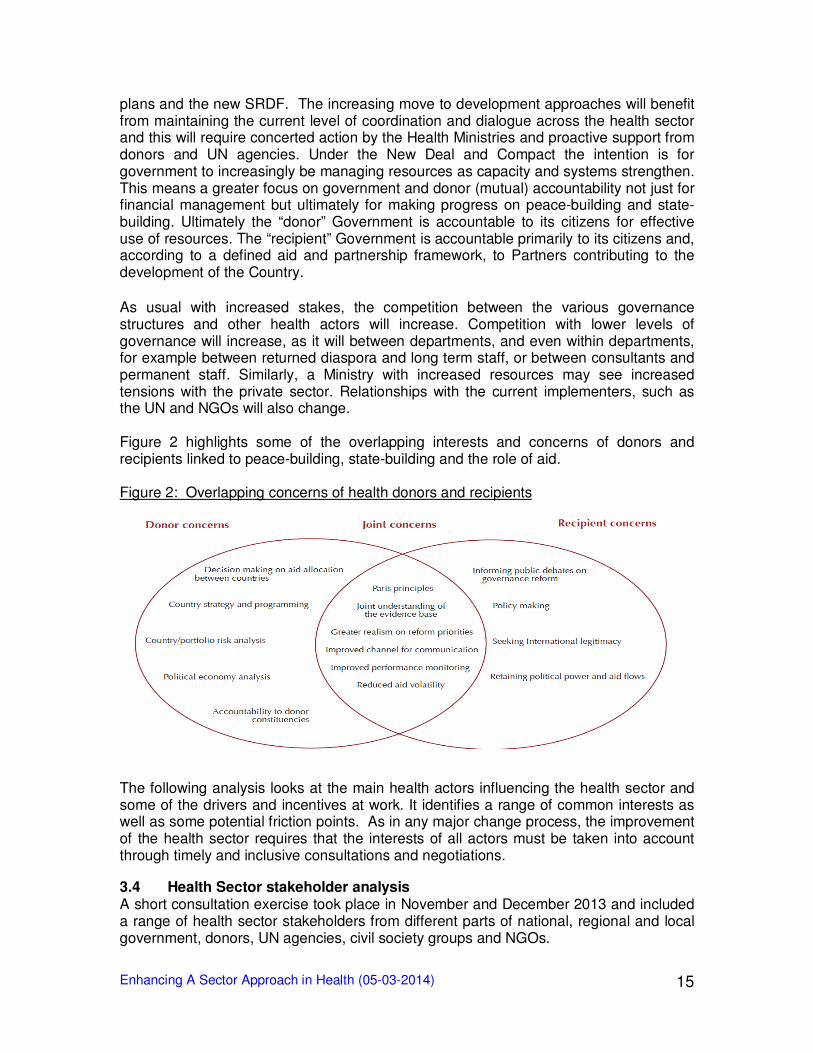
As usual with increased stakes, the competition between the various governance structures and other health actors will increase. Competition with lower levels of governance will increase, as it will between departments, and even within departments, for example between returned diaspora and long term staff, or between consultants and permanent staff. Similarly, a Ministry with increased resources may see increased tensions with the private sector. Relationships with the current implementers, such as the UN and NGOs will also change. Figure 2 highlights some of the overlapping interests and concerns of donors and recipients linked to peace-building, state-building and the role of aid. Figure 2: Overlapping concerns of health donors and recipients
The following analysis looks at the main health actors influencing the health sector and some of the drivers and incentives at work. It identifies a range of common interests as well as some potential friction points. As in any major change process, the improvement of the health sector requires that the interests of all actors must be taken into account through timely and inclusive consultations and negotiations. 3.4 Health Sector stakeholder analysis A short consultation exercise took place in November and December 2013 and included a range of health sector stakeholders from different parts of national, regional and local government, donors, UN agencies, civil society groups and NGOs.
Enhancing A Sector Approach in Health (05-03-2014)
16
While there is an abundance of analysis of the political economy of Somalia, analysis of actors in the health sector is rather sparse and fragmented. This section provides a short overview of the key stakeholders in the health sector based on consultations held in Nairobi, Hargeisa, Garowe and Mogadishu and an initial analysis of some key dynamics. Inevitably the result is a snapshot, and in the current fluid context considerable change, even in the short term, is quite possible. The main health actors considered here are: Ministries of Health; Ministries of Finance/Planning; Local health authorities; Donors; UN Agencies; (I)NGOs; Diaspora; Private health sector providers; and Al Shabaab. Some of the main issues raised in discussion with representatives (where possible) are presented below together with issues from document reviews. 3.4.1 Government Authorities Of considerable importance are the changes at the highest levels of government that have recently taken place. The FGS now has a new Prime Minister and Puntland has a new President. Both changes were peaceful and democratic, and both new incumbents are professionals from the returning diaspora, with enormous experience in governance, business as well as an understanding of how the UN and donors work. Both are also economists and expected to prioritize investment of the budget in the economy. The health authorities will have the opportunity to bring sound and measurable evidence of progress to the table in order to get health as a higher priority on the domestic budget, within the developing mutual accountability context. The Ministries of Health The public health sector can be the main winner in the compact. The three Ministries have achieved a high level of technical coordination and cooperation. Policies are well aligned as are the health strategic plans and strategies. External technical assistance played a significant role in these achievements, but the processes are clearly Somali owned. This has been helped by Partners working to ensure distribution of resources across the three zones in an acceptable way. The Ministries have had very limited influence to date on funding decisions that were largely taken at the Nairobi level by UN agencies, implementing partners and donors. Over the last few years a Health Advisory Board and a Health Sector Committee were established which allowed a greater cooperation between Ministries of Health, donors, UN agencies, implementing NGOs and civil society. The main programme that is beginning to change this dynamic is the Joint Health and Nutrition Programme (JHNP). The establishment of the Federal Government in late 2012 could have changed the dynamics in the Health Advisory Board. However, coordination has remained excellent with the three zones finalising their independent but highly aligned health sector strategies on a professional footing as de-facto equals. The Compact, with its anticipated financial flows, threatens to change the dynamics due to the wider political dialogue surrounding the New Deal. This has for instance led to Special Arrangements for Somaliland and the establishment of separate discussions on new financing facilities. The Somaliland Ministry of Health operates in a clear development mode and restructured in November 2013 under new leadership. The Government allocates 6% of internal revenue to health, with commitments to increase.
Enhancing A Sector Approach in Health (05-03-2014)
17
The Puntland Ministry of Health has been stable for several years and is building its capacity. The presidential elections conducted in January 2014 have lead to a new cabinet, a new Minister of Health was just appointed. Puntland is said to spend 4% of its domestic revenue on health, and is in transition from recovery towards development. In December 2013 there was a change of Prime Minister and in January the Federal Government of Somalia established a new cabinet of 25 Ministries; a new Minister of Health was appointed. The previous Ministry of Human Development has been working on establishing relationships with regional authorities that have recently come under government control, and working to establish Regional Health Offices. The Ministry is keen to expand its influence across the regions but recognises its limited capacity. Many areas in South and Central Somalia are still under humanitarian emergency support, with a large number of external actors providing health services with little influence of the Ministry. The Federal government budget for 2014 allocates just over one per cent of domestic revenues for health, largely to pay for Ministry staff in Mogadishu. All health actors agreed that building the capacity of all the three Ministries of Health is key to achieving progress, and that sufficient resources for this must be allocated. Governance, leadership and management has been made a priority in all HSSPs and in the zonal annual workplans and budgets for 2013 although (financial) support for this element of the plans has been limited. The Health Advisory Board and the Health Sector Committee, chaired by the Somali Health Authorities, were praised from all sides as the model for governance that was relevant beyond health, in Somalia. The Ministries of Finance and Planning Funding of the health sector has up to now taken place largely outside the view of the Ministries of Finance and Planning, and was off-budget. Somaliland is now making progress in collecting these data and presenting this as an annex to the budget, with plans to include it in the budget in future. Puntland has also started to collect data, and the FGS has plans to do so. The prospect of relatively large amounts of funding becoming available under the Compact and becoming more under the influence of government Ministries has sharply increased the attention of the Ministries of Finance. The division of resources amongst the zones has become a source of potential conflict. Somaliland already has its own separate arrangement and Puntland was holding discussions in early December 2013. The Local Health Authorities The Compact provides an excellent opportunity to bring health closer to the population and to strengthen the role of the local health authorities. The Somaliland vision for the health sector seems to be that of a centrally lead policy and a regulated public sector, implemented at district level. There is a clear decentralisation policy and all district councils should now have technical departments including one for social services with dedicated budgets under District council control. Due to resource limitations in many of the poorer districts these departments are under or non-staffed and district budgets can be minimal. NGO budgets for the district are not integrated with the district budgets as yet. Somaliland, supported by the Joint

Enhancing A Sector Approach in Health (05-03-2014)
18
Programme on Local Governance (JPLG), is experimenting with direct budget support to the district councils, and any new funding arrangement can be used to strengthen the health departments. In Puntland District councils are elected by the clan elders, and have a limited authority to collect local revenues and create budgets. There are however large differences between districts in revenue creating capacity but systemic fiscal decentralisation is still in its infancy. Districts have a variable but small health capacity. Districts have however substantial though ad hoc influence on the government as their clans play a key role in ensuring security. The vision for the health sector in Puntland seems to be a centrally planned and regulated public sector, implemented at regional level by health boards that are appointed rather than elected, supported by one NGO per region. Any new funding would likely strengthen these regional health boards, and the option of getting NGO health funding on the regional budget in some way seems viable. In South Central Somalia the situation is rather different. The authority of the Federal government is still limited due to security and is patchy across the regions. The Ministry of Health has focused on building its relationship with Regional and other local authorities as security permits. In the health sector there are a number of districts and regional health entities that do seem functional. There is evidence that some of these councils are able to operate across frontlines in both Al Shabaab and AMISOM controlled areas. Their capacity might be low, they might be highly dependent on NGO support, but they function, and could be an excellent entrance point for the federal government to gain legitimacy. This process would be greatly facilitated if the Federal health department was able to offer some substantive devolved resources and technical support. 3.4.2 Donors For the donors the Compact provides a real opportunity to make development in Somalia a reality and to help to end the conflicts. The donors in Somalia are however also facing multiple dilemmas, at a time when domestic politics force some to be increasingly risk-averse. The first is the humanitarian/development dilemma. There is an on-going need for direct service delivery and there is a need to build government capacity and the balance between these two is crucial. On the whole donor governments are increasingly interested to show results and that these results are attributable to their funding. Funding health systems capacity building work that aims to build government owned and led systems is often a more long-term endeavour and one that is slow to deliver results in service provision. More direct funding to implementing partners is often seen as a quicker way to show results especially in fragile environments where security is a problem. This is linked to the critical dilemma whether to deliver support to a state whose legitimacy is questioned beyond the capital4. Each donor faces its domestic political imperatives and geopolitical considerations, meaning that a united donor position will be very difficult to achieve and maintain. Although established under a rather rushed timetable with indications that more consultation would have been beneficial, the Compact provides an enormous opportunity and some form of unified approach will likely emerge. The important issue
4 Synthesis of country programme evaluations in fragile states, DFID Evaluation reports EV 709, 2010
Enhancing A Sector Approach in Health (05-03-2014)
19
now is for donors to back the New Deal and ensure effective programmes are established under the various development plans and financing facilities being established. Donors with an interest in health will need to work together to ensure some of the funds that will be channelled through the new financing “Windows” are allocated for the health sector. 3.4.3 United Nations The United Nations has played an enormous role in alleviating the humanitarian crisis in Somalia, particularly in the conflict affected areas in South and Central. It will now have to adapt to a changing role, with the likely loss of some of its functions. As part of this role the UN has built a formidable administrative and logistic capacity in neighbouring Kenya and arguably has been the largest humanitarian actor. More modest investments have been developed inside Somalia, mainly in Puntland and Somaliland. The continuing security concerns and strict regulations of the UN have severely limited the field presence of UN staff in the South, and much of the implementation had to be subcontracted to commercial and NGO actors. The public perception of the UN in health is generally positive, certainly in Puntland and Somaliland. The three involved UN agencies, WHO, UNICEF and UNFPA, have considerable field presence, though implementation is still largely done through NGOs and some commercial firms. The technical assistance provided by the UN was appreciated by the Ministries, although more should be done to ensure skills transfer to reduce reliance on expensive external consultants. The UN was highly praised for making the health sector strategy possible and enabling the roll-out of the EPHS. However, on a more general note the UN is also currently under criticism from government circles and the population for its lack of accountability and high overheads especially linked to its Nairobi offices. Government health authorities all called for greater transparency and more influence in funding decisions linked to the larger health development programmes. UNICEF in particular acts as a major funding channel for international support across Somalia. It role includes providing technical assistance; managing HMIS and MICS; running EPI and polio programmes; funding coordination mechanisms; and paying incentives to MoH staff. Many of these roles are MoH roles and great care should be taken to avoid conflict of interest in any new arrangement that is established. The transition from a largely humanitarian programme towards developmental programmes will have large implications for the UN including the overall size of the budget being managed. The staffing component will reduce, and change in profile from providing services to technical assistance. As staff and operations are required to move into Somalia this will present a range of organisational challenges to the UN including staff retention and recruitment. However, the UN will likely remain a major player and important actor in the coming years both for humanitarian and development operations. 3.4.4 (International) NGOs The NGOs have played a major role in delivering humanitarian services and are widely appreciated, but their role will also change. They had considerable field presence throughout Somalia and the public perception is generally positive. Thanks to this field presence NGOs also have a good sense of the realities on the ground and they tend to have good relationships with the de-facto lower levels of governance, developed through

Enhancing A Sector Approach in Health (05-03-2014)
20
long time cooperation and mutual trust. The NGOs have invested heavily in building administrative and logistical systems, largely in neighbouring Kenya. There is little evidence of joint systems between NGOs, rather a multitude of parallel systems have been established. These systems have enabled the NGOs to be effective, but due to the parallel setup also rather inefficient. The transition towards development will be difficult for many NGOs. As the government takes over more functions, the budgets of the NGOs will decrease. Systems will become more unified, meaning that the parallel systems of the NGOs will have to be dismantled. Staff redundancies will be inevitable. This will affect Kenyan staff but also Somali staff who will often have no alternative but to accept jobs in the emerging Somali systems that pay considerably lower salaries. There will also have to be considerable rightsizing at headquarter level to adjust for the loss of the Somali overheads. In the current economic climate, with reduced charity contributions, many NGOs will find this a painful adjustment. An additional issue for many NGOs is that they do not have the organisational systems, structures and capacities to be a development actor. Some, like Save the Children, straddle the continuum from emergency to development, some others are very good in humanitarian interventions, but simply lack the development experience and expertise. They might be selected in the early recovery phase because of their extensive field experience and networks of contacts, but will lose out when development is more fully established. 3.4.5 Diaspora Remittances alone make the diaspora a very significant actor in Somalia. At 1.3 billion US$ per year, plus informal remittances, this is already more than the pledges made under the Compact, and these remittances are not pledges, but solid cash delivered in a predictable manner, with limited conditions attached. Much of this money goes towards supporting livelihoods and procuring services, including health services. An unknown proportion of the remittances is also invested, amongst others in establishing private health services. The diaspora is not just a financial resource, but also increasingly a human resource for Somalia. The combination of a Somali educated abroad with a sound hard currency capital base, has established many a successful company. This initially created a lot of resentment with those who had stayed behind, but that is said to have diminished recently. It is however well described in the literature5 that diaspora involvement does not just have a positive impact on recovery and development. Loyalties to tribe, clan or family can be even stronger in the diaspora than at home, and the diaspora can also be a major influencing group both for better and worse. In both the public and private health sector the diaspora plays an important role. In the private sector they are both investors and practitioners, and tend to operate at the higher end of the health market. The Ministries of Health recognise the role of the private sector as well as the challenges ahead in ensuring this is well regulated and providing services at acceptable quality standards.
5 Diaspora in Conflict: Peace makers or peace wreckers, United nations University 2007

Enhancing A Sector Approach in Health (05-03-2014)
21
In the public health sector the diaspora also plays an important role. Young, highly foreign educated Somali are found in many Ministry positions, and they are instrumental in ensuring that any strategy, policy or procedure that is developed meets both professional standards, and has Somali ownership. Some of these returnees work at regional level and below. They have usually returned on their own initiative and often have a private sector role as well. They tend to be well integrated, but are largely invisible to the UN and donor systems. Diaspora professionals that have been placed in the public system through UN or NGO consultancy mechanisms seem to be more contentious. 3.4.6 Private Sector The private sector currently provides the majority of curative services, often through small clinics and pharmacies. Quality of training and services from many of these clinics and private pharmacies is a major concern. The situation is under discussion with work starting to develop health professional organisations that will begin some level of regulation. The roll out of the EPHS will also start to provide competition and challenge these private facilities. In Somaliland this regulatory process is already well under way and in Puntland it has started. For the private health sector, in its current form, the new funding modalities, with its emphasis on government in the lead might be a mixed blessing, specifically at the lower end. The higher end of the private sector will also experience more competition and regulation, but could be a big winner in the coming change process. Health is however also big business. Out of pocket health expenditure in Somalia exceeds all public health funding combined, and there will be forces that resist regulation. Experience, in the region and in other post-conflict situations, shows that the irregular medicine importers can be one of these factors and can be very difficult to regulate given vested interests of influential groups. HSSPs begin to discuss working with the private sector and call for both building capacity in government for commissioning as well as establishing contracts with non-state suppliers, such as for voucher schemes. Such an approach has much potential to scale up both quality and quantity of health services, but clearly still needs a lot of work. 3.4.7 Al Shabaab Al Shabaab is not often considered as an actor in health, but it is nevertheless mentioned here. Al Shabaab lost a lot of popular support by banning relief aid in the 2011-2012 famine and has definitely made health care provision by external agents very difficult. Al-Shabaab will certainly oppose federal government attempts to establish transparent and accountable services, but their renewed emphasis on hearts and minds may form an entrance point for constructive engagement with at least some factions. All stakeholders considered above are influential in the ongoing process to different extents and according to their respective interests and authority. The government authorities have considerable interest in promoting and sustaining the New Deal process and also the authority to influence its progress. This is potentially affected by conflict within government authorities operating in different levels of government, sectors, and political divisions. The New Deal process brings intrinsic peace-building and state-building potentials, the realization of which will however also depend on other actors. The donors are in many ways the architects of the New Deal and as such have invested strongly in its success. Progress will depend heavily on donor harmonisation and the
Enhancing A Sector Approach in Health (05-03-2014)
22
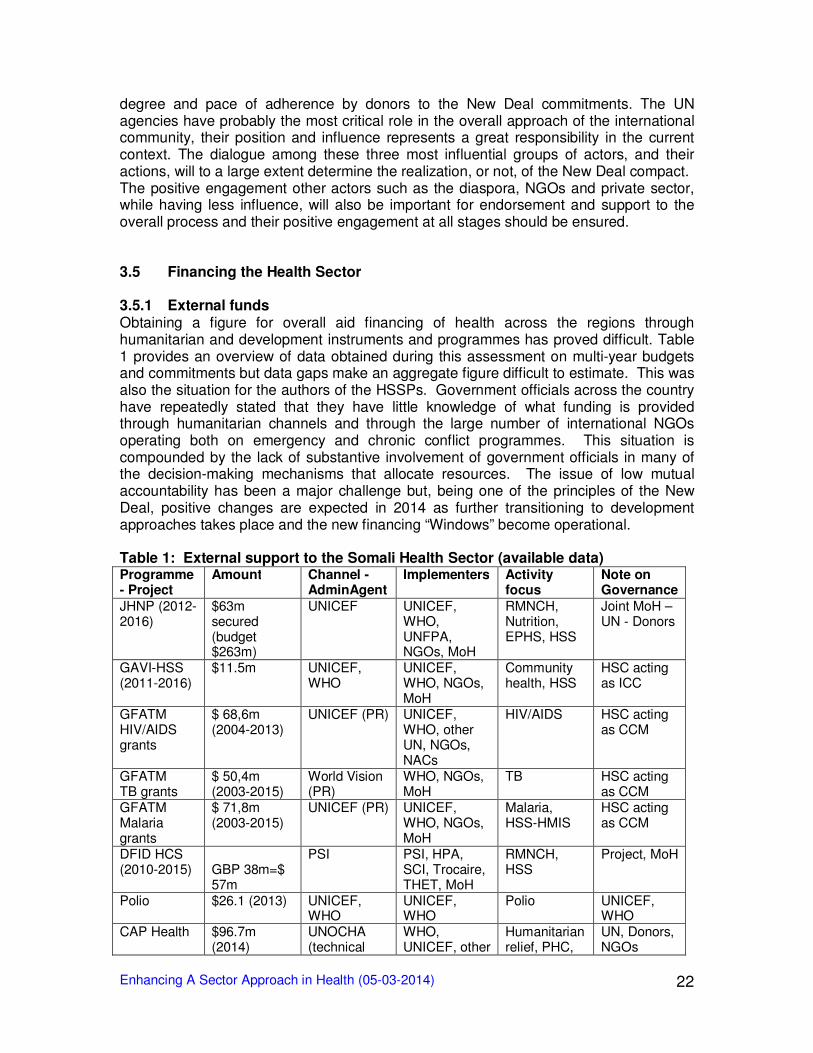
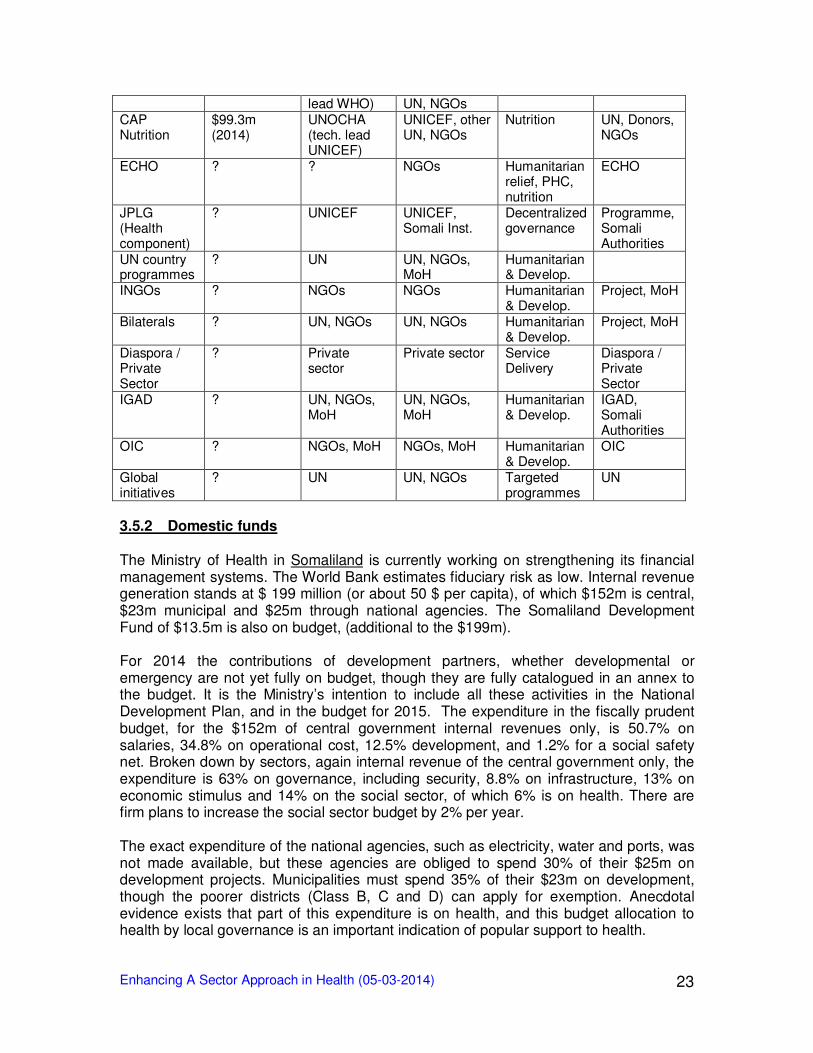
degree and pace of adherence by donors to the New Deal commitments. The UN agencies have probably the most critical role in the overall approach of the international community, their position and influence represents a great responsibility in the current context. The dialogue among these three most influential groups of actors, and their actions, will to a large extent determine the realization, or not, of the New Deal compact. The positive engagement other actors such as the diaspora, NGOs and private sector, while having less influence, will also be important for endorsement and support to the overall process and their positive engagement at all stages should be ensured. 3.5 Financing the Health Sector 3.5.1 External funds Obtaining a figure for overall aid financing of health across the regions through humanitarian and development instruments and programmes has proved difficult. Table 1 provides an overview of data obtained during this assessment on multi-year budgets and commitments but data gaps make an aggregate figure difficult to estimate. This was also the situation for the authors of the HSSPs. Government officials across the country have repeatedly stated that they have little knowledge of what funding is provided through humanitarian channels and through the large number of international NGOs operating both on emergency and chronic conflict programmes. This situation is compounded by the lack of substantive involvement of government officials in many of the decision-making mechanisms that allocate resources. The issue of low mutual accountability has been a major challenge but, being one of the principles of the New Deal, positive changes are expected in 2014 as further transitioning to development approaches takes place and the new financing “Windows” become operational. Table 1: External support to the Somali Health Sector (available data) Programme - Project
Amount Channel - AdminAgent
Implementers Activity focus
Note on Governance
JHNP (2012-2016)
$63m secured (budget $263m)
UNICEF UNICEF, WHO, UNFPA, NGOs, MoH
RMNCH, Nutrition, EPHS, HSS
Joint MoH – UN - Donors
GAVI-HSS (2011-2016)
$11.5m UNICEF, WHO
UNICEF, WHO, NGOs, MoH
Community health, HSS
HSC acting as ICC
GFATM HIV/AIDS grants
$ 68,6m (2004-2013)
UNICEF (PR) UNICEF, WHO, other UN, NGOs, NACs
HIV/AIDS HSC acting as CCM
GFATM TB grants
$ 50,4m (2003-2015)
World Vision (PR)
WHO, NGOs, MoH
TB HSC acting as CCM
GFATM Malaria grants
$ 71,8m (2003-2015)
UNICEF (PR) UNICEF, WHO, NGOs, MoH
Malaria, HSS-HMIS
HSC acting as CCM
DFID HCS (2010-2015)
GBP 38m=$ 57m
PSI PSI, HPA, SCI, Trocaire, THET, MoH
RMNCH, HSS
Project, MoH
Polio $26.1 (2013) UNICEF, WHO
UNICEF, WHO
Polio UNICEF, WHO
CAP Health $96.7m (2014)
UNOCHA (technical
WHO, UNICEF, other
Humanitarian relief, PHC,
UN, Donors, NGOs
Enhancing A Sector Approach in Health (05-03-2014)
23
lead WHO) UN, NGOs CAP Nutrition
$99.3m (2014)
UNOCHA (tech. lead UNICEF)
UNICEF, other UN, NGOs
Nutrition UN, Donors, NGOs
ECHO ? ? NGOs Humanitarian relief, PHC, nutrition
ECHO
JPLG (Health component)
? UNICEF UNICEF, Somali Inst.
Decentralized governance
Programme, Somali Authorities
UN country programmes
? UN UN, NGOs, MoH
Humanitarian & Develop.
INGOs ? NGOs NGOs Humanitarian & Develop.
Project, MoH
Bilaterals ? UN, NGOs UN, NGOs Humanitarian & Develop.
Project, MoH
Diaspora / Private Sector
? Private sector
Private sector Service Delivery
Diaspora / Private Sector
IGAD ? UN, NGOs, MoH
UN, NGOs, MoH
Humanitarian & Develop.
IGAD, Somali Authorities
OIC ? NGOs, MoH NGOs, MoH Humanitarian & Develop.
OIC
Global initiatives
? UN UN, NGOs Targeted programmes
UN
3.5.2 Domestic funds The Ministry of Health in Somaliland is currently working on strengthening its financial management systems. The World Bank estimates fiduciary risk as low. Internal revenue generation stands at $ 199 million (or about 50 $ per capita), of which $152m is central, $23m municipal and $25m through national agencies. The Somaliland Development Fund of $13.5m is also on budget, (additional to the $199m). For 2014 the contributions of development partners, whether developmental or emergency are not yet fully on budget, though they are fully catalogued in an annex to the budget. It is the Ministry’s intention to include all these activities in the National Development Plan, and in the budget for 2015. The expenditure in the fiscally prudent budget, for the $152m of central government internal revenues only, is 50.7% on salaries, 34.8% on operational cost, 12.5% development, and 1.2% for a social safety net. Broken down by sectors, again internal revenue of the central government only, the expenditure is 63% on governance, including security, 8.8% on infrastructure, 13% on economic stimulus and 14% on the social sector, of which 6% is on health. There are firm plans to increase the social sector budget by 2% per year. The exact expenditure of the national agencies, such as electricity, water and ports, was not made available, but these agencies are obliged to spend 30% of their $25m on development projects. Municipalities must spend 35% of their $23m on development, though the poorer districts (Class B, C and D) can apply for exemption. Anecdotal evidence exists that part of this expenditure is on health, and this budget allocation to health by local governance is an important indication of popular support to health.
Enhancing A Sector Approach in Health (05-03-2014)
24
Somaliland has an ambitious Health Sector Strategic Plan (HSSP) fully integrated with their National Development Plan. By late 2014 it aims to have all donor-funded projects on budget. Somaliland finance and planning ministries expect the New Deal funding, under the special Somaliland agreement, to be both on budget and on treasury, albeit earmarked. Less detailed data were made available for Puntland. The Ministries seem to be in a somewhat earlier state of development. Nevertheless the World Bank estimates the fiduciary risk as low. Domestic revenue collection was said to stand at $41m, or about $10 per capita. About 70% of this comes from in and export taxation, about 30% from other taxes and revenues. Breakdowns for budgeted expenditure were not available, and the division between recurrent and development expenditure is unknown. Education was said to account for 3.8 % and health for 4% in 2012, all recurrent expenditure, but with stated commitments to increase. The health budget also pays for at least part of the salaries of health staff in the periphery. Part of the local revenue generated is spent on health, again signifying popular prioritisation of health issues. Puntland has an ambitious HSSP integrated in the second five year Puntland Development Plan 2014-2018. The HSSP calls for an expenditure over four years in excess of $100m. In this context it must be realised that most health expenditure, HCS, JHNP and others, is currently off-budget. It is not clear how much progress is being made in at least inventorising these flows. The HSSP costing is however additional to these current externally funded expenditures. More details were available for the Federal budget. The 2013 budget totals $84 million, $54m domestic revenue and $30m donor funded. As in the other zones, most of the domestic revenue is customs based. A per capita estimate is not useful as domestic revenues can only be collected in the Benadir region. A World Bank Fiduciary Diagnostic Assessment portrayed a PFM environment of systematic and sophisticated predation of public finances, assets and international assistance to the tune of 68% of revenues under the previous TFG government. No current assessment is available. Recurrent expenditure runs at $104m (an unsustainable budget deficit of $20m), for salaries and office costs of mainly the central government institutions. Social expenditure, health and education combined, stands at $2.3m, exclusively for salaries and running costs of the ministry. Health allocation is thus difficult to estimate, but in the one to two per cent of domestic revenue range. In the South there is also anecdotal evidence that some local authorities spent part of the local revenues on health, though amounts are unknown. The Federal HSSP is again ambitious at $101m over four years for the South Central zone alone, additional to current health expenditure by external actors. For the year 2014 health needs under the humanitarian Common Appeal (CAP) were estimated at $96m. The budgets for HSSP, additional to current external health funding, are realistic given the investments being made in health from all sources (see Table 1 above). To achieve an increasing share of the domestic budget will require good evidence of progress to present to Finance Ministers and other senior officials controlling the allocation of scarce national resources. The proposed JAR will hopefully go some way to achieving this. The overall development plans (FGS ERP, Puntland 5-Year
Enhancing A Sector Approach in Health (05-03-2014)
25
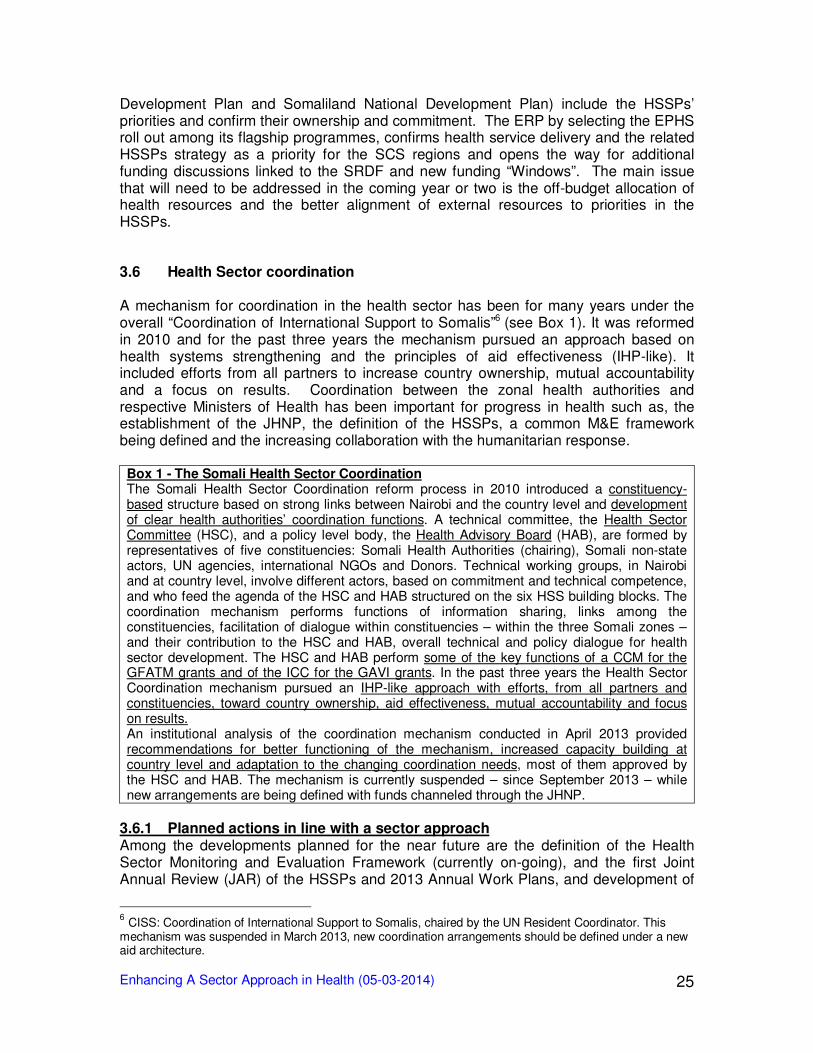
Development Plan and Somaliland National Development Plan) include the HSSPs’ priorities and confirm their ownership and commitment. The ERP by selecting the EPHS roll out among its flagship programmes, confirms health service delivery and the related HSSPs strategy as a priority for the SCS regions and opens the way for additional funding discussions linked to the SRDF and new funding “Windows”. The main issue that will need to be addressed in the coming year or two is the off-budget allocation of health resources and the better alignment of external resources to priorities in the HSSPs. 3.6 Health Sector coordination A mechanism for coordination in the health sector has been for many years under the overall “Coordination of International Support to Somalis”6 (see Box 1). It was reformed in 2010 and for the past three years the mechanism pursued an approach based on health systems strengthening and the principles of aid effectiveness (IHP-like). It included efforts from all partners to increase country ownership, mutual accountability and a focus on results. Coordination between the zonal health authorities and respective Ministers of Health has been important for progress in health such as, the establishment of the JHNP, the definition of the HSSPs, a common M&E framework being defined and the increasing collaboration with the humanitarian response.
Box 1 - The Somali Health Sector Coordination The Somali Health Sector Coordination reform process in 2010 introduced a constituency-based structure based on strong links between Nairobi and the country level and development of clear health authorities’ coordination functions. A technical committee, the Health Sector Committee (HSC), and a policy level body, the Health Advisory Board (HAB), are formed by representatives of five constituencies: Somali Health Authorities (chairing), Somali non-state actors, UN agencies, international NGOs and Donors. Technical working groups, in Nairobi and at country level, involve different actors, based on commitment and technical competence, and who feed the agenda of the HSC and HAB structured on the six HSS building blocks. The coordination mechanism performs functions of information sharing, links among the constituencies, facilitation of dialogue within constituencies – within the three Somali zones – and their contribution to the HSC and HAB, overall technical and policy dialogue for health sector development. The HSC and HAB perform some of the key functions of a CCM for the GFATM grants and of the ICC for the GAVI grants. In the past three years the Health Sector Coordination mechanism pursued an IHP-like approach with efforts, from all partners and constituencies, toward country ownership, aid effectiveness, mutual accountability and focus on results. An institutional analysis of the coordination mechanism conducted in April 2013 provided recommendations for better functioning of the mechanism, increased capacity building at country level and adaptation to the changing coordination needs, most of them approved by the HSC and HAB. The mechanism is currently suspended – since September 2013 – while new arrangements are being defined with funds channeled through the JHNP.
3.6.1 Planned actions in line with a sector approach Among the developments planned for the near future are the definition of the Health Sector Monitoring and Evaluation Framework (currently on-going), and the first Joint Annual Review (JAR) of the HSSPs and 2013 Annual Work Plans, and development of
6 CISS: Coordination of International Support to Somalis, chaired by the UN Resident Coordinator. This
mechanism was suspended in March 2013, new coordination arrangements should be defined under a new aid architecture.
Enhancing A Sector Approach in Health (05-03-2014)
26
the 2014 Work Plans. While late – these are scheduled between January and March 2014 – this review and planning exercise is seen as critical in the current phase in order to consolidate the HSSPs, in terms of process, contents and partners’ commitment, and establish the expected planning-budgeting cycle for the health sector. Although the Terms of Reference focus on the “four key aligned programmes i.e. GFATM, GAVI-HSS, JHNP and HCS” the JAR provides the opportunity to get many other partners actively on board or “on budget” in HSSP implementation. The review and planning exercise becomes even more important in the context of the New Deal. It can provide factual elements for active involvement of the health sector in devising and piloting the tools of the new aid architecture. It can provide the necessary elements for “internal” accountability within the country in relation to the government, the development plans and the other sectors. Moreover, based on the willingness expressed by most partners in a sectoral approach to health in the context of the New Deal, the JAR could be the opportunity to introduce some key aid effectiveness indicators (further pursuing the “IHP-like approach”) and start monitoring from 2014 the commitment of health authorities and development partners. Progress is being made on health systems development and some of these are relevant for a sectoral approach:
- On health financing the path to define the strategy has been drafted, including NHA - On human resources, Health Professions Councils are being established - On health information, the HMIS is being reviewed and a mapping of health facilities
and services planned, building on the health cluster tools. - The health sector coordination mechanism, currently on hold, will be revised based
on the analysis conducted and on the new overall coordination arrangements.
3.6.2 On-going programmes and alignment in the Health Sector The Joint Health and Nutrition Programme (JHNP) is a pooled funding (joint) programme based on partnership among the three Health Authorities in Somaliland, Puntland and South Central Somalia (Federal Government), Donors (DFID, SIDA, AusAID, USAID), UN agencies (WHO, UNICEF and UNFPA) and implementing partners, fully aligned to the HSSPs. It has been defined through a widely consultative process, facilitated by the coordination mechanism and it is now fully in implementation. Its focus on Reproductive, Maternal, Neonatal and Child Health (RMNCH) and Nutrition services is realized in the roll out of the EPHS in 9 selected regions and health systems strengthening activities for each of the six building blocks. Although some limitations and a number of implementation challenges, the JHNP now represents an example of a joint fund potentially aligned to the New Deal principles. As in other country contexts, a sectoral pooled fund can have relevance beyond its funding scope as a catalyser for harmonization and alignment. The establishment of the Joint Health and Nutrition Programme (JHNP) made a critical step by supporting the definition of the HSSPs. Other significant on-going programmes include the GAVI Alliance support to Immunization and to HSS; the Global Fund grants; the DFID-NGO Health Consortium Somalia; UN agencies support; a number of bilateral contributions implemented by experienced NGOs partners as well as direct INGOs contributions; humanitarian interventions; contributions from IGAD, OIC, regional and global initiatives; the Diaspora and private sector investments. Many programmes and projects are increasingly aligning to the HSSPs and collaborating with the health authorities. Most interventions on
Enhancing A Sector Approach in Health (05-03-2014)
27
Primary Health Care are now being framed according to the Essential Package of Health Services and their implementation contributes to the roll out of health service delivery within this framework. Fragmentation of interventions is still prevalent, especially in South Central Somalia where humanitarian interventions are still operational and extremely relevant in terms of funding. However, an increasing alignment to the HSSPs is bringing about a new way of working in collaboration, increasing ownership and responsibilities of the Somali health authorities and focus on results, even involving health-related humanitarian interventions and the IASC7 health cluster coordination. All these interventions and actors can contribute to the realization of the ERP flagship programme on health. 3.7 Transitioning from Humanitarian Assistance to development Humanitarian assistance has been the main channel for international assistance to health for the past 20 years providing basic health services and saving lives. In recent years this has included more developmental elements aimed at building capacities and systems. The role of the humanitarian / emergency response is still critical, especially in South Central Somalia: a three year CAP plan was launched in 2013 with an increased attention to resilience and capacity building. The CAP health budget for 20138 was $89m of which $34m was funded through the Health Cluster. The 20149 health budget requirement is estimated at around $96.7m, targeting 1.8 million people, in a collaboration of 41 partners for disease surveillance and response, immunization, PHC and EmONC according to the EPHS framework, coordination and capacity building. The nutrition budget requirement is $99.3m, targeting 660,000 people, a collaboration of 52 partners to respond to nutrition needs. Humanitarian funding is fragmented and outside government control or oversight. It continues to play an important role for conflict and harsh environment areas. Much of the aid is managed remotely by international NGOs and funds channelled through UN agencies. The extent and scope of work under humanitarian assistance is not well known to government even though information is available. The disconnect between the emerging developmental work and on-going humanitarian assistance is a cause for concern as governments and donors start to work on alignment behind HSSPs. The counter concern is that stopping humanitarian funding may result in reduction of services for some of the most vulnerable sections of the Somali population. The approach of the CAP strategic response plan, as well as the individual partners, has been to increase constructive collaboration with the Somali health authorities, firstly in Somaliland, then in Puntland and more recently with the Somalia Federal Government. Synergies between the Health Cluster and the Health Sector Coordination mechanism were being developed. The transition process is increasingly under discussion as more confidence in the health system slowly grows. 3.8 Conclusions and potential for change The fragile and disrupted context of the country and the health sector presents a number of enormous challenges for development. The need for reform is perceived by most
7 IASC: Inter-Agency Standing Committee (coordinating humanitarian assistance)
8 Somalia: Humanitarian Dashboard – October 2013
9 Somalia CAP 2014 Strategic response Plan.
http://www.unocha.org/somalia/financing/consolidated-appeal-somalia
Enhancing A Sector Approach in Health (05-03-2014)
28
actors and the opportunities are being provided by a dynamic environment created by the recent political developments and the will of Somali and external actors. However, despite the known weaknesses, the Somali health sector has definitely managed to set a trend toward development. Although not so recognised in the high political agenda and while most international emphasis was on emergency and humanitarian response, the health sector started working on principles of cooperation and aid effectiveness. Technical issues are being addressed, key assets put in place (such as the HSSPs), decision-making is moving slowly but surely into the country with increasing responsibility of the Somali authorities. The main limitation being the weak capacities and systems caused by years of protracted conflict. The health sector actors have started experiencing the benefits of country ownership as well as the related challenges. Limited but significant opportunities to bring health sector management closer to the population has shown, when local authorities are strengthened and the MoH is able to provide support, the potential for increased state legitimacy, accountability of government and trust from the population. The experience being gained in the health sector is acting as a powerful driver for change with the Somali actors increasingly identifying the way forward and willing to follow the development path. Most international partners (Donors and UN) are committed to aid effectiveness principles – from Paris to Busan HLF – and many signed the Somali compact. The current context provides the opportunity to realize this commitment, although the process implies risks and substantial changes in the approach and therefore the pace can differ among partners. Donors interested in health will have to work together to ensure funding within the new financing arrangements under the New Deal, building on a trend already visible toward the development approach. The UN role in capacity building will be critical to develop the needed skills and systems, it will require an even more decisive shift toward the country level and away from the pure humanitarian assistance of the past. Similarly, the international NGOs that have historically represented the link between the international community and the local organizations, will need to exploit their experience in a new direction, as some are already doing. The returning Diaspora and the private sector are by themselves key elements of the current dynamic environment and relevant factors for change. The role of the Somali authorities is critical in setting the direction and exploiting their leadership and governance role for the country. This analysis shows that there are fundamental elements for change in place and that there is a recognised need and space for it. The New Deal process can be exploited for health sector development, along trends already established. However, considering the set of priorities outlined in the Compact and the high political level where key discussion take place, additional efforts from health sector actors are needed to pursue a sectoral approach to development. Most discussants are well aware of this opportunity, of the priority challenge and the need to proactively engage in the process and foster health sector development. A major challenge in the near future is to build the trust between government and development partners and demonstrate this through rapidly improving mutual accountability through agreed transparent systems for sharing decision-making and information. A strong suggestion to further develop the IHP+ like approach came from several discussants, as the way to guide these efforts, building on experience and partners’ commitments.
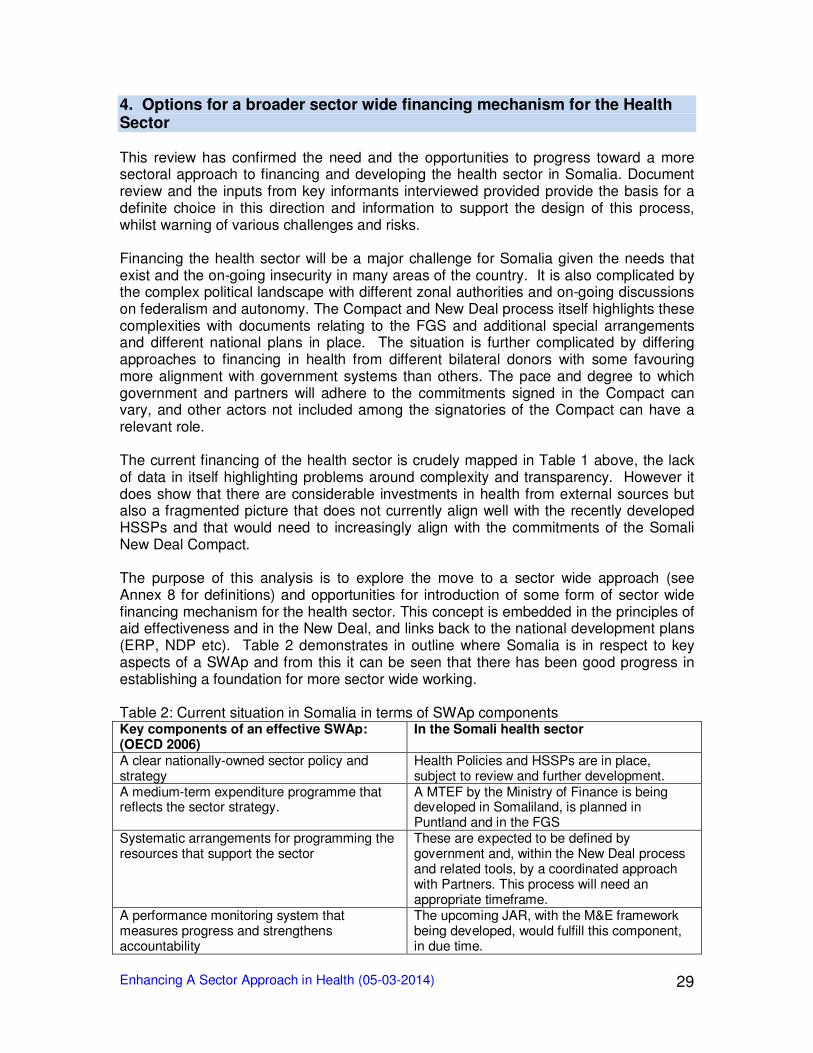
Enhancing A Sector Approach in Health (05-03-2014)
29
4. Options for a broader sector wide financing mechanism for the Health Sector This review has confirmed the need and the opportunities to progress toward a more sectoral approach to financing and developing the health sector in Somalia. Document review and the inputs from key informants interviewed provided provide the basis for a definite choice in this direction and information to support the design of this process, whilst warning of various challenges and risks. Financing the health sector will be a major challenge for Somalia given the needs that exist and the on-going insecurity in many areas of the country. It is also complicated by the complex political landscape with different zonal authorities and on-going discussions on federalism and autonomy. The Compact and New Deal process itself highlights these complexities with documents relating to the FGS and additional special arrangements and different national plans in place. The situation is further complicated by differing approaches to financing in health from different bilateral donors with some favouring more alignment with government systems than others. The pace and degree to which government and partners will adhere to the commitments signed in the Compact can vary, and other actors not included among the signatories of the Compact can have a relevant role. The current financing of the health sector is crudely mapped in Table 1 above, the lack of data in itself highlighting problems around complexity and transparency. However it does show that there are considerable investments in health from external sources but also a fragmented picture that does not currently align well with the recently developed HSSPs and that would need to increasingly align with the commitments of the Somali New Deal Compact. The purpose of this analysis is to explore the move to a sector wide approach (see Annex 8 for definitions) and opportunities for introduction of some form of sector wide financing mechanism for the health sector. This concept is embedded in the principles of aid effectiveness and in the New Deal, and links back to the national development plans (ERP, NDP etc). Table 2 demonstrates in outline where Somalia is in respect to key aspects of a SWAp and from this it can be seen that there has been good progress in establishing a foundation for more sector wide working. Table 2: Current situation in Somalia in terms of SWAp components Key components of an effective SWAp: (OECD 2006)
In the Somali health sector
A clear nationally-owned sector policy and strategy
Health Policies and HSSPs are in place, subject to review and further development.
A medium-term expenditure programme that reflects the sector strategy.
A MTEF by the Ministry of Finance is being developed in Somaliland, is planned in Puntland and in the FGS
Systematic arrangements for programming the resources that support the sector
These are expected to be defined by government and, within the New Deal process and related tools, by a coordinated approach with Partners. This process will need an appropriate timeframe.
A performance monitoring system that measures progress and strengthens accountability
The upcoming JAR, with the M&E framework being developed, would fulfill this component, in due time.

Enhancing A Sector Approach in Health (05-03-2014)
30
Broad consultation mechanisms that involve all significant stakeholders
Consultations occur on purpose, an institutionalised mechanism need to be devised, probably within the sectoral coordination in-country and with external Partners.
A formalised government-led process for aid co-ordination and dialogue at the sector level
Mechanisms and processes for aid coordination at health sector level are partially in place (developing coordination functions of the MoH, HSC and HAB) and will be reformed / developed within the New Deal process.
An agreed process for moving towards harmonised systems for reporting, budgeting, financial management and procurement.
This should be pursued, based on clear statements by Government and Partners about their commitment to move in this direction. A roadmap – living document – would serve this component.
Moving to a sector wide approach also involves increasingly using government systems. This is where there is a long way to go in Somalia. Basic systems for public financial management, although variable across the regions, remain very weak or at the design stage. This is also true for Human Resources for Health systems and health information systems. The HSSPs recognise this weakness of systems and capacity. 4.1 Health financing options for Somalia The current financing that has been described above includes major inputs from both humanitarian and development sources. These have quite different triggers and cannot be seen as a complementary package of support. If the environment is assessed as suitable for development funding then justification for the substantial and quite structural humanitarian funding may stop. The humanitarian funds through CAP and EC cannot be rechanneled for development, they are either used for humanitarian projects or not. This means that classifying the situation as suitable for transition to development may come with the challenge of how to replace short term humanitarian funding with longer term development funding. As development funding has a longer start-up phase care must be taken that this does not lead to a temporary or even extended decrease in overall health funding. This will likely impact the regions in South Central and in particular those regions not yet under government control. The extent to which conditions are in place for discussion on transition to sector wide thinking in health therefore varies across the country. The HSSPs do provide a government framework for the sector based on WHO guidelines and are developed with aid effectiveness principles (using IHP+ tools) in mind. The question being asked now is to what extent the framework can be adopted, the willingness of donors, the UN and local actors to do so, and against what timeframe. Safe to say the speed of transition should not, and does not need to be, uniform across the regions. While this complicates planning and decision-making it is an important short to medium term consideration.
There are a number of broader sector financing options available that link with the development plans of the different authorities (ERP, NDP etc). These should be considered by the government and donors, with a view to moving towards a sector approach, at a speed and scale that takes into account the variations described above. In essence the options available vary in the degree to which funding is under the control
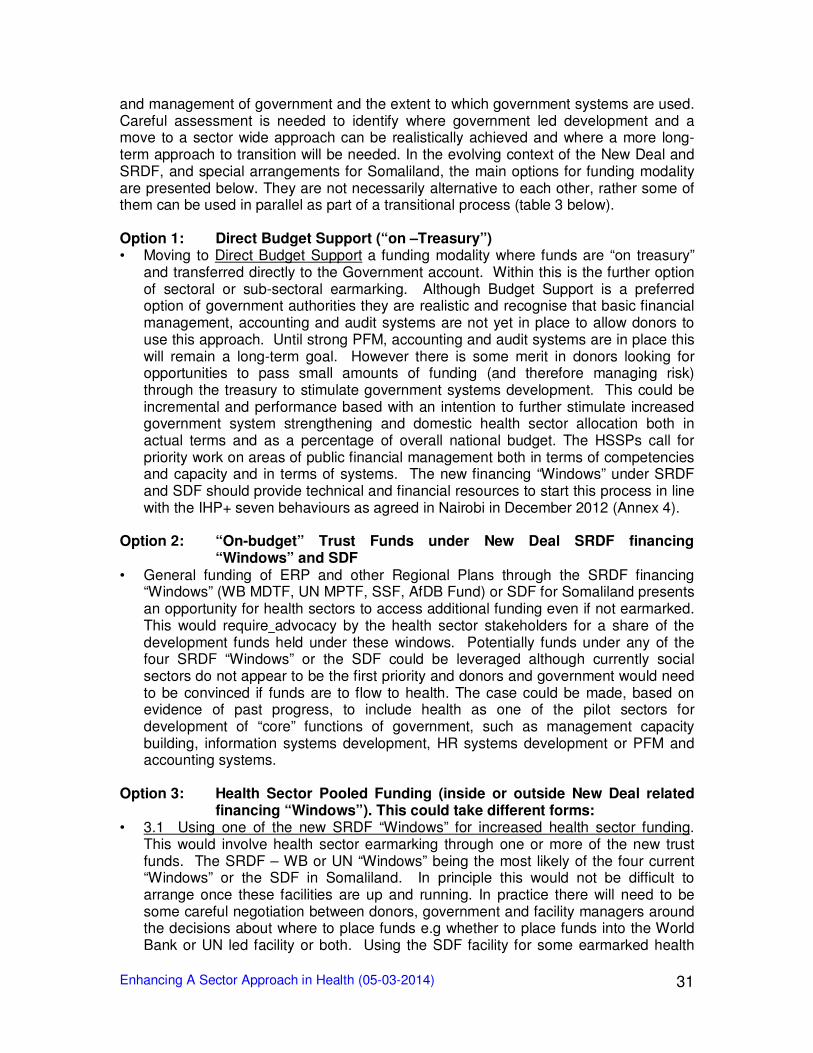
Enhancing A Sector Approach in Health (05-03-2014)
31
and management of government and the extent to which government systems are used. Careful assessment is needed to identify where government led development and a move to a sector wide approach can be realistically achieved and where a more long-term approach to transition will be needed. In the evolving context of the New Deal and SRDF, and special arrangements for Somaliland, the main options for funding modality are presented below. They are not necessarily alternative to each other, rather some of them can be used in parallel as part of a transitional process (table 3 below). Option 1: Direct Budget Support (“on –Treasury”) • Moving to Direct Budget Support a funding modality where funds are “on treasury”
and transferred directly to the Government account. Within this is the further option of sectoral or sub-sectoral earmarking. Although Budget Support is a preferred option of government authorities they are realistic and recognise that basic financial management, accounting and audit systems are not yet in place to allow donors to use this approach. Until strong PFM, accounting and audit systems are in place this will remain a long-term goal. However there is some merit in donors looking for opportunities to pass small amounts of funding (and therefore managing risk) through the treasury to stimulate government systems development. This could be incremental and performance based with an intention to further stimulate increased government system strengthening and domestic health sector allocation both in actual terms and as a percentage of overall national budget. The HSSPs call for priority work on areas of public financial management both in terms of competencies and capacity and in terms of systems. The new financing “Windows” under SRDF and SDF should provide technical and financial resources to start this process in line with the IHP+ seven behaviours as agreed in Nairobi in December 2012 (Annex 4).
Option 2: “On-budget” Trust Funds under New Deal SRDF financing
“Windows” and SDF • General funding of ERP and other Regional Plans through the SRDF financing
“Windows” (WB MDTF, UN MPTF, SSF, AfDB Fund) or SDF for Somaliland presents an opportunity for health sectors to access additional funding even if not earmarked. This would require advocacy by the health sector stakeholders for a share of the development funds held under these windows. Potentially funds under any of the four SRDF “Windows” or the SDF could be leveraged although currently social sectors do not appear to be the first priority and donors and government would need to be convinced if funds are to flow to health. The case could be made, based on evidence of past progress, to include health as one of the pilot sectors for development of “core” functions of government, such as management capacity building, information systems development, HR systems development or PFM and accounting systems.
Option 3: Health Sector Pooled Funding (inside or outside New Deal related
financing “Windows”). This could take different forms: • 3.1 Using one of the new SRDF “Windows” for increased health sector funding.
This would involve health sector earmarking through one or more of the new trust funds. The SRDF – WB or UN “Windows” being the most likely of the four current “Windows” or the SDF in Somaliland. In principle this would not be difficult to arrange once these facilities are up and running. In practice there will need to be some careful negotiation between donors, government and facility managers around the decisions about where to place funds e.g whether to place funds into the World Bank or UN led facility or both. Using the SDF facility for some earmarked health
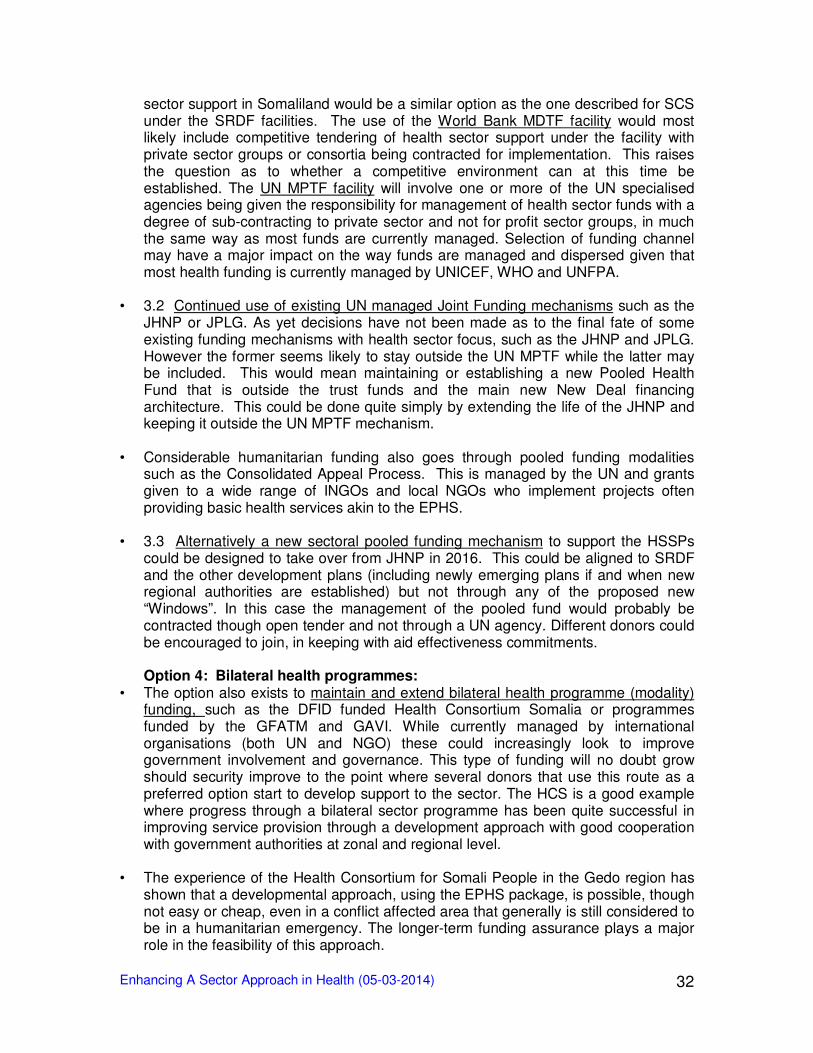
Enhancing A Sector Approach in Health (05-03-2014)
32
sector support in Somaliland would be a similar option as the one described for SCS under the SRDF facilities. The use of the World Bank MDTF facility would most likely include competitive tendering of health sector support under the facility with private sector groups or consortia being contracted for implementation. This raises the question as to whether a competitive environment can at this time be established. The UN MPTF facility will involve one or more of the UN specialised agencies being given the responsibility for management of health sector funds with a degree of sub-contracting to private sector and not for profit sector groups, in much the same way as most funds are currently managed. Selection of funding channel may have a major impact on the way funds are managed and dispersed given that most health funding is currently managed by UNICEF, WHO and UNFPA.
• 3.2 Continued use of existing UN managed Joint Funding mechanisms such as the
JHNP or JPLG. As yet decisions have not been made as to the final fate of some existing funding mechanisms with health sector focus, such as the JHNP and JPLG. However the former seems likely to stay outside the UN MPTF while the latter may be included. This would mean maintaining or establishing a new Pooled Health Fund that is outside the trust funds and the main new New Deal financing architecture. This could be done quite simply by extending the life of the JHNP and keeping it outside the UN MPTF mechanism.
• Considerable humanitarian funding also goes through pooled funding modalities
such as the Consolidated Appeal Process. This is managed by the UN and grants given to a wide range of INGOs and local NGOs who implement projects often providing basic health services akin to the EPHS.
• 3.3 Alternatively a new sectoral pooled funding mechanism to support the HSSPs
could be designed to take over from JHNP in 2016. This could be aligned to SRDF and the other development plans (including newly emerging plans if and when new regional authorities are established) but not through any of the proposed new “Windows”. In this case the management of the pooled fund would probably be contracted though open tender and not through a UN agency. Different donors could be encouraged to join, in keeping with aid effectiveness commitments.
Option 4: Bilateral health programmes:
• The option also exists to maintain and extend bilateral health programme (modality) funding, such as the DFID funded Health Consortium Somalia or programmes funded by the GFATM and GAVI. While currently managed by international organisations (both UN and NGO) these could increasingly look to improve government involvement and governance. This type of funding will no doubt grow should security improve to the point where several donors that use this route as a preferred option start to develop support to the sector. The HCS is a good example where progress through a bilateral sector programme has been quite successful in improving service provision through a development approach with good cooperation with government authorities at zonal and regional level.
• The experience of the Health Consortium for Somali People in the Gedo region has
shown that a developmental approach, using the EPHS package, is possible, though not easy or cheap, even in a conflict affected area that generally is still considered to be in a humanitarian emergency. The longer-term funding assurance plays a major role in the feasibility of this approach.
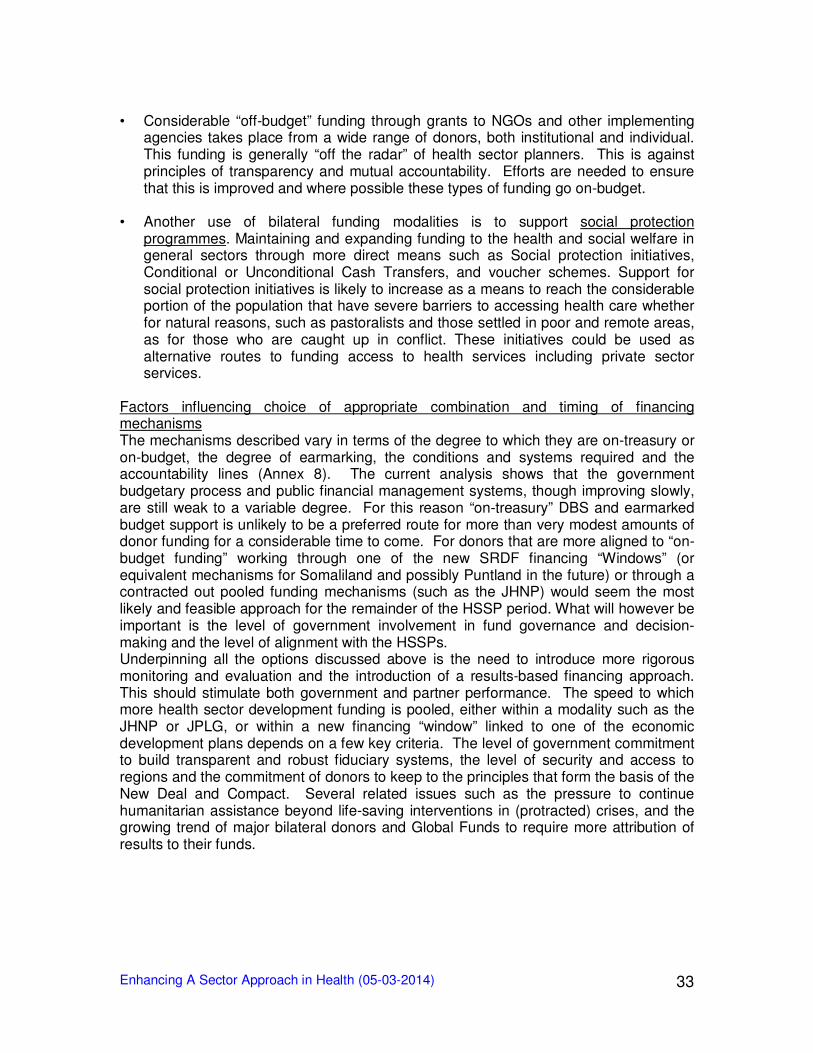
Enhancing A Sector Approach in Health (05-03-2014)
33
• Considerable “off-budget” funding through grants to NGOs and other implementing
agencies takes place from a wide range of donors, both institutional and individual. This funding is generally “off the radar” of health sector planners. This is against principles of transparency and mutual accountability. Efforts are needed to ensure that this is improved and where possible these types of funding go on-budget.
• Another use of bilateral funding modalities is to support social protection
programmes. Maintaining and expanding funding to the health and social welfare in general sectors through more direct means such as Social protection initiatives, Conditional or Unconditional Cash Transfers, and voucher schemes. Support for social protection initiatives is likely to increase as a means to reach the considerable portion of the population that have severe barriers to accessing health care whether for natural reasons, such as pastoralists and those settled in poor and remote areas, as for those who are caught up in conflict. These initiatives could be used as alternative routes to funding access to health services including private sector services.
Factors influencing choice of appropriate combination and timing of financing mechanisms The mechanisms described vary in terms of the degree to which they are on-treasury or on-budget, the degree of earmarking, the conditions and systems required and the accountability lines (Annex 8). The current analysis shows that the government budgetary process and public financial management systems, though improving slowly, are still weak to a variable degree. For this reason “on-treasury” DBS and earmarked budget support is unlikely to be a preferred route for more than very modest amounts of donor funding for a considerable time to come. For donors that are more aligned to “on-budget funding” working through one of the new SRDF financing “Windows” (or equivalent mechanisms for Somaliland and possibly Puntland in the future) or through a contracted out pooled funding mechanisms (such as the JHNP) would seem the most likely and feasible approach for the remainder of the HSSP period. What will however be important is the level of government involvement in fund governance and decision-making and the level of alignment with the HSSPs. Underpinning all the options discussed above is the need to introduce more rigorous monitoring and evaluation and the introduction of a results-based financing approach. This should stimulate both government and partner performance. The speed to which more health sector development funding is pooled, either within a modality such as the JHNP or JPLG, or within a new financing “window” linked to one of the economic development plans depends on a few key criteria. The level of government commitment to build transparent and robust fiduciary systems, the level of security and access to regions and the commitment of donors to keep to the principles that form the basis of the New Deal and Compact. Several related issues such as the pressure to continue humanitarian assistance beyond life-saving interventions in (protracted) crises, and the growing trend of major bilateral donors and Global Funds to require more attribution of results to their funds.
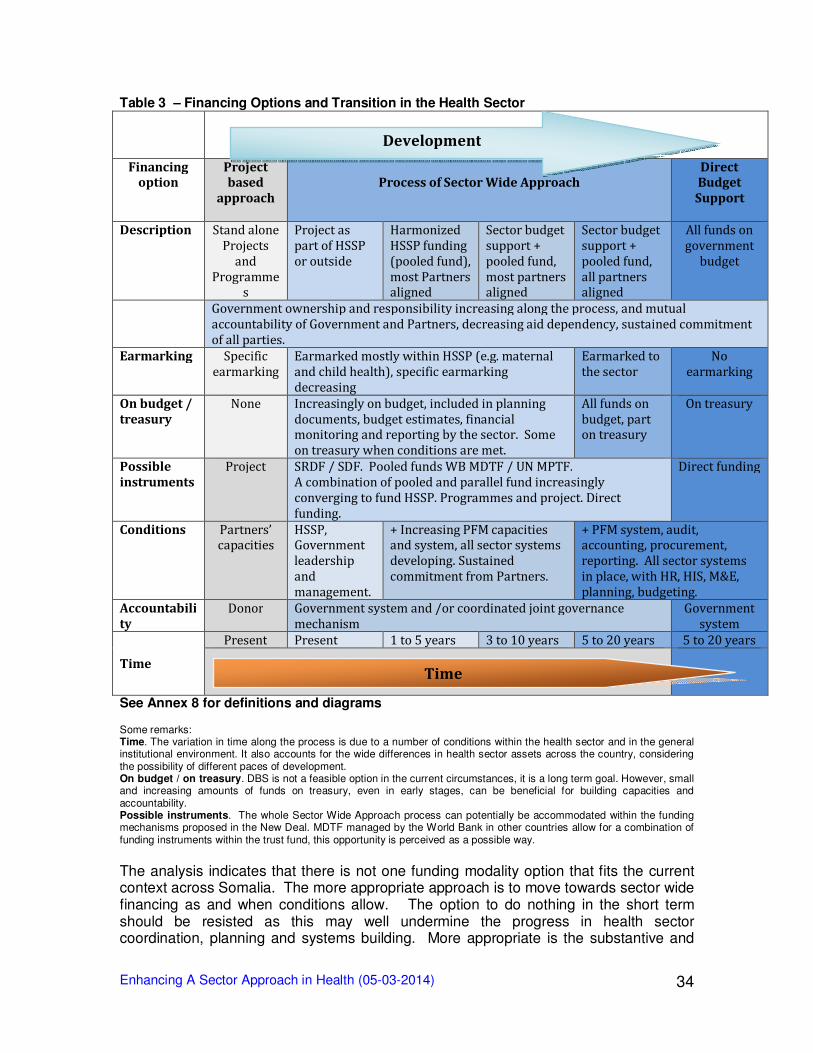
Enhancing A Sector Approach in Health (05-03-2014)
34
Table 3 – Financing Options and Transition in the Health Sector
Financing option
Project based
approach
Process of Sector Wide Approach
Direct Budget
Support
Description Stand alone
Projects
and
Programmes
Project as
part of HSSP
or outside
Harmonized
HSSP funding
(pooled fund),
most Partners aligned
Sector budget
support +
pooled fund,
most partners aligned
Sector budget
support +
pooled fund,
all partners aligned
All funds on
government
budget
Government ownership and responsibility increasing along the process, and mutual
accountability of Government and Partners, decreasing aid dependency, sustained commitment
of all parties.
Earmarking Specific
earmarking
Earmarked mostly within HSSP (e.g. maternal
and child health), specific earmarking
decreasing
Earmarked to
the sector
No
earmarking
On budget /
treasury
None Increasingly on budget, included in planning
documents, budget estimates, financial monitoring and reporting by the sector. Some
on treasury when conditions are met.
All funds on
budget, part on treasury
On treasury
Possible
instruments
Project SRDF / SDF. Pooled funds WB MDTF / UN MPTF.
A combination of pooled and parallel fund increasingly
converging to fund HSSP. Programmes and project. Direct
funding.
Direct funding
Conditions Partners’ capacities
HSSP, Government
leadership
and
management.
+ Increasing PFM capacities and system, all sector systems
developing. Sustained
commitment from Partners.
+ PFM system, audit, accounting, procurement,
reporting. All sector systems
in place, with HR, HIS, M&E,
planning, budgeting.
Accountabili
ty
Donor Government system and /or coordinated joint governance
mechanism
Government
system
Time
Present Present 1 to 5 years 3 to 10 years 5 to 20 years 5 to 20 years
See Annex 8 for definitions and diagrams Some remarks: Time. The variation in time along the process is due to a number of conditions within the health sector and in the general institutional environment. It also accounts for the wide differences in health sector assets across the country, considering the possibility of different paces of development. On budget / on treasury. DBS is not a feasible option in the current circumstances, it is a long term goal. However, small and increasing amounts of funds on treasury, even in early stages, can be beneficial for building capacities and accountability. Possible instruments. The whole Sector Wide Approach process can potentially be accommodated within the funding mechanisms proposed in the New Deal. MDTF managed by the World Bank in other countries allow for a combination of funding instruments within the trust fund, this opportunity is perceived as a possible way.
The analysis indicates that there is not one funding modality option that fits the current context across Somalia. The more appropriate approach is to move towards sector wide financing as and when conditions allow. The option to do nothing in the short term should be resisted as this may well undermine the progress in health sector coordination, planning and systems building. More appropriate is the substantive and
Development
Time
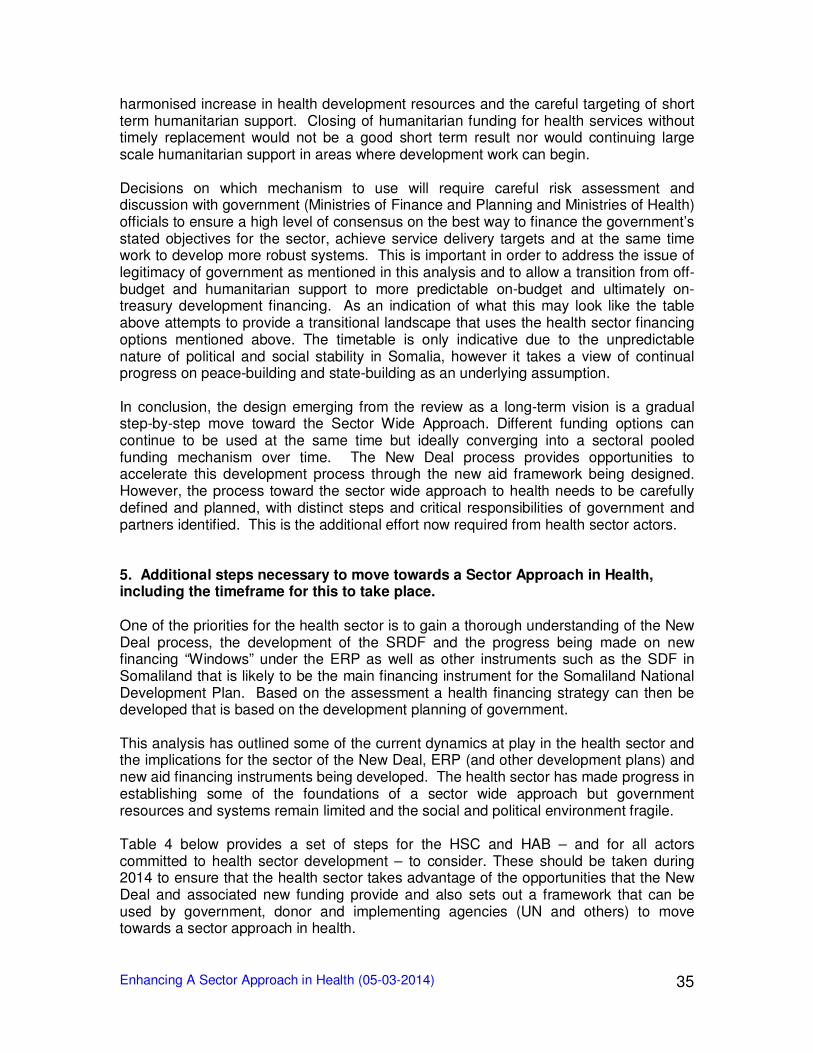
Enhancing A Sector Approach in Health (05-03-2014)
35
harmonised increase in health development resources and the careful targeting of short term humanitarian support. Closing of humanitarian funding for health services without timely replacement would not be a good short term result nor would continuing large scale humanitarian support in areas where development work can begin. Decisions on which mechanism to use will require careful risk assessment and discussion with government (Ministries of Finance and Planning and Ministries of Health) officials to ensure a high level of consensus on the best way to finance the government’s stated objectives for the sector, achieve service delivery targets and at the same time work to develop more robust systems. This is important in order to address the issue of legitimacy of government as mentioned in this analysis and to allow a transition from off-budget and humanitarian support to more predictable on-budget and ultimately on-treasury development financing. As an indication of what this may look like the table above attempts to provide a transitional landscape that uses the health sector financing options mentioned above. The timetable is only indicative due to the unpredictable nature of political and social stability in Somalia, however it takes a view of continual progress on peace-building and state-building as an underlying assumption. In conclusion, the design emerging from the review as a long-term vision is a gradual step-by-step move toward the Sector Wide Approach. Different funding options can continue to be used at the same time but ideally converging into a sectoral pooled funding mechanism over time. The New Deal process provides opportunities to accelerate this development process through the new aid framework being designed. However, the process toward the sector wide approach to health needs to be carefully defined and planned, with distinct steps and critical responsibilities of government and partners identified. This is the additional effort now required from health sector actors. 5. Additional steps necessary to move towards a Sector Approach in Health, including the timeframe for this to take place. One of the priorities for the health sector is to gain a thorough understanding of the New Deal process, the development of the SRDF and the progress being made on new financing “Windows” under the ERP as well as other instruments such as the SDF in Somaliland that is likely to be the main financing instrument for the Somaliland National Development Plan. Based on the assessment a health financing strategy can then be developed that is based on the development planning of government. This analysis has outlined some of the current dynamics at play in the health sector and the implications for the sector of the New Deal, ERP (and other development plans) and new aid financing instruments being developed. The health sector has made progress in establishing some of the foundations of a sector wide approach but government resources and systems remain limited and the social and political environment fragile. Table 4 below provides a set of steps for the HSC and HAB – and for all actors committed to health sector development – to consider. These should be taken during 2014 to ensure that the health sector takes advantage of the opportunities that the New Deal and associated new funding provide and also sets out a framework that can be used by government, donor and implementing agencies (UN and others) to move towards a sector approach in health.
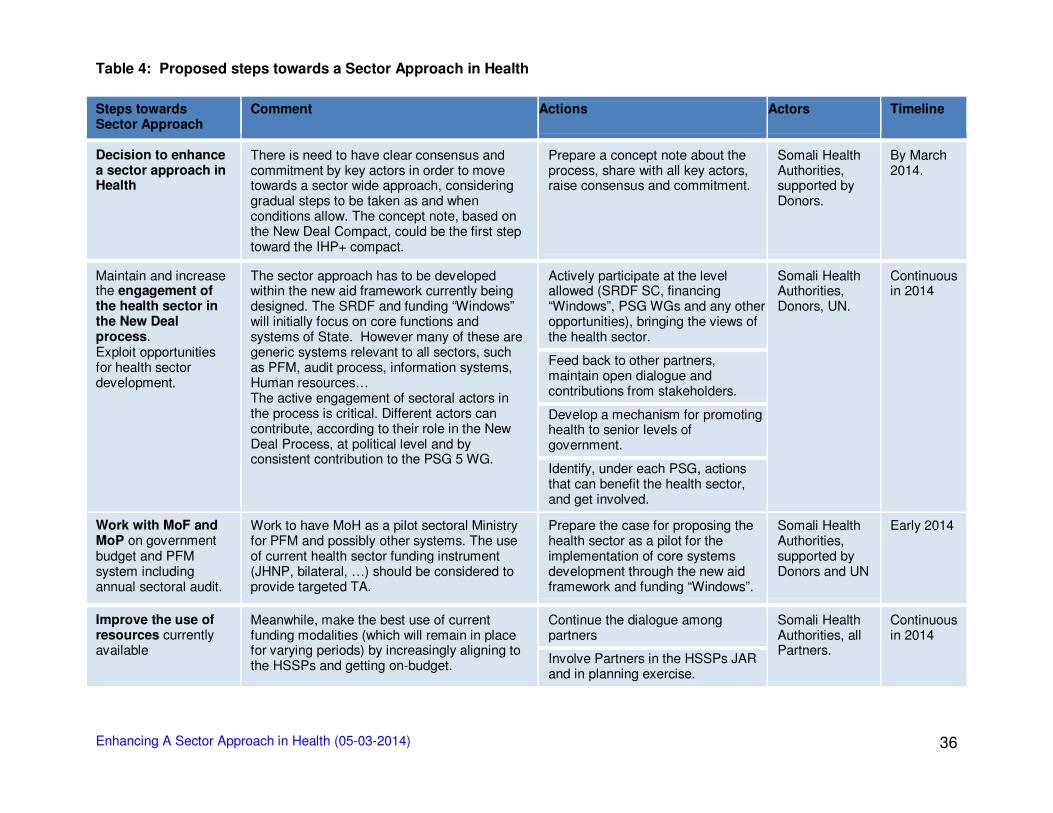
Enhancing A Sector Approach in Health (05-03-2014)
36
Table 4: Proposed steps towards a Sector Approach in Health
Steps towards Sector Approach
Comment Actions Actors Timeline
Decision to enhance a sector approach in Health
There is need to have clear consensus and commitment by key actors in order to move towards a sector wide approach, considering gradual steps to be taken as and when conditions allow. The concept note, based on the New Deal Compact, could be the first step toward the IHP+ compact.
Prepare a concept note about the process, share with all key actors, raise consensus and commitment.
Somali Health Authorities, supported by Donors.
By March 2014.
Maintain and increase the engagement of the health sector in the New Deal process. Exploit opportunities for health sector development.
The sector approach has to be developed within the new aid framework currently being designed. The SRDF and funding “Windows” will initially focus on core functions and systems of State. However many of these are generic systems relevant to all sectors, such as PFM, audit process, information systems, Human resources… The active engagement of sectoral actors in the process is critical. Different actors can contribute, according to their role in the New Deal Process, at political level and by consistent contribution to the PSG 5 WG.
Actively participate at the level allowed (SRDF SC, financing “Windows”, PSG WGs and any other opportunities), bringing the views of the health sector.
Somali Health Authorities, Donors, UN.
Continuous in 2014
Feed back to other partners, maintain open dialogue and contributions from stakeholders.
Develop a mechanism for promoting health to senior levels of government.
Identify, under each PSG, actions that can benefit the health sector, and get involved.
Work with MoF and MoP on government budget and PFM system including annual sectoral audit.
Work to have MoH as a pilot sectoral Ministry for PFM and possibly other systems. The use of current health sector funding instrument (JHNP, bilateral, …) should be considered to provide targeted TA.
Prepare the case for proposing the health sector as a pilot for the implementation of core systems development through the new aid framework and funding “Windows”.
Somali Health Authorities, supported by Donors and UN
Early 2014
Improve the use of resources currently available
Meanwhile, make the best use of current funding modalities (which will remain in place for varying periods) by increasingly aligning to the HSSPs and getting on-budget.
Continue the dialogue among partners
Somali Health Authorities, all Partners.
Continuous in 2014
Involve Partners in the HSSPs JAR and in planning exercise.
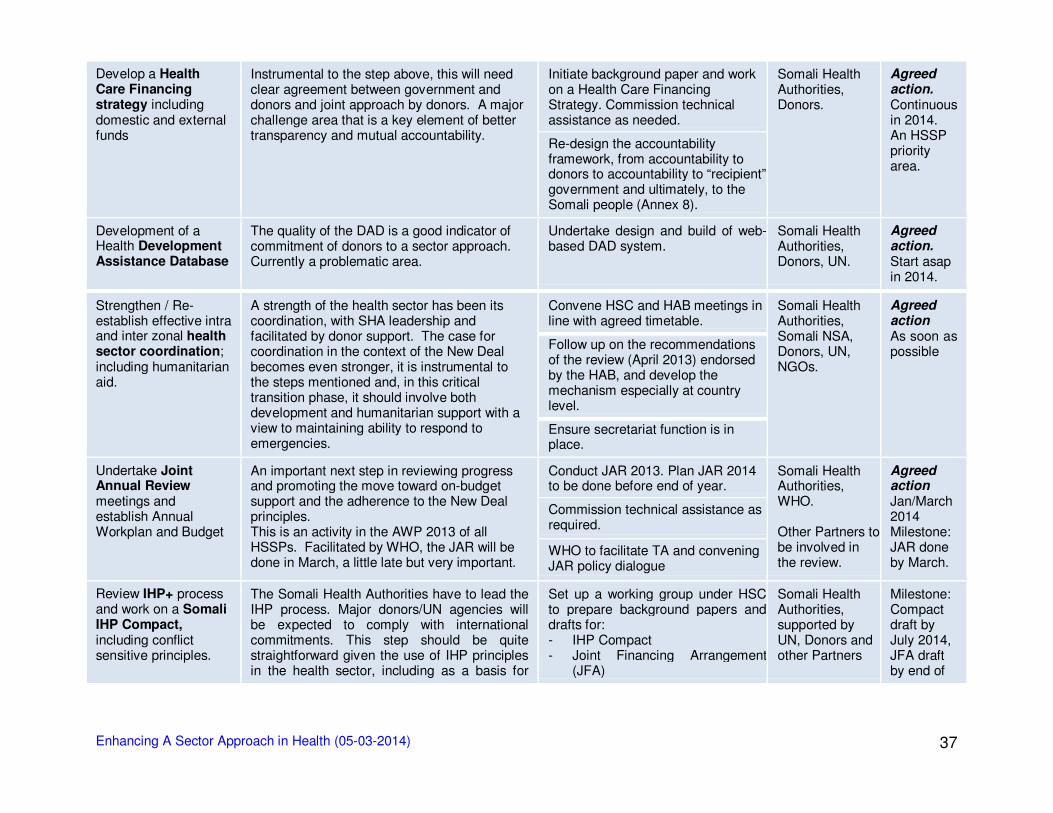
Enhancing A Sector Approach in Health (05-03-2014)
37
Develop a Health Care Financing strategy including domestic and external funds
Instrumental to the step above, this will need clear agreement between government and donors and joint approach by donors. A major challenge area that is a key element of better transparency and mutual accountability.
Initiate background paper and work on a Health Care Financing Strategy. Commission technical assistance as needed.
Somali Health Authorities, Donors.
Agreed action. Continuous in 2014. An HSSP priority area.
Re-design the accountability framework, from accountability to donors to accountability to “recipient” government and ultimately, to the Somali people (Annex 8).
Development of a Health Development Assistance Database
The quality of the DAD is a good indicator of commitment of donors to a sector approach. Currently a problematic area.
Undertake design and build of web-based DAD system.
Somali Health Authorities, Donors, UN.
Agreed action. Start asap in 2014.
Strengthen / Re-establish effective intra and inter zonal health sector coordination; including humanitarian aid.
A strength of the health sector has been its coordination, with SHA leadership and facilitated by donor support. The case for coordination in the context of the New Deal becomes even stronger, it is instrumental to the steps mentioned and, in this critical transition phase, it should involve both development and humanitarian support with a view to maintaining ability to respond to emergencies.
Convene HSC and HAB meetings in line with agreed timetable.
Somali Health Authorities, Somali NSA, Donors, UN, NGOs.
Agreed action As soon as possible
Follow up on the recommendations of the review (April 2013) endorsed by the HAB, and develop the mechanism especially at country level.
Ensure secretariat function is in place.
Undertake Joint Annual Review meetings and establish Annual Workplan and Budget
An important next step in reviewing progress and promoting the move toward on-budget support and the adherence to the New Deal principles. This is an activity in the AWP 2013 of all HSSPs. Facilitated by WHO, the JAR will be done in March, a little late but very important.
Conduct JAR 2013. Plan JAR 2014 to be done before end of year.
Somali Health Authorities, WHO. Other Partners to be involved in the review.
Agreed action Jan/March 2014 Milestone: JAR done by March.
Commission technical assistance as required.
WHO to facilitate TA and convening JAR policy dialogue
Review IHP+ process and work on a Somali IHP Compact, including conflict sensitive principles.
The Somali Health Authorities have to lead the IHP process. Major donors/UN agencies will be expected to comply with international commitments. This step should be quite straightforward given the use of IHP principles in the health sector, including as a basis for
Set up a working group under HSC to prepare background papers and drafts for: - IHP Compact - Joint Financing Arrangement
(JFA)
Somali Health Authorities, supported by UN, Donors and other Partners
Milestone: Compact draft by July 2014, JFA draft by end of
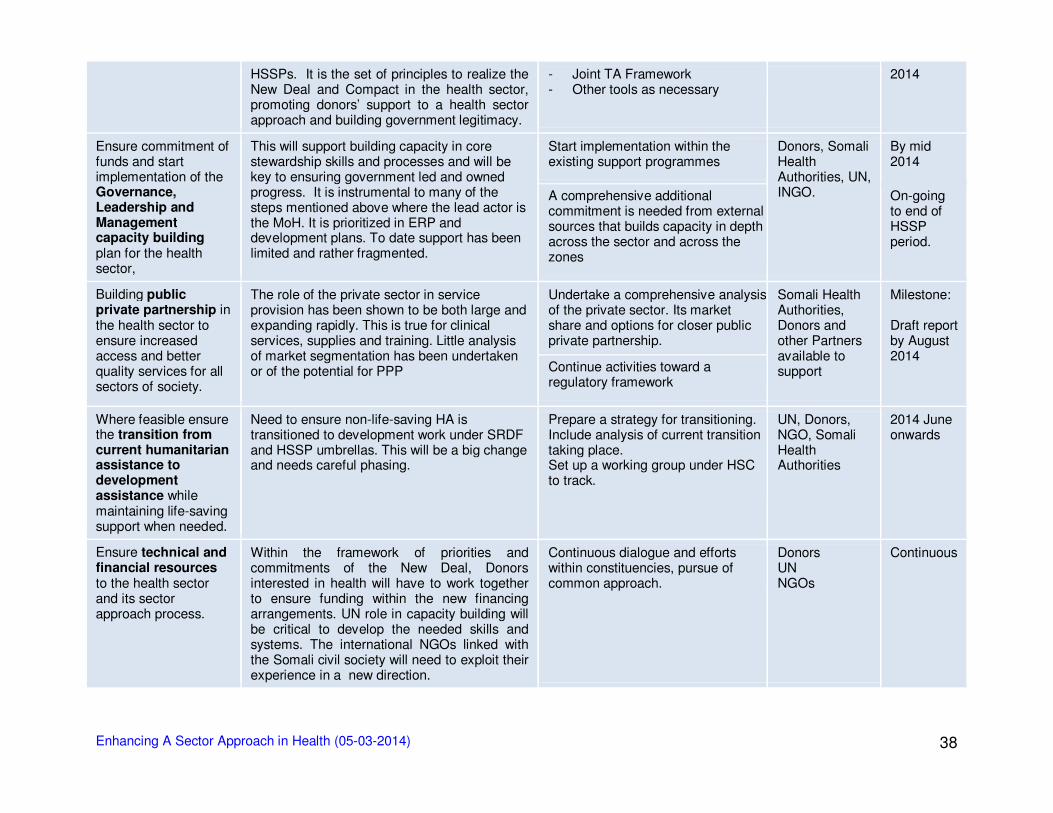
Enhancing A Sector Approach in Health (05-03-2014)
38
HSSPs. It is the set of principles to realize the New Deal and Compact in the health sector, promoting donors’ support to a health sector approach and building government legitimacy.
- Joint TA Framework - Other tools as necessary
2014
Ensure commitment of funds and start implementation of the Governance, Leadership and Management capacity building plan for the health sector,
This will support building capacity in core stewardship skills and processes and will be key to ensuring government led and owned progress. It is instrumental to many of the steps mentioned above where the lead actor is the MoH. It is prioritized in ERP and development plans. To date support has been limited and rather fragmented.
Start implementation within the existing support programmes
Donors, Somali Health Authorities, UN, INGO.
By mid 2014
A comprehensive additional commitment is needed from external sources that builds capacity in depth across the sector and across the zones
On-going to end of HSSP period.
Building public private partnership in the health sector to ensure increased access and better quality services for all sectors of society.
The role of the private sector in service provision has been shown to be both large and expanding rapidly. This is true for clinical services, supplies and training. Little analysis of market segmentation has been undertaken or of the potential for PPP
Undertake a comprehensive analysis of the private sector. Its market share and options for closer public private partnership.
Somali Health Authorities, Donors and other Partners available to support
Milestone: Draft report by August 2014
Continue activities toward a regulatory framework
Where feasible ensure the transition from current humanitarian assistance to development assistance while maintaining life-saving support when needed.
Need to ensure non-life-saving HA is transitioned to development work under SRDF and HSSP umbrellas. This will be a big change and needs careful phasing.
Prepare a strategy for transitioning. Include analysis of current transition taking place. Set up a working group under HSC to track.
UN, Donors, NGO, Somali Health Authorities
2014 June onwards
Ensure technical and financial resources to the health sector and its sector approach process.
Within the framework of priorities and commitments of the New Deal, Donors interested in health will have to work together to ensure funding within the new financing arrangements. UN role in capacity building will be critical to develop the needed skills and systems. The international NGOs linked with the Somali civil society will need to exploit their experience in a new direction.
Continuous dialogue and efforts within constituencies, pursue of common approach.
Donors UN NGOs
Continuous
Enhancing A Sector Approach in Health (05-03-2014)
39
6. Conclusion The New Deal and Compact mentions the health sector as an example where progress has been made in sectoral planning and adherence to aid effectiveness principle. While progress in the health sector has been considerable, there is also a rising awareness that health must be placed in the broader political context, and that the interests of all stakeholders must be taken into account. There is an apparent optimism that progress can be made in health both from government and donor sides. This is evident in the consultations held during this review. As new interest from the international community emerges the health sector should position itself to take advantage of the resources and expertise that this will bring. At the same time it should be recognised that the increased funding through the New Deal and the increased profile of the health sector in some of these documents could lead to more political interest in how the health sector is managed and coordinated across the country. This will grow if and when the role of health service provision is recognised as an important contributor to peace-building and State legitimacy. The Health Sector Strategic Plans and corresponding Annual Work Plans and Budgets provide a useful framework for dialogue and donors should work to ensure sufficient and predictable financing through available funding modalities. This report points to the value of donors and government using pooled funding mechanisms for those that are able to do so and through aligned “on-budget” bilateral support for those that cannot. Donors need to balance interest in demonstrating results and attribution to investments made with building government systems and avoiding the creation of parallel programmes. A challenge ahead will be to rationalise the current fragmented funding to the sector, transition away from humanitarian assistance while maintaining emergency interventions when needed and working on establishing a legitimate government regulated health system that includes a substantial private sector component. Given the current fragile environment this will all need to be done with a strong emphasis on conflict sensitive programme management. The report has considered a range of financing options available to the sector and their relative merits and feasibility in the current environment. While the New Deal should now lead to increased investment in Somalia, the weak capacities and systems of government will restrict how these funds are channelled. Limited on-treasury funding could be considered although donors are likely to be hesitant due to fiduciary risks this will entail. The main options for increased health funding are for generic systems funding to include the health sector or for pooled funding under either the WB or UN or SDF windows. The alternative is to work towards an alternative pooled funding mechanisms that is on-budget but externally managed. The report emphasises the importance of on-budget funding, including all bilateral programmes, and establishing transparent systems that will allow better planning and budgeting. The report has also developed a set of next steps that should help to reinforce the progress made in the health sector across Somalia as it develops towards a sector approach. Many of these are consistent with aid effectiveness principles that form the basis of the New Deal. The Somali Health Advisory Board, in commissioning this analysis, expressed a willingness to understand the New Deal process, to be part of it, exploit and promote opportunities for health sector development, toward a sectoral approach. This willingness was also expressed by most discussants during the analysis and should now

Enhancing A Sector Approach in Health (05-03-2014)
40
be translated into a firm commitment by the HAB members, each in their specific capacities. Somali Health Authorities, Somali non-State Actors, Donors, UN and international NGOs should all be encouraged and expected to make critical decisions, both jointly and within constituencies, building on the foundations already laid in the Somali health sector over the past few years, and pursue a substantive process towards a sector approach. This report concludes that the New Deal and Compact should bring new opportunities for increased financing of the health sector, given the substantial pledges that have been made by the international community, and for a strengthened leadership by the Somali health authorities. While these funds are aimed primarily at implementing priority activities articulated in economic development plans, this should also flow through to sectoral priorities and building core functions across all government departments in order to make this strengthened Somali leadership possible.The wide variety of stakeholders supporting health care provision need to engage proactively in the next stages of SRDF and SDF financing decisions and advocate strongly for health being included in discussions and for the health sector being selected as a pilot sector for core systems development. A major challenge in the near future is to build the trust between government and development partners and demonstrate this through rapidly improving mutual accountability through agreed transparent systems for sharing decision-making and information.
Enhancing A Sector Approach in Health (05-03-2014)
41
Annexes
Enhancing A Sector Approach in Health (05-03-2014)
42
Annex 1 – List of Persons consulted Dr. Maryam Qasim Minister FGS, Ministry of Human
Development & Public Services
Mogadishu
Mr. Duale Adam Director General FGS, DoH Mogadishu Dr. Abdi Awad Ibrahim Senior Adviser FGS, DoH Nairobi Dr. Abdihamid Ibrahim Director of Planning,
Health FGS, DoH
Mogadishu Mr. Ahmed Moallim M. Adviser FGS, DoH Nairobi Dr. Mohamed A. Farah Director of Public Health FGS, DoH Mogadishu Mr. Abdullahi Aress Aid Finance Coordinator FGS, Ministry of Finance
and Planning Mogadishu Mr. Abshir Technical Officer PL Ministry of Finance Garowe Mr. Mohamud Aidid Dirir Minister PL Ministry of Planning Garowe Mr. Farah Kulmiye Director General PL Ministry of Planning Garowe Mr. Abdirizak Abshir Director of PHC and EPI PL MoH Garowe Dr. Abdirizak Hassan Isse Director of Planning PL MoH Garowe Dr. Abdirizak Hersi Hassan
Director General PL MoH Garowe
Dr. Ali Abdullahi Warsame
Minister PL MoH Garowe
Mr. Hussein Karkaar Regional Medical Office
PL MoH Garowe
Ms. Zeinab Ugaas Vice Minister PL MoH Garowe Mr. Hussein Samantar Health Sector JPLG
consultant PL MoH
Nairobi Mr. Mohamed Hassan Barre
Chair, New Deal Commission
PL New Deal Commission Garowe
Mr. Omar Hashi Consultant PFM SL Ministry of Finance Hargeisa Mr. Abdirashid A. Guleid Director General SL Ministry of Planning Hargeisa Mr. Adan Da'ud Egal "Weli"
Director, Dept Planning and Statistics
SL Ministry of Finance Hargeisa
Mr. Abdirahman Elmi Wairah
Health Sector JPLG consultant
SL MoH Hargeisa
Mr. Ahmed Maydal Programme Officer - Coordination
SL MoH Hargeisa
Ms. Faisa Ahmed Ibrahim Head, Planning Policy and Strategic Department
SL MoH Hargeisa
Mr. Khadar M. Ahmed Former MoH Director of Planning
SL MoH Hargeisa
Dr. Ahmed Aartan Member PL - Nugal Medical Association
Garowe
Dr. Lula Hussein Executive Director SL National Health Professions Commission
Hargeisa
Ms. Roda Ali President SL Edna Adan University and SL Nurses and Midwives Association
Hargeisa
Mr. Hakan Bilgin Country Director IMC Nairobi
Dr. Caroline Mwangi-Otieno
Health Coordinator IRC Nairobi
Mr. Jama Mohamed Health Programme Manager
SCI Garowe
Mr. Osman Dhalaweyne Deputy RMO Karkaar PL MoH Garowe
Enhancing A Sector Approach in Health (05-03-2014)
43
Ms. Sirad Aden Health Programme Manager
SRCS Garowe
Mr. Martin Dwan Trocaire Nairobi
Ms. Ombretta Mazzaroni Health Programme Manager
Trocaire Nairobi
Ms. Rosemary Heenan Country Director Trocaire Nairobi
Mr. Philippe Lazzarini UN Resident and Humanitarian Coordinator
UN RC Nairobi
Ms. Jo Nickolls Strategic Planner and Head of the RC's Office
UN RC Nairobi
Dr. Achu Lordfred Maternal Health Adviser UNFPA Nairobi
Mr. Cheikh Tidiane Cisse Country Rep UNFPA Nairobi
Ms. Marieme Ba Sourang Consultant UNFPA Nairobi
Dr. Anirban Chatterjee Chief of Health UNICEF Nairobi
Ms. Esther Waters-Crane JHNP Programme and Planning Specialist
UNICEF Nairobi
Ms. Foroogh Foyouzat Deputy Country Rep UNICEF Nairobi
Dr. Raza Zaidi JHNP Senior Programme Manager
UNICEF Nairobi
Dr. Alaa Abou-Zeid Health Cluster Coordinator WHO Mogadishu
Dr. Humayun Rizwan PHC Adviser WHO Nairobi
Dr. Katja Schemionek HSS Adviser and GAVI HSS
WHO Nairobi
Ms. Amy Clancy Fund Portfolio Manager GFATM Geneva, call
Ms. Carin-marie Lacock Programme Officer GFATM Nairobi
Mr. Job Muriuki Programme Officer GFATM Nairobi
Ms. Alessia Riccardi Somalia Desk Officer Italy - Italian Cooperation Nairobi, call
Ms. Katie Bigmore Health Adviser UK - DFID & Sweden - SIDA
Nairobi
Ms. Pauline Seenan Head of Health, Wealth and Humanitarian Team
UK - DFID Nairobi
Ms. Rebecca Terzeon Deputy Head of DFID Somalia
UK - DFID Nairobi
Ms. Karen Stephenson Health Adviser UK - DFID Nairobi
Ms. Grace Miheso Senior Regional Maternal and Child Health Specialist
USA - USAID Nairobi
Ms. Marybeth McKeever Somalia Programme Advisor
USA - USAID Nairobi
Mr. Geoff Handley Economist World Bank Nairobi
Enhancing A Sector Approach in Health (05-03-2014)
44
Annex 2 – Reference Documents Key background documents Eldon J, HLSP (2013). Somali Health Sector Coordination. Institutional Analysis of Organisational and Governance Arrangements. May 2013. Somali HSC Library.
Fund for Peace - FFP (2013). Failed States Index. Somalia. http://ffp.statesindex.org/somalia.
High Level Conference “A New Deal for Somalia” (2013). Communiqué. Brussels 16/09/2013.
High Level Conference “A New Deal for Somalia” (2013). Pledges as of 16th September 2013.
Puntland Government (2013). Puntland Five Year Development Plan 2014-2018. Draft.
Puntland Ministry of Health (2013). Health Sector Strategic Plan January 2013 – December 2016.
Somali Health Sector Coordination (2013). Somali Health Sector Committee Structure and Functions. Synthesis from the official HSC Reform Report 2010. Somali HSC Library.
Somalia Federal Government (2013). Economic Recovery Plan 2014-2015. (ERP)
Somalia Federal Government (2013). The Somali Compact. Brussels, September 2013.
Somalia Federal Government, Directorate of Health (2013). Health Sector Strategic Plan January 2013 – December 2016.
Somaliland Government (2012) Somaliland National Development Plan.
Somaliland Ministry of Health (2013). Health Sector Strategic Plan 2013 – 2016.
UN Somalia RC office (2013). UN Multi-Partner Trust Fund for Somalia (Somalia UN MPTF). Draft Terms of Reference. Revised version January 2014.
World Bank (2013). New Deal Fragility Assessment Somalia: Input Paper on PSG 5 – Revenue & Services.
Selected Bibliography
Bornemisza O et al. (2010). Health Aid Governance in Fragile States: The Global Fund Experience. Global Health Governance, Vol. IV, No. 1 (fall 2010) http://www.ghgj.org.
Browne, E., & Fisher, J. (2013). Key actors mapping: Somalia. Rapid literature review. Birmingham, UK: GSDRC, University of Birmingham. November 2013.
Cassels, A (1997), A guide to sector-wide approaches for health development, World Health Organisation, Geneva. 2007.
Chapman N and Vaillant C. (2010). Synthesis of country programme evaluations conducted in fragile states, DFID Evaluation reports EV 709. February 2010.
Commins S et al. (2013). Pooled Funding to Support Service Delivery. Lessons of Experience from Fragile and Conflict-Affected States. May 2013.
Coppin E, Manuel M and McKechnie A (2011). Fragile states: measuring what makes a good pooled fund. Overseas Development Institute – ODI Project Briefing No.58. August 2011.
Coppin E. (2012). Measuring good pooled funds in fragile states. Overseas Development Institute – ODI. November 2012.
Eldon J, Waddington C and Hadi Y. (2008). Health System Reconstruction: Can it Contribute to State-building? HLSP Institute. Health and Fragile States Network. October 2008.
Foster, M (2000). New Approaches to Development Co-operation: What can we learn from experience with implementing Sector Wide Approaches?, ODI Working Paper 140. London:ODI
Enhancing A Sector Approach in Health (05-03-2014)
45
Freeman T et al. (2007). “Joint External Evaluation of the Health Sector in Tanzania, 1999-2006” Cowi, Goss Gilroy, Inc., Management Consultants, EPOS Health Consultants, October 2007.
Goldsmith C. and Muhamad A. (2013). Review of Compensation, Salaries, Incentives and Benefits for Health Personnel in Somalia. Final Report, March 2013. Somali HSC Library.
Lindley A. (2007). Remittances in Fragile Settings: a Somali Case Study. HiCN Working Paper. Institute of Development Studies (IDS) University of Sussex UK. March 2007.
McNee, E (2012), Rethinking Health Sector Wide Approaches through the lens of Aid Effectiveness, Development Policy Centre Discussion Paper #14, Crawford School of Public Policy, The Australian National University, Canberra. 2012.
Newbrander W. (2006). Providing Health Services in Fragile States. BASICS. USAID. May 2006.
OECD (2006). Harmonising Donor Practices for Effective Aid Delivery. Volume 2. Budget Support, Sector Wide Approaches and Capacity Development in Public Financial Management. DAC Guidelines and Reference Series. 2006.
OECD (2006). Harmonizing Donor Practices for Effective Aid Delivery, Volume 2. A DAC Reference Document. 2006.
OECD (2010). Peacebuilding and Statebuilding Priorities and Challenges. A synthesis of findings from seven multi-stakeholder consultations. 2010.
OECD (2012). Fragile States 2013: Resource flows and trends in a shifting world. DAC International Network on Conflict and Fragility. 2012.
OECD (2013), Gender and Statebuilding in Fragile and Conflict-affected States, Conflict and Fragility, OECD Publishing. http://dx.doi.org/10.1787/9789264202061-en
Pavignani E, Correggia R, Pearson N. (2009). Report 7: Steps towards Harmonizing External Support Health Care Provision for the Somali people. UNICEF, DFID, European Commission, Italian Development Cooperation.
Pearson N. and Khan S. (2013). Somali Package of Health Services - more essential than ever. Review of EPHS implementation in Sahil Region of Somaliland, Kaarkar region of Puntland and Gedo Region of South Central Somalia. November 2013.
Rothmann, I. and A. Canavan (2009) Assessment of readiness for a sector-wide approach in fragile states. A methodological framework. KIT Working Papers Series H4. Amsterdam: KIT
Rothmann, I., A. Canavan et al (2011) Moving towards a sector-wide approach (SWAp) for health in fragile states: Lessons learned on the state of readiness in Timor Leste, Sierra Leone and Democratic Republic of Congo. KIT Working Papers Series H5. Amsterdam: KIT
Smith H, Stares P. (2007). Diasporas in Conflict: Peacemakers or Peace Wreckers? United Nations University Press.
UNOCHA Somalia (2013). 2014 Humanitarian Needs Overview. Somalia. October 2013. UNOCHA Somalia (2013). 2014 Strategic Response Plan. Somalia. December 2013. http://unocha.org/somalia
World Bank (2009), Do health sector wide approaches achieve results? Emerging evidence and lessons from six countries, World Bank Independent Evaluation Group, Washington D.C.
World Bank (2013). New Deal Fragility Assessment Somalia: Input Papers on PSGs.
Enhancing A Sector Approach in Health (05-03-2014)
46
Annex 3 - The New Deal at a glance The “New Deal for Engagement in Fragile States” was endorsed at the Fourth High-Level Forum on Aid Effectiveness in Busan in 2011 by over 44 countries and multilateral partners. It is the official commitment to realize the principles of aid effectiveness - Paris Declaration, Accra Agenda for Action, Busan – in fragile states. . The facts
• 1.5 billion people live in conflict-affected and fragile states. • About 70% of fragile states have seen conflict since 1989. • Basic governance transformations may take 20-40 years. • 30% of Official Development Assistance (ODA) is spent in fragile and conflict-affected contexts. • These countries are furthest away from achieving the Millennium Development Goals (MDGs).
The New Deal defined five Peacebuilding and Statebuilding Goals (PSGs) as the foundation for progress and a guide for work in fragile and conflict- affected states. � PSG 1 Legitimate Politics. Foster inclusive political settlements and conflict
resolution � PSG 2 Security. Establish and strengthen people’s security � PSG 3 Justice Address injustices and increase people’s access to justice � PSG 4 Economic Foundations Generate employment and improve livelihoods � PSG 5 Revenues and Services Manage revenue and build capacity for
accountable and fair service delivery The New Deal defined five elements in the new way for engagement, supporting inclusive, country-owned and -led pathways out of fragility, summarized in the FOCUS:
F - Fragility Assessments of the causes and features of fragility, which is country-led, as the basis for one vision and one plan. O - One vision, one plan, which is country owned and led to address the PSGs and to transition out of fragility C – Compact, to implement the one vision one plan and to guide partnership between all partners to achieve the PSGs U - Use PSGs to monitor progresses S - Support political dialogue and leadership for effective peacebuilding and statebuilding.
The New Deal also defined a set of commitments to enhance transparency, manage risk to use country systems, strengthen national capacities and improve the timeliness and predictability of aid. This set is called TRUST:
T – Transparency in the use of domestic resources, enhanced and at every level R - Risk-sharing. Risk that is jointly assessed and managed for better and greater investment in fragile states. U - Use country systems building and delivering through them. S - Support capacity development of local institutions and actors to build peaceful states T - Timely and predictable aid through simplified, faster and better tailored mechanisms
http://www.newdeal4peace.org
Enhancing A Sector Approach in Health (05-03-2014)
47
Annex 4 - IHP+ Seven Behaviours At the IHP+ meeting in Nairobi, December 2012, participants identified a number of critical areas where international development partners need to change their behaviour in order to accelerate progress on the MDGs. Recent meetings of global health leaders have strongly supported renewed action on these seven behaviours which, if implemented, would bring visible results.
The seven behaviours
1. Agreement on priorities that are reflected in a single national health strategy and underpinning sub-sector strategies, through a process of inclusive development and joint assessment, and a reduction in separate exercises.
2. Resource inputs recorded on budget and in line with national priorities
3. Financial management systems harmonized and aligned; requisite capacity building done or underway, and country systems strengthened and used.
4. Procurement/supply systems harmonized and aligned, parallel systems phased out, country systems strengthened and used with a focus on best value for money. National ownership can include benefiting from global procurement.
5. Joint monitoring of process and results is based on one information and accountability platform including joint annual reviews that define actions that are implemented and reinforce mutual accountability.
6. Opportunities for systematic learning between countries developed and supported by agencies (south-south/triangular cooperation).
7. Provision of strategically planned and well-coordinated technical support.
On this basis, two separate but interrelated sets of activities are being initiated. The first is international partner change in relation to the seven behaviours, with organization-wide effect. The second is to work with countries to fast-track implementation and learn about results.
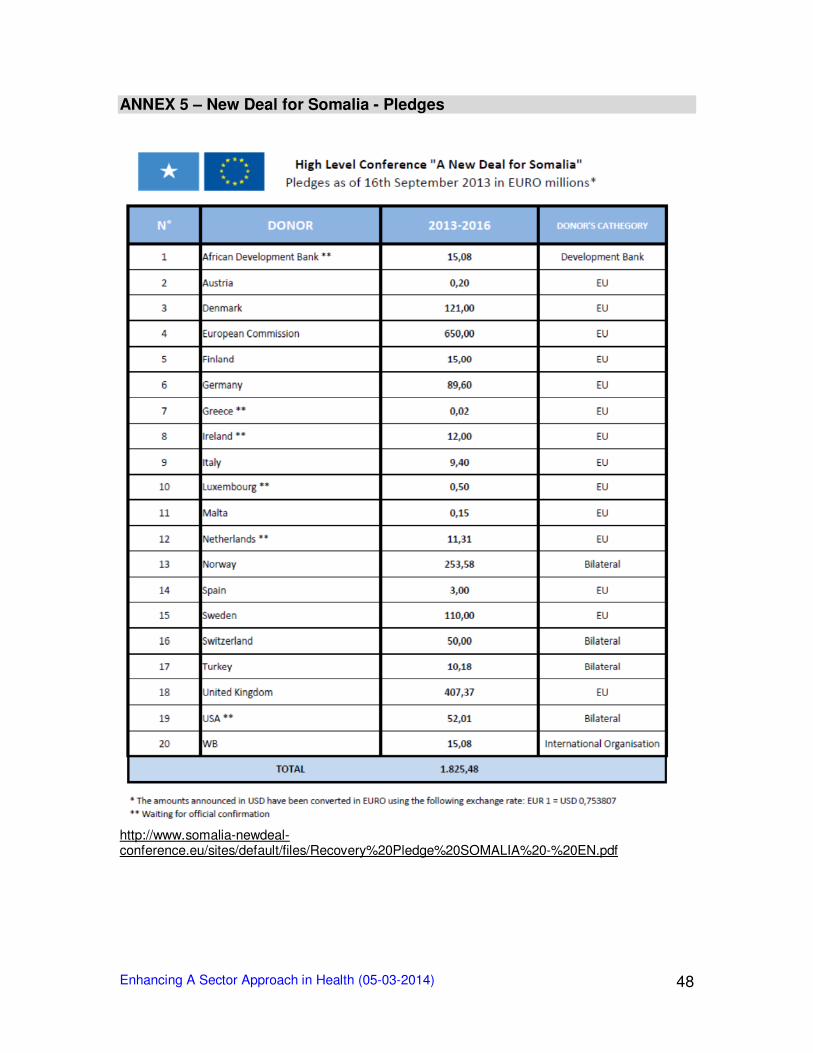
Enhancing A Sector Approach in Health (05-03-2014)
48
ANNEX 5 – New Deal for Somalia - Pledges
http://www.somalia-newdeal-conference.eu/sites/default/files/Recovery%20Pledge%20SOMALIA%20-%20EN.pdf
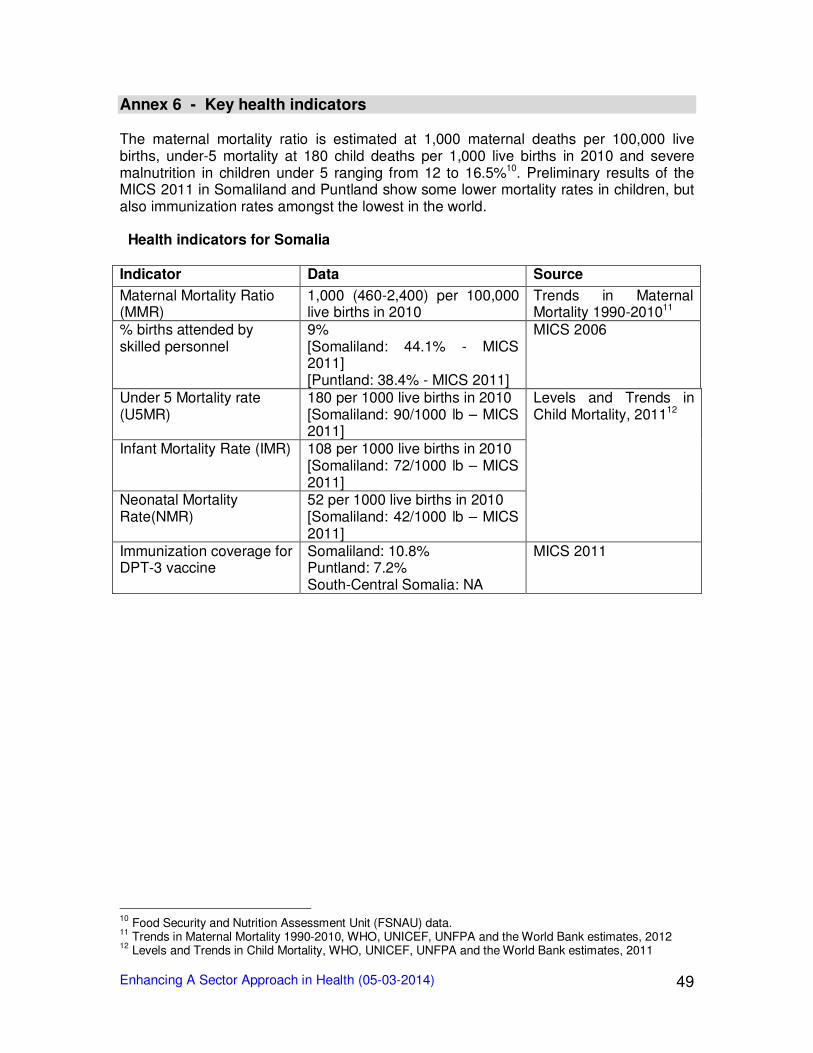
Enhancing A Sector Approach in Health (05-03-2014)
49
Annex 6 - Key health indicators The maternal mortality ratio is estimated at 1,000 maternal deaths per 100,000 live births, under-5 mortality at 180 child deaths per 1,000 live births in 2010 and severe malnutrition in children under 5 ranging from 12 to 16.5%10. Preliminary results of the MICS 2011 in Somaliland and Puntland show some lower mortality rates in children, but also immunization rates amongst the lowest in the world. Health indicators for Somalia Indicator Data Source
Maternal Mortality Ratio (MMR)
1,000 (460-2,400) per 100,000 live births in 2010
Trends in Maternal Mortality 1990-201011
% births attended by skilled personnel
9% [Somaliland: 44.1% - MICS 2011] [Puntland: 38.4% - MICS 2011]
MICS 2006
Under 5 Mortality rate (U5MR)
180 per 1000 live births in 2010 [Somaliland: 90/1000 lb – MICS 2011]
Levels and Trends in Child Mortality, 201112
Infant Mortality Rate (IMR) 108 per 1000 live births in 2010 [Somaliland: 72/1000 lb – MICS 2011]
Neonatal Mortality Rate(NMR)
52 per 1000 live births in 2010 [Somaliland: 42/1000 lb – MICS 2011]
Immunization coverage for DPT-3 vaccine
Somaliland: 10.8% Puntland: 7.2% South-Central Somalia: NA
MICS 2011
10
Food Security and Nutrition Assessment Unit (FSNAU) data. 11
Trends in Maternal Mortality 1990-2010, WHO, UNICEF, UNFPA and the World Bank estimates, 2012 12
Levels and Trends in Child Mortality, WHO, UNICEF, UNFPA and the World Bank estimates, 2011
Enhancing A Sector Approach in Health (05-03-2014)
50
Annex 7 – Definitions - Health Sector Strategic Plans (HSSPs) The HSSPs for Puntland, Somaliland and South-Central Somalia are meant to guide national and international investments in the health sector and to improve their effectiveness. The HSSPs have six strategies, based on the WHO key components of a well-functioning health system and set realistic targets for each of them. 1. Governance and leadership. Focused on increasing MoH capacities at different
level and its responsibilities – by increased ownership – on health sector development.
2. Human resources for health. Focused on effective development and management of this as the most important resources for health sector development.
3. Health service delivery. The EPHS is formally adopted as the framework for service delivery across all interventions.
4. Health financing. Focused on increasing domestic financing, national and local, and the development of systems for more effective use of domestic and international resources for the health sector, with transparency and accountability.
5. Medicines, vaccines and technologies. Focused on the need for regulation, quality control and proper use.
6. Health information. Emphasis on better information and its use for planning and management in the health sector.
The HSSP process was led by government health authorities in Hargeisa, Garowe and Mogadishu, included preparatory analysis of the health situation, systems and resources and identified major gaps in capacities and services. Consultative meetings including regional actors were led by government and inclusive roundtable planning meetings held in the three zonal capitals. Coordination between the three authorities was maintained throughout and led to an agreement on format and major objectives. The three HSSPs produced were similar in form with regional variations. A common set of indicators for the monitoring and evaluation framework was selected, again with some regional variations. Joint workshops were also carried out at strategic points in the process to discuss priorities and agree approach. These included joint presentations in Nairobi by authorities to major international partners in the sector. As part of the HSSP process was other systems related work in the sector such a “Review of Compensation, Salaries, Incentives and Benefits for Health Personnel” aimed at appropriate and harmonized HR management and the agreement on a Joint Governance, Leadership and Management plan linked to the first strategic priority in the HSSPs; this was costed and detailed work planning for 2013 undertaken. As part of the HSSP process the government teams used the Joint Assessment of National Strategies (JANS) tool of the IHP+. This was used as an independent internal check on quality and relevance of the plans as well as a way to increase confidence in the plans. The JAR was included for the 2013 workplan to start the process of tracking implementation, alignment of partners and overall performance. It was recognised that the initial JAR would provide a useful means of discussing mutual accountability and alignment behind the government’s priorities in a period where many transitional processes would be at play.
Enhancing A Sector Approach in Health (05-03-2014)
51
Annex 8 – Definitions - Sector-Wide Approach (SWAp) The SWAp defines a method of working between Government and Partners, a mechanism for co-ordinating support to public expenditure programmes. The agreed components include Government leadership on the sector programme, all significant fundings support theprogramme, common management and implementation approaches are applied by all partners, and Government procedures are used, over time, to disburse and account for funds. “An approach that involves all significant funding for the sector supporting a single sector policy and expenditure program, under government leadership, adopting common approaches across the sector, and progressing towards relying on government procedures to disburse and account for all funds”. (Cassels 1997) “An approach to a locally-owned program for a coherent sector in a comprehensive and coordinated manner, moving toward the use of country systems. SWAps represent a ...shift in the focus, relationship and behaviour of donors and governments. They involve high levels of donor and country coordination for the achievement of program goals, and can be financed through parallel financing, pooled financing, general budget support, or a combination”. (World Bank 2007) “Both Cassells’ and the World Bank definitions stress the idea of ‘moving towards’ the use of government systems, with the World Bank being explicit that sector programs can be supported via multiple modalities (parallel – i.e. projects – pooled or budget support). The key conceptual point is that the SWAp is about aid being managed in such a way that it ultimately supports government leadership of sector development, without being prescriptive about how this is achieved”. (McNee, 2012)
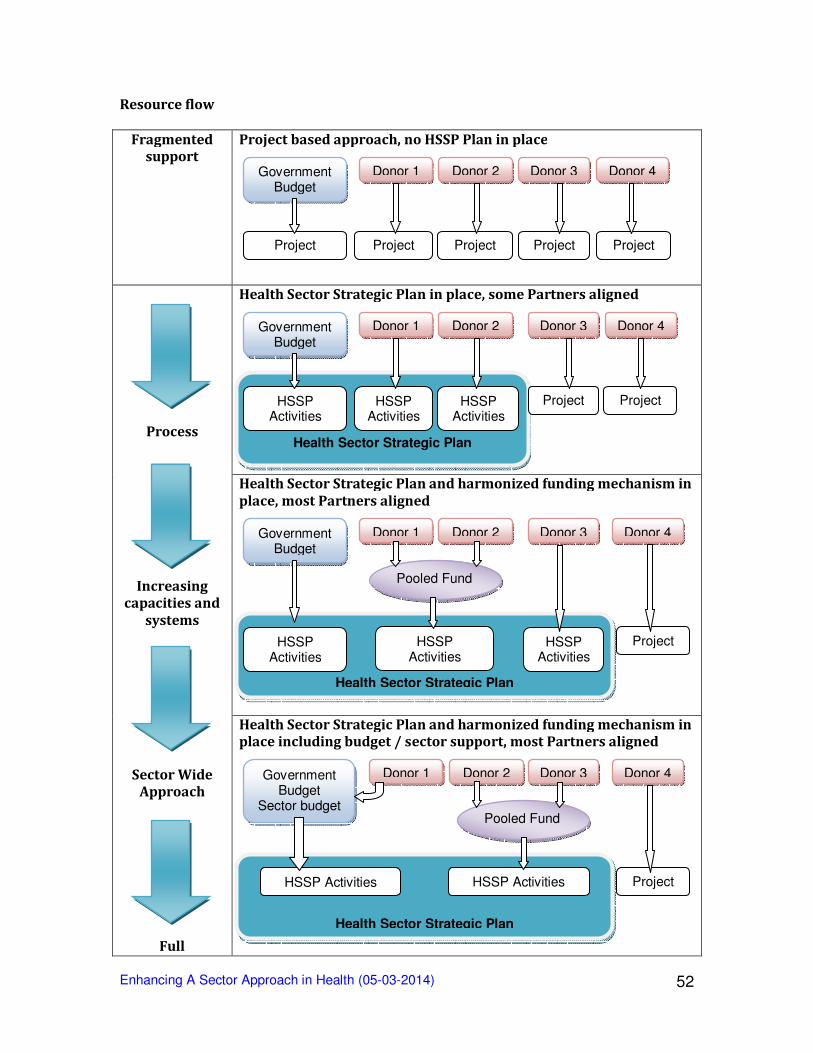
Enhancing A Sector Approach in Health (05-03-2014)
52
Resource flow
Fragmented
support
Project based approach, no HSSP Plan in place
Process
Increasing
capacities and
systems
Sector Wide
Approach
Full
Health Sector Strategic Plan in place, some Partners aligned
Health Sector Strategic Plan and harmonized funding mechanism in
place, most Partners aligned
Health Sector Strategic Plan and harmonized funding mechanism in
place including budget / sector support, most Partners aligned
Government Budget
Donor 1 Donor 2 Donor 3
Project Project Project Project
Donor 4
Project
Pooled Fund
Health Sector Strategic Plan
Government Budget
Sector budget
Donor 1 Donor 2 Donor 3
HSSP Activities HSSP Activities
Donor 4
Project
Pooled Fund
Health Sector Strategic Plan
Government Budget
Donor 1 Donor 2 Donor 3
HSSP Activities
HSSP Activities
HSSP Activities
Donor 4
Project
Health Sector Strategic Plan
Government Budget
Donor 1 Donor 2 Donor 3
HSSP Activities
HSSP Activities
HSSP Activities
Project
Donor 4
Project
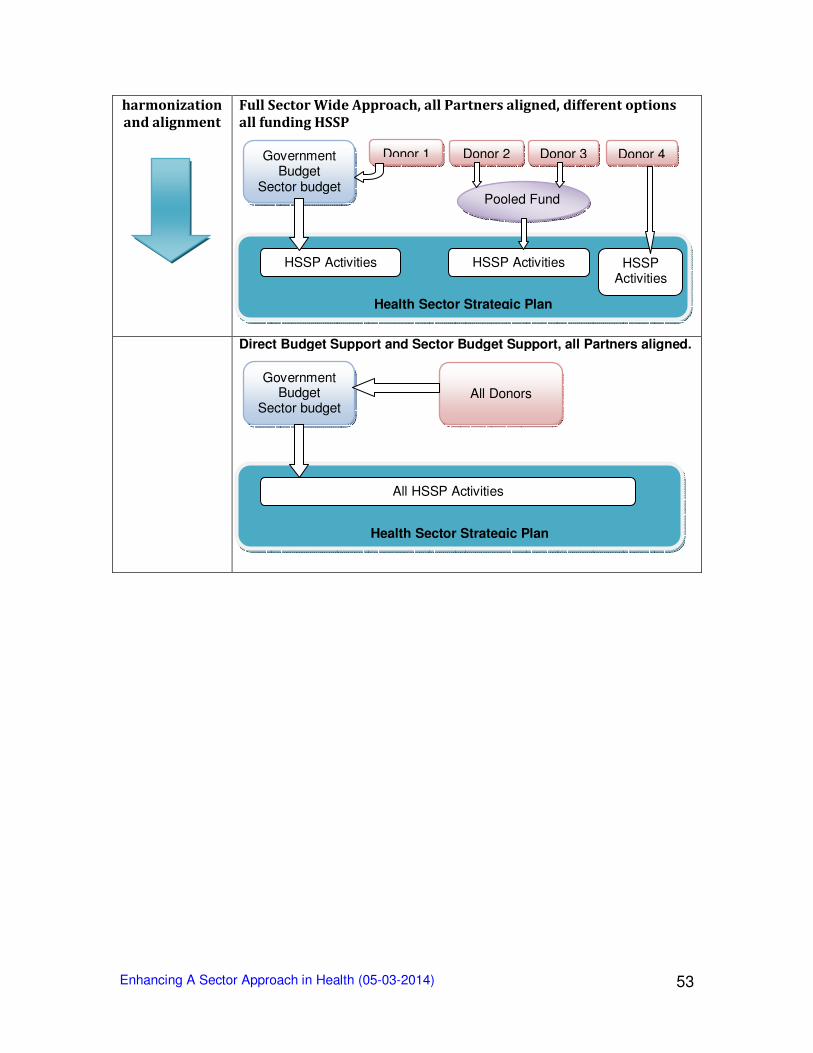
Enhancing A Sector Approach in Health (05-03-2014)
53
harmonization
and alignment
Full Sector Wide Approach, all Partners aligned, different options
all funding HSSP
Direct Budget Support and Sector Budget Support, all Partners aligned.
Health Sector Strategic Plan
Government Budget
Sector budget
All Donors
All HSSP Activities
Pooled Fund
Health Sector Strategic Plan
Government Budget
Sector budget
Donor 1 Donor 2 Donor 3
HSSP Activities HSSP Activities
Donor 4
HSSP Activities
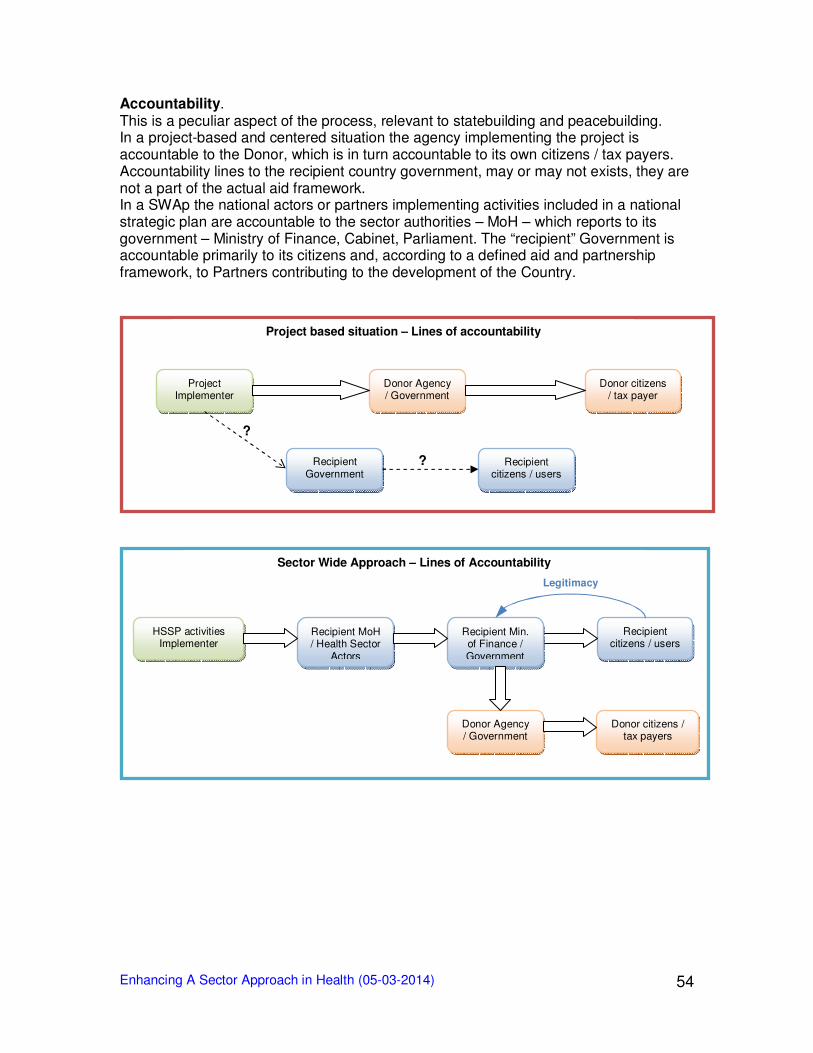
Enhancing A Sector Approach in Health (05-03-2014)
54
Accountability. This is a peculiar aspect of the process, relevant to statebuilding and peacebuilding. In a project-based and centered situation the agency implementing the project is accountable to the Donor, which is in turn accountable to its own citizens / tax payers. Accountability lines to the recipient country government, may or may not exists, they are not a part of the actual aid framework. In a SWAp the national actors or partners implementing activities included in a national strategic plan are accountable to the sector authorities – MoH – which reports to its government – Ministry of Finance, Cabinet, Parliament. The “recipient” Government is accountable primarily to its citizens and, according to a defined aid and partnership framework, to Partners contributing to the development of the Country.
Legitimacy
HSSP activities Implementer
Recipient MoH / Health Sector
Actors
Recipient citizens / users
Donor Agency / Government
Donor citizens / tax payers
Recipient Min. of Finance / Government
Sector Wide Approach – Lines of Accountability
?
?
Project Implementer
Donor Agency / Government
Donor citizens / tax payer
Recipient Government
Recipient citizens / users
Project based situation – Lines of accountability