Endurance training improves skeletal muscle electrical activity in active COPD patients
10
ABSTRACT: The effect of endurance training on muscle electrical activity during general exercise testing was investigated in physically active patients with chronic obstructive pulmonary disease (COPD). Before and after reha- bilitation, patients performed identical incremental exercise tests. Pulmonary gas exchange, venous lactate and pyruvate concentrations, and the quad- riceps electromyographic signal were sampled every minute throughout exercise testing. Three weeks of rehabilitation increased exercise capacity without modifying pulmonary function. M-wave amplitude, root mean square (RMS) of electromyographic activity, and RMS/oxygen uptake were in- creased significantly during post-rehabilitation testing at the same exercise intensity compared to pre-rehabilitation. Median frequency was significantly lower after training. These modifications reflect greater muscle excitability, greater muscle activation for the same level of exercise, and higher recruit- ment of slow-twitch fibers. Pulmonary rehabilitation in active COPD patients may normalize the electrical activity of skeletal muscles during incremental dynamic exercise. The electromyographic signal confirms neuromuscular changes after endurance training. Muscle Nerve 28: 744 –753, 2003 ENDURANCE TRAINING IMPROVES SKELETAL MUSCLE ELECTRICAL ACTIVITY IN ACTIVE COPD PATIENTS NADE ` GE GOSSELIN, PhD, 1 KAREN LAMBERT, PhD, 1 MAGALI POULAIN, PhD, 1–3 ANNE MARTIN, 3 CHRISTIAN PRE ´ FAUT, MD, 2 and ALAIN VARRAY, PhD 1 1 Laboratory “Sport, Performance, Health,” Faculty of Sport Sciences, 700 Av du Pic St Loup, 34090 Montpellier, France 2 Laboratory of Interaction Physiology, Ho ˆpital Arnaud de Villeneuve, Montpellier, France 3 Clinique du Souffle “La Solane,” Osseja, France Accepted 29 July 2003 Patients with chronic obstructive pulmonary disease (COPD) have a variable degree of exercise limita- tion, 7 caused in part by ventilatory abnormalities directly related to changes in respiratory mechanics and excessive ventilation, but also by impaired lower- limb muscle function. 2,16 Evidence of the structural and biochemical alterations to skeletal muscle in chronic respiratory disorders has accumulated. 9 These abnormalities include changes in fiber types and enzyme activities involved in energy supply for muscle contractions, leading to a reduced oxidative capacity of skeletal muscle associated with greater participation of the anaerobic glycolysis pathway. Moreover, surface electromyographic (SEMG) anal- ysis has shown alterations in the electrical activity and excitability of quadriceps muscle in COPD pa- tients compared with controls during exercise test- ing. 10 The mechanisms of these abnormalities seem to be complex and include deconditioning. The skeletal muscle alterations in COPD may be the consequences of both chronic inactivity and the pulmonary disease itself. 23 Metabolic dysfunction is potentially reversible by endurance training pro- grams in the context of pulmonary rehabilitation. 5,21 The modifications to trained muscle consist mainly of increased capillary and mitochondrial density, to- gether with increased concentrations of oxidative enzymes, 4,9,21 suggesting a shift toward increased aerobic capacity. Other possible neuromuscular changes related to endurance training have not been assessed in COPD patients and have been poorly explored in healthy subjects. In healthy pro- fessional cyclists, endurance training increased reli- ance on aerobic fibers and subsequently enhanced the recruitment of motor units. 19 Surprisingly, these Abbreviations: COPD, chronic obstructive pulmonary disease; FEV 1 , forced expiratory volume in 1 s, MF, median frequency; MVC, maximal voluntary contraction; PaO 2 and PaCO 2 , arterial oxygen and arterial carbon dioxide partial pressures; Peak V ˙ O 2 , maximal oxygen consumption measured; RMS, root mean square; SaO 2 , arterial oxygen saturation; SEMG, surface electro- myographic signal; V ˙ e peak, maximal ventilation measured; V ˙ O 2 , oxygen con- sumption measured. Key words: dynamic exercise; EMG; M-wave; pulmonary rehabilitation; respiratory disease Correspondence to: N. Gosselin; e-mail: [email protected] © 2003 Wiley Periodicals, Inc. 744 Training and Muscle Activity in COPD MUSCLE & NERVE December 2003
-
Upload
independent -
Category
Documents
-
view
1 -
download
0
Transcript of Endurance training improves skeletal muscle electrical activity in active COPD patients

ABSTRACT: The effect of endurance training on muscle electrical activityduring general exercise testing was investigated in physically active patientswith chronic obstructive pulmonary disease (COPD). Before and after reha-bilitation, patients performed identical incremental exercise tests. Pulmonarygas exchange, venous lactate and pyruvate concentrations, and the quad-riceps electromyographic signal were sampled every minute throughoutexercise testing. Three weeks of rehabilitation increased exercise capacitywithout modifying pulmonary function. M-wave amplitude, root mean square(RMS) of electromyographic activity, and RMS/oxygen uptake were in-creased significantly during post-rehabilitation testing at the same exerciseintensity compared to pre-rehabilitation. Median frequency was significantlylower after training. These modifications reflect greater muscle excitability,greater muscle activation for the same level of exercise, and higher recruit-ment of slow-twitch fibers. Pulmonary rehabilitation in active COPD patientsmay normalize the electrical activity of skeletal muscles during incrementaldynamic exercise. The electromyographic signal confirms neuromuscularchanges after endurance training.
Muscle Nerve 28: 744–753, 2003
ENDURANCE TRAINING IMPROVES SKELETALMUSCLE ELECTRICAL ACTIVITY INACTIVE COPD PATIENTS
NADEGE GOSSELIN, PhD,1 KAREN LAMBERT, PhD,1 MAGALI POULAIN, PhD,1–3
ANNE MARTIN,3 CHRISTIAN PREFAUT, MD,2 and ALAIN VARRAY, PhD1
1 Laboratory “Sport, Performance, Health,” Faculty of Sport Sciences, 700 Av du Pic St Loup, 34090 Montpellier, France2 Laboratory of Interaction Physiology, Hopital Arnaud de Villeneuve, Montpellier, France3 Clinique du Souffle “La Solane,” Osseja, France
Accepted 29 July 2003
Patients with chronic obstructive pulmonary disease(COPD) have a variable degree of exercise limita-tion,7 caused in part by ventilatory abnormalitiesdirectly related to changes in respiratory mechanicsand excessive ventilation, but also by impaired lower-limb muscle function.2,16 Evidence of the structuraland biochemical alterations to skeletal muscle inchronic respiratory disorders has accumulated.9
These abnormalities include changes in fiber typesand enzyme activities involved in energy supply formuscle contractions, leading to a reduced oxidativecapacity of skeletal muscle associated with greater
participation of the anaerobic glycolysis pathway.Moreover, surface electromyographic (SEMG) anal-ysis has shown alterations in the electrical activityand excitability of quadriceps muscle in COPD pa-tients compared with controls during exercise test-ing.10 The mechanisms of these abnormalities seemto be complex and include deconditioning.
The skeletal muscle alterations in COPD may bethe consequences of both chronic inactivity and thepulmonary disease itself.23 Metabolic dysfunction ispotentially reversible by endurance training pro-grams in the context of pulmonary rehabilitation.5,21
The modifications to trained muscle consist mainlyof increased capillary and mitochondrial density, to-gether with increased concentrations of oxidativeenzymes,4,9,21 suggesting a shift toward increasedaerobic capacity. Other possible neuromuscularchanges related to endurance training have notbeen assessed in COPD patients and have beenpoorly explored in healthy subjects. In healthy pro-fessional cyclists, endurance training increased reli-ance on aerobic fibers and subsequently enhancedthe recruitment of motor units.19 Surprisingly, these
Abbreviations: COPD, chronic obstructive pulmonary disease; FEV1, forcedexpiratory volume in 1 s, MF, median frequency; MVC, maximal voluntarycontraction; PaO2 and PaCO2, arterial oxygen and arterial carbon dioxidepartial pressures; Peak VO2, maximal oxygen consumption measured; RMS,root mean square; SaO2, arterial oxygen saturation; SEMG, surface electro-myographic signal; Ve peak, maximal ventilation measured; VO2, oxygen con-sumption measured.Key words: dynamic exercise; EMG; M-wave; pulmonary rehabilitation;respiratory diseaseCorrespondence to: N. Gosselin; e-mail: [email protected]
© 2003 Wiley Periodicals, Inc.
744 Training and Muscle Activity in COPD MUSCLE & NERVE December 2003

neuromuscular adaptations occurred in athletes whowere already well-trained before participating in theexperimental training program.
We have examined whether endurance traininghas beneficial effects on the electrical activity ofskeletal muscle of COPD patients during incremen-tal and maximal exercise testing. In order to focusonly on those neuromuscular modifications linkedessentially to pulmonary disease and not to decon-ditioning, we chose COPD patients who were physi-cally active before beginning the training sessions.
METHODS
Study Population. We studied seven COPD patients(five men and two women) recruited from amongthe patients of a medical rehabilitation center. Thediagnosis of obstructive airway disease was based onsmoking history and pulmonary function tests. Allpatients were clinically stable at the time of entryinto the exercise program. None had exercise-limit-ing cardiovascular or neuromuscular diseases, or re-quired oral steroids or supplemental oxygen. Pa-tients were following their standard medical regimenat the time of the evaluation, and this included aninhaled corticoid preparation for six patients andinhaled beta-agonists for seven patients. The studyprotocol was approved by our institutional reviewboards, and written consent to participate was ob-tained from each subject after a detailed descriptionof the procedure was given.
Experimental Arrangement. Lung Function and BloodGas Assessment. Lung function studies were doneusing a whole body plethysmograph (Vmax229;SensorMedics, Yorba Linda, California). Arterializedblood gas samples were obtained with the ear lobemicromethod (IL-1306; Instrumentation Laborato-ries, Milan, Italy).
Physical Activity Level. Physical activity was as-sessed by a questionnaire adapted for the elderly.26
The global physical activity scores took into accountscores for household activities, sports activities, andother physical leisure-time activities.
Skeletal Muscle Function Assessment. Maximal vol-untary contraction (MVC) of both quadriceps mus-cles was assessed on an exercise bench (Domyos,Decathlon, Portugal) with a strain gauge (INSERMUnit 103, Montpellier, France). With arms crossed infront of the chest and knees flexed at 90 degrees,subjects performed, after a 3-min warm-up on anunloaded cycle ergometer, three brief maximal iso-metric contractions of the quadriceps separated by 1min of rest. If the maximal values of strength were
reproducible (less of 5% of variability between val-ues), the highest strength of these contractions wasdefined as MVC.
Exercise Testing. Incremental exercise tests wereperformed on an ergometer (Ergometrics 900; Ergo-line, Bitz, Germany). Patients rested on the bicycleuntil measurements of heart rate (Cardiosoft Corina;Marquette Hellige Medical Systems, Freiburg, Germa-ny), oxygen saturation in the arterial blood (SaO2)estimated by an ear oximeter (Sat-Trak; SensorMed-ics), and expired gas concentrations were stable. Theexercise test protocol has been fully described else-where.10 Briefly, pedaling started with 3 min ofwarm-up at 20 watts. The individualized load was in-creased every minute by 5–10 watts depending on sex,age, anthropometrics, and baseline lung function mea-surements, and with the aim of completing the incre-mental phase within 8–12 min. After peak exercise, 3min of active recovery at the same workload as thewarm-up (20 watts) were followed by 12 min of passiverecovery. The ventilatory threshold was determinedaccording to the method of Beaver et al.1 The sameindividualized exercise protocol was used for each pa-tient before and after rehabilitation.
Venous Blood Collection. Venous blood sampleswere collected for determination of lactate and pyru-vate concentration during the last 20 s of the follow-ing time periods: rest; the 3rd min of warm-up, eachworkload, and maximal exercise; and the 3rd, 4th,5th, 10th, and 15th min of recovery. Collected bloodwas immediately deproteinized in 7% perchloricacid, placed in ice, and centrifuged (Jouan BR-3.11;St. Herblain, France) at the end of the exercise test.Blood pyruvate concentrations were determined us-ing an enzymatic kit (Sigma, St. Louis, Missouri) andblood lactate content was analyzed enzymatically ac-cording to the method of Gutmann and Wahle-feld.12 Capillary blood was drawn from the earlobe tomeasure pH and the arterial partial pressure of ox-ygen (PaO2) and carbon dioxide (PaCO2) (Stat Pro-file Phox; Nova Biomedical, Les Ulis, France) at restand peak exercise. Lactate and pyruvate measuresreflected venous values and arterialized blood gassamples reflected arterial values.
Surface Electromyography. The signal from vastuslateralis was recorded with an input impedance of 10M� and gain of 1000 (Bagnoli 8 EMG system; Delsys,Boston, Massachusetts) at a sampling frequency of1,024 Hz with bipolar surface electrodes fixed longitu-dinally over the muscle belly. The stimulation tech-nique and analysis of the SEMG signal have been de-scribed elsewhere.10 M-waves were evoked at constantmuscle length by supramaximal stimulations (0.1-msduration rectangular single current pulse lasting 0.1
Training and Muscle Activity in COPD MUSCLE & NERVE December 2003 745

ms) of the vastus lateralis motor point during the last5 s of every minute of exercise testing and recovery bya stimulator with an insulation box (S48K; Grass, WestWarwick, Rhode Island). M-waves were characterizedby peak amplitude of the negative phase and by dura-tion. Quantitative SEMG analysis started when the con-traction began and covered the entire contraction asdetermined by passage of the pedal over a sensor to thevertical position. Root mean square (RMS) and me-dian frequency (MF) parameters were averaged foreach contraction for every minute of exercise. Contrac-tions with stimulation superposed were removed. RMSwas divided by the concomitant body oxygen uptake(RMS/VO2 ratio) to compare the SEMG signal at thesame energetic level. M-wave amplitude was obtainedfor each of the five M-waves obtained per minute andaveraged. In order to analyze changes in RMS, RMS/VO2, and M-wave before and after rehabilitation, thecontrol or reference value was chosen to be the firstminute of warm-up, i.e., an unloaded cycling condi-tion. SEMG parameters were then normalized by thisunloaded value.
Rehabilitation Program. Rehabilitation sessionswere held in small groups of 8 to 10 subjects, 5 days/week. The program lasted for 3 successive weeks andincluded the following: (1) health education (2h/week), with information on pulmonary disease,medications, and healthy daily-living strategies, and dis-cussions on the psychological problems linked to thedisease; (2) respiratory therapy with aerosol and/ordrainage (1 h/day); and (3) personalized adaptedphysical exercise training (2 h/day), 5 days/week. Thistraining had four components: cycling, gymnastics, re-laxation, and walking. The cycling session consisted of45 min on a cycle ergometer (Monark 815 E; Varberg,Sweden) with three successive pedaling periods of 10min, separated by 5 min of active recovery. Work in-tensity was individualized for each patient using thetechnique described by our group24,25 and corre-sponded to the heart rate at the ventilatory threshold,as assessed throughout the pre-training incrementaltest. The recovery intensity was 20 watts. After cycling,patients stretched for 10 min. The gymnastics sessionsincluded 1 h of weight-training, abdominal exercise,and stretching followed by 30 min of relaxation. Thelast component was 2 h of country walking, with at least45 min at ventilatory threshold intensity. Cycling, gym-nastics, and relaxation were done in the same half-day,and walking was done in the other half-day. Heart ratewas monitored using a heart rate telemetry system(Sport-Tester PE 3000; Polar Electro, Kemple, Fin-land).
Protocol. Before and after the 3-week trainingperiod, all patients underwent the same tests in the
same order, including body composition analysis(TBF-310; Tanita, Tokyo, Japan). Resting pulmonaryfunction and MVC were evaluated 90 min beforeexercise. After SEMG installation and a 10-min restperiod following catheter insertion in a superficialbrachial vein, patients performed an incrementalexercise test until exhaustion. The test was alwaysheld at least 2 h after the same light breakfast beforeand after training. Before training, patients wereasked to respond to the questionnaire on physicalactivity.
Statistical Analysis. Data on patient characteristicsbefore and after training (plethysmographic valuesand MVC) were analyzed using Student’s pairedt-test. Physiological parameters during exercise werecompared at peak exercise and also at an identicalexercise workload corresponding to a percentage ofpre-training maximal workload. The effects of therehabilitation program (Ftraining) and exercise inten-sity on cardiorespiratory and SEMG parameters weretested for statistical differences using a two-way anal-ysis of variance with repeated measures. When theanalysis of variance F ratio was significant for exer-cise time, the different means were compared usinga least significant difference (LSD) post hoc test.The relationships between exercise tolerance param-eters (used as variables to explain), SEMG variables,and resting characteristics (used as explanatory vari-ables) were tested by multiple regression analysis. Alldata used in stepwise regressions (except SEMGdata) were the difference (�) between values ob-tained at peak exercise before and after training(pre–post). The SEMG data used in stepwise regres-sion analyses were: (1) the post-training minus pre-training difference of the greatest decrease obtainedduring exercise for MF (expressed in Hz), and dur-ing both exercise and recovery for M-wave (� mini-mal M-wave amplitude and duration, expressed as apercentage of reference value); and (2) the post-training minus pre-training difference of the great-est increase expressed in percentage of the refer-ence value obtained during exercise for RMS andRMS/VO2, and during both exercise and recoveryfor M-wave (� maximal M-wave amplitude and dura-tion). Significance was set at P � 0.05. All values areexpressed as mean � SEM.
RESULTS
Resting data. The mean values for age, height, andweight before training were 61 � 2.9 years, 167 � 0.8cm, and 69.7 � 3.9 kg, respectively. The patients hadmoderate or severe airflow obstruction and mild
746 Training and Muscle Activity in COPD MUSCLE & NERVE December 2003
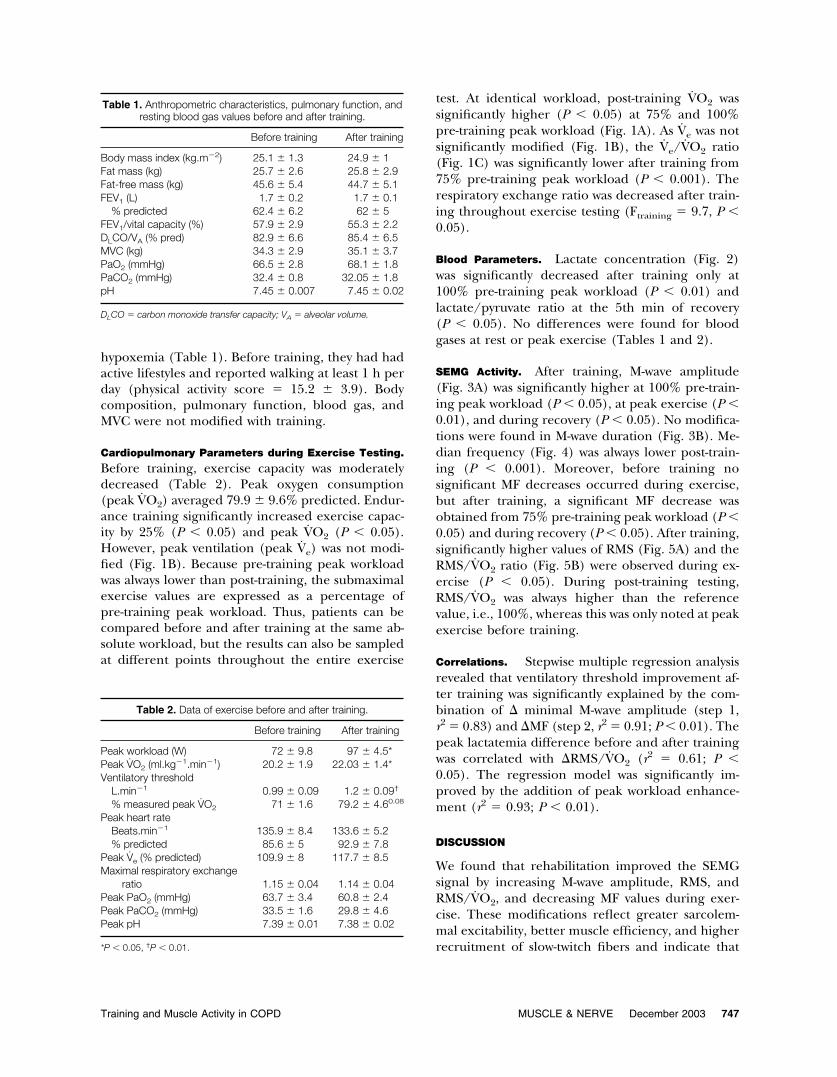
hypoxemia (Table 1). Before training, they had hadactive lifestyles and reported walking at least 1 h perday (physical activity score � 15.2 � 3.9). Bodycomposition, pulmonary function, blood gas, andMVC were not modified with training.
Cardiopulmonary Parameters during Exercise Testing.
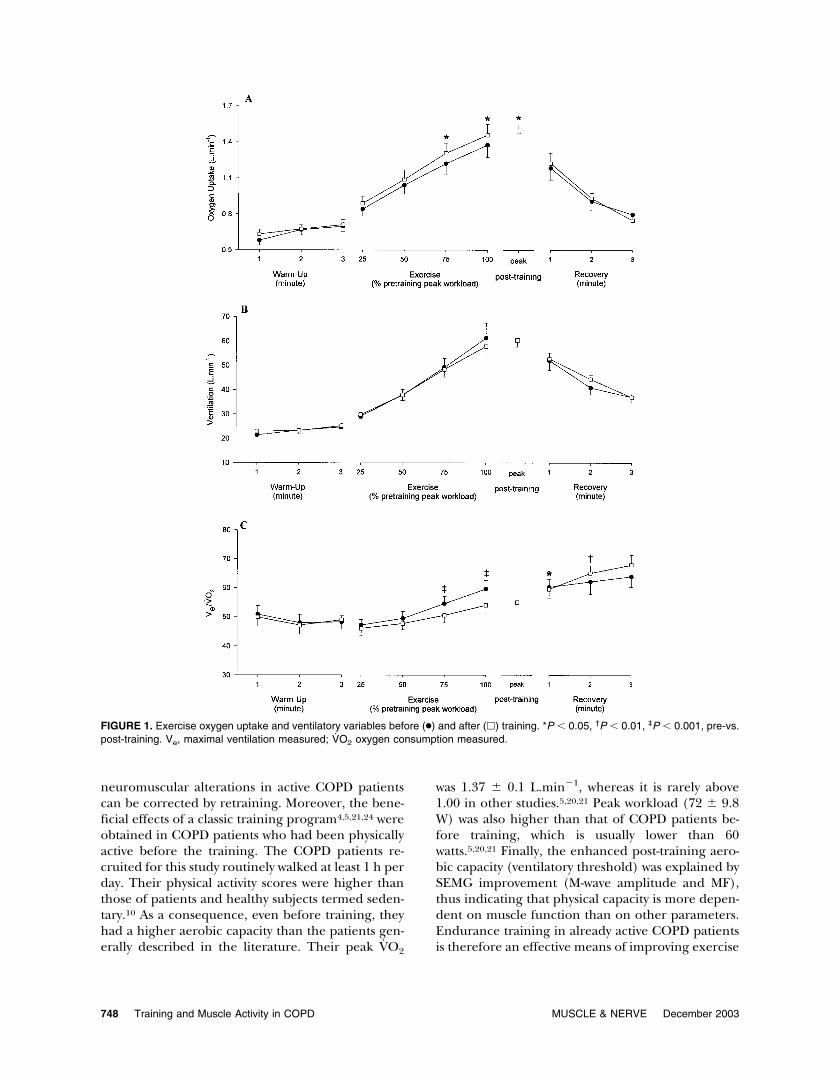
Before training, exercise capacity was moderatelydecreased (Table 2). Peak oxygen consumption(peak VO2) averaged 79.9 � 9.6% predicted. Endur-ance training significantly increased exercise capac-ity by 25% (P � 0.05) and peak VO2 (P � 0.05).However, peak ventilation (peak Ve) was not modi-fied (Fig. 1B). Because pre-training peak workloadwas always lower than post-training, the submaximalexercise values are expressed as a percentage ofpre-training peak workload. Thus, patients can becompared before and after training at the same ab-solute workload, but the results can also be sampledat different points throughout the entire exercise
test. At identical workload, post-training VO2 wassignificantly higher (P � 0.05) at 75% and 100%pre-training peak workload (Fig. 1A). As Ve was notsignificantly modified (Fig. 1B), the Ve/VO2 ratio(Fig. 1C) was significantly lower after training from75% pre-training peak workload (P � 0.001). Therespiratory exchange ratio was decreased after train-ing throughout exercise testing (Ftraining � 9.7, P �0.05).
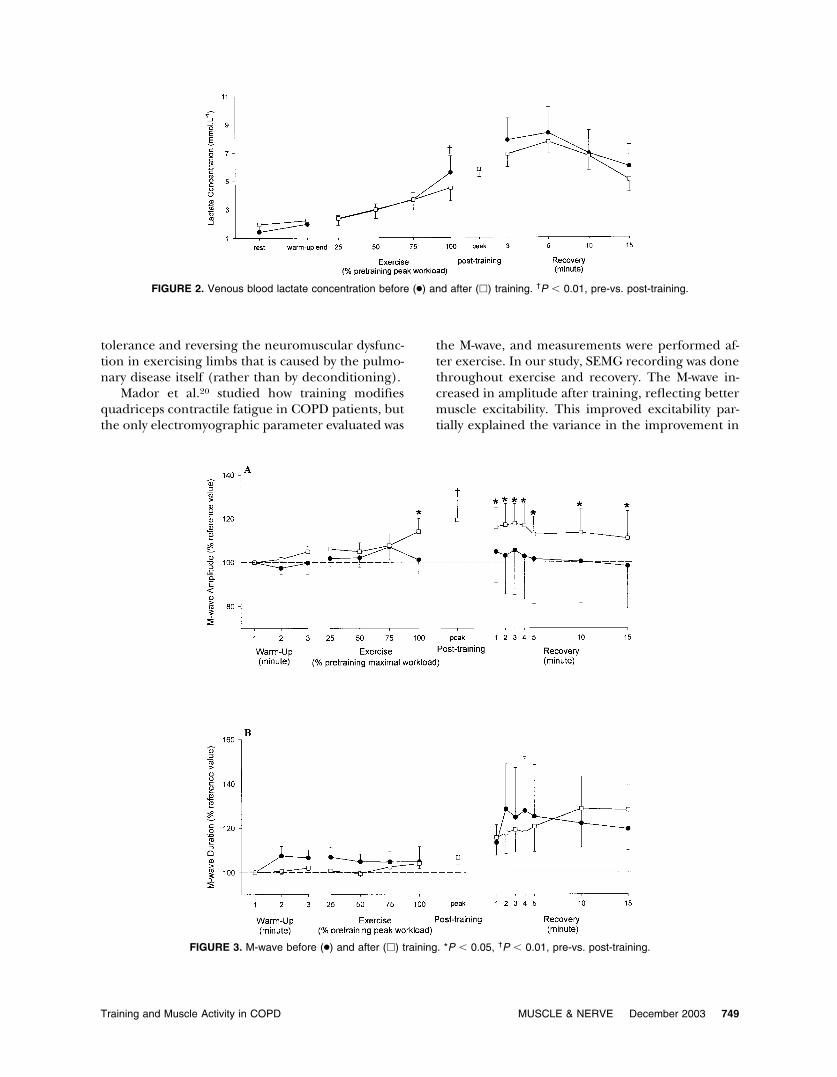
Blood Parameters. Lactate concentration (Fig. 2)was significantly decreased after training only at100% pre-training peak workload (P � 0.01) andlactate/pyruvate ratio at the 5th min of recovery(P � 0.05). No differences were found for bloodgases at rest or peak exercise (Tables 1 and 2).
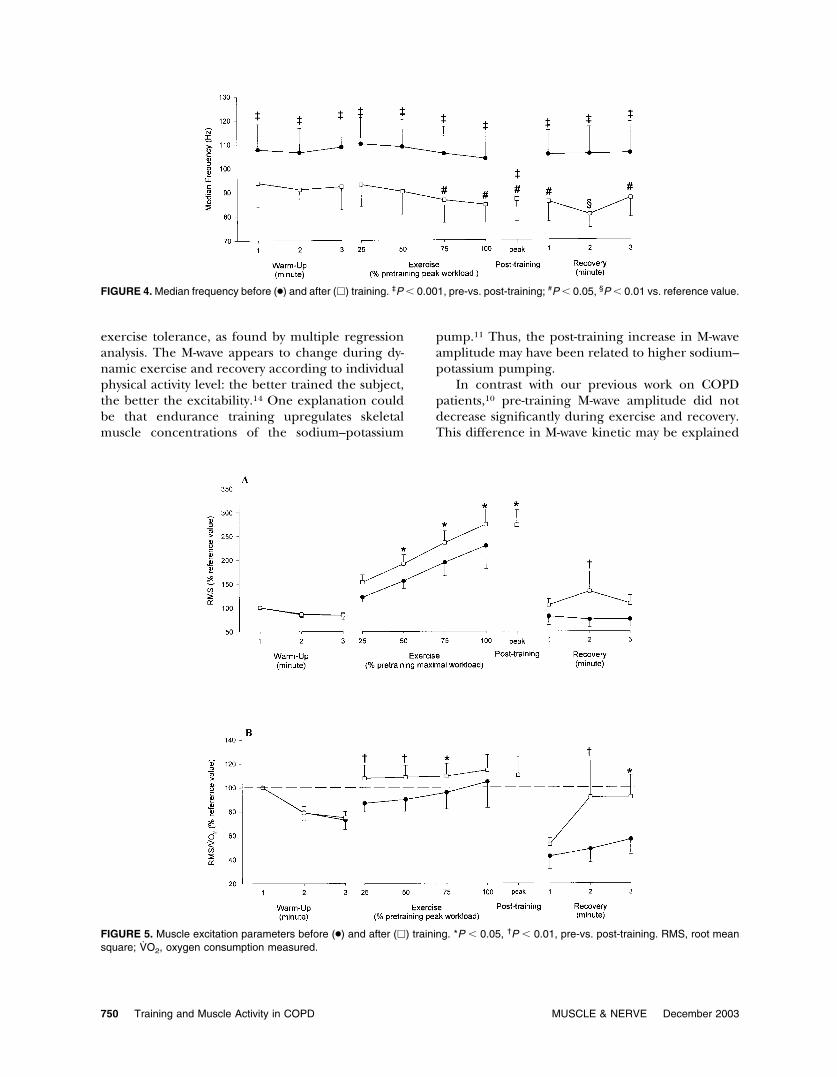
SEMG Activity. After training, M-wave amplitude(Fig. 3A) was significantly higher at 100% pre-train-ing peak workload (P � 0.05), at peak exercise (P �0.01), and during recovery (P � 0.05). No modifica-tions were found in M-wave duration (Fig. 3B). Me-dian frequency (Fig. 4) was always lower post-train-ing (P � 0.001). Moreover, before training nosignificant MF decreases occurred during exercise,but after training, a significant MF decrease wasobtained from 75% pre-training peak workload (P �0.05) and during recovery (P � 0.05). After training,significantly higher values of RMS (Fig. 5A) and theRMS/VO2 ratio (Fig. 5B) were observed during ex-ercise (P � 0.05). During post-training testing,RMS/VO2 was always higher than the referencevalue, i.e., 100%, whereas this was only noted at peakexercise before training.
Correlations. Stepwise multiple regression analysisrevealed that ventilatory threshold improvement af-ter training was significantly explained by the com-bination of � minimal M-wave amplitude (step 1,r2 � 0.83) and �MF (step 2, r2 � 0.91; P � 0.01). Thepeak lactatemia difference before and after trainingwas correlated with �RMS/VO2 (r2 � 0.61; P �0.05). The regression model was significantly im-proved by the addition of peak workload enhance-ment (r2 � 0.93; P � 0.01).
DISCUSSION
We found that rehabilitation improved the SEMGsignal by increasing M-wave amplitude, RMS, andRMS/VO2, and decreasing MF values during exer-cise. These modifications reflect greater sarcolem-mal excitability, better muscle efficiency, and higherrecruitment of slow-twitch fibers and indicate that
Table 1. Anthropometric characteristics, pulmonary function, andresting blood gas values before and after training.
Before training After training
Body mass index (kg.m�2) 25.1 � 1.3 24.9 � 1Fat mass (kg) 25.7 � 2.6 25.8 � 2.9Fat-free mass (kg) 45.6 � 5.4 44.7 � 5.1FEV1 (L) 1.7 � 0.2 1.7 � 0.1
% predicted 62.4 � 6.2 62 � 5FEV1/vital capacity (%) 57.9 � 2.9 55.3 � 2.2DLCO/VA (% pred) 82.9 � 6.6 85.4 � 6.5MVC (kg) 34.3 � 2.9 35.1 � 3.7PaO2 (mmHg) 66.5 � 2.8 68.1 � 1.8PaCO2 (mmHg) 32.4 � 0.8 32.05 � 1.8pH 7.45 � 0.007 7.45 � 0.02
DLCO � carbon monoxide transfer capacity; VA � alveolar volume.
Table 2. Data of exercise before and after training.
Before training After training
Peak workload (W) 72 � 9.8 97 � 4.5*Peak VO2 (ml.kg�1.min�1) 20.2 � 1.9 22.03 � 1.4*Ventilatory threshold
L.min�1 0.99 � 0.09 1.2 � 0.09†
% measured peak VO2 71 � 1.6 79.2 � 4.60.08
Peak heart rateBeats.min�1 135.9 � 8.4 133.6 � 5.2% predicted 85.6 � 5 92.9 � 7.8
Peak Ve (% predicted) 109.9 � 8 117.7 � 8.5Maximal respiratory exchange
ratio 1.15 � 0.04 1.14 � 0.04Peak PaO2 (mmHg) 63.7 � 3.4 60.8 � 2.4Peak PaCO2 (mmHg) 33.5 � 1.6 29.8 � 4.6Peak pH 7.39 � 0.01 7.38 � 0.02
*P � 0.05, †P � 0.01.
Training and Muscle Activity in COPD MUSCLE & NERVE December 2003 747
neuromuscular alterations in active COPD patientscan be corrected by retraining. Moreover, the bene-ficial effects of a classic training program4,5,21,24 wereobtained in COPD patients who had been physicallyactive before the training. The COPD patients re-cruited for this study routinely walked at least 1 h perday. Their physical activity scores were higher thanthose of patients and healthy subjects termed seden-tary.10 As a consequence, even before training, theyhad a higher aerobic capacity than the patients gen-erally described in the literature. Their peak VO2
was 1.37 � 0.1 L.min�1, whereas it is rarely above1.00 in other studies.5,20,21 Peak workload (72 � 9.8W) was also higher than that of COPD patients be-fore training, which is usually lower than 60watts.5,20,21 Finally, the enhanced post-training aero-bic capacity (ventilatory threshold) was explained bySEMG improvement (M-wave amplitude and MF),thus indicating that physical capacity is more depen-dent on muscle function than on other parameters.Endurance training in already active COPD patientsis therefore an effective means of improving exercise
FIGURE 1. Exercise oxygen uptake and ventilatory variables before (●) and after (�) training. *P � 0.05, †P � 0.01, ‡P � 0.001, pre-vs.post-training. Ve, maximal ventilation measured; VO2 oxygen consumption measured.
748 Training and Muscle Activity in COPD MUSCLE & NERVE December 2003
tolerance and reversing the neuromuscular dysfunc-tion in exercising limbs that is caused by the pulmo-nary disease itself (rather than by deconditioning).
Mador et al.20 studied how training modifiesquadriceps contractile fatigue in COPD patients, butthe only electromyographic parameter evaluated was
the M-wave, and measurements were performed af-ter exercise. In our study, SEMG recording was donethroughout exercise and recovery. The M-wave in-creased in amplitude after training, reflecting bettermuscle excitability. This improved excitability par-tially explained the variance in the improvement in
FIGURE 2. Venous blood lactate concentration before (●) and after (�) training. †P � 0.01, pre-vs. post-training.
FIGURE 3. M-wave before (●) and after (�) training. *P � 0.05, †P � 0.01, pre-vs. post-training.
Training and Muscle Activity in COPD MUSCLE & NERVE December 2003 749
exercise tolerance, as found by multiple regressionanalysis. The M-wave appears to change during dy-namic exercise and recovery according to individualphysical activity level: the better trained the subject,the better the excitability.14 One explanation couldbe that endurance training upregulates skeletalmuscle concentrations of the sodium–potassium
pump.11 Thus, the post-training increase in M-waveamplitude may have been related to higher sodium–potassium pumping.
In contrast with our previous work on COPDpatients,10 pre-training M-wave amplitude did notdecrease significantly during exercise and recovery.This difference in M-wave kinetic may be explained
FIGURE 4. Median frequency before (●) and after (�) training. ‡P � 0.001, pre-vs. post-training; #P � 0.05, §P � 0.01 vs. reference value.
FIGURE 5. Muscle excitation parameters before (●) and after (�) training. *P � 0.05, †P � 0.01, pre-vs. post-training. RMS, root meansquare; VO2, oxygen consumption measured.
750 Training and Muscle Activity in COPD MUSCLE & NERVE December 2003

by the more active COPD group in the present study.Because we wanted to exclude any impact of de-training status on exercising muscle, we deliberatelychose patients with a substantially more active life-style than those in the earlier work.10 This inter-pretation is supported by the work of Jammes et al.,14
who showed that M-wave parameters depend ontraining level. They found a decreased M-wave am-plitude and an increased M-wave duration in un-trained compared to trained subjects. This interpre-tation is also reinforced by the significantrelationship found in this work between M-wave am-plitude and training status (ventilatory threshold).
The lower post-training MF values for the sameworkload could be the result of different trainingmodifications. Confounding factors such as skinfoldthickness and muscle temperature are unlikely to beresponsible because body composition was not sig-nificantly modified by training, and the exercise pro-tocol was exactly the same for both tests. Modifica-tion in muscle fiber type (higher proportion of slow-twitch fibers) can also be rejected because Jobin etal.15 did not observe such modifications in COPDskeletal muscle after training. A higher recruitmentof slow-twitch fibers after training, however, is con-sistent with the lower post-training MF values. To-gether with the higher RMS values, which suggestedgreater neural activity by increased synchronizationof the motor unit firing rate or different fiber re-cruitment, this lower post-training MF could reflectthe training-induced motor program and a modifi-cation in the motor unit recruitment strategy duringexercise, independently of any changes in musclefiber proportion. Given that a higher proportion ofslow-twitch fibers may be implicated during contrac-tions and that these fibers have less force-generatingcapacity than fast-twitch fibers,18 additional motorunits would be needed for the same cycling load.The more slow-twitch fibers are recruited, the moreSEMG voltage is needed per unit force.18 The higherRMS/VO2 ratio during post-training exercise alsoaccords with the higher post-training recruitment ofslow-twitch fibers, which are more efficient than fastfibers6 (less VO2 for a given workload). The decreasein MF compared to the reference value only aftertraining should not be interpreted as a negativeeffect of training on muscle fatigue, but rather as thesign of normalized muscle activity. In fact, the MFdecrease during the last steps of an exhaustive exer-cise has previously been shown in healthy subjects3
and is consistent with recruitment strategy modifica-tion of motor units.
Motor unit recruitment strategy can be modulatedby the so-called muscle wisdom phenomenon during
exercise. This mechanism delays muscle fiber failureduring fatiguing contractions by slowing the motorunit discharge rate8 via the group III–IV muscle affer-ents. Group III–IV muscle afferents are activated by aperiod of hypoxemia13 or metabolite accumulation.17
Because COPD hypoxemia was not improved aftertraining, the first hypothesis can be excluded. Withregard to an accumulation of metabolites, training mayinduce lower muscular acidosis for the same post-train-ing exercise workload because of more efficient oxida-tive phosphorylation. Unfortunately, acidosis was mea-sured only in blood at peak exercise. Blood acidosis wasnot modified after training, but peak workloads werehigher. We can thus reasonably assume that muscleacidosis was decreased for the same submaximal work-load, which is in accordance with data22 showing thattraining delays acidosis in the muscles of COPD pa-tients. Moreover, the rise in VO2 without blood desatu-ration reflects the normalization of adenosine triphos-phate production by the aerobic metabolism. Suchimproved oxidative enzyme activity has been well de-scribed21 and the lower Ve/VO2 observed in thepresent study was consistent with this: for the samerespiratory muscle work, more oxygen was taken up.This oxygen supplement was available to the skeletalmuscles for higher aerobic metabolism, which delayedthe accumulation of muscle acidosis. After training, thelater ventilatory threshold may have been the conse-quence of the lower contribution from anaerobic gly-colysis at the beginning of exercise. Acidosis wouldthus have been lowered and the muscle afferents lessactivated.
The lower activation of muscle afferents aftertraining is consistent with higher exercise RMS andthe higher RMS/VO2 ratio. One adaptation to en-durance training in active COPD patients might bethe ability to recruit an additional number of motorunits in exercising muscle or to increase the synchro-nization of those motor units already active. Thisresult has already been found in healthy subjects:higher RMS values were recorded in trained com-pared with sedentary subjects,14 and in professionalcyclists after the competitive season.19 We can thushypothesize that the higher RMS could reflect re-cruitment of additional motor units and that thesemotor units were composed mainly of slow-twitchfibers. It is interesting to note that in sedentaryCOPD patients, the exercise RMS/VO2 was clearlylower than in our active COPD patients before train-ing. This may be due to disproportionate hyperven-tilation with respect to the real workload.16 Since theoxygen cost of breathing during exercise is increasedin COPD patients, the decreased RMS/VO2 ratio canlogically be attributed to excessive VO2 for a given
Training and Muscle Activity in COPD MUSCLE & NERVE December 2003 751

workload due to excessive hyperventilation. In ouractive patients, the higher RMS/VO2 ratio aftertraining was not due to lower ventilation (Fig. 1B),but could be attributed to RMS modifications relatedto the lower muscle afferent activation.
The lack of post-training decrease in blood lac-tate concentration in our study may be explained bythe short duration of the training program. More-over, blood lactate is an indirect measure of musclemetabolism, and our data (higher VO2 and ventila-tory threshold, same venous blood acidosis forhigher workload) are consistent with an increasedaerobic metabolism after training and a concomitantdecrease in anaerobic involvement.
Finally, training may induce energetic modifica-tions. The respiratory exchange ratio was significantlylower after training at the same submaximal intensity.Furthermore, the values recorded were below 1.00 forhigher post-training intensities. Such findings are con-sistent with those of studies in healthy subjects,19 whichconcluded that one of the main adaptations to trainingis increased fat metabolism at any submaximal intensitydue to greater reliance on the oxidative pathway. Thisadaptation is important for patients with energetic ab-normalities. Although the exact energetic modifica-tions induced by endurance training need further in-vestigation, increased fat oxidation is consistent withthe normalized aerobic pathway and muscle activityreported in this work.
In conclusion, our findings suggest that endurancetraining in already active COPD patients improvedneuromuscular function and exercise tolerance. Theelectromyographic signal reflected a different recruit-ment of motor units in active muscles, better sarcolem-mal excitability, and greater reliance on aerobic me-tabolism. SEMG normalization at the same exerciseworkload post-training is consistent with the hypothesisthat muscle afferents were less activated. From a clini-cal point of view, this study provides evidence thatexercise training should be proposed to COPD pa-tients who are not necessarily sedentary, and highlightsthe importance of skeletal muscle function in the ex-ercise tolerance of these patients.
The authors gratefully thank the medical and technical staff of theClinique du Souffle “La Solane,” particularly Francois Ceugnietand Jose Cabesudo, the patients for their cooperation with ourproject, and Mr. Denis Mottet and Ms. Catherine Stott Carmenifor valuable technical assistance.
REFERENCES
1. Beaver WL, Wasserman K, Whipp B. A new method for de-tecting anaerobic threshold by gas exchange. J Appl Physiol1986;60:2020–2027.
2. Bernard S, LeBlanc P, Whittom F, Carrier G, Jobin J, BelleauR, Maltais F. Peripheral muscle weakness in patients withchronic obstructive pulmonary disease. Am J Respir Crit CareMed 1998;158:629–634.
3. Bouissou P, Estrade PY, Goubel F, Guezennec CY, Serrurier B.Surface EMG power spectrum and intramuscular pH in hu-man vastus lateralis muscle during dynamic exercise. J ApplPhysiol 1989;67:1245–1249.
4. Casaburi R, Patessio A, Ioli A, Zanaboni S, Donner CF, Was-serman K. Reductions in exercise lactic acidosis and ventila-tion as a result of exercise training in patients with obstructivelung disease. Am Rev Respir Dis 1991;143:9–18.
5. Casaburi R, Porszasz J, Burns MR, Carithers ER, Chang RSY,Cooper CB. Physiologic benefits of exercise training in reha-bilitation of patients with severe obstructive pulmonary dis-ease. Am J Respir Crit Care Med 1997;155:1541–1551.
6. Crow MT, Kushmerick MJ. Chemical energetics of slow-andfast-twitch muscles of the mouse. J Gen Physiol 1982;79:147–166.
7. Decreamer M, Gosselink R, Troosters T, Verschueren M, EversG. Muscle weakness is related to utilization of health care re-sources in COPD patients. Eur Respir J 1997;10:417–423.
8. Enoka RM, Stuart DG. Neurobiology of muscle fatigue. J ApplPhysiol 1992;72:1631–1648.
9. Gosker HR, Wouters EFM, Van Der Vusse GJ, Schols AMWJ.Skeletal muscle dysfunction in chronic obstructive pulmonarydisease and chronic heart failure: underlying mechanismsand therapy perspectives. Am J Clin Nutr 2000;71:1033–1047.
10. Gosselin N, Matecki S, Poulain M, Ramonatxo M, Ceugniet F,Prefaut C, Varray A. Electrophysiologic changes during exer-cise testing in patients with chronic obstructive pulmonarydisease. Muscle Nerve 2003;27:170–179.
11. Green HJ, Chin ER, Ball-Burnett M, Ranney D. Increases inhuman skeletal muscle Na�-K�-ATPase concentration withshort-term training. Am J Physiol 1993;264:C1538–C1541.
12. Gutmann I, Wahlefeld M. L-(�)-lactate determination withlactate dehydrogenase and NAD. In: Bergmeyer HU, editor.Methods of enzymatic analyses. New York: Academic Press;1974. p 1464–1472.
13. Hill JM, Pickar JG, Parrish MD, Kaufman MP. Effects ofhypoxia on the discharge of group III and IV muscle afferentsin cats. J Appl Physiol 1992;73:2524–2529.
14. Jammes Y, Zattara-Hartmann MC, Caquelard F, Arnaud S,Tomei C. Electromyographic changes in vastus lateralis dur-ing dynamic exercise. Muscle Nerve 1997;20:247–249.
15. Jobin J, Maltais F, Doyon JF, LeBlanc P, Simard PM, SimardAA, Simard C. Chronic obstructive pulmonary disease: capil-larity and fiber-type characteristics of skeletal muscle. J Car-diopulm Rehabil 1998;18:432–437.
16. Killian KJ, Leblanc P, Martin DH, Summers E, Jones NL,Campbell EJM. Exercise capacity and ventilatory, circulatory,and symptom limitation in patients with chronic airflow lim-itation. Am Rev Respir Dis 1992;146:935–940.
17. Lagier-Tessonnier F, Balzamo E, Jammes Y. Comparative ef-fects of ischemia and acute hypoxemia on muscle afferentsfrom tibialis anterior in cats. Muscle Nerve 1993;16:135–141.
18. Linssen WHJP, Stegeman DF, Joosten EMG, Merks MJH, TerLaak HJ, Binkhorst RA, Notermans SLH. Force and fatigue inhuman type I muscle fibers. A surface EMG study in patientswith congenital myopathy and type I fiber predominance.Brain 1991;114:2123–2132.
19. Lucia A, Hoyos J, Pardo J, Chicharro JL. Metabolic and neu-romuscular adaptation to endurance training in professionalcyclists: a longitudinal study. Jpn J Physiol 2000;50:381–388.
20. Mador MJ, Kufel TJ, Pineda LA, Steinwald A, Aggarwal A,Upadhyay AM, Khan MA. Effect of pulmonary rehabilitationon quadriceps fatigability during exercise. Am J Respir CritCare Med 2001;163:930–935.
21. Maltais F, Leblanc P, Simard C, Jobin J, Berube C, Bruneau J,Carrier L, Belleau R. Skeletal muscle adaptation to endurancetraining in patients with chronic obstructive pulmonary dis-ease. Am J Respir Crit Care Med 1996;154:442–447.
752 Training and Muscle Activity in COPD MUSCLE & NERVE December 2003

22. Sala E, Roca J, Marrades RM, Alonso J, Gonzalez de Suso JM,Moreno A, Barbera JA, Nadal J, de Jover L, Rodriguez-RoisinR, Wagner PD. Effects of endurance training on skeletalmuscle bioenergetics in chronic obstructive pulmonary dis-ease. Am J Respir Crit Care Med 1999;159:1726–1734.
23. Serres I, Gautier V, Varray A, Prefaut C. Impaired skeletalmuscle endurance related to physical inactivity and alteredlung function in COPD patients. Chest 1998;113:900 –905.
24. Vallet G, Ahmaıdi S, Serres I, Fabre C, Bourgouin D, Desplan J,Varray A, Prefaut C. Comparison of two training programmes inchronic airway limitation patients: standardized versus individu-alized protocols. Eur Respir J 1997;10:114–122.
25. Varray A, Prefaut C. Exercise training in patients with respiratorydisease: procedures and results. Eur Respir Rev 1995;5:51–58.
26. Voorrips LE, Ravelli AC, Dongelmans PC, Deurenberg P, VanStaveren WA. A physical questionnaire for the elderly. MedSci Sports Exerc 1991;23:974–979.
Training and Muscle Activity in COPD MUSCLE & NERVE December 2003 753