Effectiveness of a Lifestyle Physical Activity Intervention in a Women's Organization
10
JOURNAL OF WOMEN’S HEALTH Volume 17, Number 3, 2008 © Mary Ann Liebert, Inc. DOI: 10.1089/jwh.2007.0464 Effectiveness of a Lifestyle Physical Activity Intervention in a Women’s Organization JOKE OPDENACKER, M.Sc., 1 FILIP BOEN, Ph.D., 1 YVES VANDEN AUWEELE, Ph.D., 1 and ILSE DE BOURDEAUDHUIJ, Ph.D. 2 ABSTRACT Objective: The objective of the present study was to evaluate the effectiveness of a minimal contact physical activity intervention that was maximally integrated into the existing struc- tures of a women’s organization. Methods: The intervention included one group meeting, a self-help booklet, and five monthly reminder letters and was implemented in four units of a rural women’s organiza- tion. Two other units served as control group. Pretest and posttest measurements were com- pleted by 81 women in the intervention group and 88 in the control group. Physical activity was assessed at baseline and at 6 months with accelerometers and the International Physical Activity Questionnaire (IPAQ). Results: There was a significant interaction between time and group for the total ac- celerometer activity counts (p 0.007). Total activity counts increased in the intervention group, whereas there was a decrease in the control group. No significant results were found with the IPAQ. Conclusions: An intervention in a women’s organization was effective in increasing the ob- jectively measured physical activity levels of its members. These results indicate that wo- men’s organizations can be valuable settings for physical activity promotion programs. The minimal number of contact hours and the use of existing structures and communication chan- nels are important strengths for later implementation. 413 INTRODUCTION T HE HEALTH BENEFITS OF developing regular physical activity are well established. Being regularly active reduces the risk of developing cardiovascular diseases and cancer, the two lead- ing causes of death in Europe. 1–3 In addition, physical activity is inversely associated with such diseases as diabetes, osteoporosis, and hyperten- sion. 4–6 It reduces depression and anxiety, and it is associated with increased well-being. 7–9 Despite all this evidence, a large proportion of the European population remains sedentary. Ac- cording to Varo et al., 10 the percentages of seden- tary adults across European countries range from 43.3% in Sweden to 87.8% in Portugal. Moreover, women are less active then men 11 and rural res- idents consistently report lower rates of physical 1 Department of Human Kinesiology, Faculty of Kinesiology and Rehabilitation Sciences, Katholieke Universiteit Leuven, 3001 Leuven, Belgium. 2 Department of Movement and Sport Sciences, Ghent University, 9000 Ghent, Belgium. This study was carried out under the authority of the Policy Research Centre “Sport, Physical Activity and Health,” with financial support of the Flemish Government.
Transcript of Effectiveness of a Lifestyle Physical Activity Intervention in a Women's Organization

JOURNAL OF WOMEN’S HEALTHVolume 17, Number 3, 2008© Mary Ann Liebert, Inc.DOI: 10.1089/jwh.2007.0464
Effectiveness of a Lifestyle Physical Activity Intervention in a Women’s Organization
JOKE OPDENACKER, M.Sc.,1 FILIP BOEN, Ph.D.,1 YVES VANDEN AUWEELE, Ph.D.,1and ILSE DE BOURDEAUDHUIJ, Ph.D.2
ABSTRACT
Objective: The objective of the present study was to evaluate the effectiveness of a minimalcontact physical activity intervention that was maximally integrated into the existing struc-tures of a women’s organization.
Methods: The intervention included one group meeting, a self-help booklet, and fivemonthly reminder letters and was implemented in four units of a rural women’s organiza-tion. Two other units served as control group. Pretest and posttest measurements were com-pleted by 81 women in the intervention group and 88 in the control group. Physical activitywas assessed at baseline and at 6 months with accelerometers and the International PhysicalActivity Questionnaire (IPAQ).
Results: There was a significant interaction between time and group for the total ac-celerometer activity counts (p � 0.007). Total activity counts increased in the interventiongroup, whereas there was a decrease in the control group. No significant results were foundwith the IPAQ.
Conclusions: An intervention in a women’s organization was effective in increasing the ob-jectively measured physical activity levels of its members. These results indicate that wo-men’s organizations can be valuable settings for physical activity promotion programs. Theminimal number of contact hours and the use of existing structures and communication chan-nels are important strengths for later implementation.
413
INTRODUCTION
THE HEALTH BENEFITS OF developing regularphysical activity are well established. Being
regularly active reduces the risk of developingcardiovascular diseases and cancer, the two lead-ing causes of death in Europe.1–3 In addition,physical activity is inversely associated with suchdiseases as diabetes, osteoporosis, and hyperten-
sion.4–6 It reduces depression and anxiety, and itis associated with increased well-being.7–9
Despite all this evidence, a large proportion ofthe European population remains sedentary. Ac-cording to Varo et al.,10 the percentages of seden-tary adults across European countries range from43.3% in Sweden to 87.8% in Portugal. Moreover,women are less active then men11 and rural res-idents consistently report lower rates of physical
1Department of Human Kinesiology, Faculty of Kinesiology and Rehabilitation Sciences, Katholieke UniversiteitLeuven, 3001 Leuven, Belgium.
2Department of Movement and Sport Sciences, Ghent University, 9000 Ghent, Belgium.This study was carried out under the authority of the Policy Research Centre “Sport, Physical Activity and Health,”
with financial support of the Flemish Government.

activity than their urban or suburban counter-parts.12,13 Possible explanations for the low lev-els of physical activity in rural women are theirlimited access to exercise facilities and their per-ception of significant barriers to physical activity,such as having no one to exercise with or lack oftime.13,14 Consequently, there is a need for effi-cient physical activity interventions that targetrural women.15
Over the past decades, numerous interventionshave been developed to promote physical activ-ity,16,17 among them so-called lifestyle physicalactivity interventions. Lifestyle interventions al-low a person to choose from a large variety ofleisure, occupational, and household activities toaccumulate the recommended 30 minutes ofmoderate-intensity physical activity each day.Research has shown that these lifestyle physicalactivity interventions are effective in increasingphysical activity and fitness levels.18 Only a lim-ited number of these interventions are imple-mented in a real life setting, however. One possible explanation is that most of these inter-ventions rely on a substantial number of contacthours with experts,19,20 which is difficult to real-ize in real life situations with small budgets. Lim-iting the number of contact hours is, therefore,one factor that can be considered with respect toimplementation possibilities.
Another factor that can facilitate implementa-tion is to embed the intervention in an alreadyexisting structure. An additional advantage of us-ing existing structures (e.g., traditional meetingplaces and times) and communication channels(e.g., monthly newsletters) is that it increases thechance of reaching sedentary people, who con-stitute an important subgroup seldom reached byresearch staff members. Worksite and primarycare interventions are examples of interventionsthat are embedded in existing structures. Theyhave been the subject of multiple studies in thepast, with mixed results.21,22
Another possibility to reach people, rather thanmedical or worksite settings to reach people, is touse other kinds of settings where people meeteach other on a regular basis, such as social orcultural organizations. Rural women are unitedin worldwide rural women’s organizations, suchas The Associated Country Women of the World,the Woman’s National Farm and Garden Associ-ation (USA), the Country Women’s association ofAustralia, and the Norwegian Society of RuralWomen. These organizations bring women to-
gether in an agreeable and socially engagingatmosphere. They stimulate social awareness, so-cial bonding, and creativity among their partici-pants and organize recreational events and meet-ings around educational and socially relevantthemes. Because of their integration in local so-cial communities, these organizations have theadditional advantage of being able to use localsocial networks and existing friendships, whichcan enhance social support during an interven-tion. To our knowledge, no systematic studies areavailable that evaluated physical activity inter-ventions in women’s organizations.
All these elements were combined in a mini-mal contact lifestyle intervention that was maxi-mally integrated into the existing structures of awomen’s organization. The main purpose of thepresent study was to examine the effectiveness ofthis intervention in increasing physical activity.
MATERIALS AND METHODS
Participants
For this study, a Catholic rural women’s orga-nization with about 117,000 members, spreadover 1048 units in Flanders (Belgium, population6 million), was contacted. Units are geographi-cally structured divisions of which the bordersusually are delineated by separate villages. Theyare under the supervision of a local board andconsist of 50–250 members. The members of thisorganization are adult women, with the majoritybeing between 35 and 65 years old.
After agreement of the national board, six unitswere asked to participate in the study. They wereselected according to their location (i.e., near theuniversity of Leuven but with a rural character),their size (i.e., not very large or small units: thenumber of members varied between 89 and 161members), and the age structure of their mem-bers (i.e., similar percentages of younger andolder members among the units). Four units wererandomly allocated to the intervention group andtwo to the control group. The study was ap-proved by the Ghent University Ethics Commit-tee.
Procedure
All members (n � 697) of the six participatingunits were personally informed about the studyin September 2005 by a member of the board of
OPDENACKER ET AL.414

their unit. Members in the intervention conditionwere told that the university would carry out anintervention on physical activity promotion dur-ing the next months and that they needed data toevaluate this intervention. If members of the in-tervention units agreed to participate, the boardmember gave them an informed consent form,the pretest questionnaires, and an invitation tothe intervention meeting.
Members in the control condition were toldthat the university would carry out an interven-tion on physical activity promotion in other unitsduring the next months and that the researchersneeded data to evaluate their intervention with aview toward nationwide implementation. Ifmembers of the control units agreed to partici-pate, the board member gave them an informedconsent form and the pretest questionnaires butno invitation to an intervention meeting.
Completed informed consent forms and ques-tionnaires were collected by the board members.A random selection of about 30 members in eachunit was contacted by telephone and asked towear an accelerometer. The number of ac-celerometers per unit was dependent on the num-ber of accelerometers available. A random selec-tion per unit was obtained by drawing theappropriate number of names, or more in casepeople refused, from a blinded box with all theparticipants’ names per unit. The accelerometerswere delivered and collected at home or at a cen-tral point in the village by a researcher. The sameprocedure for measurement was used at posttestin April 2006.
Intervention
Because the goal was to create an interventionthat could be implemented in the regular activi-ties of the organization, it was developed in closecooperation with different levels of the organiza-tion. Preparing the organization for a physical ac-tivity promotion intervention required additionalactions at the level of the organization that are be-yond the scope of this paper (e.g., informing thenational board of the scientific relevance of theresearch and convincing them of the practical ap-plicability of the intervention) but that were es-sential for the acceptance of and support for theintervention by the national board.
The intervention consisted of one interventionmeeting, a self-help booklet, and monthly re-minders. The aim was to give the women infor-
mation on why and how to incorporate morephysical activity into their daily lives.
The intervention meeting lasted 90 minutes,which is comparable to other meetings of this or-ganization. It followed the usual structure (i.e.,same starting hour, same duration including a cof-fee break, with an emphasis on both informationand interaction) and was held at their usual meeting point in the village. The meeting wasguided by a researcher and consisted of the following elements: (1) a presentation of the ben-efits of regular physical activity and the AmericanCollege of Sports Medicine/Centers for DiseaseControl (ACSM/CDC) recommendations formoderate and vigorous physical activity, (2) goalsetting exercises resulting in an individually tai-lored physical activity contract for the next 6months, (3) explanation of an exercise calendar forself-monitoring, (4) interactive discussions on bar-riers, reminders, and rewards, and (5) informationabout the use of pedometers. The self-help book-let was developed by the authors and was basedon the “Jump Start to Health” booklets by Marcuset al.23 The self-help booklet consisted of 20 color-ful pages, with many pictures and informationsimilar to that provided during the meeting (i.e.,benefits, norms, goal setting, barriers, tips formaintenance).
Afterward, participants received five monthlyreminder letters with encouragements and tips tostay physically active, in which the essential in-formation of the meeting and the self-help book-let was repeated and elaborated.
In the control condition, members did not re-ceive any of the information on physical activity.
Measurements
Background characteristics. Participants com-pleted a short questionnaire in which they wereasked to indicate their age, their height (in cm),their weight (in kg), their level of education, theirmarital status, and their employment status.
International Physical Activity Questionnaire(IPAQ). Physical activity was measured with thelong “last 7 days recall form” of the IPAQ. Thisquestionnaire assesses physical activity at work,during transportation, in leisure time, and inhousehold and yard work, together with daily sit-ting time. Acceptable measurement properties ofthe IPAQ were found in an international studyover 12 countries24 and in a Flemish sample.25
LIFESTYLE INTERVENTION IN RURAL WOMEN 415
CSA accelerometer. In a subsample of both theintervention and control groups, physical activ-ity was also measured using the Computer Sci-ence and Applications, Inc. model 7164 (CSA) ac-celerometer (Shalimar, FL). Different studies haveshown that this is a reliable and valid monitor tomeasure physical activity.26,27 Participants wereasked to wear the accelerometer during wakinghours for 5 consecutive days of the same week,starting on a Wednesday to include both weekand weekend days. The monitor was worn on theright hip and was removed only for water basedactivities and sleeping. Participants kept a diaryduring the 5 days in which they noted for what
activity they removed the monitor. These activi-ties were later incorporated into the accelerome-ter data.
Statistical analyses
All data were analyzed with SPSS 14.0 (Chicago,IL). To assess differences between groups, inde-pendent samples t tests, chi-square analyses, andone-way ANOVAs were used. Effects on physi-cal activity were analyzed with repeated mea-sures ANCOVAs, with time (within) and group(between) as factors and marital status (dummycoded) as covariate.
OPDENACKER ET AL.416
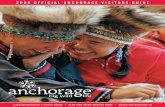
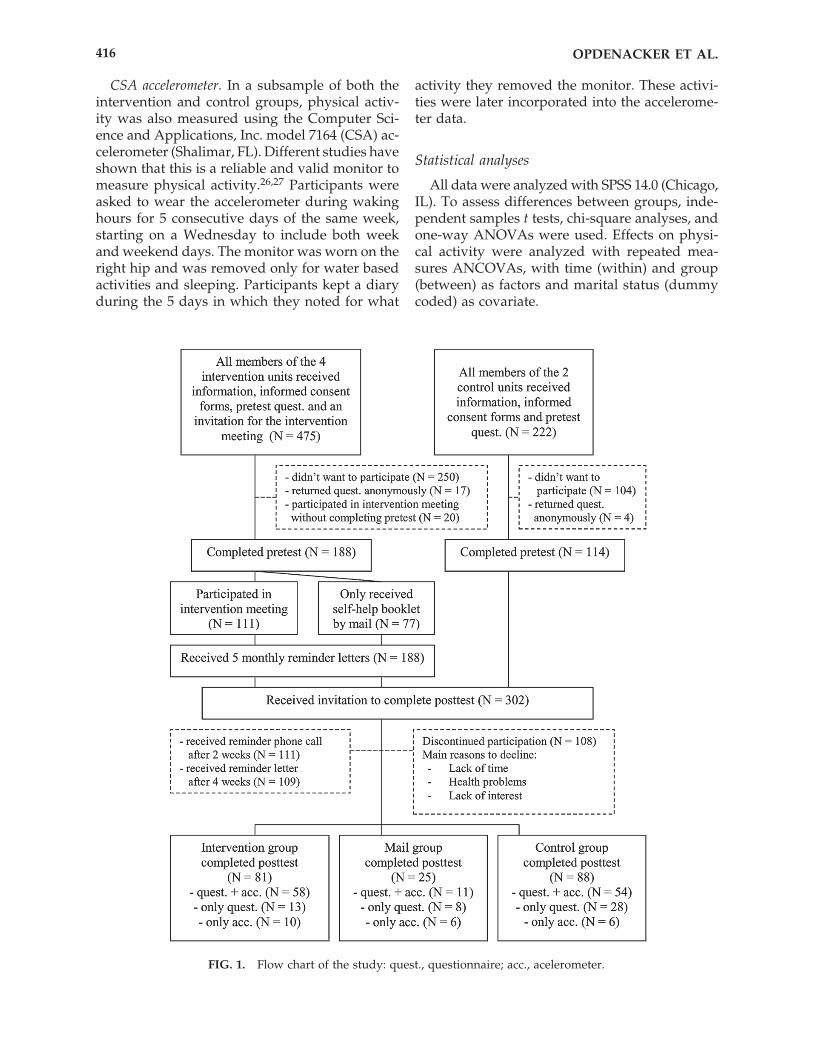
FIG. 1. Flow chart of the study: quest., questionnaire; acc., acelerometer.

RESULTS
Response rates
Figure 1 displays the response rates of thestudy. Because the group in the intervention con-dition that received information only by mail andcompleted all tests was too small (n � 25), it wasnot included in the analyses. Dropout percent-ages in the intervention (27.0%) and the controlcondition (22.8%) were not significantly different.In the intervention group, there were no pretestdifferences between dropouts and completers forany of the variables. Dropouts in the controlgroup had a significantly higher body mass in-dex (BMI) than completers (t � 3.061, p � 0.01).
Demographic variables
There were no significant differences betweenthe two groups in mean age, BMI, years of edu-cation, or employment status (Table 1). However,a significantly higher proportion of the controlgroup was married compared with the interven-tion group. This significant difference remainedwhen dropouts were included. To account for thisdifference, marital status was included as covari-ate in the repeated measures analyses.
Effect measurements
No significant pretest differences between theintervention group and the control groupemerged for any of the IPAQ or CSA measure-ments. There were also no significant differencesat pretest or posttest between the different unitswithin the intervention or control condition forany of these measurements.
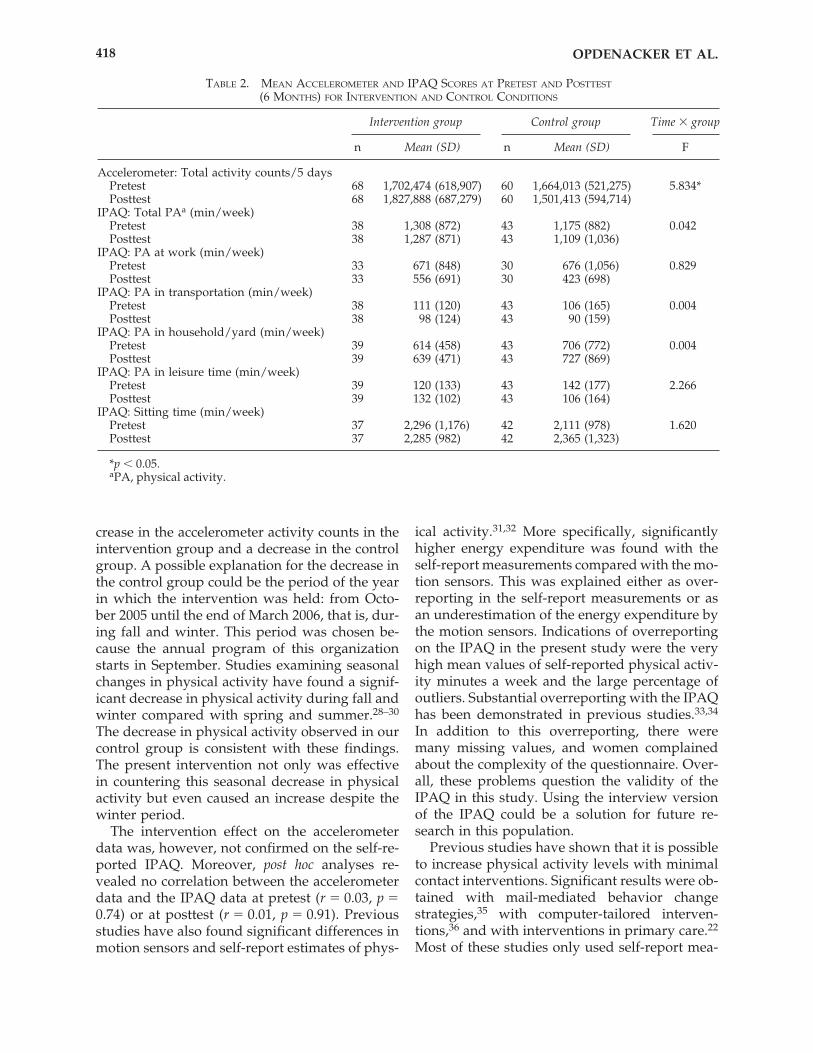
There was a significant interaction betweentime and group for the total accelerometer activ-
ity counts (Table 2). Total activity counts in-creased in the intervention group, whereas therewas a decrease in the control group. This patternwas not confirmed for the self-reported physicalactivity levels. No significant differences werefound for any of these measurements (Table 2).Overall, the mean values for the self-reportedphysical activity measurements were very high.According to the guidelines for data processingand analysis of the IPAQ (www.ipaq.ki.se), 9(12.6%) outliers in the intervention group and 12(14.6%) in the control group were excluded fromanalysis. The outliers were cases of extreme over-reporting, probably as a result of not fully un-derstanding or misinterpreting the questions.Additional t tests revealed no significant differ-ences between participants with extreme valuesand the other participants on any of the demo-graphic characteristics. Another 23 (32%) subjectsin the intervention condition and 27 (32.9%) inthe control condition were excluded because ofmissing values. This resulted in a decrease ofpower.
Comparable results (i.e., a significant interac-tion for total accelerometer counts and no signif-icant results with the IPAQ) were found with in-tention-to-treat analyses (n � 225), where nochange was assumed from pretest to posttest fordropouts.
DISCUSSION
The results of the present study showed that aminimal contact intervention embedded in theexisting structures of a rural women’s organiza-tion can have a positive effect on the objectivelymeasured physical activity levels of its members.The significant interaction effect indicated an in-
LIFESTYLE INTERVENTION IN RURAL WOMEN 417
TABLE 1. DEMOGRAPHIC CHARACTERISTICS OF THE TWO GROUPS AT PRETEST
Intervention group Control groupCharacteristic (n � 81) (n � 88) pa
Age, years 54.5 (12.0)b 53.0 (12.5) NSBody mass index 25.2 (4.3)0b 24.9 (4.0)0 NSEducation (years) 12.1 (3.0)0b 12.5 (2.9)0 NSMarital status
% Married 71.6% 89.8% �0.05Employment status
% Employed 44.3% 43.5% NS
aResult of t test or chi-square comparing intervention and control group atpretest.
bMean (SD).
crease in the accelerometer activity counts in theintervention group and a decrease in the controlgroup. A possible explanation for the decrease inthe control group could be the period of the yearin which the intervention was held: from Octo-ber 2005 until the end of March 2006, that is, dur-ing fall and winter. This period was chosen be-cause the annual program of this organizationstarts in September. Studies examining seasonalchanges in physical activity have found a signif-icant decrease in physical activity during fall andwinter compared with spring and summer.28–30
The decrease in physical activity observed in ourcontrol group is consistent with these findings.The present intervention not only was effectivein countering this seasonal decrease in physicalactivity but even caused an increase despite thewinter period.
The intervention effect on the accelerometerdata was, however, not confirmed on the self-re-ported IPAQ. Moreover, post hoc analyses re-vealed no correlation between the accelerometerdata and the IPAQ data at pretest (r � 0.03, p �0.74) or at posttest (r � 0.01, p � 0.91). Previousstudies have also found significant differences inmotion sensors and self-report estimates of phys-
ical activity.31,32 More specifically, significantlyhigher energy expenditure was found with theself-report measurements compared with the mo-tion sensors. This was explained either as over-reporting in the self-report measurements or asan underestimation of the energy expenditure bythe motion sensors. Indications of overreportingon the IPAQ in the present study were the veryhigh mean values of self-reported physical activ-ity minutes a week and the large percentage ofoutliers. Substantial overreporting with the IPAQhas been demonstrated in previous studies.33,34
In addition to this overreporting, there weremany missing values, and women complainedabout the complexity of the questionnaire. Over-all, these problems question the validity of theIPAQ in this study. Using the interview versionof the IPAQ could be a solution for future re-search in this population.
Previous studies have shown that it is possibleto increase physical activity levels with minimalcontact interventions. Significant results were ob-tained with mail-mediated behavior changestrategies,35 with computer-tailored interven-tions,36 and with interventions in primary care.22
Most of these studies only used self-report mea-
OPDENACKER ET AL.418
TABLE 2. MEAN ACCELEROMETER AND IPAQ SCORES AT PRETEST AND POSTTEST
(6 MONTHS) FOR INTERVENTION AND CONTROL CONDITIONS
Time � group
n Mean (SD) n Mean (SD) F
Accelerometer: Total activity counts/5 daysPretest 68 1,702,474 (618,907) 60 1,664,013 (521,275) 5.834*Posttest 68 1,827,888 (687,279) 60 1,501,413 (594,714)
IPAQ: Total PAa (min/week)Pretest 38 1,308 (872) 43 1,175 (882) 0.042Posttest 38 1,287 (871) 43 1,109 (1,036)
IPAQ: PA at work (min/week)Pretest 33 671 (848) 30 676 (1,056) 0.829Posttest 33 556 (691) 30 423 (698)
IPAQ: PA in transportation (min/week)Pretest 38 111 (120) 43 106 (165) 0.004Posttest 38 98 (124) 43 90 (159)
IPAQ: PA in household/yard (min/week)Pretest 39 614 (458) 43 706 (772) 0.004Posttest 39 639 (471) 43 727 (869)
IPAQ: PA in leisure time (min/week)Pretest 39 120 (133) 43 142 (177) 2.266Posttest 39 132 (102) 43 106 (164)
IPAQ: Sitting time (min/week)Pretest 37 2,296 (1,176) 42 2,111 (978) 1.620Posttest 37 2,285 (982) 42 2,365 (1,323)
*p � 0.05.aPA, physical activity.
Intervention group Control group

sures of physical activity, but some also usedmore objective measures. For example, a signifi-cant intervention effect on accelerometer activitycounts was found by Calfas et al.37 after a shortprimary care intervention. In agreement with thepresent findings, no effects were found with aself-report physical activity questionnaire. DuVall et al.38 compared the impact of three mini-mal contact lifestyle interventions on physical ac-tivity in women and found a significant increasein physical activity, measured with accelerome-ters only, in all three intervention groups.
As far as we know, no studies have been pub-lished that implemented a physical activity in-tervention in a women’s organization, althoughsome church-based health promotion programshave been described in the literature.39,40 Likewomen’s organizations, churches also have animportant link with the community and the ad-vantage of built-in social support networks. Con-sistent with our findings, Young and Stewart41
and Peterson et al.42 found no effects of theirchurch-based physical activity programs for wo-men on self-reported physical activity question-naires. Peterson et al.42 did find a significant ef-fect on VO2max, a more objective measure ofphysical fitness, which again stresses the impor-tance of including objective outcome measures inintervention studies.
Strengths and limitations
This study is the first to examine the effect of aphysical activity intervention in a rural women’sorganization. A strength of the present study isthat an effect on objectively measured physical ac-tivity was obtained with a minimal contact inter-vention. A further strength is that the interventionwas developed within the existing structures of theorganization. This required very close cooperationamong different layers of the organization, but itwas worth the time and energy with regard to laterimplementation. In this case, the national board ofthis organization decided to choose physical ac-tivity promotion for their next annual year themeand implement the intervention on a larger scale.In this way, the intervention will reach thousandsof rural women, and the costs will be completelycovered by the organization itself.
This positive consequence caused a first limi-tation. Because the national board of the organi-zation decided to implement our intervention ona national scale just 3 months after the posttest,
no follow-up was possible because the partici-pants in the control group also received infor-mation about physical activity. A second limita-tion is the considerable dropout rate: 27.0% in theintervention condition and 22.8% in the controlcondition. The only difference between dropoutsand completers, however, was found in the con-trol group, where dropouts had a significantlyhigher BMI. Comparable results were found withintention-to-treat analyses. A final limitation con-cerns the problems we experienced with the self-report version of the IPAQ, which probablycaused invalid results.
CONCLUSIONS
The present minimal contact intervention, em-bedded in a women’s organization, was effectivein increasing physical activity in comparison witha no-intervention control group. These results in-dicate that women’s organizations can be valu-able settings for physical activity promotion pro-grams. Their existing social networks and strongintegration in the community make physical ac-tivity more easily accessible, which is especiallyimportant for sedentary people like the majorityof rural women. More research is needed to as-sess the generalizability and long-term effects ofthis kind of interventions.
DISCLOSURE STATEMENT
No competing financial interests exist.
REFERENCES
1. Wannamethee SG, Shaper AG. Physical activity andcardiovascular disease. Semin Vasc Med 2002;2:257.
2. Niederlaender E. Causes of death in the EU. A reportby the EU’s statistical office, Eurostat. European Com-munities, 2006.
3. Hu G, Tuomilehto J, Silventoinen K, Barengo NC, Pel-tonen M, Jousilahti P. The effects of physical activityand body mass index on cardiovascular, cancer andall-cause mortality among 47,212 middle-agedFinnish men and women. Int J Obesity 2005;29:894.
4. Ernst E. Exercise for female osteoporosis—A system-atic review of randomised clinical trials. Sports Med1998;25:359.
5. Sigal RJ, Kenny GP, Wasserman DH, Castaneda-Sceppa C, White RD. Physical activity/exercise and
LIFESTYLE INTERVENTION IN RURAL WOMEN 419
type 2 diabetes. A consensus statement from theAmerican Diabetes Association. Diabetes Care2006;29:1433.
6. Wallace JP. Exercise in hypertension—A clinical re-view. Sports Med 2003;33:585.
7. Antunes HKM, Stella SG, Santos RF, Bueno OFA, deMello MT. Depression, anxiety and quality of lifescores in seniors after an endurance exercise program.Rev Bras Psiquiatr 2005;27:266.
8. Byrne A, Byrne DG. The effect of exercise on depres-sion, anxiety and other mood states—A review. J Psy-chosom Res 1993;37:565.
9. Stathopoulou G, Powers MB, Berry AC, Smits JAJ,Otto MW. Exercise interventions for mental health: Aquantitative and qualitative review. Clin Psychol SciPr 2006;13:179.
10. Varo JJ, Martínez-González MA, de Irala-Estévez J,Kearny J, Gibney M, Martínez JA. Distribution anddeterminants of sedentary lifestyles in the EuropeanUnion. Int J Epidemiol 2003;32:138.
11. Wijndale K, Matton L, Duvigneaud N, et al. Fysiekeactiviteit , fitheid en gezondheid in Vlaanderen [Phys-ical activity, fitness and health in Flanders]. In: SteensG, ed. Moet er nog sport zijn. Sport, beweging engezondheid in Vlaanderen 2002–2006. Antwerpen:F&G Partners, 2006:55.
12. Parks SE, Housemann RA, Brownson RC. Differentialcorrelates of physical activity in urban and ruraladults of various socioeconomic backgrounds in theUnited States. J Epidemiol Community Health2003;57:29.
13. Osuji T, Lovegreen S, Elliot M, Brownson RC. Barri-ers to physical activity among women in the ruralmidwest. Women Health 2006;44:41.
14. Sherman BJ, Gilliland G, Speckman JL, Freund KM.The effect of a primary care exercise intervention forrural women. Prev Med 2007;44:198.
15. Hageman PA, Walker SN, Pullen CH, Boecker LS,Oberdorfer MK. Physical activity and fitness amongmidlife and older rural women. J Aging Phys Act2005;13:327.
16. Hillsdon M, Foster C, Throgood M. Interventions forpromoting physical activity. Cochrane Database SystRev 2005;1:CD003180.
17. Kahn EB, Ramsey LT, Browson RC, et al. The effec-tiveness of interventions to increase physical activity.A systematic review. Am J Prev Med 2002;22:73.
18. Dunn AL, Andersen RE, Jakicic JM. Lifestyle physi-cal activity interventions: History, short- and long-term effect, and recommendations. Am J Prev Med1998;15:398.
19. Kohl HW, Dunn AL, Marcus BH, Blair SN. A ran-domized trial of physical activity interventions: De-sign and baseline data from Project Active. Med SciSports Exerc 1998;30:275.
20. Andersen RE, Wadden TA, Bartlett SJ, Zemel B, VerdeTJ, Franckowiak SC. Effects of lifestyle activity vsstructured aerobic exercise in obese women. JAMA1999;281:335.
21. Dishman RK, Oldenburg B, O’Neal H, Shephard RJ.Worksite physical activity interventions. Am J PrevMed 1998;15:344.
22. Eakin EG, Glasgow RE, Riley KM. Review of primarycare-based physical activity intervention studies. Ef-fectiveness and implications for practice and futureresearch. J Fam Practice 2000;49:158.
23. Marcus BH, Emmons KM, Simkin-Silverman LR, etal. Evaluation of motivationally tailored versus stan-dard self-help physical activity interventions at theworkplace. Am J Health Prom 1998;12:246.
24. Craig CL, Marshall AL, Sjostrom M, et al. Interna-tional Physical Activity Questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 2003;35:1381.
25. Vandelanotte C, De Bourdeaudhij I, Sallis JF, Philip-paerts R, Sjostrom M. Reliability and validity of acomputerised and Dutch version of the InternationalPhysical Activity Questionnaire (IPAQ). J Phys ActHealth 2005;2:63.
26. Freedson PS, Melanson E, Sirard J. Calibration of theComputer Science and Applications, Inc. accelerom-eter. Med Sci Sports Exerc 1998;30:777.
27. Sirard JR, Melanson EL, Li L, Freedson PS. Field eval-uation of the Computer Science and Applications, Inc.physical activity monitor. Med Sci Sports Exerc 2000;32:695.
28. Matthews CE, Freedson PS, Hebert JR, et al. Seasonalvariation in household, occupational, and leisure timephysical activity: Longitudinal analyses from the sea-sonal variation of blood cholesterol study. Am J Epi-demiol 2001;153:172.
29. Pivarnik JM, Reeves MJ, Rafferty AP. Seasonal varia-tion in adult leisure-time physical activity. Med SciSports Exerc 2003;35:1004.
30. Uitenbroek DG. Seasonal variation in leisure timephysical activity. Med Sci Sports Exerc 1993;25:755.
31. Dishman RK, Darracot CR, Lambert LT. Failure togeneralize determinants of self-reported physical ac-tivity to a motion sensor. Med Sci Sports Exerc1992;24:904.
32. Leenders NYM, Sherman WM, Nagaraja HN. Com-parisons of four methods of estimating physical ac-tivity in adult women. Med Sci Sports Exerc2000;32:1320.
33. Fogelholm M, Malmberg J, Suni J, et al. Internationalphysical activity questionnaire: Validity against fit-ness. Med Sci Sports Exerc 2006;38:753.
34. Rzewnicki R, Vanden Auweele Y, De BourdeaudhuijI. Addressing overreporting on the InternationalPhysical Activity Questionnaire (IPAQ) telephonesurvey with a population sample. Public Health Nutr2003;6:299.
35. Cardinal BJ, Sachs ML. Effects of a mail-mediated,stage-matched exercise behavior change strategies onfemale adults’ leisure-time exercise behavior. J SportsMed Phys Fitness 1996;36:100.
36. Vandelanotte C, De Bourdeaudhuij I, Sallis J, SpittaelsH, Brug J. Efficacy of sequential or simultaneous in-
OPDENACKER ET AL.420
teractive computer-tailored interventions for increas-ing physical activity and decreasing fat intake. AnnBehav Med 2005;29:138.
37. Calfas KJ, Long BJ, Sallis JF, Wooten DJ, Pratt M,Patrick K. A controlled trial of physician counselingto promote the adoption of physical activity. PrevMed 1996;25:225.
38. Du Vall C, Dinger MK, Taylor EL, Bemben D. Mini-mal-contact physical activity interventions in women:A pilot study. Am J Health Behav 2004;28:280.
39. Lasater TM, Becker DM, Hill MN, Gans KM. Synthe-sis of findings and issues from religious-based car-diovascular disease prevention trials. Ann Epidemiol1997;7:S46.
40. Peterson J, Atwood JR, Yates B. Key elements for church-based health promotion programs: Outcome-based lit-erature review. Public Health Nurs 2002;19:401.
41. Young DR, Stewart KJ. A church-based physical ac-tivity intervention for African American women. FamCommunity Health 2006;29:103.
42. Peterson JA, Yates BC, Atwood JR, Hertzog M. Effectsof a physical activity intervention for women. West-ern J Nurs Res 2005;27:93.
Address reprint requests to:Joke Opdenacker
Department of Human KinesiologyK.U.Leuven
Tervuursevest 101, 3001 Heverlee (Leuven)Belgium
E-mail: [email protected]
LIFESTYLE INTERVENTION IN RURAL WOMEN 421