Educational approaches and conditions for effective ...
331
Self-management education for patients with chronic diseases in South Africa LOVENESS DUBE FEBRUARY 2017 Thesis presented for obtaining the degree Doctor in Public Health Sciences Faculty of Public Health Université catholique de Louvain Faculty of Public Health Institute of Health and Society - Institut de recherche santé et société (IRSS) Psychological Sciences Research Institute - Institut de Recherche en Sciences Psychologiques (IPSY) Supervisors : Professor Stephan Van den Broucke (UCL) Professor William D’Hoore (UCL) Dr. Anne-Marie Bergh (University of Pretoria) Despite the high need for self-management education (SME) for chronic diseases in developing countries, existing programmes have almost exclusively been de- veloped and evaluated in developed countries. This thesis looks at the feasibility of a more context-specific approach to chronic disease SME in resource-limited settings by investigating the needs for SME in a developing country (South Afri- ca), developing a SME tool that meets these needs, and testing the conditions for its successful implementation. The thesis consists of a series of research papers investigating the current status of diabetes SME in developing countries, the characteristics of existing SME programs in South Africa, the perceived needs for self-management among chronic patients and experts, and the feasibility of a contextually adapted SME tool for diabetes and hypertension in the form of a care-plan booklet. A pilot study of the use of this tool showed positive changes in hypertension knowledge and served as a basis for a larger effect study proto- col. By adding to the knowledge on chronic disease SME in resource-limited set- tings this thesis can inform decision-makers to help integrate self-management into routine care. Loveness Dube comes from Chipinge, Zimbabwe and she completed her high school edu- cation at Mabelreign Girls High School in Harare. In 2009 she obtained a Bachelor in Social Work at the University of Fort Hare in South Africa. From 2009 to 2012, Miss Dube worked as a social worker in child protection services at Johannesburg Child Welfare. She completed a Mas- ter in Public Health at the Uni- versity of Pretoria in June 2013. From October 2013 to February 2017 she enrolled in a PhD pro- gram at the Université catho- lique de Louvain in Belgium. She authored three articles pu- blished in peer-reviewed scien- tific journals. Self-management education for patients with chronic diseases in South Africa Loveness Dube 2017 Educational approaches and conditions for effective implementation
-
Upload
khangminh22 -
Category
Documents
-
view
0 -
download
0
Transcript of Educational approaches and conditions for effective ...

Self-management education for patients with chronic diseases in South Africa
Loveness Dube
February 2017
Thesis presented for obtaining the degree Doctor in Public Health Sciences
Faculty of Public Health
Université catholique de LouvainFaculty of Public Health
Institute of Health and Society - Institut de recherche santé et société (IRSS)Psychological Sciences Research Institute - Institut de Recherche en Sciences Psychologiques (IPSY)
Supervisors : Professor Stephan Van den Broucke (UCL) Professor William D’Hoore (UCL) Dr. Anne-Marie Bergh (University of Pretoria)
Despite the high need for self-management education (SME) for chronic diseases in developing countries, existing programmes have almost exclusively been de-veloped and evaluated in developed countries. This thesis looks at the feasibility of a more context-specific approach to chronic disease SME in resource-limited settings by investigating the needs for SME in a developing country (South Afri-ca), developing a SME tool that meets these needs, and testing the conditions for its successful implementation. The thesis consists of a series of research papers investigating the current status of diabetes SME in developing countries, the characteristics of existing SME programs in South Africa, the perceived needs for self-management among chronic patients and experts, and the feasibility of a contextually adapted SME tool for diabetes and hypertension in the form of a care-plan booklet. A pilot study of the use of this tool showed positive changes in hypertension knowledge and served as a basis for a larger effect study proto-col. By adding to the knowledge on chronic disease SME in resource-limited set-tings this thesis can inform decision-makers to help integrate self-management into routine care.
Loveness Dube comes from Chipinge, Zimbabwe and she completed her high school edu-cation at Mabelreign Girls High School in Harare. In 2009 she obtained a Bachelor in Social Work at the University of Fort Hare in South Africa. From 2009 to 2012, Miss Dube worked as a social worker in child protection services at Johannesburg Child Welfare. She completed a Mas-ter in Public Health at the Uni-versity of Pretoria in June 2013. From October 2013 to February 2017 she enrolled in a PhD pro-gram at the Université catho-lique de Louvain in Belgium. She authored three articles pu-blished in peer-reviewed scien-tific journals.
Self-
man
agem
ent e
duca
tion
for p
atie
nts
with
chr
onic
dis
ease
s in
Sou
th A
fric
a
Lov
enes
s D
ube
201
7
Educational approaches and conditions for effective implementation
i
Loveness DUBE
Self-management education for patients with chronic
diseases in South Africa: Educational approaches and
conditions for effective implementation
Faculty of Public Health
Institute of Health and Society

ii
Cover picture: The Wellness Coalition©

iii
JURY
Supervisor: Prof. Stephan Van den Broucke (UCL)
Co-supervisors: Prof. William D’Hoore (UCL)
Dr. Anne-Marie Bergh (University of Pretoria)
Jury members:
Prof. Jean-Marie Degryse (President - UCL)
Prof. Isabelle Aujoulat (UCL)
Prof. Vincent Lorant (UCL)
Prof. Bernard Vandeleene (UCL)
Prof. Walter Sermeus (Katholieke Universiteit Leuven)

iv
Contact details:
Université catholique de Louvain
Institut de Recherche en Sciences Psychologiques
10 Place Cardinal Mercier
1348 Louvain-la-Neuve, Belgium
Tel: +32 (0) 10 47 80 68
Email: [email protected] / [email protected]

v
To my mom

vi
ACKNOWLEDGEMENTS
This thesis would not have been possible without the support of few individuals that
I am gratefully indebted to:
I would like to express my sincere gratitude to my co-supervisor Dr. Kirstie-Rendall
Mkosi (posthumously) who passed away before the finalization of this thesis. She
would have loved to see the end result … anyway you are greatly missed.
Very special thanks go to my supervisor Professor Van den Broucke, for your
constant support and guidance throughout the research at the Université catho-
lique de Louvain. Thank you for your faith in me that I could do this work.
To my co-supervisor Dr. Anne-Marie Bergh (University of Pretoria), you have been
there in the times of need; you have been a pillar of strength for me. Thank you for
your unwavering support and allowing me to tap into your knowledge and experi-
ence. You have been and will always be my source of inspiration.
To my co-supervisor Professor D’Hoore, thank you for everything from the
beginning, especially for those days where you had to clarify things.
Thanks to the two institutions that made this work possible; the Université
catholique de Louvain for the PhD scholarship and the University of Pretoria for the
two research assistant grants.
To the research assistants Mr Precious Hajison, Ms Petronella Mzalamba and Ms
Keabetswe Kodi, this work would have been difficult to realize without your help
with data collection.
To the staff members of the University of Pretoria; Mrs Lizeka Napoles for your
support and guidance whenever needed and to Professor Kuku Voyi, Dr. Elize
Webb, Professor Paul Rheeder and Professor Dannie VanZyl for your constant
support in the academic journey. To Nokuthula Mafutha, thanks for your assistance
and for your sacrifice even though you were also working on your own thesis.

vii
Thanks to the members of the Diabetes Literacy team, Diane Levin-Zamir, Gerard
Van der Zanden, Lucy Yardely, Peter Schwatrz, Henna Riemenschneider for your
support in reviewing manuscripts for publication and all the other members for your
support and guidance.
To Curo Health staff members, Dr. Richard Botha and Mrs Rosanne Ludick, thank
you very much for your support in the development of the care-plan booklet.
To my colleagues at the Université catholique de Louvain at Louvain-la-Neuve
campus, Dr. Marie Housiaux and Louise Schinckus, you were the first contacts in a
foreign land and thank you for your comfort and support, especially when I was
missing home. To Monica Suárez and Pablo Alonso Peña, you joined the team a
bit later but thanks for the support. And to Sophie Agboli at Woluwe campus, you
have been there through thick and thin, you were a shoulder to cry on when it
really got tough. Thank you for being there.
Special thanks also go to the members of the jury, Professor Jean-Marie Degryse
(President), Professor Isabelle Aujoulat, Professor Vincent Lorant, Professor
Bernard Vandeleene and Professor Walter Sermeus (Katholieke Universiteit
Leuven) for your critical comments, which have by far improved this work.
To my family, my father and mother, thank you for your unfailing love and support
from childhood. It was not easy to send a child to school, especially a girl child, but
you did. And here we are today; I will always love you. To my siblings, I love you
and I thank you for your continued support, especially Dr. Francis Dube and wife
for everything you have done. To my uncles, Mr Jairos Ngorima and Mr Victor
Dube (posthumously) and their families, thank you for all your support. Although
sometimes things were tough, you persevered for me. To my cousins, Miriam
Phinda, thank you for showing me direction, and also to Carol Mukove, and Charity
Makua, thanks for everything, I can’t begin to count.
Last but not least, I am grateful to God Almighty who has made this journey
possible and has been my source of strength when I was weak, without him I
wouldn’t have made it this far.

viii

ix
TABLE OF CONTENTS
LIST OF TABLES .................................................................................................... xiii
LIST OF FIGURES ..................................................................................................xiv
LIST OF ABREVIATIONS ....................................................................................... xv
GENERAL INTRODUCTION: Background and layout of thesis ................................. 1
Background ................................................................................................................................ 2
Burden of chronic diseases in developing countries .................................................. 2
The role of self-management ............................................................................................... 5
Research questions and objectives .................................................................................... 8
References ................................................................................................................................ 13
CHAPTER 1: Towards a model of self-management for chronic diseases ............ 17
Introduction ............................................................................................................................ 18
The need for self-management in chronic care.......................................................... 18
The chronic care model ....................................................................................................... 22
Models of or approaches to self-management ............................................................ 25
Conclusion ................................................................................................................................ 28
References ................................................................................................................................ 28
CHAPTER 2: The South African health context ....................................................... 31
Introduction ............................................................................................................................ 32
The formal healthcare sector in South Africa ............................................................. 33
Traditional healthcare ........................................................................................................ 39
Health literacy in South Africa .......................................................................................... 41
The context of this study ..................................................................................................... 42
Conclusion ................................................................................................................................ 43
CHAPTER 3: Systematic Review .............................................................................. 47
Abstract ..................................................................................................................................... 48
Introduction ............................................................................................................................ 49
Methods ..................................................................................................................................... 52
Results ....................................................................................................................................... 55
x
Discussion ................................................................................................................................ 75
Conclusion ................................................................................................................................ 77
References ................................................................................................................................ 78
CHAPTER 4: An audit of policies and programs .................................................... 83
Abstract ..................................................................................................................................... 84
Introduction ............................................................................................................................ 86
Design and Methods ............................................................................................................. 87
Results ....................................................................................................................................... 90
Discussion .............................................................................................................................. 103
Conclusions ............................................................................................................................ 106
References .............................................................................................................................. 107
CHAPTER 5: Self-management needs assessment ............................................ 111
Abstract ................................................................................................................................... 112
Methods ................................................................................................................................... 116
Results ..................................................................................................................................... 120
Discussion .............................................................................................................................. 127
Conclusion .............................................................................................................................. 129
References .............................................................................................................................. 130
CHAPTER 6: Development of a care-plan booklet ................................................ 135
Introduction .......................................................................................................................... 136
Printed materials for health education ....................................................................... 138
The prototype care-plan booklet .................................................................................. 142
Conclusion .............................................................................................................................. 149
References .............................................................................................................................. 150
CHAPTER 7: Feasibility study ............................................................................... 153
Summary ................................................................................................................................. 154
Introduction .......................................................................................................................... 155
Method ..................................................................................................................................... 157
Results ..................................................................................................................................... 161
Discussion .............................................................................................................................. 170

xi
Conclusion .............................................................................................................................. 173
References .............................................................................................................................. 173
CHAPTER 8: Pilot study ........................................................................................ 177
Abstract ................................................................................................................................... 178
Introduction .......................................................................................................................... 179
Method ..................................................................................................................................... 181
Results ..................................................................................................................................... 185
Discussion .............................................................................................................................. 186
Conclusion .............................................................................................................................. 187
References .............................................................................................................................. 189
CHAPTER 9 –Main findings and discussion .......................................................... 191
Introduction .......................................................................................................................... 192
Summary of main findings ............................................................................................... 192
Discussion of the main findings ..................................................................................... 198
Strengths and limitations of studies ............................................................................ 206
Conclusion .............................................................................................................................. 207
References .............................................................................................................................. 208
CHAPTER 10 - Study protocol ............................................................................... 213
Introduction .......................................................................................................................... 214
Statement of problem ........................................................................................................ 216
Aim, objectives and hypothesis ...................................................................................... 216
Method ..................................................................................................................................... 217
Conclusion .............................................................................................................................. 231
GENERAL CONCLUSION – Conditions for effective implementation ..................... 237
References .............................................................................................................................. 241
PUBLICATIONS & SCIENTIFIC COMMUNICATION ................................................ 245
APPENDICES ....................................................................................................... 247
APPENDIX A ......................................................................................................... 249
APPENDIX B ......................................................................................................... 285
APPENDIX C ........................................................................................................ 287

xii
APPENDIX D ........................................................................................................ 309

xiii
LIST OF TABLES
Table 1.1 Care differences between acute and chronic conditions 20
Table 1.2 Comparison of patient education and self-management 23
Table 3.1 Study characteristics for T2DM in low mortality developing
countries
57
Table 3.2 Study characteristics for T2DM in high mortality developing
countries
61
Table 3.3 DSME Intervention/programs characteristics for T2DM in
low mortality developing countries
64
Table 3.4 DSME Intervention/programs characteristics for T2DM in
high mortality developing countries
73
Table 4.1 Number of respondents from each province 91
Table 4.2 DSME information extracted from guidelines using the
International Standards for Diabetes Education
94
Table 4.3 Timeframes of structured programs 99
Table 4.4 Content included in programs and ad-hoc interventions 101
Table 5.1 Overview of participant characteristics, sampling and data
collection strategies
117
Table 5.2 Main themes and categories 121
Table 6.1 Differences between the Curo Health care-plan and the
new prototype care-plan booklet
143
Table 8.1 Demographic characteristics of participants completing the study 182
Table 8.2 Results of paired samples t-test 185
Table 9.1 Main themes and categories 195

xiv
LIST OF FIGURES
Figure 0.1 Double burden of disease in low- and middle-income
countries compared to high income countries
4
Figure 0.2 Self-management as the core component of care 7
Figure 0.3 Overview of the thesis 10
Figure 1.1 The chronic care model 24
Figure 3.1 Flowchart of the selection process 53
Figure 4.1 Types of providers in diabetes self-management
education
100
Figure 9.1 Complexity of self-management process 202
Figure 10.1 Trial flow chart 218
Figure 10.2 Contents of the booklet 221

xv
LIST OF ABREVIATIONS
AADE American Association of Diabetes Educators
AIDS Acquired immune deficiency syndrome
BMI Body mass index
CCM Chronic Care Model
CDSMP Chronic Disease Self-Management Program
CHC Community health center
CHW Community health worker
DCST District-based clinical specialist support team
DM Diabetes mellitus
DSME Diabetes self-management education
GDP Gross domestic product
GDS Global diabetes survey
HbA1c (A1c) Glycated hemoglobin
HBM Health Belief Model
HIV human immunodeficiency virus
ICCC Innovative Care for Chronic Conditions
ICDM Integrated chronic disease model
IDF International Diabetes Federation
IDSE International Standards for Diabetes Education
LMIC Low-and-middle income country
NCD Non-communicable disease

xvi
NGO Non-governmental organization
NHI National health insurance
PHC Primary healthcare
RCT Randomized controlled trial
SDGs Sustainable Development Goals
SMBG Self-monitoring of blood glucose
SEMDSA Society for Endocrinology, Metabolism and Diabetes of South
Africa
SME Self-management education
SSA Sub-Saharan Africa
TB Tuberculosis
T1DM Type 1 diabetes mellitus
T2DM Type 2 diabetes mellitus
UNESCO United Nations Education, Scientific and Cultural Organization
WHO World Health Organization
WBOT Ward-based outreach team

1
GENERAL INTRODUCTION: Background and layout of
thesis

2
Background
Non-communicable diseases (NCDs), also known as chronic diseases, have
become the world’s major public health threat (1). NCDs affect people in all
countries, regardless of economic status, gender and age (2). Worldwide, NCDs
are the leading causes of morbidity, mortality and disability (3). According to the
World Health Organization’s (WHO) 2015 report, NCDs were the cause of 38
million out of the 56 million deaths in 2012 globally (2). It is estimated that NCDs kill
38 million people every year and 16 million of these deaths occur prematurely
before the age of 70 (3).
NCDs are diseases that cannot be passed from one person to another; they
develop and progress slowly and are of long duration. They can be classified in
four groups of diseases: cardiovascular diseases (heart attacks and stroke),
chronic respiratory diseases (asthma and chronic obstructive pulmonary disease or
COPD), cancers, and diabetes (4, 5). These NCDs are related in the sense that
they share common risk factors that are to a large extent preventable and
modifiable. More specifically, behavioral and lifestyle factors such as: tobacco use,
physical inactivity, unhealthy diets and harmful use of alcohol have a major effect
on the onset and course of NCDs (5-8). In 2012 these four groups of diseases
accounted for 82% of all NCD deaths worldwide (4). There is currently no cure for
NCDs and without treatment they result in a slow and painful death (9).
Burden of chronic diseases in developing countries
Although NCDs are a global challenge for the twenty-first century, they are more
felt and more devastating in developing countries (2, 10). Previously, NCDs were
mainly associated with the affluent, to the extent they were sometimes referred to
as “development diseases”. However, this is no longer the case, as NCDs are
accelerating at a faster rate in developing countries than they did in the developed
countries 50 years ago (11). Of the 38 million NCD deaths, three quarters (28
million) occur in developing countries (4) and 82% of the premature deaths as a
result of NCDs occur in developing countries (3). Despite the fact that NCDs are

3
leading causes of morbidity and mortality in low- and middle-countries (LMICs), the
prevention and control of NCDs is not a priority yet for most developing countries
(12, 13). Maher et al. argue that sub-Saharan Africa (SSA) has the greatest need
to improve the health system’s response to NCDs, as it experiences major NCD
deaths and does not have enough human and economic resources to effectively
respond to the rising double burden of communicable diseases (e.g. malaria and
tuberculosis) and NCDs (6).
In SSA, NCDs are the second leading cause of death. At the moment the burden of
communicable diseases still outnumbers that of NCDs as causes of death in SSA,
with 69% of deaths caused by communicable diseases (including tuberculosis and
malaria) in 2009 (14, 15). This situation is unique and more striking in SSA than
anywhere else in the world (14). However, as the epidemiological transition from
communicable to non-communicable in SSA continues the region will witness a
growing double burden of disease (14, 16). For example, it is estimated that the
number of people with hypertension will increase by 68% from 75 million in 2008 to
126 million in 2025 (17). Figure 0.1 illustrates the size of the double burden of
disease for LMICs compared to that in high income countries.
In developing countries, NCDs and communicable diseases do not just co-exist,
but interact with each other, whereby one exacerbates the other, leading to
multimorbidity (14-16). Moreover, Albreht et al. argue that worldwide the advances
in healthcare systems have transformed previously life-threatening diseases like
the human immunodeficiency virus (HIV) into chronic conditions requiring ongoing
care (18). In 2013 SSA had an estimated 24.7 million people living with HIV and
the acquired immune deficiency syndrome (AIDS), while also still carrying the
heavy burden of malaria cases (80% of 219 million cases worldwide) (17). While
tuberculosis is a well-known preventable and curable disease, the WHO report of
2013 estimated that SSA had 8.6 million incident cases (19).

4
Source: Lopez et al. (20)
Figure 0.1 Double burden of disease in low- and middle-income countries compared to high income countries
Developed countries have made considerable progress in focusing on and
addressing the burden of NCDs, whereas the developing world has paid less
attention to them, despite their rapid increase (6, 16). This is partly due to the latter
countries’ lack of funding and resources to effectively tackle the cumulative burden
of NCDs or their individual risk factors and the burden of communicable diseases
(16). On the other hand, the authorities of developing countries have also ignored
NCDs, because they are less visible, advance more slowly and are mostly
underdiagnosed (16). According to the International Diabetes Federation report of
2015, the African region had the highest proportion of undiagnosed diabetes,
where an estimated 14.2 million adults aged 20 to 79 had diabetes and over two
thirds of people with diabetes were undiagnosed (21).

5
Because of the lower visibility it took time for country leaders and policy makers to
acknowledge the challenge of NCDs while in the background these diseases were
causing the greatest damage (21). However, the high level United Nations (UN)
meeting of 2011 which brought heads of states together to discuss the issue of
NCDs, marks an onset of more consideration towards NCD control (9). Yet the
acknowledgement of the NCD burden does not always translate into the
development and application of policies to address NCDs. The greatest contributor
to the challenge of NCDs in Africa is the lack of political will in many states.
Because communicable diseases still claim more lives than NCDs, there is a
misperception that NCDs do not contribute that much to the burden of diseases
and therefore they are rarely on the national policy agenda (14).
The rising double burden of communicable and non-communicable diseases in
SSA is also linked to the question of sustainability in the field of health and
development. Alleyne et al. argue that as long as NCDs are present, it remains a
challenge to fully achieve health as an end goal of human development (7). The
current Sustainable Development Goals (SGDs) proposed by the United Nations
address the issue of NCDs as a target on the global health agenda for the first time
(22). Goal 3.4 of the SDGs is a target to “reduce by one third, by 2030, premature
mortality from NCDs through prevention and treatment and [to] promote mental
health and well-being” (23). The inclusion of NCDs into the SDGs was due to the
fact that the burden of NCDs needed a collective effort, as no country alone can
overcome the threat of NCDs (9, 24). Because NCDs act as a barrier to poverty
alleviation in all respects through a loss of productivity, premature deaths and high
costs for treatment, it is crucial to address them so that the relevant SDG can be
attained (2).
The role of self-management
Since NCDs are different from acute conditions in terms of duration and prognosis,
they require a different treatment approach (25). The available literature suggests
that the treatment of chronic disease can only be successful if it considers

6
psychological as well as medical factors, and promotes the quality of care of
services as well as enhancement of the autonomy of patients through therapeutic
education (26). Therefore, one of the critical success factors in the treatment of
NCDs is the self-management capacity of patients.
Self-management is defined by deSilva as “the actions individuals and carers take
for themselves, their children, their families and others to stay fit and maintain good
physical and mental health; meet social and psychological needs; prevent illness or
accidents; care for minor ailments and long term conditions; and maintain health
and wellbeing after an acute illness or discharge from hospital " (27) (p.1). Self-
management support refers to the actions undertaken by health professionals to
provide information and encourage patients to maintain greater control of their
condition and become capable of monitoring themselves and taking appropriate
action (27).
Because approximately 80 to 90 percent of the care for chronic patients lies in the
hands of individuals and their families, self-care is extensively required (27).
Therefore, the capacities of patients and families to manage their own illness and
care process are regarded as a key determinant of the treatment process. In order
to enhance these capacities, self-management education and support of chronic
patients is widely recommended. This especially holds true for patients in resource-
limited settings. Figure 0.2 depicts how self-management forms the core of chronic
disease management, whereby the healthcare providers assist by supporting the
patient. Some of the self-management actions to be performed by the patient
include taking medications, physical activity, eating healthy food and coping with
symptoms of the disease (25, 27, 28).
Self-management as an area of focus will be discussed in detail in Chapter 1 –
Towards self-management of chronic diseases.

7
Source: Centre for Managing Chronic Disease (29).
Figure 0.2 Self-management as the core component of care
An extensive literature shows that chronic disease self-management support and
education by health providers improves the way patients manage their conditions,
medication adherence, healthy behavior, self-efficacy, quality of life, and clinical
outcomes (27, 30). However, given the diversity of available self-management
programs and the relative scarcity of information regarding conditions for effective
implementation, further research is necessary before large-scale implementation in
LMICs can be recommended. In addition, the bulk of the literature on the
effectiveness of self-management programs is concerned with studies carried out
in developed countries. Consequently, their effectiveness in resource-limited
settings like SSA is not proven.
Recent literature reviews of health interventions implemented in SSA revealed that,
among other factors, linking interventions to the context of the target communities
improves the ownership of programs and acts as a facilitator to sustaining
interventions (17, 31). However, these reviews also mention that currently not
much attention is paid to sustainability, that programs tailored to the context and
the broader dynamic and complex health transition should be developed and
addressed in the region (17). Issues related to context in which this study was done
will be discussed in more detail in Chapter 2 – The South African context.

8
Research questions and objectives
To address the lack of evidence-based information regarding the effectiveness of
self-management programs for chronic diseases in resource-limited settings and
the conditions in which they must be implemented in order to be effective, the
current PhD study was undertaken. The overarching research question for this
research was:
What is the current status of self-management programs for chronic
disease management education in South Africa and how can they be
made more effective?
This broad question entails the following specific questions:
1. What is the current status of type 2 diabetes self-management education
programs in developing countries, and is there a difference between
countries with high and low mortality?
2. What policies and programs for diabetes education currently exist in South
Africa?
3. What are the experiences and needs of chronic disease patients and their
carers in South Africa with regard to self-management?
4. How feasible is the implementation of a contextually adapted self-
management education and support tool for diabetes and hypertension
patients?
5. What is the effectiveness of a self-management education and support tool
for diabetes and hypertension patients?
Based on these questions, the following study objectives were formulated, and
matching study designs were chosen to reach those objectives.

9
Objective Study design
• Review the current status of type 2 diabetes self-management education programs in developing countries in terms of contextual adaptation and catering for low health literacy
Systematic literature review
• Perform an audit by type and format of the current diabetes self-management education programs in South Africa
Cross-sectional
• Perform a needs analysis for self-management among chronic patients and health professionals in South Africa.
Qualitative
• Develop and test the feasibility of a contextually adapted self-management tool for diabetes and hypertension
Qualitative
• Pilot-test the effectiveness of the self-management tool with regard to health literacy and disease-specific knowledge
Quasi-experimental
Organization of the thesis
This thesis is organized around the five research questions and contains four
sections and ten chapters. Section One, which consists of the two first chapters,
provides the background for the study, in terms of the role of self-management in
addressing NCDs and the organization of the health care system in South Africa,
respectively. Section Two, which contains Chapters 3 and 4, presents two studies
assessing the current status of diabetes self-management education in developing
countries and specifically in South Africa. Section Three, consisting of chapters 5
through 8, looks at the development and testing of a contextually adapted self-
management education tool, and Section Four provides a summary and general
discussion of the findings, and presents a comprehensive protocol for a more
refined and larger effectiveness study of the self-management care-plan booklet.
Three chapters (Chapters 3, 4 and 5) are published papers, and two chapters
(Chapters 8 and 9) are manuscripts that have been submitted for publication. The
thesis ends with a general conclusion that details some of the conditions that may

10
need to be met for embarking on a larger implementation of an intervention. A
graphic overview of the section and chapter division of the thesis is provided in
Figure 0.3.
Figure 0.3 Overview of the thesis
A more detailed description of the four sections and chapters is given as follows:
Section 1: Background (Chapters 1 and 2)
In Chapter 1, we give a brief overview on self-management education and support,
its role and current status in the approach to chronic diseases. In Chapter 2, we
provide a detailed health system background of the study country, South Africa.
This background information describes the context in which this study was
conceived and carried out.

11
Section 2: Status of current interventions (Chapters 3 and 4)
As a start of our research, we looked at the current status of type 2 diabetes self-
management education (DSME) in high- and low-mortality developing countries by
way of a systematic review. This review and its results are discussed in Chapter 3.
For this review we extracted information on educational programs for type 2
diabetes and pre-diabetes. We extracted data on the content, the intervention,
strategy, duration, providers, the training of providers and the accessibility of
programs to people with low literacy. To extract information from eligible studies
retrieved we used the template for the global initiative for diabetes data collection
named Global Diabetes Survey (GDS) (32).
Chapter 4 presents the results of an audit of DSME conducted in seven of the nine
provinces of South Africa, with the intention to review the DSME policies and
guidelines presently available in South Africa, and to characterize the existing
DSME offered in both private and public healthcare sectors. The questions
addressed in the audit were to establish what types of DSME programs were
currently offered in different settings across the country, who implemented them,
what educational approaches were used, how the programs were structured, how
accessible they were, what challenges were faced, and to what extent they were
contextually and culturally sensitive. The results of this audit present a snapshot of
the current DSME status in South Africa.
Section 3: Development and testing of a self-management tool (Chapters 5, 6,
7 and 8)
In this section we first report on a qualitative study that was performed to explore
chronic patients’ experiences and perceived support needs and the perspectives of
key informants on patient self-management, with a view to develop contextually-
appropriate disease self-management support tools for chronic patients in South
Africa (Chapter 5). Focus group and individual interviews were conducted with
patients and individual interviews with key informants to address this issue.

12
The next chapter (Chapter 6) provides a detailed description of the development of
an individual care plan booklet as a self-management tool for diabetes and
hypertension in primary care facilities. The booklet was meant for use during
consultations with healthcare providers and to inform the patient on his or her
condition and the ways to manage it.
Chapter 7 presents a qualitative study conducted to explore the feasibility of the
use of the prototype of an individual care-plan booklet as a self-management tool
for diabetes and hypertension in primary care facilities in South Africa. For this
study which addressed the question whether this care-plan tool would work, focus
group and individual interviews were held with patients and providers to solicit their
perspectives on the care-plan booklet. Bowen et al. eight focus areas for feasibility
studies were used as a point of departure (33).
Lastly in this section, Chapter 8 reports on a quasi-experimental pilot study with
diabetic and hypertensive patients to test the potential effectiveness of the use of a
care-plan booklet. This chapter answers the question: Does the use of a self-
management booklet for diabetes and hypertension have an effect on health
literacy and disease-specific knowledge?
Section 4: Main findings and comprehensive study protocol (Chapters 9 and
10)
The last section starts with Chapter 9 which summarizes and discusses the main
findings of the different studies of this thesis. Chapter 10 (last chapter) details a
comprehensive protocol for a larger study that draws on the lessons learned from
the pilot and feasibility studies. This chapter could form the basis for a
methodologically more rigorous study to test the effectiveness of the care-plan
booklet and for further development and improvement of the intervention in future
research.
It is to be noted that the empirical work reported in this thesis focuses mainly on
diabetes. Hypertension was included at a later stage to align the study more

13
closely with the recent policy changes in the country of study (South Africa).
Whereas previously chronic diseases were considered separately, the adoption of
an integrated chronic-disease model in 2011 (34) called for a more horizontal and
integrated approach that made it less obvious to distinguish between chronic
diseases in practice. Furthermore, the studies in the thesis also report mostly on
type 2 diabetes and do not consider type 1 diabetes. In South Africa, type 1
diabetic patients are seen and managed at hospital level, and only under special
circumstances would a patient be transferred to a primary care facility. Since this
project was done in primary care facilities, it made more sense to focus on type 2
diabetic patients only.
References
1. Beaglehole R, Bonita R, Horton R, Adams C, Alleyne G, Asaria P, et al.
Priority actions for the non-communicable disease crisis. Lancet. 2011;377(9775):1438-47.
2. World Health Organization. Global status report on noncommunicable diseases 2014; Geneva: World Health Organization; 2014 [cited 17 July 2016]. Available from: http://apps.who.int/iris/bitstream/10665/148114/1/9789241564854_eng.pdf?ua=1.
3. World Health Organization. Chronic diseases and health promotion: Integrated chronic disease prevention and control. Geneva: World Health Organization; 2016 [cited 20 July 2016]. Available from: http://www.who.int/chp/en/.
4. World Health Organization. Noncommunicable diseases. Fact sheet. [Internet]. 2014 [cited 07 November 2014]. Available from: http://www.who.int/mediacentre/factsheets/fs355/en/.
5. World Health Organization. Global status report on non-communicable diseases; 2010. [cited 05 August 2016]. Available from: http://apps.who.int/iris/bitstream/10665/44579/1/9789240686458_eng.pdf.
6. Maher D, Ford N, Unwin N. Priorities for developing countries in the global response to non-communicable diseases. Global Health. 2012;8:14.
7. Alleyne G, Binagwaho A, Haines A, Jahan S, Nugent R, Rojhani A, et al. Embedding non-communicable diseases in the post-2015 development agenda. Lancet. 2013;381(9866):566-74.
8. Puoane T, Tsolekile L, Sanders D, Parker W. Chronic non-communicable diseases. In: Barron P, Roma-Reardon,J, editors. South African Health Review 2008. Durban: Health Systems Trust; 2008. p. 73-87.

14
9. Beaglehole R, Bonita R, Alleyne G, Horton R, Li L, Lincoln P, et al. UN High-level meeting on non-communicable diseases: addressing four questions. Lancet. 2011;378(9789):449-55.
10. Mendis S. Research is essential for attainment of NCD targets and Sustainable Development Goals. Glob Heart. 2016;11(1):139-40.
11. World Health Organization. The global burden of disease. Geneva: World Health Organization; 2016 [cited 19 July 2016]. Available from: http://www.who.int/nutrition/topics/2_background/en/print.html.
12. Mishra SR, Neupane D, Preen D, Kallestrup P, Perry HB. Mitigation of non-communicable diseases in developing countries with community health workers. Global Health. 2015;11:43.
13. Islam SM, Purnat TD, Phuong NT, Mwingira U, Schacht K, Froschl G. Non-communicable diseases (NCDs) in developing countries: a symposium report. Global Health. 2014;10:81.
14. de-Graft Aikins A, Unwin N, Agyemang C, Allotey P, Campbell C, Arhinful D. Tackling Africa's chronic disease burden: from the local to the global. Global Health. 2010;6:5.
15. Young F, Critchley JA, Johnstone LK, Unwin NC. A review of co-morbidity between infectious and chronic disease in Sub Saharan Africa: TB and diabetes mellitus, HIV and metabolic syndrome, and the impact of globalization. Global Health. 2009;5:9.
16. Yach D, Hawkes C, Gould CL, Hofman KJ. The global burden of chronic diseases: overcoming impediments to prevention and control. JAMA. 2004;291(21):2616-22.
17. Iwelunmor J, Blackstone S, Veira D, Nwaozuru U, Airhihenbuwa C, Munodawafa D, et al. Toward the sustainability of health interventions implemented in sub-Saharan Africa: a systematic review and conceptual framework. Implement Sci. 2016;11:43.
18. Albreht T, Dyakova M, Schellevis FG, Van den Broucke S. Many diseases, one model of care. JOC. 2016;6(1):12-20.
19. World Health Organization. World malaria report 2013. Geneva: World Health Organization; 2014 [cited 17 July 2016]. Available from: http://www.who.int/malaria/publications/world_malaria_report_2013/en/.
20. Lopez A, Mathers CD, Ezzati M, Jamison,DT, Murray CJL. Global burden of disease and risk factors. Washington, DC: The World Bank Group, 2006.
21. International Diabetes Federation. IDF Diabetes Atlas, 7th edn. Brussels, Belgium: International Diabetes Federation; 2015 [cited 20 January 2016]. Available from: http://www.diabetesatlas.org/resources/2015-atlas.html.
22. Hawkes C, Popkin BM. Can the sustainable development goals reduce the burden of nutrition-related non-communicable diseases without truly addressing major food system reforms? BMC Med. 2015;13:143.
23. World Health Organization. Health in 2015 from MDGs, Millenium Development Goals to SDGs, Sustainable Development Goals. Geneva: World Health Organization 2015.
24. Buse K, Hawkes S. Health in the sustainable development goals: ready for a paradigm shift? Global Health. 2015;11:13.

15
25. Bodenheimer T, Lorig K, Holman H, Grumbach K. Patient self-management of chronic disease in primary care. JAMA. 2002;288(19):2469-75.
26. Fond-Harmant L. [Diabetes plans in six European countries and in Canada]. Santé Publique. 2011;23(1):41-53.
27. deSilva D. Evidence. Helping people help themselves. A review of evidence considering whether it is worthwhile to support self-management. London: The Health Foundation; 2011 [cited 14 March 2015]. Available from: http://www.health.org.uk/publication/evidence-helping-people-help-themselves.
28. Lawn S, Schoo A. Supporting self-management of chronic health conditions: common approaches. Patient Educ Couns. 2010;80(2):205-11.
29. Centre for Managing Chronic Disease. About chronic disease 2016 [cited 10 October 2016]. Available from: http://cmcd.sph.umich.edu/about/about-chronic-disease/.
30. Cunningham P. Patient perceptions of clinician self-management support for chronic conditions. Am J Manag Care. 2016;22(4):e125-33.
31. Amazigo U, Okeibunor J, Matovu V, Zoure H, Bump J, Seketeli A. Performance of predictors: evaluating sustainability in community-directed treatment projects of the African programme for onchocerciasis control. Soc Sci Med. 2007;64(10):2070-82.
32. Schwarz PE, Gallein G, Ebermann D, Muller A, Lindner A, Rothe U, et al. Global Diabetes Survey – an annual report on quality of diabetes care. Diabetes Res Clin Pract. 2013;100(1):11-8.
33. Bowen DJ, Kreuter M, Spring B, Cofta-Woerpel L, Linnan L, Weiner D, et al. How we design feasibility studies. Am J Prev Med. 2009;36(5):452-7.
34. Asmall S, Mahomed O. Integrated chronic diseases management manual. National Department of Health of South Africa; 2011 [cited 10 June 2014]. Available from: http://www.kznhealth.gov.za/family/Integrated-chronic-disease-management-manual.pdf.

16

17
CHAPTER 1: Towards a model of self-management for
chronic diseases

18
Introduction
In this chapter, we summarize the literature on the concept of self-management, its
introduction in the chronic care model, its current status in the management of
chronic disease and its differentiation to health education. In the general
introduction we have already introduced the concept of self-management in chronic
disease care.
The need for self-management in chronic care
Due to the growing number of chronic diseases in low-and-middle income countries
(LMICs) there is a great burden on the health system in terms of rising cost (1).
Van Olmen et al. argue that current efforts of both high-income and low-income,
developing countries are not enough to address the burden of non-communicable
diseases (NCDs) (1). They further note that the provider-centered models
introduced in high-income countries are labor intensive and therefore too
expensive and unsustainable for countries with limited resources (1). These
“paternalistic” models have been seen to produce poor results as they do not take
the chronic nature of the diseases into consideration and do not sufficiently
account for the role of the patients in the care and management of chronic
diseases (2, 3). For LMICs countries like in sub-Saharan Africa (SSA), provider-
centered models of care are not even possible because of inadequate human
resources and the high expenditures involved (1). In 2007 Anyangwe et al. pointed
out that SSA is among the regions with a highest need of healthcare but also lacks
human resources for health. As a result, SSA accommodated 11% of the world’s
population by 2007 and had a 24% share of the global burden of disease, but only
3% of the human resources to address the problem (4).
As noted earlier, NCDs are sometimes referred to as chronic diseases. According
to van Olmen et al. the definition of chronic diseases encompasses the fact that
they are “life-long conditions requiring long-term medical interventions and
adherence to medication and adjustments in life” (1) (p. 2). Although this definition
also includes conditions like the human immunodeficiency virus /acquired immune

19
deficiency syndrome (HIV/AIDS), it is a good fit for LMICs, especially in SSA, which
is currently undergoing the epidemiological transition from communicable to non-
communicable diseases (5, 6). As chronic diseases are life-long and persist over
time, there will be an increase in prevalence. This will, in turn, lead to an increasing
demand for healthcare services, thereby placing even more strain on the already
weak healthcare systems (1, 7, 8). Apart from straining costs for the healthcare
system, chronic diseases also place financial strains on families and individuals
and on society overall, as payment for hospitals care is sometimes an out-of-
pocket expense (1).
On the other hand, before the advent of chronic diseases, health systems were
focused on a paternalistic model where health professionals were the experts and
bringers of solutions, while patients were rather passive and on the receiving side
of advice from experts (9). This paternalistic model was perfect for treating acute
illnesses that are short in duration and for which medical adherence is not really a
problem, because patients know that if they stick to the regimen they will get better
(9). In contrast, chronic diseases are conditions that do not disappear and for which
affected people have to adjust their lifestyles in order to remain healthy (1). With
the advent of chronic diseases there is a change in the roles of patients from being
passive recipients of care to becoming active experts in managing their conditions,
while health service providers are partners.
Van Olmen et al. argue that people with chronic diseases are still people with
normal lives to live, having needs that are related to their conditions and also social
and economic needs. Upon diagnosis, these people have to change their lifestyles
to fit in the new element of their lives, where they have to experience the chronic
diseases every day for the rest of their lives (1). In order to get better a person has
to mobilize the available social, cultural, physical or medical resources. The
dynamic process involved after a person is diagnosed is described as “rebalancing”
(1). Table 1.1 gives an outline of differences in care between acute and chronic
conditions.

20
Table 1.1 Care differences between acute and chronic conditions
Acute care Chronic care
Cure available and expected Improvement of symptoms and impact on psycho-social life, but no cure expected
Short-term duration On-going care; often attached to stigma and discrimination
Short-term goals for a short period to achieve health outcomes
Health outcomes achieved by short-term goals for a longer period
The expert is the health professional
The patient is the expert through living with the condition
Directive and expected adherence to medication and health enhancing activities
Negotiation and cooperation is expected
Quality of life is a result of short-term professional care
Quality of life is a result of patient’s self-management and decision making and the on-going provision of support services
Source: Lawn et al. 2010 (9)
Bodenheimer et al. argue that in chronic diseases, unlike in acute conditions,
patients themselves are the principal caregivers and health professionals act as
consultants in supporting the patients (3). While patients only consult with health
professionals periodically, much of the time they are at home without the support of
health professionals and still have to constantly make choices that affect their
chronic condition (1). These decisions include, for example, whether they will
exercise, eat healthy, adhere to medication, or go for follow-up visits (1, 3, 9).
Lawn et al. argue that, therefore, an effective health service support is defined by
the existence of health professionals who understand the complexity of disease
management by patients (9). Van Olmen et al. add that the long-term nature of
chronic conditions and the effects that patients themselves have on the course of
development of their illness present an opportunity for them to learn and become
experts on their conditions (1). Shaw and Baker noted that in this “chronic condition
journey” some patients gain truly amazing experience as experts (2). It is therefore

21
clear that what patients need is not a lecture from health providers, but a web of
support that will enable them to cope and adjust their lifestyles.
Healthcare providers obviously have a great deal of knowledge about the disease
in general, but patients are experts in living with the condition itself and how it
makes them feel (1). For instance, only patients coming for medical consultations
really know what has happened prior to consultation. They know if they adhered to
the treatment or not, and for many reasons might decide not to share this
information with their health provider. In their attempt to fit in the “normative,
biomedical expectations of correctness”, patients may choose to offer socially
desirable rather than true answers during counseling or may even follow a healthy
lifestyle only a few days before the next medical consultation in order to make sure
that vital signs are in normal range (1, 10-12). In instances like these, if patients are
not taken as experts and respected for their role, the health professional will
assess patients according to his or her own expertise and make wrong decisions
for the treatment. Van Olmen et al. refer to this situation where the patient has
more information that can be used to make treatment decisions, rather than relying
only on the doctor’s knowledge only as “reverse asymmetry of information”, (1).
Therefore, people with chronic diseases not only need to be in the center of the
receiving care, but also need to be active and fully responsible for their condition.
To achieve this they need a lot of support from different stakeholders, including
families, healthcare providers and the social environment (1).
Supporting self-management in chronic care
As noted earlier, self-management support refers to the assistance that healthcare
providers and other caregivers can provide to patients in order to enable and
encourage them to make daily decisions to achieve better health (13). It
encompasses the process of making multi-level modifications in the health systems
and the community to enable patients to self-manage their disease(s) (14). In this
process, self-management education plays a pivotal role (1).

22
It is important to note that self-management education is different from patient
education, although the terms are sometimes used interchangeably. Traditional
patient education refers to providing disease-specific information to patients and
enhancing the technical skills that are necessary to control their disease, in the
assumption that better knowledge and skills will lead to better compliance with the
medical prescriptions and treatment. In contrast, self-management support
increases the health providers’ role from just giving out information to one of
helping patients and their families in building confidence and making decisions that
improve the management of the disease, which will consequently lead to better
outcomes (14). Self-management does not replace health services, but
complements them by building skills that can be applied at home and in routine
health consultations (15). Table 1.2 summarizes the difference between self-
management education and traditional patient education.
The chronic care model
The introduction of the concept of self-management in chronic diseases has to a
large extent been influenced by the chronic care model (CCM). The CCM is one of
the most significant models in chronic disease treatment and care. It is based on
the principle that, through proper training and support, many people can change
the advancement of disease by actively managing their own health (16). According
to the CCM model, certain health systems improve health outcomes through the
interactions between patients and providers (17). These health systems have
characteristics that include, among other aspects, a form of self-management
support that gives patients the priority to increase confidence and skills in
managing their own illnesses (17).

23
Table 1.2 Comparison of patient education and self-management
Patient education Self-management education
Supporting theory
Disease-specific knowledge leads to behavior change, which produces better clinical outcomes
Self-efficacy (confidence in life-improving activities) leads to better clinical outcomes
Content Technical skills and information about the condition
Skills and techniques on how to overcome problems
Formation of problems
Problems are a result of poor control of disease
Patient’s experienced problems are identified but may or may not be linked to the disease(s)
Goal of education
Patient must comply with behavior changes taught in order to improve outcomes
Patients increase self-efficacy in order to reach better outcomes
Link between education and the disease
Disease-specific education Education includes problem-solving skills in relation to chronic conditions
The educator The health professional Wide range of providers, including peers, health professionals, etc.
Source: Bodenheimer et al. 2002 (3)
The CCM model further argues that the management of chronic disease is best
achieved by productive interactions between a patient and the health system team
operating within a setting characterized by a reliable, evidence-based approach to
self-management (16). It considers six elements essential to chronic care: self-
management support, delivery system design, decision support, clinical information
systems, community resources, and healthcare organizations (17, 18). Figure 1.1
shows a graphic depiction of the CCM and its respective elements.

24
Source: Wagner, 1998 (17) Figure 1.1 The chronic care model
The self-management support element empowers and prepares patients to
manage their conditions, while emphasizing the role the patient plays in managing
his or her own health. The delivery system design assures the delivery of effective,
efficient clinical care and self-management support. The decision support promotes
clinical care consistent with scientific evidence and patient preferences. Clinical
information systems organize patient and population data to facilitate efficient and
effective care. Community resources and policies mobilize resources of the
community to meet the needs of patients. Finally, the health system creates an
organizational culture and strategies that promote safe and high quality care (17,
18).
In an effort to assist health systems in member countries to meet the increasing
challenges of chronic care, the World Health Organization (WHO) established a
framework entitled the Innovative Care for Chronic Conditions (ICCC): Building

25
Blocks for Action (19, 20). This framework and its building blocks are relevant for
both prevention and disease management for chronic diseases in healthcare
systems. The model places the patient and family, the community and the health
system in the center, with support of the larger healthcare organization, community
and policy environments (19). Although the ICCC model has been criticized
because it does not include issues of multi-morbidity, in LMICs like South Africa, it
is already applied for patients presenting with comorbidities (19).
Models of or approaches to self-management
To help implement self-management in practice, different models of self-
management have been developed and used in a variety of countries and settings
to aid health professionals to provide self-management support to patients (9).
These self-management models differ in many ways: how they are delivered;
where they are delivered; who delivers them; and how participants are recruited
(21). Despite these differences, however, they all attempt to provide a reliable,
organized approach to self-management support, while ensuring that core
minimum levels of best practice are achieved (9). Some of the more well-known
models and approaches are described below, namely motivational interviewing,
health coaching, the 5As model, the Chronic Disease Self-Management Program
(CDSMP) and the Flinders Program.
Motivational interviewing approach
Motivational interviewing is defined as “a collaborative conversation style for
strengthening a person’s own motivation and commitment to change” (22) (p. 12).
This patient-centered, non-judgmental approach was developed by specialists in
the field of addiction, especially alcohol. The principles of this approach include the
expression of empathy through reflective listening, developing a discrepancy
between where one is currently and where one wants to be, rolling with resistance,
assuming that the client is responsible for the decisions, and supporting self-
efficacy (9, 23). One of the main strengths of this approach is its potential
application in many different settings because of its flexibility and the suitability for

26
many patients with chronic diseases. Its main disadvantages are the extensive
training that is required for people who are not experienced in counseling, and the
lack a formal structure (9).
Health coaching approach
Health coaching is an approach in healthcare that uses principles of psychology,
coaching and counseling to assist people to achieve behavior change that
improves health outcomes (24). Health coaching can be done by a peer or a health
professional to support a chronic patient in becoming active in chronic disease self-
management. It can also involve telephone coaching. This approach is introduced
in a one- to two-day workshop and uses motivational interviewing and cognitive
behavioral approaches (9, 24). The flexibility of this approach and the application of
techniques at any stage of client readiness for change are some of the advantages
(9, 24).
The 5As model
Originally developed in the United States of America (USA) for smoking
interventions, the 5As model is currently used in primary care settings to provide
structure to communication between patients and healthcare providers (9). 5As
stands for:
Assess – asking about behavior
Advise – provide a clear message of reinforcement for change
Agree – establish and set goals founded upon readiness for change
Assist – in the gaining of skills, knowledge and support
Arrange – provide referrals and plan follow up
The framework can be followed by any trained professional, regardless of discipline
and level of experience. Its main disadvantage, however, is that in most cases it
can only be used as a short intervention because of time constraints (9).

27
The Stanford Chronic Disease Self-Management Program
The Chronic Disease Self-Management Program model was developed at Stanford
University’s School of Medicine in the 1990s. The program evolved from the
realization that the arthritis self-management program developed in the 1980s by
the same university had self-management skills common to a range of chronic
diseases (9, 24, 25). The CDSMP program is based on the theory of self-efficacy
and involves a peer-led, group-based approach with 10 to 15 participants meeting
for six weeks (26). Group leaders who include health professionals and peer-
leaders are trained for three days to conduct the program. The course involves
skills such as goal setting, action planning, healthy living, problem solving,
communication and working in partnership with health professionals (9).This model
is also used by the United Kingdom Expert Patient Program (27). A randomized
controlled trial evaluating the CDSMP over a three year period using self-efficacy,
healthcare utilization, health status, and self-management behaviors as outcome
indicators showed significant improvements in communication with providers,
physical activity, and less healthcare utilization (28, 29). The strengths of this
model revolve around the facilitation of empowerment through sharing and peer
learning. Its main limitations are that it is time limited and that not everyone is
comfortable in a group environment (9, 24).
The Flinders Program
The Flinders model was developed by the Flinders University’s Department of
Human Behaviour and Health Research in Australia in the 1990s (9, 30). This
program uses an individual patient-centered approach and care planning process
to facilitate behavioral change by incorporating motivational interactions between
patient and health providers. It is a one-on-one process requiring assessment and
care planning through standardized forms and tools. Providers attend a two-day
training course and submit case studies as part of training. The strength of this
model is the fact that it is individualized and person centered, whereas its main
limitation is its time-intensiveness (9, 30).

28
Conclusion
As chronic diseases require extensive self-care, self-management is crucial in
improving health and behavior outcomes. The previously “passive” patient concept
is rapidly being replaced by the “active” patient concept. As noted, self-
management does not replace care but complements the other components of
care. While different approaches to self-management exist, the end goal is always
to support patients in managing their condition. In this thesis we present studies
that look at the challenges related to the implementation of self-management
education in developing countries, using South Africa as a case exemplar. Before
doing so, however, the next chapter will outline the context in which these studies
were conducted by giving the reader an overview of the health system in South
Africa.
References
1. van Olmen J, Ku GM, Bermejo R, Kegels G, Hermann K, Van Damme W. The growing caseload of chronic life-long conditions calls for a move towards full self-management in low-income countries. Global Health. 2011;7:38.
2. Shaw J, Baker M. "Expert patient" – dream or nightmare? Br Med J (Clin Res Ed). 2004;328(7442):723-4.
3. Bodenheimer T, Lorig K, Holman H, Grumbach K. Patient self-management of chronic disease in primary care. JAMA. 2002;288(19):2469-75.
4. Anyangwe SC, Mtonga C. Inequities in the global health workforce: the greatest impediment to health in sub-Saharan Africa. Int J Environ Res Public Health. 2007;4(2):93-100.
5. Young F, Critchley JA, Johnstone LK, Unwin NC. A review of co-morbidity between infectious and chronic disease in Sub Saharan Africa: TB and diabetes mellitus, HIV and metabolic syndrome, and the impact of globalization. Global Health. 2009;5:9.
6. de-Graft Aikins A, Unwin N, Agyemang C, Allotey P, Campbell C, Arhinful D. Tackling Africa's chronic disease burden: from the local to the global. Global Health. 2010;6:5.
7. de-Graft Aikins A, Boynton P, Atanga LL. Developing effective chronic disease interventions in Africa: insights from Ghana and Cameroon. Global Health. 2010;6:6.

29
8. Barlow J, Wright C, Sheasby J, Turner A, Hainsworth J. Self-management approaches for people with chronic conditions: a review. Patient Educ Couns. 2002;48(2):177-87.
9. Lawn S, Schoo A. Supporting self-management of chronic health conditions: common approaches. Patient Educ Couns. 2010;80(2):205-11.
10. Werner A, Malterud K. It is hard work behaving as a credible patient: encounters between women with chronic pain and their doctors. Soc Sci Med. 2003;57(8):1409-19.
11. Vermeire E, Hearnshaw H, Ratsep A, Levasseur G, Petek D, van Dam H, et al. Obstacles to adherence in living with type-2 diabetes: an international qualitative study using meta-ethnography (EUROBSTACLE). Prim Care Diabetes. 2007;1(1):25-33.
12. Edwards M, Davies M, Edwards A. What are the external influences on information exchange and shared decision-making in healthcare consultations: a meta-synthesis of the literature. Patient Educ Couns. 2009;75(1):37-52.
13. Schaefer J, Miller D, Goldstein M, Simmons L. Partnering in self-management support: a toolkit for clinicians. Cambridge, MA: Institute for Healthcare Improvement; 2009 [cited 24 July 2016]. Available from: http://www.improvingchroniccare.org/downloads/selfmanagement_support_toolkit_for_clinicians_2012_update.pdf.
14. Coleman MT, Newton KS. Supporting self-management in patients with chronic illness. Am Fam Physician. 2005;72(8):1503-10.
15. deSilva D. Evidence. Helping people help themselves. A review of evidence considering whether it is worthwhile to support self-management. London: The Health Foundation; 2011 [cited 14 March 2015]. Available from: http://www.health.org.uk/publication/evidence-helping-people-help-themselves.
16. Johnston S, Liddy C, Ive SM, Soto E. Literature review on chronic diseases self-management. Toronto: SCO Health Service and Élisabeth Bruyère Research Institute; 2008 [cited 04 August 2016]. Available from: https://www.livinghealthynortheast.ca/Portals/0/Documents/Literature%20Review%20on%20Chronic%20Disease%20Self%20Management.pdf.
17. Wagner EH. Chronic disease management: what will it take to improve care for chronic illness? Eff Clin Pract. 1998;1(1):2-4.
18. Improving Chronic Illness Care (ICIC). The Chronic Care Model [cited 04 August 2016]. Available from: http://www.improvingchroniccare.org/index.php?p=The_Chronic_Care_Model&s=2.
19. Oni T, McGrath N, BeLue R, Roderick P, Colagiuri S, May CR, et al. Chronic diseases and multi-morbidity: a conceptual modification to the WHO ICCC model for countries in health transition. BMC Public Health. 2014;14:575.
20. World Health Organization. Innnovative care for chronic conditions: building blocks for action. Genevea: World Health Organization; 2002. [cited 18 January 2017]. Available from: http://www.who.int/chp/knowledge/publications/icccglobalreport.pdf?ua=1.

30
21. Lake AJ, Staiger PK. Seeking the views of health professionals on translating chronic disease self-management models into practice. Patient Educ Couns. 2010;79(1):62-8.
22. Miller W, Rollnick S. Motivational interviewing: helping people change. 3rd ed. New York: Guildford Press; 2013.
23. Emmons KM, Rollnick S. Motivational interviewing in health care settings: opportunities and limitations. Am J Prev Med. 2001;20(1):68-74.
24. Department of Health, Victoria, Australia. Common models of chronic disease self-management: a fact sheet for primary care partnerships [Internet]. [cited 04 August 2016]. Available from: http://vicpcp.org/wp-content/uploads/2015/10/Common-models-of-chronic-disease.pdf.
25. Stanford Patient Education Research Center. Chronic disease self-management program. [Internet]. 2016 [cited 04 January 2016]. Available from: http://patienteducation.stanford.edu/programs/cdsmp.html.
26. Lorig KR, Sobel DS, Stewart AL, Brown BW, Bandura A, Ritter P, et al. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: a randomized trial. Med Care. 1999;37(1):5-14.
27. Wilson PM, Kendall S, Brooks F. The Expert Patients Programme: a paradox of patient empowerment and medical dominance. Health Soc Care Community. 2007;15(5):426-38.
28. Lorig KR, Ritter P, Stewart AL, Sobel DS, Brown BW, Bandura A, et al. Chronic disease self-management program: 2-year health status and health care utilization outcomes. Med Care. 2001;39(11):1217-23.
29. Lorig KR, Ritter PL, Laurent DD, Plant K. Internet-based chronic disease self-management: a randomized trial. Med Care. 2006;44(11):964-71.
30. Flinders Human Behaviour & Health Research Unit (FHBHRU), Flinders University. The Flinders Program™ for Chronic Condtion Management; 2010 [cited 04 August 2016]. Available from: http://www.flinders.edu.au/medicine/fms/sites/FHBHRU/documents/publications/FLINDERS%20PROGRAM%20INFORMATION%20PAPER%20FINAL_M.pdf.

31
CHAPTER 2: The South African health context

32
Introduction
Although chronic conditions are generic and global, their manifestations and
determinants are largely defined by local conditions and contextual influences.
Addressing these determinants therefore requires context relevant interventions
(1). Depending on the way health problems are manifested and the resources that
are available in a country, actions that can be undertaken to tackle these problems
differ. Related to this, it is a well-known fact that patient education and self-
management education are more effective when they are adapted to the context.
The seminal work of Kreuter et al (2) on cultural tailoring shows how culturally
sensitive interventions can be developed by adapting existing materials and
programs to the needs of the population. This adaptation depends on the beliefs
people hold and what is going on around them (3, 4).
The adaptation of self-management education to the specific situation in South
Africa is at the core of the studies presented in this thesis. However, in order to be
able to adapt an intervention to the local context, an understanding of this context
is required. While the contextual needs of patients and healthcare providers will be
addressed elsewhere in specific chapters of the thesis, it is also important to have
an understanding of the healthcare system. In this chapter we will introduce the
context in which the studies presented in this thesis were performed by providing
the reader with a background of the structure of the health system in South Africa.
In their description of realist evaluation Marchal and colleagues consider context as
“actors or other factors that are external to the intervention, present or occurring
even if the intervention does not lead to an outcome, and which may have an
influence on the outcome” (5) (p. 207). Contextual factors include institutional
facilitating factors (e.g. availability of resources) and society’s influencing factors
(e.g. socio-cultural aspects) (6). The current project focused on South Africa, which
is a middle-income country with a high mortality and characterized by a limitation of
resources for healthcare.

33
Like many sub-Saharan African (SSA) countries, South Africa is currently
undergoing an epidemiological change. The simultaneous occurrence of
communicable diseases and a rapid rise of non-communicable diseases (NCDs)
seen more notably after the political independence of 1994 are complemented by a
heavy burden of perinatal and maternal conditions, injury and violence (7). In 2011,
South Africa had a gross domestic product (GDP) of US$364, and in 2009/2010,
about 8.6% GDP was used on health delivery, which is similar to developed
countries like England. However, the large investment in health does not translate
into better health outcomes (8). In 2004, the World Health Organization (WHO)
estimated that the burden of NCDs in South Africa was three to four times higher
than in developed countries and in 2012 NCDs accounted for 43% of all deaths in
South Africa (9, 10).
One element in this situation is the high prevalence of infections with human
immunodeficiency virus (HIV) in South Africa. As a result of the widespread provi-
sion of antiretroviral treatment (ART), the acquired immune deficiency syndrome
(AIDS) caused by HIV is now being approached differently. HIV/AIDS has been
transformed to a chronic disease, with infected people living longer and developing
other NCDs similar to the rest of the population. Research has also shown that
other NCDs can develop as a result of side effects from medicines used in ART
(11, 12). Because of the transformation of previously acute conditions to chronic
diseases and the co-existence of HIV/AIDS with chronic NCDs, a pattern of
multimorbidity different from developed countries is evolving in low- and middle-
income countries (LMICs) (13).
The formal healthcare sector in South Africa
South Africa has a number of healthcare systems that sometimes complement
each other or sometimes run parallel to each other. The formal healthcare sector
has two tiers, a public sector and a private sector. Parallel to the formal western-
medicine based health system is the healthcare provided by traditional healers.
Some South Africans access both formal and traditional healthcare, with the

34
National Department of Health making an effort in formal regulation of the
traditional healers (11, 14, 15).
The formal private sector in South Africa offers services to about 17% of the
population and is responsible for 48% (US$13 billion per annum) of the total
national health expenditure. On the other hand, the state-funded public healthcare
system provides care to about 83% of the population and spent about US$14.5
billion per annum in 2013/2014. Because of the major burden of management and
treatment of diseases in the public health sector, about 11% of the government’s
annual budget is spent on healthcare, which is more than the 5% recommended by
the WHO. Major contributions are currently attributed to HIV and tuberculosis (TB)
and the high burden in the public health sector is aggravated by high levels of
unemployment and poverty. However, despite major efforts in the management
and treatment of disease, health outcomes are still poor compared to other middle-
income countries (11, 15, 16).
The public health system consists of primary healthcare (PHC) and three levels of
hospitals (district, regional and tertiary hospitals). PHC institutions are the first point
of patient contact with the health system and provide services free of charge.
Patients who need advanced treatment are referred to a district hospital, from
where they may be further referred to a regional or tertiary hospital for more
advanced care. South Africa’s private health system ranks among the top four
health systems in the world after Switzerland, the Netherlands and Belgium (15).
The private health system comprises health professionals providing private
services that are mainly funded from medical aid subscriptions. Complementary to
the two-tier health system are non-governmental organizations (NGOs) that use
donor funding to provide services, especially for HIV/AIDS and TB (11, 16).
The public health system is already facing enormous challenges, including
inequitable distribution of health personnel, inefficient and inequitable resource
allocation, and a curative-oriented health service (11). According to the WHO, as
cited in Jobson (16), one clinic should serve about 10,000 people. In South Africa,

35
one clinic on average serves 13,718 people, with an average of 2.5 visits per
person per year. The private health sector includes 73% of general practitioners,
with an average of 243 patients per doctor compared to the public health sector
with one doctor serving an average of 4,219 patients (16).
The growth in population from around 21 million in 1994 to around 52 million in
2013 highlights the need for more healthcare workers. In response, community
health workers (CHWs) have been employed to fill in this void and provide
voluntary, counseling and testing, TB treatment monitoring and home-based care.
More resources are allocated to preventative measures in order to limit the number
of people who develop complications (16).
Health inequalities in South Africa
The origins of health inequalities in South Africa emanate from discrimination
based on race and gender that was embedded in the apartheid history of the
country (17). Before political independence in 1994, there were policies on political,
economic and land restrictions according to one’s race, gender and age-based
hierarchies and these significantly impacted access to basic resources like health
services (17, 18). South Africa is a multiracial country with Africans constituting
around 79.2 percent of the general population alongside the minority populations
(whites, coloreds and Indians). Due to these historical discriminations, South Africa
is one of the countries with the highest Gini coefficient (the most used indicator of
income inequality with 0 meaning no inequality and 1 signifying great inequalities).
In 2005, South Africa had 0.73 percent Gini coefficient showing great inequalities
among the population (18). The government is trying to address the impact of
poverty and unemployment through social grants and South Africa is among the
few developing countries with this kind of system (17, 19). However, despite the
existence of social grants, many households remain poor with limited access to
health services. This then called for the restructuring of the health system and the
introduction of the National Health Insurance (NHI).

36
Restructuring of the public health system
South Africa is one of the countries that are currently implementing universal health
coverage, called the National Health Insurance (NHI). Universal health coverage is
defined as “the provision of primary healthcare services that are accessible,
equitable and responsive to the needs of target communities” (20) (p. 1). As the
double burden of diseases increases in South Africa, it will be a challenge to
provide affordable and effective healthcare to the increasing number of people
affected (20, 21). The NHI is planned to be phased in over a 14-year period, with
pilot districts starting in 2012. An ideal health system is suggested to have the six
building blocks consisting of (1) human resources, (2) medicines and technology,
(3) universal health coverage, (4) information systems, (5) financing and
governance, and (6) service delivery. However, maintaining these building blocks
will be a challenge for most resource-limited settings like South Africa, as the
double burden of disease further weakens the health system (16, 20, 22).
In the NHI, PHC is being re-engineered and services are provided through three
streams:
• Municipal ward-based outreach teams (WBOTs) provide health promotion
through community involvement. Each municipal ward has a team led by a
health professional. Each team serves a specific number of the allocated
households.
• District-based clinical specialist support teams (DCSTs) comprise a team
of health specialists addressing priority health-care programs in reducing
maternal and child mortality and improve general health outcomes.
• School health services in a form of health promotion, with preventive and
curative services provided by professional nurse-led teams to address the
needs of school-going children (16).

37
The South African Integrated Chronic Disease Management model
As part of their PHC re-engineering efforts the South African government recently
adopted the Integrated Chronic Diseases Management (ICDM) model based on the
WHO’s “Innovative Care for Chronic Diseases” (ICCC) (13). The ICDM “is a model
of managed care that provides for integrated prevention, treatment and care of
chronic patients at primary healthcare level … to ensure a seamless transition to
‘assisted’ self-management within the community” (23) (p. 11). The ICDM’s aim is
to reach best clinical outcomes for patients with chronic conditions by using the
health system building blocks approach. The rationale behind the development of
this management model was to address the paradigm shift in the burden of disease
and to be able to achieve a comprehensive, appropriate and effective provision of
long-term chronic care services, while at the same time responding adequately to
acute care services (11, 23).
The ICDM model is linked to the chronic disease model (CCM) and has four
additional building blocks to the CCM (24). The ICDM building blocks are
organization of health, delivery systems re-design, clinical management support,
clinical information support, human resources, medicine supply and management,
equipment supply, health information, leadership and advocacy. The assisted self-
management element of the ICDM seeks to empower patients and create
awareness of ownership of their own health by providing access to care through
the ward-based outreach teams (11).
Alongside the ICDM, South Africa has developed and implemented its Strategic
Plan for the Prevention and Control of Non-Communicable Diseases 2013-17 in
order to address the rapidly rising NCD burden (23, 25). As can be noted, South
Africa is already moving forward in the direction of self-management and patient-
centered care.

38
Efforts towards the prevention of NCDs
South Africa was among the first countries in SSA to develop policies to fight
against NCDs. Firstly, there is the Tobacco Products Control Act (Act 83 of 1993),
amended in 1999 and 2007 (26-29). Globally, this type of legislation has come to
be one of the most effective policies. Since young adults were previously targeted
by tobacco companies, the Act now protects children and adolescents through
banning advertising. It also acknowledges the right of non-smokers to a clean envi-
ronment by protecting them against second-hand smoking (30). The Liquor Act
(Act 59 of 2003), amended in 2008, was implemented to protect the population
from advertising that attracts minors and an age restriction on selling alcohol to
minors has been enforced (31, 32). Hours of trading have also been restricted and
alcohol is heavily taxed in an effort to reduce alcohol abuse (30, 33).
The food-based dietary guidelines developed in 2001 and revised in 2013 have
been approved by the National Department of Health (34). They are revised on a
continuous basis and are used to educate people on the prevention of NCDs.
Although there are significant barriers to their implementation, such as poverty,
these guidelines could be used as a basis for a healthy eating plan to prevent
NCDs (30). Although the ICDM model has been adopted in South Africa, the self-
management aspect of this model needs to be enhanced in order to reach
optimum implementation.
On the other hand, it appears that South African citizens have not really benefited
from the anticipated progress in healthcare policies since the year 1994 due to low
quality, poor and uneven access to healthcare, which can be attributed to poor
health systems and disease burden (7, 11). The NCD burden is rising, even in rural
communities, and also affects the urban poor. This result in major repercussions in
terms of the demand for treatment and care for chronic conditions and the ability to
provide acute and chronic care services (7). Because of the rising mortality from
NCDs, especially in rural areas, and also the mounting pressure from NCDs on
healthcare services, it is evident that South Africa’s effort leaves much to be
desired and more could be done (11, 30).

39
Traditional healthcare
As noted earlier, the traditional health system runs parallel to the western health
system. In the general household survey of 2014, participants were asked on
whom they consulted first when they fell ill or got injured. Sixty-nine percent
(69.3%) of households reported that they would first go to public clinics or
hospitals, 28.9 percent said that they would first consult a private doctor, or go to a
private clinic or hospital, and 0.5 percent said they would first go to a traditional
healer. In 2002 the World Health Organization (WHO) reported that in Africa about
80% of the population used traditional medicines.
Although the two healthcare systems co-exist in a form of medical pluralism, there
are indications of controversies. The current drive to promote collaboration
between the biomedical (western) and the healing (traditional) paradigms is
surrounded by mistrust, tensions and unresolved issues (14). These conflicts and
mistrust could be one of the reasons why some traditional healers tell their patients
not to mention their consultations with a traditional healer when visiting a medical
doctor or why they advise their patients not to take western medicine at all (14, 35).
In traditional African healing, it is believed that traditional healers are the channels
through which the interconnected worlds of the physical, psychological, spiritual
and ancestral are conversed with. There are four different categories of traditional
healers and each provides a different set of services. Traditional surgeons (ingcibi)
perform circumcisions; diviners (sangoma) consult, diagnose and prepare herbs;
herbalists (inyanga) consult, identify, collect and dispense herbs; and traditional
birth attendants (abebelethisi) are consulted for conception, pregnancy and pre-
and postnatal care (36, 37).
To better understand the context of traditional healthcare in South Africa, it is
important to also explore explanations for the causes of illness and disease
through the lens of medical anthropology, the field of study describing human
health in society from a cultural context (38). One of the points of departure is that
an individual’s definitions and perceptions of health and illness are influenced by all

40
the spheres of life around him or her, including cultural factors (39). Herselman (40)
defines illness in this context as “patients’ subjective experiences and
interpretations of sickness in line with their health-belief system rooted in culture”
(p. 62). Disease is described as “a physiological or psychological process of
malfunctioning of the body manifest in specific symptoms recognized by the
medical profession which gives its identity” (40) (p. 62).
According to Herselman (40) and Nksoi (38), there are traditional explanations for
the causes of illness and disease in the population:
• Punishment for disobedience. The illness is believed to be imposed by
supernatural forces, either the ancestors or the spirit of light. As dead
people are considered important and believed to connect the living with the
creator, it is imperative to always please the ancestors and failure to
appease them will bring punishment (illness, bad luck or misfortune). When
customs are neglected, for example failure to offer an animal sacrifice after
a relative’s death will result in the ancestors withdrawing their protection
and causing illness or misfortunes. Illness will now be interpreted as a type
of communication in the form of penalty for opposing accepted norms.
Illnesses caused by supernatural forces are believed not be understood
and cannot be treated by western medicine.
• Witchcraft and sorcery. Another cause of illness and disease is believed to
be through spiritual practice that invokes spirits of darkness to be
transmitted through the spiritual world in the form of curses, words or name
calling. Witchcraft involves hateful activities of one who influences the
power inherent in a person in order to bring harm on others. Anyone could
be the witch and accusations occur between relatives or neighbors and
usually these reveal tensions consequential to competition over limited
resources for instance in polygamous relationships. Sorcery is associated
with using magical powers or spells to manipulate personal objects like the
placentas or nail pairings. This is why at child birth personal remains like
the placenta are strictly protected and buried around the house where they

41
are believed to be sheltered by the ancestors. Usually witchcraft is
considered to be aggravated by jealousy of the other person.
• Cultural norms and practice. Sometimes sickness is believed to be caused
by the violation of a taboo. For example, the Pedi (Northern Sotho) people
believe that a woman should not have sexual relations during menstruation
or during the first three months of pregnancy. If this happens the woman
becomes impure and suffers from the condition of ‘heat’, called fisa. When
someone is impure he or she is vulnerable to misfortune and must be
cleansed through a ritual called ditlhapiso. People who are ritually impure
should be avoided and any contact with them would also bring sickness to
the perpetrator.
Many South Africans practice dual consultation of both traditional healers and
medical doctors for a variety of reasons, including maximizing chances of recovery
or getting a second opinion on their condition in order to aid coping with disease.
The medical practitioner is consulted for alleviating symptoms and the traditional
healer for finding the root cause and making sure the condition does not occur
again. Relatives may also insist on visiting the traditional healer to perform healing
procedures before going to the hospital (38, 40). Although public healthcare is free
of charge, lack of transport fees may cause some people to depend on a traditional
healer situated nearby.
Health literacy in South Africa
In South Africa there is a paucity of information on healthy literacy (41). Although it
is one of the African countries with high levels of general literacy, it is also one of
the countries known to have a high burden of disease. Studies show that although
education and literacy are key determinants of health, they do not necessarily
ensure health literacy (41, 42).
A recent systematic review by Sorensen et al defined health literacy as “the
knowledge, motivation and competence [of a person] to access, understand,
appraise and apply health information in order to make judgments and take

42
decisions in everyday life concerning healthcare, disease prevention and health
promotion to maintain or improve quality of life during the life course” (43) (p. 3).
Research indicates that poor health literacy is linked to poor adherence to
treatment, higher mortality and increased use of services, less disease knowledge
and self-management skills (41, 44, 45).
As health promotion is defined as a process of enabling people to take control of
their lives, it is important that the health-literacy skills of the population are
considered, especially in resource-limited settings (41, 46).
The context of this study
The study reported in this thesis was conducted in the formal healthcare system,
mainly in the Mamelodi Township, one of the six major townships in the City of
Tshwane (also known as Pretoria). Tshwane is a metropolis established in the year
2000 and is the administrative center and the capital city of South Africa. According
to the 2011 census, Tshwane is home to about 2.9 million people, with 70 percent
of the population being between 15 and 64 years old. More than half the population
is more than 20 years of age and has formal education. There are 911,536
households in Pretoria and 80 percent of the population lives in formal dwellings.
About 76 percent of households have a flush toilet connected to a sewage pipe; 64
percent have piped water inside the house, 88 percent have electricity lighting; and
80 percent have refuse removals weekly (47).
Townships are urban living areas that were reserved for the non-white population
from the late 19th century until the end of apartheid in South Africa in 1994 (48).
The township of Mamelodi is located in the northeast part of the city and was
established in 1953. At the moment it is the second largest township in Pretoria
after Soshanguve. Mamelodi has a total population of 334,577, according to the
census of 2011 (47). The population is mostly made up of black Africans (98%),
with the most common language being Sepedi (also known as Northern Sotho)
(42%) (47).

43
Conclusion
The context in which an intervention is being delivered is important, because
behaviors are influenced by what is going on around the person and the beliefs
and traditions they hold (49). Therefore, for the effective implementation
interventions need to be adapted to suit the context for which they are meant.
The next chapter presents a study on a systematic review of literature on diabetes
self-management education in high- and low-mortality developing countries. We
started the study by looking at the broader context of developing countries. Later
we narrowed the focus to one specific resource-challenged, middle-income
country, and finally focused on a resource-limited setting within South Africa.
References
1. Van den Broucke S. How international is health promotion? Health Promot Int. 2016;31(3):491-4.
2. Kreuter MW, Lukwago SN, Bucholtz RD, Clark EM, Sanders-Thompson V. Achieving cultural appropriateness in health promotion programs: targeted and tailored approaches. Health Educ Behav. 2003;30(2):133-46.
3. Barrera M, Jr., Castro FG, Strycker LA, Toobert DJ. Cultural adaptations of behavioral health interventions: a progress report. J Consult Clin Psychol. 2013;81(2):196-205.
4. Betsch C, Bohm R, Airhihenbuwa CO, Butler R, Chapman GB, Haase N, et al. Improving medical decision making and health promotion through culture-sensitive health communication: an agenda for science and practice. Med Decis Making. 2016;36(7):811-33.
5. Marchal B, van Belle S, van Olmen J, Hoeree T, Kegels G. Is realist evaluation keeping its promise? A review of published empirical studies in the field of health systems reaserch. Evaluation. 2012;18(2):192-212.
6. Goicolea I, Vives-Cases C, San Sebastian M, Marchal B, Kegels G, Hurtig AK. How do primary health care teams learn to integrate intimate partner violence (IPV) management? A realist evaluation protocol. Implement Sci. 2013;8:36.
7. Mayosi BM, Flisher AJ, Lalloo UG, Sitas F, Tollman SM, Bradshaw D. The burden of non-communicable diseases in South Africa. Lancet. 2009;374(9693):934-47.
8. Naledi T, Barron P, Schneider H. Primary Health Care in SA since 1994 and implications of the new vision for PHC re-engineering. In: Padarath A,

44
English R, editors. South African Health Review. Durban: Health Systems Trust; 2011. p. 17-28.
9. World Health Organization. Noncommunicable diseases country profiles, 2014. Geneva: World Health Organization; 2014 [cited 18 January 2017]. Available from: http://apps.who.int/iris/bitstream/10665/128038/1/9789241507509_eng.pdf?ua=1.
10. The global burden of disease: 2004 update. Geneva: World Health Organisation; 2008 [cited 10 November 2014]. Available from: http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf?ua=1.
11. Mahomed OH, Asmall S. Development and implementation of an integrated chronic disease model in South Africa: lessons in the management of change through improving the quality of clinical practice. Int J Integr Care. 2015;15:e038.
12. Maher D, Ford N, Unwin N. Priorities for developing countries in the global response to non-communicable diseases. Global Health. 2012;8:14.
13. Oni T, McGrath N, BeLue R, Roderick P, Colagiuri S, May CR, et al. Chronic diseases and multi-morbidity: a conceptual modification to the WHO ICCC model for countries in health transition. BMC Public Health. 2014;14:575.
14. Moshabela M, Zuma T, Gaede B. Bridging the gap between biomedical and traditional health practitioners in South Africa. In: Padarath A, King J, Mackie E, Casciola J, editors. South African Health Review 2016. Durban: Health Systems Trust; 2016. p. 83-92.
15. Ramjee S, Vieyra T, Abraham M, Kaplan J, Taylor R. National Health Insurance and South Africa's private sector. S Afr Health Review. 2015;3(9).
16. Jobson M. Structure of the health system in South Africa: actions to secure the right to health in South Africa. [Internet]. Khulumani Support Group, 03 November 2015. Available from: http://www.khulumani.net/active-citizens/item/1164-the-health-system-in-south-africa-actions-to-secure-the-right-to-health-in-south-africa.html.
17. Coovadia H, Jewkes R, Barron P, Sanders D, McIntyre D. The health and health system of South Africa: historical roots of current public health challenges. Lancet. 2009;374(9692):817-34.
18. Mooney G, Mclntyre DE. South Africa: a 21st century apartheid in health and health care? MJA. 2008;189(11/12):637-40.
19. Benatar SR. The challenges of health disparities in South Africa. S Afr Med J. 2013;103(3):154-5.
20. de-Graft Aikins A, Kushitor M, Koram K, Gyamfi S, Ogedegbe G. Chronic non-communicable diseases and the challenge of universal health coverage: insights from community-based cardiovascular disease research in urban poor communities in Accra, Ghana. BMC Public Health. 2014;14 Suppl 2:S3.
21. Republic of South Africa. National Health Insurance for South Africa: towards universal health coverage (Version 40). Department of Health; 2015. Available from: https://www.health-e.org.za/wp-

45
content/uploads/2015/12/National-Health-Insurance-for-South-Africa-White-Paper.pdf
22. World Health Organization. Monitoring the bulding blocks of health systems: a handbook of indicators and their measurement strategies. Geneva: World Health Organization; 2010.
23. Asmall S, Mahomed O. Integrated chronic diseases management manual. National Department of Health of South Africa. 2011 [cited 10 June 2014]. Available from: http://www.kznhealth.gov.za/family/Integrated-chronic-disease-management-manual.pdf.
24. Wagner EH. Chronic disease management: what will it take to improve care for chronic illness? Eff Clin Pract. 1998;1(1):2-4.
25. Republic of South Africa. Strategic Plan for the Prevention and Control of Non-Communicable Diseases. Department of Health; 2013 [cited 30 May 2014]. Available from: http://www.health-e.org.za/wp-content/uploads/2013/09/NCDs-STRAT-PLAN-CONTENT-8-april-proof.pdf.
26. Republic of South Africa. Tobacco Products Control Act (Act 83 of 1993), Government Gazette. 1993;337(14916).
27. Republic of South Africa. Tobacco Products Amendment Act (Act 12 of 1999). Government Gazette. 1999;406(19926)..
28. Republic of South Africa. Tobacco Products Amendment Act (Act 23 of 2007). Government Gazette. 2008;5i2(30821).
29. Tobacco Products Control Amendment Act, 2008 (Act 63 of 2008), Government Gazette. 2008; 523(31790).
30. Puoane T, Tsolekile L, Sanders D, Parker W. Chronic non-communicable diseases In: Barron P, Roma-Reardon J, editors. South African Health Review 2008. Durban: Health Systems Trust; 2008. p. 73-87.
31. Republic of South Africa. Liquor Act, 2003 (Act 59 of 2003). Government Gazette. 2004; 466(26294).
32. Liquor Products Amendment Act, 2008 (Act 32 of 2008). Government Gazette. 2008; 521(31637).
33. Yach D, Hawkes C, Gould CL, Hofman KJ. The global burden of chronic diseases: overcoming impediments to prevention and control. JAMA. 2004;291(21):2616-22.
34. Vorster H, Badham JB, Venter CS. An introduction to the revised food-based dietary guidelines for South Africa. S Afr J Clin Nutr. 2013;26(3):S1-S164.
35. Maimela E, Van Geertruyden JP, Alberts M, Modjadji SE, Meulemans H, Fraeyman J, et al. The perceptions and perspectives of patients and health care providers on chronic diseases management in rural South Africa: a qualitative study. BMC Health Serv Res. 2015;15:143.
36. Street R. Unpacking the new proposed regulations for South Africa Traditional health practiotioners. S Afr Med J. 2016;106(4):325-6.
37. South African Tourism. Traditional healing. [Internet] 2016. Available from: http://www.southafrica.net/za/en/articles/entry/article-southafrica.net-traditional-healing1.

46
38. Nkosi B. Understanding and exploring illness and disease in the South Africa: a medical anthropology context. Int J Humanit Soc Sci. 2012;2(24):84-93.
39. de-Graft Aikins A, Boynton P, Atanga LL. Developing effective chronic disease interventions in Africa: insights from Ghana and Cameroon. Global Health. 2010;6:6.
40. Herselman S. 'Health care through a cultural lens': insights from medical anthropology. Curr Allergy Clin Im. 2007;20(2):62-5.
41. Bress J. Developing a framework to identify and respond to health literacy needs using community-based emergency first aid responders in the Lavender Hill. MSc dissertation, University of Cape Town; 2014.
42. Schrauben SJ, Wiebe DJ. Health literacy assessment in developing countries: a case study in Zambia. Health Promot Int. 2015 Dec 10. [Epub ahead of print].
43. Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80.
44. Schillinger D, Grumbach K, Piette J, Wang F, Osmond D, Daher C, et al. Association of health literacy with diabetes outcomes. JAMA. 2002;288(4):475-82.
45. Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K. Low health literacy and health outcomes: an updated systematic review. Ann Intern Med. 2011;155(2):97-107.
46. Mokwena K. Strategies to increase the health literacy needed to complement health-promoting legislation in South Africa. S Afr J Clin Nutr. 2015;28(4):197.
47. Statistics South Africa. Statistical release (Revised) p0301.4. Census 2011. [Internet] 2012. Available from: http://www.statssa.gov.za/publications/P03014/P030142011.pdf.
48. Show me. Pretoria Township Tours [Internet] 2009 [cited 20 September 2016]. Available from: http://showme.co.za/pretoria/tourism/pretoria-townships/.
49. Marsiglia FF, Booth JM. Cultural adaptation of interventions in real practice settings. Res Soc Work Pract. 2015;25(4):423-32.

47
CHAPTER 3: Systematic Review
Type 2 diabetes self-management education
programs in high and low mortality developing
countries: A systematic review
Published as:
Dube L, Van den Broucke S, Housiaux M, D’Hoore W, Rendall-Mkosi K. Type 2
diabetes self-management education programs in high and low mortality
developing countries: A systematic review. Diabetes Educator, 2015: 41(1), 69–
85. doi: 10.1177/0145721714558305.

48
Abstract
Purpose: Although self-management education is a key factor in the care for
diabetes patients, its implementation in developing countries is not well
documented. This systematic review considers the published literature on diabetes
self-management education in high and low mortality developing countries. The
aim is to provide a state of the art of current practices, assess program outcomes,
cultural sensitivity and accessibility to low literate patients.
Methods: The Cochrane Library, PubMed, MEDLINE, PsycInfo and PsycArticles
databases were searched for peer-reviewed articles on Type 2 diabetes published
in English between 2009 and 2013. The World Bank and WHO burden of disease
criteria were applied to distinguish between developing countries with high and low
mortality. Information was extracted using a validated checklist.
Results: Three reviews and 23 primary studies were identified, 18 of which were
from low mortality developing countries. Studies from high mortality countries were
mostly quasi-experimental, those from low mortality countries experimental.
Interventions were generally effective on behavior change and patients’ glycemic
control in the short term (≤9 months). While 57% of the studies mentioned cultural
tailoring of interventions, only 17% reported on training of providers, and 39% were
designed to be accessible for people with low literacy.
Conclusions: The limited studies available suggest that diabetes self-
management education programs in developing countries are effective in the short
term, but must be tailored to conform to the cultural aspects of the target
population.
Keywords: Type 2 diabetes, self-management education, cultural tailoring,
developing countries, knowledge, gaps, effectiveness, systematic review.

49
Introduction
Diabetes mellitus (DM) is one of the most common chronic diseases worldwide.1,2
While until recently it was considered a disease of the affluent, it is increasingly
becoming a burden for developing countries. Approximately 80% of people with
diabetes live in low- and middle-income countries,3 and their number is estimated
to increase by 170% between 2000 and 20254. This makes the anticipated impact
of the condition greater and more damaging in these countries than in more
affluent parts of the world.5
Developing countries face a significant rise in healthcare expenditure due to the
increasing prevalence of diabetes. In many countries, diabetes consumes 5% to
20% of the healthcare budget, and more than 50% of that cost is due to
complications.6 Together with pharmacological treatment, lifestyle changes such as
increased levels of physical activity, a healthier diet, and smoking cessation have
proven useful in altering the course of Type 2 diabetes (T2DM) and delaying the
development of complications.7 Consequently, the education of diabetes patients to
manage their illness and adopt lifestyle practices to prevent complications is widely
recommended, particularly in populations where economic resources are limited.8-
10 As such, diabetes self-management education (DSME) can be considered as a
crucial way to address the diabetes problem in developing countries.
Despite the growing body of literature demonstrating positive effects of DSME,11-15
its implementation in developing countries is a challenging task. Developing
countries are often faced with low levels of education in the adult population,
resource poor environments, and a health system designed to address infectious
diseases, being less well prepared to tackle chronic conditions like diabetes.4 As
the bulk of the literature documenting the effectiveness of DSME concerns
programs that were developed, implemented and evaluated in developed
countries,11,14,16
their direct importance to developing countries with different socio-
cultural and economic conditions is uncertain.

50
Cultural sensitivity of DSME
The challenge of addressing the diabetes epidemic in developing countries could
be partially resolved by using culturally appropriate and context relevant
interventions to delay diabetes and prevent its complications.4 Culture refers to the
behavior patterns, beliefs, arts and all other products of human work and thought,
as expressed in a particular community.17
For diabetes education to be effective in
multi-cultural societies, both the educators and the content of programs should be
culturally sensitive.18
This can be achieved through cultural tailoring, which is
defined as “the process of creating culturally sensitive interventions, often involving
the adaptation of existing materials and programs for racial/ethnic groups”.19
There are two levels of cultural sensitivity: (1) Surface structure involves matching
the intervention materials and messages to observable “superficial” (although
important) characteristics of a target population, such as familiar people, places,
language, music, food and locations; (2) Deep structure requires an understanding
of the cultural, social, historical and psychological forces that influence the target
population. Whereas surface culture only increases the acceptance of programs,
deep cultural factors have more influence on the effectiveness of programs.19
Literacy sensitivity of DSME
Literacy is defined by the United Nations Educational, Scientific and Cultural
organization (UNESCO), as the ability to identify, understand, interpret, create,
communicate and compute, using printed and written materials associated with
varying contexts.20
A challenge to DSME in developing countries is that many
patients with diabetes have low levels of literacy.21-23
Health literacy which is linked
to literacy entails people’s knowledge, motivation and competences to access,
understand, appraise and apply health information in order to make decisions in
everyday life concerning healthcare, disease prevention and health promotion to
maintain or improve quality of life during the life course.24
People with low literacy
understand little (50%) of what is told to them during medical consultations and
they may be embarrassed by their situation and hide their low level of literacy from

51
people who could possibly help (healthcare providers, family members and
friends).21,23
As a result, they have difficulties in managing their medication and
lifestyle. Screening for low literacy and tailoring DSME programs to the level of the
patients through working with communities to develop more accessible educational
materials and interventions can address this problem and enhance program
effectiveness.
DSME in developing countries
In light of the above, it appears that addressing the burden of diabetes in
developing countries requires DSME programs that are culturally and literacy
sensitive.25
To document the extent to which existing DSME programs in
developing countries meet these demands, this systematic review considers the
published literature on DSME in developing countries, looking at cultural sensitivity
and adaptation for low literacy as potential determinants of effectiveness.
To our knowledge, this is the first systematic literature review of DSME programs in
developing countries with a focus on these socio-cultural and literacy aspects. A
recent paper by Rawal et al7 reviewed the evidence for the effectiveness of DSME
in developing countries, but did not consider cultural sensitivity and low literacy.
Moreover, the review only included studies that considered blood glucose or
glycated hemoglobin A1C (A1C) as a primary outcome, thus limiting the review to
seven studies from four countries, all of which are classified as low mortality
countries. However, as the primary goal of DSME is to enable patients to integrate
self-management into their daily lives and adopt a healthier lifestyle, the core
outcomes of DSME are essentially behavioral. Hence, it makes sense to also
include studies in the review that evaluate DSME program effectiveness in terms of
behavioral outcomes, and not only in terms of A1C level changes. In addition, it is
possible that DSME programs are implemented differently in countries with a high
mortality, where the health system is often less well equipped to address chronic
conditions.

52
Therefore, this systematic review aimed to answer the following review questions:
(1) What is the current status of DSME for T2DM in developing countries? and (2)
To what extent are cultural specificity, low literacy and low health literacy
addressed in DSME programs in developing countries?
Methods
The process of conducting and reporting this review was underpinned by the
PRISMA Statement for Systematic Reviews and Meta-Analyses.26
Information sources and search terms
To find existing systematic reviews on DSME programs in developing countries,
the Cochrane Library was first consulted, but no reviews were found focusing
specifically on developing countries. Consequently PubMed, MEDLINE, PsycInfo,
PsycArticles and Google scholar were searched using combinations of the
following search terms: review, diabetes, self-management education, patient
education, programmes / programs, developing countries, Africa, Latin America
and “by country”(only in PubMed). Reference lists from the identified articles were
hand searched for additional relevant articles.
Eligibility criteria
The search was restricted to peer-reviewed articles published in English and with
full text available. The initial search was from 1980 but because of time and
resource constraints it was limited to the period 2009 until 2013 (November 13). To
define developing country status, the World Bank list for developing countries was
used. The WHO burden of disease criteria was applied to distinguish between high
and low mortality countries.27,28
Studies with a full description of the DSME
intervention, from a developing country, and focusing on T2DM or pre-diabetes
were considered for inclusion. Studies on T1DM or mixed T1DM and T2DM,
without a clear indication of the type of DM, gestational DM and whose subjects
were not diabetes patients were excluded. As no primary studies on pre-diabetes

53
were found during the search; this review focuses on T2DM only. All the articles
were selected for inclusion by the first author (LD) and a subsample of the studies
was analyzed for inclusion and exclusion by a second assessor (MH). Assessor
agreement was 100%.
Study selection
Using the abovementioned procedure, 2289 articles were identified (2171 from
electronic databases and 118 from hand search). After applying the inclusion and
exclusion criteria, 28 publications remained, 25 of which were primary articles
(representing 23 studies) and three were reviews (Fig 3.1).
Figure 3.1 Flowchart of the selection process

54
Study quality
Using a validated checklist for measuring study quality29
(question 1-10), 22 articles
were rated as having good quality, one article as fair quality and no articles as poor
quality. Good quality was said to have a score of eight and above. All articles gave
sufficient information about: study aims, outcomes measures, patient selection,
description of intervention, results and statistical details. The main limitations
observed in study quality were lack of reporting of adverse events and no report on
characteristics of patients lost to follow-up.
Data extraction
An analysis of the existing reviews was performed separately. For the analysis of
the DSME programs presented in the primary articles, the authors used a
description tool developed and validated by an international consortium.30
This tool
was developed via a multiple Delphi process for the Global Diabetes Survey
(GDS), which is a global initiative to collect data on diabetes care quality on a
yearly basis.31
It consists of an online wiki-like survey with questions
describing existing educational programs for diabetes and pre-diabetes prevention.
The items used for the purpose of this review include program content,
intervention, strategy, duration, program providers, training of the providers, and
accessibility of the program to patients with low literacy.
Although the primary interest for this systematic review was on health literacy, the
primary studies found do not give information on health literacy but literacy levels.
Due to the fact that there was only one paper on health literacy, the overall literacy
levels of the patients will be discussed in this paper. In addition, program
effectiveness on outcomes and tailoring of the program to the culture (surface and
deep cultural aspects) were assessed. An intervention was said to be culturally
sensitive (surface structure) if it was delivered in the local language, if local foods,
symbols, objects were used and if local guidelines or country guidelines were
incorporated in the design of the intervention. Deep structure was assessed as
needs assessment, an understanding of cultural history, values and norms and

55
incorporating this knowledge in the design of the program.19
Data were
summarized in tables and missing data according to the description tool were
reported as “not reported” (NR).
Data extraction from the selected articles was done by the first author. A
subsample of the articles was also evaluated by a second assessor, yielding an
assessor agreement of 95%. The assessors then discussed the differences and
consensus was reached (100%).
Results
Existing reviews
Three reviews evaluated the published literature on DSME programs in low
mortality developing countries. The first review included 7 articles on DSME
programs from 4 countries. Of these seven studies, 4 were concerned with
prevention of complications in T2DM, and 3 were focused on prevention of the
development of T2DM. While considering lifestyle and other non-pharmacological
interventions to prevent T2DM and its complications, this review only included
studies with blood glucose measure or A1C as a primary outcome.7 The main
conclusion was that the reasonably consistent and positive results are significantly
limited by the small number of studies.
The second was a systematic review of 18 reports on DSME in Iran, published
between 2002 and 2008.32
Of these 18 studies, 11 were studies on T2DM, 4 were
T1DM, 1 was mixed T1DM and T2DM and in 2 studies, the type of DM was
unknown. Whereas the interventions seemed to have a positive effect on
knowledge, self-monitoring of blood glucose and glycemic control, the review
concluded that the findings were insufficient and too conflicting to draw firm
conclusions.
The third review gave a summary of the literature on DSME in mainland China,
involving 34 studies published between 1989 and 2008.33
Of these 34 studies, 18

56
were on T2DM, 6 were on mixed T1DM and T2DM, 1 was on Gestational DM, and
in 9 studies, the type of diabetes was not mentioned. Only interventions with a
duration of at least 3 months, and involving A1C and/or behavior change as
outcome measures were included. This led to the conclusion that DSME programs
in China have positive effects on the patient’s knowledge and glycemic control, but
that the effects on behavior change and on cardiovascular risks were variable.
Long-term effects of the programs on quality of life and on medical complications
were not assessed.
Study characteristics of identified studies
Of the 23 original studies that were identified in the 25 publications, 18 (78%) were
from low mortality developing countries (Iran,23,34-41
Argentina,42,43
Turkey,44,45
South Korea,46
China,47,48
Malaysia49
and a combination of 27 selected developing
countries50,51
); five were from two high mortality developing countries (South
Africa52-54
and India55-57
) (Tables 3.1 and 3.2). Most studies from low mortality
developing countries were experimental and, except for one, those from high
mortality developing countries were quasi experimental (Tables 3.1 and 3.2). A
third of the studies (35%), only one being from high mortality developing countries,
referred to theories of behavior change as a theoretical basis for the interventions.
Sample sizes ranged from 62 to 11,384 participants.
The professional background of the educators who provided the interventions
varied across studies (reported in only eighteen studies) with nurses in 8/18 as the
most common providers, followed by physicians/doctors 7/18, dietitians/nutritionists
5/18 and community support workers or health promoters 2/18. Only 4/18 studies
reported using trained diabetes educators. The content of the educational
interventions was comprehensive in most interventions, covering almost all the
topics of diabetes education including basic knowledge of diabetes, diet, exercise,
self-monitoring blood glucose, medication taking, reducing risks, problem solving
and living with diabetes.

57
Table 3.1 Study characteristics for *T2DM in low mortality developing countries (n=18)
Reference Country Study objective Design Inclusion criteria Sample Duration
Negarandeh et al
23
Iran Explore the impact of pictorial image and teach back educational strategies on knowledge, adherence to medication and diet among patients with T2DM and low health literacy.
*RCT >6 months duration of diabetes Low health literacy (59 or lower on *TOFHLA), 18 years or older Absence of mental, visual or learning abilities Former participation in diabetes education research projects
135 9 weeks
Aliha, et al34
Iran Evaluate the effects of diabetes self-care group education and nurse- telephone follow-up on glycemic control and compliance with treatment orders in patients with T2DM attending to diabetes clinic
RCT Informed consent, access to telephone Lack of difficulty in speech, hearing and vision Absence of disease associated with physical & mental illness, excluded if admitted during study, changing treatment protocol or developing complications.
62 3 months
Samadi, et al
39
Iran Determine the effect of quality of life education on self-concept of patients with T2DM.
RCT ˃30years old, Cognitive ability to answer questions and consent given Excluded if with prior *DSME within 1 year or having complications.
123 3 months
Bayat, et al35
Iran Assess the effectiveness of educational intervention based on extended health belief model on T2DM patients
RCT Being able to read and write T2DM diagnosis by specialist
120 6 months

58
Reference Country Study objective Design Inclusion criteria Sample Duration
Farsaei, et al
36
Iran Evaluate the effect of a clinical pharmacist-led patient education program for T2DM patients
RCT With uncontrolled T2DM ˃7% Able to read and write
Were in suitable therapeutic condition Excluded if confused, unable to communicate verbally, or reached <7% during 1
st month
172 3 months
Sharifirad, et al
40
Iran Determine the effectiveness of the HBM on nutrition education in T2DM patients.
Semi-experimental study
30-60years, not to be illiterate At least 1 year attendance in Iranian Diabetes Association seminars, regulars follow-ups, No severe and chronic complication of diabetes
88 NR (only 1 month follow-up)
Hazavehei, et al
37
Iran Determine the effects of educational program based on the Belief, Attitude, Subjective Norm, and Enabling Factors (BASNEF) Model on eye care among patients with insulin independent diabetes mellitus.
Experimental study
40-60 years, 5 year duration of diabetes Exposed to danger of ocular complications
Excluded if diagnosed with ocular or cardiac complications
100 4 months
Kashfi, et al38
Iran Evaluate the effect of educational program and jogging based on HBM on sugar control in type 2 patients
prospective quasi- experimental interventional study
Without diabetes foot and cardiovascular side effects
100 3 months
Vatankhah,et al
41
Iran Evaluate the impact of a simple educational program on the knowledge and practice of people with T2DM in relation to the foot at risk
NR Excluded if unable to answer questionnaire due to dementia, psychosis or profound deafness
148 9 months (6months follow-up)

59
Reference Country Study objective Design Inclusion criteria Sample Duration
Gagliardino, et al
42
Argentina
Implement an educational program in 10 Latin American countries and to evaluate its effect on the clinical, biochemical, and therapeutic aspects as well as the economic cost of diabetes
Randomized 2x2 design
At least 2 years duration of diabetes, between 25-75 years old, excluded if *T1DM, with severe complications, alcohol or drug addiction or inability to self-care
468 42 months
Perman, et al
43
Argentina
Compare the all-cause mortality rate in elderly T2DM patients who attended self-management educational workshops compared with those who did not.
Retrospective cohort study
Diagnosis of T2DM b4 Dec 31 2003 ≥65 at Jan 1 2001 Remain an affiliate of the health plan at least for 1 year after recruitment
1730 6 years
Atak, et al44
Turkey Evaluate the effect of patient education on knowledge, self-management behaviors and self-efficacy in patients with T2DM
RCT Had attended at least 1 follow-up visit Able to give informed consent
80 1 month
Karakurt,et al
45
Turkey Determine the effect of education given to patients with T2DM mellitus on self-care
Pre-post-test experimental design
At least 6 months of *DM duration, being Literate, no serious complications , No psychiatric history volunteer to participate
100 9 months
Song, et al46
South Korea
Investigate the effects of a diabetes outpatient intensive management program (DOIMP) on A1C levels and adherence to control recommendations.
Randomized 2 group pre-post-test experimental design
Able to perform *SMBG Take oral hypoglycemic agents (OHAs) Understand the study goals
Excluded if with complications
59 3 months

60
Reference Country Study objective Design Inclusion criteria Sample Duration
Shi, et al48
China Examine the effect of a hospital-based clinic intervention on glycemic control self-efficacy and glycemic control behavior of Chinese patients with T2DM
RCT At least 1 year diagnosis Able to communicate, verbally, read & write in mandarin Willing to participate
No previous DSME
Excluded if <30, with type 1 or gestational diabetes or with complications.
157 5 months
Liu, et al47
China Develop a Chinese diabetes group visit program and to examine its effectiveness on self-management behavior, self-efficacy and health status for patients with T2DM
RCT Aged 35-80years Excluded if outside the age range or with -complications or physical disability
208 12 months
Al-haddad,et al
49
Malaysia Measure the effectiveness of two different diabetes educational programs (less structured vs. structured).
Prospective observational Study
T2DM patients Able to communicate in Malaysian National language
74 8 months
Gagliardino,et al
50,51
27 devel-oping coun-tries
Evaluate the impact of diabetes education provided to patients with T2DM in non-controlled studies (real-world conditions) on quality of care, resource consumption and conditions of employment.
Cross Sectional & longitudinal Survey
Excluded if with active participation in a clinical study or recent short-term insulin treatment
11 384 9 months
* T2DM = Type 2 diabetes mellitus, RCT = Randomized controlled trial, TOFHLA = Test of functional health literacy in adults, DSME = diabetes self-management education, T1DM = type 1 diabetes mellitus, DM = diabetes mellitus, SMBG = self-monitoring blood glucose, HBM = Health Belief Model, NR = Not reported

61
Table 3.2 Study characteristics for *T2DM in high mortality developing countries (n=5)
Reference Country Study objective Design Inclusion criteria Sample Duration
van der Does, et al
54
South Africa
Evaluate the Take Five School (TFS) group education program for patients with T2DM in South Africa.
Mixed methods -Pre-post test
*NR 84 1 month
Price, et al52,53
South Africa
Determine the long-term (4 years) glycemic outcome of a structured nurse-led intervention program for T2DM patients in rural Africa.
Cohort study NR 320 4 years
Mahant56
India Evaluate the impact of a model program of diabetes on diabetes control.
Prospective study
All included without bias for gender, age, duration of disease, severity or educational status.
1050 3 years
Mahajan, et al
55
India Improve the health and blood sugar control in T2DM by giving health education, dietary advice and encouraging them for regular blood sugar monitoring and physical exercise.
Cross-Sectional
˃40years old 300 12 months
Malathy, et al
57
India Assess the baseline levels of knowledge, attitude and practices of diabetes patients visiting two multispecialty hospitals and one private diabetes clinic regarding disease management.
*RCT ˃30years old Excluded pediatric & pregnant patients.
207 9 months
* T2DM = Type 2 diabetes mellitus, NR = Not reported, RCT = Randomized controlled trial

62
Intervention characteristics
In low mortality developing countries, the reported interventions were mostly
delivered in groups (12 of 18 studies). Three studies used a telephone follow-up.
Four interventions used face to face individual sessions and one of these included
a telephone follow-up while two interventions used both group and individual
delivery strategy (Table 3.3). Sixteen of the studies in low mortality countries were
12 months or less in duration and only two studies had duration of 42 months and
6 years (Table 3.1). Eight studies provided written literature to the intervention
group to supplement the educational sessions. Forms of teaching differed across
the interventions and included lectures, group discussions, question and answer
sessions. A few interventions used film demonstrations, illustrative materials and
role plays.
In high mortality developing countries, two interventions were delivered in groups,
two individually, and one using a combination of group and individual sessions.
Education formats included discussions, individual counseling, and providing
written literature to supplement the sessions. Only two studies had duration of
more than 1 year (Tables 3.2 and 3.4).
Tailoring to culture
Thirteen studies (57%) from both high and low mortality developing countries
reported aspects of cultural sensitivity. Nine of these studies reported programs
that were using the local language and incorporating the existing materials and
local guidelines. Two studies from low mortality countries required speaking and
understanding the local language as inclusion criteria for the program. Another
nine studies required information on needs assessment of the target population
before designing the intervention program. Two of these studies were from high
mortality countries. All the studies from high mortality countries, except one, were
accessible to people with low levels of literacy. Four studies from low mortality
countries reported access to people with low literacy; five studies reported

63
programs that excluded patients with low literacy. Other studies did not report on
this issue (Tables 3.1 and 3.2).
Outcome measures
Different outcomes were measured across studies. The most commonly measured
(in 70% of the studies) was behavior change (e.g. diet, physical exercise, self-
monitoring of blood glucose (SMBG)). A1C was measured in less than half of the
studies (49%). Other outcome measures included knowledge and other individual
dispositions, fasting blood sugar (FBS), body mass index (BMI), lipid profiles- and
psychological states (Table 3 and 4).
Effectiveness of DSME interventions
Nearly all the identified studies indicated a significant difference on outcome
measures between the intervention group and the control group or from pre-test to
post-test. Six studies (26%) did not find a significant difference between
intervention and control groups or from pre-test to post-test on some of the
outcomes measured, which included knowledge, psychological state, behavior and
BMI. The change in A1C was significant in all the studies where this indicator was
used as an outcome measure. In most studies, effectiveness of the interventions
was only considered at short-term follow-up. Four studies measured follow up over
a longer period, but in one of them (with a 6 year follow-up) it was not clear
whether the improvement was an effect of the intervention or of other factors. In the
other study, with a 4 year follow-up, glycemic slippage was observed over time,
indicating less impact at longer term follow-up.

64
Table 3.3 DSME Intervention/programs characteristics for *T2DM in low mortality developing countries
Reference Intervention for T2DM Provider Provider training
Theoretical model
Measures Main outcomes Comments
Negarandeh, et al
23
Two interventions and 1 control. Group. 1: Three weekly individual teach back sessions each lasting 20miutes. Group 2: Three weekly individual pictorial image sessions each lasting 20minutes. Control Group: received usual care-presentation of an educational brochure on diabetes control
Community health nurse
*NR NR -Level of health functional literacy Diabetes knowledge
-Adherence to medication and diet
Statistically significant differences (P<0.05) between intervention and control
The intervention was effective all measures were significant in both intervention groups than controls.

65
Reference Intervention for T2DM Provider Provider training
Theoretical model
Measures Main outcomes Comments
Aliha, et al34
Two group educational sessions for 60 minutes in 2 consecutive days using face to face lectures and film demonstration and 16 follow-up telephone calls by nurse (1st month 2 calls per week and 2nd and 3rd months 1 call per week) + booklet. Control group: Conventional care and usual education for diabetes patients
Diabetes nurse
YES NR *FBS *A1C
Blood glucose 2hours after meals Blood Sugar (2hppBS) Adherence to treatment
FBS, *2hppBS, A1C were statistically significant. Adherence increased from 6.5% to 90.3% in intervention group while in control it decreased from 12.5% to 0%.
The intervention was effective, in all measures there was a significant difference in intervention than control group.
Samadi, et al
39
Eight weekly face to face group quality of life educational sessions for 90 minutes + hand-out and 1 month telephone follow-up Control Group: received hand-out + education after follow-up.
Nurse, physiotherapist, nutritionist, orthopedist, psychologist
NR NR Self-concept Self-esteem
Body image
*BMI
BMI was statistically significant P=0.004. Increased self-esteem and self-concept.
Intervention was effective, significant differences in all outcomes were observed in the case than control group after intervention.

66
Reference Intervention for T2DM Provider Provider training
Theoretical model
Measures Main outcomes Comments
Bayat, et al
35
Two 30-40 minutes individual face to face lectures via pamphlets and question and answer method + telephone follow-up. Follow-up at 3 and 6 months
NR NR *HBM HBM constructs Self-efficacy
At 3 and 6 months follow-up
Significant impact P<0.0001on extended HBM constructs.
The intervention showed a positive and significant impact on extended health model belief constructs. However, perceived susceptibility and self-efficacy remained constant at 6 months
Farsaei, et al
36
Two group pharmacist-led educational sessions and weekly telephone follow-up and appointments for 3 months Control group: general education by nursing staff.
Pharmacist NR NR A1C FBS
A1C decreased significantly in intervention than control (p<0.001)
Intervention was effective. Glycemic control was significantly decreased in intervention than groups

67
Reference Intervention for T2DM Provider Provider training
Theoretical model
Measures Main outcomes Comments
Sharifirad, et al
40
Four group sessions each lasting 40 minutes + One month follow-up.
NR NR HBM Nutritional knowledge HBM Constructs
Nutritional practice Weight, *BMI, FBS
Statistically significant results (P<0.001) in intervention compared to control group in knowledge and perceived susceptibility. Behavior increased significantly (P<0.001) in intervention than in control.
Intervention significantly improved knowledge scores, and FBS compared to the control group but perceived severity, threat and benefits remained the same.
Hazavehei, et al
37
Six group educational sessions using lectures, question and answer and group discussions, each session lasting 55-60 minutes over 1 month + 3 month follow-up
NR NR *BASNEF Model
*BASNEF Model components A1C
FBS
Eye care practice
A1C decreased significantly (P<0.001).
The BASNEF Model components, knowledge and all other outcomes were significantly improved in the intervention group compared to the control group after follow-up.

68
Reference Intervention for T2DM Provider Provider training
Theoretical model
Measures Main outcomes Comments
Kashfi, et al
38
3 sessions (each 60 minutes) of training on jogging and control of sugar + 3 months follow-up.
NR NR
HBM HBM constructs Practices
A1C FBS
A1C decreased significantly (P<0.001).
Intervention was effective; all outcomes were significant in case than in control group after intervention.
Vatankhah, et al
41
Single 20minute individual face-to-face foot education session + Booklet and follow up after 6 months.
NR NR NR Knowledge Foot care practice
Improved knowledge and practice about diabetes foot care (p<0.0001 and P=0.011)
Intervention effective in increasing knowledge and practice scores significantly.
Gagliardino, et al
42
Group structured educational courses: Group 1: Control Group 2: Physician education only Group 3: Patient education only
Group 4: Patient and physician education Four weekly 90-120 minutes teaching sessions using illustrative materials + program book and a reinforcement session at 6 months.
Trained educators
YES NR A1C Lipid profile and *BP
Psychological state
A1C decreased significantly (p<0.05) at 42 months. Largest decrease in groups where patients and physicians were educated.
All outcomes measures were significant in case groups being largest in combined programs after intervention but psychological state was significant in both groups

69
Reference Intervention for T2DM Provider Provider training
Theoretical model
Measures Main outcomes Comments
Perman, et al
43
Four group education workshops for 2 hours per year and individual counseling on non-pharmacological treatment by physician assistants and follow- up through mails and delivery of educational material. Other “informal” education also available.
Diabetes educators (family physicians/endocrinologists)
YES Patient Empowerment Model
All-cause mortality Crude hazard ratio after adjustment was decreased from 33% to 18% (HR 0.82; 95%CI:0.61-1.08).
Workshop attendants had 33% lower all-cause mortality rate at 6 years of follow-up but impact of intervention not clear.
Atak, et al44
Two weekly group question-based patient centered sessions each lasting 45 minutes.
Researcher NR NR Knowledge self-reported self-management
Significant differences in self-reported self-management between case and control groups, p values <0.05.
Limited effect on knowledge and behavior but significant on self-efficacy.

70
Reference Intervention for T2DM Provider Provider training
Theoretical model
Measures Main outcomes Comments
Karakurt, et al
45
Individual narrative, question and answer educational sessions, each lasting 45-60 minutes. Education repeated twice every other month + booklet.
Researcher NR NR Self-care activities Metabolic control A1C
Lipid profile
A1C decreased significantly (p<0.001) from pre-test to post-test. Triglycerides were statistically significant (p<0.05) after intervention.
Only high density lipoproteins, BMI and Waist circumference were not statistically significant after intervention.
Song, et al46
2 day group and individual educational sessions + weekly telephone counseling. Patients free to call nurse at any time.
Endocrinologist, Nurse, physician, rehabilitation therapist, Dietitian, dermatologist, psychologist, pharmacist, ophthalmologist, physiotherapist
NR NR A1C Adherence to diet
A1C significantly decreased (p<0.05) in intervention group after the intervention. Significant difference in adherence (p=0.0001) was also observed in intervention after intervention.
Significant differences were observed overtime in A1C and Adherence to diet in intervention than control.

71
Reference Intervention for T2DM Provider Provider training
Theoretical model
Measures Main outcomes Comments
Shi, et al48
Group education, with 4 weekly sessions, 1-2hours per session for a month using discussions, videos, demonstrations, role plays and written literature. Telephone follow up, 2 calls each week, each 5-15 minutes for 4 months.
Researcher
NR Health Educational Strategies and Self-efficacy theory
Glycemic control self-efficacy Glycemic control behavior
Statistically significant improvements in Glycemic control self-efficacy and Glycemic control behavior (p<0.05) in experimental group compared to control group.
Intervention showed statistically significant improvement in glycemic control self-efficacy and glycemic control behavior immediately and four months after the intervention
Liu, et al47
12 monthly interactive group sessions lasting 90 minutes + I hour for individual consultation.
General practitioner Nurse Preventive doctor
YES The Cooperative Health Care Clinic Model
Behaviors Self-efficacy
Health status
Significant differences in behavior change (p<0.05) in case compared to control group.
Significant increase in self-efficacy and measures of illness. On average intervention group increased their exercise duration.

72
Reference Intervention for T2DM Provider Provider training
Theoretical model
Measures Main outcomes Comments
Al-haddad, et al
49
Group based monthly less structured versus structured teaching sessions each lasting 90-120 minutes for 4 months. Patient could call the researcher at any time.
Pharmacists Doctor Nurse
NR NR A1C BMI BP
A1C significantly decreased (p=0.004) in the structured group than in the less structured group.
Significantly increase in A1C levels was observed in the less structured group while significantly reduced in the structured group. BMI and Diastolic BP were not significant.
Gagliardino, et al
50,51
Face to face consultation and referral to ad hoc structured group education programs with different degrees of complexity and number of sessions and a 9 month longitudinal follow-up.
Nurse Dietitian Educator
NR NR Clinical- weight, height, *WC, BP, Foot Evaluation. Metabolic- A1C, lipid profile
A1C control significantly higher in case group.
Intervention significantly improved the percentage of patients achieving target values set by international guidelines.
*T2DM = type 2 diabetes mellitus, NR = Not reported, A1C = Glycated hemoglobin, FBS = Fasting blood glucose,
2hppBS = 2 hour after meals blood sugar, BMI = Body mass index, HBM = Health belief model, BASNEF = Belief, Attitude, Subjective Norm, and
Enabling Factors, BP = Blood pressure, WC = Waist circumference

73
Table 3.4 DSME Intervention/programs characteristics for *T2DM in high mortality developing countries
Reference Intervention for T2DM Provider Provider training
Theoretical model
Measures Main outcomes Comments
van der Does, et al
54
Weekly group education classes, each lasting 60 minutes for 4 weeks
Dietitian Heath Promoter Doctor
*NR NR Self-care activities
No statistically significant reduction in smoking (p=0.08)
Intervention was effective in improving adherence to a diabetes diet, physical activity, foot care and the perceived ability to teach others was seen but no significant change in smoking or adherence to medication was noticed
Price, et al
52,53
Structured group nurse-led diabetes care 3 monthly group sessions using picture based flip-charts + booklet and reinforcements per each clinic visit for 4 years.
Nurses Community support workers
NR Empowerment theory
*BMI *A1C
A1C decreased significantly compared to baseline at 6 and 18 and 24 months (P<0.001) and at 48 months it was (p=0.015)
There was significant improvement in A1C up to 18 months follow-up, but thereafter BMI was no longer significant and there was glycemic slippage.

74
Reference Intervention for T2DM Provider Provider training
Theoretical model
Measures Main outcomes Comments
Mahant56
30 minute counseling at 6 months visit for 3 years + booklet in Hindi
physician NR NR Knowledge practices Attitudes, blood glucose level A1C
A1C and blood glucose level decreased significantly (P<0.05).
The intervention was effective especially in monitoring of blood and urine glucose test and knowledge about hypoglycemia.
Mahajan, et al
55
Monthly 45-minute group education and individual consultations + comprehensive medical treatment, eye care and monitoring of blood sugar.
Dietitian Doctors
NR NR Life style Self-care practices Illness perception Glycemic status BMI
Significant improvements in lifestyle, self-care practices, illness perception and glycemic status
Intervention was effective in improving outcome measures
Malathy, et al
57
Monthly counseling sessions each lasting 20-25 minutes for 3 months + hand-outs
Pharmacist
NR NR Knowledge, Attitude, Practices (KAP), Post Prandial Blood Glucose, Lipid profile
*KAP scores of test patients improved significantly (p<0.0001)
Intervention proved to be effective
*T2DM = Type 2 diabetes mellitus, NR = Not reported, BMI = body mass index, A1C = Glycated hemoglobin, KAP = knowledge, attitude and practices

75
Discussion
The limited studies available suggest that DSME programs in developing countries
have positive effects on A1C, knowledge, glycemic control and behavioral
outcomes on short term follow-up. This finding is consistent with existing literature
which reports a positive impact on glycemic control after the delivery of
interventions in developing and developed countries.7,11-16
Despite these positive results, the review also identified shortcomings in the DSME
programs. Most interventions were provided by a range of health professionals.
While this suggests progress in the provision of DSME, it is quite clear that
developing countries are not equipped for this kind of implementation due to the
shortage of health care professionals, especially in rural areas.58
Therefore it is
advisable that where there is not enough professional capacity, peers and
community health workers can be trained to provide DSME while professional staff
like nurses can be wisely used in supervisory and training roles for the non-
professionals in these resource poor settings. This strategy has proven to be
effective.16,59-62
Only a few studies in the current review reported on the training of the providers.
This finding is consistent with the findings of the review by Lou et al, who found that
of the 34 studies reviewed from China, not a single study mentioned training of
providers.33
Without training of providers, the quality of a DSME program cannot be
guaranteed, since the information provided to patients is not adapted to the needs
of the particular target group.
Furthermore, few studies reported on accessibility of the intervention by patients
with low literacy levels. People with diabetes and low literacy are more likely to
have poor glycemic control, find it difficult to read food labels, estimate portion
sizes and therefore have low self-confidence in management of diabetes.23,63,64
In
previous studies, the use of pictorial aid and teach back strategies have been

76
shown to enhance the comprehension and recall, and adherence for people with
low literacy levels.65,66
Only a few interventions included in this review were guided by behavior change
theories yet interventions supported by a theoretical framework have been found to
have positive results on the participants.35
In addition, significant improvement still
needs to be effected with regard to the strength and rigor of the study designs used
in the interventions.
Our review suggests that DSME interventions in developing countries address the
surface cultural aspects such as language tailoring of reading materials. However,
deep cultural factors were rarely reported. The results are similar to other reviews
reporting that most interventions focus on surface structures of culture while
ignoring its deep structures.58
Rawal et al suggest that developing linguistically
appropriate and context-specific lifestyle interventions that are tailored to the
cultural, religious and socio-economic needs of the target population will enhance
the sustainability of the interventions.7
Studies from both low and high mortality developing countries differed in many
ways. There were more studies in the low mortality countries than in the high
mortality countries, implying that very little research on the topic is being done in
high mortality developing countries. Most interventions from high mortality
countries were culturally sensitive and were accessible to people with lower levels
of literacy, but did not report on provider training. Most importantly, of the entire
interventions only one from a high mortality developing country used community
support workers as providers in addition to nurses.
Limitations
There are a number of limitations of this review that should be mentioned. Firstly, it
included only studies published in peer reviewed, English journals from 2009 to
2013, thus excluding useful information which may not have been peer reviewed,
may be in other languages, published before 2009 or unpublished studies.

77
Secondly, the results of this review may also have been affected by publication
bias, in that only studies with positive results were published and those with
negative results were unavailable or unpublished. Despite these limitations,
however, we believe that the review provides a clear state of the art that may
inform DSME educators in developing countries.
Conclusion
DSME programs have been shown to be effective in these limited numbers of
studies from low and high mortality developing countries, especially on short-term
follow-up. However, there are several gaps that need to be addressed if programs
are to be sustainable. Guiding programs by behavior change theories, training
professional and non-professional providers (community health workers, health
promoters, peer support leaders), addressing the cultural sensitivity of programs,
and making them more accessible to people with low literacy. These gaps if
addressed could enhance the effectiveness of DSME programs in developing
countries.
As such, the findings of this review have important implications for diabetes
education in developing countries. Since diabetes continues to affect millions of
people in developing countries, it is imperative that health workers providing
education in developing countries continue to examine the sustainability and
effectiveness of interventions by tailoring them to the culture and literacy levels of
the target population. Many techniques can be used to address the burden of low
literacy, such as the use of pictures and teach back techniques which have
previously been proved successful.23,65,66
In addition, as professional staff should
be wisely used in resource poor settings, trained non-professionals can be included
to provide diabetes education with professional staff assuming a supervisory and
training role.
78
References
1. IDF. Position statement: Self-management education. 2011; http://www.idf.org. Accessed 16 October, 2013.
2. Pal K, Eastwood SV, Michie S, et al. Computer-based diabetes self-management interventions for adults with type 2 diabetes mellitus. Cochrane Database Syst Rev. 2013;3:Cd008776.
3. IDF. International Diabetes Federation Atlas. 2013; http://www.idf.org/diabetesatlas. Accessed 16 October, 2013.
4. Debussche X, Balcou-Debussche M, Besancon S, Traore S. Challenges to diabetes self-management in developing countries. Diabetes voice. 2009;54:12-14.
5. Paz-Pacheco E. Diabetes self management education: an effective response to the increasing burden in underserved communities. Diabetes voice. 2011;56(1):10-13.
6. WHO. Diabetes action now: An imitative of the World Health Organisation and the International Diabetes Federation. 2004; www.who.int/diabetes. Accessed 16 October, 2013.
7. Rawal LB, Tapp RJ, Williams ED, Chan C, Yasin S, Oldenburg B. Prevention of type 2 diabetes and its complications in developing countries: a review. Int J Behav Med. Jun 2012;19(2):121-133.
8. Ezenwaka C, Eckel J. Prevention of diabetes complications in developing countries: time to intensify self-management education. Arch Physiol Biochem. Dec 2011;117(5):251-253.
9. Funnell MM, Brown TL, Childs BP, et al. National standards for diabetes self-management education. Diabetes Care. Jan 2012;35 Suppl 1:S101-108.
10. AADE. Diabetes Education. 2013; www.diabeteseducator.org/export/sites/aade/_resources/pdf/Diabetes_Education_Definition.pdf. . Accessed 25 January, 2014.
11. Clement S. Diabetes self-management education. Diabetes Care. Aug 1995;18(8):1204-1214.
12. Norris SL, Engelgau MM, Narayan KM. Effectiveness of self-management training in type 2 diabetes: a systematic review of randomized controlled trials. Diabetes Care. Mar 2001;24(3):561-587.
13. Norris SL, Lau J, Smith SJ, Schmid CH, Engelgau MM. Self-management education for adults with type 2 diabetes: a meta-analysis of the effect on glycemic control. Diabetes Care. Jul 2002;25(7):1159-1171.
14. Steed L, Cooke D, Newman S. A systematic review of psychosocial outcomes following education, self-management and psychological interventions in diabetes mellitus. Patient Educ Couns. Sep 2003;51(1):5-15.
15. Deakin T, McShane CE, Cade JE, Williams RD. Group based training for self-management strategies in people with type 2 diabetes mellitus. Cochrane Database Syst Rev. 2005(2):Cd003417.
16. Clark M. Diabetes self-management education: a review of published studies. Prim Care Diabetes. Sep 2008;2(3):113-120.

79
17. Caballero AE. Diabetes in the Hispanic or Latino population: genes, environment, culture, and more. Curr Diab Rep. Jun 2005;5(3):217-225.
18. Millan-Ferro A, Caballero E. Role of Culture and Health Literacy in Diabetes Self-Management and Education. In: Weinger K, Carver C, eds. Educating your patient with diabetes. New York: Human Press; 2009.
19. AADE. Cultural sensitivity and diabetes education. Diabetes Educ. Jan-Feb 2012;38(1):137-141.
20. The Plurality of literacy and its implications for policy and programs. UNESCO Education Sector Position Paper. Paris.2004:13.
21. Boren SA. A review of health literacy and diabetes: opportunities for technology. J Diabetes Sci Technol. Jan 2009;3(1):202-209.
22. Habib SS, Aslam M. Risk factors, knowledge and health status in diabetic patients. Saudi Med J. Nov 2003;24(11):1219-1224.
23. Negarandeh R, Mahmoodi H, Noktehdan H, Heshmat R, Shakibazadeh E. Teach back and pictorial image educational strategies on knowledge about diabetes and medication/dietary adherence among low health literate patients with type 2 diabetes. Prim Care Diabetes. Jul 2013;7(2):111-118.
24. Sorensen K, Van den Broucke S, Fullam J, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80.
25. Muchiri J, Gericke G, Rheeder P. Needs and preferences for nutrition education of type 2 diabetic adults in a resource-limited setting in South Africa. Health SA Gesondheid. 2012;17(1):1-13.
26. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. Aug 18 2009;151(4):264-269, w264.
27. How we classify countries. 2013; http://data.worldbank.org/about/country-classifications. Accessed 15 October, 2013.
28. WHO. List of member states by WHO region and mortality stratum. 2013; http://www.who.int/mental_health/neurology/annexes_neuro_disorders_public_h_challenges.pdf. Accessed 09 December, 2013.
29. Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. Jun 1998;52(6):377-384.
30. Van den Broucke S, Van der Zanden G, Chang P, Doyle G, Levin D, Pelikan J, Schilinger D, Schwarz P, Sorensen K, Yardley L, Reimenschneider H. Enhancing the effectiveness of diabetes self-management education: The Diabetes Literacy project. Horm Metab Res.In press.
31. Schwarz PE, Gallein G, Ebermann D, Muller A, Lindner A, Rothe U, Nebel IT, Muller G. Global Diabetes Survey--an annual report on quality of diabetes care. Diabetes Res Clin Pract. Apr 2013;100(1):11-18.
32. Baradaran HR, Shams-Hosseini N, Noori-Hekmat S, Tehrani-Banihashemi A, Khamseh ME. Effectiveness of diabetes educational interventions in Iran: a systematic review. Diabetes Technol Ther. Apr 2010;12(4):317-331.

80
33. Lou Q, Wu L, Dai X, Cao M, Ruan Y. Diabetes education in mainland China- a systematic review of the literature. Patient Educ Couns. Dec 2011;85(3):336-347.
34. Aliha JM, Asgari M, Khayeri F, Ramazani M, Farajzadegan Z, Javaheri J. Group education and nurse-telephone follow-up effects on blood glucose control and adherence to treatment in type 2 diabetes patients. Int J Prev Med. Jul 2013;4(7):797-802.
35. Bayat F, Shojaeezadeh D, Baikpour M, Heshmat R, Baikpour M, Hosseini M. The effects of education based on extended health belief model in type 2 diabetic patients: a randomized controlled trial. J Diabetes Metab Disord. 2013;12(1):45.
36. Farsaei S, Sabzghabaee AM, Zargarzadeh AH, Amini M. Effect of pharmacist-led patient education on glycemic control of type 2 diabetics: a randomized controlled trial. J Res Med Sci. Jan 2011;16(1):43-49.
37. Hazavehei SM, Khani Jeihooni A, Hasanzadeh A, Amini S. The Effect of Educational Program Based on BASNEF Model for Eye Care in Non-insulin Dependent Diabetic Patients. J Res Health Sci. 2010;10(2):81-90.
38. Kashfi SM, Khani Jeihooni A, Rezaianzadeh A, Amini S. The effect of health belief model educational program and jogging on control of sugar in type 2 diabetic patients. Iran Red Crescent Med J. Jul 2012;14(7):442-446.
39. Samadi N SM, Mahmoodi M. Impact of quality of life education on self-concept among type 2 diabetes patients. J Diabetes Metab. 2011;2(5):1-5.
40. Sharifirad G, Entezari MH, Kamran A, Azadbakht L. The effectiveness of nutritional education on the knowledge of diabetic patients using the health belief model. J Res Med Sci. Jan 2009;14(1):1-6.
41. Vatankhah N, Khamseh ME, Noudeh YJ, Aghili R, Baradaran HR, Haeri NS. The effectiveness of foot care education on people with type 2 diabetes in Tehran, Iran. Prim Care Diabetes. May 2009;3(2):73-77.
42. Gagliardino JJ, Lapertosa S, Pfirter G, et al. Clinical, metabolic and psychological outcomes and treatment costs of a prospective randomized trial based on different educational strategies to improve diabetes care (PRODIACOR). Diabet Med. Sep 2013;30(9):1102-1111.
43. Perman G, Beratarrechea A, Aliperti V, et al. Mortality in an elderly type 2 diabetic patients' cohort who attended a self-management educational workshop. Prim Care Diabetes. Oct 2011;5(3):175-184.
44. Atak N, Gurkan T, Kose K. The effect of education on knowledge, self-management behaviours and self-efficacy of patients with type 2 diabetes. Int J Nurs Pract. 2009;18(2):170-179.
45. Karakurt P, Kasikci MK. The effect of education given to patients with type 2 diabetes mellitus on self-care. Int J Nurs Pract. Apr 2012;18(2):170-179.
46. Song MS, Kim HS. Intensive management program to improve glycosylated hemoglobin levels and adherence to diet in patients with type 2 diabetes. Appl Nurs Res. Feb 2009;22(1):42-47.
47. Liu S, Bi A, Fu D, et al. Effectiveness of using group visit model to support diabetes patient self-management in rural communities of Shanghai: a randomized controlled trial. BMC Public Health. 2012;12:1043.
48. Shi Q, Ostwald SK, Wang S. Improving glycaemic control self-efficacy and glycaemic control behaviour in Chinese patients with type 2 diabetes

81
mellitus: randomised controlled trial. J Clin Nurs. Feb 2010;19(3-4):398-404.
49. Al-haddad M, Ibrahim M, Sulaiman S, Maarup N. The impact of two diabetes educational programs on patients with diabetes in Malaysia. J Clin Diagn Res. . 2009;3:1633-1640.
50. Gagliardino JJ, Aschner P, Baik SH, et al. Patients' education, and its impact on care outcomes, resource consumption and working conditions: data from the International Diabetes Management Practices Study (IDMPS). Diabetes Metab. Apr 2012;38(2):128-134.
51. Chan JC, Gagliardino JJ, Baik SH, et al. Multifaceted determinants for achieving glycemic control: the International Diabetes Management Practice Study (IDMPS). Diabetes Care. Feb 2009;32(2):227-233.
52. Gill GV, Price C, Shandu D, Dedicoat M, Wilkinson D. An effective system of nurse-led diabetes care in rural Africa. Diabet Med. May 2008;25(5):606-611.
53. Price C, Shandu D, Dedicoat M, Wilkinson D, Gill GV. Long-term glycaemic outcome of structured nurse-led diabetes care in rural Africa. Qjm. Jul 2011;104(7):571-574.
54. van der Does AM, Mash R. Evaluation of the "Take Five School": an education programme for people with Type 2 Diabetes in the Western Cape, South Africa. Prim Care Diabetes. Dec 2013;7(4):289-295.
55. Mahajan H, Kambali T, Chokhandre M, Borle A, Padvi M. Health Intervention Impact Assessment on Glycemic Status of Diabetic Patients. International Journal of Diabetes Research. 2012;1(5):73-80.
56. Mahant S. Evaluating the impact of counseling on quality of life in type-2 diabetes mellitus patients. . Int J Pharm Bio Arch. 2013;2(6):137-141.
57. Malathy R, Narmadha M, Ramesh S, Alvin JM, Dinesh BN. Effect of a diabetes counseling programme on knowledge, attitude and practice among diabetic patients in Erode district of South India. J Young Pharm. Jan 2011;3(1):65-72.
58. Brown SA, Hanis CL. Culturally competent diabetes education for Mexican Americans: the Starr County Study. Diabetes Educ. Mar-Apr 1999;25(2):226-236.
59. Balagopal P, Kamalamma N, Patel TG, Misra R. A community-based participatory diabetes prevention and management intervention in rural India using community health workers. Diabetes Educ. Nov-Dec 2012;38(6):822-834.
60. Corkery E, Palmer C, Foley ME, Schechter CB, Frisher L, Roman SH. Effect of a bicultural community health worker on completion of diabetes education in a Hispanic population. Diabetes Care. Mar 1997;20(3):254-257.
61. Norris SL, Chowdhury FM, Van Le K, et al. Effectiveness of community health workers in the care of persons with diabetes. Diabet Med. May 2006;23(5):544-556.
62. Philis-Tsimikas A, Fortmann A, Lleva-Ocana L, Walker C, Gallo LC. Peer-led diabetes education programs in high-risk Mexican Americans improve glycemic control compared with standard approaches: a Project Dulce promotora randomized trial. Diabetes Care. Sep 2011;34(9):1926-1931.

82
63. Kandula NR, Nsiah-Kumi PA, Makoul G, et al. The relationship between health literacy and knowledge improvement after a multimedia type 2 diabetes education program. Patient Educ Couns. Jun 2009;75(3):321-327.
64. White RO, Wolff K, Cavanaugh KL, Rothman R. Addressing Health Literacy and Numeracy to Improve Diabetes Education and Care. Diabetes Spectr. Oct 2 2010;23(4):238-243.
65. Katz MG, Kripalani S, Weiss BD. Use of pictorial aids in medication instructions: a review of the literature. Am J Health Syst Pharm. Dec 1 2006;63(23):2391-2397.
66. Kripalani S, Robertson R, Love-Ghaffari MH, et al. Development of an illustrated medication schedule as a low-literacy patient education tool. Patient Educ Couns. Jun 2007;66(3):368-377.

83
CHAPTER 4: An audit of policies and programs
An audit of diabetes self-management education
programs in South Africa
Published as:
Dube L, Van den Broucke S, Rendall-Mkosi K, Kalweit K, Housiaux M, D’Hoore W.
An audit of diabetes self-management education programs in South Africa.
Journal of Public Health Research, 2015: 4(581), 176–184. doi:
10.4081/jphr.2015.581.

84
Abstract
Background
Diabetes is a significant contributor to the burden of disease worldwide. Since its
treatment requires extensive self-care, self-management education is widely
recommended, particularly in resource limited settings. This study aimed to review
the current state of policies and implementation of diabetes self-management
education (DSME) in South Africa, with a specific focus on cultural appropriate-
ness.
Design and Methods
The audit involved a review of policy documents and semi-structured
questionnaires with providers and experts in public and private health services.
Forty-four respondents were interviewed. Documents were analysed with reference
to the International Standards for Diabetes Education from the International
Diabetes Federation. Interview data were entered and analysed in excel to give a
description of the DSME programs and ad-hoc interventions.
Results
Three guidelines for Type 2 diabetes and two for chronic diseases were retrieved,
but none were specifically dedicated to DSME. Five structured programs and 22
ad-hoc interventions were identified. DSME is mostly provided by doctors, nurses
and dietitians and not consistently linked to other initiatives such as support
groups. Health education materials are mainly in English with limited availability.

85
Conclusions
DSME in South Africa is limited in scope, content and consistency, especially in the
public services. A National curricula and materials for diabetes education need to
be developed and adapted to the socio-economic context, culture and literacy
levels of the target populations. It is recommended that DSME would be addressed
in national policies and guidelines to guide the development and implementation of
standardised programs.
Significance to public health
Diabetes significantly contributes to the global burden of disease. This burden is
especially felt in developing countries, where resources are limited and the health
system simultaneously has to deal with communicable and non-communicable
diseases. While there is a growing body of literature on the development and
implementation of diabetes self-management education, nearly all programs
originate from developed countries. Very little is known about the current state of
diabetes self-management education in developing countries. By focusing on
diabetes self-management education in Southern Africa, the current paper provides
policy makers and decision makers in South Africa with information that will help
decide on where and how to intervene with regard to diabetes self-management
education. The paper also has relevance for decision makers from other
developing countries by providing recommendations on diabetes policies and
diabetes self-management education.

86
Introduction
Diabetes mellitus (DM) is a significant contributor to the burden of disease
worldwide, and its growing prevalence is a great concern for public health (1).
Recent estimates indicate that 382 million people are living with diabetes
worldwide, and that by the year 2035 this number will rise to 592 million (2). It is
also estimated that about 77% of people with diabetes live in low- and middle-
income countries where most deaths occur under the age of 60 years (2, 3). As a
result, many developing countries including South Africa are faced with the double
burden of communicable and non-communicable diseases (NCDs) (3).
According to the International Diabetes Federation (IDF), there were nearly 3
million people with diabetes in South Africa in 2013, with a prevalence of 8.27%
among the age group 20-79 years (2). The rising prevalence of diabetes is largely
due to economic development and urbanization which leads to changing lifestyles,
thereby reducing physical activity and increasing the levels of obesity and the
consumption of foods high in salt, fat and sugar (4). The prevalence of obesity is
indeed very high in South Africa, where the rates of obesity and combined
overweight and obesity (42% and 69.3%, respectively) are the highest in Sub-
Saharan Africa (5).
As diabetes requires extensive self-management related to diet, exercise and
medication in order to prevent complications, self-management education and
support are regarded as a critical element of treatment for all people with diabetes
(6). As such, diabetes self-management education (DSME) is widely
recommended and carried out where resources permit. However, despite the
great variety of DSME programs that are currently available internationally, there
is a paucity of information regarding educational interventions for the prevention of
diabetes complications in developing countries (7, 8).
The National Department of Health of South Africa has recently taken the initiative
to re-engineer the organisation of Primary Health Care (PHC) in the country and
to develop a National Health Insurance (NHI) system (9). A National Summit on

87
the prevention and control of NCDs organized in 2011 resulted in the commitment
to develop and implement different strategies to prevent and control NCDs
through preventive, health promoting, curative, rehabilitative and palliative
services at all levels (10). As such, it is important, to consider how DSME can be
integrated in this new system, and to what extent the re-engineering of PHC
provide a basis to develop and implement evidence-based programs for diabetes
self-management.
Moreover, for DSME to be effective in a multicultural society like South Africa, it is
required that both the educators and the content of programs be culturally
sensitive (11). Cultural sensitivity can be considered at two levels: surface
structure and deep structure (7). Surface structure refers to matching the
intervention materials and messages to observable “superficial” characteristics of
a target population, such as familiar people, places, language, music, food and
locations. Deep structure requires an understanding of the cultural, social,
historical and psychological forces that influence the target population.
This study sought to review the policies and guidelines presently available in
South Africa with regard to DSME, and to characterise the existing DSME offered
in both the private and the public health care services. The questions addressed
in the audit were to establish what types of DSME programs are currently offered
in different settings across the country, who implements them, what educational
approaches are used, how the programs are structured, how accessible they are,
what challenges are faced, and to what extent they are culturally sensitive. As
such, the audit provides a snapshot of the current state of DSME policies and
guidelines and of the implementation of DSME programs in South Africa.
Design and Methods
Study design and setting
An audit was conducted from March to June 2014 to explore DSME policies and
programs across the seven Provinces of South Africa. The audit involved a
document review of DSME policy and guidelines as well as interviews with health

88
service providers and experts involved in diabetes service provision, management
and research, in order to describe current DSME interventions.
Definition of terms
An intervention is referred to as a structured program when it has a clear definition,
a specific target group, a planned structure, a clear objective, a defined timeframe,
and a person/unit with formal program responsibility (Röthlin et al. Protocol for a
pre-post evaluation study on the effectiveness of existing diabetes self-
management programs, Working paper, Unpublished, The Diabetes Literacy
Project. 2014). For the purpose of this study, ad-hoc interventions were regarded
as those interventions which include educational talks in the waiting area or
spontaneous sharing of information during individual medical consultations without
planned structure and defined time frame. A public health service is one that is
provided by the national government, whereas a private health service is one
provided by the private sector and is for profit making. Providers include nurses,
doctors, health educators and experts refer to either researchers or people
involved in the field of diabetes in government, universities or private services.
Sampling
Purposive, convenience and snowball sampling were used to select respondents
aiming for diversity between public and private providers. Purposive sampling was
used to include respondents from different health sectors, as differences were
expected between private and public services. Convenience sampling was applied
by asking the organisers of the 49th Congress of the Society for Endocrinology,
Metabolism and Diabetes of South Africa (SEMDSA) the permission to recruit
participants attending this congress. Furthermore, respondents were recruited from
different settings, including selected public and private facilities and non-
governmental organisations (NGO) using snowball sampling. The first author (LD)
contacted Heads of the Provincial Health Departments of all provinces of South
Africa and asked to be referred to a focal person for chronic diseases in each
Province. Provincial focal persons were interviewed and referred the researchers to

89
relevant facilities and other NGO focal people in the area. Data were only collected
from Provinces who gave approval and from individuals who gave informed
consent to participate.
Data collection
Policy and guideline documents for the review were accessed via the website of
the National Department of Health (11). To avoid missing relevant documents,
respondents were asked for any available documents and copies were collected if
available. Only documents relating to Type 2 diabetes were included for document
analysis.
For the data collection from service providers, experts and researchers, two
questionnaires were used. The questionnaires were adapted from the Global
Diabetes Survey (GDS), which is a tool to collect data on diabetes care quality on a
yearly basis, developed and validated via a multiple Delphi process (12, 13). The
provider questionnaire collected information about existing DSME programs in
terms of the type of programs, providers, target groups, educational approach, and
challenges faced. The expert questionnaire collected information regarding DSME
policy, accreditation of DSME interventions by accrediting bodies (standardising
bodies) and suggestions for policies and guidelines. The questionnaires were
mostly self-administered but in a few cases (5 interviews) they were interviewer
administered. Additional notes were taken during the interviews.
Data management and analysis
Data from the documents were extracted using the International Standards for
Diabetes Education (ISDE) developed by the International Diabetes Federation.
These standards have been developed and revised based on experiences from
diabetes educators in both developing and developed countries, and aim to
support policy makers worldwide to develop diabetes education. They provide a
benchmark against which the quality of education delivered can be evaluated (14).
The ISDE were used by two authors (LD and MH) to independently extract

90
information on the content of DSME in the national guidelines in order to establish
the adequacy of these documents in South Africa in terms of structure, process
and outcome standards. An agreement of 90% was achieved between the authors
and through further discussion a consensus (100% agreement) was reached.
Questionnaire data were entered and analysed in excel to give an overview of the
current status of DSME in private and public services of South Africa.
Ethics
The study was approved by the Health Sciences Research Ethics Committee of the
University of Pretoria (54/2014) and the Provincial Research Ethics Committees of
each province in the public sector. Respondents gave written informed consent and
anonymity and confidentiality of their responses was assured.
Results
Distribution of participants across provinces
Forty-four respondents completed the questionnaires; 27 providers (7 from
private, 4 from NGOs and 16 public) and 17 experts. Data was collected in all
provinces except for Eastern Cape and Limpopo’s public sector where no
permission was granted. Table 4.1 shows number of respondents per province
with Gauteng having the highest number of respondents.

91
Table 4.1 Number of respondents from each province
Province Provider
questionnaire Expert
questionnaire Total
respondents
Gauteng 8 9 17
Mpumalanga 4 1 5
North West 3 1 4
Northern Cape 1 1 7
Free State 3 1 4
Western Cape 4 0 5
KwaZulu-Natal 2 3 7
Limpopo 2 1 3
Eastern Cape 0 0 0
Total 27 17 44
Policies and guidelines with regard to DSME
No policy documents were identified with regards to DSME specifically. Three
guideline documents on Type 2 diabetes were found: The Updated Management of
Type 2 Diabetes in Adults at Primary Care Level, released in 2014 (15); The
National Guidelines for the Management of Diabetes Type 1 and 2 in Adults at
Hospital Level, released in 2005 (16); and The 2012 SEMDSA Guideline for the
Management of Type 2 Diabetes (Revised) (17). The first two documents were
obtained from the National Department of Health. In these three documents,
diabetes education was minimally covered. The guidelines included information on
structure and process standards; however, this information was not
comprehensive. As shown in Table 4.2, it appears that the 2014 document from the
National Department of Health was derived using the 2012 SEMDSA guidelines as
the information included is almost the same. The 2005 document covered the least
amount of information on DSME compared to the other two guidelines.
To understand DSME in the context of chronic disease management in South
Africa, the Integrated Chronic Disease Management (ICDM) Manual (undated)(18)

92
and the Primary Care 101(19) guidelines were also taken into consideration. The
ICDM is a model of care for chronic diseases that is being implemented by the
National Department of Health of South Africa. The Primary care 101 is currently
being implemented as part of the ICDM in primary care. The disease categories
currently being addressed in this model are hypertension, diabetes, chronic
obstructive pulmonary disease, asthma, epilepsy, mental health HIV/AIDS,
tuberculosis (TB) and multi-drug resistant TB. The model contains a self-
management component which aims to empower individuals to take responsibility
for their illness through understanding the necessary preventive and promotional
actions required to decrease complications and multiple visits to the facilities. The
expected outcome is to create an informed, motivated and adherent patient.
According to this model, trained Community Health Workers (CHWs) are mandated
to provide health education to patients during home visits. Health education and
promotion strategies are applied at the individual, family and community level to
reduce the risk factors for developing chronic diseases and prevent complications
from the existing condition(s). The health education sessions include, but are not
limited to: healthy eating, active living through appropriate exercises, decrease in
alcohol intake, reduction in tobacco, snuff, alcohol, salt and risky sexual behaviour.
The primary care 101(19) guideline document is designed in such a way that for
each chronic disease, it gives some educational information which the provider
should give to the patient. For diabetes the provider is advised to encourage the
patient to adhere to medication, educate patient on recognizing and managing
hypoglycemia, and to care for their feet.
In their responses to the questionnaires, experts and providers made recommen-
dations that could be included in policies and guidelines for implementation of
DSME. These include environment related policies such as subsidization of healthy
foods and support for people with diabetes in the work place. To support patient
adherence to insulin use, policies could mandate patients to bring back an empty
insulin pen to qualify for renewal of insulin prescription. Furthermore, guidelines

93
could also include dietary recommendations appropriate for poor communities in
order to support patients to adhere to dietary recommendations. Guidelines could
consider more attention to the actual implementation of DSME, support for
educational programs, establishment of one standard-assuring body for diabetes
education and also consider recognition of the training of providers in DSME.
Description of DSME programs
Of the 27 respondents who answered the questionnaire on interventions, five
reported on structured programs and 22 reported on ad-hoc education
interventions. Sixteen of the 27 programs are in the public services whilst 11 are
in the private services and NGOs. Respondents reported that few interventions
(37%) are accredited by a professional body (Diabetes Education Society of South
Africa (DESSA), the International Diabetes Federation (IDF), the United Kingdom
Diabetes Association and Center for Diabetes Education (CDE), the Provincial
Department of Health and SEMDSA).
Of the five programs that are structured, three are in the public services and two in
the private services. All the programs are offered as initial education interventions
and have a clear start and an end with a duration of two days to eight months
(Table 4.3). At two facilities the same program is offered. Twenty-two services
offer ad-hoc education. Of these, 13 are in the public services and nine in the
private sector. Most DSME interventions (15 of 22) are incorporated into the
ICDM, whereby the diabetes patients are grouped with those with other chronic
illnesses for educational purposes. This education mostly takes place in the facility
waiting area or club rooms, or, in the case of individual counseling, sometimes
during medical consultations with the providers. DSME interventions in the public
sector are free of charge. In the private sector they are included in the
consultation fee.

94
Table 4.2 DSME information extracted from guidelines using the International Standards for Diabetes Education (14)
Domains in International Standards for Diabetes Education (14)
Criteria set by the International standards for diabetes education
The Updated Management of Type 2 Diabetes in Adults at Primary Care Level ,2014
The 2012 SEMDSA Guideline for the Management of Type 2 Diabetes, 2012
The National Guidelines for the Management of Diabetes Type 1 and 2 in Adults at Hospital Level, 2005
STRUCTURE STANDARDS
Organizational support- there is evidence of organizational/institutional support for diabetes self-management education (DSME) as an integral part of diabetes care
Not included Not included Not included
Coordination- One person responsible for the organization and administration of DSME services to ensure that the process and outcome standards are met
Not included Not included Not included
Physical space and equipment- the quality and availability of physical space and educational resources affect learning and are based on individual/community needs
Not included Not included Not included
Advisory committee- An advisory committee ensures that the views and values of all stakeholders are represented in the ongoing planning and delivery of DSME
Not included Not included Not included
The team and team work-multidisciplinary teamwork and communication are evident among those providing DSME and diabetes care services
Not included Not included All health professionals, lay health workers, traditional healers & complimentary health professionals

95
Domains in International Standards for Diabetes Education (14)
Criteria set by the International standards for diabetes education
The Updated Management of Type 2 Diabetes in Adults at Primary Care Level ,2014
The 2012 SEMDSA Guideline for the Management of Type 2 Diabetes, 2012
The National Guidelines for the Management of Diabetes Type 1 and 2 in Adults at Hospital Level, 2005
STRUCTURE STANDARDS
Professional skill and continuing education- a) personnel involved in DSME have a sound clinical understanding of diabetes, and are knowledgeable about teaching and learning methods and diabetes care b) The competence and performance of personnel involved in DSME are reviewed at least annually and an individual learning and development plan implemented to strengthen knowledge, skills and attitudes c) Professional DSME personnel are appointed based on demonstrated competences not on a rotational basis
Not Clear - Trained educators mentioned to provide education
Not clear – providers to be trained in motivational interviewing
Not included
Curriculum- Diabetes education covers topics based on individual assessment and fosters the acquisition of knowledge, skills, behaviors and coping strategies that are needed for optimal self-management of diabetes
Only topics outlined Only topics outlined Only topics outlined
Support systems- a) Strategic partnerships and referral pathways are developed in order to improve communication and the consistency of services among healthcare professionals, and to maximize the impact of diabetes resources. b) Ongoing self-management education and support are accessible to people with diabetes after the completion of initial DSME.
Not included Not included Not included

96
Domains in International Standards for Diabetes Education (14)
Criteria set by the International standards for diabetes education
The Updated Management of Type 2 Diabetes in Adults at Primary Care Level ,2014
The 2012 SEMDSA Guideline for the Management of Type 2 Diabetes, 2012
The National Guidelines for the Management of Diabetes Type 1 and 2 in Adults at Hospital Level, 2005
PROCESS STANDARDS
Community assessment- The DSME service develops based on an ongoing assessment of the needs of the population it serves.
Not included Not included Not included
Individualized plan - Plans for individual diabetes education and diabetes education programs are learner-centered and subject to ongoing review and modification.
An integrated approach to education is utilized, recognizing and acknowledging the different needs of the patient, family and / or caregiver.
Not included Not included
Implementation – a) The implementation of DSME is learner-centered and facilitates cognitive learning, behavior change, healthy coping and self-management, and is extended to families, supporters, carers and communities where appropriate. b) DSME is evidence-based and provided in a professional and ethically sound manner.
An evidence-based structured education program on diabetes self-management is offered to all patients at the time of diagnosis, and consolidated at regular intervals thereafter.
An evidence-based, structured education program should be offered to all patients at the time of diagnosis, and consolidated at regular intervals thereafter.
Not included

97
Domains in International Standards for Diabetes Education (14)
Criteria set by the International standards for diabetes education
The Updated Management of Type 2 Diabetes in Adults at Primary Care Level ,2014
The 2012 SEMDSA Guideline for the Management of Type 2 Diabetes, 2012
The National Guidelines for the Management of Diabetes Type 1 and 2 in Adults at Hospital Level, 2005
Access- a) DSME services will be recognized by and accessible to the local community. b) The DSME service leadership and team members seek strategic alliances and partnerships with relevant community services in order to increase accessibility, and advance DSME and DSMS. c) Follow-up and DSMS are accessible as needed and recommended as part of continuing education, behavioral goal-setting and action-planning, and/or reinforcement.
Not included Not included Not included
Evaluation- The effectiveness and quality of the DSME service are assessed annually, linked to outcomes, and reviewed and revised on the basis of this assessment.
A regular audit of the program, and its effect on outcomes, is advised
A regular audit of the program and its effect on outcomes is advised.
OUTCOME STANDARDS
Knowledge- People with diabetes understand the effects of diabetes, treatment modalities, management of the behavioral, psychosocial and clinical aspects of diabetes, and the significance of maintaining a healthy lifestyle in order to reduce the risks for diabetes-related complications.
Not included Not included Not included

98
Domains in International Standards for Diabetes Education (14)
Criteria set by the International standards for diabetes education
The Updated Management of Type 2 Diabetes in Adults at Primary Care Level ,2014
The 2012 SEMDSA Guideline for the Management of Type 2 Diabetes, 2012
The National Guidelines for the Management of Diabetes Type 1 and 2 in Adults at Hospital Level, 2005
Application of knowledge - People with diabetes and those at risk for diabetes make informed decisions and take deliberate action towards healthy living. These decisions occur in the context of their own values, socio-economic needs and resources, and desired quality of life.
Not included Not included Not included
Clinical outcomes- a) The physical, psychological, and emotional health of the person with diabetes is improved. b) The person with diabetes collaborates with clinical care providers to define problems, set priorities, establish goals, create action and treatment plans, and solve problems.
Not included Not included Not included
The community- primary prevention Communities are aware of risk factors for diabetes and its potential complications and actions that may delay their onset.
Not included Not included Not included
Community support- Communities are aware of the different types of diabetes and the needs of and support available for people living with diabetes.
Not included Not included Not included

99
Table 4.3 Timeframes of structured programs
Name of program Duration Number
of sessions
Duration of each
session
Period between sessions
Five steps to self-care (NGO- Gauteng)
8 months 32 30mins -2hours 1 week
Diabetic Lifestyle Education Collaboration & Action (D-LECA) (Woodstock, public facility, Western Cape)
4 months 4 2-4hours 1 month
D-LECA (Lotus river , public facility, Western Cape)
4 months 4 1-2 hours 1 month
Lifestyle management + training for T2 diabetes (Public Hospital- Gauteng)
6 weeks 6 4 hours 1 week
Youth with diabetes weekend camps (Youth with Diabetes, NGO- Gauteng)
2 days 5 30-60 minutes Annual 2 days event
Providers - For both structured programs and ad-hoc education, different
combinations of providers are employed. Most providers are health professionals,
with physicians and dietitians being the most common. Health promoters are the
only non-professional category mentioned (Figure 4.1). Respondents also
mentioned that training is essential for providers and that specific diabetes-related
training courses are necessary, including the ones provided by DESSA or CDE.

100
Figure 4.1 Types of providers in diabetes self-management education
Target population - In structured programs, the target population are patients
with either Type 1 or 2 diabetes and other chronic diseases. Only one program
addressed children and adolescents with Type 1 diabetes. The ad-hoc interven-
tions in the public services mostly target adult patients, while children are referred
to specific facilities. In the private service all age groups are addressed.
Educational interventions offered in the private services also address gestational
diabetes, while in the public service these patients are immediately referred to the
special maternity care clinics. In both structured and ad-hoc interventions,
education is designed for patients and their families or their peers. The majority of
the ad-hoc interventions were done in community based primary care, diabetes
special care and hospital settings. Of the structured programs, 3 were offered in
community based primary care, one in diabetes special care, and one in a non-
clinical setting.
Program content – Content analysis of the structured and ad-hoc interventions
was done based on the self-care behaviour topics included in the American

101
Association of Diabetes Education (AADE) (20) (i.e., healthy eating, staying
active, taking medication, monitoring of blood glucose, problem solving, reducing
risks and living with diabetes). In both the structured programs and ad-hoc
interventions, the content of the educational activities varied considerably. Table
4.4 shows the different contents of education for both structured and ad-hoc
interventions. As this table shows, across programs healthy eating, physical
activity and self-monitoring of blood glucose were most often addressed, while
glucagon administrations, self-measurement of blood pressure and dealing with
the legal aspects of the disease were least often addressed.
Table 4.4 Content included in programs and ad-hoc interventions
Topic based on AADE (20)
Sub-topic Ad-hoc Structured
Healthy eating
Meal planning 21 4
Food labelling & interpretation 17 4
Weighing 16 4
Carbohydrates counting 13 3
Physical activity Developing appropriate activity plans 21 2
Increase frequency, duration and intensity 19 4
Self-monitoring of blood glucose
Self-monitoring of blood glucose technique (skills) 22 5
Recording of blood glucose values 21 5
Equipment use and care 18 3
Taking medication
Preparation, technique and administration 20 5
Recognition, treatment & prevention of low blood glucose
20 5
Safe handling and disposal of equipment 18 4
Dose adjustment 16 3
Problem solving
Hypoglycaemia treatment 22 5
Use of blood glucose data to determine appropriate actions
21 5
Glucagon administration 7 2
Reducing risks
Self-management of blood glucose (knowledge) 19 5
Smoking cessation 20 3
Maintaining personal records 19 4
Foot exam 19 3

102
Topic based on AADE (20)
Sub-topic Ad-hoc Structured
Staying in contact with diabetes care professionals 18 4
Support in searching for further contact and help 14 4
Self-measurement of blood pressure 10 2
Living with diabetes
Goal setting/individual targets 21 4
Problem solving 20 4
Coping strategies 18 4
Action planning 18 3
Understanding own clinical picture 19 2
Self-efficacy 20 1
Dealing with depression 15 1
Dealing with legal aspects of the disease 10 0
Educational approaches - In the structured programs, education is offered in
planned group sessions with professional facilitation and sometimes with
additional individual and self-help sessions for patients with poorly controlled
diabetes. A structured written curriculum for each program is available and two of
the programs use the “I change 4 Health” lifestyle change materials developed for
patients with non-communicable diseases (21). One program has a website
available for patients. The ad-hoc educational interventions are offered in groups
in the waiting area and during individual consultation sessions with the provider.
Some ad-hoc educational interventions had written guidelines to which provider
could refer for information. Respondents reported using pamphlets and booklets
which are mainly written in English. In most cases these materials are supplied by
pharmaceutical companies free of charge but are not always available. According
to the respondents (93%) from both structured and ad-hoc interventions,
education is accessible to people with low levels of literacy through the use of the
local language, practical demonstrations, pictures and visual aids and the
encouragement of family involvement. However, deep structural aspects of culture
including individual needs assessment are rarely addressed.
Evaluations of programs - Two of the five structured programs were based on a
randomised controlled trial (RCT) that showed the program to be cost-effective in

103
the South African context (22). Two other programs are in the process of being
evaluated: one using a randomised controlled trial, and another using a
retrospective observation study. The remaining program was never evaluated.
None of the ad-hoc educational interventions have ever been evaluated.
The experts’ responses to the questionnaires revealed that core educational
principles exist on paper, yet their implementation is not guaranteed. In terms of
the perceived effectiveness of DSME programs, most experts gave a score
between 5 to7 on a scale of 1-10 (with 1 being not at all effective versus 10 being
very effective), indicating an intermediate effectiveness. When asked to identify
the aspects of DMSE that need improvement, the experts mentioned the need to
develop structured patient education programs and a need to train personnel in
chronic disease education. The introduction of chronic disease education in
schools as part of a school lifestyle and wellness was also suggested.
In their response to questionnaires, providers identified a range of problems that
affect the delivery of DSME. One problem concerned inadequate finances, which
results in a shortage of staff, long working hours, and lack of time and space for
patient education which leads to low prioritisation of DSME. A second problem is
the lack of recognition for staff after diabetes training, and a shortage of teaching
materials to give to patients. A third issue concerns the patients, who are said to
be ignorant and non-compliant. Abuse of services and misconceptions
surrounding diabetes regardless of patient education was also mentioned. A
further problem is related to poverty and the difficulty patients have in adhering to
diet recommendations due to food insecurity.
Discussion
This audit aimed to collect information on policies and the nature of existing DSME
programs in South Africa. It was revealed that although there is currently no policy
specific to DSME in South Africa, DSME is mentioned in national guidelines on
diabetes. However, much needs to be done in terms of developing and implement-
ing guidelines for DSME, in order to reach the International Standards for Diabetes

104
Education (14). As these standards are designed to provide a framework to
establish or further develop DSME, failure to meet these standards results in a
poor implementation of DSME.
A first shortcoming revealed by this audit is the absence of well-structured
programs for DSME. DSME is often delivered on an ad-hoc basis in the waiting
area or individually during consultation with the provider. Individual ad-hoc
education has its own challenges, such as the fact that the actual delivery of the
education depends on the available time of the provider (23), or that patients
receiving DSME in the waiting area are disturbed by noise, lack of privacy, and
other factors that make it difficult to concentrate on the content. The ad-hoc nature
of DSME also results in individual patients being exposed to an arbitrary choice of
topics, which may not result in the behaviour change that is required.
On the other hand, it is possible to combine ad hoc counselling with structured
group education. A model that combines behaviour change counselling with ad hoc
guidance organised around 5 “As”(assess, advise, agree, assist and arrange) has
been proposed and has shown to be effective. (24) Although the implementation of
this 5As model is currently limited, it could be used by primary care physicians in
their consultations with patients.
The providers who are responsible for DSME in South Africa are mostly
professional health care providers and only a small proportion are non-health
professionals. This is contrary to the ICDM model, which recommends that health
education should mainly be provided by CHWs and health promoters. There was
no mention of CHWs as providers in the interviews. According to a recent
systematic review, it is advisable that in resource poor settings peers and CHWs
are trained to provide DSME, while professional staff like nurses takes up
supervisory and training roles for the non-professionals (7). However, one should
note that relying more on CHWs also has its limits and is not a panacea, especially
when these are not sufficiently trained. An extensive Cochrane review revealed
limited evidence of trained lay health workers on providing effective DSME,
however, this could still be part of the solution for developing countries (25).

105
A second shortcoming emerging from this audit is that there is no continued
education for providers and a lack of recognition for providers after diabetes
training. Despite the existence of national guidelines on diabetes education, some
providers reported that they were not aware of these, which suggests a lack of
ongoing training and refresher workshops that are crucial for providers. This
confirms the findings from a previous study, indicating that current training in
behaviour change counselling for primary care providers is very limited (26). Health
professionals need access to continued education and training to stay updated on
new developments and to boost their morale and professional role (23). Moreover,
a lack of a standardised written curriculum, physical space and time presents a
challenge for the implementation of DSME programs, as has been suggested by
previous research mentioning the lack of physical space in facilities as hindering
DSME interventions (23, 26, 27).
A third point showing from this audit is the lack of cultural adaptation of DMSE and
the absence of the patient perspective. Whereas diabetes guidelines recognise
and acknowledge the different needs of patients, family and caregivers, there is
very little evidence of this taking place in practice. Although local languages are
used to communicate with patients and pictures and visual aids are used (surface
structure), there are no individual needs assessments (deep structure), and most
written materials are only available in English. Providers requested practical dietary
recommendations for people in poverty stricken areas as the current
recommendations are inappropriate. This shows that the cultural sensitivity of
existing DSME interventions still needs to be improved. For diabetes education to
be effective in multicultural societies, both the educators and the content of
programs should be culturally sensitive (7, 8, 28). Therefore, self-management
curricula should be developed and adapted to the culture and needs of the
patients. The patient education component in the Primary Care 101 document
could be expanded in order to provide advice to providers.
A fourth shortcoming is the lack of evaluation of DSME programs. It is important in
health promotion that programs be evaluated in order to contribute to the evidence

106
base (29, 30). Although the national guidelines on diabetes state that evidence-
based structured self-management must be provided to patients and that a regular
audit should be performed, this was not the case. Most DSME interventions, except
for the two structured programs derived from the RCT, have not been evaluated,
which makes it impossible to consider their effectiveness.
While this audit is the first of its kind to describe current policies and guidelines with
regard to DSME in South Africa, and to consider the way in which DSME
interventions are implemented in different settings across the country, we are
aware of its limitations. Firstly, since non-randomised sampling was used as a
method to select interventions for inclusion in the study, it is possible that we have
missed some interventions. Furthermore, because of difficulty in obtaining ethical
clearance from some facilities and authorities, and due to limited resources, some
potentially relevant documents and interventions may have been missed. Thirdly
no observation of interventions was carried out, which precludes the possibility of
triangulating the results with what respondents reported. Nevertheless, given the
recurrent findings and the high degree of consensus with regard to the information
derived from the sources that were consulted, we believe that this audit provides a
useful snapshot of the current policy and practice with regard to DSME in South
Africa.
Conclusions
DSME is rarely adequately addressed in national policies and guidelines in South
Africa, and much work still needs to be done for DSME in the country to reach
international standards. At present, DSME is mainly offered on an ad-hoc basis,
and only a few structured programs exist. For both ad-hoc and structured
interventions, health professionals are the main providers. Many barriers exist to
develop and implement more structured DSME. These include, but are not limited
to, lack of time and space, lack of finances, and lack of educational resources in
other languages than English. It is recommended that these points would be

107
addressed in national policies to guide the development and implementation of
standardised, more culturally sensitive and more effective DSME programs.
References
1. Hjelm K, Mufunda E. Zimbabwean diabetics' beliefs about health and illness: an interview study. BMC international health and human rights. 2010;10:7.
2. IDF Diabetes Atlas. Sixth edition. [Internet]. 2013 [cited 28 July 2015]. Available from: https://www.idf.org/sites/default/files/EN_6E_Atlas_Full_0.pdf.
3. Mayosi BM, Flisher AJ, Lalloo UG, Sitas F, Tollman SM, Bradshaw D. The burden of non-communicable diseases in South Africa. Lancet. 2009;374(9693):934-47.
4. Whiting DR, Guariguata L, Weil C, Shaw J. IDF diabetes atlas: global estimates of the prevalence of diabetes for 2011 and 2030. Diabetes research and clinical practice. 2011;94(3):311-21.
5. Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9945):766-81.
6. Schinckus L, Van den Broucke S, Housiaux M. Assessment of implementation fidelity in diabetes self-management education programs: A systematic review. Patient education and counseling. 2014;96(1):13-21.
7. Dube L, Van den Broucke S, Housiaux M, Dhoore W, Rendall-Mkosi K. Type 2 diabetes self-management education programs in high and low mortality developing countries: a systematic review. The Diabetes educator. 2015;41(1):69-85.
8. Ezenwaka C, Eckel J. Prevention of diabetes complications in developing countries: time to intensify self-management education. Archives of physiology and biochemistry. 2011;117(5):251-3.
9. Dennill K, Rendall-Mkosi K. Primary Health Care in South Africa. A comprehensive approach. Cape Town: Oxford University Press Southern Africa; 2012.
10. South African Declaration on the prevention and control of non-communicable diseases. [Internet]. 2011 [cited 28/07/2014]. Available from: http://www.health.uct.ac.za/usr/health/research/groupings/cdia/downloads/SA_NCD_Declaration.pdf.
11. Policy Documents. Department of Health South africa [Internet]. 2014. Available from: http://www.health.gov.za/policies.php.
12. Schwarz PE, Gallein G, Ebermann D, Muller A, Lindner A, Rothe U, et al. Global Diabetes Survey--an annual report on quality of diabetes care. Diabetes research and clinical practice. 2013;100(1):11-8.
13. Van den Broucke S, Van der Zanden G, Chang P, Doyle G, Levin D, Pelikan J, et al. Enhancing the effectiveness of diabetes self-management

108
education: the diabetes literacy project. Hormone and metabolic research = Hormon- und Stoffwechselforschung = Hormones et metabolisme. 2014;46(13):933-8.
14. International Standards for Diabetes Education. Third edition. [Internet]. 2009 [cited 1 July 2014]. Available from: http://www.idf.org/files/idf_publications/international_standards_for_diabetes_education_EN/index.html.
15. Updated management of type 2 diabetes in adults at primary care level. National Department of Health South africa. 2014.
16. National Guidelines. Management of diabetes type 1 and 2 in adults at Hospital level. The National Department of Health. 2005.
17. Amod A, Ascott-Evans BH, Berg GI BD, Brown SL, Carrihill MM, Dave JA, et al. The 2012 SEMDSA Guideline for the Management of Type 2 Diabetes (Revised). Journal of Endocrinology, Metabolism and Diabetes of South Africa. 2012;17(2):S1-S95.
18. Asmall S, Mahomed O. Integrated chronic diseases management manual. National Department of Health of South Africa. Undated.
19. Primary Care 101: Symptom-based integrated care approach to the adult in primary care. [Internet]. National Department of Health. 2013. Available from: http://knowledgetranslation.co.za/programmes/pc-101/.
20. Mulcahy K, Maryniuk M, Peeples M, Peyrot M, Tomky D, Weaver T, et al. Diabetes self-management education core outcomes measures. The Diabetes educator. 2003;29(5):768-70, 73-84, 87-8 passim.
21. Murphy K, Mash B, Malan Z. Helping people to change: the busy healthcare practitioners guide to providing brief behaviour change counselling on non-communicable diseases (NCD) lifestyle risk factors.: CIDA; 2013. Available from: http://www.ichangeforhealth.co.za/index.php/healthcare-professionals/#prettyPhoto/0/.
22. Mash R, Kroukamp R, Gaziano T, Levitt N. Cost-effectiveness of a diabetes group education program delivered by health promoters with a guiding style in underserved communities in Cape Town, South Africa. Patient education and counseling. 2015;98(5):622-6.
23. Parker WA, Steyn NP, Levitt NS, Lombard CJ. Health promotion services for patients having non-comminicable diseases: feedback from patients and health care providers in Cape Town, South Africa. BMC public health. 2012;12:503.
24. Mash R. The KM Seedat Memorial Lecture: Behaviour change counselling in the South African context. Transactions. 2014;58(1):58-62.
25. Deakin T, McShane CE, Cade JE, Williams RD. Group based training for self-management strategies in people with type 2 diabetes mellitus. The Cochrane database of systematic reviews. 2005(2):Cd003417.
26. Malan Z, Mash B, Everett-Murphy K. A situational analysis of training for behaviour change counselling for primary care providers, South Africa. African journal of primary health care & family medicine. 2015;7(1):E1-e10.
27. Mash RJ, Rhode H, Zwarenstein M, Rollnick S, Lombard C, Steyn K, et al. Effectiveness of a group diabetes education programme in under-served communities in South Africa: a pragmatic cluster randomized controlled

109
trial. Diabetic medicine : a journal of the British Diabetic Association. 2014;31(8):987-93.
28. Rawal LB, Tapp RJ, Williams ED, Chan C, Yasin S, Oldenburg B. Prevention of type 2 diabetes and its complications in developing countries: a review. International journal of behavioral medicine. 2012;19(2):121-33.
29. Green J, K. T. Heath Promotion: Planning and Strategies. London: SAGE Publications Ltd; 2010.
30. Tones K, Tilford S. Health Promotion: Effectiveness, efficiency and equity. .
3rd ed. Cheltenham: Nelson Thornes Ltd; 2001.

110

111
CHAPTER 5: Self-management needs assessment
Self-management support needs of patients with chronic
diseases in a South African township: a qualitative study
Accepted for publication as:
Dube L, Rendall-Mkosi K, Van den Broucke S, Bergh AM, Mafutha NG. Self-
management support needs of patients with chronic diseases in a South African
township: a qualitative study. Journal of Community Health Nursing.In Press

112
Abstract
Despite the need for chronic disease self-management strategies in developing
countries, few studies have aimed to contextually adapt programs; yet culture has
a direct impact on the way people view themselves and their environment. This
study aimed to explore the knowledge, attitudes and self-management needs and
practices of patients with chronic diseases. Four patient focus groups (n=32), two
patient interviews, group observations, and key informant interviews (n=12) were
conducted. Five themes emerged: health-system and service-provision challenges,
healthcare provider attitudes and behavior, adherence challenges related to
medication and lifestyle changes, patients’ personal and clinic experiences and
self-management tool preferences. The findings provide a window of opportunity
for the development of contextually adapted self-management programs for com-
munity health nursing in developing countries.
Keywords Chronic disease · Self-management support · Patient needs and
challenges · Community health nursing · South Africa

113
Introduction
Non-communicable diseases (NCDs) affect all countries, people, genders and
ages, regardless of socio-economic status; however, they are more devastating in
low-and-middle income countries (World Health Organization, 2015a). Albreht,
Dyakova, Schellevis, & Van den Broucke, (2016) argue that worldwide the
advances in health care systems have transformed previously life-threatening
diseases like HIV into chronic conditions requiring on-going care. Because of this
transformation, developing countries now face a unique double burden of
communicable and non-communicable diseases. As such, NCDs have become an
international public health threat and have now been included in global health
targets for the first time, for example in the Sustainable Development Goals
(SDGs) (World Health Organization, 2015b).
NCDs are grouped into cardiovascular diseases, cancers, diabetes and chronic
respiratory diseases, revealing their relationship with common modifiable lifestyle
risk factors such as physical inactivity, tobacco use, unhealthy diets and harmful
use of alcohol (Maher, Ford, & Unwin, 2012). They are conditions that do not
disappear and affected people have to adjust their lifestyles in order to remain
healthy (van Olmen et al. 2011). As such, self-management is generally considered
a key treatment modality for patients with chronic diseases (Dube, et al. 2015a).
De Silva describes self-management as “the actions that individuals and caregivers
take for themselves, their children, their families and others to stay fit and maintain
good physical and mental health, meet social and psychological needs, prevent
illness or accidents, care for minor ailments and long-term conditions and maintain
health and wellbeing after an acute illness or discharge from hospital” (deSilva,
2011).
People with chronic conditions or their caregivers and family perform 80 to 90 per
cent of the overall care needed. Taking up this responsibility requires collaborative
support from health service providers. Self-management support involves

114
educating patients to maintain greater control through understanding their
condition, being involved in monitoring, and taking action. This should be
complemented by support in goal setting, decision making, adopting a healthy
lifestyle and knowing when to seek help (deSilva, 2011; Lukewich, Mann,
VanDenKerkhof, & Tranmer, 2015).
There is evidence that supporting patients to improve their self-management has
positive effects on clinical outcomes, quality of life and health service use (Brady,
et al. 2013; Franek, 2013; Steinsbekk, Rygg, Lisulo, Rise & Fretheim, 2012;
Stoilkova, Janssen, & Wouters, 2013). For this reason, health programs such as
Healthy People 2020 include self-management objectives for chronic patients
(Healthy People.gov, 2014). However, in developing countries, there is a paucity of
literature related to culturally-appropriate chronic disease self-management
strategies and tools that would meet both the surface and deep structural aspects
of the societies in which they are offered and that would affect sustainable changes
in behavior (Dube, Van den Broucke, Hosiaux, Dhoore & Rendall-Mkosi, 2015b;
Choi, Walker, Ralson, & Palermo, 2014). Surface structure refers to matching
interventions to observable characteristics of a target population (people, places,
language, music), while deep structure refers to an understanding of the culture of
the target population and includes an analysis of needs (Dube et al. 2015b).
Culture has a direct impact on the way people view themselves and their
environment (Marsiglia & Booth, 2015). While overweight and obesity are major
risk factors for NCDs, increasing weight in the South African culture is associated
with success (Kirsten & Karch, 2012) and overweight women do not perceive
obesity as a health threat (Okop, Mukumbang, Mathole, Levitt & Puoane, 2016).
Other studies have found that exposure to Asian cultural cues and identification
with black culture in American women was associated with larger ideal body sizes
(Yam, 2013). In some cases chronic illness is attributed to spiritual causes and as
a result the individual is perceived as not having control over the disease (de Graft
Aikins, Anum, Agyemang, Addo & Ogedegbe, 2012). In South African culture
traditional healers play a significant role in some communities. Sometimes these

115
healers would not refer patients to western-orientated health facilities or they would
tell patients to stop taking treatment (Maimela et al. 2015). Although contextually
relevant self-management strategies are therefore required, the development and
use of such strategies are often challenged by weak health systems and human
resource shortages. As such, the adaptation of interventions to the culture and
context of the target population is still lacking in many settings (Kirsten & Karch,
2012). Self-management does not replace health services, but complements them
by building skills for application at home and in routine health consultations
(deSilva, 2011).
Self-management education, coupled with other strategies, can thus contribute to
the task of dealing with the burden of chronic diseases in resource-poor settings
like South Africa (Dube, et al, 2015a). The South African integrated disease
management model highlights “assisted” self-management as a core component of
care (Asmall & Mahomed, 2011). In South Africa, primary healthcare (PHC)
facilities are the patients’ first point of contact with the healthcare system. These
facilities focus mainly on disease prevention and assisting and empowering
patients, while also diagnosing and treating minor illnesses. In the PHC system
professional nurses are the frontline service providers to communities, whereas
medical professionals only visit healthcare facilities for rendering services
(Mahomed & Asmall, 2015).
According to the World Health Organization (2105c), there is a misunderstanding
that chronic diseases cannot be prevented, while, in fact, 80% of premature onset
of diseases such as stroke, diabetes and heart diseases are preventable. As PHC
nurses form a central part of the multidisciplinary health team, they are increasingly
taking up roles in chronic diseases management, with one systematic review
demonstrating the effectiveness of self-management interventions implemented by
PHC nurses (Sargent, Forrest, & Parker, 2012). Community health nursing,
therefore, provides opportunities for the establishment of fruitful self-management
initiatives by patients (Maimela et al. 2015).

116
Despite the importance of contextually adapted interventions, few studies have
aimed to contextually adapt programs to the needs of the target population in
developing countries (Dube et al., 2015b). Therefore, the aim of the present study
was to explore chronic patients’ experiences of self-management and their
perceived support needs and the perspectives of key informants on patient self-
management, with a view to develop contextually appropriate disease self-
management support tools for chronic patients in South Africa.
Methods
A qualitative exploratory design with a content analysis approach was used in order
to inductively formulate categories and themes that portray the experiences and
perspectives of chronic disease participants in their natural environment (Mayring,
2014).
Study setting
The study was conducted in two public primary healthcare (PHC) facilities in an
urban township in the Tshwane metropolitan area in South Africa. One is a
community health center (CHC), with a 24-hour casualty and maternity service and
five doctors for chronic patients. The second center is a PHC clinic operating on
weekdays, with two doctors and no emergency department.
Study participants and sampling
The study had two distinct participant groups: patients with chronic diseases using
the two selected clinics for care, and professional key informants working at
different levels in the health system. Purposive, convenient and snowball sampling
strategies were employed (McKenzie, Neiger, and Smeltzer, 2005). Table 5.1 gives
an overview of participant characteristics, sampling and data collection methods.
Patient inclusion criteria were males and females over the age of 18 years with one
or more of the following conditions: diabetes, hypertension, asthma, epilepsy and

117
the human immunodeficiency virus (HIV). Patients were approached for participa-
tion on the day of their visit to the facility, while waiting to see a healthcare
provider.
Table 5.1 Overview of participant characteristics, sampling and data
collection strategies
Participants Number Sampling Data collection
KEY INFORMANTS:
Health service providers (at the 2 clinics)
4 Purposive Semi-structured individual interviews (KI) Chronic disease program
managers / Coordinators 4 Purposive
Snowball
Academics / experts 4 Purposive Snowball
PATIENTS:
Male (n= 9) Female (n = 23)
32 Purposive Convenient
Focus group interviews (FG) (n=4)
Male (n=1) Female (n =1)
2 Purposive Convenient
Individual interviews (PI)
Male (n=2) Female (n =4)
6 Convenient
Observations: individual consultations
Groups in waiting area (= ± 30-40)
4 Convenient
Observations: health education group sessions
Key informants (health service providers, managers and experts) were initially
sampled purposively because of their involvement with chronic patients, chronic
disease treatment or research. Snowball sampling was added to identify additional
information-rich participants. Sampling continued until data saturation had been
reached.

118
Data collection
Focus group interviews with patients
Focus group (FG) interviews were chosen as data collection method because of
patients’ shared experiences of self-management. Two FGs were conducted per
facility in the preferred indigenous language. In two instances, individual interviews
were conducted, as sufficient patient numbers for a group were not available. All
four FGs had eight members each, with roughly three men per FG, except for one
all-female group. A female community health worker from the same cultural
background had two days of training in being the primary facilitator, with the
primary researcher (LD) and a research assistant present at all FGs. The FGs
lasted approximately 60 minutes, with individual interviews being slightly shorter.
All interviews were audio-recorded and were guided by an interview schedule with
open-ended questions.
Observations of patient consultations and group education
Ten systematic observations of the types of education patients received were
conducted (6 individual patient consultations and 4 group education sessions).
Aspects observed included educational method(s), materials used, assessment of
patient needs prior to the education, level of patient participation, recording of
information by patients, and duration of educational sessions.
Key-informant interviews
The primary researcher (LD) conducted audio-recorded interviews in English with
12 key informants, which included four health service providers at the study
facilities (1 nurse, 1 doctor and 2 health promoters), four chronic disease program
managers at district and provincial level (2 at each level), and four academic
experts in chronic disease (2 providing active care). Program managers and
academic experts were included to provide a better understanding of the context of
chronic-disease self-management promotion in the broader health system.

119
Data management and analysis
The first author (LD) transcribed the key-informant interviews and the fifth author
(NGM), with translation experience from indigenous languages to English,
transcribed and translated the patient interviews simultaneously. A second person
did a peer review of two transcripts to control for accuracy. All direct quotations in
this paper were double-checked for translation accuracy.
Inductive qualitative content analysis was used to analyze the interview transcripts
by means of Atlas.ti 7 software (Mayring, 2014; Scientific software development,
1999). Data analysis occurred in two phases. Two researchers (LD, NGM)
independently analyzed the transcripts to identify manifest content and then
reached consensus on codes and categories to be used. In the second phase, two
researchers (LD, AMB) confirmed the original interpretations and did a further
inductive thematic analysis.
Credibility of data
To ensure trustworthiness of the analysis (Shenton, 2004) several steps were
undertaken. Credibility was enhanced through letting the researchers familiarize
themselves with the research context, using different methods of data collection
and doing frequent member checks during the interviews by summarizing
participants’ contributions. Confirmability was ensured by involving three different
researchers in the data analysis. Transferability was achieved through presenting
thick descriptions and direct quotations to allow for possible application in other
settings.
Ethical considerations
The study received ethical approval from the Research Ethics Committee of the
Faculty of Health Sciences, University of Pretoria (Protocol No. 57/2015) and the
Tshwane District Department of Health (Project No. 15/2015). Participants received
an information leaflet about the study and all voluntarily gave consent, mostly

120
written, but verbally in the case of participants with limited reading abilities. The
patient participants received a small gift equivalent to R30 (±USD2) afterwards as a
token of appreciation for their time.
Results
The findings from the content analysis revealed five issues for patients with a
chronic disease(s) that could have a profound influence on their ability to achieve
self-management: (i) health-system and service-provision challenges, (ii) health-
care provider attitudes and behavior, (iii) adherence to medication and lifestyle, (iv)
patients’ personal and clinic experiences, and (iv) self-management tool prefer-
ences. Table 5.2 provides more detail on the identified themes and categories. In
the quotations below FG refers to focus group and KI to key informant.
Health-system and service-provision challenges
Both patient and key-informant participants referred to challenges related to the
health system and service provision. An important challenge was medication stock-
outs, which could have a major impact on the self-management options of patients.
“I do take treatment and I also drink my pills, but I have got one problem
with one thing. Here at the clinic they are always short of pills for a long
time. Like now, since last time they didn’t have pills. Even now we are here
to collect pills and they only give us those vitamin pills.” (Male FG4)
A further concern was the long waiting times for patients. Participants at one clinic
indirectly alluded to getting emotionally tired while waiting in the queue and saw
this as a possible reason for their high blood pressure when they finally reached
the vitals station:
“That is why you find that, in the queues you wait for a long time;
sometimes your blood pressure goes up while … waiting to be assisted

121
and sometimes they [nurses] go for their tea times and meetings.” (Female
FG4)
Table 5.2 Main themes and categories
Themes Categories
Health-system and service-provision challenges
• Medication stock-outs • Long waiting times • Lack of educational materials and equipment • Mind set of providers • Lack of structure
Healthcare provider attitudes and behavior
• Poor communication • Lack of proper check-ups and follow-up • Confidentiality breaches • Poor relations
Adherence to medication and lifestyle changes
• Inconsistency in taking treatment • Poverty • Different food choices of family • Lack of self-monitoring equipment • Financial challenges • Side-effects of medication • Lack of information
Patients’ personal and clinic experiences
• Health education set-up in clinics • Feelings of hopelessness and acceptance of disease • Coping mechanisms • Substituting medication with herbs
Self-management tool preferences
• Booklet • Content
Key informants referred to resources and approaches to care provision as
challenges to self-management. Resource issues related to lack of educational
materials (e.g. pamphlets for patients about their disease) and no dedicated space
to implement physical activity interventions or, where there was space, a lack of
equipment for patient use: “Honestly, we are suffering with chronic disease
materials … it is difficult to implement awareness interventions when we do not
have these things.” (KI-5) Some health workers even ended up photocopying
pamphlets for patients.
Another challenge was healthcare providers’ approach to the provision of care:

122
“The framework or mind-set or the model that the people [healthcare
providers] are trained here is just to give patients medicine and they hope
they will take it and get better … So self-management as a co- vital
component of care is missing in the mind-set of health practitioners [nurses
and doctors].” (KI-7)
As a result, the self-management education given to patients was “… not done in a
structured way. It is not planned; it’s haphazard, you know; it just happens when it
happens.” (KI-7) Because the education was not planned, health service providers
sometimes gave conflicting messages, and there was no adequate follow-up of
patients referred to other health service providers.
Healthcare provider attitudes and behavior
Patient participants reported several issues related to the attitudes of nurses
towards them, which had an effect on their self-management. They perceived
communication with nurses to be poor, resulting in patients not feeling free to say
how they felt. One participant commented:
“We communicate with the nurses but when we try to explain something,
they become irritable, saying, ‘You are teaching me my job’. We do not
have a voice.” (Female FG3)
Patients also complained about a lack of proper check-ups and information on their
well-being and expressed a desire for a doctor to explain their disease status:
“They [nurses] do ask us about pain and we tell them, but they do not
check us. The doctor must check us and inform us of the status of our
condition. We need to know what is happening this month.” (Female FG3)
In addition, participants reported confidentiality breaches by nurses:

123
“I once came to the clinic, I fell pregnant while my other baby was still one
year. Instead of the sister [nurse] talking to me nicely in the consulting
room, she waited for me to leave the room and said in front of other
patients: ‘Don’t you know there is something called family planning?’ Just
imagine, other patients sitting there. So it made me angry.” (Female FG4)
Poor relations between nurses and patients also resulted in patients not wanting to
visit the clinic because of the way they had been treated. In one focus group it was
explained as follows:
“One thing I am not satisfied about is that at the blood pressure side. If
they see that your blood pressure is high, they tell you that you are going
to die. This is not nice, especially for someone who does not understand
blood pressure. They might think this is their last day of life.” (Female FG4)
Adherence to medication and lifestyle changes
Patient participants highlighted several challenges regarding adherence to
medication and lifestyle changes. One dominant challenge was consistency in the
time of the day for taking medication. A major reason for this was poverty:
“Poverty is also the reason you can’t take medication, because you can’t
take medication on an empty stomach, sometimes there is no bread in the
house.” (Female FG2)
Some participants also reported that they forgot to take their medications on time:
“I sometimes forget to take my medication, like if I’m in hurry, rushing to the mall, I
forget and then take it after some time.” (Female FG1)
A further challenge was adherence to dietary recommendations hampered by
cultural expectations. When visiting other households, patients were expected to
eat the food provided and could not choose something else. At functions like
weddings, cultural expectations were described as follows:

124
“But now when you are maybe at a wedding and you don’t eat the food
there, people will start talking, ‘There he goes again, we know this type. He
doesn’t like eating other people’s food.’ When you eat that food, because
you are now a visitor that is where you make a mistake.” (Male FG2)
Diet challenges at home related to participants’ different food needs than those of
the rest of the family and the unavailability of the right types of food: “It is difficult to
make the children to eat your diet because they want this and that.” (Male FG2)
The problem could even arise at the grocery shop:
“At least at the shops they do have the food that accommodates us. But
when you go for groceries, they [other family members] don’t buy the food
that accommodates you. When you try to buy Tab [sugar-free cola drink],
they would rather buy cold drinks with bad acid in them… you end up
joining the chosen drink.” (Male FG2)
Other lifestyle-change difficulties included a lack of time to exercise and lack of
glucose or blood pressure self-monitoring equipment at home. One participant
reported that, “I was supposed to quit smoking but I didn’t” (PI-1), indicating that he
knew what was the correct thing to do.
Financial challenges existed when employed patients had to go and collect
medication, as this patient reported:
“We work casual jobs. You find that you are only working ten days and on
those ten days they give you one day off to come and collect medication
and [if] you do not get it, you are given another date [at the clinic] and you
still have to take another [day] off for you to collect your medication. And
when you check, you see that you could have actually done something
with that money you lost on the day you were absent.” (Female FG4)
Some patients mentioned not taking their medication because of side-effects: “I
don’t even take my medication if I’m going to town because I know I have to go to

125
the toilet in two hours every ten minutes.” (Female FG1) Other patients reported
coming to the clinic to collect the medication but
“… there are some high blood pills that they changed for us and they are
not treating us well. We get swollen and dizzy, so as she [other participant]
says, she throws them away. We also throw them away.” (Female FG3)
Finally, participants referred to a lack of information about the disease and the
prescribed medication as a factor influencing self-management. One key informant
was of the view, “… that is why our patients do not complete their medication
because they don’t get information, full information.” (KI-5)
Patients’ personal and clinic experiences
On arrival at the clinic, patients received their clinic record on which all the previous
information about their condition was recorded. They handed the record back to
the clerk before leaving the premises. Patients were only allowed to take home a
clinic appointment card with the next appointment date. In most instances, patients
were passive or only partially active. Individual health education in consultations
lasted about two minutes and ad-hoc waiting-area group talks lasted around 30
minutes. Patients had nowhere to record any information conveyed to them and did
not prepare questions in advance.
Patient dispositions influenced the participants’ adherence to self-management
recommendations. Some participants expressed a feeling of hopelessness
regarding their condition, with one commenting that “… there is no victory; you
must just continue like AIDS; you drink medication throughout.” (Female FG2)
Others reported learning to accept their disease(s): “Acceptance is what is helping
us; it is also what motivates us to be here and to check our conditions and take our
medication.” (Male FG2)
Participants reported different ways of coping with their condition, which in turn had
an effect on the way they managed their condition themselves. Some adopted a

126
religious approach: “I ask God and whatever they are doing to me I send it to God.”
(Female FG3) Others had learned to manage and control their emotions, so that
this should not affect their blood pressure:
“At home I stay with my boys; they are orphans and they are my
grandchildren. They are troublesome people, but in most cases I try to stay
calm and not to shout when I am with them.” (Female FG2)
There were also participants who were scared of taking tablets or who replaced
their medication with herbs in order to get better: “I don’t take medication. I drink
some herbs. I can take a week and not drink my medication.” (Female FG3)
Self-management tool preferences
Patients and key informants were also asked about the type of chronic disease
self-management tool they believed could make a difference. Most participants
mentioned a booklet for those who could read and write: “I go with a booklet
because you can sit and read. Where you don’t understand, you read again.” (Male
FG2)
Those with limited literacy could be assisted by family members or neighbors in the
“spirit of Ubuntu”, a South African humanity principle where “… most people run to
their neighbors or within the household.” (KI-3) Other suggestions included support
groups, mobile phone messages, and radio and TV programs.
In terms of content and appearance participants suggested that the booklet “…
must be written in different languages so that we can all understand …” (Male FG1)
and it “… must not be too thick because it demotivates [us] to read.” (Female FG1)
It should have pictures to assist those with low levels of literacy and should be
sufficiently motivating to share it with family members. Furthermore, the booklet
should contain information about the diseases and their complications and should
have clear instructions for patients in cases of emergencies.

127
Discussion
The sustainability of health interventions depends on the capacity of stakeholders
(patients and health professional) to participate (Maimela et al. 2015). This study
explored South African chronic patients’ experiences and key informants’
perspectives of self-management in order to identify perceived support needs. A
number of issues were identified concerning self-management education for
chronic patients in primary care. These issues relate to the health system as well
as to patients.
Several hindrances to self-management by patients originate from the health
system and service provision, such as medication stock-outs, long queues and lack
of educational materials. These are issues that the patient and the healthcare
provider do not have control of, no matter their need for self-management. These
results are also reflected in other study results in the South Africa that
demonstrated how medication stock-outs at facilities left the patients stranded
(Maimela, et al. 2015). Other studies have also reported concerns on the lack of
health promotion materials and the use of poor quality photocopies that could
discourage patients to read (Parker, Steyn, Levitt, & Lombard, 2012; Rushforth,
McCrorie, Glidewell, Midgley & Foy, 2016).
Our study highlighted the treatment-and-drug-dispensing approach of health
professionals, with a neglected focus on self-management as a vital core
component. The way in which individual consultations and ad-hoc health
information sessions were conducted – often in noisy waiting areas – highlighted
the need for better patient support for self-management. Patient health education is
haphazard and may result in conflicting or confusing messages received from
different providers. Other South African studies report on the lack of training of
primary healthcare providers in behavior-change counseling skills and recommend
effective training, accompanied by health-system reform that supports health
promotion and self-management (Dube et al, 2015a; Malan, Mash, & Everett-
Murphy, 2015; Murphy, Chuma, Mathews, Steyn & Levitt, 2015).

128
In our study, provider attitudes and behaviors in the form of poor communication
and relations presented as a concern for patients’ motivation for self-management.
Because of poor or absent patient-provider relationships, patients felt obliged to
collect their medication even if they discarded it afterwards. Primary care is the first
contact point of the community with the health system in South Africa. This
highlights the imperative of effective health communication by PHC providers to
make a major difference in self-management (Maimela et al. 2015). The current
absence of patient-centered practice hinders patient self-management, as has also
been reported elsewhere (Everett-Murphy, De Villiers, Ketterer, & Steyn, 2015; Fort
et al. 2013. Rushforth et al. (2016) argue that, although self-management has been
promoted in different settings, PHC providers continue to find it difficult to
effectively share responsibility with patients and to support them to change their
behavior.
Community health nursing lends itself to lead the integration of self-management
into a patient-centered model of care for chronic patients that complements the
other components of care. Therefore, in order to make meaningful collaborations
with patients in self-management, community health nurses need to be aware of
the needs and experiences of the specific target groups of patients they serve. In
chronic diseases, unlike in acute conditions, patients themselves are principal
caregivers and health professionals only act as consultants in supporting the
patients. Although patients may consult with the professionals periodically, much of
the time they are at their homes, making everyday choices that affect their chronic
condition (van Olmen et al. 2011).
In addition to issues within the health services, other barriers to medication and
lifestyle adherence found in our study included poverty, cultural expectations and
family dietary preferences. Participants in our study appeared to lack knowledge on
how to address immediate side-effects of their prescribed medication, resulting in
non-adherence. Patients felt a social obligation to eat whatever was presented and
were also forced to eat the available food because of financial constraints and the
attitudes of family members. Problems with losing weight as a barrier to active self-

129
management were not raised in our study, possibly because gaining weight is
associated with health, affluence and success in South African culture (Kirsten &
Karch, 2012). A lack of social support and financial resources has also been
reported in previous studies as barriers to self-care (Liddy, Blazkho, & Mill, 2014;
Muchiri, Gericke, & Rheeder, 2012).
Study limitations
Our study had a number of limitations. Firstly, patient interviews were not
conducted in English, which limited the degree of rapport building between
researcher and participants. The trained facilitator was, however, fluent in the local
vernaculars. Secondly, more women than men consented to participate. Although
we benefited from mixing genders in the focus groups and discussed topics that
might not have been raised in separate groups, other issues may have been
missed because of the gender mixing. Finally, this study was only conducted in one
part of the Tshwane metropolitan area, although the findings may resonate with the
situation in other areas in South Africa. Further research on the subject of self-
management needs is required in order to add to the knowledge base of culturally
adapted interventions in community health and to inform policy development.
Conclusion
The current study raises awareness of self-management needs and experiences of
patients and healthcare providers in one cultural context in order to improve
community health nurses’ knowledge and skills in working with these patients.
While adherence to medication and lifestyle changes are recognized as important
by patients and providers alike, the two groups have different perspectives and
experiences of treatment and self-management of chronic diseases. In this study,
patients expressed their willingness to be involved and to learn more about their
disease(s), while PHC providers were willing to assist with such an endeavor.
However, more training of community health nurses and other healthcare profes-
sionals as well as changes in the healthcare system are needed to achieve better
self-management support for patients.

130
The findings of this study provide a window of opportunity for the development and
implementation of contextually adapted, structured self-management support
interventions for community health nurses in developing countries. Although self-
management is now regarded as a pillar in the treatment of chronic diseases like
diabetes and hypertension, it is not a panacea for everything.
Acknowledgements
This work was supported by the 2012-2013 doctoral fellowships for development
cooperation of the Université catholique de Louvain and a research assistant grant
from the University of Pretoria.
References
Albreht, T., Dyakova, M., Schellevis, F. G., & Van den Broucke, S. (2016). Many diseases, one model of care. Journal of Comorbidity, 6, 12–20. doi:10.15256/joc.2016.6.xx.
Asmall, S., & Mahomed, O. (2011, June 2014). Integrated chronic diseases management manual. National Department of Health of South Africa. Retrieved June 14, 2015, from: http://www.kznhealth.gov.za/family/Integrated-chronic-disease-management-manual.pdf.
Brady, T., Murphy, L., O'Colmain, B. J., Beauchesne, D., Daniels, B., Greenberg, M., et al. (2013). A meta-analysis of health status, health behaviors, and healthcare utilization outcomes of the Chronic Disease Self-Management Program. Preventing Chronic Diseases, 10(E07), 120112. doi:10.5888/pcd10.120112.
Choi, T. S. T, Walker, K. Z., Ralson, R. A., & Palermo, C. (2014). Diabetes education needs of Chinese Australians: a qualitative study. Health Education Journal, 74, 197–208. doi:10.1177/0017896914523276.
de Graft Aikins, A., Anum, A., Agyemang, C., Addo, J., & Ogedegbe, O. (2012). Lay representations of chronic diseases in Ghana: implications for primary prevention. Ghana Medical Journal, 46(2 Suppl), 59–68.
deSilva, D. (2011, 14 March 2015). Evidence. Helping people help themselves. A review of evidence considering whether it is worthwhile to support self-management. Retrieved March 14, 2015, from: http://www.health.org.uk/publication/evidence-helping-people-help-themselves.
Dube, L., Van den Broucke, S., Rendall-Mkosi, K., Kalweit, K., Hosiaux, M., & Dhoore, W. (2015a). An audit of diabetes self-management education programs in South Africa. Journal of Public Health Research, 4, 176–184. doi: 10.4081/jphr.2015.581.

131
Dube, L., Van den Broucke, S., Hosiaux, M., Dhoore, W., & Rendall-Mkosi, K. (2015b). Type 2 diabetes self-management education programs in high and low mortality developing countries. Diabetes Educator, 41, 69–85. doi: 10.1177/0145721714558305.
Everett-Murphy, K., De Villiers, A., Ketterer, E., & Steyn, K. (2015). Using formative research to develop a nutrition education resource aimed at assisting low-income households in South Africa adopt a healthier diet. Health Education Research, 30, 882–896. doi:10.1093/her/cyv051.
Fort, M .P., Alvarado-Molina, N., Pena, L., Mendoza Montano, C., Murrillo, S., & Martinez, H. (2013). Barriers and facilitating factors for disease self-management: a qualitative analysis of perceptions of patients receiving care for type 2 diabetes and/or hypertension in San Jose, Costa Rica and Tuxtla Gutierrez, Mexico. BMC Family Practice, 14, 131. doi:10.1186/1471-2296-14-131.
Franek, J. (2013). Self-management support interventions for persons with chronic disease: an evidence-based analysis. Ontario Health Technology Assessment Series, 13(9), 1–60.
Kirsten, W., & Karch, R.C. (2012). Global perspectives in workplace health promotion. Sudbury, Masschusetts, United States of America: Jones & Barlette Learning LLC.
Liddy, C., Blazkho, V., & Mill, K. (2014). Challenges of self-management when living with multiple chronic conditions: systematic review of the qualitative literature. Canadian Family Physician, 60, 1123–1133.
Lukewich, J., Mann, E., VanDenKerkhof, E., & Tranmer, J. (2015). Self-management support for chronic pain in primary care: a cross-sectional study of patient experiences and nursing roles. Journal of Advanced Nursing, 71, 2551–2562. doi:10.1111/jan.12717.
Maher, D., Ford, N., & Unwin, N. (2012). Priorities for developing countries in the global response to non-communicable diseases. Globalization and Health, 8, 14. doi:10.1186/1744-8603-8-14.
Mahomed, O. H., & Asmall, S. (2015). Development and implementation of an integrated chronic disease model in South Africa: lessons in the management of change through improving the quality of clinical practice. International Journal of Integrated Care, 15(e038).
Maimela, E., Van Geertruyden, J. P., Alberts, M., Modjadji, S. E., Meulemans, H., Fraeyman, et al. (2015). The perceptions and perspectives of patients and health care providers on chronic diseases management in rural South Africa: a qualitative study. BMC Health Services Research, 15, 143. doi:10.1186/s12913-015-0812-5.
Malan, Z., Mash, B., & Everett-Murphy, K. (2015). A situational analysis of training for behaviour change counselling for primary care providers, South Africa. African Journal of Primary Health Care & Family Medicine, 7(1). doi:10.4102/phcfm.v7i1.731.
Marsiglia, F. F., & Booth, J. M. (2015). Cultural adaptation of interventions in real practice settings. Research on Social Work Practice, 25, 423–432. doi:10.1177/1049731514535989.

132
Mayring, P. (2014). Qualitative content analysis: theoretical foundation, basic procedures and software solution. Klagenfurt, Austria. Retrieved August 26, 2016, from: http://nbn-resolving.de/urn:nbn:de:0168-ssoar-395173.
McKenzie, J., Neiger, B., & Smeltzer, J. (2005). Planning, implementing and evaluating health promotion programs. (4th ed.). San Francisco: Pearson Education Inc.
Muchiri, J. W., Gericke, G. J., & Rheeder, P. (2012). Needs and preferences for nutrition education of type 2 diabetic adults in a resource-limited setting in South Africa. Health SA Gesondheid, 17(1), 1–13.
Murphy, K., Chuma, T., Mathews, C., Steyn, K., & Levitt, N. (2015). A qualitative study of the experiences of care and motivation for effective self-management among diabetic and hypertensive patients attending public sector primary health care services in South Africa. BMC Health Services Research, 15, 303. doi:10.1186/s12913-015-0969-y.
Okop, K. J., Mukumbang, F.C., Mathole, T., Levitt, N., & Puoane T. (2016). Perceptions of body size, obesity threat and the willingness to lose weight among black South African adults: a qualitative study. BMC Public Health, 16, 365. doi: 10.1186/s12889-016-3028-7.
Parker, W. A., Steyn, N. P., Levitt, N. S., & Lombard, C. J. (2012). Health promotion services for patients having non-communicable diseases: feedback from patients and health care providers in Cape Town, South Africa. BMC Public Health, 12, 503. doi:10.1186/1471-2458-12-503.
Rushforth, B., McCrorie, C., Glidewell, L., Midgley, E., & Foy, R. (2016). Barriers to effective management of type 2 diabetes in primary care: qualitative systematic review. The British Journal of General Practice, 66, e114–127. doi:10.3399/bjgp16X683509.
Sargent, G. M., Forrest, L. E., & Parker, R. M. (2012). Nurse delivered lifestyle interventions in primary health care to treat chronic disease risk factors associated with obesity: a systematic review. Obesity Reviews, 13, 1148–1171. doi:10.1111/j.1467-789X.2012.01029.x.
Scientific Software Development. (1999). ATLAS.ti. Version 7. Berlin, Germany: Scientific Sofware Development. Retrieved April, 2015 from http://atlasti.com/.
Shenton, K. (2004). Strategies for ensuring trustworthiness in qualitative research projects. Education for Information, 22, 63–75.
Steinsbekk, A., Rygg, LØ., Lisulo, M., Rise, MB., & Fretheim, A. (2012). Group based diabetes self-management education compared to routine treatment for people with type 2 diabetes mellitus: a systematic review with meta-analysis. BMC Health Services Research, 12, 213.
Stoilkova, A., Janssen, D. J., & Wouters, E. F. (2013). Educational programmes in COPD management interventions: a systematic review. Respiratory Medicine, 107, 1637–1650. doi:10.1016/j.rmed.2013.08.006.
Healthy People.gov. (2014). Older adults. Retrieved August 20, 2016, from: https://www.healthypeople.gov/2020/topics-objectives/topic/older-adults/objectives#4978.
van Olmen, J., Ku, G. M., Bermejo, R., Kegels, G., Hermann, K., & Van Damme, W. (2011). The growing caseload of chronic life-long conditions calls for a

133
move towards full self-management in low-income countries. Globalization and Health, 7, 38. doi:10.1186/1744-8603-7-38.
World Health Organization. (2015a). Heatlh in 2015 from MDGs, millenium development goals to SDGs, sustainable development goals. Geneva, Switzerland: World Health Organization. Retrieved January 1, 2016, from: http://apps.who.int/iris/bitstream/10665/200009/1/9789241565110_eng.pdf?ua=1.
World Health Organization. (2015b). Chronic diseases and health promotion. Overview - preventing chronic diseases: a vital investment. Geneva, Switzerland: World Health Organization. Retrieved January 7, 2016, from: http://www.who.int/chp/chronic_disease_report/part1/en/index11.html.
World Health Organization. (2015c). Global status report on noncommunicable diseases, 2014. Geneva, Switzerland: World Health Organization. Retrieved September 2, 2015, from: http://apps.who.int/iris/bitstream/10665/148114/1/9789241564854_eng.pdf?ua=1.
Yam, M. (2013). Does culture matter in body image? The effects of subjective and contextual culture on body image among bicultural women. (Doctoral dissertation). University of Michigan. Retrieved August 20, 2016, from: https://deepblue.lib.umich.edu/handle/2027.42/97941.

134

135
CHAPTER 6: Development of a care-plan booklet
Development and intended use of a prototype individual
care-plan booklet

136
Introduction
It is well accepted that the capacity of chronic patients to self-manage their illness
has positive effects on clinical outcomes, quality of life and health service use (1-4).
For this reason, self-management education is generally recommended as part of
the treatment. However, while nearly all existing self-management education
programs have been developed in western, resourceful countries, there is a paucity
of literature related to the question whether these programs also meet the needs of
patients in resource-limited countries like South Africa (5, 6). A study of the self-
management support needs of patients with chronic diseases in a South African
township (7) revealed that most patients preferred an individual booklet written in
their own language, containing information about the diseases and their complica-
tions in easy language and with visual illustrations, and with clear instructions in
cases of emergencies. This chapter describes the development of such a care-plan
booklet.
The care-plan booklet builds on the three studies reported in Chapters 3, 4 and 5.
First, the systematic review of diabetes self-management education (DSME)
programs in high- and low-mortality developing countries revealed that most
published studies on DSME were done in low-mortality developing countries, and
that only a handful of studies originated from high-mortality developing countries
(5). Moreover, only some of the programs described in these studies were
accessible to people with lower levels of literacy and for many interventions the
sustainability of the effects was of concern due to the lack of tailoring to the target
population.
Secondly, the audit of DSME in South Africa (8) gave an overview of the policies
and programs for diabetes self-management that exist in the country. This study
showed that there was no policy supporting DSME in South Africa and that DSME
was rarely mentioned in guidelines. In reality, DSME is mostly unplanned, unstruc-
tured and given on an ad-hoc basis. During consultations, patients do not have

137
anywhere to record the advice that is given by the health provider, and patients are
mostly passive recipients of this information.
Thirdly, the study on the self-management needs of chronic patients in two primary
healthcare (PHC) facilities in an urban township in South Africa (7) explored the
views of both patients and experts on the challenges to self-management, and
gave information on a preferred tool that could assist the education of self-
management skills. As reported in Chapter 5, participants in that study considered
a booklet as a preferred tool to assist them in increasing self-management skills.
The preference for a care-plan booklet as a tool for self-management education is
in line with findings in the literature that point to the usefulness of printed materials
in aiding the patient to remember some of the information given during a
consultation (9). However, simply enhancing the capacity of patients to remember
the information given by healthcare providers is not enough: as shown in the
literature, printed materials are not very effective in changing health related
behavior when they are used on their own, and only provide an added value when
they complement the interactions between patients and providers. This is
supported by the findings of our study on the self-management needs of chronic
patients presented in Chapter 5, which revealed several challenges in the
interaction between patients and providers. To address some of these challenges,
it is necessary to improve the interaction and communication between patients and
providers. Hence, the care-plan booklet that was developed for this study was not
just an information tool, but also a vehicle for facilitating the interaction between
patient and provider during a medical consultation, as well as that with family and
friends at home. To that effect, it combines health information with a care-plan.
Moreover, as low health literacy is a factor that hinders the understanding of
information and the usability of existing information supports, it was decided to
illustrate the content of the care-plan booklet with pictures. While it was also
suggested to use the local languages to help those with low levels of education,
this suggestion could not be taken up due to lack of resources. However, patients

138
who had low literacy levels indicated that they could ask their children or family
members to read for them.
This chapter introduces the prototype individual care-plan booklet for people with
type 2 diabetes mellitus and hypertension (high blood pressure). It also describes
the literature and the rationale behind the development of the care-plan booklet, its
intended use and how it was evaluated. The prototype booklet was only available
for diabetic and hypertensive patients. The assumption was that if the use of this
care-plan booklet was found to be acceptable and potentially effective in improving
the provider-patient relationship – which will in turn lead to improved health
outcomes – it could be expanded to include other chronic diseases seen at PHC
level. As a starting point, diabetes and hypertension were selected as the condi-
tions to include in the booklet, as these patients are mostly seen at PHC centers
every day.
Printed materials for health education
Health education is defined by the World Health Organization (WHO) as “any
combination of learning experiences designed to help individuals and communities
improve their health, by increasing their knowledge or influencing their attitudes”
(10). Several health communication strategies are used to assist patients in
promoting healthy behavior. These strategies include groups or individual inter-
ventions, telephone communication, websites and printed materials. For the last
part of the broader study, we focused on printed materials, as the needs assess-
ment among chronic disease patients had indicated a desire for a care-plan
booklet (see Chapter 5).
Printed materials are regarded as a necessary requirement for the participation of
patients in healthcare, although there are reservations about their potential impact
on health outcomes if used in a stand-alone fashion (11). A systematic review by
Paul and Redman indicated that printed materials can be effective in changing
behavior, knowledge and attitudes in health matters, but that the effectiveness
depends on various aspects of their implementation (12). These factors include, for

139
example, if pamphlets are used alone or as a supplementary to another
intervention. Pamphlets are likely to be more effective when used in patient
education compared to using them to influence the general public and are also
more effective in achieving knowledge and attitudes change than behavior change
(12, 13). Printed materials are also beneficial to patients even when not interacting
with physicians, because patients can seek answers from written materials and can
choose the amount of information and the level of detail that suit their coping
strategies (9).
Bonevisk and Newell (13) did a review on the effects of distributing written health
education materials and found that distribution of printed material by healthcare
professionals led to a high number of people keeping the material and recalling the
receipt of materials. It was concluded that there are higher rates of reception and
readership if pamphlets are distributed by healthcare professionals, although it is a
slower method than mailing.
While printed materials can aid in the promotion of health, their effects are
influenced by the patient’s level of health literacy. This is especially the case for
resource-limited settings, where inadequate health literacy is often endemic, but
appears to be under-researched (14, 15). As defined earlier, health literacy entails
“people’s knowledge, motivation and competence to access, understand, appraise
and apply health information in order to make judgements and take decisions in
everyday life concerning healthcare, disease prevention and health promotion to
maintain or improve quality of life during the life course” (16) (p. 3). Houts et al.
noted that understanding and using health information is challenging for people at
all levels of literacy, but even more so for people with limited literacy skills (11).
Health literacy does not only entail reading and understanding health information,
but also involves empowerment of patients (17). Low health literacy is associated
with poor health status, poor treatment adherence, high rates of hospital
admissions and poor preventive strategies (17).

140
The available evidence suggests that well-designed written information can be
useful in aiding professional consultation and improving health knowledge and
recall (17). The review by Houts et al. shows that the use of pictures helps to draw
the attention to the education materials and has a positive effect on intentions and
health-related behavior (11). Moreover, spoken information supported by pictures
is recalled better by people with low literacy levels.
Health professionals play a crucial role in the provision of educational and self-help
programs. In fact, interventions that provide information only (without the involve-
ment of health professionals) are not very successful (17). A review by Eakin et al.
indicated that programs with health professional involvement are especially more
effective for disadvantaged populations (18). Materials with health information are
also more effective when they complement rather than replace the interaction
between patients and providers. To improve self-management skills, patients need
on-going support from their health providers and this support is crucial for their
success (17).
According to Fu et al, healthcare providers are seen as primary facilitators of the
patient’s self-management skills, especially in PHC settings, as the demand for
self-management in chronic care increases (19). The collaboration between
patients and providers in self-management could be seen as a therapeutic exercise
where providers assist in validating patients’ ideas and develop individual care
plans aimed at improving patients’ health. In a study on chronic pain, patient-
provider partnerships were seen to stimulate and nurture the internal resources of
patients that led to behavior change (19).
The Health Belief Model
While the development of the care-plan booklet was triggered by an existing self-
management tool for chronic patients (see below), it was also theoretically
underpinned by the Health Belief Model (HBM). The HBM was developed in the
1950s to explain the unsuccessful efforts of the United States Public Health

141
Services in the treatment of tuberculosis. Since then the HBM has been one of the
most often-used exploratory models in health education and health promotion and
has been applied to a large range of health behaviors. The main assumption of the
HBM is that health-related behavior is determined by an individual’s beliefs about
the threats posed by a disease and the possibility to prevent these threats from
happening. The theory has four main constructs: perceived severity; perceived
susceptibility; perceived benefits; and perceived barriers. More recently, the model
has been expanded to also include cues to action, motivating factors and self-
efficacy (20-23).
Perceived severity concerns a person’s belief about the seriousness of a disease
(for instance, diabetes or hypertension) and its consequences on their life. The
consequences can include pain, financial problems, inability to work or the
development of diabetes or hypertension complications (20, 23).
Perceived susceptibility refers to an individual’s perception of the chances of
getting a disease. If the risk is greater, then there is a greater likelihood of taking up
behavior to decrease the risk. For instance, if patients perceive a greater risk of
developing diabetes or hypertension complications they are more motivated to
change their lifestyles to avoid or delay these complications. However, research
shows that sometimes the perception of susceptibility does not lead to behavior
change. For example, knowing that one has an increased risk of developing skin
cancer does not stop people from tanning (20, 24). The perception of susceptibility
combined with the perception of severity, results in a perceived threat, which can
lead to a change in behavior. For example, most children whose parents are
diabetic and who perceive a threat of developing non-insulin dependent diabetes
engage in weight control measures (25).
A perceived benefit is the belief that taking action (changing life style behavior) will
decrease the seriousness of the disease, such as diabetes or hypertension. It is
more likely that people will take up behavior when they believe that it will work for
them. Perceived barriers, on the other hand, refer to circumstances that might

142
hinder the person to take up the new behavior. Some studies suggest that out of all
the constructs of the HBM, perceived barriers is the one that most determines if
one will take up the new behavior (23). Barriers can include fear of not being
successful, or fear of embarrassment. If the benefits outweigh the costs of adopting
the new behavior, it is more likely that the person will change behavior (20, 21).
The possibility of adopting a new behavior based on the HBM is modified by
personal factors, including cues to action and self-efficacy. Cues to action are
contextual factors to which the person is exposed and which help to elicit the
action. For example, a reminder from a health service provider to exercise or a
family member developing a complication of the same disease will elicit self-
management behavior. Self-efficacy involves an individual’s confidence in his or
her capacity or ability to perform the behavior or action successfully. In principle,
individuals normally do not try out an action unless they believe that they can do it
(20, 22, 23).
The prototype care-plan booklet
Development of the booklet
The trigger for the development of the care-plan booklet was an existing general
self-management tool of Curo Health (26), a non-governmental organization (NGO)
based in Pretoria, South Africa. Their booklet is built upon the principles of the
Stanford University Chronic Disease Self-Management Programs (CDSMP) which
is based on the theory of self-efficacy (see Chapter 1). The Curo Health booklet is
a carry-home booklet for patients. In addition to information about the disease and
its management, it contains tables about which the patient and provider can
discuss during a consultation, as well as spaces where the patient can write down
questions for the provider as a preparation for the consultation. Although, the Curo
Health booklet was already used in consultations between patients and healthcare
providers in the private healthcare sector, it has never been evaluated. Moreover,
its usability in the public health sector, with patient of lower socio-economic status
and lower health literacy, could be a point of concern. Therefore, the Curo Health

143
booklet inspired the development of the new care-plan booklet which fits the
context of the target population. The HBM which underpins the development of the
current booklet (see above) is a more advanced and elaborate theory which also
improves the care-plan booklet. Table 6.1 shows the major differences between the
original care-plan booklet and the new prototype care-plan booklet. Existing
pamphlets on diabetes and hypertension available in PHC clinics were also
consulted for additional information (27, 28).
The main changes include the addition of more information on the relevant
diseases (diabetes and hypertension) and the national guidelines for normal levels
of glucose and blood pressure (for patients to compare against their own). A
section was also added for recording vital signs for patients to monitor themselves.
The latter can be used by the patient to prepare for the consultation, ask questions,
and improve the interaction with the healthcare provider. Furthermore, pictures
were added that were compatible with the township context. While the language of
the pilot care-plan booklet remained English, it is envisaged that the final version to
be used in a larger-scale project will be translated into other South African
languages.
Table 6.1 Differences between the Curo Health care-plan and the new proto-type care-plan booklet
Contents Curo Health
booklet New booklet
The pledge √
Information on how to use the booklet √
National guidelines on target values √
Definition of a chronic disease √
Tips how to make most of the medical consultation (for patients) √
Preparing for the consultation X 4 √ √
During the consultation (discussion with provider) X 4 √ √
Vitals signs table for each consultation √
Emotions chart (to assist in the discussion with the provider) √
Brief information on diabetes and high blood pressure (incl. complications)
√

144
Contents Curo Health
booklet New booklet
Health messages for both diabetes and high blood pressure √
Messages on physical activity √
Treatment record √ √
Contact details of patient √
Details of providers √
The vicious cycle of symptoms √
Unnecessary pictures √
Description of the prototype care-plan booklet
The care-plan booklet focuses on diabetes and hypertension and is intended to be
used with health service providers during consultations. It has an A5 format with
light green pages. The cover has a picture of an older couple and a space for
patients to write their name, contact number and clinic name in case the booklet
gets lost. The prototype care-plan booklet covers the following content:
• How to use the booklet
• Glossary of terms (with translations in Zulu and Sepedi)
• Making most of the medical consultation (tips for patients)
• Information on diabetes and hypertension
- Definition
- Physiology
- Signs and symptoms
- Complications
- Health education messages
• Lifestyle change messages
• Body mass index table
• Preparing for the consultation
- Tables for recording vital signs by healthcare providers
- Tables for use in provider-patient consultation
• Spaces for referral notes
• General notes by healthcare provider
• Pocket for appointment card at the inside back cover
• Emergency telephone numbers on outside back cover

145
The first part of the booklet, which consists of 18 pages, contains information about
diabetes and hypertension and their complications and advice on diet and exer-
cise. Pictures are used to aid the reader and to assist those with low levels of
literacy. Pages 19 and 20 present the national guidelines and target glucose and
blood pressure values. A table for body mass index (BMI) is also included. Pages
22 and 27 contain pages for preparation and discussion with the provider for use
during a consultation and a space is also provided for recording vital signs.
Page 28 provided tables for use by other healthcare providers to whom a patient
might be referred. The last two pages provide a space for general notes where the
healthcare provider can, for example, record the referral and results of required
tests such as foot and eye tests. The inside of back cover page is equipped with a
pocket for keeping a clinic appointment card.
Although the study on needs assessment indicated that the care-plan booklet must
preferably be written in the local language, for the purposes of this study the
prototype care-plan booklet was developed in English only. This was a decision
made for convenience: since there are 11 official languages in South Africa,
translation in all languages would have been too costly and time-consuming.
However, English is one of the official languages of South Africa and the language
of schooling, and most people comprehend basic simplified English.
Contextual issues considered in the development of the booklet
In Chapter 2 we discussed the context in which this project was carried out. This
context was an important element in the development of the care-plan booklet and
its intended use in the primary healthcare facilities. Particularly, the fact of a
westernized and traditional healthcare system running parallel to each other, both
of which can be accessed by chronic disease patients, is of interest, as it may
result in patients receiving conflicting messages (7, 29). As such, the care-plan
booklet can serve as an interactive tool that enables patients to discuss issues that
they do not understand or about which they are confused. For instance, the study
reported in the Chapter 5 revealed that because of poor communication between

146
healthcare providers and patients, the latter sometimes throw away medication
after collecting it because they believed it made them sicker (7). Other patients
indicated that they were mixing their medication with herbs. The inclusion of tables
for recording vital signs and for recording items to be discussed during
consultations allows monitoring medication use more systematically and helps in
resolving conflicting issues.
The booklet also contains practical information about the two diseases, which the
patients can discuss at home with other family members. This is important because
as a support system, family members have a strong influence on the patients’ self-
management behavior. Their knowledge about the disease and about the
appropriate actions can be an importance facilitator or barrier to the patient’s self-
management capacity. For example, a family member who is well informed about
the signs and symptoms of diabetes and of the possible complications of the
disease can help the patient decide on seeking help at the clinic facilities. In this
way, both the care-plan booklet and the communication during consultation can
counter harmful beliefs on the part of both the patients and their families, and as
such help the patients to better manage their conditions.
Since the care-plan booklet was developed to fit the context of the target
population, certain contextual features were included, for example:
Allowing to share the care-plan at home
Allowing to share the care-plan with the healthcare provider
Allowing assistance by family and friends for those with low levels of
literacy
Not including sensitive information in the booklet
Writing the booklet in simple, basic English

147
Aim and objectives of the care-plan booklet
The aim of the care-plan booklet is to enhance the interaction between patient and
provider by providing a structure for the medical consultation. The objectives are:
To provide a low-cost information tool on diabetes and hypertension
suitable for resource-limited settings
To enhance patient knowledge and health literacy to better understand
diabetes and hypertension.
To provide a vehicle to facilitate patient-provider interaction during medical
consultations to assist in self-management.
To provide a tool to help patients monitor relevant self-care behaviors.
Assumptions about the use of the care-plan booklet
The care-plan booklet is not an intervention in itself and should not be used as
such. It is meant to be part of a broader, already existing intervention for the
treatment and care of diabetic and hypertensive patients. Therefore, it would be
inappropriate to expect health outcomes changes or behavior changes on the
basis of the information provided in this care-plan booklet alone. The health service
providers involved have to be trained in behavior counseling techniques in order to
be able to make maximum use of the booklet and for the patient to benefit from
using the booklet. Therefore, the health service providers and the patients have a
role to play in using the booklet during a medical consultation. The care-plan
booklet is not provider-oriented, but can be seen as a facilitator of the
communication process that also builds or enhances the capacity and skills of the
patient. Through preparing for each consultation and by following the treatment
process, the patient can become aware of where he or she is and where he or she
needs to go.

148
The role of patients
As self-management requires patients to be more than passive receivers of
information, patients have a crucial role to play in the use of this care-plan booklet.
To begin with, the patient should bring the booklet to every medical consultation.
Patients may record questions they have and if they do not understand some of the
information, they may ask the health service providers during consultation. Patients
may also share the care-plan booklet at home with family members or neighbors to
improve their understanding of the disease.
The role of health service providers
Although the care-plan booklet is a carry-home tool for patients, healthcare
providers are expected to make active use of the booklet during consultations.
Each diabetic or hypertensive patient will bring the booklet along to each
consultation. The health service providers will record the vital-signs values in the
booklet.
When the patient consults with a professional nurse or doctor, the booklet will be
used to assist in the discussion. For example, the patient might have pre-recorded
questions to be addressed to the healthcare provider during consultation and the
booklet will serve as a reminder. A provider might also start the discussion by
focusing on the comparison of the vital signs with the recommended value and ask
the patient why he or she thinks they are like that. The emotion pictures included in
the booklet can be used as a starting point for health service providers to ask
patients how they feel and why they feel that way.
Together with the patient, the healthcare provider can use the spaces in the
booklet to draw up a care plan that can be referred to and reviewed at each visit.
The provider can also refer to the topics already included in the care-plan booklet
or explore together with the patient any difficult issues that need more explanation.

149
Conclusion
In this chapter we have presented the care-plan booklet that was developed to
provide a low-cost, context-specific self-management tool for diabetes type 2 and
hypertension that is suitable for use in resource-limited settings in South Africa.
The tool aims to enhance patient knowledge and understanding of diabetes and
hypertension while being attentive to low (health) literacy, to provide a vehicle to
facilitate patient-provider interaction during medical consultations, and to provide a
tool to help patients monitor relevant self-care behaviors, with a view to enhance
the patients’ self-management skills. This care-plan booklet is not an intervention
on its own, but a tool to be used within the structure of broader, already existing
treatment and care for diabetes or hypertension. As a basis for its development,
the literature on the use of printed materials in patient education was briefly
discussed, as well as the theoretical model that underpinned the development of
the booklet, which gave a rationale to its development. Furthermore, a description
of the care-plan booklet and of its aims and objectives was provided, as well as a
detailed description of how the care-plan booklet should be used by patients and
providers.
As a next step, the care-plan booklet was and will be evaluated in a series of
studies. The next two chapters (Chapter 7 and 8) each present a study that
addressed an aspect of that evaluation. Chapter 7 reports on the qualitative data
collected on the feasibility of implementing this care-plan booklet in PHC settings in
South Africa. Chapter 8 describes the results of a quasi-experimental study
investigating the potential effects of the care-plan booklet in patient-provider
interactions in terms of improving the health literacy and disease-specific
knowledge of diabetic and hypertensive patients. Finally, in Chapter 10, a
comprehensive protocol will be presented for a randomized controlled trial in which
the care-plan booklet will be further evaluated.

150
References
1. Brady TJ, Murphy L, O'Colmain BJ, Beauchesne D, Daniels B, Greenberg M, et al. A meta-analysis of health status, health behaviors, and healthcare utilization outcomes of the Chronic Disease Self-Management Program. Prev Chronic Dis 2013;10(E07).
2. Franek J. Self-management support interventions for persons with chronic disease: an evidence-based analysis. Ont Health Technol Assess Ser. 2013;13(9):1-60.
3. Steinsbekk A, Rygg L, Lisulo M, Rise M, Fretheim A. Group based diabetes self-management education compared to routine treatment for people with type 2 diabetes mellitus. A systematic review with meta-analysis. BMC Health Serv Res. 2012;12(213).
4. Stoilkova A, Janssen DJ, Wouters EF. Educational programmes in COPD management interventions: a systematic review. Respir Med. 2013;107(11):1637-50.
5. Dube L, Van den Broucke S, Housiaux M, D'Hoore W, Rendall-Mkosi K. Type 2 Diabetes selfmanagement education programs in high and low mortality developing countries. Diabetes Educ. 2015;41(1):69-85.
6. Choi TST, Walker KZ, Ralson RA, Palermo C. Diabetes education needs of Chinese Australians: a qualitative study. Health Educ J. 2014;74(2):197-208.
7. Dube L, Van den Broucke S, Bergh A-M, Mafutha N, Rendall-Mkosi K. Self-management support needs of patients with chronic diseases in a South African township: a qualitative study. J Community Health Nurs. In Press.
8. Dube L, Van den Broucke S, Rendall-Mkosi K, Kalweit K, Housiaux M, D'Hoore W. An audit of diabetes self-management education programs in South Africa. J Public Health Res. 2015;4(581):176-84.
9. Hoffmann T, Worrall L. Designing effective written health education materials: considerations for health professionals. Disabil Rehabil. 2004;26(19):1166-73.
10. World Health Organization. Health topics: health education [Internet]. 2016 [cited 18 October 2016]. Available from: http://www.who.int/topics/health_education/en/.
11. Houts PS, Doak CC, Doak LG, Loscalzo MJ. The role of pictures in improving health communication: a review of research on attention, comprehension, recall, and adherence. Patient Educ Couns. 2006;61(2):173-90.
12. Paul C, Redman S. A review of the effctiveness of print material in changing health-related knowledge, attitudes and behaviour. Health Promot J Austr. 1997;7:91-9.
13. Bonevski B, Newell S. Development of written health education materials: a review. New Castle: Hunter Centre for Health Advancement Research Seminar; 1999.
14. Dowse R. The limitations of current health literacy measures for use in developing countries. J Commun Healthc. 2016;9(1):4-6.

151
15. Bress J. Developing a framework to identify and respond to health literacy needs using community-based emergency first aid responders in the Lavender Hill. MSc dissertation, University of Cape Town; 2014.
16. Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80.
17. Coulter A, Ellins J. Effectiveness of strategies for informing, educating, and involving patients. BMJ (Clinical research ed). 2007;335(7609):24-7.
18. Eakin EG, Bull SS, Glasgow RE, Mason M. Reaching those most in need: a review of diabetes self-management interventions in disadvantaged populations. Diabetes Metab Res Rev. 2002;18(1):26-35.
19. Fu Y, Yu G, McNichol E, Marczewski K, Jose Closs S. The effects of patient-professional partnerships on the self-management and health outcomes for patients with chronic back pain: a quasi-experimental study. Int J Nurs Stud. 2016;59:197-207.
20. Cao ZJ, Chen Y, Wang SM. Health belief model based evaluation of school health education programme for injury prevention among high school students in the community context. BMC Public Health. 2014;14:26.
21. National Cancer Institute. Theory at a glance: a guide for health promotion practice. 2nd ed. NIH Publication No. 05-3896 [Internet]. U.S Department of Health and Human Services, National Institutes of Health; 2005 [cited 22 September 2015]. Available from: http://www.sbccimplementationkits.org/demandrmnch/wp-content/uploads/2014/02/Theory-at-a-Glance-A-Guide-For-Health-Promotion-Practice.pdf.
22. Abraham C, Sheeran, P. The Health Belief Model. In: Conner M, Norman, P, editor. Predicting and changing health behavior. 3rd ed. Berkshire: McGraw-Hill Education; 2015.
23. Raingruber B. Contemporary health promotion in nursing practice. Burlington: Jones & Bartlett Learning, LLC; 2014.
24. Lamanna LM. College students' knowledge and attitudes about cancer and perceived risks of developing skin cancer. Dermatol Nurs. 2004;16(2):161-4, 175-6.
25. Forsyth LH, Goetsch VL. Perceived threat of illness and health protective behaviors in offspring of adults with non-insulin-dependent diabetes mellitus. Behav Med. 1997;23(3):112-21.
26. Curo Health. Individual care plan booklet. 2015. 27. Department of Health, South Africa. Nutritional management of
hypertension [Pamphlet]. 28. Department of Health, South Africa. Nutritional management of diabetes
[Pamphlet]. 29. Maimela E, Van Geertruyden JP, Alberts M, Modjadji SE, Meulemans H,
Fraeyman J, et al. The perceptions and perspectives of patients and health care providers on chronic diseases management in rural South Africa: a qualitative study. BMC Health Serv Res. 2015;15:143.

152

153
CHAPTER 7: Feasibility study
Feasibility of a self-management tool for diabetes and
hypertension in South Africa
Submitted for publication as:
Dube L, Bergh A-M, Van den Broucke S, D’Hoore W. Feasibility of a self-
management tool for diabetes and hypertension in South Africa.

154
Summary
The continuous rise of non-communicable diseases, especially diabetes and
hypertension, creates a double burden of diseases in low- and middle-income
countries. As self-management support enables patients to take an active role in
managing their own condition and is a cost-effective way to address the chronic
disease burden, there is a need for contextually appropriate self-management
support tools. This qualitative study explored the feasibility of using a contextually
adapted self-management care plan booklet for diabetes and hypertension for use
in medical consultations. Focus group and individual interviews with patients and
healthcare providers were conducted in three primary healthcare facilities. Eight
focus areas for feasibility studies were used as the lens for data analysis:
acceptability, demand, implementation, practicality, adaptation, integration,
expansion and limited-efficacy testing. The study revealed a high acceptance of
the booklet by both patients and providers. Patients reported that the booklet
increased their knowledge of their conditions, indicated that they would share the
booklet with friends and families, and expressed the need to use it with their
providers. Providers mentioned that community health workers and health
promoters could play an important role in implementing the tool. The findings of this
study contribute to the knowledge base needed for the development and adoption
of the self-management component of the South African integrated chronic
diseases model. The care plan booklet can be used to stimulate the interaction
between patients, providers and/or family and friends.
Key words: cultural adaptation; self-management; diabetes and hypertension;
feasibility study; South Africa

155
Introduction
As chronic diseases continue to rise in both industrialized and non-industrialized
countries, it has become crucial for healthcare systems to shift from paternalistic
models of care to models involving a partnership between patient and healthcare
professionals (Bodenheimer et al. 2002). Partnership models focus on self-
management education and collaborative care, where patients take an active role
in the management of their own disease(s) (deSilva, 2011; Bodenheimer et al.
2002; Von Korff et al. 1997). The purpose of providing self-management support is
to enable patients to take an active role in managing their own condition, which is
different from patient education (Foster et al. 2007).
A strong focus on self-management has been shown to be cost effective and to
increase patient adherence to medication and the uptake of healthy behaviors,
which can help to improve population health (Mills et al. 2016; deSilva, 2011;
Cunningham, 2016). However, one of the challenges for self-management support
programs is their implementation in underserved communities. Not only are such
programs less often organized for these communities, even when they are
available through health centers, but the specific individual needs of chronic
patients related to their social environment and cultural background are often
neglected (Mills et al. 2016).
This also holds true for self-management programs in developing countries.
Whereas the epidemiological shift of the burden of disease from infectious to
chronic disease that has been noted in most developing countries can largely be
attributed to the transition from traditional to western lifestyles (Levin-Zamir et al.
2016), the same cannot be said for chronic disease self-management (Puoane et
al. 2008). Even relatively universal problems have to be addressed differently
because of varying socio-economic and cultural contexts (Van den Broucke, in
press). Therefore, self-management programs and materials that have been
developed in western countries need a contextual adaptation that is sensitive to the
needs of communities in developing countries before they can be implemented.

156
To find out if adaptations of programs take the cultural context sufficiently into
account, feasibility studies can be done. Feasibility studies in the field of health
promotion are often conducted to investigate if all the components of a bigger
intervention work properly in a given context, and their findings provide a basis to
decide whether an intervention is worth further testing for efficacy. Knowledge
about the feasibility and acceptability of an intervention does not guarantee
effectiveness, but can increase the possibility of an intervention being liked,
comprehensive, accepted, remembered, credible and attractive (Vandelanotte et
al. 2004). According to Bowen et al (2009), feasibility studies can focus on different
areas, including acceptability, demand, implementation, practicality, adaptation,
integration, expansion and limited-efficacy testing, depending on the research
question.
The aim of this study was to explore the feasibility of using a contextually adapted
individual care plan booklet as a self-management support tool for diabetes and
hypertension during medical consultations in a South African community. The
experiences and views of patients and healthcare providers were elicited to assess
the feasibility of the tool’s implementation. To our knowledge, no previous study
has systematically evaluated the feasibility of the use of a self-management
support tool for chronic patients in a developing country. The study built on the
findings from two previous studies (Dube et al. 2015; Dube et al. submitted) that
had acquainted the researchers with the current status with regard to diabetes self-
management education programs in South Africa and with the perceived needs of
the target population in terms of self-management support.
The intervention
The intervention involved the development of a prototype individual care plan
booklet in A5 format for use by providers and diabetic and/or hypertensive patients
during medical consultations. The content of the booklet was informed by the
needs of the patients identified in a previous study (Dube et al. 2015; Dube et al.
submitted). As revealed by this study, patients did not have an opportunity to
prepare questions for a consultation with the provider, had no means to record the

157
advice of the physician, and did not have a take-home individual care plan; while
providers did not have enough educational materials to support patients in the self-
management of their disease. The format of the booklet was informed by a more
general booklet used in South Africa (Curo Health, 2015, unpublished). Other
materials were also used, including the few already existing pamphlets on the
specific disease conditions (Department of Health South Africa, unpublished). A
first draft of the booklet was circulated to different stakeholders who commented on
its content, after which the prototype booklet was finalized for the study. The
booklet was only available in English, which is one of the official languages in
South Africa and the language of schooling.
The prototype booklet included the following topics:
• How to use the booklet
• Glossary of terms (with translations in Zulu and Sepedi)
• Making most of the medical consultation (tips for patients)
• Information on diabetes and hypertension
- definition
- physiology
- signs and symptoms
- complications
- health education messages
• Lifestyle change messages
• Body mass index table
• Preparing for the consultation
- tables for recording vital signs by healthcare providers
- tables for use in provider-patient consultation
• Spaces for referral notes
• General notes by healthcare provider
• Pocket for appointment card at the inside back cover
• Emergency telephone numbers on outside back cover
Method
The Research Ethics Committee of the Faculty of Health Sciences, University of
Pretoria (protocol 57/2016) and the Tshwane District Research Ethics Committee
(Project 15/2016) approved the research.

158
Study design
A qualitative study design was used to explore the views and perspectives of the
participants on the feasibility of using an individual care plan booklet integrated in
the consultations with providers. The study was designed to answer the question if
the intervention could work, and more particularly to understand how the use of the
booklet could fit with the daily-life activities of healthcare providers and patients
(Bowen et al. 2009).
Sampling and recruitment
The study was conducted in three community healthcare facilities and had two
distinct groups of participants, an intervention group and a ‘comments-only’ group.
The intervention group consisted of diabetic and hypertensive patients and
healthcare providers (nurses and doctors) in an urban community health center
(CHC) that had been part of the previous study on self-management needs (Dube
et al. submitted). The providers in this group were trained on the use of the booklet
with patients as part of the existing consultation process. The comments-only
group was composed of diabetic and hypertensive patients and healthcare
providers (doctors, nurses, dieticians and health promoters) recruited in a CHC in a
rural setting and in a primary healthcare clinic in the same area as the intervention
site. They were asked to provide comments on the content and possible use of the
booklet. The reason for including a comments-only group was to elicit a wider
variety of views, as it was not practically possible to include more sites and
participants in the intervention group.
The patients participating in the intervention and comments-only groups received
primary care services at the three study facilities. To be included, patients had to
be 18 years or older with diabetes and/or hypertension, and able to read and write
or have someone at home to assist with reading and writing. Health providers were
included because they are important to the success of the integration of
interventions like these (Lake and Staiger, 2010). At the intervention CHC, patients
were purposively selected to only include diabetic and/or hypertensive patients with

159
uncontrolled values and who would return for follow-up within one month. Doctors
and nurses identified qualifying patients and, after issuing the booklet, referred the
patients to the researchers who then explained the purpose of the study and
sought written informed consent. At the two facilities where comments-only
participants were sampled, diabetic and hypertensive patients were recruited from
the queue while waiting for a medical consultation. Those who gave written
informed consent were included.
All doctors and nurses caring for chronic patients in the three study facilities were
invited to participate. A sample of dieticians and health promoters were
conveniently selected for an invitation to participate. All provider participants also
gave informed consent before being included in the study.
More females than males participated in both study groups. Participants’ ages
ranged between 29 and 98 years. The majority of participants were Sepedi,
Setswana, isiZulu and isiNdebele first-language speakers. More than half the
participants were married or lived with a partner. More participants in the
intervention group completed 12 years of schooling than in the comments-only
group. Half of the intervention-group participants were employed compared to less
than one fifth in the comments-only group. Nurses were participants’ main source
of information, followed by radio, and magazines and books. Supplementary file 1
contains more information on the demographic characteristics of participants.
Data collection strategy
In both study groups, focus group and individual interviews were held with patients
and providers by means of interview guides. The choice of method was determined
by the availability of participants. Focus groups are considered an appropriate
method to collect evidence for the acceptability of an intervention (Bowen et al.
2009).
In the intervention group, the interviews took place after one month and after
patients and providers had used the booklet in consultations. Questions focusing

160
on the content and experiences of using the booklet were included in these
interviews. In the interviews with the comments-only group, the focus was on
content and potential use of the booklet. All patient participants completed a short
demographic questionnaire (see supplementary file 1).
A total of 10 focus groups and 7 individual interviews were conducted. Sixteen
patients and 8 providers in the intervention group participated, whereas there were
32 patient participants and 9 providers in the comments-only group. Interviews
lasted between 12 and 45 minutes and were audio-recorded. Audio-recordings
were transcribed and, where needed, translated and cross-checked by researchers
fluent in the vernacular languages.
Data analysis
Using a framework by Bowen et al. (2009) for the design of feasibility studies as a
point of departure, the data were first organized according to the eight focus areas
under the topic “Can the intervention work?”
• Acceptability: reaction of target population
• Demand: likelihood of using intervention
• Implementation: applicability of intervention
• Practicality: execution of intervention with limited resources
• Adaptation: altering intervention for new populations
• Integration: how new intervention can be accommodated within existing
structures
• Expansion: cost of applying the intervention in a different setting
• Limited efficacy: potential success of an intervention
For each area, a thematic analysis was conducted to explore salient topics and
develop codes within each theme. The analysis was done in a reiterative fashion,
with two authors (LD & AMB) analyzing the data independently, with regular
discussions on interpretations and provisional findings. Codes were continuously
refined and the data re-analyzed until consensus was reached. The following

161
reference codes are used for direct quotations: Prv = provider; Pat = Patients; FG =
focus group; II = individual interview; IG = intervention group; CO = comments-only
group; M = male; F = female.
Results
Not all the areas and outcomes described in Bowen et al. (2009) framework for the
design of a feasibility study were applicable to the current study, as participants
were not in a position to give a perspective on some of the health systems and
policy issues such as cost analysis and efficacy testing. Some areas of the
framework were also adapted to accommodate additional findings from our data.
Areas that stood out most were acceptability, demand, practicality, and adaptation.
Implementation, integration, expansion and limited efficacy were less prominent.
Acceptability
Both patients and providers expressed satisfaction with the content and approach
of the booklet. As effective management of chronic diseases requires the
strengthening of both pharmacological and non-pharmacological interventions, one
provider commented specifically on the holistic approach: ‘… most of the time
when we treat the chronic illnesses, we emphasize on pharmacology, but this one
is non-pharmacological.’ (Prv_FG1_IG_M)
Patients reported that the booklet improved their knowledge of their condition – ‘I
knew some of the things, but most of this I didn’t know’ (Pat_FG1_IG_F); – ‘This
booklet … opens our knowledge, because we are sick and we don’t know how to
cure ourselves’ (Pat_FG1_IG_M).
Patients also perceived the booklet as being an appropriate guide or manual for
the day-to-day self-management of chronic conditions, for which one participant
made the following comparison:

162
Like when I want to go to the driving school, they tell me this is a stop sign, a
hill sign. But when I don’t follow those rules, I am going to make an accident.
But when I follow the rules, then I will be always driving well. (Pat_FG1_IG_M)
Providers perceived the booklet as appropriate in encouraging patients to self-
manage their care and ‘… enforcing patients to get what they are actually
supposed to get’ (Prv_II2_CO_M). Providers ‘… don’t always have time to discuss
everything with them [patients]; so things that we may have left out will be in here
[in the booklet]’ (Prv_II_3_CO_F).
Providers’ perspective that ‘a book like this might make it easy for junior doctors’
(Prv_II2_CO_F) when doing routine check-ups for chronic patients fits in with the
demands of the organizational culture. The booklet was also seen as ‘a perfect and
a nice monitoring tool’ (Prv_II1_IG_F). From a patient perspective, members of the
intervention group mentioned that writing down questions for the next consultation
was an effective reminder mechanism – ‘The booklet gives us access to the
doctors, so you can ask questions concerning this book and you get a good
relationship with the doctor’ (Pat_FG1_IG_F). Others also found the more holistic
and patient-centered approach appealing – ‘Last time we would get inside, they
just write and say, ‘Go and take the pills.’ And we follow drinking those pills just like
that. This … book is better than that’ (Pat_FG1_IG_F).
Demand
Patients expressed themselves strongly on their intention to use or to continue to
use the booklet – ‘Nothing will stop me from using this book’ (Pat_FG2_IG_F), and
‘… my children will read for me and I will know what to eat, what not’
(Pat_FG2_CO_F).
Some patients viewed the booklet as a facilitator for self-managing their own care:
‘… this book … it is my life, that’s why I am going to use it’ (Pat_FG2_IG_F).
Patients in the intervention group used the booklet for reading and preparing their

163
questions for the providers, whereas providers used the booklet for communication
and answering patient questions.
Today I did ask the doctor that I wanted to chat to him and I gave him this
booklet and he asked if I was drinking or smoking ... eating correctly … if I was
sleeping okay ... So you understand that you talk with your doctor about what
is bothering you (Pat_FG2_IG_F).
Patients in the comments-only group expressed their intention to use the booklet
as a ‘passport’ (Pat_FG1_CO_F), but with reservations, for instance ‘if the doctors
would give us that chance we would use it’ (Pat_FG2_CO_F). Reasons for wanting
to use the booklet included improved knowledge and the benefit of sharing
information with family and offspring – ‘Even kids at home will see it and read it. A
book is like a history; it has things that will not disappear. It’s like a candle that
lights for them to be clever’ (Pat_FG2_CO_M).
Both patient and providers reported a perceived demand for the booklet. From the
patient’s perspective the emphasis was on the demand for information, on the
condition itself and on lifestyle changes, especially dietary guidelines.
I think this book will help many of us who did not know. If they [other family
members] read for us, since we did not learn, then we will hear what is the
disease, what we should eat and what are the mistakes (Pat_FG4_CO_M).
The demand for the booklet was perceived to go further than the patients only, as
‘everyone in this world who is alive will benefit from this booklet’ (Pat_FG2_CO_F),
and ‘since diabetes runs in the family … even if I pass away, they [other family
members] will know how to treat themselves’ (Pat_FG2_CO_F).
The study also had a ripple effect on other providers not involved in the study who
enquired about photocopying the booklet or making recommendations for using it
with community health workers.

164
Implementation
Successes and failures in using the booklet were related to the intervention group’s
patients reading and writing in the booklet – ‘I wrote whatever was my concern and
then I asked my doctor about it; so in case I forgot ... I wrote whatever complains
that’ (Pat_II1_IG_F). Participant feedback was varied, with some referring to the
following – ‘We have taken time to read it’ and ‘I did write where I understand;
where I did not understand, I did not write’ (Pat_FG2_IG_F). Apart from not
understanding, other reasons for not writing included ‘I was just lazy to write’
(Pat_FG1_IG_M), and ‘I had problems of funerals’ (Pat_FG2_IG_F). On the other
hand, the providers’ use of the booklet may have been influenced by their
assessment of the patients’ literacy levels and ability to understand English and by
the availability of family members to read for them.
Some [patients] … told us that they gave us this book … ‘I have to ask
questions … at home [to] my kids. I don’t stay with my kids.’ … We [providers]
find ourselves having this book, but patients not understanding how to use it.
(Prv_FG1_IG_M)
There was not much probing in terms of the resources that were needed to use the
booklet. However, some providers referred to the importance of including frontline
community health workers, ‘the ones that go into the families’ (Prv_FG1_IG_M), in
using the booklet. Others saw health promoters as key implementers, as ‘[t]hey will
be able to unpack the book properly for patients while they are waiting’
(Prv_FG1_IG_M). The potential of using the booklet in support groups was also
mentioned.
I think as a tool to educate the patients this book it’s out of this world. Actually
I was thinking of coming back to you to ask, ‘Do you mind if I can use this
book when I have support groups?’ It’s very good. (Prv_FG2_IG_F)
Factors mentioned that affected the ease or difficulty of implementation included
the size of the booklet.

165
Some of them [patients] … might look at it and say, ‘A book’. You know, most
people are lazy out there. These are practical ways on how people may react
to this like ‘Oh, why did they give me such a huge book with lots of tables? I
don’t have time for that.’ (Prv_II1_IG_F)
Other factors were patients’ functional literacy and proficiency in English, with
some patient participants finding ‘the English is very understandable’
(Pat_FG1_IG_F) and the glossary with the translation of key words in Zulu and
Sepedi helpful: ‘… they explain the words that they thought will be difficult for us to
understand in English’ (Pat_II1_IG_F). Cooperation of healthcare providers in the
use of the booklet was also a concern – ‘Maybe if you [researcher] haven’t talked
to them [nurses]… it will be difficult’ (Pat_FG1_CO_F).
Providers referred to ‘rural patients who never read or write’ (Prv_II3_CO_F) and
the fact that ‘most of our diabetic patients are older patients; they can’t read and
write.’ (Prv_FG2_CO_F) They also had concerns about privacy – ‘Some people,
they don’t want other relatives or family members to know what they are suffering
from.’ (Prv_II1_IG_F) One provider from the rural CHC in the comments-only
group also expected issues with difficult patients who would not want to bring their
booklets along for consultations – ‘Some patients are lazy, and … stubborn …
harsh. You will ask them, “Where is that book?” And they will start complaining’
(Prv_FG1_CO_F).
Practicality
Patients in the intervention group reported several positive and expected positive
effects of the use of the booklet. In terms of interaction with health providers, they
mentioned the reciprocal relationship in terms of asking questions – ‘I don’t think
there was a time when the doctor asked me questions like that, but now I am
happy’ (Pat_FG2_IG_F).
Some participants made decisions about lifestyle changes – ‘I got the information
from the book about my diet, so I decided to start with my diet and if I get that right

166
I will start to exercise’ (Pat_II1_IG_F). Others reported on perceived or expected
health outcomes – ‘I am better than before because I read this book’
(Pat_FG2_IG_F), and ‘My blood pressure is still high, but I believe this book is
going to help me’ (Pat_FG2_IG_F).
Providers saw the booklet as ‘an empowerment tool to get patients to take
responsibility’ (Prv_II1_CO_M), but a few doubted the ability of patients to use the
booklet effectively. As already mentioned some providers perceived some patients
as being lazy and stubborn. But some also felt that parts of the booklet would have
more value for use – ‘I think one should stress that the patient … should be able to
look on the first few pages just to get information on what is diabetes … I think
that’s really good and the health messages’ (Prv_II3_CO_F).
According to some providers, the efficiency and speed of the implementation of a
care plan booklet could be hampered by the additional consultation time needed
with the booklet and the heavy workload of staff – ‘We see a lot of patients’
(Prv_FG1_IG_M).
But now we need also to consider … patients’ waiting time, because the time
will increase. If we are used to seeing the patient for 15 minutes, this will
increase from 15 to 25 minutes because we record in the patient’s file and the
register and this [booklet]. (Prv_FG1_CO_M)

167
Adaptation
One aim of the study was to receive recommendations for the adaptation of the
content and format of the prototype booklet. Apart from translations into several
languages, the patients did not have many recommendations about the content. In
the comment-only group, patients reported that they needed more time to read and
understand the booklet – ‘Now we haven’t read it nicely to see if it has everything,
we will go and read it at home’ (Pat_FG2_CO_M). Others indicated that they had
little knowledge about the subject of the booklet, so they were happy that they got
something to teach them. There were also requests for additional information on
diet, for example, ‘I want to know about … banana … How does it affect diabetes?’
(Pat_FG2_IG_F).
Providers reported that the booklet should include a set of minimum requirements
for diabetes care to empower patients to demand the care they are supposed to
receive: ‘… a set of minimum requirements for diabetes care … you as a diabetic
patient are entitled to … at every visit, once or twice a year’ (Prv_II1_CO_M).
Others thought that there should be a simple flow chart to record vital signs for five
or ten years showing a trend so that one can easily see if target levels are met.
There were also some comments on pictures to be changed, the use of more color,
the inclusion of community resources where patients can get help, and the revision
of the body mass index table. With regard to the last recommendation one provider
commented:
I think they are doing their study mostly based on white people … you know we
are African; on weight, you know, we are big people. So if you say we are
overweight, there I don’t know. (Prv_FG1_CO_F)
Integration
For this study, integration refers to the level of system changes needed to integrate
the booklet into the day-to-day care and treatment of diabetic and hypertensive
patients. Patients’ perceptions of fit with current infrastructure related to feelings of

168
being better cared for by the system through the facilitation of communication with
healthcare providers.
We previously did not have the audacity and the right to ask questions to the
nurses and the doctors. Ours was, come and take medication and listen. And
some of them [providers] they don’t have patience. (Pat_FG3_CO_M)
Patients also felt the booklet ‘… will help even when we get home; the kids will
read for us, telling me it’s this and that.’ (Pat_FG2_CO_F)
Providers referred to how the booklet could fit in with the system – ‘So it’s a tool
that we can give to patients in the initial phases; it would get good results because
patients have something to refer to’ (Prv_FG1_IG_M). All healthcare providers
were seen to possibly benefit from the use of the booklet– ‘It’s not only doctors that
are practitioners ... most of the patients, especially in small clinics … are seen by a
nurse health practitioner’ (Prv_FG1_IG_F). However, a concern was expressed
about the ability to refer patients needing certain types of special care – ‘I do not
know if in the primary healthcare there is any psychologist. We don’t have a
podiatrist’ (Prv_II1_CO_M).
With regard to sustainability, some providers had reservations because of time
challenges – ‘I think time is the biggest issue; it needs extra time to look at the
book’ (Prv_II3_CO_F). A dietician also referred to ‘[w]e end up giving duplicate
information’ and some patients being confused because ‘they don’t gel well’
(Prv_II1_IG_F).
Expansion
As the booklet can be integrated in the current infrastructure, its use as a
communication tool between providers and patients fits in with patient-centered
care and can be said to fit with organizational goals and culture. There were some
patient requests for mass production – ‘Please make lots of them and distribute
them among clinics and provinces and go and teach people’ (Pat_FG2_CO_M).

169
The expansion of the content to include more chronic diseases treated in primary
care was also proposed – ‘I feel that the [booklet] … could actually be beneficial to
all five or six chronic conditions that we are managing’ (Prv_FG1_IG_F).
On the other hand, providers in the comments-only group, apart from seeing a
possible negative effect of the use of the booklet on their use of time, also referred
to possible positive effects on their organization of work.
For us as providers it will help us ... when we give health talk to the patients.
They will have that knowledge from this book. If we talk about diabetes and
hypertension, they already know exactly what are we talking about.
(Prv_FG1_CO_M)
Limited efficacy
Although limited efficacy could only be properly tested by using quantitative
measures, in this study participants expressed their views on the effect of the
booklet on their lives – ‘[The booklet] it’s already made a difference in my life; so I
believe it is going to have impact on even more people’ (Pat_II1_IG_F).
Providers, on their part, saw the effect of the booklet on creating an opportunity for
more holistically-orientated consultations.
I like the idea that patients need to prepare for the consultation … because we
never think of patients come to us and they didn’t think of what they want to
complain of [with regard to their chronic condition] … It’s often they complain
of things that are not related to the diabetes. So we often see patients, then
they complain of ‘flu, then that is their major problem now. But their diabetes
care problems are not addressed, because they don’t ask us about their
diabetes care. (Prv_II1_CO_M)

170
Discussion
Feasibility studies can assess whether an intervention is suitable for further testing
and provide information on whether it is relevant and sustainable (Bowen et al.
2009). This study tried to answer the question whether the self-management care
plan booklet that was adapted for patients with diabetes and/or hypertension in
South-African communities would work. The results indicate that both from the
perspective of the patients and of the healthcare providers the care plan booklet
was considered to have a good chance of success, if the potential pitfalls could be
factored in. These pitfalls can be addressed in a bigger study in which the focus
areas of expansion and efficacy testing should get more attention.
This study revealed a high acceptability of the care plan booklet by both patients
and providers in facilitating the collaboration in self-management. The acceptance
of the booklet is probably motivated by the patients’ lack of sufficient information
about their conditions (Dube et al. submitted; Parker et al. 2012) and by the current
lack of context specific health education material. Some comments relating to
organizational culture fit in well with the emphasis on ‘assisted self-management
support’ in the integrated chronic diseases model (ICDM) adopted for South Africa
(Mahomed and Asmall, 2015).
The study also highlighted the value of the individual care plan booklet in
increasing the patients’ knowledge and improving the communication between
patients and their health providers during consultations. This confirms the finding
from previous research that healthcare providers in South Africa mostly have a
treatment-and-drug dispensing approach, while neglecting the self-management
component of care (Dube et al. submitted). The current shift in the provision of care
from paternalistic to partnership models requires patients to become part of the
treatment process (Bodenheimer et al. 2002; Von Korff et al. 1997) in which their
voices are heard and their needs attended to by the healthcare providers in a more
holistic manner. Bodenheimer et al. (2002) assert that it can be an eye opening
experience to allow patients to define their problems.

171
The demand for a care plan booklet was illustrated by patients wanting to share the
booklet with family members and even neighbors. This demonstrates that the
booklet could be used as a vehicle for communication, not only with providers but
also with family and friends. A study on maternal handbooks in Cambodia also
found that women were willing to share manuals with family members and that they
saw records as a valuable source of health information (Yanagisawa et al. 2015).
Although patients in our study referred to the actual and intended use of the care
plan booklet, most of them expressed the need for health service providers to
cooperate with them. This points to the need for partnership in the treatment of
chronic diseases necessitated by the epidemiological shift in lifestyles. Having a
care plan booklet could be a good start for many developing countries, as patients
need to understand their changing role from being dependent on healthcare
providers to becoming active agents of their own treatment (Von Korff et al. 1997;
Bodenheimer et al. 2002).
The booklet was regarded as easy to implement, as the people who would be
instrumental in any role-out were already available. Community health workers
(CHWs) who conduct home visits and health promoters who engage with patients
in the waiting area were seen as key stakeholders. In many low-to-middle income
countries like South Africa, the use of CHWs has been accelerated, especially due
to a shortage of health service professionals (Mishra et al. 2015). CHWs act as a
link between the community and the health facilities. Research in Iran indicated
that trained CHWs were effective in the control of diabetes and hypertension
(Farzadfar et al. 2012). However, while the use CHWs might sound like a good
opportunity for task shifting, this suggestion should be approached with caution.
There are challenges such as overburdening the CHWs, thereby reducing the
quality of their work in communities. CHWs will need proper training and adequate
provision of equipment and support if they are to be involved NCD care (Mishra et
al. 2015).
A small number of exceptions notwithstanding, patients in the intervention group of
the present study generally managed to use the booklet. The fact that some
172
patients did not use it may reflect certain characteristics of the population whereby
socio-cultural obligations are put before one’s own health needs, in such a way that
the booklet became second to other ‘important tasks’. Betsch et al (2015) also
point out that the cultural background of an individual affects his or her attitude
towards behavior. Again, this tendency could be due to the socialization of people
to the medical model of care whereby patients expect the health service provider to
be responsible for everything and don’t give themselves a role to play
(Bodenheimer et al. 2002).
In general, the care plan booklet was perceived as something that was practical
and that could easily be integrated in the treatment plan. This is a positive sign in
the light of South Africa’s current drive to re-engineer primary healthcare and to
integrate the chronic care model that includes self-management as an equal
component of care (Mahomed and Asmall, 2015; Wagner, 1998). Although
providers voiced the issue of time and long queues in the primary healthcare
facilities as possible barriers to the integration of the booklet in the treatment, the
general opinion was that it could be sustainable. The latter is crucial in view of the
double burden of disease in the developing countries (Iwelunmor et al. 2016).
Finally, several points were mentioned related to possible adaptations of the care
plan booklet. Participants’ suggestions that the booklet should be provided in their
own language reveals a need for interventions to be contextually adapted to the
target population. On the other hand, the providers’ complaint that the body mass
index scale is not appropriate for African people demonstrates the salient influence
of context on the beliefs about health (Dube et al, submitted).
Limitations of the study
This study yielded insightful views about the feasibility of the use of an individual
care plan booklet for diabetic and hypertensive patients. However, some limitations
must be acknowledged. A major limitation was the short time for the study and the
limited availability of some of the participants. Interviews were done at the facilities
providing care for the participants and some patients were in a rush to finish their

173
interviews. This hampered our ability to get a good sense of the real potential of the
longer-term utilization of the care booklet by patients and their families or in
medical consultations. Secondly, the potential impact of existing knowledge about
the disease and of health literacy was not explored in depth. The prototype booklet
was only printed in English. While this was due to limited resources, many patients
would have preferred the tool to be available in their first language. The short
duration of the study made it difficult to collect data on health outcomes, which
highlights to the needs for more research in this regard.
Conclusion
This study provides relevant information for the development and adoption of the
self-management component of the ICDM that is currently being implemented in
South Africa. The care plan booklet can be used as a vehicle to improve the
interaction between patients and their providers and/or family and friends. Although
participants accepted the booklet and saw it as an empowerment tool, more needs
to be done to further adhere to the health providers’ recommendations and to
enhance the capabilities of patients to self-manage their disease more effectively.
Conflict of interest
The authors declare no conflict of interest.
References
Barron, P. and Roma-Reardon J. (eds) (2008) South African Health Review 2008. Health Systems Trust, Durban.
Bodenheimer, T., Lorig, K., Holman, H. and Grumbach, K. (2002) Patient self-management of chronic disease in primary care. Journal of the American Medical Assosciation, 288, 2469–75.
Bowen, D. J., Kreuter, M., Spring, B., Cofta-Woerpel, L., Linnan, L., Weiner, D., et al. (2009) How we design feasibility studies. American Journal of Preventive Medicine, 36, 452–7.
Cunningham, P. (2016) Patient perceptions of clinician self-management support for chronic conditions. American Journal of Managed Care, 22, e125–33.
Desilva, D. (2011) Evidence. Helping people help themselves. A review of evidence considering whether it is worthwhile to support self-management.

174
The Health Foundation. http://www.health.org.uk/publication/evidence-helping-people-help-themselves (last accessed 2 December 2015).
Dube, L., Van Den Broucke, S., Rendall-Mkosi, K., Kalweit, K., Hosiaux, M and Dhoore, W. (2015) An audit of diabetes self-management education programs in South Africa. Journal Public Health Research, 4, 176–84.
Farzadfar, F., Murray, C. J., Gakidou, E., Bossert, T., Namdaritabar, H., Alikhani, S., et al. (2012) Effectiveness of diabetes and hypertension management by rural primary health-care workers (behvarz workers) in Iran: A nationally representative observational study. Lancet, 379, 47–54.
Iwelunmor, J., Blackstone, S., Veira, D., Nwaozuru, U., Airhihenbuwa, C., Munodawafa, D., et al. (2016) Toward the sustainability of health interventions implemented in sub-Saharan Africa: A systematic review and conceptual framework. Implementation Science, 11, 43.
Lake, A. J. and Staiger, P. K. (2010) Seeking the views of health professionals on translating chronic disease self-management models into practice. Patient Education and Counseling, 79, 62–8.
Levin-Zamir, D., Badarne, S., Najami, M., Gan Noy, S., Poraz, I., Shapira, M., et al. (2016) The use of focus groups as a basis for planning and implementing culturally appropriate health promotion among people with diabetes in the Arab community. Global Health Promotion, 23, 5–14.
Mahomed, O. H. and Asmall, S. (2015) Development and implementation of an integrated chronic disease model in south africa: Lessons in the management of change through improving the quality of clinical practice. International Journal of Integrated Care, 15, e038.
Mills, S. L., Brady, T. J., Jayanthan, J., Ziabakhsh, S. and Sargious, P. M. (2016) Toward consensus on self-management support: The international chronic condition self-management support framework. Health Promotion International, May 30, 2016: 10.1093/heapro/daw030.
Mishra, S. R., Neupane, D., Preen, D., Kallestrup, P. and Perry, H. B. (2015) Mitigation of non-communicable diseases in developing countries with community health workers. Globalization and Health, 11, 43.
Parker, W. A., Steyn, N. P., Levitt, N. S. & Lombard, C. J. (2012) Health promotion services for patients having non-comminicable diseases: Feedback from patients and health care providers in Cape Town, South Africa. BMC Public Health, 12, 503.
Vandelanotte, C., De Bourdeaudhuij, I. and Brug, J. (2004) Acceptability and feasibility of an interactive computer-tailored fat intake intervention in belgium. Health Promotion International, 19, 463–70.
Von Korff, M., Gruman, J., Schaefer, J., Curry, S. J. & Wagner, E. H. (1997) Collaborative management of chronic illness. Annals of Internal Medicine, 127, 1097–102.
Wagner, E. H. (1998) Chronic disease management: What will it take to improve care for chronic illness? Effective Clinical Practice, 1, 2–4.
Yanagisawa, S., Soyano, A., Igarashi, H., Ura, M. & Nakamura, Y. (2015) Effect of a maternal and child health handbook on maternal knowledge and behaviour: A community-based controlled trial in rural cambodia. Health Policy and Planning, 30, 1184–92.

175
Supplementary file
Demographic characteristics of patient participants

176

177
CHAPTER 8: Pilot study
Enhancing diabetes and hypertension health literacy in
a South African township: a pilot study
To be submitted for publication as:
Dube L, Van den Broucke S, Berg, AM, D’Hoore W. Enhancing diabetes and
hypertension health literacy in a South African township: a pilot study.

178
Abstract
Several programs have been developed to assist in self-management of chronic
diseases and generally have positive outcomes. However, their effectiveness may
depend on various patient characteristics like health literacy, especially in
resource-limited settings. Health literacy is currently an under-researched subject
in resource-limited settings, despite the possibility of a higher prevalence of low
health literacy. A pilot study was conducted with the aim to explore changes in
disease-specific knowledge and health literacy among diabetic and hypertensive
patients who had received self-management education using an individual care-
plan booklet to be used in a healthcare consultation. Participants were diabetic and
hypertensive patients from a community health center, in a South African township.
Forty-four (83%) of the 53 recruited participants completed the post-questionnaire
(one month follow-up). Paired samples t-test revealed a significant difference in
knowledge about hypertension from pre- to post-test (p 0.013), but no significant
change in diabetes knowledge and functional and communicative health literacy.
As existing health promoting activities will yield limited results among people with
limited health literacy, further research on improving the health literacy of the
population in developing countries is recommended.
Key words: healthy literacy, knowledge, diabetes, hypertension, South Africa.

179
Introduction
Self-management education refers to behavioral interventions aimed at facilitating
the knowledge, skills, and abilities that are necessary for the day-to-day manage-
ment of a chronic disease. As chronic diseases require daily self-care, a patient’s
capacity to manage his or her disease is generally considered to be a key
determinant of treatment outcomes and of health-related costs. Consequently, a
range of psychoeducational and self-management education programs have been
developed for a variety of chronic diseases (1, 2).
While these programs generally have positive outcomes (3) their effectiveness may
depend on various patient characteristics. One of these characteristics is health
literacy (4). Health literacy can be defined as “people’s knowledge, motivation and
competences to access, understand, appraise and apply health information in
order to make judgements and take decisions in everyday life concerning being ill,
being at risk and staying healthy” (5) (p. 3). A low level of health literacy has been
associated with a range of outcomes related to health, including poor access to
healthcare, inadequate use of healthcare services, a lower likelihood to engage in
health-promoting behaviors, poor knowledge of diseases, decreased medication
adherence, and poor adherence to self-care management, as well as poor general
health and higher mortality (6).
The self-management activities that must be performed by persons suffering from a
chronic disease, such as taking medication, respecting dietary restrictions, staying
physically active, or monitoring blood glucose or blood pressure can be challenging
for someone who has limited health literacy (4, 7). Furthermore, people with low
health literacy often feel ashamed of their difficulty to understand information and
hide this from their doctors (8-10).
Nutbeam et al. (11) proposed a model discriminating between three types of health
literacy. Functional health literacy refers to the basic skills, including reading and
writing, which are required to access and understand information that is relevant to
one’s health. Communicative health literacy involves more advanced skills that

180
enable the extraction of information, defining meaning and applying that
information to everyday life. Critical health literacy requires a set of more advanced
skills to evaluate information from different sources and use it to take charge of
one’s life (11, 12).
Most self-management support programs for chronic patients provide information
about the condition, and enhance the patient’s competences and skills to manage
it on a day-to-day basis. A direct expected outcome of these programs is therefore
an increase of disease-specific (mainly functional) health literacy. On the other
hand, self-management education programs also make use of health information in
different formats (print, internet, oral) to help patients self-manage their condition
(2, 12). As such, a patient’s level of general health literacy is critical for under-
standing the information that is provided and for developing the skills to participate
in the management of their condition.
While the role of health literacy for self-management education of chronic diseases
is increasingly recognized, very few studies have actually investigated its impact on
the effectiveness of self-management programs. To our knowledge, only two
studies have examined whether health literacy moderated the effects of self-
management education (13, 14), demonstrating an improvement of self-care
behaviors in both high- and low- health literate patients. Moreover, very few studies
have investigated health literacy in developing countries (15), and so far no studies
have explicitly focused on disease-specific health literacy as an outcome of self-
management education.
This pilot study aimed to investigate the effectiveness of a self-management
education intervention for diabetes and hypertension on health literacy and
disease-specific knowledge. Specifically, it evaluated the effects of using a context-
specific care-plan booklet by patients and healthcare professionals during medical
consultations. To our knowledge, this is one of the first outcome studies of self-
management education in a developing country using a care-plan booklet as an

181
intervention and considering disease-specific health literacy as an outcome
indicator.
Method
Sample
The study was part of a larger study on the development and testing of a self-
management support tool for chronic patients, and took place in a community
health center (CHC) in a township of the Tshwane metropolitan area in South
Africa. A convenience sample of 53 diabetes and/or hypertensive patients with
uncontrolled values for glucose and blood pressure who received treatment and
care at this CHC were included in the study. Male and female patients 18 years
and older who were able to read and write or who had someone at home to assist
with reading were recruited. All participants gave written informed consent. The
study was approved by the Research Ethics Committee of the Faculty of Health
Sciences, University of Pretoria (protocol 57/2016) and the Tshwane District
Research Ethics Committee (Project 15/2016).
Forty-four (83%) of the 53 recruited participants completed the post-questionnaire.
Nine patients were lost to follow-up, mostly as a result of the timing of the follow-up
dates which were directly before and after major public holidays in South Africa.
Table 8.1 gives a summary of the demographic characteristics of participants. Their
age ranged from 29 to 75 years. More than half of the participants were women
(59%). One quarter of participants completed some years of primary school
education, whereas the rest had completed junior (grade 8-10) and senior (grade
11 -12) high school education.

182
Table 8.1 Demographic characteristics of participants completing the study (n=44)
Intervention
The study consisted of a pre-post comparison looking at disease-specific health
literacy and knowledge before the introduction of an individual care-plan booklet for
collaborative use by providers and diabetic and/or hypertensive patients during
medical consultations, and after one month follow-up. The care-plan booklet was

183
not the intervention by itself, but was used to complement or enhance the already
existing doctor-patient consultations. Patients consult with their health service
providers (nurses or doctors) every one to three months. The development of a
care-plan booklet was informed by the results of a previous study of patient and
provider needs, revealing that patients were mostly passive recipients of
information and did not have a place to record the advice given by health service
providers. A booklet could assist them in retaining messages and enhancing the
self-management of their chronic conditions. Providers also did not have a tool to
support patients with self-management (16).
The concept for the development of the care-plan booklet was triggered by an
existing self-management tool used by Curo Health (17), a non-governmental or-
ganization (NGO) based in Pretoria, South Africa. Their care-plan booklet was
developed based on the Stanford University Chronic Disease Self-Management
Programs (CDSMP(18). Although the booklet was already used in consultations
between patients and health service providers in the private healthcare sector, it
had not yet been evaluated. Moreover, its usefulness in the public health sector,
with patient of lower socio-economic status and lower health literacy, was of
concern. Therefore, the existing booklet had to be adapted to fit the context of the
target population. Other pamphlets on diabetes and hypertension available in PHC
clinics were also consulted for additional information to include in a contextually-
appropriate booklet for this study (19, 20).
The care-plan booklet contains information on diabetes and hypertension, their
complications, examples of lifestyle changes and target values for blood glucose
and blood pressure. The part to be used during a consultation has spaces for the
patient to pre-record observations and questions for the health provider, a space
for vital signs, different emotional faces to be used by the health service provider to
probe how the patient was feeling and discussion questions on diet, exercise,
medication, smoking and alcohol consumption.

184
For the purpose of this study, health service providers issued the care-plan booklet
to eligible patients. After one month patients brought back the booklet which was
then used in aiding communication during the medical consultation.
Questionnaires
A pre-post questionnaire was used to collect data. Health literacy was measured
via an adaptation of Ishakawa’s Health Literacy (HL) questionnaire which
measures functional, communicative and critical health literacy in diabetes patients
(12). Only the items on functional and communicative health literacy were used, as
the items on critical health literacy were considered too difficult, given the lower
educational level of the participants and their preference for verbal interaction. The
items were adapted to be relevant for hypertensive patients. The internal
consistency analysis (Cronbach’s alpha) gave high levels of internal consistency
both for functional health literacy (0.90) and for communicative health literacy
(0.84). Diabetes knowledge was measured via Eigenmann’s tool on diabetes
knowledge (21). The seven most relevant items for the South-African context were
included in the questionnaire. For hypertension knowledge questions, the five most
relevant items were selected from Schapira’s 14-item questionnaire (22).
Data collection
In order to reach as many participants as possible, patients were contacted by
mobile phone a day before their scheduled consultation to remind them of the date
and to bring the booklet with them. Participants who could not complete the post-
questionnaire at the CHC (n = 9) were contacted by telephone and the researcher
completed this questionnaire with them telephonically. The questionnaires were
handed to the participants when they came to consultation. In some instances
where the patients needed assistance, the questionnaire was interviewer-
administered. A trained research assistant fluent in the local vernaculars
administered the questionnaire to patients who preferred to respond in their own
language.

185
Although most of the items were adapted from pre-existing tools (12, 21, 22), any
questionnaire had to be kept very simple and short. Patients in the study came
from a verbal culture and English was not their first language. Participants were
mostly older patients, with whom there is a preference for verbal communication.
Data analysis
Data were analyzed with the Statistical Package for Social Sciences (SPSS version
12) (23). To establish the reliability of the health literacy scales, Cronbach’s alpha
was calculated. Descriptive statistics (means and frequencies) were generated and
paired samples t-test were used to compare the scores before and after the
intervention.
Results
Health literacy
Paired samples t-test on the health literacy scales revealed no significant change in
functional health literacy from pre- to post-test. For communicative health literacy, a
moderate difference was observed between the scores on the pre-test and post-
test, but the t-test again revealed no significant difference (Table 8.2).
Table 8.2 Results of paired samples t-test
Health literacy and knowledge levels
Pre-test Mean (SD)
Post-test Mean (SD)
t p
Functional health literacy 2.19 (0.622) 2.21 (0.652) -0.086 0.932
Communicative health literacy 1.57 (0.521) 1.72 (0.669) -1.102 0.280
Diabetes knowledge 2.79 (1.010) 3.12 (0.907) -0.899 0.388
Hypertension knowledge 2.17 (1.022) 2.70 (1.078) -2.594 0.013
Twelve participants completed the diabetes knowledge questionnaire in both pre-
and post-tests. No significant change was found in the knowledge of patients as a

186
result of the intervention. For hypertension, 41 participants answered the
questionnaire. As shown in Table 8.2, there was a significant change in knowledge
of hypertensive patients from pre- to post-test (p = 0.013).
Discussion
To our knowledge, this study is the first one to evaluate the effects on health
literacy and disease-specific knowledge of using a care-plan booklet in South
Africa. There is a paucity of information regarding health literacy in developing
countries, as the vast majority of publications on health literacy concern developed
countries (15, 24). However, developing countries are in need of research, as it can
be assumed that health literacy is generally low (15) given the link between health
literacy and overall literacy (5). Although South Africa has one of the highest
general literacy rates in Africa (24), it also suffers from a double burden of disease,
i.e. communicable diseases (e.g. malaria and tuberculosis) and non-communicable
diseases (e.g. diabetes, hypertension, asthma, and epilepsy) (25). Given the
complexity of issues that patients have to deal with in the self-management of their
conditions, low health literacy creates a huge challenge for the management of
chronic conditions.
As this was a small pilot study, its results have to be interpreted with caution.
Specifically, the low power of the study due to the small sample size should be
acknowledged, particularly for the participants with diabetes (n=12). Furthermore,
the time between the pre- and posttest was limited. So, while the only significant
change observed was the improvement in hypertension-specific knowledge, it is
unlikely to expect major changes in health literacy after a short-term intervention of
one month with a small sample. It is possible that the results would have been
different over a longer period of time and with a larger sample.
Another limitation concerns the fact that the care-plan booklet was only available in
English. Ideally, it should be made available in the patients’ own language (26), but
for this feasibility study it was not possible to translate the booklet into the
languages spoken by participants. Similarly, the evaluation questionnaire was

187
administered in English, although the option of translation in participants’ own
language was provided. This may explain some of the missing responses where
patients either chose not to respond to a particular item or not having understood
the item.
Furthermore, this pilot study did not include a process evaluation, which would
have been useful to explore how the booklet was used and to explain some of the
results. Further research on the usability of the care-plan booklet in view of its
wider dissemination should pay specific attention to translation and language
issues, as South Africa has 11 official languages and in most communities multiple
languages are used for communication.
Lastly, to decide on the use of the care-plan booklet, its impact on health literacy
and self-management behavior should be investigated in a more comprehensive
and controlled way. An effect study should not only use a more stringent design
and include health-related and behavioral outcome measures, but also involve a
longer time frame of at least three to six months to ensure sufficient opportunities
for consultations during which the booklet can be used. Furthermore, an effect
study should be complemented with a process evaluation component to better
understand why and how the care-plan booklet has been used and explain the
results.
Conclusion
As Africa continues to face a critical but neglected burden of chronic diseases,
health literacy is an important aspect that warrants attention. Currently, the South
African government is making major strides in providing information on health
related lifestyle factors, both for the general public and for chronic patients. A
sufficient level of health literacy is a critical condition for chronic disease patients to
be able to interpret and understand such health information (27, 28). Health
promotion and self-management education will achieve little in the absence of
sufficient health literacy. Further research on self-management education initiatives

188
and tools that are accessible and effective for patients with limited levels of health
literacy are therefore recommended.
Conflict of interest
The researchers declare no conflict of interest.

189
References
1. Van den Broucke S, Van der Zanden G, Chang P, Doyle G, Levin D, Pelikan J, et al. Enhancing the effectiveness of diabetes self-management education: the diabetes literacy project. Horm Metab Res. 2014;46(13):933-8.
2. deSilva D. Evidence. Helping people help themselves. A review of evidence considering whether it is worthwhile to support self-management: London: The Health Foundation; 2011 [cited 14 March 2015]. Available from: http://www.health.org.uk/publication/evidence-helping-people-help-themselves.
3. Lorig KR, Holman H. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1-7.
4. Boren SA. A review of health literacy and diabetes: opportunities for technology. J Diabetes Sci Technol. 2009;3(1):202-9.
5. Sørensen K, Van den Broucke S, Fullam J, Doyle G, Pelikan J, Slonska Z, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80.
6. Van den Broucke S. Health literacy: a critical concept for public health. Arch Public Health. 2014;72(1):10.
7. Negarandeh R, Mahmoodi H, Noktehdan H, Heshmat R, Shakibazadeh E. Teach back and pictorial image educational strategies on knowledge about diabetes and medication/dietary adherence among low health literate patients with type 2 diabetes. Prim Care Diabetes. 2013;7(2):111-8.
8. Heijmans M, Waverijn G, Rademakers J, van der Vaart R, Rijken M. Functional, communicative and critical health literacy of chronic disease patients and their importance for self-management. Patient Educ Couns. 2015;98(1):41-8.
9. Moodley L, Rambiritch, V. An assessment of the level of knowledge about diabetes mellitus among diabetic patients in a primary healthcare setting. SA Fam Pract. 2007;49(10):16.
10. Habib SS, Aslam M. Risk factors, knowledge and health status in diabetic patients. Saudi Med J. 2003;24(11):1219-24.
11. Nutbeam D. Evaluating health promotion: progress, problems and solutions. Health Promot Int. 1998;13(1):27-44.
12. Ishikawa H, Takeuchi T, Yano E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care. 2008;31(5):874-9.
13. Kim S, Love F, Quistberg DA, Shea JA. Association of health literacy with self-management behavior in patients with diabetes. Diabetes Care. 2004;27(12):2980-2.
14. Peer S, Ganahl K, Roethlin F, Baumann L, Pelikan J, Chang P, et al. Relative effectiveness of diabetes self-management education programs using different modes of delivery. Submitted.
15. Dowse R. The limitations of current health literacy measures for use in developing countries. J Commun Healthc. 2016;9(1):4-6.

190
16. Dube L, Van den Broucke S, Bergh A-M, Mafutha N, Rendall-Mkosi K. Self-management support needs of patients with chronic diseases in a South African township: a qualitative study. J Community Health Nurs. In Press.
17. Curo Health. Individual care plan booklet. 2015. 18. Stanford Patient Education Research Center. Chronic disease self-
management program. [Internet]. 2016 [cited 04 January 2016]. Available from: http://patienteducation.stanford.edu/programs/cdsmp.html.
19. Department of Health, South Africa. Nutritional management of hypertension [Pamphlet].
20. Department of Health, South Africa. Nutritional management of diabetes [Pamphlet].
21. Eigenmann C, Colagiuri R, Skinner T. Development and validation of a diabetes knowledge questionnaire. Pract Diab Int. 2011;28(4):166-70.
22. Schapira MM, Fletcher KE, Hayes A, Eastwood D, Patterson L, Ertl K, et al. The development and validation of the hypertension evaluation of lifestyle and management knowledge scale. J Clin Hypertens (Greenwich). 2012;14(7):461-6.
23. IBM Corp. IBM SPSS Statistics for Windows, Version 22.0. Released 2013. New York: IBM Corp; 2013.
24. Bress J. Developing a framework to identify and respond to health literacy needs using community-based emergency first aid responders in the Lavender Hill. MSc dissertation, University of Cape Town; 2014.
25. Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9945):766-81.
26. Dube L, Bergh A-M, Van de Broucke S, D'Hoore W. Feasibility of a self-management tool for diabetes and hypertension in South Africa. Submitted.
27. de-Graft Aikins A, Boynton P, Atanga LL. Developing effective chronic disease interventions in Africa: insights from Ghana and Cameroon. Global Health. 2010;6:6.
28. Mokwena K. Strategies to increase the health literacy needed to complement health-promoting legislation in South Africa. S Afr J Clin Nutr. 2015;28(4):197.

191
CHAPTER 9 –Main findings and discussion

192
Introduction
Self-management is regarded as a key component of care for people with chronic
diseases, especially in resource-limited settings in countries like South Africa. How-
ever, to date, most self-management programs reported in the literature have been
developed, implemented and evaluated in high-income countries. Because low-
and middle-income countries have a different context, the effectiveness of these
programs in resource-limited settings is uncertain (1-4). To address this problem,
the research presented in this PhD thesis focuses on self-management education
for chronic disease patients in a developing country: South Africa. Specifically, it
intended to analyze the status of chronic disease self-management education in
South Africa, and to investigate how the existing offer of programs can be better
adapted to the specific context of the country and its health system. For the latter, a
self-management tool in the form of a care-plan booklet that is context specific and
that can be used as part of a medical consultation in a middle-income country was
developed and tested for its feasibility and preliminary effects.
This chapter is divided into three sections. First, we give a summary of the main
findings of the studies composing this thesis. Secondly, we will discuss the main
findings and their implications for research and practice. Finally, we will come to an
overall conclusion of the findings.
Summary of main findings
The aim of this PhD study was to provide evidence-based information regarding
the current status of self-management education programs for chronic disease
patients in South Africa, and to investigate how the existing offer of programs can
be better adapted to the specific context of the country and its health system.
To investigate these issues, we first answered the question regarding the current
status of type 2 diabetes self-management education programs in high- and
low-mortality developing countries. To that effect, we performed a systematic

193
review of the available literature regarding diabetes self-management education
(DSME) programs in developing countries, using the World Health Organization
(WHO) and World Bank criteria to differentiate between high- and low-mortality
developing countries (5, 6). The review, which is reported in Chapter 3, showed
that there is only a limited number of published studies from developing countries
that describe or test DSME programs (n=23 original studies in 25 publications).
Most studies (n=18) are from low-mortality developing countries. In terms of
program characteristics, we found that most programs (n=14) were delivered in
groups. Thirteen publications reported on the cultural adaptation of the
interventions, of which nine involved a needs assessment of the target population
prior to designing the intervention. Only nine of the evaluated programs were
accessible for people with lower levels of literacy, whereas five programs excluded
low literate patients and the remainder of studies did not present information on this
matter.
In terms of effectiveness, significant changes were found in most studies on a
variety of outcome measures, including behavior change, body mass index, HbA1c
and fasting blood glucose. Where HbA1c was used as an outcome, the effects of
the programs were found to be significant at short term follow-up. In contrast,
studies that also looked at long-term effectiveness did not find any significant
changes except for one study which reported effects even after a six year follow-
up, but this improvement could have been attributable to other factors. In six
studies, no significant change was found between the control and intervention
groups with regard to knowledge, behavior change, body mass index and
psychological state.
A second question addressed in this thesis is what type of policies and
programs for diabetes education currently exist in South Africa, as an
example of a high mortality developing country. To answer this question, we
performed an audit of the DSME policies and guidelines that are currently used in
South Africa for self-management education of type 2 diabetes patients. The study,
which is reported in Chapter 4, used document analysis in combination with a key

194
informant interview approach to look at the characteristics of existing DSME
programs in both the public and the private healthcare services. The International
Standards for Diabetes Education (ISDE) developed by the International Diabetes
Federation (IDF) (7) was used for document analysis. The ISDE serves as a
benchmark for diabetes education in all IDF countries, which include South Africa.
No formal policy documents were identified, but three guideline documents could
be found, two from the National Department of Health of South Africa and the other
from the Society of Endocrinology, Metabolism and Diabetes of South Africa (8-10).
Compared to the ISDE, a lot of information was missing in the guideline
documents. To get a better understanding of the background of DSME, two more
documents from the National Department of Health (11, 12) were analyzed. It came
to light that the country had just adopted the Integrated Chronic Disease Model
(ICDM) that calls for the integration of the management of chronic diseases instead
of running a silo system. Integrated into the ICDM, the Primary Care 101 document
aids the health service provider with information to be given to the patient.
With regard to existing DSME programs, 27 key informants (educators, and
program officers) from seven provinces gave information about DSME programs
used in South Africa using a semi-structured questionnaire. Of the 27 programs
identified, five reported on structured programs and 22 can be considered as ad-
hoc education interventions. In the public healthcare services, DSME was mixed
with educational interventions for other chronic diseases. The most common
providers of DSME in both public and private healthcare settings were healthcare
professionals (physicians and dietitians). Only in a few cases the education was
given by health promoters. The content of programs included the self-care behavior
topics recommended by the American Association of Diabetes Education (AADE)
(13). In ad-hoc interventions, education was typically given in waiting rooms and
sometimes involved handing out educational pamphlets, most of which had been
developed by pharmaceutical companies. Through the use of the local language,
pictures and visual aids and practical demonstrations education was considered to
be accessible to people with low levels of literacy. A few surface structural aspects
of culture were addressed (notably local language), but deep structural aspects of

195
culture were rarely considered. Some of the structured programs had been
evaluated, but none of the ad-hoc interventions. In sum, an important finding of this
study was that the existing DSME interventions in South Africa were often
unstructured, not very sensitive to the local context and to deep structural aspects
of culture, and in most cases not evaluated, whereas they do consider literacy to
some extent.
The third question addressed in this thesis concerns the self-management needs
of chronic disease patients in South Africa. The study detailed in Chapter 5
explored the needs and experiences of patients, healthcare providers and experts
in the field of chronic diseases with regard to self-management. The five themes
and their categories that emerged from this study are summarized in Table 9.1.
Table 9.1 Main themes and categories
Themes Categories
Health-system and service-provision challenges
• Medication stock-outs • Waiting times at facilities • Educational materials and equipment • Mind set of providers • Structure of self-management
Healthcare provider attitudes and behavior
• Communication and relations with providers • Check-ups and follow-up • Confidentiality breaches
Adherence to medication and lifestyle changes
• Inconsistency in taking treatment • Poverty and financial challenges • Different food choices of family • Self-monitoring equipment at home • Side-effects of medication • Information provision
Patients’ personal and clinic experiences
• Health education set-up in clinics • Feelings of hopelessness and acceptance of disease • Coping mechanisms • Substituting medication with herbs
Self-management tool preferences
• Booklet • Content

196
The first theme is health-system and service-provision challenges, where both
patients and key informants reported on several barriers that hinder patients from
achieving maximum self-management. The second theme concerns healthcare
provider attitudes and behavior. For the third theme, both participant groups
mentioned challenges related to adherence and lifestyle changes. Poverty, cultural
expectations, dietary issues with families and the effect on side effects were
mentioned as factors that contributed to medication adherence difficulties. In some
cases, lack of information about the disease contributed to the inability to change
lifestyle. The fourth theme involved the patients’ personal and clinic experiences.
Patients did not have anywhere to record the health education and consultation
advice on self-management of their diseases that they had received. Some
patients expressed a feeling of hopelessness in managing their disease while
some mixed tablets with herbs. The last theme related to self-management
strategies and patients’ preferred for a booklet which they could use with their
families and friends and even their healthcare providers. The healthcare providers
supported the idea, mentioning that even those who could not read or write would
be assisted by their relatives or their providers during medical consultations to
understand the booklet. So, in order to answer some of the existing challenges,
patients preferred a booklet to support their self-management, and health service
providers were willing to be involved in self-management activities. This provided a
window of opportunity for the development of contextually adapted self-manage-
ment programs for community health nursing.
The next question addressed in this thesis concerns the feasibility of implement-
ing a contextually adapted self-management education and support tool.
Triggered by an existing care-plan booklet already used in the private health care
in South Africa (14), a contextually adapted care-plan booklet for diabetes and
hypertension was developed for use in medical consultations in the public health
care system. The development of this tool as well as its theoretical basis and main
characteristics are described in Chapter 6. The qualitative study reported in
Chapter 7 explored the feasibility of implementing this booklet with chronic patients
in South-Africa, using focus groups and individual interviews with patients and

197
healthcare providers. The eight areas of feasibility testing described by Bowen et
al. (15) were used as areas of focus for the data analysis. Although not all the eight
areas could be confirmed, the results of this study indicated that there was a high
acceptability of the proposed intervention (booklet used in medical consultations)
from both participant groups. A higher demand of the care-plan booklet could be
inferred from the patients’ and provider’s intention to continue to use or use of the
booklet, with some patient mentioning that they wanted to use the booklet as a
“passport”. Concerning the actual implementation of the care-plan booklet by both
participant groups, it was noted that some patients had managed to use the
booklet with their providers, while others had failed for different reasons, including
“attending funerals”. Providers indicated that the high number of patients they see
per day could affect the efficiency and speed of implementation. It was noted that
the implementation of the proposed intervention with patients was practical,
indicating the positive and expected positive effects of using the care-plan booklet.
Other providers, however, expressed concern about some patients being lazy in
terms of using the booklet effectively.
Both patient and provider groups gave useful information on further adapting the
care-plan booklet to meet their needs. Patients needed more information,
especially with regard to diet, while providers suggested adding more information
that could further empower patients, for example, a set of minimum requirements
for diabetes care that would allow patients to know what services they were
supposed to receive legally per annum. If patients did not receive these services,
they had a right to remind their health service providers. It was also found that the
use of the care-plan booklet could easily be integrated within the current
infrastructure, thanks to the ICDM that encourages self-management as a core
component of care (11, 16). In terms of expansion, some patients suggested a
wider distribution of the care-plan booklet and providers indicated that the same
kind of care-plan could be beneficial to patients with other chronic conditions seen
at primary care. While the efficacy of the care plan booklet should be tested by
means of a more rigorous design, the participants in our study perceived the use of
the care-plan booklet to be effective and believed that it could also have an effect

198
on other patients with the same chronic conditions. We can conclude that the care-
plan booklet was acceptable and could be used as a vehicle to improve the inter-
action between patients and their providers and/or their families and friends.
The last question addressed in the thesis concerns the effect of using the self-
management tool for diabetes and hypertension patients. A pilot-test of the
effectiveness of the care-plan booklet in terms of altering the participants’ disease
specific knowledge and health literacy was presented in Chapter 8. It concerns a
quasi-experimental study using adapted versions of questionnaires measuring
knowledge with regard to diabetes and hypertension as well as disease-specific
health literacy (17, 18) to assess the effect of using the tool at one month follow-up.
A total of 53 participants completed the pre-test questionnaire, 44 (83%) of whom
completed the post-test. A comparison between the scores before and after
starting to use the booklet indicated a significant increase of the knowledge about
hypertension from pre-test to post-test, but no significant changes of knowledge
about diabetes or of disease-specific health literacy. The limited effect, however,
can probably be explained by the small number of participants, especially of
diabetic patients, and the short time span, which does not lend itself to observe
changes in health literacy. We can thus conclude that using the care-plan booklet
is effective in increasing hypertension disease specific knowledge, but that in order
to enhance diabetes knowledge or hypertension or diabetes-specific health literacy
the use of the booklet over a longer period of time is necessary, and that a larger
sample of patients should be studied to evaluate the effects. .
Discussion of the main findings
Shortcomings of diabetes self-management education programs in high- and
low-mortality developing countries
The first part of this thesis aimed to explore the existing self-management
programs in high- and low-mortality developing countries, and more particularly in
one specific resource-limited middle-income country (South Africa). The results of

199
these studies indicated some gaps that, if addressed appropriately, could enhance
the implementation and effectiveness of DSME programs in developing countries.
As the research literature does not provide much information about self-
management programs from high-mortality developing countries, especially from
sub-Saharan Africa (except for South Africa), there is an urgent need for the
design, implementation and evaluation of such programs in order to achieve
evidence-based practice informed by local research. Our results are similar to other
studies that highlighted the fact that most available research is conducted in
developed countries, while developing countries carry the larger share of the NCD
burden (4, 19). Although the current research capacity, infrastructure and outputs
from low- and high-mortality developing countries are insufficient and scarce (20,
21), there remains a need for locally-based country research capacity building in
low- and middle-income countries (22, 23).
The systematic review also revealed a lack of programs that were tailored to the
context and needs of the populations thy work with. According to the literature,
tailoring of interventions to the context of the intended population increases the
ownership of interventions by the local people, thereby increasing the chances that
the interventions lead to sustainable change (24). The context is defined by
Marchal et al. (25) as “actors or other factors that are external to the intervention,
present or occurring even if the intervention does not lead to an outcome, and
which may have an influence on the outcome” (p. 207). These contextual factors
include institutional facilitating factors (e.g. the availability of resources) and
society’s influencing factors (e.g. socio-cultural aspects) (26).
The question of sustainability is crucial for developing countries, especially in SSA,
where there are huge health gains that have been achieved in the last 20 years,
including the decline of under-five mortality (24). However, these gains have now
been overtaken by the global disease burden that the region is carrying. Given the
fact that most funding to implement programs and intervention in developing
countries is donor-funded; the crucial question is what happens when donor-

200
funding dries-up (24). To address that issue, interventions have to be contextually
adapted. Yet while tailoring interventions to the culture of the target population is
critical for their success, other studies have reported that cultural-competent
programs create inequalities in healthcare (27). This aspect warrants attention, and
further research is needed, especially in resource-limited settings where many
other factors also play a role. One of these factors is the level of health literacy
among the population. Although empirical evidence about the level of health
literacy in SSA is lacking, it is likely that a large share of the population has limited
or insufficient levels of health literacy. This implies that low health literacy must be
taken into account, also in chronic disease self-management education. To that
effect, many techniques can be used, such as the uses of pictures and teach-back
techniques, which have previously been proved successful (28-30).
Another issue raised in the studies is that in most programs professional healthcare
staff members were the providers or facilitators of health education programs.
Although using professional staff is often considered as an indicator of
improvement in healthcare, low- and middle-income countries cannot afford such
kind of investment because of the lack of human resources for healthcare. De-
Graft-Aikins pointed out that despite the global disease burden being huge in SSA
(24%), this region has the smallest number (3%) of the global health workforce to
deal with this burden (19). It is therefore vital that professional staff be wisely used
in resource-limited settings. In this case, trained non-professionals can be included
to provide chronic disease health education, with professional staff assuming a
supervisory and training role.
In South Africa, community health workers (CHWs) have been recruited and
trained to assist in healthcare provision to address the shortage of human
resources for health (31). It is, therefore, advisable that non-professional health
workers like CHWs and health promoters deliver programs, while nurses occupy
supervisory roles (32-34). However, while the use CHWs might seem a good
opportunity for task shifting, it should be approached with caution as it poses
several challenges. One challenge is overburdening the CHWs, thereby reducing

201
the quality of their work in communities. Another challenge is the need for CHWs to
get appropriate training and adequate provision of equipment and support if they
are to be involved in NCD care (31). Since NCDs are not only a health issue but a
human development issue, and as they continue to affect millions of people in
developing countries, it is imperative that these points be addressed.
Our second study revealed that self-management education for diabetes is rarely
addressed in national policies and guidelines of South Africa and that few
structured programs exist, while the majority are mainly ad-hoc interventions. Ad-
hoc interventions were defined in the study as those interventions which include
educational talks in the waiting area or spontaneous sharing of information during
individual medical consultations without a planned structure and defined time
frame. The findings of this study are supported by others which note that
governments in developing countries are not up to date with formulating policies,
legislation and infrastructure to deal with NCDs (19, 35). Unlike other low- and
middle-income countries, South Africa has made great progress in addressing
NCDs in national policies and guidelines, but these efforts are still not adequate in
terms of self-management (11, 36). Self-management education should be
regarded as a core component of care and should be treated as such in practice.
This includes the development of guidelines for self-management education
programs that are based on evidence, for example the International Standards for
Diabetes Education that were developed by the International Diabetes Federation
(IDF) (7).
Self-management needs of patients with chronic diseases in a South African
township
Non-communicable diseases are sometimes referred to as chronic diseases.
According to Lawn et al., this definition reflects the fact that they are conditions of a
lifetime that require long-term interventions and adjustments in life (37). In addition,
as noted earlier in the introduction of the thesis, the classification of NCDs is linked
to the fact that they share common preventable and modifiable risk factors, namely

202
tobacco use, physical inactivity, unhealthy diets and harmful use of alcohol (38-41).
As such, self-management is regarded as a critical factor in the management of
conditions like diabetes and hypertension, conditions that require extensive self-
care (42-44). It is, therefore, important to invest in the education of patients in order
to improve their self-management capacities.
As noted before, developing sustainable self-management interventions builds on
the capacity of the stakeholders and conducting a needs assessment is a way of
involving primary and secondary stakeholders (45). The third study reported in this
thesis (Chapter 5) showed that there is an opportunity for the development and use
of self-management programs by PHC nurses. As PHC facilities are the first point
of contact with the community, they are important in the prevention of NCDs.
However, to achieve optimal self-management by patients, several barriers need to
be addressed. The study on patient needs for self-management support also
revealed the complex processes in self-management, which include the dynamics
and interactions within and between social and health systems (Figure 9.1).
Figure 9.1 Complexity of self-management process

203
The lack of health promotion materials and drug stock-outs in facilities could be
explained by the lack of financial resources in developing countries, but could also
be due to the lower priority assigned to NCDs. Despite the heavy costs that may be
felt in addressing NCDs, it is worthwhile to invest in the interventions to prevent
and treat NCDs, as in the long run the economic gains will be higher (46). The
gains of investing in prevention could lead to a healthy working population and an
increase in the life expectancy of the population.
The results of our study reported in Chapter 5 also revealed that patients preferred
a booklet to assist them with self-management of chronic diseases, while providers
preferred a booklet to be part of a more comprehensive package to be used during
medical consultations. Although different approaches to self-management exist,
including cell phone, web and group interventions (44, 47), a booklet was chosen
for our study because the patients perceived it as useful for sharing at home with
family members and for keeping it for later use. E-health technologies could also
serve the same purpose, but their application in a low-resource context is
expensive and not practical.
Written or printed health education materials have been long criticized for having
less impact on health outcomes. However, the available evidence suggest that
written information that is well designed can be useful in aiding professional
consultation and improving health knowledge and recall (48). A review by Houts et
al. revealed that the use of pictures assisted in drawing attention to the health
education materials, and that they had an effect on the health intentions and
behavior (49). Furthermore, spoken information aided by pictures was recalled
better by people with low literacy levels. Thus, the critical role of health service
providers in the use of the care-plan booklet developed as part of our study cannot
be underestimated (48). The roles for health service providers include supporting
patients in self-management and placing the patient at the center of care.
Patient-centered care is considered as re-organization of services around patients’
needs and can also be viewed as patient-perceived needs, priorities and expecta-

204
tions of healthcare (50) (51). Kolosa noted that, in patient-centered care, time spent
with the patient is crucial in order to achieve meaningful outcomes. However, in
reality, patient-centeredness is often forgotten or not possible in many settings (52,
53). South Africa has made considerable effort to encourage patient-centered care
in the health system. This has been achieved through legislature, for example the
White Paper on the Transformation of the Public Service (Batho Pele) introduced in
1997 (50, 54). The eight Batho Pele principles include: (1) Consultation, where
patients should be asked about the level of service they get and they should be
given a choice; (2) Information concerns patients being given full access to
information regarding the services they are entitled to get; (3) Access- means that
all patients should have full access to services; (4) Openness and transparency
involves patients having access to reports and information; (5) Redress is the
consideration of the people’s concerns and complaints regarding care or service
that is promised but is not available to them; (6) Value for money is concerned with
efficiency to provide a value for money to the patients; (7) Courtesy concerns the
realization that patients are worthy of being treated with dignity, consideration and
respect; and lastly (8) Service standards involves people being informed on what
services quality they should expect.
However, despite the availability of the Batho Pele principles, gaps in patient-
centered care still exist in South Africa. In 2013, Loveday et al. conducted a case
study following tuberculosis patients to see if they received patient-centered care
(55). The results concluded that the patients had received sub-optimal treatment
and solutions were needed both at national and provincial levels. The obstacles
from the health system included pharmaceutical services, laboratory performance
and provider performance. A study by Madigare also concluded that patients’ and
nurses’ lack of knowledge was the major barrier to patient-centered care.
Furthermore, patients and their families were reluctant to be involved in their self-
care, while the lack of information made it difficult to make good healthy choices
(50).

205
Feasibility of using a care-plan booklet for diabetes and hypertension self-
management support
In Chapters 7 and 8 of this thesis, we demonstrated that it is feasible to implement
a care-plan booklet in resource-limited settings and that this tool can be effective in
increasing hypertension-specific knowledge. Testing the feasibility of interventions
is a critical step in the development of health promotion interventions. As noted in
Chapter 7, having some sense of the potential feasibility of an intervention can
increase the possibility of it being accepted or remembered by the target population
(56). Our study showed a high acceptability of the care-plan booklet by the
participants, which can be considered as a positive starting point.
Since health promotion and patient education interventions, amongst other things,
aim to influence health related behavior, an investigation into the feasibility of an
intervention is crucial (57, 58). Psychological theories of behavior change such as
the theory of planned behavior (TPB) state that a person’s perception of a behavior
as being feasible promotes the carrying out of the behavior. More specifically, the
TPB asserts that behavior is determined by a person’s behavioral intention, which
in turn is influenced by the person’s attitude towards behavior, the subjective norm
regarding the behavior, and the perceived behavioral control. The latter relates to
the fact that in many situations people’s intentions and behavior can be influenced
by external factors, and that the perception of being able to change these
behaviors significantly contributes to behavioral change. So, if a person has a
positive attitude and a positive subjective norm towards the behavior but feels less
in control of the situation, the behavior will not be carried out (58, 59). On the
analogy, the perception of a tool being usable will contribute to it being effectively
used. In our study patients reported that the booklet was welcomed by the
significant others, but expressed a desire that healthcare providers would also
agree to use it with them.
While the feasibility study indicated that the use of the care-plan booklet was
considered as feasible, the pilot study indicated that its use can also be effective, in

206
terms of increasing disease-specific knowledge – more specifically with regard to
hypertension. Although disease-specific health literacy did not significantly increase
due to the use of the booklet, there was a trend towards positive change which
could be more significant if more time would be given to using the booklet over a
longer period of time involving more consultations. In that way, the results of the
two studies reported in Chapters 7 and 8 can inform a larger effectiveness study
planned for the future (Chapter 10). As there are not many studies from high-
mortality developing countries that are experimental, a future study would ideally
be a cluster randomized controlled trial on a larger sample that can produce strong
evidence.
As indicated in Chapter 2, South Africa’s healthcare is characterized by public and
private healthcare sectors, with the private sector having the quality of care
equivalent to that of developed countries like Belgium, the United Kingdom and the
Netherlands (60). The fact that the care-plan booklet was triggered by a concept
tool already used in the private sector and adapted for integration into the public
sector is interesting, as it illustrates the potential for low-resource settings to benefit
from well-structured practices being implemented in the private healthcare sector.
As the care-plan booklet facilitates and enhances the communication between
patients and providers, whereby even patients with low health literacy are able to
benefit from it, it can make an essential contribution to the public health care
sector, even more so as it is a low-cost intervention which the government can
modify and implement on a larger scale.
Strengths and limitations of studies
Each published or submitted article included in this thesis reported on the strengths
and limitations of the individual studies. However, the whole thesis project also had
some strengths and limitations.
The strengths of this thesis include the fact that, to our knowledge, this is the first
time the issue of self-management education and a specific tool to support self-

207
management for chronic patients was explored in a middle-income country. As
such, this thesis contributes to the literature and creates a basis for further
research in the field of chronic disease self-management in low- and middle-
income countries. Although some parts of this thesis report on quantitative studies,
most of the work reported here emanated from studies using qualitative methodolo-
gies. A qualitative research approach allowed us to explore issues, describe
people’s personal experiences and gain an understanding thereof. By analyzing
the data involving two or three researchers, we managed to ascertain the rigor of
the research in order to minimize subjectivity.
Although this work was the first of its kind, it also had its limitations. On the one
hand, findings from qualitative studies have limited generalizability, as they can
only be applied to a specific context or a specific kind of population. On the other
hand, the constraints in terms of time and resources also limited the scope and
power of the quantitative study we performed on the effects of the care-plan
booklet (Chapter 8). However, to compensate for these limitations, a cluster
randomized controlled trial is planned for the future to evaluate the effectiveness of
the care-plan booklet more rigorously, on a larger sample and over a longer period
of time. In that way, the studies presented in the thesis paved the way for a more
rigorous study, the detailed protocol for which forms the last Chapter of this thesis
(Chapter 10). Awaiting the results of that study, the present thesis, by focusing on
chronic self-management education in south Africa, already provides policy makers
and decision makers in South Africa with information that can help decide on where
and how to intervene with regard to chronic disease self-management education.
Conclusion
Self-management is regarded as a cornerstone in the management of chronic
diseases, and evidence-informed programs are important in health promotion and
patient education. This thesis contributes to the scarce literature on self-
management in South Africa and other developing countries. Although further
research is required on the subject of health literacy, this work adds to the small

208
amount of information on self-management education and health literacy that is
available for South Africa. Despite its limitations, this work has opened new
avenues for future studies. If adequate funding can be provided, the study protocol
presented in the last chapter of this thesis can be one of those studies.
NCDs will continue to rise in low- and middle-income countries and strategies are
needed to put in place to deal with them. The curative health systems that have
been put in place to address acute conditions are not useful to address the
challenge of NCDs. In addition, healthcare providers need to change their mindset
from a sole focus on dealing with acute conditions to the inclusion of the
management of chronic conditions, in which patients are required to be active
participants and not just passive recipients of care. The care-plan booklet
developed and tested in this thesis will assist in this interaction between patients
and providers.
References
1. Brady TJ, Murphy L, O'Colmain BJ, Beauchesne D, Daniels B, Greenberg M, et al. A meta-analysis of health status, health behaviors, and healthcare utilization outcomes of the Chronic Disease Self-Management Program. Prev Chronic Dis 2013;10(E07).
2. Franek J. Self-management support interventions for persons with chronic disease: an evidence-based analysis. Ont Health Technol Assess Ser. 2013;13(9):1-60.
3. Stoilkova A, Janssen DJ, Wouters EF. Educational programmes in COPD management interventions: a systematic review. Respir Med. 2013;107(11):1637-50.
4. Mendis S. Research is essential for attainment of NCD targets and Sustainable Development Goals. Glob Heart. 2016;11(1):139-40.
5. World Health Organization. List of Member States by WHO region and mortality stratum. 2013 In: World Health Organization. Neurological disorders: public health challenges. Geneva: World Health Organization; 2006. p183-4. [cited 9 December 2013]. Available from: http://www.who.int/mental_health/neurology/annexes_neuro_disorders_public_h_challenges.pdf.
6. The World Bank. How does the World Bank classify countries? [cited 15 October 2013]. Available from:

209
https://datahelpdesk.worldbank.org/knowledgebase/articles/378834-how-does-the-world-bank-classify-countries.
7. International Diabetes Federation. International Standards for Diabetes Education. 3rd ed. Brussels, Belgium: International Diabetes Federation; 2009 [cited 1 July 2014]. Available from: http://www.idf.org/webdata/docs/INTNL-STANDARDS-EN.pdf.
8. National Department of Health, South Africa. Updated management of type 2 diabetes in adults at primary care level. 2014.Unpublished.
9. Amod A, Ascott-Evans BH, Berg GI BD, Brown SL, Carrihill MM, Dave JA, et al. The 2012 SEMDSA Guideline for the Management of Type 2 Diabetes (Revised). JEMDSA. 2012;17(2):S1-S95.
10. National Department of Health, South Africa. National Guidelines. Management of diabetes type 1 and 2 in adults at hospital level. 2005. Unpublished.
11. Asmall S, Mahomed O. Integrated chronic diseases management manual. National Department of Health, South Africa; 2011 [cited 10 June 2014]. Available from: http://www.kznhealth.gov.za/family/Integrated-chronic-disease-management-manual.pdf.
12. Republic of South Africa, Department of Health. Primary care 101: Symptom-based integrated approach to the adult in primary care, 2013/14. [Internet]. 2013. Available from: https://www.health-e.org.za/wp-content/uploads/2015/04/PC-101-Guideline-v2-2013-14-2.pdf.
13. Mulcahy K, Maryniuk M, Peeples M, Peyrot M, Tomky D, Weaver T, et al. Diabetes self-management education core outcomes measures. Diabetes Educ. 2003;29(5):768-70, 73-84, 87-8. .
14. Curo Health. Individual care plan booklet. 2015. 15. Bowen DJ, Kreuter M, Spring B, Cofta-Woerpel L, Linnan L, Weiner D, et
al. How we design feasibility studies. Am J Prev Med. 2009;36(5):452-7. 16. Wagner EH. Chronic disease management: what will it take to improve
care for chronic illness? Eff Clin Pract. 1998;1(1):2-4. 17. Schapira MM, Fletcher KE, Hayes A, Eastwood D, Patterson L, Ertl K, et
al. The development and validation of the hypertension evaluation of lifestyle and management knowledge scale. J Clin Hypertens (Greenwich). 2012;14(7):461-6.
18. Eigenmann C, Colagiuri R, Skinner T. Development and validation of a diabetes knowledge questionnaire. Pract Diab Int. 2011;28(4):166-70.
19. de-Graft Aikins A, Unwin N, Agyemang C, Allotey P, Campbell C, Arhinful D. Tackling Africa's chronic disease burden: from the local to the global. Global Health. 2010;6:5.
20. Engelgau MM, El-Saharty S, Kudesia P, Rajan V, Rosenhouse S, Okamoto K. Capitalizing on the demographic transition: tackling noncommunicable diseases in South Asia. Conference edition. The World Bank; 2011 [cited 11 November 2016]. Available from: http://siteresources.worldbank.org/SOUTHASIAEXT/Resources/223546-1296680097256/7707437-1296680114157/NCDs_South_Asia_February_2011.pdf.
21. Bloomfield GS, Baldridge A, Agarwal A, Huffman MD, Colantonio LD, Bahiru E, et al. Disparities in cardiovascular research output and citations

210
from 52 African countries: a time-trend, bibliometric analysis (1999-2008). J Am Heart Assoc. 2015;4(4).
22. Engelgau MM, Sampson UK, Rabadan-Diehl C, Smith R, Miranda J, Bloomfield GS, et al. Tackling NCD in LMIC: Achievements and lessons learned from the NHLBI-UnitedHealth Global Health Centers of Excellence Program. Glob Heart. 2016;11(1):5-15.
23. World Health Organization. Global action plan for the prevention and control of noncommunicable diseases 2013-2020. Geneva: World Health Organization; 2013 [cited 10 October 2016]. Available from: http://apps.who.int/iris/bitstream/10665/94384/1/9789241506236_eng.pdf.
24. Iwelunmor J, Blackstone S, Veira D, Nwaozuru U, Airhihenbuwa C, Munodawafa D, et al. Toward the sustainability of health interventions implemented in sub-Saharan Africa: a systematic review and conceptual framework. Implement Sci. 2016;11:43.
25. Marchal B, van Belle S, van Olmen J, Hoeree T, Kegels G. Is realist evaluation keeping its promise? A review of published empirical studies in the field of health systems reaserch. Evaluation. 2012;18(2):192-212.
26. Goicolea I, Vives-Cases C, San Sebastian M, Marchal B, Kegels G, Hurtig AK. How do primary health care teams learn to integrate intimate partner violence (IPV) management? A realist evaluation protocol. Implement Sci. 2013;8:36.
27. Dauvrin M, Lorant V. Culturally competent interventions in type 2 diabetes mellitus management: an equity-oriented literature review. Ethn Health. 2014;19(6):579-600.
28. Katz MG, Kripalani S, Weiss BD. Use of pictorial aids in medication instructions: a review of the literature. Am J Health Syst Pharm. 2006;63(23):2391-7.
29. Kripalani S, Robertson R, Love-Ghaffari MH, Henderson LE, Praska J, Strawder A, et al. Development of an illustrated medication schedule as a low-literacy patient education tool. Patient Educ Couns. 2007;66(3):368-77.
30. Negarandeh R, Mahmoodi H, Noktehdan H, Heshmat R, Shakibazadeh E. Teach back and pictorial image educational strategies on knowledge about diabetes and medication/dietary adherence among low health literate patients with type 2 diabetes. Prim Care Diabetes. 2013;7(2):111-8.
31. Mishra SR, Neupane D, Preen D, Kallestrup P, Perry HB. Mitigation of non-communicable diseases in developing countries with community health workers. Global Health. 2015;11:43.
32. Deakin T, McShane CE, Cade JE, Williams RD. Group based training for self-management strategies in people with type 2 diabetes mellitus. Cochrane Database Syst Rev. 2005(2):Cd003417.
33. Balagopal P, Kamalamma N, Patel TG, Misra R. A community-based participatory diabetes prevention and management intervention in rural India using community health workers. Diabetes Educ. 2012;38(6):822-34.
34. Philis-Tsimikas A, Fortmann A, Lleva-Ocana L, Walker C, Gallo LC. Peer-led diabetes education programs in high-risk Mexican Americans improve glycemic control compared with standard approaches: a Project Dulce promotora randomized trial. Diabetes Care. 2011;34(9):1926-31.

211
35. Islam SM, Purnat TD, Phuong NT, Mwingira U, Schacht K, Froschl G. Non-communicable diseases (NCDs) in developing countries: a symposium report. Global Health. 2014;10:81.
36. Non-communicable diseases: a strategic vision. National Guideline. National Department of Health, South Africa. Unpublished.
37. Lawn S, Schoo A. Supporting self-management of chronic health conditions: common approaches. Patient Educ Couns. 2010;80(2):205-11.
38. World Health Organization. Global status report on noncommunicable diseases 2014; Geneva: World Health Organization; 2014 [cited 17 July 2016]. Available from: http://apps.who.int/iris/bitstream/10665/148114/1/9789241564854_eng.pdf?ua=1.
39. Maher D, Ford N, Unwin N. Priorities for developing countries in the global response to non-communicable diseases. Global Health. 2012;8:14.
40. Alleyne G, Binagwaho A, Haines A, Jahan S, Nugent R, Rojhani A, et al. Embedding non-communicable diseases in the post-2015 development agenda. Lancet. 2013;381(9866):566-74.
41. Puoane T, Tsolekile L, Sanders D, Parker W. Chronic non-communicable diseases In: Barron P, Roma-Reardon J, editors. South African Health Review 2008. Durban: Health Systems Trust; 2008. p. 73-87.
42. Van den Broucke S, Van der Zanden G, Chang P, Doyle G, Levin D, Pelikan J, et al. Enhancing the effectiveness of diabetes self-management education: the diabetes literacy project. Horm Metab Res. 2014;46(13):933-8.
43. Schinckus L, Van den Broucke S, Housiaux M. Assessment of implementation fidelity in diabetes self-management education programs: a systematic review. Patient Educ Couns. 2014;96(1):13-21.
44. Huygens MW, Vermeulen J, Swinkels IC, Friele RD, van Schayck OC, de Witte LP. Expectations and needs of patients with a chronic disease toward self-management and eHealth for self-management purposes. BMC Health Serv Res. 2016;16:232.
45. Maimela E, Van Geertruyden JP, Alberts M, Modjadji SE, Meulemans H, Fraeyman J, et al. The perceptions and perspectives of patients and health care providers on chronic diseases management in rural South Africa: a qualitative study. BMC Health Serv Res. 2015;15:143.
46. Beaglehole R, Bonita R, Alleyne G, Horton R, Li L, Lincoln P, et al. UN high-level meeting on non-communicable diseases: addressing four questions. Lancet. 2011;378(9789):449-55.
47. Lorig KR, Ritter PL, Laurent DD, Plant K. Internet-based chronic disease self-management: a randomized trial. Med Care. 2006;44(11):964-71.
48. Coulter A, Ellins J. Effectiveness of strategies for informing, educating, and involving patients. BMJ (Clinical research ed). 2007;335(7609):24-7.
49. Houts PS, Doak CC, Doak LG, Loscalzo MJ. The role of pictures in improving health communication: a review of research on attention, comprehension, recall, and adherence. Patient Educ Couns. 2006;61(2):173-90.
50. Madigage MM. The perception of professional nurses on patient centered care MA dissertation, University of South Africa; 2005.[cited 18 January

212
2017]. Available from; http://uir.unisa.ac.za/bitstream/handle/10500/2301/dissertation.pdf?sequence=1&isAllowed=y
51. Riley BH, White J, Graham S, Alexandrov A. Traditional/restrictive vs patient-centered intensive care unit visitation: perceptions of patients' family members, physicians, and nurses. Am J Crit Care. 2014;23(4):316-24.
52. Kolosa M. Patient-centered care in primary health care. SA Fam Pract. 2005;47(8):3-4.
53. Weiland S, Koczela, S. The time is now for patient-centred innovation. The Lancet Global Health Blog;, 7 October 2014 [cited 18 January 2017]. Available from: http://globalhealth.thelancet.com/2014/10/07/time-now-patient-centred-innovation.
54. SA Health. Patient and consumer centred care [Internet]. 2016 [cited 09 September 2016]. Available from: http://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/clinical+resources/safety+and+quality/partnering+with+consumers+and++the+community/patient+and+consumer+centred+care.
55. Loveday M, Padayatchi N, Voce A, Brust J, Wallengren K. The treatment journey of a patient with multidrug-resistant tuberculosis in South Africa: is it patient-centred? Int J Tuberc Lung Dis. 2013;17(10 Suppl 1):56-9.
56. Vandelanotte C, De Bourdeaudhuij I, Brug J. Acceptability and feasibility of an interactive computer-tailored fat intake intervention in Belgium. Health Promot Int. 2004;19(4):463-70.
57. Betsch C, Bohm R, Airhihenbuwa CO, Butler R, Chapman GB, Haase N, et al. Improving medical decision making and health promotion through culture-sensitive health communication: an agenda for science and practice. Med Decis Making. 2016;36(7):811-33..
58. National Cancer Institute. Theory at a glance: a guide for health promotion practice. 2nd ed. NIH Publication No. 05-3896 [Internet]. U.S Department of Health and Human Services, National Institutes of Health; 2005 [cited 22 September 2015]. Available from: http://www.sbccimplementationkits.org/demandrmnch/wp-content/uploads/2014/02/Theory-at-a-Glance-A-Guide-For-Health-Promotion-Practice.pdf.
59. Ajzen I. The Theory of Planned Behaviour. Organizational Behaviour and Human Decision Process. 1991;50:179-211.
60. Ramjee S, Vieyra T, Abraham M, Kaplan J, Taylor R. National Health Insurance and South Africa's private sector. In: Padarath A, English R, editors. South African Health Review 2013/14. Durban: Health Systems Trust; 2014. p. 93-104.

213
CHAPTER 10 - Study protocol
Effectiveness of using a care-plan booklet for people
with diabetes: A cluster randomized controlled trial

214
Introduction
Southern Africa suffers a double burden of communicable and non-communicable
diseases (NCDs) due to a demographic and socio-economic transition
characterized by rapid unplanned urbanization and a proliferation of unhealthy
lifestyles. The chronic disease burden is much felt in low- and middle-income
countries, where it is estimated to further increase as a result of the effects of
demographic change, globalization and urbanization (1). It is estimated that about
80% of deaths from chronic diseases worldwide occur in developing countries. By
the year 2040 the number of people living with diabetes in Africa is expected to
increase from 415 million in 2015 to 612 million (2). However, in sub-Saharan
Africa (SSA), little consideration is given to address this problem, which could be
explained by the fact that the leading risks of morbidity and mortality are still
undernutrition and unsafe sex (3-5).
Of the countries in SSA, South Africa has the highest level of obesity in women
aged 20 years or more, and consequently faces a great problem of chronic
diseases (6). It is estimated that the NCD burden in South Africa is two to three
times higher than in high-income countries (7).
Among the chronic diseases, type 2 diabetes is one of the leading NCDs in South
Africa (1, 8). The International Diabetes Federation (IDF) reported in 2015 that
South Africa had a 7.0 percent national prevalence of diabetes in the age group 20
to 79 (2). As a result, of all the conditions seen in public primary healthcare (PHC)
in South Africa, type 2 diabetes ranks the fourth most common condition (1). South
Africa and Cameroon are also among the top countries in Africa where diabetes
leads to complications, which is the case in 50 percent of diabetic cases. Around
25 percent of people with diabetes type 2 were found to already have retinopathy
at the time of diagnosis, and around 49 percent of all neuropathic complications
consisted of erectile dysfunction (3).

215
Self-management of chronic diseases
Beaglehole et al argue that in order to overcome the burden of chronic conditions
like diabetes, developing countries have to reinforce the drug treatment, education
and continuous care of patients (9). Indeed, effective management of chronic
diseases like diabetes not only requires adequate medication use, but also self-
management by the patient and his or her family or other informal caregivers (10).
Therefore, self-management is highly recommended, especially in resources-poor
settings in countries like South Africa. It is estimated that 80 to 90 percent of overall
care for chronic patients is performed by the patients themselves or their informal
caregivers (11). This responsibility demanded from individuals requires support
from health service providers. Self-management of a chronic disease is achieved
when a patient takes a lead role in managing his or her chronic condition. To
accomplish effective self-management, it is therefore crucial that health providers
work collaboratively with patients and their families to support and empower them
(11, 12).
In South Africa, many of the patients with diabetes are seen at the public health
facilities. Annually approximately 17 million cases treated at public health facilities
are cases of diabetes and/or hypertension (7, 13, 14). However, despite the fact
that they receive medication and care, many of the diabetic patients are struggling
to achieve treatment targets (15). Structured group education programs can
support the patients in their efforts. The results of a randomized controlled trial by
Mash et al evaluating the effectiveness of a structured group education program for
type 2 diabetes patients in Cape Town, South Africa concluded that a structured
group education program was cost effective (1). The group intervention had one
session monthly, each with a 60 minute duration. Seventeen community health
centers participated and were randomized into intervention and control centers.

216
Statement of problem
While the evidence shows that self-management education for chronic disease
patients is effective, the vast majority of existing self-management education
programs have been developed, implemented and evaluated in developed
countries. As such, the applicability of these findings to developing countries is
uncertain (16). In South Africa, the Integrated Chronic Disease Management
(ICDM) model acknowledges that self-management should be an integral
component of chronic disease care and treatment, but in reality this component of
care is still neglected by healthcare providers (17). Recent qualitative studies
exploring the experiences of chronic patients and their motivation for self-
management found many barriers for patients to achieve effective self-
management (8, 18). These include healthcare provider attitudes, low health
literacy, lack of educational materials, medication stock-outs, lack of self-efficacy
and a perceived lack of social support (8, 18, 19). To address these barriers,
patients and providers alike have suggested that a take-home booklet combining
information about the disease and its treatment with space to monitor progress and
note questions to prepare for consultations would be a useful adjunct to treatment
(18). A pilot study revealed that such a care-plan booklet was indeed effective in
increasing hypertension knowledge in a resource-limited setting (Chapter 8).
Aim, objectives and hypothesis
The aim of this study is to evaluate the effectiveness of using a diabetes care-plan
booklet during consultations between patients and healthcare providers (profes-
sional nurses and physicians) in PHC facilities of Tshwane district, South Africa.
The study has four objectives:
Objective 1: To evaluate the effectiveness of using the care-plan booklet during
consultations by assessing group changes with regard to the following outcomes:

217
Primary outcome: HbA1c values
Secondary outcomes:
Individual dispositions: health literacy, diabetes knowledge, attitudes to
diabetes, self-efficacy, locus of control
Behavior outcomes: healthy eating, self-monitoring of blood glucose, taking
medication, problem solving, risk reduction and healthy coping
Health-related outcomes: means for blood pressure, fasting blood glucose,
total cholesterol, waist circumference and mean weight loss, and quality of
life and wellbeing
Objective 2: To explore the experiences of patients who received and used the
care-plan booklet with their healthcare providers during medical consultations.
Objective 3: To explore the experiences of healthcare provides who used the
care-plan booklet with their patients. (Healthcare providers include doctors, nurses,
health promoters, dieticians, and community health workers).
Objective 4: To evaluate the fidelity of using the care-plan booklet with diabetic
patients.
The hypothesis for this study is as follows:
Patients who use the booklet during medical consultations with their healthcare
providers will experience improved patient-provider interaction and will have
improved glycemic control as measured by the HbA1c test.
Method
Study design
To test the hypothesis, a cluster randomized controlled trial accompanied by a
qualitative process evaluation will be employed. The Consolidated Standards of
Reporting Trials (CONSORT) 2010 statement: extension to cluster randomized

218
trials were applied in the design of this study (20). The trial design is shown in
Figure 10.2. The trial will be registered in an appropriate registry, for example the
International Standard Randomized Controlled Trials Number (ISRCTN) registry,
which is recognized by the World Health Organization (WHO) and the International
Committee of Medical Journal Editors (ICMJE) (21).
Figure 10.1 Trial flow chart
Setting
The study will take place in PHC clinics in Tshwane district, South Africa. A cluster
is defined as a group of patients being attended to by one physician or professional
nurse at each clinic.

219
Inclusion and exclusion criteria
Inclusion criteria will be patients with type 2 diabetes, seen by a specific healthcare
provider. Patients should be 18 years or older and should have signed the
informed consent document, regardless of whether they are on insulin or oral medi-
cation.
Exclusion criteria will be patients not willing to participate, type 1 diabetic patients,
and patients with mental illness, dementia or acute conditions.
The intervention
The intervention will be described according to the template developed for
Intervention Description and Replication (TIDieR) guidelines by Hoffmann et al.
(22).
Brief name of the intervention:
A care-plan booklet for patients with diabetes for use in medical consultations with
health service providers in South Africa
Why implement the intervention?
Self-management of patients with chronic diseases can lead to improved clinical
outcomes, fewer emergency room visits, increased patient responsibility and en-
hanced adherence to treatment (23-25). A pilot study in a resource-limited setting
in South Africa has indicated that the use of the care-plan booklet with healthcare
providers during medical consultation improves disease specific knowledge for
hypertension (26).
What materials will be used?
The intervention is underpinned by the Health Belief Model (HBM) and involves the
use of an A5 care-plan booklet (Appendix A) by diabetic patients and their health-

220
care providers during consultation. An existing care-plan booklet used in the private
health sector served as a model for developing a more focused and contextually
adapted care-plan booklet to fit a target population with a low socio-economic
status and attending public health facilities. The results of three previous studies
(17, 18, 27) and existing educational materials for diabetes informed the structure
and content of the booklet (28). A first draft of the current version of the booklet
was circulated among different stakeholders who commented on its content, after
which a prototype booklet was finalized.
The prototype booklet was then tested for feasibility in a qualitative study, which led
to further adaptations of cover and the contents of the booklet using the feedback
by patients and healthcare providers (29). A professional graphic designer will be
assigned to provide the final layout and design of the booklet manuscript presented
in Appendix A. As the prototype version of the booklet was only available in
English, one of the official languages in South Africa and the language of
schooling, the booklet will also be translated into the major indigenous languages
spoken by the target study population, for example isi Zulu, Sepedi and Setswana,
to better take the needs of patients and providers into account. The contents of the
final booklet are presented in Figure 10.1.
The HBM is a theory of health behavior extensively used in health education and
patient education. The HBM is based on the assumption that behavior change is
influenced by an individual’s beliefs or perceptions about the disease(s) and
available ways of preventing the disease from occurring. The theory has four main
constructs: perceived severity, perceived susceptibility, perceived benefits, and
perceived barriers. More recently, the theory has been expanded to also include
cues to action, motivating factors and self-efficacy (30-33). Using this theory, we
assume that the use of the care-plan booklet during consultation with healthcare
providers will improve the patients’ awareness of the perceived seriousness,
susceptibility, benefits and at the same time overcome the barriers to change. This
will then lead to behavior change that will improve the health and behavior-related
outcomes.

221
What the booklet is all about
Making most of the medical consultation (tips for patients)
A set of minimum tests per patient per year
Preparing for the consultation: spaces for recording vital signs and for use in provider-patient consultations
Vital signs flow chart
Annual vital signs flow chart
General notes by healthcare provider
National guidelines for glucose values
Information on diabetes: definition, physiology, signs and symptoms, complications, health education messages
Lifestyle change messages
Activity diary
Pocket for appointment card at the inside back cover
Emergency telephone numbers on outside back cover
Figure 10.2 Contents of the booklet
What procedures will be followed?
The booklets in the intervention clusters will be delivered to the patients by the
health service providers (doctors/nurses) at the month zero consultation. The
health promoters will introduce the booklet to the patients in the waiting area,
explaining in detail how it can be used by both the patient and the health service
provider. At this time in the waiting area the researchers will explain the study and
the informed consent form in detail. During consultation the nurse/doctor will ask
the patient if he or she wants to participate. If the patient agrees to participate, the
booklet will be issued and the patient will be requested to complete the informed
consent form outside. Once the patient leaves the consultation room with the book-
let the researchers will request the patient to complete the informed consent form.
A baseline questionnaire collecting demographic data will be administered by the
researchers at month zero in the intervention and the control groups. The patients
in the intervention group will be informed to bring the booklet every time they have
a medical consultation. The providers will then use the booklet with the patients
during the next consultations. If patients have questions that are recorded in the

222
booklet, they record the answers next to the questions. Short-term follow-up will be
done at six months and long-term follow-up will be done at one year follow-up.
Who will provide the intervention?
Previous studies (18, 29) reported that in the Public Health System of South Africa
health service is provided to chronic patients by a multidisciplinary team, including
doctors, nurses, dieticians, health promoters and community health workers
(CHWs). All participating healthcare providers in the intervention arm will be trained
in a one-day workshop focused on the structure of the intervention, how to use the
care-plan booklet with patients and the provider log sheet (Appendix B), and
communication skills. Soon after training, patient recruitment will begin. In addition,
training will include brief behavior change counselling skills to all the providers in
the intervention. Previous research has indicated that training primary care
providers in brief behavior change counseling changes their clinical practice (34).
How will the intervention be implemented?
Because of the nature of the intervention, the booklet will be used on a one-on-one
basis with a health service provider during medical consultation. Patients can share
the booklet at home with friends and family and if need be record their questions in
the booklet. Upon consulting with the doctor the patient may use the booklet in
order to recall the questions. The nurses taking the vital signs will also double
record the vital signs in the patient’s booklet, so that there is a trend to which the
patient and the health provider can refer to during consultations.
Health promoters will be involved in explaining the use for the booklet to the patient
during the waiting time and also during their consultation with the patients.
Community health workers will be involved in assisting patients to use the booklets
or explaining it to the patients at their homes during the CHWs’ routine visits.
Dieticians and other health service providers will also be involved in using the
booklet with patients during individual consultation if necessary. As an additional

223
use, the information in the booklet can be used during patient support group to
motivate members to self-manage their illnesses.
Where will the intervention occur?
The intervention will take place in different locations throughout the journey of the
patient at the intervention facility at the time for a medical consultation. Firstly, the
intervention will take place in the waiting area where the health promoter will
explain or reinforce the use and importance of the self-management booklet to
patients. Secondly, during the taking of vital signs, the nurses will also record the
vital signs observations in the patients’ booklet. Thirdly, during the medical
consultation with the doctor or nurse, the booklet will serve as a vehicle of
interaction between the patient and the health service provider. Fourthly, the book-
let will be used in the health facility and at the patient’s home – in the health facility
with other health service providers like health promoters, dieticians or during
support groups, and at home with family and friends.
When and how much?
Since the use of the care-plan booklet with the health service provider depends on
the appointments made and on the level of control of patients in terms of vital
signs, there is no set number of times when the patient and provider should use the
booklet during consultation. A patient whose vital signs are under control normally
sees a doctor once every three months, but those whose vital signs are not under
control will return to the health facility within one or two months, depending on the
level of control. A minimum of two-follow-up visits will be required for each patient
at six months follow-up and at least four times at one year follow-up. The log sheet
will indicate how many times a patient has been seen.
How will the intervention be tailored?
The intervention will be tailored to the target population in different ways. Firstly,
the care-plan booklet will be translated into the indigenous language(s) of the

224
target population in the areas where the study will take place, thus meeting the
requests of patients in previous studies (18, 29). Secondly, the booklet will be
further adapted to include the pictures and content that patients requested. Thirdly,
questionnaires will be in English and will be simplified for the target population.
Interpretation assistance and assistance with completion of the questionnaire will
be available for patients with limited English proficiency or functional literacy. The
booklet will also be sent to a graphic designer for giving it a professional
appearance.
Modifications?
More information on implementation fidelity will be reported after the trial has been
conducted.
How well (planned) and how well (actual)?
Information on fidelity on the implementation of the intervention will be reported
after the intervention has been implemented. However, fidelity will be assured by
training the health service providers who will be responsible for delivering the
intervention.
Sample size calculation
A previous study from Tshwane district, our target district, reported a mean HbA1c
of 8.8% (SD=2.4) and an intra-cluster correlation coefficient (ICC) of 0.05 (35).
These figures were used to calculate the cluster number and sample size for each
cluster for a 1.5% reduction in HbA1c. Two scenarios were observed, both based
on the 0.05 level of significance but with different levels of power.
Firstly, at power of 0.8, the study will require 8 clusters in each arm with 10
patients per cluster. The total sample size for the first scenario would
therefore be 16 clusters (physicians) and 160 patients.

225
Secondly, at power of 0.9, the study will require 11 clusters in each arm
with 10 patients per cluster. The total sample size would be 22 clusters and
220 patients.
The second scenario was selected as more feasible. To cover for loss to follow-up,
15 patients will be recruited per cluster, giving a total sample size of 270 patients.
The target district has a total 24 City of Tshwane PHC clinics that could be involved
in the study.
Randomization
The PHC clinics will be the unit of randomization in order to avoid contamination
and a trained, independent team will conduct the randomization. All clinics that
agree to participate will be allocated randomly by computer generated random
numbers. A cluster is a group of patients seen by one specific healthcare provider
who will be involved in the study. The patients in the control group will receive
usual care at their respective clinics. Usual care consists of medical consultations
without the care-plan booklet.
Measurements
Measurements will include HbA1c, blood pressure, fasting blood glucose, triglycer-
ides, cholesterol and body weight. In addition, a questionnaire (Appendix C) will be
used to collect data on the following:
Demographics
Demographic data will be collected with questionnaire items on gender, age, length
of time since diabetes diagnosis, marital status, living situation, education level,
language, employment status, type of medication and duration since diagnosis.

226
Individual dispositions
General health literacy: The questionnaire developed by Ishikawa et al focusing on
functional, communicative and critical health literacy will be used (36). Functional
literacy requires basic reading and writing skills. Communicative literacy involves
advanced skills that enable the extraction of information, defining meaning and
applying that information to everyday life. Critical literacy requires a set of more
advanced skills in order to evaluate information from different sources and use it to
take charge of one’s life (36, 37).
Diabetes knowledge: A 24-item questionnaire developed by Garcia et al will be
used to collect information on diabetes knowledge (38). This tool was chosen
because it is a generic version and does not need any adaptations, except for
question 8 where 210mg/dl is replaced by 11.65mmol/L to fit the country of study’s
standard of measurement.
Diabetes attitudes: The revised diabetes attitudes scale-III (DAS-III) will be used to
collect information on attitudes to diabetes (39). This is a 33 Likert-item scale with a
scoring between one (strongly disagree) and five (strongly agree). The items
measure the psychosocial impact of diabetes and patient autonomy, attitudes
pertaining to needs for special training for professionals, and seriousness of the
disease. This questionnaire has previously been used in South Africa (40).
Self-efficacy: The questionnaire developed by the Stanford University on diabetes
self-management will be used (41), as it has been previously applied in South
Africa (42, 43). (Self-efficacy relates to a patient’s confidence in his/her ability to
perform self-management activities.)
Locus of control: A questionnaire developed by Trento et al will be used to collect
information on locus of control (44). This questionnaire has also been used
successfully in the South African context (42, 43). (Locus of control refers to a
person’s belief in his/her ability to control his/her illness [internal locus of control]
versus the belief that he/she cannot control his/her illness with this control being

227
placed in the hands of others [external locus of control] or the belief that the ability
to control is based on luck [chance locus of control].)
Behavioral outcomes
Diabetes behaviors: A questionnaire developed based on the diabetes behaviors of
the American Association of Diabetes Education (AADE) and previously used by
the Diabetes Literacy project will be used in this proposed study (45, 46). (There
are seven diabetes behavioral outcomes: healthy eating, being active, monitoring
of blood glucose, taking medication, problem solving, reducing risks and healthy
coping.)
Health outcomes
Disease-related outcomes: HbA1c, fasting blood glucose and cholesterol levels will
be measured.
Reduced health risks: Body weight, waist circumference, cholesterol, triglycerides,
high density lipoprotein (HDL), low density lipoprotein (LDL) and blood pressure will
be measured.
Health-related quality of life and wellbeing will be measured using a previously
validated questionnaire for the Diabetes Literacy project (46).
Provider outcomes
Provider outcomes of this intervention include:
Improved communication with patients
Use of the booklet during medical consultation

228
Process evaluation
Process evaluation aims to monitor, improve progress and increase the chances of
the intervention being successful (47). Process evaluation makes it possible to
identify effective components of an intervention, the circumstances that make an
intervention effective, and the beneficiaries of an intervention (to whom the
intervention is effective) (48). This type of evaluation is important to improve and
maintain successful public health interventions.
In this proposed study, the experiences of healthcare providers who used the care-
plan booklet during consultation will be assessed by means of conducting focus
group discussions at six and twelve months follow-up. Four focus groups will be
held, two at each time interval. Provider focus groups will take place at venues
convenient for the participants.
Patient experiences will be evaluated by means of in-depth interviews with two
patients per clinic and convenient sampling will be used to recruit patients. The
venue(s) for conducting patient interviews will be decided upon according to the
patients’ preference, either at the facility or in their homes. The interviews with the
patients will also be done at the two time intervals of six and twelve months follow-
up. A semi-structured interview guide will be used (Appendix D).
Data collection
Data will be collected at baseline, six and twelve months follow-up. Hired nurses
will be collecting blood and taking physical measurements. Standard operating
procedures will be used in measuring waist circumference by tape measures,
weight by electronic scales and blood pressure by the Omron digital blood pressure
monitor or similar device. HbA1c and total cholesterol will be sent to the
laboratories servicing the public health facilities (National Health Laboratory
Service). Research assistants will receive one day of training to administer
questionnaires and will be supervised by the project coordinator throughout the
research period. Focus group discussions and interviews with providers and
229
patients will be conducted by the primary investigator. Blinding will not be
applicable in this kind of study.
Data analysis
Descriptive statistics (means and frequencies) will be used to describe the data. In
addition an intent-to-treat analysis will be used to evaluate primary and secondary
outcomes. Anova with a fixed effect (i.e. intervention) and a random effect (i.e.
cluster) will be performed (SAS procedure MIXED). Qualitative data from interviews
and focus group discussions will be transcribed and translated and analyzed using
Atlas.ti or similar software.

230
Logistical issues
Time frame

231
Budget and resources
Item description ZAR
Transport R 5 000
Computers (x3) R 15 000
Printing and photocopying R 2 000
Research assistants (x11) R 55 000
Data capture and analysis R 50 000
Dissemination of results R 100 000
Other
Total cost R227 000
Contributors and authorship
The ICMJE criteria will be used to define the role of authors and contributors (49).
Conclusion
There is paucity of literature on the effectiveness of diabetes self-management
programs in developing countries, as the vast majority of intervention programs
have been developed, implemented and evaluated in developing countries (16).
However, as diabetes continues to affect millions of people in developing countries,
it is imperative that self-management programs also be developed and imple-
mented in resource-challenged countries like South Africa.
Results from existing research highlight the fact that very little effort has been
devoted to the prevention of chronic conditions like diabetes in developing
countries (50, 51). This study will contribute to the much needed literature on the
effectiveness of self-management programs in resource-limited countries and will
add to evidence-informed practice. The results of this study will provide information
to governments and policy makers from resource-limited settings on potential

232
implementation strategies to embark on in the prevention and control of diabetes
and other chronic conditions, with specific emphasis on self-management.
References
1. Mash R, Kroukamp R, Gaziano T, Levitt N. Cost-effectiveness of a diabetes group education program delivered by health promoters with a guiding style in underserved communities in Cape Town, South Africa. Patient Educ Couns. 2015;98(5):622-6.
2. International Diabetes Federation. IDF Diabetes Atlas, 7th edn. Brussels, Belgium: International Diabetes Federation; 2015 [cited 20 January 2016]. Available from: http://www.diabetesatlas.org/resources/2015-atlas.html.
3. de-Graft Aikins A. Africa's neglected epidemic:multidisciplinary research, intervention and policy for chronic diseases. Conference report May 2010. London: British Academy; 2010. [cited 18 January 2017]. Available from: https://ncdalliance.org/sites/default/files/resource_files/Africa's%20Neglected%20Epidemic%20-%20British%20Academy%20Report%202010.pdf.
4. World Health Organization. The global burden of chronic. [Internet]. [cited 10 August 2015]. Available from: http://www.who.int/nutrition/topics/2_background/en/.
5. Forouzanfar MH, Alexander L, Anderson HR, Bachman VF, Biryukov S, Brauer M, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(10010):2287-323.
6. Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2014;384(9945):766-81.
7. Lalkhen H, Mash R. Multimorbidity in non-communicable diseases in South African primary healthcare. S Afr Med J. 2015;105(2):134-8.
8. Murphy K, Chuma T, Mathews C, Steyn K, Levitt N. A qualitative study of the experiences of care and motivation for effective self-management among diabetic and hypertensive patients attending public sector primary health care services in South Africa. BMC Health Serv Res. 2015;15:303.
9. Beaglehole R, Epping-Jordan J, Patel V, Chopra M, Ebrahim S, Kidd M, et al. Improving the prevention and management of chronic disease in low-income and middle-income countries: a priority for primary health care. Lancet. 2008;372(9642):940-9.
10. Van den Broucke S, Van der Zanden G, Chang P, Doyle G, Levin D, Pelikan J, et al. Enhancing the effectiveness of diabetes self-management

233
education: the diabetes literacy project. Horm Metab Res. 2014;46(13):933-8.
11. deSilva D. Evidence. Helping people help themselves. A review of evidence considering whether it is worthwhile to support self-management: London: The Health Foundation; 2011 [cited 14 March 2015]. Available from: http://www.health.org.uk/publication/evidence-helping-people-help-themselves.
12. Lukewich J, Mann E, VanDenKerkhof E, Tranmer J. Self-management support for chronic pain in primary care: a cross-sectional study of patient experiences and nursing roles. J Adv Nurs. 2015;71(11):2551-62.
13. Republic of South Africa. Strategic Plan for the Prevention and Control of Non-Communicable Diseases. Department of Health; 2013 [cited 30 May 2014]. Available from: http://www.health-e.org.za/wp-content/uploads/2013/09/NCDs-STRAT-PLAN-CONTENT-8-april-proof.pdf.
14. Folb N, Timmerman V, Levitt NS, Steyn K, Bachmann MO, Lund C, et al. Multimorbidity, control and treatment of noncommunicable diseases among primary healthcare attenders in the Western Cape, South Africa. S Afr Med J. 2015;105(8):642-7.
15. Bradshaw D, Levitt N, Nojilana B. Non-communicable disease: a race against time. Policy brief. South African Medical Research Council; 2011 (updated 2014) [cited 12 December 2015]. Available from: http://www.mrc.ac.za/policybriefs/raceagainst.pdf.
16. Mendis S. Research Is essential for attainment of NCD targets and Sustainable Development Goals. Glob Heart. 2016;11(1):139-40.
17. Dube L, Van den Broucke S, Rendall-Mkosi K, Kalweit K, Housiaux M, D'Hoore W. An audit of diabetes self-management education programs in South Africa. J Public Health Res. 2015;4(581):176-84.
18. Dube L, Van den Broucke S, Bergh A-M, Mafutha N, Rendall-Mkosi K. Self-management support needs of patients with chronic diseases in a South African township: a qualitative study. J Community Health Nurs. In Press.
19. Parker W A, Steyn N P, Levitt N S, Lombard C J. Health promotion services for patients having non-communicable diseases: feedback from patients and health care providers in Cape Town, South Africa. BMC Public Health. 2012;12:503.
20. Campbell MK, Piaggio G, Elbourne DR, Altman DG. Consort 2010 statement: extension to cluster randomised trials. BMJ. 2012;345:e5661.
21. BioMed Central.International Standards Randomised Controlled Trials Number (ISRCTN) registry. [Internet]. 2016 [cited 05 January 2017]. Available from: http://www.isrctn.com/.
22. Hoffmann TC, Glasziou PP, Boutron I, Milne R, Perera R, Moher D, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687.
23. Lorig K R, Ritter P, Stewart A L, Sobel D S, Jr. BBW, Bandura A, et al. Chronic disease self-management program: 2-year health status and health care utilization outcomes. Med Care. 2001;39(11):1217-23.

234
24. Lorig K R, Ritter P L, Laurent D D, Plant K. Internet-based chronic disease self-management: a randomized trial. Med Care. 2006;44(11):964-71.
25. Lorig KR, Holman H. Self-management education: history, definition, outcomes, and mechanisms. Ann Behav Med. 2003;26(1):1-7.
26. Dube L, Van den Broucke S, Bergh, A-M, D'Hoore W. Enhancing diabetes and hypertension health literacy in a South African township: a pilot study. Submitted.
27. Dube L, Van den Broucke S, Housiaux M, D'Hoore W, Rendall-Mkosi K. Type 2 Diabetes selfmanagement education programs in high and low mortality developing countries. Diabetes Educ. 2015;41(1):69-85.
28. Department of Health, South Africa. Nutritional management of diabetes [Pamphlet].
29. Dube L, Bergh A-M, Van de Broucke S, D'Hoore W. Feasibility of a self-management tool for diabetes and hypertension in South Africa. Submitted.
30. Cao ZJ, Chen Y, Wang SM. Health belief model based evaluation of school health education programme for injury prevention among high school students in the community context. BMC Public Health. 2014;14:26.
31. National Cancer Institute. Theory at a glance: a guide for health promotion practice. 2nd ed. NIH Publication No. 05-3896 [Internet]. U.S Department of Health and Human Services, National Institutes of Health; 2005 [cited 22 September 2015]. Available from: http://www.sbccimplementationkits.org/demandrmnch/wp-content/uploads/2014/02/Theory-at-a-Glance-A-Guide-For-Health-Promotion-Practice.pdf.
32. Abraham C, Sheeran, P. The Health Belief Model. In: Conner M, Norman, P, editors. Predicting and changing health behavior. 3rd ed. Berkshire: McGraw-Hill Education; 2015.
33. Raingruber B. Contemporary health promotion in nursing practice. Burlington: Jones & Bartlett Learning, LLC; 2014.
34. Malan Z, Mash B, Everett-Murphy K. Evaluation of a training programme for primary care providers to offer brief behaviour change counselling on risk factors for non-communicable diseases in South Africa. Patient Educ Couns. 2016;99(1):125-31.
35. Webb EM, Rheeder P, Van Zyl DG. Diabetes care and complications in primary care in the Tshwane district of South Africa. Prim Care Diabetes. 2015;9(2):147-54.
36. Ishikawa H, Takeuchi T, Yano E. Measuring functional, communicative, and critical health literacy among diabetic patients. Diabetes Care. 2008;31(5):874-9.
37. Nutbeam D. Evaluating health promotion: progress, problems and solutions. Health Promot Int. 1998;13(1):27-44.
38. Garcia AA, Villagomez ET, Brown SA, Kouzekanani K, Hanis CL. The Starr County Diabetes Education Study: development of the Spanish-language diabetes knowledge questionnaire. Diabetes Care. 2001;24(1):16-21.
39. Anderson RM, Fitzgerald JT, Funnell MM, Gruppen LD. The third version of the Diabetes Attitude Scale. Diabetes Care. 1998;21(9):1403-7.

235
40. Muchiri J, Gericke, GJ, Rheeder P. Impact of nutrition education on diabetes knowledge and attitudes of adults with type 2 diabetes living in a resource-limited setting in South Africa: a randomised controlled trial. JEMDSA. 2016;21(2):26-34.
41. Stanford Patient Education Research Center. Diabetes Self-Efficacy Scale [Internet]. [cited 18 October 2016]. Available from: http://patienteducation.stanford.edu/research/sediabetes.html.
42. Mash B, Levitt N, Steyn K, Zwarenstein M, Rollnick S. Effectiveness of a group diabetes education programme in underserved communities in South Africa: pragmatic cluster randomized control trial. BMC Fam Pract. 2012;13:126.
43. Mash RJ, Rhode H, Zwarenstein M, Rollnick S, Lombard C, Steyn K, et al. Effectiveness of a group diabetes education programme in under-served communities in South Africa: a pragmatic cluster randomized controlled trial. Diabet Med. 2014;31(8):987-93.
44. Trento M, Passera P, Miselli V, Bajardi M, Borgo E, Tomelini M, et al. Evaluation of the locus of control in patients with type 2 diabetes after long-term management by group care. Diabetes Metab. 2006;32(1):77-81.
45. Mulcahy K, Maryniuk M, Peeples M, Peyrot M, Tomky D, Weaver T, et al. Diabetes self-management education core outcomes measures. Diabetes Educ. 2003;29(5):768-70, 73-84, 87-8. .
46. Röthlin F, Pelikan J, Ganahl K. Protocol for a pre-post evaluation study on the effectiveness of existing DSM programs. .Working paper. The Diabetes Literacy Project; 2014. Unpublished.
47. Executive Agency for Health and Consumers (EAHC). Project management in public health in Europe; 2011 [cited 02 January 2017]. Available from: http://ec.europa.eu/chafea/documents/health/leaflet/project_management2.pdf.
48. Linnan L, Steckler A, editors. Process evaluation for public health interventions and research. San Francisco, CA: John Woley & Sons; 2002.
49. International Committee of Medicl Journal Editors (ICMJE). Defining the role of authors and contributors; 2017 [cited 05 January 2017]. Available from: http://www.icmje.org/recommendations/browse/roles-and-responsibilities/defining-the-role-of-authors-and-contributors.html.
50. de-Graft Aikins A, Boynton P, Atanga LL. Developing effective chronic disease interventions in Africa: insights from Ghana and Cameroon. Global Health. 2010;6:6.
51. Unwin N, Setel P, Rashid S, Mugusi F, Mbanya JC, Kitange H, et al. Noncommunicable diseases in sub-Saharan Africa: where do they feature in the health research agenda? Bull World Health Organ. 2001;79(10):947-53.

236

237
GENERAL CONCLUSION – Conditions for effective
implementation

238
The essence of this thesis revolves around the current status of self-management
education programs for chronic diseases in South Africa and the conditions for their
effective implementation. The underlying aim was to contribute to the scarce
literature on education for self-management of chronic diseases in developing
countries, especially in sub-Saharan Africa (SSA). By way of conclusion, we would
like to draw upon the lessons learnt from the studies presented in this thesis to
further assist the implementation of chronic disease self-management programs in
resource-limited settings. These conditions include, but are not limited to, the
attention that is paid to the context and characteristics of the target population, the
capacities of health promoters and community health workers, a healthcare system
that functions at some minimal level, networking and liaising at different levels, and
most importantly a staggered implementation.
As highlighted in Chapter 2 of this thesis, the context in which the target population
lives is a crucial element to be considered since, among other factors, contextual
factors affect the development of chronic diseases and the way they can be
managed (1). We also discussed the health context of South Africa and referred to
the two healthcare systems (formal-westernized and informal-traditional) that
operate in parallel (2), illustrating how these two systems can complement or be in
direct conflict with each other (3). As a consequence, self-management education
in South Africa must take account of the fact that the target population, apart from
receiving messages from the primary healthcare (PHC) facilities, may also receive
information from other sources which may conflict with the received messages.
The language in which self-management education is provided is also an important
element. South Africa has 11 official languages, and it is important to align
language(s) and education materials with the specific target populations for which
the intervention is meant. Nevertheless, it is possible to make some trade-offs in
terms of choice of language, as seven of the South African languages belong to
two main language families – the Nguni and Sotho families – and mutual
comprehension is often possible. Nguni languages include isiZulu, isiXhosa,

239
isiNdebele and siSwati. Sotho languages include Sesotho sa Leboa/Sepedi,
Setwana and Sesotho (4).
In terms of capacity building, it is imperative that health promoters and community
health workers (CHWs) are trained in chronic diseases self-management and that
they are brought on board. The shortage of human resources which is
characteristic of resource-limited setting was noted in Chapters 3 and 4. One way
to address this problem is to involve community health workers and let them play
an important part in the roll-out of a program, with professionals fulfilling
supervisory roles (5, 6). In the study reported in Chapter 7, health service providers
referred to the significant role CHWs and health promoters could play in the
implementation of the care-plan booklet (7). However, for CHWs and health
promoters to take up this role they need to be trained and their capacity to act in
complex roles should be strengthened, thereby ensuring quality of care (8, 9). Not
only non-professional health workers will need to be trained, but also the capacities
of professional health service providers’ (doctors and nurses) will need to be
enhanced. Other studies have already pointed out the need for the training of
primary care providers in brief behavior change counseling and motivational
interviewing in South Africa’s primary care facilities (10, 11). This can be extended
with adequate training in chronic diseases self-management education techniques.
As noted in the studies reported in this thesis, the implementation of chronic
disease self-management education interventions in primary care settings requires
a healthcare system that functions at a minimal level. In many instances,
healthcare facilities in resource-limited settings, especially in the public health
system, are lacking in many areas, such as staff and materials for educating
patients (12, 13). However, this shortage can partly be overcome through task-
shifting (e.g., by assigning some tasks to CHWs as outlined above) and through
liaison at and between different levels of the health system and during the different
stages of the intervention. Such task shifting could ensure the smooth
implementation of self-management education interventions and at the same time
identify problem and solutions.

240
Many developing countries are at the moment facing a double burden of
communicable and non-communicable diseases (14-16). Addressing this double
burden calls for an integrated approach, especially in view of the problem of
comorbidities (16). The “old” approach of dealing with diseases in vertical silos no
longer provides a solution. South Africa, the country focused upon in this thesis,
has recently changed its policy to dealing with chronic conditions from a vertical to
an integrated approach (17, 18). This needs to be taken into consideration when
planning, designing and implementing chronic disease self-management
interventions in resource-limited settings. Although a broad and large-scale
implementation of self-management for all chronic diseases is not feasible, a
staggered implementation of self-management education may be necessary to
ensure that all aspects are covered. Such an approach, which uses a staged
implementation process, also has other advantages, such as the reduction of risk,
allowing extra time to make improvements to the program, and engaging
stakeholders to get them on board with the change.
As self-management education is not a panacea for the treatment and
management of chronic disease, the care-plan booklet of which the development
was described in this thesis does not have the ambition to be the answer to all the
problems and challenges that patients face in their self-management (7, 19). Some
of these challenges, as noted in Chapter 5, are not related to the booklet but
pertain more to problems in the healthcare system itself (12). However, the care-
plan booklet can be seen as a tool to improve the communication and interaction
between the healthcare providers, the patients and/their or families. It builds on
and enhances the capacity of the patients to prepare for medical consultations and
to communicate during these consultations.
The care-plan booklet may seem more provider-oriented than patient-oriented, but
there is ample room for improving the booklet in further studies. Using the booklet
in conjunction with other interventions, including cell-phone or web-based
interventions, could also be explored. However, where resources are limited, the
booklet is a simple, low-cost intervention that can assist in ensuring that messages
are uniform in the consultations between providers and patients. The set of

241
minimum requirement for each patient per visit and per annum may also serve to
improve accountability of healthcare providers.
The care-plan booklet can also assist healthcare providers in complying with some
of the Batho Pele principles discussed in Chapter 9 (20). For example, the principle
of courtesy is where patients are seen as worthy to be treated with dignity,
consideration and respect. As a vehicle for interaction between patients and
providers, the booklet may assist in the communication process and encourage the
patients and the providers to interact. This communication on its own can already
be meaningful for the patients, as a lack of communication between patients and
providers was seen as a barrier to chronic disease self-management (12).
In summary, the different aspects of the contexts should be taken into
consideration when developing and implementing self-management education
programs for developing countries facing a unique double burden of disease.
Taking the above-mentioned conditions into consideration can assist in this
endeavor. However, further research is needed to fully understand the conditions
that co-determine the effectiveness of self-management education in resource-
limited settings and to find ways to enhance the effectiveness by aligning programs
and interventions to the targeted population.
References
1. Van den Broucke S. How international is health promotion? Health Promot Int. 2016;31(3):491-4.
2. Moshabela M, Zuma T, Gaede B. Bridging the gap between biomedical and traditional health practitioners in South Africa. In: Padarath A, King J, Mackie E, Casciola J, editors. South African Health Review. 2016. Durban: Health Systems Trust; 2016. p. 83-92.
3. Maimela E, Van Geertruyden JP, Alberts M, Modjadji SE, Meulemans H, Fraeyman J, et al. The perceptions and perspectives of patients and health care providers on chronic diseases management in rural South Africa: a qualitative study. BMC Health Serv Res. 2015;15:143.
4. Wikipedia. Languages of South Africa [Internet]. 2016 [cited 02 January 2017]. Available from: https://en.wikipedia.org/wiki/Languages_of_South_Africa.

242
5. Dube L, Van den Broucke S, Housiaux M, D'Hoore W, Rendall-Mkosi K. Type 2 diabetes selfmanagement education programs in high and low mortality developing countries. Diabetes Educ. 2015;41(1):69-85.
6. Dube L, Van den Broucke S, Rendall-Mkosi K, Kalweit K, Housiaux M, D'Hoore W. An audit of diabetes self-management education programs in South Africa. J Public Health Res. 2015;4(581):176-84.
7. Dube L, Bergh A-M, Van de Broucke S, D'Hoore W. Feasibility of a self-management tool for diabetes and hypertension in South Africa. Submitted.
8. Mishra SR, Neupane D, Preen D, Kallestrup P, Perry HB. Mitigation of non-communicable diseases in developing countries with community health workers. Global Health. 2015;11:43.
9. Tsolekile LP, Puoane T, Schneider H, Levitt NS, Steyn K. The roles of community health workers in management of non-communicable diseases in an urban township. Afr J Prim Health Care Fam Med. 2014;6(1).
10. Malan Z, Mash B, Everett-Murphy K. Evaluation of a training programme for primary care providers to offer brief behaviour change counselling on risk factors for non-communicable diseases in South Africa. Patient Educ Couns. 2016;99(1):125-31.
11. Mash R. The KM Seedat Memorial Lecture: Behaviour change counselling in the South African context. Transactions. 2014;58(1):58-62.
12. Dube L, Van den Broucke S, Bergh A-M, Mafutha N, Rendall-Mkosi K. Self-management support needs of patients with chronic diseases in a South African township: a qualitative study. J Community Health Nurs. In Press.
13. Parker WA, Steyn NP, Levitt NS, Lombard CJ. Health promotion services for patients having non-communicable diseases: feedback from patients and health care providers in Cape Town, South Africa. BMC Public Health. 2012;12:503.
14. Lopez A, Mathers, CD., Ezzati, M., Jamison, DT., Murray, CJL. Global burden of disease and risk factors. Washington, DC: The World Bank Group; 2006.
15. de-Graft Aikins A, Unwin N, Agyemang C, Allotey P, Campbell C, Arhinful D. Tackling Africa's chronic disease burden: from the local to the global. Global Health. 2010;6:5.
16. Young F, Critchley JA, Johnstone LK, Unwin NC. A review of co-morbidity between infectious and chronic disease in Sub Saharan Africa: TB and diabetes mellitus, HIV and metabolic syndrome, and the impact of globalization. Global Health. 2009;5:9.
17. Asmall S, Mahomed O. Integrated chronic diseases management manual. National Department of Health, South Africa; 2011 [cited 10 June 2014]. Available from: http://www.kznhealth.gov.za/family/Integrated-chronic-disease-management-manual.pdf.
18. Mahomed OH, Asmall S. Development and implementation of an integrated chronic disease model in South Africa: lessons in the management of change through improving the quality of clinical practice. Int J Integr Care. 2015;15:e038.

243
19. Dube L, Van den Broucke S, Bergh A-M, D'Hoore W. Enhancing diabetes and hypertension health literacy in a South African township: a pilot study. Submitted.
20. SA Health. Patient and consumer centred care [Internet]. 2016 [cited 09 September 2016]. Available from: http://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/clinical+resources/safety+and+quality/partnering+with+consumers+and++the+community/patient+and+consumer+centred+care.

244

245
PUBLICATIONS & SCIENTIFIC COMMUNICATION
Publications
1. Dube L, Van den Broucke S, Housiaux M, D'Hoore W, Rendall-Mkosi K.
Type 2 Diabetes selfmanagement education programs in high and low
mortality developing countries. Diabetes Educator. 2015;41(1):69-85
2. Dube L, Van Den Broucke S, Rendall-Mkosi K, Kalweit, K, Hosiaux M,
Dhoore W. (2015) An audit of diabetes self-management education
programs in South Africa. Journal Public Health Research. 4(581), 176–
84
3. Dube L, Rendall-Mkosi K, Van den Broucke S, Bergh A, Mafutha N. Self-
management support needs of patients with chronic diseases in a South
African township: a qualitative study. Journal of Community Health
Nursing. In Press
4. Dube L, Bergh A-M, Van den Broucke S, D’Hoore W. Feasibility of a self-
management tool for diabetes and hypertension in South Africa,
Submitted.
5. Dube L, Van den Broucke S, Bergh AM, D’Hoore W. Enhancing diabetes
and hypertension health literacy in a South African township: a pilot study.
To be submitted.
Scientific communication
Type 2 Diabetes selfmanagement education programs in high and low
mortality developing countries. Poster presentation. 49th Society of
Endocrinology, Metabolism and Diabetes of South Africa (SEMDSA),
Durban, South Africa. Dube L, Van den Broucke S, Housiaux M, D'Hoore
W, Rendall-Mkosi K.
An audit of diabetes self-management education programs in South Africa.
Oral Presentation. PhD day, ULB. Brussels, Belgium. Dube L, Van Den
Broucke S, Rendall-Mkosi K, Kalweit K, Hosiaux M, Dhoore W.

246
An audit of diabetes self-management education programs in South Africa.
Oral Presentation. Chronic disease Initiative for Africa: Annual network
meeting. Cape Town, South Africa. Dube L, Van Den Broucke S, Rendall-
Mkosi K, Kalweit K, Hosiaux M, Dhoore W.
An audit of diabetes self-management education programs in South Africa.
Poster Presentation.World Diabetes Congress.Vancouver, Canada. Dube
L, Van Den Broucke S, Rendall-Mkosi K, Kalweit K, Hosiaux M, Dhoore
W.
Self-management support needs of patients with chronic diseases in a
South African township: a qualitative study. Poster Presentation. Curitiba,
Brazil. Dube L, Rendall-Mkosi K, Van den Broucke S, Bergh A, Mafutha N.
Individial care-plan booklet for chronic patients – a feasibility study (South
Africa). Poster Presentation. 9th European Public Health Conference.
Vienna, Austria. Dube L, Bergh A-M, Van den Broucke S, D’Hoore W.

247
APPENDICES
• Appendix A – The care-plan booklet
• Appendix B – Providers’ log sheet
• Appendix C – Questionnaire (pre & post)
• Appendix D – Semi-structured interview guide

248

249
APPENDIX A

250
Page intentionally left blank!

251

252
Page intentionally left blank!

253

254

255

256

257

258

259

260

261

262

263

264

265

266

267

268

269

270
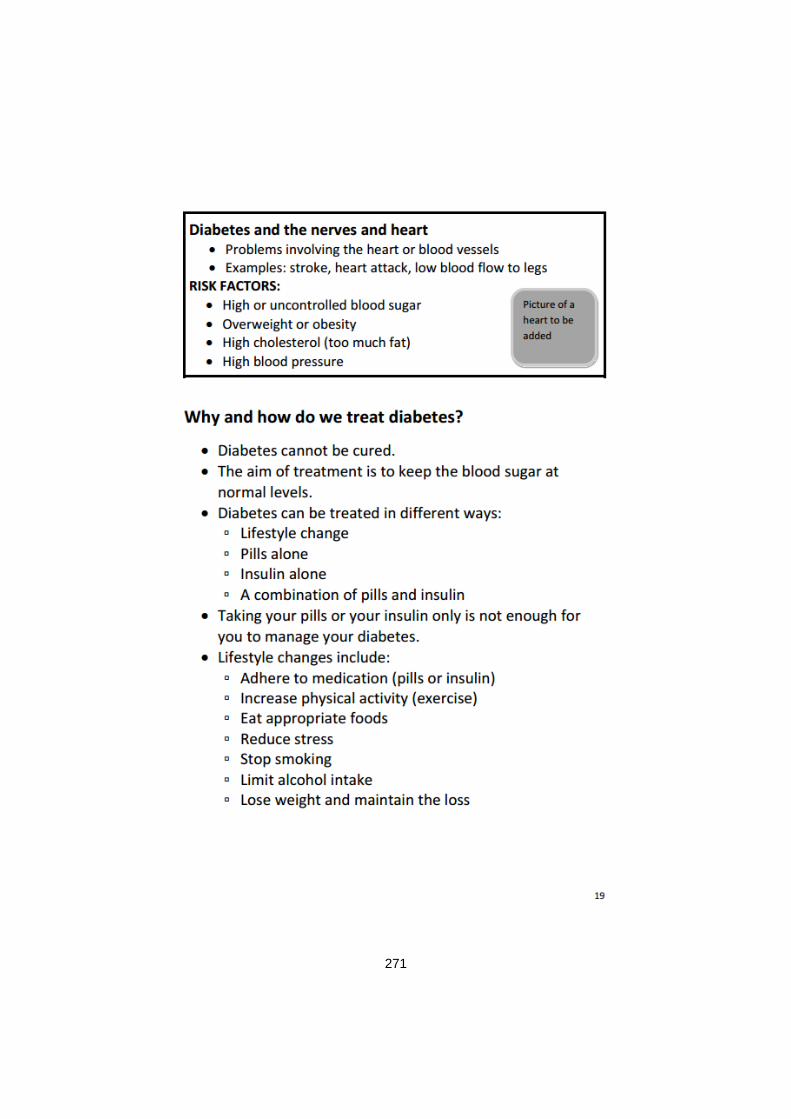
271

272

273

274

275

276

277

278

279

280

281

282
Page intentionally left blank!

283

284

285
APPENDIX B
PROVIDER LOG SHEET
Facility name or facility code ………………………………………………………….
Provider name or code …………………………………………………………………
Patient
name or
code
Months of consultations
(Tick at each month if seen during medical consultation)
0 1 2 3 4 5 6 7 8 9 10 11 12
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12
13.
14.
15

286

287
APPENDIX C
PRE- & POST-TEST PATIENT QUESTIONNAIRE
Participant number: ……………………..……… Date: ………………………………
PRE- & POST-TEST PATIENT QUESTIONNAIRE
PART A: DEMOGRAPHIC INFORMATION (only for pre questionnaire)
We would first like to get some more information about yourself.
A.1 What is your name?
Surname: ………………………………. First name: …………………………….
A.2. Would you mind to give your cell number? We need it for follow-up purposes,
Phone number: ………………………………….
A.3 Home address
Street number: …………………………………. Zone: …………………………….
A.4 Gender
1 Male 2 Female
A.5 When were you born?
Date of birth: …………………………………………………..……|_Y_|_Y_|_Y_|_Y_| |_M_|_M_| |_D_| _D_|
A.6 What is your marital status?
1 Married 2 Divorced/separated
3 Single
4 Living with partner 5 Other (Please specify)
…….…………………………………………………………..

288
A.7 Whom do you stay with?
1 Family 3 Other (Please specify)
2 Alone ……..………………………………………………..
A.8 What is you first language?
1 Sepedi 5 isiZulu
9 Afrikaans
2 Setswana 6 isiXhosa
10 Tshivenda
3 Sesotho 7 isiNdebele
11 Xitsonga
4 English 8 SiSwati
12 Other (Please specify)
……………………………………………………………….
A.9 What other languages do you speak at home?
1 Sepedi 5 isiZulu
9 Afrikaans
2 Setswana 6 isiXhosa
10 Tshivenda
3 Sesotho 7 isiNdebele
11 Xitsonga
4 English 8 SiSwati
12 Other (Please specify)
……………………………………………………………….
A.10 How far did you go with your school education?
0 No schooling 4 Grade 4 7 Grade 7
10 Grade 10
1 Grade 1 5 Grade 5 8 Grade 8
11 Grade 11
2 Grade 2 6 Grade 6 9 Grade 9
12 Grade 12
3 Grade 3
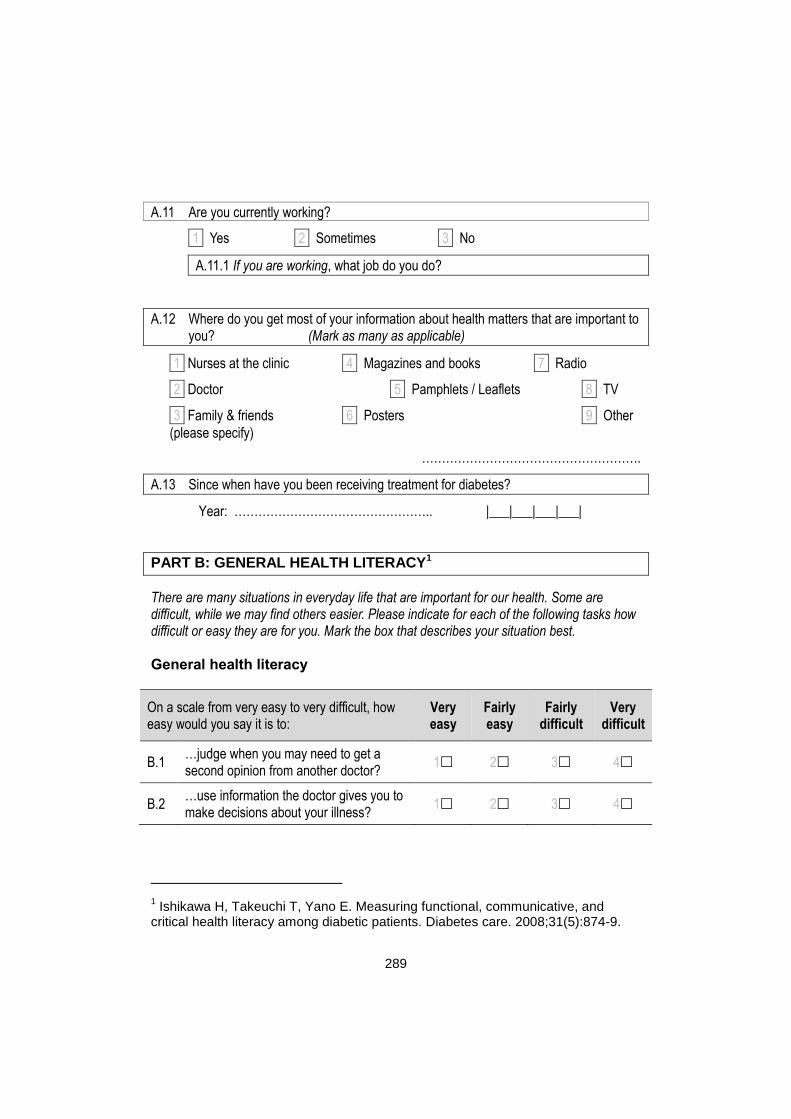
289
A.11 Are you currently working?
1 Yes 2 Sometimes 3 No
A.11.1 If you are working, what job do you do?
A.12 Where do you get most of your information about health matters that are important to you? (Mark as many as applicable)
1 Nurses at the clinic 4 Magazines and books 7 Radio
2 Doctor 5 Pamphlets / Leaflets 8 TV
3 Family & friends 6 Posters 9 Other
(please specify)
……………………………………………….
A.13 Since when have you been receiving treatment for diabetes?
Year: ………………………………………….. |___|___|___|___|
PART B: GENERAL HEALTH LITERACY1
There are many situations in everyday life that are important for our health. Some are difficult, while we may find others easier. Please indicate for each of the following tasks how difficult or easy they are for you. Mark the box that describes your situation best. General health literacy
On a scale from very easy to very difficult, how easy would you say it is to:
Very easy
Fairly easy
Fairly difficult
Very difficult
B.1 …judge when you may need to get a second opinion from another doctor?
1 2 3 4
B.2 …use information the doctor gives you to make decisions about your illness?
1 2 3 4
1 Ishikawa H, Takeuchi T, Yano E. Measuring functional, communicative, and
critical health literacy among diabetic patients. Diabetes care. 2008;31(5):874-9.

290
On a scale from very easy to very difficult, how easy would you say it is to:
Very easy
Fairly easy
Fairly difficult
Very difficult
B.3 …find information on how to manage mental health problems like stress or depression?
1 2 3 4
B.4 …judge if the information on health risks in the media is reliable? (Examples: TV, Internet or other media)
1 2 3 4
B.5 …find out about activities that are good for your mental well-being? (Examples: meditation, exercise, walking, pilates etc.)
1 2 3 4
B.6 …understand information in the media on how to get healthier?(Examples: internet, newspapers, magazines)
1 2 3 4
Diabetes-specific health literacy
The next questions ask about how often you have had certain experiences as a patient and as a diabetic. Mark the box that describes your situation best.
In reading instructions or leaflets from hospitals/pharmacies, you…
Never Seldom Sometimes Often
B.7 …found that the print was too small to read. 1 2 3 4
B.8 …found characters and words that you did not know.
1 2 3 4
B.9 …found that the content was too difficult. 1 2 3 4
B.10 …needed a long time to read and understand them.
1 2 3 4
B.11 …needed someone to help you read them. 1 2 3 4
Since being diagnosed with diabetes, you have… Never Seldom Sometimes Often
B.12 …collected information from various sources.
1 2 3 4

291
Since being diagnosed with diabetes, you have… Never Seldom Sometimes Often
B.13 …extracted the information you wanted. 1 2 3 4
B.14 … understood the obtained information. 1 2 3 4
B.15 …communicated your thoughts about
your illness to someone. 1 2 3 4
B.16 …applied the obtained information to your daily life.
1 2 3 4
B.17 …considered whether the information was
applicable to your situation. 1 2 3 4
B.18 …considered the credibility of the information.
1 2 3 4
B.19 …checked whether the information was
valid and reliable. 1 2 3 4
B.20 …collected information to make health-
related decisions. 1 2 3 4
PART C: INDIVIDUAL PATIENT DISPOSITIONS
Diabetes knowledge2 Mark the box that you think is the correct answer to each statement.
Question Yes No Don’t know
C.1 Eating too much sugar and other sweet foods is a cause of diabetes
2 √1 0
C.2 The usual cause of diabetes is lack of effective insulin in the body
√2 1 0
2 Garcia AA, Villagomez ET, Brown SA, Kouzekanani K, Hanis CL. The Starr
County Diabetes Education Study: development of the Spanish-language diabetes knowledge questionnaire. Diabetes Care. 2001;24(1):16-21.

292
Question Yes No Don’t know
C.3 Diabetes is caused by failure of the kidneys to keep sugar out of the urine
2 √1 0
C.4 Kidneys produce insulin 2 √1 0
C.5 In untreated diabetes, the amount of sugar in the blood usually increases.
√2 1 0
C.6 If I am diabetic, my children have a higher chance of being diabetic.
√2 1 0
C.7 Diabetes can be cured. 2 √1 0
C.8 A fasting blood sugar level of 11.65mmol/l is too high. √2 1 0
C.9 The best way to check my diabetes is by testing my urine. 2 √1 0
C.10 Regular exercise will increase the need for insulin or other diabetic medication.
2 √1 0
C.11 There are two main types of diabetes: Type 1 (insulin--dependent) and Type 2 (non-insulin dependent).
√2 1 0
C.12 An insulin reaction is caused by too much food. 2 √1 0
C.13 Medication is more important than diet and exercise to control my diabetes.
2 √1 0
C.14 Diabetes often causes poor circulation. √2 1 0
C.15 Cuts and abrasions on diabetes heal more slowly. √2 1 0
C.16 Diabetics should take extra care when cutting their toenails.
√2 1 0
C.17 A person with diabetes should cleanse a cut with iodine and alcohol.
2 √1 0
C.18 The way I prepare my food is as important as the foods I eat.
√2 1 0
C.19 Diabetes can damage my kidneys. √2 1 0
C.20 Diabetes can cause loss of feeling in my hands, fingers and feet.
√2 1 0
C.21 Shaking and sweating are signs of high blood sugar. 2 √1 0
C.22 Frequent urination and thirst are signs of low blood sugar. 2 √1 0

293
Question Yes No Don’t know
C.23 Tight elastic hose or socks are not bad for diabetics. 2 √1 0
C.24 A healthy diet consists mostly of special foods. 2 √1 0
Diabetes attitudes3
Below are some statements about diabetes. Each numbered statement finishes the sentence “In general, I believe that...” You may believe that a statement is true for one person but not for another person or may be true one time but not be true another time. Mark the answer that you believe is true most of the time or is true for most people. Place a check mark in the box below the word or phrase that is closest to your opinion about each statement. It is important that you answer every statement. Note: The term “health care professionals” in this survey refers to doctors, nurses, and dietitians.
In general I believe that…
Strongly agree
Agree Neutral Disagree Strongly disagree
C.25 ...health care professionals who treat people with diabetes should be trained to communicate well with their patients.
5 4 3 2 1
C.26 ...people who do not need to take insulin to treat their diabetes have a pretty mild disease.
5 4 3 2 1
3 Anderson RM, Fitzgerald JT, Funnell MM, Gruppen LD. The third version of the
Diabetes Attitude Scale. Diabetes Care. 1998;21(9):1403-7.

294
In general I believe that…
Strongly agree
Agree Neutral Disagree Strongly disagree
C.27 ...there is not much use in trying to have good blood sugar control because the complications of diabetes will happen anyway.
5 4 3 2 1
C.28 ...diabetes affects almost every part of a diabetic person’s life.
5 4 3 2 1
C.29 ...the important decisions regarding daily diabetes care should be made by the person with diabetes.
5 4 3 2 1
C.30 ...health care professionals should be taught how daily diabetes care affects patients’ lives.
5 4 3 2 1
C.31 ...older people with Type
2* diabetes do not usually get complications.
5 4 3 2 1
C.32 ...keeping the blood sugar close to normal can help to prevent the complications of diabetes.
5 4 3 2 1
C.33 ...health care professionals should help patients make informed choices about their care plans.
5 4 3 2 1

295
In general I believe that…
Strongly agree
Agree Neutral Disagree Strongly disagree
C.34 ...it is important for the nurses and dietitians who teach people with diabetes to learn counseling skills.
5 4 3 2 1
C.35 ...people whose diabetes is treated by just a diet do not have to worry about getting many long-term complications
5 4 3 2 1
C.36 ...almost everyone with diabetes should do whatever it takes to keep their blood sugar close to normal.
5 4 3 2 1
C.37 ...the emotional effects of diabetes are pretty small.
5 4 3 2 1
C.38 ...people with diabetes should have the final say in setting their blood glucose goals
5 4 3 2 1
C.39 ...blood sugar testing is not needed for people
with Type 2* diabetes.
5 4 3 2 1
C.40 ..low blood sugar reactions make tight control too risky for most people.
5 4 3 2 1
C.41 ...health care professionals should learn how to set goals with patients, not just tell them what to do.
5 4 3 2 1

296
In general I believe that…
Strongly agree
Agree Neutral Disagree Strongly disagree
C.42 ...diabetes is hard because you never get a break from it.
5 4 3 2 1
C.43 ...the person with diabetes is the most important member of the diabetes care team.
5 4 3 2 1
C.44 ...to do a good job, diabetes educators should learn a lot about being teachers
5 4 3 2 1
C.45 ...Type 2* diabetes is a very serious disease.
5 4 3 2 1
C.46 ...having diabetes changes a person’s outlook on life.
5 4 3 2 1
C.47 ...people who have Type
2*diabetes will probably not get much payoff from tight control of their blood sugars.
5 4 3 2 1
C.48 ...people with diabetes should learn a lot about the disease so that they can be in charge of their own diabetes care.
5 4 3 2 1
C.49 ...Type 2* is as serious
as Type 1† diabetes. 5 4 3 2 1
C.50 ...tight control is too much work.
5 4 3 2 1

297
In general I believe that…
Strongly agree
Agree Neutral Disagree Strongly disagree
C.51e
...what the patient does has more effect on the outcome of diabetes care than anything a health professional does.
5 4 3 2 1
C.52 ...tight control of blood sugar makes sense only for people with Type 1 diabetes.
5 4 3 2 1
C.53 ...it is frustrating for people with diabetes to take care of their disease.
5 4 3 2 1
C.54 ...people with diabetes have a right to decide how hard they will work to control their blood sugar.
5 4 3 2 1
C.55 ...people who take diabetes pills should be as concerned about their blood sugar as people who take insulin.
5 4 3 2 1
C.56 ...people with diabetes have the right not to take good care of their diabetes.
5 4 3 2 1
C.57 ...support from family and friends is important in dealing with diabetes.
5 4 3 2 1

298
Self-efficacy for diabetes4
We would like to know how confident you are in doing certain activities. For each of the following questions, please circle the number that corresponds to your confidence that you can do the tasks regularly at the present time.
C.58 How confident do you feel that you can eat three regular meals every day?
C.59 How confident do you feel that you can eat healthy food when you have to prepare or share food with other people who do not have diabetes?
C.60 How confident do you feel that you can choose appropriate healthy foods to eat?
C.61 How confident do you feel that you can get healthy food to eat every day?
C.62 How confident do you feel that you can do moderate physical activity for 15 to 30 minutes, 4 to 5 times a week? (Moderate physical activity makes your heart beat faster or gives you a slight sweat)
C.63 How confident do you feel that you know when your blood sugar is low and what to do about it?
C.64 How confident do you feel that you can take your medication according to your prescription every day?
4 Diabetes Self-Efficacy Scale [Internet]. [cited 18 October 2016]. Available from:
http://patienteducation.stanford.edu/research/sediabetes.html.

299
C.65 How confident do you feel that you can judge when you are ill from your diabetes and should visit the clinic?
C.66 How confident do you feel that you can control your diabetes so that it does not interfere with the things you want to do in your daily life?
Diabetes-specific locus of control questionnaire5
Please tick the answer that best represents how much you agree or disagree with each of the following statements with regard to your diabetes.
Statement
Str
on
gly
dia
gre
e
Dis
agre
e
Mild
ly
dia
gre
e
Mild
ly
agre
e
Ag
ree
Str
on
gly
agre
e C.67 I can avoid complications 1 2 3 4 5 6
C.68 When my sugar is high it’s because of something I’ve done
1 2 3 4 5 6
C.69 Good health is a matter of luck 1 2 3 4 5 6
C.70 Regular clinic visits avoid problems 1 2 3 4 5 6
C.71 What I do is the main influence on my health
1 2 3 4 5 6
C.72 Avoiding complications is a matter of luck
1 2 3 4 5 6
C.73 I should visit the clinic whenever I feel sick
1 2 3 4 5 6
C.74 My blood sugars levels are out of 1 2 3 4 5 6
5 Trento M, Passera P, Miselli V, Bajardi M, Borgo E, Tomelini M, et al. Evaluation
of the locus of control in patients with type 2 diabetes after long-term management by group care. Diabetes Metab. 2006;32(1):77-81.

300
Statement
Str
on
gly
dia
gre
e
Dis
agre
e
Mild
ly
dia
gre
e
Mild
ly
agre
e
Ag
ree
Str
on
gly
agre
e
my control
C.75 Blood sugars are controlled by luck 1 2 3 4 5 6
C.76 I should only do what my doctor or nurse tells me
1 2 3 4 5 6
C.77 I never know why my diabetes is out of control
1 2 3 4 5 6
C.78 I rely on the doctor or nurse to keep me healthy
1 2 3 4 5 6
C.79 My family is a big help in controlling my diabetes
1 2 3 4 5 6
C.80 When my blood sugar is high it’s because I’ve made a mistake
1 2 3 4 5 6
C.81 Good control of my diabetes is a matter of luck
1 2 3 4 5 6
C.82 Complications are the result of my carelessness
1 2 3 4 5 6
C.83 I am responsible for looking after my diabetes
1 2 3 4 5 6
C.84 Other people have a big responsibility for looking after my diabetes
1 2 3 4 5 6
PART D: DIABETES BEHAVIORS6
The following questions ask about your diabetes self-care activities during the past 7 days. If you were sick during the past 7 days, please think back to the last 7 days that you were not sick.
6 Mulcahy K, Maryniuk M, Peeples M, Peyrot M, Tomky D, Weaver T, et al.
Diabetes self-management education core outcomes measures. Diabetes Educ. 2003;29(5):768-70.

301
Diet
D.1 How many of the last SEVEN DAYS have you followed a healthful eating plan?
0 1 2 3 4 5 6 7
D.2 On average, over the past month, how many DAYS PER WEEK have you followed your eating plan?
0 1 2 3 4 5 6 7
D.3 On how many of the last SEVEN DAYS did you eat five or more servings of fruits and vegetables?
0 1 2 3 4 5 6 7
D.4 On how many of the last SEVEN DAYS did you eat high fat foods such as red meat or full-fat dairy products?
0 1 2 3 4 5 6 7
D.5 On how many of the last SEVEN DAYS did you space carbohydrates evenly through the day?
0 1 2 3 4 5 6 7
Exercise
D.6 On how many of the last SEVEN DAYS did you participate in at least 30 minutes of physical activity? (Total minutes of continuous activity, including walking).
0 1 2 3 4 5 6 7
D.7 On how many of the last SEVEN DAYS did you participate in a specific exercise session (such as swimming, walking, biking) other than what you do around the house or as part of your work?
0 1 2 3 4 5 6 7
Blood sugar testing
D.8 On how many of the last SEVEN DAYS did you test your blood sugar?
0 1 2 3 4 5 6 7
D.9 On how many of the last SEVEN DAYS did you test your blood sugar the number of times recommended by your health care provider?
0 1 2 3 4 5 6 7

302
Medications
D.10 Has insulin injection been recommended to you?
YES No
D.10.1 If YES: On how many of the last SEVEN DAYS did you take your recommended insulin injections?
0 1 2 3 4 5 6 7
D.11 Have diabetes pills been recommended to you?
YES No
D.11.1 If YES: On how many of the last SEVEN DAYS did you take your recommended number of diabetes pills?
0 1 2 3 4 5 6 7
Foot care
D.12 On how many of the last SEVEN DAYS did you check your feet?
0 1 2 3 4 5 6 7
D.13 On how many of the last SEVEN DAYS did you inspect the inside of your shoes?
0 1 2 3 4 5 6 7
D.14 On how many of the last SEVEN DAYS did you wash your feet?
0 1 2 3 4 5 6 7
D.15 On how many of the last SEVEN DAYS did you soak your feet?
0 1 2 3 4 5 6 7
D.16 On how many of the last SEVEN DAYS did you dry between your toes after washing?
0 1 2 3 4 5 6 7
Smoking
D.17 Have you smoked a cigarette—even one puff—during the past SEVEN DAYS?
0 No 1 Yes

303
D.17.1 If Yes, how many cigarettes did you smoke on an average day?
Number of cigarettes:............................................
D.17.2 When did you last smoke a cigarette?
1 More than two years ago, or never smoked 2 One to two years ago 3 Four to twelve months ago 4 One to three months ago 5 Within the last month 6 Today
Problem solving
The next questions ask about which of the following diabetes issues are currently a problem for you? Tick the number that best describes your degree of difficulty. Please provide an answer for each question.
D.18 Feeling scared when you think about living with diabetes?
Not a problem
Minor problem
Moderate problem
Somewhat serious problem
Serious problem
0 1 2 3 4
D.19 Feeling depressed when you think about living with diabetes?
Not a problem
Minor problem
Moderate problem
Somewhat serious problem
Serious problem
0 1 2 3 4
D.20 Worrying about the future and the possibility of serious complications?
Not a problem Minor
problem Moderate problem
Somewhat serious problem
Serious problem
0 1 2 3 4
D.21 Feeling that diabetes is taking up too much of your mental and physical energy every day?
Not a problem Minor
problem Moderate problem
Somewhat serious problem
Serious problem
0 1 2 3 4

304
D.22 Coping with complications of diabetes?
Not a problem
Minor problem
Moderate problem
Somewhat serious problem
Serious problem
0 1 2 3 4
Coping
People differ in their thoughts and feelings about having diabetes. We would like to know how you feel about having diabetes. Therefore, please circle the answer to each question which is closest to the way you feel. Please give your honest feelings – we are interested in how you feel, not what your doctor or family may think.
D.23 How upsetting is having diabetes for you?
Not at all Slightly upsetting
Moderately upsetting
Very upsetting Extremely upsetting
1 2 3 4 5
D.24 How much control over your diabetes do you have?
None at all Slight
amount Moderate amount Large amount Total amount
1 2 3 4 5
D.25 How much uncertainty do you currently experience in your life as a result of being diabetic?
None at all Slight
amount Moderate amount Large amount
Extremely large amount
1 2 3 4 5
D.26 How likely is your diabetes to worsen over the next several years? (Try to give an estimate based on your personal feeling rather than based on a rational judgment.)
Not likely at all
Slightly likely
Moderately likely Very likely Extremely likely
1 2 3 4 5
D.27 Do you believe that achieving good diabetic control is due to your efforts as compared to factors which are beyond your control?
Totally because of
me
Mostly because
of me
Partly because of me and partly
because of other factors
Mostly because of other factors
Totally because of other factors
1 2 3 4 5

305
D.28 How effective are you in coping with your diabetes?
Not at all Slightly effective
Moderately effective Very effective Extremely effective
1 2 3 4 5
D.29 To what degree does your diabetes get in the way of your developing life goals?
None at all Slight
amount Moderate amount Large amount
Extremely large amount
1 2 3 4 5
PART E: HEALTH OUTCOMES
E.1 HbA1c value
.
Medication
The next question asks about your current diabetes medication.
E.2 Which of the following medications for your diabetes has your doctor [actually] prescribed? Please mark all that apply:
1 An insulin shot 1 or 2 times a day.
2 An insulin shot 3 or more times a day.
3 Diabetes pills to control my blood sugar level.
4 Other – please specify: .....................................................................................
5 I have been prescribed neither insulin nor pills for my diabetes.

306
Bodyweight
The next two questions deal with your bodyweight and Body Mass Index (BMI) (relation of body weight and body height).
E.3 How tall are you? (approximately)
…………………………………………….. cm
E.4 How much do you weigh? (approximately)
…………………………………………….. kg
General health and well-being7
The next 5 questions ask about your general health.
E.5 In general, would you say your health is:
Excellent Very good Good Fair Poor 1 2 3 4 5
E.6 I seem to get sick a little easier than other people
Definitely true Mostly true Don’t know Mostly false Definitely false 1 2 3 4 5
E.7 I am as healthy as anybody I know
Definitely true Mostly true Don’t know Mostly false Definitely false 1 2 3 4 5
E.8 I expect my health to get worse
Definitely true Mostly true Don’t know Mostly false Definitely false 1 2 3 4 5
E.9 My health is excellent
Definitely true Mostly true Don’t know Mostly false Definitely false 1 2 3 4 5
7 Röthlin FP, Jürgen M.; Ganahl, Kristin. . Protocol for a pre-post evaluation study
on the effectiveness of existing DSM programs. (Working paper, The diabetes literacy project. 2014.

307
Well-being
The next 5 questions ask about your well-being. Please indicate for each of the five statements, which is closest to how you have been feeling over the last two weeks.
E.10 I have felt cheerful and in good spirits
All of the time
Most of the time
More than half of the
time
Less than half of the time
Some of the time
At no time
5 4 3 2 1 0
E.11 I have felt calm and relaxed
All of the time
Most of the time
More than half of the
time
Less than half of the time
Some of the time
At no time
5 4 3 2 1 0
E.12 I have felt active and vigorous
All of the time
Most of the time
More than half of the
time
Less than half of the time
Some of the time
At no time
5 4 3 2 1 0
E.13 I woke up feeling fresh and rested
All of the time
Most of the time
More than half of the
time
Less than half of the time
Some of the time
At no time
5 4 3 2 1 0
E.14 My daily life has been filled with things that interest me
All of the time
Most of the time
More than half of the
time
Less than half of the time
Some of the time
At no time
5 4 3 2 1 0

308

309
APPENDIX D
INTERVIEW GUIDE: CARE-PLAN BOOKLET
AND MEDICAL CONSULTATION EVALUATION
PART A: FOR PATIENTS
Notes to the interviewer:
Make sure participant(s) have their booklets with them, as there may be
points where you or a participant may want to refer to a specific page in the
booklet.
Use probes only if the information or viewpoints on that specific topic has
not been spontaneously divulged in any of the participant(s)’ responses to
previous questions.
1. Icebreaker: Tell me a bit more about what you think of diabetes.
Probes:
- How long ago were you diagnosed with diabetes?
- What was your reaction when you heard your diagnosis?
- Do you have any children or grandchildren?
- Do you have any worries about diabetes?
2. Did you use the care-plan booklet?
Probes:
If Yes:
- How did your use it?
- Did you write any questions or advice from provider?
- Which part was most interesting to you?
- Which part did you like most?
- What did you not like about the whole intervention?
If No:
- What made you to not use the care-plan booklet?
- Do you think you can overcome these barriers?
3. Tell me something that you learnt from using the booklet?

310
Probes:
- While at home or during consultation
4. Did your health provider use the booklet with you during the medical
consultations?
Probes:
If Yes:
- How did it feel/ did you like discussion?
- Do you think you can continue doing it?
- What are the potential barriers that could stop you?
- What could make it easier?
If No:
- What do you think made the provider not to use the booklet?
- Do you think these barriers could be avoided?
5. Did you always bring the booklet for consultation?
Probes:
If Yes:
- What made it easy for you?
If No:
- What made you not to bring the booklet to consultations?
6. Did you use the booklet at home?
Probes:
If Yes:
- Did you share the booklet with anyone?
If No:,
- What made you not to use the booklet at home?
7. Was the booklet useful to you?
Probes:
If Yes:
- How was the booklet useful?
If No:
- How was the booklet not useful?
8. Tell me what you think about the booklet?
Probes:
- Colour
- Content
- Pictures

311
9. Do you think there is information that you would have liked to know
but was not covered? Please explain.
10. Was the booklet easy to use?
If Yes: How?
If No: How?
11. Have you received any of your annual check-ups?
If Yes: Which ones?
If No: Do you know when you will get them?
12. Tell me about the changes you have made in your lifestyle?
13. What advice would you give us if we were to develop another
booklet?

312
PART B: FOR HEALTH CARE PROVIDERS
Notes to the interviewer:
Make sure participant(s) have their booklets with them, as there may be
points where you or a participant may want to refer to a specific page in the
booklet.
Use probes only if the information or viewpoints on that specific topic has
not been spontaneously divulged in any of the participant(s)’ responses to
previous questions.
1. What do you think about using the booklet during consultations?
Probes:
- Was it easy?
- What made it easy
- What made it difficult?
2. Did you follow the guidelines of using the booklet?
Probes:
- What made it easy to follow guidelines
- What made it difficult
3. Was the booklet useful during consultation?
Probes:
- How was it useful?
- How was it not useful?
4. Did any of the patients forget their booklet at home?
Probes:
- Did you remind patients to produce the booklet?
- What do you think made them to forget?
5. Tell me about what you think can make the use of this booklet easier?
6. What do you think of the booklet?
Probes:
- The content
- The pictures

313
7. How much time do you spent with the patient when using the
booklet?
8. Do you think this booklet can be implemented on a larger scale?
9. Do you think we can add or remove some information?
10. What advice would you give us if we were to develop another
booklet?
11. Are you going to continue using the booklet?

314