
Theory-Based Approaches to Understanding Public Emergency Preparedness: Implications for Effective...
18
PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [Michigan State University] On: 28 July 2010 Access details: Access Details: [subscription number 918013331] Publisher Taylor & Francis Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37- 41 Mortimer Street, London W1T 3JH, UK Journal of Health Communication Publication details, including instructions for authors and subscription information: http://www.informaworld.com/smpp/title~content=t713666566 Theory-Based Approaches to Understanding Public Emergency Preparedness: Implications for Effective Health and Risk Communication Hye-Jin Paek a ; Karen Hilyard b ; Vicki Freimuth c ; J. Kevin Barge d ; Michele Mindlin e a Department of Advertising, Public Relations, & Retailing, College of Communications Arts & Sciences, Michigan State University, East Lansing, Michigan, USA b School of Advertising & Public Relations, College of Communication and Information, University of Tennessee, Knoxville, Tennessee, USA c Department of Speech Communication and the Grady School of Journalism and Mass Communication, University of Georgia, Athens, Georgia, USA d Department of Communication, Texas A&M University, College Station, Texas, USA e Georgia Division of Public Health, Atlanta, Georgia, USA Online publication date: 21 June 2010 To cite this Article Paek, Hye-Jin , Hilyard, Karen , Freimuth, Vicki , Barge, J. Kevin and Mindlin, Michele(2010) 'Theory- Based Approaches to Understanding Public Emergency Preparedness: Implications for Effective Health and Risk Communication', Journal of Health Communication, 15: 4, 428 — 444 To link to this Article: DOI: 10.1080/10810731003753083 URL: http://dx.doi.org/10.1080/10810731003753083 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
Transcript of Theory-Based Approaches to Understanding Public Emergency Preparedness: Implications for Effective...
PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [Michigan State University]On: 28 July 2010Access details: Access Details: [subscription number 918013331]Publisher Taylor & FrancisInforma Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Journal of Health CommunicationPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713666566
Theory-Based Approaches to Understanding Public EmergencyPreparedness: Implications for Effective Health and Risk CommunicationHye-Jin Paeka; Karen Hilyardb; Vicki Freimuthc; J. Kevin Barged; Michele Mindline
a Department of Advertising, Public Relations, & Retailing, College of Communications Arts &Sciences, Michigan State University, East Lansing, Michigan, USA b School of Advertising & PublicRelations, College of Communication and Information, University of Tennessee, Knoxville, Tennessee,USA c Department of Speech Communication and the Grady School of Journalism and MassCommunication, University of Georgia, Athens, Georgia, USA d Department of Communication, TexasA&M University, College Station, Texas, USA e Georgia Division of Public Health, Atlanta, Georgia,USA
Online publication date: 21 June 2010
To cite this Article Paek, Hye-Jin , Hilyard, Karen , Freimuth, Vicki , Barge, J. Kevin and Mindlin, Michele(2010) 'Theory-Based Approaches to Understanding Public Emergency Preparedness: Implications for Effective Health and RiskCommunication', Journal of Health Communication, 15: 4, 428 — 444To link to this Article: DOI: 10.1080/10810731003753083URL: http://dx.doi.org/10.1080/10810731003753083
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

Theory-Based Approaches to Understanding PublicEmergency Preparedness: Implications for Effective
Health and Risk Communication
HYE-JIN PAEK
Department of Advertising, Public Relations, & Retailing,College of Communications Arts & Sciences, Michigan State University,East Lansing, Michigan, USA
KAREN HILYARD
School of Advertising & Public Relations, College of Communicationand Information, University of Tennessee, Knoxville,Tennessee, USA
VICKI FREIMUTH
Department of Speech Communication and the Grady Schoolof Journalism and Mass Communication, University of Georgia,Athens, Georgia, USA
J. KEVIN BARGE
Department of Communication, Texas A&M University,College Station, Texas, USA
MICHELE MINDLIN
Georgia Division of Public Health, Atlanta, Georgia, USA
Recent natural and human-caused disasters have awakened public health officials tothe importance of emergency preparedness. Guided by health behavior and mediaeffects theories, the analysis of a statewide survey in Georgia reveals thatself-efficacy, subjective norm, and emergency news exposure are positively associa-ted with the respondents’ possession of emergency items and their stages of emerg-ency preparedness. Practical implications suggest less focus on demographics as thesole predictor of emergency preparedness and more comprehensive measures of
This research is a part of emergency and disaster preparedness project, supported by theGeorgia Department of Human Resources–Public Health Division, with funds from the U.S.Department of Health and Human Services, Centers for Disease Control and Prevention. Anearlier version of this article was presented at the 2008 National Communication AnnualConvention in San Diego, CA, November 21–24.
Address correspondence to Hye-Jin Paek, Department of Advertising, Public Relations,& Retailing, College of Communication Arts & Science, Michigan State University, 320 CAS,East Lansing, MI 48824, USA. E-mail: [email protected]
Journal of Health Communication, 15:428–444, 2010Copyright # Taylor & Francis Group, LLCISSN: 1081-0730 print=1087-0415 onlineDOI: 10.1080/10810731003753083
428
Downloaded By: [Michigan State University] At: 00:40 28 July 2010

preparedness, including both a person’s cognitive stage of preparedness andchecklists of emergency items on hand. We highlight the utility of theory-basedapproaches for understanding and predicting public emergency preparedness as away to enable more effective health and risk communication.
Following a series of natural and human-caused disasters ranging from HurricaneKatrina to 9=11 to epidemic disease outbreaks such as West Nile virus and avianflu, the public’s level of emergency preparedness is capturing the attention of pub-lic health officials, risk communicators, and academicians. The Federal EmergencyManagement Agency (2007) has allocated more than $16 billion for state and localgovernment initiatives to prepare for terrorism and more than $7 billion to preparethe nation for pandemic flu (Morse, Garwin, & Olsiewski, 2006) and establishednew protocols such as the National Incident Management System (NIMS) toenhance government response to disaster. Despite the intense interest in emergencyplanning and preparedness, relatively little is known about the determinants of thepublic’s level of emergency preparedness beyond demographic characteristics. Thisstudy explores the extent to which three key predictors—efficacy, perceived norm,and attention to emergency-related news media—are related to levels of emergencypreparedness. Drawing on literature from social psychology, persuasion, publichealth, and mass communication, we highlight the theoretical rationale for select-ing these three predictors. Our analysis of a statewide emergency preparedness sur-vey provides several practical implications for public health officials and riskcommunication practitioners when designing messages to promote emergency pre-paredness.
Emergency Preparedness as a Critical Public Health and Safety Issue
Emergency preparedness refers to the capability of individuals, as well as public healthand risk organizations and communities, ‘‘to prevent, protect against, quickly respondto, and recover from emergencies’’ (Nelson, Lurie, Wasserman, & Zakowski, 2007,p. S9). The term ‘‘emergency’’ connotes the sense of a sudden and unexpected onsetof a disaster, but it also can be applied to other situations, which may not reach the levelof ‘‘disaster.’’ From a public health perspective, emergencies tend to be characterized bydisruptions in essential services, such as utilities, transportation, and food supply; thepotential damage or destruction of dwellings and businesses; and the need for evacu-ation or rescue. Although many different checklists exist to help citizens prepare, themost common emergencies such as fires, floods, hurricanes, and earthquakes requirea similar set of supplies; human-caused emergencies such as terrorism and industrialaccidents often build on the same lists. Accordingly, we take this broader conceptionof emergency and consider preparedness as a coordinated and continuous process ofplanning to take corrective action (Nelson et al., 2007).
The majority of research related to emergency management deals with responserather than preparation (McEntire & Myers, 2004). Studies of emergency prepared-ness behavior among the public primarily have been confined to descriptive statisticsof degrees of preparedness or to scrutinizing government actions, with little attentionbeing paid to predictors other than demographic characteristics. Also absent in theresearch is any examination of preparedness campaigns within the context of a con-tinuum or staged process—a critical oversight, given that being prepared for an
Public Emergency Preparedness 429
Downloaded By: [Michigan State University] At: 00:40 28 July 2010

emergency is not an all-or-nothing proposition, but a process in which people mayadopt recommended precautions incrementally.
Existing literature reveals that Americans generally are not well prepared foremergencies, although there are some differences in preparedness levels amongparticular demographic groups (Eisenman et al., 2006; Enarson, 1998; Fothergill& Peek, 2004). For example, in a February 2007 poll, the American Public HealthAssociation (2007) found that 23% of the public had taken no steps to prepare foran emergency; 27% claimed to be prepared, but only half that group had a 3-daysupply of food, water, and medicine. First aid kits and cash on hand also were lack-ing, but even low- or no-cost preparations were overlooked, such as planning how tocommunicate with family members in an emergency. Other nationwide polls foundsimilar results, with about 23–28% of respondents not prepared at all (e.g.,American Red Cross and the Council for Excellence in Government, 2007; HarrisInteractive, 2007).
Generally, it is the poor, the elderly, and households headed by women that arebelieved to be the least likely to be prepared for emergencies (American Red Cross,2007; Morrow, 1999). Post-Hurricane Katrina studies have examined demographicdifferences in perceptions of community preparedness and the ability of the govern-ment to respond to disasters, but the same data do not exist with regard to individualor household preparedness (Perry & Lindell, 2003; Sattler, Kaiser, & Hittner, 2000;Tierney, Lindell, & Perry, 2001).
It seems that personal vulnerability and resilience also contribute to individualvariance in preparedness. Other influences on preparedness, however, appear coun-terintuitive. For example, awareness of risk is not associated with increased levels ofpreparedness. A 2002 poll of more than 8,000 residents of Los Angeles Countyshowed that despite high perceived risk in which 60% believed a terrorist attackwas likely within the next year, only 37% had emergency supplies or plans. As mightbe expected, young people and single people were found to be the least prepared.One unexpected finding was that the disabled, African Americans, and residentsborn outside the United States tended to be prepared better than other groups(Eisenman et al., 2006). This contrasts with conventional wisdom that these popula-tions are inherently more vulnerable to emergencies due to language barriers or lackof resources, indicating a need for further research.
Lessons Learned from the Past Studies: Toward Theory-BasedUnderstanding and Prediction
Inherent in many of the typical preparedness surveys such as those detailed aboveare two measures of emergency preparedness: One is defined by a checklist of howmany items have been gathered or plans made; and another describes the cognitiveprocess behind preparedness behavior, including reflexive perceptions of prepared-ness. There are both practical and theoretical reasons to discern two types ofemergency preparedness. Practically, the first measure (counting the number ofemergency items) has been employed as an indicator of preparedness by many publichealth organizations (e.g., American Red Cross, King County Office of EmergencyManagement). This measure does not capture whether people own certain emerg-ency items coincidentally or whether they deliberately have collected these items toprepare for an emergency. As a result, a measure of how mindful people are of plan-ning for emergencies may better describe, explain, and predict the public’s level of
430 H.-J. Paek et al.
Downloaded By: [Michigan State University] At: 00:40 28 July 2010

emergency preparedness. The utility of measuring the respondent’s self-appraisal ofdeliberate planning and preparation is also supported by the Transtheoretical Model(TTM). The TTM posits that people change their behavior through stages of action(Glanz, 1997; Prochaska & DiClemente, 1983; Prochaska, DiClemente, & Norcross,1992). The number of stages of action has changed over time and may vary acrosshealth contexts, but most research incorporates some version of the following fivestages: (1) precontemplation—the stage where people have no intention to changebehavior in the near future; (2) contemplation—where people are aware that a prob-lem exists and are seriously thinking about overcoming it, but they have not yetmade a commitment to take an action; (3) preparation—where people intend to takeaction and have started to make some changes; (4) action—where individuals modifytheir behavior or environment to overcome problems and reach certain goals; and (5)maintenance—in which people maintain behavior changes for at least 6 months ormore (Prochaska & DiClemente, 1983).
The TTM suggests that communication messages should be different forpeople in different stages of change. For example, action-oriented messagesmay be quite effective with individuals who are in the decision or actionstages, but these same campaigns may be ineffective with individuals inprecontemplation or contemplation stages. These individuals may not yet beaware of a need to prepare, or they may not yet be persuaded of the urgencyor efficacy of preparation (Prochaska et al., 1992). Research has shown theimportance of targeting each stage in the process to produce incrementalchange. Even moving just one stage initially, for example, from precontempla-tion to contemplation or contemplation to preparation can double the chance ofan individual’s likelihood of getting to the action stage within 6 months or inthe ‘‘near future’’ (Prochaska & Norcross, 2001). The model successfully hasbeen applied to many health contexts including smoking and drug cessation,weight control, condom use, and mammography screening (Prochaska et al.,1994).
In this study, we apply the TTM in two ways. First, we use the stages-of-change model to construct the dependent variable measuring the stage of emerg-ency preparedness actions. This allows us to examine the degrees by which peopleconsider, learn, prepare, maintain, and update emergency supplies and plans. Itmakes sense to examine behavior as it is associated with these stages, becauseresponse to emergency preparedness campaigns often is incremental or graduatedin nature, a phenomenon similar to that documented in literature from many dis-ciplines (Marcus et al., 1992; Nigg et al., 1999; Prochaska & DiClemente, 1983).Second, we use the TTM to examine some of the key theoretical concepts ordeterminants that are related to both the number of emergency items that indivi-duals have and the individual’s stage of emergency preparedness. Three importanttheoretical determinants are identified in the TTM that cut across several theoriesof behavioral change (see Slater, 1999): (1) self-efficacy; (2) normative influence;and (3) media effects.
Efficacy Hypothesis
In order to take action, a person must first recognize the existence of the problemand a need to improve the situation (also see Situational Theory in public relationsliterature; Grunig & Hunt, 1984). Second, the person must take into account any
Public Emergency Preparedness 431
Downloaded By: [Michigan State University] At: 00:40 28 July 2010

constraints that might limit their control over the situation. This idea is closelyrelated to perceived self-efficacy, which has been defined in Social Cognitive Theory(SCT; Bandura, 1997) and others (Witte, 1992) as an individual’s belief that he or sheis capable of executing a particular behavior.1 The Extended Parallel Process Model(EPPM; Witte, 1992) and Protection Motivation Theory (Rogers, 1983) also proposethat people must have the confidence to undertake the recommended behaviors.Finally, the Theory of Planned Behavior (TPB; Ajzen, 1985) also notes the signifi-cant role of perceived behavioral control in predicting behavioral intention. Similarto self-efficacy, perceived behavioral control is defined as an individual’s perceptionsof his or her ability or feelings of self-efficacy to perform a behavior. Numerousstudies have tested and confirmed that self-efficacy is a significant predictor ofbehavior or behavior change in various health and risk contexts (Glanz et al.,2002; Maddux, 1991).
Based on conceptual and empirical support from SCT, EPPM, and TPB, weoffer the following hypothesis:
H1. Self-efficacy is positively related to emergency preparedness.
Normative Influence Hypothesis
Although self-efficacy serves as an internal driving force to make people adopt arecommended risk reduction behavior (like emergency preparedness), people alsooften follow what is acceptable in society and among their significant others. Theidea of normative influence is reflected most prominently in the Theory of ReasonedAction (TRA)=Theory of Planned Behavior (TPB; Ajzen, 1985; Fishbein & Ajzen,1975). Both theories explain how behavior is influenced by the interplay amongbeliefs, attitudes, and behavioral intentions. That is, behavior is dependent onintention, which is determined by an individual’s attitude (i.e., beliefs and valuesabout the outcome of the behavior) and subjective norm (i.e., a belief about howone’s significant others think she or he should engage in the behavior). Althoughattitudes may best explain behavioral intention, subjective norm also has beenfound to explain behavioral intention to a significant extent (Gottlieb, Gingiss, &Weinstein, 1992).
While the subjective norm identified in TRA and TPB is limited in scope to aperson’s ‘‘significant others’’ (e.g., parents, close friends, spouses, children),another line of normative influence literature embraces perceived norm inbroader terms: an individual’s perception about what most people do or whatis typical or normal (also called descriptive norm by Cialdini, Reno, & Kallgren,1990). Whether subjective norm or perceived norm, the idea behind this norma-tive influence is that people are influenced by what others think and how othersbehave (Paek & Gunther, 2007).
Guided by the normative influence literature, varying levels of emergencypreparedness among individuals are likely tied to their perception of what their
1SCT proposes causal, triadic interactions among the environment (both social and physi-cal), people (and their intrinsic cognitive, affective, and biological traits), and the behavior(Bandura, 1997). In this theory, self-efficacy is critical to performing a particular behaviorsuccessfully (Glanz, Rimer, & Lewis, 2002).
432 H.-J. Paek et al.
Downloaded By: [Michigan State University] At: 00:40 28 July 2010

significant others approve of or what a majority of Americans think and do. Thus,this study proposes the following normative influence hypothesis:
H2. Subjective norm (H2–1) and perceived norm (H2–2) are positivelyrelated to emergency preparedness.
Media Effects Hypothesis
People can learn from the news media about current disasters and emergencies andhow to prepare for them. First, one of the main functions of media, ‘‘surveillance,’’ isthe watchdog function to keep people informed of what is happening in the environ-ment and aware of threats or dangers. With media monitoring the world and gath-ering and summarizing important information, people can go about their daily lives,knowing they will be alerted when something relevant or dangerous needs theirattention (Perse, 2001).
Second, through agenda setting and priming, the media play a key role not onlyin making certain issues more salient (McCombs & Reynolds, 2002) but also in alter-ing criteria for evaluating political leaders and government policies (Iyengar, 1991).
Third, media expand the boundary of an individual’s experiences, allowing themto vicariously experience various human-caused and natural emergencies such asHurricane Katrina, 9=11, and anthrax (Mutz, 1998). The vicarious experience ideaalso is supported by the SCT, which posits that people observe and learn from rolemodels and respond to an environment, in this case provided by media (Bandura,1994).
Studies of disaster news have examined its functions in communicating warningsand directives to individuals directly affected, as well as the policy implications, edu-cational potential, and emotional impact of coverage on a wider audience (Garner &Huff, 1997; Keselman, Slaughter, & Patel, 2005). While emergency-related news maymake disaster more salient to the public, coverage that emphasizes the random nat-ure of disaster may result in higher levels of fatalistic thinking (McClure, Sutton, &Sibley, 2007; Tierney et al., 2001). Therefore, the third hypothesis explores therelationship between attention to the emergency-related news and preparednessbehavior:
H3. Exposure to emergency-related media news is positively related toemergency preparedness.
Methods
Data
The study analyzed a state-representative telephone survey of 1,302 adult respon-dents age 18 and older conducted in the state of Georgia in July 2006. Georgiamay be an ideal microcosm for the study of emergencies and disasters in general,because it experiences the same disasters that many other states do, yet there is nosingle overwhelming threat like earthquakes or hurricanes that might dominate resi-dents’ thoughts. While many areas of Georgia are rural, Atlanta is the ninth largestmetropolitan statistical area in the United States. The city’s size and the presence ofinstitutions such as the Centers for Disease Control and Prevention (CDC) and
Public Emergency Preparedness 433
Downloaded By: [Michigan State University] At: 00:40 28 July 2010

Cable News Network (CNN) make it a possible terrorist target, and its importanceas a travel hub makes it a potential vector for disease.
A professional research firmwas employed to conduct the 15-minute telephone sur-vey, collected through a stratified, list-assisted, random digit-dialing (RDD) samplingmethod among the state’s general population.2 The CASRO response rate was40.5%.3 Compared with the 2006 census data, the sample appeared to slightly over-represent females (62%), Whites (69.6%), older citizens (M¼ 48.59, SD¼ 15.53), andthe better-educated (M¼ 5.06—some college education, SD¼ 1.02).
Measures
The variables used in the present analysis can be categorized into five groups, withone group serving as criterion variables and the four other groups serving as inde-pendent variables: (1) criterion variables; (a) the number of emergency items and(b) stage of emergency preparedness; (2) control variables: (a) demographics (gender,race, age, and the number of children at home), (b) social structural variables (socialstatus, home ownership), (c) residential area, and (d) past experience; and (3) mainpredictors: (a) respondents’ own beliefs and perceptions—self-efficacy, subjectivenorm, and perceived norm regarding emergency preparedness; and (b) exposure toemergency-related media news. Question items were drawn from existing literatureand modified to fit the study context. Appendix A reports the individual questionitems used to operationalize the variables. Table 1 reports descriptive statistics forall the variables used in the study.
The number of emergency items was measured by counting the number ofactual emergency supplies people possessed. The survey asked a series of ‘‘yes’’or ‘‘no’’ questions about specific preparedness behaviors and supplies. Thequestion items were drawn from other emergency preparedness programs (e.g.,King County Office of Emergency Management; American Red Cross) and con-firmed by public health officials. Due to the limited time of a telephone interview,the Computer-Aided-Telephone-Interview (CATI) system randomly divided thesample into two groups (N¼ 654 and 648), each of which was asked either 10
2Using a multistage sampling method, all possible telephone numbers were divided intoblocks that were defined by the last two digits of a 10-digit phone number. Strict procedureswere implemented to improve response rate and to ensure that the hard-to-reach respondentshad a chance to be interviewed, including the following: (1) a requirement of distributing callattempts by each interviewer at different times across different days; and (2) strict call-backrules stipulating that a number could not be abandoned unless it had been verified as beinginvalid or attempted at least 25 times. Within each household, the interviewer randomly selec-ted the adult in the household who most recently celebrated a birthday in order to randomizewithin-household selection and to prevent bias associated with only speaking to the personwho answers the telephone. The survey was composed of two sections: (a) one about emerg-ency preparedness in general; and (b) the other soliciting citizens’ knowledge and perceptionsof avian flu and pandemic flu. The present analysis is based on the first section of the survey,where respondents were asked about their media use and attention related to emergency news,their perceptions and self-reported knowledge about emergency preparedness, various emerg-ency supplies that they currently owned, and their stages of emergency preparedness.
3The CASRO rate is a formula suggested by the Council of American Survey ResearchOrganizations (CASRO) and is largely used in nationwide and statewide surveys (e.g., Beha-vioral Risk Factor Surveillance System). Similar to American Association for Public OpinionResearch (AAPOR) response rate formula 3, the CASRO rate was calculated as the number ofinterviews divided by the number of known and unknown eligible cases.
434 H.-J. Paek et al.
Downloaded By: [Michigan State University] At: 00:40 28 July 2010
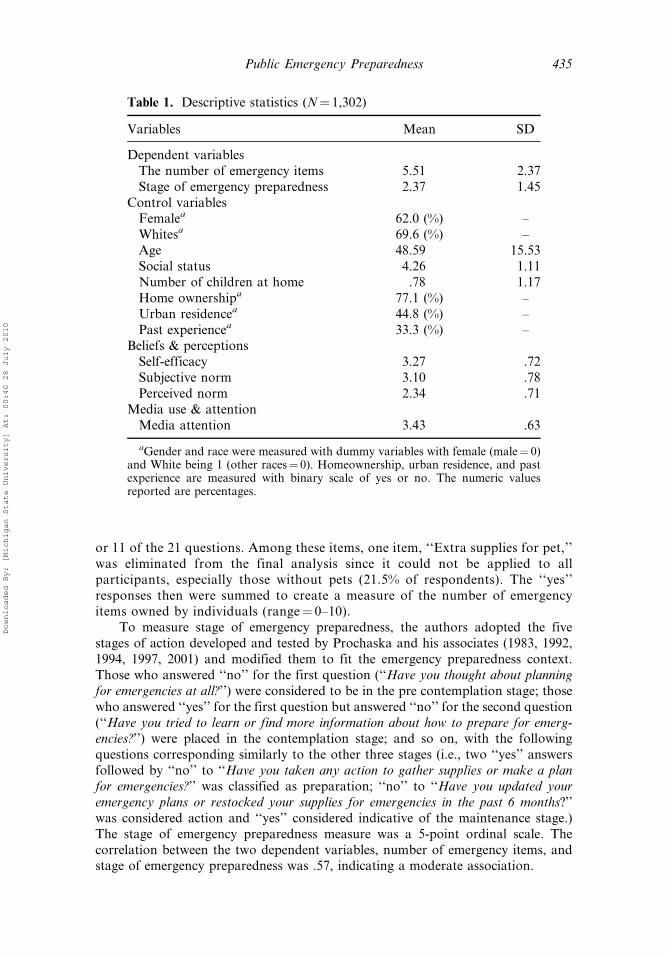
or 11 of the 21 questions. Among these items, one item, ‘‘Extra supplies for pet,’’was eliminated from the final analysis since it could not be applied to allparticipants, especially those without pets (21.5% of respondents). The ‘‘yes’’responses then were summed to create a measure of the number of emergencyitems owned by individuals (range¼ 0–10).
To measure stage of emergency preparedness, the authors adopted the fivestages of action developed and tested by Prochaska and his associates (1983, 1992,1994, 1997, 2001) and modified them to fit the emergency preparedness context.Those who answered ‘‘no’’ for the first question (‘‘Have you thought about planningfor emergencies at all?’’) were considered to be in the pre contemplation stage; thosewho answered ‘‘yes’’ for the first question but answered ‘‘no’’ for the second question(‘‘Have you tried to learn or find more information about how to prepare for emerg-encies?’’) were placed in the contemplation stage; and so on, with the followingquestions corresponding similarly to the other three stages (i.e., two ‘‘yes’’ answersfollowed by ‘‘no’’ to ‘‘Have you taken any action to gather supplies or make a planfor emergencies?’’ was classified as preparation; ‘‘no’’ to ‘‘Have you updated youremergency plans or restocked your supplies for emergencies in the past 6 months?’’was considered action and ‘‘yes’’ considered indicative of the maintenance stage.)The stage of emergency preparedness measure was a 5-point ordinal scale. Thecorrelation between the two dependent variables, number of emergency items, andstage of emergency preparedness was .57, indicating a moderate association.
Table 1. Descriptive statistics (N¼ 1,302)
Variables Mean SD
Dependent variablesThe number of emergency items 5.51 2.37Stage of emergency preparedness 2.37 1.45
Control variablesFemalea 62.0 (%) –Whitesa 69.6 (%) –Age 48.59 15.53Social status 4.26 1.11Number of children at home .78 1.17Home ownershipa 77.1 (%) –Urban residencea 44.8 (%) –Past experiencea 33.3 (%) –
Beliefs & perceptionsSelf-efficacy 3.27 .72Subjective norm 3.10 .78Perceived norm 2.34 .71
Media use & attentionMedia attention 3.43 .63
aGender and race were measured with dummy variables with female (male¼ 0)and White being 1 (other races¼ 0). Homeownership, urban residence, and pastexperience are measured with binary scale of yes or no. The numeric valuesreported are percentages.
Public Emergency Preparedness 435
Downloaded By: [Michigan State University] At: 00:40 28 July 2010

Self-efficacy was measured with a single item, ‘‘How confident are you aboutyour own ability to manage an emergency?’’ with a 4-point scale ranging from‘‘not at all confident (1)’’ to ‘‘very much confident (4).’’
Subjective norm was measured with a single item, ‘‘To what extent do most ofyour family or friends think you personally should prepare for an emergency?’’ witha 4-point scale ranging from ‘‘not at all (1)’’ to ‘‘very much (4).’’
Perceived norm was measured with a one-item question, ‘‘How well prepared doyou think most people in the U.S. are for an emergency?’’ with a 4-point scaleranging from ‘‘not at all prepared (1)’’ to ‘‘very much prepared (4).’’
To measure media use, participants were asked about the amount of attentionthey paid to emergency preparedness news using a 4-point scale (1¼‘‘no attentionat all,’’ to 4¼ ‘‘very close attention’’). The Exploratory Factor Analysis (EFA) resultshows that the four items clearly constituted one factor explaining 59.8% of the totalvariance (Cronbach’s alpha¼ .76). The four items were averaged to create an indexof attention to emergency news, with a higher score indicating a higher level ofattention.
For control variables, guided by existing risk communication literature (e.g.,Griffin & Dunwoody, 2000), the authors included gender, age, race (White as adummy variable), number of children at home, social status, home ownership, resi-dential area (i.e., urban=rural), and past experiences with various emergency situa-tions (see Paek, Yoon, & Shah, 2005; Tierney et al., 2001, for the relevant rationales).
For social status, an averaging index of education and income was created(6-point scale), because the two variables often represent individuals’ socioeconomicstatus and are highly correlated (inter-item correlation¼ .50; see Griffin &Dunwoody, 2000, for the same measure).
Analytic Strategy
First, the variables were evaluated to see if they violated normality assumptions thatmight threaten the results. Diagnostic statistics using skewness and kurtosis showedthat the normality assumption was not violated.
Second, two hierarchical multiple regression models were computed to assess thepredictive value of all the variables on the two dependent variables, the number ofemergency items and stage of emergency preparedness. In the regression models,predictors were entered in the following order: control variables (demographics,social structural variables, and past experience), respondents’ own beliefs andperceptions, and then media attention variables (see Table 2). Although the stage ofemergency preparedness is measured with an ordinal scale (that is not truly an intervalscale), the diagnostic statistics indicate normal distributions without any outliers ortruncation of the data. Ordinary least squares (OLS) regression was used because ityields results similar to those from ordinal techniques such as probit or logit modelsbut allows clearer interpretations (Fox, 1991; Knoke & Bohrnstedt, 1994).
Results
H1. Efficacy Hypothesis
Hypothesis 1 predicted that the more confident people are about their ability to pre-pare for an emergency, the more likely they will have emergency items and the higher
436 H.-J. Paek et al.
Downloaded By: [Michigan State University] At: 00:40 28 July 2010
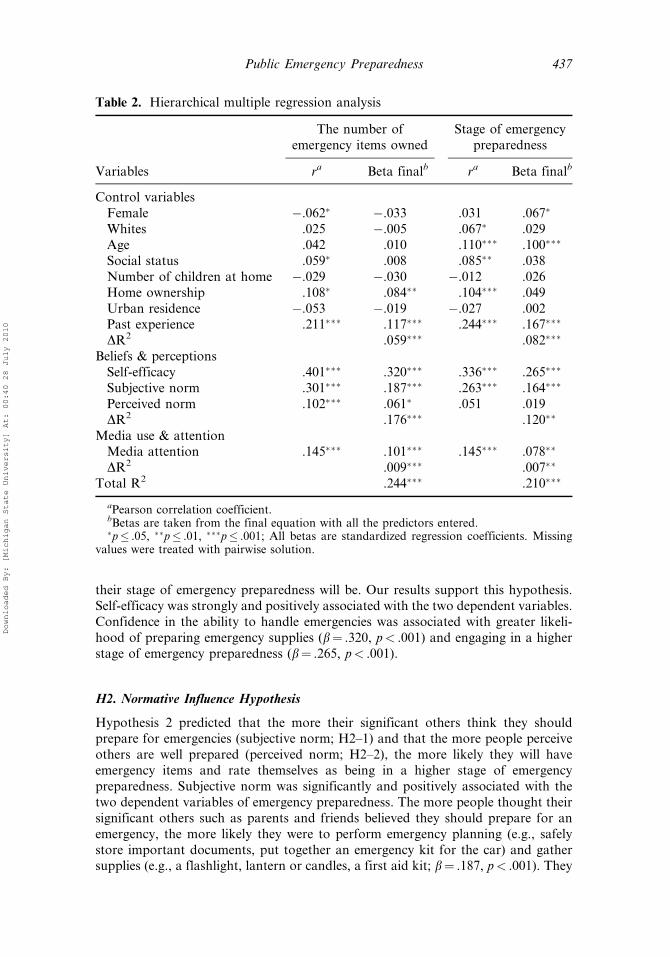
their stage of emergency preparedness will be. Our results support this hypothesis.Self-efficacy was strongly and positively associated with the two dependent variables.Confidence in the ability to handle emergencies was associated with greater likeli-hood of preparing emergency supplies (b¼ .320, p< .001) and engaging in a higherstage of emergency preparedness (b¼ .265, p< .001).
H2. Normative Influence Hypothesis
Hypothesis 2 predicted that the more their significant others think they shouldprepare for emergencies (subjective norm; H2–1) and that the more people perceiveothers are well prepared (perceived norm; H2–2), the more likely they will haveemergency items and rate themselves as being in a higher stage of emergencypreparedness. Subjective norm was significantly and positively associated with thetwo dependent variables of emergency preparedness. The more people thought theirsignificant others such as parents and friends believed they should prepare for anemergency, the more likely they were to perform emergency planning (e.g., safelystore important documents, put together an emergency kit for the car) and gathersupplies (e.g., a flashlight, lantern or candles, a first aid kit; b¼ .187, p< .001). They
Table 2. Hierarchical multiple regression analysis
The number ofemergency items owned
Stage of emergencypreparedness
Variables ra Beta finalb ra Beta finalb
Control variablesFemale �.062� �.033 .031 .067�
Whites .025 �.005 .067� .029Age .042 .010 .110��� .100���
Social status .059� .008 .085�� .038Number of children at home �.029 �.030 �.012 .026Home ownership .108� .084�� .104��� .049Urban residence �.053 �.019 �.027 .002Past experience .211��� .117��� .244��� .167���
DR2 .059��� .082���
Beliefs & perceptionsSelf-efficacy .401��� .320��� .336��� .265���
Subjective norm .301��� .187��� .263��� .164���
Perceived norm .102��� .061� .051 .019DR2 .176��� .120��
Media use & attentionMedia attention .145��� .101��� .145��� .078��
DR2 .009��� .007��
Total R2 .244��� .210���
aPearson correlation coefficient.bBetas are taken from the final equation with all the predictors entered.�p� .05, ��p� .01, ���p� .001; All betas are standardized regression coefficients. Missing
values were treated with pairwise solution.
Public Emergency Preparedness 437
Downloaded By: [Michigan State University] At: 00:40 28 July 2010
were also in a higher stage of emergency preparedness (b¼ .164, p< .001). Bycontrast, the respondents’ perception that average Americans were well preparedwas positively related to the number of emergency items (b¼ .061, p< .05), butnot to the stage of emergency preparedness (b¼ .019, p¼ ns). Even at a bivariatelevel, perceived norm was only marginally significantly related to the stage ofemergency preparedness (r¼ .051, p¼ .068) and became nonsignificant when theother predictors were controlled in the model.
H3. Media Effects Hypothesis
Last, Hypotheses 3 predicted that the more people are exposed to emergency-relatednews in media, the more likely they will have emergency items and rate themselves asbeing in a stage of emergency preparedness. This hypothesis was strongly supported.The more attentive people were to news about various emergencies delivered by tele-vision, radio, newspaper, and the Internet, the more likely they were to have emerg-ency items (b¼ .101, p< .001) and to engage in a higher stage of preparation actions(b¼ .078, p< .01). Although the variance explained by the media exposure variablewas small, it significantly contributed to the regression models (DR2¼ .009 for thenumber of emergency items model and DR2¼ .007 for the stage of emergency pre-paredness model).
Overall, the two regression models, respectively, accounted for more than 24%and 21% of total variance explained in the two dependent variables.
Discussion
This study explored three promising theoretical concepts (i.e., self-efficacy, subjectiveand perceived norm) and media exposure as critical determinants of the public’semergency preparedness. Two emergency preparedness variables were constructed,one for the number of emergency items that individuals actually possessed and theother for stage of emergency preparedness based on the TTM.
The findings suggest that, in general, only about half the respondents tended toprepare with specific emergency supplies, consistent with the Readiness QuotientPublic Opinion Survey that reported a less-than-desired level of emergency prepared-ness (American Red Cross, 2007). The finding may imply that the public is not clearabout what to prepare other than basic emergency kits, or some emergency items(e.g., flashlight, first aid kit) may be more easily purchased and prepared, whileothers (e.g., dust mask, generator) may not. Measuring level of emergency prepared-ness using the number of emergency items, however, may not capture the deliberateintention to prepare better. Employing the stage of emergency preparedness guidedby TTM may provide a more nuanced and alternative way of assessing the public’semergency preparedness.
Indeed, the stage of emergency preparedness shows a somewhat different picturefrom the number of emergency items that the respondents actually own. The data showthat more than half of the respondents have taken some action related to emergency pre-paredness (action: 24.0%) or updated their emergency plans, restocked emergency sup-plies, or both activities in the past 6 months (maintenance: 30.5%). About one-third ofthe respondents however, said that they have either not thought about preparing foremergencies at all or have thought about it but have not sought more information abouthow to prepare. Given that consideration or information seeking is a necessary step for
438 H.-J. Paek et al.
Downloaded By: [Michigan State University] At: 00:40 28 July 2010
an individual to engage in actual emergency preparation behaviors (Prochaska et al.,1992, 1994), these pre-contemplative individuals may constitute a much different audi-ence than those who are at later stages of action.
Beyond the description of how well people are prepared, the main focus was toidentify predictors of emergency preparedness. The data demonstrate that most ofthe theoretical concepts tested in this study contribute to predicting respondents’possession of emergency items and stage of emergency preparedness but with somedifferent patterns: subjective norm was strongly related to both dependent variables,but perceived norm was related only to possession of emergency items, not stage ofpreparedness. This reflects the relatively stronger predictive value of subjective normover perceived norm documented in empirical studies (Campo et al., 2003) and thetendency to follow reference group or in-group norms rather than nonreference orout-group norms (Hyman, 1968; Sherif & Sherif, 1964). The nonsignificant associ-ation between perceived norm and stage of emergency preparedness in our studymay be due to the referent (i.e., people in the United States) that was provided toparticipants in the survey question. According to the peer proximity and socialdistance premises, people seemed more influenced by perception of ‘‘others’’ whoare more similar to themselves in terms of demographic and psychographiccharacteristics (Paek & Gunther, 2007). The results may have been different if weused more similar and closer others, such as residents of the same state or eventhe same neighborhood. Future research should investigate this possibility in variousemergency contexts.
Last, attention to media news about emergencies such as human-caused andnatural disasters and pandemic flu seems to play a significantly positive role inemergency preparedness. It may imply that news media can inform and educatethe public about what should be prepared for emergencies (Bryant & Thompson,2002; Perse, 2001). Media also can play an agenda-setting role, alerting the publicto the importance of emergency preparedness (McCombs & Reynolds, 2002), whichmakes it critical that public health and risk communication practitioners sustainmedia interest in this topic.
Limitations
First, some of the single-item measures may lack reliability, and an importantdirection for future research will be developing and testing more robust measuresof the most important variables in an emergency preparedness context.
Second, although Georgia experiences many types of natural disasters (tor-nadoes, hurricanes, flooding, wildfires), it is not as disaster prone as states such asthose in tornado alley, near earthquake faults, or on the hurricane-prone Gulf Coast;therefore, our results may not be generalizable to those areas.
Third, due to the nature of the cross-sectional data, all the findings should beinterpreted as correlation rather than causation. For example, those who pay themost attention to news coverage of emergencies may be a self-selecting group whoalready think or worry more about emergencies. Regarding self-efficacy, peoplemay feel more confident about their ability to handle emergencies because they havedone more preparation, rather than the other way around, although literature hasshown self-efficacy is an important precursor to behavior change (Kvalem & Træen,2000; Schwarzer & Fuchs, 1995; Stuart, Borland, & McMurray, 1994). Last,regarding normative influence, people who are prepared with more emergency
Public Emergency Preparedness 439
Downloaded By: [Michigan State University] At: 00:40 28 July 2010

supplies may perceive that average Americans are better prepared accordingly (thisargument is also related to false consensus effect; Prentice & Miller, 1993). More rig-orous evidence of a causal relationship is beyond the data, but it should be pursuedin future studies using longitudinal data.
Implications
First, public information campaigns focusing on increasing individuals’ perceptionsof self-efficacy or subjective norm may be an effective approach for improving thepublic emergency preparedness (e.g., ‘‘What will your friends do=your family wantin an emergency?’’).
Second, campaigns should be focused on more than simply gathering emergencysupplies; increasing the stage of preparation should also be a critical goal. Forexample, this study demonstrated that the effects of perceived norm on the twodependent variables could diverge. Some demographic characteristics also predicteddifferently the two types of emergency preparedness measures (see Table 2). From apragmatic point of view, differences may appear in real preparedness between some-one who happens to have some emergency supplies on hand and an individual whohas gathered them purposefully; there are further real differences between the indi-vidual whose supplies and plans are out of date (possible even for someone in the‘‘action’’ stage) and those who recently have restocked pantries and updated phonelists or knowledge of evacuation routes (those in the ‘‘maintenance’’ stage). Pro-gression from even one stage to the next is a step in the right direction, but stoppingshort of the maintenance stage may give both individuals and community organizersa false sense of security. Therefore, efforts should be aimed not just at usheringpeople from contemplation to action, but from action to maintenance. This kindof stage-of-action approach to understanding and promoting emergency prepared-ness may provide more feasible and effective programs to public health and riskcommunication practitioners.
References
Ajzen, I. (1985). From intentions to actions: A theory of planned behavior. In J. Kuhl &J. Beckman (Eds.), Action-control: From cognition to behavior (pp. 11–39). Heidelberg:Springer.
American Public Health Association. (2007). National opinion survey to determine levels ofpreparedness for a public health crisis. Washington, DC: Author.
American Red Cross and the Council for Excellence in Government. (2007). Readiness Quo-tient Public Opinion Survey. Washington, DC: Author.
Bandura, A. (1994). Social cognitive theory of mass communication. In J. B. D. Zillmann(Ed.), Media effects: Advances in theory and research (pp. 121–153). Hillsdale, NJ:Lawrence Erlbaum.
Bandura, A. (1997). Self-efficacy: The exercise of control. New York: W.H. Freeman.Bryant, J., & Thomson, S. (2002). Fundamentals of media effects. Boston: McGraw Hill.Campo, S., Brossard, D., Frazer, M. S., Marchell, T., Lewis, D., & Talbot, J. (2003). Are
social norms campaigns really magic bullets? Assessing the effects of students’ mispercep-tions on drinking behavior. Health Communication, 15, 481–497.
Cialdini, R. B., Reno, R. R., & Kallgren, C. A. (1990). A focus theory of normative conduct:Recycling the concept of norms to reduce littering in public places. Journal of Personalityand Social Psychology, 58, 1015–1026.
440 H.-J. Paek et al.
Downloaded By: [Michigan State University] At: 00:40 28 July 2010

Eisenman, D. P., Wold, C. (2007). Fielding, J., Long, A., Setodji, C., Hickey, S., et al. (2006).Differences in individual-level terrorism preparedness in Los Angeles County. AmericanJournal of Preventive Medicine, 30(1), 1–6.
Enarson, E. (1998). Through women’s eyes: A gendered research agenda for disaster socialscience. Disasters, 22(2), 157–173.
Federal Emergency Management Agency. (2007). Welcome to the National Integration Center(NIC) Incident Management Systems Division. Retrieved January 16, 2008, from http://www.fema.gov/emergency/nims/
Fishbein, M., & Ajzen, I. (1975). Belief, attitude, intention, and behavior: An introduction totheory and research. Reading, MA: Addison-Wesley.
Fothergill, A., & Peek, L. A. (2004). Poverty and disasters in the United States: A review ofrecent sociological findings. Natural Hazards, 32(1), 89–110.
Fox, J. (1991). Regression diagnostics. New York: Sage Publications.Garner, A. C., & Huff, W. A. K. (1997). The wreck of Amtrak’s Sunset Limited: News cover-
age of a mass transport disaster. Disasters, 21(1), 4–19.Glanz, K. (1997). Behavioral research contributions and needs in cancer prevention and
control: Dietary change. Preventive Medicine, 26(5), S43–S55.Glanz, K., Rimer, B. K., & Lewis, F. M. (2002). Health behavior and health education: Theory,
research and practice. San Francisco: Wiley & Sons.Gottlieb, N. H., Gingiss, P. L., & Weinstein, R. P. (1992). Attitudes, subjective norms and
models of use for smokeless tobacco among college athletes—implications for preventionand cessation programming. Health Education Research, 7(3), 359–368.
Griffin, R. J., & Dunwoody, S. (2000). The relation of communication to risk judgment andpreventive behavior related to lead in tap water. Health Communication, 12(1), 81–81.
Grunig, J. E., & Hunt, T. (1984). Managing public relations. New York: Rinehart andWilson.
Harris Interactive. (2007). Harris Poll #54. Rochester, NY: Author. Conducted April 10–16,2007.
Hyman, H. H. (1968). Readings in reference group theory and research. New York: Free Press.Iyengar, S. (1991). Is anyone responsible? How television frames political issues. Chicago:
University of Chicago Press.Keselman, A., Slaughter, L., & Patel, V. L. (2005). Toward a framework for understanding lay
public’s comprehension of disaster and bioterrorism information. Journal of BiomedicalInformatics, 38(4), 331–344.
Knoke, D., & Bohrnstedt, G. W. (1994). Statistics for social data analysis. Itasca, IL: PeacockPublishers.
Kvalem, I. L., & Træen, B. (2000). Self-efficacy, scripts of love and intention to use condomsamong Norwegian adolescents. Journal of Youth and Adolescence, 29, 337–353.
Maddux, J. E. (1991). Self-efficacy. In C. R. Snyder & D. R. Forsyth (Eds.), Handbook ofsocial and clinical psychology: The health perspective (pp. 57–78). New York: PergamonPress.
Marcus, B. H., Banspach, S. W., Lefebvre, R. C., Rossi, J. S., Carleton, R. A., & Abrams,D. B. (1992). Using the stages of change model to increase the adoption of physicalactivity among community participants. American Journal of Health Promotion, 6,424–429.
McClure, J., Sutton, R. M., & Sibley, C. G. (2007). Listening to reporters or engineers? Howinstance-based messages about building design affect earthquake fatalism. Journal ofApplied Social Psychology, 37(9), 1956–1973.
McCombs, M. E., & Reynolds, A. (2002). News influence on our pictures of the world. InJ. Bryant & D. Zillmann (Eds.), Media effects: Advances in theory and research(pp. 1–18). Mahwah, NJ: Lawrence Erlbaum.
McEntire, D. A., & Myers, A. (2004). Preparing communities for disasters: Issues andprocesses for government readiness. Disaster Prevention and Management, 13(2), 140–152.
Public Emergency Preparedness 441
Downloaded By: [Michigan State University] At: 00:40 28 July 2010

Morrow, B. H. (1999). Identifying and mapping community vulnerability. Disasters, 23(1), 1.Morse, S. S., Garwin, R. L., & Olsiewski, P. J. (2006). Public health: Next flu pandemic: What
to do until the vaccine arrives? Science, 314(5801), 929.Mutz, D. C. (1998). Impersonal influence: How perceptions of mass collectives affect political
attitudes. Cambridge: Cambridge University Press.Nelson, C., Lurie, N., Wasserman, J., & Zakowski, S. (2007). Conceptualizing and
defining public health emergency preparedness. American Journal of Public Health, 97,S9–S11.
Nigg, C. R., Burbank, P. M., Padula, C., Dufresne, R., Rossi, J. S., Velicer, W. F., et al.(1999). Stages of change across ten health risk behaviors for older adults. Gerontologist,39, 473–482.
Paek, H.-J., & Gunther, A. C. (2007). How peer proximity moderates indirect media influenceon adolescent smoking. Communication Research, 34, 407–432.
Paek, H.-J., Yoon, S., & Shah, D. V. (2005). Local news, social integration, and communityparticipation: hierarchical linear modeling of contextual and cross-level effects. Journal-ism & Mass Communication Quarterly, 82, 587–606.
Perry, R. W., & Lindell, M. K. (2003). Preparedness for emergency response: Guidelines forthe emergency planning process. Disasters, 27, 336–350.
Perse, E. M. (2001). Media effects and society. New York: Lawrence Erlbaum.Prentice, D. A., & Miller, D. T. (1993). Pluralistic ignorance and alcohol use on campus: Some
consequences of misperceiving the social norm. Journal of Personality and SocialPsychology, 64, 243–256.
Prochaska, J. O., & DiClemente, C. C. (1983). Stages and processes of self-change of smoking:Toward an integrative model of change. Journal of Consulting and Clinical Psychology,51, 390–395.
Prochaska, J. O., DiClemente, C. C., & Norcross, J. C. (1992). In search of how peoplechange: Applications to addictive behaviors. American Psychologist, 47, 1102–1114.
Prochaska, J. O., & Norcross, J. C. (2001). Stages of change. Psychotherapy, 38, 443–448.Prochaska, J. O., & Velicer, W. F. (1997). The transtheoretical model of health behavior
change. American Journal of Health Promotion, 97(12), 38–48.Prochaska, J. O., Velicer, W. F., Rossi, J. S., Goldstein, M. G., Marcus, B. H., Rakowski, W.,
et al. (1994). Stages of change and decisional balance for 12 problem behaviors. HealthPsychology, 13(1), 39–46.
Rogers, R. W. (1983). Cognitive and psychological processes in fear appeals and attitude change.New York: Guilford.
Sattler, D. N., Kaiser, C. F., & Hittner, J. B. (2000). Disaster preparedness: Relationshipsamong prior experience, personal characteristics, and distress. Journal of Applied SocialPsychology, 30, 1396–1420.
Schwarzer, R., & Fuchs, R. (1995). Changing risk behaviors and adopting health behaviors: Therole of self-efficacy beliefs. New York: Cambridge University Press.
Sherif, M., & Sherif, C. W. (1964). Reference groups: Exploration into conformity and deviationof adolescents. New York: Harper.
Slater, M. D. (1999). Integrating application of media effects, persuasion, and behavior changetheories to communication campaigns: A stages-of-change framework. Health Communi-cation, 11, 335–354.
Stuart, K., Borland, R., & McMurray, N. (1994). Self-efficacy, health locus of control, andsmoking cessation. Addictive Behaviors, 19(1), 1–12.
Tierney, K. J., Lindell, M. K., & Perry, R. W. (2001). Facing the unexpected disaster prepared-ness and response in the United States. Washington, DC: Joseph Henry Press.
Witte, K. (1992). Putting the fear back into fear appeals—The Extended Parallel ProcessModel. Communication Monographs, 59, 329–349.
442 H.-J. Paek et al.
Downloaded By: [Michigan State University] At: 00:40 28 July 2010
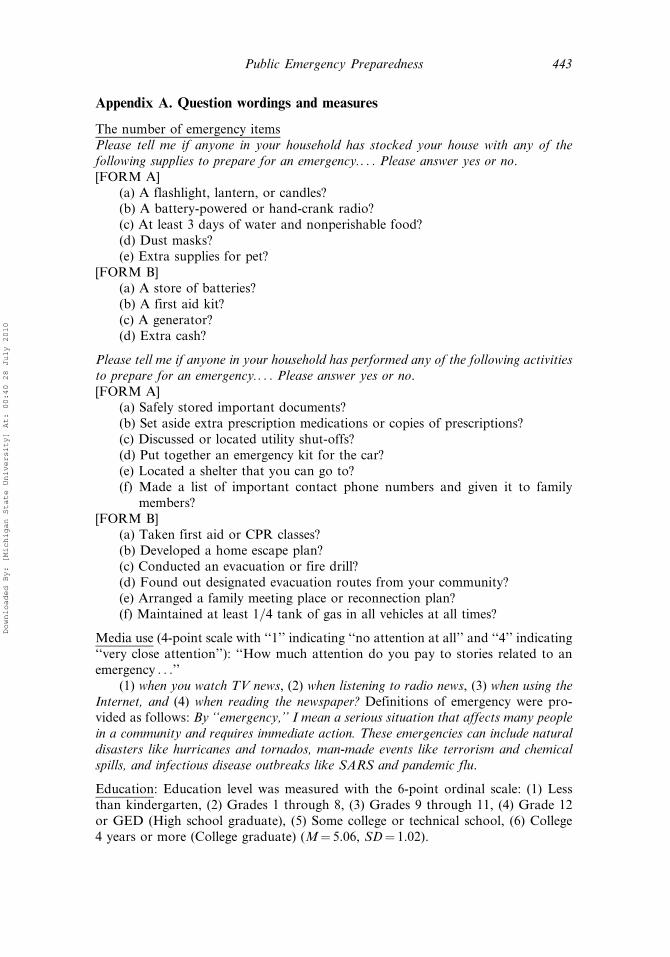
Appendix A. Question wordings and measures
The number of emergency itemsPlease tell me if anyone in your household has stocked your house with any of thefollowing supplies to prepare for an emergency.. . . Please answer yes or no.[FORM A]
(a) A flashlight, lantern, or candles?(b) A battery-powered or hand-crank radio?(c) At least 3 days of water and nonperishable food?(d) Dust masks?(e) Extra supplies for pet?
[FORM B](a) A store of batteries?(b) A first aid kit?(c) A generator?(d) Extra cash?
Please tell me if anyone in your household has performed any of the following activitiesto prepare for an emergency.. . . Please answer yes or no.[FORM A]
(a) Safely stored important documents?(b) Set aside extra prescription medications or copies of prescriptions?(c) Discussed or located utility shut-offs?(d) Put together an emergency kit for the car?(e) Located a shelter that you can go to?(f) Made a list of important contact phone numbers and given it to family
members?[FORM B]
(a) Taken first aid or CPR classes?(b) Developed a home escape plan?(c) Conducted an evacuation or fire drill?(d) Found out designated evacuation routes from your community?(e) Arranged a family meeting place or reconnection plan?(f) Maintained at least 1=4 tank of gas in all vehicles at all times?
Media use (4-point scale with ‘‘1’’ indicating ‘‘no attention at all’’ and ‘‘4’’ indicating‘‘very close attention’’): ‘‘How much attention do you pay to stories related to anemergency . . .’’
(1) when you watch TV news, (2) when listening to radio news, (3) when using theInternet, and (4) when reading the newspaper? Definitions of emergency were pro-vided as follows: By ‘‘emergency,’’ I mean a serious situation that affects many peoplein a community and requires immediate action. These emergencies can include naturaldisasters like hurricanes and tornados, man-made events like terrorism and chemicalspills, and infectious disease outbreaks like SARS and pandemic flu.
Education: Education level was measured with the 6-point ordinal scale: (1) Lessthan kindergarten, (2) Grades 1 through 8, (3) Grades 9 through 11, (4) Grade 12or GED (High school graduate), (5) Some college or technical school, (6) College4 years or more (College graduate) (M¼ 5.06, SD¼ 1.02).
Public Emergency Preparedness 443
Downloaded By: [Michigan State University] At: 00:40 28 July 2010
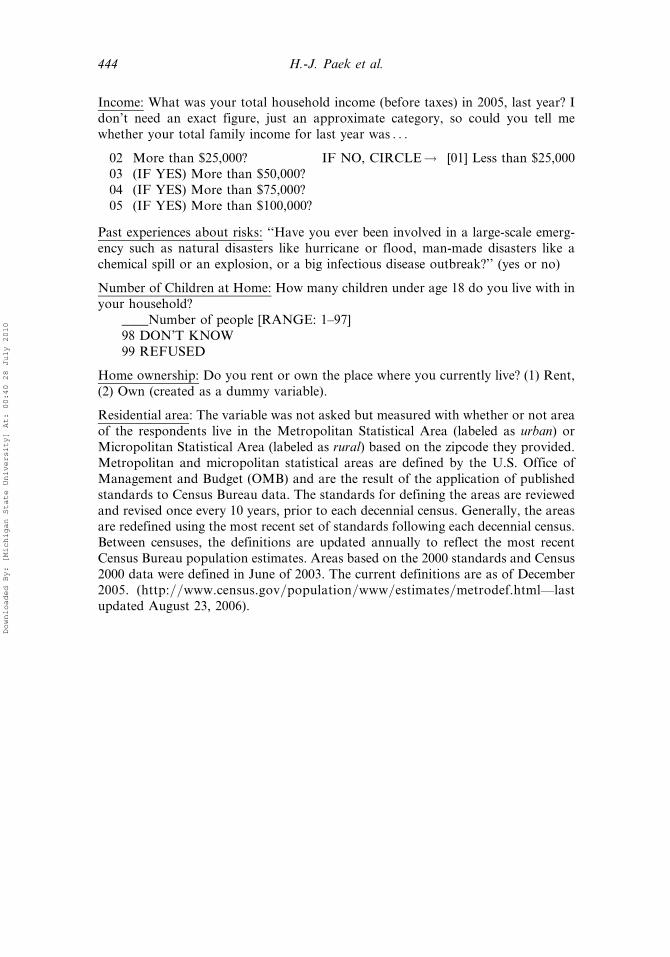
Income: What was your total household income (before taxes) in 2005, last year? Idon’t need an exact figure, just an approximate category, so could you tell mewhether your total family income for last year was . . .
02 More than $25,000? IF NO, CIRCLE! [01] Less than $25,00003 (IF YES) More than $50,000?04 (IF YES) More than $75,000?05 (IF YES) More than $100,000?
Past experiences about risks: ‘‘Have you ever been involved in a large-scale emerg-ency such as natural disasters like hurricane or flood, man-made disasters like achemical spill or an explosion, or a big infectious disease outbreak?’’ (yes or no)
Number of Children at Home: How many children under age 18 do you live with inyour household?
____Number of people [RANGE: 1–97]98 DON’T KNOW99 REFUSED
Home ownership: Do you rent or own the place where you currently live? (1) Rent,(2) Own (created as a dummy variable).
Residential area: The variable was not asked but measured with whether or not areaof the respondents live in the Metropolitan Statistical Area (labeled as urban) orMicropolitan Statistical Area (labeled as rural) based on the zipcode they provided.Metropolitan and micropolitan statistical areas are defined by the U.S. Office ofManagement and Budget (OMB) and are the result of the application of publishedstandards to Census Bureau data. The standards for defining the areas are reviewedand revised once every 10 years, prior to each decennial census. Generally, the areasare redefined using the most recent set of standards following each decennial census.Between censuses, the definitions are updated annually to reflect the most recentCensus Bureau population estimates. Areas based on the 2000 standards and Census2000 data were defined in June of 2003. The current definitions are as of December2005. (http://www.census.gov/population/www/estimates/metrodef.html—lastupdated August 23, 2006).
444 H.-J. Paek et al.
Downloaded By: [Michigan State University] At: 00:40 28 July 2010




















