Dysfunctional visual word form processing in progressive alexia
14
BRAIN A JOURNAL OF NEUROLOGY Dysfunctional visual word form processing in progressive alexia Stephen M. Wilson, 1,2 Kindle Rising, 1 Matthew T. Stib, 1 Steven Z. Rapcsak 1,2 and Pe ´lagie M. Beeson 1,2 1 Department of Speech, Language and Hearing Sciences, University of Arizona, Tucson, AZ, USA 2 Department of Neurology, University of Arizona, Tucson, AZ, USA Correspondence to: Stephen M. Wilson, Ph.D. Department of Speech, Language and Hearing Sciences, P.O. Box 210071, Tucson, AZ 85721, USA E-mail: [email protected]. Progressive alexia is an acquired reading deficit caused by degeneration of brain regions that are essential for written word processing. Functional imaging studies have shown that early processing of the visual word form depends on a hierarchical posterior-to-anterior processing stream in occipito-temporal cortex, whereby successive areas code increasingly larger and more complex perceptual attributes of the letter string. A region located in the left lateral occipito-temporal sulcus and adjacent fusiform gyrus shows maximal selectivity for words and has been dubbed the ‘visual word form area’. We studied two patients with progressive alexia in order to determine whether their reading deficits were associated with structural and/or functional abnormalities in this visual word form system. Voxel-based morphometry showed left-lateralized occipito-temporal atrophy in both patients, very mild in one, but moderate to severe in the other. The two patients, along with 10 control subjects, were scanned with functional magnetic resonance imaging as they viewed rapidly presented words, false font strings, or a fixation crosshair. This paradigm was optimized to reliably map brain regions involved in orthographic processing in individual subjects. All 10 control subjects showed a posterior-to-anterior gradient of selectivity for words, and all 10 showed a functionally defined visual word form area in the left hemisphere that was activated for words relative to false font strings. In contrast, neither of the two patients with progressive alexia showed any evidence for a selectivity gradient or for word-specific activation of the visual word form area. The patient with mild atrophy showed normal responses to both words and false font strings in the posterior part of the visual word form system, but a failure to develop selectivity for words in the more anterior part of the system. In contrast, the patient with moderate to severe atrophy showed minimal activation of any part of the visual word form system for either words or false font strings. Our results suggest that progressive alexia is associated with a dysfunctional visual word form system, with or without substantial cortical atrophy. Furthermore, these findings demonstrate that functional MRI has the potential to reveal the neural bases of cognitive deficits in neurodegenerative patients at very early stages, in some cases before the development of extensive atrophy. Keywords: progressive alexia; letter-by-letter reading; posterior cortical atrophy; logopenic primary progressive aphasia; visual word form system Abbreviations: PCA = posterior cortical atrophy; VWFA = visual word form area doi:10.1093/brain/awt034 Brain 2013: 136; 1260–1273 | 1260 Received June 13, 2012. Revised December 11, 2012. Accepted December 29, 2013 ß The Author (2013). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved. For Permissions, please email: [email protected] by guest on February 29, 2016 http://brain.oxfordjournals.org/ Downloaded from
-
Upload
independent -
Category
Documents
-
view
0 -
download
0
Transcript of Dysfunctional visual word form processing in progressive alexia

BRAINA JOURNAL OF NEUROLOGY
Dysfunctional visual word form processing inprogressive alexiaStephen M. Wilson,1,2 Kindle Rising,1 Matthew T. Stib,1 Steven Z. Rapcsak1,2 andPelagie M. Beeson1,2
1 Department of Speech, Language and Hearing Sciences, University of Arizona, Tucson, AZ, USA
2 Department of Neurology, University of Arizona, Tucson, AZ, USA
Correspondence to: Stephen M. Wilson, Ph.D.
Department of Speech, Language and Hearing Sciences,
P.O. Box 210071, Tucson, AZ 85721, USA
E-mail: [email protected].
Progressive alexia is an acquired reading deficit caused by degeneration of brain regions that are essential for written word
processing. Functional imaging studies have shown that early processing of the visual word form depends on a hierarchical
posterior-to-anterior processing stream in occipito-temporal cortex, whereby successive areas code increasingly larger and more
complex perceptual attributes of the letter string. A region located in the left lateral occipito-temporal sulcus and adjacent
fusiform gyrus shows maximal selectivity for words and has been dubbed the ‘visual word form area’. We studied two patients
with progressive alexia in order to determine whether their reading deficits were associated with structural and/or functional
abnormalities in this visual word form system. Voxel-based morphometry showed left-lateralized occipito-temporal atrophy in
both patients, very mild in one, but moderate to severe in the other. The two patients, along with 10 control subjects, were
scanned with functional magnetic resonance imaging as they viewed rapidly presented words, false font strings, or a fixation
crosshair. This paradigm was optimized to reliably map brain regions involved in orthographic processing in individual subjects.
All 10 control subjects showed a posterior-to-anterior gradient of selectivity for words, and all 10 showed a functionally defined
visual word form area in the left hemisphere that was activated for words relative to false font strings. In contrast, neither of the
two patients with progressive alexia showed any evidence for a selectivity gradient or for word-specific activation of the visual
word form area. The patient with mild atrophy showed normal responses to both words and false font strings in the posterior
part of the visual word form system, but a failure to develop selectivity for words in the more anterior part of the system. In
contrast, the patient with moderate to severe atrophy showed minimal activation of any part of the visual word form system for
either words or false font strings. Our results suggest that progressive alexia is associated with a dysfunctional visual word form
system, with or without substantial cortical atrophy. Furthermore, these findings demonstrate that functional MRI has the
potential to reveal the neural bases of cognitive deficits in neurodegenerative patients at very early stages, in some cases
before the development of extensive atrophy.
Keywords: progressive alexia; letter-by-letter reading; posterior cortical atrophy; logopenic primary progressive aphasia; visual wordform system
Abbreviations: PCA = posterior cortical atrophy; VWFA = visual word form area
doi:10.1093/brain/awt034 Brain 2013: 136; 1260–1273 | 1260
Received June 13, 2012. Revised December 11, 2012. Accepted December 29, 2013
� The Author (2013). Published by Oxford University Press on behalf of the Guarantors of Brain. All rights reserved.
For Permissions, please email: [email protected]
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

IntroductionReading involves a complex mapping from a pattern of light on
the retina to an abstract visual word form that is invariant for
features such as size, location, case and font (Warrington and
Shallice, 1980). Functional imaging studies suggest that this map-
ping depends on a hierarchical posterior-to-anterior gradient of
processing in the ventral visual stream, with successive regions
coding increasingly larger and more complex perceptual attributes
of the letter string (Cohen et al., 2003; Grainger and Whitney,
2004; Dehaene et al., 2005; Vinckier et al., 2007). Collectively,
the cortical network of visual areas that support reading has been
referred to as the visual word form system (Vinckier et al., 2007).
The earlier stages of processing are bilateral; primary visual cortex
represents simple features such as oriented bars, and extrastriate
visual areas extract local contours and then letter shapes. The
culmination of this stream of processing is an abstract visual
word form in a left-lateralized region located in the lateral
occipito-temporal sulcus and/or adjacent fusiform gyrus (Binder
and Mohr, 1992; Cohen et al., 2000, 2002; Molko et al., 2002;
Clarke, 2003; Cohen et al., 2003; Dehaene et al., 2005; Vinckier
et al., 2007; Epelbaum et al., 2008; Dehaene and Cohen, 2011).
This region has been termed the ‘visual word form area’ (VWFA)
(Cohen et al., 2000). Although its functional specificity continues
to be debated (Price and Devlin, 2003, 2011; Dehaene and
Cohen, 2011; Vogel et al., 2012), researchers concur that the
VWFA plays an important role in reading.
Acquired reading deficits are traditionally divided into peripheral
and central alexias. Peripheral alexias involve deficits in mapping
visual inputs to visual word forms, whereas central alexias involve
damage to orthographic representations or the mapping from or-
thography to phonological and/or semantic representations. When
the visual word form system is damaged, words can no longer be
recognized quickly and automatically. Reading is often possible to
some extent, but it is characterized by a slow and effortful serial
strategy referred to as letter-by-letter reading (Dejerine, 1892;
Damasio and Damasio, 1983; Binder and Mohr, 1992;
Beversdorf et al., 1997; Cohen et al., 2003; Leff et al., 2006;
Mani et al., 2008; Pflugshaupt et al., 2009). Although
letter-by-letter reading is generally considered the most archetypal
form of peripheral alexia, it should be noted that many patients
with letter-by-letter reading also exhibit central orthographic pro-
cessing deficits that may affect both reading and spelling
(Behrmann et al., 1998; Rapcsak and Beeson, 2004; Tsapkini
and Rapp, 2010).
Acquired alexia due to neurodegenerative disease is termed
‘progressive alexia’. Its onset is insidious and deficits become pro-
gressively worse over time (Mendez et al., 2007). Acquired per-
ipheral alexias are most commonly associated with the clinical
neurodegenerative syndrome of posterior cortical atrophy (PCA)
(Benson et al., 1988), which usually reflects Alzheimer’s pathology
(Hof et al., 1997; Tang-Wai et al., 2004) though other aetiologies
have been reported (Victoroff et al., 1994). PCA is characterized
by progressive deficits of visual and visuospatial functioning.
Peripheral alexias are a prominent early symptom in most, if not
all cases with PCA, often constituting the first clinical
manifestation of the disease (Benson et al., 1988; McMonagle
et al., 2006). Patients with PCA have been reported to present
with a variety of types of peripheral alexia including not only
letter-by-letter reading, but also neglect alexia, attentional alexia,
and alexia secondary to simultanagnosia (Cogan, 1985; De Renzi,
1986; Benson et al., 1988; Freedman et al., 1991; Freedman and
Costa, 1992; Graff-Radford et al., 1993; Ardila et al., 1997;
Beversdorf and Heilman, 1998; Mendez and Cherrier, 1998;
Mendez et al., 2002; Tang-Wai et al., 2004; McMonagle et al.,
2006; Crutch and Warrington, 2007; Mendez et al., 2007; Crutch
and Warrington, 2009; Giovagnoli et al., 2009; Catricala et al.,
2011; Fragassi et al., 2011). Alexia is typically out of proportion to
any other language deficits that may occur, such as anomia or
transcortical sensory aphasia (McMonagle et al., 2006).
Although progressive peripheral alexia most frequently occurs in
patients with PCA, it is also occasionally seen in cases of primary
progressive aphasia. For instance, several patients with semantic
dementia have been reported with letter-by-letter reading
(Hodges et al., 1992; Patterson and Hodges, 1992; Noble et al.,
2000). However, peripheral alexias are not common in primary
progressive aphasia; more commonly seen are central alexias
involving deficits in linking visual word forms to semantic or
phonological representations (Hodges et al., 1992; Patterson and
Hodges, 1992; Mendez, 2002; Jefferies et al., 2004; Brambati
et al., 2009; Wilson et al., 2009; Henry et al., 2012; Snowden
et al., 2012).
Relatively little is known about the neural substrates of progres-
sive peripheral alexias with letter-by-letter reading. Most patients
with clinically defined PCA have atrophy and/or hypometabolism
of bilateral occipito-parietal and/or occipito-temporal cortex
(Benson et al., 1988; Graff-Radford et al., 1993; Mendez et al.,
2002; Tang-Wei et al., 2004; Whitwell et al., 2007); however,
imaging abnormalities are not apparent in all individuals
(McMonagle et al., 2006). Several cases have been reported in
which alexia was the most prominent symptom and in which at-
rophy and/or hypometabolism were more pronounced in left than
right posterior brain regions (Freedman et al., 1991; Beversdorf
and Heilman, 1998; Giovagnoli et al., 2009; Fragassi et al., 2011).
There have also been suggestions that alexia in PCA may be
related to ventral rather than dorsal pathology (Beversdorf and
Heilman, 1998; Mendez and Cherrier, 1998). However, no struc-
tural or functional imaging studies have been carried out to iden-
tify which regions are specifically responsible for progressive alexia
in PCA. Similarly, in primary progressive aphasia, although several
studies have investigated the neural basis of central alexias
(Brambati et al., 2009; Wilson et al., 2009; Henry et al., 2012),
it is not known which regions are implicated in the occasional
patients with primary progressive aphasia whose alexia includes
a peripheral component.
In this study, we investigated the structural and functional status
of the visual word form system, including the VWFA, in two pa-
tients with progressive alexia and a profile of letter-by-letter read-
ing. One patient was diagnosed with PCA and the other with
logopenic variant primary progressive aphasia. We used a func-
tional MRI paradigm that was optimized to detect the
posterior-to-anterior gradient of selectivity for word forms, culmi-
nating in word-specific activity in the VWFA, in every individual
Visual word form processing in progressive alexia Brain 2013: 136; 1260–1273 | 1261
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

healthy control participant. We hypothesized that the visual word
form system would be functionally abnormal in the two patients
with progressive alexia, and by comparing the patients to healthy
control subjects, we sought to characterize the nature of any func-
tional abnormalities.
Previous functional imaging studies of patients with
letter-by-letter reading due to stroke or surgical resection have
revealed abnormal or absent neural activation when the VWFA
is damaged or disconnected from its visual inputs (Cohen et al.,
2000, 2003, 2004; Henry et al., 2005; Gaillard et al., 2006;
Epelbaum et al., 2008; Ino et al., 2008; Tsapkini et al., 2011).
All of these cases had frank structural damage to the visual word
form system. In contrast, although our two patients had different
degrees of atrophy in the visual word form system, no regions
were completely destroyed, raising the question of whether
functional abnormalities can be identified in such cases.
Materials and methods
ParticipantsTwo individuals with progressive alexia participated in the study. Both
were male, and aged 71 and 74, respectively, when they were
scanned. Before scanning both patients completed a comprehensive
battery of language, neuropsychological and reading evaluations,
described below.
Control data for the functional imaging study were acquired from
10 healthy control participants who were primarily recruited from
newspaper advertisements or flyers. These included five males and
five females, with a mean age of 67 years (range: 50–77). In particu-
lar, there were four control males who were similar in age (72, 74, 75
and 77 years) to the two patients.
As control subjects for voxel-based morphometry, we used 9 of
these 10 control subjects (the youngest, aged 50, was not used),
plus an additional 13 age-matched control subjects who had been
scanned on the same scanner for a different study, for a total of 22
control subjects. These included nine males and 13 females, with a
mean age of 71 years (range: 63–77).
All participants gave written informed consent, and were compen-
sated for taking part in the study. The study was approved by the
University of Arizona Institutional Review Board.
Patient J: Case history and evaluationsPatient J was a left-handed male who was first seen in November
2010, at which time he was 70 years old. He had a masters degree
in Fine Arts, had worked as an artist and art teacher, and continued to
work part-time facilitating art classes. He described a 4 to 5-year his-
tory of progressive reading difficulties.
Because Patient J was left-handed, we used a standard clinical lan-
guage mapping paradigm (picture naming) to determine whether his
language areas were left-lateralized. This study revealed clear left lat-
eralization for language processing (Supplementary Fig. 1). Because
lateralization for reading tends to match lateralization for spoken lan-
guage (Van der Haegen et al., 2012), it is reasonable to assume that in
Patient J, reading would probably also have been premorbidly
left-lateralized.
Patient J’s spoken language was largely intact (Table 1). In conver-
sation, his output was fluent but characterized by mild anomia. In
formal testing, this was reflected in a score of 46 out of 60 on the
Boston Naming Test. His comprehension of conversational speech was
very good but there was a mild deficit on formal testing of single word
comprehension; he made three semantic errors on spoken
word-picture matching (PALPA 47); in each case, he chose
semantically-related foils, e.g. he chose ‘tiara’ in response to ‘crown’.
He did not show any significant cognitive, executive or memory
deficits (Table 1). He performed poorly only on the Trail Making
Test, which was presumably due to the fact that this test requires
reading of letters and digits. He exhibited only mild visuospatial def-
icits; he performed well on copy and delayed copy of a modified
Rey-Osterrieth figure (Fig. 1B and C) and well on face matching.
However, he missed 3 of 10 items on the number location subtest
from the Visual Object and Space Perception battery (VOSP)
(Warrington and James, 1991), in which participants are asked to
identify which of 16 digits in a square correspond to the location of
a dot in an adjacent square.
Patient J was severely alexic (Table 2). Although he was highly
educated, he was no longer reading at all in daily life. He was com-
pensating through the use of books on tape and a computerized read-
ing program. He had deficits at the single letter level, with errors on
case matching, letter naming, and matching spoken-to-written letters
(Table 2). He read single words extremely slowly with a letter-by-letter
strategy, subvocally mouthing the individual letter names before even-
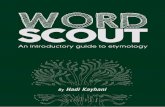
tually producing a response. His reading time increased as a function
of word length (Fig. 2), a typical pattern in letter-by-letter readers.
Because his single letter naming was error-prone, his letter-by-letter
strategy was often not successful; overall, he read 70% of words and
50% of pseudowords correctly. His most frequent error types were
visually similar words (46%, e.g. ‘stale’ for ‘slate’, ‘bride’ for ‘bribe’,
‘circus’ for ‘circuit’), probably reflecting his deficits at the single letter
level. Other frequent error types were lack of any response (33%) and
unrelated words (17%, e.g. ‘step’ for ‘chef’, ‘huge’ for ‘laugh’).
Paragraph reading was extremely slow. Patient J took 202 s to read
the first two lines of a second grade level passage (18 words, 11.2 s
per word), and he read only 11 of the 18 words correctly.
Patient J’s written spelling was also impaired; he spelled 80% of
regular real words, 60% of irregular real words, and 85% of pseudo-
words correctly. Direct copy of single words was good (96% letters
correct), whereas case conversion was poor (58% correct), suggesting
an allographic impairment, i.e. an impairment in mapping graphemes
to letter shapes.
We evaluated Patient J again in June 2011, 7 months later. His anomia
had progressed only slightly; he scored 42 out of 60 on the Boston
Naming Test. In contrast, his reading was now dramatically worse.
He read only 28% of words and 5% of pseudowords correctly. His
most common error type was not to respond (73%, e.g. ‘I don’t
know’), followed by visually similar words (22%, e.g. ‘dump’ for
‘bump’, ‘comfort’ for ‘compact’). However, testing in the oral modality
revealed strikingly spared orthographic knowledge. He was able to rec-
ognize 98% of words that were spelled out loud for him, and 90% of
pseudowords.
Patient J’s written spelling had further deteriorated; he now spelled
only 55% of regular real words, 33% of irregular real words, and 65%
of pseudowords correctly. However, he performed much better in oral
testing, correctly spelling out loud 95% of regular words, 70% of
irregular words, and 100% of pseudowords. The superior performance
in oral spelling suggests a significant allographic impairment, whereas
the pattern of surface agraphia in both modalities suggested mild
damage to central orthographic representations.
In summary, Patient J presented with severe progressive alexia that
was predominantly peripheral in nature, as evidenced by his very slow
1262 | Brain 2013: 136; 1260–1273 S. M. Wilson et al.
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

and error-prone letter-by-letter reading. In addition, he showed a sig-
nificant allographic impairment and mild damage to central ortho-
graphic representations. Patient J met criteria for the clinical
syndrome of PCA (Tang-Wei et al., 2004). We scanned him in June
2011, shortly after this second evaluation.
Patient B: Case history and evaluationPatient B was a right-handed male who was first seen in June 2010, at
which time he was 73-years-old. He had an eighth grade education,
had worked as a construction foreman, and was the owner of a
company involved in the mining industry. He described an
�18-month history of difficulty expressing himself, which he first
noticed as a difficulty in telling jokes, and progressive reading difficul-
ties over the same period.
His spoken language was characterized by prominent anomia, cir-
cumlocutions, and retracings, and mild comprehension difficulties were
evident in conversation. Language testing resulted in a clinical diagno-
sis of logopenic progressive aphasia (Gorno-Tempini et al., 2011),
supported by anomia in spontaneous speech and confrontation
naming, impaired repetition, and preserved single word comprehen-
sion, motor speech, and grammatical function (Table 1).
Table 1 Language and neuropsychological measures in the two progressive alexic patients
Patient J
Nov 2010 June 2011 Patient B
Diagnosis Progressive alexia Progressive alexia
and mild anomia and logopenic PPA
Age 70 71 73
MMSE (/30) 27 25 20
Handedness left-handed right-handed
Language measures
Western Aphasia Battery Aphasia Quotiant (/100) 97.5 — 82.2
WAB classification Anomic — Anomic
Content (/10) 10 — 9
Fluency (/10) 10 — 8
Comprehension (/10) 9.85 — 9.8
Repetition (/10) 10 — 7.4
Naming (/10) 8.9 — 6.9
Boston naming test (/60) 46 42 22
Phonemic verbal fluency (generate words starting with d) 10 10 7
Semantic verbal fluency (generate animal names) 9 7 11
Pyramids and Palm Trees (pictures) 52 51 45
Pyramids and Palm Trees (written) discontinued too impaired discontinued
Spoken word-picture match (PALPA 47, 5AFC, /40) 37 34 40
Arizona Phonological Battery (/100) 94 — 45
Cognitive/Executive/Memory
Raven’s Progressive Coloured Matrices (/36) 31 31 21
Trail Making Test A* 81 s — 45 s
Trail Making Test B* 4300 s — discontinued
Digits forward 8 + 7 5
Digits backwards 5 3 —
Visuospatial tests**
Modified Rey-Osterrieth copy (/17) — 13 13
Modified Rey-Osterrieth delayed copy (/17) — 13 6
Modified Rey-Osterrieth recognition (yes/no) — yes yes
Number location (VOSP) (/10) — 7 8
Face matching (CATS) (/12) — 11 11
MMSE = Mini-Mental State Examination (Folstein et al., 1975); WAB = Western Aphasia Battery (Kertesz, 1982); PALPA = Psycholinguistic Assessments of LanguageProcessing in Aphasia (Kay et al., 1992); VOSP = number location subtest from the Visual Object and Space Perception battery (Warrington and James, 1991); CATS = facematching subtest from the Comprehensive Affect Testing System (Froming et al., 2006).Boston Naming Test (Kaplan et al., 1983); Pyramids and Palm Trees (Howard and Patterson, 1992); Arizona Phonological Battery (Rapcsak et al., 2009); Raven’s
Progressive Colored Matrices (Raven et al., 1990); modified Rey-Osterrieth figure copy and recall (Possin et al., 2011).— = not tested.5AFC = 5-alternative forced choice.* Performance on the Trail Making Test was presumably compromised by reading deficits. Normal performance on Trails A in this age range is 40 � 14 s (education4 12 years, as for Patient J) or 42 � 15 s (education4 12 years, as for Patient B). Normal performance on Trails B is 86 � 24 s (education4 12 years) or 110 � 35 s(education4 12 years) (Tombaugh, 2004).** Visuospatial tests were performed several months later than the other tests.
Visual word form processing in progressive alexia Brain 2013: 136; 1260–1273 | 1263
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

Table 2 Orthographic, reading, writing and spelling measures in the two progressive alexic patients
Patient J
Nov 2010 June 2011 Patient B
Single letter tasks
Mirror reversal (PALPA 18, 2AFC, /36) 35 35 32
Case matching (PALPA 19/20, 2AFC, /52) 47 46 37
Letter naming (PALPA 22, /26) 20 17 —
Spoken letter-written letter match (PALPA 23, 4AFC, /26) 23 22 21
Reading
Lexical decision, illicit foils (PALPA 24, 2AFC, /60) 51 49 54
Lexical decision, plausible foils (PALPA 25, 2AFC, /60) discontinued too impaired 36
Orthographic choice (2AFC, /40) 22 too impaired 30
Oral reading of regular words (ABRS) (/40) 31 13 7
Oral reading of irregular words (ABRS) (/40) 25 9 9
Oral reading of pseudowords (ABRS) (/20) 10 1 0
Oral ‘reading’ of regular words spelled out loud (/40) — 39 —
Oral ‘reading’ of irregular words spelled out loud (/40) — 39 —
Oral ‘reading’ of pseudowords spelled out loud (/20) — 18 —
Written word-picture match (PALPA 48, 5AFC, /40) 37 23 29
Writing and spelling
Direct copy of single words (% letters correct) 96% 87% 90%
Case conversion (/52) 30 30 37
Written spelling of regular words (ABRS) (/40) 32 22 12
Written spelling of irregular words (ABRS) (/40) 24 13 5
Written spelling of pseudowords (ABRS) (/20) 17 13 2
Oral spelling of regular words (ABRS) (/40) — 38 —
Oral spelling of irregular words (ABRS) (/40) — 28 —
Oral spelling of pseudowords (ABRS) (/20) — 20 —
PALPA = Psycholinguistic Assessments of Language Processing in Aphasia (Kay et al., 1992); ABRS = Arizona Battery for Reading and Spelling (Henry et al., 2007; Rapcsaket al., 2009; Beeson et al., 2010).Control subjects make only occasional sporadic errors and are at ceiling for all measures (Beeson et al., 2010).— = not tested.nAFC = n-alternative forced choice.
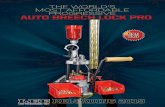
Figure 1 Preserved figure copy and delayed copy in the
two patients with progressive alexia. (A) The modified
Rey-Osterrieth figure (Possin et al., 2011). (B) Patient J’s copy of
the figure. (C) Patient J’s delayed copy of the figure after 10 min.
(D) Patient B’s copy of the figure. (E) Patient B’s delayed copy of
the figure after 10 min.
Figure 2 Reading time increased as a function of word length
in Patient J, a pattern that is characteristic of letter-by-letter
reading.
1264 | Brain 2013: 136; 1260–1273 S. M. Wilson et al.
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

Mr. B showed moderate cognitive deficits, as evidenced by poor
performance on Raven’s progressive coloured matrices (Table 1). He
performed poorly on the Trail Making Test but, as noted above, this
test requires reading of letters and digits. He exhibited only mild visuo-
spatial deficits; he performed well on copy and moderately well on
delayed copy of a modified Rey-Osterrieth figure (Fig. 1D and E). He
missed 2 of the 10 items on the number location subtest from the
Visual Object and Space Perception battery, but he did well on face
matching.
Patient B reportedly had never been much of a reader, but he had
read the Bible and trade magazines. He described reading less and less
as he had found it becoming increasingly difficult. Patient B’s reading
was severely impaired (Table 2), with deficits at the single letter level
evident in errors on discrimination of mirror-reversed letters, case
matching, and case conversion. He employed a laborious
letter-by-letter reading strategy that was often unsuccessful due to
his difficulties in the identification of individual letters. The following
examples are typical of his attempts to read single words:
(1) [target: reach] B R E A T H, berneath, bearth, I dunno, that’s
not it
(2) [target: shove] S H O P E sharp, no
(3) [target: choir] cough, C O U M D, cough, that don’t sound right,
cough, C O U, no that’s not C O, C H O I R, cough, no, it’s C O
U something, C H O I R.
Overall, single words were read correctly just 20% of the time, and no
pseudowords were read correctly. The most common error types were
unrelated words (30%, e.g. ‘touch’ for ‘doubt’) and visually similar words
(22%, e.g. ‘change’ for ‘charge’). Too few of his responses were correct
to permit the calculation of reaction time.
Patient B was generally unable to pronounce words that were
spelled out loud for him, but this was not formally tested (note that
the phonological short-term memory deficits of logopenic primary pro-
gressive aphasia would make this challenging even if orthographic
representations were intact). Written spelling was also very poor for
both words and pseudowords.
In sum, patient B showed severe progressive alexia with a significant
peripheral component, as evidenced by his slow and error-prone
letter-by-letter reading. His spelling impairment for both words and
pseudowords indicated damage to lexical-semantic and sublexical spel-
ling mechanisms. In addition, Patient B demonstrated prominent
spoken language deficits, meeting diagnostic criteria for logopenic pri-
mary progressive aphasia (Gorno-Tempini et al., 2011). We scanned
Patient B �1 year after we first saw him, in June 2011.
Functional magnetic resonance imagingexperimental designThe aim of our functional imaging study was to determine whether the
visual word form system was functionally normal in the two patients
with progressive alexia, therefore it was important to optimize our
paradigm such that the functional organization of the visual word
form system could be robustly mapped in each individual healthy con-
trol participant. Otherwise a seemingly abnormal pattern in the pa-
tients might just reflect interindividual variability, and would be difficult
to interpret. Pilot studies suggested that four design features were
important to reliably map the visual word form system: (i) a block
design to maximize signal to noise; (ii) a control condition closely
matched for low-level visual features; (iii) a rapid presentation rate;
and (iv) an attentionally demanding non-linguistic task. It is likely that
these last two features minimize semantic processing and other higher
level processing of the stimuli, and thus are more effective in revealing
lower level processes, which are more consistent across subjects than
higher level processes. Rapid presentation rates and attentionally de-
manding tasks have been used in previous studies aimed at mapping
response selectivity in occipito-temporal cortex (Vinckier et al., 2007).
We used false font strings rather than non-word orthographic strings
as the control condition, because activation levels for non-word strings
depend heavily on the orthographic plausibility of the non-word
strings. Implausible non-words behave like false fonts, whereas
plausible non-words produce similar levels of activity to real words
(Vinckier et al., 2007).
Participants were scanned with functional MRI as they viewed
blocks of rapidly presented words, false font strings, or a fixation
crosshair, while performing an attentionally demanding non-linguistic
task. Each block was 20 s long, and in each run there were six repe-
titions of each of the three conditions, presented in pseudorandom
order, for a total run length of 6 min, plus 8 s to acquire four additional
volumes that were discarded. Participants completed two runs each,
except for one control participant, who completed only one run.
The stimulus words were nouns and adjectives selected from the
Medical Research Council database (Coltheart, 1981). They were all
six letters long and medium frequency, with Kucera-Francis frequen-
cies ranging from 10 to 110. Proper names and some emotive words
were excluded. Words were shown in Times New Roman font, all
capitals, centred on a fixation cross. Words were presented in white
on a grey background for 100 ms, then a white fixation cross was
displayed for 200 ms, then the next word was presented. There
were 67 words in each 20-s block.
The false font stimuli were created using letters from alphabetic
orthographies other than English. These stimuli were presented with
the same timing and visual parameters as the words.
The task was to detect occasional words or false font strings pre-
sented in red instead of white, and then press a button on a response
pad as quickly as possible. These catch trials were presented pseudo-
randomly in four of the six word blocks, and four of the six false
font blocks.
Participants were familiarized with the stimuli and practiced the task,
before being placed in the scanner.
Neuroimaging protocolParticipants were scanned as they lay supine in a General Electric 3 T
HD Signa Excite scanner at the University of Arizona Medical Centre.
They viewed the stimuli through magnetic resonance-compatible gog-
gles (Resonance Technology, Inc), and wore padded headphones and
earplugs to attenuate scanner noise.
For anatomical reference and registration, a T1-weighted 3D spoiled
gradient recalled inversion recovery sequence was acquired with
the following parameters: 160 sagittal slices; slice thickness = 1 mm;
field of view = 256 � 256 mm; matrix = 256 �256 mm; repetition
time = 7.5 ms; echo time = 3.0 ms; inversion time = 500 ms; flip
angle = 15�.
For the functional imaging paradigm, 184 blood oxygen level-
dependent T2*-weighted volumes were acquired using a single-shot
spiral pulse sequence (Glover and Law, 2001) with the following par-
ameters: 30 anterior commissure/posterior commissure-aligned axial
slices in sequential order; slice thickness = 4 mm with no gap; field of
view = 240 � 240 mm; matrix = 64 � 64; repetition time = 2000 ms;
echo time = 30 ms; flip angle = 90�.
Visual stimuli were presented with PsychToolbox 3.0.8 (Brainard,
1997; Pelli, 1997) running under MATLAB 7.11 (Mathworks) on a
Windows PC.
Visual word form processing in progressive alexia Brain 2013: 136; 1260–1273 | 1265
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

Voxel-based morphometryThe T1-weighted structural images were bias-corrected, segmented
into grey matter, white matter and CSF, and normalized to MNI
space using the unified segmentation algorithm in SPM (version
SPM5; http://www.fil.ion.ucl.ac.uk/spm; Ashburner and Friston,
2005). Grey matter and white matter probability maps were scaled
by Jacobians, smoothed with a Gaussian kernel of 10 mm full-width
half-maximum, then summed together to obtain a map of brain par-
enchyma (Wilson et al., 2010). Each of the two patients was com-
pared to the 22 control subjects, with age, sex and total intracranial
volume included as covariates. Statistical maps were thresholded at
voxelwise P5 0.005, with a minimum cluster size of 1500 mm3.
Functional magnetic resonance imagingdata analysisThe functional imaging data were preprocessed with AFNI (version
2011-06-22; http://afni.nimh.nih.gov/afni; Cox, 1996). The data
were corrected for slice timing differences, realigned to account for
head movement, smoothed with a Gaussian kernel of 4 mm full-width
half-maximum, high pass filtered (cut-off = 0.006 Hz) and detrended
(Legendre polynomials of order up to and including two). A general
linear model was fit at each voxel using the ‘fmrilm’ procedure from
FMRISTAT (version 2006-06-02; http://www.math.mcgill.ca/keith/
fmristat; Worsley et al., 2002), modelling temporal autocorrelation
as an autoregressive process of degree one.
The design matrix contained one explanatory variable for word
blocks and one for false font blocks, each convolved with a
canonical haemodynamic reference function modelled as a difference
of two gamma functions. Six head motion parameters, slow drift par-
ameters, and the global whole-brain signal were included as covariates
of no interest. Each subject’s two runs were combined with a fixed
effects model using the ‘multistat’ procedure from FMRISTAT.
Functional images were initially coregistered to structural images
using SPM5, then manually realigned for greater accuracy.
Anatomical images were transformed to MNI space with SPM5, and
this transformation was then applied to the statistical images.
To identify the VWFA in each individual subject, we contrasted
words to false font strings at voxelwise P5 0.05, masked by the con-
trast of words to fixation at P5 0.0001 (cf. Glezer et al., 2009). We
considered only clusters with a centre of mass within 15 mm of the
published VWFA coordinates of (–42, –57, –15) (Cohen et al., 2002).
Whole brain random effects group analyses were carried out after
applying a second smoothing kernel (6 mm full-width half-maximum)
to the individual effect size images. To identify the VWFA in the 10
control subjects, we contrasted words to false font strings. This ana-
lysis was thresholded at voxel-wise P5 0.005 and corrected for mul-
tiple comparisons at P5 0.05 based on cluster extent (Worsley et al.,
1996). To identify regions where the two patients showed less activa-
tion than the 10 control subjects, we compared the contrast of words
to false font strings between the patients and control subjects using a
two-sample t-test with pooled variance. This analysis was thresholded
at voxelwise P5 0.005, then corrected for multiple comparisons
(Friston et al., 1997) based on the extent of the closest cluster to
the published coordinates of the VWFA, which was the region
hypothesized to show reduced activation in patients.
Previous studies have demonstrated a posterior-to-anterior gradient
of visual word form processing in the ventral visual stream, with suc-
cessively anterior regions increasingly selective for words (Vinckier
et al., 2007). To identify this selectivity gradient in each individual
subject, we created images showing the signal for false font strings
as a proportion of the signal for words, in regions that were active for
words versus fixation at P5 0.0001. We also plotted the mean signal
for words and false font strings in occipito-temporal cortex in each
hemisphere as a function of y coordinate (i.e. posterior-to-anterior), by
averaging across a region of interest defined by the control group
activation for words versus rest thresholded as described above (vox-
elwise P5 0.005 and corrected for multiple comparisons at P5 0.05).
Results
Voxel-based morphometryVoxel-based morphometry showed that Patient J had very mild
atrophy of the left posterior inferior temporal gyrus, and widening
of the left sylvian fissure (Fig. 3A, Table 3).
Patient B had much more extensive atrophy of the left inferior
and middle temporal gyri, the left fusiform gyrus, the white matter
underlying these regions, and a smaller region of the right poster-
ior inferior temporal gyrus (Fig. 3B, Table 3).
Behavioural data collected duringfunctional magnetic resonance imagingControl subjects responded to 90.5% � 15.8% (SD) of the catch
trials (occasional words or false font strings coloured red instead of
white). Patient J responded to 87.5% of the catch trials, and
Patient B responded to 100% of the catch trials. Most participants
also made occasional false positive responses.
Functional magnetic resonance imagingAll 10 control subjects showed a VWFA that responded more to
words than false font strings according to our criteria (Fig. 4A–C,
Table 4). For the more basic contrasts of words versus fixation and
false font strings versus fixation, all control subjects showed bilat-
eral occipito-temporal activation (Fig. 4A–C).
Unlike the control subjects, neither of the two patients with
progressive alexia showed a VWFA according to our criteria
(Fig. 4D and E, Table 4). For the more basic contrasts relative to
fixation, the two patients differed from one another. Patient
J showed typical robust bilateral occipito-temporal activation for
both of these contrasts (Fig. 4D). Patient B showed much weaker
activation for these contrasts, with more activity in the right than
the left hemisphere (Fig. 4E).
We next checked whether loosening our criteria for the VWFA
(i.e. words versus false font strings P50.05, words versus fixation
P50.0001, within 15 mm of published coordinates) would reveal
any evidence for a VWFA in either patient. For Patient J, there
were two single voxels meeting the voxel-wise criteria in left
occipito-temporal cortex; however, the closest to the VWFA was
27 mm away at (–52, –82, –14). In right occipito-temporal cortex
there was a cluster of 39 voxels with centre of mass (41, –57, 2),
which is 17 mm from the right hemisphere homologue of the
VWFA. We then examined the contrast of words versus false
fonts without the mask of words versus rest, and observed a clus-
ter of 44 voxels with centre of mass (–60, –56, –11), which is
1266 | Brain 2013: 136; 1260–1273 S. M. Wilson et al.
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

18 mm from the VWFA. However, activation at that location was
slightly negative for all words relative to rest, suggesting that the
cluster arose due to a deactivation for false font strings. A failure
to activate for words relative to rest is inconsistent with the re-
sponse properties of the VWFA. For Patient B, there were no
voxels meeting the voxel-wise criteria in left occipito-temporal
cortex. In right occipito-temporal cortex there were a few scat-
tered voxels meeting the voxel-wise criteria, but none were close
to the right homologue of the VWFA; the closest was located at
(–40, –72, –2), which is 20 mm from the right hemisphere homo-
logue of the VWFA. We then examined the contrast of words
versus false fonts without the mask of words versus rest, and
observed a small cluster of nine voxels with centre of mass
(–50, –43, –10), which is 17 mm from the VWFA. But activation
at that location was slightly negative for all words relative to
rest, inconsistent with the response properties of the VWFA.
In summary, neither patient showed any activation resembling a
typical VWFA, even when the criteria were relaxed.
We next performed a whole-brain random effects analysis con-
trasting words to false font strings in the 10 control subjects. The
VWFA was the only region activated (centre of mass: –43, –50, –18;
extent = 6312 mm3; corrected P50.001) (Fig. 5A). We then
directly compared the two patients to the 10 control subjects. The
patients showed significantly less activation than control subjects
in the VWFA (centre of mass: –39, –45, –19; extent = 1000 mm3;
corrected P = 0.034) (Fig. 5B). This was the largest cluster observed,
and no other clusters reached significance.
To reveal the anticipated posterior–anterior gradient of selectiv-
ity for words, we plotted the signal to false font strings as a pro-
portion of the signal to words, in regions that were active for
words versus fixation (Fig. 6). We found evidence for this gradient
in each of the 10 control subjects (Fig. 6A–J). There was some
individual variability, for instance, Control Subject 4 (who was
left-handed) showed a typical gradient in the left hemisphere,
but an even stronger gradient in the right hemisphere; Control
Subject 5 showed rather weak activity for both conditions relative
to rest; and Control Subject 9 showed an additional word-selective
region more posteriorly. However, despite this variability, left
hemisphere posterior-anterior gradients were evident in all control
subjects.
In contrast, neither of the two patients with progressive alexia
exhibited a posterior-anterior gradient of selectivity for words
(Fig. 6K and L). Both patients had small regions in the right hemi-
sphere that were selective for words at P50.05, but in both cases
these were considerably dorsal to the right hemisphere homologue
of the VWFA (Fig. 6K and L).
We also plotted the mean signal for words and false font strings
in occipito-temporal cortex in each hemisphere as a function of
Figure 3 Structural images of the two progressive alexic
patients. Regions of tissue loss as revealed by voxel-based
morphometry (voxel-wise P50.005, minimum cluster
extent = 1500 mm3) are shown with red outlines (white in
printed version). (A) Patient J showed mild atrophy of the left
posterior inferior temporal gyrus. (B) Patient B showed much
more extensive atrophy of left temporal cortex.
VBM = voxel-based morphometry.
Table 3 Voxel based morphometry showing tissue loss inthe two progressive alexic patients
Brain region MNI coordinates Max t Extent(mm3)
x y z
Patient J
Left posteriorinferior temporalgyrus
�56 �55 �16 4.75 1680
Left sylvian fissure(widening)
�40 2 2 4.72 5880
Patient B
Left inferior andmiddle temporalgyri and fusiformgyrus
�44 �40 �9 9.67 80032
Right posteriorinferior temporalgyrus
57 �58 �15 5.20 2368
Thresholded at voxel-wise P50.005, cluster extent41500 mm3. Extent is thesize of the region in which there was significant tissue loss (voxel-wise P5 0.005)compared with control subjects.
Visual word form processing in progressive alexia Brain 2013: 136; 1260–1273 | 1267
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

y coordinate (i.e. posterior-to-anterior) (Fig. 6). This analysis high-
lighted a notable difference between the two patients. Patient
J showed normal responses to both words and false font strings
in posterior occipito-temporal cortex, but unlike control subjects,
he showed no emergence of selectivity for words more anteriorly.
In fact, he showed somewhat less activity for words than false
font strings in the vicinity of the VWFA. In contrast, Patient B
showed minimal activation for either words or false font strings
in any part of occipito-temporal cortex. In this respect, Patient B
differed from Patient J and the control subjects, all of whom
showed robust responses for both words and false font strings
relative to rest.
Figure 4 Functional identification of the visual word form area. (A, B and C) In three typical control subjects, viewing words or false font
strings relative to fixation activated bilateral occipital and posterior temporal regions (voxel-wise P50.0001). The contrast of words
versus false font strings (voxel-wise P50.05) masked by the contrast of words versus rest (voxel-wise P50.0001) revealed the VWFA in
each of the 10 control participants. (D) Patient J showed typical bilateral occipito-temporal activation for words or false font strings relative
to fixation, however there were no regions activated for words versus false font strings. (E) Patient B showed weak right-lateralized
activation for words or false font strings relative to fixation, and no regions activated for words versus false font strings.
Table 4 Localization of VWFA with functional MRI
Subject MNI coordinates of VWFA Distance Max t Extent
x y z (mm) (mm3)
Control 1 �37 �45 �23 15 2.89 928
Control 2 �44 �54 �16 4 5.25 3432
Control 3 �45 �56 �9 6 4.05 2704
Control 4 �35 �45 �20 15 2.90 616
Control 5 �45 �56 �15 3 2.34 96
Control 6 �41 �60 �12 4 3.72 4328
Control 7 �51 �51 �14 11 5.45 3416
Control 8 �42 �52 �13 6 5.99 3184
Control 9 �43 �52 �12 6 6.56 N/A*
Control 10 �43 �52 �14 5 4.63 N/A*
Patient J None
Patient B None
Distance is the distance from the VWFA coordinates of (�42, �57, �15)reported by Cohen et al. (2002).*Clusters for these subjects were contiguous with other clusters outsidethe VWFA, so cluster extent could not be determined. The t threshold wasraised until the clusters separated to determine the centre of mass of the VWFA
cluster.
Figure 5 The visual word form area in control subjects and
patients. (A) In the control group, the contrast of words versus
false font strings (voxel-wise P50.005, corrected for multiple
comparisons at P50.05) revealed the visual word form area.
(B) Activation for this contrast was reduced in the patients
relative to the control subjects (voxel-wise P50.005, corrected
for multiple comparisons at P5 0.05).
1268 | Brain 2013: 136; 1260–1273 S. M. Wilson et al.
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

DiscussionThe goal of this study was to investigate the structural and func-
tional status of the visual word form system, including the VWFA,
in two patients with progressive alexia. Structural imaging showed
left-lateralized occipito-temporal atrophy in both patients, mild in
one (Patient J) but moderate to severe in the other (Patient B).
Functional imaging in control subjects revealed a posterior-to-
anterior gradient of selectivity for words, and all 10 showed a
functionally defined VWFA that was activated for words relative
Figure 6 The typical anterior-posterior gradient of selectivity for words in occipito-temporal cortex was abnormal in the two patients with
progressive alexia. (A–J) In all control subjects, posterior occipito-temporal cortex responded as much for false font strings as for words,
whereas more anterior regions showed greater responses to words than false font strings. This pattern was also apparent (arrowheads)
when plotting mean occipito-temporal responses in each hemisphere to words and false font strings as a function of y coordinate, as
shown in the line graphs below each image. (K and L) This selectivity gradient for words was not apparent in either of the two progressive
alexic patients. Additional slices are shown to demonstrate that both patients showed small regions that were selectively responsive to
words more dorsally in the right hemisphere. The black outlines show regions that responded more to words than false font strings
(voxel-wise P50.05) and more to words than fixation (voxel-wise P50.0001). The red outlines show regions in the two patients that
VBM showed to be atrophic (voxel-wise P5 0.005, minimum cluster extent = 1500 mm3). F = female; M = male.
Visual word form processing in progressive alexia Brain 2013: 136; 1260–1273 | 1269
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

to false font strings. In contrast, neither of the two patients
showed any evidence for a selectivity gradient or for word-specific
activation of the VWFA. These findings support our hypothesis
that the visual word form system would be functionally abnormal
in progressive alexia.
Patient J showed normal bilateral occipito-temporal responses
for words relative to rest and false fonts relative to rest, whereas
Patient B showed reduced activation even in these basic contrasts.
This may be related to the degree of occipito-temporal atrophy,
which was much greater in Patient B. Because Patient B showed
abnormal activity even in basic contrasts in regions posterior to the
VWFA, it seems clear that early processing stages in the visual
word form system were implicated in his reading deficit, consistent
with the fact that his deficits extended even to the single letter
level. Patient J, in contrast, did not lack activation of regions pos-
terior to the VWFA. Rather, he lacked any emergence of select-
ivity for words. Whereas the dysfunction of his visual word form
system was more subtle than that of Patient B, regions posterior to
the VWFA may likewise be implicated as Patient J also had deficits
at the single letter level. Although our data suggest that functional
abnormalities arise posterior to the VWFA in both patients, it
should be emphasized that neither patient had severe visual per-
ceptual deficits, and object recognition was intact. Both patients’
deficits were quite specific for reading.
A crucial methodological aspect of our study was the optimiza-
tion of a paradigm that would reliably activate the VWFA in every
individual normal control subject. Otherwise, failure to detect the
VWFA in the patients with progressive alexia might simply reflect
a lack of statistical power. We used a block design with false font
control stimuli, rapid presentation, and an attentionally demanding
task in order to maximize power, minimize visual confounds, and
minimize higher level semantic processing. This design was quite
similar to that used by Vinckier et al. (2007). Our pilot testing
showed that with slower presentation rates, there was consider-
able interindividual variability presumably related to higher level
processing, and words did not necessarily activate the VWFA
more than visually matched non-word stimuli such as false fonts
or consonant strings. Others have made similar observations
(Tagamets et al., 2000; Cohen et al., 2003). Our optimized para-
digm was successful in identifying the VWFA and mapping the
posterior-to-anterior gradient of selectivity for words in all 10 of
our healthy control participants. Because of this consistency, we
can be confident that the abnormal functionality of the visual
word form system in the two patients is unlikely to reflect
normal individual variability. A direct comparison between the
two patients and the 10 control subjects provided further support
for this conclusion.
Previous functional imaging studies of the VWFA and earlier
visual processing areas in patients have shown that the VWFA
does not show typical activation for word reading or selectivity
for words when it is damaged or disconnected from its inputs
[Cohen et al., 2003, 2004 (Patient F), Henry et al., 2005;
Gaillard et al., 2006; Epelbaum et al., 2008]. Sometimes rather
precise disconnections have been demonstrated. For instance,
damage to the white matter in the splenium of the corpus callo-
sum or its continuation in the forceps major disconnects the VWFA
from right hemisphere visual processing areas, resulting in
hemialexia in the left visual field; in these patients, the VWFA is
not activated by words presented in the left visual field [Cohen
et al., 2000, 2003 (Patient D)]. Damage to earlier visual process-
ing regions in the left hemisphere does not result in alexia if right
hemisphere regions are intact and interhemispheric connectivity is
preserved; in these cases, the VWFA is activated normally [Cohen
et al., 2003 (Patient M)]. The importance of the VWFA at the
anterior endpoint of the visual word form processing stream has
been highlighted in particular by two studies. Ino et al. (2008)
reported a patient who became alexic after haemorrhage in the
vicinity of the VFWA. The patient lacked functional activity in the
VWFA, but 6 weeks later his reading had recovered, and the
VWFA showed functional activity for reading again. Tsapkini
et al. (2011) showed that VWFA-like activation was displaced
posteriorly in a patient with a left fusiform resection, resulting in
a limited reading deficit. Our two cases differ from all of these
previous cases of acquired alexia in that the VWFA was neither
completely destroyed nor deafferented by a frank structural lesion.
However, our results converge with findings of abnormal function-
ality in the visual word form system in children and adults with
developmental dyslexia, in whom there may be structural abnorm-
alities but there are no frank lesions (Salmelin et al., 1996;
Rumsey et al., 1997; McCrory et al., 2005; van der Mark et al.,
2009, 2011).
Our two patients with progressive alexia met criteria for differ-
ent clinical syndromes. Patient J likely represents an early case of
PCA, whereas Patient B met diagnostic criteria for logopenic
primary progressive aphasia. Here we consider our findings for
each patient in the context of their broader clinical syndrome.
Patient J met clinical criteria for PCA, in that his presenting dif-
ficulty was the insideous onset of a primary visual dysfunction
(Tang-Wai et al., 2004). It is not uncommon that the first visual
dysfunction in PCA is progressive peripheral alexia (Benson et al.,
1988; McMonagle et al., 2006; Mendez et al., 2007). Patient
J did not have any other significant visual or visuospatial deficits,
although he made some errors on the number location subtest
from the Visual Object and Space Perception battery, which
may be a harbinger of the emergence of a more generalized
visual impairment.
Some authors have proposed that distinct variants of PCA dif-
ferentially involve dorsal and ventral visual streams (Caselli, 1995;
Mackenzie Ross et al., 1996; Beversdorf and Heilman, 1998;
Mendez and Cherrier, 1998; Migliaccio et al., 2012) or that
there is a continuum between dorsal and ventral forms
(Lehmann et al., 2011), whereas others have argued that the
dorsal stream is generally more affected than the ventral stream
(McMonagle et al., 2006). Mendez and Cherrier (1998) reported
two cases of PCA in which alexia with letter-by-letter reading was
the first symptom, but both patients eventually developed a more
general ventral simultanagnosia and eventually dorsal simultanag-
nosia. In contrast, Mendez (2001) reported another patient with
PCA with deficits primarily affecting visual localization and visuo-
spatial integration, in whom reading was largely preserved. PET
showed bilateral occipito-parietal hypometabolism. In another pa-
tient with occipito-parietal degeneration, Vinckier et al. (2006)
showed that reading was preserved, except in situations that
make particular demands on visuospatial processing, such as
1270 | Brain 2013: 136; 1260–1273 S. M. Wilson et al.
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

rotated words, or words with spaces between the letters. Taken
together, these cases suggest that peripheral alexia with
letter-by-letter reading in PCA is related to dysfunction of ventral
rather than dorsal visual regions (Mendez and Cherrier, 1998;
Mendez, 2001).
Our findings with Patient J are consistent with this view. The
functional abnormalities we observed were ventral, as was the
mild structural atrophy, consistent with progressive alexia being
the only prominent symptom in this case. We concur with previ-
ous researchers that there are multiple variants of PCA depending
on the particular regions affected (Caselli, 1995; Mackenzie Ross
et al., 1996; Lehmann et al., 2011; Migliaccio et al., 2012), and
that cases in which alexia is the first and most prominent symptom
reflect a ventral variant (Beversdorf and Heilman, 1998; Mendez
and Cherrier, 1998).
Patient B met clinical criteria for logopenic primary progressive
aphasia. He showed progressive alexia with a prominent peripheral
component, as evidenced by letter-by-letter reading, as well as a
central spelling deficit, and significant aphasia. Although logopenic
primary progressive aphasia is associated with reading deficits
(Brambati et al., 2009; Henry et al., 2012), such deficits are typically
central in nature; to our knowledge, no previous cases have been
reported with significant peripheral deficits as well. Patient B’s
unique pattern of impairment can be explained in terms of his atro-
phy, which encompassed both posterior perisylvian cortex,
accounting for spoken language deficits and possibly contributing
to his spelling impairment, as well as occipito-temporal regions, ac-
counting for peripheral alexia. Patient B’s atrophy was also strongly
left-lateralized, which is consistent with his relatively spared visuo-
spatial functions. It has been suggested that PCA and logopenic pri-
mary progressive aphasia have much in common as atypical
Alzheimer’s variants, and may differ primarily in relative lateralization
of posterior atrophy (Migliaccio et al., 2009).
In conclusion, we have shown that the visual word form system
was functionally abnormal in two cases of progressive alexia,
despite the fact that the VWFA was neither completely destroyed
nor were there any frank lesions that would disconnect it from its
afferents. This functional abnormality was accompanied by sub-
stantial atrophy in only one of the two cases, indicating that
defective activation of the visual word form system resulting in
profound alexia may precede significant atrophy.
AcknowledgementsWe thank Scott Squire, Sarah Andersen, Ashley Chavez and Adam
Gendreau for assistance with functional imaging data collection,
Kate Possin for help with visuospatial assessments, Cyma Van
Petten, Elena Plante and Dianne Patterson for sharing control
structural data, three anonymous reviewers for their constructive
comments, and the individuals who participated in our study,
especially Patient J and Patient B for their time and patience.
FundingThis work was supported by the National Institutes of Health
[DC010878 to S.M.W., DC007646 to P.B., DC008286 to S.Z.R.
and P.B., AG014792 to Cyma Van Petten] and the University of
Arizona.
Supplementary materialSupplementary material is available at Brain online.
ReferencesArdila A, Rosselli M, Arvizu L, Kuljis RO. Alexia and agraphia in posterior
cortical atrophy. Neuropsychiatry Neuropsychol Behav Neurol 1997;
10: 52–9.
Ashburner J, Friston KJ. Unified segmentation. Neuroimage 2005; 26:
839–51.Beeson PM, Rising K, Kim ES, Rapcsak SZ. A treatment sequence for
phonological alexia/agraphia. J. Speech Lang Hear Res 2010; 53:
450–68.
Behrmann M, Plaut DC, Nelson J. A literature review and new datasupporting an interactive account of letter-by-letter reading. Cogn
Neuropsychol 1998; 15: 7–51.
Benson DF, Davis RJ, Snyder BD. Posterior cortical atrophy. Arch Neurol
1988; 45: 789–93.Beversdorf DQ, Heilman KM. Progressive ventral posterior cortical
degeneration presenting as alexia for music and words. Neurology
1998; 50: 657–9.
Beversdorf DQ, Ratcliffe NR, Rhodes CH, Reeves AG. Pure alexia:
clinical-pathologic evidence for a lateralized visual language associationcortex. Clin Neuropathol 1997; 16: 328–31.
Binder JR, Mohr JP. The topography of callosal reading pathways. A
case-control analysis. Brain 1992; 115: 1807–26.
Brainard DH. The psychophysics toolbox. Spat Vis 1997; 10: 433–6.Brambati SM, Ogar J, Neuhaus J, Miller BL, Gorno-Tempini ML. Reading
disorders in primary progressive aphasia: a behavioral and neuroima-
ging study. Neuropsychologia 2009; 47: 1893–1900.
Caselli RJ. Focal and asymmetric cortical degeneration synfromes.Neurologist 1995; 1: 1–19.
Catricala E, Rosa PAD, Ortelli P, Ginex V, Marcone A, Perani D, et al.
The evolution of alexia in two cases of posterior cortical atrophy.
Behav Neurol 2011; 24: 229–36.
Clarke S. The role of homotopic and heterotopic callosal connections inhumans. In: Zaidel E, Iacoboni M, editors. The Parallel Brain.
Cambridge, MA: MIT Press; 2003. p. 461–72.
Cogan DG. Visual disturbances with focal progressive dementing disease.
Am J Ophthalmol 1985; 100: 68–72.Cohen L, Dehaene S, Naccache L, Lehericy S, Dehaene-Lambertz G,
Henaff MA, et al. The visual word form area: spatial and temporal
characterization of an initial stage of reading in normal subjects and
posterior split-brain patients. Brain 2000; 123: 291–307.Cohen L, Henry C, Dehaene S, Martinaud O, Lehericy S, Lemer C, et al.
The pathophysiology of letter-by-letter reading. Neuropsychologia
2004; 42: 1768–80.
Cohen L, Lehericy S, Chochon F, Lemer C, Rivaud S, Dehaene S.
Language-specific tuning of visual cortex? Functional properties ofthe Visual Word Form Area. Brain 2002; 125: 1054–69.
Cohen L, Martinaud O, Lemer C, Lehericy S, Samson Y, Obadia M, et al.
Visual word recognition in the left and right hemispheres: anatomical
and functional correlates of peripheral alexias. Cereb Cortex 2003; 13:1313–33.
Coltheart M. The MRC psycholinguistic database. Q J Exp Psychol A
1981; 33A: 497–505.
Cox RW. AFNI: software for analysis and visualization of functional mag-
netic resonance neuroimages. Comput Biomed Res 1996; 29: 162–173.Crutch SJ, Warrington EK. Foveal crowding in posterior cortical atrophy:
a specific early-visual-processing deficit affecting word reading. Cogn
Neuropsychol 2007; 24: 843–66.
Visual word form processing in progressive alexia Brain 2013: 136; 1260–1273 | 1271
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

Crutch SJ, Warrington EK. The relationship between visual crowding and
letter confusability: towards an understanding of dyslexia in posterior
cortical atrophy. Cogn Neuropsychol 2009; 26: 471–98.
Damasio AR, Damasio H. The anatomic basis of pure alexia. Neurology
1983; 33: 1573–83.De Renzi E. Slowly progressive visual agnosia or apraxia without demen-
tia. Cortex 1986; 22: 171–80.Dehaene S, Cohen L. The unique role of the visual word form area in
reading. Trends Cogn Sci 2011; 15: 254–62.Dehaene S, Cohen L, Sigman M, Vinckier F. The neural code for written
words: a proposal. Trends Cogn 2005; 9: 335–41.
Dejerine J. Contribution a l’etude anatomo-pathologique et clinique des
differentes varietes de cecite-verbale. Memoires Societe Biologique
1892; 4: 61–90.
Epelbaum S, Pinel P, Gaillard R, Delmaire C, Perrin M, Dupont S, et al.
Pure alexia as a disconnection syndrome: new diffusion imaging
evidence for an old concept. Cortex 2008; 44: 962–74.Folstein MF, Folstein SE, McHugh PR. ‘Mini-mental state’: A practical
method for grading the cognitive state of patients for the clinician.
J Psychiat Res 1975; 12: 189–98.
Fragassi NA, Chiacchio L, Errichiello L, Pappata S, Tedeschi MR,
Striano P, et al. Posterior cortical atrophy with prominent alexia with-
out agraphia in a Tourette syndrome. Neurol Sci 2011; 32: 1129–33.Freedman L, Costa L. Pure alexia and right hemiachromatopsia in pos-
terior dementia. J Neurol Neurosurg Psychiatr 1992; 55: 500–2.Freedman L, Selchen DH, Black SE, Kaplan R, Garnett ES, Nahmias C.
Posterior cortical dementia with alexia: neurobehavioural, MRI, and
PET findings. J Neurol Neurosurg Psychiatr 1991; 54: 443–8.
Friston KJ. Testing for anatomically specified regional effects. Hum Brain
Mapp 1997; 5: 133–136.
Froming K, Levy M, Schaffer S, Ekman P. The comprehensive affect
testing system. psychology software, Inc 2006.
Gaillard R, Naccache L, Pinel P, Clemenceau S, Volle E, Hasboun D, et al.
Direct intracranial, FMRI, and lesion evidence for the causal role of left
inferotemporal cortex in reading. Neuron 2006; 50: 191–204.
Giovagnoli AR, Aresi A, Reati F, Riva A, Gobbo C, Bizzi A. The neuro-
psychological and neuroradiological correlates of slowly progressive
visual agnosia. Neurol Sci 2009; 30: 123–31.
Glezer LS, Jiang X, Riesenhuber M. Evidence for highly selective neuronal
tuning to whole words in the ‘visual word form area’. Neuron 2009;
62: 199–204.Glover GH, Law CS. Spiral-in/out BOLD fMRI for increased SNR
and reduced susceptibility artifacts. Magn Reson Med 2001; 46:
515–22.
Gorno-Tempini M L, Hillis AE, Weintraub S, Kertesz A, Mendez M,
Cappa SF, et al. Classification of primary progressive aphasia and its
variants. Neurology 2011; 76: 1006–14.Graff-Radford NR, Bolling JP, Earnest F 4th, Shuster EA, Caselli RJ,
Brazis PW. Simultanagnosia as the initial sign of degenerative demen-
tia. Mayo Clin Proc 1993; 68: 955–64.
Grainger J, Whitney C. Does the huamn mnid raed wrods as a wlohe?
Trends Cogn Sci 2004; 8: 58–9.
Henry C, Gaillard Raphael, Volle E, Chiras J, Ferrieux S,
Dehaene Stanislas, et al. Brain activations during letter-by-letter read-
ing: a follow-up study. Neuropsychologia 2005; 43: 1983–1989.Henry ML, Beeson PM, Alexander GE, Rapcsak SZ. Written language
impairments in primary progressive aphasia: a reflection of damage
to central semantic and phonological processes. J Cogn Neurosci
2012; 24: 261–75.
Henry ML, Beeson PM, Stark AJ, Rapcsak SZ. The role of left perisylvian
cortical regions in spelling. Brain Lang 2007; 100: 44–52.
Hodges JR, Patterson K, Oxbury S, Funnell E. Semantic dementia.
Progressive fluent aphasia with temporal lobe atrophy. Brain 1992;
115: 1783–806.
Hof PR, Vogt BA, Bouras C, Morrison JH. Atypical form of Alzheimer’s
disease with prominent posterior cortical atrophy: a review of lesion
distribution and circuit disconnection in cortical visual pathways. Vision
Res 1997; 37: 3609–25.
Ino T, Tokumoto K, Usami K, Kimura T, Hashimoto Y, Fukuyama H.
Longitudinal fMRI study of reading in a patient with letter-by-letter
reading. Cortex 2008; 44: 773–81.
Jefferies E, Lambon Ralph MA, Jones R, Bateman D, Patterson K. Surface
dyslexia in semantic dementia: a comparison of the influence of
consistency and regularity. Neurocase 2004; 10: 290–9.
Kaplan EF, Goodglass H, Weintraub S. The Boston naming test. 2nd edn.
Philadelphia: Lea and Febiger; 1983.
Kay J, Lesser R, Coltheart M. PALPA: Psycholinguistic assessments of
language processing in aphasia. Hove: Lawrence Erlbaum Associates;
1992.
Kertesz A. Western aphasia battery. New York: Grune and Stratton;
1982.Leff AP, Spitsyna G, Plant GT, Wise RJS. Structural anatomy of pure and
hemianopic alexia. J Neurol Neurosurg Psychiatr 2006; 77: 1004–7.Lehmann M, Barnes J, Ridgway GR, Wattam-Bell J, Warrington
Elizabeth K, Fox NC, et al. Basic visual function and cortical thickness
patterns in posterior cortical atrophy. Cereb Cortex 2011; 21:
2122–32.
Mackenzie Ross SJ, Graham N, Stuart-Green L, Prins M, Xuereb J,
Patterson K, et al. Progressive biparietal atrophy: an atypical presen-
tation of Alzheimer’s disease. J Neurol. Neurosurg Psychiatr 1996; 61:
388–95.
Mani J, Diehl B, Piao Z, Schuele SS, Lapresto E, Liu P, et al. Evidence for
a basal temporal visual language center: cortical stimulation producing
pure alexia. Neurology 2008; 71: 1621–7.McCrory EJ, Mechelli A, Frith U, Price CJ. More than words: a common
neural basis for reading and naming deficits in developmental dyslexia?
Brain 2005; 128: 261–7.
McMonagle P, Deering F, Berliner Y, Kertesz A. The cognitive profile of
posterior cortical atrophy. Neurology 2006; 66: 331–8.
Mendez MF. Visuospatial deficits with preserved reading ability in a
patient with posterior cortical atrophy. Cortex 2001; 37: 535–43.
Mendez MF. Slowly progressive alexia. J Neuropsychiatry Clin Neurosci
2002; 14: 84.
Mendez MF, Cherrier MM. The evolution of alexia and simultanagnosia
in posterior cortical atrophy. Neuropsychiatry Neuropsychol Behav
Neurol 1998; 11: 76–82.
Mendez MF, Ghajarania M, Perryman KM. Posterior cortical atrophy:
clinical characteristics and differences compared to Alzheimer’s disease.
Dement Geriatr Cogn Disord 2002; 14: 33–40.
Mendez MF, Shapira JS, Clark DG. ‘Apperceptive’ alexia in posterior
cortical atrophy. Cortex 2007; 43: 264–70.
Migliaccio R, Agosta F, Rascovsky K, Karydas A, Bonasera S,
Rabinovici GD, et al. Clinical syndromes associated with posterior
atrophy: early age at onset AD spectrum. Neurology 2009; 73:
1571–8.
Migliaccio R, Agosta F, Scola E, Magnani G, Cappa SF, Pagani E, et al.
Ventral and dorsal visual streams in posterior cortical atrophy: A DT
MRI. Neurobiol Aging 2012; 33: 2572–84.Molko N, Cohen L, Mangin JF, Chochon F, Lehericy S, Le Bihan D, et al.
Visualizing the neural bases of a disconnection syndrome with diffu-
sion tensor imaging. J Cogn Neurosci 2002; 14: 629–36.
Noble K, Glosser G, Grossman M. Oral reading in dementia. Brain Lang
2000; 74: 48–69.
Patterson K, Hodges JR. Deterioration of word meaning: implications for
reading. Neuropsychologia 1992; 30: 1025–40.
Pelli DG. The VideoToolbox software for visual psychophysics: transform-
ing numbers into movies. Spat Vis 1997; 10: 437–42.
Pflugshaupt T, Gutbrod K, Wurtz P, von Wartburg R, Nyffeler T,
de Haan B, et al. About the role of visual field defects in pure
alexia. Brain 2009; 132: 1907–17.
Possin KL, Laluz VR, Alcantar OZ, Miller BL, Kramer JH. Distinct neuro-
anatomical substrates and cognitive mechanisms of figure copy per-
formance in Alzheimer’s disease and behavioral variant frontotemporal
dementia. Neuropsychologia 2011; 49: 43–8.Price CJ, Devlin JT. The myth of the visual word form area. Neuroimage
2003; 19: 473–81.
1272 | Brain 2013: 136; 1260–1273 S. M. Wilson et al.
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from

Price CJ, Devlin JT. The interactive account of ventral occipitotemporalcontributions to reading. Trends Cogn Sci 2011; 15: 246–53.
Rapcsak SZ, Beeson PM. The role of left posterior inferior temporal
cortex in spelling. Neurology 2004; 62: 2221–9.
Rapcsak SZ, Beeson PM, Henry ML, Leyden A, Kim E, Rising K, et al.Phonological dyslexia and dysgraphia: cognitive mechanisms and
neural substrates. Cortex 2009; 45: 575–91.
Raven JC, Court JH, Raven J. Coloured progressive matrices. Oxford:
Oxford Psychologists Press; 1990.Rumsey JM, Nace K, Donohue B, Wise D, Maisog JM, Andreason P. A
positron emission tomographic study of impaired word recognition and
phonological processing in dyslexic men. Arch Neurol 1997; 54: 562–73.Salmelin R, Service E, Kiesila P, Uutela K, Salonen O. Impaired visual
word processing in dyslexia revealed with magnetoencephalography.
Ann Neurol 1996; 40: 157–62.
Snowden JS, Kindell J, Thompson JC, Richardson AMT, Neary D.Progressive aphasia presenting with deep dyslexia and dysgraphia.
Cortex 2012; 48: 1234–9.
Tagamets MA, Novick JM, Chalmers ML, Friedman RB. A parametric
approach to orthographic processing in the brain: an fMRI study.J Cogn Neurosci 2000; 12: 281–97.
Tang-Wai DF, Graff-Radford NR, Boeve BF, Dickson DW, Parisi JE,
Crook R, et al. Clinical, genetic, and neuropathologic characteristics
of posterior cortical atrophy. Neurology 2004; 63: 1168–74.Tombaugh TN. Trail Making Test A and B: normative data stratified by
age and education. Arch Clin Neuropsychol 2004; 19: 203–214.
Tsapkini K, Rapp B. The orthography-specific functions of the leftfusiform gyrus: evidence of modality and category specificity. Cortex
2010; 46: 185–205.
Tsapkini K, Vindiola M, Rapp B. Patterns of brain reorganization subse-
quent to left fusiform damage: fMRI evidence from visual processingof words and pseudowords, faces and objects. Neuroimage 2011; 55:
1357–72.
Van der Haegen L, Cai Q, Brysbaert M. Colateralization of Broca’s area
and the visual word form area in left-handers: fMRI evidence. BrainLang 2012; 122: 171–178.
van der Mark S, Bucher K, Maurer U, Schulz E, Brem S, Buckelmuller J,
et al. Children with dyslexia lack multiple specializations along thevisual word-form (VWF) system. Neuroimage 2009; 47: 1940–9.
van der Mark S, Klaver P, Bucher K, Maurer U, Schulz E, Brem S,et al. The left occipitotemporal system in reading: disruption of
focal fMRI connectivity to left inferior frontal and inferior parietal
language areas in children with dyslexia. Neuroimage 2011; 54:
2426–36.Victoroff J, Ross GW, Benson DF, Verity MA, Vinters HV. Posterior
cortical atrophy. Neuropathologic correlations. Arch Neurol 1994; 51:
269–74.
Vinckier F, Dehaene S, Jobert A, Dubus JP, Sigman M, Cohen L.Hierarchical coding of letter strings in the ventral stream: dissecting
the inner organization of the visual word-form system. Neuron 2007;
55: 143–56.Vinckier F, Naccache L, Papeix C, Forget J, Hahn-Barma V, Dehaene S,
et al. ‘What’ and ‘where’ in word reading: ventral coding of written
words revealed by parietal atrophy. J Cogn Neurosci 2006; 18:
1998–2012.Vogel AC, Petersen SE, Schlaggar BL. The left occipitotemporal cortex
does not show preferential activity for words. Cereb Cortex 2012; 22:
2715–32.
Warrington E K, James M. Visual Object and Space Perception Battery.Bury St Edmunds: Thames Valley; 1991.
Warrington EK, Shallice T. Word-form dyslexia. Brain 1980; 103:
99–112.
Whitwell JL, Jack CR Jr, Kantarci K, Weigand SD, Boeve BF,Knopman DS, et al. Imaging correlates of posterior cortical atrophy.
Neurobiol Aging 2007; 28: 1051–61.
Wilson SM, Brambati SM, Henry RG, Handwerker DA, Agosta F,Miller BL, et al. The neural basis of surface dyslexia in semantic
dementia. Brain 2009; 132: 71–86.
Wilson SM, Henry ML, Besbris M, Ogar JM, Dronkers NF, Jarrold W,
et al. Connected speech production in three variants of primaryprogressive aphasia. Brain 2010; 133: 2069–88.
Worsley KJ, Liao CH, Aston J, Petre V, Duncan GH, Morales F, et al.
A general statistical analysis for fMRI data. Neuroimage 2002; 15:
1–15.Worsley KJ, Marrett S, Neelin P, Vandal AC, Friston KJ, Evans AC,
et al. A unified statistical approach for determining significant sig-
nals in images of cerebral activation. Hum Brain Mapp 1996; 4:58–73.
Visual word form processing in progressive alexia Brain 2013: 136; 1260–1273 | 1273
by guest on February 29, 2016http://brain.oxfordjournals.org/
Dow
nloaded from