Dr. Priyadarshani Kadus.pdf
185
-
Upload
khangminh22 -
Category
Documents
-
view
2 -
download
0
Transcript of Dr. Priyadarshani Kadus.pdf
BHARATI VIDYAPEETH DEEMED UNIVERSITY
COLLEGE OF AYURVED, PUNE- 43
CERTIFICATE
This is to certify that Dr. Priyadarshani A. Kadus, a Ph.D scholar in
the speciality of Panchakarma has successfully completed her thesis
entitled „ STUDY OF ANUVASAN BASTI AS AN ALTERNATIVE
PURVAKARM FOR SNEHAPAN IN VAMAN AND VIRECHAN.‟ for the
degree of Ayurved Varidhi (Doctor of Philosophy) Under the direct
supervision and guidance of Prof. Dr. Surendra M. Vedpathak.
The scholar has presented her research work before the experts
committee of Institutional Research and Ethical Committee (IREC) and
in Pre-Ph.D seminar on 6th January 2011 and 2nd July 2014
respectively. The suggestions given by the subject expert are
incorporated in this thesis.
The scholar has put up hard work in bringing about this thesis after
making an intensive study of the subject on the subject from
Ayurvedic and allied literature for the conceptual as well as clinical
study. This work makes a distinct advance on scientific lines in this
subject. This is further certified that she has completed all the
formalities laid down in the regulations governing the award of
„Ayurved Varidhi‟ Ph.D Degree of Bharati Vidyapeeth deemed
university, Pune.
Hence, her thesis is recommended for being submitted to the
adjudication for the award of Ph.D degree in Panchakarma.
Place: Pune Prof. Dr.A.B.Patil Date: Dean and Principal B.A.M.S.,D.T.F.M.Ph.D
Bharati Vidyapeeth Deemed University
College of Ayurved Pune-43
BHARATI VIDYAPEETH DEEMED UNIVERSITY
COLLEGE OF AYURVED, PUNE- 43
DEPARTMENT OF PANCHAKARMA
CERTIFICATE OF THE GUIDE
This is to certify that the work incorporated in the thesis
„STUDY OF ANUVASAN BASTI AS AN ALTERNATIVE
PURVAKARM FOR SNEHAPAN IN VAMAN AND
VIRECHAN.‟ Submitted by Dr. Priyadarshani A. Kadus, was
carried out under my supervision/ guidance. Such material
as has been obtained from other sources has been duly
acknowledged in the thesis.
Place :-Pune Guide
Date :- Prof. Dr.S.M.Vedpathak
MD (Ayu),Ph.D,MBA(HR)
Head Department of Panchakarma
Vice Principal, BVDU,
College of Ayurved, Pune-43
DECLARATION BY THE CANDIDATE
I declare that the thesis entitled „STUDY OF ANUVASAN BASTI
AS AN ALTERNATIVE PURVAKARM FOR SNEHAPAN IN VAMAN
AND VIRECHAN.‟ submitted by me for the degree of Doctor of
Philosophy is the record of work carried out by me during
the period from 5th August 2010 to 2nd July 2014 under the
guidance of Prof. Dr.S.M.Vedpathak and has not formed the
basis for the award of any degree, diploma, associate ship,
fellowship, titles in this or any other university or other
institution of higher learning.
I further declare that the material obtained from other
sources has been duly acknowledged in the thesis.
Place: Pune
Date:
Dr. Priyadarshani Arvind Kadus
Research Scholar

INDEX
No. Name of the Topic Page No. Acknowledgement
Key to Transliteration
Abbreviation
Introduction Section A Conceptual Study 01-56
I Historical review of Snehana 01-02
II Literary review of Snehapāna 03-18
III Historical review of Basti Karma 19-20
IV Literary review of Anuvāsana Basti
21-33
V Pharmacodynamics of Basti 34-35
VI Drug review 36-37
VII Review of previous work done 38-39
VIII Concept of Anuvāsana Basti as an
alternative for Snehapāna.
40-41
IX References 42-56
Section:B Clinical Study 57-118
I Aim and Objectives 57
II Materials and Methods 58-62
III Observations and Results 63-118
Section:C Discussion. 119-134
I Discussion 119-129
II Further scope of study 130
III References 131-134
Section:D Conclusion 135
Section:E Summary 136
Section:F Bibliography 137-139
Section:G Annexure
Case paper with Prakṛti, Koṣṭha
and Agni Parikṣaṇa and written
consent.
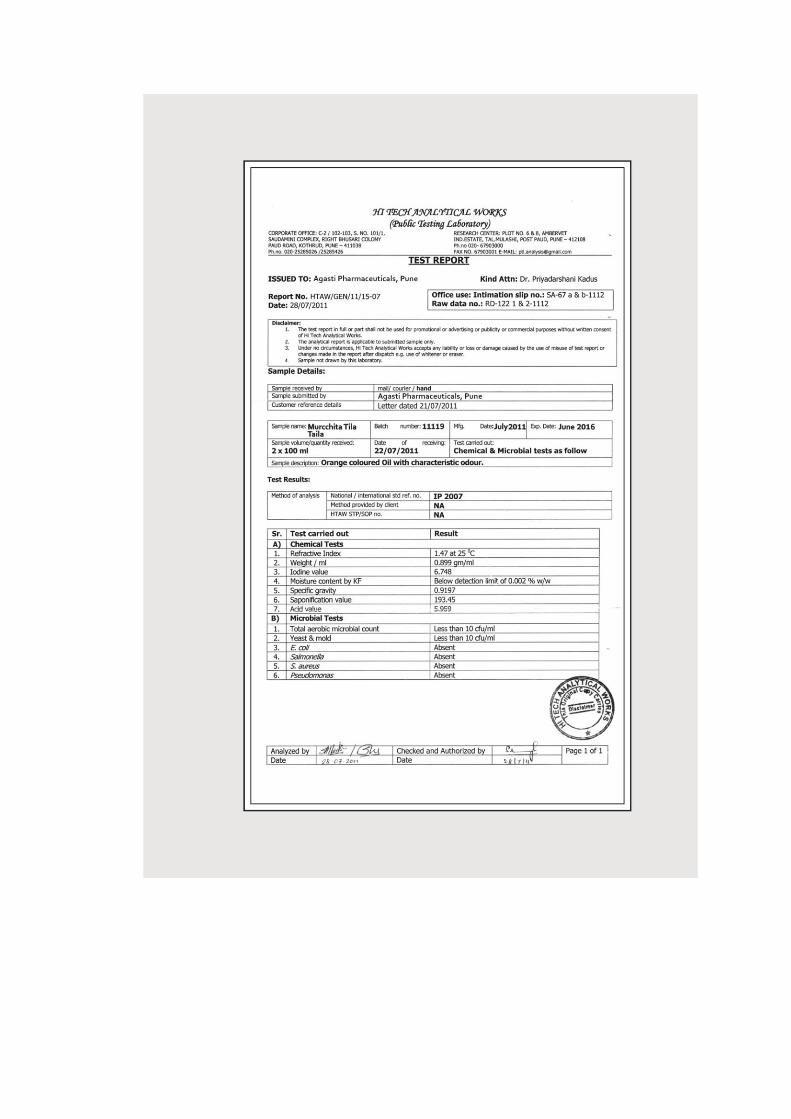
Letter of Standardization of Mūrcchita Tila Taila.
ACKNOWLEDGEMENT
Firstly I salute God of Vaidyas, Lord Dhanvantari and God of
intelligence Ganesha and Saraswati for bringing about the completion
of this project smoothly.
It is with heart full of gratitude that I acknowledge my guide Dr.
Surendra Vedpathak, Professor and Head Department of
Panchakarma, for his constant inspiration and guidance befitted me to
complete this creative work.
I solicit my gratitude to Chancellor, BVDU, Dr. Patangarao Kadam
and Vice Chancellor, BVDU, Dr. Shivajirao Kadam for giving me
opportunity to seek Ph. D degree from this university.
I am thankful to Dr. Abhijit Patil, Principal, Dr. V.V.Bhalsing and Dr.
S.M.Vedpathak, Vice- Principal, BVDU, College of Ayurved and Dr.
Shubhangi Katkar, Director, Bharati Ayurved Hospital, for providing
me best available facilities for the work.
I am deeply indebted to my Guru Dr. Vivek Sane for his timely
encouragement for selection of this topic for Ph. D.
With deep sense of gratitude, I convey my thanks to Dr. S.M. Sathye
for his guidance.
I wish to extend my special thanks to Dr. Supriya Bhalerao, research
scientist, IRSHA, for her efforts to bring perfection in this work.
I aknowledge Dr. Arvind Kadus, Propritor, Agasti Pharmaceuticals,
Pune for providing specially prepaired Basti pouches with required
quantity of Mūrcchita Tila Taila and Saindhava.
I must give my sincere thanks to all my patients who have actively
participated in the clinical trial, without them this work would not
have been successful.
I am thankful to my departmental colleagues Dr. Santosh Chavan and
Dr. Minaj Kulkarni for their support. I express my gratitude to Dr.
Manju Chavan, Dr. Sunanda Ghare, Dr. Snehalata Salunke, Dr.
Seema Gholap, Dr. Mrudula Kulkarni, Dr. Rahul Gujrathi who
believed me and provided their patients for this trial due to which this
study could take a shape.
Male and female therapists of our department gave their best for
administration of Anuvāsana Basti as per the protocol of this work. It‟s

my duty to convey my thanks to our therapists; Jyothi, Seema,
Vanita, Swati, Ravi, Ramdas, Sunil and Kumbhar.
I am thankful to my students; Dr. Bharati, Parag , Archana, Amit,
Abhishek, Pratik, Mayur, Jaydatt for observing and proper counselling
the patients.
I am grateful to Dr. Asavari Kanade and Dr. Gauri Joshi for providing
me accurate statistics required for this study.
I am also thankful to my friends Dr. Swapnali and Dr. Suwarna who
always kept me alert and fresh.
My sincere thanks to Mr. Rakesh, Swami Enterprises for his
appropriate art work and designing which made this work presentable.
I experience the blessings of the god in my parents, Mrs. Sandhya
Bapat and late Mr. Avdhut Bapat. My vocabulary falls short to express
my regards to them.
My other family members, my sisters Mrs. Rashmi, Mrs. Nita and
Shilpa, my brother in law Mr. Sanjay, Mr. Bhalchandra, Mr. Atul, Mr.
Avinash, my sister in law Mrs. Arti and Mrs. Rohini always supported
me in every way to complete this work. I must express my sincere
thanks to them.
Even though my kids Arya and Parth are too small to understand the
meaning and importance of this work, they gave me constant
encouragement and support in their own innocent way, which helped
me to stabilize my mind.
My inner strength, really none other than my husband, Dr. Arvind,
whose timely encouragement made me aware of my aims and
capacities without which it was impossible for me to reach this stage
of life. He gave me unshaken support, care and stood solidly besides
me in each and every movement of my life. It is really beyond the
reach of my language to express my gratitude for him.

KEY TO TRANSLITERATION
A a Aa ā [ i
[- ī ] u } ū
e e eO ai Aao o
AaO au AM aṃ A: aḥ
k ka K kha ga ga
Ga gha = ṅa
ca ca C cha ja ja
Ja jha Ha ña
T ṭa z ṭha D ḍa
Z ḍha Na ṇa
t ta qa tha d da
Qa dha na na
p pa f pha ba ba
Ba bha ma ma
ya ya r ra la la
va va Sa śa Ya ṣa
sa sa h ha L la
xa kṣa & jña
? ṛa Ea ṣra
ABBREVIATION
Aṣtanga Hṛday A.). Vātānulomana VA
Caraka Saṃhitā ca. Angalāghava AL
Cakradatta cak`. Asaṃhata Varca AV
Sutra Sthāna saU. Klama KL
Kalpa Sthāna k. Snigdha Twak ST
Nidāna Sthāna ina. Samyak Snigdhatā Lakṣaṇa
SSL
Vimāna Sthāna iva. Anuvāsana Basti AB
Aṣtanga Saṃgraha A.saM Vāta Pitta Prakṛti VP
Suśruta Saṃhitā sau. Vāta Kapha Prakṛti VK
Kaśyapa Saṃhitā ka. Pitta Vāta Prakṛti PV
Cikitsā Sthāna ica. Pitta Kapha Prakṛti PK
Siddhi Sthāna isa. Kapha Vāta Prakṛti KV
Uttar Tantra ]. tM. Kapha Pitta Prakṛti KP
Uttama Śuddhi US
Madhyama Śuddhi MS
Hīna Śuddhi HS

INTRODUCTION
Pañcakarma is not merely a Śodhana therapy as it is understood, but
also having larger range of therapeutics such as Snehana, Swedana,
Stambhana etc. Out of these internal and external Snehana and
Swedana are considered as preparatory procedures or Purvakarma of
Śodhana. Ābhyantar Snehana is in practice since ancient times which
aims to prepare the body for expelling out the Doṣa and to protect the
body from Vātaprakopa after Śodhana.
In present days Ᾱyurveda physicians are showing much interest in
Śodhana Cikitsā, but many times they come across some difficulties in
administrating Purvakarma i.e. Snehapāna. They often experience a
poor compliance for oral administration of medicated fats (Snehapāna)
Patients are not ready to take Sneha orally even though they are
willing to undergo Vamana or Virecana. Patients have the major
problem in terms of quantity, taste, smell and oiliness of Sneha. In
our experience, at least 10 – 15 % patients are seen complaining about
having Sneha orally. It has also been observed that some patients
drop this treatment during the course. Incomplete Snehapāna or
premature development of Snehodwega cause discontinuation of
Snehapāna. All these conditions ultimately pose a problem for a
physician to prepare the patient for Śodhana process.
In other words, to convince the patient for taking Sneha orally is a
major problem for an Ᾱyurveda practitioner. These inconveniencies
made us think about effective alternative to counter drawbacks of
Snehapāna. Obviously, the alternative for having medicated fat orally
needs to be „Patient Friendly‟. Development of such alternative is the
need for today‟s era. This may further help popularising „Pañcakarma
processes‟ among the patients. Hence the present study was planned
to evaluate whether sign and symptoms of proper Snehana could be
achieved by administration of Anuvāsana Basti instead of Snehapāna.
There are no direct references available in texts which can point out
the use of Anuvāsana Basti as an alternative for Snehapāna; but with
the help of Yuktī Pramāṇa, it was taken into consideration that
Anuvāsana Basti can be used instead of Snehapāna. As the original
dose of Anuvāsana Basti is 120 ml; constant dose was administered in
one group. Generally dose of Ābhyantar Snehapāna is kept escalating;
hence Anuvāsana Basti was also administered in the escalating dose
in another group.
The scope of this study is,
Convenient for the patients who have aversion to Snehapāna.
The major problem for the doctors, to convince the patient
regarding Snehapān can be solved.
In this present study, Anuvāsana Basti is used as an alternative for
Snehapāna. Mūrcchit Tila Taila has been used along with Saindhava
for Anuvāsana Basti.
Hypothesis
Even though, Basti is a rectal rout of drug administration; it is
considered as an internal route of drug administration by Dalhaṇa. It
was therefore thought that Anuvāsana Basti of Mūrcchita Tila Taila
along with Saindhava can prove as an effective modality to achieve
symptoms of proper Snehana.
In this study; the subject has been elaborated as follows:-
Introduction: - Significance and scope of present study, hypothesis,
are discussed in the topic of introduction. Overall concept of the study
is put forth.
Conceptual Study:-
Review of literature: - In this topic review of Snehapāna Vidhī,
Vicāraṇā Sneha, Anuvāsana Basti, Tila Taila, Saindhava is taken
from various Saṃhitā. Previous work related to the subject has
been studied. Rectal route of administration of drug is also
studied available on web sites. On the basis of all these
references a concept of Anuvāsana Basti as an alternative for
Snehapāna has been discussed.
Clinical Study:-
Aim and objectives: Aim of the study regarding achieving
Samyak Snigdha Lakṣhaṇa by administration of Anuvāsana
Basti and objectives related to Koṣṭha are written in this topic.
Materials and Methods: In this section, material used for
Anuvāsana Basti with SOP of Anuvāsana Basti, inclusion and
exclusion criteria, drug administration criteria are discussed.
Scoring pattern and grades of Samyak Snigdhatā are also noted
in this topic. Two groups have been made. In group A dose of
Anuvāsana Basti was kept constant for minimum 3 and
maximum 7 days i.e. 120ml Murchita Tila Taila + 500mg
Saindhava. In group B, the dose was kept escalating i.e. 120ml
Murchita Tila Taila + 500mg Saindhava on 1st day increasing
with 25ml Murchita Tila Taila + 100mg Saindhava every day
minimum for 3 days and maximum for 7 days.
Observations and Results: Results have been drawn by
considering various observations. Observations are based upon
the statistical analysis of symptoms of Samyak Snigdhata;
Vātānulomana, Angalāghava, Asaṃhata Varca, Klama and
Snigdha Twak. Various statistical tests like Chi square test,
paired and unpaired t test have been applied to analyse the
data. To our surprise, in Gp. B i.e. in escalating dose of
Anuvāsana Basti, 58% patients showed symptoms of Pravara
Snigdhatā. No one was observed Asnigdha in this group.
Outcomes of Vamana and Virecana were also observed.
Discussion: The observations are discussed elaborately
according to various references. Main topics for discussion are;

Vicāraṇā Sneha, mode of action and Utkleśana Karma of
Anuvāsana Basti, Samyak Snigdhatā Lakśaṇa and consideration
of Basti Karma as an internal route of drug administration.
Observations are also discussed in this topic. Some limitations
and further scope regarding this study have been discussed
here.
Conclusion: On the basis of observations and discussions,
conclusions have been drawn. Anuvāsana Basti especially in
escalating dose can be a trend alternative for Snehapāna.
Summary: - The whole study has been summarised in this
topic, as Anuvāsana Basti is considered as an internal route of
drug administration; Snehana is possible through this route. In
the present study, this is proved.
Bibliography: According to the APA format, bibliography has
been written.


I. HISTORICAL REVIEW OF SNEHANA
(A) Veda
1) Ṛgveda:- the word Ghṛta is used as a synonym for nutritious
diet. Capacity of Ghṛta to inflame Agni is also described.
2) Atharvaveda: Ghṛta has been much complemented.
(B) Purāṇa
In Mārkandeya Purāna; Ghṛta, Taila, Vasā and Majjā were quoted as
Snehadravya.
(C) Saṃhitā Kāla
Caraka Saṃhitā
Contains a lot of information regarding Snehapāna but in scattered
manner.
Sūtra Sthāna:-
First chapter contains Mahāsneha, Guṇa and Karma of Caturvidha
Sneha.
Second chapter denotes Snehana and Swedana as a Purvakarma of
Pañcakarma.
Thirteenth chapter is totally devoted for Sneha. The sources, qualities
of Sneha, proper season of uses of each Sneha, concept of Vicaranā,
indications, contraindications of Sneha, dosage form of Sneha and
classification are described.
Twentysecond chapter contains six fold treatments with definition of
Snehana.
Vimāna Sthāna:-
Sixth chapter describes Snehana as a treatment of Vāta and Pitta.
Cikitsā Sthāna:-
Many references are available in the form of Sneha preparations and
as a treatment of Vātavyādhī.
Siddhī Sthāna:-
In first chapter, qualities of Saṃśodhanārtha Snehapāna are described
along with maximum period required for Snehana.
Suśruta Saṃhitā
The description about Pañcakarma is started from Snehopayogitā
Cikitsā Adhyāya of Cikitsā Sthāna. All information regarding all types
of Sneha is quoted.
Aṣtāṅga Saṃgraha and Aṣtāṅga Hṛdaya
In Snehādhyāya, total Sneha Vidhī is described in elaborated manner.
Śārangadhara Saṃhitā
In Uttarakhanḍa, a separate chapter is devoted for Snehanakarma, in
which Snehana Vidhī, dose, duration, indications, contraindications,
Samyak Yogadī Lakṣaṇa are described. The numerical values of Sneha
i.e. Pala, Karṣa are given.
Bhāvaprakāśa
A full description on Snehapāna Vidhī has been given in Purvakhanḍa.
The days for Snehana and Mātrā are discussed on the basis of types of
Koṣṭha and Agni.
Kaśyapa Saṃhitā
Kaśyapa has devoted total Adhyāya for Snehana Karma. Snehana
types, discussion on Śamana and Śodhana Sneha has been done.
Bhela Saṃhitā
In fourteenth chapter of Sutrasthāna, Snehana Karma has been
described. The mode of action of Snehapāna as a Purvakarma is
beautifully narrated. Bhela has given simily that the water flows from
upper side to lower level, likewise after Snehana, Doṣā come to Koṣṭha
from Śākhā.
Cakradatta
In chapter of Snehādhikāra; Snehana procedure is described.
Vangasena
In Snehapānādhikara chapter, the entire dose schedule of Jaghanya,
Madhyama and Uttama Mātra is given. Vardhamāna Mātrā of Sneha
for Śodhana is first time discussed.

II. LITERARY REVIEW OF SNEHAPĀNA
Śodhanārth Ābhyantara Snehapāna:
Śodhana therapy is meant for purification of body, through which all
the morbid Doshās are expelled out to maintain the proper functioning
of the body. This is the specialty of Āyurveda.
Śodhana procedure especially Vamana and Virecana is three fold
therapy. Certain preparatory procedures known as Purvakarma are
preceded by main procedures i.e. Pradhāna Karma followed by post
operative i.e. Paścāta Karma. The whole Śodhana procedure depends
upon the proper mobilization of Doṣas from Śākhā to Koṣṭha and
Utkleśa of Doṣas which are to be achieved by Snehana and Swedana.
Out of these two; Snehana has got importance which helps Doṣas to
move towards Koṣṭha by Vṛddhī and Abhiṣyanda of Doṣas.(1,2)
Etymology of the word „Sneha‟:
The word „Sneha‟ is derived from the ‘isnah\’ with iNaca\ p`%yaya. (vaacasp%yama\)
It has two meanings. One being „Snih-prītau‟ means to render affection
and the other „Snih-Snehane‟ meaning to render lubrication.
Snehana:
Snehana is the word to denote a therapy which promotes mainly
Snigdha Guṇa in a body. In Śabdastoma Mahānidhī, the term
Snehana is used only for external application of Sneha to the body.
Where as in Āyurvedic texts it is often used for internal administration
of Sneha.
Nirūkti / Definition:
The procedure by which Snigdhatā, Viṣyandana, Mārdavatā, and
Kledana are brought about is known as Snehana.(3) This particular
quotation has got extreme importance regarding Śodhanārtha
Ābhyantara Snehpāna. Snehana indicates Snigdhatā i.e. unctuousness, oiliness. Viṣyandana refers to Vilayana; i.e. dissolution
or diffusion, fluidity or liquification. After diffusion; excretion and
overflowing of Sneha is known as Viṣyandana. Mārdavata means
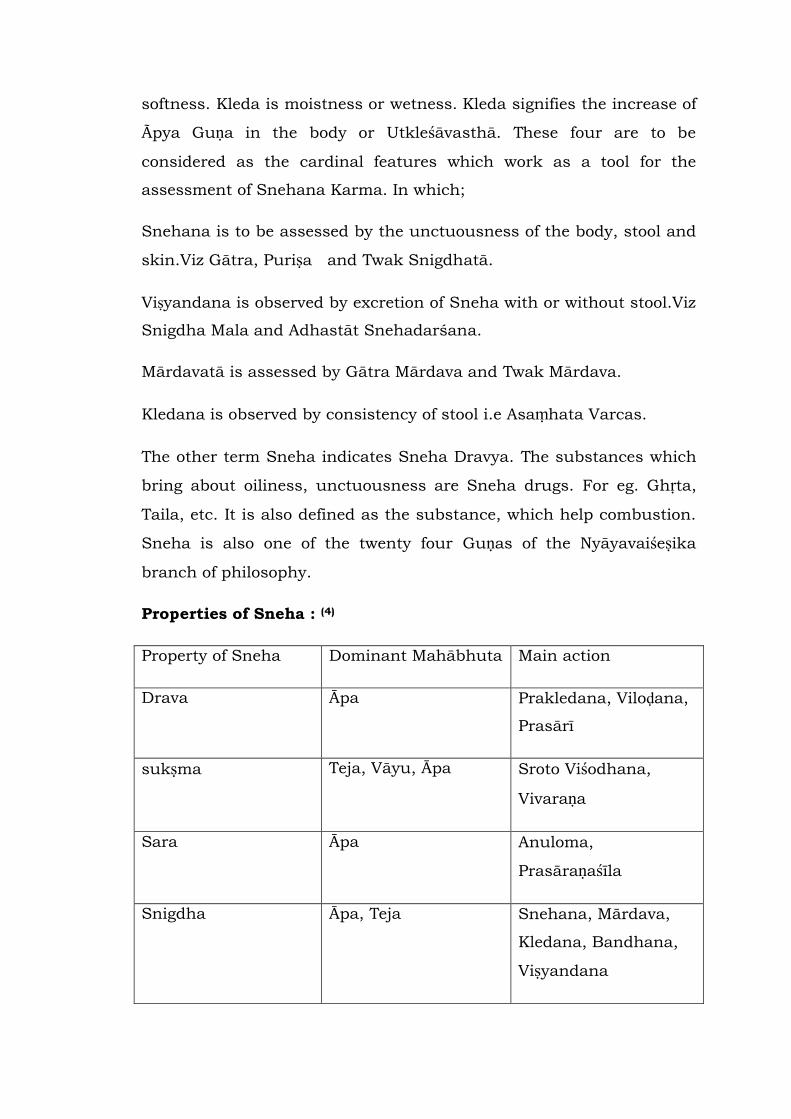
softness. Kleda is moistness or wetness. Kleda signifies the increase of
Ãpya Guṇa in the body or Utkleśāvasthā. These four are to be
considered as the cardinal features which work as a tool for the
assessment of Snehana Karma. In which;
Snehana is to be assessed by the unctuousness of the body, stool and
skin.Viz Gātra, Puriṣa and Twak Snigdhatā.
Viṣyandana is observed by excretion of Sneha with or without stool.Viz
Snigdha Mala and Adhastāt Snehadarśana.
Mārdavatā is assessed by Gātra Mārdava and Twak Mārdava.
Kledana is observed by consistency of stool i.e Asaṃhata Varcas.
The other term Sneha indicates Sneha Dravya. The substances which
bring about oiliness, unctuousness are Sneha drugs. For eg. Ghṛta,
Taila, etc. It is also defined as the substance, which help combustion.
Sneha is also one of the twenty four Guṇas of the Nyāyavaiśeṣika
branch of philosophy.
Properties of Sneha : (4)
Property of Sneha Dominant Mahābhuta Main action
Drava Āpa Prakledana, Viloḍana,
Prasārī
sukṣma Teja, Vāyu, Āpa Sroto Viśodhana,
Vivaraṇa
Sara Āpa Anuloma,
Prasāraṇaśīla
Snigdha Āpa, Teja Snehana, Mārdava,
Kledana, Bandhana,
Viṣyandana
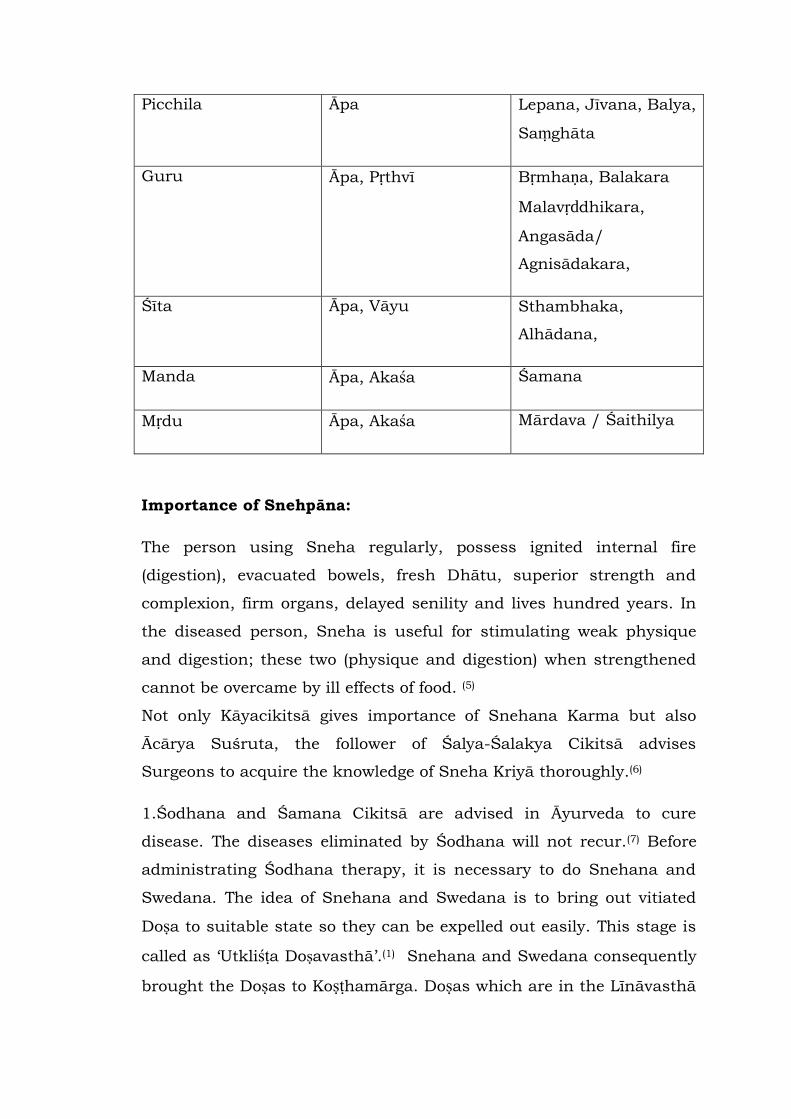
Picchila Āpa Lepana, Jīvana, Balya,
Saṃghāta
Guru Āpa, Pṛthvī Bṛmhaṇa, Balakara
Malavṛddhikara,
Angasāda/
Agnisādakara,
Śīta Āpa, Vāyu Sthambhaka,
Alhādana,
Manda Āpa, Akaśa Śamana
Mṛdu Āpa, Akaśa Mārdava / Śaithilya
Importance of Snehpāna:
The person using Sneha regularly, possess ignited internal fire
(digestion), evacuated bowels, fresh Dhātu, superior strength and
complexion, firm organs, delayed senility and lives hundred years. In
the diseased person, Sneha is useful for stimulating weak physique
and digestion; these two (physique and digestion) when strengthened
cannot be overcame by ill effects of food. (5)
Not only Kāyacikitsā gives importance of Snehana Karma but also
Ācārya Suśruta, the follower of Śalya-Śalakya Cikitsā advises
Surgeons to acquire the knowledge of Sneha Kriyā thoroughly.(6)
1.Śodhana and Śamana Cikitsā are advised in Āyurveda to cure
disease. The diseases eliminated by Śodhana will not recur.(7) Before
administrating Śodhana therapy, it is necessary to do Snehana and
Swedana. The idea of Snehana and Swedana is to bring out vitiated
Doṣa to suitable state so they can be expelled out easily. This stage is
called as „Utkliśṭa Doṣavasthā‟.(1) Snehana and Swedana consequently
brought the Doṣas to Koṣṭhamārga. Doṣas which are in the Līnāvasthā
(the deep seated Doṣa) change to Pravāhaṇa Avasthā, due to which
they could be removed easily.(8,9) The Doṣas become moistened with
Sneha, and liquefied by Swedana. Thus it becomes easy to expel them
by Śodhana.(10)
2. Ācārya Vāgbhaṭa has classified treatment into two categories. They
are, Santarpaṇa Cikitsā and Aptarpaṇa Cikitsā. Rūkṣana, Swedana
and Langhana come under Aptarpaṇa Cikitsā while Snehana ,
Stambhana and Bṛṃhaṇa come under Santarpaṇa Cikitsā.(11) These six
are called as Ṣadupakramas (six therapeutic principles). By this it can
be well understood that Snehana is one of the fundamental
therapeutic measure in Āyurveda.
3. As the body is originated from Śukra and Ãrtava which are
Snehatama Dhātus of the body; it has got a special affinity towards
Sneha. So body is considered as „Sneha Sāra‟.(12) Morever from the
childhood Snigdha Āhāra are habituated. A person who can be called
as „Snehasāra‟ may not be susceptible to diseases like Rājayaksmā etc
(13)
4. Pitta and Kapha are two Doṣas which have Snigdha Guṇa.(14)
Vitiation of Vāta especially by Rūkṣaṇa gets pacified by Sneha Kriyā.
5. Rasa, Rakta, Māṃsa, Meda, Majjā and Śukra Dhātus have Snigdha
Guṇa. These Dhātus maintain the normal body function by their
Snigdha property. Snigdha Guṇa increases as the Dhātus get
upgraded from Rasa to Śukra.(15)
6. The Upadhātus namely Vasā, Stanya and Oja have dominance of
Snigdha. Malas like Puriṣa, Mūtra, and Sweda are also having Snigdha
Guṇa and its deficiency indicates disease.(16,17)
7. In Bāla Cikitsā, the young children are considered always being
oleated because they are fed mainly with Shigdha Āhāra like breast

milk, or cow‟s milk, Ghī etc. So they are directly subjected to Śodhana
Cikitsā (mild) when necessary.
In nutshell, Sneha Guṇa exists in Doṣa, Dhātu, Upadhātu and Mala
which constitute our body.
Classification of sneha:
1. Classification of Sneha Dravya according to their
origin(18,19)
Sthāvara :- (Plant origin)
Seed eg. Tila, Eranda, Atasī, Karanja
Bark eg. Twak (Dālchinī)
Core eg. Chandan
Leaf eg. Eucalyptus, Lemon grass
Suśruta has described 12 Sthāvara Sneha with different functions (20)
Virecanopaga : Eranda, Tilwak, Jaypal
Vamanopayogī : Jimutaka, Kutaj
Śirovirecanopayogī : Vidanga, Jyotiṣmati
Duṣta Vraṇopayogī : Karanja, Puti Karanja
Mahāvyādhyupayogī : Bhallātaka, Kampillaka
Mutrasaṅga : Kuṣmāṇḍa
Aśmarīghna : Harītakī
Pramehopayogī : Sarṣapa, Nīma
In Pitta saṃsṛṣṭa Vāyu : Nārikela, Priyal
Kṛṣṇikaraṇopayogī : Bibhītaka, Bhallataka
Pāndukaraṇopayogī : Ṣyonaka, Priyangu
Dadru/ Kitibha kuṣthaghna : Agaru, Devadāru
Jaṅgama :- (Animal origin)(19)
Animal source of oils and fat (Jangama Sneha) ; Matsya (fish toothed
animals), Pakṣī (avians), constitute the animals fats.
Dadhī (curd), Kṣīra (milk), Ghṛta (Ghī), Amiṣa (meat), Vasā (fat), Majjā
(bone marrow) of these animals and birds.
2. Classification of the Snehana on the basis of their route of
administration (21,22,23,24)
a) Abhayantara –
Pāna
Basti
Nasya
Bhojana
b) Bāhya –
Abhyanga
Lepa
Mardana
Udvaratana
Saṃvāhana
Pādāghāta
Murdhataila
Ganduṣa
Karṇa Pūraṇa
Akṣī Pūraṇa
Parīṣeka
Picu
3. Classification of Sneha on the basis of Mātrā (25)
1) Hraswa Mātrā is that Mātrā which is digested in 6hrs.
2) Madhyam Mātrā is digested in 12hrs.
3) Uttama Mātrā is digested in 24hrs.
4) Hrasīyasī Mātrā is described by Vāgbhaṭa. The Mātrā which
would digest in half time of Hraswa Mātrā that means in 3hrs is
called as Hrasīyasī.
4.Classification of Sneha on the basis of their combination(26)
1) Yamaka Sneha- the combination of two Sneha. E.g.
Sarpi+Taila, Taila+Majjā etc.
2) Trivṛta Sneha- the combination of three Sneha. E.g.
Sarpi+Taila+Vasā.
3) Mahā Sneha- the combination of four Sneha. E.g.
Sarpi+Taila+Vasā+Majjā.
5. Classification of Sneha on the basis of its preparation
1) Accha Sneha
Accha Sneha is one, when it is used internally as it is i.e.unmixed and
in large quantity. The external application of unmixed Sneha, is not
Accha Sneha as it does not come in contact of Jāṭharāgni directly.(26)
In Amara Kośa the meaning of word „Accha‟ is given as clear and
clean. Accha also means that which is not solid (Aghana). The
synonym of Accha Sneha is Kevala Sneha which means a medicated
or not medicated (Samskṛtam- Asamskaṛtam va) Sneha when given
alone (27)
Accha Peya is of two types-
Saṃśodhan Accha Snehas (Purificatory simple oleation )
Saṃśamana Accha Peya (Palliative simple oleation)
Accha Sneha is administered in persons, who are Sātmya to Sneha
and those who can sustain physical strain. This is administered in
such a period, when it is neither Śīta nor Uṣṇa.(28)
2. Vicāraṇā Sneha (29)
Sneha along with various preparations like with Odana, Vilepī,
Yavāgu.
Route of administration is different than oral. Eg. Abhyanga,
Anuvāsana Basti, Karṇa Tarpaṇa.
Vicāraṇā Sneha is prescribed to those persons who have aversion for
taking Sneha substances, those who are in the habit of Madyapāna,
those who are having Mṛdu Koṣṭha, those who cannot resist to physical
strain.(30) Suśruta further added as this should also prescribed in the
condition of Tṛṣṇa and in Uṣṇa Kāla.(31)
6. Classification of Sneha on the basis of Kārmukatā (32)
1. Śodhana Sneha-
Sneha- employed as the preparatory procedure for Śodhana Karma. It
is to be given in more quantity, in the morning when the meal taken
in the previous night gets digested.
2. Śamana Sneha-
The one, which will not increase or decrease the Doṣa is called as
Śamana. The Sneha employed for Kuṣṭha, Duṣṭa Vraṇa, Pāṇdu etc.
comes under this type. The Śamana Sneha is administered when the
person feels hungry. It is given in Madhyama Mātrā.
It kindles the Agni, cleanses the Koṣṭha, increases Dhātu, Bala, Varṇa.
Due to Śamana Sneha; Indriya becomes strong, aging process
delays.(5)
3. Bṛṃhaṇa Sneha-
The Sneha which is administered for Bṛṃhaṇa of body is called as
Bṛṃhaṇa Sneha. It is given with Māṃsa, Madya or with meal, in Alpa
Mātrā.
It is indicated in Bāla, Vṛddha, Pipasārta, Snehadweṣī, Madyaśīla.
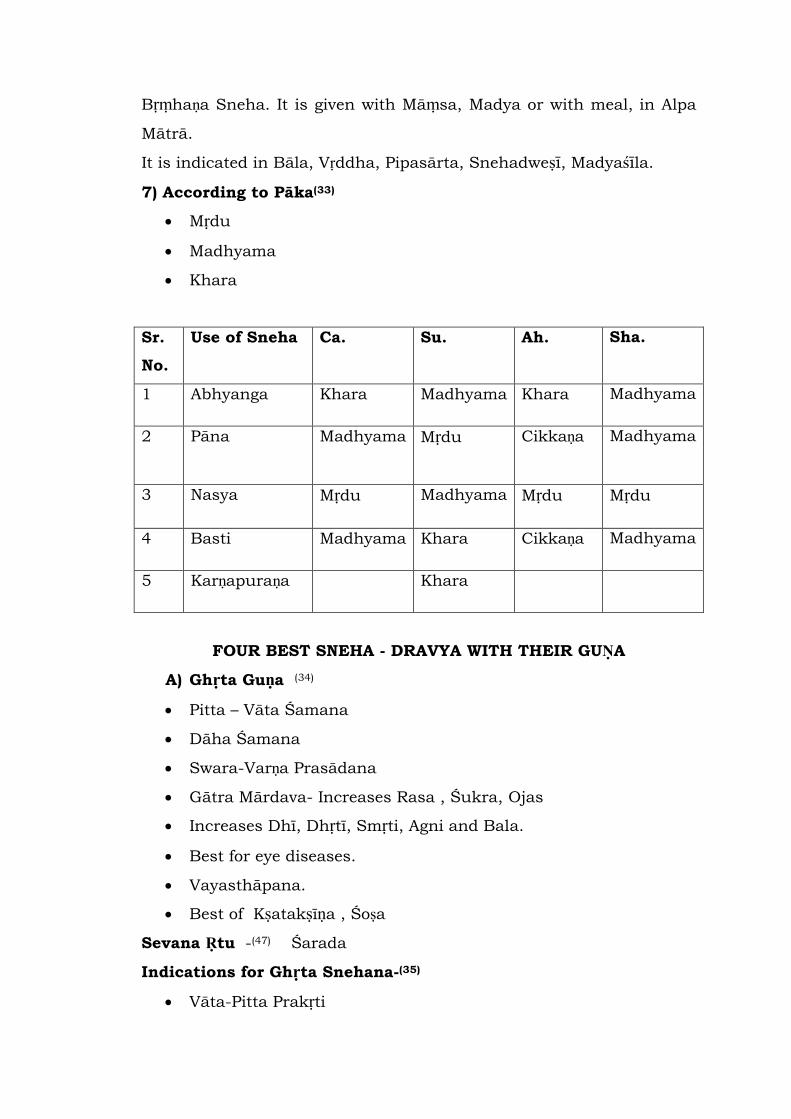
7) According to Pāka(33)
Mṛdu
Madhyama
Khara
Sr.
No.
Use of Sneha Ca. Su. Ah. Sha.
1 Abhyanga Khara Madhyama Khara Madhyama
2 Pāna Madhyama Mṛdu
Cikkaṇa Madhyama
3 Nasya Mṛdu Madhyama Mṛdu Mṛdu
4 Basti Madhyama Khara Cikkaṇa Madhyama
5 Karṇapuraṇa Khara
FOUR BEST SNEHA - DRAVYA WITH THEIR GUṆA
A) Ghṛta Guṇa (34)
Pitta – Vāta Śamana
Dāha Śamana
Swara-Varṇa Prasādana
Gātra Mārdava- Increases Rasa , Śukra, Ojas
Increases Dhī, Dhṛtī, Smṛti, Agni and Bala.
Best for eye diseases.
Vayasthāpana.
Best of Kṣatakṣīṇa , Śoṣa
Sevana Ṛtu -(47) Śarada
Indications for Ghṛta Snehana-(35)
Vāta-Pitta Prakṛti
Vāta-Pitta Vikārī
Cakṣukāmā
Kṣatakṣīṇa
Vṛddha, Bāla
Abala
Āyuprakarśakāmī
Bala-Varṇa-Swarārthinah
Puṣtikāmā.
Prajākāma.
Saukumāryārthina.
Dāha-Śastra-Viśa Pidita etc.
B) Taila Guṇa(36)
Āgneya, Uṣṇa, Tīkṣṇa, Madhura Vipāki, Vyavāyi, Sukṣma,
Viśada,Vikāsī, Guru, Sara, Lekhana.
Vāta Kapha Naśaka.
Twacya, Netrya, Kṛmighna.
Yoni - Sirā - Garbhāśaya Śulaghna.
Karṇa Śulaghna.
Śarira Mārdavakara, Māṃsabalya.
Sevana Kāla(47) – Pravṛṣa, Śitala Kāla .
Indications of Taila Snehana –(37)
Pravṛddha Sleṣma Medaska
Cala Sthula Gala Udar
Vātavyādhi
Vāta Prakṛti
For Bala, Tanutwa, Laghutā, Dṛḍhatā Sthir Gātratā
Kṛmi Koṣṭha
Krūra Koṣṭha
Nādivraṇa
C) Vasā Guṇa (38)
It is the Updhātu of Māṃsa Dhātu
Vasā of Grāmya, Anupa, Audaka animals is Guru, Uṣṇa, Madhura,
Vātaghna. Vasā of Jāṅgala, Ekasapha, Kravyāda animals is Śita,
Laghu, Kaṣaya, Raktapittanāśaka, Vasā of Pratuda and Viṣkira is
Kaphanāśaka.
Sevana Kāla(47) - Mādhava
Indications for Vasā Snehana – (39,40)
Vātātapasahā
Rukṣa
Bhārādhwa Karśita
Rujā in Asthi, Sandhi, Snāyu, Marma, Koṣṭha.
Āvaraṇa of Balawāna Vāyu on the Srotasa
Saṃśuṣka Retas, Rudhira
Nispīta Kapha Medas.
Mahat Agnibala
Vasā Sātmya
D) Majjā Guṇa (41)
Majjā is situated deeply inside the Asthi. The main function of it is
Purāṇa.
Guru among all the Snehas
Bāla Vardhaka
Rasa-Kapha-Majjā Vardhaka.
Asthi Dṛḍhikarṇa
Sevana Kāla(47) – Mādhava
Indications of Majjā Snehana – (42)
Dīptāgni
Kleśasaha
Ghasmara
Snehsevi
Vātarakta
Krura Koṣṭha
Snehana, Jīvana, Varnya, Bala-Upacaya Vardhana and Kaphāpaha.(43)
According to Kāśyapa, among all the four Uttama Snehas – Ghṛta,
Taila, Vasā, and Majjā are the Śreṣṭha Purvāpurvo which means Ghṛta
is best among all. Taila comes after Ghṛta then Vasā and Majjā in
sequences.(44) In the same manner they are Pittaśāmaka.(45) Majjā has
got the most Guru property than Ghṛta.(46)
Indications of Snehapāna :(48)
All fit for Sweda and Śodhana.
Vāta Roga: Rukṣa Guṇa. Eg. Ati Vyavāya, Ati Madyapāna, Ati
Cintā.
With Rukṣa and Cala Guṇa. Eg. Ati Vyāyāma.
Kṣīṇa Dhātu
Aged/ children/ ladies
Contra- indications of Snehana :(49)
Agni Vikṛtī : Ati Mandāgni, Tikṣṇāgni
Āmaja Vikāra : Atisāra, Chardī, Apaprasūta, Aruci, Tṛṣṇā
Kapha dominant / Srotorodhajanya diseases: Urustambha, Udara,
Sthaulya
Madya / Gara Viṣapidita
Immediate after Śodhana like Virecana, Nasya, Basti
Samyak Snigdha Lakṣaṇa: (50)
Careful assessment of Samyak Snigdha Lakṣaṇa is very important for

deciding further Śodhana procedures.
Vātānulomana: Proper Evacuation of flatus, faeces and urine
Diptogni: proper ignition of Agni
Snigdha Varca along with Asaṃhata Varca: it denotes the saturation of
Sneha in Varca.
Klama: exausion without much exersion.
Twak Snigdhatā/ Gātra Mārdavatā:
Asnigdha Lakṣaṇa: (51)
Appearance of symptoms like Grathita and Rukṣa Purīṣa, Vāta
Pratilomatā, Agnimāndya, Gātra Rukṣatā/ Kharatā etc during
Snehapāna is known as Asnigdha Lakṣaṇa. Actually these symptoms
may be present prior to Snehana therapy, but when Snehana is
not done properly, these symptoms persist.
Atisnigdha Lakṣaṇa: (52)
If Snehapāna is given in larger dose even after appearance of Samyak
Snigdhatā; Atisnigdha Lakṣaṇa may appear.
Pāṇdutā, Gaurava, Jāḍya, Avipakwa Puriśa, Tandrā, Aruci and Utkleśa
are some symptoms of Atisnigdhatā.
Sneha Jīrṇājīrṇa Lakṣaṇa:(53)
During the period of digestion of Sneha, some symptoms are produced
which are called as Sneha- Jīryamaṇa Lakṣaṇa. These symptoms
disappear after digestion of Sneha and don‟t require any sort of
therapeutic intervention. In case of doubt regarding digestion or
indigestion of Sneha, one should take hot water which brings Śuddha
Udgāra.
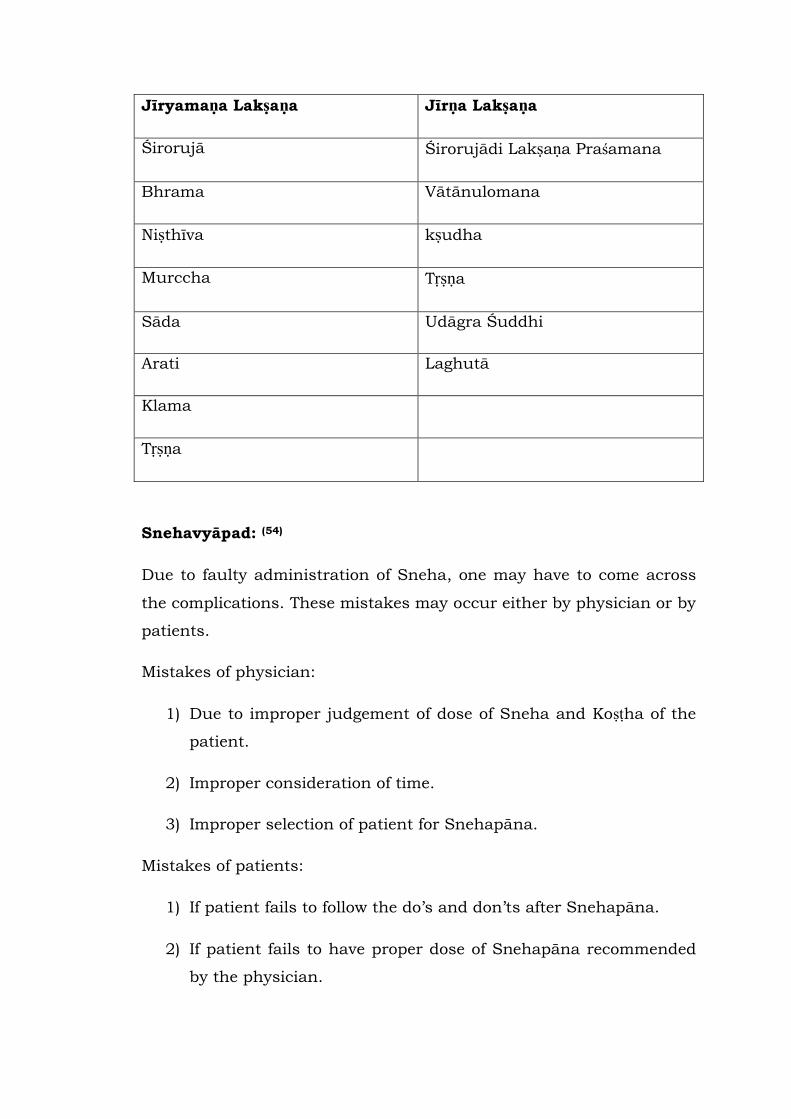
Jīryamaṇa Lakṣaṇa Jīrṇa Lakṣaṇa
Śirorujā Śirorujādi Lakṣaṇa Praśamana
Bhrama Vātānulomana
Niṣthīva kṣudha
Murccha Tṛṣṇa
Sāda Udāgra Śuddhi
Arati Laghutā
Klama
Tṛṣṇa
Snehavyāpad: (54)
Due to faulty administration of Sneha, one may have to come across
the complications. These mistakes may occur either by physician or by
patients.
Mistakes of physician:
1) Due to improper judgement of dose of Sneha and Koṣṭha of the
patient.
2) Improper consideration of time.
3) Improper selection of patient for Snehapāna.
Mistakes of patients:
1) If patient fails to follow the do‟s and don‟ts after Snehapāna.
2) If patient fails to have proper dose of Snehapāna recommended
by the physician.
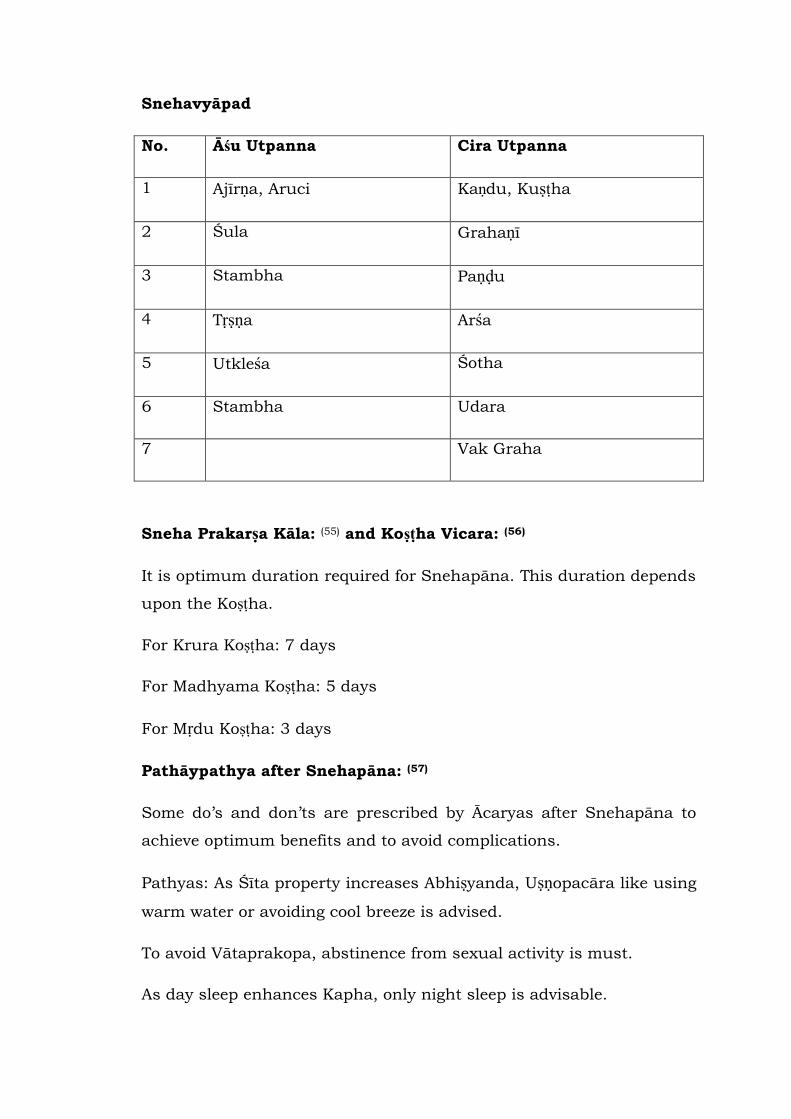
Snehavyāpad
No. Āśu Utpanna Cira Utpanna
1 Ajīrṇa, Aruci Kaṇdu, Kuṣṭha
2 Śula Grahaṇī
3 Stambha Paṇḍu
4 Tṛṣṇa Arśa
5 Utkleśa Śotha
6 Stambha Udara
7 Vak Graha
Sneha Prakarṣa Kāla: (55) and Koṣṭha Vicara: (56)
It is optimum duration required for Snehapāna. This duration depends
upon the Koṣṭha.
For Krura Koṣṭha: 7 days
For Madhyama Koṣṭha: 5 days
For Mṛdu Koṣṭha: 3 days
Pathāypathya after Snehapāna: (57)
Some do‟s and don‟ts are prescribed by Ācaryas after Snehapāna to
achieve optimum benefits and to avoid complications.
Pathyas: As Śīta property increases Abhiṣyanda, Uṣṇopacāra like using
warm water or avoiding cool breeze is advised.
To avoid Vātaprakopa, abstinence from sexual activity is must.
As day sleep enhances Kapha, only night sleep is advisable.
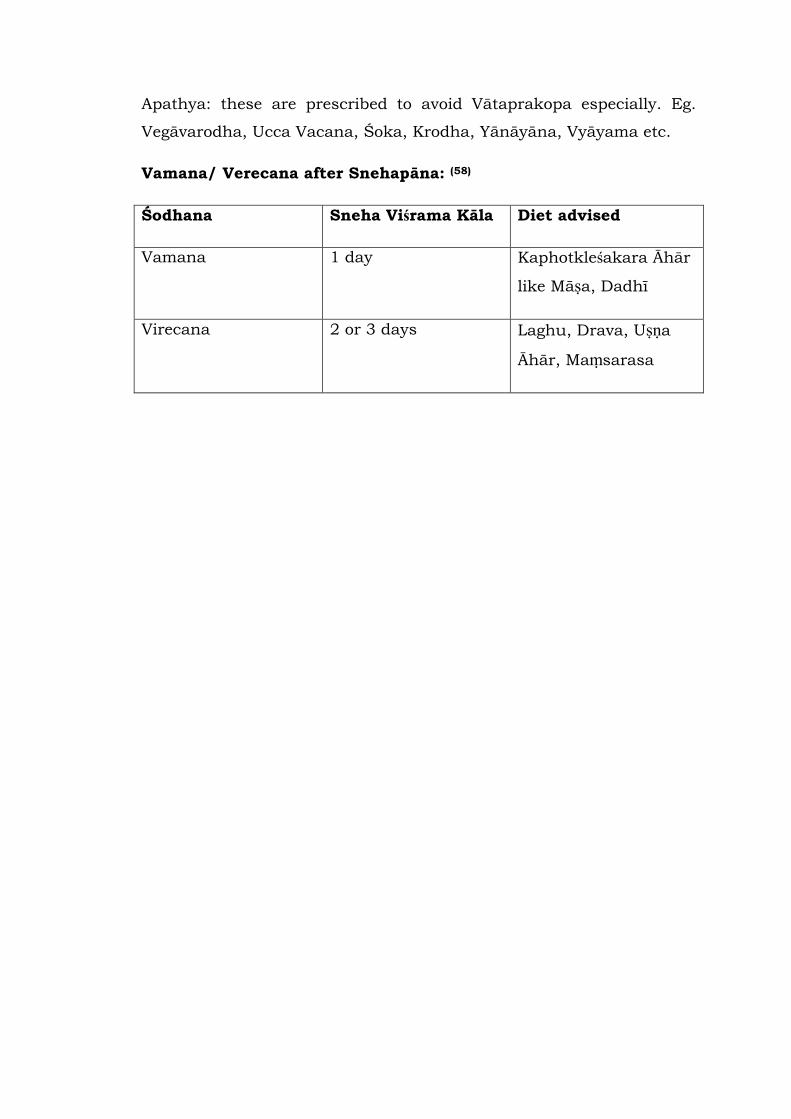
Apathya: these are prescribed to avoid Vātaprakopa especially. Eg.
Vegāvarodha, Ucca Vacana, Śoka, Krodha, Yānāyāna, Vyāyama etc.
Vamana/ Verecana after Snehapāna: (58)
Śodhana Sneha Viśrama Kāla Diet advised
Vamana 1 day Kaphotkleśakara Āhār
like Māṣa, Dadhī
Virecana 2 or 3 days Laghu, Drava, Uṣṇa
Āhār, Maṃsarasa

III. HISTORICAL REVIEW OF BASTI KARMA
(A) Veda
The Kauśika Sutra of Atharvaveda, Basti is indicated as a substitute
for minor operation. (K.S. Darila 25/127).
(B) Purāṇa
In Agnipurāṇa, Basti is indicated as a principle treatment in
complaints marked by predominance of Vāta (A. P. 279/63). In Aśwa
Cikitsā Kathana, Taila Basti is recommended in horses to relieve their
fatigue immediately (A. P. 284/14). It is also stated that according to
season different Sneha should be used for Basti (A. P. 289/46).
(C)Yogic Literature
Gheraṇḍa Sam hitā
Basti is included in Ṣaṭkarma. Two kinds of Bastis are described there.
Procedure of Basti explained in detail in [1/44-48]
1) Jala Basti – To be done in water
2) Suşka Basti – To be done always on land.
(D) Saṃhitā Kāla
Caraka Sam hitā
The scattered references regarding Basti are available in various
chapters of Caraka Sam hitā, but in Siddhīsthāna out of 12 chapters, 8
chapters are devoted to Basti. First two chapters of Siddhīsthāna deals
with properties of Basti, Samyakyoga, Atiyoga, Ayoga Lakṣaṇas,
indications and contraindications of Basti.This denotes the importance
of Basti in the field of Kāyacikitsā.
Suśruta Sam hitā
In Sus ruta Sam hitā, four chapters have been devoted completely for
the description of the Basti in Cikitsāsthāna. In these chapters, detail
information regarding Bastinetra, indication, contra-indications,
complications, classification of Basti etc. are available. Other various
references of Basti are also available in this Sam hitā.

Aştāṅga Saṃgraha
In 19th chapter of Sutrasthāna classification, indication, contra-
indication, Dosage, process of administration etc. have been described
in detail. Also four chapters of Kalpasthāna have been contributed to
Basti. In these chapters, description regarding importance of Basti,
different types of Basti, Sneha Basti Vyāpada etc. are available.
Aştāṅga Hṛdaya
In 19th chapter of Sutrasthāna, Basti Vidhī is described. In 4th and
5th chapter of Kalpasthāna named as Basti Kalpa and Basti Vyāpada
Siddhī respectively, every aspect of Basti has been explained.
Kaśyapa Samhitā
In Kaśyapa Sam hitā, Basti has been explained in detail in
Siddhīsthāna and Khilasthāna.
Bhela Sam hita
In Bastimātrīya Siddhī, Upakalpa Siddhī, Phala Mātrā Siddhī and
Doṣa Vyāpadikā Basti Siddhī of Siddhīsthāna description of Basti is
available.
Hārita Saṃhitā
In this text, only 3rd chapter of Sūtrasthāna deals with Basti.
Cakradatta
In this text, two chapters named Anuvāsanādhikāra and
Niruhādhikāra are dealt with Anuvāsana and Niruha Basti
respectively.
Śārañgadhara Saṃhitā
In Uttara Khaṇḍa 5th, 6th, 7th chapter, description of Basti is
available in detail. Some of the contributions are like Paribhāṣā of
Basti, Āsthāpana etc are noted.
Bhāva Prakāśa
Basti is explained in detail in Pūrvakhaṇḍa. Most of the explanations
are similar to Suśruta and Śārangadhara.

IV. LITERARY REVIEW OF ANUVĀSANA BASTI
Derivation of Basti:
vasau inavaasao vasa\ AacCadnao vasa\ vaasanao sauriBakrNao |
baist: basto: AavaRNaaoit maUHama\ | naaBao: AQaaoBaagao maUHaaQaaro sqaanao |
It means to lie or to reside.
It means to cover.
Basti is that which covers Mūtra.
Niruktī /Defination of Basti(59,60)
1) The treatment which is given by using Basti, i.e. urinary bladder
of animal is called as Basti.
2) Basti means Mutrāśaya i.e bladder. The process in which
Mutrāśaya is used is called as Basti.
3) Basti word is used to demonstrate anatomical organ bladder.
4) Ācārya Caraka mentioned that, the process through which
medicine reaches up to Kaṭī Pārśva, Kukṣī, spreads and oleates
the body, destroys Bandha of Doṣas and Malas and expelled
them out from the body, is called as Basti.
Types of Basti
According to Adhiṣhṭhāna:
1. Internal: Pakwāśayagata, Mutrāśayagata, Garbhāśayagata
(uttarabasti), Vraṇabasti.
3. External: In this type medicated oil is retained over the affected
part for a prescribed time therefore it is called as Basti.
According to the body part, the names are given eg. Śirobasti,
Katibasti etc.
According to Basti Dravya (61)
1. Niruh: decoction or any Drava-dravya is used eg Yāpana Basti,
Picchā Basti, Kṣāra Basti, Takra Basti, Kṣīra Basti, Mam sarasa
Basti, Gomūtra Basti, Dadhimastu Basti, Amlakāñjī Basti,
Prasannā/ Surā/ Āsava Basti.
2. Anuvāsana Basti: in which Snehadravya is used.
According to Sankhya : (62)
1. Karma: 18 Anuvāsana+12 Niruha = 30 Basti
2. Kala: 10 Anuvāsana+ 6Niruha = 16 Basti
3. Yoga: 5 Anuvāsana+ 3Niruha = 8 Basti
According to Matra: (63)
1. Dvādaśa Prāsṛta Basti
2. Ekādaśa Prāsṛta Basti
3. Nava Prāsṛta Basti
4. Aṣṭa Prāsṛta Basti
5. Sapta Prāsṛta Basti
6. Ṣaḍ Prāsṛta Basti
7. Pañca Prāsṛta Basti
8. Catuh Prāsṛta Basti
On the basis of the Rasa of the Basti Dravya: (64)
1. Madhura Rasa Dravya Basti
2. Āmla Rasa Dravya Basti
3. Lavaṇa Rasa Dravya Basti
4. Kaṭu Rasa Skandha Basti
5. Tikta Rasa Skandha Basti
6. Kaṣāya Rasa Dravya Basti
On the basis of the nature of the Basti Dravya: (65)
1. Mṛdu Basti: Snehadravyas are used.
2. Madhyama Basti: Decoctions like Erandamūla are used.
3. Tīkṣṇa Basti: Tīkṣna Dravyas like Gomutra, Kañjī are used.
On the basis of action on Doşa:
1. Utkleśana Basti
2. Śodhana Basti
3. Śamana Basti
4. Vātahara Basti
5. Pittahara Basti
6. Kaphahara Basti
7. Doṣa-Sansargahara Basti
8. Śoṇita Doṣahara Basti
9. Snehana Basti
10. Bṛṃhaṇa Basti
11. Sangrāhika Basti
12. Vājīkaraṇa Basti
13. Rasāyana Basti
14. Balavarṇakṛta Basti
15. Dīpana Basti
16. Pakvāśaya Śodhana Basti
17. Lēkhana Basti
18. Cakṣuṣya Basti
19. Raktapittahara Basti
20. Pramehahara Basti
21. Kuṣṭhahara Basti
22. Visarpahara Basti
23. Vātaraktahara Basti
24. Abhiśyandahara Basti
25. Dāhaghna Basti
26. Kṛmihara Basti
27. Mūtrakṛcchrahara Basti
28. Parīkartikāhara Basti
On the basis of speciality of names:
1. Mādhutailika Basti
2. Siddha Basti
3. Yuktaratha Basti
4. Yāpana Basti
5. Picchā Basti
6. Vaitaraṇa Basti
7. Picchīla Basti
These classifications are based on different aspects of Basti. But
practically only Niruha and Sneha Basti are main two types which
include all above classification. As this work deals with Anuvāsana
Basti; details of Anuvāsana Basti are mentioned.
Definition of Anuvāsana Basti: (66)
Anuvāsana literally means that which remains in the body for some
time without causing any adverse effect and it can be given every day.
Anuvāsana Basti means administration of Sneha through Basti.
According to Caraka, there are three dosage forms of Anuvāsana Basti.
They are as follows :( 67)
1. Sneha Basti:
Ācārya Suśruta and Caraka mentioned the dose of Sneha Basti as
1∕4th of Niruha Basti.(68) It is considered as Uttama Mātrā of
Anuvāsana Basti.
2. Anuvāsana Basti:
Basti which is given in half dose of Sneha Basti is called as Anuvāsana
Basti.(69)
3. Mātrā Basti:
Mātrā Basti is a type of Snēha Basti/ Anuvāsana Basti. The dose of
Snēha used in it is very less as compared to the dose of Snēha Basti.
Acārya Vāgbhaṭa has defined the Mātrā Basti as the Basti in which
the dose of Snēha is equal to Hrasva Mātrā of Snehapāna.(70)
Ācārya Suśruta mentioned Basti which is given in half dose of
Anuvāsana Basti is called as Mātrā Basti.
Points to be considered for administration of Anuvāsana Basti:
1. Kāla Vicāra:
A. Anuvāsana Basti yogya Kāla: (71)
It should be administered during day time; as Agni is in its normal
state and Srotomukha are open to receive the Vīrya of Sneha.
B.Anuvāsana Basti Ayogya Kāla: (72,73)
Anuvāsana Basti is not advisable to give at night as Srotomukha
are closed; the Vīrya of Sneha can‟t spread throughout the body.
As night is Śīta by nature; Utkleśa of Doṣa takes place.
C. Kāla Viśeṣa Vicāra:
In Śīta and Vasanta Rṛtu: in day time (74)
Śarada and Griṣma: in night ( Prathama Prahara)
If patient is suffering from Tīvra Rujā with extreme vitiation of
Vāta; then Anuvāsana Basti can be administered at any time after
consuming the food.
Anuvāsana Basti can be given daily in the conditions like Rukṣa
and Bahuvātāvasthā. (75)
2. Agni Vicāra:
Even though; Anuvāsana Basti is administered in Pakwāśaya, the
consideration of Jātharāgni is very necessary. Proper functioning
of Anuvāsana Basti depends upon the absorption capacity of Agni
present in Pakwāśya.(76) This capacity is ignited and supported by
Jātharāgni itself. Further digestion and assimilation of Sneha
depends upon the proper condition of Dhātvāgni and Bhutāgni.
3. Rules to be followed regarding position:
A. Significance of Vāma Pārśva/ left lateral position: (77)
There are three valves in the rectum. Out of that, middle valve is
important anatomically, physiologically and functionally also. It is
situated in the right side of the rectum. It plays important role in
the defecation process. Any injury to this valve may cause fecal
incontinence.
Lying on the left lateral keeps the sphincters submerged into the
musculature. This position helps in gravity because of the
anatomical slope which facilitates passing of Basti Dravyas across
the rectum to other areas.
The absorptive area of mucosa is also more on the left side.
B. The table on which patient takes the left lateral position
should not be too high or too low. Head of the patient must be
towards east. It should be sufficient to accommodate the patient
with soft and clean covering. (78)
4. Indications of Anuvāsana Basti:
Those who are indicated for Āsthāpana Basti are indicated for
Anuvāsana Basti also. (79)
Sarvāngagata Vāta, Ekānga Vāta, Varca- Mutra Sanga, Karṇaśula,
Hṛday, Pṛṣtha, Katigraha, Pliha, Gulma, Hṛdroga, Bhagandara,
Unmāda etc. Especially Rukṣa, Tīkṣṇāgni, Kevala Vāta Roga. (80)
5. Contraindications of Anuvāsana Basti:
Those who are contraindicated for Āsthāpana Basti are
contraindicated for Anuvāsana Basti also. (81)
Navajwara, Pāṇdū, Kāmalā, Meha, Arśa, Pratiśyāya, Pīnasa,
Plīhāroga, Atisāra, Kaphodara, Gurukoṣṭha, Ślīpada, Galadaṇḍa,
Apaci, Abhiśyanda, Atikṛśa, Sthula, Kṛmikoṣṭha, and Abhukta.
6. Rules to be followed before administration of Anuvāsana
Basti:
A. Patient should be asked to evacuate faeces and urine prior to
Anuvāsana Basti so that it can entre without any obstruction. (82)
B. Anuvāsana Basti should be given after having food. Sneha has
got Vyavāyī, Tīkṣṇa, Uṣṇa and Sukṣma properties due to which the
Sneha will move to the upper part of the colon and can destroy the
digestive power. It will cause some adverse effects like
Agnimāndya, Cardī, Bhrama etc. (83) Suśruta emphasizes to give
Anuvāsana Basti immediate after having food by quoting the
specific word Ādrapāṇī i.e. immediate after having food when
palms are wet. If it is given in the Vidagdhāvasthā of Anna; Jwara
can be seen. Even it should not be administered after having
Snigdha food as it may cause Mada and Mūrcchā. Alpa Snigdha
food is advisable before it‟s administration as Rukṣa food destroys
Bala and Varṇa. It is better to consume 1/4th less amount of food
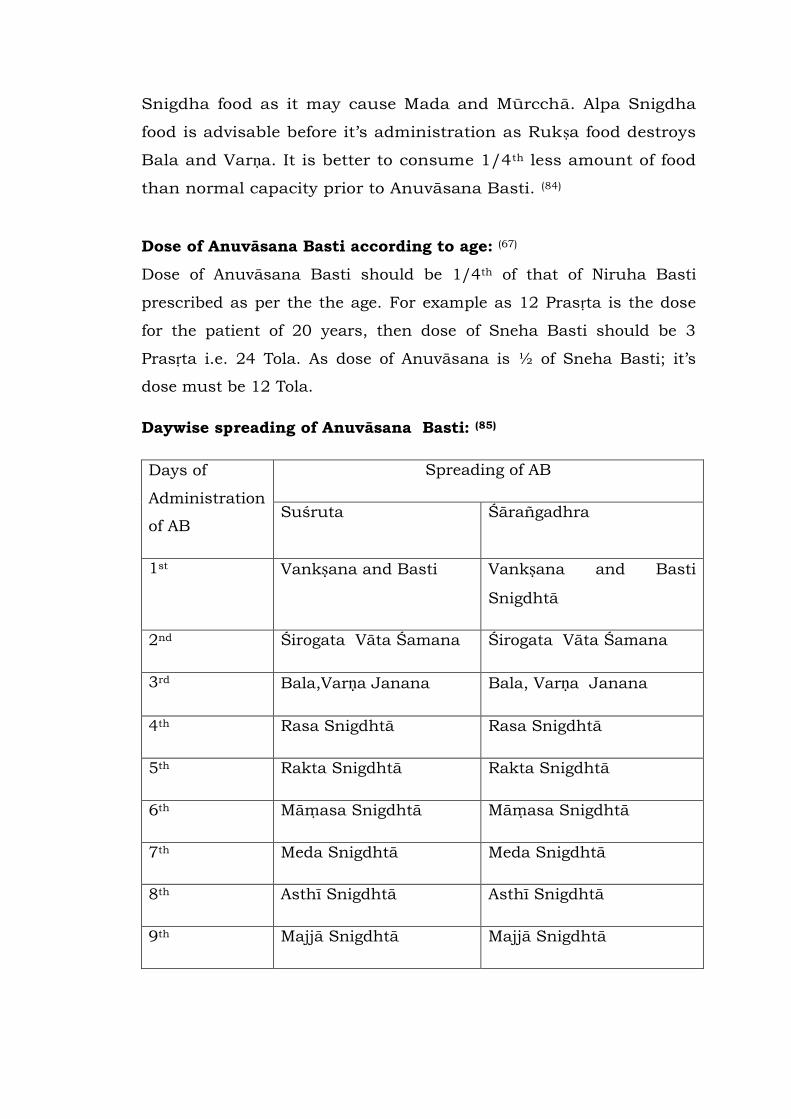
than normal capacity prior to Anuvāsana Basti. (84)
Dose of Anuvāsana Basti according to age: (67)
Dose of Anuvāsana Basti should be 1/4th of that of Niruha Basti
prescribed as per the the age. For example as 12 Prasṛta is the dose
for the patient of 20 years, then dose of Sneha Basti should be 3
Prasṛta i.e. 24 Tola. As dose of Anuvāsana is ½ of Sneha Basti; it‟s
dose must be 12 Tola.
Daywise spreading of Anuvāsana Basti: (85)
Days of
Administration
of AB
Spreading of AB
Suśruta Śārañgadhra
1st Vankṣana and Basti Vankṣana and Basti
Snigdhtā
2nd Śirogata Vāta Śamana Śirogata Vāta Śamana
3rd Bala,Varṇa Janana Bala, Varṇa Janana
4th Rasa Snigdhtā Rasa Snigdhtā
5th Rakta Snigdhtā Rakta Snigdhtā
6th Mām asa Snigdhtā Māmasa Snigdhtā
7th Meda Snigdhtā Meda Snigdhtā
8th Asthī Snigdhtā Asthī Snigdhtā
9th Majjā Snigdhtā Majjā Snigdhtā
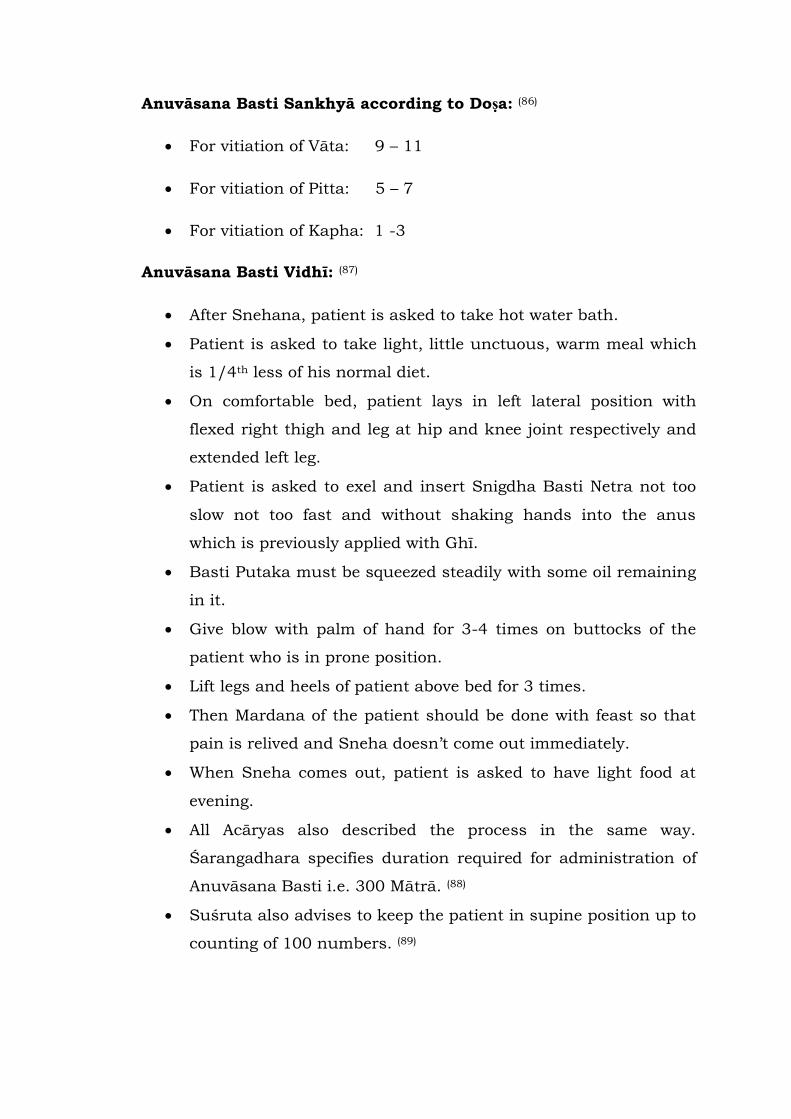
Anuvāsana Basti Sankhyā according to Doṣa: (86)
For vitiation of Vāta: 9 – 11
For vitiation of Pitta: 5 – 7
For vitiation of Kapha: 1 -3
Anuvāsana Basti Vidhī: (87)
After Snehana, patient is asked to take hot water bath.
Patient is asked to take light, little unctuous, warm meal which
is 1/4th less of his normal diet.
On comfortable bed, patient lays in left lateral position with
flexed right thigh and leg at hip and knee joint respectively and
extended left leg.
Patient is asked to exel and insert Snigdha Basti Netra not too
slow not too fast and without shaking hands into the anus
which is previously applied with Ghī.
Basti Putaka must be squeezed steadily with some oil remaining
in it.
Give blow with palm of hand for 3-4 times on buttocks of the
patient who is in prone position.
Lift legs and heels of patient above bed for 3 times.
Then Mardana of the patient should be done with feast so that
pain is relived and Sneha doesn‟t come out immediately.
When Sneha comes out, patient is asked to have light food at
evening.
All Acāryas also described the process in the same way.
Śarangadhara specifies duration required for administration of
Anuvāsana Basti i.e. 300 Mātrā. (88)
Suśruta also advises to keep the patient in supine position up to
counting of 100 numbers. (89)
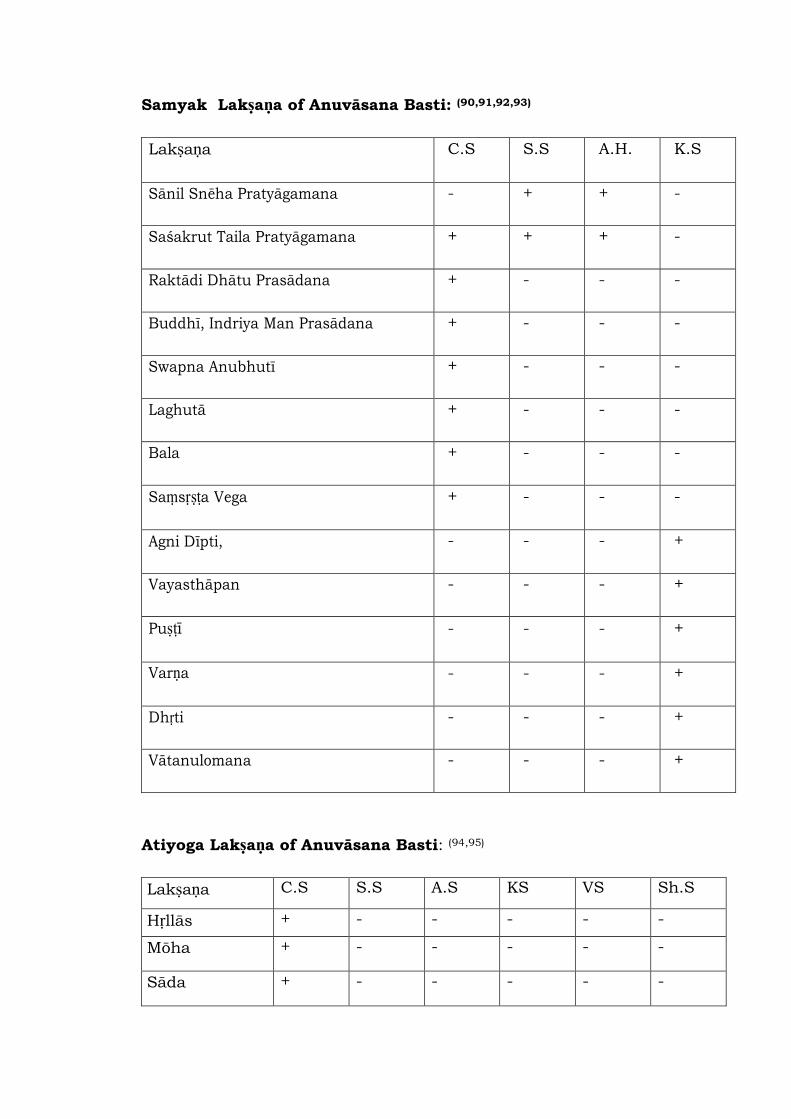
Samyak Lakṣaṇa of Anuvāsana Basti: (90,91,92,93)
Lakṣaṇa C.S S.S A.H. K.S
Sānil Snēha Pratyāgamana - + + -
Saśakrut Taila Pratyāgamana + + + -
Raktādi Dhātu Prasādana + - - -
Buddhī, Indriya Man Prasādana + - - -
Swapna Anubhutī + - - -
Laghutā + - - -
Bala + - - -
Saṃsṛṣṭa Vega + - - -
Agni Dīpti, - - - +
Vayasthāpan - - - +
Puṣṭī - - - +
Varṇa - - - +
Dhṛti - - - +
Vātanulomana - - - +
Atiyoga Lakṣaṇa of Anuvāsana Basti: (94,95)
Lakṣaṇa C.S S.S A.S KS VS Sh.S
Hṛllās + - - - - -
Mōha + - - - - -
Sāda + - - - - -
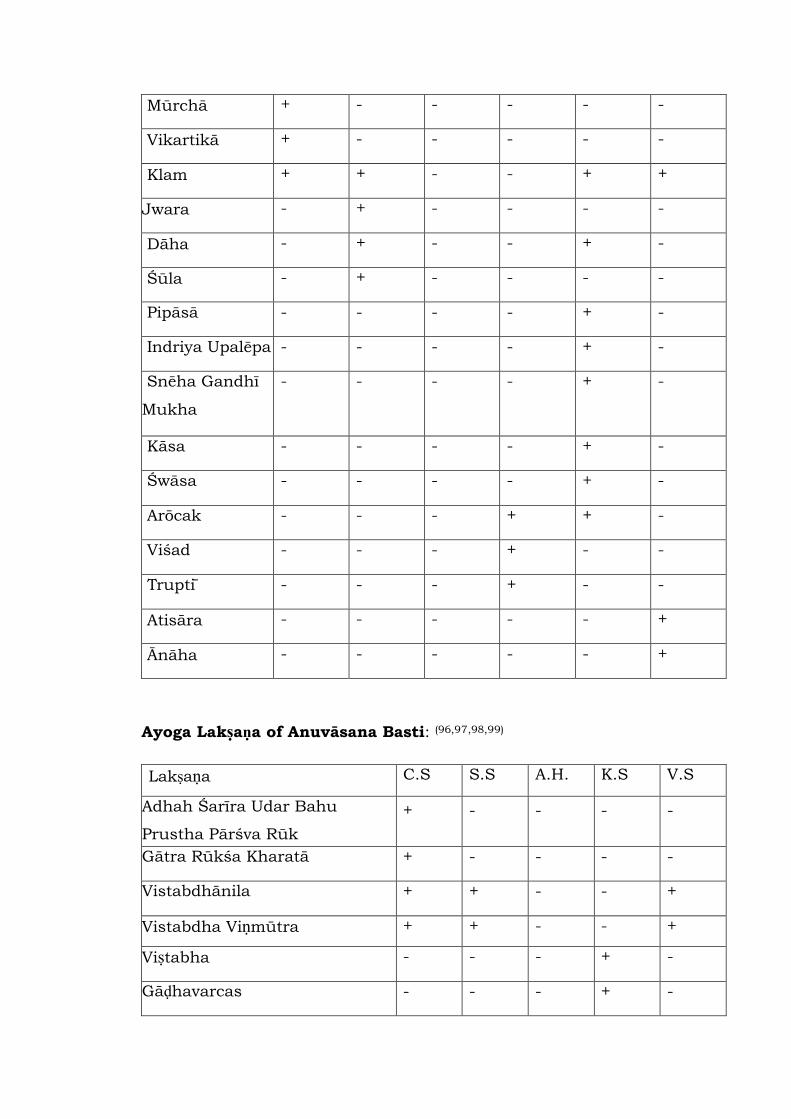
Mūrchā + - - - - -
Vikartikā + - - - - -
Klam + + - - + +
Jwara - + - - - -
Dāha - + - - + -
Śūla - + - - - -
Pipāsā
- - - - + -
Indriya Upalēpa
- - - - + -
Snēha Gandhī
Mukha
- - - - + -
Kāsa
- - - - + -
Śwāsa
- - - - + -
Arōcak
- - - + + -
Viśad
- - - + - -
Trupti
- - - + - -
Atisāra - - - - - +
Ānāha - - - - - +
Ayoga Lakṣaṇa of Anuvāsana Basti: (96,97,98,99)
Lakṣaṇa C.S S.S A.H. K.S V.S
Adhah Śarīra Udar Bahu
Prustha Pārśva Rūk
+ - - - -
Gātra Rūkśa Kharatā
+ - - - -
Vistabdhānila
+ + - - +
Vistabdha Viṇmūtra
+ + - - +
Viṣtabha
- - - + -
Gāḍhavarcas
- - - + -
Rogvṛddhī
- - - + -
Vivarṇata - - - + -
Vepathu - - - + -
Vāta Vṛddhī
- - - + -
Retention period of Anuvāsana Basti: (100)
The normal Pratyāgamana Kāla of Anuvāsana Basti is 3 Yāma i.e. 9
hours. There is no harm if Anuvāsana Basti retains for a whole day.
If Anuvāsana Basti comes out immediately, another Basti can be given
to get better Snehana.
Sneha Basti Vyāpad (101, 102)
Complications may produce if Doṣas present in Koṣṭha are dominant
and Anuvāsana Basti has got Alpa Vīrya. The another cause is Mithyā
Praṇihita Basti i.e. administration of Anuvāsana Basti without proper
precausions as prescribed earlier.
Vyāpad Causes Symptoms Treatment
Vāta
Avṛta
Sneha
When
Koṣṭha is
full of Vāta,
and Basti is
given with
cold Sneha
or in small
quantity.
Aṅgamarda,
Jwara,
Ādhmāna,
Stambha, Urah,
Parsvaśūla
Niruha Basti of Pañcamula
Kwātha and Gomūtra,
Rāsnā Taila prepared by
Pitadāru, Tilvak, Surā,
Sauviraka, Kola, Kulattha,
Yava, Kwātha mixed with
Kalka of Snigdha, Uṣṇa, Āmla,
Lavaṇa Dravya is given to
eliminate the Vātavṛta Sneha
Pitta
Avṛta
If excessive
Basti is
Udara Dāha,
Raga, Truşņā,
Niruha Basti prepared with
Madhura and Tikta Dravyas

Sneha given in
Pitta
dominance
Moha,
Tamakaśvāsa
and Jwara.
should be given.
Kapha
Avṛta
Sneha
If Mṛdu
Basti is
given in
condition of
dominance
of Kapha.
Tandrā, Jwara,
Ālasya,
Praseka, Arucī,
Gaurva,
Mūrchā and
Glānī
Anuvāsana Basti of Tila Taila
prepared by Kaṣāya, Kaţu,
Tīkṣṇa and Uṣṇa Dravya, Surā
Gomūtra and mixed with
Madana Phala and Āmla
Dravya Kalka is given.
Anna
Avṛta
Sneha
After having
a heavy
meal; Basti
administere
d which is
prepared
with Guru
Dravya.
Chardī,
Mūrchā, Arucī,
Glāni, Śūla,
Nidrā,
Agnimāndya
and Āma
Lakṣaṇa, Dāha.
For proper digestion, Kaṣāya
and Cūrṇa of Kaţu
Dravya with Lavaṇa should be
given.
Mṛdu Virecana should be
given.
The treatment for Āma should
be done.
Purīṣa
Avṛta
Sneha
Anuvāsana
Basti
of Alpa
Bala is
administere
d, when
Mala
Sañcaya is
present in
Pakwāśaya
Purīṣasanga,
Mūtrasanga,
Vātasanga,
Śūla, Gaurava,
Ādhmāna and
Hṛdroga.
Snehana, Swedana should be
done.
Guḍa vartī should be placed in
anus. Anuvāsana Basti and
Niruha Basti prepared with
Śyāmā, Bilva, Daśamula
Kaṣāya and Kalka should be
given.
Abhukt
āvasthā
Basti is
given in a
It reaches up to
throat and
Niruha Basti and Anuvāsana
Basti of Sneha prepared with
Basti
Vyāpad
person with
empty
stomach.
may come out
from the
mouth.
Gomūtra, Śyāmā, Trivṛtta,
Yava, Kola, Kulattha should
be given.
Little pressure should be
given on throat.
Tīkṣṇa Virecana should be
given.
Treatment prescribed for
Vamana should be given.

V. PHARMACODYNAMICS OF BASTI
Basti is one of the important therapies amongst all the treatments of
Āyurveda. Hence it can be used in various diseases and conditions. As
it‟s action is multidimensional; it can be used not only for Vātavyādhī;
but for Pittaja, Raktaja, Sannipātaja and Saṃsargajanya Vyādhi
also.(117)
In Āyurvedic classics Ācaryas have tried to explain actions of Basti
hypothetically with suitable analogies. Recent studies also show
similarities in the concept of absorption of Basti. They are:
As tree irrigated in its root level attains branches with beautiful
tender leaves, flowers and fruits; in the same way Basti which is
administered in rectum performs significant results up to head
to toe. ( Āpāda Mastaka )(113)
Ācarya Parāśara opined that Guda is the main root of the body
and having blood vessels in it. Basti administered in the rectum
nourishes all the limbs and organs of the body through these
blood vessels.(118)
While describing action of Basti; Ācarya Suśruta says that Sun
stands millions of kilometres away from the Earth evaporates
the water with powerful sun rays, in the same manner Basti
retains in Pakwāśaya and dwells Doṣas from all over the
body..(119)
Suśruta explains the importance of Basti and says that Basti
only can pacifies the provocated Vāta like cyclonic storm is
sustained and controlled by waves of the sea.(120)
Recent studies shows that, the rectal administration has become
more popular since the side effects of the intra-muscular
injection are noted. “ Noboru yata” et al (1985) reported that the
tight junction of the epithelia of the rectum will be markedly
influenced by the pressure of adjuvant especially in the
hypotonic solution. Further he explains that volume of secreted
fluids in the rectum is generally considered to be small. In that
situation the osmolarity of the secreted fluids will be increased
by dissolving the drugs and adjuvant. The increased osmolarity
of the rectal fluids may influence the absorption promoting the
effect of the drug.(121)
Medicines which are administered through rectal route are
absorbed in rectum and large intestine. The rectum has rich
blood and lymph supply and drugs can cross through the rectal
mucosa like other lipid membranes. The portion which is
absorbed from upper part rectal mucosa is carried by the
Superior Haemorrhoidal vein into the portal circulation, where
as the Middle and Inferior Haemorrhoidal veins absorb from the
lower rectal mucosa enters directly into Systemic circulation.
The rectum with its vascularity and venous plexus provides a
good absorbing surface and many soluble substances produce
their effect more quickly without passing the liver where they
may be destroyed.(121) This was investigated and proved with
lidocaine, a hepatic high clearance drug.(122)
Absorption of drugs from rectal epithelium involves two
transport routes: the trans cellular and para cellular. An uptake
mechanism in trans cellular route depends on lipophilicity
where para cellular route is drug diffusion through a space
between epithelial cells.(122)


VI. DRUG REVIEW
Mūrcchita Tila Tail and Saindhava were used in Anuvāsana Basti as a
Sneha Dravya. Mūrcchana of Tila Taila is done by Manjiṣṭhā and
Harīdrā to reduce its Sāmatā according to Āyurved Sāra Saṃgraha.(123)
Therefore review of Tila Tail and Saindhava have been taken.
REVIEW OF TILA TAILA:
The term Taila is derived from Tila itself. ( itlaat\ tOlama\ )
It is a type of Sthāvara Sneha which is taken out by seeds. Tila Taila is
the main Sneha among Sthāvara Sneha. (103)
Properties of Tila: (104)
Rasa :Tikta, Katu, Kaṣāya, Madhura
Vīrya :Uṣṇa
Vipāka :Katu
Guṇa :Guru,
Karma :Vātaghna, Kapha- Pitta Kara
Twacya, Keśya, Balya, Medhakṛta, Agnivardhaka,
Alpamutrakara, Hima Sparśa.
Latin Name :Sesamum indicum
Properties of Tila Taila: (105)
Rasa: Madhura, Tikta, Kaṣaya
Vīrya: Uṣṇa
Vipāka: Madhura
Guṇa: Guru, Tīkśṇa, Vyavāyī, Viṣada, Vikāsi, Sara, Sukṣma,
Karma: Vāta- Kaphaghna, Twacya, Keśya, Balya, Medhākṛta,
Agnivardhaka, Varṇya, Bṛṃhaṇa, Alpamutrakara, Karṇa
Śulaghna, Śarīra Mārdavakara, Maṃsabalya, Kṛmighna,
Lekhana, Cakṣuṣya, Pācana, Yoni, Śira, Karṇa
Śulapraśamana, Bhagnahara, Kṣāra, Agnidagdhahara
Uses: Basti, Pāna, Nasya, Karṇa- Akṣipuraṇa
Caraka also describes the same properties of Tila Taila. But he
adds Saṃyoga Saṃskārānuvarti property of Tila Taila. (106)
Mahābhuta: Agni, Āpa
Indications for Snehana by Tila Tail: (37)
Pravṛddha Śleśma- Meda
Cala Sthula Gala Udara
Vātavyādhī
Vātaprakṛti
For Bala, Laghutā, Tanutwa, Dṛdhatā, Sthiragātratā
In Kṛmikoṣṭha, Krurakoṣṭha and Nādivraṇa.
REVIEW OF SAINDHAVA:
Saindhava is considered as the best among all Lavaṇa. (107,108,109)
Rasa: Lavaṇa, Madhura
Vipāka: Madhura
Virya: Uṣṇa/ Śīta/ Anuṣṇa
Guṇa: Snigdha, Laghu
Doṣaghnatā: Tridoṣaghna
Karma: Rocana, Dīpana, Vṛṣya, Cakṣuṣya, Avidāhī , Hṛdya,
Rucya, Agnidīpana, Pathyakara
If it is mixed with Sneha, Snehana takes place earlier. Hence it
is used in preparations of Sadyosnehana.(110)
As it is Sukṣma, Arukṣa, Uṣṇa, Vyavāyi and Doṣasanghāta
Vicchedaka; it is used along with Sneha.(111)

VII. REVIEW OF PREVIOUS WORK DONE
Previous work related with this topic was studied. Some concepts like
anal route of drug administration, Utkleśana Karma of Basti were
studied available from MD or Ph.D work and even from internet also.
1. To ascertain the mode of action of Utklesion Basti with reference
to it‟s indications and contraindications.
By Vd. Monika Vanarase, Guide: Vd. Vilas Nanal. Pune, (MD
work). 2000.
In this work, Utkleśana Basti was given instead of Utkleśaka
āhara prior to Vamana and Virecana. It was given in Sadyo
Vamana also as a Snehana. Oil was prepared with Suśrutokta
Utkleśana Basti Dravya. Utkleśana Karma was observed in the
diseases like Śwasa, Udara and Āmavātā.
2. Arohanakrama Mātrā Basti an effective alternate for Snehapāna.
By Dr. Basavajyoti, Guide: Dr. Sudhir, Bangalore, (MD work).
2005
In this study, Mātrā Basti is given in Arohaṇa Mātrā starting
from 24 ml upto 72 ml. and Utkleśana was observed.
3. Study of organs during Basti Karma w. s. r. to Rachana and
Kriya.
By Dr. Kanthi G. Manappa. Guide Dr. Doiphode, ( Ph.D. Work ).
In this work, Yoga Basti was administered and anatomical
involvement of organs like Pakwaśaya was studied.
4. Lakshmi P. J., Deepthi B., Rama Rao N. Rectal drug delivery: A
promising route for enhancing drug absorption. Asian J. Res.
Pharm. Sci. 2012;

Available from:
http://www.asianpharmaonline.org/AJPS/6_AJPS_2_4_2012.p
df
5. Mirteimouri M , Tara F, Teimouri B, Sakhavar N and Vaezi A.
Efficacy of Rectal Misoprostol for Prevention of Postpartum
Haemorrhage. Iran J Pharm Res. 2013 Spring.
Available from:
http://www.ncbi.nlm.nih.gov/pubmed/24250623
Recent researches have suggested that rectal absorption can prove the
good alternative rout of drug administration as it provides partial
avoidance of first portal pass metabolism. It has been demonstrated
that the rectal rout is more efficient than even intravenous route.

VIII. CONCEPT OF ANUVĀSANA BASTI AS AN ALTERNATIVE FOR
SNEHAPĀNA IN VAMANA AND VIRECANA.
Many methods of Snehana like Abhyaṅga, Pāna, Anuvāsana Basti,
Māstiṣkya etc. are described by Suśruta.(22) It is clearly mentioned that
out of these; the proper method of Snehana should be chose by using
Yuktī Pramāṇa.(23) It means according to Doṣa, Duṣya, physical and
mental condition of the patient, the method of Snehana can vary.
Vicāraṇā Sneha is a concept in which Accha Snehapāna has been
substituted by adding some dietary items with Sneha, for eg. Yavāgu
or by changing the route of administration of Sneha for eg.
Anuvāsana Basti through anus.(29)
While describing indications of Vicārana Sneha.; Caraka quotes that
the patients who have aversion for Sneha are fit for Vicārana Sneha.
This study deals with these patients only.(30)
As Anuvāsana Basti is not only one of the method of Snehana and
Vicārana, but rectal route is considered as an internal route of drug
administration; it can be considered as an alternative for
Snehapāna.(24)
Definition of Basti clearly indicates the spreading and oleating
properties of Basti. It also mentions the Vilodana of Doṣas through
Basti.(60)
Suśruta even explains the spreading of Vīrya of Basti according to
days.(85) This suggests, Sneha present in Anuvāsana Basti can reach
throughout the body. To support this phenomena, Suśruta says, even
though roots of a tree are irrigated; the tender leaves, flowers and
fruits get nourished.(113) In the same manner even though Basti is
administered in rectum, the Vīrya of Basti spreads and acts on every
Srotasa, Dhātu and subtle elements.
Anuvāsana Basti gets absorbed by Apāna and gradually by Samāna,
Vyāna, Udāna and Prāṇa.(116) Hence Vīrya of Basti can reach
throughout the body and can act on Śākhāgata Doṣa which may be in
Līnāvasthā.
Vṛddhī, Abhiśyanda, Kledana and ultimetly Utkleśa of Doṣa are
expected when Śodhanānga Snehapāna is given(2,112) so that Doṣas
present in Śākhā are forced to move towards Koṣṭha. Jātharāgni,
Dhātvāgni and Bhutāgni digest the Sneha taken orally and thus
Sneha spreads all over the body.
Utkleśana of Doṣa is possible through Anuvāsana Basti also if it is
given continuously.(114) It has got capacity to control Vāta Doṣa in
Koṣṭha which is expected in Śodhanānga Snehapāna. Suśruta has
described Utkleśana Basti, Śodhana Basti and Śamana Basti in a
sequence. It indicates Śodhana of Doṣa after Utkleśana and Śamana of
Doṣa after Śodhana.(115) This process is exactly same as that of
Śodhanānga Snehapāna, Śodhana and Śamana Cikitsā thereafter.
Anuvāsana Basti doesn‟t get digested by Jātharāgni directly. Śoṣaṇa
Karma of Jātharāgni can be seen in Pakwāśaya.(76) Hence without
actual digestion, Basti can reach throughout the body. This
phenomenon is already explained in the chapter Pharmacodynamics of
Basti. From the point of view of anatomy and physiology also this can
be explained. Superior, Middle and Inferior Rectal Veins are present
in rectum. Out of these three; Middle and Inferior Rectal Veins directly
drains into Inferior Vena Cava. Hence Basti can directly reach in
systemic circulation and may act fast. Only Superior Rectal Vein
drains into the Portal vein and subsequently into the liver. It indicates
that very little amount of Vīrya of Basti spreads through Portal
circulation.
Collectively we can say that Anuvāsana Basti can be considered as an
alternative for Snehapāna.

IX. REFERENCES
1 isnagQa isvannasya BaOYajyaodao-YastU%@laoiSatao balaat\ I
inalaaoyato na maagao-Yau isnagQao BaaND [vaaodkma\ I I sau.ica. 33/40
2 snaohsvaodp`cailata rsaO : isnagQaO$dIirta : I
daoYaa : kaoYzgata jantao : sauKa ht-uM ivaSaaoQanaO : I I sau.ica. 33/47
3 snaohnaM snaoh ivaYyandM maad-vaM @laodkarkma\ I ca.saU. 22/11
4 d`vaM saUxmaM sarM isnagQaM ipicClaM gau$ SaItlama\ I
p`ayaao mandM maRduM ca yat\ d`vyaM snaohnamaucyato II ca. saU. 22/15
5 dIPtantraigna : pirSaud\QakaoYz :
p`%yaga`Qaatuba-lavaNa-yau@t : I
dZoMind`yaao mandjar : Satayau :
snaohaopsaovaI pu$Ya : pidYT : I I A.).saU. 16/46
6 snaohao ihtao duba-lavai*nadoh sanQauxaNaovyaaiQainapIiDtasya I
balaainvataO BaaojanadaoYajaatO: p`maid-tuM taO sahsaa na saaQyaaO I I sau.ica. 31/57
7 daoYaa : kadaica%kuPyaint ijata la=GanapacanaO :
ijata : saMSaaoQanaOyao - tu na toYaaM puna$d\Bava : I I ca.saU. 16/20
8 pacanaOdI-pnaO: snaohostansvaodOSca pirYkRtana\ I
SaaoQayaocCaoQanaO: kalao yaqaasannaM yaqaabalama\ I I A.).sau. 13/ 28,29
9 tanyaupisqatdaoYaaNaaM snaohsvaodaoppadnaO :
pHcakmaa-iNa kuvaI-t maa~akalaaO ivacaaryana\ I I ca.saU. 2/15
10 isnagQaat\ pa~ayaqaa taoyamaya%naona p`Naudyato I
kfadya : pNaudyanto isnagQaa_oha<aqaaOYaQaO : I I
Aad-M kaYzM yaqaa vai*naiva-Yyandyait sava-t : I
yaqaa isnagQasya vaO daoYaana\ svaodao ivaYyandyaot\ isqarana\ I I
i@laYTM vaasaao yaqaao%@laoSya mala : saMSaaoQyato | mBasaa I
snaohsvaodOstqaao%@laoSya SaaoQyato SaaoQanaOma-la : I I ca.isa. 6/11 – 13
11 snaohnaM $xaNaM kma- svaodnaM stMBanaM ca yat\ l
BaUtanaaM tdip dvaOQyaaid\vatyaM naaitvat-to l l A.).saU. 14 /3
12 snaoohsaarao|yaM pu$Ya : paNaaSca snaohBaUiyaYTa : snaohsaaQyaaSca Bavaint l
13 saahsaM vaogasaMraoQa : Sauk`aOja : snaohsaMxaya :
AnnapanaivaiQa%yaagaSca%vaarstsya hotva : l l A.).ina. 5 /4
14 ip<aM sasnaohtIxNaaoYNaM laGau ivasaM sarM dvama\ l
isnagQa : SaItao gau$ma-nd : SlaxNaao : maR%sna : isqar : kf : l l A.).saU. 1 /11
15 t~asqaina isqatao vaayau : ip<aM tu svaodr>yaao : l
SlaoYmaa SaoYaoYau tonaOYaamaaEayaaEaiyaNaaM imaqa : l l A.*.saU. 11 /26
16 Aaoja : saaomaa%makM isnagQaM Sau@laM SaItM isqarM sarma\
ivaiva>M maRdu maR%snaM ca Pa`aNaayatnamau<amama\ l l sau.saU. 15 /21
17 SaoYaoYau rsamaaMsamaodaomajjaaSaukmaU~purIYaaidYau l A.*.saU. 11 /26 iTka Aayauvao-drsaayana
homaaid`
18 Aqa t%saMSayacCo<aa p%yauvaaca punava-sau : I
snaohanaaM idvaivaQaa saaOmya yaaoina : sqaavarja=maa I I ca.saU.13/9
19 t~ jaMgamaoByaao gavyaM GaRtM p`QaanaM sqaavaroByaaistlatOlaM p`Qaanaimait I sau. ica.31/4
20 At }Qva-M yaqaapyaaojanaM yaqaapQaanaM ca sqaavarsnaohanaupdoxyaama : I sau. ica.31/5
21 ]pyaaojanama\ ]pyaaogaao baa*ya AaByantrSca t~ baa*yaao|Bya=gaaid : AaByantr : panaaid l
sau. ica.31/2 DlhNa
22 snaohao ih panaanauvaasanamaistYkiSaraobas%yau%trbaistnasyakNa-
pUrNagaa~aByaMgaBaaojanaoYaUpyaaojya : l sau. ica.31/3
23 yau@%yaa|vacaaryao%snaohM BaxyaaVnnaona baistiBa : l
nasyaaByaMjanagaNDUYamaUw-kNaa-ixatp-NaO : ll A.).saU. 16/14
24 t~ baa*ya : snaohsvaodaBya=gapirYaokaopnaahiSaraobaistnasyaaid : AaByantrstu
snaohpanaanauvaasanaina$haid : l sau. ].26/2,3 DlhNa
25 WaByaaM catuiBa-rYTaiBayaamaOjaI-ya-it yaa kmaat\ l
*svamaQyaao%tmaa: maa~astastaByaSca *saIyasaIma\ I A.).saU.16/17,18
26 WaByaaM i~iBaScatuiBa-stOya-makis~vaRtao mahana\ I A.).saU. 16/4
26 AcCpoyastu ya: snaohao na tamaahuiva-caarNaama\ l
snaohsya sa iBaYagdRYT klp p`aqama kilpk: ll ca.saU. 13/26
27 kovalamacCpoyama\ l sau. ica.31/21 DlhNa
28 snaoho saa%mya: @laoSasah: kalao naa%yauYNa SaItlao I
AcCmaova ipbaot\ snaohM AcCpanaM ih pUijatma\ I I ica.31/21
29 AaodnaSca ivalaopI ca rsaao maaMsa pyaao diQa l
yavaagaU: saUpSaakaO ca kambailak: KD: l
sa>vaistlaipYTM ca maVM laohastqaOva ca l
BaxyamaByaHjanaM baiststqaa caao<arbastya: l
gaNDUYa: kNa-tOlaM ca nast: kNaa-ixatPa-Nama\ l
catuiva-MSaitir%yaota: snaohsya pivacaarNaa: l l ca.saU.13 /23,25
30 snaohiWYa: snaohina%yaa maRdukaoYzaSca yao nara: l
@laoYaasaha maVina%yaastoYaaimaYTa ivacaarNaa l l ca.saU. 13 /82
31 saukumaarM kRSaM vaRwM iSaSauM snaohiWYaM tqaa l
tRYNaa<a-mauYNakalao ca sah Ba@tona payayaot\ l l sau. ica.31/ 37
32 *yastnao jaINa- evaannao snaohao|cC: Sauwyao bahu: I I
Samana: xauWtao|nannaao maQyamaa~Sca Sasyato I
baRMhNaao rsamaVaVO: saBa>ao|lp: I
baalavaRd\Qaippasaat-snaohiWramaVSaIilaYau I A.).saU.16/19, ca.saU.13 /61
33 KraoByaMga : smaRt : pakao maRduna-st : ik`yaasau ca I
maQyapakM tu panaaqao- bastI ca ivainayaaojayaot\ l l ca.k. 12 /201
34 GaRtM ip%tainalahrM rsaSauk`aOjasaaM ihtma\ I
inavaa-pNaM maRdukrM svarvaNa-psaadnama\ l l ca.saU. 13 /14
35 vaatip<ap`kRtyaao vaatip<aivakairNa: I
caxau:kamaa: xata: xaINaa vaRwa baalaastaqaa|balaa: I
Aaya:pkYa-kamaaSca balavaNa-svaraiqa-na: I
puiYTkamaa: pjaakamaa: saaOkumaayaa-iqa-naSca yao I
dIPtaoja: smaRitmaoQaaignabauwIindyabalaaiqa-na: I
ipbaoyau: saip-rata-Sca dahSas~ivaYaaignaiBa: I I ca.saU. 13 /43, 44
36 maa$tGnaM na ca SlaoYmavaw-naM balavaQa-nama\ I
%vacyamauYNaM isqarkrM tOlaM yaaoinaivaSaaoQanama\ I I ca.saU. 13 /15
37 p`vaRwSlaoYmamaodskaScalasqaUlagalaaodra: I
vaatvyaaiQaiBaraivaYTa vaatp`kRtyaSca yao I

balaM tnau%vaM laGautaM dRZtaM isqargaa~tama\ I
isnagQaSlaxNatnau%va>aM yao ca kaMxaint doihna: I
kRimakaoYza : k`urkaoYzastqaa naaDIiBarid-ta: I
ipbaoyau : SaItlao kalao tOlaM tOlaaoicataSca yao I I ca.saU. 13 /45,46
38 ga`amyaanaUpaOdkanaaM ca vasaamaodaomajjaanaao gau$YNamaQauravaatGnaa :
jaa=galaOkSafk`vyaadadInaaM laGauSaItkYaayaa r>ip<aGnaa : ptudivaiYkraNaaM SlaoYmaGnaa I
sau. saU. 45 /131
39 vaatatpsaha yao ca $xaaBaaraQvakiSa-ta: I
saMSauYkrotao$iQara inaYpItkfmaodsa: I
AisqasaMiQaisarasnaayaumama-kaoYzmaha$ja: I
balavaanmaa$tao yaoYaaM Kaina caavaR%ya itYzit I
mahccaaignabalaM yaoYaaM vasaasaa%myaaSca yao nara: I
toYaaM snaohiyatvyaanaaM vasaapanaM ivaQaIyato I I ca.saU. 13 /47-49
40 ivawBagnaahtBaYTyaaoinakNa-iSarao$ija I
paO$Yaao pcayao snaoho vyaayaamao caoYyato vasaa I I ca.saU. 13 /16
41 balaSaukrsaSlaoYmamaodaomajjaivavaw-na : I
majjaa ivaSaoYatao|sqnaaM ca balakR%snaohnao iht : I I ca.saU. 13 /27
42 dIPtagnaya : @laoSasaha Gasmara : snaohsaoivana: I
vaatata- : kurkaoYzaSca snao*yaa majjaanamaaPnauyau: I ca.saU. 13 /50
43 snaohnaa jaIvanaa vaNyaa- balaaopcayavaQa-naa :
snaoha *yaoto ca ivaihta vaatip<akfapha : I I ca.saU. 1 /88
44 GaRttOlavasaamajjaaM pUva- : pUvaao- varao|nyaoBya : I ka.saU. 22
45 ip<aGnaasto yaqaapUva-imatrGnaa yaqaao<arma\ I A.).saU.16/3
46 GaRta<aOlaM gau$ vasaa tOlaanmajjaa ttao|ip ca I A.).saU.16/4
47 saip- : Sarid patvyaM vasaa majjaa ca maaQavao I
tOlaM p`avaRiYa naa%yauYNaSaIto snaohM ipbaonnar : I I ca.saU. 13 /18
48 svaoVsaMSaaoQyamaVs~I vyaayaamaasa@ticaMtka: l
vaRwbaalaabala $xaa kRSaa xaINaasarotsa: l
vaatat-syaand itimar da$Na: pitbaaoiQana: ll A.).saU. 16/56
49 snao*yaa
na %vaitmandaignatIxNaaignasqaUladuba-laa: I
}$stMBaaitsaaramagalaraogagaraodrO: I I
maUcCa-cCV-$icaSlaoYmatRYNaamaVOScapIiDta: I
App`saUta yau>o ca nasyao bastaO ivarocanao I I A.).saU. 16/6,7
50 vaatanaulaaomyaM idPtao|ignava-ca-O: isnagQamasaMhtma\ l
maad-vaM isnagQata caaMgao isnagQaanaamaupjaayato l l ca.saU.13 / 57
51 paNDUta gaaOrvaM jaaDyaM puirYasyaaivap@vata l
tnd`a$ica$%@laoSa: syaaditisnagQasyalaxaNama\ l l ca.saU.13 / 58
52 puirYaM gaiqatM $xaM vaayaurp`gauNaao maRdu: l
p@ta Kr%vaM raOxyaM ca gaa~syaaisnagQa laxaNama\ l l ca.saU.13 / 59
53 tRNmaUcCa-mauKSaaoYaO : SabdWoYaa=gamad-jaRmBaaiBa :
tnd`IvaagdohsaadO : snaohjaa jaIya-tI%yaah
]dgaarsya ivaSauwI : kaMxaa isqarta laGau%vamaivaYaad :
Balavaaigaind`yasaMpjjaINao- snaoho balasauKo ca
kNaa-ixap`aNabalaM smaRitkoSaaojasaaM vaRiw QaRitpuiYT :
Saaintstd\vyaaQaInaaM Bau@%vaa|nau snaohpItsya l l ka.saU.22 / 41
54 tnd`a saao%@laoSa Aanaahao jvar : stMBaao ivasaM&ta l
kuYzaina kNDU : paNDU%vaM SaaofaSaa-Msya$icastRYaa l l
jazrM gahNaIdaoYa stOima%yaM vaa@yainagah : l
SaUlamaamapdaoYaaSca jaayanto snaohivaBa`maat\ l l ca.saU.13 /75,76
55 snaohsya p`kYaaO- tu saPtra~ai~ra~kaO
ekamuau<amaa poyaa Hyahmaova tu maQyamaa l l ca.saU.13 / 51
56 maRdukaoYzis~ra~oNa isna*ya%yacCaopsaovayaa l
isna*yait kUrkaoYzstu saPtra~oNa maanava : l l ca.saU.13 / 65
57 ]YNaaodkaopcaarI syaat\ ba`*macaarI xapaxaya: I
SakRnmaU~ainalaaod\gaaranaudINaa-MSca na Qaaryaot\ I
vyaayaamamauccaOva-canaM kaoQaSaaokaO ihmaatpaO I
vaja-yaodpvaatM ca saovaot Sayanaasanama\ II ca.saU.13/62,63
58 ekahaoprtstWdBau@%vaa pcCd-naM ipbaot\ I
snaohat\ p`skndnaM jantuis~ra~aoprt : ipbaot\ I
snaohvad\d`vamauYNaM ca ~yahM Bau@%vaa rsaaOdnama\ II ca.saU.13/80
59 baistiBadI-yato yasmaat\ tsmaad\ baistiritsmaRt : I Saa. ]. 4
60 naaiBap`doSaM kiTpaSva-kuixaM l
ga%vaa SakRd\daoYacayaM ivalaaoDya l
saMsnao( kayaM sapuirYadaoYa: l
samyak\ sauKonaOit ca ya: sa baist: l ca.isa. 1/40
61 t~ iWivaQaao baist : naO$ihk : snaOihkSca l sau. ica. 35/18
62 i~MSanmat : kma- nau bastyaao ih l
kalasttao | Qao-na ttSca yaaoga : l
saanvaasanaa WadSa vaO ina$ha : l
p`ak\ snaoh ek : prtSca pMca l
kalao ~yaao | nto purststqaOk : l
snaoha ina$hantirtaSca YaT\syau : l
yaaogao ina$has~ya eva doya : l
snaohaSca pMcaOva praid maQyaa : l l ca.isa. 1/47-49
63 Aqaomaana\ saukumaaraNaaM ina$hana\ snaohnaana\ maRdUna\
kma-Naa ivaPlautanaaM ca vaxyaaima p`saRtO : pRqak\ l l ca.isa. 8/3
64 YaD\ vagaa- : pirsaM#yaata ya eto rsaBaodt :
AasqaapnamaiBapo%ya tainvaVa%saava-yaaoigakana\ l l ca.iva. 8/148
65 tIxNa%vaM maU~pIlvaisnalavaNaxaarsaYa-pO :
P`aaPtkalaM ivaQaatvyaM xaIraVOmaa-d-vaM tqaa l l ca.isa. 7/63
66 Anauvasana\ Aip na duYya%yanauidvasaM vaa dIyat [it Anauvaasana: l sau.ica.35/18
67 ina$hpadaMSasamaonatOlaonaoit ina$hpadpmaaNaona , catuiva-MSaitplao ina$ho YaT\plaona
snaohonao%yaqa- : , [yaM caao<amamaa~a | nauvaasanasya, ]@tM (nya~ ]<amaa YaT\plaIp`ao@ta
maQyamaai~plaI Bavaot\ l knaIyasaIsaaQa-plaa, i~Qaamaa~a | nauvaasanao [it l
sauEauto | Pyaotavanmaanamaova snaohsyaanauvaasanamaa~a maa~abaistivaBaagaonaanauvaasanao ]@tma \ l
cak`paiNa
68 yaqaavayaao ina$haNaaM yaa maa~a : pirkIit-ta :
padavakRYTasta : kayaa- : snaohbaistYau doihnaama\ l sau.ica.37/4
69 ]<amaa syaa%plaO : YaD\iBama-Qyamaa syaa%plaOis~iBa : l
tdwo-na ca hInaa syaai~Qaamaa~anauvaasanao l l cak`d<a
70 )svayaa snaohpanasya maa~ayaa yaaoijat: sama:
maa~abaist : smart : snaoh : l l A.).saU. 19 /67
71 Ainhsqaanaisqato daoYao vanhaO caannarsaainvato l
sfuT saaotaomauKo doho snaohaOja: pirsap-it l l sau.ica.37 / 48
72 ra~aO baistM na dVa%tu daoYaao%@laoSaao ih ra~Ija: l
snaohvaIya-yaut: kuyaa-daQmaanaM gaaOrvaM jvarma\ l l sau.ica.37 /47
73 na ra~aO p`Nayaod\baistM snaohao%@laoSaao ih ra~Ija :
snaohvaIya- yaut : kuyaa-daQmaanaM gaaOrvaM jvarma\ l l A.saM.saU. 28 / 25
74 SaIto vasanto ca idvaa | nauvaasyaao
ra~aO Sard\ga`IYmaGanaagamaoYau l
tanaova daoYaana\ pirrxata yao
snaohsya panao pirkIit-ta : p`ak\ l l ca.isa.1 /22,23
75 Ahaora~sya kalaoYau savao -YvaovaainalaaiQakma\
tIva`ayaaM $ija jaINaa-nnaM Baaojaiya%vaa | nauvaasayaot\ l l sau.ica.37 /52
76 p@vaaSayaM tu p`aPtsya SaaoYyamaaNasya vainhnaa l ca.ica.15 /11
p@vaaSayaM tu p`aPtsyaoit mala$ptyaa p@vaaSayaM gatsya l SaaoYyamaaNasya vainhnaoit
yaVPyaUQva-dahxamaao vai*na : , tqaa | PyasyaaQaaogatsya vai*nana SaaoYyamaaNa%vaM
p@vaaSayagatsyaaPyauppnnama\ l yatScaaQaaogamanao samyagvai*navyaaparao naaist At :
‘ pcyamaanasya ’ [it pdM pir%yajya ‘ SaaoYyamaaNasya ’ [it kRtma\ l ca.ica.15 /11
cak`paiNa
77 vaamaaEayao ih ga`hNaIgaudo ca
tt\ paSva-saMsqasya sau#aaoplaibQa : l l
laIyant evaM valayaSca tsmaat\
savyaM Sayaanaao |h-it baistdanama\ l ca.isa.3 /24
78 naa%yauicC/tM naaPyaitnaIcapadM
sapadpIzM SayanaM p`Sastma\ l l ca.isa.3 /33
p`QaanamaRWastrNaaoppnnaM
p`ak\SaIYa-kM Sau@lapTao<arIyama\ l
79 evaasqaaPyaast evaanauvaasyaa: ivaSaoYatstu $xatIxNaagnaya: kovalavaatraogaat-Sca ll
ca.isa.2 /16
80 SaoYaas%vaasqaaPyaa : ivaSaoYatstu savaa-M=gaOka=gakuixaraogavaatvacaao -
maU~Sauk`sa=gabalamaaMsarot : xayadaoYaaQmaanaa=gasauiPtik`imakaoYzaodavat-Sauwaitsaarpva-
BaodaiBatapiPlahgaulmaSaUla*Rd`aogaBagandraonmaadjvarba`GnaiSar : kNa-SaUla*RdyapaSva-
pRYzkTIga`hvaodnaaxaopkgaaOrvaaitlaaGavarja:xayaat-
ivaYamaaignaisfgjaanauja=Gaao$gaulfpaiYNa-p`pdyaaoinbaa*va=gauilastnaantdntnaKpvaa-
isqaSaUlaSaaoYastmBaan~kUjanapirkit-kalpalpsaSabdaoga`ganQaao%qaanaadyaao vaatvyaaQayaao
ivaSaoYaoNa maharaogaaQyaayaao>aSca etoYvaasqaapnaM p`Qaanatmaima%yau@tM
vanaspitmaUlacCodvat\ l l ca.isa.2 /16
81 ya evaanaasqaaPyaast evaananauvaasyaa: syau: ivaSaoYats%vaBau@tBa@tnavajvarpaNDuraoga
kamalaapmaohaSa-: p`itSyaayaaraocakmandaignaduba-laPlaIhkfaodrrao$stMBavacaao -Baod ivaYa
garpItip<akfaiBaYyandgau$kaoYz SlaIpd galgaNDapicaik`imakaoiYzna: ll
ca.isa.2 /17
82 ]%saRYTainalaivaNmaU~o naro baistM ivaQaapyaot\
etOih- ivaht: snaohao naOvaant p`itpVto l l sau.ica. 37 /5
83 na caaBau@tvat: snaoh: p`iNaQaoya: kqaMcana
Sauw%vaacCUnyakaoYzsya snaoh }Qva-M samau%ptot\ l l sau.ica. 37 /53
84 sada|nauvaasayaoccaaip Baaojaiya%vaa||d`-paiNanama\
jvarM ivadgQaBau@tsya kuyaa-t\ snaoh: p`yaaoijat:
na caait isnagQa SamanaM Baaojaiya%vaa|nauvaasayaot\
madM maUcCa- ca janayaod\ iWQaa snaoh: p`yaaoijat:
$xaM Bau@tvatao (nnaM balaM vaNa- ca hapyaot\
yau@tsnaohmatao jantuM Baaojaiya%vaa|nauvaasayaot\
yaUYaxaIrrsaOstsmaaVqaavyaaiQa samaIxya vaa
yaqaaoicatat\ padhInaM Baaojaiya%vaa|nauvaasayaot\ l l sau.ica. 37 /54-58
85 d<astu p`qamaao baist: snaohyaod\baistva=xaNaaO
samyagdtaO iWtIyastu maUQa-sqamainalaM jayaot\
janayaod\balavaNaaO- ca tRtIyastu p`yaaoijat:
rsaM catuqaao- r@tM tu pMcama: snaohyao<aqaa
YaYzstu snaohyaonmaaMsaM maod: saPtma eva ca
AYTmaao navamaScaaisqa majjaanaM ca yaqaak`mama\
evaM Sauk`gatana\ daoYaana\ iWgauNa: saaQau saaQayaot\ l l sau.ica. 37 /71-74
86 ekM tqaa ~Ina\ kfjao ivakaro
ip<aa%mako pMca tu saPt vaa|ip l
vaato navaOkadSa vaa punavaa-
bastInayaugmaana\ kuSalaao ivadQyaat\ l l ca.isa.1/25
87 naa%yauicC/to na caaocCIYao - saMivaYTM vaamapaSva-t: I
sa=kaocya dixaNaM sai@qa p`saaya- ca ttao|prma\ I I
Aqaasya nao~M p`Nayaoi%snagQao isnagQamauKM gaudo I
]cCvaasya bastova-dnao bawo hstmakmpyana\ I I
pRYzvaMSaM p`it ttao naaitd`utivalaimbatma\ I
naaitvaogaM na vaa mandM sakRdova p`pIDyaot\ I I
saavaSaoYaM ca kuvaI-t vaayau: SaoYao ih itYzit I
d<ao tU<aanadohsya paiNanaa taDyaoi%sfjaaO I I
t%paiYNa-ByaaM tqaa SayyaaM padtSca i~$i%xapot\ I
tt: p`saairta=gasya saaopQaanasya paiYNa-ko I I
AahnyaanmauiYTnaa|=gaM ca snaohonaaByajya mad-yaot\ I
vaodnaat-imait snaohao na ih SaIGa`M inavat-to I I
Yaaojya: SaIGa`M inavaR<ao|nya: snaohao|itYznnakaya-kRt\ I
dIPtaignaM %vaagatsnaohM saayaa*Nao BaaojayaollaGau I I A.).saU. 19/23-30
88 i~MSanmaa~aimat: kala: p`ao@tao bastostu pIDnao
tta: p`iNaiht: snaoh ]<aanaao vaa@SatM Bavaot\ I I Saa.saM.
89 tt: p`iNaihtsnaoh ]<aanaao vaak\SatM Bavaot\ I I sau.ica. 37/60
90 p`%yao%yasa@tM saSakRcca tOlaM
r@taidbauwIind`ya saMp`saad: l
svaPnaanauvaRi<ala-Gauta balaM ca
saRYTaSca vaogaa: svanauvaaisato syau: l l ca.isa.1/44
91 saainala: sapuirYaSca snaoh: p`%yaoit yasya tu l
AaoYacaaoYaaO ivanaa SaIGa`M sa samyaganauvaaisat: I I sau.ica. 37/67
92 ikMica%kalaM isqatao yaSca sapurIYaao inavat-to l
saa|naulaaomaa|inala: snaohsti%sawmanauvaasanama\ I I A.).saU. 19/42
93 AignadIiPtva-ya: sqaanaM puiYTvaNaao- QaRitba-lama\
vaatanaulaaomata Saaint : svanauvaaisatlaxaNama\ I I ka.saM. 2
94 )llaasamaaoh@lamasaadmaUcCa-
ivakit-ka caa%yanauvaaisatsya l l ca.isa.1/46
95 dahjvar ippasaait-krScaa%yaanauvaasanao I I sau.ica. 37/66
96 AQa: SarIraodrbaahupRYzpaSvao-Yau $xaKrM ca gaa~ma\ l
ga`hSca ivaNmaU~samaIrNaanaamasamyagaotanyauvaaisatsya l l ca.isa.1/45
97 ivaYTbQaainala ivaNmaU~: snaohao hInao|nauvaasanao l sau.ica. 37/66
98 tsya hIna samyagaityaaogaa: snaoh pItvat\ l
samyagQaInaaityaaogaaSca tsya syau: snaohpItvat\ I I A.).saU. 19/41
99 ivaYTmBaao gaaZvaca-s%vaM raogavaRiwiva-vaNa-ta l
vaopqauvaa-tvaRiwSca $paM durnauvaaisato l l ka.isa. 2
100 yasyaoh yaamaananauvat-to ~Ina\
snaohao nar: syaat\ sa ivaSauw doh: l
AaSvaagato|nyaostu punaiva-Qaoya:
snaohao na saMsnaoh yait *yaitYzna\ l l ca.isa.1/46
101 balavantao yada daoYaa: kaoYzo syaurinalaadya: l
AlpvaIya-M tda snaohmaiBaBauya pRqaigvaQaana l l sau.ica. 37/82
102 vaatip<akfa%yanna puirYaOravaRtsya ca l
ABau@to ca p`NaItsya snaohbasto: YaDapda: l l ca.isa.4/24
103 sqaavaroByaistlatOlaM p`Qaanaimait l sau.ica. 31/3
104 ]YNas%vacyaao ihma: spSao- koSyaao balyaistlaao gau$:
AlpmaU~ : kTu : pako maoQaa|ignakfip<akRt\ I I A.).saU. 6/23
105 tOlaM %vaagnaoyamauYNaM tIxNaM maQaurM maQaurivapakM baRMhNaM vyavaaiya saUxmaM ivaSadM gau$
sarM ivakaisa vaRYyaM %vak\p`saadnaM maoQaamaad-vamaaMsasqaOya-vaNa-balakrM caxauYyaM bawmaU~M
laoKnaM it@tkYaayaanaursaM pacanamainalabalaasaxayakrM ik`imaGnamaiSatip<ajananaM
yaaoinaiSar:kNa-SaUlap`SamanaM gaBaa-SayaSaaoQanaM ca tqaa iCnnaiBannaivawaoi%pYTcyaut
maiqatxatipiccatBagna sfuiTtxaaraignadgQaivaiSlaYTdairtaiBahtduBa-
gnamaRgavyaalaivadYTp`BaRitYau ca pirYaokaBya=gaavagaahaidYau itlatOlaM p`Sasyato l l
td\baistYau ca panaoYau nasyao kNaa-ixapUrNao l
AnnapanaivaQaaO caaip p`yaaojyaM vaatSaantyao l l sau.saU. 45/112,113
106 tOlaM saMyaaogasaMskarat\ sava-raogaaphM matma\ l l ca.saU. 27/287
107 raocanaM dIpnaM vaRYyaM caxauYyamaivadaih ca l
i~daoYaQnaM samaQaurM saOMQavaM lavaNaao<amama\ l l ca.saU. 27/300
108 caxauYyaM saOMQavaM *RdyaM $cyaM laGvaignadIpnama \
isnagQaM samaQaurM vaRYyaM SaItM daoYaGnamau<amama\ l l sau.saU. 46/314
109 saOMQavaM t~ sasvaadu vaRYyaM *RdyaM i~daoYanaut\
laGvanauYNaM dRSa : pqyamaivada*yaignadIpnama\ I I A.).saU. 6/144
110 saPtOt snaohnaa: saV: snaohaSca lavaNaaolbaNaa: I I A.).saU. 16/42
111 lavaNaaopihta : snaoha: snaohyan%yaicarannarma\
twyaiBaYyanV$xaM ca saUxmamauYNaM vyavaaiya ca l l ca.saU. 14/98
112 vaRwyaa ivaYyandnaa%pakat\ sa`aotaomau#aivaSaaoQanaat\ l
Saa#aaM mau@%vaa malaa: kaoYzM yaaint vaayaaoSca inagahat\ l l ca.saU. 28/47
113 p@vaaSayaad\baistvaIya-M KOdo-hmanausaip-it l
vaRxamaUlao inaiYa@tanaamapaM vaIya-imava dumama\ l l sau.ica. 35/25
114 snaohbaistM ina$hM vaa naOkmaovaaitSaIlayaot\ l
snaohadignavaQaa%@laoSaaO ina$hat\ pvanaad\Bayama\ l l sau.ica. 37/77
115 dVadu%@laoSanaM pUva-M maQyao daoYahrM puna : l
pScaat\ saMSamanaIyaM ca dVaWistM ivacaxaNa : l l sau.ica. 38/92
116 ya<a~aOYaQa vaIya-M ih tdpanaona vaayaunaa l
Payaa-Ptmaicaradova samaana : pitpVto l l
samaanaadU<arM caOvaM vyaanaaVa : pvanaakmaat\ l
to tRPta : pkRitM yaaint SarIranaugaho isqata : l l A.).isa. 5
117 baistvaa-to ca ip<ao ca kfo r@to ca Sasyato
saMsagao- sainnapato ca baistrova iht: sada l l sau.ica. 35/6
118 ]@tM ih praSaro maUlaM gaudM Sairrsya isarst~ p`itiYzta :
sava- SarIrM puYNaait maUQaa-naM yaavadaiEata : l l ca. isa.9/50
119 vaIyao-Na baistrad<ao daoYaanaapadmastkat\
p@vaaSayasqaao|mbargaao BaUmaorkao- rsaainava l l sau.ica. 35/28
120 vaayaaoiva-Yahto vaogaM naanyaa basto?-toik`yaa
pvanaaivaw taoyasya vaolaa balamaaraogyamaayauYa : l l sau.ica. 35/30
121 Clinical Pañcakarma by Dr. Yadaiah Polepally Pg No. 93, 94.
122 Laxmi Prasanna J. Rectal drug delivery: a promising route for
enhancing drug absorption. From: www.asianpharmaonline.org,
vol.2,issue 4, page 143-149.
123 Ayurved Sara Sangraha, 20th edition, Pg. No. 678.

I. AIM AND OBJECTIVES
Aim of the research work
To evaluate Samyak Snigdha Lakṣaṇa achieved by
administration of Anuvāsan Basti.
Research objectives
To study the dose and duration of Anuvāsana Basti according to
Koṣṭha.
To evaluate Samyak Śuddhi Lakṣaṇas of Vamana and Virecana
after administration of Anuvāsana Basti as an alternative for
Snehapāna.

II. MATERIALS AND METHODS
Materials:
Mūrcchita Tila Taila (Batch No 11119) was purchased from Agasti
Pharmaceuticals, Pune. Standardization was done in Hi – Tech Lab,
Pune. Some physico-chemical tests like Refractive Index (1.47 at
250C), Iodine value (6.748), Moisture content (below detection limit),
Saponification value (193.45), Microbial tests like tests for pathogens
like E. Coli, Salmonella, S. aureus etc. were done. The oil found free
from pathogens.
Special Basti Puṭakas (Basti pouches attached with catheter) were
prepared according to quantity required of Mūrcchita Tila Taila and
Saindhava by Agasti Pharmaceuticals, Pune.
Special case paper was prepared, in which Daṣavidha, Aṣtavidha and
Srotasa Parīkṣaṇa were done. Separate questions were asked to the
patients to assess Prakṛti, Agni and Koṣṭha.
Total plan of the treatment was explained to patients in their own
language.
Written consent was taken by the patient.
Methodology:
After obtaining Institutional Ethic committee Ethical permission, a
randomized open label clinical study was carried out. The study has
been registered with CTRI (No CTRI/2013/07/003832).
This study was carried out in two steps:
I. Pilot study was carried out in 10 patients. Two groups of 5 patients
each were done. On the basis of conceptual study; it was taken into
granted that Anuvāsana Basti could be given as an alternative for
Snehapāna. So group A was kept as a control group in which
Anuvāsana Basti was given with constant dose of 120 ml of Tila Taila
along with 500 mg Saindhava for minimum 3 and maximum 7 days.
Group B was experimental group, in which escalating dose of
Anuvāsana Basti was administered. In this group starting dose of
Anuvāsana Basti was 120 ml Tila Taila with 500 mg Saindhava
increasing with 25 ml Tila Taila and 100 mg Saindhava daily for
minimum 3 days and maximum 7 days. As Anuvāsana Basti is
considered as an internal route of drug administration, maximum
period of administration of Anuvāsana Basti was kept 7 days i.e. same
as that of Sneha Prakarṣa Kāla.
Symptoms of Samyak Snigdhatā of either group were observed.
Adverse effects (Vyāpad of Anuvāsana Basti) if any were studied. No
patient was found having any adverse effect of Anuvāsana Basti.
II. Total 105 patients were allocated for this study. Group A was
observed with constant dose and Group B with escalating dose of
Anuvāsana Basti. In group A, 52 patients were enrolled; but 2 patients
discontinued the treatment. In group B, 53 patients were allocated.
Out of these, 3 patients were dropped out. Thus two groups of 50
patients each were done.
Inclusion criteria:-
1. Patients between age group of 20 to 60 yrs.
2. Patients of either gender.
3. Patients who were advised Vamana or Virecana treatment
irrespective of the disease and especially having aversion for
Snehapāna. (Patients with Bahudoṣāvasthā or Utkliṣṭa
Doṣāvasthā.)
Exclusion criteria:-
1. Patients who were suffering from anal diseases like Arśa,
Bhagandara, Parīkartikā etc. (which have been described as
contra-indications for Basti)
2. Patients with Alpadoṣāvasthā.
Daṣavidha and Aṣṭavidha Parikṣaṇa were done in every patient.
Diagnosis of the disease along with Doṣāvasthā was assist. If
Samāvasthā of Jivhā was observed; Hingvāṣṭaka Cūrṇa in the dose of
1gm was given before meal for 3 to 5 days.
Gandharva Harītakī in the dose of 5 gms was given to the patient
before bed time to assess the Koṣṭha.
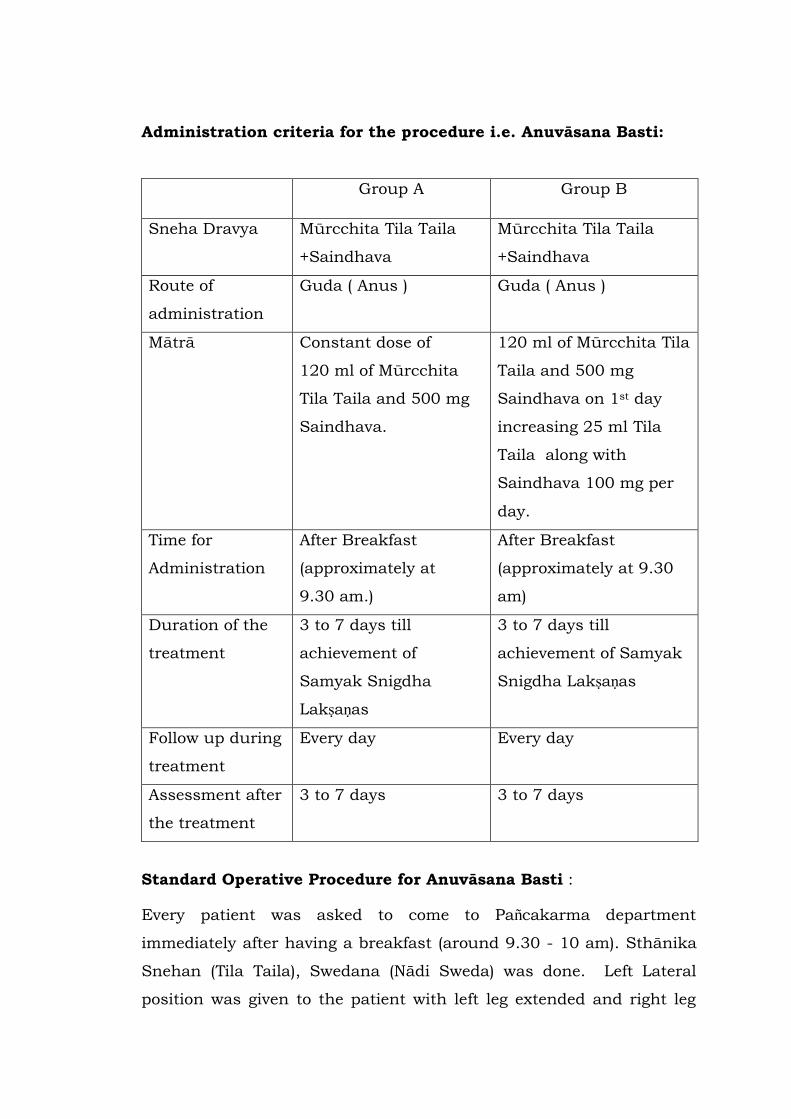
Administration criteria for the procedure i.e. Anuvāsana Basti:
Group A Group B
Sneha Dravya Mūrcchita Tila Taila
+Saindhava
Mūrcchita Tila Taila
+Saindhava
Route of
administration
Guda ( Anus ) Guda ( Anus )
Mātrā Constant dose of
120 ml of Mūrcchita
Tila Taila and 500 mg
Saindhava.
120 ml of Mūrcchita Tila
Taila and 500 mg
Saindhava on 1st day
increasing 25 ml Tila
Taila along with
Saindhava 100 mg per
day.
Time for
Administration
After Breakfast
(approximately at
9.30 am.)
After Breakfast
(approximately at 9.30
am)
Duration of the
treatment
3 to 7 days till
achievement of
Samyak Snigdha
Lakṣaṇas
3 to 7 days till
achievement of Samyak
Snigdha Lakṣaṇas
Follow up during
treatment
Every day Every day
Assessment after
the treatment
3 to 7 days 3 to 7 days
Standard Operative Procedure for Anuvāsana Basti :
Every patient was asked to come to Pañcakarma department
immediately after having a breakfast (around 9.30 - 10 am). Sthānika
Snehan (Tila Taila), Swedana (Nādi Sweda) was done. Left Lateral
position was given to the patient with left leg extended and right leg
flexed at knee joint. Specially designed Basti pouch with prescribed
quantity of Mūrcchita Tila Taila and Saindhava was kept in warm
water for 15 minutes to make the contents warm.
Lubricated Basti Netra was inserted inside the anus up to four Angula.
Oil was pushed inside slowly and steadily. Buttocks were patted 3 to 4
times. Patient was asked to lie on the bed with his legs in elevated
position for 5 to 10 minutes. Patient was advised to drink warm water
throughout the day and immediate after administration of Anuvāsana
Basti. Kṣudbodha of every patient was observed and accordingly he
was advised to have light diet preferably Mudga Yuṣa whenever he
feels hungry. Dhāraṇa Kāla of Anuvāsana Basti i.e. retention period
was noted. Daily assessment was done for the symptoms of Samyak
Snigdhatā.
Other procedures like Viṣrāma, Doṣotkleśaka Āhara, Bāhya Snehana
and Swedana were carried out in the same manner as that of our
routine Vamana and Virecana. For Vamana, oil application and
fomentation were carried out on the last day of Anuvāsana Basti, one
day prior to Vamana and on Vamana day. The patients were asked to
eat curd, jaggery, and banana with milk for aggravation of Kapha or as
Doṣotkleśaka Āhara. This diet facilitates elimination of Doṣas through
Vamana. For Virecana, oil application and fomentation were carried
out for three days, after completion of administration of Anuvāsana
Basti. On the third day of oil application and fomentation; patient had
asked to include Kokam Śerbet in his diet which is considered as
Anulomaka i.e. helpful for therapeutic purgation. Vamana or Virecana
was given with appropriate medicines according to the disease. For
Vamana, Madanaphala and Yashtīmadhū Kaṣāya were used. For
Virecana, Abhayādi Modaka or Trivṛta Leham with Virecana Kaṣaya
was used.
Assessment was done on the basis of Samyak Snigdha Lakṣaṇas.
Agnidīpti and Varca Snigdhatā were excluded from assessment.


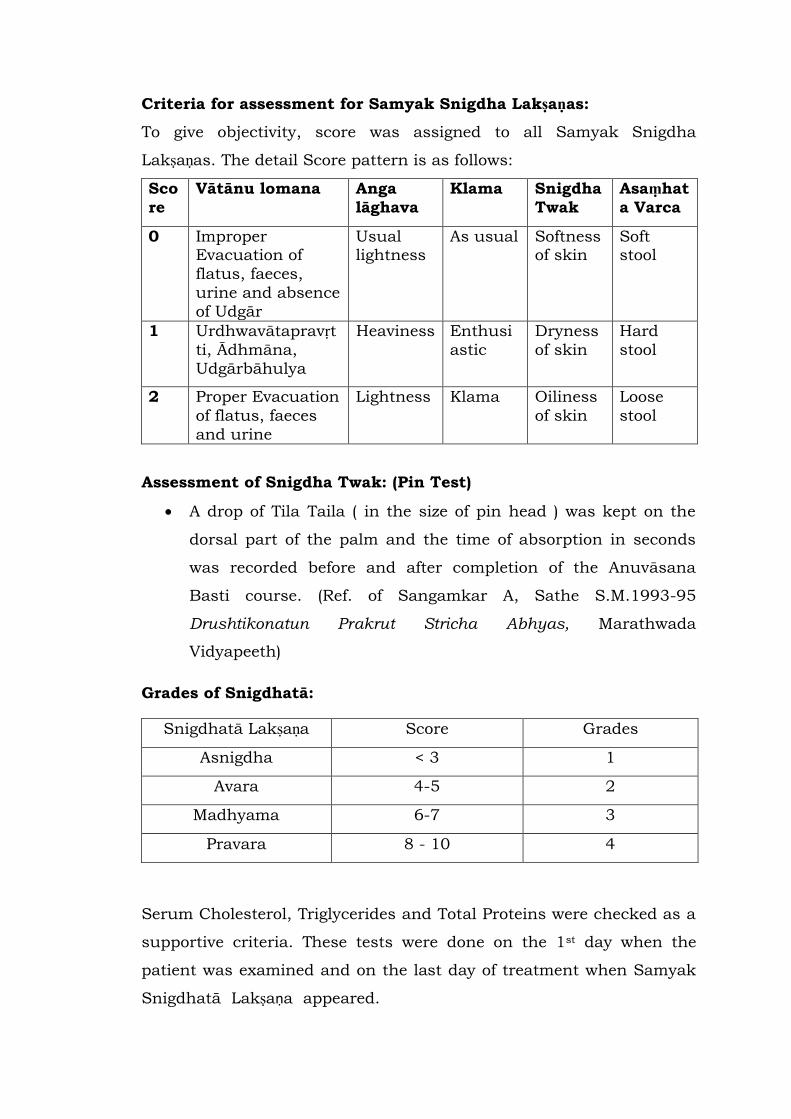
Criteria for assessment for Samyak Snigdha Lakṣaṇas:
To give objectivity, score was assigned to all Samyak Snigdha
Lakṣaṇas. The detail Score pattern is as follows:
Sco
re
Vātānu lomana Anga
lāghava
Klama Snigdha
Twak
Asaṃhat
a Varca
0 Improper Evacuation of
flatus, faeces,
urine and absence
of Udgār
Usual lightness
As usual Softness of skin
Soft stool
1 Urdhwavātapravṛt
ti, Ādhmāna,
Udgārbāhulya
Heaviness Enthusi
astic
Dryness
of skin
Hard
stool
2 Proper Evacuation
of flatus, faeces
and urine
Lightness Klama Oiliness
of skin
Loose
stool
Assessment of Snigdha Twak: (Pin Test)
A drop of Tila Taila ( in the size of pin head ) was kept on the
dorsal part of the palm and the time of absorption in seconds
was recorded before and after completion of the Anuvāsana
Basti course. (Ref. of Sangamkar A, Sathe S.M.1993-95
Drushtikonatun Prakrut Stricha Abhyas, Marathwada
Vidyapeeth)
Grades of Snigdhatā:
Snigdhatā Lakṣaṇa Score Grades
Asnigdha < 3 1
Avara 4-5 2
Madhyama 6-7 3
Pravara 8 - 10 4
Serum Cholesterol, Triglycerides and Total Proteins were checked as a
supportive criteria. These tests were done on the 1st day when the
patient was examined and on the last day of treatment when Samyak
Snigdhatā Lakṣaṇa appeared.

III. OBSERVATIONS AND RESULTS
In the present study, Samyak Snigdhatā Lakṣaṇas were observed after
administration of Anuvāsana Basti prior to Vamana and Virecana.
Vātānulomana, Angalāghava, Asaṃhata Varca, Klama and Twak
Snigdhatā were observed as they are Samyak Snigdhatā Lakṣaṇas.
These symptoms were observed within Prakṛti, Agni and Koṣṭha.
Scores were given to each symptom and grades of Snigdhatā were
drawn.
To examine the association between Samyak Snigdhatā Lakṣaṇa and
Treatment groups Chi-square test was used.
Paired t test was used to find significance of Twak Snigdhatā in each
group before and after the treatment.
Inter group Twak Snigdhatā was assessed by using unpaired t test.
To find significance association of Samyak Snigdhatā Lakṣaṇa,
unpaired t test and Z test for proportion were used.
Student‟s t test was applied for two independent groups for Dhāraṇa
Kāla of Anuvāsana Basti.
Paired t test was used to find significance of values of Sr. Cholesterol,
Triglycerides and Total Proteins in each group before and after the
treatment.
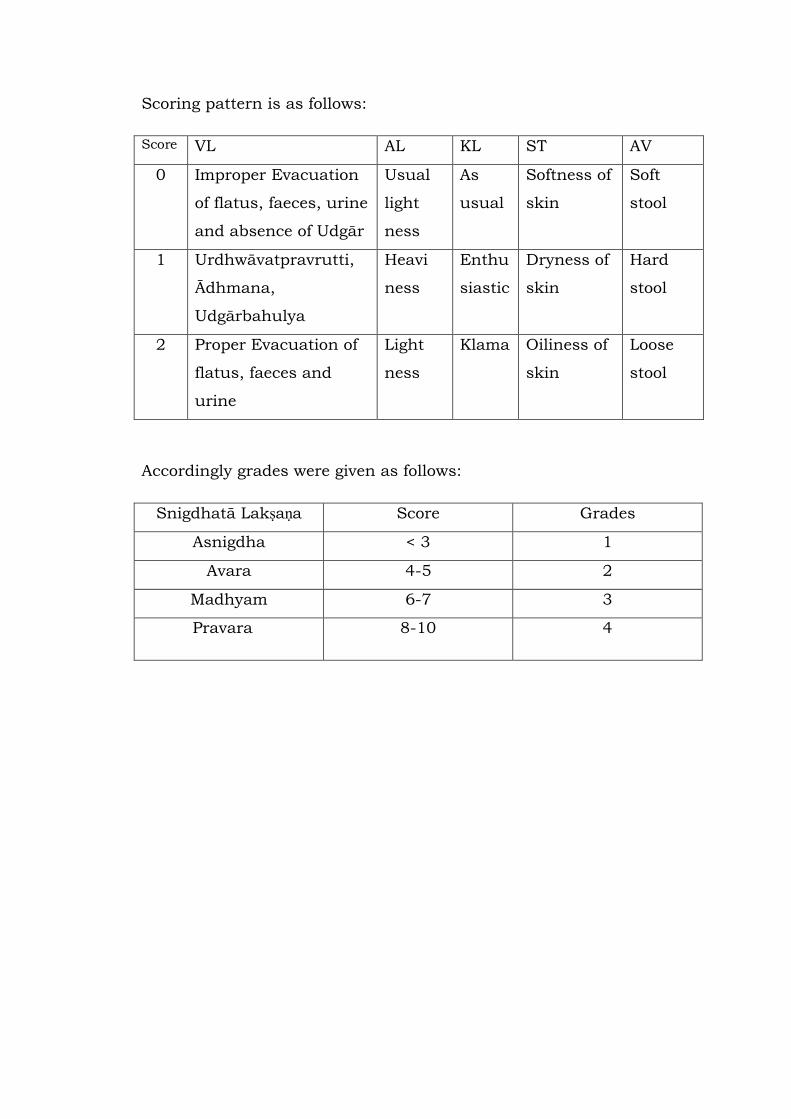
Scoring pattern is as follows:
Score VL AL KL ST AV
0 Improper Evacuation
of flatus, faeces, urine
and absence of Udgār
Usual
light
ness
As
usual
Softness of
skin
Soft
stool
1 Urdhwāvatpravrutti,
Ādhmana,
Udgārbahulya
Heavi
ness
Enthu
siastic
Dryness of
skin
Hard
stool
2 Proper Evacuation of
flatus, faeces and
urine
Light
ness
Klama Oiliness of
skin
Loose
stool
Accordingly grades were given as follows:
Snigdhatā Lakṣaṇa Score Grades
Asnigdha < 3 1
Avara 4-5 2
Madhyam 6-7 3
Pravara 8-10 4
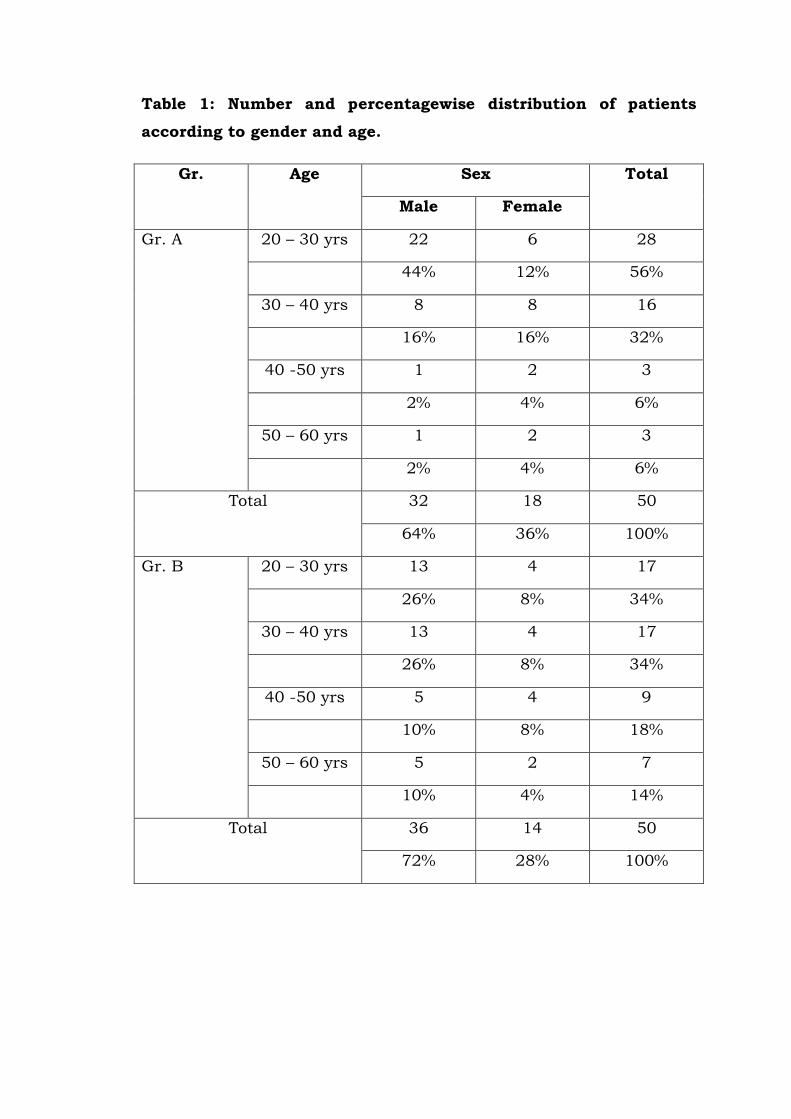
Table 1: Number and percentagewise distribution of patients
according to gender and age.
Gr. Age Sex Total
Male Female
Gr. A 20 – 30 yrs 22 6 28
44% 12% 56%
30 – 40 yrs 8 8 16
16% 16% 32%
40 -50 yrs 1 2 3
2% 4% 6%
50 – 60 yrs 1 2 3
2% 4% 6%
Total 32 18 50
64% 36% 100%
Gr. B 20 – 30 yrs 13 4 17
26% 8% 34%
30 – 40 yrs 13 4 17
26% 8% 34%
40 -50 yrs 5 4 9
10% 8% 18%
50 – 60 yrs 5 2 7
10% 4% 14%
Total 36 14 50
72% 28% 100%
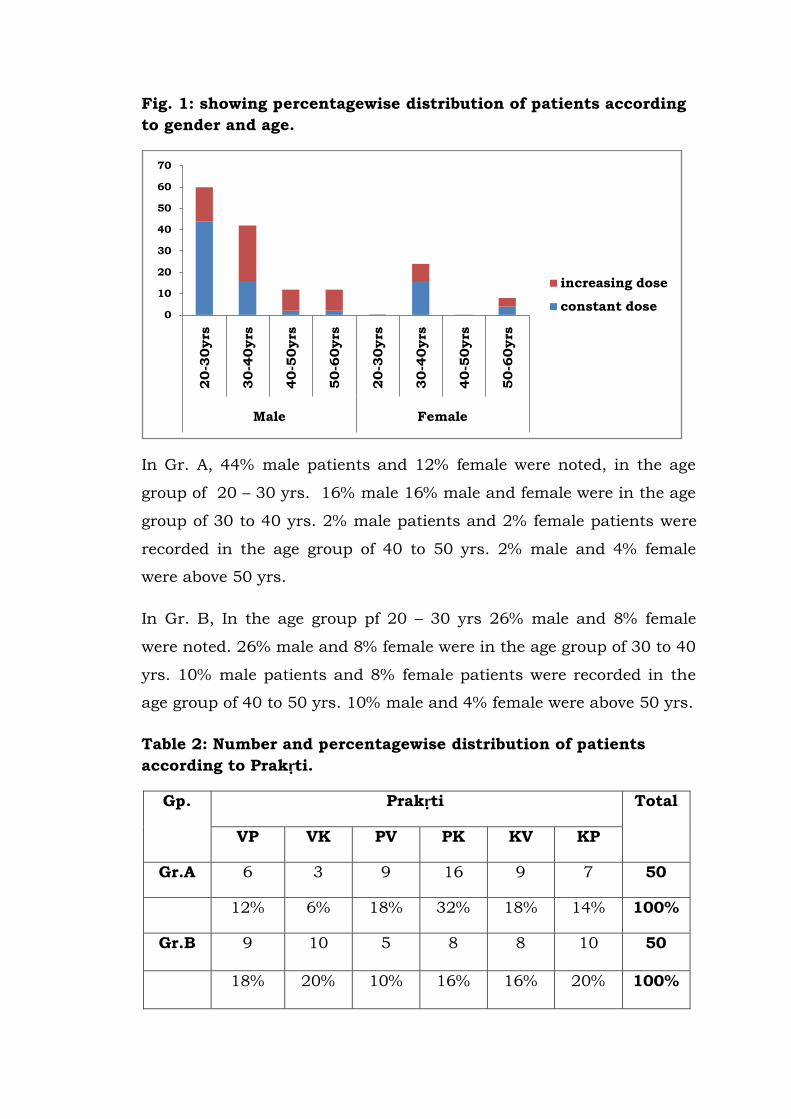
Fig. 1: showing percentagewise distribution of patients according
to gender and age.
In Gr. A, 44% male patients and 12% female were noted, in the age
group of 20 – 30 yrs. 16% male 16% male and female were in the age
group of 30 to 40 yrs. 2% male patients and 2% female patients were
recorded in the age group of 40 to 50 yrs. 2% male and 4% female
were above 50 yrs.
In Gr. B, In the age group pf 20 – 30 yrs 26% male and 8% female
were noted. 26% male and 8% female were in the age group of 30 to 40
yrs. 10% male patients and 8% female patients were recorded in the
age group of 40 to 50 yrs. 10% male and 4% female were above 50 yrs.
Table 2: Number and percentagewise distribution of patients
according to Prakṛti.
Gp. Prakṛti Total
VP VK PV PK KV KP
Gr.A 6 3 9 16 9 7 50
12% 6% 18% 32% 18% 14% 100%
Gr.B 9 10 5 8 8 10 50
18% 20% 10% 16% 16% 20% 100%
0
10
20
30
40
50
60
70
20-3
0yrs
30-4
0yrs
40-5
0yrs
50-6
0yrs
20-3
0yrs
30-4
0yrs
40-5
0yrs
50-6
0yrs
Male Female
increasing dose
constant dose
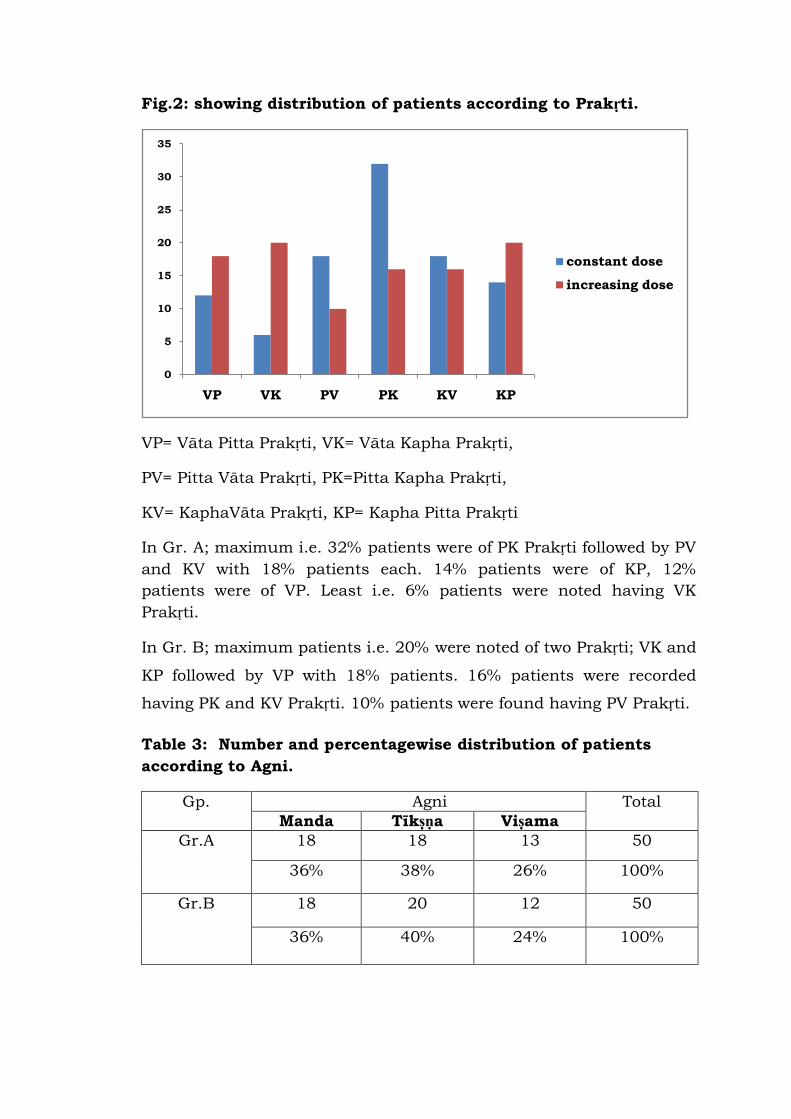
Fig.2: showing distribution of patients according to Prakṛti.
VP= Vāta Pitta Prakṛti, VK= Vāta Kapha Prakṛti,
PV= Pitta Vāta Prakṛti, PK=Pitta Kapha Prakṛti,
KV= KaphaVāta Prakṛti, KP= Kapha Pitta Prakṛti
In Gr. A; maximum i.e. 32% patients were of PK Prakṛti followed by PV
and KV with 18% patients each. 14% patients were of KP, 12%
patients were of VP. Least i.e. 6% patients were noted having VK
Prakṛti.
In Gr. B; maximum patients i.e. 20% were noted of two Prakṛti; VK and
KP followed by VP with 18% patients. 16% patients were recorded
having PK and KV Prakṛti. 10% patients were found having PV Prakṛti.
Table 3: Number and percentagewise distribution of patients
according to Agni.
Gp. Agni Total
Manda Tīkṣṇa Viṣama
Gr.A 18 18 13 50
36% 38% 26% 100%
Gr.B 18 20 12 50
36% 40% 24% 100%
0
5
10
15
20
25
30
35
VP VK PV PK KV KP
constant dose
increasing dose
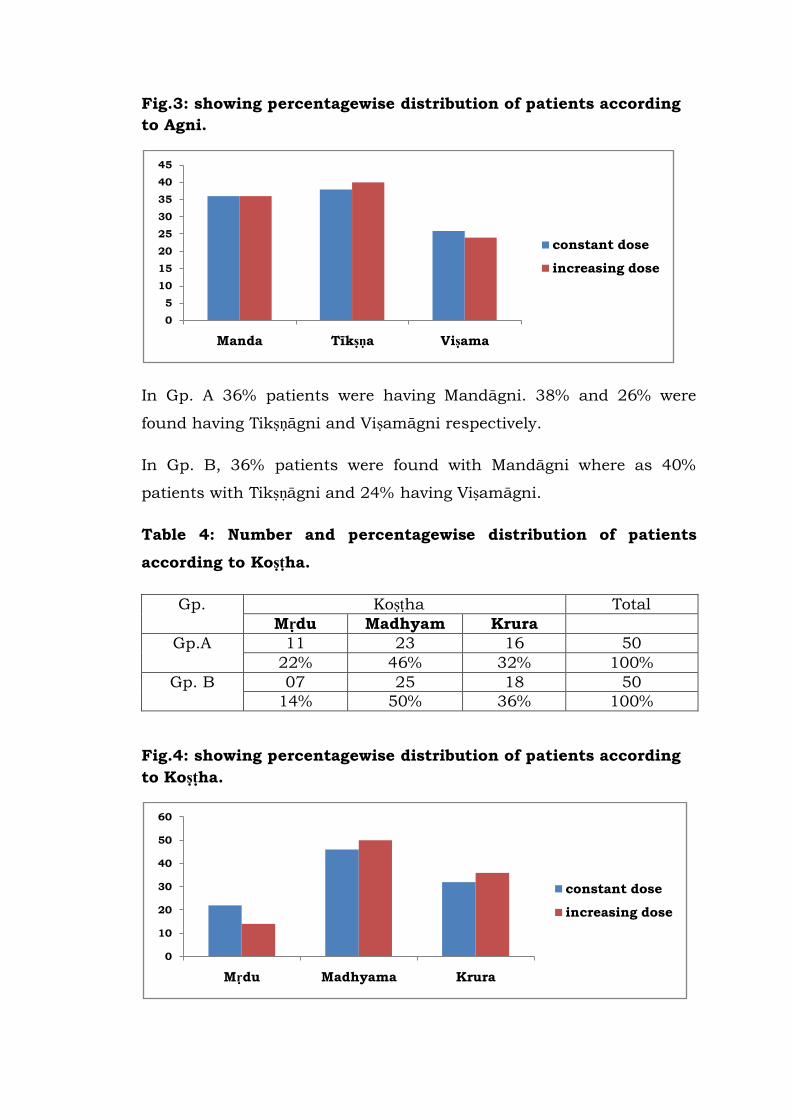
Fig.3: showing percentagewise distribution of patients according
to Agni.
In Gp. A 36% patients were having Mandāgni. 38% and 26% were
found having Tikṣṇāgni and Viṣamāgni respectively.
In Gp. B, 36% patients were found with Mandāgni where as 40%
patients with Tikṣṇāgni and 24% having Viṣamāgni.
Table 4: Number and percentagewise distribution of patients
according to Koṣṭha.
Gp. Koṣṭha Total
Mṛdu Madhyam Krura
Gp.A 11 23 16 50
22% 46% 32% 100%
Gp. B 07 25 18 50
14% 50% 36% 100%
Fig.4: showing percentagewise distribution of patients according
to Koṣṭha.
0
5
10
15
20
25
30
35
40
45
Manda Tīkṣṇa Viṣama
constant dose
increasing dose
0
10
20
30
40
50
60
Mṛdu Madhyama Krura
constant dose
increasing dose
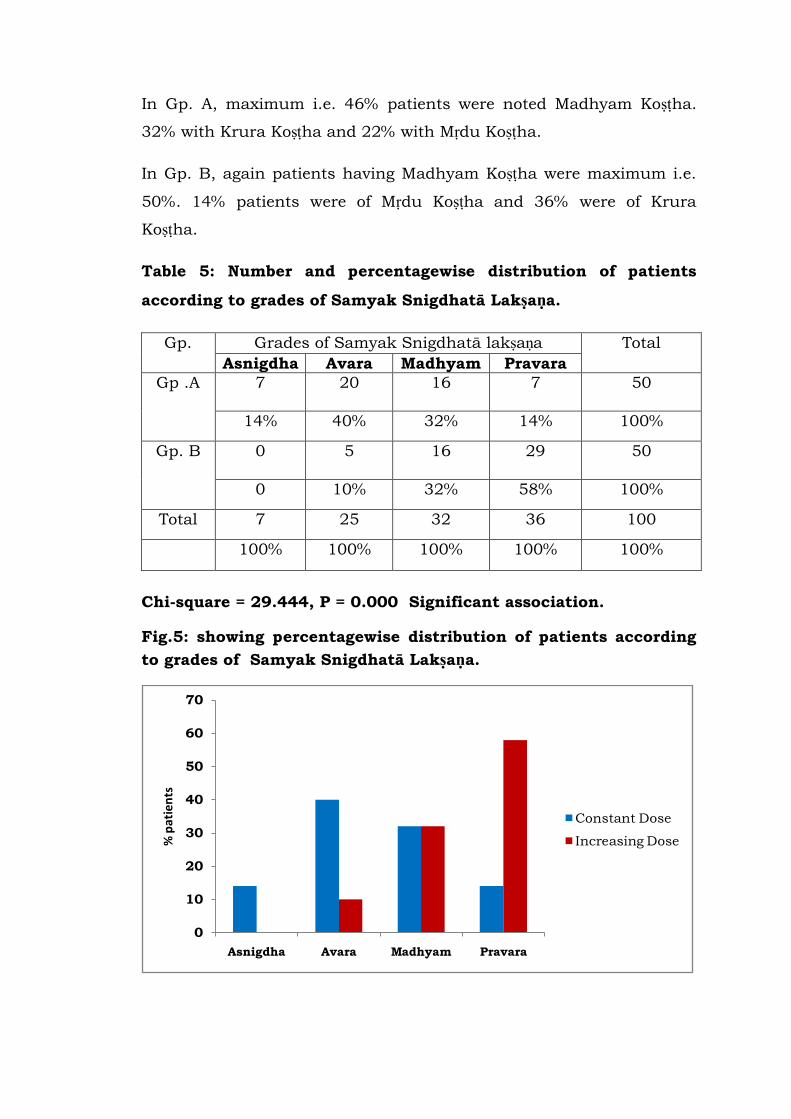
In Gp. A, maximum i.e. 46% patients were noted Madhyam Koṣṭha.
32% with Krura Koṣṭha and 22% with Mṛdu Koṣṭha.
In Gp. B, again patients having Madhyam Koṣṭha were maximum i.e.
50%. 14% patients were of Mṛdu Koṣṭha and 36% were of Krura
Koṣṭha.
Table 5: Number and percentagewise distribution of patients
according to grades of Samyak Snigdhatā Lakṣaṇa.
Gp. Grades of Samyak Snigdhatā lakṣaṇa Total
Asnigdha Avara Madhyam Pravara
Gp .A 7
20
16
7
50
14% 40% 32% 14% 100%
Gp. B 0 5
16
29
50
0 10% 32% 58% 100%
Total 7 25 32 36 100
100% 100% 100% 100% 100%
Chi-square = 29.444, P = 0.000 Significant association.
Fig.5: showing percentagewise distribution of patients according
to grades of Samyak Snigdhatā Lakṣaṇa.
0
10
20
30
40
50
60
70
Asnigdha Avara Madhyam Pravara
% p
atie
nts
Constant Dose
Increasing Dose
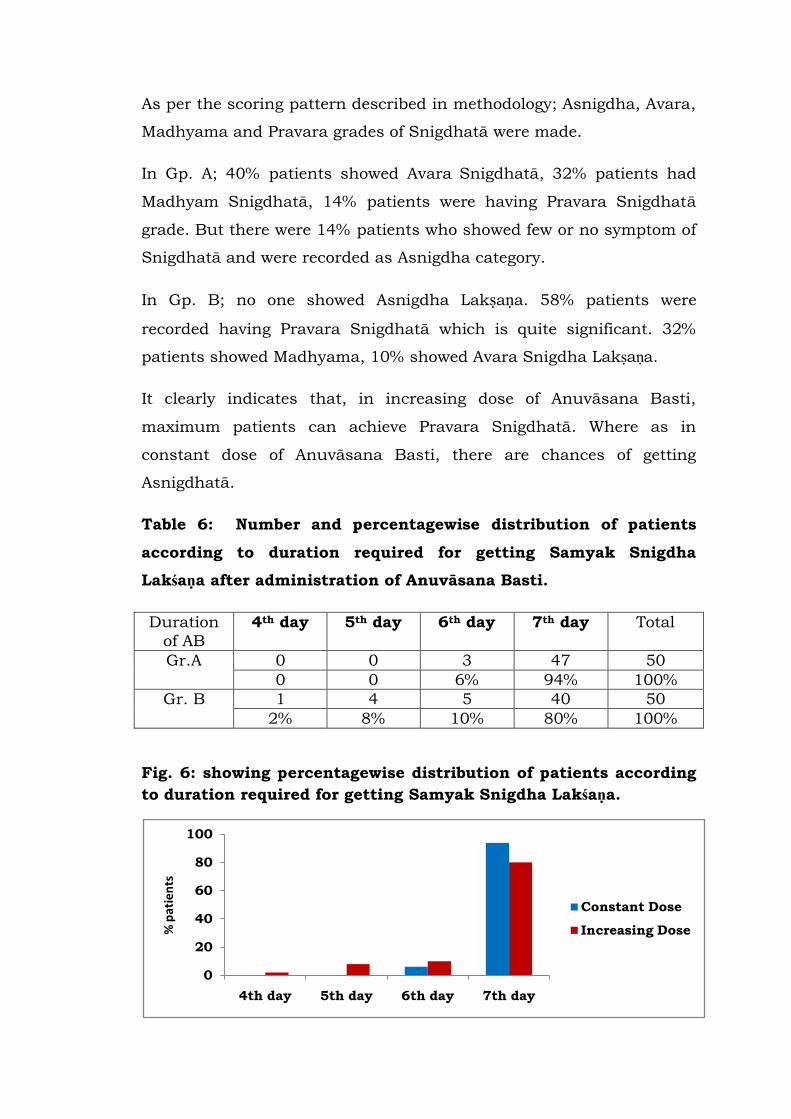
As per the scoring pattern described in methodology; Asnigdha, Avara,
Madhyama and Pravara grades of Snigdhatā were made.
In Gp. A; 40% patients showed Avara Snigdhatā, 32% patients had
Madhyam Snigdhatā, 14% patients were having Pravara Snigdhatā
grade. But there were 14% patients who showed few or no symptom of
Snigdhatā and were recorded as Asnigdha category.
In Gp. B; no one showed Asnigdha Lakṣaṇa. 58% patients were
recorded having Pravara Snigdhatā which is quite significant. 32%
patients showed Madhyama, 10% showed Avara Snigdha Lakṣaṇa.
It clearly indicates that, in increasing dose of Anuvāsana Basti,
maximum patients can achieve Pravara Snigdhatā. Where as in
constant dose of Anuvāsana Basti, there are chances of getting
Asnigdhatā.
Table 6: Number and percentagewise distribution of patients
according to duration required for getting Samyak Snigdha
Lakśaṇa after administration of Anuvāsana Basti.
Duration
of AB
4th day 5th day 6th day 7th day Total
Gr.A 0 0 3 47 50
0 0 6% 94% 100%
Gr. B 1 4 5 40 50
2% 8% 10% 80% 100%
Fig. 6: showing percentagewise distribution of patients according
to duration required for getting Samyak Snigdha Lakśaṇa.
0
20
40
60
80
100
4th day 5th day 6th day 7th day
% p
atie
nts
Constant Dose
Increasing Dose
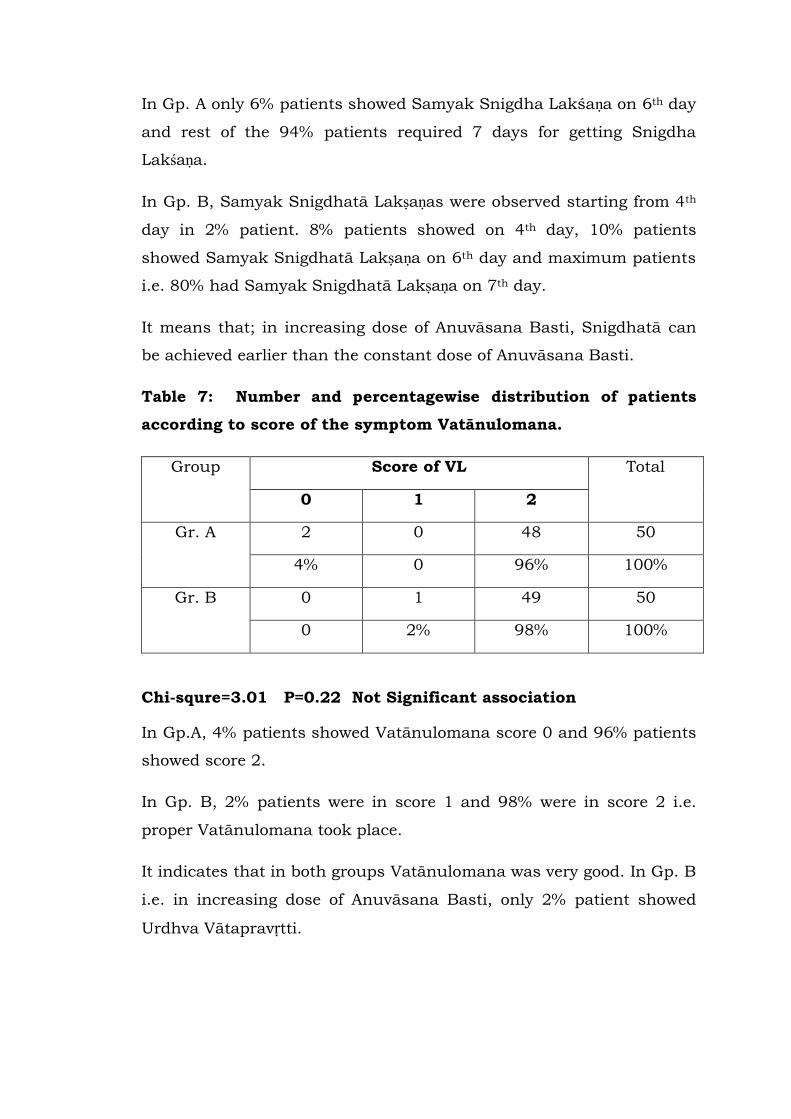
In Gp. A only 6% patients showed Samyak Snigdha Lakśaṇa on 6th day
and rest of the 94% patients required 7 days for getting Snigdha
Lakśaṇa.
In Gp. B, Samyak Snigdhatā Lakṣaṇas were observed starting from 4th
day in 2% patient. 8% patients showed on 4th day, 10% patients
showed Samyak Snigdhatā Lakṣaṇa on 6th day and maximum patients
i.e. 80% had Samyak Snigdhatā Lakṣaṇa on 7th day.
It means that; in increasing dose of Anuvāsana Basti, Snigdhatā can
be achieved earlier than the constant dose of Anuvāsana Basti.
Table 7: Number and percentagewise distribution of patients
according to score of the symptom Vatānulomana.
Group Score of VL Total
0 1 2
Gr. A 2 0 48 50
4% 0 96% 100%
Gr. B 0 1 49 50
0 2% 98% 100%
Chi-squre=3.01 P=0.22 Not Significant association
In Gp.A, 4% patients showed Vatānulomana score 0 and 96% patients
showed score 2.
In Gp. B, 2% patients were in score 1 and 98% were in score 2 i.e.
proper Vatānulomana took place.
It indicates that in both groups Vatānulomana was very good. In Gp. B
i.e. in increasing dose of Anuvāsana Basti, only 2% patient showed
Urdhva Vātapravṛtti.

Table 8: Number and percentagewise distribution of patients
according to score of the symptom Angalāghava.
Group Score of AL Total
0 1 2
Gr. A 28 3 19 50
56% 6% 38% 100%
Gr. B 15 20 15 50
30% 40% 30% 100%
Chi-squre=16.97 P=0.000 Significant association
In Gp. A, 56% patients showed no change in Angalāghava i.e. score 0
where as 6% patients showed Angagaurava and 38% patients were
noted Angalāghava.
In Gp. B, 30% patients feels as usual i.e. score 0, 40% patients
recorded Angagaurava and 30% patients had Angalāghava.
It means in Gp. B may be due to the larger quantity, patients felt
Angagaurava.
Table 9: Number and percentagewise distribution of patients
according to score of the symptom Asaṃhata Varca.
Group Score of AV Total
0 1 2
Gr. A 20 0 30 50
40 0 60% 100%
Gr. B 3 1 46 50
6% 2% 92% 100%
Chi-square=16.93 P=0.000 Significant association
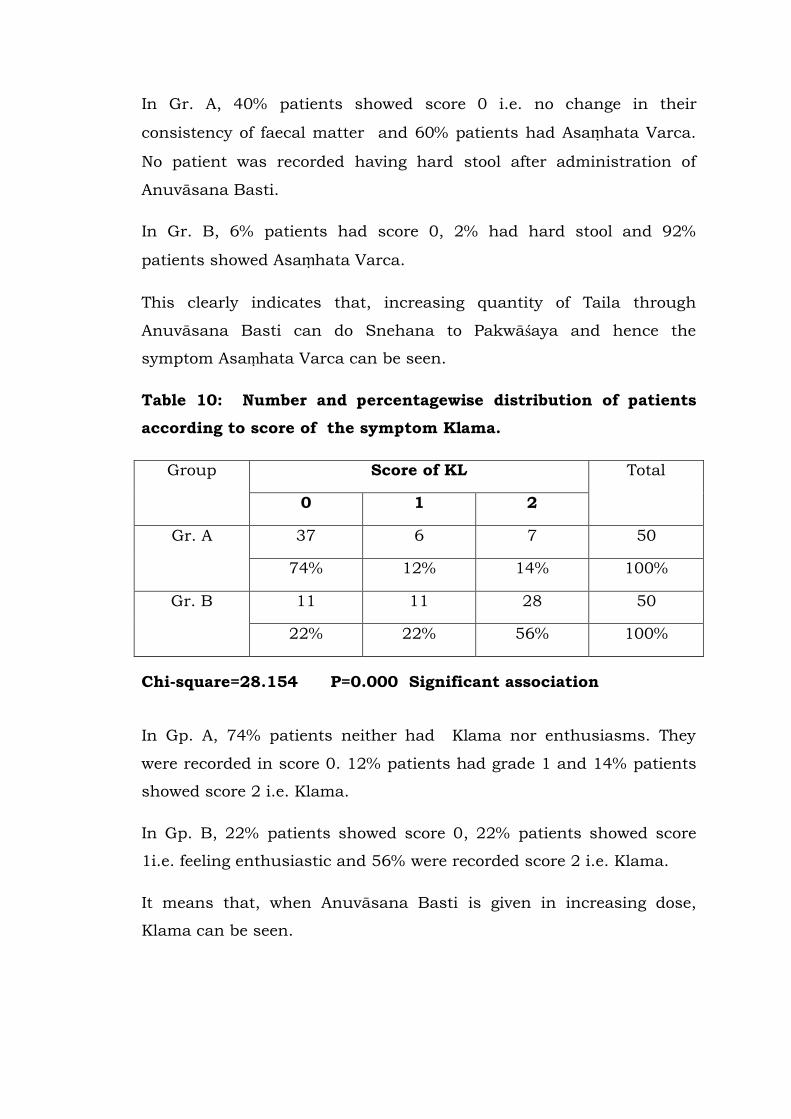
In Gr. A, 40% patients showed score 0 i.e. no change in their
consistency of faecal matter and 60% patients had Asaṃhata Varca.
No patient was recorded having hard stool after administration of
Anuvāsana Basti.
In Gr. B, 6% patients had score 0, 2% had hard stool and 92%
patients showed Asaṃhata Varca.
This clearly indicates that, increasing quantity of Taila through
Anuvāsana Basti can do Snehana to Pakwāśaya and hence the
symptom Asaṃhata Varca can be seen.
Table 10: Number and percentagewise distribution of patients
according to score of the symptom Klama.
Group Score of KL Total
0 1 2
Gr. A 37 6 7 50
74% 12% 14% 100%
Gr. B 11 11 28 50
22% 22% 56% 100%
Chi-square=28.154 P=0.000 Significant association
In Gp. A, 74% patients neither had Klama nor enthusiasms. They
were recorded in score 0. 12% patients had grade 1 and 14% patients
showed score 2 i.e. Klama.
In Gp. B, 22% patients showed score 0, 22% patients showed score
1i.e. feeling enthusiastic and 56% were recorded score 2 i.e. Klama.
It means that, when Anuvāsana Basti is given in increasing dose,
Klama can be seen.
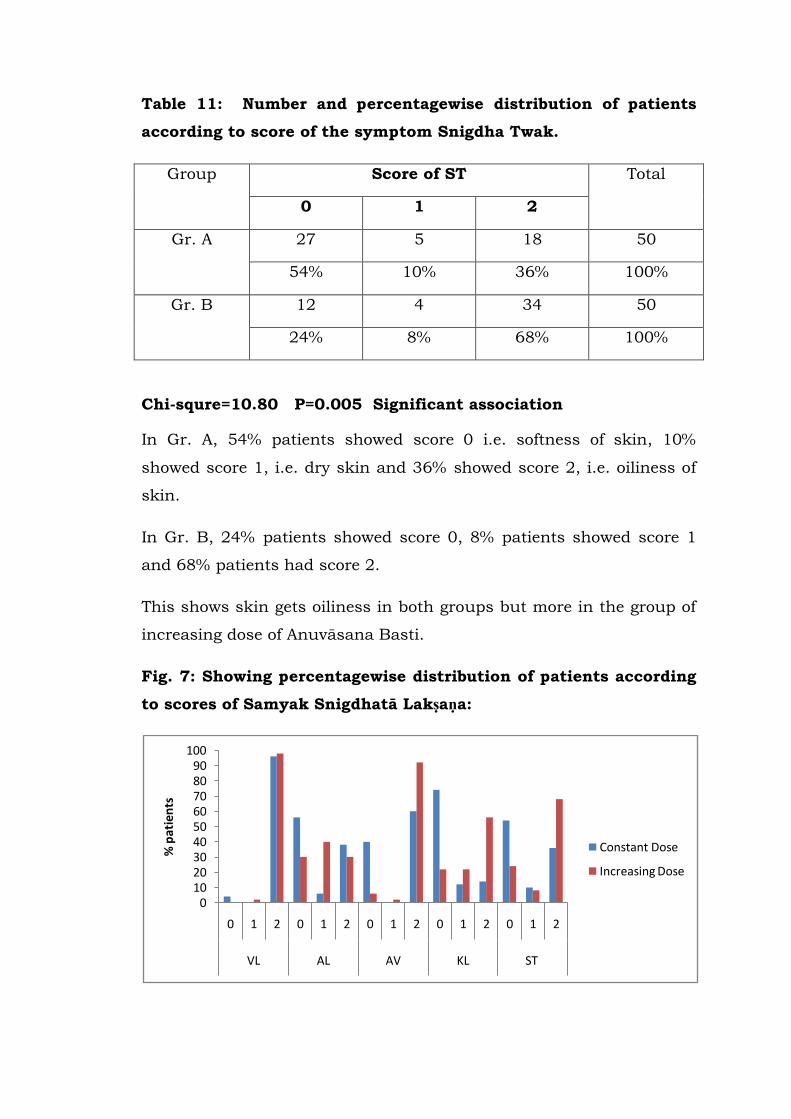
Table 11: Number and percentagewise distribution of patients
according to score of the symptom Snigdha Twak.
Group Score of ST Total
0 1 2
Gr. A 27 5 18 50
54% 10% 36% 100%
Gr. B 12 4 34 50
24% 8% 68% 100%
Chi-squre=10.80 P=0.005 Significant association
In Gr. A, 54% patients showed score 0 i.e. softness of skin, 10%
showed score 1, i.e. dry skin and 36% showed score 2, i.e. oiliness of
skin.
In Gr. B, 24% patients showed score 0, 8% patients showed score 1
and 68% patients had score 2.
This shows skin gets oiliness in both groups but more in the group of
increasing dose of Anuvāsana Basti.
Fig. 7: Showing percentagewise distribution of patients according
to scores of Samyak Snigdhatā Lakṣaṇa:
0102030405060708090
100
0 1 2 0 1 2 0 1 2 0 1 2 0 1 2
VL AL AV KL ST
% p
atie
nts
Constant Dose
Increasing Dose
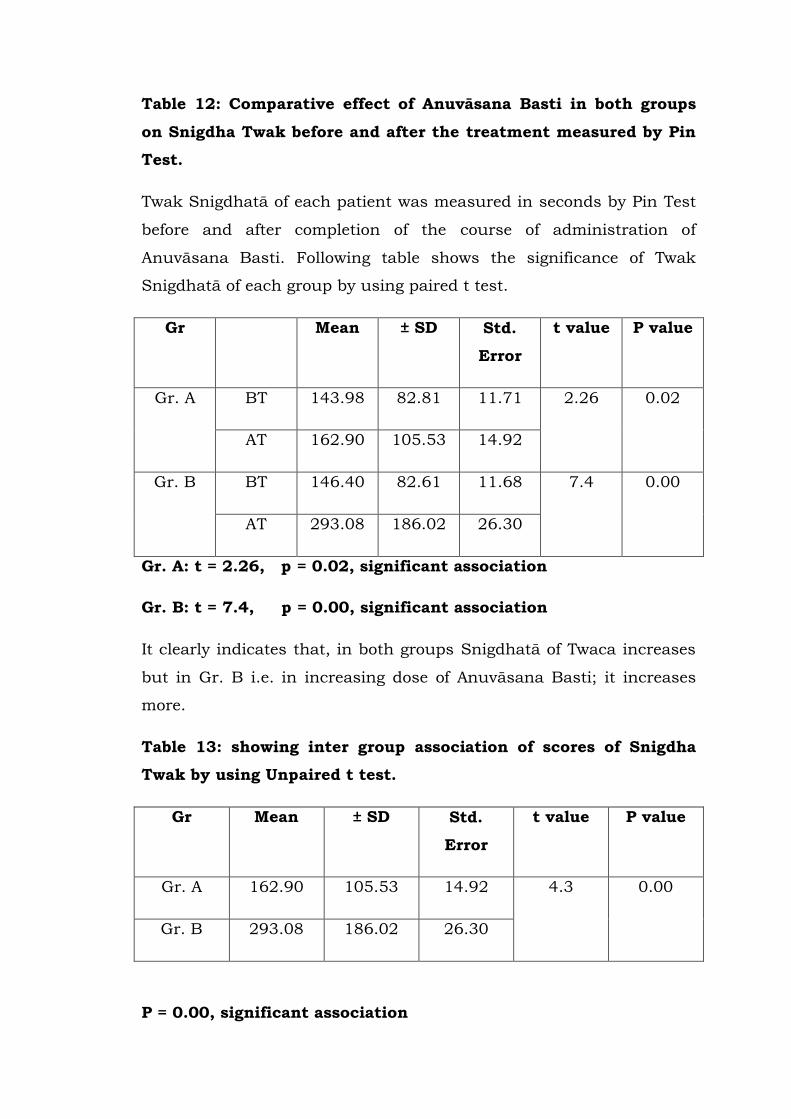
Table 12: Comparative effect of Anuvāsana Basti in both groups
on Snigdha Twak before and after the treatment measured by Pin
Test.
Twak Snigdhatā of each patient was measured in seconds by Pin Test
before and after completion of the course of administration of
Anuvāsana Basti. Following table shows the significance of Twak
Snigdhatā of each group by using paired t test.
Gr Mean ± SD Std.
Error
t value P value
Gr. A BT 143.98 82.81 11.71 2.26 0.02
AT 162.90 105.53 14.92
Gr. B BT 146.40 82.61 11.68 7.4 0.00
AT 293.08 186.02 26.30
Gr. A: t = 2.26, p = 0.02, significant association
Gr. B: t = 7.4, p = 0.00, significant association
It clearly indicates that, in both groups Snigdhatā of Twaca increases
but in Gr. B i.e. in increasing dose of Anuvāsana Basti; it increases
more.
Table 13: showing inter group association of scores of Snigdha
Twak by using Unpaired t test.
Gr Mean ± SD Std.
Error
t value P value
Gr. A 162.90 105.53 14.92 4.3 0.00
Gr. B 293.08 186.02 26.30
P = 0.00, significant association
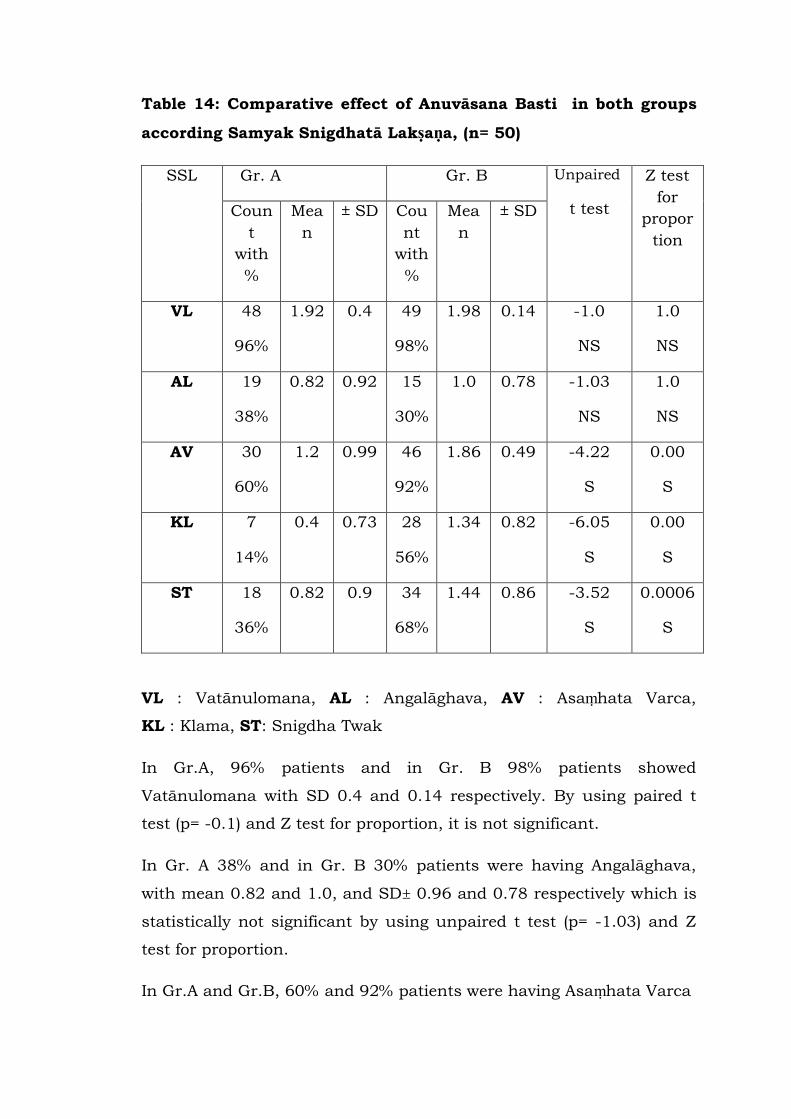
Table 14: Comparative effect of Anuvāsana Basti in both groups
according Samyak Snigdhatā Lakṣaṇa, (n= 50)
SSL Gr. A Gr. B Unpaired
t test
Z test
for
propor
tion
Coun
t
with
%
Mea
n
± SD Cou
nt
with
%
Mea
n
± SD
VL 48
96%
1.92 0.4 49
98%
1.98 0.14 -1.0
NS
1.0
NS
AL 19
38%
0.82 0.92 15
30%
1.0 0.78 -1.03
NS
1.0
NS
AV 30
60%
1.2 0.99 46
92%
1.86 0.49 -4.22
S
0.00
S
KL 7
14%
0.4 0.73 28
56%
1.34 0.82 -6.05
S
0.00
S
ST 18
36%
0.82 0.9 34
68%
1.44 0.86 -3.52
S
0.0006
S
VL : Vatānulomana, AL : Angalāghava, AV : Asaṃhata Varca,
KL : Klama, ST: Snigdha Twak
In Gr.A, 96% patients and in Gr. B 98% patients showed
Vatānulomana with SD 0.4 and 0.14 respectively. By using paired t
test (p= -0.1) and Z test for proportion, it is not significant.
In Gr. A 38% and in Gr. B 30% patients were having Angalāghava,
with mean 0.82 and 1.0, and SD± 0.96 and 0.78 respectively which is
statistically not significant by using unpaired t test (p= -1.03) and Z
test for proportion.
In Gr.A and Gr.B, 60% and 92% patients were having Asaṃhata Varca
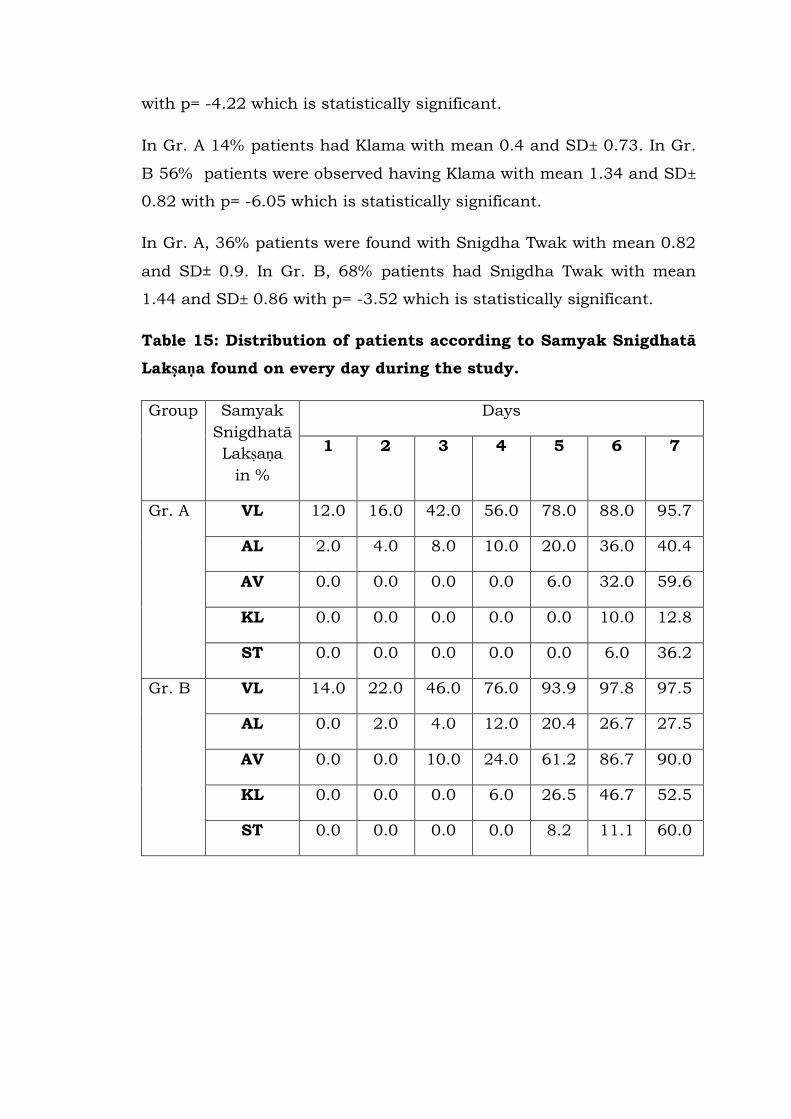
with p= -4.22 which is statistically significant.
In Gr. A 14% patients had Klama with mean 0.4 and SD± 0.73. In Gr.
B 56% patients were observed having Klama with mean 1.34 and SD±
0.82 with p= -6.05 which is statistically significant.
In Gr. A, 36% patients were found with Snigdha Twak with mean 0.82
and SD± 0.9. In Gr. B, 68% patients had Snigdha Twak with mean
1.44 and SD± 0.86 with p= -3.52 which is statistically significant.
Table 15: Distribution of patients according to Samyak Snigdhatā
Lakṣaṇa found on every day during the study.
Group Samyak
Snigdhatā
Lakṣaṇa
in %
Days
1 2 3 4 5 6 7
Gr. A VL 12.0 16.0 42.0 56.0 78.0 88.0 95.7
AL 2.0 4.0 8.0 10.0 20.0 36.0 40.4
AV 0.0 0.0 0.0 0.0 6.0 32.0 59.6
KL 0.0 0.0 0.0 0.0 0.0 10.0 12.8
ST 0.0 0.0 0.0 0.0 0.0 6.0 36.2
Gr. B VL 14.0 22.0 46.0 76.0 93.9 97.8 97.5
AL 0.0 2.0 4.0 12.0 20.4 26.7 27.5
AV 0.0 0.0 10.0 24.0 61.2 86.7 90.0
KL 0.0 0.0 0.0 6.0 26.5 46.7 52.5
ST 0.0 0.0 0.0 0.0 8.2 11.1 60.0

Fig.8: showing percentagewise distribution of the appearanceof Snigdhatā Lakṣaṇa according to days.
0
10
20
30
40
50
60
70
80
90
100
1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7 1 2 3 4 5 6 7
VL AL AV KL ST
% p
atie
nts
Constant Dose
Increasing Dose

In Gr. A, the pattern of Samyak Snigdhatā Lakṣaṇa found with respect
of duration of Anuvāsana Basti as follows Vatānulomana was seen in
12% of subjects on 1st day.16%, 42%, 56%, 78%, 88% and 95.7% on
subsequent days.
Angalāghava was noted 2%, 4%, 8%, 10%, 20%, 36% and 40.4% on
1st to 7th day respectively.
Asaṃhata Varca was observed from 5th day of administration of
Anuvāsana Basti. 6% patients were found on 5th day followed by 32%
and 59.6% on subsequent days.
10% patients showed Klama on 6th day and 12.8% patients on 7th day
of Anuvāsana Basti.
Twak Snigdhatā was found 6% on 6th day and 36.2% on 7th day of
administration of Anuvāsana Basti.
In Gr. B, the pattern of Samyak Snigdhatā Lakṣaṇa found with respect
of duration of Anuvāsana Basti as follows Vatānulomanā was seen in
14% of subjects on 1st day.22%, 46%, 76%, 93%, 97.8% and 97.5% on
subsequent days.
Angalāghava was noted 2%, 4%, 12%, 20.4%, 26.7% and 27.5% on
2nd to 7th day respectively.
Asaṃhata Varca was observed from 3rd day of administration of
Anuvāsana Basti. 10%, 24%,61.2%, 86.7% and 90% patients were
found on 3rd to 7th day respectively.
6% patients showed Klama on 4th day,26.5% patients on 5th day,
46.7% on 6th day and 52.5% on 7th day of Anuvāsana Basti.
Twak Snigdhatā was found 8.2%% on 5th day. 11.1% and 60.0% on
6th and 7th day of administration of Anuvāsana Basti respectively.
It means symptoms of Samyak Snigdhatā do not appear on the same
day but as Snehana process goes on through Anuvāsana Basti, the
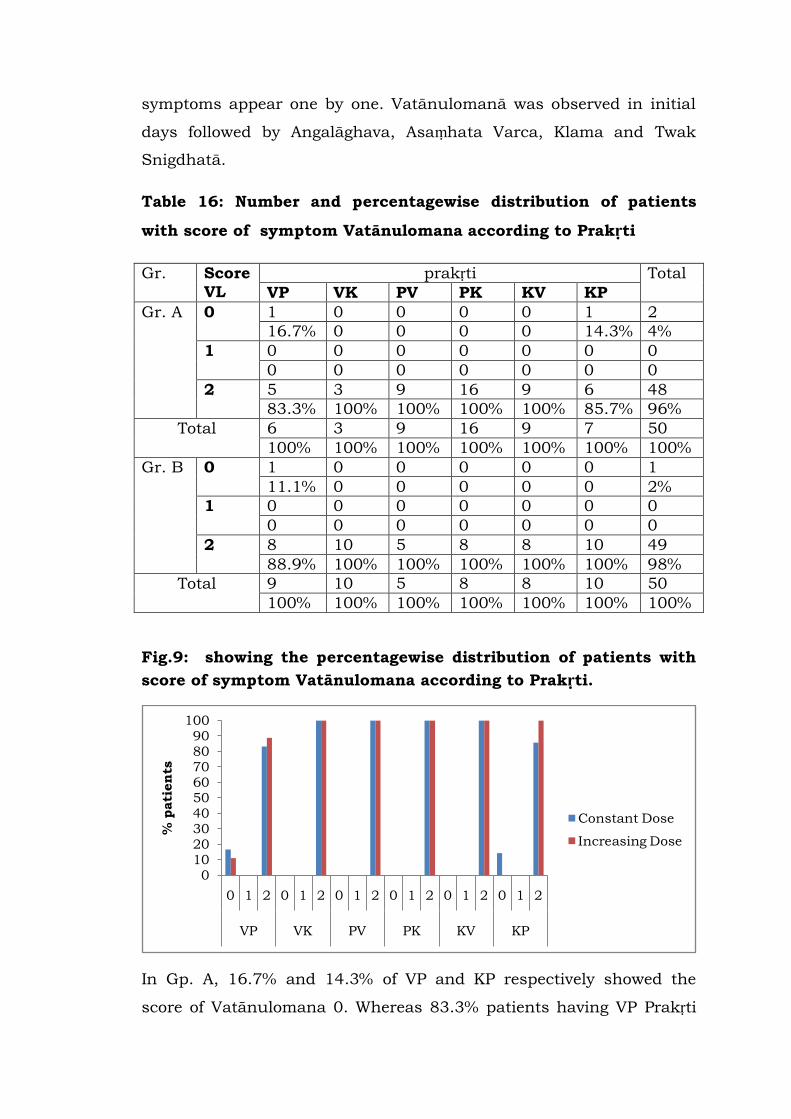
symptoms appear one by one. Vatānulomanā was observed in initial
days followed by Angalāghava, Asaṃhata Varca, Klama and Twak
Snigdhatā.
Table 16: Number and percentagewise distribution of patients
with score of symptom Vatānulomana according to Prakṛti
Gr. Score
VL
prakṛti Total
VP VK PV PK KV KP
Gr. A 0 1 0 0 0 0 1 2
16.7% 0 0 0 0 14.3% 4%
1 0 0 0 0 0 0 0
0 0 0 0 0 0 0
2 5 3 9 16 9 6 48
83.3% 100% 100% 100% 100% 85.7% 96%
Total 6 3 9 16 9 7 50
100% 100% 100% 100% 100% 100% 100%
Gr. B 0 1 0 0 0 0 0 1
11.1% 0 0 0 0 0 2%
1 0 0 0 0 0 0 0
0 0 0 0 0 0 0
2 8 10 5 8 8 10 49
88.9% 100% 100% 100% 100% 100% 98%
Total 9 10 5 8 8 10 50
100% 100% 100% 100% 100% 100% 100%
Fig.9: showing the percentagewise distribution of patients with
score of symptom Vatānulomana according to Prakṛti.
In Gp. A, 16.7% and 14.3% of VP and KP respectively showed the
score of Vatānulomana 0. Whereas 83.3% patients having VP Prakṛti
0102030405060708090
100
0 1 2 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2
VP VK PV PK KV KP
% p
ati
en
ts
Constant Dose
Increasing Dose

and 85.7% patients having KP Prakṛti showed score 2. All other
patients having VK, PV, PK, KV Prakṛti had score 2.
In Gp. B, 11.2% and 88.9% of VP Prakṛti showed score 0 and 2
respectively. Score 2 was obtained by remaining five Prakṛti.
It shows that irrespective of Prkṛti and dose of Anuvāsana Basti,
Vatānulomana can be obtained.
Table 17: Distribution of patients with score of symptom
Angalāghava within Prakṛti
Gp. Score
AL
Prakṛti Total
Gr. A
VP VK PV PK KV KP
0 5 3 6 7 4 3 28
83.3% 100% 66.7% 43.8% 44.4% 42.9% 56%
1 0 0 1 1 0 1 3
0 0 11.1% 6.3% 0 14.3% 6%
2 1 0 2 8 5 3 19
16.7% 0 22.2% 50% 55.6% 42.9% 38%
Total 6 3 9 16 9 7 50
100% 100% 100% 100% 100% 100% 100%
Gp.
B
0 2 3 2 4 2 2 15
22.2% 30% 40% 50% 25% 20% 30%
1 4 7 0 3 2 4 20
44.4% 70% 0 37.5% 25% 40% 40%
2 3 0 3 1 4 4 15
33.3% 0 60% 12.5% 50% 40% 30%
Total 9 10 5 8 8 10 50
100% 100% 100% 100% 100% 100% 100%
Fig.10: showing percentagewise distribution of patients with
score of symptom Angalāghava within Prakṛti.
0102030405060708090
100
0 1 2 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2
VP VK PV PK KV KP
% p
ati
en
ts
Constant Dose
Increasing Dose
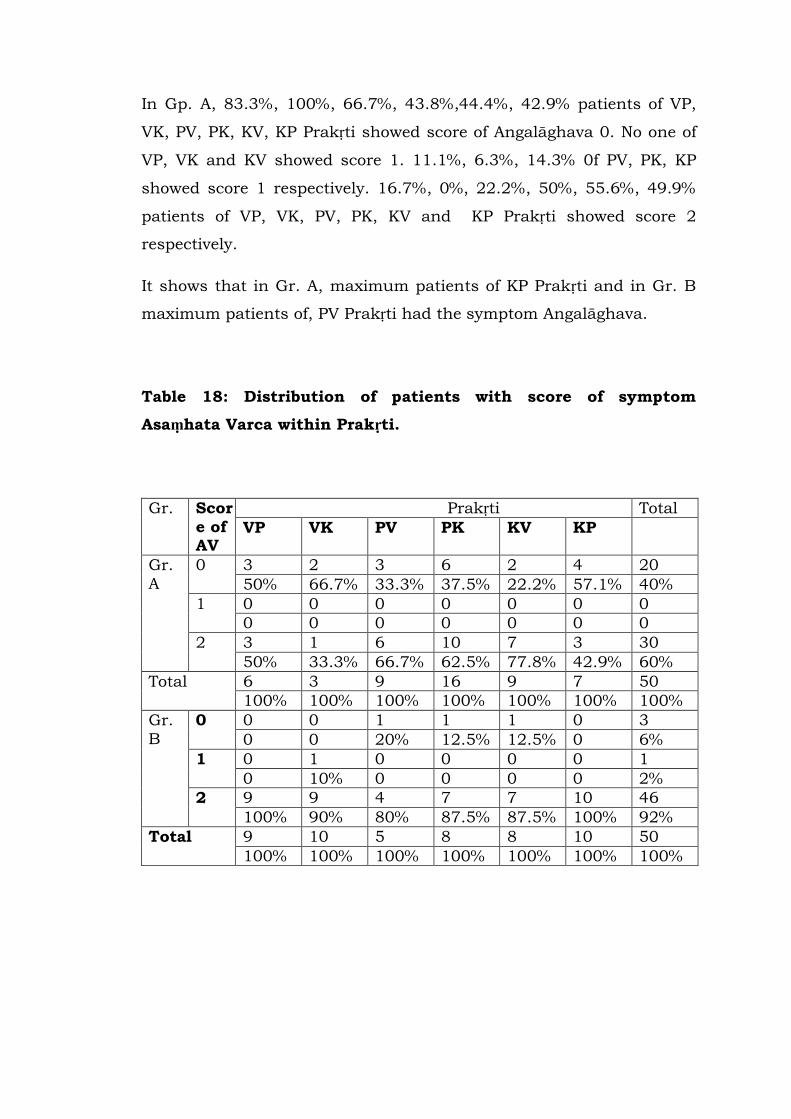
In Gp. A, 83.3%, 100%, 66.7%, 43.8%,44.4%, 42.9% patients of VP,
VK, PV, PK, KV, KP Prakṛti showed score of Angalāghava 0. No one of
VP, VK and KV showed score 1. 11.1%, 6.3%, 14.3% 0f PV, PK, KP
showed score 1 respectively. 16.7%, 0%, 22.2%, 50%, 55.6%, 49.9%
patients of VP, VK, PV, PK, KV and KP Prakṛti showed score 2
respectively.
It shows that in Gr. A, maximum patients of KP Prakṛti and in Gr. B
maximum patients of, PV Prakṛti had the symptom Angalāghava.
Table 18: Distribution of patients with score of symptom
Asaṃhata Varca within Prakṛti.
Gr. Scor
e of AV
Prakṛti Total
VP VK PV PK KV KP
Gr.
A
0 3 2 3 6 2 4 20
50% 66.7% 33.3% 37.5% 22.2% 57.1% 40%
1 0 0 0 0 0 0 0
0 0 0 0 0 0 0
2 3 1 6 10 7 3 30
50% 33.3% 66.7% 62.5% 77.8% 42.9% 60%
Total 6 3 9 16 9 7 50
100% 100% 100% 100% 100% 100% 100%
Gr.
B
0 0 0 1 1 1 0 3
0 0 20% 12.5% 12.5% 0 6%
1 0 1 0 0 0 0 1
0 10% 0 0 0 0 2%
2 9 9 4 7 7 10 46
100% 90% 80% 87.5% 87.5% 100% 92%
Total 9 10 5 8 8 10 50
100% 100% 100% 100% 100% 100% 100%
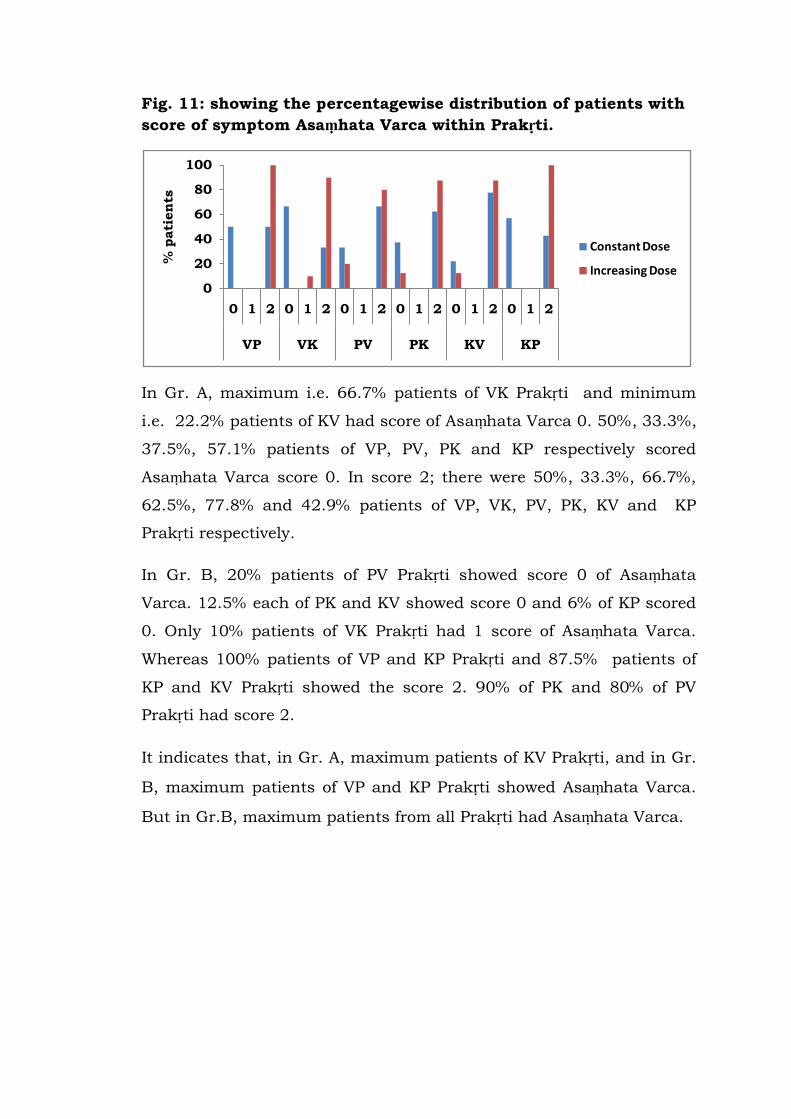
Fig. 11: showing the percentagewise distribution of patients with
score of symptom Asaṃhata Varca within Prakṛti.
In Gr. A, maximum i.e. 66.7% patients of VK Prakṛti and minimum
i.e. 22.2% patients of KV had score of Asaṃhata Varca 0. 50%, 33.3%,
37.5%, 57.1% patients of VP, PV, PK and KP respectively scored
Asaṃhata Varca score 0. In score 2; there were 50%, 33.3%, 66.7%,
62.5%, 77.8% and 42.9% patients of VP, VK, PV, PK, KV and KP
Prakṛti respectively.
In Gr. B, 20% patients of PV Prakṛti showed score 0 of Asaṃhata
Varca. 12.5% each of PK and KV showed score 0 and 6% of KP scored
0. Only 10% patients of VK Prakṛti had 1 score of Asaṃhata Varca.
Whereas 100% patients of VP and KP Prakṛti and 87.5% patients of
KP and KV Prakṛti showed the score 2. 90% of PK and 80% of PV
Prakṛti had score 2.
It indicates that, in Gr. A, maximum patients of KV Prakṛti, and in Gr.
B, maximum patients of VP and KP Prakṛti showed Asaṃhata Varca.
But in Gr.B, maximum patients from all Prakṛti had Asaṃhata Varca.
0
20
40
60
80
100
0 1 2 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2
VP VK PV PK KV KP
% p
ati
en
ts
Constant Dose
Increasing Dose
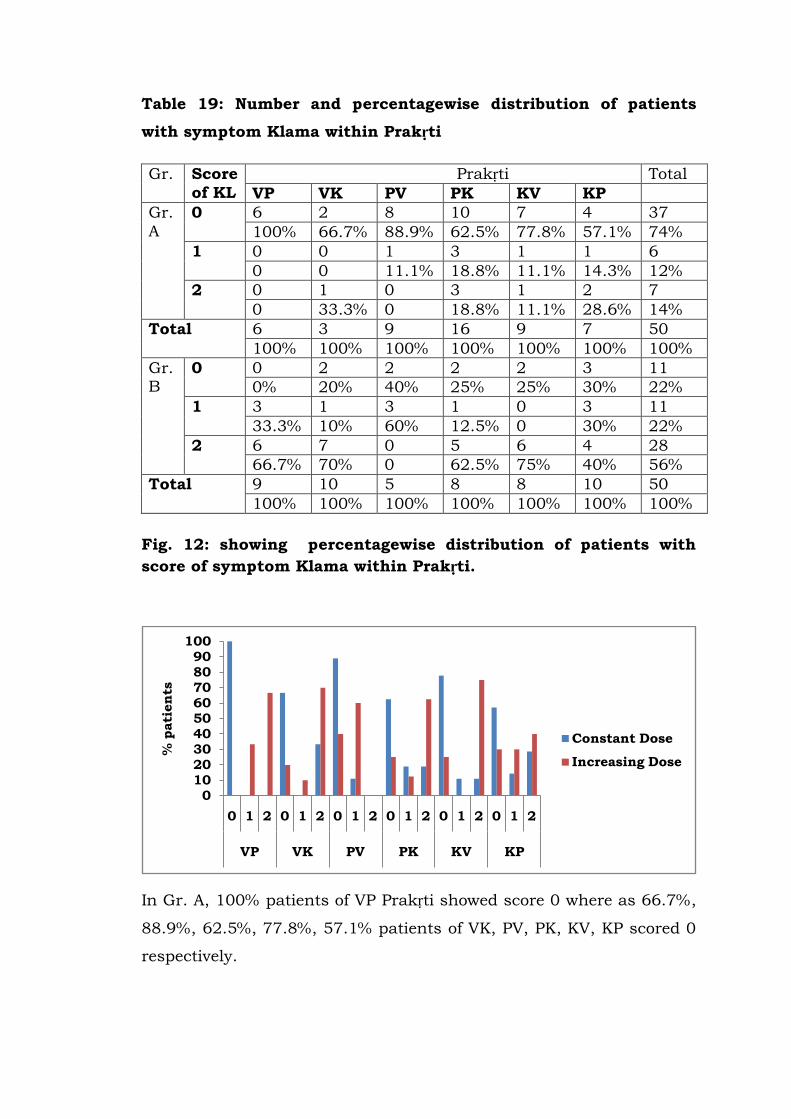
Table 19: Number and percentagewise distribution of patients
with symptom Klama within Prakṛti
Gr. Score
of KL
Prakṛti Total
VP VK PV PK KV KP
Gr.
A
0 6 2 8 10 7 4 37
100% 66.7% 88.9% 62.5% 77.8% 57.1% 74%
1 0 0 1 3 1 1 6
0 0 11.1% 18.8% 11.1% 14.3% 12%
2 0 1 0 3 1 2 7
0 33.3% 0 18.8% 11.1% 28.6% 14%
Total 6 3 9 16 9 7 50
100% 100% 100% 100% 100% 100% 100%
Gr. B
0 0 2 2 2 2 3 11
0% 20% 40% 25% 25% 30% 22%
1 3 1 3 1 0 3 11
33.3% 10% 60% 12.5% 0 30% 22%
2 6 7 0 5 6 4 28
66.7% 70% 0 62.5% 75% 40% 56%
Total 9 10 5 8 8 10 50
100% 100% 100% 100% 100% 100% 100%
Fig. 12: showing percentagewise distribution of patients with
score of symptom Klama within Prakṛti.
In Gr. A, 100% patients of VP Prakṛti showed score 0 where as 66.7%,
88.9%, 62.5%, 77.8%, 57.1% patients of VK, PV, PK, KV, KP scored 0
respectively.
0102030405060708090
100
0 1 2 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2
VP VK PV PK KV KP
% p
ati
en
ts
Constant Dose
Increasing Dose
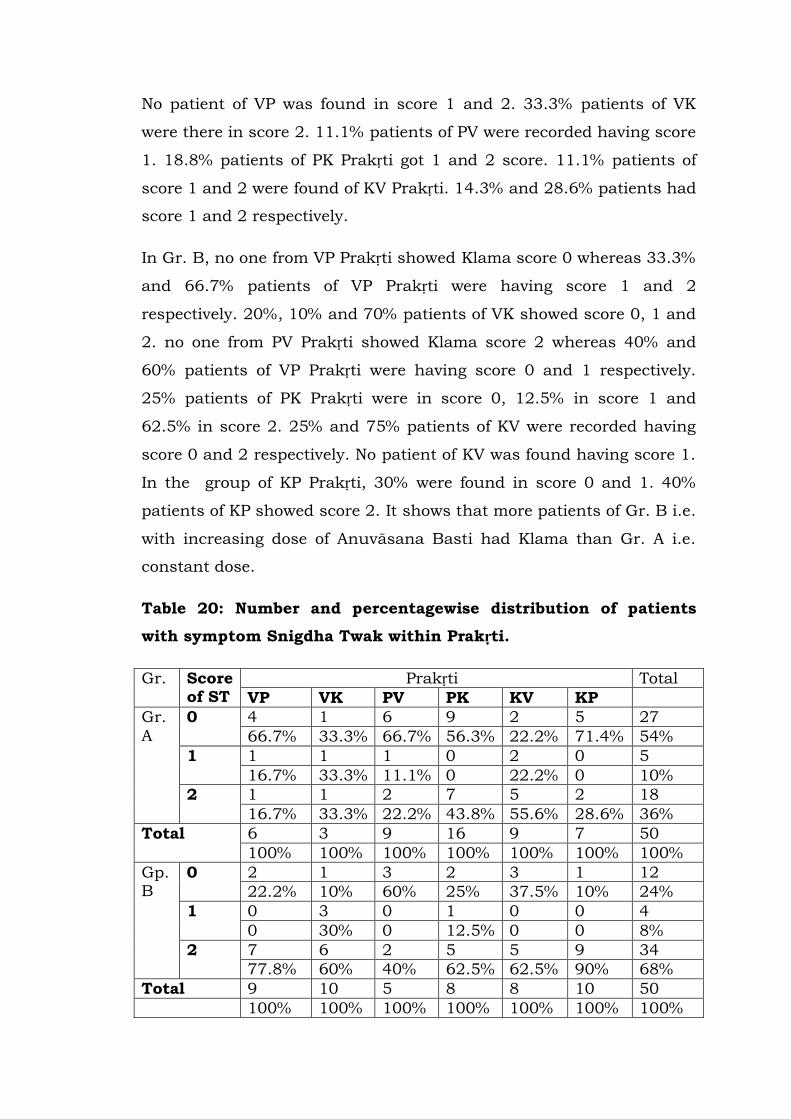
No patient of VP was found in score 1 and 2. 33.3% patients of VK
were there in score 2. 11.1% patients of PV were recorded having score
1. 18.8% patients of PK Prakṛti got 1 and 2 score. 11.1% patients of
score 1 and 2 were found of KV Prakṛti. 14.3% and 28.6% patients had
score 1 and 2 respectively.
In Gr. B, no one from VP Prakṛti showed Klama score 0 whereas 33.3%
and 66.7% patients of VP Prakṛti were having score 1 and 2
respectively. 20%, 10% and 70% patients of VK showed score 0, 1 and
2. no one from PV Prakṛti showed Klama score 2 whereas 40% and
60% patients of VP Prakṛti were having score 0 and 1 respectively.
25% patients of PK Prakṛti were in score 0, 12.5% in score 1 and
62.5% in score 2. 25% and 75% patients of KV were recorded having
score 0 and 2 respectively. No patient of KV was found having score 1.
In the group of KP Prakṛti, 30% were found in score 0 and 1. 40%
patients of KP showed score 2. It shows that more patients of Gr. B i.e.
with increasing dose of Anuvāsana Basti had Klama than Gr. A i.e.
constant dose.
Table 20: Number and percentagewise distribution of patients
with symptom Snigdha Twak within Prakṛti.
Gr. Score of ST
Prakṛti Total
VP VK PV PK KV KP
Gr.
A
0 4 1 6 9 2 5 27
66.7% 33.3% 66.7% 56.3% 22.2% 71.4% 54%
1 1 1 1 0 2 0 5
16.7% 33.3% 11.1% 0 22.2% 0 10%
2 1 1 2 7 5 2 18
16.7% 33.3% 22.2% 43.8% 55.6% 28.6% 36%
Total 6 3 9 16 9 7 50
100% 100% 100% 100% 100% 100% 100%
Gp. B
0 2 1 3 2 3 1 12
22.2% 10% 60% 25% 37.5% 10% 24%
1 0 3 0 1 0 0 4
0 30% 0 12.5% 0 0 8%
2 7 6 2 5 5 9 34
77.8% 60% 40% 62.5% 62.5% 90% 68%
Total 9 10 5 8 8 10 50
100% 100% 100% 100% 100% 100% 100%
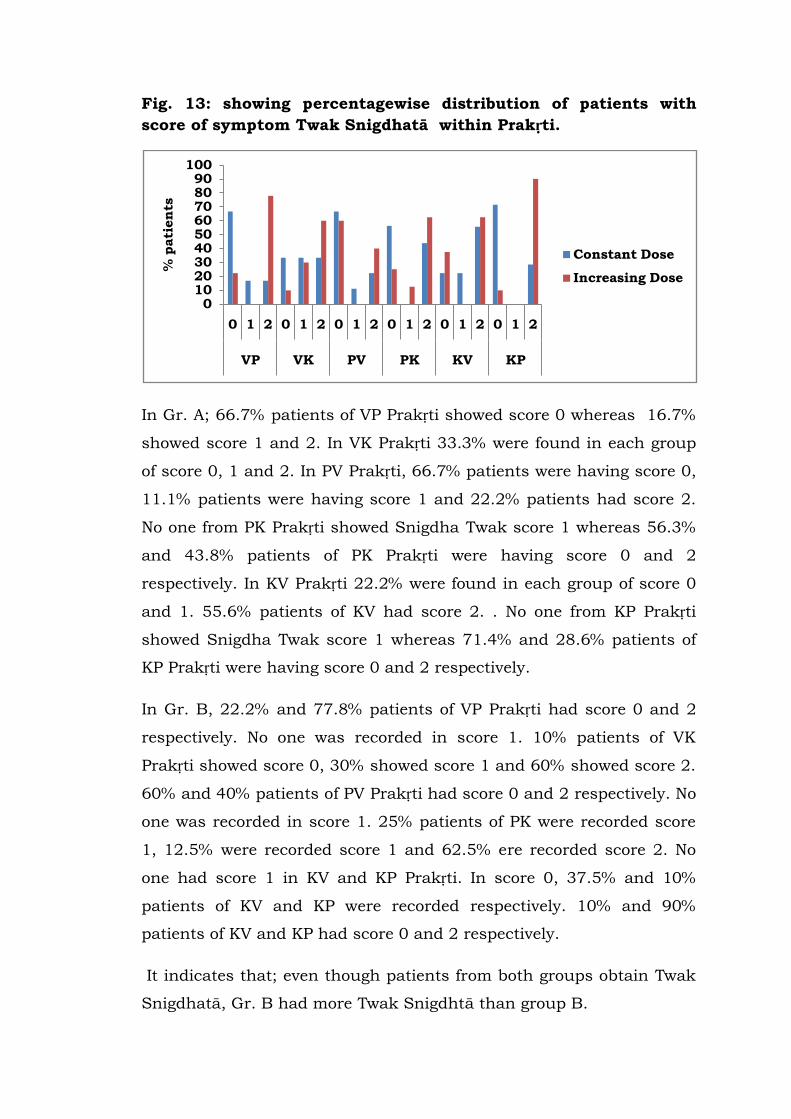
Fig. 13: showing percentagewise distribution of patients with
score of symptom Twak Snigdhatā within Prakṛti.
In Gr. A; 66.7% patients of VP Prakṛti showed score 0 whereas 16.7%
showed score 1 and 2. In VK Prakṛti 33.3% were found in each group
of score 0, 1 and 2. In PV Prakṛti, 66.7% patients were having score 0,
11.1% patients were having score 1 and 22.2% patients had score 2.
No one from PK Prakṛti showed Snigdha Twak score 1 whereas 56.3%
and 43.8% patients of PK Prakṛti were having score 0 and 2
respectively. In KV Prakṛti 22.2% were found in each group of score 0
and 1. 55.6% patients of KV had score 2. . No one from KP Prakṛti
showed Snigdha Twak score 1 whereas 71.4% and 28.6% patients of
KP Prakṛti were having score 0 and 2 respectively.
In Gr. B, 22.2% and 77.8% patients of VP Prakṛti had score 0 and 2
respectively. No one was recorded in score 1. 10% patients of VK
Prakṛti showed score 0, 30% showed score 1 and 60% showed score 2.
60% and 40% patients of PV Prakṛti had score 0 and 2 respectively. No
one was recorded in score 1. 25% patients of PK were recorded score
1, 12.5% were recorded score 1 and 62.5% ere recorded score 2. No
one had score 1 in KV and KP Prakṛti. In score 0, 37.5% and 10%
patients of KV and KP were recorded respectively. 10% and 90%
patients of KV and KP had score 0 and 2 respectively.
It indicates that; even though patients from both groups obtain Twak
Snigdhatā, Gr. B had more Twak Snigdhtā than group B.
0102030405060708090
100
0 1 2 0 1 2 0 1 2 0 1 2 0 1 2 0 1 2
VP VK PV PK KV KP
% p
ati
en
ts
Constant Dose
Increasing Dose
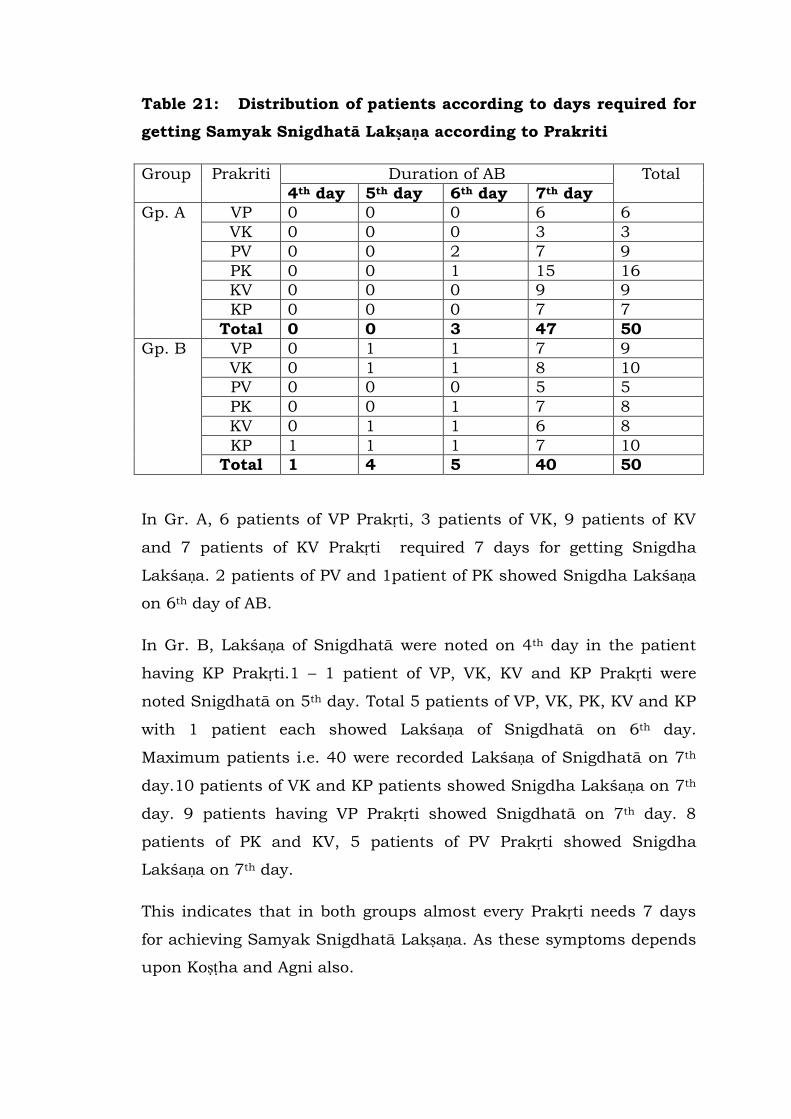
Table 21: Distribution of patients according to days required for
getting Samyak Snigdhatā Lakṣaṇa according to Prakriti
Group Prakriti Duration of AB Total
4th day 5th day 6th day 7th day
Gp. A VP 0 0 0 6 6
VK 0 0 0 3 3
PV 0 0 2 7 9
PK 0 0 1 15 16
KV 0 0 0 9 9
KP 0 0 0 7 7
Total 0 0 3 47 50
Gp. B VP 0 1 1 7 9
VK 0 1 1 8 10
PV 0 0 0 5 5
PK 0 0 1 7 8
KV 0 1 1 6 8
KP 1 1 1 7 10
Total 1 4 5 40 50
In Gr. A, 6 patients of VP Prakṛti, 3 patients of VK, 9 patients of KV
and 7 patients of KV Prakṛti required 7 days for getting Snigdha
Lakśaṇa. 2 patients of PV and 1patient of PK showed Snigdha Lakśaṇa
on 6th day of AB.
In Gr. B, Lakśaṇa of Snigdhatā were noted on 4th day in the patient
having KP Prakṛti.1 – 1 patient of VP, VK, KV and KP Prakṛti were
noted Snigdhatā on 5th day. Total 5 patients of VP, VK, PK, KV and KP
with 1 patient each showed Lakśaṇa of Snigdhatā on 6th day.
Maximum patients i.e. 40 were recorded Lakśaṇa of Snigdhatā on 7th
day.10 patients of VK and KP patients showed Snigdha Lakśaṇa on 7th
day. 9 patients having VP Prakṛti showed Snigdhatā on 7th day. 8
patients of PK and KV, 5 patients of PV Prakṛti showed Snigdha
Lakśaṇa on 7th day.
This indicates that in both groups almost every Prakṛti needs 7 days
for achieving Samyak Snigdhatā Lakṣaṇa. As these symptoms depends
upon Koṣṭha and Agni also.

Table 22: Distribution of patients according to grades of Samyak
Snigdhatā Lakṣaṇa within Prakṛti
G
r.
SSL Prakṛti Total
VP VK PV PK KV KP
G
r.
A
Asnig
dha
2 1 2 0 0 2 7
33.3% 33.3% 22.2% 0% 0% 28.6% 14%
Avara 3 1 4 8 2 2 20
50.0% 33.3% 44.4% 50% 22.2% 28.6% 40%
Madh
yam
1 1 3 4 5 2 16
16.7% 33.3% 33.3% 25% 55.6% 28.6% 32%
Prava
ra
0 0 0 4 2 1 7
0 0 0 25% 22.2% 14.3% 14%
Total 6 3 9 16 9 7 50
100% 100% 100% 100% 100% 100% 100%
G
r.
B
Asnig
dha
0 0 0 0 0 0 0
0 0 0 0 0 0 0
Avara 0 0 2 2 1 0 5
0 0 40% 25% 12.5% 0% 10%
Madh
yam
2 4 2 1 3 4 16
22.2% 40% 40% 12.5% 37.5% 40% 32%
Prava
ra
7 6 1 5 4 6 29
77.8% 60.0% 20.0% 62.5% 50.0% 60.0% 58.0%
Total 9 10 5 8 8 10 50
100% 100% 100% 100% 100% 100% 100%
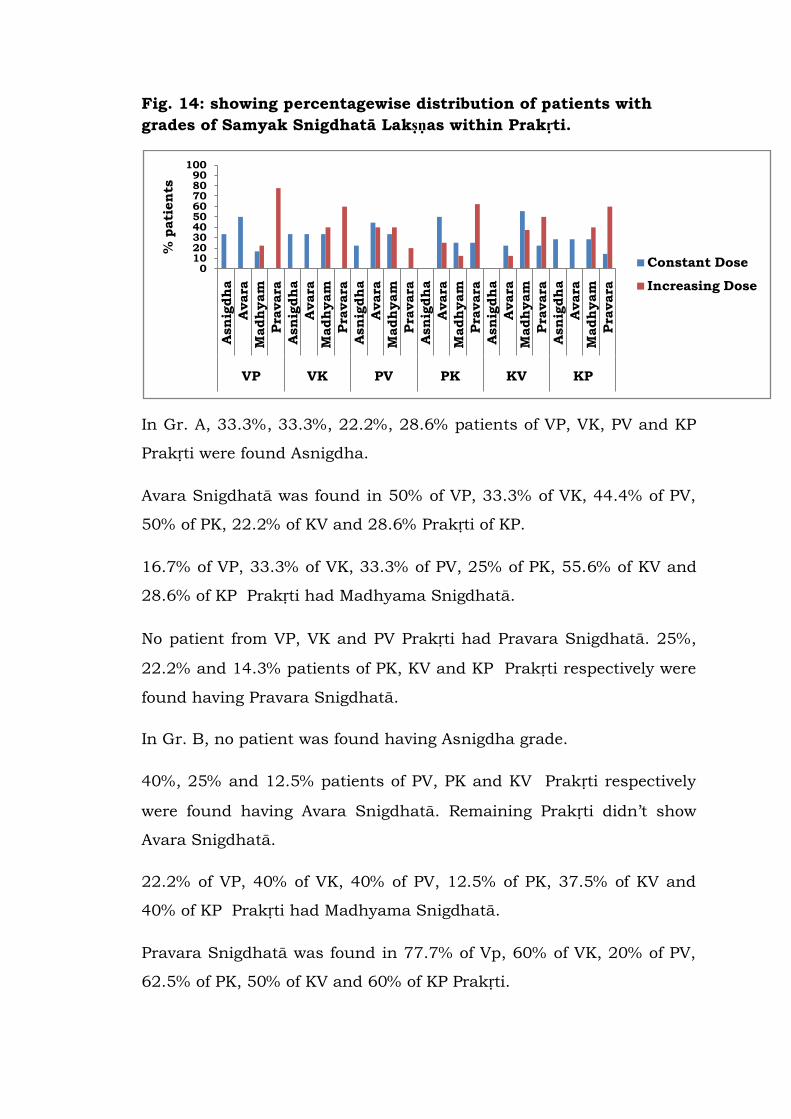
Fig. 14: showing percentagewise distribution of patients with
grades of Samyak Snigdhatā Lakṣṇas within Prakṛti.
In Gr. A, 33.3%, 33.3%, 22.2%, 28.6% patients of VP, VK, PV and KP
Prakṛti were found Asnigdha.
Avara Snigdhatā was found in 50% of VP, 33.3% of VK, 44.4% of PV,
50% of PK, 22.2% of KV and 28.6% Prakṛti of KP.
16.7% of VP, 33.3% of VK, 33.3% of PV, 25% of PK, 55.6% of KV and
28.6% of KP Prakṛti had Madhyama Snigdhatā.
No patient from VP, VK and PV Prakṛti had Pravara Snigdhatā. 25%,
22.2% and 14.3% patients of PK, KV and KP Prakṛti respectively were
found having Pravara Snigdhatā.
In Gr. B, no patient was found having Asnigdha grade.
40%, 25% and 12.5% patients of PV, PK and KV Prakṛti respectively
were found having Avara Snigdhatā. Remaining Prakṛti didn‟t show
Avara Snigdhatā.
22.2% of VP, 40% of VK, 40% of PV, 12.5% of PK, 37.5% of KV and
40% of KP Prakṛti had Madhyama Snigdhatā.
Pravara Snigdhatā was found in 77.7% of Vp, 60% of VK, 20% of PV,
62.5% of PK, 50% of KV and 60% of KP Prakṛti.
0102030405060708090
100
Asn
igdh
a
Avara
Madh
yam
Pra
vara
Asn
igdh
a
Avara
Madh
yam
Pra
vara
Asn
igdh
a
Avara
Madh
yam
Pra
vara
Asn
igdh
a
Avara
Madh
yam
Pra
vara
Asn
igdh
a
Avara
Madh
yam
Pra
vara
Asn
igdh
a
Avara
Madh
yam
Pra
vara
VP VK PV PK KV KP
% p
ati
en
ts
Constant Dose
Increasing Dose
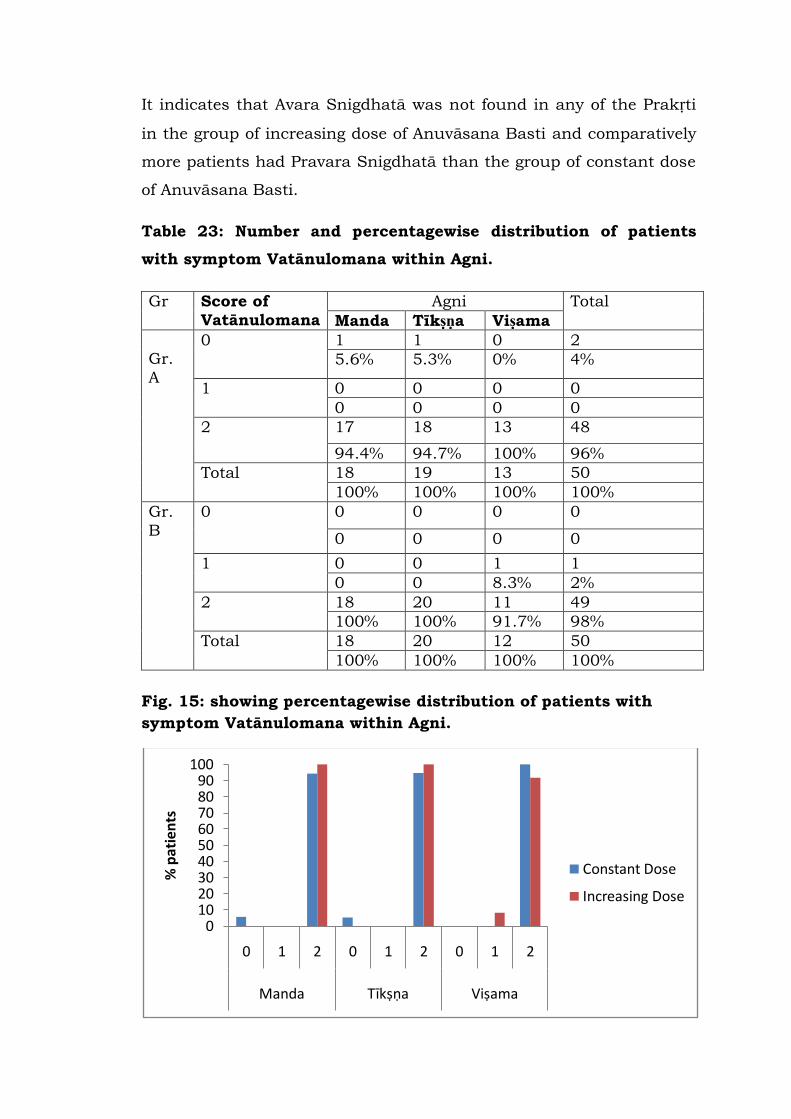
It indicates that Avara Snigdhatā was not found in any of the Prakṛti
in the group of increasing dose of Anuvāsana Basti and comparatively
more patients had Pravara Snigdhatā than the group of constant dose
of Anuvāsana Basti.
Table 23: Number and percentagewise distribution of patients
with symptom Vatānulomana within Agni.
Gr Score of
Vatānulomana
Agni Total
Manda Tīkṣṇa Viṣama
Gr.
A
0 1 1 0 2
5.6% 5.3% 0% 4%
1 0 0 0 0
0 0 0 0
2 17 18 13 48
94.4% 94.7% 100% 96%
Total 18 19 13 50
100% 100% 100% 100%
Gr.
B
0 0 0 0 0
0 0 0 0
1 0 0 1 1
0 0 8.3% 2%
2 18 20 11 49
100% 100% 91.7% 98%
Total 18 20 12 50
100% 100% 100% 100%
Fig. 15: showing percentagewise distribution of patients with
symptom Vatānulomana within Agni.
0102030405060708090
100
0 1 2 0 1 2 0 1 2
Manda Tīkṣṇa Viṣama
% p
atie
nts
Constant Dose
Increasing Dose
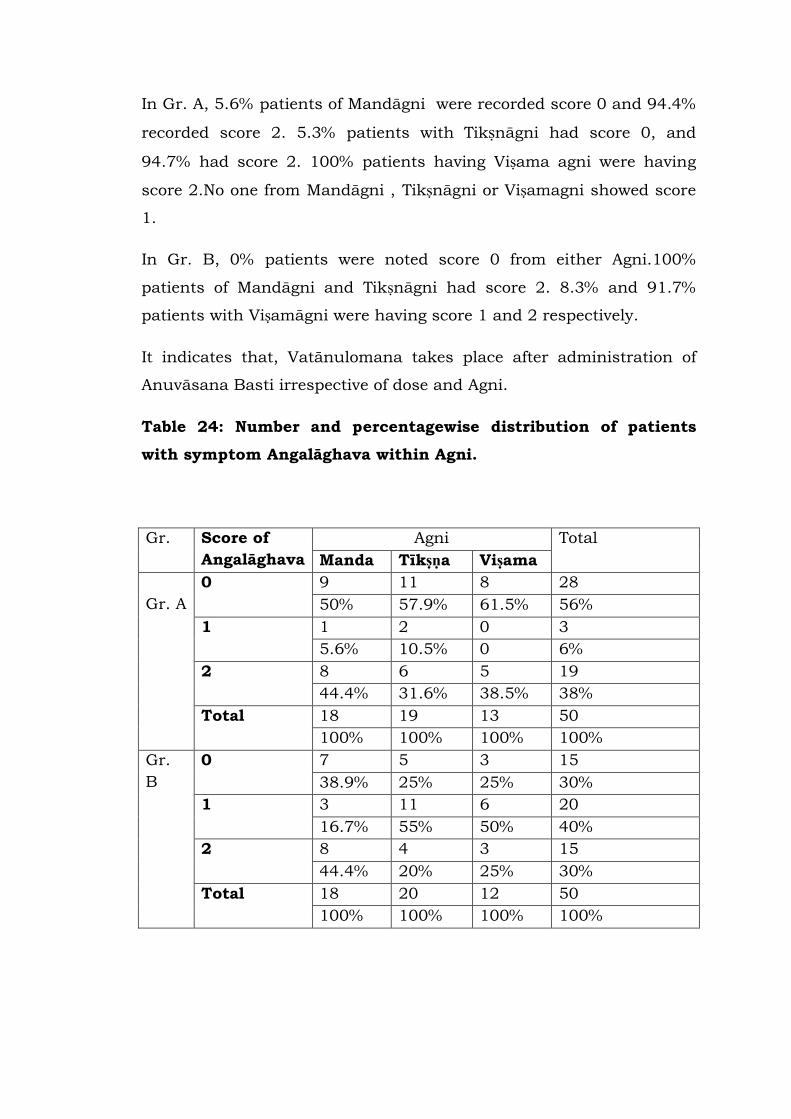
In Gr. A, 5.6% patients of Mandāgni were recorded score 0 and 94.4%
recorded score 2. 5.3% patients with Tikṣnāgni had score 0, and
94.7% had score 2. 100% patients having Viṣama agni were having
score 2.No one from Mandāgni , Tikṣnāgni or Viṣamagni showed score
1.
In Gr. B, 0% patients were noted score 0 from either Agni.100%
patients of Mandāgni and Tikṣnāgni had score 2. 8.3% and 91.7%
patients with Viṣamāgni were having score 1 and 2 respectively.
It indicates that, Vatānulomana takes place after administration of
Anuvāsana Basti irrespective of dose and Agni.
Table 24: Number and percentagewise distribution of patients
with symptom Angalāghava within Agni.
Gr. Score of
Angalāghava
Agni Total
Manda Tīkṣṇa Viṣama
Gr. A
0 9 11 8 28
50% 57.9% 61.5% 56%
1 1 2 0 3
5.6% 10.5% 0 6%
2 8 6 5 19
44.4% 31.6% 38.5% 38%
Total 18 19 13 50
100% 100% 100% 100%
Gr.
B
0 7 5 3 15
38.9% 25% 25% 30%
1 3 11 6 20
16.7% 55% 50% 40%
2 8 4 3 15
44.4% 20% 25% 30%
Total 18 20 12 50
100% 100% 100% 100%
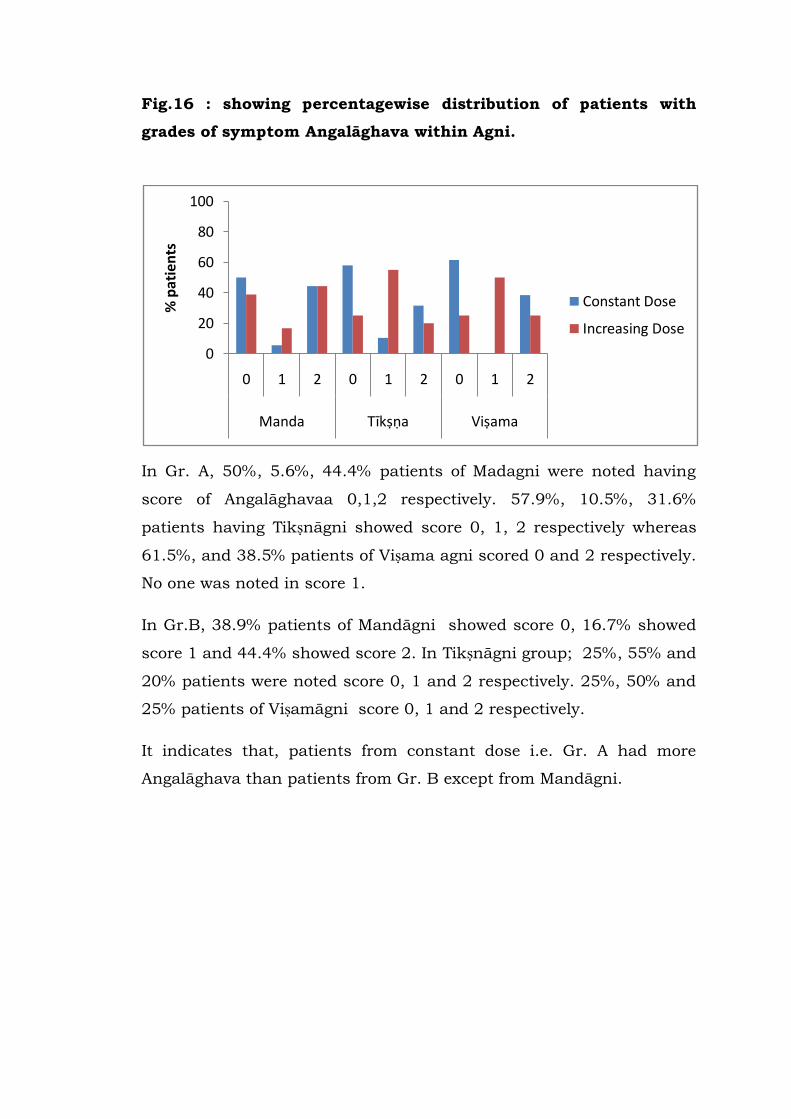
Fig.16 : showing percentagewise distribution of patients with
grades of symptom Angalāghava within Agni.
In Gr. A, 50%, 5.6%, 44.4% patients of Madagni were noted having
score of Angalāghavaa 0,1,2 respectively. 57.9%, 10.5%, 31.6%
patients having Tikṣnāgni showed score 0, 1, 2 respectively whereas
61.5%, and 38.5% patients of Viṣama agni scored 0 and 2 respectively.
No one was noted in score 1.
In Gr.B, 38.9% patients of Mandāgni showed score 0, 16.7% showed
score 1 and 44.4% showed score 2. In Tikṣnāgni group; 25%, 55% and
20% patients were noted score 0, 1 and 2 respectively. 25%, 50% and
25% patients of Viṣamāgni score 0, 1 and 2 respectively.
It indicates that, patients from constant dose i.e. Gr. A had more
Angalāghava than patients from Gr. B except from Mandāgni.
0
20
40
60
80
100
0 1 2 0 1 2 0 1 2
Manda Tīkṣṇa Viṣama
% p
ati
ents
Constant Dose
Increasing Dose
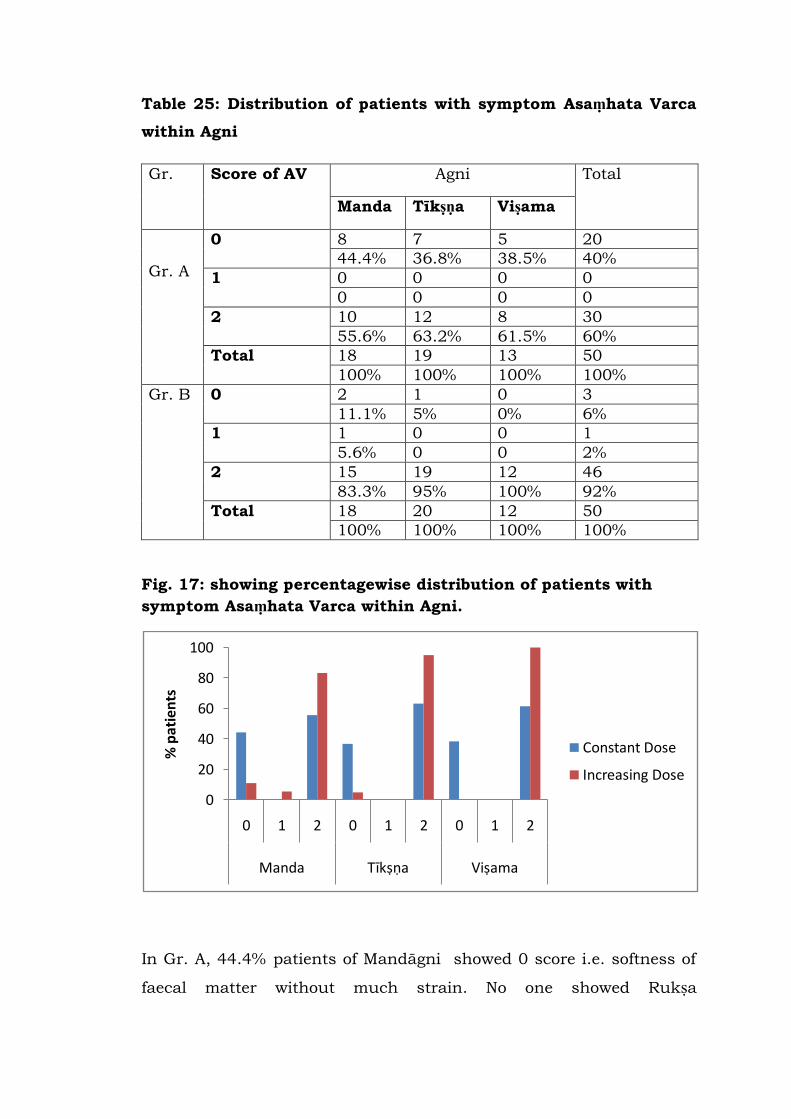
Table 25: Distribution of patients with symptom Asaṃhata Varca
within Agni
Gr. Score of AV Agni Total
Manda Tīkṣṇa Viṣama
Gr. A
0 8 7 5 20
44.4% 36.8% 38.5% 40%
1 0 0 0 0
0 0 0 0
2 10 12 8 30
55.6% 63.2% 61.5% 60%
Total 18 19 13 50
100% 100% 100% 100%
Gr. B 0 2 1 0 3
11.1% 5% 0% 6%
1 1 0 0 1
5.6% 0 0 2%
2 15 19 12 46
83.3% 95% 100% 92%
Total 18 20 12 50
100% 100% 100% 100%
Fig. 17: showing percentagewise distribution of patients with
symptom Asaṃhata Varca within Agni.
In Gr. A, 44.4% patients of Mandāgni showed 0 score i.e. softness of
faecal matter without much strain. No one showed Rukṣa
0
20
40
60
80
100
0 1 2 0 1 2 0 1 2
Manda Tīkṣṇa Viṣama
% p
atie
nts
Constant Dose
Increasing Dose
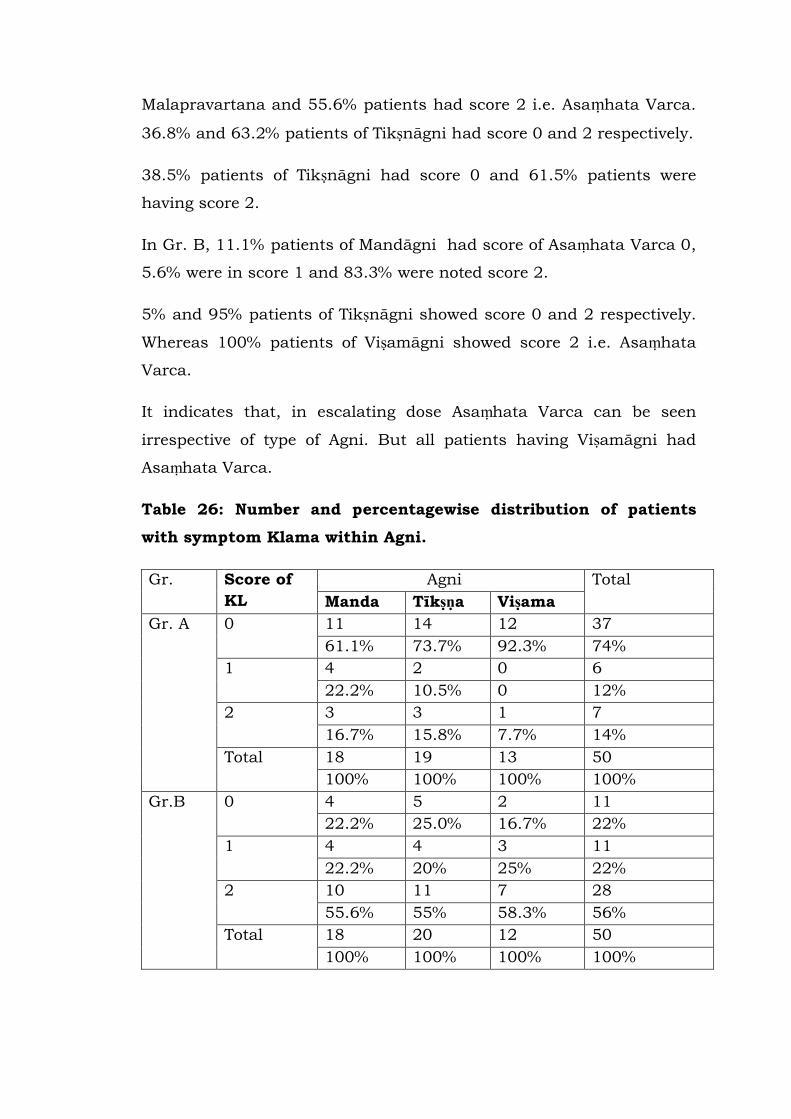
Malapravartana and 55.6% patients had score 2 i.e. Asaṃhata Varca.
36.8% and 63.2% patients of Tikṣnāgni had score 0 and 2 respectively.
38.5% patients of Tikṣnāgni had score 0 and 61.5% patients were
having score 2.
In Gr. B, 11.1% patients of Mandāgni had score of Asaṃhata Varca 0,
5.6% were in score 1 and 83.3% were noted score 2.
5% and 95% patients of Tikṣnāgni showed score 0 and 2 respectively.
Whereas 100% patients of Viṣamāgni showed score 2 i.e. Asaṃhata
Varca.
It indicates that, in escalating dose Asaṃhata Varca can be seen
irrespective of type of Agni. But all patients having Viṣamāgni had
Asaṃhata Varca.
Table 26: Number and percentagewise distribution of patients
with symptom Klama within Agni.
Gr. Score of
KL
Agni Total
Manda Tīkṣṇa Viṣama
Gr. A 0 11 14 12 37
61.1% 73.7% 92.3% 74%
1 4 2 0 6
22.2% 10.5% 0 12%
2 3 3 1 7
16.7% 15.8% 7.7% 14%
Total 18 19 13 50
100% 100% 100% 100%
Gr.B 0 4 5 2 11
22.2% 25.0% 16.7% 22%
1 4 4 3 11
22.2% 20% 25% 22%
2 10 11 7 28
55.6% 55% 58.3% 56%
Total 18 20 12 50
100% 100% 100% 100%
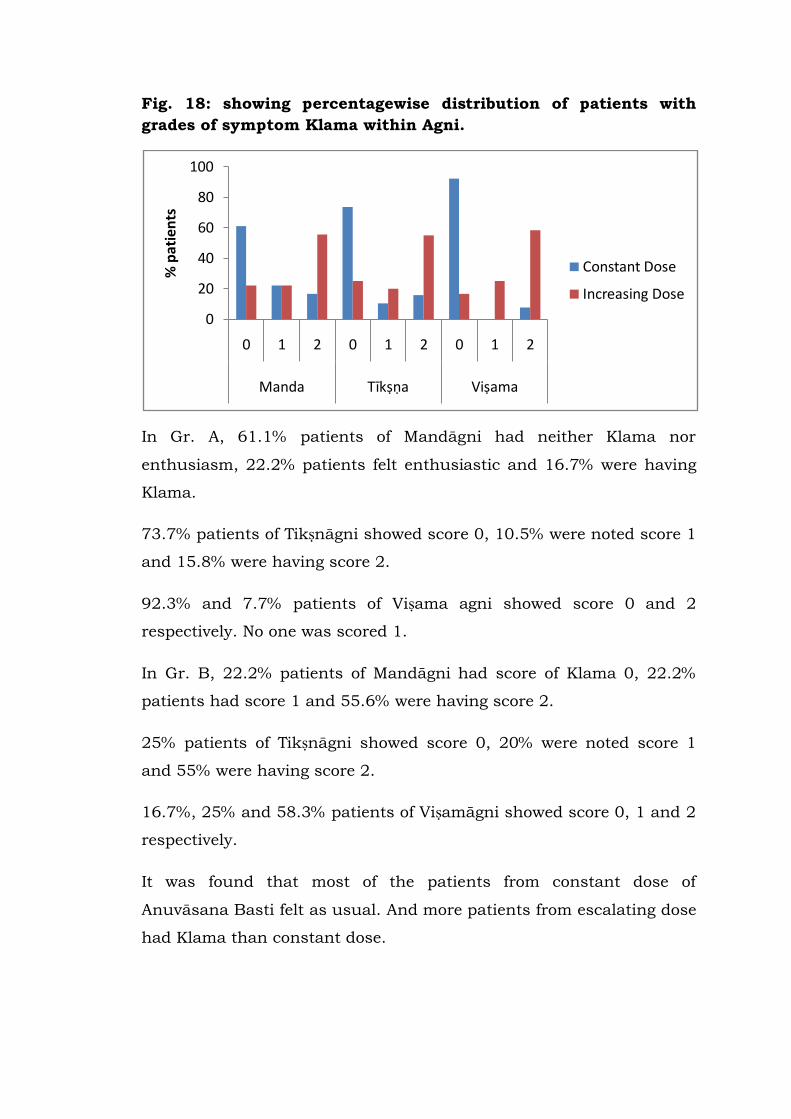
Fig. 18: showing percentagewise distribution of patients with
grades of symptom Klama within Agni.
In Gr. A, 61.1% patients of Mandāgni had neither Klama nor
enthusiasm, 22.2% patients felt enthusiastic and 16.7% were having
Klama.
73.7% patients of Tikṣnāgni showed score 0, 10.5% were noted score 1
and 15.8% were having score 2.
92.3% and 7.7% patients of Viṣama agni showed score 0 and 2
respectively. No one was scored 1.
In Gr. B, 22.2% patients of Mandāgni had score of Klama 0, 22.2%
patients had score 1 and 55.6% were having score 2.
25% patients of Tikṣnāgni showed score 0, 20% were noted score 1
and 55% were having score 2.
16.7%, 25% and 58.3% patients of Viṣamāgni showed score 0, 1 and 2
respectively.
It was found that most of the patients from constant dose of
Anuvāsana Basti felt as usual. And more patients from escalating dose
had Klama than constant dose.
0
20
40
60
80
100
0 1 2 0 1 2 0 1 2
Manda Tīkṣṇa Viṣama
% p
ati
ents
Constant Dose
Increasing Dose
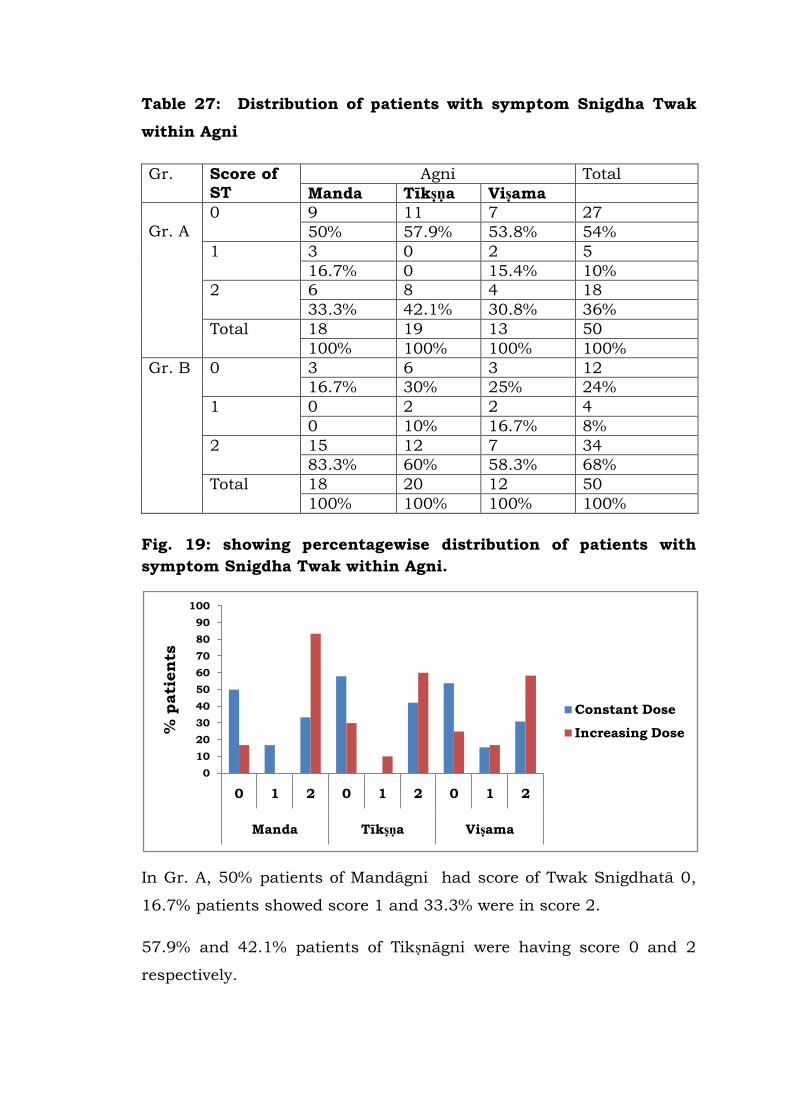
Table 27: Distribution of patients with symptom Snigdha Twak
within Agni
Gr. Score of
ST
Agni Total
Manda Tīkṣṇa Viṣama
Gr. A
0 9 11 7 27
50% 57.9% 53.8% 54%
1 3 0 2 5
16.7% 0 15.4% 10%
2 6 8 4 18
33.3% 42.1% 30.8% 36%
Total 18 19 13 50
100% 100% 100% 100%
Gr. B 0 3 6 3 12
16.7% 30% 25% 24%
1 0 2 2 4
0 10% 16.7% 8%
2 15 12 7 34
83.3% 60% 58.3% 68%
Total 18 20 12 50
100% 100% 100% 100%
Fig. 19: showing percentagewise distribution of patients with
symptom Snigdha Twak within Agni.
In Gr. A, 50% patients of Mandāgni had score of Twak Snigdhatā 0,
16.7% patients showed score 1 and 33.3% were in score 2.
57.9% and 42.1% patients of Tikṣnāgni were having score 0 and 2
respectively.
0
10
20
30
40
50
60
70
80
90
100
0 1 2 0 1 2 0 1 2
Manda Tīkṣṇa Viṣama
% p
ati
en
ts
Constant Dose
Increasing Dose
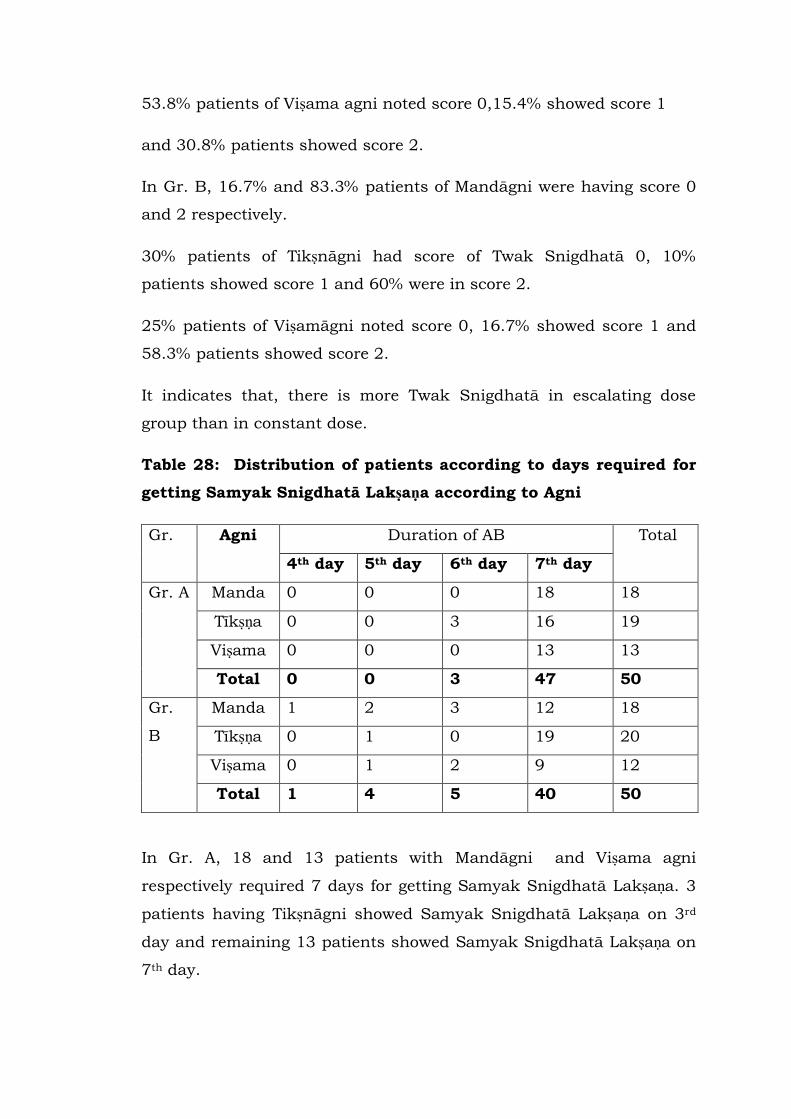
53.8% patients of Viṣama agni noted score 0,15.4% showed score 1
and 30.8% patients showed score 2.
In Gr. B, 16.7% and 83.3% patients of Mandāgni were having score 0
and 2 respectively.
30% patients of Tikṣnāgni had score of Twak Snigdhatā 0, 10%
patients showed score 1 and 60% were in score 2.
25% patients of Viṣamāgni noted score 0, 16.7% showed score 1 and
58.3% patients showed score 2.
It indicates that, there is more Twak Snigdhatā in escalating dose
group than in constant dose.
Table 28: Distribution of patients according to days required for
getting Samyak Snigdhatā Lakṣaṇa according to Agni
Gr. Agni Duration of AB Total
4th day 5th day 6th day 7th day
Gr. A Manda 0 0 0 18 18
Tīkṣṇa 0 0 3 16 19
Viṣama 0 0 0 13 13
Total 0 0 3 47 50
Gr.
B
Manda 1 2 3 12 18
Tīkṣṇa 0 1 0 19 20
Viṣama 0 1 2 9 12
Total 1 4 5 40 50
In Gr. A, 18 and 13 patients with Mandāgni and Viṣama agni
respectively required 7 days for getting Samyak Snigdhatā Lakṣaṇa. 3
patients having Tikṣnāgni showed Samyak Snigdhatā Lakṣaṇa on 3rd
day and remaining 13 patients showed Samyak Snigdhatā Lakṣaṇa on
7th day.

In Gr. B, 1patient of Mandāgni showed Samyak Snigdhatā Lakṣaṇa on
4th day, 2 patients on 5th day, 3 patients on 6th day and 12 patients
on 7th day. 1 patient of Tikṣnāgni was noted Samyak Snigdhatā
Lakṣaṇa on 5th day, 19 patients on 7th day. 1,2 and 9 patients of
Viṣama agni showed Samyak Snigdhatā Lakṣaṇa on 5th ,6th, 7th day
respectively.
In the group of increasing dose of AB, Samyak Snigdhatā Lakṣaṇa
started on 4th day in a patient of Mandāgni .
Table 29: Distribution of patients according to grades of Samyak
Snigdhatā Lakṣaṇa within Agni.
Gr. SSL Agni Total
Manda Tīkṣṇa Viṣama
Gr. A Asnigdha 3 3 1 7
16.7% 15.8% 7.7% 14%
Avara 6 8 6 20
33.3% 42.1% 46.2% 40%
Madhyam 7 3 6 16
38.9% 15.8% 46.2% 32%
Pravara 2 5 0 7
11.1% 26.3% 0% 14%
Total 18 19 13 50
100% 100% 100% 100%
Gp. B Asnigdha 0 0 0 0
0 0 0 0
Avara 1 3 1 5
5.6% 15% 8.3% 10%
Madhyam 7 6 3 16
38.9% 30% 25% 32%
Pravara 10 11 8 29
55.6% 55% 66.7% 58%
Total 18 20 12 50
100% 100% 100% 100%
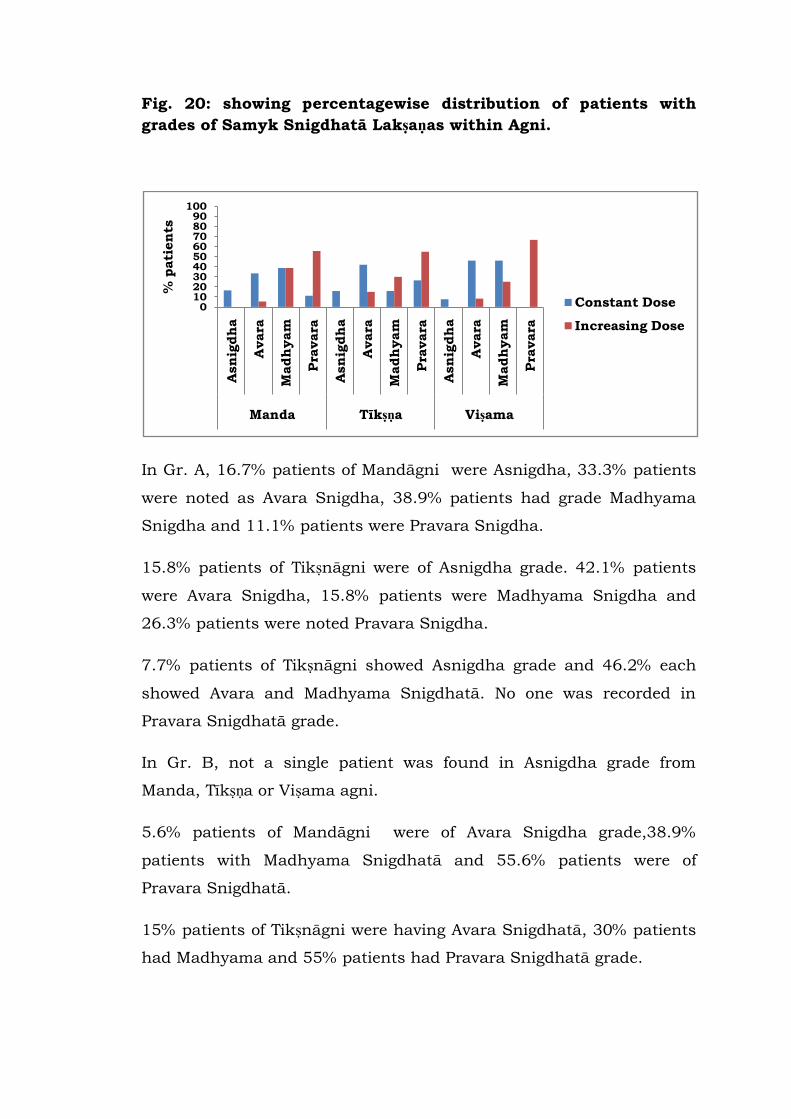
Fig. 20: showing percentagewise distribution of patients with
grades of Samyk Snigdhatā Lakṣaṇas within Agni.
In Gr. A, 16.7% patients of Mandāgni were Asnigdha, 33.3% patients
were noted as Avara Snigdha, 38.9% patients had grade Madhyama
Snigdha and 11.1% patients were Pravara Snigdha.
15.8% patients of Tikṣnāgni were of Asnigdha grade. 42.1% patients
were Avara Snigdha, 15.8% patients were Madhyama Snigdha and
26.3% patients were noted Pravara Snigdha.
7.7% patients of Tikṣnāgni showed Asnigdha grade and 46.2% each
showed Avara and Madhyama Snigdhatā. No one was recorded in
Pravara Snigdhatā grade.
In Gr. B, not a single patient was found in Asnigdha grade from
Manda, Tīkṣṇa or Viṣama agni.
5.6% patients of Mandāgni were of Avara Snigdha grade,38.9%
patients with Madhyama Snigdhatā and 55.6% patients were of
Pravara Snigdhatā.
15% patients of Tikṣnāgni were having Avara Snigdhatā, 30% patients
had Madhyama and 55% patients had Pravara Snigdhatā grade.
0102030405060708090
100
Asn
igdh
a
Avara
Madh
yam
Pra
vara
Asn
igdh
a
Avara
Madh
yam
Pra
vara
Asn
igdh
a
Avara
Madh
yam
Pra
vara
Manda Tīkṣṇa Viṣama
% p
ati
en
ts
Constant Dose
Increasing Dose
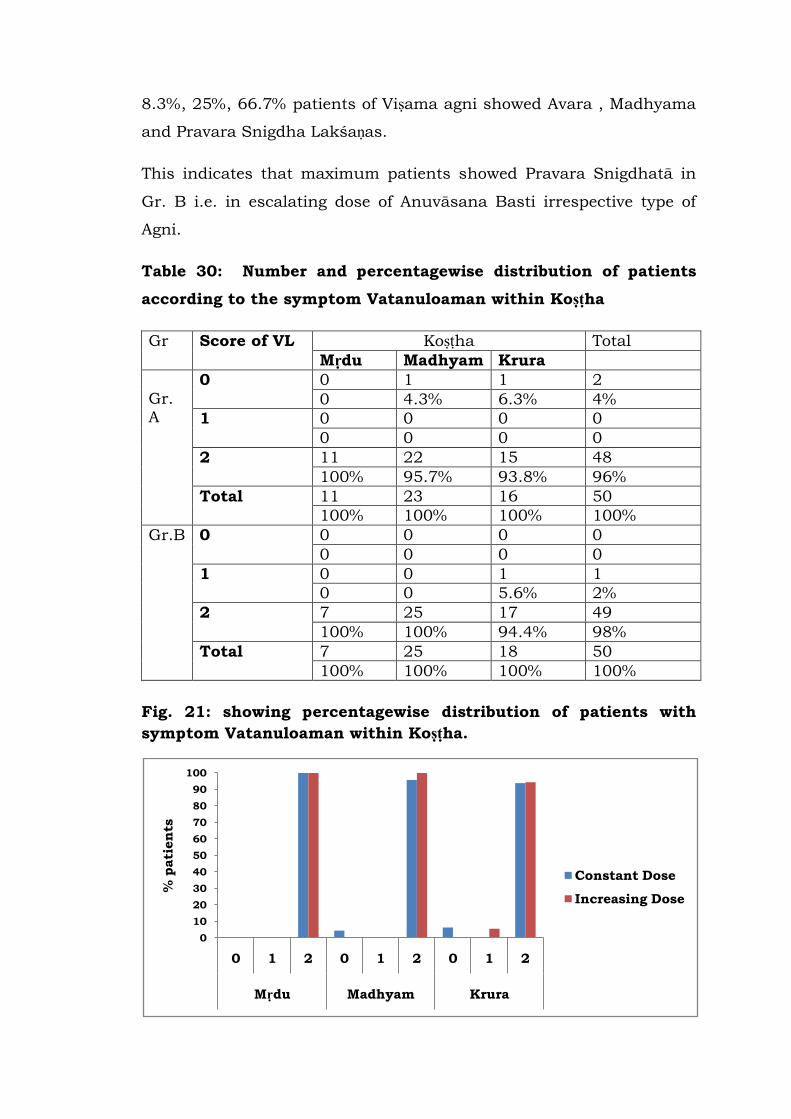
8.3%, 25%, 66.7% patients of Viṣama agni showed Avara , Madhyama
and Pravara Snigdha Lakśaṇas.
This indicates that maximum patients showed Pravara Snigdhatā in
Gr. B i.e. in escalating dose of Anuvāsana Basti irrespective type of
Agni.
Table 30: Number and percentagewise distribution of patients
according to the symptom Vatanuloaman within Koṣṭha
Gr Score of VL Koṣṭha Total
Mṛdu Madhyam Krura
Gr. A
0 0 1 1 2
0 4.3% 6.3% 4%
1 0 0 0 0
0 0 0 0
2 11 22 15 48
100% 95.7% 93.8% 96%
Total 11 23 16 50
100% 100% 100% 100%
Gr.B 0 0 0 0 0
0 0 0 0
1 0 0 1 1
0 0 5.6% 2%
2 7 25 17 49
100% 100% 94.4% 98%
Total 7 25 18 50
100% 100% 100% 100%
Fig. 21: showing percentagewise distribution of patients with
symptom Vatanuloaman within Koṣṭha.
0
10
20
30
40
50
60
70
80
90
100
0 1 2 0 1 2 0 1 2
Mṛdu Madhyam Krura
% p
ati
en
ts
Constant Dose
Increasing Dose
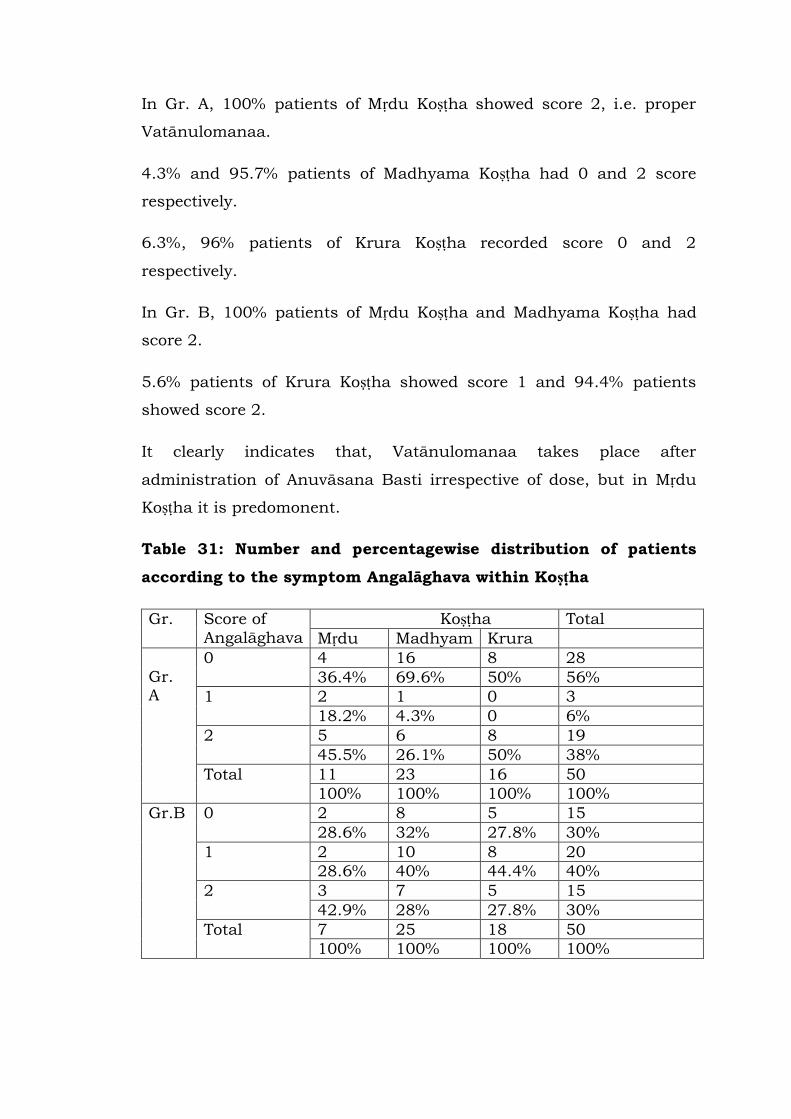
In Gr. A, 100% patients of Mṛdu Koṣṭha showed score 2, i.e. proper
Vatānulomanaa.
4.3% and 95.7% patients of Madhyama Koṣṭha had 0 and 2 score
respectively.
6.3%, 96% patients of Krura Koṣṭha recorded score 0 and 2
respectively.
In Gr. B, 100% patients of Mṛdu Koṣṭha and Madhyama Koṣṭha had
score 2.
5.6% patients of Krura Koṣṭha showed score 1 and 94.4% patients
showed score 2.
It clearly indicates that, Vatānulomanaa takes place after
administration of Anuvāsana Basti irrespective of dose, but in Mṛdu
Koṣṭha it is predomonent.
Table 31: Number and percentagewise distribution of patients
according to the symptom Angalāghava within Koṣṭha
Gr. Score of
Angalāghava
Koṣṭha Total
Mṛdu Madhyam Krura
Gr. A
0 4 16 8 28
36.4% 69.6% 50% 56%
1 2 1 0 3
18.2% 4.3% 0 6%
2 5 6 8 19
45.5% 26.1% 50% 38%
Total 11 23 16 50
100% 100% 100% 100%
Gr.B 0 2 8 5 15
28.6% 32% 27.8% 30%
1 2 10 8 20
28.6% 40% 44.4% 40%
2 3 7 5 15
42.9% 28% 27.8% 30%
Total 7 25 18 50
100% 100% 100% 100%
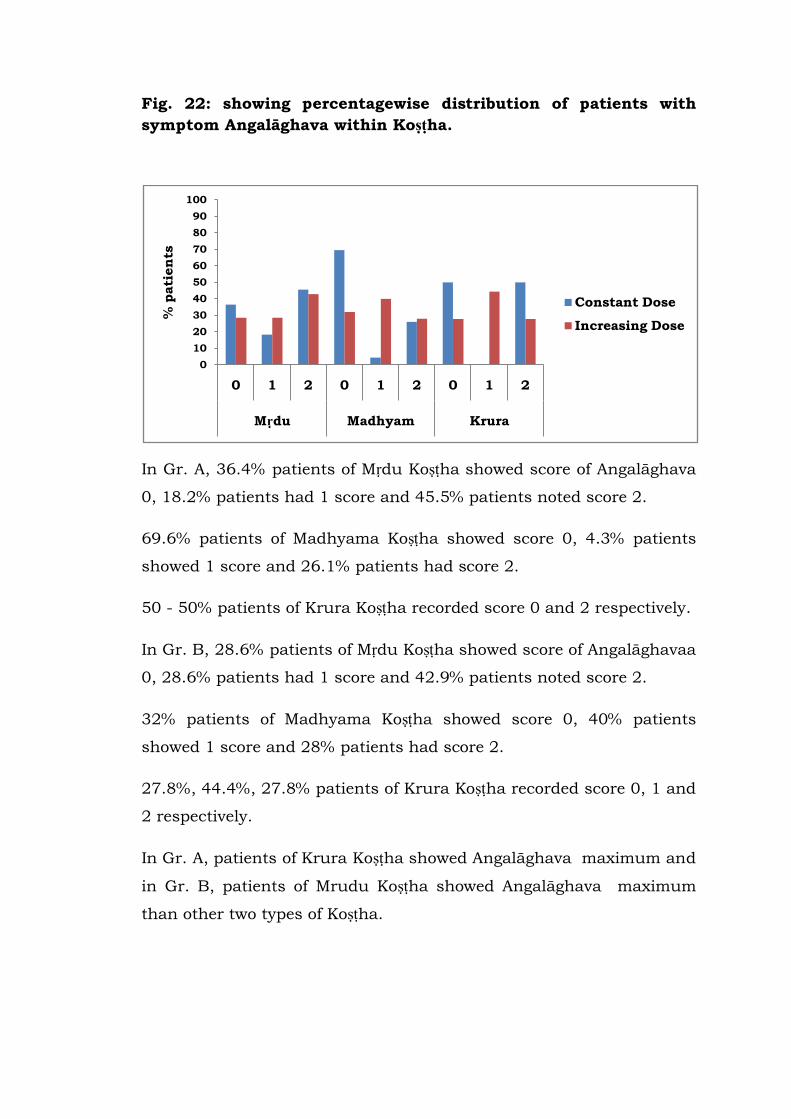
Fig. 22: showing percentagewise distribution of patients with
symptom Angalāghava within Koṣṭha.
In Gr. A, 36.4% patients of Mṛdu Koṣṭha showed score of Angalāghava
0, 18.2% patients had 1 score and 45.5% patients noted score 2.
69.6% patients of Madhyama Koṣṭha showed score 0, 4.3% patients
showed 1 score and 26.1% patients had score 2.
50 - 50% patients of Krura Koṣṭha recorded score 0 and 2 respectively.
In Gr. B, 28.6% patients of Mṛdu Koṣṭha showed score of Angalāghavaa
0, 28.6% patients had 1 score and 42.9% patients noted score 2.
32% patients of Madhyama Koṣṭha showed score 0, 40% patients
showed 1 score and 28% patients had score 2.
27.8%, 44.4%, 27.8% patients of Krura Koṣṭha recorded score 0, 1 and
2 respectively.
In Gr. A, patients of Krura Koṣṭha showed Angalāghava maximum and
in Gr. B, patients of Mrudu Koṣṭha showed Angalāghava maximum
than other two types of Koṣṭha.
0
10
20
30
40
50
60
70
80
90
100
0 1 2 0 1 2 0 1 2
Mṛdu Madhyam Krura
% p
ati
en
ts
Constant Dose
Increasing Dose
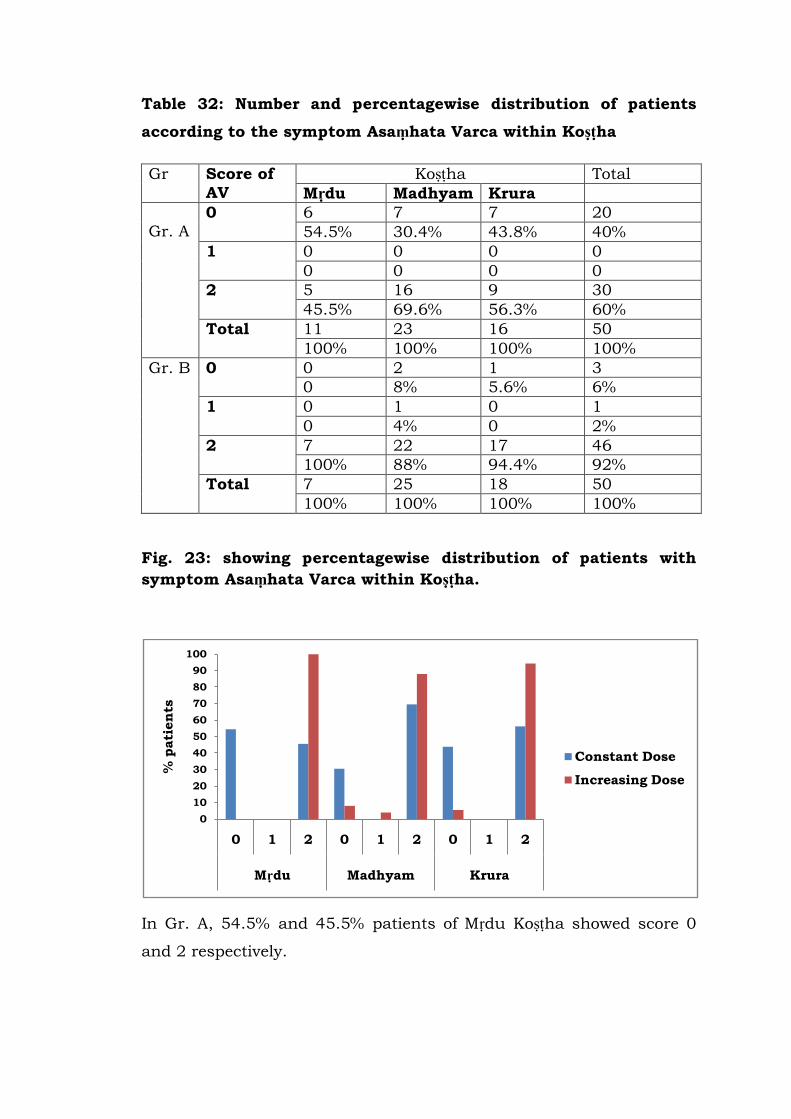
Table 32: Number and percentagewise distribution of patients
according to the symptom Asaṃhata Varca within Koṣṭha
Gr Score of
AV
Koṣṭha Total
Mṛdu Madhyam Krura
Gr. A
0 6 7 7 20
54.5% 30.4% 43.8% 40%
1 0 0 0 0
0 0 0 0
2 5 16 9 30
45.5% 69.6% 56.3% 60%
Total 11 23 16 50
100% 100% 100% 100%
Gr. B 0 0 2 1 3
0 8% 5.6% 6%
1 0 1 0 1
0 4% 0 2%
2 7 22 17 46
100% 88% 94.4% 92%
Total 7 25 18 50
100% 100% 100% 100%
Fig. 23: showing percentagewise distribution of patients with
symptom Asaṃhata Varca within Koṣṭha.
In Gr. A, 54.5% and 45.5% patients of Mṛdu Koṣṭha showed score 0
and 2 respectively.
0
10
20
30
40
50
60
70
80
90
100
0 1 2 0 1 2 0 1 2
Mṛdu Madhyam Krura
% p
ati
en
ts
Constant Dose
Increasing Dose
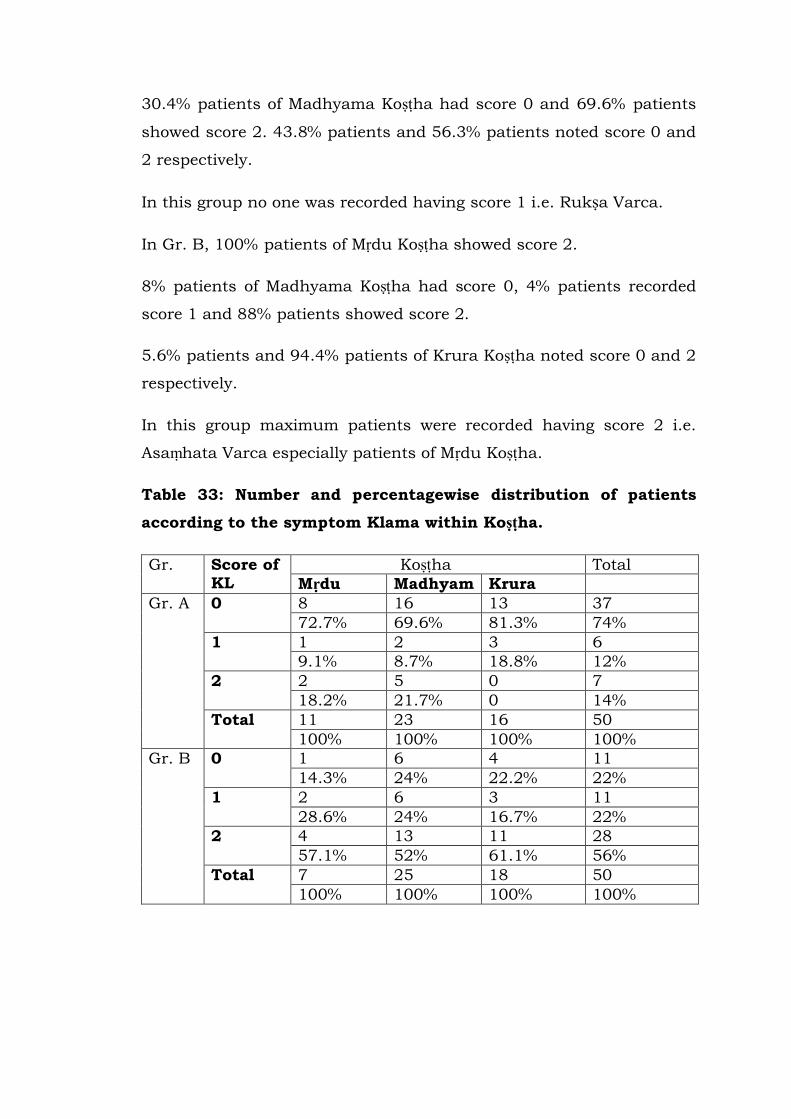
30.4% patients of Madhyama Koṣṭha had score 0 and 69.6% patients
showed score 2. 43.8% patients and 56.3% patients noted score 0 and
2 respectively.
In this group no one was recorded having score 1 i.e. Rukṣa Varca.
In Gr. B, 100% patients of Mṛdu Koṣṭha showed score 2.
8% patients of Madhyama Koṣṭha had score 0, 4% patients recorded
score 1 and 88% patients showed score 2.
5.6% patients and 94.4% patients of Krura Koṣṭha noted score 0 and 2
respectively.
In this group maximum patients were recorded having score 2 i.e.
Asaṃhata Varca especially patients of Mṛdu Koṣṭha.
Table 33: Number and percentagewise distribution of patients
according to the symptom Klama within Koṣṭha.
Gr. Score of KL
Koṣṭha Total
Mṛdu Madhyam Krura
Gr. A 0 8 16 13 37
72.7% 69.6% 81.3% 74%
1 1 2 3 6
9.1% 8.7% 18.8% 12%
2 2 5 0 7
18.2% 21.7% 0 14%
Total 11 23 16 50
100% 100% 100% 100%
Gr. B 0 1 6 4 11
14.3% 24% 22.2% 22%
1 2 6 3 11
28.6% 24% 16.7% 22%
2 4 13 11 28
57.1% 52% 61.1% 56%
Total 7 25 18 50
100% 100% 100% 100%
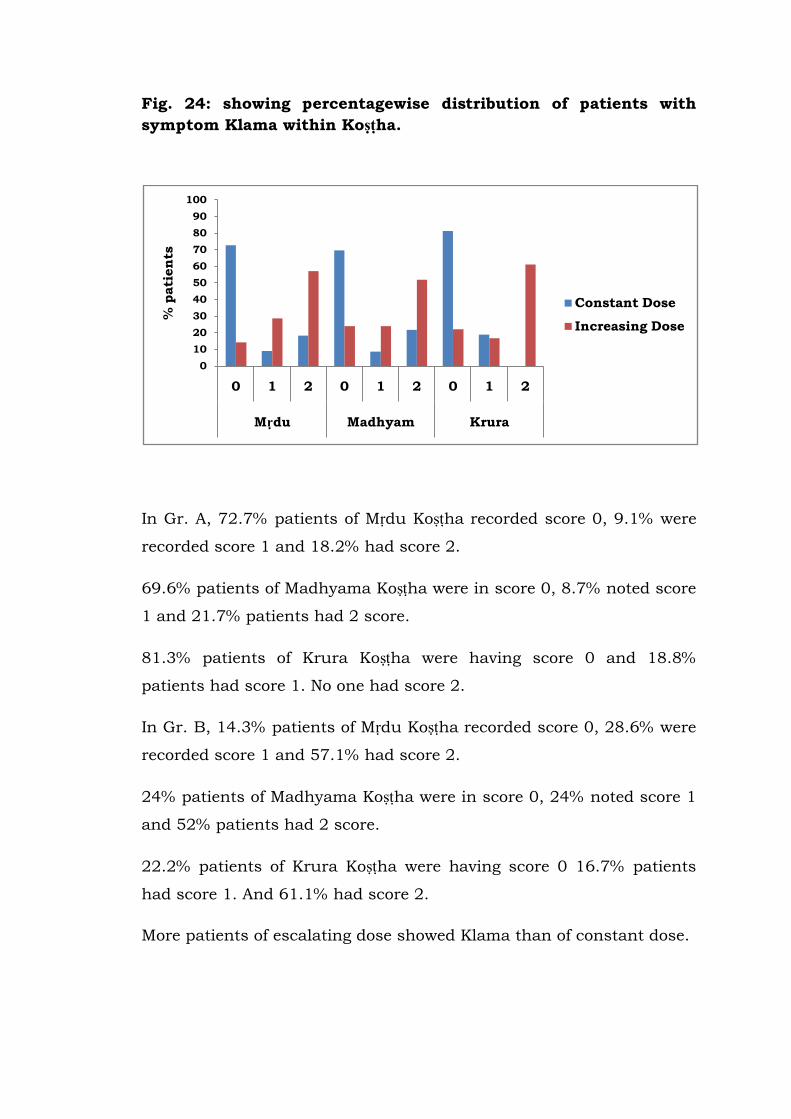
Fig. 24: showing percentagewise distribution of patients with
symptom Klama within Koṣṭha.
In Gr. A, 72.7% patients of Mṛdu Koṣṭha recorded score 0, 9.1% were
recorded score 1 and 18.2% had score 2.
69.6% patients of Madhyama Koṣṭha were in score 0, 8.7% noted score
1 and 21.7% patients had 2 score.
81.3% patients of Krura Koṣṭha were having score 0 and 18.8%
patients had score 1. No one had score 2.
In Gr. B, 14.3% patients of Mṛdu Koṣṭha recorded score 0, 28.6% were
recorded score 1 and 57.1% had score 2.
24% patients of Madhyama Koṣṭha were in score 0, 24% noted score 1
and 52% patients had 2 score.
22.2% patients of Krura Koṣṭha were having score 0 16.7% patients
had score 1. And 61.1% had score 2.
More patients of escalating dose showed Klama than of constant dose.
0
10
20
30
40
50
60
70
80
90
100
0 1 2 0 1 2 0 1 2
Mṛdu Madhyam Krura
% p
ati
en
ts
Constant Dose
Increasing Dose
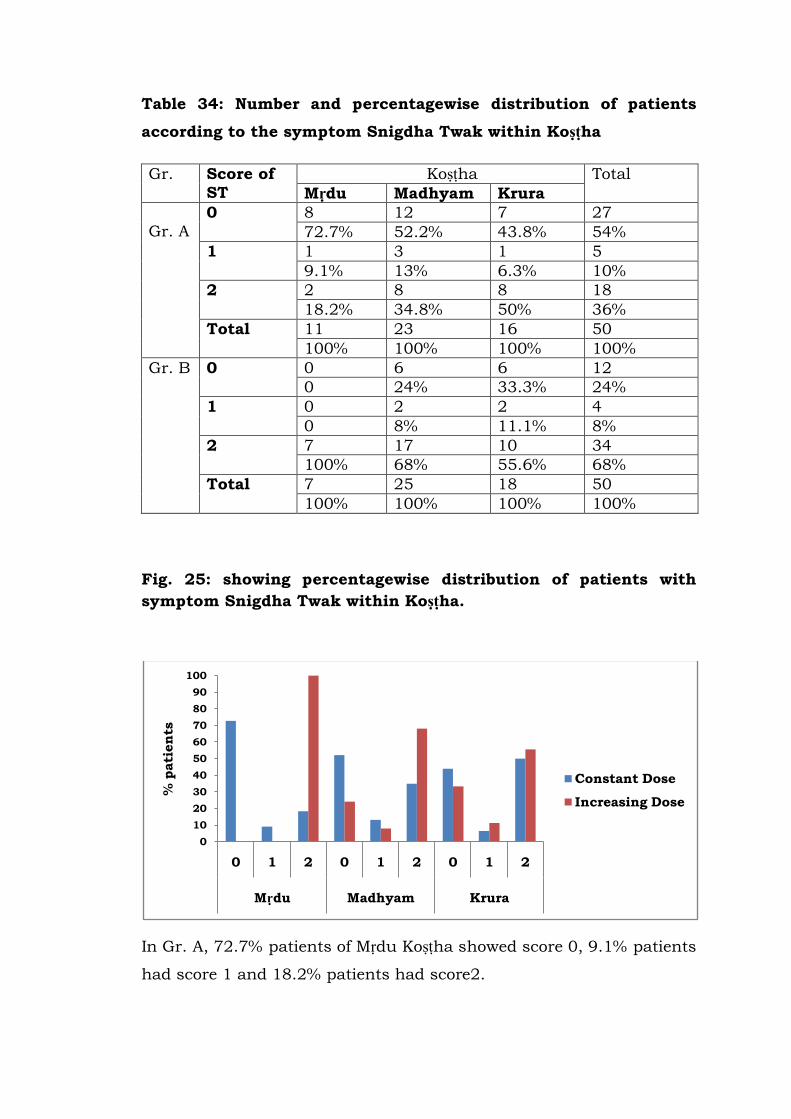
Table 34: Number and percentagewise distribution of patients
according to the symptom Snigdha Twak within Koṣṭha
Gr. Score of
ST
Koṣṭha Total
Mṛdu Madhyam Krura
Gr. A
0 8 12 7 27
72.7% 52.2% 43.8% 54%
1 1 3 1 5
9.1% 13% 6.3% 10%
2 2 8 8 18
18.2% 34.8% 50% 36%
Total 11 23 16 50
100% 100% 100% 100%
Gr. B 0 0 6 6 12
0 24% 33.3% 24%
1 0 2 2 4
0 8% 11.1% 8%
2 7 17 10 34
100% 68% 55.6% 68%
Total 7 25 18 50
100% 100% 100% 100%
Fig. 25: showing percentagewise distribution of patients with
symptom Snigdha Twak within Koṣṭha.
In Gr. A, 72.7% patients of Mṛdu Koṣṭha showed score 0, 9.1% patients
had score 1 and 18.2% patients had score2.
0
10
20
30
40
50
60
70
80
90
100
0 1 2 0 1 2 0 1 2
Mṛdu Madhyam Krura
% p
ati
en
ts
Constant Dose
Increasing Dose
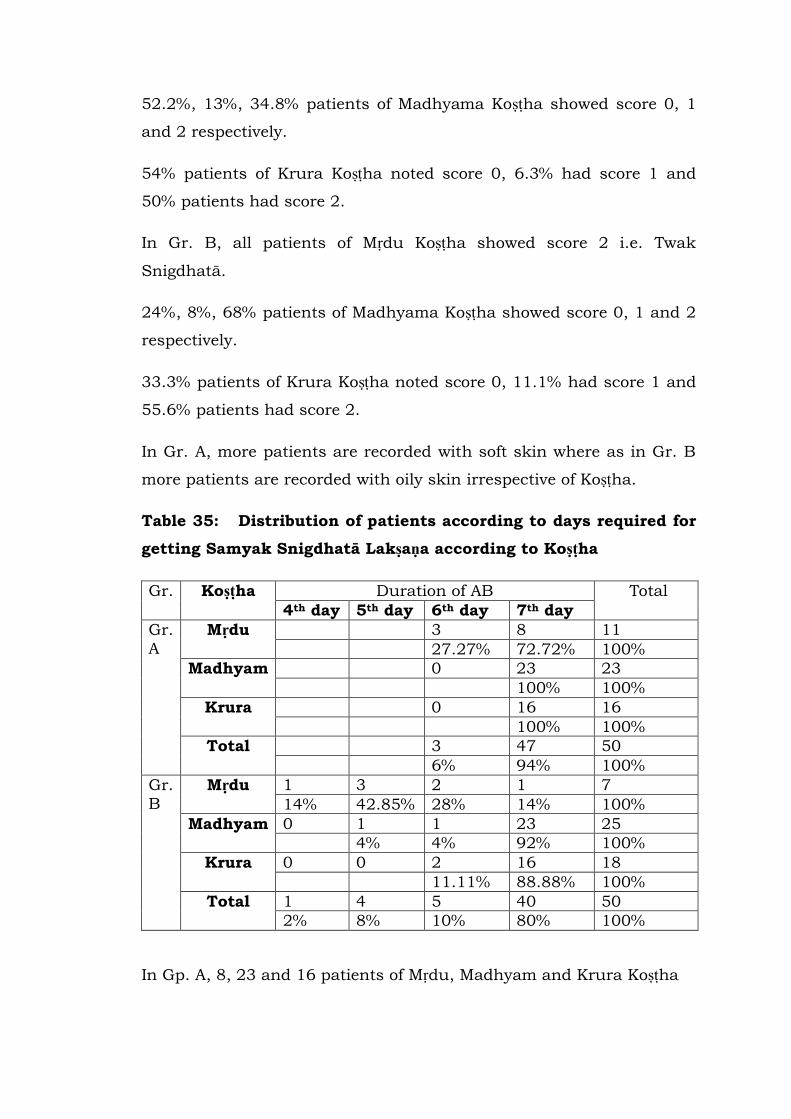
52.2%, 13%, 34.8% patients of Madhyama Koṣṭha showed score 0, 1
and 2 respectively.
54% patients of Krura Koṣṭha noted score 0, 6.3% had score 1 and
50% patients had score 2.
In Gr. B, all patients of Mṛdu Koṣṭha showed score 2 i.e. Twak
Snigdhatā.
24%, 8%, 68% patients of Madhyama Koṣṭha showed score 0, 1 and 2
respectively.
33.3% patients of Krura Koṣṭha noted score 0, 11.1% had score 1 and
55.6% patients had score 2.
In Gr. A, more patients are recorded with soft skin where as in Gr. B
more patients are recorded with oily skin irrespective of Koṣṭha.
Table 35: Distribution of patients according to days required for
getting Samyak Snigdhatā Lakṣaṇa according to Koṣṭha
Gr. Koṣṭha Duration of AB Total
4th day 5th day 6th day 7th day
Gr.
A
Mṛdu 3 8 11
27.27% 72.72% 100%
Madhyam 0 23 23
100% 100%
Krura 0 16 16
100% 100%
Total 3 47 50
6% 94% 100%
Gr.
B
Mṛdu 1 3 2 1 7
14% 42.85% 28% 14% 100%
Madhyam 0 1 1 23 25
4% 4% 92% 100%
Krura 0 0 2 16 18
11.11% 88.88% 100%
Total 1 4 5 40 50
2% 8% 10% 80% 100%
In Gp. A, 8, 23 and 16 patients of Mṛdu, Madhyam and Krura Koṣṭha
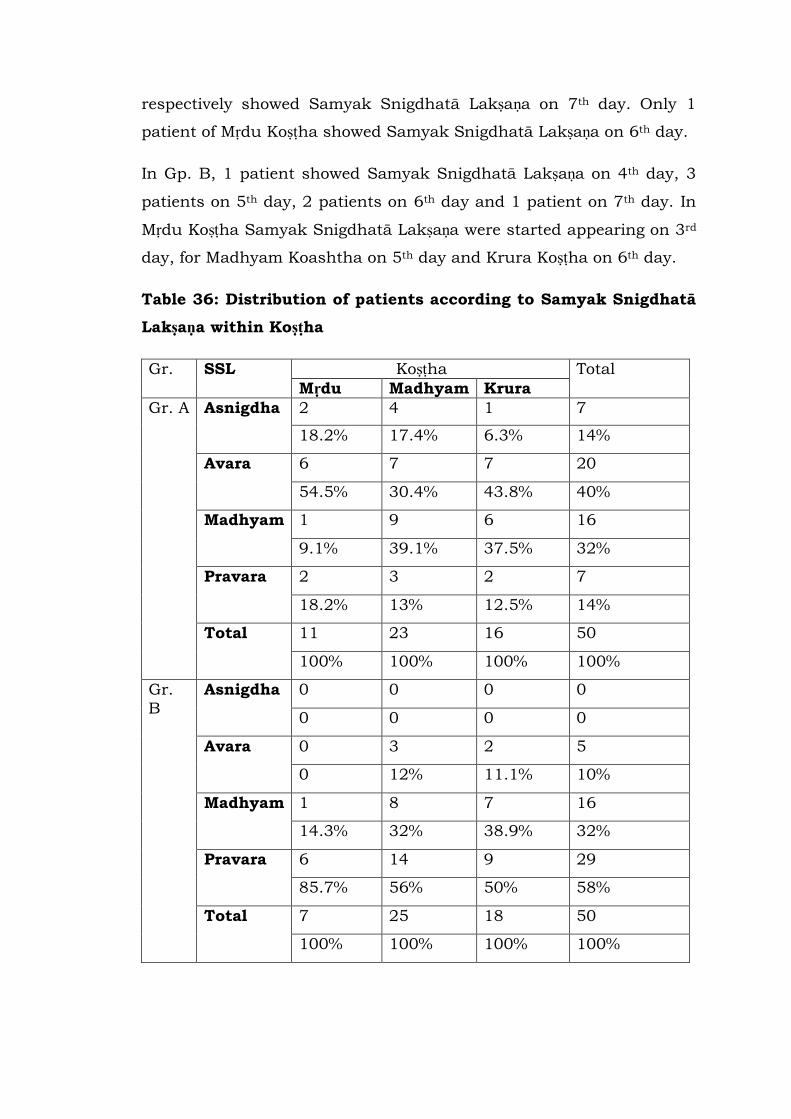
respectively showed Samyak Snigdhatā Lakṣaṇa on 7th day. Only 1
patient of Mṛdu Koṣṭha showed Samyak Snigdhatā Lakṣaṇa on 6th day.
In Gp. B, 1 patient showed Samyak Snigdhatā Lakṣaṇa on 4th day, 3
patients on 5th day, 2 patients on 6th day and 1 patient on 7th day. In
Mṛdu Koṣṭha Samyak Snigdhatā Lakṣaṇa were started appearing on 3rd
day, for Madhyam Koashtha on 5th day and Krura Koṣṭha on 6th day.
Table 36: Distribution of patients according to Samyak Snigdhatā
Lakṣaṇa within Koṣṭha
Gr. SSL Koṣṭha Total
Mṛdu Madhyam Krura
Gr. A Asnigdha 2 4 1 7
18.2% 17.4% 6.3% 14%
Avara 6 7 7 20
54.5% 30.4% 43.8% 40%
Madhyam 1 9 6 16
9.1% 39.1% 37.5% 32%
Pravara 2 3 2 7
18.2% 13% 12.5% 14%
Total 11 23 16 50
100% 100% 100% 100%
Gr.
B
Asnigdha 0 0 0 0
0 0 0 0
Avara 0 3 2 5
0 12% 11.1% 10%
Madhyam 1 8 7 16
14.3% 32% 38.9% 32%
Pravara 6 14 9 29
85.7% 56% 50% 58%
Total 7 25 18 50
100% 100% 100% 100%
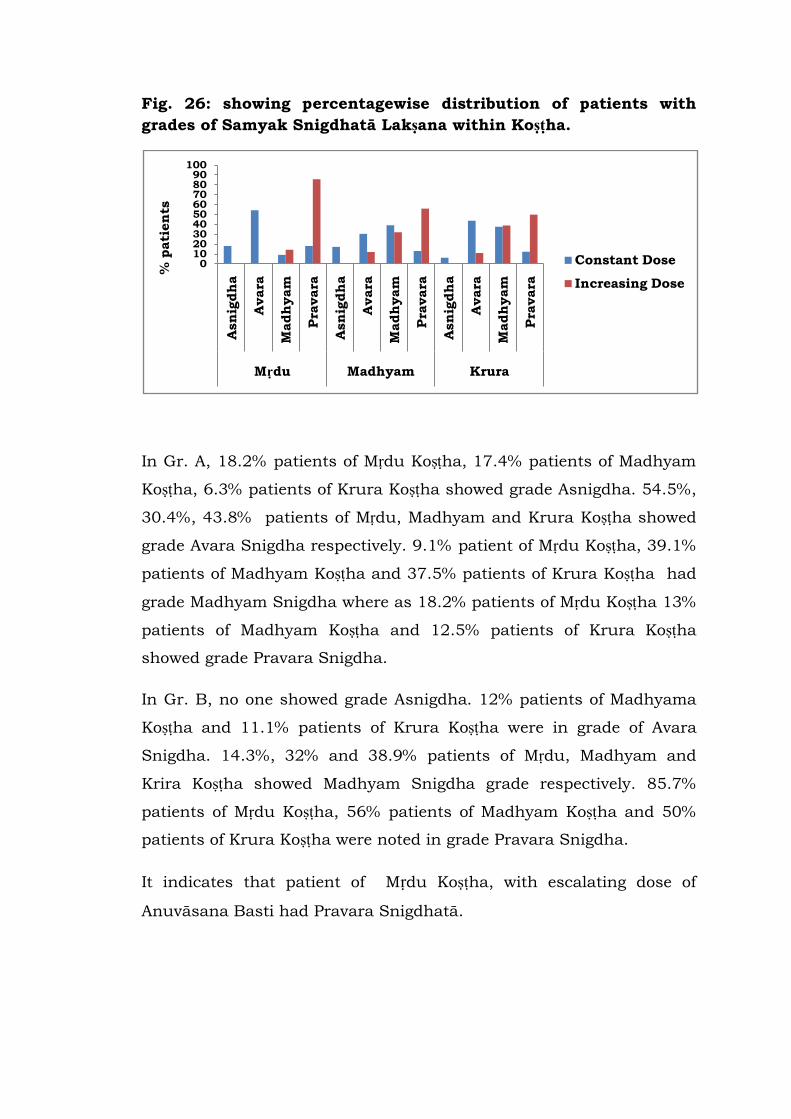
Fig. 26: showing percentagewise distribution of patients with
grades of Samyak Snigdhatā Lakṣana within Koṣṭha.
In Gr. A, 18.2% patients of Mṛdu Koṣṭha, 17.4% patients of Madhyam
Koṣṭha, 6.3% patients of Krura Koṣṭha showed grade Asnigdha. 54.5%,
30.4%, 43.8% patients of Mṛdu, Madhyam and Krura Koṣṭha showed
grade Avara Snigdha respectively. 9.1% patient of Mṛdu Koṣṭha, 39.1%
patients of Madhyam Koṣṭha and 37.5% patients of Krura Koṣṭha had
grade Madhyam Snigdha where as 18.2% patients of Mṛdu Koṣṭha 13%
patients of Madhyam Koṣṭha and 12.5% patients of Krura Koṣṭha
showed grade Pravara Snigdha.
In Gr. B, no one showed grade Asnigdha. 12% patients of Madhyama
Koṣṭha and 11.1% patients of Krura Koṣṭha were in grade of Avara
Snigdha. 14.3%, 32% and 38.9% patients of Mṛdu, Madhyam and
Krira Koṣṭha showed Madhyam Snigdha grade respectively. 85.7%
patients of Mṛdu Koṣṭha, 56% patients of Madhyam Koṣṭha and 50%
patients of Krura Koṣṭha were noted in grade Pravara Snigdha.
It indicates that patient of Mṛdu Koṣṭha, with escalating dose of
Anuvāsana Basti had Pravara Snigdhatā.
0102030405060708090
100
Asn
igdh
a
Avara
Madh
yam
Pra
vara
Asn
igdh
a
Avara
Madh
yam
Pra
vara
Asn
igdh
a
Avara
Madh
yam
Pra
vara
Mṛdu Madhyam Krura
% p
ati
en
ts
Constant Dose
Increasing Dose
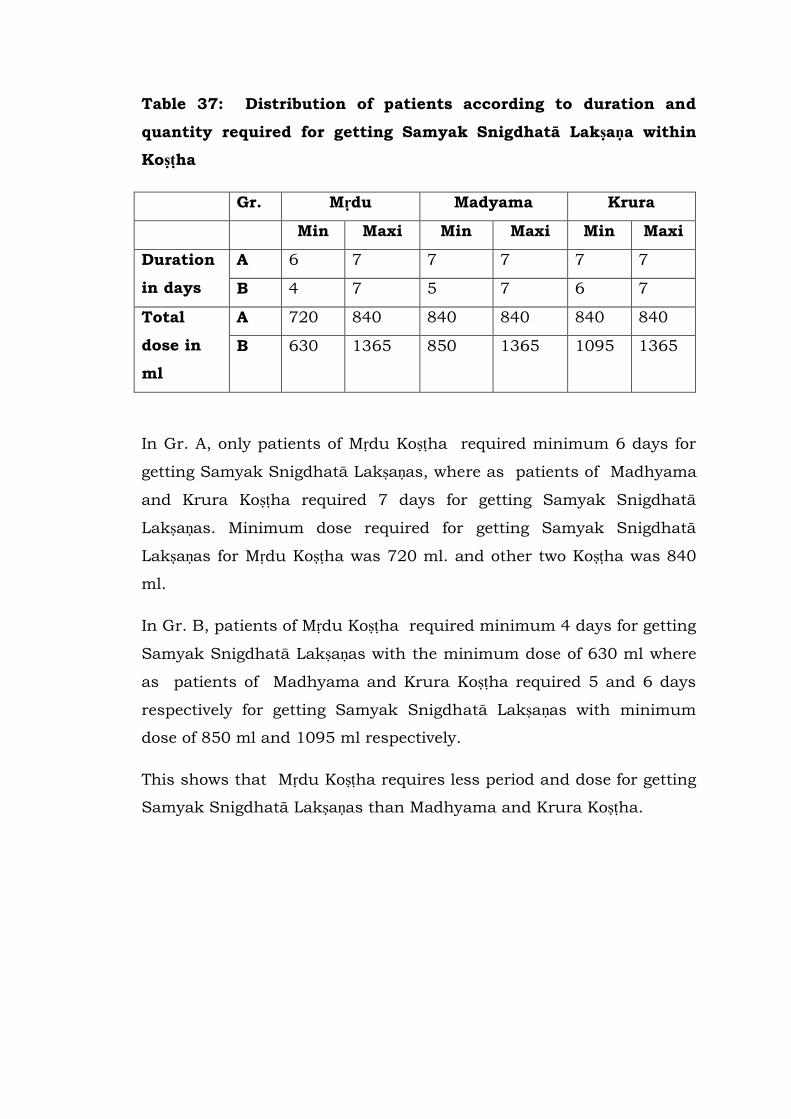
Table 37: Distribution of patients according to duration and
quantity required for getting Samyak Snigdhatā Lakṣaṇa within
Koṣṭha
Gr. Mṛdu Madyama Krura
Min Maxi Min Maxi Min Maxi
Duration
in days
A 6 7 7 7 7 7
B 4 7 5 7 6 7
Total
dose in
ml
A 720 840 840 840 840 840
B 630 1365 850 1365 1095 1365
In Gr. A, only patients of Mṛdu Koṣṭha required minimum 6 days for
getting Samyak Snigdhatā Lakṣaṇas, where as patients of Madhyama
and Krura Koṣṭha required 7 days for getting Samyak Snigdhatā
Lakṣaṇas. Minimum dose required for getting Samyak Snigdhatā
Lakṣaṇas for Mṛdu Koṣṭha was 720 ml. and other two Koṣṭha was 840
ml.
In Gr. B, patients of Mṛdu Koṣṭha required minimum 4 days for getting
Samyak Snigdhatā Lakṣaṇas with the minimum dose of 630 ml where
as patients of Madhyama and Krura Koṣṭha required 5 and 6 days
respectively for getting Samyak Snigdhatā Lakṣaṇas with minimum
dose of 850 ml and 1095 ml respectively.
This shows that Mṛdu Koṣṭha requires less period and dose for getting
Samyak Snigdhatā Lakṣaṇas than Madhyama and Krura Koṣṭha.
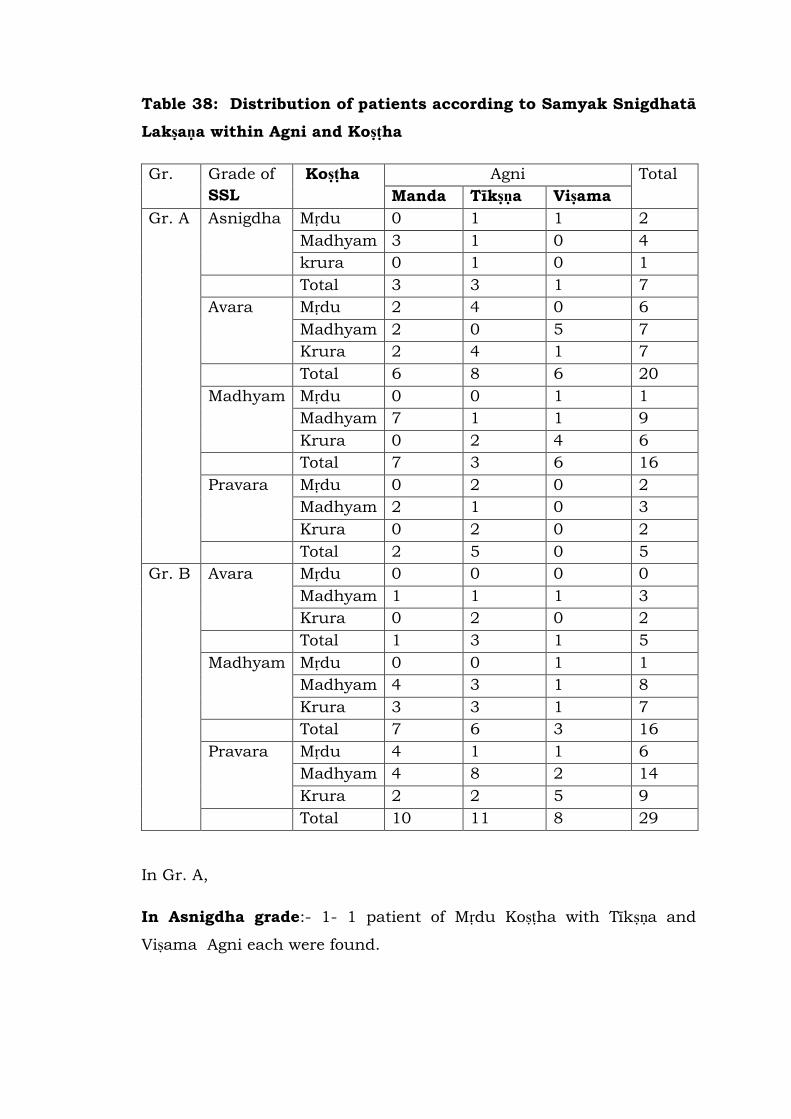
Table 38: Distribution of patients according to Samyak Snigdhatā
Lakṣaṇa within Agni and Koṣṭha
Gr. Grade of
SSL
Koṣṭha Agni Total
Manda Tīkṣṇa Viṣama
Gr. A Asnigdha Mṛdu 0 1 1 2
Madhyam 3 1 0 4
krura 0 1 0 1
Total 3 3 1 7
Avara Mṛdu 2 4 0 6
Madhyam 2 0 5 7
Krura 2 4 1 7
Total 6 8 6 20
Madhyam Mṛdu 0 0 1 1
Madhyam 7 1 1 9
Krura 0 2 4 6
Total 7 3 6 16
Pravara Mṛdu 0 2 0 2
Madhyam 2 1 0 3
Krura 0 2 0 2
Total 2 5 0 5
Gr. B Avara Mṛdu 0 0 0 0
Madhyam 1 1 1 3
Krura 0 2 0 2
Total 1 3 1 5
Madhyam Mṛdu 0 0 1 1
Madhyam 4 3 1 8
Krura 3 3 1 7
Total 7 6 3 16
Pravara Mṛdu 4 1 1 6
Madhyam 4 8 2 14
Krura 2 2 5 9
Total 10 11 8 29
In Gr. A,
In Asnigdha grade:- 1- 1 patient of Mṛdu Koṣṭha with Tīkṣṇa and
Viṣama Agni each were found.
3 patients of Mandāgni and 1 of Tikṣnāgni with Madhyama Koṣṭha
were noted.
Only 1 patient of Tikṣnāgni with Krura Koṣṭha was recorded.
In Avara Snigdhatā grade:- 2 patient of Mṛdu Koṣṭha with Tīkṣṇa and
4 patients of Viṣama Agni were found.
2 patients of Mandāgni and 5 of Viṣama agni with Madhyama Koṣṭha
were noted.
2,4 and 1 patient of Mandāgni , Tikṣnāgni and Viṣama agni with Krura
Koṣṭha were recorded.
In Madhyama Snigdhatā grade:- only 1 patient of Mṛdu Koṣṭha with
Viṣama a Agni was found.
7, 1 and 1 patient of Mandāgni , Tikṣnāgni and Viṣama agni with
Madhyama Koṣṭha were recorded respectively.
2 patients of Tikṣnāgni and 4 of Viṣama agni with Krura Koṣṭha were
noted.
In Pravara Snigdhatā Grade :- only 2 patients of Mṛdu Koṣṭha with
Mandāgni was found.
2 and 1 patient of Manda and Tīkṣṇa Agni respectively with
Madhyama Koṣṭha were recorded.
2 patients of Tikṣṇāgni with Krura Koṣṭha was noted.
In Gr. B,
In Asnigdha grade:- no patient of Mṛdu Koṣṭha with Manda, Tīkṣṇa
and Viṣama Agni was found.
1,1,1 patient of Madhyama Koṣṭha with Manda, Tīkṣṇa and Viṣama
Agni were noted.
Only 2 patients of Tikṣnāgni with Krura Koṣṭha was recorded.
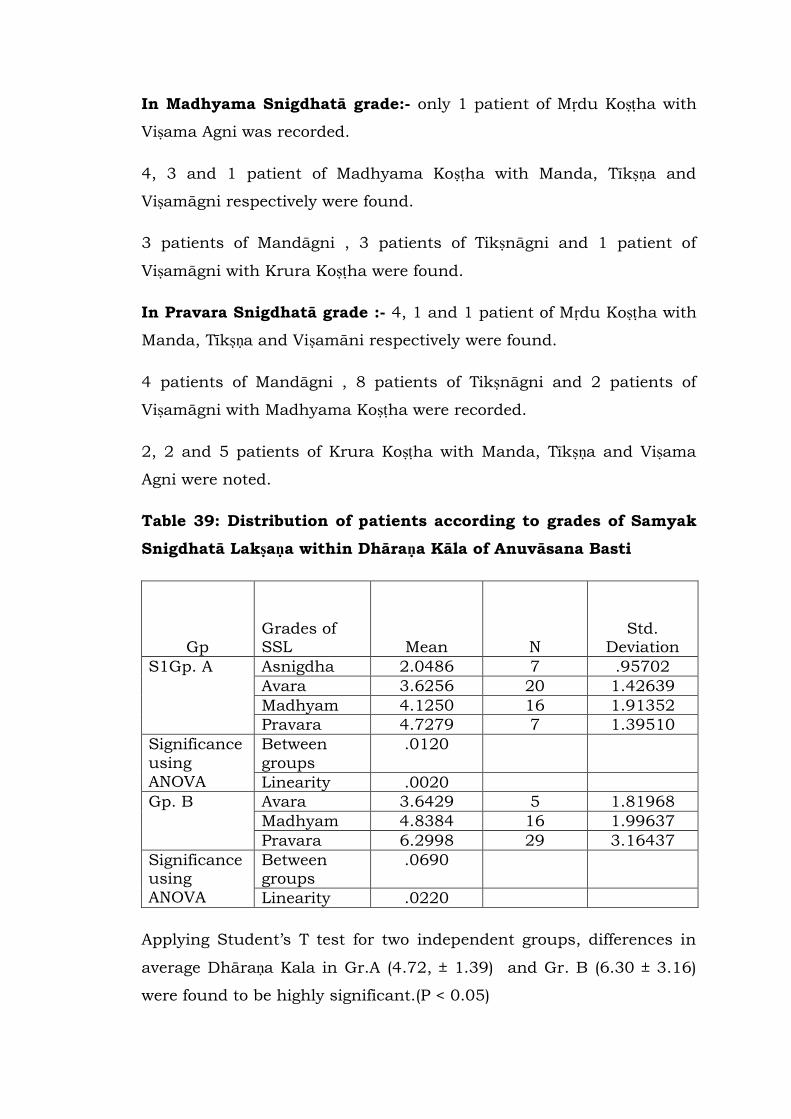
In Madhyama Snigdhatā grade:- only 1 patient of Mṛdu Koṣṭha with
Viṣama Agni was recorded.
4, 3 and 1 patient of Madhyama Koṣṭha with Manda, Tīkṣṇa and
Viṣamāgni respectively were found.
3 patients of Mandāgni , 3 patients of Tikṣnāgni and 1 patient of
Viṣamāgni with Krura Koṣṭha were found.
In Pravara Snigdhatā grade :- 4, 1 and 1 patient of Mṛdu Koṣṭha with
Manda, Tīkṣṇa and Viṣamāni respectively were found.
4 patients of Mandāgni , 8 patients of Tikṣnāgni and 2 patients of
Viṣamāgni with Madhyama Koṣṭha were recorded.
2, 2 and 5 patients of Krura Koṣṭha with Manda, Tīkṣṇa and Viṣama
Agni were noted.
Table 39: Distribution of patients according to grades of Samyak
Snigdhatā Lakṣaṇa within Dhāraṇa Kāla of Anuvāsana Basti
Gp
Grades of SSL Mean N
Std. Deviation
S1Gp. A Asnigdha 2.0486 7 .95702
Avara 3.6256 20 1.42639
Madhyam 4.1250 16 1.91352
Pravara 4.7279 7 1.39510
Significance
using
ANOVA
Between
groups
.0120
Linearity .0020
Gp. B Avara 3.6429 5 1.81968
Madhyam 4.8384 16 1.99637
Pravara 6.2998 29 3.16437
Significance using
ANOVA
Between groups
.0690
Linearity .0220
Applying Student‟s T test for two independent groups, differences in
average Dhāraṇa Kala in Gr.A (4.72, ± 1.39) and Gr. B (6.30 ± 3.16)
were found to be highly significant.(P < 0.05)
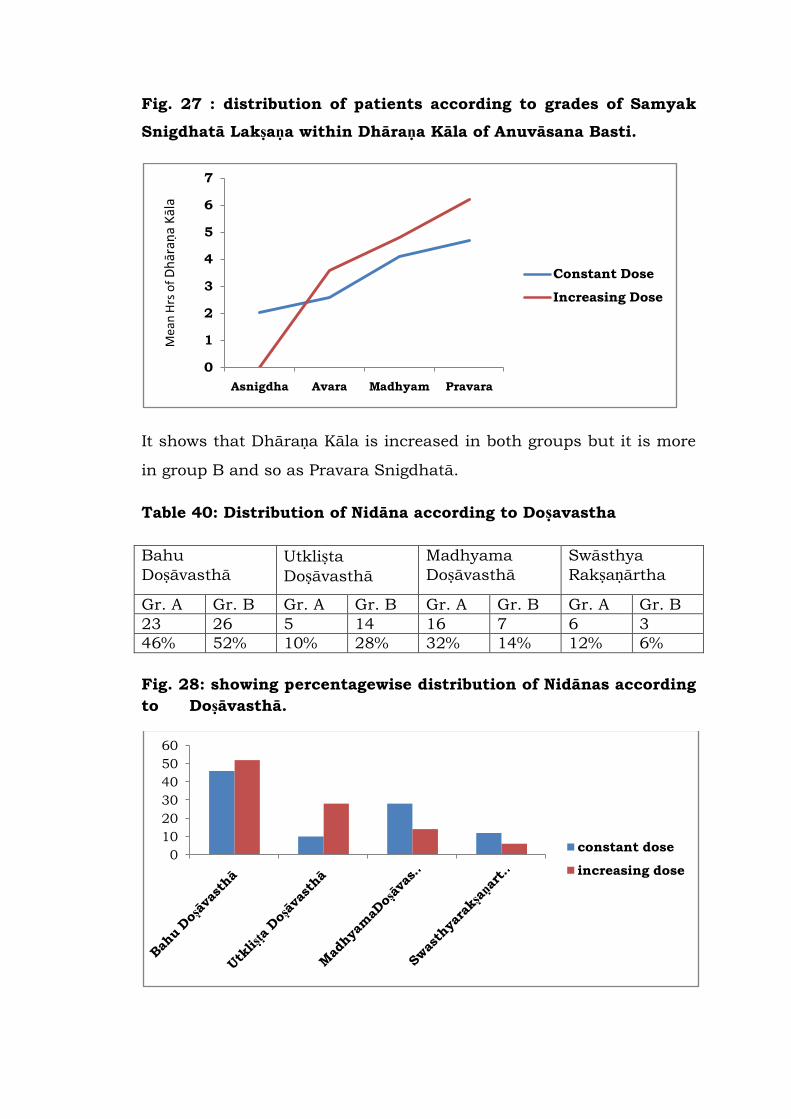
Fig. 27 : distribution of patients according to grades of Samyak
Snigdhatā Lakṣaṇa within Dhāraṇa Kāla of Anuvāsana Basti.
It shows that Dhāraṇa Kāla is increased in both groups but it is more
in group B and so as Pravara Snigdhatā.
Table 40: Distribution of Nidāna according to Doṣavastha
Bahu
Doṣāvasthā Utkliṣta
Doṣāvasthā
Madhyama
Doṣāvasthā
Swāsthya
Rakṣaṇārtha
Gr. A Gr. B Gr. A Gr. B Gr. A Gr. B Gr. A Gr. B
23 26 5 14 16 7 6 3
46% 52% 10% 28% 32% 14% 12% 6%
Fig. 28: showing percentagewise distribution of Nidānas according
to Doṣāvasthā.
0
1
2
3
4
5
6
7
Asnigdha Avara Madhyam Pravara
Mea
n H
rs o
f D
hār
aṇa
Kāl
a
Constant Dose
Increasing Dose
0
10
20
30
40
50
60
constant dose
increasing dose
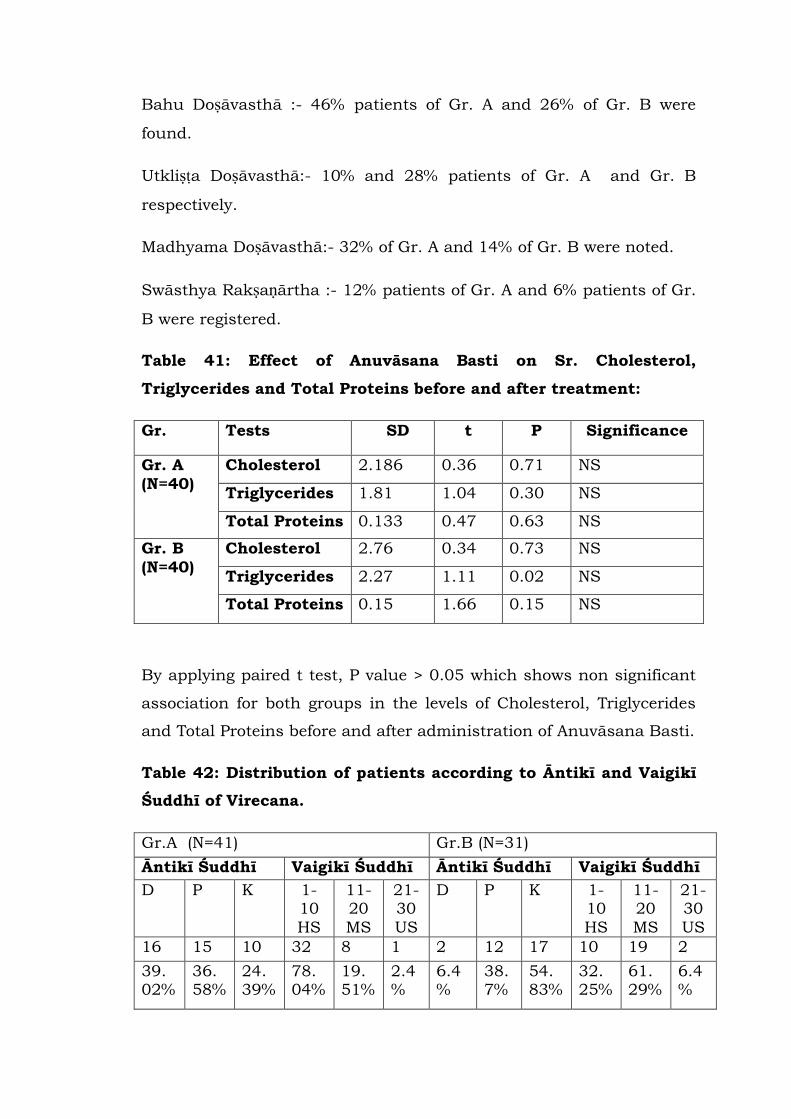
Bahu Doṣāvasthā :- 46% patients of Gr. A and 26% of Gr. B were
found.
Utkliṣṭa Doṣāvasthā:- 10% and 28% patients of Gr. A and Gr. B
respectively.
Madhyama Doṣāvasthā:- 32% of Gr. A and 14% of Gr. B were noted.
Swāsthya Rakṣaṇārtha :- 12% patients of Gr. A and 6% patients of Gr.
B were registered.
Table 41: Effect of Anuvāsana Basti on Sr. Cholesterol,
Triglycerides and Total Proteins before and after treatment:
Gr. Tests SD t P Significance
Gr. A
(N=40)
Cholesterol 2.186 0.36 0.71 NS
Triglycerides 1.81 1.04 0.30 NS
Total Proteins 0.133 0.47 0.63 NS
Gr. B
(N=40)
Cholesterol 2.76 0.34 0.73 NS
Triglycerides 2.27 1.11 0.02 NS
Total Proteins 0.15 1.66 0.15 NS
By applying paired t test, P value > 0.05 which shows non significant
association for both groups in the levels of Cholesterol, Triglycerides
and Total Proteins before and after administration of Anuvāsana Basti.
Table 42: Distribution of patients according to Āntikī and Vaigikī
Śuddhī of Virecana.
Gr.A (N=41) Gr.B (N=31)
Āntikī Śuddhī Vaigikī Śuddhī Āntikī Śuddhī Vaigikī Śuddhī
D P K 1-10
HS
11-20
MS
21-30
US
D P K 1-10
HS
11-20
MS
21-30
US
16 15 10 32 8 1 2 12 17 10 19 2
39. 02%
36. 58%
24. 39%
78. 04%
19. 51%
2.4 %
6.4 %
38. 7%
54. 83%
32. 25%
61. 29%
6.4 %
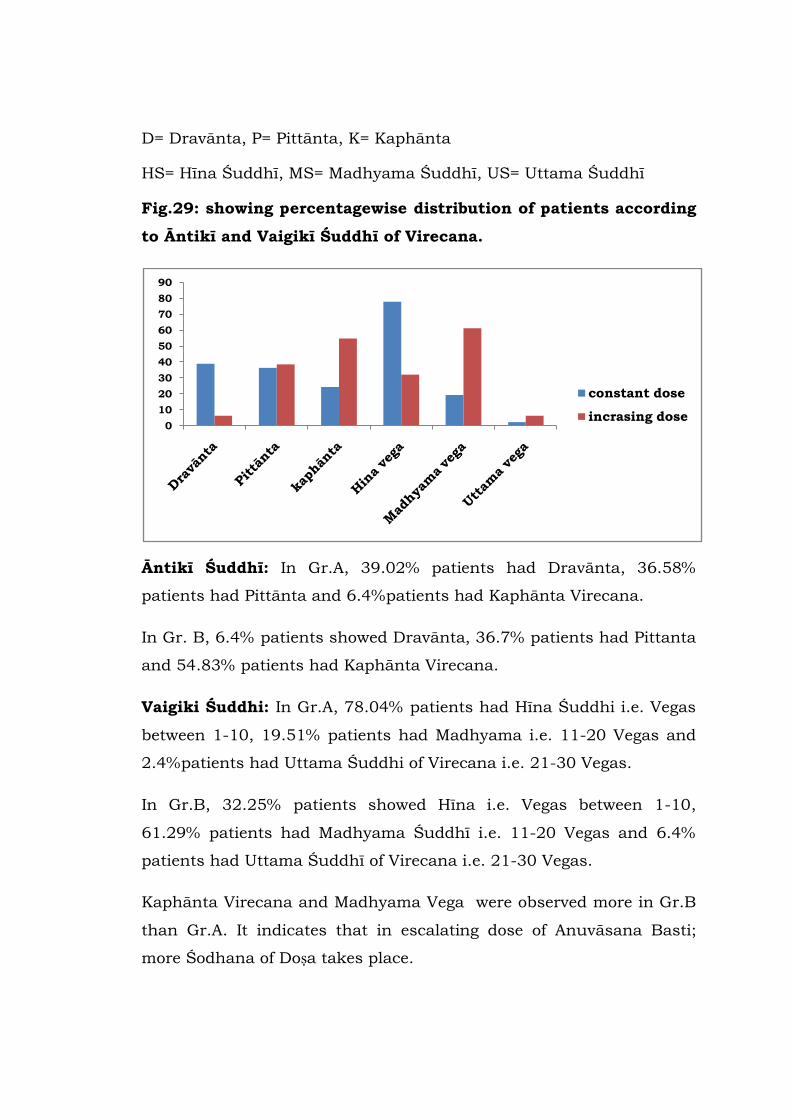
D= Dravānta, P= Pittānta, K= Kaphānta
HS= Hīna Śuddhī, MS= Madhyama Śuddhī, US= Uttama Śuddhī
Fig.29: showing percentagewise distribution of patients according
to Āntikī and Vaigikī Śuddhī of Virecana.
Āntikī Śuddhī: In Gr.A, 39.02% patients had Dravānta, 36.58%
patients had Pittānta and 6.4%patients had Kaphānta Virecana.
In Gr. B, 6.4% patients showed Dravānta, 36.7% patients had Pittanta
and 54.83% patients had Kaphānta Virecana.
Vaigiki Śuddhi: In Gr.A, 78.04% patients had Hīna Śuddhi i.e. Vegas
between 1-10, 19.51% patients had Madhyama i.e. 11-20 Vegas and
2.4%patients had Uttama Śuddhi of Virecana i.e. 21-30 Vegas.
In Gr.B, 32.25% patients showed Hīna i.e. Vegas between 1-10,
61.29% patients had Madhyama Śuddhī i.e. 11-20 Vegas and 6.4%
patients had Uttama Śuddhī of Virecana i.e. 21-30 Vegas.
Kaphānta Virecana and Madhyama Vega were observed more in Gr.B
than Gr.A. It indicates that in escalating dose of Anuvāsana Basti;
more Śodhana of Doṣa takes place.
0
10
20
30
40
50
60
70
80
90
constant dose
incrasing dose
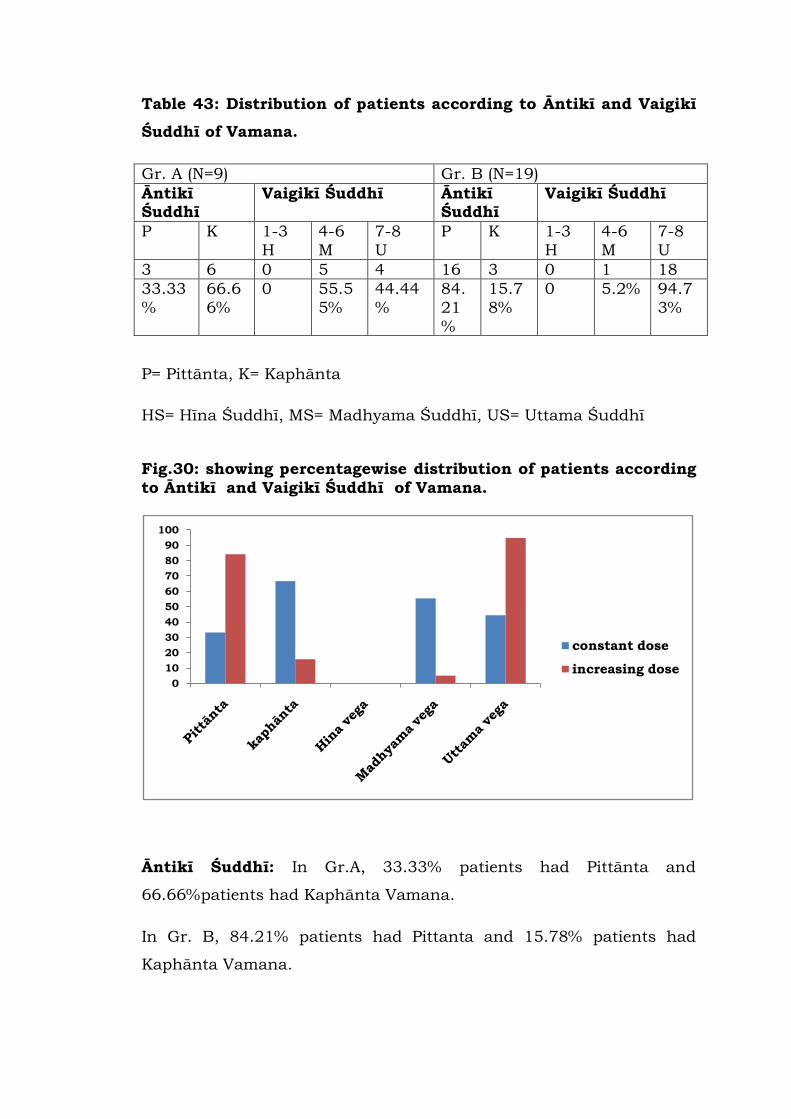
Table 43: Distribution of patients according to Āntikī and Vaigikī
Śuddhī of Vamana.
Gr. A (N=9) Gr. B (N=19)
Āntikī Śuddhī
Vaigikī Śuddhī Āntikī Śuddhī
Vaigikī Śuddhī
P K 1-3
H
4-6
M
7-8
U
P K 1-3
H
4-6
M
7-8
U
3 6 0 5 4 16 3 0 1 18
33.33
%
66.6
6%
0 55.5
5%
44.44
%
84.
21
%
15.7
8%
0 5.2% 94.7
3%
P= Pittānta, K= Kaphānta
HS= Hīna Śuddhī, MS= Madhyama Śuddhī, US= Uttama Śuddhī
Fig.30: showing percentagewise distribution of patients according
to Āntikī and Vaigikī Śuddhī of Vamana.
Āntikī Śuddhī: In Gr.A, 33.33% patients had Pittānta and
66.66%patients had Kaphānta Vamana.
In Gr. B, 84.21% patients had Pittanta and 15.78% patients had
Kaphānta Vamana.
0
10
20
30
40
50
60
70
80
90
100
constant dose
increasing dose
Vaigikī Śuddhī: In Gr.A, no one was found having Hīna Śuddhi,
55.5% patients had Madhyama i.e. 4-6 Vegas and 44.4%patients had
Uttama Śuddhī of Vamana i.e. 7-8 Vegas.
In Gr.B, no one showed Hīna Śuddhī, i.e. Vegas between 1-3, 5.2%
patients had Madhyama Śuddhī i.e. 4-6 Vegas and 94.73% patients
had Uttama Śuddhī of Vamana i.e.7-8 Vegas.
Pittānta Vamana and Uttama Vega were observed more in Gr.B than
Gr.A. It indicates that in escalating dose of Anuvāsana Basti; more
Śodhana of Doṣa takes place.


I. DISCUSSION
Snehapāna as a preparatory procedure is extremely necessary prior to
Vamana and Virecana.(1) The purpose of Snehapāna prior to Śodhana
Karma is Snehana, Viṣyandana, Mārdava and Kledan of Doṣa.(2) Sneha
spreads all over the body through various Srotas and brings the Doṣa
from Śakhā to Koṣṭha so that they can be expelled out easily. This is
achieved by Vṛddhi and Abhiṣyanda of morbid Doṣas.(3) Caraka gives
simily that, as from a smooth container, contents easily separate
without any effort, similarly Kaphādi Doṣas are expelled out easily
from the Snigdha body.(4) As morbid Malas of any cloth is easily
washed by water, if we loosen them from its site, in the similar way
Malas are expelled out by Śodhana if we make them Utkliṣṭa by
Snehana and Swedana.(5) In the present study, efforts have been
made to observe the symptoms of Samyak Snigdhatā through
administration of Anuvāsana Basti.
As Basti is described as an internal route of drug administration by
Dalhaṇa [6], here anal route is considered as an alternative to oral
route so as Anuvāsana Basti to Snehapāna.
In this study, we observed symptoms of Samyak Snehana by
administration of Anuvāsana Basti in constant and escalating doses
instead of Snehapāna. Symptoms like Vātānulomana, Angalāghava,
Asaṃhata Varca, Klama and Snigdha Twak were observed.(7) Other
symptoms of Utkleśa of Doṣa were also noted.
By scrutinizing the symptoms of Snigdhatā carefully; it is clear that
they are obtained from following:-
1) Changes in the movement of Vāyu in Koṣṭha.
2) Changes produced in physical orientation like Angalāghava.
3) Changes occurred in consistency and Snigdhatā of Puriṣa.
4) Mental orientation like Glāni, Sāda, Klama.
5) Changes related to lustre and texture of skin.
6) Changes pertaining to Agni.
(1) Changes in the movement of Vāyu in Koṣṭha:-
Vātānulomana i.e. proper evacuation of flatus, faeces and urine.
Vātapratilomatā i.e. Urdhwavātapravṛtti, Udgāra Bāhulya and
Ādhmāna.
Improper evacuation of flatus, faeces and urine.
These symptoms are the result of movements in Koṣṭha. Sneha present
in Anuvāsana Basti; have the cardinal property of Snigdhatā which
acts on the exactly opposite property of Vāta i.e. Rukṣatā.
Vātānulomana is very first symptom quoted by Ācaryas in the list of
Samyak Snigdhatā . Practically also this symptom appeared on very
first day of Anuvāsana Basti in both groups. (Table No.15 ) It was
observed that on 3rd, 4th and 5th day; Vātānulomana was higher in Gr.
B. On 6th and 7th day both groups achieved Vātānulomana. It was
seen that, total 96% in gr. A and 98% patients in gr. B achieved
Vātānulomana ( Table No.7 ) As Vātānulomana is the main symptom
of proper administration of Anuvāsana Basti irrespective of it‟s dose;
in both groups Vātānulomana had been seen predoninently.(8)
Snigdha and Sara Guṇa of Tila Taila help in bringing Vātānulomana.
Tila Taila along with Saindhava lubricates and oliates Puriṣavaha
Srotas so as Pakwāśaya. It helps the fecal matter, urine and flatulance
to pass through with ease. As we know due to Rukṣatā, faecal matter
becomes hard and obstructs Vāta Gati, which in turn produces
Pratiloma Gati of Vāta. If the quantity of Sneha in Anuvāsana Basti is
not sufficient and Rukṣatā remains as it is, Vāta Pratilomatā takes
place with Udgāra, Ādhmāna or improper evacuation. These symptoms
are listed under Asnigdha Lakṣaṇas.(9)

Vātānulomana not only indicates the proper Gati of Vāyu but it
indicates Vāta Nigraha in Koṣṭha which helps Doṣa to move towards
Koṣṭha from Śakha.(3)
(2) Changes produced in physical orientation like Angalāghava:-
Following factors were considered to study this symptom.
Feeling of lightness in the body.
Feeling as usual.
Heaviness in body.
Angalāghava was seen in Gr. A on the 1st day which was observed
increasing on the following days. In Gr. B it was observed from 2nd
day. (Table No.15) Over all in Gr. A, 38% patients and in Gr. B, 30%
patients showed Angalāghava. On the contrary, 40% patients from Gr.
B had Angagaurava may be due to Guru property and large quantity of
Tila Taila administered through Anuvāsana Basti. (Table No.8)
(3) Changes occured in consistency and Snigdhatā to Puriṣa:
Following criterias were considered to check the consistency of Puriṣa.
Asaṃhata Varca.
Mṛdu Varca (Soft stool) without much straining.
Rukṣa Varca with straining.
Due to Snigdha property of Tila Taila; Pakwāśaya and Puriṣa becomes
Snigdha where as due to Sara and Drava properties, Puriṣa gets
loosened.
Asaṃhata Varca is a state of saturation of Sneha in faeces.
Eventhough in both groups Asaṃhata Varca was oberved; in Gr. B it
was seen earlier than Gr. A, i.e. on 3rd day. (Table No15 ) In Gr. A,
total 60% patients and in Gr. B total 92% patients showed the
symptom Asaṃhata Varca.(Table No.9) It indicates that, the saturation
of Sneha in the Puriṣa is more in escalating dose of Anuvāsana Basti.
When Sneha is administered in larger quantity through Anuvāsana
Basti, Śoṣyamaṇa Vanhī present in Pakwāśaya fails to absorb it
completly, hence Asaṃhata Varca and excretion of Sneha through anal
route can be observed. In Gr. A, 40% patients didn‟t show any change
in consistancy and frequency of faeces, but proper defication without
any strain was seen in these patients. It is again the Samyak Lakṣaṇas
of Anuvāsana Basti as the dose given was 120ml constantly.(8)
Vīrya of Anuvāsana Basti is absorbed by Apāna and immediately
taken up by Samāna Vāyu which in tern starts oliating Annavaha
Srotas.(10) Asaṃhata Varca indicates Snehana of Annavaha and
Purishavaha Srotas i.e. Snigdhatā of Koṣṭha in general.
The Rukṣa, Grathita, Śuṣka and Kṛcchra Varcapravāhaṇa is enlisted
under Asnigdha Lakṣaṇas, which denotes the quantity of Sneha given
is too less to overcome the Rukṣatā of Koṣṭha.(9)
In this study, we came across one limitation of observing the symptom
Snigdha Varca. In the process of Snehapāna, after certain period, stool
becomes oily due to saturation of Sneha in Koṣṭha. Whenever
defecation takes place after administration of Anuvāsana Basti of Tila
Taila, patient could not differentiate between oiliness of stool and stool
along with oil.
(4) Changes produced in mental orientation like Klama:-
Tiredness or exhaustion without much exertion.
Reasonably active as usual.
Enthusiastic
These factors were considered to assess Klama.
In Gr. B, Klama was seen on 4th day onwards. Whereas in Gr. A, it was
observed on 6th day. (Table No.15 )
Tiredness or exhaustion without much exertion may occur due to
obstruction in the way of perception of sense organs. This lassitude
develops due to Guru and Manda properties with large quantity of
Sneha and may be observed during digestion of Sneha. Over all 14%
and 56%patients from Gr. A and Gr. B respectively showed the
symptom Klama. Whereas 74% patients in gr. A were enthusiastic
after administration of Anuvāsana Basti in the dose of 120 ml
constantly. (Table No.10) This may happened due to proper excretion
of fecal matter, urine and flatulance and can be considered as Samyak
Anuvāsana Lakṣaṇa.(8a,8b,8c,8d)
(5) Changes related to lustre and texture of skin:-
Following symptoms were studied in this factor.
Proper oiliness of Skin.
Softness of skin.
Dryness of skin.
Interesting observation in the study was that, oiliness of skin was seen
in 68% patients of gr. B and 36% patients of gr. A. (Table No11) In the
present study, Snigdhatā of skin was measured before starting and
after completion the Anuvāsana Basti by Pin Test. The logic behind
that is; as oiliness of skin increases the absorption time of oil will also
increase. Interestingly we observed increased duration of absorption of
oil through skin in both groups. (Table No.12) In Gr. B, may be due to
gradually increasing dose of Tila Taila in Anuvāsana Basti, Twak
Snigdhatā was found significant. (Table No.13) Suśruta supports this
phenomenon by stating that as tree irrigated in its root level attains
branches with leaves, flowers and fruits. [11] In the same way;
Anuvāsana Basti administered into the rectum spreads and performs
significant results up to head to toe in human body. Vīrya (potency) of
Basti spreads all over the body even though it is administered in
rectum. [12] Suśruta further quotes day wise spreading of Basti. On 4th
day Basti reaches up to Rasa Dhātu and on 5th day up to Maṃsa
Dhātu. It indicates that Sneha can reach up to skin within 5 days as
skin is Upadhātu of Maṃsa and Vyaktīsthāna (site of manifestation)
of Rasa.(13) Vīrya of Anuvāsana Basti spreads all over the body through
Apāna, Samāna, Vyāna, Prāṇa and Udāna.(10) Hence Twak Snigdhatā
can be observed after administration of Anuvāsana Basti.
According to Sāmānya- Viśeṣa Siddhānta, Snigdha, Picchila and Mṛdu
properties of Tila Taila, enhances the same qualities in the body hence
Twak Snigdhatā and Mārdava can be seen.(14) Twak Prasadakara is a
quality of Tila Taila which is again one of the cause of Twak
Snigdhatā.(15)
In this study, Twak Snigdhatā was observed from 6th day in Gr. A
(Table No.15) and from 5th day in Gr. B. In Gr. A, 54% patients had
Rukṣa Twak which were observed unchanged after administration of
Anuvāsana Basti in constant dose of 120ml. It indicates the
significance of dose of Anuvāsana Basti in attaining Twak Snigdhatā .
(Table No.11)
(6) Changes pertaining to Agni:-
Agnidiptī is the symptom enlisted in the symptoms of Samyak
Snigdhatā . After proper Anulomana of Apāna Vāyu and Samāna Vāyu
Pacaka Pitta works properly. Even though Sneha is Āpa Mahābhuta
Pradhāna; it works as a fuel especially when the dose is low. But when
it is administerd in a larger quantity as a preparatory procedure for
Śodhana; Kṣudhāmandya is observed upto digestion of Sneha. In this
study we face some difficulties in assessing Agnidiptī; as Snehapāna is
done in empty stomach and Anuvāsana has to be given after having
food. In Snehapāna process Agni digests the Sneha only but in this
study Agni has to digest not only Sneha but food also. Hence
observation of Agnidīpti was the limitation of our study. Some
patients showed the symtom Kṣudhāmāndya from 4th – 5th day of
Anuvāsana Basti in Gr. B as dose of Anuvāsana increased. But no one
complaind Avipāka, Bhaktadweṣa or Aruci which can be considered as
symptoms of Asnigdha.
(7) Symptoms of Utkleśa:
In Gr. B, few patients showed Urdhvaga Utkleśa with symptoms like
Hṛllās, Kanthopalepa, Śirogaurava. To our surprise, two patients were
observed with Netra Mala Vṛddhi. This shows that effect of Basti is not
restricted to ano-rectal region locally. In this context, Chakrapāṇi
states that Basti reaches up to duodenum. (16) This statement is
supported by Best and Taylor who states “materials introduced by
enema, may in some instances pass through the valve into the ileum.
Such incompetence may permit the enema fluid to reach the
duodenum.”[17] However, considering the symptoms observed in our
study, we may infer that the effect of Basti can be seen even beyond
duodenum. It should be however noted that the extent of vitiated
Doṣa, season and other elements in the body also play the major role
in the process of Utkleśa. According to Caraka, Utkleśa of Doṣa and
Agnivadha are manifested if Anuvāsana Basti is administered
continuously.(18) Here Anuvāsana Basti was administered not only for
many days but also in escalating dose. Due to administration of oil in
large quantity, Utkleśa of Doṣa may take place. But in this study, both
groups were administered Anuvāsana Basti maximum for seven days
which is indicated as the limit of Ābhyantara Snehapāna.(19) Hence the
symptom Agnivadha may not be observed in this study.
Role of Agni in Snehana Karma through Anuvāsana Basti:
Even though Basti is administered in rectum, the Jāṭharāgni must be
in it‟s normal state. Absorption of Basti in Pakwāśaya is possible only
when Jāṭharāgni is in it‟s normal state and so as Dhātvāgni and
Bhutāgni. Digestion, absorption and assimilation of Sneha present in
Anuvāsana Basti is possible when these Agnis are in their proper
working capacity.
As observed in this study, in Gr. A, where the dose of Anuvāsana Basti
was constant, days required to achieve Samyak Snigdhatā are more
for Mandāgni and Viṣamāgni than Tikṣṇāgni. It underlines the
importance of pattern of Agni in absorption of Basti.(Table No.28) But
in gr. B, where the dose was escalating; 1 patient of Mandāgni showed
symptom of Snigdhatā earlier than other two Agni. This may
happened due to other factors like Koṣṭha and Prakṛti.
Agni plays major roll in absorption of Sneha in Anuvāsana Basti. As
Śoṣyamaṇa Karma is expected in Pakwāśaya, the proper working
capacity of Jāṭharāgni should be present.(20) Hence discrimination of
all symptoms of Samyak Snigdhatā were present in both groups
irrespective of their type. As in Gr. B, dose was escalating, Śoṣaṇa of
Sneha decreases and hence the symptom Asaṃhata Varca was
observed more in all types of Agni than in Gr. A.(Table No. 25) No
specific observations were found according to the grades of symptoms
of Samyak Snigdhatā. (Table No.29)
Roll of Koṣṭha in Snehana Karma through Anuvāsana Basti:
Types of Koṣṭha are dependent upon the dominance of properties of
Doṣa present in the Koṣṭha which are responsible for the tendency of a
person to pass stool.
The data shows that, in Gr.A, i.e. in constant dose, Snigdhatā
Lakṣaṇas appeared on 6th day of Anuvāsana in the patients of Mṛdu
Koṣṭha where as for Madhyama and Krura Koṣṭha, symptoms appeared
on 7th day. (Table No. 35)
In Gr. B, i.e. in escalating dose, 14% patients with Mṛdu Koṣṭha
showed symptoms of Snigdhatā on 4th day, 42.85% on 5th day, 28% on
6th day and 14% on last day. Patients having Madhyama Koṣṭha also
started showing symptoms of Snigdhatā earlier i.e. on 5th and 6th
day. Patients of Krura Koṣṭha showed Snigdhatā on 6th day
onwards.(Table No. 35) Surprisingly the data shows that the duration

required for achieving symptoms of proper Snehana after
administration of Anuvāsana Basti was similar to the textual reference
of Snehapāna. [21]
Even Pravara grade of Snigdhatā was achieved maximum i.e. in 85%
of patients with Mṛdu Koṣṭha in Gr. B and 18% in Gr. A (Table No.36)
Mṛdu Koṣṭha has a dominance of Pitta with Sara and Snigdha
properties. It may be the cause that Vātānulomana, Asaṃhata Varca
appeared earlier in the patients of Mrudu Koṣṭha. (Tabla No. 15) While
describing indications of Vicaraṇā Sneha, Caraka has maintioned
patients having Mṛdu Koṣṭha.(22) In this study the same results were
obtained.
Roll of Prakṛti in Snehana Karma through Anuvāsana Basti:
As Agni and Koṣṭha are two major components in defining Prakṛti, no
specific relationship was found between Prakṛti and symptoms of
Samyak Snigdhatā. (Table No. 16-22) Discrimination of all three Doṣas
is present in each, but dominating Doṣas are considered to define the
Prakṛti. This may be the cause that we could not relate Prakṛti with
symptoms of Samyak Snigdhatā.
Roll of Dhāraṇa Kāla in Snehana Karma through Anuvāsana Basti:
Dhāraṇa Kāla of Anuvāsana Basti and symptoms of Samyak Snigdhatā
were correlated. In both groups it was observed that as Dāraṇa Kāla
increases, grades of Samyak Snigdhatā also get increased. (TableNo.
39) Suśruta clearly mentions that, if Anuvāsana Basti doesn‟t retain
inside the rectum; then it is unable to provide proper Snigdhatā to
Pakwāśaya and may not avail expected results.(23) In Gr.B, Dhāraṇa
Kāla of Anuvāsana Basti was found more than that of Gr.A. This may
be the reason that, Pravara Snigdhatā was found more in that group.
Śuddhi of Virecana and Vamana after administration of
Anuvāsana Basti as an alternative for Snehapāna prior to Virecana
and Vamana:
In both groups Kaphānta Virecanas were observed. But more patients
were found in Gr.B having Kaphānta Virecana. In group A, patients
had Dravānta Virecana more than Kaphānta or Pittānta. In Gr. B more
patients were found having Virecana Vega between 11-20 i.e.
Madhyama Śuddhī. Hence by considering Āntikī and Vaigikī Śuddhī, it
is clear that, Asnigdha or Avara Snigdhatā cause improper Śuddhī of
Virecana.(24,25) (Table No.42)
For Vamana also same phenomenon was observed. (Table No.43)
Āntikī and Vaigikī Śuddhī were seen more in Gr. B may be due to
achievement of Samyak Snigdhatā. Proper Snigdhatā of the body,
cause Koṣṭhagati of Doṣa which in turn causes proper expulsion of
Doṣa without having Vātaprakopa.
In the present study also; very positive results were obtained in terms
of Vaigikī, Mānikī and Laingikī Śuddhi especially in Gr. B. Laingikī
Śuddhī was observed in both groups with relief obtained immediate
after Śodhana procedure and relief obtained in the symtoms of the
disease. Śarīra Lāghava, Indriya-Mana Prasannatā, Kṣudha Vṛddhī etc.
were found as immediate symptoms of Samyak Śodhana in both
groups. Maximum relief was found more in the diseases with
Bahudoṣāvasthā and Utklīṣṭa Doṣāvasthā for eg. In Vicarcikā; Kandu
and Srāva were discreased. Patients with Sthaulya, lost their weight
from 1 to 4 kg. Patients having Samprāpti related to Apāna Kṣetra, eg.
Vibandha, Urdhvaga Āmlapitta due to Vibandha, PCOD, Aniyamīta
Rajapravartana, Kaṣtārtava etc. had very good results irrespective of
way of Śodhana i.e. Vamana or Virecana and dose of Anuvāsana Basti.
As in the present study all diseases indicated for Vamana or Virecana
were included and allocated randomly in both groups; no significant
comparison was done in terms of results.
Biochemical Parameters like Serum Cholesterol, Serum Triglycerides
and Serum total Protein were observed. No significant changes in
these parameters were found in both groups. (Table No.41) As Basti
gets absorbs directly in systemic circulation and has portal bypass;
observations of these parameters were very important.

In the present study, a concept of Snehana Karma through Anuvāsana
Basti is put forth on the basis of Yuktī Pramāṇa. Even though
digestion of Sneha taken orally and through anal route is different,
Samyak Snigdhatā Lakṣanas were assessed here after administration
of Anuvāsana Basti. Surprisingly 58% patients who were administered
Anuvāsana Basti in increasing dose showed Pravara Snigdhatā. It
indicates the absorption of Sneha through anus. On the basis of
clinical study, the concept of Anuvāsana Basti as an alternative to
Snehapāna is seemed to be proved.
Even though all Ācaryas affirm the importance of Acchapāna; this
attempt has been made for those patients who may deprive the
benefits of Śodhana procedures; only because of aversion of
Snehapana. Hence considering some limitations and further scope
regarding this alternative; we have tried utmost.

II. FURTHER SCOPE OF THE STUDY
Study can be done with various Siddha Taila or Ghṛta according
to Vyādhīs.
Various doses of Anuvāsana Basti can be studied.
Study can be carried out with specific variable like Koṣṭha.
Study can be done according to proper Kāla for Śodhana, i.e. in
Vasanta Rṛtu- Vamana.
Study can be done with specific Siddha Sneha in specific
disease by keeping the variables identical like Ṛtu, Koṣṭha, Agni
etc.
Study can be done with bio- markers.

III. REFERENCES
1. snaohsvaodpcailata rsaO : isnagQaO$dIirta : I
daoYaa : kaoYzgata jantao : sauKa ht-uM ivaSaaoQanaO : I I sau.ica. 33/47
2. snaohnaM snaoh ivaYyandM maad-vaM @laodkarkma\ I ca.saU. 22/11
isnagQaat\ pa~ayaqaa taoyamaya%naona pNaudyato I
3. vaRdQyaa ivaYyaMdnaat\ pakat\ sa`aotaomauKivaSaaoQanaat\
SaaKaM %ya@%vaa malaa : kaoYzM yaaint vaayaaoSca inagahat\ I vaa.saU. 13/11
4. isnagQaat\ pa~aVqaataoyamaya%naona p`NauVto I
kfadya : pNaudyanto isnagQaa_oha<aqaaOYaQaO : I I ca.isa. 6/11
5.Aad`-M kaYzM yaqaa vai*naiva-Yyandyait sava-t : I
yaqaa isnagQasya vaO daoYaana\ svaodao ivaYyandyaot\ isqarana\ I I
i@laYTM vaasaao yaqaao%@laoSya mala : saMSaaoQyato | mBasaa I
snaohsvaodOstqaao%@laoSya SaaoQyato SaaoQanaOma-la : I I ca.isa. 6/12 – 13
6.t~ baa*ya : snaohsvaodaBya=gapirYaokaopnaahiSaraobaistnasyaaid : AaByantrstu
snaohpanaanauvaasanaina$haid : l sau. ].26/2,3 DlhNa
7. vaatanaulaaomyaM idPtao|ignava-ca-O: isnagQamasaMhtma\ l
maad-vaM isnagQata caaMgao isnagQaanaamaupjaayato l l ca.saU.13 / 57
8a.p`%yao%yasa@tM saSakRcca tOlaM
r@taidbauwIind`ya saMp`saad: l
svaPnaanauvaRi<ala-Gauta balaM ca
saRYTaSca vaogaa: svanauvaaisato syau: l l ca.isa.1/44
8b. saainala: sapuirYaSca snaoh: p`%yaoit yasya tu l
AaoYacaaoYaaO ivanaa SaIGa`M sa samyaganauvaaisat: I I sau.ica. 37/67
8c.ikMica%kalaM isqatao yaSca sapurIYaao inavat-to l
saa|naulaaomaa|inala: snaohsti%sawmanauvaasanama\ I I A.).saU. 19/42
8d.AignadIiPtva-ya: sqaanaM puiYTvaNaao- QaRitba-lama\
vaatanaulaaomata Saaint : svanauvaaisatlaxaNama\ I I ka.saM. 2
9. puirYaM gaiqatM $xaM vaayaurp`gauNaao maRdu: l
p@ta Kr%vaM raOxyaM ca gaa~syaaisnagQa laxaNama\ l l ca.saU.13 / 59
10. ya<a~aOYaQa vaIya-M ih tdpanaona vaayaunaa l
Payaa-Ptmaicaradova samaana : pitpVto l l
samaanaadU<arM caOvaM vyaanaaVa : pvanaakmaat\ l
to tRPta : pkRitM yaaint SarIranaugaho isqata : l l A.).isa. 5
11. p@vaaSayaad\baistvaIya-M KOdo-hmanausaip-it l
vaRxamaUlao inaiYa@tanaamapaM vaIya-imava dumama\ l l sau.ica. 35/25
12. naaiBapdoSaM kiTpaSva-kuixaM l
ga%vaa SakRd\daoYacayaM ivalaaoDya l
saMsnao( kayaM sapuirYadaoYa: l
samyak\ sauKonaOit ca ya: sa baist: l ca.isa. 1/40
13. d<astu p`qamaao baist: snaohyaod\baistva=xaNaaO
samyagdtaO iWtIyastu maUQa-sqamainalaM jayaot\
janayaod\balavaNaaO- ca tRtIyastu p`yaaoijat:
rsaM catuqaao- r@tM tu pMcama: snaohyao<aqaa
YaYzstu snaohyaonmaaMsaM maod: saPtma eva ca
AYTmaao navamaScaaisqa majjaanaM ca yaqaak`mama\
evaM Sauk`gatana\ daoYaana\ iWgauNa: saaQau saaQayaot\ l l sau.ica. 37 /71-74
14. vaRiw : samaanaO : savao-YaaM ivaprItOiva-pya-ya : l l A.).sau. 1/13
15. maa$tGnaM na ca SlaoYmavaw-naM balavaQa-nama\ I
%vacyamauYNaM isqarkrM tOlaM yaaoinaivaSaaoQanama\ I I ca.saU. 13 /15
16. vaamaaEayao ih ga`hNaIgaudo ca
tt\ paSva-saMsqasya sau#aaoplaibQa : l l
laIyant evaM valayaSca tsmaat\
savyaM Sayaanaao |h-it baistdanama\ l ca.isa.3 /24
17. Aayauvao-idya pMcakma- iva&ana ksturo hirdasa EaI baOd\yanaaqa Aayauvao-d Bavana p`ayavaoT
ila. saPtma saMskrNa pRYz k`. 469
18. snaohbaistM ina$hM vaa naOkmaovaaitSaIlayaot\ l
snaohadignavaQaa%@laoSaaO ina$hat\ pvanaad\Bayama\ l l sau.ica. 37/77
19. snaohsya p`kYaaO- tu saPtra~ai~ra~kaO
ekamuau<amaa poyaa Hyahmaova tu maQyamaa l l ca.saU.13 / 51
20. p@vaaSayaM tu p`aPtsya SaaoYyamaaNasya vainhnaa l ca.ica.15 /11
p@vaaSayaM tu p`aPtsyaoit mala$ptyaa p@vaaSayaM gatsya l SaaoYyamaaNasya vainhnaoit
yaVPyaUQva-dahxamaao vai*na : , tqaa | PyasyaaQaaogatsya vai*nana SaaoYyamaaNa%vaM
p@vaaSayagatsyaaPyauppnnama\ l yatScaaQaaogamanao samyagvai*navyaaparao naaist At :
‘ pcyamaanasya ’ [it pdM pir%yajya ‘ SaaoYyamaaNasya ’ [it kRtma\ l ca.ica.15 /11
21. maRdukaoYzis~ra~oNa isna*ya%yacCaopsaovayaa l
isna*yait kUrkaoYzstu saPtra~oNa maanava : l l ca.saU.13 / 65
22. snaohiWYa: snaohina%yaa maRdukaoYzaSca yao nara: l
@laoYaasaha maVina%yaastoYaaimaYTa ivacaarNaa l l ca.saU. 13 /82
23. yasyaoh yaamaananauvat-to ~Ina\
snaohao nar: syaat\ sa ivaSauw doh: l
AaSvaagato|nyaostu punaiva-Qaoya:
snaohao na saMsnaoh yait *yaitYzna\ l l ca.isa.1/46
24. AisnagQa isvanna dohsya$xasyaanavamaaOYaQama\ daoYaanaui%@laSya inah-tu-M ASa@tM
janayaoMdgadana\ l l ca.isa.6/38
25. AisnagQaisvannaonaalpgauNaM vaa BaoYajamaupyau@tM Alpana\ daoYaana\ hint l sau.ica. 34/7

CONCLUSION
Symptoms of Samyak Snigdhatā can be achieved after
administration of Anuvāsana Basti.
They can be developed better especially after administration of
escalating dose of Anuvāsana Basti.
Anuvāsana Basti in escalating dose can definitely be used as an
alternative for Snehapāna prior to Śodhana, i.e. Vamana and
Virecana.
Patients with Mṛdu Koṣṭha required minimum dose and duration for
getting symptoms of Samyak Snigdhatā, Madhyama Koṣṭha required
medium dose and duration, where as Krura Koṣṭha required
maximum dose and duration for getting Samyak Snigdhatā if dose
of Anuvāsana Basti is kept increasing.
Śuddhi Lakṣaṇas of Vamana and Virecana in terms of Vaigiki, Āntiki
and Laingiki were very promising. Madhyama to Uttama Śuddhi of
Vamana and Virecana can be observed, if Anuvāsana Basti is
administered in escalating dose.
SUMMARY
Anuvāsana Basti, Snehapāna and Rectal drug delivery described in
moderm medicine were studied at the length.
On the basis of the study; hypothetically it was confirmed that,
Anuvāsana Basti can be administered as an alternative for
Snehapāna in Vamana and Virecana as it is considered as internal
route of drug administration.
As Anuvāsana Basti was compaired with Snehapāna; maximum
duration for administration of Anuvāsana Basti was kept 7 days.
As no references were found regarding the concern topic; two groups
were made on the basis of dosage form: A group with constant dose
of Anuvāsana Basti of Mūrcchita Tila Taila (120ml) and Saindhava
(500mg) considered as control grop. B group with escalating dose.
Concept of escalating dose of Anuvāsana Basti was adopted as the
dose of Snehapāna used for Śodhana also gets increased. Hrasīyasī
Mātrā of Snehapāna is 25 to 30ml. By considering the same dose,
we decided to increase the dose of Anuvāsana Basti by 25ml daily.
As the dose of Saindhava is not mentioned in texts, 500mg dose was
decided on the 1st day with increase of 100mg daily for minimum 3
and maximum 7 days.
Symtoms of Samyak Snigdhatā except Agnidīpti and Snigdha Varca
were observed and statistically analysed. 58% patients of Gr. B had
Pravara Snigdhatā.
Samyak Śuddhi Lakṣaṇas of Vamana and Virecana were also
observed. These observations were discussed in detailed.
On the basis of conceptual study, observations, results and
discussion; conclusions were drawn.
The hypothesis which was drawn from a conceptual study i.e.
Anuvāsana Basti with Murcchita Tila Taila and Saindhava can be
used as an alternative for Snehapāna in Vamana and Virecana is
seemed to be proved as said by Dalhaṇa, especially in escalating
dose of Anuvāsana Basti.
BIBLIOGRAPHY
Jadavaji T. Acarya.( 1981,4th edition). Caraka Saṃhitā of
Agnivesa. New Delhi: Munshiram Manoharlal Publishers Pvt.
Ltd.
Jadavaji T. Acarya.( 1992,5th edition). Suśruta Saṃhitā of
Suśruta. Varanasi: Chaukhamba Orientalia.
Gupta K.A. (1993, 2nd edition). Aṣtāanga Saṃgraha with Hindi
commentary. Varanasi: Krishnadas academy.
Gadre G.K. (1983, 7th edition). Vāgbhat Kṛta Aṣtāṅga Hṛday with
Marāthi translation. Dadar, Mumbai: Gajanana Book Depot.
Kunte A.M. (1982, 7th edition). Shrīmad Vāgbhat Viracitam
Aṣtāṅga Hṛdayam. Varanasi: Chaukhamba Orientalia.
Vajpeyi J.S. (2002, 4th edition). Chakradatta. Mumbai: Shri
Vyankateśwara Press.
Pandita Śārgadharācaryā. (1985) Śārangadhara Saṃhitā.
Varanasi: Krishnadas Academy.
Sharma H.,Satyapala Bhishagacharya (1988, 4th edition).
Kāśyapa Saṃhitā. Varanasi: Choukhamba Sanskrit Sansthan.
Chunekar K. (2010). Shrimad Bhāvmiśra Praṇita Bhavprakāśa
Nighantu, (Indian Materia Medica). Varanasi: Choukhamba
Bharati Academy.
Krishnamurthi K.H. Dr. (2005). Bhela Saṃhitā text with English
translation. Varanasi: Choukhamba Vishwabharati.
Jadavaji T. Acarya.( 1999,5th edition). Madhavanidana.
Varanasi: Chaukhamba Orientalia.
Shastri Ramvallabha. (1985, 1st edition ). Harita Samhita.
Varanasi: Prachya Prakashan.
Vaiṣya S. (2003). Vangasena with Hindi commentary. Bombay:
Khemraja Shreekrishnadasa Prakashana.
Upadhyaya B. (1966). Shrimanmahrshi Krishnasvaipayana
Vyasa praṇitam Shree Agni Puraṇam. Varanasi: Chaukhamba
Sanskriti series office.

Narker C. Dr. (1995). Gheranda Saṃhita. Dharwad: Medha
Publications.
Ugradhityaacharya, edited by Vardhamman. (1940).
Kalyāṇkārakam. Solapur: Shet Govindaji Raoji Doshee.
Compiled by Vachaspatya T.T. Vachaspatya Bṛhat
Sankṛtabidanam. Varanasi: Chokhamba Sanskrit series office.
Kasture H.S. (1993, 4th edition). Āyurvediya Pañcakarma
Vidnyāna. Nāgpur: Shri Baidyanath Āyurved Bhavan.
Dwivedi M. (2008, 2nd edition). Āyurvediya Pañcakarma Cikitsā.
Delhi: Chokhamba Sanskrit Pratiṣthāna.
Nanal R. (1985). Madhu Jīvana, Grahaṇī Roga Viśeṣanka.
Mumbai: Mādhavī Prakaśana.
Patil V. (2008, 1st edition). Snehana Therapy in Āyurveda. New
Delhi: Chaukhamba Publications.
Yadaiah P. (2008, 2nd edition). Clinical Panchakarma. Hydrabad:
Jaya Publications.
Vasudevan Nampoorthiri M.R., Mahadevan L. (2006, 1st edition).
Principles and Practice of Vasti. Kanyakumari: Shri Sarada
Ayurvedic Hospital.
Ayurved Sara Sangraha (2004, 20th edition).Shri Baidyanath
Ayurved Bhavan Ltd.
Basavajyoti, Sudhir (2005) Arohanakrama matra basti an
effective alternate for Snehapan. MD level work. Bangalore,
Karnataka, India.
Vanarase M., Nanal V. (June 2001) To ascertain the mode of
action of Utklesion Basti with reference to it’s indications and
contraindications. MD level work. Pune, Maharashtra, India.
Badve V.B., Bhogal M.J., Singh G. (March 2000) A clinical study
on standardization of Śodhanārtha Ābhyantara Snehapāna. MD
level work. Jamnagar, Gujrat, India.
Sangamkar A., Sathe S.M. (1993-95) Drushtikonatun Prakrut
Stricha Abhyas, MD level work. Marathwada Vidyapeeth,
Maharashtra, India.
Kanthi G. M., Doiphode V.V. Study of organs during Basti Karma
w. s. r. to Rachana and Kriya. Ph.D. Work. Pune, Maharashtra,
India.
Chaurasia B. D. (1974, 1st edition) Human anatomy, Vol. 2.
Delhi: CBS Publishers and Distributors.
Guyton C, John E Hall. (1996, 9th edition). Text Book of Medical
Physiology. Bangalore: Prism Books (Pvt.) Ltd.
Lakshmi Prasanna J. (Oct.-Nov.2012) Rectal drug delivery : A
promising route for enhancing drug absorption; Vol.2: Issue 4,
Pg 143-149. Retrieved November 4th, 2012, from http://
www.asianpharmaonline.org/Asian pharma press/ Asian J. Res.
Pharma. Sci. 2012;
Gupta P.K.( January 2001) A conceptual study on Vasti Effect;
Vol.XX, Pg 54-59. Retrieved October 28th 2000. From
http://www.ancientscienceoflife.org
Savrikar S.S. (Jan.-Mar. 2010) Study of Preparation and
Standardization of „ Madhutailik Basti‟ with special reference to
Emulsion Stability; Vol.31, Issue 1, Pg 1-6. Retrieved November
8th 2013, from http://www.ayujournal.org;
Mirteimouri M , Tara F, Teimouri B, Sakhavar N and Vaezi A.
Efficacy of Rectal Misoprostol for Prevention of Postpartum
Haemorrhage. Iran J Pharm Res. 2013 Spring. From:
http://www.ncbi.nlm.nih.gov/pubmed/24250623

B.V.M.F.‟s BHARATI AYURVED HOSPITAL
PUNE 43
Case paper for the research project
“Study of Anuvāsana Basti as an alternative Purvakarm for
Snehapan in Vaman and Virechan.”
Scholar: Dr. Priyadarshani Kadus. Guide: Dr. S.M. Vedpathak
Name:- Date:-
Age:- Gender:-M/F.
Address:- Wt.:-
Occupation:- Religion:-
OPD No:- IPD No:-
Vedana Vishesh:-
Purvavrutta:-
Kulavrutta:-
Samanya Parikshana:-
Nadi:-
Mala Pravrutti:-
Mutra Pravrutti:-
Jivha:-
Shabda:-
Sparsha:-
Druk:-
Akruti:-
B.P.
Menstrual History:-
Obstetrical History :-
Pakruti Parikshan:-
Sara:-
Samhanana:-
Satva:-
Satmya:-
Bala:-
Koshtha Parikshan:-
Agni Parikshan:-
Vikrut Srotas Parikshan:-
Dosh:-
Dushya:-
Srotas:-
Vyadhimarga:-
Vyadhi Avastha:-
Nidan:-
Chikitsa:- Vaman / Virechan
Purvakama:- Anuvāsana Basti. Gp.A / Gp.B
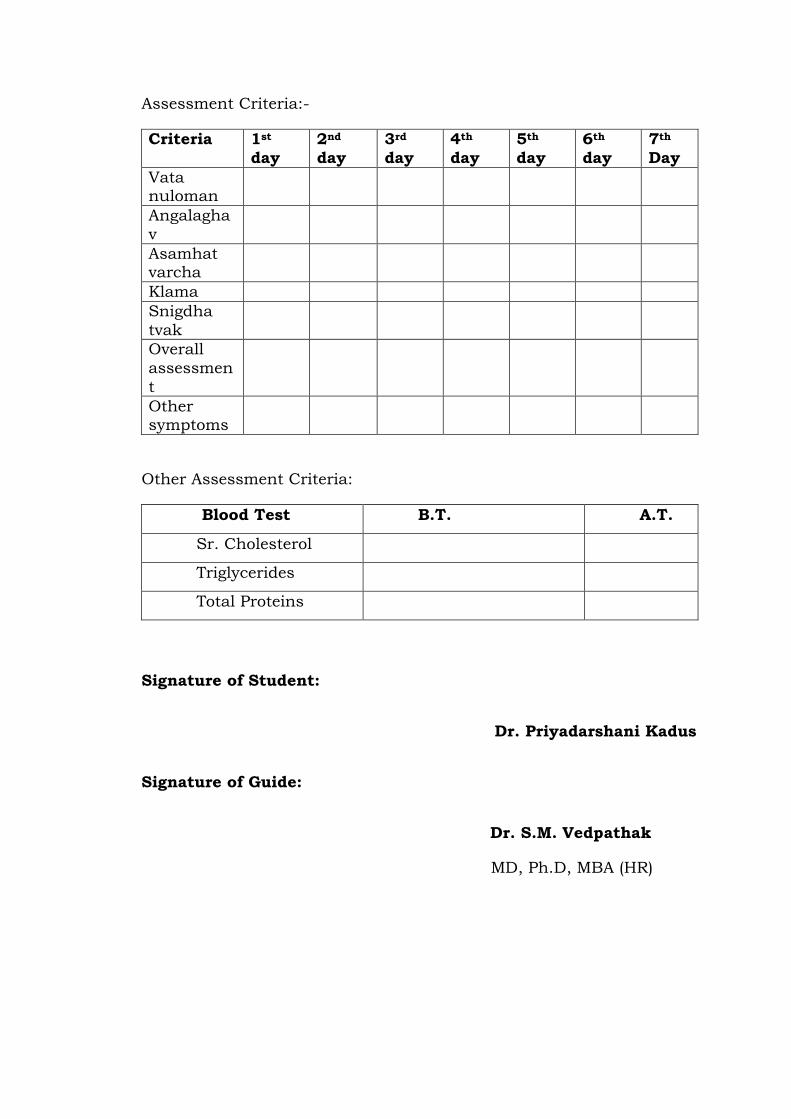
Assessment Criteria:-
Criteria 1st
day
2nd
day
3rd
day
4th
day
5th
day
6th
day
7th
Day
Vata nuloman
Angalagha
v
Asamhat varcha
Klama
Snigdha
tvak
Overall
assessmen
t
Other symptoms
Other Assessment Criteria:
Blood Test B.T. A.T.
Sr. Cholesterol
Triglycerides
Total Proteins
Signature of Student:
Dr. Priyadarshani Kadus
Signature of Guide:
Dr. S.M. Vedpathak
MD, Ph.D, MBA (HR)
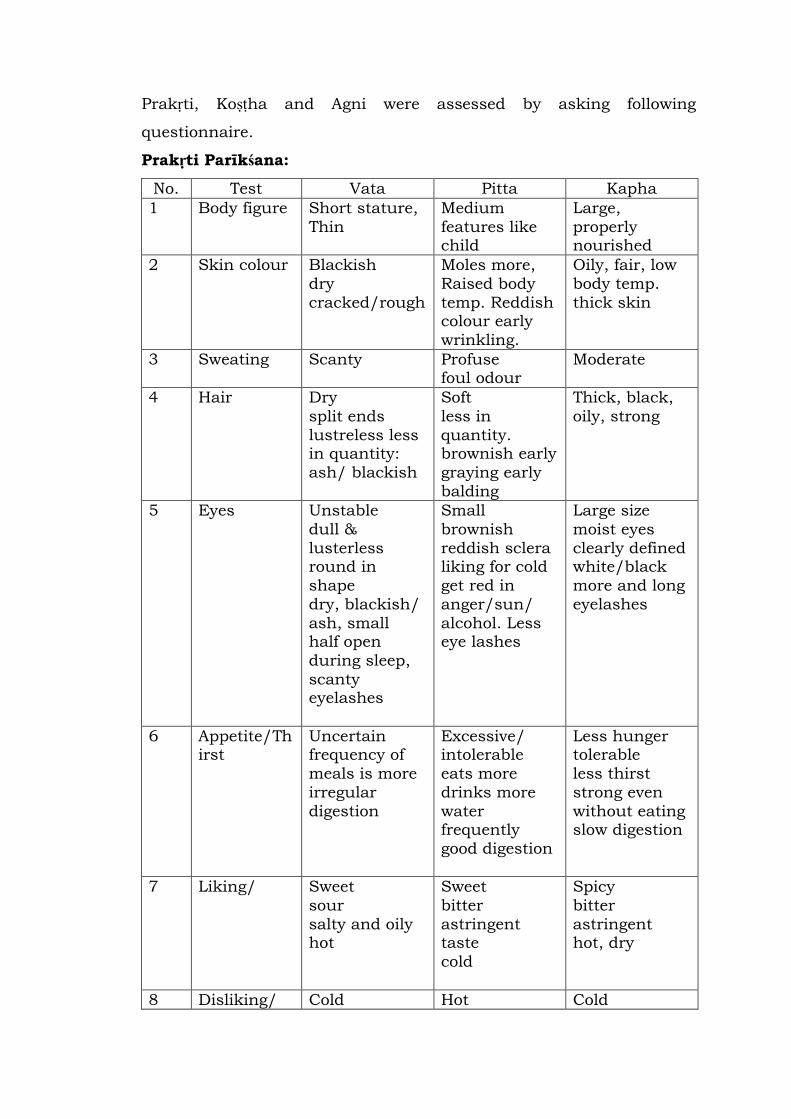
Prakṛti, Koṣṭha and Agni were assessed by asking following
questionnaire.
Prakṛti Parīkśana:
No. Test Vata Pitta Kapha
1 Body figure Short stature,
Thin
Medium
features like child
Large,
properly nourished
2 Skin colour Blackish
dry
cracked/rough
Moles more,
Raised body
temp. Reddish colour early
wrinkling.
Oily, fair, low
body temp.
thick skin
3 Sweating Scanty Profuse foul odour
Moderate
4 Hair Dry
split ends
lustreless less in quantity:
ash/ blackish
Soft
less in
quantity. brownish early
graying early
balding
Thick, black,
oily, strong
5 Eyes Unstable
dull &
lusterless round in
shape
dry, blackish/
ash, small half open
during sleep,
scanty eyelashes
Small
brownish
reddish sclera liking for cold
get red in
anger/sun/
alcohol. Less eye lashes
Large size
moist eyes
clearly defined white/black
more and long
eyelashes
6 Appetite/Thirst
Uncertain frequency of
meals is more
irregular
digestion
Excessive/ intolerable
eats more
drinks more
water frequently
good digestion
Less hunger tolerable
less thirst
strong even
without eating slow digestion
7 Liking/ Sweet
sour
salty and oily hot
Sweet
bitter
astringent taste
cold
Spicy
bitter
astringent hot, dry
8 Disliking/ Cold Hot Cold
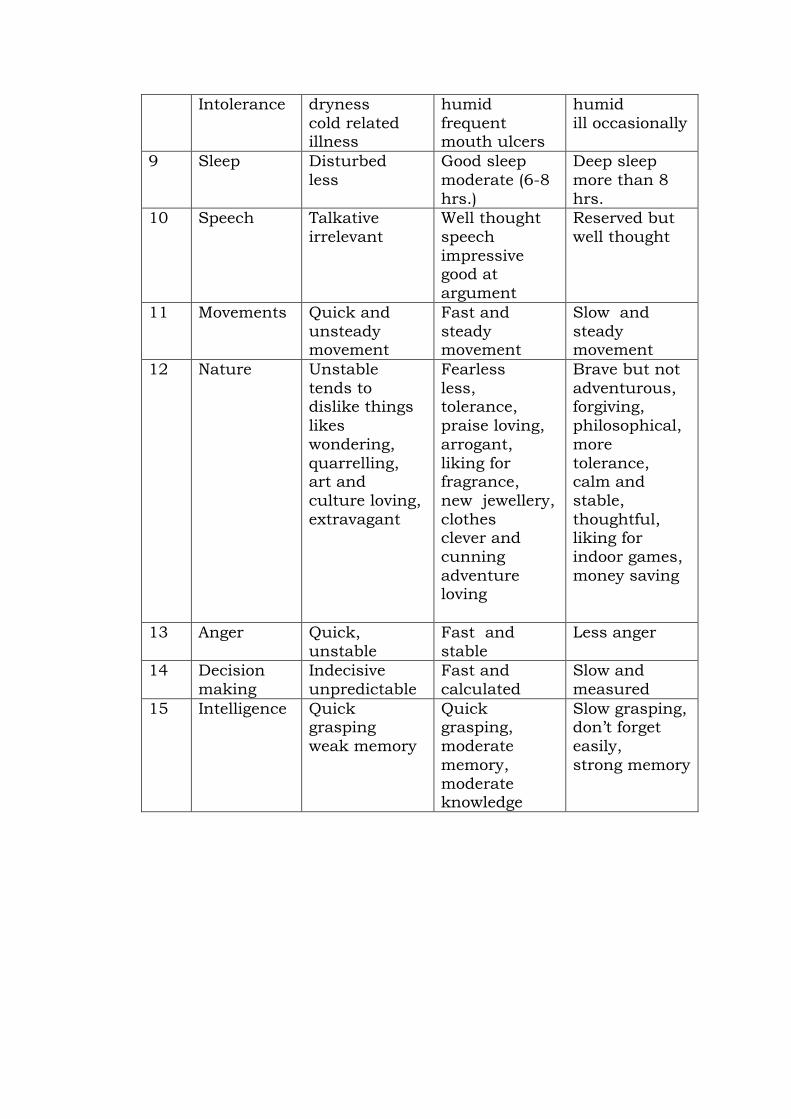
Intolerance dryness
cold related illness
humid
frequent mouth ulcers
humid
ill occasionally
9 Sleep Disturbed
less
Good sleep
moderate (6-8
hrs.)
Deep sleep
more than 8
hrs.
10 Speech Talkative
irrelevant
Well thought
speech
impressive good at
argument
Reserved but
well thought
11 Movements Quick and
unsteady movement
Fast and
steady movement
Slow and
steady movement
12 Nature Unstable
tends to dislike things
likes
wondering,
quarrelling, art and
culture loving,
extravagant
Fearless
less, tolerance,
praise loving,
arrogant,
liking for fragrance,
new jewellery,
clothes clever and
cunning
adventure loving
Brave but not
adventurous, forgiving,
philosophical,
more
tolerance, calm and
stable,
thoughtful, liking for
indoor games,
money saving
13 Anger Quick,
unstable
Fast and
stable
Less anger
14 Decision
making
Indecisive
unpredictable
Fast and
calculated
Slow and
measured
15 Intelligence Quick grasping
weak memory
Quick grasping,
moderate
memory,
moderate knowledge
Slow grasping, don‟t forget
easily,
strong memory
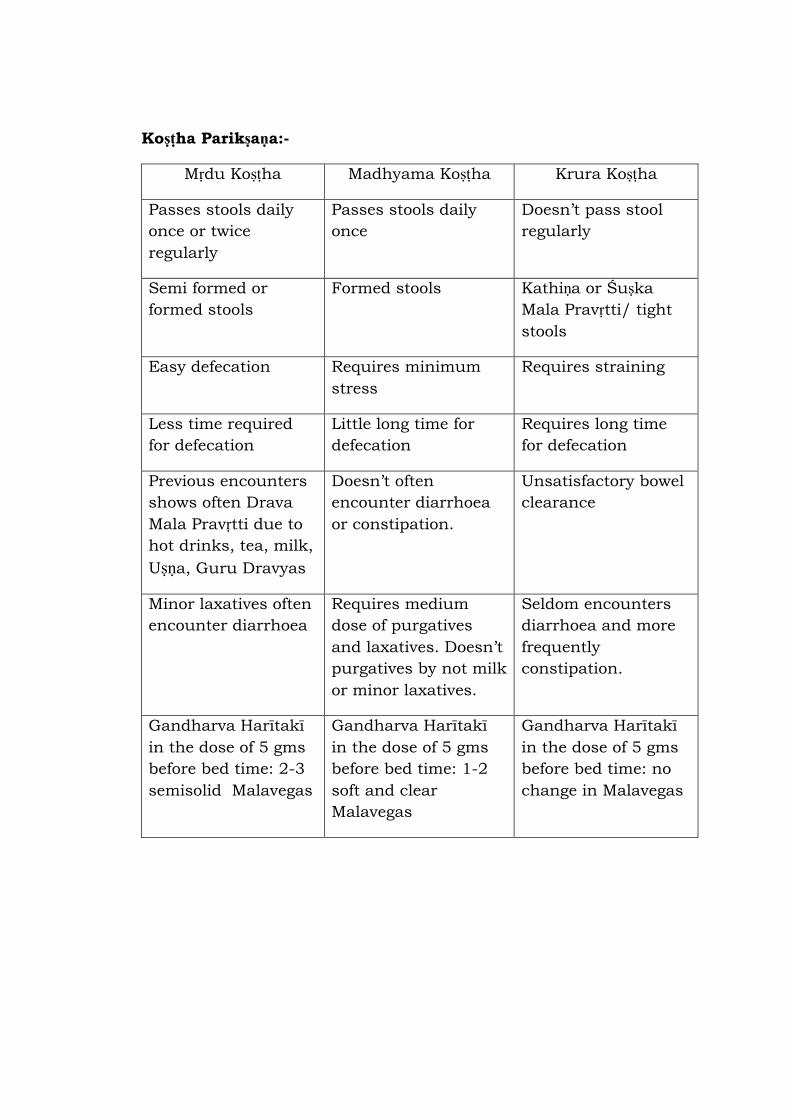
Koṣṭha Parikṣaṇa:-
Mṛdu Koṣṭha Madhyama Koṣṭha Krura Koṣṭha
Passes stools daily
once or twice
regularly
Passes stools daily
once
Doesn‟t pass stool
regularly
Semi formed or
formed stools
Formed stools Kathiṇa or Śuṣka
Mala Pravṛtti/ tight
stools
Easy defecation Requires minimum
stress
Requires straining
Less time required
for defecation
Little long time for
defecation
Requires long time
for defecation
Previous encounters
shows often Drava
Mala Pravṛtti due to
hot drinks, tea, milk,
Uṣṇa, Guru Dravyas
Doesn‟t often
encounter diarrhoea
or constipation.
Unsatisfactory bowel
clearance
Minor laxatives often
encounter diarrhoea
Requires medium
dose of purgatives
and laxatives. Doesn‟t
purgatives by not milk
or minor laxatives.
Seldom encounters
diarrhoea and more
frequently
constipation.
Gandharva Harītakī
in the dose of 5 gms
before bed time: 2-3
semisolid Malavegas
Gandharva Harītakī
in the dose of 5 gms
before bed time: 1-2
soft and clear
Malavegas
Gandharva Harītakī
in the dose of 5 gms
before bed time: no
change in Malavegas
Assessment of Agni:
As Agni is assessed by evaluating Jaraṇa Śaktī, Abhyavaharaṇa Śaktī
and Ruci; questions were asked to the patients and pattern of Agni
was decided.
To evaluation of Jaraṇa Śaktī (capacity to digest) questions were asked
to the patient regarding Jīrṇa Āhar Lakṣaṇa like 1.Utsāha 2. Laghutā
3. Udgāra Śuddhi 4. Kṣudha Tṛṣṇā Pravṛtti 5. Yathocita Malotsarga
To assess Abhyavaharaṇa Śakti (capacity to eat) quantity and
frequency of intake of food per day were asked to the patient.
B.V.M.F.‟s BHARATI AYURVED HOSPITAL
PUNE 43
INFORMED CONSENT
I, Mr./ Mrs./ Miss ………………………………………………age……..yrs.
hereby give my consent to undergo examination and subsequent
treatment in the project “Study of Anuvāsana Basti as an
alternative Purvakarm for Snehapan in Vaman and Virechan.”
Undertaken by Dr. Priyadarshani Kadus.
The project has been explained to me and I have fully understood it. I
give my consent to participate in the project as volunteer in complete
consciousness and without being under any pressure.
Date: sign/ thumb
saMmatIp~
maI KalaIla sahI krNaar EaI. / saaO
........…………………………………………………………..................vaya………
vaYao- ilahUna doto dotao kI, Da. ip`yadSa-naI kDUsa yaaMcyaa Aayauvao -d vaairQaI AByaasak`maaMtga-t
AnausaMQaana p`baMQaamaQyao ‚Anauvaasana baistcaa vamana ivarocanaacyaa pUva -kmaa-maQyao snaohpanaaeovajaI
]pyaaoga‛ yaa AByaasaasaazI icaik%saa krNaosa maaJaI puNa - tyaarI Aaho. yaa saMSaaoQana
p`klpamaQyao svat:hUna sahBaagaI haot AsaUna maaJaI tpasaNaI AaiNa ]pcaar krNyaasa
prvaanagaI dot Aaho.
Anauvaasana baist dotovaoLI ikMvaa kolyaanaMtr haoNaayaa pirNaamaaMcaI malaa Da@TraMnaI pUNa-
klpnaa idlaI Aaho AaiNa %yaasaaZI maaJaI tyaarI Aaho. kaoNa%yaahI AimaYaalaa ikMvaa
dDpNaalaa baLI na pDta malaa saMSaaoQana p`klpat saaimala k$na GaoNyaasa prvaanagaI dot
Aaho.
idnaaMk : sahI / AMgaza